
Notes
Article history
The research reported in this issue of the journal was commissioned and funded by the HTA programme on behalf of NICE as project number 08/06/01. The protocol was agreed in June 2008. The assessment report began editorial review in January 2009 and was accepted for publication in April 2009. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the referees for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
None
Permissions
Copyright statement
© 2009 Queen’s Printer and Controller of HMSO. This monograph may be freely reproduced for the purposes of private research and study and may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NETSCC, Health Technology Assessment, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2009 Queen’s Printer and Controller of HMSO
Chapter 1 Background
Description of health problem
Aetiology (cause of disease)
The development of obesity, at a simple level, occurs when energy taken into the body as food exceeds the amount of energy expended by the body. However, in reality, obesity is the outcome of a heterogeneous collection of disorders arising from a number of different causes. There is a complex interplay between genetic,1 biochemical, neural and psychological factors, and external aspects such as environmental, social and economic factors. 2
Natural history
Overweight and obesity are defined as abnormal or excessive fat accumulation that may impair health. However, the natural history of weight gain over time and progression to the development of overweight, obesity or morbid obesity have not been well documented. Some people are able to maintain a healthy weight throughout their life, but others will be at risk for weight gain. The age of onset and rate of progression of weight gain varies between individuals. Longitudinal studies have shown that age, sex and ethnicity are key risk factors for weight gain. 3–5 Such studies also suggest that, without intervention, reversal of overweight and obesity is uncommon. 4,6
Classification (measurement of disease)
The most commonly used measure for classifying overweight and obesity is the Body Mass Index (BMI). This is a simple index of weight-for-height that is defined as the weight in kilograms divided by the square of the height in metres (kg/m2). In adults overweight is most commonly defined as a BMI of 25 or over, obesity as a BMI of 30 or over, and severe or morbid obesity as a BMI of 40 or over (Table 1). 7,8 BMI (adjusted for age and gender) is also recommended by the National Institute for Health and Clinical Excellence (NICE) guideline on obesity9 as a practical estimate of overweight in children and young people, but the guideline points out that this needs to be interpreted with caution because it is not a direct measure of adiposity (the amount of body fat). For children and young people, overweight and obesity are not defined according to a particular BMI. The NICE obesity guideline recommends instead that tailored clinical intervention should be considered for children with a BMI at or above the 91st centile and assessment of comorbidity should be considered for children with a BMI at or above the 98th centile.
| Classification | BMI | Risk of comorbidities |
|---|---|---|
| Underweight | < 18.5 | Low (but risk of other clinical problems increased) |
| Normal range | 18.50–24.99 | Average |
| Overweight | ≥ 25.00 | |
| Preobese | 25.00–29.99 | Increased |
| Obese | ≥ 30.00 | |
| Obese class I | 30.00–34.99 | Moderate |
| Obese class II | 35.00–39.99 | Severe |
| Obese class III (morbid obesity) a | ≥ 40.00 | Very severe |
Epidemiology
Incidence
There is a large body of work reporting on the prevalence of obesity (see below), but much less information regarding the incidence of obesity. The published information regarding the incidence of obesity relates to the USA and Sweden, but no information has been found that is specific for the UK.
Adults
A recent study10 evaluated trends in the incidence of overweight and obesity in the USA from 1950 to 2000 using data from the Framingham study participants. The results indicated that the overall incidence rates of overweight increased twofold, and that of obesity more than threefold over five decades. Per decade, there was an increase in the incidence of overweight of 25% in women and 20% in men. The corresponding per decade increases in women and men were 34% and 29% for the incidence of obesity, and 31% and 97% for the incidence of class II obesity.
A second study has compared trends in the incidence of overweight and obesity in a rural population from Sweden, and one from the USA between 1989 and 1999. 11 The 10-year incidence of overweight was similar in the two countries (337/1000 in Sweden, 336/1000 in the USA). However, the 10-year incidence of obesity was greater in the USA (173/1000) where 21.3% were obese in 1989 rising to 32.3% in 1999, than in Sweden (120/1000) where the prevalence of obesity was lower at both time points (9.6% in 1989 and 18.4% in 1999).
Adolescents and children
Calculating the incidence of overweight or obesity in adolescents and children is particularly problematic. For adolescents who are approaching adulthood the difficulty lies in ensuring that the data sets employed in the study have used a definition of obesity that is comparable for the age groups of interest. Gordon-Larsen and colleagues6 have used data from a longitudinal, nationally representative, school-based study of US adolescents and estimated that obesity incidence over the five-year study period was 12.7%. In contrast, fewer than 2% of the total sample of young adults who were obese as adolescents became non-obese.
The generalisability of the findings reported above to adults and children in the UK is unknown.
Prevalence
Adults
The World Health Organization (WHO)’s projections indicated that globally in 2005 approximately 1.6 billion adults (age 15 +) were overweight and at least 400 million adults were obese. 12 In England in 2006 the prevalence of overweight in people aged 16 and over was 38% (approximately 15.4 million people), with 24% obese (approximately 9.8 million people). 13 In Wales in 2007, 57% of adults were classified as overweight or obese, including 21% obese. 14
The prevalence of obesity (BMI > 30) among adults in England and Wales is increasing. In 2006 reported obesity prevalence in England was 23.7% for men and 24.2% for women. The increase was clear when the 2006 figures are compared with those for 1998 which were 17.3% for men and 21.2% for women. 15 The 2006 prevalence of morbid obesity (BMI > 40)16 was 2.1% (just under 863,000 people) with women being more likely to be morbidly obese than men (2.7% of women versus 1.5% of men). In comparison, the 1998 figures for morbid obesity were 0.6% for men and 1.9% for women. For a standard primary-care trust (PCT) population of 250,000, there would be 5250 cases of morbid obesity (based on the overall 2006 population value for England of 2.1% morbid obesity).
Prevalence of obesity increases with age, until age 55–64 years in men and until age 65–74 years in women, when it begins to decline16 (Table 2). The number of men and women with obesity in England is shown in Table 3. 17,18 Obesity in women is more common in households where the current or former occupation of the household reference person is classified as routine and manual than in those households classified as intermediate, or managerial and professional (Table 4). 16 For morbid obesity in women the prevalence was 1.6% in managerial and professional households, but 4.0% in routine and manual households. Differences for men by category based on occupation was less marked. 16 Data from the Welsh Health Survey also indicate a rise in obesity among people aged 16 years and over from 18% in 2003–4 to 19% in 2005–6. 19
| Age (years) | Total | |||||||
|---|---|---|---|---|---|---|---|---|
| 16–24 | 25–34 | 35–44 | 45–54 | 55–64 | 65–74 | 75 + | ||
| % | % | % | % | % | % | % | % | |
| Men | ||||||||
| Underweight | 5.5 | 0.2 | 0.4 | 0.1 | 0.5 | 0.4 | 0.6 | 1.2 |
| Normal | 60.8 | 37.7 | 26.5 | 23.7 | 19.9 | 19.2 | 30.5 | 31.7 |
| Overweight | 24.7 | 41.3 | 48.1 | 48.1 | 46.6 | 49.4 | 51.0 | 43.4 |
| Obese | 9.0 | 20.7 | 25.0 | 28.1 | 33.0 | 31.1 | 17.8 | 23.7 |
| Overweight including obese | 33.7 | 62.0 | 73.1 | 76.2 | 79.6 | 80.4 | 68.8 | 67.1 |
| Morbidly obese | 0.9 | 1.1 | 1.6 | 1.7 | 2.7 | 1.2 | 0.2 | 1.5 |
| Mean BMI | 24.1 | 26.7 | 27.8 | 28.0 | 28.6 | 28.3 | 27.0 | 27.2 |
| Women | ||||||||
| Underweight | 6.5 | 2.2 | 1.0 | 0.7 | 1.2 | 1.3 | 2.3 | 2.1 |
| Normal | 61.8 | 50.3 | 45.2 | 36.9 | 33.0 | 26.5 | 28.7 | 41.8 |
| Overweight | 19.7 | 29.2 | 30.1 | 35.2 | 35.7 | 37.5 | 41.6 | 31.9 |
| Obese | 12.0 | 18.2 | 23.7 | 27.2 | 30.2 | 34.7 | 27.4 | 24.2 |
| Overweight including obese | 31.7 | 47.5 | 53.8 | 62.4 | 65.9 | 72.2 | 69.0 | 56.1 |
| Morbidly obese | 1.4 | 2.0 | 3.1 | 3.1 | 3.4 | 3.6 | 1.6 | 2.7 |
| Mean BMI | 24.0 | 25.9 | 26.8 | 27.6 | 28.0 | 28.6 | 27.5 | 26.8 |
| Age (years) | Total | ||||
|---|---|---|---|---|---|
| 16–34 | 35–54 | 55–74 | 75 + | ||
| Men | |||||
| Overweight | 2,066,211 | 3,281,310 | 2,349,520 | 706,323 | 8,403,365 |
| Obese | 851,769 | 1,848,110 | 1,305,710 | 296,998 | 4,302,588 |
| Overweight including obese | 2,917,981 | 5,129,420 | 3,655,231 | 1,003,321 | 12,705,953 |
| Women | |||||
| Overweight | 1,470,007 | 2,329,645 | 2,021,398 | 951,706 | 6,772,757 |
| Obese | 980,440 | 1,695,650 | 1,455,904 | 622,087 | 4,754,080 |
| Overweight including obese | 2,450,447 | 4,025,295 | 3,477,302 | 1,573,793 | 11,526,837 |
| BMI | Men | Women | ||||||
|---|---|---|---|---|---|---|---|---|
| Occupation of head of householda | Occupation of head of household | |||||||
| All adults (%) | Managerial and professional (%) | Intermediate (%) | Routine and manual (%) | All adults (%) | Managerial and professional (%) | Intermediate (%) | Routine and manual (%) | |
| Underweight | 1.4 | 1.3 | 0.6 | 1.9 | 2.1 | 2.1 | 1.3 | 2.3 |
| Normal | 33.2 | 32.1 | 33.0 | 34.6 | 42.3 | 48.1 | 43.0 | 36.2 |
| Overweight | 43.2 | 45.8 | 42.3 | 40.8 | 32.6 | 31.1 | 36.1 | 32.5 |
| Obese | 21.2 | 20.2 | 22.9 | 21.6 | 20.1 | 17.0 | 17.0 | 25.0 |
| Morbidly obese | 1.0 | 0.7 | 1.2 | 1.1 | 2.9 | 1.6 | 2.6 | 4.0 |
| Overweight including obese | 65.4 | 66.6 | 66.4 | 63.5 | 56.0 | 49.8 | 55.7 | 61.5 |
The prevalence of obesity is predicted to rise in the future. WHO has projected that by 2015 more than 700 million adults will be obese. In the UK, the Foresight programme provides visions of the future using science-based methods. The Foresight project ‘Tackling Obesities: Future Choices’ produced a report made up of a number of documents which forms a long-term vision of how a sustainable response to obesity can be delivered in the UK over the next 40 years. The modelling section of the Foresight Report predicts that in England, if current trends persist, 36% of men and 28% of women aged 21 to 60 will be obese in 2015. 20 Predicting trends in morbid obesity is more problematic. The Foresight modelling projection to 2050 suggests figures of 1% for males and 4% for females. 20 In contrast a different Foresight project output has estimated that the proportion of morbidly obese English males and females will reach nearly 3% and 6%, respectively, in 2030. 21
Children
As noted, overweight and obesity in children and young people are not defined according to a particular BMI. This means that varying prevalences of overweight and obesity in children and young people will be obtained depending on the particular definitions used. 22 This not only makes it difficult to obtain an accurate prevalence estimate, but also creates problems when trying to compare prevalences reported by studies employing different definitions. The NICE obesity guideline states that BMI measurement in children and young people should be related to the UK 1990 BMI charts to give age- and gender-specific information. 9
Despite the difficulties in assessing the prevalence of overweight and obesity in children and young people there is general agreement that these are increasing. The National Statistics for England16 report that between 1995 and 2005 the proportion of boys aged 2 to 15 years who were obese increased from 10.9% to 18.3%. For girls a similar pattern was seen with the proportion of obese 2–15-year-olds increasing from 12.0% in 1995 to 18.3% in 2005 (Table 5). In the 11–15 years age group the prevalence of obesity in 2005 was very similar in boys and girls at 20.4% and 20.8% respectively. In general the proportion of children who are obese increases with age until age 13–15 (Table 6). 16 These prevalence figures were derived using the UK National BMI percentile classification to describe childhood overweight and obesity. This uses a BMI threshold for each age above which a child is considered overweight or obese. The classification estimates were produced by calculating the percentage of boys and girls who were over the 85th (overweight) or 95th (obese) BMI percentiles based on the 1990 UK reference population.
| Overweight | Obese | Overweight including obese | ||||
|---|---|---|---|---|---|---|
| 1995 | 2005a | 1995 | 2005a | 1995 | 2005a | |
| Boys | ||||||
| Aged 2–10 | 12.9 | 16.1 | 9.6 | 16.9 | 22.5 | 33.0 |
| Aged 11–15 | 13.4 | 15.0 | 13.5 | 20.4 | 26.9 | 35.3 |
| Aged 2–15 | 13.1 | 15.7 | 10.9 | 18.3 | 24.0 | 33.9 |
| Girls | ||||||
| Aged 2–10 | 12.6 | 12.2 | 10.3 | 16.8 | 22.9 | 29.0 |
| Aged 11–15 | 13.9 | 14.1 | 15.4 | 20.8 | 29.3 | 34.9 |
| Aged 2–15 | 13.1 | 12.9 | 12.0 | 18.3 | 25.0 | 31.2 |
| Age (years) | 2002–2004a | |
|---|---|---|
| Obese % | Overweight including obese % | |
| 2–3 | 11.6 | 25.2 |
| 4–5 | 12.8 | 27.2 |
| 6–7 | 13.5 | 26.7 |
| 8–10 | 18.7 | 31.8 |
| 11–12 | 22.0 | 37.6 |
| 13–15 | 19.5 | 34.1 |
Impact of health problem
Obesity can have a variety of adverse health consequences including a risk of death. An increased risk of health problems starts when someone is only very slightly overweight, and the likelihood of adverse health consequences increases as someone becomes progressively more overweight and obese. 12 The risks of obesity also apply to children as childhood obesity is associated with a higher chance of premature death and disability in adulthood. 12 The health consequences associated with obesity, such as those listed in Table 7, impose a considerable economic burden on society.
| Disease | Relative riska – women (England)24 | Relative riska – men (England)24 | WHO estimate of increased risk (men and women worldwide)8 |
|---|---|---|---|
| Type 2 diabetes | 12.7 | 5.2 | Greatly increased |
| Dyslipidaemia | – | – | Greatly increased |
| Insulin resistance | – | – | Greatly increased |
| Breathlessness | – | – | Greatly increased |
| Sleep apnoea | – | – | Greatly increased |
| Cardiovascular disease | – | – | Moderately increased |
| Myocardial infarction | 3.2 | 1.5 | |
| Angina | 1.8 | 1.8 | |
| Stroke | 1.3 | 1.3 | |
| Hypertension | 4.2 | 2.6 | Moderately increased |
| Cancer of the colon | 2.7 | 3.0 | Slightly increased |
| Gall bladder diseases | 1.8 | 1.8 | Greatly increased |
| Osteoarthritis | 1.4 | 1.9 | Moderately increased (knees) |
| Hyperuricaemia and gout | – | – | Moderately increased |
| Ovarian cancer | 1.7 | – | |
| Breast cancer in postmenopausal women | – | – | Slightly increased |
| Endometrial cancer | – | – | Slightly increased |
| Reproductive hormone abnormalities | – | – | Slightly increased |
| Polycystic ovary syndrome | – | – | Slightly increased |
| Impaired fertility | – | – | Slightly increased |
| Fetal defects associated with maternal obesity | – | – | Slightly increased |
| Low back pain due to obesity | – | – | Slightly increased |
| Risk of anaesthesia complications | – | – | Slightly increased |
Health risks of overweight and obesity
The current NICE guideline on obesity9 recommends that the assessment of the health risks associated with overweight and obesity in adults should be based on BMI and waist circumference (Table 8). The proportion of English men and women who fall into different health risk categories as defined in the NICE guidelines have been estimated by the National Statistics Information Centre (Table 9). 16
Health consequences of overweight and obesity
The counterweight program, which has been developed and evaluated to be an effective model for obesity management with general practice in the UK, undertook a cross-sectional survey of the records of 6150 obese adults. It found that obese patients made significantly more visits to their general practitioner (GP), practice nurse and hospital outpatient departments than patients classified as normal weight, even after adjustments had been made for confounding factors. 23 Over the last 10 years there were 17,458 Finished Consultant Episodes with a primary diagnosis of obesity. Almost a quarter of these (4068) occurred in 2006–7. 16
Health consequences in adults
The predominant serious health consequences associated with overweight and obesity in adults include Type 2 diabetes, cardiovascular disease (CVD) (mainly heart disease and stroke), musculoskeletal disorders such as osteoarthritis, and certain cancers (Table 7) and are discussed in more detail below. As indicated in Table 8 and Table 9 the risk of serious health consequences increases with increasing obesity (greater detail is provided in Chapter 5, Data sources, Effectiveness data). Some of these health consequences may constitute the principal cause of death, e.g. heart disease, stroke, some cancers; whereas, others such as Type 2 diabetes lead to a reduced life expectancy. Other important health consequences that have a negative impact on quality of life (QoL) are obstructive sleep apnoea, infertility, obstetric complications and psychiatric comorbidity.
| Men | Women | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Over-weight | Obesity I | Obesity II | Obesity III | All | Over-weight | Obesity I | Obesity II | Obesity III | All | |
| No increased risk | 13 | 45 | 4 | 45 | ||||||
| Increased risk | 19 | 0 | 20 | 12 | 0 | 14 | ||||
| High risk | 11 | 3 | 13 | 15 | 1 | 16 | ||||
| Very high risk | 15 | 4 | 1 | 21 | 14 | 6 | 3 | 23 | ||
The WHO finds that the relative risks of particular disease in obese people, compared with lean people, are fairly similar throughout the world and have classified these into three broad categories: greatly increased risk (relative risk much greater than 3); moderately increased risk (relative risk 2–3); and slightly increased risk (relative risk 1–2) (Table 7). 8 The best estimates of the increased disease risk due to obesity for the English population were calculated from international studies by the National Audit Office24 for a number of these conditions and these risk estimates are also shown alongside the WHO estimates in Table 7. Although the results should be interpreted with some caution (some studies that contributed data used an alternative cut-off point for obesity instead of the widely used definition of a BMI of 30 or above) they do provide a broad indication of the strength of the association between obesity and disease.
Increased mortality
Obesity significantly increases the risk of mortality at any given age (including after adjustment for other risk factors such as smoking) and those who have been overweight for the longest are at the highest risk. The National Audit Office (NAO) has reported that evidence from studies suggests that young adults with a BMI of 30 have a mortality risk that is about 50% higher than that of a young adult with a healthy BMI (18.5–25). 24 For a young adult with a BMI of 35 the mortality risk is more than doubled. One study reported that 40-year-old obese (BMI greater than or equal to 30) women and men lost 7.1 and 5.8 years of life, respectively, compared with 40-year-old non-smoking women and men of normal weight. 25 In 2004, a House of Commons Select Committee report estimated that 6.8% of all deaths in England were attributable to obesity. 26
Type 2 diabetes
Type 2 diabetes is the most common form of diabetes, accounting for over 90% of all diabetes in the UK. 13 It is characterised by insulin resistance and is a serious life-shortening condition. The ‘first-line’ treatment is diet, weight control and physical activity but drug therapy, e.g. with metformin, sulphonylurea drugs, thiazolidinediones (commonly called glitazones), or insulin therapy may become necessary. The risk of developing diabetes rises with increasing BMI even below the threshold of clinical obesity. The Health Survey for England (HSE) data have been used to examine the association between a number of risk factors and Type 2 diabetes in adults aged 35 years and over. Men and women who were obese had approximately double the odds of having Type 2 diabetes compared with those who had a BMI of less than 25 (after adjusting for other factors). A raised waist circumference was also linked to increased odds of having Type 2 diabetes, in men the odds were doubled, whereas women with a raised waist circumference were four times more likely to have Type 2 diabetes than those without a raised waist circumference measurement. 13
Cardiovascular disease and CVD risk factors
The term CVD encompasses ischaemic heart disease (IHD) [also known as coronary heart disease (CHD)], stroke and peripheral vascular disease. Obesity is an independent risk factor for CVD. Data from the HSE 200317 demonstrate that a relationship between IHD and BMI is present in men and women. The prevalence of IHD or stroke was lowest among people with a normal BMI, but increased for people in the overweight category and was highest among obese women and men. However, in women, the higher prevalence in the obese was no longer significant following age standardisation (Table 10). A raised waist circumference is also linked to an increased prevalence of CVD in men and women.
| Observed prevalence 2003 | Age-standardised prevalence 2003 | |||
|---|---|---|---|---|
| Any CVD (%) | IHD or stroke | Any CVD (%) | IHD or stroke | |
| Men | ||||
| Normal range | 10 | 4 | 10 | 5 |
| Overweight | 14 | 8 | 11 | 6 |
| Obese | 17 | 10 | 13 | 8 |
| Women | ||||
| Normal range | 10 | 3 | 11 | 4 |
| Overweight | 13 | 6 | 12 | 5 |
| Obese | 16 | 7 | 14 | 6 |
Hypertension is a key risk factor for CVD and the positive association between blood pressure and BMI is well documented. Data from the HSE 200317 shows that overweight men and women (BMI between 25 to less than 30) and obese men and women (BMI 30 or more) both have a higher blood pressure than those with a normal BMI (Table 11). The link between high blood pressure and obesity was also observed during the HSE 2005 which focused on people aged 65 years and over. 27 In this age group hypertension was twice as common in obese men and women, and more prevalent in overweight women, compared with those with a weight in the normal range.
| Difference from the reference category mmHg (95% CI) | |
|---|---|
| Men | |
| Reference category: normal range | 0 |
| Overweight | 2.86 (1.15 to 4.21) |
| Obese | 6.22 (4.71 to 7.73) |
| Women | |
| Reference category: normal range | 0 |
| Overweight | 3.32 (2.29 to 4.34) |
| Obese | 6.02 (4.76 to 7.29) |
Abnormalities in serum lipid levels [raised total cholesterol, triglycerides and low-density lipoprotein (LDL), with reduced high-density lipoprotein (HDL)] are a further risk factor for CVD. The National Health and Nutrition Examination Survey (NHANES) III28 found that the prevalence of raised cholesterol (≥ 240 mg/dl) in obese men and women was 22% and 27%, respectively, compared with 13% of adults with BMI < 25. HDL-cholesterol decreased with increasing BMI. The prevalence of low HDL-cholesterol (< 35 mg/dl men, < 45 mg/dl women) in obese adults was 31% of men and 41% of women compared with 9% and 17%, respectively, in adults with desirable weight. A more recent publication employing data from the survey of health, ageing and retirement in Europe (SHARE) also found that the odds ratios for high cholesterol were significantly increased for overweight and obese adults. 29
Cancer
A systematic review and meta-analysis of prospective observational studies reported that in men, a 5 kg/m2 increase in BMI was strongly associated with oesophageal adenocarcinoma [relative risk (RR) 1·52, p < 0·0001] as well as thyroid (1·33, p = 0·02), colon (1·24, p < 0·0001) and renal (1·24, p < 0·0001) cancers. For women, the strong associations were between a 5 kg/m2 increase in BMI and endometrial (1·59, p < 0·0001), gall bladder (1·59, p = 0.04), oesophageal adenocarcinoma (1·51, p < 0·0001) and renal (1·34, p < 0·0001) cancers. There were also weaker positive associations between increased BMI and some other cancers in both men and women. 30 As health risks increase with increasing obesity, increases in BMI greater than 5 kg/m2 may be associated with greater cancer risks.
A study assessing the cost of obesity to the UK estimated that the cancers with some relationship with overweight and obesity (breast cancer, colon/rectum cancer and corpus uteri cancer) were responsible for 6.2% of all mortality. 31
Osteoarthritis
Osteoarthritis, or degenerative disease of the knee and other weight-bearing joints, and lower back pain are common in obesity. Some effects are thought to be the result of excess weight; BMI has been associated with the incidence and progression of knee osteoarthritis, but not associated with the incidence and progression of hip osteoarthritis. However, it has also been postulated that some obesity-related osteoarthritis may be the result of a metabolic effect. 32,33 Whatever the cause, an estimated 27% of hip replacements and 69% of knee replacements in middle-aged women in the UK are attributable to obesity. 34
Respiratory disorders
Respiratory disorders such as obstructive sleep apnoea are associated with obesity. It has been estimated that approximately 17% of adults aged 30–69 years in the USA have sleep-disordered breathing graded as ‘mild or worse’ and it is further estimated that in 41% of these adults their sleep-disordered breathing can be attributed to having a BMI ≥ 25. The study has similarly estimated that 5.7% of adults have sleep-disordered breathing graded ‘moderate or worse’ which in 58% of cases may be attributed to excess weight. 35
Reproductive disorders
Reproductive disorders are common in obesity, occurring in both women and men. Cohort studies have identified obese women as having a higher risk of complications during pregnancy, such as pregnancy-induced hypertension, antepartum venous thromboembolism, induction of labour, caesarean delivery and wound infection, pre-eclampsia, premature labour, gestational diabetes and macrosomia (large-for-date fetuses). 36–40 Some studies have found evidence for an increased risk of adverse pregnancy outcomes such as perinatal death,41 but others have not found evidence for an increased risk. 38
Health consequences in children and young people
Overweight and obese children and young people are at high risk of developing comorbidities, either while still young, or as they progress into adulthood. The current NICE Obesity guideline recommends that assessment of comorbidity should be considered for children with a BMI at or above the 98th centile.
It is not surprising that studies reporting on the health consequences of overweight and obesity in children and young people have found many of the comorbid conditions described above for adults. 42–45 However, caution should be exercised in applying findings from one population to another. One recent study aimed to investigate the prevalence of comorbidity in a population representative of the general obese childhood population in the UK and found that the prevalence of abnormal blood test results (e.g. for insulin, glucose, triglycerides and cholesterol) may be lower than those published in the USA and from a UK tertiary referral centre (Great Ormond Street, London, UK). 46
Other health consequences
There are likely to be a number of other potential health consequences that have not been mentioned above which are associated with overweight and obesity but for which, at the moment, there are insufficient data to enable the health risks to be robustly estimated. For example, there is emerging evidence that suggests obese people are more likely than people of normal weight to develop various types of infection, including postoperative infections. 47
Benefits of weight loss
Although the success of weight loss interventions are often expressed in terms of the amount of weight lost, improvements in QoL and comorbidities are generally a more meaningful indication of success for individuals. 48–50 A systematic review of the long-term effects of obesity treatments on body weight, risk factors for disease and disease51 found that weight loss from surgical and non-surgical interventions for people suffering from obesity was associated with decreased risk of development of diabetes, and a reduction in LDL-cholesterol, total cholesterol and blood pressure, in the long term. The effects of bariatric (weight loss) surgery on weight and Type 2 diabetes have also been reviewed. 52 The authors reported that bariatric surgery not only led to weight reduction, but also that preoperative diabetes resolved postsurgery in more than 75% of cases. A further systematic review of the long-term weight loss effects on all-cause mortality in overweight/obese populations53 concludes that there is some evidence that intentional weight loss has long-term benefits on all-cause mortality for women and more so for people with diabetes. However, the long-term effects for men are not clear. Weight loss in obese patients with knee osteoarthritis has also been systematically reviewed and the results of meta-analysis indicated that disability could be significantly improved when weight was reduced over 5.1%, or at the rate of > 0.24% reduction per week. 54 Weight loss has not been found to have a beneficial effect on risk of stroke. 55
Adverse effects of weight loss
It is important that obese patients are made aware of the potential adverse effects of weight loss so that they can come to a judgement about the balance between the risks and benefits of the approaches to weight loss that they are considering. 49,50,56 Not only are adverse effects associated with the various pharmaceutical and surgical interventions for achieving weight loss, but adverse effects are also associated with dietary regimens. In particular rapid weight loss is an important risk factor for gallstone development, there is evidence that obese women who lose 4–10 kg in weight have a 44% increase in risk of gallstones caused by the increase in circulating cholesterol. 8 However, it has been estimated that the incidence of gallstone formation is unchanged below rates of weight loss of 1.5 kg per week. 57 Weight loss may also decrease bone density. 8 Contradictory evidence has been published with regard to the effect of weight loss and mortality. A recent review of the evidence has suggested that the impact of weight loss may be gender specific, there was some evidence for long-term benefits on mortality in women, but the long-term effects for men were not clear. 53
Current service provision
Management of disease
Non-surgical interventions are the cornerstone of overweight and obesity treatment. The intensity of management for overweight and obesity will depend on the level of risk of health problems and the potential to gain benefit from weight loss.
Adults
Management initially takes place within the general practice setting provided by the GP or practice nurse. As the degree of overweight increases, and depending on the presence or absence of comorbidities, intensity of management should increase to include dietary, physical exercise and lifestyle advice. The current NICE obesity guideline9 states that multicomponent interventions are the treatment of choice. Weight management programmes should include behaviour change strategies to increase people’s physical activity levels or decrease inactivity, improve eating behaviour and the quality of the person’s diet and reduce energy intake. 9 The NICE guideline suggests that in adults a prescription for drugs for weight control should be considered for people who are overweight with obesity-related comorbidities (BMI 25.00–29.99) or who meet the criteria for class I obesity (BMI 30.00–34.99) with obesity-related comorbidities, or who meet the criteria for class II obesity (BMI 35.00–39.99). The currently approved drugs are orlistat, sibutramine and, for obese people who have tried orlistat and sibutramine or who are unable to tolerate these two drugs, rimonabant. The NICE obesity guideline lists the situations when onward referral to specialist care should be considered:
-
the underlying causes of overweight and obesity need to be assessed
-
the person has complex disease states and/or needs that cannot be managed adequately in either primary or secondary care
-
conventional treatment has failed in primary or secondary care
-
drug therapy is being considered for a person with a BMI more than 50
-
specialist interventions [such as a very-low-calorie diet (VLCD) for extended periods] may be needed
-
surgery is being considered.
Surgery is usually considered a last resort intervention. NICE obesity guidelines recommend bariatric surgery as a treatment option only when all of the listed criteria are fulfilled:
-
the person has a BMI of 40 or more, or a BMI between 35 and 40 and other significant disease (for example, Type 2 diabetes or high blood pressure) that could be improved with weight loss
-
all appropriate non-surgical measures have been tried but have failed to achieve or maintain adequate, clinically beneficial weight loss for at least six months
-
the person has been receiving or will receive intensive management in a specialist obesity service
-
the person is generally fit for anaesthesia and surgery
-
the person commits to the need for long-term follow-up.
The guidelines also recommend bariatric surgery as a first-line option (instead of lifestyle interventions or drug treatment) for adults with a BMI of more than 50 in whom surgical intervention is considered appropriate.
Children and young people
As with adults, management initially takes place within the general practice setting provided by the GP or practice nurse. The NICE Obesity guideline9 indicates that BMI measurement in children and young people should be related to the UK 1990 BMI charts to give age- and gender-specific information. A tailored clinical intervention should be considered for children with a BMI at or above the 91st centile, depending on the needs of the individual child and family. NICE guidelines do not recommend a dietary approach alone for children and young people. Instead any dietary recommendations must be part of a multicomponent intervention. For children with a BMI at or above the 98th centile an assessment of comorbidity should be considered.
Referral to an appropriate specialist should be considered for children who are overweight or obese and have significant comorbidity or complex needs (for example, learning or educational difficulties). In secondary care, the assessment of overweight or obese children and young people should include assessment of associated comorbidities and possible aetiology. This can include investigations of blood pressure, fasting lipid profile, fasting insulin and glucose levels and liver and endocrine functions.
Orlistat and sibutramine do not have UK marketing authorisation for use in children; however, the NICE obesity guideline does not preclude their use in children. In children younger than 12 years, drug treatment may be used only in exceptional circumstances, e.g. if severe life-threatening comorbidities are present, and only in specialist paediatric settings. In children aged 12 years and older, treatment with orlistat or sibutramine may be started in a specialist paediatric setting by multidisciplinary teams experienced in prescribing for this age group. However, treatment is only recommended if physical comorbidities or severe psychological comorbidities are present. Rimonabant has recently been approved by NICE for use in adults when certain conditions are met, but it is not approved for use in children.
NICE obesity guidelines do not recommend bariatric surgery as a general treatment option for obese children and young people. However, the guideline acknowledges that there may be exceptional circumstances in which bariatric surgery can be considered providing the young person has achieved, or nearly achieved physiological maturity.
Current service cost
A recent study has estimated the direct cost of overweight and obesity to the NHS at £3.2 billion. 31 The majority of the costs attributable to overweight and obesity were the result of stroke, CHD, hypertensive disease and diabetes mellitus. This study was based on including people with a BMI of 22 and above, and because cost estimates are very sensitive to the BMI cut-off point chosen, the cost estimate from this study is higher than those of other studies.
A House of Commons Health Committee report26 estimated the direct treatment costs of obesity for 2002 were between £46 million and £49 million. The costs included in calculating this estimate were those for GP consultations, ordinary admissions, day cases, outpatient attendances and prescriptions. The cost estimate for treating the consequences of obesity (comorbidities) in 2002 was between £945 million and £1075 million. When the direct treatment costs and consequences of obesity costs were combined the total range for the direct costs of treating obesity and its consequences for 2002 was £990 to 1225 million (2.3–2.6% of net NHS expenditure in 2001–2). These figures were based on including people with a BMI of 25 and over, this is one reason why the estimate may be lower than for the more recent study above. However, it must be acknowledged that the Health Committee report stresses that these figures are still likely to underestimate the true cost of treating obesity and its consequences.
Relevant national guidelines
Three pieces of guidance with relevance to the UK are:
-
Obesity: the prevention, identification, assessment and management of overweight and obesity in adults and children. NICE clinical guideline 43. Issue date: December 2006. 9 This guideline replaces three earlier pieces of NICE guidance [TA22 Obesity – orlistat, TA31 Obesity – sibutramine and TA46 Obesity (morbid) – surgery] and largely supersedes the 2003 Royal College of Physicians report ‘Anti-obesity drugs. Guidance on appropriate prescribing and management’. 58
-
Rimonabant for the treatment of overweight and obese patients. NICE Technology appraisal. Issue date June 2008. 59 NICE has temporarily withdrawn its guidance on the use of rimonabant for the treatment of overweight and obese patients. The withdrawal of this guidance follows the decision of the European Medicines Agency (EMEA) in October 2008 to recommend suspension of the marketing authorisation for rimonabant. The EMEA concluded that the benefits of rimonabant no longer outweigh its risks. NICE will continue to review the status of its guidance in light of any further changes to rimonabant’s marketing authorisation.
-
The Scottish Intercollegiate Guidelines Network (SIGN) is in the process of updating it guidance on obesity.
Description of technologies under assessment
Surgical procedures for those with obesity aim to reduce weight and maintain any loss through restriction of intake and/or malabsorption of food. It is hoped that as a consequence eating behaviour is modified, with patients consuming smaller quantities of food more slowly. In addition to modifying eating habits, patients are encouraged to commit to daily exercise as part of a wider change in lifestyle. Surgery for obesity is a major surgical intervention with a risk of significant early and late morbidity and of perioperative mortality. Contraindications for bariatric surgery include poor myocardial reserve, significant chronic obstructive airways disease or respiratory dysfunction, non-compliance of medical treatment and psychological disorders of a significant degree.
Before surgery, patients should be made aware of the nature of the procedure and how it fits into the overall management programme for morbid obesity. Particularly important before surgery are the preoperative breathing exercises to reduce the incidence and severity of postoperative pulmonary insufficiency and assessment through spirometry. Patients may require antibiotic prophylaxis at anaesthesia and prophylactic measures to guard against perioperative thromboembolic disease. It is rare that patients will require ventilatory support and many, particularly if the surgery has been conducted laparoscopically, will not require intensive care nursing in a high dependency unit.
Several different surgical procedures have been used for people with morbid obesity. This review will focus on the principal types of surgical procedure that are in current use, including gastric bypass, gastric banding, biliopancreatic diversion and vertical banded gastroplasty. Of the procedures in current use gastric bypass and gastric banding are much more commonly performed than the others. Procedures that are no longer practised, such as jejunoileal bypass and horizontal gastroplasty, are not considered by this report. The following section briefly discusses these procedures and their complications. The section does not provide a comprehensive discussion of the many variants of these procedures that have developed. Intragastric balloons are not discussed because these are considered a short-term or temporary measure and not a comparator for the other surgical procedures.
Gastric bypass
The Roux-en-Y and resectional gastric bypass procedures combine restriction and malabsorption techniques, creating both a small gastric pouch and a bypass that prevents the patient from absorbing all they have eaten. 15 The Roux-en-Y procedure entails partition of the upper part of the stomach using surgical staples to create a small pouch (50 ml or less) with a small outlet (gastroenterostomy stoma) to the intestine that is attached to the pouch. The Roux-en-Y technique is used to avoid loop gastroenterostomy and the bile reflux that may ensue. Adaptations of the procedure include lengthening of the Roux-en-Y limb to 100–150 cm and use of retrocolic and retrogastric routing of the gastrojejunostomy. Often a prosthetic band, such as a Silastic ring or Gortex band, is positioned above the junction of the gastric pouch and small intestine to stabilise the gastroenterostomy, preventing late stretching of the opening and improving long-term weight control. Banded gastric bypass is not undertaken in the UK and because there is some disagreement as to whether it constitutes a separate procedure it is considered separately in this review. It is technically possible to reverse a gastric bypass. All patients who undergo gastric bypass procedures need long-term vitamin B12 replacement and oral iron therapy. Patients may be at risk from postgastrectomy bone disease. Advice on diet suggests a liquid diet for several weeks after the operation and improved eating habits involving small meals and multivitamin supplementation. Typically gastric bypasses which are performed laparoscopically require up to three to five days of inpatient stay (the open procedure, which is rarely undertaken now, requires a longer inpatient stay), with most patients unable to go back to work until after one month following surgery.
Complications associated with gastric bypass include failure of the staple partition, leaks at the junction of the stomach and small intestine, acute gastric dilatation, delayed gastric emptying either spontaneously or secondary to a blockage of the efferent limb. Failures of the staple line have been overcome by either transection of the stomach (staple line is divided and the cut ends over sewn) or superimposed staple rows causing firm scarring along the staple line. Other complications may occur following surgery including: vomiting caused by narrowing of the stoma as the result of scar tissue development, correctable through stretching by use of an endoscopic balloon dilatation as a day case; wound hernias and intestinal obstruction; anaemia as a result of lack absorption of iron and vitamin B12 and calcium deficiency (all are overcome by supplements). Dumping syndrome can also occur (an adverse event caused by eating refined sugar, symptoms of which include rapid heart rate, nausea, tremor, faint feeling and diarrhoea). It is thought that the dumping syndrome aids weight loss by conditioning the patient against eating sweets.
Adjustable gastric banding
Gastric banding is the least invasive of the purely restrictive bariatric surgery procedures. It limits food intake by placing a constricting ring completely around the top end (fundus) of the stomach, below the junction of the stomach and oesophagus. While early bands were non-adjustable, those used currently incorporate an inflatable balloon within their lining to allow adjustment of the size of the stoma to regulate food intake. Adjustment is undertaken without the need for surgery by adding or removing saline through a subcutaneous access port. As a restrictive procedure, gastric banding avoids the problems associated with malabsorptive techniques. Gastric banding is technically a reversible procedure. Surgery to fit an adjustable gastric band is typically undertaken laparoscopically and involves a short hospital stay, usually a maximum of two or three days. Following surgery, patients are usually seen regularly until they achieve their target weight and then on an infrequent basis thereafter. Often patients will be advised on nutrition postoperatively.
Complications include those associated with the operative procedure, splenic injury, oesophageal injury, wound infection, band slippage, band erosion (or migration), reservoir deflation/leak, persistent vomiting, failure to lose weight and acid reflux. Some studies have documented a high need for revisional or band-removal surgery as a result of complications,60 with major reoperations required by over 20% of patients after mean follow-up periods of about five years. 61,62 Expert opinion suggests that band failure rate may be greater than this, possibly approaching 30%.
Biliopancreatic diversion
Biliopancreatic diversion was first reported in 1978 by Scopinaro. 63 It has become popular in Europe and is primarily a malabsorptive procedure. The standard procedure involves the removal of part of the stomach (a limited horizontal gastrectomy) to limit oral intake and induce weight loss. The gastric pouch which is created is larger than that of gastric bypass or the restrictive procedures therefore allowing larger meals, and patients remain on a less restricted diet than would be the case following gastric bypass. Part of the small intestine is also bypassed (the malabsorptive component) by the construction of a long limb Roux-en-Y anastomosis with a short common ‘alimentary’ channel of 50 cm length. As the procedure does not defunctionalise any part of the small intestine fewer liver problems are caused than occurred with jejunoileal bypass procedures. 64 Biliopancreatic diversion is only a partially reversible procedure. The combination of biliopancreatic diversion with duodenal switch is an additional adaptation of the standard procedure. It has a sleeve gastrectomy rather than a horizontal gastrectomy. Length of hospital stay for biliopancreatic diversion ranges between two and seven days.
Biliopancreatic diversion is considered to be a technically demanding procedure with an operative mortality of 2% and major perioperative morbidity of 10%. 65 Side effects of the procedure include loose stools, stomal ulcers, offensive body odour and foul smelling stools and flatus. Serious complications include anastomotic leak and anastomotic ulceration (3%–10%), protein malnutrition (3%–4%), hypoalbuminaemia, anaemia (< 5%), oedema, asthenia (lack of energy) and alopecia (hair loss). 65,66 In some instances patients require further hospitalisation and hyperalimentation. As a result of malabsorption, patients usually need calcium and vitamin supplements and lifelong follow-up. In an attempt to overcome these complications, particularly stomal ulceration and diarrhoea, several variants of the procedure have been developed. Sleeve resection of the stomach maintains continuity of the gastric lesser curve while the duodenal switch maintains continuity of the gastroduodeno–jejunal axis.
Sleeve gastrectomy
For some patients who are at high risk from bariatric surgery a sleeve gastrectomy is considered. This is generally seen as the first part of a two-part surgical procedure, being followed at a later date by a conversion to either a gastric bypass or a duodenal switch. However, for some, enough weight is lost with the sleeve gastrectomy alone. The sleeve gastrectomy divides the stomach vertically to reduce its size to about 25%. It leaves the pyloric valve at the bottom of the stomach intact, which means that the stomach function remains unaltered and digestion is therefore unaltered. After 6–12 months the stomach may have expanded and does not restrict intake as much, this is when the gastric bypass can then be added if necessary. The sleeve gastrectomy is not reversible.
Complications are reduced because digestion is unaffected; however, patients are at risk from leaking from the newly formed stomach or vomiting as a result of over-eating. As with all surgery, there is a risk from postoperative complications such as postoperative bleeding and small bowel obstruction.
This operation is relatively quick to perform, which reduces the risk from complications. Hospital stay is normally one or two days.
Vertical banded gastroplasty
Vertical banded gastroplasty is now used infrequently; however, it has been used in a number of studies as the comparator intervention and hence is included here. Vertical banded gastroplasty partitions the stomach, using surgical staples, to create a small segment at the top of the stomach which is partially separated from the remainder of the stomach, with only a small gap (stoma) remaining. In addition, a polypropylene band may be used around the lower end of the vertical pouch to prevent stretching. The intention is to cause the person to have the sensation of fullness from a limited intake of food. This procedure has the advantage of being a restrictive procedure with no malabsorption component or dumping, but weight regain is common. The only restrictions are that people should chew food thoroughly to avoid vomiting and high-calorie liquids should be avoided. Vertical banded gastroplasty usually requires similar inpatient stay and time to return to work as gastric bypass, up to 10 days hospitalisation and return to work after at least a month.
Complications are relatively rare, with a low postoperative mortality rate (1%). Revision rates requiring further surgical intervention are often high at approximately 30%. Specific complications include bolus obstruction and there are few instances of anaemia or calcium or vitamin deficiencies. Other complications associated with the operative procedure include leakage, stenosis, ulcer, incisional hernia, wound infection, staple-line disruption, pouch dilatation and band erosion.
Laparoscopic versus open procedures
Laparoscopic surgery has become a major advance for bariatric surgery. The learning curve is long, the technique is challenging, and there may be differences in open and laparoscopic versions of particular procedures. Nevertheless, gastric banding, gastric bypass, vertical banded gastroplasty and sleeve gastrectomy procedures are increasingly undertaken laparoscopically. This decreases the time spent in hospital and the recovery time for the patient. In the current review comparisons of laparoscopic and open procedures have been included.
Place in the treatment pathway
As noted in the Current service provision section, bariatric surgery for morbid obesity is usually only considered after patients have attempted other forms of weight loss such as behaviour change, increased physical activity and drug therapy, but without achieving permanent weight loss. The exception to this is adults with a BMI of more than 50 where NICE guidelines recommend bariatric surgery as a first-line option (instead of lifestyle interventions or drug treatment) if surgical intervention is considered appropriate. The NICE guideline indicates that patients being considered for surgery should receive intensive management in a specialist obesity clinic. These clinics offer a combination of interventions, including drug therapy, VLCDs and sometimes psychologist input as well as surgery. An NAO report24 cites an unpublished survey carried out by the NHS Clinical Obesity Group in 1998. This identified 12 obesity clinics in England, eight of which were run by physicians and four by surgeons. In addition, four physicians and 28 surgeons in England were seeing patients for their obesity outside obesity clinics. These data are now 10 years out of date and expert opinion suggests that there are many more specialist obesity clinics now. The British Obesity Surgery Patients Association (BOSPA) website provides a UK surgery directory which in June 2008 listed NHS hospitals in about 50 English and Welsh towns and cities where a surgeon can be contacted regarding referral for NHS bariatric surgery. In addition, contact details are provided for surgeons who only undertake private practice work.
Following surgery, patients require ongoing dietary advice and support. Those who have had an adjustable gastric band fitted will need access to a band adjustment service.
Current usage in the NHS
A recent assessment of obesity surgery in England between 1996 and 2005 found that the rate of obesity surgery had risen from 72 procedures in 1996 to 347 procedures in 2004 (equivalent to a rate of seven per million population). 67 Additional information68 published alongside the NICE obesity guideline included results of a survey of surgeons performing bariatric surgery in England in 2006 (survey by BariatricEdge, a division of Ethicon Endo Surgery: a Johnson & Johnson company, unpublished data). This survey estimated that the total average rate of bariatric surgery was 6.5 per 100,000 population, of which around three per 100,000 population were funded by the NHS. Both the published study67 and the unpublished survey reported variable levels of bariatric surgery occurring in different parts of the country, but these variations did not mirror regional differences in estimated levels of morbid obesity. This suggests that the intervention is not uniformly available across the country and there may be inequalities in service delivery.
BOSPA69 have undertaken an audit of the criteria that PCTs use to approve funding for surgery. In June 2008 more than half of the 151 PCTs listed were basing their funding decisions on NICE criteria, but more than a fifth of the PCTs were using criteria that were more stringent than the NICE criteria and information was not available for a further fifth of the PCTs listed. A minority of PCTs use criteria that are not based on a particular BMI.
Expert opinion indicates that in addition to inequalities in availability of bariatric surgery, band adjustment services are also not uniformly available across the country.
Anticipated costs associated with intervention
Bariatric surgery is a highly specialised and low volume activity and is not included in the NHS Reference Costs returns. Costings developed for this review estimate the cost of the surgical procedures alone at £6985 for laparoscopic gastric bypass and £4304 for laparoscopic adjustable gastric banding. Approximately £1200 to £2000 of these costs are associated with high-cost consumables (including staples used in gastric bypass procedures and the gastric bands, and a range of single-use equipment). In addition to the procedure costs the estimate for costs of preoperative assessments is £1114, while postdischarge care of surgical patients will cost up to £1800 in the two years following gastric bypass surgery and up to £1900 following gastric banding (if costs of band fill and adjustments are included). Overall the anticipated costs for laparoscopic gastric bypass are £11,462 and for laparoscopic adjustable gastric banding are £8762. These overall costs include estimates of additional resource use arising from adverse events during the initial hospitalisation, reoperations within two years for patients whose initial surgery was unsuccessful, abdominal hernia procedures and additional cholecystectomies in patients within two years of a bariatric procedure.
The cost estimates developed for this review may not reflect the scarcity of surgeons with appropriate training and experience to perform bariatric procedures. The previous review15 developed a scenario to assess the impact of involving surgeons at an early stage of the learning curve – the likely impacts that directly affect treatment costs were identified as being reflected in longer operating times (50% higher), a doubling in revision rates. Including these effects raises the estimated cost of gastric bypass surgery to £14,787 (of which the procedure cost is £8795), while the estimated cost of adjustable gastric banding increases to £11,310 (of which £5510 is the procedure cost). Additional impacts of involving less experienced surgeons, that are not directly reflected in cost estimates, were identified in an increased risk of surgical mortality and a likelihood of poorer outcomes (in terms of percentage weight loss following surgery).
Rationale for this study
The prevalence of obesity (BMI > 30) and morbid obesity (BMI ≥ 40) among adults is increasing. A similar pattern of increasing prevalence of obesity is seen in children and young people. A systematic review and economic evaluation of surgery for morbid obesity was conducted in 200215 and it found that although surgery appeared effective in terms of weight change, there was limited evidence addressing the long-term consequences and its influence on the QoL of patients. The economic evaluation was based on several assumptions because of the limitations of the data available, and it found that surgery offered additional quality-adjusted life-years (QALYs) at an additional cost when compared with non-surgical management over a 20-year period, but comparison of the different procedures suggested that the difference in cost per QALY was less clear. The review found that there were few economic evaluations comparing the different surgical interventions, and the availability of costing and resource-use data was limited. The systematic review of clinical effectiveness was also published as a Cochrane review70 which was updated in 2005,71 when further trials were identified, but an economic evaluation was not undertaken.
The earlier reviews15,70,71 identified needs for further research. There was a need for good-quality randomised controlled trials (RCTs) comparing either surgery with non-surgical interventions, or comparing one type of surgical procedure with another surgical procedure. Further key implications for research were the need for an assessment of outcomes over longer time periods (at least five years) and the need to include QoL outcomes. Further good quality economic evaluations were also needed.
An update of the systematic review and economic evaluation is therefore required which will include data from more recent trials, including any that may have assessed new bariatric surgical techniques. Any good-quality research that has assessed bariatric surgery for young obese people will be considered for inclusion in the review because some current guidelines9,64 do not rule out surgical intervention for young people. Furthermore the updated review will include people with lower BMIs than the previous reviews15,72 (BMI > 30), to take account of the emerging literature that possible benefits of early intervention (particularly in reducing obesity-related comorbidity) outweigh the potential harms. This is reflected in one guideline64 that allows for surgery in people with a BMI greater than 30 and serious comorbid disease.
Chapter 2 Definition of the decision problem
Decision problem
Obesity is associated with increased morbidity and mortality. Bariatric (weight loss) surgery for obesity is considered when other treatments have failed. The aim of this health technology assessment is to assess the clinical effectiveness and cost-effectiveness of bariatric surgery in the obese. This report is an update of a previously published systematic review and economic evaluation. 15,70,71 To ensure that the systematic review remains relevant to current practice, some small changes have been made to the eligibility criteria at each update. The changes made to the eligibility criteria for this update are discussed below.
Population including subgroups
The original review was restricted to adults aged 18 years or over with BMI greater than 40 or BMI greater than 35 with serious comorbid disease. 15,70,71 The present review has been broadened to include people of all ages undergoing surgery for obesity, in order to reflect some current guidelines which do not rule out surgical intervention in young people9,64 and indications from the literature that weight loss surgery is undertaken in young people under 18 years of age. The present review also includes people with a BMI greater than 30 with serious comorbid disease, again to reflect changing guidelines from the American Society for Bariatric Surgery64 and emerging literature suggesting that benefits may outweigh the harms in this group.
