

Notes
Article history
The research reported here is the product of an HS&DR Evidence Synthesis Centre, contracted to provide rapid evidence syntheses on issues of relevance to the health service, and to inform future HS&DR calls for new research around identified gaps in evidence. Other reviews by the Evidence Synthesis Centres are also available in the HS&DR journal.
The research reported in this issue of the journal was funded by the HS&DR programme or one of its preceding programmes as project numbers 16/47/22, 16/47/17, 16/47/11. The contractual start date was in April 2017. The final report began editorial review in March 2021 and was accepted for publication in May 2021. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HS&DR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Permissions
Copyright statement
Copyright © 2021 Anderson et al. This work was produced by Anderson et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaption in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2021 Anderson et al.
Chapter 1 Background
Systematic reviews for policy and service improvement
For systematic reviews to be useful, rigorous and deliverable within given resources, they need to articulate a well-defined review question. The bold advice in one of the more authoritative methods textbooks in the field is ‘Never start a systematic review until a clear question (or clear questions) can be framed’. 1 Useful, deliverable systematic reviews also require an appropriately bounded set of inclusion criteria that together describe the nature of the evidence and types of studies that should answer the review question. 1–3 The review question and inclusion criteria form the core information of systematic review protocols, driving the specification of subsequent aspects of the methods (i.e. search strategies, data extraction plans, tools for study quality assessment and strategy for evidence synthesis). In turn, prespecified and registered systematic review protocols seek to assure rigour and transparency in the conduct of systematic reviews. 4
Policy-makers and service commissioners frequently express a desire to use evidence, but acknowledge that they often lack the time or relevant skills to explore and specify which type of research evidence would best inform a policy or service commissioning choice. Therefore, teams of experienced systematic reviewers and information specialists are often commissioned to undertake such responsive review work with and for them. The model of having university-based research centres, commissioned for a number of years to conduct highly applied work for the Department for Health and Social Care (DHSC), National Institute for Health and Care Excellence (NICE) or the National Institute for Health Research (NIHR), is a key feature of the applied ‘evidence ecosystem’ to inform UK health services and policy. For example, there are long-term arrangements for commissioning systematic reviews or model-based economic evaluations to support NICE technology appraisals and policy-making in the DHSC (e.g. Policy Research Programme evidence review facilities).
The NIHR’s Health Services and Delivery Research (HSDR) programme first commissioned two evidence synthesis centres in 2013, and then three centres from 2017 to 2020 [the University of Exeter (Exeter, UK), University of Sheffield (Sheffield, UK) and University of York (York, UK)-based teams that produced this report]. 5 The aim of these centres has been to ‘produce evidence syntheses which will be of immediate use to the NHS in order to improve the quality, effectiveness and accessibility of the NHS including delivery of services’. 5 The review topics are specified by the HSDR programme, and:
. . . will be areas of importance to the service, where there is a reasonable level of published evidence but these may be dispersed, with useful lessons for the NHS from other sectors, countries or a broad range of literature. The finished products are designed to summarise key evidence for busy managers and clinical leaders, while evaluating the quality of information and strength of findings. The aim is for an authoritative single-source document, which provides simple top-line messages in complex areas.
. . . The output will be an evidence synthesis – that is, a comprehensive review of published literature with explicit search strategy, appropriate range of sources and critical assessment of quality of evidence and strength of findings.
Between 2017 and 2020, our three research centres were commissioned to conduct evidence syntheses that respond to specific health policy-makers’ and service commissioners’ needs. Typically, we were tasked, at short notice, to conduct a systematic/rapid review of evidence on a service delivery/design health-care topic, following the identification of a need for evidence on that topic by a policy or commissioning lead or team within the DHSC or NHS England.
Scoping within systematic reviews
The scoping stage of a review comprises those initial processes that aim to establish or refine the review questions and determine the review’s scope, such as its area of focus, key terms and types of studies to be included. (It is potentially confusing that a scoping review is a particular type of review method and evidence end-product.) In general, the scoping stage seeks to reconcile the twin goals of asking the ‘right review question’ (to best address user needs) and making the best use of available research and other evidence. To be useful, systematic reviews frequently have to negotiate a compromise between these two goals, answering questions that are close to the user’s needs, but also being confident that evidence of adequate quantity and quality exists. This report aims to share the lessons learned from our varied experiences of managing this compromise within the NIHR HSDR programme’s remit, primarily to inform health-care commissioning and delivery in the UK.
This report's focus was initially suggested by the lead author (RA) at our annual HSDR Evidence Synthesis Centres meeting, in May 2019. After further discussion by e-mail, we chose this focus for our joint final report because we felt, collectively, that question formulation and review scoping are (1) critically important stages and processes in ensuring the quality and usefulness of responsive reviews, (2) review stages for which few explicit ‘methods’ or detailed guidance exists (see next section), and they are also (3) rarely described in journal articles or reports of reviews and systematic reviews. We also wanted to explore, for the benefit of our own teams and others that conduct policy-/service-responsive reviews, whether or not it is possible to specify ‘best practice’ principles and approaches to question formulation and review scoping on the basis of our experiences.
Established principles for scoping and developing review questions
This section summarises the guidance from established textbooks and guides on the methodology and conduct of high-quality systematic reviews in the health-care field or more broadly in the social sciences. Table 1 shows the degree of coverage of methods or principles for question formulation and scoping provided in the established textbooks and guides most used by and familiar to the members of the three review teams.
| Source | Coverage of how to develop or decide review questions? | Other guidance on best practice for scoping? |
|---|---|---|
| Boland et al.6 | Contains an 18-page chapter on ‘defining my review question and identifying inclusion and exclusion criteria’. Outlines a six-step process from identifying a topic of interest to writing a review protocol | ‘Consider contacting experts in the topic area’ is only step five of six scoping steps, revealing the student-oriented focus of the text |
| Booth et al.7 | Contains a 24-page chapter ‘Defining your scope’ (pp. 83–107), which includes defining your scope with an audience in mind, the specific requirements for complex interventions, further defining your scope (mapping and data mining) and challenges and pitfalls | Chapter 3 on ‘Choosing your review methods’ includes a box (box 3.1) on ‘what do we mean by scoping’? |
| Higgins et al.8 | Contains a chapter (chapter 2) on determining the scope of the review and the questions it will address (pp. 13–32) | Chapter 2 also includes brief coverage of involvement of stakeholders and use of conceptual models |
| CRD9 | Contains a four-page section on ‘Review question and inclusion criteria’ (under ‘Key areas to cover in a review protocol’), but describes how good effectiveness review questions should be framed and presented, rather than the process of how to develop them | Contains a section on conducting scoping searches to check that a systematic review of the same or overlapping question has not already been conducted |
| Gough et al.10 | Chapter 4, ‘Getting started with a review’, of Gough et al.10 (pp. 71–92) includes building the scope through use of conceptual frameworks and choosing review methods, scale and timescale | Includes a complete chapter on stakeholder perspectives and participation in reviews, and covers the entire review process, including clarifying the problem and question |
| Petticrew and Roberts1 | Contains a seven-page section on ‘Framing the review question’ (pp. 28–34) and includes a section on ‘Framing policy issues and answerable questions’ |
Chapter 2 is titled ‘Starting the review: refining the question and defining the boundaries’ Other sections in chapter 2 consider when a systematic review should be carried out and when they are most valuable |
Although most methodological guidance on the conduct of systematic reviews offer coverage and consideration of how to develop review questions and agree the scope of a review, others start with the review question as already given. For example, both the Centre for Reviews and Dissemination guidance9 on conducting systematic reviews in health care and the Cochrane handbook by Higgens et al. 8 give very little guidance on scoping and developing review questions, beyond the need to conduct searches to confirm that an identical or overlapping systematic review is not already published or in progress.
Petticrew and Roberts1 indicate the importance of asking the ‘right review question’ when deciding whether or not a new systematic review would be appropriate and useful. The authors also list situations when conducting a systematic review may not be appropriate (Box 1).
-
High-quality systematic reviews already exist on the same topic.
-
A systematic review on the same topic is already being conducted.
-
The review question is too vague/broad.
-
The review question is too narrowly scoped and, therefore, unlikely to be useful.
-
There are insufficient resources to conduct a reliable systematic review.
Summary of box 2.2 in Pettigrew and Roberts. 1
More positively, Petticrew and Roberts1 describe the importance of finding and using previous systematic reviews and, if resources allow, conducting scoping searches to see what sorts of studies and what number of primary studies exist in relation to a potential review question. They go on to assert that policy questions may often be quite broad and that work is usually required to decide which questions it would be most useful to answer. The authors imply that this often involves ‘working back’ from the types of available evidence and the disciplines that have produced them. 1
Advice offered by these texts often also includes breaking down the question into common components. Typically, for effectiveness review questions, these are its PICOS [population (or patient type), intervention, comparator, outcomes, study types] components. 2,3,7 This exploration and breaking down is also framed as developing a conceptual framework for a systematic review. 3 To give direction and corroboration to these decisions, several authors strongly suggest setting review questions jointly with the intended users of the review and also involving them in developing the review protocol. 1,3 However, beyond such general advice, the texts offer limited specific, practical guidance on the principles or process of negotiating a path to the ‘right’ review question and inclusion criteria. Our experience as systematic reviewers within our teams also underlines that we have never been ‘taught’ or learned ‘formal methods’ for conducting these important stages of reviews, but have mainly learned through experience of conducting many commissioned and responsive reviews and engaging directly with the intended review users/commissioners.
An initial model for understanding the scoping process
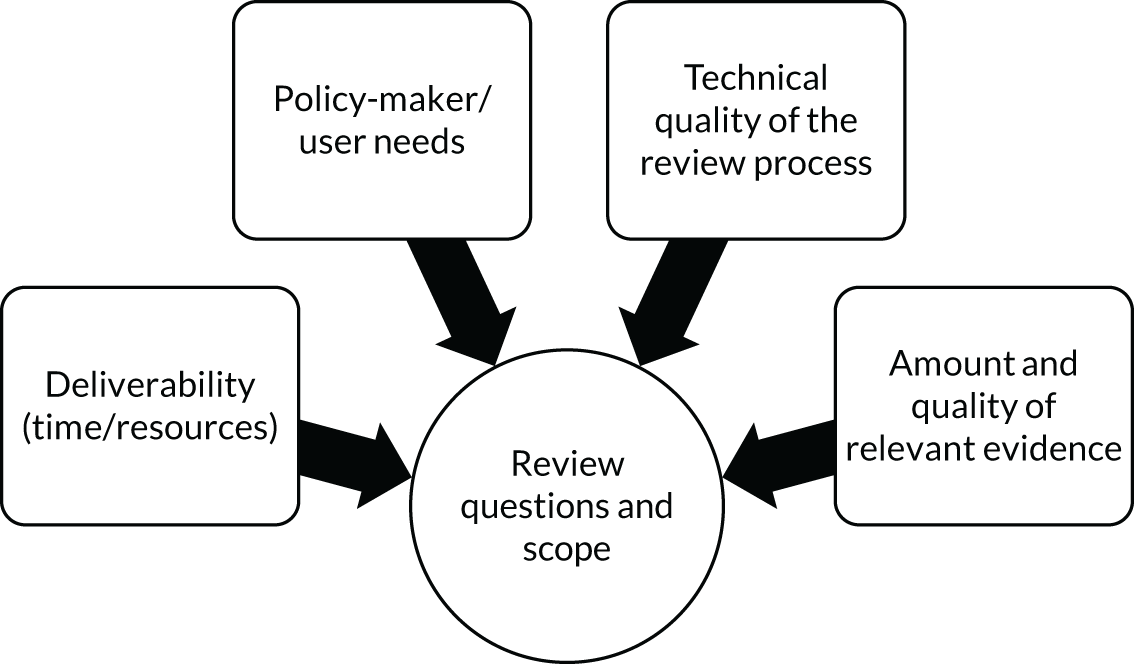
To help guide our descriptions, discussions and reflections on scoping processes, we devised a simple model to depict the interaction of the stakeholder and other main considerations that determine review questions and review scope (Figure 1). Essentially, this combines the drivers associated with rigour (i.e. technical quality) and relevance (to policy-maker and user needs), alongside logistic concerns relating to deliverability (i.e. time/resources) and empirical considerations (i.e. amount and quality of relevant evidence). Acknowledging that quality extends beyond technical quality to include the perceptions of the policy-makers and users of the utility of each review product, the model can be seen to partly embody a specific application of the reconciliation of time, quality and money (as previously identified in Booth et al. 7).
FIGURE 1.
Basic model of key factors in systematic review scoping.
Aim of this report
The aims of this work and report were to:
-
describe six or more varied examples of recent scoping processes that were required to shape and specify responsive systematic reviews conducted by the three HSDR evidence synthesis centres
-
provide reflective commentary on the different choices, sources of information and advice that shaped the review question(s) and scope for each review
-
provide an overarching summary and set of principles or lessons for effective scoping of rapid and responsive systematic reviews.
We intended that these principles would apply to reviews when they are commissioned at short notice and with limited time for completion, and to meet specific health-care policy/commissioning needs. We sought to compare these principles and lessons with current authoritative advice on developing review questions and the scoping stage of systematic reviews.
Discussion of these aims revealed a shared interest in the need to reconcile, on the one hand, technical or ‘data-driven’ aspects of scoping the evidence for potentially answerable questions and, on the other hand, the collective learning processes required to develop an understanding of a new topic, and to build relationships with stakeholders and potential users of the review. As one co-author framed it, we sought to cover:
. . . technical issues of scoping (e.g. scoping searches and preliminary desk research) and the softer issues of consultation as they specifically relate to topic identification and scoping and could include our relationships with variously the generator of the initial topics (as appropriate), the HSDR team, patient/public representatives and those delivering services.
Personal communication between authors (Anderson et al. ), 2020
At the same time, we were mindful that the previous report and paper, which was based on these centres’ work (from 2014 to 2017), had mainly reflected on the role of stakeholder engagement in such responsive and service-/policy-oriented reviews. 11 The main findings from that previous review of the HSDR centres’ earlier review projects are shown in Box 2.
Rapid production of high-quality outputs is facilitated by initial evidence mapping and topic scoping.
Barriers to prioritising the topic and defining the scope were: review team knowledge of the wider NHS/policy context; ability to define a scope that was both relevant and manageable.
Staying on track with the review was facilitated by: the ability in the team to deal with unexpected findings or problems; the commitment of individuals to support the project (especially external stakeholders).
Responsive working with stakeholders was also facilitated by: producing and disseminating appropriate outputs; the timeliness and topicality of outputs; producing or capturing evidence of impact.
Involvement of stakeholders at key stages maximises value and potential for impact but the impact of evidence on decision-making remains poorly documented.
Responsive evidence synthesis programmes should seek the optimum balance between decision-makers’ needs for rapid and efficient evidence synthesis and the time and resource requirements of rigorous systematic reviews.
Reproduced with permission from Chambers et al. 11 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/. The box includes minor additions and formatting changes to the original.
We aimed for our new collective methodological reflection to complement rather than duplicate that work. We believed that new and valuable insights might emerge from a systematic focus on the processes of topic scoping and review question formulation, which are rarely described in academic outputs of systematic reviews.
For the purposes of this reflective exercise, the scoping processes of a review were specified as those that occurred between the time of first notification of a new review topic and the final agreement of the review protocol (with the NIHR HSDR programme and policy customer), including final review questions, inclusion criteria and the type of planned evidence synthesis.
Chapter 2 Methods
Overview
This report presents, discusses and reflects on the experiences of the three research centres that conducted evidence syntheses to inform health and social care service organisation and delivery in the UK between April 2017 and June 2020. These responsive and often rapid reviews were commissioned by the NIHR HSDR programme, although the direct customers and audiences of different reviews included policy-makers, service commissioners, service providers and managers, or particular types of care professionals working in the UK health and social care sector.
This discussion and reflection on our experiences of the process of review scoping and review question formulation is based on the following:
-
the collation and writing of eight descriptive case studies of selected reviews within each of the three teams
-
a broad and basic thematic analysis of key issues or common considerations that shaped the processes of review scoping and question formulation
-
a discussion and reflection on the overall process and practice of scoping for such policy, service and practice-responsive evidence syntheses.
The process comprised within-centre reviewing of documents, review team recollection, reflection and discussion (to produce the descriptive case studies) and between-centre discussion and reflection on our shared experience of scoping selected review topics, primarily through consideration of each other’s experiences, as written in the case studies.
We did not explicitly aim to document how our centres and teams differ in academic experience, team organisation or working practices; however, from past collaborations and experience (e.g. on public health reviews and technology assessments) we typically learned that we worked in similar ways in most respects. The HSDR centres at Exeter and York had smaller core teams that conducted most of the work on every review project; however, the Sheffield team typically made use of a wider group of researchers, with different people working on different reviews. Otherwise, we were not aware of major differences in how review teams within the three centres worked.
Choice of case study reviews
In May 2020, all researchers (the co-authors) in each of the three centres were e-mailed and asked to select two or three examples of their reviews, commissioned since April 2017, where ‘the scoping was challenging, interesting, and demonstrates a variety of approaches, or where the teams believe it was particularly critical to the ultimate delivery, quality and usefulness of the review’. The final number provided by each centre reflected the diversity of topics covered and challenges faced, but also the capacity and time resources of the researchers within teams to create these retrospective accounts of scoping. All case studies suggested by centres were written up and included.
Data sources and process
Exploration of the scoping processes for each case study drew on a combination of researcher recollection, review of notes and meeting minutes (e.g. with expert stakeholders) from within teams, e-mail correspondence with stakeholders, scoping searches and search results, from first allocation of a review topic through to review protocol agreement (with the NIHR HSDR programme or the policy customer). However, the extent to which the case study was grounded in or checked against documentary evidence (e.g. notes of meetings with service commissioners or HSDR contacts), rather than the recollections of review team members, was not rigorously documented. In most cases, the initial draft was written by one lead researcher, before elaboration and revision by other members of that review’s team.
Case study content
To simplify the process of writing and to best enable cross-case comparisons, we sought a similar structure and level of content for each case study. A draft case study was prepared by the Exeter team and shared across all three teams with a proposed set of headings and content:
-
introduction of the basic context and origin of each review and topic (identifying the review team, the supporting protocol and main academic output)
-
a statement of the final review questions or aims
-
a description of the key challenges or choices during scoping, plus key decisions made in response to them, to illustrate how the team moved from an original review topic to specific review questions and the detailed review approach
-
a (within-case) reflection and discussion section.
This broad structure was agreed by all co-authors for use in all case studies, although identification of key challenges and key decisions was not constrained to the subheadings.
Thematic analysis
Drafts of all eight case studies were shared across the three teams prior to a joint teleconference. One of the co-authors (AB) drafted a provisional thematic analysis based on reading these drafts. This framework of 14 distinct scoping considerations was informed by earlier conversations on the focus of the report, which had identified the combined influence and inter-relationships between stakeholder-/user-related factors and review team/technical factors. It also drew on factors identified in a systematic review of evidence use by policy-makers12 and sought to reflect the twin emphases of an associated report for policy-makers and systematic reviewers. 13 Finally, the conceptual model was informed by the RETREAT (Review question, Epistemology, Time/Timescale, Resources, Expertise, Audience and purpose, Type of data) framework of review considerations, with review question, epistemology, and audience and purpose collectively reflecting the user-related factors; and time, resources, expertise and type of data capturing the technical requirements. 14 The RETREAT framework was developed (by co-author AB) from an analysis of the attributes of qualitative evidence synthesis methods in 26 methodological papers, and has been shown to both distinguish and inform selection of synthesis approaches. 15
The initial tabulation of scoping considerations organised themes according to whether or not they primarily related to:
-
consultative issues (i.e. externally generated issues relating to input from commissioners, stakeholders, experts and patient groups to inform the planned evidence synthesis product)
-
interface issues (i.e. issues relating to the interaction between the technical processes of the review team and the requirements of the review user)
-
technical issues (i.e. internally managed issues relating to the conduct of the review, as experienced within the review team).
The first draft of the thematic framework was shared with all co-authors and commented on using e-mail and tracked changes. It was also discussed in a teleconference. This led to several revisions of wording and clarified definitions, but all 14 originally suggested considerations in the framework were retained and no new ones added. The framework was used by the lead author to allow similarities and differences in scoping processes and outcomes to be more easily identified as a basis for drafting this report’s discussion. Co-authors were also encouraged to consider the framework in relation to reviews that they had contributed to, which enabled further mapping of these scoping considerations to the case study reviews.
Ethics considerations
As this report is not based on any formal process of data collection and analysis, and did not formally recruit any participants from which data were obtained (e.g. interviews), it would not be defined as research and, therefore, did not require research ethics approval. The main contributors were the team members and co-authors of this report. Nevertheless, the scoping processes described in this report sometimes closely involved other individuals within the NIHR, DHSC and other national and regional organisations linked to NHS service commissioning and delivery. Although such individuals are potentially identifiable from the report and the underlying review reports of the eight case study reviews, in all cases, we ensured that the degree of anonymity in this report was the same as in the report already in the public domain.
Chapter 3 Results
The eight case studies feature the scoping stages of evidence syntheses conducted by the HSDR Evidence Synthesis Centres between 2017 and 2020: three cases from the University of Exeter, three from the University of Sheffield and two from the University of York. Table 2 shows the considerable diversity of topics and types of synthesis method that these case studies covered. Please note that for ‘synthesis type’ we have used the terminology used in the source project and report, and that there is some variation and overlap in use of terms. In particular, evidence maps and mapping reviews are essentially the same in purpose and final product, and scoping reviews (as a defined product) should be distinguished from the scoping stage and processes that are the focus of all of the case studies. In addition, most of these named subtypes of evidence synthesis are also systematic reviews (in the sense that they had clearly defined questions and explicit methods for identifying, assessing and summarising included evidence sources). We have decided to retain the terms as used in each case study review, rather than to retrospectively impose a standardised typology. Further details of the specific synthesis methods used in each case study review, the rationale for their choice and any patient and public involvement (PPI) are in Appendix 1, Table 13.
| Short name | Centre | Population | Intervention/phenomenon | Comparator | Outcome/domain of performance | Study or publication types included | Synthesis type |
|---|---|---|---|---|---|---|---|
| 1. Digital-First Primary Care | York | Primary care medical staff and patients (or their caregivers) | Digital/non-face-to-face systems for accessing primary care and receiving care | Conventional systems | Effectiveness and safety, patient access/convenience, system-level efficiencies and related issues, such as workforce retention, training and satisfaction | Systematic reviews, meta-analyses and other forms of evidence syntheses |
Scoping evidence map Rapid evidence synthesis |
| 2. MHA | Exeter | People detained under the MHA, their family and carers and the individuals involved with their care | Specific legal provisions for involving trusted relatives or friends in decisions about detention or care | Not applicable | Experiences of care, especially dignity, confidentiality and feeling supported | Qualitative research studies | Rapid framework synthesis |
| 3. Integrated care regulation and inspection | York | Any users of integrated health and social care | Regulation and inspection of integrated care, including integration between primary and secondary care | No/less regulation/inspection (implicit) |
Effectiveness (any outcome relevant to integrated care) Implementation (barriers and enablers) Description of innovative regulatory models or frameworks |
Empirical publications (qualitative and quantitative) and non-empirical publications | Rapid scoping review and evidence map |
| 4. Social care access and diversity | Sheffield | Ethnic minorities and LGBT+ people with social care needs | Personal, social and cultural factors | Any or no comparison | Access to social care | Any study design | Rapid realist review |
| 5. Strengths-based approaches | Exeter | People being supported by social workers or adult social care teams | Strengths-based approaches to social work practice | Any area, service or teams of social workers that have not adopted the given strengths-based approach |
Any effectiveness measure used (intended outcomes) Markers of implementation |
Comparative empirical evaluations (question 1) Qualitative or mixed-methods studies (question 2) |
Framework synthesis |
| 6. Reducing length of stay | Exeter | Hospital inpatients (planned admissions) aged ≥ 60 years | Multicomponent hospital-led interventions that aimed to reduce length of stay or enhance recovery | Any type of control group or comparator (e.g. usual hospital care) | Effectiveness and cost-effectiveness | RCTs, controlled before-and-after studies and interrupted time series | Systematic review of effectiveness and cost-effectiveness |
| 7. Interventions to reduce preventable hospital admissions | Sheffield | Adults with a cardiovascular or respiratory condition (not cancer) | Implementation of evidence-based interventions to reduce preventable hospital admissions (or re-admissions, or combinations of these interventions) | Any or no comparator | Implementation in the context of the NHS at the patient, GP and health system level (e.g. barriers and facilitators, staff or patient views/experiences) |
UK experimental intervention studies Sampling from mapping review and wider evidence base (including controlled/uncontrolled observational studies, qualitative studies and systematic reviews) |
Mapping review and realist synthesis |
| 8. Access to services for adults with IDs | Sheffield | People aged ≥ 16 years with IDs | Actions, interventions or models of service provision in primary health-care services | The general population | Access to primary health-care services and barriers to and facilitators of accessing and using services | Qualitative research, comparative literature, evaluation studies and systematic reviews | Mapping review and systematic review |
The case studies that started with a clearly known policy customer/decision-maker and with a clearly stated review question or evidence gap/need are presented first, through to those that had neither a clearly stated policy customer nor a clear initial question. In this way, the order of presentation of the case studies should, in principle, move from those with clearer predefined initial scopes to those with more open-ended and uncertain scopes. The classification of case studies according to these two criteria is presented in Table 3.
| Degree of clarity in initially stated review question | Known main policy customer/decision-maker | Unspecified main policy customer/decision-maker |
|---|---|---|
| Very clear |
Digital-First Primary Care (York HSDR Evidence Synthesis Centre) MHA16 (Exeter HSDR Evidence Synthesis Centre) |
Integrated care regulation and inspection (York HSDR Evidence Synthesis Centre) |
| Some clarity |
Social care access and diversity (Sheffield HSDR Evidence Synthesis Centre) Strength-based approaches (Exeter HSDR Evidence Synthesis Centre) |
|
| Unclear (just a topic area) |
Reducing length of stay (Exeter HSDR Evidence Synthesis Centre) Interventions to reduce preventable hospital admissions (Sheffield HSDR Evidence Synthesis Centre) Access to services for adults with IDs (Sheffield HSDR Evidence Synthesis Centre) |
Case study 1: rapid evidence synthesis of ‘Digital-First Primary Care’
This topic was given to the HSDR Evidence Synthesis Centre at York, having been identified as an urgent topic from an NHS England primary care workshop that focused on digital aspects of care. The York team had not been involved in the workshop and so sought further information from NHS England about evidence requirements and scope. Following initial clarification and discussion with representatives from NHS England in June 2018, the team undertook a rapid, responsive evidence synthesis between July and December 2018. Throughout the project, the York team maintained e-mail and telephone contact with a senior policy lead in the new business models team of NHS England’s Strategy and Innovation Directorate. This person co-ordinated the involvement of representatives from other teams (e.g. primary care).
