

Notes
Article history
The research reported in this issue of the journal was funded by the EME programme as project number 14/202/03. The contractual start date was in January 2016. The final report began editorial review in October 2017 and was accepted for publication in June 2018. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The EME editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
none
Disclaimer
This report contains transcripts from group session recordings obtained in the course of the research and contains language that may offend some readers.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2019. This work was produced by Borek et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2019 Queen’s Printer and Controller of HMSO
Chapter 1 Introduction
Background
Optimising the effectiveness of health-related behaviour change interventions is contingent on understanding the mechanisms by which such interventions can bring about change and developing techniques to alter processes underpinning this change. Recent work on behaviour change has led to the identification, classification and integration of > 80 behaviour change theories1,2 and > 90 categories of behaviour change techniques. 3,4 Some techniques are frequently employed in behaviour change interventions and can be reliably identified from descriptions of interventions. 5 Evidence indicating which theorised mechanisms and which types of techniques might improve intervention effectiveness when targeting particular behaviours is accumulating. 6–8 For example, self-regulatory behaviour change techniques, such as goal-setting and self-monitoring, have been found to be associated with increased effectiveness in interventions targeting diet and physical activity. 6,8 However, the majority of the theorised mechanisms and technique types studied to date focus on individual-level, intrapersonal change, with little or no consideration of social, interpersonal or group-based processes and factors that shape health-related behaviour patterns. Furthermore, these mechanisms and techniques are often assumed to work similarly in interventions regardless of their delivery mode or setting (e.g. when self-delivered, delivered one to one, through group sessions, online or over the telephone).
For decades, small groups have been used to facilitate personal change in health-care, community, commercial and work settings. Theories explaining, and research into, how such groups work have developed over many years and across multiple disciplines. Research has demonstrated that groups are not just an intervention delivery mode (that allow delivery of an intervention simultaneously to many people) but, additionally, provide ‘active ingredients’ in facilitating personal change. For example, as early as 1905, Joseph Pratt highlighted the importance of group identification (or group ‘spirit’), social support and shared hope in psychotherapy groups for tuberculosis patients. 9 In addition to psychotherapy,10 groups have also been used to promote personal change in human relations training (also called sensitivity training or ‘T’ groups)11,12 and self-help and support programmes. 13 More recently, many health promotion and health-related behaviour change programmes have been delivered in groups. For example, interventions supporting self-management of chronic conditions,14–16 including type 2 diabetes mellitus17 and cancer,18 are commonly delivered in groups. Groups have also been used in preventative contexts to promote breastfeeding,19 walking and physical activity,20,21 smoking cessation22 and weight loss. 23,24
There is increasing evidence from systematic reviews that group-based interventions are effective for supporting change in a number of behavioural targets. 17,22,23 Indeed, particularly for weight loss, group interventions appear to be more effective than similar interventions delivered individually. 24 Group-based interventions therefore provide a time-effective and potentially cost-effective way to address important health challenges, including those related to growing rates of overweight and obesity that are contributing to the increasing burden of chronic conditions.
Group-based interventions show wide variation in their design and delivery. Perhaps because of this, there is still limited understanding of, and evidence on, which mechanisms lead to personal change in group interventions, how short- and long-term behaviour change is best facilitated in groups and what design features, change processes or delivery methods optimise the effectiveness of group interventions. Identifying important design features, change processes occurring in groups and techniques that can be used to facilitate changes is, therefore, a first step towards improving the effectiveness of group-based interventions. Group-based delivery provides an ideal opportunity for use of change techniques involving interpersonal interaction, such as ‘providing opportunities for social comparison’ or ‘prompting identification as a role model’. 3 Furthermore, some types of change techniques are unique to group settings, such as ‘engage group support’ or ‘communicate group member identities’. 25 It is unclear, however, how pre-categorised change techniques and processes operate in groups and how they are influenced by group characteristics, context and facilitation, and which currently undefined, group-specific techniques and processes may support personal change in groups. Therefore, the lack of clarity about what works and how is even more acute in group-based than individual behaviour change interventions.
Understanding change processes in groups is crucial to the design and evaluation of group-based health interventions. Medical Research Council (MRC) guidance26,27 on developing complex health interventions highlights key questions that intervention designers need to ask, including about what the intervention aims to achieve and change, and how. Considering groups only as a delivery mode limits their potential to contribute to the theoretical underpinnings, often represented in a logic model explaining the mechanisms by which the intervention works. MRC process evaluation guidance28,29 further emphasises that, in order to understand how complex interventions work, it is important to describe and assess (1) how they are delivered and implemented (fidelity and quality of implementation), (2) their mechanisms of action (causal processes generating change) and (3) whether or not, and how, they may work differently across settings and contexts (contextual influences). As shown in Figure 1, all three of these domains have implications for delivering health interventions in groups.
FIGURE 1.
Logic model of components influencing behaviour change and outcomes in group interventions. Note: the figure draws on logic model framework presented in MRC process evaluation guidance28,29 showing generic processes that may occur in group-based interventions that are broadly organised into the key commonly included process evaluation elements of context, implementation, mechanisms of action (i.e. how interventions produce change in participants) and outcomes. 28,29
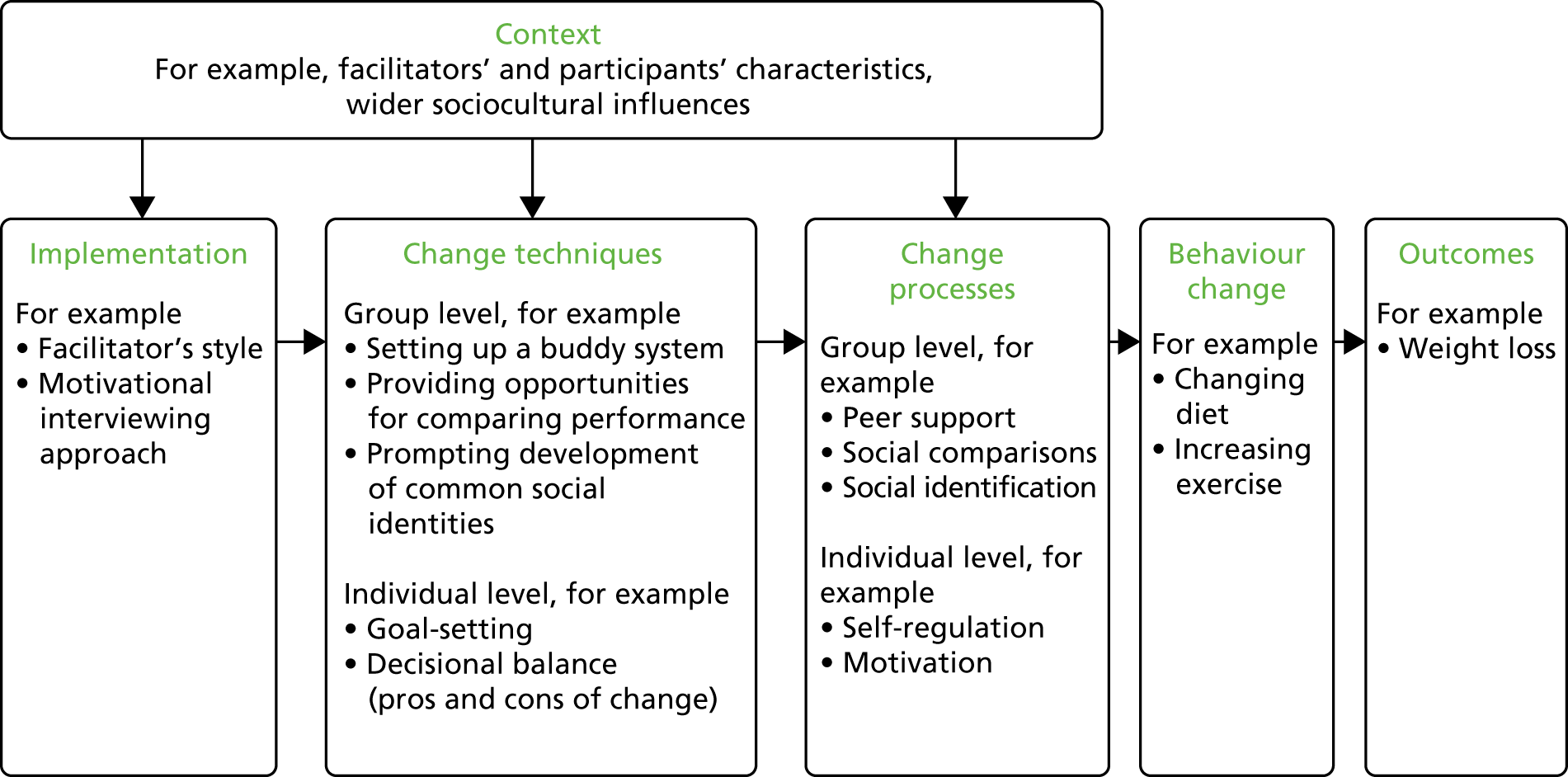
First, it is important to document and investigate how interventions are implemented in groups, including the amount (‘dose’) and pattern of group contact, training of facilitators, resources used, fidelity of delivery and if, or what, adaptations in delivery are made when the same group-based intervention is replicated in different contexts. It may also be important to explore differences between groups in relation to facilitator delivery style and participant engagement and interaction. Second, investigating change processes in groups is important in understanding mechanisms by which they have an impact on psychological and behaviour change, including potentially unexpected or adverse processes and consequences. Third, group interventions may be affected by contextual factors, including the wider sociocultural environment (e.g. social norms and values), organisational context (e.g. climate, setting or type of organisation) or individual characteristics and circumstances that participants and facilitators bring to groups (e.g. gender, available external support and social networks). These group-related moderators of intervention effects are often omitted in studies that focus on mechanisms or mediators of intervention effects in isolation, such as studies in which change techniques are considered separately from aspects of implementation and context. 30
The lack of understanding about how behaviour change interventions work, particularly when delivered in groups, is further compounded by reliance on systematic reviews and meta-analyses to explore quantitative relationships between intervention features and outcomes across previous studies. 6,8,31 Despite the importance of synthesising data across multiple studies, this type of research assumes that descriptions of interventions, which are often brief in journal articles or design protocols, are complete and accurate reflections of what was delivered in practice. A critical limitation of this approach is that it cannot account for differences in fidelity (i.e. the extent to which the intervention was delivered in line with the protocol) or style of delivery. This review of group-based weight loss interventions has shown that details of fidelity assessment in group session delivery, the methods used to facilitate groups, group processes observed and change techniques employed are rarely reported. 23 A review of group studies in nursing journals showed that information on the conduct of groups and attempts to account for group-level effects in analyses were largely absent. 32 This makes it impossible to identify the ‘active ingredients’ and change mechanisms in group interventions from study reports included in systematic reviews. It also makes it difficult to accurately replicate effective group-based interventions.
In addition, meta-analytic data are only as good as the categories used to group and differentiate between the included interventions. Consequently, if the categories are too inclusive (i.e. they count interventions as having similar features when they are, in reality, different), then the results can be misleading. This has been referred to as the ‘apples and oranges’ problem. Abraham33 illustrated how this problem may affect interpretation of meta-analytic studies in which the authors sought to identify techniques designed to alter psychological processes in behaviour change interventions. Consider, for example, a category of change techniques such as ‘encouraging social support’. This refers to a variety of facilitation techniques designed to prompt change in interpersonal relationships between the target person and some other person(s). Yet we know that there are many different types of social support that can be provided by many different people and evidence shows that these have quite different psychological effects on the receiver. 34 Similarly, meta-analytic studies may generate misleading findings if they do not include categories of techniques that are critical to real-world change. For example, a review of 72 evaluations of interventions designed to alter eating behaviour identified 19 categories of techniques employed to modify or manage impulsive processes associated with unhealthy eating behaviour, many of which had not been used in previous meta-analyses of healthy eating interventions. 35 There is, therefore, a need for research to enrich understanding and enhance specificity of how similarities and differences between behaviour change interventions are conceptualised.
This need is especially evident in relation to group-based health-related behaviour change interventions, for which research is needed to identify what processes underpin personal change in such groups and which techniques, or groups of techniques, can be employed to modify those processes. Such research can draw on an extensive literature from social psychology, education and organisational studies on how groups in general work and how they influence individuals. Unfortunately, however, this literature has been largely ignored in designing and evaluating group-based health interventions. 36 In particular, social psychological literature on group dynamics from which more specialist fields evolved (e.g. work-related teams and educational groups) describes how both intrapersonal and interpersonal processes operate in groups. 37–39 A review of this literature40 has identified a number of theories describing change processes in groups, such as social comparisons,41 social learning,42 social identity43 and social facilitation44 theories, that could be used to enhance our understanding of how groups influence individuals and how group context and facilitation can enhance or inhibit change in health interventions. Moreover, the ‘social cure’ approach to health applies social identity theory to conceptualise links between group membership and improved health. 45,46 Qualitative studies with group participants and facilitators also highlight the importance of the group context in influencing engagement with health interventions and behaviour change. For example, interviews conducted with participants in three different group-based health interventions showed that making social comparisons, developing a shared social identity and creating a supportive and friendly group context were important factors that facilitated participants’ engagement with the interventions and lifestyle changes. 47–49 Effective facilitation of groups to promote these group-level processes can be challenging, particularly for lay leaders,50 and it requires specific competencies. For example, 23 facilitator competencies, such as ‘encourage group discussions’ or ‘encourage mutual support’, have been identified as being required to deliver group-based smoking cessation interventions. 51 However, there is little evidence on which (and how) skills and competencies are employed in practice, which might lead to inadequate training of group facilitators.
The importance of employing systematic approaches to designing and evaluating group-based health interventions has been stressed previously. 36 This provided an important first step by identifying some of the key factors in group interventions related to group leaders, participants, community and environment. However, it does not show how these factors are related to change techniques and mechanisms of change. Borek and Abraham40 present a conceptual model linking our understanding of group processes and personal change to change mechanisms in group interventions. The work reported in this study extends that model and seeks to identify change techniques that may optimise the effectiveness of group interventions.
In contrast to many of the recent approaches to behaviour change, we began with an assumption – based on wider research on groups – that change processes can be influenced by, or even unique to, group delivery. Therefore, the promotion of individual change in groups may be critically different from that in individual behaviour change interventions because the former activate distinct interpersonal change processes. More generally, different delivery modes (e.g. internet based vs. face to face) may prompt different change processes and so affect effectiveness even when intervention content appears similar.
Groups provide opportunities for enhancing individual change processes and instigating social change processes, but may also impede some change processes or have adverse or unintended negative consequences. For example, groups may enhance individual problem-solving by providing opportunities to share and draw from others’ ideas, access peer support and identify with people in a similar situation. However, lack of time and/or tailoring to individual needs in a group might impede individual goal-setting and review, negative group dynamics might impede engagement and/or attendance, and poorer performance compared with other group members might lead to decreases in self-efficacy. Moreover, group facilitators’ characteristics and skills may improve effectiveness for one group but decrease effectiveness for another, depending on relationships between the facilitators and group members. 52 Techniques to alter normative beliefs may promote behaviour change among young people but reduce intervention effectiveness for older recipients. 53 Group climate and group cohesion may increase attendance and self-efficacy (in exercise classes). 54 The use of humour may help engage middle-aged men in a weight loss intervention55 but have an opposite effect among young women in a sexual health intervention. 56 Furthermore, many health-related behaviour patterns are influenced by sociocultural contexts (e.g. social norms) and are social practices enacted in social contexts (e.g. eating with others, eating out) with attached meanings, norms and values. Groups can, therefore, help change behaviour patterns that are both individual and social. For example, they can help change individual perceptions of social norms, identify solutions to common barriers encountered in social contexts, change meanings and values attached to social practices, or provide opportunities to practise relevant social skills, such as communication skills. Consequently, sophisticated models of group operation including specification of change mechanisms, group composition, facilitator characteristics and techniques employed by facilitators to promote personal change, as well as other influences of group implementation and context, are needed to optimise group-based interventions.
In summary, although group interventions are effective and commonly used in health-care and public health contexts, their mechanisms of action, representing how and why they work, have not been systematically explored. It is therefore not clear how groups operate and group processes function to engender or impede personal change, and what factors related to implementation and context influence mechanisms of change and intervention outcomes. Most current thinking about mechanisms that underpin behaviour change is based on individual-level theories. Moreover, meta-analyses of intervention components associated with effectiveness are mainly based on descriptions of interventions, which, particularly for group interventions, are limited by a lack of comprehensive reporting and inadequate categorisation of the real-world differences between interventions. Distinctions between group implementation, facilitation, change processes, change techniques and contextual factors are rarely clarified in a way consistent with the MRC framework for process evaluation,28,29 and there is little evidence on how these components are manifested in practice. The most modifiable elements of group-based interventions are the change techniques that facilitators use and their style of delivery. We do not, however, have a conceptual framework for systematically investigating what processes and techniques operate, and are effective, in group interventions, or for identifying facilitators’ delivery techniques and styles, and their influences on these processes. This is problematic for the construction of logic models in intervention development, the design of process evaluations and the training of facilitators in intervention delivery. Only with a better understanding of the change mechanisms in group interventions, and guidance on how important processes can be activated and facilitated, will we be able to guide development and delivery of interventions to optimise effectiveness. Starting with the MRC process evaluation guidance28,29 and existing literature on groups, this study is a step towards addressing these gaps in the research.
Study aims and objectives
This Mechanisms of Action in Group-based Interventions (MAGI) study aimed to develop a better understanding of mechanisms of action in group-based health-related behaviour change interventions by identifying, describing and synthesising possible processes of change in groups. It also aimed to develop and illustrate methods for exploring the influence of change processes in group-based behaviour change interventions (GB-BCIs). We focused on the example of group-based weight loss interventions targeting diet and physical activity. Our hypothesis was that behaviour change interventions delivered in groups involve change techniques and change processes that are specific to the group setting, and that may be influenced by implementation and contextual factors. The successful initiation and facilitation of these change techniques and processes would lead to increased engagement with the intervention and more effectively promote behaviour change (e.g. diet and physical activity), thereby improving intervention outcomes (e.g. weight loss). Overall, the project aimed to increase understanding in order to guide the future design, delivery and evaluation of GB-BCIs.
In order to achieve this aim, the study had three more specific objectives. These were to:
-
develop a generalisable framework of mechanisms of action in GB-BCIs by identifying, defining and categorising potentially important group design features, group processes, facilitation techniques and contextual factors in groups
-
test and refine the framework, using a coding schema derived from it, as a tool for identifying these group features, processes and facilitation techniques in the recordings of sessions from three GB-BCIs (focused on diet, physical activity and weight loss), and to provide examples to illustrate framework elements
-
develop mixed-methods approaches based on the framework to explore why some groups may be more or less successful than others, and to illustrate their use with available qualitative and quantitative data from a GB-BCI.
Study outline
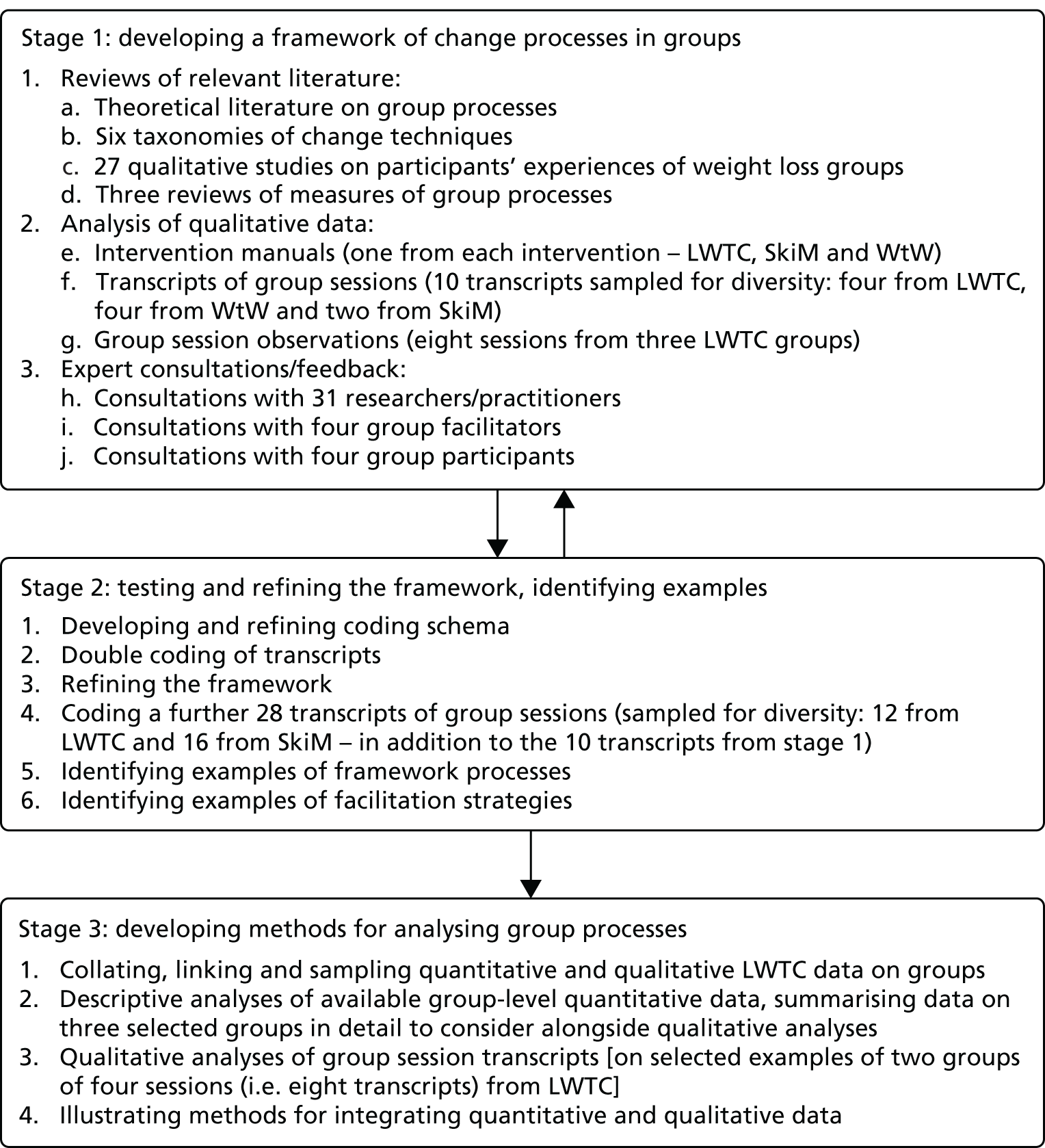
These three objectives were addressed in three stages, which are reported in the subsequent chapters: Chapter 2 provides a description of the framework and its development (objective 1), Chapter 3 reports on the development and use of a coding scheme derived from the framework for analysing group sessions and provides examples of the concepts, processes and techniques included in the framework (objective 2), and Chapter 4 reports on the development of methods for applying the framework to analyse how groups work in a weight loss intervention and how such methods might be employed to explore potential links with outcomes (objective 3). Figure 2 outlines the tasks completed in the three stages over 20 months between January 2016 and August 2017.
FIGURE 2.
Outline of the key stages of the MAGI study. LWTC, Living Well Taking Control; SkiM, Skills for weight loss Maintenance; WtW, Waste the Waist.
Sources of data: three group-based interventions
The MAGI study builds on three studies of GB-BCIs: the ongoing (at the time of conducting this study) Community-based Prevention of Diabetes (ComPoD) trial (Jane Rebecca Smith, University of Exeter Medical School, September 2017, personal communication) that evaluated the Living Well Taking Control (LWTC) programme and the Skills for weight loss Maintenance (SkiM) study (Colin Greaves, University of Exeter Medical School, September 2017, personal communication), and the completed Waste the Waist (WtW) study. 57–59 All three were primarily delivered in South West England and targeted adults who were overweight [average body mass index (BMI) in the obese range]. The ComPoD and WtW studies targeted other risk factors for chronic disease, and recruited samples that were older but otherwise broadly representative of local populations in terms of their gender mix and low numbers of participants from non-white British backgrounds. The interventions all targeted lifestyle changes, such as improving diet and increasing physical activity, in order to achieve or maintain a healthy weight and prevent obesity-related diseases (i.e. type 2 diabetes, cardiovascular diseases). The interventions were delivered in small groups (up to 12 participants) by facilitators with backgrounds in health promotion, and in accordance with intervention delivery manuals. In this study, we used secondary data that were already available or able to be collected as part of the ongoing studies, including intervention delivery manuals, audio-recordings of group sessions and outcome data. In particular, we used audio-recordings made as part of the process evaluations and quality assurance in the three studies (ComPoD: ≈80 sessions, SkiM: ≈88 sessions, and WtW: ≈36 sessions). The three studies had received research ethics committee approvals (ComPoD: 14/NW/1113, SkiM: 5/SW/0126, WtW: 10/H0206/74) with participants giving consent for audio-recording the sessions for use in research. In the following sections, we describe each study, and Table 1 summarises the key details of the interventions and data used from each study.
| Study details | Intervention | ||
|---|---|---|---|
| LWTC/ComPoD | SkiM | WtW | |
| Intervention details | |||
| Aim | Improve diet, increase physical activity and improve well-being to promote weight loss and prevention/management of type 2 diabetes in those at risk/newly diagnosed | Address weight loss maintenance issues in obese adults accessing weight management services | Promote healthy eating, physical activity and weight loss for people with high cardiovascular risk in primary care |
| Setting, venue | Community venues in and around Exeter and Birmingham | Community venues in Devon | Community venues in Bath and North East Somerset |
| Provider | Westbank Community Health and Care, westbank.org.uk (Exeter); Health Exchange, healthexchange.org.uk (Birmingham) | Westbank Community Health and Care, and the Healthy Lifestyles service of Torbay and South Devon NHS Foundation Trust | Local, community-based facilitators recruited for the research study |
| Contact time | Four weekly 1- to 2-hour group sessions plus five follow-up support contacts at 2, 3, 6, 9 and 12 months (varying in delivery format across time points/sites) and access to ≥ 5 hours of classes/activities (e.g. exercise classes, walking groups, cooking classes) | 14 fortnightly 1.5-hour sessions | Four weekly 2-hour sessions plus five 1.5-hour follow-up sessions, up to 1 year |
| Main content | Information and addressing common misconceptions around type 2 diabetes, clinical risk factors (e.g. HbA1c levels) and lifestyle changes | Address weight loss maintenance issues based on principles including the personal assessment and management of sources of ‘tension’ caused by making lifestyle changes and managing internal and external influences on this tension | Promotion of healthy eating, physical activity and weight loss, plus motivation, social support, self-regulation and understanding of the behaviour change process |
| Participants’ materials | Participant handbook, self-monitoring diaries | Participant handbook, self-monitoring diaries, automated telephone text reminder service | Participant handbook, self-monitoring diaries |
| Group composition and allocation of participants | Up to 12 participants (partners could attend), allocated to groups based on location/time | Up to 15 participants | 8–12 participants (partners could attend), allocated to groups based on location |
| Number and professional background of facilitators | One facilitator per group with nutrition or physical activity background | One facilitator with weight loss management background and | Two co-facilitators per group, with nutrition, physical activity, fitness or health promotion background |
| One assistant per group with visiting experts (dietitian, fitness trainer) in some sessions | |||
| Facilitator training and materials | 1-day training in intervention delivery; facilitator manual | 2-day training in intervention delivery, person-centred counselling style and group facilitation; feedback meetings every 2 months to discuss progress and to problem-solve any barriers to delivery; facilitator manual | 2.5-day training in intervention delivery and person-centred counselling style; feedback meetings every 2 months to problem-solve any barriers to delivery; facilitator manual and slides |
| Data used in the MAGI study | |||
| Delivery manuals | LWTC – Pre-diabetes Training Manual (v4, August 2013, 52 pages); authors: Westbank and Health Exchange, with advice from Colin Greaves, University of Exeter Medical School, (unpublished, available from authors on request) | SkiM weight management programme – Programme Manual (v1, March 2016, 185 pages); authors: Colin Greaves, University of Exeter Medical School, and Leon Poltawski (unpublished, available from authors on request) | WtW – Lifestyle Coaches Manual (2011, 73 pages); authors: Colin Greaves, University of Exeter Medical School, Afroditi Stathi and Fiona Gillison (unpublished, available from authors on request) |
| Session recordings (see Appendix 1) | 24 in total | 18 in total | 4 in total |
| Stage 1 | Four transcripts: two from two groups, delivered by two facilitators | Two transcripts from one group, delivered by one facilitator | Four transcripts: two from two groups, co-delivered by two of five facilitators |
| Stage 2 | 12 transcripts from eight groups, delivered by four facilitators | 16 transcripts: four from four groups, delivered by two facilitators | |
| Stage 3 | Eight transcripts from two groups, delivered by two facilitators | ||
| Session observations | In stage 1: eight sessions from three groups | None | None |
| Quantitative data | In stage 3: participant characteristics, attendance and outcomes collected by providers as part of programme | None used | None used |
Living Well Taking Control programme in the Community-based Prevention of Diabetes trial (www.isrctn.com/ISRCTN7022167060,61)
The LWTC programme was an existing community-based diabetes prevention and management programme delivered by voluntary sector organisations from late 2013. The structure, content and delivery of LWTC were intended to be compliant with all 11 recommendations of the National Institute for Health and Care Excellence (NICE) guidance for diabetes prevention interventions. 62 A before-and-after service evaluation of the LWTC programme led by the University of the West of England was completed in September 2016. 60 The clinical outcomes and cost-effectiveness of the diabetes prevention component were evaluated in the ComPoD trial, which was a randomised waiting list controlled trial completed in March 2017. In the ComPoD trial, 314 adults at a high risk of developing type 2 diabetes were recruited via general practices and randomised to receive the LWTC programme either immediately (intervention group) or after 6 months (waiting list control group). The study primary outcome was objective weight loss, and secondary outcomes included changes in physical activity (assessed via accelerometers), blood glucose levels [indicated by levels of glycated haemoglobin (HbA1c)] and self-reported diet and well-being at 6 months, with observational follow-up at 12 months of the intervention group only.
Skills for weight loss Maintenance study (www.isrctn.com/ISRCTN45134679)
The SkiM study is a feasibility study using an action research design and observational (pre–post) evaluation of weight outcomes, which was ongoing at the time of writing. The aim is to develop intervention materials that specifically address weight loss maintenance and integrate them into existing weight management services. The study aims to inform development of a future trial that will be used to evaluate the resulting intervention programme. A total of 45 adults with a BMI of > 30 kg/m2 were recruited in the first round of intervention delivery. They had agreed to take part in one of two existing tier 2 community-based weight loss programmes delivered by local participating voluntary sector and NHS-based service providers. As well as feasibility measures for a future trial (e.g. recruitment, attendance, retention rates), the study outcomes include change in weight at 6, 12 and 18 months, physical activity (assessed via accelerometers), BMI, waist circumference and self-reported health status. A process evaluation assesses engagement, processes of change, intervention fidelity and ways in which the intervention could be improved using participant and provider interviews, questionnaires, session recordings and observations. Data gathered during a first presentation of the intervention was used to refine the intervention, then evaluated in a second iteration.
Waste the Waist study (www.isrctn.com/ISRCTN1070789957–59)
The WtW study, completed in 2013, was a pilot randomised controlled trial of a theory-based group intervention. A total of 108 adults at a high risk of type 2 diabetes or heart disease were randomised to the group-based intervention plus usual care or to usual care alone. The primary outcome was change in objective measures of weight at 12 months. Secondary outcomes included changes in diet, physical activity (assessed via accelerometers), markers of cardiovascular risk (e.g. blood pressure, blood glucose) and quality of life at 4 and 12 months.
Key terms
Throughout this report, we use a number of key terms, some of which are defined in Table 2. Other terms, in particular those derived from the literature reviews, are defined in Table 3.
| Key terms | Definitions |
|---|---|
| Mechanisms of action | Components of interventions in health behaviour change interventions, including change techniques and change processes, through which an intervention has its effect, in our examples leading to changes in participants’ behaviour and health outcomes |
| Change processes | Processes that are theorised to lead to individual behaviour or other psychological change, and thus, other intervention outcomes; they may instigate and facilitate change, or impede it. For example, motivational, learning processes |
| Interpersonal change processes | Change processes that are instigated through interaction with, or presence of, one or more other people |
| Intrapersonal change processes | Psychological processes that occur within individuals to bring about personal change |
| Change techniques | Techniques that facilitators can use, or prompt participants to use, to instigate or support change processes. Although these are commonly referred to as ‘behaviour change techniques’, we refer to them as ‘change techniques’ because they initially instigate psychological change that may or may not lead directly to behaviour change. For example, use of ‘if–then’ plans is initially an intrapersonal change that may/may not lead to change in behaviour patterns. Note too that when we refer to change techniques, we really mean a set of categories or types of technique because, for example, if–then plans take many different forms |
| Facilitation techniques | Techniques that facilitators use to facilitate groups, group interaction and change processes. They may include change techniques or more generic techniques to facilitate interaction. For example, facilitating group discussion, prompting individual introductions in groups |
| Interventions | Interventions, programmes or treatments that aim to facilitate individual health-related change processes, and thus improve health or prevent illness |
| Modes of delivery | Overall approach to how an intervention is delivered, such as through one-to-one consultations, groups, self-delivery (e.g. manuals, apps or websites), in person or online |
| Group | At least three people who interact with each other |
| Group-based interventions | Interventions partly or fully delivered in groups, that is, including at least three participants (or group members) and usually at least one facilitator (or leader) |
| Behaviour change interventions | Interventions, or programmes, that aim to bring about changes in individual behaviours |
| Group-specific change techniques/processes | Processes or techniques that are delivered through interaction between two or more people, and, thus, may be unique, or particularly suitable, to group-based delivery. For example, buddying up, peer support |
| Group-sensitive change techniques/processes | Processes or techniques that can be self-delivered on one’s own, one on one or in a group setting, but when delivered in groups, they may be affected by the group interactions. For example, problem-solving or goal-setting – conducted individually vs. discussed in a group (e.g. involving sharing ideas, suggestions, modelling) |
Chapter 2 Development of the Mechanisms of Action in Group-based Interventions framework (stage 1)
Background and rationale
As noted in Chapter 1, there is a wealth of research on group processes and how groups affect individuals,37,38,64,65 and a long tradition of using small groups to support personal change, promote health and deliver education (e.g. in group psychotherapy and counselling,10,12,66 self-help and support groups,13 chronic disease self-management programmes,14,17 health-promoting interventions20–22 and team-based learning initiatives67). Delivery of health interventions in groups allows people to support and learn from each other and takes better account of the fact that many health-related behaviours are performed with, or in the presence of, other people and are subject to social influences. With the increased prevalence and social and economic burden of preventable, lifestyle-related diseases, groups therefore offer a suitable and potentially cost-effective way to deliver health-related behaviour change interventions.
To date, theories specifying processes capable of regulating and changing behaviour patterns and techniques that may be used to modify those processes have focused on intrapersonal change, occurring within individuals. However, change processes are often initiated and facilitated through social interaction, and are affected by social context, including group settings. Thus, social, interpersonal processes may direct and alter intrapersonal processes. Yet our understanding of how interpersonal interaction in groups initiates and shapes intrapersonal change is limited. This might be because research into group-promoted personal change and research into intrapersonal change processes that explain changes in individual behaviour have developed in parallel with little cross-fertilisation of ideas. Further research is needed to ascertain how health behaviour change interventions work in group settings, how intrapersonal change processes might be shaped by group context and which interpersonal change processes are critical to group effectiveness. Such research would be greatly facilitated by a synthesis of the current knowledge of group processes and change mechanisms in groups. Therefore, in the first stage of this study, we aimed to identify important elements related to the design, implementation, context and change processes operating in GB-BCIs. Drawing on existing research, we aimed to develop a framework to bring together and categorise potentially important intervention components, and change processes and techniques that explain the mechanisms of action in GB-BCIs.
Methods
We developed a framework of change processes in group-based interventions by bringing together findings from three approaches. We focused in particular on face-to-face, adult groups that target health-related behaviour and other psychological change. First, we built on reviews of relevant literature, including theoretical literature on group dynamics and group change processes, taxonomies of categories of change techniques, qualitative studies of participants’ experiences of group-based weight loss interventions, and measures of group processes. Second, we qualitatively coded the content of delivery manuals and recordings of group sessions from three recent GB-BCIs targeting weight loss. Third, we consulted experts, including group participants, facilitators and researchers. The findings from each approach helped to develop, refine and revise the framework in an iterative fashion. For an outline of this stage of the research, and how it fits in with other stages of the study, see Chapter 1. The three approaches used and how findings from them were brought together are described in detail in the following sections.
Reviews of relevant literature
Foundational previous research
The initial concepts used in the framework were based on an earlier programme of work on GB-BCIs,68 in particular a checklist for reporting of GB-BCIs69 and a conceptual review and model of change processes in groups. 40 In this work, we identified and reviewed relevant theoretical literature on how groups work and how group processes can enhance or impede individual change.
A systematic review of theoretical literature on change processes in groups was not feasible because of the extensiveness of this literature, which spanned a number of decades and disciplines. A search for ‘group dynamics’ in MEDLINE in early 2016 resulted in over 33,000 references, and searching and screening of The British Library catalogue identified > 160 potentially relevant books. 40 Consequently, we employed a pragmatic approach to identify and integrate relevant concepts, processes and theories. We began with a previously developed model of change processes in groups (see Appendix 2)40 and key books summarising research on groups. 10,12,37,64,70 We conducted further selective searches of electronic databases (e.g. MEDLINE, PsycINFO) for this study using key search terms relevant to specific processes included in the previous model (e.g. ‘social support’) and types of groups (e.g. ‘support groups’). We also hand-searched for relevant, useful articles in recent issues of the following journals: Psychological Review, Psychological Bulletin, Social Science & Medicine, Sociological Review, Educational Review, Journal for Specialists in Group Work and Group Dynamics: Theory, Research and Practice. Concepts or processes identified in these sources were compared with, and added to, the earlier concepts, resulting in the development of an initial framework. We also used the key books and articles on groups37,38,71 to extract definitions of key concepts, which were then discussed and agreed on with the study team members.
The earlier research40 resulted in a conceptual model identifying five categories of interacting processes: (1) group development processes, (2) dynamic group processes and properties, (3) social change processes, (4) personal change processes and (5) group design and operating parameters. Each of these categories encompasses a variety of theorised mechanisms explaining individual change in small groups. Key change processes included in each of these categories are shown in Appendix 2. This work provided a conceptual foundation for stage 1 of the MAGI study.
Taxonomies of change techniques
A series of taxonomies have defined categories of change techniques3,4,35,53,72 and some have linked these to change mechanisms specified by empirically tested theories. 3,53,72 These categories refer to sets of techniques that may differ in implementation across interventions. For example, ‘encouraging social support’, ‘inducing cognitive dissonance’ or ‘facilitating formation of if–then plans’ can be implemented in quite distinct ways and so refer to different practices in different interventions. 33 Nonetheless, we will use the term ‘technique’ as shorthand for a defined category of potentially effective actions or practices assumed to influence a specified change mechanism that, consequently, may/may not be effective in prompting behaviour change in particular contexts. 23,33
Taxonomies of change techniques were used as a source of potentially important change processes and techniques in group settings. One researcher (AJB) initially used the taxonomies to select techniques that were likely to be specific to group-based delivery (i.e. group specific) or that could be affected by group delivery (i.e. group sensitive) and incorporated them into the developing framework. Then, after the framework was further developed, two researchers (AJB and CA) reviewed each taxonomy again and compared each technique category included in these taxonomies for correspondence with the draft framework. Any additional techniques were considered for relevance to GB-BCIs (being either specific or sensitive to group setting) and, when relevant, added to the framework.
Qualitative studies
One researcher (AJB) searched electronic databases (MEDLINE, PsycINFO, PsycARTICLES, EMBASE, Social Policy and Practice accessed via Ovid platform) between January 2000 and June 2016 using a detailed search strategy [based on the PICOS (participants, interventions, comparisons, outcomes, study design) model,73 see Appendix 3] to identify qualitative studies of participants’ experiences or perceptions of group-based weight loss programmes. We included qualitative studies of lifestyle-based weight loss interventions for overweight or obese adults that reported findings related to group-based delivery (e.g. participants’ perceptions of groups, how the group setting might have influenced their experience of the intervention, behaviour change or weight loss). The included reports were uploaded to NVivo software, versions 10 and 11 (QSR International, Warrington, UK), in which the findings were coded for themes common across studies. The identified themes were compared with and, when relevant, added to the developing framework. After the framework was further refined (following stage 2, see Chapter 3), the themes developed from the qualitative studies were revised to correspond with the structure of the framework and, when appropriate, individual codes were renamed to match the framework categories. For further details of the review of qualitative studies, see Appendix 3.
Measures of group processes
We initially intended to search electronic databases for individual measures of group processes. However, our scoping searches identified existing reviews of such measures. Consequently, we used these reviews to extract details of, and references to, measures of group processes and change in groups. We then compared the concepts operationalised in these measures with the developing framework, and any new concepts or processes were considered for inclusion in the framework. Following this, we decided not to conduct further specific database searches for individual measures.
Analysis of qualitative data
In order to include in the framework categories that would apply to ‘real-life’ GB-BCIs and to help clarify and refine the definitions of the framework categories, we conducted qualitative coding of the content of intervention manuals and group sessions sampled from three recent GB-BCIs: LWTC, SkiM and WtW (see Table 1). The secondary data from these interventions were uploaded to, and coded in, NVivo software (v10/11).
Intervention manuals
We selected one primary intervention manual from each study. The manuals provided information to be used by the group facilitators as the basis for delivering the intervention. The content of the manuals was coded thematically, and the emerging coding schema was compared with the developing framework. Any additional concepts or processes relevant to group-based delivery that were not captured by the framework were considered for adding to the framework. After the framework was developed, the coding of the manuals was revised to make it consistent with the framework’s headings and structure.
Recordings of group sessions
We sampled 10 audio-recordings of group sessions for diversity, representing all three interventions, different stages of the group programmes (beginning, middle and end sessions) and different facilitators (for details of all transcripts used, see Appendix 1). Recordings were transcribed verbatim by a transcription company, and one researcher (AJB) checked the transcripts against the original recordings for accuracy and as part of data familiarisation, paying attention to elements that were not transcribed (e.g. tone of voice indicating engagement, laughter, speaking over each other, etc.). One researcher (AJB) then coded the transcripts inductively (i.e. bottom up, without using the a priori framework) to capture what happened in the group sessions. The codes were then compared with the developing framework and matched with the framework categories, prompting revisions to the framework and to the coding schema. Further revisions to the framework were conducted following stage 2 of the research that involved coding additional transcripts of group sessions (see Chapter 3). In brief, stage 2 involved deductive coding (using a coding schema derived from the draft framework) of 28 additional transcripts of sessions from the LWTC and SkiM interventions, also sampled for diversity. The two stages were iterative but the framework presented in Results is the final version revised in stage 2.
Observations of group sessions
Our analyses of the intervention manuals and group session recordings were supplemented with observations of ongoing group sessions in the LWTC programme. One researcher (AJB) observed eight sessions from three different groups, taking notes about what happened in the sessions and how participants interacted with each other and the facilitator. These observations provided additional insight into processes that could not be ascertained from, or identified in, the intervention manuals, audio-recordings or transcripts of group sessions, for example seating arrangements, what happened when the audio-recorder was turned off (i.e. at the beginning and end of sessions) and non-verbal behaviour of participants and facilitators. These observations were not conducted in a structured manner and were not formally coded or analysed; instead, they provided supplementary insights that facilitated interpretation of the more formal data analyses.
Consultations with experts
Throughout the study, we discussed the developing framework with experts, including researchers working with group-based interventions, group facilitators and group participants. The aims of these consultations were to (1) identify important elements that should be included in the framework, (2) collect examples and insights helpful for defining the framework categories and hypothesising about links between techniques, processes and outcomes, and (3) seek feedback on the developing framework. For a full list and details of the conducted consultations see Appendix 4. In summary, in the early stages of the study we conducted two meetings with participants who had attended the LWTC groups, and we met with two group facilitators (from the LWTC and SkiM interventions). Throughout the study, we sought feedback from researchers and practitioners at relevant conferences, and we sought feedback at an internal seminar and an external workshop, which we organised. In the final stage of the study, we met with four group facilitators (from the LWTC and SkiM interventions) and sought written feedback from researchers and practitioners on the near-final version of the framework. We discussed with each group of experts their understanding of how groups might facilitate or impede behaviour changes and other outcomes (e.g. weight loss), and what the important processes in groups might be (including different facilitation techniques, and benefits and challenges of the group setting). We also sought feedback on the emerging framework and suggestions for any new components, or potential links between the framework categories.
Developing and revising the framework
We followed a process drawing on the ‘best fit’ approach to framework synthesis. 74 We used a conceptual model developed in our previous work40 as an a priori framework. We then used the other sources (i.e. literature reviews, data analyses and consultations) and the expertise of the study team to identify (through coding concepts and processes described in these sources) and list all potentially important processes, concepts and design elements. Each identified relevant ‘candidate’ element was compared with the a priori (and then revised) framework, and added to the framework, combined or separated, and sorted into a category. We then defined categories, described the hypothesised relationships between them and developed diagrams to summarise the framework. Further refinements to the framework were made following its application to code additional transcripts of session recordings in stage 2 (see Chapter 3), so this was an iterative process that extended throughout the study. The process of developing and refining the framework, including decisions about the framework categories and their definitions, involved extensive discussions with the study team members, all of whom have relevant experience and expertise (for details of study team meetings, see Appendix 4).
Results
Findings from relevant literature
Theoretical literature
Before developing the framework, we identified and defined the key concepts used in this study, as relevant to the intended framework. In doing so, we drew on the expertise of our study team members and on selected summaries of theoretical literature. 37,38 We discussed and agreed on the key concepts and their ‘working definitions’ in meetings with, and through written feedback from, team members. The terms related to theoretical conceptualisations of groups are reported in Table 3; other relevant terms were defined in Chapter 1.
| Terms | Definitions/descriptions |
|---|---|
| Group | An entity that is more than a collection of individuals: ‘a collection of individuals who have relations to one another that make them interdependent to some significant degree’ (p. 46)37 |
The following characteristics are commonly cited as distinguishing a group from a collection of individuals:37,75
|
|
| Types of groups | Groups can be classified in different ways; for example, they can be based on:
|
| Based on the above classification, a goals-and-process matrix for groups classifies groups based on goal (i.e. a purpose that guides the direction of a group) and process (i.e. the type of interaction characteristic of the working stage of the group)76,77 | |
|
|
|
|
| Group dynamics and group processes | ‘Group dynamics’ is often used in different ways, referring to:
|
| We use ‘group dynamics’ to refer to group properties and within-group processes that help explain how groups work and change | |
For clarity, we distinguish between ‘group dynamics’ and:
|
These definitions of key concepts provided a basis for the framework and helped establish its scope and focus. For example, based on the experience and expertise of the study team, we agreed that GB-BCIs are most likely to be small, psychoeducational or counselling groups with shared personal goals and led by professional or peer facilitators. Therefore, in developing the framework we focused on the literature, processes and concepts most relevant to these types of groups, rather than, for example, work groups, sports teams or large groups that have different characteristics and types of group processes operating. Moreover, we included some of the defining characteristics of groups (e.g. group identification, goals, cohesion) that were relevant to GB-BCIs in the framework.
We began developing the framework of change processes in groups by listing potential change processes identified in our previous work40,69 and in selected other helpful summaries of theoretical literature on group processes and personal change in group interventions. 9,10,12,36,38,64,71,75,78,79 We kept a record of helpful references (available on request) including > 160 books on groups, and > 335 articles and book chapters, which were classified and filed for reference depending on the topic (e.g. concept, process or theory). These were also used as a source of framework elements. The theoretical literature on groups can be divided into three categories related to how groups function (we refer to this type of theory/process as ‘group dynamics’), how groups generate individual psychological or behavioural change (we refer to this as ‘change processes in groups’) and how factors external to a group may affect a group and its members (we refer to this as ‘contextual factors’). These categories broadly map onto the MRC’s process evaluation model,28,29 which refers to ‘implementation’ (mapping onto group delivery and group dynamics), ‘mechanisms of impact’ (covering change processes in groups) and ‘context’ (covering ‘contextual factors’). This provided initial ‘scaffolding’ for the MAGI framework and all processes and concepts that were identified in the theoretical literature and, through other sources, were used to populate these overarching categories.
Taxonomies of change techniques
We selected and reviewed six taxonomies of change techniques listing categories of techniques designed to bring about psychological change, which we considered to be the most established, widely used and relevant to our study. These included the initial taxonomy developed by Abraham and Michie,3 the CALO-RE (Coventry, Aberdeen & London – Refined) taxonomy for diet and physical activity interventions,80 the Behaviour Change Technique Taxonomy v1 (BCTTv1)4, the Intervention Mapping taxonomy,72 the Oxford Food and Activity Behaviours (OxFAB) taxonomy of techniques used by participants for weight loss81 and a taxonomy of group-specific techniques used in smoking cessation programmes. 25 In these taxonomies, we identified very few group-specific categories of change techniques (i.e. techniques that are unique to groups or particularly suitable to be delivered in group settings, and that facilitate interpersonal change processes), but a larger number of techniques that could be sensitive to group delivery (i.e. techniques that can be delivered in other ways than groups, but may be adapted to, or affected by, group delivery in how they facilitate personal change). Selected examples are presented in Table 4.
| Group-specific change techniques | Group-sensitive change techniques and their possible adaptations to engage group processes | |
|---|---|---|
|
|
Delivered in groups through group discussion and sharing of information and ideas |
|
Delivered in groups through group participants sharing experiences, information and ideas, and modelling behaviours of other group participants | |
|
Delivered in groups through group activities, group demonstrations/modelling and group discussions | |
Qualitative studies
The searches for qualitative studies of participants’ experiences of group-based weight loss groups resulted in the identification of > 4000 potentially relevant references (see Appendix 3, Figure 19). After screening 57 full texts, 27 articles49,82–152 were included. Common themes related to participants’ perceptions of, and experiences in, weight loss groups were identified (see Appendix 3). These included factors affecting participants’ experiences of groups and behaviour change and weight loss [i.e. factors related to individuals (e.g. previous experiences of weight loss), group design (e.g. contact time, venue), facilitators (e.g. personal and professional qualities), group context (e.g. group climate), change processes (e.g. accountability to the group, peer pressure), and practical delivery techniques and content (e.g. group activities and topics)]. These lower-level categories were added to the developing framework or were used to refine framework categories. The content of the coded themes and subthemes from the reviewed qualitative studies provided additional insights that contributed to the framework, defining the framework categories and hypotheses around the potential importance of, and relationships between, the framework concepts and processes (see Appendix 3 for more details of this review).
Measures of group processes
We identified and used three reviews of measures of group processes. 108–110 and looked up other potentially relevant measures. 54,111–119 The identified measures could be divided into four types: (1) screening tools used with participants to assess their suitability for, or fit with, the group, (2) measures to assess group facilitators’ skills and behaviours, (3) measures to assess group interaction (used by researchers, observers or coders) and (4) questionnaires to assess participants’ perceptions of groups and group processes. In addition, qualitative approaches, such as interviews with participants, were identified as a way of assessing participants’ experiences and perceptions of the groups. The measures identified in these reviews were listed, and the concepts and processes that these measures focused on were mapped onto the developing framework (see Appendix 5 for details and examples of measures.).
Findings from analysis of qualitative data
One researcher (AJB) coded three facilitator manuals (two of which were co-authored by one of the study team members: CJG) and 10 transcripts of group session recordings, including four sessions from the LWTC programme (with two different facilitators), two sessions from SkiM (with one facilitator) and four sessions from WtW (with five different facilitators, cofacilitating the sessions) as shown in Table 1, with further details on the transcripts provided in Appendix 1. The coding resulted in identification of categories from the transcripts, which were compared with, and helped to refine, the a priori framework. The coding was supplemented with notes from observations of eight group sessions (e.g. checking whether or not any other potentially important elements were missing). The inductively developed codes are reported in Appendix 6. In an iterative manner, the evolving framework underpinned the further coding of group sessions presented in Chapter 3 but findings from this also informed the later versions of the framework.
Findings from consultations with experts
Feedback received in the expert consultations was incorporated into the framework by adding new elements, or contributed to defining framework categories and relationships between them. The details of the consultations and main changes in the framework resulting from these are reported in Appendix 4 and can be matched with the evolving versions of the framework presented in Appendix 2.