People with a BMI 30 to 35 do not meet the current NICE guideline for bariatric surgery,9 therefore this subgroup will be considered separately where appropriate and if data allow. A further subgroup of people with BMI greater than 50 (super-obese) will also be considered separately where appropriate.
Interventions
Surgical procedures in current use are included, such as gastric bypass, biliopancreatic diversion sleeve gastrectomy, vertical banded gastroplasty and adjustable gastric banding. Four procedures that are not in current use have been excluded:
-
Jejunoileal bypass was included in the original review,15 but was excluded from the Cochrane reviews70,71 and the present update because this procedure is not in current practice as a result of unacceptably high morbidity and mortality. Three studies (seven publications) of jejunoileal bypass that were included in the original review15 were excluded from later updates70,71 and the present review.
-
Horizontal gastroplasty was included in the previous versions of this review. 15,70,71 However, this surgical intervention is not currently practiced and the most recent trial was published over 20 years ago. Seven studies (13 publications) of horizontal gastroplasty were therefore excluded from this update.
-
One study included in previous versions of this review assessed vertical gastroplasty that was not banded. 15,70,71 This intervention has also been excluded because it is no longer practiced.
-
Non-adjustable gastric banding. One study published as an abstract only73 and included in the Cochrane reviews70,71 included a non-adjustable gastric band as one of three interventions assessed. All bands in current use are adjustable so this arm of the trial has been excluded from the current review. The surgical cohort of the Swedish Obese Subjects (SOS) study includes a minority of participants who received either adjustable or non-adjustable gastric bands. However, this study is included in the current review because those who received gastric banding of any type make up less than a fifth of the surgical cohort and much of the data are reported for the surgical cohort as a whole.
Relevant comparators
As bariatric surgery is usually an intervention of last resort when all other methods have failed, much of the published evidence reports comparisons between one type of bariatric surgery and another. It is anticipated that there will be few RCTs comparing surgery with no surgery (no treatment, medical management, e.g. VLCD or drugs such as orlistat or sibutramine or usual care), therefore prospective cohort studies are also included for these comparisons. Open surgery compared with laparoscopic surgery for the same procedure is also assessed. Comparisons of variations of surgical techniques rather than different procedures are excluded.
Outcomes
The primary outcomes of interest are measures of weight change, QoL, perioperative and postoperative mortality and morbidity, change in obesity-related comorbidities, and cost-effectiveness. It will be necessary to identify the resource implications of interventions and comparators, for example time in surgery, because these factors will help to inform the economic model. It is anticipated that the principal outcome of the economic model will be expressed in terms of incremental cost per QALY gained.
Overall aims and objectives of assessment
The aim of this report was to assess the clinical effectiveness and cost-effectiveness of bariatric surgery for obesity by updating and expanding the previous systematic review and economic evaluation of surgery for morbid obesity. 15,70,71
The objectives were to:
-
summarise the evidence of clinical effectiveness and cost-effectiveness of surgery when compared with no surgery (medical management, usual care or no treatment)
-
summarise the evidence of clinical effectiveness and cost-effectiveness comparing different surgical procedures in current use
-
develop, where appropriate, an economic model adapting an existing cost-effectiveness model or constructing a new model using best available evidence to determine cost-effectiveness in the UK
-
identify priorities for future research.
Chapter 3 Methods for the systematic review of clinical effectiveness and cost-effectiveness
This report is an update of a previously published systematic review and economic evaluation. 15,70,71 The a priori methods for systematically reviewing the evidence of clinical and cost-effectiveness are described in the research protocol (Appendix 1). The protocol was sent to experts for comment; although helpful comments were received relating to the general content of the research protocol, there were none that identified specific problems with the methods of the review. The methods outlined in the protocol are briefly summarised below.
Search strategy
The search strategy for the update review was refined by an experienced information scientist. Separate searches were conducted to identify studies of clinical effectiveness, cost-effectiveness, QoL, resource use/costs and epidemiology/natural history. Sources of information and search terms are provided in Appendix 2, and a flow chart of identification of studies can be seen in Appendix 3. The most recent search was carried out in August 2008.
Searches for clinical effectiveness and cost-effectiveness literature were undertaken from the date of the last search of the previous review. 71 Electronic databases searched included: MEDLINE; EMBASE; PreMedline In-Process & Other Non-Indexed Citations; The Cochrane Library including the Cochrane Systematic Reviews Database, Cochrane Controlled Trials Register, DARE, NHS EED and HTA databases; Web of Knowledge Science Citation Index (SCI); Web of Knowledge ISI Proceedings; PsycInfo; CRD databases; BIOSIS; and databases listing ongoing clinical trials. A total of 17 electronic resources were searched: 12 resources (encompassing 15 databases) listing published papers and abstracts and five databases listing ongoing clinical studies. Searches were not restricted by language and conference abstracts were not excluded from the search strategy (see Inclusion criteria section, this chapter, for inclusion criteria on language and conference abstracts as these differed between the reviews of clinical effectiveness and cost-effectiveness studies). Bibliographies of related papers were screened for relevant studies, and the expert advisory group was also contacted for advice and peer review, and to identify additional published and unpublished references.
Inclusion and data extraction process
Titles and abstracts identified by the search strategy for the clinical effectiveness section of the review were assessed for possible eligibility by two reviewers independently. The full texts of relevant papers were then obtained and inclusion criteria were again applied by two reviewers independently using a standardised form. Any disagreements over eligibility were resolved by consensus or by recourse to a third reviewer. Data were extracted by one reviewer using a standardised data extraction form and independently checked by two further reviewers.
Titles and abstracts identified by the search strategy for the cost-effectiveness section of the review were assessed for potential eligibility by two health economists. Economic evaluations were considered for inclusion if they reported both health-service costs and effectiveness, or presented a systematic review of such evaluations. Full papers were formally assessed by one health economist with respect to their potential relevance to the research question.
Quality assessment
Within the clinical effectiveness section of the review the quality of included cohort studies was assessed using criteria recommended by NHS Centre for Reviews and Dissemination (CRD)74 (Appendix 4). RCTs were assessed using the Cochrane criteria for judging risk of bias (Appendix 4). 75 These criteria include consideration of the following factors:
-
sequence generation
-
allocation concealment
-
blinding of participants, personnel and outcome assessors
-
incomplete outcome data
-
selective outcome reporting
-
topic-specific, design-specific or other potential threats to validity.
Quality criteria were applied independently by two reviewers. At each stage, any differences in opinion were resolved through discussion or consultation with a third reviewer.
For the cost-effectiveness section of the review the included studies were summarised and critically appraised by two health economists to identify:
-
the number and characteristics of alternative surgical interventions included in economic evaluations
-
the choice of a comparator treatment
-
population to whom the results of the economic evaluations apply
-
approach and assumptions used in decision analytic models
-
methods used in transforming clinical and economic data to the needs of economic modelling
-
methods of dealing with uncertainties and potential bias in estimated results
-
other issues as recommended by the checklist for economic evaluation publications (Drummond and Jefferson76) and the guidelines for good practice in decision-analytic modelling in health technology (Phillips and colleagues77).
Inclusion criteria
The eligibility criteria for the systematic review of clinical effectiveness differ slightly from those of the previously published versions of the review;15,70,71 these differences are described in Chapter 2, Decision problem section. The inclusion criteria for the present review are described below.
Patients
-
Adult patients fulfilling the standard definition of obese, i.e. people with a BMI of 30 or over.
-
Young people who fulfil the definition of obesity for their age, sex and height.
-
Where data were available, clinical effectiveness and cost-effectiveness will be reported separately for patients who meet current NICE guidelines for bariatric surgery, those with a lower BMI who would not currently meet the NICE criteria for bariatric surgery, and young people.
Interventions
-
Open and laparoscopic bariatric surgical procedures in widespread current use. Clinical experts were consulted to ensure that the included procedures are those which are most relevant to current clinical practice. The procedures included are gastric bypass, biliopancreatic diversion (including biliopancreatic diversion with duodenal switch), sleeve gastrectomy, adjustable gastric banding and vertical banded gastroplasty.
Comparators
-
Surgical procedures in current use in comparison with one another.
-
Open surgery compared with laparoscopic surgery for the same procedure.
-
Surgical procedures in current use compared to non-surgical interventions. These non-surgical interventions may have included drugs such as orlistat and sibutramine, dietary interventions, exercise and combinations of non-surgical interventions such as diet and exercise, or no surgery.
Outcomes
-
To be included, studies must have reported outcomes following a minimum of 12 months of follow-up.
-
Included studies had to have reported on at least one of the following outcomes: measures of weight change, QoL, perioperative and postoperative mortality and morbidity, change in obesity-related comorbidities, cost-effectiveness (i.e. both costs and outcomes should be reported). For cost-effectiveness, intermediate outcomes (in BMI) had to have been converted to final outcomes [i.e. either life-years (LYs) or QALYs], cost-effectiveness studies where results were reported only with respect to intermediate outcomes other than BMI (e.g. cost per kg of excess weight loss; cost per adverse event avoided) were not eligible for inclusion.
Types of studies
-
Systematic review of clinical effectiveness: RCTs were eligible for inclusion. For the comparisons of surgical procedures with non-surgical procedures controlled clinical trials and prospective cohort studies (with a control cohort) were also eligible for inclusion (because it was anticipated that few or no RCTs would be found).
-
Systematic review of cost-effectiveness: full cost-effectiveness analyses, cost–utility analyses, cost–benefit analyses and cost–consequence analyses. Only publications in English were eligible for inclusion in the systematic review of cost-effectiveness.
-
Studies published as abstracts or conference presentations were eligible for inclusion in the clinical effectiveness section if sufficient details were presented to allow an appraisal of the methodology and the assessment of results to be undertaken. Conference abstracts were not eligible for inclusion in the cost-effectiveness section.
Data synthesis
Data were synthesised through a narrative review with tabulation of results of all included studies. Full data extraction forms are presented in Appendix 5 to Appendix 15. Within the clinical effectiveness section studies using similar surgical procedures were grouped together to aid interpretation. However, within these groupings there may be differences in procedures, such as modifications of procedures (for example variations of gastric bypass), or open or laparoscopic procedures. These are noted where appropriate. It was not considered appropriate to combine the included RCTs in a meta-analysis because of the heterogeneity in the patient groups, comparator treatments and outcomes (see Chapter 4, Assessment of clinical effectiveness and Chapter 7 Strengths and limitations of the assessment).
Chapter 4 Clinical effectiveness
Quantity and quality of research available
Studies identified
As this report is an update of a systematic review and economic evaluation originally published in 2002,15 with the review of clinical effectiveness updated for the Cochrane Library in 200370 and 2005,71 searching and screening have been conducted on a number of occasions. Moreover, each version update differs slightly in the studies included as the review has evolved. Appendix 3 explains how the review has evolved and notes the main differences between the reviews with respect to the eligibility criteria and studies included in each publication. A flow chart of the identification of studies at each stage can also be seen in Appendix 3.
In summary, a total of 5386 references were identified through the previous and current searches. Twenty-six studies reported in 52 publications met the current inclusion criteria.
Assessment of inter-rater agreement
Inter-rater agreement for study selection was excellent (Cohen’s kappa = 0.84). Initial disagreements were resolved though discussion in all cases.
Excluded studies
The reasons for excluding 32 studies after examination of the full papers from the 2005 and 2008 updated searches can be seen in Appendix 16. Studies excluded from the original searches have been described previously. 15,70 Studies were often excluded for more than one reason, but the most common reason for exclusion was a study design other than an RCT for comparisons of surgical procedures, or a controlled prospective cohort study for comparisons of surgery versus non-surgical management. Four studies published as abstracts only were excluded because of inadequate length of follow-up. 78–81 The authors of these trials were contacted to determine if further follow-up was available, but no replies were received.
Characteristics of included studies
Twenty-three of the 26 included studies were RCTs. One study (SOS) was a prospective multicentre cohort study with matched concurrent controls. This study has multiple publications, 20 of which have been included in this review. 82–101 Throughout the review, this study will be referred to as the SOS study, with specific references cited where appropriate. Two studies had prospective cohort designs (Stoeckli and colleagues102–104 and Buddeberg-Fischer and colleagues105). Two of the included studies were reported as abstracts only. 73,106 Table 12 summarises the comparisons identified by the searches.
| Comparisona | Study |
|---|---|
| Surgery vs non-surgical interventions (RCTs and prospective cohort studies) | |
| Laparoscopic adjustable gastric banding vs conventional therapy117 OR Intensive medical programme115,116 OR No surgery102–104 (vs open gastric bypass102–104) | 1. Dixon et al., 2008,117 RCT; 2. O’Brien et al., 2006,115,116 RCT; 3. Stoeckli et al., 2004,102–104 Cohort study |
| Biliopancreatic diversion vs diet | 1. Mingrone et al., 2002,119 RCT |
| Surgery (various) vs conventional treatment83–90 | 1. SOS 1997 to 2007,82–101 Cohort study; 2. Buddeberg-Fischer et al., 2006,105 Cohort study |
| Comparisons of different surgical procedures (RCTs) | |
| Gastric bypass vs vertical banded gastroplasty | 1. Howard et al., 1995120; 2. VanWoert et al., 1992106; 3. MacLean et al., 1995121,122; 4. Sugerman et al., 1987123; 5. Lee et al., 2004124; 6. Olbers et al., 2005108,109; 7. Agren and Naslund, 198973,b |
| Gastric bypass (non-banded) vs banded gastric bypass | 1. Bessler et al., 2007118 |
| Laparoscopic gastric bypass vs laparoscopic adjustable gastric banding | 1. Angrisani et al., 2007107 |
| Laparoscopic Roux-en-Y gastric bypass vs laparoscopic sleeve gastrectomy | 1. Karamanakos et al., 2008125 |
| Vertical banded gastroplasty vs adjustable gastric banding | 1. Nilsell et al., 2001126; 2. Morino et al., 2003110; 3. van Dielen et al., 2005127,128 |
| Laparoscopic adjustable gastric banding vs laparoscopic isolated sleeve gastrectomy | 1. Himpens et al., 2006129 |
| Open gastric bypass vs laparoscopic gastric bypass | 1. Puzziferri et al., 2006113,114; 2. Lujan et al., 2004130; 3.Westling and Gustavsson, 2001131; 4. Sundbom and Gustavsson, 2004112 |
| Open vertical banded gastroplasty vs laparoscopic vertical banded gastroplasty | 1. Davila-Cervantes et al., 2002111 |
| Open adjustable silicone gastric banding vs laparoscopic adjustable silicone gastric banding | 1. de Wit et al., 1999132 |
Participants
Most studies included participants with morbid obesity, and where this was described further, a definition of BMI greater than 40 was commonly used, often with the additional criteria of BMI greater than 35 or 37 with comorbid disease (Table 13). However, Angrisani and colleagues107 included participants with BMI greater than 35, and the SOS study included men and women with a BMI greater than or equal to 34 and 38 respectively. A maximum of BMI of 50, 107,108,109,110,111 55,112 or 60113,114 was also specified by some studies.
| Study details | Intervention | Target population and selected baseline characteristics (mean and SD unless stated otherwise) |
|---|---|---|
| Surgery versus non-surgical interventions (RCTs and prospective cohort studies) | ||
|
Dixon, 2008117 Australia RCT, follow-up: 24 months |
1. LAGB (n = 30) 2. Con therapy (n = 30) |
Target pop: Type 2 diabetes, BMI 30–40, age 20–60 years AGE, years: LAGB 46.6 (7.4); con therapy 47.1 (8.7) SEX (M : F): LAGB 15 : 15, con therapy 13 : 17 BMI: LAGB 37.0 (2.7); con therapy 37.2 (2.5) |
|
Australia RCT, follow-up: 24 months |
1. LAGB (n = 40) 2. Intensive non-surgical programme (n = 40) |
Target pop: BMI 30 to 35 with comorbidities, age 20–50 years AGE, years: LAGB 41.8 (6.4); non-surgical 40.7 (7.0) SEX (M : F): LAGB 10 : 30; non-surgical 9 : 31 BMI: LAGB 33.7 (1.8); non-surgical 33.5 (1.4) |
|
Mingrone, 2002119 Italy RCT, follow-up: 1 year |
1. BPD (n = 46) 2. Diet (n = 33) |
Target pop: morbidly obese AGE, years: 30–45 SEX (M : F): BPD 15 : 31, diet 12 : 21 BMI: women, diet 48.4 (8.9), BPD 48.3 (6.3). men, diet 47.8 (8.8), BPD 48.0 (5.4) |
|
Sweden Multicentre, cohort study, follow-up: up to 10 years |
1. Surgery (VBG, Gband or GBP) (n = 2010) 2. Controls: conventional treatment, not standardised, best non-surgical options available at the time (n = 2037) |
Target pop: BMI ≥ 34 (men) and ≥ 38 (women), 37–60 years AGE, years: surgery 47.2 (5.9), control 48.7 (6.3) SEX: (M : F) surgery 590 : 1420, control 590 : 447 BMI: surgery 42.4 (4.5), control 40.1 (4.7) (all data here taken from most recently published study) |
|
Switzerland Cohort study, follow-up: 24 months |
1. LAGB (n = 8) 2. Open RYGBP (n = 5) 3. Control (n = 7) |
Target pop: morbid obesity (BMI > 37) AGE, years (SE): LAGB 41.1 (2.6), RYGBP 43.8 (4.4), controls 49.9 (2.6) SEX (M : F): LAGB 2 : 6, RYGBP 0 : 5, controls 2 : 5 BMI: LAGB 41.7 (1.0), RYGBP 43.6 (2.0), controls 41.1 (1.0) |
|
Buddeberg-Fischer, 2006105 Switzerland Cohort study Mean follow-up 3.2 years (SD 1.3, range 0.28–5.8) |
1. Surgery (LAGB, LRYGBP) (n = 63) 2. No surgery (n = 30) |
Target pop: BMI > 40, or > 35 with substantial comorbidity AGE, years 43.5 (9.8, range 21.65) SEX (M : F) 23 : 70 BMI: surgery, 44.7 (6.1) [LRYGBP (n = 23), 47.3 (7.8); LAGB (n = 40), 43.4 (4.5)]; no surgery 42.9 (5.5) |
| Comparisons of different surgical procedures (all RCTs) | ||
|
Howard, 1995120 USA Follow-up: 12 to 78 months |
1. GBP (n = 20) 2. VBG (n = 22) |
Target pop: Class IV obesity (BMI > 40); < 50 years old AGE, years: GBP 38.1 (SE 1.9), VBG 36.5 (SE 2.3) SEX (M : F): GBP 5 : 15, VBG 4 : 18 BMI: not reported |
|
VanWoert, 1992106 USA (abstract) Follow-up: 36 months |
1. GBP (n = 15) 2. VBG (n = 17) |
Target pop: BMI > 40 AGE, years: GBP 38 (8), VBG 38 (10) SEX (M : F): GBP 4 : 11, VBG 3 : 14 BMI: GBP 52 (SD 10), VBG 51 (SD 6) |
|
Canada Follow-up: up to 6.5 years |
1. VBG (n = 54) 2. RYGBP (n = 52) |
Target pop: target population not stated AGE, years: VBG 38.8 (9.5), RYGBP 40.1 (7.7) SEX: not reported BMI: VBG 48.2 (6.5), RYGBP 49.9 (7.4) |
|
Sugerman, 1987123 USA Follow-up: 3 years |
1. RYGBP (n = 20) 2. VBG (n = 20) |
Target pop: more than 100 lb (45.5 kg) above ideal weight AGE, years: RYGBP 38 (11), VBG 38 (9) SEX (M : F): RYGBP 2 : 18, VBG 2 : 18 BMI: not reported |
|
Lee, 2004124 Taiwan Follow-up: Mean 20 months (range 18 to 30) |
1. LVBG (n = 40) 2. LRYGBP (n = 40) |
Target pop: significant obesity > 5 years, BMI > 40 or BMI > 35 with comorbidities, age 18–59 AGE, years: LVBG 32.5 (7.8), LRYGBP 31.6 (8.6) SEX (M : F): LVBG 11 : 29, LRYGBP 13 : 27 BMI: LVBG 43.14 (6.1), LRYGBP 43.18 (7.5) |
|
Sweden Follow-up: 24 months |
1. LRYGBP (n = 37) 2. LVBG (n = 46) |
Target pop: BMI > 40 or > 35 with obesity-associated morbidity, BMI < 50 AGE (median, range), years: LRYGBP 37 (34–61); LVBG 34 (26–60) SEX (M : F): LRYGBP 12 : 25; LVBG 10 : 36 BMI: LRYGBP 42.7 (4.0); LVBG 42.1 (4.2) |
|
Agren and Naslund, 198973 Sweden Follow-up: 18 months |
1. VBG (n = 27) 2. Loop GBP (n = 25) |
Target pop: morbidly obese AGE: not reported SEX: not reported BMI 42.8 |
|
Bessler, 2007118 USA Follow-up: up to 36 months |
1.Banded long-limb GBP (n = 46) 2. Non-banded long-limb GBP (n = 44) |
Target pop: BMI > 50 AGE, years: banded GBP 40.6 (7.4); non-banded GBP 42.6 (7.2) SEX (M : F): banded GBP 20 : 26; non-banded GBP 12 : 32 BMI: banded GBP 59.4 ± 7.3; non-banded GBP 59.7 ± 7.1 |
|
Angrisani, 2007107 Italy Follow-up: 60 months |
1. LRYGBP (n = 24) 2. LAGB (n = 27) |
Target pop: BMI > 35 to < 50, age > 16 years but < 50 years AGE, years: LRYGBP 34.1 (8.9); LAGB 33.8 (9.1) SEX (M : F): LRYGBP 4 : 20; LAGB 5 : 22 BMI (range): LRYGBP 43.8 ± 4.1 (38.9–48.9); LAGB 43.4 ± 4.2 (38.1–49.2) |
|
Nilsell, 2001126 Sweden Follow-up: 4–5 years |
1. AGB (n = 29) 2. VBG (n = 30) |
Target pop: BMI > 40 or BMI >37 with obesity associated comorbidity AGE, years: AGB 38 (20–58), VBG 39 (19–59) SEX (M : F): AGB 8 : 21, VBG 6 : 24 BMI: AGB 42.8 (5.4), VBG 43.9 (3.8) |
|
Morino, 2003110 Italy Follow-up: mean 33.1 months (range 24–46) |
1. LAGB (n = 49) 2. LVBG (n = 51) |
Target pop: BMI 40–50, aged 18–60 years AGE, years: LAGB 37.2 (20–55), LVBG 38.2 (21–58) SEX (M : F): LAGB 11 : 38, LVBG 8 : 43 BMI: LAGB 44.7 (40.1–50.0), LVBG 44.2 (40.0–50.0) |
|
The Netherlands Follow-up: 24 months and 84 months |
1. Open VBG (n = 50) 2. LAGB (n = 50) |
Target pop: BMI > 40 or > 35 with comorbidities; age 18–60 years AGE: VBG 39 (8.5) years; LAGB 37.2 (9.7) years SEX (M : F): Open VBG 10 : 40; LAGB 10 : 40 BMI: VBG 46.6 (6.4); LAGB 46.7 (6.1) |
|
Karamanakos, 2008125 Greece Follow-up: 1 year |
1. LRYGBP (n = 16) 2. LSG (n = 16) |
Target pop: not reported AGE, years: LRYGBP 37 (8.25), LSG 30.6 (7.8), p = 0.023 SEX (M : F): LRYGBP 4 : 12, LSG 1 : 15 BMI: LRYGBP 46.6 (3.7), LSG 45.1 (3.6) |
|
Himpens, 2006129 Belgium Follow-up: 36 months |
1. LAGB (n = 40) 2. LISG (n = 40) |
Target pop: not stated AGE (median, range), years: LAGB 36 (20–61); LISG 40 (22–65) SEX (M : F): LAGB 7 : 33; LISG 9 : 31 BMI (median, range): LAGB 37 (30–47); LISG 39 (30–53) |
|
USA Follow-up: 36 months |
1. LRYGBP (n = 79) 2. Open RYGBP (n = 76) |
Target pop: BMI 40–60; age 21–60 years AGE: LRYGBP 40 years (± 8), RYGBP 42 years (± 9) SEX (M : F): LRYGBP 7 : 72, RYGBP 9 : 67 BMI: LRYGBP 47.6 (± 4.7), RYGBP 48.4 (± 5.4) |
|
Lujan, 2004130 Spain Follow-up: mean 23 months |
1. LGBP (n = 53) 2. Open GBP (n = 51) |
Target pop: BMI > 40 or BMI > 35 with coexisting pathologic disorders AGE, years: LGBP 37 (18–64), GBP 38 (20–63) SEX (M : F): LGBP 10 : 43, GBP 13 : 38 BMI: LGBP 48.53 (36–78), GBP 52.20 (37–80) |
|
Westling and Gustavsson, 2001131 Sweden (abstract) Follow-up: 1 year |
1. LRYGBP (n = 30) 2. Open RYGBP (n = 21) |
Target pop: BMI > 40 or BMI > 35 with significant comorbidity AGE overall group: 36 years (SD 9) SEX overall group: 94% female BMI LRYGBP 41 (SD 4), RYGBP 44 (SD 4) |
|
Sundbom and Gustavsson, 2004112 Sweden Follow-up: 1 year |
1. Hand-LRYGBP (n = 25) 2. Open RYGBP (n = 25) |
Target pop: BMI < 50. minimum BMI not reported AGE (range), years: hand-LRYGBP 37 (19–54), RYGBP 38 (24–54) SEX (M : F): hand-LRYGBP 2 : 23, RYGBP 3 : 22 BMI: hand-LRYGBP 44 (range 36–54), RYGBP 45 (range 34–54) |
|
Davila-Cervantes, 2002111 Mexico Follow-up: 1 year |
1. Open VBG (n = 14) 2. LVBG (n = 16) |
Target pop: BMI 40–50 AGE median (range), years: VBG 36.5 (22–56), LVBG 34.5 (24–46) SEX (M : F) VBG 1 : 13, LVBG 2 : 14 BMI median (range): VBG 43 (37–50), LVBG 45 (38–50) |
|
de Wit, 1999132 The Netherlands Follow-up: 1 year |
1. Open AGB (n = 25) 2. LAGB (n = 25) |
Target pop: BMI > 40, aged 18–55 years AGE: not reported SEX (M : F): LAGB 8 : 17, AGB 8 : 17 BMI: LAGB 51.3 (10.4), AGB 49.7 (5.6) |
Three studies included participants notably different from the rest of the studies in this review; with two studies focusing on the lower side of the obesity continuum, and one focusing on the upper side. O’Brien and colleagues115,116 included participants with a BMI of 30 to 35 (Class I obesity) and identifiable comorbidities. Dixon and colleagues117 limited inclusion to people diagnosed with Type 2 diabetes and a BMI of 30 to 40. At the other extreme, Bessler and colleagues118 required participants to have a BMI greater than 50.
The individual study sample size ranged from 20102–104 to 4047 (SOS study); however, the number of participants included in the analysis of the SOS study depended on the length of follow-up which varied for the different outcomes reported in different publications.
The majority of participants in the studies were female, the proportion of female participants in studies ranged from 53% to 94% where reported. Mean age ranged from 31 years in one arm of the RCT by Karamanakos and colleagues125 to 49 years in the SOS study (Table 13). Excluding the three studies with notably different inclusion criteria, mean baseline BMI ranged from 37 in the RCT by Himpens and colleagues129 (inclusion criteria were not reported by this study) to 52 in the study by vanWoert and colleagues. 106 Baseline BMI in the study focusing on Class I obesity was 34 in each group,115,116 and was 37 in each group in the study focusing on Type 2 diabetes. 117 The study by Bessler and colleagues,118 which focused on participants with BMI greater than 50, had a mean baseline BMI of 59.4 in the banded gastric bypass group and 59.7 in the non-banded group.
Baseline characteristics were similar between groups in most of the studies. However, the SOS study involved an interval of about nine months between matching of controls and the start of treatment (surgery) that led to significant differences in weight and other possible risk factors. The surgical group were younger than controls, had a higher prevalence of hypertension, and had increased BMI, blood pressure and energy intake at the time of surgery. The authors state that dissimilarities between groups at inclusion were adjusted for in the calculations. Sundbom and Gustavsson112 stated that groups were well matched for age, sex, BMI, previous abdominal surgery and comorbid conditions; however, comorbidity appears to be higher in the open surgery group. Patients in the study by Karamanakos and colleagues125 had a statistically significant difference in mean age between groups {37 years [standard deviation (SD 8.25)] versus 30.6 years (SD 7.8), p = 0.023}.
Interventions
The included studies compared a variety of interventions, which are summarised in Table 12 and displayed visually in Figure 1. Although these studies have been grouped according to the type of surgery for the purposes of this systematic review, there may be variations in surgical technique or procedure within the groupings. Three RCTs and three cohort studies (one cohort study had three arms) compared surgery with non-surgical interventions. The remaining 20 RCTs compared different surgical procedures, including various types of gastric bypass, vertical banded gastroplasty, adjustable gastric banding and isolated sleeve gastrectomy, performed with open or laparoscopic surgery. Gastric bypass (usually Roux-en-Y gastric bypass) and vertical banded gastroplasty were the most commonly investigated procedures and formed the majority of the evidence base. Comparisons of open versus laparoscopic surgery for gastric bypass (four RCTs), vertical banded gastroplasty (one RCT) and adjustable gastric banding (one RCT) were also assessed.
FIGURE 1.
Network of comparisons of surgical interventions for obesity. Note: The lines between interventions represent comparisons (either trials or pairs of trial arms where a study has compared more than two procedures). The numbers along the lines indicate the number of trials (or pairs of trial arms) for that comparison. Trials are RCTs unless otherwise stated. AGB, adjustable gastric banding; BPD, biliopancreatic diversion; GBP, gastric bypass; lap, laparoscopic surgery; LSG, laparoscopic sleeve gastrectomy; open, open surgery; RCT, randomised controlled trial; VBG, vertical banded gastroplasty.
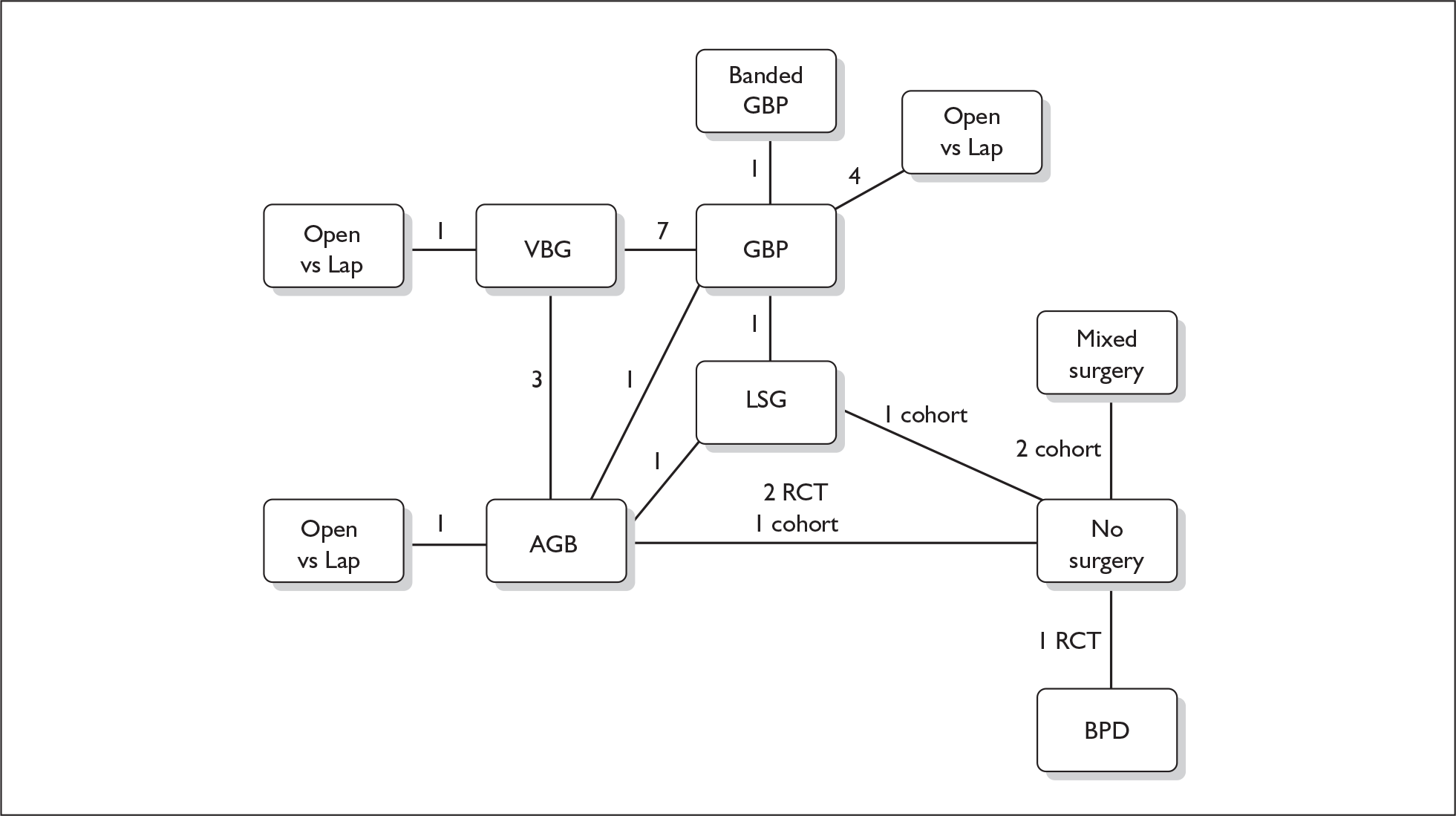
Outcomes
Several different measures of weight change were reported by the studies, namely BMI, change in BMI, weight, weight loss, per cent weight loss, per cent excess weight loss, fat mass, fat free mass, per cent ideal body weight and proportion of ‘successes’. Some of the studies did not report measures of variability such as confidence intervals or standard deviations.
QoL was reported by just five studies,86,100,105,113–116,124 (three RCTs and two cohort studies) and comorbidities were reported by eight studies88,89,97,107,113–118,127,129 (seven RCTs and one cohort study).
Mortality, adverse events and/or additional procedures were reported by most studies.
Follow-up
The minimum duration of follow-up for inclusion in this review was 12 months, and most studies followed participants for 12, 24 or 36 months. Studies with longer follow-up periods included Nilsell and colleagues126 (four to five years), Angrisani and colleagues107 (60 months), Howard and colleagues120 (12 to 78 months), MacLean and colleagues121,122 (6.5 years), van Dielen and colleagues127,128 (24 months and 84 months). The longest follow-up was for 10 years by the SOS study (Table 13). It should be noted that some studies did not follow all participants for the given length of time.
Country
Six studies, including the SOS study, were conducted in Sweden73,108,109,112,126,131 and five studies were conducted in the USA. 106,113,114,118,120,123 Three studies were conducted in Italy. 107,110,119 Two studies were conducted in each of Switzerland,102–105 the Netherlands127,128,132 and Australia. 115–117 One study was conducted in Belgium,134 Canada,121,122 Mexico,111 Spain,130 Taiwan124 and Greece. 125
Risk of bias in included studies
Randomised controlled trials
The summary of risk of bias assessment of RCTs can be seen in Table 14.
| Adequate sequence generation? | Allocation concealment? | Blinding of outcome assessors? | Blinding of participants on self-reported outcomes? | Incomplete outcome data addressed? (weight loss) | Incomplete outcome data addressed? (QoL) | Incomplete outcome data addressed? (comorbidity) | Free of selective reporting? | Free of other bias? | |
|---|---|---|---|---|---|---|---|---|---|
| Agren and Naslund, 198973 | ? | ? | ? | n/a | ? | n/a | n/a | ? | ? |
| Angrisani, 2007107 | ? | ? | ? | n/a | + | n/a | + | ? | ? |
| Bessler, 2007118 | ? | + | ? | ? | ? | n/a | ? | – | ? |
| Davilla-Cervantes, 2002111 | ? | ? | ? | n/a | + | n/a | n/a | ? | ? |
| de Wit, 1999132 | + | + | ? | n/a | + | n/a | n/a | ? | ? |
| Dixon, 2008117 | + | ? | – | n/a | + | n/a | + | ? | – |
| Himpens, 2006129 | ? | ? | ? | n/a | ? | n/a | ? | ? | ? |
| Howard, 1995120 | ? | ? | ? | n/a | + | n/a | n/a | ? | ? |
| Karamanakos, 2008125 | + | ? | + | n/a | + | n/a | n/a | ? | ? |
| Lee, 2004124 | ? | ? | ? | ? | ? | ? | n/a | ? | ? |
| Lujan, 2004130 | + | + | ? | n/a | ? | n/a | n/a | ? | ? |
| MacLean, 1995121,122 | ? | ? | ? | n/a | ? | n/a | n/a | ? | ? |
| Mingrone, 2002119 | ? | ? | ? | n/a | + | n/a | n/a | ? | ? |
| Morino, 2003110 | + | + | ? | n/a | + | n/a | n/a | ? | ? |
| Nilsell, 2001126 | ? | ? | – | – | + | n/a | n/a | ? | ? |
| O’Brien, 2006115,116 | + | + | – | – | ? | ? | ? | ? | ? |
| Olbers, 2005108,109 | + | ? | ? | n/a | + | n/a | n/a | ? | ? |
| Puzziferri, 2001113,114 | ? | ? | ? | – | ? | ? | ? | ? | – |
| Sugerman, 1987123 | + | ? | ? | n/a | + | n/a | n/a | ? | – |
| Sundbom and Gustavsson, 2004112 | ? | ? | ? | n/a | + | n/a | n/a | ? | – |
| Van Dielen, 2005127,128 | + | ? | ? | n/a | + | n/a | + | ? | ? |
| VanWoert, 1992106 | ? | ? | ? | n/a | ? | n/a | n/a | ? | ? |
| Westling and Gustavsson, 2001131 | ? | ? | ? | – | + | n/a | n/a | ? | – |
Allocation
Nine of 23 RCTs described adequate allocation sequence generation,108–110,115–117,123,125,127,128,130,132 and just five had adequate concealment of allocation. 110,115,116,118,130,132 The method of allocation sequence generation and concealment was not reported by the remaining studies, therefore they were judged to be of uncertain risk of bias.
Blinding
Only one RCT reported that outcome assessors were blinded to the intervention assignment. 125 Outcome assessors were not blinded to the intervention assignments in three RCTs,115–117,126 therefore they were judged to be at high risk of bias. This information was not reported by the remaining RCTs.
Six RCTs assessed outcomes self-reported by participants. In four of these studies participants were not blinded to the intervention received,113–116,126,131 and in two studies blinding of participants was not reported or was unclear. 118,124
Incomplete outcome data
Incomplete outcome data for weight loss were adequately addressed by 14 RCTs (Table 14.3). 107–110,112,117,119,120,123,125–129,131,132 The remaining nine RCTs were judged to be at uncertain risk of bias. The withdrawals in the study by O’Brien and colleagues115,116 were uneven between groups, but as reasons were not provided for all withdrawals it was not clear whether withdrawals were related to outcome. In the studies by Lujan and colleagues130 and Bessler and colleagues,118 the number of participants included at each follow-up was not reported. The study by Puzziferri and colleagues was reported in two publications,113,114 the most recent of which contained a smaller number of participants, but no explanation for this was given. Information in the study by MacLean and colleagues121,122 was contradictory between tables and text. Presence or absence of missing outcome data was not reported by four studies. 73,106,124,129
Three RCTs assessed QoL. 113–116,124 Incomplete outcome data for QoL were not reported by Lee and colleagues. 124 O’Brien and colleagues115,116 analysed QoL data only for those who completed the study, which suffered from uneven withdrawals between the groups as previously stated. QoL in the study by Puzziferri and colleagues113,114 was reported only for 44 of 155 patients originally randomised, with no explanation given.
Comorbidity was assessed by seven RCTs. Incomplete outcome data for comorbidity were adequately addressed by three studies,107,117,127,128,132 but the remaining four studies were judged to be of uncertain risk of bias. 113–116,118,129
Selective reporting
The study by Bessler and colleagues118 was judged not to be free of selective outcome reporting, as per cent excess weight loss was reported at 6, 12, 24 and 36 months follow-up (with a statistically significant difference at 36 months), while BMI was reported at 12 and 24 months only, with no measure of variance or statistical analysis. The remaining studies were judged to be of uncertain risk of bias. For example, the studies by Agren and Naslund73 and VanWoert and colleagues106 are reported as abstracts only, therefore limited data were provided. Lujan and colleagues130 reported BMI in a figure only, with no exact data reported and no measure of variance. Mingrone and colleagues119 did not report adverse effects.
Other potential sources of bias
Four RCTs were judged to be at high risk of bias because they used block randomisation in an unblinded trial which can mean it is possible to predict future assignments. 113,114,117,123,131 In addition, recruitment to the RCT by Sugerman and colleagues123 was stopped early (after nine months) following an a priori stopping rule which stated that when a significant difference (p < 0.05) in weight loss was noted for either treatment, patient recruitment would cease until patients had achieved the same follow-up after surgery. The study would have reopened if statistical significance p < 0.01 was not present when all patients had reached an equivalent time frame after surgery. Studies that are stopped early are more likely to show extreme treatment effects than those that continue to the end. 135 Sundbom and Gustavsson112 was also judged to be at high risk of bias, as there appeared to be higher comorbidity on one of the treatment arms. The remaining RCTs were judged to be of uncertain risk of bias, because there was either insufficient information to assess whether an important risk of bias exists, or insufficient rationale or evidence that an identified problem will introduce bias. For example, Olbers and colleagues108,109 excluded 17 patients after randomisation either because they expressed a preference about the surgery they received, or were found to have a BMI > 50; the effect of the exclusion of these patients was unclear. Also, Angrisani and colleagues107 reported that they were in the early phase of the learning curve for one intervention, whereas the senior author had more experience with the comparator.
Prospective cohort studies
The summary of quality assessment of three included cohort studies can be seen in Table 15. The SOS study and the study by Stoeckli and colleagues102–104 adequately described the groups and the distribution of prognostic factors. Buddeberg-Fischer and colleagues105 did not report baseline characteristics separately for each group, therefore it was uncertain whether the groups were comparable on all important confounding factors. Although the groups in the SOS study were not comparable on all important factors, these were adjusted for in the analysis. The groups in the study by Stoeckli and colleagues102–104 were judged to be comparable. It was not clear in any of the studies whether the groups were assembled at a similar point in their disease progression. Outcome assessors were not blind to the intervention in the SOS study or in the study by Buddeberg-Fischer and colleagues,105 in which all measures, including BMI, were self-reported by participants. Blinding was not reported by Stoeckli and colleagues. 102–104 Dropout rates for each group and reasons for dropout were not reported by any of the studies.
| Quality item | Buddeberg- Fischer, 2006105 | SOS study | Stoeckli, 2004102–104 |
|---|---|---|---|
| Is there sufficient description of the groups and the distribution of prognostic factors? | No | Yes – differences between groups | Yes |
| Are the groups assembled at a similar point in their disease progression? | Uncertain | Unclear | Uncertain |
| Is the intervention/treatment reliably ascertained? | Yes | Yes | Yes |
| Were the groups comparable on all important confounding factors? | Uncertain | No – significant differences between groups | Yes |
| Was there adequate adjustment for the effects of these confounding variables? | No | Yes – states adjustments made where appropriate | Not applicable |
| Was outcome assessment blind to exposure status? | No. All measures, including BMI, were self-reported | No | Uncertain |
| Was follow-up long enough for the outcomes to occur? | Yes | Yes | Yes |
| What proportion of the cohort was followed up? | 119/131 at first follow-up, 93/131 at second follow-up. | At 2 years: 84% surgical, 93% control At 8 years: 73% of surgical, 67% control | Uncertain |
| Were dropout rates and reasons for dropout similar across intervention and unexposed groups? | No | Unclear – numbers and reasons not given | Uncertain |
Allocation of participants in the cohort studies
In the SOS study, participants could volunteer for conventional or surgical treatment. For each surgical case a control was matched by computer taking into account 18 variables. The study by Stoeckli and colleagues102–104 included participants opting for surgical treatment, choosing either adjustable silicone gastric banding or gastric bypass. The control group were patients attending diet consultation, although the reasons for the patients not undergoing surgery are not given. Buddeberg-Fischer and colleagues105 included patients applying for bariatric surgery. However, the comparability of the surgery and no-surgery groups is unclear because although one paper states that all but three participants met the criteria for surgery (one had BMI 31.6, two were aged > 60 years),105 about nine participants in an earlier publication said that the reason for not undergoing surgical treatment was that their BMI was under the limit for morbid obesity. 133
Missing outcome data due to participant withdrawals and losses to follow-up
Reporting of missing outcome data formed part of the quality assessment of the included studies (see Risk of bias in included studies, this chapter). Here, two factors contributing to missing outcome data within RCTs: participant withdrawals from studies, and losses to follow-up are addressed. Reporting of these factors within the RCTs included in this review was variable. Only two RCTs specifically reported on study withdrawals. In the study by Dixon and colleagues117 one participant (3.3%) withdrew in the LAGB group and four participants (13.3%) withdrew in the conservative therapy group, leading to an overall follow-up of 55 of 60 participants (92%) at two years. O’Brien and colleagues115,116 reported the withdrawal of one participant (2.5%) in the surgical group and five withdrawals (12.5%) from the non-surgical group, leading to an overall follow-up of 74 of 80 participants (93%) at two years. O’Brien and colleagues also reported that two (5%) participants were lost to follow-up from the non-surgical group because they moved overseas. There was therefore an overall loss to follow-up in this study of 2.5% at two years. Seven further RCTs also reported on participants lost to follow-up (Table 16) with these losses ranging from 1% to 9% for the overall study population. Five RCTs reported that no patients were lost to follow-up (Karamanakos and colleagues,125 Lujan and colleagues,130 Westling and Gustavsson,131 Sundbom and Gustavsson112 and Davila-Cervantes and colleagues111). One RCT (Lee and colleagues124) states that an intention-to-treat (ITT) analysis was conducted, but it is unclear if this applied to the weight loss at two years outcome where a figure suggests less than two-thirds of the participants contribute data and no information is provided regarding patients lost to follow-up. The number of participants contributing data is observed to decrease over time in four RCTs but no reasons are provided for this. 110,113,114,118,120 In the remaining four RCTs losses, to follow-up are not reported and it is not possible to ascertain how many patients contribute data at each follow-up time point. 73,106,119,134
| Study arm A | Study arm B | Overall | Other comments | |
|---|---|---|---|---|
| Withdrawals | ||||
| Dixon, 2008117 | LAGB: 1/30 (3.3%) | Conservative therapy: 4/30 (13.3%) | 5/60 (8%) at 2 years | ITT analysis |
| O’Brien, 2006115,116 | Surgical: 1/40 (2.5%) | Non-surgical: 5/40 (12.5%) | 6/80 (7%) at 2 years | Lost to follow-up also reported, but no other missing data |
| Lost to follow-up | ||||
| O’Brien, 2006115,116 | Surgical: 0 | Non-surgical: 2/40 (5%) | 2/80 (2.5%) at 2 years | Withdrawals also reported, but no other missing data |
| Maclean, 1995121,122 | GBP/VBG: 1 participant (study arm not stated) | 1/106 (1%) at 3 years | Other outcome data missing. Reasons not stated | |
| Sugerman, 1987123 | GBP: 0 | VBG: 1/20 (5%) | 1/40 (2.5%) at 3 years | Reasons for other missing data provided |
| Olbers, 2005108,109 | LGBP: 1/37 (2.7%) | LVBG: 2/46 (4.3%) | 3/83 (3.6%) at 2 years | Reasons for other missing data provided |
| Angrisani, 2007107 | LAGB: 1/27 (3.7%) | LGBP: 0/24 | 1/51 (2%) at 5 years | States not ITT. Unclear how many participants contribute data at each time point. |
| Nilsell, 2001126 | VBG: 2/30 (6.7%) | AGB: 3/29 (10.3%) | 5/59 (8.5%) at 5 years | Not all participants followed up at every time point. |
| Van Dielen, 2005127,128 | Open VBG | LAGB | 9% at 7 yearsa | |
| de Wit, 1999132 | Open AGB: 1/25 (4%) | Lap AGB: 0/25 | 1/50 (2%) at 1 year | |
Assessment of clinical effectiveness evidence
Meta-analysis was considered inappropriate. In some cases, a comparison of surgical procedures (such as gastric bypass versus adjustable gastric banding, or adjustable gastric banding versus isolated sleeve gastrectomy) was assessed by just one study. Where the same procedures were compared by more than one RCT, there were often differences in the outcomes reported or the patient groups. The studies comparing surgery with non-surgical interventions also differed in the surgical procedures and the non-surgical comparators. Standard deviations (or any data by which to calculate them) were not reported by the majority of studies. This is discussed further in Chapter 7, Strengths and limitations of the assessment.
Surgery versus non-surgical interventions
Three RCTs and three cohort studies compared surgery with non-surgical interventions; however, the types of surgery or the comparators differed between the studies. The results below are discussed according to study design.