The protocol was posted on the team’s webpage,17 as it was not eligible for registration in PROSPERO. The final report was published in full18 and a brief evidence summary produced. 19
The original questions articulated at the workshop were as follows:
-
What are the most effective automated systems management approaches that result in high levels of general practitioner (GP) engagement?
-
How do you present data to ensure change in practice?
-
What are the barriers to and motivators of using digital technology that drive cultural and behavioural change within primary care practitioners?
Following initial discussions with NHS England, which identified a broad and far-reaching list of themes and questions, an iterative production process was agreed to undertake the work in stages. We presented the findings after each stage to discuss progression onto the next stage. After the discussions that followed the second stage, the work was concluded and the report completed.
The rapid responsive evidence synthesis was undertaken to inform NHS England policy in ‘Digital-First Primary Care’. The principles and some aspects of systematic review methodology were applied to ensure transparency and reproducibility. The two stages of the synthesis consisted of (1) scoping the published review evidence and (2) addressing a refined set of questions produced by NHS England from the evidence retrieved during the scoping stage. Given that ‘a full systematic review was not possible, given the time and resources available’, the team ‘conducted a rapid synthesis of the most relevant evidence identified during the scoping exercise (stage 1) to establish if and to what extent these questions can be answered by the identified research’. 18 Patient and public representatives were not directly involved in the development of the synthesis aims, methods or interpretation.
The following questions were addressed in the second stage:
-
What are the benefits – to patients, GPs and the system – of digital modes and models of engagement between patients and primary care?
-
As GP workload and workforce is the main threat to primary care, how do we use these innovations to alleviate this, rather than only increasing patient convenience and improving their experience?
-
Which patients can benefit from digital (online) modes and models of engagement between patients and primary care?
-
What channels work best for different patient needs and conditions?
-
Are there differences in synchronous and asynchronous models?
-
-
How do you integrate ‘digital first’ models of accessing primary care within wider existing face-to-face models?
-
How do you contract such models and how do you deliver them (what geography size, population size)?
The final inclusion criteria were as follows:
-
population – any primary care medical staff and patients (or their caregivers) of any age and/or other medical professionals
-
interventions – as the known literature rarely conceptualised interventions as ‘digital primary care’, any form of non-face-to-face interaction, including e-mail, online/video, messaging and artificial intelligence-led systems or triage (or any of these alongside telephone consultation)
-
outcomes – impact on care in terms of effectiveness and safety, patient access/convenience (including which patients are able to use digital consultations and what conditions are appropriate for non-face-to-face engagement), system-level efficiencies and related issues, such as workforce retention, training and satisfaction
-
study design – systematic reviews, meta-analyses and other forms of evidence syntheses (any related primary studies encountered were included where relevant, although primary research evidence was not systematically searched).
Summary of key challenges/choices and scoping decisions
Challenge 1: clarifying the questions of interest and deciding the most appropriate method of synthesis
The brief topic outline we were given at the start of the project was broadened and expanded during the initial communications with NHS England. They were interested in patient-focused digital innovation in primary care and identified four broad themes and nearly 20 separate questions for which they wanted answers. The questions were wide-ranging, covering issues of contracting and implementation, as well as effectiveness, cost-effectiveness, benefits and risks. They reflected the interests and priorities of the various sections of NHS England involved in implementing ‘Digital-First Primary Care’.
It became clear in these discussions that it was not possible, at that stage, to identify a clear and focused research question (or questions) of high priority to NHS England that was amenable to evidence synthesis. Instead, we identified the need for a responsive and iterative approach to support the needs of the policy-makers.
We adopted a multistage approach to the work. We began by searching the research literature to scope available evidence syntheses. We extracted the key characteristics of all included documents and produced an interactive database of published and ongoing evidence that could be ordered or filtered according to these characteristics, incorporating links to the full-text versions where available. We produced an interim report that summarised the key evidence identified in this scoping exercise, along with an annotated bibliography and the interactive spreadsheet.
We presented the interim report to NHS England and asked them to decide whether it provided the information they needed or if a gap remained to be addressed by further rapid evidence synthesis. NHS England responded with seven questions that reflected specific ‘live’ policy areas in which they were most interested. Therefore, we undertook a second stage and conducted a rapid synthesis of the relevant evidence identified from the stage 1 scoping exercise with the seven research questions identified by NHS England, forming the basis of a thematic framework. Critical appraisal of included evidence was facilitated by relevant assessment tools and reporting standards used to inform judgements about the internal and external validity of included research results presented in the thematic synthesis.
We produced a report that combined both the initial scoping exercise and the rapid synthesis undertaken at stage 2. Again, we presented the findings through a summary report and teleconference to representatives from various NHS England teams (e.g. new business models, primary care, digital and workforce). Following this presentation, and the subsequent discussions, the topic was concluded.
Summary of response to challenge
We needed to adopt an iterative, responsive approach to this topic and revise our methodology accordingly. The initial scoping exercise was undertaken to provide a high-level overview of the available evidence, followed by a rapid evidence synthesis. A full systematic review was not possible, but aspects of systematic review research methodology (such as a priori inclusion criteria, critical appraisal of included evidence, and process measures to avoid bias and errors) were applied to introduce a level of transparency and reproducibility.
Challenge 2: identifying and incorporating recent and ongoing research
As a result of the initial scoping exercise and discussions with other researchers working in the field, we became aware of recent and ongoing projects, as well as two open NIHR calls for a proposal relevant to the topic. Although we searched for evidence syntheses, we incidentally identified some recent or ongoing primary research studies.
We were keen to ensure that we did not duplicate effort and also to alert NHS England to academic groups actively researching the topic. Therefore, we made contact with the researchers who were eager to engage, providing early sight of their draft reports in confidence to be included in our work. They were also keen to engage further with NHS England to inform ongoing policy work.
Summary of response to challenge
To avoid duplication of effort and to ensure that policy was informed by the most recent research, we highlighted the ongoing work alongside review evidence and facilitated contact between NHS England and the research authors.
Reflections and lessons
Multiple stakeholders from different areas within the same organisation identified a broad and far-reaching list of themes and questions that reflected the differing remits and priorities of the stakeholders. This required an iterative production process, undertaking the work in stages and presenting the findings at each stage to support their needs. We identified a tension between ongoing engagement with busy and changing stakeholders and fast-moving policy in an area of rapid and ongoing innovation. This required pragmatic adaptation of methods to meet the needs of stakeholders to balance methodological rigour with the usefulness of outputs, while maintaining transparency. In addition, in an area of rapid and ongoing innovation where peer-reviewed evidence may not be currently available, it was helpful to highlight ongoing work and academic colleagues working in the area for further direct dialogue with the stakeholder.
Disseminating the outputs from this multistage project was problematic. To respond to the stakeholder needs, we produced an interactive database of published and ongoing evidence (i.e. enabling sorting and filtering of the evidence base on key characteristics, accessing direct links to full publications and/or contact details of researchers). Reducing this to a final textual HSDR report stripped away this functionality and obscured much of the underlying work.
Case study 2: review of experiences of the ‘nearest relative’ provisions of the Mental Health Act 1983
Origin and context of the review topic
This evidence review topic was initially notified by the NIHR HSDR programme in direct response to an urgent request for help in gathering evidence for the independent review of the Mental Health Act 1983 (MHA),16 which was being conducted during 2018. In the UK, the MHA16 is the central piece of legislation that determines the circumstances and processes for when and how people experiencing mental distress can be compulsorily detained for assessment or treatment.
For the Exeter centre, it was the most rapid of the rapid systematic reviews that we had conducted during the contract period, as well as our first review project that was specifically about a piece of legislation (rather than a health-care intervention or model of health service delivery). We got our first indication of the review topic on 3 January 2018 and submitted the final report by the end of March 2018. The scoping process was, therefore, compressed and pragmatic, for example relying closely on the knowledge and stated needs of the main policy contact within the team conducting the independent review. Although we could identify a time point when the review questions and inclusion criteria were agreed, in other respects the scoping stage was less distinguishable from the main searches and review. In effect, it was a ‘live’ review protocol and the review was shaped and delivered through regular ongoing contact with the policy customer.
The scoping and systematic review was conducted by the HSDR evidence synthesis team at Exeter, and the full review protocol was published on the PROSPERO database (CRD42018088237). 20
The review topic was initially stated as one of several very brief issues or aspects of the MHA16 sent to the team by NIHR. The subtopics that the policy leads initially prioritised as ‘the most pressing’ were:
-
the rights of relatives
-
consent and capacity
-
the criminal justice system (tribunals and restricted patients)
-
legal clarifications.
Our work was steered towards the first topic and, specifically, the ‘nearest relative’ provisions of the MHA. 16 These are the legal requirements and associated practices that govern the involvement of the spouse or close biological relatives (i.e. the ‘nearest relative’) of a person who is being detained compulsorily for mental health reasons under the MHA16 (sometimes referred to as ‘being sectioned’). These persons are involved primarily as an advocate and support for the person in mental distress, especially in relation to decisions about care.
Although we had no specific review question, the remit of the independent review of the MHA16 included specific questions that it wanted to answer (Box 3) and these usefully shaped the possible directions of our rapid evidence review.
Overarching question: are the powers of the nearest relative within the MHA16 appropriate?
What is the role of the nearest relative under the MHA?16
What rights are available for nearest relatives and are these appropriate?
What are service users’ and carers’ experiences of nearest relative provision?
What is the impact on (1) service users’ access to family and carer support and (2) the experiences of families and carers involved in a person’s care?
How does this role impact information sharing and confidentiality?
Are there any possible alternative models (e.g. international best practice)?
Our contact person in the independent review team expressed the purpose of the needed review as the following main review question:
-
Are the powers under the MHA16 relating to the appointment and involvement of the nearest relative appropriate (i.e. working)?
By the time we completed scoping the topic and finalised our review protocol, the planned systematic review aimed to address the following question:
-
What are the experiences of services users, family members, carers and professionals of the use of the ‘nearest relative’ provisions in the compulsory detention and ongoing care of people under the MHA?
However, the remit and context of the independent review, together with guidance from the policy customer about the main perceived problems with the current legislation, revealed specific stages or aspects of these provisions that were of particular interest. These included the processes of identification of the nearest relative, displacement (i.e. replacement) of the assigned nearest relative, decisions about care, service users having access to support from those carers and loved ones who they wanted support from, and issues of patient confidentiality and information sharing. These stages/aspects were expressed in the PROSPERO protocol under the ‘outcomes’ of interest (see Table 8). 20
We aimed to answer this question by identifying, summarising and synthesising evidence from studies that met specific inclusion criteria. Table 4 summarises how the scoping process refined review questions and defined the inclusion criteria, compared with the initial, briefly stated review topic. The ultimate choice of a rapid form of qualitative evidence synthesis (i.e. framework synthesis) was mainly dictated by the review question’s focus on people’s experiences, combined with the very short time frame. Although there was some PPI in interpreting and writing up this rapid evidence synthesis, people or carers who had been directly affected by the nearest relative provisions were not involved in scoping the review or its questions.
| Criterion | Original topic or question | Final question about experiences of the nearest relative provisions |
|---|---|---|
| Population/sample | People affected by the MHA16 |
People detained under Section 2 or 3 of the MHA,16 their family and carers and the individuals involved with their care who work within the remit of the MHA16 Excluding those detained for criminal purposes |
| Intervention/phenomenon of interest | The MHA16 | Experiences of or attitudes towards the application of the nearest relative provision of the MHA.16 This includes any experiences in relation to the involvement of relatives, carers or professionals in the care of or decisions about a compulsorily detained person |
| Comparator | Uncertain if relevant | Not applicable |
| Outcomes domain of interest | Patient and carer experiences |
Explore experiences:Issues related to decisions about care during detention and after discharge, including to a community treatment order Issues related to service users having access to support from those carers and loved ones who they want to be involved with or informed about their care Issues relating to patient confidentiality and information sharing, relating to all aspects of compulsory detention |
| Study designs | Not stated | Qualitative research studies (e.g. based on analysing data from interviews or focus group discussions with patients) |
| Geographical scope | Not stated | UK-only evidence (i.e. legal jurisdictions of England, Wales, Scotland and Northern Ireland) |
| Date limits | Not stated | Evidence published from 1998 onwards |
Summary of key challenges/choices and scoping decisions
Key challenge 1: uncertainty about the type of evidence that would best answer the questions
The first question was whether or not any prior research had focused on patient and carer experiences of the nearest relative provisions within UK legislation. The questions of interest seemed so specific that we doubted if research would address them. Our review group’s contract and work remit extended to the potential for primary research or surveys, where such methods best answer policy-maker or NIHR HSDR questions. However, two early discoveries enabled us to focus on the evidence review component, rather than primary research. First, we identified a 2017 survey of people’s experiences of the MHA by the Mental Health Alliance and Rethink Mental Illness (London, UK). 21 Second, we learned that the independent review team were, themselves, conducting a survey of carer experiences.
It became important to know early on whether the policy customer expected the review team to summarise research evidence or, given the distinct possibility of finding no or very little research, to extend coverage to other relevant non-research forms of evidence in the public domain (e.g. blogs, online discussion forums). Our first teleconference with the policy customer revealed a clear preference for research-based evidence, if available. This was to ‘reduce possible bias’ and achieve a breadth of evidence in the review process, given the other information sources and consultation on which the independent review processes would be drawing.
Therefore, the policy customer gave us a clear and early steer to search for and synthesise research evidence only. Nevertheless, at that time, we were not sure if there would be sufficient, or even any, good-quality UK-based research evidence on patient and carer experiences of the nearest relative provisions. Therefore, we also noted that, later, we might need to extend the scope to grey literature and less research-based sources of evidence, or include evidence from beyond the UK. This highlights pervasive uncertainty about the available evidence for answering alternative potential questions, and the motivation to make best use of a review team’s core skills and resources in responsive, commissioned policy-informing reviews.
Decision 1: to limit to research evidence only
The response of the team was to commit to reviewing evidence from research only. However, we also made some aspects of the review scope and protocol conditional (i.e. on the amount and quality of research evidence found). For such reviews, the scope and protocol are live and adjustable plans that are expected to change in response to the evidence that is found. They often lay out sequences of possible scopes, iteratively refined, realigned and renegotiated. Had the team found only one or two includable research studies, this decision may have been revisited. This kept options open within a very rapid review timescale.
Key challenge 2: deliverability within 8 weeks
This was the overarching challenge and a non-negotiable constraint, against which the other challenges and decisions were all weighed. The deliverability of any review would critically depend on the number, richness/quality and, therefore, amenability to formal synthesis of the studies found, and this would not be known until 4–6 weeks before the report submission deadline. Concerns about this were compounded by our awareness that synthesising qualitative research, usually being an interpretative process, takes time and requires a team approach. We had team discussions about the value of also searching for and including survey research (i.e. which may not be qualitative). However, having found enough qualitative research, we did not ultimately search for survey studies. (In any case, such a review would be unlikely to provide more recent and relevant evidence than a reanalysis of the 2017 Mental Health Alliance survey responses.)
Decision 2: manage expectations of the policy customer through regular contact and review of progress
We had teleconferences with the policy customer every 1 or 2 weeks, at a minimum, during the first half of the review. This was not so much a decision, but a direct response to our uncertainty (i.e. to keep open communications with the policy customer about whether or not we were finding evidence and what evidence we were finding). Had there been too much evidence to synthesise, there would be discussions during these teleconferences as to what evidence we should focus on. The short time frame of the review, undoubtedly, also played a part in us choosing not to look for evidence from beyond the UK or prior to 1998 (see Key challenge 3: how old and from which other jurisdictions would evidence be relevant to experiences of the UK Mental Health Act? and Decision 3: to include only UK evidence and evidence after 1998).
Key challenge 3: how old and from which other jurisdictions would evidence be relevant to experiences of the UK Mental Health Act?
As mentioned, this was our first review of an aspect of legislation. Although people in other countries might have experience of equivalent legislation and practices for including family members of close friends in decision-making for people experiencing severe mental distress, only people from the UK (i.e. the jurisdiction of application of the MHA16) would have directly relevant experience of the nearest relative provisions.
Decision 3: to include only UK evidence and evidence from after 1998
This was an early and relatively easy decision (i.e. to not include evidence from beyond the UK). The legislation and the nearest relative provisions within it were so specific to the jurisdiction of the UK that evidence from elsewhere would have very little applicability to the UK legislative and mental health-care context. It was also because the broad context of this review – and the scope of the interim report of the independent review of the MHA16 that it was to inform – was the creation of a fuller understanding of the current and past problems with legislation and its use. Had the review context required a stronger understanding of potential alternatives and legislative solutions, then perhaps an international and comparative review of equivalent provisions in mental health legislation in other countries may have been useful. Another factor that may have informed this decision was that we knew that some research evidence would originate from Scotland, where an alternative to the nearest relative provisions was already current practice. It was, therefore, likely that this evidence, and its comparison with studies in England and Wales, would be more likely to inform the independent review than studies from mainland Europe or North America.
The cut-off date of 1998 was partly to limit the size of the screening task (i.e. to address deliverability in 8 weeks) and partly because our stakeholders confirmed that the experience of the nearest relative provisions would have differed before and after the adoption of the Human Rights Act 199822 in the UK. Therefore, only evidence about experience of the mental health legislation after 1998 was judged as relevant to future possible legislation.
Key challenge 4: conducting rapid synthesis of qualitative research evidence
Given the extremely tight timelines, and the researcher-intensive nature of qualitative evidence synthesis, we were very nervous about the possibility of finding too many studies that met our inclusion criteria. This would have risked making the review undeliverable, rushed and of reduced quality, or having to retrospectively exclude studies.
Decision 4: using ‘framework synthesis’ and prioritising conceptually richer studies within the synthesis
Although a full thematic synthesis would have been the preferred approach, this would not have been possible within the limited time frame of this review. However, committing to conducting a rapid synthesis of qualitative research was less risky and more feasible because a streamlined, pragmatic approach to qualitative evidence synthesis was available, which could be applied to a modest number of studies. Fortunately, we found 35 papers from 20 studies; however, 22 papers provided only half a page of qualitative evidence relevant to the five study objectives.
This meant that we could, with some adaptations and innovations to the method, conduct a pragmatic, rapid, best-fit framework synthesis of the qualitative studies within the 6-week time frame. Within the method, a three-stage approach was used. First, relevant data were extracted according to the research objectives of our review from the 22 papers with half a page of relevant qualitative evidence. This process identified the six richest studies that contained the most data relevant to our research questions. Themes were selected from these studies to further refine the framework. In the third and final stage of the synthesis, thematic synthesis of the data enabled the corroboration and extension of the framework. 23
Reflection and lessons
In this review, where review scoping and the conduct of the review overlapped almost completely, regular contact with the policy customer was an important way of staying responsive to the state of the evidence as it emerged. Fine-tuning of the review in response to the evidence needed to be in keeping with the overall protocol and fit with the available time and resources. These were decisions that could largely be manage from our side. However, the review also needed to be relevant to the policy customer’s needs, which demanded a close working relationship in such a rapidly evolving review.
The development of search strategies to scope the literature and identify pockets of evidence that were amenable to review underpinned many of the decisions that were made in the early stages. Scoping searches using Google Search and Google Scholar (Google Inc., Mountain View, CA, USA), and the initial bibliographic search development, played a key role in the decisions to exclude experiences of the MHA16 via criminal justice proceedings and to focus on research published after the 1998 Human Rights Act. 22 Throughout this process, the integration of the information specialist in the review team was crucial. The pressing requirement to rapidly scope the available literature meant that our bibliographic database search strategy was developed and ready to run as soon as the final focus of the review was agreed. Supplementary searches were iterative and responsive to the emerging literature, within the prespecified boundaries set out in the protocol. In particular, this included iterative citation searching or ‘snowballing’ of key primary studies. Indeed, this approach to searching is a core part of qualitative searching, but the rapid nature of this review brought to the foreground the importance of this type of searching.
The searches also determined that there were no available frameworks or theories directly relevant to our research objectives that we could use to inform the initial framework for our framework synthesis. This informed our decision to structure our initial framework based on our initial research objectives, and then refine the framework using the themes from the primary studies included in our reviews, followed by thematic synthesis.
Case study 3: regulating and inspecting integrated health and social care in the UK
In 2018, the NIHR conducted a topic identification exercise within the broad area of professional regulation in UK health care. The exercise generated approximately 30 possible research topics, with some articulated as research questions and others as stated areas thought to be lacking in evidence. The NIHR assessed each topic and prioritised the following questions for referral to the York HSDR review team:
-
What factors enable delivery of an effective system of regulation and inspection in an environment where services are increasingly being provided on a multiagency (including third sector) and local basis in or close to people’s own homes?
-
How can we overcome the barriers to delivering effective joint regulation and inspection in a way that makes sense from the perspective of the individual accessing the care and services? To what extent is it possible to achieve this without the need for major legislative or structural change?
The research team conducted extensive stakeholder consultation to shape these questions into research questions, define terms and adapt the scope where necessary (see Summary of key challenges/choices and scoping decisions). There was some PPI in the review project, but at the report-writing and dissemination stages only. Ultimately, we planned to conduct a rapid scoping review to identify and classify published material that could potentially address four key questions:
-
What models of regulation and inspection of integrated care have been proposed (including approaches taken in other countries)?
-
What evidence is available on the effectiveness of such models?
-
What are the barriers to and enablers of effective regulation and inspection of integrated care?
-
Can barriers to effective regulation and inspection be overcome without legislative change?
The rationale for conducting a scoping review was based on these mainly descriptive, rather than evaluative, review questions (especially questions 1–3). The protocol was posted on the team’s webpage,24 as it was not eligible for registration in PROSPERO. The final report was published in full25 and a brief evidence summary produced. 26
As can be seen by the above contrasting sets of questions, consulting with diverse stakeholders resulted in a broader scope, with a series of research questions focusing on the extent and nature of the evidence that were best suited to a scoping review. A map of the evidence was created, underpinned by the following inclusion criteria:
-
Publication type – both empirical and non-empirical publications were eligible for inclusion. Empirical studies could be of a qualitative or quantitative design. Non-empirical publications could include discussion or theory papers, as well as other descriptive pieces, such as editorials. Letters or news articles were excluded, as were publications that reported the findings from inspections of care services.
-
Setting – publications were primarily focused on the integration of health and social care provision, for example services delivered jointly by NHS providers and local authorities. However, publications could also focus on care provision that is delivered across other settings/sectors by different professional groups working together, for example across primary or secondary care. Care providers could be in the public, private or third sector, and services could be aimed at both adults and children.
-
Focus – publications needed to have a primary focus on the regulation and/or inspection of integrated care. Reference to the governance of services more broadly was not sufficient for inclusion. Integration could be either horizontal or vertical in type and be at a macro-, meso- or micro-level.
-
Outcomes – empirical studies could report on any outcome relevant to the regulation and/or inspection of integrated care. This could include issues related to implementation, such as views about barriers and enabling factors. Non-empirical publications could focus on any relevant issue, including proposed models of regulation or outcome frameworks.
Each included publication was coded on various key characteristics, including topic (i.e. regulation or inspection), country, population/setting and document type (e.g. empirical research, models or frameworks, or theoretical). This information was used to produce a high-level descriptive overview, which characterised the nature of current literature on the regulation and inspection of integrated health and social care in the UK, as well as identifying research gaps.
Summary of key challenges/choices and scoping decisions
Key challenge 1: reconciling multiple independent stakeholder consultations
The original questions prioritised by the NIHR originated from Health Inspectorate Wales (Merthyr Tydfil, Wales). A teleconference held between the York team and representatives of both Health Inspectorate Wales and Care Inspectorate Wales (Merthyr Tydfil, Wales), provided background and context to their proposed questions. However, before this teleconference could be arranged, the research team had already consulted other key stakeholders about the proposed questions.
