
Notes
Article history
The research reported in this issue of the journal was funded by the HS&DR programme or one of its proceeding programmes as project number 09/1809/1075. The contractual start date was in January 2010. The final report began editorial review in April 2013 and was accepted for publication in October 2013. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HS&DR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
John Powell is a member of the NIHR Journals Library Board.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2014. This work was produced by Scarbrough et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction and aims
The Collaboration for Leadership in Applied Health Research and Care (CLAHRC) initiative was developed by the National Institute for Health Research (NIHR) in response to a new research and development (R&D) strategy in the NHS: ‘Best Research for Best Health’. This response focused on the ‘second gap in translation’ identified by the Cooksey review;1 namely, the need to translate clinical research into practice. As specified by the NIHR’s briefing document on CLAHRCs, a crucial stage in translating research into practice was seen to be ‘the evaluation and identification of those new interventions that are effective and appropriate for everyday use in the NHS, and the process of their implementation into routine clinical practice’ (p. 1).
The research presented in this report was funded by the NIHR as one of four uniquely focused projects aimed at evaluating the CLAHRC initiative. The ‘external evaluation’ reported here was designed to complement the internal evaluations being carried out within each CLAHRC. Its particular focus was on CLAHRCs as a new form of ‘networked innovation’. Following a start-up meeting of the evaluation projects in October 2009, our study commenced January 2010.
Aims of the Collaboration for Leadership in Applied Health Research and Care initiative
The NIHR established nine CLAHRCs as partnerships between at least one university and surrounding NHS and other organisations in October 2008. The CLAHRCs were selected through open competition, by an independent international selection panel. The objectives for the CLAHRCs as set out in the original call for proposals were as follows:
-
to develop an innovative model for conducting applied health research and translating research findings into improved outcomes for patients
-
to create a new, distributed model for the conduct and application of applied health research that links those who conduct applied health research with all those who use it in practice across the health community covered by the collaboration
-
to create and embed approaches to research and its dissemination that are specifically designed to take account of the way that health care is increasingly delivered across sectors and across a wide geographical area
-
to increase the country’s capacity to conduct high-quality applied health research focused on the needs of patients, and particularly research targeted at chronic disease and public health interventions; and
-
to improve patient outcomes across the geographic area covered by the collaboration.
The core funding for this initiative was around £50M, with each CLAHRC being funded £5–10M over 5 years by the NIHR, with added ‘matched funding’ by local partners.
Aims of our study
Our research design was developed in response to a call for proposals issued by the Service Delivery Organisation (SDO) of the NIHR (www.nets.nihr.ac.uk/__data/assets/pdf_file/0005/81572/CB-09-1809-1072.pdf). While certain broad areas were identified within this call, it did not specify particular research questions but exhorted researchers ‘to capitalise on the opportunity provided by the CLAHRCs to evaluate this new initiative and in doing so to make a substantial contribution to learning for the CLAHRCs themselves and for the NHS as a whole’ (p. 5). The call specified that evaluations should be well theorised, and should be able to contribute to ‘the wider evidence base on how best to foster the application of research findings in practice settings’. In response to this call, the aims for our study were specified as follows:
-
to provide an independent and theory-based evaluation of CLAHRCs as a new form of networked innovation in the health sector
-
to support the organisational learning and improvement of CLAHRCs by providing comparative evidence and insights on their innovation capabilities within both a national and an international context
-
to support improved patient outcomes by adding to the evidence base on networked innovation within the UK health sector, especially with respect to management and governance mechanisms, and how this compares with leading international examples
-
to increase the NHS’s capability for networked approaches to innovation by developing a more comprehensive theoretical framework
-
to make recommendations on improving the evaluation of KT through greater appreciation of the role of networks; and
-
to contribute to the international knowledge base on research use through cross-national comparisons, and the cross-fertilisation of academic literatures.
These aims have remained unchanged since the beginning of the study.
Chapter 2 Review of existing literature
The knowledge translation problem in health care
As outlined above, the challenge facing the CLAHRCs was defined in terms of overcoming a ‘translational gap’ between research and practice. This notion of a gap between the knowledge developed by research communities in health care and health-care practice itself is the subject of an extensive literature. 2–5 A perceived gap between research and practice is not confined to health-care organisations; other work has identified it more broadly as a major societal and organisational challenge. 6 The implications of such a gap, however, are seen as extremely serious in the health-care setting where the ‘non-adoption’ of new research evidence and/or the lack of spread of new forms of improved practice may have significant adverse consequences for patient well-being. 3,7,8 These concerns were articulated by the Cooksey report,1 which sought to address the relationship between research and practice as a continuum of activities. As noted above, Cooksey’s analysis of the translational gap within that continuum helped to inform the establishment of the CLAHRC initiative.
The analysis of the knowledge translation (KT) challenge in health care in terms of a metaphorical ‘gap’ has had important implications for the development of theoretical models and, beyond that, policy initiatives in this area. While it has long been argued that the translation of research into practice is problematic, traditionally this has been viewed in terms of linear and unidirectional movement, from the production of research (and other forms of knowledge) to its use in practice. 9 In effect, there was an assumption that research findings would be disseminated from the laboratory through applied research and development and then into practice.
This assumed linear path from the production of knowledge to its use – signified in the term ‘gap’ – has since been subject to lengthy debate and criticism in the health-care sphere. 10–12 Some scholars have even questioned the continued use of the term ‘translation’, given the one-way direction of knowledge flow and conversion that it often implies. 13 In the period leading up to the establishment of the CLAHRCs, then, a new set of approaches were emerging that highlighted the importance of ongoing interaction and trust-based relationships between researchers and practitioners in meeting the challenge of translation. 14–16 These approaches moved away from a linear view of translation to one which gave greater recognition of the complex, multifaceted interactions involved in developing and implementing research in practice. 17,18 At the same time, within the wider literature of organisation studies, a further stream of research focused on explaining the processes and practices through which knowledge is translated across different settings. 19,20 Leaving aside any notational issues, such approaches depict KT as crucially important for improving health care as this is the process whereby research evidence comes to inform and impact health-care policy and practice and vice versa. 21
In the health-care setting, the notion of KT was given greater prominence among policy makers by the work of the Canadian Institutes for Health Research (CIHR). The World Health Organization subsequently adapted the CIHR’s work and defined KT as ‘the synthesis, exchange, and application of knowledge by relevant stakeholders to accelerate the benefits of global and local innovation in strengthening health systems and improving people’s health’ (p. 2).
Responding to the knowledge translation problem: policy interventions
Policy-makers now recognise that, as collaborative working practices facilitate the process through which research findings can come to inform policy and practice,22 deliberate institutional strategies for collaboration can be used to support the utilisation of knowledge. 5 Policy interventions designed to support KT in health care, and to connect innovations with practical improvements, have taken a wide variety of forms. One approach taken by health research funding agencies has been to commission collaborative entities in which academic researchers work closely with other stakeholder groups (such as health-care practitioners, patients, industry and policy representatives). Canada has been at the forefront of such initiatives. An early example was a grant programme developed by the Quebec Social Research Council (CQRS) in the 1990s to encourage the building of research partnerships between researchers, decision-makers and practitioners. 23 A second Canadian example is the Need to Know project funded by the CIHR. 24 A notable example in the USA has been the Quality Enhancement Research Initiative (QUERI) of the US Veterans Administration. 25
These policy interventions represent examples of system-level KT interventions, where an environment is created to support the production and application of health-care evidence in influencing policy and practice. 26 In the UK, various centres and networks (including CLAHRCs, Biomedical Research Centres, Patient Safety Translational Research Centres and, most recently, Diagnostic Evidence Co-operatives) already form a crucial part of the NIHR infrastructure, and the recently established academic health science networks are intended to play a major role in connecting innovation with improvement in the NHS, and have a brief to work with CLAHRCs on translating research and learning into practice. Each programme is characterised by a strategic approach of assembling mechanisms and processes to support KT across the boundaries of stakeholder groups, such as between the ‘producers’ (i.e. academic researchers) and the ‘users’ (i.e. practitioners, commissioners and patients) of health-care evidence in policy and practice. While it is the ‘external-directed’ boundary between the diversely different communities of the ‘producers’ (academics) and ‘users’ (practitioners and policy makers) of health-care research27 that is most often recognised as the focus of these interventions, they can also be directed ‘internally’, such as within the boundaries of a profession28,29 and/or between members of the same organisational entity. 30
These kinds of policy interventions, while being many and varied, are all premised on the assumption that supporting new forms of highly networked, collaborative working across boundaries (organisational and/or epistemic) will result in better knowledge sharing and, as a result, the speedier translation of new ideas into (and from) actionable solutions. These interventions, including the CLAHRCs, can be framed, then, as initiatives aimed at ‘networked innovation’; that is, ‘innovation that occurs through relationships that are negotiated in an ongoing communicative process, where control cannot rely on either market or hierarchy alone’ (p. 916). 31 Our evaluation of the CLAHRCs is thus able to be positioned, more broadly, as an evaluation of an initiative aimed at networked innovation.
The premise underpinning networked innovation initiatives is that network-based organisational forms are more effective at knowledge sharing and, therefore, better for innovative performance, than either markets or hierarchies. The features which enable such effectiveness, however, are the subject of ongoing research. Work on some of the recent initiatives highlighted above, for example, has highlighted features such as the importance of leadership, culture, and context (e.g. CQRS);23 the need to build relationships between groups to support KT (e.g. Need to Know);24 and the long time scales needed to show health benefit (QUERI). 25 Even the benefits of the network form itself are open to question. A recent systematic review of knowledge mobilisation in health-care organisations found that the superiority of networked organisation designs for knowledge sharing and performance rested on the quality of the relationships more than the network structure. 32 For example, low-trust relationships in networks can lead to poorer knowledge sharing than high-trust relationships in hierarchies. 32 Put simply, ‘relationships trump design’ (p. 173). 32 The broad conclusion of this review was that the benefits of network arrangements for KT cannot be taken for granted.
We need, then, to better understand what it is that makes networks actually work. This means asking questions about the social relationships and boundary-spanning activities underpinning knowledge sharing in networked settings, the beliefs and interests of those involved, and the governance and management mechanisms deployed in specific contexts for particular ends.
Conceptual framework
Our perspective involved viewing the work of the CLAHRCs and their partners as involving a process of networked innovation. 31 This perspective begins from the important point that the KT efforts of the CLAHRCs are aimed, ultimately, at achieving innovative outcomes. They exist, in other words, for a specific purpose, which is to encourage the sharing of knowledge aimed at translating new ideas into improved practices. As is well recognised, however, this innovation task is problematic. 33 The requisite knowledge is distributed across the boundaries of expertise, professional groups and organisations. 20,34 As a result, innovation requires the progressive exchange, transformation and ‘co-production’ of knowledge by collaborating groups. 16 Moreover, because the CLAHRCs entail novel forms of collaboration, the roles, accountabilities and management of these groups also need to be worked out. Our conceptual framework thus needed to incorporate particular processes found in previous research to shape the ability of such distributed groups to work together in KT endeavours. These include the following.
Overcoming boundaries to access distributed knowledge
As work in the innovation field has highlighted, the knowledge required to develop and implement innovation is increasingly distributed across different groups and organisations. 35 This finding is also echoed in studies within health care. McAneney et al. ,36 for example, note that ‘the knowledge which is needed to solve problems and bring about changes is likely to be distributed throughout organisations and to come from many different sources’ (p. 1498). Recognition of the need to span boundaries is a long-established theme in innovation studies, and research has focused to a great extent on organisational boundaries. 37 However, the importance of accessing distributed forms of knowledge underlines not only the need for translation between different organisations, but also the need to circumvent what recent work has termed the ‘knowledge boundaries’ that constrain the flow of knowledge between different epistemic groups and communities.
Knowledge boundaries naturally arise, according to Carlile, because of the embeddedness of knowledge in practice – knowledge sticks at the boundaries of practice and is shared where practices are shared. 20 Such boundaries can be analysed in terms of syntactic (shared or different language), semantic (shared or different meanings) and pragmatic (shared or different practices) dimensions. 20 The value of this analysis is that it highlights the multifaceted and relational character of KT. 38 It thus provides a broader view of the challenges of translation that highlights the extent to which particular groups, such as researchers, policy-makers and practitioners, are connected or divided by their respective contexts, language and (politically invested) practice. These different groups can be viewed as ‘epistemic communities’, which are characterised by shared language, values and world views. 39
A number of studies have sought to establish the types of mechanisms and processes that can be used to support KT across knowledge boundaries in health care. 27,40 These studies build on an understanding that knowledge cannot easily be translated into a comprehensible form from one community for utilisation by another dissimilar community:41,42 knowledge, in other words, is embedded or ‘sticky’,43 as the producers and users of knowledge inhabit different worlds. 44 Knowledge is also politically invested,20,45 so there is a pressure within networked innovation initiatives for more collaborative forms of knowledge production to revert to (or even be undermined by) long-established modes of producing knowledge based on professional demarcations. 46
Given that the challenges of translating knowledge across the boundaries of diverse groups and communities are especially stark within the health-care field, attention has been placed on developing, managing and evaluating interventions that can facilitate this process. Among the mechanisms highlighted in the existing literature is the creation of boundary-spanning or ‘knowledge broker’ roles for individuals to link discrete communities;47–49 organisational-level activities (such as using forums and meetings) as places for the exchange of ideas between groups;50,51 and integrated KT processes and end-of-grant activities in which findings are translated for other audiences. 52
Considerable attention has been placed on understanding the process of ‘boundary spanning’ across organisational and epistemic groups within health care. While some research has highlighted the importance of material objects in bridging diverse groups,39 boundary spanning can also be achieved by individuals who, either formally or informally, enact a ‘knowledge broker’ role. Such individual boundary spanners have been described as performing functions such as acting in leadership and network-building roles, fostering relationships, and contributing an innovative perspective,53,54 suggesting that boundary-spanning individuals are those with experience of and credibility in both ‘camps’, such that they can move back and forth and broker understandings between different thought worlds. Such knowledge-brokering strategies can be used to address the language and cultural barriers between the worlds of research and decision-making by translating research and other evidence into different vocabularies. 55 The knowledge-broker role is designed so that individuals can act as facilitators of collaboration and ‘translators’ of knowledge from one community to another. Indeed, as the use of interpersonal contacts and good communication skills in the context of partnerships and research collaborations is emphasised in knowledge brokering, it has been described as particularly suitable for linking upstream research with downstream practice. 48 Therefore, one important strand of our work is on roles enacted by individuals to support the translation of knowledge across groups.
While much attention has been given to individuals performing boundary-spanning activities as brokers between diverse groups, previous studies also indicate that knowledge brokering can be enabled by organisations and structures, such as a whole network of ties or collaborative strategies. 56 These types of boundary-spanning mechanisms are about structures, activities or processes that an initiative may develop in order to facilitate KT within a collaborative community. For example, explicit strategies that have been described include initiative-wide activities developed to provide a ‘space’ for face-to-face interaction and discussion, such as consultation sessions, interactive multidisciplinary workshops, steering committees and the formal creation of networks and communities of practice. 57 The CIHR’s influential global integrated KT approach represents an organisational-wide strategy to support activities that are conducive for KT across the boundaries of the producers and users of research. 58 This approach is about building a structure and interlinking activities at the level of a whole initiative that is able to facilitate sharing knowledge across the boundaries of a wide range of actors, including health professionals, researchers, the public, policy-makers and research funders. 59 It may also include the formal allocation of resource to individual knowledge brokers.
Developing social networks to enable the translation of knowledge
In the recent period, recognition of the importance of boundaries between groups has been complemented by greater awareness of the central importance of social networks in enabling innovation that spans communities or practice groups. 31 Studies focusing on the analysis of network ties have highlighted the importance of network structures in shaping the flow of knowledge and information within and between organisations. 34,60 Here, the focus is less on individuals and more on the nature of the relationships and information flows across individuals and groups: their interconnectedness, in other words. Network analysts use a range of well-developed concepts (e.g. ‘nodes’ to denote position or location, and ‘ties’ to denote relationships or links among these positions) and methods [in particular, social network analysis (SNA)] to link the patterns of relationships in the network to the behaviours that arise from it. 61 Such tools allow analysts to reveal and represent the informal social relationships within and across organisations that shape work-related outcomes. This now-extensive body of work links helps to underline the impact, for example, on innovation of brokering across ‘structural holes’62 between different groups, as well as the pivotal roles of boundary-spanning groups and gatekeepers. It also highlights the different roles played by different kinds of social ties in knowledge sharing, with weak ties being linked to the sourcing of information and strong ties being linked to the establishment of trust and the sharing of tacit knowledge. 63 Importantly, social networks provide a relational form of governance (the ‘informal structure’) whereby an individual or group’s position (centrality) in a network relative to others plays a key role in their ability to exercise power. This informal structure has been found to be especially important in networked innovation settings (such as the CLAHRCs) where the exercise of power requires extensive boundary spanning and where sources of power influence innovation outcomes. 64
The attention paid to social networks in studies of innovation more generally has not so far been matched by work in the health-care management field. Here, recent studies, with relatively few exceptions, have focused on networks as formal, quasi-organisational entities, frequently associated with policy interventions. 65 As McAneney et al. 36 note, relatively few studies have addressed the implications of network structure for KT. Only in more recent work do we find social network analytical techniques being applied to uncovering the latent structure of ties between groups and individuals. Thus, a study by Currie and White66 uses SNA to identify the interplay between knowledge brokering and professional hierarchy. The authors argue that such brokering both is influenced by, and helps to mitigate, the impact of such hierarchy on knowledge mobilisation. They also highlight the role of groups in such brokering as against the actions of specific individuals.
Bringing together different interpretations: the role of cognitive maps
The importance of cognition and the underlying belief structures that groups and individuals bring to their interpretation of new situations has been identified as central to networked innovation and collaborative work. 67,68 Furthermore, work has shown how underlying cognitive structures or belief systems – sometimes termed ‘cognitive maps’ – are implicated in sense-making and decision-making processes. 69 However, while a number of studies have addressed the role of such cognitive maps in the actions of managerial groups,70 less attention has been paid to their importance in health-care settings. One exception here is the work of Sutherland and Dawson,71 who adopt a ‘sense-making’ approach to behavioural change among clinicians. They use the notion of cognitive maps to highlight the way in which actors ‘apportion meaning to situations, relationships, roles, and objects, and store such interpretations and understanding in cognitive structures, often in the form of “taken-for-granted” knowledge’ (p. 53). 71 Such structures or maps in turn influence how novel events or ‘equivocal’ situations are interpreted. 72
The arguments coming from this strand of work effectively underline the relevance of cognitive structures to the outcomes of networked innovation initiatives such as the CLAHRCs. As we highlighted at the beginning of this report, the notion of KT, which informed the original funding initiative for the CLAHRCs, was broadly defined and ‘equivocal’ in the sense that it was open to multiple interpretations. Organisational models and mechanisms of KT and its effectiveness within different contexts remain highly debated. It follows from this that the cognitive maps which different CLAHRC groups bring to this KT endeavour – what it means, and how it can or should be operationalised – may vary significantly across CLAHRCs, and may have important consequences for the way in which policy-inspired models are interpreted and enacted. A crucial question here has to do with participants’ ‘causal maps’ – that is, the associations they make between particular phenomena and particular outcomes. This is because such causal maps and their characteristics (e.g. cognitive complexity) have been closely linked to strategic visions and intentions and decision-making. 70 We recognise, of course, that intentions and cause–effect beliefs do not necessarily translate directly into behaviours and actions. 73 However, drawing the role of cognition and cognitive maps into our conceptual framework provides a useful complement to the emphasis on social interaction seen in previous research on networked innovation and collaborative work.
Management, governance and organisation
Much of the literature on KT tends to focus on the process by which this occurs, thus emphasising the micro-dynamics of interactions between individuals and groups. Viewing this process in the abstract, however, tends to neglect the important, if often antecedent, effect of the way in which that process is designed, directed and resourced.
Previous work has shown that efforts to engineer a process of KT may fail because management and governance are inappropriate to the task at hand. Relevant here is a study of the management and organisation of the Genetics Knowledge Parks initiative – a policy intervention designed to speed the translation of genetics and genomics science into clinical practice through the establishment of regionally based ‘knowledge parks’, where academic researchers, health-care practitioners and industry would work collaboratively. 74,75 This study found that the ambiguity that was inherent in these novel forms of collaboration generated uncertainties about its evaluation and the extent to which it was delivering against broadly defined, but extremely ambitious, objectives. This uncertainty prompted governing bodies (funders and policy bodies) to try to more tightly monitor and evaluate the work, thus creating burdensome reporting requirements and constraints on innovation.
This example raises an important issue of governance – that is, management practices often assume a linear model of innovation (i.e. planning and monitoring against predefined objectives and targets) whereas networked innovation is inherently an emergent and iterative process. 76,77 Equally, this example may reflect inappropriate forms of accountability and organisation being applied to a policy intervention. 74 The importance of management and organisation was fully recognised in the CLAHRC call for proposals, however, which highlighted the need to specify a director, management arrangements and explicit strategies for managing the collaborative partnerships involved in the CLAHRC.
The impact of the institutional and policy context
The example of the Genetics Knowledge Parks, outlined above, shows how the translation work occurring at the micro level within networked innovation initiatives is shaped by the wider institutional and policy context. The impact of the institutional and policy context on innovations in health care is widely reflected in the existing literature. 40,65,78,79 One conclusion here, then, is that, while much can be learned from models of KT in other nations, we must also be sensitive to the need to adapt and appropriate such models for the UK health-care setting.
Complementing this recognition of the importance of context at a macro level, there is a growing body of work on the ways in which context may shape more localised efforts to translate knowledge into health-care practice. Studies have shown, for example, that the same evidence may lead to different outcomes in different decision-making contexts,80 or that some translational activities, such as knowledge-broker roles, may be adaptable to different contexts. 49 At the same time, there remains a gap within the existing literature on how contextual features influence the KT process. This has driven calls for further research to address the influence of context as a prerequisite for developing more effective approaches in this area. 81,82
Development of capabilities for networked innovation
One perspective on the influence of context which has emerged in the literature focuses on the development of capabilities for networked innovation. Such innovation is seen as taking place at the interstices of organisations and of professional communities, thereby demanding new capabilities on the part of participating organisations. 61 Two forms of capability have been identified as crucial to the translation of scientific research and evidence into practical applications. ‘Relational capability’ denotes an organisation’s ability to work with diverse others in an innovation system. ‘Integrative capability’ is defined in terms of the ability of individuals and groups to move back and forth between science and the locus of practice. 83
The emergence of these capabilities is seen as being influenced by the institutional context for innovation. A study of networked forms of biomedical innovation, for example, highlights the influence of the national institutional context on UK firms’ capabilities as compared with their US counterparts, highlighting in particular the constraints on the development of more ‘hybrid’ roles that combine scientific and entrepreneurial skills. 79
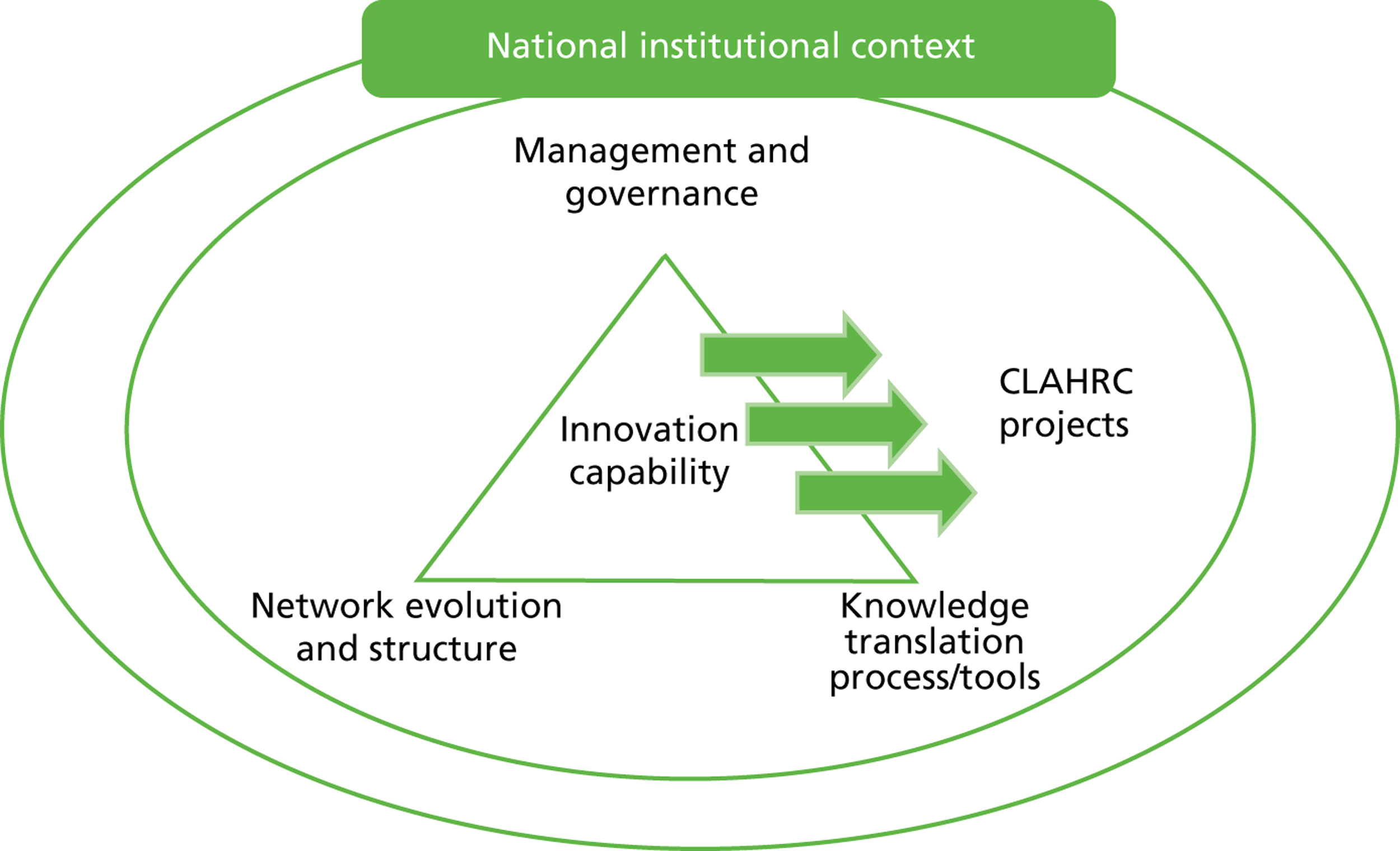
Taken together, these different strands in our analysis of the literature helped us to develop a conceptual framework for our study, as outlined in Figure 1 .
FIGURE 1.
Conceptual framework.
Research objectives of the empirical study
Integrating this conceptual framework with the wider aims identified for the study helped us to frame the specific research objectives to be addressed by the empirical study. These were specified as follows:
-
Identify the micro-level relationships between researchers, intermediary groups and practitioners which enable the translation of knowledge from research into practical settings.
-
Map the evolving structure of social and interorganisational networks that underpin CLAHRCs, including the emergence of boundary-spanning groups and gatekeeper individuals, and brokering across ‘structural holes’ between communities.
-
Examine the impact of policy and governance arrangements within which such networks are situated on translations of knowledge between research and practice.
-
Compare the UK CLAHRC initiative with similarly intentioned networked innovation initiatives in the USA and Canada, with a view to learning from these experiences while also recognising their distinctive institutional contexts.
Chapter 3 Research methods
The study uses a mixed-methods approach for a comparative case study of six collaborative initiatives designed to facilitate the translation of research evidence into health-care policy and practice. This chapter describes the research design that was used and reflects on the methodological considerations of our approach, including how we applied our networked innovation conceptual framework to support the amalgamation and analysis of the data collected from the different components of this study.
Stages of the research process
The overall study design was comparative case study involving a temporally phased data collection process conducted across three case sites based in the UK and three sites in North America over a period of 36 months ( Figure 2 ). The UK fieldwork was conducted over two partially overlapping phases of work in order to support our research objectives of mapping the evolving structure and social relationships that underpinned the development of the CLAHRCs over time (objectives 1 and 2, Chapter 2 ), as well as the impact of different models of governance and management implemented by the CLAHRCs (objective 3, Chapter 2 ). The two phases allowed us to identify how, under ostensibly the same policy initiative, the CLAHRCS developed different types of structures, relationships and activities and to trace the ways in which these supported or engendered different elements of their vision(s) and the KT process.
FIGURE 2.
Research plan.
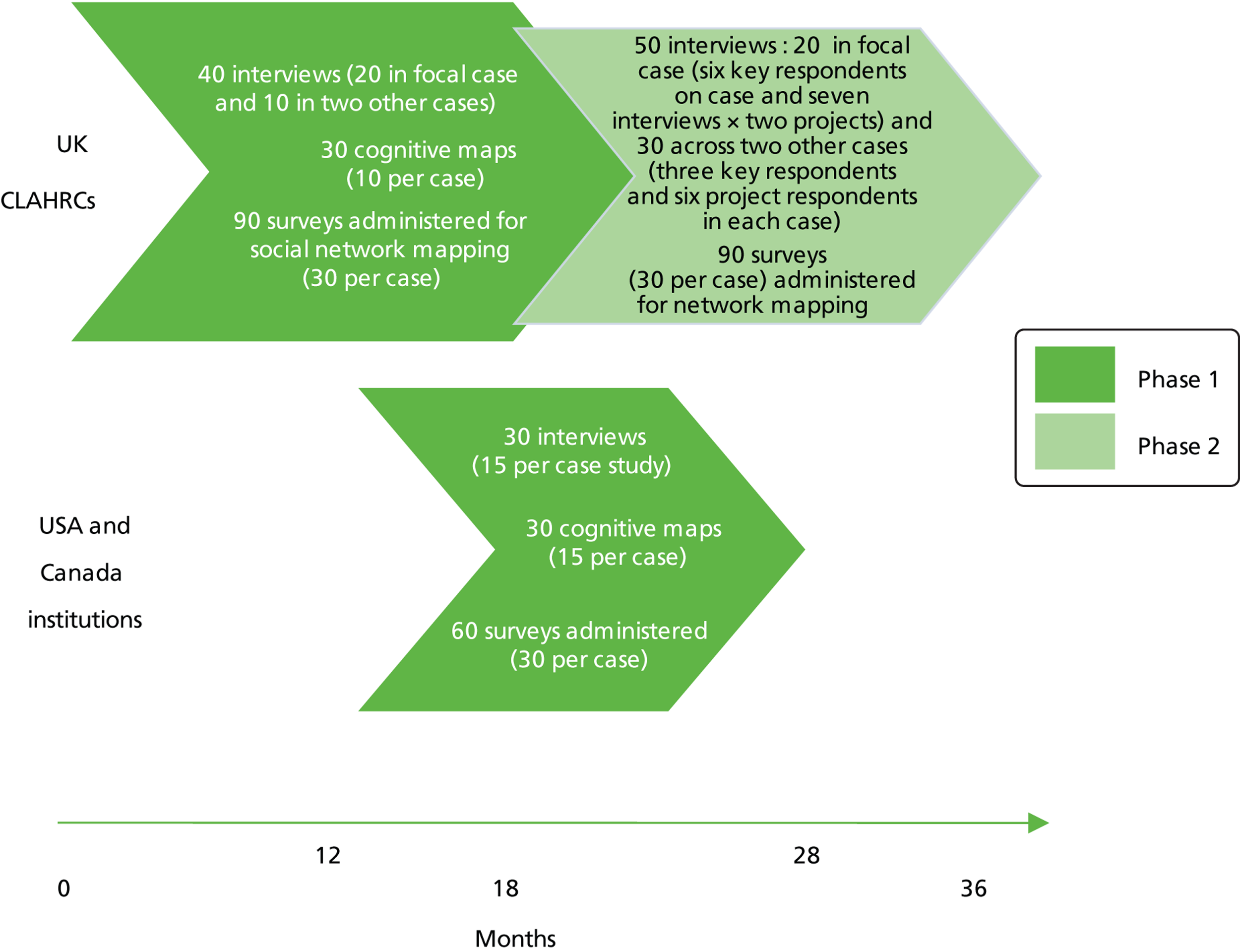
The fieldwork in North America was conducted in one phase. The data collection here was designed to meet objective 4 – that is, to allow a comparison of the CLAHRC initiative with similarly intentioned networked innovation initiatives in the USA and Canada, with a view to learning from these experiences while also recognising their distinctive contexts.
Before we commenced the study, the protocol was reviewed by the University of Warwick ethics committee. In addition, before the data collection with NHS participants commenced, the UK study was reviewed by the West Midlands research ethics committee (REC) and received a favourable opinion in July 2010 (REC ref. 10/H1208/30) allowing data collection to include employees of NHS organisations in addition to those holding university contracts.
The study was also guided by a scientific advisory board, whose membership included individuals with direct experience of CLAHRC operations, external experts, and a service user representative.
To operationalise our comparative case study design, we utilised three major sets of research methods:
-
qualitative investigation based on a comparative approach and involving the use of semistructured interviews with key participants across cases
-
social network analysis via the use of survey instruments
-
analysis of cognitions via the use of a cognitive mapping tool (Cognizer®, Mandrake Technology Limited, Leeds, UK).
The rationale and application of these different methods is outlined next.
Qualitative investigation
Data were collected using a case study approach, comprising three sites based in the UK and three based in North America. A case study design was considered appropriate for this study as this method supports the exploratory aims of this study, which are ‘how’ and ‘why’ questions related to the development of organisations over time through the interaction and relationships between individuals and communities within programmes of work. 84 In particular, this approach allows evaluation of the contextual conditions (at both the micro and the institutional level) that influence how the different modes of organising developed and deployed by CLAHRCs are able to support their KT endeavours.
It is important to note that the aim of our study was not to compare the CLAHRCs in terms of their overall ‘success’; it was recognised from the outset that, given the very broad remit of the CLAHRCs, and the different originating contexts, what counted as ‘success’ would be context-specific and would require a different kind of evaluation. 78 Rather, the aim of the comparison was exploratory and developmental – that is, to trace the ways in which different kinds of activities with similar objectives could support (or sometimes constrain) particular aspects of KT and innovative performance within certain contexts, and to compare lessons learned across cases. Thus, it is appropriate for this type of exploratory study to use a purposive sampling frame to select cases, as the aim is to use the distinctive features of each case to support our analysis by highlighting the role of particular case attributes and context in influencing how innovation is achieved, and the challenges and issues experienced.
The international dimension of the study was motivated by the (then) SDO call itself and by the benefits of international comparison in this field. We selected reference sites in the USA and Canada because these countries were highlighted in the Cooksey report8 as relevant international comparators for the UK. These are also countries that are recognised as leaders in health-care innovation, but which are facing, or have recently faced, similar challenges in terms of demands for translation. In addition, both the USA and Canada have undergone significant institutional reforms in recent years aimed at achieving more effective translation.
The three UK cases selected had all successfully bid for funding under the UK NIHR CLAHRCs programme. However, each initiative had enjoyed extensive flexibility in how they interpreted the remit. As a result, the visions which their leaders brought to the CLAHRC mission, and the associated governance and management structures which were put in place, varied significantly. We chose the three case study sites as they each represented different ‘experimental’ models of how institutional support can be used to develop collaborative networks to facilitate translational research. This allowed us to explore how the different approaches and attributes of each model related to the development of different types of capabilities for supporting innovation within a networked context. In particular, it allowed an analysis of how the characteristics of each case – such as its vision, its management approach, its structure and organisation – related to the capabilities it had for supporting an innovative programme of work. In addition, by conceptualising each case study as a ‘network of connections’, this approach enabled comparative study of how social ties supported KT between actors involved with the initiative.
To support our aim of identifying the interplay between the national or institutional context and the micro-level relationships which enable KT, within each case site it was important to contextualise how macro-level attributes of each initiative (e.g. management, governance, structure, vision) shaped how the various programmes of work within each initiative were achieved in practice. Therefore, for each UK case site, we selected three to four clinical projects to act as ‘micro-cases’ for us to explore in greater detail how project teams were able to achieve their work within the context of how each initiative was envisaged. In order to select projects that would be complementary across all three case sites, we first developed a selection framework tool to collect information about the background and aims of each clinical project, such as whether or not the project was developed from a pre-existing area of work, the type of organisations involved with the team, and the type of innovation the project work involved. The tool was completed by the CLAHRC core management, and projects were selected that fitted into three broad clinical topic areas (mental health, stroke and community services), as they represented complementary features across the three case studies.
The three North American initiatives are not part of the same funding programme. Instead, they were funded by different regional entities and by foundations (as per the two Canadian initiatives) or by federal money (as per the US initiative). Further details about the funding programs of each North America initiative are provided in the next section (see Qualitative data collection). In terms of the selection of specific clinical projects, the criteria varied across the initiatives. The Canada–Coordination initiative is a relatively small project that focuses on improving co-ordination among four health-care players located in the Ottawa metropolitan area and the clinical focus is on improving the quality of care of children with complex care problems. The Canada–Translation initiative involves a number of clinical themes ranging from mental health to the management of the relationships between doctors and patients. For this second case, we decided to focus on the creation of processes and practices promoting KT due to the fact that the initiative is relatively young and tangible research output on specific themes was not available at the time of our fieldwork. The US–Health initiative includes a broad range of clinical themes. In our qualitative analysis we present examples involving the management of the relationships between health-care structures and end users (i.e. the patients).
Qualitative data collection
Semistructured interviews were conducted face to face with individual members from three CLAHRC organisations within the UK as well as from the three North American initiatives. This was guided by an interview schedule, which was framed in terms of discussion of the three broad topics captured by the theoretical framework depicted in Figure 1 – that is, management and governance, KT processes/tools, and the development of social networks and relationships. Questioning encouraged interviewees to discuss specific examples of collaborative working (e.g. prompts such as ‘tell us about a situation where you have worked together well/where you have found it challenging’). The length of interviews was approximately 45–60 minutes, and the audio recordings were subsequently transcribed, providing texts of data for analysis. The interviews were supplemented by observational data and the collation of key documents, for the purpose of providing greater insight into the work taking place within the initiatives. This included attending meetings, including core management meetings, knowledge exchange, dissemination and engagement events. In addition, with respect to the UK CLAHRCs, original bid documents and NIHR interim reports were also collected. At the project level, in addition to attending project meetings, where opportunity arose, we also observed other activities, such as advisory board meetings and engagement events. We also collected written information about the projects, such as project outlines, information for participants, publications and other outputs.
In terms of the UK CLAHRCS, the first interviews conducted were with core members/founders of each CLAHRC initiative, such as the director, programme managers and other core members, and these members were reinterviewed in phase 2. Interviews were also conducted with members of the sample ‘micro-case’ project teams, which focused on three or four of the projects from each CLAHRC. The interviewees selected for phase 1 purposively targeted data collection from those in a variety of different types of roles (team leaders, managers, research and clinical professionals). Additional interviews were conducted with members of ‘specialist support services’, which were areas where each CLAHRC demonstrated particular types of expertise, such as academic advice in the form of economics and statistics support, KT and implementation expertise, and practitioner insight into areas of clinical services, commissioning, policy-making and capacity building. Depending on the different model of each CLAHRC, some of these members belonged to the clinical project teams, with others positioned in other parts of the initiative, such as central support and ‘cross-cutting themes’. Because of this variation, interviews with individuals in these types of roles were particularly important for understanding the distinctive ‘flavour’ of the vision of each CLAHRC model. In phase 2, follow-up interviews were targeted to be conducted with, primarily, the same representatives as from phase 1. However, owing to changes in personnel, particularly at the researcher level, these interviews typically focused on those in leadership and managerial positions from both central CLAHRC and project level, and also clinical professionals involved in project work.
In the first phase, interviews focused on the start-up of each CLAHRC, such as its set-up, aspirations, plans and initial formation of contacts. Documentary evidence, such as the NIHR funding application forms, website information and project-specific documents (such as study protocols), was used to provide additional information on these aspects and to reduce potential problems of retrospective accounting. In the second phase, interviews focused on what types of outcomes had been achieved, and the discussion focused on reflection about the experience of conducting a work programme within the CLAHRC context. In addition, textual information, such as interim reports and examples of outputs and dissemination activity, were used to supplement examination of the types of outcomes being demonstrated by each CLAHRC. In total, 67 interviews were conducted in phase 1 (Bluetown, 24; Greentown, 21; Browntown, 22) and 42 in phase 2 (Bluetown, 16; Greentown, 12; Browntown, 14).
In terms of the North American initiatives, we conducted a few preliminary interviews with the leaders of each initiative. Following a snowball approach, we were able to gain access to additional people involved in the various projects and to collect documents including presentations from steering and working committees and minutes of meetings. We were also able to attend (and record and transcribe) several meetings. The North American fieldwork was conducted in a single phase spanning September 2010 to March 2012. In total, we conducted 49 interviews and observations (27 with Canada-Coordination, 11 with Canada-Translation and 11 with US-Health). The criteria to select the sample followed the UK CLAHRCs (as one aim of the North American study is to compare the results with the UK CLAHRCs). Therefore, we adopted similar criteria and focused on people who were involved in the initiatives from the beginning, having a broad view of the overall initiative and, in most cases, decision-making responsibility.
Social network survey and research design
The use of SNA as an analytical tool within health-care research is still relatively limited, though there is growing recognition of the effect of social networks on the spread of certain medical conditions. 85 To inform our social network survey design, therefore, we drew primarily on a critique of the existing literature in the organisational and management studies fields. 86,87 In relation to the UK CLAHRCs, we wanted to know with whom CLAHRC individuals translate knowledge relevant to their CLAHRC work and from this construct an informal knowledge network for each CLAHRC organisation within the context of formal management structures. The following name generator question was used to yield a list of knowledge contacts: ‘Who are the most important (people) for you to have contact with in order to be effective in your CLAHRC work?’. We invited respondents to name contacts within their CLAHRC team, in the CLAHRC as a whole and external to the CLAHRC, with up to five names per category.
Following other studies of informal advice-giving and -seeking activities as the key processes of KT in professional settings,38,88 we also investigated the type of knowledge resources provided by CLAHRC network contacts. We asked respondents to describe the type of benefit provided by their contacts using the following knowledge resource categories: organisational/professional backing, technical advice, access to groups and/individuals, practical advice, management advice, or other. The survey also questioned the intensity/quality of knowledge-related ties based on emotional closeness and frequency of interaction and previous collaboration between contacts.
Our original proposal did not include undertaking SNA in North America, but we took the opportunity to conduct a SNA study at Canada-Coordination. To ensure comparability and validity, we adopted similar design and sample criteria to the CLAHRC study.
Collecting network data
The first task was therefore to identify individual members of each KT initiative through discussion with the health-care initiatives. Administrators of each KT initiative provided a membership roster. These lists were checked to remove individuals for whom participation in the study was not relevant. This included individuals who were no longer involved or employed by the organisation or who were on leave (i.e. sick/maternity/sabbatical). Delineation of each network sample was therefore defined by the criteria of CLAHRC membership. We then surveyed all individuals who we believed to be members of each CLAHRC. The same method was applied to our Canadian case site, Canada–Coordination.
With knowledge of who was in the network as well as demographic information on these individuals, it was then possible to assess the structure of KT between individuals in each health-care setting. An online survey was developed and individuals were sent an e-mail containing a web-link to access. The roster of CLAHRC member names was built into the electronic survey so that respondents were able to see the names of other CLAHRC members via a drop-down menu. Respondents were also able to name external contacts so that we were able to study KT relations beyond the CLAHRC. To show the development and changes of CLAHRC knowledge networks over time, the SNA survey ran for two data collection waves, providing data snapshots, which we refer to as time 1 and time 2.
Piloting
Prior to the official online release date, the survey was piloted, including testing and retesting, by a subsample of CLAHRC members and also members of the research team not involved with the SNA component of the study.
Response rates
The social network survey was sent to a total of 325 individuals across three CLAHRC health-care initiatives in the UK and 39 members of the Canada-Coordination initiative. The average response rate for the CLAHRCs was 71% at time 1 and 63% at time 2. The response rate from Canada-Coordination was lower than for the CLAHRCs. A breakdown of the response rates is provided in Table 1 .
| Health-care initiative | Time 1 | Time 2 | ||
|---|---|---|---|---|
| Respondents/sample (n/N) | Response rate (%) | Respondents/sample (n/N) | Response rate (%) | |
| Greentown | 75/109 | 69 | 68/102 | 67 |
| Bluetown | 93/123 | 76 | 54/100 | 54 |
| Browntown | 93/135 | 68 | 89/131 | 68 |
| Canada-Coordination | 39/77 | 51 | N/A | N/A |
Non-response and partial completions
Reminder prompts were sent to individuals who had not responded or who had provided a partial completion of the survey. The use of personalised e-mail prompts, telephone calls and reminders by CLAHRC leadership helped to achieve an increased response rate from members.
Validity
Our interim feedback reports and presentations to the KT initiatives allowed us to cross-check that the network ‘story’ that was being built made sense and resonated with CLAHRC members. In all cases, we received positive responses and helpful critical questions from the CLAHRCs. We also triangulated SNA and qualitative data sources.
Visualisation and analysis
Social network analysis was conducted using UCINET (Analytic Technologies, Lexington, KY, USA), with descriptive statistics and graphs in SPSS (SPSS Inc., Chicago, IL, USA) and Microsoft Excel (Microsoft Corporation, Redmond, WA, USA). In network visualisations, each ‘node’ represents a survey respondent/KT initiative member.
Limitations
Generalisability
We attempt to provide comparative analysis of the KT networks but, as per our research design, we do acknowledge that KT activities may be influenced by specific contexts.
Missing data and network size
Social network analysis is sensitive to missing data,88 and this inevitably impacts on our study (more so for time 2 data). Social network data are notoriously difficult to collect. The study was ambitious and we relied on building and maintaining strong, positive relationships with the CLAHRCs and frequent communication and interim feedback of findings. Time 2 data collection occurred during the period prior to CLAHRC refunding, which may help to explain the lower response rate. To help overcome the issue of missing data we assumed symmetry for relations where it made sense to do so in our analysis. 89 We acknowledge the effects of network size on other structural metrics such as density,90 particularly for the smallest Canada-Coordination network.