Weight change
Randomised controlled trials
The two RCTs that compared laparoscopic adjustable gastric banding with non-surgical interventions in obese people (BMI 40 or less) with identifiable comorbidities, reported statistically significant benefit on measures of weight change for those receiving laparoscopic adjustable gastric banding115–117 (Table 17). In a comparison of laparoscopic adjustable gastric banding with non-surgical interventions in people with a BMI ranging from 30 to 35 and identifiable comorbidities, O’Brien and colleagues115,116 reported a statistically significant (p < 0.001) difference in the weight of participants at 12, 18 and 24 months. While people in the laparoscopic adjustable gastric banding group consistently lost weight during the two-year follow-up, those in the non-surgical group increased in weight, despite an initial loss of weight at six months. The differences in weight change were reflected in their respective BMIs, with statistically significant (p < 0.001) differences at beyond the six-month follow-up. Participants in the laparoscopic adjustable gastric banding group experienced a decrease in their BMI from 33.7 at baseline to 26.4 at two years compared with a decrease from a BMI of 33.5 at baseline to 31.5 at two years for those in the non-surgical group. By two years people receiving laparoscopic adjustable gastric banding had lost 87.2% of excess weight, statistically significantly (p < 0.001) more than the 21.8% lost by people in the non-surgical group. Some 98% of those people with a laparoscopic adjustable gastric banding had achieved a satisfactory weight loss (greater than 25% of excess weight loss) at two years, compared with 35% of people in the non-surgical group.
| Dixon, 2008117 | LAGB (n = 30) | Con therapy (n = 30) | Effect size/p-value (95% CI) | |
|---|---|---|---|---|
| % initial weight loss at 2 years | 20.0 (± 9.4) | 1.4 (± 4.9) | p < 0.001 | |
| % excess weight loss at 2 years | 62.5 | 4.3 | ||
| Weight loss (kg) at 2 years | – 21.1 (± 10.5) | – 1.5 (± 5.4) | Difference –19.6 (–23.8 to – 15.2) p < 0.001 | |
| Reduction in BMI at 2 years | from 36.9 to 29.5 | from 37.1 to 36.6 | ||
| O’Brien, 2006115,116 | LAGB (n = 40) | Non surgical (n = 40) | ||
| Weight at 12 months [mean (95% CI) kg] | 76.3 (74.1–78.5) | 85.3 (83.0–87.5) | p < 0.00 1 | |
| Weight at 18 months [mean (95% CI) kg] | 75.2 (73.1–77.4) | 87.7 (79.9–83.0) | p < 0.001 | |
| Weight at 24 months [mean (95% CI) kg] | 74.5 (72.4–76.7) | 89.5 (80.5–83.6) | p < 0.001 | |
| BMI at 12 months [mean (95% CI)] | 27.0 (26.2–27.8) | 29.9 (29.1–30.8) | p < 0.001 | |
| BMI at 18 months [mean (95% CI)] | 26.7 (25.9–27.5) | 30.9 (30.0–31.8) | p < 0.001 | |
| BMI at 24 months [mean (95% CI)] | 26.4 (25.6–27.2) | 31.5 (30.6–32.4) | p < 0.001 | |
| % of initial weight lost at 2 years [mean (95% CI)] | 21.6 (19.3–23.9) | 5.5 (3.2–7.9) | ||
| % excess weight lost at 12 months [mean (95% CI)] | 78.6 (69.2–88.1) | 41.1 (31.2–50.9) | p < 0.001 | |
| % excess weight lost at 2 years [mean (95% CI)] | 87.2 (77.7–96.6) | 21.8 (11.9–31.6) | p < 0.001 | |
| Proportion achieving excess weight loss > 50% at 2 years | 33/39 (85%) | 8/31 (26%) | p < 0.001 | |
|
Proportion achieving satisfactory weight loss (> 25% excess weight lost) |
39/40 (98%) | 14/40 (35%) | p < 0.001 | |
| Mingrone, 2002119 | BPD (n = 46) | Diet (n = 33) | ||
| Weight (kg) women | ||||
| Baseline | 125.3 (± 12.8) | 121.6 (± 24.1) | ||
| 1 year, p-value vs baseline | 90.2 (± 15.0), p < 0.0001 | 114.5 (± 24.5) | ||
| Weight (kg) men | ||||
| Baseline | 151.8 (± 17.1) | 147.3 (± 26.8) | ||
| 1 year, p-value vs baseline | 99.7 (± 7.0), p < 0.0001 | 138.2 (± 27.1) | ||
| BMI women | ||||
| Baseline | 48.3 (± 6.3) | 48.4 (± 8.9) | ||
| 1 year, p-value vs baseline | 35.2 (± 7.6), p < 0.0001 | 43.8 (± 7.7) | ||
| BMI men | ||||
| Baseline | 48.0 (± 5.4) | 47.8 (± 8.8) | ||
| 1 year, p-value vs baseline | 30.4 (± 3.5), p < 0.0001 | 44.8 (± 8.4) | ||
| Fat-free mass (kg) women | ||||
| Baseline | 59.3 (± 5.6) | 58.3 (± 8.8) | ||
| 1 year, p-value vs baseline | 50.5 (± 4.7), p < 0.0001 | 56.7 (± 8.8) | ||
| Fat-free mass (kg) men | ||||
| Baseline | 88.7 (± 8.1) | 87.3 (± 11.4) | ||
| 1 year, p-value vs baseline | 74.2 (± 5.4), p < 0.0001 | 83.7 (± 11.8) | ||
| Fat mass (kg) women | ||||
| Baseline | 65.9 (± 10.2) | 63.3 (± 16.2) | ||
| 1 year, p-value vs baseline | 39.8 (± 12.7), p < 0.0001 | 57.8 (± 16.5) | ||
| Fat mass (kg) men | ||||
| Baseline | 63.1 (± 10.2) | 60.0 (± 15.6) | ||
| 1 year, p-value vs baseline | 25.5 (± 2.7), p < 0.0001 | 54.6 (± 15.6) | ||
| SOS study, 1997–200797,99,100 | Surgery | Control | ||
| % weight change at 2 years97 | – 23.4 (n = 1845) | 0.1 (n = 1660) | Difference 22.2 (21.6 to 22.8), p < 0.001 | |
| % BMI change at 2 years97 | – 23.3 (n = 1845) | 0.1 (n = 1845) | 22.1 (21.5 to 22.7), p < 0.001 | |
| Weight at 10 years, kg100 | 100.5 (± 17.7) (n = 655) | 115.2 (± 19.9) (n = 621) | p < 0.0001 | |
| Weight change at 10 years (kg)100 | – 19.7 (± 15.8) (n = 655) | 1.3 (± 13.8) (n = 621) | p < 0.0001 | |
| Weight % change at 10 years100 | – 16 (± 12.1) (n = 655) | 1.5 (± 9.9) (n = 621) | ||
| BMI at 10 years100 | 35.3 (± 5.4) (n = 655) | 40.6 (± 5.9) (n = 621) | ||
| Change in BMI at 10 years100 | – 6.7 (± 5.4) (n = 655) | 0.7 (± 4.9) (n = 621) | p < 0.0001 | |
| Buddeberg-Fischer, 2006105 | Surgery (n = 63) | No surgery (n = 30) | ||
| BMI at mean 3.2 years | 34.9 (± 5.5) | 40.6 (± 7.4) | p < 0.09 | |
| BMI change at mean 3.2 years | – 21.0 (± 13.4) | – 5.5 (± 11.1) | p < 0.001 | |
| % EWL at mean 3.2 years | 42.2 (± 23.4) | 11.5 (± 25.8) | p < 0.001 | |
| Stoeckli, 2004102–104 | LAGB (n = 8) | Open RYGBP (n = 5) | Controls (n = 7) | |
| BMI | ||||
| Baseline | 41.7 (± 2.8) | 43.6 (± 4.4) | 41.1 (± 2.6) | |
| 24 months | 33.2 (± 4.7)* | 32.9 (± 6.7)* | 41.0 (± 3.4) | * vs control p < 0.001 |
| Weight, mean (SEM) kg | ||||
| Baseline | 117.2 (2.5) | 113.3 (4.9) | 113.5 (4.9) | |
| % change | –16.0 (3.2) p < 0.01 | – 28.6 (3.6) | + 0.5 (1.2) | |
| Total fat mass, mean (SEM) kg | ||||
| Baseline | 63.7 (2.2) | 63.6 (2.2) | 64.8 (4.7) | |
| % change | – 33.9 (5.3) p < 0.001 | – 51.0 (5.2) | + 2.5 (3.3) | |
Dixon and colleagues,117 who assessed the effectiveness of laparoscopic adjustable gastric banding and conventional therapy on obese people (BMI 30 to 40) diagnosed with Type 2 diabetes at two years follow-up, found a statistically significantly (p< 0.001) greater mean percentage weight loss following laparoscopic adjustable gastric banding (20.0%) compared with conventional therapy (1.4%). This equated to a statistically significant (p < 0.001) difference in mean weight loss with those receiving laparoscopic adjustable gastric banding losing an additional 19.6 kg. The change in weight resulted in a reduction in the mean BMI for people in the laparoscopic adjustable gastric banding group from 36.9 to 29.5, while those in the conventional therapy group declined from a BMI 37.1 to 36.6. Dixon and colleagues reported that the loss of weight represented a loss of 62.5% of excess weight (using BMI 25 as ideal weight) for people with the laparoscopic adjustable gastric banding and 4.3% for people receiving conventional therapy. Similar benefits were noted on measures of waist circumference and waist : hip ratio for those in the laparoscopic adjustable gastric banding group compared with the conventional therapy group (Appendix 5).
Mingrone and colleagues119 randomised patients to either biliopancreatic diversion or a diet of 20 kcal/kg fat-free mass, 55% carbohydrates and 15% proteins that was modified every six months according to analysis of fat-free mass. Weight, BMI, fat-free mass and fat mass were significantly reduced in both men and women 12 months following biliopancreatic diversion compared with baseline (p < 0.0001). Weight loss in women and men following surgery was 35 kg and 52 kg, respectively, and 7 kg and 9 kg, respectively, following the diet. The study did not present a statistical comparison of surgery versus diet, and because the results reflect a before and after comparison only they should be treated with caution.
Cohort studies
In 3505 participants who completed two years follow-up, the SOS study reported a significantly greater weight loss among gastric surgery patients (23.4%) than for those receiving conventional treatment (0.1% gain) [difference 22.2, 95% confidence interval (CI) 21.6 to 22.8, p < 0.001]97 (Table 17). Among 1276 patients followed for 10 years, patients in the surgical group had a 16% (SD 12.1) weight loss compared with a 1.5% (SD 9.9) gain in weight for patients receiving conventional treatment. This equates to a mean reduction in weight and BMI of – 19.7 kg (SD 15.8) and – 6.7 (SD 5.4), respectively, for the surgical group versus a gain in weight and BMI of 1.3 kg (SD 13.8) and 0.7 (SD 4.9), respectively for the conventional treatment group, a statistically significant difference between groups (p < 0.0001). 100 Weight loss after 10 years was greater following gastric bypass (25%, SD 11) than following vertical banded gastroplasty (16%, SD 11) or gastric banding (adjustable or non-adjustable) (14%, SD 14), although it should be noted that this was not tested statistically and may be subject to selection bias (systematic differences between the groups) as the groups were not randomised. After 15 years, the weight loss was 27% (SD 12), 18% (SD 11) and 13% (SD 14), for the three surgical groups respectively; although it should be noted that the numbers followed for this duration were much smaller (Appendix 5). 99
One small cohort study, reported by Buddeberg-Fischer and colleagues,105 compared participants undergoing laparoscopic gastric banding or laparoscopic gastric bypass (surgery group) with a no-surgery control group. While mean BMI was not shown to be statistically significantly different between the two groups at end point (mean 3.2 years follow-up), the mean change in BMI was (p < 0.001), indicating greater BMI reduction in the surgery group (Table 4.6). The percentage of excess weight loss was also seen to be statistically significantly better in the surgery group compared with the no-surgery group (p < 0.001). It should be noted, however, that there is some potential for bias as these measures were self-reported and the rates of dropout were different between the two groups over time. The study also assessed BMI and percentage excess weight loss between the two types of surgical procedures used within the surgery arm. The study showed that the mean change in BMI was greater in those undergoing laparoscopic gastric bypass than those undergoing laparoscopic gastric banding [– 27.7 (SD 12.6) versus –17.2 (SD 12.5) for the two groups respectively, p = 0.002], and that the percentage excess weight loss was greater in the laparoscopic gastric bypass subgroup than the laparoscopic gastric banding group [52.8% (SD 17.0) versus 36.0% (SD 24.5) respectively, p = 0.005] (Appendix 5). Care should be used when interpreting these results, however, because the sample sizes were small, there was some degree of crossover between surgical options, this was not a planned comparison, and the surgical groups were not randomised and therefore were subject to selection bias.
The small cohort study with just 20 participants, reported by Stoeckli and colleagues,102–104 also found a statistically significant lower mean BMI two years following surgery [gastric bypass 32.9 (SD 6.7); laparoscopic adjustable silicone gastric banding 33.2 (SD 4.7); compared with a control group who did not undergo surgery 41.0 (SD 3.4)].
Quality of life
Randomised controlled trials
O’Brien and colleagues compared changes in the short-form health survey (SF-36) domain scores from baseline to two years follow-up for people undergoing laparoscopic adjustable gastric banding and non-surgical therapy. 115,116 Although no point estimates were reported, O’Brien and colleagues noted improvements in scores on all eight domains for the laparoscopic adjustable gastric banding group and on three domains (physical function, vitality and mental health) for the non-surgical therapy group. Statistically significantly greater improvements were reported for five of the eight domains for laparoscopic adjustable gastric banding compared with the non-surgical group (Table 18).
| O’Brien, 2006115,116 | LAGB (n = 39) | Non-surgical (n = 33) | Effect size/p-value |
|---|---|---|---|
| Mean SF-36 domain scores,a at 2 years | |||
| Physical function | 90 | 87 | p < 0.05 |
| Physical role | 92 | 70 | p < 0.05 |
| Pain | 83 | 78 | p = ns |
| General health | 73 | 68 | p < 0.05 |
| Vitality | 66 | 57 | p < 0.05 |
| Social functioning | 85 | 81 | p = ns |
| Emotional role | 92 | 72 | p < 0.05 |
| Mental health | 76 | 72 | p = ns |
| SOS study, 1997–2007100 b | Surgery (n = 655) | Control (n = 621) | |
| Current health perceptionc | |||
| 1-year follow-up,% improvement | 48% | 7% | |
| 10-year follow-up | 57.5 (± 26.8) | 55.4 (± 25.1) | p = ns |
| 10-year change | 5.8 (± 27.6) (11% improvement) | – 3.4 (± 25.2) | p < 0.0001 |
| Effect size of change | 0.21 | – 0.13 | |
| Obesity-related problemsd | |||
| 1-year follow-up,% improvement | ~ 63% | 7% | |
| 10-year follow-up | 29.7 (± 27.3) | 31.3 (± 25.5) | p = ns |
| 10-year change | 28.3 (± 28.3) | 9.6 (± 22.6) | p < 0.0001 |
| Effect size of change | 1.00 | 0.42 | |
| Social interactione | |||
| 1-year follow-up,% improvement | ~60% | 7% | |
| 10-year follow-up | 8.4 (± 12.4) | 7.7 (± 11.1) | p = ns |
| 10-year change | – 3.2 (± 13.0) | 0.5 (± 10.0) | p < 0.01 |
| Effect size of change | 0.25 | – 0.05 | |
| MACL Overall moodf | |||
| 10-year follow-up | 3.06 (± 0.59) | 3.11 (± 0.56) | p = ns |
| 10-year change | 0.14 (± 0.56) | 0.05 (± 0.51) | p = ns |
| Effect size of change | 0.25 | 0.10 | |
| HADS Depressiong | |||
| 10-year follow-up | 3.7 (± 3.7) | 3.7 (± 3.5) | p = ns |
| 10-year change | – 1.4 (± 3.9) | – 0.5 (± 3.4) | p < 0.05 |
| Effect size of change | 0.35 | 0.14 | |
| HADS Anxietyg | |||
| 10-year follow-up | 4.6 (± 4.4) | 4.0 (± 4.2) | p < 0.01 |
| 10-year change | – 1.4 (± 4.3) | – 1.4 (± 3.9) | p = ns |
| Effect size of change | 0.33 | 0.35 | |
| Buddeberg-Fischer, 2006105 | Surgery (n = 63) | No surgery (n = 30) | |
| HADS – Anxiety Scoreg: mean 3.2 years follow-up | 5.76 (± 4.27) | 6.53 (± 4.29) | p = 0.21 |
| HADS – Depression Scoreg: mean 3.2 years follow-up | 4.67 (± 4.58) | 4.33 (± 3.01) | p = 0.65 |
| BSQ Scoreh: mean 3.2 years follow-up | 7.16 (± 9.68) | 8.87 (± 9.52) | p = 0.55 |
| PassQ Scorei: mean 3.2 years follow-up | 2.11 (± 2.04) | 1.87 (± 2.08) | p = 0.99 |
Quality of life was not reported by either Dixon and colleagues117 or Mingrone and colleagues. 119
Cohort studies
The SOS study assessed Health Related Quality of Life (HRQoL) using several measures, including general health perceptions from the General Health Rating Index, social interaction from the Sickness Impact Profile, overall mood from the Mood Adjective Check List (MACL), the obesity-related problems scale and the Hospital Anxiety and Depression scale. At baseline the patients in the surgery group had generally worse HRQoL than those in the conventional treatment group. 86,100 These differences may reflect the significant differences in BMI and prevalence of hypertension that developed between matching of controls and start of treatment, or may indicate bias in the selection of patients for surgery.
The two-year results of 974 participants have been tabulated and discussed in the previous report15 and can be seen in Appendix 5. In brief, at two years follow-up gastric surgery patients had significant improvements in all HRQoL measures compared with patients receiving conventional treatment. These changes were significantly related to the magnitude of the weight loss and may have been expected given that the patients in the surgical group had significantly higher BMI at the time of treatment compared with the controls. 86
A more recent report of 1276 participants found that improvements in HRQoL, which peaked one year after surgery, were followed by a gradual decline between one and six years, and then observations were relatively stable between six and ten years follow-up. 100 All HRQoL measures were improved at 10 years compared with baseline for the surgery group, but for the conventional group some had improved while others had worsened. After 10 years follow-up, the mean level of current health perception, social interaction, obesity-related problems, overall mood and depression did not differ significantly between the surgery and conventional treatment groups, although the surgery group had more anxiety (p < 0.01). However, statistically significantly greater 10-year change was observed in the surgery group for current health perceptions, social interaction, obesity-related problems and depression. There was no statistically significant difference in 10-year change for overall mood and anxiety (Table 18).
Buddeberg-Fischer and colleagues105 applied a range of validated questionnaires related to quality of life to participants via telephone interview. The study reported that the Psychosocial Stress and Symptom Questionnaire (PSSQ) was used which incorporated the Hospital Anxiety and Depression Scale (HADS), the Bing Scale Questionnaire (BSQ) and the Psychosocial Assessment Questionnaire (PAssQ), although no results were reported for the overall PSSQ questionnaire. After a mean follow-up of 3.2 years there were no statistically significant differences between groups on mean scores from any of the three questionnaires (Table 18).
Buddeberg-Fischer and colleagues105 also presented self-reported assessment of overall physical and mental health. This was also undertaken via telephone interview and while the results give an indication of the individuals’ perception of their health this was not a validated measure and is likely to be measuring the state of the individual at that particular point in time only. Higher proportions of participants in the surgical group (79.3%) rated their physical health as good compared with the no-surgery group (64.5%), but this was not statistically significantly different (p = 0.10). A similar pattern emerged for ratings of mental health (77.6% versus 67.7% for the two groups respectively, p = 0.22). No analysis was presented of the proportions rating their health as poor (Appendix 5).
Quality of life was not reported by Stoeckli and colleagues. 102–104
Comorbidities
Randomised controlled trials
Dixon and colleagues assessed the effects of laparoscopic adjustable gastric banding compared with conventional therapy on measures of glycaemic control and use of diabetes medication among 60 obese people with Type 2 diabetes. 117 Remission of Type 2 diabetes at two years follow-up was statistically significantly (p < 0.001) higher following laparoscopic adjustable gastric banding (73%) than conventional therapy (13%) (RR 5.5; 95% CI 2.2, 14.00) (Table 19). Similarly, people undergoing laparoscopic adjustable gastric banding were statistically significantly less likely to suffer from metabolic syndrome (70% versus 13%, p < 0.001). Measures of glycaemic control improved more following laparoscopic adjustable gastric banding than conventional therapy with statistically significantly greater decreases in mean levels of HbA1c (glycosylated haemoglobin; difference – 1.43, 95% CI – 2.1 to 0.80, p < 0.001), plasma glucose (difference – 31.8, 95% CI – 53.1 to – 12.3, p = 0.002), plasma insulin (difference – 13.4, 95% CI – 19.6 to – 7.3, p < 0.001), and HDL-cholesterol (difference 10.0, 95% CI 5.8 to 14.2, p < 0.001). There were greater improvements in other indices of glycaemic control (e.g. blood pressure, total cholesterol) for the laparoscopic adjustable gastric banding group compared with the conventional therapy group, although these were not statistically significant (Appendix 5). The benefits of laparoscopic adjustable gastric banding compared with conventional therapy were evident in the reduction in the use of diabetes medication. At two years follow-up a greater proportion of those receiving laparoscopic adjustable gastric banding no longer required diabetes medication compared with conventional therapy (change from baseline 83% versus 15% respectively, not tested for statistical significance). There were similar improvements from baseline to two years follow-up for those in the laparoscopic adjustable gastric banding group compared to the conventional therapy group in their use of metformin (86.3% versus 30.8%), other hypoglycaemics (27.6% versus 3.2%), insulin (3.4% versus 11.5%), anti-hypertensives (48% versus 0%) and lipid-lowering agents (27.6% versus 3.9%) although these differences between the groups were also not tested for statistical significance.
| Dixon, 2008117 | LAGB (n = 30) | Con therapy (n = 30) | Effect size/p-value (95% CI) |
|---|---|---|---|
| Remission of Type 2 diabetes at 2 years | 22/30 (73%) | 4/30 (13%) | RR 5.5 (95% CI 2.2 to 14.0) p < 0.001 |
| Metabolic syndromea | |||
| At baseline | 1 (3%) | 1 (3%) | |
| At 2 years | 21 (70%); p < 0.001 | 4 (13%); p = 0.22 | p < 0.001 |
| No diabetes medication | |||
| At baseline | 2/29 (6.9%) | 4/26 (15.4%) | |
| At 2 years | 26/29 (89.7%) | 8/26 (30.8%) | |
| Metformin use | |||
| At baseline | 28/29 (96.6%) | 26/26 (100%) | |
| At 2 years | 3/29 (10.3%) | 18/26 (69.2%) | |
| Other hypoglycaemic use | |||
| At baseline | 9/29 (31%) | 8/26 (30.8%) | |
| At 2 years | 1/29 (3.4%) | 7/26 (26.9%) | |
| Insulin use | |||
| At baseline | 1/29 (3.4%) | 0 | |
| At 2 years | 0 | 3/26 (11.5%) | |
| Antihypertensive agents | |||
| At baseline | 20/29 (70%) | 15/26 (57.7%) | |
| At 2 years | 6/29 (20.7%) | 15/26 (57.7%) | |
| Lipid-lowering agents | |||
| At baseline | 12/29 (41.4%) | 8/26 (30.8%) | |
| At 2 years | 4/29 (13.8%) | 7/26 (26.9%) | |
| O’Brien, 2006115,116 | LAGB (n = 39) | Non-surgical (n = 33) | |
| Metabolic syndrome | |||
| Before treatment | 15/40 (37.5%) | 15/40 (37.5%) | |
| 2 years after treatment | 1/39 (2.7%) | 8/33 (24%) | p = 0.006 |
| SOS study, 1997–200796,97,136,b | Surgery | Controls | |
| Incidence of diabetes at 2 years | 15/1489 (1%) | 112/1402 (8%) | OR 0.14 (0.08 to 0.24), p < 0.001 |
| Incidence of diabetes at 10 years | 36/517 (7%) | 129/539 (24%) | OR 0.25 (0.17 to 0.38), p < 0.001 |
| Recovery of diabetes at 2 years | 246/342 (72%) | 52/248 (21%) | OR 8.42 (5.68 to 12.5), p < 0.001 |
| Recovery of diabetes at 10 years | 42/118 (36%) | 11/84 (13%) | 3.45 (1.64 to 7.28), p < 0.001 |
| No. on diabetes medication136 at baseline | (n=32) | (n=21) | |
| % at 2 years | 56.2 | 100.0 | RR 0.56 (0.41 to 0.76), p < 0.05 |
| % at 6 years | 68.8 | 100.0 | RR 0.71 (0.56 to 0.89), p < 0.05 |
| No. not on diabetes medication136 at baseline | (n=478) | (n=434) | |
| % at 2 years | 0.2 | 3.7 | RR 0.08 (0.01 to 0.58), p < 0.05 |
| % at 6 years | 2.1 | 11.3 | RR 0.20 (0.10 to 0.38), p < 0.05 |
| Incidence of hypertension at 2 years | 149/623 (24%) | 223/770 (29%) | OR 0.78 (0.60 to 1.01), p = 0.06 |
| Incidence of hypertension at 10 years | 88/215 (41%) | 137/279 (49%) | OR 0.75 (0.52 to 1.08), p = 0.13 |
| Recovery from hypertension at 2 years | 409/1204 (34%) | 185/880 (21%) | 1.72 (1.40 to 2.12), p < 0.001 |
| Recovery from hypertension at 10 years | 81/424 (19%) | 38/342 (11%) | OR 1.68 (1.09 to 2.58), p = 0.02 |
| Incidence of hypertriglyceridaemia at 2 years | 58/731 (8%) | 176/801 (22%) | OR 0.29 (0.21 to 0.41), p < 0.001 |
| Incidence of hypertriglyceridaemia at 10 years | 38/225 (17%) | 75/281 (27%) | OR 0.61 (0.39 to 0.95), p = 0.03 |
| Recovery from hypertriglyceridaemia at 2 years | 683/1102 (62%) | 187/850 (22%) | OR 5.28 (4.29 to 6.49), p < 0.001 |
| Recovery from hypertriglyceridaemia at 10 years | 185/402 (46%) | 79/331 (24%) | OR 2.57 (1.85 to 3.57), p < 0.001 |
| Incidence of low HDL-cholesterol at 2 years | 25/1293 (2%) | 117/1174 (10%) | OR 0.21 (0.14 to 0.32), p < 0.001 |
| Incidence of low HDL-cholesterol at 10 years | 13/431 (3%) | 26/440 (6%) | OR 0.57 (0.29 to 1.15), p = 0.12 |
| Recovery from low HDL-cholesterol at 2 years | 338/445 (76%) | 154/396 (39%) | 5.28 (3.85 to 7.23), p < 0.001 |
| Recovery from low HDL-cholesterol at 10 years | 123/169 (73%) | 88/166 (53%) | 2.35 (1.44 to 3.84), p < 0.001 |
| Incidence of hypercholesterolaemia at 2 years | 136/504 (27%) | 143/596 (24%) | OR 1.27 (0.95 to 1.69), p = 0.11 |
| Incidence of hypercholesterolaemia at 10 years | 40/135 (30%) | 51/188 (27%) | OR 1.16 (0.69 to 1.95), p = 0.57 |
| Recovery from hypercholesterolaemia at 2 years | 292/1327 (22%) | 178/1048 (17%) | 1.22 (0.98 to 1.51), p = 0.07 |
| Recovery from hypercholesterolaemia at 10 years | 105/498 (21%) | 74/435 (17%) | OR 1.30 (0.92 to 1.83), p = 0.14 |
| Incidence of hyperuricaemia at 2 years | 42/1044 (4%) | 163/1017 (16%) | OR 0.22 (0.15 to 0.31), p < 0.001 |
| Incidence of hyperuricaemia at 10 years | 58/342 (17%) | 107/382 (28%) | OR 0.49 (0.34 to 0.71), p < 0.001 |
| Recovery from hyperuricaemia at 2 years | 562/792 (71%) | 197/637 (31%) | OR 5.36 (4.23 to 6.78), p < 0.001 |
| Recovery from hyperuricaemia at 10 years | 140/292 (48%) | 66/243 (27%) | OR 2.37 (1.61 to 3.47), p < 0.001 |
| Biliary disease and pancreatitis frequencies over 2 years (%)96 | |||
| (n = 1422) | (n = 1260) | ||
| Cholelithiasis | |||
| Men | 4.0 | 1.2 | OR 4.2 (1.5 to 12.0), p = 0.011 |
| Women | 5.5 | 4.5 | OR 1.1 (0.7 to 1.8), p = 0.328 |
| Cholecystitis | |||
| Men | 2.5 | 0.7 | OR 4.5 (1.2 to 17.1), p = 0.058 |
| Women | 3.3 | 2.5 | OR 1.4 (0.7 to 2.5), p = 0.379 |
| Cholecystectomy | |||
| Men | 3.4 | 0.7 | OR 5.4 (1.5 to 19.6), p = 0.008 |
| Women | 3.5 | 2.3 | OR 1.6 (0.9 to 3.0), p = 0.191 |
| Total biliary disease | |||
| Men | 4.1 | 1.5 | OR 3.5 (1.3 to 9.2), p = 0.024 |
| Women | 6.8 | 5.3 | OR 1.2 (0.8 to 1.9), p = 0.223 |
| Pancreatitis | |||
| Men | 1.1 | 0.2 | OR 3.6 (0.4 to 31.2), p = 0.219 |
| Women | 0.7 | 0.4 | OR 1.8 (0.4 to 7.6) p = 0.514 |
| Cardiovascular disease medication136 | |||
| On medication at baseline | n = 150 | n = 125 | |
| % on medication at 2 years | 61.7 | 91.2 | RR 0.69 (0.60 to 0.80), p < 0.05 |
| % on medication at 6 years | 64.7 | 86.4 | RR 0.77 (0.67 to 0.88), p < 0.0 5 |
| Not on medication at baseline | n = 360 | n = 330 | |
| % on medication at 2 years | 3.1 | 10.1 | RR 0.28 (0.14 to 0.56), p < 0.05 |
| % on medication at 6 years | 13.3 | 16.7 | RR 0.80 (0.56 to 1.16) |
| Buddeberg-Fischer, 2006105 | Surgery (n = 59/63) | No surgery (n = 30/30) | |
| Number of different drugs at mean 3.2 years for [mean, median (range)]: | |||
| Obesity | 0.03, 0 (0–1) | 0.32, 0 (0–2) | p < 0.001 |
| Somatic comorbidity | 2.29, 2 (0–15) | 2.10, 1 (0–9) | p = 0.98 |
| Psychiatric comorbidity | 0.17, 0 (0–3) | 0.6, 0 (0–2) | p = 0.25 |
O’Brien and colleagues noted that the group receiving laparoscopic adjustable gastric banding experienced a statistically significant reduction in the proportion of people with metabolic syndrome at two years follow-up (baseline 37.5%, two years 2.7%, p < 0.001). 115,116 For those in the non-surgical group the proportion with metabolic syndrome decreased, but not significantly (baseline 37.5%, two years 24%, p = 0.22). There was a statistically significant difference in the number of participants with metabolic syndrome between the two interventions, at two years p = 0.006 (Table 19).
Comorbidities were not reported by Mingrone and colleagues. 119
Cohort studies
Earlier publications from the SOS study of two-year and eight-year data on the incidence of diabetes and hypertension in 483 participants89 and two-year data on lipid disturbances in 1449 participants88 have been summarised previously15 and can be seen in Appendix 5. More recently reported data including 3505 participants at two-year follow-up and 1268 participants at 10-year follow-up97 are discussed here.
The incidence of diabetes (2 years: 1% versus 8%, p < 0.001; 10 years: 7% versus 24%, p < 0.001), hypertriglyceridaemia (2 years: 8% versus 22%, p < 0.001; 10 years: 17% versus 27%, p = 0.03) and hyperuricaemia (2 years: 4% versus 16%, p < 0.001; 10 years: 17% versus 28%, p < 0.001) was significantly lower in the surgery group at both 2 and 10 years follow-up (Table 19). The incidence of low HDL-cholesterol was significantly lower in the surgery group at two years (2% versus 10%, p < 0.001), but not 10 years (3% versus 6%, p = 0.12) follow-up, and there was no statistically significant difference in the incidence of hypertension (2 years: 24% versus 29%, p = 0.06; 10 years: 41% versus 49%, p = 0.13) and hypercholesterolaemia (2 years: 27% versus 24%, p = 0.11; 10 years: 30% versus 27%, p = 0.57) at 2 or 10 years follow-up. Participants who underwent surgery were more likely to recover from diabetes (2 years: 72% recovered versus 21%, p < 0.001; 10 years: 36% versus 13%, p < 0.001), hypertension (2 years: 34% recovered versus 21%, p < 0.001; 10 years: 19% versus 11%, p = 0.02), hypertriglyceridaemia (2 years: 62% recovered versus 22%, p < 0.001; 10 years: 46% versus 24%, p < 0.001), low HDL-cholesterol (2 years: 76% recovered versus 39%, p < 0.001; 10 years: 73% versus 53%, p < 0.001) and hyperuricaemia (2 years: 71% recovered versus 31%, p < 0.001; 10 years: 48% versus 27%, p < 0.001) than those with conventional treatment, at 2 and 10 years follow-up, but there was no statistically significant difference in recovery from hypercholesterolaemia between groups (2 years: 22% recovered versus 17%, p = 0.07; 10 years: 21% versus 17%, p = 0.14) (Table 19).
Of patients who were on diabetes medication at baseline, significantly fewer surgery patients were on diabetes medication at six years follow-up compared with controls [68.8% versus 100%, RR 0.71 (95% CI 0.56 to 0.89), p < 0.05]. This was also the case for patients who were not on diabetes medication at baseline [2.1% versus 11.3%, RR 0.20 (95% CI 0.10 to 0.38), p < 0.05]. 136
Of patients who were on CVD medication at baseline, significantly fewer surgery patients were on CVD medication at six years follow-up compared with controls [64.7% versus 86.4%, RR 0.77 (95% CI 0.67 to 0.88), p < 0.05]. Of patients who were not on medication at baseline, the difference in the proportion on medication was statistically significant at two years follow-up [surgery 3.1%, control 10.1%, RR 0.28 (95% CI 0.14 to 0.56), p < 0.05], but not at six years follow-up [surgery 13.3%, control 16.7%, RR 0.80 (95% CI 0.56 to 1.16)]. 136
At two years follow-up, men with surgery had more cholelithiasis [4.0% versus 1.2%, p = 0.011, OR 4.2 (95% CI 1.5 to 12.0)], cholecystectomy [3.4% versus 0.7%, p = 0.008, OR 5.4 (95% CI 1.5 to 19.6], cholecystitis [2.5% versus 0.7%, p = 0.058, OR 4.5 (95% CI 1.2 to 17.1)] and total biliary disease [4.1% versus 1.5%, p = 0.024, OR 3.5 (95% CI 1.3 to 9.2)] than male controls. There was no difference in pancreatitis among men, and there were no statistically significant differences in these diseases among women. 96
Incidence of cancer during an average of 11 years follow-up in the SOS study has been reported in a recent abstract. 101 In the surgery group (n = 2010) there were 126 cases of first-time cancers and in the control group (n = 2037) there were 173 cases. The unadjusted hazard ratio for overall cancer incidence was 0.71 (p = 0.003) and the hazard ratio adjusted for risk factors was 0.74 (p = 0.011). The unadjusted hazard ratio for men (n = 1178) was 0.98 (95% CI 0.63–1.51, p = 0.91) and for women (n = 2867) was 0.63 (95% CI 0.48–0.82, p = 0.001) (Appendix 5).
Only data on medication use were reported by Buddeberg-Fischer and colleagues. 105 In the last three months of the study those in the surgery group were found to use statistically significantly fewer numbers of different obesity-related drugs than those in the no-surgery group (p < 0.001). There were no statistically significant differences in the number of different medications being taken for somatic comorbidity or psychiatric comorbidity (Table 19). Caution is required in interpreting these outcomes as these were medications used only in the last three months of a study with a mean of 3.2 years follow-up, no measures of variance around the mean values were reported, results were based on self-reports and no further definition of the drugs was given.
Comorbidities were not reported by Stoeckli and colleagues. 102–104
Complications and additional operative procedures
Randomised controlled trials
O’Brien and colleagues found a higher proportion of adverse events among those people in the non-surgical therapy group (58%, n = 31) than in the laparoscopic adjustable gastric banding group (18%, n = 39)115,116 (Table 20). For those receiving non-surgical therapy the most common adverse events were intolerance to orlistat (26%), acute cholecystitis (13%), the need for operative interventions (13%) and intolerance to a VLCD (3%). Adverse events reported by people in the laparoscopic adjustable gastric banding group included operative interventions (13%), laparoscopic revision (prolapse or posterior) (10%), 5-mm port site infection (2.6%) and acute cholecystitis (2.6%). Loss to follow-up was higher in the non-surgical group (16%) compared with the laparoscopic adjustable gastric banding group (2.6%) (but reasons were not given).
| Dixon, 2008117 | LAGB (n = 30) | Conventional therapy (n = 30) |
|---|---|---|
| Mean procedure time (SD, range) | 54 minutes (10.8, 40 to 74) | |
| Length of hospital stay | ||
| 1 day | 23 (80%) | |
| 2 day | 5 (17%) | |
| 4 days | 1 (3%) | |
| Adverse events (n) | ||
| Superficial wound infection | 1 | |
| Gastric pouch enlargement at 10 months | 2 | |
| Band removal | 1 | |
| Febrile episodes | 1 | |
| Minor hypoglycaemic episode | 1 | |
| Intolerance to metformin | 1 | |
| Minor gastrointestinal tract adverse events | 2 | |
| Persistent diarrhoea with metformin | 1 | |
| Vasculitic rash | 1 | |
| Multiple hypoglycaemic episodes | 1 | |
| Angina and transient cerebral ischaemic episode | 1 | |
| Intolerant to very low-calorie meal replacement | 2 | |
| O’Brien, 2006115,116 | LAGB (n = 39) | Non-surgical (n = 31) |
| Total of adverse events (%) | 7/39 (18) | 18/31 (58) |
| 5-mm port site infection (%) | 1/39 (2.6) | n/a |
| Acute cholecystitis (%) | 1/39 (2.6) | 4/31 (13) |
| Prolapse, posterior (laparoscopic revision) (%) | 4/39 (10) | n/a |
| Intolerance to very-low-calorie diet (%) | n/a | 1/31 (3) |
| Intolerance to orlistat (%) | n/a | 8/31 (26) |
| Operative interventions (%) | 5/39 (13)a | 4/31 (13)b |
| SOS study, 1997–200799 | Surgery (n = 2010) | Control (n = 2037) |
| Deaths within 90 days of surgery | 5 (0.25%) (four peritonitis with organ failure, one sudden death) | 2 (0.10%) (one pancreatic cancer, one alcohol-related causes) |
| Peri/postoperative complications97,137 | (n = 1164) | |
| No. of patients with complications (%) | 151 (13%) | |
| Total no. of complications | 193 | |
| Bleeding | 0.9% | |
| Thromboembolic events | 0.8% | |
| Wound complications | 1.8% | |
| Abdominal infection | 2.1% | |
| Pulmonary symptoms | 6.2% | |
| Miscellaneous | 4.8% | |
| Postoperative complications requiring reoperation | 26 patients (2.2%) | |
| Surgical reoperations or conversions (excluding operations caused by postoperative complications) in those followed up for at least 10 years | (n = 1338); banding 31%, VBG 21%, GBP 17% | |
| Buddeberg-Fischer, 2006105 | Surgery (n = 56) | No surgery (n = 37) |
| Reoperation | 7/56; LAGB (n = 47) conversion to RYGBP 5, reversed (debanding) 2; RYGBP (n = 9) 0 | Underwent RYGBP 9/37 |
Dixon and colleagues reported several adverse events among people in the laparoscopic adjustable gastric banding group (n = 30), including a superficial wound infection (one patient), gastric pouch enlargement requiring revisional surgery (two patients), eating difficulties and persistent regurgitation requiring band removal (one patient), postoperative febrile episode (one patient), hypoglycaemic episode (one patient) and gastrointestinal tract intolerance to metformin (one patient)117 (Table 20). People in the conventional therapy group (n = 30) suffered minor adverse events associated with their medication which resolved following discontinuation of treatment, including gastrointestinal problems (two patients), persistent diarrhoea with metformin (one patient), and vasculitic rash (one patient). Other adverse events included multiple hypoglycaemic episodes (one patient), angina and transient cerebral ischaemic episode requiring admission to hospital (one patient) and intolerance to very-low-calorie meal replacement (two patients). Dixon and colleagues noted that the mean procedure time for placement of the laparoscopic adjustable gastric banding was 54 minutes and that 80% of patients were kept in hospital for only one day.
Complications and additional operative procedures were not reported by Mingrone and colleagues. 119
Cohort studies
Within 90 days of surgery in the SOS study there were five deaths (0.25%) in the surgery group (four from peritonitis with organ failure, one from sudden death) and two deaths in the control group (one from pancreatic cancer, one from alcohol-related causes). 99
Perioperative complications were experienced by 13% of 1164 patients in the SOS study, these included bleeding (0.9%), thromboembolic events (0.8%), wound complications (1.8%), abdominal infection (2.1%), pulmonary symptoms (6.2%) and miscellaneous (4.8%) (Table 20). Postoperative complications requiring reoperation were experienced by 2.2% of patients in the surgery group. The patients in the SOS study underwent vertical banded gastroplasty, gastric banding or gastric bypass, but the complications are only reported for the surgery group as a whole. Surgical reoperations or conversions (excluding operations caused by postoperative complications) were reported for 1338 patients followed for at least 10 years, and occurred in 31% of gastric banding patients, 21% of vertical banded gastroplasty patients and 17% of gastric bypass patients.
The Buddeberg-Fischer and colleagues105 cohort study reported reoperations only. Seven of 69 participants in the surgery group were reported to have a reoperation; five participants with laparoscopic gastric banding were converted to Roux-en-Y gastric bypass and two had their bands removed. Nine patients in the no-surgery group underwent gastric bypass. No further details are reported.
Complications and additional operative procedures were not reported by Stoeckli and colleagues. 102–104
Cumulative overall mortality
The SOS study reported cumulative overall mortality during a period of up to 16 years (mean 10.9 years follow-up). 99 The hazard ratio of the surgery group compared with the control group was 0.76 [(95% CI 0.59 to 0.99) p = 0.04]. There were 101 (5%) deaths in the surgery group and 129 deaths (6.3%) in the control group. Table 21 displays the causes of death; the most common causes of death were cancer (surgery 29 cases, control 47 cases), sudden death (surgery 20 cases, control 14 cases) and myocardial infarction (surgery 13 cases, control 25 cases).
| SOS study99 | Surgery (n = 2010) | Control (n = 2037) |
|---|---|---|
| Number of deaths (%) | 101/2010 (5.0%) | 129/2037 (6.3%) |
| Cause of death: cardiovascular condition | ||
| Any event (number of subjects) | 43 | 53 |
| Cardiaca | 35 | 44 |
| Stroke | 6 | 6 |
| Other | 2 | 3 |
| Cause of death: non-cardiovascular | ||
| Any event (number of subjects) | 58 | 76 |
| Tumour | 29 (all cancer) | 48 (47 cancer, 1 non-malignant) |
| Infection | 12 | 3 |
| Thromboembolic disease | 5 | 7 |
| Other | 12 | 18 |
Summary
Three RCTs (one with a low risk of selection bias, one with a high risk of selection bias and one of uncertain risk of bias) and three cohort studies (of variable size and quality) were included. Regardless of the surgical intervention used or the type of patients included, all studies reporting a statistical comparison found statistically significant benefits on measures of weight change compared with no surgery at two to three years follow-up. A large cohort study found weight loss was still significantly greater at 10 years follow-up compared with conventional treatment. One RCT found statistically significantly greater improvements in five of eight domains of the SF-36 following laparoscopic adjustable gastric banding compared with no surgery, but one cohort study found no statistically significant difference in mean scores of the PSSQ between surgery and no-surgery groups. The SOS study found mixed results in HRQoL at 10 years follow-up, with significantly greater 10-year change following surgery observed in some measures, but not others. The RCT of people with Type 2 diabetes found significantly higher remission of the disease following laparoscopic adjustable gastric banding than conventional therapy, and two RCTs reporting metabolic syndrome found significantly fewer people with the syndrome two years after surgery. The SOS study found a statistically significant reduction in the incidence in three of six comorbidities assessed at 10-year follow-up after surgery compared with conventional therapy. Significantly fewer surgery patients than conventional therapy patients were on diabetes medication at two and six years follow-up, and on CVD medication at two, but not six years follow-up. Two RCTs reported adverse events from following surgery (e.g. operative interventions, revisional surgery, port-site infection) and from conventional therapy (e.g. intolerance to medication, acute cholecystitis, need for operative intervention, gastrointestinal problems). Within 90 days of surgery in the SOS study there were five deaths (0.25%) in the surgery group and two deaths in the control group. Perioperative complications occurred in 13% of patients.
Comparisons of different surgical procedures
Gastric bypass versus vertical banded gastroplasty
Weight change
Three of the seven RCTs that compared vertical banded gastroplasty with gastric bypass (open or laparoscopic surgery) demonstrated statistically significantly greater percentage of excess weight loss with gastric bypass108,109,120,123 (Table 22). Howard and colleagues120 found that patients with open gastric bypass (n = 20) had 78% excess weight loss compared with 52% excess weight loss for patients undergoing open vertical banded gastroplasty (n = 22) (p < 0.05) at 12 months follow-up. At five years excess weight loss was 70% and 37% for gastric bypass and vertical banded gastroplasty, respectively (p < 0.05), although only six patients in each group were followed for this length of time. All gastric bypass patients had lost at least 50% of excess weight at 12 months and 60 months follow-up, whereas only 55% of vertical banded gastroplasty patients had achieved this at 12 months, and none by 60 months (p-value not stated, Appendix 6). Sugerman and colleagues123 found that excess weight loss for open gastric bypass was significantly greater than for open vertical banded gastroplasty at 12 months [68% (SD 17) versus 43% (SD 18), p < 0.001], 24 months [66% (SD 29) versus 39% (SD 24), p < 0.001] and 36 months [62% (SD 18) versus 37% (SD 19), p < 0.001]. As previously stated, this study has a high risk of bias because recruitment was stopped early when a significant difference (p < 0.05) in weight loss was noted in favour of gastric bypass. At this point 20 patients had been recruited to each arm of the study, and were followed up for three years. Before surgery, Sugerman and colleagues classified patients as ‘sweets eaters’ or ‘non-sweets eaters’. They noted that gastric bypass surgery led to a significantly greater excess weight loss for sweets eaters than did vertical banded gastroplasty (p < 0.0001). For non-sweets eaters gastric bypass caused greater decreases in excess weight compared with vertical banded gastroplasty, but differences were not significant [p = ns (not statistically significant)] (Appendix 6). The authors attribute this difference to the development of dumping syndrome symptoms in sweets eaters with gastric bypass. However, caution is required when interpreting these results because sample sizes were small and the comparisons were not randomised. A third study, Olbers and colleagues,108,109 which compared laparoscopic gastric bypass with laparoscopic vertical banded gastroplasty also reported that excess weight loss for gastric bypass was significantly greater than for vertical banded gastroplasty at 12 months [78.3% (SD 20) versus 62.9% (SD 28.4), p = 0.009], and at 24 months [84.4% (SD 22.1) versus 59.8% (SD 29.6), p < 0.001]. A greater proportion of patients (34 of 36) who received laparoscopic gastric bypass achieved an excess weight loss of at least 50% without remedial surgery, in comparison to those receiving laparoscopic vertical banded gastroplasty (21 of 35) (Appendix 6). Weight loss was also reflected in mean BMI values which had fallen to 29 in the laparoscopic Roux-en-Y gastric bypass group and 32 in the laparoscopic vertical banded gastroplasty group (p-value not reported), but there was little further change at two years when BMI values were 28 and 32, respectively (p-value not reported).
| Howard, 1995120 | GBP (n = 20) | VBG (n = 22) | p-value |
|---|---|---|---|
| % excess weight loss 1 yeara | 78 (n = 20) | 52 (n = 20) | p < 0.05 |
| % excess weight loss 5 yearsa | 70 (n = 6) | 37 (n = 6) | p < 0.05 |
| Patients with at least 50% of excess weight loss | |||
| 12 months | 100% | 55% | p not stated |
| 60 months | 100% (n = 6) | 0% (n = 6) | p not stated |
| Patients with more than 75% of excess weight loss | |||
| 12 months | 60% | 18% | p not stated |
| 60 months | 50% (n = 6) | 0% (n = 6) | p not stated |
| Sugerman, 1987123 | RYGBP (n = 20) | VBG (n = 20) | |
| % excess weight loss 1 year | 68 (± 17) n = 19 | 43 (± 18) n = 18 | p < 0.001 |
| % excess weight loss 2 yearsa | 66 (± 29) n = 18 | 39 (± 24) n = 17 | p < 0.001 |
| % excess weight loss 3 yearsa | 62 (± 18) n = 18 | 37 (± 19) n = 16 | p < 0.001 |
| % ideal body weight 12 months | 138 (± 32) n = 19 | 176 (± 41) n = 18 | p < 0.01 |
| % ideal body weight 24 months | 139 (± 32) n = 18 | 178 (± 41) n = 17 | p < 0.01 |
| % ideal body weight 36 months | 142 (± 37) n = 18 | 180 (± 44) n = 16 | p < 0.01 |
| Weight loss (kg) 12 months | 43.5 (± 11.3) n = 19 | 32.2 (± 10.9) n = 18 | p < 0.001 |
| Weight loss (kg) 24 months | 43.5 (± 15.4) n = 18 | 30.4 (± 12.2) n = 17 | p < 0.001 |
| Weight loss (kg) 36 months | 41.3 (± 12.7) n = 18 | 27.2 (± 14.5) | p < 0.01 |
| % weight lost 12 months | 33 (± 7) n = 19 | 22 (± 8) n = 18 | p < 0.001 |
| % weight lost 24 months | 33 (± 9) n = 18 | 22 (± 9) n = 17 | p < 0.001 |
| % weight lost 36 months | 32 (± 9) n = 18 | 20 (± 10) n = 16 | p < 0.01 |
| Olbers, 2005108,109 | LRYGBP (n = 37) | LVBG (n = 46) | |
| % excess weight loss 1 year | 78.3 (± 20.0) n = 36 | 62.9 (± 28.4) n = 39 | p = 0.009 |
| % excess weight loss 2 years | 84.4 (± 22.1) n = 36 | 59.8 (± 29.6) n = 35 | p < 0.001 |
| BMI at 1 yeara | 29 (n = 36) | 32 (n = 39) | |
| BMI at 2 yearsa | 28 (n = 36) | 32 (n = 35) | |
| Proportion achieving excess weight loss of at least 50% without remedial surgery after 2 years | 34/36 (94.4%) | 21/35 (60%) | |
| Agren and Naslund, 198973 | Loop GBP (n = 25) | VBG (n = 27) | |
| % excess weight loss 1 year | 76.6 | 58.3 | |
| % excess weight loss 18 months | 76.6 | 59.8 | |
| Lee, 2004124 | LRYGBP (n = 40) | LVBG (n = 40) | |
| % excess weight loss 1 year | 62.9 (n = 40) | 55.4 (n = 40) | |
| % excess weight lost 2 years | 71.4 (n = 26) | 53.1 (n = 27) | |
| BMI 1 year | 29.6 | 31.1 | |
| BMI 2 years | 28.5 | 31.9 | |
| VanWoert, 1992106 | GBP (n = 15) | VBG (n = 17) | |
| % ideal body weight at 3 years | 121% | 123% | p = ns |
| MacLean, 1995, 1993121,122 | RYGBP (n = 52) | VBG (n = 54) | |
| Success rateb ~ 3 years | 30 (58%) | 21 (39%) | p = 0.08 |
| Success rate up to 6.5 years | 16 (34%) | 9 (16%) | p = 0.112 |
Two of the seven trials reported greater weight loss in the gastric bypass group, but did not indicate whether or not this difference was statistically significant (Table 22). The trial by Agren and Naslund,73 which was reported only as an abstract, found greater mean excess weight loss with loop gastric bypass (76.6%) than with vertical banded gastroplasty (59.8%) at 18 months follow-up. Lee and colleagues124 compared laparoscopic gastric bypass and laparoscopic vertical banded gastroplasty and reported that at two years follow-up the gastric bypass group had lower BMI (28.5 versus 31.9) and greater excess weight loss (71.4% versus 53.1%).
The remaining two trials that compared gastric bypass with vertical banded gastroplasty found that there was no significant difference in weight loss between the groups (Table 22). VanWoert and colleagues106 reported, in an abstract only, per cent of ideal body weight at 36 months to be 121% in the gastric bypass group, and 123% in the vertical banded gastroplasty group. Success rates, defined as a BMI < 35 or < 50% excess weight and reoperation not required, were compared for Roux-en-Y gastric bypass and vertical banded gastroplasty with surgical isolation of the gastric pouch by MacLean and colleagues. 121,122 When compared at three years and five to six years follow-up, there was no significant difference in success rates between gastric bypass and vertical banded gastroplasty [about three years: 58% versus 39% (p = 0.08); five to six years: 34% versus 16%, (p = 0.112)]. Failures were converted to isolated gastric bypass, which had a success rate of 63% at five to six years. Although comparisons of the three procedures were reported to show a significantly greater success rate for isolated gastric bypass compared with gastric bypass (p < 0.0009) and vertical banded gastroplasty (p = 0.0001), these were not valid because the periods of follow-up differed.
Quality of life and comorbidities
Only one RCT comparing gastric bypass with vertical banded gastroplasty reported on QoL measures, and this study performed both procedures laparoscopically. 124 Using the gastrointestinal quality of life index (GIQLI), patients in both groups had significant improvements in physical function, emotional function and social function domains, but patients with vertical banded gastroplasty had a significant decrease in the domain of symptoms (p-values not reported) (Table 23). Patients with gastric bypass scored significantly better on seven of 19 symptom items, four of five emotional items, one of seven physical items and two of five social items (p-values ranged from p = 0.04 to p < 0.001, see Appendix 6). Patients with vertical banded gastroplasty scored better on the symptom of abdominal flatulence (p = 0.02).
| Lee, 2004124 | LRYGBP (n = 40) | LVBG (n = 40) | p-value |
|---|---|---|---|
| Mean GIQLI domain score at 12 months: | |||
| Symptoms (baseline 63.7) | 60.9 | 54.3 | |
| Physical function (baseline 16.1) | 24 | 20.9 | |
| Emotional function (baseline 12.8) | 17.7 | 14.7 | |
| Social function (baseline 14.3) | 18.4 | 16.5 | |
| Overall score (baseline 106.9) | 121 | 106.4 | |
Data on comorbidities were not assessed.
