
Notes
Article history
The research reported in this issue of the journal was funded by the HTA programme as project number 03/37/06. The contractual start date was in January 2005. The draft report began editorial review in February 2007 and was accepted for publication in March 2008. As the funder, by devising a commissioning brief, the HTA Programme specified the research question and study design. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the referees for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
None
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2008. This work was produced by Woodman et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2008 Queen’s Printer and Controller of HMSO
Chapter 1 Background
Definition and burden of physical abuse
Physical abuse was defined in 2006 in the UK government’s Green Paper Working together to safeguard children as follows: ‘Physical abuse may involve hitting, shaking, throwing, poisoning, burning or scalding, drowning, suffocating, or otherwise causing physical harm to a child. Physical harm may also be caused when a parent or carer fabricates the symptoms of, or deliberately induces, illness in a child’ (Section 1.30). 2 In addition, local authorities have a duty under the 1989 Children Act to take any action to safeguard or promote a child’s welfare when they ‘have reasonable cause to suspect that a child who lives, or is found, in their area is suffering, or is likely to suffer, significant harm’. 5 This requirement recognises that physical abuse may occur as a result of physical violence, whether or not the child is injured.
The recent United Nationsworld report on violence against children published in 2006 left no room for doubt about the scale and impact of the global burden of violence against children. 5,6 Across the world, an estimated 80–98% of children suffered physical punishment in their homes, with one-third or more experiencing severe physical punishment resulting from the use of implements. The report emphasised that only a small proportion of the widespread violence is detected and reported to children’s services because of the hidden nature of abuse, fears of the child and family members, and stigma or mistrust of social services and others in authority. 6 These factors make the true incidence and characteristics of physical abuse difficult to measure.
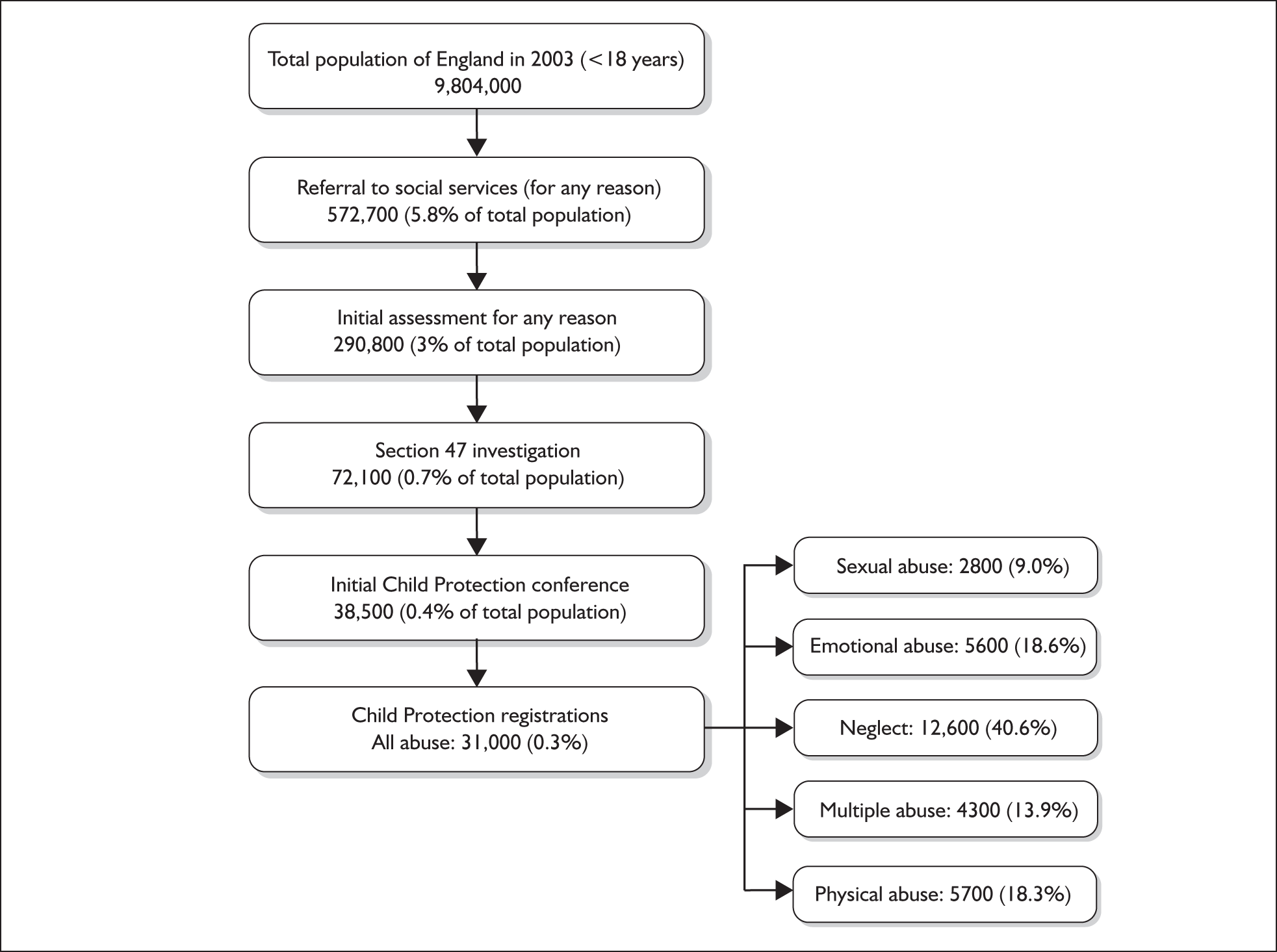
Even when physical abuse is suspected and reported it can be difficult to quantify because of problems with thresholds for confirmation and lack of routinely collected data. Currently in the UK, the child protection register (CPR) offers the only routine data on the incidence of physical abuse. As Figure 1 shows, registration is the final stage of child protection proceedings in the UK and represents a very high threshold for defining physical abuse. In 2003, only 0.1% of the child population under 16 years was newly registered on the CPR under the category of physical or multiple abuse (Figure 1). This figure substantially underestimates the incidence of physical abuse in the UK.
The impact of violence against children is often long term, resulting in increased susceptibility to adverse social, emotional, cognitive and health outcomes, and huge economic costs to society. 7 Social services costs alone are considerable. The annual survey of local authorities’ social services child and family teams estimated that in 2005 44% of their budget, or £30.5 million per week, was spent on child abuse and neglect, equivalent to £1.6 billion per year. 8
Policy in the UK
The tragic death of Victoria Climbié in 2000 highlighted the ineffective and muddled detection of abuse by agencies in the UK. In his inquiry into Victoria’s death, Lord Laming identified an ‘institutional malaise’ in children’s services and specified that the major failings were inefficient detection of abuse, failure to act appropriately when there were concerns, poor record keeping and poor communication within and between agencies. 10
In response to Lord Laming’s recommendations10 the government published a Green Paper, Every child matters. This committed the government to strengthening coordination of services and interagency communication by establishing local safeguarding boards, mandating a duty of cooperation between agencies, and integrating children’s services at a local level through the establishment of children’s trusts and Contact Point (previously known as the Information Sharing Index), an index of all children that documents their needs and contacts with agencies. 11 The Children Act 2004 (Sections 11 and 12)12 provided the legislative basis for these changes. Contact Point and the Common Assessment Framework (CAF) will be fully implemented in all areas of England by mid 2009; they have cost £224 million to implement with an anticipated £41 million running costs each year. 13
The Children Act 2004 mandated training in the recognition of and response to child abuse and neglect for all staff in contact with children. Professional bodies responded by publishing guidelines and competences for their members, which are designed to protect both children and the professional. 3,14–17 All accident and emergency (A&E) staff are expected to receive training in child protection, which ranges from hourly training sessions to a compulsory 3 days a year, depending on their level of contact with children and child protection responsibilities. 3,12,18 The process of screening, assessment and referral of children with suspected physical abuse in A&E is summarised in Table 1.
| Child attends A&E | Clerk notes demographic details and generates a medical record (sometimes electronic). This may include information on previous A&E attendances |
| Clinical screening assessment | A triage nurse and/or A&E senior house officer (SHO) take a history and examine the child. In children’s A&E departments, staff may be paediatric trained |
| Paediatric assessment | If abuse is suspected the child is referred for assessment by a paediatrician (usually on-call registrar or above). The paediatrician may be on site in children’s A&E. If the paediatric team suspect abuse the child will usually be admitted for further assessment. This may include the designated paediatrician and the hospital social worker. The child may be discharged if the paediatric consultant and social work team judge that the child is at no further risk of harm. If abuse is considered likely the paediatrician will contact the child’s local social services department. In some cases referral is preceded by discussion with social services about the appropriateness of referral |
| After discharge | A record of A&E attendance is sent to the GP for all children. In some departments this record is also sent to the health visitor or school nurse. In most departments, records of all children attending A&E are scrutinised the next day by a community liaison nurse (CLN) for social or child protection issues that may have been missed by A&E staff. Children with concerns are discussed at a weekly or monthly meeting involving the CLN and paediatric, A&E and social work staff at the hospital |
The recognition of the need for better training has focused attention on the signs and symptoms that staff should be trained to look for. The Royal College of Paediatricians and Child Health (RCPCH) recently produced guidelines on the detection and management of child abuse and neglect and highlighted the poor quality of the evidence underpinning many of the recommendations and the need for more research. 14 Signs and symptoms suggestive of physical abuse cited by the report included injury in infants, vague, unwitnessed, inconsistent or discrepant history, unexplained injuries, delayed presentation, injuries not consistent with a child’s development, repeated attendance for injury, and multiple bruises in certain areas such as the face, head and neck. In some cases the evidence underpinning these markers of abuse is based on case series of abused children or on comparisons between definitely abused children and healthy children seen in routine child health clinics. 19,20
Despite the uncertain evidence on the performance of these features for predicting physical abuse, they are being increasingly used in checklists, aide-memoires and protocols in A&E departments to improve detection by front-line A&E staff. 14,20–23 To date, no systematic evaluation has determined which factors are most predictive of physical abuse and which might overwhelm the paediatric team with false-positive referrals of non-abused children. The aim of this study was to address this gap in the evidence by evaluating the performance of screening tests for physical abuse in A&E.
Chapter 2 Aims, objectives and overview of methods
We aimed to determine the clinical effectiveness of screening tests for physical abuse in children attending A&E departments in the UK. The four specific objectives were to determine:
-
the burden of physical abuse among children in the community
-
the incidence of attendance at A&E with injury and the characteristics of attendees
-
the accuracy of screening tests for physical abuse in A&E
-
optimal screening strategies based on a clinical effectiveness model.
Overview of systematic review methods
We carried out a series of systematic reviews to address objectives (1), (2) and (3). Because of the paucity of valid and relevant evidence we adopted an ‘exploratory’ approach to each review question. We used broad inclusion criteria to select studies for review because we could not anticipate all of the important elements of the study methods that could affect validity and applicability. This approach allowed us to examine the relationship between study quality and results and helped to define limits within which the true estimate might lie. We selected studies to inform the parameters for the clinical effectiveness model using epidemiological principles. By making explicit the rationale for the estimates used in the clinical effectiveness model, readers can use the data to test alternative interpretations.
Clinical effectiveness model
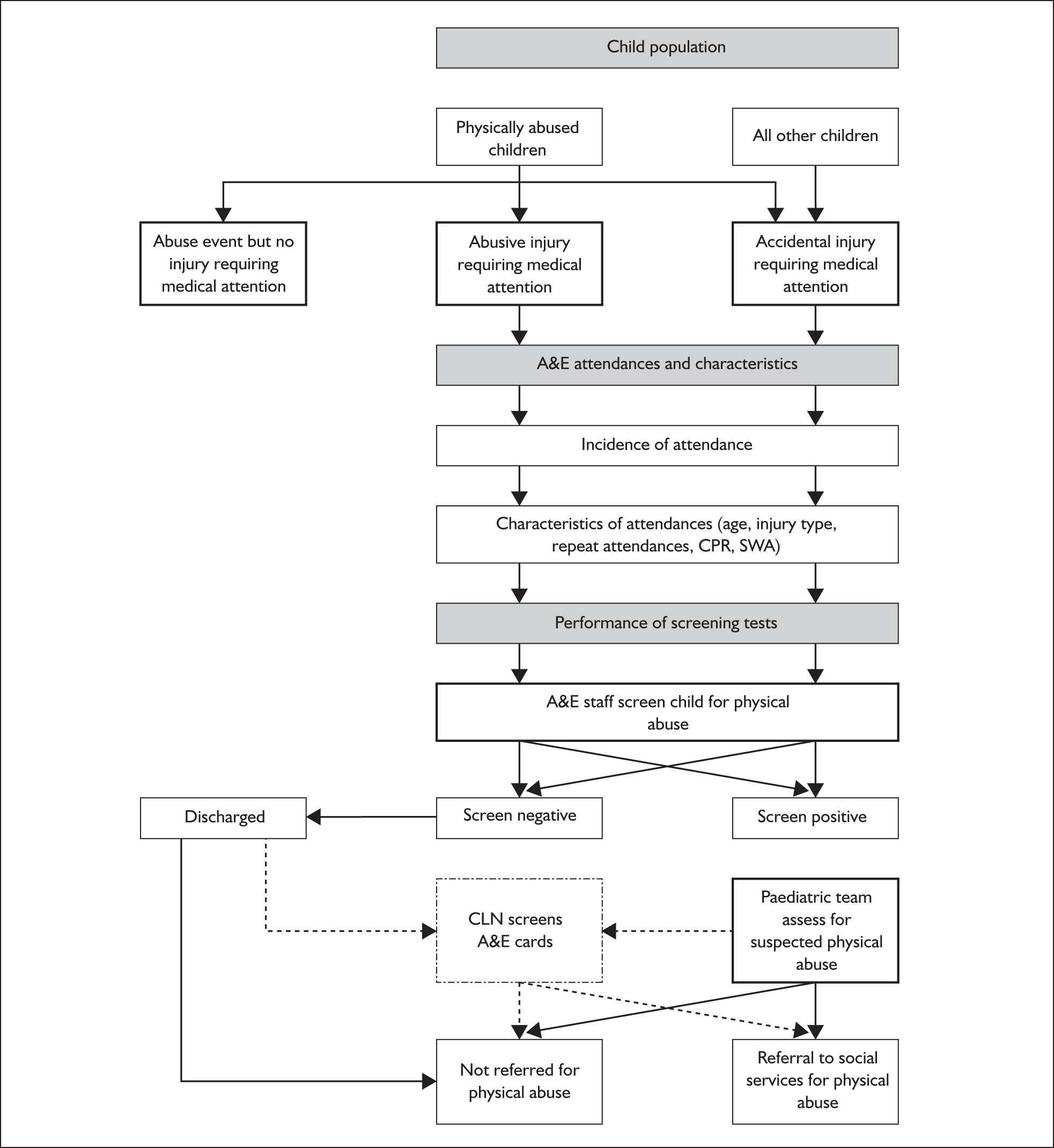
We developed a simple clinical effectiveness model based on a scoping review of the literature and discussions with health and social services providers (Figure 2). The model was based on a hypothetical population of children (< 16 years) in the UK and provides a simplified representation of the occurrence of physical abuse, the risk of resulting injury requiring medical attention, attendance at A&E of physically abused and non-abused injured children, detection by screening in A&E, and referral or not to social services. Injury was defined as head injury, fractures, burns, bruises or ‘other’ and excluded poisoning, foreign bodies and fabricated illness. More details on the classification of injuries are given in Table 10. Physical abuse was defined as at least one act of severe violence (kick, bite, scald/burn, ‘beat up’, hit with object, shake a young child, or threaten to use a weapon) from a parent or carer towards a child. 5
FIGURE 2.
Flow diagram showing the steps included in the model. CLN, community liaison nurse; CPR, child protection register; SWA, social work active.
Parameters defining the probability of outcomes at each step of this pathway were obtained from the systematic reviews (Chapter 4) and entered into the model using Microsoft Excel®. The model then multiplied the parameters to generate the probabilities of the outcomes used to measure the clinical effectiveness of screening: the proportion of abused children detected in A&E and referred to social services, and the proportion of non-abused children unnecessarily referred to social services for suspected abuse. We assumed that all referrals from doctors in A&E to social services would result in an ‘initial assessment’ as required under Section 47 of the 1989 Children Act. 5
Screening tests
We defined screening tests as any criterion or ‘test’ that would be universally applied to all injured children to detect those with suspected physical abuse. We accepted any characteristic or form of assessment provided that it was universally applied. We selected screening strategies based on existing A&E protocols or tests used in UK A&E departments, as revealed in a review of the published literature and interviews with staff in five A&E departments. 14,20–23 We added one further protocol, whether the child is social work active (systematic review 8, Table 12). Although not yet in use, this information will be recorded on Contact Point in all local authorities in England by 2009. 13,24
The types of screening strategies examined are listed in Table 2. The base-case strategy, standard care, comprised the history and examination of an injured child conducted by A&E staff. We sought evidence on two other clinical screening tests: the use of a checklist to enhance the initial clinical screening assessment and the use of a community liaison nurse to scrutinise all child attendance records for children with possible abuse missed by A&E staff. We then evaluated the effectiveness of adding screening protocols, based on characteristics of the child, to the clinical assessment screen.
| Type of strategy | Description | |
|---|---|---|
| Clinical screening tests | ||
| 1 | Standard care | Base-case strategy. Screening involves the standard history and examination by A&E staff |
| 2 | Checklist for abuse | Used by the clinician who first examines the child. Usually a five-point checklist, e.g. explanation consistent with the injury, consistencies in explanations, delay in presentation, interaction between carer and child appropriate |
| 3 | Community liaison nurse (CLN) | The CLN scrutinises A&E attendance records for at-risk children who were not referred by A&E staff |
| Screening protocols | ||
| 4 | Age group | e.g. All infants referred for paediatric assessment |
| 5 | Injury type | e.g. Referral to paediatrician if head injury or fracture in infants |
| 6 | Repeat attendance | Repeat attendances at A&E for injury in the last year |
| 7 | Social work active (ISA) | The child is recorded on Contact Point as social work active.24 This means that the child is currently (or has been in the last 12 months) allocated to a social worker or duty social work team27 |
| 8 | Child protection register (CPR) | The child is currently on the CPR for any reason |
The study had three main limitations. First, it was restricted to physical abuse, the remit given by the funders, even though this is frequently linked to other forms of abuse. Second, we included only injured children, who account for about one-third of all A&E attendees. 25,26 Third, we did not consider the important policy question of whether screening reduces the adverse consequences of physical abuse over the child’s lifetime and improves their quality of life. This would require information on the benefits and harms of detection, failure to detect abuse and false-positive referrals, and the benefits and harms of interventions offered by social services and other agencies. These questions were beyond the scope of our study.
Chapter 3 Searches and study selection
Methods
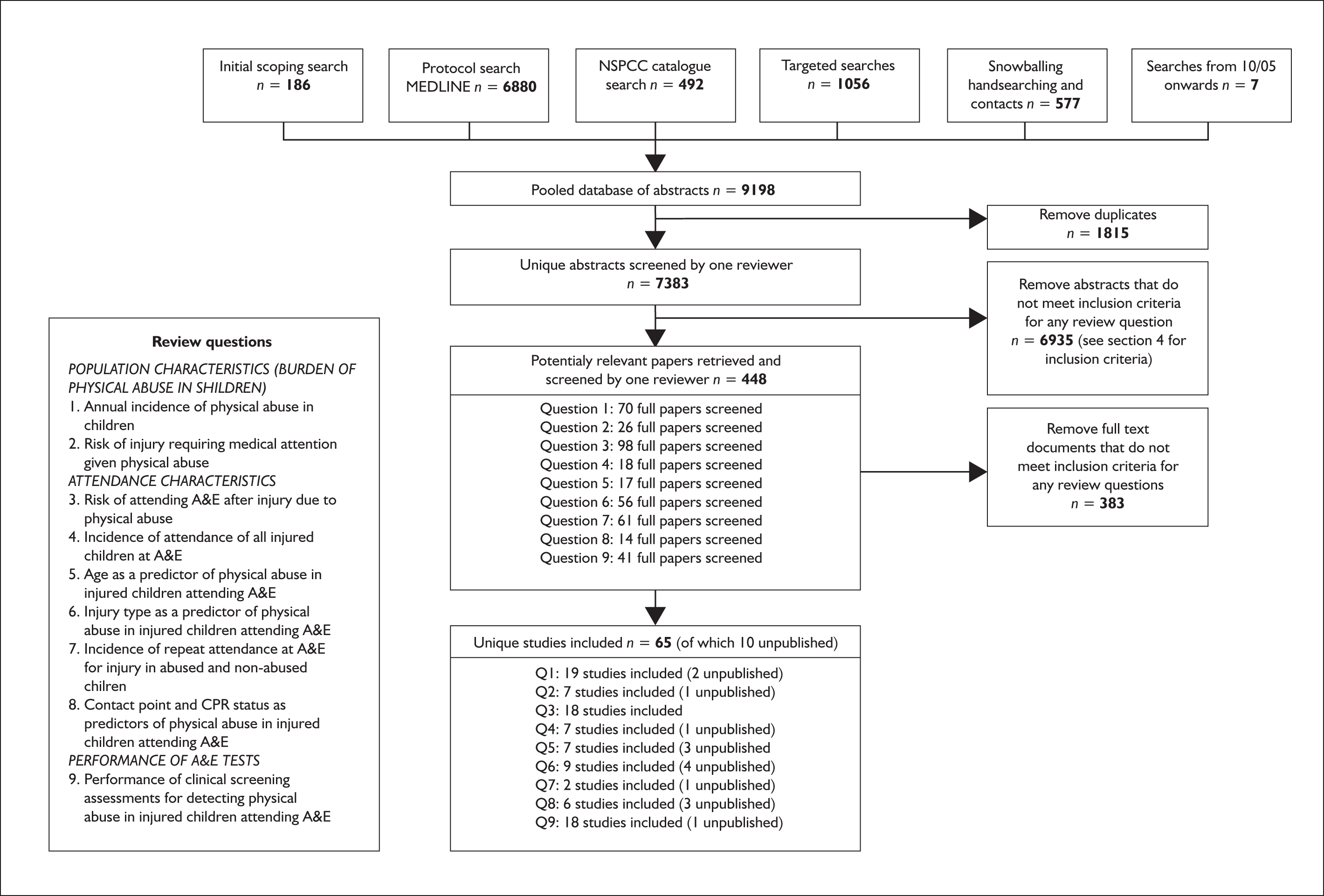
We developed a database of abstracts based on the six methods shown in Figure 3. Searches were limited to studies published after 1974 when major changes in the way that child abuse was managed were instituted in the UK (see Inclusion criteria). Start dates for each method are given below. Further details of the search methods are reported in Appendix 1.
-
Method 1: The initial scoping search was carried out in August 2004 and was based on Medical Subject Headings (MeSH) and text word terms for child, abuse, maltreatment, violence and punishment. The search yielded 186 references.
-
Method 2: We developed a more detailed search strategy that was used on MEDLINE in October 2005. This search yielded 6880 references.
-
Methods 3: The third source was the publications catalogue of the National Society for the Prevention of Cruelty to Children (NSPCC), which was searched in September 2005. We included any references that appeared to be relevant to physical abuse. This search yielded 492 references.
-
Method 4: As the type of evidence sought was complex and heterogeneous and could relate to clinical, management or policy issues in health or social care, we complemented the protocol-driven search (method 2) by carrying out four types of ‘targeted search’ in January 2006 (Appendix 1, Table 25). 28
-
First, we listed the most valuable studies found from the scoping search (‘gold standard’ papers, n = 16). Using the Web of Science we found all subsequently published papers that cited each source paper.
-
Second, using the ‘related articles’ search on the Web of Science we found papers (previously or subsequently published) that shared references with each source paper.
-
Third, we identified papers with the same subject terms, headings or MeSH terms as each of our source papers by using the ‘related articles’ algorithm on PubMed. We imported the 20 most relevant papers and those other papers identified by our search terms.
-
In the fourth step we applied search terms across databases [including Department of Health database (DH-Data), British Nursing Index and Cumulative Index to Nursing and Allied Health (CINAHL)] that were not covered by our main protocol-driven search. These four search techniques yielded 1216 references (deduplicated, n = 1056).
-
-
Method 5: The third search method was snowballing. This involved judgement and was based on scanning reference lists, hand searching journals, searching the internet and chasing up professional contacts for unpublished data. This method is especially useful for identifying high-quality studies in obscure locations. 28 This search yielded 577 references.
-
Method 6: Finally, we carried out a search of three key journals (Pediatrics, Child Abuse and Neglect and Child Abuse Review) in October 2006 to identify any relevant studies published since the original protocol search was carried out in October 2005. Inclusion of studies in the database relied on the researcher’s judgement. This search yielded an additional seven studies.
FIGURE 3.
Flow diagram summarising methods used for identification of studies to include in the nine reviews.
Inclusion criteria
The inclusion criteria are reported separately for each review question in Chapter 4. Two inclusion criteria applied to all review questions. First, studies had to be published after 1974, as this was the year of the inquiry into the death of Maria Colwell, who died from injuries inflicted by her stepfather in 1973. The report made recommendations for child protection procedures that have formed the basis for child protection in the UK over the last 30 years. These recommendations included the establishment of area child protection committees (now replaced by local safeguarding boards),10 the establishment of a child protection register and the system of multidisciplinary case conferences. The Maria Colwell report identified inadequacies in the handling of the case by services and emphasised the need for professional accountability and multidisciplinary communication. 29 Second, we excluded studies relating to developing countries because recognition of child abuse and services for dealing with abuse are likely to differ from the UK setting.
All abstracts were scanned by a single reviewer (JW) who determined whether they were potentially relevant to one or more of the review questions. The full article was retrieved for all potentially eligible studies and separately appraised for each review question by one reviewer (JW). A second reviewer then appraised all included studies and any borderline decisions (RG).
Chapter 4 Systematic reviews
Methods, results and model parameters
In this chapter we report the methods and findings of a series of systematic reviews that informed parameter estimates at each step of the assessment pathway (see Figure 2). For each review question we report the inclusion criteria, the quality of the included studies and the results of the review. The derivation of the relevant parameters for the clinical effectiveness model is reported in Chapter 5. All forest plots are based on fixed-effects meta-analyses and show proportions and 95% confidence intervals.
The systematic reviews can be considered in three parts, representing the burden of abuse, the incidence and characteristics of attendees at A&E, and the performance of clinical screening tests.
Burden of abuse
Two reviews were conducted to determine the incidence of severe parental violence and the consequent risks of injury requiring medical attention. We classified severe violence from a parent or carer (defined as punching, kicking, biting, hitting with a hard object, inflicting a scald or burn, shaking a young child, or threatening with a weapon) as physical abuse. Over 80% of physical abuse is perpetrated by a parent, parental figure or non-professional carer and this figure remains constant across all age groups under 16 years. 30 Consequently, our definition captures the large majority of physical abuse cases. The definition also includes children at risk of injury as well as those actually injured and is therefore consistent with the minimum threshold for mandatory investigation as laid out in Section 47 of the 1989 UK Children Act5 and definitions of physical abuse used in recent reports by the World Health Organization and the United Nations. 6,31 In this study we assume that severe parental violence is equivalent to physical abuse.
Systematic review 1: Incidence of physical abuse
Review methods
The review aimed to determine the age-specific incidence of physical abuse. We included studies that reported any measure of physical abuse or severe physical punishment or discipline perpetrated by parents or carers which could be used to derive the annual incidence of physical abuse.
To aid comparison between studies we classified the results into two categories:
-
severe violence (assumed to be equivalent to physical abuse): kick, bite, scald/burn, ‘beat up’, hit with object, shake a young child, (threaten to) use a weapon
-
physical abuse (severity of abuse unknown) reported by agencies involved in child protection.
We grouped all included studies according to the reporting source: parents, self-report and agency. To assist analysis of the variation between the included studies we report additional results for minor violence [slap, spank, slap, push, grab, shove (no injury/lasting marks)] and for violence over the child’s lifetime. Table 27 in Appendix 2 shows excluded studies that reported physical abuse over the child’s lifetime but not in the past year.
Review results
A total of 19 studies were identified (Table 3). Five were based on parental reports, three on self-reports and 11 on agency reports (including two unpublished studies). Methods and results for the two unpublished studies30,32 are reported in Appendix 4. All studies underestimated the incidence of physical abuse as they reported the prevalence of children with one or more episodes of severe violence in the previous 12 months. Further reasons for underestimation of abuse from these studies are poor response to surveys, under-reporting by parents and misclassification of abuse as accidents in agency figures. One further UK study was excluded as it was based on violence perpetrated by mothers of 8-month-old babies. 33
| First author, country, year of publication | Methods | Risk of violence (% of total child population) |
|---|---|---|
| Parent reports | ||
| Ghate, UK, 200234 |
A total of 1249 parents with a child < 13 years, randomly selected from the 1991 UK census, had face-to-face interviews about discipline in the past 12 months (59.3% responded). Violence was measured by the Misbehaviour Response Scale. We classified punching, kicking and hitting with a hard object as consistent with physical abuse, and smacking, slapping on the arms or legs, grabbing and pushing as minor violence Minor violence in the past year [overall 868/1222 (71.0%)]: 0–1 years: 8%; 1–2 years: 61%; 2–4 years: 82.7%; 5–7 years: 64.7%; 8–10 years: 54.7%; 11–13 years: 37%; total < 13 years: 705/1222 (57.7%) The age-specific incidence as entered into our model gives a weighted average of 8.8% |
Physical abuse in the past year: 0–1 years: 7/203 (3.45%); 2–4 years: 34/292 (11.6%); 5–7 years: 25/261 (9.6%); 8–10 years: 30/261 (11.5%); 11–13 years: 15/205 (7.3%); total < 13 years: 111/1222 (9.1%) Physical abuse during childhood < 13 years: 134/1222 (11.0%) |
| Bardi, Italy, 200135 |
A total of 2388 families with school-age children < 13 years in Tuscany completed an anonymous questionnaire sent out through schools in 1998 (50% responded). Violence was measured using the Conflict Tactics scale (CT scale). 48,49 We classified punching, kicking and hitting with a hard object as physical abuse, and smacking, slapping on the arms or legs, grabbing or pushing as minor abuse Minor abuse over 12 months: 1877/2388 (78.6%) |
Physical abuse in the past year: 198/2388 (8.3%) |
| Theodore, USA, 200536 | A total of 1435 mothers (≥ 18 years) with an index child under 18 years in Carolina, USA, identified by random sampling, were interviewed anonymously by telephone in 2002 about discipline (52% responded). We classified punching, kicking, hitting with a hard object or shaking a child under 2 years as physical abuse. Only violence inflicted by the mother was recorded | Physical abuse in the past year: < 5 years: 10/365 (2.8%); 5–8 years: 17/321 (5.3%); 9–12 years: 18/298 (5.9%); 13–17 years: 17/448 (3.9%); total < 18 years: 62/1435 (4.3%) |
| Wolfner, USA, 199337 |
A total of 3232 parents (18–85 years) with a child < 18 years were identified by random sampling and interviewed by telephone in 1985 (84% responded). Measurement of violence was based on the CT scale. We classified violence intended to cause injury as physical abuse, including kicking, biting, hitting with an object and threatening with or using a knife or gun Minor physical abuse in past year: overall < 18 years: 2001/3232 (61.9%); < 2 years: 323/567 (57%); 3–6 years: 659/740 (88.8%); 7–12 years: 553/771 (71.7%); 13–17 years: 406/1149 (35.3%) |
Physical abuse in past year: < 2 years: 45/567 (7.9%); 3–6 years: 106/740 (14.3%); 7–12 years: 96/771 (12.5%); 13–17 years: 102/1149 (8.9%); total < 18 years: 356/3232 (11.0%) |
| Gelles, USA and Sweden, 198638 |
USA: 1146 two-parent families with children between 3 and 17 years; Sweden: nationally representative sample of 1105 single and two-parent families with children between 3 and 17 years in 1980 Parents were interviewed face to face at home about family violence (CT scale). Physical abuse: kicking, biting, hitting with an object, threatening with or using a knife or gun |
Physical abuse in the last year: USA: 162/1146 (14.2%); Sweden: 51/1105 (4.6%) |
| Self-reports | ||
| Sebre, Baltic/Eastern Europe, 200441 | A total of 1145 children (10–14 years) in Latvia, Lithuania, Macedonia and Moldova were randomly selected to complete a questionnaire about ‘thought, feelings and relationships’ in 1998–2000. Violence was measured using the CT scale. Frequent minor violence such as slapping or being hit with an object, kicked, punched or burned/scalded was considered equivalent to physical abuse | Physical abuse in past year: 244/1145 (21.3%) |
| Sariola, Finland, 199242 |
Classes including 7435 students aged 14–15 years were randomly sampled and given questionnaires distributed by the school nurse (96% responded). Violence was measured using the CT scale. Hitting with a fist/object, kicking, biting and threatening/using a knife/weapon were classified as physical abuse; slapping, hitting and grabbing were classified as minor physical abuse Minor physical abuse: in the last year: 1344/7264 (18.5%); during childhood: 5223/7264 (71.9%) |
Physical abuse in past year: 334/7264 (4.6%); physical abuse during childhood < 15 years: 559/7264 (7.7%) |
| Nelson, USA, 199543 | A total of 1957 school students aged 14–18 years in 25 schools, randomly selected across Atlanta state, completed an adolescent survey questionnaire in 1993 including three questions about ‘physical abuse’ by parents (82% responded of whom 75% answered questions on physical abuse). We classified hitting with an object and punching and kicking as physical abuse | Physical abuse in past year: 319/1957 (16.3%); physical abuse during childhood < 18 years: 550/1957 (28.1%) |
| Agency reports | ||
| Social services data for Hammersmith and Fulham, 2005 (unpublished audit; see Appendix 4)32 |
Audit of initial assessments by social services for suspected physical abuse in children (< 18 years) in one referral centre during 3 months in 2005 (153 initial assessments, missing data for a further 28). Reports ranged from slapping to obvious injury The incidence of initial assessment for physical abuse was estimated as 13.6% times the incidence of initial assessments for any reason in England (290,800/9,804,000 = 0.29%)9 |
Initial assessment for physical abuse over 12 months: 17/153 (11.1%) |
| Metropolitan Police, UK (London), 2005 (unpublished)30 | All children < 16 years reported to London Metropolitan Police child protection unit in 12 months (2005) for ‘violence against the person’ by any perpetrator. We classified ‘acts of violence’ as physical abuse. We assumed that children comprised 19.5% of the total population of 7.2 million (based on census projections for London 2002). Some children may have been reported more than once | Physical abuse (reported to police) in the last year: 0–2 years: 317/184320 (0.20%); 2–4 years: 547/276480 (0.20%); 5–9 years: 1300/471600 (0.28%); 10–15 years: 2271/4716000 (0.48%); total < 16 years: 4435/1404000 (0.32%) |
| Child protection register (CPR), England, 20049 | Registrations on the CPR for physical abuse or ‘multiple abuse’ from 2003 to 2004. Denominator population taken from England Office for National Statistics 2003 figures.50 We derived the age distribution of new registrations by assuming it was equitable with the age distribution of children on the register on 31 March 2004 | CPR (new cases): < 1 year:1283/575000 (0.22%); 1–4 years: 2981/2273000 (0.013%); 5–9 years: 2794/3150000 (0.09%); 10–15 years: 2941/3780000 (0.08%); total < 16 years: 10000/9778000 (0.10%) |
| Creighton, UK, 200445 | Systematic review of sexual and physical abuse from substantiated reports to official agencies in 2003–4. Denominator estimates taken from national websites51 | CPR (12 months): USA: 145550/60646000 (0.24%); Australia: 7560/3978800 (0.19%) |
| Sibert, UK, 200252 | Consultant paediatricians and senior clinical medical officers in Wales returned cards about children < 14 years diagnosed with an injury (grievous bodily harm) following physical abuse in Wales 1996–8. Reports for babies < 1 year were supplemented by cases on the CPR. We have adjusted the data (reduced by 50%) to report cases over 12 months | Severe injury reported by senior medical staff over 12 months: < 1 year: 26/35200 (0.074%); 1–4 years: 13/141200 (0.0092%); 5–13 years: 2/424500 (0.00047%); total < 14 years: 41/600900 (0.007%) |
| Creighton, UK, 198553 | Children placed on CPR for physical abuse in 1981 in parts of England and Wales. Denominator population calculated from rates. All children were registered for physical abuse | CPR (over 12 months): < 16 years: 6532/10,910,300 (0.06%) |
| Lindell, Sweden, 200154 | Physical abuse in children (< 15 years) by a parent or carer reported to the police in one district in 1986 and 1996 and substantiated by/registered with official agencies. Denominator based on police district | Substantiated physical abuse in the past year (to police): 145/27724 (0.05%) |
| Christensen, Denmark, 199939 | Health visitors returned questionnaires reporting visible signs of parental violence in children. The study covered 80% of infants in Denmark in 1991 (83% response rate). Health visitors visit children 5–6 times in their first year | Visible injury reported by health visitor over 12 months: < 1 year: 502/50151 (1%); 1–2 years: 361/18042 (1%); 2–3 years: 136/6798 (2%); 3–4 years: 73/3634 (2%); total < 4 years: 1072/78625 (1.4%) |
| US Department of Health and Human Services, USA, 2006 (NIS-3)44 | New cases of suspected physical abuse identified by 5800 professionals involved in child protection in 42 counties in 1993 (Table 3–1 in NIS-3 report). Children were classified as physically abused according to the harm standard (requires demonstrable harm) or the endangerment standard (includes children at risk of injury). Overall there are an estimated additional 1,261,800 children defined as abused under the endangerment standard. Denominators calculated from the rate (difference caused by rounding) | New cases of physical abuse (harm) reported in all US children within 12 months: 381,700/66,964,912 (0.57%); physical abuse (endangerment): 614,100/67,483,516 (0.91%) |
| Trocmé, Canada, 200346 | Children (< 16 years) on the Canadian CPR for physical abuse in 1998 | On CPR for physical abuse (point prevalence): 15,300/5,583,942 (0.25%) |
| Gessner, Alaska, 200455 | Deaths or hospital admissions due to physical abuse in infants (< 1 year) born between 1994 and 2000 (n = 70,842) in four states, using linked databases. A total of 72 of the 325 reports of physical abuse led to hospitalisation (n = 58), death (n = 4) or both (n = 10) | Physical abuse (reported to social services) over 12 months: < 1 year: 325/70,842 (0.46%) |
Parent-reported physical abuse
Figure 4 shows the proportion of parents who reported one or more episodes of physical abuse in the previous 12 months. Data were collected by telephone or face-to-face interviews except for one study35 based on anonymous questionnaires (see Table 3).
FIGURE 4.
Prevalence of parent-reported physical abuse in the past year.
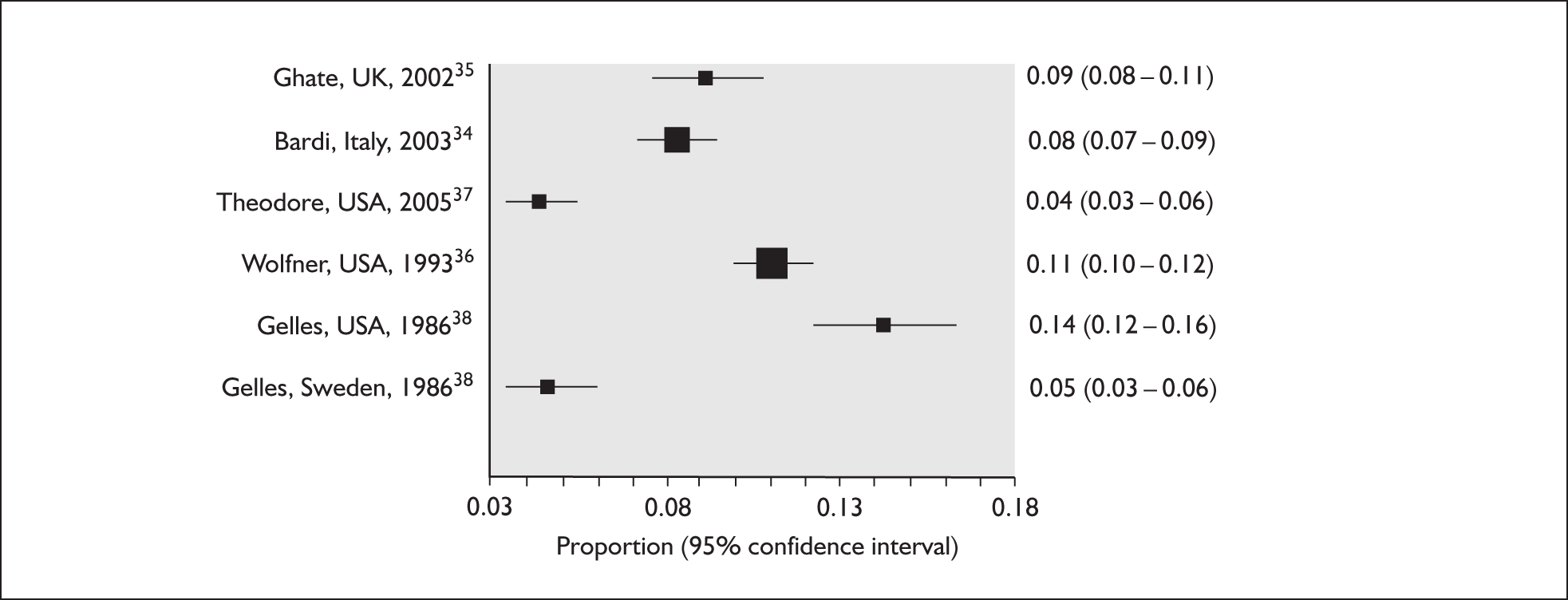
The prevalence of 9.1% reported by Ghate et al. 34 in the UK study (age-adjusted figure for UK is 8.8%) was consistent with studies in the US (11%36) and Italy (8.3%34) but higher than a US study (4.3%36) in which only maternal violence was recorded. The relatively low rate of severe physical abuse in Sweden (4.6%38) may reflect long-standing legislation prohibiting physical punishment in the home. All but two studies37,39 had relatively low response rates (50–60%).
The annual prevalence of physical abuse reported in the UK study was similar to the rate reported for the child’s lifetime by May-Chahal and Cawson40 (7%), although different methods were used (see Appendix 2, Table 27). In studies using the same methods, the lifetime prevalence of abuse was close to but higher than the annual prevalence (Appendix 2, Table 27).
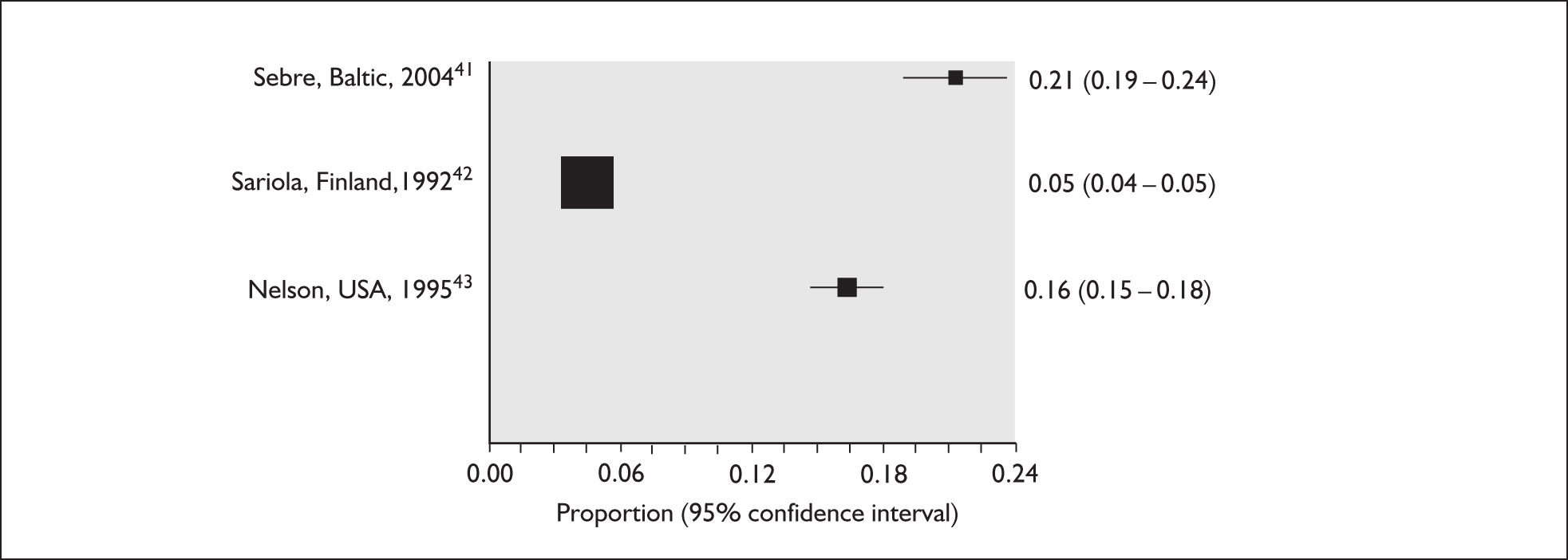
Self-reported physical abuse in the past year
Figure 5 shows results for three studies of self-reported physical abuse. All were based on questionnaires completed by adolescents. The annual incidence ranged from 4.6% to 21.3% and was highest in Eastern Europe41 and lowest in Finland. 42 One US study43 reported slightly higher rates of severe physical abuse (16.3%) than the parent-reported incidence for adolescents in the US national study37 (11%). This may reflect differences in the study populations, methods and definitions, as well as variation according to reporting source (see Table 3).
FIGURE 5.
Prevalence of self-reported physical abuse in the last year.
Agency-reported physical abuse in the past year
Figure 6 shows the prevalence of parent or carer physical abuse reported by agencies. Results varied enormously depending on the agency, their criteria for notification and the event reported (child affected by one or more episodes, as with the CPR figures,9 or individual episodes, as in the Metropolitan Police audit30).
FIGURE 6.
Incidence of agency-reported physical abuse in the past year.
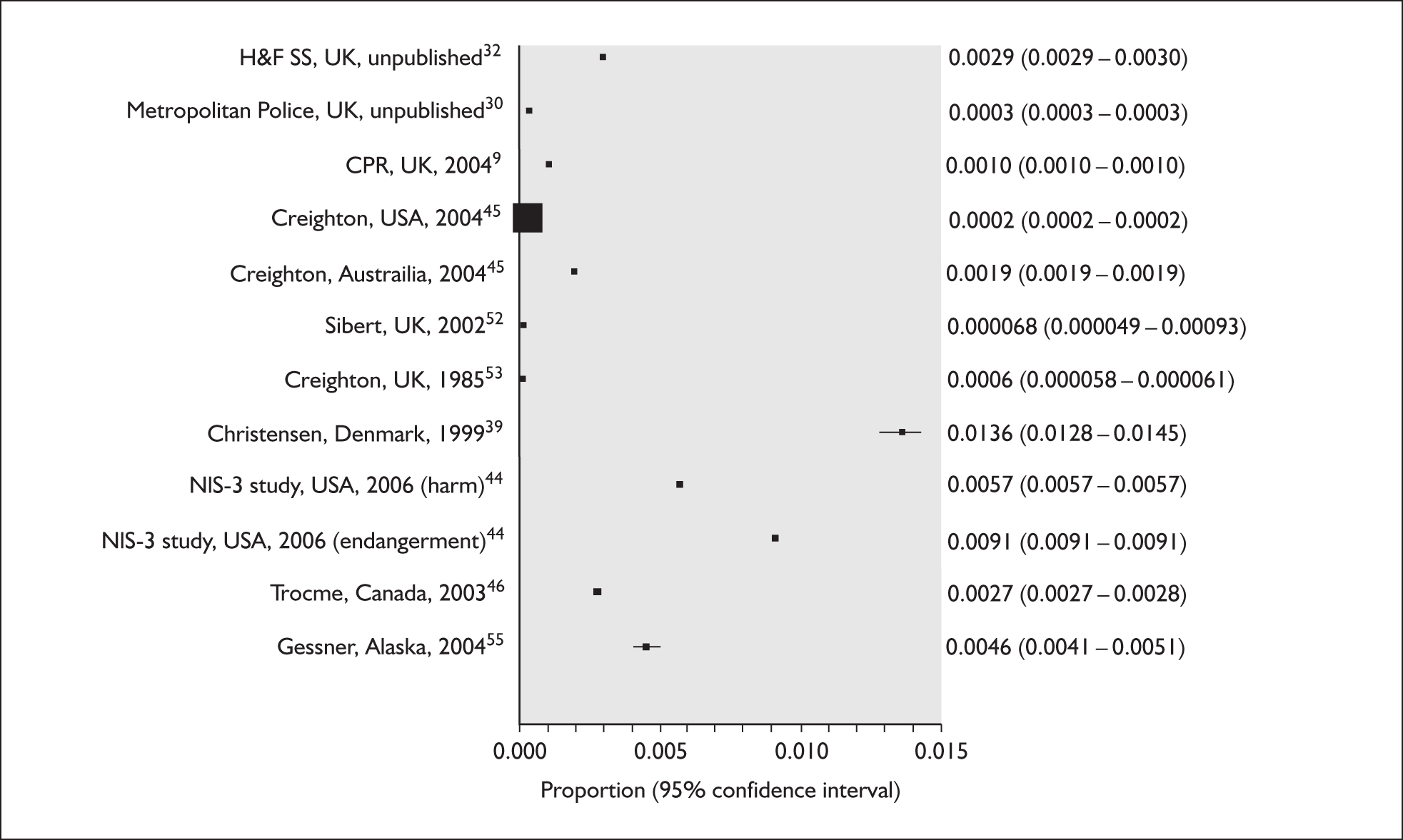
In the UK, agencies reported substantially fewer children than the 8.8% subjected to physical abuse each year based on parent reports. The Metropolitan Police found 0.38 reports per 100 child-years in 2005. 30 This is roughly equivalent to 1 in 23 physically abused children, assuming both studies were drawn from the same population and that no children were reported to the police twice in 1 year [i.e. 1/(0.38/8.8)]. A similar rate was found for social services in an unpublished audit of one London borough. During 3 months in 2005, 11.1% (17/153) of ‘initial assessments’ for children under 18 years were for physical abuse. Extrapolating to the national rate of initial assessments (2.9%9), approximately 0.39% of children would undergo an initial assessment each year for physical abuse (see Table 3). The proportion of reports that were common to social services and police records is not known and we found no UK figures on the incidence of physical abuse suspected by professionals, referred to social services or investigated.