Other issues
Beyond general issues related to inaccurate survey response (i.e. respondent misunderstanding questions), we highlight that network studies can be affected by the accuracy of respondent recall. 91 However, omission of contacts seems to be an issue for studies on weak or distant ties92 and this study focuses on ‘most important’ ties for KT activities, relations which are likely to be more obvious.
The boundary specification problem is a common issue when studying social networks with unclear boundaries, that is, where it is not entirely clear who is in the network. For this study, the network boundary was defined by CLAHRC membership. Our survey also permitted the inclusion of external knowledge contacts if these people were deemed important to respondents in the context of their CLAHRC KT work. A fixed vertex degree research design limited the number of contacts respondents were able to name to up to five external contacts. This restriction was chosen to yield data on the most important ties in KT contexts both internal and external to the CLAHRC, and to prevent people from simply recalling contacts from memory, which would likely result in bias towards most frequent and recent ties.
We considered the trade-off between respondent fatigue and a survey of the whole organisation and concluded that asking for relations between all CLAHRC members would have been too burdensome on respondents. Our fixed vertex research design urged respondents to think about whom to include and exclude rather than freely name everyone, or name too few.
Cognitive and causal mapping approach
A number of studies on cognitive mapping highlight that this technique allows the identification of frames, schemas, and mental paths that characterise individuals as well as groups of people. 93,94 Causal maps (the tool adopted in this research) are a particular cognitive mapping method that highlight cause–effect relationships between a priori established ‘entities’ (or constructs) that play a role in a project/initiative. A common approach,95 and one followed in this study, is to identify inputs (i.e. drivers, factors or triggers) and outputs (i.e. aims, objectives or targets) of a project. The inputs are those elements that contribute towards reaching the outputs. It is clear that both inputs and outputs can vary and might be not clear to (or shared among) all participants in the project.
Scholars who apply causal mapping techniques are interested in knowing more about the beliefs of the participants in order to establish, for example, whether or not there is alignment between inputs and outputs. Alignment (or misalignment) of the participant’s beliefs does not always mirror the success (or the failure) of a project. However, knowing more about collective beliefs (as we do in this research) might help in understanding the development of a project. Therefore, we chose to adopt the causal mapping tool to (1) identify (common) perceptions of inputs and outputs of the five initiatives that we studied and (2) map perceived causal links between inputs and outputs.
As outlined in Table 2 , we were able to identify 28 constructs using a content analysis method applied to official documents of the three CLAHRCs (the bids) and similar documents of the two Canadian initiatives supplemented with data drawn from initial interviews with those involved in the initiatives. We used these constructs to develop individual and then collective causal maps for each initiative, using Cognizer®, a software tool that manages the causal mapping exercise.
| Focus | Governance and management | Design | Processes | Networks | Dissemination of findings | Outcomes |
|---|---|---|---|---|---|---|
| Conduct research that fits with national policy priorities | Have patient and public involvement | Design studies based on literature review | Conduct formative research | Enable collaboration within the agencies involved in the project | Disseminate findings to practitioners | Build capacity for health-care service delivery change |
| Conduct research that is focused on patient needs | Involve experts from multidisciplinary backgrounds | Conduct longitudinal research | Conduct ongoing review and evaluation of projects | Enable cross-fertilisation with similar local initiatives | Publish findings in academic journals and conferences | Improve the efficiency of health-care service delivery |
| Conduct research that considers local priorities | Have governance structure to oversee and co-ordinate activities | Use mixed methods (qualitative and quantitative) | Compare findings to national/international health-care standards | Enable collaboration between researchers and practitioners | Implement findings in practice locally | Improve the quality of health-care service delivery |
| Conduct research that fills research gaps in the literature | Use information technology for project management | Conduct applied research | Identify barriers to service change and redesign | Enable collaboration with external organisations (e.g. police, social services) | Implement findings in practice nationally | Reduce inequalities in health-care access |
Below, we provide a detailed description of the method adopted. The four steps follow Clarkson and Hodgkinson. 95
Step 1: We performed content analysis of a number of documents and interviews [using NVivo (QSR International, Warrington, UK)] of the three CLAHRCs and the two sites in Canada. The content analysis concentrated on gathering information regarding two main themes: (1) What are the factors that will lead to the success of the particular health-care initiative? and (2) What will constitute success for the particular initiative? We focused the content analysis on input–output constructs and identified unique codes (initially 516) for each sentence that corresponded to a statement linking an input and an output.
Step 2: We reduced the 516 codes to 28 constructs, cross-matching multiple sources of data. We performed a confirmatory test involving two academics experts in health care as well as six health-care practitioners from the various initiatives involved in this research, obtaining 95% overlapping results.
Step 3: Three independent researchers grouped the 28 constructs into seven categories, including four outcome constructs. As these are derived from a process of analysis of documents and interviews of the five initiatives where health-care systems are sufficiently different (Canada vs. the UK), we can argue that the identified constructs could be applied to most health-care service redesign innovation initiatives. In terms of using these constructs in a causal mapping exercise, the following process was undertaken (step 4).
Step 4: Using Cognizer®, software designed to produce causal maps, we involved people across the three CLAHRCS and the two Canadian initiatives. Following the approach identified in previous studies,96 we selected people who (1) led the initiative, (2) were decision makers and (3) were involved in one or more project committees. The participants to the causal mapping exercise were asked to (1) select 8 of 28 constructs (we removed the four outcome constructs from the list of available constructs), (2) rank order these selected constructs in terms of their importance to the initiative (we refer to this as the survey part of the exercise); and (3) rate the relationship between the selected constructs (we refer to this as the causal mapping part of the exercise). In terms of this last task, we elicited causal maps using Cognizer®, following the steps outlined by Clarkson and Hodgkinson. 95
Chapter 4 Empirical analysis and findings: qualitative investigation
Introduction
As noted previously, to be able to address the different dimensions of CLAHRC activity relevant to our study, we adopted a ‘multilevel’ approach in our fieldwork and analysis97 that sought to integrate evidence from both our CLAHRC-level and our project-level data collection to provide a coherent, narratively structured account of the CLAHRCs’ development.
The overall approach that we adopted to data analysis incorporated a hybrid process combining both inductive and deductive thematic analysis of interview data. 98 At a basic level, thematic analysis of interview data is simply where coding ‘is used to break up and segment the data into simpler, general categories and expand and tease out the data in order to formulate new questions and levels of interpretation’ (p. 30). 99 It was important to recognise that, in building our study on a theoretical concern with networked innovation,31,79 we had already made assumptions and developed ideas about the focus for the analysis. However, it was also important to allow our analysis to be data driven to allow new ideas to emerge during the process of coding. Therefore, we needed to develop an approach that allowed us to make use of our preconceived ideas and theoretical underpinning, while still maintaining the inductive flexibility of an approach that supports the generation and development of new ideas.
As interpretive research still needs to demonstrate credibility and trustworthiness through being founded on a systematic evidence of the research process, our data analysis was supported by a structured method that combined steps in which we were ‘data driven’ and inductively developed codes based on interesting ideas and themes that emerged from our study of transcripts, together with incorporating phases of review in which we reflected on how these ideas fitted in with the overall objectives of our study. Therefore, although our research analysis was based on a linear ‘step-by-step’ procedure, this still facilitated an iterative and reflexive process. 98 However, in following a structured approach, we were able to continually reframe our analysis both based on ideas from inductive study, and allowing our theoretical grounding to be an integral part of the generation of codes.
We used NVivo to support our data analysis. While NVivo can be used to support a more objective and logical categorisation of codes, we should recognise that this is only an aid to the organisation of the material and is not in itself an interpretive device.
To structure the individual case narratives outlined below, we have adopted three major headings which reflect our conceptual framework and support critical concerns around the development of the CLAHRCs. These headings are as follows: governance, management and organisation; collaboration and networks; and KT. To begin our account, however, we focus on the way in which the goals of the CLAHRC initiative were appropriated by individual CLAHRCs in terms of the vision which they defined for themselves.
The vision of the Collaborations for Leadership in Applied Health Research and Care
As the three case sites of translational initiatives within the UK were all created through the same UK NIHR funding programme, they were all designed to meet the same aim and generic mission. However, there was significant flexibility in the way in which this mission was interpreted by the leaders of different CLAHRCs. We term these interpretive acts of leadership as different ‘visions’ of collaborative translational research. Within our study we have explored how the vision of each CLAHRC has emerged from and interacted with the structuring of the initiative, particularly in terms of management and governance. By studying the CLAHRCs’ development over time, then, the qualitative fieldwork has been able to explore how these distinctive features of each CLAHRC influence their approach to KT.
Bluetown Collaboration for Leadership in Applied Health Research and Care
The Bluetown CLAHRC is based on a partnership with organisations from a large urban area. It is led by a university hospital with an established strong reputation in conducting research. The health-care partners are representative of a range of organisation types, including acute hospital, primary care and mental health trusts, which includes both organisations with extensive research experience and those that have been previously less involved. The CLAHRC was originally established around a simple ‘hub-and-spoke’ model of a small central management team and nine clinical project teams. The core of the CLAHRC, including its management team and several of the clinical project teams, is centred on a traditional medical school public health department with high-profile academic expertise in clinical sciences research, and historic links with the lead NHS site. Each project team is largely composed of members based in the same geographical base, with a number of teams based at the university, and other clinical project teams are located within one of the health-care partnership organisations. Specialist support services were included as a CLAHRC-wide resource, providing each clinical project team with access to people who could contribute medical sociology, health economics, methods such as systematic reviewing, and statistical expertise.
The director was integral to developing the vision for this CLAHRC and for embedding this within the different clinical projects. Throughout the development of this CLAHRC, his vision has been strongly influential on the form that the work programmes within the CLAHRC have taken as they have progressed. In particular, a clinical scientific tradition was incorporated into the design of study protocols at the start of the programme, with particular attention being placed on scientific methodological rigour, especially the production of outputs suitable for top-quality, peer-reviewed academic publication. In particular, all of the clinical projects were designed as prospective evaluation clinical-academic research studies and, therefore, constituted a set of work programmes all linked by a common scientific approach.
It’s to prospectively evaluate service delivery as it happens. And where possible to interact, you know, with managers and how the service delivery takes place. So that the product will be examples where this has happened prospectively and good examples that have been published in good places. In the process of doing that to export the idea or develop the idea in the local area.
BLUETOWN001
This illustrates a cornerstone of the Bluetown CLAHRC model: the vision emphasises that the quality of the evidence being produced is crucial to its ultimate impact. As a result, the vision of this CLAHRC was founded on the view that any programme of work should first be grounded in a rigorous scientific approach, as only high-quality evidence should be taken up within health-care policy and practice.
Management, governance and organisation
The CLAHRC was originally formed around a small central leadership team, with the vision of the director strongly influencing the focus and direction of the CLAHRC model. As the director had a historically strong reputation in the local area, this helped to legitimise the CLAHRC as something that was perceived as of value by those in senior positions within the partner organisations.
The vision of the core management team has been strongly influential on the approach that each programme of work uses. Each programme of work is expected to use a rigorous scientific design and methodology in order to produce robust evidence that is suitable for publication in high-quality academic journals. Therefore, the model builds on the approach to scientific work that was historically conducted by the lead organisations, with the CLAHRC emphasising that through these work programmes the teams should foster collaborative relationships with relevant service areas. This vision is emphasised through the role of the leaders within each of the project teams, who provide scientific and methodological direction to the programme of work. However, although there is recognition of the overarching objectives expected from each team by the central management, there is no CLAHRC-wide strategy for how each team should be structured or how collaborative relationships should be formed and developed. As a result, the lead of each project team has been provided with extensive flexibility on how their individual programme is organised. As a consequence, each team tended to foster relationships with particular groups and communities as relevant to the local services on which they were gathering evaluative evidence. The influence of the CLAHRC was important here in formalising and legitimising this collaboration between clinical academics and targeted groups in the NHS.
Without CLAHRC, we would have some of those connections but I think the momentum, thrust and energy that’s going into current programme really wouldn’t be there . . . associating with individuals from other fields, groups that we wouldn’t normally be part of. This has really allowed us to reflect more objectively on work, and the direction we’re going.
BLUETOWN022
Structural features of the CLAHRC were used to communicate the overarching objectives of central management to the clinical project teams. This involved regular interactions between the centre and projects, management representation at project team meetings, and programmed meetings for project leaders and project managers. The positions which project members held in other environments (i.e. outside of their own team environment) were typically construed as ‘honorary’ – that is, not part of the main role which project members perform within their clinical team or central management group ( Box 1 ).
Observation of the interactions within a project meeting illustrated how the vision of the overall initiative is emphasised through the presence of a member of the core management at clinical project meetings. The core of the project team is based in a different location to the central CLAHRC. However, the team also have a number of affiliated members who contribute different types of expertise, such as health economics and clinical-academic insight. At the outset of the meeting, the advisory member recounted how she had earlier met with members of the central CLAHRC and discussed the overall objectives of the CLAHRC. She was asked to stress the core management group’s strategy and approach for the CLAHRC, and in particular the need for the team to consider where findings from the programme of work could be published in academic journals. She describes her role within the project meetings as ‘to remind the project team of central management’s priorities and viewpoints for the vision of the initiative’.
Although the majority of clinical project team members share similar types of disciplinary expertise, with most having clinical–academic experience, the structural organisation of the initiative provides access to other types of expertise. The extent of the CLAHRC-wide resources means that individuals with expertise such as health economics, statistics, systematic reviewing, sociology and communication are easily available for project teams to access. With the sociology theme, for example, each project team allocated a small proportion of their own resources to support the employment of a select number of people with this type of expertise. Although these team members come from different working cultures from the majority of the CLAHRC members, it is clear to the clinical project teams that the director values and respects the expertise that these individuals can provide. This helps to legitimise their contribution within the teams, even in sociological territory, which such teams would not normally view as part of their remit. At the start of CLAHRC, the cross-cutting activity for sociology was an undefined programme of work, but this provided an opportunity for these members to liaise with the clinical project teams to identify how they could support their programme of work. As relationships were built up, they quickly identified certain project teams where they could add value to the other work that was already planned by the team lead.
We are officially termed as a cross-cutting theme but we’re also embedded in the individual research, as in our jobs are paid out of individual projects.
BLUETOWN003
This cross-cutting work has become an embedded part of a proportion of the clinical project teams. Although they provide a different type of expertise to the clinical projects, the members of this cross-cutting theme enact their role in such a way as to fit in with the overall work programme. While, overall, the cross-cutting theme constitutes only a small part of the CLAHRC, resources were deliberately allocated so that the members of this group would be highly skilled and experienced, and therefore able to achieve this. They have also been able to contribute guidance to more junior members of the project teams who are involved with areas that overlap with their area of expertise, such as qualitative components. Observation from in-depth studies of the four clinical themes indicates that this approach has facilitated the ‘embedding’ of the cross-cutting theme members within the project teams.
Networks and collaboration
The qualitative interviews demonstrated that from the early stages of the CLAHRC’s development, a clear objective was understood to focus on working with stakeholder groups, such as collaborating with NHS practitioners and managers within the clinical project work. There was also acknowledgement that this required some compromise with established academic work practices, with some effort being required to produce work that is suitable for practitioners.
Getting researchers to understand practitioners is a covert aim of CLAHRC. So that you don’t go away for five years and then tell them what they should have done in the first place because practitioners don’t want to hear that.
CMBLUETOWN007
The activity of each of the clinical project teams means that they create links to defined health-care organisations involved in the CLAHRC partnership. The interaction between members of the project team (e.g. the project lead) is integral to fostering the relationships among the official partner organisations of the CLAHRC. As many senior CLAHRC members had pre-existing collaborative relationships with NHS trusts, they were able to enact ‘senior’ boundary-spanning roles. Many of the theme leads were in clinical–academic dual activity roles and held honorary contract positions with NHS organisations. However, their leadership typically reflected the wider ‘epistemic’ community of a university setting, emphasising academic values rather than the practical concerns seen in the health service environment. For university-based teams, the collaborative interaction was framed by the values of the academic community, with high-level academic publication considered as important for demonstrating value to these groups. This was seen as consistent with the vision of the CLAHRC, in that the collaboration is seen as creating a culture within health-care settings which is more receptive to high-quality scientific evidence.
It’s nonsense to say . . . the PCT health, local authority or the voluntary sector don’t consider evidence. They do. They just consider evidence perhaps in a different way than you or I perhaps might consider evidence . . . The CLAHRC process is about the better, the optimal decision making that we can bring, the greater rigour, to set different parameters for making the decision. That is the value.
BLUETOWN014
Thus, the CLAHRC emphasises clinical–academic evaluation of service delivery in terms of producing high-quality evidence. As a result, the CLAHRC’s applied health research is conducted on the terms set by the clinical–academic community, to which other groups must be able to fit in. At the same time, the CLAHRC’s strong scientific reputation within certain fields helps it to build links with communities that value this type of evidence, such as national policy groups and certain local clinical groups. Certain groups of health-care managers and policy makers were perceived as valuing exactly this type of evidence.
Publishing all this information in top quality journals as absolutely, absolutely key. Not just to the academic credibility of CLAHRC but to the managerial credibility of CLAHRC . . . dealing with managers, when they want to know how good somebody is the first thing they do is see whether other academics respect that person. And one method of that is you publish in the top journals. They don’t want to deal with somebody who’s not up there at the cutting edge. They want to be with the front people.
BLUETOWN001
The work taking place within these themes tends to be dominated by the traditions of the theme lead and the culture where the theme is physically located. Non-health care-based teams do use ‘in-built boundary spanners’, pre-existing contacts and mechanisms such as advisory boards to draw on insights about the local health-care context ( Box 2 ). This approach enables the teams to focus on their own academic areas of expertise but perhaps supports depth rather than breadth of approach.
Although this CLAHRC did not have a formalised structure within its functional design to facilitate connections between clinical project teams, the flexibility provided for each subgroup in how they organised their day-to-day work meant that each team developed a tailored strategy to facilitate collaborative working for their own programme of work. The teams that were based within the university were faced with a challenge of how to develop and maintain collaborative working relationships with the NHS organisations involved in their study. One approach that supported work was the inclusion of NHS practitioners who took on a research role as part of an opportunity:
It’s much easier for me to go in to do data collection at the Trust I belong to, because I know the people or I can very easily find the right people to talk to, to point me in the right direction of people to contact . . . I think being a clinician has made it easier for me to build a rapport with the clinicians, what I’m actually finding really difficult is trying to get, you know, working ties with the nursing staff.
BLUETOWN012
It is significant that in this example that, as the practitioner involved was a clinician, they felt that they could naturally interact with other members of their profession even when they belonged to a different NHS organisation. However, they felt that it was more difficult to perform similar roles with those from different clinical professions, such as nursing staff.
Bluetown CLAHRC also includes a number of themes based directly in health-care organisations. As the teams working on these themes are closer to the issues of practice, their work has the potential to more easily impact on health-care practice. In ‘speaking the same language’ as the practice and community groups they intend to impact, they are in a better position to integrate the perspectives of these groups. This should facilitate the implementation of findings and local impact that these groups will have. However, as these teams are further away from the core CLAHRC, greater attention has been required to ensure that these themes feel part of the Bluetown CLAHRC community.
Knowledge translation
Bluetown CLAHRC was not built on an explicit CLAHRC-wide strategy for KT. However, as each project team was provided with extensive flexibility in how they organised their clinical study, each individual theme has developed their own strategy for dissemination of outputs, with a flexibility to interpret the aims of the CLAHRC to fit their own clinical context. As a result, the themes have developed their own tailored approaches to relating their findings to local health-care practice and policy. These are not, however, related to an overall CLAHRC plan or strategy for this approach to the work. Additionally, these approaches do not appear to be shared between the themes, and their context-specific design may potentially limit wider application.
Overall, the Bluetown CLAHRC is formed from members who represent both academic disciplines and health-care professional groups. This means that the cumulative work of Bluetown CLAHRC has the potential to innovatively incorporate many different perspectives and draw from different types of expertise. However, currently, these tend to focus on project–team connections, which limit the potential of a co-ordinated Bluetown CLAHRC effect across the region. The lack of a co-ordinated strategy to link with the different types and levels of the Bluetown partners may have limited the capacity-building of the CLAHRC as a whole, notwithstanding the benefit of the strong relationships fostered by each individual team.
As the CLAHRC developed, a new theme of knowledge management was developed by the central CLAHRC management team. This was designed as a high-level cross-cutting theme. The activity was separate from the clinical project work.
But having said all that I am very keen to in addition add a specific knowledge management function to the CLAHRC but I am very clear this is not based on discoveries made in the CLAHRC, although I would not exclude those, but it’s not based on that, it’s based on the knowledge out there in the world, what can we make of that. So knowledge exchange if you like.
BLUETOWN001
However, it drew on the infrastructure that the teams had used and fostered during the early stages of the CLAHRC. In particular, it was felt that, as the clinical project teams had demonstrated activity within the NHS organisations at an early stage, NHS managers and executives valued the work of the CLAHRC, and that this facilitated buy-in for this new venture.
Due to the financial model of the CLAHRC, no specific funding was allocated to this area. However, NIHR Flexibility and Sustainability Funding money was allocated to this activity. As part of this, the core management team was expanded to include support for the clinical teams and CLAHRC as a whole with external engagement and communication and dissemination activities. In addition, a knowledge-exchange forum was developed. This was targeted at high-level managers within NHS and local authority organisations. The meetings acted as a place where NHS organisations could discuss issues that they considered important areas for further work, and the CLAHRC team developed these ideas into discrete programmes of work in which they provided the resource for tailored evidence to be produced.
In this sense, as led by the director, this CLAHRC has evolved to incorporate new objectives as it has developed over time. However, the original vision of the CLAHRC model has been central to supporting the development of these new components. In particular, the knowledge-exchange forum has drawn on the connections fostered by the clinical teams, and the reputation established within partner organisations and beyond. This has allowed them to generate a membership of executive-level personnel who are in decision-making and management positions within their own organisations. Overall, the conceptual vision of the CLAHRC has helped to expand the CLAHRC programme of work beyond the initial set of clinical projects ( Box 3 ).
Theme 1 was built on what they describe as ‘a unique opportunity offered by these changes to carry out longitudinal studies into the interaction between changing drivers (physical, cultural, and financial, sometimes encouraging, often constraining) and service redesign’. The collaborations between the university-based team and the three health-care organisations were new, and the central CLAHRC formal partnerships were important in legitimising their initial formation. However, considerable attention was required by the team to be given to fostering these relationships.
Although the work of the theme was initially focused on evaluating particular areas of health-care services, the design of the work package was always aimed to be able to be easily applied to other areas. The model of work was specifically designed to be generic to all service areas with the aim of producing a product that could be offered to support the redesign of any services through their evaluation approach.
For sustainability, our theme is much more generic, it’s about any clinical system that is looking at redesign. We have a model that if we can get awareness high enough we create a market if you like for ourselves. And because we have these capabilities which is clinical area neutral, we can do it for anything. The approach is generic.
BLUETOWN011
As the work programme has progressed, it has been important for the team to use the connections they have developed in order to realise their aim of offering this ‘product’ to develop future programmes of work that the health-care organisations themselves have identified as important.
This theme, started off as being a theme that was tracking the development of hospital services over three hospital sites. Now we’re getting much more involved in working with hospitals on determining what it is that they might want to improve in the future and evaluate it.
P2BLUETOWN204
Reflections on the Bluetown Collaboration for Leadership in Applied Health Research and Care model and its development over time
The Bluetown CLAHRC’s vision and structure enables it to collaborate readily with those communities that are more aligned with the working practices of its members. The partner organisations and the members involved in the initiative, therefore, tend to support the principle that only rigorous evidence should be used to inform service developments. However, within this constraint, the Bluetown initiative does support new operational approaches, and in particular emphasises that project teams need to develop collaborative relationships with external communities, especially management and decision-makers.
With no overarching CLAHRC-wide strategy to support KT activity, each theme has developed approaches tailored to their own local communities and clinical context to support the mobilisation of the knowledge produced through their programme of work. However, as the CLAHRC has progressed over time, central management have augmented the original structure to develop new aspects to support overall Bluetown CLAHRC work. For example, they identified that CLAHRC-wide support was required to support the dissemination activities of the individual project teams. As a result, new central support was established to facilitate engagement of the project teams with end-users of their research, and to support the translation of research findings through a CLAHRC-wide communication strategy within the region.
Greentown Collaboration for Leadership in Applied Health Research and Care
The Greentown CLAHRC is led by a mental health trust, and the core of the initiative builds on established academic-research links between this health-care trust, a university hospital acute trust, and a university institution. However, an aim of this CLAHRC is to spread beyond the organisations that have traditionally been involved with research in order to build research capacity in localities further away from this core. As such, partner organisations are spread over a large geographical area, comprising a mix of urban and rural areas. The overall aim of the CLAHRC is to use an organisational learning model to facilitate a change in how research is conducted and utilised within the region. One key component of the model of this CLAHRC is about using the research experience of members from the ‘core’ organisations as a foundation from which this expertise can be dispersed and built on in other areas that have not traditionally worked in this way.
One of the things that CLAHRC was trying to do is move outside traditional university clinical centres, that would be located in this region . . . So it was not just about getting research into practice per se but broadening research into practice . . . In [another area] it’s red neck territory . . . best practice isn’t as evident over there as it is around the university, the trusts closely located to the university.
GREENTOWN001
The CLAHRC model is built on an organisational learning approach which aims to close the gap between academia and practice. Within this approach, the vision of this CLAHRC is to develop the initiative in such a way that it can bring about a ‘step-change’ in how research is delivered and services are designed by facilitating a change in how the different communities involved conceptualise and undertake these types of activities. From the outset, the Greentown CLAHRC model created a number of structural features which were intended to embed this vision into its operational organisation. Key features include the clustering of work programmes within a small number of defined clinical themes, which support the building of communities around these clinical areas. There was also resourcing of dedicated ‘knowledge broker’ roles, through which a selected group of practitioners would support KT from project teams to the wider NHS. Cross-cutting themes were formed with the aim of providing clinical project team members with specialist forms of expertise in areas such as KT, synthesis of evidence, external engagement and communication, and statistical support. A CLAHRC-wide approach guided a similar constitution for all project teams, which included explicit mechanisms to support boundary spanning between different communities, through incorporating links within the structure of the CLAHRC to support the contact academics have with practitioners and managers in health services. This illustrates a key attribute of the Greentown vision for the CLAHRC in which the model that is being developed is designed to close the gap between research and practice by changing the working culture of the various stakeholder groups involved. However, as the CLAHRC has progressed, issues with the original approach were recognised, and amendments to this vision have been undertaken.
Management, governance and organisation
Greentown CLAHRC has had several changes in leadership since the decision to apply for a CLAHRC was made, with each one bringing different types of professional expertise to the role, ranging from clinical–academic, through business school academic, to health-services executive management. These changes in leadership are reflected in the ways in which the vision and approach of the CLAHRC has evolved from its conception and funding application through to its latter stages. Each new director has contributed a particular characteristic to the CLAHRC through their leadership. As the first director of the CLAHRC observed, the novelty of the role itself created a need for it to be ‘interpreted’ and ‘enacted’:
Even if they’d had a visible leadership role before the structured things were set up the brokering, engagement, it can be quite intangible. These sort of things have come to the fore . . . I am doing a leadership role that’s much more strategic and autonomous and I think there will be a degree of variability and interpretation of what the role is and how it’s enacted. My first port of call was to get practice on board. Those chief execs are quite frightening people sometimes. So get practice on board. So I went round every trust board that was a partner in CLAHRC and presented the CLAHRC.
GREENTOWN001
As this suggests, the agency demonstrated by the leadership of the CLAHRC has been important in shaping its approach to KT. The original head of the CLAHRC bid was a clinical academic with a strong reputation in mental health research. A change in leadership was made to a specialist in organisational studies, with the aim of emphasising that the CLAHRC model was about a different way of working compared with traditional, standalone clinical–academic projects.
Overall, however, Greentown CLAHRC is structured around a set of clinical research programmes of work designed by clinical academics (i.e. typically a professor from one of the medical school clinical subdisciplines). These focus on applied health research issues to do with the delivery of services for chronic and mental health conditions. Although the basic form of the clinical themes persisted over time, they were eventually complemented by the creation of explicit structures for cross-cutting work. A considerable proportion of the finance was reallocated away from clinical research into implementation science to emphasise the integral role of this approach to their proposal. This process of evolving the planned model for the CLAHRC has generally been viewed as a positive process that enabled the CLAHRC strategy to be well defined by the time it started, supporting earlier progress.
And I mean, that letter and the feedback, you know, it was fairly explicit and it provided a platform for the reworking in the bid. You know, along implementation lines and gave me legitimacy to lead it . . . And I think that referral process was really useful for us. I think we were able to hit the ground running to a much greater extent than the other CLAHRCs.
GREENTOWN001
Initiative-wide structures connected each clinical project team to members who provided specialist academic expertise, such as KT or statistical support. These fitted in with CLAHRC-wide activities, and were incorporated into the Greentown CLAHRC organisational model as a way of facilitating the sharing of different types of expertise with members from varied disciplinary and professional backgrounds.
This incorporation of this greater emphasis on implementation work was included after the majority of the core individuals had already ‘signed up’ to be part of the bid, and at a point when much of the focus for the clinical research projects had already been decided. In effect, the new KT strategy was grafted onto a CLAHRC structure that had evolved around a more traditional clinical–academic research model. Therefore, this new emphasis on an explicit implementation strategy had to be adopted by CLAHRC members with established interpretations of their roles, and where much of the content of the CLAHRC’s work programme had already been specified.
The majority of CLAHRC members are employed by the university, and many are co-located. However, as the CLAHRC spans multiple university departments, bringing together academics from a clinical–academic background within community health sciences, and social sciences from business and sociology departments, it created significant challenges for members with different types of expertise trying to work together.
For the clinical scientists this is a completely new way for them to do any work . . . They’ve never thought about the wider implementation aspects and actually how do you physically get research into practice.
GREENTOWN002
As Greentown CLAHRC is built on a cross-disciplinary academic collaboration, this CLAHRC has faced additional challenges of working across the academic norms and practices of several different academic disciplines, including clinical sciences, nursing and allied health, and management and social sciences. In practice, it has sometimes been difficult to align these different spheres, especially in relating the conceptual remit of the cross-cutting themes. A further change to the leadership was made in the middle phase of the CLAHRC’s time frame, bringing in a director with a background in NHS executive management. This move helped to bring about a shift towards greater engagement with different types and levels of NHS organisations, in order to make the CLAHRC more NHS facing. At the same time, a key part of the restructuring from the mid-term review of Greentown was designed to combat uncertainty about the role of different programme components, and particularly the cross-cutting themes. In particular, as the CLAHRC’s vision emphasised new ways of working, it had been difficult for individuals to comprehend what their role should involve, or to fit this into traditional career trajectories.
As part of this restructuring, roles were divided into academic and non-academic parts, with the aim of allowing each member to focus on their own form of expertise, and to provide clear access to other types of skills. As a result, the CLAHRC was able to become more NHS facing, with a clearly defined team to assist with the delivery of research to practitioner and policy communities.
Networks and collaboration
A typical configuration for the arrangement of positions within project teams had been designed by central management and was used across the initiative. Each core team was established around the team leader, which generally involved other colleagues from within the same academic subdivisions, and the employment of other team members who had trained within similar academic areas to fill designated roles for research and management of the programme of work. Additionally, management created a team structure that aimed to create connections between the core members of each project team, and other team members who could contribute different forms of expertise. These included ‘knowledge broker’ roles aimed at facilitating externally directed ties within health-care or community organisations. These acted as an explicit mechanism to support KT between different communities. An account provided by one team member who had taken on one such externally focused ‘knowledge brokering’ position describes some of her responsibilities within the team, and highlights how working across boundaries was achieved. She describes how an important part of this aspiration is for the team members in the designated brokering positions to spend time with external groups who are relevant stakeholders for to the intervention they are studying.
I did a lot of meetings etc., doing a presentation, explaining about the project. You need to tell them what’s happening with the project and how it’s going to be implemented locally, what the practice can have on them. And they’re a key part of making it work. Whether you . . . take their ideas up or we’re bringing ideas from the [initiative] to them, I just think it works both ways. So that won’t work or this won’t work and what about these participants, how is that going to work? Is there any money for that and then have we got stuff for that. Stuff that people in the university don’t understand.
Members in defined boundary-spanning roles within academic-centred project teams describe how they use team meetings to, for example, bring in insights about public health issues to the academic core team members. We observed in one discussion how project meetings were used as a place where the implications of the information provided by external groups was incorporated into a discussion on developing a sustainable implementation of the intervention which the project team were researching. Senior academic members of the team integrated this information by aligning it with the scientific and methodological approach for the project work, such as considering how this related to the study design, and the implications changes to the protocol would have on demonstrating the academic rigour required for high-quality journal publications.
I think a CLAHRC is about doing things differently to what’s been done before. I think the only way to do that is to bring in people who have different backgrounds and different experiences, who understand the world in a different way. Because I think one of the problems that the CLAHRCs are set up to address is that academic research is done for academics and clinical research is done for clinicians and the twain don’t meet. And I think this CLAHRC has been sensible in bringing in people from different backgrounds.
GREENTOWN002
The structure of Greentown is centred on themes defined by related clinical areas. This supports the achievement of collaboration between CLAHRC members and relevant stakeholders in the local area. The commonality of many activities covering mental health, and related projects within the stroke rehabilitation theme, has provided an opportunity for CLAHRC members to develop communities around these clinical areas. In building on the formal roles to link project teams with external groups, efforts were made from the project team leadership to develop relationships with communities relevant to their research topic. With the senior leaders already having a reputation within their field, this provided a platform for connecting with stakeholders from within the local region, and in presenting a body of ‘CLAHRC-type’ work to national clinical groups.
As part of the CLAHRC-wide strategy, the building of ‘communities of practice’ is actively promoted as an approach which can ultimately support the implementation of evidence into local policy and practice. Four groups are perceived as particularly important: academics, clinical practitioners, health services decision-makers (managers and commissioners) and service user representatives. In particular, creating connections and building on links of existing networks of practitioners is viewed as a strategy to support this aim. In addition, the importance of developing relationships with opinion leaders within the local area has been described as an important part of the implementation process. The CLAHRC has developed an inclusive register of associates, where anyone who is interested in the CLAHRC work can sign up to receive updates about the CLAHRC work and are invited to events. Many of the activities and events are formed around the clinical topics that are of mutual interest, which forms an emergent community for people within the local area to connect to certain groups within the CLAHRC.
Knowledge translation
Greentown adopted an explicitly translational approach for informing external communities, such as commissioners, decision-makers and clinical practitioners, about the results of the clinical teams’ programme of work. This was based on a standard template and style of writing which emphasises the implications for policy and practice. These ‘bite-sized’ outputs operate as a tool to support KT of the work of the CLAHRC to the local practitioner and commissioning community. They require the academic teams (with assistance from specialist support members of the CLAHRC, and those with insight into practice) to tailor the way in which their work is presented for different types of audiences ( Box 4 ).
A clinical project team organised a workshop to share interim findings from their programme of work. This both acted as a strategic tool for the dissemination of the study interim findings and allowed the team to receive feedback to inform the direction of the next stages of the programme of work. The vision of the initiative was described as ‘formalising the working arrangements’ between researchers and external groups, with many of the teams developing connections with pre-existing networks of relevant stakeholders within the clinical area they were studying, and incorporating representatives of these communities into advisory boards. It is clear that members of the initiative considered that these connections facilitated the form and utilisation of the outputs that the teams ultimately produced.
Somehow the clinical link is usually missing. Sometimes research is done in academia and is not always pertinent to what’s happening on the ground. But in developing [the output from our study] we looked at the Cochrane database, and went through all the statements and things that we were doing in clinical practice that weren’t necessarily in the database. And then I took it back to the clinical team and asked them their opinion. So I suppose that was the link between the clinical team and the researchers.
GREENTOWN013
The workshop helped to create an environment where the boundaries between the academic world and that of policy and practice could be spanned. The use of such events by this team facilitated the sharing of information and insight between the different communities involved with the initiative, who through their normal day-to-day working approach would otherwise not interact with other groups in a way that would allow them to consider knowledge from different perspectives.
In addition to organisational-level mechanisms, roles performed by individuals acted as bridges to support KT between different communities. Members in defined boundary-spanning roles within academic-centred project teams describe how they use team meetings to bring insight to the academic core team members relating to issues about using the public health intervention in a community setting:
I add an ability to look at things from an outsider’s perspective and say, ‘why are you doing it that way?’ And I think there’s as much challenge to academia as there is to the NHS. I think this CLAHRC along with the others were set up with ‘we’re the academics, we’ve got the knowledge, we’re going to tell you what you need to know’. And actually one of the biggest shifts that’s happening here is that academics have to get a sort of understanding of a new process around the democratisation of research.
GREENTOWN009
Ultimately, these individuals were able to work with the academic team by enacting roles, such as ‘translating’ how information should be presented for different audiences. They also acted as ‘interpreters’ when providing insights into the practical implications of particular implementations of interventions, and helped to negotiate or legitimise the CLAHRC’s work in non-academic settings:
One of the goals was to try and encourage evidence based practice, and it’s using people like [the clinical practitioner who is a team member] to try and overcome some of the barriers. He’s very useful, as being a clinician he would command quite a lot of respect.
GREENTOWN018
However, this KT occurred very much at the periphery of the project team’s work, with little impact on academic work practices. The creation of explicit knowledge-broker roles provided a formalised link for the team to work with those with academic expertise, and we observed how the project team meetings were used by its members as a focused time and space in which the insight and knowledge of those from beyond the community of the core team, such as academic advisors, and those representing the vision of the central management of the initiative, could be considered.
Reflections on the Greentown Collaboration for Leadership in Applied Health Research and Care model and its development over time
As noted, this CLAHRC has explicitly aimed at developing a model in which its members work in new and different ways. However, the qualitative data suggest that, in practice, there have been issues with the effectiveness of the CLAHRC’s original model. Some members (including leads) have failed to fully engage with the work of the CLAHRC (a key objective of the CLAHRC model), as they have struggled to understand the purpose and remit of certain elements of this CLAHRC’s structure (e.g. what the purpose of the implementation theme is; what the role of knowledge brokers is), and how they can integrate the CLAHRC model into achieving clinical sciences programmes of work.
The changes that took place in the mid-term of the CLAHRC’s life cycle were designed to take these challenges into account. Overall, the vision of the CLAHRC was reaffirmed, including the organisational learning model and its structural features and roles. However, it was recognised that the original CLAHRC model had led to some confusion about the contribution of particular roles and themes. As a result, the restructuring involved redefining roles to emphasise the specialisms of particular members, while providing greater resources for individuals with the expertise to make the CLAHRC more ‘NHS facing’.
Browntown Collaboration for Leadership in Applied Health Research and Care
Browntown CLAHRC is based on a partnership between the universities and health-care organisations within a region that comprises several metropolitan boroughs. The core activity of the initiative is centred on organisations based within the same city that have historically been engaged with research activity. Many of the CLAHRC members are employed either by the universities or by the acute health-care organisation within this city, but the CLAHRC was also designed to build extensive numbers of new collaborative relationships between different communities based across these organisations. In particular, the initiative brings together academics from across different departments and universities who have not previously worked together. In addition, a range of health-care organisations are involved as partners, including acute hospital trusts, primary trusts and mental health services.
This vision of the CLAHRC is described as bringing about a step-change in the way research evidence is used, so as to influence the design of health-care services within the region and to improve their quality and effectiveness.
I initially thought the initiative would have been that the content and the research questions that were there, although soon I began to realise that although they’re important, it was about a much bigger transformation in the way that things are done. To get a paradigm shift really.
BROWNTOWN014
The metropolitan area has a high level of health inequalities, and the CLAHRC programme of work is structured around groupings of clinical research projects for various long-term conditions which are undertaken using an applied health approach. In addition, there are a number of separate activities that use KT approaches to undertake later-stage implementation programmes of work designed to directly interact with and impact current health-care policy and services. There is a strong emphasis on capacity building within the various partner organisations across the region in relation to developing expertise on how evidence is handled. Overall, both the clinical research projects and the KT programmes of work are based on a model of integrating members from both research and practice by embedding a focus on practice-based issues.
It’s about addressing the second gap in translation. So it’s about getting research very close to practice or as part of practice. So it’s about undertaking applied research or making sure that research is implemented into practice . . . I don’t think it’s on practice, it’s research with practice . . . really integrating research as practice almost to improve services as you go along through reflection and action. The implementation arm is exactly the same, it’s really trying to get research so close to practice that you can’t really see a difference. So I think it’s about the full bridge really. So it’s about not saying research is one place and practice is another, it’s about trying to make things a lot more connected and integrated.
BROWNTOWN021
The CLAHRC’s leadership is largely from an allied health and nursing background, with the CLAHRC membership including a high percentage of academic researchers and health-care practitioners with an allied health background. The vision of this CLAHRC is consequently informed by the practice-based approaches traditionally used within allied health professions, including an operating model centred on applied activities that aim to seamlessly integrate research and practice. However, while the approach of this CLAHRC fits well with the working practices of the allied health professions (both research and practice), it faces greater challenges to involve other groups, such as academics from other disciplines.
Management, governance and organisation
Browntown CLAHRC is built around a novel collaboration between the two main academic centres within the region: one which focuses on traditional forms of clinical science work, and another with expertise in allied health. This allied health ethos is reflected in the types of partnerships that are being built with the NHS, with strong links with senior and middle-level management in nursing and allied health within the partner trusts. These have been influential in informing the Browntown programmes of work.
This is not centric about the university. This is about an NHS collaboration that is distributed across a health environment, a health economy . . . It is about long-term conditions, and about knowledge mobilisation.
BROWNTOWN002
In practice, this CLAHRC model faced challenges in creating a coherent overall programme of work that integrated members from a wide range of professional and disciplinary backgrounds, including different types of academics, and different groups of health-care practitioners. Nevertheless, especially at the core management level, the overall emphasis of the CLAHRC is to develop integrated work programmes involving both academic and NHS groups, and for these connections to be across different levels (i.e. to create links at high- and medium-level health-care management, and also NHS practice-level participation), and also to build the work of the CLAHRC across the whole Browntown region. In particular, the capacity-building objective of the CLAHRC is about building up the skills and expertise in all partner organisations, and ultimately bringing about an evidence-based applied health research culture across the Browntown region.
Overall, Browntown CLAHRC is formed from members of a wide mixture of academic disciplines and different groups of health-care professionals. This heterogeneous composition means that the work of Browntown CLAHRC has the potential to innovatively incorporate many different perspectives and draw from different types of expertise. This provides this CLAHRC with a strong foundation to develop a novel approach for an inclusive and collaborative model of applied research – one better able to span the boundaries between the ‘producers’ and ‘users’ and research. The clinical project work is structured into a small number of clusters which each constitute a programme of work within a common clinical topic. This deployment of members into relatively large subcommunities helps to foster collaboration between members who come from different departments and organisations. On being involved in a project that was one of a set within a larger programme of work, one respondent comments about the benefits of belonging to the translational initiative, as opposed to doing standalone project work:
It was a group of like-minded people where we could work together, because often we would all be doing independent things and not working together. So it was an opportunity for people to work together in some sort of funded activity which would have more power and influence than an individual academic working on their own.
BROWNTOWN010
It was felt that having an interlinked set of projects could potentially have a greater impact. The overall programmes of work were often designed to inform different levels or aspects of health services for the same clinical areas. This more ‘holistic’ package of activity was perceived to have the potential to have a greater impact. In belonging to a larger team, there could be a co-ordinated presentation of activities to policy groups, with team members able to draw on the established connections with other groups to legitimise their own work through the high reputation of other colleagues. However, as members remain part of their ‘home’ organisation, this presents some operational challenges, as limited day-to-day interaction can mean that some members cannot easily access tacit information, or do not have a day-to-day reinforcement of the CLAHRC ‘approach’.
Many of the team members have several roles across different parts of the initiative, such as being members of clinical project teams while holding positions within the core management of the initiative. The central management team comprises a large group of CLAHRC members, meaning that internally the CLAHRC adheres to a distributed leadership style. This helps to support the diffusion of the values and aspirations of the central management team within the project work, and helps to reinforce the vision of the CLAHRC across the whole work programme. Many senior CLAHRC members, both from within the core management and the theme leads, are implicit boundary spanners – sometimes by dint of having ‘dual contracts’ with both NHS and university bodies – who contribute hybrid expertise and ‘belong’ to more than one community. They help to support the aim that the various programmes of work should incorporate different perspectives. The overlap between a large core management group and those in positions of leadership within the project teams helps to spread this vision. A smaller core group co-ordinates the overall CLAHRC-wide organisation, and presents the external-facing view of this CLAHRC model, and is influential in driving the vision throughout the CLAHRC. Overall, the onus is on project leadership to co-ordinate the different types of knowledge into one coherent programme. The leaders of the CLAHRC itself view their role as one of facilitating a new form of collaboration, rather than providing specific scientific or methodological expertise ( Box 5 ).
The role of the project leader is to co-ordinate different areas of work that are producing knowledge aligned to different disciplines, with the aim of producing one coherent programme of work. In working with a heterogeneous team, the lead will not necessarily share the same scientific and methodological expertise as their colleagues and, therefore, will not seek to guide the technical aspects of the programme of work.
On the face of it, I don’t fully connect with all of these projects. There are ones within that programme that I’m very interested in and so it was about being able to do some primary research in these areas. I knew that the initiatives were obviously about second gap translation and networks and so on but I think once I started working in role that became the primary focus.
BROWNTOWN014
The work taking place within these themes or project work is not dominated by the vision or traditions of one individual (e.g. the theme lead), but a culture has been created where individuals can contribute from their own perspective. As there is no one dominant culture influencing the approach of the work programmes, members with ‘specialist’ types of expertise are integrated members of project teams, allowing different types of knowledge to routinely inform the programme of work.
In [this translational initiative] you’re going into situations all the time where everyone in the room has got lots of different roles. That can be a bit of a challenge at times with people having to approach things from lots of different perspectives. It’s very much going in and out of roles sometimes.