Initial contact with representatives from the Professional Standards Authority (London, UK) and Care Quality Commission (London, UK) provided the team with an overview of health-care regulation in the UK and associated research. They expressed a willingness to assist with the proposed work and arranged for researchers to attend (1) the Professional Standards Authority’s Policy and Research Forum and (2) a meeting of the health and social care regulators. The former included representatives from the Professional Standards Authority and various regulatory organisations [e.g. the General Pharmaceutical Council (London, UK), the General Chiropractic Council (London, UK), the Health and Care Professions Council (London, UK), the General Optical Council (London, UK), the General Osteopathic Council (London, UK), the General Medical Council (London, UK), the General Dental Council (London, UK) and the Nursing and Midwifery Council (London, UK)]. The latter included senior managers from the Care Quality Commission, DHSC, the General Dental Council, the Health and Care Professions Council, the Local Government and Social Care Ombudsman (Coventry, UK), the Nursing and Midwifery Council, the General Pharmaceutical Council, the Parliamentary and Health Service Ombudsman (London, UK), the Professional Standards Authority, the Medicines and Healthcare products Regulatory Agency (London, UK), Social Work England (Sheffield, UK) and the General Medical Council. The research team also held a separate teleconference with a representative of the General Medical Council.
In each case, different stakeholders emphasised slightly different areas of interest, deviating to a greater or lesser extent from the original questions. The Health and Social Care Regulators suggested that interdisciplinary regulation of online primary care was the topic of interest. The diverse disciplines and regulatory organisations providing online care provoked questions about effective regulatory oversight and complaints related to care. The potential relevance and utility of the international evidence was particularly emphasised.
The General Medical Council agreed that, even given the differences in the regulatory architecture and frameworks across countries, there was scope to learn from other health and social care systems that face similar issues and potential risks. Of particular interest was multidisciplinary team working: understanding the barriers to, enablers of and issues around responsibility, given joint working and multidisciplinary collaboration.
The representatives of Healthcare Inspectorate Wales and Care Inspectorate Wales described recent policy initiatives to promote the integration of health and social care in Wales and the implications of such policies for regulators. They elaborated on their initial questions to pose a series of fundamental questions about the regulation and inspection of integrated health and social care provision, including what models exist, their effectiveness, the barriers to their implementation and non-legislative means of overcoming these barriers.
Decision 1: share all scoping conversations among the stakeholders and encourage ongoing engagement
It can be seen that – when given exactly the same information to scope a rapid evidence review – different stakeholders proposed differing but inter-related research questions. As these stakeholders are the likely audience for the review, we felt it crucial that they remain engaged with its development. Consequently, as part of the protocol development process, we shared our individual stakeholder discussions with the wider group. An introduction to the draft protocol outlined how these shared discussions informed the basis of a draft scope, which the stakeholders were then invited to further comment on and amend, as appropriate. Each of the stakeholder groups responded positively to this invitation.
Beginning with two detailed questions derived from a prioritisation exercise may have been a barrier to initial engagement from some stakeholders. Some stakeholders would defer to the questions as worded, focusing on interpreting the authors’ intentions rather than expressing their own perception of research priorities. The research team, therefore, encouraged stakeholders to use the initial questions as a starting point for the discussion about research priorities.
Key challenge 2: not all stakeholders are familiar with rapid evidence synthesis
It was clear that stakeholders’ experience and knowledge of rapid evidence synthesis varied widely, particularly in relation to formulating implementable research questions. We wanted to avoid the potential hazard of arriving at a scope that was simply amenable to evidence synthesis rather than reflecting a genuine stakeholder knowledge need.
Decision 2: empower stakeholders to take advantage of the available resource
The research team began each stakeholder group consultation with a presentation to ensure a common level of understanding before beginning the scoping work. This presentation covered:
-
the nature of the work conducted by the HSDR Evidence Synthesis Centres
-
the types of evidence synthesis and the related research processes
-
the role of stakeholder involvement in evidence synthesis
-
required stakeholder input for this specific project [e.g. helping develop the scope of the research question(s)].
The presentation aimed to create conditions in which stakeholders could lead the discussion, speak with confidence about their evidence needs and describe how rapid evidence synthesis might serve those needs. The research team could outline the types of research method that might be feasible or suitable for proposed research questions, but were careful not to influence topic-specific discussions. It became clear that stakeholders’ information needs were best served by quickly identifying and organising the apparently diffuse and disparate literature on regulation and inspection of integrated care. Consequently, a rapid scoping review was considered the most appropriate starting point.
Reflections and lessons
Successful scoping of rapid evidence synthesis questions requires the involvement of stakeholders who are knowledgeable, enthusiastic and engaged. However, it also requires researchers to developa framework in which stakeholders can lead conversations about the scope while remaining within the parameters of what can be achieved by a rapid evidence synthesis. This requires researchers to focus on listening and facilitation in the early stages of consultation, moving towards providing stronger guidance on possible methodologies once a level of consensus among stakeholders has been achieved. The time and effort required to develop these processes and practise these skills should not be underestimated.
Case study 4: social care access for BAME and LGBT+ populations – a rapid realist review
This evidence review topic was initially proposed by the Research Programmes Branch – Health and Care Section within the UK’s DHSC. The scoping and subsequent rapid realist synthesis was conducted by the HSDR Evidence Synthesis Centre at the School of Health and Related Research (ScHARR), University of Sheffield. The protocol was published on PROSPERO (CRD42019158250) and was also made publicly accessible on the NIHR’s published Sheffield Evidence Synthesis Centre web page (URL: https://njl-admin.nihr.ac.uk/document/download/2031791; accessed 21 June 2021). The review was conducted between November 2019 and the end of June 2020 and was published in 2021. 27
The review focus was initially stated as the following topic:
-
addressing diversity and inequalities in access to social care services.
Access to social care services had featured as a dominant theme within the James Lind Alliance’s Adult Social Work Top 10,28 reflecting a recent priority setting exercise. Rather than representing a specific priority from the James Lind Alliance exercise, this theme encapsulated several priorities. It was, therefore, felt by the NIHR and the DHSC that coverage of these priorities could be interpreted and understood by targeting the review at groups for whom access to social care could be particularly challenging. Initial discussion with the contacts at the DHSC focused on two particular groups of interest: ethnic minorities, and lesbian, gay, bisexual, transgender plus (LGBT+) people with social care needs. This process emphasises how a broad theme may be refined to particular populations, both as a specific target for policy initiatives and in the assumption that by addressing issues in access for specific groups, this can have wider implications for other population subgroups.
Rather untypically, the review customer (the DHSC) had already conducted a preliminary literature scoping around race disparities in the use of social care. The review team, therefore, faced two particular challenges: (1) how to add value to the initial literature review by complementary activity and (2) how to inform the social care access literature from the extensive work completed in health care. Both of these considerations shaped our subsequent approach to scoping the literature. In addition, the review scope and the perceived relevance of the review was discussed with members of the Sheffield Evidence Synthesis Centre’s PPI Group.
Although classic scoping of effectiveness review questions involves population (or patient type), intervention, comparator and outcomes, with the subsequent addition of study types (i.e. PICOS), once the quantity and quality of available literature has been established by scoping, we have identified the need for addition of a further ‘S’ [population (or patient type), intervention, comparator, outcome, study types, synthesis method (PICOSS)]. This additional ‘S’ relates to the type of ‘synthesis’ (i.e. a preliminary assessment of the literature allows us to identify what type of synthesis will be possible and useful to match the requirements of the topic to the needs of the commissioner). In this instance, we identified that realist methods would extend the evidence base beyond the descriptive literature review that the DHSC team had already explored to gain an understanding of how ‘access’ worked (or did not work) for different groups.
As part of the scoping, our jointly trained lead reviewer/information specialist identified a realist review on the topic of access in primary care. 29 Our team was interested in the extent to which the conceptual models from that study might transfer to social care, particularly in relation to a trajectory or pathway of access.
Our initial scoping identified a significant number of data relating to the use of social care services by refugees and asylum seekers, particular by those with poor mental health. Checking with policy colleagues, via our direct point of contact, revealed that these groups would be included among the identified populations of interest. It further revealed a particular interest in the intersectionality between our two populations: ethnic minorities and LGBT+ people.
Following these explorations, discussions with the DHSC resolved the specifics of the review to the following research questions:
-
What are the barriers to and facilitators of accessing social care for (1) ethnic minorities and (2) LGBT+ populations?
-
Using ‘if–then–leading to’ statements (i.e. context–mechanism–outcome configurations), can we map access to social care against access pathways to health care (Ford et al. 29) to provide additional explanations for what influences access to social care?
We aimed to obtain answers to these questions by identifying, summarising and synthesising evidence from studies that met specific inclusion criteria, using a realist review approach. The rationale for conducting a realist review was to address the primary interest ‘for whom’ (or for which groups) access to social care works, as rapid realist methods have been specifically developed for work with policy-makers and realist methods also allow us to look at the contexts of access to social care and the role of mechanisms in determining the outcomes around access (see also table 13 in Booth et al. 27). In addition, the DHSC acknowledged that the characteristics of their topic, which the team matched to the required review type (i.e. limited existing explanatory literature, mainly descriptive), were previously ‘reviewed’ in the UK literature and they were looking for added value from the evidence.
A key feature of realist approaches, however, involves prioritising studies or sources that can inform and develop candidate programme theories (i.e. provisional explanations of how interventions work). In this sense, even though the original research questions were suitably specified for developing the protocol, we continued to refine the focus of the scope as we started to interpret the evidence. An interim remote meeting was arranged between the ScHARR team and the DHSC to prioritise four or five programme theories to be addressed by the review. A notable feature of the review was the need to specify certain concepts early in the process. Table 5 summarises how the scoping process defined the inclusion criteria and shaped the scope.
| Concept | Definition | Source of definition | Type of definition |
|---|---|---|---|
| Diversity and inclusion (population) | The following characteristics as protected from discrimination in the workplace and wider society: age, sex, gender reassignment, disability, ethnicity, sexuality, religion, pregnancy and marriage | Equality Act 201030 | Legislative definition |
| Access (intervention/phenomenon of interest) | Defined in terms of candidacy, not as a static and fixed relationship:Candidacy describes the ways in which people’s eligibility for . . . attention and intervention is jointly negotiated between individuals and . . . services . . .31 | Dixon-Woods et al.31 | Academic (theoretical) definition |
| Comparison | Any or no comparison | ||
| Adult social care (outcome) | . . . care and support for people who need it because of age, illness, disability or other circumstances . . . Social care can be provided in people’s homes, to enable independent living or help with recovery after illness and . . . , provide a safe space for people to live in supported housing, residential or nursing homesReproduced with permission from The Health Foundation322018The Health Foundation | Thorlby et al.32 | Working definition from the literature |
| Study designs | Any research design | Quantitative, qualitative or mixed-methods studies | |
| Synthesis type | Rapid realist synthesis | Saul et al.33 | Research methodology |
| Geographical scope | UK only, focusing primarily on England followed by the devolved nations | ||
| Date limits | 2009–20 | ||
Key challenges/choices and scoping decisions
Key challenge 1: the role of definitions in specifying relevant concepts
Dixon-Woods et al. 34 make the distinction between an integrative synthesis ‘where the focus is on summarising data, and where the concepts (or variables) under which data are to be summarised are assumed to be largely secure and well specified’ and an interpretive synthesis with its concern with ‘the development of concepts, and with the development and specification of theories that integrate those concepts’. The reviews specified by the NIHR HSDR programme typically include at least one concept that has to be ‘discovered’ during the course of the review, whether that be unpacking the constituents of an intervention, the diversity of outcomes or, as in this case, in exploring if a health-oriented concept of access and candidacy could usefully be translated to social care. Elsewhere, Dixon-Woods et al. 31 cite the distinction between the question as an ‘anchor’ [i.e. where four elements of population (or patient type), intervention, comparator and outcomes are prescribed and pinned down] and where the question is a ‘compass’ [i.e. where one element is pinned down (e.g. ‘adult social care’) and the implications of variation in the remaining concepts is explored during the course of the review].
These archetypal uses of review questions are, of course, end points of a continuum of approaches between having highly fixed inclusion criteria and questions and very fluid/flexible criteria and questions. Although the concepts of compass and anchor continue to offer useful heuristics at the question-generation stage, additional conceptual development could usefully explore their further utility and application, as they clearly also link to the core trade-off between the importance of the question(s) and the availability of relevant research to answer it (them).
In reality, when working on a review, we can recognise that all concepts are potentially either ‘compasses’ or ‘anchors’. Furthermore, definitions may be semisecure, such as the working definition provided in Thorlby et al. 32 (see Table 5), or bound by statute, such as the Equality Act30 definitions associated with protected characteristics. Definitions may come from one of many different types of source (Table 6). Our lead reviewer for this project leads for diversity and inclusion at a faculty level and so was already familiar with the scope and variety of terms and concepts within this topic.
| Type of definition | Source of definition |
|---|---|
| Authoritative definition | Term taken from a definitive source (official, legislative, user or academic definition) |
| Working technical definition | How the review team and/or the review commissioners agree to interpreta term |
| Working user definition | How professionals or expert patients use a term (i.e. in defining what it includes/excludes), also known as ‘user warrant’ |
| Author labels | How authors use a term in the literature (i.e. as retrieved from abstract or full-text searching), regardless of how accurately the term is used (also known as ‘literary warrant’) |
| No definition | Where a term is progressively refined through exploration, either through following related articles/references or through a formal concept analysis |
Key challenge 2: adding to the value of previous review work
Frequently, the review work that we undertake involves updating or complementing a previous review. In this case, the DHSC had already undertaken a rapid descriptive literature review. Part of our PICOSS challenge was to convey the added value of our preferred form of synthesis for this particular question. This can be conceived as a two-way dynamic flow between review commissioner and review team, in which the commissioner shares details of topic and research question and, in return, the review team seeks to communicate the synthesis methodology. Scoping, therefore, involved identifying existing evidence syntheses (such as Ford et al. 29) that could communicate the potential of our planned review, act as templates for our own methods and outputs, and introduce the methods to be used.
Key to this process is the requirement to be familiar with diverse review methods so that matching between topic/question and methodology can be managed effectively. The emerging science of reviewing research (‘reviewology’) involves familiarisation with different review choices and engaging in an informed negotiation with the review commissioner. Evidence Synthesis Centres, therefore, need to include or have good access to experienced synthesis methodologists to perform this integral function.
Key challenge 3: scope and protocol as a work in progress
As mentioned above, the review team had a final opportunity to determine the scope of the rapid realist synthesis following completion of a process of sensitisation and rapid data extraction that preceded the interim remote meeting with the DHSC staff. The review team prepared and shared 13 candidate programme theories in a technical document, with accompanying illustrative extracts. At a subsequent meeting, the team at the DHSC indicated the relative priority of these programme theories and then confirmed these with policy colleagues. Engaging with such a vivid exemplification of the review scope in practice helped in finally determining the limits of the work. From January 2020 onwards, the review team worked within the scope of each of the five prioritised individual programme theories, selected by DHSC from the initial list, to organise analyse and interpret data within what are essentially ‘mini-reviews’ based on each programme theory. As befits an interpretative review, the parameters of the review product were determined relatively late and from within a wider sampling frame. Furthermore, the limits of the mini-reviews continued to emerge as decisions were made on the scope of each programme theory and their degree of complementarity, synergy or overlap.
Reflection and lessons
The scoping process involves extended negotiations, involving transactions and exchange of ideas, knowledge, references and topical and methodological artefacts between review commissioner and review team in moving to a shared understanding of the problem and its potential for resolution. The choice of review synthesis approach is not a decision to be made once the scope has been finalised. It represents an integral part of the scoping process (i.e. as an additional ‘S’ to the traditional PICOS framework).
More fundamentally, scoping also includes determining the extent to which concepts should be predefined or the extent to which they should be left to emerge from the review process or studies found. Concepts can themselves be viewed individually as ‘anchors’ or ‘compasses’ and definitions may be prespecified (i.e. temporarily fixed for the purposes of the review) or emerge from and give direction to an interpretive review method as part of the ‘findings’.
Case study 5: review of the effectiveness and implementation of strengths-based approaches to adult social work
This evidence review topic was initially proposed by the Chief Social Worker for Adults within the UK’s DHSC, in August 2019. The scoping and systematic review was conducted by the HSDR Evidence Synthesis team at Exeter and the full review protocol was published on the PROSPERO database (CRD42020166870). 35 The review was conducted between November 2019 and the end of June 2020.
The review topic was initially stated as the following brief question:
-
Different models of social work practice: what social work practice works best?
This directly translates into the more precise, typical language of systematic review questions as ‘What is the effectiveness of different models of social work practice?’
By the time we completed scoping the topic and finalised our review protocol, the planned systematic review aimed to address the following two questions:
-
What is the effectiveness of different strengths-based approaches used within adult social work?
-
What factors enable or inhibit the implementation of different strengths-based approaches in adult social work within the UK?
In other words, we had expanded the initial focus on effectiveness (i.e. ‘what works’) to include evidence on the implementation or embedding of strengths-based approaches into routine social work practice, and this case study mainly explores how that expanded focus arose. Ultimately, the review asked people with lived experience of using adult social care services to comment on research summaries and no service users were involved early enough in the process to shape the review questions and scope.
We aimed to obtain answers to these two questions by identifying, summarising and synthesising evidence from studies that met specific inclusion criteria. Table 7 summarises how the scoping process refined the review questions and defined the inclusion criteria, compared with the initial, briefly stated review topic. Ultimately, as no effectiveness studies that met our inclusion criteria were found, it became a rapid synthesis of qualitative studies of implementation and (as with the review in case study 2) used framework synthesis because of its pragmatic aims and proven value for applied health care and informing policy.
| Criterion | Original topic or question | Question 1 (effectiveness question) | Question 2 (implementation question) |
|---|---|---|---|
| Population/sample | Not stated | People being supported by social workers or adult social care teams | Social workers or people leading or managing adult social care teams |
| Intervention/phenomenon of interest | Models of social work practice | Strengths-based approaches to practising social work | Strengths-based approaches to practising social work |
| Comparator | Alternative models of social work practice | Any area, service or team of social workers that have not adopted the given strengths-based approach or before they adopted the given subsidiary approach | Not applicable |
| Outcomes domain of interest | Effectiveness (‘what models . . . work best?’) | Effectiveness (intended outcomes for people, families or communities being supported) | Markers or perceptions of implementation |
| Study designs | Not stated | Comparative outcome evaluations | Qualitative or mixed-methods studies |
| Geographical scope | Not stated | UK | UK |
| Date limits | Not stated | None | None |
Summary of key challenges/choices and scoping decisions
Key challenge 1: specifying the phenomenon of interest
Although the initially stated topic made no mention of specific models of social work practice, the earliest communications with the Chief Social Worker for Adults usefully and quickly clarified that one broad ‘model’ of social work practice was of most interest, that is strengths-based approaches. Such approaches had been enshrined in policy as part of the Care Act 2014,36 and were already strongly supported and promoted by the DHSC, the Social Care Institute for Excellence (SCIE) and NICE.
However, from expert advice and reading key reports, it quickly became clear that a strengths-based approach is not a single, well-defined ‘intervention’ or model of practice. Rather, it is a holistic way of working, with a multidimensional set of core ideas and principles about how social care can be effectively and positively provided in a way that respects people’s rights, desires, life and family circumstances, and draws on the capabilities and strengths of the individuals being supported, their families and the communities in which they live. At the same time, we had also been sent a table by the Chief Social Worker for Adults (i.e. the policy customer), which listed various subsidiary approaches, theories and models of practice, on which she had marked ‘those that more clearly fit under strengths-based approaches’.
Therefore, by 3 October 2019, when corresponding with NICE (about key challenge 2), we wrote:
We are aware from our previous scoping searches that there will be few, if any, comparative empirical evaluations of using strengths-based approaches vs. using traditional/usual approaches to social work practice. So we have provisionally, instead, decided to conduct a systematic review of some of the component therapeutic approaches or specific tools that are commonly seen as ways of delivering social work within a strengths-based approach.
Rob Anderson, University of Exeter Medical School, 2019, personal communication
In the likely absence of comparative, empirical evidence of the effectiveness of the overall strengths-based approach (based on our own scoping searches), the team had briefly considered conducting a theory-driven review (e.g. a realist review) to better specify the supposed underlying principles and mechanisms of strengths-based approaches (i.e. how the strengths-based approach improves social work outcomes). However, rather than using a review to better understand the effectiveness of strengths-based approaches from a theoretical perspective, we instead chose a more pragmatic approach to meeting the user’s stated evidence need.
Decision 1: focusing on subsidiary, named approaches aligned to strengths-based principles and practice
Mindful of the relatively short (5-month) timeline, we chose to conduct a systematic review of 17 named subsidiary approaches (i.e. models of social work practice and service change that are widely believed to be closely aligned with or to exemplify a strengths-based approach). As well as reflecting the reality of how strengths-based approaches were being fostered and adopted in different local authority adult social care teams, basing our review around such a list of named strengths-based approaches would enable targeted literature searches and give us flexibility at the evidence synthesis stage to not conduct syntheses where studies were either too few in number or too poor in quality. Our review protocol explicitly stated that the rapid review:
. . . will ultimately only include studies evaluating a selection of the approaches which are seen as a priority by the policy customer [DHSC], and [which] have an adequate number of studies for the synthesis to be more valuable.
Anderson et al. 35
The Chief Social Worker for Adults initially sent the team a table of named approaches and theories of social work (that had been produced by one local authority), and they had marked those that they saw as most aligned to a strengths-based approach. We supplemented this with an appraisal of named approaches within recent presentations/webinars, government reports and a roundtable meeting report about strengths-based approaches to social work. The final list of 17 strengths-based approaches that formed the basis of our searches and review were based on a table produced from these sources and, subsequently, corroborated by social work/social care expert stakeholders who had commented on the review protocol. Although acknowledging that the list was not exhaustive, the team believed it to capture the main subsidiary approaches that foster a strengths-based approach to practice or organisational change.
In summary, the nebulous definition of strengths-based approaches, being derived from various principles and an approach of how to work with vulnerable people rather than a single distinct model, offered two competing alternatives. We needed to focus on these underlying defining principles and, therefore, how strengths-based approaches improve outcomes (e.g. using a realist review), or focus on selected, named subsidiary approaches that are believed to foster or encapsulate a strengths-based approach, and effectively conduct a systematic review of each of these. For the reasons described above, we chose the latter approach.
Key challenge 2: rapidly becoming familiar with a new domain of policy and practice
The review team have primarily worked within health care and health policy research, and so the world of adult social care and social workers as a specific professional group was unfamiliar to all members of the review team at the beginning of this review. This meant that more time than usual had to be invested in talking to experts and reading key background reports to get to grips with the language, key concepts and basic context, such as what is adult social care? What is social work and social work practice? What are the types of adults and families in the UK who typically need support from social workers?
Decision 2: recruiting a wider group of stakeholders and involving experienced social workers in the review team
Rather than being an identifiable decision, this was a conscious ongoing effort to reach out to academics, practitioners and service leads in the social work field and adult social care services. It was boosted by two significant examples of collegial generosity and luck. First, a professor of social work who had co-authored one of the key recent government reports of strengths-based working was keen to help us in our work. The professor provided detailed commentary and e-mail feedback on emerging sections of the report and synthesis. Second, a health researcher from the Institute of Health Research (University of Exeter Medical School, Exeter, UK) who was a former social worker and had also been a leader and manager of adult social care services in two different local authorities assisted with the review.
Key challenge 3: assuring that we would not duplicate ongoing or recent evidence reviews by others
By following various leads in the literature and a tip-off from our policy customer about ‘a similar piece of work’, we became aware of (1) a recent policy document from NICE and the SCIE,37 which could have been based on a review of research evidence similar to our emerging topic, and (2) another university-based group conducting a review of the evidence relating to strengths-based approaches to social work. We, therefore, investigated both possibilities, through e-mails and telephone calls, to ensure that our planned review of the evidence relating to strengths-based approaches had not already been conducted.
In 2019, NICE and SCIE had jointly published Evidence for Strengths and Asset-Based Outcomes: A Quick Guide for Social Workers. 37 Knowing that NICE evidence products are typically based on commissioned or internally produced systematic reviews, the review team contacted the Quick Guide authors at NICE to find out what evidence this guide was based on. Ultimately, e-mails and telephone conversations with two members of the social care and leadership team at NICE confirmed that no new or specific systematic reviews had been conducted to inform the Quick Guide. Rather, the evidence comprised a collation of evidence-based recommendations drawn from NICE, SCIE and other authoritative sources.
The second potential duplication of our planned review involved a small team based at the University of Kent (Kent, UK) that we had been told was ‘involved in developing a research proposal with others on strengths-based social work, through NIHR’. We spoke with both the principal investigator and the main researcher on this work to gain a clearer picture of their planned work. They confirmed that an ongoing project, conducted by the Adults Social Care Outcomes Unit (a DHSC policy research unit), involved exploring ‘strengths-based practice in social care’.
However, discussions with the lead researcher clarified that this was effectively a scoping review of relevant literature. We concluded that a broader focus and different methods (e.g. no specific study designs or inclusion criteria, etc.) meant that, notwithstanding shared inclusion of some studies, our systematic review would have a sufficiently different focus and methods (i.e. on effectiveness studies, and on specific, selected subapproaches within a strengths-based approach) to be both distinctive and valuable.
Key challenge 4: avoiding an empty review
A frequent criticism of systematic reviews is the apparently high prevalence of so-called ‘empty reviews’. Although empty reviews may give research commissioners impetus to fund more primary research to fill research gaps and give service commissioners greater freedom to encourage service innovations based on experiential knowledge and theory, they typically have less value in the immediate decision-making context of users of rapid reviews.
Decision 4: to extend the focus of the review to include the implementation of strengths-based approaches
The decision to add a second focus and review question about the implementation of strengths-based approaches was informed by three considerations. These were as follows:
-
Our scoping searches and advice from others with much greater experience in the field of social care research, indicated there would be no or, at best, very few comparative effectiveness studies of different strengths-based approaches. We judged that a review addressing the effectiveness question only would likely be an ‘empty review’ (i.e. no studies meeting our inclusion criteria).