Complications and additional operative procedures
Of the seven RCTs comparing vertical banded gastroplasty with gastric bypass surgery, five reported no deaths. 106,108,109,120–122,124 Three of these trials were comparisons of open procedures,106,120–122 the other two were comparisons of laparoscopic procedures. 108,109,124 One trial reported no deaths in the vertical banded gastroplasty group but two deaths (10%) in the gastric bypass group, occurring after three days and 13 months as the result of assumed arrhythmia. 123 Agren and Naslund73 reported one death, but did not state when this occurred or whether following gastric bypass, vertical banded gastroplasty or gastric banding (unbanded, intervention not included in systematic review) (Table 24).
| Howard, 1995120 | GBP (n = 20) | VBG (n = 22) | p-value |
|---|---|---|---|
| Deaths | 0 | 0 | |
| Early complication: wound infection | 1 (2%) super-obese patient | ||
| Late complication: symptomatic ulcer disease | 25% (half required surgical intervention) | 0% | |
| Intraoperative cholecystectomya | 20% | 14% | |
| Late complication: postoperative cholecystectomy | 29% | 29% | |
| Sugerman, 1987123 | RYGBP (n = 20) | VBG (n = 20) | |
| Deaths | 2/20 (10%) | 0 | |
| Conversions VBG to RYGBP | 1/20 (5%) at 1 month; 1/20 (5%) at 18 months; 2/20 (10%) at 38 months | ||
| Intractable vomiting and stomal stenosis | 5/20 (25%) | ||
| Marginal ulcer of jejunal side of gastrojejunostomy | 1/20 (5%) | ||
| Superficial stomal erosion | 1/20 (5%) | ||
| Vitamin B12 at 24 months, pg/ml [mean (SD)] | 286 (± 149) | 461 (± 226) | p < 0.05 |
| Olbers, 2005108,109 | LRYGBP (n = 37) | LVBG (n = 46) | |
| Deaths | 0 | 0 | |
| Conversions to open surgery | 0 | 0 | |
| Operating time [mean (SD)] | 138 (± 41) minutes | 105 (± 35) minutes | p < 0.001 |
| Early reoperation (n) | 5 | 1 | p = 0.080 |
| Haemorrhage | 3 | 0 | |
| Stenosis | 1 | 0 | |
| Suspected leak | 1 | 1 | |
| Perioperative complications (n)b | |||
| Minor bleeding | 2 | 4 | |
| Deep infection | 1 | 1 | |
| Thrombotic complications | 0 | 0 | |
| Pulmonary complications | States no difference between groups | p = 0.888 | |
| Median hospital stay, days | 3 (range 2–15) | 3 (range 1–16) | |
| Remedial surgical intervention (n, conversion to RYGBP) | 0 | 8 | |
| Due to migration of outlet restricting band | 1 | ||
| Vomiting and insufficient weight loss | 5 | ||
| Vomiting and excessive weight loss | 2 | ||
| Intra-abdominal abscess after discharge (n) | 1 | 0 | |
| Agren and Naslund, 198973 | Loop GBP (n = 25) | VBG (n = 27) | |
| Deaths | 1 (group not statedc) | ||
| Reoperation | 1/27 (4%) | ||
| Lee, 2004124 | LRYGBP (n = 40) | LVBG (n = 40) | |
| Deaths | 0 | 0 | p = ns |
| Conversions to open surgery | 1/40 (2.5%) | 0 | p = ns |
| Mean operative time (minutes) | 209 (± 50) | 126 (± 38) | p < 0.001 |
| Intraoperative blood loss (ml) | 35 (± 26) | 31 (± 77) | p = ns |
| Postoperative flatus passage (days) | 2.5 (± 1.2) | 1.9 (± 0.6) | p < 0.01 |
| Early postoperative complication | 7/40 (17.5%) | 1/40 (2.5%) | p < 0.05 |
| Major early complication (n)d | 3 | 0 | |
| Anastomotic leakage | 2 (reoperation) | ||
| Abdominal abscess | 1 | ||
| Minor early complication (n) | 4 | 1 | |
| Included upper gastrointestinal bleeding, a sutured nasogastric tube, and minor leakage from a drainage tube | 4 | ||
| Wound infection | 1 | ||
| Analgesic use (units) | 2.4 (± 3.0) | 1.4 (± 1.5) | p < 0.05 |
| Postoperative stay (days) | 5.7 (± 2.2) | 3.5 (± 0.9) | p < 0.001 |
| Late complications (readmission) | 4/40 (10%) | 2/40 (5%) | p = ns |
| Anastomotic stricture | 1 | ||
| Marginal ulcer | 2 | ||
| Pyothorax | 1 | ||
| Reflux oesophagitis | 2 (1 laparoscopic revision surgery) | ||
| VanWoert, 1992106 | GBP (n = 15) | VBG (n = 17) | |
| Deaths | 0 | 0 | |
| Major late complication: cholelithiasis | 13% | 24% | |
| Major late complication: peptic gastro-oesophagitis | 33% | 18% | |
| MacLean, 1995, 1993121,122 | RYGBP (n = 52) | VBG (n = 54) | |
| Deaths | 0 | 0 | |
| Conversions at approx. 3 years | 0 to normal; 12/52 (23%) to IGBP | 5/54 (9%) to normal; 18/54 (33%) to IGBP | |
| Conversions up to 6.5 years | 1/52 (2%) to normal; 19/52 (37%) to IGBP. | 5/54 (9%) to normal; 24/54 (44%) to IGBP | |
| Reoperations | 12/52 (23%) | 23/54 (43%) | |
| Stenosis | 0 | 11 (20%) | |
| Enlarged orifice | 0 | 7 (13%) | |
| Staple-line disruption | 12 (23%) | 2 (4%) | |
| Clinical failure | 0 | 2 (4%) | |
| Stomal ulcere | 7 (13%) | 0 | |
| Abscess | 0 | 1 (2%) | |
Complications were not reported by all studies, but when they were reported they differed between the various surgical procedures (Table 24).
Of the two studies that compared laparoscopic procedures, Olbers and colleagues108,109 reported no conversions to open surgery, but Lee and colleagues124 reported that conversion to open surgery occurred in one (2.5%) patient with laparoscopic gastric bypass and none of the patients with laparoscopic vertical banded gastroplasty (p = ns). Operative time was significantly less with laparoscopic vertical banded gastroplasty in both studies [126 minutes (SD 38) versus 209 minutes (SD 50), p < 0.001124, and 105 minutes (SD 35) versus 138 minutes (SD 41), p < 0.001108,109]. In one study mean postoperative stay was also significantly shorter for the laparoscopic vertical-banded gastroplasty group [3.5 days (0.9) versus 5.7 days (2.2), p < 0.001124], whereas in the other study there appeared to be little difference in the length of hospital stay (LOS) [median three days (range 1–16 days) versus three days (range 2–15 days)108,109].
In one study124 early postoperative complications were significantly more common following laparoscopic gastric bypass (17.5%, seven patients) than laparoscopic vertical banded gastroplasty (2.5%, one patient). Three of the seven early postoperative complications experienced by laparoscopic gastric bypass patients were major complications. These required interventional management and hospitalisation for over 14 days. Two with anastomotic leakage required reoperation, the third had an abdominal abscess. The remaining four early postoperative complications in this group were classed as minor and included upper gastrointestinal bleeding, a sutured nasogastric tube, and minor leakage from a drainage tube. Only one early postoperative complication occurred in the laparoscopic vertical banded gastroplasty group and this was a wound infection that was classed as a minor complication. Analgesic use was also higher [2.4 units (3.0) versus 1.4 units (1.5), respectively (p < 0.05)] in this study. 124 The second study that compared laparoscopic procedures108,109 reported five early reoperations in the gastric bypass group (three for haemorrhage, one for stenosis and one for suspected leak) and one early reoperation in the vertical banded gastroplasty group (for suspected leak), but this difference was not significant (p = 0.080). A statistical comparison of the perioperative complications reported by Olbers and colleagues108,109 (in addition to the reoperations) is not provided, but these appear similar (gastric bypass group: two minor bleeding, one deep infection; vertical banded gastroplasty group: four minor bleeding, one deep infection) (Table 24). Neither group experienced a thrombotic complication, and there was no difference in the incidence of pulmonary complications between the groups (p = 0.888). One patient in the laparoscopic Roux-en-Y gastric bypass group experienced an intra-abdominal abscess after discharge.
Readmission for late complications reported by Lee and colleagues124 was similar between the laparoscopic procedures (10% versus 5%, p = ns). Late complications associated with laparoscopic gastric bypass included marginal ulcer requiring blood transfusion (two patients), anastomotic stricture (one patient), and pyothorax (pus in the chest cavity) (one patient). Two patients (5%) with laparoscopic vertical banded gastroplasty experienced the late complication of reflux oesophagitis, one of which required laparoscopic revision surgery. Olbers and colleagues,108,109 however, reported that remedial surgical intervention was required for eight participants in the vertical banded gastroplasty group (four in the first year and four in the second year, all conversion to Roux-en-Y gastric bypass, due to: one migration of outlet restricting band, five vomiting and insufficient weight loss, two vomiting and excessive weight loss), but for none in the gastric bypass group.
In the comparisons of open procedures73,106,120–123 gastric bypass patients suffered from symptomatic ulcer disease (25% of patients),120 staple-line fistula (23%),121,122 stomal ulcers (13% of patients),121,122 intractable vomiting and stomal stenosis (25%),123 marginal ulcer of jejunal side of gastrojejunostomy (5%),123 cholelithiasis (gallstone formation) (13%),106 and peptic gastro-oesophagitis (33%). 106 Vertical banded gastroplasty patients suffered stenosis (20%),121,122 enlarged orifice (13%),121,122 staple-line fistula (4%),121,122 clinical failure (4%),121,122 abscess (2%),121,122 superficial stomal erosions (5%),123 cholelithiasis (24%)106 and peptic gastro-oesophagitis (18%). 106 Intraoperative cholecystectomy and postoperative cholecystectomy were reported for gastric bypass (20% and 29% respectively) and vertical banded gastroplasty (14% and 29% respectively) (Table 24). 120
In the trial by MacLean and colleagues,121,122 failures of vertical banded gastroplasty (due to stenosis and enlargement of the gastroplasty orifice), and failures of gastric bypass (due to perforation of the vertical staple line), were converted to normal (9% versus 2%) or isolated gastric bypass (44% versus 37%). In another trial by Sugerman and colleagues,123 a total of four (20%) vertical banded gastroplasty patients were converted to Roux-en-Y gastric bypass. One patient was converted at one month due to staple-line disruption, and a further three patients were converted due to a failure to lose weight, one at 18 months, and two at 38 months following surgery. After 2 years there were no significant deficiencies in most vitamins, electrolytes, renal or liver function tests. However, vitamin B12 levels were lower in patients with Roux-en-Y gastric bypass than those with vertical banded gastroplasty (286 pg/ml versus 461 pg/ml, p <0.05) (Appendix 6). Agren and Naslund73 found just one patient (4%) with vertical banded gastroplasty required reoperation for staple-line disruption. Agren and Naslund73 reported that morbidity was low and not significantly different between the groups, but no data were presented.
Summary
Seven RCTs were included. Six trials were of uncertain risk of bias as many factors were not reported. One study by Sugerman and colleagues had a high risk of bias because of an a priori stopping rule. On measures of weight, participants who underwent gastric bypass had a better outcome, particularly at later time points, in five of the seven trials than those who underwent vertical banded gastroplasty (although a statistically significant difference was only reported in three of these trials). Only Lee and colleagues reported on QoL, which they found to be better for the gastric bypass group. Data on comorbidities were not assessed. Reporting of complications varied between studies. Evidence from two studies108,109,124 suggests that the laparoscopic vertical banded gastroplasty surgery is quicker, and is associated with fewer early postoperative complications than laparoscopic gastric bypass surgery. However, two studies of open surgery121–123 report that after approximately three years, conversions to an alternative bariatric procedure occurred more often in the vertical banded gastroplasty groups, but neither study tested this for statistical significance.
Gastric bypass (non-banded) versus banded gastric bypass
One RCT118 compared non-banded long limb gastric bypass with banded long limb gastric bypass in participants with BMI greater than 50. Banded gastric bypass (which is not undertaken in the UK) is considered separately in this review, although there is some disagreement among surgeons about whether it constitutes a distinct procedure, or whether it is a variation of the standard gastric bypass procedure.
Weight change
At one and two years follow-up, Bessler and colleagues118 reported per cent excess weight loss was greater for participants undergoing banded than non-banded long limb gastric bypass, but the differences were not statistically significant (Table 25). After three years, the per cent excess weight loss was statistically significantly higher in the banded gastric bypass group compared with the non-banded gastric bypass group (p < 0.05). There is however an uncertain risk of bias for this outcome as the paper reports that this was based on the small number of patients reaching the 36-month follow-up period (numbers not presented). The proportion achieving a BMI of less than 35 was higher in the banded gastric bypass groups than the non-banded gastric bypass groups at one and two years follow-up but the difference was not statistically significant. No rates were reported for the three-year follow-up.
| Bessler, 2007118 | Banded GBP (n = 46) | Non-banded GBP (n = 44) | p-value |
|---|---|---|---|
| % EWL at 12 months | 64 | 57.4 | p = ns |
| % EWL at 24 months | 64.2 | 57.2 | p = ns |
| % EWL at 36 months | 73.4 (small n, not reported) | 57.7 (small n, not reported) | p < 0.05 |
| Achieving a BMI of < 35 at 12 months (%): | 47.8 | 41.0 | |
| Achieving a BMI of < 35 at 24 months (%) | 52.9 | 37.5 |
Quality of life and comorbidities
Data on QoL were not assessed. Comorbidities were reported by Bessler and colleagues. 118 The study reported baseline values for stated comorbidities and the proportion with resolution of these comorbidities; however, the study does not state which follow-up period is being reported, or give any numerators and denominators for these calculations.
The proportion of participants with resolution of their respective comorbidities was not shown to be statistically significantly different between the two interventions (Table 26).
| Bessler, 2007118 | Banded GBP (n = 46) | Non-banded GBP (n = 44) | p-value |
|---|---|---|---|
| Resolution of hypertension (%) | 79 | 90 | p = ns |
| Resolution of diabetes (%) | 92 | 98 | p = ns |
| Resolution of hyperlipidaemia (%) | 50 | 62 | p = ns |
| Resolution of arthritis (%) | 76 | 91 | p = ns |
| Resolution of gastro-oesophageal reflux disease (%) | 94 | 83 | p = ns |
| Resolution of stress urinary incontinence (%) | 83 | 93 | p = ns |
Complications and additional operative procedures
There were no deaths reported in the study by Bessler and colleagues118 and no statistically significant differences between banded gastric bypass and non-banded gastric bypass in rates of any postoperative complications. Postoperative gastrointestinal symptoms were scored according to a subjective scale where 0 = none, 1 = mild, 2 = moderate, 3 = severe. In this study only the scores for emesis were statistically significantly better (lower score) in the non-banded gastric bypass group than in the banded gastric bypass participants (0.35 versus 0.13 respectively, p = 0.0002) (Table 27). No other gastrointestinal symptoms were statistically significantly different between the two interventions. The proportion of participants with food intolerance was higher in the banded gastric bypass group (79% versus 33%, p < 0.05). Care is required in the interpretation of these results, not only because of the subjective nature of these outcomes, but also because the study does not state which follow-up period is being reported or what the participant numbers were for these outcomes.
| Bessler, 2007118 | Banded GBP (n = 46) | Non-banded GBP (n = 44) | p-value |
|---|---|---|---|
| Mortality | 0 | 0 | |
| Total complications | 12/46 (26%) | 13/44 (29.5%) | p = ns |
| Wound infection | 7/46 (15.2%) | 5/44 (11%) | p = ns |
| Anastomotic leak | 0 | 2/44 (4.8%) | p = ns |
| Pneumonia | 1/46 (2.1%) | 1/44 (2.2%) | p = ns |
| Pulmonary embolism | 0 | 0 | |
| Small bowel obstruction | 1/46 (2.1%) | 1/44 (2.2%) | p = ns |
| Band erosion/slippage/removal | 0 | n/a | |
| Other | 3/46 (6.5%) | 4/44 (9.0%) | p = ns |
| Gastrointestinal symptoms (average scores) | |||
| Dumping | 0.12 | 0.05 | p = ns |
| Emesis | 0.35 | 0.13 | p = 0.0002 |
| Diarrhoea | 0.11 | 0.13 | p = ns |
| Constipation | 0.07 | 0.08 | p = ns |
| Flatulence | 0.22 | 0.13 | p = ns |
| Abdominal pain | 0.04 | 0.06 | p = ns |
| Food intolerance (%) | 79 | 33 | p < 0.05 |
Summary
One study (with a low risk of selection bias but at high risk of bias through selective reporting) found similar weight loss after banded and non-banded gastric bypass in people with BMI greater than 50. Although a statistically significant difference in BMI was found at 36 months follow-up, this was based on a small number of participants. Rates of improvement of existing comorbidities were not different between the two groups and complications were also generally similar. The evidence suggests that in these high BMI participants there is little added benefit from the addition of banding to the intervention.
Laparoscopic gastric bypass versus laparoscopic adjustable gastric banding
One RCT119 compared laparoscopic Roux-en-Y gastric bypass with laparoscopic adjustable gastric banding.
Weight change
At one and three years of follow-up Angrisani and colleagues107 found that the per cent excess weight loss was greater for those undergoing laparoscopic Roux-en-Y gastric bypass than laparoscopic adjustable gastric banding, but no statistical significance was reported (Table 28). After 5 years of follow-up the per cent excess weight loss and mean weight were statistically significantly better for participants in the laparoscopic Roux-en-Y gastric bypass group compared with those in the laparoscopic adjustable gastric banding group (p < 0.001 for both outcomes). At one and three years follow-up the mean BMI was also lower in the laparoscopic Roux-en-Y gastric bypass group (but no p-values were reported) than the laparoscopic adjustable gastric banding group. After five years the mean BMI was statistically significantly better in the laparoscopic Roux-en-Y gastric bypass group than the laparoscopic adjustable gastric banding group (p < 0.001). The proportion classed as weight loss failures, defined as those with a BMI > 35 at 5 years, were statistically significantly lower in the laparoscopic Roux-en-Y gastric bypass than the laparoscopic adjustable gastric banding group (p < 0.001) and the proportion with a BMI of less than 30 at 5 years were statistically significantly higher in the laparoscopic Roux-en-Y gastric bypass group (p < 0.001) than in the laparoscopic adjustable gastric banding group.
| Angrisani, 2007107 | LAGB (n = 27) | LRYGBP (n = 24) | p-value |
|---|---|---|---|
| % excess weight loss at 12 months | 34.7 | 51.3 | |
| % excess weight loss at 36 months | 47.3 | 67.3 | |
| % excess weight loss at 5 years (range 60–66 months) | 47.5 | 66.6 | p < 0.001 |
| Mean weight (kg) at 12 months | 102.4 | 92.8 | |
| Mean weight (kg) at 36 months | 98.7 | 83.5 | |
| Mean weight (kg) at 5 years (range 60–66 months) | 97.9 | 84 | p < 0.001 |
| Mean BMI at 12 months | 38.7 | 35.4 | |
| Mean BMI at 36 months | 35.6 | 29.1 | |
| Mean BMI at 5 years (range 60–66 months) | 34.9 | 29.8 | p < 0.001 |
| Weight loss failure (BMI > 35 at 5 years) | 9/26 (34.6%) | 1/24 (4.2%) | p < 0.001 |
| BMI < 30 at 5 years | 3/26 (11.5%) | 15/24 (62.5%) | p < 0.001 |
Quality of life and comorbidities
QoL was not assessed by Angrisani and colleagues. 107 Baseline rates of comorbidities were low in this study, with two participants in the laparoscopic Roux-en-Y gastric bypass group having hyperlipaemia, one hypertension and one Type 2 diabetes. In the laparoscopic adjustable gastric banding group three participants had hypertension and one sleep apnoea. The study reports that at five years there was resolution of the diabetes and hyperlipaemia (in the laparoscopic Roux-en-Y gastric bypass group) and the sleep apnoea (in the laparoscopic adjustable gastric banding group) (Appendix 8).
Complications and additional operative procedures
No deaths were noted in either group of the Angrisani and colleagues study119 (Table 29). Operative time for laparoscopic adjustable gastric banding was significantly shorter than for laparoscopic Roux-en-Y gastric bypass [mean 60 (SD 20) minutes versus mean 220 (SD 100) minutes, p < 0.001]. Four (15.2%) participants in the laparoscopic adjustable gastric banding group underwent a reoperation (two pouch dilatation, two band removal because of inadequate weight loss: one of these was converted to biliopancreatic diversion, three waiting list for laparoscopic Roux-en-Y gastric bypass) and three (12.5%) from the laparoscopic Roux-en-Y gastric bypass group underwent a reoperation (for potentially lethal complications not further specified). Early complications requiring surgery in the laparoscopic Roux-en-Y gastric bypass group occurred in two (8.4%) [one posterior pouch leak intraoperatively causing conversion to open surgery, one (4.2%) sepsis caused by jejunal perforation (sutured and intestine resected)]. No early complications requiring surgery were noted in the laparoscopic adjustable gastric banding group. One participant undergoing laparoscopic Roux-en-Y gastric bypass had a late complication (small bowel obstruction as the result of internal hernia) and two participants undergoing laparoscopic adjustable gastric banding had gastric pouch dilatation (which was treated by band removal). No significance testing was undertaken for reoperation rates, or early or late complication rates between groups. Mean hospital stay was statistically significantly longer in the laparoscopic Roux-en-Y gastric bypass group than the laparoscopic adjustable gastric banding group [4 days (SD 2) versus 2 days (SD 1) for the two groups respectively, p < 0.05], although one participant in the laparoscopic Roux-en-Y gastric bypass group required an intensive care stay of 40 days (Appendix 8).
| Angrisani, 2007107 | LAGB (n = 27) | LRYGBP (n = 24) | p-value |
|---|---|---|---|
| Mortality | 0 | 0 | |
| Reoperationa | 4/26 (15.2%) | 3/24 (12.5%) | |
| Gastric pouch dilatation | 2 | ||
| Unsatisfactory weight loss (band removal) | 2 | ||
| Early complications (with reoperation) | 0 | 2 (8.4%) | |
| Posterior pouch leak | 1 (conversion to open) | ||
| Sepsis (jejunal perforation) | 0 | 1 | |
| Late complication | 2/26 (7.6%) | 1/24 (4.2%) | |
| Small bowel obstruction due to internal hernia | 1 | ||
| Pouch dilatation (band removal) | 2 | ||
| Hospital stay, days [mean (SD)] | 2 (± 1) | 4 (± 2) | p < 0.05 |
| Operative time, mins [mean (SD)] | 60 (± 20) | 220 (± 100) | p < 0.001 |
Summary
On a variety of measures of weight this small study showed that laparoscopic Roux-en-Y gastric bypass was superior to laparoscopic adjustable gastric banding. Reoperation rates were similar between the two interventions, and comorbidities were similar and few. Early complications requiring reoperation were seen in more participants undergoing laparoscopic Roux-en-Y than laparoscopic adjustable gastric banding, but the numbers were small and not tested for statistical significance. The risk of bias for this study is uncertain, although the risk of bias from incomplete outcome data for weight loss and comorbidities is likely to be low.
Laparoscopic gastric bypass versus laparoscopic sleeve gastrectomy
One RCT compared laparoscopic Roux-en-Y gastric bypass with laparoscopic sleeve gastrectomy. 125
Weight loss
There were no statistically significant differences in BMI or weight loss between the two procedures at 12 months follow-up. However, laparoscopic sleeve gastrectomy led to a greater per cent excess weight loss at 12 months [69.7% (SD 14.6) versus 60.5% (SD 10.7), p = 0.05] in this small RCT (Table 30).
| Karamanakos, 2008125 | LRYGBP (n = 16) | LSG (n = 16) | p-value |
|---|---|---|---|
| BMI at 12 months | 31.5 (± 3.4) | 28.9 (± 3.6) | p = 0.41 |
| % EWL at 12 months | 60.5 (± 10.7) | 69.7 (± 14.6) | p = 0.05 |
| Weight loss at 12 months (kg) | 40.0 (± 8.3) | 43.6 (± 11.7) | p = 0.322 |
Quality of life and comorbidities
QoL was not assessed by this study. Two patients had diabetes at baseline (both in the laparoscopic Roux-en-Y gastric bypass group); this was resolved at 12 months in both patients. The outcome of other comorbidities noted at baseline (see Appendix 9) was not reported.
Complications and additional operative procedures
Karamanakos and colleagues reported that there were no conversions to open surgery and no intraoperative and postoperative complications. No further details were reported.
Summary
In this small RCT with uncertain risk of bias, BMI and weight loss at 12 months follow-up were similar between laparoscopic Roux-en-Y gastric bypass and sleeve gastrectomy. per cent excess weight loss was greater with sleeve gastrectomy at 12 months (p = 0.05).
Vertical banded gastroplasty versus adjustable gastric banding
One study126 compared open vertical banded gastroplasty with open adjustable gastric banding, one study110 compared laparoscopic vertical banded gastroplasty with laparoscopic adjustable silicone gastric banding, and one study127,128 compared open vertical banded gastroplasty with laparoscopic adjustable banding.
Weight change
At one year follow-up, Nilsell and colleagues126 found that weight loss was greater for the vertical banded gastroplasty group, but these patients then began to regain weight. The patients with adjustable gastric banding experienced lower initial weight loss, but this continued over five years resulting in a weight reduction of 43 kg at five years compared with 35 kg for vertical banded gastroplasty (statistical significance not given) (Table 31).
| Nilsell, 2001126 | VBG (n = 30) | AGB (n = 29) | p-value |
|---|---|---|---|
| Mean weight (kg) baseline (SEM) | 123 (30) | 124 (29) | |
| Mean weight (kg) 1 year (SEM)a | 82 (25) | 98 (28) | |
| Mean weight (kg) 2 year (SEM)a | 85 (29) | 88 (23) | |
| Mean weight (kg) 3 year (SEM)a | 90 (15) | 85 (13) | |
| Mean weight (kg) 4 year (SEM)a | 95 (15) | 86 (17) | |
| Mean weight (kg) 5 years (SEM) | 88 (16) | 81 (16) | |
| Morino, 2003110 | LVBG (n = 51) | LAGB (n = 49) | |
| BMI 1 year | 30.1 | 35.5 | p < 0.05 |
| BMI 2 years | 29.7 | 34.8 | p = ns |
| BMI 3 years | 30.7 | 35.7 | p = ns |
| % excess weight loss 1 year | 62.3 | 39.2 | p < 0.05 |
| % excess weight loss 2 years | 63.5 | 41.4 | p = ns |
| % excess weight loss 3 years | 58.9 | 39.0 | p = ns |
| Patients with an excellent or good resultb 2 years | 74% | 35% | p < 0.001 |
| Patients with an excellent or good result 3 years | 63% | 25% | p = 0.056 |
| van Dielen, 2005127,128 | Open VBG (n = 50) | LAGB (n = 50) | p-value |
| Mean BMI at 1 year (± SD) | 31.1 (± 6.2) | 35.0 (± 6.3) | |
| Mean BMI at 2 years (± SD) | 31.0 (± 6.0) | 34.6 (± 6.5) | p ≤ 0.002 |
| % excess weight loss at 1 year (± SD) | 71.1 (± 24.0) | 53.3 (± 21.2) | p ≤ 0.001 |
| % excess weight loss at 2 years (± SD) | 70.1 (± 25.5) | 54.9 (± 23.3) | p ≤ 0.001 |
| % excess BMI loss at mean 84 months | 68.8% | 56.9% |
When comparing laparoscopic procedures, Morino and colleagues110 also found significantly lower BMI with vertical banded gastroplasty at one year follow-up (30.1 versus 35.5, p < 0.05), but at two and three years follow-up the difference was not statistically significant (two years: 29.7 versus 34.8; three years: 30.7 versus 35.7). A similar result was seen in terms of percentage excess weight loss which was significantly greater with vertical banded gastroplasty at one year follow-up (62.3% versus 39.2%, p < 0.05), but was not statistically significantly different at later follow-up (two years: 63.5% versus 41.4%, three years: 58.9% versus 39.0%, p-values not reported). At three years follow-up, 25% of patients with laparoscopic adjustable silicone gastric banding and 63% of patients with laparoscopic vertical banded gastroplasty had an excellent or good result (residual excess weight < 50%, p = 0.056).
Van Dielen and colleagues127,128 reported a comparison of open vertical banded gastroplasty and laparoscopic adjustable gastric banding at one and two years follow-up, with data at a mean of 84 months follow-up reported in a recent abstract128 (Table 31). At one year, mean BMI was lower in the open vertical banded gastroplasty group than in the laparoscopic adjustable gastric banding group [31.1 (SD 6.2) versus 35.0 (SD 6.3), no p-value reported] and statistically significantly lower at the two-year follow-up [31.0 (SD 6.0) versus 34.6 (SD 6.5), p ≤ 0.002]. Percentage excess weight loss was statistically significantly greater in the open vertical banded gastroplasty group in comparison to the laparoscopic adjustable gastric banding group at both one and two years [one year: 71.1% (SD 24.0) versus 53.3% (SD 21.2), p ≤ 0.001; two years: 70.1% (SD 25.5) versus 54.9% (SD 23.3), p ≤ 0.001]. The difference was maintained at a mean of 84 months follow-up (per cent excess BMI loss 68.8% versus 56.9%, respectively). 128 However, it should be noted that at this time point 59% of vertical banded gastroplasty participants had been converted to gastric bypass, and 11% of laparoscopic adjustable gastric banding participants had been converted to another procedure. From the limited information presented in the abstract reporting these results128 it is not clear whether this has been taken into consideration.
Quality of life and comorbidities
One study assessed patient satisfaction126 and one study reported on comorbidities,127 whereas one study did not report QoL or comorbidity outcomes. 110 At five years follow-up, patients were asked if they were satisfied with, or regretted having undergone, the operation. 126 Only 56% of vertical banded gastroplasty patients were satisfied with the result of the operation, while 81% of the patients with adjustable gastric banding were satisfied (statistical significance not given). The comparison of open vertical banded gastroplasty and laparoscopic adjustable gastric banding127 revealed that although the overall number of patients with comorbidity in both groups significantly decreased following surgery at one and two years follow-up, no differences in comorbidities were observed between groups (open vertical banded gastroplasty: 82% at baseline, 30.4% at one year, 47.9%, at two years, p ≤ 0.001 versus baseline; laparoscopic adjustable gastric banding 78% at baseline, one year 37.5% at one year, 40% at two years, p ≤ 0.001 versus baseline) (Table 32). Significant improvements in both groups were seen in joint problems (p ≤ 0.001 compared with preoperative), pulmonary problems (p ≤ 0.05 compared to preoperative) and diabetes mellitus (p ≤ 0.05 compared with preoperative). No improvement in either group was observed between the percentage of patients with preoperative and postoperative hypertension, cardiovascular problems, hypercholesterolaemia, reflux disease, sleep apnoea or neurological problems (Appendix 10). After a mean of 84 months follow-up comorbidities had all significantly decreased except for gastro-oesophageal reflux disease (GERD), which increased in both groups, although no numerical data are provided in the abstract reporting these results. 128
| van Dielen, 2005127 | Open VBG (n = 50) | LAGB (n = 50) | p-value |
|---|---|---|---|
| Preoperative patients with comorbidity | 41 (82%) | 39 (78%) | |
| Joint problems | 29 (58%) | 28 (56%) | |
| Pulmonary problems | 8 (16%) | 9 (18%) | |
| Hypertension | 10 (20%) | 7 (14%) | |
| Diabetes mellitus | 7 (14%) | 5 (10%) | |
| Cardiovascular problems | 3 (6%) | 2 (4%) | |
| Hypercholesterolaemia | 2 (4%) | 2 (4%) | |
| Reflux disease | 2 (4%) | 3 (6%) | |
| Sleep apnoea | 1 (2%) | 1 (2%) | |
| Neurological problems | 0 (0%) | 1 (2%) | |
| At 1 year patients with comorbidity | 14 (30.4%)a | 18 (37.5%)a | |
| Joint problems | 7 (15.2%)a | 10 (20.8%)a | |
| Pulmonary problems | 3 (6.5%)b | 3 (6.3%)b | |
| Hypertension | 8 (17.4%) | 5 (10.4%) | |
| Diabetes mellitus | 1 (2.2%)b | 1 (2.1%)b | |
| Cardiovascular problems | 2 (4.3%) | 2 (4.2%) | |
| Hypercholesterolaemia | 1 (2.2%) | 2 (4.2%) | |
| Reflux disease | 0 (0%) | 0 (0%) | |
| Sleep apnoea | 0 (0%) | 0 (0%) | |
| Neurological problems | 0 (0%) | 1 (2.1%) | |
| At 2 years patients with comorbidity | 23 (47.9%)a | 20 (40%)a | |
| Joint problems | 13 (27.1%)a | 12 (24%)a | |
| Pulmonary problems | 3 (6.3%)b | 1 (2%)b | |
| Hypertension | 7 (14.6%) | 5 (10%) | |
| Diabetes mellitus | 1 (2.1%)b | 1 (2%)b | |
| Cardiovascular problems | 1 (2.1%) | 3 (6%) | |
| Hypercholesterolaemia | 1 (2.1%) | 1 (2%) | |
| Reflux disease | 0 (0%) | 0 (0%) | |
| Sleep apnoea | 0 (0%) | 0 (0%) | |
| Neurological problems | 1 (2.1%) | 1 (2%) |
Complications and additional operative procedures
Van Dielen and colleagues127 report that two deaths (4%) occurred, both in the open vertical banded gastroplasty group, one from sepsis in the first postoperative week, and one as the result of a pre-existing pneumonia that had not been reported to the surgeon preoperatively. No postoperative deaths occurred in the other two studies,110,126 and although one patient from each group died during follow-up in the study by Nilsell and colleagues,126 these deaths are reported to be unrelated to the surgery (Table 33).
| Nilsell, 2001126 | VBG (n = 30) | AGB (n = 29) | p-value |
|---|---|---|---|
| Postoperative deaths | 0 | 0 | |
| Deaths | 1 | 1 | |
| Reoperation: anastomotic leak (n) | 1 | 0 | |
| Late reoperations | 10/27 (37%) | 3/26 (11.5%) | |
| Removal of band | 4 | 1 | |
| Gastrogastrostomy | 3 | 0 | |
| Longer band | 1 | 0 | |
| Gastric banding | 2 | 0 | |
| Replacement of band | 0 | 2 | |
| Gastro-oesophageal reflux disease | 4/27 (14.8%) | 3/26 (11.5%) | |
| Staple-line disruption | 5/27 (18.5%) | ||
| Morino, 2003110 | LVBG (n = 51) | LAGB (n = 49) | |
| Mortality | 0 | 0 | |
| Operative time, minutes [mean (range)] | 94.2 (40–270) | 65.4 (35–120) | p < 0.05 |
| Hospital stay, days [mean (range)] | 6.6 (3–58) | 3.7 (2–6) | p < 0.05 |
| Conversion to open surgery | 0 | 0 | |
|
Associated procedures Cholecystectomies Lymph node biopsy |
5 (10%) 4 1 |
5 (10%) 5 0 |
|
| Early morbidity | 5/51 (9.8%) | 3/49 (6.1%) | p < 0.754 |
| Band slippage | 1 | ||
| Port infection | 1 | ||
| Haematoma at port site | 1 | ||
| Fistula at staple line | 1 | ||
| Prolonged postoperative pyrexia | 2 | ||
| Respiratory failures | 2 | ||
| Late complications | 7/50 (14%) | 16/49 (32.7%) | p < 0.05 |
| Band slippage | 9 | ||
| Symptomatic reflux disease | 4 | 3 | |
| Complete food intolerance | 1 | ||
| Poor compliance | 1 | ||
| Port infection | 1 | ||
| Port twisted | 1 | ||
| Pouch dilatation | 1 | ||
| Asymptomatic pouch to fundus fistula | 1 | ||
| Gastric bezoar | 1 | ||
| Morino, 2003110 | LVBG (n = 51) | LAGB (n = 49) | |
| Late reoperations | 0/50 | 12/49 (24.5%) | p < 0.001 |
| Band removed | 8 | ||
| For slipping | 6 | ||
| For severe reflux oesophagitis | 1 | ||
| For poor compliance | 1 | ||
| Slipped band replaced laparoscopically | 1 | ||
| Gastric bypass (due to food intolerance) | 1 | ||
| Port repositioned | 1 | ||
| Port removed | 1 | ||
| van Dielen, 2005127 | Open VBG (n = 50) | LAGB (n = 50) | |
| Mortality | 2/50 (4%) | 0 | |
| Mean length of hospital stay, days (± SD; range) | 6.8 (± 10.4; 2–56) | 3.5(± 1.5; 2–9) | p < 0.001 |
| Conversion to open surgery | n/a | 2 (4%) to open procedure; 1 (2%) to gastric bypass | |
| Immediate postoperative complications | 9/50 (18%) | 3 conversions as noted above | |
| Leakage (reoperation required) | 3 | ||
| Splenectomy | 2 | ||
| Obstruction (gastroscopy required) | 2 | ||
| Infections | 7 in 5 (10%) patients | 0 | |
| Sepsisa | 3 | ||
| Urinary tract infection | 1 | ||
| Pneumoniaa | 3 | ||
| Wound infection | 1 | ||
| Late complications requiring further surgery (detailed below) | 26/50 (52%)b | 20/50 (40%)c | |
| Revisional surgery (conversion to gastric bypass) | 18/50 (36%) | ||
| Due to vertical staple-line disruption | 15 | ||
| Due to narrow outlet | 2 | ||
| Due to insufficient weight loss | 1 | ||
| Surgical repair of incisional hernia | 8/50 (16%) | ||
| Major reoperations | 16 (32%) | ||
| Pouch dilatation/pouch slippage | 12 | ||
| Band leakage | 2 | ||
| Band erosion | 2 | ||
| Minor reoperations | 4/50 (8%) | ||
| Outlet stenosis or obstruction requiring gastroscopy | 6/50 (12%) |
Operative time was shorter with laparoscopic adjustable silicone gastric banding than laparoscopic vertical banded gastroplasty [65.4 minutes (35–120) versus 94.2 minutes (40–270), p < 0.05], as was hospital stay [3.7 days (2 to 6), versus 6.6 days (3 to 58), p < 0.05] in the Morino and colleagues study. 110 Hospital stay was also shorter for laparoscopic adjustable gastric banding than open vertical banded gastroplasty [mean 3.5 days (SD 1.5), range 2–9 days, versus mean 6.8 days (SD 10.4) days, range 2–56 days; p < 0.001] in the study by van Dielen and colleagues. 127
One reoperation on the third postoperative day because of an anastomotic leak in the vertical banded gastroplasty group is reported by Nilsell and colleagues. 126 Morino and colleagues110 found that early morbidity was similar between the two laparoscopic procedures (laparoscopic adjustable gastric banding 6.1% versus laparoscopic vertical gastric banding 9.8%, p = 0.754) and there were no conversions to open surgery. One patient experienced early postoperative band slippage (laparoscopically repositioned). There was also one port infection and one haematoma at the port site in the laparoscopic adjustable gastric banding group. In the vertical banded gastroplasty group there was one fistula at the staple line (treated with open gastric bypass), two instances of prolonged postoperative pyrexia, and two respiratory failures without evidence of pulmonary embolism. Van Dielen and colleagues127 reported that two conversions to open surgery were necessary in the laparoscopic adjustable banding group, and in an additional patient a conversion to gastric bypass was necessary. In the open vertical banded gastroplasty group nine patients experienced immediate postoperative complications: leakage in three patients required reoperation, two splenectomies were performed, and in two patients an obstruction that necessitated gastroscopy occurred. There were no infections in the laparoscopic adjustable banding group, but there were seven infections in five patients (including the two patients who died) in the open vertical banded gastroplasty group.
Nilsell and colleagues126 reported that late reoperations were necessary in a third of vertical banded gastroplasty patients because of staple-line disruption with rapid weight regain or strictures of the stoma with vomiting or intolerance of solid food. The total incidence of staple-line disruption was 18.5% (five patients), but three patients were not reoperated on for various reasons. 126 Three (11.5%) adjustable gastric banding patients were reoperated; two as the result of dilatation of the gastric pouch, and one patient requested that their band be removed for reasons that were unclear. Morino and colleagues,110 found that late complications were more common following laparoscopic adjustable silicone gastric banding (32.7% versus 14%, p < 0.05). However, no patients with laparoscopic vertical banded gastroplasty required late reoperation, whereas 24.5% of patients required late reoperation following laparoscopic adjustable silicone gastric banding (p < 0.001), most commonly because of bands slipping. The percentage of late complications occurring in the open vertical banded gastroplasty group and the laparoscopic gastric bypass group appear similar in van Dielen and colleagues127 (no statistical comparison reported). Revisional surgery (conversion to gastric bypass) was necessary in 36% of those who had undergone open vertical banded gastroplasty, in most cases (15/18) this was the result of vertical staple-line disruption. A further eight (16%) patients required a surgical repair of an incisional hernia. Six patients (12%) required gastroscopy at least once for outlet stenosis or obstruction. In the laparoscopic adjustable gastric banding group, 40% of participants required reoperation. The majority of reoperations (16/20) were major reoperations for pouch dilatation or slippage, band leakage, or band erosion. At a mean of 84 months follow-up, the authors reported that long-term complications ‘were mainly’ staple-line disruption (51%) and incisional hernia (27%) for patients with open vertical banded gastroplasty, and pouch dilatation (24%) and anterior slippage (15%) for patients with laparoscopic adjustable gastric banding. 128 Major reoperation was required in 59% of vertical banded gastroplasty patients, who required conversions to gastric bypass, and in 46% of laparoscopic adjustable gastric banding patients, who required refixation or band replacements (35%) or conversion to another procedure (11%). 128
GERD was slightly more common in patients with vertical banded gastroplasty (14.8%) than adjustable gastric banding (11.5%) in the study by Nilsell and colleagues. 126
Summary
Three studies were included: one had a low risk of selection bias and two were of uncertain risk of bias for several items, although missing outcome data for weight loss were adequately addressed. Weight loss results were inconclusive. One study found that weight loss was initially greater with vertical banded gastroplasty, but weight regain meant that by three years patients with adjustable gastric banding had a lower mean weight, and this was still the case at five years (statistical significance not reported). The second study found lower BMI and greater per cent excess weight loss following laparoscopic vertical banded gastroplasty, but this was statistically significant only at year one and not at years two or three. The third study found statistically significant lower BMI and greater per cent excess weight loss at one and two years following open vertical banded gastroplasty, and greater per cent excess BMI loss seven years after open vertical banded gastroplasty (statistical significance not reported). However, the impact of participants being converted to another procedure in this study is unclear. More patients who had undergone adjustable gastric banding reported being satisfied with the results at five years, but this apparent superiority was not tested statistically. Resolution of comorbidities was similar in the two groups in the only study that reported on this outcome. 127 It is difficult to draw conclusions regarding complications and additional operative procedures because one study compared two open procedures, one two laparoscopic procedures, and one compared an open procedure with a laparoscopic procedure. In the comparison of open procedures more reoperations were necessary following open vertical banded gastroplasty than open adjustable gastric banding, but a statistical comparison was not reported. Laparoscopic adjustable gastric banding was associated with a statistically shorter operative time and hospital stay than laparoscopic vertical banded gastroplasty, but there were statistically more late complications and reoperations. The third comparison found laparoscopic adjustable gastric banding was associated with a statistically significant shorter hospital stay while open vertical banded gastroplasty led to more infections. Late complications requiring further surgery were similar but a statistical comparison was not reported.
Laparoscopic adjustable gastric banding versus laparoscopic isolated sleeve gastrectomy
One RCT129 compared laparoscopic adjustable gastric banding with laparoscopic isolated sleeve gastrectomy.
Weight loss
In this study Himpens and colleagues129 report that the proportion of excess weight loss was statistically significantly greater in participants in the laparoscopic isolated sleeve gastrectomy group than the laparoscopic adjustable gastric banding group at one year (57.7% versus 41.4%, p = 0.0004) and three years (66% versus 48% p = 0.0025) (Table 34). Weight loss (three years: 29.5 kg versus 17 kg, p < 0.0001) and reduction in BMI (three years: 27.5 versus 18, p < 0.0001) were statistically significantly improved in laparoscopic isolated sleeve gastrectomy participants in comparison with the laparoscopic adjustable gastric banding participants. All of these data were presented by the trial authors as median and range so care should be taken when interpreting the results.
| Himpens, 2006129 | LAGB (n = 40) | LISG (n = 40) | p-value |
|---|---|---|---|
| % EWL at 1 year (median, range) | 41.4 (– 11.8 to 130.5) | 57.7 (0 to 125.5) | p = 0.0004 |
| % EWL at 3 years (median, range) | 48 (0 to 124.8) | 66 (– 3.1 to 152.4) | p = 0.0025 |
| Weight loss at 1 year (kg, median, range) | 14 (– 5 to 38) | 26 (0 to 46) | p < 0.0001 |
| Weight loss at 3 years (kg, median, range) | 17 (0 to 40) | 29.5 (1 to 48) | p < 0.0001 |
| BMI decrease at 1 year (median, range) | 15.5 (5 to 39) | 25 (0 to 45) | p < 0.0001 |
| BMI decrease at 3 years (median, range) | 18 (0 to 39) | 27.5 (0 to 48) | p = 0.0004 |
Quality of life and comorbidities
QoL was not assessed in this study. At baseline in the Himpens and colleagues129 study GERD requiring drug therapy with proton pump inhibitors was a problem for 15% (6/40) of the laparoscopic adjustable gastric banding participants and 20% (8/40) of the participants in the laparoscopic isolated sleeve gastrectomy group. After one year GERD had disappeared in 83% and 75% of these participants in the two groups respectively, and this remained the same at three years. Statistical significance was not reported. In those without GERD at baseline, no statistically significant differences in rates of appearance of GERD between the intervention groups were observed at one year [laparoscopic adjustable gastric banding 3/34 (8.8%), versus laparoscopic isolated sleeve gastrectomy 7/32 (21.8%), p = ns] or three years [laparoscopic adjustable gastric banding 7/34 (20.5%) versus laparoscopic isolated sleeve gastrectomy 1/32 (3.1%), p = ns] (Appendix 11).
Complications and additional operative procedures
No early postoperative complications were seen in the laparoscopic adjustable gastric banding group of the Himpens and colleagues129 study, two participants in the laparoscopic isolated sleeve gastrectomy group had an early postoperative complication, both required revisional surgery, in one this was a total gastrectomy for gastric ischaemia (Table 35). Late complications requiring surgery were observed in the laparoscopic adjustable gastric banding participants, with three pouch dilatations (treated with band removal in two and conversion to Roux-en-Y gastric bypass in one); one gastric erosion (treated with Roux-en-Y gastric bypass) and three disconnections of the port (treated with reconnection). There were no late complications requiring surgery in the laparoscopic isolated sleeve gastrectomy group. Complications not requiring surgery that were observed at one and three years can be seen in Table 35. There appeared to be higher frequencies of complications in the laparoscopic adjustable gastric banding group than in the laparoscopic isolated sleeve gastrectomy group but this is based on observation of the data only, no statistical analysis was undertaken.
| Himpens, 2006129 | LAGB (n = 40) | LISG (n = 40) |
|---|---|---|
| Early postoperative complications (requiring surgery) | 0 | 2/40 (5%) |
| Intraperitoneal bleed requiring laparoscopy | 1 | |
| Gastric ischaemia requiring total gastrectomy | 1 | |
| Late complications requiring surgery | 7/40 (17.5%) | 0 |
| Pouch dilatation leading to band removal | 2 | |
| Pouch dilatation leading to conversion to RYGBP | 1 | |
| Gastric erosion leading to conversion to RYGBP | 1 | |
| Port disconnections, reconnected | 3 | |
| Conversion due to insufficient weight loss | 2/40 (5%) to RYGBP | 2/40 (5%) to laparoscopic duodenal switch |
| Complications at 1 year (not requiring surgery) | ||
| Shoulder pain | 3/40 (7.5%) | |
| Frequent vomiting | 6/40 (15%) | 1/40 (2.5%) |
| Poor choice of alimentation | 2/40 (5%) | |
| Gastric pain | 2/40 (5%) | |
| Mineral deficiency | 2/40 (5%) | |
| Complications at 3 years (not requiring surgery)a | ||
| Shoulder pain | 3 (8.5%) | |
| Frequent vomiting | 10 (28.5%) | 5 (16.6%) |
| Poor choice of alimentation | 17 (48.5%) | 8 (26.6%) |
| Gastric ulcer | 1 (2.8%) | |
| Mineral deficiency | 3 (10%) |
In addition, two participants in each group had ‘insufficient weight loss’ noted as a complication in the Himpens and colleagues129 study. The two participants in the laparoscopic adjustable gastric banding group were converted to Roux-en-Y gastric bypass and the two participants in the laparoscopic isolated sleeve gastrectomy group were converted to laparoscopic duodenal switch.
Summary
On measures of weight, participants undergoing laparoscopic isolated sleeve gastrectomy showed more improvement than participants undergoing laparoscopic adjustable gastric banding in one study with an uncertain risk of bias. Rates of complications were observed to be lower in the laparoscopic isolated sleeve gastrectomy group, apart from rates of early postoperative complications.
Open versus laparoscopic gastric bypass
Three RCTs compared open gastric bypass with laparoscopic gastric bypass113,114,130,131 and another RCT compared open gastric bypass with hand-assisted laparoscopic gastric bypass. 112
Weight change
Puzziferri and colleagues113,114 demonstrated a slightly higher percentage of excess body weight loss following laparoscopic gastric bypass (one year: 68%, SD 15) compared with open gastric bypass (one year: 62%, SD 14), but the difference was not statistically significant at one year (p = 0.07) or at the three-year or four-year follow-ups114 (Table 36). Similarly, a non-significant difference in reduction of BMI was found at one year by Westling and Gustavsson131 [laparoscopic 14 (SD 3), open 13 (SD 3)], Sundbom and Gustavsson112 (BMI reduction of 15 in both groups, BMI: laparoscopic 29, open 30) and at three years follow-up by Lujan and colleagues130 (laparoscopic 31, open 35.5). Incomplete weight loss outcome data were adequately addressed by Westling and Gustavsson131 and by Sundbom and Gustavsson. 112 However, the risk of bias from incomplete weight loss data was uncertain in the studies by Lujan and colleagues130 and Puzziferri and colleagues. 113,114
| Open versus laparoscopic gastric bypass | |||
|---|---|---|---|
| Puzziferri, 2006113,114 | Open RYGBP (n = 76) | LRYGBP (n = 79) | p-value |
| % excess body weight loss 12 months | 62 (± 14) (n = 25) | 68 (± 15) (n = 29) | p = 0.07 |
| % excess body weight loss 3 years | 67 (± 21) (n = 33) | 77 (± 22) (n = 30) | p = ns |
| % excess body weight lost 4 years | 71 (± 25) (n = 18) | 76 (± 19) (n = 22) | p = ns |
| Westling and Gustavsson, 2001131 | Open RYGBP (n = 21) | LRYGBP (n = 30) | |
| BMI 1 year | 30.6 (± 4) | 27 (± 4) | |
| Change in BMI 1 year | 13 (± 3) | 14 (± 3) | p = ns |
| Lujan, 2004130 | Open GBP (n = 51) | LGBP (n = 53) | |
| BMI 12 months (estimated from figure) | 37 | 33 | p = ns |
| BMI 18 months (estimated from figure) | 36 | 31 | p = ns |
| BMI 24 months (estimated from figure) | 35 | 32 | p = ns |
| BMI 36 months (estimated from figure) | 35.5 | 31 | p = ns |
| Sundbom, 2004112 | Open RYGBP (n = 25) | Hand-LRYGBP (n = 25) | |
| Weight reduction at 1 year, median (range) | 41 kg (26–57) | 39 kg (23–57) | |
| BMI at 1 year, median | 30 | 29 | |
| Reduction in BMI | 15 | 15 | |
| Open versus laparoscopic vertical banded gastroplasty | |||
| Davila-Cervantes, 2002111 | Open VBG (n = 14) | LVBG (n = 16) | p-value |
| Excess body weight loss at 12 months | 55% (30–88) | 47% (22–97) | |
| BMI at 12 months, median (estimated from figure) | 33 | 33 | |
| Open versus laparoscopic adjustable silicone gastric banding | |||
| de Wit, 1999132 | Open AGB (n = 25) | LAGB (n = 25) | p-value |
| Mean weight loss (12 months) | 34.4 kg | 35 kg | p = ns |
| BMI reduction (12 months) | 10.6 | 11.6 | p = ns |
Quality of life and comorbidities
The one- to six-month QoL outcomes for Puzziferri and colleagues113 have been tabulated and discussed previously,15 and can be seen in Appendix 12. In brief, early differences in some components of the SF-36 score (at one month) and Moorehead–Ardelt quality of life questionnaire (MAQoL) (at three months) were no longer significant at three months or six months respectively. At the three-year follow-up there continued to be no significant difference in MAQoL scores, and there was also no significant difference in the proportion of participants with Bariatric Analysis and Reporting Outcome System (BAROS) scores of good, very good or excellent (Table 37).
| Open versus laparoscopic gastric bypass | |||
|---|---|---|---|
| Puzziferri, 2006114 | Open RYGBP (n = 22) | LRYGBP (n = 22) | p-value |
| MAQoL scores 3 years | |||
| Self-esteem | 0.88 | 0.89 | p = ns |
| Physical activity | 0.36 | 0.40 | p = ns |
| Social life | 0.33 | 0.34 | p = ns |
| Labour or work conditions | 0.25 | 0.33 | p = ns |
| Sexual interest/activity | 0.24 | 0.20 | p = ns |
| BAROS scores (%) 3 years | |||
| Fair | 9.1% | 4.5% | |
| Good, very good or excellent | 86.4% | 95.5% | p = ns |
Westling and Gustavsson131 reported that 92% of all patients described themselves as ‘very satisfied’ with the result of the operation after one year, while the remaining patients described themselves as ‘satisfied’. The authors report no significant difference between the groups, but data were not provided.