BROWNTOWN013
Members within the Browntown CLAHRC typically evolved more flexible and overlapping roles, reflecting the need for expertise to support different aspects of the work programme across the initiative.
Networks and collaboration
Although the overall theme of each programme of work remained largely unchanged during the study period, the CLAHRC model and leadership in Browntown has allowed different groups to shape the focus and direction of the work packages. By collaboratively working with other stakeholder groups, the work packages were shaped by the values and insight of different communities, in what one respondent describes as an ‘organic process’.
It’s a tool for facilitating research, applied healthcare research. To enable patients and clinicians and commissioners to make sense of decisions about what to, about what types of treatment to provide . . . The overall structure of the research design didn’t change but it was such an organic process really, what we set out to do is what we’re doing, but their support and interest and feedback was important.
CMBROWNTOWN002
In describing the work programme within the clinical theme, the participant highlights the flexibility of the plans for the project work, and how this allowed the integration of insights from different groups to inform and shape the direction of the work ( Box 6 ).
In this example, we observed a situation where a project team responded to external groups’ requests for outputs to inform their service development by refocusing their research from a PhD project into a more applied piece of work. Through discussion, it was identified that, as an academic study, it would take too long for useful evidence to become available for these groups, and so the programme of work was reorganised to incorporate a tailored component that could produce outputs more quickly.
We had planned a PhD around this raising awareness project. But, clearly, as the pace has changed, it doesn’t fit well with the PhD. The PhD will be invaluable in looking at the way in which information is shared around social networks. But the NHS board wanted some quick and dirty evaluation of this campaign that they’re doing. So we’ve been able to use some money again to devise a slightly separate, parallel piece of work that is very much about going in and working with the groups of people involved in that social marketing campaign, to conduct some process work.
BROWNTOWN014
This example of how the funding for a programme of work was distributed demonstrates that the requirements of external groups were clearly influential. A member of the same team describes how, for a systematic literature review that they conducted, they worked in a different way to the traditional academic approach. In particular, they produced the outputs more quickly in order to have an impact on services through ‘real-time’ information. This helped the outputs to be more relevant and usable for informing policy and practice.
One of the opportunities for us is what the clinicians might bring to our research or that service users might bring. I think one thing that the researchers can do technically very well is appraise literature and have a position on it. For me, CLAHRC is a very powerful bringing together of different knowledge sets . . . We conducted a review very quickly in order to get key messages out that we can then use locally. This informed the way in which that was undertaken. And that’s contributed to some really good outcomes. Had we just gone ahead and just done that normally, I’m not sure we’d have engaged in the right way.
BROWNTOWN014
The project teams across the CLAHRC were composed of a mix of academics from different disciplines and clinical practitioners. The senior management group actively encouraged teams to continue developing their original proposals based on discussion and dialogue with stakeholder groups. This more emergent approach was enabled by certain features of the CLAHRC model and membership. Within the project team, for example, several of the team members were what we will term ‘hybrid’ individuals, that is, they were affiliated to both academic and practitioner communities, and they helped to foster an environment where no one group dominated the direction of work programmes. Instead, all team members were encouraged to actively interact with other groups, and to be flexible in doing their project work. Thus, the vision of the CLAHRC fostered an environment where members were encouraged to develop new work practices and build relationships, rather than to conform to particular disciplinary approaches.
Across the Browntown CLAHRC, many of the members were able to act as boundary spanners precisely by virtue of their ‘hybrid’ academic and health practitioner background. This supported a more fluid integration between research and practice and the building of sustainable relationships, as the overlapping roles conferred membership of both the CLAHRC community and of external groups of managers and commissioners. At the same time, those in leadership positions helped to create an environment where knowledge from different perspectives was routinely shared across teams. Boundary-spanning mechanisms, such as project meetings, were used to support the fluid integration of different perspectives into the various components of work involved.
You see everyone has got a different perspective. Whether you’re a commissioner, you know, perhaps coming from a public health or social services background, but you’re commissioning. Or a manager in the NHS, perhaps social services seconded to NHS. Or a doctor or a nurse or a psychologist or a GP or a service user. You’ve all got a different understanding of what the care pathway is and what needs to be done to improve it. And so very much we deliberately wanted to incorporate a collaborative project between all those different groups.
BROWNTOWN008
Knowledge translation
This CLAHRC’s KT approach drew from an established implementation model, the Canadian ‘knowledge into action’ cycle. In particular, many of the members of Browntown CLAHRC come from the NHS partner organisations, and many of the academics involved with this CLAHRC also hold NHS contracts and have been practically involved with roles at the local NHS organisations. In this sense, the CLAHRC organisation itself acts as a key mechanism to support the translation of knowledge between different communities.
I think CLAHRC is a boundary spanner. That’s its job, that’s what it is. Because the organisations, the NHS organisations, I mean, they do talk to each other because of, you know, Department of Health policy and stuff but they all have different ways of implementing policy. And so they don’t necessarily talk to each other but through us there’s work happening that can be, you know, translated across the different organisations. So we do act as kind of a, it’s almost like a phone exchange.
BROWNTOWN017
The Browntown CLAHRC model included a number of work programmes which were designed from the outset to focus on explicit late-stage implementation activity that would produce tangible impact at an early stage in the CLAHRC time frame. These themes were not designed to produce new research evidence, but were intended to align with the NIHR aim of learning more about KT by conducting implementation activity.
We need to demonstrate progress with implementation from the start of CLAHRC. They are implementation projects using research methods, as well as making a difference to practice, and we’re very much committed to adding to the body of knowledge about knowledge translation . . . Implementation work is really a cross between action research and participatory research, and you need to shape the projects as you work with the key stakeholders.
BROWNTOWN001
The implementation programmes of work were designed to produce results and impact on practice at an early stage. Thus, although they drew on established research expertise, they also emphasised collaboration with the local partners, including at all levels (executives, middle-management and ground-level staff) with whom the activities were taking place. These strands of work thus helped to reinforce and promote the expectation that all programmes of work, including the research themes, would generate outputs that could be applied to inform health-care practice.
The KT themes, in particular, focus on developing evidence that will help to make a practical difference to local health-care services. The clinical priorities for implementation are identified collaboratively, and the project work is seen as socially embedded in the organisations where change is happening. This facilitates the effective translation of knowledge into action by individuals and teams.
There’s a sense in which often researchers come to the NHS with their research ideas and then you try and get sign-up from them to take a project forward. This is turning the coin over completely and it’s saying, ‘we’re a resource; we want to work with you. What are your priorities?’ It’s been getting that ownership that I think has meant that we work in a different way, but also we get a different response back from NHS managers and clinicians. But also seeing, I guess it’s the role of brokers in all of this.
BROWNTOWN001
The main focus of the work of these themes is on piloting and evaluating innovative strategies for implementation, which are then planned to be rolled out across the NIHR CLAHRC for Browntown partnership (with further evaluation of their impact). One key mechanism in this effort involves focusing resources on individuals who are employed by the health-care trusts. A role was designed for these members to act as ‘facilitators’ to build up research activity within their organisations based on the priorities and general ethos of Browntown CLAHRC-type work.
We have what are called ‘research and development facilitators’. The model which was developed was to actively engage each partner healthcare organisation by having a person working within them. So we would bring CLAHRC to these organisations. My role is to bring research evidence to my organisation, and encourage people to use the research evidence much more determining the way that work is completed. And also to help people here to articulate some of their, some of the issues which they have which could have a research solution. They could find a solution through research or at least some preliminary studies.
BROWNTOWN022
It is clear from our analysis that members from throughout the CLAHRC recognise that there is an underlying strategy for this initiative to facilitate KT, and that this is conceptualised as involving an integrated, collaborative approach between academics, health-care practitioners and managers in order to facilitate implementation work. Thus, although the CLAHRC does designate certain work packages as ‘implementation’ projects, the vision enacted throughout the CLAHRC emphasises the need to bridge the second translational gap, and not limit KT activity to discrete programmes of work.
It’s not that simple as just having an implementation arm in CLAHRC . . . I think that a lot of people have been practitioners and have done research, there are very few pure academics who have never really linked in and have been in practice or not in the NHS . . . if you look at nearly every lead they’ve either been a practitioner or had a role in the NHS before as well as doing research. They’re all boundary spanners.
BROWNTOWN021
However, while this priority given to KT is very apparent at the core management level of the CLAHRC, it is perhaps more difficult for this type of approach to radically influence all areas of the CLAHRC work, and in particular for innovation approaches to inform the approach of the research-focused clinical theme work. In addition, the challenges of conducting implementation research are also highlighted, as the inductive co-production approach here differs from the design of conventional academic projects. Thus, while achieving KT through the seamless integration of research and practice is an important part of the Browntown CLAHRC vision, it depends heavily on the contribution of those occupying ‘hybrid roles’. Crucially, the individuals within these roles are not deemed peripheral to the project teams, but are well positioned to incorporate insights from different community perspectives into the work of the teams.
I work between a number of different organisations, so principally the NHS and academia. It was useful that I am actually from an academic background myself. It makes it a little bit easier in terms of understanding what academic opportunities there might be which the NHS might be able to tap into . . . I work with the initiative really because I work for the NHS and ensure that the CLAHRC work is embedded within this NHS organisation. So it’s very much that boundary-spanning role, I have two identities.
BROWNTOWN022
Reflections on the Browntown Collaboration for Leadership in Applied Health Research and Care model and its development over time
The vision of the Browntown CLAHRC collaboration aims to foster a change in the culture of members across the partner organisations by building the capacity of its members to engage with applied health activities. The fact that the core of the CLAHRC is not university-centric, but is instead based on the traditions of allied health academics and practitioners, has helped to privilege health services’ concerns in shaping the programme of work. Although discrete KT activities were established at its inception, the vision of the Browntown CLAHRC is for all programmes of work to engage with diverse perspectives and traditions. In this way, the CLAHRC builds capacity for innovation through a work environment where work practices are able to draw on a diverse range of perspectives.
The Browntown CLAHRC has evolved incrementally over time as new activities have been developed in response to partner need. From its inception, the CLAHRC has emphasised the scope for such incremental growth both through grafting on new programmes of work and through the expansion of the CLAHRC community to include new types of partners. Although not emphasised in the original bid, collaboration with industry has also emerged as an important strand of this evolution. One result of this approach has been the ability of the CLAHRC Browntown model to adapt to a changing policy landscape, as the ‘organisational memory’ of relationships with the primary care trusts has been used to forge relationships with new commissioning organisations.
Comparative analysis of Collaboration for Leadership in Applied Health Research and Care models and their enactments
The CLAHRCs were given extensive flexibility in interpreting the NIHR remit. They thus represent a ‘natural experiment’ in how to focus, organise and manage applied health research, which will have an impact on a local health-care environment. Our study of three CLAHRCs has highlighted how it has been necessary for each model to be tailored to their own local context.
The senior management of Bluetown CLAHRC strongly emphasises a common vision throughout its work, and contributes technical scientific support to work programmes. The ambition here is to produce high-quality scientific evidence through a rigorous methodological approach. Within this broad remit, each project team has extensive flexibility in the operational management of their work programmes. Instead of drawing on a CLAHRC-wide approach for KT, each project team here developed their own approach to translating the findings from their work programmes into practice. In this sense, the Bluetown model for KT is about supporting the operational autonomy of each project team to develop its own locally tailored approach.
Greentown CLAHRC draws on an explicit CLAHRC-wide organisational structure to facilitate KT activity. This structure emphasises a common operational management championed by the core leadership. The overall approach draws on a cross-disciplinary conceptual model which integrates different types of knowledge, including both clinical and social science academic traditions. However, each project team develops its own approach to accessing and developing requisite scientific and technical expertise, which allows team members to retain their pre-existing working practices.
The Browntown CLAHRC model was based on adapting the explicit Canadian framework for KT. Operationally, the CLAHRC work was situated within heterogeneous teams embedded within the local partner organisations. This, together with features such as overlapping community memberships and hybrid roles, helped to support the fluid, and often tacit, integration of different types of knowledge across all work programmes.
Notably, all three of the CLAHRCs we studied were able to develop and adapt their model over the 5-year funding time frame. The focus of these developments, and the extent to which modifications occurred, varied depending on each CLAHRC context. Bluetown CLAHRC started with a conventional model of the relationship between research and practice, which allowed work activity to commence straight away, and did not require radical changes to the working practices of its members. However, as the CLAHRC developed over time, new activities were introduced to support KT and knowledge management and engagement activities. Importantly, the established relationships of the early CLAHRC model are credited with helping to gain support for these new types of activities.
Greentown CLAHRC has experienced several changes in leadership since the initial formation of its model. Its development over time has particularly focused on refining the original organisational learning model in order to improve effectiveness. As such, this CLAHRC has engaged in changes to its operational management by restructuring the groups within the CLAHRC, and, in particular, making adaptations to the work of the specialist support services to support the clinical project teams more effectively.
The model of Browntown CLAHRC has evolved incrementally and has maintained consistent support for capacity building across local health-care communities. In particular, this CLAHRC has sought to develop and integrate new work programmes reflective of its overall vision into its CLAHRC community. It has continually expanded its engagement with its original health-care partners, and also new types of stakeholder groups, such as industry. In keeping with its distributed leadership style, the central management team itself grew over time, so as to assimilate representatives of different work components and incorporate their views into the organisation of the CLAHRC’s work. Our study of the three different CLAHRC helps to explain the way in which the broad CLAHRC remit has been appropriated in distinctive ways, according to the social networks and local contexts which have shaped the CLAHRCs’ development. In the process, we have observed also the generative effect of leadership and vision. These variations in the interpretation and enactment of the CLAHRC mission underlines the importance of their differing network structures and sense-making cognitions as addressed through the other research strands in our study (and succeeding sections of this report). In respect of KT, it is clear that each CLAHRC has developed its own distinctive approach, some aspects of which are managed and articulated at senior management level, while others (e.g. the implications of hybrid roles) make a more implicit contribution.
USA and Canada qualitative analysis
The next part of the report will describe, analyse and discuss the three North American cases. The first case is the Canada-Coordination, an initiative involving a number of health-care players in the Ottawa district, Ontario (Canada), and aiming to improve the co-ordination and quality of health-care delivery. The initiative is specifically addressed to a small number of children with complex care needs (these children have at least five different specialists who follow them). At the time of our fieldwork, the Canada-Coordination initiative included 23 such children. The second case is the Canada-Translation, an initiative involving a community hospital (Com-Hospital) and a large university (Uni-Canada) in the same city in Quebec, aiming to promote KT processes from academic (Uni-Canada) to practitioners (Com-Hospital) and, more generally, aiming to increase collaboration and cross-fertilisation activities between the hospital and the university. The third case is US-Health, an initiative involving a number of universities, hospitals and consultant companies specialising in health-care management and applied research and aiming to promote implementation research across the USA.
All three initiatives are different to the CLAHRCs in terms of size, being either somewhat smaller (e.g. the Canada-Translation) or larger (US-Health). In addition, their thematic focus and governance arrangements are necessarily different to the CLAHRCs’ (e.g. the Canada-Coordination is more focused on KT and collaboration across existing health-care organisations). However, these three cases were chosen because they are all organised to promote implementation research and KT processes on a networked basis, by exploiting existing networks and/or facilitating the creation of new collaborative networks.
The qualitative analysis of the North American cases, in line with the CLAHRCs analysis, is structured as follows (for each case): firstly, we introduce the case; secondly, we break down the analysis into the three main theoretical elements (or dimensions) of the framework supporting this study (governance and management aspects, networks and collaborations, and KT); and, thirdly, we discuss the implications of the case. As with the CLAHRCs qualitative analysis, each case involves three case examples, one for each dimension of the framework. We conclude this section with a discussion of the three initiatives and a comparison between these (North American) cases and the UK CLAHRCs.
Canada-Coordination pilot project
Canada-Coordination is a pilot project housed at the White Hospital, located in Ottawa, ON, Canada, and involves the hospital itself (a world-class tertiary paediatric centre), and several paediatric organisations and agencies in the Ottawa community.
Management, governance and organisation
The pilot project involves four main players (organisations): (1) the Regional Community Care Access Centre (RCAC), which is a community health provider that organises home, school, and hospital care, developing customised ‘care plans’ and providing support from health-care professionals, nurses, physiotherapists, social workers, registered dieticians, occupational therapists, speech therapists, and personal support workers to provide a range of care and support services; (2) the Ottawa Association to Support Children (OASC), which is another community health provider that provides specialised care for children and youth in Ontario with multiple physical, developmental, and associated behavioural needs; (3) the social services (SS), which is an agency that develops case resolution mechanisms to provide recommendations and referrals for families with children with complex care needs who are experiencing difficulties accessing support and services in the community; and (4) the White Hospital, which is the ‘hub’ of the project in that the children with complex care needs are patients of the hospital and, therefore, the main treatments are provided at the White Hospital.
The pilot project funds three key people to manage the project: (1) a project manager, (2) the most responsible physician and (3) the nurse co-ordinator. The project manager supervises the pilot project: she ensures that processes, communication pathways and flow maps have been developed; conducts staff training sessions; co-ordinates the meetings and presentations for the steering and advisory committees; and prepares reports. The most responsible physician reviews the overall complex medical needs of each child and co-ordinates communication with all the specialists at the White Hospital, other tertiary paediatric centres specialists, and the community physicians. The nurse co-ordinator works very closely with the most responsible physician, interfacing between the doctors, nurses, and managers at the White Hospital, and the other agencies; the nurse co-ordinator is the link person for all of the families of the children in the project. Interestingly, along with a solid governance structure, informal relationships played a central role in the pilot project, as is outlined in the example below ( Box 7 ).
The governance structure of the pilot project is relatively formal including steering and advisory committees that meet monthly in addition to an external entity – the White Hospital Research Institute – that evaluates the progress of the project and provides written reports to the board of the hospital. However, according to the people who lead the pilot project, the success of the initiative lies in the informal relationships among the managers/directors. In fact, for instance, the directors of RCAC, OASC, and SS have been working together for many years in the Ottawa community and know each other very well. The quote below is from the director of RCAC, who explains how personal relationships mattered during the initial phase of the pilot project.
I think the difficult part when you study it, however, is to isolate the relationship factor. I think from my perspective, I’ve been in the community a long time, I worked in children’s health for almost twenty years, I think the reality is sometimes that’s not easily captured. It isn’t just who is involved but it’s also the relationships that have been built between . . . And that’s the piece that’s sometimes really hard to catch is that I have the utmost respect for [the OASC Director]. [The OASC director] and I may not always agree but working with her is wonderful. Same with [the most responsible physician], the same applies with [the project manager], the same applies with [a colleague].
From the case example in Box 7 , it is clear that informal relationships facilitated tight collaborations and promoted trust among the players involved in the pilot project. The development of trust, as we will show below, was also a relevant element in supporting the health-care network of the Ottawa community.
Networks and collaboration
The pilot project exploits existing networks between the players involved including RCAC, OASC, SS, independent paediatricians, and the White Hospital personnel (doctors, nurses and staff). In fact, while the project involved hiring some key people who could facilitate collaboration among the players, many of the relationships between, for example, social services (RCAC) and the nurses and doctors in the hospital (the White Hospital) were already tight. This aspect (prior networks) has positively affected the overall project because while formal networks are relatively easy to establish, it takes time for people to begin working together productively. Interestingly, the pilot project network developed collaborations aimed at improving the quality of health-care delivery that were not limited to the players that were involved in the initial project. In fact, the managers (of the four agencies) soon realised that in order to clearly identify the needs of the children involved in the pilot project, it was important to involve the patients directly. Therefore, the project manager, in accordance with the directors of RCAC, OASC, and SS, decided to involve the parents of two children involved in the project. This involvement included having the parents sitting in the steering committee of the project that meets monthly and makes decisions regarding how the co-ordination of care at the White Hospital and across its network can be improved.
As the project manager highlighted regarding the evaluation process of the project: ‘So the two parents from family forum that also sit on our steering committee for this Pilot Project reviewed our questionnaires and helped us get to the questions we wanted so that it’s more a participatory evaluation approach’. This quote underlines a collaborative climate where actors belonging to different networks are willing to bring their contributions and are supported by a common aim: to identify ways to improve the quality of health-care delivery services for children with complex care needs. One of the most relevant issues that emerged from the feedback with the (two) families who sit in the steering committee was the difficulty of having all of the different community services up to date with the most recent changes regarding the children’s condition – this problem was made very challenging by the fact that each child is frequently seen by a number of specialists.
Knowledge translation
Knowledge translation within Canada-Coordination was focused on relations between clinicians and with family members of the children involved. It was facilitated not only by direct interactions among these groups, but also by the development of artefacts that could help span the boundaries between them. In this context, the introduction of the Single Point of Care (SPOC) document is an important example because it radically improved the relationship between the White Hospital and the health-care networks. The SPOC is a paper-based medical sheet including all basic information about a child’s health, such as current health status, current treatments (medications), and any other detail that can be helpful at school (e.g. current allergies) or in emergency situations (particular drugs that the child needs to take if his/her condition suddenly becomes severe or life-threatening). The SPOC is issued by the White Hospital and is carried by the families, who now no longer have the difficult and at times confusing task of collating themselves all the medical information related to their children produced by different specialists. The SPOC is also shared with a number of organisations in the Ottawa community, such as police and schools. In particular, it is very relevant that, for example, if the child develops a new allergy or changes one medication, the school nurse is aware of the changes. While the creation of the SPOC will be broadly discussed in the next section – the SPOC being a KT tool – the following case is meaningful in highlighting how SPOC contributed to promoting networks and collaboration across different players in the Ottawa community ( Box 8 ).
The SPOC originated from discussions between the families of the children involved in the pilot project and the doctors and managers during steering committee sessions. Its value is highlighted here through the example of Karen. Karen is the mother of Jane, a child with severe conditions ranging from kidney failures to breathing difficulties whose causes are, thus far, mostly unknown. Due to the ongoing investigations about Jane’s medical conditions, her situation is particularly at risk because, due to the child’s unstable condition, urgent care needs occur frequently. Moreover, in the last few months Jane (who at the time of our fieldwork was 7 years old) has started developing allergies to a number of different medications. However, since the SPOC was introduced and was shared with Jane’s school, Karen feels more confident that the school nurses are constantly updated on Jane’s changing conditions (and new reactions to drugs, e.g. new allergies). Karen is also confident that in case her daughter develops a health issue at school, the personnel can take appropriate actions:
They know who to call. So they have [the nurse coordinator]’s number and [the most responsible physician]’s number at White Hospital, and they know if there’s an emergency just call 911 which is our emergency services here in Canada. So they, and they have a plan and they have a copy of a document of the Complex Care Program, it’s called the Single Point of Care document.
The SPOC also helped to reduce redundant examinations because the parents show the medical sheet to each specialist who would edit it as appropriate and gather information about forthcoming tests. In sum, the introduction of the SPOC improved efficiency (being a co-ordination mechanism for different specialists) and provided the families with more awareness about the conditions of their children. In fact, while on the one hand the SPOC is acknowledged by any doctor as an official document because it is issued by a hospital, on the other hand, the (simple) way the SPOC is structured allows the family to interpret (in general terms) the health status of their child.
In sum, according to the project founders (the leaders of RCAC, OASC and SS), the involvement of the parents had produced significant benefits. This point was also confirmed by a number of interviews that we conducted with the families of the children involved in the pilot project because a number of issues of the families in terms of co-ordination emerged that could be brought up for discussion in the project meetings (steering committee).
Reflections on the pilot project model and its development over time
The pilot project is an example of how informal networks are effective in promoting KT and collaboration across community partners, including health-care partners such as a hospital and the SS, yet also including also non-health-care partners such as the police department and the schools. The management of the project includes periodic controls undertaken by an independent entity that is the White Hospital Research Institute. The White Hospital Research Institute surveys doctors and families of the children involved in the project and makes sure that co-ordination and health-care delivery services are continuously improved. This is evidenced by feedback from both clinicians and patient families.
Canada-Translation Centre
The Canada-Translation Centre is an initiative that originates at Com-Hospital, a community and university affiliated health centre in Quebec, Canada, and that serves a multicultural population in southern Quebec.
Management, governance and organisation
The Canada-Translation Centre started in 2010 with the aim to promote and co-ordinate clinical research carried out by clinicians who work at Com-Hospital and are also appointed by Uni-Canada, a university in Quebec. According to the regulatory framework of the Canada-Translation Centre, it carries out clinical, epidemiological, and health services research studies, provides consultation to other researchers in the hospital, and provides educational services, including seminars and workshops, related to research.
The Canada-Translation Centre is led by Johanna, Associate Professor at Uni-Canada and the vice president (VP) of Academic Affairs at Com-Hospital. The Canada-Translation Centre organises monthly meetings (last Thursday of every month) that are held in the hospital. As at the time of our research the Canada-Translation Centre was in its initial stage of development, the main objective of the meetings that we observed involved the establishment of guidelines and systems.
From a governance perspective, the three main bodies that collaborate with the Canada-Translation Centre are (a) the REC, which is responsible for reviewing the scientific and ethical aspects of all research projects involving human subjects; (b) the research review office, which is co-ordinated by the research administrative secretary and provides administrative support to both the EC and the REC; and (c) the Quality Assessment (QA) Unit, which provides assistance to hospital staff on various aspects of QA analysis and evaluation, that is, projects that assess current performance or practice.
The governance aspects of the Canada-Translation Centre are extremely formalised, reflecting the interest of the academics at Uni-Canada to secure control of the development of the project, especially in its early stages. The board of directors supervises all research activities, while the VP of Academic Affairs (who is also the Canada-Translation Centre’s Director) supervises all main research committees. The Quality and Risk Management Committee is an independent body chaired by the VP of Professional Services. According to an interview with Johanna, the rationale of this design lies in the desire to have objective control of research activities by an independent body (the Quality Committee).
Networks and collaboration
The network of the Canada-Translation Centre is formed by people who work in the hospital who also have at least a teaching appointment or, more often, a professorial appointment, at Uni-Canada. The design of the three key bodies of the centre sought to promote collaboration and cross-fertilisation between the hospital and Uni-Canada. In particular, within Family Medicine at Uni-Canada there are four departments that have been always very independent and loosely coupled; however, with the start of the Canada-Translation Centre, members of these four departments started meeting twice a month to try and pursue common research objectives. In sum, the main objectives of the Canada-Translation Centre are to (1) tighten the collaboration between Uni-Canada and Com-Hospital by promoting networks and (2) bring in expertise from external collaborations.
In terms of improving the network within the Canada-Translation Centre (Com-Hospital and Uni-Canada) one of the initial challenges was to try to build relationships between key actors who had no experience of working together. For instance, quality and risk management staff rarely interacted with academics prior to the start of the project. This group quickly became committed to collaborating with the academic groups, as highlighted by the director of the quality and risk management at Com-Hospital:
And I convinced Johanna that the uniqueness of the relationship between Quality and Research here has to live somehow and has to be formalised in whatever plan she does. And I think she saw that as an opportunity. If it were someone else here than me I don’t know if it would work the same. It’s just because I started out working in Research and I, you know, I did that for ten, twelve years and I know the language and I know their challenges and I know, you know, how they think and how they . . . operate.
While it is important that people within Com-Hospital are able to work together (e.g. the research team and the quality and risk management department, as per what was highlighted above), it is also relevant that the (more practice-oriented) researchers at Com-Hospital collaborate and develop networks with the professors at Uni-Canada. The associate dean of Inter-Hospital Affairs plays a role in doing this by trying to promote fruitful collaborations between the hospital and the university. As he highlighted to us:
It was a natural thing to develop research along these lines. Again my role has been to facilitate communication between the hospital and the university, both with the Dean of Medicine and with other research leaders within the university. I’m not a researcher myself. My role is mainly to put people together. And to use the links that we have with the Ministries to help support what the hospitals do. The other way in which I interplay with the hospital is I’m on the board of directors. So being on the board of directors of course some of these initiatives to fund this research infrastructure comes to the board and at times I speak to it in a supportive fashion in order to help promote this venture for the hospital.
Knowledge translation
Included in the Canada-Translation Centre mission for the period 2010–15 there are five main domains of research to be pursued:
-
to support and conduct high quality clinical and health services research relevant to the patients and services provided by Com-Hospital
-
to promote KT and exchange activities to support evidence-informed decision-making in practice, management and policy
-
to provide decision support for clinical and management leaders through high-quality rapid systematic reviews of scientific evidence
-
to support the application of evidence through quality improvement and other implementation initiatives
-
to provide a high-quality training programme and environment for students interested in research careers.
From the above it is clear that the Canada-Translation Centre has a specific focus on KT. In fact, each research member (i.e. a professor) must also be a clinician (i.e. he/she needs to spend a minimum number of hours per week in the hospital), a rule which is aimed at promoting applied research. As outlined by the case example below ( Box 9 ), one of the strategies that the Canada-Translation Centre adopts for promoting implementation research is to work on small projects whose short-term tangible results are directly testable in the hospital environment.
One example of how the Canada-Translation Centre promotes implementation research is to try to develop very small projects where implementation requires months if not just weeks. Through the exploitation of a network involving academics and a number of physician practitioners (at Com-Hospital), the Canada-Translation Centre is able to deliver small but relevant projects that are implemented in practice in the short term. Below is a quote from an interview with the CEO of Com-Hospital (Dr Thomas) who highlights this strategy:
I think for me the important thing is that we do meaningful research. Healthcare systems research, population-based research. That we are actually are able to collaborate and participate in meaningful research which is applicable. Which is applicable in the short term. We are not in bench research, you know, we don’t do phase one, phase two, phase three, phase four clinical trials. There are other institutions that are very good at it and do it very well. So, you know, we are not into the development of designer drugs . . . But the type of lab we are to put it very bluntly is exactly the type of lab that we can say, look, you know, we think we can make small but important transformational changes at the micro and the mid level, which hopefully the macro will see and say whoa, that’s interesting. Especially if we have a good collaborating network, so that’s in a broad sense what the précis is.
Reflections on the Canada-Translation Center model and its development over time
In contrast with the pilot project in Ottawa, this initiative is much more complex and involves more than 50 people including Com-Hospital physicians, Uni-Canada’s academics, and administrative personnel. Staff involved are fully aware of the barriers between academics and practitioners and between people who work in different departments (in the case of Com-Hospital) and in different institutions (at the hospital and at Uni-Canada). Therefore, specific boundary spanners – such as the associate dean of Inter-Hospital affairs – were identified to connect people with different background, professional and personal interests.
US-Health
US-Health is a model of field-based research designed to promote innovation in health-care delivery by promoting the diffusion of research into practice. The US-Health initiative promotes innovation in health-care delivery by speeding up the development, implementation, diffusion, and uptake of evidence-based tools, strategies, and findings. In particular, US-Health develops and aims to disseminate scientific evidence to improve health-care delivery systems.
The US-Health network includes a number of large partnerships (the ‘contractors’) and collaborating organisations that provide health care to more than 100 million Americans and is a 5-year implementation model of research that is field based and that fosters public–private collaboration aiming to provide concrete results in the short term. The US-Health partnerships involve most US states and provide access to large numbers of providers, major health plans, hospitals, long-term care facilities, ambulatory care settings, and other health-care structures. Each partnership includes health-care systems with large, robust databases, clinical and research expertise, and the authority to implement health-care innovations.
US-Health focuses on a wide variety of demand-driven, practical, applied topics of interest to the partnerships’ own operational leaders as well as the project funders. The programme emphasises projects that are addressed to user needs and operational interests and which, ideally, are expected to be generalisable across a number of settings.
US-Health partnerships operate under multi-year contracts. Proposals are bid on a rolling basis throughout each 5-year cycle. Projects need to be undertaken in the short term; they are awarded under separate task orders and are completed within 12–24 months. Also, the US-Health network is promoted by a national health agency called Federal-Health. Federal-Health’s mission is to improve the quality, safety, efficiency, and effectiveness of US health care. Federal-Health supports research that helps people make more informed decisions and improves the quality of health-care services.
US-Health’s research has two main characteristics: it is practice based and implementation oriented. Thus, it supports field-based research to explore practical, applied topics that are responsive to diverse user needs and operational interests. By testing innovations directly in the practical settings in which they are intended to be adopted, US-Health increases the likelihood of their eventual successful uptake. US-Health research is also designed to increase knowledge about the process of implementing innovations and the contextual factors influencing implementation. It aims to promote understanding of how and why specific strategies work or fail.
Management, governance and organisation
The governance structure of US-Health is relatively flat. Federal-Health is the government organisation that manages the tendering process for contracts, and US-Health (the network) is one of the recipients of these contracts. Informal relationships between Federal-Health and its collaborations over time, however, help to ensure that contracts are tailored to the strengths of members of the US-Health network. For example, Federal-Health frequently discusses potential research projects with the contractors of previous bids to elicit their interest.
Once a contract is signed, a project officer is assigned to each contractor; there are few project officers who manage multiple contracts nationwide. The main task of the project officer is to make sure that all milestones are met during the very short period of the contract. Moreover, the project officer can review ongoing documents, can come to visit a contractor to see how the research project progresses, and can provide suggestions and indications. The project officers need to write periodic reports for Federal-Health; therefore, Federal-Health can closely monitor each contractor (and each research project). The way a contractor (e.g. a member of the US-Health network) manages the research project is very subjective. While a proposal on how they will reach the objectives needs to be provided to Federal-Health, no specific guidelines on how to undertake the research are given. However, the contracts (and the research projects) are generally very specific in their objectives and concrete results. Very often, the research output is a ‘toolkit’, that is, a document with specific recommendations on how to manage a health-care problem in practice.
Many of the people whom we interviewed and who were involved in one or more US-Health research projects (i.e. contracts) highlighted that the success of the project depended to a large extent on the project officer. The effects of the project officer role can be both positive and negative, as shown by the example below ( Box 10 ).
This interview was undertaken with a professor in a department of family medicine who has been involved in a Federal-Health project for several years. She describes with examples points of strength and weakness of the monitoring activities of different project officers.
We have a new project officer, our first person left. She was lovely. The new person I think was a little better in terms of working with us around being flexible and understanding that health centres don’t want this, you’ve got to work with us. There was more back and forth and less just telling you what to do . . . The ones who don’t know the content they’re just monitoring for compliance.
Networks and collaboration
US-Health has a very complex network including, as we previously noted, a number of large partnerships. In this section we provide some insights that focus on two main partnerships where we were able to conduct interviews: Health-partnership and Health-Consulting. We chose these two networks because they are very different (one is a partnership whose participants are academics while the other is a consultant company with expertise in health care). Although collaboration on bid writing between partners was limited by a lack of funding, some collaboration did take place across US-Health contractors.
Health-partnership (primary contractor) is a partnership led by a US university (name not disclosed) which managed some 10 contracts with Federal-Health within US-Health. The contracts of Health-partnership involve themes such as improving hepatitis C virus-screening practices and testing uptake in select primary care providers, preventing pressure ulcers in hospitals, co-ordinating care across primary care practices, using innovative communication technology to improve the health of minorities, avoiding readmissions in hospitals using technology, and reducing infections caused by particular bacteria.
Health-Consulting is a much smaller entity, being a private consultancy company with some 15 senior consultants. As a result, it is not in a position to develop clinical research involving patients. Health-Consulting’s strategy within US-Health was, therefore, to find collaborators (subcontractors) who could undertake implementation research in health-care structures. To do this, they drew on a wide network of subcontractors. The contracts managed by Health-Consulting focused on the relationship between patient information management in hospitals and risks of complications and mortality while patients are hospitalised (this contract investigates both electronic and paper-based medical records) and on the development of performance measures for injurious falls in nursing homes and rehospitalisation of patients discharged from hospitals to home care. Although collaboration on bid writing between partners was limited by a lack of funding, some collaboration did take place across US-Health contractors.
Knowledge translation
With the overall goal of translating research into practice, US-Health links many of the largest health-care systems in the USA with top health services researchers who are identified through a tendering process and are managed through short- to medium-term contracts.
It provides a network of delivery-affiliated researchers and sites with a means of testing the application and uptake of research knowledge. US-Health is the successor to another large-scale initiative which was completed in 2005. All of the large partnerships (i.e. the prime contractors who work with a specified range of other organisations) have a demonstrated capacity to turn research into practice for proven interventions, targeting those who manage, deliver or receive health-care services. As per the above, both Health-partnership and Health-Consulting develop research that is focused on a wide variety of demand-driven, practical, applied topics which are of interest to the partnerships’ own operational leaders as well as to the project funders. The overall programme (US-Health) emphasises projects that are broadly responsive to user needs and operational interests and which are expected to be generalisable across a number of settings. An example of implementation research conducted by Health-Consulting is outlined in the case example below ( Box 11 ).
Health-Consulting developed a tool to improve pharmacists’ communications with patients. This was informed by evidence that only 12% of US adults understand and use health information effectively and more than one-third of adults have basic or below basic health literacy, The tools instruct pharmacists on how to create pill cards or medication records for patients, improve communication skills, and assess pharmacies’ health literacy practices, among other activities.
Federal-Health contracted with Health-Consulting to widely disseminate the tools and research the factors affecting their adoption and implementation by pharmacies. Health-Consulting completed a set of comparative case studies of diverse pharmacies across the country to understand the pharmacies’ experiences with the tool. The case study found that pharmacies successfully implemented the tool with the participation of pharmacy students and residents or college of pharmacy faculty.
Reflections on the US-Health model and its development over time
The US-Health case, if compared with the two other North American cases, involves a number of partnerships, each partnership involving a number of organisations and players. Moreover, the funding model is quite unique, depending on bids for contracts (very often agreed between parties – e.g. Federal-Health and, in our case, US-Health). Even though there was little interaction across the US-Health network as a whole, collaborations proliferated within partnerships. Moreover, most projects have been successful and some projects were adopted nationwide.
Chapter 5 Empirical analysis and findings: social network study
Introduction
We use SNA to investigate our case study networks at two time points and to illustrate comparative differences and similarities between CLAHRCs. In our analysis, we take into account the structure (or shape) of each CLAHRC network as well as the composition (characteristics) of relations (ties) within. We summarise our UK findings below with more detailed analysis of the networks and a full glossary of measures provided in Appendix 1 . The more limited social network study of one of our North America sites (Canada-Coordination) at one time period is also outlined and compared with our UK findings in Appendix 1 .
Ambidextrous networks: brokerage and closure
Research indicates that developing and maintaining social network ties can be costly in terms of both time and energy. 100 Therefore, a structure whereby everyone is connected to each other is not viable. Instead, it is preferable to have small clusters of individuals with high levels of network connectivity (closure) that promote implementation and embedding knowledge into practice, for example in work teams or communities of practice. 101 Clusters working in isolation, however, limit the development and transfer of novel information. 62 Thus, it is also important for there to be ‘brokering’ or ‘boundary-spanning’ ties; networks that connect between work team clusters as well as ties that connect to other people outside of an organisation or entity. 102,103 Closure and brokerage, therefore, offer different benefits for KT. 104,105 We describe this ability to reconcile structures of brokerage and closure as ‘network ambidexterity’. In our study, we assess the extent to which the CLAHRC KT networks feature such ambidexterity by incorporating elements of brokerage and closure ( Box 12 ).
Networks featuring ‘brokerage’ and ‘closure’ provide contrasting, but important, capabilities for KT activity. Brokerage structures are found in loose or fragmented networks and support the generation of new ideas. Structures of closure are formed within tight-knit networks and are suited to capturing and embedding knowledge into practice. We describe the ability to reconcile structures of brokerage and closure as ‘network ambidexterity’.
Structures for generating new ideas (brokerage)
Brokerage structures have been associated with the opportunity to ‘bridge’ between distinct knowledge camps. This offers potential access to new, in other words ‘non-redundant’, information, as well as to support the fusion of new ideas from different information sources.
Structural holes are ‘gaps’ in a network created where there is a lack of connectivity between actors. Structural holes present opportunities for knowledge brokerage because brokers are positioned at these network gaps. The network gaps presented by structural holes encourage the formation of separate pockets of information and ideas, and so opportunities for boundary spanning between distinct knowledge camps are enhanced. Bridging offers similar opportunities for innovative knowledge transfer. Here, there are two individuals who are not directly connected but, unlike structural holes where the gap remains, the gap has already been bridged by a broker who acts as an intermediary between parties.
Three main SNA metrics tap into this notion of brokerage: Gould and Fernandez brokerage,106 actor-level betweenness107 and structural holes. 108 Table 3 presents average brokerage, betweenness and structural holes scores for each CLAHRC at two time points.
| Network metric | Time 1 | Time 2 | ||||
|---|---|---|---|---|---|---|
| Greentown | Bluetown | Browntown | Greentown | Bluetown | Browntown | |
| Gould and Fernandez brokeragea | 0.50 | 0.44 | 0.39 | 0.43 | 0.45 | 0.45 |
| Ego betweennessb | 19.10 | 12.01 | 10.68 | 10.73 | 12.54 | 12.10 |
| Structural holesc | ||||||
| Efficiency | 0.69 | 0.72 | 0.63 | 0.68 | 0.68 | 0.70 |
| Constraint | 0.64 | 0.69 | 0.65 | 0.61 | 0.79 | 0.63 |
We analysed the extent to which the CLAHRC networks provided brokerage opportunity, with the results presented in Table 3 . The greatest difference between CLAHRCs is at time 1. Greentown had the highest betweenness and Gould and Fernandez brokerage scores, meaning that there were more individuals in this CLAHRC acting as ‘bridges’ and more disconnected pairs of contacts than in CLAHRCs Bluetown and Browntown. At both time points, efficiency scores show that CLAHRC members had a relatively high proportion of non-redundant ties that provided access to structural holes. However, the constraint scores suggest that a significant proportion of these relational investments were focused around a single contact rather than many different pockets of knowledge. By time 2, brokerage, betweenness and structural hole scores became more similar and there was less variance between CLAHRCs.
Structures for embedding knowledge (closure)
Closure in tight-knit (dense) networks has been associated with the ability to build trust and stability, which in turn helps to create an evironment that supports embedding and implementing knowledge. 101,109
The simplest measure of network structure with which network connectivity or closure can be assessed is network density. Density is the actual number of ties divided by the possible number of ties. As outlined in Table 4 , in the Greentown CLAHRC, density was 8.6% at time 1, decreasing to 7.8% at time 2, the most connected of the three CLAHRCs. Browntown was the least connected of the CLAHRCs at both time points (5.3% at time 1, 6.7% at time 2). Greentown’s density decreased over time whereas Bluetown and Browntown densities increased. The results show that there was not a high level or connectivity or closure across any of the CLAHRCs. This is positive for knowledge innovation at the level of the CLAHRC entity level because the too much connectivity would have a negative effect on diversity of knowledge (more redundant information).
| Network metric | Time 1 | Time 2 | ||||
|---|---|---|---|---|---|---|
| Greentown | Bluetown | Browntown | Greentown | Bluetown | Browntown | |
| People in network | 109 | 123 | 135 | 102 | 100 | 131 |
| Respondents | 75 | 93 | 92 | 68 | 54 | 89 |
| Ties | 1018 | 940 | 960 | 808 | 764 | 1134 |
| Ties per respondent | 13.6 | 10.1 | 10.4 | 11.9 | 14.1 | 12.7 |
| Density | 8.6% | 6.3% | 5.3% | 7.8% | 7.7% | 6.7% |
| Geodesic distance | 2.6 | 2.9 | 3.0 | 2.7 | 2.7 | 2.7 |
| Reciprocitya | 24% | 22% | 20% | 21% | 20% | 18% |
While density is a frequently used measure of overall connectivity, it is possible to have a densely connected network that is actually fragmented into two or more subgroups. As a check on fragmentation we also calculated geodesic distance measures for each network. Geodesic distance is the average number of links between one person and every other person in the network. This network measure has been popularised by the notion of six degrees of separation that examines how closely connected any two people are. 110,111 At time 1, we find that the Greentown CLAHRC is the most connected as it has the lowest average geodesic distance score (2.6, compared with 3.0 for Browntown). Therefore, there are, on average, 2.6 connections between every person in the Greentown network. Our findings for geodesic distance are in line with those for density, with Greentown being the most connected and Browntown the least connected. At time 2, the CLAHRCs have established equal geodesic distances between members. Everyone in each of the three CLAHRCs can reach each other within an average of 2.7 links, and this indicates that the KT networks are not fragmented despite the low global density scores.
The third structural measure that we report is reciprocity ( Figure 3 ). This measures the extent to which relations are two-way, so that, where a nominates b as a knowledge contact, b also names a in return. Reciprocity of ties is often used as a proxy for trust, which has been shown to be associated with the sharing of knowledge within a network. 112 Figure 3 provides a visual illustration of reciprocal KT ties in each of the CLAHRC networks at time 1. The data suggest that Greentown members at both time points have a very slightly higher level of trust in each other than in the other two CLAHRCs. At time 2, the level of reciprocity has fallen slightly in each of the CLAHRCs. This is partly attributable to the fact that not everyone responded to our survey.
FIGURE 3.
Reciprocal KT ties in the CLAHRC networks (reciprocal ties in red). (a) Greentown; (b) Bluetown; and (c) Browntown.