The fact that agencies detect far less abuse than is reported by parents or victims has been well established by North American studies. The large US National Incidence Study of Child Abuse and Neglect (NIS-3),44 which surveyed 5600 professionals involved in detecting child abuse in 42 counties, found that professionals reported one or more episodes of physical abuse in 0.58% of children each year, but estimated that only 28% of all types of abuse identified by professionals were investigated by child protection services. A similar discrepancy between identification and reporting is suggested by the high rate (1.4%) of visible evidence of physical abuse reported by health visitors in Denmark. 39 One explanation for these disparities is that some abused children may be followed up by social services for other reasons. An audit of consecutive initial assessments by social services in one London borough found 16 children undergoing initial assessment for suspected physical abuse, but a further 11 with currently documented parental violence were referred for other reasons and only 3 out of the 11 were investigated for other types of abuse (unpublished audit;32 Table 3 and Appendix 4).
Further decrement occurs in the frequency of investigation of physical abuse if agency reports are based on substantiated rather than suspected abuse. In the UK, the proportion of children placed on the CPR for physical abuse is less than 1 in 100 of those abused and less than one in three of the children who undergo initial assessment (per year: 0.08% of all children are on the CPR, 0.33% have initial assessment, 8.8% are physically abused). Similarly, Figure 6 shows that studies reporting suspected physical abuse found approximately twice as many cases as those reporting substantiated abuse in the US45 (0.24% versus 0.4%) and Canada46 (0.27% versus 0.5%). The US NIS-3 study found that 60% of all types of abuse investigated were unsubstantiated. 44,47 This is partly due to insufficient evidence or concern about further serious harm to warrant substantiation in abused children. In addition, children with accidental injuries may be falsely labelled as abused. There are few data on the proportion of false positives but expert opinion elicited for this study suggests that they account for only 10–20% of children undergoing initial assessment for physical abuse. An audit of social service referrals in the London Borough of Camden suggested that, among consecutive children referred for initial assessment for physical abuse to social services, only 3/26 index children (excluding siblings) were false positives (RE Gilbert, unpublished audit, Camden Social Services; Table 3 and Appendix 4).
The average figures reported in Table 3 hide substantial variation in overall rates of social services investigations according to locality8 and differences in age distributions according to agency. According to parent and self-report studies, the incidence of severe physical abuse is as high, or higher, in school-age children as in preschool children. Notification to the police follows a similar pattern. 30 However, the rate of child protection registration for physical abuse decreases markedly in school-age children. 9
In summary, these results provide strong evidence that parental physical abuse is poorly reported by agencies. As self-reported abuse is limited by the age of children who can be surveyed, parent reports provide the most reliable evidence of parent-inflicted physical abuse. The rates from such studies for severe parental violence in the past year are moderately consistent. 34–36 In the UK, approximately 1 in 11 children (8.8%) were subjected to violence each year of a severity consistent with physical abuse (Table 3).
Systematic review 2: Risk of injury requiring medical attention due to physical abuse
Review methods
The aim of the review was to determine the risk of injury requiring medical attention in children subjected to physical abuse. We included studies of physically abused children that reported the risk of injury after an episode of abuse. Although less representative of all abused children in the community, we restricted studies to agency reports of children presenting to services as the assessment of injury was likely to be objective. We excluded studies based on parent reports or self-reports as assessments of injury and the need for medical attention are less likely to be objective and parents may be reluctant to admit to injury. We defined injuries requiring medical attention as severe cuts or lacerations, fractures, severe burns, head injuries and internal injuries, or according to the author’s classification of injuries needing medical attention. As the data were limited we included high- or low-risk groups of children reported to services.
Review results
Seven studies met the inclusion criteria (Table 4 and Figure 7). All involved physically abused children referred to child protection services.
| First author, country, year of publication | Methods | Risk of injury |
|---|---|---|
| Suspected physical abuse | ||
| Metropolitan Police, UK (London), 2005 (unpublished data, Wareing 2006)30 |
Duty officer classified severity of injury in 5188 children (< 16 years) reported to the Metropolitan Police child protection unit in 2005 for physical abuse by parents. Injuries coded by police as moderate or serious were classified as requiring medical attention Any injury (minor or worse): < 2 years: 46.0%; 2–4 years: 39.3%; 5–9 years: 48.7%; 10–15 years: 64.7%; overall < 16 years: 55.5% |
Injury requiring medical attention: < 2 years: 88/317 (27.8%); 2–4 years: 79/574 (14.4%); 5–9 years: 172/1300 (13.2%); 10–15 years: 341/2271 (15.01%); total < 16 years: 680/4435(15.3%) |
| English, USA, 200060 | Children (< 18 years) with suspected physical abuse reported to social services and considered not to require further investigation. All (n = 862) were referred to a voluntary community-based support organisation. Injury ascertained by staff using a standard severity rating | Injury (> minor): 4/862 (0.46%) |
| Substantiated physical abuse | ||
| Gibbons, UK, 199556 | A total of 170 children (< 6 years) placed on NSPCC register for physical abuse in 1981. Injuries requiring medical attention (fractures, head injury, internal injury, severe burns or toxic ingestion) were documented from case conference reports | Injury requiring medical attention: 27/170 (16%) |
| Creighton, UK, 198553 | A total of 4329 children (< 18 years) placed on NSPCC register for physical abuse between 1977 and 1982. Injuries requiring medical attention (fractures, head injury, internal injury, severe burns or toxic ingestion) were documented from case conference reports | Injury requiring medical attention: 519/4329 (12%) |
| Lindell, Sweden, 200154 | A total of 145 children (< 15 years) with substantiated physical abuse reported to police (1986 and 1996). Fractures, burns and head or mouth injury were classified as requiring medical attention. Any injury reported in 75/145 (51.7%) | Injury requiring medical attention: 7/145 (4.8%) |
| Trocmé, Canada, 200357 | Nationally representative sample of 7672 children (< 16 years) reported to Canadian social services for suspected child abuse or neglect in 1998. A total of 3780 had substantiated abuse, of whom 1010 had physical abuse. Injury was reported by age group for 3780 children, classified as minor or requiring medical attention. Any injury reported in 379/1010 (37.5%) with physical abuse | Injury requiring medical attention: physical abuse: 70/1010 (6.9%); any abuse: < 1 year: 34/230 (14.8%); 1–3 years: 33/604 (5.5%); 4–7 years: 29/991 (2.9%); 8–11 years: 23/916 (2.5%); 12–15 years: 32/1012 (3.2%); < 16 years: 151/3753 (4%) |
| Zuravin, USA, 199461 | A total of 789 out of 2944 children reported to Child Protection Services in Baltimore City in 1984 for physical abuse were analysed. Injury classified as requiring medical attention included same or worse than sprain, mild concussion, broken teeth, cuts requiring sutures, second-degree burns, fractures or more than two ‘mild’ injuries on any body part. Any injury, including mild, reported in 497/789(63.0%) | Injury requiring medical attention: 146/789 (18.5%) |
FIGURE 7.
Risk of injury requiring medical attention given a single physical abuse event.
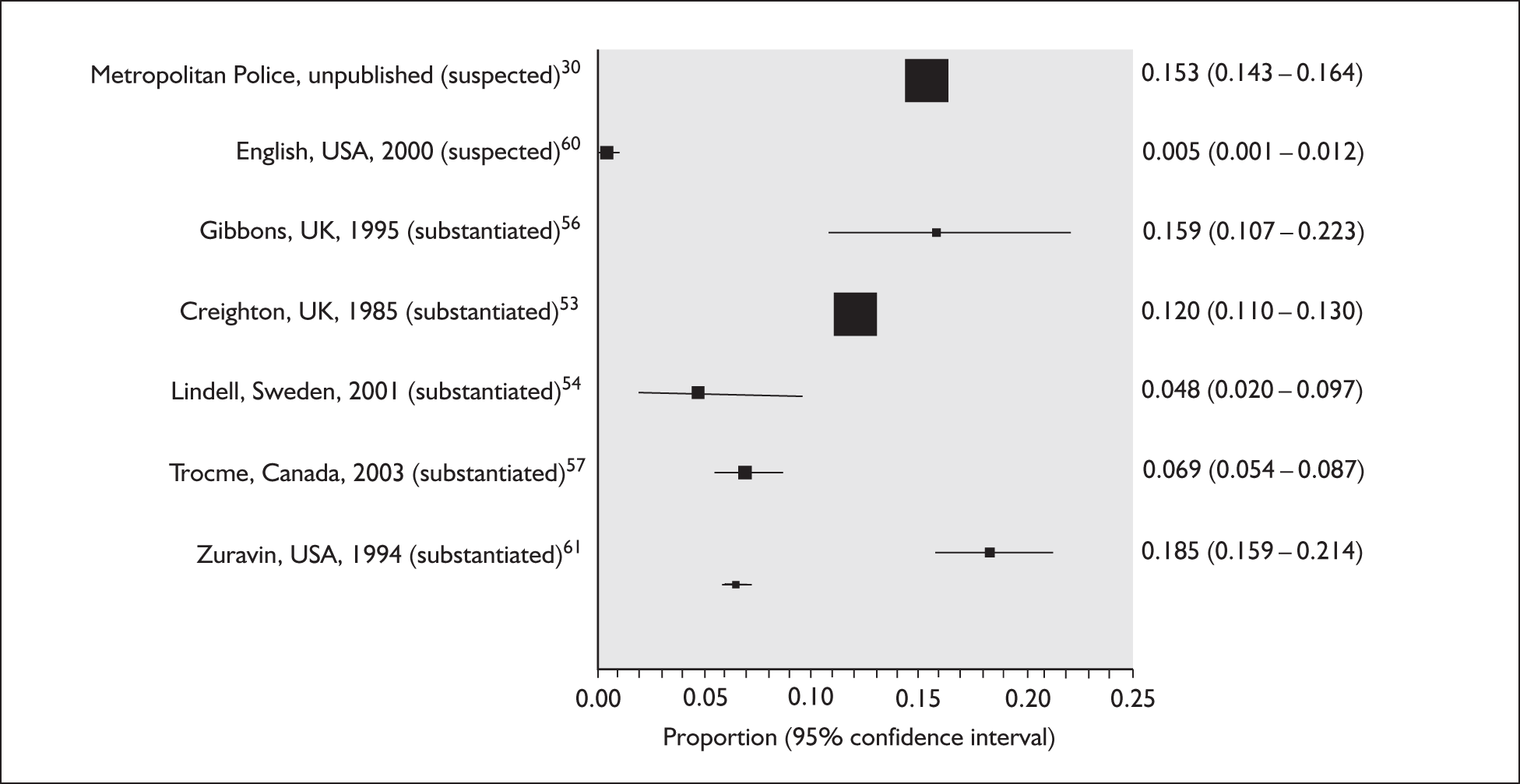
Of the included studies, all three UK studies reported high rates of injury compared with recent studies elsewhere. The high rate in the Metropolitan Police study (15.3%) (2006, unpublished data30) may reflect increased police involvement when there is a visible injury, better recording of marks by police than by other agencies or, in the absence of guidelines, overestimation of the need for medical attention. The other two UK studies were based on children registered in the early 1980s (injury prevalence 12%53 and 16%56) and may reflect more severe abuse 25 years ago than currently or a higher threshold of severity before cases were registered.
The risk of injury was moderately consistent in the two most recent studies in Canada57 (6.9%) and Sweden54 (4.8%). Excluded studies based on self-reported injury occurring over a period ranging from 12 months to the whole of childhood reported high rates of injury requiring medical attention (from 14%58 to 26%59). In contrast, the study by Ghate et al. 34 found a very low rate of reported visible injury suggesting parental reluctance to disclose inflicted injury. Only four parents (out of 1249) responded to the question ‘Have you ever inflicted any injury on your child that required medical attention?’ All four parents said ‘No’.
Attendance at A&E
In this section we report a series of systematic reviews to determine the incidence of attendance at A&E and how the characteristics of the child vary according to whether or not the injury was due to physical abuse.
Systematic review 3: Risk of attending A&E after injury due to physical abuse
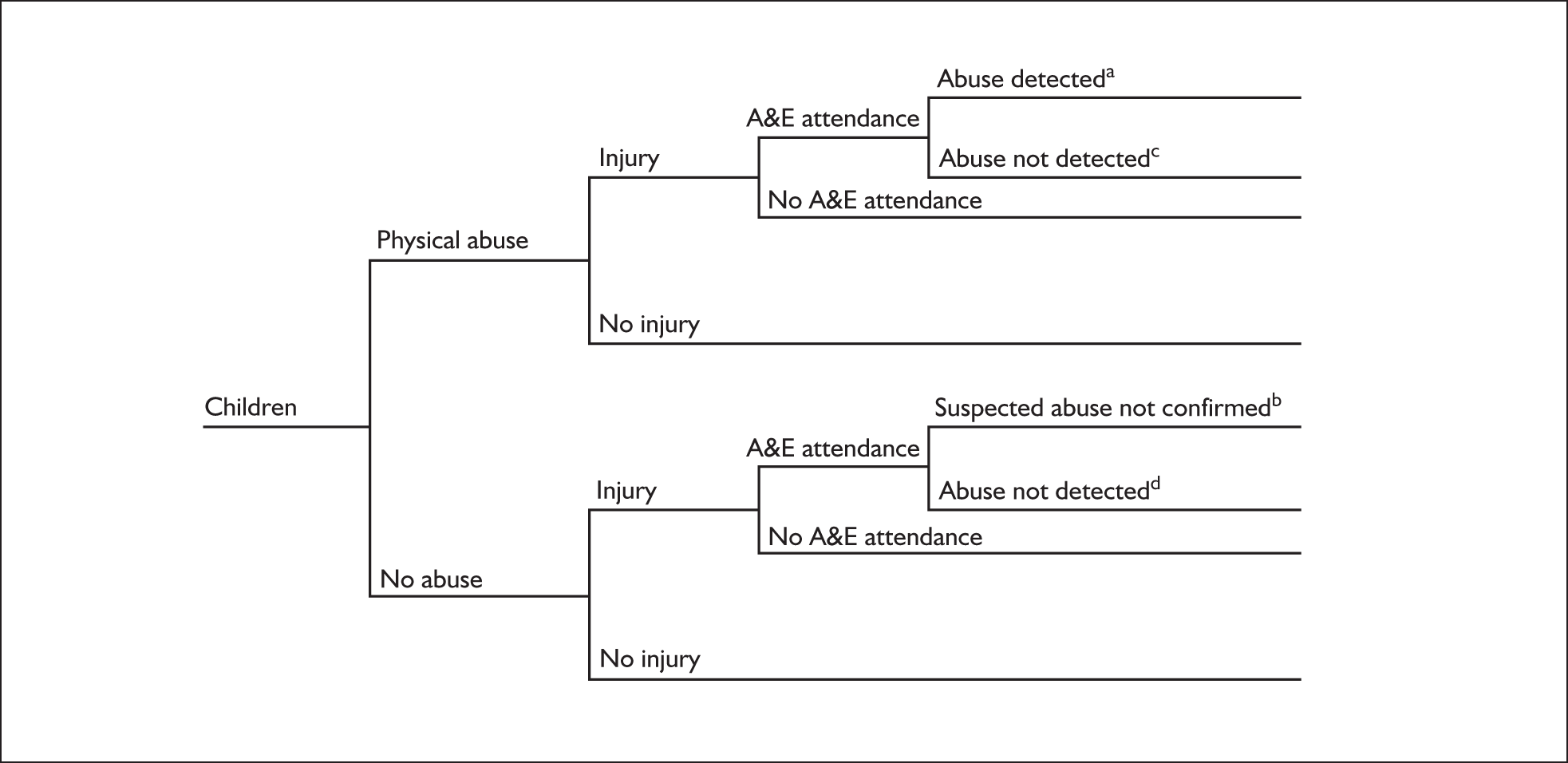
Direct measurement of the risk of a physically abused child attending A&E is difficult as some abused children may never be detected. Instead, we estimated this parameter indirectly (see Chapter 5) by addressing the following four questions, which can be mapped onto the tree in Figure 8:
-
What is the prevalence of A&E attendance in physically abused children who are injured [(a + c)/all abused and injured in Figure 8]?
-
What is the prevalence of confirmed physical abuse in all injured children attending A&E [a/(a + b + c + d) in Figure 8]?
-
What is the prevalence of confirmed and suspected physical abuse in injured children attending A&E [(a + b)/(a + b + c + d) in Figure 8]?
-
What is the prevalence of confirmed abuse in injured children with suspected physical abuse attending A&E [a/(a + b) in Figure 8]?
FIGURE 8.
Diagram showing how review questions (b)–(d) indirectly inform the probability of A&E attendance in injured, physically abused children [question (a)].
Review 3(a): Risk of A&E attendance in physically abused and injured children
Review methods
We included any study that reported presentation for medical services in children with confirmed physical abuse.
Review results
We found one study in which 4695 undergraduate students were interviewed and asked to recall any episodes of physical abuse by their parents (defined as injury due to parental violence) and whether they received medical attention (Table 5). A total of 592/4695 (12.6%) respondents reported one or more episodes of physical abuse, of which 146 involved fractures or head injury and were likely to have required medical attention. A total of 94 (0.16%) students reported having received medical attention for an abusive injury. If all A&E attendances were related to severe injuries (this is unclear in the report), 64% (94/146) of those with severe injury attended.
| First author, country, year of publication | Methods | Results |
|---|---|---|
| (a) Risk of A&E attendance in physically abused and injured children, (a + c)/all abused and injured | ||
| Berger, USA, 198889 | A representative sample of psychology undergraduates (n = 4695) completed a questionnaire including questions on parental violence during childhood, specific injuries resulting from violence and whether they ever received medical attention. A total of 592/4695 (12.6%) reported any injury due to parental violence in childhood, of which 55% were bruises, 18.1% cuts, 4.7% dental injuries, 7.6% burns, 6.7% broken bones and 10.5% head injury. We classified burns, broken bones and head injuries as likely to require medical attention (n = 146). A total of 94 attended A&E but it is not known for which type of injury | Risk of injury receiving medical attention: all injuries: 94/592 (15.9%); severe injuries: 94/146 (64.4%) |
| (b) Prevalence of confirmed physical abuse in all injured children attending A&E, a/(a + b + c + d) | ||
| Macgregor, UK (Scotland), 200362 | Records of 434 children < 1 year who presented to A&E with injury in 2000 were reviewed. Abuse was measured by referral to social services for suspected abuse | Confirmed abuse: 6/434 (1.3%) |
| Moore, UK (Liverpool), 199266 | A total of 110 children < 16 years presenting to children’s A&E in 1988 and claiming assault were interviewed by researchers. Abuse was based on disclosure by the child or caretaker (n = 15). We assumed that 27% (3767) of the 13,951 A&E attendances were for injury25,26,65 | Disclosed abuse: 15/3767 (0.40%) |
| Chang, USA, 200564 | Discharge records of 58,558 children (< 15 years) attending or admitted to hospital for injury in 1997 or 1998 were analysed for child abuse E-codes. We assumed that children with abuse recorded on the discharge database would have been referred to social services. ‘All centres’ includes non-trauma centre hospitals (n = 31,681) and data collected from a level 1 paediatric trauma centre during the development phase of the study (n = 11,919) | Abuse recorded on discharge: paediatric trauma centres: 65/551 (1.24%); trauma centres also serving adults: 158/21,326 (0.7%); total (all centres): 447/58,558 (0.76%) |
| Pless, Canada, 198765 | A total of 2211 children (< 6 years) attending children’s A&E with injury or poisoning in 1976. Specially trained nurses screened children using a checklist, full undressed examination, and discussion with physician (n = 1563). Abuse confirmed by hospital child protection team (resulting in referral to social services) | Confirmed abuse: 14/2211 (0.6%) |
| (c) Prevalence of suspected physical abuse in injured children attending A&E, (a + b)/(a + b + c + d) | ||
| Suspected abuse defined by referral to the paediatric team | ||
| Benger, UK (Bristol), 200221 | A total of 1000 injured children < 5 years consecutively attending a children’s A&E department. Referral to senior medical staff for suspected abuse recorded retrospectively from records | Referral to paediatrician: 6/1000 (0.6%) |
| Pless, Canada, 198765 | Children < 6 years attending A&E for injury/poisoning during 18 weeks in 1976 [see review 3(b)]. Referrals for suspected abuse to hospital child protection team | Suspect and confirmed: 36/2211 (1.6%) |
| Suspected abuse defined by a risk score | ||
| Palazzi, Italy, 200578 | A total of 10,175 children (< 15 years) presenting to 19 children’s A&E departments on random census days in 2000. Staff used a six-point suspicion index for all children. A score of equal to or more than 4 positive points indicated suspected abuse (n = 204). Of 204, 18% (36/204) were for suspected physical/sexual abuse | High score for physical/sexual abuse: 36/10175 (0.4%) |
| Johnson, USA, 198679 | A total of 333 children < 5 years presenting with injury to A&E (1981–2). Abuse (any) based on retrospective classification of inadequately explained/unexplained injury (45 children with incomplete records excluded) | Suspected abuse: 3/288 (1.0%) |
Review 3(b): Prevalence of confirmed physical abuse in all injured children attending A&E
Review methods
We included studies that reported confirmation of physical abuse in children attending A&E with any type of injury. We excluded studies that confined abuse detection to specific type of injuries (e.g. burns or fractures) as these are not representative of all attendances at A&E. We judged referral to social services to be an adequate marker of confirmation of physical abuse.
Review results
Four studies62–66 were included (Table 5; Figure 9, confirmed studies). The prevalence of confirmed physical abuse among injured children ranged from 0.37% to 1.38% (Figure 10). There were two UK studies. One,62 limited to injured infants attending A&E (1.3% had confirmed physical abuse), overestimates the risk for all children as infants are at higher risk of abuse. The other UK study by Moore and Robson66 likely underestimates the risk of abuse as detection of abuse required disclosure of parental assault. In a large US study by Chang et al. ,64 based on attendances for injury and discharge diagnoses at 1196 hospitals, the overall prevalence of confirmed abuse was 0.76%; however, the prevalence was higher in paediatric trauma centres, presumably because staff were more alert to the possibility of abuse. A similar prevalence of abuse (0.64%) was reported in a study by Pless et al. 65 from Canada in 1976, which was restricted to children under 6 years of age.
FIGURE 9.
Prevalence of confirmed and confirmed plus suspected physical abuse in all injured children attending A&E: systematic reviews 3(b) and 3(c). Note: confirmed abuse = a/(a + b + c + d), review 3(b); confirmed and suspected abuse = (a + b)/(a + b +c + d), review 3(c).
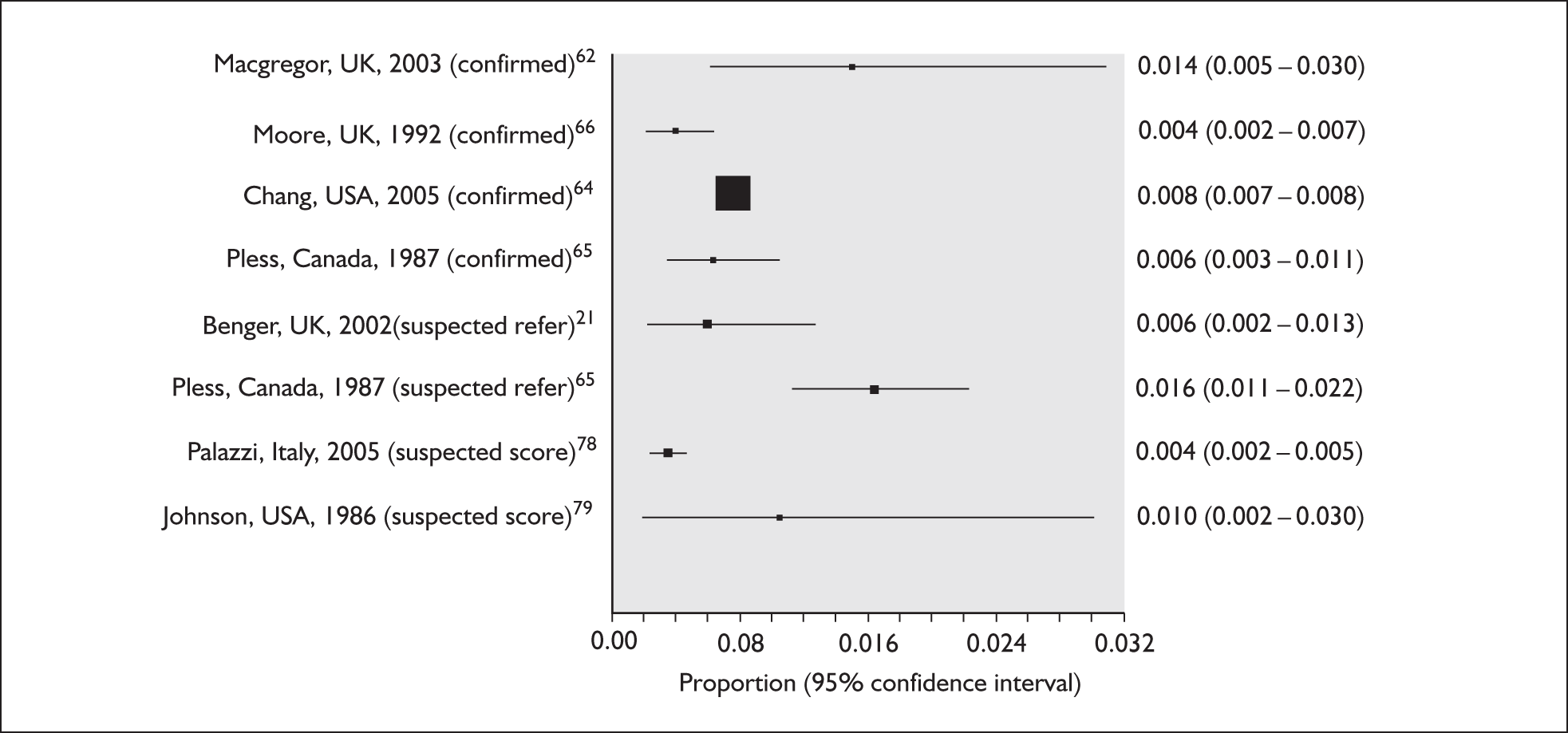
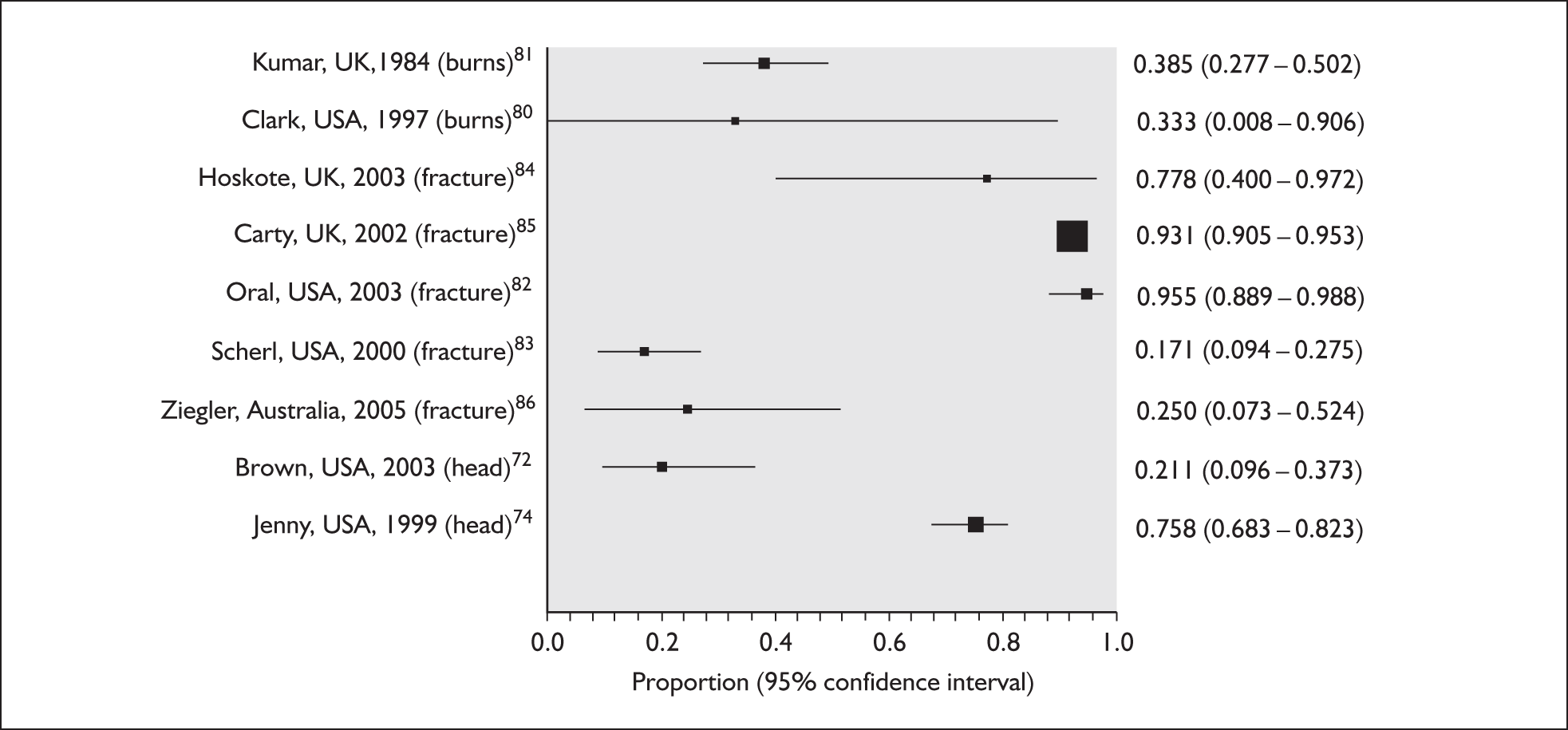
FIGURE 10.
Prevalence of confirmed abuse in injured children referred for suspected physical abuse [a/(a + b) in Figure 8]: systematic review 3(d).
These figures contrast with results from studies of high-risk patients or studies with low thresholds for measuring abuse that were excluded from this review. For example, in studies looking at fractures in children between birth and 3 years of age, the prevalence of abuse in injured children ranged from 23% to as high as 83% for children under 2 years with rib fractures. 67–70 The prevalence of abuse in young children with head injury was also high, ranging from 14% to 70% depending on the age of the child, the type and severity of head injury and the measurement of physical abuse. 71–76
Systematic review 3(c): Prevalence of confirmed and suspected physical abuse in injured children attending A&E
Review methods
We included studies that reported any measure of suspected abuse in children attending A&E for injury. Studies restricted to specific injuries were excluded. We included studies that did not differentiate between injury due to physical abuse or neglect, provided that they included physical abuse.
Review results
We found four studies, of which one (Pless et al. 65) was included in review 3(b) of confirmed physical abuse (see Table 5, Figure 9). These are analysed below according to the criteria for defining suspected abuse. 21,65,77–79
Two studies measured suspected abuse by referral to a paediatrician or the child abuse team within the hospital. 21,65 Benger and Pearce21 found that 0.6% of injured children under 5 years attending a UK children’s A&E department were referred to a paediatrician. Similar results were found in a Canadian children’s A&E department: between 0.6% and 1.4% of injured children under 6 years were referred to the hospital child protection team for any abuse, and about half of these were for physical abuse (i.e. 0.3–0.8% from 1976 to 1984; the figure for 1976 of 0.64% is used in Figure 9). 65
Two studies78,79 used a risk score to identify children with suspected abuse, although a suspicious score did not necessarily result in referral. Palazzi et al. 78 conducted a multicentre study in 19 A&E departments in Italy and found that 0.35% of 10,175 injured children had a high score (≥ 4 points) for physical abuse.
Systematic review 3(d): Prevalence of confirmed abuse in injured children referred for suspected physical abuse from A&E
Information on the probability of confirmed abuse in injured children referred from A&E can be used to validate estimates used in the clinical effectiveness model for the prevalence of confirmed abuse in injured children attending A&E [a/(a + b + c + d)]. This information, known as the positive predictive value or post-test probability, may be drawn from studies that follow up referrals for suspected abuse or from the paediatrician’s experience. Consequently, we addressed this question using published studies and estimates from experts.
Review methods
We included any study that reported any measure of confirmation of physical abuse (separately from other types of abuse) in children with any type of injury who were referred for suspected physical abuse. We assumed that ‘inflicted’ injury or ‘non-accidental’ injury referred to physical abuse, and ‘abuse’ (with no further definition) referred to all types of abuse and neglect. As few studies reported referrals from A&E we accepted any hospital setting. We sought expert opinion from three paediatricians who assess referrals from A&E.
Review results
We found nine studies (Table 6). 72,74,80–86 Post-test probability varied between 20% and 95% depending on the type and severity of injury, the threshold for referral, the criteria for confirmation of abuse and the accuracy of clinicians who decided which children to refer. All of the included studies were based on specific injury groups that would be classified post hoc, after investigation, and which are therefore likely to be based on highly selected populations, at higher risk of abuse than the average injured child attending A&E. 65,70,87 The included studies suggest some consistency in the risk of abuse for burns80,81 but not for other types of injury.
| First author, country, year of publication | Age | Admitted (Y/N) | Injury, setting, time | Test for abuse | Confirmation of abuse | Confirmed physical abuse (%) |
|---|---|---|---|---|---|---|
| Burns | ||||||
| Kumar, UK, 198481 | < 9 years | Y | Burns unit, 1977–81 | Referral to SS | SS confirm | 30/78 (38.5%) |
| Clark, USA, 199780 | < 16 years | N | Burns, A&E, 1990–1 | Referral to SS (standard care) | SS confirm | 1/3 (33.3%) |
| < 18 years | N | Burns, A&E, 1992–3 | Referral to SS (checklist) | SS confirm | 7/26 (26.9%) | |
| Fractures | ||||||
| Hoskote, UK, 200384 | < 1 year | N | Fracture, A&E, 1993–4 | Referral to SS | Children registered on CPR | 7/9 (77.8%) |
| Carty, UK, 200285 | < 16 years | N | Fracture, radiology department, 1984–96 | Referral to SS | Admitted/court confirm | 435/467 (83.2%) |
| Oral, USA, 200382 | < 3 years | N | Fracture, children’s emergency department, 1995–8 | Referral to SS | Researchers confirm | 85/89 (95.5%) |
| Scherl, USA, 200083 | < 6 years | Y | Diaphyseal femur fracture, children’s hospital, 1986–96 | Referral to SS | SS confirm | 13/76 (17.1%) |
| Ziegler, Australia, 200586 | < 3 years | N | Fracture, emergency department (tertiary), 2001–2 | Referral to SS | SS confirm | 4/16 (25%) |
| Head injury | ||||||
| Brown, USA, 200372 | < 4 years | Y | Head injury, 1993–9 | Referral to SS/police | Hospital, SS, police confirm | 8/38 (21.0%) |
| Jenny, USA,199974 | < 3 years | Y | Head injury, children’s hospital, 1993–6 | Referral to hospital CAP team | CAP team confirm | 119/173 (68.8%) |
Three consultant paediatricians gave their opinion on the risk of confirmed physical abuse in injured children referred by A&E staff to the paediatric team, usually a paediatric registrar, for assessment. The estimates were 5–10%, higher than 2–10%, and 50–60%. Such variation reflects recall bias, variation in feedback about the outcome of referrals and knowledge about referrals to the paediatric team as a whole, as well as real differences in the skills of A&E staff, the threshold for referral and the populations studied. 35,57,64,88,89
Systematic review 4: Incidence of attendance of all injured children at A&E
Review methods
To determine the annual incidence of attendance of injured children at A&E according to age group we included any UK study that reported the number of attendances for all injuries at A&E in any age group and the denominator population. We excluded studies from outside the UK as patterns of primary care and emergency care provision differ across countries. We accepted attendances for accidents as equivalent to attendances for injury but excluded reports of all attendances as the proportion due to injury varies by age group and may be affected by relative ease of access to primary care and A&E. 25,26
Review results
We found seven studies (Table 7 and Figure 11). 62,88,90–94 Two studies from Norwich91,92 were combined as they used the same geographic population and methods but studied different age groups. All six studies were based on children attending A&E after 1989 and all but one were based on routine hospital coding of the principal reason for attendance. The largest and most nationally representative study was based on unpublished data provided by the Royal Society for the Prevention of Accidents (RoSPA) for A&E departments across the UK in 2000–2. 88 The RoSPA used interviews with patients in A&E departments to categorise reasons for attendance. The Norwich study estimated the denominator population based on person-years of residence using child health records. 91,92 All other studies estimated the denominator population from point prevalence census data. 62,88,90,93,94
| First author, place, year of publication | Methods | Number of injury attendances/denominator (rate per 100 child-years) |
|---|---|---|
| Brownscome, Bath, 200490 | Resident children (< 5 years) attending A&E for accidents, including those found to have no injury (n = 165), identified by A&E audit (1997–2000) | < 5 years: 2300/4245 (13.1 per 100 child-years) |
| MacGregor, Aberdeen, 200362 | Infants (< 1 year) attending A&E for injury were identified by case note review (2000). Population estimated. These data are not represented in Figure 11 as they are only for children under 1 year | < 1 year: 434/6000 (7.2 per 100 child-years) |
| Royal Society for the Prevention of Accidents (RoSPA), UK, 2002 (unpublished)88 | Patients interviewed at 16 representative A&E departments (2000–2). Numerator assumed to be approximately 5% of all UK attendances. We calculated denominator based on mid-population estimates for 2002. Accident attendances with foreign bodies or ‘no injury’ were excluded (5% of total accidents). The age-specific incidence entered into our model gives a weighted average of 19.0 per 100 child-years | < 1 year: 3322/32,244 (10.3 per 100 child-years); 1–4 years: 26,791/134,293 (20.0 per 100 child-years); 5–9 years: 26,637/185,390 (16.9 per 100 child-years); 10–15 years 46,423/216,673 (21.4 per 100 child-years); total < 16 years: 103,173/568,600 (18.1 per 100 child-years) |
| Reading, Norwich, 199992 and Haynes, Norwich, 200391 | Resident children identified from A&E records and injury classified by researchers (0–4 years in 1994; 5–14 years in 1999). Poisoning or foreign bodies were excluded. Denominator recorded as person-time of residence from child health records | 0–4 years: 2012.02/18,693 (10.76 per 100 child-years); 5–10 years: 1829/12,868.2 (14.2 per 100 child-years); 11–14 years: 1636/8575.8 (19.1 per 100 child-years); total < 15 years: 5477/40,140 (13.6 per 100 child-years) |
| Walsh, Newcastle, 199694 | Random sample of resident children attending two A&E departments for accidental injury (< 16 years), identified from A&E records and classified by researchers (1990). Denominator based on census | < 5 years: (22.5 per 100 child-years); 5–9 years: (19.0 per 100 child-years); 10–15 years: (27.5 per 100 child-years); total < 16 years: 11,682/54,400 (21.5 per 100 child-years) |
| Lyons, South Wales, 199593 | Resident children (< 15 years) attending three A&E departments for injury (1993). Denominator based on census | < 15 years: 10117/55,588 (18.2 per 100 child-years) |
FIGURE 11.
Incidence of attendance of all injured children at A&E (per 100 child-years).
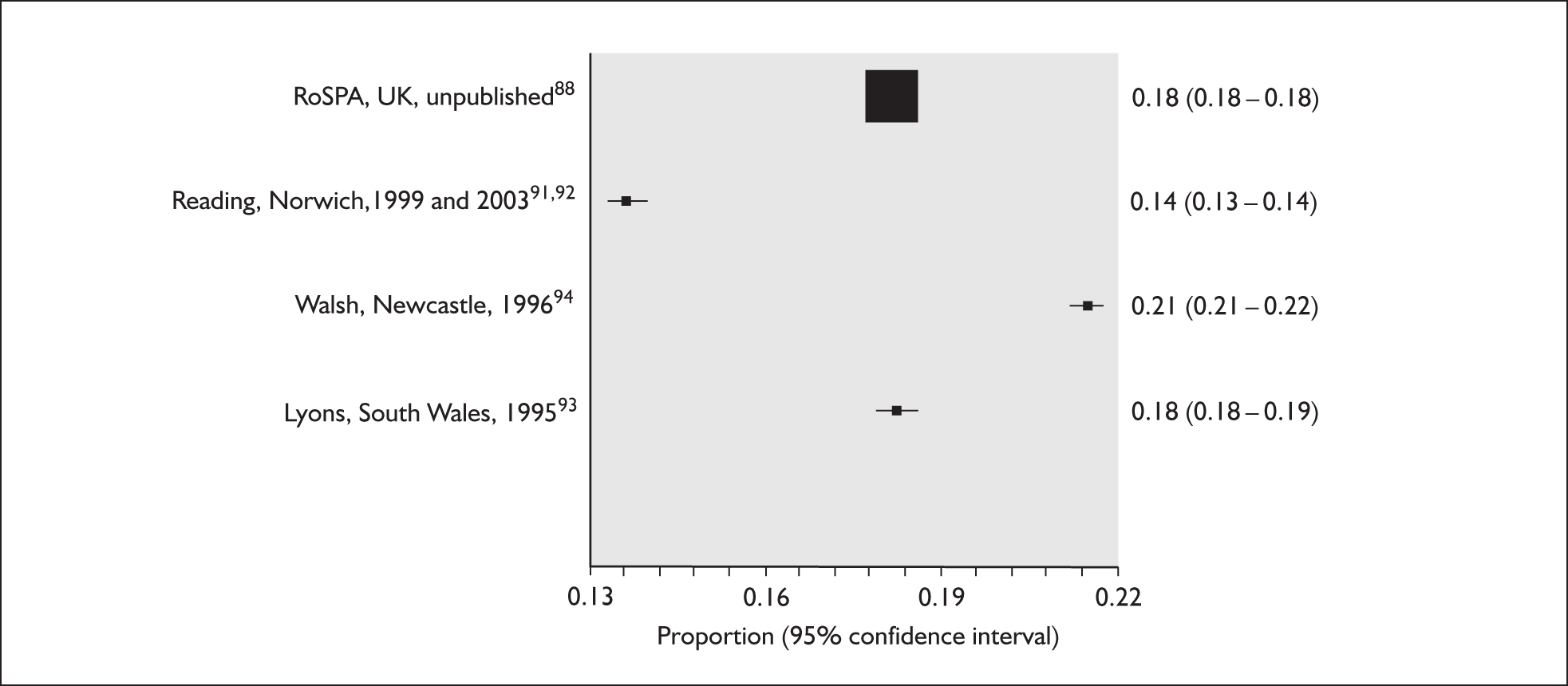
In the four studies that reported results for all ages, the incidence of attendance ranged from 13.6 per 100 child-years in Norwich to 21.5 per 100 child-years in Newcastle. 91,92,94 The RoSPA reported an incidence for the UK of 18.1 per 100 child-years. 88 The low rate of injury attendances in Norwich,79,80 Bath90 and Aberdeen62 may reflect better access to or a preference for primary care services in these areas. 88
Characteristics of children attending A&E for injury
In this section we review the evidence on the performance of a range of child characteristics or markers that have been used in screening protocols to determine which children should be referred directly to the paediatricians for assessment of suspected child abuse. Characteristics that have been used to date include young age (e.g. infants or children under 2 years), fractures or head injury in young children,22 children currently on the CPR,22,95 and repeated attendance for injury (Ian Maconochie, St Mary’s Hospital, London, February 2006, and Ben Lloyd and Jane Mattison, Royal Free Hospital, London, January 2006, personal communication). 1,20,96,97
Several potentially important characteristics were not evaluated because of a lack of UK data. These include presentation during night-time hours,98,99 parental mental illness and drug abuse, and domestic violence, all of which are factors evaluated by the community liaison nurse (Ben Lloyd, January 2006, personal communication).
As the prevalence of physical abuse in injured children attending A&E is very low (about 1%), only characteristics that are very strongly associated with abuse will have any appreciable impact on the probability of abuse. Consequently, although the quality of the research literature relating to this question was generally poor, strong associations should nevertheless be apparent.
Systematic review 5: Age as a predictor of physical abuse in injured children attending A&E
We aimed to determine the performance of the child’s age as a predictor of physical abuse. The results were used to derive a likelihood ratio (LR), a measure of diagnostic test performance, that estimates how many times as likely is a test result (e.g. age under 1 year) in abused compared with non-abused children. 100 LRs are preferable to sensitivity and specificity as they capture test performance for a specific marker (e.g. infancy) when multiple markers are possible (e.g. four different age groups).
The LR was calculated as:
The LR can be used to calculate the post-test probability of abuse in a specific age group using Bayes’ theorem (pre-test odds × LR = post-test odds). 100
Because of a paucity of evidence we evaluated two types of study. Those that:
-
directly compared abused and non-abused injured children
-
reported the age distribution of injuries in abused children or all children but which could be assumed to be drawn from a similar population (indirect comparison).
Systematic review 5(a): Studies that directly compared abused and non-abused injured children
Review methods
We included any study that reported age groups for children attending A&E for injury categorised into physically abused and non-abused using any measure.
Review results
Three studies were found (Table 8). Only one study,101 conducted in Hawaii, was based on all injured children attending A&E. Two other studies75,98 were based on a subset of children admitted with severe injuries.
| First author, place, year of publication | Methods | Results | ||||
|---|---|---|---|---|---|---|
| (a) Studies comparing abused and non-abused children | Age | Abused | Non-abused | LR | Probability a | |
| Yamamoto, Hawaii, 1991101 | Children (< 16 years) seen in A&E with injury (not burns) in 1987–8. Suspicion of physical abuse by clinicians was recorded in a prospective survey | < 1 year | 11 (6.6%) | 171 (4.3%) | 1.54 | 6.0% |
| 1–5 years | 48 (28.9%) | 1953 (24.1%) | 1.12 | 2.5% | ||
| 6–10 years | 34 (20.5%) | 1047 (26.3%) | 0.78 | 3.2% | ||
| 11–15 years | 73 (44.0%) | 806 (20.7%) | 2.13 | 8.8% | ||
| < 16 years | 166 | 3977 | 4.0% | |||
| TARNlet, UK (unpublished)75 | Very severely injured children (< 16 years) admitted to 20 hospitals (30–50% of all trusts in England and Wales) between 1996 and 2004. Injury coding and classification of abuse was based on examination of records for the whole admission. We estimated that TARNlet comprises approximately 0.2–0.35% of all injury attendances in the UK in children | < 1 year | 231 (57.0%) | 754 (4.38%) | 13.0 | 23.5% |
| 1–4 years | 161 (39.8%) | 3286 (18.8%) | 2.1 | 4.7% | ||
| 5–9 years | 9 (2.2%) | 4486 (26.0%) | 0.09 | 0.2% | ||
| 10–15 years | 1 (0.2%) | 8712 (50.6% | 0.004 | 0.01% | ||
| < 16 years | 405 | 17,229 | 2.3% | |||
| Chang, USA, 200498 | Children (< 16 years) attending a level 1 paediatric trauma centre (1990–2002). Data retrospectively extracted from trauma registry. Abuse was defined by routine diagnostic codes | < 1 year | 97 (56.7%) | 873 (7.4%) | 7.7 | 11.1% |
| 1–5 years | 55 (32.2%) | 3111 (26.6%) | 1.2 | 1.7% | ||
| 5–15 years | 19 (11.1%) | 7867 (66.4%) | 0.2 | 0.2% | ||
| < 16 years | 171 | 11,851 | 1.4% | |||
| (b) Indirect comparison of age distributions in abused and non-abused injured children attending A&E | ||||||
| Abused children | ||||||
| Shrivastava, Coventry, 1988 (PhD thesis)102 | Injured children (≤ 16 years) admitted from A&E because of suspected abuse (1983–7, n = 126; abuse confirmed in 108), identified by retrospective review of admission charts | < 1 year: 29/126 (23%); 1–2 years: 19/126 (15.1%); 3 years: 15/126 (11.9%); 4–5 years:13/126 (10.3%); 6–7 years: 14/126 (11.1%); 8–10 years: 5/126 (4.0%); 11–15 years: 15/126 (11.9%); 16 years: 16/126 (12.7%) | ||||
| Roberton, Nottingham, 1982103 | Injured children (< 12 years) admitted from A&E with disclosed (n = 35) or suspected abuse (n = 49) in 1981. Retrospective record review | < 3 years: 37/84 (44.0%); 4–11 years: 47/84 (56.0%) | ||||
| Non-abused children | ||||||
| University College London Hospital, UK, 2003–5 (unpublished)25 | Children (< 16 years) attending general A&E for injury (2003–5). Routine records of primary reason for attendance | < 1 year: 235/5165 (4.6%); 1–4 years: 1599/5165 (31.0%); 5–10 years: 1660/5165 (32.1%); 11–15 years: 1671/5165 (32.4%) | ||||
| Royal Society for the Prevention of Accidents (RoSPA), UK, 2002 (unpublished)88 | Children (< 16 years) attending 16 representative A&Es. Reasons for attendance based on interviews with patients. See www.hassandlass.org.uk/query/reports/2000_2002.pdf | < 1 year: 73431/2,427,303 (3.0%); 1–4 years: 610,510/2,427,303 (25.2%); 5–9 years: 632,568/2,427,303 (26.1%); 10–15 years 1,110,793/2,427,303 (45.7%) | ||||
The results show marked differences depending on the severity of injury. In the Hawaiian study, which reported a clinical suspicion of physical abuse in 4% of injured children, the LRs for age groups were all close to 1.0 and the post-test probability did not vary much between age groups. 101 In the two studies based on severe injury, infancy was predictive of abuse.