Only one study reported on comorbidities. 114 At the three-year follow-up the improvement of obesity-related comorbidities was significantly different between the two groups for only two of the reported comorbidities: osteoarthritis symptoms improved more in the laparoscopic gastric bypass group than the open gastric bypass group (p < 0.05), whereas the open gastric bypass group experienced a greater improvement of dyslipidaemia (p < 0.01). For other obesity-related comorbidities improvements were not statistically significantly different between the groups (Table 38).
| Open versus laparoscopic gastric bypass | |||
|---|---|---|---|
| Puzziferri, 2006114 | Open RYGBP (n = 57) | LRYGBP (n = 59) | |
| Osteoarthritis | |||
| Baseline | 31 (54%) | 30 (51%) | p = ns |
| Improvement/resolution at 3 years | 19 (61%) | 24 (80%) | p < 0.05 |
| Hypertension | |||
| Baseline | 28 (49%) | 18 (31%) | p = ns |
| Improvement/resolution at 3 years | 28 (100%) | 15 (83%) | p = ns |
| Depression | |||
| Baseline | 17 (30%) | 17 (29%) | p = ns |
| Improvement/resolution at 3 years | 12 (71%) | 13 (76%) | p = ns |
| Gastro-oesophageal reflux | |||
| Baseline | 21 (37%) | 14 (24%) | p = ns |
| Improvement/resolution at 3 years | 21 (100%) | 14 (100%) | p = ns |
| Dyslipidaemia | |||
| Baseline | 14 (25%) | 8 (14%) | p = ns |
| Improvement/resolution at 3 years | 14 (100%) | 7 (88%) | p < 0.01 |
| Sleep apnoea | |||
| Baseline | 15 (26%) | 5 (8%) | p < 0.05 |
| Improvement/resolution at 3 years | 12 (86%) | 5 (100%) | p = ns |
| Diabetes mellitus | |||
| Baseline | 8 (14%) | 5 (8%) | p = ns |
| Improvement/resolution at 3 years | 7 (88%) | 5 (100%) | p = ns |
| Infertility | |||
| Baseline | 5 (9%) | 7 (12%) | p = ns |
| Improvement/resolution at 3 years | 2 (40%) | 2 (29%) | p = ns |
| Urinary incontinence | |||
| Baseline | 4 (7%) | 8 (14%) | p = ns |
| Improvement/resolution at 3 years | 4 (100%) | 7 (88%) | p = ns |
| Lower extremity oedema | |||
| Baseline | 3 (5%) | 2 (3%) | p = ns |
| Improvement/resolution at 3 years | 3 (100%) | 1 (50%) | p = ns |
Complications and additional operative procedures
One postoperative death in the laparoscopic gastric bypass group was reported by Westling and Gustavsson;131 this was the result of malignant hyperthermia which developed during surgery leading to the death of the patient one week later. Lujan and colleagues130 reported three postoperative deaths. Two occurred in the laparoscopic group, one on postoperative day 32, and the other (unrelated to surgery) six months after surgery. One death occurred in the open surgery group within the first 30 postoperative days. No postoperative deaths occurred in the open versus laparoscopic113,114 or open versus hand-assisted laparoscopic112 gastric bypass studies (Table 39).
| Open versus laparoscopic gastric bypass | |||
|---|---|---|---|
| Puzziferri, 2006113,114 | Open RYGBP (n = 76) | LRYGBP (n = 79) | p-value |
| Perioperative deaths | 0 | 0 | |
| Late deaths | 0 | 0 | |
| Conversion from LGBP to GBP | n/a | 2.5% | |
| Operative time (minutes) | 195 (± 41) | 225 (± 40) | p < 0.001 |
| Estimated blood loss (ml) | 395 (± 284) | 137 (± 79) | p < 0.001 |
| Intraoperative transfusion | 3.9% | 0 | |
| Proportion requiring intensive-care unit stay | 21.1% | 7.6% | p = 0.03 |
| Median length of hospital stay (days) | 4 (IQR 2) | 3 (IQR 1) | p < 0.001 |
| Reoperation | 6.6% | 7.6% | p = ns |
| Return to activities of daily living (days) | 17.7 (± 19.1) | 8.4 (± 8.6) | p < 0.001 |
| Return to work (days) | 46.1 (± 20.6) | 32.2 (± 19.8) | p = 0.02 |
| Early major complications (total) | 9.2% | 7.6% | p = 0.78 |
| Anastomotic leak | 1 | 1 | |
| Gastric pouch outlet obstruction | 1 | 0 | |
| Hypopharyngeal perforation | 0 | 1 | |
| Jejunojejunostomy obstruction | 0 | 3 | |
| Pulmonary embolism | 1 | 0 | |
| Respiratory failure | 1 | 0 | |
| Gastrointestinal bleeding | 0 | 1 | |
| Wound infection | 2 | 0 | |
| Retained laparotomy sponge | 1 | 0 | |
| Early minor complications (total) | 11.8% | 7.6% | p = 0.42 |
| Ileus | 0 | 1 | |
| Clostridium difficile colitis | 0 | 1 | |
| Gastrogastric fistula | 1 | 0 | |
| Leak (asymptomatic) | 1 | 0 | |
| Gastrointestinal bleeding | 0 | 2 | |
| Wound infection | 6 | 1 | |
| Deep venous thrombosis | 1 | 1 | |
| Late complications (total)113 | 15.8% | 18.9% | p = 0.52 |
| Anastomotic stricture | 2 | 9 | p = 0.06 |
| Prolonged nausea vomiting | 2 | 1 | |
| Small bowel obstruction | 0 | 1 | |
| Cholelithiasis | 0 | 3 | |
| Ventral hernia | 6 | 0 | p = 0.01 |
| Anaemia | 2 | 0 | |
| Protein-calorie malnutrition | 0 | 1 | |
| Late complications at 3 years114 | Open RYGBP (n = 57) | LRYGBP (n = 59) | |
| Incisional hernia | 22 (39%) | 3 (5%) | p < 0.01 |
| Anaemia | 3 (5%) | 8 (14%) | p = ns |
| Vitamin B12 deficiency | 6 (11%) | 3 (5%) | p = ns |
| Chronic nausea vomiting | 2 (4%) | 3 (5%) | p = ns |
| Chronic abdominal pain | 1 (2%) | 2 (3%) | p = ns |
| Marginal ulcer | 1 (2%) | 0 | p = ns |
| Small bowel obstruction | 1 (2%) | 2 (3%) | p = ns |
| Cholecystectomy (excludes those with previous Cholecystectomy) | 2/40 (5%) | 12/43 (28%) | p = ns |
| Late deaths | 0 | 0 | p = 0.03 |
| Westling and Gustavsson, 2001131 | Open RYGBP (n = 21) | LRYGBP (n = 30) | |
| Deaths | 1/30 (3%) | ||
| Conversions to open surgery | n/a | 7/30 (23%) | |
| Duration (minutes), median (range) | 100 (70–150) (n = 21) | 245 (135–390) (n = 30) | |
| Preoperative bleeding (ml), median (range) | 300 (200–500) (n = 21) | 250 (50–1500) (n = 30) | |
| Pain – morphine dose (mg) | 140 (± 90) (n = 21) | 98 (± 71.5) (n = 29); conversions excluded 69 (± 46.4) (n = 22) |
(p = ns); p < 0.005 |
| Hospital stay (days) | 6 (± 3.8) (n = 21) | 4.5 (± 1.2) (n = 29); conversions excluded 4 (± 0.8) (n = 22) |
p = ns; p = 0.025 |
| Sick leave (weeks) | 5 (± 3.3) (n = 14) | 3.9 (± 2.1) (n = 24); conversions excluded 2.8 (± 1.8) (n = 18) |
p = ns; p = 0.025 |
| Reoperations | 1/21 (4.8%)a | 6/30 (20%)b | |
| Gastrointestinal symptoms (dumping, vomiting, diarrhoea) | 5% of all patients | ||
| Complications (n) | |||
| Incisional hernia | 1 | ||
| Small embolus | 1 | ||
| Colicky pain and vomiting | 6b | ||
| Leakage | 1a | ||
| Jejunal ulcers | 2 | 3 | p = ns |
| Stricture in gastrojejunostomy | 1 | ||
| Superficial wound infection | 3 | ||
| Readmission | 1/21 (4.8%) | 3/30 (10%) | |
| Unexplained fever | 1 | ||
| Pneumonia | 1 | ||
| Epigastric pain and/or vomiting | 2 | ||
| Lujan, 2004130 | Open GBP (n = 51) | LGBP (n = 53) | |
| Postoperative mortality | 1/51 (2%) | 2 (3.8%)(1 unrelated to surgery) | |
| Conversions to laparotomy | n/a | 4/53 (8%) | |
| Intraoperative complications | 4/51 (8%) | ||
| Splenectomies | 3 | ||
| Splenic vein tear requiring suture | 1 | ||
| Mean operating time, minutes | 201.7 (129–310) | 186.4 (125–290) | p < 0.05 |
| Mean hospital stay, days | 7.9 (2–28) | 5.2 (1–13) | p < 0.05 |
| Early complications (< 30 days) | 15 (29.4%) | 12 (22.6%) | p = ns |
| Intestinal subocclusions | 3 | ||
| Asymptomatic leaks | 2 | ||
| Intra-abdominal bleeding | 2 | ||
| Upper gastrointestinal haemorrhage | 2 | 3 | |
| Lower gastrointestinal haemorrhage | 1 | ||
| Thrombophlebitis | 1 | ||
| Stenosis of gastro-entero-anastomosis | 1 | ||
| Subphrenic abscess | 4 | ||
| Wound infection | 4 | ||
| Respiratory infection | 3 | ||
| Eviscerationc | 1 | ||
| Late complications (> 30 days) | 12 (24%) | 6 (11%) | p < 0.05 |
| Intestinal obstructionc | 3 (1 reoperation) | 1 (reoperation) | |
| Pancreatitis/cholecystectomy | 2 | ||
| Sudden death (possible pulmonary thromboembolism) | 1 | ||
| Eventration | 10 | ||
| Subphrenic abscess | 1 | ||
| Sundbom, 2004112 | Open RYGBP (n = 25) | Hand-LRYGP (n = 25) | |
| Deaths within 30 days postoperative | 0 | 0 | |
| Laparoscopic conversions to laparotomy | n/a | 0 | |
| Duration of surgery, minutes [Median (range)] | 85 (60–150) | 150 (110–265) | p < 0.001 |
| Peroperative bleeding, ml [Median (range)] | 250 (0–900) | 250 (0–1300) | |
| Intra-abdominal bleeding (oozing) | 3 | ||
| Intense intraluminal bleeding | 2 | ||
| Patients requiring blood transfusion due to post operative anaemia | 1 (2 units) | 1 (2 units) | |
| Patients with postoperative respiratory symptoms requiring prolonged antibiotic treatment and physiotherapy treatment | 5 | 8 | |
| Postoperative deep venous thrombosis, pulmonary embolism, or wound dehiscence | 0 | 0 | |
| Length of hospital stay, days [Median (range)] | 6 (3–7) | 6 (4–14) | |
| Morphine requirement, mg: | |||
| Day 1 [Median (range)] | 32 (6–150) (n = 25) | 48 (12–148) (n = 25) | |
| Day 2 [Median (range)] | 30 (12–118) (n = 22) | 36 (14–123) (n = 20) | |
| Day 3 [Median (range)] | 25 (10–62) (n = 11) | 28 (12–99) (n = 16) | |
| Total days 1–3 [Median (range)] | 66 (6–318) | 98 (12–370) | |
| Reoperation | 0 | 1/25 (4%) | |
| Complications at 1 month follow-up, (n) | |||
| Dysphagia (various grades) | 18 (group not stated) | ||
| Narrow anastomosis | 4 | 2 | |
| Wound infection with pus | 0 | 1 | |
| Abnormal secretions | 4 (group not stated) | ||
| Total sick leave, days, median (range). (10 patients retired or on long-term sick leave excluded) | 37 (19–95) | 30 (15–59) | |
| Complications at 1-year follow-up, (n) | |||
| Anaemia requiring intensive treatment | 2 (group not stated) | ||
| Symptomatic incisional hernia | 1 | 0 | |
| Short-term treatment with proton pump inhibitor | 3 | 3 | |
| Small stomal ulcer | 1 | 0 | |
| Open versus laparoscopic vertical banded gastroplasty | |||
| Davila-Cervantes, 2002111 | Open VBG (n = 14) | LVBG (n = 16) | p-value |
| Surgical details (median, min-max) | |||
| Surgical time | 1.45 hours (1.1–2.5) | 2.1 hours (1.5–4.0) | p < 0.002 |
| Blood transfusions | 0 | 0 | |
| Conversion to open surgery | n/a | 0 | |
| Hospitalisationd | 4 days (3–42) | 4 days (3–97) | p = ns |
| Complications (number of patients) | |||
| Wound problems (seroma, dehiscence or infection) | 6 | 1 | |
| Pulmonary atelectasis requiring physical therapy | 1 | ||
| Number of extra doses of analgesics: (median, min.–max.) | |||
| 1st postoperative day | 2 (0–3) | 1 (0–2) | p = 0.04 |
| 2nd postoperative day | 1 (0–1) | 2 (0–2) | p = 0.78 |
| 3rd postoperative day | 1 (0–1) | 0 (0) | p = 0.46 |
| 12 months follow-up | |||
| Number with pathological scare | 12 | 5 | p = 0.002 |
| Developed abdominal wall hernias | 2 | 0 | |
| Open versus laparoscopic adjustable silicone gastric banding | |||
| de Wit, 1999132 | Open AGB (n = 25) | LAGB (n = 25) | |
| Conversions | Lap to open procedure: 8% | ||
| Surgical time | 76 minutes (SD 20) | 150 minutes (SD 48) | p < 0.05 |
| Mean days in hospital | 7.2 (range 5–13) | 5.9 (range 4–10) | p < 0.05 |
| Early postoperative complications (lap vs open) | |||
| Cholecystectomy | 5/25 (20%) | 2/25 (8%) | |
| Adhesiolysis | 1/25 (4%) | ||
| Gall bladder puncture (to obtain samples for study purposes) | 7/25 (28%) | 0 | |
| Pulmonary complications | 2/25 (8%) | 2/25 (8%) | |
| Urinary infection | 0 | 2/25 (8%) | |
| Rhabdomyolysis | 0 | 1/25 (4%) | |
| Neurological complication (neuropraxis) | 1/25 (4%) | 1/25 (4%) | |
| Perforation pouch | 1/25 (4%) | 0 | |
| Wound abscess | 1/25 (4%) | 0 | |
| Fever | 2/25 (8%) | 0 | |
| Gout | 1/25 (4%) | 0 | |
| First year surgical complications | |||
| Incisional hernia | 7 (28%), in 3 (12%) patients | 0 | p = ns |
| Migration band | 1/24 (4%) | 0 | p = ns |
| Umbilical hernia | 0%, | 1/25 (4%) | p = ns |
| Access port complications | 6 (24%) in 5 (20%) patients | 7 (28%), in 5 (20%) patients | p = ns |
| Readmissions | |||
| Patients | 7/24 (28%) | 5/25 (20%) | p = ns |
| Total readmissions | 15/24 | 6/25 | p < 0.05 |
| Overall length of hospital stay in the first year, days | 11.8 (SD 10.5) | 7.8 (SD 6) | p < 0.05 |
Conversion from laparoscopy to open procedure occurred in 2.5%,113 8% (all in the first 20 patients),130 and 23% of patients. 131 None of the patients with hand-assisted laparoscopy required conversion. 112 Reoperation was required in 4%,112 7.6%113 and 20%131 of laparoscopy patients, and none112 to 6.6%113 of patients with open gastric bypass.
In two of the studies, operative time was longer for laparoscopy [225 minutes (SD 40)113 to 245 minutes (range 135–190)131] than open gastric bypass (100 minutes (range 70–150)131 to 195 minutes (SD 41), p < 0.001113]. This was also the case for hand-assisted laparoscopy112 (150 minutes, 110–265; open 85 minutes, 60–150, p < 0.01]. However, Lujan and colleagues130 found operative time was longer for open (201.7 minutes, 129–310) than for laparoscopic gastric bypass (186.4 minutes, 125–290), p < 0.05.
Puzziferri and colleagues113 found significantly less blood loss with laparoscopy (137 ml, SD 79 versus 395 ml, SD 284, p < 0.001), whereas Westling and Gustavsson131 found only a slight reduction in blood loss [250 ml (50–1500) versus 300 ml (200–500), p = ns), and Sundbom and Gustavsson112 found no difference between hand-assisted laparoscopy [median 250 ml, (0–1300)] and open surgery [median 250 ml (0–900)].
When excluding patients who were converted to open procedures, Westling and Gustavsson131 found significant reductions in postoperative pain indicated by morphine dose, hospital stay and sick leave with laparoscopy, although the observations were not significant when using ITT analysis. Similarly, Sundbom and Gustavsson112 found no difference in the median LOS between open and hand-assisted laparoscopic gastric bypass [open six days (range 3–7), laparoscopy six days (range 4–14)], and the amount of morphine required during the first three days was similar for the two procedures. Total sick leave was slightly higher following open surgery [hand-assisted laparoscopy 30 days (15–59), open 37 days (19–95)]. Puzziferri and colleagues,113 however, found significant reductions in the proportion requiring intensive-care unit (ITU) stay (7.6% versus 21.1%, p = 0.03), median LOS {three days [inter quartile range, (IQR), 1] versus four days (IQR 2), p < 0.001}, days to return to activities of daily living [8.4 days (SD 8.6) versus 17.7 days (SD 19.1), p < 0.001], and days to return to work [32.2 days (SD 19.8) versus 46.1 days (SD 20.6), p = 0.02] following laparoscopy. Lujan and colleagues130 also found a shorter mean hospital stay following laparoscopy [5.2 days (1–13) versus 7.9 days (2–28), p < 0.05].
The reporting of complications varied between studies, but in all studies most complications affected a small proportion of patients. Early major complications reported by Puzziferri and colleagues113 occurred in 9.2% of open gastric bypass patients and 7.6% of laparoscopy patients (p = 0.78). The most common complication in the laparoscopic group was jejunojejunostomy obstruction (3.8%) with other patients experiencing either an anastomotic leak (1.3%), hypopharyngeal perforation (1.3%), or gastrointestinal bleeding (1.3%). Participants receiving open surgery experienced wound infection (2.6%), anastomotic leak (1.3%), gastric pouch outlet obstruction (1.3%), pulmonary embolism (1.3%), respiratory failure and a retained laparotomy sponge (1.3%). Early minor complications, were similar following the open procedure (11.8% versus 7.6%, p = 0.42), although minor wound infections were more common following the open procedure (six patients versus one patient). Late complications were also similar (open: 15.8% versus laparoscopic: 18.9%, p = 0.52). Among the late complications reported by Puzziferri and colleagues113 anastomotic stricture occurred more often after laparoscopic gastric bypass than open surgery but the difference was not statistically significant (laparoscopy 8.9% versus open 2.4%, p = 0.06), whereas ventral hernia was statistically significantly more frequent in the open surgical group (laparoscopy 0%, open 7.9%, p = 0.01). The difference in occurrence of hernias was still apparent at the three-year follow-up, which reports statistically significantly more patients in the open gastric banding group developed an incisional hernia than in the laparoscopic gastric banding group [22 (39%) versus 3 (5%), p < 0.001]. In addition, significantly more participants in the laparoscopic group required a cholecystectomy [12/43 (28%) versus 2/40 (5%), p = 0.03]. At three years the late complication of incisional hernia was still statistically significantly more frequent in the open surgical group (laparoscopy 5%, open 39%, p < 0.01), but there were no significant differences in the other complications reported at three years, and there were no late deaths (Table 39). In contrast to Puzziferri and colleagues,113 Lujan and colleagues130 reported four intraoperative complications in the open gastric bypass group and none in the laparoscopic group. They also found that while there was no significant difference between early complications (laparoscopy 22.6%, open 29.4%), late complications (> 30 days) were more common following open gastric bypass (11% versus 24%, p < 0.05). The most common early complications for laparoscopy included intestinal subocclusions (5.7%), asymptomatic leaks (3.8%), intra-abdominal bleeding (3.8%) and upper gastrointestinal haemorrhage (3.8%). For open surgery these included subphrenic abscesses (7.8%), wound infections (7.8%), upper gastrointestinal haemorrhage (5.9%) and respiratory infection (5.9%). The most common late complications reported by Lujan and colleagues130 included intestinal obstructions (5.7% of laparoscopy patients) and eventrations (protrusion of intestines through wound) (19.6% of open surgery patients). Late complications led to two reoperations, one in each group. Sundbom and Gustavsson112 reported that postoperative respiratory symptoms requiring prolonged antibiotic treatment and physiotherapy treatment occurred in 32% of hand-assisted laparoscopy patients and 20% of open surgery patients. Other complications included various grades of dysphagia (36% of patients, group not stated), narrow anastomosis (hand-assisted laparoscopy 8%, open 16%), and short-term treatment with a proton pump inhibitor (12% of each group). Westling and Gustavsson131 did not report early and late postoperative complications separately. The most commonly reported complications occurring after surgery were reoperations (discussed earlier), most often as the result of stricture of the tunnel through the mesocolon causing colicky pain and vomiting, jejunal ulcers (laparoscopy 10.3%, open 9.5%), and superficial wound infection (open 14.3%). There were four readmissions in the first year (laparoscopy 10.3%, open 4.7%) and one participant (4.7%) who had received open surgery developed an incisional hernia (Table 39).
Gastrointestinal symptoms reported at one year, such as dumping, vomiting or diarrhoea, were experienced by 5% of all patients in Westling and Gustavsson. 131
Summary
Four trials were included. The risk of selection bias was high in one trial, low in one trial and uncertain in two trials, and the risk of bias from other sources was mostly uncertain as many factors were not reported. Weight loss and QoL were similar between open and laparoscopic gastric bypass. Only one study reported on comorbidities and improvements were similar between the procedures except for two of the comorbidities. Statistically significant differences were found in favour of laparoscopic gastric bypass for a number of operative characteristics, particularly hospital stay in some studies. Complications in the two groups were in general reported to be not significantly different or were reported without a statistical comparison having been made.
Open versus laparoscopic vertical banded gastroplasty
One RCT compared open vertical banded gastroplasty with laparoscopic vertical banded gastroplasty. 129
Weight change
Davila-Cervantes and colleagues111 reported similar excess weight loss at 12 months (open 55% versus laparoscopic 47%, statistical significance not reported), resulting in a median BMI of 33 in both groups. In addition data were presented by the trial authors as median and range so care should be taken when interpreting the results (Table 36).
Quality of life and comorbidities
Data on QoL or comorbidities were not assessed. The median patient satisfaction score at 12 months was higher among the patients undergoing laparoscopic surgery [median score 2 (0–2) versus 1 (0–2), p = 0.006].
Complications and additional operative procedures
There were no conversions from laparoscopic to open surgery. Surgical time was longer with laparoscopy [median 2.1 hours (1.5–4.0) versus 1.45 hours (1.1–2.5), p < 0.002], but there was no statistically significant difference in LOS (median four days in both groups). Patients undergoing open surgery required more extra doses of analgesics on the first postoperative day [open median 2 (0–3), laparoscopic median 1 (0–2), p = 0.04], but not the second or third day. Wound problems such as seroma (accumulation of fluid), dehiscence (opening of wound) or infection were experienced by 43% of the open surgery group, whereas 6% of the laparoscopy group experienced wound infection and 6% experienced pulmonary atelectasis requiring physical therapy. One patient in each group developed a fistula at the gastric partition which required reoperation and prolonged hospital stay. Fewer laparoscopic patients had a pathologic scar at 12 months (five patients versus 12 patients, p = 0.002). Two patients (14%) with open surgery developed abdominal wall hernias (Table 39).
Summary
Similar excess weight loss occurred following open and laparoscopic vertical banded gastroplasty and LOS was not significantly different between the two groups. Operative time was statistically significantly shorter for the open surgery group but after surgery fewer laparoscopic patients had wound problems and at 12 months fewer had a pathological scar. Laparoscopic patients had a higher patient satisfaction score at 12 months. This small RCT has an uncertain risk of bias as many factors were not reported.
Open versus laparoscopic adjustable silicone gastric banding
One RCT compared open adjustable silicone gastric banding with laparoscopic adjustable silicone gastric banding. 132
Weight change
De Wit and colleagues132 demonstrated no significant difference in weight loss between the procedures 12 months after surgery (p = ns). However, both laparoscopic and open adjustable silicone gastric banding were associated with a significant reduction in weight compared with baseline (35 kg and 34.4 kg respectively, p < 0.05) (Table 36).
Quality of life and comorbidities
Data on QoL or comorbidities were not assessed.
Complications and additional operative procedures
Surgical complications and access port complications did not differ significantly between the two procedures, although patients undergoing the open procedure had higher proportions of incisional hernia complications compared with laparoscopy (12% versus 0%, p = ns). Similarly early postoperative complications differed little between open and laparoscopic adjustable silicone gastric banding, although there were greater proportions of cholecystectomy among those undergoing open procedures (20% versus 8%). Readmissions (15 among 7/24 open patients versus six among 5/25 laparoscopic surgical patients, p < 0.05) following open and laparoscopic surgery, respectively, and mean overall LOS in the first year (11.8 days versus 7.8 days, p < 0.05) were significantly higher in those undergoing open compared to laparoscopic procedures (Table 39).
Two (8%) patients were converted from laparoscopic to open procedure because of an inability to obtain a pneumoperitoneum. Laparoscopic surgery was rated as more difficult than open surgery (p < 0.05), and took longer to perform [150 minutes (SD 48) versus 76 minutes (SD 20), p < 0.05] (Table 39). Difficulty of surgery was rated on a subjective scale from 1 = easy to 10 = could not be performed or had to be converted, and therefore the finding should be treated with some caution.
Summary
Open and laparoscopic surgeries to fit adjustable silicone gastric banding led to similar degrees of significant weight loss. Operative time was statistically significantly shorter for the open surgery group. However, participants undergoing open procedures had a significantly longer hospital stay and were significantly more likely to be readmitted to hospital. Early postoperative complications were similar between the groups, but incisional hernia complications were experienced by 12% of patients who received the open procedure and by none of the laparoscopic surgical group. This study had a low risk of selection bias and a low risk of bias from incomplete weight loss data.
Summary of clinical effectiveness
Many of the included RCTs had an uncertain risk of bias because the reporting was unclear. Just five RCTs reported adequate allocation concealment and were, therefore, at low risk of selection bias. Most studies did not mention whether outcomes assessors were blinded to intervention assignments. The reporting of incomplete outcome data for weight loss, QoL or comorbidity was unclear for almost half of the studies. Other sources of bias included the use of block randomisation in non-blinded trials, making it possible to predict future assignments. The included cohort studies were of variable size and quality. Most study participants were women so it is uncertain how generalisable the results are to men. All the studies included in this review were conducted in countries other than the UK. It is difficult to determine how generalisable the results of the included studies are to the ethnically diverse population within the UK.
Clinical effectiveness of surgery versus non-surgical interventions
Three RCTs and three cohort studies contributed evidence on the comparison of surgical versus non-surgical interventions for obesity. All the studies reported that surgery results in greater weight loss than a non-surgical weight loss intervention even though they varied in the types of surgery undertaken, the non-surgical comparator, and the participants included. Two RCTs focused on participants at the lower side of the obesity continuum, one was judged to have a high risk of selection bias, and the other a low risk of selection bias, but at an uncertain risk of other sources of bias. These trials reported mean percentage excess weight loss at two years of 62.5% and 87.2% following surgery, but only 4.3% and 21.8% excess weight loss in participants in the non-surgical groups of these trials. The third RCT, judged to have an uncertain risk of bias, focused on people with morbid obesity, but again weight loss in men and women participants was greater one year following surgery (35 kg and 52 kg) than following diet (7 kg and 9 kg). Bias is inherently more likely within cohort studies than RCTs for a variety of reasons, but chiefly because there is a risk that confounding factors (both known and unknown) are distributed unevenly between the cohorts and the lack of randomisation provides an opportunity for selection bias to take place. The possible effect of these biases must therefore be kept in mind when interpreting the results of such studies. As noted above all the included cohort studies reported greater weight loss following surgical intervention than a non-surgical alternative. One of the three cohort studies, the large SOS study, has also reported the longest follow-up of all the included studies and therefore provides some evidence for the maintenance of the difference in weight loss for as long as 10 years.
Quality of life characteristics were reported by one of the RCTs and two of the cohort studies. The RCT provided evidence for an improvement in some aspects of QoL at two years in patients who had undergone surgery, whereas one of the cohort studies found that after 3.2 years there were no significant differences between the groups. In contrast the larger SOS cohort study reported that all HRQoL measures were improved at 10 years compared with baseline for the surgery group, but for the conventional group some had improved while others had worsened.
One of the RCTs focused on participants at the lower side of the obesity continuum who also had Type 2 diabetes. In this study, remission of Type 2 diabetes at two years was significantly higher in the surgery group than in the conventional therapy group and surgically treated participants were less likely to have metabolic syndrome. The other RCT focusing on participants at the lower end of the obesity continuum also reported a statistically significant reduction in the proportion of surgically treated participants with metabolic syndrome at two years. The SOS cohort study again provides evidence that improvements in comorbidities such as Type 2 diabetes and metabolic syndrome can be maintained at least for 10 years. Another weight-related comorbidity, hypertension, was improved in one of the RCTs at two years and in the SOS study at 10 years, but the difference was not statistically significant at these time points.
Two of the RCTs reported that there were adverse events associated with both surgical and non-surgical interventions and the SOS cohort study reported on complications and adverse events for the surgical group only, as well as overall mortality for both groups. The SOS study reported five deaths (0.25%) within 90 days of surgery in the surgical group in comparison with two deaths (0.10%) that occurred during the same period in the non-surgical group. During long-term follow-up (of mean duration 10.9 years) 5% of the surgical group died in comparison with 6.3% of the non-surgical group.
Clinical effectiveness of different surgical interventions
The clinical effectiveness of different surgical interventions was assessed by 20 RCTs which between them focused on nine different comparisons: six comparisons of different types of bariatric surgery and three comparisons of open and laparoscopic approaches to bariatric surgery. Among the six comparisons of different types of bariatric surgery there were three comparisons of procedures combining restrictive and malabsorption components with restrictive procedures (gastric bypass versus vertical banded gastroplasty; gastric bypass versus adjustable gastric band, and gastric bypass versus laparoscopic sleeve gastrectomy), two comparisons between restrictive procedures (vertical banded gastroplasty versus adjustable gastric band, and adjustable gastric band versus laparoscopic isolated sleeve gastrectomy), and one comparison between unbanded gastric bypass and banded gastric bypass.
Four comparisons included gastric bypass compared with either vertical banded gastroplasty (seven RCTs), banded gastric bypass (one RCT), adjustable gastric banding (one RCT), or laparoscopic sleeve gastrectomy (one RCT). On measures of weight change gastric bypass, which combines restrictive and malabsorption components, was superior to the purely restrictive procedures of vertical banded gastroplasty, and laparoscopic adjustable gastric banding. The comparison with laparoscopic sleeve gastrectomy was inconclusive. For people with a BMI over 50, banded gastric bypass was similar to non-banded gastric bypass.
The comparisons between restrictive procedures included three RCTs which contributed evidence on the comparison between vertical banded gastroplasty and adjustable gastric banding, and the results were inconclusive. All studies found greater initial weight loss following vertical banded gastroplasty, but one study found no statistically significant difference at two or three years follow-up, one study found that vertical banded gastroplasty patients regained weight, so that at three to five years follow-up weight loss was greater following adjustable gastric banding (statistical significance not reported), and one study found that per cent excess BMI loss was greater with vertical banded gastroplasty at the seven-year follow-up (statistical significance not reported). The final comparison of different types of bariatric surgery, laparoscopic adjustable gastric banding versus laparoscopic isolated sleeve gastrectomy (both restrictive procedures) was assessed by only one RCT that reported weight-related outcomes at one and three years. All the data were reported as median and range and at both time points the participants who had received isolated sleeve gastrectomy showed more improvement than participants who had received adjustable gastric banding.
The comparisons of open versus laparoscopic gastric bypass (four RCTs), open versus laparoscopic vertical banded gastroplasty (one RCT), and open versus laparoscopic adjustable silicone gastric banding (one RCT) all found that there were no significant differences in weight loss outcomes between the open and laparoscopic surgical approaches, both groups lost similar amounts of weight.
Only two RCTs comparing surgical procedures assessed QoL. One RCT reported that following surgery QoL was better in the gastric bypass group than in the vertical banded gastroplasty group on some items. The other RCT assessed people who had received either open or laparoscopic gastric bypass and found that there was no significant difference between the groups in QoL measures.
Five of the 20 RCTs assessing the clinical effectiveness of different surgical interventions reported on changes in comorbidities after surgery. In general comorbidities improved in all groups with no significant differences in improvements observed between different surgical interventions.
Reporting of adverse events, complications and operative variables varied greatly between studies and statistical comparisons between the groups were not often made. In general, adverse events and complications affected few participants. Fourteen of the 20 RCTs reported no deaths during or shortly after surgery and the remaining six RCTs reported very few deaths. Where deaths were reported separately for each trial arm, mortality ranged from 2% (one death within the first 30 postoperative days among 51 patients receiving open gastric bypass surgery) to 10% (two deaths among 20 patients receiving open Roux-en-Y gastric bypass; one on the fourth postoperative day and one after 13 months).
Two studies provided evidence that laparoscopic vertical banded gastroplasty surgery is quicker, and is associated with fewer early postoperative complications than laparoscopic gastric bypass surgery. However, approximately three years following open surgery to provide a vertical banded gastroplasty, conversions to an alternative bariatric procedure occurred more often than after open gastric bypass, but neither of the two studies reporting this comparison tested the outcome for statistical significance. Complications were generally similar for banded and unbanded gastric bypass apart from emesis and food intolerance, which were statistically significantly worse in the banded gastric bypass group. Laparoscopic gastric bypass was associated with a similar level of early complications and reoperations as laparoscopic adjustable gastric banding in the one RCT that compared these procedures. A further small RCT that compared laparoscopic gastric bypass with laparoscopic sleeve gastrectomy reported no intraoperative or postoperative complications in either group. Operative time was shorter for laparoscopic adjustable gastric banding than for laparoscopic vertical banded gastroplasty and hospital stay was also shorter than for laparoscopic or open vertical banded gastroplasty. However, there were statistically significantly more late complications following laparoscopic adjustable gastric banding than laparoscopic vertical banded gastroplasty in the trial that reported this comparison. Open vertical banded gastroplasty was associated with more infections than laparoscopic adjustable gastric banding. In the RCT that compared laparoscopic isolated sleeve gastrectomy with laparoscopic adjustable gastric banding there were more early postoperative complications with laparoscopic isolated sleeve gastrectomy, but late complications were higher in the laparoscopic adjustable gastric banding group. The comparisons of open and laparoscopic procedures in general favour the laparoscopic procedure for a number of operative characteristics, particularly hospital stay, and with fewer laparoscopic patients experiencing wound problems or incisional hernia complications.
Chapter 5 Assessment of cost-effectiveness
Introduction
The aim of this section is to assess the cost-effectiveness of multiple types of surgical treatments for adults with morbid obesity (i.e. with BMI > 40), compared with non-surgical treatments, as well as a comparison of surgical treatments to each other. The cost-effectiveness of surgical treatment of obese patients (i.e. with BMI more than 35, but less than 40) with significant comorbidities is also analysed. The definition of the obese population here is consistent with the definition in the NICE Guidelines9 and with the general criteria of eligibility for bariatric surgery, as used in the cost-effectiveness studies138–142 presented below. The obese population here is therefore defined according to narrower criteria than those used for clinical effectiveness (see Chapter 3, Inclusion criteria).
The following types of surgical intervention treatments were included:
-
open gastric bypass
-
laparoscopic gastric bypass
-
vertical banded gastroplasty
-
laparoscopic adjustable gastric banding
-
biliopancreatic diversion and duodenal switch.
Results
Results of the literature search
A total of 448 reports of studies on the economics of surgical treatments were identified from which 36 citations were retrieved as potentially eligible for inclusion and the full papers were obtained. Two systematic reviews51,143 of economic analyses of surgical interventions and five original economic evaluations138–142 that met the inclusion/exclusion criteria described in Chapter 3, Inclusion criteria were identified from the full reports (listed below). The reasons for excluding 29 studies after examination of the full papers can be seen in Appendix 17.
Included systematic reviews of cost-effectiveness of bariatric surgery
-
Relevant parts of Chapter 4 in the ‘Systematic review of the long-term effects and economic consequences of treatments for obesity and implications for health improvement’ by Avenell and colleagues. 51
-
‘Are bariatric surgical outcomes worth their cost? A systematic review’ by Salem and colleagues. 143
The two systematic reviews listed above were used as sources for economic evaluations published since searches were undertaken in 2001 for the previous review published in 2002. 15 The final search for economic evaluation studies in the systematic review by Avenell and colleagues51 does not include any reports published after 2001. The systematic review by Salem and colleagues143 identified only three publications that reported the cost-effectiveness of bariatric surgery as cost per QALY, including our previous 2002 systematic review and economic evaluation. 15 Only one of these three economic evaluation studies140 was published after 2001. This study is included in the list below of five newly identified original economic evaluations published after 2001. In addition to this study,140 four other original economic evaluations that met the inclusion/exclusion criteria were identified and appraised.
Original economic evaluations of bariatric surgeries included in the current review
-
Ackroyd R, Mouiel J, Chevallier JM, Daoud F. ‘Cost-effectiveness and budget impact of obesity surgery in patients with type-2 diabetes in three European countries’. 138
-
van Mastrigt GA, van Dielen FM, Severens JL, Voss GB, Greve JW. ‘One-year cost-effectiveness of surgical treatment of morbid obesity: vertical banded gastroplasty versus Lap-Band’. 139
-
Craig BM, Tseng DS. ‘Cost-effectiveness of gastric bypass for severe obesity’. 140
-
Jensen C, Flum DR. ‘The costs of nonsurgical and surgical weight loss interventions: is an ounce of prevention really worth a pound of cure?’. 141
-
Salem L, Devlin A, Sullivan SD, Flum DR. ‘Cost-effectiveness analysis of laparoscopic gastric bypass, adjustable gastric banding, and nonoperative weight loss interventions’. 142
Four of the identified studies were designed to estimate the cost-effectiveness of bariatric surgery in comparison with non-surgical treatment138,140–142 and one study, by van Mastrigt and colleagues139, conducted a head-to-head comparison of clinical and economic effectiveness of two surgical alternatives. The study by van Mastrigt and colleagues139 is an economic evaluation alongside a clinical trial conducted over a one-year time interval. In this study the utility values were directly obtained from the trial participants. The four other studies are based on a decision analytic model that extrapolated the time horizon beyond the duration of clinical trials used as a source of clinical effectiveness and transformed an intermediate outcome (a body-weight reduction) into the final outcome (QALY or LY). Three out of the four modelled economic evaluations140–142 have a lifetime horizon and one138 has a five-year horizon.
The studies differ with respect to: characteristics of the populations included in economic models (e.g. the baseline age, BMI and presence of comorbidities); perspectives of the evaluations (i.e. of a health-care system, a payer’s or a societal perspective); and, the source of clinical and epidemiological evidence. The study by van Mastrigt and colleagues139 has been undertaken from the societal perspective (the Netherlands). The only other study conducted from the societal (the USA) perspective is Jensen and Flum. 141 This and two other studies140–142 use the same published US clinical, epidemiological and economic data. 144 Only one study, by Ackroyd and colleagues,138 used UK data along with data from Germany and France. These issues are further elaborated in subsequent sections.
Description of the identified studies
Table 40 shows a list of surgical and non-surgical interventions from the identified studies and maps them across the list of surgical interventions included in the economic evaluation undertaken for this report.
| Study | Type of treatment strategies | ||||
|---|---|---|---|---|---|
| Non-surgical treatment (description) | Open gastric bypass (Open GBP) | Laparoscopic gastric bypass (LGBP) | Open vertical banded gastroplasty (VBG) | Laparoscopic adjustable gastric banding (LAGB) | |
| Ackroyd and colleagues138,a | Conventional treatment for obese Type 2 diabetes patientsb | X | X | ||
| van Mastrigt and colleagues139 | – | X | X | ||
| Craig and Tseng140 | No treatmentc | X | |||
| Jensen and Flum141 | Diet and exercise | X | |||
| Salem and colleagues142,a | Non-operative weight loss interventionsd | X | X | ||
Table 40 shows that none of the economic evaluations involved the whole range of treatment alternatives for obesity. None of the identified studies included biliopancreatic diversion and duodenal switch, so this type of bariatric surgery was excluded from further consideration. Two studies, Craig and Tseng140 and Jensen and Flum,141 compared open gastric bypass with non-surgical treatment, although the definitions of non-surgical treatment differ in these two studies. Two other studies, by Ackroyd and colleagues138 and Salem and colleagues,142 reported pair-wise comparisons of laparoscopic gastric bypass with a no-treatment strategy and laparoscopic adjustable gastric banding with a no-treatment strategy respectively. These studies differ with respect to the population included (only patients with Type 2 diabetes were included in Ackroyd and colleagues138) and the health-care systems where the intervention took place. Ackroyd and colleagues138 conducted economic evaluations using data from three European countries – the UK, Germany and France – whereas Salem and colleagues142 used clinical, epidemiological, cost and economic outcomes data from the USA. The only study that conducted a head-to-head comparison of two alternative surgical interventions was an economic evaluation alongside a clinical trial undertaken in a single Netherlands hospital. 139
The studies were summarised and critically appraised according to the methods described in Chapter 3, Quality assessment. The studies are characterised by large variations across the characteristics of the population, the interventions and the countries where the interventions took place so no formal quantitative systematic analysis of the results is possible. However, the strengths and weaknesses of the studies are presented in the Summary section of this chapter and the appraisal allowed us to make some judgements about the credibility of reported results and recommendations that the authors of identified studies had made.
Table 41 provides a summary of the characteristics of the five included published economic evaluations of surgical treatment alternatives for obesity (see Appendix 15 for full data extractions and critical appraisal of each study).
| Author | Ackroyd and colleagues138 | van Mastrigt and colleagues139 | Craig and Tseng140 | Jensen and Flum141 | Salem and colleagues142 |
|---|---|---|---|---|---|
| Publication year | 2006 | 2006 | 2002 | 2005 | 2008 |
| Country | UK, Germany and France | the Netherlands | USA | USA | USA |
| Currency base | 2005 British pound in UK analysis and 2005 Euro in German and French analysesa | The resources were first assessed in 1999 Netherlands guilders and then converted to eurosb | 2001 US dollars | 2004 US dollars | 2004 US dollars |
| Study type | CEA and CUA | CEA and CUA | CEA and CUA | CUA | CUA |
| Study perspective | The payers’ perspective (i.e. NHS in the case of UK) | A societal perspective | The payers’ perspective (i.e. the insurers’ + patients’ copayments) | A societal perspective | The payers’ perspective (i.e. the insurers’ + patients’ copayments) |
|
Study population (definition of obesity/eligibility for surgery) |
BMI > 35 and Type 2 diabetes. Eligible patients need to fail at least one prior year of medical treatment. The mean age of the target population is not reported | BMI > 40 or BMI between 35–40 and a significant comorbidity. VBG mean age 38.9 (SD = 8.53). LAGB mean age 37.2 (SD = 9.64) | BMI 40 to 50. Non-smoking males and females 35–55 years of age without a cardiovascular disease, who failed conservative therapies of dieting, exercise, behaviour therapy and pharmacotherapyc | The cohort of white female patients enter each arm of the model at the age of 18 with BMI of 33 or 35.d The patients in the surgical intervention arm undergo open GBP at the age of 40 and BMI ≥ 40 | BMI of 40 to 60. Males and females 35–55 years of age without any obesity-related comorbidity at the baseline |
| Surgical intervention(s) and the comparator treatment | LAGB vs conventional treatment and LGBP vs Conventional treatment | Head-to-head comparison of VBG with LAGB | Open GBP vs no treatment | Open GBP vs diet and exercise | LAGB vs no treatment and LGBP vs no treatment |
| The primary clinical treatment effects modelled/assessed | 1 kg/m2 of BMI reduction (or increase) and Type 2 diabetes prevalence | Reduction in % EWL, operative mortality | Operative mortality; rates of revision surgery and reversal surgery; % EWLe | Mortality rates from immediate complications; BMI reduction; | Operative mortality; % EWLe |
| Source of clinical evidence for the primary effect | For LAGB the data on BMI reduction and Type 2 diabetes prevalence were taken from Clegg and colleagues;15 NICE guidelines9 and 13 publications including non-randomised cohort studies and case series. For LGBP the data on BMI reduction and Type 2 diabetes prevalence were extracted from 11 publications. | The clinical data were collected from 100 patients (50 in each arm) enrolled in a RCT comparing clinical and cost-effectiveness of VBG and LAGB. The clinical outcomes are reported in van Dielen and colleagues147 | Primary source of clinical effectiveness data (BMI, mortality and complication rates) is a case series study of 608 morbidly obese patients followed up for 14 years with a 96.3% follow-up rate (Pories and colleagues148); Rates of reversal surgeries were taken from RCT of open GBP vs laparoscopic VBG by Hall and colleagues149 | BMI reduction and complication rates were taken from the SOS study89 346 surgical patients were matched with 346 non-surgical controls and followed up for eight years. For the comparator data on BMI reduction were taken from Heshka and colleagues.150 | Operative mortality was taken from the systematic literature review of LAGB by Chapman and colleagues.151 Estimates of the primary clinical end points (% EWL) were taken from the range of studies including cohort and case series studies. |
| For the comparator the BMI reduction data and Type 2 diabetes prevalence over three years were taken from the Swedish HTA systematic review and the US Clinical guidelines145,146 and extrapolated for the years 4 and 5 of the time horizon in the model. | 211 patients undergoing a diet and exercise commercial programme were matched with 212 controls undergoing a self-help programme and followed up for two years. | ||||
| Secondary treatment effects (e.g. safety of surgical procedure) | The rates of revision and reversal surgeries and complications that do not require surgery were not included on the outcome side of the cost-effectiveness calculations, but were included on the cost side. The operative- and obesity-specific and all courses mortality was implicitly assumed to be zero. | The differential operative mortality rates were recorded. | The differential non-surgical complications were not consistently included in the ICER (i.e. the associated disutility was omitted from the outcome side of the cost-effectiveness calculations) | It is not clear how immediate complications are defined and whether mortality associated with both revision and reversal surgeries was included in the LY estimate. It does not appear that the treatment of subsequent complications (e.g. cholecystectomy and abdominoplasty) undertaken within two to five years after surgery was included in the model | The differential non-surgical complications were not consistently included in the ICER (i.e. the associated disutility was omitted from the outcome side of the cost-effectiveness calculations) |
| Outcomes used in CEA (if applicable) | Incremental cost per BMI × year; incremental cost per Type 2 diabetes-free year | Incremental cost per 1% of extra weight loss – EWL | Incremental cost per life-year saved | Not applicable | Not applicable |
| Final outcomes (i.e. QALY or LY) | QALY | QALY | LY, QALY | QALY | QALY |
| Discounting (and values) | Costs and QALYs were discounted at 3.5%; outcomes used in CEA were not discounted | Not applicable, the duration of the RCT and economic evaluation was one year | Cost and outcomes are discounted at 3% | Discounting of costs or outcomes seems to have been conducted but the discounting rate(s) are not reported | Cost and outcomes are discounted at 3% |
The target population.
The studies presented in Table 41 are consistent with respect to the definition of the obese population for whom a surgical intervention is recommended according to NICE guidelines:9 patients with BMI ≥ 40 or with BMI between 35 and 40 and with a significant disease such as Type 2 diabetes or high blood pressure. At the same time the studies differ with respect to baseline characteristics of the target population such as age (ranging from 35 to 55 years old) and the presence or absence of comorbidities. Craig and Tseng140 and Salem and colleagues142 have assumed that the population of obese patients with BMI ≥ 40 have no comorbidities at baseline, which may not be a realistic assumption and would limit the generalisability of results. Likewise, the outcomes reported in Ackroyd and colleagues138 are only applicable to the population of obese patients with Type 2 diabetes. The outcomes reported in Jensen and Flum141 are applicable only to white female patients who were obese at the age of 18 with BMI ≥ 33 (or 35) (see Table 41, footnote d). The population enrolled in the study by van Mastrigt and colleagues139 appears to be the closest to the population typically presented in (European) clinical practice for bariatric surgery as it consists of both male and female patients with a mix of obesity-related comorbidities.
Sources of clinical evidence for weight reduction used in the modelled economic evaluations.
Four modelled economic evaluations138,140–142 used the primary clinical end point of reduction in BMI (or per cent excess weight loss converted into BMI values). In all four studies the BMI values were taken from the published evidence; however, it does not appear that a systematic literature search and evidence synthesis was conducted in these studies. The economic analysis reported in Craig and Tseng140 and Jensen and Flum141 was based on bariatric surgery outcomes obtained from a single published source of evidence (a case series study by Pories and colleagues148 and a case–control longitudinal study by Sjostrom and colleagues,89 respectively). The likelihood of a biased estimate of clinical outcomes is the highest in the case of a single and/or uncontrolled clinical study, which potentially affects validity of the estimate of the differential weight loss and generalisability of the results.
Primary and secondary clinical outcome(s) used in the modelled economic evaluations.
The short-term intervention period (which is defined differently across the studies) is also characterised by the likelihood of an operative mortality and possible immediate and subsequent complications, some of which may result in surgical revisions (see Assumptions of economic evaluations, this chapter). Differential operative mortality rates (including mortality in revision and/or reversal surgeries) are translated into the different life expectancy in the intervention and the comparator arms. Some patients also require reversal surgery (e.g. a band removal after laparoscopic adjustable gastric banding). The study by Jensen and Flum141 includes only immediate (unspecified) postsurgical complications and associated mortality. The studies by Ackroyd and colleagues,138 Craig and Tseng,140 and Salem and colleagues142 include a fairly complete list of both immediate and subsequent complications (e.g. cholecystectomy, abdominoplasty).