-
Several of our expert stakeholders indicated that the research needs of adult social care teams were now less to do with whether or not strengths-based approaches are effective and more about how they can be effectively implemented by adult social care teams or individual social workers.
-
The view, shared by stakeholders and present in recent publications, that most social workers and other professionals working in social care ‘fundamentally supported a strengths-based approach within adult social work and social care, but often found it difficult to demonstrate, evidence and practice such an approach in practice’. Initial indications that local evaluations of models of strengths-based practice had included a focus on implementation (e.g. to identify enablers of or barriers to the adoption of the particular strengths-based approach).
Reflection and lessons
The fact that strengths-based approaches were already fully promoted by government and other agencies, that they are also widely assumed by social workers to be a positive and beneficial approach (reflecting the core goals and values of the profession) and the likelihood of there being no high-quality effectiveness studies of the overall approach led to us scoping a more useful review in two ways.
First, we added the second focus on the implementation of strengths-based approaches. This meant that if the effectiveness review was empty, we would have still provided a valuable evidence synthesis. Second, and relatedly, we avoided the challenge of defining what comprises or defines a strengths-based approach to social work practice by asking other stakeholders to identify named initiatives and subsidiary approaches that they deemed to be reflecting or fostering a strengths-based approach.
Scoping searches, therefore, played a critical role in defining what potentially synthesisable evidence existed, which fed back into the specification of productive review questions. Owing to the rapid timelines of this review, our main stakeholder at the beginning was the policy customer who was engaged with the process and setting the review goals. However, we were able to corroborate and expand our understanding of the evidence needs and which named initiatives were deemed to foster or exemplify strengths-based working by working with other social care and social work experts during the review, and by building on recent roundtable reports and webinars on strengths-based working. Without this broader engagement, we would have been less confident in the choice of the 17 strengths-based approaches that we ultimately included and less aware of the important differences between them (and, therefore, also less aware of limitations in the ultimate applicability of our findings). The lesson from this is that, even when you have a very engaged and knowledgeable policy customer, it is important to form a balanced view of the evidence needs using a broader range of experts and documentary sources.
Case study 6: review of hospital-led interventions to reduce the length of hospital stay for planned admissions of older people
Origin and context of the review topic
This case example was conducted by the Exeter HSDR Evidence Synthesis Centre. The review protocol was published on the PROSPERO database (CRD42017080637). 38 The review was conducted between September 2017 and October 2018 and published in 2020 (with a pause of 3 months in early 2018 to address an urgent policy question) (see Case study 2: review of experiences of the ‘nearest relative’ provisions of the Mental Health Act 1983). 39
The scope of the review was initially discussed at a teleconference between the review team and the scientific adviser at NIHR HSDR. The aims of the meeting were to obtain a preliminary understanding of (1) the background to the decision to prioritise the topic for review, (2) the main areas of uncertainty and (3) the purpose of the proposed review.
Two key aspects of the discussion informed our next steps:
-
Although the decision to focus on this area had partly been informed by key published references, the topic was considered a priority for the HSDR programme, with no other identifiable policy customer.
-
There was recognition that systems beyond hospitals often have an impact on timely discharge after unplanned care, but this should not necessarily be the case following planned admission. Potential topics of interest included –
-
admission avoidance and non-emergency (hospital) care
-
organisation of hospitals (i.e. hospital elements of control for planned care)
-
population groups for which reducing length of stay may be particularly relevant (e.g. people receiving palliative care, people with dementia or delirium and people with learning disabilities).
-
Following a teleconference with the NIHR commissioners, a member of the review team ‘suggested that intervention or programme ideas could be looked at for [intended impacts on] length of stay – although narrow’ and it was agreed that this focus could extend to evidence on other outcomes of initiatives with this aim. This helped confirm the focus for our further exploration and scoping searches (i.e. a focus on interventions that explicitly aimed to reduce length of stay).
Given considerable uncertainty about the most useful review topic, our next steps were to familiarise ourselves with the topic and the body of evidence available. We (1) conducted broad scoping searches and (2) contacted local clinical experts with knowledge and expertise of caring for patients during planned hospital admission. The review team also met on three occasions with a group of four adults aged > 60 years, including one meeting on checking the review’s planned focus. Each individual had experience of being admitted to hospital overnight for a planned procedure.
On completion of scoping the topic and finalising the review protocol, the planned systematic review aimed to address the following two questions:
-
What is the effectiveness of hospital-led multicomponent interventions to reduce length of inpatient stay in hospitals for older adults following planned admission?
-
What is the cost-effectiveness of hospital-based multicomponent interventions to reduce length of inpatient stay in hospitals for older adults following planned admission?
We aimed to obtain answers to these two questions by identifying, summarising and synthesising evidence from studies that met specific inclusion criteria that are typical of systematic reviews of effectiveness and cost-effectiveness, seeking quantitative outcome data from rigorous comparative evaluations [such as randomised controlled trials (RCTs)]. 9 Table 8 summarises how the scoping process refined the review questions and defined the inclusion criteria, compared with the initially stated review topic.
| Criterion | Original topic or question | Question 1 (clinical effectiveness question) | Question 2 (cost-effectiveness question) |
|---|---|---|---|
| Population/sample | Hospital patients. Probably for planned care | Older adults (where the mean age of the sample is ≥ 60 years) undergoing planned (i.e. elective) treatment that requires an overnight stay in a hospital | |
| Intervention/phenomenon of interest | Interventions to shorten length of stay (or equivalent goals – ‘accelerate recovery’) | Any multicomponent hospital-based intervention or strategy for patients receiving planned care as an inpatient, which explicitly aims to reduce length of stay in hospital or aims to improve/enhance recovery (or equivalent language in the aims of the strategy, e.g. accelerate rehabilitation) | |
| Comparator | Unclear: usual previous/alternative care | Any type of control group or comparator. In many cases this may be described as ‘usual hospital care’ or ‘usual best clinical practice’ for a given type of hospital admission | |
| Outcomes domain of interest | Effectiveness (‘what models . . . work best?’) | Effectiveness (intended outcomes for people, families or communities being supported) | Cost and cost-effectiveness |
| Study designs | Not stated | Comparative effectiveness studies | Economic evaluations or comparative cost studies |
| Geographical scope | Not stated | High-income countries | High-income countries |
| Date limits | Not stated | None | None |
Summary of key challenges and decisions during scoping
Key challenge 1: absence of an explicit policy customer or question
With no explicit policy customer, it was not easy to identify a clear and specific clinical or policy need or evidence gap, within a given population. Our initial consultations with the HSDR programme provided insight into specific populations of interest; however, we did not know what evidence already existed for these populations or the scale and importance of the problems relating to their planned hospital admissions. Conversely, several relatively recent, high-quality systematic reviews indicated where there was an abundance of research and also which evidence had already been synthesised. We were also informed by our research commissioners about another review that was being conducted, which focused on ‘early discharge’-style interventions and mainly encompassed hospital-at-home and social care interventions after patients left hospital.
Decision 1: conduct broad and targeted literature searches to try and identify an unsynthesised body of relevant primary research
With a broad domain of health services only (planned hospital admissions) and a general perceived need for better evidence relating to it, we decided to conduct scoping searches to identify what questions, patient groups and hospital procedures had been the focus of primary research, and which evidence had already been effectively summarised and synthesised by others. This very quickly led to a second challenge.
Key challenge 2: lots of previous research and quite a few previous systematic reviews of it – but was there a gap?
Owing to the substantial cost of hospital admissions within all modern health systems, there has been a focus for decades on implementing and evaluating various types of service changes that aim to avoid hospital admissions in the first place (i.e. admissions avoidance) or shorten them by enabling people to be discharged earlier and supported at home or in other non-hospital settings. Increasingly, such intermediate care, hospital-at-home and early supported discharge schemes have also been seen as ways to further policy goals of person-centred care and, relatedly, providing care closer to or in people’s homes.
This has produced a wealth of research and also systematic reviews of that research. However, our research commissioners had felt that an evidence need remained in relation to this topic, but it was not clear if that need had already been met by primary research or syntheses. Early scoping activity centred on three population groups believed, by our commissioner, to exhibit greater uncertainty: (1) people with learning disabilities, (2) palliative care and (3) people with dementia or delirium.
Initial scoping searches of Ovid MEDLINE and Google Scholar identified several systematic reviews of the effectiveness of enhanced recovery after surgery and enhanced recovery programme interventions. However, we found no reviews that specifically focused on the three population groups of interest. We followed up this finding in two different ways. First, we searched for primary studies to ascertain whether or not a review of interventions focusing on these population groups would be feasible. Second, because we were unsure whether or not primary research would have been conducted specifically on these population groups, we considered the possibility of conducting a review of reviews, using subgroup analyses of the population groups of interest within systematic reviews of primary studies of general population groups. We also initiated discussions with external experts, colleagues and stakeholders about our proposed question.
Decision 2: focusing on hospital admissions of older people
These discussions guided us towards our final decision to focus on older people in our review, enabling us to consider evidence relating to at least two of the three population groups of interest: (1) people with dementia or delirium and (2) palliative care:
-
A research associate at the Nuffield Trust (London, UK), and author of their related report,40 thought that achieving shorter hospital stays for older people was highly important because they are the most vulnerable to hospital-acquired harms.
-
A professor of ageing and rehabilitation at the University of Exeter emphasised that older people would not necessarily receive an intervention unless it was deemed effective enough and, for this reason, enhanced recovery programmes could be an important option not being considered often enough for older people.
-
A consultant geriatrician at Royal Devon and Exeter NHS Foundation Trust (Exeter, UK) suggested that we consider the need for evidence to inform ‘doing the right thing for the person’ in the treatment of older people with comorbidities, where interventions may not add much to quality of life. This was based on the assumption that enhanced recovery programmes are generally accepted as safe and effective, based on research evidence in younger and less complex patients.
Therefore, although the effectiveness of enhanced recovery programmes and similar initiatives to enable people to leave hospital earlier seemed to be accepted in general, there was shared uncertainty about whether or not such programmes would always be appropriate and effective in older people and, if not, for whom they would be effective. Returning to our scoping activity, we confirmed a gap in the synthesised research literature around organisational (i.e. hospital-based or hospital-led) interventions aiming to reduce the length of stay for older people following planned procedures.
Key challenge 3: defining and operationalising hospital-led ‘organisational interventions’ that aimed to reduce length of stay
Searching for evaluations of hospital-based interventions and hospital-led interventions to reduce length of stay revealed numerous studies that compared specific treatments or procedures. For example, many evaluations compared different drugs or protocols for anaesthesia, laparoscopic surgery with open surgery or different types of postoperative physiotherapy. Therefore, the team needed to distinguish ‘treatment interventions’ from broader ‘organisational interventions’ and changes in how whole teams work to support earlier discharge. In line with Medical Research Council definitions of complex interventions (as comprising multiple components41), checklists for describing components of enhanced recovery after surgery protocols42 and Cochrane Effective Practice and Organisation of Care group checklists,43 we decided to distinguish our interventions of interest as multicomponent interventions, as follows:
-
Intervention has multiple components. As defined in the guidance for using the Intervention Complexity Assessment Tool for systematic reviews (iCAT_SR), commissioned by Cochrane, an intervention component is ‘a discrete, active element of an intervention that could be implemented independently of other elements’ (p. 6). 43 Therefore, for inclusion, interventions should contain more than one component (e.g. education and exercise).
Therefore, organisational (multicomponent) hospital-based or hospital-led interventions in older people became the ultimate focus for our systematic review, and distinguished this review from those focusing explicitly on alternatives to hospital care or those focusing on single-component interventions (e.g. laparoscopic vs. open surgery or comparing different regimes for anaesthesia and analgesia for planned surgery). We also excluded strategies that were focused on discharge planning or pre-treatment assessment only (e.g. comprehensive geriatric assessment alone), as these do not affect other stages of the hospital stay.
In the absence of reliable intervention labels, the second challenging aspect of defining our included interventions was how to decide when an intervention aimed to reduce length of hospital stay (and, ideally, in a way that could be plausibly identified from a journal paper’s abstract). Our two main options were (1) to include only those papers that explicitly stated that its intention was to reduce length of stay (i.e. including papers in which length of hospital stay was the stated primary outcome), or (2) to also include those in which the aims implied that a reduction in length of stay was one of the aims [e.g. if the paper stated that it aimed to ‘improve’ or ‘enhance’ recovery (or equivalent language, e.g. ‘accelerate rehabilitation’)].
Reflection and lessons
The scoping of this systematic review exemplified many of our HSDR reviews in requiring iteration between the ‘technical’ (or data-driven, bottom-up) process of defining and refining searches to quantify research on different potential questions, and the ‘collective learning’ of a small group of reviewers working with clinical or research commissioner stakeholders to ‘home in’ on the most useful review questions (as a top-down process).
From both the searches and suggestions from the research commissioners, key published sources informed our understanding of the context of the review (e.g. the possible specification of organisational interventions), highlighted key pre-existing evidence syntheses on reducing patient length of stay and helped to develop our own search strategy. However, it was the combined views of several clinical and policy stakeholders that, on top of our learning from the searches, provided the critical decision and narrower focus (i.e. on older people). This decision allowed the scope to really take shape and helped to identify the main evidence gap to be addressed by our review. As one of our reviewers later reflected, such suggestions ‘stopped it becoming an academic exercise’. Our clinical stakeholders also aided our understanding of the stages of the patient journey through hospital and how these may differ according to age group and urgency of procedure. Again, this insight supported our definition of multicomponent, hospital-led interventions.
In conclusion, after reflection by the team, this scoping exercise was considered to have been ‘evidence’ rather than question driven. It started without a clearly defined question and the final scope and questions were based on scoping searches that showed a considerable body of unsynthesised research evidence related to stated evidence needs. In the absence of a clearly specified question at the beginning or a well-defined service delivery or policy area of uncertainty, it represented a general hunch about a lack of clear evidence relating to interventions that aimed to shorten the length of hospital stays for planned hospital admissions. This hunch was explored through considerable iteration between scoping searches and consulting clinical stakeholders. The ‘breakthrough’ decision, which provided an answerable review question that would likely yield useful evidence without too many included studies, was to focus on older people. All other decisions, including to focus on multicomponent and comprehensive models of care, such as enhanced recovery programmes, can be seen as following this main decision on the patient group. As a bonus, the focus on older people enabled the review to seek evidence in relation to people with dementia or delirium (another priority group mentioned by our commissioners).
Case study 7: implementation of interventions to reduce preventable hospital admissions for cardiovascular or respiratory conditions – an evidence map and realist synthesis
This evidence review topic was initially proposed by the HSDR programme, with no direct identifiable policy customer. Negotiations about the scope, therefore, took place with the HSDR technical adviser. Scoping and the subsequent evidence map and realist synthesis was conducted by the HSDR Evidence Synthesis team at ScHARR. The review was conducted in multiple stages between September 2017 and April 2019 and published in 2020. 44
The review topic was initially stated in broad terms:
-
interventions for preventing unnecessary hospital admissions.
Given that comparatively little primary research had focused on how to support the implementation of interventions to reduce preventable hospital admissions, an evidence map and realist synthesis was designed to address the following research question:
-
With regard to the implementation of interventions to reduce preventable hospital admissions for cardiovascular and respiratory conditions, what works, for whom, how and in what circumstances?
The rationale for conducting a realist review was that the review’s commissioners (i.e. the NIHR HSDR programme) asked the team to consider the interventions as ‘proven interventions’ and, therefore, to provide greater understanding of how interventions that have been shown to reduce admissions for cardiovascular and respiratory conditions work in practice. The preceding mapping review was primarily to inform the sampling frame for the realist review.
Considerable effort and energy was expended at the beginning of the review to define the term ‘unnecessary’ (hospital admissions) from the originally stated review topic. Eventually, the team decided that conceptualising ‘unnecessary’ in terms of appropriateness was the realistic approach. The team and HSDR adviser agreed to focus on conditions characterised as ambulatory or primary care sensitive conditions (ACSCs). Ambulatory services are those services, like hospital outpatient services, where people attend and leave the appointments during the same day, and patients are, therefore, not classed as admitted patients and do not need an overnight stay. The logic is that where the severity or risk of acute episodes of a chronic condition is sensitive to the amount or quality of primary care or ambulatory care, then escalations and admissions to hospital can be prevented.
Table 9 summarises how the commissioned review sought to broaden and interpret the earlier review by Purdy et al. 45
| PICOSS criterion | Purdy et al.45 review | HSDR review | Principal differences? |
|---|---|---|---|
| Population/sample | ACSCs | Cardiovascular or respiratory conditions | HSDR focuses on conditions with prior evidence of high effectiveness |
| Intervention/phenomenon of interest | Interventions to reduce preventable admissions | Interventions to reduce preventable admissions | None |
| Comparator | Non-intervention | Non-intervention | None |
| Outcomes domain of interest | Effectiveness (‘what works best?’) | Mechanisms of effect (what works for whom under what circumstances) | HSDR reivew seeks to be explanatory |
| Study designs | Research evidence (in general) | Any research design plus grey literature on current practice | HSDR review has broader scope to capture candidate interventions |
| Synthesis type | Overview of research evidence | Evidence map and realist synthesis | HSDR review uses systematic methods |
| Geographical scope | International | UK | HSDR review privileges relevance to NHS |
| Date limits | Not stated (up to 2010) | 2010–October 2017 | HSDR review targets currency |
Summary of key challenges/choices and scoping decisions
Key challenge 1: targeting a representative part from a larger ‘whole’
An initial challenge was to select, from a long list of ACSCs on the DHSC website, a suitably productive focus to exemplify and, hopefully, to encapsulate issues for conditions generally. A frequent criticism is that realist syntheses fail to capitalise on the inherent analytical capacity of ‘what works for whom under what circumstances’ by failing to link qualitative insights to ‘what works’ (i.e. the effectiveness information). To avoid this pitfall, the team explicitly constructed a table (Table 10) that mapped the interim conclusions on effectiveness to different ACSCs. It immediately became apparent that cardiovascular or respiratory conditions had been sufficiently explored and adequately supported as effective to make these an appropriate focus for a realist inquiry. A telephone conversation with the technical adviser at the HSDR programme examined the case for each of the candidate conditions, in turn, to finally resolve the review scope. This approach to scoping, which resolves the coverage of a review by optimising both relevance and the likely explanatory power of the evidence, represents a risk-averse strategy when commissioning rapid reviews.
| Intervention | Positive | No effect | Negative |
|---|---|---|---|
| 1. Case management | Heart failure | Older people, COPD | |
| 2. Specialist clinics | Heart failure | Older people, asthma | |
| 3. Community interventions | Acutely at-risk populations (e.g. failure to thrive infants, heart failure) | Older people, mother and child health and heart disease | |
| 4. Care pathways and guidelines | General conditions, specific diseases (e.g. gastrointestinal surgery, stroke and asthma) | ||
| 5. Medication review | Older people, heart failure or asthma | ||
| 6. Education and self-management | |||
| 6a. Education | Heart failure | ||
| 6b. Self-management | Adults with asthma, COPD | Children with asthma | |
| 7. Exercise and rehabilitation | |||
| 7a. Pulmonary rehabilitation | COPD | ||
| 7b. Exercise-based cardiac rehabilitation | Coronary heart disease | ||
| 7c. Therapy-based rehabilitation | Stroke | ||
| 7d. Fall prevention interventions | Older people | ||
| 8. Telemedicine | Heart disease, diabetes, hypertension, older people | ||
| 9. Vaccine programs | |||
| 9a. Influenza vaccinations | Asthma, older people | ||
| 9b. Health worker influenza vaccination | Older people | ||
| 10. Hospital at home | Older people | ||
| 11. Finance schemes | Insufficient data | ||
| 12. Emergency department interventions | Insufficient data | ||
| 13. Continuity of care | Insufficient data | ||
Realist synthesis typically requires prioritisation of programme theory to explore the phenomenon of interest in sufficient depth. The team had to ensure that, having identified review capacity to explore up to three chosen candidate programme theories, they optimised the analytical and explanatory power of their chosen foci. In consultation with the technical adviser from HSDR and the ScHARR Standing Advisory Group on Public Participation, the team selected foci to represent patient, carer and GP perspectives, respectively, within the candidate programme theory.
Key challenge 2: establishing comparability with the target population across diverse study populations
In a realist synthesis, evidence is excluded only if it does not relate to or inform the development of the programme theory. The practical focus of this review required that we exclude evidence with limited transferability to the NHS, such as avoidable admissions in low- and middle-income countries. In line with this decision, we prespecified five countries from which to derive direct evidence to the review, namely the UK, USA, Australia, Canada and New Zealand. These ‘big five’ were selected because of comparable health-care systems to the UK setting. The team continued to engage with the wider evidence base through systematic reviews, opinion pieces and direct reference to individual study reports, particularly where authors connected interventions to the UK context.
Key challenge 3: maximising the utility of review outputs
Much of the emphasis of published descriptions of scoping focuses on determining the conceptual boundaries, methodology options and logistic constraints of an individual review. In comparison, little attention has focused on the role of scoping in shaping the knowledge end product from the very beginning of the process. The scoping process offers an opportunity for commissioners and stakeholders, through their engagement, to exert an early influence on tailoring the final product to their requirements. So, for example, the focus on cardiovascular and respiratory conditions was not determined by evidence on effectiveness only, but also from the commissioner perspective, as articulated by the NIHR programme staff. For the review team, the resultant risk-averse strategy minimises the chances of producing a product that is neither useful nor appropriate. Scoping different options is one way of modelling different review configurations without embarking too far down a particular route.
Unlike other review processes that typically prioritise rigour and reproducibility (e.g. the internationally regarded NICE evidence synthesis products, with their explicit interest in effectiveness and cost-effectiveness), the emphasis of the HSDR programme has generally been to optimise a third ‘R’ of relevance (e.g. encompassing feasibility of implementation, acceptability and sustainability in different organisational contexts). This must continue to be underpinned by the preceding considerations of rigour/reproducibility. Scoping offers an early opportunity to sensitise the context within which the review is eventually situated. In this connection, subsequent attempts by the centres to further improve their working relationships with the patients, public and commissioners is particularly germane. Necessarily, this process of shaping review outputs does not simply involve determining the content, but also entails stimulating receptivity for the form of the final review. Review teams spend a significant amount of time, both in conversations and through the written protocol, cultivating the expectations of the commissioners with regard to less-standard review products, such as realist syntheses.
Reflection and lessons
In a research arena that is increasingly populated by systematic reviews and other types of evidence synthesis, this review and case study has demonstrated the increasingly frequent call to build on the foundations provided by a previous review. Previous reviews can be used in numerous ways (likened to the choice between bulldozing and reusing materials from an existing structure, building an extension or constructing a separate and adjacent annexe). In this particular case, the extension model was most evident. The review shaped the choice of a specific subset of studies that were extended and examined closely. Data on the viability of the chosen conditions, and the likelihood of their achieving an effect, drove the subsequent realist inquiry into how these interventions work. A long list of potential conditions to be examined was slimmed down rapidly into a short list of ambulatory sensitive conditions of potential interest. Conversely, this ‘extension’ approach required good familiarity with the original review, its implications and the definitions encapsulated within its methods.
The existence of a relevant systematic review also reduced some of the synthesis workload, allowing the team valuable time for exploring experimental initiatives reported in the grey literature or located in the ‘.nhs.uk’ internet domain. HSDR topics typically exhibit a shared concern with the established and evaluated, and the innovative and experimental. Although it is important to preserve the separate contributions of these two types of evidence, variously privileging rigour or relevance, the prior existence of a systematic review of effectiveness studies45 released search effort for exploration of ephemeral contributions. Potentially, NHS service initiatives extend the evaluation horizon by showcasing locally developed solutions with the, as yet unevaluated, potential to deliver health benefit. Faced with concentrated timescales, it is tempting to prioritise a formal scoping search of one or more bibliographic databases when the contribution of web sources may also be important.
Case study 8: access to primary and community health-care services for adults with intellectual disabilities – a mapping and targeted systematic review
This evidence review topic was initially proposed at the annual review meeting of the three evidence synthesis centres with members of the NIHR HSDR programme. The meeting forms the first stage of the process of scoping, where the teams identify prior experience and expertise in relation to a long list of topics generated by the HSDR priority generation process. At this time, the ScHARR review team identified a key researcher with expertise and networks in intellectual disabilities (IDs) to work with the review team to deliver against the identified topic.
The exact timing of this review was negotiated around the availability of the researcher and a joint reviewer/information scientist was scheduled to project manage the topic. As the review eventually took the form of an extensive mapping review, it was not formally included on PROSPERO. However, the protocol is published as a supplementary appendix to the final report. The review protocol was finalised in May 2018, following 2 months of scoping and iteration with the HSDR team, and the final report was delivered in December 2018 and published in 2020. 46
The review topic was initially stated as follows:
-
access and quality of health services for people with learning disability.
Within the context of the NIHR HSDR programme, this was a landmark topic, returning to the scene of a previous review by its predecessor, the Service Delivery and Organisation programme. 47–50 The ‘footprint’ of this preceding review influenced several subsequent reviewing decisions, emphasising how each new synthesis fits within the evidence landscape. Indeed, even the title of the original review illustrates how both the topic and methodology had advanced. The title identified the output generically as a ‘literature review’, compared with our ‘mapping and targeted systematic review’, and the topic was described as ‘learning disabilities’ compared with the recent ‘IDs’.