In the UK TARNlet study,75 which was restricted to the most severely injured 0.34% of all A&E attendances for injury, age was predictive of abuse for children under 1 year (risk of abuse increased) and over 5 years (risk of abuse decreased). In total, 2.3% of all children in the TARNlet study were recorded as injured because of physical abuse, but this rose to 23.5% for infants (Table 8). 75 Similar trends were reported by Chang et al. 98
In summary, we found no direct evidence that age is predictive of physical abuse in all injured children attending A&E, but admission with severe injury in infancy was moderately predictive of abuse.
Systematic review 5(b): Indirect comparison of age distributions in abused and non-abused injured children attending A&E
Review methods
We included any study that reported the age distribution of physically abused and injured children, or all injured children, attending A&E. We compared the age distributions in abused and non-abused children by assuming that they were drawn from the same population. Consequently, we included only UK studies.
Review results
We found two studies102,103 based on physically abused children (Table 8) and used two datasets25,88 based on routine A&E attendances to determine the age distribution for all injured children attending A&E.
Both UK studies were conducted in the 1980s. Both found that the youngest children accounted for the highest proportion of abuse cases per year of age. 102,103 As abuse was recorded only in injured children who were admitted from A&E, this may over-represent younger children as older children may not always be admitted. The age distributions in the two UK datasets (RoSPA and a central London trust) were remarkably consistent, showing a static rate of injury attendance in children over 1 year of age and a much lower rate for infants. 25,88
In summary, injured children under 1 year attending A&E appear to be more likely to have been abused than older children. 88,102
Systematic review 6: Type of injury as a predictor of physical abuse in children attending A&E
We determined the performance of five broad categories of injury for predicting physical abuse: head injury, fracture, bruises, burns and other. Because of the paucity of published evidence we conducted two reviews:
-
direct comparisons within study of the type of injury in abused and non-abused injured children
-
an indirect comparison of studies reporting type of injury in abused or all children.
Systematic review 6(a): Studies reporting a direct comparison of type of injury in abused and non-abused children
Review methods
We included studies that reported the type of injury in abused and non-abused injured children attending A&E. Studies based on children admitted to hospital were excluded.
Review results
We found no published studies that met our inclusion criteria. We included one unpublished UK national audit based on injured children admitted from A&E who met predefined severity criteria (TARNlet,75 described in Table 8). Table 9 shows that the LRs for injury type within each age group are all close to 1.0 (range 0.2–3.6) and the probability of physical abuse given each type of injury is similar to the probability for the age group overall (last column). Values for older school-age children were based on small numbers of abused children and were therefore very uncertain. These results indicate that, after taking age into account, type of injury is not a good predictor of physical abuse in this severely injured population.
| Age | Data | Head injury | Fractures | Bruises | Burns | Other injury | Total diagnoses (abused/all) | Total children (abused/all) |
|---|---|---|---|---|---|---|---|---|
| < 1 year | Diagnoses (abused/all) | 172/460 | 79/454 | 85/208 | 6/92 | 0/10 | 324/1224 | 231/985 |
| LRa (95% CI) | 1.5 (1.3–1.8) | 0.5 (0.4–0.6) | 1.8 (1.4–2.3) | 0.2 (0.1–0.4) | 0.0b | |||
| Probability of abuse | 37.4% | 17.4% | 40.9% | 6.5% | 0%b | 27.9% | 23.5% | |
| 1–4 years | Diagnoses (abused/all) | 93/994 | 72/2032 | 56/482 | 17/475 | 1/89 | 239/4072 | 161/3447 |
| LR (95% CI) | 1.7 (1.4–2.0) | 0.6 (0.5–0.7) | 2.1 (1.6–2.7) | 0.6 (0.4–0.9) | 0.2 (0.03–1.3) | |||
| Probability of abuse | 9.4% | 3.5% | 11.6% | 3.6% | 1.1% | 5.9% | 4.6% | |
| 5–9 years | Diagnoses (abused/all) | 3/1325 | 4/3103 | 3/629 | 1/145 | 1/198 | 12/5400 | 9/4495 |
| LR (95% CI) | 1.0 (0.4–2.7) | 0.6 (0.3–1.3) | 2.2 (0.8–5.7) | 3.1 (0.5–20.5) | 2.3 (0.3–15.0) | |||
| Probability of abuse | 0.23% | 0.1% | 0.5% | 0.7% | 0.5% | 0.2% | 0.2% | |
| 10–15 years | Diagnoses (abused/all) | 1/2413 | 0/6432 | 0/1200 | 0/151 | 0/386 | 1/10582 | 1/8713 |
| LR (95% CI) | 4.4 (4.2–4.5) | 0.0 | 0.0 | 0.0 | 0.0b | |||
| Probability of abuse | 0.04% | 0%b | 0%b | 0%b | 0%b | 0%b | 0.01% | |
| Total < 16 years | Diagnoses (abused/all) | 269/5192 | 155/12021 | 144/2519 | 24/863 | 2/683 | 594/21278 | 402/17640 |
| LR (95% CI) | 1.9 (1.7–2.1) | 0.5 (0.4–0.5) | 2.1 (1.8–2.4) | 0.1 (0.7–1.5) | 0.1 (0.03–0.4) | |||
| Probability of abuse | 5.2% | 1.3% | 5.7% | 2.8% | 0.3% | 2.8% | 2.3% |
Systematic review 6(b): Indirect comparison of studies reporting type of injury
Review methods
We included any UK study that reported the frequency of the principal type of injury in physically abused or all injured children attending A&E. The type of injury was grouped into five categories (bruises, fractures, head injury, burns, other) by one reviewer (JW). For studies reporting abused children we accepted any measure of physical abuse.
Review results
We found one study based on children with suspected physical abuse admitted from A&E in Coventry that reported the type of injury but in which cases were not subdivided by age group (Table 10). 102 We excluded one further study of children under 8 years as it was based in France (n = 197). 104 We found three published studies91,92,94,105 and four primary datasets that reported the type of injury in all children attending A&E. 25,26,88 Most reported the principal injury although the RoSPA reported 21% more injuries (n = 130,647) than children (n = 108,259). 88
| First author, place, date of publication | Methods | Proportion with each type of injury (%) | |||||
|---|---|---|---|---|---|---|---|
| Abused children | |||||||
| Shrivastava, Coventry, 1988 (PhD thesis)102 | Injured children (< 16 years) admitted from A&E for suspected physical abuse in Coventry (1983–7). See Table 8 for more details. Results for injury type not given by age group | Head injury: 3/131 (2.3%) | |||||
| Fracture: 32/131 (24.4%) | |||||||
| Bruises: 79/131 (60.3%) | |||||||
| Burns: 14/131 (10.7%) | |||||||
| Other: 3/131 (2.3%) | |||||||
| All injured children attending A&E | < 1 year | 1–4 years | 5–9 years | 10–15 years | All ages | ||
| Downing, West Midlands, 2006105 | Children (< 16 years) attending A&E in 16 hospitals (2002–4). We classified injury types as follows:a head injury (head injury); fractures (dislocation, fracture, joint injury, amputation); bruises (laceration, contusion, abrasion, soft tissue injury, sprains, vascular injury); burns (burns, electrocutions), other (other injury) | Head injury | 2027 (17.8%) | 4314 (16.9%) | 6489 (9.8%) | 5890 (5.3%) | 18,720 (6.8%) |
| Fracture | 154 (1.3%) | 5515 (6.5%) | 8427 (12.7%) | 18,313 (16.5%) | 32,409 (11.9%) | ||
| Bruises | 1101 (9.5%) | 40,578 (48.1%) | 41,632 (63%) | 73,122 (65.8%) | 156,433 (57.2%) | ||
| Burns | 198 (1.7%) | 3020 (3.6%) | 927 (1.4%) | 896 (0.8%) | 5041 (1.8%) | ||
| Other | 8110 (69.7%) | 21011 (24.9%) | 8680 (13.1%) | 12,934 (11.6%) | 50,735 (18.6%) | ||
| Total | 11,636 | 84,439 | 66,156 | 111,156 | 273,387 | ||
| University College London Hospital, UK, 2006 (unpublished)25 | Routine data from a general A&E department (2003–5). Exclusive injury categories used. Injuries classified as: head injury (closed head injury); fractures (dislocation, fracture, joint injury, amputation); bruises (laceration, contusion, abrasion, soft tissue injury, sprains/ligament injury, muscle/tendon injury, nerve injury); burns (burns, electrocutions), other (vascular injury, internal injury) | Head injury | 63 (26.8%) | 105 (6.6%) | 80 (4.8%) | 42 (2.5%) | 290 (5.6%) |
| Fracture | 12 (5.1%) | 193 (12.1%) | 371 (22.3%) | 400 (23.9%) | 976 (18.9%) | ||
| Bruises | 136 (57.8%) | 1232 (77.0%) | 1177 (70.9%) | 1209 (73.4%) | 3754 (72.7%) | ||
| Burns | 24 (10.2%) | 68 (4.3%) | 32 (1.9%) | 20 (1.2%) | 144 (2.8%) | ||
| Other | 0 (0%) | 1 (0.1%) | 0 (0%) | 0 (0%) | 1 (0%) | ||
| Total | 253 | 1599 | 1660 | 1671 | 5165 | ||
| Electronic Child Health Register, North East London, 2006 unpublished26 | Routine A&E attendance data for children (< 8 years) attending five London Hospitals (2000–6; average 4.4 years). Exclusive injury categories used. Injuries classified as: head injury (closed head injury); fractures (dislocation, fracture, joint injury, amputation); bruises (laceration, contusion, abrasion, soft tissue injury, sprains, vascular injury); burns (burns, electrocutions), other (other injury) | < 1 year | 1–4 years | 5–7 years | All ages | ||
| Head injury | 79 (13.9%) | 206 (8.2%) | 92 (7.7%) | 377 (8.8%) | |||
| Fracture | 59 (10.4%) | 337 (13.5%) | 171 (14.3%) | 567 (13.3%) | |||
| Bruises | 386 (68.0%) | 1751 (70.0%) | 872 (72.9%) | 3009 (70.6%) | |||
| Burns | 20 (3.5%) | 85 (4.4%) | 22 (1.8%) | 127 (3.0%) | |||
| Other | 24 (4.2%) | 123 (4.9%) | 38 (3.2%) | 185 (4.3%) | |||
| Total | 568 | 2502 | 1195 | 4265 | |||
| Royal Society for the Prevention of Accidents (RoSPA), UK, 2002 (unpublished)88 | Details elsewhere (see Table 7). Each patient could have up to five injuries recorded but multiple injuries not identifiable in dataset. There are 21% more injuries than patients. Injuries classified as: head injury (concussion, unconsciousness); fractures (bone injury); bruises (open wound, contusion/bruise, other soft tissue injury, superficial injury, joint/tendon injury); burns (burn), other (other injury, chemical injury, systemic injury, unspecified injury) | < 1 year | 1–4 years | 5–9 years | 10–15 years | All ages | |
| Head injury | 652 (18.2%) | 2624 (8.8%) | 1624 (5.3%) | 1391 (2.6%) | 6291 (5.3%) | ||
| Fracture | 127 (3.5%) | 2128 (7.1%) | 4547 (14.7%) | 9716 (17.9%) | 16,518 (14.0%) | ||
| Bruises | 1906 (53.2%) | 19,627 (65.9%) | 22,040 (71.4%) | 39,469 (72.8%) | 83,042 (70.1%) | ||
| Burns | 324 (9.0%) | 1425 (4.8%) | 406 (1.3%) | 4529 (1.0%) | 6684 (5.6%) | ||
| Other | 573 (16.0%) | 3977 (13.4%) | 2240 (7.3%) | 3080 (5.7%) | 9870 (8.3%) | ||
| Total | 3582 | 29,781 | 30,857 | 54,185 | 118,405 | ||
| Reading, Norwich, 199992 and Haynes, Norwich, 200391 | Details elsewhere (see Table 7). Exclusive injury categories used. Injuries classified as: head injury (head injury); fractures (fractures, dislocation); bruises (lacerations, bite, piercing, soft tissue inflammation: sprain, crush, bruises); burns (burn, scald, smoke inhalation), other (other injury, unknown) | 0–4 years | 10–15 years | All ages | |||
| Head injury | 22 (1.3%) | 17 (1.0%) | 39 (1.2%) | ||||
| Fracture | 320 (18.4%) | 420 (25.7%) | 740 (21.9%) | ||||
| Bruises | 1340 (77.1%) | 1160 (77.1%) | 2500 (74.1%) | ||||
| Burns | 30 (1.7%) | 9 (0.6%) | 39 (1.2%) | ||||
| Other | 25 (1.4%) | 30 (1.8%) | 55 (1.6%) | ||||
| Total | 1737 | 1636 | 3373 | ||||
| Walsh, Newcastle, 199694 | Details elsewhere (Table 7). Injuries classified as: head injury (head injury); fractures (fractures, dislocation); bruises (lacerations, foreign body orifice, soft tissue injury, sprains, etc.); burns (burn), other (poisoning) | All ages | |||||
| Head injury | 2510 (21.5%) | ||||||
| Fracture | 1450 (12.4%) | ||||||
| Bruises | 6925 (59.3%) | ||||||
| Burns | 270 (2.5%) | ||||||
| Other | 527 (4.5%) | ||||||
| Total | 11,682 | ||||||
Bruises accounted for the large majority of injuries in physically abused children (60%)102 and all children attending A&E (range from 59%105 to 74%91,92). Fractures were the second most common injury in abused children102 and in all injured children of school age. 25,26,88,91,92,105 Burns appeared to be more common in abused children but this finding may be confounded by there being more young children in the abused group than in the studies of all children. The distribution of each type of injury was remarkably similar in the three studies that reported results for all ages. 25,75,88,105
Systematic review 7: Incidence of repeat attendance at A&E for injury
We determined the performance of repeated attendance at A&E for injury as a marker for physical abuse by (a) conducting a review of studies that directly compared abused and non-abused children and (b) indirectly comparing studies reporting results for abused or all children.
Systematic review 7(a): Direct comparison of repeat attendances in abused and non-abused injured children
Review methods
We included studies that reported repeat attendances at A&E for injury in physically abused and non-abused injured children.
Review results
We found no relevant studies. We excluded three large studies because they were based on abused children identified through social services106 or hospital admissions,107 or they reported repeat attendances at A&E for any reason78 (see Table 11). We report the results for the three studies that we excluded. In two studies the relative risk for re-attendance was significantly increased in abused compared with non-abused children. 78,107 However, the study by Friedlaender et al. ,106 based on record linkage of children registered for Medicaid in the US, found that the relative risk for re-attendance in abused compared with non-abused children was close to 1.0 after taking into account cash eligibility, race and chronic disease. These findings indicate that the incidence of re-attendance is strongly confounded by socioeconomic factors, which are associated with both recurrent attendance and physical abuse.
| First author, place, year of publication | Methods | Results | |||
|---|---|---|---|---|---|
| Direct comparison – excluded studies | |||||
| DiScala, USA, 2000107 | Data extracted from the National Pediatric Trauma Registry database on preceding attendances for any medical conditions during the child’s lifetime in 18,828 children admitted for injury under 5 years (1997–8). Children with ‘established abuse’ compared with remainder. Odds ratio adjusted for age and sex | Previous medical attendance: abused: 1058/1988 (53%); non-abused: 2366/16831 (14.1%) | |||
| Adjusted odds ratio: 6.33 (95% CI 5.69–7.07) | |||||
| Unadjusted LR for abuse: 3.79 (95% CI 3.59–3.99) | |||||
| Friedlaender, USA, 2005106 | Nested case–control study of children aged from 6 months to 5 years enrolled in fee-for-service Medicaid (1994–6). Children placed in foster care within 2 weeks of their first substantiated report of serious physical abuse or neglect (157 cases) were compared with matched control subjects with no record of maltreatment (628 cases). Odds ratio for abuse associated with any visit to A&E in the previous 12 months was adjusted for race, cash eligibility and chronic disease | Previous A&E attendance: abused: 25/157 (15.9%); non-abused: 30/628 (4.8%) | |||
| Adjusted odds ratio: 0.80 (correct to two decimal places) (95% CI 0.53–1.16) | |||||
| Unadjusted LR for abuse: 3.33 (95% CI 2.02–5.47) | |||||
| Palazzi, Italy, 200578 | Previous attendance within 12 months compared in children (< 14 years) seen in A&E for any reason according to whether or not the child scored ≥ 4 using an abuse risk score | Previous A&E attendance: abused: 44/188 (23.4%); non-abused: 1346/9498 (14.2%) | |||
| LR: 1.65 (95% CI 1.26–2.12) | |||||
| Indirect comparison: abused children – included studies | |||||
| Shrivastava, Coventry, 1988 (PhD thesis)102 | Records reviewed of injured children (< 16 years) admitted for suspected physical abuse (1983–7). Research identified previous A&E attendance for injury during child’s lifetime that resulted in admission due to suspected abuse. Average time at risk and re-attendance without admission were not reported | One or more previous admissions 22/108 (20.4%); one re-admission: 17/108 (15.7%); two re-admissions: 3/108 (2.8%); ≥ three admissions: 2/108 (1.9%) | |||
| 11/108 (10.2%) had previous injury admissions due to accidents | |||||
| Indirect comparison: all children – included studies | |||||
| Electronic Child Health Register, North East London, 2006 (unpublished)26 | Children (< 8 years) attending five inner London A&E departments for injury (2000–6; further details in Table 10). Subsequent attendance for injury within 12 months was recorded at any of the five hospitals, excluding re-attendances within 7 days as attendances for follow-up care, such as dressing change, could not be differentiated from acute attendances. As all attendances are linked to a unique child identifier, double counting of attendances by the same child at multiple sites should be avoided | Visits in 12 months | < 1 year | 1–4 years | 5–7 years |
| One visit only | 734/1436 (51.1%) | 2897/5348 (54.2%) | 2271/3043 (74.6%) | ||
| Two visits | 305/1436 (21.2%) | 876/5348 (16.4%) | 476/3043 (11.8%) | ||
| Three visits | 183/1436 (12.7%) | 434/5348 (8.1%) | 189/3043 (6.2%) | ||
| Four visits | 100/1436 (7.0%) | 538/5348 (10.1%) | 70/3043 (2.3%) | ||
| > Four visits | 113/1436 (7.8%) | 602/5348 (11.3%) | 37/3043 (0.9%) | ||
| > One visit | 702/1436 (48.9%) | 2451/5348 (45.8%) | 763/3043 (25.1%) | ||
Systematic review 7(b): Indirect comparison of repeat attendances in abused or all children
Review methods
We included studies that reported repeat attendances at A&E for injury in abused or all children. We restricted our criteria to the UK as the indirect comparison requires the assumption that abused and all children were from the same population.
Review results
We found one study,102 published in a PhD thesis, that reported previous admissions from A&E for injury in children admitted from A&E with suspected physical abuse in Coventry, UK (Table 11). Using retrospective case note reviews, the risk of re-admission for any injury was found to be 20.4% (22/108) over the period that the child had been resident in Coventry. The 22 children with more than one admission for suspected physical abuse generated 62 admissions following an injury during their lifetimes, 51 (82.3%) of which were for suspected physical abuse.
We excluded a large number of studies that reported repeated injuries in abused children but which did not report attendance at A&E. It was difficult to compare rates of repeat abuse in these studies as the measurement of physical abuse or all abuse differed, and the populations and time at risk varied. Overall, these studies found that repeated episodes of physical abuse within the next 12 months occurred in 7–25% of physically abused children who came to the attention of social services or police. 108–113 The reported recurrence rate increased to between 40% and 80% in studies looking at high-risk children, or an extended time at risk, or in studies with a low threshold for recording abuse. 54,112,114,115 Only a minority of repeated episodes of suspected abuse were substantiated116 or referred to social services,117 and few attended hospital. In a randomised controlled trial of home visiting for children with substantiated physical abuse conducted in Canada, 47% of 160 children followed for 3 years had at least one recurrent physical abuse event but none of these children attended hospital. 118
We found no published studies but did find one unpublished A&E dataset26 from which we could derive the incidence of repeated A&E attendance in all children (see Table 10). Between 20% and 49% of injured pre-school children seen in A&E re-attended for injury within 12 months, and 13–21% had two or more repeat attendances (i.e. three visits within 1 year) The re-attendance rate for school-age children appeared to be slightly lower (25%) but was limited to children under 8 years old. 26 These relatively high rates of re-attendance at inner city hospitals may reflect local patterns of primary care and A&E use. In addition, rates of re-attendance may increase with growing usage of A&E. In Manchester, A&E attendance by children increased by 13.5% between 2002 and 2005 (Martin Smith, Fiona Lecky, Trauma Audit Research Network, January 2007, personal communication).
Systematic review 8: Child protection registration or being social work active as markers of physical abuse
The CPR is a national register that lists the names of children under 18 years old who are considered to be at high risk of abuse or neglect. 1 In 2003, 0.3% of children were placed on the CPR, of which 32.2% were for physical (18.3%) or mixed abuse (13.9%) (see Figure 1). 9
Government guidelines specify that A&E staff should be familiar with local procedures for checking children against the relevant CPR. 2 One study reported that only 30% of 190 UK A&E departments surveyed routinely checked all children against the CPR. 119 Others have reported that CPR checking detects a small minority of children on the CPR who attend A&E. 120
In the long term the CPR will be replaced in the UK by the Integrated Children’s System (ICS), a nationwide database of children’s social services records. The ICS will provide information on children at all stages of social services investigations, for all local authorities, and should be kept up to date. It will be accessible only by social workers. The CPR is to be renamed the child protection plan in 2008.
A parallel data system, previously called the Information Sharing Index and now called Contact Point, will operate as an information sharing tool between key professionals and agencies that offer assessments and services to children in the UK (social workers, health professionals, teachers, youth workers, etc.). Designated hospital staff will be able to access the system to identify children who are social work active (allocated to a social worker or the duty team currently or in the last 12 months). Further details will be obtained by contacting the named lead professional. Eventually, Contact Point should list information on every child (under 18 years) in the UK using education, social services, Sure Start and health records. 121 It is currently being evaluated in 11 trailblazing groups, covering 15 local authorities across the UK. 24,122
We wanted to determine the performance of the CPR and identification of children as social work active as markers of physical abuse in injured children seen in A&E. Ignoring feasibility issues (including compliance), we assumed that information on whether a child was social work active could be used as a screening marker for all injured children attending A&E.
Review methods
We first sought studies that compared the performance of the CPR or social work active status in abused and non-abused children. As only one study was found we also sought studies that reported the incidence of subsequent physical abuse in children placed on the CPR or followed up by social services, and those reporting CPR or social work active status in children identified with physical abuse.
The results were used to estimate relative risks for CPR and for social work active status in abused compared with non-abused children.
Review results
Comparative studies of the performance of CPR/social work active status for abuse
We found one study78 based in 19 A&E departments in Italy that classified any type of suspected abuse based on a risk score (Table 12). Children at high risk of abuse were four times more likely to have had previous contact with social services or mental health services than low-risk children. Whether these estimates can be applied to social work active status among physically abused children in the UK is difficult to judge.
| First author, place, year of publication | Methods | Results |
|---|---|---|
| Comparison of social work active status in abused versus non-abused | ||
| Palazzi, Italy, 200578 | Children (< 14 years) attending A&E for any reason in 19 hospitals in Italy. Trained researchers completed a six-point suspicion checklist and recorded previous contact with social or mental health services using data from medical notes, the accompanying adult and examination at presentation. Children scoring ≥ 4 were considered to be ‘abused’ | Contact with social/mental health services: high risk for abuse: 27/192 (14.1%); low risk for abuse: 320/9278 (3.4%) |
| LR: 4.1 (95% CI 2.8–5.8) | ||
| Incidence of subsequent physical abuse if CPR or social work active | ||
| Gorin, London, 2002 (NSPCC; unpublished)123 | A total of 136 children of 75 families on the CPR were studied in 2001. Physical punishment was determined from social work and case conference records. Most children suffered multiple episodes but time interval during which events recorded was not given | Risk of physical punishment: on CPR for physical abuse: 10/15 (66.7%); on CPR for other abuse: 23/121 (19%) |
| Brandon, London, 1997127 and 2005 (NSPCC; unpublished)124 | A total of 77 of 105 consecutive children from separate families at risk of significant harm assessed using interviews and social work records (28 could not be traced). Re-abuse or neglect, sufficient to warrant a supervision order or CPR registration, was recorded during the subsequent 12 months (44/77; 57%). No separate results given for physical abuse | Re-abuse or neglect in 12 months: 32/77 (42%) |
| CPR or social work active status in children identified with physical abuse | ||
| Johnson, UK, 2003 (NSPCC; unpublished)125 | A total of 291 children calling the NSPCC child protection helpline were referred to social services, who were asked to complete a feedback questionnaire on whether the child was currently social work active or had any previous referrals to social services for any reason. Response rate by social services was 64% | Social work active: 45/291 (15.5%); previously known: 170 (58.4%) |
| Macmillan, Canada, 2003126 | In face-to-face interviews, a random sample of residents (≥ 15 years) who self-reported physical abuse in 1990 were asked about any contact with social services (including ‘talked to’) during childhood. Severe physical abuse: frequent kicking, punching or hit with an object, choked, burned or scalded more than once in childhood. Physical abuse: pushing, shoving and objects being thrown at the child | Severe physical abuse: 79/917 (8.6%); physical abuse: 116/2275 (5.1%) |
| Trocmé, Canada, 2001128 | Children (< 18 years) investigated by child protection services for physical abuse. Previous social services investigations for abuse or anything else recorded. The weighted estimates are based on a representative subset of 5235 children (all types of abuse) with available information. Actual number of physical abuse cases not given | Previous abuse investigation in children with physical abuse: 42.1%; family received previous social services investigation for reasons other than abuse: 15.9% |
Incidence of subsequent physical abuse in children placed on the CPR or followed up by social services
We found two unpublished studies,123,124 both undertaken for the NSPCC (Table 12). Neither directly addressed the review question. Gorin123 reported moderate and severe physical punishment during an unspecified period, and it was not clear whether events reported were in addition to the original episode leading to CPR registration. In contrast, Brandon et al. 124 only reported incidents of neglect or abuse leading to further supervision orders of registration, but did not differentiate physical abuse. We also sought expert opinion from two community professionals. Both stated that they thought physical abuse was more likely in children allocated to social services than in the general population.
CPR or social work active status in children identified with physical abuse
We found three studies46,125,126 that reported the prevalence of previous social work involvement among abused children. The only UK study, an unpublished report,125 found that 15.5% of 291 children ringing the NSPCC child protection helpline because of any type of abuse were currently social work active and 58% of children had had previous contact. These findings concur with the view expressed by social workers whom we interviewed during the study that abused children or their families are frequently known to social services.
The two other studies were from Canada (Table 12). One study,126 based on self-reported physical abuse in young adults, found that only 5% recalled any previous contact with social services, and only 9% of those reporting severe physical abuse. The other study,46 based on children investigated for any type of abuse by social services, found that 42% had had previous investigations by social services. Although these very different results may reflect recall bias in the first study, they raise the possibility that detection is focused on a particular subpopulation of abused children while a large majority remain undetected.
Performance of clinical screening assessments for detecting physical abuse in A&E
We defined a screening test as any test that could be applied in routine practice to all injured children. We assumed that a positive screen test would result in referral to the paediatric team for investigation of suspected abuse, whereas a negative result would lead to no referral. The paediatric team would undertake one or more assessments to confirm or exclude physical abuse. Confirmation of physical abuse by paediatricians would result in referral to social services for suspected abuse. We report test performance in terms of sensitivity and specificity as some studies reported one or other but not both. A further reason for not reporting LRs in this section is that the clinical threshold for determining suspicion or not was not explicit or reproducible in any of studies. 4
In the previous sections we reviewed the performance of characteristics in the child that could be used as markers in screening protocols to determine which children are at sufficiently high risk of abuse to warrant direct referral to the paediatrician. In this section we report the findings of systematic reviews to determine the performance of clinical screening assessments based on the initial history and examination in A&E. These were defined as:
-
Standard Care. Initial history and examination by a triage nurse and/or A&E doctor.
-
Checklist. Use of a checklist to enhance recall of the key elements of the history and examination that should be considered as part of standard care.
-
Community liaison nurse (CLN). The CLN would scrutinise all child attendance records to detect suspected abuse missed by A&E staff.
The review sought studies that simultaneously measured sensitivity and the false-positive rate. Two subsequent reviews analysed studies that separately reported sensitivity or specificity. These were used to provide corroborative evidence for levels of sensitivity and the false-positive rate seen in practice.
Systematic review 9: Performance of clinical screening assessments for detecting physical abuse
Systematic review 9(a): Studies reporting sensitivity and false-positive rates
Review methods
We included any study that reported the results of any type of clinical assessment for physical abuse in injured children attending hospital, and reported the results of any type of reference standard for confirming or excluding physical abuse. Because of the paucity of studies we included studies based on injured children admitted to hospital and those restricted to specific age groups or type of injury.
Review results
Three studies met the inclusion criteria (Table 13). Two were based on standard care72,82 and one involved the addition of a checklist and a full undressed examination of the child. 65 We f ound one unpublished audit reporting outcomes for suspected child abuse detected by the CLN in addition to standard care. 18
| First author, country, year of publication | Methods | Results | ||
|---|---|---|---|---|
| Studies reporting sensitivity and false-positive rates | ||||
| Oral, USA, 200382 |
Population: all children < 3 years diagnosed with a fracture (including skull) seen in A&E/orthopaedic clinic in a tertiary hospital (1995–8) Test: referral to social services or not Reference standard: risk score for abuse based on retrospective examination of records; physical abuse includes children with inadequate documentation to rule out abuse (n = 151) |
Test: referral | Physical abuse | Non-abuse |
| Yes | 85 | 4 | ||
| No | 151 | 413 | ||
| Total | 236 | 417 | ||
| Sensitivity: 85/236 (36%); false positives: 4/417 (0.96%); abuse prevalence: 236/653 (36%) | ||||
| Brown, USA 200372 |
Population: children < 4 years admitted for head injury (1993–6) Test: immediate referral (on admission) or delayed/no referral (a few days after admission) Reference standard: abuse confirmed by hospital, social services, police or chief medical examiner investigation; classified as non-abuse if not investigated or not confirmed |
Test: referral | Physical abuse | Non-abuse |
| Immediate | 8 | 30 | ||
| Delayed/no referral | 4 | 43 | ||
| Total | 12 | 73 | ||
| Sensitivity: 8/12 (67%); false positives: 30/73 (41%); abuse prevalence: 12/85 (14%) | ||||
| Pless, Canada, 198765 |
Population: children < 6 years attending A&E at a children’s hospital for injury or poisoning during 18-week period in 1976 Test: immediate referral to hospital child protection team for physical abuse or neglect based on a checklist, full undressed examination for bruises and cuts by specially trained nurses, and discussion with physician (received by 70% of eligible children); or referral for assessment by public health nurse after scrutiny of records by researchers; or no referral Reference standard: child protection team case conference confirmed or excluded abuse or neglect, or exclusion of abuse after assessment by public health nurse; non-abuse also defined by non-referral |
Test: referral | Physical abuse/neglect | Non-abuse |
| Immediate | 25 | 11 | ||
| From record review | 3 | 24 | ||
| No | 0a | 2148 | ||
| Total | 28 | 2183 | ||
| Sensitivity: 25/28 (89%); false positives: 2172/2183 (0.5%); abuse/neglect prevalence: 28/2183 (1.3%) | ||||
| Audit at the Royal Free Hospital, UK (London), 2005 (unpublished)18 |
Population: all children attending A&E at a central London Hospital in 2005 Test: referral to social services for abuse or neglect or no referral by A&E or inpatient medical services, referral by the CLN, or no referral Reference standard: referral or not to social services, or for CLN test; non-abuse based on decision by weekly child protection safety net meeting |
Test: referral | Physical abuse/neglect | Non-abuse |
| Immediate | 25.3 | Unknown | ||
| CLN referral | 9 | 421 | ||
| No | Unknown | Unknown | ||
| Total | 34.3 | 10,886 | ||
| Abuse prevalence: 34.3/10,886 (0.3%); 9/430 (2.1%) of CLN referrals. CLN increased sensitivity of standard care by (43.5%/25.3) × 9 = 15.5% | ||||
| Studies reporting sensitivity | ||||
| Ziegler, Australia, 200586 |
Population: all children < 3 years presenting in A&E with confirmed fracture (2001–2; n = 99) Test: referral to social services for suspected abuse by treating doctor Reference standard: high risk of abuse based on retrospective review of A&E records; 26 cases with inadequate records excluded |
Sensitivity: 12/18 (66%); abuse prevalence: 18/99 (18%) | ||
| Trokel, USA, 2006131 |
Population: random sample of children < 2 years on a multistate hospital database admitted with fractured femur, fracture or traumatic brain injury to a children’s hospital (CH, n = 1086), a children’s unit in a general hospital (CUGH, n = 589) or a general hospital (GH, n = 1086) Test: child abuse recorded as mechanism of injury on database Reference standard: expected rate of child abuse in children’s hospitals |
Sensitivity | Prevalence | |
| CH | 100%b | 29% | ||
| CUGH | 64% | 19% | ||
| GH | 60% | 13% | ||
| Carty, UK, 200285 |
Population: case series of children < 2 years assessed by single radiologist (1984–96; n = 435); includes patients referred for second opinion Test: immediate referral at first presentation or delayed referral with subsequent injury Reference standard: admission of assault, court decision, medical evidence, or signs interpreted retrospectively from records by investigator |
Sensitivity: 384/435 (88.3%); abuse prevalence not known | ||
| Jenny, USA, 199974 |
Population: children < 3 years referred to hospital child protection team (CPT) after admission to intensive care unit with serious head injury (1990–5) Test: immediate referral or delayed referral Reference standard: confirmation of abuse by CPT assessment (required consensus) |
Sensitivity: 119/173 (68.8%); abuse prevalence not given | ||
| Studies reporting false-positive rates | ||||
| Standard threshold for confirming abuse | ||||
| Kumar, UK, 198481 |
Population: admissions < 9 years to burns unit (1977–81); 30 cases of physical abuse/neglect represented 2% of burns admissions (estimated to be 1500) Test: referral to child protection paediatrician and social worker Reference standard: not referred, referred and no case conference, or abuse excluded at case conference |
False-positive rate: 48/1500 (3.2%); abuse prevalence: 30/1578 (2%) | ||
| Hobson, UK, 1994132 |
Population: children < 3 years admitted with burns Test: referral to paediatrician or social services by A&E or ward staff Reference standard: abuse or neglect excluded by paediatrician (n = 11) or social services (n = 6), or abuse not suspected |
False-positive rate: 17/260 (6.5%); prevalence abuse/neglect: 9/269 (3.3%) | ||
| Clark, USA, 199780 |
Population: children < 18 years with burns seen in A&E (1990–1) Test: referral to social services or not based on clinical assessment that included a checklist Reference standard: abuse not substantiated by social services or not referred |
False-positive rate: 19/208 (8.8%); abuse prevalence: 7/215 (3.3%) | ||
| Skellern, Australia, 2000133 |
Population: all children < 1 year with a fracture seen in A&E in a children’s hospital Test: suspected abuse or not based on retrospective record review Reference standard: abuse unfounded based on medical review and subsequent social services or police investigations |
False-positive rate: 7/80 (8.8%); abuse prevalence: 15 + 4 indeterminate/99 (30%) | ||
| High threshold for confirming abuse | ||||
| Scherl, USA, 200083 |
Population: admissions < 6 years with closed diaphyseal femur fracture (1986–96) Test: referral to social services for suspected abuse Reference standard: abuse excluded if not referred to social services, referred but not investigated, or investigated and child not removed from home |
False-positive rate: 131/194 (67.5%); abuse prevalence: 13/207 (6.3%) | ||
| Schwend, USA, 2000134 |
Population: children < 4 years with fractured femur (1993–7) Test: referral to social services Reference standard: abuse excluded if not referred or not offered intervention by social services |
False-positive rate: 27/128 (21.1%); abuse prevalence: 7/139 (7.9%) | ||
Both studies on the performance of standard care were conducted in the US. Neither adequately reflected the clinical screening assessment in A&E, the reference standard of referral or not to social services for suspected physical abuse, or the population of all injured children attending A&E. Further major flaws were the lack of independence and blinding between the clinical assessment and the reference standard and use of a different reference standard in children referred and not referred. As shown in Table 28 (Appendix 3), these studies failed to meet all but two of the 12 quality criteria listed in the QUADAS tool129 modified by Martin et al. 130
Oral et al. 82 evaluated children under 3 years seen with a fracture in A&E or orthopaedic clinic (sensitivity 36%, false-positive rate 1%). Referral to the paediatricians (test positive) or not (test negative) was compared in children with probable abuse or inadequate documentation to exclude abuse (reference standard classification for abuse) and in children in whom abuse was excluded by researchers using medical records. As the threshold for categorising a child as abused was low, the prevalence of possible abuse was very high (36%) and the false-positive rate was low (1%).
Brown and Malone72 studied children under 5 years admitted with a head injury (sensitivity 67%, false-positive rate 41%). Immediate referral to paediatricians (test positive) or referral on subsequent visits or no referral (test negative) was analysed according to whether abuse was confirmed by social services or police (reference standard for abuse) or not confirmed or not assessed (reference standard for non-abuse). Given this stringent reference standard for abuse, the false-positive rate was high. Sensitivity was overestimated as children not referred to paediatricians were assumed to be true negatives. The high prevalence of abuse (12/85; 14%) may be because the study was restricted to children admitted with head injury.
The only study to report the performance of a checklist was conducted in 1976 in children under 6 years seen with an injury or poisoning in a children’s A&E department (sensitivity 89%, false-positive rate 1%). 65 The clinical assessment comprised examination by specially trained nurses who fully undressed all children to search for bruises, burns and cuts, completed a 10-point checklist, discussed their findings with the physician, and undertook a further assessment if necessary. Children with suspected abuse were referred to the hospital child protection team (test positive). To ascertain false negatives (abused children not referred), all A&E records were reviewed by researchers and any additional cases were interviewed by a public health nurse at a special home or hospital visit and, if concerns persisted, referred to the child protection team. The reference standard was confirmation or exclusion of abuse by the child protection team, or non-referral to the team. The high sensitivity and low false-positive rates may reflect the series of screening and diagnostic assessments by the nurse and physician, rather than a single screening assessment. Specificity may have been further improved if the A&E team had consulted with the on-site child protection team before making a referral, thereby further blurring the boundaries between screening, diagnosis and the reference test.
Indirect evidence that checklists may improve the sensitivity of the standard care clinical screening assessment comes from studies that evaluated changes in the referral rate for suspected abuse after introduction of a checklist (Table 14). All studies showed an increase in referrals with introduction of a checklist, but whether these are entirely false-positive cases or include additional true positives is not known as none reported confirmation or exclusion of abuse.
| First author, country, year of publication | Methods | Number (%) of children with suspected abuse |
|---|---|---|
| Studies reporting an increase in referrals for suspected physical abuse using a checklist | ||
| Benger, UK, 200221 |
Population: children < 5 years attending A&E for any injury Test: five-point flow chart placed in child’s records |
Referrals to senior doctor before: 6/1000 (0.6%); with checklist: 14/1000 (1.4%) |
| Benger, UK, 2001135 |
Population: A&E attendees < 6 years for burns (n = 200) Test: four-point checklist in records and training |
Referrals to senior doctor before: 0/100 (0.0%); with checklist: 3/60 (5.0%) |
| Sidebotham, UK, 199722 |
Population: children attending A&E for injury Test: revision of five-point checklist |
Referrals to paediatric registrar before: 50/1357 (3.7%); with revised version: 40/988 (4.0%) |
| Clark, USA, 199780 |
Population: children attending A&E for burn injury (1990–3) Test: 13-point risk indicator checklist attached to records; the checklist was not completed in 46 of 215 cases (24%) and 22 of the 105 files from 1990–1 could not be located (21%) |
Referrals to social services before: 3/87 (3.4%); with checklist: 26/215 (12.1%) |
| Pless, Canada, 198765 |
Population: A&E attendees < 6 years with injury or poisoning Test: fully undressed examination and 10-point checklist |
Referrals to child protection team before (same calendar period): 19/1555 (1.2%); with checklist: 26/1555 (1.8%) |
The included studies did not analyse which component of a checklist was most predictive of abuse. Palazzi et al. 78 reported that perceived developmental delay in the child and inconsistency between the history and examination were the characteristics most strongly associated with a high score for any type of abuse.
We found no published studies but one unpublished audit of cases detected by the CLN during 2005 in one central London A&E department (see Table 13). The CLN scrutinised A&E attendance records for all children not already referred to paediatricians or social services for investigation of any form of child abuse or neglect. Records of children with possible child protection concerns were reviewed at a weekly child protection safety net meeting attended by the CLN, consultant paediatrician, hospital social worker and other staff (Ben Lloyd, January 2006, personal communication) At the safety net meeting it was decided whether or not to refer the child to social services (reference standard) or whether other action was needed such as contacting the GP, health visitor or school. CLN scrutiny resulted in referral of an additional nine children to social services (increase of 36%; 9/25.3), compared with the 25.3 already referred (note figures for total referrals are based on 9 months of data extrapolated to the whole of 2005). A total of 421 records were false positives (children discussed who did not have child protection concerns). The low post-test probability of CLN scrutiny (2.1%, 9/430 of CLN referrals had child protection concerns) is explained by the fact that the population excluded high-risk children referred directly to paediatricians or social services. It is worth noting that discussion of false-positive records at a meeting has minimal adverse effects on the family.
In summary, the validity and applicability of the three included studies was poor. The results provided no more than a description of the range of performance of clinical assessment of injured children. Use of a checklist appeared to be associated with improved performance. There was weak evidence that the addition of the CLN improved the detection of abuse or neglect at a cost of increased false-positive assessments.
Systematic review 9(b): Studies reporting sensitivity of clinical assessments
As few studies reported both sensitivity and the false-positive rate, we sought studies that reported these outcomes separately. The aims were to provide quantitative evidence of the frequencies with which physically abused and injured children are detected by clinical assessors (sensitivity) and non-abused children are referred to social services or other agencies for suspected abuse (false-positive rate).
Review methods
We included studies that reported any measure of suspected abuse including referral compared with delayed referral or no referral to paediatricians or social services. We accepted any measure of confirmation of physical abuse as the reference standard, whether based on medical or social services investigations or opinion. We assumed that confirmation of abuse meant physical abuse although, in practice, children with injuries may be referred to child protection services because of other types of abuse such as neglect (see Appendix 5, Table 32). Sensitivity was defined as the proportion of all children with confirmed abuse who were referred, or referred immediately, or reached a threshold of suspicion likely to warrant referral.
Review results
We found no studies that compared the outcome of clinical screening (referral or not for suspected physical abuse) with a separate professional assessment of the child in all cases tested (reference standard) (see Table 13). One study compared the clinical screening test in children under 3 years with fractures with a risk score (reference standard) applied retrospectively to records by researchers. 82 Such studies suffer from inadequate documentation of the history, and lack independence and blinding, as the reference standard and test are based on the same information.
We found one study that compared rates of referral of children with a head injury or femur fracture in a children’s hospital (reference standard) with rates of referral for the same condition in two other hospitals. 131 The results underestimated sensitivity as no missed cases were documented at the children’s hospital. The higher rate of detection at the children’s hospital may be the result of a higher rate of false positives, a lower threshold for referral because of better access to child protection professionals, a higher prevalence of abuse, attendance by more severely injured abused children or differences in coding.
Three studies72,74,85 examined immediate or delayed referral of children in whom abuse was eventually confirmed (see Table 13). As all three studies overestimated sensitivity because abused children who were never referred were not included in the denominator, they provide an upper limit for sensitivity in the hospital setting (69%,74 67%72 and 88%85). In the study by Carty and Pierce85 (88%), inclusion of children with repeated suspicious injuries and those referred for child protection medicals would have grossly overestimated sensitivity.
In summary, we found strong evidence that abused children are missed by clinicians even when they are admitted to hospital and subject to repeated clinical assessments. Sensitivity ranged from 36% to 89%. None of the studies reported the false-positive rate making it hard to generalise the performance of the assessment to other settings. Biases due to the poor study quality may under- or overestimate sensitivity.
Systematic review 9(c): Studies reporting the false-positive rate of clinical assessments
Review methods
We included studies that reported any measure of referral for suspected abuse by clinicians (the clinical screening test) to a paediatric team, social services or other type of child protection agency, in injured children attending hospital. Any measure for excluding physical abuse was accepted as the reference standard, including the assumption that children who were not referred were not abused. The false-positive rate was defined as the proportion of all accidentally injured children who were referred or investigated for suspected abuse.
Review results
We found six studies80,81,83,132–134 (see Table 13). All categorised no referral for physical abuse as one of the criteria for excluding physical abuse (i.e. children not referred for abuse were not subjected to further investigations). Although such studies overestimated specificity, because false-negative cases (not referred but abused) were classified as true negatives (not referred and not abused), the number misclassified in this way would have been small relative to total true negatives.
Variation in the false-positive rate from 41% to 1% is likely to reflect variation in the thresholds for referral and for confirming and excluding abuse, as well as differences in the spectrum of abuse. For example, the false-positive rate was low if criteria for ruling out abuse were stringent,82 and high if abuse was considered to be present only if confirmed by removal of the child from his/her home,83 or if the family received an intervention for abuse. 134
Studies based on a reference standard of referral or not to social services or confirmation or exclusion of abuse by the hospital child protection team were most representative of the outcome considered in our clinical effectiveness analyses (referral or not to social services for physical abuse, see Chapter 5). 80,81,132,133 The results suggest that a relatively high false-positive rate (3–10%) may operate in routine hospital practice, at least for young children with a burn or fracture (see Table 13). 18,21,65,72,82
Chapter 5 Clinical effectiveness model and results
Methods
We used a clinical effectiveness model to illustrate the impact of different markers or clinical screening assessments on the effectiveness of screening in A&E. The findings do not provide a reliable quantification of the relative performance of screening strategies for physical abuse because of the poor quality of the studies and their limited applicability to the UK. Given these problems we did not model the uncertainty in the parameters using a probabilistic approach. Instead, we used point estimates for all parameters. The findings do provide information about the rank order of strategies.
We used a simple decision-analytic model to determine the clinical effectiveness of screening tests for physical abuse in children attending A&E. The structure of the model, shown in Figure 12, was based on a review of the literature and discussion with experts. The model had three main elements: a hypothetical population of physically abused and non-abused children and their attributes (e.g. age), the annual incidence of attendance at A&E for injury with characteristics of attendees based on the population subgroups, and the performance of screening and confirmatory testing in A&E.
FIGURE 12.
Flow diagram for detection in the accident and emergency department. The population section divides the overall population into subgroups based on demographic data [e.g. age, social work active (SWA) and child protection registration (CPR) status]. The attendance section generates representative annual A&E attendances for each population subgroup (age, injury type, repeat attendance, SWA, CPR) based on attendance data. The testing section calculates the percentage of attendances referred at each level of screening and confirmatory testing for each attendance category based on test data.