The study by Ackroyd and colleagues138 seems to have implicitly assumed a zero mortality rate (i.e. operative mortality, all-cause mortality and mortality associated with obesity-specific comorbidities, were all assumed to be zero) in all treatment options over the entire five years of the modelled time interval. It effectively implies that the differential operative mortality in the interventions (laparoscopic adjustable gastric banding and laparoscopic gastric bypass) and the comparator arms (non-surgical treatment) do not have an effect on the estimates of LYs and QALYs. The same also applies to the differential rates of postsurgical complications, including revision and reversal surgeries. These implicit assumptions do not seem to be reasonable and may potentially affect the validity of the estimate of the LYs gained and the generalisability of the results.
All modelled economic evaluations applied a discounting rate to both costs and outcomes although Jensen and Flum141 did not specify the value of the discounting rate.
Critical appraisal of economic evaluations
Table 42 outlines the approaches used in the identified cost-effectiveness studies. For completeness, the only economic evaluation that was not based on a decision analytic model139 is also included.
| Author | Ackroyd and colleagues138 | van Mastrigt and colleagues139 | Craig and Tseng140 | Jensen and Flum141 | Salem and colleagues142 |
|---|---|---|---|---|---|
| New model | Yes | Not applicable | Yes | Yes | Adapted from Craig and Tseng |
| Type of the economic evaluation | Deterministic decision analytic model | Economic evaluation alongside a clinical trial | Deterministic decision analytic model (a decision tree) | Deterministic decision analytic model (a decision tree) | Deterministic decision analytic model (a decision tree) |
| Time horizon/duration of the study | Five years | One year | Lifetime (unspecified) | Lifetime (unspecified) | Lifetime (unspecified) |
| Baseline cohort | At the baseline in both arms of the model 100% of patients have Type 2 diabetes and BMI > 35 | Not applicable | Cost-effectiveness analysis seems to have been conducted separately for cohorts of men and women in the different age categories (between 35 and 55 years with 10-year increments) and different baseline BMI values (between 40 and 50 with an increment of 5 units) | Open GBP group: white women; baseline age 18 years; surgery at the age of 40 and BMI of ≥ 40. Diet and exercise group: white women; age 18 years; baseline BMI of 33 (or 35)b | A set of ICER estimates comparing LGBP with no-treatment and LAGB with no-treatment have been conducted separately for cohorts of men and women: aged 35 with BMI = 40; aged 45 with BMI = 50; aged 55 with BMI = 60 |
| Assumption, main clinical outcomes and how the intermediate outcomes are translated into the final outcomes | Outcomes of bariatric surgery are assessed in terms of weight loss and Type 2 diabetes remission. The probability of developing other obesity-related comorbidities and corresponding changes in life expectancy are implicitly assumed to be the same as in the non-surgical treatment arm. Operative, all cause and comorbidity-related mortality rates are implicitly assumed to be zero. In each year in each arm of the model the Type 2 diabetes outcome is independently assessed as a change from the baseline in proportion of patients free of Type 2 diabetes. This is called an ‘annual marginal Type 2 diabetes-free-year gained at a particular year’. | In this non-modelled economic evaluation the EQ-5Dc utility values were collected from each surviving patient at the baseline, and at 3, 6 and 12 months. To obtain a QALY for each patient the EQ-5D scores were multiplied by the duration of time to which these scores related. The mean QALY values for each of the treatment alternatives are used in the ICER. The direct and indirect medical cost data were collected from the observational study undertaken to estimate the cost of surgeries, the hospital’s billing system, and patients’ diaries. | In the no-treatment arm of the model it was assumed that patients do not lose or gain weight, i.e. they remain at the baseline BMI. Life expectancy depends on: (1) BMI value (reduced as a result of a successful surgery and stabilised at five years after surgery, or reversed to the baseline value as a result of a reversal surgery); (2) gender; and (3) the age at which the surgery was undertaken. Life expectancy was adjusted for the estimated operative mortality. Utility values (also differentiated by BMI, gender, and age) are applied to the estimated LYs spent with the eventual BMI to obtain QALYs. | Life expectancy depends on the BMI, which increases with age, following a trajectory of the obese population (at the rate observed in general USA population in the 95th percentile for weight). In the base case this rate is applied to all surviving patients in each branch of the decision tree. However, the BMI reduction obtained as a result of the GBP (at the age of 40) or a diet and exercise programme (as a result of a one- year programme undertaken at the age of 18) is retained for life. As a result the BMI in such patients, although increasing at the above rate, is always reduced by the incremental BMI value observed after the intervention. | In the no-treatment arm of the model it was assumed that patients do not lose or gain weight, i.e. they remain at the baseline BMI. Life expectancy depends on: (1) BMI value (reduced as result of a successful surgery and stabilised at three years after surgery, or reversed to the baseline value as a result of a reversal surgery); (2) gender; and (3) the age at which the surgery was undertaken. Life expectancy was adjusted for the estimated operative mortality. Utility values (also differentiated by BMI, gender and age) are applied to the estimated LYs spent with the eventual BMI to obtain QALYs. |
| The cumulative Type 2 diabetes-free years are calculated by aggregating the proportion of patients free from Type 2 diabetes in each year over 5 years.a Utility weights are derived from the linear combination of BMI values and the Type 2 diabetes status. QALYs are obtained by aggregating the estimated utility values (according to the BMI and % of Type 2 diabetes-free patients observed in each year) over five years. | The productivity loss was estimated using the friction cost method (not elaborated). The total cost for each patient was calculated as direct and indirect medical cost and the mean total costs for each of the treatment alternatives are used in the ICER. | The arbitrary assigned utility values are applied to the period of time spent in the hospital and in recovering. It was also assumed that the patients who underwent the reversal surgery have ‘never [psychologically] recovered completely’. A 50% reduction in utility weights was applied to these patients for the rest of their lives. |
Utility values (as a function of BMI) are taken from the published literature. 152 Utility values are assigned according to the BMI observed in each year to obtain QALYs. |
The values are taken directly from the study by Craig and Tseng, 2002.140 | |
| Structure of the model | Not reported. It appears that the cost and effectiveness parameters are assigned to each year independently and then aggregated over five years producing either years free from Type 2 diabetes or QALYs. The cost data were collected from the published literature and expert opinion and assigned to the first year (intervention). | Not applicable | The open GBP arm of the decision tree model assumes four surgery outcomes that occur in the first instance: successful surgery, revision surgery, reversal surgery and death. Revision surgery and reversal surgery are in turn associated with probability of a postsurgical death, while the former may be followed by a subsequent reversal surgery, which is also associated with the probability of death. It is implicitly assumed that the initial and subsequent interventions take place within five years after which the reduced postsurgical BMI is either stabilised or reversed to the baseline value in the unsuccessful surviving patients. | The open GBP arm of the decision tree model assumes two outcomes of the intervention: surgery with immediate complications (undefined), and surgery without immediate complications. Both outcomes are associated with probability of death. The surviving patients may have a reduced BMI or remain with their initial BMI. The diet and exercise arm of the decision tree model assumes that no patient experiences complications associated with death. The surviving patients from the control arm follow the pathway corresponding to the no-complication branch in the open GBP arm of the decision tree. | Both surgery intervention arms of the model assume two outcomes that occur in the first instance: successful surgery, and death. In the LGBP arm the surviving patients may need to undergo a revision surgery, which can be successful or can result in the death of a patient. In the LAGB arm the surviving patients may need to undergo a reversal surgery (band removal), which is not associated with the risk of death. All surviving patients in both arms (except those who underwent a reversal surgery) achieve weight loss specific to the type of surgery. |
| Parameters used in sensitivity/scenario analysis (if any) | Simultaneously BMI reduction; % patients free of Type 2 diabetes; (by implication the utility weights have also changed). | Only cost estimates were subjected to the set of one-way sensitivity analyses. These were: operation room personnel cost per minute and unit price of an inpatient day. | % of excess weight lost; reimbursement rate; lifetime medical cost; life expectancy (it was assumed that life expectancy is not affected by the weight loss – i.e. the estimate that corresponds to the baseline weight were apparently used); regression coefficients in the (unreported) multiple regression equation for the utility values were decreased by 25%; operative mortality; complication rates. In the two-way sensitivity analysis the discount rate was increased from 3% to 5% while the lifetime medical cost was assumed to be zero. Another two-way sensitivity analysis varied the estimate of weight loss and the medical cost adjusted for the different reimbursement rates. | A series of one-way sensitivity analyses were performed (the list of parameters tested was not provided). The results proved to be sensitive to the estimated cost of complications (the range tested in the sensitivity analysis was not reported) and the discount rate (neither the value nor the range were reported). | % of excess weight lost; cost of the surgical procedure; number of times a band adjustment was required in the LAGB arm; rates of abdominoplasty; rates of cholecystectomy; operative mortality; rates of revision surgery; rates of reversal surgery in the LAGB arm; a two-way sensitivity analysis was conducted where clinical effect (% EWL) was varied simultaneously in both arms of the models comparing LAGB with no treatment and LGBP with no treatment. |
| Scenario analysis | The simultaneous reduction in both effectiveness estimates by 20% is called a ‘worst case scenario’, which is in fact a two-way sensitivity analysis. Both the weight loss (in BMI) and decreased Type 2 diabetes prevalence were reduced by 20% (which is equivalent to assigning a zero benefit in terms of Type 2 diabetes to a non-surgical treatment arm). Cost estimates seem to have been excluded from the scenario/sensitivity analysis. | The base-case analysis was conducted from the societal perspective. An alternative perspective (presumably that of the Netherlands health-care system) was undertaken when non-medical costs (paid and unpaid help + productivity change) were excluded and the sensitivity of the outcomes to the change of the perspective in the economic evaluation was tested. | The total cost incurred by the payer(s) (the third party + patient’s contributions?) was reduced by the median reimbursement rate, which is effectively an equivalent to the change of the perspective of economic evaluation from the unspecified payer’s to that of the individually insured patient (who contributes copayments to the total cost). | Best case scenario: patients remained at the exact BMI that they had achieved at the end of the follow-up. Worst case scenario: all weight lost was regained within three years, and the weight gain trajectory of the upper 4.4% was then followed. | None reported |
The economic evaluation alongside a clinical trial reported by van Mastrigt and colleagues139 and the deterministic models reported in the other studies138,140–142 are two different methods of assessing the cost-effectiveness of bariatric surgery, and therefore cannot be directly compared across the whole range of criteria used for critical appraisal of decision analytic models. 77 Nevertheless, as reported below, some selected criteria can be used across the entire range of the identified economic evaluations.
Assumptions of economic evaluations
Time horizon
The time horizon of the economic evaluation in van Mastrigt and colleagues139 is only one year. The authors have acknowledged the short-term horizon as one of the limitations of the study. In particular, the two types of bariatric surgery (laparoscopic adjustable gastric banding and vertical banded gastroplasty) compared in the study are characterised by the differential speed at which patients lose weight during the first 12 months. This is because the laparoscopic adjustable gastric banding patients need to undertake a few band adjustments in the first year following surgery, therefore losing weight in a more gradual fashion. The authors suggested that it is reasonable to expect that the patients in the laparoscopic adjustable gastric banding arm will continue to lose weight in the following postoperative years (up to five years), while the weight loss trend in the vertical banded gastroplasty arm will reach a plateau or even reverse after the first year. 126
The five-year time interval, as opposed to one year, was recommended in Clegg and colleagues15 as appropriate for assessing the (short-term) effectiveness of a surgical intervention. This statement was used as a rationale for selecting a five-year time horizon in the model reported by Ackroyd and colleagues. 138 However, the long-term consequences of weight loss may extend beyond the five-year time interval, and result in reduced rates of lifetime mortality and morbidity. 153 Therefore, the lifetime horizon in the models reported in Craig and Tseng,140 Jensen and Flum141 and Salem and colleagues142 is more appropriate for assessing the long-term benefits of bariatric surgery. However, as explained below, these models differ with respect to assumptions about the short-term consequences of bariatric surgery.
Baseline cohort
Van Mastrigt and colleagues139 reported the baseline characteristics (gender, age, BMI and comorbidities) of the population enrolled in the clinical trial that provided evidence for the economic evaluation of open vertical banded gastroplasty as compared with laparoscopic adjustable gastric banding. Although the population is reasonably well matched across the arms with respect to most of the clinical parameters, there are differences (possibly statistically significant) in relation to the proportion of people in paid employment and (conversely) on disability benefits. In particular, the number of patients claiming disability benefits at baseline was four times higher in the open vertical banded gastroplasty than in the laparoscopic adjustable gastric banding arm. There appears to be a statistically significant difference in the baseline utility values in favour of the laparoscopic adjustable gastric banding arm that may reflect the difference in the level of disability observed at the baseline.
The clinical effectiveness data in the two arms of the model presented in Jensen and Flum141 were collected from populations of different ages and from different countries. 89,150 It is not clear whether the data for the open gastric bypass arm of the model came from the subgroup of the open GBP patients or from patients who underwent any type of bariatric surgery. 89 The authors acknowledged that the strong assumption of the model is that 18-year-old women with BMI > 33 (or 35) (see Table 41, footnote d) are the same individuals who continue gaining weight until they reach BMI > 40 at the age of 40, at which point they undergo open GBP.
In the study by Craig and Tseng140 the baseline cohort is described as non-smoking adults without a CVD, drug addiction or major psychological disorder and who failed conservative therapies consisting of dieting, exercise, behaviour therapy and pharmacotherapy. The age of the patients is said to be between 35 and 55 years and BMI > 40 and < 50. However, the clinical evidence for the open gastric bypass arm was obtained from a single case series study involving 608 obese patients with BMI ≥ 40 or BMI ≥ 35 with comorbidities such as diabetes, arthritis or cardiopulmonary failure. 148 The age of the patients in this study ranged from 14 to 64 (mean age at the time of surgery was 37.3 years). This inconsistency between the definition of the target population for whom bariatric surgery is typically recommended and characteristics of the population used as a source of clinical evidence is likely to undermine the internal validity of the results of the study.
Both Craig and Tseng140 and Salem and colleagues142 assumed that patients in the non-surgical treatment arm retain the baseline weight for life. The same assumption, beginning from the second year, was also made in the model reported in Ackroyd and colleagues. 138 This may not be a realistic assumption because patients in the non-treatment arm are likely to continue gaining weight during their lifetime, as assumed in the model reported by Jensen and Flum. 141 The assumption of zero weight gain over the modelled time interval in patients in the non-surgical treatment arm is likely to bias the cost-effectiveness estimates although the direction of the potential bias is uncertain.
Assumptions about the short-term and long-term consequences of surgical interventions
The immediate consequences of surgical interventions are associated with the risk of operative death and complications that may occur during the postsurgery recovery such as deep venous thrombosis and wound infection, which do not typically require a surgical intervention. Other complications such as staple-line disruption or dehiscence may require a revision or even a reversal surgery. Reversal surgery is also required when patients cannot restrict their diets sufficiently following surgery and develop intractable dumping syndrome. In addition, nearly a quarter of patients require treatment for incisional hernia within two years after hospital discharge. Some patients require treatment for cholelithiasis two years after discharge and abdominoplasty five years after discharge. 140
Ackroyd and colleagues138 do not model the differential rates of postsurgical complications for laparoscopic adjustable gastric banding, open gastric bypass and non-surgical treatment (where they are, by definition, zero). However, the differential use of resources is included in the cost side of the cost-effectiveness estimate. The decision analytic models reported by Jensen and Flum,141 Salem and colleagues,142 and Craig and Tseng140 all include differential probabilities associated with operative mortality and complications, especially those that require surgical interventions and are associated with the risk of death. Jensen and Flum141 only include immediate (unspecified) complications while Salem and colleagues142 and Craig and Tseng142 model postoperative complications over three-year and five-year time intervals, respectively. In these studies the operative mortality is factored into calculations of LY estimates.
The postoperative complications in surviving patients are likely to result in a temporary reduction in QoL. The study by Craig and Tseng was the only one that attributed disutility values to patients who experienced postoperative complications, but only to those complications that required a surgical intervention (see section on Translation of short-term outcomes into final outcomes, this chapter). Other modelled economic evaluations do not fully incorporate the differential rate of postoperative complications in surviving patients.
The long-term outcomes of bariatric surgery include the reduced probability of developing an obesity-related disease. In particular, remission of Type 2 diabetes is frequently observed in obese patients who successfully underwent bariatric surgery. In Ackroyd and colleagues,138 which includes only patients with Type 2 diabetes at baseline, the clinical effectiveness data for each of the five years appear to have been extracted from the various studies with different cut-off points and different characteristics of the obese population. It appears that the implicit assumption of the model is that for each patient the probability of Type 2 diabetes remission in each year does not depend on the Type 2 diabetes status in the previous year or on the BMI. This assumption may not be reasonable.
Jensen and Flum,141 Salem and colleagues142 and Craig and Tseng140 do not explicitly model the differential probabilities of developing an obesity-related disease. However, the gender- and age-specific life expectancy estimates used in these studies are taken from the published model by Thompson and colleagues144 that includes the lifetime risks of hypertension, hypercholesterolemia, Type 2 diabetes, coronary heart disease (CHD) and stroke in relation to BMI.
Translation of short-term outcomes into final outcomes
Typically, to obtain final outcomes such as QALYs the duration of time that a patient spends in a particular health state is ‘weighted’ using a utility estimate (typically ranging from 0 = death to 1 = perfect health) that corresponds to this health state. This approach was used in assessing the cost-effectiveness of pharmacotherapies for obesity treatment as compared to non-pharmaceutical treatment options. 154
The modelled economic evaluations of bariatric surgery do not explicitly define health states in terms of disease progression but either derive the utility estimates from the regression analysis that estimated the relationship between utility [measured in European Quality Of Life-5 Dimensions (EQ-5D) values] and BMI values while accounting for the Type 2 diabetes status,138 or used the published utility estimates for the general population,155 and for the overweight population. 152 The utility weights are then applied to the cohort of surviving obese patients as they progress through the modelled time interval.
The second component (life expectancy) that is required to calculate QALYs in the modelled economic evaluations with a lifetime horizon140–142 was obtained from a single published source,144 which reports life expectancy for the US population categorised by age and BMI.
Estimation of utility values
There are variations between the studies in the methods adopted for estimating utility values.
In van Mastrigt and colleagues139 the EQ-5D utility values were collected from each surviving patient at the baseline, and at three, six and 12 months. To obtain a QALY for each patient the EQ-5D scores were multiplied by the duration of time (as a proportion of the 12-month time interval) to which these scores related. The mean QALY values for each of the treatment alternatives were used in the denominator of the ICER.
Ackroyd and colleagues138 utility values were estimated using the empirical data on the representative sample of the UK population (n = 13,500), that included both obese and non-obese individuals. 156 The data were used to estimate a linear relationship between the EQ-5D values and BMI values. The authors do not justify the linearity assumption in their estimate of the relationship between the observed utility and BMI values. As is evident from Figure 1 in Ackroyd and colleagues,138 while this assumption may be true in the general UK population, in relation to the obese population with BMI > 35, a more complex form of regression equation may be more appropriate.
It appears that at first the coefficients in the linear regression of utility values on BMI values were estimated separately for Type 2 diabetes and non-Type 2 diabetes subgroups. The authors then assumed that there was no statistically significant difference in the estimated regression coefficients (slopes) in these two equations. Therefore the alternative (not reported) regression equations were used to estimate utility values in both subgroups. It seems that the modified regression equations have different constant terms (from the original equations), but the same slope equal to the weighted average of the slopes in regression equations for two separate subgroups. This is not a correct way of deriving utility estimates that may vary with respect to both BMI and Type 2 diabetes. A multiple regression of utility values on BMI values and Type 2 diabetes status and an interaction term (BMI × Type 2 diabetes) would be more appropriate.
The QALY outcomes in the study by Ackroyd and colleagues138 were obtained by combining the utility estimates for the mean BMI reduction observed in any particular year in Type 2 diabetes and non-Type 2 diabetes patients and then aggregating the calculated values over the five-year time interval.
Craig and Tseng140 do not report clearly the method used for obtaining utility values for the specified cohorts of men and women in the different age categories and baseline BMI values. From their reference it can be deduced that utility values might have been elicited using the published algorithm which employed data from the 1997 USA National Health Interview Survey. 155 The population-based mean values describing the Activity Limitations and Perceived Health Status were then interpreted as single attribute scores of a two-dimensional generic QoL instrument. A modelling technique was used to obtain the missing multiple attribute scores (e.g. for the combination of Activity Limitations and Perceived Health Status values). The resulting utility values are assumed to reflect HRQoL in the US general population. These values were not available for the population categorised by age, gender and BMI, which limited the possibility of using the estimates of life expectancy for the general population categorised by gender, age and BMI values. 144
It is not clear whether Craig and Tseng140 fully replicated the complex modelled calculations reported in Erickson and colleagues155 with respect to the population data stratified by age, gender and BMI. It is possible that some methodological shortcomings were overlooked in the process. For example, Erickson and colleagues estimated that in the US general population of 35–40 years old the utility value is 0.89. According to Craig and Tseng,140 the overweight 35-year-old men and women (i.e. with BMI of 25) have utility values of 0.93 and 0.91 respectively. It then follows that the overweight population in this age group has a higher HRQoL than the general US population. This contradicts the authors’ statement that their findings indicate that there is a negative relation between HRQoL and BMI.
Nevertheless, the newly estimated utility values were then applied to the estimated age/gender/BMI-specific life expectancy144 to obtain QALYs. The shortcoming of this approach is that first, the utility weights were not obtained using one of the conventional techniques for eliciting population-based health preferences (standard gamble or time trade-off) and second, that the utility weights were not elicited from the obese population, whose health-related preferences may be different from those of the general population.
The study by Craig and Tseng140 was the only one among the identified modelled economic evaluations that attempted to incorporate the differential rates of surgical complications on both the cost and the effectiveness sides of the ICER. It was reasonably assumed that there is a reduction in QoL (disutility) associated with postsurgical complications. In the absence of published evidence, Craig and Tseng140 assigned some arbitrary utility values to the period of time spent in hospital and in postsurgery recovery. It was implicitly assumed that non-surgical complications are not associated with a reduction in QoL. For the period of a hospital admission the corresponding age/gender/BMI-specific utility value was reduced by 200% (assuming that being in hospital is equivalent to a health state which is significantly ‘worse than death’). The utility value associated with the recovery time was 50% of the applicable utility value. The utility weights which apply to the remaining years of life in patients who underwent a reversal surgery were also reduced by 50% (it is assumed that patients never recovered completely from reversal surgery because of its psychological effects). No justification for the choice of these values was provided.
Salem and colleagues142 replicated the method of converting the intermediate clinical outcomes (weight reduction) into QALYs introduced by Craig and Tseng140 and used the utility values from their study. Therefore the methodological shortcomings that characterise the study by Craig and Tseng140 also apply to the study by Salem and colleagues. 142
In both studies by Craig and Tseng140 and by Salem and colleagues142 the gender-specific utility weights change over time as the age of the cohort increases. However, utility weights do not change with respect to the BMI value that remained fixed at the baseline level in the non-surgical treatment arm, and in the surgery arm, at the level achieved when the postsurgical interventions (e.g. band adjustments, revision and reversal surgeries) are completed.
In contrast, the study by Jensen and Flum141 does not make an assumption about the BMI values remaining unchanged during the patients’ lifetime. The trajectory of weight increase was estimated from the data on the BMI distribution in the US white female population stratified by age. 157 In the base-case scenario BMI values increase from one year to another at the rate observed in the general USA population in the 95.6th percentile for weight (a cut-off point for BMI > 40, which corresponds to 4.4% of the population at age 40). In the base case this rate is applied to all surviving patients in each branch of the decision tree. However, the BMI reduction obtained as a result of the open GBP or a diet and exercise programme is retained for life. As a result, the BMI in such patients, although increasing at the above rate, is always reduced by the incremental BMI value observed after the intervention. Utility values used in this study were obtained from the study by Hakim and colleagues,152 who estimated a utility gain associated with each unit of BMI lost. The utility values were then combined with life expectancy data. 144 QALYs gained in each arm of the model are totalled each year. The authors commented that this yearly calculation, rather than assigning a single estimate of the life expectancy based on the BMI observed at the end of the intervention period, is necessary because the interventions take place at different times and BMI is assumed to be increasing over time. 141
Life expectancy and lifetime medical cost estimates
As was mentioned before, all modelled economic evaluations with the lifetime horizon140–142 applied utility values to the life expectancy estimates for the US population categorised by age, gender and BMI. 144 Thompson and colleagues144 reported both the life expectancy estimates and the lifetime medical cost estimates that were also used in all modelled economic evaluations. The estimates are based on the USA Third National Health and Nutrition Examination Survey (1988–94) that was provided separately for men and women categorised by age groups from 35 to 64 years in 10-year increments. However, Thompson and colleagues144 report the life expectancy estimates only up to BMI of 37.5, which is below the range of BMI values assessed in the modelled economic evaluations.
Craig and Tseng140 and Salem and colleagues142 applied what they described as ‘a simple linear approximation’ to obtain life expectancy for the BMI values beyond the range reported in Thompson and colleagues. 144 Although no further details were provided, it appears that the method was insufficient to obtain reliable estimates of life expectancy. For example, Thompson and colleagues144 reported life expectancy of men aged 59.5 years (midpoint in the age group of 55–64 years) with BMI of 37.5 to be 18.3 years. It is reasonable to assume that the life expectancy of men aged 55 with BMI of 37.5 is likely to be higher than this.
According to the calculations by Craig and Tseng,140 life expectancy of 55 year old men with BMI of 40 from the ‘no treatment’ arm is 16.15 years. This implies that the additional weight of 2.5 BMI is associated with the loss of at least 2.15 years of life. According to Thompson and colleagues144 for men in the 55–64-year age group the additional weight gain of five BMI units (from 32.5 to 37.5 kg/m2) is associated with the loss of just 0.5 years of life (from 18.8 to 18.3 years). Although it is possible that the lesser increments in weight gain when applied to the higher BMI values are associated with the accelerated loss of years of life, the difference in the estimates of additional LYs lost as the result of obesity is too large to be plausible and is more likely to relate to a deficiency in the methods used by Craig and Tseng140 to extrapolate life expectancy values to the higher BMI categories. It is therefore likely that the study by Craig and Tseng140 has produced biased estimates of the final outcomes.
Salem and colleagues142 do not report the estimated life expectancy values obtained by method of ‘a simple linear approximation’, so it is not possible to assess their validity.
Jensen and Flum141 also used a ‘linear approximation’ to obtain life expectancy for each BMI value not reported in Thompson and colleagues. 144 The linear regression equation that relates the remaining years of life to the BMI value is provided. It appears that only a subset of the data reported in Thompson and colleagues144 (i.e. the life expectancy data for women in the 45–54-year-old category) was used in the regression. How accurate the linear fit is in relation to other subgroups of the female population is not clear.
The final outcomes (LYs and QALYs) reported in the identified economic evaluations are presented in Tables 45 to 47 in the section on Results reported in the identified economic evaluations of bariatric surgeries in this chapter.
Structure of the models
The structure of the decision tree models reported in the studies by Craig and Tseng,140 Jensen and Flum141 and Salem and colleagues142 are presented in a graphical format. The study by Ackroyd and colleagues138 does not explicitly present the structure of their deterministic model.
Craig and Tseng140 have assumed that in the first instance four alternative outcomes of open gastric bypass can occur simultaneously: a successful surgery, a revision surgery, a reversal surgery and death. Revision surgery and reversal surgery are in turn associated with the probability of a postsurgical death, while the former may be followed by a subsequent reversal surgery, which is also associated with the probability of death. Although it may be reasonable to assume that in some patients revision surgery may be undertaken immediately to correct the complications arising in the course of the initial surgery, other surgical interventions (e.g. abdominoplasty) may occur over a period of three to five years. It is not clear how these later surgeries are incorporated into the model. Also, the decision to undertake a reversal surgery may be separated in time from the initial surgery. The modelling assumptions in Craig and Tseng140 may not correspond to current clinical practice.
The structure of the model presented in Salem and colleagues142 seemed to be an improvement in comparison to the structure of the model presented in Craig and Tseng. 140 Salem and colleagues142 have assumed that the immediate outcome of bariatric surgery is either survival or death, therefore the probabilities of revision or reversal surgeries apply only to the surviving patients.
The decision tree model reported in Jensen and Flum141 has the following options: ‘Intervention with immediate complications’; ‘Intervention without immediate complications’; ‘Death’; ‘Alive with reduced BMI’; and ‘Alive with baseline BMI’. The probability values associated with each outcome are not reported. No details on the types of immediate complications are provided. It is reasonably assumed in the diet and exercise arm of the decision tree that no patient experiences complications associated with death. The surviving patients in both arms of the model may have a reduced BMI or remain with their initial BMI.
The shortcoming of the model is the exclusion of non-immediate complications, which among other things, rules out the probability of revision surgeries that occur later in time and are also associated with the risk of death. Therefore the modelling assumptions in Jensen and Flum141 may not correspond to current clinical practice.
Estimation of costs within economic evaluations
Cost of bariatric surgeries
A comprehensive itemised list of health-care resources used and the corresponding unit costs were not provided in the identified studies on economic evaluation of bariatric surgery. The most detailed account of health-care resources used in laparoscopic gastric bypass and laparoscopic adjustable gastric banding is reported in Ackroyd and colleagues. 138 It seems that for each type of surgical intervention the range of resource items was identified, checked with experts and multiplied by the corresponding unit costs. However, the list of resource components in natural units does not include the itemised cost of complications. It is not clear how the cost of postsurgical complications was estimated.
Ackroyd and colleagues138 employed different methods for producing the cost estimates in relation to three European countries, which makes the comparison of cost data across these countries problematic. Therefore, only the UK cost data as reported in Ackroyd and colleagues138 are included in this section.
Van Mastrigt and colleagues139 estimated resources used in laparoscopic adjustable gastric banding and open vertical banded gastroplasty in natural units by conducting an observational study of 10 surgical procedures of both types of surgery. Other hospital costs were obtained from the hospital’s billing system. Health-resource items used outside the hospital (e.g. medications used during the follow-up) were obtained from the patients’ cost-diaries. The cost of each of the postsurgical complications was not reported. However, the aggregated mean cost of rehospitalisations is provided and is likely to relate to the number and seriousness of postsurgical complications associated with each surgery.
Table 43 summarises the cost data in terms of the natural units and the corresponding unit costs because this is a conventional approach to reporting cost data. Cost data by unit costs for the selected cost items are reported in Ackroyd and colleagues138 and in van Mastrigt and colleagues139 along with other cost data that are reported in more aggregated cost categories. These are also included for completeness.
| Cost components | Type of health-care resources by the type of surgery | Mean number of units (source) | Unit cost (source) | Aggregated costs: laparoscopic gastric bypass (source) | Aggregated costs: laparoscopic adjustable gastric banding (source) | Aggregated costs: vertical banded gastroplasty (source) |
|---|---|---|---|---|---|---|
| Preoperative evaluation | n/a | n/a | n/a | £610138 | £610138 | n/a |
| Diagnostic procedures | n/a | n/a | n/a | £187138 | £492138 | n/a |
| Hospital stay for the initial surgery | Bed use (LGBP) | LOS = 4.88138 | Cost per day = £235138 | 235 × 4.88 = £1147138 | ||
| Bed use (LAGB) | LOS = 5138 | Cost per day = £241138 | 241 × 5 = £1205138 | |||
| Bed use (LAGB) | LOS = 5.56a,139 | Cost per day = €332139 (LAGB and VBG) | 332 × 5.56 = €1846 | |||
| Bed use (VBG) | LOS = 6.78a,139 | €2251139 | ||||
| Operating room costs | Hours (LGBP) | 3.84138 | Operating theatre personnel cost per minute was not reported | n/a | n/a | n/a |
| Hours (LAGB) | 1.9138 | |||||
| Hours (LAGB) | 3.26139 | Operating theatre personnel cost per minute = €2.96139 (LAGB and VBG) | €579 | n/a | ||
| Hours (VBG) | 2.50139 | €444 | ||||
| Operating room overheads | n/a | n/a | n/a | £187138 | £492138; €87139 | €87139 |
| Surgery specific equipment | Implants (LGBP) | 1138 | £2591138 | Total cost of surgery-specific equipment and materials is not reported by Ackroyd and colleagues138 | Total cost of surgery-specific equipment and materials is not reported by Ackroyd and colleagues138 | n/a |
| Implants (LAGB) | 1138 | £1175138 | ||||
| Surgery specific materials (unspecified)b | n/a | n/a | n/a | n/a | €2143139 | €691139 |
| Subtotal: cost of initial surgery | n/a | n/a | n/a | n/a | €3861139 | €1676139 |
| Subtotal: cost of initial hospitalisationc | £4456138 | £3315138; €5954139 | €5258139 | |||
| Cost of unspecified complications | n/a | n/a | n/a | £45138 | £296138 | |
| Cost of rehospitalisations | n/a | n/a | n/a | n/a | €724139 | €599139 |
| Cost of follow-up | n/a | n/a | n/a | £312138 | £439138; €1479139 | €1426139 |
| Total health-care (medical) cost of bariatric surgeryd,e | £6346138 | £6060138; €7336139 | €8105139 |
Craig and Tseng140 and Salem and colleagues142 reported aggregated cost categories for bariatric surgery, postsurgical complications, revision and reversal surgery using the US Healthcare Cost and Utilisation project database (1997). 158 The costs were then adjusted for inflation using a medical-care component of the consumer price index. No further details were reported.
Jensen and Flum141 used the published cost data from a single study comparing open gastric bypass with laparoscopic gastric bypass. 113 The missing estimate of the cost(s) of complications was set to be $5000 per complication, which appears to be an underestimate. The costs were then adjusted for inflation to 2004 US prices using the Bureau of Labour Statistics Inflation calculator. It is not clear whether this method is an equivalent to the correct method of using a medical-care component of the consumer price index as in the other US studies. 140,142 Costs for the comparator treatment – a one-year programme of diet and exercise – were taken from the US case–control longitudinal study by Heshka and colleagues. 150 Health-care resources and the corresponding unit costs are reported only for the comparator arm of the model and no direct medical costs of bariatric surgery are reported, therefore this study is excluded from the cost data analysis presented below.
It should be noted that although in different studies the same name may be used to identify an aggregated cost component, the health-care resources included under this category may be quite different. Therefore, no meaningful comparison across the studies with respect to the individual cost items can be made. Comparisons with respect to the total costs are also limited because of differences in the nature of the health-care systems (i.e. private versus public) and because of differences in the currencies in which costs are reported (see Table 41).
According to Ackroyd and colleagues,138 the direct medical costs of laparoscopic gastric bypass and laparoscopic adjustable gastric banding over five years do not appear to be different. Likewise, van Mastrigt and colleagues139 found no statistically significant difference in the mean costs of laparoscopic adjustable gastric banding and vertical banded gastroplasty over a one-year time interval.
Only a very limited number of cost components, (i.e. those reported in natural units) are available for direct comparison between the studies. According to Ackroyd and colleagues,138 the mean LOS for the initial surgery is not very different between laparoscopic gastric bypass and laparoscopic adjustable gastric banding and is about five days. The study by van Mastrigt and colleagues139 reported the mean estimate of the LOS for the initial laparoscopic adjustable gastric banding as 5.56 days, which is about 0.5 days longer than the corresponding LOS reported in Ackroyd and colleagues. 138 However, van Mastrigt and colleagues139 found that the median LOS was only four days, which is one day shorter than the mean LOS reported in Ackroyd and colleagues. 138 The discrepancy between the mean and median LOS reported in van Mastrigt and colleagues139 is likely to have resulted from the relatively small sample of the population participating in the study (50 patients in each arm). The sample size used in the LOS estimate in Ackroyd and colleagues138 was not reported. It is therefore uncertain which of the estimates is more accurate. The same concern also applies to the duration of the operating theatre time to conduct laparoscopic adjustable gastric banding surgery, which is reported as 1.9 hours and 3.26 hours, respectively, in the studies by Ackroyd and colleagues138 and van Mastrigt and colleagues. 139
Table 44 summarises the cost data as reported in two US studies by Craig and Tseng140 and by Salem and colleagues. 142 In comparison to Ackroyd and colleagues138 and van Mastrigt and colleagues,139 the US studies140,142 provide a more elaborate list of postsurgical complications and associated direct medical costs. Direct comparison of the cost estimates across these studies is not possible because they do not involve a common surgical intervention and employ different formats for reporting cost estimates: Craig and Tseng140 report the costs by gender categories while Salem and colleagues142 do not differentiate the costs by gender. Both studies140,142 report health-care resources used in bariatric surgery by aggregated cost categories, the only resource reported in natural units is the number of follow-up visits, which is three times a year for three years for open gastric bypass according to Craig and Tseng140 and twice a year for three years for laparoscopic gastric bypass according to Salem and colleagues. 142 The latter study also reported that the expected number of band adjustments over three years following laparoscopic adjustable gastric banding is 10. Both studies report only point estimates without a 95% CI, which limits the possibility of establishing the statistical significance of the difference in costs of bariatric surgeries.
| Resource category | Type of resources by aggregated cost categories | Cost estimate of resources used in open GBP (Craig and Tseng140) (US$2001) | Cost estimate of resources used in LGBP (Salem and colleagues142) (US$2004) | Cost estimate of resources used in LAGB (Salem and colleagues142) (US$2004) | |
|---|---|---|---|---|---|
| Men | Women | Obese population | Obese population | ||
| Cost of surgery | $26,100 | $20,500 | $27,560 | $16,200 | |
| Band adjustment | n/a | $150 per visit × 10 visits over 3 years | |||
| Cost of immediate complications requiring surgery | Revision surgery | $38,500 | $25,600 | $10,000 | $5000 |
| Reversal surgery (band removal) | n/a | n/a | n/a | $6000 | |
| Reversal surgery GBP | $38,500 | $25,600 | N/R | n/a | |
| Cost of subsequent complications | Minor wound infection | $192 | $192 | $204 | $204 |
| Major wound infection | $20,600 | $19,200 | $11,236 | $11,236 | |
| Deep venous thrombosis | $8700 | $8100 | $9222 | $9222 | |
| Pulmonary embolism | $14,700 | $13,900 | $15,582 | $15,582 | |
| Leak non-operative | n/r | n/r | $50,000 | n/a | |
| Cholecystectomy | $27,100 | $22,700 | $16,000 | $16,000 | |
| Incisional hernia | $13,200 | $12,500 | $14,416 | $14,416 | |
| Abdominoplasty | $13,600 | $12,200 | $13,992 | $13,992 | |
| Postoperative death | $27,600 | $29,000 | n/r | n/r | |
| Follow-up cost | $150 per visit × 3 visits a year | $150 per visit × 3 visits a year | $159 per visit × 2 visits a year | None required except for the scheduled band adjustment visits | |
| Lifetime cost of pharmaceuticals | $68 | $68 | $72 | $0 | |
Neither Craig and Tseng140 nor Salem and colleagues142 report the estimated cost of bariatric surgery that would apply to the general population. The total cost estimates are available only with respect to the subgroups of the population with the selected combination of gender/age/BMI value and no comorbidities at the baseline. Craig and Tseng140 reported that sex-specific cost estimates were consistently higher in men than in women except for postoperative death, but did not offer any explanation as to the possible reason for the observed cost differences.
The US cost estimates in Table 44 are not consistent with the cost data presented in Table 43 in that the mean total cost of laparoscopic gastric bypass appears to be higher than the mean total cost of laparoscopic adjustable gastric banding although whether this difference reaches the level of statistical significance is uncertain.
There is a large difference in costs of revision surgeries with open gastric bypass revision in men being four times more expensive than laparoscopic gastric bypass revision and eight times more expensive than laparoscopic adjustable gastric banding revision. 140,142 The cost difference is likely to be the result of the differences between the open and laparoscopic surgeries, and other differences in surgical techniques employed across the bariatric surgeries.
Cost of non-surgical treatment (comparator)
It appears that Craig and Tseng140 and Salem and colleagues142 have implicitly assumed that the short-term cost of non-surgical treatment alternatives (such as diet and exercise) is zero. This assumption, although it may not be realistic, is conservative and is likely to bias the ICER in favour of the comparator.
Jensen and Flum141 provided a detailed account of the health-care resources in natural units and the corresponding unit costs for the comparator treatment – a one-year diet and exercise programme. However, the cost of a single privately run diet and exercise programme undertaken by predominantly white females residing in the USA may be of limited generalisability.
Ackroyd and colleagues138 provided a fairly comprehensive list of health-care resources used in the comparator arm – a conventional treatment that typically involves dieting (see Table 40, footnote b). The resource use is reported in natural units (e.g. number of GP and dietitian consultations; number of district and practice nurse consultations; number of laboratory assessments and number of food substitutes) and the corresponding unit costs as well as in aggregated cost-categories (an annual cost of outpatient visits, pharmaceuticals and hospital admissions).
The study by Ackroyd and colleagues138 was the only one among the modelled economic evaluations that explicitly modelled the prevalence of Type 2 diabetes in non-surgical and surgical treatment arms. The cost of treatment of obesity-related Type 2 diabetes was taken from the CODE-2 (The Cost of Diabetes in Europe – Type II) survey which used the 1999 prices,159 while the cost of surgical interventions is expressed in 2005 prices. It does not appear likely that the cost of a comparator in terms of treatment of Type 2 diabetes was converted into 2005 prices using the health price index. This approach is likely to produce a bias in the cost-effectiveness estimate in favour of surgical treatments.
Long-term costs
The studies by van Mastrigt and colleagues139 and by Ackroyd and colleagues138 limited their time horizons to one year and five years, respectively, and did not include any long-term costs and the outcomes of bariatric surgeries.
Three other studies140–142 used the same published source of the lifetime medical costs for the different subgroups of the US population categorised by age/gender/BMI. 144 These costs were applied to both the surgical and non-surgical treatments. As already mentioned in the section on Translation of short-term outcomes into final outcomes, this chapter, Thompson and colleagues144 reported the lifetime medical cost estimates separately for men and women categorised by age groups from 35 to 64 years old in 10-year increments. However, the published lifetime medical-cost estimates are available only up to BMI of 37.5 which is below the range of BMI values assessed in the modelled economic evaluations. All authors used a linear extrapolation method to obtain the estimates of the lifetime medical cost for BMI values above the range reported in Thompson and colleagues. 144 Although no actual values of the estimated lifetime medical cost are reported in the studies, the same concerns about the methods used in extrapolating life expectancy estimates, that were outlined earlier may also apply to extrapolating lifetime medical costs.
Results reported in the identified economic evaluations of bariatric surgeries
Tables 45 to 47 present the estimated costs, outcomes and ICERs as reported in the identified studies. Three tables were designed to accommodate the inconsistency in the format of reporting incremental costs and incremental outcomes across the studies. Some studies (most notably Jensen and Flum141) do not report costs and outcomes separately for each treatment alternative.
| Type of treatment strategies | Results | ||||
|---|---|---|---|---|---|
| Intervention and comparator | Cost of the interventiona | Cost of the comparatora | QALYs interventiona | QALYs comparatora | ICER (Incremental cost over incremental outcome) |
| LGBP vs conventional treatment138 | £9121b | £7083b | 3.34b | 2.00b | 2033/1.34 = £1517/QALY |
| LAGB vs conventional treatment138 | £9072b | £7088b | 3.03b | 2.00b | 1984/1.03 = £1929/QALY |
| VBG vs LAGB (assumed to be a comparator)139 | €8105c | €7336c | 0.76d (SD = 0.2) | 0.81d (SD = 0.13) | LAGB dominates open VBG |
| Type of treatment strategies | Results: Open GBP vs non-surgical treatment | ||
|---|---|---|---|
| Incremental cost | Incremental outcome (additional LY gained)a | ICER | |
| Open GBP vs diet and exercise141 | US$4600 | 0.61 | US$7126/QALY |
| Subgroup | Cost of intervention (Open GBP) | Cost of comparator (non-surgical treatment) | QALY interventiona | QALY comparator (non-surgical treatment) | ICER | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Results: Open GBP vs non-surgical treatment140 | ||||||||||
| Men 35 years; BMI 40 | US$68,600 | US$38,500 | 19.56 | 18.51 | US$28,600/QALY | |||||
| Men 35 years; BMI 50 | US$75,000 | US$53,200 | 18.87 | 16.83 | US$10,700/QALY | |||||
| Men 55 years; BMI 40 | US$77,600 | US$47,900 | 13.32 | 12.48 | US$35,600/QALY | |||||
| Men 55 years; BMI 50 | US$85,300 | US$63,500 | 12.81 | 11.17 | US$13,300/QALY | |||||
| Women 35 years; BMI 40 | US$59,000 | US$35,300 | 19.82 | 18.21 | US$14,700/QALY | |||||
| Women 35 years; BMI 50 | US$64,800 | US$48,500 | 18.88 | 16.03 | US$5700/QALY | |||||
| Women 55 years; BMI 40 | US$69,600 | US$48,200 | 13.94 | 12.62 | US$16,100/QALY | |||||
| Women 55 years BMI 50 | US$77,000 | US$64,100 | 13.23 | 10.88 | US$5400/QALY | |||||
| Results: LGBP vs non-surgical treatment142 | ||||||||||
| Men 35 years; BMI 40 | US$27,560 | n/r | n/r | n/r | US$18,543/QALY | |||||
| Women 35 years; BMI 40 | US$27,560 | n/r | n/r | n/r | US$14,680/QALY | |||||
| Results: LAGB vs non-surgical treatment142 | ||||||||||
| Men 35 years; BMI 40 | US$16,200 | n/r | n/r | n/r | US$11,604/QALY | |||||
| Women 35 years; BMI 40 | US$16,200 | n/r | n/r | n/r | US$8878/QALY | |||||
Results reported in Ackroyd and colleagues138 and van Mastrigt and colleagues139
Table 45 presents results reported in Ackroyd and colleagues138 and van Mastrigt and colleagues139 with respect to costs and outcomes expressed in QALYs. These two studies adopt different perspectives: Ackroyd and colleagues138 adopted a payer’s perspective (i.e. the NHS in the case of UK) and van Mastrigt and colleagues139 adopted a societal perspective. The costs in van Mastrigt and colleagues139 were reduced by us by the amount of non-direct costs to make the results of these two studies comparable (see Table 43, footnote e). Both studies undertook cost-effectiveness analyses (CEA) in addition to cost–utility analyses (CUA). These are discussed below.
Ackroyd and colleagues138 reported that in comparison to non-surgical treatment laparoscopic gastric bypass is associated with an incremental cost of £1517 per QALY, and laparoscopic adjustable gastric banding is associated with an incremental cost of £1929 per QALY. Both costs and outcomes are discounted at 3.5%. With respect to diabetes mellitus outcome, laparoscopic gastric bypass is associated with an additional 2.6 years free of Type 2 diabetes or incremental cost of £776 per Type 2 diabetes-free year, and laparoscopic adjustable gastric banding is associated with an additional 2.5 years free of Type 2 diabetes or incremental cost of £810 per Type 2 diabetes-free year. The outcomes in terms of the Type 2 diabetes prevalence observed over five years were not discounted. It is not clear whether discounted or undiscounted costs were used in calculating ICERs with respect to the Type 2 diabetes prevalence. Ackroyd and colleagues138 suggested that at five-year follow-up both laparoscopic gastric bypass and laparoscopic adjustable gastric banding are cost-effective in comparison to a non-surgical treatments in patients with Type 2 diabetes and a baseline BMI > 35.
Van Mastrigt and colleagues139 used the observational data collected alongside an RCT involving 100 patients undertaking either laparoscopic adjustable gastric banding or open vertical banded gastroplasty and reported the 12-month outcomes in terms of % excess weight loss (EWL) and QALYs. A bootstrap analysis of the joint distribution of incremental costs and outcomes involving 1000 replications identified that in 86% of trials laparoscopic adjustable gastric banding was both less effective and less expensive in comparison to open vertical banded gastroplasty, and in 14% of trials it was less effective and more expensive (i.e. dominated by open vertical banded gastroplasty). The authors erroneously claimed that moving from open vertical banded gastroplasty to laparoscopic adjustable gastric banding would involve an additional amount of €105.80 per each additional % EWL. In fact, this amount is what society would be spending for choosing not to switch from open vertical banded gastroplasty to laparoscopic adjustable gastric banding, i.e. replacing open vertical banded gastroplasty with laparoscopic adjustable gastric banding would involve a saving of €105.80 for each per cent of extra weight retained.
With respect to the outcomes expressed in QALYs a different (and somewhat contradictory) result was reported: laparoscopic adjustable gastric banding appears to be both less expensive and more effective than open vertical banded gastroplasty (i.e. a dominant strategy). A bootstrap analysis showed that in 79% of trials laparoscopic adjustable gastric banding was both more effective and less expensive in comparison to open vertical banded gastroplasty (i.e. dominant); and in 14% of trials it was more effective but also more expensive. There was a negligible probability of open vertical banded gastroplasty being dominant (3%) or being both less effective and less expensive (4%).
The authors suggested that the difference in QALYs at 12 months after surgery was not statistically significant between the open vertical banded gastroplasty and laparoscopic adjustable gastric banding arms. Although the observed utility scores at 12 months do appear very similar between the arms these values do not reflect the baseline difference (see discussion in section on Assumptions of economic evaluations, this chapter). The absolute utility values were not reported, but as is evident from Figure 3 in van Mastrigt and colleagues,139 the incremental utility gain over 12 months appears to be larger in the open vertical banded gastroplasty arm. Without the long-term data it is not possible to say whether the larger incremental gain associated with open vertical banded gastroplasty would extend beyond the first year. However, these considerations undermine the long-term validity of the authors’ conclusions of no incremental gain in QALYs between the open vertical banded gastroplasty and laparoscopic adjustable gastric banding and the laparoscopic adjustable gastric banding dominance with respect to open vertical banded gastroplasty.
Inconsistently with the results of their CEA the authors concluded that at 12 months the costs and QALYs outcomes of two alternative surgical interventions were found to be equal. 139 Therefore the selection of the procedure should be based on the clinical aspects, efficacy and safety at one year.
Results reported in the US studies by Jensen and Flum,141 Craig and Tseng140 and Salem and colleagues142
Table 46 presents results reported in Jensen and Flum. 141 The studies by Craig and Tseng140 and Salem and colleagues142 are reported separately in Table 47.
On the basis of the results reported in Jensen and Flum,141 open gastric bypass appears to be cost-effective at the incremental cost of $7126 per QALY, although the incremental effect is reported in terms of additional LYs gained rather than QALYs. The ICER reported by Jensen and Flum141 comparing open bastric bypass undertaken by white females at the age of 40 (BMI > 40) with a diet and exercise programme undertaken at the age of 18 [BMI > 33(or 35); see Table 41, footnote d] falls within the range of ICERs reported by Craig and Tseng for the subgroups of females aged 35 or 55 and with the baseline BMI of 40 or 50 (see Table 47).
Table 47 presents results reported in Craig and Tseng140 and Salem and colleagues. 142 The results are reported with respect to subgroups of population with the specified baseline characteristics of gender/age/BMI.
The results reported by Craig and Tseng140 are characterised by large variability with respect to baseline demographic characteristics of the obese population. The ICER varies from US$5400 per QALY in 55-year-old females with BMI of 50 to US$35,600 per QALY in 55-year-old males with a baseline BMI of 40.
Salem and colleagues142 do not report the results across the same subgroups as Craig and Tseng,140 which makes it impossible to compare variability of estimates of incremental cost-effectiveness in various subgroups of the obese population. However, the authors reported that both bariatric procedures in comparison to non-surgical treatment were cost-effective at < $25,000 per QALY for all base-case scenarios (i.e. the combinations of baseline age of either 35, 45, or 55 years and BMI of either 40, 50 or 60).
Salem and colleagues142 concluded that laparoscopic adjustable gastric banding is more cost-effective than laparoscopic gastric bypass for all base-case scenarios. However, this conclusion is based on the ICERs individually comparing laparoscopic gastric bypass with non-surgical treatment and laparoscopic adjustable gastric banding with non-surgical treatment, whereas the direct comparison of these two surgical interventions in terms of incremental costs and QALYs was not reported. Therefore this conclusion may not be true for every subgroup of the obese population.