By the time we undertook this review, we had consolidated lessons learned from the previous 3-year work programme. 11 This endorsed a three-stage review process for most evidence synthesis topics, namely mapping, scoping and then systematic review. 51 Although some researchers use mapping and scoping interchangeably, these processes are becoming distinct as their respective methods evolve. Mapping represents an attempt to obtain one’s bearings and take stock of the nature and quantity of research within a defined wider area of potential study, often with a view to identifying synthesis gaps where a subsequent potential review might be located. Scoping represents a process for identifying the limits or bounds to a specific planned review, whereby the implications in terms of both logistics and conceptual scope are explored, the limits and quantities of likely literature gauged and potential inclusion and exclusion criteria piloted. Therefore, scoping can be likened to drawing a line to describe the boundary of a review (i.e. deciding what is inside and what is outside its scope), whereas mapping is more about exploring and describing what studies are within particular bounds.
Although not every review requires a formal output at all three stages, these processes of mapping, scoping and reviewing feature in almost all of the three evidence synthesis teams’ projects. Therefore, we authored a protocol that involved two components: (1) a mapping review to offer breadth and then, following focused scoping, (2) a targeted systematic review to complement this with depth.
The mapping review aimed to address the following questions:
-
What are the gaps in evidence about access to primary and community health care for people with ID?
-
What are the barriers to accessing primary and community health-care services for people with ID and their carers?
-
What actions, interventions or models of service provision improve access to health services for people with ID and their carers?
One feature of this scoping process was consulting people with IDs, family carers and formal paid carers so that the review could be informed by the views and experiences of stakeholders (for more details, see Appendix 1, Table 13). This consultation had multiple aims, namely to:
-
illuminate the model of access to health care for people with IDs
-
inform and refine our search strategies by identifying barriers to accessing health care and any solutions developed
-
identify gaps in the literature.
We contacted the clinical director and senior commissioning manager of a Clinical Commissioning Group for services for people with IDs and asked them to identify relevant community groups for people with IDs and their carers. We sent information about the review to these groups and asked to visit them to discuss their experiences of accessing health care. Discussions were loosely guided by a topic guide, drawn from the previous review, covering how people identify a health need, what actions they take, the issues influencing their decision to take a particular course of action and the barriers to and facilitators of their access and use of the chosen service. The barriers and facilitators were used to identify relevant search terms and for future comparison with the barriers and facilitators identified in the qualitative literature.
Other scoping decisions proved important to the direction of the review. The original review distinguished between access and efficiency in focusing on ability to use a service (i.e. access), rather than whether or not the service was provided to a high standard (i.e. efficiency/effectiveness). In contrast, the update review sought studies reporting the effectiveness of any measures or interventions designed to improve access to the relevant services. Comparing the scopes of the original and more recent reviews illustrates how the HSDR programme, and its associated science, has developed and expanded how it conceptualises accessibility and related aspects of service delivery over the last decade or so.
The subsequent targeted systematic review focused on evidence from the UK, building on the findings of the mapping review. Key elements of the targeted systematic review were:
-
development of the research questions based on the findings of the mapping review and information from PPI meetings
-
a focused systematic database search following inspection of the mapping review findings;
-
a full data extraction of relevant studies
-
a quality assessment of included full peer-reviewed papers and no formal quality assessment of conference abstracts or grey literature.
Summary of key challenges/choices and scoping decisions
Key challenge 1: defining ‘relevance’
This review would include evidence from the UK only. This decision was taken to ensure relevance and to assist in managing the large volume of literature on this topic. A key scoping decision is which interpretation of relevance and context makes most sense in relating the study populations to the target population within each review. In some reviews, relevance is defined simplistically, as either geographical or chronological proximity. In other situations, relevance relates to similarities in how interventions work (i.e. conceptual homogeneity). For example, primary care settings for this review represent a ‘first point of contact’ for ID patients or their carers. In either case, the review team has to determine how to incorporate relevance into their review,7 either formatively, by methods used in the review, or summatively, in using one of many tools available for transferability or applicability. 52,53
Key challenge 2: ‘mapping as scoping’
Broad topics are often characterised by uncertainties in relation to the quantity and quality of research. With limited time, the review team must decide how best to optimise the review resource. ‘Empty’ reviews are not helpful to decision-making, and yet overpopulated reviews are likely to either overrun timewise or prove superficial in their analysis and interpretation. A mapping review offers the possibility to offer breadth before the depth of a targeted systematic review. For this mapping review, initial descriptive analysis took place based on title and abstracts only. Subsequently, a subset (of approximately 20%) of the overall studies was sifted from the original retrieval results, supplemented by grey literature searches to form the data set for the targeted review. This approach keeps the scope as elastic as possible until informed decisions on coverage have been made. At this point, a formal protocol is finalised to provide the necessary scientific rigour. A further benefit of this staged approach is that it diversifies review outputs for different target audiences. Those requiring broad coverage can use the mapping review and those requiring a filtered approach that includes quality assessment are presented with a conventional systematic review.
Key challenge 3: building on previous systematic reviews
Although it may seem attractive to build on previous systematic reviews, the complexity of review decisions may offer minimal advantage from starting a review de novo. As illustrated by this review, not only had the preferred terminology changed, but also different fundamental assumptions about how to interpret ‘access’ shaped the subsequent review. Search terms need to be checked for new index terms and for the emergence of new terminology around the user community. Searches must be specified from the date of last search (not from publication date) together with overlap to avoid key items falling down a gap between reviews. Will the original data sources be replicated for fidelity to the original review? In the case of this particular review, the information specialist revisited the original list of sources to modify, and even improve, the original research. They also checked new index terms and terminology to ensure that the strategies continued to meet the requirements of the current review. This tension between comparability and contemporaneity needs to be managed according to the intended purpose of the review. Above all, the review team needs to decide whether to build on the foundation of the previous review, dismantle the previous review and reuse its original studies only alongside recent additions, or simply construct their own review, overlapping with the previous review.
Reflection and lessons
This review and case study has shown the value of recognising the distinct processes of mapping, scoping and systematic reviewing in managing the overall review, regardless of whether or not these lead to formal nominated review outputs. In general, unless the review customer has already conducted reliable searches and scoping of what evidence exists, some initial mapping and/or scoping needs to be conducted before any useful systematic review can be planned and conducted.
The case study also showed the potential contribution of different stakeholders in informing the scope and coverage of the review, including members of the public (in this case, adults with IDs). Stakeholder involvement included helping to identify gaps in the literature.
The case study also highlighted challenges that arise from changes in terminology and, importantly, adjustments in conceptualisation, as reflected in successive versions of related reviews. This may mean that a previous related systematic review cannot simply be updated, and the focus and intended value of the new review has to be carefully articulated. Even, as here, where the new systematic review is justified as updating and complementing previous reviews, the additional time and effort remains considerable compared with starting a new review from scratch.
Chapter 4 Discussion
Shared learning
In total, 14 scoping considerations were identified, each evident in two or more of the eight case studies. (The development of this framework of 14 scoping considerations is described in Chapter 2, Thematic analysis.) These were then checked and (where necessary) refined by case study authors at each centre, and so should not be viewed as a formal or rigorous qualitative thematic analysis. Table 11 shows the final 14 scoping considerations together with the case studies that illustrate them.
| Concept | Explanation | Case studies |
|---|---|---|
| Consultative issues: externally generated issues relating to input from commissioners, stakeholders, experts and patient groups to inform the planned evidence synthesis product | ||
| Managing and deciding priorities (C1) | How the review team manages and negotiates with NIHR, stakeholders and other customers to ensure that priorities are addressed within resource constraints | Case studies 2, 3 and 6 |
| Reconciling different priorities/perspectives (C2) | How the review team manages potentially competing tensions between what different groups or stakeholders may want to achieve within the overall project remit | Case studies 3 and 6 |
| Achieving buy-in and engagement (C3) | How the review team secures input into the scoping and prioritising process from stakeholders and sustains this throughout the project to include reception of the deliverables | Case studies 3 and 4 |
| Educating the end-user about synthesis process and products (C4) | How the review team communicates aspects of review methodology and different synthesis outputs to the potential users/audience, particularly in terms of what they will deliver | Case studies 3 and 4 |
| Managing stakeholder expectations (C5) | How the review team communicates what the review project will and will not be able to achieve within the available resources and time frame, particularly when the review will ‘fall short’ of the conventional systematic review standards | Case studies 2–5 |
| Interface issues: issues relating to the interaction between the technical processes of the review team and the requirements of the review user | ||
| Identifying the niche/gap and optimising added value (I1) | How the review team positions the intended synthesis product within previous literature or reviews and in addressing users’ specific needs | Case studies 1, 2, 4–6 and 8 |
| Rigour/reliability (reproducibility)/relevance (usefulness) (I2) | How the review team manages potentially competing tensions of scientific quality, confidence in the review output and utility to the intended users within the constraints of remit and resources | Case studies 1, 2, 6 and 7 |
| Transferability/applicability of study evidence to policy/service user context (I3) | How the review team manages the need to provide UK-specific interpretation from an evidence base that may have to be drawn from other countries and contexts | Case studies 2, 3 and 5–8 |
| Technical issues: internally managed issues relating to the conduct of the review as experienced within the review team | ||
| Choosing the method(s) of synthesis (PICOSS) (T1) | How the review team explores different options and makes an informed decision about which type of synthesis product will best meet the needs of the intended users | Case studies 1–4, 6 and 7 |
| Balancing fixed vs. fluid questions/components/definitions (T2) | The extent to which the question as a whole and/or its individual PICO components are predefined and predetermined or if they emerge during exploration of the literature | Case studies 1, 2 and 4–8 |
| Taking stock of (and building on) what is already out there (T3) | How the review team explores the quantity, quality and characteristics of primary studies and/or reviews in determining which output will be both feasible and useful | Case studies 1, 5, 6 and 8 |
| Mapping vs. scoping vs. reviewing (T4) | How the review team manages and intersects the relationship between exploring the characteristics of the evidence base (mapping), determining the parameters of the specific synthesis (scoping) and conducting the synthesis (reviewing), and the extent to which these processes transform into discrete project deliverables | Case studies 1 and 8 |
| Scoping/relevance as a continuous process, not just at initiation (T5) | The extent to which the scoping process is used as an opportunity to precondition the users to the content and form of the final synthesis product | Case studies 2, 4 and 7 |
| Calibrating general vs. specific and broad vs. deep (T6) | How the review team makes decisions regarding whether to cover an entire topic or to select one or more subtopics as exemplars of the whole, and the extent to which they optimise coverage vs. detail (e.g. description vs. analysis) | Case studies 2, 5, 7 and 8 |
Consultative/external issues in scoping and question formulation
Consultative/external issues relate to liaison with either the commissioner (i.e. HSDR), the direct client (e.g. NHS England) or the stakeholders of a review. Typically, these issues involved communication, engagement, negotiations, managing expectations, conceptualisation and definitions.
Managing and deciding priorities (consultative issue 1)
This theme captured how the review team manages and negotiates with NIHR, policy stakeholders and other customers to ensure that priorities are addressed within resource constraints. In most review scoping processes, the choices made represent trade-offs between various competing goals, especially between the duration/timeliness and comprehensiveness of a review (i.e. resources) and its rigour and relevance. Where a policy or health service customer of a review is identifiable, it is important to ensure that they are aware of these trade-offs and the scoping decisions that affect them.
A clear example of this need to manage trade-offs comes from the rapid review to inform the independent review of the MHA16 (i.e. case study 2). The initial question was expressed as a policy question rather than a research question, and would conventionally be answered by finding comparative quantitative effectiveness studies. Our preliminary searches revealed few, if any, such studies of this kind. To both reduce and share the risk with the policy customer, the review team expanded their focus and question to patient, carer and professional experiences of the ‘nearest relative’ provisions and, at the same time, made some aspects of the review scope and protocol conditional on how much evidence we found. This process was achieved through close and regular consultation with the policy customer.
These discussions and negotiations also taught the review team about particular aspects of reviewing evidence about legislation (as opposed to health interventions). Legislation, by definition, is jurisdiction specific and so this reduces the value of research evidence about similar legislation in other countries. Similarly, sometimes the legal context changes so significantly at a particular time point that any evidence from before then becomes far less relevant. In this rapid review, this gave us a defensible rationale to exclude evidence from before 1998, which was when the UK’s Human Rights Act22 came into law (and, we were advised, this significantly altered the operation of the MHA16).
The key point, perhaps magnified in the context of such a rapid review, is that trade-offs between rigour and relevance, timeliness and deliverability of the review, and all of these with closeness to the perceived original evidence need, have to be carefully negotiated with and fully involve the policy customer. Where the main policy customer is identifiable, the review team needs to present these choices, and their likely implications for these trade-offs, as far as they can be anticipated in the early review stages. Outlining the available choices is also helpful when a network or group of key stakeholders are the main users or audience of the review, as in the review of the regulation and inspection of health and social care, although it makes the process for agreeing the review’s aims more complicated. This consultative issue, therefore, links to all three interface issues and the two-way discussions between stakeholders and the review team that often take place to identify the important gap in synthesised evidence to balance rigour and relevance and to maximise applicability (for our teams, to the UK health and social care context)
Reconciling different priorities/perspectives (consultative issue 2)
This theme captured how the review team manages potentially competing tensions between what different groups or stakeholders may want to achieve within the overall project remit. The need to reconcile priorities was perhaps most evident in the review of the regulation and inspection of health social care (i.e. case study 3), where the diverse stakeholders included both national service regulatory bodies (such as the Care Quality Commission and Health Inspectorate Wales) and the regulatory bodies of different types of care professionals. The review team noted that ‘the stakeholders emphasised slightly different areas of interest, deviating to a greater or lesser extent from the original questions’.
In the review of hospital-led intervention to reduce length of stay for planned admissions (i.e. case study 6), individual (rather than institutional) stakeholders had different reasons for agreeing on the overall importance of the review topic for older people. One stakeholder noted the overall importance of the goal of reducing the length of hospital stays for older people to reduce the risks of hospital-acquired harms, like falls or infections. Another stakeholder felt that older people may often be excluded from enhanced recovery programmes, perhaps because of perceptions that evidence of benefit was lacking in this patient group. However, a clinical stakeholder was aware of the opposite risk (i.e. older people might be subject to enhanced recovery protocols without evidence that it is safe for them or the protocols may not take account of more complex needs). Therefore, in this case study, the differing stakeholder views did not pull the review scope in different directions, but rather reflected the underlying uncertainty of the initial topic, specifically in relation to older hospital patients (in this case, helping to confirm a narrower focus of shared interest).
Achieving buy-in and engagement (consultative issue 3)
This theme captured how a review team secures input from stakeholders into the scoping and topic prioritisation process. Although the focus is on the initial review stages and on developing a detailed review scope and protocol, we acknowledge that these processes have importance beyond scoping and question formulation.
Although often implicit within our case studies, an important incentive for a stakeholder to engage in question refinement and topic scoping is when their organisation has proposed the need for the review. For example, in the review of the regulation and inspection of integrated care (i.e. case study 3), the topic had originated from Health Inspectorate Wales, and this organisation and Care Inspectorate Wales were strongly engaged with the review throughout. This case study suggests another potential incentive – for buy-in and engagement from equivalent agencies in the different devolved nations of the UK – and so, ultimately, the scoping of this project also involved the Care Quality Commission (for England) and the Professional Standards Authority [for the UK (health professionals) or England (social workers)]. We further speculate that securing the input of lead agencies in relevant jurisdictions may incentivise equivalent agencies in other jurisdictions or subsidiary agencies to ‘not be left out’ and to represent their constituencies.
A review team needs to reconcile different priorities and perspectives held by wider groups of relevant stakeholders, often with equivalent or overlapping remits [see Reconciling different priorities/perspectives (consultative issue)]. Although this could present a challenge to scoping, it may also secure greater engagement, overall, by intentionally using a transparent and collective/group engagement process. Such engagement could be achieved by meeting as a stakeholder group or, as in the review of regulation and inspection of integrated care, by sharing individual stakeholder discussions with the wider group of stakeholders. Engagement could also be achieved by ensuring that stakeholders understand that the initially specified questions may not be the ones that best serve user needs.
In contrast, the realist review of access to social care for ethnic minority and LGBT+ populations (i.e. case study 4) had a single identified stakeholder (the DHSC) and was conducted within the context of a scope that was evolving throughout the review process. Here, early and ongoing engagement seemed to be aided by the DHSC’s close involvement in shaping the core concepts that would provide the ‘anchors’ or ‘compass’ of the review. Similarly, as the review progressed, the DHSC were closely involved in discussing and shaping the emerging programme theories. However, it is unclear from this case study whether the promise of involvement throughout a review process acts as an incentive or a disincentive to close involvement in scoping and question formulation. Conceivably, there may be some policy or service stakeholders who invest time in the early stages of scoping and question specification in the hope that this will mean a need for less subsequent engagement and effort. Overall, it seems that factors that determine the strength of stakeholder engagement will be varied, complex and context specific, and may exist at an organisational level or be steered by the interest and commitment of individual policy-makers or commissioners.
Educating the end-user about synthesis process and products (consultative issue 4)
A related consultative issue in many review scoping processes is how the review team explains to stakeholders about review methodology and the choice of different potential synthesis outputs produced (e.g. given different prioritised questions or different available evidence). This closely relates to the technical scoping issues of choosing the different methods of synthesis (technical issue 1) and balancing the goals of mapping, scoping or reviewing previous research (technical issue 3). This dialogue also strongly influences the consultative issue of managing stakeholder expectations [see Managing stakeholder expectations (consultative issue 5)].
Most service, clinical professional or policy stakeholders are most aware of systematic reviews that use quantitative research, such as clinical trials, to produce integrative syntheses of evidence, for instance overall summaries of effectiveness of well-defined interventions. The review of access to social care for ethnic minorities and LGBT+ people (i.e. case study 4) involved working with the DHSC to show how a realist review might use diverse sources of research evidence and provide richer explanations of how ‘access’ worked or did not work for different groups. More generally, it involved conveying to the end-user that not all types of review have to be prespecified and that the concepts guiding them can evolve during the review, including studies that can expand to enable relevant explanations (in this case, by including refugees and asylum seekers).
Another recurrent feature of HSDR reviews experienced across the teams, and one the stakeholders needed to be aware of, was the two- or three-stage nature of many review projects. They would begin with searches and a type of rapid scoping review, and then work with stakeholders to reassess what kind of synthesis, or perhaps just mapping or description, would be feasible and useful on the basis of the number and types of studies known to exist [this common sequencing is further explored as Mapping versus scoping versus reviewing (technical issue 4)].
Managing stakeholder expectations (consultative issue 5)
This theme captured how the review team communicates what the review project will and will not be able to achieve within the available resources and time frame, particularly when the deliverable is likely to ‘fall short’ of the conventional systematic review goals (e.g. of providing a summary answer to effectiveness or cost-effectiveness questions).
A key expectation is often around the fixed or fluid nature of the review question itself [see Balancing fixed versus fluid questions/components/definitions (technical issue 2)]. In the realist review of access to social care for ethnic minority and LGBT+ groups (i.e. case study 4), uncertainty related to the definition of key terms and concepts, and in the recognition that the review would have to refocus at a later stage (in this case, in a realist review, when a smaller set of programme theories are chosen as the basis for the rest of the review). In addition, with realist reviews, the synthesis and end product comprises a set of refined and empirically grounded programme theories.
It is important to have early conversations with stakeholders about the variety of possible synthesis methods, their relative suitability for answering different types of review question and the expected content and format of their findings [see Choosing the methods of synthesis (technical issue 1)]. At the same time, the review team needs as much clarity as possible about the other PICOS elements that define the boundaries of a review’s scope [i.e. population, intervention (phenomenon), comparator, outcomes and study type]. Perhaps the basic strategy for managing expectations about a review is to develop the review protocol iteratively and collaboratively with the main stakeholders or user.
Interface issues in scoping and question formulation
Interface issues concern how scoping and question formulation occur in transactions and negotiations between the review team and other interested parties. Negotiations may require translation (as between the languages of policy and research), interpretation or the realignment of the time and quality and/or resource implications of the review. As such interactions involve identifying and agreeing the niche/gap that meets users’ needs while seeking to complement previous reviews, and balancing rigour, relevance and applicability, these considerations were evident, to some degree, in all our case studies. Only in situations with no identifiable review user and little stakeholder engagement would interface issues not be prominent.
Identifying the niche/gap and optimising added value (interface issue 1)
This theme captured how the review team positions the intended synthesis product within previous literature or reviews and in addressing users’ specific needs. This builds on the principle that a new systematic review adds most value in situations where:
-
the potential review question matches or is very similar to a current and important policy or health service question
-
a sufficient number of primary research studies have directly or indirectly generated evidence to answer the potential review question
-
no recent, high-quality systematic review has sought to answer the same or a very similar review question.
Where any one of these three conditions is not met, the value of a new, high-quality systematic review is significantly diminished. Many scoping processes can be viewed, in retrospect, as an iterative process of trying to establish these conditions. Nevertheless, the central interaction between the review team and the review users is based around condition (a), whereas conditions (b) and (c) are technical and data driven and do not require much input from review users.
The review of access to health care for adults with IDs (i.e. case study 8) illustrated the complexity of building on or filling gaps between previous systematic reviews. Although, ostensibly, the earlier systematic review had addressed a similar question and ‘simply’ needed updating, concepts and terminology relating to ID and to accessibility had changed considerably. This meant that search strategies had to be redesigned and the scopes of the earlier and the new review carefully reconciled. In addition, the methods and, by current standards, the quality of much older systematic reviews may mean that a review update that replicates the methods of the earlier review would be neither useful to stakeholders nor appealing to academic review teams.
In situations where a recent high-quality systematic review exists, the implied gap or opportunity for justifying a new systematic review may lie in asking different questions within the same topic (intervention, population and outcome) boundaries inhabited by a documented body of research evidence. For example, in the review of interventions to reduce preventable hospital admissions (i.e. case study 7), the earlier (2012) systematic review of effectiveness by Purdy et al. 45 showed where and in which specific patient groups there was sufficient evidence of effectiveness for a realist review to add value. Apparent similarities between previous and currently planned reviews, or apparent gaps/differences between high-quality systematic reviews, requires careful exploration to confirm the existence of genuine gaps and a clear need for an updated or new systematic review.
The review of digital innovations in primary care (i.e. case study 1) illustrated challenges related to identifying the gap/niche and meeting user needs. In this case, the user (i.e. NHS England) had identified numerous needs (nearly 20 questions within four themes), which led to an iterative, multistage approach with interim evidence synthesis products to inform potential next stages. This included an initial report, presenting a scoping review, which helped to focus the final stage synthesis on a narrower and more manageable set of prioritised questions.
Finally, both review teams and review users should be open to the possibility that no clear niche or gap might usefully be filled by a new evidence synthesis within a given topic. Such a situation exists when no primary research addresses the main questions and uncertainties of the policy customer, or where such primary research does exist and has already been summarised and synthesised in a high-quality systematic review. This issue links to earlier consultative issues on managing stakeholder expectations (consultative issue 5) and educating the end-user about synthesis processes and products (consultative issue 4).
Balancing rigour/reliability (reproducibility)/relevance (interface issue 2)
This theme captured how the review team manages potentially competing tensions of scientific quality, confidence in the review output and utility to the intended users within the constraints of remit and resources.
The review of digital innovations in primary care (i.e. case study 1) showed how meeting user’s needs might involve departing from conventional standards of academic rigour and reporting. They chose to meet their user’s needs not by conducting a ‘full systematic review’, but, instead, by adopting systematic review methodology wherever feasible. This decision ultimately meant that their evidence synthesis products were also less conventional, going beyond the summary and synthesis of previously published research within a written report. For example, they produced an interactive resource (i.e. a type of evidence map) for identifying relevant evidence, alongside information on ongoing relevant research and links to academic researchers active in the fast-changing area of service innovation.
Similarly, the evidence map about access to health care for adults with IDs (i.e. case study 8) traded-off the quantity of literature covered against data validity. The team constructed their evidence map using evidence from study titles and abstracts, without verifying the abstracts against the full text of the included sources. Such trade-offs are common when seeking to achieve timely and deliverable review products that still have credible quality.
Transferability/applicability of study evidence to the policy/service/service user context (interface issue 3)
This theme captured how the review team manages the need to provide UK-specific interpretation from evidence bases drawn from other countries and contexts. A key and commonly negotiated choice, evident in several of the case studies, relates to whether to include international evidence or restrict to studies conducted in UK health-care and social care settings.
Case studies 2 and 5 both identified specific policy customers and a phenomenon of interest that was explicitly based in legislation or the application and use of legislation (respectively, the MHA’s provisions for involving trusted relatives or friends in compulsory detention16 and the strengths-based working by social workers as promoted by the Care Act 201436). This meant that applicable evidence was likely to be jurisdiction specific, and studies from outside the UK were likely to be of limited relevance. Both of these reviews were commissioned within tight, externally imposed timelines (2 and 6 months, respectively), adding a further pragmatic reason to consider restricting to UK studies. However, in both cases, this presumption had to be discussed and confirmed with policy stakeholders. In case study 2, to inform reform of the MHA,16 interest in looking at international evidence was balanced by existing variation in both relevant legislation and in related evidence between the UK’s four devolved nations.