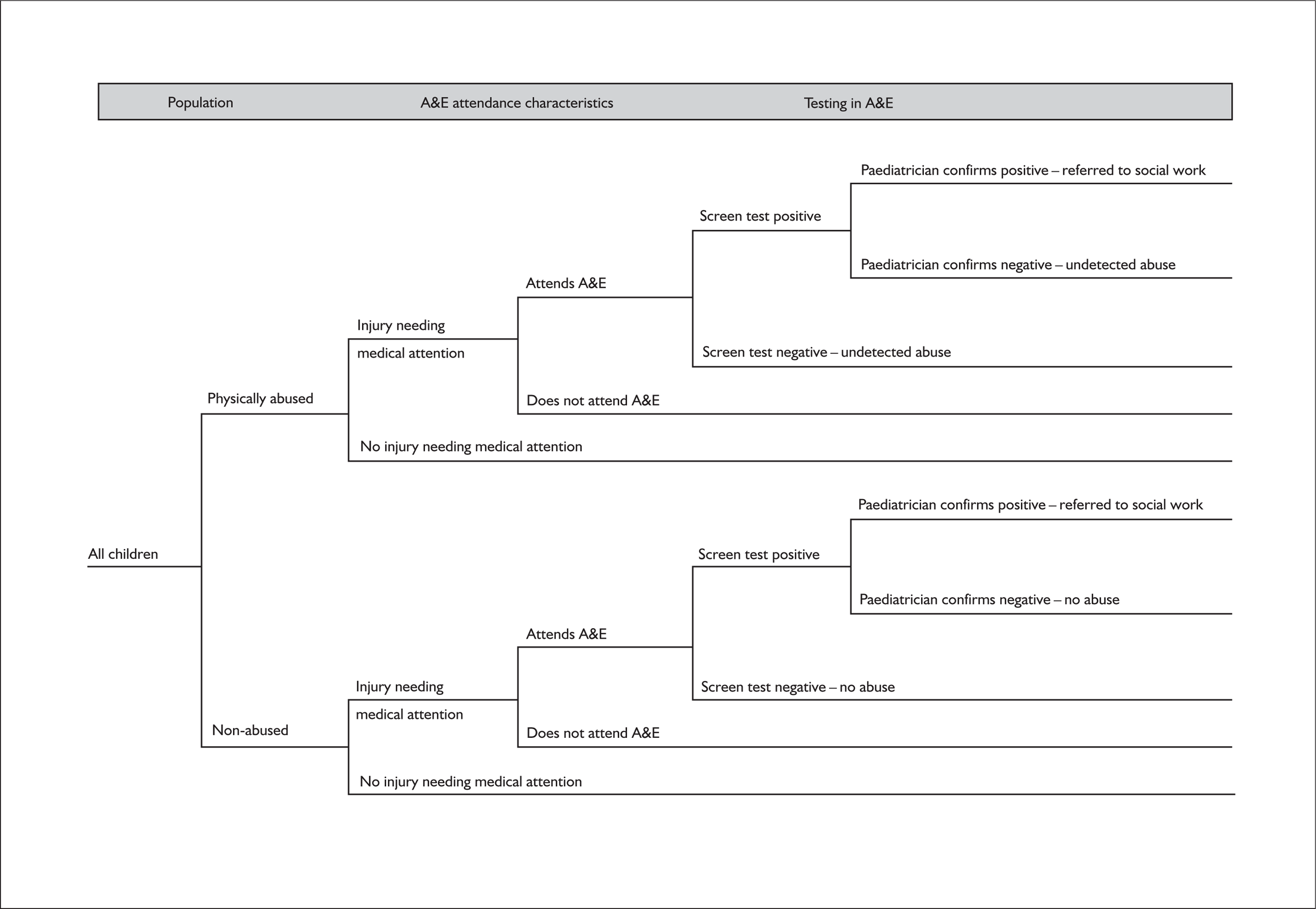
We assumed that the main outcomes of concern to service providers would be to maximise detection of physical abuse while minimising false-positive referrals. We also recorded intermediary outcomes that could be audited in practice. These were the proportion of all injured children referred to the paediatric team and the proportion of children assessed by paediatricians and social services who were truly abused. From a societal perspective, the proportion of injured abused children who receive appropriate medical attention would be a further concern. This outcome raises questions about other agencies, apart from A&E, that detect physical abuse in the community, and is discussed briefly in systematic review 10.
Derivation of parameters used in the model
The parameters used in the model are listed in Table 15. We derived the parameters using the following methods.
| Parameter | Input value | Numbers | Source | |
|---|---|---|---|---|
| Population characteristics | ||||
| Child population in the UK | ||||
| 1 | All children < 16 years | 100% | 11,597,500 | UK population mid 200550 |
| 2 | Infants < 1year | 6.2% | 715,914 | |
| 3 | 1–4 years | 23.4% | 271,161 | |
| 4 | 5–9 years | 30.7% | 3,560,432 | |
| 5 | 10–15 years | 39.7% | 4,609,542 | |
| Annual prevalence of physical abuse in children in the UK | ||||
| 6 | Infants < 1 year | 4.3% | 8.75/203 | UK study of parent-reported severe violence35 (systematic review 1). Weighted average = 8.8% |
| 7 | 1–4 years | 11.6% | 34/292 | |
| 8 | 5–9 years | 9.6% | 25/261 | |
| 9 | 10–15 years | 7.3% | 15/205 | |
| Risk of injury requiring medical attention after a single physical abuse event | ||||
| 10 | Infants < 1 year | 25.5% | NA | Canadian study of children with substantiated physical abuse57 (systematic review 2). Weighted average = 6.9% |
| 11 | 1–4 years | 9.4% | NA | |
| 12 | 5–9 years | 5.0% | NA | |
| 13 | 10–15 years | 4.9% | NA | |
| Characteristics of children attending A&E | ||||
| Prevalence of physical abuse in A&E attendances for injury | ||||
| 14 | All children < 16 years | 1% | Researcher opinion based on systematic reviews 3b, 3c64 | |
| Annual incidence of A&E attendance for injury per 100 child-years | ||||
| 15 | Infants < 1 year | 10.3 | 3322/32,244 | RoSPA study in the UK88 and population estimates for 2002 (systematic review 4)9. Weighted average = 19.0 per 100 child-years |
| 16 | 1–4 years | 20.0 | 26,791/134,293 | |
| 17 | 5–9 years | 16.9 | 26,637/185,390 | |
| 18 | 10–15 years | 21.4 | 46,423/216,673 | |
| Likelihood ratio for age group | ||||
| 19 | Infants < 1 year | 9.45 | NA | Indirect estimate from two UK studies (systematic review 5b)88,102 |
| 20 | 1–4 years | 1.71 | NA | |
| 21 | 5–9 years | 0.66 | NA | |
| 22 | 10–15 years | 0.3 | NA | |
| Prevalence of type of injury in all injured children attending A&E | ||||
| Infants < 1 year | 235 | Unpublished dataset from one London A&E 2003–5 (systematic review 6)26,102 | ||
| 23 | Head injury | 26.8% | 63 | |
| 24 | Fracture | 5.1% | 12 | |
| 25 | Burns | 57.9% | 136 | |
| 26 | Bruises | 10.1% | 24 | |
| 27 | Other | 0.0% | 0 | |
| 1–4 years | 1599 | |||
| 28 | Head injury | 6.6% | 105 | |
| 29 | Fracture | 120.1% | 193 | |
| 30 | Burns | 77.1% | 1232 | |
| 31 | Bruises | 4.3% | 68 | |
| 32 | Other | 0.0% | ||
| 5–9 years | 1660 | |||
| 33 | Head injury | 4.8% | 80 | |
| 34 | Fracture | 22.4% | 371 | |
| 35 | Burns | 70.9% | 1177 | |
| 36 | Bruises | 1.9% | 32 | |
| 37 | Other | 0.0% | ||
| 10–15 years | 1671 | |||
| 38 | Head injury | 2.9% | 42 | |
| 39 | Fracture | 23.7% | 400 | |
| 40 | Burns | 72.0% | 1209 | |
| 41 | Bruises | 1.3% | 20 | |
| 42 | Other | 0.3% | 0 | |
| Likelihood ratio for type of injury | ||||
| 43 | Head injury < 16 years | 1 | NA | Researcher opinion based on direct and indirect comparisons88 (systematic reviews 6a, 6b)26,75,102 |
| 44 | Fracture < 16 years | 1 | NA | |
| 45 | Burns < 16 years | 1 | NA | |
| 46 | Bruises < 16 years | 1 | NA | |
| 47 | Other < 16 years | 1 | NA | |
| Prevelance of repeat attendance for injury at A&E | ||||
| Infants < 1 year | 2928 | Unpublished data from five London A&E departments from 2000 to 200626,106 | ||
| 48 | Single attendance | 51.2% | 1499 | |
| 49 | Second/third attendances | 37.6% | 1103 | |
| 50 | Fourth+ attendances | 11.1% | 326 | |
| 1–4 years | 11,560 | |||
| 51 | Single attendance | 49.0% | 5668 | |
| 52 | Second/third attendances | 35.9% | 4148 | |
| 53 | Fourth+ attendances | 15.1% | 1744 | |
| 5–9 years | 4387 | |||
| 54 | Single attendance | 72.2% | 3166 | |
| 55 | Second/third attendances | 24.5% | 1077 | |
| 56 | Fourth+ attendances | 3.3% | 144 | |
| 10–15 years | 4387 | |||
| 57 | Single attendance | 72.2% | 3166 | |
| 58 | Second/third attendances | 24.5% | 1077 | |
| 59 | Fourth+ attendances | 3.3% | 144 | |
| Likelihood ratio for repeat attendance for injury | ||||
| 60 | All children < 16 years | 1 | NA | US study with adjustment for social factors and researcher opinion [systematic review 7(a)]106 |
| Prevalence of being social work active (SWA) | ||||
| 61 | Infants < 1 year | 2.7% | 15,249/2,273,000 | Uses rate of SWA for all children (2.1%, 2004) and ONS population data (2002).50 Weighted average = 2.16% |
| 62 | 1–4 years | 2.1% | 46,913/3,150,000 | |
| 63 | 5–9 years | 1.8% | 55,173/3,780,000 | |
| 64 | 10–15 years | 2.3% | 88,002/3,780,000 | |
| Likelihood ratio for being SWA | ||||
| 65 | Infants < 1 year | 7.19 | Indirectly derived (systematic review 8) | |
| 66 | 1–4 years | 2.46 | ||
| 67 | 5–9 years | 3.04 | ||
| 68 | 10–15 years | 4.10 | ||
| Prevalence of being on child protection register (CPR) | ||||
| 69 | Infants < 1 year | 0.62% | 3539/8909 | All registrations at March 2004 (n = 31,000)9 and ONS population data for the same year50 Average = 0.33% |
| 70 | 1–4 years | 0.39% | 8909/3,150,000 | |
| 71 | 5–9 years | 0.29% | 9276/3,150,000 | |
| 72 | 10–15 years | 0.18% | 9276/5,041,200 | |
| Likelihood ratio for being on CPR | ||||
| 73 | Infants < 1 year | 12.68 | Indirectly derived (systematic review 8) | |
| 74 | 1–4 years | 4.10 | ||
| 75 | 5–9 years | 4.72 | ||
| 76 | 10–15 years | 6.58 | ||
| Test performance of clinical assessments in A&E | ||||
| Standard care | ||||
| 77 | Sensitivity | 43.5% | Derived as midpoint between two studies.72,82 Estimate extremely uncertain | |
| 78 | False-positive rate | 5.0% | ||
| Community liaison nurse | ||||
| 79 | % Abused cases | 15.5% | (43.5%/25.3) × 9 | Increase in sensitivity and false-positive rate assuming parameters 78 and 79. Unpublished audit in one London A&E18 |
| 80 | False-positive rate | 3.9% | 421/10885.7 | |
| Paediatric assessment of screen-positive cases | ||||
| 81 | Sensitivity | 90.0% | Researcher opinion – highly optimistic and uncertain | |
| 82 | False-positive rate | 2.5% | ||
Population characteristics
Child population in the UK (parameters 1–5)
We used the estimated mid-year population for the UK for 2005 published by the Office of National Statistics grouped by the age categories shown in Table 15 (URL: www.statistics.gov.uk/downloads/theme_population/KPVS32_2005/KPVS2005.pdf).
Annual prevalence of physical abuse in children in the UK (parameters 6–9; based on systematic review 1)
We used the rate of parent-reported physical abuse by Ghate et al. 35 because the findings were most relevant to the UK, most recent and most consistent with other parent-reported studies. 36,37 As we lacked data on the frequency of multiple episodes of abuse we assumed that the prevalence rate was equivalent to the incidence rate (i.e. each child suffered only one episode of abuse per year). 35
We derived incidence rates of abuse for each age group using unpublished data provided by Ghate et al. (see Table 3). The data were manipulated to match the age groups used in the model as follows. We applied the rate for the 0–1 year olds to infants less than 1 year, the rate for 2–4 year olds to children aged 1–4 years, the rate for 5–10 year olds to children aged 5–9 years, and the rate for 11–13 year olds to children aged 10–15 years. We increased the rate for infants by 25% to take into account the fact that approximately 25% of children in this age group would have been less than 12 months at interview. On average, standardising for the age distribution in the UK we estimated that 8.8% of children are physically abused each year.
Risk of injury requiring medical attention following a single physical abuse event (parameters 10–13; based on systematic review 2)
We used the results reported by Trocmé et al. 57 (6.9%) as the best available estimate for the risk of injury in all physically abused children. This study was recent, the results were consistent with a similar study in Sweden,54 and social services routinely recorded whether children required medical attention, regardless of whether or not they saw a doctor. As data were not presented in the form that we needed, we used the average prevalence rate of injury requiring medical attention due to physical abuse and the age distribution for any maltreatment, including neglect (Table 4). We used the data of Trocmé et al. for 1–3 year-olds for our 1- to 4-year-old group, the data for 4–7 year-olds for our 5- to 9-year-old group and an average of the results for 8–11 and 12–15 year-olds for our group aged from 10 to 15 years.
As expected, the younger the child, and hence the more vulnerable, the higher the risk of injury requiring medical attention (see Table 4). Trocmé and colleagues commented on the surprisingly low rate of injury in children with substantiated physical abuse, 57% of whom had no injury at all but were nevertheless considered to be at significant risk of harm. Absence of injury may be even more common for physically abused children in the community than among children with substantiated abuse. Consequently, the estimate used in the model is very uncertain.
Characteristics of children attending A&E
Prevalence of physical abuse in A&E attendances for injury [parameter 14; based on systematic reviews 3(b) and 3(c) using notation (a + c)/(a + b + c + d) from Figure 8]
We used results from the two most representative studies reporting the prevalence of confirmed abuse in injured children attending A&E or admitted to hospital [a/(a + b + c + d) from Figure 8]. Chang et al. 64 reported an overall prevalence of 0.76% and Pless et al. 65 a prevalence of 0.6%. These figures exclude an unknown number of abused children who were not detected (false negatives). Surprisingly, the study based in 19 Italian A&E departments78 of suspected abuse in injured children reported a much lower prevalence (0.4%), despite including false-positive referrals and using a low threshold for detection based on a clinical score. On balance, we judged that the prevalence of physical abuse in injured children attending A&E is 1% or less. This estimate is uncertain and takes no account of variation by age.
Annual incidence of A&E attendance for injury per 100 child-years (parameters 15–18; based on systematic review 4)
We used the age-specific incidence rates reported by RoSPA. 88 This was most likely to be nationally representative and was within the range of estimates reported by other studies. 9
Likelihood ratio for age group [parameters 19–22; based on systematic reviews 5(a) and 5(b)]
We defined four age groups based on broad developmental criteria (under 1 year olds are mostly unable to walk) and schooling: infants (under 1 year), preschool (1–4 years), primary school (5–9 years) and secondary school (10–15 years). Only two studies reported age groups in abused and non-abused children attending A&E78,101 and only one study,101 from Hawaii, reported separate results for infants and preschool children. As we doubted the applicability of the findings in Hawaii to the UK setting, we indirectly compared the age distribution reported for abused and injured children by Shrivastava102 with the nationally representative RoSPA dataset88 (Table 8), making the arguable assumption that they were drawn from the same population. We then estimated the LRs for each age group, assuming that the overall prevalence of physical abuse was 1% (Table 16). The results are similar to the LRs reported for severely injured children admitted to hospital (Table 8). Although the best available estimates, they are flawed for at least three reasons. First, children were not from the same population or assessed in the same way in both studies. Second, the RoSPA data includes some abused children. Third, expectation that infancy is a predictor of abuse would have affected detection in the study by Shrivastava. Consequently, the results of the clinical effectiveness analysis are likely to overestimate the performance of infancy as a marker for abuse.
| Age group | Abuseda | Non-abuseda | All (RoSPA) | Likelihood ratio | Post-test probability |
|---|---|---|---|---|---|
| Under 1 year | 6399.249 | 67,031.75 | 73431 | 9.45 | 8.7% |
| 1–4 years | 10,371.2 | 600,138.8 | 610,510 | 1.71 | 1.7% |
| 5–9 years | 4192.612 | 628,375.4 | 632,568 | 0.66 | 0.7% |
| 10–15 years | 3309.957 | 1,107,483 | 1,110,792.5 | 0.30 | 0.3% |
| < 16 years | 24,273.02 | 2,403,028 | 2,427,302 | 1.0 | 1.0% |
Prevalence of type of injury in all injured children attending A&E [parameters 23–42; based on systematic review 6(b)]
We used unpublished data25 on 5165 injured children attending an inner London A&E department (University College Hospital London; Table 10) as this reported results for all age groups and had few attendances classified as ‘other’. The distribution of the type of injury by age group was similar to two other studies reporting results for all age groups. 88,105
Likelihood ratio for type of injury [parameters 43–47; based on systematic reviews 6(a) and 6(b)]
We found no clear evidence that the type of injury was associated with the risk of physical abuse. There was weak evidence from the direct comparison of abused and non-abused children in the TARNlet study to suggest that age confounded any association between type of injury and abuse. This was confirmed by indirect comparisons showing similar distributions of type of injury in abused children and in all injured children (see Table 8). 75 We therefore assumed that the LR was 1.0 for all types of injury in the clinical effectiveness model.
Prevalence of repeat attendance for injury at A&E [parameters 48–59; based on systematic review 7(b)]
We used unpublished data from five inner London A&E departments to determine the prevalence of repeated attendance for injury (see Table 11). 26
Likelihood ratio for repeat attendance for injury [parameter 60; based on systematic review 7(a)]
We judged that there was no association between repeat attendance and physical abuse, based on a US study that took into account socioeconomic status. 106 Weak, but statistically significant, associations were found for two other studies (see Table 11). 78,107
Prevalence of being social work active or on the CPR (parameters 61–64 and 69–72)
We used national figures for the number of children who were SWA or on the CPR in England during 2003–4. 9,50 For CPR we used published figures for children newly registered or re-registered for any reason during 12 months in 2003–4. The figure, 31,000, was higher than the point prevalence of children on the CPR during 1 week in 2003, but we reasoned that health professionals might be able to obtain information about current and recent CPR status. Being SWA is a marker indicating that a child is currently or has been in the last 12 months allocated to a social worker or to the duty team. We assumed that this status would apply to children undergoing an initial assessment, at least temporarily, and we therefore used national data on the incidence of initial assessments. As statistical returns for initial assessments do not include information on age or reason for referral, we extrapolated the age distribution from the CPR data. We assumed that 11% of all initial assessments are for physical abused based on an audit in two London local authorities, supported by expert opinion (see Appendix 4).
Likelihood ratio for being social work active or on the CPR (parameters 65–68 and 73–76; based on systematic review 8)
In the absence of more robust data we assumed that the estimates provided by Gorin123 reflected the prevalence of physical abuse in the subsequent year for children on the CPR for physical abuse (67%). We assumed the same risk applied to children who are SWA.
We calculated the LRs as shown in Table 17 using the notation in Figure 13. The prevalence of physical abuse in all children [(a1 + c1)/(a1 + b1 + c1 + d1)] was assumed to be 8.8% (weighted average from Ghate et al. ,34 systematic review 1). The overall prevalence of children on the CPR, 0.32% [(a1 + b1)/(a1 + b1 + c1 + d1)], was based on national figures (see previous section). 9,50 The proportion of children on the CPR experiencing subsequent physical abuse over the next year was estimated to be 34.4% [a/(a + b)], based on a risk of 66% in children registered for physical or mixed abuse (29% of 0.32% on the CPR) and a risk of 19% in those registered for other reasons. 9,123 The estimates vary for each age group because of the varying prevalence of CPR- or SWA-positive status (Table 17). The LR for being SWA for all children was 3.5, consistent with the LR of 4.1 observed by Palazzi et al. (see Table 12). 78,89
| Notation | All | Under 1 year | 1–4 years | 5–9 years | 10–15 years | Data source | |
|---|---|---|---|---|---|---|---|
| Number of children in England (2005) | a1 + b1 + c1 + d1 | 9,720,800 | 606,400 | 2,286,900 | 2,981,500 | 3,846,000 | Office for National Statistics, 2005, Series VS, No. 32, PP1, No. 28 |
| Prevalence of physical abuse in all children (%) | (a1 + c1)/(a1 + b1 + c1 + d1) | 8.8 | 4.3 | 11.6 | 9.6 | 7.3 | Based on parent-reported severe violence in 12 months (Ghate, 200235) |
| Child protection registration (CPR+) | |||||||
| Number on CPR at any one time (any abuse) | a1 + b1 | 31,000 | 3539 | 8909 | 9276 | 9276 | Tables 5a and 5b, National Statistics, 2004, DfES; new or re-registrations during the 12 months 2003–4 |
| Prevalence of CPR+ among all children (%) | (a1 + b1)/(a1 + b1 + c1 + d1) | 0.32 | 0.58 | 0.39 | 0.31 | 0.24 | Parameters 69–72, Table 15 |
| Data to estimate prevalance of physical abuse in CPR+ in 12 months | |||||||
| Proportion CPR+ for physical or mixed abuse (%) | 32.3 | 36.3 | 33.5 | 30.1 | 31.7 | Table 4c, National Statistics, 2004, DfES | |
| Prevalence of physical abuse in 12 months in children CPR+ (%) | a1/(a1 + b1) | 34.4 | 36.3 | 35.0 | 33.4 | 34.1 | Assumed risk of severe violence in next 12 months is 66% for children registered for physical abuse and 19% for others (see text) |
| Derived variables | |||||||
| Probability of CPR+ in children exposed to physical abuse (%) | a1/(a1 + c1) | 1.25 | 4.93 | 1.17 | 1.08 | 1.13 | |
| Likelihood ratio for CPR+ | (a1/(a1 + c1))/(b1/(b1 + d1) | 5.43 | 12.68 | 4.10 | 4.72 | 6.58 | Parameters 73–76, Table 15 |
| Social work active (SWA+) | |||||||
| Prevalence of SWA+ among all children (%) | (a2 + c2)/(a2 + b2 + c2 + d2) | 2.10 | 2.65 | 2.06 | 1.75 | 2.33 |
Table 7b, National Statistics, 2004, DfES: proportion of children undergoing initial assessment during 12 months (age breakdown extrapolated from CPR) Parameters 61–64, Table 15 |
| Data to estimate prevalence of physical abuse in SWA+ in 12 months | |||||||
| Proportion of SWA+ children referred for physical abuse (%) | 11.1 | 11.1 | 11.1 | 11.1 | 11.1 | Based on audit of initial assessments | |
| Prevalence of physical abuse in 12 months in children on CPR (%) | a2/(a2 + b2) | 24.3 | 24.3 | 24.3 | 24.3 | 24.3 | Assumed risk of severe violence in next 12 months is 66% for children registered for physical abuse and 19% for others (see text) |
| Derived variables | |||||||
| Probability of SWA+ in children exposed to physical abuse (%) | a2/(a2 + c2 ) | 6.03 | 15.06 | 4.35 | 4.46 | 7.79 | |
| Likelihood ratio for SWA+ | (a2/(a2 + c2 ))/(b2/(b2 + d2 )) | 3.467 | 7.19 | 2.46 | 3.04 | 4.10 | Parameters 59–65, Table 15 |
FIGURE 13.
Child protection registration (CPR) status in abused and non-abused children.
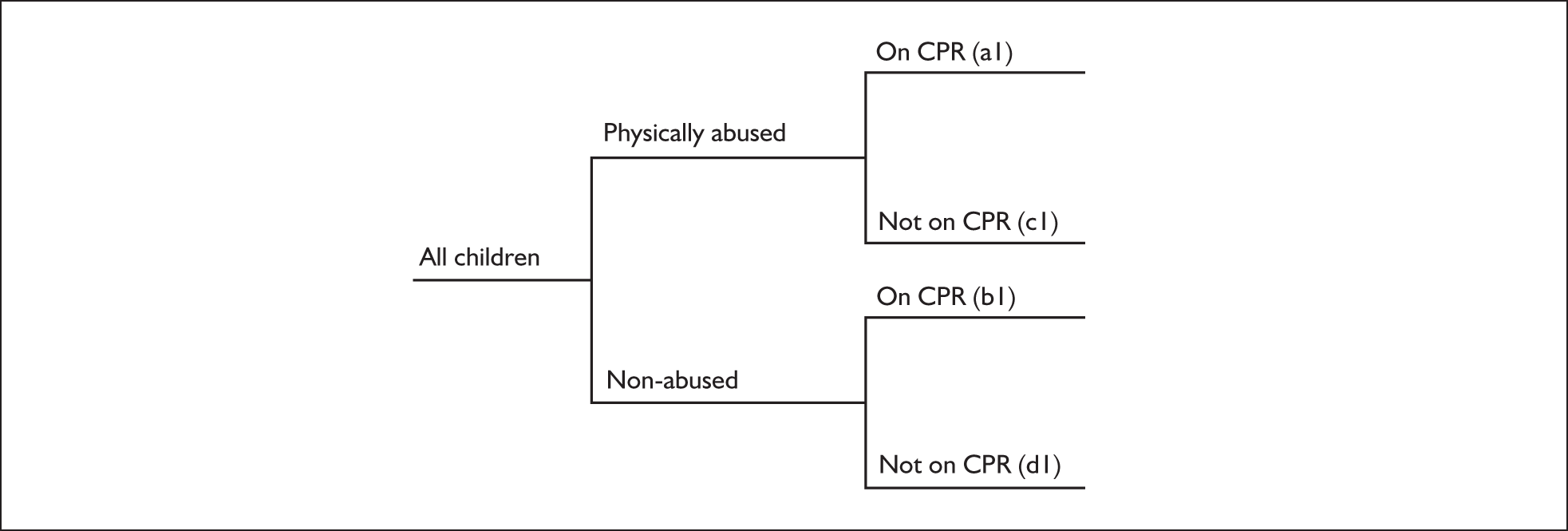
Test performance of clinical assessments in A&E
Standard care: sensitivity and false-positive rate (parameters 77 and 78; Table 15)
The estimated sensitivity and false-positive rate for standard care are very uncertain, being based on poor-quality data interpreted as follows. First, we fixed the false-positive rate at 5%, although, in practice, this will vary according to the threshold for referral to paediatricians, which in turn is determined by the availability of paediatricians and the experience of the clinical screening assessors. A rate of 5% is lower than that reported in many studies based on routine practice [systematic review 9(c)],65,72,82 but higher than the 2% considered feasible for all injured children in a UK children’s A&E department (Jonathan Benger, United Bristol NHS Healthcare Trust and University of the West of England, August 2006, personal communication). 21
Second, we estimated sensitivity for a 5% false-positive rate for the only two studies that reported sensitivity and a false-positive rate for standard care [systematic review 9(a); see Table 13]. 72,82 Receiver operator curves (ROCs) were derived using the diagnostic odds ratio and assuming that the curve was symmetrical (Figure 14; diagnostic odds ratio = odds sensitivity/odds false-positive rate). 4 Third, we derived a curve for the midpoint for sensitivity, at a 5% false-positive rate, between these two studies (Figure 14). Weaknesses of this method include the assumption that the results of the two studies are comparable, that the ROC curve is symmetrical, and that there is a continuous scale of detection that could correspond to a 5% false-positive rate. The sensitivity was estimated as 43.5% for a 5% false-positive rate.
FIGURE 14.
Sensitivity and false-positive rate of clinical screening assessments. In the receiver operating curves, squares show actual study results.
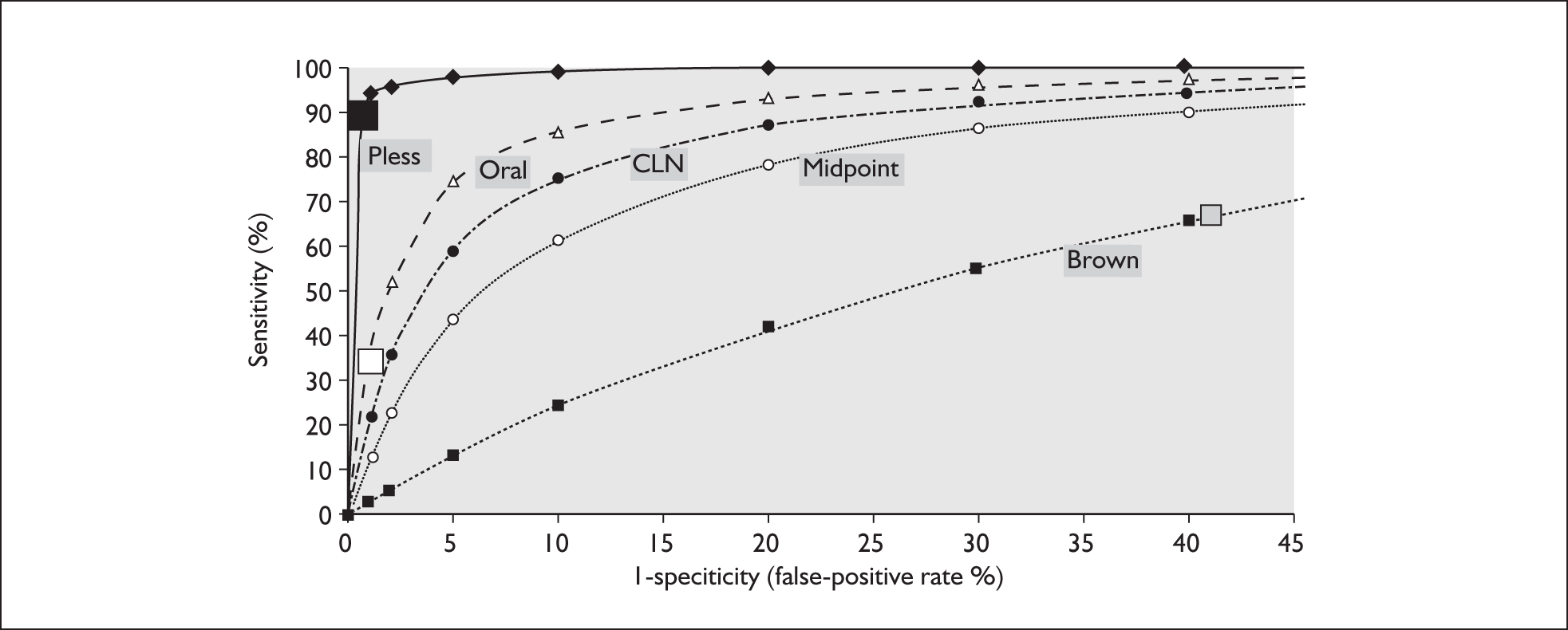
We attempted to address the weaknesses of the method above by indirectly comparing the result with other studies. Although higher rates for sensitivity were reported by seven out of eight studies (60–89%), it is likely that many operated at much higher false-positive rates. All were biased in favour of overestimation of sensitivity [systematic review 9(b); see Table 13]. Findings from before and after studies showed that detection rates more than doubled in three of five studies, although what proportion was due to false-positive cases is not known (see Table 14). Taking all these data into account, the research team accepted the estimates for standard care as reasonable but uncertain.
Community liaison nurse: sensitivity and false-positive rate (parameters 79 and 80)
To estimate the sensitivity for the CLN in addition to standard care, we assumed that the sensitivity of standard care in the study by Lloyd was equivalent to the base-case scenario of 43.5% (25.3 cases detected). We estimated that sensitivity increased to 59.0% with the addition of CLN screening [43.5% × (1 + (9/25.3)); see systematic review 9(a)]. 18 The false-positive rate increased from 5% to 8.9% (Figure 14 and see Table 13).
Paediatric assessment of screen-positive cases: sensitivity and false-positive rate (parameters 81 and 82)
The performance of the paediatric assessment was held constant at a sensitivity of 90% and a false-positive rate of 2.5%. In practice, the performance of confirmatory testing (the paediatric assessment) would be expected to change with the probability of abuse in children referred from A&E, but we found no data to quantify such variation.
Strategies analysed
We analysed 11 strategies (Tables 18 and 19). Our starting point was the base-case strategy, assumed to be closest to current practice. The additional number of abused children detected and children falsely labelled as abused was determined relative to standard care for 10 strategies involving a CLN (strategy 2) or protocols that stipulated children who should be directly assessed by a paediatrician (strategies 3–11). For all strategies we assumed that, overall, 8.8% of all children were physically abused each year and 6.9% of these required medical attention (Table 15 shows age breakdown).
| Strategy | Type of strategy |
|---|---|
| 1 | Standard care |
| In addition to standard care | |
| 2 | Community liaison nurse (CLN) |
| 3 | All under 1 year (all infants) |
| 4 | Head injury and fractures in children under 1 year (HI/FR infants) |
| 5 | Head injury and fractures in children under 5 years (HI/FR < 5 years) |
| 6 | Repeat attendance ≥ 2 at A&E in past 12 months (repeat visit ≥ 2) |
| 7 | Repeat attendance ≥ 3 at A&E in past 12 months (repeat visit ≥ 3) |
| 8 | Social work active (SWA) – allocated to social work/duty team in past 12 months |
| 9 | Currently on child protection register (CPR) |
| 10 | SWA+ all infants |
| 11 | CPR+ all infants |
| A&E | Referred to paediatric team | Referred to social services | Abuse detected (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | Strategy | Sensitivity (%) | False-positives (%) | Abused | Non-abused | Injured (%) | Assessed as abused (%) | Abused | Non-abused | Abused (%) | In A&E | In population |
| 1 | Standard care | 43.5 | 5.0 | 9629 | 109,104 | 5.4 | 8.1 | 8666 | 2728 | 76.1 | 39.2 | 0.8 |
| 2 | CLN | 59.0 | 8.9 | 13,060 | 194,205 | 9.4 | 6.3 | 11,754 | 4855 | 70.8 | 53.1 | 1.1 |
| 3 | All infants | 49.9 | 6.5 | 11,049 | 176,768 | 8.5 | 5.9 | 9944 | 4419 | 69.2 | 44.9 | 1.0 |
| 4 | Fracture + HI infants | 45.5 | 5.5 | 10,082 | 130,693 | 6.4 | 7.2 | 9074 | 3267 | 73.5 | 41.0 | 0.9 |
| 5 | Fracture + HI < 5 years | 50.4 | 11.1 | 11,163 | 224,909 | 10.7 | 4.7 | 10,047 | 5623 | 64.1 | 45.4 | 1.0 |
| 6 | Repeat visit ≥ 3 | 48.8 | 11.8 | 10,806 | 242,450 | 11.5 | 4.3 | 9725 | 6061 | 61.6 | 43.9 | 1.0 |
| 7 | Repeat visit ≥ 2 | 66.5 | 38.8 | 14,717 | 816,815 | 37.7 | 1.8 | 13,246 | 20,420 | 39.3 | 59.8 | 1.3 |
| 8 | SWA | 47.1 | 6.6 | 10,416 | 145,437 | 7.1 | 6.7 | 9375 | 3636 | 72.1 | 42.4 | 0.9 |
| 9 | CPR | 44.4 | 5.2 | 9821 | 113,289 | 5.6 | 8.0 | 8839 | 2832 | 75.7 | 39.9 | 0.9 |
| 10 | SWA + all infants | 52.5 | 8.1 | 11,623 | 211,686 | 10.1 | 5.2 | 10,461 | 5292 | 66.4 | 47.3 | 1.0 |
| 11 | CPR + all infants | 50.5 | 6.7 | 11,167 | 180,676 | 8.7 | 5.8 | 10,051 | 4517 | 69.0 | 45.4 | 1.0 |
Results
Table 19 depicts the results of the clinical effectiveness analyses for the base-case strategy and the increase in sensitivity and false-positive rates from adding screening by a CLN or a protocol stipulating markers that should result in direct assessment by the paediatrician. The proportion of all injured children assessed by the paediatrician ranges from 5.4% (standard care) to 38% if all children with two or more repeated attendances at A&E for injury within the last 12 months are referred (strategy 7). The proportion of injured children assessed by the paediatrician can be readily audited and provides critical information on the need for paediatric services to respond to A&E referrals.
The other critical outcome is the prevalence of abuse among children referred to social services. Most estimates range between 64% and 76% (Table 19, column 11). These figures concur with opinions from paediatricians and social workers. This marker could be audited, given feedback from social services on the outcome of the initial assessment, and would provide an important measure of the performance of A&E screening and paediatric assessments. The high ratio of abused to non-abused false-positive referrals is achieved because the paediatrician is assumed to have a very low false-positive rate (2.5%). In practice, this will depend on their experience and workload. Overall, the proportion of all abused children attending A&E with injury who are referred to social services is less than 60%, or around 1% of all injury episodes (Table 19, column 13) due to abuse each year in the community.
Table 20 lists strategies in rank order of increasing detection of abused children relative to standard care. The CLN and the strategy involving referral of all children with two or more previous A&E attendances detect the most cases. The latter strategy would overwhelm paediatric services, with assessments needed of an estimated 38% of all injured children seen in A&E. Consequently, the CLN appears to be the best option.
| Strategy | Type of strategya | Number abused | % of total in A&E | Number non-abused | Additional referrals to social services (vs standard care) | ||
|---|---|---|---|---|---|---|---|
| Number abused | Number non-abused | Additional abused/non-abusedb | |||||
| 1 | Standard care | 8666 | 39.2 | 2728 | |||
| 9 | CPR | 8839 | 39.9 | 2832 | 173 | 105 | 0.60 |
| 4 | HI/FR infants | 9074 | 41.0 | 3267 | 408 | 540 | 1.32 |
| 8 | SWA | 9375 | 42.4 | 3636 | 709 | 908 | 1.28 |
| 6 | Repeat visit ≥ 3 | 9725 | 43.9 | 6061 | 1059 | 3334 | 3.15 |
| 3 | All infants | 9944 | 44.9 | 4419 | 1278 | 1692 | 1.32 |
| 5 | HI/FR < 5 years | 10,047 | 45.4 | 5623 | 1381 | 2895 | 2.10 |
| 11 | CPR+ all infants | 10,051 | 45.4 | 4517 | 1385 | 1789 | 1.29 |
| 10 | SWA+ all infants | 10,461 | 47.3 | 5292 | 1794 | 2565 | 1.43 |
| 2 | CLN | 11,754 | 53.1 | 4855 | 3088 | 2128 | 0.69 |
| 7 | Repeat visit ≥ 2 | 13,246 | 59.8 | 20,420 | 4579 | 17,693 | 3.86 |
Scenario analyses
As can be readily predicted, the benefits of adding protocols or the CLN diminish as sensitivity of standard care increases. At the extreme assumption of 99% sensitivity for standard care, screening protocols offer virtually no benefit and only increase the number of false positives referred. In practical terms this suggests that screening protocols offer most benefit when A&E is staffed by inexperienced clinical assessors.
Results for overall detection of abuse
Our findings suggest that, of the 8.8% of children subjected to severe parental violence each year, approximately 7% sustain injuries requiring medical attention. Model estimates suggest that, if 1% of all injured children attend A&E because of physical abuse, this would amount to 38% of all physically abused children in the community requiring medical attention. Although these results are very uncertain, they raise the possibility that the majority of abused and injured children requiring medical attention do not present to A&E and may not receive medical attention at all.
Chapter 6 Which agencies detect physical abuse?
Our remit was to evaluate the effectiveness of screening tests in A&E for physical abuse. We estimated that A&E refers about 1% of all physically abused children to social services each year. This extremely low level of detection raises the question of whether or not physically abused children are detected by other agencies, and how A&E can contribute to improving detection overall.
We carried out a systematic review to estimate the overall level of detection of physical abuse in the UK and to measure the contributions made by different agencies.
Systematic review 10: How much physical abuse is detected overall and what is the contribution of different agencies?
Review methods
We included any study that reported the proportion of physical abuse detected by different agencies. We defined ‘detected’ as any notification to any official agency or to the study itself. We included unsubstantiated and uninvestigated referrals to social services, the police or the team coordinating the study and accepted any number of sources of detection, as long as they gave separate figures for hospital detection. We included studies that measured detection of physical abuse either separately or combined with other types of abuse.
Review results
We found four published44,136–138 and three unpublished30,32,139 studies that met our inclusion criteria (Table 21). Four studies were based in the UK. 44,136–138
| First author, place, year of publication | Methods | Reports by source (%) |
|---|---|---|
| Unpublished audit, Hammersmith and Fulham Social Services, London, 200532 | Referral source extracted for all social services initial assessments for physical abuse in one district during 3 months in 2005 (n = 17 children and families). Community health referrals comprised: one GP; one midwife; one mental health worker | A&E 2/17 (11.8%); community heath: 3/17 (17.6%); education: 2/17 (11.8%); police: 4/17 (23.5%); individuals 1/17 (5.9%); social services 3/17 (17.6%); other: 2/17 (11.8%) |
| Unpublished analyses, Metropolitan Police London, 200530 | Analyses of referrals made to the London Metropolitan Police Child Abuse Investigation Command in 2005 by source (n = 7498). The source was electronically logged at the time of referral | Hospital: 38/7498 (0.5%); education: 108/7948 (1.4%); police: 318/7498 (4.2%); individuals: 3665/7498 (48.9%); social services 3357/7948 (42.3%); unknown: 12/7498 (0.2%) |
| Unpublished audit, Camden Social Services, London, 2005139 | Audit of social services case files for children under 16 years newly referred for physical abuse to social services in one district during 3 months in 2005 (n = 58 from 26 families). A further 10 files were unavailable for audit. The source of referral was captured for all children referred for physical abuse (n = 29). Community health referrals comprised: one GP; one health visitor; three community midwives | A&E: 2/26 (7.7%); community health: 5/26 (19.2%); education: 8/29 (27.6%); police: 4/29 (13.8%); individuals 2/29 (7.7%); NSPCC 1/29(3.8%); residential care 2/29(7.7%); community groups 2/29 (7.7%) |
| Miller, UK, 1993136 | Children referred to a rural local authority for any abuse in 12 months (1989–90). In total, 20% of referrals were for siblings; 48 referrals by health professionals were from health visitors | Health professionals: 136/817 (16.6%); education: 148/817 (18.1%); police: 55/817 (6.7%); individuals: 298/817 (36.5%); social services/local authority: 122/817 (14.9%); other: 56/817 (6.9%); missing 2/817 |
| US Department of Health and Human Services, USA, 200644 | Nationally representative sample of over 5600 professionals in 842 agencies in 42 US counties in 1993. In total, 1.55 million reports by professionals met harm standard (demonstrable harm of a severe level for neglect and moderate level for other abuse). A total of 28% of reports were investigated by child protection services | Probation: 36,600 (2.4%); police: 111,500 (7.2%); public health: 27,500 (1.8%); hospitals: 113,200 (7.3%); schools: 920,000 (59.2%); day care: 59,700 (3.9%); mental health: 50,900 (3.3%); social services: 96,000 (6.7%); welfare: 15,000 (1.0%); other agency: 7000 (0.5%); all other: 116,400 (7.5%) |
| Drake, USA, 1995137 | All child physical abuse referrals to Missouri social services in 1992 | Medical personnel: 1110 (9.0%); mental health: 544 (4.4%); school: 1856 (15.1%); law enforcement: 1246 (10.1%); other professionals: 3567 (29.0%); anonymous: 2278 (18.5%); care providers: 438 (3.6%) |
| Kaufman, USA, 1991138 | Proportion of telephone ‘contacts’ made by hospitals to County Children Services Board in Ohio about physical and sexual abuse, neglect, unruly and dependent children and delinquents (1985–6) | Contacts by hospitals: 1700/45246 (3.8%) |
Of the four studies that separately reported findings for physical abuse, the contribution of hospitals or A&E ranged from 0.5%, reported by the Metropolitan Police,30 to 17% for all health professionals. 5 The low rate reported by the police may be because social services usually contact the police for children identified by hospitals. The proportion of cases reported by hospitals was low for all types of abuse. Overall, these results suggest that hospitals or A&E contribute to between 7% and 12% of the cases of abuse referred to child protection agencies. The main sources of referral in the UK were police, education, community health professionals and individuals. In the US, schools were one of the main sources. 44,137
Chapter 7 Discussion
Key findings
We found consistent evidence that physical abuse affects 1 in 11 children in the UK each year. The proportion of abused children who require medical attention is small but poorly quantified. We estimated that approximately 1% of all child attendances at A&E for injury are for physical abuse, amounting to just under 1 in 50 of all physical abuse episodes in the community.
We found clear evidence that physically abused children who do attend A&E are missed but that the performance of the clinical screening assessment was poorly quantified. We found no evidence that any test was highly predictive of physical abuse. There was weak evidence that use of a checklist or a CLN improved the performance of the screening assessment in A&E. We estimated that the best strategy involved the standard clinical assessment screen combined with a CLN. This option would result in referral to social services of about half of the abused children attending A&E. Given the poor quality of the data, this result is highly uncertain.
The addition of protocols stipulating immediate paediatric assessment of children with specific markers plus clinical screening assessment of those without these markers offered only marginal benefits and the number of additional false-positive referrals exceeded the number of additional abused children detected (see Table 20). The most effective protocol involved referral of all injured infants and all injured children who were social work active. The benefits of protocols declined as the clinical screening assessment improved. We found no clear evidence that repeated A&E attendance, type of injury or age group, apart from infancy, were predictive of physical abuse.
Our findings show that few incidents of physical abuse are investigated by social services or police and, of these, a small minority are detected in A&E.
Strengths and limitations of the study
A major strength of the study was the use of a simple model to explain the rationale for the review questions and the way that the results were integrated. We used broad inclusion criteria for each review, thereby allowing examination of the range of results and factors contributing to variation between studies. We also took into account the fact that abused children attend A&E for accidents. We left no review questions unanswered, although the answer was sometimes very uncertain and based on indirect evidence.
The main limitation was the poor quality of the source data. As a result, the estimates generated by the model were very uncertain. We did not attempt to model the uncertainty using a probabilistic model as this would not have addressed the far greater problems of bias and questionable applicability to the UK of many of the studies. We selected parameter inputs for the model using epidemiological principles to judge threats to validity and applicability. The potential for bias was compounded by the use of indirect evidence to derive some parameter estimates (e.g. in the estimation of the prevalence of injured, abused children attending A&E). As far as possible we examined the face validity of model outputs by comparison with expert opinion and external data not used in the model.
A second limitation is that the burden of physical abuse inevitably depends on how it is defined, which in turn hinges on the level of violence towards children that society regards as acceptable. We used a widely accepted definition for severe parental violence to define the annual prevalence of physical abuse in children in the community. The figure of 9% was consistent with other studies. Even if the lowest reported estimate were used (4%), our findings of a huge gap between the occurrence and detection of abuse would be unchanged.
Third, we limited the study by focusing on screening tests for physical abuse in injured children despite the fact that physical abuse often occurs in association with other forms of abuse and neglect and that the pathway of referral to social services is similar. Benefits of detection of one type of abuse impinge on other types, as well as on other social problems, but this was outside the scope of our study. We further limited the study to detection of physical abuse in injured children, despite the fact that physical abuse may be found during examination of children for medical problems such as asthma.
Fourth, we did not investigate several potential screening tests because of lack of data. The timing of attendance at A&E (night-time) and the severity of the injury are both associated with physical abuse and warrant further investigation. 75,98,99 Bruising to the head or face may also offer a feasible screening test without requiring a fully undressed examination, but its performance needs to be assessed in the A&E population. 19 We could not evaluate direct questioning of school-age children as we found no relevant studies, despite the recommendation by Lord Laming that children with suspected abuse be questioned about the injury. 10 Finally, we evaluated checklists as a composite test as there were insufficient data to determine the performance of individual questions. Others have suggested that the most predictive question relates to inconsistency between the explanation and injury;140 however, this question is likely to be highly operator dependent as experience is required to know which events constitute a consistent explanation.
A fifth limitation was the use of fixed performance characteristics for the paediatric confirmatory assessment. In practice, paediatric scrutiny will vary depending on the threshold for referral by the A&E screeners. In addition, ward staff may make an important contribution to the overall detection of abuse by the hospital by identifying abused children, particularly those with severe injuries, who were not referred by A&E staff. We ignored this contribution as our focus was on A&E.
Finally, the Victoria Climbié inquiry identified poor coordination between services as one of the main problems that could have averted her death, rather than failure to identify physical abuse. We limited our analyses by not considering failures in the chain of referrals, as we aimed to reflect the optimal decision options facing service providers rather than implementation issues.