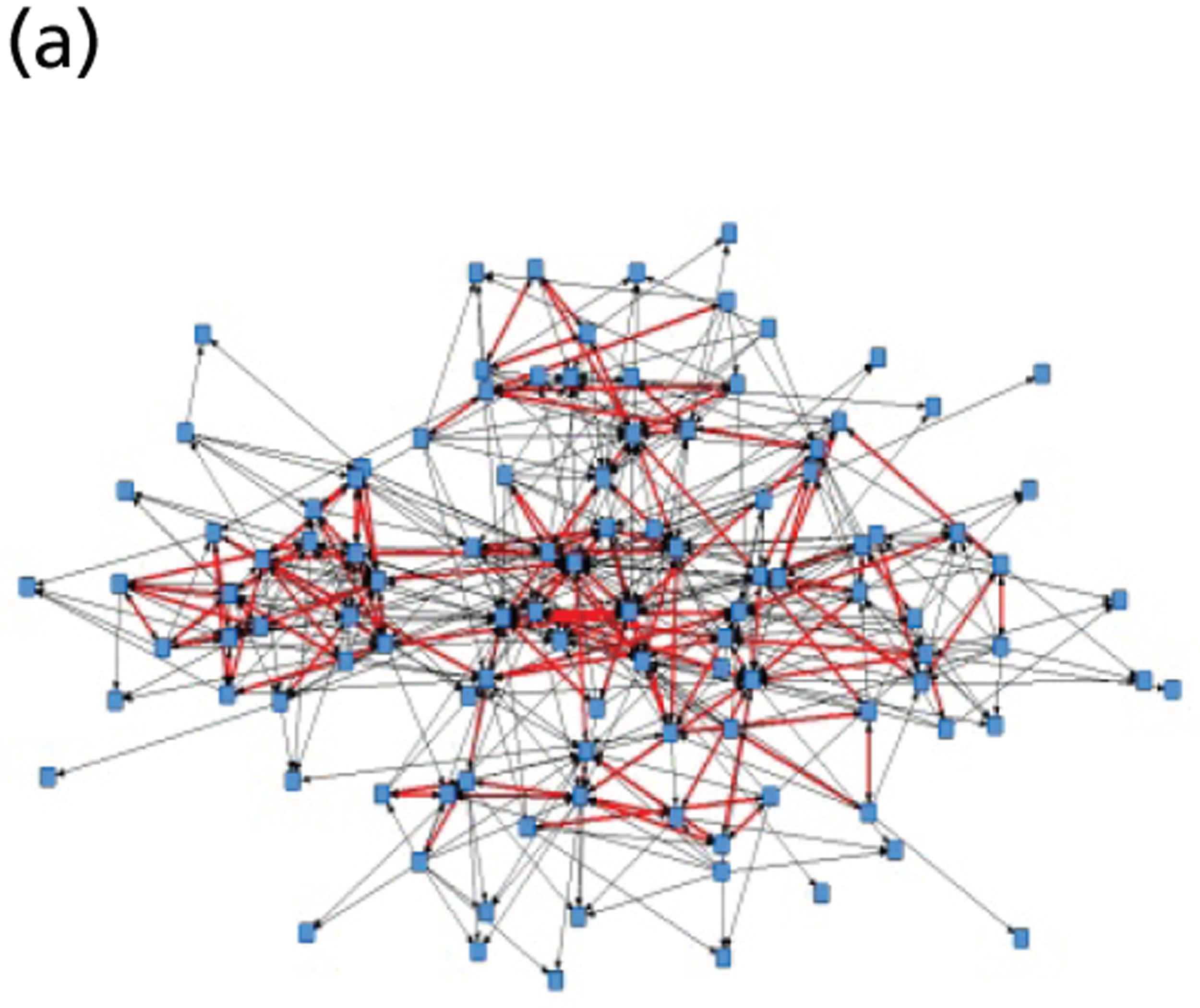
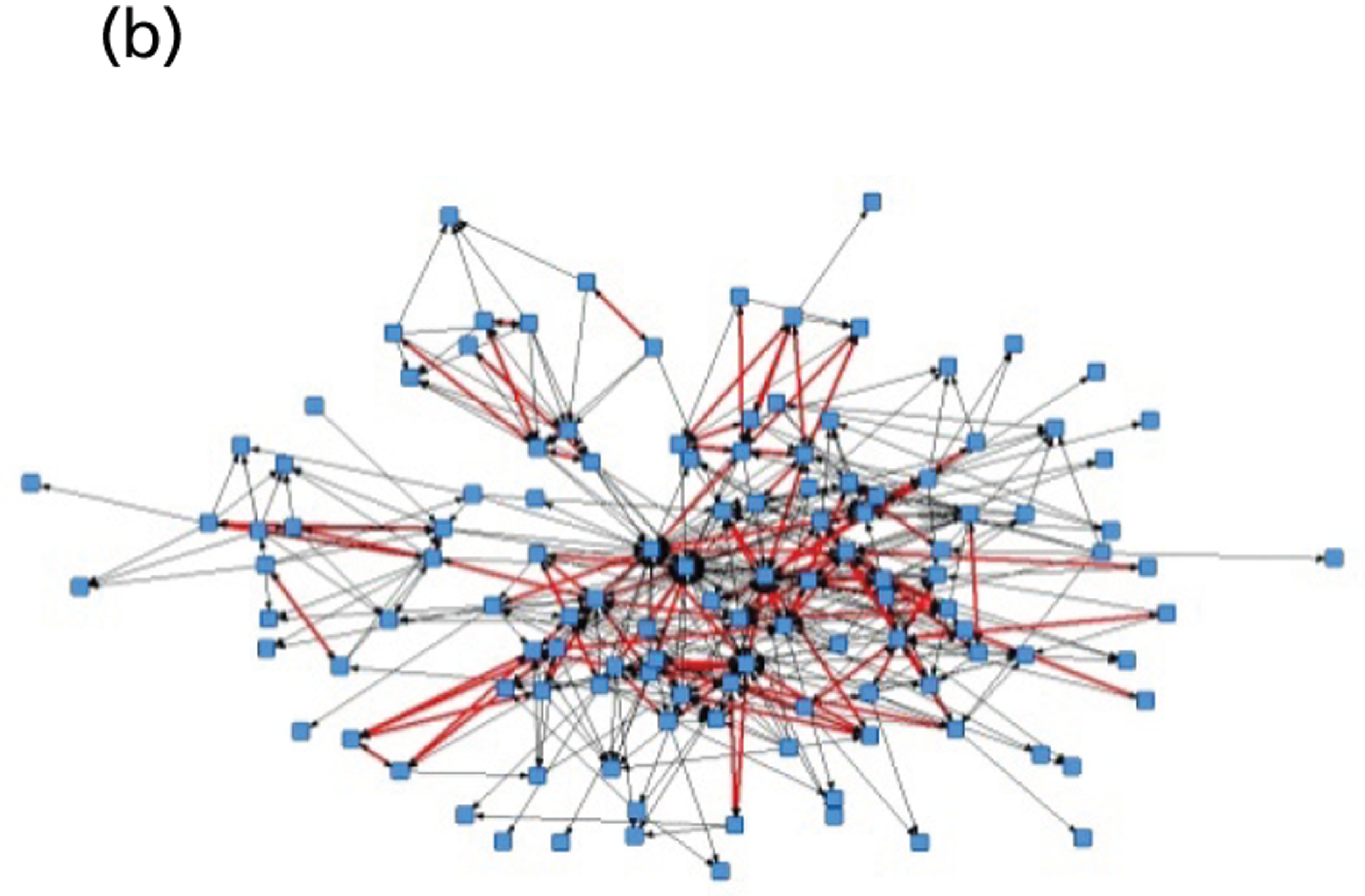
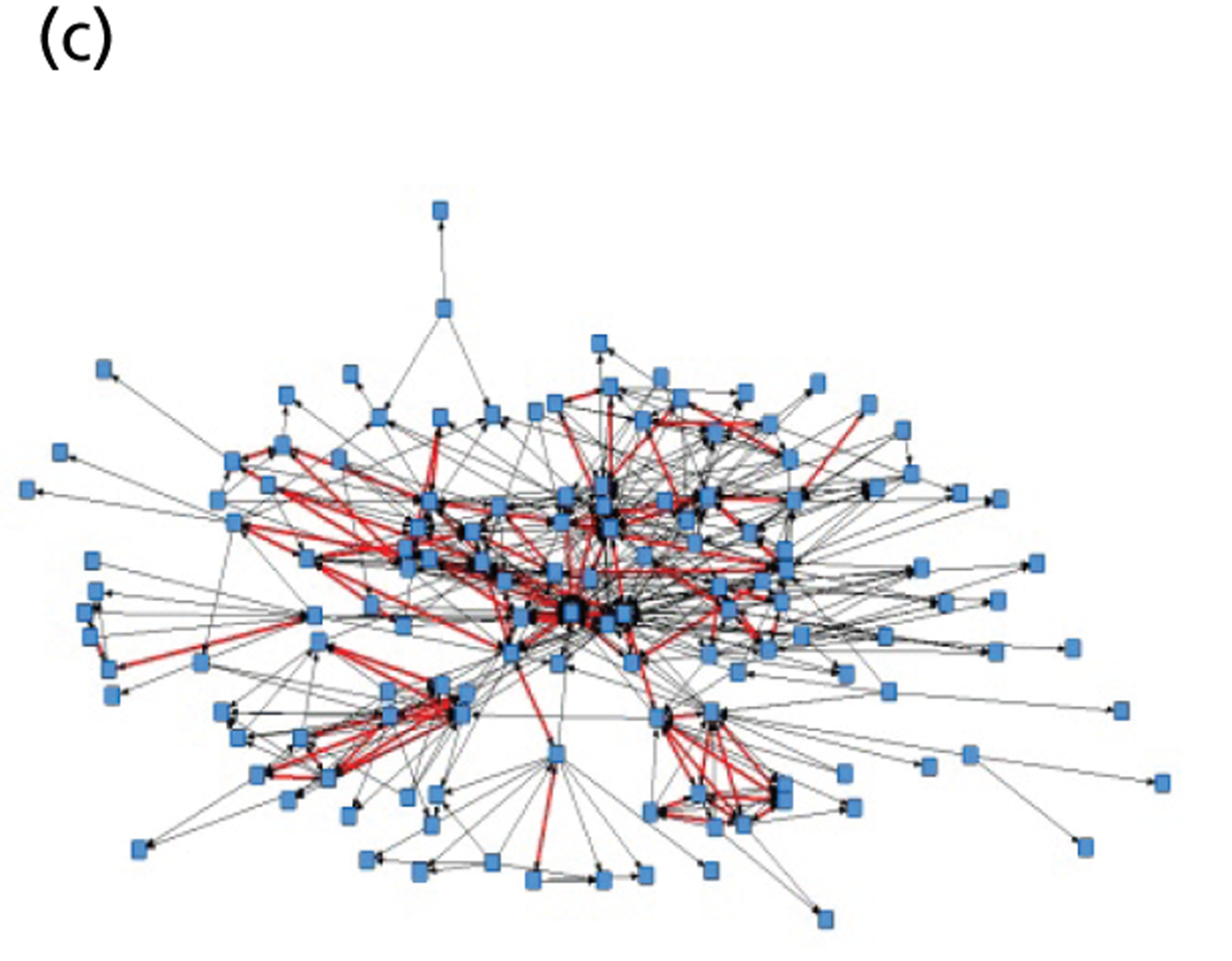
Implications of brokerage and closure for knowledge translation policy and practice
Network size is most often deemed to be a positive factor in exchange networks. The more knowledge contacts a person has relationships with, the greater the chance that one of them has the resource he or she needs. Density, that is the overall cohesiveness of a network, will have a curvilinear effect on KT. 113 By definition, some connectivity is required for a network to be a network rather than a set of isolated people. Dense networks are more ‘cohesive’ and ‘tight-knit’ than they are fragmented, and, for KT purposes, such a structure is functional in a way that ensures that network members will be held together (be it through common purpose, shared goals or mutual trust). The speed of KT will be positively impacted by network density. Indeed, research in health-care settings has shown that knowledge will diffuse more effectively in a community of practice. 6,114 In a highly connected KT network, short distances between contacts will provide faster access to knowledge and accurate transmission of information, while long distances (where individuals are not directly connected or even disconnected) can delay and distort the information. Given the limits on the number of ties that can be maintained, it is of course negative if all individuals are directly connected to each other in a KT network because knowledge obtained in such circles or cliques will likely be redundant rather than novel information. 115 In these instances of closure, the network becomes closed off from external influences. It is important for KT networks to feature brokerage via structural holes and bridging because the converse, a knowledge network where all individuals are directly connected, will more likely encourage individuals to conform to accepted ideas and practice rather than develop diverse and innovative ideas. Thus, there is a ‘trade-off’ or curvilinear effect to the amount of closure and brokerage optimally required for a KT network to be effective. 104,105 Table 5 summarises the implications of brokerage and closure for KT while Box 13 gives an example of ambidexterity.
| Features of KT | Brokerage | Closure |
|---|---|---|
| Network structure | Loose (fragmented), longer distances | Tight-knit (dense), short distances |
| Actors (network composition) | Different backgrounds/social circles, competing views | Same or similar backgrounds/social circles, shared outlook |
| Knowledge forms supported | Abstract, developmental, creative, merged perspectives | Embedded, grounded in accepted principles (i.e. technical/scientific methodology) |
| Implications for KT network | Collaboration, boundary spanning, idea generation, innovation | Co-operation, trust, implementation, concrete deliverables |
| Fluidity/risk | Hegemony, normative practice |
A clinical researcher requires knowledge that will keep him well informed about cases of recent research being used to assist patients with chronic obstructive pulmonary disease (COPD). He decides to link up with other COPD researchers both within the CLAHRC and externally. This brokerage allows him to build new contacts and widens his pool of knowledge. He then brings these new ideas back to his theme group and together they develop a protocol on best practice, which becomes embedded in the implementation work of the team.
In sum, brokerage and closure are network structures that can support KT. The usefulness of each will depend on specific KT contexts. It is important that the CLAHRC as a KT initiative features both brokerage and closure so that the social capital resources associated with these ties can be activated when needed.
Overall, we find no indication of fragmentation into separate clusters within the CLAHRCs. The CLAHRC knowledge-sharing networks were, however, not particularly closed or ‘tight-knit’, either (in the sense where all CLAHRC members are connected to each other), nor did they display a high degree of reciprocity. We found some notable changes in levels of closure over time. Overall, density, geodesic distances and reciprocity became more similar over time. The Greentown CLAHRC became slightly less connected, whereas the Bluetown and Browntown CLAHRCs saw an increase in their connectedness.
Taken together, our SNA metrics suggest that there had been some organisational restructuring of KT ties over time to moderately improve the capability for CLAHRC knowledge brokering. In doing so, the CLAHRC KT networks also became more similar. However, constraint did not decrease greatly over time which is likely to be because many structural holes would inevitably have been bridged as the CLAHRC developed. In particular, Bluetown had fewer structural hole opportunities at time 2 (efficiency decreased and constraint increased). We explore the actual changes in knowledge ties in the next section.
Information search strategies: translating knowledge across boundaries
Our social relationships with others can act as banks of resources, or ‘social capital’. 116 The portfolio of social capital resources we have access to will depend very much on the quality of our social networks. Arguably, networks that span organisational and professional boundaries will support ‘knowledge brokering’ because they bridge across information camps. 117
The CLAHRCs were organised into working teams referred to as ‘themes’. Each theme had a specific health-care focus and members of each theme therefore shared common reference points in terms of research/implementation goals, projects, working practices and sometimes co-located office space. Each CLAHRC had a different number and set of themes. We analysed the extent to which KT occurred within and between these thematic groups. We measure connectivity between themes as evidence of boundary spanning within the CLAHRC (where individuals seek knowledge from other themes more often than from colleagues of the same theme). Table 6 provides proportions of knowledge ties within and between CLAHRC themes at two time points (see Appendix 1 for a detailed breakdown).
| CLAHRC | Time 1 | Time 2 | ||||
|---|---|---|---|---|---|---|
| No. of ties | Per cent within theme | Per cent other themes | No. of ties | Per cent within theme | Per cent other themes | |
| Greentown | 629 | 59.1 | 40.9 | 488 | 49.8 | 50.2 |
| Bluetown | 575 | 59.7 | 40.2 | 439 | 51.0 | 49.0 |
| Browntown | 358 | 55.6 | 44.4 | 584 | 55.3 | 44.7 |
When we consider the total percentage of ties within and between themes, we find that each of the CLAHRC networks has a relatively balanced proportion of ties. At time 1, 60% of Bluetown’s ties are within theme, which is slightly higher than the proportion for Greentown (59%) and Browntown (56%). By time 2, Greentown and Bluetown had increased the proportion of cross-theme ties, while Browntown’s proportions were unchanged. It is important to note the reorganisation of theme groupings in CLAHRCs Bluetown and Greentown between time points, whereas Browntown theme groups stayed constant over time.
Rather than focus on the total of within- and between-theme ties per CLAHRC, we felt it more necessary to highlight the networks of individual themes and ask CLAHRC members to consider the appropriateness of this activity given the remit of each theme. Proportions of cross-theme ties were reported back to the CLAHRCs as part of our stage 1 feedback. We detail the pattern of ties in the figures below, which capture cross-theme ties by theme group at two time points. Themes that were disbanded between time points have been omitted from the figures below.
In Greentown ( Figure 4 ), the programme management theme had the highest level of cross-theme ties over time (time 1: 90.0%; time 2: 94.4%). The most internally connected themes in CLAHRC Greentown at time 1 were stroke, children and young people (CYP), and primary care (with 20.6%, 32.5% and 33.8% of cross-theme ties, respectively). At time 2, the Greentown network saw an increase in the proportion of cross-theme ties for all themes (especially stroke and primary care, which became less internally focused).
FIGURE 4.
Greentown CLAHRC proportion of cross-theme knowledge ties per theme at two time frames. CYP, children and young people; RDSU, Research Delivery and Support Unit.
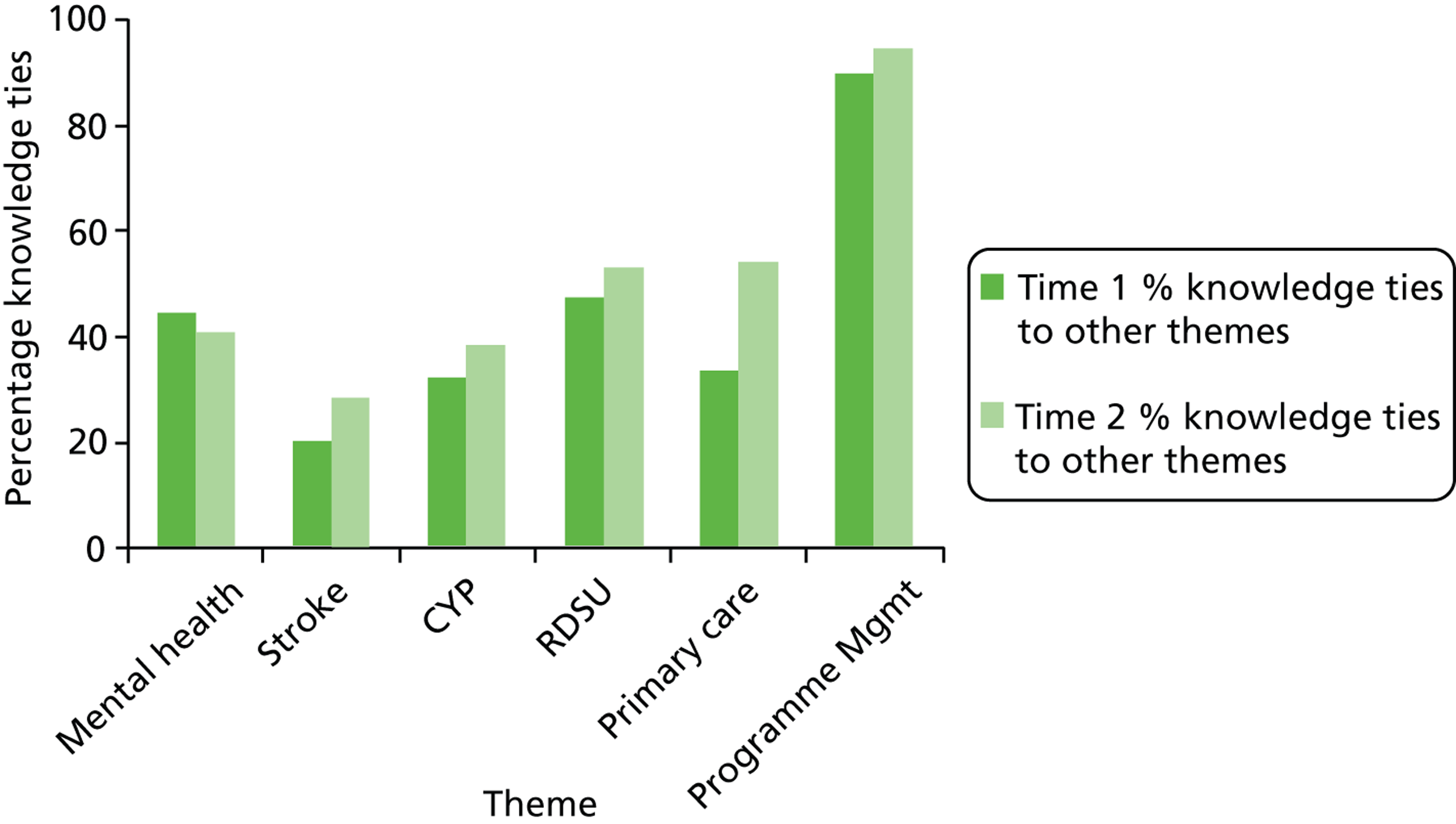
In Bluetown ( Figure 5 ), core team/programme management and cross-cutting themes had the highest level of cross-theme knowledge ties over time. The most internally connected themes in the CLAHRC Bluetown network at time 1 were stroke and transient ischaemic attack (TIA), pyschosis and maternity support (percentage of cross-theme ties 13.0%, 18.2% and 31.0%, respectively). At time 2, the Bluetown network saw an increase in the proportion of cross-theme ties. Psychosis, maternity support, and stroke became less internally focused. The cross-cutting themes maintained a high proportion of cross-theme brokering ties at both time frames (82.4% at time 1, 73.5% at time 2). The core/programme management team became more externally facing over time increasing its ties to other themes from 60.4% to 73.9%.
FIGURE 5.
Bluetown CLAHRC proportion of cross-theme knowledge ties per theme at two time frames. TIA, transient ischaemic attack.
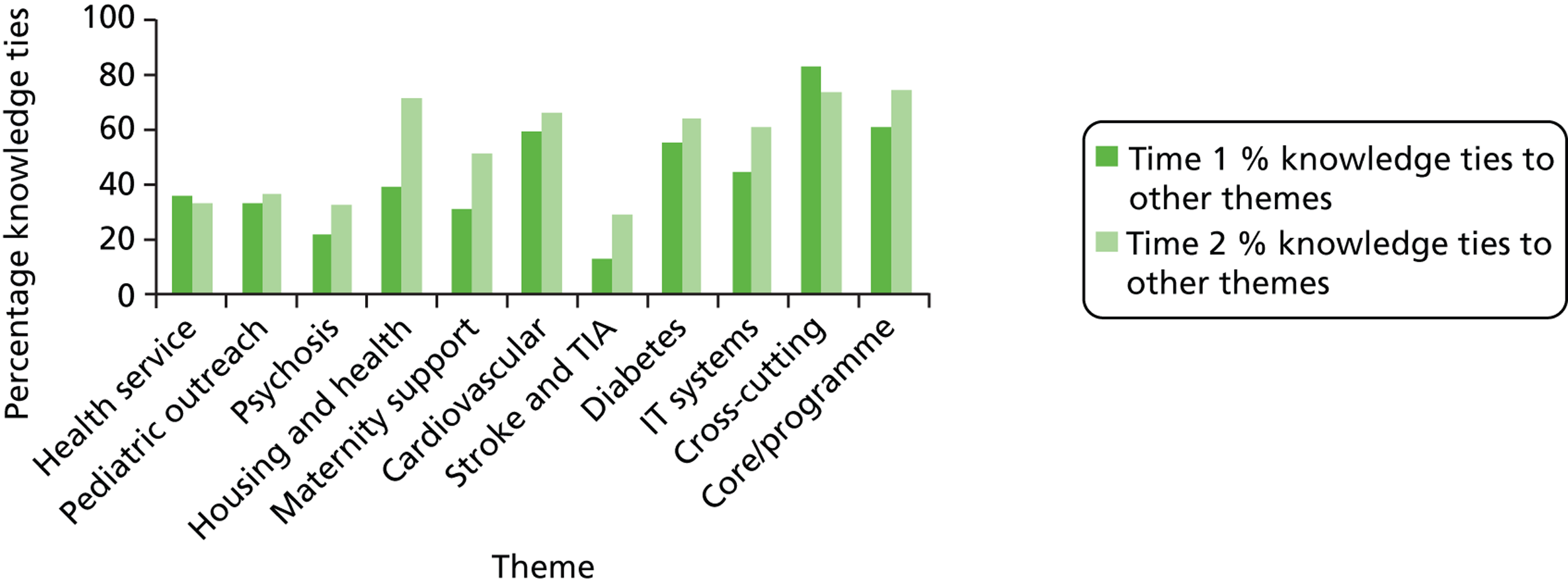
The Browntown KT network ( Figure 6 ) had a similar proportion of cross-theme ties in each time period (44.4% at time 1 and 44.7% at time 2). At time 1, the themes with the lowest proportion of in-theme ties were diabetes (22.9%), depression (26.1%) and obesity (32.1%). At time 2, genetics, chronic obstructive pulmonary disease and obesity became much less internally focused. Core team, TaCT (Telehealth & Care Technologies) and IntelComm became more internally focused.
FIGURE 6.
Browntown CLAHRC proportion of cross-theme knowledge ties per theme at two time frames. UCHD, user-centred health-care design. TaCT, Telehealth & Care Technologies.
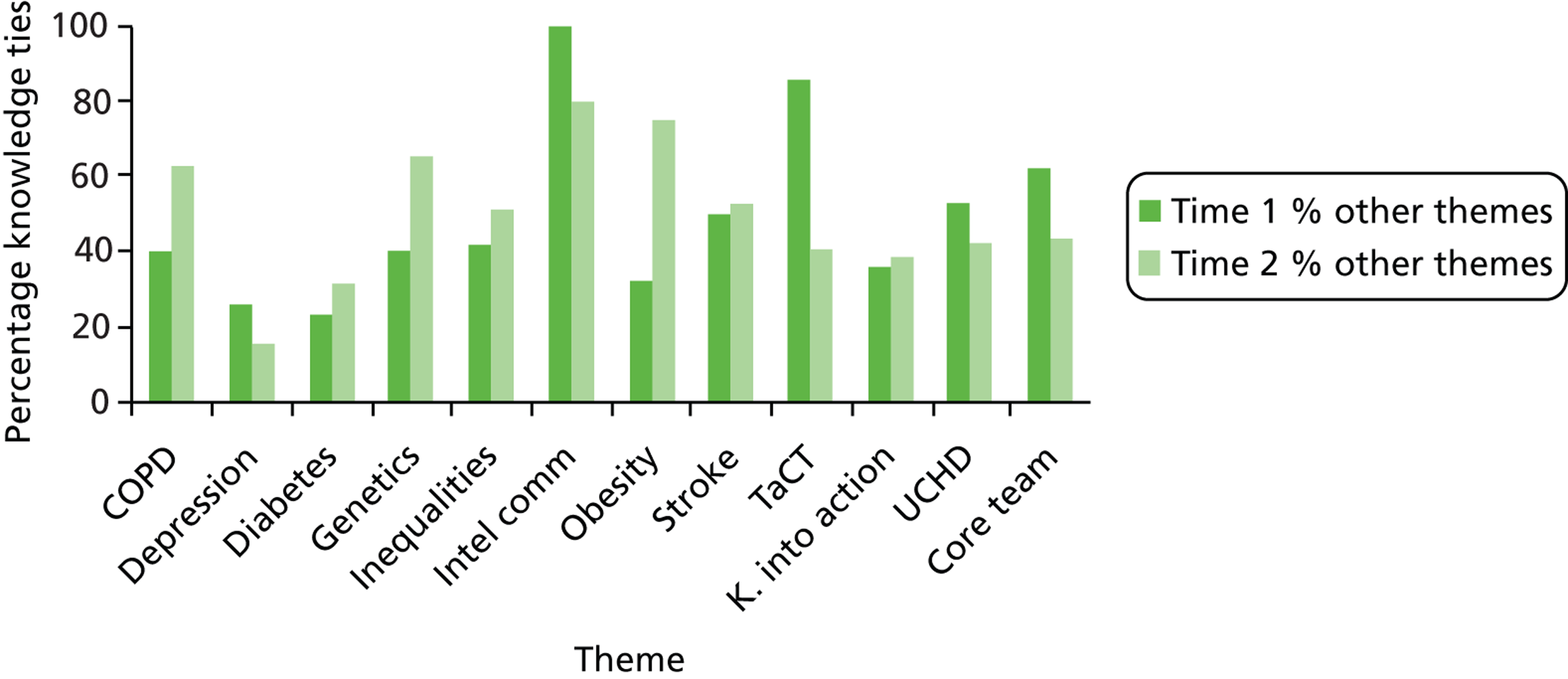
Drawing on internal and external knowledge ties
Table 7 compares ties with people inside and outside of the CLAHRC. At time 1, all of the CLAHRCs used an expansive information search strategy – networks were diverse and knowledge came in a variety of forms from multiple sources. In general, external ties were important for accessing new contacts and obtaining practical advice. CLAHRC members had previously collaborated with most of their external contacts and, therefore, brought these network resources into the CLAHRC. At time 1, members of the Greentown CLAHRC had the highest number of internal and external ties (average number of knowledge contacts per respondent).
| CLAHRC | Time period | External people | External ties | Average no. of external ties | Internal ties | Average no. of internal ties |
|---|---|---|---|---|---|---|
| Greentown | 1 | 174 | 241 | 3.01 | 641 | 8.01 |
| 2 | 125 | 168 | 2.47 | 488 | 7.18 | |
| Bluetown | 1 | 86 | 214 | 2.46 | 575 | 6.61 |
| 2 | 100 | 104 | 1.93 | 457 | 8.46 | |
| Browntown | 1 | 216 | 271 | 2.95 | 574 | 6.30 |
| 2 | 178 | 203 | 2.25 | 664 | 7.38 |
By time 2, external knowledge ties became less important. Instead, individuals prefered to draw on knowledge from CLAHRC colleagues as the CLAHRC matured. There was a reduction in Greentown members’ number of internal and external KT ties. While the numbers of external KT ties also dropped for the Bluetown and Browntown CLAHRCs, these reductions were compensated by increases in the average number of internal KT ties as the CLAHRCs matured. At time 2, the Bluetown and Browntown CLAHRCs had adopted a more targeted information search strategy – internal ties with CLAHRC colleagues became most important. External ties that were maintained became closer at time 2.
As part of our survey of CLAHRC members, we asked respondents to indicate the institutional affiliation of their knowledge contacts. At time 1, based on number of ties, the NHS was the dominant institution for Browntown and Bluetown, whereas academia was the dominant institution for Greentown. At time 2, academia was the dominant institution for all CLAHRCs. At time 1, all CLAHRC knowledge networks included ties beyond the NHS and academia – to local authorities, central government, the private industry, third sector and service users. By time 2, Browntown had increased its number of ties to non-NHS/academic contacts, whereas Greentown and Bluetown had reduced theirs, which illustrates a greater focus on NHS–academic collaborations within these two CLAHRCs.
Types of knowledge resources provided by internal and external ties
We analysed how the KT networks provided different forms of knowledge resources to the CLAHRCs. The types of information sought out from internal ties within the CLAHRC at time 2 are relatively similar ( Figure 7 ) (for a more detailed analysis see Appendix 1 ). One exception is that of the Bluetown CLAHRC, which has a higher ratio of technical advice sought out internally. There are considerable differences in the external ties ( Figure 8 ). There is a much higher desire for advice on organisational backing and access to groups in Greentown than in the other CLAHRCs. In contrast, there is less desire for practical advice. The other notable difference is a greater search for management advice from external ties by the Bluetown CLAHRC compared with the other two.
FIGURE 7.
Knowledge resources provided by internal ties (percentage of CLAHRC total at time 2).
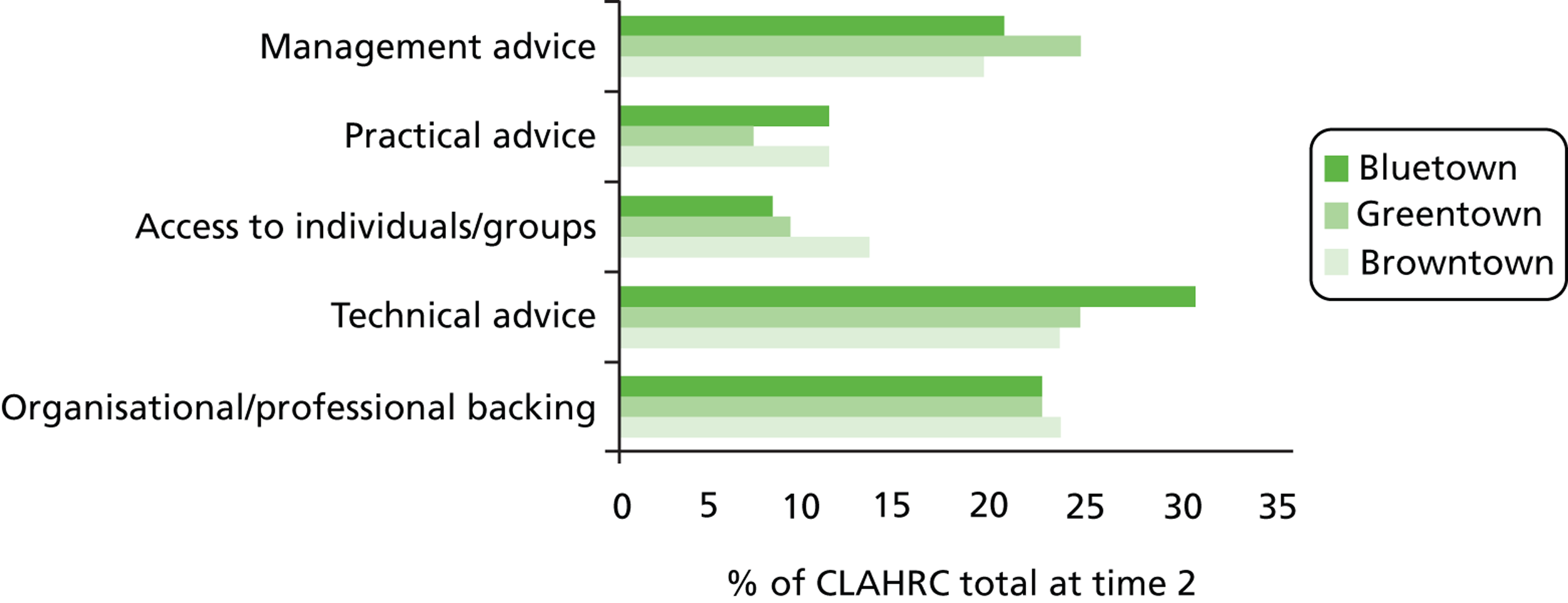
FIGURE 8.
Knowledge resources provided by external ties (percentage of CLAHRC total at time 2).
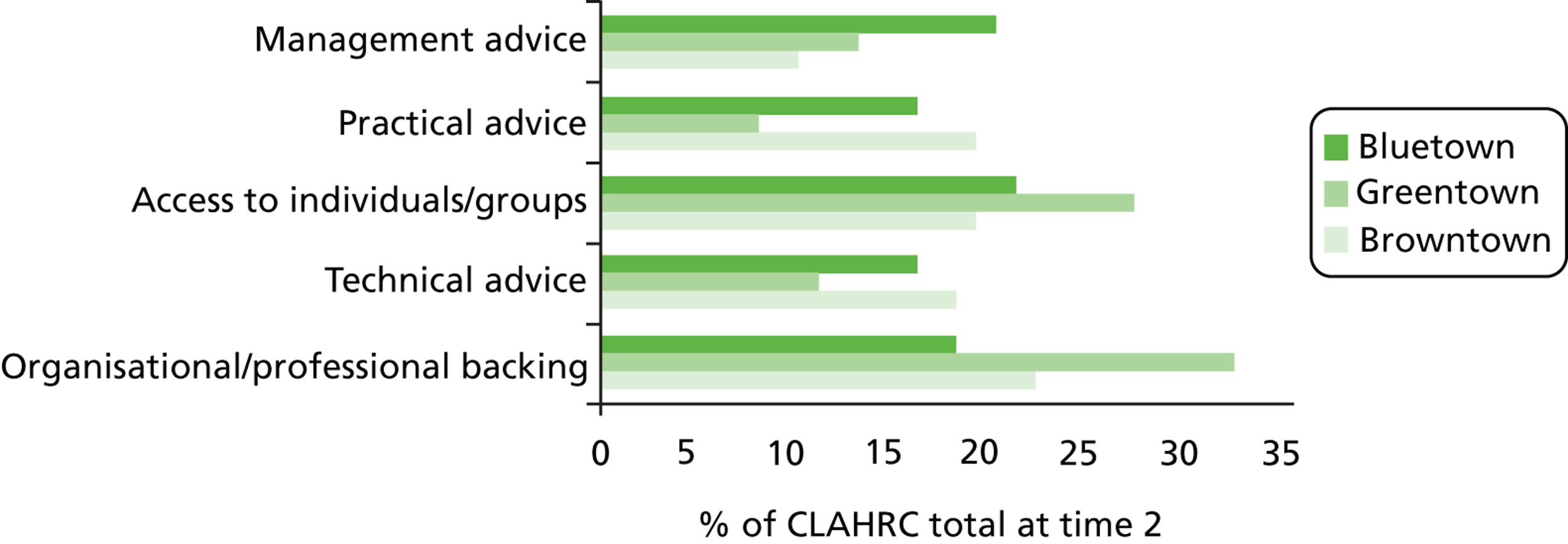
In Greentown, within-theme ties were used to obtain scientific advice, inside-CLAHRC ties mostly provided scientific advice, and outside-CLAHRC ties provided access to other groups, practical advice, and management advice. For Bluetown, within-theme ties were frequently used to obtain practical and technical advice, inside-CLAHRC ties were most often used to obtain management and technical advice, and outside-CLAHRC ties provided access to other groups. For CLAHRC Browntown at time 2, we found variance in the types of resources that were important to which themes. There is also variance in terms of where people within each theme go for resources. For example, those in Core Team, Obesity and Stroke sought practical advice from outside of the CLAHRC, whereas those in Depression and Knowledge into Action looked within their own theme for the same resource.
Epistemic boundary spanners
In this section we analyse instances where individuals act as brokers because they connect across professional disciplines in a KT network. This definition takes into account the attributes of brokers as well as their network position. (Non-participant actors have been removed from the original network because this analysis requires answers to survey questions about CLAHRC members’ discipline.) We use the attribute ‘professional discipline expertise’ to code CLAHRC actors into three epistemic groups: clinical practitioner (medicine, nursing, allied health), academic researcher (social sciences, pure sciences, medicine, health sciences) and business functions (management, commissioning and administration). Table 8 gives a breakdown of the composition of each group. The sociograms in Figure 9 represent KT networks between CLAHRC individuals, colour-coded by discipline.
| Professional group | Time 1 | Time 2 | ||||
|---|---|---|---|---|---|---|
| Greentown | Bluetown | Browntown | Greentown | Bluetown | Browntown | |
| Clinical practitioner | 25 (22.7) | 21 (18.9) | 32 (23.9) | 26 (21.5) | 24 (21.1) | 39 (23.2) |
| Academic researcher | 54 (49.1) | 51 (45.9) | 48 (35.8) | 58 (47.9) | 57 (50.0) | 76 (45.2) |
| Business function | 28 (25.5) | 27 (24.3) | 29 (21.6) | 16 (13.2) | 21 (18.4) | 24 (14.3) |
| Missing | 3 (2.7) | 12 (10.8) | 25 (18.7) | 21 (17.4) | 12 (10.5) | 29 (17.2) |
| Total | 110 (100.0) | 111 (100.0) | 134 (100.0) | 121 (100.0) | 114 (100.0) | 168 (100.0) |
FIGURE 9.
CLAHRC knowledge translation networks at time 2 (nodes coded by discipline). (Cases with missing attribute data were removed from the sociograms and excluded from the External-Internal Index analysis.) (a) Bluetown CLAHRC (102 nodes, 716 ties); (b) Greentown CLAHRC (101 nodes, 603 ties); and (c) Browntown CLAHRC (139 nodes, 1034 ties).
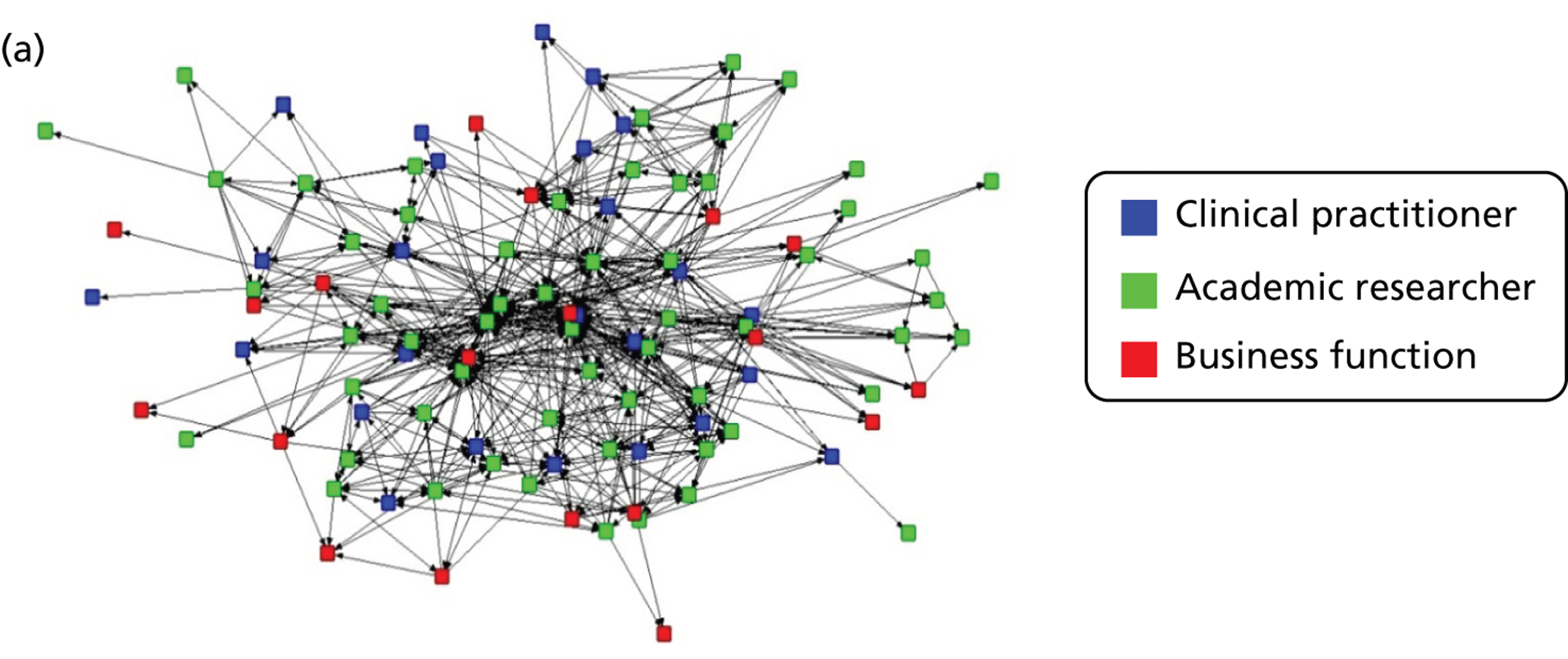
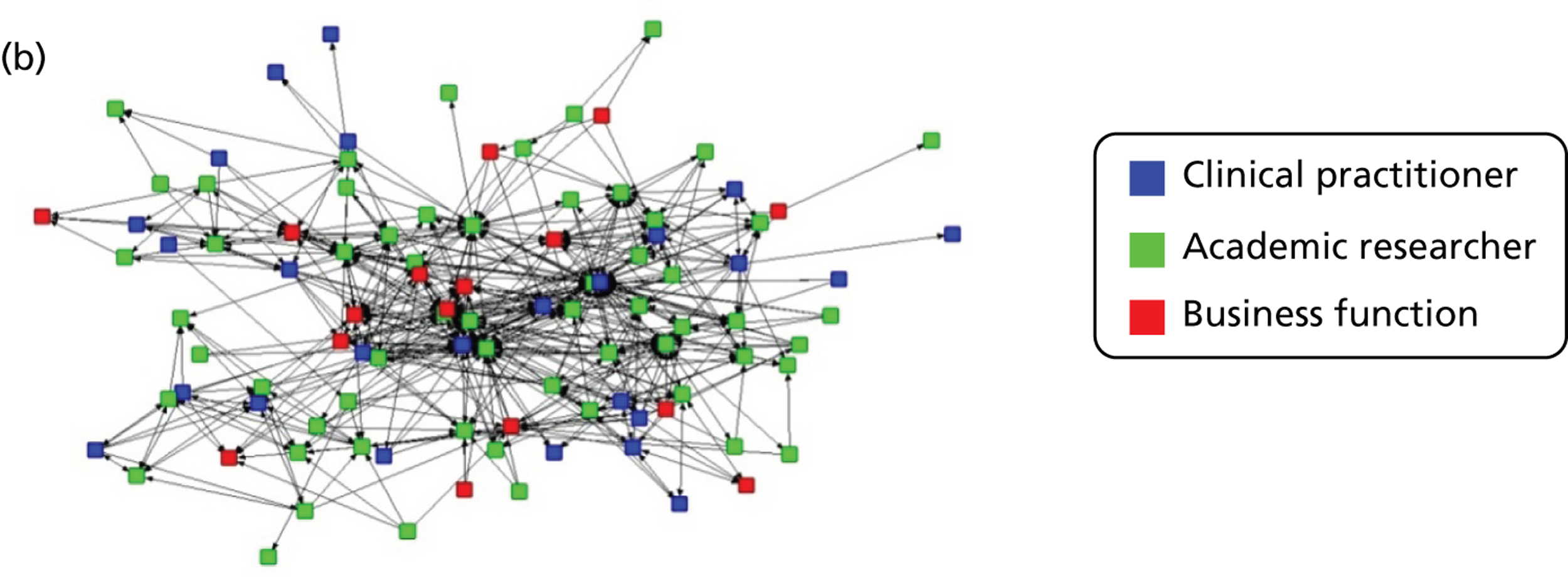
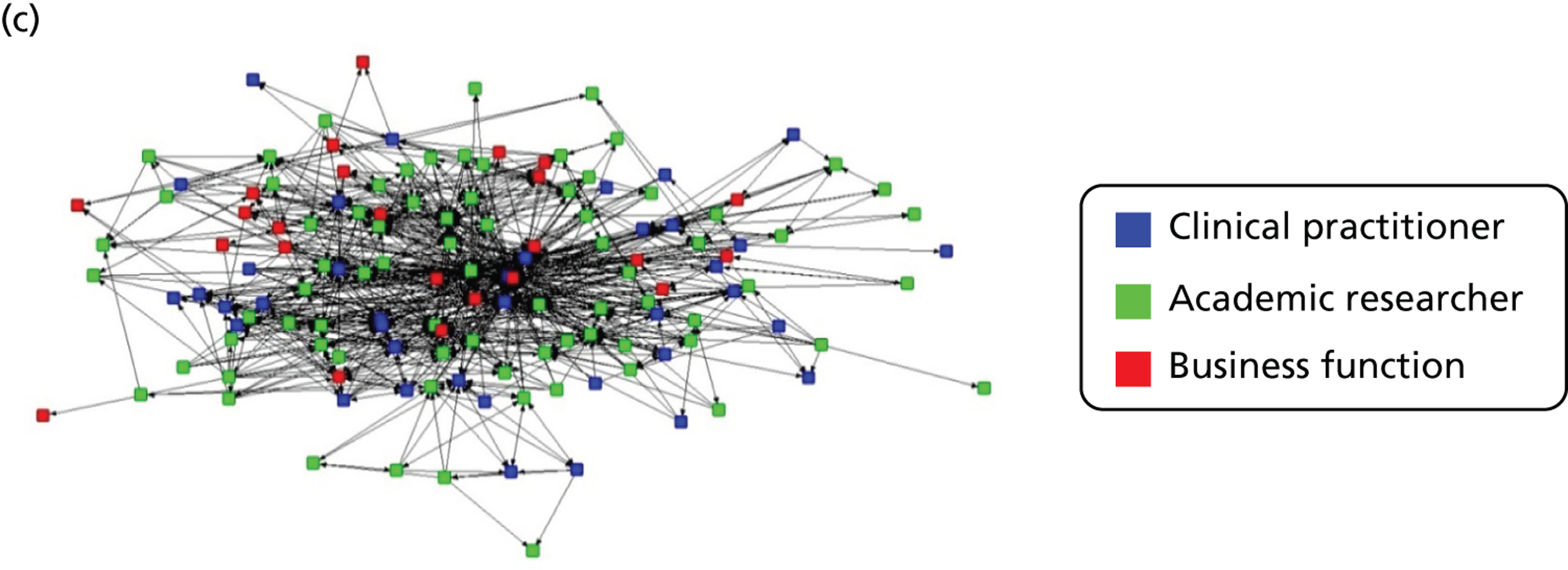
Using the External-Internal (E-I) Index routine118 in the UCINET software package, we measured the extent to which people with expertise in multiple disciplines have more heterophilous KT networks than individuals with single-discipline expertise. We found clear evidence of epistemic differences influencing KT networks. Scores are reported in Table 9 .
| Scores | Greentown | Bluetown | Browntown |
|---|---|---|---|
| Network level | |||
| E-I rescaled | –0.071 | 0.191 | 0.252 |
| E-I expected | –0.154 | 0.156 | 0.270 |
| Group level | |||
| Single-discipline expertise | –0.370 | –0.051 | 0.039 |
| Multiple-discipline expertise | 0.582 | 0.350 | 0.399 |
The results in the table indicate a tendency towards heterophily for individuals with multiple-discipline expertise, with more homophily found for individuals with single-discipline expertise. People with single-discipline expertise tend to translate knowledge to others with single-discipline expertise more than they do to those with multiple-discipline expertise. Conversely, people with more than one discipline specialism were found to translate knowledge to individuals with both single- and multiple-discipline expertise. We therefore suggest that individuals with multiple-discipline expertise are ‘epistemic boundary spanners’ by nature of their KT practices.