Sensitivity analysis
Eight one-way sensitivity analyses undertaken by van Mastrigt and colleagues139 were undertaken to test the sensitivity of the outcomes associated with variability of cost estimates used in CEA (with outcomes expressed in % EWL) and CUA. The cost of operating-theatre personnel time (€2.96 per minute) was substituted in turn for the maximum and minimum values of €3.56 and €2.66 per minute respectively. Also the per diem cost (€332 per day in hospital) was substituted for the maximum and minimum values of €432 and €232 per day respectively. The results reported in terms of the outcomes of bootstrapping analyses of joint distribution of incremental costs and outcomes are very robust with respect to variations in unit cost estimates. A scenario analysis from the alternative health-care system perspective (rather than the societal perspective used in the original economic evaluation) was also undertaken. With respect to the QALY outcome exclusion of non-medical costs, that represent 39% and 35% of open vertical banded gastroplasty and laparoscopic adjustable gastric banding costs, respectively, has reduced the probability of laparoscopic adjustable gastric banding being a dominant strategy (from 79% to 68%) and increased the probability of laparoscopic adjustable gastric banding being more effective and more expensive (from 14% to 27%). van Mastrigt and colleagues139 did not test the uncertainty associated with clinical effectiveness or utility estimates observed in the RCT.
Ackroyd and colleagues138 do not seem to test the variability in cost estimates using a sensitivity analysis. Instead the authors conducted a two-way sensitivity analysis where clinical effectiveness of laparoscopic adjustable gastric banding and laparoscopic gastric bypass with respect to both BMI reduction and Type 2 diabetes prevalence was reduced by 20% in each arm of the model, which is equivalent to assigning zero Type 2 diabetes benefits from a non-surgical treatment in the first year. The ICER for laparoscopic adjustable gastric banding compared with non-surgical treatment changed from £1929 to £3251 per QALY. The ICER for laparoscopic gastric bypass compared to non-surgical treatment changed from £1517 to £2599 per QALY. The ICERs appear to be very sensitive to variability in clinical effectiveness estimates. The sensitivity of results to the variations in utility estimates was not tested in this study.
Jensen and Flum141 conducted a series of one-way sensitivity analyses and the outcomes are reported to be sensitive to the estimated cost of complications (although the range was not reported) and the discount rate (neither the value nor the range were reported).
Craig and Tseng140 conducted a series of one-way sensitivity analyses that varied the short-term clinical effectiveness parameters (% EWL, mortality rates and complication rates) and the long-term outcomes (LYs lost as the result of the elevated BMI). Another sensitivity analysis was conducted to assess the impact of variability in utility estimates. However, instead of varying the utility values, the regression coefficients in the (unreported) multiple regression equation (see the section on Translation of short-term outcomes into final outcomes, this chapter) used to obtain utility values were decreased by 25%. It is not clear how the actual utility values were affected.
Two-way sensitivity analysis varying both the lifetime medical cost and the discount rate was undertaken by Craig and Tseng. 140 Another two-way sensitivity analysis varied the estimated % EWL and the reimbursement rates for the insured patients. These parameters were also used in the threshold analysis for the subgroup of insured 55-year-old men with the baseline BMI of 40 with the ICER of $50,000 per QALY as a threshold. The results indicated that under the base-case assumptions about the 67% reimbursement rate, the loss of excess weight greater than 46% is sufficient for the incremental cost per incremental QALY to be below US$50,000. The threshold analysis implicitly assumed the change of the perspective of the economic evaluation from that of the health-care system (where the cost of medical care is covered by both the third party and the patients’ copayments) to the perspective of the individually insured patients. It was also implicitly assumed that for any payer (Government, the third party or an insured individual) the same criterion of value for money is applied (i.e. the threshold of $50,000 per QALY). This may not be a reasonable assumption.
Craig and Tseng140 concluded that the results reported in Table 47 appear to be robust to all parameter variations for the subgroups of women and younger more obese men. An open gastric bypass may not be cost-effective for some subgroups of older and less obese men as the ICER exceeds US$50,000 per QALY when the base-case assumptions about some clinical effectiveness parameters are varied.
Salem and colleagues142 investigated the uncertainty associated with parameter estimates in the model, but the source of the ranges in parameter estimates, and the methods used to derive them, were not clear. A series of one-way sensitivity analyses were performed and results are said to be sensitive to the value of the primary clinical outcome (% EWL), cost of the surgical procedure, number of times the band adjustment was required for the laparoscopic adjustable gastric banding procedure and the estimated rate of operative mortality for laparoscopic gastric bypass.
To summarise, none of the identified studies undertook a probabilistic sensitivity analysis. The rationale for choosing the model parameters and the ranges included in the sensitivity analysis is not clear in some studies. 138,139 In other studies results of the sensitivity analyses are not fully reported. 140,141 Nevertheless, based on the reported set of one-way and two-way sensitivity analyses, the results in the identified economic evaluations of bariatric surgeries appear to be fairly robust with respect to the variation in (the tested) parameter estimates.
Summary of the results reported in economic evaluations of bariatric surgeries
As discussed in the previous sections, all identified studies138–142 are characterised by various methodological shortcomings that undermine the validity and generalisability of the reported results. Most importantly, the natural disease progression was not explicitly modelled in terms of probabilities of obesity-related diseases. Only one study138 has modelled a Type 2 diabetes outcome explicitly and accounted for it in the final outcomes (QALYs); however, this model is limited to the five-year horizon and has numerous methodological problems and results are only relevant to the obese population with Type 2 diabetes at the baseline. Other modelled economic evaluations138,140–142 are based on the lifetime horizon, but do not incorporate separate differential probabilities of developing/reversing obesity-related diseases. Instead, the published estimates of life expectancy and lifetime costs for the US population categorised by age, gender and BMI (up to 37.5) were used. 144 As discussed in the section on Translation of short-term outcomes into final outcomes (this Chapter) extrapolation of the life expectancy and lifetime cost estimates to include BMI values higher than 37.5 is likely to have produced unreliable estimates. Also, the unspecified method of deriving utility estimates, which was reported by Craig and Tseng140 and replicated in Salem and colleagues,142 may not be of sufficient methodological rigour to produce reliable estimates of QALYs. Other assumptions also appear not to correspond to the clinical evidence. In particular, the assumptions of no weight gain in the comparator arm140,142 does not seem to be realistic.
It appears that none of the identified modelled economic evaluations has provided a reliable and generalisable estimate of the incremental cost-effectiveness of bariatric surgeries in comparison to a non-surgical treatment. However, some of the assumptions in the identified studies are reasonable and need to be considered in the future economic evaluations:
-
differential time in gaining full benefits from the different types of bariatric surgery139
-
differential rates of short-term mortality and morbidity associated with different types of bariatric surgery140
-
postsurgical interventions may be required immediately after the surgery140,141 and over the longer time interval (up to five years)138,142
-
differential rate of regaining the lost weight over the lifetime associated with the bariatric surgery and the non-surgical treatment141
-
differential probabilities of developing/reversing obese-related diseases as a function of changes in BMI140–142
-
use of utility weights that relate to the changes in BMI. 141
To summarise, none of the identified studies undertook an economic evaluation across the entire range of bariatric surgery. All modelled economic evaluations138–142 found the bariatric surgery evaluated to be cost-effective in comparison to non-surgical treatment, although the variability in estimates of costs and outcomes is large. The choice and the range of model parameter estimates used in the sensitivity analyses were not justified. Nevertheless, with respect to the selected parameters the results appear to be robust to parameter variations in most of the CEA. The only exception, as reported by Craig and Tseng,140 are some subgroups of older and less obese men for whom an open gastric bypass may not be cost-effective (i.e. exceeding US$50,000 per QALY) when the base-case assumptions about some clinical effectiveness parameters are varied.
It should also be noted that numerous methodological shortcomings discussed in the previous sections are likely to have resulted in biased estimates of the incremental cost-effectiveness of bariatric surgeries in comparison with the non-surgical treatment. The head-to-head RCT of two bariatric surgical procedures,139 although being methodologically sound, was nevertheless compromised by the discrepancies in the baseline characteristics of the population randomised to the laparoscopic adjustable gastric banding and open vertical banded gastroplasty that resulted in the difference in the baseline utility values in two intervention groups. This difference is likely to be the major reason for the contradicting results of the CEA and CUA undertaken within this study.
Uncertainties and the source of biases within economic evaluations of bariatric surgery
Clinical evidence used to obtain the primary outcomes (weight reduction)
In all four studies the BMI values were taken from the published evidence; however, it does not appear that any study conducted a systematic literature search and evidence analysis. Two studies, Craig and Tseng140 and Jensen and Flum,141 used the outcomes from a single published source of evidence which may affect validity of the estimate of the differential weight loss in the alternative treatments and the generalisability of results. Generalisability of results is also impaired by the choice of evidence that applies only to a subgroup of the obese population: the population of obese patients with Type 2 diabetes as in Ackroyd and colleagues138 and white female patients who were obese at the age of 18 with BMI > 33 (or 35) (see Table 41, footnote d) as in Jensen and Flum. 141
Assumptions about the target population
Craig and Tseng140 and Salem and colleagues142 have assumed that the cohort of obese patients with BMI > 40 have no comorbidities at the baseline, which may not be a realistic assumption.
Assumptions about the outcomes of bariatric surgeries
Ackroyd and colleagues138 implicitly assumed that there is no differential operative mortality and postoperative morbidity between the two surgical treatments and the non-surgical treatment comparator. This is not likely to be a realistic assumption. The same is also true with respect to the assumption of a zero weight gain over the modelled time horizon in patients in the non-surgical treatment arm in Ackroyd and colleagues,138 Craig and Tseng140 and Salem and colleagues. 142
Utility estimates
Utility estimates reported in Ackroyd and colleagues138 were also used in Craig and Tseng140 and Salem and colleagues. 142 However, these are not likely to be unbiased estimates of the HRQoL because of the multiple methodological shortcomings in the way they were derived from the available data. In addition, the source data relate to the general population whose health-related preferences may differ from those of the obese population.
SHTAC economic model
Statement of the decision problem and perspective for the cost-effectiveness analysis
We developed a model to estimate the cost-effectiveness of bariatric surgery comparing surgical procedures against each other and against non-surgical comparators, for a UK cohort of adults meeting the NICE criteria for bariatric surgery. The perspective of the CEA is that of the NHS and Personal Social Services (PSS).
Strategies/comparators
Interventions included in the economic model are gastric bypass and gastric banding. Surgical procedures are compared with a non-surgical comparator. For patients with morbid obesity the non-surgical comparator, as in the previous report15 consists primarily of monitoring rather than active treatment, because NICE guidance9 specifies that patients offered bariatric surgery should have failed to achieve (or maintain) an adequate and clinically beneficial weight loss for at least six months on all appropriate non-surgical alternatives. We assume that procedures are performed laparoscopically, where possible, but that conversion to open procedures may be required.
Methods
Summary of methods and results of economic modelling in the previous assessment report15
The previous assessment report15 presented estimates of the cost-effectiveness of gastric bypass, vertical banded gastroplasty and adjustable silicone gastric banding using a simple economic model. Surgical procedures were compared with each other, as well as a non-surgical comparator. It has not been possible to repeat all of the methodological detail of the model here. Readers are therefore encouraged to consult the original report which is freely available for download (http://www.ncchta.org/fullmono/mon612.pdf).
The model in the previous report was not developed as a state transition model. However, conceptually it contained four health states: no comorbidity, remission of comorbidity, Type 2 diabetes and death. The remission of comorbidity health state was included in the model to allow for the fact that people with Type 2 diabetes may revert to normoglycaemia following successful treatment for obesity. Comorbidities other than Type 2 diabetes, such as myocardial infarction, angina and stroke, were not included. The model was used to extrapolate long-term outcomes (in terms of QALYs up to 20 years following surgery) and lifetime costs (in terms of costs of managing diabetes in addition to intervention costs) based on intermediate outcomes reported in the clinical effectiveness review (per cent weight reduction, operative mortality, percentage of people with Type 2 diabetes reverting to normoglycaemia, diabetes incidence in surgical and non-surgical patients).
In the model it was assumed that weight reduction (36% with gastric bypass, 25% to 17% for vertical banded gastroplasty, 20% to 33% with adjustable silicone gastric banding) occurred over five years following surgery, but that patients then reverted to their baseline weight of 135 kg. Operative mortality was based on a combination of trial evidence and expert opinion and was assumed to be 1% for gastric bypass, 0.5% for vertical banded gastroplasty and 0% for adjustable silicone gastric banding. Baseline diabetes prevalence in the model was 10%. Based on evidence from the Adelaide study149 it was assumed that 75% of people with diabetes revert to normoglycaemia and remain off medication for eight years (based on follow-up from the SOS study89,90) – after eight years these patients revert to medication. Different diabetes incidence rates were applied to surgical and non-surgical patients (2.3% per annum for non-surgical and 0.45% per annum for surgical patients) based on data from the SOS study89,90 – after eight years surgical patients revert to the incidence rate for non-surgical patients. Reversion to normoglycaemia and incidence rates were applied on the basis of whether patients had or had not undergone surgery and were not directly related to their weight loss or assumed BMI.
HRQoL in the model was entirely dependent on BMI (using data from an unpublished study). There were no adjustments to these utility values for patients who developed Type 2 diabetes or for people with Type 2 diabetes who reverted to normoglycaemia.
Intervention costs for non-surgical management consisted of primary-care and dietitian contacts, with a VLCD (for 12 weeks) every three years. This continued for all patients for the model time horizon. Intervention costs for surgery consisted of preoperative assessment (including outpatient and dietitian appointments as well as psychological assessment), surgery (based on theatre time, length of ward stay, admission to an ITU or high-dependency unit (HDU), and percentage of reoperations) and postdischarge management (consisting of outpatient follow-up, community dietitian contacts, psychology consultations and primary care). Disease management costs in the model were limited to those associated with diabetes, using the assumptions on diabetes prevalence, reversion to normoglycaemia and diabetes incidence for surgical and non-surgical patients described earlier. Annual cost per person with Type 2 diabetes was taken from the CODE-2 study. 160
The model had a 20-year time horizon and the analysis adopted the perspective of the NHS and personal social services. The baseline cohort in the model was 90% female, had an average age of 40, average body weight of 135 kg and an average BMI of 45. The baseline model assumed no change in life expectancy and only included postoperative mortality; all-cause or disease-specific mortality was not included in the model.
Table 48 reports the base-case cost-effectiveness estimates from the previous report. 15 On the basis of these results the report concluded that surgery was a cost-effective alternative to non-surgical management and that gastric bypass may be the preferred option. The conclusion, that surgery was cost-effective was robust to changes in a series of scenario analyses. However, the report cautioned against interpreting these results as conclusive given limited data available for some of the surgical options.
| Intervention | ||||
|---|---|---|---|---|
| VBG | AGB | GBP | ||
| Comparator | Non-surgical | £2663; 0.26 QALY; £10237 | £3831; 0.45 QALY; £8527 | £2800; 0.45 QALY; £6289 |
| Vertical banded gastroplasty | ||||
| Adjustable silicone gastric band | £1168; 0.19 QALY; £6,176 | |||
| Gastric bypass | £137; 0.19 QALY; £742 | £1031; 0.004 QALY; £256,856 | ||
Summary of findings of current review and implications for economic model
This update has identified:
-
The model developed for the previous assessment report15 based QoL entirely on BMI and took no account of the effect of comorbidity on QoL. Since the publication of the previous assessment report15 a systematic review on patient utilities related to body weight and a number of additional models has been published, in some cases suggesting a larger reduction in QoL in relation to BMI. For this report we intend adopting an estimate of the impact of BMI on utility, and including additional state-specific utility decrements for patients experiencing comorbidities (Type 2 diabetes and CVD).
-
The model developed for the previous assessment report15 included Type 2 diabetes as the only comorbidity of obesity. This was based on evidence from included studies that weight loss following bariatric surgery was associated with:
-
– reversion to normoglycaemia or cessation of medication for patients with pre-existing Type 2 diabetes;89,149,161
-
– reduced incidence of diabetes [0% versus 4.7% at two years (corresponding to annual incidence of 0% versus 2.41% using the declining exponential approximation to life expectancy, or DEALE, method162) and 3.6% versus 18.5% at eight years (corresponding to annual incidence of 0.45% versus 2.56% using the DEALE method) for surgical and control patients respectively];89
-
-
Adopting a deliberately conservative approach the previous review limited the scope of comorbidities considered to Type 2 diabetes. As discussed earlier, the impact of Type 2 diabetes was limited to the cost impact, no estimate of the impact on QoL was included in the model.
For the analysis in this report we adopt a set of BMI-specific Type 2 diabetes incidence estimates and include estimates of cardiovascular comorbidities, where trial data support such estimates (see section on Data sources, Effectiveness data, this chapter, for details and discussion).
-
Costings developed for the previous assessment report15 were predominantly based on expert opinion, in terms of preoperative assessments, surgical costs and postdischarge management. Since the publication of the previous assessment report15 a number of economic evaluations have been published reporting costs or resource use assumptions for different types of bariatric surgery. For this report we intend updating the cost assumptions in relation to bariatric surgery, where published evidence or expert opinion suggests there have been substantial changes since the publication of the previous assessment report. 15
-
Methodological guidance and accepted practice in discounting have changed since the publication of the previous assessment report,15 where costs and outcomes were each discounted at 6%. Updated estimates, using the original model, are presented in Appendix 18 using the current practice of discounting both costs and outcomes each at 3.5%. Where this has a substantial impact on the results of the analysis, this will be discussed in the conclusions of this report.
Model type and rationale for the model structure
For this report we have sought to expand the conceptual model adopted for the previous assessment report, to include CHD and stroke. Figure 2 shows the state transition diagram for the model developed for this review. In this diagram ellipses indicate health states and arrows indicate allowable transitions. Patients may enter the model in any of the grey-shaded ellipses – i.e. they may have already developed Type 2 diabetes as a result of their obesity, they may resolve diabetes (temporarily or permanently) as a result of treatment for their obesity or they may enter the model free of diabetes. We assume that patients are free of CHD and have not experienced stroke before treatment.
FIGURE 2.
State transition diagram. CHD, coronary heart disease.
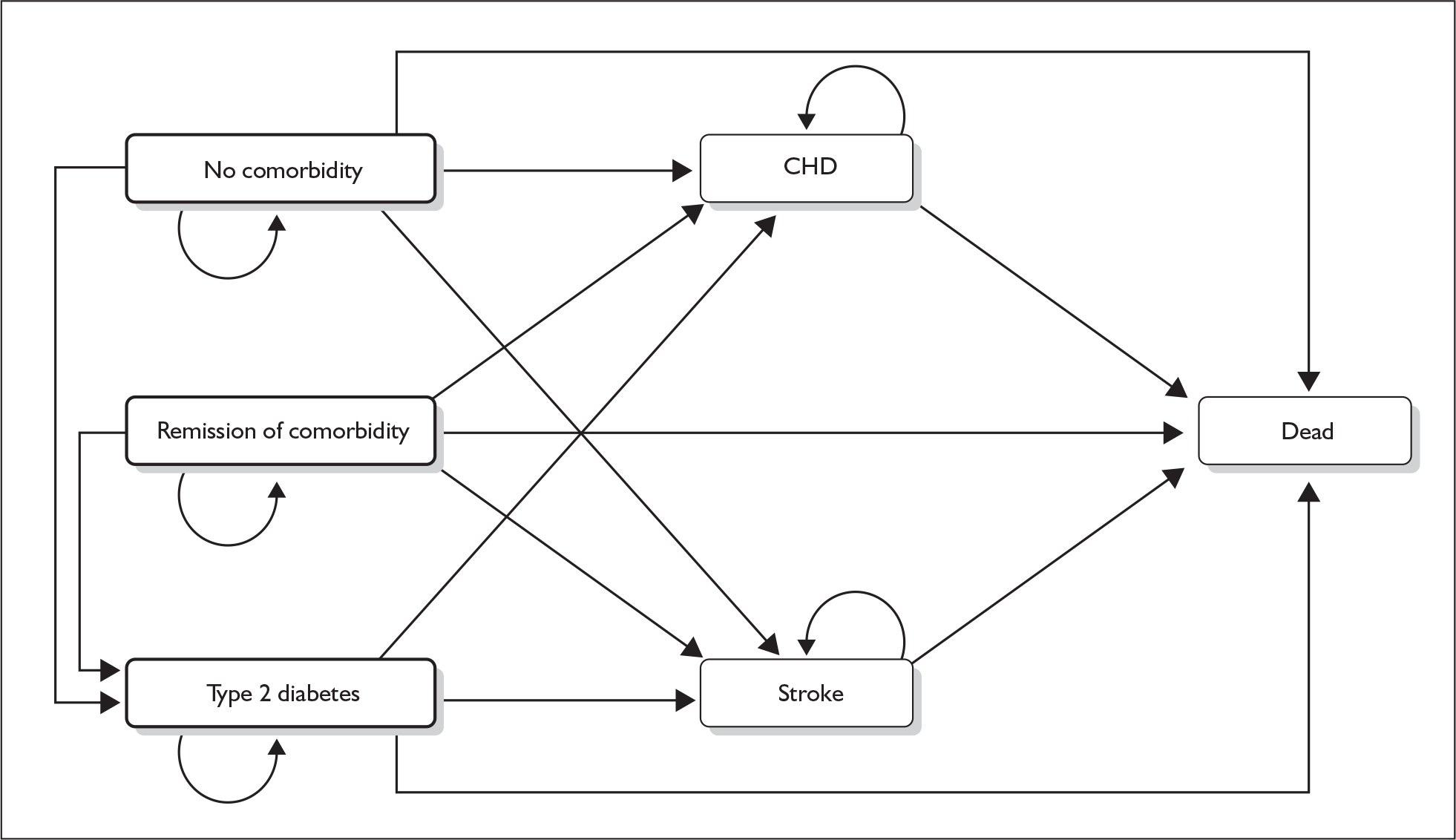
The primary outcomes reported for clinical trials included in this review are typically related to change in body weight (total weight change from baseline, change in excess weight or change in BMI) so data to model transitions between health states would ideally be based on a standardised, weight-related measure such as BMI. However, body weight may not be an ideal parameter for predicting some comorbidities associated with obesity – for example, CHD and stroke are more typically modelled using blood pressure and lipid measurements rather than BMI. The reporting of these additional measures is not complete in all studies. Where these additional parameters are not available in trial reports it may not be possible to apply the full model described before – in that situation a more limited model, similar to that adopted for the previous report will be used.
The models have a maximum time horizon of 20 years, as adopted in the previous assessment report, to allow for some extrapolation of trends in weight loss beyond the end of trial follow-up. This time horizon represents a trade-off between allowing the benefits of continued weight reduction (compared with baseline) to accrue and the limited long-term follow-up data, uncertainty over its applicability to current clinical practice and surgical technology (including the absence of reliable data on long-term reoperation rates and conversions). In the analyses conducted using the updated model cost-effectiveness results are presented for three time horizons – trial-only (two years), intermediate extrapolation (to five years) and a longer term extrapolation (to 20 years). The purpose of this is to identify how far the extrapolation of benefits, beyond the trial period, affects the cost-effectiveness estimates.
Baseline cohort of patients with morbid obesity
The baseline cohort consists of patients with morbid obesity, with a BMI of 45, 90% of which are female, with a mean age of 40, and all have failed to achieve or maintain adequate, clinically beneficial weight loss for at least six months using appropriate non-surgical measures. This is similar to the baseline cohort for the previous report and is consistent with current NICE guidance. 9 It is estimated that 10% of morbidly obese patients, eligible for treatment, have Type 2 diabetes before the start of treatment with surgical or non-surgical treatment to promote weight loss.
Additional analyses will be undertaken for a cohort of obese patients, mean BMI of 37 with Type 2 diabetes (adopting the baseline characteristics of the trial reported by Dixon and colleagues117). Treatment outcomes from the trial reported by Dixon and colleagues107 will be applied to estimate the cost-effectiveness of bariatric surgery in this group of patients. These patients meet the NICE criteria in having a BMI greater than 35 and other significant disease (Type 2 diabetes) that could be improved if they lost weight. However, it is not clear from the trial report whether these patients had previously failed to achieve or maintain weight loss with non-surgical interventions. Analyses will also be presented based on characteristics and clinical outcomes for patients recruited to the trial reported by O’Brien and colleagues,115 which selected patients with moderate obesity (baseline BMI between 30 and 35) and are therefore outside the scope of the NICE guideline.
Data sources
Effectiveness data
We have reported on the findings from our systematic review on the clinical effectiveness of bariatric surgery (see Chapter 4, Assessment of clinical effectiveness evidence) and also the findings of the review of natural history models and clinical effectiveness data used in economic evaluations of interventions included in this report (Results, this chapter). The clinical effectiveness review concluded that it was not appropriate to conduct a meta-analysis because of the limited number of studies for comparison of surgical procedures, differences in surgical and non-surgical comparators, heterogeneity of patient populations, and poor reporting (no reporting of standard deviations or equivalent measures of variation). In the absence of formally analysed, robust estimates of the relative effectiveness of surgical and non-surgical approaches, based on all relevant studies included in the clinical effectiveness review, the effectiveness data for this economic evaluation have been derived from five sources:
-
effectiveness estimates adopted in the previous assessment report15
-
a prospective randomised trial of laparoscopic adjustable gastric banding and laparoscopic Roux-en-Y gastric bypass107
-
an RCT of laparoscopic adjustable gastric banding and conventional therapy for patients with BMI of greater than 30 and less than 40, with Type 2 diabetes117
-
an RCT of laparoscopic adjustable gastric banding and an intensive medical programme for patients with BMI of greater than 30 and less than 35115
-
trends in weight reduction for surgical patients and non-surgical controls, over 10 years, from the SOS study. 97
The previous assessment report estimated a percentage weight reduction for bariatric surgery procedures separately, with an underlying assumption that long-term weight loss was very unlikely to occur in patients undergoing non-surgical management, based on data from the SOS study. The baseline assumption for Roux-en-Y gastric bypass, on the basis of a visual inspection of the percentage weight loss from baseline in eight studies, was that patients lose 36% of initial weight and that this weight loss is maintained for five years following surgery. There was more limited evidence on weight reduction following adjustable gastric banding – the baseline assumption corresponded to the percentage weight loss reported in an RCT of adjustable gastric banding and vertical banded gastroplasty. 126
Table 49 reports the baseline weight (or BMI where weight reduction was not reported) for included trials of gastric bypass and the absolute change in weight or BMI reported for each year of follow-up in the trial.
| Study | Baseline | Year 1 | Year 2 | Year 3 | Year 4 | Year 5 |
|---|---|---|---|---|---|---|
| Absolute weight reduction (kg) | ||||||
| Howard120 | 154 | 55 | 53 | 54 | 50 | |
| Sugerman123 | 132 | 44 | 44 | 41 | ||
| Angrisani107 | 118 | 25 | 35 | 34 | ||
| Absolute reduction in BMI (kg/m2) | ||||||
| Stoeckli102 | 43.6 | 10.7 | ||||
| Olbers108 | 42.7 | 13.7 | 14.7 | |||
| Lee124 | 43.18 | 13.6 | 14.7 | |||
Table 50 reports the percentage weight reduction (or percentage reduction in BMI where weight reduction was not reported) calculated from the values reported in Table 49. The baseline assumption of a 36% reduction in weight for gastric bypass, adopted in the previous assessment report, is at the upper extreme of the values reported in Table 50.
| Study | Year 1 | Year 2 | Year 3 | Year 4 | Year 5 |
|---|---|---|---|---|---|
| Percentage weight reduction | |||||
| Howard120 | 36% | 34% | 35% | 32% | |
| Sugerman123 | 33% | 33% | 31% | ||
| Angrisani107 | 21% | 29% | 29% | ||
| Percentage reduction in BMI | |||||
| Stoeckli102 | 25% | ||||
| Olbers108 | 32% | 34% | |||
| Lee124 | 31% | 34% | |||
For consistency, the percentage weight reduction adopted in the previous report will be used in this evaluation – these represent the most optimistic assumptions for weight reduction following gastric bypass. A second set of effectiveness estimates, based on percentage weight reduction reported by Angrisani and colleagues,107 will also be reported. These represent the least optimistic assumptions for weight reduction following gastric bypass.
Table 51 reports the baseline weight (or BMI where weight reduction was not reported) for included trials of adjustable gastric banding and the absolute change in weight or BMI reported for each year of follow-up in the trial.
| Study | Baseline | Year 1 | Year 2 | Year 3 | Year 4 | Year 5 |
|---|---|---|---|---|---|---|
| Absolute weight reduction (kg) | ||||||
| Angrisani107 | 117 | 15 | 19 | 19 | ||
| Nilsell126 | 124 | 26 | 36 | 39 | 38 | 43 |
| De Wit132 | 152 | 35 | ||||
| Absolute reduction in BMI (kg/m2) | ||||||
| Stoeckli102 | 41.7 | 8.0 | 8.5 | |||
| Morino110 | 44.7 | 9.2 | 9.9 | 9.0 | ||
| Van Dielen127 | 46.7 | 11.7 | 12.1 | |||
Table 52 reports the percentage weight reduction (or percentage reduction in BMI where weight reduction was not reported) calculated from values reported in Table 51. The baseline assumption of an initial 20% reduction in weight in the first year rising to a 33% weight reduction at five years, adopted in the previous assessment report, is the most optimistic set of assumptions for weight reduction following adjustable gastric banding and contrasts starkly with the results of the trial reported by Angrisani and colleagues. 107 For consistency the percentage weight reduction adopted in the previous report will be used in this evaluation. However a second set of effectiveness estimates, based on percentage weight reduction reported by Angrisani and colleagues107 will also be reported, representing the least optimistic assumptions for weight reduction following adjustable gastric banding.
| Study | Year 1 | Year 2 | Year 3 | Year 4 | Year 5 |
|---|---|---|---|---|---|
| Percentage weight reduction | |||||
| Angrisani107 | 13% | 16% | 16% | ||
| Nilsell126 | 21% | 29% | 31% | 31% | 35% |
| De Wit132 | 23% | ||||
| Percentage reduction in BMI | |||||
| Stoeckli102 | 19% | 20% | |||
| Morino110 | 21% | 22% | 20% | ||
| Van Dielen127 | 25% | 26% | |||
Data on trends in weight reduction for surgical patients and non-surgical controls, over 10 years, from the SOS study97 are used to extrapolate beyond five years of follow-up. Percentage weight reduction for gastric bypass patients was estimated to decline by 17.7% from five to 10 years of follow-up (estimated from Sjostrom and colleagues97, see Figure 1of their article). The equivalent decline for adjustable gastric banding patients was estimated to be 14.7%.
Table 53 reports the percentage weight reduction applied in the model for each intervention and comparator for morbidly obese patients. Where values were not reported for each year (Angrisani and colleagues reported trial outcomes at year 1, year 3 and year 5) values were estimated by linear interpolation.
| Time (years) | Non-surgical management | Gastric bypass | Adjustable gastric banding | ||
|---|---|---|---|---|---|
| Optimistic | Pessimistic | Optimistic | Pessimistic | ||
| 0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| 1 | 0.0 | – 36.0 | – 21.4 | – 21.0 | – 12.6 |
| 2 | 0.0 | – 36.0 | – 25.3 | – 29.0 | – 14.4 |
| 3 | 0.0 | – 36.0 | – 29.2 | – 31.5 | – 16.2 |
| 4 | 0.0 | – 36.0 | – 29.0 | – 30.6 | – 16.3 |
| 5 | 0.0 | – 36.0 | – 28.8 | – 34.7 | – 16.4 |
| 6 | 0.0 | – 34.7 | – 27.8 | – 33.7 | – 15.9 |
| 7 | 0.0 | – 33.5 | – 26.8 | – 32.6 | – 15.4 |
| 8 | 0.0 | – 32.2 | – 25.8 | – 31.6 | – 15.0 |
| 9 | 0.0 | – 30.9 | – 24.7 | – 30.6 | – 14.5 |
| 10 | 0.0 | – 29.6 | – 23.7 | – 29.6 | – 14.0 |
Table 54 reports the weight loss from baseline for patients followed up for two years following surgery using laparoscopic adjustable gastric banding compared with conventional diabetes care with a focus on weight loss by lifestyle change in the trial reported by Dixon and colleagues. 117
| Intervention | Weight loss (standard error) | BMI |
|---|---|---|
| Surgical | 21.1 (1.9170) | 29.6 |
| Non-surgical | 1.5 (0.9859) | 36.6 |
For the base-case analysis it is assumed that the reduction in BMI occurs from entry to the study and persists for two years with reversion to baseline BMI of 37 kg/m2 at the end of the study period (two years). An additional analysis will be reported, extrapolating the percentage weight reduction over 10 years using data on trends in weight reduction for patients undergoing gastric banding from the SOS study,97 which suggest that the percentage weight reduction from baseline reduces by one-third from two to 10 years following surgery.
Table 55 reports the percentage weight loss from baseline at four observation points for moderately obese patients followed up for two years following surgery using laparoscopic adjustable gastric banding compared with a non-surgical programme using behaviour modification, VLCDs and pharmacotherapy.
| Intervention | 6 months | 12 months | 18 months | 24 months | ||||
|---|---|---|---|---|---|---|---|---|
| Weight loss (%) | BMI | Weight loss (%) | BMI | Weight loss (%) | BMI | Weight loss (%) | BMI | |
| Surgical | 14.1 | 28.8 | 19.7 | 26.9 | 20.8 | 26.5 | 21.6 | 26.3 |
| Non-surgical | 13.9 | 28.8 | 10.0 | 30.1 | 7.5 | 31.0 | 5.6 | 31.6 |
For the base-case analysis it is assumed that the reduction in BMI follows the pattern described by the solid lines in Figure 3, showing the estimated BMI over time for surgical and non-surgical cohorts. This figure reproduces Figure 3 from the original trial report115 except that it plots estimated BMI (reported in Table 54), rather than per cent weight loss from baseline. For the base-case analysis both cohorts revert to baseline BMI at the end of two years, i.e. applying data from the clinical trial report with no extrapolation of effect beyond the trial duration. Inspection of Figure 3 suggests that BMI for the non-surgical cohort is already reverting toward the baseline level at two years, whereas for the surgical cohort the BMI appears to be stabilising around a value 20% below the baseline level.
An additional scenario is considered:
-
As illustrated using the dashed lines in Figure 3, a linear extrapolation has been estimated using the final two BMI values (month 18 and month 24) for the non-surgical cohort. This suggests that BMI is reverting to its baseline value at a rate of 0.106 points per month. On this basis the estimated BMI reverts to its baseline value 18 months after the end of the two-year study period. Applying the same rate of increase for the surgical cohort implies that BMI reverts to its baseline value 68 months (52/3 years) after the end of the two-year study period.
FIGURE 3.
Estimated BMI for moderately obese subjects over two years surgical and non-surgical treatment. BMI, body mass index.
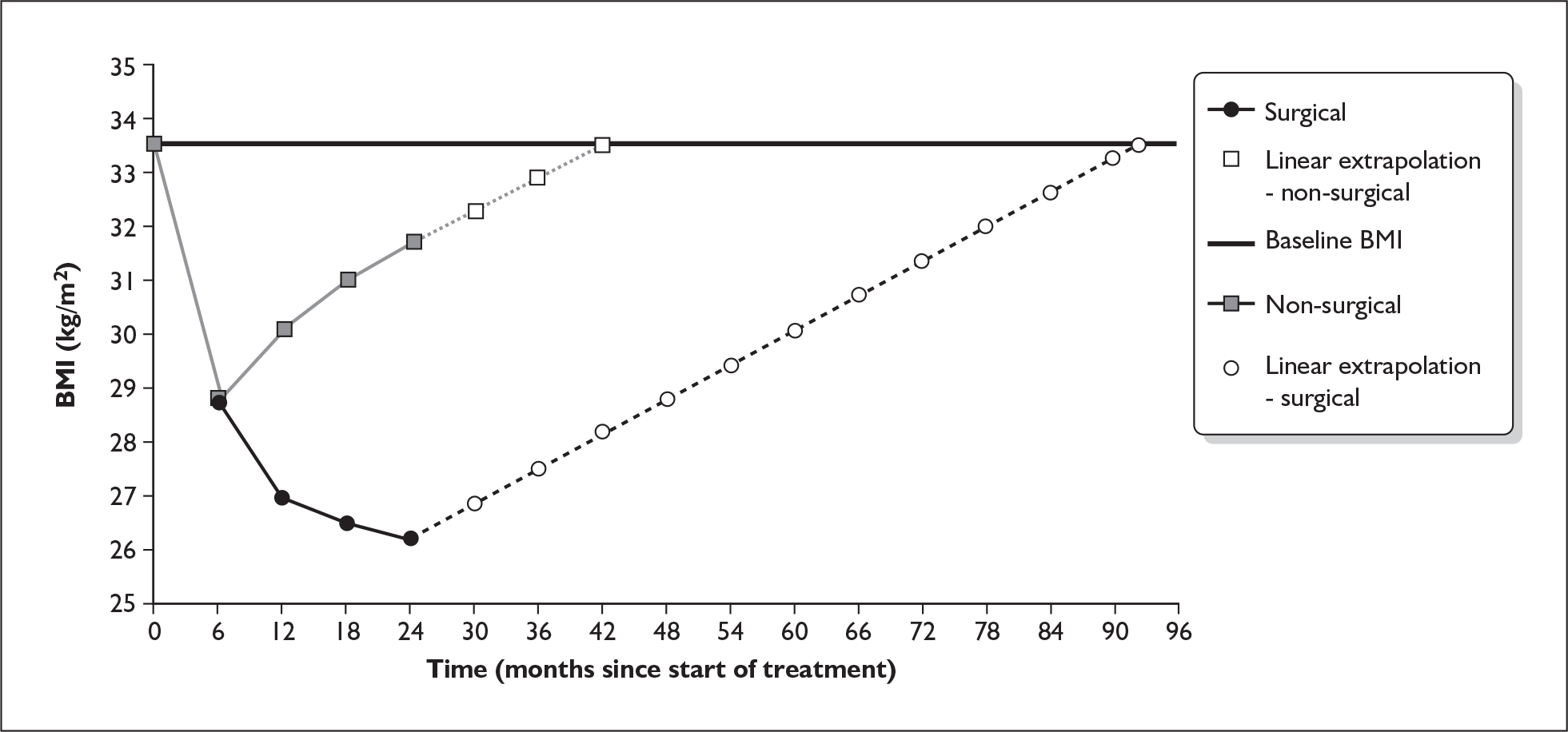
The previous assessment report estimated the proportion of morbidly obese patients with existing Type 2 diabetes who revert to normoglycaemia following bariatric surgery as 75%, based on the proportion of patients who were off medication at three years reported by Hall and colleagues. 149 Similar proportions have been reported for patients with Type 2 diabetes in the SOS study (72% recovery from diabetes at two years)97 and Dixon and colleagues117 (73% remission of diabetes in surgical patients versus 13% in conventionally treated patients, though these were patients with a lower BMI of between 30 and 40). At 10 years of follow-up the SOS study97 reported that 36% of patients who had had Type 2 diabetes at baseline, were in remission following bariatric surgery. For the base case we adopt the assumption that 75% of prevalent Type 2 diabetes cases revert to normoglycaemia up to two years following bariatric surgery and that 36% are in recovery at 10 years – the percentage of patients for intermediate years is estimated using linear interpolation. The proportion of patients in the control cohort in the SOS study97 is used to estimate recovery from Type 2 diabetes with non-surgical management. These values are 21% at two years and 13% at 10 years – as with the surgically managed patients the values for intermediate years are estimated using linear interpolation.
Table 56 reports the percentage of patients with Type 2 diabetes at baseline, who were in remission at two years following surgery using laparoscopic adjustable gastric banding compared with conventional diabetes care in the trial reported by Dixon and colleagues. 117
| Intervention | per cent of patients resolving diabetes (standard error) |
|---|---|
| Surgical | 73.3 (0.0811) |
| Non-surgical | 13.3 (0.0614) |
For the base-case analysis it is assumed that the resolution of diabetes occurs from entry to the study and persists for two years with reversion to Type 2 diabetes at the end of the study period (two years).
The effect of bariatric surgery on blood pressure and lipids is not included in the model for morbidly obese patients because the baseline ratio of total to HDL-cholesterol and change from baseline over time was not reported in any of the included studies. Hence the model for morbidly obese patients does not include an estimate of the effect of bariatric surgery on cardiovascular morbidity or mortality.
Table 57 reports the change in systolic blood pressure and change in the ratio of total to HDL-cholesterol from baseline for patients followed up for two years following surgery using laparoscopic adjustable gastric banding compared with conventional diabetes care in the trial reported by Dixon and colleagues. 117
| Intervention | Change in systolic blood pressure, mmHg (standard error) | Change in the ratio of total to HDL-cholesterol (standard error) |
|---|---|---|
| Surgical | – 6.0 (3.2681) | – 0.82 (0.3469) |
| Non-surgical | – 1.7 (2.5926) | – 0.14 (0.1899) |
For the base-case analysis it is assumed that the change in systolic blood pressure (from a baseline value of 135 mmHg) and change in ratio of total to HDL-cholesterol (from a baseline ratio of 4.4) occurs from entry to the study and persists for two years with reversion to baseline values at the end of the study period (two years).
Table 58 reports the change in systolic blood pressure and change in the ratio of total to HDL-cholesterol from baseline at four observation points for moderately obese patients followed up for two years following surgery using laparoscopic adjustable gastric banding compared with a non-surgical programme using behaviour modification, VLCDs and pharmacotherapy.
| Intervention | Change in systolic blood pressure % (standard error) | Change in the ratio of total to HDL- cholesterol % (standard error) |
|---|---|---|
| Surgical | – 10.8 (1.7294) | – 21.3 (2.4019) |
| Non-surgical | – 7.2 (1.7422) | – 8.0 (2.8198) |
For the base-case analysis it is assumed that the change in systolic blood pressure (from a baseline of 131 mmHg) and change in ratio of total to HDL-cholesterol (from a baseline ratio of 4.3) occurs from entry to the study and persists for two years with reversion to baseline values at the end of the study period (two years). For the alternative scenarios – where reduction in BMI below baseline levels is assumed to persist beyond two years (up to 18 months for non-surgical and 68 months for the surgical cohort in the first scenario, and up to 14 months for the second) – the same duration of effect is assumed for changes in systolic blood pressure and ratio of total to HDL-cholesterol. Values between the observed changes at two years and the assumed date of reversion to baseline are estimated by linear interpolation.
The Description of health problem section in chapter 1 of this report briefly reviewed epidemiological evidence for the association between BMI and Type 2 diabetes, indicating an approximate doubling of the odds of Type 2 diabetes for obese subjects compared with those with a BMI less than 25. Targeted searches were undertaken to identify studies reporting diabetes incidence by BMI. Economic evaluations of interventions to promote weight reduction were also identified and searched for data relating BMI and diabetes incidence.
Column two of Table 59 reports estimates of diabetes incidence by BMI, derived by Warren and colleagues. 163 These are based on data reported by Colditz and colleagues164 (column one Table 59), which reported diabetes incidence by bounded categories, up to a BMI value of 34.9, with the final incidence rate applied to an unbounded BMI category of 35 and over. Warren and colleagues163 extrapolated for values beyond 35 kg/m2 using data from Sjostrom and colleagues,88 which reported two-year incidence in control patients (who did not lose weight and had average BMI of 40) of 6.3% versus a diabetes incidence of 0.2% in treated patients, who achieved an average weight reduction of 27.8 kg (reducing average BMI from 42.1 to 32.4 kg/m2).
| BMI | Colditz and colleagues164 Age standardised risk per 100,000 persons | Warren and colleagues163 % annual incidence | Polynomial regression using estimates of Colditz and colleagues164 |
|---|---|---|---|
| 22–22.9 | 37.4 | 0.04 | 0.04 |
| 23–23.9 | 54.9 | 0.05 | 0.05 |
| 24–24.9 | 62.9 | 0.06 | 0.07 |
| 25–26.9 | 103.5 | 0.10 | 0.11 |
| 27–28.9 | 200.4 | 0.20 | 0.21 |
| 29–30.9 | 354.5 | 0.35 | 0.34 |
| 31–32.9 | 521.2 | 0.52 | 0.51 |
| 33–34.9 | 703.6 | 0.70 | 0.71 |
| 35–36.9 | 1190.5a | 1.19 | 0.95 |
| 37–38.9 | 1.55 | 1.23 | |
| 39–40.9 | 2.00 | 1.55 | |
| 41–42.9 | 2.50 | 1.90 | |
| 43–44.9 | 3.15 | 2.28 |
Comparing the incidence rates estimated by Warren and colleagues163 with those adopted in the previous report [2.3% without surgery (BMI of 45) and 0.45% with surgery (BMI between 29 and 38)] suggests that adopting these BMI-specific values would estimate a greater difference in diabetes incidence than would be the case with the original model. For example, the original model predicted that, in cohorts of 100 patients with an initial BMI of 45, an initial Type 2 diabetes prevalence of 10%, and a reduction in BMI of 16 points (over five years) following surgery compared with no reduction for non-surgical management, 43% treated non-surgically and 35% treated with gastric bypass would have Type 2 diabetes after 20 years. The equivalent values using the same baseline assumptions as in the original model, but using the BMI-specific incidences, are 53% and 41% respectively. The difference in diabetes incidence between the two cohorts is therefore 9% in the original model and 12% using the incidence rates adopted by Warren and colleagues. 163
An alternative method for estimating BMI-specific diabetes incidence for values of BMI beyond 35 would be to fit a regression line. Table 59 reports the results of fitting a polynomial regression, using the mid-points of the BMI categories, to the age-standardised incidences for the bounded categories up to 34.9. The regression equation is then used to extrapolate values beyond BMI of 35. This gives an estimated incidence of 2.5% for a BMI of 45, which is more consistent with values adopted for the model used in the previous report. 15 Repeating the comparison described earlier, in cohorts of 100 patients with an initial BMI of 45, an initial Type 2 diabetes prevalence of 10%, and a reduction in BMI of 16 points (over five years) following surgery compared with no reduction for non-surgical management, 46% treated non-surgically and 36% treated with gastric bypass would have Type 2 diabetes after 20 years. The difference in diabetes incidence between the two cohorts is therefore 9% in the original model and 10% using the polynomial regression for extrapolation.
We adopt the extrapolation based on the polynomial regression for the base case in the model, applying the values estimated by Warren and colleagues163 in a sensitivity analysis.
Targeted searches failed to find reliable published estimates relating CHD [acute myocardial infarction (AMI) or angina] to BMI alone. Where data were identified they related to CHD mortality165–167 rather than incidence or CHD events and used BMI categories that were of little benefit in populating the model (e.g. upper BMI categories set at greater than or equal to 32 or greater than or equal to 35).
To estimate CHD for patients with and without diabetes the Framingham Heart Study (FHS) accelerated failure time risk equations are used,168 which predict first cardiovascular events. The hazard of CHD events is estimated based on sex, age, systolic blood pressure, smoking status, total cholesterol to HDL-cholesterol ratio (TC : HDL). These equations are typically used to derive 10-year risks. However, a reparameterisation, as proposed by Caro and colleagues169 has been adopted to estimate hazards for each model cycle (see Appendix 19 for details).
The Framingham equation for myocardial infarction only, is used in the model, therefore the model does not predict angina in the modelled cohorts.
To apply the FHS risk equations, information on baseline systolic blood pressure and TC : HDL and also changes from baseline are required for included clinical trials. These data are not available for all trials and therefore predictions of CHD risk may not be available for all comparisons. In that situation a more limited version of the model, similar to that adopted for the previous report,15 will be used.
Targeted searches identified studies describing associations between total stroke risk (also broken down by ischaemic and haemorrhagic stroke) by BMI for both men170 and women. 171 Both studies found significantly higher stroke risk for participants with greater BMI. The relative risk was 2.00 (95% CI 1.48 to 2.71) for total stroke, 1.95 (95% CI 1.398 to 2.72) for ischaemic stroke and 2.25 (95% CI 1.01 to 5.01) for haemorrhagic stroke in men with BMI of 30 or more compared with those with a BMI less than 23. In women the relative risks of ischaemic stroke were 1.75 (95% CI 1.17 to 2.59) for BMI of 27 to 28.9, 1.90 (95% CI 1.28 to 2.82) for BMI of 29 to 31.9 and 2.37 (95% CI 1.60 to 3.50) for BMI of 32 or more, compared with those with a BMI less than 21. For haemorrhagic stroke, in women, there was a non-significant inverse association between risk and obesity. However, as with studies reporting associations between BMI and CHD mortality, the BMI categories reported in these studies were of little benefit in populating the model (e.g. upper BMI categories set at greater than or equal to 30 or greater than or equal to 32). In addition, the reported relative risks did not distinguish between subjects with or without diabetes.
As for CHD, stroke risk for patients with and without diabetes will be estimated using the FHS risk equations,168 which predict first stroke events, based on sex, age, systolic blood pressure, smoking status and TC : HDL. The same reparameterisation, as adopted for CHD, will be used for predicting stroke risk. However, there is no adjustment for BMI applied in calculating the stroke risks.
As discussed earlier, where baseline systolic blood pressure and TC : HDL and also changes from baseline are not reported for the included clinical trials these risks cannot be computed and a more limited version of the model, similar to that adopted for the previous report,15 will be used.
Health state values/utilities
A targeted search was conducted to identify published utility estimates for the BMI values relevant to the obese population included in the models. The search aimed to identify estimates of the change in utility scores based on the unit change in BMI values. Utility estimates were only considered where they used a validated, multiattribute utility scale (e.g. EQ-5D) or appropriate methodology (e.g. standard gamble or time trade-off techniques) and provided a clear definition of utility scores anchors 0 and 1 (Table 60). Utility values within a broader scope than is relevant to the current economic model can be found in a recent systematic review of the impact of body weight on patient utilities with or without Type 2 diabetes. 172 This systematic review does not include utility estimates associated with specific surgical interventions. Critical appraisal of utility estimates used in economic evaluations of bariatric surgeries is presented in the Translation of short-term outcomes into final outcomes section in this chapter. A systematic review of published utility estimates in the obese population,173 published in 2004, identified only one study that assessed the change in utility scores as a function of change in BMI. 152 This study is described below.
| Men | Women | People with diabetes | People without diabetes | Tool used | Source and comments | |
|---|---|---|---|---|---|---|
| Change in utility per one unit change in BMI | 0.01665 | 0.0264 | 0.0285 | 0.017 | TTO | Hakim and colleagues152 derived utility values from the data on the cohort of 621 patients predominantly female (78%) and white (91%) with the mean age of 42 years and mean BMI of 35 kg/m2 controlling for age, gender and the health preference value at the beginning of the year |
| Change in utility per one unit change in BMI | With no diabetes-related complications: 0.01; with diabetes-related complications: 0.016 | EQ-5D | Currie and colleagues178 derived utility values from the hospitalised patients with mean BMI of 29 kg/m2 controlling for age and peripheral neuropathy | |||
| Change in utility per one unit change in BMI | 0.0168 | Dixon and colleagues173 derived utility values from 13,152 inpatients and outpatients. Mean BMI was not reported for the entire sample. The results are estimated for patients with BMI> 25 kg/m2 | ||||
| Change in utility per one unit change in BMI | 0.01 | 0.0079 | EQ-5D | Lee and colleagues179 derived utility values from regression analysis controlling for age but not for gender. The data on inpatients and outpatients included 24,250 people without and 2575 patients with Type 2 diabetes with mean age of 59 and 68 in patients without and with Type 2 diabetes, respectively. The patients were predominantly white (>95%) with mean BMI of 26 kg/m2 and 29 kg/m2 in patients without and with Type 2 diabetes, respectively. | ||
Some of the identified studies indicated that obesity is an independent predictor of the health-related preferences with the utility scores as a function of BMI decreasing (in absolute values) as the number of covariates included in the model increases. 174,175 The search failed to identify the change in utility values specific to an obese population with CHD. However, some studies estimated the change in utility scores in obese populations with and without diabetes. 152,179 For example, Hakim and colleagues152 found that a one-unit decrease in BMI, over a period of one year, was associated with a gain of 0.017, which was independent of age or gender. However, overweight patients with Type 2 diabetes appear to have the greatest gain in utility for a given change in BMI over one year (0.0285).