Implications for practice
A small minority of physically abused children present to A&E, and some abused and injured children may not receive the medical care that they need. Any efforts to improve detection of physical abuse in A&E should not discourage presentation of injured children for medical attention. The priority should be for abused children to be able to access medical attention if they need it.
Our findings suggest that improving the clinical screening assessment, based on a clinical synthesis of findings in the history and examination, is likely to be more useful than protocols, except where the paediatric expertise of assessors is minimal. All of the strategies examined involved referral of at least 5% of injured children to paediatricians, which may exceed existing capacity. Lower rates of referral to paediatricians would substantially diminish the proportion of abused children detected.
Improvements in the performance of the clinical assessment depend on training, feedback and experience, and might be enhanced by paediatric or other child protection expertise on site. Whether policy should focus on input by paediatricians or CLNs, or both, is unclear.
Further improvements in the overall detection of physical abuse by A&E might be achievable by taking action for the large number of abused children referred to paediatricians for suspected abuse who fail to reach the high level of certainty of abuse required to justify referral to social services. Such children fail to have the suspicion of abuse put on record for access by other professionals and, most importantly, fail to access supportive interventions. Lowering the threshold for action for such children could result in referral to social services to address the child’s social needs (i.e. as a ‘child in need’ referral) rather than referral solely on the grounds of abuse. Alternatively, the paediatrician could refer the child and family directly to supportive services in the community (e.g. Sure Start, parenting training). Completion of the CAF form will be used as a vehicle to record concerns about additional needs for information sharing but the practicalities of clinicians in A&E filling in an eight-page form need to be addressed. 141 Finally, standardised recording and coding of the clinical diagnosis or suspicion of abuse or neglect, whether or not children are referred to social services, would greatly enhance the potential for identifying children at risk by allowing clinicians to establish a cumulative record of abuse or neglect.
We found a lack of feedback about the outcome of suspected physical abuse within the hospital and from social services to A&E staff. All CLNs that we spoke to relied on their handwritten records of cases that they identified. Routinely compiled electronic records could provide invaluable feedback to staff at all levels and allow audits of the rate of referral for suspected abuse. Feedback implemented via regular multidisciplinary meetings to review child protection cases in A&E, outpatients and inpatients could be used as a model to offer opportunities for training, ensure that data are up to date and improve multidisciplinary working (Ben Lloyd, January 2006, personal communication). 18
Every paediatrician that we interviewed complained of a lack of feedback from some social services departments about whether children underwent an initial assessment at all and what further action was taken. In the clinical effectiveness model we assumed that all referrals from paediatric to social services for physical abuse would be investigated, as stipulated in Working together,2 but this may not be the case. 142 We received anecdotal reports that, during preliminary discussions with social services, doctors had to ‘choose their words carefully’ to avoid being deterred from making a formal referral. There was a perception that services were so stretched that new referrals were discouraged or that investigations might be limited. Many professionals who we interviewed expressed the need for telephone access to experienced social services advice to assist with judgements about referral and management of potential abuse. Several commented that they felt the existing services did not meet this need. Consideration could be given to making such advice centrally available.
Feedback to medical staff is mandatory for children proceeding to a Section 47 inquiry. However, we found anecdotal evidence that Section 47 inquiries occur in a minority of children considered to have been physically abused. Similar concerns were echoed in a recent Department of Health report142 that highlighted the continuing problem of varying thresholds for investigation. This view is supported by a recent report143 on costs and outcomes of children’s social care that highlighted the drastic rationing that takes place when children are referred, with cases closed after initial assessment despite high levels of need.
Various interventions or classification as a ‘child in need’ may pre-empt the need for a Section 47 inquiry and may offer the most beneficial approach for the child and family. However, lack of investigation for physical abuse can be construed as evidence that social services considered abuse had not occurred. The extent of this problem is hard to fathom as, although routine statistics record referrals to social services, initial assessments and subsequent investigations, they record the principal reason for investigation only at the end point, CPR. Hence, the burden of abuse measured by referrals and subsequent management cannot be determined. There also appears to be an undue emphasis on CPR as this is the only point at which abuse is coded, whereas the vast majority of abused children investigated by social services never reach this stage.
Consideration needs to be given to the feasibility of accessing information on whether a child is social work active from Contact Point (previously known as the Information Sharing Index), which member of staff will do this, and how the time taken for access (currently 2–3 minutes) can be reduced. We found strong evidence that the CPR was suboptimally used routinely and for individual children in A&E because of difficulties in access and unclear policy. 119,120 Contact Point could offer benefits for multidisciplinary working that extend beyond physical abuse, but ease of access to a reliable, up-to-date record will be key.
Wider burden and detection of abuse
Physical abuse usually goes undetected. We estimated that a small minority (about 1 in 31) of children subjected to severe parental violence each year undergo an initial assessment by social services for physical abuse. Similar findings have been reported by others. 6,37
Most physically abused children referred to social services were reported by neighbours, police, schools and community health workers. Efforts to improve detection of abuse may be most effective if focused on the range of agencies involved with children. Existing training programmes in child abuse may partly address this need. 11 Strategies to reduce the public’s tolerance of violence to children could be effective for both detection and prevention.
It was striking how few cases of physical abuse were reported by GPs. Lack of reporting by GPs was acknowledged in a recent Royal College of General Practitioners (RCGP) report17 which stated that GPs see themselves outside the child protection services and have traditionally ‘enjoyed non-engagement’ with child protection. They may choose not to recognise the abuse, put the needs of the parent first or manage the abuse themselves and follow up the family until they are sure. Some may not know how to report or may not trust the advice from social services. 17 Although addressed by the recent RCGP report, the apparent dislocation of GPs from child protection services should be a major policy concern, especially as evidence suggests that training and interventions can substantially increase the engagement of GPs with child protection issues and the reporting of suspected abuse. 144
Child protection registrations focus on infants and pre-school children and there is a perception among health-care staff that physical abuse is predominantly a problem of the pre-school years. Although children under 5 years may have an increased risk of injury from abuse, population-based studies and police reports show that more children over 5 years are affected by parental or carer physical abuse. 30,35
Research recommendations
It was striking how little high-quality research had been generated in the UK compared with North America. Part of the reason may be the lack of electronic databases that allow linkage between social services and health databases. With the current enormous investment in data systems in both arenas in the UK there is scope for large-scale studies.
-
Well-designed, large-scale studies are required to evaluate the effectiveness of assessments that are currently used in A&E for identifying abused children and initiating appropriate interventions. In particular, the role and effectiveness of the CLN warrants further research. Investigation is also required into which information obtained from other sources in the community is most effective for informing decisions about management of possible abuse or neglect.
-
Studies are needed to evaluate the feasibility, acceptability and effectiveness of new tests such as direct questioning of school-age children about injuries, assessment of bruising on the head and face, timing of attendance at A&E, information from the cumulative record of health-care use, and information from agencies outside health.
-
Monitoring is needed of the incidence of abuse identified by professionals working with children and how this is changing over time. National data on reasons for CPR should be extended to referrals to social services and analysed alongside studies of abuse identified by professionals to determine how much is referred.
-
Research is required to investigate the reasons for referral to social services and for completion of the CAF form, subsequent actions and re-referrals. Such a study would be important to gain a more accurate picture of the extent of abuse dealt with by social services, much of which may be labelled under non-abuse categories, or dealt with by information sharing via CAFs without involvement of social services.
-
Periodic local hospital A&E audits of patients with suspected abuse or neglect, actions taken within hospital, and contacts made with other agencies should be encouraged.
-
A working party should be established to determine the research priorities across health services, social services, education and police. With the introduction of electronic records in health and social services there will be considerable scope for high-quality large-scale studies, based on a combination of routine records and primary data collection. The working group should include expertise in population research and epidemiology, the different service areas and policy priorities, and should build on and complement the existing research agenda developed by the Department for Children, Schools and Families. For too long, interventions in child abuse have followed investigations of high-profile cases. A population-based approach is needed to generate high-quality research to underpin the effectiveness of the extremely costly services that exist to address this serious and common condition.
Acknowledgements
Information about service provision
We are grateful to the following individuals who contributed to the study. They facilitated site visits, discussed the child protection procedures in their departments, gave their expert opinions about the model structure or specific parameters and/or provided feedback on preliminary results.
Chelsea and Westminster Hospital NHS Foundation Trust
Paul Hargreaves, Consultant Paediatrician and Designated Doctor for Child Protection.
East and North Hertfordshire NHS Trust
Dominic Croft, Community Paediatrician and Named Doctor for Child Protection.
Great Ormond Street Hospital for Children NHS Trust
Danya Glaser, Consultant Child and Adolescent Psychiatrist.
Hampstead NHS Trust
Ben Lloyd, Consultant Paediatrician and Named Doctor for Child Protection.
London Borough of Camden
Cathy Doll, Information Sharing and Assessment Programme Manager; Mina Epelle, Camden Safeguarding and Social Care; Bodil Mlynarska, Head of Children’s Quality Assurance Unit. Primary care: Kathy Hoffman, GP.
London Borough of Hammersmith and Fulham
Children’s Services: Emma Clements, Senior Social Worker Referral and Assessment Team and link worker for Queen Charlotte’s Hospital; Tim Deacon, Head of Review and Quality Assurance Unit; Lynne Jones, Designated Child Protection Nurse; Nicky Love, Named Nurse For Child Protection; Bev Sharpe, Service Manager for Family Support and Child Protection.
Primary care: Louise Kelly, Named GP For Child Protection.
Southwark Primary Care Trust
Beatrice Cooper, Consultant Community Paediatrician and Designated Doctor for Looked After Children; Ros Healy, Designated Doctor for Child Protection.
Data contributed
We are very grateful to the following individuals who contributed datasets or specific analyses based on unpublished data. They did so free of charge and responded in full to queries. As far as we are aware they gain no academic recognition for this.
Analyses from study on family violence and discipline: Dr Deborah Ghate provided unpublished analyses from a study of parent-reported violence to children.
Child Protection Report (Royal Free Hospital, London), 2005: Dr Ben Lloyd (Royal Free Hampstead NHS Trust) provided two unpublished audits conducted at the Trust: one of abused children referred to social services during 9 months in 2005; the other on the outcome of children detected by the community liaison nurse for A&E.
Dataset for study using a reminder flowchart: Dr Jonathan Benger provided the datasets for an audit of the use of a reminder flowchart in the A&E department of Frenchay Hospital, Bristol. These data were not analysed in our project as they did not contain information on the outcome of children referred.
Evidence that doctors often fail to diagnose child abuse and neglect: Dr Russell Dominic Croft (East and North Hertfordshire NHS Trust) provided us with his unpublished paper of a personal case series of missed diagnoses of child abuse and neglect between 1994 and 2006.
Electronic Child Health Register database: Brent Taylor (University College Hospital) and Graeme Hall (Royal Free Hospital) provided a database of over 55,000 children under 8 years who attended five London Hospitals between 2000 and 2006 (average period of data contribution 4.4 years).
Home and Leisure Accident Surveillance System (HASS) database: the Royal Society for the Prevention of Accidents provided specific analyses of the HASS survey of patients attending 18 UK A&E departments in 2002.
London Borough of Camden: Bodil Mlynarska and Paul Bain collaborated with an audit of children referred to social services for physical abuse.
Identifying children at risk of abuse by using a risk assessment form at University College London Hospital A&E department: Ella Rachamin (SHO, UCH), Deborah Hodes (Consultant Community Paediatrician, Camden PCT), Leona Bull (Psychologist, Institute of Child Health), Ann Lloyd (Liaison Health Visitor, UCH), Sonia Jenkins (Child Protection Advisor, UCH), Ann Kilby (Consultant Paediatrician and the paediatric team, UCH), Claire Walford (A&E Consultant, UCH), Dr Rao (Paediatric Registrar, UCH) and Gayle Davies (Ward Clerk on Paediatric Ward, UCH) collaborated with an audit of referrals to the paediatric team using a checklist for all children attending UCLH A&E department over 8 weeks in 2005. These data were not included in the analyses.
London Borough of Hammersmith and Fulham Children’s Services: Tim Deacon, Etiene Steyn, Ann Harvey, Marcelino Radcliffe, Debbie Grusin, Ross Tuckley and Ivy Sseruma collaborated with an audit of the primary reason for initial assessment of children by social services.
London Metropolitan Police: Caroline Wareing, Martin Arnold, Carly Mellin and Ken Shuttlewood at the London Metropolitan Police Child Abuse Investigation Command provided aggregate data on the number of children referred for physical abuse in 2004 and 2005 (n = 5395).
Norwich Accident Project database: Richard Reading and Robin Haynes (University of East Anglia) supplied the original databases used for two papers on A&E department attendances at one hospital by children resident in Norwich city in 1994 and 1999.
TARNlet: Fiona Lecky, Omar Bouamra and Martin Smith on behalf of the Trauma and Audit Research Network provided analyses of data on 17,640 children attending 20 core hospitals in England and Wales and admitted with severe trauma between 1996 and 2004. The data were analysed according to age group, diagnosis of abuse and type of injury. Data were also provided on time trends in A&E attendances.
University College Hospital London NHS Trust: Information services provided data on the number of A&E attendances by age and injury type.
Co-investigators
Dr Jill Ellis (Institute of Child Health) and Professor Ken Stein (Peninsula Medical School, University of Exeter) were co-applicants and helped to develop the original application and gave feedback on the model in the early stages.
We are grateful to the following collaborators: Melissa Harden (Centre for Paediatric Evidence Based Medicine, Institute of Child Health) who carried out scoping searches and provided support and advice on further searches and referencing; Sam Hellmuth (Centre for Paediatric Evidence Based Medicine, Institute of Child Health) who carried out the main searches for all of the systematic reviews; Leona Bull (Centre for Paediatric Evidence Based Medicine, Institute of Child Health) who contributed as a research fellow in the early stages of the study.
Contribution of authors
Jenny Woodman carried out the systematic reviews of the literature and analyses of primary data and the decision-analytic model and, together with Ruth Gilbert, wrote the report. Martin Pitt designed and developed the decision model and contributed to the analyses. Deborah Hodes contributed to the design of the study and commented on results and drafts of the report. Brent Taylor contributed to the design of the study and commented on results and drafts of the report. Reinhard Wentz carried out the ‘targeted’ searches and gave feedback on the searches chapter of the report. Ruth Gilbert was the principal investigator for the project and had overall responsibility for all aspects of the study.
Disclaimers
The views expressed in this publication are those of the authors and not necessarily those of the HTA Programme or the Department of Health.
References
- Department of Health, Home Office, Department for Education and Employment . Working Together to Safeguard Children 1999.
- Department for Education and Skills . Working Together to Safeguard Children: An Interagency Guide to Safeguard and Promote the Welfare of Children 2006.
- Royal College of Paediatrics and Child Health . Safeguarding Children and Young People: Roles and Competencies for Health Care Staff 2006.
- Glas A, Lijmer J, Prins M, Bonsel G, Bossuyt P. The diagnostic odds ratio: a single indicator of test performance. J Clin Epidemiol 2003;56:1129-35.
- Children Act 1989 1989.
- Secretary General of the UN . United Nations World Report on Violence Against Children 2006.
- Collishaw S, Pickles A, Messer J, Rutter M, Shearer C, Maughan B. Resilience to adult psychopathology following childhood maltreatment: evidence from a community sample. Child Abuse Negl 2007;31:211-29.
- Department for Education and Skills . Statistics of Education: Referrals, Assessments and Children and Young People on Child Protection Registers: Year Ending 31 March 2006 2006.
- Department for Education and Skills . Statistics of Education: Referrals, Assessments and Children and Young People on Child Protection Registers: Year Ending 2004 2004.
- Lord Laming . The Victoria Climbié Inquiry 2003.
- Department for Education and Skills . Every Child Matters 2003.
- Children Act 2004 2004.
- House of Lords Select Committee on Merits of Statutory Instruments . Analysis of Time Saved by Practitioners: Supplementary Memorandum by the Department for Children, Schools and Families 2007. www.publications.parliament.uk/pa/ld200607/ldselect/ldmerit/146/14606.htm.
- Royal College of Paediatrics and Child Health . Child Protection Companion 2006.
- Royal College of Paediatrics and Child Health . Survey Shows That Paediatricians Are Deterred from Vital Child Protection Work 2004.
- Royal College of Nursing . Child Protection: Every nurse’s Responsibility (guidance for Nursing Staff) 2002.
- Royal College of General Practitioners . ‘Keep Me safe’: The Royal College of General Practitioners Strategy for Child Protection 2005.
- Lloyd B, Swarbrick H, Mattison J. Royal Free Hampstead NHS Trust Child Protection Report – 2005 n.d. www.royalfree.org.uk/doc/260106/appendix%20J.doc (accessed 1 May 2007).
- Dunstan FD, Guildea ZE, Kontos K, Kemp AM, Sibert JR. A scoring system for bruise patterns: a tool for identifying abuse. Arch Dis Child 2002;86:330-3.
- Sidebotham P, Biu T, Goldsworthy L. Child protection procedures in emergency departments. Emerg Med J 2007;24:831-5.
- Benger JR, Pearce AV. Simple interventions to improve detection of child abuse in emergency departments. BMJ 2002;324:780-2.
- Sidebotham P, Pearce A. Audit of child protection procedures in accident and emergency department to identify children at risk of abuse. BMJ 1997;315:855-6.
- McKinney A, Lane G, Hickey F. Detection of non-accidental injuries presenting at emergency departments. Emerg Med 2004;21:562-4.
- Every child matters. ICS, CAF and Contact Point – an overview. London: Department for Children, Schools and Families; 2007.
- University College London Hospital Data Management Team . Routine Data on Children under 16 Years Attending the A&Amp;E Department Between 2003 and 2005 2006.
- Taylor B, Hall G. Electronic Child Health Register (eCHR) (data from Five London A&Amp;E Departments from 2000 to 2006) 2006.
- Camden Information Tracking and Referral Team . Integrated Services for Children and Young People: A practitioner’s Guide 2004.
- Greenhalgh T, Peacock R. Information in practice. BMJ 2005;331.
- Parton N. From Maria Colwell to Victoria Climbié: reflections on public inquiries into child abuse a generation apart. Child Abuse Rev 2004;13:80-94.
- Wareing C, Shuttlewood K. PIB’s CRIME Unit . An Unpublished Audit of Victims of Violence Against the Person in 2005, Aged 0 to 16, Investigated by the Child Abuse Investigation Command (London Metropolitan Police) 2006.
- World Health Organization . Report on Violence and Health 2002.
- Steyn E, Radcliffe M, Deacon T, Woodman J, Gilbert R. An Audit of Initial Assessments Carried Out by Hammersmith and Fulham’s children’s Referral and Assessment Team over Three Months 2005.
- Sidebotham P. The ALSPAC study team . Patterns of child abuse in early childhood, a cohort study of the ‘children of the nineties’. Child Abuse Rev 2000;9:311-20.
- Ghate D, Creighton S, Field J. A national study of parents, children and discipline. London: Economic and Social Research Council; 2002.
- Bardi M, Borgognini-Tarli S. A survey on parent–child conflict resolution: intra family violence in Italy. Child Abuse Negl 2001;25:839-53.
- Theodore A, Chang J, Runyan D, Hunter W, Bangdiwala SI, Agans R. Epidemiologic features of the physical and sexual maltreatment of children in the Carolinas. Pediatrics 2005;115.
- Wolfner GD, Gelles RJ. A profile of violence towards children: a National study. Child Abuse Negl 1993;17:197-212.
- Gelles RJ, Edfeldt AW. Violence toward children in the United States and Sweden. Child Abuse Negl 1986;10:501-10.
- Christensen E. The prevalence and nature of abuse and neglect in children under four: a national survey. Child Abuse Rev 1999;8:109-19.
- May-Chahal C, Cawson P. Measuring child maltreatment in the United Kingdom: a study of the prevalence of child abuse and neglect. Child Abuse Negl 2005;29:949-51.
- Sebre S, Sprugevica I, Novotni A, Bonevski D, Pakalniskiene V, Popescu D, et al. Cross-cultural comparisons of child-reported emotional and physical abuse: rates, risk factors and psychosocial symptoms. Child Abuse Negl 2004;28:113-27.
- Sariola H, Uutela A. The prevalence and context of family violence against children in Finland. Child Abuse Negl 1992;16:823-32.
- Nelson DE, Higginson GK, Grant-Worley JA. Physical abuse among high school students. Prevalence and correlation with other health behaviors. Arch Pediatr Adolesc Med 1995;149:1254-8.
- US Department of Health and Human Services . The Third National Incidence Study of Child Abuse and Neglect (NIS-3) 2006.
- Creighton SJ. Prevalence and incidence of child abuse: international comparisons. London: NSPCC; 2004.
- Trocmé N, Tourigny M, MacLaurin B, Fallon B. Major findings from the Canadian incidence study of reported child abuse and neglect. Child Abuse Negl 2003;27:1427-39.
- King G, Trocmé N, Thatte N. Substantiation as a multitier process: the results of a NIS-3 analysis. Child Maltreat 2003;8:173-8.
- Straus MA, Hamby SL, Boney-McCoy S, Sugarman DB. The revised Conflicts Tactics Scales (CTS2): development and preliminary psychometric data. J Fam Iss 1996;17:283-316.
- Straus M, Hamby S, Boney-McCoy S, Sugarman DB, Finklehor D, Moore Dea. Conflicts Tactics Scale: handbook and revised forms. Los Angeles: Western Psychology Services; 1979.
- Office of National Statistics . Population Trends 2006.
- US Census Bureau . Resident Population by Age and Sex 1980–2002. 2003. www.census.gov/prod/2004pubs/03statab/pop.pdf (accessed 30 January 2007).
- Sibert JR, Payne EH, Kemp AM, Barber M, Rolfe K, Morgan RJH, et al. The incidence of severe physical child abuse in Wales. Child Abuse Negl 2002;26:267-76.
- Creighton SJ. An epidemiological study of abused children and their families in the United Kingdom between 1977 and 1982. Child Abuse Negl 1985;9:441-8.
- Lindell C, Svedin CG. Physical child abuse in Sweden: a study of police reports between 1986 and 1996. Soc Psychiatry Psychiatr Epidemiol 2001;36:150-7.
- Gessner BD, Moore M, Hamilton B, Muth PT. The incidence of infant physical abuse in Alaska. Child Abuse Negl 2004;28:9-23.
- Gibbons J, Gallager B, Bell C, Gordon D. Development after physical abuse in early childhood. London: HMSO; 1995.
- Trocmé N, MacMillan H, Fallon B, De M. Nature and severity of physical harm caused by child abuse and neglect: results from the Canadian Incidence Study. CMAJ 2003;169:911-5.
- Berrien FB, Aprelkov G, Ivanova T, Zhmurov V, Buzhicheeva V. Child abuse prevalence in Russian urban population: a preliminary report. Child Abuse Negl 1995;19:261-4.
- Youssef RM, Attia MS, Kamel MI. Children experiencing violence. I. Parental use of corporal punishment. Child Abuse Negl 1998;22:959-73.
- English DJ, Wingard T, Marshall D, Orme M, Orme A. Alternative responses to child protective services: emerging issues and concerns. Child Abuse Negl 2000;24:375-88.
- Zuravin SJ, Orme JG, Hegar RL. Predicting severity of child abuse injuries with ordinal probit regression. Soc Work Res 1994;18:131-8.
- Macgregor DM. Accident and emergency attendances by children under the age of 1 year as a result of injury. Emerg Med J 2003;20:21-4.
- Keshavarz R, Kawashima R, Low C. Child abuse and neglect presentations to a pediatric emergency department. J Emerg Med 2002;23:341-5.
- Chang DC, Knight VM, Ziegfeld S, Haider A, Paidas C. The multi-institutional validation of the new screening index for physical child abuse. J Pediatr Surg 2005;40:114-19.
- Pless IB, Sibald AD, Smith MA, Russell MD. A reappraisal of the frequency of child abuse seen in pediatric emergency rooms. Child Abuse Negl 1987;11:193-200.
- Moore RS, Robson WJ. Cases of assault attending a children’s accident and emergency department: an epidemiological study. Arch Emerg Med 1992;9:239-43.
- Barsness KA, Cha ES, Bensard DD, Calkins CM, Partrick DA, Karrer FM, et al. The positive predictive value of rib fractures as an indicator of nonaccidental trauma in children. J Trauma 2003;54:1107-10.
- Kowal-Vern A, Paxton TP, Ros SP, Lietz H, Fitzgerald M, Gamelli RL. Fractures in the under-3-year-old age cohort. Clin Pediatr (Phila) 1992;31:653-9.
- Cadzow SP, Armstrong KL. Rib fractures in infants: red alert! The clinical features, investigations and child protection outcomes. J Paediatr Child Health 2000;36:322-6.
- Bulloch B, Schubert CJ, Brophy PD, Johnson N, Reed MH, Shapiro RA. Cause and clinical characteristics of rib fractures in infants. Pediatrics 2000;105.
- Bechtel K, Stoessel K, Leventhal JM, Ogle E, Teague B, Lavietes S, et al. Characteristics that distinguish accidental from abusive injury in hospitalized young children with head trauma. Pediatrics 2004;114:165-8.
- Brown GW, Malone P. Child head injuries: review of pattern from abusive and unintentional causes resulting in hospitalization. Alaska Med 2003;45:9-13.
- Keenan H, Runyan D, Marshall S, Nocera M, Merten D, Sinal S. A population-based study of inflicted traumatic brain injury in young children. JAMA 2003;290:621-6.
- Jenny C, Hymel KP, Ritzen A, Reinert SE, Hay TC. Analysis of missed cases of abusive head trauma. JAMA 1999;281:621-6.
- Lecky F, Maconochie I, Smith M, Bouamra O. Trauma Audit Research Network . Children Admitted With Severe Trauma Between 1996 and 2004 2005.
- Jayawant S, Rawlinson A, Gibbon F, Price J, Schulte J, Sharples P, et al. Subdural haemorrhages in infants: population based study. BMJ 1998;317:1558-61.
- Johnson CF, Showers J. Injury variables in child abuse. Child Abuse Negl 1985;9:207-15.
- Palazzi S, de Girolamo G, Liverani T. Observational study of suspected maltreatment in Italian paediatric emergency departments. Arch Dis Child 2005;90:406-10.
- Johnson CF, Apolo J, Joseph JA, Corbitt T. Child abuse diagnosis and the emergency department chart. Pediatr Emerg Care 1986;2:6-9.
- Clark KD, Tepper D, Jenny C. Effect of a screening profile on the diagnosis of nonaccidental burns in children. Pediatr Emerg Care 1997;13:259-61.
- Kumar P. Child abuse by thermal injury – a retrospective survey. Burns 1984;10:344-8.
- Oral R, Blum KL, Johnson C. Fractures in young children: are physicians in the emergency department and orthopedic clinics adequately screening for possible abuse?. Pediatr Emerg Care 2003;19:148-53.
- Scherl SA, Miller L, Lively N, Russinoff S, Sullivan CM, Tornetta P. Accidental and nonaccidental femur fractures in children. Clin Orthop Relat Res 2000;376:96-105.
- Hoskote A, Martin K, Hormbrey P, Burns CE. Fractures in infants: one in four is non-accidental. Child Abuse Rev 2003;12:384-91.
- Carty H, Pierce A. Non-accidental injury: a retrospective study of a large cohort. Eurol Radiol 2002;12.
- Ziegler D, Sammut J, Piper A. Assessment and follow-up of suspected child abuse in preschool children with fractures seen in a general hospital emergency department. J Paediatr Child Health 2005;41:251-5.
- Berger DK, Rolon Y, Sachs J, Wilson B. Child abuse and neglect: an instrument to assist with case referral decision making. Health Soc Work 1989;14:60-73.
- RoSPA . Attendances at A&Amp;E Departments Due to Accidents 2002.
- Berger AM, Knutson JF, Mehm JG, Perkins KA. The self-report of punitive childhood experiences of young adults and adolescents. Child Abuse Negl 1988;12:251-62.
- Brownscombe J, Simpson N, Lenton S, Davis R, Barby T. The potential of emergency department injury surveillance data: an illustration using descriptive analysis of data in 0–4 years olds from the Bath injury surveillance system. Child Care Health Dev 2004;30:161-6.
- Haynes R, Reading R, Gale S. Household and neighbourhood risks for injury to 5–14 year old children. Soc Sci Med 2003;57:625-36.
- Reading R, Langford IH, Haynes R, Lovett A. Accidents to pre-school children: comparing family and neighbourhood risk factors. Soc Sci Med 1999;48:321-30.
- Lyons RA, Lo SV, Heaven M, Littlepage BN. Injury surveillance in children – usefulness of a centralised database of accident and emergency attendances. Inj Prev 1995;1:173-6.
- Walsh SSM, Jarvis SN, Towner EM, Aynsley-Green A. Annual incidence of unintentional injury among 5400 children. Inj Prev 1996;2.
- King W, Reid C. National audit of emergency department child protection procedures. Emerg Med J 2003;20:222-4.
- Royal College of Paediatrics and Child Health . Accident and Emergency Services for Children – Report of a Multidisciplinary Working Party 1999.
- Royal College of General Practitioners . Services for Children in Emergency Departments: Report of the Intercollegiate Committee for Services for Children in Emergency Departments 2007.
- Chang DC, Knight V, Ziegfeld S, Haider A, Warfield D, Paidas C. The tip of the iceberg for child abuse: the critical roles of the pediatric trauma service and its registry. J Trauma 2004;57:1189-98.
- Pellai A, Sannino A, Ceratti F. Child abuse cases in the emergency room: a retrospective study. J Prev Med Hyg 1995;36:69-73.
- Knottnerus J, van Wheel C, Muris J. Evaluation of diagnostic procedures. BMJ 2002;324:477-80.
- Yamamoto LG, Wiebe RA, Matthews WJ. A one-year prospective ED cohort of pediatric trauma. Pediatr Emerg Care 1991;7:267-74.
- Shrivastava RJ. Non-Accidental Injuries 1988.
- Roberton DM, Barbor P, Hull D. Unusual injury? Recent injury in normal children and children with suspected non-accidental injury. Br Med J (Clin Res Ed) 1982;285:1399-401.
- Matrille L, Catteno C, Dorandeu A, Baccino E. A multicentre and prospective study of suspected cases of child physical abuse. Int J Legal Med 2006;120:73-8.
- Downing A, Rudge G. A study of childhood attendance at emergency departments in the West Midlands region. Emerg Med J 2006;23:391-3.
- Friedlaender E, Rubin DM, Alpern ER, Mandell DS, Christian CW, Alessandrini EA. Patterns of health care use that may identify young children who are at risk for maltreatment. Pediatrics 2005;116:1303-8.
- DiScala C, Sege R, Li GH, Reece RM. Child abuse and unintentional injuries – a 10-year retrospective. Arch Pediatr Adolesc Med 2000;154:16-22.
- Hamilton CE, Browne KD. Recurrent maltreatment during childhood: a survey of referrals to police and child protection units in England. Child Maltreat 1999;4:275-86.
- Lipien L, Forthofer MS. An event history analysis of recurrent child maltreatment reports in Florida. Child Abuse Negl 2004;28:947-66.
- Fluke JD, Yuan YYT, Edwards M. Recurrence of maltreatment: an application of the National Child Abuse and Neglect Data System (NCANDS). Child Abuse Negl 1999;23:633-50.
- Levy HB, Markovic J, Chaudhry U, Ahart S, Torres H. Reabuse rates in a sample of children followed for 5 years after discharge from a child-abuse inpatient assessment program. Child Abuse Negl 1995;19:1363-77.
- DePanfilis D, Zuravin SJ. Epidemiology of child maltreatment recurrences. Soc Serv Rev 1999;73:218-39.
- Fryer GE, Miyoshi TJ. A survival analysis of the revictimization of children: the case of Colorado. Child Abuse Negl 1994;18:1063-71.
- Jellinek MS, Murphy JM, Poitrast F, Quinn D, Bishop SJ, Goshko M. Serious child mistreatment in Massachusetts: the course of 206 children through the courts. Child Abuse Negl 1992;16:179-85.
- MacMillan HL, Thomas BH. Public health nurse home visitation for the tertiary prevention of child maltreatment: results of a pilot study. Can J Psychiatry 1993;38:436-42.
- Drake B, Jonson-Reid M, Way I, Chung S. Substantiation and recidivism. Child Maltreat 2003;8:248-60.
- Ferleger N, Glenwick DS, Gaines RR, Green AH. Identifying correlates of reabuse in maltreating parents. Child Abuse Negl 1988;12:41-9.
- MacMillan HL, Thomas BH, Jamieson E, Walsh HA, Boyle MH, Shannon HS, et al. Effectiveness of home visitation by public-health nurses in prevention of the recurrence of child physical abuse and neglect: a randomised controlled trial. Lancet 2005;365:1786-93.
- Quin G, Evans R. Accident and emergency department access to the child protection register: a questionnaire survey. Emerg Med J 2002;19:136-7.
- Flanagan NM, MacLeod C, Jenkins MG, Wylie R. The child protection register: a tool in the accident and emergency department?. Emerg Med J 2002;19:229-30.
- Department for Education and Skills . The Information and Sharing Assessment Index 2005. www.everychildmatters.gov.uk/_files/9AC3B0507A9BB06B054EC358D63FDE27.doc (accessed 1 January 2007).
- Department for Education and Skills . Learning from Information Sharing and Assessment Trail Blazers 2005. www everychildmatters.gov.uk.
- Gorin SD. A pilot study of child protection, family characteristics and physical punishment. London: NSPCC; 2002.
- Brandon M, Thoburn J, Rose S, Belderson P. Living with significant harm: a follow up study. London: NSPCC; 2005.
- Johnson A. A study of the outcomes of NSPCC child protection helpline referrals. London: NSPCC; 2003.
- MacMillan HL, Jamieson E, Walsh CA. Reported contact with child protection services among those reporting child physical and sexual abuse: results from a community survey. Child Abuse Negl 2003;27:1397-408.
- Brandon M, Howe D, Black J, Dodsworth J. Safeguarding Children With the Children Act 1989 1999.
- Trocmé N, MacLaurin B, Fallon B, Dacuik J, Billingsley D, Tourigny M, et al. Canadian Incidence Study of Reported Abuse and Neglect: Final Report 2001.
- Whiting P, Rutjes A, Dinnes J, Reitsma J, Bossuyt P, Kleijen J. Development and validation of methods for assessing the quality of diagnostic accuracy studies. Health Technol Assess 2004;8.
- Martin J, Williams K, Abrams K, Turner D, Sutton A, Chapple C, et al. Systematic review and evaluation of methods of assessing urinary incontinence. Health Technol Assess 2006;10.
- Trokel M, Waddimba A, Griffith J, Sege R. Variation in the diagnosis of child abuse in severely injured childern. Pediatrics 2006;117:722-8.
- Hobson MI, Evans J, Stewart IP. An audit of non-accidental injury in burned children. Burns 1994;20:442-5.
- Skellern CY, Wood DO, Murphy A, Crawford M. Non-accidental fractures in infants: risk of further abuse. J Paediatr Child Health 2000;36:590-2.
- Schwend RM, Werth C, Johnston A. Femur shaft fractures in toddlers and young children: rarely from child abuse. J Pediatr Orthop 2000;20:475-81.
- Benger J, McCabe S. Burns and scalds in pre-school children attending accident and emergency: accident or abuse?. Emerg Med J 2001;18:172-4.
- Miller LB, Fisher T, Sinclair I. Decisions to register children as at risk of abuse. Soc Work Soc Sci Rev 1993;4:101-18.
- Drake B. Associations between reporter type and assessment outcomes in child protective services referrals. Child Youth Serv Rev 1995;17:503-22.
- Kaufman KL, Rudy L. Future directions in the treatment of physical child abuse. Crim Justice Behav 1991;18:82-97.
- Rachamin E, Bull L, Hodes D. Audit of new referrals to Camden Social Services for child physical abuse over 12 months 2004–2005. London: University College Hospitals NHS Trust; 2005.
- Laming L. We owe it to Victoria’s memory. (Impact of new Green Paper Every child matters on the work of health and social services in protecting children from abuse). Community Care 2003;18:40-1.
- Department for Education and Skills . Common Assessment Framework Form 2005. www everychildmatters.gov.uk/resources-and-practice/TP00004/ (accessed 1 January 2007).
- Department of Health . Safeguarding Children: A Joint Chief Inspector’s Report on Arrangements to Safeguard Children 2002.
- Cleaver H, Walker S, Meadows P. Assessing children’s needs and circumstances: the impact of the assessment framework. London: Jessica Kingsley Publishers; 2003.
- Wright I, Epstein E, HIkmet F, Hodes D. Improving the Involvement of GPs at Initial Child Protection Case Conferences in an Inner City Borough: An Audit n.d.
- Bethea L. Primary prevention of child abuse. Am Fam Physician 1999;59:1577-2.
- Browne K. Preventing child maltreatment through community nursing. J Adv Nurs 1995;21:57-63.
- DePanfilis D, Zuravin SJ. The effect of services on the recurrence of child maltreatment. Child Abuse Negl 2002;26:187-205.
- Fryer GE, Miyoshi TJ. The role of the environment in the etiology of child maltreatment. Aggress Violent Behav 1996;1:317-26.
- Hamilton CE, Falshaw L, Browne KD. The link between recurrent maltreatment and offending behaviour. Int J Offender Ther Comp Criminol 2002;46:75-94.
- Kibayashi K, Shojo H. Patterned injuries in children who have suffered repeated physical abuse. Pediatrics Int 2003;45:193-5.
- Nobes G, Smith M. Family structure and the physical punishment of children. J Fam Iss 2002;23:349-73.
- Taitz J, Moran K, O’Meara M. Long bone fractures in children under 3 years of age: is abuse being missed in emergency department presentations?. J Paediatr Child Health 2004;40:170-4.
- Nobes G, Smith MA. Physical punishment of children in two parent families. Clin Child Fam Psychol Rev 1997;2:271-81.
- Newson J, Newson E. The extent of physical punishment in the UK. London: APPROACH; 1989.
- Reigstad B, Jorgensen K, Wichstorm L. Diagnosed and self-reported childhood abuse in national and regional samples of child and adolescent pyschiatric patients: prevalences and correlates. Nord J Psychiatry 2006;60:58-66.
- MacMillan HL, Fleming JE, Trocmé N, Boyle MH, Wong M, Racine YA, et al. Prevalence of child physical and sexual abuse in the community. Results from the Ontario Health Supplement. JAMA 1997;278:131-5.
- Millichamp J, Martin J, Langley J. On the receiving end: young adults describe their parents’ use of physical punishment and other disciplinary measures during childhood. NZ Med J 2006;119.
- Scher CD, Forde DR, McQuaid JR, Stein MB. Prevalence and demographic correlates of childhood maltreatment in an adult community sample. Child Abuse Negl 2004;28:167-80.
- Briere J, Elliott DM. Prevalence and psychological sequelae of self-reported childhood physical and sexual abuse in a general population sample of men and women. Child Abuse Negl 2003;27:1205-22.
- Cawson P, Wattam C, Brooker S, Kelly G. Child maltreatment in the United Kingdom: a study of the prevalence of child abuse and neglect. London: NSPCC; 2000.
- Carlin AS, Kemper K, Ward NG, Sowell H, Gustafson B, Stevens N. The effect of differences in objective and subjective definitions of childhood physical abuse on estimates of its incidence and relationship to psychopathology. Child Abuse Negl 1994;18:393-9.
- Sack WH, Mason R, Higgins JE. The single-parent family and abusive child punishment. Am J Othorpsychiatry 1985;55:252-9.
- McGuigan WM, Pratt CC. The predictive impact of domestic violence on three types of child maltreatment. Child Abuse Negl 2001;25:869-83.
- Croft R. Evidence that doctors often fail to diagnose child abuse and neglect. Stevenage: East and North Hertfordshire NHS Trust; 2006.
- Paradise JE, Bass J, Forman SD, Berkowitz J, Greenberg DB, Mehta K. Minimum criteria for reporting child abuse from health care settings. Del Med J 1997;69:357-63.
- Benzel E, Hadden T. Neurological manifestations of child abuse. South Med J 1989;82:1347-51.
- Sinclair R, Bullock R. Learning from past experience – a review of serious case reviews. London: Department of Health; 2002.
- Chester DL, Jose RM, Aldlyami E, King H, Moiemen NS. Non-accidental burns in children – are we neglecting neglect?. Burns 2006;32:222-8.
- Department for Education and Skills . Child in Need in England: Preliminary Results of a Survey of Activity and Expenditure As Reported by Local Authority Social services’ Children and Families Teams for a Survey Week in Feburary 2005 2005. www.dfes.gov.uk/rsgateway/DB/SFR/s000620/SFR52-2005.pdf (accessed 1 May 2007).
- Department for Education and Employment, Home Office . Framework for the Assessment of Children in Need and Their Families 2000. www.archive.official-documents.co.uk/document/doh/facn/fw-02%20htm#2.13 (accessed 12 February 2007).
Appendix 1 Additional material on search methods and results relating to Chapter 3
The searches involved six different strategies:
-
Scoping search (186 papers)
-
Protocol-based search of MEDLINE (6880 papers):
-
Step 1. Focused search (4130 papers including duplicates)
-
Step 2. Generation of large RevMan database
-
-
NSPCC library search (492 papers)
-
Targeted search (1052 papers):
-
Step 1. Forward citation search
-
Step 2. Articles sharing same references using Web of Science
-
Step 3. PubMed ‘related articles’
-
Step 4. Cross-database search
-
-
Snowballing and hand searching (577 papers)
-
Update search of key journals (7 papers).
Further details are reported in the following sections for some of these methods.
Scoping search (method 1)
The scoping search was carried out by MH in August 2004. The sources and terms used are listed in Table 22.
| Databases | Search formulation |
|---|---|
| National Electronic Library for Health (NeLH) guidelines finder (URL: www.library.nhs.uk/guidelinesfinder/). All sites under international guidelines | ((non-accidental injury) OR (child abuse) OR (physical abuse) OR (maltreatment)) AND (accident OR injury OR (accident and emergency)) |
| MEDLINE Plus (URL: http://medlineplus.gov/) | For Cochrane Library revised to: (physical abuse) OR (child abuse) OR (neglect) OR (maltreatment) OR (torture) OR (Violence) OR (accident) OR (injury) OR (wound) OR (bruis) OR (burn) OR (scald) OR (fracture) OR (trauma) OR (bite) |
| Turning Research Into Practice database (URL: www.tripdatabase.com/index.html) | |
| Cochrane Library (with a CRD filter to limit to reviews) (URL: www.thecochranelibrary.com) | |
| Other sites searched: | |
| Campbell Collaboration database (URL: www.campbellcollaboration.org/index.asp) | |
| US National Guidelines Clearing House (URL: www.guideline.gov/) | |
| Child Welfare Information Gateway, Children’s Bureau, Administration for Children and Families, US Dept of Health and Human Services (URL: www.childwelfare.gov/) | |
| Criminal Justice Abstracts (URL: www.ncjrs.gov/abstractdb/Search.asp) | |
Protocol-based search of MEDLINE (method 2)
Step 1: A search was carried out on MEDLINE on 24 October 2005. Terms are listed in Table 23. Concepts were combined as: ((Child AND abuse)) AND social-services AND (prevalence-study OR substantiated OR retrospective OR (retrospective-study AND A&E)) OR A&E) OR (child AND repeated).
| Concept | Free text terms | MeSH terms |
|---|---|---|
| Child | child* | child# |
| baby, babies | adolescent | |
| newborn, neonat* | infant# | |
| infant* | pediatrics | |
| toddler* | ||
| teenage* | ||
| juvenile* | ||
| adolescent* | ||
| young people | ||
| youngster*, youth* | ||
| kid* | ||
| offspring* | ||
| paediatric, pediatric | ||
| Abuse | neglect | child-abuse |
| (child/physical) abuse | child-welfare | |
| maltreat* | violence | |
| violent* | mandatory-reporting | |
| torture | aggression | |
| domestic violence | domestic-violence | |
| deliberate/abusive injur* | ||
| shaken baby syndrome | ||
| munchausen syndrome by proxy | ||
| Social-services | social service/s | social-work |
| social support | social-welfare | |
| social work | child-welfare | |
| social welfare | infant-welfare | |
| hospital social work department | social-work-department-hospital | |
| mandatory reporting | mandatory-reporting | |
| child protection | child-abuse | |
| child (abuse/neglect/maltreat*/mistreat*) (investigat*/assess*) | child-advocacy | |
| Prevalence-study | case control study/ies | risk-assessment |
| cohort study/ies | mass-screening | |
| case series study/ies | epidemiologic-studies | |
| cross section* study/ies | case-control-studies | |
| population based study/ies | cohort-studies | |
| epidemiol* | cross-sectional-studies | |
| incidence prevalence | ||
| prevalence | ||
| Retrospective-study | retrospective question* | questionnaires |
| retrospective | risk-assessment | |
| A&E | accident AND emergency | emergency-service-hospital |
| casualty | emergency-services | |
| triage | emergency-treatment | |
| accident emergency department | emergency-nursing | |
| accident emergency | emergency-medicine | |
| emergency room | triage | |
| emergency medical service/s | trauma-centers | |
| emergency health centre/s | ||
| trauma centre/s | ||
| Repeated | previous/repeated child abuse | |
| previous/repeated physical abuse | ||
| reinjur*/re-injur* | ||
| reabuse*/re-abuse* | ||
| reattend*/re-attend* | ||
| rereferr*/re-referr* | ||
| subsequent abuse/injur*/referr* | ||
| previous abuse/injur*/referr* | ||
| further abuse/injur*/referr* | ||
| second abuse/injur*/referr* | ||
| prior abuse/injur*/referr* | ||
| multiple incidents of abuse | ||
| repeat/multiple victimization |
Step 2: We generated a large database of 14,000 records using the terms listed in Table 24. The concepts were combined as follows: (Abuse(revised) OR injury(revised)) AND (study-type(revised) OR study-type2(revised)).
| Concept | Terms |
|---|---|
| Abuse (revised) | ((non-accidental[All Fields] AND (“injuries”[Subheading] OR (“wounds and injuries”[TIAB] NOT Medline[SB]) OR “wounds and injuries”[MeSH Terms] OR injuries[Text Word])) OR (“child abuse”[MeSH Terms] OR child abuse[Text Word]) OR (“battered child syndrome”[MeSH Terms] OR battered child syndrome[Text Word])) |
| Injury (revised) | (((injur[ti] OR injure[ti] OR injured[ti] OR injured/infected[ti] OR injured/regenerating[ti] OR injured’s[ti] OR injureis[ti] OR injurer[ti] OR injurers[ti] OR injures[ti] OR injurie[ti] OR injuried[ti] OR injurier[ti] OR injuries[ti] OR injuries/diseases[ti] OR injuries/general[ti] OR injuries/hepatitis[ti] OR injuries/illness[ti] OR injuries’[ti] OR injuriesat[ti] OR injurin[ti] OR injuring[ti] OR injurious[ti] OR injuriousness[ti] OR injuris[ti] OR injurles[ti] OR injurof[ti] OR injurous[ti] OR injurt[ti] OR injurues[ti] OR injury[ti] OR injury/choosing[ti] OR injury/contamination[ti] OR injury/disorders[ti] OR injury/immune[ti] OR injury/lipopolysaccharide[ti] OR injury/neural[ti] OR injury/spina[ti] OR injury’[ti] OR injurying[ti] OR injuryproducing[ti]) OR (violence[ti] OR violence/lesions[ti] OR violence/therapist[ti] OR violence/threat[ti] OR violence’[ti] OR violencia[ti] OR violene[ti] OR violens[ti] OR violent[ti] OR violent/destructive[ti] OR violent’[ti] OR violently[ti] OR violentum[ti])) |
| Child (revised) | (child[ti] OR child/elderly[ti] OR child/pet[ti] OR child’[ti] OR child’s[ti] OR child’stalk[ti] OR childbearers[ti] OR childbearing[ti] OR childbed[ti] OR childbirt[ti] OR childbirth[ti] OR childbirth/parenthood[ti] OR childbirth’[ti] OR childbirthing[ti] OR childbirths[ti] OR childblains[ti] OR childbood[ti] OR childbrith[ti] OR childcare[ti] OR childcare’s[ti] OR childcaring[ti] OR childe[ti] OR childed[ti] OR childeen[ti] OR childen[ti] OR childen’s[ti] OR childeren[ti] OR childern[ti] OR childers[ti] OR childes[ti] OR childfeeding[ti] OR childfile[ti] OR childfree[ti] OR childhealth[ti] OR childhhod[ti] OR childhod[ti] OR childhodd[ti] OR childhold[ti] OR childhoo[ti] OR childhood[ti] OR childhood/congenital[ti] OR childhood/early[ti] OR childhood’[ti] OR childhood’s[ti] OR childhoods[ti] OR childhoof[ti] OR childhoofd[ti] OR childhool[ti] OR childhoold[ti] OR childhoood[ti] OR childhoos[ti] OR childhren[ti] OR childia[ti] OR childish[ti] OR childishness[ti] OR childism[ti] OR childlen[ti] OR childless[ti] OR childlessness[ti] OR childlike[ti] OR childline[ti] OR childminders[ti] OR childminders’[ti] OR childminding[ti] OR childmother[ti] OR childness[ti] OR childnood[ti] OR childonium[ti] OR childood[ti] OR childparent[ti] OR childproof[ti] OR childproofing[ti] OR childproofing’[ti] OR childpsychiatric[ti] OR childre[ti] OR childreach[ti] OR childrearing[ti] OR childred[ti] OR childrelationships[ti] OR childrem[ti] OR children[ti] OR children/les[ti] OR children/national[ti] OR children/youngsters[ti] OR children/yourself[ti] OR children’[ti] OR children’s[ti] OR children’s/tertiary[ti] OR children’s’[ti] OR children’scatalgine[ti] OR childrenae[ti] OR childrenand[ti] OR childrenduring[ti] OR childrenese[ti] OR childrenin[ti] OR childreninterview[ti] OR childrens[ti] OR childrens’[ti] OR childrens’s[ti] OR childrensuspected[ti] OR childreq[ti] OR childress[ti] OR childrn[ti] OR childrn’s[ti] OR childrne[ti] OR childrren[ti] OR childs[ti] OR childs’[ti] OR childsafe[ti] OR childsaving[ti] OR childsight[ti] OR childspacing[ti] OR childsubtotal[ti] OR childwatch[ti])) |
| Study-type (revised) | ((“diagnosis”[Subheading] OR “diagnosis”[MeSH Terms] OR diagnosis[Text Word]) OR (“statistics”[MeSH Terms] OR statistics[Text Word]) OR (“classification”[Subheading] OR “classification”[MeSH Terms] OR classification[Text Word]) OR (“registries”[MeSH Terms] OR registries[Text Word]) OR (“epidemiology”[Subheading] OR “epidemiology”[MeSH Terms] OR epidemiology[Text Word]) |
| Study-type 2 (revised) | (cohort[All Fields] OR follow-up[All Fields] OR case-control[All Fields] OR retrospective[All Fields] OR longitudinal[All Fields] OR cross-sectional[All Fields] OR “epidemiologic studies”[MeSH Terms] OR epidemiologic studies[Text Word])) |
The results were imported into a RevMan database and searched using the following terms: school OR police OR NSPCC; OR (health AND visitor) OR (GP OR general AND practitioner) OR (social AND work*) (1173 references identified). Additional keyword searches identified a further 1586 references: Missed diagnosis, Emergency[ti], Recurrence, Social work, Primary care, Detect*[ti], “registries” [MeSH terms], “registries” [MeSH terms] AND Great Britain, “registries” [MeSH terms] AND North America, Validat*[ti], “[predictive value of tests” [MeSH terms], “longitudinal studies” [MeSH terms], Temporal correlates.