It makes prima facie sense that epistemic boundary spanners would have more diverse interactions than single-discipline specialists. In fact, these interaction preferences were related to social network structure. Epistemic boundary spanning was negatively correlated with ego-network density (r = –0.229, p = 0.00) and positively correlated with normalised brokerage (r = 0.295, p = 0.00). This meant that, in comparison with those with single-discipline expertise, CLAHRC members with multiple-discipline expertise had looser knowledge-sharing networks and often found themselves acting as brokers between people who were not themselves connected. Moreover, individuals with multiple-discipline expertise were also more highly engaged with the CLAHRC initiative than those with single-discipline expertise (r = 0.250, p = 0.00).
Implications of boundary spanning for knowledge translation policy and practice
Our findings highlight the different information search strategies undertaken by members of the KT initiatives and the social capital generated in support of boundary-spanning activities. Firstly, the knowledge networks at CLAHRC-theme level varied. Some themes were internally facing where team members mostly relied on theme colleagues for the translation of knowledge. Other themes were externally facing, with team members preferring to span theme boundaries in doing CLAHRC translation work. Team density will be intrinsically related to the nature of the work involved, the specific remit of each group and where the theme’s priorities lie on the research–practice spectrum. In our feedback to the CLAHRCs, we highlighted the network activities of themes and invited members to reflect on the network structure of each work group. Secondly, we also highlighted the change in information search from ‘expansive’ to ‘targeted’ strategies. At time 1, the CLAHRCs employed expansive information search strategies using diverse networks to draw on multiple sources of knowledge. By time 2, internal ties became more important and the search for information in the KT initiatives became much more targeted. The CLAHRC itself becomes a networked resource bank for KT as it matured over time.
Thirdly, there were also variances between CLAHRCs in terms of the use of internal and external ties, and where different types of knowledge resources were drawn from. KT networks were adapted as the CLAHRCs’ need for knowledge resources changed over time. Fourthly, the epistemic make-up of CLAHRC members was important for boundary spanning, particularly for the translation of knowledge across professional boundaries. We found that individuals with more than one disciplinary expertise had more diverse knowledge-sharing networks – translating to/from individuals with both single- and multiple-discipline expertise and, therefore, acting as ‘epistemic boundary spanners’. The results show that epistemic attributes and network position are related characteristics and that these factors influence preferences for in-/out-group KT across professional disciplines.
Governance co-ordination and control
In our analysis, we explored the extent to which the CLAHRC KT networks were centralised/decentralised and if a dominant ‘core’ set of actor could be identified. These factors would have direct implications for co-ordination and control of the networks and, thus, implications for the translation of knowledge.
Centralised knowledge networks feature hierarchy due to an asymmetric, or unequal, distribution of ties. Decentralised networks feature a more equitable distribution of knowledge ties, and so are more egalitarian in nature ( Box 14 ). Core actors are a set of dominant individuals in a network who frequently translate knowledge to each other, in contrast to peripheral actors who translate only to the core (on an unreciprocated basis) and not to each other ( Box 15 ). 119
High centralisation occurs when KT networks are distributed hierarchically so that central individuals dominate the network and have the potential to control knowledge flow. Conversely, decentralised KT networks offer more equal access to knowledge because individuals have relatively equitable proportions of network ties.
Core actors are a set of dominant individuals in a network who frequently translate knowledge to each other, in contrast to peripheral actors who translate only to the core (on an unreciprocated basis) but not to each other. The presence of a set of core actors indicates that some individuals dominate the KT network and the skills and experiences of more peripheral actors may be relegated as a consequence.
The distribution of knowledge ties varied between CLAHRCs. As outlined in Table 10 , at time 1 Bluetown and Browntown had comparably more centralised (hierarchical) knowledge networks, in that many ties went to a small number of people in the centre of the network while there were fewer ties between peripheral individuals. In contrast, Greentown had the most decentralised network (where members had relatively equal access to and control over knowledge) at time 1. Refering back to Figure 3 , it is interesting to note that the structural location of reciprocal ties differs between CLAHRCs. Greentown’s decentralised network has reciprocal ties spread across the whole network, while reciprocal ties in CLAHRCs Browntown and Bluetown cluster at the centre of the network.
| Network metric | Time 1 | Time 2 | ||||
|---|---|---|---|---|---|---|
| Greentown | Bluetown | Browntown | Greentown | Bluetown | Browntown | |
| Core–periphery | 0.33 | 0.34 | 0.35 | 0.40 | 0.32 | 0.31 |
| Centralisation | ||||||
| Degree (prestige) | 10.2% | 34.5% | 28.7% | 21.3% | 22.0% | 20.4% |
| Betweenness (control) | 11.1% | 37.6% | 37.5% | 9.5% | 15.1% | 35.2% |
| Closeness (access) | 30.8% | 49.0% | 46.6% | 29.2% | 35.2% | 49.8% |
| Eigenvector (global) | 36.0% | 52.7% | 51.1% | 35.3% | 37.0% | 51.2% |
| Flow betweenness (alternate path) | 2.8% | 4.2% | 8.1% | 5.4% | 6.6% | 7.9% |
The network structures did not remain constant, and by time 2 the Greentown and Bluetown CLAHRCs had adjusted their levels of centralisation up/down and so became similar to each other. With the lowering of the Bluetown CLAHRC’s level of centralisation, Browntown became the most centralised CLAHRC at time 2.
At both time points, a set of individuals leading KT could be identified. Using a core–periphery algorithm,119 it was possible to ascertain how focused each CLAHRC was around a ‘core’ of individuals and who the core individuals in each network were. The composition of core actors in terms of their organisational role is important in identifying the professional types leading the knowledge network.
The results revealed similar core–periphery structures between CLAHRCs across the two time frames (a more detailed summary of the changes in network structures over time is provided in Appendix 1 ). For the Bluetown and Browntown CLAHRCs, senior CLAHRC members (directors or programme/theme leads) were found to be the most dominant core actors, suggesting some vertical control over KT relating to organisational hierarchy. Conversely, we found that the Greentown knowledge network ‘core’ was the least dominated by senior managers, reflecting its decentralised network structure. Here, core actors occupied a mix of organisational roles (predominantly theme leads, project managers and support staff) and this network diversity was suggestive of an organisational ethos of inclusiveness in a horizontally governed KT model. By time 2, the structure of Greentown’s network had transformed to be more aligned with that of the other two CLAHRCs, both structurally (more centralised) and compositionally (with more senior level CLAHRC members in the core).
Implications of network co-ordination and control for knowledge translation policy and practice
Although neither organisational form is inherently superior, there are strengths and weaknesses to each and accompanying impacts for the governance of KT models. Centralisation can enhance internal efficiency, co-ordination and dissemination of information and persuasive messages. 120–122 Networks that are centralised and/or have a core–periphery structure are easier to co-ordinate because the hierarchical structure supports the communication of directives, standardisation of practice and operational clarity. 123 Network centralisation, therefore, creates a backbone for the provision of certain elements of knowledge governance. However, the limitation is that some individuals will likely dominate the knowledge network and the skills and experiences of more peripheral actors may be relegated as a consequence, which will have serious implications for the translation of knowledge ( Box 16 ).
A CLAHRC director consults regularly with her five theme leads on management issues. The meetings involve a two-way dialogue whereby the director updates on policy and health research developments and the theme leads report on the activities of their work groups. To ensure that management messages are consistently received throughout the wider CLAHRC, the outcomes of the strategy meeting are then disseminated to members via a monthly e-bulletin and theme leads’ feedback to their project teams individually.
In the same CLAHRC, a different set of individuals who are ‘experts’ in palliative care form a knowledge core on the topic and CLAHRC colleagues can consult these core individuals when required. Although the CLAHRC director supports a centralised network for management knowledge, she feels that technical knowledge should be organised differently so that it forms a network that is open to peripheral or less dominant perspectives. As such, she decides that membership of the knowledge core should not be fixed. She introduces a place on the panel for a newcomer in the field to sit alongside established experts for 6 months at a time. An early-career researcher takes the first placement.
In sum, centralised, core–periphery networks are easier to co-ordinate than fractioned networks because they can be controlled by a set of central, well-connected individuals. However, the views of opinions of marginal or peripheral individuals may be overlooked as a result.
In the absence of control benefits, decentralised networks are actually more robust than centralised networks. This is because knowledge ties are more equitably shared across the initiative so the network is not as dependent on key (central) actors. This is arguably one of the reasons that the Greentown CLAHRC was able to avoid factioning (or even collapse) during several changes in leadership. The drawback is that decentralised networks, lacking a strong structure for internal co-ordination, may be susceptible to mixed messages that may result in role confusion124 [as our per our qualitative findings for the Greentown CLAHRC (see Chapter 4 )].
Social network analysis summary
We draw out some CLAHRC-specific findings from our research:
-
The CLAHRCs built ‘ambidextrous’ KT networks with the capacity for both ‘brokerage’ and ‘closure’, network structures that are conducive to generating new knowledge as well as capturing of knowledge to support implementation into practice.
-
The CLAHRCs varied in their use of internal and external ties to source different types of knowledge resources. Our findings highlight the changing nature of knowledge ties as KT networks activate social capital resources according to need. Knowledge ties within and between themes may be assessed according to remit; for example, whether or not there are insufficient ties between departments that must collaborate for the CLAHRC to work effectively.
-
The disciplinary background of CLAHRC members was important in the translation of knowledge across professional boundaries. We found that individuals with more than one disciplinary expertise had more diverse knowledge sharing networks and acted as ‘epistemic boundary spanners’.
-
Centralisation and decentralisation in a network has direct implications for the governance of KT models and the nature of knowledge translated. Particularly important is who dominates the network and whose views are sidelined.
-
The CLAHRC KT networks became more similar to each other over time (particularly in terms of information search strategies, co-ordination and control, and network ambidexterity).
Social network analysis can add value to policy insight by characterising the linkages between individuals practising KT, particularly to discern the shape (or structure) of networks and the extent to which knowledge flow is dominated by central actors, and to illustrate the type of information exchanged. 125 Such analyses are useful in highlighting the potential for generating new ideas through brokerage or boundary spanning as well as embedding more explicit forms of knowledge into practical implementation within teams. In our analysis, we draw on several network measures of social capital to operationalise the capacity for KT in each of the initiatives and use this evidence to highlight some implications for KT policy and practice. We would encourage more research into the organisational forms of KT collaborations and on how KT activities are impacted by network structures and professional-epistemic characteristics. Another interesting avenue for further research would be to qualitatively explore the isomorphism, or convergence, that we found between CLAHRC networks at time 2.
Chapter 6 Empirical analysis and findings: cognitive mapping
Introduction
In this section we synthesise the major results of the cognitive mapping exercise. Cognitive or causal maps can be analysed using a qualitative and descriptive approach as indicated in Tyler and Gnyawali;126 also, statistical techniques can be applied to the maps following Clarkson and Hodgkinson. 95
The detailed analysis of the collective maps is provided in Appendix 2 , which outlines both the qualitative and the quantitative analyses of these maps. In the remainder of this section, we provide the collective maps themselves ( Figures 10 – 14 ), and outline a summary of major findings resulting from their analysis. The results show cause–effect relationships to each other and to the outcome constructs among the eight constructs that were chosen by the participants. The individual maps of each initiative were then combined to produce five collective maps127 that represent collective beliefs within each initiative.
FIGURE 10.
Collective causal map: Bluetown CLAHRC.
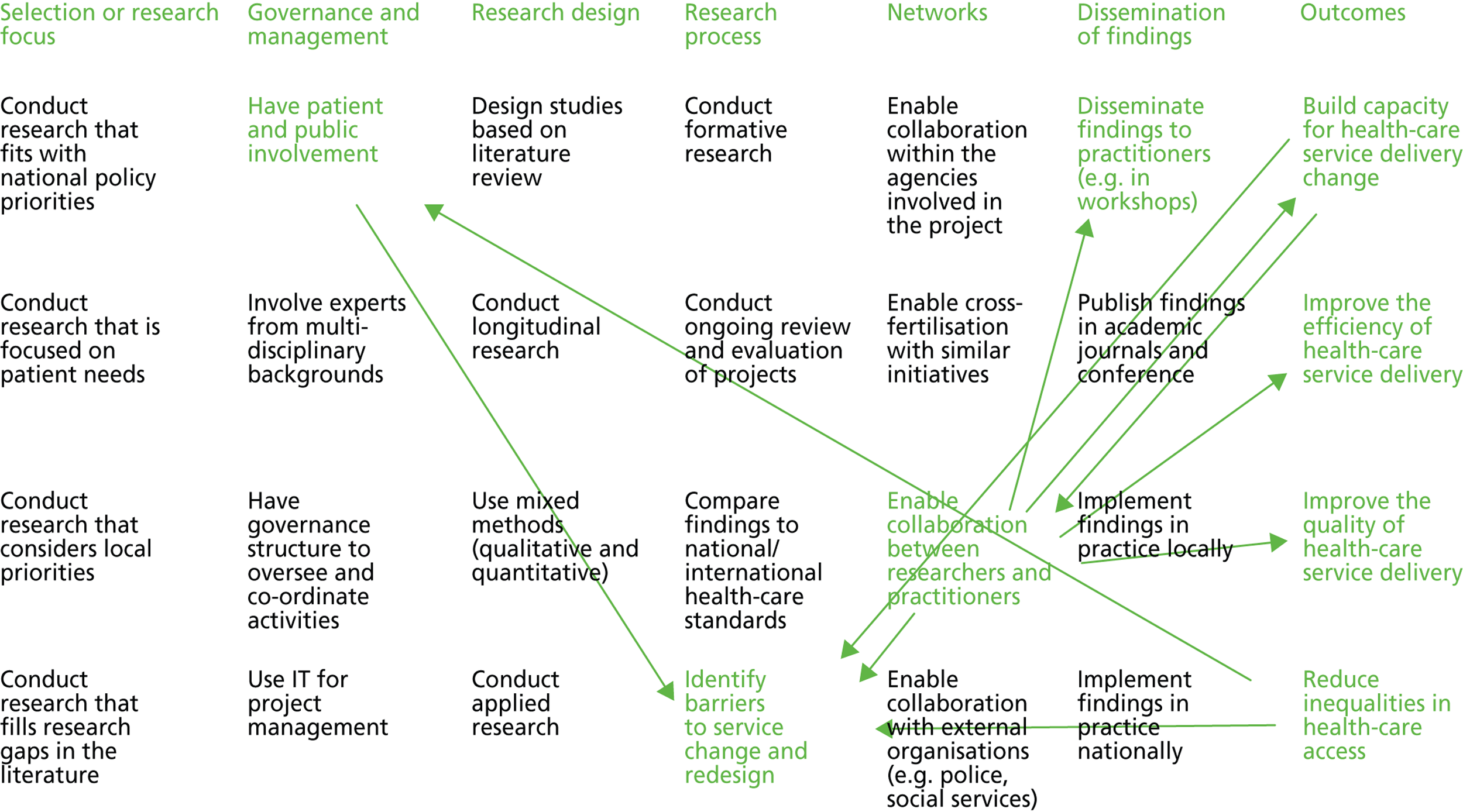
FIGURE 11.
Collective causal map: Greentown CLAHRC.
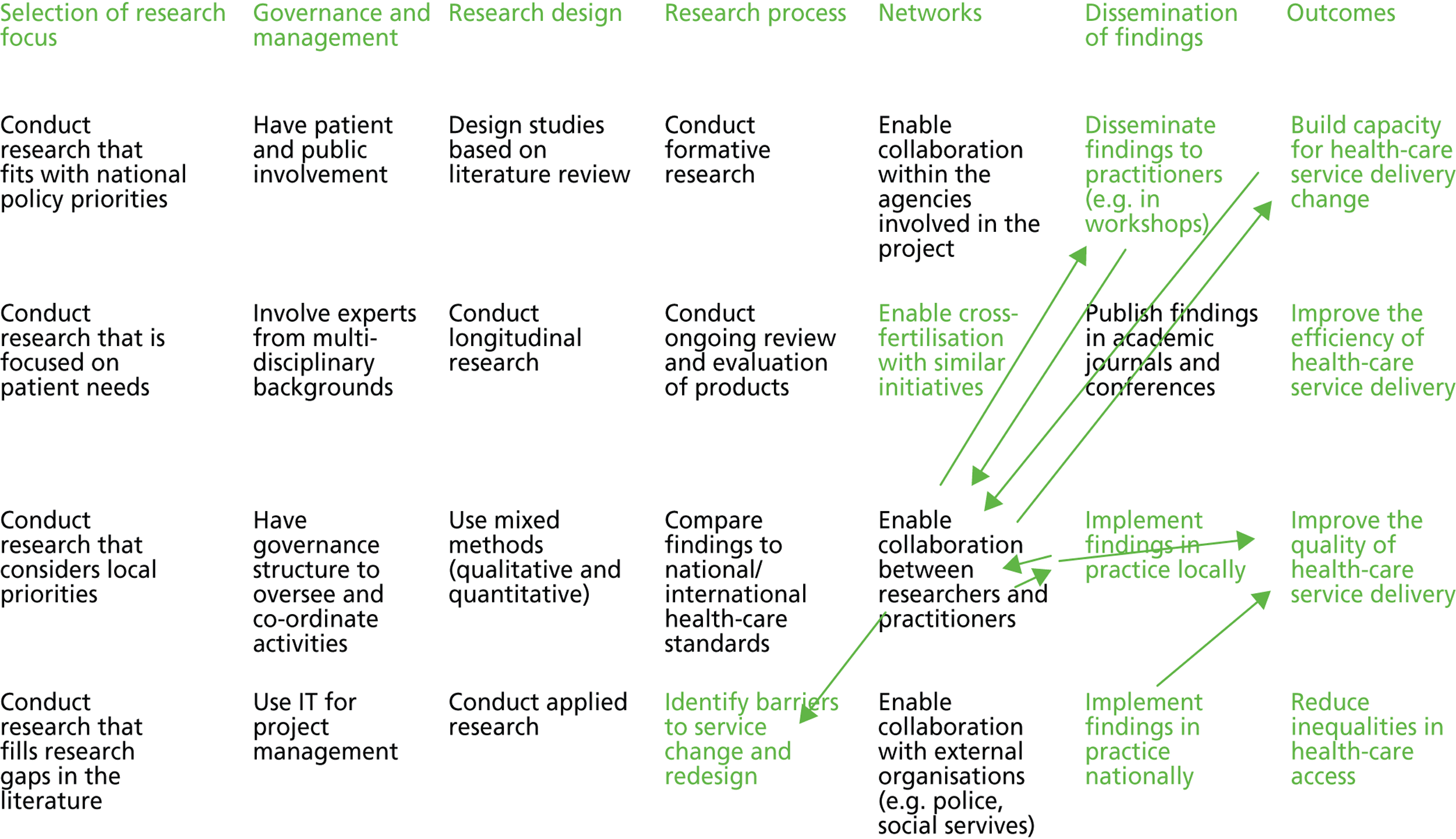
FIGURE 12.
Collective causal map: Browntown CLAHRC.
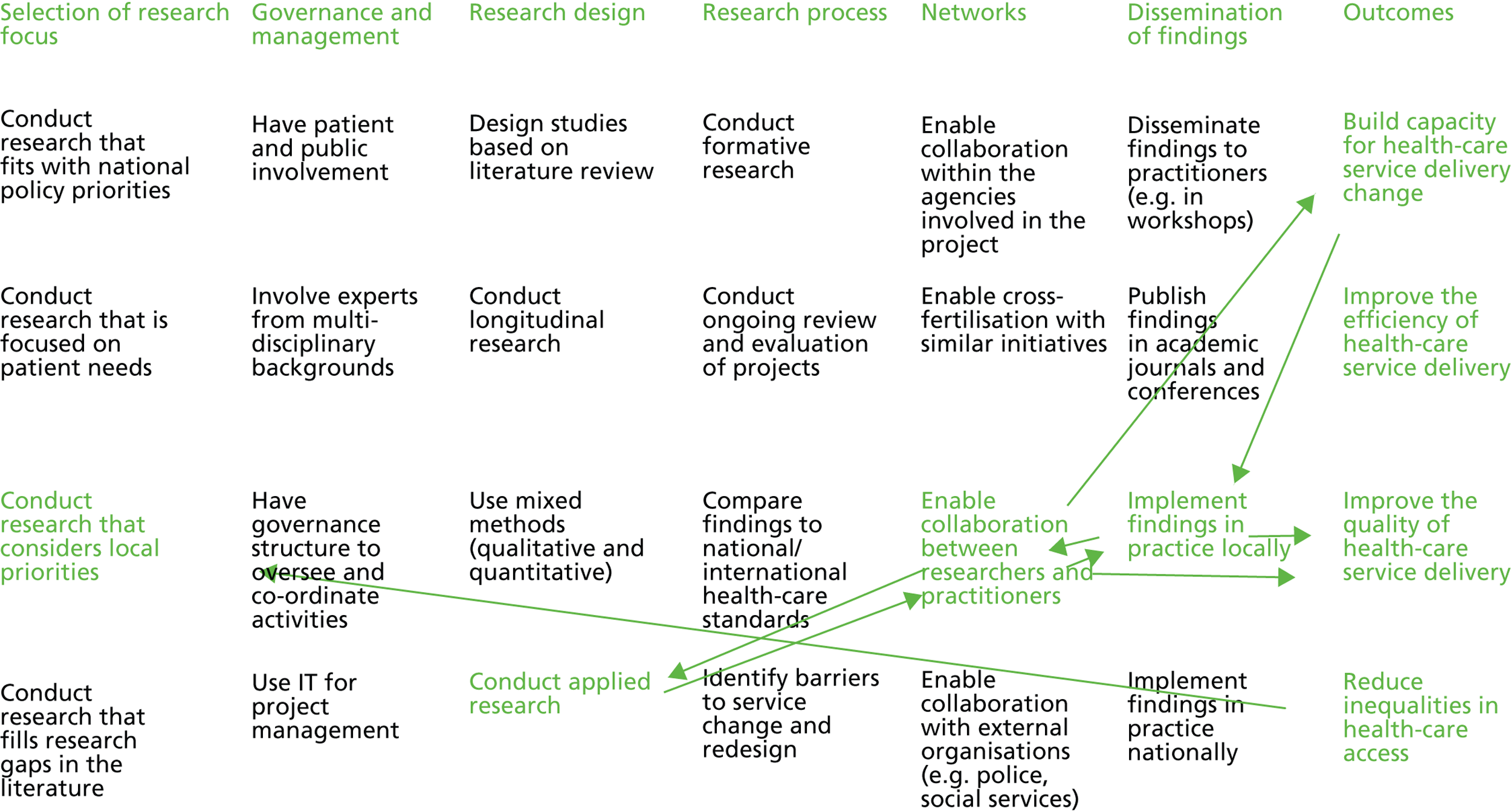
FIGURE 13.
Canada-Coordination collective map (10 participants).
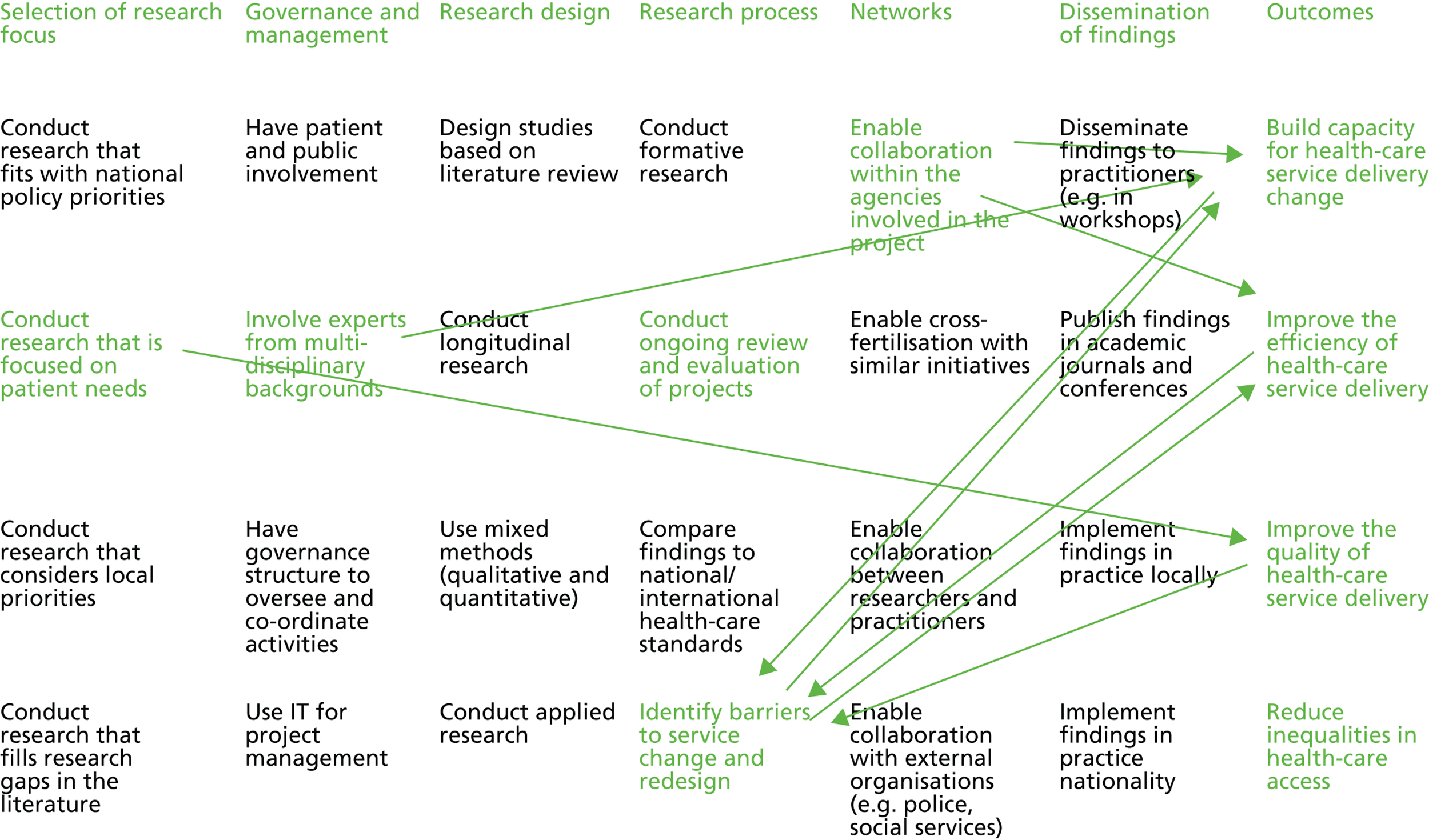
FIGURE 14.
The Canada-Translation collective map (11 participants).
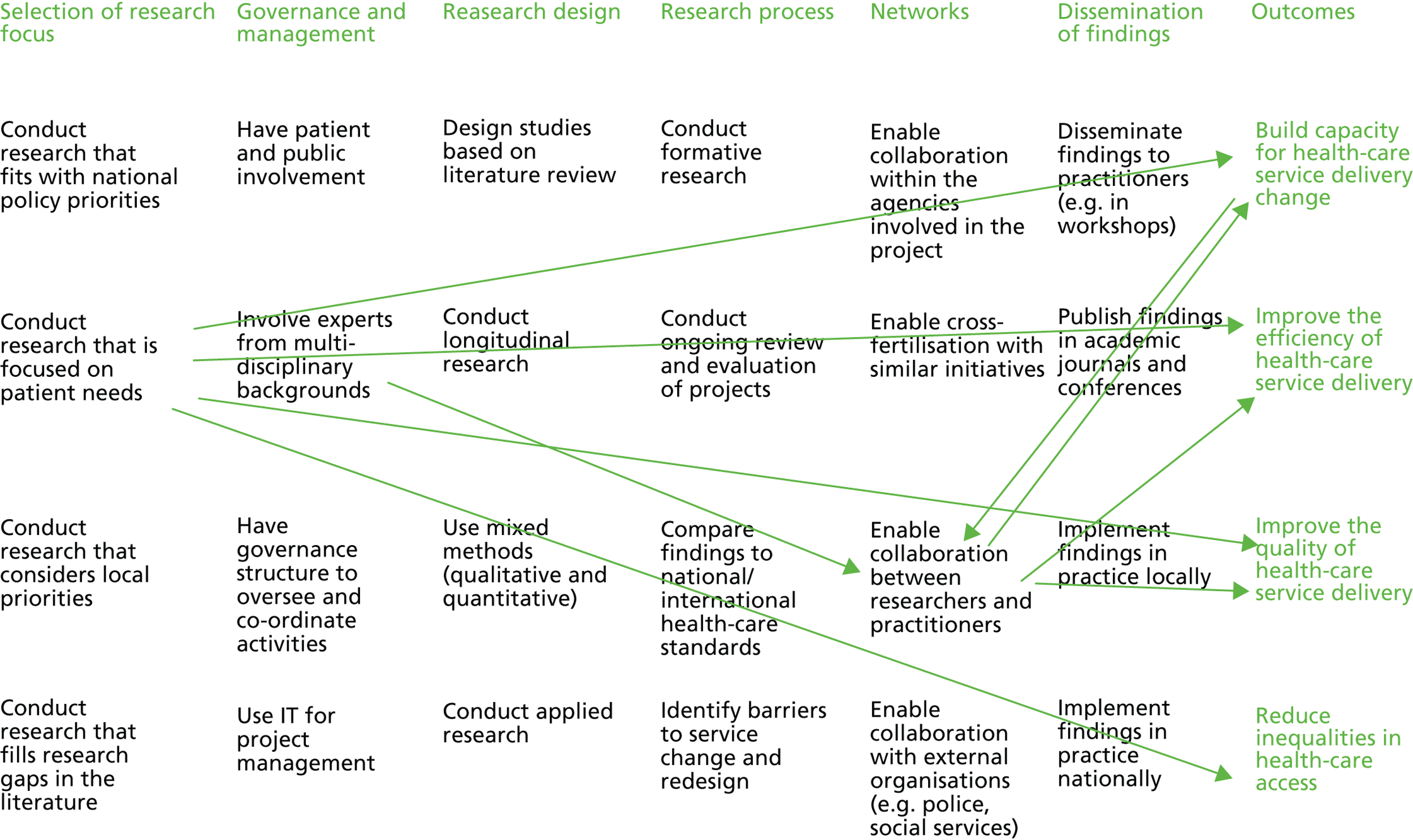
The comparison of the five causal maps produced by our study suggests that while some constructs are acknowledged to be relevant in all initiatives, some constructs are initiative specific. This could be associated with particular objectives of an initiative as well as with the members involved in an initiative (and their background, i.e. more academic or more professional). Further, some maps indicate clear cause–effect relations between constructs while other maps include two-way relationships. One- versus two-way relationships might be associated with governance structures that involve (or do not involve) feedback loop processes. Certain country-specific constructs were identified. For instance, themes associated with collaboration between different health-care partners and with the relevance of having a patient-centric approach were found in the Canadian initiatives while a focus on implementation research was found in the CLAHRCs. This suggests that different institutional contexts influence how such networked innovation initiatives play out in practice.
Comparative analysis
The participants of each initiative were asked to identify the most relevant constructs among the ones identified in Table 2 . Table 11 shows these results.
| Construct | Bluetown | Greentown | Browntown | Canada-Coordination | Canada-Translation | Sum | Variance |
|---|---|---|---|---|---|---|---|
| 1. Involvement of health care and user representatives | 3.1 | 2.3 | 3.1 | 3.9 | 2.9 | 15.3 | 0.3 |
| 2. Collaboration between partner organisations involved in the initiative | 1.3 | 2.9 | 2.3 | 4.7 | 3.4 | 14.6 | 1.6 |
| 3. Identification of barriers to service change and redesign | 3.2 | 2.1 | 2.8 | 4.4 | 1.7 | 14.2 | 1.1 |
| 4. Implementation of findings in practice locally | 3.4 | 3.1 | 4.1 | 1.4 | 1.0 | 12.9 | 1.7 |
| 5. Involvement of experts from multidisciplinary backgrounds | 1.3 | 3.4 | 2.2 | 3.6 | 2.4 | 12.9 | 0.9 |
| 6. Conduct of research that is focused on patient needs | 0.8 | 1.9 | 1.1 | 3.1 | 4.3 | 11.2 | 2.1 |
| 7. Collaboration with external organisations (e.g. local authority, third sector) | 1.9 | 2.4 | 0.9 | 3.2 | 1.5 | 9.9 | 0.8 |
| 8. Dissemination of findings to practitioners (e.g. in workshops) | 2.2 | 3.5 | 1.9 | 0.7 | 1.4 | 9.7 | 1.1 |
| 9. Conduct of research that considers local priorities | 1.6 | 1.4 | 3.0 | 0.3 | 3.2 | 9.4 | 1.5 |
| 10. Publication of findings in academic journals and conferences | 3.1 | 2.1 | 1.4 | 0.4 | 1.8 | 8.8 | 0.9 |
| 11. Collaboration between researchers and practitioners | 2.2 | 3.2 | 2.1 | 0.1 | 0.7 | 8.3 | 1.5 |
| 12. Use of mixed methods (qualitative and quantitative) | 3.4 | 0.7 | 0.8 | 1.0 | 0.9 | 6.8 | 1.3 |
Table 11 indicates that the most relevant constructs are the involvement of health-care professionals and patients, the exploitation of collaboration across partners, and the identification of barriers to change. Some constructs were found to be important (or not important) for all initiatives; some are initiative specific; and some others are country-specific. The first construct (involvement of health-care professionals and patients) is almost equally relevant for all initiatives (the variance is very low: 0.3). The second construct (collaboration across partners) is very important for the Canadian initiatives [average per country (Canada) = 4.05] while it is only quite important for the UK initiatives [average per country (UK) = 2.16]; the diversity across countries is confirmed by the total variance, which is high (1.6). The third construct (identification of barriers) is very relevant for only one of the two Canadian initiatives (Canada-Translation = 4.4) and for only one of the three UK initiatives (Bluetown = 3.2); the variance is relatively high (1.1).
Other country-specific constructs that emerged are implementation of findings in practice locally (construct number 4), which is very relevant for the UK initiatives while only relatively important for the Canadian initiatives (and the variance = 1.7) – this reflects the tendency in the UK to develop high-quality health-care services in local settings. Another example is that taking a patient-centric approach (construct number 6) is very important for the Canadian initiatives while it is relatively unimportant for the UK initiatives (and the variance = 2.1). This reflects a country-specific health-care policy; in Canada, the Ministry of Health in 2011 suggested that health-care change should focus on two main issues: being patient centric and reducing waiting time in the emergency room (Ontario Ministry of Health and Long-term Care, 2012, a policy report, available at http://health.gov.on.ca). 128 Construct number 11 clearly shows that the UK initiatives tend to give importance to the collaboration between researchers and practitioners (UK average = 2.8), while this need is less perceived in the Canadian initiatives (Canada average = 0.4).
In conclusion, Table 11 points to those constructs that, according to the participants of each initiative, are more relevant. Table 11 indicates that while some constructs are generally acknowledged as relevant, some others are initiative specific. Our analysis also suggests that there are not just initiative specific but also country-specific differences, and that this might be associated with different institutional contexts and factors. However, the sample size and the way the sample was chosen (i.e. with the aim to focus on particular types of health-care projects to investigate networked innovation) suggest that further investigation with a wider and more randomised sample is needed to assess whether or not there are statistically significant differences, supporting country-specificity claims.
Maps analysis
Figure 15 provides an overview of the causal maps of the five initiatives. The arrangement of the constructs is by thematic area and the arrows represent a selection of the links shown in the collective maps generated with Cognizer®. In fact, while the software provides all links that have emerged from the causal mapping exercise, for clarity reasons only the three top rated links per each initiative are reported (considering both the number of times the link was chosen and the ‘strength’ of each link).
FIGURE 15.
Comparison of collective maps.
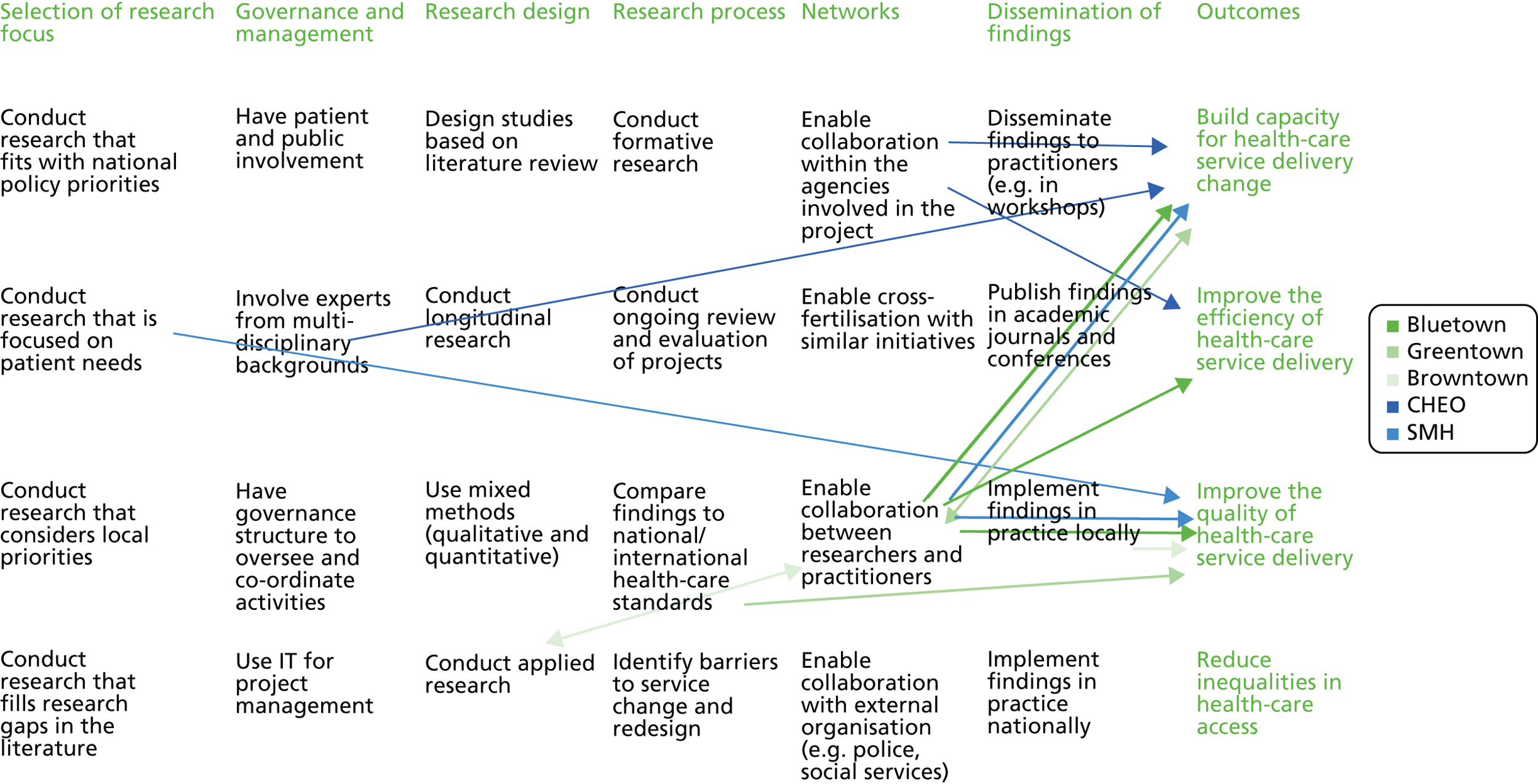
Figure 15 highlights the following. Firstly, two-way arrows occurred in two out of three CLAHRCs while none occurred in either the Canada-Coordination or Canada-Translation. Although this result is not statistically significant due to the small sample, it does suggest that in the UK CLAHRCs there was more appreciation of the inter-relations between factors that influence health-care innovation initiatives, rather than seeing simple cause–effect relationships. Given the size and publicity associated with the overall CLAHRC initiative, it is possible that this has led those involved in health-care innovation projects in the UK to better appreciate the complexity associated with developing, mobilising and using knowledge in ways that improve practice. In the more isolated contexts of the two Canadian initiatives that we consider here, this complexity may be masked by the focus on getting the research done and applied in practice. It is also possible to relate one- versus two-way relationships between themes with the particular composition of health-care teams. For instance, the CLAHRCs teams were mainly formed by clinicians, that is, some doctors are team leaders; they act as managers and co-ordinators yet they have a clinician background. In contrast, in Canada, while a few of the managers are also doctors of medicine, others have a business background (this occurred in both the Canada-Coordination and Canada-Translation).
There are several implications from the comparative analysis based on the causal mapping exercise. Firstly, the pool of (28) constructs can be used in similar health-care initiatives to map the beliefs of those involved. We contend that the constructs identified here have relevance across settings, given the diversity included in our research.
Secondly, from a methodological perspective, the focus on aggregated indexes in collective maps provides information on whether or not a team/project’s beliefs are aligned. For instance, from the links density and their variance it emerges that beliefs among participants in some projects, for instance the Greentown CLAHRC and Canada-Translation, are more aligned than in others.
Finally, we showed that causal mapping techniques are able to identify relevant constructs from document and interview analysis (see Table 2 ); they can reveal perceptions of relevant characteristics of projects at the collective level (see Figure 15 ); and they can be effectively applied to health-care settings to provide relevant insights for practitioners.
Chapter 7 Discussion and conclusions
Qualitative investigation
Our work on the CLAHRCs contributes to a growing literature on the limitations of established views of KT. 11,13 Previous work on overcoming the translational gap between research and practice (and especially the CIHR model so influential in the development of CLAHRCs) has been criticised in a recent study for assumptions of universality and consensus in KT. Such universality is seen as reflected in a lack of attention to the institutional contexts, partnering relationships and histories of KT efforts. 41 The authors of the study argue that future research should avoid the blanket use of knowledge-transfer notions, but focus instead on ‘better understanding the ways in which different types of “knowledge” become enacted, negotiated and legitimated in practice’ (p. 17). 41
As highlighted in Chapter 4 (see The vision of the Collaborations for Leadership in Applied Health Research and Care), we found that the different ‘visions’ for each of the CLAHRCs in our study were associated with different leadership and management arrangements, and even different structures in their social networks. This finding challenges the universalist view of KT. It reinforces the view that collaborative relationships and boundary-spanning activities may be more critical to KT efforts than structural forms. 14,32
In line with this view that KT needs to be seen as enacted and negotiated within particular contexts, the qualitative strand of our study highlighted in particular the need to differentiate between boundary-spanning mechanisms. As we highlighted in Chapter 4 , one result of the different enactments of the CLAHRC model in our case studies was distinctively different approaches to boundary spanning.