Mechanisms of Action in Group-based Interventions framework
The literature reviews, qualitative analyses and consultations were used as sources for developing the MAGI framework. Appendix 7 includes a summary of the framework categories matched with the sources that they were identified from. Appendix 2 provides the evolving framework diagrams and tables, illustrating the process of refinement. The full version of the framework, which is intended to be a stand-alone document, is presented in Report Supplementary Material 1.
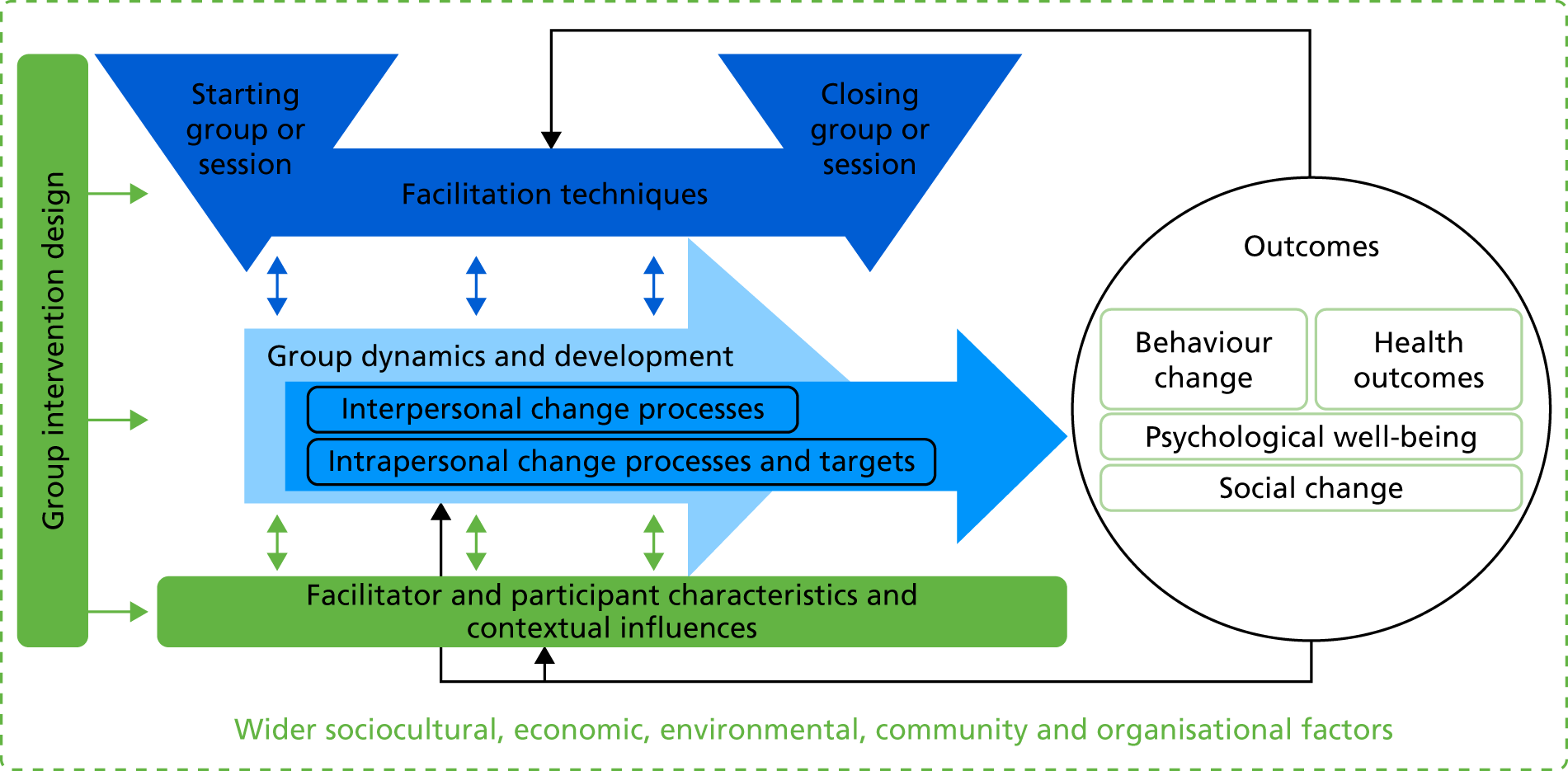
The identified processes, techniques and concepts helpful in explaining the mechanisms were grouped into six overarching categories: (1) group intervention design, (2) facilitation techniques, (3) group dynamics and development, (4) interpersonal change processes, (5) intrapersonal change processes and targets and (6) facilitator characteristics, participant characteristics and other contextual influences. On the basis of the reviewed literature and expert consultations, we hypothesise that the group features, processes, change targets, and techniques included in these categories are critical to the operation of groups and the mechanisms by which groups generate individual and collective psychological and behavioural change. The structure of the framework is illustrated in Figure 3 and described in the following sections.
FIGURE 3.
Main MAGI framework categories and relationships between them. Note: the green boxes (corresponding with categories 1 and 6 described below) and the green line around the diagram represent external influences on the group (e.g. design prior to group sessions, influences from outside the group sessions); the blue triangles and box between them (referring to category 2) represent the techniques that facilitators use to facilitate the group and instigate or support group processes; the blue arrows (categories 3, 4 and 5) represent within-group processes leading to change, that is, what happens during a group-based intervention to bring about behaviour change and other outcomes. Reproduced from Borek et al. 63 © 2019 The Author(s). Published by Informa UK Limited, trading as Taylor & Francis Group. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Category 1: group intervention design elements
These are features of the design of group-based interventions that are important for the functioning of the group and facilitation of change processes. These features should be considered during the intervention design stage (i.e. before the groups are set up) and decided on in alignment with the intervention logic model and intended change processes. When a group intervention is delivered, these features are likely to affect other elements of the intervention implementation (group facilitation, group dynamics and development) and change processes in the group.
Category 2: facilitation techniques
These refer to techniques that facilitators can use to facilitate the group and particular change-inducing interactions within the group. In Figure 3, we highlight the techniques, or tasks, that are important when establishing groups and starting group sessions, and when closing groups or sessions (these specific time points are emphasised by the blue triangles). The techniques for starting the groups or sessions are particularly important for establishing an interpersonal context conducive to engaging participants and inducing change processes, whereas techniques for closing the groups or sessions might help reinforce participants’ commitment to return to the next session, change processes and maintenance of behaviour change. Other techniques can also be used and their deployment determines how a group works (i.e. group dynamics and development) and which inter- and intra-personal change processes are initiated and sustained within the group. Facilitation techniques might change over time; for example, the facilitators might adapt which techniques they use, and how, depending on the needs and characteristics of the group, emerging group dynamics and change processes, or participants’ characteristics and their progress in achieving goals and intervention outcomes (this is represented in Figure 3 by the dark-blue two-way arrows).
Category 3: group dynamic and development processes
These refer to generic group properties and processes used to describe how groups work and change over time (i.e. this time change is represented by the light-blue arrow). These processes are group specific (i.e. unique to a group setting) and are relevant to any type of group, regardless of whether or not they target personal change. Positive group dynamics, and a successful progression into a cohesive group that works collaboratively to achieve group goals (the so-called performing stage of group development), optimises the social environment conducive to the operation of change processes. Conversely, negative group dynamics or impeded development may inhibit change processes and negatively affect participants’ experiences of the group (potentially also leading to low attendance or drop-out). Therefore, group dynamics and development are conceptualised as underpinning change processes in groups (in Figure 3 this is represented by the darker blue arrow being on top of the ‘group dynamics’ arrow). Group dynamics can be affected by facilitation techniques, including how groups are set up, by facilitator and participant characteristics (including the relationship and interaction between facilitators and participants) and by other contextual influences (e.g. social norms). These influences could include both planned changes (e.g. in facilitation techniques) and unplanned influences on group dynamics that the group responds to (e.g. progress of group members or attendance rates).
Categories 4 and 5: interpersonal and intrapersonal change processes
Interpersonal change processes are instigated in social or group contexts and through social or group interactions, whereas intrapersonal change processes and targets operate within an individual and may extend beyond the duration of a group session or a group (i.e. time is represented by the dark-blue arrow, which extends beyond the duration of the group and the associated ‘group dynamics’ arrow). Indeed, that this lasting change extends beyond the group is the aim of GB-BCIs. Interpersonal change processes might prompt or influence intrapersonal change processes or they may happen simultaneously. For example, when people are talking with others in the group, they engage both inter- and intrapersonal processes, as any conversation does. Both of these types of change processes may be affected by, and affect, the group dynamics and development when facilitated in groups (as opposed to other modes of delivery). As the arrows represent, they may also be instigated or facilitated by facilitator techniques, and may be influenced by facilitator and participant characteristics and the wider sociocultural context within which the groups operate.
Category 6: facilitator and participant characteristics, and other contextual influences
These refer to factors external to the group that may influence, and be influenced by, what happens in the groups. They include characteristics of group facilitators and group participants, which they ‘bring’ to the group, for example individual cognitive (e.g. beliefs) and emotional factors (e.g. anxieties), previous experiences (e.g. of groups, weight loss) and health conditions. These may influence participants’ interactions and the development of relationships in the groups. In particular, participants’ experience of, and engagement with, the intervention and behaviour change might be influenced by the relationship with, degree of rapport with, and perceptions of the facilitator. Other contextual factors, such as available support networks or social norms, may also influence the groups, and change processes. These factors and participants’ and facilitators’ characteristics may change over time as a result of participating in, or facilitating, the groups (e.g. increased assertiveness, confidence, skills; see Outcomes), which is represented by the arrows in Figure 3.
Outcomes
The outcomes of group-based health interventions include a range of intended and unintended consequences, for example changes in psychological processes (e.g. cognitions) underpinning behaviours, behaviours (e.g. diet), health-related outcomes (e.g. outcomes), well-being or quality of life (e.g. resulting from social connection), or social change across a collection of individuals (e.g. social norms or practices). Outcomes of group-based interventions may be affected, directly or indirectly, through change processes, and the underlying group context and dynamics. Moreover, observing or receiving feedback on outcomes, or progress towards them, can create a feedback loop, affecting the group dynamics, change processes, the use of facilitation techniques, and individual characteristics and contextual factors (this is represented by the black arrows going from outcomes back to the group, facilitation techniques, and facilitator and participant characteristics). Because the (targeted or unintended) outcomes are specific to each intervention, we do not further describe or discuss the different outcomes. Methods that can be used to explore potential links between group processes and outcomes are described in Chapter 4.
Wider influencing factors
Finally, wider influencing factors, such as sociocultural, economic, environmental, community and organisational factors, may influence all aspects of GB-BCIs, including their design, implementation, processes, facilitators and participants, and outcomes. For example, economic factors may affect participants (e.g. costs of accessing the group or buying health food) or intervention design and implementation (e.g. prespecified requirements set, or resources provided, by programme commissioners). Although we acknowledge that these wider determinants are very important, and recognise their impact on group functioning, these are beyond the focus of our study (and hence are not further discussed).
The MAGI framework provides conceptual guidance on questions of how key change agents shape group processes and change processes in GB-BCIs. This is illustrated in Figure 4, which highlights who these agents are, what they do and what they bring to group-based intervention design and operation. For example, group intervention designers have control over, and responsibility for, decisions about intervention design, which affect group dynamics, development and change processes. Group facilitators bring to the group their own characteristics (e.g. beliefs, experiences), professional and interpersonal skills, and facilitation techniques. Group participants also bring their own characteristics, social contexts and change-related factors (e.g. motivation, readiness to change). All of these influence, and contribute to, what happens in the group sessions, including group dynamics and change processes (represented by the blue circles in Figure 4) that lead to outcomes.
FIGURE 4.
Agency and processes in group-based interventions. Note: green boxes represent external influences on the group (e.g. design prior to group sessions, participants’ influences from outside the group sessions); the blue box represents the techniques that facilitators use to facilitate the group and instigate or support group processes; and the light and dark blue circles represent within-group processes leading to change (i.e. what happens during a group to bring about the outcomes).
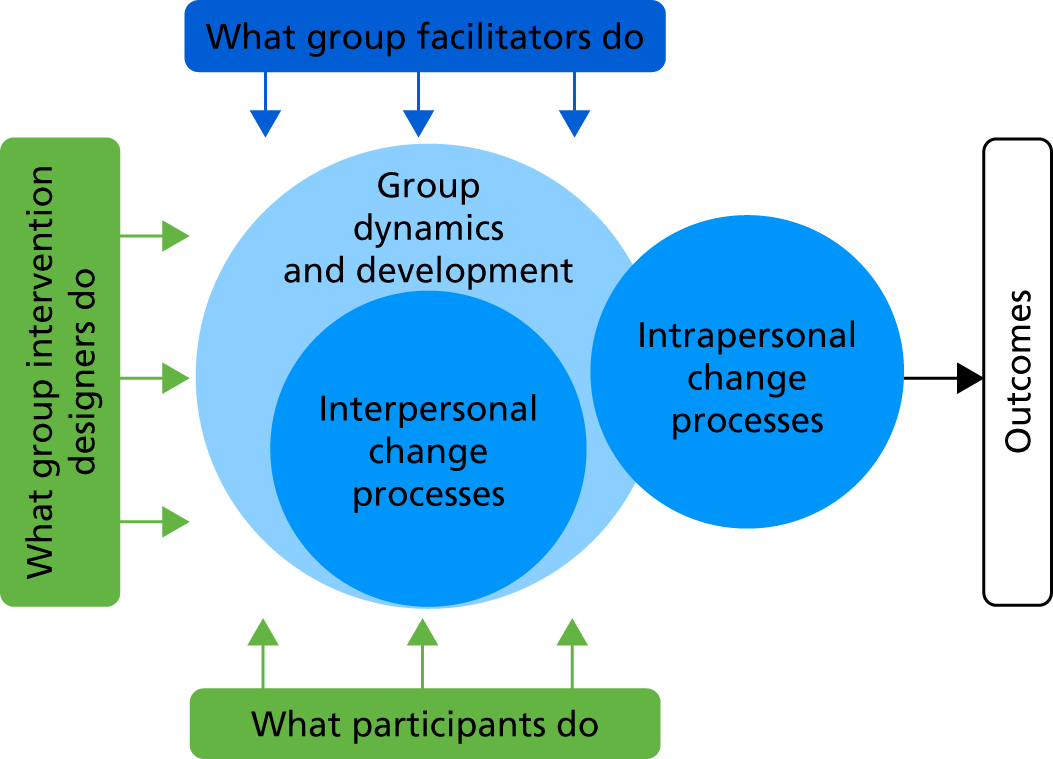
Table 5 summarises group features, processes, targets and techniques included in the framework categories described above. Detailed definitions, with descriptions of their importance and hypothesised links between them (based on the literature and expert consultations), are fully reported in Report Supplementary Material 1 and are summarised below.
| 1. Group intervention design | 2. Facilitation techniques | |||||
|---|---|---|---|---|---|---|
| 2.1. Techniques to start the group/session | 2.2. Generic facilitation techniques | 2.3. Techniques to facilitate group dynamics | 2.4. Techniques to facilitate interpersonal change processes | 2.5. Techniques to facilitate intrapersonal change processes | 2.6. Techniques to end the group/session | |
|
3. Group dynamic and development processes | |||||
|
|
|
||||
| 4. Interpersonal change processes | 5. Example intrapersonal change processes and targets | |||||
|
|
|
||||
| 6. Facilitator and participant characteristics and contextual influences | ||||||
| 6.1. Facilitator characteristics | 6.2. Participant characteristics | 6.3. Other contextual influences | ||||
1. Group intervention design
These elements of GB-BCIs can be predesigned and should be carefully planned before groups are set up and delivered as they can influence all aspects of implementation and change processes. Intervention designers need to carefully consider 1.1 intended changes and processes and outcomes during planning of GB-BCIs. They should pay particular attention to the 1.2 purpose and benefits of using a group format and deployment of interpersonal change processes so that the potential impact of group participation on planned outcomes is maximised. For example, a group setting might be used to facilitate peer support in order to enhance the quality of social relationships of members during and after the intervention. If the intended change processes are primarily intrapersonal (e.g. changes in individual knowledge, attitudes and motivation), designers should consider whether the intervention could be better delivered individually or self-delivered. In addition, designers should consider how facilitation and change techniques may need to be adapted so that they operate optimally in relation to the interpersonal processes foundational to group operation. Designers need to also consider the potential impact of 1.3 group characteristics, such as group size, processes of becoming group members, continuity of group membership and incentives, rewards or payments to attend, on group dynamics, interaction and engagement. 1.4 Participant selection and group composition, including demographic (e.g. age, gender) and condition-related (e.g. at risk of diabetes) characteristics, and attendance of any accompanying persons (e.g. partners), may affect how cohesive the group is, and can facilitate or impede establishment of common goals in the group. 1.5 Facilitator selection and training, especially professional and personal characteristics and skills (e.g. including whether they are selected as peers or professionals), and training in the use of facilitation and change techniques, are crucial in how well the intervention is delivered, how the group works (group dynamics) and how inter- and intrapersonal change processes operate, interact and are sustained. For example, facilitators whom participants consider to be credible sources, whom they identify with (e.g. peer facilitators) and who have strong interpersonal skills are more likely to instigate interpersonal change processes, such as social influence. Moreover, intervention designers need to plan 1.6 intervention content, such as participant and facilitator materials, session content, group activities, any tasks to do between sessions, any additional relevant resources (classes, facilities, etc.), and any additional information and contact outside the group. The designers need to also decide about the intervention 1.7 setting and venue, considering how these might affect participants’ expectations of, and experiences in, the programme (e.g. different implications of delivering groups in a community or hospital), and any practical issues that might affect engagement or attendance (e.g. room set-up or venue accessibility). Finally, 1.8 group set-up and delivery need to be planned, involving decisions regarding contact time, and the intended facilitation or delivery style, which should be consistent with the intended change processes. Considering and planning these elements before the group starts can help to ensure that the intended, positive group dynamics and change processes occur.
2. Facilitation techniques
These should be considered during intervention design and implementation. As group leaders, facilitators have an important role in the group and, in particular, in 2.1 techniques to start the group/session. Setting up or starting the group is a crucial stage as it provides a basis for the group dynamics and group development, and, consequently, the initiation and establishment of change processes, including members’ initial identification with the group. Starting sessions may be different in form, but equally important, in ongoing, open groups as in time-bound, closed groups; for example, similar tasks, such as personal introductions, need to be completed at the beginning of the first session in a closed group (which can be minimised or skipped in subsequent sessions) and at the beginning of each session in an open group (when there might be different new participants in each session). Beyond starting the groups or sessions, facilitators shape interaction and activities in the group, deliver intervention content and facilitate positive, while managing any negative, group processes. Thus, they need to be skilled with a range of facilitation techniques to meet these challenges, including 2.2 generic facilitation techniques to facilitate group interaction and engagement, and 2.3 techniques to facilitate group dynamics. They also need to know how to use 2.4. techniques to facilitate interpersonal change processes and 2.5 techniques to facilitate intrapersonal change processes (for examples of these facilitation techniques, see Chapter 3). Finally, at the end of the group, or at the end of the session (if it is an ongoing group), the facilitators need to positively end the group or session. 2.6. Techniques to end the group/session can help to ensure that participants leave the session with positive impressions, remembering what was covered, with motivation to continue with behaviour change after or between sessions, and/or to establish independence from the group. Although some, or most, of these techniques and tasks might be used throughout the intervention, the facilitators should ensure that, by the end of the group or session, these have been sufficiently covered and reinforced, as they are critical to maintenance of change. Examples of techniques, or tasks, important to starting and closing the groups or sessions are presented in Table 6.
| Techniques for starting the group/session | Techniques for closing the group/session |
|---|---|
| Introduce people, icebreaker | Review the session/programme |
| Manage expectations | Review individual progress and provide feedback |
| Identify/specify and agree group goals | Plan for long-term and relapse prevention |
| Prompt and facilitate group/social identification | Prompt practice skills and habit formation |
| Identify/specify and agree group rules | Prompt social support and social connections outside the group |
| Negotiate and manage group roles/responsibilities | Signpost to expert advice/facilities |
| Establish a positive group climate | Explain tailing-off of group contact/follow-up group sessions |
| Explain the programme | |
| Recap previous session | |
| Outline the session |
3. Group dynamic and development processes
These include emerging and changeable (thus ‘dynamic’) group processes and properties used to describe how groups work. They include 3.1 group goals (i.e. a purpose or task for the group), 3.2 identification with/as a group (i.e. a perception of constituting a group and being a group member), 3.3 group cohesion and attraction (i.e. a bond with the group, and wanting to belong to the group which fulfils one’s needs or goals), 3.4 group climate (i.e. socioemotional context), 3.5 group engagement (i.e. active participation in group activities), 3.6 communication patterns (i.e. patterns of how participants communicate with each other and with the facilitators, and how cofacilitators interact), 3.7 group norms (i.e. norms about acceptable group behaviour), 3.8 group roles (i.e. a structure of members’ functions and responsibilities) and, finally, 3.9 group development over time, that is, moving through forming, storming (insecurities, tensions), norming (establishing patters and relations), performing (working towards group goals) and (for most groups) adjourning stages. These group properties and processes are closely linked together, and affect overall group experience and group-related outcomes. For example, identifying with the group is closely related to identifying a common group goal and creating a sense of group cohesion, and, at the same time, group cohesion may be measured through a sense of identification with the group and perceptions of common group goals. Such group dynamics are present in any type of a group and they emerge regardless of the facilitator’s actions. However, facilitators can actively promote positive group dynamics, such as by identifying and agreeing on rules for working together, and helping resolve any negative dynamics, such as conflicts or tensions. Promoting positive group dynamics and minimising negative ones helps create a group environment that is conducive to, and underpins, the operation of change processes critical to the planned outcomes of the intervention.
4. Interpersonal change processes
These include a range of processes that operate through interaction with other people in a group and that may prompt people to change. They might be influenced by group dynamics, for example establishment of a common goal or purpose, a sense of identification and cohesion, and norms and climate that are conducive to psychological change (e.g. confidential, trusting and supportive). Many behaviour change groups are psychoeducational, interactive groups, in which the prevalent interpersonal change processes include 4.1 sharing experiences and 4.2 social learning that occurs by exchanging information, advice and ideas, and modelling or vicarious learning. These processes are often facilitated through group discussions and group activities that encourage, and provide opportunities for, participants to learn from each other. Group interaction can be also a source of 4.3 social influence processes, whereby participants influence each other’s beliefs or behaviours, for example by referring to own past experiences and expertise, health-promoting or resistant talk (e.g. in motivational interviewing terms, change or resistance or sustain talk120), using persuasion, or providing encouragement or pressure. Participants may also influence each other and their intrapersonal change through 4.4 agreeing or disagreeing with, or challenging, each other. Many health-related groups are also described as ‘support groups’ as they offer opportunities for 4.5 social support in the group, which can involve peer informational, emotional or practical support (e.g. encouragement, buddying up). Groups also provide opportunities for making social connections and enjoying the social aspects of the group, thus reducing negative effects of isolation or lack of a support network outside the group. Participants might also benefit from providing support to others and reciprocity in the groups. Groups can provide opportunities for 4.6 social validation of participants’ experiences. This might help people realise that they are not alone with a problem or challenge, thus validating or normalising individual experiences, and helping to increase one’s self-efficacy and self-esteem.
Change processes may be reinforced through 4.7 social identification with others who are perceived as belonging to similar social groups or categories. This may involve both recognition of pre-established shared identities that members import from outside the group and the development of a new group identity among members. This is especially important if the group member identities promote or impede health-related social norms and behaviours. Identifying with health-promoting identities can enhance behaviour change and health, whereas health-impeding identities may need to be explored and redefined in the group. So, for example, becoming an ex-user of a particular service or substance may involve redefining the social self in ways that can bolster maintained behaviour change. Being with and interacting with people in a group can also create opportunities for 4.8 social comparisons, which involve upwards or downwards comparisons with ‘similar’ others, and identifying or becoming role models. Group members might also feel 4.9 accountability to the group for achieving individual or group goals, which might motivate them to take action. Similarly, 4.10 competition might be a source of motivation to perform, with either others in a group or other groups. Conversely, participants may 4.11 co-operate in the group to achieve group or individual goals, for example by working together, and supporting and encouraging each other. Change processes can also be amplified and maintained by collaborative 4.12 group problem-solving, and by providing 4.13 group-level feedback on the group performance (thus reinforcing common group goals and co-operation). Finally, being in a group might prompt 4.14 social facilitation, whereby people’s performance on simple or well-trained tasks improves by being in the presence of others. This can, unfortunately, also undermine individual performance of poorly established skills.
Interpersonal change processes, like group dynamics, are inter-related and can affect each other and/or co-occur. Some of these processes may have negative effects on psychological or behaviour change. For example, identifying with social groups that are stigmatised or that do not have health-promoting social norms might impede health or engagement with health-related behaviours. Social comparisons or intragroup competition might negatively affect underperformers and may decrease their motivation, self-efficacy and self-esteem. Thus, it is crucial for group facilitators to help facilitate these interpersonal change processes in ways that increase their potential for positive effects and minimise the negative effects.
5. Intrapersonal change processes and targets
These can be generated and supported outside groups. This category includes processes (such as developing understanding) as well as psychological targets (such as normative beliefs) that can be influenced and changed by different, often multiple, change processes. When generated in the groups, intrapersonal processes are very likely to be shaped by interpersonal change processes operating in groups and by group dynamics (e.g. group cohesion and climate). Group sessions require considerable time and effort so participants need to 5.1 commit to attend the group, which can be linked with motivation for making changes and working towards group goals. Participants might also 5.2 develop and express understanding, or lack of understanding, which can be addressed by social learning processes. Interacting in a group with a health-related purpose might affect the way that people 5.3 self-present themselves (e.g. as health-oriented) and their health-related 5.4 normative beliefs. In the group, participants are also likely to express their health-related 5.5 attitudes, 5.6 attributions, 5.8 intervention outcome expectations, 5.9 motivation or 5.10 self-efficacy and sense (or lack) of personal control; they may acknowledge changes in these targets. These, in turn, can be affected by the group and other people’s expressions. Expressing beliefs in the group that are different from participants’ usual behaviour patterns might lead to 5.7 cognitive dissonance, which (in order to reduce inconsistency) could prompt attitude change that, in turn, may change motivation and indeed behaviour.
Many behaviour change groups involve participants 5.11 setting goals, 5.12 reviewing goals or progress, 5.14 identifying individual barriers and problem-solving and receiving 5.16 individual-level feedback. These techniques can be facilitated in groups collaboratively by engaging group participants, discussing their goals, progress or barriers, and thus facilitating interpersonal change processes, such as sharing experiences, social learning or accountability. Groups also provide a context for 5.13 developing and practising new skills and behaviours that can prompt modelling. Group interaction and sharing can help with 5.17 developing self-insight or a better self-understanding, and might affect an 5.18 identity shift (e.g. becoming a ‘new’, healthy person). Groups can also be good platforms for discussing and sharing ideas for 5.15 self-monitoring, 5.20 associative learning (e.g. using rewards or incentives), 5.19 using self-talk and discussing 5.21 forming habits (and changing old habits) or 5.22 managing stress and emotions. This is not an exhaustive list; many more intrapersonal processes involved in behaviour change have been identified. Here, we highlighted intrapersonal change processes that are commonly targeted in GB-BCIs, and that are particularly sensitive to group delivery.
6. Facilitator and participant characteristics and contextual factors
These might influence all the processes in groups, that is, group dynamics and inter- and intrapersonal change processes. 6.1 Facilitator characteristics include their demographic, professional or personal characteristics that facilitators bring to the group. For example, their ability to build rapport with participants and engage with the group, or their own experiences (e.g. of weight loss or other behaviours relevant to the group) and beliefs, may affect the group interaction and change processes. Some characteristics may be controlled at the design stage, whereas others are more difficult to control but could be explored (e.g. interpersonal skills, experiences or beliefs). Similarly, 6.2 participant characteristics, such as their social identities, individual personalities, cognitive or emotional characteristics, experiences and existing health conditions, might affect how the group operates and whether or not, and how, people change. In addition, contextual, social factors that are external to the group might affect people’s lives and their individual behaviour change as part of the group. These might include social support and negative influences of others in participants’ social networks, social events or circumstances, or social norms that affect people’s health-related behaviours. All of these factors have an impact on participants outside the group who may be brought into, and discussed in, the group, thus providing opportunities for interpersonal change processes (e.g. sharing experiences, social learning or validation).
Discussion
We identified a wide range of concepts, processes and techniques from a number of sources, including reviews of relevant literature, qualitative analyses of data and expert consultations. These were integrated in a framework that highlights how these various components might affect the outcomes of group-based interventions, in particular individual behaviour change. The framework consists of six overarching categories, and the relationships between key categories illustrate the proposed mechanisms of action in group-based health interventions. These six overarching categories comprise 62 more specific group features and processes that help explain how groups work and effect change. These provide a basis for designing, delivering and evaluating group-based interventions.
Group-based behaviour change interventions vary greatly in their design, implementation or targeted change mechanisms. Thus, the relevance and importance of different concepts, processes and techniques included in the MAGI framework will vary across interventions. The framework offers a set of concepts and processes, all of which are, potentially, more or less important for facilitating individual change during and beyond group participation. Practical limitations might make it difficult, or impossible, to control all of these elements in intervention design or implementation, and time and resource limitations may prevent investigation of all these processes in process evaluations. Thus, the framework provides a resource, or a ‘catalogue’, for designers, facilitators or evaluators of GB-BCIs to choose from. They can select which processes or concepts are critical in a given intervention and specifically focus on and target them when designing, delivering and evaluating GB-BCIs.
The presented framework is somewhat complex, but at the same time may not be complex enough to fully represent the complexity of within-group processes and relationships between them. The described links between concepts, processes and techniques are hypotheses based on the reviewed literature, expert consultations and our earlier research. There is a variable amount and quality of evidence supporting each process and hypothesised link, which we were unable to appraise in detail, and some processes still need to be empirically tested. In the same way as the periodic table has changed considerably since its initial development, the categorisation system that the MAGI framework represents will probably evolve as empirical evidence accumulates on how changes in group interventions occur. The framework can guide work to generate this.
In the framework, we distinguished between different categories to highlight the key domains of GB-BCIs, and distinguished between different concepts, processes, targets and techniques to aid clarity and understanding. However, these are not mutually exclusive categories; in fact, the processes categorised and described separately may co-occur and influence each other. For example, the process of sharing experiences might be closely linked with social learning (i.e. participants learning from each other’s experiences) and social validation (i.e. which may be evoked by sharing experience). Moreover, each of the interpersonal change processes happens between as well as within individuals (i.e. an individual learns, receives support, feels accountable, etc.), so they could also be facilitated in one-to-one consultations. However, these processes are likely to be reinforced by the interpersonal, social context of a group. Learning may be reinforced if it involves learning from each other, social support might be reinforced if it involves mutual peer support (thus providing benefits of providing and receiving support) and accountability might be reinforced if it involves striving to ‘not let the group down’, especially if the group has a common goal. Similarly, intrapersonal change processes also occur within the interpersonal, group context and, thus, can be affected by it; for example, goal-setting might be reinforced by sharing and discussing one’s goals with the group or impeded by not having the time or opportunity in a group to sufficiently focus and reflect on individual goals and needs. Within ‘intrapersonal change processes’, we included some examples of only individual-level change processes and targets that are particularly common to GB-BCIs or that may be particularly sensitive to group context and delivery. Intrapersonal change processes, targets and techniques have been extensively described in psychological literature and other classifications of these exist. 3,4,72,81
The inter- and intrapersonal change processes could be also facilitated in one-to-one interactions (e.g. in pairs of participants, or between a participant and a counsellor) but are likely to be affected by the group (i.e. are group sensitive). We also identified group dynamic and development processes, which are unique to the group setting (i.e. are group specific). These processes underpin change processes, and may especially affect engagement with the intervention, session attendance and drop-out rates. It is these that designers, facilitators and evaluators of GB-BCIs need to focus more on when working with group-based interventions.
Strengths and limitations
Founded on the previous research40 the MAGI framework is, to our knowledge, the most comprehensive synthesis of concepts and processes used to understand how GB-BCIs may influence behavioural and possibly other psychological change. We drew on a wide range of sources and multiple methods to identify relevant concepts and processes, including reviews of diverse literature, qualitative data analyses, and consultations with group participants, facilitators, researchers and practitioners. By combining and triangulating results from these diverse methods, we achieved a more comprehensive approach to synthesis of theories than previous studies. 1,121,122 This has allowed us to incorporate different perspectives on how group-based interventions work, including those of group participants and facilitators, and provide evidence of these processes from recordings and observations of group sessions, rather than including only theoretical accounts. We also kept audit records of decisions involved in the framework development and its refinements.
In developing the framework, we took a broad approach to identifying and mapping as many group features and processes as we could from the diverse sources used. We drew on extensive social psychological literature on groups as this underpins more recent, specialist developments, for example in organisational psychology or education. Because research on groups is so extensive, developed over many decades and across different disciplines, it was not feasible to review all existing, potentially relevant literature. Thus, we did not specifically review research on, for example, work/business/sports teams as they differ from personal change groups in their types of goals (although the basic group features and group dynamics, included in the framework, are probably similar between all types of small groups). Similarly, we did not specifically review and incorporate individual-level change theories (as other such taxonomies exist3,4,72,81) or other existing frameworks or tools for analysing interaction in health contexts (e.g. Roter Interactional Analysis System,116 specific to coding doctor–patient interaction, or motivational interviewing coding systems,123,124 for one-to-one behaviour change counselling), but we did include examples of these when they were pertinent to group settings under intrapersonal change processes in the framework and in the summary of measures in Appendix 5. Our broad approach meant that systematic review methodology involving in-depth analysis and appraisal of the evidence was not feasible within the scope of this project. Separate systematic reviews could be conducted around each of the many concepts and processes included in the framework. Future research could map out and evaluate the evidence in support of the framework concepts and processes, identifying where more evidence or empirical research is needed.
We aimed to develop a framework that would be comprehensive and potentially generalisable across different settings, targets and populations but focused on the concepts most relevant to health behaviour change interventions because we aimed to bridge a gap between the extensive existing literature on group functioning and the current (sometimes poorly conceptualised) use of groups in health-related interventions. Although we incorporated a large number of concepts, we might have missed some important characteristics, processes and techniques. For example, we developed the framework by focusing on weight loss interventions, and, thus, we might have missed elements that are present in other types of group-based health interventions. For example, additional external influences might affect group participants and processes in stigmatised groups, or groups addressing addiction to tobacco or alcohol. Finally, we focused on face-to-face groups for adults and have not explored how these processes apply to, or what other processes might be relevant in, other types of groups (e.g. online) or populations (e.g. children or families). Thus, the framework is unlikely to be an exhaustive list of all relevant processes and techniques, but provides the most up-to-date and comprehensive synthesis and model of GB-BCIs that researchers can build on and adapt to different types of group interventions.
It is also important to note limitations in mapping our sources with the framework categories, in particular when reviewing taxonomies of change techniques, measures of group processes, or qualitative studies. Different studies sometimes define and operationalise concepts or processes differently, despite using the same terminology. For example, although we define group cohesion in the MAGI framework similarly to how it is defined in a measure of group environment,54 the measure operationalises group cohesion as an overarching process, comprising elements (and questionnaire items) related to group task and social elements of the group, which in the framework would map onto ‘group goals’ and social connections within ‘social support’ processes. Moreover, coding qualitative studies involved our interpretation of the authors’ own interpretations of their data; this ‘double’ interpretation might constitute a source of bias or inconsistency. Measures and qualitative studies refer to specific types of therapy groups and weight loss interventions; thus, the applicability and transferability of their results might be limited. Finally, when coding the initial 10 transcripts, one researcher (AJB) attempted to undertake as inductive an approach as possible by coding directly from transcripts without using a prespecified coding schema. However, the coding was probably influenced by AB’s previous research on groups, concurrent reviews of literature and involvement in development of the draft framework.
Implications for designing, delivering and evaluating group-based behaviour change interventions
The framework was developed to provide a comprehensive resource for researchers and practitioners working with group-based interventions focused on diet and physical activity and potentially other health behaviour change interventions. It can be used at all stages of intervention design, implementation and evaluation.
Design
The framework provides a list of elements that can be considered when designing GB-BCIs. Decisions about group design affect the intervention implementation and change processes. Thus, groups should be considered not a ‘delivery method’ per se but a crucible of interpersonal change processes that generate and direct intrapersonal change processes critical to planned outcomes. Interpersonal change processes crucial to change will not necessarily ensue because people meet in a group; these processes need to be facilitated by use of group management or facilitation techniques. Intervention designers need to consider how positive group dynamics can be facilitated in their intervention, and which interpersonal change processes the intervention will target and how. For example, an intervention might specifically target social identification processes by facilitating emergence of a shared social identity in the group via particular group design and facilitation methods,125 or it might target changes in health-related normative beliefs through changing group norms, facilitated by specific group activities, such as group discussions and role plays,126 or both. By providing an overview of key change processes operating in groups, the MAGI framework extends existing guidance on designing health behaviour change interventions and we recommend that it is used in conjunction with them when planning GB-BCIs. 26,36,127,128
Delivery
The framework highlights the role of facilitators, their characteristics and skills in using facilitation techniques and how these might affect the operation and maintenance of change processes critical to intervention outcomes. The importance of facilitators’ training129 and of facilitators’ competencies in delivering behaviour change and group-based interventions51,130 and their prior experience of delivering group programmes has been acknowledged previously. 50,131,132 Facilitators of group-based interventions need to be trained and prepared to deliver the intervention content, facilitate the groups and promote change processes. Identifying, training and sharing effective facilitation techniques to support group dynamics (in particular to manage any negative group dynamics) and the intended change processes would be helpful. The framework is a resource for group facilitators to improve their understanding of group processes and how facilitation techniques can instigate and reinforce these. It could be used when training facilitators, discussing or reflecting on any issues arising in the groups, as a starting point or for exploring and learning about specific concepts and processes in more detail. It could also be used to provide structured feedback to facilitators and enhance their awareness of using, or under-using, various techniques. Finally, the framework highlights for facilitators the importance of, and their role in, ensuring that there is sufficient time and opportunities to instigate positive group dynamics (e.g. learning and using participants’ names) and interpersonal change processes (e.g. facilitating learning from each other, rather than just providing information). The importance of creating a group context conducive to group performance and change processes is highlighted in the framework, as are techniques and tasks for facilitators when starting and closing the groups or sessions.
Evaluation
The framework can be used to inform process evaluation of GB-BCIs, for example by guiding group session observations, analyses of session recordings (see Chapters 3 and 4), participant and facilitator interviews or the use and design of questionnaires evaluating participant and/or facilitator perceptions and experiences. Investigating the potential role and impact of specific design elements and group processes, either predesigned or unintended, can help explain how intervention outcomes were affected. For example, investigating characteristics of the venue and setting (e.g. organisational culture and its impact on facilitators and participants),133 group dynamics (e.g. group conflicts)134 or communication patterns (e.g. facilitator–participant talk ratios)135 might help explain variations in intervention outcomes.
Conclusions
The MAGI framework offers a synthesis of concepts and processes important to our understanding of how group-based diet and physical activity, and potentially other health behaviour change interventions, work. It captures how group intervention design, facilitation techniques, group dynamics and development, interpersonal and intrapersonal change processes, and facilitator and participant characteristics and contextual influences might affect each other and affect the outcomes of group-based interventions. It also highlights processes that may facilitate or impede the effectiveness of interventions, and, thus, should be considered when designing, delivering and evaluating group-based health interventions. The framework provides a basis for future research to explore and generate evidence for precise links between these processes, and how they might optimise intervention effectiveness.
Chapter 3 Change processes and facilitation techniques in group-based behaviour change interventions: a qualitative analysis based on the Mechanisms of Action in Group-based Interventions framework
Introduction
There are many possible pathways to psychological and behavioural change in GB-BCIs, as outlined in the MAGI framework (see Chapter 2). Identifying which of these processes occur in interventions, and how they are instigated and facilitated, is critical to investigating links between interventions and outcomes, and developing an evidence base on what works and how in GB-BCIs. The MAGI framework includes group characteristics, processes, targets and techniques relevant to understanding how GB-BCIs work. However, it does not provide illustrations or examples of how these processes are instigated or supported by group facilitators, in actual group-based interventions. It is also unclear how the framework could be used in practice to identify and analyse these processes and techniques.
The MRC guidance on process evaluation28,29 emphasises the importance of exploring the role of change mechanisms (how change is intended to be produced), implementation (how change mechanisms are facilitated) and context (how contextual factors affect change mechanisms, implementation and outcomes). A range of methods may be useful to do this in GB-BCIs. They can include quantitative methods, such as measuring ‘dose’ of the delivered intervention (e.g. time in groups), the presence and quality of delivery of intervention components and techniques58 or using questionnaires to measure perceptions of group processes [e.g. group dynamics134 (assessed using the Group Climate Questionnaire Short Form153)]. Qualitative methods can also be used, such as observing group sessions, interviewing group participants and facilitators48,49,97,100 or using ethnographic approaches. 133 Some studies have used qualitative methods in a focused way to test pre-existing theory on processes of change in behaviour change interventions. e.g,136 However, it is unclear how the MAGI framework and its components could inform qualitative analyses of group-based interventions.
Research aims
In this second stage of the study, it was intended to use the MAGI framework to identify examples of change processes and their facilitation in recordings of real-world GB-BCI sessions, with a view to providing initial validation of the framework. The second stage of the study addressed the following objectives:
-
Develop and test a coding schema that could be used in future studies of GB-BCIs for applying the MAGI framework in qualitative analyses of group sessions.
-
Identify examples of the MAGI framework categories in transcripts of group sessions to illustrate and provide evidence for the processes included in the framework.
-
Identify examples of facilitation techniques, used in our selected GB-BCIs, to initiate and manage the processes included in the MAGI framework.
Methods
Data sources and sampling
We used audio-recordings of group sessions from the three studies of GB-BCIs targeting diet, physical activity and weight loss (LWTC, SkiM, WtW) described in Table 1. We originally attempted to sample group session recordings to ensure sample diversity (i.e. across the three interventions, facilitators and in early, mid- and late stages of the groups). However, we found that most of the recordings from the WtW study were of insufficient quality to produce good-quality transcripts. Thus, we used only four of the best-quality recordings from this study, which were sampled in stage 1. In the stage 2 analysis, we used the 10 recordings selected in stage 1 (see Chapter 2) and an additional 28 recordings (38 transcripts in total). In stage 2, we selected more recordings of first sessions to allow identification of elements related to group set-up and formation. Tables 7 and 8, and Appendix 1, include details of the sampled recordings.
| Session number | Intervention (n) | Total (n) | ||
|---|---|---|---|---|
| LWTC/ComPoD | SkiM | WtW | ||
| 1 | 7 | 3 | 1 | 11 |
| 2 | 2 | 2 | – | 4 |
| 3 | 2 | 2 | 1 | 5 |
| 4 | 5 (final) | 2 | 1 | 8 |
| 5 | N/A | 2 | – | 2 |
| 6 | N/A | 2 | – | 2 |
| 7 | N/A | 1 | 1 | 2 |
| 8 | N/A | 1 | – | 1 |
| 9 | N/A | 1 | – (final) | 1 |
| 10 | N/A | 1 | N/A | 1 |
| 14 | N/A | 1 (final) | N/A | 1 |
| Stage 1 | 4 | 2 | 4 | 10 |
| Stage 2 | 12 | 16 | 0 | 28 |
| Total | 16 | 18 | 4 | 38 |
| Facilitators (n = 11) (gender, background, site) | Number of sessions (N = 38) | Intervention |
|---|---|---|
| 1 (female, exercise, site 1) | 12 | 4 LWTC and 8 SkiM |
| 2 (female, diet, site 2) | 10 | SkiM |
| 3 (female, diet, site 1) | 6 | LWTC |
| 4 (female, diet, site 1) | 2 | LWTC |
| 5 (female, unknown, site 3) | 2 | LWTC |
| 6 (female, unknown, site 3) | 2 | LWTC |
| 7 (male, exercise, site 4)a | 2 | WtW |
| 8 (female, diet, site 4)a | 1 | WtW |
| 9 (male, behaviour change, site 4)a | 1 | WtW |
| 10 (female, health promotion, site 5)a | 2 | WtW |
| 11 (female, behaviour change, site 5)a | 2 | WtW |
All 38 audio-recordings were transcribed verbatim by professional transcribing services. One researcher (AJB) checked them for accuracy against the recordings as part of the data familiarisation process. The transcripts included notes on non-verbal behaviours (e.g. laughter, moving chairs/tables) and group activities (e.g. subgroup discussions). However, it was not possible to indicate when specific group participants spoke, so the speakers were labelled only as ‘male’, ‘female’ or ‘facilitator’.
Developing a coding schema
The first 10 transcripts from stage 1 were coded without using a pre-existing coding schema (see Appendix 6), which served as the basis for the MAGI framework. In stage 2, we used the MAGI framework (see Report Supplementary Material 1) to develop more specific coding instructions. To do that, the framework definitions were shortened and instructions on how to identify these categories in transcripts of group sessions were formulated.
After this initial ‘draft’ coding schema was developed, a researcher (AJB) used it to code six transcripts sampled in stage 2. During this process, additional subcategories were identified from the transcripts and, when helpful for more precise coding, were added to the coding schema. Examples of techniques recurrently used by facilitators in the groups were also identified.
The draft version of the coding schema was then used by a researcher (JRS) to code two transcripts and by other study team members (FG, SMT and CA) and one researcher external to this study (LP, involved in the SkiM study) to independently code one transcript each (i.e. six transcripts were independently coded). During the independent coding, the coders recorded any issues related to coding, definitions of categories or coding instructions. The double-coded transcripts were then compared with AB’s initial coding. Differences in coding and any recorded issues were discussed and clarified among study team members. In addition, other study team members (CG, MT and RM) provided comments on the draft coding schema. All comments and suggestions were used to revise the coding schema (e.g. by clarifying the categories and coding instructions, removing overlaps between categories) until an agreement was reached. These revisions were also used, when applicable, to revise the framework categories and definitions. After the revisions, the study team members further checked, and agreed on, the revised version of the coding schema.
Applying the coding schema and identifying examples
The revised coding schema was then applied by a researcher (AJB) to code the remaining group session transcripts sampled in stage 2 (and to recode the already analysed transcripts) to identify examples of the MAGI framework processes and facilitation techniques. After identifying several examples for some of the framework categories, the later transcripts were coded more selectively by focusing on identifying examples of less prevalent categories and on identifying only particularly interesting or different examples of processes or facilitation techniques for which there already were many examples.
In the coding of transcripts, we also identified some recurrent techniques used by facilitators in the sessions to facilitate group interaction and change processes. We reviewed the examples of the coded group dynamic processes, interpersonal and intrapersonal change processes, and identified any patterns, or techniques, linked to how the facilitators initiated or managed (e.g. responded to) them. On this basis, we developed a list of facilitation techniques used to facilitate group processes.
Results
Coding schema for the Mechanisms of Action in Group-based Interventions framework
In Report Supplementary Material 2, we provide the full, detailed coding schema that we developed based on the MAGI framework for coding transcripts of group sessions in GB-BCIs. It includes the framework categories, brief definitions and instructions for coding. The framework and the coding instructions include different types of categories, which require different approaches to coding. Here, we highlight these, by reporting on the main differences between the framework and the coding schema.
First, in the coding schema we distinguished lower-level ‘subcategories’ to allow for more precise identification and categorisation. For example, category 1.6 intervention content includes multiple subcategories in the coding schema, such as 1.6.5 group activities, some of which, in turn, are subdivided into more specific sub-subcategories, in the case of group activities indicating different types of activities (e.g. 1.6.5.1 whole-group activities, 1.6.5.2. subgroup activities and 1.6.5.3. individual activities). Category 3.4 group climate includes 3.4.1 laughter/humour and 3.4.2 informal talk (which might be indicative of a positive group climate) and category 4.1 sharing experiences includes 4.1.1. self-disclosures of personal or emotional issues and 4.2.2. self-disclosure of transgressive behaviour (see Report Supplementary Material 2).
Second, the framework includes categories, such as design features or group dynamics, that might not be explicit in the recorded group interactions or identifiable in the transcripts. For example, the framework’s 1 group intervention design elements involve predesigned features of group interventions, such as 1.5.5 training of facilitators or 1.8.1 time structure of intervention, which are likely to have an impact on group processes, but may not be identifiable in the data. Other categories, such as 3.9 group development or 4.14 social facilitation processes, are likely to occur but may not be easily recognised in the session recordings or transcripts (as they are unlikely to be verbalised in sessions).
Consequently, the coding instructions evolved to allow for the coding of three different types of content: (1) explicit processes or uses of techniques, (2) implicit processes and (3) the content of talk (e.g. talking about group dynamics or intrapersonal change processes/targets, but not implementing them). First, there are processes that can be identified in verbal interaction, and thus coded explicitly, or semantically (answering the question of ‘what is being done in this moment in the session?’). This type of code includes, for example, sharing experiences, social learning processes (e.g. exchanging information, ideas, advice), providing social validation (e.g. expressing empathy), providing feedback, goal-setting and goal-reviewing. Second, processes may occur that are implicit or based on a coder’s perceptions and, thus, may not be identifiable in verbal interaction. Thus, these processes need to be coded interpretatively or latently (based on the coder asking ‘what processes do I think might be happening in this moment in the session?’). This type of category includes, for example, group climate (which is based on people’s perceptions, and may be different for different people in the same group), social influence, social identification processes, social comparisons and many intrapersonal change processes (e.g. cognitive dissonance). Third, all concepts, processes and techniques included in the MAGI framework may be talked about in the groups, and in these cases the codes can be applied to the content of the talk. For example, participants and facilitators might discuss intervention design elements (e.g. comment on the venue), group dynamics (e.g. reflect on what the group climate is like), interpersonal change processes (e.g. talk about group competition), intrapersonal change processes (e.g. discuss the importance of, or reasons for, motivation), or participant contextual influences (e.g. discuss the role of social support outside the group). Therefore, the coding instructions include prompts to identify whether each category is likely to be applied in coding explicitly, interpretatively or to the content of talk.
Examples of Mechanisms of Action in Group-based Interventions framework processes and facilitation techniques
In this section, we provide examples of the framework processes and facilitation techniques identified in coding transcripts of the group sessions. For brevity, we do not report on all framework categories; instead, we describe categories with particularly high or low prevalence or those that are most pertinent to the group setting. A document containing further illustrative excerpts (‘quotes’) from the coded session transcripts for the three GB-BCIs (LWTC, SkiM and WtW) within subcategories for which examples were identified is available on request from the authors. These provide illustrations of, and evidence for, the processes and techniques included in the MAGI framework. The excerpts and examples are reported under numbered headings corresponding with the MAGI framework. At the end of the sections describing group dynamics and intrapersonal and interpersonal change processes, we provide tables with summaries of the examples of facilitation techniques identified for these processes, as well as indicating their prevalence. We describe the techniques as ‘frequent’ if multiple (e.g. more than seven) instances were identified in the analysed transcripts, ‘occasional’ if there were several examples (e.g. three to seven) within a transcript or across a few transcripts, ‘rare’ if we identified very few examples (e.g. fewer than three) across the data set, and ‘none’ if we identified no clear examples in the data set. These are broad indicators of prevalence, rather than specific measures.
1 Group intervention design elements
1.2 Purpose or benefits of using group format
A few times a positive perception of, and expectation from, the group was created or reinforced by discussing the purpose or benefits of the group. In the first sessions of the WtW and SkiM interventions, facilitators discussed the benefits of being in a group and by doing so created an expectation of helpful group processes (e.g. group support). In a few other groups, participants reflected on the benefits of groups in general or in relation to their own group. Facilitators can use such instances to understand how participants want, or expect, to benefit from the group (e.g. how the group views accountability or competition) and what the important processes for them are, thus allowing the facilitators to focus on facilitating and reinforcing these processes. We identified no instances of discussing or addressing any negative expectations of groups. Although these might not be openly expressed until trust is established, we identified an example when, at the end of the first session, a participant expressed relief that she enjoyed the group session and admitted that she had been anxious about coming. Facilitators could manage such anxiety or insecurity by pre-emptively acknowledging it at the beginning of the first session. Another related strategy could involve discussing participants’ previous experiences of groups, and explaining any differences or similarities between other types of groups and the intervention (e.g. we identified participants reporting and comparing the current programme with commercial weight loss groups).