Targeted search (method 4)
The targeted methods cannot be reproduced because of the continual publication of new material (and therefore changing hierarchy of relevancy) and judgement involved in selecting relevant papers. One limitation of this method is that, given our understanding of the literature after completing the study, our ‘gold standard’ papers would be different now to those selected at the time of the search.
Targeted search step 1: forward citation search. We used the Web of Knowledge search engine to identify subsequent papers that cited each of 16 ‘gold standard’ papers (listed in Table 25; Figure 15, item C). Figure 15 shows the search record for the first of the gold standard papers. We clicked on ‘times cited’ (labelled C) to view all studies that had referenced gold standard paper 1. All of these papers were added to our ‘marked’ list in preparation for exporting them to the RevMan database at a later stage.
| Gold standard papers: first author, place, year of publication | Web of Science | PubMed | ||
|---|---|---|---|---|
| Column 1: ‘cited treferences’ | Column 2: ‘related records’a | Column 3: ‘related articles’b | Column 4: search formulation used to identify additional papersc | |
| 1. Benger, UK, 200221 | 7 | 6 (10–2) | 364 (30) | (detection[ti] OR emergency[ti] OR improve[ti]) and abuse and (review or trial) (13) |
| 2. Bethea, USA, 1999145 | 7 | 6 (39–4) | 462 (62) | Primary prevention[ti] and abuse (15) |
| 3. Browne, UK, 1995146 | 12 | 9 (37–3) | 481 (83) | nursing and abuse and review (8) |
| 4. Chang, USA, 200498 | 3 | 1 (12–8) | 105 (108) | review AND abuse (10) |
| 5. DePanfilis, USA, 2002147 | 8 | 10 (42–4) | 176 (136) | (recurren* OR repeat* or recidivism) and abuse (19) |
| 6. Flanagan, USA, 2002120 | 0 | 4 (6–1) | 151 (55) | (regist*[ti] or protect*[ti] or document*[ti] or identify[ti]) and abuse (15) |
| 7. Fryer, USA, 19968 | 21 | 2 (7–2) | 149 (178) | (survival analysis OR population Surveillance) and abuse (15) |
| 8. Hamilton, UK, 2002149 | 0 | 37 (76–5) | 144 (208) | (offen* [ti] or behavior or prisoners) and abuse and (review OR follow-up OR cohort) (14) |
| 9. Jayawant, UK 199876 | 56 | 56 (23–4) | 322 (239) | (haemorrhage or head injuries) and (abuse OR non-accidental) AND review (20) |
| 10. Keshavarz, USA, 200263 | 2 | 8 (2–2) | 1590 (262) | (emergency[ti] or acute[ti] or burn*[ti]) and abuse and review (23) |
| 11. Kibayashi, USA, 2003150 | 1 | 47 (7–1) | 232 (291) | (pattern*[ti] or injur*[ti]) and (abuse or shaken-baby) AND review (11) |
| 12. Levy, USA, 1995111 | 21 | 40 (37–2) | 104 (299) | [not ‘first 20’] abuse and (reabuse or recurrence or time factors) (12) |
| 13. MacMillan, Canada, 2003126 | 0 | 30 (20–3) | 685 (355) | (child welfare OR social services) and abuse and review (47) |
| 14. Sidebotham, UK, 199722 | 7 | 4 (3–1) | 214 (369) | (medical audit OR risk) and abuse and (review OR follow-up) (8) |
| 15. Skellern, Australia, 2000133 | 7 | 29 (11–2) | 255 (395) | (fractures or recurrence or risk[ti]) and abuse and (review) (33) |
| 16. Taitz, Australia, 2004152 | 3 | 66 (31–4) | 2363 (414) | (fracture*[ti] OR Miss*[ti] or emergency[ti]) and abuse and review (37) |
| Total | 155 | 306 | 414 | |
FIGURE 15.
Web of Science record for targeted search method.
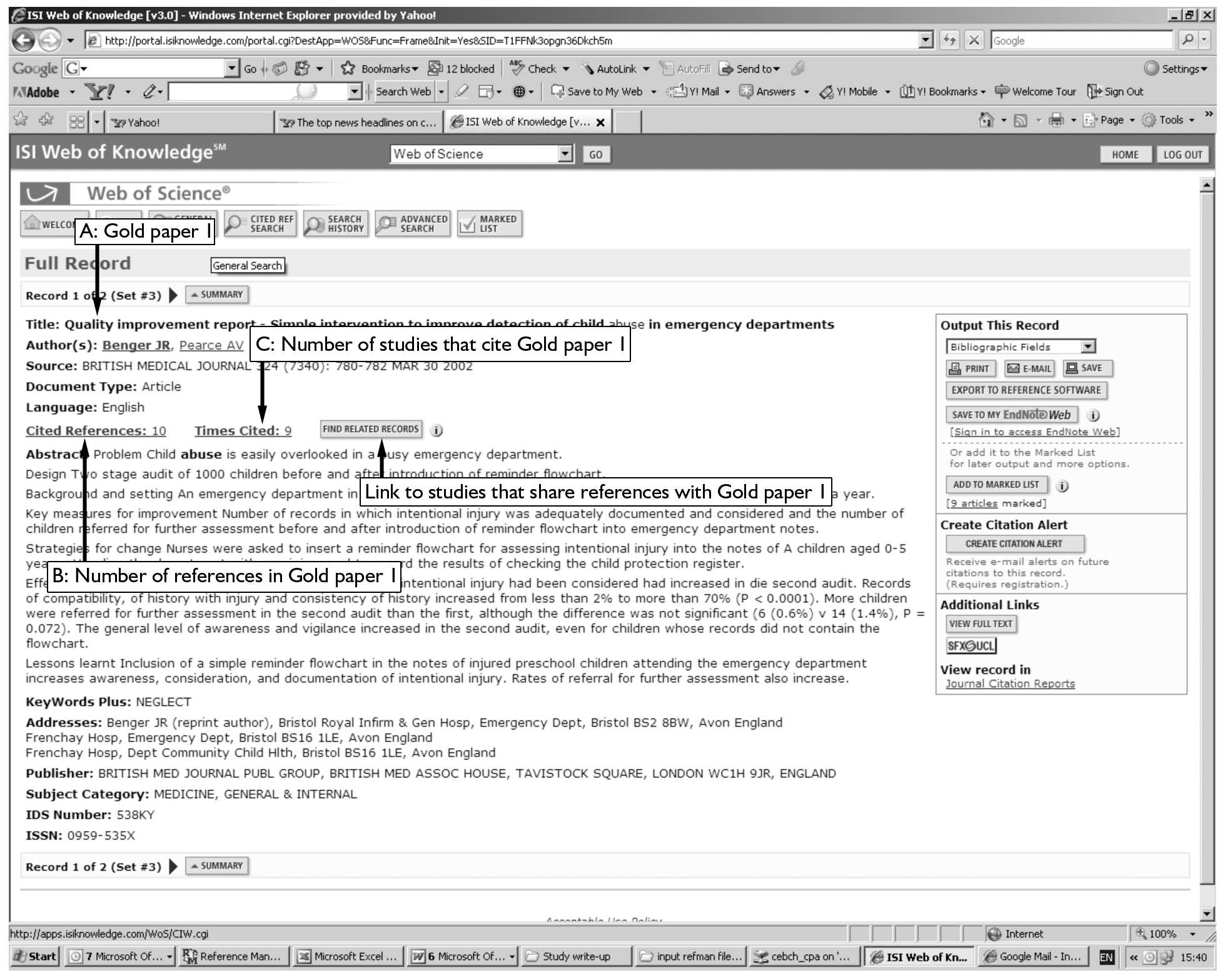
Targeted search step 2: articles sharing the same references. We clicked on ‘related records’ (labelled D in Figure 15) to view studies that shared at least one reference with gold standard paper 1. The list of studies is displayed in Figure 16 (labelled E) with the most relevant, that with the highest number of shared references, listed first. The cut-off for the number of shared references was judged by the researcher and is shown for each gold standard paper as the final number in column 2 of Table 25.
FIGURE 16.
Targeted search step 2: identification of articles with shared references using the Web of Science search engine.
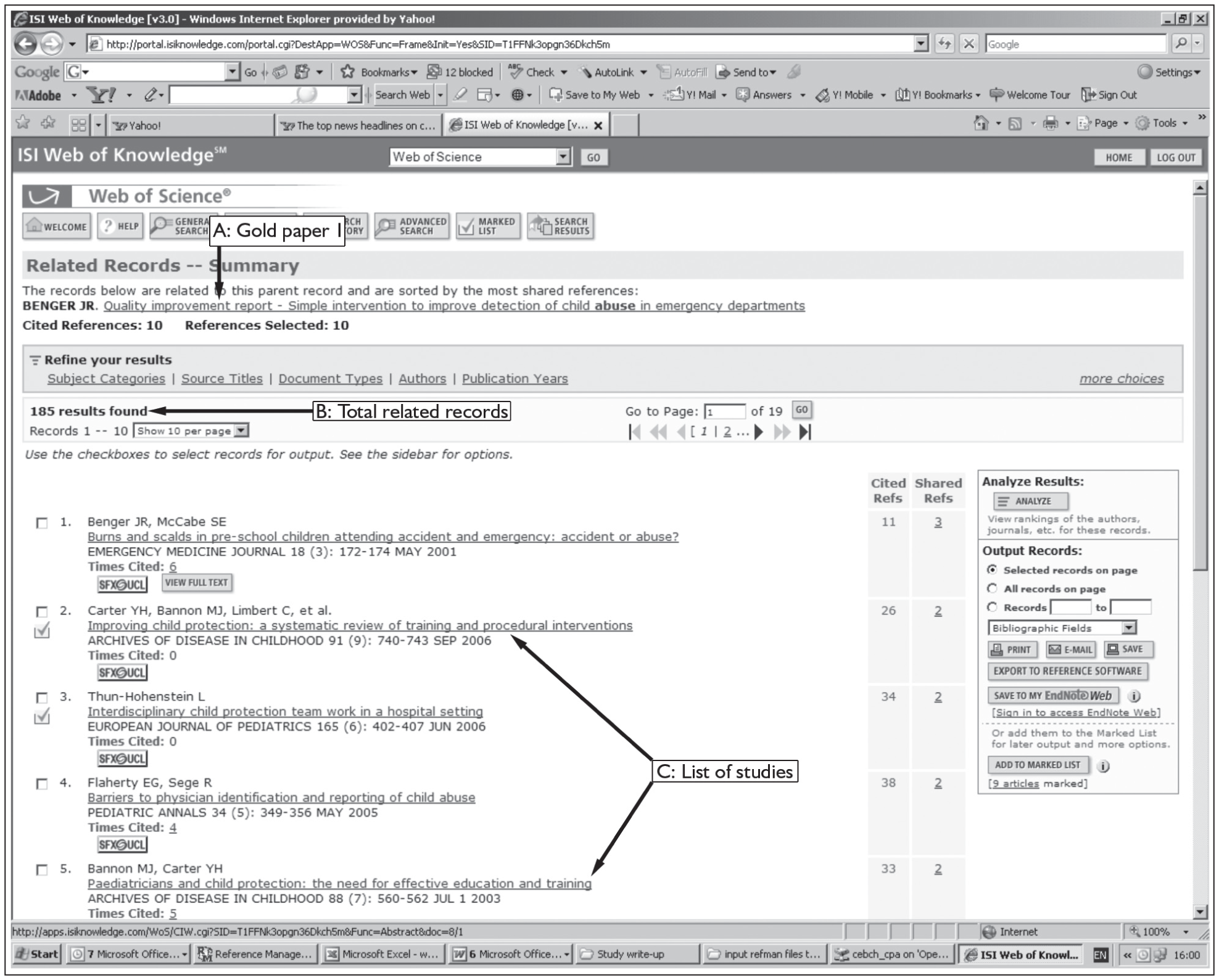
Targeted search step 3: PubMed ‘related articles’. The ‘related articles’ algorithm on PubMed identifies papers that share MeSH terms and text words with the gold standard paper. We located each gold standard article on PubMed and then clicked on related articles (Figure 17). Usually about 100 or more references are listed, which are ranked by level of relatedness. This number is shown in column 3 of Table 25 (first number). We routinely downloaded the first 20 related articles. Each set of related articles was then transferred to the clipboard and searched using a specific search formulation (column 4, Table 25) for references not among the first 20 references. The additional articles were then added to the first 20 (column 3, second number, Table 25). These methods identified an additional 414 unique records.
FIGURE 17.
Targeted search step 3: PubMed ‘related articles’.
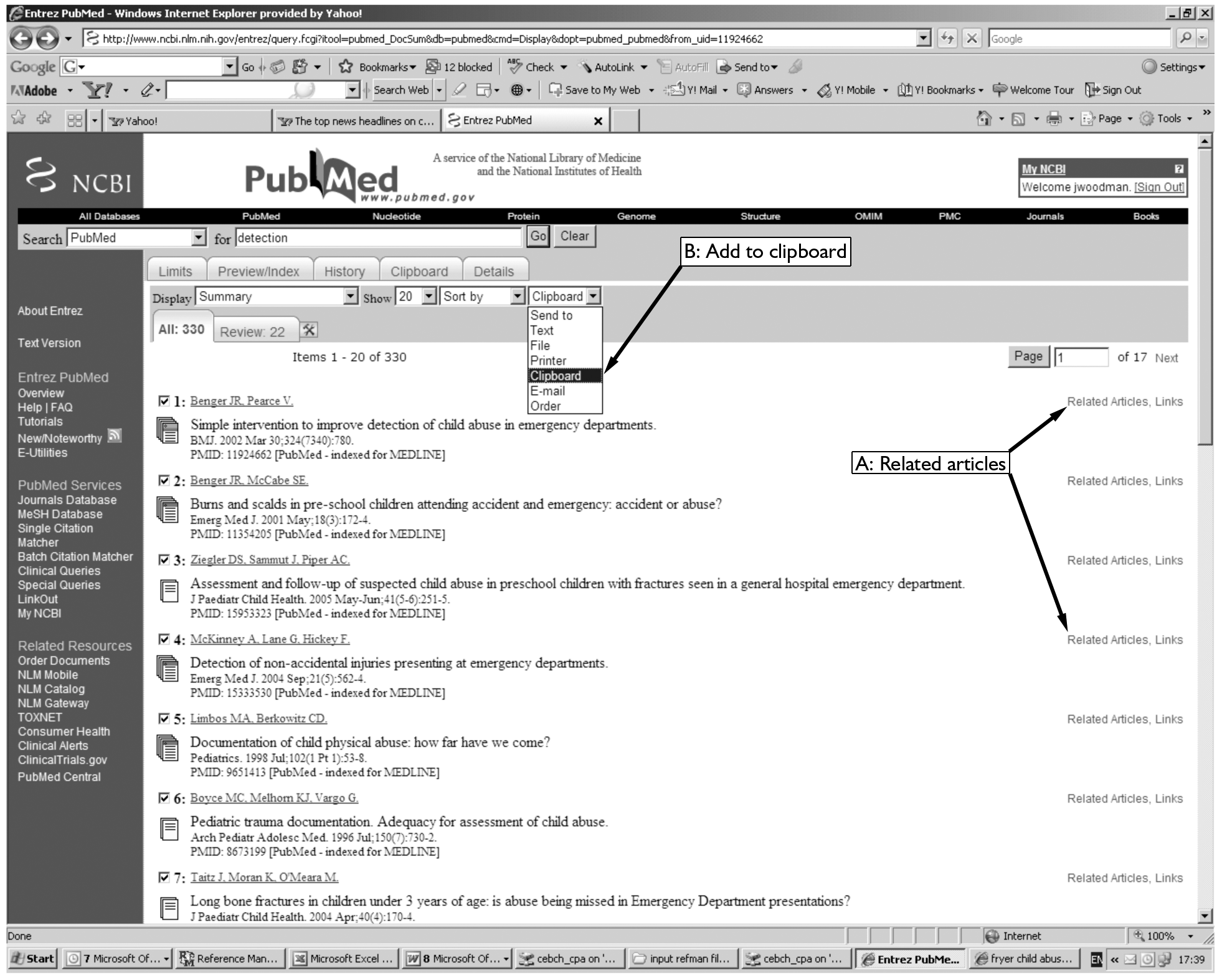
Targeted search step 4: Cross-database search – articles sharing the same references. We searched MEDLINE and five other databases on 19 October 2005 [Department of Health database (DH-Data), EMBASE, PsychInfo, British Nursing Index and the Cumulative Index to Nursing and Allied Health (CINAHL) database]. The search terms, shown in Table 26, were designed to complement the MEDLINE protocol search.
| Search formulation | Number of records |
|---|---|
| (child or children or infant or infants).ti. and (abuse or maltreatment or mistreatment or non-accidental).ti. and (social work or social worker or social service or social services).ti. | 116 |
| (child or children or infant or infants).ti. and (abuse or maltreatment or mistreatment or non-accidental).ti. and (referral or referrals or referred).ti. | 41 |
| (child or children or infants or infant).ti. and (abuse or maltreatment or mistreatment or non-accidental).ti. and (missed or error or erroneous or truly or mistake).ti. | 9 |
| (child or children or infant or infants).ti. and (abuse or maltreatment or mistreatment or non-accidental).ti. and (emergency or casualty or A E).ti. | 80 |
| (child or children or infant or infants).ti. and (abuse or maltreatment or mistreatment or non-accidental).ti. and (screening or screened or test or tests).ti. | 60 |
| (child or children or infant or infants).ti. and (abuse or maltreatment or mistreatment or non-accidental).ti. and (recur or recurrence or recurrent or again or re-admitted or repeat or repeated).ti. | 35 |
Appendix 2 Additional material on the burden of abuse: systematic review 1
We included any study that measured the prevalence of one or more episodes of severe violence during childhood. Severe violence included hitting with an object, punching, kicking, biting or worse. Results are shown in Table 27.
| First author, country, date of publication | Population and methods | Physically abused/total (%) |
|---|---|---|
| Studies based on parental reports | ||
| Nobes, UK, 2002151 | Single mothers, children < 12 years. Methods as Nobes153 | 10/57 (17.5%) |
| Nobes, UK,1997153 | Two-parent families with children < 12 years, parents interviewed separately at home about child punishment. Definition of abuse is hit with implement | 20/99 (20.0%) |
| Newson, UK, 1989154 | A total of 700 mothers interviewed at home about child discipline for ages 1, 4, 7, 11 and 16 years (1985) | 154/700 (22.0%) |
| Self-reports | ||
| May-Chahal, UK, 200540 | Young adults (14–18 years) sampled using census data, interviewed face-to-face on many aspects of childhood. Response rate 69% | 201/2869 (7.0%) |
| Reigstad, Norway, 2006155 | Psychiatric outpatients 12–18 years, 2001–2. Written questionnaire | 40/118 (33.9%) |
| Youssef, Egypt, 199859 | A total of 2170 school students 10–20 years completed written questionnaire. Physical abuse defined as injured | 210/2170 (9.7%) |
| MacMillan, Canada, 1997156 | Ontario residents > 15 years, face-to-face interview in 1990. A total of 2629 reported ‘minor’ violence over childhood (26.6%) | 997/9953 (10.0%) |
| Nelson, USA, 199543 | School students 14–18 years in 25 schools across Atlanta completed a written questionnaire. A total of 82% responded but 25% did not answer physical abuse questions | 550/1957 (28.1%) |
| Berrien, Russia, 199558 | School students 11–16 years, intellectually gifted but (often) socially disadvantaged. Written questionnaire | 108/375 (28.9%) |
| Sariola, Finland, 199242 | School students 14–15 years, classes randomly sampled. Written questionnaires, response rate 96%. Reports of minor violence in 71.9% (5223/7264) | 559/7264 (7.7%) |
| Retrospective self-reports | ||
| Millichamp, New Zealand, 2006157 | Adults 26 years from Dunedin longitudinal cohort. Face-to-face interviews in 1988–9. A total of 431 reported minor violence (44.8%) | 282/962 (29.3%) |
| Scher, USA, 2004158 | Residents of Memphis/Tennessee 18–65 years. Telephone interviews, 1997 | 234/1007 (23.2%) |
| Briere, Canada, 2003159 | US residents 18–90 years. Written questionnaire | 196/935 (20.9%) |
| Cawson, UK, 2000160 | Random sample of adults 18–24 years interviewed by telephone. A total of 402 reported minor violence (14%) | 201/2869 (7.0%) |
| Carlin, USA 1994161 | Women 18 years or over, English speaking at a university-based family medicine clinic, selected from waiting room. Response rate 82.1%; 32 also self-defined physical abuse over childhood (11.4%) | 79/280 (28.2%) |
| Berger, USA, 198889 | A total of 4695 students at Iowa University. Written questionnaire | 568/4695 (12.1%) |
| Sack, USA, 1985162 | A total of 805 Oregon residents > 18 years. Face-to-face interview in 1978 | 48/805 (6.0%) |
| Official state/agency statistics | ||
| McGuigan, USA, 2001163 | Non-accidental injury confirmed by child protective services in children who were part of the Healthy Start initiative in 1992. Children aged between 1 month and 38 months at time of confirmed abuse | 25/2544 (1.0%) |
Appendix 3 Additional material on the performance of the clinical screening assessment: systematic review 9
| Assessment criteria | Studies evaluated | ||
|---|---|---|---|
| Oral 200382 | Brown 200372 | Pless 198765 | |
| 1. Was the spectrum of patients representative of the patients who will receive the test in practice? | No | No | No |
| 2. Were selection criteria clearly described? | No | No | No |
| 3. Is the reference standard likely to correctly classify the condition? | No | No | No |
| 4. Is the time period between reference standard and index tests short enough? | Yes | Yes | Yes |
| 5. Did the whole sample or a random selection of the sample receive verification using a reference standard? | No | No | No |
| 6. Did patients receive the same reference standard regardless of the index test results? | No | No | No |
| 7. Was the reference standard independent of the index test? | No | No | No |
| 8. Was the execution of the (a) index test and (b) reference standard test described in sufficient detail to permit replication of the tests? | (a) No; (b) No | (a) No; (b) No | (a) No; (b) No |
| 9. (a) Were the index test results interpreted without knowledge of the results of the reference standard? (b) Was the reference test interpreted without knowledge of the results of the index test? | (a) Unclear; (b) No | (a) Unclear; (b) No | (a) Unclear; (b) No |
| 10. Were the same clinical data available when test results were interpreted as would be available when the test is used in practice? | Yes | Yes | No |
| 11. Were uninterpretable/intermediate test results reported? | Unclear | Unclear | Unclear |
| 12. Were withdrawals from the study explained? | Unclear | Unclear | Unclear |
| First author, country, year of publication | Methods and reason for exclusion | Sensitivity |
|---|---|---|
| Croft, UK,164 unpublished | Case series of referrals to social services for abuse. Excluded as delayed referrals not systematically ascertained and no ascertainment of non-referrals. Denominator estimated | Delayed/all referrals: 108/134 (80.6%) |
| Expert opinions (elicited 2006) | Estimated | |
| Designated doctor for child protection | 98–99% | |
| Child protection named nurse | 21/25 (84%) – 27/30 (90%) | |
| Consultant in paediatric emergency medicine | 20/25 (80%) – 45/50 (90%) | |
| A&E consultant | One case missed in 5 years’ experience | |
| Paediatric registrar | ‘Very very few’ missed | |
| Community paediatrician (very experienced) | 67% | |
| Paradise, USA, 1997165 | Hospital records of children with confirmed abuse analysed for likely abuse/not. Excluded as subsample of all referred children | Previous referral/all likely previous abuse: 10/25 (40%) |
| Benzel, USA, 1989166 | Children < 6 years referred to social services for inflicted head injury who had previous hospital visits (1982–6; n = 23). Excluded as analysed subsample with multiple hospital visits | Previous referral/previous visits: 0/9 |
| Chang, USA, 200564 | Analysis of 447 children with abuse diagnosis on hospital database. Positive score on the SIPCA screening tool applied retrospectively to medical notes. Excluded as assumes 100% sensitivity of abuse detection in paediatric centres and constant prevalence of abuse across centres (1.24%) | Adult/adult and paediatric centres: 158/264 (59.8%); non-trauma centres: 220/392 (56.1%) |
| Sinclair, UK, 2002167 | Analysis of sample of 40 serious case reviews (Part 8 reviews; 1998 and 2001) (n = 20). Excluded as involvement with A&E noted but no clearly defined test evaluated | 9/40 children had been ‘involved’ with A&E in the 2 years prior to their Part 8 review (two had ‘substantial’ involvement) |
Appendix 4 Additional material on unpublished studies
London Metropolitan Police30
The London Metropolitan Police Child Abuse Investigation Command and Performance Analysts extracted data in October 2006 on children (under 16 years) reported in 2005 with physical abuse or assault (5395 reported and 4142 reports confirmed). 30 A total of 80% of cases were assault or abuse by ‘parent’ perpetrators (see column 1 in Table 30). Data were recorded at the time of the abuse report by the officer assessing the case. The total denominator was approximately 7,200,000 (including adults) and we estimated the proportion under 16 years using census data for London in 2002. 168
| Categories included in ‘parent’ perpetrator | Other categories |
|---|---|
| Parent(s) | Sibling(s) |
| Parent(s) and step-parents/partners | Sibling(s) and other |
| Parent(s) and sibling(s) | Care provider |
| Parent(s) and foster parent(s) (including ex) | Other childcare |
| Parent(s) and other | Other childcare and other |
| Parent(s) and other childcare | Teacher |
| Parent(s) and other family | Teacher and other |
| Step-parents/partners | School worker |
| Step-parents/partners and other | Unrecorded |
| Step-parents/partners and other family | Other |
| Sibling(s) and other family | |
| Sibling(s) and step-parents/partners | |
| Other family | |
| Other family and foster parent(s) (including ex) | |
| Other family and other | |
| Other family and other childcare | |
| Foster parent(s) (including ex) |
We classified injuries reported as moderate, serious or fatal as requiring medical attention based on discussion with the Metropolitan Police. We recategorised the data on reporting source into five simplified categories (Table 31).
| Simplified category | Police categorisation of reporting source |
|---|---|
| Individuals | Telephone call made to police building other than information room |
| Telephone call made to information room | |
| Reported direct to officer on duty and away from station | |
| Reported by person calling at police building | |
| Initial detail taken by telephone crime recording unit | |
| Received from third-party report sites | |
| Education | Reported to police by school, education authority |
| Social services | Reported to police by social services |
| Health | Reported to police by doctor, hospital, etc. |
| Police | Reported by other means, e.g. letter, prisoner already in custody |
| Referred by police to Child Abuse Investigation Command | |
| Discovered by police | |
| Automatic alarm message to security organisation | |
| Automatic alarm message to information room |
Audit of Hammersmith and Fulham Social Services initial assessments32
We audited initial assessments in one of two centres in the London Borough of Hammersmith and Fulham Social Services Department. The children’s services team identified children (under 18 years) who had an initial assessment during 3 months in 2005 from the database of referrals. They identified 181 children, retrieved 132 complete files and printed out limited data from initial assessment forms from an electronic database of a further 21 children. We audited 153/181 initial assessments (missing data 15.4%).
We extracted data on the primary reason for the initial assessment and captured any other ‘mention’ of physical violence to the child from the parent or carer. We used the ‘reason for referral’ on the initial assessment referral form to identify the primary reason for assessment. The whole paper file was scanned for any mention of violence in the household, which was categorised as current (within 6 months of initial assessment) or previous (more than 6 months before the initial assessment), and by perpetrator. We reported results only for parental or carer violence. We defined violence as any recorded aggressive physical contact between the parent or carer and child. Consequently, the ‘violence’ we report ranges form slaps, pinches and hair pulling to high levels of physical abuse such as throwing an infant. Data on ‘previous’ violence were not available in the 21 cases without full paper files.
Audit of referrals to Camden Social Services for physical abuse139
We audited case notes of 59 children from 26 families referred for physical abuse to one centre in Camden during 12 months (2004–5). A further 10 files were not available. All referrals underwent an initial assessment. In total, 29/59 children were victims of abuse, rather than the siblings of victims. We analysed 26 index cases, one for each family. The source of the initial referral was extracted from records.
Appendix 5 Additional material (relevant to discussion)
| First author, region, year of publication | Methods | % of referrals for physical abuse |
|---|---|---|
| Chester, West Midlands, 2006168 | Children under 16 years admitted to burns unit 2000–2 and referred to social services for abuse/neglect | Physical abuse: 4/45 (8.9%); neglect: 41/45 (91.1%) |
| Hobson, Plymouth, 1994132 | Children under 5 years admitted to burns unit 1989–2002 and referred to hospital abuse team (n = 26; nine placed on CPR because of confirmed abuse/neglect) | Physical abuse: 2/9 (22.2%) |
| Audit at the Royal Free Hospital, London, unpublished18 | Children under 16 years referred to social services for abuse/neglect from hospital in 2005 | Under 1 year: 9/14a (64.3%); 1–4 years: 2/2 (100%); 5–9 years: 0/0 (0%); 10–15 years: 0/3 (0%); total 0–15 years: 11/19 (57.9%) |
Appendix 6 UK National Screening Committee: criteria for appraising the viability, effectiveness and appropriateness of a screening programme
Ideally, all of the following criteria should be met before screening for a condition is initiated.
The condition
-
The condition should be an important health problem The true incidence of physical child abuse is difficult to quantify. Studies based on parental reports suggest that each year approximately 9% of children under 16 years in the UK are subjected to at least one episode of severe violence by a parent or carer that would be equivalent to physical abuse under the definition used by Working together to safeguard children 20062 and which meets the threshold for local authority investigation as laid out in Section 47 of the 1989 Children Act. 5
-
The epidemiology and natural history of the condition, including development from latent to declared disease, should be adequately understood and there should be a detectable risk factor, disease marker, latent period or early symptomatic stage The impact of violence against children is often long term, resulting in increased susceptibility to adverse social, emotional, cognitive and health outcomes. However, these consequences are poorly quantified. 169
-
All the cost-effective primary prevention interventions should have been implemented as far as practicable Prevention of child abuse and neglect by early intervention is one of the aims of reforms laid out in the government Green Paper Every child matters. 140 Changes resulting from the Green Paper are currently being enacted through the implementation of systems for collating, recording and using data on children referred to social services through the Integrated Children’s System, and for allowing cross-agency information sharing for all children via the Information Sharing Index. A standardised Common Assessment Framework has been introduced to make referrals and identification of children’s needs more effective. 11
-
If the carriers of a mutation are identified as a result of screening the natural history of people with this status should be understood, including the psychological implications Not applicable.
The test
-
There should be a simple, safe, precise and validated screening test There is no such test. A clinical screening assessment is performed by A&E staff but it is hard to define exactly what this entails. Checklists for indicators of abuse are used in some departments as are protocols stating which children should be referred directly to paediatricians for assessment (e.g. all infants or all young children with fractures). None of these tests have been adequately validated.
-
The distribution of test values in the target population should be known and a suitable cut-off level defined and agreed None of the screening tests have been adequately validated.
-
The test should be acceptable to the population We found no evidence on whether screening tests were acceptable. As checklists and protocols have been used by many A&E departments, this may indicate some level of acceptability to staff.
-
There should be an agreed policy on the further diagnostic investigation of individuals with a positive test result and on the choices available to those individuals Children who screen positive are referred to the paediatric team for further assessment and, if abuse is confirmed, they are referred to social services who carry out an initial investigation.
-
If the test is for mutations the criteria used to select the subset of mutations to be covered by screening, if all possible mutations are not being tested, should be clearly set out Not applicable.
The treatment
-
There should be an effective treatment or intervention for patients identified through early detection, with evidence of early treatment leading to better outcomes than late treatment The study did not investigate the effectiveness of social services interventions on outcomes in referred children.
-
There should be agreed evidence-based policies covering which individuals should be offered treatment and the appropriate treatment to be offered Interventions are determined by social services based on an assessment of the needs of each individual case. There are, however, agreed policies about the threshold for various levels of investigation by children’s services. 2,5 For health professionals there is a legal obligation to safeguard children (Section 11, Children Act 2004), which includes making appropriate referrals to social services when abuse or neglect is suspected. 2,12
-
Clinical management of the condition and patient outcomes should be optimised in all health-care providers prior to participation in a screening programme Information is lacking on cases of suspected abuse detected in A&E, whether children are referred to social services, whether social services confirms or excludes abuse and what actions are taken. It is therefore impossible to know whether clinical management is optimal. Suspected abuse needs to be recorded at all levels in A&E, in other hospital records and at all levels in social services.
The screening programme
-
There should be evidence from high-quality randomised controlled trials that the screening programme is effective in reducing mortality or morbidity. Where screening is aimed solely at providing information to allow the person being screened to make an ‘informed choice’ (e.g. Down syndrome, cystic fibrosis carrier screening), there must be evidence from high-quality trials that the test accurately measures risk. The information that is provided about the test and its outcome must be of value and readily understood by the individual being screened There are no controlled trials of universal screening.
-
There should be evidence that the complete screening programme (test, diagnostic procedures, treatment/intervention) is clinically, socially and ethically acceptable to health professionals and the public Detection of physical child abuse is a clinical, social, ethical and legal duty for health-care professionals. Failure to fill paediatric posts in child protection may indicate a lack of acceptability of the consequences of detecting abuse, particularly the legal consequences. Referral of suspected abuse to social services entails an additional workload for health professionals who complain of a ‘loss of control’, lack of feedback and failure to appreciate that the diagnosis of abuse is probabilistic rather than 100% certain. For the public, referral to social services for suspected abuse is traumatic for abused and non-abused children.
-
The benefit from the screening programme should outweigh the physical and psychological harm (caused by the test, diagnostic procedures and treatment) The study was confined to examination of test performance and did not investigate the harms and benefits of interventions arising from test results.
-
The opportunity cost of the screening programme (including testing, diagnosis and treatment, administration, training and quality assurance) should be economically balanced in relation to expenditure on medical care as a whole (i.e. value for money) As above for question 15.
-
There should be a plan for managing and monitoring the screening programme and an agreed set of quality assurance standards As above for question 12. We found no evidence of routine electronic record systems that allowed monitoring of detection and outcomes of suspected abuse.
-
Adequate staffing and facilities for testing, diagnosis, treatment and programme Use of protocols will substantially increase the workload for the paediatric team and may exceed capacity. Consequences for staffing cannot be determined without evidence on the performance of clinical screening in the UK.
-
All other options for managing the condition should have been considered (e.g. improving treatment, providing other services) to ensure that no more cost-effective intervention could be introduced or current interventions increased within the resources available See answer to question 5. There is a lack of information on the performance of standard clinical screening assessment. We found weak evidence to suggest that this could be improved by the inclusion of a community liaison nurse.
-
Evidence-based information, explaining the consequences of testing, investigation and treatment, should be made available to potential participants to assist them in making an informed choice In our view it would not be acceptable for parents to choose whether or not to undergo screening for physical abuse.
-
Public pressure for widening the eligibility criteria for reducing the screening interval, and for increasing the sensitivity of the testing process, should be anticipated. Decisions about these parameters should be scientifically justifiable to the public Given recent government initiatives and the Children Act, it is widely accepted that detection of physical abuse is not the remit of a one-off screening test implemented by A&E staff but is part of the assessment of children by professionals at all levels, whether they are involved in health, social services, education or the police. These documents emphasise the need for constant vigilance to detect possible abuse at all stages of care, even when other professionals have ruled out the possibility, for example in a previous attendance. A further issue is that recent initiatives have recognised the need to improve detection of all types of abuse and neglect along with identification of all levels of social need. This approach is the basis of the Common Assessment Framework, which is designed to allow assessment of each child’s level and type of need (including abuse) in the context of their development, parent, carers and family and wider environment. 170
-
If screening is for a mutation the programme should be acceptable to people identified as carriers and to other family members Not applicable.
Glossary
- A&E team
- The front-line staff (senior house officers or triage nurses) who are the first to assess and treat patients attending accident and emergency departments.
- Agencies
- Any public or voluntary agency charged with identifying child abuse or carrying out child abuse investigations (e.g. social services, police, schools, hospitals, NSPCC).
- Allocated social worker
- The named social worker responsible for managing a child’s social services investigation and interventions.
- Child
- Under 16 years of age.
- Child abuse
- All types of maltreatment – physical abuse, sexual abuse, emotional abuse and all forms of neglect perpetrated by a parent or carer – towards a child.
- Child protection register
- National register listing children who are at high risk of further abuse. Due to be phased out in favour of the child protection plan.
- Common Assessment Framework
- A standardised method for assessing and sharing information with other agencies about children who give rise to concerns. The system should be universally used by all professionals in England by the end of 2008. See www.everychildmatters.gov.uk/deliveringservices/caf/.
- Community liaison nurse
- Someone who has had training in children’s nursing or health visiting. Among other duties, the community liaison nurse scrutinises the attendance records of every child who attends A&E to identify children with child protection or social concerns who may have been missed by A&E staff. Usually these cases will be discussed at a weekly meeting with other clinical staff.
- Contact Point
- Contact Point is a database that will be implemented throughout England by mid 2009. It will contain basic demographic data on every child, contact details for practitioners providing additional services to the child, and information on whether the child has an allocated social worker or a completed Common Assessment Framework form (see above). This technology aims to support information sharing by professionals caring for children. See www.everychildmatters.gov.uk/deliveringservices/integratedworking/.
- Designated doctor/nurse
- Each primary care trust should have doctors/nurses with designated child protection roles and responsibilities, including offering support and advice to local safeguarding children’s boards and named professionals.1–3
- Diagnostic odds ratio
- The ratio of the odds of disease in test positives divided by the odds of disease in test negatives. The odds of disease is the number with the disease divided by the number without the disease.4
- Integrated Children’s System
- A conceptual framework, method of practice and business process to support practitioners and managers in undertaking the key tasks of assessment, planning, intervention and review. Designed to be supported by an electronic case record system that will store Common Assessment Framework forms. See www.everychildmatters.gov.uk/socialcare/integratedchildrenssystem/about/.
- Likelihood ratio
- The proportion of all those with a condition who test positive divided by the proportion of all those without the condition who test positive. It is a measure of test performance.
- Maltreatment
- All types of maltreatment – physical abuse, sexual abuse, emotional abuse and all forms of neglect – perpetrated by a parent or carer towards a child.
- Named doctor/nurse
- Each NHS trust/foundation trust/primary care trust should have named doctors/nurses with specific child protection roles and responsibilities.1–3
- NIS-3
- Third National Incidence Study (USA) – data from 1993 and published in 2006. See www.nis4.org/NIS_History.pdf.
- Paediatric team
- Considered to include all specialist paediatric or child abuse hospital staff (paediatric registrars, consultants, hospital social workers and community liaison nurses).
- Parent or carer
- Biological mother or father; parent figure (mother’s or father’s partner) regardless of live-in status or person who takes significant responsibility for the day-to-day needs of the child.
- Physical abuse
- At least one act of severe violence from a parent or carer towards a child. Severe violence is defined as a kick, a bite, a scald/burn, ‘beating up’, hitting with an object, shaking a young child, or threatening to use a weapon. Physical abuse is also defined by reporting of physical abuse by agencies involved in child protection, based on the agency’s criteria.
- Post-test probability
- The probability of child abuse for a given screen or diagnostic test result.
- Senior house officer
- A junior and non-specialist hospital doctor who initially sees and assesses the patients at accident and emergency departments.
- Social work active
- A child who has an allocated social worker or who is allocated to the duty social work team, currently or within the last 12 months.
- Substantiated reports
- An American term for a report of maltreatment that has been verified by the child protection agency in accordance with state law. If an investigator finds that abuse or neglect occurred then the report is substantiated or founded. In some states reports can be also be indicated (suggests maltreatment occurred but without the necessary level of proof to be substantiated according to state law). See www.reason.org/ps262.html#39.
List of abbreviations
- A&E
- accident and emergency (department)
- CAF
- Common Assessment Framework
- CAP team
- child abuse and protection team
- CLN
- community liaison nurse
- CPR
- child protection register
- ICS
- Integrated Children’s System
- LR
- likelihood ratio
- MeSH
- Medical Subject Headings
- NSPCC
- National Society for the Prevention of Cruelty to Children
- ONS
- Office of National Statistics
- RCPCH
- Royal College of Paediatricians and Child Health
- RoSPA
- Royal Society for the Prevention of Accidents
- SHO
- senior house officer
- SWA
- social work active
- TARN
- Trauma Audit and Research Network
- TARNlet
- children’s sector of the Trauma Audit and Research Network
All abbreviations that have been used in this report are listed here unless the abbreviation is well known (e.g. NHS) or it has been used only once or it is a non-standard abbreviation used only in figures/tables/appendices, in which case the abbreviation is defined in the figure legend or in the notes at the end of the table.
Notes
Health Technology Assessment reports published to date
-
Home parenteral nutrition: a systematic review.
By Richards DM, Deeks JJ, Sheldon TA, Shaffer JL.
-
Diagnosis, management and screening of early localised prostate cancer.
A review by Selley S, Donovan J, Faulkner A, Coast J, Gillatt D.
-
The diagnosis, management, treatment and costs of prostate cancer in England and Wales.
A review by Chamberlain J, Melia J, Moss S, Brown J.
-
Screening for fragile X syndrome.
A review by Murray J, Cuckle H, Taylor G, Hewison J.
-
A review of near patient testing in primary care.
By Hobbs FDR, Delaney BC, Fitzmaurice DA, Wilson S, Hyde CJ, Thorpe GH, et al.
-
Systematic review of outpatient services for chronic pain control.
By McQuay HJ, Moore RA, Eccleston C, Morley S, de C Williams AC.
-
Neonatal screening for inborn errors of metabolism: cost, yield and outcome.
A review by Pollitt RJ, Green A, McCabe CJ, Booth A, Cooper NJ, Leonard JV, et al.
-
Preschool vision screening.
A review by Snowdon SK, Stewart-Brown SL.
-
Implications of socio-cultural contexts for the ethics of clinical trials.
A review by Ashcroft RE, Chadwick DW, Clark SRL, Edwards RHT, Frith L, Hutton JL.
-
A critical review of the role of neonatal hearing screening in the detection of congenital hearing impairment.
By Davis A, Bamford J, Wilson I, Ramkalawan T, Forshaw M, Wright S.
-
Newborn screening for inborn errors of metabolism: a systematic review.
By Seymour CA, Thomason MJ, Chalmers RA, Addison GM, Bain MD, Cockburn F, et al.
-
Routine preoperative testing: a systematic review of the evidence.
By Munro J, Booth A, Nicholl J.
-
Systematic review of the effectiveness of laxatives in the elderly.
By Petticrew M, Watt I, Sheldon T.
-
When and how to assess fast-changing technologies: a comparative study of medical applications of four generic technologies.
A review by Mowatt G, Bower DJ, Brebner JA, Cairns JA, Grant AM, McKee L.
-
Antenatal screening for Down’s syndrome.
A review by Wald NJ, Kennard A, Hackshaw A, McGuire A.
-
Screening for ovarian cancer: a systematic review.
By Bell R, Petticrew M, Luengo S, Sheldon TA.
-
Consensus development methods, and their use in clinical guideline development.
A review by Murphy MK, Black NA, Lamping DL, McKee CM, Sanderson CFB, Askham J, et al.
-
A cost–utility analysis of interferon beta for multiple sclerosis.
By Parkin D, McNamee P, Jacoby A, Miller P, Thomas S, Bates D.
-
Effectiveness and efficiency of methods of dialysis therapy for end-stage renal disease: systematic reviews.
By MacLeod A, Grant A, Donaldson C, Khan I, Campbell M, Daly C, et al.
-
Effectiveness of hip prostheses in primary total hip replacement: a critical review of evidence and an economic model.
By Faulkner A, Kennedy LG, Baxter K, Donovan J, Wilkinson M, Bevan G.
-
Antimicrobial prophylaxis in colorectal surgery: a systematic review of randomised controlled trials.
By Song F, Glenny AM.
-
Bone marrow and peripheral blood stem cell transplantation for malignancy.
A review by Johnson PWM, Simnett SJ, Sweetenham JW, Morgan GJ, Stewart LA.
-
Screening for speech and language delay: a systematic review of the literature.
By Law J, Boyle J, Harris F, Harkness A, Nye C.
-
Resource allocation for chronic stable angina: a systematic review of effectiveness, costs and cost-effectiveness of alternative interventions.
By Sculpher MJ, Petticrew M, Kelland JL, Elliott RA, Holdright DR, Buxton MJ.
-
Detection, adherence and control of hypertension for the prevention of stroke: a systematic review.
By Ebrahim S.
-
Postoperative analgesia and vomiting, with special reference to day-case surgery: a systematic review.
By McQuay HJ, Moore RA.
-
Choosing between randomised and nonrandomised studies: a systematic review.
By Britton A, McKee M, Black N, McPherson K, Sanderson C, Bain C.
-
Evaluating patient-based outcome measures for use in clinical trials.
A review by Fitzpatrick R, Davey C, Buxton MJ, Jones DR.
-
Ethical issues in the design and conduct of randomised controlled trials.
A review by Edwards SJL, Lilford RJ, Braunholtz DA, Jackson JC, Hewison J, Thornton J.
-
Qualitative research methods in health technology assessment: a review of the literature.
By Murphy E, Dingwall R, Greatbatch D, Parker S, Watson P.
-
The costs and benefits of paramedic skills in pre-hospital trauma care.
By Nicholl J, Hughes S, Dixon S, Turner J, Yates D.
-
Systematic review of endoscopic ultrasound in gastro-oesophageal cancer.
By Harris KM, Kelly S, Berry E, Hutton J, Roderick P, Cullingworth J, et al.
-
Systematic reviews of trials and other studies.
By Sutton AJ, Abrams KR, Jones DR, Sheldon TA, Song F.
-
Primary total hip replacement surgery: a systematic review of outcomes and modelling of cost-effectiveness associated with different prostheses.
A review by Fitzpatrick R, Shortall E, Sculpher M, Murray D, Morris R, Lodge M, et al.
-
Informed decision making: an annotated bibliography and systematic review.
By Bekker H, Thornton JG, Airey CM, Connelly JB, Hewison J, Robinson MB, et al.
-
Handling uncertainty when performing economic evaluation of healthcare interventions.
A review by Briggs AH, Gray AM.
-
The role of expectancies in the placebo effect and their use in the delivery of health care: a systematic review.
By Crow R, Gage H, Hampson S, Hart J, Kimber A, Thomas H.
-
A randomised controlled trial of different approaches to universal antenatal HIV testing: uptake and acceptability. Annex: Antenatal HIV testing – assessment of a routine voluntary approach.