Boundary spanning and knowledge translation
Our study suggests that it may be helpful to distinguish between different forms of boundary spanning in order to provide a greater understanding of how KT can take place across the boundaries of different groups within translational research initiatives. In considering the different types of mechanisms that have been used by project teams within our case study sites, we have identified that these can be categorised into two different types of boundary spanning – ‘bridging’ and ‘blurring’. With ‘bridging’ mechanisms to span boundaries, an intermediary (a person, event or object) acts as a facilitator for the translation of knowledge between one setting and another. In particular, there is frequent use of mechanisms explicitly designed to facilitate knowledge flow between different groups.
The ‘bridging’ approach was exemplified by Bluetown CLAHRC, where, as noted, themes were led by university-based clinical-academics, who typically held honorary roles within local health-care organisations. Although team members such as these generally had prior experience as health-care professionals, within the context of the CLAHRC, these individuals constructed their identity as belonging to a clinical–academic community. The team leader was influential in directing the subprogrammes of work, resulting in the traditions of a clinical–academic environment being the dominant ideology within the clinical project teams. However, at CLAHRC level, collaboration between clinical–academics and those from other academic disciplines, and between the project teams and local health-care providers and commissioners, was also strongly encouraged as part of the process of making research evidence more useful for health-care policy and practice.
Structural features within this model had been designed with the explicit purpose of linking the clinical project teams with specialist types of academic expertise (such as economics, statistical support and KT and dissemination skills). It was clear from our study that these individuals were required to be flexible in the approaches that they followed for doing their work. One participant from a specialist support service team described how she felt that the clinical team that she had been allocated to work with did not initially understand the type of perspective her expertise could provide, or how her role could usefully contribute to the programme of work that had already been planned within their theme. In working through this challenge, it was important that the individual was willing to be flexible in the type of working traditions that were followed. Although the initiative-wide strategy had initially aspired to the greater ‘blurring’ of knowledge from different academic perspectives, the challenges experienced meant that a ‘bridging’ approach for KT was more widely applied in practice.
In contrast to the Bluetown CLAHRC, our study within Browntown CLAHRC highlighted how boundaries were ‘blurred’. In this case, project teams were drawn from a more diverse set of groups, representing different disciplines and professional groups. However, rather than the more polarised differences seen in Bluetown, there was a greater degree of overlap or ‘redundancy’ between the types of disciplines and professional expertise represented in teams. For example, many of the academics involved were from professional sciences rather than disciplinary sciences, and so were closer to the epistemic concerns of team members who were health-care practitioners. 129 Our data showed that that there was a willingness to incorporate insight from team members from quite different perspectives, and that these ideas could be more fluidly translated into shared practices within the teams. As a result, the outputs from the work programme could be more easily understood within a health-care policy and practice context, without a reliance on a ‘bridging’ type mechanism to facilitate translation.
The contrast between the bridging and blurring approaches identified in our study is summarised in Table 12 .
| Organisational form and processes | Bridging – explicit boundary spanning | Blurring – implicit boundary spanning |
|---|---|---|
| Context for project team boundary spanning | ||
| Framing of project team work | The programme of work of a project team is informed by one dominant approach, which provides a clear vision for the type of work being undertaken | There is no dominant approach for the project team’s programme of work, but different elements may be informed by the traditions/methods of different team members |
| Team composition | Team members are predominantly from similar backgrounds, where they do not typically have to span organisational, disciplinary or professional boundaries to share knowledge internally within the team | The team is constituted of heterogeneous members, which means that project team members are spanning organisational, professional, disciplinary and geographic boundaries internally within the team |
| Process for interaction between team members | The majority of team members are co-located within one organisational setting, where day-to-day interaction can take place, and members are in a position to easily access knowledge from other similar types of people to develop greater depth of expertise | Team members are not generally co-located but are based in different organisations. Interaction requires additional ‘office space’ away from their ‘home’ environment, or team members may have more than one location for their work. This allows members to draw on their insight from these different settings and to share this information with the team to inform the programme of work |
| Processes created through organisational mechanisms | ||
| Arrangement to connect clinical project teams with core management | Members from one group move to the space of the other group to interact, and then go back to their ‘home’ environment, e.g. attendance at core management meetings and management representation at project team meetings | Individuals have dual roles which generates a blurred identity of which parts of the initiative they ‘belong’ to, e.g. have ‘real’ positions in core management and clinical project teams |
| Processes to access to expertise within the initiative | The structural organisation of the initiative emphasises a formal distinction between clinical project teams and other services. Where connections are made, individuals with ‘specialist’ sit on the edge of the team, and act as a connection between their world and that of the project team. Mechanisms such as official team meetings are used to create a space where project team members can meet with specialist support services | Members with ‘specialist’ types of expertise are integrated members of project teams, rather than sitting on the edge of clinical project work. This allows more seamless movement of different types of knowledge to inform the programme of work. Mechanisms such as organised project meetings and informal days when team member spend time in the same location are used to create a practice environment where knowledge from the different perspectives can be practically shared |
| Processes to support the project teams to develop connections outside of the initiative | Planned arrangements to create a ‘separate space’ for different types of knowledge to be considered, before returning back to project team context, e.g. advisory boards/stakeholder meetings; clinical-academics with ‘honorary’ positions at health-care organisations | Project team members seamlessly interact with other types of knowledge through ‘hybrid’ positions, e.g. clinical-academics who hold ‘active and extensive’ positions in both academic and health-care settings; members who have roles with other stakeholder groups that were not explicitly taken up because of the clinical project work |
| Formal structures for linking evidence to practice | ||
| Knowledge brokering roles performed by individuals | ||
| External-focused boundary-spanning roles | Boundary-spanning role is enacted by individuals who sit on the ‘edge’ of the project team. These individuals naturally belong in another environment, but compromise their approach to working to fit in with the approach of the project team. They enact a role to connect the project team to their ‘home’ context, and act as facilitators for knowledge flow between these settings | Individuals who have hybrid roles, naturally belong to more than one community, and can easily relate to these different perspectives |
| This role allows the team member to contribute knowledge from these different perspectives | ||
| Roles to support interaction within the initiative | Members from one group move to the space of the other group to interact, and then go back to their ‘home’ environment – ‘honorary roles in other environments’, e.g. attendance at core management meetings, management representation at project team meetings | Individuals have dual roles which generates a blurred identity of which parts of the initiative they ‘belong’ to, e.g. have ‘real’ positions in core management and clinical project teams |
Bridging versus blurring as approaches to boundary spanning
As Table 12 suggests, ‘bridging’ emerges from and sustains an environment in which little compromise or negotiation is required by collaborating groups around their epistemic differences. Instead, the emphasis is on the mechanism of the bridge as a translational process, in order for knowledge to be able to be understood in a different context. In ‘bridging’ approaches, the emphasis is on an intermediary enacting the translation process themselves. They perform roles, such as ‘translator’ and ‘interpreter’ of knowledge, between the environment of the clinical project team and their ‘home’ context. In this case, the emphasis is on the boundary-spanning mechanisms to possess the requisite capability, such as an individual adapting their own comprehension of different situations, or a meeting space which has an appropriate environment to stimulate two-way discussion.
With ‘bridging’ mechanisms, the project team themselves are not required to radically alter how they work. As a result, they can develop knowledge based on the traditions and norms of their own community. As has been previously highlighted,130 an advantage of mechanisms that focus on trusted intermediaries enacting knowledge-brokerage roles is that there is less pressure on researchers to develop a new set of skills for KT, as instead they rely on the broker to carry out this work. However, as power balances and legitimacy battles between epistemic groups influence KT and mobilisation,28 facilitation by the senior management of the CLAHRC can be important in creating an environment of openness to engage and interact with the ‘bridging’ mechanism.
Viewed positively, ‘bridging’ approaches may have the advantage that university-based teams are able to produce high-quality publications, while still meeting CLAHRC objectives on informing health-care policy and practice. In this sense, ‘bridging’ mechanisms can be useful as they provide a supportive structure for groups and communities with markedly different practices and forms of expertise. However, the extent to which this knowledge can be transformed into novel forms can be limited, as it is reliant on what can be achieved by the bridging mechanisms.
Our analysis of ‘blurring’ forms of boundary spanning illustrated an environment where knowledge could be more readily mobilised across organisational, discipline and professional boundaries. Where the epistemic differences across these groups are not great, knowledge can be co-produced through subtle transformation, to incorporate ideas and expertise from different perspectives. In this sense, ‘blurring’ forms of boundary spanning have the potential to develop ‘novel’ types of knowledge that are not embedded in traditionally established specialist domains. Although explicit mechanisms were not used to support this type of boundary spanning, implicit organisational features and processes were important in supporting KT through this boundary-spanning approach. Particularly important here were ‘hybrid’ individuals with dual positions who could act as boundary spanners, and also organisational processes that enabled members to take on multiple positions within the initiative. By creating teams that span a variety of diverse groups, this approach has the potential to develop an innovative programme of work, creating capacity for innovation through the co-production of knowledge at the interstices of many different perspectives. 34 For ‘blurring’ mechanisms, ‘figureheads’ did not have the same importance as has been shown for ‘bridging’ mechanisms,79 as there was a greater onus on all members of the initiative to be flexible in their work practices and epistemic commitments. At the same time, support from CLAHRC senior management was crucial to creating an environment where the perspectives of diverse groups were respected and were enabled to inform the direction and focus of the work programme.
Social network study
In this strand of our study, we reinforced and elaborated on the qualitative findings to a significant extent. Our findings on network ties, for example, reflected the above-noted need to view KT efforts as situated within a particular historical and institutional context. Thus, we found that CLAHRC KT networks are embedded in, and influenced by, wider organisational, institutional and social factors. Further, reflecting our findings on the different enactments of the CLAHRC model seen in our cases, we observed in the social network study variation between CLAHRCs’ social networks reflecting difference in governance and approaches to KT.
An important concern for our study, as noted previously, was to identify the different routes to achieving networked innovation navigated by our three CLAHRC cases. Here, our social network research highlighted the importance of what we termed ‘ambidextrous networks’ to the pursuit of such innovation.
The importance of ambidextrous networks
In advancing the networked perspective on innovation, scholars have drawn on theorists of social networks and social capital, notably Burt and Coleman, to better understand the ways in which knowledge is created and shared through social networks. 131,132 This work has emphasised the related structural features of ‘brokerage’ and ‘closure’ as playing vital roles in generating different forms of social capital which contribute to the innovation process.
The extent to which individuals are connected to others who are not themselves connected is known as brokerage within the SNA literature. Brokerage thus describes the potential for actors located at structural holes (in disconnected groups) to connect and exchange non-redundant (new) information. 62,131 From the standpoint of innovation, it represents an important mechanism through which new knowledge can be created via novel combinations of existing knowledge.
If measures of individual brokerage are aggregated, it is possible to find the extent to which a governance network contains these phenomena. In our study, we find that the CLAHRCs had somewhat similar levels of brokerage at time 1. The exception was the Greentown CLAHRC, which had slightly more people acting as knowledge brokers between disconnected others in the network. By time 2, we see very similar brokerage scores for each of the CLAHRCs, indicating convergence in network structure. The level of brokerage within each of the CLAHRCs was conducive to the fusing together of novel information sources through individuals brokering across the loosely connected structure of the network between the themes.
By way of contrast, closure occurs in cohesive groups and describes situations where subsets of actors in a network are structurally positioned so that they have a tendency to be closed off from others. In an organisational setting, this may be akin to an established work team of colleagues with shared interests, motivations and goals or a community of practice. Closure is linked to density, reciprocity and trust,101 structural conditions that facilitate action, and ‘getting things done’ in practice. It thus helps to account for the role of networks in ‘embedding’ new knowledge.
The CLAHRC networks were loosely knit structures, especially between the themes. Within the themes, however, there was a much higher level of closure. We argue that this has a prima facie logic because social processes occurring at the local group level are likely to develop closure over brokerage. Each CLAHRC thus acted as a space to bring together various individuals and clusters around different themes under a common KT vision. We observed slightly different levels of closure between CLAHRCs at time 1. In the first time period, the Greentown KT network had a higher level of closure than that of the other CLAHRCs. In network analyses terms, we found that the Greentown CLAHRC had higher density and reciprocity and lower average distance between contacts. At time 2, the CLAHRCs became more similar in terms of their levels of closure.
It is important to recognise, however, that brokerage and closure only represent local network conditions; that is, phenomena which emerge within one part of a wider network. Existing studies have tended to focus on these local conditions as discrete phenomena133 – focusing, in particular, on knowledge creation via brokerage – and have not addressed their implications for the innovation process as a whole. A process view of innovation defines it as a temporally and episodically structured, highly iterative design and decision process involving the creation, diffusion, blending and implementation of new ideas and knowledge at different stages. 134 From this standpoint, innovation is seen as involving not only brokerage across structural holes to facilitate idea generation, but closure within cohesive groups to implement and embed these ideas. It follows that addressing the role of networks in the innovation process involves developing a better theoretical understanding of how they might simultaneously support brokerage and closure conditions.
In simple terms, the need for both brokerage and closure can be understood in terms of their relative costs and benefits. Previous research indicates that there are costs to having social network ties in both time and energy. Therefore, a structure whereby everyone is connected to each other is not viable. Instead, it is preferable to have small clusters of individuals with high levels of network connectivity that promotes embedding knowledge into practice. Clusters working in isolation, however, limit the transfer of novel information. Therefore, it is also important for there to be brokering ties that connect clusters as well as there being ties to other people outside of an organisation or entity. We found that the CLAHRCs were successful in building ambidextrous networks encompassing areas within the network that had high levels of closure (well-connected KT network structures suited to embedding knowledge into practice) and loose network structures containing ‘structural holes’ that supported the fusing together of novel information sources through individuals brokering across the structural holes. This network ambidexterity was maintained at both time points.
The importance of this ‘ambidextrous’ character in social networks is particularly relevant to KT networks. In this respect, the discussion here helps to draw out the implications of our findings on the CLAHRCs for wider theorising and practical intervention in the health-care domain. Thus, an important finding of our study was that each of the CLAHRCs had built KT networks with the capacity for both brokerage (ties conducive to generating new, innovative knowledge) and closure (tie structures suited to capturing knowledge to implement or embed into practice). The CLAHRC networks were able to achieve such ambidexterity, moreover, despite manifesting significant differences in their structural forms in terms of their degrees of hierarchy and centralisation.
Development of networks over time
One important contribution of our study to our theorising of the role of networks in KT is the extent to which our study was able to identify changes in the CLAHRCs’ networks over time. Research to date has tended to view networks primarily in structural terms, as channels, conduits or ‘pipelines’ through which knowledge is transferred. 135 The more limited research available, focusing on networking processes, crucially establishes that networks are not static, but are dynamic and evolving as circumstances unfold. 136 Yet relatively little attention has been paid to understanding and explaining the social and political processes underpinning the formation and effectiveness of network relationships specifically as they relate to innovation. Nor is there sufficient understanding of the ways in which processes of networking relate to the formation, and transformation, of new network structures across institutional, scientific and professional boundaries – structures which may, in turn, enable or constrain further processes of innovation. 137
In this respect, our findings are significant in demonstrating the scope and implications of change in networks over time. In particular, we observed a significant pattern of convergence – that the CLAHRC KT networks became more similar to each other over time. We also found that the CLAHRCs became more self-reliant and self-referential as social networks. Thus, in our initial study, we found that the CLAHRCs had adopted ‘expansive’ information search strategies. CLAHRC members had previously collaborated with most of their external contacts and external ties were important for access to new contacts and practical advice. In our second-phase work, we found that all three CLAHRCs had more ‘targeted’ information search strategies. External knowledge ties had become less important, as members drew on knowledge from CLAHRC colleagues.
Causal mapping
In our findings, we showed that causal mapping techniques are able to identify relevant constructs from document and interview analysis, and that they can reveal perceptions of relevant characteristics of projects at the collective level. Our study thus suggests that they can be effectively applied to health-care settings to provide relevant insights for practitioners. In particular, the pool of (28) constructs identified here can be used in similar health-care initiatives to map the beliefs of those involved. We contend that the constructs identified here have relevance across settings, given the diversity included in our research.
Our comparative analysis of the cognitive maps of the CLAHRC and transatlantic initiatives in our study found both commonality and variation in the constructs viewed as important by their members. Variation here seems to be associated with the particular objectives of an initiative (reflecting, and maybe helping to generate differences in the way in which KT is enacted). At the same time, we found expected variation which reflected differences in the occupational background of participants (as between academic and professional groupings).
Differences in the relative complexity of the maps elicited from initiative members are more difficult to attribute. We found that some maps indicate unilinear cause–effect relations between constructs while other maps include two-way relationships. A possible factor here is that one- versus two-way relationships may be associated with the extent of feedback and organisational learning enabled by different management and governance structures.
We also found some differences which may be related to national and institutional contexts. For instance, themes associated with collaboration between different health-care partners and having a patient-centric approach were found in the Canadian initiatives. In contrast, a focus on implementation research was found in the CLAHRCs. This adds further evidence to our argument that different contexts influence how such networked innovation initiatives play out in practice.
An important application of this method to health-care settings has to do with ascertaining the relative alignment of objectives across different groups. Causal maps can shed light on the extent to which the beliefs of the people involved in a health-care network are aligned. More importantly, the analysis of individual and collective maps can clearly identify whether or not an alignment has been reached among the participants. Thus, our focus on aggregated indexes in collective maps provides information on whether or not a team/project’s beliefs are aligned. For instance, from the links density and their variance it emerges that beliefs among participants in some projects – for instance the Greentown CLAHRC and Canada-Translation are more aligned than in others. In the case that an alignment in a network’s map is not achieved (i.e. different constructs are selected by different participants), it is also possible to identify constructs that are organisation specific and that are not in line with the overall objectives of an initiative.
Comparative case analysis: developing capabilities for networked innovation
In this section, we integrate the different strands of our study to develop a higher-level and comparative analysis of our cases. As discussed previously, as a form of networked innovation, these initiatives can be evaluated comparatively in respect of the development of their organisational capabilities. Two forms of capability have been identified as crucial to the translation of scientific research into practice: relational and integrative. 83 As outlined earlier, in the conceptual model developed for our study, integrative capabilities refer to the ability to move knowledge back and forth between scientific research and the world of practical application. Relational capabilities arise from the links between different organisations that enable groups and individuals to work together.
In terms of our original research model, then, we can link relational capabilities to network evolution and structure and integrative capabilities to the KT process (with management and governance providing the context which influences how these capabilities develop). Relational capabilities are, thus, evidenced by a capacity to span organisational boundaries, while integrative capabilities are observed at the more micro level, as individuals and groups working on particular projects seek to span the epistemic boundaries between them. Evidence on such capabilities in our study was produced from two main strands of research. Our SNA study shows primarily the extent of links within each case, but also their links to external bodies. This provides evidence on their relational capabilities. Our qualitative study focused on the KT practices of each case organisation. This speaks directly to the extent of integrative capabilities in each case.
Drawing on the qualitative strand of our research suggests that relational capability may be built in different ways. Network structures spanning boundaries may be developed through episodic and instrumental activity focused on a specific pre-defined goal – collaborative partners are sought out through networks to provide resources for a pre-specified purpose. On the other hand, the activities producing these boundary-spanning networks may be more open-ended and long term in focus, with more emergent relationships being developed. In other words, our cases suggest that it may be useful to make a distinction between (a) relational capability that is developed in a directive way between collaborating organisations, and that involves exploiting networks instrumentally to access particular types of resources (which we can term ‘directive relational capability’) and (b) the capability which arises from a more emergent and longer-term approach to network development (which we can term ‘emergent relational capability’).
In terms of our cases, we observe from our case analysis how the Bluetown CLAHRC was more focused on ‘using’ networks top-down, for a specific purpose, and how they developed the directive form of relational capability, while Browntown adopted a more ‘bottom-up’ and emergent approach to building sustainable networks, resulting in a more emergent form of relational capability. However, as highlighted by our SNA and qualitative work, we also saw over time that there was some convergence between the CLAHRCs.
In contrast, in the three North American initiatives there was very little progress towards a more emergent form of relational capability. This was the case even for the US-Health initiative, which was explicitly based on the partnership model. However, as we noted in our qualitative account, through collaborative responses to the tendering process particular organisations did network instrumentally with other organisations to provide resources (knowledge, skill and access) for the particular project that was being proposed. In Canada-Coordination, while there was some emergent relational capability built between the specific team of people representing the different organisations directly involved in the pilot project, this did not extend beyond the project and so failed to build any significant sustainable relational capability between the different organisations and specialisations. Finally, in Canada-Translation we see that the intent was to build relationships between the organisations involved in order to develop a longer-term relational capability, but there was insufficient evidence during the time period of our study to establish what would materialise in practice.
We can also derive from our case analysis significant differences in approaches to KT at the more micro level that were consequential for the integrative capabilities of these entities; that is, the ways in which, and extent to which, different types of knowledge could be brought to bear on a problem. In this respect, the previously mentioned distinction between bridging and blurring comes into focus. Bridging activities, being more discrete, purposive and focused in character, were often led by one group or organisation, for example being either practitioner led or research led. This approach seems to have limited the form of integrative capability developed due to the political implications – for example, as we noted of Bluetown CLAHRC, the more peripheral role or status afforded boundary-spanning individuals within project teams – and the privileging of one epistemic community over another. Integrative capability was thus more limited in scope.
This can be contrasted with our network findings on the importance of ‘hybrid’ roles (e.g. as in Browntown CLAHRC) in promoting links across multiple disciplines, and by our findings on the blurring approach to KT at the project level. As we observed, such features tended to encourage integrative capabilities centred on the co-production of knowledge among the parties concerned. As in the Browntown case, we found members of different epistemic communities becoming more aware of the usefulness of different perspectives and the limitations of their own view of the world. Over time, however, in all three CLAHRCs there was evidence of the development of this more inclusive form of integrative capability.
When we assess the integrative capability of the North American cases, we observe one clear example of a practitioner-led approach (Canada-Coordination) and one example of a researcher-led initiative (Canada-Translation). In contrast, the US-Health initiative shows more evidence of integrative capability centred on co-production.
Figure 16 summarises our analysis by outlining indicative positions of our case sites within the linked dimensions of relational and integrative capability outlined above. First, there are those initiatives where organisational networking is approached instrumentally and top-down as a series of independent projects with pre-defined aims and objectives (directive relational capability), leading very often to projects being led at the local level by either an academic or a practitioner (bridging integrative capability). Such initiatives can produce very useful short-term knowledge; if they are practitioner led they can result in the successful translation of knowledge (as with the Canada-Coordination case, from patients to clinicians and vice versa), and if they are academic led they can result in successful research on implementation that can be written up in academic publications, even while its practical significance may be less apparent (Bluetown in its original manifestation). Then, there are initiatives which are still organised in a fairly top-down way with organisational networks used instrumentally but where there is greater capability co-produce knowledge through a more blurred approach to KT and/or hybrid roles. Of our cases, US-Health was probably the best example, and the focus was on a programme of work (although divided into individual projects) which could produce research to develop implementation methodologies more generally. Given the instrumental use of the networks, however, the sustainability of such initiatives may be difficult because the diffusion of knowledge is not facilitated by long-term organisational collaboration.
FIGURE 16.
Comparative analysis and indicative mapping of innovation capabilities.
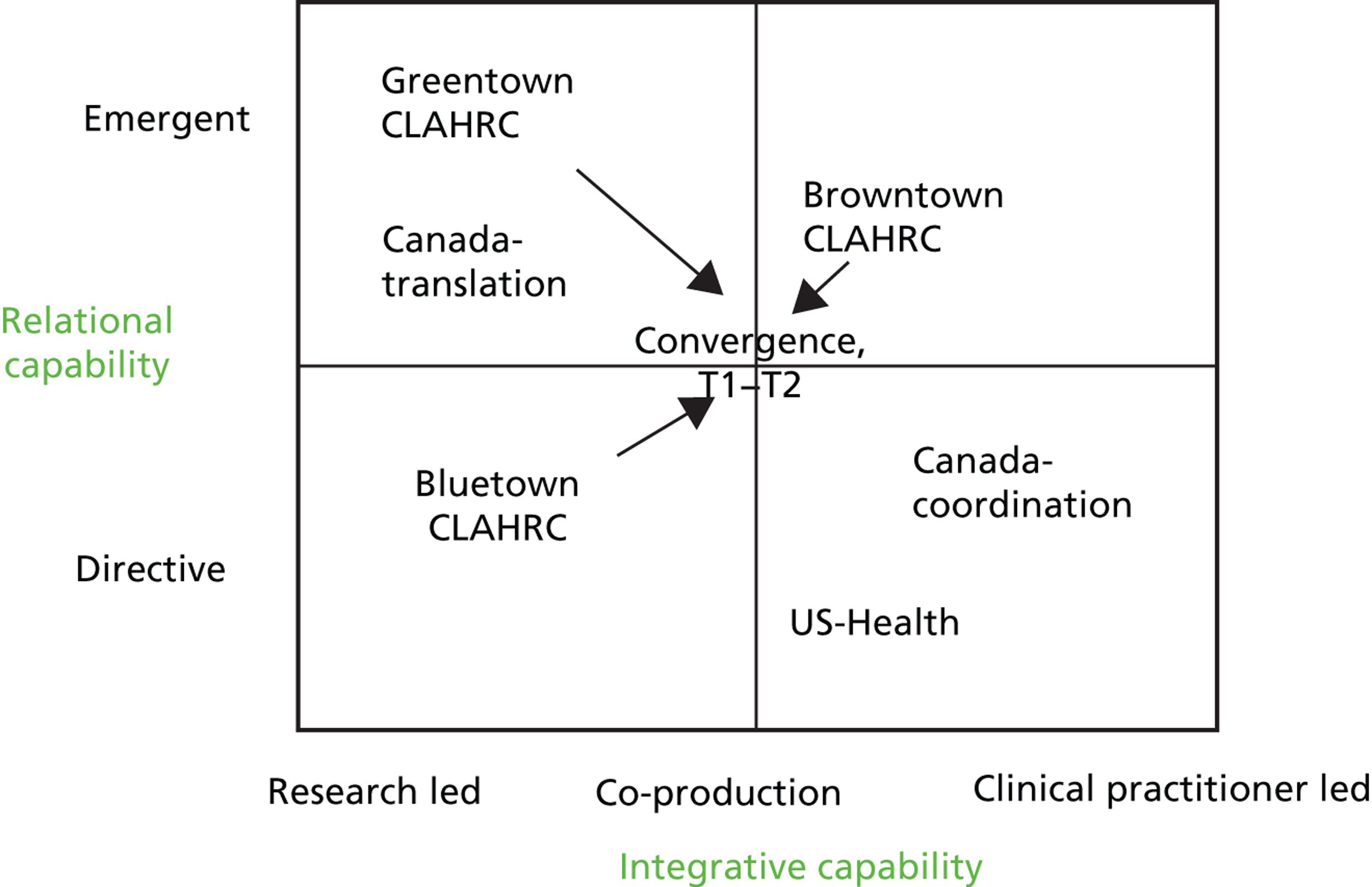
Finally, there are those initiatives where organisational networks are built bottom-up (as well as top-down), which are more emergent than directed, and which involve more equal forms of collaboration between academics and practitioners, thereby enabling the co-production of knowledge. Both Greentown and Browntown CLAHRCs show some evidence of these capabilities, although, as outlined in our analysis, both qualitative and social network data suggest greater convergence of all the CLAHRCs initiatives towards this position over time.
Institutional factors
There appeared to be a number of institutional factors that affected the management and governance of the initiatives and that helped to account for the differences between the North American initiatives and the CLAHRCs in terms of their development of a more emergent (vs. directive) relational capability and in terms of their development of a more blurred, co-production (vs. research- or practitioner-led) approach to the development of integrative capabilities. First, the longer-term and more open-ended funding for the CLAHRCs meant that they could be more receptive to emergent forms of networking (encouraging networking between organisations with no clear idea as to what this would lead to) rather than being narrowly focused on networking to secure resources to meet a pre-defined problem. Second, because CLAHRCs were required to provide matched funding, they had a vested interest in building some long-term relationships between the organisations involved. Finally, the CLAHRCs had a more specific remit to promote co-production with stakeholder groups.
Conclusions
Our evaluation of three CLAHRC initiatives makes a number of important contributions to our understanding of the means by which the second translational gap can be overcome. We evaluated the CLAHRCs through the lens of ‘networked innovation’. This involved a focus in our empirical study on the way in which the knowledge distributed across different organisations and epistemic communities was mobilised through project-based collaboration to create new practices and services. This theorisation of the CLAHRCs’ role differs from established models of KT, which arguably privilege the process of translation over the importance of collaborative relationships between groups, and the leadership and management activities which foster such relationships.
In our qualitative investigation, we found that the mechanisms of KT developed by the CLAHRCs were influenced by the ‘vision’, that is the interpretation of the CLAHRC’s ethos and identity, as promoted by the leadership of each CLAHRC. This highlights the specificity of the process of KT and the extent to which it is shaped by leadership and management practices, as well as by the beliefs inculcated and spread through such practices. We found that where the vision for a CLAHRC framed KT as essentially involving the dissemination of high-quality evidence into practice (as with the Bluetown CLAHRC), ‘bridging mechanisms’ of KT were utilised to overcome the boundaries between research and practice. In contrast, where the vision placed greater emphasis on the integration of research practices with practical concerns (as in Browntown), ‘blurring’ of boundaries occurred to a much greater extent. Significantly, reliance on these different mechanisms seems to reflect the relative extent of ‘epistemic’ differences between the communities involved.
Our qualitative analysis of the differences between the CLAHRCs ‘enactment’ of their missions can also be related to the importance of shared beliefs about the causal relationships involved in KT. This aspect of the CLAHRCs was explored in greater detail through our use of cognitive mapping techniques. Findings here further underline the context-specificity of KT efforts, showing how beliefs about the efficacy of particular constructs may be shared across initiatives, thereby reinforcing or constraining different approaches. This strand of our study also supported a wider, international comparison of experience with translational initiatives, helping us to identify not only the differences between CLAHRCs but also their commonalities when compared with initiatives in the USA and Canada. This comparison was revealing as to the influence exerted by the UK’s particular institutional context, and how this made possible the level of investment and policy intervention that underpinned the CLAHRC ‘experiment’.
Our understanding of the areas of commonality and difference between CLAHRCs was further extended by the analysis of their social networks. Here, our focus on networked innovation highlights certain contributions of the structure and distribution of social ties which are not currently addressed in work on KT. In particular, our analysis highlights the importance of both ‘closure’ (dense social ties within particular areas) and ‘brokerage’ (bridging ties across different groups) to a networked process of innovation. We develop the notion of ‘ambidextrous’ networks to capture the need for both these network formations in supporting the process of innovation. The importance of such ambidexterity has not been adequately covered in the previous literature on KT, as this has focused primarily on brokerage. We found, however, that the CLAHRCs in our study were characterised by such ambidextrous network forms. Moreover, they had been able to achieve such ambidexterity despite manifesting significant differences in other aspects of their social networks.
Finally, we developed a higher-level analysis (see Figure 16 ) of the cases in our study by investigating the innovation capabilities which they had developed as a result of the particular visions, social network formations, and KT practices outlined above. By integrating the findings from our different research strands, this analysis helps to unpack our cases’ acquisition of distinctively different capabilities. This analysis provides a useful framework for policy and practice in assessing the capacity of particular types of KT initiative to produce different outcomes.
Implications for further research
In moving beyond the abstract models of KT currently available in the literature, our study highlights the need for further research to better understand the way in which KT activities are grounded in particular settings. Certain of the methods developed for this study, notably the social network survey instrument and the application of cognitive mapping techniques, represent valuable methodological contributions, which can be applied and developed in future studies.
The present study, however, is based on a small sample of UK initiatives, and the limited comparison made possible by our case sites in the USA and Canada. Our findings on the importance of the ‘vision’, and shared causal beliefs, in the enactments of KT by particular initiatives could be usefully extended and deepened by a wider international study, capable of encompassing a larger number of entities in a systematic way.
Likewise, our analysis of social networks reveals significant areas of difference and commonality across the CLAHRCs, and provides a more analytical approach to the relationship between network structures and innovation processes. Although limited in scope, the longitudinal analysis of network evolution presented here suggests that future studies of the role of social networks in KT could usefully incorporate a longitudinal dimension that would enable a greater understanding of the benefits and limitations of development and adaptation by such networks over time.
Finally, the evaluative focus of our study was on how the CLAHRCs developed capacity and mechanisms to support networked innovation, rather than the outcomes from their efforts. As noted earlier, evaluating outcomes from KT initiatives may be problematic due to the time scales involved and the lack of counterfactual evidence. However, future studies capable of overcoming these problems should be able to contribute to a wider evidence base on the outcomes and wider benefits of KT initiatives, and through comparative analysis might provide systematic evidence on the relative merits of the different ‘visions’, network patterns and belief structures exhibited by such initiatives.
Acknowledgements
Contributions of authors
All members of the team were involved in the empirical study to some extent, including involvement in fieldwork, project team meetings, etc. However, the principal roles carried out by different members of the team were as follows:
Dr Daniela D’Andreta (Research Fellow, Warwick Business School) (with support from consultant Andrew Parker) conducted the social network study, fieldwork, analysis and write-up.
Dr Sarah Evans (Research Fellow, Warwick University) was primarily responsible for the data collection, analysis and write-up of the qualitative investigation.
Dr Marco Marabelli (Research Fellow) and Professor Sue Newell (co-investigator and Professor, Bentley College, USA, and Warwick University, UK) carried out the fieldwork in North America, and conducted, analysed and wrote up the causal mapping exercise and the qualitative analysis related to the North American cases.
Professor John Powell, co-investigator (Senior Clinical Researcher, Oxford University), advised on the research design, dissemination and implications for practice.
Professor Harry Scarbrough, principal investigator (Professor, Keele University, and formerly Warwick University), provided overall project management and leadership, liaison with the SDO/NETSCC and CLAHRC partners, and edited the final report.
Professor Jacky Swan, co-investigator (Professor, Warwick Business School), advised on the research design, and contributed particularly to the causal mapping exercise and editing of the final report.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health.
References
- Cooksey D. A Review of UK Health Research Funding. London: HM Treasury; 2006.
- Tetroe JM, Graham ID, Foy R, Robinson N, Eccles MP, Wensing M, et al. Health research funding agencies’ support and promotion of knowledge translation: an international study. Milbank Q 2008;86:125-55.
- Lomas J. Connecting research and policy. Can J Policy Res 2000;1:140-4.
- Gkeredakis E, Swan J, Powell J, Nicolini D, Scarbrough H, Roginski C, et al. Mind the gap: understanding utilisation of evidence and policy in health care management practice. J Health Organ Manag 2011;25:298-314.
- Walshe K, Rundall TG. Evidence-based management: from theory to practice in health care. Milbank Q 2001;79:429-57. http://dx.doi.org/10.1111/1468-0009.00214.
- Rynes SL, Bartunek JM, Daft RL. Across the great divide: knowledge creation and transfer between practitioners and academics. Acad Manag J 2001;44:340-55.
- Ferlie E, Fitzgerald L, Wood M, Hawkins C. The nonspread of innovations: the mediating role of professionals. Acad Manag J 2005;48:117-34. http://dx.doi.org/10.5465/AMJ.2005.15993150.
- Dopson S, Fitzgerald L. Knowledge to Action? Evidence-based Health Care in Context. Oxford: Oxford University Press; 2005.
- Weiss CH. The many meanings of research utilization. Public Adm Rev 1979;39:426-31. http://dx.doi.org/10.2307/3109916.
- Newell S, Edelman L, Scarbrough H, Swan J, Bresnen M. ‘Best practice’ development and transfer in the NHS: the importance of process as well as product knowledge. Health Serv Manag Res 2003;16:1-12. http://dx.doi.org/10.1258/095148403762539095.
- Davies H, Nutley S, Walter I. Why ‘knowledge transfer’ is misconceived for applied social research. J Health Serv Res Policy 2008;13:188-90. http://dx.doi.org/10.1258/jhsrp.2008.008055.
- Gabbay J, Le May A. Practice-based Evidence for Healthcare: Clinical Mindlines. Abingdon: Routledge; 2010.
- Greenhalgh T, Wieringa S. Is it time to drop the ‘knowledge translation’ metaphor? A critical literature review. JRSM 2011;104:501-9. http://dx.doi.org/10.1258/jrsm.2011.110285.
- Crilly T, Jashapara A, Ferlie E. Report for the National Institute for Health Research Service Delivery and Organisation Programme. Southampton: NIHR SDO; 2010.
- Ferlie E, Crilly T, Jashapara A, Peckham A. Knowledge mobilisation in healthcare: a critical review of health sector and generic management literature. Soc Sci Med 2012;74:1297-304. http://dx.doi.org/10.1016/j.socscimed.2011.11.042.
- Swan J, Clarke A, Nicolini D, Powell J, Scarbrough H, Roginski C, et al. Evidence in Management Decisions (EMD)-Advancing Knowledge Utilization in Healthcare Management. Final Report. NIHR Service and Delivery Organisation Programme 2012.
- Graham ID, Logan J, Harrison MB, Straus SE, Tetroe J, Caswell W, et al. Lost in knowledge translation: time for a map?. J Continuing Educ Health Prof 2006;26:13-24. http://dx.doi.org/10.1002/chp.47.
- Knights D, Scarbrough H. In search of relevance: perspectives on the contribution of academic–practitioner networks. Organ Stud 2010;31:1287-309. http://dx.doi.org/10.1177/0170840610374398.
- Nicolini D, Mengis J, Swan J. Understanding the role of objects in cross-disciplinary collaboration. Organ Sci 2012;23:612-29. http://dx.doi.org/10.1287/orsc.1110.0664.
- Carlile PR. A pragmatic view of knowledge and boundaries: boundary objects in new product development. Organ Sci 2002;13:442-55. http://dx.doi.org/10.1287/orsc.13.4.442.2953.
- Lang ES, Wyer PC, Haynes RB. Knowledge translation: closing the evidence-to-practice gap. Ann Emerg Med 2007;49:355-63. http://dx.doi.org/10.1016/j.annemergmed.2006.08.022.
- Denis JL, Lomas J. Convergent evolution: the academic and policy roots of collaborative research. J Health Serv Res Policy 2003;8. http://dx.doi.org/10.1258/135581903322405108.
- Antil T, Desrochers M, Joubert P, Bouchard C. Implementation of an innovative grant programme to build partnerships between researchers, decision-makers and practitioners: the experience of the Quebec Social Research Council. J Health Serv Res Policy 2003;8:35-43. http://dx.doi.org/10.1258/135581903322405153.
- Bowen S, Martens P. Demystifying knowledge translation: learning from the community. J Health Serv Res Policy 2005;10:203-11. http://dx.doi.org/10.1258/135581905774414213.
- Graham ID, Tetroe J. Learning from the US Department of Veterans Affairs Quality Enhancement Research Initiative: QUERI series. Implement Sci 2009;4.
- Boyko J, Lavis J, Abelson J, Dobbins M, Carter N. Deliberative dialogues as a mechanism for knowledge translation and exchange in health systems decision-making. Soc Sci Med 2012;75:1938-45. http://dx.doi.org/10.1016/j.socscimed.2012.06.016.
- Bartunek J, Trullen J, Bonet E, Sauquet A. Sharing and expanding academic and practitioner knowledge in health care. J Health Serv Res Policy 2003;8:62-8. http://dx.doi.org/10.1258/135581903322405199.
- Martin GP, Currie G, Finn R. Reconfiguring or reproducing intra-professional boundaries? Specialist expertise, generalist knowledge and the modernization of the medical workforce. Soc Sci Med 2009;68:1191-8. http://dx.doi.org/10.1016/j.socscimed.2009.01.006.
- Powell A, Davies H. The struggle to improve patient care in the face of professional boundaries. Soc Sci Med 2012;75:807-14. http://dx.doi.org/10.1016/j.socscimed.2012.03.049.
- Bate P. Changing the culture of a hospital: from hierarchy to networked community. Public Adm 2000;78:485-512.
- Swan J, Scarbrough H. The politics of networked innovation. Hum Relations 2005;58:913-43. http://dx.doi.org/10.1177/0018726705057811.
- Crilly T, Jashapara A, Trenholm MS, Peckham MA, Currie G, Ferlie E. Knowledge Mobilisation in Healthcare Organisations: Synthesising the Evidence and Theory using Perspectives of Organisational Form, Resource Based View of the Firm and Critical Theory. NIHR Service Delivery and Organisation Programme 2013.
- Greenhalgh T, Robert G, MacFarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organizations: systematic review and recommendations. Milbank Q 2004;82:581-629. http://dx.doi.org/10.1111/j.0887-378X.2004.00325.x.
- Powell WW, Koput KW. Interorganizational collaboration and the locus of innovation: networks of learning in biotechnology. Adm Sci Q 1996;41. http://dx.doi.org/10.2307/2393988.
- Coombs R, Harvey M, Tether BS. Analysing distributed processes of provision and innovation. Indust Corporate Change 2003;12:1125-55. http://dx.doi.org/10.1093/icc/12.6.1125.
- McAneney H, McCann J, Prior L, Wilde J, Kee F. Translating evidence into practice: a shared priority in public health?. Soc Sci Med 2010;70:1492-500. http://dx.doi.org/10.1016/j.socscimed.2010.01.038.
- Tushman M, Scanlon T. Boundary spanning individuals: their role in information transfer and their antecendents. Acad Manag J 1981;24:289-305. http://dx.doi.org/10.2307/255842.
- Borgatti SP, Cross R. A relational view of information seeking and learning in social networks. Manag Sci 2003;49:432-45. http://dx.doi.org/10.1287/mnsc.49.4.432.14428.
- Swan J, Bresnen M, Newell S, Robertson M. The object of knowledge: the role of objects in biomedical innovation. Hum Relations 2007;60:1809-37. http://dx.doi.org/10.1177/0018726707084915.
- Currie G, Suhomlinova O. The impact of institutional forces upon knowledge sharing in the UK NHS: the triumph of professional power and the inconsistency of policy. Public Adm 2006;84:1-30. http://dx.doi.org/10.1111/j.0033-3298.2006.00491.x.
- Oborn E, Barrett M, Racko G. Knowledge Translation in Healthcare: A Review of the Literature. Cambridge: Judge Business School; 2010.
- Carlile PR. Transferring, translating, and transforming: an integrative framework for managing knowledge across boundaries. Organ Sci 2004;15:555-68. http://dx.doi.org/10.1287/orsc.1040.0094.
- Szulanski G. The process of knowledge transfer: a diachronic analysis of stickiness. Organ Behav Hum Decis Processes 2000;82:9-27. http://dx.doi.org/10.1006/obhd.2000.2884.
- Caplan N. The two-communities theory and knowledge utilization. Am Behav Sci 1979;22:459-70. http://dx.doi.org/10.1177/000276427902200308.
- Oborn E, Dawson S. Knowledge and practice in multidisciplinary teams: struggle, accommodation and privilege. Hum Relations 2010;63:1835-57. http://dx.doi.org/10.1177/0018726710371237.
- Swan J, Scarbrough H, Newell S. Why don’t (or do) organizations learn from projects?. Manag Learn 2010;41:325-44. http://dx.doi.org/10.1177/1350507609357003.
- Ward V, House A, Hamer S. Knowledge brokering: the missing link in the evidence to action chain?. Evidence Policy 2009;5:267-79. http://dx.doi.org/10.1332/174426409X463811.
- Lomas J. The in-between world of knowledge brokering. BMJ 2007;334:129-32. http://dx.doi.org/10.1136/bmj.39038.593380.AE.
- Dobbins M, Robeson P, Ciliska D, Hanna S, Cameron R, O’Mara L, et al. A description of a knowledge broker role implemented as part of a randomized controlled trial evaluating three knowledge translation strategies. Implement Sci 2009;4. http://dx.doi.org/10.1186/1748-5908-4-23.
- Baumbusch JL, Kirkham SR, Khan KB, McDonald H, Semeniuk P, Tan E, et al. Pursuing common agendas: a collaborative model for knowledge translation between research and practice in clinical settings. Res Nurs Health 2008;31:130-40. http://dx.doi.org/10.1002/nur.20242.
- Lavis JN. Research, public policymaking, and knowledge-translation processes: Canadian efforts to build bridges. J Continuing Educ Health Prof 2006;26:37-45.
- Davison C, OJah P. Knowledge Utilization, Diffusion, Implementation, Transfer, and Translation: New Directions for Evaluation. Hoboken, NJ: John Wiley & Sons; 2009.
- Williams P. The competent boundary spanner. Public Adm 2002;80:103-24. http://dx.doi.org/10.1111/1467-9299.00296.
- Bartunek JM. Academic-practitioner collaboration need not require joint or relevant research: toward a relational scholarship of integration. Acad Manag J 2007;50:1323-33. http://dx.doi.org/10.5465/AMJ.2007.28165912.
- Sin CH. The role of intermediaries in getting evidence into policy and practice: some useful lessons from examining consultancyclient relationships. Evidence Policy 2008;4:85-103.
- Ward V, House A, Hamer S. Developing a framework for transferring knowledge into action: a thematic analysis of the literature. J Health Serv Res Policy 2009;14:156-64. http://dx.doi.org/10.1258/jhsrp.2009.008120.
- Mitton C, Adair CE, McKenzie E, Patten SB, Perry BW. Knowledge transfer and exchange: review and synthesis of the literature. Milbank Q 2007;85:729-68. http://dx.doi.org/10.1111/j.1468-0009.2007.00506.x.
- Graham ID, Tetroe J. How to translate health research knowledge into effective healthcare action. Healthcare Q 2007;10:20-2.
- Grimshaw JM, Ward J, Eccles M, Pencheon DGC, Melzer D, Gray JAM. Oxford Handbook of Public Health. Oxford: Oxford University Press; 2001.