1.3.1 Group size
This was discussed in the context of the dwindling number of attending participants in some groups. Fewer participants attending the sessions may create a negative perception of the group, making it appear as less attractive or helpful and, therefore, negatively influencing perceptions of group cohesion, attractiveness and individual commitment to attend. In the identified examples, facilitators addressed this by reporting reasons for absence (e.g. illness) and by reinforcing perceived benefits of a smaller group (e.g. more time to discuss individual experiences). Combining groups when they get too small is another common strategy (used in SkiM groups) to try to maintain positive group dynamics (and efficient use of resources). Cohesion of the new, combined group needs to be promoted by the use of specific techniques, such as those used for starting a group.
1.6.5 Group activities
The vast majority of time in the analysed groups was spent on whole-group discussions, with fewer subgroup discussions and brainstorming activities. This reflects the small size of the groups and high prevalence of engaging social learning processes (see 4.2 Social learning), for which group discussions and brainstorming are particularly suitable. Whole-group discussions were the main way that facilitators engaged interpersonal change processes by exchanging information, advice and ideas, and by eliciting sharing experiences, ideas and social validation. However, the majority of these discussions and exchanges were conducted between the facilitator(s) and individual participants, and participants engaged directly with each other less frequently (e.g. asking questions of, or responding directly to, each other). To facilitate between-participant interaction and encourage participation, the facilitators used generic techniques (see 2.2 Generic facilitation techniques below). Using subgroup discussions or brainstorming (although rarely possible to transcribe because of overlapping voices) also allowed more individuals to engage directly with each other (e.g. including those who were quieter in whole-group discussions). This provided opportunities for exchanges of ideas between participants, group problem-solving and making social connections. Individual activities were also used to prompt participants to set and write individual goals and individually reflect on their behaviours or emotions, which were then sometimes discussed in the groups. Such individual activities are particularly suited for tasks that require reflection, and in some cases they were set as ‘take-away’ tasks to do individually at home. Finally, we identified ‘practical’ activities that involved participants actively doing something in the sessions, rather than only talking, for example reading food labels and sorting out foods in order of sugar content or measuring out the amounts of sugar, sorting out food products into different food groups, diet quizzes (e.g. assessing fat or fibre intake and calculating scores) or having a ‘taster’ of activities (e.g. relaxation or exercises that can be done while sitting). These practical activities provided a way to energise and engage participants, which helped to create a positive, ‘fun’ group climate and opportunities for co-operation, vicarious learning, modelling, social comparisons and practice of skills and behaviours.
2 Facilitation techniques
2.1 Starting the group or session (Table 9)
In all first sessions, the facilitators introduced themselves, giving their name and, in most cases, professional background. In most first sessions (although this was not identified in all transcripts), participants were asked to introduce themselves by name and, more rarely, share additional information about themselves (e.g. why they are in the group). Remembering the names of multiple participants can be difficult (which was commented on in some groups), so in rare examples facilitators repeated the name introductions in the second session. In another example, a facilitator acknowledged this difficulty and asked participants not to get offended if someone does not remember their name.
| Examples of 2.1 techniques to start the group/session | Prevalence in the coded transcripts |
|---|---|
| 2.1.1. Introducing people, icebreaking | Frequent |
| 2.1.2. Managing expectations | Occasional |
| 2.1.3. Identifying/specifying and agreeing group goals | None explicitly for the group, but frequent as goals for individuals |
| 2.1.4. Prompting and facilitating group/social identification | Rare |
| 2.1.5. Identifying/specifying and agreeing group rules | Occasional |
| 2.1.6. Negotiating and managing group roles, responsibilities | Occasional (mainly facilitator role) |
| 2.1.7. Establishing a positive group climate | See ‘Group climate’ in Table 12 |
| 2.1.8. Explaining the intervention | Frequent |
| 2.1.9. Recapping any previous session | Frequent |
| 2.1.10. Outlining the current session | Frequent |
In most first sessions, facilitators also asked participants to discuss their expectations of the programme (hopes and fears, or reasons for why they were there). This tended to lead participants to report their programme outcome expectations (e.g. to lose weight, get healthier, fitter), which facilitators drew on in explaining the intervention goals, content and structure. We identified no examples of identifying or specifying a group goal (i.e. a common goal for the whole group); rather, the intended intervention outcomes (e.g. weight loss, changing diet and physical activity) served as individual goals for participants that they had in common. In a very few instances, facilitators prompted identification with a group. To do that, they drew on the similarities between participants’ condition and common goals, such as all group participants having pre-diabetes and aiming to prevent type 2 diabetes. When groups included a mix of people with and without diabetes, or overweight and normal-weight participants, the focus was on the commonality of goals as the basis for the group (i.e. making healthier lifestyle changes). Moreover, at the beginning of a number of first sessions, facilitators discussed and asked participants to agree on group rules. The identified techniques included ‘telling’ participants about pre-set group rules (e.g. confidentiality) or asking participants to come up with their own rules. We also identified examples of facilitators introducing formal group roles, such as being a facilitator or ‘visiting’ expert, and defining responsibilities, such as facilitators delivering the content and organisational aspects (e.g. paperwork), and participants engaging and interacting. We identified no specific techniques for establishing a positive group climate at the beginning of the sessions or intervention, other than engaging in informal chatting or offering drinks (see 3.4 Group climate). Finally, session initiation often involved a more or less structured explanation or outline of the interventions, current sessions and (from session 2) review of the content of previous sessions.
2.2 Generic facilitation techniques (Table 10)
| Examples of 2.2 generic facilitation techniques | Prevalence in the coded transcripts |
|---|---|
| 2.2.1. Encouraging participation, for example: | Frequent |
| Asking open and closed questions | Frequent |
| Commenting/reflecting on participation | Occasional |
| Encouraging specific participants to participate | Occasional |
| 2.2.2. Managing time/activities, for example: | Frequent |
| Stating the time constraints/need to move on | Occasional |
| Refocusing/referring back to topic/activity | Occasional |
| 2.2.3. Checking understanding | Frequent |
| 2.2.4. Requesting elaboration | Frequent |
| 2.2.5. Providing clarification | Frequent |
| 2.2.6. Directing a question back to the group | Rare |
| 2.2.7. Providing illustrations | Occasional |
| 2.2.8. Summarising | Frequent |
| 2.2.9. Paraphrasing | Frequent |
| 2.2.10. Referring to what participants said before | Occasional |
| 2.2.11. Reframing | Frequent |
| 2.2.12. Reinforcing | Frequent |
In addition to techniques that facilitators used to facilitate group dynamics and change processes, some ‘generic’ techniques were identified that could be used to facilitate general group interaction and multiple processes. Facilitators encouraged group participation by asking the group open and closed questions, but also by commenting or reflecting on active participation, or lack of it, and by encouraging specific participants or groups of participants to contribute. They managed time in the sessions and group activities by stating a need to move on to the next activity or discussion, commenting on limited time remaining to cover the necessary content, and by refocusing on the activity or topic (e.g. using phrases such as ‘all right’, ‘so now we’re going to’). Facilitators used strategies, such as checking understanding, requesting elaboration and providing clarifications, as part of different processes, in particular social learning processes, sharing experiences and problem-solving. Rarely, facilitators directed participants’ questions (for information or ideas) back to the group, allowing other participants to answer them, rather than providing answers. This promoted participants’ interaction and engagement, learning from each other and peer support.
Facilitators used different ways to enhance understanding and memory of the content of discussions by providing illustrations, summaries and paraphrases. ‘Providing illustrations’ involved comparisons or metaphors with everyday examples that participants could relate to, such as comparing the number of calories in high-calorie food with equivalent amounts of healthier, low-calorie food, or with the time walking required to burn off the high-calorie food. ‘Summarising’ involved offering summaries of group discussions (e.g. of shared common experiences or recommendations/advice discussed) and programme content (e.g. key messages). ‘Paraphrasing’ involved partially or inexactly summarising what was said in the group, in order to draw out particular points or aspects of that (e.g. to highlight ‘learning points’, techniques or programme messages). Closely related techniques were referring to what participants said before, reframing and reinforcing. ‘Referring to something that participants said previously’, either earlier in the current or in the previous session (e.g. provided examples or shared experiences) not only showed facilitators’ attention and active listening, but also was a way to relate the information, advice or problem-solving to participants’ own experiences and individual situations. In some cases, it highlighted positive behaviours and role models. ‘Reframing’ was often used together with summarising, paraphrasing or referring to what participants said. It involved reinterpreting or drawing on small, positive aspects of what participants said (e.g. when reviewing goals/progress). For example, when participants reported perceived ‘failures’ of not (fully) meeting goals for healthy behaviour change, the facilitators focused on the smallest positive aspect of their report (e.g. ‘at least’ they did not put weight on, or they did whatever they could). The technique was intended to provide encouragement and reassurance and to help sustain motivation and commitment, but in some cases (e.g. when participants did not meet their goals), a challenge, exploring barriers and problem-solving might have been more constructive. Finally, ‘reinforcement’ was a strategy that involved repeating or summarising with the aim of emphasising the key messages or approaches promoted in the intervention.
2.6 Closing the group or session (Table 11)
The majority of session closings involved the facilitator explicitly stating that they had come to the end of the session. In most cases, this also occurred immediately before or after goal-setting. In several sessions, the facilitators reviewed the session or the programme (in the final session) by asking the group what the key messages were or what they would take away. In some cases, the facilitator provided a summary of the key content covered. At the end of the groups, we identified very few instances of reinforcing long-term planning, relapse prevention, prompting practice and habit formation, engaging social support and making connections outside the group. These techniques were discussed within the interventions, rather than specifically at the end. On the contrary, there were many examples of (sometimes extensive) discussions about access to additional resources and facilities as part of the intervention (e.g. vouchers for or free activity classes) and outside the intervention (e.g. signposting to, or sharing information about, activities and facilities available locally). At the end of the sessions and programme, facilitators also explained what happens next (e.g. when the next session is, or when any follow-up review sessions are).
| Examples of 2.6 techniques (or sets of techniques) to end the group/session | Prevalence in the coded transcripts |
|---|---|
| 2.6.1. Review the session/intervention | Occasional |
| 2.6.2. Review individual/group progress and provide feedback | Frequent (only individual progress review and feedback) |
| 2.6.3. Plan for long-term and relapse prevention | Rare (in the final sessions) |
| 2.6.4. Prompt practice of skills and habit formation | Rare (in the final sessions) |
| 2.6.5. Prompt social support/social connections outside group | Rare (in the final sessions) |
| 2.6.6. Signpost to expert advice/facilities | Frequent |
| 2.6.7. Explain tailing off of group contact/follow-up sessions | Frequent |
3 Group dynamics (Table 12)
| Examples of 2.3 techniques (or sets of techniques) to facilitate group dynamics | Prevalence in the coded transcripts |
|---|---|
| 2.3.1. Identifying/referring to common, programme or individual goals | Frequent (but common as individual/programme, not groups goals) |
| 2.3.2. Referring to the group as ‘we’ | Occasional |
| 2.3.3. Referring to/distinguishing from other groups | Rare |
| 2.3.4. Presenting the group as attractive | Rare |
| 2.3.5. Reflecting on the positive aspects of the group | Occasional |
| 2.3.6. Using names | Occasional |
| 2.3.7. Using humour | Frequent |
| 2.3.8. Providing opportunities for/engaging in informal talk | Occasional |
| 2.3.9. Encouraging/managing group interaction | See Table 10 |
| 2.3.10. Discussing/reflecting on group engagement or intended interaction style | Occasional |
| 2.3.11. Referring to/reinforcing group rules | Rare |
| 2.3.12. Addressing/managing disruptive, negative behaviour | Rare |
| 2.3.13. Prompting selection of informal group roles | Rare |
3.1 and 3.2 Group goals and identifying with/as a group
As reported above, we did not identify any examples of setting common goals for the groups; instead, we found individual outcome goals set for the intervention that the participants had in common (e.g. losing weight, preventing diabetes, becoming healthier). These goals were linked closely with the reasons why people were invited to the group and, together, these provided a basis for identifying as a group (i.e. being a group for people at risk of diabetes and wanting to prevent it). Facilitators instigated and reinforced these group goals and a sense of identification with the group by referring to the programme goals. In instances when participants had different goals (e.g. maintaining weight, managing rather than preventing diabetes), the facilitators referred to the common goal of making healthy lifestyle changes. Furthermore, sometimes facilitators and participants referred to the groups as ‘we’ and (more rarely) referred to, and suggested differences from, other groups (e.g. in the programme or other types commercial weight loss groups). This might be indicative of identification with a group (i.e. through ‘us’ vs. ‘them’ distinctions) and a perception of common goals and shared understanding (e.g. commitment to improving health rather than only losing weight).
3.3 Group cohesion and attraction
These are difficult to code as they relate to participants’ perceptions (which were rarely explicitly vocalised) rather than aspects of a group that can be observed in transcripts. However, we identified some examples that may facilitate or reflect group cohesion and attraction. Facilitators sometimes talked about the research base for the interventions or referred to the successes of previous participants, which presented the group as attractive and may have promoted participants’ attraction to, and willingness to be part of, the group. Facilitators (and participants) also reflected on the group and its positive aspects (e.g. helpfulness, being a ‘lovely’, supportive group) and used each other’s names, which may indicate a level of cohesion or bond within the group.
3.4 Group climate
Similarly to group cohesion, it was difficult to identify examples of group climate in transcripts; it would be more feasible to assess participants’ perceptions of group climate via questionnaires or qualitative interviewing. We identified no explicit references to the group climate (but some of the examples reported in 3.3 Group cohesion and attraction as indicative of cohesion might also relate to group climate). We identified instances of laughter/humour and informal interaction as possible indicators of group climate. Instances of group laughter occurred in certain situations. This included when participants made jokes, admitted to ‘unhealthy’ or ‘transgressive’ behaviours, created shared understandings (especially related to barriers to healthy behaviours, e.g. food cravings) and when referring to group-specific knowledge (e.g. previously shared experiences, in-group jokes). Facilitators joined in laughing with the group and sometimes also used humour. Informal interaction involved participants talking about personal or general topics, unrelated to the intervention. This often occurred before the session or during breaks and, in some groups, throughout the sessions (i.e. off-topic talk). Facilitators enabled or promoted such informal interaction by organising session breaks, offering drinks and engaging in informal talk with participants. Group climate can also encompass creating a safe, trusting and confidential setting, which is linked with the established group norms (see 3.7 and 3.8 Group norms and roles).
3.5 and 3.6 Group engagement and communication patterns
These could not be coded as separate examples as they refer to patterns of interaction in groups. Throughout the sessions, facilitators used generic facilitation techniques to encourage and manage group interaction (see Table 10). In a few examples, facilitators explicitly described the sessions as ‘interactive’, which indicated the expected engagement and intended communication patterns in the group. In a few rare instances, participants reflected on the communication style in the group, for example praising the fact that they were not provided just with instructions for behaviour, but rather were given opportunities for sharing and discussing ideas. In many groups, there seemed to be some participants who were more vocal and willing to share than others in the group, and in a few groups individual participants seemed to dominate the discussions, drawing the facilitators’ time and attention to personal issues or experiences (e.g. health problems or specific individual barriers). This, however, was difficult to capture and code in the transcripts of single sessions because (1) the transcripts did not indicate when the same participants spoke (this can be identified in audio-recordings only to a limited extent) and (2) these kinds of patterns may emerge over time (this could be more easily identified when looking for patterns between sessions). Communication patterns may also be explored by coding and comparing proportions of interaction. We conducted exploratory coding of 10 transcripts, which suggested that, in the analysed groups, the facilitators had more ‘turns’ speaking than participants, and between 50% and 78% of transcripts covered facilitators’ talk. Moreover, despite there generally being fewer men than women in the mixed-gender groups, men had, on average, slightly higher number of ‘turns’ and proportion of talk than women. We did not further pursue using this approach owing to time constraints; for details and exploratory findings, see Appendix 8.
3.7 and 3.8 Group norms and roles
It was hard to identify explicit examples of group norms because of their implicit nature and gradual formation. Instead, we identified examples of interaction that may indicate or influence group norms. In some groups, facilitators and participants agreed group rules in the first session (see 2.1 Starting the group or session), for example starting the sessions promptly or switching off mobile phones. However, we identified no further references to these and no examples of facilitators managing situations when group rules were breached (e.g. when repeatedly ringing mobile phones or late-arriving participants disrupted the sessions). Similarly to group norms, group roles emerge over time and, thus, may be difficult to capture in transcripts. In some groups, we identified examples of informal ‘functional’ roles emerging, such as a ‘writer’ or ‘reporter’ in subgroup activities. In very few transcripts, we also identified instances that would suggest ‘dysfunctional’ roles. This involved participant behaviour that was disruptive to the group and its goals, such as joking repeatedly and/or inappropriately, undermining the facilitator or other participants, or repeatedly countering facilitators’ health-related talk with resistance or disagreement. We identified no examples of facilitators directly managing, or responding to, such behaviours, except for facilitators addressing expressed resistance (see 2.4.3. facilitating social influences in Table 13). The facilitators in our consultations reported that they found managing such participants particularly challenging (highlighting the need for more training in this) and that in at least one case they addressed the ‘difficult’ participants outside the sessions. It was also not possible to assess from the transcripts whether or not, or to what extent, breaching group rules or disruptive behaviour promoted negative group norms (e.g. they might be disapproved of via non-verbal means).
4 Interpersonal change processes (Table 13)
| Examples of 2.4. techniques (or sets of techniques) for facilitating interpersonal change processes | Prevalence in the coded transcripts |
|---|---|
| 2.4.1. Facilitating sharing experiences | Frequent |
| Prompting sharing of experiences | Frequent |
| Using participants’ experience to provide information/advice | Frequent |
| Referring information or advice to participants’ experiences | Frequent |
| Sharing facilitators’ own experiences | Rare |
| Acknowledging sharing experiences or self-disclosures | Rare |
| 2.4.2. Facilitating social learning | Frequent |
| Providing information, explaining (didactic) | Frequent |
| Exchanging information interactively (e.g. asking questions to elicit information, then summarising or correcting) | Frequent |
| Providing advice/recommendations | Frequent |
| Exchanging advice/recommendations interactively | Frequent |
| Facilitating brainstorming of ideas | Frequent |
| Demonstrating behaviours | Occasional |
| Asking participants to demonstrate behaviours | Rare |
| Prompting modelling | Occasional |
| Providing instructions how to perform behaviours | Occasional |
| 2.4.3. Facilitating social influences | Frequent |
| Appealing to credible sources or evidence | Occasional |
| Using persuasive arguments | Occasional |
| Eliciting positive influences, change talk (e.g. eliciting reports of positive experiences/emotions, reports of practice of behaviours/skills) | Frequent |
| Addressing negative influences, resistance (e.g. using humour, challenging, ‘rolling with resistance’) | Occasional |
| 2.4.4. Facilitating agreements, disagreements, challenges | Frequent |
| Eliciting agreements | Occasional |
| Prompting self-reflection in response to disagreements (e.g. using open questions, ‘rolling with resistance’, i.e. exploring reasons, motivations, reinforcing autonomy) | Occasional |
| Challenging/’correcting’ misconceptions (e.g. providing information or referring to credible sources of information) | Occasional |
| Providing positive counter-statements of ‘reframing’ | Frequent |
| Using humour (e.g. exaggerating, referring to common knowledge/examples from media or celebrities, raising confidence) | Occasional |
| 2.4.5. Facilitating social support in groups | Frequent |
| Discussing, encouraging group/peer support | Occasional |
| Describing support as part of the role of facilitators/group | Occasional |
| Reinforcing participants’ talk about group support | Occasional |
| Explicitly offering support | Occasional |
| Providing praise | Frequent |
| Providing reassurance | Frequent |
| Providing encouragement | Occasional |
| Discussing, encouraging buddying up | Rare |
| Providing opportunities for making social connections (e.g. informal talking about things in common) | Occasional |
| 2.4.6. Facilitating social validation | Occasional |
| Providing personal validation | Occasional |
| Normalising | Occasional |
| Expressing empathy, understanding | Occasional |
| 2.4.7. Facilitating social identification | Rare |
| Referring to common participants’ social categories/identities | Rare |
| 2.4.8. Providing opportunities for social comparisons | Occasional |
| Prompting participants to share information about comparable behaviours | Occasional |
| Prompting participants to share self-assessments | Occasional |
| Referring to participants as role models or good examples | Rare |
| 2.4.9. Facilitating accountability | Occasional |
| Discussing accountability | Rare |
| Asking to share goals with the group | Occasional |
| Prompting a public promise/commitment to goals | Rare |
| Taking objective measures of progress | Occasional |
| 2.4.10. Facilitating competition | Rare |
| Providing opportunities for participants to compare objective measures of progress | Occasional |
| Discussing, explaining competition | Rare |
| Discouraging competition | Rare |
| 2.4.11. Facilitating co-operation | Occasional |
| Prompting/providing opportunities for group work | Occasional |
| 2.4.12. Facilitating group problem-solving | Occasional |
| Facilitating discussions of general barriers | Occasional |
| Facilitating sharing ideas for problem-solving | Occasional |
| 2.4.13. Providing group-level feedback (i.e. including information on performance) | None |
| Providing group-level praise on performance | Rare |
4.1 Sharing experiences
Participants sharing their experiences and opinions constituted large proportions of every group session. This involved different types of disclosure including sharing experiences of, and opinions about, everyday health-related practices and behaviours, experiencing and dealing with factors affecting health and health-related behaviours, and interactions with other people (both positive and negative). Sharing experiences had different functions and, thus, helped facilitate different change processes. This generic process seemed to underpin multiple change processes in groups. For example, participants shared experiences to provide (1) context for asking a related question or requesting clarification, (2) illustrations and examples that helped relate information, advice or ideas to personal situations and (3) ideas or advice to others. All of these processes can also be seen as facilitating social learning processes. Moreover, discussing experiences provided an opportunity to create shared understandings and realise commonality of experiences, thus facilitating social validation and potentially contributing to group cohesion. Participants shared experiences of engaging in health-related behaviours and achieving (or not achieving) goals, and self-disclosed ‘transgressive’ behaviours that were at odds with the health recommendations or participants’ goals (e.g. eating unhealthy foods, overeating or overdrinking). This provided opportunities for facilitating social support (e.g. praise, reassurance), social comparisons, accountability and individual feedback. Many of the sharing experiences were initiated by participants or occurred as part of ongoing group discussions. Facilitators elicited sharing explicitly by inviting participants to share or tell the group about their experiences, or implicitly by providing information or advice that was responded to by participants sharing personal experiences. Conversely, facilitators sometimes used participants’ shared experiences to provide related information or advice. More rarely, the facilitators shared their own experiences. This also offered opportunities for providing information, advice or personal validation of participants’ experiences. Sometimes participants self-disclosed personal, potentially sensitive or emotional issues, such as current or past mental health and severe health issues (e.g. depression, anxiety, cancer, eating disorders). We found such disclosures in several groups, but very few instances of the facilitator explicitly acknowledging such disclosure (‘thank you for [sharing] that’).
4.2 Social learning
Social learning was facilitated by a number of techniques that involved both facilitators and participants. Providing and exchanging information was one of the most prevalent techniques used in the groups. Facilitators, following the intervention manuals, provided information, explained relevant issues and answered participants’ questions; some in a more interactive manner than others. The degree of interactivity and amount of participant-initiated exchange of information differed between interventions, facilitators, groups and sessions (see Appendix 8). Exchanges of information were also prevalent as part of recapping current or previous sessions. Together with providing information and explanations, the facilitators used generic techniques, such as checking understanding and illustrating. Another way to facilitate social learning was by facilitators and participants providing advice, for example by referring to official guidelines and recommendations (e.g. dietary guidelines) or making suggestions (e.g. what one should or should not do). Providing advice and referring to guidelines were especially prevalent among ‘expert’ facilitators (e.g. dietitians) and when discussing healthy diet. Facilitators initiated discussions in which participants came up with and shared ideas (e.g. listing ideas about benefits of physical activity, ways to be active or relax) as whole-group or subgroup activities. It also involved participants offering ideas to other participants, often as part of discussions on problem-solving. Demonstrating and modelling behaviours were not very common in the analysed groups. We identified few examples of facilitators demonstrating specific behaviours and one instance of a participant demonstrating how to measure blood pressure. There were also very few instances of participants modelling the intended behaviours (e.g. modelling exercises, reading labels), perhaps not surprisingly considering the nature of the targeted behaviours (e.g. diet, physical activity). Finally, facilitators (mainly) and participants (rarely) provided verbal instructions on how to perform behaviours, such as how to start running or use relaxation techniques.
4.3 Social influence processes
Social influence processes can be facilitated through group interaction and other interpersonal change processes (e.g. sharing experiences, social learning) as well as discussing intrapersonal change in groups – all of which can influence participants’ beliefs and behaviours. More specifically, facilitators instigated social influence processes by appealing to credible sources or evidence (e.g. research evidence, national guidelines) and by using persuasive arguments. Participants, in turn, could also have positive or negative social influence on each other. Participants could have a positive social influence through expressing ‘change talk’, positive expectations for (or experiences of) health-related change and health-promoting beliefs, or a negative social influence by expressing resistance, expressing negativity or undermining health-promoting beliefs and ideas. The identified examples of negative influences in some cases could be linked with dysfunctional behaviours or roles. Although such negative influences were not commonly addressed or responded to by the facilitators, we identified some examples of facilitators countering such talk, for example by using humour/riposte or challenge.
4.4 Agreeing, disagreeing and challenging
Throughout group discussions, participants expressed agreement or (more rarely) disagreement with the facilitators or (even more rarely) with other participants. Disagreements seemed to serve as challenges to others’ beliefs (e.g. challenging their perceptions of barriers, low confidence or no motivation to engage in health behaviours). Facilitators elicited agreements from participants in relation to the provided information or explanations (e.g. ‘do we all agree that . . .’). They also sometimes challenged participants’ views, for example (1) by asking open questions to prompt self-reflection (e.g. asking why participants might not be able to do something, or ‘rolling with resistance’), (2) by challenging or ‘correcting’ misconceptions (e.g. by providing information or referring to credible sources of information), (3) by providing positive counter statements or ‘reframing’ (see 2.2 generic facilitation techniques in Table 10) or (4) by using humour. In consultations, however, the facilitators reported that they mostly avoided directly challenging, or disagreeing with, the participants to minimise the risks of losing participants, conflict and having a negative impact on group dynamics.
4.5 Social support in groups
This was mainly promoted by facilitators through (1) explicitly discussing it, (2) reinforcing participants’ talk about it (e.g. reflecting on how supportive the group is, encouraging peer support), (3) offering support to the group or individual participants and (4) describing ‘providing support’ as part of their role. Moreover, they provided emotional support through techniques, such as providing praise, reassurance and encouragement, and by using social validation techniques (see 4.6 Social validation processes). Participants emotionally supported each other by providing praise, encouragement and social validation, and offered practical support by volunteering practical ideas and information (e.g. about available exercise classes). We identified very few examples of participants initiating discussions about, and facilitators encouraging, buddying up (i.e. to do activities together). It was unclear whether or not these were taken outside the group (although the facilitators confirmed in our consultations that this was the case in some instances). Participants also made new social connections with each other by informally chatting about issues that they had in common but that were unrelated to the group (e.g. where they lived or common acquaintances). Facilitators provided opportunities for this by allowing time for, or instigating, informal interaction (e.g. before the session began). We identified no comments about potential benefits of providing support or reciprocity.
4.6 Social validation processes
These processes were enabled by either facilitators or participants in three main ways: (1) offering personal validation, (2) normalising (3) and expressing empathy or understanding. Personal validation usually involved participants saying that they also had a similar experience, which was sometimes followed by sharing their experiences or feelings. Normalising involved mainly facilitators responding to participants’ disclosures by saying that it was ‘normal’ to experience that or that the shared experience was common (e.g. ‘we all do that’). In the identified examples, such normalisations were positively intended and served as reassurances, creating a perception of universality of experiences, in particular barriers and difficulties. However, it is also possible that expressing such normalisations could be perceived as underplaying one’s difficulties. Finally, both participants and facilitators expressed understanding and empathy in response to participants’ disclosures, without personal validations or normalisations (e.g. ‘I can understand that’).
4.7 Social identification
Participants expressed perceptions of similarities between themselves and other members of the group, or social connections that suggested identification with common social categories, or shared identities. For example, they talked about being retired or belonging to the same general practices. In a few instances, facilitators made some of these social identities salient during sessions by referring to participants in terms of common social categories (e.g. ‘foodies’).
4.8 Social comparisons
Social comparisons within groups are most likely to be implicit, so they could not be easily coded. However, we identified some interactions that provided opportunities for making social comparisons. For example, facilitators asked participants to share comparable information about their experiences or practices (e.g. what they had for breakfast, how much physical activity they did) and about their self-assessments (e.g. sharing self-assessments of confidence or scores on diet quizzes). Participants also shared information about their performance or outcomes (e.g. increases in the number of steps, weight loss) that could be used as a basis for social comparisons. Such disclosures were usually volunteered by participants rather than requested by facilitators. Moreover, in a few sessions facilitators highlighted some participants as good examples (or role models) of engaging in health behaviours, but role modelling was also more likely to be an implicit process.
4.9 and 4.10 Accountability and competition
There were a few identified examples of participants and facilitators discussing the need for, or potential positive or negative effects of, accountability and competition. Some participants reported that they valued feeling accountable to others or the competitive element of groups. Accountability was indirectly facilitated by sharing individual goals in the group (or publicly stating goals and intentions) and then referring to them in goal or progress reviews in the following sessions (see 5.11, 5.12 and 5.16 Setting goals, reviewing progress and individual-level feedback). Facilitators provided opportunities for accountability and competition by taking objective measures of progress or enabling self-monitoring of these in the sessions (e.g. weighing or having scales for participants to use) or by eliciting participants’ reports of comparable progress or goal achievement (e.g. number of steps). However, in most cases accountability and competition did not seem to be specifically facilitated by group facilitators, and we identified no examples of intergroup competition.
4.12 Group problem-solving
In some sessions, facilitators encouraged discussions that were focused on identifying barriers to health behaviours and generating potential solutions as a group. Interestingly, not all instances of identifying barriers were followed by problem-solving. Moreover, engaging a group in discussing barriers and problem-solving was less common than participants reporting individual barriers, and facilitators prompting individual participants to problem-solve. We also identified some examples of facilitators promoting 4.11 co-operation through organising group activities in which participants worked together. We identified no examples of facilitators providing 4.13 group-level feedback (i.e. that included measurable detail regarding progress), which most likely reflected a lack of group-level goals in these interventions. However, we identified few examples of facilitators providing praise to the whole group. Finally, we coded no examples of 4.14 social facilitation as is it is an implicit process, which might have occurred through practical activities and modelling.
5 Selected intrapersonal change processes and targets (Table 14)
| Examples of 2.5. techniques (or sets of techniques) to facilitate intrapersonal change processes | Prevalence in the coded transcripts |
|---|---|
| 2.5.1. Facilitating commitment to attend sessions | Occasional |
| Acknowledging presence/absence of participants | Occasional |
| Providing opportunities to attend sessions with another group | Occasional |
| Reporting reasons for participants’ absences, low attendance | Rare |
| Providing praise to present participants | Occasional |
| Emphasising benefits of attending | Rare |
| 2.5.2. Facilitating understanding | Frequent |
| Reviewing previously covered content | Occasional |
| Checking understanding | Frequent |
| Correcting misunderstanding or lack of understanding | Occasional |
| 2.5.8–10. Discussing intervention outcomes expectations, motivation and self-efficacy | Frequent |
| 2.5.11. Facilitating setting goals | Frequent |
| Explaining goal-setting | Occasional |
| Asking to set individual goals, write action plans | Frequent |
| Asking to share, discuss goals with others | Occasional |
| Prompting setting specific (SMART) goals | Occasional |
| Prompting setting small or smaller, achievable goals | Frequent |
| Prompting setting (more) challenging goals | Rare |
| Prompting setting long-term, sustainable goals | Frequent |
| 2.5.12. Facilitating progress review | Frequent |
| Asking for review of specific goals | Occasional |
| Asking for general review of progress | Frequent |
| Taking objective measures | Occasional |
| 2.5.14. Facilitating individual barrier identification and problem-solving | Frequent |
| Prompt reporting of individual barriers | Frequent |
| Prompt individual problem-solving of individual barriers | Occasional |
| Prompt group problem-solving of individual barriers | Rare |
| 2.5.16. Providing individual-level feedback | Occasional |
5.1 Commitment to attend group sessions
This commitment was expressed by participants in some groups and was also evident when participants could not attend certain sessions and tried to arrange to attend the session with another group (which the facilitators allowed and offered). In some groups, the facilitators acknowledged presence or absence of specific participants in the sessions. However, some groups experienced low attendance or dropout, which was discussed at the beginning of sessions. Facilitators reinforced present members’ commitment to attend the sessions by stating reasons for other participants’ absences (e.g. illness), providing praise or positive reinforcement to the present participants, and by offering benefits of tailoring to, and focus on, present participants.
5.2 Developing understanding
A majority of the time in groups was spent on group discussions and learning; facilitators regularly checked participants’ understanding throughout the sessions and, in particular, when recapping the previous sessions. This was conducted through question and answer sequences, and, when participants’ disclosed misunderstanding, or lack of understanding, the facilitators provided corrections or additional explanations.
5.8–5.10 Intervention outcomes expectations, motivation and self-efficacy
These outcomes were commonly discussed in the group sessions. Participants expressed generally positive expectations of the outcomes that they hoped to achieve in the programme. Many claimed to be motivated to change and achieve these outcomes, reported various reasons for this motivation (most were health related) and expressed perceptions of a high importance of making relevant lifestyle changes. Such expressions promoted positive social influences in the group. However, some participants expressed difficulties with maintaining motivation to engage in healthy, or avoid unhealthy, behaviours outside, or after the end of, the groups, and some expressed low confidence for making relevant changes. In some instances, facilitators addressed these by reinforcing group support, providing reassurance (e.g. that later in the programme their confidence or motivation might increase) or by challenging participants to think what might help them become more motivated or confident.
5.11, 5.12 and 5.16 Setting goals, reviewing progress and individual-level feedback
In most sessions, participants were asked to set goals for making changes to their diet and/or physical activity. In some sessions, goals were not set because there was not enough time in the session and, in these cases, facilitators asked participants to set goals at home. However, facilitators’ approaches to delivering this technique differed. In some, but not all, first sessions, the facilitators discussed or explained the benefits of goal-setting, and what SMART (specific, measurable, achievable, relevant and time-bound; in SkiM participants were asked to set goals that were also Enjoyable) goals or action plans are. All goal-setting was facilitated via individual activities (i.e. participants were asked to set and write down individual goals). In some sessions, the facilitators circulated around the room offering individual advice, asked participants to discuss their goals in pairs or sometimes asked participants to share their goals with the whole group. Sharing goals with the group provided opportunities to engage interpersonal processes (i.e. learning from each other, sharing ideas or suggestions, accountability) and for the facilitators to help (re)formulate the goals as SMART goals. However, this was not always the case, and in many instances participants set non-specific goals, or expressed general intentions rather than goals, which were not challenged by the facilitators. Facilitators also began most sessions with a review of progress or goals but, again, the delivery of this technique varied from instigating generic sharing of experiences (e.g. ‘how did you do last week?’) to asking whether or not, and how, participants met their goals (and referring to these goals specifically). In some cases, the facilitators remembered or referred to the goals that participants set and shared in the previous session, thus engaging accountability and showing active listening. In many goal reviews, participants responded to facilitators by reporting barriers to healthy behaviours or external circumstances that prevented them from meeting their goals. Facilitators tended to respond by reframing, providing reassurance, normalising or expressing empathy/understanding. They also referred to setting small (or smaller), realistic goals (i.e. opposite to challenging them). More rarely facilitators responded by instigating problem-solving or providing challenge to participants. In the final session of the LWTC programme, the facilitators took objective measures of progress (e.g. weight, body fat). Reviews of specific goals and taking objective measures provided opportunities to provide specific individual-level feedback (including also praise, reassurance or challenge) and for accountability.
5.14 Individual barriers and problem-solving
Although, in some instances, general barriers to behaviours were discussed and groups generated ideas for problem-solving, in the majority of cases participants reported individual barriers and facilitators prompted individual-level problem-solving (rather than asking the group to collaboratively identify potential solutions). Moreover, in many instances of participants reporting barriers to their behaviours, these were reported during progress reviews as reasons for not meeting their goals, and facilitators rarely followed such reports with prompts for problem-solving or with challenge.
Acknowledging change
Although participants did not usually report change in their motivation, attitudes, identity or self-efficacy, they talked about making changes and progress, and expressed better self-understanding. Some praised themselves for this positive change, whereas others praised the facilitators. We see this as constituting a positive feedback loop in the group, facilitating positive social influences and role modelling. Facilitators provided praise to participants reporting positive outcomes, and provided reassurance and reframing to participants who reported feeling more negative about their progress.
6 Participant characteristics and contextual influences
Participants shared and discussed, in the groups, influences from outside the group on their behaviours and health. These included health-related conditions that were often reported as limiting ability to engage in health-related behaviours (e.g. physical activity). In a sense, these were particular barriers to behaviours, but such that they could not be problem-solved in the groups. Participants also discussed contextual social influences on their health and behaviours. For example, they discussed the importance of supportive social networks, reported receiving social support, or lack of support, from their partners or friends. In some instances where supportive connections were lacking, participants expressed wanting to extend the support received in the programme (from the group or participants) outside it. In such situations, the facilitators could promote making social connections or buddying up with group members beyond the sessions. Participants also discussed negative influences of other people outside the group on their health-related behaviours and motivation, for example sabotaging or undermining attempts at changing behaviours, demotivating them or promoting unhealthy behaviours. They also discussed the negative influences of social situations or events and social norms on health behaviours, for example social norms related to unhealthy eating during celebrations or festivals. In a few of these situations, the groups provided opportunities for developing shared understanding and social validation, and identifying strategies to deal with these influences (e.g. group brainstorming or problem-solving).
Discussion
In this stage of the MAGI study, we developed a coding schema to enable identification of the MAGI framework categories in transcripts of group sessions. This includes specific instructions on identifying and coding framework categories, and additional lower-level subcategories for precise coding of group interactions and processes. We coded 38 transcripts (10 sampled in stage 1 and 28 in stage 2) of group sessions from three GB-BCIs (LWTC, SkiM and WtW) and identified examples of the framework categories from these interventions. These examples provide evidence for the occurrence of the framework processes in ‘real-world’ groups and illustrate the framework categories. We also identified examples of techniques used by group facilitators to instigate and facilitate group dynamics and change processes.
The majority of the processes included in the framework were well evidenced, with multiple examples identified across transcripts (showing good levels of data saturation). Our findings show that facilitators use a wide array of techniques (or sets of techniques) to facilitate and manage groups. The most prevalent processes in the analysed interventions involved social learning processes and sharing of experiences, and facilitation techniques linked to these (e.g. providing or interactively exchanging information, prompting participants to relate information to shared experiences). We also identified good evidence of social influences (positive and negative, from facilitators and participants) and social support (mainly emotional) in the groups. We identified fewer examples related to other interpersonal change processes (i.e. social identification, social comparisons, accountability, competition, co-operation) and to some group dynamics (i.e. identifying with/as a group, group cohesion, climate, norms). These processes with fewer coded examples probably reflect their implicit nature (i.e. that they might not be verbalised even if they occur). Thus, other methods might need to be used to identify them in groups (e.g. participants’ self-report). They may also reflect less focus in the analysed interventions on these processes (and a primary focus on exchanging and explaining health-related information and recommendations). Finally, many intrapersonal change processes and techniques were often delivered in ways that did not fully engage the group; for example, goal-setting, problem-solving and feedback were predominantly delivered individually or between participants and facilitators, rather than through group interaction (e.g. discussing goals could engage social learning and accountability to the group).
These identified examples of processes and techniques, of course, might be different in other types of interventions or groups, depending on the intended/targeted processes and changes or participant characteristics. For example, support or self-management groups might focus more on sharing experiences, social validation and peer support (rather than provision of information), whereas some weight loss groups might engage more social comparisons, accountability and competition (e.g. through public weighing). Currently, we still lack evidence for which of these processes may optimise effectiveness in behaviour change groups, but identifying which of them occur and with what prevalence in GB-BCIs (as shown in this stage of the MAGI study) may be a useful first step to developing such evidence.
Strengths and limitations
The coding schema was developed by using multiple, complementary approaches, including existing theory, expert opinion and content coding of empirical data. It was applied to a relatively large data set (including 38 transcripts, and hundreds of pages of transcripts) and data saturation was achieved for many of the framework categories. Some categories were not populated because they describe processes that are implicit rather than explicit. Thus, they could not be identified in this type of data. A number of transcripts were independently double-coded, which contributed to the refinement of the coding schema (and the MAGI framework). Inter-rater agreement would be difficult to calculate because codes could be applied to different lengths of excerpts (e.g. words, turns or whole sequences) and included ‘interpretative’ approaches (i.e. not only semantic-level content coding more suitable for assessments of inter-rater agreements). Such assessments are also not typical in this type of qualitative analysis. Moreover, the coding involves > 160 subcategories, some of which might be applied to the same excerpts and may require specialist knowledge and understanding of the coded processes. Thus, we suggest that the framework and the coding schema are used as ‘catalogues’ from which researchers can select categories of interest to focus on in the coding.
In this study, we used data from only three, quite similar, interventions and a relatively small number of facilitators (i.e. 11). Thus, the generalisability of the coding schema is limited. Future research could use similar methods to apply the coding schema to other types of interventions, groups or different types of data (e.g. observations, videos of group sessions). Furthermore, the examples identified and provided, including additional excerpts available from the authors, are limited by the quality of the available recordings and transcripts (e.g. many of the WtW recordings were of insufficient quality to be included in the sampling) and the type of data. For example, it was not possible to transcribe overlapping conversations or to identify different speakers from audio-recordings. Finally, the use of audio-recordings meant that non-verbal behaviours could not be considered and that examples of some framework processes could not be identified, as they may not be expressed verbally (e.g. social facilitation). Thus, different types of data and methods are needed to fully validate these elements of the framework. Suitable methods might include video-recordings, coding of intervention manuals or the use of participant questionnaires to capture changes in specific hypothesised processes (see Chapter 4). Finally, participants might perceive and interpret the situations or interaction differently to an external coder. For example, a coder might identify examples of dysfunctional/disruptive group role or behaviour, whereas participants might not perceive that as a negative influence on the group.
Implications
The examples identified provide practical illustrations of the framework processes and techniques and may enhance understanding of their definitions and the associations between them. The developed coding schema can be used to code transcripts of group sessions as part of process evaluations of group-based interventions. Such coding may also be used to generate feedback for group facilitators. The examples extracted could be useful to illustrate good or poor practice when training future facilitators (or updating training for existing facilitators). As the coding schema encompasses a large number of categories and subcategories, the precision and reliability of coding could be improved by focusing on aspects of the framework that are crucial to particular investigations. So depending on the research questions pursued, only subsets of the defined categories might be used. Researchers could also, in the future, adapt the coding schema for use with specific types of groups and interventions, and develop additional framework categories and subcategories. Furthermore, the checklist could also be used to analyse group sessions directly from audio- or video-recordings or session observations.
These findings show that some potentially useful interpersonal processes were used infrequently, at least in the specific interventions studied. This kind of finding could be used to train and provide feedback to the facilitators to increase their awareness of the wider range of group dynamic and interpersonal processes that can be specifically targeted and facilitated in the groups, and the range of available facilitation techniques for doing so.
Conclusions
In stage 2 of the MAGI study, a coding schema was developed and used to code a range of group sessions from three GB-BCIs. The coding identified examples of most of the framework processes and techniques ‘in action’. This provides evidence for the existence of the processes and techniques proposed in the MAGI framework, and confirms its content validity in the context of our GB-BCIs focused on diet, physical activity and weight loss. The methods developed here may be useful for process evaluation of group-based interventions, as well as for informing the training of facilitators to improve their competencies in delivering GB-BCIs. Future research should apply the framework and the coding schema to other types of groups and interventions to provide more generalisable evidence of change processes in groups, and develop methods for linking these analyses of processes with intervention outcomes.
Chapter 4 Assessing and analysing relationships between mechanisms of action and outcomes in group interventions (stage 3)
Introduction
In the previous chapters, we first described the development of a comprehensive framework of mechanisms of action in group-based interventions (the MAGI framework) and presented definitions and details of the framework components (stage 1). Next, we used the framework as the basis for developing qualitative methods to identify and analyse change processes in GB-BCIs, and to provide examples of framework components and facilitation techniques (stage 2). Evidence of many components was found, thus providing a preliminary validation of the framework. We were also able to estimate the frequency with which many processes occurred and with which facilitation techniques were used. Two further developments of this work are envisaged: first, exploring the applicability of the framework to other types of GB-BCIs and, second, investigating which facilitation techniques and processes in the framework are most important for maximising group engagement/attendance and outcomes for participants.
As highlighted previously, MRC process evaluation guidance28,29 emphasises the importance of exploring implementation, mechanisms of change, and context. These can be represented in a logic model that describes how interventions and their important components are related to each other and work to influence outcomes. The logic model articulates the ‘theory of change’ of the intervention and, in GB-BCIs, group processes identified in the MAGI framework should be included if they are thought to affect outcomes. As recommended in the guidance, a range and mix of methods, drawing on both qualitative and quantitative data, could be used in process evaluations of GB-BCIs to explore these aspects and advance understanding about what makes these interventions effective (or not).
The MAGI framework identifies a large number of, potentially interacting, processes and influences in GB-BCIs, which may vary depending on contextual characteristics. Therefore, sophisticated methods, integrating data from qualitative and quantitative sources, are important when investigating how group dynamics and processes operate and influence outcomes. As shown in Chapters 2 and 3, qualitative methods could involve observing or analysing audio- or video-recordings of group sessions. Facilitators’ or participants’ perceptions of group dynamics and change processes in groups can be also investigated through interviews and focus groups,47–49,100,125 and ethnographic methods. 133 Quantitative methods might be used in assessing the content or ‘dose’ of the delivered intervention,58 quantifying occurrences of particular types of interactions or processes, characterising different groups to provide information on contextual factors, or using questionnaires to measure participants’ perceptions of group processes (e.g. social identification, group cohesion46,54). Mixed-methods approaches to process evaluation of GB-BCIs are recommended, but it is unclear when researchers should employ particular methods, how they should mix or integrate these methods and how group-level data can be collected and presented meaningfully. These are the issues that this third and final stage of the MAGI study explored.
In the context of our three GB-BCIs, and in the light of the framework presented in Chapter 2 and data presented in Chapter 3, the hypothesis guiding this stage of the study was that the successful initiation and facilitation of key group processes leads to increased participant engagement, changes in intrapersonal change targets (e.g. motivation, self-efficacy and planning for change) and, thus, behaviour change (e.g. improved diet, physical activity) that can generate improved health outcomes (e.g. weight loss) and, potentially, other unplanned benefits (e.g. social connectedness). Hence, groups developing positive group dynamics and demonstrating a wide range of interpersonal change processes are postulated to be more effective in engaging participants and facilitating outcomes than groups where there is evidence of negative group dynamics (e.g. with dysfunctional or disruptive behaviours) and limited interpersonal change processes (e.g. focusing on provision rather than exchange of information). Indeed, some group-related factors have previously been found to be associated with improved intervention outcomes, including the use of specific change techniques,6,8,31,137 change talk,138,139 social support140,141 and social identification. 142 For example, participants’ perceptions of group dynamics have been associated with weight loss outcomes,134 and group norms have been associated with group members’ body perceptions and dieting intentions. 126 Moreover, session attendance (indicating engagement with the group and intervention) has been associated with weight loss outcomes in group interventions. 143,144
Our initial plan for stage 3 of the study was, therefore, to combine further qualitative data on processes and techniques based on the MAGI framework with quantitative data on attendance and outcomes in a sample of the groups studied, to explore why some groups were more successful than others. By characterising and comparing more and less effective groups, we hoped to provide initial evidence of, and explanations for, links between what happens in group sessions, on the one hand, and attendance, behaviour change and health outcomes (e.g. weight loss), on the other. It would also generate further hypotheses that might be explored in wider secondary data sets available from the three studies used in our research, or in future research.
Meaningful linkage of group-level qualitative data on the operation of many complex, interacting processes with quantitative data on individual-level attendance and outcomes may be impossible if appropriate data are not collected. Moreover, variation in individual outcomes within groups may be as great as variation across different groups, making it difficult to attribute outcome differences to qualitative differences in group operation. For these reasons, we did not anticipate being able to undertake meaningful quantitative analyses that could predict outcome differences. Furthermore, as the study progressed, we became aware of further limitations in the data available to us for secondary analyses (see Availability of qualitative data and revised sampling). Therefore, the aims of this final stage were reviewed and refined.
Aims
Our refined aim for this stage of the study was to apply mixed methods, based on the MAGI framework, to illustrate how we can explore why some groups may be more or less successful than others in GB-BCIs.
We planned to provide guidance and a resource for researchers to facilitate future research on GB-BCIs using the MAGI framework to formulate hypotheses, and to collect, analyse and integrate mixed-methods data to address specific research questions.
Methods
Planned methods
Our original plan, as outlined in our protocol [www.journalslibrary.nihr.ac.uk/programmes/eme/1420203/#/ (accessed 18 December 2018)], was for a researcher who was not involved in the prior qualitative coding and analysis (see Chapter 3) to examine quantitative data from groups for which recordings from all sessions were held and to sample groups characterised by good or poor engagement (i.e. attendance) and group-level outcomes (e.g. weight loss). We planned to select six groups, most likely from the LWTC programme, for which most data were available: three with good engagement/outcomes and three with poor engagement/outcomes. We planned to use the framework to code transcripts from all sessions linked to these (e.g. six groups of four sessions each, making 24 sessions in total for LWTC groups). We then intended to undertake framework analysis145 to construct ‘group narratives’ for these groups, providing a higher-level analysis across sessions (to capture features that emerge only when considering groups over time, such as group development processes146) and across groups (to highlight differences between groups), including key group processes and facilitator techniques. We also planned to code participants’ verbalised responses to their group experiences, for example in the form of ‘change talk’ [as outlined in analysis of motivational interviewing interventions (e.g. using the Motivational Interviewing Skill Code124)], and to indicate changes in motivation as a precursor to changes in behaviour and outcomes. Using these narratives and higher-level descriptions, we planned to develop a sophisticated characterisation of groups within and across each session. This would allow us to examine whether or not differences between groups in terms of framework components provided plausible explanations for differences in engagement and outcomes (i.e. between the successful and not so successful groups), thereby identifying specific processes and techniques as potential predictors or moderators of intervention outcomes.
Availability of qualitative data and revised sampling
Full, adequate-quality recordings for all sessions were available for only seven groups from the LWTC programme at the Exeter site examined in the ComPoD trial. Other groups had less than the full four sessions recorded, or incomplete or poor-quality recordings. Furthermore, the SkiM intervention sessions were ongoing at the time of analysis, and WtW intervention recordings were generally of very poor quality. Thus, we could not apply the intended sampling strategy and, instead, randomly selected six groups from these seven and sent all associated session recordings for transcription. We suspected that among these there would not be sufficient variability to enable comparison of groups that were more or less successful, undermining the intention to explore links between differences in group processes and facilitation techniques to differences in attendance and outcomes. Nonetheless, we believed that the analyses of transcripts of all sessions across six groups would provide a good illustration of how the MAGI framework could be applied to future data sets to do this.
Availability and linkage of quantitative data
As it was an ongoing programme, the recordings of LWTC group sessions extended to groups delivered outside the timeframe of the ComPoD trial intervention period and groups could include trial and non-trial participants, including people with newly diagnosed diabetes. For the purposes of this study, the trial data set that had high rates of follow-up at 6 months (91%) and low levels of missing data for participants with pre-diabetes was supplemented with data (see details in Quantitative analyses of data from the Living Well Taking Control programme) for all LWTC participants (i.e. including those entering the programme outside the trial, and with diabetes) that had been collected and entered by the programme providers at the Exeter site. These data were initially collected for a parallel before-and-after service evaluation, which provided a report on participants entering the programme up until April 2015, with < 60% of these providing follow-up data by October 2015. 60 Data continued to be collected alongside programme delivery beyond this and the data set provided to us contained details of participants entering the programme (but not necessarily due follow-up) until February 2016, so we were aware that levels of missing data may be high.