Other contexts where international evidence may have less applicability might include accessibility and patient experience, especially when linked to cultural, ethnic or demographic factors (as in case study 4, about access to social care for ethnic minorities or LGBT+ people). In contrast, it is often presumed that hospital-based care systems are similar across high-income countries and, therefore, evidence is applicable between them. For example, in case study 7 (a review of the implementation of interventions to reduce hospital admissions), evidence was sought from the major anglophone high-income countries: the UK, USA, Australia, Canada and New Zealand. However, both case studies (4 and 7) involved realist approaches to synthesis, in which the transferability of evidence between studies, and from studies to the intended review user’s setting, is achieved through identifying shared theoretical mechanisms across different contexts. Therefore, applicability and transferability of research evidence is not a static, inherent property of the evidence itself and where it has come from. Rather, it is judged in relation to the models of causality on which the particular synthesis methods are based. Consequently, some ‘configurative’ methods – like realist synthesis – require studies from diverse contexts to develop their outputs, which is in contrast to conventional ‘aggregative’ methods (like quantitative meta-analysis) that work best when between-study heterogeneity is minimal.
Technical/internal (review team) issues in scoping and question formulation
This broad category of scoping considerations relates to how issues of method and reporting, which are typically outlined conceptually in textbooks and handbooks on systematic review methodology, work out in practice. Technical issues relate to choice of methods, depth of analysis and format of presentation of review findings. These considerations seek to inform methodological choices that are both rigorous and appropriate to the review question, audience and types of data/study available. These issues are technical in the sense that they rely more, but not exclusively, on the skills and experience of reviewers and information specialists in matching the detailed review methods to the review questions, and to the quantity and quality of available evidence. These considerations, therefore, include what might be called the ‘science’ of scoping, drawing on shared and established principles and research methods.
Choosing the methods of synthesis (technical issue 1)
This theme captured how the review team explores different options and makes an informed decision about which type of synthesis product will best meet the needs of the intended users. The steps to arriving at a particular method of synthesis varied considerably between the reviews in our case studies, as did the final type of evidence synthesis delivered. These eight case studies comprised effectiveness reviews (typically, narrative syntheses), realist reviews, scoping reviews, evidence maps and reviews of qualitative evidence. The outcomes of interest spanned effectiveness, cost-effectiveness, patient and carer experiences, accessibility and implementation.
In general, the starting point for choosing the method of synthesis was the review question, based on translating the policy customer’s evidence need into a specific outcome of interest (e.g. ‘what works?’ becomes ‘what is the effectiveness of . . . ?’). Within the review question, the explicit or implied outcome of interest was a key determinant of whether quantitative or qualitative evidence was sought and synthesised. For example, in case study 6, the study of hospital-led approaches to reduce length of stay for planned admissions, the review questions were framed around evaluating the clinical effectiveness and cost-effectiveness of alternative approaches. These questions can be validly and reliably answered using only quantitative comparative evaluations, like RCTs, and evidence synthesis methods, like narrative synthesis alongside meta-analysis, typically using an integrative approach to synthesis (i.e. ideally, to produce a generalisable summary answer to the question).
In case study 1, to synthesise evidence on Digital First Primary Care, the questions were so broad and the potentially relevant research so diverse, that a thematic synthesis approach was adopted, largely to accommodate multiple questions and types of evidence. The York team described this as not being a full systematic review, but a process of transparently identifying, critically appraising and summarising the research evidence relating to these questions.
The second main consideration that drove the choice of synthesis method was the quantity and design of available primary research studies. For example, in case study 2, the focus was on patient and carer experiences (of the ‘nearest relative’ provisions) and the scoping searches mainly identified qualitative research studies. Therefore, some type of rapid/pragmatic qualitative synthesis was required. That the synthesis method cannot always be rigidly specified at the protocol stage is further underlined by case study 4. The Sheffield team reflected that ‘The choice of review synthesis approach is not a decision to be made once the scope has been finalised – it represents an integral part of the scoping process (PICOSS)’ and this underlines a wider blurring of the conventional separation of scoping and protocol agreement and commencement of the systematic review [see Scoping as a continuous process through to shaping the end product (technical issue 5)].
Conversely, certain approaches to evidence synthesis are seen as too labour-intensive and time-consuming to do well in the context of rapid and policy-responsive review teams, notably meta-ethnography for reviewing qualitative evidence (although rapid meta-ethnographies have been conducted). In addition, of the eight case studies presented here, only one (i.e. case study 6, on strategies for reducing hospital length of stay in older people) addressed an effectiveness question where a sufficient number of high-quality randomised studies existed for meta-analysis to be feasible. However, even in this systematic review, the meta-analyses included only a smaller subset of all studies comparing the relevant alternatives.
Balancing fixed versus fluid questions/components/definitions (technical issue 2)
This theme captured the extent to which the question as a whole and/or its individual PICOS components are predefined or if they emerge during exploration of the literature. This balancing act seems to be a dominant trade-off for responsive reviews in the health and social care services and policy field, as exemplified in seven of our eight case studies. This technical issue is linked to the consultative issue of managing stakeholder expectations (consultative issue 5) and the technical issue of determining which review activity, of mapping, scoping and reviewing, will take place. Responsive, rapid reviews for policy-makers are multistage and, unlike RCTs, offer valuable opportunities for review and interim revisions of aims and methods.
A key example of this balancing act is case study 6, in which the plans for evidence synthesis had to be significantly adapted when > 100 effectiveness studies were identified (according to the original inclusion criteria). This led to a revised plan for evidence synthesis that sought to balance rigour and applicability. The review included two evidence syntheses: one of comparative effectiveness studies from the UK only (but of all high-quality comparative designs) and the other of studies from any high-income country, but RCTs only. This hybrid approach meant that review users interested in applicability to the UK could use the first synthesis and those interested in the most scientifically rigorous (internally valid) evidence across diverse contexts could use the second synthesis. As a result, the review avoided the effort of having to data extract, quality assess and synthesise the less rigorous evidence from beyond the UK. The realist review of access to social care for ethnic minority and LGBT+ populations (i.e. case study 4) was also conducted within the context of a scope that evolved throughout the review process.
In short, although review protocols are drafted and initial inclusion criteria and synthesis plans are prespecified (and even published, e.g. in PROSPERO), it is acknowledged that they will likely change. Moreover, even where the question remains fixed, learning and clarity about key concepts and terms within it are expected to emerge throughout the review. These technical aspects, therefore, go hand in hand with interface and consultative issues as the evolving protocol for the review is transparently revised, especially in consultation with the ultimate policy end-user.
Taking stock of (and building on) what studies exist (technical issue 3)
This theme captured how the review team explores the quantity, quality and characteristics of primary studies and/or reviews in determining which output will be both feasible and useful.
Sometimes, as in case studies 7 and 8, a key previous review offers a starting point for the new review. In the review of interventions to reduce preventable hospital admissions, the effectiveness review by Purdy et al. 45 provided a useful sampling frame of medical conditions on which the realist review might focus in depth. In contrast, in their review of access to care for people with IDs, the much older review by Alborz et al. ,49 ostensibly on the same topic, did provide some reusable resources (such as an interview schedule). However, it largely seemed to serve as a marker of how concepts of disability, notions of access and frameworks for understanding the performance of health services have all advanced significantly since 2003, and that the focus and intended value of the new review had to be carefully articulated.
In other reviews, taking stock is directly a process of assessing the diversity and quantity of available evidence and tailoring the planned synthesis to make the best of what evidence is available, in relation to the review’s questions. However, these decisions necessarily occur once searching and screening is mostly complete and so may not strictly constitute the topic-scoping phase.
Mapping versus scoping versus reviewing (technical issue 4)
This theme captured how the review team manages the relationship between exploring the characteristics of the evidence base (mapping), determining the parameters of the specific planned synthesis (scoping) and conducting the synthesis (reviewing), and the extent to which these processes transform into discrete project deliverables. This common three-stage sequence of responsive reviews is partly a response to the risks of overspecifying the planned final evidence synthesis at the beginning (and also relates to technical issue 2 of balancing fixed vs. fluid questions). 11 Although they are conceptually useful, we recognise that, in practice, scoping, mapping and reviewing are processes that necessarily interact and often overlap, as well as being labels applied to review outputs that may signal a formal end or transition of a stage in a continuous process.
Scoping as a continuous process through to shaping the end product (technical issue 5)
This theme captured the extent to which the scoping process is used as an opportunity to precondition the users to the content and form of the final synthesis product. Through their potential engagement, the scoping process offers an opportunity for commissioners and stakeholders to have an early influence on tailoring the final product to their requirements
Therefore, in case study 7, the focus on cardiovascular and respiratory conditions was determined not only by evidence on effectiveness, but also from the commissioner perspective, as articulated by the NIHR programme staff. For the review team, it is also part of a risk-averse strategy that minimises the chances of producing a product that is neither useful nor appropriate. In case study 4, the review team shared a previous similar realist review of access to care for a different marginalised group (i.e. older people in rural areas) to show the end-users the kind of findings that a realist review can produce [similar to the earlier consultative issue of ‘educating the end-user about synthesis process and products’ (consultative issue 4)].
Choosing between general and specific and broad and deep focus (technical issue 6)
This theme captured how the review team decides whether to cover an entire topic or to select one or more subtopics as exemplars of the whole, and the extent which they optimise coverage compared with detail. This includes decisions about whether to primarily describe and not to synthesise studies (as in an evidence map), or to also critically appraise and analyse included studies within a formal synthesis (e.g. a framework synthesis or narrative synthesis).
In the review of experiences of strengths-based approaches to social work (i.e. case study 5), this decision involved a choice between reviewing evidence explicitly about strengths-based practice and working itself, although it is a nebulous and loosely bounded set of principles and concepts, and ‘deconstructing’ or ‘representing’ strengths-based working as a collection of specific programmes and initiatives that are widely seen as fostering or exemplifying strengths-based working. Through tabulating documentary sources and consulting with diverse stakeholders, we ultimately identified 17 subsidiary approaches and programmes that were seen as fostering strengths-based working. Although this made searching for named programmes more straightforward, it did, however, risk treating the 17 approaches/programmes as equally strengths based in approach (i.e. not appreciating the substantial differences between them).
The review of interventions to prevent avoidable hospital admissions (i.e. case study 7) also showed the challenges to review teams of selecting a representative and manageable body of evidence to synthesise from a larger whole. The challenge in this case lay in the plentiful ACSCs and the solution was to choose a smaller selection to be reviewed in detail as useful exemplars for understanding others (e.g. cardiovascular and respiratory conditions). These two conditions had been sufficiently explored, and adequately supported as effective, to make these an appropriate focus for a realist inquiry.
Summary of the findings
This report has presented the scoping stages of diverse review projects commissioned or conducted in direct response to the expressed or perceived needs of health policy-makers or health and social care service commissioners. Despite the diversity of topics and goals, and their being conducted by three independent university-based research teams, they reveal similar challenges and draw on common principles and processes developed to scope topics and formulate review questions.
Iteration and perseverance
Several case studies highlight that effective topic scoping and question formulation takes time and effort. Reviewers should not expect the ‘optimal’ review question to emerge from a single cycle of scoping searches and stakeholder consultation. Related to this, it is important to involve as many members of the review team as possible in the discussions (or shared notes) from stakeholder meetings, reading key sources and the screening and discussion of scoping searches. This maximises the chances of identifying recurrent needs or uncertainties in previous reports or stakeholder opinions about where clearer evidence is needed. It also creates a shared understanding of the key terms, service/policy contexts and complexities relevant to a particular review.
Another time-consuming, but ultimately productive, element of many of the scoping processes described is the time taken to identify, approach and build relationships with the key stakeholders. This often includes following false leads and the use of multiple strategies (e.g. e-mail, telephone) to contact people in relevant organisations who are able and willing to share their experience and knowledge.
Navigating between ‘the two fears’
One way of understanding scoping processes is as a process of navigating between ‘two fears’ or averting two risks: (1) the fear of finding and having to summarise and synthesise too much research (posing a risk to deliverability) and (2) the fear of finding too little or no research (posing a risk to the usefulness of the review findings). Many decisions made during scoping try to anticipate and avoid these two extremes to produce a review that is deliverable, on time and within resources, but that is also as useful as possible in addressing policy-makers’, service commissioners’ or clinicians’ evidence needs. Nevertheless, ‘too much’ evidence is also defined in relation to the (typically fixed) size of the review team, and the general expectations that a review and report will be produced in a certain time frame (e.g. 6, 8 or 12 months). These trade-offs were typically shared and discussed with the policy customers as the ultimate arbiters of what combination of scope (i.e. size), timeliness and relevance of review would be most useful to them. This key tension between finding ‘too much’ evidence or finding ‘too little’ has also been noted in relation to systematic reviews as student projects. 2
Although finding sufficient high-quality studies to create a useful answer is the ideal, there are circumstances where producing an ‘empty review’ (i.e. finding no good-quality studies to answer a particular question) remains useful to policy-makers. Authoritatively concluding an absence of reliable scientific evidence on currently implemented service designs or policies may legitimise innovative service and policy change, or fully justify the need for funding rigorous research and evaluation of current and new services. Given the considerable time and other resources involved in producing an empty review, it is worth establishing in advance, from the main policy customer(s), that such an outcome would still be valuable. The review team will also inevitably be aware that an empty review is less publishable.
Negotiation or not negotiation?
Team members were divided over the extent to which the process of determining and agreeing the scope should be considered ‘negotiation’. Some resisted the business or commercial implications of ‘negotiation’ and drew attention to mutual interests, of research team and research commissioners, in seeking to deliver a rapid review that meets a genuine health service need in a way that minimises inefficiency and duplication and optimises the use of public funding. Certainly, the teams considered it helpful that negotiations did not start from an adversarial standpoint. In this sense, resolution of the negotiations comes not necessarily in agreeing a review protocol, but in a necessary prerequisite of reaching a common understanding. Our teams found that the protocol only loosely served as a contractual safety net, but more often served as a snapshot of an intended direction, and perhaps had most value through the process of sharing and negotiating it to develop a shared understanding.
From this shared platform, both review team and review commissioner can then adopt a position from which to take forward detailed plans for the review. This understanding did not simply relate to the topic under review, but extended to acknowledgement of what might reasonably be achieved within the resources available. Others saw the process from a public health perspective of negotiation, in recognising that negotiating and influencing are particularly important when these skills offer the only route by which to deal with external organisations and partners.
Managing stakeholder expectations (consultative issue 5) was seen as particularly important and the tension between underselling the potential value of the review and overpromising on what might be delivered needs to be handled within each individual project and each year’s programme as a whole. A key challenge is helping the commissioners of a review to gain clarity about what a review might be expected to address. The teams reflected on classic models of information needs and negotiation, whereby such a lack of clarity might be accompanied by a need for ‘sense-making’ by which to resolve ‘questions, confusions, muddles, riddles and angst’. 54 This explains why careful defining of terms and of the research problem constitutes an essential first step.
Another resonance with negotiation occurs where the NIHR HSDR programme staff act as intermediaries, or even mediators, between the review teams and diverse stakeholders, in managing stakeholder expectations (consultative issue 5). End-users may not realise the resource implications of different review methods or their suitability for their questions. In contrast, the funders, as more experienced users of reviews, could help other agencies to revise their expectations more realistically.
The teams shared recognition that the process typically began at an earlier stage than negotiation (i.e. a more open-ended stage of ‘pre negotiation’ that some preferred to describe as ‘information sharing’). At this point, neither review commissioner nor review team knows fully what they might realistically achieve in connection with the underlying information need. Sharing of priorities and perspectives is a necessary prequel to reconciling those different priorities/perspectives (consultative issue 2). Some team members felt that the review team held particular influence because they were able to propose both review methodology and the associated resources to accompany each topic. At the same time, the NIHR programme team are themselves able to build up experience and knowledge on what might be achieved and expected, and are able to use this in agreeing the final ‘sign-off’.
Review teams have previously seen themselves as having an ‘honest broker’ role when interpreting topics with which they have not specifically engaged. The reality is that reviewers will also seek to optimise the benefits of the chosen review for themselves and their academic organisations, alongside meeting the needs of the review commissioners and of the health and care services. For example, review teams may privilege a given review method, from multiple options, that might offer the possibility of methodological innovation or experimentation. Alternatively, they may seek to make the review output as publishable as possible. Viewed in this micro-context, the model of negotiation – the classic ‘win–win’ situation – is seen to exert an influence on outcomes from the scoping process.
Co-production? To what extent and, if so, with whom?
The teams also discussed whether or not the questions and scopes of these reviews were actually developed through a process of ‘co-production’. 55,56 Co-production, in the context of research, is the process whereby stakeholders – those who may use or be affected by the outcomes of research – work as partners with researchers to create, shape and deliver research (or, indeed, syntheses of research evidence). Co-production does not necessarily refer exclusively to the relationship between researchers and the potential end-users of the service, as most commonly discussed, but might also relate to the relationship between the funder and research team.
Related to this, one of the models the group discussed related to the researcher-in-residence model, which held particular parallels with aspects of having ‘on-call’ review teams. 57 Although the review teams were not physically co-located in the NIHR commissioning organisation, they did engage and interact in numerous ways to acquire a more complete understanding of the review commissioner’s needs. The teams saw three-way co-production between funders, researchers and users as an important aspiration that could yield benefits for all parties. Although all could point to instances of successful co-production, for example in including service users or care professionals as co-researchers and as co-authors on the reports, there was general recognition of the potential to extend this further. However, this was accompanied by an awareness that the brief and episodic interaction with some of the stakeholders often impairs more genuine or intensive co-production.
The team concluded by reflecting on the extent to which ‘true’ co-production can ever be possible within a rapid response review programme when faced with such accelerated timescales. Again, managing expectations extends to being open and honest with PPI representatives about their roles in informing the direction of reviews, and making it clear to other advisory panels and stakeholders that they are coming in on a process that has already undergone considerable stakeholder involvement and/or consultation. The teams highlighted the difference between informing the topic and informing the review. They also identified how the protocol was a genuine product of co-production, albeit within the context of being more important to the review team, but of relatively little detailed interest to the review users or policy customer (who were mainly interested in the final review output).
Interestingly, we did not directly discuss how we made our choices about how much and what content or service/policy context was required for each review project, although these choices clearly greatly influence the relevance of the scopes and the final review products. In general, each project team obtained as much and as diverse, relevant and co-operative content expertise as we could, given time and other resource constraints. However, efforts to identify and secure further or more specific expert knowledge after the agreement of the protocol would, inevitably, over time compete with efforts to deliver the work itself. This aspect of conducting rapid, responsive reviews is worthy of more explicit and prospective evaluation.
Although we did not discuss it in detail, it is possible that learning materials or templates could be developed that quickly clarify and communicate these typical expectations around scoping, explain key review terminology and provide ‘bite-size’ learning about common evidence synthesis methods and products. This was achieved, to some extent, by pointing new policy or service delivery stakeholders to our websites or relevant previous reviews. Within the case study projects, such knowledge sharing with the synthesis end-users happened in a more responsive and ad hoc way (i.e. in e-mails and teleconferences), which may have led to inconsistencies and duplicated effort. However, the time constraints on the senior health policy and service delivery professionals to use such learning materials would probably also mean a more bespoke and informal process of learning from the review team would prevail.
‘Pinning down’ versus ‘keeping open’
The teams recognised that, in contrast to a systematic review, where the review protocol is an opportunity to pin down and specify the intended final review, a responsive rapid review programme needs to build in contingency and conditionality. Although specifying the work to be carried out and the timescales and milestones within which it will be accomplished is a necessary part of negotiations, it was considered important to reserve the right, for both parties, to modify overall plans if necessary. This could be seen in changing the emphasis of results, prioritising a particular subquestion for earlier delivery or renegotiating the final review methodology. The three-phased mapping–scoping–review model, referred to in our previous report,11,58 not only optimised different methodologies for different stages of the question, but also offered multiple time points beyond which further plans might be framed conditionally.
Teams felt that the symbolic status of the protocol – analogous to a handshake to seal a deal – was often as important as the explicit technical information specified within it. Stakeholders, whether policy-makers or the public, often revealed little interest in the finalised protocols and the team and review commissioners tended to attach more value to the formative process rather than to the document as final artefact. Viewed in such a context, the scoping process is less a discernible phase of the review and more a pervasive issue that offers less flexibility as one nears the point of delivery. This also meant that the protocol was seen more as a ‘snapshot’ of the planned review and its intended direction at a point in this process (rather than a fixed blueprint for producing the defined end product). If this were a highly commercial contract between different parties wanting different goals, this would be a problem. However, in a context where the goals of the review teams and the policy customers are closely aligned (respectively, to produce and to receive a useful, independent and academically rigorous review of relevant evidence), such formal ‘contractual’ purposes of the protocol seem secondary. Scientifically, however, review protocols are also intended to minimise bias in review findings (through prespecifying and publishing the detailed aims and planned methods) and so the review protocols still fulfilled this important function.
Members from across the teams also pointed out how a similar, contingent need to keep plans open related to the involvement of stakeholders, whereby revisiting the consultative process might lead to further revision, refinement or reconceptualisation, ideally as a planned, transparent and documented activity. The teams reflected that this served to distinguish these commissioned review programmes from ‘classic’ research. They saw this contingent quality as an essential feature of policy support, more reflective of consultancy activities. Indeed, the team would also adopt the role of consultant when educating the end-user about synthesis process and products (consultative issue 4). This is seen when the review teams lay out the range of review products that they can provide and then advise the review commissioners on what might be most appropriate given the available time.
The role of the information specialist
Interestingly, within our case studies, less prominence was given to the contribution that different disciplines and skills provide within the scoping process. Information specialists on our teams could identify clear parallels between the skills they customarily employ when interacting, as internal knowledge brokers within a review team, and those that they utilised, as external knowledge brokers, as a ‘translator’ within discussions with the review commissioners. The different teams utilised diverse models of information specialist involvement (from nominated to the programme, through being dedicated to the programme and involvement in hybrid information specialist/reviewer roles). However, all three centres confirmed the need to ‘embed’ the information specialist within the scoping process and subsequent ‘negotiation’ to some degree or other. Distinct advantages were recognised from ensuring continuity in the information staff involved, particularly given that the types of topics explored through the NIHR HSDR contracts differed in their nature and requirements from ‘conventional’ systematic review topics. Indeed, an information specialist’s recognition of the ‘differentness’ of the review requirements could be as important as their technical knowledge in designing and conducting searches.
Although the need to involve information specialists in reviews, especially rapid reviews, has almost become a mantra in recent years, it is particularly interesting to isolate this specific contribution of their professional skills set beyond the technical knowledge of terminology, sources and databases. Information models associated with sense-making and the satisfying of information needs59 recognise the importance of relationship building, as evidenced in these review scoping processes. On the other hand, an information science perspective confirmed a recent observation that models of information need, typically spotlighted within information science, almost exclusively focus on an individual information need and not on the collective information transfer required by review teams. 60
Abbreviated/accelerated review commissioning?
The review teams discussed the ‘upstream pipeline’ from ideas to commissioning briefs, as well as the ‘downstream’ pipeline from commissioning briefs to rapid review outputs. The constraints and practical, organisational and political considerations involved in managing and deciding priorities (consultative issue 1) within the review commissioning process contrast with the flexibility and agility that review teams can achieve once the topic is adopted in-house and comes within their control. Team members speculated if, ultimately, review commissioning might mirror the technical production of rapid reviews (i.e. in the form of abbreviated and accelerated versions of commissioning to match the concepts of abbreviated and accelerated review processes).
Team members expressed the view that the most satisfying and successful reviews in which they had participated typically involved a rapid path from ideas to briefs, such that the review outputs were contemporary, relevant and used in decision-making. In contrast, ‘testing the water’ with stakeholders as part of the scoping process sometimes revealed that they had not previously shaped the priority, or that time may have elapsed and priorities shifted. Team members felt that it could be useful to ‘check back the narrative’ (i.e. to ask if a previous high-priority question advanced for a review could be reaffirmed as a current high priority). On the other hand, the team recognised the need to reach a point at which a review question can be anchored and a protocol produced to draw a ‘line in the sand’, given that it would not be feasible to engage in a continual cycle of revisit, rescope and reprioritise. In some cases, the team may have invested considerable ‘sunk costs’ into the scoping process and may find it more feasible to make an existing priority work – by tailoring the scope – rather than pursue a de novo topic. In short, although review teams should understand that policy processes and priorities are often and necessarily dynamic, complex and political, review commissioners and users have to accept that a high-quality evidence synthesis can only be produced from a brief and question that, at some point in the review process, has to be fixed.
The ethics of commissioned reviews
The discussion concluded by reflecting on the ethics aspects of the scoping process. Team members felt a responsibility to produce reviews that genuinely meet the needs of health and social care services to avoid duplication and to ensure that public funding is effectively and efficiently spent. Reference was made to the Royal Society’s four ‘principles for good evidence synthesis for policy’: transparent, inclusive, accessible and rigorous. 61 One of the centres had formally adopted these (with the addition of ‘appropriate’) as core values for use in its internal annual reviews. Reviewers have a responsibility to identify if a review might already exist or if a topic may be conceived too soon or articulated too late to be valuable. In such cases, the review commissioner might accept the availability and interpretation of evidence as it currently exists, commission primary research to meet the evidence need or set a time point when the value of a potential evidence review can be reconsidered. Note that none of the reviews that form the basis of our eight case studies required or obtained research ethics approval. This is accepted good research practice for systematic review projects (where the research ‘data’ is invariably already in the public domain).
Both a technical and a social process
Discussion within the teams agreed that the rapid review process extended beyond being a technical and exclusively information-driven process. Essentially, the relationship with commissioners of the reviews, whether the NIHR programme team or the end-users, is a social process that requires high-level social/research skills. The five themes (consultative issues 1–5) attest to the importance and prominence of this aspect of the rapid review commissioning process. This echoed the findings of Moore et al. ,62 who identified 35 different skills, many of which were required at an experienced or very experienced level by knowledge brokers involved in a rapid review commissioning programme in New South Wales.