- Hansen MT. Knowledge networks: explaining effective knowledge sharing in multiunit companies. Organ Sci 2002;13:232-48. http://dx.doi.org/10.1287/orsc.13.3.232.2771.
- Powell W, Koput K, Smith-Doerr L. Interorganizational collaboration and the locus of innovation: networks of learning in biotechnology. Adm Sci Q 1996;41:116-45. http://dx.doi.org/10.2307/2393988.
- Burt RS. The network structure of social capital. Res Organ Behav 2000;22:345-423. http://dx.doi.org/10.1016/S0191-3085(00)22009-1.
- Hansen MT. The search transfer problem: the role of weak ties in sharing knowledge across organizational sub-units. Adm Sci Q 1999;44:82-111.
- Ibarra H. Network centrality, power, and innovation involvement. Determinants of technical and administrative roles. Acad Manag J 1993;36:471-50. http://dx.doi.org/10.2307/256589.
- Martin GP, Currie G, Finn R. Leadership, service reform, and public-service networks: the case of cancer-genetics pilots in the English NHS. J Public Adm Res Theory 2009;19:769-94. http://dx.doi.org/10.1093/jopart/mun016.
- Currie G, White L. Inter-professional barriers and knowledge brokering in an organizational context: the case of healthcare. Organ Studies 2012;33:1333-61. http://dx.doi.org/10.1177/0170840612457617.
- Dougherty D. Interpretative barriers to successful product innovation in large firms. Organ Sci 1992;3:179-202.
- Boland RJ, Tenkasi RV. Perspective making and perspective taking in communities of knowing. Organ Sci 1995;6:350-63. http://dx.doi.org/10.1287/orsc.6.4.350.
- Swan J, Clark PA. Organizational decision-making in the appropriation of technological innovation: cognitive and political dimension. Eur Work Organ Psychologist 1992;2:103-27. http://dx.doi.org/10.1080/09602009208408538.
- Huff A, Jenkins M. Mapping Strategic Knowledge. London: Sage Publications; 2002.
- Sutherland K, Dawson S. Making sense in practice: doctors at work. Int Stud Manag Organ n.d.:51-69.
- Weick KE. The Social Psychology of Organizing. Reading, MA: Addison-Wesley; 1979.
- Swan J. Using cognitive mapping in management research: decisions about technical innovation. Br J Manag 1997;8:183-98. http://dx.doi.org/10.1111/1467-8551.0050.
- Robertson M. Translating breakthroughs in genetics into biomedical innovation: the case of UK genetic knowledge parks. Technol Anal Strategic Manag 2007;19:189-204. http://dx.doi.org/10.1080/09537320601168136.
- Swan J, Bresnen M, Robertson M, Newell S, Dopson S. When policy meets practice: colliding logics and the challenges of ‘mode 2’ initiatives in the translation of academic knowledge. Organ Stud 2010;31:1311-40. http://dx.doi.org/10.1177/0170840610374402.
- Tidd J, Bodley K. The influence of project novelty on the new product development process. Res Develop Manag 2002;32:127-38. http://dx.doi.org/10.1111/1467-9310.00245.
- Dougherty D, Dunne DD. Digital science and knowledge boundaries in complex innovation. Organ Sci 2011;23:1467-84. http://dx.doi.org/10.1287/orsc.1110.0700.
- Swan J, Newell S, Robertson M, Goussevskaia A, Bresnen M. The role of institutional differences in biomedical innovation processes: a comparison of the UK and US. Int J Healthcare Technol Manag 2007;8:333-53. http://dx.doi.org/10.1504/IJHTM.2007.013167.
- Swan J, Goussevskaia A, Newell S, Robertson M, Bresnen M, Obembe A. Modes of organizing biomedical innovation in the UK and US and the role of integrative and relational capabilities. Res Policy 2007;36:529-47. http://dx.doi.org/10.1016/j.respol.2007.02.014.
- Dobrow MJ, Goel V, Lemieux-Charles L, Black NA. The impact of context on evidence utilization: a framework for expert groups developing health policy recommendations. Soc Sci Med 2006;63:1811-24. http://dx.doi.org/10.1016/j.socscimed.2006.04.020.
- Contandriopoulos D, Lemire M, Denis JL, Tremblay É. Knowledge exchange processes in organizations and policy arenas: a narrative systematic review of the literature. Milbank Q 2010;88:444-83. http://dx.doi.org/10.1111/j.1468-0009.2010.00608.x.
- Ward V, Smith S, House A, Hamer S. Exploring knowledge exchange: a useful framework for practice and policy. Soc Sci Med 2012;74:297-304. http://dx.doi.org/10.1016/j.socscimed.2011.09.021.
- Owen-Smith J, Riccaboni M, Pammolli F, Powell WW. A comparison of US and European university–industry relations in the life sciences. Manag Sci 2002;48:24-43.
- Yin R. Case Study Research. Thousand Oaks, CA: Sage Publishing; 2003.
- Christakis NA, Fowler JH. The spread of obesity in a large social network over 32 years. N Engl J Med 2007;357:370-9. http://dx.doi.org/10.1056/NEJMsa066082.
- Cross R, Parker A, Prusak L, Borgatti SP. Knowing what we know: supporting knowledge creation and sharing in social networks. Organ Dynamics 2001;30:100-20. http://dx.doi.org/10.1093/0195165128.003.0005.
- Cross R, Cummings JN. Tie and network correlates of individual performance in knowledge-intensive work. Acad Manag J 2004;47:928-37. http://dx.doi.org/10.2307/20159632.
- Borgatti SP, Carley KM, Krackhardt D. On the robustness of centrality measures under conditions of imperfect data. Soc Networks 2006;28:124-36. http://dx.doi.org/10.1016/j.socnet.2005.05.001.
- Newman M, Durlauf SN, Blume LE. The New Palgrave Dictionary of Economics. Basingstoke: Palgrave Macmillan; 2008.
- Dunn AG, Westbrook JI. Interpreting social network metrics in healthcare organisations: a review and guide to validating small networks. Soc Sci Med 2011;72:1064-8. http://dx.doi.org/10.1016/j.socscimed.2011.01.029.
- Brewer DD, Webster CM. Forgetting of friends and its effects on measuring friendship networks. Soc Networks 2000;21:361-73. http://dx.doi.org/10.1016/S0378-8733(99)00018-0.
- Burt RS. A note on missing network data in the general social survey* 1. Soc Networks 1987;9:63-7. http://dx.doi.org/10.1016/0378-8733(87)90018-9.
- Hodgkinson GP, Maule AJ, Bown NJ. Causal cognitive mapping in the organizational strategy field: a comparison of alternative elicitation procedures. Organ Res Methods 2004;7:3-26. http://dx.doi.org/10.1177/1094428103259556.
- Langfield-Smith K. Exploring the need for a shared cognitive map. J Manag Stud 1992;29:349-68. http://dx.doi.org/10.1111/j.1467-6486.1992.tb00669.x.
- Clarkson GP, Hodgkinson GP. Introducing Cognizer™: a comprehensive computer package for the elicitation and analysis of cause maps. Organ Res Methods 2005;8:317-41.
- Nakayama V, Armstrong DJ. Causal mapping for research in information Technology. Hershey, PA: Idea Group Publishing; 2005.
- Gittell JH, Weiss L. Coordination networks within and across organizations: a multi-level framework. J Manag Studies 2004;41:127-53. http://dx.doi.org/10.1111/j.1467-6486.2004.00424.x.
- Fereday J, Muir-Cochrane E. Demonstrating rigor using thematic analysis: a hybrid approach of inductive and deductive coding and theme development. Int J Qual Methods 2008;5:80-92.
- Coffey AJ, Atkinson PA. Making Sense of Qualitative Data: Complementary Research Strategies. Thousand Oaks, CA: Sage Publications Inc.; 1996.
- Dunbar RI. Coevolution of neocortical size, group size and language in humans. Behav Brain Sci 1993;16:681-93. http://dx.doi.org/10.1017/S0140525X00032325.
- Coleman JS. Social capital in the creation of human capital. Am J Sociol 1988;84:S95-120. http://dx.doi.org/10.1086/228943.
- Ahuja G. Collaboration networks, structural holes, and innovation: a longitudinal study. Adm Sci Q 2000;45:425-55. http://dx.doi.org/10.2307/2667105.
- Burt RS. Structural holes and good ideas. Am J Sociol 2004:349-99. http://dx.doi.org/10.1086/421787.
- Reagans R, McEvily B. Contradictory or compatible? Reconsidering the ‘trade-off’ between brokerage and closure on knowledge sharing. Adv Strat Manag 2008;25:275-313. http://dx.doi.org/10.1016/S0742-3322(08)25008-4.
- Burt RS. Brokerage and Closure: An Introduction to Social Capital. New York, NY: Oxford University Press, USA; 2005.
- Gould RV, Fernandez RM. Structures of mediation: a formal approach to brokerage in transaction networks. Sociol Methodol 1989;19:89-126. http://dx.doi.org/10.2307/270949.
- Freeman LC. Centrality in social networks conceptual clarification. Social Networks 1979;1:215-39. http://dx.doi.org/10.1016/0378-8733(78)90021-7.
- Burt RS. Structural Holes: the Social Structure of Competition. Cambridge, MA: Harvard University Press; 1995.
- Coleman JS, Katz E, Menzel H. Medical Innovation: A Diffusion Study. New York, NY: Bobbs-Merrill Company; 1966.
- Watts DJ, Strogatz SH. Collective dynamics of ‘small-world’ networks. Nature 1998;393:440-2.
- Milgram S. The small world problem. Psychol Today 1967;2:60-7.
- Dirks KT, Ferrin DL. Trust in leadership: meta-analytic findings and implications for research and practice. J Appl Psychol 2002;87:611-28. http://dx.doi.org/10.1037//0021-9010.87.4.611.
- Harary F. Graph Theory. Reading, MA: Addison-Wesley; 1969.
- Swan J, Scarbrough H, Robertson M. The construction of ‘communities of practice’ in the management of innovation. Manag Learn 2002;33:477-96. http://dx.doi.org/10.1177/1350507602334005.
- Burt RS. The social structure of competition. Networks Organ 1992:57-91.
- Lin N. Building a network theory of social capital. Connections 1999;22:28-51.
- Lomas J. The in-between world of knowledge brokering. BMJ 2007;334:129-32. http://dx.doi.org/10.1136/bmj.39038.593380.AE.
- Krackhardt D, Stern RN. Informal networks and organizational crises: an experimental simulation. Soc Psychol Q 1988;51:123-40. http://dx.doi.org/10.2307/2786835.
- Borgatti SP, Everett MG. Models of core/periphery structures. Soc Networks 2000;21:375-95. http://dx.doi.org/10.1016/S0378-8733(99)00019-2.
- Tichy NM, Tushman ML, Fombrun C. Social network analysis for organizations. Acad Manag Rev 1979;4:507-19. http://dx.doi.org/10.2307/257851.
- Turk H. Organizations in Modern Life. San Francisco, CA: Jossey-Bass; 1977.
- West E, Barron DN, Dowsett J, Newton JN. Hierarchies and cliques in the social networks of health care professionals: implications for the design of dissemination strategies. Soc Sci Med 1999;48:633-46. http://dx.doi.org/10.1016/S0277-9536(98)00361-X.
- Baldassarri D, Diani M. The integrative power of civic networks. Am J Sociol 2007;113:735-80. http://dx.doi.org/10.1086/521839.
- Friedkin NE. A Structural Theory of Social Influence. Cambridge: Cambridge University Press; 2006.
- Scott J, Tallia A, Crosson JC, Orzano AJ, Stroebel C, DiCicco-Bloom B, et al. Social network analysis as an analytic tool for interaction patterns in primary care practices. Ann Fam Med 2005;3:443-8. http://dx.doi.org/10.1370/afm.344.
- Tyler BB, Gnyawali DR. Managerial collective cognitions: an examination of similarities and differences of cultural orientations. J Manag Stud 2009;46:93-126. http://dx.doi.org/10.1111/j.1467-6486.2008.00795.x.
- Swan JA. Exploring knowledge and cognitions in decisions about technological innovation: mapping managerial cognitions. Hum Relations 1995;48:1241-70. http://dx.doi.org/10.1177/001872679504801101.
- Ontario Ministry of Health and Long-term Care . Ontario’s Action Plan for Healthcare 2012. http://health.gov.on.ca. (accessed 10 February 2012).
- Landry R, Amara N, Lamari M. Utilization of social science research knowledge in Canada. Res Policy 2001;30:333-49. http://dx.doi.org/10.1016/S0048-7333(00)00081-0.
- Lavis JN, Robertson D, Woodside JM, McLeod CB, Abelson J. How can research organizations more effectively transfer research knowledge to decision makers?. Milbank Q 2003;81:221-48. http://dx.doi.org/10.1111/1468-0009.t01-1-00052.
- Burt RS. The contingent value of social capital. Adm Sci Q 1997;42:339-65. http://dx.doi.org/10.2307/2393923.
- Coleman J. Foundations of Social Theory. Cambridge, MA: Harvard University Press; 2000.
- Oliver AL, Ebers M. Networking network studies: an analysis of conceptual configurations in the study of inter-organizational relationships. Organ Stud 1998;19:549-83. http://dx.doi.org/10.1177/017084069801900402.
- Van de Ven AH. The Innovation Journey. New York, NY: Oxford University Press; 1999.
- Owen-Smith J, Powell WW. Knowledge networks as channels and conduits: the effects of spillovers in the Boston biotechnology community. Organ Sci 2004;15:5-22. http://dx.doi.org/10.1287/orsc.1030.0054.
- Grandori A, Soda G. Inter-firm networks: antecedents, mechanisms and forms. Organ Stud 1995;16:184-21. http://dx.doi.org/10.1177/017084069501600201.
- Lam A. Embedded firms, embedded knowledge: problems of collaboration and knowledge transfer in global cooperative ventures. Organ Stud 1997;18:973-96. http://dx.doi.org/10.1177/017084069701800604.
- Nohria N, Ghoshal S. The Differentiated Network: Organizing Multinational Corporations for Value Creation. San Francisco, CA: Jossey-Bass; 1997.
- Gulati R, Nohria N, Zaheer A. Strategic networks. Strat Manag J 2000;21:203-15. http://dx.doi.org/10.1002/(SICI)1097-0266(200003)21:3%3C203::AID-SMJ102%3E3.0.CO;2-K.
- Zaheer A, Bell GG. Benefiting from network position: firm capabilities, structural holes, and performance. Strat Manag J 2005;26:809-25. http://dx.doi.org/10.1002/smj.482.
- Kilduff M, Tsai W. Social Networks and Organizations. London: Sage Publications Limited; 2003.
- Eden C, Ackermann F, Cropper S. The analysis of cause maps. J Manag Studies 1992;29:309-24. http://dx.doi.org/10.1111/j.1467-6486.1992.tb00667.x.
- Langfield-Smith K, Wirth A. Measuring differences between cognitive maps. J Oper Res Soc 1992;43:1135-50. http://dx.doi.org/10.2307/2584270.
Appendix 1 Social network analysis
A glossary of the technical terms used in SNA is provided at the end of this section.
Social network analysis epistemology and ontology
Knowledge networks exist at multiple levels and can be analysed, for example, through a focus on internal intraorganisational ties,138 interorganisational ties133,139 or both. 140 Kilduff and Tsai141 argue that taking such a multilevel approach can lead to a better understanding of organisational network behaviours, which necessarily culminates in high-level theoretical abstractions. We try to adopt and develop this approach in our methodology by conducting analyses of the KT networks at three distinct levels of analysis: governance/organisational level (ties between CLAHRC members), interinstitutional level (knowledge ties beyond the CLAHRC), and meso level (ties between epistemic groups). We have converted some individual-level measures into network-level averages (i.e. normalised brokerage and betweenness for each CLAHRC), but as an ethical issue we have largely avoided individual-level analysis of data in order to maintain the confidentiality of respondents (i.e. it was not appropriate to identify CLAHRC members with the most network ties – highest centrality).
In our analysis we provide sets of summative scores for the CLAHRC networks. Many standard inferential statistics do not apply to SNA because social network data violate case independency criteria; respondents are not sampled independently from their population – rather, they are sampled as a whole population. Instead, permutation approaches are applied to calculate sampling distributions of statistics directly from observed networks using random assignment/matrix manipulation across thousands of trials under the assumption that null hypotheses are true. In addition, it is worth noting that some network measures were not applicable to the study of external ties (i.e. centralisation, density, reciprocity) because external contacts were not surveyed and so these connections could not be assumed to have two-way capability.
Rather than make direct comparisons between CLAHRCs, we recognise that these networks are case-study contextualisations so the data have been interpreted in a way that acknowledges the governance structure and is sensitive to the CLAHRC culture in which these interactions are embedded.
International comparison: Canada-Coordination network structure
We compare the CLAHRC experiences with those of the Canadian initiative, Canada-Coordination. There were some structural and compositional differences between network samples, which we acknowledge in our analysis.
Around half of CLAHRC respondents were employed in permanent positions, compared with 90% for Canada-Coordination. Most members taking part in the study indicated that they had an additional job role affiliation to that within the KT initiative (Canada-Coordination, 85%; Browntown, 73%; Bluetown, 69%; Greentown, 63%). CLAHRC members tended to fall most heavily into the minimum or maximum ‘working days per week’ categories (‘1 day or less’ or ‘4–5 days’ per week). A large proportion of Canada-Coordination members worked on a small pro-rata basis, with 84.8% spending just up to 1 day per week on the project. In all CLAHRCs, a notable portion of respondents falling into the ‘up to 1 day per week’ category actually worked very few hours for the CLAHRC, with comments such as, ‘not officially contracted’, ‘voluntary’, ‘as and when required’, ‘involvement at steering group meetings only’. As with the CLAHRCs, some Canada-Coordination members were not formally contracted to work on Canada-Coordination projects and described their frequency of input as ‘a few hours a month’, ‘when time allows’, ‘hardly ever’, ‘once every couple of months’, ‘very little’. There was similarity in levels of expertise across KT initiatives; 58% of Canada-Coordination respondents had over 16 years’ experience in their field alongside 51.4% in Greentown, 42.0% in Browntown and 40.3% in Bluetown. There was a gender and ethnic bias in all of the sample populations. Of CLAHRC respondents, 62–72% were female and 73–97% were white (100% on both counts for Canada-Coordination). There was a fair distribution of respondents across categories for age (but no respondents under 25 years of age for Browntown and Canada-Coordination).
The Canada–Coordination network had 77 people and 364 ties. The Canada-Coordination network was smaller than the CLAHRC KT networks and we account for this in our interpretation of network structure. Closure in the Canada-Coordination network was assessed in the same ways as the CLAHRCs, using a set of indicators that measured the connectedness of the network. At 6.2%, the density measure was similar to the CLAHRC scores; the Canada-Coordination network was not tight-knit. The proportion of reciprocal (two-way) knowledge-sharing ties was also similar to the CLAHRCs at 17% (closest to the Browntown network). Given the comparably smaller size of the Canada-Coordination network, we would have expected density to be somewhat higher in the former. (Density is often found to increase in small networks and decrease in large networks, the logic being that each person can sustain only a limited number of connections, and so networks with a large number of nodes tend to feature more fragmentation than networks with a small number of nodes.) It is therefore reasonable to state that the CLAHRCs had comparably more two-way knowledge-sharing ties and, from this claim, that there were arguably higher levels of trust in the CLAHRC KT networks ( Figure 17 ).
FIGURE 17.
Reciprocity in the Canada-Coordination KT network (reciprocal ties in red).
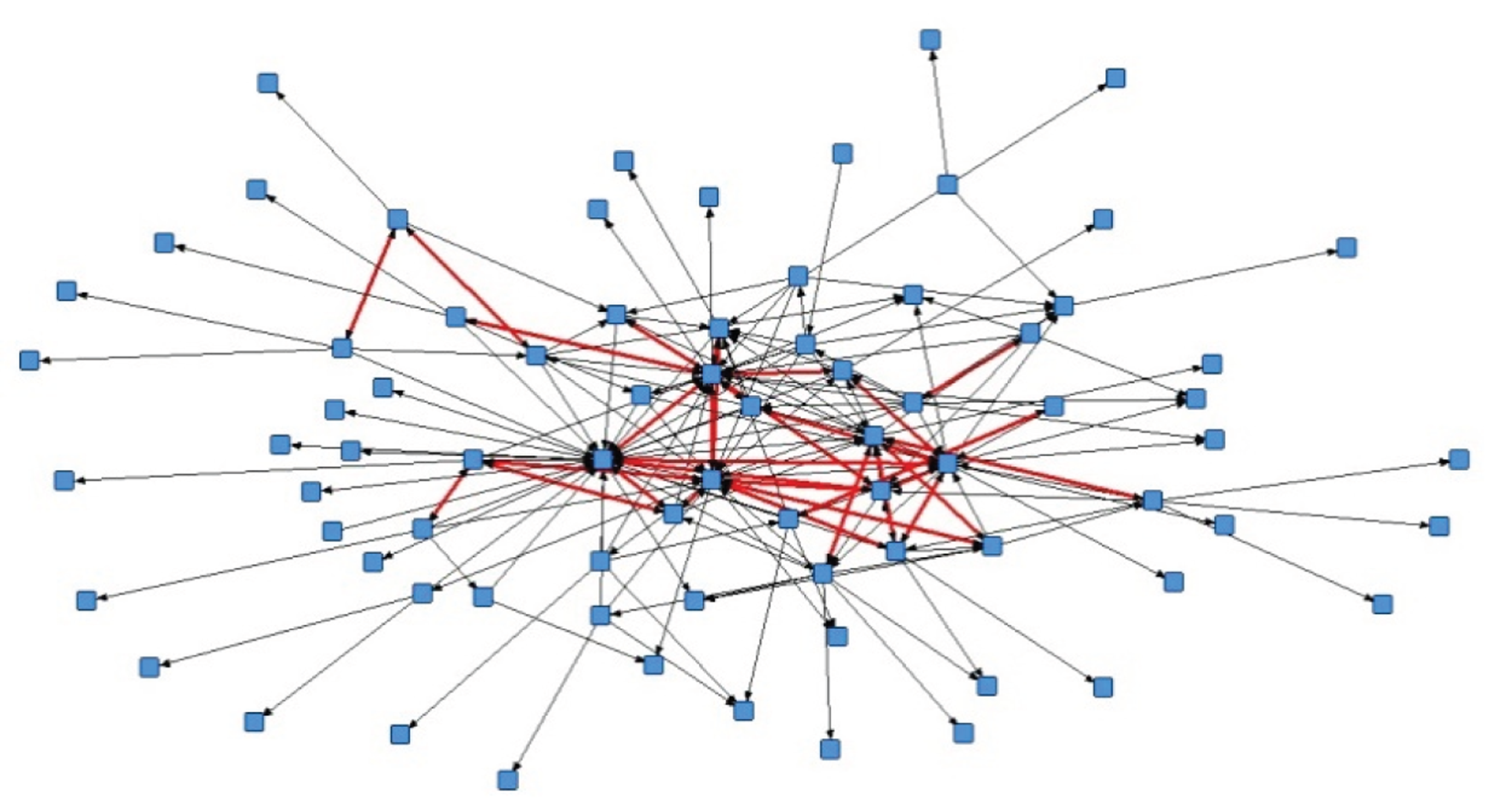
There were differences in terms of levels of engagement between Canada-Coordination and the CLAHRCs ( Figures 18 and 19 ). The three CLAHRCs exhibited fairly comparable levels of member engagement. In particular, most respondents described their engagement with their theme (team) as ‘very high’ or ‘high’ (Greentown = 78%, Bluetown = 77.1%, Browntown = 81.7%). Overall, CLAHRC members were more engaged at team level than at the level of the wider initiative. Canada-Coordination members were less engaged than CLAHRC members and slightly more engaged with the initiative than their team, with 30.4% and 27.3% of respondents indicating a ‘very high’ or ‘high’ level of engagement with team and initiative respectively.
FIGURE 18.
Member engagement at team level.
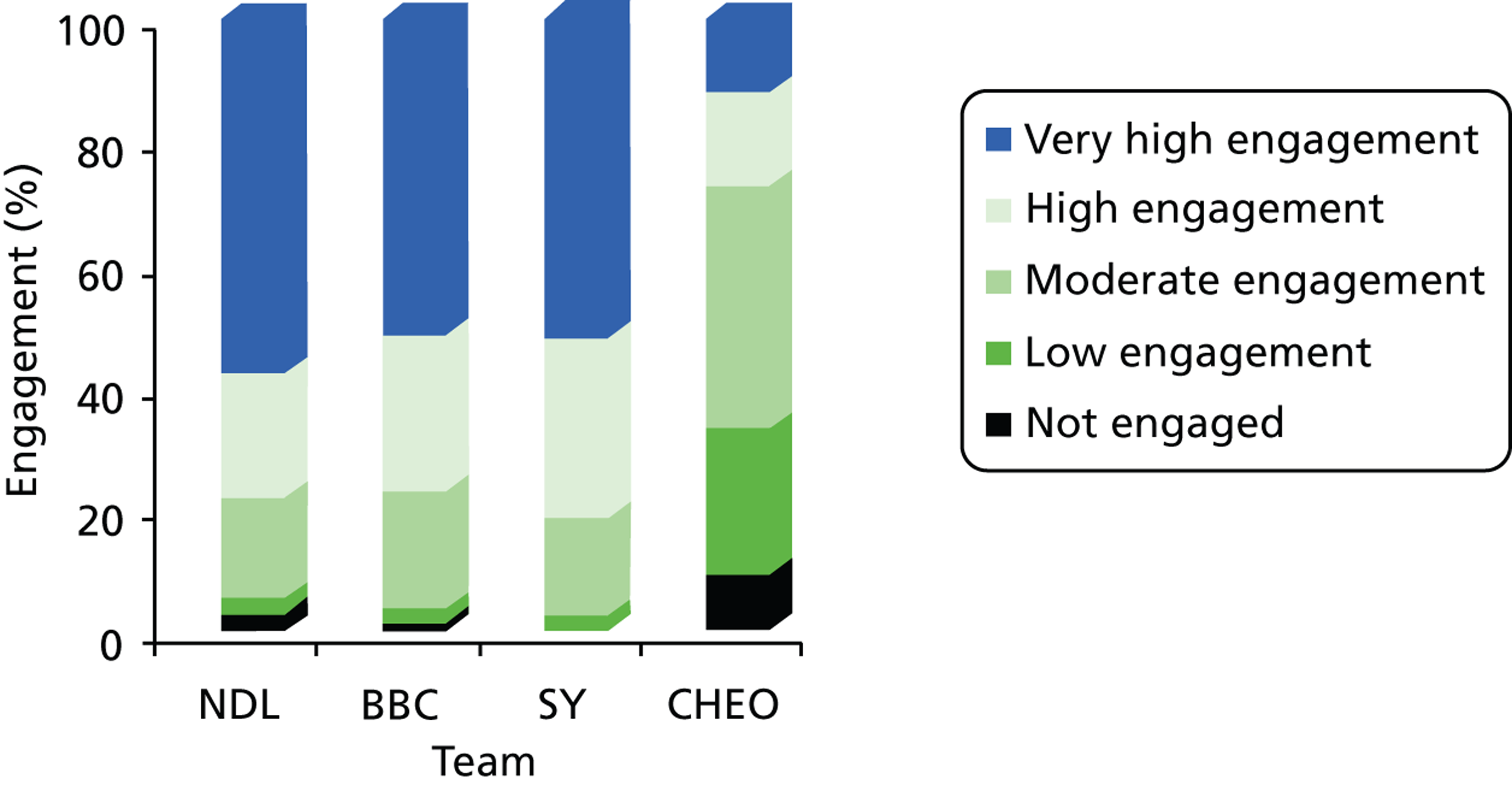
FIGURE 19.
Member engagement at initiative level.
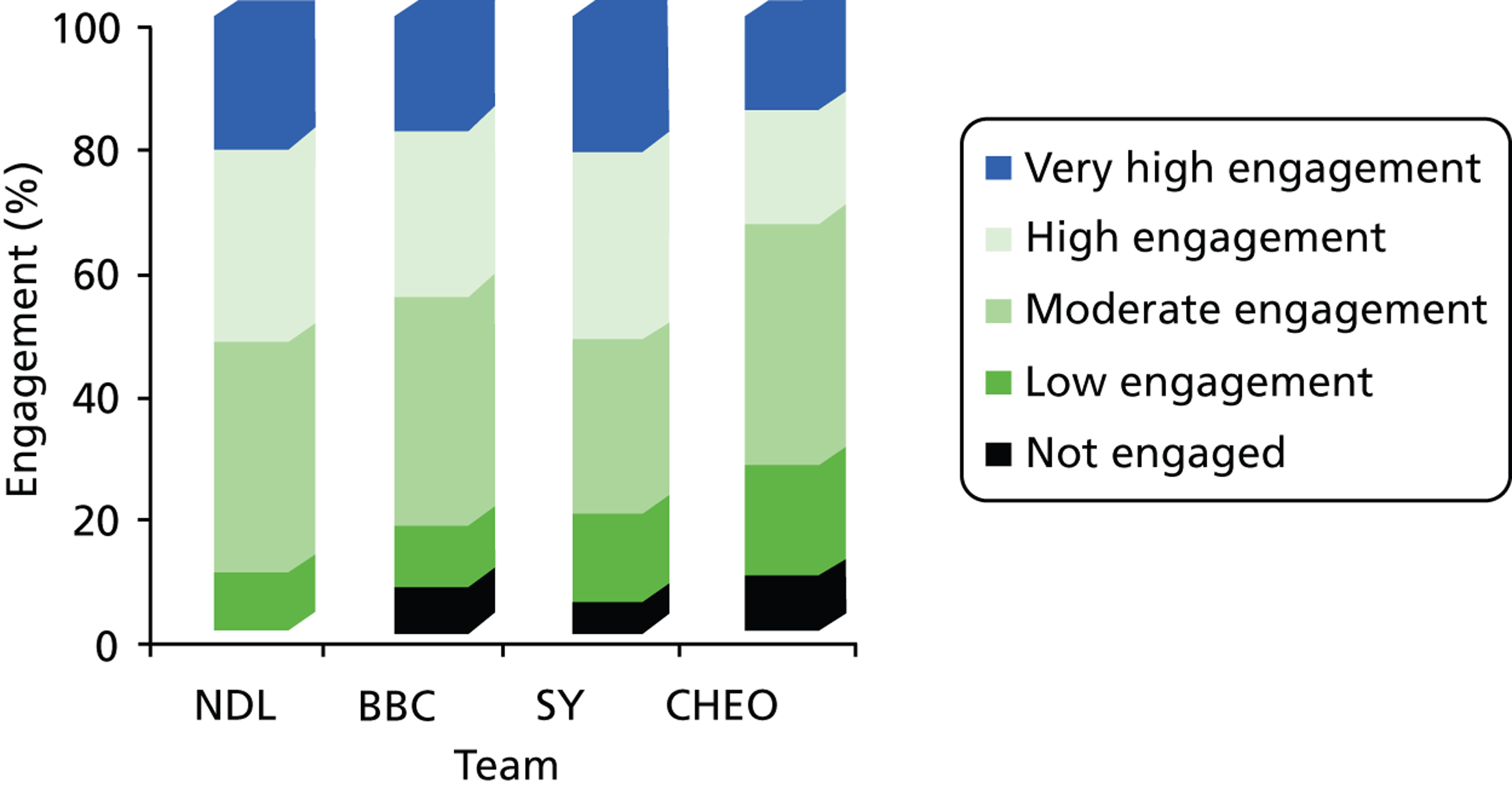
The Canada-Coordination network had a stronger core–periphery structure than the CLAHRCs (0.45), with higher centralisation scores. Reciprocal ties in Canada-Coordination were mostly between core members (at the centre of the network) but also extended towards some peripheral individuals (see Figure 17 ). There are high scores across all types of centralisation, which suggests power differences between Canada-Coordination members relating to KT. Individuals within Canada-Coordination differed from each other in terms of the number of connections (degree), control over information (betweenness) and access to knowledge contacts (closeness) and access to alternative knowledge paths (flow betweenness). The Canada-Coordination degree centralisation scores were more in line with those found by Scott et al. 125 in their study of interaction patterns in primary care settings in the USA. As with the CLAHRCs, the Canada-Coordination network indicated a high degree of structural efficiency alongside high constraint.
Across all knowledge types, Canada-Coordination members were most likely to rate their relationship with knowledge contacts as ‘close’ (50.7%) or ‘less than close’ (27.1%). Knowledge sharing in the Canada-Coordination network occurred more frequently between individuals who had previously collaborated. Interestingly, Canada-Coordination members had many ties for practical advice and fewer ties for scientific/technical advice (the opposite pattern was found for the CLAHRCs).
In sum and in comparison with the CLAHRCs, the Canada-Coordination network was less connected with a lower proportion two-way knowledge-sharing ties. A stronger core–periphery structure and higher centralisation was found for the Canada-Coordination network than for the CLAHRCs. This indicates that the distribution of knowledge ties was more unequal in the Canadian network. Reciprocal ties, commonly used as a proxy for trust, were mostly found between actors at the centre of the knowledge network.
Knowledge sharing in the Canada-Coordination network occurred more frequently between individuals who had previously collaborated. Interestingly, Canada-Coordination members had many ties for practical advice and fewer ties for scientific/technical advice (the opposite pattern was found for the CLAHRCs).
Overall, Canada-Coordination members were less engaged than CLAHRC members and slightly more engaged with the initiative than their team. A large proportion of Canada-Coordination members worked on a small pro-rata basis and this may have influenced both network structure and engagement scores.
Knowledge translation within and between organisational teams (Collaboration for Leadership in Applied Health Research and Care themes)
Greentown Collaboration for Leadership in Applied Health Research and Care
The most internally connected themes in CLAHRC Greentown at time 1 were stroke, CYP and primary care (79.4%, 67.5% and 66.2% of within-theme ties, repectively). At time 2, the Greentown network saw an increase in the proportion of cross-theme ties, with stroke, CYP and primary care becoming slightly less internally focused.
| Theme | Time 1 | Time 2 | ||||
|---|---|---|---|---|---|---|
| No. of ties | Per cent within theme | Per cent other themes | No. of ties | Per cent within theme | Per cent other themes | |
| Mental health | 128 | 55.5 | 44.5 | 112 | 58.9 | 41.1 |
| Implementation | 56 | 37.5 | 62.5 | N/A | – | – |
| Stroke | 155 | 79.4 | 20.6 | 77 | 71.4 | 28.6 |
| CYP | 83 | 67.5 | 32.5 | 55 | 61.8 | 38.2 |
| RDSU | 99 | 52.5 | 47.5 | 94 | 46.8 | 53.2 |
| Primary care | 71 | 66.2 | 33.8 | 94 | 45.7 | 54.3 |
| Programme management | 20 | 10.0 | 90.0 | 18 | 5.6 | 94.4 |
| Director/core team | 17 | 0.0 | 100.0 | – | – | – |
| Other | – | – | – | 38 | 0.0 | 100.0 |
| Total | 629 | 59.1 | 40.9 | 488 | 49.8 | 50.2 |
Bluetown Collaboration for Leadership in Applied Health Research and Care
At time 1, the most internally connected themes in the CLAHRC Bluetown network were stroke and TIA, pyschosis and maternity support (percentage of ties within themes: 87.0%, 81.8% and 69.0%, respectively). At time 2, the Bluetown network saw an increase in the proportion of cross-theme ties. Psychosis, maternity support, and stroke became less internally focused. The cross-cutting themes maintained a high proportion of cross-theme brokering ties at both time frames (82.4% at time 1, 73.5% at time 2). The Core team became less internally focused at time 2.
| Theme | Time 1 | Time 2 | ||||
|---|---|---|---|---|---|---|
| No. of ties | Per cent within theme | Per cent other themes | No. of ties | Per cent within theme | Per cent other themes | |
| Health service | 120 | 64.2 | 35.8 | 45 | 66.7 | 33.3 |
| Paediatric outreach | 90 | 66.7 | 33.3 | 49 | 63.3 | 36.7 |
| Psychosis | 44 | 81.8 | 18.2 | 52 | 67.3 | 32.7 |
| Housing and health | 43 | 60.5 | 39.5 | 7 | 28.6 | 71.4 |
| Maternity support | 42 | 69.0 | 31.0 | 33 | 48.5 | 51.5 |
| Cardiovascular | 42 | 40.5 | 59.5 | 47 | 34.0 | 66.0 |
| Stroke and TIA | 46 | 87.0 | 13.0 | 75 | 70.7 | 29.3 |
| Diabetes | 27 | 44.4 | 55.6 | 36 | 36.1 | 63.9 |
| IT systems | 38 | 55.3 | 44.7 | 23 | 39.1 | 60.9 |
| Cross-cutting themes | 34 | 17.6 | 82.4 | 49 | 26.5 | 73.5 |
| Core/programme | 48 | 39.6 | 60.4 | 23 | 26.1 | 73.9 |
| Total | 575 | 59.7 | 40.2 | 439 | 51.0 | 49.0 |
Browntown Collaboration for Leadership in Applied Health Research and Care
The Browntown network has a similar proportion of cross-theme ties in each time period (44.4% at time 1 and 44.7% at time 2). At time 1, the themes with the highest proportion of in-theme ties were diabetes (77.1%), depression (73.9%) and obesity (67.9%). At time 2, genetics and inequalities became less internally focused. Core team and TaCT became more internally focused. (Note: some theme data are missing.)
| Theme | Time 1 | Time 2 | ||||
|---|---|---|---|---|---|---|
| No. of ties | Per cent within theme | Per cent other themes | No. of ties | Per cent within theme | Per cent other themes | |
| COPD | 5 | 60.0 | 40.0 | 8 | 37.5 | 62.5 |
| Depression | 23 | 73.9 | 26.1 | 51 | 84.3 | 15.7 |
| Diabetes | 35 | 77.1 | 22.9 | 48 | 68.8 | 31.3 |
| Genetics | 10 | 60.0 | 40.0 | 23 | 34.8 | 65.2 |
| Inequalities | 62 | 58.1 | 41.9 | 100 | 49.0 | 51.0 |
| Intel comm | 1 | 0.0 | 100.0 | 10 | 20.0 | 80.0 |
| Obesity | 28 | 67.9 | 32.1 | 28 | 25.0 | 75.0 |
| Stroke | 60 | 50.0 | 50.0 | 68 | 47.1 | 52.9 |
| TaCT | 14 | 14.3 | 85.7 | 42 | 59.5 | 40.5 |
| Knowledge into action | 39 | 64.1 | 35.9 | 83 | 61.4 | 38.6 |
| UCHD | 36 | 47.2 | 52.8 | 54 | 57.4 | 42.6 |
| Core team | 45 | 37.8 | 62.2 | 69 | 56.5 | 43.5 |
| Total | 358 | 55.6 | 44.4 | 584 | 55.3 | 44.7 |
Types of knowledge translated
Browntown Collaboration for Leadership in Applied Health Research and Care
At time 1, 32% of ties are outside the CLAHRC; this decreases to 23% in time 2 ( Tables 16 and 17 ). People tend to go outside the CLAHRC to gain access to groups and individuals. This is especially the case at time 1. In time 2, we see an increase in the number of ties outside the CLAHRC providing practical advice. At time 1 people have a relatively high percentage of ties outside the CLAHRC in which they had previously collaborated. This drops in time 2. This highlights the switch from external to internal ties as the CLAHRC matures.
At time 1, ties outside of the CLAHRC were, on average, not very close, whereas by time 2 the outside-CLAHRC ties that remained were considered much closer. Not surprisingly, ties to people within the CLAHRC were more frequent than those to people outside the CLAHRC.
| Type of tie | Ties inside CLAHRC | Ties outside CLAHRC | Total ties | Per cent inside CLAHRC | Per cent outside CLAHRC |
|---|---|---|---|---|---|
| All ties | 574 | 271 | 845 | 0.68 | 0.32 |
| Benefits | |||||
| Organisational/professional backing | 93 | 50 | 143 | 0.65 | 0.35 |
| Technical advice | 116 | 58 | 174 | 0.67 | 0.33 |
| Access to groups/individuals | 57 | 60 | 117 | 0.49 | 0.51 |
| Practical advice | 77 | 35 | 112 | 0.69 | 0.31 |
| Management advice | 88 | 20 | 108 | 0.81 | 0.19 |
| Other benefit | 52 | 22 | 74 | 0.70 | 0.30 |
| Closeness | |||||
| Distant | 26 | 25 | 51 | 0.51 | 0.49 |
| Less than close | 134 | 114 | 248 | 0.54 | 0.46 |
| Close | 232 | 94 | 326 | 0.71 | 0.29 |
| Especially close | 89 | 28 | 117 | 0.76 | 0.24 |
| Frequency | |||||
| Less than once in 6 months | 22 | 27 | 49 | 0.45 | 0.55 |
| A few times in 6 months | 119 | 115 | 234 | 0.51 | 0.49 |
| Few times per month | 167 | 82 | 249 | 0.67 | 0.33 |
| Once or twice per week | 113 | 24 | 137 | 0.82 | 0.18 |
| Nearly every day | 67 | 13 | 80 | 0.84 | 0.16 |
| Type of tie | Ties inside CLAHRC | Ties outside CLAHRC | Total ties | Per cent inside CLAHRC | Per cent outside CLAHRC |
|---|---|---|---|---|---|
| All ties | 664 | 203 | 867 | 0.77 | 0.23 |
| Benefits | |||||
| Organisational/professional backing | 152 | 44 | 196 | 0.78 | 0.22 |
| Technical advice | 152 | 36 | 188 | 0.81 | 0.19 |
| Access to groups/individuals | 86 | 39 | 125 | 0.69 | 0.31 |
| Practical advice | 71 | 38 | 109 | 0.65 | 0.35 |
| Management advice | 127 | 21 | 148 | 0.86 | 0.14 |
| Other benefit | 69 | 24 | 93 | 0.74 | 0.26 |
| Closeness | |||||
| Distant | 120 | 29 | 149 | 0.81 | 0.19 |
| Less than close | 283 | 86 | 369 | 0.77 | 0.23 |
| Close | 209 | 70 | 279 | 0.75 | 0.25 |
| Especially close | 37 | 17 | 54 | 0.69 | 0.31 |
| Frequency | |||||
| Less than once every 6 months | 53 | 16 | 69 | 0.77 | 0.23 |
| A few times in 6 months | 169 | 78 | 247 | 0.68 | 0.32 |
| Few times per month | 228 | 64 | 292 | 0.78 | 0.22 |
| Once or twice per week | 116 | 27 | 143 | 0.81 | 0.19 |
| Nearly every day | 92 | 15 | 107 | 0.86 | 0.14 |
Greentown Collaboration for Leadership in Applied Health Research and Care
At time 1, 27% of ties are outside the CLAHRC; this decreases very slightly to 26% in time 2. At time 1, people tended to go outside the CLAHRC to gain access to groups and individuals and for practical advice. By time 2, there was much less searching for practical advice outside the CLAHRC.
At time 1, people have a relatively high percentage of ties outside the CLAHRC in which they had previously collaborated. This drops in time 2. This highlights the switch from external to internal ties as the CLAHRC matures.
At time 1, ties outside of the CLAHRC were, on average, not very close, whereas by time 2 the outside-CLAHRC ties that remained were considered much closer. Not surprisingly, ties to people within the CLAHRC were more frequent than those to people outside the CLAHRC.
| Type of tie | Ties inside CLAHRC | Ties outside CLAHRC | Total ties | Per cent inside CLAHRC | Per cent outside CLAHRC |
|---|---|---|---|---|---|
| All ties | 641 | 241 | 882 | 0.73 | 0.27 |
| Benefits | |||||
| Organisational/professional backing | 126 | 56 | 182 | 0.69 | 0.31 |
| Technical advice | 158 | 33 | 191 | 0.83 | 0.17 |
| Access to groups/individuals | 84 | 60 | 144 | 0.58 | 0.42 |
| Practical advice | 72 | 45 | 117 | 0.62 | 0.38 |
| Management advice | 145 | 26 | 171 | 0.85 | 0.15 |
| Other benefit | 54 | 21 | 75 | 0.72 | 0.28 |
| Closeness | |||||
| Distant | 62 | 30 | 92 | 0.67 | 0.33 |
| Less than close | 184 | 95 | 279 | 0.66 | 0.34 |
| Close | 294 | 87 | 381 | 0.77 | 0.23 |
| Especially close | 99 | 29 | 128 | 0.77 | 0.23 |
| Frequency | |||||
| Less than once every 6 months | 39 | 19 | 58 | 0.67 | 0.33 |
| A few times in 6-month time frame | 130 | 98 | 228 | 0.57 | 0.43 |
| Few times per month | 184 | 90 | 274 | 0.67 | 0.33 |
| Once or twice per week | 157 | 23 | 180 | 0.87 | 0.13 |
| Nearly every day | 130 | 10 | 140 | 0.93 | 0.07 |
| Type of tie | Ties inside CLAHRC | Ties outside CLAHRC | Total ties | Per cent inside CLAHRC | Per cent outside CLAHRC |
|---|---|---|---|---|---|
| All ties | 488 | 168 | 656 | 0.74 | 0.26 |
| Benefits | |||||
| Organisational/professional backing | 106 | 51 | 157 | 0.68 | 0.32 |
| Technical advice | 115 | 18 | 133 | 0.86 | 0.14 |
| Access to groups/individuals | 43 | 43 | 86 | 0.50 | 0.50 |
| Practical advice | 35 | 12 | 47 | 0.74 | 0.26 |
| Management advice | 115 | 20 | 135 | 0.85 | 0.15 |
| Other benefit | 65 | 15 | 80 | 0.81 | 0.19 |
| Closeness | |||||
| Distant | 73 | 9 | 82 | 0.89 | 0.11 |
| Less than close | 193 | 60 | 253 | 0.76 | 0.24 |
| Close | 162 | 67 | 229 | 0.71 | 0.29 |
| Especially close | 28 | 16 | 44 | 0.64 | 0.36 |
| Frequency | |||||
| Less than once every 6 months | 20 | 17 | 37 | 0.54 | 0.46 |
| A few times in 6-month time frame | 112 | 65 | 177 | 0.63 | 0.37 |
| Few times per month | 137 | 56 | 193 | 0.71 | 0.29 |
| Once or twice per week | 103 | 16 | 119 | 0.87 | 0.13 |
| Nearly every day | 109 | 14 | 123 | 0.89 | 0.11 |
Bluetown Collaboration for Leadership in Applied Health Research and Care
At time 1, 27% of ties are outside the CLAHRC; this decreases to 19% at time 2. At time 1, people tended to go outside the CLAHRC to gain access to groups and individuals and for practical advice. In time 2, this remained the same.