On attempting to link individual-level quantitative data on baseline characteristics, session attendance, perceptions of group sessions and outcomes (e.g. weight loss) for participants in the six groups selected for qualitative analyses, we became aware of limitations with the quantitative data. As shown in Table 15, no attendance or follow-up data were available for two out of the six selected groups, and one further group had follow-up data on only 3 out of 10 participants. This left three groups for which some follow-up data were available for at least half of the six to eight participants in each of the groups (shaded rows in Table 15). The data available from trial and provider data sets are shown in the final two columns.
| Group identifier | Session number | Facilitator | Minutes transcribed | Number of group participants (including those taking part in the linked trial) with baseline data available | Number of group participants with follow-up data availablea |
|---|---|---|---|---|---|
| Group 1 | 1 | A | 53 | 8 (3 in trial) | 6 (3 in trial) |
| 2 | A | 127 | |||
| 3 | A | 114 | |||
| 4 | A | 75 | |||
| Group 2 | 1 | B | 50 | 7 (3 in trial) | 4 (3 in trial) |
| 2 | B | 122 | |||
| 3 | B | 115 | |||
| 4 | B | 56 | |||
| Group 3 | 1 | B | 49 | 10 (1 in trial) | 3 (0 in trial) |
| 2 | B | 119 | |||
| 3 | B | 106 | |||
| 4 | B | 36 | |||
| Group 4 | 1 | B | 47 | 6 (5 in trial) | 5 (5 in trial) |
| 2 | B | 121 | |||
| 3 | B | 88 | |||
| 4 | B | 49 | |||
| Group 5 | 1 | B | 58 | 6 (1 in trial controla) | 0 |
| 2 | B | 109 | |||
| 3 | B | 104 | |||
| 4 | B | 49 | |||
| Group 6 | 1 | C | 67 | 7 (4 in trial controlsa) | 0 |
| 2 | C | 127 | |||
| 3 | C | 95 | |||
| 4 | C | 65 |
Final sample
For illustration purposes, quantitative data on characteristics and outcomes for the three groups highlighted above were summarised at group level (see In-depth summary of quantitative data for three Living Well Taking Control programme groups). The first two groups, which had two different facilitators, were then selected to illustrate higher-level qualitative analyses (see Qualitative analyses of group processes in two Living Well Taking Control programme groups), and links were made between the quantitative and qualitative data for these groups. Summaries of the quantitative and qualitative data were generated independently by two separate researchers (JRS and AJB) without access to the other data set. In addition, this limited sample was supplemented with presentation of further available group-level quantitative data from the entire LWTC data set (see Quantitative analyses of data from the Living Well Taking Control programme).
Quantitative data and analysis
We produced descriptive summaries on group-level characteristics, attendance and outcomes from all available LWTC data, to demonstrate methods for presenting and summarising such data, to explore variability between groups and group-level factors that might be considered in relation to group processes and outcomes, and to identify hypotheses that could be investigated with reference to qualitative data. Groups were included in analyses if data for the variable of interest were available for at least half of the participants in the group (when this exceeded three). Variables selected for analyses were those for which there were low levels of missing data. These included group size, group composition in terms of key sociodemographic (e.g. gender, age, ethnicity) and socioeconomic characteristics (e.g. education level, employment status), BMI (at baseline), weight loss (at 6-month follow-up), self-reported health status assessed as a percentage score using the EuroQol-5 Dimensions thermometer147 (at baseline and follow-up), and participants’ ratings of the perceived importance of, and their confidence in, achieving recommended levels of physical activity and a healthy diet (at baseline and follow-up). These provided an indication of participants’ levels of motivation and were assessed using four single-item rating scales scored from 1 (not at all important/confident) to 10 (extremely important/confident). 148 We had originally planned to summarise self-reported behavioural outcomes (physical activity149 and dietary behaviour150) but found that the questionnaires assessing these had not been consistently completed.
We also conducted descriptive analyses of available data on participant perceptions of key group processes collected at the end of the group sessions (at approximately 1-month follow-up) available for a subsample of LWTC participants. The questionnaire (see Appendix 9) included 12 items to which participants responded on Likert scales scoring from one to seven and labelled from ‘very strongly disagree’ to ‘very strongly agree’. Mean scores were calculated across three four-item scales assessing (1) ‘group support’ (i.e. participants’ perceptions of support within the group, such as ‘I can count on other members in the group meetings when things go wrong’), (2) ‘group identification’ (i.e. their sense of identification with the group, such as ‘I feel strong ties with other members in my group’) and (3) ‘other social identities’ brought to the group reflecting connections with external groups (e.g. ‘I have friends who are members of lots of different groups’). Higher scores indicated greater perceived group support, group identification and connectedness/identities stemming from external groups.
As indicated above, quantitative data on participant characteristics, engagement (indicated by session attendance), and key outcomes (e.g. weight loss) were also summarised and tabulated for the three groups matched to qualitative data, and observations about similarities and differences were made.
Qualitative coding and analysis
All analyses of transcripts were undertaken without insight into the available quantitative data for each group. Although limited to only two groups (with four sessions each), these qualitative analyses proceeded as originally planned and involved three steps:
-
data familiarisation
-
detailed coding and analysis of session transcripts using the coding schema (see Chapter 3)
-
summarising sessions and groups, which involved the development of ‘group narratives’ based around the key framework processes and facilitation techniques, and comparison of these summaries between groups (this encompassed investigating the occurrence of ‘change talk’ and ‘resistance talk’).
Integration of qualitative and quantitative data
We illustrated three main approaches to integrating quantitative and qualitative data127 using our data sets:
-
‘triangulation’, which involved comparing findings from different data sources/methods with each other to check for agreement or divergence
-
‘following a thread’, in which hypotheses generated from one data set are explored in another
-
a ‘matrix approach’ in which data from the same group from different sources were aligned, compared and integrated in a table to identify patterns.
Results
Overview
First, we present descriptive data characterising groups and participants across all groups for which data were available in the LWTC programme data set including group size, group composition and participants’ levels of motivation. All of these elements are captured in the MAGI framework (primarily under ‘group intervention design’ and ‘participant characteristics’). This provides a context for the later, in-depth quantitative and qualitative analyses of selected groups for which all session recordings and adequate follow-up data were available. It also illustrates variability across and within groups and potential hypotheses that might be explored. Second, we illustrate the steps undertaken in the qualitative analyses and summarise findings from these analyses in relation to the two groups studied in depth. This illustrates how such analyses might be used in future research. Finally, we provide examples using our data of mixed-methods approaches to integrating data.
Quantitative analyses of data from the Living Well Taking Control programme
Baseline characteristics of Living Well Taking Control programme groups
There were records for 565 LWTC participants, with at least some further baseline and/or follow-up data available for 538 participants (95%). Of these, 445 (83%) participants had an identifier indicating to which group they belonged and a further 35 (7%) participants without an identifier had follow-up data suggesting that they did participate in a group but that this information had not been recorded.
There were records for 75 groups in total, but only 67 (including 431 participants) had some data available for at least three participants. These were considered in further analyses. Twenty (30%) of these groups comprised participants with newly diagnosed type 2 diabetes; the rest were for participants with pre-diabetes. Figure 5 shows the number of groups of different sizes based on available records (we are uncertain whether or not any participants were missing records, for example if they did not consent to having measures recorded). Across the 67 groups, records were available for an average of six, and up to 12, participants, with over one-third of groups including six or seven participants (not including partners or supporters present, for whom no data were held).
FIGURE 5.
Number of groups of different sizes (as indicated by available records, which may be different from the actual group sizes) in the LWTC programme.
Table 16 summarises available baseline data on key group and participant characteristics. Overall, 42% of participants in the groups were men. There was one all-male group, 25 (37%) groups comprised a majority of men, two included equal numbers of men and women, half comprised a majority of women, and there were five all-female groups. The average age of participants across all groups was 64 years, but this ranged from an average of 47 years to 74 years for individual groups, with participants across the entire sample ranging from 28 years to 91 years. Twenty-eight groups (42%) included at least one participant who was aged < 50 years. The average age difference between the oldest and youngest participants in the same group was 25 years, suggesting high within-group variability. However, in some groups, participants were of a similar age (e.g. in seven groups, the age difference was < 10 years) and in other groups the age difference was very large (e.g. in another seven groups, the age difference was > 40 years).
| Summary data | Characteristic | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Group size (n) | Gender (% male) | Age (years) | BMI (kg/m2) | Self-rated health (%) | Importance of physical activity (1–10)a | Confidence in physical activity (1–10)a | Importance of healthy diet (1–10)a | Confidence in healthy diet (1–10)a | |
| Number of groups (%) for which data were available | 67 (100) | 67 (100) | 67 (100) | 67 (100) | 62 (93) | 56 (84) | 54 (81) | 58 (87) | 57 (85) |
| Number of participants (%) for whom data were available | 431 (100) | 431 (100) | 415 (96) | 397 (92) | 363 (84) | 344 (80) | 343 (80) | 349 (81) | 348 (81) |
| Mean (SD) across groups | 6.4 (2.2) | 42 (24) | 63.9 (5.6) | 31.3 (2.5) | 72 (9.6) | 7.0 (1.0) | 6.5 (1.3) | 8.6 (0.6) | 7.6 (0.8) |
| Range in means across groups | 3–12 | 0–100 | 47–74 | 26–37 | 47–88 | 5.6–9.3 | 2.7–9.1 | 7.3–9.9 | 5.6–10.0 |
| Range across entire sample | N/A | 28–91 | 19–56 | 7–100 | 0–10 | 0–10 | 2–10 | 1–10 | |
Owing to the geographical location for intervention delivery (Exeter, UK), the sample were overall predominantly from a white British background. However, 12 groups had at least one non-white British participant and, in one group, four out of the eight participants were from other ethnic backgrounds. The LWTC data set analysed for the purposes of the before-and-after evaluation of the programme60 included information on participants at the Birmingham site, where nearly half of participants were from an ethnic minority background. However, in the data set from the Birmingham provider, participants did not have a group identifier, making it impossible to conduct any further group-level analyses of these data, including examination of the influence of ethnic background on group mechanisms as a means of explaining some observed differences in engagement and weight loss between those from white British and other backgrounds. 61
All but seven groups (90%) included at least one participant who was retired, with an average of three retired participants per group. Fifty-five groups (82%) included at least one participant who was working, but the number of participants working was low in many groups. However, there were two groups (probably held in the evening) in which all participants were working. Larger numbers of participants and groups had missing data on education levels, so these data were not analysed in detail; but among the groups for which data were available, two-thirds included at least one participant who was degree educated, and there was wide variation in education levels within most groups.
In three-quarters of groups (50/67 groups), the average BMI of participants was at the lower end of the obese range, but in 17 groups it was in the overweight range. In 24 groups (36%), at least one participant was severely obese (i.e. a BMI of > 40 kg/m2) and in 29 (43%) groups at least one member was in the healthy weight range (ComPoD trial entry criterion of being overweight as represented by a BMI of > 25 kg/m2 did not apply to the diabetes groups and was not so stringently applied for entry to the LWTC programme outside the trial).
Participants’ perceptions of their health and ratings of life satisfaction also varied considerably within and across groups. For example, among the 61 groups with adequate data, the average self-rated health status across groups was 72%. However, this ranged from an average of 45% to 87% for individual groups and was highly variable within groups, with only six groups having ratings for all members that were < 20% apart and differences in other groups ranging from 0% to 87% (mean 44%) between the highest- and lowest-scoring group members.
Participants’ perceptions of the importance of, and their confidence in achieving, adequate physical activity and a healthy diet varied greatly across the entire sample and to a lesser extent across the groups, with most variability across groups in perceptions of the importance of physical activity. This suggests that some groups (e.g. those in which average scores were above 9 out of 10 for these items) were highly motivated, and others (e.g. with average scores of six or below for one or more items) less so. There was also evidence from 12 groups of mismatches between one or more individual participants’ ratings and that of the wider group, particularly in relation to confidence in achieving physical activity and a healthy diet. As described below, qualitative analyses demonstrated that participants’ motivations, reflected in their perceptions of importance and confidence, were explicitly revisited in the sessions, allowing triangulation of these data and insight into potential links with group processes.
These baseline data indicate variability in the size and sociodemographic, socioeconomic and health-related characteristics across the groups (i.e. between-group variability), and in the make-up of individual groups (i.e. within-group variability). Some of this variability might be explained by ‘group intervention design’ features in the framework related to 1.4 participant selection and group composition and 1.3.2 process of becoming a group member under 1.3 group characteristics. These varying characteristics could be further explored in relation to their influence on group dynamics (e.g. group engagement, cohesion), interpersonal change processes (e.g. social support) and intervention outcomes (e.g. weight loss). They could also be examined in relation to other design (e.g. venue) and contextual features (e.g. facilitator characteristics) not recorded in this data set. It is worth noting that, although facilitator details were not recorded here, the facilitator represents another level of clustering within the data set. If such data were available, potential links between participant and facilitator characteristics, and the impact that these may have on interaction and group processes, would be worth exploring. 52
In future research, groups with different features (e.g. small or large group size; high or low average BMI, and scores of importance and confidence among participants; differing numbers of members with certain characteristics) or with different levels of heterogeneity within groups (e.g. comparing more homogeneous with heterogeneous groups in terms of sociodemographic, socioeconomic or clinical characteristics) could be sampled and then analysed using qualitative methods, to explore potential differences in group processes (as described in Qualitative analyses of group processes in two Living Well Taking Control programme groups). Relationships between group-level characteristics and self-reported perceptions of group processes could also be explored via multivariate analyses. ‘Outlier’ members (e.g. the only younger person, a severely obese participant) and the impact this status has on these participants’ perceptions of the group and on wider group processes might also be explored.
Engagement and perceptions of group processes in the Living Well Taking Control programme
Table 17 summarises descriptive data on participants’ engagement (assessed via session attendance) and self-reported perceptions of group processes (i.e. group support, group identification, other social identities) in the LWTC groups. Attendance data were relatively complete (sufficient data available for 87% of groups with baseline data) and attendance at group sessions was, in general, very high (75% of participants across the whole sample attended all sessions), with little variability apparent across groups. However, there were 16 groups (28%) that included one or more participants who dropped out after the first or second session. Although we are aware from the ComPoD trial that some of these may be for reasons external to the group (e.g. ill health), it would be interesting to explore further data on the characteristics of these dropouts in comparison with other group members, and to explore whether or not qualitative analyses could illuminate how dropouts affected, and were affected by, group processes.
| Summary data | Attendance | Perception of groups (1–7) | |||
|---|---|---|---|---|---|
| Number of sessions attended (1–4) | Attended all sessions | Group support | Group identification | Connections/social identities outside the group | |
| Number (%) of groups for which data were available | 58 (87) | 58 (87) | 48 (72) | 48 (72) | 48 (72) |
| Number (%) of participants for whom data were available | 360 (84) | 360 (84) | 260 (60) | 266 (62) | 253 (59) |
| Mean (SD) across groups | 3.8 (0.3) | 82 (18) | 4.9 (0.5) | 5.3 (0.5) | 4.1 (0.7) |
| Range in means across groups | 3–4 | 25–100 | 3.7–6.2 | 4.0–6.2 | 2.3–5.8 |
| Range across entire sample | 0–4 | 1–7 | 1–7 | 1–7 | |
Of the 306 participants (54%) across the whole LWTC data set who had completed the questionnaire on group perceptions, 253 (83%) had a group identifier for a group included in this analysis, and adequate data on this measure were available for 72% of the original 67 groups. Perceptions of ‘group support’ and ‘group identification’ both averaged close to 5 out of 7 on the scale, indicating that the participants generally perceived the group as supportive and experienced a sense of psychological connection to the group. There was also evidence that, overall, participants were moderately well connected outside the LWTC group setting, with scores for ‘other social identities’ averaging 4 out of 7. Inevitably, there was some variability in these group-level variables, and 10 groups included an individual whose scores on the group support and/or identification scales were low (less than 3), sometimes in contrast to the rest of the group. Thus, unsurprisingly, not every participant experienced their group in the same way.
These measures could be linked directly to outcome data in order to test, for example, hypotheses relating perceived group support and social identification to weight loss. 134 Haslam et al. 45 present testable hypotheses concerning links between such group processes and health, and Appendix 5 provides a summary of existing measures for assessing different aspects of groups from the reviews identified during our literature searches (see Chapter 2). In the current sample, 150 participants had a group identifier, data on perceptions of the group and complete baseline and follow-up weight, permitting calculation of weight loss. These data made such an analysis possible, but this was beyond the scope of the current study. Information from these measures could also be linked to qualitative data using the methods described further in Qualitative analyses of group processes in two Living Well Taking Control programme groups.
Motivation and outcomes at follow-up in Living Well Taking Control programme groups
Relatively complete 6-month follow-up data (i.e. for at least half the group and a minimum of three participants) on selected outcomes were available for 37 groups (55%) (a minimum of 225, or 52% of, participants). As shown in Table 18, there were generally small increases from baseline in participants’ perceptions of the importance of, and their confidence in, achieving healthy lifestyles. However, there remained considerable variability in these indicators of motivation between groups and participants, with divergent scores within at least six groups, particularly in relation to confidence in achieving adequate physical activity. Health status measures were also slightly improved from baseline (as per ComPoD trial results61) but remained highly variable across groups, with differences between the highest- and lowest-scoring participants within groups ranging from 7% to 88% (mean 37%). There was also little indication that groups became less heterogeneous in terms of measures of motivation or health status as time progressed.
| Summary data | Importance of activity (1–10)a | Confidence in activity (1–10)a | Importance of diet (1–10)a | Confidence in diet (1–10)a | Self-rated health | Weight loss (kg) |
|---|---|---|---|---|---|---|
| Number (%) of groups for which data were available | 37 (55) | 37 (55) | 37 (55) | 37 (55) | 37 (55) | 37 (55) |
| Number (%) of participants for whom data were available | 227 (53) | 230 (53) | 230 (53) | 230 (53) | 227 (53) | 225 (52) |
| Mean (SD) across groups | 8.0 (1.0) | 6.9 (1.2) | 8.8 (0.7) | 7.7 (0.8) | 76 (9) | –2.2 (2.03) |
| Range in means across groups | 5.4–9.7 | 4.3–9.0 | 7–10 | 5.2–9.0 | 55–89 | –7.6–1.7 |
| Range across entire sample | 0–10 | 0–10 | 3–10 | 2–10 | 10–100 | –16.3–19.2 |
The average weight loss in the current sample (2.2 kg) is slightly greater than in the ComPoD trial61 and LWTC evaluation60 (in which it was around 1.8 kg). This is not surprising given high loss to follow-up in this data set and suggests that this sample is not fully representative of the entire population of LWTC participants. There is considerable variability across groups in terms of average weight loss, ranging from weight loss of 7.6 kg per participant in the most successful and weight gain of 1.7 kg in the least successful. It should be noted that a few identified outliers, whose weight loss/gain could be attributed to other factors (e.g. diagnosis of another condition), are likely to account for some of this observed variation owing to the small numbers within groups, which is a factor that would need to be considered in further analyses of group-level outcomes.
There were eight ‘successful’ groups whose participants on average lost > 4 kg, and, in six of these, all participants lost at least some weight. In contrast, there were 10 ‘less successful’ groups whose participants on average lost < 1 kg or, in four of these, gained weight. In 8 out of these 10 groups there were still examples of one or two participants who lost > 2 kg, meaning that they were not necessarily ‘less successful’ groups for these people. This suggests that our original plan to sample more or less successful groups on the basis of weight loss outcomes, and then to characterise and compare these groups through in-depth qualitative analyses, would have been feasible. However, how more and less successful groups are defined would need careful consideration.
In-depth summary of quantitative data for three Living Well Taking Control programme groups
Tables 19 and 20 present in-depth summaries of key quantitative variables for three of the six groups sampled for in-depth analysis as described in Methods, building on the data presented above and including further details. Two of these with different facilitators are subsequently considered in the qualitative analyses below.
| Group | Characteristics | Weight status | Other groups | Other measures | Activity/diet | ||
|---|---|---|---|---|---|---|---|
| Sociodemographic | Socioeconomic | Clinical | |||||
| 1a FAC: A | Eight participants: six female, two male | Five out of eight had an existing condition | Average BMI of 33 kg/m2 (range 27–39 kg/m2) | Three out of eight attending other groups | Average 57% health rating (range 22–92%) | Average ratings (out of 10) for PA: 7 importance (range 1–10), 7 confidence (range 1–10) | |
| Average age 67 (range 42–80) years; two younger, six olderb | Two employed, six retired | Two high blood pressure | Two overweight, five obese | Average 8/10 life satisfaction rating (range 5–10) | Average rating (out of 10) for diet: 9 importance (range 7–10), 8 confidence (range 5–10) | ||
| All white British | Three school to 16 years, one school to 18 years, one professional training, two degree or above (one missing) | Three out of seven had HbA1c levels in pre-diabetes range | |||||
| One smoker | |||||||
| 2a FAC: B | Seven participants: four female, three male | One employed, three retired, one carer, one student | Six or seven existing condition | Average BMI of 34 kg/m2 (range 29–40 kg/m2) | One out of four attending other groups | Average 70% health rating (range 49–97%) | Average ratings (out of 10) for PA: 9 importance (range 7–10), 7 confidence (range 5–8) |
| Average age 61 (range 48–77) years; two younger, two middle-aged, two olderb (one missing) | One school to 16 years, two professional training, three degree (1 missing) | Three high blood pressure | |||||
| Three out of seven HbA1c levelsin pre-diabetes range | Three overweight, three obese, one severely obese | Average 6/10 life satisfaction rating (range 4–9) | Average rating (out of 10) for diet: 9 importance (range 7–10), 8 confidence (range 5–10) | ||||
| One Asian participant | One smoker | ||||||
| 3 FAC: A | Six participants: two female, four male | One employed, four retired, one unemployed | Two out of six had an existing chronic condition | Average BMI of 33 kg/m2 (range 28–38 kg/m2) | Two out of six attending other groups | Average 85% health rating (range 70–100%) | Average ratings (out of 10) for PA: 9 importance (range 8–10), 9 confidence (range 7–10) |
| Average age 65 (range 54–73) years; one younger, two middle-aged, three olderb | One school to 16 years, two professional training, three degree | Two high blood pressure | Two overweight, four obese | Average 8/10 life satisfaction rating (range 5–10) | Average rating (out of 10) for diet: 9 importance (range 7–10), 9 confidence (range 7–10) | ||
| One white/Asian participant | No HbA1c levels in pre-diabetes range | ||||||
| One smoker | |||||||
| Similarities | Group sizes of six to eight participants | Majority retired/not working | One smoker in all groups | Average BMI in obese range (33–34 kg/m2) | Minority attending other groups (mostly exercise) | On average saw healthy PA and diet as important, and were confident in achieving | |
| Average age 61–67 years; one or two younger in all groups | Mixed levels of education (school to at least degree) | Two or three high blood pressure in all groups | |||||
| All or majority white British | |||||||
| Differences | One majority female, one majority male, one mixed | Two groups in which at least half of participants were educated to degree level | In two, majority have existing condition; in one, majority healthy | Some variation in health status and life satisfaction across groups | Some variation across groups | ||
| Two majority older, one mixed-aged | Two have participants with HbA1c levels in pre-diabetes range | One group with participant with low PA importance and confidence scores | |||||
| Two groups with one or two participants with maximum scores | |||||||
| Group | Attendance | Weight loss | Other weight loss outcomes | Other measures | Activity/diet | Perceptions of group |
|---|---|---|---|---|---|---|
| 1a five out of eight with follow-up | No clear dropout Average 3.9 sessions attended (range 3–4) | Average 5.9 kg (range 16.3 kg to 0.5 kg loss) although one with large weight loss may be due to cancer diagnosis;b when excluded, the average is 3.3 kg | Average 2.2 kg/m2 reduction in BMI (1.3 kg/m2 excluding outlier, range –5.7 to 0.2 kg/m2 reduction), taking group average down to overweight/obese cut-off point | Average 64% health rating (range 49–96%), reflecting some improvement from baselinec | Average ratings (out of 10) for PA: 5 importance (range 0–10), 5 confidence (range 0–10), reflecting some reduction from baseline | Average ratings of 4.3 (range 2.8–5.8), 5.1 (range 4–5.8), 5.2 (4–6.3) (out of 7) on measures of group support, group identification and other social identities |
| Six out of eight attended all | Average 7.7 cm reduction in waist (5.9 cm excluding outlier, range 2.0–15.5 cm) | Average 7/10 life satisfaction rating (range 5–9), reflecting small reduction from baseline | Average rating (out of 10) for diet: 9 importance (range 8–10), 7 confidence (range 5–9), reflecting little change from baseline | All reported benefits, one mentioning group aspects (being in group) | ||
| Two participants missed one session each (sessions 3 and 4) | ||||||
| 2a four out of seven with follow-up | No clear dropout Average 3.4 sessions attended (range 2–4 sessions) | Average 3.9 kg (range 8.4 kg loss to 1.2 kg gain) | Average 1.5 kg/m2 reduction in BMI (range 3.2 reduction to 0.4 increase), taking group average down to bottom end of obese range | Average 74% health rating (range 48–91%), reflecting little change from baseline | Average ratings (out of 10) for PA: insufficient data to explore (< 3 participants) | Average ratings of 4.6 (range 3.5–5.5), 4.9 (range 4.5–6), 5.3 (3.5–7) (out of 7) on measures of group support, group identification and other social identities |
| Five out of seven attended all | Average 5.3 cm reduction in waist (range 0.5–9 cm) | Average 7/10 life satisfaction rating (range 5–8), reflecting small improvement from baseline | Average rating (out of 10) for diet: 8 importance (range 7–10), 7 confidence (range 6–8), reflecting little change from baseline | All reported benefits, three mentioning group aspects (discussion, sharing) | ||
| Two participants missed two sessions each (one participant missed sessions 2 and 3, one participant missed sessions 2 and 4) | ||||||
| 3 five out of six with follow-up | One no data = dropout? | Average 2.0 kg (range 5.1 kg loss to no change) | Average 1.0 kg/m2 reduction in BMI (range 1.7 to 0.1 kg/m2 reduction), with group average still in obese range | Average 60% health rating (range 48–91%), reflecting some reduction from baseline | Average rating (out of 10) for PA: 9 importance (range 8–10), 8 confidence (range 8–9), possibly reflecting small reduction in confidence (although n = 3) | Average ratings of 5.4 (range 4.5–6), 5.7 (range 5–6), 4.9 (2.8–6) (out of 7) on measures of group support, group identification and other social identities |
| Three out of five participants attended all | ||||||
| Average 3.6 sessions attended (range 3–4 sessions) | Average 2.0 cm reduction in waist (range 2.3 cm increase to 4.3 cm reduction) | Average 7/10 life satisfaction rating (range 3–10), reflecting small reduction from baseline | Average rating (out of 10) for diet: 9 importance (all 9), 8 confidence (range 7–9), possibly reflecting small reduction in confidence (although n = 3) | All reported benefits, three mentioning group aspects (being in group, discussion) | ||
| Two participants missed one session each (sessions 3 and 4) | ||||||
| Similarities | High attendance overall | Large variation in weight loss within groups | Most people in all groups saw improvements in BMI and waist | None improved from baseline, although all started high | All reported benefits | |
| Differences | One dropout in one group (reported 100% health, satisfaction and importance/confidence at baseline)? | Some variation in weight loss between groups | Some groups show possible reduction in perceptions of health/life satisfaction (although may be due to more healthy missing data?) | Some groups show possible reductions, especially in confidence (although may be due to missing data from more confident participants?) | Two or three groups more emphasis on group aspects by some |
The groups highlighted here were chosen on the basis of data availability rather than purposefully to represent the sample, or on the basis of presence/absence of certain characteristics. As shown in Table 19, they appear to be fairly typical groups in terms of participants’ age, employment status, education level and BMI, and somewhat atypical in having generally high levels of motivation. They also illustrate the wider between-group diversity in terms of gender mix and ethnic background. Two of the three groups might be classified as ‘successful’ groups on the basis of the average weight loss achieved. However, from exploring the data at this level, the outcomes in one of the groups are known to be influenced by an outlier who lost a large amount of weight due to an unrelated condition. None could be classified as ‘less successful’ groups.
It is difficult to make any meaningful observations about the participants’ perceptions of the groups (i.e. group support and identification); however, the third group appear to have, on average, slightly lower scores for ‘other social identities’ and somewhat more positive perceptions of ‘group support’ and ‘group identification’, despite there being possible evidence of a participant who dropped out of this group (attendance data for one participant are missing for the later sessions).
The last column of Table 20 highlights additional qualitative data available from open questions (‘What did you like the most?’ and ‘What did you like the most’) on a programme satisfaction questionnaire (not analysed further in the context of this study), demonstrating that participants frequently provided (mostly positive) comments about their experiences in the group. These could provide useful insight on differing views, for example by providing explanations for differences in perceptions of the group. A single open question such as this, or more specifically focused on the group experience, has potential to provide an insight into perceptions of the group for a large number of participants.
In summary, this part of the results illustrated methods for summarising quantitative data on characteristics and outcomes for groups and group participants. We analysed data for a large sample descriptively, demonstrating between- and within-group variability, and provided examples of how these and similar data could be used for developing and exploring hypotheses about potential links between group features, group processes and outcomes. A more detailed descriptive summary of quantitative data was provided for three groups, selected on the basis of availability of quantitative data that could be linked to qualitative analyses of all session recordings.
Qualitative analyses of group processes in two Living Well Taking Control programme groups
This section describes how we developed and applied qualitative methods for analysing transcripts of group sessions (using the MAGI framework) addressing the question of ‘how can qualitative methods be used to explore potential links between group processes and intervention outcomes?’. For illustration purposes, and owing to the time-consuming nature of these analyses, we selected two out of the three groups for which data were summarised above, which had two different facilitators. We describe the steps that can be helpful in such qualitative analyses. Later, in Integration of qualitative and quantitative data, we consider mixed-methods approaches for integrating the qualitative and quantitative data.
Data familiarisation
A first step involved data familiarisation through reading session transcripts and listening to recordings. This allowed the transcripts to be checked and corrected, adding any details that might be helpful in analysing group processes, such as the amount of time spent on group activities, overlapping talk or indications of non-verbal behaviours. It also helped to gain an overall impression of the group dynamics and interaction, and to interpret and understand some non-verbal interaction (e.g. laughter, moving chairs for specific activities). Notes were made on these initial observations about each group session.
Detailed coding and analysis of sessions using the Mechanisms of Action in Group-based Interventions framework
In the second step, we analysed each transcript using the MAGI framework coding schema (see Chapter 3 and Report Supplementary Material 2). This involved two simultaneous tasks: coding transcripts and writing summaries of each session.
First, we coded the transcripts deductively in Microsoft Word (Microsoft Corporation, Redmond, WA, USA) documents (i.e. by inserting comments, e.g. Figure 6) using the coding schema (see Chapter 3). In this coding, all framework categories can be used, or there can be a focus on specific categories of interest (e.g. included in a prior logic model for the intervention, or selected on the basis of other data, such as that presented above). The coding of transcripts can also be undertaken using qualitative data analysis software (i.e. NVivo version 11, e.g. Figure 7). Using NVivo can help facilitate easy access to transcript excerpts within each coded category and can automatically display data on prevalence (e.g. which categories were used in coding and how many times). Coding within text documents can help to retain a more holistic view of the sessions; it is easier to follow the progression of longer sequences of group discussions (involving multiple processes and techniques) rather than by fragmenting them using separate codes. Thus, it can help focus on co-occurrence between framework categories that may be interrelated (e.g. between exchanging information and sharing experiences).
FIGURE 6.
Example of a group session transcript coded in Microsoft Word document.
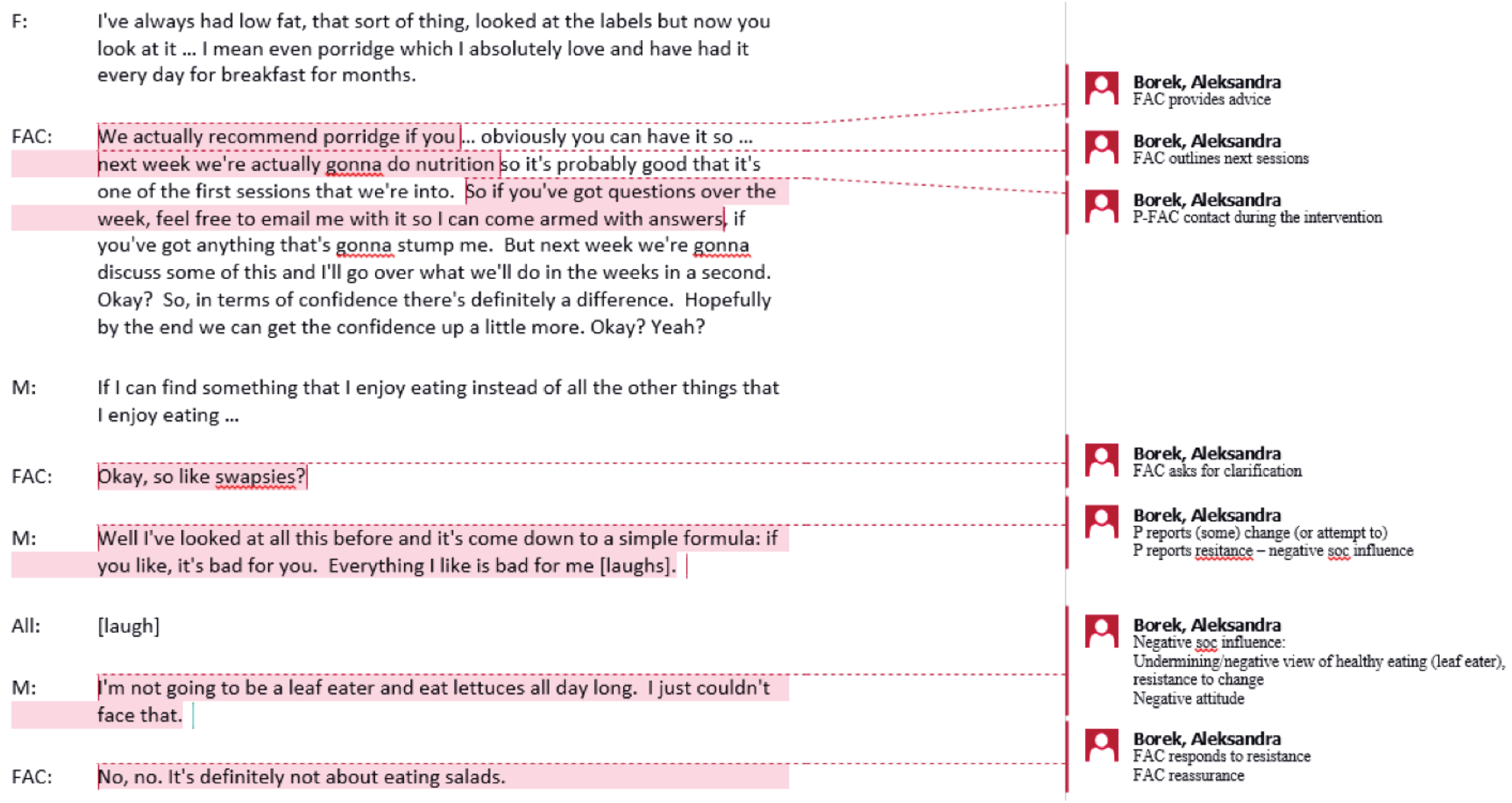
FIGURE 7.
Example of a group session transcript coded in NVivo.
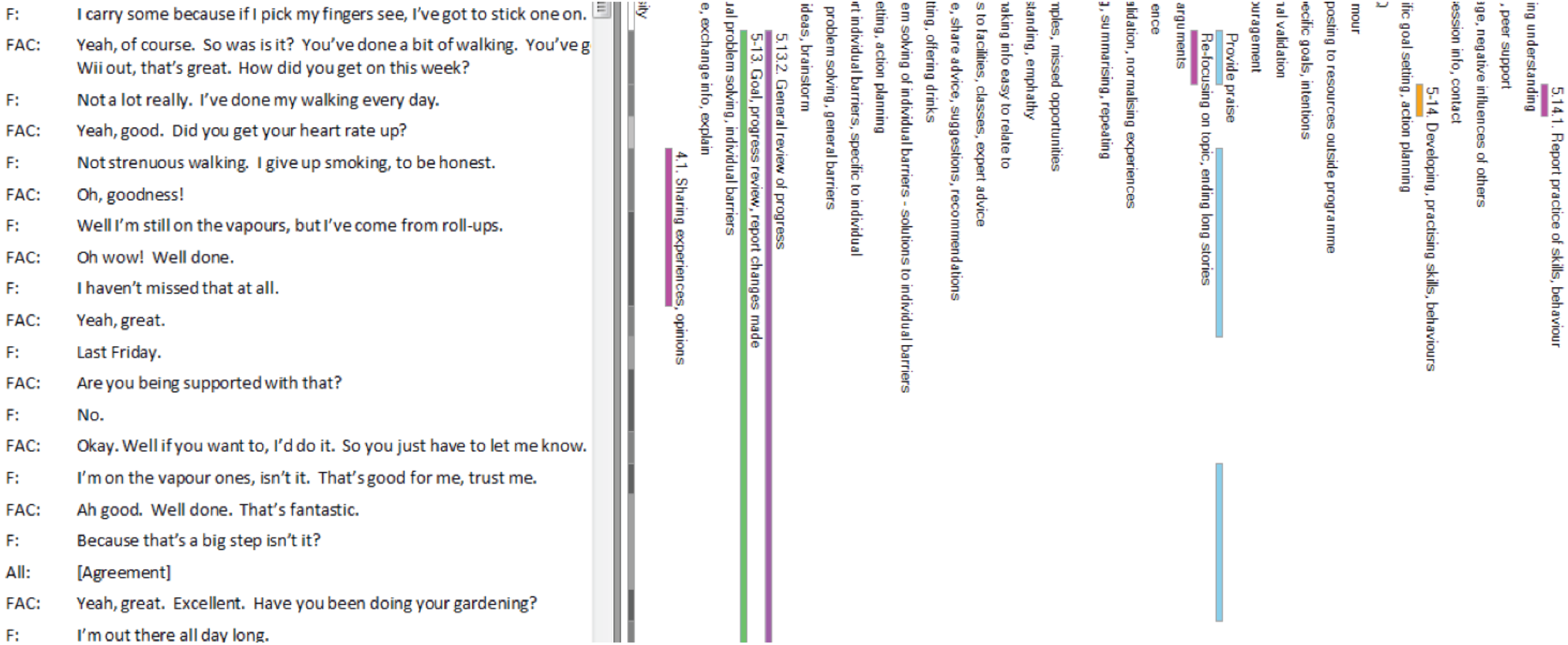
Second, to help characterise sessions, we wrote detailed summaries of each session (Box 1 shows an example). This involved listing distinguishable session activities (i.e. sequences of interaction focused on the same topic, or discernible group/subgroup activities) and adding brief descriptions of the framework processes and facilitation techniques.
-
P–P interaction: P shares experience of buying low-fat ice-cream, another P asks where to get it, so P shares information/advice. FAC draws on P experience to reinforce key message on small portions.
-
FAC provides information in interactive way – by asking questions and then confirming information (e.g. about calcium, fat in cheese). Ps ask questions; FAC draws answers out; FAC directs P’s question back to the group. Few instances of P–P interaction.
-
Whole-group practical activity – sugar game (ordering foods in order of sugar content, based on reading labels), including practice of skills in the session (reading labels) and providing illustrations (visual equivalents of the amount of sugar in foods). Quite a bit of P–P interaction and collaboration (working together, agreeing on the order of foods). Ps express surprise about the amount of sugar in food and develop understanding; Ps develop shared understanding/shared experiences.
-
FAC offers extra sessions as part of the intervention to explore more diet-related topics.
-
FAC prompts individual goal-setting. F shows resistance (says she’s already healthy and does not set a goal) – M challenges F (‘But we are all here because we aren’t as healthy as we could be’).
-
FAC asks for self-assessments of importance of diet – Ps report high importance (8–10), one F does not know (it depends on mood if she cares about it or not, suggesting resistant talk). FAC asks about confidence – Ps report lower confidence than importance (7, 5). M expresses self-understanding of where his main problem is (evening snacking). F expresses negativity.
-
FAC prompts review of the current session. M talks about reading labels but perhaps a bit sarcastically (it will hold people in a queue).
-
F shares a goal (intention), another shares a goal and together (FAC, M) make suggestions to make it realistic.
-
FAC outlines next session.
F, female participant; FAC, facilitator; M, male participant; P, participant.
This step resulted in in-depth coding, initial analyses and summaries of the session transcripts, providing details of the content of the sessions (e.g. group activities), indications of group dynamics and interpersonal and intrapersonal change processes occurring in the sessions. This enables an in-depth understanding of how the groups worked and how within-group processes developed. However, it does not allow for easy comparisons between groups.
Summary of sessions and groups
To facilitate comparisons between groups, and help develop and explore potential hypotheses, a third step aimed to further summarise and condense the analysis of group activities, processes and techniques. This involved summarising the presence or absence of a set of group processes and techniques in a table based on the MAGI framework (Table 21 shows an excerpt, and the full table can be found in Appendix 10). Based on the coding and detailed summaries developed in step 2 (as described in Detailed coding and analysis of sessions using the Mechanisms of Action in Group-based Interventions framework), we began to narrow our focus on processes and techniques that were of particular interest. For illustration, we summarised coding of group dynamics (to explore potential differences between groups in group dynamics and development), interpersonal change processes (to explore which of these were more or less prevalent between groups and sessions), and selected other elements that were predesigned and/or comparable between sessions (e.g. group activities, facilitation techniques, motivation and self-efficacy, goal-setting and goal-reviewing). Future researchers might select fewer or more categories for comparison. For example, if the analysis is exploratory, more or all categories used in coding in step 2 could be included. On the other hand, there may be a focus on fewer categories if there are already preliminary hypotheses (e.g. based on a logic model or quantitative data analysis). In the table, we also indicated the prevalence of processes and techniques, as a count or in terms of being rare (once or twice in the session), occasional (a few times in the session) or frequent (many times throughout the session). Constructing Table 21 allowed us to explore the occurrence (presence/absence) and prevalence of different processes between sessions and groups.
| MAGI framework elements | Group session | |||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | |||||||
| S1 | S2 | S3 | S4 | S1 | S2 | S3 | S4 | |
| 3. Group dynamics, development | ||||||||
| 3.6. Communication patterns | ||||||||
| P–P interaction/exchanges | ≈4 | ≈30 | ≈14 | ≈20 | ≈2 | ≈15 | ≈23 | ≈15 |
| 4. Interpersonal change processes | ||||||||
| 4.1. Sharing experiences | F | F | F | F | F | F | F | F |
| Self-disclosure of personal issues | O | |||||||
| Self-disclosure of transgressive behaviour | O | R | R | R | R | |||
| 4.2. Social learning | ||||||||
| Providing, exchanging information | F | F | F | F | F | F | F | F |
| Providing, sharing advice | O | O | O | R | F | F | O | |
| Brainstorming, sharing ideas | O | F | F | F | F | F | ||
| Group problem-solving, barriers | R | O | R | R | R | R | ||
| Demonstrating, modelling | O | |||||||
| Providing instructions how to perform behaviour | O | |||||||
| 4.3. Social influence | ||||||||
| FAC appeals to credible source | R | R | R | R | ||||
| FAC uses persuasive arguments | O | R | R | |||||
| Negative social influences in group | ≈8 | ≈17 | ≈8 | ≈3 | ≈4 | ≈5 | ≈3 | 0 |
| FAC addresses resistance | F | F | F | O | F | F | R | |
| Positive social influences in group | ≈4 | ≈2 | ≈9 | ≈2 | ≈4 | ≈3 | ≈5 | ≈10 |
| 4.5. Social support in the group | ||||||||
| Peer support | R | R | R | R | R | |||
| Buddy up | ||||||||
| Social connections | R | R | O | O | R | R | R | |
| FAC encourages peer support | R | R | ||||||
| FAC offers support | R | R | R | |||||
| FAC provides praise | O | O | O | O | O | O | O | O |
| FAC provides reassurance | O | R | R | O | O | O | ||
| FAC provides encouragement | O | R | R | R | R | O | ||
| 5. Intrapersonal change processes/targets | ||||||||
| 5.9. Motivation (importance) | ||||||||
| Expression of motivation | R | F | R | R | R | R | R | R |
| Expression of no motivation | R | R | F | |||||
| High importance of changes | F | O | ||||||
| Low importance of changes | O | |||||||
| 5.10. Self-efficacy (confidence) | ||||||||
| Change in self-efficacy | F | F | O | O | F | O | R | |
| High self-efficacy | F | O | R | |||||
| Low self-efficacy | ||||||||
| 5.13. Developing/practising skills and behaviours | ||||||||
| Ps report practice/behaviour | O | O | O | O | O | O | O | F |
| Ps practise skills/behaviours in session | R | R | ||||||
We also created tables with short, descriptive summaries of each of the sessions and overall summaries of each of the groups according to the main framework categories (i.e. group dynamics, interpersonal and intrapersonal change processes, facilitation techniques). Table 22 provides an example summary of, and comparison between, two groups. This table complements Table 21 and helps to compare the groups, focusing on key similarities and differences. For example, analysing our two groups, we made the following observations.
| Group | Group dynamics and development | Interpersonal change processes | Intrapersonal change processes | FAC techniques |
|---|---|---|---|---|
| 1 |
|
|
|
|
| 2 |
|
|
|
|
Group dynamics and development
Both groups provided evidence of positive group dynamics including high levels of participant participation, direct between-participant interaction or exchanges, humour or laughter, and informal interaction. However, in group 1 there was more informal and, at times, off-topic chatting than in group 2. Group 2 seemed more focused on the session topics, but also, unlike group 1, they had breaks in the sessions, which allowed for ‘scheduled’ informal chatting and social interaction. The number of between-participant interactions, including peer support (e.g. participants praising, encouraging or making suggestions to each other), increased after session 1 in both groups. This could indicate that participants in both groups felt more comfortable with, and concerned for, each other over time, suggesting positive group development. In both groups, the majority of group activities involved whole-group discussions and there were very few subgroup or practical activities. In both groups, there were a couple of participants who were more vocal than others, but there was no indication of dominating or disruptive participants. Overall, there seemed to be no major differences between these groups in their dynamics or development.
Analyses of techniques that facilitators used to start the groups/sessions and facilitate group dynamics could be used as the basis for feedback to facilitators. For example, some techniques, such as managing expectations or agreeing group rules, were not used in either group, whereas others, such as identifying, agreeing and referring to common group goals, might have been underutilised because facilitators referred only to the overall aims or key messages of the programme, rather than common goals.
Interpersonal change processes
In both groups, the majority of sessions involved interactive exchanges of information, advice and ideas (i.e. social learning processes) and participants sharing experiences or reporting on their (typical or changed) behaviours. Facilitators provided information and explanations (e.g. about pre-diabetes, measures taken, healthy diet), provided advice and recommendations (e.g. about portion sizes, amounts of physical activity) and answered participants’ questions related to health behaviours and measures. This was particularly true in session 1 (focused on explaining measures, e.g. visceral fat), in which there were fewer participant contributions than in other sessions. In the following sessions, the facilitators delivered information more interactively (e.g. by asking questions, then providing explanations) and facilitated brainstorming activities, in which participants shared ideas (e.g. for different ways to be active or relax). This focus on group discussions and exchanging information and ideas reflected the type of intervention and the delivery manual. However, other interpersonal change processes also occurred (although they were less specifically or actively facilitated by the facilitators). For example, in both groups, the participants offered each other more support over time (e.g. praise/compliments, encouragement, practical suggestions) and were involved in more talk indicative of making social connections. Throughout both groups, participants shared similar experiences, provided personal validations and expressed a sense of shared understanding (social validation). However, the groups differed slightly in the expressed negativity or positivity towards health-related behaviours and behaviour change. In group 1, the participants seemed to express more ‘resistance talk’ (e.g. expressing negative attitudes towards or undermining healthy behaviours, expressing no intention to change) than in group 2. In contrast, participants in group 2 seemed to express more ‘change talk’ (e.g. expressing positive attitudes towards healthy behaviours, and motivation to change and engage in healthy behaviours). This sense of expressed negativity or positivity might have facilitated different prevalent social influences in these two groups. Of interest, in both groups the facilitators addressed most, or all, of the identified negative, ‘resistance’ talk.
Intrapersonal change processes
In analysing intrapersonal change processes evident in group interaction, we focused selectively on those that were most comparable between the two groups. The two groups different slightly in participants’ verbal expressions of motivation and confidence to engage in and change health behaviours. In group 1, some participants expressed motivation to improve health and change, but some expressed no motivation or intention to change and most of them expressed low confidence in being able to change. In group 2, some participants expressed motivation to improve health and change, no one expressed lack of such motivation and only a few expressed low self-efficacy. In group 1, participants shared more reports of unhealthy (or ‘transgressive’) behaviours than in group 2, but in both groups participants reported practice of health-related behaviours or skills. In both groups, facilitators briefly explained how to set goals but ran out of time to prompt goal-setting in the final session. In both groups, most goals that participants shared seemed to be non-specific, general intentions (rather than specific goals/action plans). Finally, in group 1 there was no goal or progress review, and in group 2 there was mainly general review of progress (based around reporting behaviours rather than referring to goals that people set).
These analyses provide an example of how group processes can be analysed at a micro-level, describing what happened in each group and in each session, and summarising the information about occurrence and prevalence of the MAGI framework processes and techniques. This work allowed us to compare between sessions (thus exploring change in groups over time) and between groups (thus exploring variability between groups). Here, for illustration, we focused on only two groups, but this process could be repeated for more groups and potentially allow grouping on the basis of certain criteria (e.g. with positive vs. negative group dynamics or social influences) to link micro-level analysis to macro-level observations, such as those based on quantitative analyses. In the next section, we describe how the results of this type of qualitative analysis can be combined with quantitative data.
Integration of qualitative and quantitative data
This section outlines three data integration strategies (based on previous research151) that can be used to bring together qualitative and quantitative data. It illustrates their application to data sets used in the MAGI study, and might also be applied to other data sets to understand processes within and between groups, and explore how these are related to intervention outcomes.
Triangulation
Qualitative analysis of session transcripts can be triangulated with the results from other types of data, for example comparing the results from analyses of participants’ questionnaires and qualitative data from coding of transcripts of group sessions. We used data that enabled us to triangulate findings from participant questionnaires on group dynamics and self-assessments of importance and confidence in making health-related changes.
Triangulating qualitative and quantitative data on group dynamics
Through qualitative analysis of session transcripts, we found that there were generally positive group dynamics. In particular, we identified signs of positive group climate (indicated by the amount of humour and informal interaction) and group engagement (indicated by the amount of between-participant interaction and active participation in the sessions, such as by asking questions and providing ideas). We also found that there were no instances of disruptive group roles or behaviours, or negative group dynamics (e.g. conflict). However, our qualitative analysis of group dynamic processes was limited by the fact that many of these processes might not be verbalised. For example, we identified no specific mention of, or discussions about, the group climate or group cohesion (or reflections on the groups). We also found that facilitators used no specific techniques to make group goals or group identification salient. Therefore, assessing group dynamics might be better explored by asking participants directly about their perceptions of the groups and group dynamics via questionnaires or interviews. 47
Our quantitative data showed that, in both of these groups, participants reported similar positive perceptions of the groups and groups dynamics (i.e. on average group 1 scored 4.3 and 4.6, respectively, on measures of group support and identification with the group, whereas group 2 scored 5.1 and 4.9, respectively; see Table 20). These triangulated findings from quantitative and qualitative analyses of group dynamics support and complement each other. This kind of triangulation of data on group dynamics might be particularly important in some cases to assess the impact of negative group dynamics, such as disruptive group behaviour or negative interactions (e.g. conflict). Such negative group dynamics, reflected in participants’ perceptions of groups (assessed through questionnaires), may inhibit progression through the programme and intervention outcomes. 134
Triangulating qualitative and quantitative data on self-assessments of importance and confidence
In session transcripts, we identified sequences of group interaction that focused on self-assessments of the importance of health-related behaviours or behaviour change, and confidence in engaging in, or changing, these behaviours. Participants were asked similar questions in the baseline and follow-up questionnaires, as reported above (see Tables 19–20). In Table 23, we duplicate these quantitative data to make comparisons with the qualitative data.
| Group | Baseline activity/diet (quantitative measures)a | Verbal expressions during group sessions on healthy lifestyle/activity/diet (qualitative ‘talk’b) | Follow-up activity/diet (quantitative measures)a |
|---|---|---|---|
| 1 | Overall healthy lifestyle: most reported high importance (10) but low confidence (2–3), one reported zero importance | ||
| Diet: 9 importance (range 7–10), 8 confidence (range 5–10) | Diet: high importance (10), lower confidence (5, 7) | Diet: 9 importance (range 8–10), 7 confidence (range 5–9), reflecting little change from baseline | |
| Activity: 7 importance (range 1–10), 7 confidence (range 1–10) | Activity: low importance and confidence, but increased at the end of the session | Activity: 5 importance (range 0–10), 5 confidence (range 0–10), reflecting small reduction | |
| 2 | Overall healthy lifestyle: high importance (10) and confidence, but lower confidence for maintenance of change | ||
| Diet: 9 importance (range 7–10), 8 confidence (range 5–10) | Diet: high importance and confidence (both 7–9), one reported feeling more confident about diet than activity | Diet: 8 importance (range 8–10), 7 confidence (range 7–8), reflecting little change from baseline | |
| Activity: 9 importance (range 7–10), 7 confidence (range 5–8) | Activity: unclear but both importance and confidence seem lower (than diet) | Activity: insufficient data to explore (fewer than three participants) |
In group 1, session 1, a majority of participants verbally reported the high importance (10 out of 10) of changing lifestyle but low confidence in doing so (2 or 3 out of 10). One female participant reported that she did not intend to change because she was already ‘very careful’ and had made some changes. Of interest, her negative response might have prompted another participant to lower, or ‘qualify’, his score in relation to confidence:
So, if we stick a number on it. We go 0 being ‘not important at all’ and 10 being ‘yeah, it’s really important’ . . . change my lifestyle, try and prevent developing diabetes. What would we do?