By Simpson WM, Johnstone FD, Boyd FM, Goldberg DJ, Hart GJ, Gormley SM, et al.
-
Methods for evaluating area-wide and organisation-based interventions in health and health care: a systematic review.
By Ukoumunne OC, Gulliford MC, Chinn S, Sterne JAC, Burney PGJ.
-
Assessing the costs of healthcare technologies in clinical trials.
A review by Johnston K, Buxton MJ, Jones DR, Fitzpatrick R.
-
Cooperatives and their primary care emergency centres: organisation and impact.
By Hallam L, Henthorne K.
-
Screening for cystic fibrosis.
A review by Murray J, Cuckle H, Taylor G, Littlewood J, Hewison J.
-
A review of the use of health status measures in economic evaluation.
By Brazier J, Deverill M, Green C, Harper R, Booth A.
-
Methods for the analysis of quality-of-life and survival data in health technology assessment.
A review by Billingham LJ, Abrams KR, Jones DR.
-
Antenatal and neonatal haemoglobinopathy screening in the UK: review and economic analysis.
By Zeuner D, Ades AE, Karnon J, Brown J, Dezateux C, Anionwu EN.
-
Assessing the quality of reports of randomised trials: implications for the conduct of meta-analyses.
A review by Moher D, Cook DJ, Jadad AR, Tugwell P, Moher M, Jones A, et al.
-
‘Early warning systems’ for identifying new healthcare technologies.
By Robert G, Stevens A, Gabbay J.
-
A systematic review of the role of human papillomavirus testing within a cervical screening programme.
By Cuzick J, Sasieni P, Davies P, Adams J, Normand C, Frater A, et al.
-
Near patient testing in diabetes clinics: appraising the costs and outcomes.
By Grieve R, Beech R, Vincent J, Mazurkiewicz J.
-
Positron emission tomography: establishing priorities for health technology assessment.
A review by Robert G, Milne R.
-
The debridement of chronic wounds: a systematic review.
By Bradley M, Cullum N, Sheldon T.
-
Systematic reviews of wound care management: (2) Dressings and topical agents used in the healing of chronic wounds.
By Bradley M, Cullum N, Nelson EA, Petticrew M, Sheldon T, Torgerson D.
-
A systematic literature review of spiral and electron beam computed tomography: with particular reference to clinical applications in hepatic lesions, pulmonary embolus and coronary artery disease.
By Berry E, Kelly S, Hutton J, Harris KM, Roderick P, Boyce JC, et al.
-
What role for statins? A review and economic model.
By Ebrahim S, Davey Smith G, McCabe C, Payne N, Pickin M, Sheldon TA, et al.
-
Factors that limit the quality, number and progress of randomised controlled trials.
A review by Prescott RJ, Counsell CE, Gillespie WJ, Grant AM, Russell IT, Kiauka S, et al.
-
Antimicrobial prophylaxis in total hip replacement: a systematic review.
By Glenny AM, Song F.
-
Health promoting schools and health promotion in schools: two systematic reviews.
By Lister-Sharp D, Chapman S, Stewart-Brown S, Sowden A.
-
Economic evaluation of a primary care-based education programme for patients with osteoarthritis of the knee.
A review by Lord J, Victor C, Littlejohns P, Ross FM, Axford JS.
-
The estimation of marginal time preference in a UK-wide sample (TEMPUS) project.
A review by Cairns JA, van der Pol MM.
-
Geriatric rehabilitation following fractures in older people: a systematic review.
By Cameron I, Crotty M, Currie C, Finnegan T, Gillespie L, Gillespie W, et al.
-
Screening for sickle cell disease and thalassaemia: a systematic review with supplementary research.
By Davies SC, Cronin E, Gill M, Greengross P, Hickman M, Normand C.
-
Community provision of hearing aids and related audiology services.
A review by Reeves DJ, Alborz A, Hickson FS, Bamford JM.
-
False-negative results in screening programmes: systematic review of impact and implications.
By Petticrew MP, Sowden AJ, Lister-Sharp D, Wright K.
-
Costs and benefits of community postnatal support workers: a randomised controlled trial.
By Morrell CJ, Spiby H, Stewart P, Walters S, Morgan A.
-
Implantable contraceptives (subdermal implants and hormonally impregnated intrauterine systems) versus other forms of reversible contraceptives: two systematic reviews to assess relative effectiveness, acceptability, tolerability and cost-effectiveness.
By French RS, Cowan FM, Mansour DJA, Morris S, Procter T, Hughes D, et al.
-
An introduction to statistical methods for health technology assessment.
A review by White SJ, Ashby D, Brown PJ.
-
Disease-modifying drugs for multiple sclerosis: a rapid and systematic review.
By Clegg A, Bryant J, Milne R.
-
Publication and related biases.
A review by Song F, Eastwood AJ, Gilbody S, Duley L, Sutton AJ.
-
Cost and outcome implications of the organisation of vascular services.
By Michaels J, Brazier J, Palfreyman S, Shackley P, Slack R.
-
Monitoring blood glucose control in diabetes mellitus: a systematic review.
By Coster S, Gulliford MC, Seed PT, Powrie JK, Swaminathan R.
-
The effectiveness of domiciliary health visiting: a systematic review of international studies and a selective review of the British literature.
By Elkan R, Kendrick D, Hewitt M, Robinson JJA, Tolley K, Blair M, et al.
-
The determinants of screening uptake and interventions for increasing uptake: a systematic review.
By Jepson R, Clegg A, Forbes C, Lewis R, Sowden A, Kleijnen J.
-
The effectiveness and cost-effectiveness of prophylactic removal of wisdom teeth.
A rapid review by Song F, O’Meara S, Wilson P, Golder S, Kleijnen J.
-
Ultrasound screening in pregnancy: a systematic review of the clinical effectiveness, cost-effectiveness and women’s views.
By Bricker L, Garcia J, Henderson J, Mugford M, Neilson J, Roberts T, et al.
-
A rapid and systematic review of the effectiveness and cost-effectiveness of the taxanes used in the treatment of advanced breast and ovarian cancer.
By Lister-Sharp D, McDonagh MS, Khan KS, Kleijnen J.
-
Liquid-based cytology in cervical screening: a rapid and systematic review.
By Payne N, Chilcott J, McGoogan E.
-
Randomised controlled trial of non-directive counselling, cognitive–behaviour therapy and usual general practitioner care in the management of depression as well as mixed anxiety and depression in primary care.
By King M, Sibbald B, Ward E, Bower P, Lloyd M, Gabbay M, et al.
-
Routine referral for radiography of patients presenting with low back pain: is patients’ outcome influenced by GPs’ referral for plain radiography?
By Kerry S, Hilton S, Patel S, Dundas D, Rink E, Lord J.
-
Systematic reviews of wound care management: (3) antimicrobial agents for chronic wounds; (4) diabetic foot ulceration.
By O’Meara S, Cullum N, Majid M, Sheldon T.
-
Using routine data to complement and enhance the results of randomised controlled trials.
By Lewsey JD, Leyland AH, Murray GD, Boddy FA.
-
Coronary artery stents in the treatment of ischaemic heart disease: a rapid and systematic review.
By Meads C, Cummins C, Jolly K, Stevens A, Burls A, Hyde C.
-
Outcome measures for adult critical care: a systematic review.
By Hayes JA, Black NA, Jenkinson C, Young JD, Rowan KM, Daly K, et al.
-
A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding.
By Fairbank L, O’Meara S, Renfrew MJ, Woolridge M, Sowden AJ, Lister-Sharp D.
-
Implantable cardioverter defibrillators: arrhythmias. A rapid and systematic review.
By Parkes J, Bryant J, Milne R.
-
Treatments for fatigue in multiple sclerosis: a rapid and systematic review.
By Brañas P, Jordan R, Fry-Smith A, Burls A, Hyde C.
-
Early asthma prophylaxis, natural history, skeletal development and economy (EASE): a pilot randomised controlled trial.
By Baxter-Jones ADG, Helms PJ, Russell G, Grant A, Ross S, Cairns JA, et al.
-
Screening for hypercholesterolaemia versus case finding for familial hypercholesterolaemia: a systematic review and cost-effectiveness analysis.
By Marks D, Wonderling D, Thorogood M, Lambert H, Humphries SE, Neil HAW.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of glycoprotein IIb/IIIa antagonists in the medical management of unstable angina.
By McDonagh MS, Bachmann LM, Golder S, Kleijnen J, ter Riet G.
-
A randomised controlled trial of prehospital intravenous fluid replacement therapy in serious trauma.
By Turner J, Nicholl J, Webber L, Cox H, Dixon S, Yates D.
-
Intrathecal pumps for giving opioids in chronic pain: a systematic review.
By Williams JE, Louw G, Towlerton G.
-
Combination therapy (interferon alfa and ribavirin) in the treatment of chronic hepatitis C: a rapid and systematic review.
By Shepherd J, Waugh N, Hewitson P.
-
A systematic review of comparisons of effect sizes derived from randomised and non-randomised studies.
By MacLehose RR, Reeves BC, Harvey IM, Sheldon TA, Russell IT, Black AMS.
-
Intravascular ultrasound-guided interventions in coronary artery disease: a systematic literature review, with decision-analytic modelling, of outcomes and cost-effectiveness.
By Berry E, Kelly S, Hutton J, Lindsay HSJ, Blaxill JM, Evans JA, et al.
-
A randomised controlled trial to evaluate the effectiveness and cost-effectiveness of counselling patients with chronic depression.
By Simpson S, Corney R, Fitzgerald P, Beecham J.
-
Systematic review of treatments for atopic eczema.
By Hoare C, Li Wan Po A, Williams H.
-
Bayesian methods in health technology assessment: a review.
By Spiegelhalter DJ, Myles JP, Jones DR, Abrams KR.
-
The management of dyspepsia: a systematic review.
By Delaney B, Moayyedi P, Deeks J, Innes M, Soo S, Barton P, et al.
-
A systematic review of treatments for severe psoriasis.
By Griffiths CEM, Clark CM, Chalmers RJG, Li Wan Po A, Williams HC.
-
Clinical and cost-effectiveness of donepezil, rivastigmine and galantamine for Alzheimer’s disease: a rapid and systematic review.
By Clegg A, Bryant J, Nicholson T, McIntyre L, De Broe S, Gerard K, et al.
-
The clinical effectiveness and cost-effectiveness of riluzole for motor neurone disease: a rapid and systematic review.
By Stewart A, Sandercock J, Bryan S, Hyde C, Barton PM, Fry-Smith A, et al.
-
Equity and the economic evaluation of healthcare.
By Sassi F, Archard L, Le Grand J.
-
Quality-of-life measures in chronic diseases of childhood.
By Eiser C, Morse R.
-
Eliciting public preferences for healthcare: a systematic review of techniques.
By Ryan M, Scott DA, Reeves C, Bate A, van Teijlingen ER, Russell EM, et al.
-
General health status measures for people with cognitive impairment: learning disability and acquired brain injury.
By Riemsma RP, Forbes CA, Glanville JM, Eastwood AJ, Kleijnen J.
-
An assessment of screening strategies for fragile X syndrome in the UK.
By Pembrey ME, Barnicoat AJ, Carmichael B, Bobrow M, Turner G.
-
Issues in methodological research: perspectives from researchers and commissioners.
By Lilford RJ, Richardson A, Stevens A, Fitzpatrick R, Edwards S, Rock F, et al.
-
Systematic reviews of wound care management: (5) beds; (6) compression; (7) laser therapy, therapeutic ultrasound, electrotherapy and electromagnetic therapy.
By Cullum N, Nelson EA, Flemming K, Sheldon T.
-
Effects of educational and psychosocial interventions for adolescents with diabetes mellitus: a systematic review.
By Hampson SE, Skinner TC, Hart J, Storey L, Gage H, Foxcroft D, et al.
-
Effectiveness of autologous chondrocyte transplantation for hyaline cartilage defects in knees: a rapid and systematic review.
By Jobanputra P, Parry D, Fry-Smith A, Burls A.
-
Statistical assessment of the learning curves of health technologies.
By Ramsay CR, Grant AM, Wallace SA, Garthwaite PH, Monk AF, Russell IT.
-
The effectiveness and cost-effectiveness of temozolomide for the treatment of recurrent malignant glioma: a rapid and systematic review.
By Dinnes J, Cave C, Huang S, Major K, Milne R.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of debriding agents in treating surgical wounds healing by secondary intention.
By Lewis R, Whiting P, ter Riet G, O’Meara S, Glanville J.
-
Home treatment for mental health problems: a systematic review.
By Burns T, Knapp M, Catty J, Healey A, Henderson J, Watt H, et al.
-
How to develop cost-conscious guidelines.
By Eccles M, Mason J.
-
The role of specialist nurses in multiple sclerosis: a rapid and systematic review.
By De Broe S, Christopher F, Waugh N.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of orlistat in the management of obesity.
By O’Meara S, Riemsma R, Shirran L, Mather L, ter Riet G.
-
The clinical effectiveness and cost-effectiveness of pioglitazone for type 2 diabetes mellitus: a rapid and systematic review.
By Chilcott J, Wight J, Lloyd Jones M, Tappenden P.
-
Extended scope of nursing practice: a multicentre randomised controlled trial of appropriately trained nurses and preregistration house officers in preoperative assessment in elective general surgery.
By Kinley H, Czoski-Murray C, George S, McCabe C, Primrose J, Reilly C, et al.
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) Acute day hospital versus admission; (2) Vocational rehabilitation; (3) Day hospital versus outpatient care.
By Marshall M, Crowther R, Almaraz- Serrano A, Creed F, Sledge W, Kluiter H, et al.
-
The measurement and monitoring of surgical adverse events.
By Bruce J, Russell EM, Mollison J, Krukowski ZH.
-
Action research: a systematic review and guidance for assessment.
By Waterman H, Tillen D, Dickson R, de Koning K.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of gemcitabine for the treatment of pancreatic cancer.
By Ward S, Morris E, Bansback N, Calvert N, Crellin A, Forman D, et al.
-
A rapid and systematic review of the evidence for the clinical effectiveness and cost-effectiveness of irinotecan, oxaliplatin and raltitrexed for the treatment of advanced colorectal cancer.
By Lloyd Jones M, Hummel S, Bansback N, Orr B, Seymour M.
-
Comparison of the effectiveness of inhaler devices in asthma and chronic obstructive airways disease: a systematic review of the literature.
By Brocklebank D, Ram F, Wright J, Barry P, Cates C, Davies L, et al.
-
The cost-effectiveness of magnetic resonance imaging for investigation of the knee joint.
By Bryan S, Weatherburn G, Bungay H, Hatrick C, Salas C, Parry D, et al.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.
By Forbes C, Shirran L, Bagnall A-M, Duffy S, ter Riet G.
-
Superseded by a report published in a later volume.
-
The role of radiography in primary care patients with low back pain of at least 6 weeks duration: a randomised (unblinded) controlled trial.
By Kendrick D, Fielding K, Bentley E, Miller P, Kerslake R, Pringle M.
-
Design and use of questionnaires: a review of best practice applicable to surveys of health service staff and patients.
By McColl E, Jacoby A, Thomas L, Soutter J, Bamford C, Steen N, et al.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.
By Clegg A, Scott DA, Sidhu M, Hewitson P, Waugh N.
-
Subgroup analyses in randomised controlled trials: quantifying the risks of false-positives and false-negatives.
By Brookes ST, Whitley E, Peters TJ, Mulheran PA, Egger M, Davey Smith G.
-
Depot antipsychotic medication in the treatment of patients with schizophrenia: (1) Meta-review; (2) Patient and nurse attitudes.
By David AS, Adams C.
-
A systematic review of controlled trials of the effectiveness and cost-effectiveness of brief psychological treatments for depression.
By Churchill R, Hunot V, Corney R, Knapp M, McGuire H, Tylee A, et al.
-
Cost analysis of child health surveillance.
By Sanderson D, Wright D, Acton C, Duree D.
-
A study of the methods used to select review criteria for clinical audit.
By Hearnshaw H, Harker R, Cheater F, Baker R, Grimshaw G.
-
Fludarabine as second-line therapy for B cell chronic lymphocytic leukaemia: a technology assessment.
By Hyde C, Wake B, Bryan S, Barton P, Fry-Smith A, Davenport C, et al.
-
Rituximab as third-line treatment for refractory or recurrent Stage III or IV follicular non-Hodgkin’s lymphoma: a systematic review and economic evaluation.
By Wake B, Hyde C, Bryan S, Barton P, Song F, Fry-Smith A, et al.
-
A systematic review of discharge arrangements for older people.
By Parker SG, Peet SM, McPherson A, Cannaby AM, Baker R, Wilson A, et al.
-
The clinical effectiveness and cost-effectiveness of inhaler devices used in the routine management of chronic asthma in older children: a systematic review and economic evaluation.
By Peters J, Stevenson M, Beverley C, Lim J, Smith S.
-
The clinical effectiveness and cost-effectiveness of sibutramine in the management of obesity: a technology assessment.
By O’Meara S, Riemsma R, Shirran L, Mather L, ter Riet G.
-
The cost-effectiveness of magnetic resonance angiography for carotid artery stenosis and peripheral vascular disease: a systematic review.
By Berry E, Kelly S, Westwood ME, Davies LM, Gough MJ, Bamford JM, et al.
-
Promoting physical activity in South Asian Muslim women through ‘exercise on prescription’.
By Carroll B, Ali N, Azam N.
-
Zanamivir for the treatment of influenza in adults: a systematic review and economic evaluation.
By Burls A, Clark W, Stewart T, Preston C, Bryan S, Jefferson T, et al.
-
A review of the natural history and epidemiology of multiple sclerosis: implications for resource allocation and health economic models.
By Richards RG, Sampson FC, Beard SM, Tappenden P.
-
Screening for gestational diabetes: a systematic review and economic evaluation.
By Scott DA, Loveman E, McIntyre L, Waugh N.
-
The clinical effectiveness and cost-effectiveness of surgery for people with morbid obesity: a systematic review and economic evaluation.
By Clegg AJ, Colquitt J, Sidhu MK, Royle P, Loveman E, Walker A.
-
The clinical effectiveness of trastuzumab for breast cancer: a systematic review.
By Lewis R, Bagnall A-M, Forbes C, Shirran E, Duffy S, Kleijnen J, et al.
-
The clinical effectiveness and cost-effectiveness of vinorelbine for breast cancer: a systematic review and economic evaluation.
By Lewis R, Bagnall A-M, King S, Woolacott N, Forbes C, Shirran L, et al.
-
A systematic review of the effectiveness and cost-effectiveness of metal-on-metal hip resurfacing arthroplasty for treatment of hip disease.
By Vale L, Wyness L, McCormack K, McKenzie L, Brazzelli M, Stearns SC.
-
The clinical effectiveness and cost-effectiveness of bupropion and nicotine replacement therapy for smoking cessation: a systematic review and economic evaluation.
By Woolacott NF, Jones L, Forbes CA, Mather LC, Sowden AJ, Song FJ, et al.
-
A systematic review of effectiveness and economic evaluation of new drug treatments for juvenile idiopathic arthritis: etanercept.
By Cummins C, Connock M, Fry-Smith A, Burls A.
-
Clinical effectiveness and cost-effectiveness of growth hormone in children: a systematic review and economic evaluation.
By Bryant J, Cave C, Mihaylova B, Chase D, McIntyre L, Gerard K, et al.
-
Clinical effectiveness and cost-effectiveness of growth hormone in adults in relation to impact on quality of life: a systematic review and economic evaluation.
By Bryant J, Loveman E, Chase D, Mihaylova B, Cave C, Gerard K, et al.
-
Clinical medication review by a pharmacist of patients on repeat prescriptions in general practice: a randomised controlled trial.
By Zermansky AG, Petty DR, Raynor DK, Lowe CJ, Freementle N, Vail A.
-
The effectiveness of infliximab and etanercept for the treatment of rheumatoid arthritis: a systematic review and economic evaluation.
By Jobanputra P, Barton P, Bryan S, Burls A.
-
A systematic review and economic evaluation of computerised cognitive behaviour therapy for depression and anxiety.
By Kaltenthaler E, Shackley P, Stevens K, Beverley C, Parry G, Chilcott J.
-
A systematic review and economic evaluation of pegylated liposomal doxorubicin hydrochloride for ovarian cancer.
By Forbes C, Wilby J, Richardson G, Sculpher M, Mather L, Reimsma R.
-
A systematic review of the effectiveness of interventions based on a stages-of-change approach to promote individual behaviour change.
By Riemsma RP, Pattenden J, Bridle C, Sowden AJ, Mather L, Watt IS, et al.
-
A systematic review update of the clinical effectiveness and cost-effectiveness of glycoprotein IIb/IIIa antagonists.
By Robinson M, Ginnelly L, Sculpher M, Jones L, Riemsma R, Palmer S, et al.
-
A systematic review of the effectiveness, cost-effectiveness and barriers to implementation of thrombolytic and neuroprotective therapy for acute ischaemic stroke in the NHS.
By Sandercock P, Berge E, Dennis M, Forbes J, Hand P, Kwan J, et al.
-
A randomised controlled crossover trial of nurse practitioner versus doctor-led outpatient care in a bronchiectasis clinic.
By Caine N, Sharples LD, Hollingworth W, French J, Keogan M, Exley A, et al.
-
Clinical effectiveness and cost – consequences of selective serotonin reuptake inhibitors in the treatment of sex offenders.
By Adi Y, Ashcroft D, Browne K, Beech A, Fry-Smith A, Hyde C.
-
Treatment of established osteoporosis: a systematic review and cost–utility analysis.
By Kanis JA, Brazier JE, Stevenson M, Calvert NW, Lloyd Jones M.
-
Which anaesthetic agents are cost-effective in day surgery? Literature review, national survey of practice and randomised controlled trial.
By Elliott RA Payne K, Moore JK, Davies LM, Harper NJN, St Leger AS, et al.
-
Screening for hepatitis C among injecting drug users and in genitourinary medicine clinics: systematic reviews of effectiveness, modelling study and national survey of current practice.
By Stein K, Dalziel K, Walker A, McIntyre L, Jenkins B, Horne J, et al.
-
The measurement of satisfaction with healthcare: implications for practice from a systematic review of the literature.
By Crow R, Gage H, Hampson S, Hart J, Kimber A, Storey L, et al.
-
The effectiveness and cost-effectiveness of imatinib in chronic myeloid leukaemia: a systematic review.
By Garside R, Round A, Dalziel K, Stein K, Royle R.
-
A comparative study of hypertonic saline, daily and alternate-day rhDNase in children with cystic fibrosis.
By Suri R, Wallis C, Bush A, Thompson S, Normand C, Flather M, et al.
-
A systematic review of the costs and effectiveness of different models of paediatric home care.
By Parker G, Bhakta P, Lovett CA, Paisley S, Olsen R, Turner D, et al.
-
How important are comprehensive literature searches and the assessment of trial quality in systematic reviews? Empirical study.
By Egger M, Jüni P, Bartlett C, Holenstein F, Sterne J.
-
Systematic review of the effectiveness and cost-effectiveness, and economic evaluation, of home versus hospital or satellite unit haemodialysis for people with end-stage renal failure.
By Mowatt G, Vale L, Perez J, Wyness L, Fraser C, MacLeod A, et al.
-
Systematic review and economic evaluation of the effectiveness of infliximab for the treatment of Crohn’s disease.
By Clark W, Raftery J, Barton P, Song F, Fry-Smith A, Burls A.
-
A review of the clinical effectiveness and cost-effectiveness of routine anti-D prophylaxis for pregnant women who are rhesus negative.
By Chilcott J, Lloyd Jones M, Wight J, Forman K, Wray J, Beverley C, et al.
-
Systematic review and evaluation of the use of tumour markers in paediatric oncology: Ewing’s sarcoma and neuroblastoma.
By Riley RD, Burchill SA, Abrams KR, Heney D, Lambert PC, Jones DR, et al.
-
The cost-effectiveness of screening for Helicobacter pylori to reduce mortality and morbidity from gastric cancer and peptic ulcer disease: a discrete-event simulation model.
By Roderick P, Davies R, Raftery J, Crabbe D, Pearce R, Bhandari P, et al.
-
The clinical effectiveness and cost-effectiveness of routine dental checks: a systematic review and economic evaluation.
By Davenport C, Elley K, Salas C, Taylor-Weetman CL, Fry-Smith A, Bryan S, et al.
-
A multicentre randomised controlled trial assessing the costs and benefits of using structured information and analysis of women’s preferences in the management of menorrhagia.
By Kennedy ADM, Sculpher MJ, Coulter A, Dwyer N, Rees M, Horsley S, et al.
-
Clinical effectiveness and cost–utility of photodynamic therapy for wet age-related macular degeneration: a systematic review and economic evaluation.
By Meads C, Salas C, Roberts T, Moore D, Fry-Smith A, Hyde C.
-
Evaluation of molecular tests for prenatal diagnosis of chromosome abnormalities.
By Grimshaw GM, Szczepura A, Hultén M, MacDonald F, Nevin NC, Sutton F, et al.
-
First and second trimester antenatal screening for Down’s syndrome: the results of the Serum, Urine and Ultrasound Screening Study (SURUSS).
By Wald NJ, Rodeck C, Hackshaw AK, Walters J, Chitty L, Mackinson AM.
-
The effectiveness and cost-effectiveness of ultrasound locating devices for central venous access: a systematic review and economic evaluation.
By Calvert N, Hind D, McWilliams RG, Thomas SM, Beverley C, Davidson A.
-
A systematic review of atypical antipsychotics in schizophrenia.
By Bagnall A-M, Jones L, Lewis R, Ginnelly L, Glanville J, Torgerson D, et al.
-
Prostate Testing for Cancer and Treatment (ProtecT) feasibility study.
By Donovan J, Hamdy F, Neal D, Peters T, Oliver S, Brindle L, et al.
-
Early thrombolysis for the treatment of acute myocardial infarction: a systematic review and economic evaluation.
By Boland A, Dundar Y, Bagust A, Haycox A, Hill R, Mujica Mota R, et al.
-
Screening for fragile X syndrome: a literature review and modelling.
By Song FJ, Barton P, Sleightholme V, Yao GL, Fry-Smith A.
-
Systematic review of endoscopic sinus surgery for nasal polyps.
By Dalziel K, Stein K, Round A, Garside R, Royle P.
-
Towards efficient guidelines: how to monitor guideline use in primary care.
By Hutchinson A, McIntosh A, Cox S, Gilbert C.
-
Effectiveness and cost-effectiveness of acute hospital-based spinal cord injuries services: systematic review.
By Bagnall A-M, Jones L, Richardson G, Duffy S, Riemsma R.
-
Prioritisation of health technology assessment. The PATHS model: methods and case studies.
By Townsend J, Buxton M, Harper G.
-
Systematic review of the clinical effectiveness and cost-effectiveness of tension-free vaginal tape for treatment of urinary stress incontinence.
By Cody J, Wyness L, Wallace S, Glazener C, Kilonzo M, Stearns S, et al.
-
The clinical and cost-effectiveness of patient education models for diabetes: a systematic review and economic evaluation.
By Loveman E, Cave C, Green C, Royle P, Dunn N, Waugh N.
-
The role of modelling in prioritising and planning clinical trials.
By Chilcott J, Brennan A, Booth A, Karnon J, Tappenden P.
-
Cost–benefit evaluation of routine influenza immunisation in people 65–74 years of age.
By Allsup S, Gosney M, Haycox A, Regan M.
-
The clinical and cost-effectiveness of pulsatile machine perfusion versus cold storage of kidneys for transplantation retrieved from heart-beating and non-heart-beating donors.
By Wight J, Chilcott J, Holmes M, Brewer N.
-
Can randomised trials rely on existing electronic data? A feasibility study to explore the value of routine data in health technology assessment.
By Williams JG, Cheung WY, Cohen DR, Hutchings HA, Longo MF, Russell IT.
-
Evaluating non-randomised intervention studies.
By Deeks JJ, Dinnes J, D’Amico R, Sowden AJ, Sakarovitch C, Song F, et al.
-
A randomised controlled trial to assess the impact of a package comprising a patient-orientated, evidence-based self- help guidebook and patient-centred consultations on disease management and satisfaction in inflammatory bowel disease.
By Kennedy A, Nelson E, Reeves D, Richardson G, Roberts C, Robinson A, et al.
-
The effectiveness of diagnostic tests for the assessment of shoulder pain due to soft tissue disorders: a systematic review.
By Dinnes J, Loveman E, McIntyre L, Waugh N.
-
The value of digital imaging in diabetic retinopathy.
By Sharp PF, Olson J, Strachan F, Hipwell J, Ludbrook A, O’Donnell M, et al.
-
Lowering blood pressure to prevent myocardial infarction and stroke: a new preventive strategy.
By Law M, Wald N, Morris J.
-
Clinical and cost-effectiveness of capecitabine and tegafur with uracil for the treatment of metastatic colorectal cancer: systematic review and economic evaluation.
By Ward S, Kaltenthaler E, Cowan J, Brewer N.
-
Clinical and cost-effectiveness of new and emerging technologies for early localised prostate cancer: a systematic review.
By Hummel S, Paisley S, Morgan A, Currie E, Brewer N.
-
Literature searching for clinical and cost-effectiveness studies used in health technology assessment reports carried out for the National Institute for Clinical Excellence appraisal system.
By Royle P, Waugh N.
-
Systematic review and economic decision modelling for the prevention and treatment of influenza A and B.
By Turner D, Wailoo A, Nicholson K, Cooper N, Sutton A, Abrams K.
-
A randomised controlled trial to evaluate the clinical and cost-effectiveness of Hickman line insertions in adult cancer patients by nurses.
By Boland A, Haycox A, Bagust A, Fitzsimmons L.
-
Redesigning postnatal care: a randomised controlled trial of protocol-based midwifery-led care focused on individual women’s physical and psychological health needs.
By MacArthur C, Winter HR, Bick DE, Lilford RJ, Lancashire RJ, Knowles H, et al.
-
Estimating implied rates of discount in healthcare decision-making.
By West RR, McNabb R, Thompson AGH, Sheldon TA, Grimley Evans J.
-
Systematic review of isolation policies in the hospital management of methicillin-resistant Staphylococcus aureus: a review of the literature with epidemiological and economic modelling.
By Cooper BS, Stone SP, Kibbler CC, Cookson BD, Roberts JA, Medley GF, et al.
-
Treatments for spasticity and pain in multiple sclerosis: a systematic review.
By Beard S, Hunn A, Wight J.
-
The inclusion of reports of randomised trials published in languages other than English in systematic reviews.
By Moher D, Pham B, Lawson ML, Klassen TP.
-
The impact of screening on future health-promoting behaviours and health beliefs: a systematic review.
By Bankhead CR, Brett J, Bukach C, Webster P, Stewart-Brown S, Munafo M, et al.
-
What is the best imaging strategy for acute stroke?
By Wardlaw JM, Keir SL, Seymour J, Lewis S, Sandercock PAG, Dennis MS, et al.
-
Systematic review and modelling of the investigation of acute and chronic chest pain presenting in primary care.
By Mant J, McManus RJ, Oakes RAL, Delaney BC, Barton PM, Deeks JJ, et al.
-
The effectiveness and cost-effectiveness of microwave and thermal balloon endometrial ablation for heavy menstrual bleeding: a systematic review and economic modelling.
By Garside R, Stein K, Wyatt K, Round A, Price A.
-
A systematic review of the role of bisphosphonates in metastatic disease.
By Ross JR, Saunders Y, Edmonds PM, Patel S, Wonderling D, Normand C, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of capecitabine (Xeloda®) for locally advanced and/or metastatic breast cancer.
By Jones L, Hawkins N, Westwood M, Wright K, Richardson G, Riemsma R.
-
Effectiveness and efficiency of guideline dissemination and implementation strategies.
By Grimshaw JM, Thomas RE, MacLennan G, Fraser C, Ramsay CR, Vale L, et al.
-
Clinical effectiveness and costs of the Sugarbaker procedure for the treatment of pseudomyxoma peritonei.
By Bryant J, Clegg AJ, Sidhu MK, Brodin H, Royle P, Davidson P.
-
Psychological treatment for insomnia in the regulation of long-term hypnotic drug use.
By Morgan K, Dixon S, Mathers N, Thompson J, Tomeny M.
-
Improving the evaluation of therapeutic interventions in multiple sclerosis: development of a patient-based measure of outcome.
By Hobart JC, Riazi A, Lamping DL, Fitzpatrick R, Thompson AJ.
-
A systematic review and economic evaluation of magnetic resonance cholangiopancreatography compared with diagnostic endoscopic retrograde cholangiopancreatography.
By Kaltenthaler E, Bravo Vergel Y, Chilcott J, Thomas S, Blakeborough T, Walters SJ, et al.
-
The use of modelling to evaluate new drugs for patients with a chronic condition: the case of antibodies against tumour necrosis factor in rheumatoid arthritis.
By Barton P, Jobanputra P, Wilson J, Bryan S, Burls A.
-
Clinical effectiveness and cost-effectiveness of neonatal screening for inborn errors of metabolism using tandem mass spectrometry: a systematic review.
By Pandor A, Eastham J, Beverley C, Chilcott J, Paisley S.
-
Clinical effectiveness and cost-effectiveness of pioglitazone and rosiglitazone in the treatment of type 2 diabetes: a systematic review and economic evaluation.
By Czoski-Murray C, Warren E, Chilcott J, Beverley C, Psyllaki MA, Cowan J.
-
Routine examination of the newborn: the EMREN study. Evaluation of an extension of the midwife role including a randomised controlled trial of appropriately trained midwives and paediatric senior house officers.
By Townsend J, Wolke D, Hayes J, Davé S, Rogers C, Bloomfield L, et al.
-
Involving consumers in research and development agenda setting for the NHS: developing an evidence-based approach.
By Oliver S, Clarke-Jones L, Rees R, Milne R, Buchanan P, Gabbay J, et al.
-
A multi-centre randomised controlled trial of minimally invasive direct coronary bypass grafting versus percutaneous transluminal coronary angioplasty with stenting for proximal stenosis of the left anterior descending coronary artery.
By Reeves BC, Angelini GD, Bryan AJ, Taylor FC, Cripps T, Spyt TJ, et al.
-
Does early magnetic resonance imaging influence management or improve outcome in patients referred to secondary care with low back pain? A pragmatic randomised controlled trial.
By Gilbert FJ, Grant AM, Gillan MGC, Vale L, Scott NW, Campbell MK, et al.
-
The clinical and cost-effectiveness of anakinra for the treatment of rheumatoid arthritis in adults: a systematic review and economic analysis.
By Clark W, Jobanputra P, Barton P, Burls A.
-
A rapid and systematic review and economic evaluation of the clinical and cost-effectiveness of newer drugs for treatment of mania associated with bipolar affective disorder.
By Bridle C, Palmer S, Bagnall A-M, Darba J, Duffy S, Sculpher M, et al.
-
Liquid-based cytology in cervical screening: an updated rapid and systematic review and economic analysis.
By Karnon J, Peters J, Platt J, Chilcott J, McGoogan E, Brewer N.
-
Systematic review of the long-term effects and economic consequences of treatments for obesity and implications for health improvement.
By Avenell A, Broom J, Brown TJ, Poobalan A, Aucott L, Stearns SC, et al.
-
Autoantibody testing in children with newly diagnosed type 1 diabetes mellitus.
By Dretzke J, Cummins C, Sandercock J, Fry-Smith A, Barrett T, Burls A.
-
Clinical effectiveness and cost-effectiveness of prehospital intravenous fluids in trauma patients.
By Dretzke J, Sandercock J, Bayliss S, Burls A.
-
Newer hypnotic drugs for the short-term management of insomnia: a systematic review and economic evaluation.
By Dündar Y, Boland A, Strobl J, Dodd S, Haycox A, Bagust A, et al.
-
Development and validation of methods for assessing the quality of diagnostic accuracy studies.
By Whiting P, Rutjes AWS, Dinnes J, Reitsma JB, Bossuyt PMM, Kleijnen J.
-
EVALUATE hysterectomy trial: a multicentre randomised trial comparing abdominal, vaginal and laparoscopic methods of hysterectomy.
By Garry R, Fountain J, Brown J, Manca A, Mason S, Sculpher M, et al.
-
Methods for expected value of information analysis in complex health economic models: developments on the health economics of interferon-β and glatiramer acetate for multiple sclerosis.
By Tappenden P, Chilcott JB, Eggington S, Oakley J, McCabe C.
-
Effectiveness and cost-effectiveness of imatinib for first-line treatment of chronic myeloid leukaemia in chronic phase: a systematic review and economic analysis.
By Dalziel K, Round A, Stein K, Garside R, Price A.
-
VenUS I: a randomised controlled trial of two types of bandage for treating venous leg ulcers.
By Iglesias C, Nelson EA, Cullum NA, Torgerson DJ, on behalf of the VenUS Team.
-
Systematic review of the effectiveness and cost-effectiveness, and economic evaluation, of myocardial perfusion scintigraphy for the diagnosis and management of angina and myocardial infarction.
By Mowatt G, Vale L, Brazzelli M, Hernandez R, Murray A, Scott N, et al.
-
A pilot study on the use of decision theory and value of information analysis as part of the NHS Health Technology Assessment programme.
By Claxton K, Ginnelly L, Sculpher M, Philips Z, Palmer S.
-
The Social Support and Family Health Study: a randomised controlled trial and economic evaluation of two alternative forms of postnatal support for mothers living in disadvantaged inner-city areas.
By Wiggins M, Oakley A, Roberts I, Turner H, Rajan L, Austerberry H, et al.
-
Psychosocial aspects of genetic screening of pregnant women and newborns: a systematic review.
By Green JM, Hewison J, Bekker HL, Bryant, Cuckle HS.
-
Evaluation of abnormal uterine bleeding: comparison of three outpatient procedures within cohorts defined by age and menopausal status.
By Critchley HOD, Warner P, Lee AJ, Brechin S, Guise J, Graham B.
-
Coronary artery stents: a rapid systematic review and economic evaluation.
By Hill R, Bagust A, Bakhai A, Dickson R, Dündar Y, Haycox A, et al.
-
Review of guidelines for good practice in decision-analytic modelling in health technology assessment.
By Philips Z, Ginnelly L, Sculpher M, Claxton K, Golder S, Riemsma R, et al.
-
Rituximab (MabThera®) for aggressive non-Hodgkin’s lymphoma: systematic review and economic evaluation.
By Knight C, Hind D, Brewer N, Abbott V.
-
Clinical effectiveness and cost-effectiveness of clopidogrel and modified-release dipyridamole in the secondary prevention of occlusive vascular events: a systematic review and economic evaluation.
By Jones L, Griffin S, Palmer S, Main C, Orton V, Sculpher M, et al.
-
Pegylated interferon α-2a and -2b in combination with ribavirin in the treatment of chronic hepatitis C: a systematic review and economic evaluation.
By Shepherd J, Brodin H, Cave C, Waugh N, Price A, Gabbay J.
-
Clopidogrel used in combination with aspirin compared with aspirin alone in the treatment of non-ST-segment- elevation acute coronary syndromes: a systematic review and economic evaluation.
By Main C, Palmer S, Griffin S, Jones L, Orton V, Sculpher M, et al.
-
Provision, uptake and cost of cardiac rehabilitation programmes: improving services to under-represented groups.
By Beswick AD, Rees K, Griebsch I, Taylor FC, Burke M, West RR, et al.
-
Involving South Asian patients in clinical trials.
By Hussain-Gambles M, Leese B, Atkin K, Brown J, Mason S, Tovey P.
-
Clinical and cost-effectiveness of continuous subcutaneous insulin infusion for diabetes.
By Colquitt JL, Green C, Sidhu MK, Hartwell D, Waugh N.
-
Identification and assessment of ongoing trials in health technology assessment reviews.
By Song FJ, Fry-Smith A, Davenport C, Bayliss S, Adi Y, Wilson JS, et al.
-
Systematic review and economic evaluation of a long-acting insulin analogue, insulin glargine
By Warren E, Weatherley-Jones E, Chilcott J, Beverley C.
-
Supplementation of a home-based exercise programme with a class-based programme for people with osteoarthritis of the knees: a randomised controlled trial and health economic analysis.
By McCarthy CJ, Mills PM, Pullen R, Richardson G, Hawkins N, Roberts CR, et al.
-
Clinical and cost-effectiveness of once-daily versus more frequent use of same potency topical corticosteroids for atopic eczema: a systematic review and economic evaluation.
By Green C, Colquitt JL, Kirby J, Davidson P, Payne E.
-
Acupuncture of chronic headache disorders in primary care: randomised controlled trial and economic analysis.
By Vickers AJ, Rees RW, Zollman CE, McCarney R, Smith CM, Ellis N, et al.
-
Generalisability in economic evaluation studies in healthcare: a review and case studies.
By Sculpher MJ, Pang FS, Manca A, Drummond MF, Golder S, Urdahl H, et al.
-
Virtual outreach: a randomised controlled trial and economic evaluation of joint teleconferenced medical consultations.
By Wallace P, Barber J, Clayton W, Currell R, Fleming K, Garner P, et al.
-
Randomised controlled multiple treatment comparison to provide a cost-effectiveness rationale for the selection of antimicrobial therapy in acne.
By Ozolins M, Eady EA, Avery A, Cunliffe WJ, O’Neill C, Simpson NB, et al.
-
Do the findings of case series studies vary significantly according to methodological characteristics?
By Dalziel K, Round A, Stein K, Garside R, Castelnuovo E, Payne L.
-
Improving the referral process for familial breast cancer genetic counselling: findings of three randomised controlled trials of two interventions.
By Wilson BJ, Torrance N, Mollison J, Wordsworth S, Gray JR, Haites NE, et al.
-
Randomised evaluation of alternative electrosurgical modalities to treat bladder outflow obstruction in men with benign prostatic hyperplasia.
By Fowler C, McAllister W, Plail R, Karim O, Yang Q.
-
A pragmatic randomised controlled trial of the cost-effectiveness of palliative therapies for patients with inoperable oesophageal cancer.
By Shenfine J, McNamee P, Steen N, Bond J, Griffin SM.
-
Impact of computer-aided detection prompts on the sensitivity and specificity of screening mammography.
By Taylor P, Champness J, Given- Wilson R, Johnston K, Potts H.
-
Issues in data monitoring and interim analysis of trials.
By Grant AM, Altman DG, Babiker AB, Campbell MK, Clemens FJ, Darbyshire JH, et al.
-
Lay public’s understanding of equipoise and randomisation in randomised controlled trials.
By Robinson EJ, Kerr CEP, Stevens AJ, Lilford RJ, Braunholtz DA, Edwards SJ, et al.
-
Clinical and cost-effectiveness of electroconvulsive therapy for depressive illness, schizophrenia, catatonia and mania: systematic reviews and economic modelling studies.
By Greenhalgh J, Knight C, Hind D, Beverley C, Walters S.
-
Measurement of health-related quality of life for people with dementia: development of a new instrument (DEMQOL) and an evaluation of current methodology.
By Smith SC, Lamping DL, Banerjee S, Harwood R, Foley B, Smith P, et al.
-
Clinical effectiveness and cost-effectiveness of drotrecogin alfa (activated) (Xigris®) for the treatment of severe sepsis in adults: a systematic review and economic evaluation.
By Green C, Dinnes J, Takeda A, Shepherd J, Hartwell D, Cave C, et al.
-
A methodological review of how heterogeneity has been examined in systematic reviews of diagnostic test accuracy.
By Dinnes J, Deeks J, Kirby J, Roderick P.
-
Cervical screening programmes: can automation help? Evidence from systematic reviews, an economic analysis and a simulation modelling exercise applied to the UK.
By Willis BH, Barton P, Pearmain P, Bryan S, Hyde C.
-
Laparoscopic surgery for inguinal hernia repair: systematic review of effectiveness and economic evaluation.
By McCormack K, Wake B, Perez J, Fraser C, Cook J, McIntosh E, et al.
-
Clinical effectiveness, tolerability and cost-effectiveness of newer drugs for epilepsy in adults: a systematic review and economic evaluation.
By Wilby J, Kainth A, Hawkins N, Epstein D, McIntosh H, McDaid C, et al.
-
A randomised controlled trial to compare the cost-effectiveness of tricyclic antidepressants, selective serotonin reuptake inhibitors and lofepramine.
By Peveler R, Kendrick T, Buxton M, Longworth L, Baldwin D, Moore M, et al.
-
Clinical effectiveness and cost-effectiveness of immediate angioplasty for acute myocardial infarction: systematic review and economic evaluation.
By Hartwell D, Colquitt J, Loveman E, Clegg AJ, Brodin H, Waugh N, et al.
-
A randomised controlled comparison of alternative strategies in stroke care.
By Kalra L, Evans A, Perez I, Knapp M, Swift C, Donaldson N.
-
The investigation and analysis of critical incidents and adverse events in healthcare.
By Woloshynowych M, Rogers S, Taylor-Adams S, Vincent C.
-
Potential use of routine databases in health technology assessment.
By Raftery J, Roderick P, Stevens A.
-
Clinical and cost-effectiveness of newer immunosuppressive regimens in renal transplantation: a systematic review and modelling study.
By Woodroffe R, Yao GL, Meads C, Bayliss S, Ready A, Raftery J, et al.
-
A systematic review and economic evaluation of alendronate, etidronate, risedronate, raloxifene and teriparatide for the prevention and treatment of postmenopausal osteoporosis.
By Stevenson M, Lloyd Jones M, De Nigris E, Brewer N, Davis S, Oakley J.
-
A systematic review to examine the impact of psycho-educational interventions on health outcomes and costs in adults and children with difficult asthma.
By Smith JR, Mugford M, Holland R, Candy B, Noble MJ, Harrison BDW, et al.
-
An evaluation of the costs, effectiveness and quality of renal replacement therapy provision in renal satellite units in England and Wales.
By Roderick P, Nicholson T, Armitage A, Mehta R, Mullee M, Gerard K, et al.
-
Imatinib for the treatment of patients with unresectable and/or metastatic gastrointestinal stromal tumours: systematic review and economic evaluation.
By Wilson J, Connock M, Song F, Yao G, Fry-Smith A, Raftery J, et al.
-
Indirect comparisons of competing interventions.
By Glenny AM, Altman DG, Song F, Sakarovitch C, Deeks JJ, D’Amico R, et al.
-
Cost-effectiveness of alternative strategies for the initial medical management of non-ST elevation acute coronary syndrome: systematic review and decision-analytical modelling.
By Robinson M, Palmer S, Sculpher M, Philips Z, Ginnelly L, Bowens A, et al.
-
Outcomes of electrically stimulated gracilis neosphincter surgery.
By Tillin T, Chambers M, Feldman R.
-
The effectiveness and cost-effectiveness of pimecrolimus and tacrolimus for atopic eczema: a systematic review and economic evaluation.
By Garside R, Stein K, Castelnuovo E, Pitt M, Ashcroft D, Dimmock P, et al.
-
Systematic review on urine albumin testing for early detection of diabetic complications.
By Newman DJ, Mattock MB, Dawnay ABS, Kerry S, McGuire A, Yaqoob M, et al.
-
Randomised controlled trial of the cost-effectiveness of water-based therapy for lower limb osteoarthritis.
By Cochrane T, Davey RC, Matthes Edwards SM.
-
Longer term clinical and economic benefits of offering acupuncture care to patients with chronic low back pain.
By Thomas KJ, MacPherson H, Ratcliffe J, Thorpe L, Brazier J, Campbell M, et al.
-
Cost-effectiveness and safety of epidural steroids in the management of sciatica.
By Price C, Arden N, Coglan L, Rogers P.
-
The British Rheumatoid Outcome Study Group (BROSG) randomised controlled trial to compare the effectiveness and cost-effectiveness of aggressive versus symptomatic therapy in established rheumatoid arthritis.
By Symmons D, Tricker K, Roberts C, Davies L, Dawes P, Scott DL.
-
Conceptual framework and systematic review of the effects of participants’ and professionals’ preferences in randomised controlled trials.
By King M, Nazareth I, Lampe F, Bower P, Chandler M, Morou M, et al.
-
The clinical and cost-effectiveness of implantable cardioverter defibrillators: a systematic review.
By Bryant J, Brodin H, Loveman E, Payne E, Clegg A.
-
A trial of problem-solving by community mental health nurses for anxiety, depression and life difficulties among general practice patients. The CPN-GP study.
By Kendrick T, Simons L, Mynors-Wallis L, Gray A, Lathlean J, Pickering R, et al.
-
The causes and effects of socio-demographic exclusions from clinical trials.
By Bartlett C, Doyal L, Ebrahim S, Davey P, Bachmann M, Egger M, et al.
-
Is hydrotherapy cost-effective? A randomised controlled trial of combined hydrotherapy programmes compared with physiotherapy land techniques in children with juvenile idiopathic arthritis.
By Epps H, Ginnelly L, Utley M, Southwood T, Gallivan S, Sculpher M, et al.
-
A randomised controlled trial and cost-effectiveness study of systematic screening (targeted and total population screening) versus routine practice for the detection of atrial fibrillation in people aged 65 and over. The SAFE study.