At time 1, people have a relatively high percentage of ties outside the CLAHRC in which they had previously collaborated. This drops at time 2. This highlights the switch from external to internal ties as the CLAHRC matures.
At time 1, ties outside of the CLAHRC were, on average, not very close, whereas by time 2 there was an increase in the ratio of outside-CLAHRC ties that were especially close. Not surprisingly, ties to people within the CLAHRC were more frequent than those to people outside the CLAHRC.
| Type of tie | Ties inside CLAHRC | Ties outside CLAHRC | Total ties | Per cent inside CLAHRC | Per cent outside CLAHRC |
|---|---|---|---|---|---|
| All ties | 575 | 214 | 789 | 0.73 | 0.27 |
| Benefits | |||||
| Organisational/professional backing | 134 | 59 | 193 | 0.69 | 0.31 |
| Technical advice | 169 | 51 | 220 | 0.77 | 0.23 |
| Access to groups/individuals | 58 | 30 | 88 | 0.66 | 0.34 |
| Practical advice | 58 | 34 | 92 | 0.63 | 0.37 |
| Management advice | 111 | 23 | 134 | 0.83 | 0.17 |
| Other benefit | 45 | 17 | 62 | 0.73 | 0.27 |
| Closeness | |||||
| Distant | 66 | 27 | 93 | 0.71 | 0.29 |
| Less than close | 149 | 77 | 226 | 0.66 | 0.34 |
| Close | 252 | 83 | 335 | 0.75 | 0.25 |
| Especially close | 108 | 27 | 135 | 0.80 | 0.20 |
| Frequency | |||||
| Less than once every 6 months | 50 | 31 | 81 | 0.62 | 0.38 |
| A few times in 6-month time frame | 158 | 71 | 229 | 0.69 | 0.31 |
| Few times per month | 153 | 56 | 209 | 0.73 | 0.27 |
| Once or twice per week | 129 | 35 | 164 | 0.79 | 0.21 |
| Nearly every day | 85 | 21 | 106 | 0.80 | 0.20 |
| Type of tie | Ties inside CLAHRC | Ties outside CLAHRC | Total ties | Per cent inside CLAHRC | Per cent outside CLAHRC |
|---|---|---|---|---|---|
| All ties | 457 | 104 | 561 | 0.81 | 0.19 |
| Benefits | |||||
| Organisational/professional backing | 99 | 19 | 118 | 0.84 | 0.16 |
| Technical advice | 135 | 16 | 151 | 0.89 | 0.11 |
| Access to groups/individuals | 38 | 22 | 60 | 0.63 | 0.37 |
| Practical advice | 49 | 16 | 65 | 0.75 | 0.25 |
| Management advice | 89 | 21 | 110 | 0.81 | 0.19 |
| Other benefit | 41 | 9 | 50 | 0.82 | 0.18 |
| Closeness | |||||
| Distant | 88 | 19 | 107 | 0.82 | 0.18 |
| Less than close | 189 | 42 | 231 | 0.82 | 0.18 |
| Close | 138 | 28 | 166 | 0.83 | 0.17 |
| Especially close | 33 | 14 | 47 | 0.70 | 0.30 |
| Frequency | |||||
| Less than once every 6 months | 53 | 10 | 63 | 0.84 | 0.16 |
| A few times in 6-month time frame | 130 | 34 | 164 | 0.79 | 0.21 |
| Few times per month | 121 | 29 | 150 | 0.81 | 0.19 |
| Once or twice per week | 79 | 18 | 97 | 0.81 | 0.19 |
| Nearly every day | 66 | 12 | 78 | 0.85 | 0.15 |
| KT features | T1 | T2 |
|---|---|---|
| Governance co-ordination and control | Bluetown (most centralised), Greentown (least centralised). C-P observed in all, Greentown slightly weaker C-P structure | Browntown (most centralised), Greentown (least centralised). Greentown and Bluetown most similar by T2 |
| Knowledge core comprises senior management in Bluetown and Browntown | Greentown: increase in C-P measure indicates that the knowledge-sharing network is more heavily focused on a group of key individuals. C-P also observed in Browntown and Bluetown but slightly weaker than at T1 | |
| Diverse knowledge-core membership in Greentown CLAHRC | ||
| Structures for embedding knowledge (closure) | Similar global density and reciprocity (highest scores for Greentown, lowest for Bluetown) | Same ranks as T1 but even more score similarity for global density, reciprocity and distance |
| Browntown furthest distances across network | ||
| Structures for accessing new knowledge (brokerage) | High efficiency at both whole and ego-network level, most constrained at ego-network level | The CLAHRC networks generally became more efficient at whole-network level at time period 2, suggesting some organisational restructuring of KT ties over time to improve the capability for knowledge brokering |
| This means that it was more difficult to exploit structural hole opportunities within people’s personal networks than across the CLAHRC as a whole | A further evening out of both betweenness and brokerage scores across CLAHRCs | |
| Quite similar brokerage scores across CLAHRCs at T1. At T1, Greentown has the highest betweenness score, which means that there are more individuals in this CLAHRC acting as ‘bridges’ between two disconnected others than in CLAHRCs Bluetown and Browntown | ||
| Information search | Expansive information search strategies adopted by all | Targeted information search by Bluetown and Browntown. Increased reliance on internal ties |
| External ties important for access to new contacts and practical advice. CLAHRC members had previously collaborated with most of their external contacts | External knowledge ties become less important – instead, members prefer to draw on knowledge from CLAHRC colleagues as the CLAHRC matures. External ties that are maintained become closer | |
| All CLAHRCs built networks beyond NHS–academic collaborations | Browntown increases networks to non-NHS/non-academic contacts. Bluetown and Greentown decrease theirs | |
| Bluetown and Browntown NHS facing, Greentown is academia facing | ||
| Organisational teams (CLAHRC themes) | Greentown and Bluetown had increased the proportion of cross-theme ties. Browntown maintained an equal split of within- and between-theme KT |
| SNA metric | Definition | Implications for KT |
|---|---|---|
| Centralisation (Freeman 1979)107 | Function of the heterogeneity in the centralities of the individual actors in the network The extent to which the KT network is focused around a few central actors |
Co-ordination and control, dissemination of information, key messages, standardisation of practice, operational clarity Some individuals may dominate the KT network and the skills and experiences of more peripheral actors may be relegated as a consequence |
| Core–periphery (Borgatti and Everett 2000)119 | The extent to which knowledge relations are dominated by a core group of individuals who frequently translate knowledge to each other (core actors) | |
| Brokerage | Occurs when pairs of individuals are not already directly connected. Normalised brokerage calculates the percentage of time an actor acts as a broker relative to network size | A broker may act as the ‘go-between’ between his/her disconnected contacts possibly to obtain new, ‘non-redundant’ information |
| Ego betweenness (Freeman 1979)107 | Individuals will have a high betweenness score if they are positioned on the shortest (geodesic) directed path ‘between’ two other actors | Individuals with high betweenness scores will be powerful in their own local network neighbourhood because their contacts will be largely disconnected from one another |
| Structural holes: efficiency (Burt 1992)115 | The extent to which an individual’s connections are ‘non-redundant’ (ties to others who are not directly connected). Taps level of impact individuals get from investing in their networks | Structural holes offer the potential for brokerage across networks |
| Structural holes: constraint (Burt 1992)115 | The extent to which an individual’s KT interactions are invested in a single alter | High constraint in KT relations can mean that although an individual is supplied knowledge by many contacts, the information may not be novel because of the interconnectivity between suppliers |
| Size (degree) (Freeman 1979)107 | The number of direct KT connections (ties) | Positive. The more people you have relationships with, the greater the chance that one of them has the resource you need |
| Density (Harary 1969)113 | The proportion of group members who are tied (with a ‘positive’ relation, ‘translates knowledge to/from’). It summarises the level of cohesiveness in a network or part of a network. In our CLAHRC study, a high density score describes tight-knit set of relations where every individual translates knowledge to everyone else | Positive; curvilinear for intellectual conflict relations, negative for personal conflict relations. But if all alters are connected, negative because has a negative effect on diversity of knowledge (more redundant information) |
| Geodesic distance (Harary 1969)113 | The average number of ‘links’ between all actors, i.e. degrees of separation | Speed of translation. Short distances between network contacts allow faster access to knowledge and accurate transmission of information, while long distances can delay and distort the information |
| Reciprocity | The extent to which relations are two-way, where if A shares knowledge with B, then B also shares knowledge with A | A proxy for trust |
| E-I Index (Krackhardt and Stern 1988)118 | The extent to which KT is internal or external to epistemic groups (homophily = score of up to –1 where CLAHRC members connect with others who are similar to themselves, or heterophily = score of up to +1) | Influence of professional expertise on KT Heterophily should mean greater exposure to a wider range of ideas. However, homophily may improve communication and trust, possibly resulting in a curvilinear relationship |
Appendix 2 Causal mapping
In terms of the qualitative analysis, we show the most chosen constructs for each initiative and highlight the main associations between inputs and outputs. Following the qualitative analysis, we introduce some figures that represent, with arrows, the top 10 relationships between constructs, per initiative ( Figures 20–24 ).
In terms of the statistical analysis, the following indexes are reported and discussed for each initiative.
Mean link strength: this index is the arithmetic mean of all link strengths within a collective map. The ‘strength’ includes numeric values between 1 and 3 and is chosen by the participant when he or she performs the causal map exercise: 1 represents a weak link between two constructs; 2 represents an average link between two constructs; 3 represents a strong link between two constructs. The strength can be also negative: –1 represents a weak negative link between two constructs; –2 represents an average negative link between two constructs; and –3 represents a strong negative link between two constructs.
Mean ABS (absolute value) link strength: this index is the arithmetic mean of the absolute values for all link strengths within a collective map. This excludes the negative relationships that are selected. However, in all cases, as we see below, there is little different between mean link strength and ABS mean length strength, reflecting the fact that very few participants selected a negative relationships, and where they did, it was typically only a low-strength (i.e. –1) relationship.
Standard deviation ABS link strength: this index is the standard deviation of absolute values for all link strengths within a collective map. This index reflects the variance among all link strengths and helps reading the previous index (mean ABS link strength).
Link density: this index provides a value that is the number of links selected divided by the number constructs. This provides an absolute value of the ‘density’ of a map, that is, whether many or few relationships between links are chosen. If link density has a high value, this means that participants tended to choose a relationship between an input and a list of (potential) outputs; if link density has a low value, participants more often chose ‘no relationship’. This index (link density) was developed in Eden et al. 142
Link strength density: this index provides a value that is the sum of all link strengths divided by the number of mapped constructs. The difference between this index and the previous (link density) is that link strength density considers not only whether or not a participant picked a relationship (rather than leaving a relationship neutral) but also whether the value of a relationship is 1, 2 or 3. Many links that are valued as strong cause–effect relationships increase the index. Many links that are valued as weak cause–effect relationships decrease the index. This index was developed in Langfield-Smith and Wirth. 143
Map density: this index provides a value that is the number of links divided by the theoretical number of maximum links between constructs [i.e. number of constructs × (number of constructs – 1)]. This index was developed in Goldberg (Cranfield University, Bedford, 1996).
Bluetown Collaboration for Leadership in Applied Health Research and Care
This map comprises 19 participants; the most relevant input constructs that were selected and rated by the users during the initial survey (see Chapter 3, Research methods) are the following:
-
using mixed methods
-
implementation of findings in practice locally
-
identification of barriers to service change and redesign
-
involvement of health-care and user representatives
-
collaboration between researchers and practitioners.
The most selected input constructs in the causal mapping exercise – that is, the constructs that are considered the most important drivers to achieve the objectives of the Bluetown CLAHRC – are the following:
-
involvement of health-care and user representatives
-
collaboration between researchers and practitioners
-
identification of barriers to service change and redesign
-
dissemination of findings to practitioners.
As expected, there is overlap between the constructs that have been selected as most relevant and the constructs that were most associated with the achievement of the outcomes of the initiative. In particular, the Bluetown collective map indicates that:
-
The involvement of health-care and user representatives helps in identifying barriers to service change and redesign.
-
Enabling collaboration between researchers and practitioners promotes the dissemination of findings in practical settings.
-
Collaboration between researchers and practitioners leads to (a) the identification of barriers to service change and redesign; (b) building capacity; (c) improving efficiency; and (d) improving quality.
Interestingly, two outputs have been chosen as drivers to achieve other constructs (that in our maps are inputs): according to the Bluetown collective map, reduction of inequalities (output) leads to the involvement of health-care and user representatives; and building capacity leads to the identification of barriers to service change and redesign.
The map of the Bluetown CLAHRC is presented in Figure 20 , where the arrows indicate participants’ most highly selected causal links selected.
FIGURE 20.
Bluetown CLAHRC collective map (19 participants).
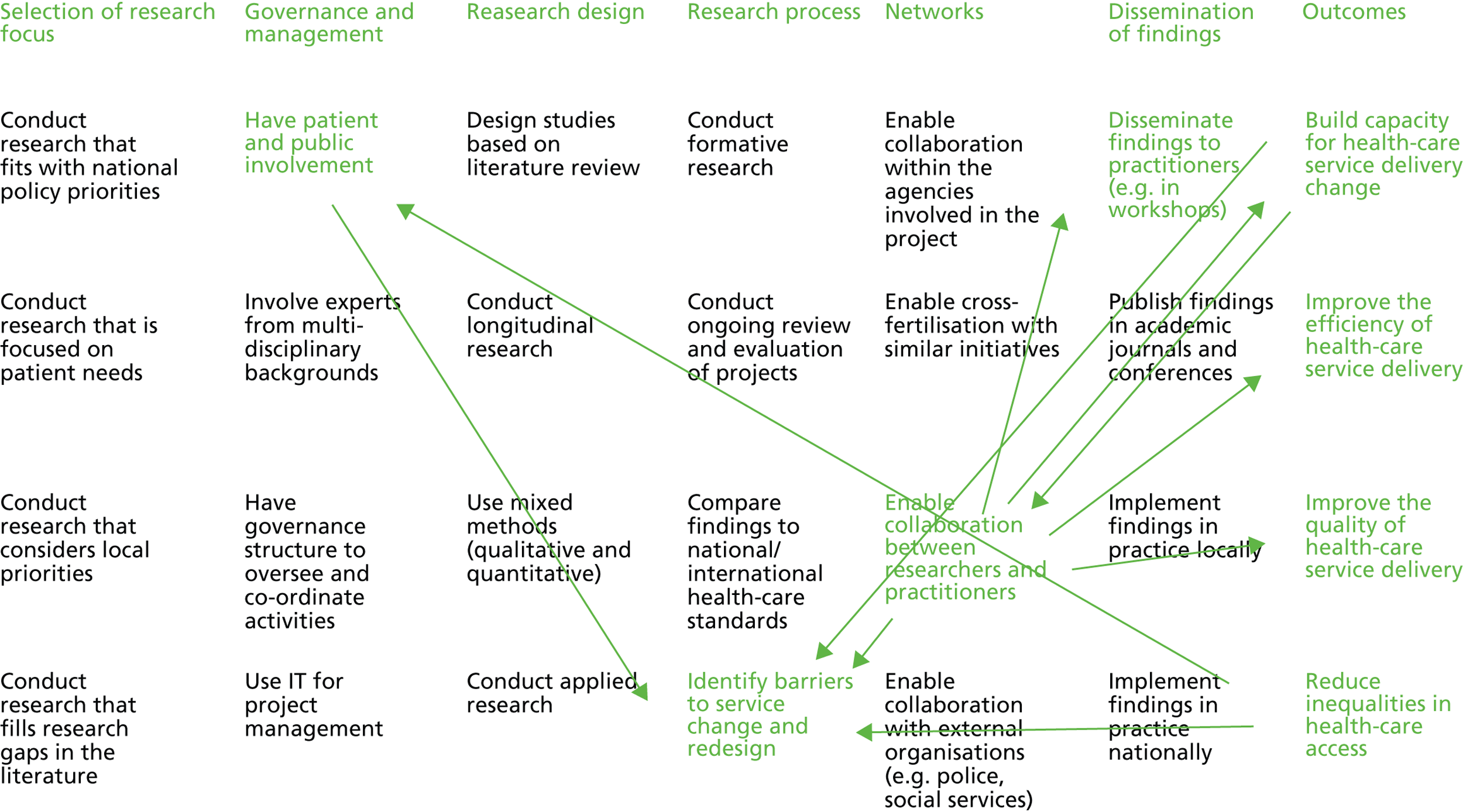
In terms of a quantitative approach, Table 24 illustrates the main statistics of the Bluetown CLAHRC and also provides the average scores across all initiatives for comparison purposes.
| Index | Bluetown | Mean of all initiatives |
|---|---|---|
| Mean links strength | 6.05 | 5.244 |
| Mean ABS links strength | 6.08 | 5.265 |
| Standard deviation ABS links strength | 5.84 | 4.586 |
| Link density | 18.54 | 15.450 |
| Link strength density | 112.11 | 82.024 |
| Map density | 0.69 | 0.572 |
Table 24 indicates that the participants of the Bluetown CLAHRC have selected a relatively high number of links (and strengths). This is shown by the first three indexes. Moreover, the link density (and the link strength density) is high. The overall map density is objectively high (it can be a value between 0 and 1) and it is also higher than the mean of the initiatives (0.690 vs. 0.572).
The statistical analysis can be interpreted as follows: (1) the similarity between the mean links strength and the mean ABS links strength shows that only few negative relationships were selected; (2) the first two indexes of the table show also that there are relatively strong links between the constructs (high mean link strength, and high mean ABS); (3) relatively high standard deviation (if compared with the mean of the standard deviation for initiatives) indicates that the range of the values (1, 2 or 3) for the relationships of the construct is wider than the mean of all initiatives (more 2 and 3 than 1); (4) high scores on link density, strength density, and map density (which were all above the mean of the initiatives) show that participants perceive more causal relationships between constructs (i.e. inputs and outputs) and perceive these relationships as being stronger than across other initiatives.
Greentown Collaboration for Leadership in Applied Health Research and Care
This map comprises 18 participants; the most relevant input constructs that were selected by the users during the initial survey (see Chapter 3, Research methods) are the following:
-
involvement of health-care and user representatives
-
collaboration between researchers and practitioners
-
identification of barriers to service change and redesign
-
dissemination of findings to practitioners.
The most selected input constructs – that is, the constructs that are perceived as the most important drivers to achieve the objectives of the Greentown CLAHRC – are:
-
identify barriers to service change and redesign
-
collaboration between researchers and practitioners
-
dissemination of findings to practitioners
-
implementation of findings in practice locally
-
implementation of findings in practice nationally.
In the Greentown CLAHRC, there is, again, (partial) overlap between the constructs that have been chosen as particularly relevant and the constructs that were most associated with the achievement of the outcomes of the initiative. In particular, the Greentown collective map indicates that participants perceive that:
-
Enabling collaboration between researchers and practitioners is a central construct (seen as both an input and an output), leading to the identification of barriers to service change and redesign, to building capacity, to improving the quality of health-care delivery, and disseminating findings to practitioners.
-
Implementing findings in practice nationally is helpful for improving quality.
-
Building capacity is helpful for implementing findings in practice locally.
-
Collaboration between researchers and practitioners (the central construct for this initiative) is enabled by building capacity (which is seen as an input as well as an output in the Greentown CLAHRC), by implementing findings in practice locally, and by disseminating findings to practitioners.
-
Collaboration between researchers and practitioners is seen as an aim of the initiative.
-
Moreover, this map incorporates a number of two-way links between constructs, as shown in Figure 21 .
FIGURE 21.
Greentown CLAHRC collective map (17 participants).
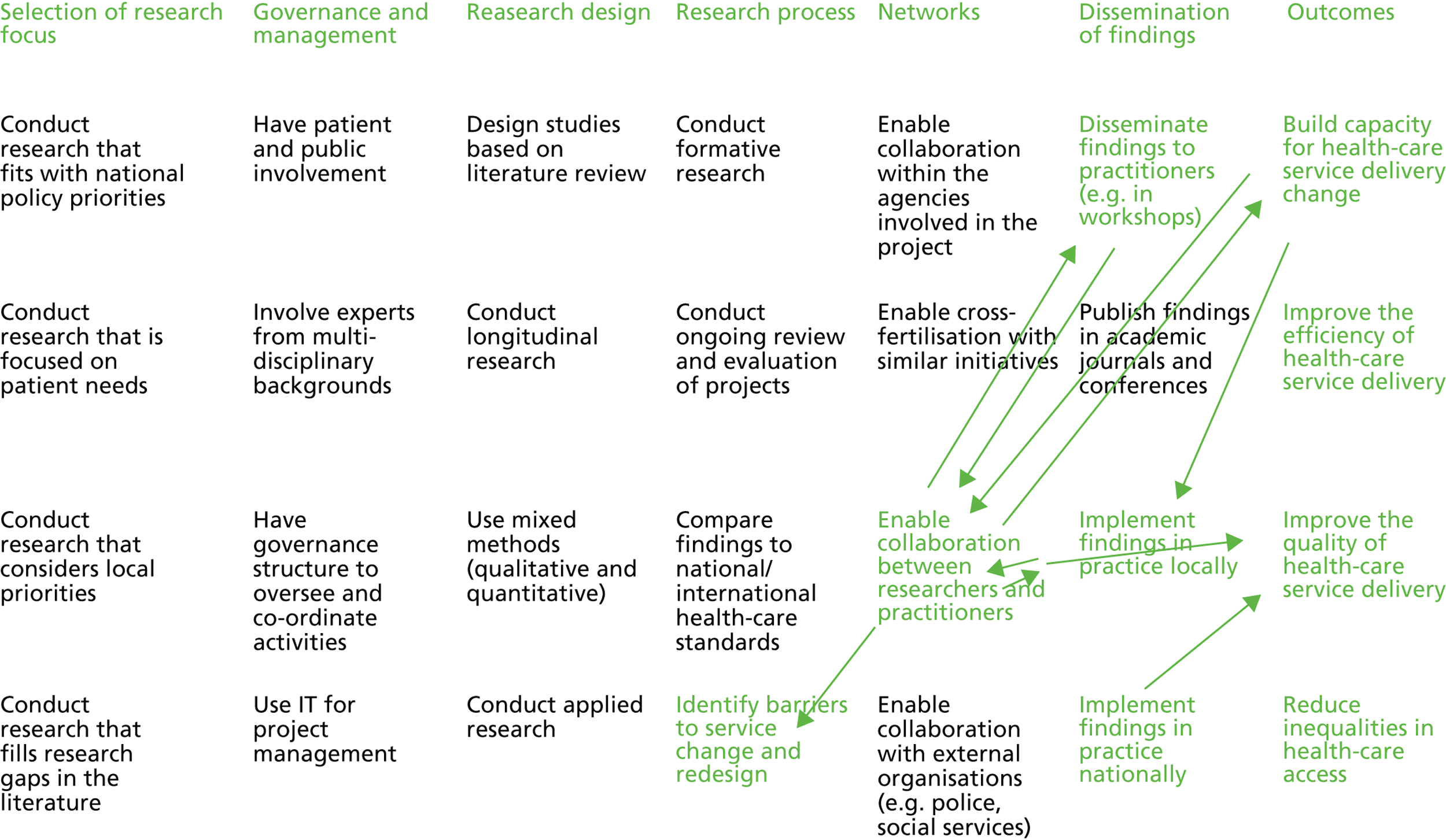
In terms of the quantitative approach, Table 25 illustrates the main statistics of the Greentown CLAHRC and also presents the mean scores across all initiatives for comparison.
| Index | Greentown | Mean of all initiatives |
|---|---|---|
| Mean links strength | 5.15 | 5.244 |
| Mean ABS links strength | 5.16 | 5.265 |
| Standard deviation ABS links strength | 3.67 | 4.586 |
| Link density | 13.21 | 15.450 |
| Link strength density | 68.11 | 82.024 |
| Map density | 0.49 | 0.572 |
Table 25 indicates that the participants of the Greentown CLAHRC have selected a relatively low number of links (and strengths). This is shown by the first three indexes. Moreover, the link density (and the link strength density) is low. The overall map density is objectively low (it is a value between 0 and 1) and it is also lower than the mean of the initiatives (0.690 vs. 0.572).
The statistical analysis can be interpreted as follows: (1) the similarity between the mean links strength and the mean ABS links strength shows that only few negative relationships were selected; (2) the first two indexes of the table show also that there are relatively weak links between the constructs (low mean link strength, and low mean ABS); (3) relatively low standard deviation (if compared with the mean of the standard deviation for initiatives) indicates that the range of the values (1, 2 or 3) for the relationships of the construct is less wide than the mean of all initiatives (more 1 and 2 rather than 3); (4) low link density, link strength density and map density (below the mean of the initiatives) indicates that fewer than average of the input–output links are perceived as relevant, and where they are considered relevant they are considered only to have medium or weak relationships.
Browntown Collaboration for Leadership in Applied Health Research and Care
This map comprises 16 participants; the most relevant input constructs that were selected by the users during the initial survey (see Chapter 3, Research methods) are:
-
involvement of health-care and user representatives
-
implementation of findings in practice locally
-
conducting research that considers local priorities
-
conducting applied research
-
identification of barriers to service change and redesign.
The most selected input constructs – that is, the constructs that are the most important drivers to achieve the objective of the Browntown CLAHRC – are:
-
conducting research that considers local priorities
-
conducting applied research
-
collaboration between researchers and practitioners
-
implementation of findings in practice locally.
In the Browntown CLAHRC, there is, again, (partial) overlap between the constructs that have been chosen as relevant and the constructs that were most associated with the achievement of the outcomes of the initiative. Interestingly, in the Browntown CLAHRC, the construct ‘conducting applied research’ is perceived to be a relevant causal factor whereas it is not considered to be relevant in the Bluetown and Greentown CLAHRCs. In particular, the Browntown collective map indicates that:
-
There is a two-way relationship between conducting applied research and collaboration between researchers and practitioners.
-
There is a two-way relationship between collaboration between researchers and practitioners and implementing findings in practice locally.
-
Collaboration between researchers and practitioners (a very central construct in this initiative) also leads to building capacity and to improving the quality of health care.
-
Reducing inequalities helps conducting research that considers local priorities.
-
Building capacity leads to implementing findings in practice locally.
Figure 22 portrays the relationships previously described.
FIGURE 22.
Browntown CLAHRC collective map (16 participants).
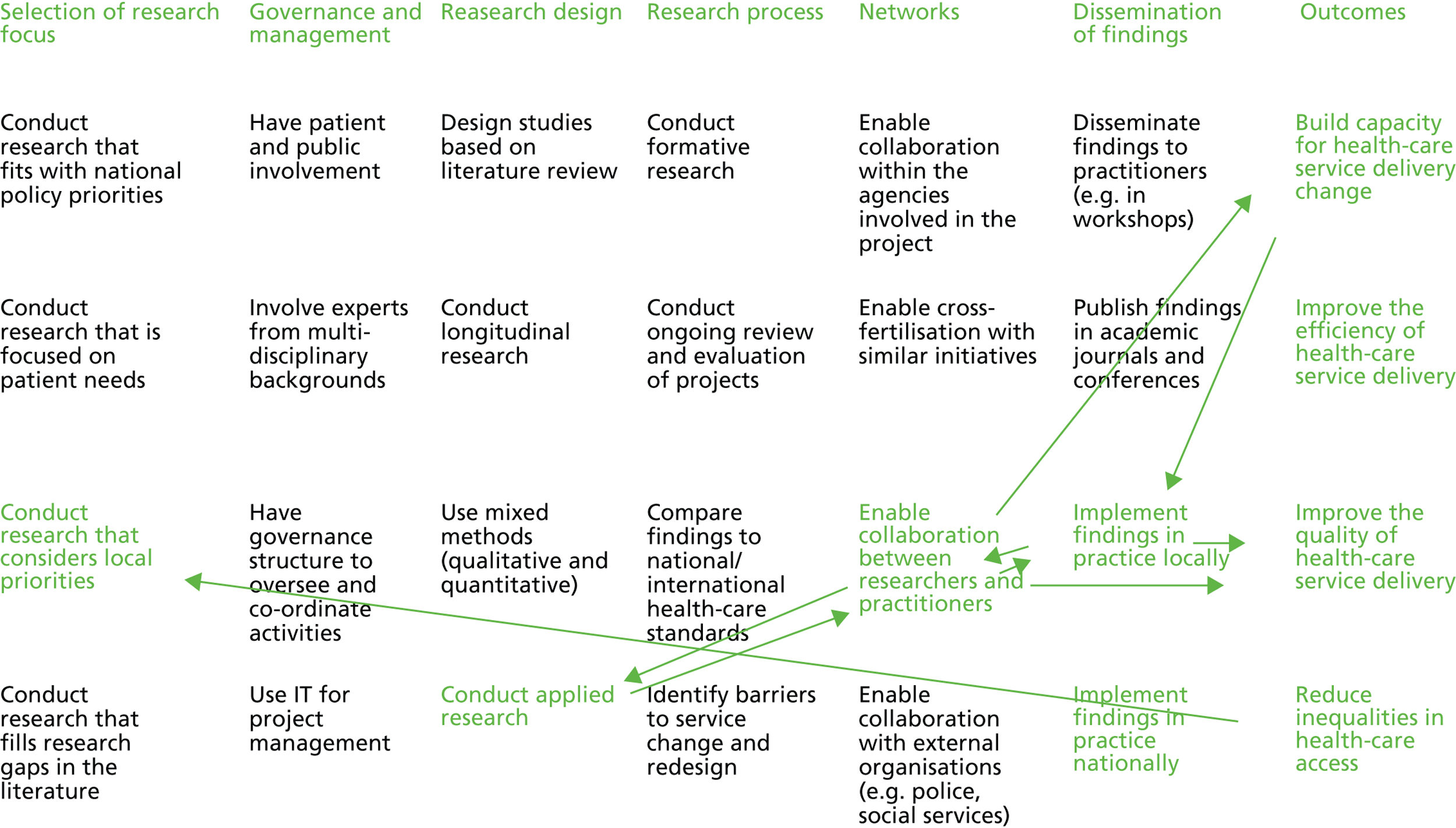
In terms of the quantitative approach, Table 26 illustrates the main statistics of the Browntown CLAHRC and compares this with the mean of all initiatives.
| Index | Browntown | Mean of all initiatives |
|---|---|---|
| Mean links strength | 6.05 | 5.244 |
| Mean ABS links strength | 6.05 | 5.265 |
| Standard deviation ABS links strength | 5.72 | 4.586 |
| Link density | 16.32 | 15.450 |
| Link strength density | 98.75 | 82.024 |
| Map density | 0.60 | 0.572 |
Table 26 indicates that the participants of the Browntown CLAHRC, similar to those of the Bluetown CLAHRC, have selected a relatively high number of links (and strengths). This is shown by the first three indexes. Moreover, the link density (and the link strength density) is high. The overall map density is objectively high (it is a value between 0 and 1) and it is also higher than the mean of the initiatives (0.600 vs. 0.572).
The statistical analysis can be interpreted as follows: (1) the similarity between the mean links strength and the mean ABS links strength shows that only few negative relationships were selected; (2) the first two indexes of the table show also that there are relatively strong links between the constructs (high mean link strength and high mean ABS); (3) relatively high standard deviation (if compared with the mean of the standard deviation for initiatives) indicates that the range of the values (1, 2, or 3) for the relationships of the construct is wider than the mean of all initiatives (more 2 and 3 rather than 1); this is similar to the Bluetown CLAHRC and differs from the Greentown CLAHRC; (4) the link density, link strength density and map density (above the mean of the initiatives) show that higher than average number of links are perceived as causally relevant, and where links are perceived as relevant they tended to be perceived as having a strong relationship (i.e. between inputs and outputs).
The Canada-Coordination pilot project, Ottawa
This map comprises 10 participants; the most relevant input constructs that were selected by the participants during the initial survey (see Chapter 3 , Research methods) are:
-
collaboration between partner organisations in the project
-
identification of barriers to service change and redesign
-
involvement of health-care and user representatives
-
involvement of experts from multidisciplinary backgrounds
-
conduct research that is focused on patient needs.
The most selected input constructs – that is, the constructs that are the most important drivers to achieve the objective of the pilot project – are:
-
conduct research that is focused on patient needs
-
involvement of experts from multidisciplinary background
-
conducting ongoing review and evaluation of the project
-
identify barriers to service change and redesign
-
collaboration between partner organisations in the project.
In the pilot project map, again, there is (partial) overlap between the constructs that have been chosen as relevant and the constructs that were most associated with the achievement of the outcomes of the initiative. In particular, the pilot project collective map indicates that:
-
Conducting research that focuses on patient needs leads to quality improvement.
-
Involving experts from multidisciplinary backgrounds leads to building capacity.
-
Collaboration within the agencies involved in the initiative leads to building capacity and improving efficiency.
-
There are two-way relationships between building capacity and identifying barriers to service change and redesign and between improving efficiency and identifying barriers to service change and redesign.
-
Conducting an ongoing review of the project helps improving the quality of health-care service delivery.
Figure 23 illustrates the relationships above described.
FIGURE 23.
Canada-Coordination collective map (10 participants).
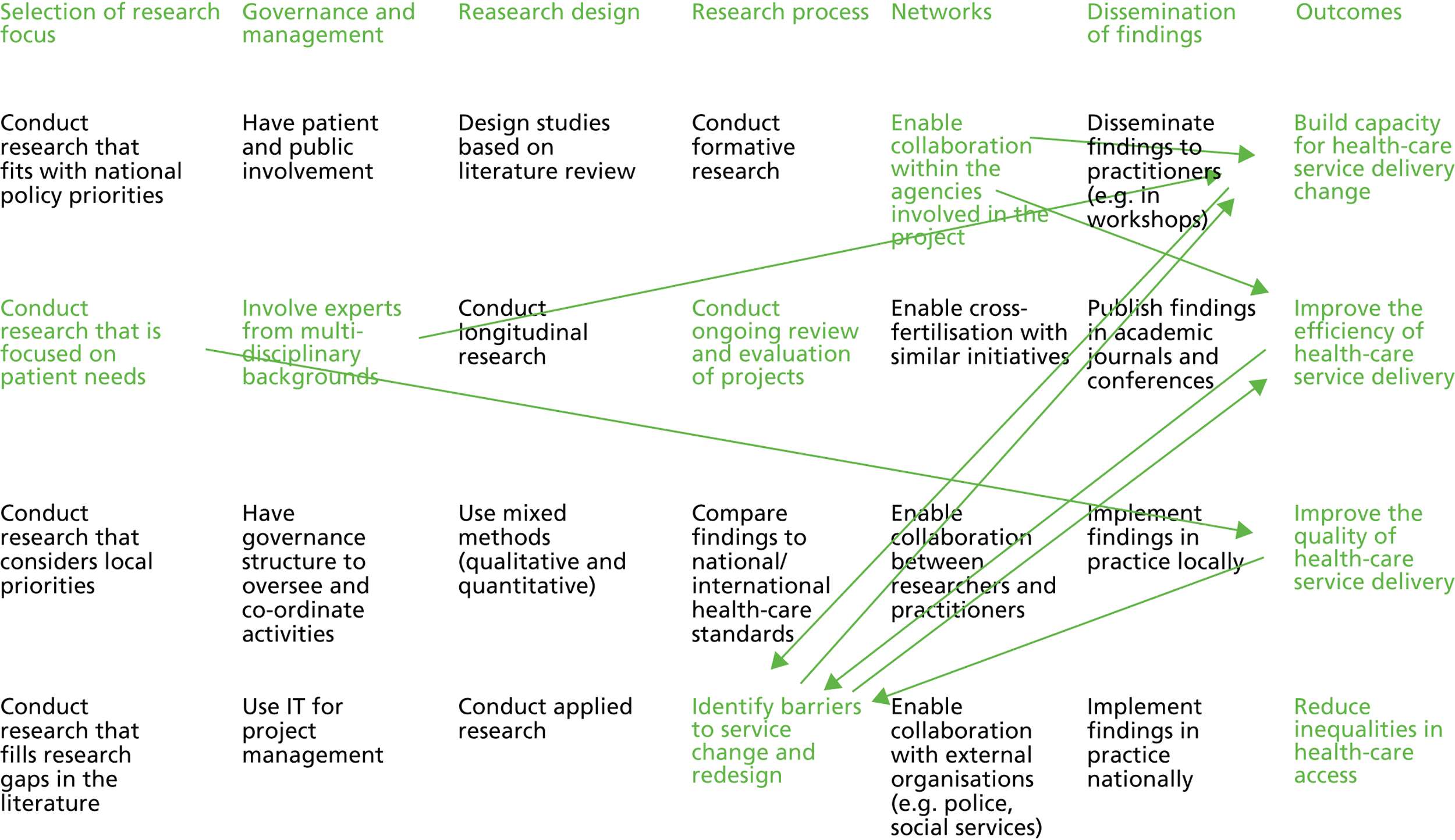
In terms of the quantitative approach, Table 27 illustrates the main statistics of the pilot project and compares this with the mean of all initiatives.
| Index | Canada-Coordination | Mean of all initiatives |
|---|---|---|
| Mean links strength | 4.81 | 5.244 |
| Mean ABS links strength | 4.81 | 5.265 |
| Standard deviation ABS links strength | 4.25 | 4.586 |
| Link density | 15.04 | 15.450 |
| Link strength density | 72.29 | 82.024 |
| Map density | 0.56 | 0.572 |
Table 27 indicates that the participants of the pilot project have selected a relatively low number of links (and strengths). This is shown by the first three indexes, which are all below the mean of all initiatives. Moreover, the link density (and the link strength density) is low. The overall map density is ‘average’ if compared with the other initiatives.
The statistical analysis can be interpreted as follows: (1) the equivalence between the mean links strength and the mean ABS links strength shows that almost no negative relationships were selected; (2) the first two indexes of the table show also that there are relatively weak links between the constructs (low mean link strength and low mean ABS); (3) relatively low standard deviation (if compared with the mean of the standard deviation for initiatives) indicates that the range of the values (1, 2 or 3) for the relationships of the construct is less wide than the mean of all initiatives (more 1 and 2 rather than 3); (4) link density, link strength density and map density are lower than average (compared with the other maps). This suggests that few associations were chosen and most of the associations that were chosen had low values (i.e. weak relationship between inputs and outputs).
Canada-Translation
This map comprises 11 participants; the most relevant input constructs that were selected by the users during the initial survey (see Chapter 3, Research methods) are:
-
conduct research that is focused on patient needs
-
involvement of experts from multidisciplinary background
-
collaboration between researchers and practitioners
-
conduct research that considers local priorities
-
involvement of health-care and user representatives.
The most selected input constructs – that is, these construct that are the most important drivers to achieve the objective of the pilot project – are:
-
conduct research that is focused on patient needs
-
involvement of experts from multidisciplinary backgrounds
-
collaboration between researchers and practitioners.
In the Canada-Translation map, there is complete overlap between the constructs that have been chosen as relevant and the constructs that were most associated with the achievement of the outcomes of the initiative. In particular, the Canada-Translation collective map indicates that:
-
Conducting research that focuses on patient needs is a central input; in fact, it leads to reducing inequalities, improving the quality, improving efficiency, and building capacity.
-
Involving experts promotes collaboration between researchers and practitioners and collaboration between researchers and practitioners helps to improve efficiency.
-
There is a two-way relationship between building capacity and enabling collaboration between researchers and practitioners.
Figure 24 illustrates the relationships described above.
FIGURE 24.
The Canada-Translation collective map (11 participants).
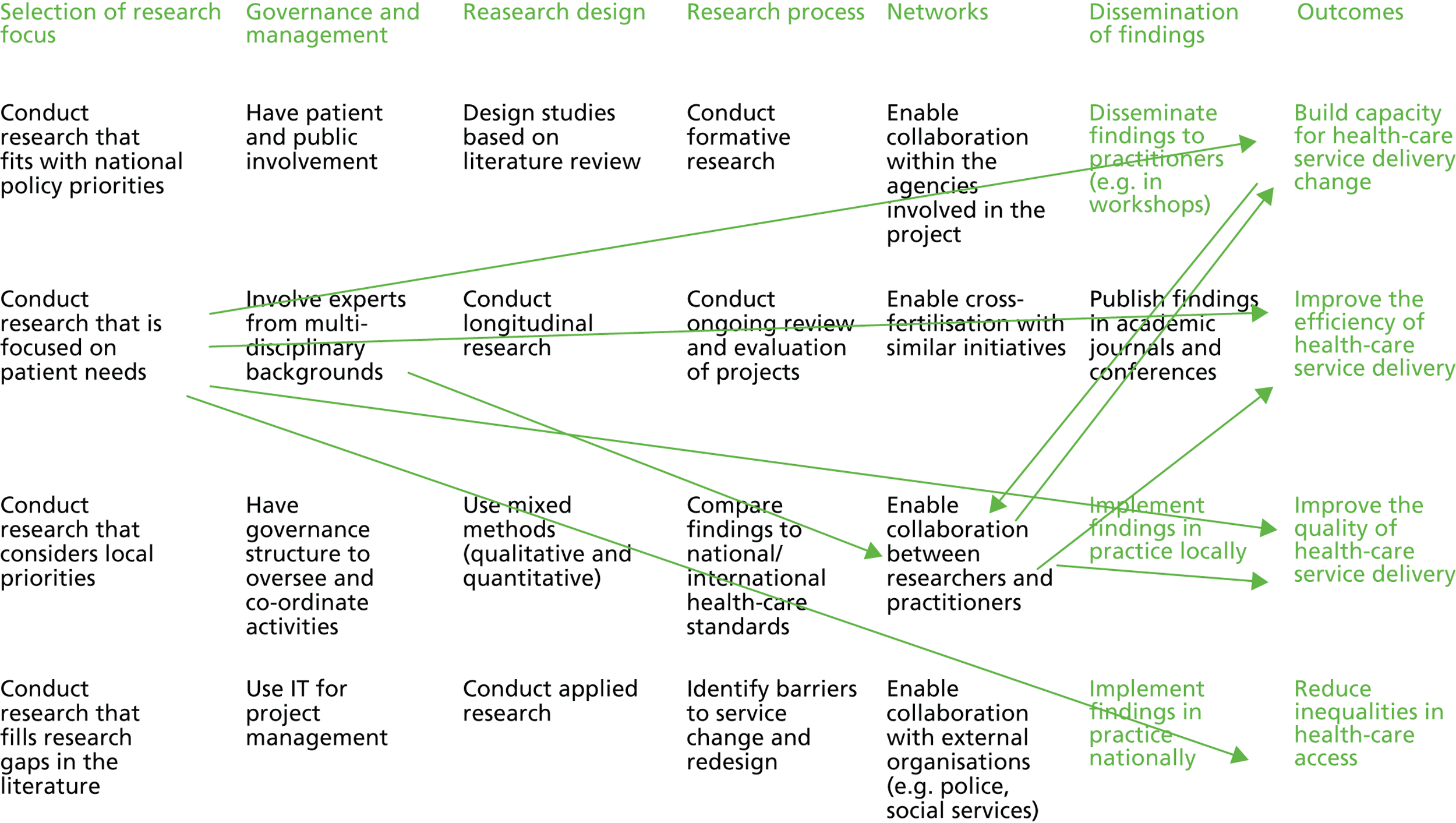
In terms of the quantitative approach, Table 28 illustrates the main statistics of Canada-Translation and compares this with the mean of all initiatives.
| Index | Canada-Translation | Mean all initiatives |
|---|---|---|
| Mean links strength | 4.16 | 5.244 |
| Mean ABS links strength | 4.18 | 5.265 |
| Standard deviation ABS links strength | 3.45 | 4.586 |
| Link density | 14.14 | 15.450 |
| Link strength density | 58.86 | 82.024 |
| Map density | 0.52 | 0.572 |
Table 28 indicates that the participants of Canada-Translation have selected a relatively low number of links (and strengths). This is shown by the first three indexes which are all below the mean of all initiatives. Moreover, the link density (and the link strength density) is low. The overall map density is the lowest if compared with the other initiatives.
The statistical analysis can be interpreted as follows: (1) the similarity between the mean links strength and the mean ABS links strength shows that only few negative relationships were selected; (2) the first two indexes of the table show also that there are relatively weak links between the constructs (low mean link strength, and low mean ABS); (3) low standard deviation (if compared with the mean of the standard deviation for initiatives) indicates that the range of the values (1, 2 or 3) for the relationships of the construct is less wide than the mean of all initiatives (more 1 and 2 rather than 3); (4) with respect to the other maps, the link density, the link strength density and map density are very low. This suggests that fewer than average associations were chosen and most of the associations that were chosen had low values (weak and medium relationships between inputs and outputs).
List of abbreviations
- ABS
- absolute value
- CIHR
- Canadian Institutes for Health Research
- CLAHRC
- Collaboration for Leadership in Applied Health Research and Care
- COPD
- chronic obstructive pulmonary disease
- CQRS
- Quebec Social Research Council
- CYP
- children and young people
- E-I
- external-internal
- KT
- knowledge translation
- NIHR
- National Institute for Health Research
- OASC
- Ottawa Association to Support Children
- QA
- quality assessment
- QUERI
- Quality Enhancement Research Initiative
- RCAC
- Regional Community Care Access Centre (Canada)
- REC
- research ethics committee
- SDO
- Service Delivery Organisation
- SNA
- social network analysis
- SPOC
- single point of care
- SS
- Social Services (Canada)
- TaCT
- Telehealth & Care Technologies
- TIA
- transient ischaemic attack
- VP
- vice president