10.
It’s got to be 10.
[General agreement.]
What do we reckon [name]? Is yours high or . . .?
No. I don’t think I would be changing very much to be honest because I’m very careful what I do anyway.
OK, OK.
When I said 10, I didn’t think I was going to be able to achieve it, I was . . .
Ah, that’ll be the next question. Don’t worry.
It’s very hard, I know.
I’m hoping to make a few changes but 10 is merely an idea that I really don’t want diabetes. So, whatever it takes.
In session 2 (which focused on diet), most participants reported high importance (9 or 10) of having a healthy diet but low confidence (5 or 7 out of 10, when stated by participants). Again, one female participant seemed to be unsure of whether or not she found a healthy diet important (‘It depends on what mood you’re in whether you care or not’). In session 3 (which focused on physical activity), the first participant expressed low importance of activity because of barriers. Other participants generally agreed that health and age had a negative impact on their scores, but they saw physical activity as ‘important’. Interestingly, when asked again about this at the end of the session, after the practice of exercises, the participants reported higher importance and confidence:
So if I re-ask the question. So, everything we have done, how important is physical activity for you?
I’m going to say 9.
[Agreement.]
Because that was easier than I thought.
OK. Importance. This is importance, not . . . confidence? Has it changed from the beginning?
[Agreement.]
You were really good. At first I did not think you were into it, but actually you did really well.
In group 2, session 1, all participants reported perception of high importance (10) of making lifestyle changes. They were also confident that they could make changes in the short term, but less confident that they could maintain them in the long term. In session 2, participants also reported high importance (7–9) of a healthy diet and high confidence that they could achieve this (7–9). One female participant commented that she felt more confident achieving a healthy diet than adequate physical activity. Indeed, in session 3, participants generally seemed less convinced about the importance of, and their confidence in, being physically active.
Both qualitative and quantitative data showed that participants perceived healthy behaviours as important (more so for diet than for physical activity) but that they were less confident in their ability to perform them (especially for physical activity). Qualitative data showed that this was reported to be due to perceived barriers and difficulties with longer-term maintenance of behaviour change. The comparisons between groups, from both qualitative and quantitative data, showed that group 2 expressed slightly higher perceptions of importance and confidence than group 1. The example from group 1 showed how participants sharing their perceptions in the group may influence each other. Thus, the qualitative data confirmed the quantitative data about importance and confidence levels, and also expanded on them by providing detail about why participants experienced low confidence, and how this changed over time.
Following a thread
Findings from initial analyses of one data set (quantitative or qualitative) could be used in an approach known as ‘following a thread’151 where ‘researchers select a question or theme from one component and follow it across the other components’,151 which could be an alternative (qualitative or quantitative) data set.
In our study and previous research, quantitative data suggest that motivation to engage in healthy behaviours leads to behaviour change and improved health outcomes. 154 On this basis, we followed a thread around motivation by analysing participants’ ‘change talk’ in the sessions as being indicative of their intentions and motivation, and explored how this changed across sessions and the impact it had on the sessions. Our qualitative analysis of transcripts suggested some differences between sessions and groups in terms of participants’ negativity or positivity towards the discussed health behaviours or behaviour change. This was proven in participants’ negative or positive talk or, as conceptualised in motivational interviewing, in ‘resistance talk’ or ‘change talk’. 120 Positive (change) or negative (resistance) talk relates to health behaviours that were expressed in groups, which can facilitate social influences on others in the group, and can affect the overall sense of positivity or negativity in the group.
In the MAGI framework we defined social influence in the groups as a process of ‘influencing, or ability to influence, others’ norms, beliefs or behaviours’ (see Report Supplementary Material 1). Such social influences can be positive (e.g. promoting healthy behaviours) or negative (e.g. promoting unhealthy behaviours or discouraging others from healthy behaviours). Here, we focused only on participants’ interactions and expressions that could potentially be a source of positive or negative influences on others in the groups. As positive social influences, we considered examples of ‘change talk’, which included positive expressions about healthy behaviours (e.g. positive attitudes), negative expressions about unhealthy behaviours, or expressions of intentions and motivation to make health-improving changes. As negative social influences we considered examples of ‘resistance talk’, including negative expressions about healthy behaviours (e.g. negative attitudes), positive expressions about unhealthy behaviours, expressions of lack of intention or motivation to change or engage in healthy behaviours, or expressions of intention or willingness to engage in unhealthy behaviours. Below we present examples of the positive and negative influences identified in the two groups.
In group 1, session 1, there were several instances of negative social influences and resistance talk, such as expressing no intention to change, focusing on the expected difficulties, or expressing negative attitudes towards healthy behaviours. For example:
Well I’ve looked at all this before and it’s come down to a simple formula: if you like, it’s bad for you. Everything I like is bad for me. [Laughs.]
[Laugh.]
I’m not going to be a leaf eater and eat lettuces all day long. I just could not face that.
No, no. It’s definitely not about eating salads.
There were also instances of positive change talk, although fewer than for negative talk (e.g. ‘. . . that sounds interesting . . . maybe I should try . . . I’m very interested in exercise’). Resistance talk remained prevalent in the following session on diet. For example, participants continued to make negative references to healthy foods and to the promoted health behaviours (e.g. reading labels) and one participant explicitly expressed no intention to change (e.g. ‘I’ve got the knowledge though and I just don’t care’). There were only a few instances of positive expressions related to diet. Although this group continued to express some negative talk, over time (in particular, in session 3, which focused on physical activity) participants expressed more positive talk related to exercise. For example:
So you were saying, when you came in, you were looking forward to this session. Why?
Well because . . . to learn more about exercise.
Why do you want to learn?
Well because I do. I want to lose weight and exercise is sort of . . . what . . . 75% of . . . not quite so much as that, isn’t it?
Some participants also expressed intentions or goals for physical activity and were more confident in being able to do it, especially after practising exercises in the session. In the final session, there were examples of both positive and negative change talk: a couple of participants reported not ‘seeing’ any difference despite being more active (but these examples also suggested that they engaged in physical activity), whereas others reported positive experiences of practising the exercises learned in the previous session (‘I’ve been loving the exercise’).
Participants in group 2 initially seemed generally more motivated and positive about making changes than those in group 1. They expressed no overt negative, resistant talk towards healthy behaviours or making changes. Although they expressed negative emotions (‘stressed’, ‘anxious’) about the measures discussed in the session (e.g. BMI, fat levels), they also saw them as a positive source of motivation to change, for example:
. . . so you’re all quite shocked, but are you feeling quite motivated to make some lifestyle changes?
Yes.
[General agreement.]
Ooh that’s good.
Very.
. . .
I think it’s just going to be hard, but it’s achievable.
This group also voiced very few negative statements about healthy foods or disliking them in session 2 (we identified four instances of negative talk in group 2 compared with 15 instances in group 1) and expressed intentions to make dietary changes.
In session 3 in this group, we identified only two instances of ‘resistance’ talk referring to diet (e.g. ‘But I love my high-fat foods’), and no negative (and a few positive) statements regarding physical activity. These included reporting positive experiences of, and attitudes towards, exercise classes, and intentions to try some activities (e.g. ‘I was thinking of joining the bowls club’), for example:
I’d say sod ‘em. [Laughs.] Go ahead, be brave [inaudible]. I don’t care what I look like, just go and do it. Well what I did find is – you know, I’ll be honest, I’ve never joined a gym in my life and I always thought I never would, never be a gym bunny, and I just thought there’d be loads of posers in there, loads of people running about thinking this is not for me, no way. Well it’s great actually, they are in there, everyone – all sorts of shapes and sizes, all they want to do and everybody just wants to help you get fit, get well. I think it’s great and I think it – if you get yourself stuck in there, you can kind of get rid of the self-consciousness and to think I will not look as good as everybody else and all that sort of stuff.
[General agreement.]
In the final session for group 2, there were some instances of positive social influences and no identified instances of negative influences. For example, participants reported confidence and positive experiences of making dietary changes and expressed intentions to make further changes (e.g. ‘That’s a really good idea. Oh I’m going to do that’). They also reported engaging in physical activity and intentions to continue. There was also an example of one older participant explicitly encouraging and motivating (positively influencing) another, younger, participant to make lifestyle changes; this example captured a sense of positive influences and peer support that was characteristic of group 2:
Oh there’s a thought going through my mind.
What do you think?
What you do today will affect you later on in life.
If they stop stocking that at Marks and Sparks [Marks and Spencer plc, London, UK] I’m going to have a bad, bad life. [Laughs].
[Laugh.]
No, no, no think of it this way, if you – if we do what we’re supposed to do be doing today, when we get to my age, I am 63, and you’re 20 what?
Six.
26, well you’ve got 40 years to go and those 40 years if you develop the pattern of good living today, when you get to my age you will not have so many problems. Physically.
Yeah that’s what I need to do. Yeah that’s what I’m really hoping to do. ’Cause I do worry, you know, ’cause one day I can’t sort myself out and you know.
Overall, qualitative analysis showed that both groups included expressions of positive, change talk as well as negative, resistance, talk. In both groups, the amount of negativity and resistance decreased with time. In the later stages of the intervention, there were also more positive influence in the groups resulting from some participants reporting changes and positive experiences of new healthy behaviours. These kinds of positive or negative expressions can be a source of influence for group participants on each other and may contribute to establishing group norms promoting or hindering health behaviour change. The impact of these influences on individual participants may, of course, depend also on other factors, such as the strength of the source of influence, social identification or group cohesion.
In summary, through the detailed qualitative analysis of transcripts, we were able to identify how the groups developed over time (e.g. increasing amount of between-participant interaction, social interaction and peer support) and how similar or different the groups were (e.g. in the expressions of positive/change and negative/resistance talk). The two groups analysed here for illustration showed different levels of positive and negative talk. Both engaged a number of inter- and intrapersonal change processes, and both were characterised by generally positive group dynamics (and lack of negative group dynamics). Both groups included a majority of participants who were motivated to change and, with time, the participants expressed more positive, and less negative, talk towards health behaviours and behaviour change. Although we were unable to formally explore links with outcomes, there were some differences between the groups as shown in both qualitative and quantitative analyses. Table 18 showed that the differences in average weight loss between these two groups were small (3.3 kg in group 1, after excluding the outlier result that was caused by illness, compared with 3.9 kg in group 2), but both appeared to be ‘moderately successful’ groups compared with groups in the sample as a whole (where average weight loss was closer to 2 kg). All but one participant across both groups lost some weight (ranging from 0.5 kg to 8.5 kg, excluding the known outlier). This kind of qualitative analysis, to explore a ‘thread’ or hypothesis, conducted on a larger number of diverse groups, might be able to map expressed differences in motivation to differences in outcomes. The ‘following a thread’ approach could be used to follow up qualitative findings: qualitative findings on positive/negative talk could lead to a new hypothesis about the relationship between positive/negative talk and outcomes, which could then be tested by comparing outcomes between groups identified as displaying varying degrees of positive/negative talk.
Matrix and other case-based approaches
In our final example, we illustrate how considering groups as ‘cases’ and using a matrix or similar approach can help bring together and allow simultaneous analyses of both qualitative and quantitative data to describe groups and group processes. Table 24 illustrates an example of a matrix table in which quantitative data on key group characteristics and weight loss and qualitative data on group processes for differing cases (i.e. groups) are brought together. Although this is for illustration only and no conclusions can be drawn from the limited data, this approach could be used to identify patterns in the data with a larger number of differing cases. Tables can be constructed in different ways to bring together different types of qualitative and quantitative data. With larger samples, prespecified, or post hoc defined, subgroups of cases based on characteristics such as those described above can be used to split the table (e.g. cases could be arranged according to good and poor outcomes). Analyses of such tables can be carried out using an inductive approach based on factors that emerge from the data, or using a deductive approach based on prespecified hypotheses. Matrix tables provide ways to explore emerging hypotheses and also causes and effect, potentially taking into account contextual factors (in subgroups). For example, an emerging hypothesis about positive/negative group dynamics developed from the qualitative data could be that the dynamics are related to the size and gender composition of the group. This hypothesis could be tested using a table similar to Table 24 (with a larger number of cases). An alternative mixed-methods approach to comparing links between outcomes and processes across differing cases (i.e. groups) is Qualitative Comparative Analysis. This might be useful with a sample that is large enough to make in-depth qualitative analysis too demanding, but not large enough to provide sufficient data for multivariate statistical analyses (e.g. a sample size of 10–50). 152
| Group | Data type | |||||
|---|---|---|---|---|---|---|
| Quantitative | Quantitative and qualitative | Qualitative | ||||
| Demographic characteristics | Weight status | Weight loss | Perceptions of group | Group dynamics and development | Interpersonal change processes | |
| 3 Five out of eight with follow-up |
|
|
Average 5.9 kg loss (range 16.3 kg to 0.5 kg loss). One participant’s large weight loss may be due to cancer diagnosis; when excluded, the average is 3.3 kg |
|
|
|
| 5 Four out of seven with follow-up |
|
|
Average 3.9 kg loss (range 8.4 kg loss to 1.2 kg gain) |
|
|
|
In summary, this final section of results illustrated mixed-methods approaches for bringing together group-level quantitative and qualitative data, using our data. Because the sample size was too small to allow purposive selection to ensure variation between the groups examined in detail, we were unable to draw any conclusions, but made observations that could form the basis of future hypotheses. We also demonstrated that these are potentially useful approaches for future exploration of links between group characteristics, processes and outcomes.
Discussion
In this final stage of the MAGI study, we developed and illustrated application of quantitative and qualitative methods and developed mixed-methods approaches, based on the MAGI framework, to explore differences between groups and potential links between group characteristics, processes and outcomes. We applied these methods to secondary, quantitative and qualitative data sets from an existing GB-BCI: the LWTC programme promoting weight loss through changes in diet and physical activity for the prevention or management of type 2 diabetes. We analysed quantitative data to illustrate between- and within-group differences in group and participants’ characteristics, perceptions of group processes and outcomes and made suggestions for how these might be further explored. We also showed how in-depth analyses of qualitative data (transcripts of group sessions) could identify group dynamics and processes. The final aim was to provide examples of mixed-methods approaches that could be used in future research to address questions about which group processes are most predictive of behavioural outcomes. To do this, we used the example of two groups, combining qualitative with quantitative data to illustrate how differences and similarities between groups in group dynamics and interpersonal and intrapersonal change processes can be summarised and explored, in order to make links between these processes, and with outcomes. By doing this, we demonstrated how the MAGI framework [a model of mechanisms of action in group-based interventions (see Chapter 2)] and a coding schema that supports its use in data analyses (see Chapter 3) can be applied in the context of future process evaluations of GB-BCIs.
Across 67 groups in the LWTC programme, there was considerable variability in group features indicative of MAGI framework components, and outcomes. This suggests that sampling to allow qualitative comparisons of groups on the basis of differences in these features or outcomes (as was originally planned) is likely to be feasible if the quantity and quality of data on groups are sufficient. Sampling could be based on differences in (1) group-level baseline characteristics (e.g. group size, high/low average BMI or scores for motivation) to explore how this influences subsequent group processes; (2) heterogeneity within groups in terms of sociodemographic or socioeconomic features, clinical characteristics and intrapersonal processes (such as motivation, to explore the impact of differences between group members on group processes and potentially how this affects outcomes for participants who are different from other group members); and (3) outcomes (e.g. more/less successful groups in terms of weight loss or attendance) to explore how group processes might explain differences. Using a questionnaire assessing participants’ perceptions of aspects of the group (e.g. group support, identification), we demonstrated that there is scope for group-level quantitative analyses to examine links between group characteristics and processes, and processes and outcomes in GB-BCIs. We also showed that detailed, descriptive summaries of quantitative data relating to group characteristics, group processes and outcomes for small numbers of selected groups could be useful for consideration alongside summaries of group-level findings from qualitative analyses and shed light on limitations of purely quantitative approaches (e.g. that a single ‘outlier’ in a group, which might be missed in larger-scale quantitative analysis, can have a big influence on a group average).
We found that qualitative analysis based on the MAGI framework can, first, provide context that enhances interpretation and understanding of the quantitative data, and, second, illuminate how groups work in practice (i.e. which processes occur and are facilitated to bring about intended changes relative to intended protocols). Moreover, we demonstrated that mixed-methods approaches have the potential to provide a more complete assessment of some elements of the MAGI framework; for example, components that may not be easily observed (e.g. group dynamics) can be measured via self-report, whereas other parts that are difficult to capture via self-report (e.g. occurrence and prevalence of interpersonal change processes) can be assessed through qualitative analysis of observations. Our illustrations of triangulation, following a thread, and matrix approaches to data integration provide examples of ways in which group-level quantitative and quantitative data can be brought together to explore links between framework components and outcomes. They further highlight the complexity surrounding how groups work, and suggest ways forward to unravel some of the mechanisms underpinning change in GB-BCIs.
Strengths and limitations
A primary strength of this project was the use of large, real-life secondary data sets, collected within a naturalistic setting (i.e. data were not collected with the purposes of this study in mind) from an ongoing community-based programme, which was designed and delivered outside a research context. The findings are, therefore, likely to be reflective of the reality of what happens in such groups, and generalisable to similar routinely delivered programmes in comparable contexts [e.g. the NHS Diabetes Prevention Programme (NHS DPP)155]. We employed systematic, detailed, macro- and micro-level approaches to the analysis of both quantitative and qualitative data. Furthermore, the quantitative and qualitative analyses were conducted independently by two researchers who did not communicate about the findings until both types of data analyses and write-up were complete, so as to minimise potential bias. As far as we are aware, our methods for integrating quantitative and qualitative analyses are relatively novel in the context of process evaluation of GB-BCIs. Despite recognition of the importance of considering group-level factors in any analyses of group-based studies,32 there are few existing robust descriptions and analyses of quantitative group-level data for GB-BCIs in the literature.
There are several limitations to this study. First, as described earlier, the availability and quality of the secondary data for analysis were poorer than anticipated: with some recordings were of poor quality, there were session recordings and group identifiers missing in qualitative and quantitative data sets, and there were higher than anticipated levels of missing quantitative data, particularly at follow-up, because some were collected outside the confines of the ComPoD trial. Our plans (as described in the protocol), therefore, had to be adapted to the available data and to ensure feasibility within the study timescale. As we would have been unable to draw robust conclusions from the available sample of three groups with complete qualitative and quantitative data, we focused instead on developing methods and hypotheses for future research by examining in detail two groups, with differing facilitators (to maximise potential differences). The measure used to assess participants’ perceptions of groups (i.e. support, identification) has also not been validated in this context.
An additional limitation was the restriction of observed data to audio-recordings, which could not provide insight into potentially important group features, such as room layout, conversations in the time before and after sessions for informal interactions (which were not recorded) and non-verbal behaviours. Furthermore, in the recordings it was also sometimes difficult to distinguish between participants, and we were unable to ascertain from either data set whether or not participants had partners/supporters with them in the groups. In this stage of the research, we used a deductive, confirmatory (rather than inductive, exploratory) approach to analysis, using the framework-based coding schema, which allowed us to pursue prespecified themes, but did not allow for identification of new ‘threads’, phenomena or unexpected findings. However, because the LWTC programme was designed, and already being delivered, outside the context of our research, there was no logic model to guide the focus of our analyses in terms of what group features and processes might be most important and are being manipulated in the intervention. This meant that the in-depth coding, even of only two groups across all sessions, aimed to cover all key aspects of the framework and proved very time-consuming: a major limitation of this approach. However, when used in future research, the coding could be used selectively to test specific hypotheses. Finally, we were not able to incorporate facilitators’ perceptions of group dynamics and change processes into our analyses, but this would provide a further opportunity for triangulation and validation of our methods.
Implications and recommendations for research
The challenges faced in this stage of the MAGI study, and our work to develop methods for future research, identify implications and recommendations for designing and evaluating GB-BCIs.
A broad implication is the need for further research to describe and evaluate potential links between group characteristics, processes (as outlined in the MAGI framework) and intervention outcomes in GB-BCIs; we were ultimately unable to do this in our study and, in retrospect, this was probably overly ambitious. Reports of group-based weight loss interventions often lack details related to group design that would allow potential comparison between GB-BCIs with different features or processes on an aggregate level (e.g. in systematic reviews and meta-analyses),23,69 so primary research is important. Key precursors to this are clear hypotheses, adequate data and adequate methods.
Clear hypotheses related to the various potential links between group characteristics, processes, techniques and outcomes (aligned with definitions in the MAGI framework) are needed to direct research, as groups are so complex and their features so numerous that all possible permutations cannot be assessed simultaneously. Such hypotheses can be prespecified on the basis of previous research or observations, or may be formulated on the basis of emerging data.
As well as a large theoretical literature (see Chapters 1 and 2), there is growing work on exploring group-level processes in health interventions that can guide the focus of future research. For example, there is considerable research linking social identification processes with health, including as part of group interventions, and measures and methods for investigating these links are available45,46 (see Appendix 5). Other types of interpersonal change processes and certain types of groups appear less well researched, which suggests avenues for further exploration. For example, with a few exceptions,126,134,144 there are limited examples of group-level analyses in weight loss and lifestyle-related GB-BCIs.
Prespecified hypotheses can be incorporated into a logic model28,29 and our earlier findings suggest that for a GB-BCI this should include hypotheses as to the role of group processes as part of the mechanisms of action (i.e. to explain how the intervention achieves its effects), and also explore the impact of facilitation techniques in implementation and other group features, such as contextual factors. Selected framework components from within one or more of these domains may be included depending on the focus and theory of change for the intervention. Our summary diagram of the MAGI framework maps closely on to the MRC framework for process evaluation28,29 and, thus, could be used as a starting point for such logic models. As well as being used in designing or describing the intervention, logic models can guide process evaluation and subsequent selection of appropriate methods (quantitative, qualitative), measures (for components that can be assessed quantitatively, e.g. social identification) and analyses (mediator and moderator analyses, framework analyses, mixed-methods approaches).
Hypotheses relating to group processes could also be derived from exploratory analyses of qualitative data (e.g. investigating within-group processes) and/or quantitative data (e.g. indicating between-group differences or variability in engagement/outcomes for different subgroups in the sample), such as that presented here. Indeed, our exploratory analyses have resulted in a number of potential research questions for future exploration.
To ensure that future data sets on GB-BCIs can be used to undertake group-level descriptive, quantitative and qualitative analyses, we suggest collection of a minimum data set on group factors, including:
-
a group identifier for all participants (so that individual-level participant characteristics, and any baseline measures and outcome data can be linked to groups and analysed at group level)
-
a facilitator identifier that can, ideally, be linked to more information about the facilitator (to allow for facilitator-level analyses, and relationships between facilitator and group participants’ characteristics to be explored)
-
information on the presence of an accompanying person within the group (when relevant)
-
attendance data broken down by session.
Any information on continuity of membership, including whether it is a rolling group with new members regularly joining (e.g. Weight Watchers®, New York, NY, USA), and details of any mergers of groups would also be helpful, but this may be more difficult to obtain/document in a way that allows linking to participant-level data.
When studies or interventions use self-report measures, we also feel it would be useful to include one or more open questions to prompt feedback about participants’ general experiences in the group (e.g. generic, such as ‘What did you like most/least about the programme?’, or more specific, such as ‘How was your experience of the group?’). Ideally guided by a prespecified logic model for the intervention/process evaluation that considers group features (as previously described), further data on participants’ (and/or facilitators’) perceptions of the groups could be collected. Appendix 5 summarises existing measures for many of the more difficult to observe aspects of group dynamics and processes, but a useful extension to our study would be to map these more directly to components of our framework, and document their psychometric properties, undertaking further validation or development work where indicated. A systematic review110 could form the starting point for this.
When collecting qualitative data, researchers should consider whether it would be feasible to collect video rather than audio-recordings as these might provide additional information about context (e.g. venue set-up) and non-verbal behaviour that can enhance qualitative analysis and data interpretation (even without planning a detailed analysis of the non-verbal behaviour, which would be very time-consuming). Practical issues with collecting qualitative data also include ensuring good-quality data (e.g. minimising background noises, positioning recorders so that all participants’ voices are recorded) and making sure that recordings can be linked to group identifiers (i.e. through filenames, or as a statement at the beginning of the recording). As recordings contain potentially identifiable and sensitive information, consent for research purposes (including potential use beyond the immediate reasons for collection, such as checking fidelity), maintaining confidentiality, data storage and data-sharing all need careful consideration.
We were unable to undertake meaningful predictive analyses to explore hypotheses linking group dynamics and processes to outcomes because of limited data and timescales. Nonetheless, this chapter provides a resource for researchers on methods for presenting and analysing quantitative and qualitative data on groups, and mixed-methods approaches for bringing data sets together. We did not undertake statistical analyses of available quantitative data, for example to explore links between participants’ perceptions of groups and engagement or outcomes, but this is possible with our data set and there are some examples of such approaches in the literature. 126,134 More sophisticated approaches to presenting, describing and taking account of within- and between-group variability, including individual participant characteristics and potential outliers in groups, may be needed to properly examine the impact of group-level factors. A previous commentary32 argues that any analyses of effects in group-based interventions should account for group-level clustering and characteristics and the interaction of these with participant characteristics, due to non-independence of data [i.e. group members are influenced by the facilitator (shared across multiple groups), each other and the group as a whole]. However, methods for doing so do not appear to be well developed or apparent in the literature. Lessons can be learned from cluster analysis and multilevel modelling approaches,156 but analysis models may be complex if they potentially need to account for clustering by delivery site (for multicentre programmes), local delivery venue and facilitator, as well as group. This, and considering implications of group-level analyses for sample sizes given demonstrated potential for large numbers of missing data when multiple variables are considered at group level, is an area for future development.
A perennial problem in research involves gaining information on participants who drop out from studies, but information on dropouts, and reasons for dropping out, are particularly important in exploring any potential effects of group features, group dynamics or other change processes in group-based interventions. For example, one hypothesis is that negative group dynamics might be linked with lower attendance, higher drop-out rate and worse outcomes, as shown previously. 134 It would be worth further exploration to identify other factors and processes that may explain why some groups develop such negative group dynamics that lead to dropouts, and how they could be managed by group facilitators.
In terms of qualitative methods, if the aim of analysing group data is to develop hypotheses, as per many of our examples above, then inductive approaches to coding may be appropriate, but these are time-consuming. Deductive approaches, which could be based on sections of our framework-based coding schema, may therefore be more appropriate and time efficient whether or not specific hypotheses have been set.
We have illustrated methods for linking qualitative and quantitative data. For example, if there are sufficient qualitative and quantitative data on a large and varied enough number of groups, sampling relatively small numbers of groups with particular characteristics, selected on the basis of quantitative data (e.g. with different gender mix, good or poor outcomes) or qualitative data (e.g. demonstrating positive or negative group dynamics), allows comparisons to be made between groups to find explanations for differences in the other data set. For example, comparing groups with good and poor (or more or less homogeneous) outcomes (e.g. weight loss) using qualitative data on group processes and facilitation, may provide explanations for why some groups are more or less successful. However, from our data it should be noted that how ‘success’ is defined may require careful consideration, as what appears to be a successful (or unsuccessful) group, on average, may still include individuals whose outcomes do not match those of the rest of the group. When, for example, baseline measures or characteristics are explicitly discussed in groups (e.g. motivation, weight), we demonstrated how triangulation can use qualitative data to provide greater insights into quantitative data (or vice versa). Using an existing hypothesis based on qualitative or quantitative data, or if exploratory analyses in one data set highlight potentially interesting or unanticipated findings, then ‘following a thread’ can be used to explore data on the phenomenon of interest in the other data set, as we illustrated for our hypotheses about change talk and resistance (see Following a thread). Finally, matrix approaches can help to bring summary quantitative and qualitative data on individual groups alongside each other to look for patterns or differences between subgroups.
As well as exploring links between group characteristics, processes and outcomes, the methods described can also be used as part of wider aspects of process evaluations for GB-BCIs. This might include assessing and improving fidelity and quality of delivery, for example by assessing facilitators’ delivery and use of facilitation techniques and providing them with feedback. It might also include analyses of delivery to inform adaptations, for example by identifying which intervention elements and processes were delivered or occurred through group interaction, and how. The MAGI framework could help structure this type of analysis and feedback, using both quantitative and qualitative methods.
Conclusions
In conclusion, stage 3 of the MAGI study illustrated the potential applicability of the MAGI framework (see Chapter 2) and coding schema (see Chapter 3) in generating and exploring hypotheses that would allow further development of evidence on the mechanisms of action in group-based interventions. This work illustrated how quantitative and qualitative methods separately, and mixed-methods approaches for combining quantitative and qualitative data, can be employed to understand the operation of GB-BCIs. We have also presented practical recommendations for future research practices that could develop a sound evidence base to investigate the operation and effectiveness of GB-BCIs. However, our data also demonstrated the complexity of groups and that, potentially, even with a large data set it may be difficult to generalise from one group to another, let alone to other types of groups, in terms of what mechanisms are important, or what facilitation techniques should be used. This may depend on the aims of intervention, facilitator skills, participants in the group and potentially other contextual factors.
Chapter 5 Discussion, implications and conclusions
In this chapter, we summarise our findings across the three stages of our study with reference to our three objectives, and discuss key strengths and limitations. We then highlight possible implications for practice and future research, including research recommendations.
Summary of findings
The overall aim of this study was to enhance understanding of mechanisms of action in GB-BCIs. We focused on health-related interventions that targeted diet, physical activity and weight loss because data from groups conducted as part of these interventions were available to us and the evidence suggests that GB-BCIs may be particularly effective in helping participants lose weight. We intended, however, to develop a theoretical understanding of the operation of GB-BCIs more generally.
We defined three study objectives that divided our research into three stages, namely to:
-
develop a generalisable framework of mechanisms of action in GB-BCIs by identifying, defining and categorising potentially important group design features, group processes, facilitation techniques and contextual factors in groups
-
test and refine the framework, using a coding schema derived from it, as a tool for identifying these group features, processes and facilitation techniques in the recordings of sessions from three GB-BCIs (focused on diet, physical activity and weight loss), and provide examples to illustrate framework elements
-
develop mixed-methods approaches based on the framework, to explore why some groups may be more or less successful than others, and illustrate their use with available qualitative and quantitative data from a GB-BCI.
In stage 1 (addressing objective 1), the MAGI framework was developed to identify, categorise and define group features and processes. Our overarching diagrammatic representation of the framework (see Figure 3) presents some of the postulated complex, bidirectional relationships between key aspects of groups over the lifetime of an intervention. The central, blue-coloured boxes and arrows represent types of mechanisms by which interaction in groups is able lead to, initiate and support individual changes in proximal (e.g. behaviour change) and distal (e.g. improved health) outcomes. These reflect mechanisms of change based in the group itself (‘group dynamics and development’), interactions between members of the group, including facilitators (‘interpersonal change processes’), and within individual participants (‘intrapersonal change processes’). The surrounding boxes represent influences on these mechanisms resulting from the initial ‘group intervention design’ (in green), ‘facilitation techniques’ used by group facilitators (in dark blue), and factors from outside the group which influence group interaction (‘facilitator and participant characteristics and other contextual influences’ from participants’ immediate social environment). All aspects represented in the framework sit within, and may be influenced by, the ‘wider sociocultural, economic, environmental, community and organisational’ context.
Our summary table of the framework (see Table 5) and definitions underpinning it (see Report Supplementary Material 1) detail between 3 and 22 subcategories within each of the six categories. These subcategories include specific mechanisms underpinning group dynamics and development (e.g. group goals, group cohesion) as well as interpersonal (e.g. social support, social comparisons) and intrapersonal change processes (e.g. developing understanding, setting goals). Intrapersonal change processes were not the key focus for this study because they have already been extensively discussed in the psychology literature. Nonetheless, as our research suggests that a considerable portion of time in GB-BCI sessions is focused on initiating such intrapersonal change, we included a non-exhaustive list of subcategories representing intrapersonal change processes and psychological change targets that may be observed and influenced in GB-BCIs. For example, enhancing participants’ attitudes towards, or their self-efficacy in relation to, a specified behaviour change may be seen as prerequisites to generating behaviour change in GB-BCIs.
The inductive qualitative analyses of 10 diverse group sessions conducted during stage 1 generated codes that mapped onto initial framework elements stemming from the reviews of the literature and early consultations, providing preliminary support for its applicability. The coding schema (see Report Supplementary Material 2), developed alongside the framework during stage 2, includes further lower-level subcategories reflecting different ways in which subcategories were manifested in the group sessions examined (e.g. for social support, peer support, buddy-up, social connections, reciprocity). However, these codes are likely to be indicative rather than exhaustive and, for this reason, were not included in the framework itself. The framework definitions (see Report Supplementary Material 1) also include some observations and hypotheses stemming from the literature, consultations and analyses of group sessions about links, interactions and interdependencies between specific framework elements. In stage 2, facilitation techniques identified through coding of transcripts were mapped onto group dynamic, inter- and intrapersonal change processes they appeared to instigate or facilitate, providing initial evidence for mechanistic links.
In stage 2, the coding schema developed from the framework was used to identify and document the frequency with which different framework subcategories from across all of the broad framework categories were observed, and ‘real-life’ examples of facilitation techniques were used to initiate or support them in a group-based weight loss intervention (addressing objective 2). No empirical examples were identified that could not be categorised within the final framework categories. It should be noted, however, that the analyses of transcripts, development of the coding schema and further consultations contributed, in an iterative manner, to the refinement and evolution of the framework. The framework categories and many of the subcategories (1) were apparent to a greater or lesser extent in intervention manuals and session transcripts, (2) paralleled aspects of groups highlighted by facilitators, (3) linked to hypotheses generated from analyses of data in stage 3 and (4) were not questioned by researchers consulted about the framework. This is indicative of overall content validity of the framework, at least for interventions focused on diet, physical activity and weight loss.
The stage 2 analyses demonstrated that the majority of group sessions involved predesigned whole-group discussions and social learning processes, in particular exchanging information, advice and ideas, and sharing of experiences. Some group processes were less common, for example establishing shared group goals or providing group-level feedback. Commonly observed intrapersonal processes, for example goal-setting, problem-solving and feedback, were predominantly facilitated on an individual basis within the group, rather than through wider group interaction. As well as examples of group features and processes, stage 2 analyses identified a wide range of techniques used by the facilitators to instigate, facilitate and manage group dynamics and inter- and intrapersonal change processes. In the framework, these were divided into (1) techniques for starting the group or session (included to highlight tasks for setting up a group and to make this generalisable to rolling groups where new members potentially join at each session), (2) generic facilitation technique types, (3) techniques for facilitating group dynamics, (4) techniques for facilitating interpersonal change processes, (5) techniques for intrapersonal change processes and (6) techniques for closing the group or session (including techniques designed to promote maintenance of behaviour change beyond the group intervention).
Some ‘group dynamics’ subcategories (e.g. group goals, cohesion and climate) and ‘interpersonal change processes’ (e.g. social comparisons, group competition and co-operation) were rarely or never observed in the session recordings. This may reflect the nature of the groups studied (e.g. little focus on developing group dynamics, or certain interpersonal processes) and difficulties in identifying processes from audio-recordings. Such processes may be better captured via participants’, facilitators’ or, potentially, observers’ perceptions. For example, in stage 3 we illustrated how a questionnaire assessing participants’ perceptions of three aspects of the group that mapped onto framework elements (i.e. group support, group identification and external social identities) can be used to generate data on key group processes. Appendix 5 includes examples of other questionnaires that can be used to assess processes defined by the framework.
The framework was developed on the basis of a broad conceptual review of the literature. 40 Consequently, although the framework was tested using GB-BCIs targeting diet and physical activity, literature on groups shows that the group features, facilitation techniques and mechanisms that we have defined are probably relevant to a wide range of GB-BCIs (e.g. to groups providing mental health support, education, team-building). Our in-depth consultations with group participants and facilitators were confined to those involved in the interventions studied here but feedback from other experts indicated that the framework captured their broader experiences of groups.
In stage 3, although our data did not permit formal investigation of group features and mechanisms that could distinguish between more or less effective groups (as originally planned), we were able to suggest questions, illustrate novel applications of mixed-methods approaches for integrating qualitative and quantitative data based on our framework and provide a resource for undertaking future detailed work to do this in future research (addressing objective 3). The additional quantitative data on up to 67 groups in the LWTC programme demonstrated large variability across groups in terms of their features (e.g. group size, mix of participants with different characteristics within groups), participants’ perceptions of interpersonal change processes (e.g. group support, group identification) and group-level outcomes. This was true to a lesser extent for attendance, which was generally high across all groups. For key characteristics and outcomes, we were able to identify groups in which the make-up of participants was more or less homogeneous, and groups that were typical or atypical in relation to the wider sample, for example single-gender groups, groups with drop-out and groups that were more or less successful in terms of their group-level weight loss outcomes. As per our original plan, we suggest that groups of different types or with different levels of success could be sampled on the basis of these group-level features, analysed qualitatively and compared to explore whether or not there are any potential differences with regard to group dynamics, use of particular facilitation techniques or occurrence of interpersonal change processes. We illustrated mixed-methods approaches to integrating quantitative and qualitative data to generate and address hypotheses including triangulation, ‘following a thread’ and matrix or other case-based approaches. We also recommended minimum data that should be collected for any group programme to allow such analyses in future research.
Strengths
A key strength of this research is that, building on our prior conceptual review of decades of multidisciplinary research,40 we incorporated key theoretical explanations of personal change in groups into a manageable framework that can be used to guide good practice and adequate data collection. As our aim was to identify and map all potentially relevant concepts, we did not plan to conduct systematic reviews to identify, select and appraise evidence on all of the ≥ 90 group features and processes that ultimately featured in our framework owing to the diverse nature and size of the literature, uncertainty regarding what would count as evidence to support their inclusion and time constraints. However, we used systematic approaches to selecting constructs when building the framework and employed systematic methods when searching the smaller literature on qualitative studies on people’s experiences of weight loss groups.
A further strength was the consultative checking for content and face validity and refinement of category definitions with around 40 experts and non-experts, including group participants, facilitators and researchers (see Appendix 4). We disseminated the framework more widely than initially proposed to gain feedback at practitioner- and researcher-focused conferences and internal seminars. The feedback we received at all stages was overwhelmingly positive, emphasising the importance of the work in the health field and beyond, and potential usefulness of the framework for a variety of purposes (e.g. ‘I think this level of detail is fantastic. This will be really useful for those reading it moving forward’; see Appendix 4). In a further extension to what was originally planned, we also began to explore, via informal discussions with colleagues in education, psychology and management, potential applications to small group-learning and research teams.
In our qualitative analyses, great care was taken to check transcripts and discuss interpretations within the team, and in the early stages we drew on as large and varied a sample of transcripts as were available. This represented a relatively large sample for a qualitative study of this type, given how complex, in-depth and time-consuming the data and analyses were. An inductive approach was initially taken in the analyses, to ensure that observations stemmed from the data and were not constrained by the framework developing from the reviews of literature. The approach to analysis became more deductive as the study progressed and the framework was iteratively refined and expanded on the basis of observations from the coding. In stage 3, analyses of quantitative and qualitative data were undertaken by separate researchers without insight into the other data set to minimise bias, before the data sets were brought together.
The development of a formal, potentially widely applicable, coding schema for our framework provides a usable resource to supplement the framework. The coding schema was applied independently to one or more transcripts by five researchers, one of whom was not directly involved in the study and one of whom had limited experience in qualitative analysis. This demonstrated that the coding procedures can be learned by coders with some level of expertise and facilitated refinement of instructions for use. Similarly, our revised stage 3 work illustrated some of the practical challenges of generating and linking meaningful group-level data and conducting mixed-methods analyses of these. We also developed a training workshop on implications and potential uses of the framework for designers, facilitators and evaluators of GB-BCIs. This resource can underpin future dissemination and application of the framework for a range of audiences.
Limitations and further considerations
When using the group session recordings in stages 1 and 2, the cataloguing, checking, transcribing and analyses proved more time-consuming and resource intensive than anticipated. The stage 2 analyses combined transcripts used in stage 1 as well as newly sampled stage 2 transcripts to maximise the number of sessions from which examples of facilitation techniques and group processes could be drawn. In stage 1, we also trialled coding of different types of interactions in the sessions (i.e. when facilitators, female and male participants spoke) and quantified the amount of interaction (i.e. numbers of ‘turns’ and proportions of transcripts in which these participants spoke). We were unable, in the time available, to undertake such coding with further transcripts but future research could expand this approach.
In stage 2, our experience of coding, double-coding and relating the codes to the framework revealed multiple ways in which transcripts of group sessions can be coded. For example, words, phrases or multiple talk sequences can be coded and, for many sections of text, multiple codes apply. This makes reliability of the coding difficult to assess, but higher-level reliability between coders in terms of presence/absence or frequency of identification of codes could be investigated in future applications. The coding of transcripts relied primarily on one researcher (AJB), although others double-coded a selection, which helped to assess general ability to identify the framework categories in the transcripts, and led to refinements to coding categories and improved instructions for use. The expertise of coders in understanding distinctions between psychological constructs used to understand group process may also have an impact on reliability. Coders also need to understand (1) the level at which they are coding (i.e. whether they focus on identifying more general processes, such as (4.2) social learning, or more precise examples of these processes, such as (4.2.1) providing, exchanging information) and (2) the different approaches to coding (i.e. implicit/interpretative or explicit/semantic). By their very nature, coding systems specify a priori a particular meaning or function to the phenomenon being studied and involve some level of abstraction from the specific context. This is both an advantage and a disadvantage of coding systems: they enable quantification of essentially qualitative communication processes but the code may not quite capture what is seen in the data or multiple codes may be potentially applicable. 157,158
Some of the researchers involved in the design of the interventions and intervention manuals (CG: ComPoD, SkiM, WtW; FG: WtW; LP: SkiM) were also involved in the framework development and coding. This might have influenced their coding of the intervention content and intended processes, but is unlikely to have biased the content or shape of the MAGI framework (which was developed from a range of sources and in consultation with over 31 consultees), or the coding of transcripts (which was primarily conducted by AJB and JRS, the researchers without prior involvement in the analysed interventions). We acknowledge, however, that common intervention designers (e.g. across WtW and SkiM) and facilitators (between the ComPoD and SkiM studies) probably make these interventions more similar to each other than other weight loss interventions; future research should test and validate the framework in a wider range of weight loss and other GB-BCIs.
We have already described limitations in the data available for the stage 3 analyses (see Chapter 4), which necessitated a shift from our original plan. Potential issues with the quality and completeness of the session recordings (e.g. poor quality of WtW recordings, only seven LWTC groups for which all session recordings were available) and whether or not they would allow us to sample more and less successful groups (as originally intended) were flagged up early in the study. It was only later that the lack of quantitative data to link to for the groups with full session recordings became apparent. However, qualitative and mixed-methods studies commonly use adaptive designs, as subsequent steps can be dependent on earlier data, analyses and findings. These limitations were not unexpected given our reliance on secondary data, collected in one study by intervention providers operating outside a research context, and not for the purpose for which the data were used here. In future, this can be addressed by better recording of group identifiers for group programmes, and prospective data collection for process evaluation alongside GB-BCIs in research contexts with analyses of group features in mind.
The framework, its constituent definitions and the coding schema were designed to be comprehensive while at the same time presenting a manageable, easy-to-understand representation of the complexity of groups. We hope that as a result of its gradual refinement the framework and coding schema may be used as ‘catalogues’ of options from which different audiences can select broad categories to focus on (e.g. group intervention design, facilitation techniques) depending on their purpose (e.g. designing an intervention, training facilitators). Researchers might also select categories on the basis of hypotheses about prespecified group-level mechanisms (e.g. guided by a logic model) or stemming from initial findings about important aspects from the interventions studied.
The framework represents the dependency of some group processes on others (e.g. certain intra- and inter-personal change processes may happen simultaneously) and the potentially multiple, bidirectional and iterative links between processes over the course of a group session or intervention. Consequently, the group dynamics and interpersonal subcategories are, to some extent, ordered to reflect dependencies and definitions. Nonetheless, the framework is inevitably a simplification of the mechanisms of change at work in GB-BCIs.
We did not conduct a formal Delphi consensus exercise to agree on framework components and categorisations, but feedback from researchers on the near-final version of the framework highlighted some overlap and confusion between change targets, processes of change, and change techniques, which we subsequently tried to define more clearly. For example, the intrapersonal change category in our framework includes cognitive processes, such as goal-setting and self-monitoring, that are also listed as change techniques in taxonomies4 despite the fact that in definitions it is clear that the techniques actually involve ‘prompting’ or ‘encouraging’ goal-setting/self-monitoring (as change processes). 3 We have tried to be clear to distinguish facilitation techniques from the change processes that they instigate or support on the basis of evidence-based explanations of how altering change targets leads to behavioural change. 3 We recognise that some of the change targets, such as increased self-efficacy or motivation, are inter-related and influenced by multiple inter- and intrapersonal change processes and, therefore, may be difficult to separate in practice. However, they are retained as separate subcategories in the framework because they are well defined and conceptually distinct in the literature. Such individual-level change targets may also be viewed as mediating or intermediary outcomes of GB-BCIs in process evaluations,28,29 potentially able to explain subsequent behaviour changes. This highlights the complexity, but also the need for better conceptual clarity and careful use of terminology, in the wider field.
A final limitation of our study, which we were aware of from the outset, is that some of the processes included in the framework may not be identifiable directly from recordings of group sessions (i.e. through verbalised expressions). For example, ‘group cohesion’, a key subcategory of group dynamics underpinning other group dynamic and interpersonal processes, cannot easily be determined from audio-recordings. Interviews, observations or video-recordings of groups may provide further insight (e.g. SkiM groups were video-recorded, subsequent to our analyses, to explore this possibility). As highlighted in stage 3, participant and facilitator self-reports of these more abstract concepts may also be useful as a substitute for, or in addition to qualitative assessments, providing scope for triangulation.
Implications
Implications for designers of group-based interventions
Our research suggests, in the context of the interventions studied here, that little explicit consideration is given to group processes in the design of interventions, and further work suggests that this is a widespread trend in GB-BCIs. 69 There was limited mention of group dynamics, group development, specific interpersonal change processes or facilitation techniques in the intervention manuals. This translated into limited evidence of some subcategories of ‘group dynamics’ in most of the sessions and also facilitators’ expressed lack of confidence in supporting these during our consultations with them.
Within any constraints placed on programme design by the delivery context and commissioning or research specifications, our framework can be considered a ‘catalogue’ of elements for designers to consider when developing GB-BCIs. ‘Group intervention design’, over which designers have a high degree of control, underpins all other aspects. Specific ‘facilitation techniques’ can be designed to create group dynamics that support personal change and group development that is conducive to such change. However, at present, many GB-BCI designers appear to leave group dynamics and development to chance. Our observations and consultations with facilitators indicated that ensuring sufficient time, and flexibility, for group interaction was important, potentially instead of delivering large quantities of ‘content’ (which could be delivered, at least partly, in other ways, e.g. via written information, online).
When GB-BCIs are merely regarded as a cost-effective delivery mode for change techniques that could be delivered in other ways,159 as is the case in most existing frameworks used to guide intervention development,127,128,160 their potential to induce and support personal change is underestimated or unseen. As we have argued elsewhere, design of GB-BCIs should begin with the rationale for using group-based delivery. 69 Our framework could then facilitate the development of logic models explaining how facilitation techniques will prompt group dynamics and group processes that optimise personal change. This planning could be usefully undertaken within an Intervention Mapping framework. 127 Such logic models would also allow specification of hypotheses, data collection approaches and analyses that can test whether or not postulated group mechanisms differentiate between groups that are more or less effective in engendering behaviour change among participants. This would advance the empirical science of mapping mechanisms in GB-BCIs.
Implications for group participants
Our framework, data on dropouts from groups in our study and the wider literature suggest that an enhanced understanding of how group processes engender personal change could also support better preparation of participants who are waiting to start or contemplating enrolment in GB-BCIs. For example, making clearer the rationale for using groups, setting up expectations about what happens in groups and what is expected of participants (potentially including prior specification of ground rules, group roles, etc.) may ease anxiety (evidence of which was observed in our analyses) and help participants get the most out of the group. Such preparation may also help participants decide whether or not they are suited to a particular type of group, or a group is appropriate for them, allowing screening out of those who are unlikely to engage with, or benefit from, a GB-BCI. Such selection could reduce resistance and the time facilitators spend on disengaged members, potentially improving the functioning of GB-BCIs.
Implications for group facilitators and trainers
Our framework, the background literature and our qualitative analyses suggest that to maximise participant engagement and optimise change processes in GB-BCIs, a wide range of specific facilitation techniques should be employed. However, in our consultations, facilitators sometimes expressed a lack of awareness, skills or confidence in using these. The framework and examples could be used to develop training for facilitators and also (particularly in ongoing programmes) provide the basis for giving structured, formative feedback to facilitators focused around key framework components linked to the focus of the intervention. Linked to this, there are developing examples of research on skills and competencies of facilitators in GB-BCIs (e.g. Avery et al. 130 and James Nobles, Leeds Beckett University, 2017, personal communication).
Informal discussions with educationalists co-ordinating and delivering small group education sessions (e.g. problem-based learning groups) have indicated that our framework and broader research may also have implications for designing and delivering these. To advance this work, it would be useful to compare current conceptual models used in educational settings with the conceptual structure of our framework161,162 and assess potential overlaps and differences.
This research, therefore, also suggests that more resources may need to be invested in training facilitators in the specifics of group facilitation and allowing more scope and time in group interventions for group processes to be supported and developed. This additional investment would be marginal in the context of overall costs of setting up and delivering an intervention. Moreover, this would have potential to further increase the cost-effectiveness of group-based interventions, which are often assumed to be more cost-effective than other modes of delivering similar content. 163 Components of our framework could, for example, be given consideration in the specification documents for commissioning GB-BCIs. However, more evidence, building on our research, showing whether or not the presence and facilitation of group processes can improve engagement and outcomes would probably be required for decision-makers. In the meantime, we hope to share our learning from this study with providers and commissioners of large-scale GB-BCIs, such as the NHS Diabetes Prevention Programme (NHS DPP). 155
Recommendations for research
This study implies a series of recommendations for research development and practice:
-
Specification of minimum data sets for group-based interventions. To facilitate future research and capitalise on opportunities for secondary analyses of data sets, research funders and commissioners should insist on provision of minimum data sets for group-based interventions delivered within, and ideally outside, research contexts, that include in each participant record:
-
a group identifier, which allows linkage of groups to individual records on participant characteristics (e.g. sociodemographic, socioeconomic, clinical), baseline measures and outcomes
-
a facilitator identifier that links to participant or group identifiers, ideally, with further key information on the facilitator (e.g. demographics, background, experience)
-
information on presence of a supporter in the group (when relevant)
-
attendance or absence at individual group sessions
-
ideally, one or more open questions on the experience of the group where this can be incorporated into self-report measures.
-
In line with recommendations for reporting of group-based69 and other interventions,164 intervention manuals should also outline key group intervention design features and intended facilitation techniques/style so that these can also be examined in retrospect.