Where possible, all of the review team should be included as part of the ‘negotiation’ of scope. Staff described an ‘all hands on deck’ scenario at the initiation of projects when getting from the initial question, which may be difficult to deconstruct and translate, to a feasible review question. Team members needed to share and harness their collective experience so that they were able to recognise the specific requirements of this type of review work and have the confidence to propose and explore alternative methods and types of review. This could only happen through the social process of dialogue within the team about emerging understandings, misconceptions, confusions, anomalies and realisations, in relation to both the evidence and the end-user’s perspectives and needs.
Potentially, individual centre staff face a challenge in managing a personal portfolio that includes commissioned rapid review work that is potentially high impact, alongside more deliberative conventional academic projects and outputs for research excellence. Correspondingly, centre directors need to balance continuity, achieved through a small and focused team, with capacity, which may require access to a larger, more flexible and diffuse team. Continuity was needed to build up relationships internally within the team and with the commissioners, but also in terms of consolidating and extending skills in handling these complex and unclear types of topics. However, continuity could be delivered in diverse ways, from project direction and the assignment of dedicated staff across all projects through to standard involvement of the methodologists and identification of clear roles on each project. Capacity could also work out at an individual level as staff move from intensive involvement at particular stages of the project and then relinquish or re-engage at subsequent stages of the review pathway. These different team configurations to balance continuity and capacity influence the information exchange and topic-immersion aspects of conducting a review, and the trust and strength of relationships built with stakeholders.
Strengths and limitations
Strengths
This report builds on the detailed research experiences and insights from researchers working in three independent, university-based systematic review teams that were directly commissioned to conduct rapid and responsive evidence review projects to meet diverse policy and health service needs. The eight reviews from which we generated our shared reflections were on a diverse range of health and social care topics, and variously focused on effectiveness, cost-effectiveness, accessibility, implementation and patient and carer experiences. Some had well-specified initial review questions or topics and a clearly identified policy customer or end-user, others did not. For some reviewers and information specialists in all three teams, this work builds on experiences of developing and conducting rapid and responsive evidence syntheses for UK health policy organisations (such as the DHSC, NICE, Public Health England, Health Promotion Wales and the National Screening Committee) over several decades. This will inevitably have shaped how we work, and how we perceive and justify how we work, in this report.
Although this report has presented and reflected on the more recent experiences and lessons from eight review projects conducted between 2017 and 2020, for the York and Sheffield teams, this further builds on the experiences and a previous methodological report from similar commissioned roles between 2014 and 2017. 11 However, in relation to review scoping processes, the previous methodological report11 highlighted three lessons: (1) the value of using a two-stage review approach (literature mapping/scoping, then review/synthesis), (2) the importance of disseminating review protocols as widely as possible and (3) the need ‘where feasible’ to include PPI in scoping reviews to ‘ensure their usefulness and relevance’. Although the first two of these emerged among our identified issues, it is conspicuous that PPI did not (see Limitations).
We have used an explicit process for describing, sharing and discussing our experiences of review scoping and question formulation (case studies described using a standardised approach). We have identified and structured our reflections using a simple framework based in previous research (of consultative, interactive and technical issues). In addition, we have situated our reflections and the proposed ‘lessons learned’ in relation to existing methods guidance on these early stages of systematic reviews.
We have endeavoured to identify common or recurring issues and principles and express them as useful lessons for others, but we have also sought to acknowledge complexity; in particular, the diversity of review user/decision-maker needs, the specificity or breadth of topics/uncertainties and the diverse and uncertain nature of available evidence. From the beginning, those involved in undertaking this work and writing this report have been open about and interested in the tension between scoping and systematic reviews as a technical and primarily information-driven process (i.e. scoping as ‘science’), and scoping as a collective social process of learning, negotiation and relationship building (i.e. scoping as ‘craft’) to create mutual understanding between reviewers, the intended review users and other stakeholders. Therefore, we hope it may also inform wider debates, such as those in science and technology studies, which seek to understand the interplay between formalised/standardised and informal practices in science,63,64 and between explicit, research-based evidence and the role of tacit, experience-based forms of knowledge in policy and practice. 65
Limitations
Inevitably, our recollections and reflections may have suppressed or selectively reported negative experiences of stakeholder engagement or communication from research commissioners. Potential conflicts of interest relate to the need to preserve relations with stakeholders who might be important collaborators or commissioners in the future. Where this relates to the input of particular individuals, review teams took steps to anonymise those individuals and organisations with which we engaged. However, in general, such individuals are acknowledged in, and therefore identifiable from, the publication of the review.
More generally, this report describes and discusses the experiences and observations of researchers (review teams) working in a particular context (i.e. to produce commissioned, rapid reviews to respond to policy and health service users) in relation to the critical early stages of conducting systematic review (i.e. topic scoping and question formulation). Unlike the review scoping processes themselves, we have not involved the ultimate review users in this reflective exercise and they might have identified different issues, challenges and solutions. A prospective study of such processes should aim for greater cross-validation from different stakeholders and reflections from others external to the team. However, this would also require the scoping processes and choices to be more fully documented for others to be able to comment or reflect on them.
Although we prespecified some issues using a plausible framework, and used these to spot similarities and differences between the case studies, this was neither a formal thematic analysis nor a comparative case study. In addition, although our initial basic four-factor model (see Figure 1) usefully shaped our early discussions and consensus across the teams, and was not contradicted by what we found, it proved too basic and was effectively superseded by the 14 more specific scoping process considerations. This report cannot be considered ‘research evidence’ or judged against the usual standards of rigour and relevance. Nevertheless, given the transparency and reflexivity with which we have described and shared our experiences, both within this report and in the discussions that enabled us to produce it, we hope that it is an authentic, readable and useful account of the principles and key issues of scoping that have emerged within our experienced community of practice.
Some readers may express surprise at the apparent lack of PPI in the case studies presented here. All of the centres view PPI as a key contributor to the overall review process. However, we also acknowledge that opportunities to elicit patient and public experiences and preferences are perhaps more limited and, indeed, more challenging during scoping than at other stages in the process. Of the eight review projects that are the focus of this report, all but one included some PPI. However, of those that did make use of PPI, patients or the public were involved in review scoping and informing questions in only four case study reviews (case studies 4, 6, 7 and 8) (see Appendix 1, Table 13). Topics, as presented to the team, had, in many cases, already undergone input from PPI representation at earlier points of the process. Some topics (such as case study 5 in the adult social care field) were operationalised within patient/service areas where major national research prioritisation exercises involving patients and the public had recently concluded (such as James Lind Alliance Priority Setting Partnerships). Topic selection processes within the DHSC and the NIHR HSDR programme seek to include PPI or lay member input before being allocated to the review team. At the point of scoping, these topics were only ‘semi-malleable’, recognising the primary purpose of our centres in summarising and synthesising evidence to inform health and social care policy and service commissioning.
Rapid reviews, by definition, include rapid scoping processes, and identifying and recruiting appropriate patients or carers to any rapid project is challenging. At least one of the centres maintains a standing group of trained and pre-identified PPI representatives. However, ensuring that representation captures the values and perspectives of target populations, such as those with IDs or carers of those from ethnic minority populations, is challenging and may require specific targeted responses. Indeed, some reviews may not have narrowed their remit to particular types of patients or members of the public, making it difficult to prespecify what experiences, of conditions or of health and social care use, it would be appropriate to involve.
These possible explanations for little mention of PPI stakeholders in our case studies should not detract from the imperative of exploring and conducting PPI as soon as feasible within topic scoping. Indeed, where an immediate primary policy/service stakeholder has not been identified, or amid many and competing priorities, PPI representatives demonstrate the potential to provide critical insights about where the need for better research evidence is greatest.
We have not explored as much as we could the ultimate question of how and why the nature of the main subject of our reviews – essentially, different ways of organising and delivering health and social care services – is associated with specific challenges in formulating review questions and devising what review scope and approach to synthesis will best meet users’ needs. There is a growing literature on the challenges of evidence synthesis of complex interventions, including the issue of developing good review questions and review scopes. 66–68 Such debates and emergent guidance encompass the recurring tensions in systematic review methods, such as how to capture and explain (vs. suppress) heterogeneity, how to capture the impact of contexts, ‘lumping’ versus ‘splitting’, whether to focus on the whole package/intervention or try to uncover associations with underlying components and mechanisms, and the critical role of theory and logic models in evidence synthesis. We recognise all of these features of complexity in the reviews we have conducted and the diverse, messy, imperfect real-world evidence of which we have sought to make sense. It would probably take a prospective research study, or at least a series of workshops among reviewers who do this kind of work, to tease out and refine the connections and lessons from our work to build on these complex interventions synthesis ideas.
Lessons learned
Our conclusions have been expressed as ‘lessons learned’, practical principles and suggestions, and as reminders to ourselves and guidance to others for improving scoping processes in the context of conducting rapid reviews for policy-makers and service commissioners and managers. Some are specific to how review teams can be more effective at question formulation and topic scoping, and others may be useful for review users and commissioners. Others simply (and humbly) describe challenges or common constraints in conducting reviews for policy and service delivery. We contend that if these lessons were more widely acknowledged – by evidence reviewers, prospective evidence users and others who may be affected by any decisions informed – these might foster more realistic expectations.
We present the lessons learned as a table (Table 12), mapping them to particular issues identified across our case studies. Particular lessons can be traced back to Chapter 4 and Table 11 to identify the case studies and reflections from which they are drawn.
| Explanation | Lessons/recommendations |
|---|---|
| Consultative issues: externally generated issues relating to input from commissioners, stakeholders, experts and patient groups to inform the planned evidence synthesis product | |
| How the review team manages and negotiates with NIHR, stakeholders and other customers to ensure that priorities are addressed within resource constraints (C1) |
Where a review team can identify a policy or health service customer for the review, they should be sure to carefully negotiate and make explicit the impact of potential scoping decisions on competing goals (e.g. review duration, resources, comprehensiveness, rigour, relevance). (Synergy with I2) Review teams and review commissioners should mutually seek to optimise the three tensions of the topic (i.e. research question, type of data), the objective (i.e. the audience and purpose, epistemology) and the logistics (i.e. time, resources, expertise) (RETREAT)14 |
| How the review team manages potentially competing tensions between what different groups and stakeholders may want to achieve within the overall project remit (C2) |
Where there are multiple stakeholders or potential review users, the review team should ensure that they have transparent processes of consultation and negotiation, such that potential review users can influence the focus and purpose of a review, and the review team can acknowledge and, where possible, reconcile different views Where the review team demonstrate an explicit commitment to openness in stakeholder discussions, this fosters high-quality engagement by stakeholders It is helpful for the review team to include multiple perspectives (from information specialists, project managers, reviewers and methodologists) in scoping discussions. Senior negotiation skills are typically required at initial discussions with the review commissioners |
| How the review team secures input into the scoping and prioritising process from stakeholders and sustains this throughout the project to include reception of the deliverables (C3) |
Where the review team demonstrate an explicit commitment to openness in stakeholder discussions, this fosters high-quality engagement by stakeholders For stakeholders’ willing to engage, the review team should make it clear when, and in what ways, stakeholders can usefully engage with the review work |
| How the review team communicates aspects of review methodology and different synthesis outputs to the potential users/audience, particularly in terms of what they will deliver (C4) |
Review teams may need to explain the variety of potentially applicable synthesis methods and the typical content, format and use of their findings Review teams need to explain the potential value of one or more of scoping, mapping and/or reviewing of evidence |
| How the review team communicates what the review project will and will not be able to achieve within the available resources and time frame, particularly when the review will ‘fall short’ of the conventional systematic review standards (C5) |
A core strategy by which a review team manages expectations about a review is to develop the review protocol iteratively and collaboratively with stakeholders or user(s) Even though the protocol adds precision to the review scope, review teams should be honest about the fixed/fluid nature of questions and how this may have an impact on the methods and scope |
| Interface issues: issues relating to the interaction between the technical processes of the review team and the requirements of the review user | |
| How the review team positions the intended synthesis product within previous literature or reviews and in addressing users’ specific needs (I1) |
The most useful responsive reviews target evidence gaps that meet three conditions:Effective scoping processes often involve an iterative process for establishing these three conditions, including the production of interim outputs, such as scoping and mapping reviews Apparent similarities between existing and planned reviews, or apparent differences between existing high-quality systematic reviews, require careful exploration to confirm the existence of genuine gaps and a clear need for an updated review or a new systematic review. This requires critical appreciation of possible shifts over time in the meaning of key concepts, evaluation and synthesis methods, and the implementation context of policies or services Throughout review scoping, both review teams and potential review users should recognise when no clear niche or gap is filled by a new evidence synthesis. In such cases, innovative or tailored ‘evidence products’ may offer an alternative use of the review team’s skills to meet user needs. Products could include interactive tools to access evidence or – in volatile areas of policy or service delivery – information on ongoing research or contact lists of active/leading researchers in the field |
| How the review team manages potentially competing tensions of scientific quality, confidence in the review output and utility to the intended users within the constraints of remit and resources (I2) | Where a review team can identify a policy or health service customer for the review, they should be sure to carefully negotiate and make explicit the impact of potential scoping decisions on competing goals (e.g. review duration, resources, comprehensiveness, rigour, relevance) (Synergy with C1) |
| How the review team manages the need to provide UK-specific interpretation from an evidence base that may have to be drawn from other countries and contexts (I3) |
Discussions between review teams and review users should recognise that the applicability and transferability of research evidence is not a static, inherent property of the evidence itself (e.g. where it has come from or how old it is). It is also dependent on the specific contexts and decisions to which the evidence is likely to be applied Review teams should always seek to meet the challenge of judging the applicability and transferability of research evidence, either for each included study and/or as a stakeholder consultation exercise about the findings |
| Technical issues: internally managed issues relating to the conduct of the review as experienced within the review team | |
| How the review team explores different options and makes an informed decision about which type of synthesis product will best meet the needs of the intended users (T1) | Review teams conducting rapid, responsive reviews for informing policy and service delivery need to access experience/expertise in diverse evidence synthesis methods, and have a detailed understanding of how they can be used to answer different types of question and how to handle different types and amounts of available evidence |
| The extent to which the question as a whole and/or its individual PICO components are predefined and predetermined or if they emerge during exploration of the literature (T2) |
Review teams conducting rapid, responsive reviews for informing policy and service delivery should expect and plan to review and revise the methods, and sometimes the questions, at key time points. Review teams should revisit all PICOS components, but, specifically, the planned approach to evidence synthesis should be reviewed once searching and full-text screening is complete Review teams should plan for potential changes in scope that may require sophisticated screening methods (e.g. fuller coding against inclusion and exclusion criteria) that include retrospective application of revised inclusion criteria Review teams should be aware of the ‘reversibility’ and resource implications of specific inclusion/exclusion choices when they scope rapid, responsive reviews. Some choices can be kept open for longer and commit less resources should they turn out not to be useful Review teams and review commissioners should be aware that, even in reviews where the review question and inclusion criteria remain fixed from early in the review process, review team learning about key concepts and the service/policy context continues to grow throughout the review. This collective understanding may legitimately change the planned methods for synthesis, presentation of findings or other aspects of the review (i.e. within-review changes are not solely data/evidence driven) |
| How the review team explores the quantity, quality and characteristics of primary studies and/or reviews in determining which output will be both feasible and useful (T3) | Review teams should search a limited, but appropriate, selection of resources, either as representative or purposive results, and feedback a complete and accurate picture of findings from the scoping search to review commissioners and/or stakeholders |
| How the review team manages and intersects the relationship between exploring the characteristics of the evidence base (mapping), determining the parameters of the specific synthesis (scoping) and conducting the synthesis (reviewing), and the extent to which these processes transform into discrete project deliverables (T4) | Review teams should avoid overcommitting/overspecifying evidence synthesis outputs by operationalising the distinct phases and goals of (1) exploring the characteristics of the evidence base (mapping), (2) determining the parameters of the specific planned synthesis (scoping) and conducting the synthesis (reviewing), and (3) acknowledging the discrete and valuable contribution of each as a potential project deliverable |
| The extent to which the scoping process is used as an opportunity to precondition the users to the content and form of the final synthesis product (T5) | All parties should recognise that scoping within rapid, responsive reviews extends beyond early prespecification of the review questions, review methods and ‘signing off’ of a review protocol (i.e. as a ‘contract’ between the review producer and the review user, and as a hypothesis-based research plan to minimise bias) |
| All parties should recognise that scoping is a social and symbolic process of information exchange; negotiation and trust-building; and shared learning between the review team, review users and other stakeholders, to establish the direction, concepts and principles that bind the project over time | |
| How the review team makes decisions regarding whether to cover an entire topic or to select one or more subtopics as exemplars of the whole, and the extent to which they optimise coverage vs. detail (e.g. description vs. analysis) (T6) | For the review team to add value, in the context of existing primary research and systematic reviews, they should decide whether to go deeper (i.e. more specific) or to go broader (i.e. more general) than existing knowledge. To inform these decisions, review teams should explicitly consider not just the amount and diversity of relevant research studies in relation to a question and context of use, but also the relative value of identifying vs. describing (e.g. mapping) studies, describing vs. critically appraising them, collating the descriptions vs. synthesising and analysing them, and using informal (e.g. narrative) vs. formal or theory-informed methods of synthesis |
Chapter 5 Conclusions
The needs of a commissioned, rapid and responsive evidence synthesis programme extend beyond the sound technical and scientific practices of a review team. Relationship building and social processes are key to the scoping and shared learning process between the review commissioners and the review team, between the review team and diverse stakeholders (including PPI representatives) and within the review team itself. In some cases, the intended users are identifiable, offering a focus for consultation, but this adds a requirement for relationship management by the review team and NIHR commissioners. Rapid evidence synthesis programmes require experienced research staff to broker the relationship between objective, product and the needs of intended users throughout the scoping and question definition process. Relationships should be conducted within agreed principles for good evidence synthesis for policy. From the shared experiences and reflections from the three centres, from 2017 to 2020, we have identified common issues and suggested lessons for improving scoping processes to inform similar commissioned and responsive review programmes.
More prospective, methodological research conducted alongside such rapid and responsive review teams could be used to validate the considerations and competing goals of scoping identified in this report, and potentially develop strategies and tools for managing them more effectively. Such research will need to recognise the inevitable interplay between formalised/standardised and informal practices in science, and also the role of more tacit, experience-based forms of knowledge in policy and practice alongside explicit research-based knowledge.
Acknowledgements
We are grateful to many current and former colleagues in each of our centres for their academic expertise, collegiality and dedication to producing high-quality and useful evidence syntheses as part of this commissioned programme. They include Jane Dalton, Gillian Parker, Andrew Street, Kath Wright, Sue Whiffin, Jenny Lowe, Anna Price, Latika Ahuja, Alison Bethel, Elizabeth Croot, Maxine Johnson, Ruth Wong and Susan K Baxter. We thank the Families Lobbying & Advising Sheffield (FLASh) carers group (Sheffield, UK), the Royal Mencap Society’s ‘Treat Me Well’ group (London, UK), staff employed by Mencap support unit and Speakup Self Advocacy (Rotherham, UK) for contributions to the intellectual disabilities project. We thank Emma Hock and Lesley Uttley on the Access to Social Care project. We thank members of the Public Advisory Group for the Sheffield Health Services and Delivery Evidence Synthesis Centre and their convener, Susan K Baxter, for input across all three Sheffield case studies. We would also like to thank the staff at the NIHR HSDR programme for their expert advice and flexibility, not just in commissioning these projects, but in enabling us to conduct them in a genuine spirit of partnership and collaboration with all stakeholders.
Rob Anderson would also like to thank Dr Ingemar Bohlin (University of Gothenburg, Gothenburg, Sweden) for the invitation to attend and present at the International Workshop on Formalised Procedures and Informality in Research Practices, 28 February–1 March 2018, Gothenburg, Sweden, which partly inspired the suggested focus and informed some of the reflections in this report.
Contributions of authors
Rob Anderson (https://orcid.org/0000-0002-3523-8559) (Professor of Health Services and Implementation Research) initially proposed the focus and methods for this reflective report; drafted the Exeter case studies; wrote the discussion section, partly based on an online ‘sandpit’ meeting about the case studies and the draft discussion section; and read, provided feedback and approved the final submitted version.
Andrew Booth (https://orcid.org/0000-0003-4808-3880) (Reader in Evidence-Based Information Practice) drafted the Sheffield case studies with input from the other Sheffield synthesis centre members; wrote the discussion section, partly based on an online ‘sandpit’ meeting about the case studies and the draft discussion section; and read, provided feedback and approved the final submitted version.
Alison Eastwood (https://orcid.org/0000-0003-1079-7781) (Professor of Research) wrote the two York case studies with input from their wider team; was involved in an online ‘sandpit’ meeting about the case studies and the draft discussion section; and read, provided feedback and approved the final submitted version.
Mark Rodgers (https://orcid.org/0000-0002-5196-9239) (Research Fellow, evidence synthesis) wrote the two York case studies with input from their wider team; was involved in an online ‘sandpit’ meeting about the case studies and the draft discussion section; and read, provided feedback and approved the final submitted version.
Liz Shaw (https://orcid.org/0000-0002-6092-5019) (Research Fellow, systematic reviews) drafted the Exeter case studies; was involved in an online ‘sandpit’ meeting about the case studies and the draft discussion section; and read, provided feedback and approved the final submitted version.
Jo Thompson Coon (https://orcid.org/0000-0002-5161-0234) (Professor of Evidence Synthesis and Health Policy) drafted the Exeter case studies; was involved in an online ‘sandpit’ meeting about the case studies and the draft discussion section; read, provided feedback and approved the final submitted version.
Simon Briscoe (https://orcid.org/0000-0002-6982-4521) (Information Specialist) drafted the Exeter case studies and read, provided feedback and approved the final submitted version.
Anna Cantrell (https://orcid.org/0000-0003-0040-9853) (Research Fellow, evidence synthesis) provided input for the Sheffield case studies and read, provided feedback and approved the final submitted version.
Duncan Chambers (https://orcid.org/0000-0002-0154-0469) (Research Fellow, evidence synthesis) provided input for the Sheffield case studies and read, provided feedback and approved the final submitted version.
Elizabeth Goyder (https://orcid.org/0000-0003-3691-1888) (Professor of Public Health) provided input for the Sheffield case studies and read, provided feedback and approved the final submitted version.
Michael Nunns (https://orcid.org/0000-0001-5500-0911) (Research Fellow, systematic reviews) drafted the Exeter case studies and read, provided feedback and approved the final submitted version.
Louise Preston (https://orcid.org/0000-0001-7477-4517) (Senior Research Fellow) provided input for the Sheffield case studies and read, provided feedback and approved the final submitted version.
Gary Raine (https://orcid.org/0000-0002-0354-0518) (Research Fellow, Evidence Synthesis) provided input for the two York case studies and read, provided feedback and approved the final submitted version.
Sian Thomas (https://orcid.org/0000-0003-0917-0068) (former Research Fellow, Evidence Synthesis) provided input for the two York case studies and read, provided feedback and approved the final submitted version.
Data-sharing statement
Requests for access to data should be addressed to the corresponding author or, if appropriate, to the corresponding author of the case study reviews. Access to anonymised data may be granted following review.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health and Social Care.
References
- Petticrew M, Roberts H, Petticrew M, Roberts H. Systematic Reviews in the Social Sciences: A Practical Guide. Oxford: Wiley; 2006.
- Cherry M, Dickson R, Cherry M, Dickson R. Doing a Systematic Review: A Student’s Guide. London: SAGE Publications Ltd; 2014.
- Oliver S, Dickson K, Bangpan M, Newman M, Gough D, Oliver S, et al. An Introduction to Systematic Reviews. London: SAGE Publications Ltd; 2017.
- Booth A, Clarke M, Ghersi D, Moher D, Petticrew M, Stewart L. An international registry of systematic-review protocols. Lancet 2011;377:108-9. https://doi.org/10.1016/S0140-6736(10)60903-8.
- NIHR Health Services and Delivery Research Programme . Specification Document 16 47 – Call for Expressions of Interest: Production of Evidence Syntheses for the HS&Amp;DR Programme (May 2016) 2016. https://njl-admin.nihr.ac.uk/document/download/2026058 (accessed 16 June 2021).
- Boland A, Cherry M, Dickson R. Doing a Systematic Review: A Student’s Guide. London: SAGE Publications Ltd; 2017.
- Booth A, Sutton A, Papaioannou D. Systematic Approaches to a Successful Literature Review. London: SAGE Publications Ltd; 2016.
- Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane Handbook for Systematic Reviews of Interventions. Chichester: John Wiley & Sons; 2019.
- Centre for Reviews and Dissemination . Systematic Reviews. CRD’s Guidance for Undertaking Reviews in Healthcare 2009.
- Gough D, Oliver S, Thomas J. An Introduction to Systematic Reviews. London: SAGE Publications Ltd; 2017.
- Chambers D, Booth A, Rodgers M, Preston L, Dalton J, Goyder E, et al. Evidence to support delivery of effective health services: a responsive programme of rapid evidence synthesis. Evid Policy 2020;17:173-87. https://doi.org/10.1332/174426419X15468574223221.
- Oliver K, Innvar S, Lorenc T, Woodman J, Thomas J. A systematic review of barriers to and facilitators of the use of evidence by policymakers. BMC Health Serv Res 2014;14. https://doi.org/10.1186/1472-6963-14-2.
- Oliver S, Dickson K, Bangpan M. Systematic Reviews: Making Them Policy Relevant. A Briefing for Policy Makers and Systematic Reviewers. London: EPPI-Centre, Social Science Research Unit, Institute of Education, University College London; 2015.