By Hobbs FDR, Fitzmaurice DA, Mant J, Murray E, Jowett S, Bryan S, et al.
-
Displaced intracapsular hip fractures in fit, older people: a randomised comparison of reduction and fixation, bipolar hemiarthroplasty and total hip arthroplasty.
By Keating JF, Grant A, Masson M, Scott NW, Forbes JF.
-
Long-term outcome of cognitive behaviour therapy clinical trials in central Scotland.
By Durham RC, Chambers JA, Power KG, Sharp DM, Macdonald RR, Major KA, et al.
-
The effectiveness and cost-effectiveness of dual-chamber pacemakers compared with single-chamber pacemakers for bradycardia due to atrioventricular block or sick sinus syndrome: systematic review and economic evaluation.
By Castelnuovo E, Stein K, Pitt M, Garside R, Payne E.
-
Newborn screening for congenital heart defects: a systematic review and cost-effectiveness analysis.
By Knowles R, Griebsch I, Dezateux C, Brown J, Bull C, Wren C.
-
The clinical and cost-effectiveness of left ventricular assist devices for end-stage heart failure: a systematic review and economic evaluation.
By Clegg AJ, Scott DA, Loveman E, Colquitt J, Hutchinson J, Royle P, et al.
-
The effectiveness of the Heidelberg Retina Tomograph and laser diagnostic glaucoma scanning system (GDx) in detecting and monitoring glaucoma.
By Kwartz AJ, Henson DB, Harper RA, Spencer AF, McLeod D.
-
Clinical and cost-effectiveness of autologous chondrocyte implantation for cartilage defects in knee joints: systematic review and economic evaluation.
By Clar C, Cummins E, McIntyre L, Thomas S, Lamb J, Bain L, et al.
-
Systematic review of effectiveness of different treatments for childhood retinoblastoma.
By McDaid C, Hartley S, Bagnall A-M, Ritchie G, Light K, Riemsma R.
-
Towards evidence-based guidelines for the prevention of venous thromboembolism: systematic reviews of mechanical methods, oral anticoagulation, dextran and regional anaesthesia as thromboprophylaxis.
By Roderick P, Ferris G, Wilson K, Halls H, Jackson D, Collins R, et al.
-
The effectiveness and cost-effectiveness of parent training/education programmes for the treatment of conduct disorder, including oppositional defiant disorder, in children.
By Dretzke J, Frew E, Davenport C, Barlow J, Stewart-Brown S, Sandercock J, et al.
-
The clinical and cost-effectiveness of donepezil, rivastigmine, galantamine and memantine for Alzheimer’s disease.
By Loveman E, Green C, Kirby J, Takeda A, Picot J, Payne E, et al.
-
FOOD: a multicentre randomised trial evaluating feeding policies in patients admitted to hospital with a recent stroke.
By Dennis M, Lewis S, Cranswick G, Forbes J.
-
The clinical effectiveness and cost-effectiveness of computed tomography screening for lung cancer: systematic reviews.
By Black C, Bagust A, Boland A, Walker S, McLeod C, De Verteuil R, et al.
-
A systematic review of the effectiveness and cost-effectiveness of neuroimaging assessments used to visualise the seizure focus in people with refractory epilepsy being considered for surgery.
By Whiting P, Gupta R, Burch J, Mujica Mota RE, Wright K, Marson A, et al.
-
Comparison of conference abstracts and presentations with full-text articles in the health technology assessments of rapidly evolving technologies.
By Dundar Y, Dodd S, Dickson R, Walley T, Haycox A, Williamson PR.
-
Systematic review and evaluation of methods of assessing urinary incontinence.
By Martin JL, Williams KS, Abrams KR, Turner DA, Sutton AJ, Chapple C, et al.
-
The clinical effectiveness and cost-effectiveness of newer drugs for children with epilepsy. A systematic review.
By Connock M, Frew E, Evans B-W, Bryan S, Cummins C, Fry-Smith A, et al.
-
Surveillance of Barrett’s oesophagus: exploring the uncertainty through systematic review, expert workshop and economic modelling.
By Garside R, Pitt M, Somerville M, Stein K, Price A, Gilbert N.
-
Topotecan, pegylated liposomal doxorubicin hydrochloride and paclitaxel for second-line or subsequent treatment of advanced ovarian cancer: a systematic review and economic evaluation.
By Main C, Bojke L, Griffin S, Norman G, Barbieri M, Mather L, et al.
-
Evaluation of molecular techniques in prediction and diagnosis of cytomegalovirus disease in immunocompromised patients.
By Szczepura A, Westmoreland D, Vinogradova Y, Fox J, Clark M.
-
Screening for thrombophilia in high-risk situations: systematic review and cost-effectiveness analysis. The Thrombosis: Risk and Economic Assessment of Thrombophilia Screening (TREATS) study.
By Wu O, Robertson L, Twaddle S, Lowe GDO, Clark P, Greaves M, et al.
-
A series of systematic reviews to inform a decision analysis for sampling and treating infected diabetic foot ulcers.
By Nelson EA, O’Meara S, Craig D, Iglesias C, Golder S, Dalton J, et al.
-
Randomised clinical trial, observational study and assessment of cost-effectiveness of the treatment of varicose veins (REACTIV trial).
By Michaels JA, Campbell WB, Brazier JE, MacIntyre JB, Palfreyman SJ, Ratcliffe J, et al.
-
The cost-effectiveness of screening for oral cancer in primary care.
By Speight PM, Palmer S, Moles DR, Downer MC, Smith DH, Henriksson M, et al.
-
Measurement of the clinical and cost-effectiveness of non-invasive diagnostic testing strategies for deep vein thrombosis.
By Goodacre S, Sampson F, Stevenson M, Wailoo A, Sutton A, Thomas S, et al.
-
Systematic review of the effectiveness and cost-effectiveness of HealOzone® for the treatment of occlusal pit/fissure caries and root caries.
By Brazzelli M, McKenzie L, Fielding S, Fraser C, Clarkson J, Kilonzo M, et al.
-
Randomised controlled trials of conventional antipsychotic versus new atypical drugs, and new atypical drugs versus clozapine, in people with schizophrenia responding poorly to, or intolerant of, current drug treatment.
By Lewis SW, Davies L, Jones PB, Barnes TRE, Murray RM, Kerwin R, et al.
-
Diagnostic tests and algorithms used in the investigation of haematuria: systematic reviews and economic evaluation.
By Rodgers M, Nixon J, Hempel S, Aho T, Kelly J, Neal D, et al.
-
Cognitive behavioural therapy in addition to antispasmodic therapy for irritable bowel syndrome in primary care: randomised controlled trial.
By Kennedy TM, Chalder T, McCrone P, Darnley S, Knapp M, Jones RH, et al.
-
A systematic review of the clinical effectiveness and cost-effectiveness of enzyme replacement therapies for Fabry’s disease and mucopolysaccharidosis type 1.
By Connock M, Juarez-Garcia A, Frew E, Mans A, Dretzke J, Fry-Smith A, et al.
-
Health benefits of antiviral therapy for mild chronic hepatitis C: randomised controlled trial and economic evaluation.
By Wright M, Grieve R, Roberts J, Main J, Thomas HC, on behalf of the UK Mild Hepatitis C Trial Investigators.
-
Pressure relieving support surfaces: a randomised evaluation.
By Nixon J, Nelson EA, Cranny G, Iglesias CP, Hawkins K, Cullum NA, et al.
-
A systematic review and economic model of the effectiveness and cost-effectiveness of methylphenidate, dexamfetamine and atomoxetine for the treatment of attention deficit hyperactivity disorder in children and adolescents.
By King S, Griffin S, Hodges Z, Weatherly H, Asseburg C, Richardson G, et al.
-
The clinical effectiveness and cost-effectiveness of enzyme replacement therapy for Gaucher’s disease: a systematic review.
By Connock M, Burls A, Frew E, Fry-Smith A, Juarez-Garcia A, McCabe C, et al.
-
Effectiveness and cost-effectiveness of salicylic acid and cryotherapy for cutaneous warts. An economic decision model.
By Thomas KS, Keogh-Brown MR, Chalmers JR, Fordham RJ, Holland RC, Armstrong SJ, et al.
-
A systematic literature review of the effectiveness of non-pharmacological interventions to prevent wandering in dementia and evaluation of the ethical implications and acceptability of their use.
By Robinson L, Hutchings D, Corner L, Beyer F, Dickinson H, Vanoli A, et al.
-
A review of the evidence on the effects and costs of implantable cardioverter defibrillator therapy in different patient groups, and modelling of cost-effectiveness and cost–utility for these groups in a UK context.
By Buxton M, Caine N, Chase D, Connelly D, Grace A, Jackson C, et al.
-
Adefovir dipivoxil and pegylated interferon alfa-2a for the treatment of chronic hepatitis B: a systematic review and economic evaluation.
By Shepherd J, Jones J, Takeda A, Davidson P, Price A.
-
An evaluation of the clinical and cost-effectiveness of pulmonary artery catheters in patient management in intensive care: a systematic review and a randomised controlled trial.
By Harvey S, Stevens K, Harrison D, Young D, Brampton W, McCabe C, et al.
-
Accurate, practical and cost-effective assessment of carotid stenosis in the UK.
By Wardlaw JM, Chappell FM, Stevenson M, De Nigris E, Thomas S, Gillard J, et al.
-
Etanercept and infliximab for the treatment of psoriatic arthritis: a systematic review and economic evaluation.
By Woolacott N, Bravo Vergel Y, Hawkins N, Kainth A, Khadjesari Z, Misso K, et al.
-
The cost-effectiveness of testing for hepatitis C in former injecting drug users.
By Castelnuovo E, Thompson-Coon J, Pitt M, Cramp M, Siebert U, Price A, et al.
-
Computerised cognitive behaviour therapy for depression and anxiety update: a systematic review and economic evaluation.
By Kaltenthaler E, Brazier J, De Nigris E, Tumur I, Ferriter M, Beverley C, et al.
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.
By Williams C, Brunskill S, Altman D, Briggs A, Campbell H, Clarke M, et al.
-
Psychological therapies including dialectical behaviour therapy for borderline personality disorder: a systematic review and preliminary economic evaluation.
By Brazier J, Tumur I, Holmes M, Ferriter M, Parry G, Dent-Brown K, et al.
-
Clinical effectiveness and cost-effectiveness of tests for the diagnosis and investigation of urinary tract infection in children: a systematic review and economic model.
By Whiting P, Westwood M, Bojke L, Palmer S, Richardson G, Cooper J, et al.
-
Cognitive behavioural therapy in chronic fatigue syndrome: a randomised controlled trial of an outpatient group programme.
By O’Dowd H, Gladwell P, Rogers CA, Hollinghurst S, Gregory A.
-
A comparison of the cost-effectiveness of five strategies for the prevention of nonsteroidal anti-inflammatory drug-induced gastrointestinal toxicity: a systematic review with economic modelling.
By Brown TJ, Hooper L, Elliott RA, Payne K, Webb R, Roberts C, et al.
-
The effectiveness and cost-effectiveness of computed tomography screening for coronary artery disease: systematic review.
By Waugh N, Black C, Walker S, McIntyre L, Cummins E, Hillis G.
-
What are the clinical outcome and cost-effectiveness of endoscopy undertaken by nurses when compared with doctors? A Multi-Institution Nurse Endoscopy Trial (MINuET).
By Williams J, Russell I, Durai D, Cheung W-Y, Farrin A, Bloor K, et al.
-
The clinical and cost-effectiveness of oxaliplatin and capecitabine for the adjuvant treatment of colon cancer: systematic review and economic evaluation.
By Pandor A, Eggington S, Paisley S, Tappenden P, Sutcliffe P.
-
A systematic review of the effectiveness of adalimumab, etanercept and infliximab for the treatment of rheumatoid arthritis in adults and an economic evaluation of their cost-effectiveness.
By Chen Y-F, Jobanputra P, Barton P, Jowett S, Bryan S, Clark W, et al.
-
Telemedicine in dermatology: a randomised controlled trial.
By Bowns IR, Collins K, Walters SJ, McDonagh AJG.
-
Cost-effectiveness of cell salvage and alternative methods of minimising perioperative allogeneic blood transfusion: a systematic review and economic model.
By Davies L, Brown TJ, Haynes S, Payne K, Elliott RA, McCollum C.
-
Clinical effectiveness and cost-effectiveness of laparoscopic surgery for colorectal cancer: systematic reviews and economic evaluation.
By Murray A, Lourenco T, de Verteuil R, Hernandez R, Fraser C, McKinley A, et al.
-
Etanercept and efalizumab for the treatment of psoriasis: a systematic review.
By Woolacott N, Hawkins N, Mason A, Kainth A, Khadjesari Z, Bravo Vergel Y, et al.
-
Systematic reviews of clinical decision tools for acute abdominal pain.
By Liu JLY, Wyatt JC, Deeks JJ, Clamp S, Keen J, Verde P, et al.
-
Evaluation of the ventricular assist device programme in the UK.
By Sharples L, Buxton M, Caine N, Cafferty F, Demiris N, Dyer M, et al.
-
A systematic review and economic model of the clinical and cost-effectiveness of immunosuppressive therapy for renal transplantation in children.
By Yao G, Albon E, Adi Y, Milford D, Bayliss S, Ready A, et al.
-
Amniocentesis results: investigation of anxiety. The ARIA trial.
By Hewison J, Nixon J, Fountain J, Cocks K, Jones C, Mason G, et al.
-
Pemetrexed disodium for the treatment of malignant pleural mesothelioma: a systematic review and economic evaluation.
By Dundar Y, Bagust A, Dickson R, Dodd S, Green J, Haycox A, et al.
-
A systematic review and economic model of the clinical effectiveness and cost-effectiveness of docetaxel in combination with prednisone or prednisolone for the treatment of hormone-refractory metastatic prostate cancer.
By Collins R, Fenwick E, Trowman R, Perard R, Norman G, Light K, et al.
-
A systematic review of rapid diagnostic tests for the detection of tuberculosis infection.
By Dinnes J, Deeks J, Kunst H, Gibson A, Cummins E, Waugh N, et al.
-
The clinical effectiveness and cost-effectiveness of strontium ranelate for the prevention of osteoporotic fragility fractures in postmenopausal women.
By Stevenson M, Davis S, Lloyd-Jones M, Beverley C.
-
A systematic review of quantitative and qualitative research on the role and effectiveness of written information available to patients about individual medicines.
By Raynor DK, Blenkinsopp A, Knapp P, Grime J, Nicolson DJ, Pollock K, et al.
-
Oral naltrexone as a treatment for relapse prevention in formerly opioid-dependent drug users: a systematic review and economic evaluation.
By Adi Y, Juarez-Garcia A, Wang D, Jowett S, Frew E, Day E, et al.
-
Glucocorticoid-induced osteoporosis: a systematic review and cost–utility analysis.
By Kanis JA, Stevenson M, McCloskey EV, Davis S, Lloyd-Jones M.
-
Epidemiological, social, diagnostic and economic evaluation of population screening for genital chlamydial infection.
By Low N, McCarthy A, Macleod J, Salisbury C, Campbell R, Roberts TE, et al.
-
Methadone and buprenorphine for the management of opioid dependence: a systematic review and economic evaluation.
By Connock M, Juarez-Garcia A, Jowett S, Frew E, Liu Z, Taylor RJ, et al.
-
Exercise Evaluation Randomised Trial (EXERT): a randomised trial comparing GP referral for leisure centre-based exercise, community-based walking and advice only.
By Isaacs AJ, Critchley JA, See Tai S, Buckingham K, Westley D, Harridge SDR, et al.
-
Interferon alfa (pegylated and non-pegylated) and ribavirin for the treatment of mild chronic hepatitis C: a systematic review and economic evaluation.
By Shepherd J, Jones J, Hartwell D, Davidson P, Price A, Waugh N.
-
Systematic review and economic evaluation of bevacizumab and cetuximab for the treatment of metastatic colorectal cancer.
By Tappenden P, Jones R, Paisley S, Carroll C.
-
A systematic review and economic evaluation of epoetin alfa, epoetin beta and darbepoetin alfa in anaemia associated with cancer, especially that attributable to cancer treatment.
By Wilson J, Yao GL, Raftery J, Bohlius J, Brunskill S, Sandercock J, et al.
-
A systematic review and economic evaluation of statins for the prevention of coronary events.
By Ward S, Lloyd Jones M, Pandor A, Holmes M, Ara R, Ryan A, et al.
-
A systematic review of the effectiveness and cost-effectiveness of different models of community-based respite care for frail older people and their carers.
By Mason A, Weatherly H, Spilsbury K, Arksey H, Golder S, Adamson J, et al.
-
Additional therapy for young children with spastic cerebral palsy: a randomised controlled trial.
By Weindling AM, Cunningham CC, Glenn SM, Edwards RT, Reeves DJ.
-
Screening for type 2 diabetes: literature review and economic modelling.
By Waugh N, Scotland G, McNamee P, Gillett M, Brennan A, Goyder E, et al.
-
The effectiveness and cost-effectiveness of cinacalcet for secondary hyperparathyroidism in end-stage renal disease patients on dialysis: a systematic review and economic evaluation.
By Garside R, Pitt M, Anderson R, Mealing S, Roome C, Snaith A, et al.
-
The clinical effectiveness and cost-effectiveness of gemcitabine for metastatic breast cancer: a systematic review and economic evaluation.
By Takeda AL, Jones J, Loveman E, Tan SC, Clegg AJ.
-
A systematic review of duplex ultrasound, magnetic resonance angiography and computed tomography angiography for the diagnosis and assessment of symptomatic, lower limb peripheral arterial disease.
By Collins R, Cranny G, Burch J, Aguiar-Ibáñez R, Craig D, Wright K, et al.
-
The clinical effectiveness and cost-effectiveness of treatments for children with idiopathic steroid-resistant nephrotic syndrome: a systematic review.
By Colquitt JL, Kirby J, Green C, Cooper K, Trompeter RS.
-
A systematic review of the routine monitoring of growth in children of primary school age to identify growth-related conditions.
By Fayter D, Nixon J, Hartley S, Rithalia A, Butler G, Rudolf M, et al.
-
Systematic review of the effectiveness of preventing and treating Staphylococcus aureus carriage in reducing peritoneal catheter-related infections.
By McCormack K, Rabindranath K, Kilonzo M, Vale L, Fraser C, McIntyre L, et al.
-
The clinical effectiveness and cost of repetitive transcranial magnetic stimulation versus electroconvulsive therapy in severe depression: a multicentre pragmatic randomised controlled trial and economic analysis.
By McLoughlin DM, Mogg A, Eranti S, Pluck G, Purvis R, Edwards D, et al.
-
A randomised controlled trial and economic evaluation of direct versus indirect and individual versus group modes of speech and language therapy for children with primary language impairment.
By Boyle J, McCartney E, Forbes J, O’Hare A.
-
Hormonal therapies for early breast cancer: systematic review and economic evaluation.
By Hind D, Ward S, De Nigris E, Simpson E, Carroll C, Wyld L.
-
Cardioprotection against the toxic effects of anthracyclines given to children with cancer: a systematic review.
By Bryant J, Picot J, Levitt G, Sullivan I, Baxter L, Clegg A.
-
Adalimumab, etanercept and infliximab for the treatment of ankylosing spondylitis: a systematic review and economic evaluation.
By McLeod C, Bagust A, Boland A, Dagenais P, Dickson R, Dundar Y, et al.
-
Prenatal screening and treatment strategies to prevent group B streptococcal and other bacterial infections in early infancy: cost-effectiveness and expected value of information analyses.
By Colbourn T, Asseburg C, Bojke L, Philips Z, Claxton K, Ades AE, et al.
-
Clinical effectiveness and cost-effectiveness of bone morphogenetic proteins in the non-healing of fractures and spinal fusion: a systematic review.
By Garrison KR, Donell S, Ryder J, Shemilt I, Mugford M, Harvey I, et al.
-
A randomised controlled trial of postoperative radiotherapy following breast-conserving surgery in a minimum-risk older population. The PRIME trial.
By Prescott RJ, Kunkler IH, Williams LJ, King CC, Jack W, van der Pol M, et al.
-
Current practice, accuracy, effectiveness and cost-effectiveness of the school entry hearing screen.
By Bamford J, Fortnum H, Bristow K, Smith J, Vamvakas G, Davies L, et al.
-
The clinical effectiveness and cost-effectiveness of inhaled insulin in diabetes mellitus: a systematic review and economic evaluation.
By Black C, Cummins E, Royle P, Philip S, Waugh N.
-
Surveillance of cirrhosis for hepatocellular carcinoma: systematic review and economic analysis.
By Thompson Coon J, Rogers G, Hewson P, Wright D, Anderson R, Cramp M, et al.
-
The Birmingham Rehabilitation Uptake Maximisation Study (BRUM). Homebased compared with hospital-based cardiac rehabilitation in a multi-ethnic population: cost-effectiveness and patient adherence.
By Jolly K, Taylor R, Lip GYH, Greenfield S, Raftery J, Mant J, et al.
-
A systematic review of the clinical, public health and cost-effectiveness of rapid diagnostic tests for the detection and identification of bacterial intestinal pathogens in faeces and food.
By Abubakar I, Irvine L, Aldus CF, Wyatt GM, Fordham R, Schelenz S, et al.
-
A randomised controlled trial examining the longer-term outcomes of standard versus new antiepileptic drugs. The SANAD trial.
By Marson AG, Appleton R, Baker GA, Chadwick DW, Doughty J, Eaton B, et al.
-
Clinical effectiveness and cost-effectiveness of different models of managing long-term oral anti-coagulation therapy: a systematic review and economic modelling.
By Connock M, Stevens C, Fry-Smith A, Jowett S, Fitzmaurice D, Moore D, et al.
-
A systematic review and economic model of the clinical effectiveness and cost-effectiveness of interventions for preventing relapse in people with bipolar disorder.
By Soares-Weiser K, Bravo Vergel Y, Beynon S, Dunn G, Barbieri M, Duffy S, et al.
-
Taxanes for the adjuvant treatment of early breast cancer: systematic review and economic evaluation.
By Ward S, Simpson E, Davis S, Hind D, Rees A, Wilkinson A.
-
The clinical effectiveness and cost-effectiveness of screening for open angle glaucoma: a systematic review and economic evaluation.
By Burr JM, Mowatt G, Hernández R, Siddiqui MAR, Cook J, Lourenco T, et al.
-
Acceptability, benefit and costs of early screening for hearing disability: a study of potential screening tests and models.
By Davis A, Smith P, Ferguson M, Stephens D, Gianopoulos I.
-
Contamination in trials of educational interventions.
By Keogh-Brown MR, Bachmann MO, Shepstone L, Hewitt C, Howe A, Ramsay CR, et al.
-
Overview of the clinical effectiveness of positron emission tomography imaging in selected cancers.
By Facey K, Bradbury I, Laking G, Payne E.
-
The effectiveness and cost-effectiveness of carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma: a systematic review and economic evaluation.
By Garside R, Pitt M, Anderson R, Rogers G, Dyer M, Mealing S, et al.
-
Drug-eluting stents: a systematic review and economic evaluation.
By Hill RA, Boland A, Dickson R, Dündar Y, Haycox A, McLeod C, et al.
-
The clinical effectiveness and cost-effectiveness of cardiac resynchronisation (biventricular pacing) for heart failure: systematic review and economic model.
By Fox M, Mealing S, Anderson R, Dean J, Stein K, Price A, et al.
-
Recruitment to randomised trials: strategies for trial enrolment and participation study. The STEPS study.
By Campbell MK, Snowdon C, Francis D, Elbourne D, McDonald AM, Knight R, et al.
-
Cost-effectiveness of functional cardiac testing in the diagnosis and management of coronary artery disease: a randomised controlled trial. The CECaT trial.
By Sharples L, Hughes V, Crean A, Dyer M, Buxton M, Goldsmith K, et al.
-
Evaluation of diagnostic tests when there is no gold standard. A review of methods.
By Rutjes AWS, Reitsma JB, Coomarasamy A, Khan KS, Bossuyt PMM.
-
Systematic reviews of the clinical effectiveness and cost-effectiveness of proton pump inhibitors in acute upper gastrointestinal bleeding.
By Leontiadis GI, Sreedharan A, Dorward S, Barton P, Delaney B, Howden CW, et al.
-
A review and critique of modelling in prioritising and designing screening programmes.
By Karnon J, Goyder E, Tappenden P, McPhie S, Towers I, Brazier J, et al.
-
An assessment of the impact of the NHS Health Technology Assessment Programme.
By Hanney S, Buxton M, Green C, Coulson D, Raftery J.
-
A systematic review and economic model of switching from nonglycopeptide to glycopeptide antibiotic prophylaxis for surgery.
By Cranny G, Elliott R, Weatherly H, Chambers D, Hawkins N, Myers L, et al.
-
‘Cut down to quit’ with nicotine replacement therapies in smoking cessation: a systematic review of effectiveness and economic analysis.
By Wang D, Connock M, Barton P, Fry-Smith A, Aveyard P, Moore D.
-
A systematic review of the effectiveness of strategies for reducing fracture risk in children with juvenile idiopathic arthritis with additional data on long-term risk of fracture and cost of disease management.
By Thornton J, Ashcroft D, O’Neill T, Elliott R, Adams J, Roberts C, et al.
-
Does befriending by trained lay workers improve psychological well-being and quality of life for carers of people with dementia, and at what cost? A randomised controlled trial.
By Charlesworth G, Shepstone L, Wilson E, Thalanany M, Mugford M, Poland F.
-
A multi-centre retrospective cohort study comparing the efficacy, safety and cost-effectiveness of hysterectomy and uterine artery embolisation for the treatment of symptomatic uterine fibroids. The HOPEFUL study.
By Hirst A, Dutton S, Wu O, Briggs A, Edwards C, Waldenmaier L, et al.
-
Methods of prediction and prevention of pre-eclampsia: systematic reviews of accuracy and effectiveness literature with economic modelling.
By Meads CA, Cnossen JS, Meher S, Juarez-Garcia A, ter Riet G, Duley L, et al.
-
The use of economic evaluations in NHS decision-making: a review and empirical investigation.
By Williams I, McIver S, Moore D, Bryan S.
-
Stapled haemorrhoidectomy (haemorrhoidopexy) for the treatment of haemorrhoids: a systematic review and economic evaluation.
By Burch J, Epstein D, Baba-Akbari A, Weatherly H, Fox D, Golder S, et al.
-
The clinical effectiveness of diabetes education models for Type 2 diabetes: a systematic review.
By Loveman E, Frampton GK, Clegg AJ.
-
Payment to healthcare professionals for patient recruitment to trials: systematic review and qualitative study.
By Raftery J, Bryant J, Powell J, Kerr C, Hawker S.
-
Cyclooxygenase-2 selective non-steroidal anti-inflammatory drugs (etodolac, meloxicam, celecoxib, rofecoxib, etoricoxib, valdecoxib and lumiracoxib) for osteoarthritis and rheumatoid arthritis: a systematic review and economic evaluation.
By Chen Y-F, Jobanputra P, Barton P, Bryan S, Fry-Smith A, Harris G, et al.
-
The clinical effectiveness and cost-effectiveness of central venous catheters treated with anti-infective agents in preventing bloodstream infections: a systematic review and economic evaluation.
By Hockenhull JC, Dwan K, Boland A, Smith G, Bagust A, Dundar Y, et al.
-
Stepped treatment of older adults on laxatives. The STOOL trial.
By Mihaylov S, Stark C, McColl E, Steen N, Vanoli A, Rubin G, et al.
-
A randomised controlled trial of cognitive behaviour therapy in adolescents with major depression treated by selective serotonin reuptake inhibitors. The ADAPT trial.
By Goodyer IM, Dubicka B, Wilkinson P, Kelvin R, Roberts C, Byford S, et al.
-
The use of irinotecan, oxaliplatin and raltitrexed for the treatment of advanced colorectal cancer: systematic review and economic evaluation.
By Hind D, Tappenden P, Tumur I, Eggington E, Sutcliffe P, Ryan A.
-
Ranibizumab and pegaptanib for the treatment of age-related macular degeneration: a systematic review and economic evaluation.
By Colquitt JL, Jones J, Tan SC, Takeda A, Clegg AJ, Price A.
-
Systematic review of the clinical effectiveness and cost-effectiveness of 64-slice or higher computed tomography angiography as an alternative to invasive coronary angiography in the investigation of coronary artery disease.
By Mowatt G, Cummins E, Waugh N, Walker S, Cook J, Jia X, et al.
-
Structural neuroimaging in psychosis: a systematic review and economic evaluation.
By Albon E, Tsourapas A, Frew E, Davenport C, Oyebode F, Bayliss S, et al.
-
Systematic review and economic analysis of the comparative effectiveness of different inhaled corticosteroids and their usage with long-acting beta2 agonists for the treatment of chronic asthma in adults and children aged 12 years and over.
By Shepherd J, Rogers G, Anderson R, Main C, Thompson-Coon J, Hartwell D, et al.
-
Systematic review and economic analysis of the comparative effectiveness of different inhaled corticosteroids and their usage with long-acting beta2 agonists for the treatment of chronic asthma in children under the age of 12 years.
By Main C, Shepherd J, Anderson R, Rogers G, Thompson-Coon J, Liu Z, et al.
-
Ezetimibe for the treatment of hypercholesterolaemia: a systematic review and economic evaluation.
By Ara R, Tumur I, Pandor A, Duenas A, Williams R, Wilkinson A, et al.
-
Topical or oral ibuprofen for chronic knee pain in older people. The TOIB study.
By Underwood M, Ashby D, Carnes D, Castelnuovo E, Cross P, Harding G, et al.
-
A prospective randomised comparison of minor surgery in primary and secondary care. The MiSTIC trial.
By George S, Pockney P, Primrose J, Smith H, Little P, Kinley H, et al.
-
A review and critical appraisal of measures of therapist–patient interactions in mental health settings.
By Cahill J, Barkham M, Hardy G, Gilbody S, Richards D, Bower P, et al.
-
The clinical effectiveness and cost-effectiveness of screening programmes for amblyopia and strabismus in children up to the age of 4–5 years: a systematic review and economic evaluation.
By Carlton J, Karnon J, Czoski-Murray C, Smith KJ, Marr J.
-
A systematic review of the clinical effectiveness and cost-effectiveness and economic modelling of minimal incision total hip replacement approaches in the management of arthritic disease of the hip.
By de Verteuil R, Imamura M, Zhu S, Glazener C, Fraser C, Munro N, et al.
-
A preliminary model-based assessment of the cost–utility of a screening programme for early age-related macular degeneration.
By Karnon J, Czoski-Murray C, Smith K, Brand C, Chakravarthy U, Davis S, et al.
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.
By Shepherd J, Jones J, Frampton GK, Tanajewski L, Turner D, Price A.
-
Absorbent products for urinary/faecal incontinence: a comparative evaluation of key product categories.
By Fader M, Cottenden A, Getliffe K, Gage H, Clarke-O’Neill S, Jamieson K, et al.
-
A systematic review of repetitive functional task practice with modelling of resource use, costs and effectiveness.
By French B, Leathley M, Sutton C, McAdam J, Thomas L, Forster A, et al.
-
The effectiveness and cost-effectivness of minimal access surgery amongst people with gastro-oesophageal reflux disease – a UK collaborative study. The reflux trial.
By Grant A, Wileman S, Ramsay C, Bojke L, Epstein D, Sculpher M, et al.
-
Time to full publication of studies of anti-cancer medicines for breast cancer and the potential for publication bias: a short systematic review.
By Takeda A, Loveman E, Harris P, Hartwell D, Welch K.
Health Technology Assessment Programme
-
Director, NIHR HTA Programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Medical Care Research Unit, University of Sheffield
Prioritisation Strategy Group
-
Director, NIHR HTA Programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Medical Care Research Unit, University of Sheffield
-
Dr Bob Coates, Consultant Advisor, NCCHTA
-
Dr Andrew Cook, Consultant Advisor, NCCHTA
-
Dr Peter Davidson, Director of Science Support, NCCHTA
-
Professor Robin E Ferner, Consultant Physician and Director, West Midlands Centre for Adverse Drug Reactions, City Hospital NHS Trust, Birmingham
-
Professor Paul Glasziou, Professor of Evidence-Based Medicine, University of Oxford
-
Dr Nick Hicks, Director of NHS Support, NCCHTA
-
Dr Edmund Jessop, Medical Adviser, National Specialist, National Commissioning Group (NCG), Department of Health, London
-
Ms Lynn Kerridge, Chief Executive Officer, NETSCC and NCCHTA
-
Dr Ruairidh Milne, Director of Strategy and Development, NETSCC
-
Ms Kay Pattison, Section Head, NHS R&D Programme, Department of Health
-
Ms Pamela Young, Specialist Programme Manager, NCCHTA
HTA Commissioning Board
-
Director, NIHR HTA Programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Medical Care Research Unit, University of Sheffield
-
Senior Lecturer in General Practice, Department of Primary Health Care, University of Oxford
-
Professor Ann Ashburn, Professor of Rehabilitation and Head of Research, Southampton General Hospital
-
Professor Deborah Ashby, Professor of Medical Statistics, Queen Mary, University of London
-
Professor John Cairns, Professor of Health Economics, London School of Hygiene and Tropical Medicine
-
Professor Peter Croft, Director of Primary Care Sciences Research Centre, Keele University
-
Professor Nicky Cullum, Director of Centre for Evidence-Based Nursing, University of York
-
Professor Jenny Donovan, Professor of Social Medicine, University of Bristol
-
Professor Steve Halligan, Professor of Gastrointestinal Radiology, University College Hospital, London
-
Professor Freddie Hamdy, Professor of Urology, University of Sheffield
-
Professor Allan House, Professor of Liaison Psychiatry, University of Leeds
-
Dr Martin J Landray, Reader in Epidemiology, Honorary Consultant Physician, Clinical Trial Service Unit, University of Oxford
-
Professor Stuart Logan, Director of Health & Social Care Research, The Peninsula Medical School, Universities of Exeter and Plymouth
-
Dr Rafael Perera, Lecturer in Medical Statisitics, Department of Primary Health Care, Univeristy of Oxford
-
Professor Ian Roberts, Professor of Epidemiology & Public Health, London School of Hygiene and Tropical Medicine
-
Professor Mark Sculpher, Professor of Health Economics, University of York
-
Professor Helen Smith, Professor of Primary Care, University of Brighton
-
Professor Kate Thomas, Professor of Complementary & Alternative Medicine Research, University of Leeds
-
Professor David John Torgerson, Director of York Trials Unit, University of York
-
Professor Hywel Williams, Professor of Dermato-Epidemiology, University of Nottingham
-
Ms Kay Pattison, Section Head, NHS R&D Programmes, Research and Development Directorate, Department of Health
-
Dr Morven Roberts, Clinical Trials Manager, Medical Research Council
Diagnostic Technologies & Screening Panel
-
Professor of Evidence-Based Medicine, University of Oxford
-
Consultant Paediatrician and Honorary Senior Lecturer, Great Ormond Street Hospital, London
-
Professor Judith E Adams, Consultant Radiologist, Manchester Royal Infirmary, Central Manchester & Manchester Children’s University Hospitals NHS Trust, and Professor of Diagnostic Radiology, Imaging Science and Biomedical Engineering, Cancer & Imaging Sciences, University of Manchester
-
Ms Jane Bates, Consultant Ultrasound Practitioner, Ultrasound Department, Leeds Teaching Hospital NHS Trust
-
Dr Stephanie Dancer, Consultant Microbiologist, Hairmyres Hospital, East Kilbride
-
Professor Glyn Elwyn, Primary Medical Care Research Group, Swansea Clinical School, University of Wales
-
Dr Ron Gray, Consultant Clinical Epidemiologist, Department of Public Health, University of Oxford
-
Professor Paul D Griffiths, Professor of Radiology, University of Sheffield
-
Dr Jennifer J Kurinczuk, Consultant Clinical Epidemiologist, National Perinatal Epidemiology Unit, Oxford
-
Dr Susanne M Ludgate, Medical Director, Medicines & Healthcare Products Regulatory Agency, London
-
Dr Anne Mackie, Director of Programmes, UK National Screening Committee
-
Dr Michael Millar, Consultant Senior Lecturer in Microbiology, Barts and The London NHS Trust, Royal London Hospital
-
Mr Stephen Pilling, Director, Centre for Outcomes, Research & Effectiveness, Joint Director, National Collaborating Centre for Mental Health, University College London
-
Mrs Una Rennard, Service User Representative
-
Dr Phil Shackley, Senior Lecturer in Health Economics, School of Population and Health Sciences, University of Newcastle upon Tyne
-
Dr W Stuart A Smellie, Consultant in Chemical Pathology, Bishop Auckland General Hospital
-
Dr Nicholas Summerton, Consultant Clinical and Public Health Advisor, NICE
-
Ms Dawn Talbot, Service User Representative
-
Dr Graham Taylor, Scientific Advisor, Regional DNA Laboratory, St James’s University Hospital, Leeds
-
Professor Lindsay Wilson Turnbull, Scientific Director of the Centre for Magnetic Resonance Investigations and YCR Professor of Radiology, Hull Royal Infirmary
-
Dr Tim Elliott, Team Leader, Cancer Screening, Department of Health
-
Dr Catherine Moody, Programme Manager, Neuroscience and Mental Health Board
-
Dr Ursula Wells, Principal Research Officer, Department of Health
Pharmaceuticals Panel
-
Consultant Physician and Director, West Midlands Centre for Adverse Drug Reactions, City Hospital NHS Trust, Birmingham
-
Professor in Child Health, University of Nottingham
-
Mrs Nicola Carey, Senior Research Fellow, School of Health and Social Care, The University of Reading
-
Mr John Chapman, Service User Representative
-
Dr Peter Elton, Director of Public Health, Bury Primary Care Trust
-
Dr Ben Goldacre, Research Fellow, Division of Psychological Medicine and Psychiatry, King’s College London
-
Mrs Barbara Greggains, Service User Representative
-
Dr Bill Gutteridge, Medical Adviser, London Strategic Health Authority
-
Dr Dyfrig Hughes, Reader in Pharmacoeconomics and Deputy Director, Centre for Economics and Policy in Health, IMSCaR, Bangor University
-
Professor Jonathan Ledermann, Professor of Medical Oncology and Director of the Cancer Research UK and University College London Cancer Trials Centre
-
Dr Yoon K Loke, Senior Lecturer in Clinical Pharmacology, University of East Anglia
-
Professor Femi Oyebode, Consultant Psychiatrist and Head of Department, University of Birmingham
-
Dr Andrew Prentice, Senior Lecturer and Consultant Obstetrician and Gynaecologist, The Rosie Hospital, University of Cambridge
-
Dr Martin Shelly, General Practitioner, Leeds, and Associate Director, NHS Clinical Governance Support Team, Leicester
-
Dr Gillian Shepherd, Director, Health and Clinical Excellence, Merck Serono Ltd
-
Mrs Katrina Simister, Assistant Director New Medicines, National Prescribing Centre, Liverpool
-
Mr David Symes, Service User Representative
-
Dr Lesley Wise, Unit Manager, Pharmacoepidemiology Research Unit, VRMM, Medicines & Healthcare Products Regulatory Agency
-
Ms Kay Pattison, Section Head, NHS R&D Programme, Department of Health
-
Mr Simon Reeve, Head of Clinical and Cost-Effectiveness, Medicines, Pharmacy and Industry Group, Department of Health
-
Dr Heike Weber, Programme Manager, Medical Research Council
-
Dr Ursula Wells, Principal Research Officer, Department of Health
Therapeutic Procedures Panel
-
Consultant Physician, North Bristol NHS Trust
-
Professor of Psychiatry, Division of Health in the Community, University of Warwick, Coventry
-
Ms Maree Barnett, Acting Branch Head of Vascular Programme, Department of Health
-
Professor Jane Barlow, Professor of Public Health in the Early Years, Health Sciences Research Institute, Warwick Medical School, Coventry
-
Mrs Val Carlill, Service User Representative
-
Mrs Anthea De Barton-Watson, Service User Representative
-
Mr Mark Emberton, Senior Lecturer in Oncological Urology, Institute of Urology, University College Hospital, London
-
Professor Steve Goodacre, Professor of Emergency Medicine, University of Sheffield
-
Professor Christopher Griffiths, Professor of Primary Care, Barts and The London School of Medicine and Dentistry
-
Mr Paul Hilton, Consultant Gynaecologist and Urogynaecologist, Royal Victoria Infirmary, Newcastle upon Tyne
-
Professor Nicholas James, Professor of Clinical Oncology, University of Birmingham, and Consultant in Clinical Oncology, Queen Elizabeth Hospital
-
Dr Peter Martin, Consultant Neurologist, Addenbrooke’s Hospital, Cambridge
-
Dr Kate Radford, Senior Lecturer (Research), Clinical Practice Research Unit, University of Central Lancashire, Preston
-
Mr Jim Reece Service User Representative
-
Dr Karen Roberts, Nurse Consultant, Dunston Hill Hospital Cottages
-
Dr Phillip Leech, Principal Medical Officer for Primary Care, Department of Health
-
Ms Kay Pattison, Section Head, NHS R&D Programme, Department of Health
-
Dr Morven Roberts, Clinical Trials Manager, Medical Research Council
-
Professor Tom Walley, Director, NIHR HTA Programme, Professor of Clinical Pharmacology, University of Liverpool
-
Dr Ursula Wells, Principal Research Officer, Department of Health
Disease Prevention Panel
-
Medical Adviser, National Specialist, National Commissioning Group (NCG), London
-
Director, NHS Sustainable Development Unit, Cambridge
-
Dr Elizabeth Fellow-Smith, Medical Director, West London Mental Health Trust, Middlesex
-
Dr John Jackson, General Practitioner, Parkway Medical Centre, Newcastle upon Tyne
-
Professor Mike Kelly, Director, Centre for Public Health Excellence, NICE, London
-
Dr Chris McCall, General Practitioner, The Hadleigh Practice, Corfe Mullen, Dorset
-
Ms Jeanett Martin, Director of Nursing, BarnDoc Limited, Lewisham Primary Care Trust
-
Dr Julie Mytton, Locum Consultant in Public Health Medicine, Bristol Primary Care Trust
-
Miss Nicky Mullany, Service User Representative
-
Professor Ian Roberts, Professor of Epidemiology and Public Health, London School of Hygiene & Tropical Medicine
-
Professor Ken Stein, Senior Clinical Lecturer in Public Health, University of Exeter
-
Dr Kieran Sweeney, Honorary Clinical Senior Lecturer, Peninsula College of Medicine and Dentistry, Universities of Exeter and Plymouth
-
Professor Carol Tannahill, Glasgow Centre for Population Health
-
Professor Margaret Thorogood, Professor of Epidemiology, University of Warwick Medical School, Coventry
-
Ms Christine McGuire, Research & Development, Department of Health
-
Dr Caroline Stone, Programme Manager, Medical Research Council
Expert Advisory Network
-
Professor Douglas Altman, Professor of Statistics in Medicine, Centre for Statistics in Medicine, University of Oxford
-
Professor John Bond, Professor of Social Gerontology & Health Services Research, University of Newcastle upon Tyne
-
Professor Andrew Bradbury, Professor of Vascular Surgery, Solihull Hospital, Birmingham
-
Mr Shaun Brogan, Chief Executive, Ridgeway Primary Care Group, Aylesbury
-
Mrs Stella Burnside OBE, Chief Executive, Regulation and Improvement Authority, Belfast
-
Ms Tracy Bury, Project Manager, World Confederation for Physical Therapy, London
-
Professor Iain T Cameron, Professor of Obstetrics and Gynaecology and Head of the School of Medicine, University of Southampton
-
Dr Christine Clark, Medical Writer and Consultant Pharmacist, Rossendale
-
Professor Collette Clifford, Professor of Nursing and Head of Research, The Medical School, University of Birmingham
-
Professor Barry Cookson, Director, Laboratory of Hospital Infection, Public Health Laboratory Service, London
-
Dr Carl Counsell, Clinical Senior Lecturer in Neurology, University of Aberdeen
-
Professor Howard Cuckle, Professor of Reproductive Epidemiology, Department of Paediatrics, Obstetrics & Gynaecology, University of Leeds
-
Dr Katherine Darton, Information Unit, MIND – The Mental Health Charity, London
-
Professor Carol Dezateux, Professor of Paediatric Epidemiology, Institute of Child Health, London
-
Mr John Dunning, Consultant Cardiothoracic Surgeon, Papworth Hospital NHS Trust, Cambridge
-
Mr Jonothan Earnshaw, Consultant Vascular Surgeon, Gloucestershire Royal Hospital, Gloucester
-
Professor Martin Eccles, Professor of Clinical Effectiveness, Centre for Health Services Research, University of Newcastle upon Tyne
-
Professor Pam Enderby, Dean of Faculty of Medicine, Institute of General Practice and Primary Care, University of Sheffield
-
Professor Gene Feder, Professor of Primary Care Research & Development, Centre for Health Sciences, Barts and The London School of Medicine and Dentistry
-
Mr Leonard R Fenwick, Chief Executive, Freeman Hospital, Newcastle upon Tyne
-
Mrs Gillian Fletcher, Antenatal Teacher and Tutor and President, National Childbirth Trust, Henfield
-
Professor Jayne Franklyn, Professor of Medicine, University of Birmingham
-
Mr Tam Fry, Honorary Chairman, Child Growth Foundation, London
-
Professor Fiona Gilbert, Consultant Radiologist and NCRN Member, University of Aberdeen
-
Professor Paul Gregg, Professor of Orthopaedic Surgical Science, South Tees Hospital NHS Trust
-
Bec Hanley, Co-director, TwoCan Associates, West Sussex
-
Dr Maryann L Hardy, Senior Lecturer, University of Bradford
-
Mrs Sharon Hart, Healthcare Management Consultant, Reading
-
Professor Robert E Hawkins, CRC Professor and Director of Medical Oncology, Christie CRC Research Centre, Christie Hospital NHS Trust, Manchester
-
Professor Richard Hobbs, Head of Department of Primary Care & General Practice, University of Birmingham
-
Professor Alan Horwich, Dean and Section Chairman, The Institute of Cancer Research, London
-
Professor Allen Hutchinson, Director of Public Health and Deputy Dean of ScHARR, University of Sheffield
-
Professor Peter Jones, Professor of Psychiatry, University of Cambridge, Cambridge
-
Professor Stan Kaye, Cancer Research UK Professor of Medical Oncology, Royal Marsden Hospital and Institute of Cancer Research, Surrey
-
Dr Duncan Keeley, General Practitioner (Dr Burch & Ptnrs), The Health Centre, Thame
-
Dr Donna Lamping, Research Degrees Programme Director and Reader in Psychology, Health Services Research Unit, London School of Hygiene and Tropical Medicine, London
-
Mr George Levvy, Chief Executive, Motor Neurone Disease Association, Northampton
-
Professor James Lindesay, Professor of Psychiatry for the Elderly, University of Leicester
-
Professor Julian Little, Professor of Human Genome Epidemiology, University of Ottawa
-
Professor Alistaire McGuire, Professor of Health Economics, London School of Economics
-
Professor Rajan Madhok, Medical Director and Director of Public Health, Directorate of Clinical Strategy & Public Health, North & East Yorkshire & Northern Lincolnshire Health Authority, York
-
Professor Alexander Markham, Director, Molecular Medicine Unit, St James’s University Hospital, Leeds
-
Dr Peter Moore, Freelance Science Writer, Ashtead
-
Dr Andrew Mortimore, Public Health Director, Southampton City Primary Care Trust
-
Dr Sue Moss, Associate Director, Cancer Screening Evaluation Unit, Institute of Cancer Research, Sutton
-
Professor Miranda Mugford, Professor of Health Economics and Group Co-ordinator, University of East Anglia
-
Professor Jim Neilson, Head of School of Reproductive & Developmental Medicine and Professor of Obstetrics and Gynaecology, University of Liverpool
-
Mrs Julietta Patnick, National Co-ordinator, NHS Cancer Screening Programmes, Sheffield
-
Professor Robert Peveler, Professor of Liaison Psychiatry, Royal South Hants Hospital, Southampton
-
Professor Chris Price, Director of Clinical Research, Bayer Diagnostics Europe, Stoke Poges
-
Professor William Rosenberg, Professor of Hepatology and Consultant Physician, University of Southampton
-
Professor Peter Sandercock, Professor of Medical Neurology, Department of Clinical Neurosciences, University of Edinburgh
-
Dr Susan Schonfield, Consultant in Public Health, Hillingdon Primary Care Trust, Middlesex
-
Dr Eamonn Sheridan, Consultant in Clinical Genetics, St James’s University Hospital, Leeds
-
Dr Margaret Somerville, Director of Public Health Learning, Peninsula Medical School, University of Plymouth
-
Professor Sarah Stewart-Brown, Professor of Public Health, Division of Health in the Community, University of Warwick, Coventry
-
Professor Ala Szczepura, Professor of Health Service Research, Centre for Health Services Studies, University of Warwick, Coventry
-
Mrs Joan Webster, Consumer Member, Southern Derbyshire Community Health Council
-
Professor Martin Whittle, Clinical Co-director, National Co-ordinating Centre for Women’s and Children’s Health, Lymington