-
Conduct systematic reviews to appraise evidence related to the framework concepts, and synthesise qualitative studies exploring group-based interventions. We identified a vast literature on group features and processes that informed our framework but further reviews could systematically appraise the evidence underpinning each concept to justify its inclusion or estimate its importance. A series of in-depth studies of participants’ experiences of weight loss groups were identified and it would be useful to undertake a formal systematic review and qualitative synthesis of these and qualitative studies examining participants’ experiences of other types of groups (e.g. for disease self-management goups165). Such reviews could be used to examine the robustness and comprehensiveness of our framework across different GB-BCIs and thereby lead to extensions and refinements.
-
Mapping available quantitative measures of group dynamics and processes. We identified measures, including questionnaires and multi-item scales, that allow characterisation of group characteristics, functioning and processes that are difficult to observe in group sessions but may be captured via participants’ self-reports. Mapping how these correspond to framework components would reveal the extent to which measures are available or, alternatively, need to be developed to adequately assess key group processes. Further work on assessing the conceptual clarity and psychometric properties of these measures would guide selection for use in research and clarify measures in need of refinement or further development.
-
Further developing qualitative methods for coding and analysing group sessions. Our coding schema from stage 2, methods for in-depth qualitative analysis demonstrated in stage 3, and preliminary approaches to coding interaction patterns in groups (see Appendix 8), could be further developed and tested. For example, it would be important to establish methods to assess reliability of the coding, determine whether or not this can be improved through training, and check reliability across different types of group interventions. Our coding approaches could also be adapted/extended for use with video-recordings and observations of group sessions.
-
Further developing mixed-methods and other research approaches to exploring group mechanisms. Building on stage 3 of our research, further specification and examples of how to integrate quantitative and qualitative data (e.g. using triangulation, following a thread, matrices) would facilitate more detailed and sophisticated analyses of mechanisms of action in GB-BCIs. Consideration could also be given to the need for more complex, systems-based approaches to researching groups and the role of realist approaches.
-
Exploring group mechanisms through process evaluations. The MAGI framework maps closely onto the summary diagram in the MRC process evaluation guidance,28,29 highlighting the potential importance of this work for evaluators of GB-BCIs. With some development (recommendations 3–5), our suggested qualitative, quantitative and mixed-methods approaches could be used by researchers to analyse group sessions by focusing on all or certain framework categories/components selected on the basis of logic models, prior hypotheses, previous research (recommendation 2) or data from other sources (e.g. facilitator observations) for the particular type of intervention being studied. As originally planned in our study, and demonstrated in stage 3, sampling could be used to make comparisons between different groups or facilitators to generate explanations for differences in engagement or outcomes, and so build evidence on what works, when and for whom in GB-BCIs. In feasibility studies, or ongoing interventions, such information might also be fed back to facilitators to improve delivery, or to designers to make adaptations.
-
Undertaking further quantitative group-level analyses using our own, and other, existing large secondary data sets from GB-BCIs, and other group interventions where a group identifier has been included. This work should:
-
establish and apply appropriate statistical techniques (e.g. multilevel modelling) to account for and explore group-level, and potentially facilitator-level, influences on outcomes
-
address specific research questions about mechanisms of action in these interventions, for example around how group size, group composition (within- or between-group variability in gender, age, clinical characteristics, etc.) may affect perceptions of group dynamics, interpersonal processes (e.g. social identification) and outcomes.
-
-
Adapting/extending the MAGI framework to other groups and populations. Work such as that described above could clarify whether or not the framework requires extension and refinement when applied to other types of GB-BCIs (e.g. targeting smoking, alcohol use, management of chronic illness) or in other contexts (e.g. mental health, education settings, research teams166) and populations (e.g. children, families, adults of different ages), including virtual/online groups.
-
Exploring the impact of group facilitators’ characteristics and skills/competencies on outcomes. Examining how facilitator characteristics and facilitation approaches (including techniques used, communication style, fidelity to protocol, and adaptation or tailoring to different groups) determine the potential of GB-BCIs to instigate personal change can help to answer questions concerning who should facilitate which groups, and what kind of training is needed to optimise outcomes.
-
Developing and evaluating group facilitator training toolkits. The above would provide the foundation for applied research that could develop and pilot training programmes, including online resources, to help facilitators identify and competently employ specific techniques designed to optimise participant engagement, group dynamics and interpersonal processes in GB-BCIs. These could be evaluated as add-ons to planned trials of GB-BCIs, or potentially in stand-alone trials.
Conclusions
The research reported here enhances our understanding of mechanisms of action in group-based interventions. The proposed MAGI framework identifies, categorises and defines group features, group processes (group dynamics, inter- and intra-personal change processes) and contextual influences, which can affect each other and facilitate or impede engagement, personal change, alteration of behaviour patterns and other intervention outcomes. The study provides evidence of these processes and examples of techniques used to facilitate them in ‘real-life’ GB-BCIs focused on diet, physical activity and weight loss, validating the framework in this context. Hypotheses and methods for further exploring potential relationships between group processes and outcomes are also proposed and illustrated. Thus, the framework and methods provide a comprehensive resource for designers, facilitators and evaluators of GB-BCIs, and further implications of our work for these and other audiences (e.g. group participants, commissioners and policy-makers) are outlined.
Acknowledgements
We would like to thank all of the facilitators and participants in the three group-based interventions from which we used data. We would also like to thank the following people for their support of the study, and insights and feedback that helped shape the framework.
Other co-applicants on the original grant
Mrs Jaine Keable from Westbank and Associate Professor Matthew Jones from the University of the West of England for their support in the early stages of the study, and for providing access to additional data on the LWTC programme.
Group participants
Mrs Sue Sedgman, Mrs Jackie Morant, Mr Douglas Osman and Mr Andrew Wilkie.
Group facilitators/programme providers
Miss Amy Clarke, Miss Sian Derrick, Mrs Ruby Entwistle and Mrs Anna Murch.
Researchers/practitioners
Dr Amanda Avery, Dr Yael Bar-Zeev, Dr Enzo Di Battista, Dr Tegan Cruwys, Dr Liz Glidewell, Dr Cindy Gray, Dr Marta Moreira Marques, Dr James Nobles and others who provided us with feedback at seminars and conferences.
We would especially like to thank Dr Leon Poltawski for his helpful advice throughout the study, his feedback on the framework and coding schema, his participation in the double coding and for his help with accessing the SkiM data.
We also thank the ComPoD Trial Steering Committee (chairperson: Professor Sharon Simpson) for their oversight of the study.
Contributions of authors
Dr Aleksandra J Borek (Postdoctoral Research Associate in Psychology Applied to Health, MAGI Study Researcher and co-applicant) contributed to study design, conducted the literature reviews, led development and revision of the framework and coding schema, coded the transcripts, undertook all qualitative analyses and data interpretation, led consultations, drafted most of the report [summaries (Abstract, Plain English summary and Scientific summary), background (Chapter 1), stage 1 (Chapter 2), stage 2 (Chapter 3) and qualitative part of stage 3 (Chapter 4)] and revised draft and final versions. The initial framework built on a previous conceptual review developed as part of Dr Borek’s doctoral research.
Dr Jane R Smith (Senior Lecturer in Primary Care, MAGI Study Chief Investigator) led the funding application and development of the original protocol, managed the study and oversaw all aspects of the research, contributed to the development of the framework, participated in the double-coding of transcripts, undertook analyses of quantitative data, contributed to interpretation of data, supported consultations, drafted sections of the report [stage 3 (Chapter 4) and Discussion (Chapter 5)] and revised draft and final versions.
Professor Colin J Greaves (Professor in Psychology Applied to Health, MAGI Study co-applicant) co-supervised Aleksandra Borek’s doctoral work on which this study is built, contributed to the study design and development of the framework (particularly identification of facilitation techniques), provided access to data, commented on the coding schema, contributed to interpretation of data and provided comments on most sections of the report.
Dr Fiona Gillison (Senior Lecturer in Exercise & Health Psychology, MAGI Study co-applicant) contributed to study design and development of the framework (particularly identification of facilitation techniques), commented on the coding schema, participated in double coding of transcripts, advised on analysis, contributed to interpretation of data and provided comments on all sections of the report.
Dr Mark Tarrant (Senior Lecturer in Psychology Applied to Health, MAGI Study co-applicant) co-supervised Aleksandra Borek’s doctoral work on which this study built, contributed to study design and development of the framework (particularly in relation to social psychological theoretical literature), commented on the coding schema, advised on quantitative analyses, contributed to interpretation of data and provided comments on most sections of the report.
Dr Sarah Morgan-Trimmer (Research Fellow in Process Evaluation, MAGI Study co-applicant) contributed to study design and the development of the framework, participated in the double-coding of transcripts, advised on qualitative and mixed-methods analyses, contributed to interpretation of data and provided comments on most sections of the report.
Professor Rose McCabe (Professor of Clinical Communication, MAGI Study co-applicant) contributed to the study design and reviewed the framework, commented on the coding schema, advised on qualitative analyses and approved the final report.
Professor Charles Abraham (Professor of Social & Health Psychology, MAGI Study co-applicant) was the senior supervising researcher for the MAGI study. The project was an extension of the doctoral programme of Aleksandra Borek and the MAGI framework is an extension of the framework developed during that work. 40 Charles Abraham designed, won funding for, and was lead supervisor for this doctoral programme. He contributed to the MAGI study design and, with Aleksandra Borek, led the conceptual development of the framework. He co-authored and edited the final study report.
Authors are listed in order of their contribution to the study and report, apart from Charles Abraham, whose designation as last author reflects his role as the senior supervising researcher, providing overall oversight of the programme of work.
Publication
Borek AJ, Abraham C, Greaves CJ, Gillison F, Tarrant M, Morgan-Trimmer S, McCabe R, Smith JR. Identifying change processes in group-based health behaviour-change interventions: development of the mechanisms of action in group-based interventions (MAGI) framework [published online ahead of print June 13 2019]. Health Psychol Rev 2019.
Data-sharing statement
This is a primarily qualitative study using secondary data and, therefore, there are no data available for further access or sharing. All available data are contained within the report. All queries should be submitted to the corresponding authors.
Patient data
This work uses data provided by patients and collected by the NHS as part of their care and support. Using patient data is vital to improve health and care for everyone. There is huge potential to make better use of information from people’s patient records, to understand more about disease, develop new treatments, monitor safety, and plan NHS services. Patient data should be kept safe and secure, to protect everyone’s privacy, and it’s important that there are safeguards to make sure that it is stored and used responsibly. Everyone should be able to find out about how patient data are used. #datasaveslives You can find out more about the background to this citation here: https://understandingpatientdata.org.uk/data-citation.
Disclaimers
This report presents independent research. The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the MRC, NETSCC, the EME programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the EME programme or the Department of Health and Social Care.
References
- Davis R, Campbell R, Hildon Z, Hobbs L, Michie S. Theories of behaviour and behaviour change across the social and behavioural sciences: a scoping review. Health Psychol Rev 2015;9:323-44. https://doi.org/10.1080/17437199.2014.941722.
- Michie S, West R, Campbell R, Brown J, Gainforth H. ABC of Behaviour Change Theories: An Essential Resource for Researchers, Policy Makers and Practitioners. London: Silverback Publishing; 2014.
- Abraham C, Michie S. A taxonomy of behavior change techniques used in interventions. Health Psychol 2008;27:379-87. https://doi.org/10.1037/0278-6133.27.3.379.
- Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med 2013;46:81-95. https://doi.org/10.1007/s12160-013-9486-6.
- Abraham C, Wood CE, Johnston M, Francis J, Hardeman W, Richardson M, et al. Reliability of identification of behavior change techniques in intervention descriptions. Ann Behav Med 2015;49:885-900. https://doi.org/10.1007/s12160-015-9727-y.
- Dombrowski SU, Sniehotta FF, Avenell A, Johnston M, MacLennan G, Araújo-Soares V. Identifying active ingredients in complex behavioural interventions for obese adults with obesity-related co-morbidities or additional risk factors for co-morbidities: a systematic review. Health Psychol Rev 2012;6:7-32. https://doi.org/10.1080/17437199.2010.513298.
- Hartmann-Boyce J, Johns DJ, Jebb SA, Aveyard P. Behavioural Weight Management Review Group . Effect of behavioural techniques and delivery mode on effectiveness of weight management: systematic review, meta-analysis and meta-regression. Obes Rev 2014;15:598-609. https://doi.org/10.1111/obr.12165.
- Michie S, Abraham C, Whittington C, McAteer J, Gupta S. Effective techniques in healthy eating and physical activity interventions: a meta-regression. Health Psychol 2009;28:690-701. https://doi.org/10.1037/a0016136.
- Horne AM, Rosenthal R. Research in group work: how did we get where we are?. J Spec Group Work 1997;22:228-40. https://doi.org/10.1080/01933929708415527.
- Yalom ID, Leszcz M. Theory and Practice of Group Psychotherapy. New York, NY: Basic Books; 2005.
- Lieberman M, Yalom I, Miles M. Encounter Groups: First Facts. New York, NY: Basic Books; 1973.
- Smith PB. Group Processes and Personal Change. London: Harper and Row; 1980.
- Kurtz LF. Self-Help and Support Groups: A Handbook for Practitioners. Thousand Oaks, CA: SAGE Publications Inc.; 1997.
- Booth A, Cantrell A, Preston L, Chambers D, Goyder E. What is the evidence for the effectiveness, appropriateness and feasibility of group clinics for patients with chronic conditions? A systematic review. Health Serv Deliv Res 2015;3.
- Griffiths C, Foster G, Ramsay J, Eldridge S, Taylor S. How effective are expert patient (lay led) education programmes for chronic disease?. BMJ 2007;334:1254-6. https://doi.org/10.1136/bmj.39227.698785.47.
- Sidhu MS, Gale NK, Gill P, Marshall T, Taylor B, Jolly K. A systematic review of lay-led group-based self-management interventions for minority ethnic populations diagnosed with long-term conditions in high-income countries. Divers Equal Health Care 2014;11:225-36.
- Deakin T, McShane CE, Cade JE, Williams RD. Group based training for self-management strategies in people with type 2 diabetes mellitus. Cochrane Database Syst Rev 2005;2. https://doi.org/10.1002/14651858.CD003417.pub2.
- Smith-Turchyn J, Morgan A, Richardson J. The effectiveness of group-based self-management programmes to improve physical and psychological outcomes in patients with cancer: a systematic review and meta-analysis of randomised controlled trials. Clin Oncol 2016;28:292-305. https://doi.org/10.1016/j.clon.2015.10.003.
- Kaunonen M, Hannula L, Tarkka MT. A systematic review of peer support interventions for breastfeeding. J Clin Nurs 2012;21:1943-54. https://doi.org/10.1111/j.1365-2702.2012.04071.x.
- Hanson S, Jones A. Is there evidence that walking groups have health benefits? A systematic review and meta-analysis. Br J Sports Med 2015;49:710-15. https://doi.org/10.1136/bjsports-2014-094157.
- Harden SM, McEwan D, Sylvester BD, Kaulius M, Ruissen G, Burke SM, et al. Understanding for whom, under what conditions, and how group-based physical activity interventions are successful: a realist review. BMC Public Health 2015;15. https://doi.org/10.1186/s12889-015-2270-8.
- Stead LF, Lancaster T. Group behaviour therapy programmes for smoking cessation. Cochrane Database Syst Rev 2000;2.
- Borek AJ, Abraham C, Greaves CJ, Tarrant M. Group-based diet and physical activity weight-loss interventions: a systematic review and meta-analysis of randomised controlled trials. Appl Psychol Health Well Being 2018;10:62-86. https://doi.org/10.1111/aphw.12121.
- Paul-Ebhohimhen V, Avenell A. A systematic review of the effectiveness of group versus individual treatments for adult obesity. Obes Facts 2009;2:17-24. https://doi.org/10.1159/000186144.
- West R, Walia A, Hyder N, Shahab L, Michie S. Behavior change techniques used by the English Stop Smoking Services and their associations with short-term quit outcomes. Nicotine Tob Res 2010;12:742-7. https://doi.org/10.1093/ntr/ntq074.
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Medical Research Council Guidance . Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ 2008;337. https://doi.org/10.1136/bmj.a1655.
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and Evaluating Complex Interventions: New Guidance. London: Medical Research Council; 2008.
- Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process Evaluation of Complex Interventions: Medical Research Council Guidance. London: MRC Population Health Science Research Network; 2014.
- Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015;350. https://doi.org/10.1136/bmj.h1258.
- Moore GF, Evans RE. What theory, for whom and in which context? Reflections on the application of theory in the development and evaluation of complex population health interventions. SSM Popul Health 2017;3:132-5. https://doi.org/10.1016/j.ssmph.2016.12.005.
- Greaves CJ, Sheppard KE, Abraham C, Hardeman W, Roden M, Evans PH, et al. IMAGE Study Group . Systematic review of reviews of intervention components associated with increased effectiveness in dietary and physical activity interventions. BMC Public Health 2011;11. https://doi.org/10.1186/1471-2458-11-119.
- Murphy SA, Johnson LC. Methodological issues associated with group intervention research. Arch Psychiatr Nurs 2006;20:276-81. https://doi.org/10.1016/j.apnu.2006.05.003.
- Abraham C. Charting variability to ensure conceptual and design precision: a comment on Ogden (2016). Health Psychol Rev 2016;10:260-4. https://doi.org/10.1080/17437199.2016.1190293.
- Peirce RS, Frone MR, Russell M, Cooper ML. Financial stress, social support, and alcohol involvement: a longitudinal test of the buffering hypothesis in a general population survey. Health Psychol 1996;15:38-47. https://doi.org/10.1037/0278-6133.15.1.38.
- van Beurden SB, Greaves CJ, Smith JR, Abraham C. Techniques for modifying impulsive processes associated with unhealthy eating: a systematic review. Health Psychol 2016;35:793-806. https://doi.org/10.1037/hea0000337.
- Hoddinott P, Allan K, Avenell A, Britten J. Group interventions to improve health outcomes: a framework for their design and delivery. BMC Public Health 2010;10. https://doi.org/10.1186/1471-2458-10-800.
- Cartwright D, Zander AF. Group Dynamics: Research and Theory. London: Tavistock; 1968.
- Brown R. Group Processes: Dynamics Within and Between Groups. Cambridge, MA: Basil Blackwell; 1993.
- Smith PB. Small Groups and Personal Change. London: Methuen; 1980.
- Borek AJ, Abraham C. How do small groups promote behaviour change? An integrative conceptual review of explanatory mechanisms. Appl Psychol Health Well Being 2018;10:30-61. https://doi.org/10.1111/aphw.12120.
- Festinger L. A theory of social comparison processes. Hum Relat 1954;7:117-40. https://doi.org/10.1177/001872675400700202.
- Bandura A. Social Learning Theory. New York, NY: General Learning Press; 1977.
- Tajfel H, Turner JC, Wrochel S, Austin WG. Psychology of Intergroup Relations. Chicago, IL: Nelson-Hall Publishers; 1986.
- Zajonc RB. Social facilitation. Science 1965;149:269-74. https://doi.org/10.1126/science.149.3681.269.
- Haslam C, Jetten J, Cruwys T, Dingle G, Haslam SA. The New Psychology of Health: Unlocking the Social Cure. Oxford: Taylor & Francis; 2018.
- Jetten J, Haslam C, Haslam SA. The Social Cure: Identity, Health and Well-Being. Hove and New York, NY: Psychology Press; 2011.
- Abraham C, Gardner B. What psychological and behaviour changes are initiated by ‘expert patient’ training and what training techniques are most helpful?. Psychol Health 2009;24:1153-65. https://doi.org/10.1080/08870440802521110.
- Borek A, Abraham C, Greaves CJ, Tarrant M. ‘We’re All in the Same Boat’: Participants’ Perceptions of How Groups Helped Them Make Lifestyle Changes in Two Interventions for Prevention of Diabetes and Cardiovascular Diseases n.d.
- Tarrant M, Khan SS, Farrow CV, Shah P, Daly M, Kos K. Patient experiences of a bariatric group programme for managing obesity: a qualitative interview study. Br J Health Psychol 2017;22:77-93. https://doi.org/10.1111/bjhp.12218.
- Barlow JH, Bancroft GV, Turner AP. Volunteer, lay tutors’ experiences of the Chronic Disease Self-Management Course: being valued and adding value. Health Educ Res 2005;20:128-36. https://doi.org/10.1093/her/cyg112.
- Michie S, Churchill S, West R. Identifying evidence-based competences required to deliver behavioural support for smoking cessation. Ann Behav Med 2011;41:59-70. https://doi.org/10.1007/s12160-010-9235-z.
- Durantini MR, Albarracín D, Mitchell AL, Earl AN, Gillette JC. Conceptualizing the influence of social agents of behavior change: a meta-analysis of the effectiveness of HIV-prevention interventionists for different groups. Psychol Bull 2006;132:212-48. https://doi.org/10.1037/0033-2909.132.2.212.
- Albarracín D, Gillette JC, Earl AN, Glasman LR, Durantini MR, Ho MH. A test of major assumptions about behavior change: a comprehensive look at the effects of passive and active HIV-prevention interventions since the beginning of the epidemic. Psychol Bull 2005;131:856-97. https://doi.org/10.1037/0033-2909.131.6.856.
- Estabrooks PA, Carron AV. The physical activity group environment questionnaire: an instrument for the assessment of cohesion in exercise classes. Group Dyn Theory Res Pract 2000;4:230-43. https://doi.org/10.1037//1089-2699.4.3.230.
- Hunt K, Wyke S, Gray CM, Anderson AS, Brady A, Bunn C, et al. A gender-sensitised weight loss and healthy living programme for overweight and obese men delivered by Scottish Premier League football clubs (FFIT): a pragmatic randomised controlled trial. Lancet 2014;383:1211-21. https://doi.org/10.1016/S0140-6736(13)62420-4.
- Campo S, Askelson NM, Spies EL, Losch M. Caution, the use of humor may lead to confusion: evaluation of a video podcast of the midwest teen sex show. Am J Sex Educ 2010;5:201-16. https://doi.org/10.1080/15546128.2010.503857.
- Gillison F, Greaves C, Stathi A, Ramsay R, Bennett P, Taylor G, et al. ‘Waste the Waist’: the development of an intervention to promote changes in diet and physical activity for people with high cardiovascular risk. Br J Health Psychol 2012;17:327-45. https://doi.org/10.1111/j.2044-8287.2011.02040.x.
- Gillison F, Stathi A, Reddy P, Perry R, Taylor G, Bennett P, et al. Processes of behavior change and weight loss in a theory-based weight loss intervention program: a test of the process model for lifestyle behavior change. Int J Behav Nutr Phys Act 2015;12. https://doi.org/10.1186/s12966-014-0160-6.
- Greaves C, Gillison F, Stathi A, Bennett P, Reddy P, Dunbar J, et al. Waste the waist: a pilot randomised controlled trial of a primary care based intervention to support lifestyle change in people with high cardiovascular risk. Int J Behav Nutr Phys Act 2015;12. https://doi.org/10.1186/s12966-014-0159-z.
- Kok M, Solomon-Moore E, Greaves C, Smith JR, Kimberlee R, Jones M. Evaluation of Living Well, Taking Control: A Community-based Diabetes Prevention and Management Programme. Bristol: University of the West of England; 2016.
- Smith JR, Greaves CJ, Thompson J, Taylor R, Jones M, Armstrong R, et al. The Community-Based Prevention of Diabetes (ComPoD) Study: A Randomised, Waiting List Controlled Trial of a Voluntary Sector-Led Diabetes Prevention Programme n.d.
- Type 2 Diabetes: Prevention in People at High Risk. Public Health Guideline 38. London: NICE; 2012.
- Borek AJ, Abraham C, Greaves CJ, Gillison F, Tarrant M, Morgan-Trimmer S, et al. Identifying change processes in group-based health behaviour-change interventions: development of the mechanisms of action in group-based interventions (MAGI) framework [published online ahead of print June 13 2019]. Health Psychol Rev 2019. https://doi.org/10.1080/17437199.2019.1625282.
- Johnson DW, Johnson FP. Joining Together: Group Theory and Group Skills. London: Prentice-Hall; 1991.
- Wheelan SA. Facilitating Training Groups: A Guide to Leadership and Verbal Intervention Skills. Westport: Greenwood Publishing Group; 1990.
- Burlingame GM, Fuhriman A, Mosier J. The differential effectiveness of group psychotherapy: a meta-analytic perspective. Group Dyn Theory Res Pract 2003;7. https://doi.org/10.1037/1089-2699.7.1.3.
- Mannix EA, Neale MA. Looking Back, Moving Forwards: A Review of Group and Team-Based Research. Bingley: Emerald Group Publishing; 2012.
- Borek AJ. Understanding How Participation in Groups Promotes Health-Related Psychological and Behaviour Change 2016.
- Borek AJ, Abraham C, Smith JR, Greaves CJ, Tarrant M. A checklist to improve reporting of group-based behaviour-change interventions. BMC Public Health 2015;15. https://doi.org/10.1186/s12889-015-2300-6.
- Elwyn G, Greenhalgh T, Macfarlane F. Groups: A Guide to Small Group Work in Healthcare, Management, Education and Research. Abingdon: Radcliffe Publishing; 2001.
- Association for Specialists in Group Work . Association for specialists in group work professional standards for the training of group workers. J Spec Group Work 2000;25:327-42. https://doi.org/10.1080/01933920008411677.
- Kok G, Gottlieb NH, Peters GJ, Mullen PD, Parcel GS, Ruiter RA, et al. A taxonomy of behaviour change methods: an Intervention Mapping approach. Health Psychol Rev 2016;10:297-312. https://doi.org/10.1080/17437199.2015.1077155.
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLOS Med 2009;6. https://doi.org/10.1371/journal.pmed.1000100.
- Carroll C, Booth A, Leaviss J, Rick J. ‘Best fit’ framework synthesis: refining the method. BMC Med Res Methodol 2013;13. https://doi.org/10.1186/1471-2288-13-37.
- Jaques D, Salmon G. Learning in Groups: A Handbook for Face-To-Face and Online Environments. London: Routledge; 2007.
- Bauman S, Waldo M. Improving the goals and process (GAP) matrix for groups: incorporating feedback from the field. J Spec Group Work 1998;23:215-24. https://doi.org/10.1080/01933929808411395.
- Waldo M, Bauman S. Regrouping the categorization of group work a goals and process (GAP) matrix for groups. J Spec Group Work 1998;23:164-76. https://doi.org/10.1080/01933929808411388.
- Knowles MS, Knowles H. Introduction to Group Dynamics. New York, NY: Association Press; 1972.
- McGrath JE, Arrow H, Berdahl JL. The study of groups: past, present, and future. Personal Soc Psychol Rev 2000;4:95-105. https://doi.org/10.1207/S15327957PSPR0401_8.
- Michie S, Ashford S, Sniehotta FF, Dombrowski SU, Bishop A, French DP. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: the CALO-RE taxonomy. Psychol Health 2011;26:1479-98. https://doi.org/10.1080/08870446.2010.540664.
- Hartmann-Boyce J, Aveyard P, Koshiaris C, Jebb SA. Development of tools to study personal weight control strategies: OxFAB taxonomy. Obesity 2016;24:314-20. https://doi.org/10.1002/oby.21341.
- Adolfsson B, Carlson A, Undén AL, Rössner S. Treating obesity: a qualitative evaluation of a lifestyle intervention for weight reduction. Health Edu J 2002;61:244-58. https://doi.org/10.1177/001789690206100306.
- Ahern AL, Boyland EJ, Jebb SA, Cohn SR. Participants’ explanatory model of being overweight and their experiences of 2 weight loss interventions. Ann Fam Med 2013;11:251-7. https://doi.org/10.1370/afm.1446.
- Ahlgren C, Hammarström A, Sandberg S, Lindahl B, Olsson T, Larsson C, et al. Engagement in new dietary habits – obese women’s experiences from participating in a 2-year diet intervention. Int J Behav Med 2016;23:84-93. https://doi.org/10.1007/s12529-015-9495-x.
- Allen JT, Cohn SR, Ahern AL. Experiences of a commercial weight-loss programme after primary care referral: a qualitative study. Br J Gen Pract 2015;65:e248-55. https://doi.org/10.3399/bjgp15X684409.
- Befort CA, Thomas JL, Daley CM, Rhode PC, Ahluwalia JS. Perceptions and beliefs about body size, weight, and weight loss among obese African American women: a qualitative inquiry. Health Educ Behav 2008;35:410-26. https://doi.org/10.1177/1090198106290398.
- Cifuentes M, Polsky S, Mitchell NS. Perspectives of older African American women on a community based weight loss program: qualitative findings from SWITCH. J Am Geriatrics Soc 2014;62:1996-8. https://doi.org/10.1111/jgs.13040.
- Diaz VA, Mainous AG, Pope C. Cultural conflicts in the weight loss experience of overweight Latinos. Int J Obes 2007;31:328-33. https://doi.org/10.1038/sj.ijo.0803387.
- Fogel S, Young L, McPherson JB. The experience of group weight loss efforts among lesbians. Women Health 2009;49:540-54. https://doi.org/10.1080/03630240903424012.
- Gallagher R, Kirkness A, Armari E, Davidson PM. Participants’ perspectives of a multi-component, group-based weight loss programme supplement for cardiac rehabilitation: a qualitative study. Int J Nurs Pract 2012;18:28-35. https://doi.org/10.1111/j.1440-172X.2011.01988.x.
- Gamsu D, Sutton M, Bennett L, Ward J. The development of a psychoeducational group intervention for overweight women with type 2 diabetes mellitus: a service evaluation. Pract Diab Int 2002;19:43-50. https://doi.org/10.1002/pdi.279.
- Gimlin D. Constructions of ageing and narrative resistance in a commercial slimming group. Ageing Soc 2007;27:407-24. https://doi.org/10.1017/S0144686X06005757.
- Gray CM, Hunt K, Mutrie N, Anderson AS, Leishman J, Dalgarno L, et al. Football Fans in Training: the development and optimization of an intervention delivered through professional sports clubs to help men lose weight, become more active and adopt healthier eating habits. BMC Public Health 2013;13. https://doi.org/10.1186/1471-2458-13-232.
- Groven KS, Engelsrud G. Dilemmas in the process of weight reduction: exploring how women experience training as a means of losing weight. Int J Qual Stud Health Well-Being 2010;5. https://doi.org/10.3402/qhw.v5i2.5125.
- Hammarström A, Wiklund AF, Lindahl B, Larsson C, Ahlgren C. Experiences of barriers and facilitators to weight-loss in a diet intervention – a qualitative study of women in northern Sweden. BMC Womens Health 2014;14. https://doi.org/10.1186/1472-6874-14-59.
- Hansen NV, Brændgaard P, Hjørnholm C, la Cour S. Qualitative research building real-life interventions: user-involving development of a mindfulness-based lifestyle change support program for overweight citizens. Eur J Clin Nutr 2014;68:1129-33. https://doi.org/10.1038/ejcn.2014.106.
- Hunt K, Gray CM, Maclean A, Smillie S, Bunn C, Wyke S. Do weight management programmes delivered at professional football clubs attract and engage high risk men? A mixed-methods study. BMC Public Health 2014;14. https://doi.org/10.1186/1471-2458-14-50.
- Kidd LI, Graor CH, Murrock CJ. A mindful eating group intervention for obese women: a mixed methods feasibility study. Arch Psychiatr Nurs 2013;27:211-18. https://doi.org/10.1016/j.apnu.2013.05.004.
- Ljung S, Olsson C, Rask M, Lindahl B. Patient experiences of a theory-based lifestyle-focused group treatment in the prevention of cardiovascular diseases and type 2 diabetes. Int J Behav Med 2013;20:378-84. https://doi.org/10.1007/s12529-012-9252-3.
- McMahon NE, Visram S, Connell LA. Mechanisms of change of a novel weight loss programme provided by a third sector organisation: a qualitative interview study. BMC Public Health 2016;16. https://doi.org/10.1186/s12889-016-3063-4.
- Metzgar CJ, Preston AG, Miller DL, Nickols-Richardson SM. Facilitators and barriers to weight loss and weight loss maintenance: a qualitative exploration. J Hum Nutr Diet 2015;28:593-60. https://doi.org/10.1111/jhn.12273.
- Östberg AL, Wikstrand I, Bengtsson Boström K. Group treatment of obesity in primary care practice: a qualitative study of patients’ perspectives. Scand J Public Health 2011;39:98-105. https://doi.org/10.1177/1403494810391524.
- Penn L, Dombrowski SU, Sniehotta FF, White M. Participants’ perspectives on making and maintaining behavioural changes in a lifestyle intervention for type 2 diabetes prevention: a qualitative study using the theory domain framework. BMJ Open 2013;3. https://doi.org/10.1136/bmjopen-2013-002949.
- Penn L, Dombrowski SU, Sniehotta FF, White M. Perspectives of UK Pakistani women on their behaviour change to prevent type 2 diabetes: qualitative study using the theory domain framework. BMJ Open 2014;4. https://doi.org/10.1136/bmjopen-2013-004530.
- Piana N, Battistini D, Urbani L, Romani G, Fatone C, Pazzagli C, et al. Multidisciplinary lifestyle intervention in the obese: its impact on patients’ perception of the disease, food and physical exercise. Nutr Metab Cardiovasc Dis 2013;23:337-43. https://doi.org/10.1016/j.numecd.2011.12.008.
- Sheppard VB, Hicks J, Makambi K, Hurtado-de-Mendoza A, Demark-Wahnefried W, Adams-Campbell L. The feasibility and acceptability of a diet and exercise trial in overweight and obese black breast cancer survivors: the Stepping STONE study. Contemp Clin Trials 2016;46:106-13. https://doi.org/10.1016/j.cct.2015.12.005.
- Walker LO, Sterling BS, Latimer L, Kim SH, Garcia AA, Fowles ER. Ethnic-specific weight-loss interventions for low-income postpartum women: findings and lessons. West J Nurs Res 2012;34:654-76. https://doi.org/10.1177/0193945911403775.
- Cahill J, Barkham M, Hardy G, Gilbody S, Richards D, Bower P, et al. A review and critical appraisal of measures of therapist-patient interactions in mental health settings. Health Technol Assess 2008;12. https://doi.org/10.3310/hta12240.
- Delucia-Waack JL. Measuring the effectiveness of group work: a review and analysis of process and outcome measures. J Spec Group Work 1997;22:277-93. https://doi.org/10.1080/01933929708415531.
- Orfanos S. Measures of Group Processes: A Review of Questionnaire-based, Interactional-analysis and Qualitative Approaches. Group Therapies for Schizophrenia: Identifying and Linking Group Interactions and Group Experiences With Outcomes 2016.
- Bales RF. Interaction Process Analysis: A Method for the Study of Small Groups. Oxford: Addison-Wesley; 1950.
- Beck AP, Lewis CM. The Process of Group Psychotherapy: Systems for Analyzing Change. Washington, DC: American Psychological Association; 2000.
- Chapman CL, Baker EL, Porter G, Thayer SD, Burlingame GM. Rating group therapist interventions: the validation of the group psychotherapy intervention rating scale. Group Dyn Theory Res Pract 2010;14. https://doi.org/10.1037/a0016628.
- Kiesler DJ. Manual for the Checklist of Interpersonal Transactions-Revised (CLOIT-R) and Checklist of Psychotherapy Transactions-Revised (CLOPT-R): A 2004 Update. Richmond, VA: Virginia Commonwealth University; 2004.
- Lee SM, Koopman J, Hollenbeck JR, Wang LC, Lanaj K. The Team Descriptive Index (TDI): a multidimensional scaling approach for team description. Acad Manag Discov 2015;1:91-116. https://doi.org/10.5465/amd.2013.0001.
- Roter D, Larson S. The Roter interaction analysis system (RIAS): utility and flexibility for analysis of medical interactions. Patient Educ Couns 2002;46:243-51. https://doi.org/10.1016/S0738-3991(02)00012-5.
- Tate KA, Rivera ET, Conwill WL, Miller MD, Puig A. Conceptualizing group dynamics from our clients’ perspective: development of the conceptualization of group dynamics inventory. J Spec Group Work 2013;38:146-68. https://doi.org/10.1080/01933922.2013.775206.
- Wilson PA, Hansen NB, Tarakeshwar N, Neufeld S, Kochman A, Sikkema KJ. scale development of a measure to assess community-based and clinical intervention group environments. J Community Psychol 2008;36:271-88. https://doi.org/10.1002/jcop.20193.
- Wölfer R, Faber NS, Hewstone M. Social network analysis in the science of groups: cross-sectional and longitudinal applications for studying intra- and intergroup behavior. Group Dyn Theory Res Pract 2015;19:45-61. https://doi.org/10.1037/gdn0000021.
- Miller WR, Rollnick S. Motivational Interviewing: Preparing People for Change. New York, NY: Guilford Press; 2002.
- Grant A, Treweek S, Dreischulte T, Foy R, Guthrie B. Process evaluations for cluster-randomised trials of complex interventions: a proposed framework for design and reporting. Trials 2013;14. https://doi.org/10.1186/1745-6215-14-15.
- Pound P, Campbell R. Exploring the feasibility of theory synthesis: a worked example in the field of health related risk-taking. Soc Sci Med 2015;124:57-65. https://doi.org/10.1016/j.socscimed.2014.11.029.
- Moyers TB, Rowell LN, Manuel JK, Ernst D, Houck JM. The Motivational Interviewing Treatment Integrity code (MITI 4): rationale, preliminary reliability and validity. J Subst Abuse Treat 2016;65:36-42. https://doi.org/10.1016/j.jsat.2016.01.001.
- Miller WR. Motivational Interviewing Skill Code (MISC): Coder’s Manual. Albuquerque, NM: University of New Mexico; 2000.
- Tarrant M, Warmoth K, Code C, Dean S, Goodwin VA, Stein K, et al. Creating psychological connections between intervention recipients: development and focus group evaluation of a group singing session for people with aphasia. BMJ Open 2016;6. https://doi.org/10.1136/bmjopen-2015-009652.
- Cruwys T, Haslam SA, Fox NE, McMahon H. ‘That’s not what we do’: evidence that normative change is a mechanism of action in group interventions. Behav Res Ther 2015;65:11-7. https://doi.org/10.1016/j.brat.2014.12.003.
- Bartholomew LK, Parcel GS, Kok G, Gottlieb NH, Fernandez ME. Planning Health Promotion Programs: An Intervention Mapping Approach. San Francisco, CA: Jossey-Bass; 2016.
- Wight D, Wimbush E, Jepson R, Doi L. Six steps in quality intervention development (6SQuID). J Epidemiol Community Health 2016;70:520-5. https://doi.org/10.1136/jech-2015-205952.
- Reddy P, Vaughan C, Dunbar J, Schwarz P, Reddy P, Greaves C, et al. Diabetes Prevention Practice. Dresden: Tumaini Institute for Prevention Management; 2010.
- Avery A, Whitehead K, Halliday V. How to Facilitate Lifestyle Change: Applying Group Education in Healthcare. Hoboken, NJ: John Wiley & Sons; 2016.
- Catalano T, Kendall E, Vandenberg A, Hunter B. The experiences of leaders of self-management courses in Queensland: exploring health professional and peer leaders’ perceptions of working together. Health Soc Care Community 2009;17:105-15. https://doi.org/10.1111/j.1365-2524.2008.00801.x.
- Hipwell A, Turner A, Barlow J. ‘We’re not fully aware of their cultural needs’: tutors’ experiences of delivering the expert patients programme to South Asian attendees. Divers Health Soc Care 2008;5:281-90.
- Hoddinott P, Britten J, Pill R. Why do interventions work in some places and not others: a breastfeeding support group trial. Soc Sci Med 2010;70:769-78. https://doi.org/10.1016/j.socscimed.2009.10.067.
- Nackers LM, Dubyak PJ, Lu X, Anton SD, Dutton GR, Perri MG. Group dynamics are associated with weight loss in the behavioral treatment of obesity. Obesity 2015;23:1563-9. https://doi.org/10.1002/oby.21148.
- Stenov V, Henriksen JE, Folker AP, Skinner TC, Willaing I. Educator talk ratio as a quality indicator in group-based patient education. Health Educ J 2016;75:259-69. https://doi.org/10.1177/0017896915574556.
- Denford S, Campbell JL, Frost J, Greaves CJ. Processes of change in an asthma self-care intervention. Qual Health Res 2013;23:1419-29. https://doi.org/10.1177/1049732313507376.
- Hankonen N, Sutton S, Prevost AT, Simmons RK, Griffin SJ, Kinmonth AL, et al. Which behavior change techniques are associated with changes in physical activity, diet and body mass index in people with recently diagnosed diabetes?. Ann Behav Med 2015;49:7-17. https://doi.org/10.1007/s12160-014-9624-9.
- Amrhein PC, Miller WR, Yahne CE, Palmer M, Fulcher L. Client commitment language during motivational interviewing predicts drug use outcomes. J Consult Clin Psychol 2003;71:862-78. https://doi.org/10.1037/0022-006X.71.5.862.
- Moyers TB, Miller WR, Hendrickson SML. How does motivational interviewing work? Therapist interpersonal skill predicts client involvement within motivational interviewing sessions. J Consult Clin Psychol 2005;73:590-8. https://doi.org/10.1037/0022-006X.73.4.590.
- Livhits M, Mercado C, Yermilov I, Parikh JA, Dutson E, Mehran A, et al. Is social support associated with greater weight loss after bariatric surgery?: a systematic review. Obes Rev 2011;12:142-8. https://doi.org/10.1111/j.1467-789X.2010.00720.x.
- Kiser LJ. Social support measurement and intervention: a guide for health and social scientists. J Nerv Ment Dis 2001;189:801-2. https://doi.org/10.1097/00005053-200111000-00015.
- Cruwys T, Alexander Haslam S, Dingle GA, Jetten J, Hornsey MJ, Desdemona Chong EM, et al. Feeling connected again: interventions that increase social identification reduce depression symptoms in community and clinical settings. J Affect Disord 2014;159:139-46. https://doi.org/10.1016/j.jad.2014.02.019.
- Orth WS, Madan AK, Taddeucci RJ, Coday M, Tichansky DS. Support group meeting attendance is associated with better weight loss. Obes Surg 2008;18:391-4. https://doi.org/10.1007/s11695-008-9444-8.
- Simon GE, Rohde P, Ludman EJ, Jeffery RW, Linde JA, Operskalski BH, et al. Is success in weight loss treatment contagious (do attendance and outcomes cluster within treatment groups)?. Obes Res Clin Pract 2010;4:e283-91. https://doi.org/10.1016/j.orcp.2010.09.179.
- Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol 2013;13. https://doi.org/10.1186/1471-2288-13-117.
- Tuckman BW, Jensen MAC. Stages of small-group development revisited. Group Organ Manag 1977;2:419-27. https://doi.org/10.1177/105960117700200404.
- EuroQol Group . EuroQol – a new facility for the measurement of health-related quality of life. Health Policy 1990;16:199-208. https://doi.org/10.1016/0168-8510(90)90421-9.
- Miller WR, Johnson WR. A natural language screening measure for motivation to change. Addict Behav 2008;33:1177-82. https://doi.org/10.1016/j.addbeh.2008.04.018.
- McLean G, Tobias M. The New Zealand Physical Activity Questionnaires: Report on the Validation and use of the NZPAQ-LF and NZPAQ-SF Self-Report Physical Activity Survey Instruments. Wellington: SPARC; 2004.
- Shannon J, Kristal AR, Curry SJ, Beresford SA. Application of a behavioral approach to measuring dietary change: the fat- and fiber-related diet behavior questionnaire. Cancer Epidemiol Biomarkers Prev 1997;6:355-61.
- O’Cathain A, Murphy E, Nicholl J. Three techniques for integrating data in mixed methods studies. BMJ 2010;341. https://doi.org/10.1136/bmj.c4587.
- Kane H, Lewis MA, Williams PA, Kahwati LC. Using qualitative comparative analysis to understand and quantify translation and implementation. Transl Behav Med 2014;4:201-8. https://doi.org/10.1007/s13142-014-0251-6.
- MacKenzie KR, Dies RR, MacKenzie KR. Advances in Group Psychotherapy. Intergrating Research and Practice. New York, NY: International Universities Press; 1983.
- Conner M, Norman P. Predicting Health Behaviour. Maidenhead: McGraw Hill; 2005.
- NHS Diabetes Prevention Programme (NHS DPP). London: NHS England; n.d.
- Fidell LS, Tabachnick BG. Using Multivariate Statistics. Boston, MA: Pearson; 2007.
- Heritage J, Maynard DW. Problems and prospects in the study of physician-patient interaction: 30 years of research. Annu Rev Sociol 2006;32:351-74. https://doi.org/10.1146/annurev.soc.32.082905.093959.
- McCabe R, Slade M, Priebe S. Choosing Methods in Mental Health Research. London: Brunner-Routledge; 2006.
- Dombrowski SU, O’Carroll RE, Williams B. Form of delivery as a key ‘active ingredient’ in behaviour change interventions. Br J Health Psychol 2016;21:733-40. https://doi.org/10.1111/bjhp.12203.
- Michie S, Atkins L, West R. The Behaviour Change Wheel: A Guide to Designing Interventions. London: Silverback Publishing; 2014.
- Lichtenberg J, London M. A Framework for diagnosing, implementing, and evaluating group interventions. Group Facil Res Appl J 2008;9:37-48.
- Haidet P, Levine RE, Parmelee DX, Crow S, Kennedy F, Kelly PA, et al. Perspective: guidelines for reporting team-based learning activities in the medical and health sciences education literature. Acad Med 2012;87:292-9. https://doi.org/10.1097/ACM.0b013e318244759e.
- Greaves CJ, Campbell JL. Supporting self-care in general practice. Br J Gen Pract 2007;57:814-21.
- Hoffmann TC, Glasziou P, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014;348. https://doi.org/10.1136/bmj.g1687.
- Hughes S, Lewis S, Willis K, Rogers A, Wyke S, Smith L. The experience of facilitators and participants of long term condition self-management group programmes: a qualitative synthesis. Patient Educ Couns 2017;100:2244-54. https://doi.org/10.1016/j.pec.2017.06.035.
- Curry LA, O’Cathain A, Clark VLP, Aroni R, Fetters M, Berg D. The role of group dynamics in mixed methods health sciences research teams. J Mix Methods Res 2012;6:5-20. https://doi.org/10.1177/1558689811416941.
- Keyserling TC, Ammerman AS, Samuel-Hodge CD, Ingram AF, Skelly AH, Elasy TA, et al. A diabetes management program for African American women with type 2 diabetes. Diabetes Educ 2000;26:796-805. https://doi.org/10.1177/014572170002600508.
- Corey MS, Corey G. Group Counselling: Process and Practice. Monterey, CA: Brooks/Cole; 1992.
- Tinsley HEA, Roth JA, Lease SH. Dimensions of leadership and leadership style among group intervention specialists. J Couns Psychol 1989;36:58-3. https://doi.org/10.1037/0022-0167.36.1.48.
- Bolman L. Some effects of trainers on their T groups. J Appl Behav Science 1971;7. https://doi.org/10.1177/002188637100700303.
- Stinchfield RD, Burlingame GM. Development and use of the directives rating system in group therapy. J Couns Psychol 1991;38:251-7. https://doi.org/10.1037/0022-0167.38.3.251.
- Bales RF, Cohen SP, Williams SA. SYMLOG: A System for the Multiple Level Observation of Groups. New York, NY: Free Press; 1979.
- Hill WF. The Hill interaction matrix. Pers Guid J 1971;49:619-22. https://doi.org/10.1002/j.2164-4918.1971.tb03693.x.
- Hill F. Hill Interaction Matrix (HIM): the conceptual framework, derived rating scales, and an updated bibliography. Small Group Behav 1977;8:251-68. https://doi.org/10.1177/104649647700800301.
- Budman SH, Soldz S, Demby A, Davis M, Merry J. What is cohesiveness? An empirical examination. Small Gr Res 1993;24:199-216. https://doi.org/10.1177/1046496493242003.
- Soldz S, Budman S, Davis M, Demby A. Beyond the interpersonal circumplex in group psychotherapy: the structure and relationship to outcome of the Individual Group Member Interpersonal Process Scale. J Clin Psychol 1993;49:551-63. https://doi.org/10.1002/1097-4679(199307)49:4<551::AID-JCLP2270490413>3.0.CO;2-5.
- Shadish WR. The validity of a measure of intimate behavior. Small Group Behav 1986;17:113-20. https://doi.org/10.1177/104649648601700110.
- Cooney NL, Kadden RM, Litt MD, Getter H. Matching alcoholics to coping skills or interactional therapies: two-year follow-up results. J Consult Clin Psychol 1991;59:598-601. https://doi.org/10.1037/0022-006X.59.4.598.
- Getter H, Litt MD, Kadden RM, Cooney NL. Measuring treatment process in coping skills and interactional group therapies for alcoholism. Int J Group Psychother 1992;42:419-30. https://doi.org/10.1080/00207284.1992.11490709.
- Caruso R, Grassi L, Biancosino B, Marmai L, Bonatti L, Moscara M, et al. Exploration of experiences in therapeutic groups for patients with severe mental illness: development of the Ferrara group experiences scale (FE-GES). BMC Psychiatry 2013;13. https://doi.org/10.1186/1471-244X-13-242.
- McGuire JM, Taylor DR, Broome DH, Blau BI, Abbott DW. Group structuring techniques and their influence on process involvement in a group counseling training group. J Couns Psychol 1986;33:270-5. https://doi.org/10.1037/0022-0167.33.3.270.
- Moos RH. Group Environment Scale Manual. Palo Alto, CA: Consulting Psychologists Press; 1986.
- Krogel J, Burlingame G, Chapman C, Renshaw T, Gleave R, Beecher M, et al. The Group Questionnaire: a clinical and empirically derived measure of group relationship. Psychother Res 2013;23:344-54. https://doi.org/10.1080/10503307.2012.729868.
- Macgowan MJ. The group engagement measure: a review of its conceptual and empirical properties. J Groups Addict Recover 2006;1:33-52. https://doi.org/10.1300/J384v01n02_04.
- Butler T, Fuhriman A. Level of functioning and length of time in treatment variables influencing patient’s therapeutic experience in group psychotherapy. Int J Group Psychother 1983;33:489-504. https://doi.org/10.1080/00207284.1983.11491347.
- Lese K, MacNair-Semands RR. The therapeutic factors inventory: development of a scale. Group 2000;24:303-17. https://doi.org/10.1023/A:1026616626780.
- Kivlighan DM, Goldfine DC. Endorsement of therapeutic factors as a function of stage of group development and participant interpersonal attitudes. J Couns Psychol 1991;38:150-8. https://doi.org/10.1037/0022-0167.38.2.150.
- Stone MH, Lewis CM, Beck AP. The structure of Yalom’s Curative Factors Scale. Int J Group Psychother 1994;44:239-45. https://doi.org/10.1080/00207284.1994.11490745.