- Booth A, Noyes J, Flemming K, Gerhardus A, Wahlster P, Van Der Wilt GJ, et al. Guidance on Choosing Qualitative Evidence Synthesis Methods for Use in Health Technology Assessments of Complex Interventions 2016. www.integrate-hta.eu/wp-content/uploads/2016/02/Guidance-on-choosing-qualitative-evidence-synthesis-methods-for-use-in-HTA-of-complex-interventions.pdf (accessed 16 June 2021).
- Booth A, Noyes J, Flemming K, Gerhardus A, Wahlster P, van der Wilt GJ, et al. Structured methodology review identified seven (RETREAT) criteria for selecting qualitative evidence synthesis approaches. J Clin Epidemiol 2018;99:41-52. https://doi.org/10.1016/j.jclinepi.2018.03.003.
- Great Britain . Mental Health Act 1983 1983.
- Centre for Reviews and Dissemination . Digital-First Primary Care: A Rapid Evidence Synthesis Initial Scoping Work and Protocol 2018. www.york.ac.uk/media/crd/Protocol-digital-primary-care.pdf (accessed 11 February 2021).
- Rodgers M, Raine G, Thomas S, Harden M, Eastwood A. Informing NHS policy in ‘digital-first primary care’: a rapid evidence synthesis. Health Serv Deliv Res 2019;7. https://doi.org/10.3310/hsdr07410.
- Centre for Reviews and Dissemination . Evidence Summary – Digital-First Primary Care: A Rapid Responsive Evidence Synthesis 2020. www.york.ac.uk/media/crd/Evidence-summary-digital-primary-care.pdf (accessed 15 October 2020).
- Shaw L, Nunns M, Briscoe S, Thompson-Coon J, Anderson R. The Experiences of Services Users, Family Members, Carers and Professionals of the Use of the ‘Nearest Relative’ Provisions in the Compulsory Detention and Ongoing Care of People Under the Mental Health Act: A Rapid Systematic Review 2018. www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42018088237 (accessed 11 February 2021).
- Mental Health Alliance . A Mental Health Act Fit for Tomorrow: An Agenda for Reform 2017. https://www.rethink.org/media/2594/a-mental-health-act-fit-for-tomorrow.pdf (accessed 21 June 2020).
- Great Britain . Human Rights Act 1998 1998.
- Shaw L, Nunns M, Briscoe S, Anderson R, Thompson Coon J. Experiences of the ‘nearest relative’ provisions in the compulsory detention of people under the Mental Health Act: a rapid systematic review. Health Serv Deliv Res 2018;6. https://doi.org/10.3310/hsdr06390.
- Centre for Reviews and Dissemination . Regulating and Inspecting Integrated Health and Social Care in the UK: Scoping the Literature [Review Protocol] 2020. www.york.ac.uk/media/crd/Protocol-reg-inspec-integrated-care.pdf (accessed 11 February 2021).
- Rodgers M, Raine G, Harden M, Eastwood A. Regulating and Inspecting Integrated Health and Social Care in the UK: Scoping the Literature. Southampton: National Institute for Health Research; 2020.
- Centre for Reviews and Dissemination . Evidence Summary – Regulating and Inspecting Integrated Health and Social Care in the UK: Scoping the Literature 2020. www.york.ac.uk/media/crd/Evidence-summary-regulating-integrated-care.pdf (accessed 15 October 2020).
- Booth A, Hock E, Preston L, Uttley L. Social Care Access for Adult BAME and LGBT+ Populations: A Rapid Realist Review. Southampton: National Institute for Health Research; 2021.
- James Lind Alliance . Adult Social Work Top 10. n.d. www.jla.nihr.ac.uk/priority-setting-partnerships/adult-social-work/top-10-priorities.htm (accessed 16 June 2021).
- Ford JA, Wong G, Jones AP, Steel N. Access to primary care for socioeconomically disadvantaged older people in rural areas: a realist review. BMJ Open 2016;6. https://doi.org/10.1136/bmjopen-2015-010652.
- Great Britain . Equality Act 2010 2010.
- Dixon-Woods M, Cavers D, Agarwal S, Annandale E, Arthur A, Harvey J, et al. Conducting a critical interpretive synthesis of the literature on access to healthcare by vulnerable groups. BMC Med Res Methodol 2006;6. https://doi.org/10.1186/1471-2288-6-35.
- Thorlby R, Starling A, Turtin C, Watt T. NHS at 70: What’s the Problem with Social Care, and Why Do We Need To Do Better. London: The Health Foundation; 2018.
- Saul JE, Willis CD, Bitz J, Best A. A time-responsive tool for informing policy making: rapid realist review. Implement Sci 2013;8. https://doi.org/10.1186/1748-5908-8-103.
- Dixon-Woods M, Agarwal S, Jones D, Young B, Sutton A. Synthesising qualitative and quantitative evidence: a review of possible methods. J Health Serv Res Policy 2005;10:45-53. https://doi.org/10.1177/135581960501000110.
- Anderson R, Price A, Ahuja L, Bramwell C, Briscoe S, Shaw L, et al. Strategies for Fostering a Strengths-Based Approach Within Adult Social Work: A Systematic Review of Effectiveness and Implementation Studies 2020. https://fundingawards.nihr.ac.uk/award/NIHR130867 (accessed 11 February 2021).
- Great Britain . Care Act 2014 2014.
- National Institute for Health and Care Excellence . Evidence for Strengths and Asset-Based Outcomes: A Quick Guide for Social Workers n.d. www.nice.org.uk/about/nice-communities/social-care/quick-guides/evidence-for-strengths-and-asset-based-outcomes (accessed 16 June 2021).
- Nunns M, Shaw L, Briscoe S, Thompson Coon J, Anderson R. What Is the Effectiveness and Cost-Effectiveness of Hospital-Based Multi-Component Strategies to Reduce the Length of Stay of Planned Inpatient Admissions of Older Adults 2017. www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42017080637 (accessed 11 February 2021).
- Nunns M, Shaw L, Briscoe S, Thompson Coon J, Hemsley A, McGrath JS, et al. Multicomponent hospital-led interventions to reduce hospital stay for older adults following elective surgery: a systematic review. Health Serv Deliv Res 2019;7. https://doi.org/10.3310/hsdr07400.
- Nuffield Trust . Reducing Length of Stay 2014.
- Medical Research Council . Developing and Evaluating Complex Interventions 2006.
- ERAS Society . List of Guidelines n.d. http://erassociety.org/guidelines/list-of-guidelines/ (accessed 18 September 2018).
- Lewin S, Hendry M, Chandler J, Oxman A, Michie S, Shepperd S, et al. Guidance for Using the iCAT_SR: Intervention Complexity Assessment Tool for Systematic Reviews 2016. https://methods.cochrane.org/sites/default/files/public/uploads/icat_sr_additional_file_4_2016_12_27.pdf (accessed 16 June 2021).
- Chambers D, Cantrell A, Booth A. Implementation of interventions to reduce preventable hospital admissions for cardiovascular or respiratory conditions: an evidence map and realist synthesis. Health Serv Deliv Res 2020;8. https://doi.org/10.3310/hsdr08020.
- Purdy S, Paranjothy S, Huntley A, Thomas RL, Mann MK, Huws DW, et al. Interventions to Reduce Unplanned Hospital Admission: A Series of Systematic Reviews. Bristol: University of Bristol; 2012.
- Cantrell A, Croot E, Johnson M, Wong R, Chambers D, Baxter SK, et al. Access to primary and community health-care services for people 16 years and over with intellectual disabilities: a mapping and targeted systematic review. Health Serv Deliv Res 2020;8. https://doi.org/10.3310/hsdr08050.
- Alborz A, McNally R, Glendinning C. Access to health care for people with learning disabilities in the UK: mapping the issues and reviewing the evidence. J Health Serv Res Policy 2005;10:173-82. https://doi.org/10.1258/1355819054338997.
- Alborz A, McNally R. Developing methods for systematic reviewing in health services delivery and organization: an example from a review of access to health care for people with learning disabilities. Part 2. Evaluation of the literature – a practical guide. Health Info Libr J 2004;21:227-36.
- Alborz A, McNally R, Swallow A, Glendinning C. From the Cradle to the Grave: A Literature Review of Access to Health Care for People With Learning Disabilities Across the Lifespan 2003. https://njl-admin.nihr.ac.uk (accessed 16 June 2021).
- McNally R, Alborz A. Developing methods for systematic reviewing in health services delivery and organization: an example from a review of access to health care for people with learning disabilities. Part 1. Identifying the literature. Health Info Libr J 2004;21:182-92. https://doi.org/10.1111/j.1471-1842.2004.00512.x.
- Rebelo Da Silva N, Zaranyika H, Langer L, Randall N, Muchiri E, Stewart R. Making the most of what we already know: a three-stage approach to systematic reviewing. Eval Rev 2017;41:155-72. https://doi.org/10.1177/0193841X16666363.
- Baxter S, Johnson M, Chambers D, Sutton A, Goyder E, Booth A. Towards greater understanding of implementation during systematic reviews of complex healthcare interventions: the framework for implementation transferability applicability reporting (FITAR). BMC Med Res Methodol 2019;19. https://doi.org/10.1186/s12874-019-0723-y.
- Munthe-Kaas H, Nøkleby H, Lewin S, Glenton C. The TRANSFER approach for assessing the transferability of systematic review findings. BMC Med Res Methodol 2020;20. https://doi.org/10.1186/s12874-019-0834-5.
- Dervin B. Sense-making theory and practice: an overview of user interests in knowledge seeking and use. J Knowl Manag 1998;2:36-4. https://doi.org/10.1108/13673279810249369.
- Martin S. Co-production of social research: strategies for engaged scholarship. Public Money Manage 2010;30:211-18. https://doi.org/10.1080/09540962.2010.492180.
- Vindrola-Padros C, Eyre L, Baxter H, Cramer H, George B, Wye L, et al. Addressing the challenges of knowledge co-production in quality improvement: learning from the implementation of the researcher-in-residence model. BMJ Qual Saf 2019;28:67-73. https://doi.org/10.1136/bmjqs-2017-007127.
- Marshall M, Pagel C, French C, Utley M, Allwood D, Fulop N, et al. Moving improvement research closer to practice: the researcher-in-residence model. BMJ Qual Saf 2014;23:801-5. https://doi.org/10.1136/bmjqs-2013-002779.
- Chambers D, Booth A, Rodgers M, Preston L, Baxter S, Dalton J, et al. NIHR HS&DR Evidence Synthesis Centres: Achievements and Learning From the First Three Year Programme, 2014–17. Southampton: NIHR Journals Library; 2017.
- Godbold N. Beyond information seeking: towards a general model of information behaviour. Inform Res 2006;11.
- Cooper C. Improving Literature Searching in Systematic Reviews: The Application of Tailored Literature Searching Compared to ‘the Conventional Approach’ 2019.
- Donnelly CA, Boyd I, Campbell P, Craig C, Vallance P, Walport M, et al. Four principles to make evidence synthesis more useful for policy. Nature 2018;558:361-4. https://doi.org/10.1038/d41586-018-05414-4.
- Moore G, Redman S, Butow P, Haynes A. Deconstructing knowledge brokering for commissioned rapid reviews: an observational study. Health Res Policy Syst 2018;16. https://doi.org/10.1186/s12961-018-0389-7.
- Bohlin I. Formalizing syntheses of medical knowledge: the rise of meta-analysis and systematic reviews. Perspect Sci 2012;20:273-309. https://doi.org/10.1162/POSC_a_00075.
- Sager M, Pistone I. Mismatches in the production of a scoping review: highlighting the interplay of (in)formalities. J Eval Clin Pract 2019;25:930-7. https://doi.org/10.1111/jep.13251.
- Greenhalgh T. How to Implement Evidence-Based Healthcare. Oxford: Wiley; 2018.
- Kelly MP, Noyes J, Kane RL, Chang C, Uhl S, Robinson KA, et al. AHRQ series on complex intervention systematic reviews-paper 2: defining complexity, formulating scope, and questions. J Clin Epidemiol 2017;90:11-8. https://doi.org/10.1016/j.jclinepi.2017.06.012.
- Petticrew M, Rehfuess E, Noyes J, Higgins JP, Mayhew A, Pantoja T, et al. Synthesizing evidence on complex interventions: how meta-analytical, qualitative, and mixed-method approaches can contribute. J Clin Epidemiol 2013;66:1230-43. https://doi.org/10.1016/j.jclinepi.2013.06.005.
- Squires JE, Valentine JC, Grimshaw JM. Systematic reviews of complex interventions: framing the review question. J Clin Epidemiol 2013;66:1215-22. https://doi.org/10.1016/j.jclinepi.2013.05.013.
- Price A, Ahuja L, Bramwell C, Briscoe S, Shaw L, Nunns M, et al. Research Evidence on Different Strengths-Based Approaches Within Adult Social Work: A Systematic Review. Southampton: National Institute for Health Research; 2020.
Appendix 1 Description of synthesis methods and patient and public involvement in each case study review
| Short name | Synthesis methods description | Explanation of choice of synthesis method | PPI |
|---|---|---|---|
|
1. Digital-First Primary Care Rodgers et al. 18 |
Stage 1 (scoping and summary of evidence) did not involve synthesis Stage 2 ‘rapid evidence synthesis’Reproduced with permission from Rodgers et al. 18 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/2019Rodgers et al. https://creativecommons.org/licenses/by/4.0/ |
For stage 2, ‘NHS England requested a very rapid, brief and high-level overview of the evidence retrieved in stage 1’18 In relation to seven questions and given that ‘a full systematic review was not possible, given the time and resources available’, the team ‘conducted a rapid synthesis of the most relevant evidence identified during the scoping exercise (stage 1) to establish if and to what extent these questions can be answered by the identified research’18 |
Although this report summarises some evidence relating to patient and public views, patient and public representatives were not directly involved in the development of this work18 |
|
2. MHA16 Shaw et al. 23 |
Given the time available, a pragmatic decision was made to undertake a framework synthesis of qualitative studies, which involved four stagesFirst, relevant data extracted from prioritised qualitative studies were entered into a framework that had been developed based on the five research objectives. In the second stage of synthesis, the studies that contributed the most data across all five research objectives were then searched for themes pertaining to each research objective. The studies contributing the most relevant data were then explored for relevant themes, which were then used to refine the framework. Finally, the content of each of the preliminary themes was examined and subthemes were developed using an inductive, iterative approach. The relationships between these themes were then describedReproduced with permission from Shaw et al.23 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/2018Shaw et al.https://creativecommons.org/licenses/by/4.0/ | A review of qualitative evidence was chosen because the main review questions concerned different aspects of patient, carer and professional experiences of the nearest relative provisions:A pragmatic decision was made to prioritise studies that contained more than a few paragraphs of relevant primary qualitative data for inclusion in the framework synthesis. With more time, all included studies would have been considered for inclusion in the synthesisA framework approach was used for the synthesis of included studies. The period available for synthesis of the prioritised studies (1–2 weeks) did not lend itself to the preferred method of synthesis, which would have used an iterative, inductive approach. For this reason, the findings of this review are largely descriptive in nature, and are not able to reflect on the nuance and underlying issues identified by the included studiesReproduced with permission from Shaw et al.23 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/2018Shaw et al.https://creativecommons.org/licenses/by/4.0/ | One carer with experience of the NR [nearest relative] provisions provided feedback on the themes and subthemes identified by the synthesis and commented on the write-up of the results within this report23 |
|
3. Integrated care regulation and inspection Rodgers et al. 25 |
Rapid scoping review of the literature:Documents were coded based on key characteristics, and a descriptive summary of the literature produced. No attempt was made to assess the quality or synthesise the findings of the retrieved evidenceReproduced with permission from Rodgers et al.25 Contains information licensed under the Non-Commercial Government Licence v2.02020Rodgers et al.http://www.nationalarchives.gov.uk/doc/non-commercial-government-licence/version/2/ |
Mainly descriptive rather than evaluative review questions, implied need for a scoping review:Reproduced with permission from Rodgers et al. 25 Contains information licensed under the Non-Commercial Government Licence v2.02020Rodgers et al. http://www.nationalarchives.gov.uk/doc/non-commercial-government-licence/version/2/ However:Reproduced with permission from Rodgers et al. 25 Contains information licensed under the Non-Commercial Government Licence v2.02020Rodgers et al. http://www.nationalarchives.gov.uk/doc/non-commercial-government-licence/version/2/ |
Two PPI advisors were recruited and ‘were invited to comment on the project report with a particular emphasis on accessibility of the content to public users’ (Reproduced with permission from Rodgers et al.25 Contains information licensed under the Non-Commercial Government Licence v2.0). They were also invited to participate in dissemination activity |
|
4. Social care access and diversity Booth et al. 27 |
The research project was a rapid realist synthesis that was divided into four parts:
|
The realist review element was related to the third, inherently explanatory, review objective:Reproduced with permission from Booth et al. 27 Contains information licensed under the Non-Commercial Government Licence v2.02021Booth et al. http://www.nationalarchives.gov.uk/doc/non-commercial-government-licence/version/2/ The rationale for undertaking a rapid realist review was described as:Reproduced with permission from Booth et al. 27 Contains information licensed under the Non-Commercial Government Licence v2.02021Booth et al. http://www.nationalarchives.gov.uk/doc/non-commercial-government-licence/version/2/ |
The emergent programme theories in the realist review were shared, discussed and endorsed by the Sheffield Evidence Synthesis Centre’s PPI group. They had also reflected on four early questions as part of scoping the review and commented of the relevance of the review There were also plans to validate findings from the realist review with a panel that was representative of the experience of social care. However, the COVID-19 pandemic meant this was ultimately not possible |
|
5. Strengths-based approaches Price et al. 69 |
Intended method: systematic review to summarise and synthesise evidence on the effectiveness and implementation of strengths-based approaches used in the area of adult social care in the UK –To assess effectiveness research we aimed to include all comparative evaluation study designs (e.g., randomised and non-randomised controlled trials)To assess factors influencing implementation of the strengths-based approaches, we sought qualitative evaluative studies that included a focus on the process of implementation of the strengths-based approachesFramework synthesis was used to synthesise qualitative evidence relevant to research question two. Themes and subthemes within the initial framework were based on the main domains of the Consolidated Framework for Implementation Research (CFIR)Reproduced with permission from Price et al.69 Contains information licensed under the Non-Commercial Government Licence v2.02020Price et al.http://www.nationalarchives.gov.uk/doc/non-commercial-government-licence/version/2/ |
Reproduced with permission from Price et al. 69 Contains information licensed under the Non-Commercial Government Licence v2.02020Price et al. http://www.nationalarchives.gov.uk/doc/non-commercial-government-licence/version/2/ However, no effectiveness studies met our inclusion criteria:Reproduced with permission from Price et al. 69 Contains information licensed under the Non-Commercial Government Licence v2.02020Price et al. http://www.nationalarchives.gov.uk/doc/non-commercial-government-licence/version/2/ |
In the section on limitations of our review methods:The small level of [patient or public] involvement was related to a lack of resource available to the team, plus challenges recruiting people at short notice from potentially vulnerable groups. However, we are very grateful to the small group of people with lived experience of using adult social care services who have commented on the plain English summary of this reportReproduced with permission from Price et al.69 Contains information licensed under the Non-Commercial Government Licence v2.02020Price et al.http://www.nationalarchives.gov.uk/doc/non-commercial-government-licence/version/2/ |
|
6. Reducing length of stay Nunns et al. 39 |
Systematic review, including narrative synthesis supported by tabulated data, of the comparative quantitative outcomes, after grouping studies by anatomical location of the planned procedures. Limited meta-analysis on outcome data from similar RCTs where feasible:Within each procedural group, the intervention and outcomes of each study was summarised visually within a table to aid comparison across multiple outcomes and intervention types. The data for each type of intervention within a procedural grouping were examined to see if any differences between the sample, intervention characteristics or study quality could be related to the effectiveness of the interventionReproduced with permission from Nunns et al.39 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/2019Nunns et al.https://creativecommons.org/licenses/by/4.0/ | The synthesis methods chosen are directly determined by the nature of the two prioritised review questions to assess the effectiveness and cost-effectiveness of multicomponent hospital-based interventions to reduce length of stay of older adults | The review team:. . . met with a group of four adults aged > 60 years for three 2-hour meetings during this review. Each individual had experience of being admitted to hospital overnight for a planned procedure. We planned to learn from their knowledge and experiences to help us identify important outcomes and aspects of care, particularly where they may have been overlooked in the included evidenceReproduced with permission from Nunns et al.39 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/2019Nunns et al.https://creativecommons.org/licenses/by/4.0/ |
| These meetings covered checking the review’s focus, feedback on initial findings and dissemination activities | |||
|
7. Interventions to reduce preventable hospital admissions Chambers et al. 44 |
1. A mapping review of 569 publications about cardiorespiratory interventions for reducing preventable admissions:Then producing a summary of key characteristics of the included studies, presented in summary tables (using EPPI-Reviewer 4; Evidence for Policy and Practice Information and Co-ordinating Centre, University of London, London, UK) 2. Realist synthesis. Data extraction was based on an existing implementation framework (PARIHS), an intervention template and a realist logic template (if–then–leading to) for eliciting programme theory Then:Reproduced with permission from Chambers et al. 44 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/2020Chambers et al. https://creativecommons.org/licenses/by/4.0/ |
The mapping review: The rationale for conducting a realist synthesis was that: |
The review made use of the pre-existing Sheffield HSDR Evidence Synthesis Centre Public Involvement Advisory Group, which provided input at various stages. (How many, and how they were selected for consulting about this review was not stated.) During three meetings, members of the group were involved in exploration of study parameters and the identification of initial ‘problem points’, refining and shaping the programme theories and emerging findings, drafting the Plain English summary and helping with disseminating the study findings |
|
8. Access to services for adults with IDs Cantrell et al. 46 |
Two stages:
|
A mapping review is a logical first step in any area to find out what research exists within a broader topic:The targeted systematic review also focused on evidence from the UK only No further explanation of this narrower focus is provided |
The team consulted people with IDs, family carers and formal paid carers ‘to ensure that the review was informed by their perspectives’46 This informed both the searches and informed discussion of the main findings and recommendations The team:Reproduced with permission from Cantrell et al. 46 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/2020Cantrell et al. https://creativecommons.org/licenses/by/4.0/ |
Glossary
- Ambulatory
- Those services or conditions that do not require hospital admission or overnight stays. Patients are generally walking and do not require a bed to be assessed or treated. Term more commonly used in health care in North America.
- Evidence synthesis
- An end product of research that is a systematic summary and integration (synthesis) of evidence from multiple studies or sources. Synonymous with evidence review of a systematic review. Can sometimes be used to refer to the stage of analysis within a review process that brings evidence together to pool the results or make joint sense of their findings (see Synthesis).
- Mapping
- To obtain one’s bearings and take stock of research within a wider area of potential study, often with a view to identifying synthesis gaps where a subsequent potential review might be located.
- Mapping review
- Systematic reviews to gain an understanding of the breadth, purpose and quantity of research activity in an area. Sometimes called ‘evidence gap maps’, and often graphically and interactively presented.
- PROSPERO
- The International Prospective Register of Systematic reviews. Hosted by the National Institute for Health Research [URL: www.crd.york.ac.uk/prospero/ (accessed 14 June 2021)].
- Protocol
- The research plan of a systematic review, including specification of the review questions, inclusion and exclusion criteria, search strategy, plans for data extraction, study quality assessment, synthesis of data and dissemination plans.
- Realist review
- A type of systematic review that is based on realist methodological ideas and seeks to identify and refine programme theory that explains how, why, for whom and in what circumstances programmes or interventions are effective.
- Scoping
- The processes in an individual review that aim to establish or refine the review questions and determine its scope (e.g. area of focus, key terms and types of studies to be included). The logistics and conceptual scope are explored, alternative potential inclusion and exclusion criteria piloted, and the quantities of likely literature gauged.
- Scoping review
- Review to describe the extent and nature of research on a topic, without any explicit intention to assess the quality or synthesise the findings of the studies identified (although it may summarise them to some extent). Can form part of the scoping processes of a fuller systematic review and synthesis.
- Synthesis
- The stage of a review or systematic review that involves combining or integrating insights or data across included studies (e.g. narratively, using text and tables, or statistically pooling numerical estimates of effect using meta-analysis). Synthesis is also used as shorthand for the whole review output (i.e. as a synonym of review or systematic review).
- Systematic review
- In principle, a systematic review is any review of any types of documentary evidence that (1) aims to answer a defined question and (2) uses explicit methods to identify, assess and summarise the findings of included studies or evidence sources. In practice, the term systematic review is often used as shorthand for systematic reviews of quantitative studies of the effectiveness of interventions. In this narrower sense, a systematic review is often also presumed to require prespecification of methods (e.g. a review protocol), reproducible searches, standardised data extraction, quality assessment of included studies and formal strategies for evidence synthesis.
List of abbreviations
- ACSC
- ambulatory or primary care sensitive condition
- DHSC
- Department for Health and Social Care
- GP
- general practitioner
- HSDR
- Health Services and Delivery Research
- ID
- intellectual disability
- LGBT+
- lesbian, gay, bisexual, transgender plus
- MHA
- Mental Health Act 1983
- NICE
- National Institute for Health and Care Excellence
- NIHR
- National Institute for Health Research
- PICOS
- population (or patient type), intervention, comparator, outcomes, study types
- PICOSS
- population (or patient type), intervention, comparator, outcome, study types, synthesis method
- PPI
- patient and public involvement
- RCT
- randomised controlled trial
- RETREAT
- Review question, Epistemology, Time/Timescale, Resources, Expertise, Audience and purpose, Type of data
- ScHARR
- School of Health and Related Research
- SCIE
- Social Care Institute for Excellence