Appendix 1 Details of group session recordings used in the Mechanisms of Action in Group-based Interventions study
| Number | Sampled for study stage | Intervention | Group number | Session number | Facilitatorsa | Length of transcribed recordings (minutes) |
|---|---|---|---|---|---|---|
| 1 | 1 | LWTC | 1 | 2 | 5 | 88 |
| 2 | 1 | LWTC | 1 | 3 | 5 | 88 |
| 3 | 1 | LWTC | 2 | 3 | 1 | 127 |
| 4 | 1 | LWTC | 2 | 4 | 1 | 90 |
| 5 | 1 | SkiM | 3 | 2 | 2 | 90 |
| 6 | 1 | SkiM | 3 | 5 | 2 | 88 |
| 7 | 1 | WtW | 4 | 1 | 7 and 8 | 105 |
| 8 | 1 | WtW | 4 | 3 | 7 and 9 | 124 |
| 9 | 1 | WtW | 5 | 4 | 10 and 11 | 123 |
| 10 | 1 | WtW | 5 | 7 | 10 and 11 | 123 |
| 11 | 2 | LWTC | 6 | 1 | 6 | 128 |
| 12 | 2 | LWTC | 6 | 4 | 6 | 99 |
| 13 | 2 | LWTC | 7 | 1 | 3 | 59 |
| 14 | 2 | LWTC | 7 | 4 | 3 | 41 |
| 15 | 2 | LWTC | 8 | 1 | 3 | 38 |
| 16 | 2 | LWTC | 8 | 4 | 3 | 48 |
| 17 | 2 | LWTC | 9 | 1 | 1 | 66 |
| 18 | 2 | LWTC | 10 | 4 | 3 | 37 |
| 19 | 2 | LWTC | 11 | 1 | 3 | 63 |
| 20 | 2 | LWTC | 12 | 1 | 4 | 49 |
| 21 | 2 | LWTC | 12 | 2 | 4 | 91 |
| 22 | 2 | LWTC | 13 | 1 | 1 | 62 |
| 23 | 2 | SkiM | 14 | 1 | 2 | 86 |
| 24 | 2 | SkiM | 14 | 3 | 2 | 91 |
| 25 | 2 | SkiM | 14 | 4 | 2 | 86 |
| 26 | 2 | SkiM | 14 | 5 | 2 | 88 |
| 27 | 2 | SkiM | 15 (combined 3 and 14) | 6 | 2 | 89 |
| 28 | 2 | SkiM | 15 (combined 3 and 14) | 9 | 2 | 83 |
| 29 | 2 | SkiM | 15 (combined 3 and 14) | 10 | 2 | 94 |
| 30 | 2 | SkiM | 15 (combined 3 and 14) | 14 | 2 | 94 |
| 31 | 2 | SkiM | 16 | 1 | 1 | 110 |
| 32 | 2 | SkiM | 16 | 2 | 1 | 103 |
| 33 | 2 | SkiM | 16 | 7 | 1 | 97 |
| 34 | 2 | SkiM | 16 | 8 | 1 | 115 |
| 35 | 2 | SkiM | 17 | 1 | 1 | 74 |
| 36 | 2 | SkiM | 17 | 3 | 1 | 100 |
| 37 | 2 | SkiM | 17 | 4 | 1 | 92 |
| 38 | 2 | SkiM | 17 | 8 | 1 | 93 |
| 1 | 3 | LWTC | 18 | 1 | 1 | 53 |
| 2 | 3 | LWTC | 18 | 2 | 1 | 127 |
| 3 | 3 | LWTC | 18 | 3 | 1 | 114 |
| 4 | 3 | LWTC | 18 | 4 | 1 | 75 |
| 5 | 3 | LWTC | 19 | 1 | 3 | 49 |
| 6 | 3 | LWTC | 19 | 2 | 3 | 122 |
| 7 | 3 | LWTC | 19 | 3 | 3 | 115 |
| 8 | 3 | LWTC | 19 | 4 | 3 | 56 |
Appendix 2 Evolution of the Mechanisms of Action in Group-based Interventions framework
A diagram was used to illustrate the main categories of the MAGI framework elements and relationships between them. It evolved throughout the study, based on the results from the sources and study team discussions. In addition to these changes to the main categories, the lists of subcategories (i.e. concepts and processes relevant to facilitating change in groups) were also refined during the process.
The MAGI framework and diagram built on our earlier work,40,68 which provided the conceptual basis for the framework. Figure 8 and Table 26 below were developed in this earlier work.
FIGURE 8.
Initial conceptual model developed in Borek and Abraham. 40 © 2018 The Authors. Applied Psychology: Health and Well-Being published by John Wiley & Sons Ltd on behalf of International Association of Applied Psychology. This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/.
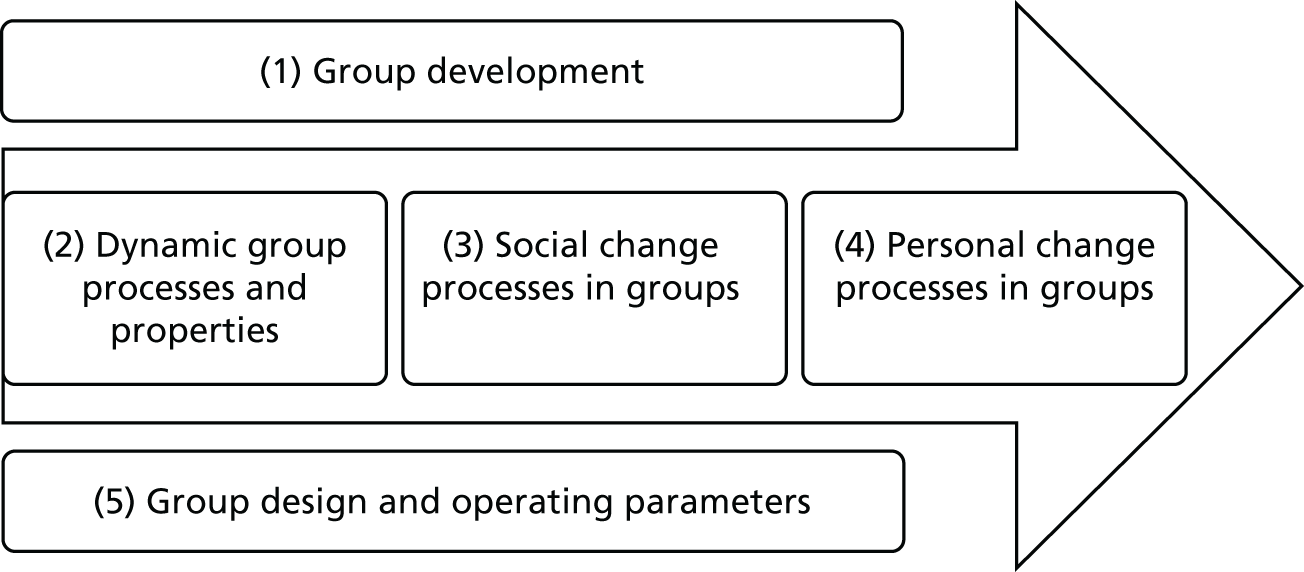
| 1. Group development | 2. Dynamic group processes and properties | 3. Social change processes | 4. Personal change processes | 5. Group design and operating parameters |
|---|---|---|---|---|
| 1. Forming | 1. Social identification | 1. Social comparison | 1. Individual cognitive change | 1. Group purpose |
| 2. Storming | 2. Group cohesion | 2. Social facilitation | 2. Individual skill acquisition | 2. Group size and composition |
| 3. Norming | 3. Group norms | 3. Modelling, imitation and social learning | 3. Self-disclosure, feedback and challenge | 3. Leadership processes |
| 4. Performing | 4. Group roles and statuses | 4. Social power and influence | 4. Facilitator characteristics | |
| 5. Adjourning | 5. Group climate | 5. Social support | 5. Group and interaction management |
The diagrams and tables below illustrate the development of the framework in the MAGI study.
Version 1 of the MAGI framework (Figure 9) was discussed and adapted in the following consultations:
-
University’s internal seminar (June 2016): participating researchers suggested the following: adding participant personal characteristics, distinguishing between time structure of the programme and (adding) time structure of the sessions (of activities within sessions), adding individual problem-solving and adding motivation building.
-
Consultation with group participants (June 2016): details were added to (1) group set-up – facilitation style/approach, accessibility of the location, communication patterns, tailoring/flexibility, pre-session information and contact, participant and facilitator materials, access to facilities, formal group roles; (2) group dynamics: informal group roles; (3) interpersonal change processes: learning styles, intergroup competition; (4) intrapersonal change processes: receipt of information/learning; and (5) group closure – individual feedback on progress.
-
Study team meeting (June 2016): the version of the framework, including changes from the above consultations, were discussed and agreed.
-
Consultation with two group facilitators (August 2016): no specific categories were suggested for addition but many categories were illustrated by examples from the facilitators’ practice.
FIGURE 9.
MAGI framework, version 1 (June 2016).
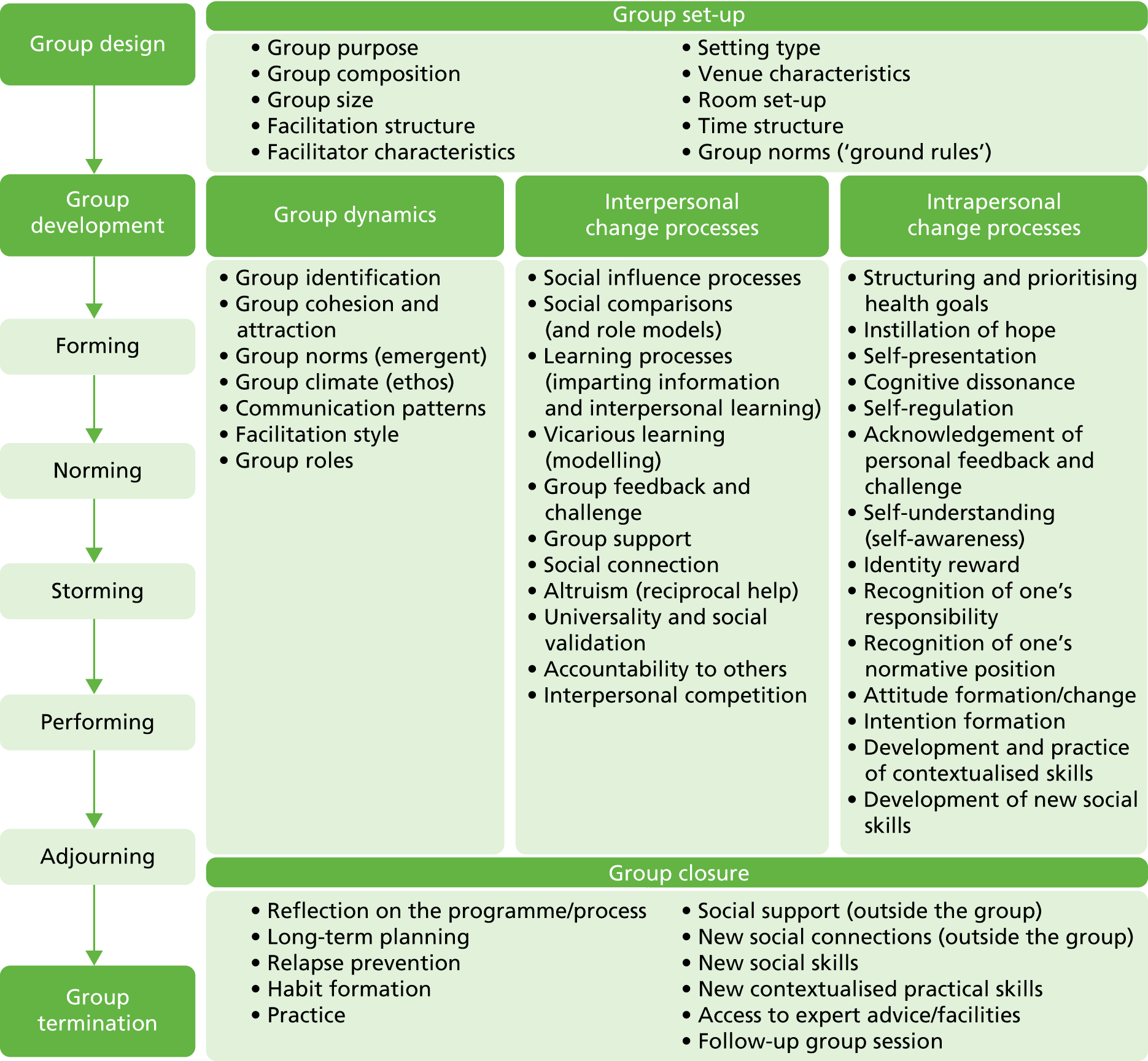
An updated version (Table 27) was presented at the Congress on Obesity conference (Nottingham, September 2016). A diagram (Figure 10) was developed at this stage to better illustrate the framework, and was revised following discussions with team members (Figures 11–14).
| Group set-up | Group dynamics | Interpersonal processes | Intrapersonal processes (examples) | Group closure |
|---|---|---|---|---|
|
|
|
|
|
| Group development | ||||
| Forming → Storming → Norming → Performing → Adjourning | ||||
FIGURE 10.
Diagram version 1 (September 2016).
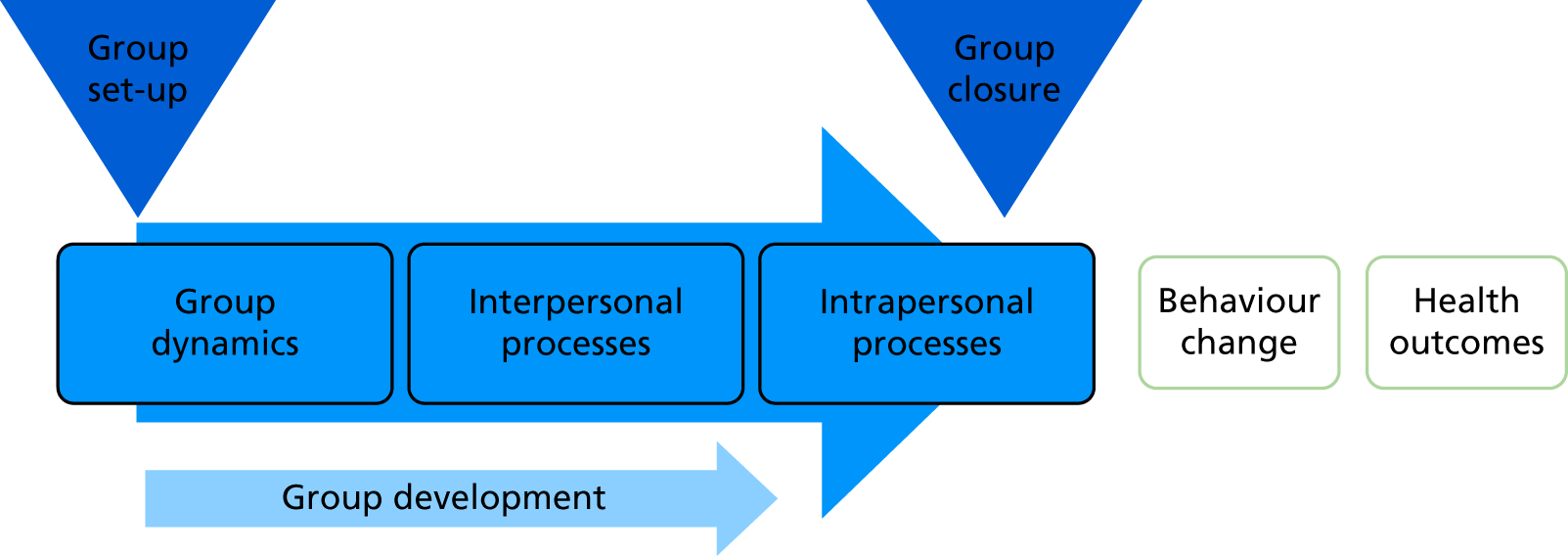
FIGURE 11.
Diagram version 2 (October 2016, following consultations with study team members, including RM).
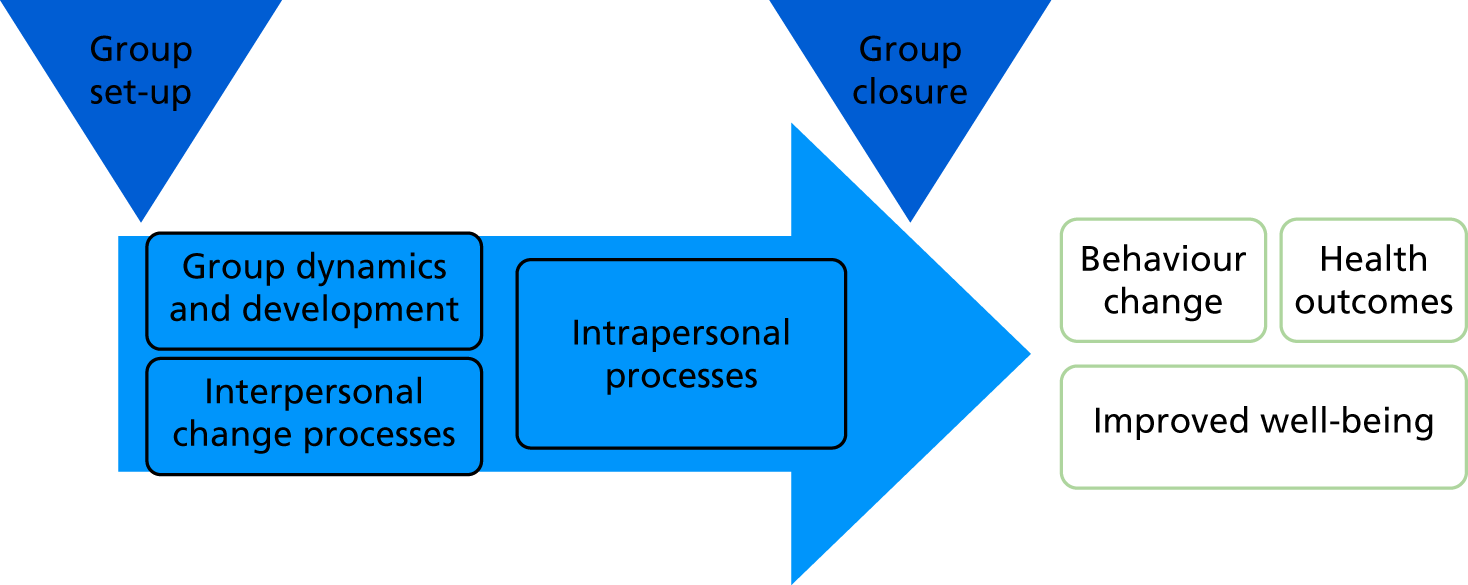
FIGURE 12.
Diagram version 3 (October 2016, following consultations with study team members, including FG).
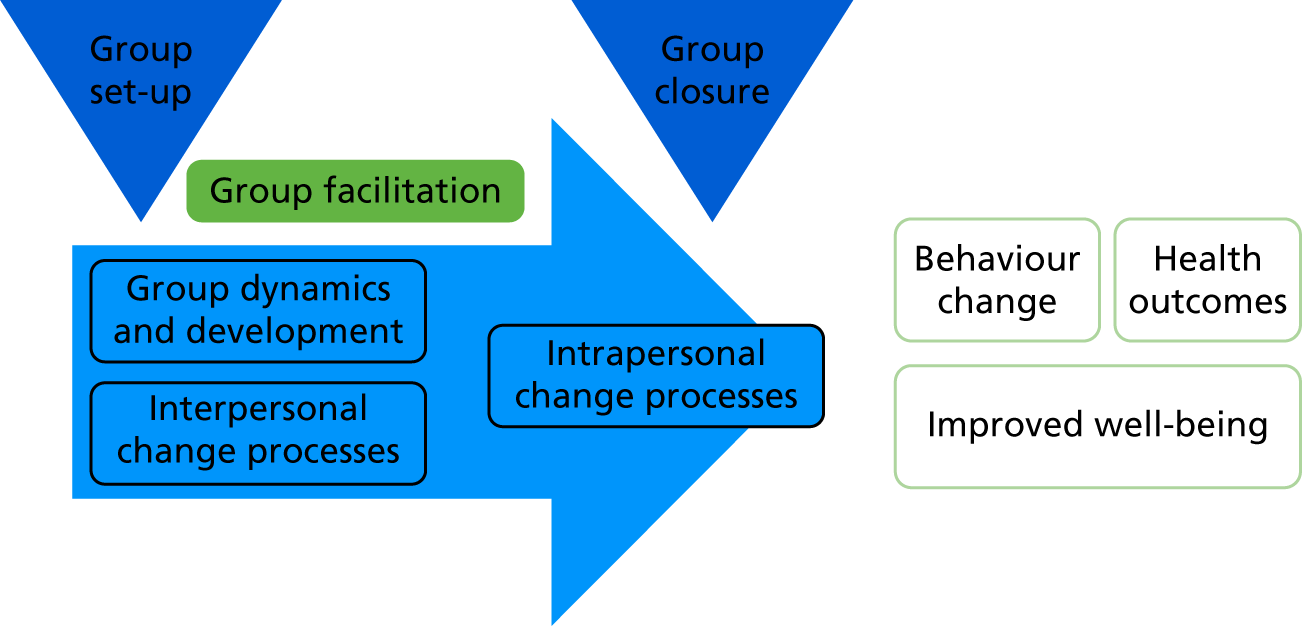
FIGURE 13.
Diagram version 4 (October 2016, following consultations with study team members, including MT).
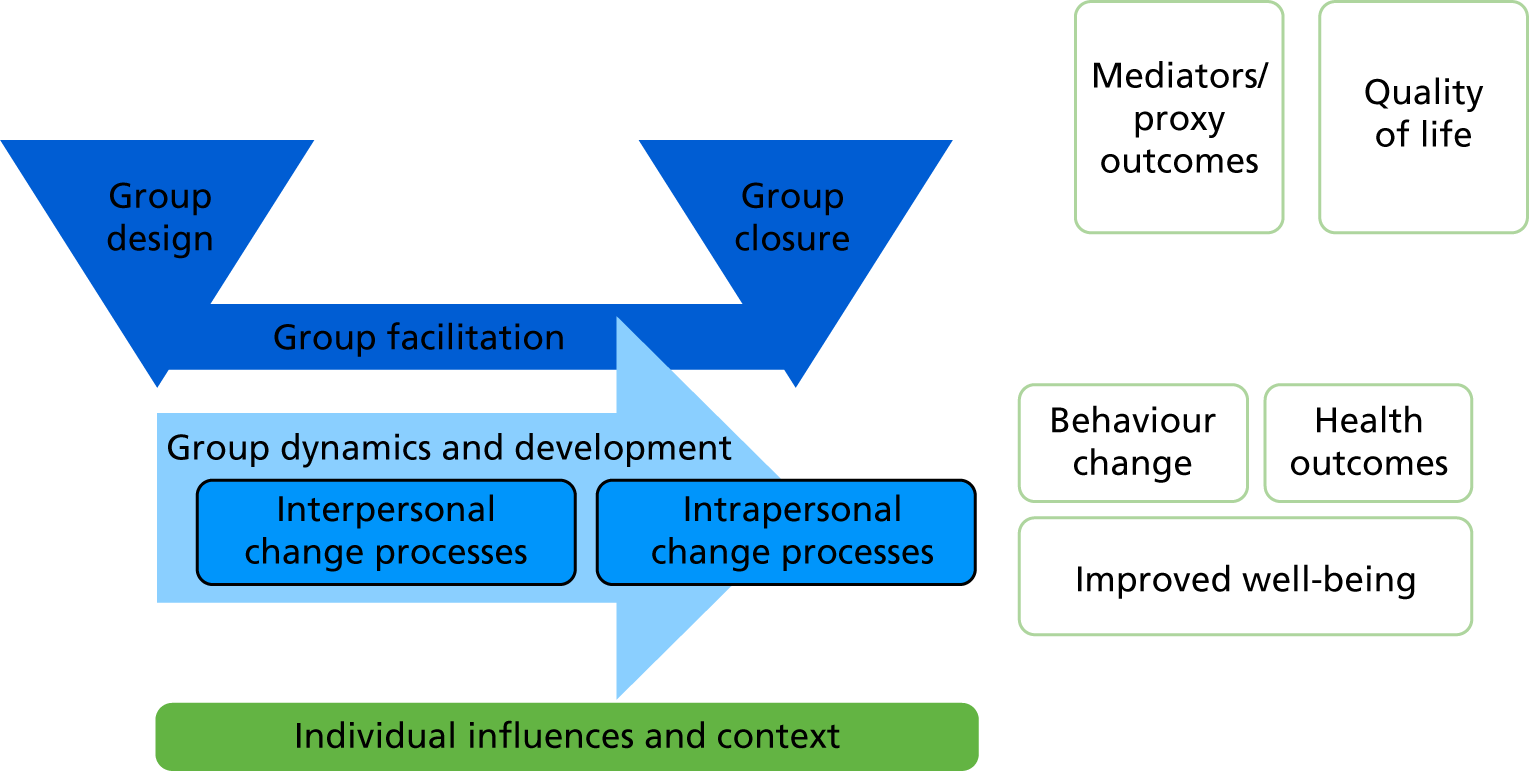
FIGURE 14.
Diagram version 5 (October 2016, following consultations with study team members, including CA).

Corresponding with the changes in the diagram, we also made changes in the framework, resulting in version 3 (Table 28).
| Group design elements | Group forming tasks | Group facilitation strategies | Group closure tasks |
|---|---|---|---|
|
Group dynamic and development processes | ||
|
|||
| Interpersonal change processes | Intrapersonal change processes | ||
|
|
||
| Individual characteristics and background | |||
Diagram version 5 and framework version 3 were presented to group participants at the ComPoD/MAGI Patient and Public Involvement meeting (31 October 2016). No new categories were added, but many were illustrated by examples of participants’ experiences in groups.
Diagram version 6 (Figure 15) and framework version 4 (Table 29) were discussed at the study team meeting 3 (November 2016), presented and discussed at the pre-conference workshop (UK Society for Behavioural Medicine, Cardiff, November 2016) and were presented at the International Congress of Behavioural Medicine (Melbourne, VIC, December 2016). The diagram and framework were then revised further following qualitative coding of transcripts, study team discussions and wider consultations, as indicated in Figures 16–18 and Tables 30 and 31.
FIGURE 15.
Diagram version 6 (November 2016, following consultations with study team members, including CG and CA).
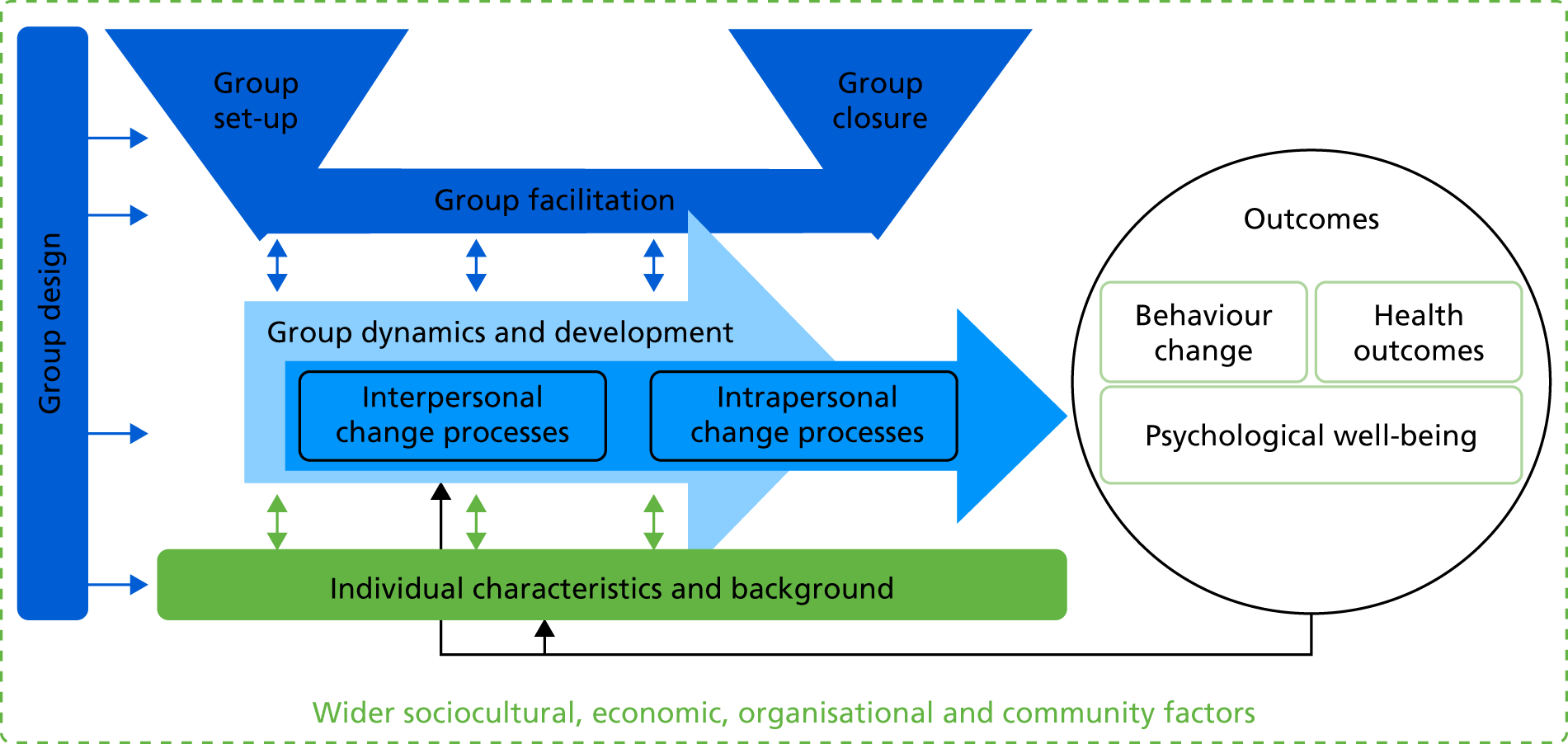
| Group design elements | Group set-up tasks | Group facilitation strategies | Group closure tasks | |
|---|---|---|---|---|
|
|
Group dynamic and development processes
|
|
|
Interpersonal change processes
|
Intrapersonal change processes
|
|||
Individual characteristics and background
|
||||
FIGURE 16.
Diagram version 7 (May 2017; diagram revised following development of the coding schema, double-coding of transcripts and refinements to the coding schema and the framework).
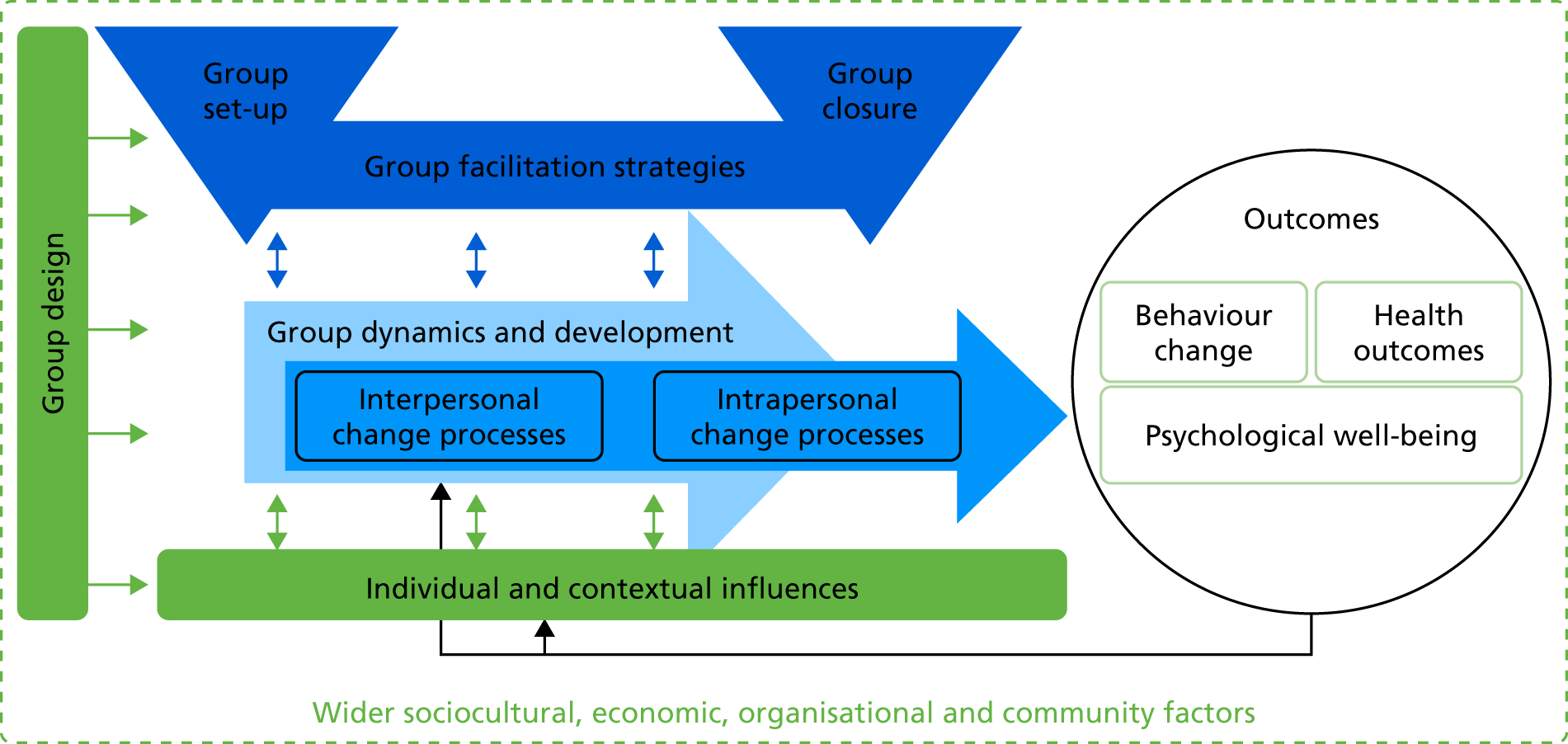
FIGURE 17.
Diagram version 8 (July 2017, continued discussions with study team members).
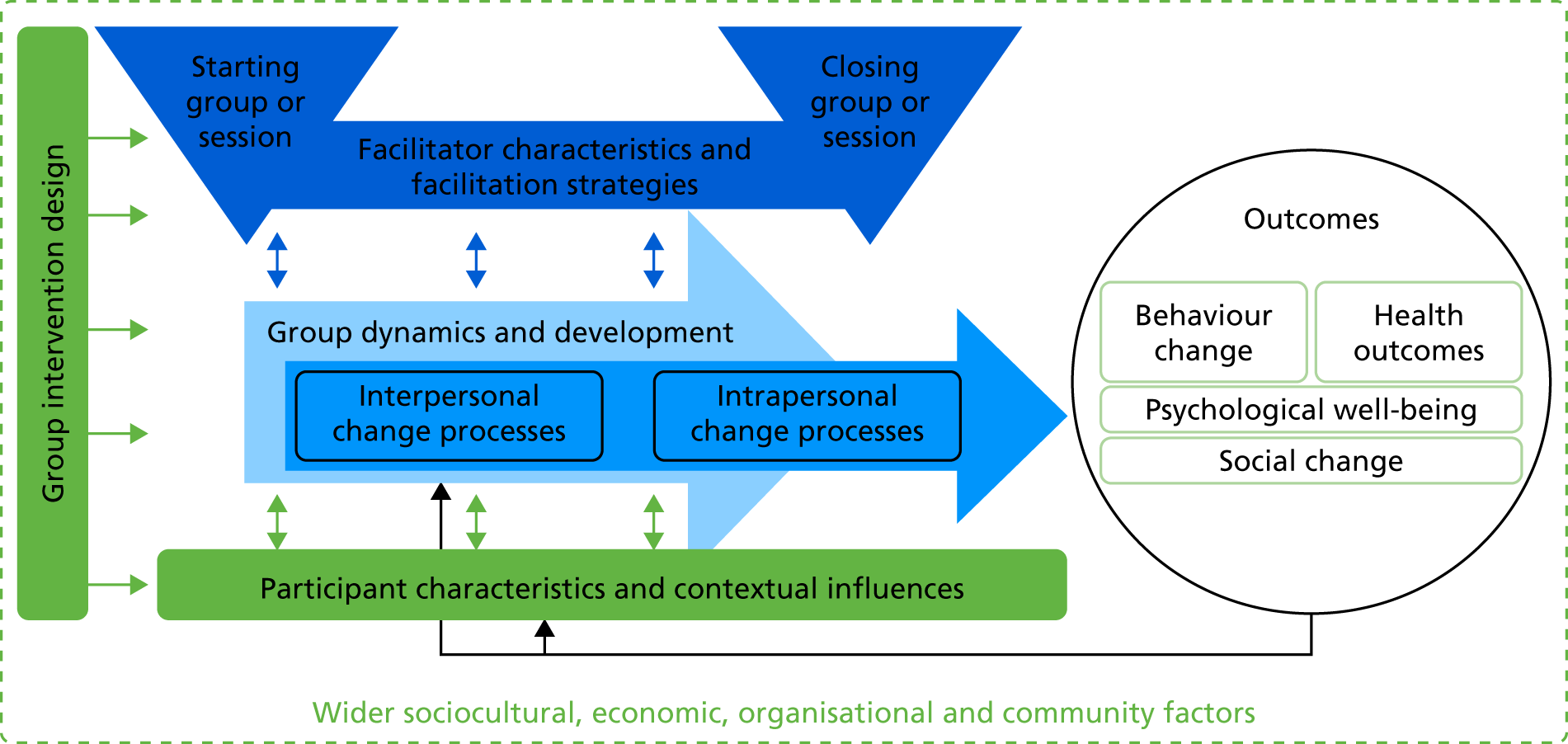
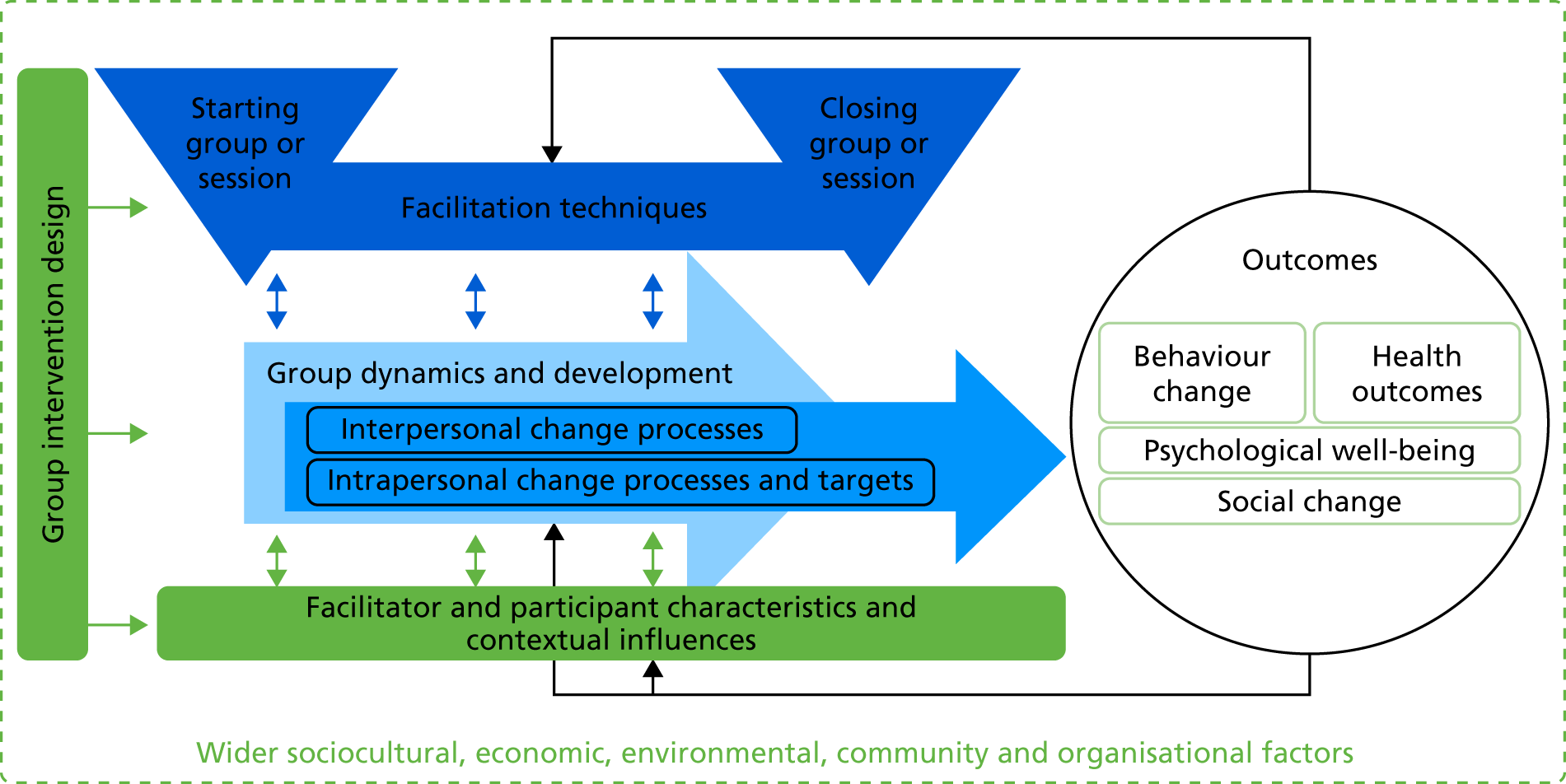
| 1. Group intervention design | 2. Facilitator characteristics and facilitation strategies | |||
|---|---|---|---|---|
| 2.1. Facilitator characteristics | 2.2. Tasks for starting the group/session | 2.3. Facilitation strategies | 2.4. Tasks for closing the group/session | |
| 1.1. Intended changes and processes | 3. Group dynamic and development processes | |||
|
|
|
||
| 4. Interpersonal change processes | 5. Intrapersonal change processes | |||
|
|
|
||
| 6. Participant characteristics and contextual influences | ||||
| 6.1. Individual personality, cognitive and emotional characteristics | 6.2. Contextual social influences | |||
| 1. Group intervention design | 2. Facilitator characteristics and facilitation strategies | |||
|---|---|---|---|---|
| 2.1. Facilitator characteristics | 2.2. Tasks for starting the group/session | 2.3. Facilitation strategies | 2.4. Tasks for closing the group/session | |
| 1.1. Intended changes and processes | 3. Group dynamic and development processes | |||
|
|
|
||
| 4. Interpersonal change processes | 5. Intrapersonal change processes | |||
|
|
|
||
| 6. Participant characteristics and contextual influences | ||||
| 6.1. Individual psychosocial and clinical characteristics | 6.2. Contextual social influences | |||
Appendix 3 Details of the review of qualitative studies
This document reports the details of the methods and results of the review of qualitative studies of participants’ experiences of group-based weight loss interventions.
Study selection criteria
Population
-
Overweight, obese.
-
Can be at risk of, or with, type 2 diabetes or cardiovascular diseases.
-
Adults (at least 18 years of age).
-
Exclude: interventions that are specific to pregnant women, or people with mental health problems, learning difficulties or eating disorders.
Intervention type
-
Lifestyle, behaviour change, education.
-
AND targeting changes in diet and/or physical activity.
-
AND weight loss (interventions for prevention of diabetes or cardiovascular disease through weight loss and changes in diet/PA should be also included).
-
AND group-based (minimum of two sessions, minimum of three participants and minimum of one facilitator).
-
Exclude: prevention of weight gain, weight maintenance only, focused on eating disorders.
Comparators
-
Not applicable.
Outcomes
-
Participants’ experiences or perceptions of a group-based weight loss programme.
-
Exclude: when general experiences are reported only (e.g. of obesity, weight loss, diabetes, cardiovascular disease, barriers to/facilitators of weight loss or behaviour change) without reporting experiences/perceptions related to the group/group setting.
Study design
-
Qualitative (interviews, focus groups, narratives, observations).
-
Include also when qualitative methods are used as part of process evaluation and reported alongside quantitative results.
Other
-
Available in English.
-
Published in a peer reviewed journal from year 2000.
-
Excluded: conference abstracts, dissertations.
Search strategy
Databases (accessed via Ovid)
-
PsycARTICLES Full Text.
-
EMBASE.
-
Ovid MEDLINE In-Process & Other Non-Indexed Citations and Ovid MEDLINE.
-
Ovid MEDLINE Daily update.
-
Ovid MEDLINE Epub Ahead of Print.
-
PsycINFO.
-
Social Policy and Practice.
Dates
Searched from year 2000 to 28 June 2016 (date of last search).
Search strategy*
-
overweight.ti,ab
-
obese.ti,ab
-
1 or 2
-
lifestyle.ti,ab
-
diet.ti,ab
-
‘physical activity’.ti,ab
-
exercise.ti,ab
-
‘weight loss’.ti,ab
-
4 or 5 or 6 or 7 or 8
-
qualitative.ti,ab
-
interview$.ti,ab
-
10 or 11
-
3 and 9 and 12
-
Limit 13 to English language (limit not valid in Journals@Ovid, Social Policy and Practice; records were retained)
-
Limit 14 to human (limit not valid in Journals@Ovid, Social Policy and Practice; records were retained)
-
Limit 15 to humans (limit not valid in Journals@Ovid, Social Policy and Practice; records were retained)
-
Limit 16 to yr = ‘2000-Current’
-
Remove duplicates from 17.
*Following a reviewer’s suggestion, we also ran this search with the search term ‘focus group$.ti,ab’. The search returned four papers, one167 of which was potentially suitable for inclusion. However, on the basis of the full text, the study would not be included in the review as it did not include results of the focus groups (which were used as part of intervention development and are only mentioned in the methods section of the paper reporting the results of the intervention trial). Another of the four identified papers reported a survey and two were conducted with children/adolescents, so are also not suitable for inclusion.
FIGURE 19.
Flow diagram of selection of qualitative studies.
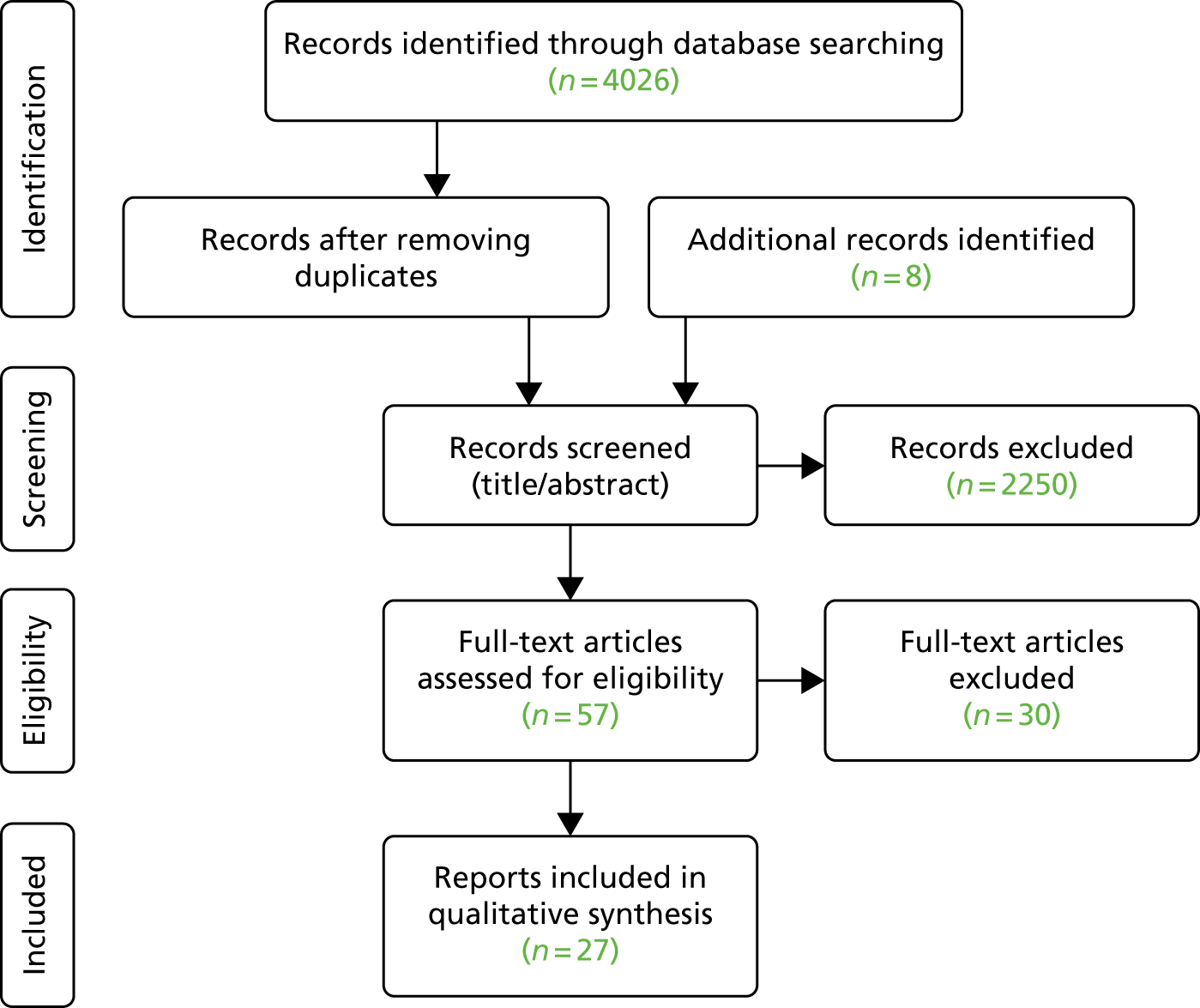
References of the included qualitative studies (numbers in superscript correspond with the reference numbers in the main list of References):
1. Adolfsson B, Carlson A, Undén AL, Rössner S. Treating obesity: a qualitative evaluation of a lifestyle intervention for weight reduction. Health Edu J 2002;61:244–58. https://doi.org/10.1177/00178969020610030682
2. Ahern AL, Boyland EJ, Jebb SA, Cohn SR. Participants’ explanatory model of being overweight and their experiences of 2 weight loss interventions. Ann Fam Med 2013;11:251–7. https://doi.org/10.1370/afm.144683
3. Ahlgren C, Hammarström A, Sandberg S, Lindahl B, Olsson T, Larsson C, Fjellman-Wiklund A. Engagement in new dietary habits – obese women’s experiences from participating in a 2-year diet intervention. Int J Behav Med 2016;23:84–93. https://doi.org/10.1007/s12529-015-9495-x84
4. Allen JT, Cohn SR, Ahern AL. Experiences of a commercial weight-loss programme after primary care referral: a qualitative study. Br J Gen Pract 2015;65:e248–55. https://doi.org/10.3399/bjgp15X68440985
5. Befort CA, Thomas JL, Daley CM, Rhode PC, Ahluwalia JS. Perceptions and beliefs about body size, weight, and weight loss among obese African American women: a qualitative inquiry. Health Educ Behav 2008;35:410–26. 86
6. Cifuentes M, Polsky S, Mitchell NS. Perspectives of older African American women on a community based weight loss program: qualitative findings from SWITCH. J Am Geriatr Soc 2014;62:1996–8. https://doi.org/10.1111/jgs.1304087
7. Diaz VA, Mainous AG, Pope C. Cultural conflicts in the weight loss experience of overweight Latinos. Int J Obes 2007;31:328–33. 88
8. Fogel S, Young L, McPherson JB. The experience of group weight loss efforts among lesbians. Women Health 2009;49:540–54. https://doi.org/10.1080/0363024090342401289
9. Gallagher R, Kirkness A, Armari E, Davidson PM. Participants’ perspectives of a multi-component, group-based weight loss programme supplement for cardiac rehabilitation: a qualitative study. Int J Nurs Pract 2012;18:28–35. https://doi.org/10.1111/j.1440-172X.2011.01988.x90
10. Gamsu D, Sutton M, Bennett L, Ward J. The development of a psychoeducational group intervention for overweight women with type 2 diabetes mellitus: a service evaluation. Pract Diab Int 2002;19:43–50. https://doi.org/10.1002/pdi.27991
11. Gimlin D. Constructions of ageing and narrative resistance in a commercial slimming group. Ageing Soc 2007;27:407–24. https://doi.org/10.1017/S0144686X0600575792
12. Gray CM, Hunt K, Mutrie N, Anderson AS, Leishman J, Dalgarno L, Wyke S. Football Fans in Training: the development and optimization of an intervention delivered through professional sports clubs to help men lose weight, become more active and adopt healthier eating habits. BMC Public Health 2013;13:232. https://doi.org/10.1186/1471-2458-13-23293
13. Groven KS, Engelsrud G. Dilemmas in the process of weight reduction: exploring how women experience training as a means of losing weight. Int J Qual Stud Health Well-being 2010;5:5125. https://doi.org/10.3402/qhw.v5i2.512594
14. Hammarström A, Wiklund AF, Lindahl B, Larsson C, Ahlgren C. Experiences of barriers and facilitators to weight-loss in a diet intervention – a qualitative study of women in northern Sweden. BMC Womens Health 2014;14:59. https://doi.org/10.1186/1472-6874-14-5995
15. Hansen NV, Brændgaard P, Hjørnholm C, la Cour S. Qualitative research building real-life interventions: user-involving development of a mindfulness-based lifestyle change support program for overweight citizens. Eur J Clin Nutr 2014;68:1129–33. https://doi.org/10.1038/ejcn.2014.10696
16. Hunt K, Gray CM, Maclean A, Smillie S, Bunn C, Wyke S. Do weight management programmes delivered at professional football clubs attract and engage high risk men? A mixed-methods study. BMC Public Health 2014;14:50. https://doi.org/10.1186/1471-2458-14-5097
17. Kidd LI, Graor CH, Murrock CJ. A mindful eating group intervention for obese women: a mixed methods feasibility study. Arch Psychiatr Nurs 2013;27:211–18. https://doi.org/10.1016/j.apnu.2013.05.00498
18. Ljung S, Olsson C, Rask M, Lindahl B. Patient experiences of a theory-based lifestyle-focused group treatment in the prevention of cardiovascular diseases and type 2 diabetes. Int J Behav Med 2013;20:378–84. https://doi.org/10.1007/s12529-012-9252-399
19. McMahon NE, Visram S, Connell LA. Mechanisms of change of a novel weight loss programme provided by a third sector organisation: a qualitative interview study. BMC Public Health 2016;16:378. https://doi.org/10.1186/s12889-016-3063-4100
20. Metzgar CJ, Preston AG, Miller DL, Nickols-Richardson SM. Facilitators and barriers to weight loss and weight loss maintenance: a qualitative exploration. J Hum Nutr Diet 2015;28:593–603. https://doi.org/10.1111/jhn.12273101
21. Östberg AL, Wikstrand I, Bengtsson Boström K. Group treatment of obesity in primary care practice: a qualitative study of patients’ perspectives. Scand J Public Health 2011;39:98–105. https://doi.org/10.1177/1403494810391524102
22. Penn L, Dombrowski SU, Sniehotta FF, White M. Participants’ perspectives on making and maintaining behavioural changes in a lifestyle intervention for type 2 diabetes prevention: a qualitative study using the theory domain framework. BMJ Open 2013;3:e002949. https://doi.org/10.1136/bmjopen-2013-002949103
23. Penn L, Dombrowski SU, Sniehotta FF, White M. Perspectives of UK Pakistani women on their behaviour change to prevent type 2 diabetes: qualitative study using the theory domain framework. BMJ Open 2014;4:e004530. https://doi.org/10.1136/bmjopen-2013-004530104
24. Piana N, Battistini D, Urbani L, Romani G, Fatone C, Pazzagli C, et al. Multidisciplinary lifestyle intervention in the obese: its impact on patients’ perception of the disease, food and physical exercise. Nutr Metab Cardiovasc Dis 2013;23:337–43. https://doi.org/10.1016/j.numecd.2011.12.008105
25. Sheppard VB, Hicks J, Makambi K, Hurtado-de-Mendoza A, Demark-Wahnefried W, Adams-Campbell L. The feasibility and acceptability of a diet and exercise trial in overweight and obese black breast cancer survivors: the Stepping STONE study. Contemp Clin Trials 2016;46:106–13. 106
26. Tarrant M, Khan SS, Farrow CV, Shah P, Daly M, Kos K. Patient experiences of a bariatric group programme for managing obesity: a qualitative interview study. Br J Health Psychol 2017;22:77–93. https://doi.org/10.1111/bjhp.1221849
27. Walker LO, Sterling BS, Latimer L, Kim SH, Garcia AA, Fowles ER. Ethnic-specific weight-loss interventions for low-income postpartum women: findings and lessons. West J Nurs Res 2012;34:654–76. https://doi.org/10.1177/0193945911403775107
The themes and subthemes reported in Table 32 were derived from coding the results of the qualitative studies. The themes and subthemes were subsequently refined to match with the refined version of the MAGI framework (in structure and naming of categories), and the qualitative studies were re-coded when necessary.
| Higher organising themes (factors affecting participants’ experiences of weight loss groups) | Identified subthemes (concepts and processes) [studies in which they were identified (numbers correspond with the list above)] |
|---|---|
| Individual factors that may affect experiences of groups and weight loss) | Beliefs about reasons for obesity, barriers to change [1, 4, 5, 10, 11, 21 and 24] |
| Comparing types of interventions [1, 2, 4, 5, 8, 10, 11, 13, 16, 21 and 24] | |
| Expectations of the programme or weight loss [1, 7, 12 and 16] | |
| Motivation for participation, weight loss, or barriers (costs, diagnosis/tipping point, health vs. attractiveness) [1–9, 11, 16, 17, 19, 21, 24 and 26] | |
| Perceptions of groups or weight loss [4, 8, 24 and 27] | |
| Preference for groups, views about benefits of groups [2, 5, 7, 10 and 15] | |
| Social support outside the group [1–3, 5, 7, 11, 14, 19–21, 24, 25 and 27] | |
| Taking responsibility (agency, locus of control) [2] | |
| Group design factors that can/should be decided on before the group start) | Access to other facilities [9, 12 and 21] |
| Contact time – during the programme [1–5, 9, 12, 14, 25 and 27] | |
| Contact time – at the end of the programme, follow-up [1, 2, 5, 6, 12, 25 and 27] | |
| First (few) sessions [12 and 16] | |
| Group composition [8, 9, 12, 13, 16 and 18] | |
| Group size [12] | |
| Long-term approach, weight loss maintenance [2, 6, 9 and 18] | |
| Participation in research study [2–4, 9, 17, 21 and 27] | |
| Significant others attending the group [1, 7 and 9] | |
| Structuring, flexibility of delivery [6, 8 and 9] | |
| Tailoring [2, 5, 6, 7, 8, 9, 12, 18, 21 and 25] | |
| Venue [2, 8, 12, 16 and 27] | |
| Facilitator-related factors (affecting group delivery and participants’ experiences) | Facilitators and facilitation (interpersonal qualities, professional qualities, facilitation style/approach, facilitator social identity) [2, 6, 8, 10, 12, 13, 16, 18 and 24–27] |
| Group context (factors related to group context but not directly related to change) | Group climate [2, 8, 9, 10, 12, 13, 15, 16, 17, 24 and 26] |
| Group cohesion [2, 8, 12, 13, 16, 17, 19, 21 and 25] | |
| Humour [12, 15 and 16] | |
| Identification (like-mindedness, shared experiences/problems, social identities) [1, 5, 7, 8, 9, 10, 12, 13, 16, 17, 18, 21, 24, 25 and 26] | |
| Socialising, ‘me time’ [13, 16, 24 and 27] | |
| Change processes (factors related to change in groups, benefits of group participation) | Accountability [2–4, 5, 6, 8, 13, 17, 20, 21 and 25] |
| Competitiveness [7, 9 and 21] | |
| Feedback, measurements [4, 9, 12, 13, 17 and 27] | |
| Information, knowledge (learning) [1, 2, 7, 9, 10, 12, 18, 19 and 24–27] | |
| Learning from each other, imitation (social learning) [2, 3, 6, 7, 9, 18, 19 and 26] | |
| Motivation in the group [1, 2, 5, 6, 7, 12, 13, 21 and 24] | |
| Peer, group pressure [1, 2, 18 and 21] | |
| Problem-solving [1 and 2] | |
| Role models, social comparisons [7, 12, 13, 18 and 19] | |
| Sharing, interaction [1, 2, 8–13, 15, 17, 21, 24 and 25] | |
| Social support in the group [1–3, 5–15, 17–21 and 25–27] | |
| Practical delivery strategies and content (used in delivering weight loss groups) | Activities, practical skills [1, 3, 6, 10, 12, 14, 15, 21, 25 and 26] |
| Content of intervention or sessions [1, 2, 6, 8, 10, 12, 21 and 27] | |
| Homework [1] | |
| Participants’ materials [6, 9 and 25] | |
| Weighing [2–4, 8, 11, 12, 13 and 27] |
Appendix 4 Details of expert consultations
This appendix includes details of expert consultations undertaken in the MAGI study.
These consultations were conducted with researchers/practitioners (with experience in group-based health interventions), group facilitators, and group participants.
The aims of these consultations were to:
-
identify potentially important factors (e.g. processes, techniques) that may affect the delivery of outcomes of group-based health interventions in order to include them in the MAGI framework
-
seek feedback on the MAGI framework (the included, and potentially missing, processes and techniques, framework presentation and its potential usefulness).
Meeting notes were kept from each of the consultations and can be provided on request. Below we summarise the details of the consultations, including type, date, participants and key implications.
Consultations with researchers and practitioners
Internal seminar at the University of Exeter Medical School, Exeter [June 2016, after initial draft framework was developed (version 1)]:
-
The seminar was advertised in the department and was open to all staff members.
-
Eleven participants (and four study team members) had expertise in behaviour change or experience of research in group-based health interventions.
-
In the seminar, we presented the emerging framework and discussed each of the framework categories, including their importance, implications and examples. The discussions validated the emerging framework, and provided examples used in the framework definitions.
-
The participants highlighted (with examples from own studies) the importance of group composition, shared social identities (in particular if they are stigmatised), characteristics of facilitators (e.g. being overweight themselves), setting group rules, participants’ contact outside the groups (e.g. setting up social media groups).
-
They also raised the issue of whether or not, and how, the framework might apply to other types of groups (e.g. online, knitting groups).
Pre-conference workshop, UK Society for Behavioural Medicine, Cardiff [November 2016, after draft framework was developed and revised (version 2)]:
-
The workshop was advertised on the conference website and was open to any interested participants.
-
Nine participants attended, including researchers and practitioners.
-
The participants were initially asked to brainstorm important, in their opinion, components and processes in group-based interventions. The identified elements were compared with the emerging framework, which was presented in the workshop. All of the components and processes identified by the workshop participants could be matched with the framework elements. The processes and components were discussed, and participants shared examples from their own research and practice supporting the importance of framework components and providing suggestions about links between them. The participants brainstormed facilitation techniques that could be used to facilitate selected group dynamics and change processes.
-
The feedback on the framework, collected at the end of the workshop, was generally positive and validated the framework. For example, the participants gave an average of 6.3 (out of 7) to the question of how useful they through the framework was to them. Some provided positive overall feedback (e.g. ‘Really interesting workshop and discussion. Chimes with a lot of issues raised in my recent work.’). They also identified potential applications of the framework for design/development and evaluation of group-based interventions, and as a resource to learn about processes in groups (e.g. ‘[The framework is] very useful – putting a name to all the group processes helps to know exactly where to intervene and how we might be able to manipulate these factors’).
-
Key implications: validation of the framework; suggestions for how the framework could be used in design, delivery and evaluation of group-based interventions.
-
E-mail and in-person consultations with/feedback from an internal researcher (from the University of Exeter Medical School; August and September 2017, after near-final version of the framework was ready).
-
We shared the framework and the coding schema with Dr Poltawski, who has expertise in group dynamics, group-based health interventions and was involved in the SkiM study.
-
He used the coding schema to code a session transcript, and provided feedback on the framework categories and definitions.
-
The feedback was used to refine definitions of several of the framework definitions and coding schema (including facilitation techniques). Dr Poltawski raised also few important points that were incorporated in our write-up.
E-mail consultations with/feedback from external researchers/practitioners (August to September 2017, the near-final version of the framework – the final version was developed on the basis of the comments from researchers and facilitators):
-
We contacted 12 researchers with expertise in group-based/behaviour change interventions who we met during the conferences where we presented the framework (see below) and who expressed interest and relevant expertise in GB-BCIs. Eleven of them replied agreeing to provide feedback, and we received feedback from eight researchers: Dr Amanda Avery, Dr Yael Bar-Zeev, Dr Enzo Di Battista, Dr Tegan Cruwys, Dr Liz Glidewell, Dr Cindy Gray, Dr Marta Moreira Marques and Dr James Nobles.
-
The framework was shared and feedback (either more general or very detailed, depending on availability) was invited.
-
All provided feedback was carefully considered, discussed with the study team, and when agreed, changes were made to the framework or framework definitions. We used the feedback to clarify distinctions between, and consistency of, the terminology (e.g. techniques, processes), made revisions to the writing of the results of stage 1 (e.g. adding clarifications and points raised in the feedback), and made some changes to the diagram [see difference between Figure 17 (diagram 8) and Figure 18 (the final diagram 9)]. A detailed record of the changes made in result of these consultations was kept.
-
We also asked for general feedback on the framework and about potentials usefulness and applicability of the framework. The views about the framework were generally positive (e.g. ‘I think this level of detail is fantastic. This will be really useful for those reading it moving forward . . . To me, this really highlights the complexity of a group-based programme and the factors at play throughout the intervention time frames. Therefore, this will be beneficial to research teams and also to practitioners, however the level of detail required by all will vary – hence why I really like the definitions and explanations, very useful!’).
-
The researchers identified potential applicability of the framework to the following:
-
designing group interventions
-
characterising and reporting of group interventions and their content and processes
-
recruiting and training facilitators (in an adapted form)
-
evaluating complex group interventions and their specific components.
-
Consultations with group facilitators
Consultation with LWTC/SkiM facilitators [August 2016, after initial draft framework was developed (version 1)]:
-
The facilitators included Miss Amy Clarke and Miss Sian Derrick, who were personally invited to the consultations as they were delivering the LWTC and SkiM group sessions at the time of this study.
-
This meeting involved an open discussion about facilitating groups, how they work, important processes that occur, techniques that facilitators use, challenges to facilitation and facilitators’ training needs.
-
The facilitators provided many examples of different groups, group processes, and techniques that they use. For example, they reported on the importance of certain processes, such as managing disagreements, conflicts and ‘difficult’, disruptive participants; benefits and challenges of co-facilitation; homogeneous group composition (seen as helping with group cohesion); and participants making social connections with each other (also outside the groups). They reported using particular techniques with quiet groups and groups that were not engaging, such as using room layout (participants facing each other), subgroup discussions and activities, and practical activities (e.g. doing simple exercises). They raised the issue of positive or negative effects of successful participants (‘role models’) and social comparisons (e.g. those doing much better than the rest of the group seemed to be ‘excluded’ from the group rather than seen as role models). They also highlighted a need for facilitator training in managing difficult participants and in responding to self-disclosures of mental health issues.
-
The notes from the meeting were then compared and matched with the emerging framework to validate the framework, checking for any new processes/concepts and contribute to writing the framework definitions.
Consultation with LWTC/SkiM facilitators (September 2017, the near-final version of the framework – the final version was developed on the basis of the comments from researchers and facilitators):
-
The facilitators were Miss Amy Clarke, Miss Sian Derrick, Mrs Anna Murch and Mrs Ruby Entwistle, who were personally invited to the consultations as they were past and current facilitators of the LWTC or SkiM interventions.
-
The framework, and the identified facilitator techniques, were shared and discussed with the facilitators in detail.
-
The facilitators provided feedback, and further examples of how the framework processes occur in the groups and of what facilitation techniques they use. They highlighted the importance of many framework components. They also identified ways in which the framework could be helpful to facilitators, which included training new facilitators (raising awareness of many available processes and techniques), training (or ‘refresher’ training) existing or experienced facilitators (giving them ‘names’ to capture the processes and techniques that they know from experience, and raising awareness of ways to further improve their understanding of certain processes), using it to structure feedback to existing facilitators (or co-facilitators’ feedback to each other), and preparing participants for what to expect from groups. They also reflected on the impact that facilitating groups had on themselves (e.g. prompting them in making changes in their own lifestyles of careers). They also recognised the importance of the wider societal factors, or determinants, affecting health and well-being (outside the groups).
Consultations with group participants
Patient and public involvement representatives from the ComPoD trial [June 2016, after initial draft framework was developed (version 1)]:
-
Including Mrs Sue Sedgman and Mr Douglas Osman, both of whom were personally invited to the consultations as they participated in the LWTC programme and acted as Patient and Public Representatives in the ComPoD trial.
-
The emerging framework was shared with the participants and discussed in detail. The participants provided examples from the groups that illustrated (or could be matched with) the framework processes. They also described how these elements might have influenced each other and outcomes. They highlighted group goals and facilitation style/techniques as particularly important.
-
Based on this consultation some elements were added to the framework (e.g. pre-session information and contact, participants’ and facilitators’ materials).
Patient and public involvement representative from the ComPoD trial [October 2016, after draft framework was developed and revised (version 2)]:
-
Included four patient and public involvement representatives, all of whom were personally invited to the consultations as participants and patient and public representatives in the ComPoD trial.
-
The framework and MAGI study was briefly explained, and participants shared their experiences of attending the groups and opinions about how they thought the groups worked, and what processes or components were most important. They highlighted the importance of pre-session information/contact; experiences of dealing with research staff and facilitators (i.e. importance of positive characteristics of facilitators); and positive expectations of the intervention and outcomes (e.g. they felt that the programme should be advertised as having much wider positive impact on health and well-being than just prevention of diabetes or weight loss). Other elements were discussed as important, such confidence and responsibility for self, setting and venue, purpose and benefits of using groups, group composition, social comparisons and competition, and facilitator characteristics.
-
The notes were compared with the MAGI framework to match with the framework categories and check for any new categories.
Consultations and discussions with the study team members
-
Pre-study planning meeting (December 2015).
-
Study team meeting 1 (January 2016).
-
Study team meeting 2 (June 2016).
-
Study team meeting 3 (November 2016).
-
Study team meeting 4 (June 2017).
-
Study team meeting 5 (September 2017).
-
Between study team meetings, Jane R Smith and Aleksandra J Borek consulted individual study team members (CA, CG, FG, MT, SMT and RMC).
In addition, the MAGI framework was presented at the following conferences, which offered opportunities for additional discussions with researchers and practitioners:
-
Congress on obesity conference, Nottingham (September 2016, oral presentation): Table 27 (framework version 2) and Figure 10 (version 1) were presented.
-
International Congress of Behavioual Medicine conference, Melbourne, VIC (December 2016, oral presentation): Table 29 (framework version 4) and Figure 15 (version 6) were presented.
-
International Society for Behavioral Nutrition and Physical Activity conference, Victoria, BC (June 2017, oral presentation): Table 31 (near-final framework version 6) and Figure 18 (final, version 9) were presented.
-
European Health Psychology Society conference, Padua (August 2017, poster): Table 31 (near-final framework version 6) and Figure 18 (final, version 9) were presented.
-
Society for Social Medicine conference, Manchester (September 2017, poster): Table 31 (near-final framework version 6) and Figure 18 (final, version 9) were presented.
Appendix 5 Measures of group processes
This document includes a summary of the measures of group processes. We identified and used helpful reviews of measures of group processes,108–110 which reported the measures listed below. For details of the measures, please refer to the reviews or the original reports of the measures. The measures might not correspond exactly with the MAGI framework categories (i.e. they might be operationalised differently in the measures and in the framework.) They were used to identify the key approaches to assessing group processes and to identify key concepts and processes.
-
Measures of facilitators’ skills and behaviour, for example:
-
General measures of interpersonal processes and interaction in groups, for example:
-
Interaction Process Analysis111 and System for Multiple Level Observation of Groups172 – Group interaction, group roles, interpersonal behaviour and relationships.
-
Hill Interaction Matrix173,174 – group interaction, group processes and group development.
-
Individual Group Member Interpersonal Process Scale175,176 – group cohesion and interaction.
-
Interpersonal Relations Scale177 – group knowledge, skills and interaction.
-
Group Sessions Rating Scale178,179 – coping skills, problem-solving, interpersonal learning.
-
Ferrara Group Experiences Scale180 – group experiences, including sharing, relationships, learning processes.
-
-
Self-disclosure and feedback behaviours. 181
-
Social identification processes: measures of identity, health, and well-being. 46
-
Group dynamics (group climate, cohesion, engagement), for example:
-
Group Climate Questionnaire153 – group climate (engagement, avoidance, conflict).
-
Group Environment Scale182 – dimensions of group environment: relationship, personal growth, system maintenance and change.
-
Group Environment Questionnaire54 – cohesion in exercise groups, based on four dimensions: attraction to group task, attraction to the group social, group integration social, group integration task.
-
Group Questionnaire183– therapeutic relationships.
-
Group Cohesiveness Scale175 – group cohesion defined as connectedness (withdrawal, self-absorption, interest, involvement, mistrust/trust, disruption/co-operation, abusiveness/caring, unfocused/focused).
-
Group Engagement Measure. 184
-
-
Measures of Yalom’s therapeutic factors, for example:
References of the identified measures:
1. Bales RF. Interaction Process Analysis: A Method for the Study of Small Groups. Vol. XI. Oxford: Addison-Wesley; 1950. 111
2. Bales RF, Cohen SP, Williams SA. SYMLOG: A System for the Multiple Level Observation of Groups. New York, NY: Free Press; 1979. 172
3. Bolman L. Some effects of trainers on their T groups. J Appl Behav Sci 1971;7:309–25. 170
4. Budman SH, Soldz S, Demby A, Davis M, Merry J. What is cohesiveness? An empirical examination. Small Gr Res 1993;24:199–216. 175
5. Butler T, Fuhriman A. Level of functioning and length of time in treatment variables influencing patient’s therapeutic experience in group psychotherapy. Int J Group Psychother 1983;33:489–504. 185
6. Cahill J, Barkham M, Hardy G, Gilbody S, Richards D, Bower P, et al. A review and critical appraisal of measures of therapist-patient interactions in mental health settings. Health Technol Assess 2008;12(24). 108
7. Caruso R, Grassi L, Biancosino B, Marmai L, Bonatti L, Moscara M, et al. Exploration of experiences in therapeutic groups for patients with severe mental illness: development of the Ferrara Group Experiences Scale (FE-GES). BMC Psychiatry 2013;13:242. 180
8. Cooney NL, Kadden RM, Litt MD, Getter H. Matching alcoholics to coping skills or interactional therapies: two year follow up results. J Consult Clin Psychol 1991;59:598–601. 178
9. Corey MS, Corey G. Group Counseling: Process and Practice, 4th edn. Monterey, CA: Brooks/Cole; 1992. 168
10. Delucia-Waack JL. Measuring the effectiveness of group work: a review and analysis of process and outcome measures. J Spec Group Work 1997;22:277–93. https://doi.org/10.1080/01933929708415531109
11. Estabrooks PA, Carron AV. The physical activity group environment questionnaire: an instrument for the assessment of cohesion in exercise classes. Group Dyn: Theory Res Pract 2000;4:230–43. 54
12. Getter H, Litt MD, Kadden RM, Cooney NL. Measuring treatment process in coping skills and interactional group therapies for alcoholism. Int J Group Psychother 1992;42:419–30. 179
13. Hill WF. The Hill Interaction Matrix. Pers Guid J 1971;49:619–22. 173
14. Hill F. Hill Interaction Matrix (HIM): the conceptual framework, derived rating scales, and an updated bibliography. Small Group Behav 1977;8:251–68. 174
15. Jetten J, Haslam C, Haslam SA. The Social Cure: Identity, Health and Well-Being. Hove and New York, NY: Psychology Press; 2011. 46
16. Kivlighan DM, Goldfine DC. Endorsement of therapeutic factors as a function of stage of group development and participant interpersonal attitudes. J Couns Psychol 1999;38:150–8. 187
17. Krogel J, Burlingame G, Chapman C, Renshaw T, Gleave R, Beecher M, Macnair-Semands R. The Group Questionnaire: a clinical and empirically derived measure of group relationship. Psychother Res 2013;23:344–54. https://doi.org/10.1080/10503307.2012.729868183
18. Lese K, MacNair-Semands RR. The therapeutic factors inventory: development of a scale. Group 2000;24:303–17. 186
19. MacKenzie KR. The Clinical Application of a Group Climate Measure. In Dies RR, MacKenzie KR, editors. Advances in Group Psychotherapy: Integrating Research and Practice. New York, NY: International Universities Press; 1983. pp. 159–170. 153
20. Macgowan MJ. The group engagement measure: a review of its conceptual and empirical properties. J Groups Addict Recover 2006;1:33–52. 184
21. McGuire JM, Taylor DR, Broome DH, Blau BI, Abbott DW. Group structuring techniques and their influence on process involvement in a group counseling training group. J Couns Psychol 1986;33:270–5. 181
22. Moos RH. Group Environment Scale Manual. Palo Alto, CA: Consulting Psychologists Press; 1986. 182
23. Orfanos S. Measures of Group Processes: A Review of Questionnaire-Based, Interactional-Analysis and Qualitative Approaches. Group Therapies for Schizophrenia: Identifying and Linking Group Interactions and Group Experiences with Outcomes. PhD Thesis. London: Queen Mary University of London; 2016. 110
24. Shadish WR. The validity of a measure of intimate behavior. Small Group Behav 1986;17:113–20. 177
25. Soldz S, Budman S, Davis M, Demby A. Beyond the interpersonal circumplex in group psychotherapy: the structure and relationship to outcome of the Individual Group Member Interpersonal Process Scale. J Clin Psychol 1993;49:551–63. 176
26. Stinchfield RD, Burlingame GM. Development and use of the directives rating system in group therapy. J Couns Psychol 1991;38:251–7. 171
27. Stone MH, Lewis CM, Beck AP. The structure of Yalom’s Curative Factors Scale. Int J Group Psychother 1994;44:239–45. 188
28. Tinsley HEA, Roth JA, Lease SH. Dimensions of leadership and leadership style among group intervention specialists. J Couns Psychol 1989;36:58–3. 169
Appendix 6 Initial coding categories developed from manuals and transcripts
This appendix includes the initial coding schema developed by inductively (bottom-up) coding of interventions manuals and the first 10 transcripts of group sessions. The categories are reported in alphabetical order (as they were listed and named in NVivo).
Initial coding schema developed during coding of intervention manuals:
-
Group set-up –
-
absences (dealing with)
-
access to facilities
-
contact participants – facilitators (outside groups)
-
degree of tailoring, flexibility of delivery
-
facilitator’s role
-
intended facilitation, delivery style
-
materials for facilitators
-
time structure
-
venue.
-
-
Group, session opening –
-
benefits of group work
-
hopes and fears of the programme
-
introducing the programme
-
introducing the session
-
introductions, icebreakers
-
recap of previous session.
-
-
Group dynamics –
-
dealing with challenges, disruptive participants
-
group climate
-
group cohesion, attraction
-
group goals
-
group identification
-
group norms, rules
-
participants’ roles.
-
-
Self-regulatory techniques –
-
goal-setting, action-planning
-
goals, progress review
-
problem-solving, barriers identification
-
self-monitoring.
-
-
What happens in the sessions –
-
ASK – discussing, participation, sharing, brainstorming
-
TELL – providing information, advice, instructions
-
activities in groups
-
competition, co-operation
-
development, practice of skills
-
instillation of hope, reassurance
-
praise, reinforcement
-
providing opportunities for social comparisons
-
social support in the group
-
weighing.
-
-
Group, session closing –
-
closing session, reflecting
-
closing the programme, reflecting
-
follow up
-
reminders
-
tasks to do between sessions.
-
-
Other.
Initial coding schema developed during coding of first 10 transcripts of group sessions:
-
Accountability.
-
Competition.
-
Discussion, learning, sharing –
-
advice, suggestions
-
providing, exchanging information, explaining
-
referring to common knowledge, media, confusing information
-
sharing ideas, brainstorming
-
sharing personal experiences, opinions.
-
-
Facilitation strategies –
-
clarifying
-
demonstrating
-
directing a question back to the group
-
encouraging participation
-
ending long stories, re-focusing on topic
-
indicating communication patterns, delivery style
-
individual tailoring, providing individual counselling
-
normalising, empathising
-
paraphrasing, summarising
-
remembering, referring to what participants said before.
-
-
Group identity, cohesion –
-
referring to group composition
-
referring to groups as ‘we’, similarities, shared identity
-
referring to missing, present members
-
referring to other groups
-
referring to, using names
-
reflecting on group, positive aspects of group.
-
-
Humour, laughter.
-
Motivation.
-
Opportunities for social comparisons.
-
Positive affect (expressed in the group).
-
Providing challenge, disagreement.
-
Resistance, surprise regarding information, recommendations.
-
Self-disclosing sensitive information about oneself.
-
Session components –
-
barriers, problem-solving
-
decisional balance
-
goal-setting, planning new behaviours
-
goals – discussing programme goals
-
group activities
-
group rules (discussing)
-
informal chatting, offering drinks
-
introducing, opening session
-
introductions, welcome to the session, programme
-
offering, referring to other classes, vouchers for activities
-
programme expectations, opinions, concerns (discussing)
-
progress review, reporting changes made
-
reviewing previous session
-
self-assessing
-
self-monitoring
-
session, group closing
-
take away tasks
-
taking measures.
-
-
Social norms.
-
Support, encouragement, praise –
-
peer support
-
praise
-
reassurance, hope
-
social support outside the group.
-
-
Other.
-
Bad examples, missed opportunities.
-
Good examples.
Appendix 7 Sources of the Mechanisms of Action in Group-based Interventions framework categories
This appendix reports the sources in which the MAGI framework categories were identified. All sources used in the development of the MAGI framework (see Chapter 2) include:
-
Theoretical literature.
All of the framework categories (including processes and concepts) were initially derived from, and have been described in, the theoretical literature on intervention design, group dynamics, change processes in groups, and individual change processes. The initial MAGI framework was based on summaries of the relevant literature,36–38,69 and in particular on a conceptual review of processes of change in groups. 40
-
Taxonomies of change techniques.
We reviewed six taxonomies: Abraham and Michie3 [A]; Michie et al. ,80 (CALO-RE) [M1]; Michie et al. ,4 (BCTTv1) [M2]; Kok et al. ,72 (intervention mapping taxonomy) [K]; Hartmann-Boyce et al.,81 (OxFAB) [H]; West et al. ,25 (group BCTs) [W]. Letter in square brackets correspond with the letters in Table 33, indicating in which taxonomy a similar category was identified.
-
Qualitative studies of participants’ experiences of weight loss groups.
We reviewed 27 reports of qualitative studies49,82–107 (see Appendix 2). Numbers in Table 33 indicate the number of studies in which a theme corresponding with the MAGI framework category was identified.
-
Measures of group processes.
We identified reviews of measures of group processes108–110 and used them to extract details of the available measures that could be used to measure group processes and interaction, some of them corresponding with the MAGI framework. For details see Appendix 5.
-
Intervention manuals from LWTC, SkiM, and WtW interventions.
We coded facilitator manuals from three interventions: LWTC [L], SkiM [S] and Waste the Waist [W]. The letters in square brackets correspond with those used in Table 33 and indicate in which manual we identified content matched with the MAGI framework categories.
-
Transcripts of group sessions from LWTC, SkiM and WtW interventions.
We coded 10 transcripts of group sessions from the LWTC, SkiM and WtW interventions. The numbers used in Table 33 indicate the number of session transcripts in which the corresponding MAGI framework categories were identified.
-
Consultations with group participants, facilitators and researchers.
We conducted consultations group participants, facilitators and researchers. The letters used in Table 33 indicate which groups of consulted experts raised the issues related to the corresponding framework categories (i.e. researchers [R], group participants [P] or group facilitators [F]).
| MAGI framework categories | Technique taxonomies (n = 6) | Qualitative studies (n = 27) | Consultations | Intervention manuals | Transcripts of group sessions (n = 10) |
|---|---|---|---|---|---|
| 1. Group intervention design | |||||
| 1.1. Intended changes and processes | R | L, S, W | 3 | ||
| 1.2. Purpose/benefits of using group format | 5 | R, F | S, W | 2 | |
| 1.3. Group characteristics | 3 | R, P, F | L, S, W | 2 | |
| 1.4. Participant selection/group composition | W | 10 | R, P, F | 5 | |
| 1.5. Facilitator selection/training | M2, K | 8 | R, P | S, W | 2 |
| 1.6. Intervention content | K, M1 | 10 | R, P, F | L, S, W | 10 |
| 1.7. Setting and venue | M1, M2, K, W | 5 | R, P, F | L | 2 |
| 1.8. Group set-up and delivery | K | 9 | R, P, F | L, S, W | 9 |
| 2. Facilitation techniques | |||||
| 2.1. Techniques for starting the group/session | 4 | R, P, F | L, S, W | 10 | |
| 2.2. Generic facilitation techniques | A, M1, K, W | 4 | R, P, F | L, S, W | 10 |
| 2.3. Techniques to facilitate group dynamics | 4 | R, P, F | L, S, W | 10 | |
| 2.4. Techniques to facilitate interpersonal change processes | A, M1, M2, K, H, W | R, P, F | L, S, W | 10 | |
| 2.5. Techniques to facilitate intrapersonal change processes | A, M1, M2, K, H, W | R, P, F | L, S, W | 10 | |
| 2.6. Techniques for closing the group/session | R, P, F | L, S, W | 10 | ||
| 3. Group dynamic and development processes | |||||
| 3.1. Group goals | 3 | S, W | |||
| 3.2. Identifying with/as a group | 8 | P | S, W | 5 | |
| 3.3. Group cohesion and attraction | W | 9 | R, P, F | W | 7 |
| 3.4. Group climate | 13 | F | W | ||
| 3.5. Group engagement | R, P, F | S, W | 10 | ||
| 3.6. Communication patterns | P | W | 10 | ||
| 3.7. Group norms | 2 | R, P, F | L, S, W | 6 | |
| 3.8. Group roles | R, F | L, W | 4 | ||
| 3.9. Group development | R, F | ||||
| 4. Interpersonal change processes | |||||
| 4.1. Sharing experiences | K, W | 20 | R, F | S, W | 10 |
| 4.2. Social learning | A, M1, M2, K, H, W | 16 | P, R, F | L, S, W | 10 |
| 4.3. Social influence (in the group) | M2, K | 8 | F | S, W | 3 |
| 4.4. Agreeing, disagreeing, challenge | K | F | 10 | ||
| 4.5. Social support (in the group) | A, M1, M2, K, H, W | 22 | R, F | L, S, W | 7 |
| 4.6. Social validation | K | 5 | R, P, F | 6 | |
| 4.7. Social identification | M2, K, W | 18 | R, F | 3 | |
| 4.8. Social comparisons | A, M1, M2, K, W | 7 | R, P, F | L, S, W | 10 |
| 4.9. Accountability to the group | M2, K, H, W | 11 | R, F | 3 | |
| 4.10. Competition | 3 | P, F | W | 1 | |
| 4.11. Co-operation | K | 1 | |||
| 4.12. Group problem-solving | A, M1, M2, K | R | L, S, W | 10 | |
| 4.13. Group-level feedback | F | W | 1 | ||
| 4.14. Social facilitation (from theoretical literature) | |||||
| 5. Intrapersonal change processes and targets | |||||
| 5.1. Committing to attend | M2 | 6 | P, F | S | 5 |
| 5.2. Developing understanding | 3 | P | L, S, W | 4 | |
| 5.3. Self-presenting | P | 5 | |||
| 5.4. Normative beliefs | A, M1, M2, K | 1 | 2 | ||
| 5.5. Attitudes | K | P | 2 | ||
| 5.6. Attributions | M2, K | 8 | S | ||
| 5.7. Cognitive dissonance | M2 | ||||
| 5.8. Intervention outcome expectations | 3 | R, P, F | L, S, W | 4 | |
| 5.9. Motivation | H | 19 | R, P, F | S, W | 10 |
| 5.10. Self-efficacy and personal control | A, M2, K | 5 | R, P | L, S, W | 6 |
| 5.11. Setting goals | A, M1, M2, K, H | 5 | R, F | L, S, W | 10 |
| 5.12. Reviewing goals/progress | A, M1, M2 | 3 | F | L, S, W | 10 |
| 5.13. Developing/practising skills and behaviours | A, M1, M2, K | 4 | L, S, W | ||
| 5.14. Individual barriers and problem-solving | A, M1, M2, K | 5 | R, F | L, S, W | 10 |
| 5.15. Self-monitoring | A, M1, M2, K, H | 6 | L, S, W | 10 | |
| 5.16. Individual-level feedback | A, M1, M2, K | 8 | R | 7 | |
| 5.17. Developing self-insight | H | 2 | R | 3 | |
| 5.18. Identity shift | M2, K | 4 | S | 2 | |
| 5.19. Using self-talk | A, M1, M2 | S | 1 | ||
| 5.20. Associative learning | A, M1, M2, K, H | S | 4 | ||
| 5.21. Forming habits | M2 | 5 | S | 6 | |
| 5.22. Managing stress, emotions | A, M1 | 1 | L, S, W | ||
| 6. Facilitator and participant characteristics and contextual influences | |||||
| 6.1. Facilitator characteristics | 13 | R, P | |||
| 6.2. Participant characteristics | 2 | R, F | |||
| 6.3. Other contextual influences | A, M1, M2, K, H, W | 15 | R, P, F | L, S, W | 10 |
Appendix 8 Trialled methods for exploring communication patterns
This document includes results of an exploratory analysis of communication patterns in 10 transcripts of group sessions (sampled in stage 1 of the MAGI study). In doing this, we coded in NVivo (v10) every turn of speech of the facilitators, female and male participants. NVivo provides numbers of the codes, which here indicate the numbers of turns of for each analysed group and each type of speaker. It also calculated percentage of the whole transcript coding using each category (in Table 34 this is reported as % of transcript). In this analysis we did not account for any group interaction that was not transcribed (e.g. overlapping talk, or talk during subgroup activities). This analysis was only exploratory and the findings presented here are only for illustration purposes (i.e. as an example of one of the potential methods that would allow to capture and compare patterns of interactions in groups that we trialled); thus, they should be interpreted with caution. We did not pursue this method further because of time limitations and the time-consuming nature of this type of analysis.
| Group session intervention | Facilitators | Participants | ||||||
|---|---|---|---|---|---|---|---|---|
| All | Female | Male | ||||||
| % of transcript | Number of turns | % of transcript | Number of turns | % of transcript | Number of turns | % of transcript | Number of turns | |
| Gr 1, S1, L | 70 | 394 | 20 | 437 | 4 | 115 | 16 | 322 |
| Gr 1, S3, L | 73 | 293 | 19 | 355 | 3 | 107 | 15 | 248 |
| Gr 2, S3, L | 59 | 390 | 28 | 695 | 8 | 303 | 20 | 392 |
| Gr 2, S4, L | 50 | 316 | 38 | 586 | 14 | 299 | 24 | 287 |
| Gr 3, S2, Sk | 62 | 351 | 28 | 428 | 28 | 428 | (no male) | n/a |
| Gr 3, S5, Sk | 57 | 665 | 30 | 750 | 30 | 750 | (no male) | n/a |
| Gr 4, S1, W | 77 | 296 | 16 | 226 | 5 | 87 | 11 | 139 |
| Gr 4, S3, W | 75 | 455 | 18 | 382 | 6 | 159 | 12 | 223 |
| Gr 5, S4, W | 61 | 503 | 26 | 786 | 14 | 475 | 12 | 311 |
| Gr 5, S7, W | 78 | 191 | 15 | 312 | 12 | 196 | 6 | 116 |
| Average | 66% | 385 | 24% | 496 | 13% | 292 | 15% | 255 |
Appendix 9 Group identity measure (used in the Living Well Taking Control/Community-based Prevention of Diabetes trials)
This appendix includes a measure used in the LWTC programme, evaluated in the ComPoD trial, to assess participants’ perceptions of group support, identification with the group, and other social identities resulting from connections with groups outside the programme.
| Being part of a group | |||||||
|---|---|---|---|---|---|---|---|
|
The following statements are about your experiences with being part of a group during the ‘Living Well Taking Control’ (LWTC) programme Read each statement carefully, and indicate how you feel about each one by ticking the box that most accurately represents how you feel |
|||||||
| The following statements are about your experiences with other members in the group meetings as part of the ‘Living Well, Taking Control’ (LWTC) programme | |||||||
| Very strongly disagree | Strongly disagree | Mildly disagree | Neutral | Mildly agree | Strongly agree | Very strongly agree | |
| a) Other members in the group meetings at LWTC really try to help me | □ | □ | □ | □ | □ | □ | □ |
| b) I can count on other members in the group meetings at LWTC when things go wrong | □ | □ | □ | □ | □ | □ | □ |
| c) There are other members in the group meetings at LWTC with whom I can share my joys and sorrows | □ | □ | □ | □ | □ | □ | □ |
| d) I can talk about my problems with other members in the group meetings at LWTC | □ | □ | □ | □ | □ | □ | □ |
| The following statements concern how you feel about being a member of your group as part of the ‘Living Well, Taking Control’ (LWTC) programme | |||||||
| Very strongly disagree | Strongly disagree | Mildly disagree | Neutral | Mildly agree | Strongly agree | Very strongly agree | |
| e) I identify with other members in my group at LWTC | □ | □ | □ | □ | □ | □ | □ |
| f) I see myself as a LWTC group member | □ | □ | □ | □ | □ | □ | □ |
| g) I am glad to be a member of my group at LWTC | □ | □ | □ | □ | □ | □ | □ |
| h) I feel strong ties with other members in my group at LWTC | □ | □ | □ | □ | □ | □ | □ |
| The following statements are about your membership of different groups outside the ‘Living Well, Taking Control’ (LWTC) programme (e.g., groups may be charity, sports, community groups, etc.). Any group other than the Living Well, Taking Control programme may be included | |||||||
| Very strongly disagree | Strongly disagree | Mildly disagree | Neutral | Mildly agree | Strongly agree | Very strongly agree | |
| i) I belong to lots of different groups outside LWTC | □ | □ | □ | □ | □ | □ | □ |
| j) I join in the activities of lots of different groups outside LWTC | □ | □ | □ | □ | □ | □ | □ |
| k) I have friends who are members of lots of different groups | □ | □ | □ | □ | □ | □ | □ |
| l) I have strong ties with lots of different groups outside LWTC | □ | □ | □ | □ | □ | □ | □ |
Appendix 10 Full table summarising coding of Mechanisms of Action in Group-based Interventions framework elements in two groups
This appendix includes a full table summarising the coding of the MAGI framework elements in the two groups analysed in stage 3 of the MAGI study. It is an expanded version of Table 21 (see Chapter 4).
| MAGI framework categories | Group | |||||||
|---|---|---|---|---|---|---|---|---|
| 1 | 1 | 1 | 1 | 2 | 2 | 2 | 2 | |
| S1 | S2 | S3 | S4 | S1 | S2 | S3 | S4 | |
| 1. Group intervention design | ||||||||
| 1.6.5. Group activities | ||||||||
| Whole-group activities | F | F | F | F | F | F | F | F |
| Subgroup activities | R (1) | R (1) | R (1) | R (2) | ||||
| Individual activities | R (1) | R (1) | ||||||
| Discussion-based activities | F | F | F | F | F | F | F | F |
| Practical activities | R (1) | R (2) | R (1) | |||||
| 2. Facilitation techniques | ||||||||
| 2.1. Techniques to start the group/session | ||||||||
| 2.1.1. Introduce people, icebreak | Yes | Yes | Yes | |||||
| 2.1.2. Manage expectations | ||||||||
| 2.1.3. Identify, specify, agree group goals | Yes | Yes | ||||||
| 2.1.4. Prompt group/social identification | ||||||||
| 2.1.5. Identify, specify, agree group rules | ||||||||
| 2.1.6. Discuss group roles, responsibilities | ||||||||
| 2.1.7. Establish a positive group climate | Yes | Yes | Yes | |||||
| 2.1.8. Explain the intervention | Yes | Yes | Yes | |||||
| 2.1.9. Recap any previous session | Yes | Yes | Yes | Yes | ||||
| 2.1.10. Outline the current session | Yes | Yes | Yes | Yes | Yes | Yes | ||
| 2.2. Generic facilitation techniques | ||||||||
| 2.2.1. Encourage participation (explicitly) | R | F | R | O | ||||
| 2.2.2. Manage time, activities/move on | R | F | O | O | R | |||
| 2.2.3. Check participants’ understanding | O | O | O | R | O | O | O | O |
| 2.2.4. Request elaboration, clarification | R | R | ||||||
| 2.2.5. Provide clarification | O | R | O | O | ||||
| 2.2.6. Direct a question back to group | R | |||||||
| 2.2.7. Provide illustration | R | R | O | R | ||||
| 2.2.8. Summarise, paraphrase | O | O | R | R | R | |||
| 2.2.9. Refer to what participant said before | R | O | O | R | O | R | ||
| 2.2.10. Reframe | O | O | O | R | O | R | R | R |
| 2.2.11. Reinforce | O | F | F | O | R | O | O | O |
| 2.3. Techniques for group dynamics | ||||||||
| 2.3.1. Use names | R | R | O | R | R | |||
| 2.3.2. Identify, refer to common goals | R | R | ||||||
| 2.3.3. Refer to the group as ‘we’ | ||||||||
| 2.3.4. Refer to other groups | R | |||||||
| 2.3.5. Present the group as attractive | R | |||||||
| 2.3.6. Reflect on positive aspects of group | ||||||||
| 2.3.7. Refer to group rules | R | |||||||
| 2.3.8. Prompt selecting informal group roles | R | R | R | |||||
| 2.3.9. Address disruptive behaviour | ||||||||
| 2.3.10. Use humour | R | R | R | R | R | R | R | R |
| 2.3.11. Provide opportunities for informal chat | R | R | ||||||
| 2.3.12. Discuss, reflect on interaction style | R | |||||||
| 3. Group dynamics and development | ||||||||
| 3.1. Group goals | R | R | ||||||
| 3.2. Group identification | R | R | ||||||
| 3.3. Group cohesion and attraction | ||||||||
| 3.3.1. Participants reflect on the group | ||||||||
| 3.4. Emergent group norms | O | |||||||
| 3.5. Group climate | ||||||||
| 3.5.1. Laughter, humour | 34 | 82 | 48 | 22 | 27 | 56 | 38 | 33 |
| 3.5.2. Informal talk | R | O | O | O | O | |||
| 3.6. Emergent group roles | ||||||||
| 3.6.1. Dysfunctional group roles | ||||||||
| 3.7. Communication patterns | ||||||||
| P–P interaction/exchanges | ≈4 | ≈30 | ≈14 | ≈20 | ≈2 | ≈15 | ≈23 | ≈15 |
| 4. Interpersonal change processes | ||||||||
| 4.1. Sharing experiences | F | F | F | F | F | F | F | F |
| 4.1.1. Self-disclosure of personal issues | O | |||||||
| 4.1.2. Self-disclosure of transgressive behaviour | O | R | R | R | R | |||
| FAC shares own experience | O | R | O | |||||
| FAC acknowledges Ps’ sharing/self-disclose | R | |||||||
| 4.2. Social learning | ||||||||
| 4.2.1. Providing, exchanging information | F | F | F | F | F | F | F | F |
| FAC provides information, explains | F | F | F | F | F | F | F | F |
| FAC prompts Ps interactive exchange | F | F | F | F | O | F | F | F |
| 4.2.2. Providing, sharing advice | O | O | O | R | F | F | O | |
| FAC provides advice, recommendation | O | O | O | R | F | F | O | |
| FAC prompts Ps exchange of advice | R | R | ||||||
| Ps provide advice, recommendations | O | R | O | O | O | |||
| 4.2.3. Brainstorming, sharing ideas | O | F | F | F | F | F | ||
| FAC prompts brainstorming of ideas | O | F | F | F | F | F | ||
| FAC offers ideas | O | O | O | R | R | |||
| Ps offer ideas | O | O | F | F | F | F | F | |
| 4.2.4. Group problem-solving | R | O | R | R | R | R | ||
| FAC prompts barrier identification | R | O | R | |||||
| FAC prompts problem-solving | R | O | R | |||||
| Ps identify general barriers | O | O | R | R | R | R | ||
| Ps offer solutions | R | R | R | |||||
| 4.2.5. Demonstrating, modelling behaviour | ||||||||
| FAC demonstrates behaviours | O | |||||||
| Ps model behaviours | O | |||||||
| Ps demonstrate behaviours | ||||||||
| 4.2.6. Providing instructions how to perform behaviour | ||||||||
| FAC provides instructions | O | |||||||
| Ps provide instructions | ||||||||
| 4.3. Social influence | ||||||||
| 4.3.1. FAC appeals to credible source | R | R | R | R | ||||
| 4.3.2. FAC uses persuasive arguments | O | R | R | |||||
| 4.3.3. Negative social influences in group, resistance talk | ≈8 | ≈17 | ≈8 | ≈3 | ≈4 | ≈5 | ≈3 | 0 |
| FAC addresses resistance | F | F | F | O | F | F | R | |
| 4.3.4. Positive social influences in group, change talk | ≈3 | ≈2 | ≈9 | ≈2 | ≈4 | ≈3 | ≈5 | ≈10 |
| 4.4. Agreeing, disagreeing, challenging | ||||||||
| Participants express agreement | R | O | R | O | O | |||
| Ps express disagreement, challenge | R | R | R | R | ||||
| FAC provides challenge to participant | R | R | ||||||
| 4.5. Social support in the group | ||||||||
| 4.5.1. Peer support | ||||||||
| P–P praise | R | R | R | R | R | |||
| P–P encouragement | R | R | R | |||||
| 4.5.2. Buddy up | ||||||||
| 4.5.3. Social connections | R | R | O | O | R | R | R | |
| FAC discusses, encourages peer support | R | R | ||||||
| FAC offers support | R | R | R | |||||
| FAC provides praise | O | O | O | O | O | O | O | O |
| FAC provides reassurance | O | R | R | O | O | O | ||
| FAC provides encouragement | O | R | R | R | R | O | ||
| 4.6. Social validation | ||||||||
| 4.6.1. Personal validation (P–P) | R | R | R | |||||
| FAC offers personal validation | ||||||||
| 4.6.2. Normalising (P–P) | ||||||||
| FAC normalises | ||||||||
| 4.6.2. Empathy (P–P) | R | |||||||
| FAC expresses empathy | R | R | R | |||||
| Ps express shared experience, understanding | R | O | R | R | R | R | O | R |
| 4.7. Social identification | ||||||||
| FAC refers to common Ps’ social categories | R | |||||||
| 4.8. Social comparisons | ||||||||
| Ps share comparable information on behaviour/performance | R | R | O | R | ||||
| FAC prompts sharing comparable information about behaviours/performance | O | R | ||||||
| FAC asks for self-assessments | R (1) | R (1) | R (2) | R (1) | R (1) | R (1) | R | R |
| FAC uses Ps as role models or good examples | O | R | ||||||
| 4.9. Accountability to the group | ||||||||
| 4.9.1. Public promise/statement (P) | R | |||||||
| FAC prompts sharing goals in public | Yes | Yes | ||||||
| FAC prompts public promise | ||||||||
| FAC takes objective measures of progress | Yes | Yes | Yes | Yes | ||||
| 4.10. Competition | ||||||||
| 4.13. Group-level feedback | ||||||||
| 5. Intrapersonal change processes | ||||||||
| 5.9. Motivation (importance of change): | ||||||||
|
R | R | R | R | R | R | R | |
|
R | R | ||||||
|
F | F | O | F | ||||
|
O | |||||||
| 5.10. Self-efficacy | ||||||||
|
O | R (1) | ||||||
|
F | O | F | R (1) | ||||
|
F | F | O | O | ||||
| 5.11. Goal-setting | ||||||||
| 5.11.1. Specific goal-setting (Ps) | R | O | R | R | ||||
| 5.11.2. Unspecific goals, intentions (P) | O | R | R | R | O | O | O | |
| 5.11.3. Achievable, small goals (Ps/FAC) | O | R | R | |||||
| 5.11.3. (More) challenging goals (Ps/FAC) | R | R | ||||||
| 5.11.4. Long-term, sustainable goals (Ps/FAC) | R | R | ||||||
| FAC explains goal-setting | Yes | Yes | ||||||
| FAC prompts individual goal-setting | Yes | Yes | Yes | Yes | Yes | Yes | ||
| FAC discusses individual goals in/with group | Yes | Yes | Yes | Yes | ||||
| 5.12. Goal/progress review | ||||||||
| 5.12.1. Review of specific goals (Ps) | R | |||||||
| 5.12.2. General review of progress (Ps) | Yes | Yes | Yes | |||||
| 5.12.3. Objective measures | Yes | Yes | ||||||
| FAC prompts review of specific goals | ||||||||
| FAC prompts general progress review | Yes | Yes | Yes | |||||
| 5.13. Developing, practising skills and behaviours | ||||||||
| 5.13.1. Ps report practice of skills/behaviour | O | O | O | O | O | O | O | F |
| 5.13.2. Ps report no practice of skills/behaviour | ||||||||
| 5.13.3. Ps practise skills/behaviour in the session | R | R | ||||||
| 5.13.4. Ps identify pre-requisite skills | R | |||||||
| 5.14. Individual barriers and problem-solving | ||||||||
| 5.14.1. Ps report individual barriers | R | R | R | R | R | O | O | |
| 5.14.2. Individual problem-solving (Ps) | R | R | R | |||||
| 5.14.3. Relapse prevention | ||||||||
| FAC prompts individual barrier identification | R | |||||||
| FAC prompts individual problem-solving | R | R | R | |||||
| 5.16. Individual-level feedback | ||||||||
| FAC provides individual feedback | ||||||||
| P–P feedback | ||||||||
List of abbreviations
- BCTTv1
- Behaviour Change Technique Taxonomy v1
- BMI
- body mass index
- ComPoD
- Community-based Prevention of Diabetes
- GB-BCI
- group-based behaviour change intervention
- LWTC
- Living Well Taking Control
- MAGI
- Mechanisms of Action in Group-based Interventions
- MRC
- Medical Research Council
- OxFAB
- Oxford Food and Activity Behaviours
- SkiM
- Skills for weight loss Maintenance
- SMART
- specific, measurable, achievable, relevant and time-bound
- WtW
- Waste the Waist