There is a large variation in the estimated change in utility with the unit change in BMI. This is likely to relate to the differences in characteristics of the population and the number of covariates included in the analysis. Recent cost-effectiveness studies in obesity141,176 have employed the utility values reported by Hakim and colleagues152 as these are derived from the obese (rather than overweight) population, have a time-frame of one year (which is consistent with the typical cycle duration used in the model) and explicitly control for baseline utility values. The disadvantage of these values is that the assumption of the linear relationship between the change in utility and the change in BMI may have produced biased estimates of utility gain over the range of extreme BMI values.
We adopt the values reported by Hakim and colleagues152 in this report, as they represent the most methodologically sound estimates derived from subjects across a wide range of obesity levels. The sensitivity of cost-effectiveness estimates to alternative assumptions regarding health-state utility is tested in a sensitivity analysis.
Cost data
Costs in the model were developed in two stages. First the additional resource use, in terms of preoperative assessments, hospital admissions for surgery, managing adverse events and postdischarge care were identified based on estimates developed for the previous review,15 published literature, discussion with surgical specialists and a costing developed for Aberdeen specialist obesity services (U. Kulkarni, NHS Grampian, 2008, personal communication). Resource use associated with non-surgical interventions was estimated using a similar approach. The resource use estimates were combined with unit costs provided by the finance department at Southampton University Hospital Trust, and from routine published sources,177 to provide estimates of the costs of surgical and non-surgical weight loss programmes. These are described below as intervention costs. Second, literature describing the costs of health states associated with obesity was reviewed and appropriate estimates, applicable to the UK setting, were extracted and used in the analysis. These are described below as health-state costs.
Resource use associated with bariatric surgery procedures has been estimated based on estimates developed for the previous review,15 duration of operative procedures and total length of stay used in published economic evaluations, in addition to clinical studies reviewed in Chapter 4, Assessment of clinical effectiveness evidence and discussion with surgical specialists. These are reported in Table 61. In the base case we estimate costs for each procedure assuming that they will be conducted laparoscopically wherever possible, using the breakdown of open and laparoscopic procedures as in the previous review (see Table 62).
| Resource use | Unit cost | Open | Laparoscopic |
|---|---|---|---|
| Gastric bypass | |||
| Time in theatre (minutes) | £16 per minute | 180 | 180 |
| Surgeons operating time (per hour) | Consultant: £87.11 | 2 | 2 |
| Anaesthetists time (per hour) | Consultant: £72.64 | 3 | 3 |
| High cost consumables | £2040 per procedure | 1 | 1 |
| Days on ward | £261 per day | 5 | 5 |
| Days in ITU | £1986 per day | 21.1% | 7.5% |
| Days in HDU | £497 per day | 78.9% | 0 |
| Specialist dietitian | £32 per hour | 2 | 2 |
| Physiotherapy | £38 per hour | 1 | 1 |
| Total cost gastric bypass | £7705 | £7042 | |
| Adjustable gastric banding | |||
| Time in theatre (minutes) | £16 per minute | 120 | 120 |
| Surgeons operating time (per hour) | Consultant: £87.11 | 1 | 1 |
| Anaesthetists time (per hour) | Consultant: £72.64 | 2 | 2 |
| High cost consumables | £1440 per procedure | 1 | 1 |
| Days on ward | £261 per day | 5 | 2 |
| Days in ITU | £1986 per day | 0 | 0 |
| Days in HDU | £497 per day | 100% | 0 |
| Specialist dietitian | £32 per hour | 2 | 2 |
| Physiotherapy | £38 per hour | 1 | 1 |
| Total cost adjustable gastric banding | £5584 | £4304 | |
| Gastric bypass | Adjustable gastric banding | |
|---|---|---|
| Proportion open procedures | 10% | 8% |
The resource use estimates differ from those adopted for the previous review. 15 Duration of surgery and length of stay for laparoscopic gastric bypass and laparoscopic gastric banding are lower than the previous values [235 minutes and six days for laparoscopic gastric bypass (operating time and total length of stay, respectively) and 150 minutes and six days for laparoscopic adjustable gastric banding]. The costings adopted here assume a lower use of high-dependency care following surgery. In the previous review all patients were assumed to spend one day in either HDU or ITU, whereas clinical advice for this update suggested that patients undergoing laparoscopic procedures typically recover on the ward unless they experience perioperative complications requiring admission to ITU. Patients undergoing open operations are estimated to spend one day in HDU following surgery.
In contrast to the costings developed for the previous review, gastric bypass is estimated to cost more than adjustable gastric banding. The previously estimated values for gastric bypass were £3286 and £3174 for laparoscopic and open procedures, respectively (using values for the 1999/2000 financial year). The equivalent values for adjustable gastric banding were £3751 and £3645.
Unit costs applied to the resource use estimates were provided by the finance department at Southampton University Hospital Trust. The ITU, HDU and ward unit costs are based on 2006/7 Reference Costs uprated to 2007/8 values. Ward unit costs are based on the excess cost per bed day for general surgery. Staff costs are based on a consultant anaesthetist with discretionary points, consultant surgeon with discretionary points (MC10) and a specialist registrar (MN25). There is a large difference in the unit cost for theatre time in this review (£960 per hour) compared with the previous review15 which estimated theatre time at £335 per hour (approximately £470 per hour at 2007/8 prices, uprated using the Hospital and Community Health Services Pay and Prices Index177). Specialist dietitian and hospital physiotherapist unit costs were taken from the Unit costs of Health and Social Care. 177
The included clinical trials provide little additional information on conversion from laparoscopic to open surgery. Moreover it is difficult to generalise the results from clinical trials, which are likely to be undertaken in more specialist centres, with more experience which may be less likely to convert to open procedures than would be the case in other centres. The proportion of cases converting to open procedures is 0%108 to 23%131 for laparoscopic Roux-en-Y gastric bypass. For laparoscopic adjustable gastric banding the range in trials reporting conversions is narrower: 0%110 to 4%. 127 Given the limited additional data on the rate of conversion from laparoscopic to open procedures reported in the included trials, we used the values adopted in the previous review, see Table 62.
Resource use assumptions for costing non-surgical management of morbidly obese patients have been taken from the previous review,15 see Table 63. Unit costs have been updated using Unit Costs of Health and Social Care. 177
| Resource use | Unit cost | Contacts per year |
|---|---|---|
| General practitioner | £30 | 4 |
| Community dietitian | £48 | 2 |
| Practice nurse | £9 | 2 |
| District nurse | £24 | 2 |
| Total cost of non-surgical management | £282 | |
Resource use assumptions for moderately obese patients undergoing the non-surgical weight reduction programme were based on the description of the programme in the clinical trial report by O’Brien and colleagues. 115 The programme consisted of an intensive six-month period of VLCD and pharmacotherapy as well as specialist dietary advice. The resource use assumptions extracted from the clinical trial report and the unit costs applied to the resource estimates are reported in Table 64.
| Resource category | Phase of programme | Unit cost | Contacts per period |
|---|---|---|---|
| Contact with physician (in out-patients, every two weeks for intensive phase and every six weeks for remainder) | Intensive phase (0 – 6 months) |
First visit: £144 Subsequent: £99 |
1 13a |
| Months 7–12 | £99 | 4b | |
| Months 13–24 | £99 | 9b | |
| Total cost of medical management for non-surgical weight loss programme | £2718 | ||
| Resource category | Phase of programme | Unit cost | Resource Use |
| Intensive management (diet and pharmacotherapy) | Very-low-calorie diet (0–12 weeks) |
£1.27 (1 packet optifast) |
168 (2 per day) |
| Transition phase (weeks 13–16) |
£1.27 (1 packet optifast) £0.40 (120 mg orlistat) |
28 (1 per day) 28 (1 per day) |
|
| Pharmacotherapy only (weeks 17–26) |
£0.40 (120 mg orlistat) |
210 (3 per day) |
|
| Postintensive management | Months 7–24 |
£0.40 (120 mg orlistat) |
1057c (3 per day) |
| Total cost of very-low-calorie diet and pharmacotherapy for non-surgical weight loss programme | £767 | ||
The frequency of patients attendance for hospital or primary care, associated with each intervention, was based on estimates developed for the previous review,15 published literature, discussion with surgical specialists and a costing developed for Aberdeen specialist obesity services (U. Kulkarni, NHS Grampian, 2008, personal communication). All new patients are evaluated in the outpatient department and receive an electrocardiogram. In the previous review the preoperative assessment schedule assumed that, for every patient undergoing surgery, four patients are screened for eligibility and two undergo workup (by VLCD) to assess suitability for treatment, based on figures reported in Andersen and colleagues. 180 This corresponded to seven outpatient visits, four dietitian consultations and one session with a psychologist. The unit costs and estimated cost per patient undergoing surgery are listed in Table 65.
| Category of resource use | Frequency | Unit cost (£) | Total cost | |
|---|---|---|---|---|
| Preoperative assessment | 7 outpatient visits | 4 × 144; 3 × 99 | £1114 | |
| 4 dietitian consultationsa | 32 per hour | |||
| 4 dietitian consultationsb | 32 per hour | |||
| 1 session with a psychologistc | 67 per hour | |||
| Postdischarge | Primary care in month following discharge | 6 GP visits | 32 per visit | £306 |
| 2 practice nurse visits | 9 per visit | |||
| 4 district nurse visits | 24 per visit | |||
| Follow-up care | Year 1 | 4 outpatient visits | 99 per visit | £849 |
| 12 community dietitian contactsd | 48 per hour | |||
| 2 psychology consultations | 67 per hour | |||
| Year 2 | 4 outpatient visits | 99 per visit | £636 | |
| 4 community dietitian contactsd | 48 per hour | |||
| 2 psychology consultations | 67 per hour | |||
| Year 3 and beyond | 2 outpatient visits | 99 per visit | £318 | |
| 2 community dietitian contactsd | 48 per hour | |||
| 1 psychology consultations | 67 per hour |
Based on the costing developed in Aberdeen, it was assumed that patients undergoing adjustable gastric banding would make four additional attendances for the initial fill and band adjustments and that they would have additional specialist dietitian consultations associated with these band adjustments. These additional attendances add £428 to the costs of follow-up for patients undergoing adjustable gastric banding.
The costs of managing adverse events were taken into account in our analyses by identifying the proportion of patients having major perioperative complications requiring ITU admission, and the proportion of patients having early reoperation (within 30 days) because of failure of the original operation (typically band slippage for patients undergoing adjustable gastric band procedures or bleeding, stenosis or leakage in patients undergoing gastric bypass). Revision surgery was estimated to cost the same as the original surgical procedure. Complications requiring admission to ITU were costed using the estimated length of ITU admission and the per diem cost (£1986) reported in Table 61. The costs were applied to the proportion of patients experiencing perioperative complications requiring ITU admission (7.5% of laparoscopic gastric bypass patients113,124) and to the proportion of patients requiring surgical revision (2% for laparoscopic adjustable gastric bypass110 and 13.5% for gastric bypass107,108).
Patients are likely to undergo a number of additional surgical procedures as a result of undergoing bariatric surgery, even when the original operation was successful. Expert opinion suggested that 5% of patients undergoing laparoscopic gastric bypass would require an additional operation for repair of internal hernia. Additionally, patients undergoing active weight reduction are at risk of developing gallstones, and may require cholecystectomy. It has been suggested that 35–38% of patients with morbid obesity develop gallstones as they lose weight following bariatric surgery181–183 (which has led some surgeons to advocate performing cholecystectomy during bariatric surgery). Miller and colleagues184 observed 12 cholecystectomies in 60 placebo-treated patients during two years follow-up in their trial of prophylaxis against gallstone formation for patients following vertical banded gastroplasty and adjustable gastric banding (patients had a mean preoperative BMI of 44.3 and were 85% female). De Wit and colleagues reported 8% of patients having a cholecystectomy within one year of bariatric surgery. 132 In the model we assume that 20% of morbidly obese patients undergo cholecystectomy within two years of a bariatric procedure (8% in the first year and 12% in the second, reflecting the observation that the peak incidence of symptomatic gallstones is 16 months after surgery).
Health-state costs
The model, as described in the section Model type and rationale for the model structure, this chapter, consists of five health states (excluding death). Costs for the health state labelled ‘no comorbidity’ in the state transition diagram, Figure 2, consists only of ongoing monitoring for postsurgical patients, or routine follow-up for patients receiving non-surgical intervention. No additional, state-specific, costs are applied to this state. The same assumption holds for the ‘remission of comorbidity’ health state.
Table 66 reports the health-state costs adopted in the model. The Type 2 diabetes cost is based on the CODE-2 UK160 estimate of health-care resource use and costs applied in the economic model developed for the previous report. The average cost per patient year (£1505) reported for CODE-2 UK, with a cost year of 1998–9, has been inflated to 2007–8 prices using the Hospital and Community Health Services (HCHS) Pay and Prices Index. 177 The breakdown of costs reported for CODE-2 UK was that 36.2% of costs were attributable to hospital admissions and 37.7% to ambulatory care, with the remainder attributable to drug treatment (22.5%) and insulin (3.5%).
| Health state | Acute (£) | Chronic (£) | Source |
|---|---|---|---|
| Diabetes | 2197 | Williams and colleagues160 | |
| AMI | 1613 | 565 | Southampton CHD treatment model |
| Stroke | 9540a | 2565 | Ward and colleagues186 |
Health-state costs for AMI were based on inputs to the Southampton CHD treatment model (K. Cooper, University of Southampton, 2008, personal communication). The acute costs are based on NHS Reference Costs for non-elective inpatient admission with AMI. Costs for the post-MI health state are based on daily dosage and estimated use of a range of drugs (statins, calcium channel blockers, beta blockers, acetylcholinesterase inhibitors and nitrates) combined with unit costs from the British National Formulary, as well as health-care utilisation data from the Health Survey for England17 combined appropriate unit costs. 177 All costs were estimated for the 2005–6 financial year and have been inflated to 2007–8 prices using the HCHS Pay and Prices Index.
Health-state costs for stroke were based on costs applied in a recent HTA of statins for the prevention of coronary events. 186 These were derived from a published study187 estimating the economic burden of stroke in the UK. The acute cost of a stroke was estimated using the cost of acute events reported by Youman and colleagues187 (mild stroke £5099, moderate stroke £4816 and severe stroke £10,555), weighted by the distribution of severity of strokes. The costs reported by Ward and colleagues186 were for the financial year 2004–5 and have been inflated to 2007–8 prices using the HCHS Pay and Prices Index.
Discounting of future costs and benefits
A discount rate of 3.5% has been applied to future costs and benefits in line with current guidance. Discount rates of 0% and 6% for costs and 0% and 1.5% for outcomes have been applied in the sensitivity analyses.
Presentation of results
We report findings on the cost-effectiveness of interventions based on analysis of a cohort of patients having baseline age, sex and weight characteristics, as discussed earlier. Surgical procedures are compared with appropriate non-surgical comparators.
We report the results of these comparisons in terms of the incremental gain in QALYs and the incremental costs determined in the cohort analysis.
Assessment of uncertainty in the SHTAC analysis (sensitivity analysis)
Parameter uncertainty in the updated model is addressed using probabilistic sensitivity analysis. Probability distributions are assigned to the point estimates used in the base-case analysis. Appendix 20 reports the variables included in the probabilistic sensitivity analyses, the form of distribution used for sampling and the parameters of the distribution.
In the absence of a robust, pooled estimate of treatment effect (with associated estimate of variability) we felt it was inappropriate to undertake probabilistic sensitivity analysis using the original model. In both models deterministic sensitivity analysis is used to address particular areas of uncertainty in the model related to:
-
model structure
-
methodological assumptions
-
parameters around which there is considerable uncertainty or which may be expected, a priori, to have disproportionate impact on study results.
The purpose of this analysis is to identify clearly the impact of this uncertainty and to test the robustness of the cost-effectiveness results to variation in structural assumptions and parameter inputs.
SHTAC cost-effectiveness model – summary of methods
-
The model developed for the previous assessment report was assessed against other published models for completeness and relevance, and the conceptual model was extended to include CHD and stroke. The ability to include these additional health states in the economic model depends on the methods adopted to estimate transitions to these states, which are not typically based on weight-related measures (such as BMI), but use blood pressure and lipid measurements. Where such measurements are reported, the expanded version of the model may be relevant. We propose using the FHS equations to model cardiovascular risks for the expanded model, which require values for blood pressure (systolic or diastolic) and the TC : HDL ratio as well as patients’ age, sex, smoking status and whether they have developed diabetes. However, not all studies will report changes in blood pressure and lipid measurements, hence the expanded model may not be applicable to all studies.
-
The analysis was developed for three patient populations covered by studies included in the clinical effectiveness review:
-
– patients with morbid (Class III, BMI ≥ 40) obesity undergoing adjustable gastric banding or gastric bypass – as in the previous review
-
– patients with severe (Class II, BMI ≥ 30 and < 40) obesity with significant comorbidity at baseline (Type 2 diabetes) undergoing adjustable gastric banding, based on data from a single trial117
-
– patients with moderate (Class I, BMI ≥ 30 and < 35) obesity undergoing adjustable gastric banding, based on data from a single trial. 115
-
-
The clinical effectiveness review concluded that meta-analysis was not appropriate, hence the model for patients with morbid obesity is not based on robust data synthesis of effectiveness – there was no statistically pooled estimate of each surgical procedure on weight loss and no robust estimate of variability. As a result, the economic model adopted two estimates of the effect of gastric bypass and adjustable gastric banding on weight loss – these were identified as ‘optimistic’ estimates (based on the previous assessment report) and an alternative ‘pessimistic’ estimate (based on a recently published trial comparing gastric bypass and adjustable gastric banding). Outcomes, in terms of weight loss at five years following surgery, were extrapolated using data from the SOS study. 97
-
Included trials for patients with morbid obesity did not report change in both blood pressure and suitable lipid measurements – hence the model developed for the previous assessment report has been used for this population, with updated assumptions on costs, diabetes incidence, permanency of diabetes remission following surgery and on the impact of BMI on health-state utility.
-
The clinical trials reporting the use of adjustable gastric banding for severely obese (BMI ≥ 30 and < 40) patients with Type 2 diabetes and for moderately obese (BMI ≥ 30 and < 35) patients reported sufficient information, up to two years of follow-up, to apply the new model. The analysis for these patients will initially be undertaken for the period of the trial follow-up only, and will then use extrapolations based on data from the SOS study, where relevant, or on the basis of data reported in the trial.
-
In the absence of a robust, pooled estimate of treatment effect (with associated estimate of variability) we felt it was inappropriate to undertake probabilistic sensitivity analysis using the original model. The robustness of the model results to variation in assumptions and parameter values was assessed using deterministic sensitivity analysis. Probabilistic sensitivity analysis would be used for the updated model, but would primarily address uncertainty in parameter values – uncertainty over model structure and methods for extrapolating trial results would be addressed using deterministic sensitivity analysis.
Results
The first of the next eight section reports results for the base-case analysis of adjustable gastric banding and gastric bypass compared with non-surgical management for patients with morbid obesity (BMI ≥ 40), using baseline characteristics described in the section Baseline cohort of patients with morbid obesity, this chapter. Total costs for all management strategies are reported, as are the total QALYs under the optimistic and pessimistic assumptions regarding weight loss. ICERs are reported for both surgical procedures relative to non-surgical management. The principal differences between the results of this analysis and the previous assessment report are identified and explanations provided. The deterministic sensitivity analysis of adjustable gastric banding and gastric bypass compared with non-surgical management for patients with morbid obesity is then discussed. In the absence of a robust, pooled estimate of treatment effect (with associated estimate of variability) we felt it was inappropriate to undertake probabilistic sensitivity analysis using the original model.
The third section reports on results for the base-case analysis of adjustable gastric banding compared with non-surgical management for patients with moderate-to-severe obesity (BMI ≥ 30 and < 40) and Type 2 diabetes, based on the trial reported by Dixon and colleagues. 117 The following two sections report the deterministic sensitivity analysis and a probabilistic sensitivity analysis of adjustable gastric banding compared with non-surgical management for patients with moderate-to-severe obesity (BMI ≥ 30 and < 40) and Type 2 diabetes. The probabilistic sensitivity analysis primarily addresses uncertainty in parameter values – uncertainty over model structure and methods for extrapolating trial results is addressed using deterministic sensitivity analysis.
Results for the base-case analysis of adjustable gastric banding compared with an intensive management programme for patients with moderate obesity (BMI ≥ 30 and < 35) are reported, based on the trial reported by O’Brien and colleagues. 115 Finally, the deterministic sensitivity analysis and a probabilistic sensitivity analysis are reported. As stated above, the probabilistic sensitivity analysis primarily addresses uncertainty in parameter values – uncertainty over model structure and methods for extrapolating trial results is addressed using deterministic sensitivity analysis.
Cost-effectiveness of bariatric surgery (gastric bypass or adjustable gastric banding) for morbid obesity (BMI ≥ 40) – base-case analysis
Table 67 reports the total costs and total QALYs for the baseline cohort of morbidly obese patients undergoing gastric bypass, adjustable gastric banding and non-surgical management, using the updated assumptions with regard to surgery cost, efficacy (in terms of weight reduction, impact on diabetes incidence and on remission of Type 2 diabetes) and health-state utility. The model has been estimated over a 20-year time horizon, as in the previous assessment report. All costs and outcomes are discounted at 3.5%.
| Treatment | Total cost (£) | QALYsa | QALYsb |
|---|---|---|---|
| Non-surgical management | 13,561 | 10.80 | 10.80 |
| Adjustable gastric banding | 17,126 | 12.68 | 11.72 |
| Gastric bypass | 19,824 | 12.78 | 12.32 |
Surgical management of obesity is estimated to be more costly than non-surgical management, but results in improved outcomes (in terms of QALYs) over the modelled 20-year time horizon. Two scenarios are modelled that effect outcomes, but not cost. Assumptions on weight loss, up to five years, adopted in the previous assessment report have been extrapolated to 10 years using data for gastric bypass and gastric banding from the SOS study. 97 An alternative scenario was constructed using data, with five years follow-up, from the trial reported by Angrisani and colleagues107 with a similar extrapolation to 10 years using data from the SOS study. 97 This gave generally less favourable estimates in terms of weight loss, particularly for gastric banding.
Compared with the previous assessment report, total QALYs associated with non-surgical management are lower, while the total QALYs for surgical management are higher. This is the result of changes in discounting practice, updated assumptions on duration of weight reduction and alternative assumptions regarding the health gain associated with weight loss. The effect of change in discounting practice, alone, would be to reduce the QALYs associated with each treatment strategy by approximately 1.7 QALYs. Extrapolating weight loss assumptions up to 10 years, alone, increases the total QALYs associated with surgical intervention by approximately 4% (with no impact on outcomes for non-surgical management because the baseline assumption is that patients receiving non-surgical management neither gain nor lose weight). Updated assumptions on the utility gain associated with weight loss increases the total QALYs associated with non-surgical management by approximately 13% and increases the total QALYs associated with surgical management by approximately 18%.
Total costs of non-surgical management and gastric bypass are approximately double the estimates included in the previous assessment report, while costs for adjustable gastric banding are approximately 60% higher. The increase in total costs is the result of a combination of changes in discounting practice, updated assumptions regarding incidence and remission of Type 2 diabetes in patients undergoing surgery and receiving non-surgical management and updated costing assumptions. For non-surgical management 36% of the difference can be attributed to changes in discounting practice alone and 44% to changes in costs alone, whereas for gastric bypass 22% of the difference can be attributed to changes in discounting practice and 73% to changes in costing assumptions. Aside from the general increase in the estimated total costs for each strategy, the other main difference from the previous assessment report is that total costs for gastric bypass are approximately £2600 higher than for adjustable gastric banding, whereas total costs for adjustable gastric banding were approximately £1000 higher than for gastric bypass in the previous report. This is primarily the result of the shorter duration of surgery for adjustable gastric banding (60 minutes versus 120 minutes for laparoscopic gastric bypass) and shorter LOS (two days for adjustable gastric banding versus five days for gastric bypass).
Table 68 reports the incremental cost-effectiveness of gastric bypass and adjustable gastric banding each compared with non-surgical management.
| Intervention | Incremental cost (£) | ‘Optimistic’ weight reduction from previous assessment report188 | ‘Pessimistic’ weight reduction from Angrisani and colleagues107 | ||
|---|---|---|---|---|---|
| Incremental QALYs | ICER (£) | Incremental QALYs | ICER (£) | ||
| AGB | 3566 | 1.88 | 1897 | 0.92 | 3863 |
| GBP | 6263 | 1.98 | 3160 | 1.52 | 4127 |
Surgical management of morbid obesity, using adjustable gastric banding or gastric bypass provides additional QALYs at additional cost under both scenarios – extrapolating weight reduction to 10 years based on data from the previous assessment report188 and the trial reported by Angrisani and colleagues. 107 The ICERs range between £1897 and £4127 per QALY gained, which are within the range conventionally deemed as cost-effective from an NHS decision-making perspective.
The incremental cost for gastric bypass is around 60% greater than for adjustable gastric banding, which contrasts with the previous assessment report, where gastric bypass was less costly than adjustable gastric banding. This is largely the result of changes in assumptions over duration of surgery, which have affected adjustable gastric banding disproportionately (duration of laparoscopic adjustable gastric banding was assumed to be 60 minutes, in contrast with 150 minutes in the previous report, whereas duration of laparoscopic gastric bypass was assumed to be 120 minutes, in contrast with 235 minutes in the previous report) and length of stay (length of stay for laparoscopic adjustable gastric banding was assumed to be two days, in contrast with five days in the previous report, whereas length of stay for laparoscopic gastric bypass was assumed to be five days, in contrast with six days in the previous report).
The QALY gain associated with surgical management of morbid obesity is approximately two, when based on assumptions on weight reduction adopted in the previous report and between 1 and 1.5 when based on the results of the trial reported by Angrisani and colleagues. These QALY gains are larger than those estimated in the previous report (0.45 QALYs when compared with non-surgical management). These differences are primarily the result of extrapolating the weight reduction assumptions up to 10 years (resulting in an approximate doubling of the QALY gain) and updated assumptions on the utility gain associated with reduction in BMI. The impact of alternative assumptions on the utility gain associated with reduction in BMI is explored in a deterministic sensitivity analysis.
Cost-effectiveness of bariatric surgery (gastric bypass or adjustable gastric banding) for morbid obesity (BMI ≥ 40) – deterministic sensitivity analysis
A series of one-way sensitivity analyses were conducted using the updated model. These are reported in Table 69, which also includes results for some scenario analyses presented in the previous assessment report (for example, Scenario five from the previous report which examined the impact of involving surgeons with less experience of bariatric surgery on the cost-effectiveness of surgical management of morbid obesity – see rows titled ‘Surgeon experience’ in Table 69). Other scenarios considered in the sensitivity analysis include:
-
altering assumptions for operative mortality from 1% to 0.5% for gastric bypass and from 0% to 0.05% for adjustable gastric banding
-
reducing the change in utility associated with a unit change in BMI (from 0.0166 to 0.0075)
-
applying BMI-specific incidence of Type 2 diabetes, rather than values for the surgical (all surgery, not specific to gastric bypass or adjustable gastric banding) and non-surgical cohorts from the SOS study97
-
allowing band adjustments in the second and/or third year rather than four only in year one
-
considering the impact of surgeon inexperience – on duration of surgery, on revision rates and on outcome (in terms of weight reduction)
-
increasing elements of surgical cost by 20%
-
varying costs of health-service contacts for patients on the intensive programme
-
consider the cost impact of a higher rate of abdominoplasty following surgically-induced weight loss and including cost impact of complications of abdominoplasty.
| Incremental cost (£) | ‘Optimistic’ weight reduction from previous assessment report188 | ‘Pessimistic’ weight reduction from Angrisani and colleagues107 | ||||
|---|---|---|---|---|---|---|
| Incremental QALYs | ICER (£) | Incremental QALYs | ICER (£) | |||
| Base case | AGB | 3566 | 1.88 | 1897 | 0.92 | 3863 |
| GBP | 6263 | 1.98 | 3160 | 1.52 | 4127 | |
|
Operative mortality (AGB = 0.05%; GBP = 0.5%) |
AGB | 3559 | 1.87 | 1906 | 0.91 | 3905 |
| GBP | 6293 | 2.05 | 3075 | 1.58 | 3983 | |
|
Health-state utility (0.0075 gain per unit BMI reduction) |
AGB | 3566 | 0.85 | 4215 | 0.42 | 8584 |
| GBP | 6263 | 0.85 | 7412 | 0.64 | 9845 | |
| Use BMI-specific incidence of Type 2 diabetes (see Table 59) | AGB | 3873 | 1.88 | 2060 | ||
| GBP | 6297 | 1.98 | 3177 | |||
| AGB | 5307 | 0.92 | 5749 | |||
| GBP | 6814 | 1.52 | 4490 | |||
| Increase cost of preoperative assessment by 20% | AGB | 3788 | 1.88 | 2015 | 0.92 | 4104 |
| GBP | 6486 | 1.98 | 3272 | 1.52 | 4273 | |
| Increase operative costs by 20% | AGB | 4542 | 1.88 | 2416 | 0.92 | 4921 |
| GBP | 7855 | 1.98 | 3963 | 1.52 | 5176 | |
| Increase postoperative costs by 20% | AGB | 4848 | 1.88 | 2579 | 0.92 | 5252 |
| GBP | 7448 | 1.98 | 3758 | 1.52 | 4908 | |
| Increase all costs by 20% | AGB | 6048 | 1.88 | 3217 | 0.92 | 6551 |
| GBP | 9262 | 1.98 | 4674 | 1.52 | 6103 | |
| Band adjustments in second year (four) | AGB | 3965 | 1.88 | 2109 | 0.92 | 4295 |
| GBP | 6263 | 1.98 | 3160 | 1.52 | 4127 | |
| Band adjustments in second year (four) and third year (two) | AGB | 4152 | 1.88 | 2208 | 0.92 | 4497 |
| GBP | 6263 | 1.98 | 3160 | 1.52 | 4127 | |
| Late reoperations for AGB continue over 10 years (6%) | AGB | 5240 | 1.88 | 2787 | 0.92 | 5676 |
| GBP | 6263 | 1.98 | 3160 | 1.52 | 4127 | |
| Late reoperations for AGB continue over 10 years (2.5%) | AGB | 3957 | 1.88 | 2105 | 0.92 | 4286 |
| GBP | 6263 | 1.98 | 3160 | 1.52 | 4127 | |
| Surgeon experience: increase duration of surgery (50%) and double revision rates | AGB | 5685 | 1.88 | 3024 | 0.92 | 6159 |
| GBP | 9588 | 1.98 | 4838 | 1.52 | 6318 | |
| Surgeon experience: double operative mortality; (GBP = 2% AGB = 0%) | AGB | 5685 | 1.88 | 3024 | 0.92 | 6159 |
| GBP | 9528 | 1.85 | 5143 | 1.39 | 6839 | |
| Surgeon experience: reduce estimated weight loss by 25% | AGB | 5685 | 1.41 | 4019 | 0.70 | 8091 |
| GBP | 9528 | 1.34 | 7135 | 0.99 | 9631 | |
| Cost cholecystectomy as a day case | AGB | 3445 | 1.88 | 1833 | 0.92 | 3732 |
| GBP | 6143 | 1.98 | 3099 | 1.52 | 4048 | |
| Cost abdominal hernia procedures as day case | AGB | 3566 | 1.88 | 1897 | 0.92 | 3863 |
| GBP | 6205 | 1.98 | 3131 | 1.52 | 4088 | |
| Adjust abdominoplasty cost for complications (25% with intermediate complication and 5% with major complication) | AGB | 3589 | 1.88 | 1909 | 0.92 | 3888 |
| GBP | 6286 | 1.98 | 3172 | 1.52 | 4142 | |
| Higher rate of apronectomy | AGB | 3901 | 1.88 | 2075 | 0.92 | 4226 |
| GBP | 6599 | 1.98 | 3330 | 1.52 | 4348 | |
| Patients recover in HDU (1 day) rather than on ward | AGB | 3766 | 1.88 | 2003 | 0.92 | 4079 |
| GBP | 6426 | 1.98 | 3243 | 1.52 | 4234 | |
| Include conversion to open procedures | AGB | 3677 | 1.88 | 1956 | 0.92 | 3983 |
| GBP | 6329 | 1.98 | 3194 | 1.52 | 4170 | |
In general the results are robust to changes in assumptions, reported in Table 69, and in all cases the ICERs remain within the range conventionally deemed as cost-effective from an NHS decision-making perspective. However, changes in some key assumptions produce less favourable cost-effectiveness estimates than the base case adopted for this analysis:
-
Adopting a lower utility gain for reductions in BMI has a large impact on the QALY gain associated with surgical management; reducing from 1.88 to 0.85 for adjustable gastric banding and from 1.98 to 0.85 for gastric bypass, for the optimistic assumption on weight reduction, when the utility gain per unit BMI reduction is reduced from 0.017 to 0.0075. Equivalent values using pessimistic assumptions are a reduction from 0.92 to 0.42 and from 1.52 to 0.64 for adjustable gastric banding and gastric bypass respectively.
-
Using BMI-specific incidence of Type 2 diabetes has a greater impact on incremental costs for adjustable gastric banding when using weight reduction from the trial reported by Angrisani and colleagues107 than is the case for gastric bypass (or for either approach to surgical management when using assumptions for weight reduction adopted in the previous assessment report). The effect of using BMI-specific diabetes incidence is to increase incremental costs for adjustable gastric banding by approximately £1750 so that the ICER rises from £3863 to £5749.
-
Increasing operative costs by 20% increases incremental costs for adjustable gastric banding by approximately £1000 and gastric bypass by approximately £1500. This increases the ICER for adjustable gastric banding from £1897 to £2416 using assumptions for weight reduction adopted in the previous assessment report, and from £3863 to £4921 based on the trial results reported by Angrisani and colleagues. 107 The equivalent changes for gastric bypass are from £3160 to £3963, and from £4127 to £5176.
-
Increasing postoperative costs by 20% increases incremental costs by between £1200 and £1300. This increases the ICER for adjustable gastric banding to £2579 using assumptions for weight reduction adopted in the previous assessment report, and to £5252 based on the trial results reported by Angrisani and colleagues. 107 The equivalent changes for gastric bypass are an increase to £3758, and to £4908.
-
Increasing all surgery-related costs by 20% leads to a higher proportionate increase for adjustable gastric banding, with incremental costs increasing by approximately £2500 (70% increase). The equivalent value for gastric bypass is approximately £3000 (48% increase). The ICER for adjustable gastric banding increases to £3217 using assumptions for weight reduction adopted in the previous assessment report, and to £6551 based on the trial results reported by Angrisani and colleagues. 107 The equivalent changes for gastric bypass are an increase to £4674, and to £6103.
-
Repeating the scenario analysis, presented in the previous assessment report, for surgical experience leads to increased costs (because of increased duration in surgery and increases in the rate of revision) and poorer outcomes (i.e. reduced QALYs because of increased operative mortality and lower weight reduction). The effect of these altered assumptions is shown cumulatively, with the effects on costs considered first. Increasing duration of surgery and revision rates leads to similar proportionate increases in incremental costs [increase of approximately £2200 (59% increase) for adjustable gastric banding and £3325 (54% increase) for gastric bypass]. The ICER for adjustable gastric banding increases to £3024 using assumptions for weight reduction adopted in the previous assessment report, and to £6159 based on the trial results reported by Angrisani and colleagues. 107 The equivalent changes for gastric bypass are an increase to £4838, and to £6318. Doubling operative mortality has no effect on adjustable gastric banding (because operative mortality was assumed to be zero), but reduces the QALY gain for gastric bypass to 1.85 using weight loss assumptions from the previous report and 1.39 using assumptions based on Angrisani and colleagues. 107 Reducing estimated weight loss by 25% reduces the QALY for surgical management by around 0.5 QALYs (using weight loss assumptions from the previous report) resulting in an ICER of £4019 for adjustable gastric banding and £7135 for gastric bypass. The equivalent values using assumptions based on Angrisani and colleagues are £8091 for adjustable gastric banding and £9631 for gastric bypass.
Cost-effectiveness of bariatric surgery (adjustable gastric banding) for moderate to severe obesity (BMI ≥ 30 and < 40), with Type 2 diabetes – base-case analysis
Table 70 reports the total costs and total QALYs for the baseline cohort of moderately-to-severely obese patients (BMI ≥ 30 and < 40) undergoing adjustable gastric banding and non-surgical management – see section on Baseline cohort of patients, this chapter, with morbid obesity for the assumptions made for this cohort. All costs and outcomes are discounted at 3.5%.
| Model time horizon | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 2 years | 5 years | 20 years | |||||||
| Non-surgical | Surgical | Difference | Non-surgical | Surgical | Difference | Non-surgical | Surgical | Difference | |
| Cost (£) | 4842 | 9874 | 5032 | 10,628 | 13,425 | 2796 | 31,683 | 33,182 | 1500 |
| QALYs | 1.47 | 1.74 | 0.27 | 3.48 | 4.09 | 0.61 | 10.39 | 11.49 | 1.10 |
| ICER (£) | 18,930 | 4580 | 1367 | ||||||
The estimated cost of surgery is based on the assumptions outlined in Table 61, with regard to operating time, length of stay and costs of consumables. Costs associated with reoperations as the result of failure of the initial surgery or reoperation because of late complications were based on complication rates reported for the trial population (3.3% reoperations caused by initial failures and 6.7% reoperation for late complications). 117 Costs for the conventional-therapy programme were based on the trial report, which stated that patients met with a member of the team (general physician, dietitian, nurse or diabetes educator) every six weeks throughout the two years of the trial. It was assumed, as with the postdischarge routine for surgical patients, that non-surgical patients would have more frequent consultations with dietitians than with general medical support – hence it was assumed that the conventional therapy programme consisted of six additional consultations with a dietitian and three additional outpatient visits. The components of the programme that were related to patients’ diabetes care was assumed to be included in the health-state costs for diabetes.
Table 70 reports results for three time horizons:
-
two years, which corresponds to the duration of the clinical trial report117
-
five years, where outcomes reported in the clinical trial have been extrapolated beyond two years, based on data on trends in weight reduction over time reported for the gastric banding cohort in the SOS study97 and on reported durability of diabetes remission reported for all surgically managed patients in the SOS study (discussed in the Effectiveness – diabetes resolution section, this chapter)
-
twenty years, where outcomes reported in the clinical trial have been extrapolated up to 10 years following surgery using trends reported for the SOS study,97 as discussed above. At 10 years following surgery it is assumed that weight, blood pressure and lipid measurements return to their baseline levels. It is also assumed that all patients who previously resolved Type 2 diabetes, either following surgery or through conventional treatment, and remained in the postdiabetic state up to 10 years would then relapse and return to the diabetic health state.
Surgical management of moderate-to-severe obesity (BMI ≥ 30 and < 40) in patients with Type 2 diabetes is estimated to be more costly, but also results in improved outcomes (in terms of QALYs) over each of the modelled time horizons. Costs for the surgical cohort are approximately double the costs for the non-surgical cohort, when adopting a two-year time horizon. However, as the time horizon increases, the proportionate difference and the absolute difference in costs between the surgical and non-surgical cohorts decreases. This is largely because of the dominant effect of diabetes-related costs for the non-surgical cohort, where only 13% of the cohort achieve remission of Type 2 diabetes in contrast with 73% of the surgically-treated cohort, and where 83% of total costs are associated with the diabetes health state cost. As a result of this, total costs for the non-surgical cohort increase by over 100% moving from the two-year to the five-year time horizon, whereas the increase is around 36% for the surgical cohort. The proportionate increase, when moving from the five-year to the 20-year time horizon, is more similar between the two cohorts, because differences in diabetes resolution and weight loss are only extrapolated up to 10 years in the model – at that point patients in both cohorts are assumed to revert to baseline values.
The total discounted QALYs with surgical management are greater than with non-surgical management for each of the time horizons modelled, with the incremental gain increasing with increasing time horizon. The proportionate increase, for surgical over non-surgical management, is approximately the same for a two-year and five-year time horizon (18.4% at two years and 17.5% at five years), but drops slightly for the 20-year time horizon (10.6%). As with the costs, this reflects the fact that trial outcomes are extrapolated up to 10 years, with both cohorts reverting to baseline values at that point.
Cost-effectiveness of bariatric surgery (adjustable gastric banding) for moderate to severe obesity (BMI ≥ 30 and < 40), with Type 2 diabetes – deterministic sensitivity analysis
A series of one-way sensitivity analyses were conducted for each time horizon. These are reported in Table 71. In all cases the least favourable ICERs are associated with the short model time horizon, ranging from around £19,000 per QALY gained up to £35,000 per QALY gained. More favourable ICERs are found for the five-year and 20-year time horizons, ranging from around £1300 per QALY gained up to £10,000 per QALY gained. In all scenarios, for longer time horizons, the ICERs remain within the range conventionally deemed as cost-effective from an NHS decision-making perspective.
| Model time horizon | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 2 years | 5 years | 20 years | |||||||
| Incr. cost (£) | Incr. QALYs | ICER (£) | Incr. cost (£) | Incr. QALYs | ICER (£) | Incr. cost (£) | Incr. QALYs | ICER (£) | |
| Base case | 5032 | 0.27 | 18,930 | 2796 | 0.61 | 4580 | 1500 | 1.10 | 1367 |
| Gradual decline in weight (base on proportions at six-month intervals in trial reported by O’Brien and colleagues115) | 5032 | 0.21 | 23,746 | 2796 | 0.56 | 5024 | 1500 | 1.04 | 1438 |
| Health-state utility (0.0075 gain per unit reduction in BMI) | 5032 | 0.14 | 34,990 | 2796 | 0.33 | 8538 | 1500 | 0.61 | 2455 |
| Operative mortality (0.1%) | 5029 | 0.26 | 19,039 | 2789 | 0.61 | 4599 | 1473 | 1.09 | 1357 |
| Operative mortality (0.05%) | |||||||||
| Band adjustments in second year (4) | 5446 | 0.27 | 20,486 | 3210 | 0.61 | 5257 | 1913 | 1.10 | 1744 |
| Band adjustments third year (2) | 5645 | 0.27 | 21,237 | 3409 | 0.61 | 5585 | 2113 | 1.10 | 1926 |
| Surgeon experience: increase duration of surgery (50%) and double revision rates | 6900 | 0.27 | 25,958 | 4664 | 0.61 | 7641 | 3368 | 1.10 | 3070 |
| Surgeon experience: reduce estimated weight loss by 25% | 6900 | 0.21 | 33,273 | 4664 | 0.48 | 9813 | 3368 | 0.87 | 3866 |
| Increase cost of preoperative assessment by 20% | 5255 | 0.27 | 19,768 | 3019 | 0.61 | 4945 | 1723 | 1.10 | 1570 |
| Increase operative cost by 20% | 5977 | 0.27 | 22,484 | 3741 | 0.61 | 6128 | 2445 | 1.10 | 2228 |
| Increase postoperative costs by 20% | 5379 | 0.27 | 20,235 | 3314 | 0.61 | 5428 | 2610 | 1.10 | 2379 |
| Increase all costs by 20% | 6546 | 0.27 | 24,627 | 4481 | 0.61 | 7341 | 3778 | 1.10 | 3443 |
| Reduction in SBP (increase by 50% for surgical patients) | 5024 | 0.27 | 18,897 | 2790 | 0.61 | 4566 | 1524 | 1.10 | 1380 |
| Reduction in TC : HDL ratio (increase by 50% for surgical patients) | 5024 | 0.27 | 18,887 | 2793 | 0.61 | 4563 | 1579 | 1.12 | 1413 |
| Reduction in SBP and TC : HDL ratio (increase by 50% for surgical patients) | 5017 | 0.27 | 18,855 | 2787 | 0.61 | 4550 | 1601 | 1.12 | 1424 |
| Reduce diabetes health state cost by 50% | 6184 | 0.27 | 23,265 | 5165 | 0.61 | 8461 | 4863 | 1.10 | 4432 |
In general the sensitivity analyses are similar to those described in the previous section. However, some entries in Table 71 may require further explanation. The first entry in the table, labelled ‘Gradual decline in weight’, tests the influence of the assumption that the weight reduction reported at two years following surgery occurs immediately following surgery. This assumption may not be realistic, given the data reported in Table 52 for percentage weight reduction following gastric banding over time (in trials of patients with morbid obesity) or the data reported in Table 55 (percentage weight reduction following gastric banding over time in patients with moderate obesity) which show a gradual decline over the first year following surgery. To estimate this gradual decline, the proportion of total weight loss at six-month intervals (up to two years) was estimated from the trial reported by O’Brien and colleagues. 115 These proportions were then applied to the total weight loss observed at two years in the trial reported by Dixon and colleagues,117 where patients with moderate obesity lost 21.6% of their baseline weight by two years. The proportion of total weight loss at six-month periods reported by O’Brien and colleagues115 was 65% at six months, 91% at 12 months, 97% at 18 months and 100% at 24 months. The two different assumptions on percentage of weight lost are illustrated in Figure 4.
Other scenarios considered in the sensitivity analysis include:
-
reducing the change in utility associated with a unit change in BMI (from 0.0166 to 0.0075)
-
including a low operative mortality for surgery (0.05% rather than zero in the base case)
-
allowing band adjustments in the second and/or third year rather than four only in year one
-
considering the impact of surgeon inexperience – on duration of surgery, on revision rates and on outcome (in terms of weight reduction).
FIGURE 4.
Base-case assumption on weight reduction contrasted with gradual decline in weight for moderate to severely obese patients (BMI ≥ 30 and < 40), with Type 2 diabetes undergoing adjustable gastric banding.
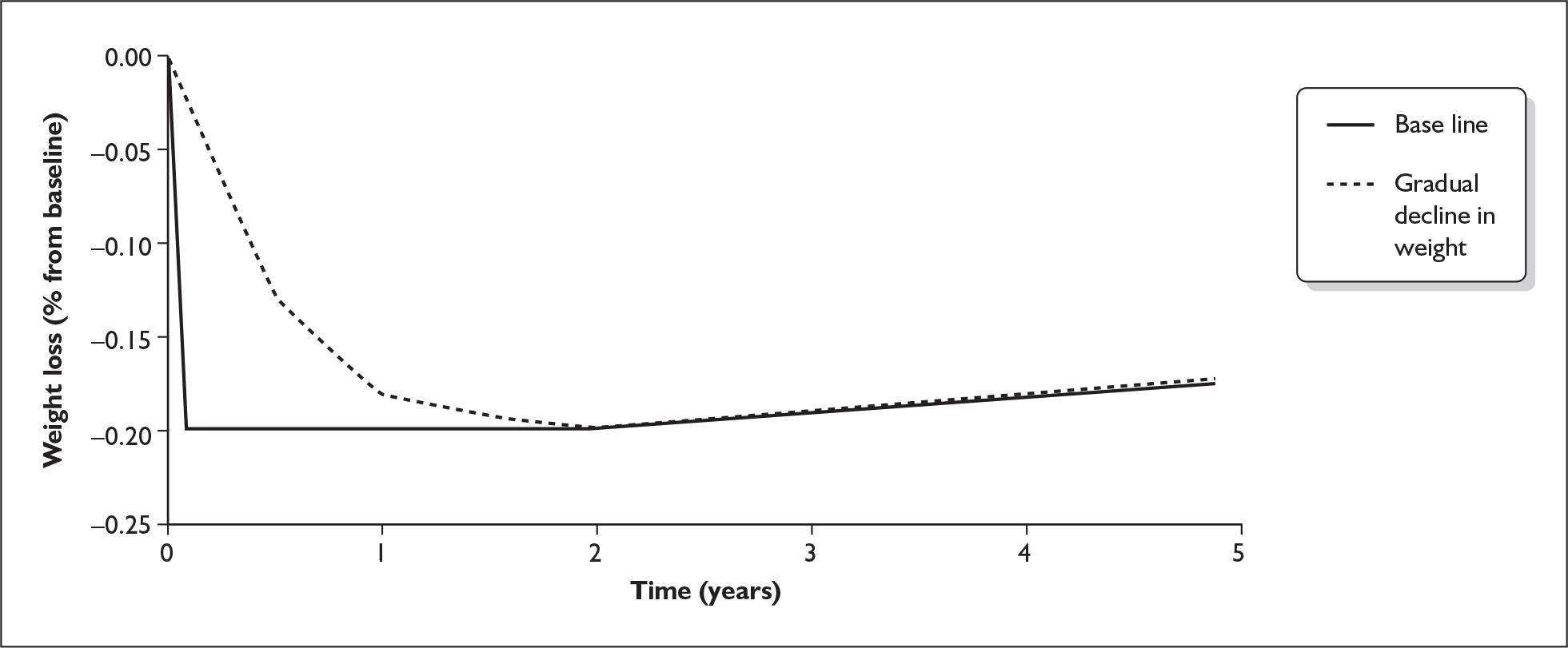
In general the results are robust to changes in assumptions. However, changes in some key assumptions produce less favourable cost-effectiveness estimates than the base case adopted for this analysis.
-
Assuming a gradual decline in weight, rather than applying the reduction observed at two years immediately following surgery, has a large impact on the ICER at two years (by reducing the QALY gain with surgery by around 20%). However, the effect of this changed assumption is greatly reduced when longer time horizons are considered;
-
Applying a lower utility gain for reduction in BMI has a large impact on the QALY gain associated with surgery, reducing from 0.27 to 0.14 at two years (applying a utility gain per unit BMI reduction of 0.0075, the value adopted in the previous review). This effect is maintained over the varying time horizons of the model, with the QALY gain being reduced by between 45% and 48%. The effect of this is to raise the ICER at two years to £35,000 per QALY gained, above a cost-effectiveness threshold considered acceptable from an NHS decision-making perspective.
-
Repeating the scenario analysis described earlier for surgical experience leads to increased costs (because of increased duration in surgery and increases in the rate of revision) and poorer outcomes (i.e. reduced QALYs because of lower weight reduction). The effect of these altered assumptions is shown cumulatively, with the effects on costs considered first. Increasing duration of surgery and revision rates leads to an increase in incremental costs of approximately £1900, an increase of 37% at two years and 125% increase at 20 years. The ICER increases to £25,958 at two years and £3070 at 20 years. Reducing estimated weight loss by 25% reduces the QALY for surgical management by around 0.06 QALYs at two years and 0.23 QALYs at 20 years (approximately 22% and 21% reduction, respectively) resulting in an ICER of £33,273 at two years and £3866 at 20 years.
-
Increasing operative costs by 20% increases incremental costs for surgery by approximately £950 increasing the ICER at two years to £22,484 (£2228 at 20 years). Increasing postoperative costs by 20% increases incremental costs by approximately £350, increasing the ICER to £20,235 at two years and £2379 at 20 years. Increasing all surgery-related costs by 20% leads to an increase in incremental costs increasing by approximately £1500, increasing the ICER to £24,627 at two years and £3443 at 20 years.
-
The impact of decreasing the diabetes health state cost by 50% on incremental costs is larger as the model time horizon increases. The proportionate increase in incremental cost at two years is 23%, whereas at 20 years it is 224%. This arises from the dominant effect of diabetes costs in the non-surgical cohort, in conjunction with the assumption that surgically treated patients who resolve Type 2 diabetes will achieve a maximum remission of 10 years.
Cost-effectiveness of bariatric surgery (adjustable gastric banding) for moderate to severe obesity (BMI ≥ 30 and < 40), with Type 2 diabetes – probabilistic sensitivity analysis
In a probabilistic sensitivity analysis, where percentage weight loss, reduction in systolic blood pressure and TC : HDL ratio, proportion of patients with remission of Type 2 diabetes (and rate of relapse up to 10 years), health-state utility and health-state costs were sampled probabilistically, all simulations produced incremental cost-effectiveness estimates that were in the north-east quadrant of the cost-effectiveness map when adopting a two-year time horizon (Figure 5). That is, all simulations are associated with increased QALYs, but also increased costs. However, when the time horizon was extended to 20 years, while all simulations showed increased QALYs a proportion have negative incremental costs (total discounted costs for the surgical cohort are lower than for the non-surgical cohort). Simulations where costs for the surgically treated cohort are lower than for the non-surgical cohort are most likely to be associated with high proportions of patients with remission of Type 2 diabetes.
FIGURE 5.
Cost-effectiveness plane – incremental costs and incremental QALYs for patients with moderate to severe obesity (BMI ≥ 30 and < 40), with Type 2 diabetes, undergoing adjustable gastric banding compared with conventional treatment. QALYs, quality-adjusted life-years.
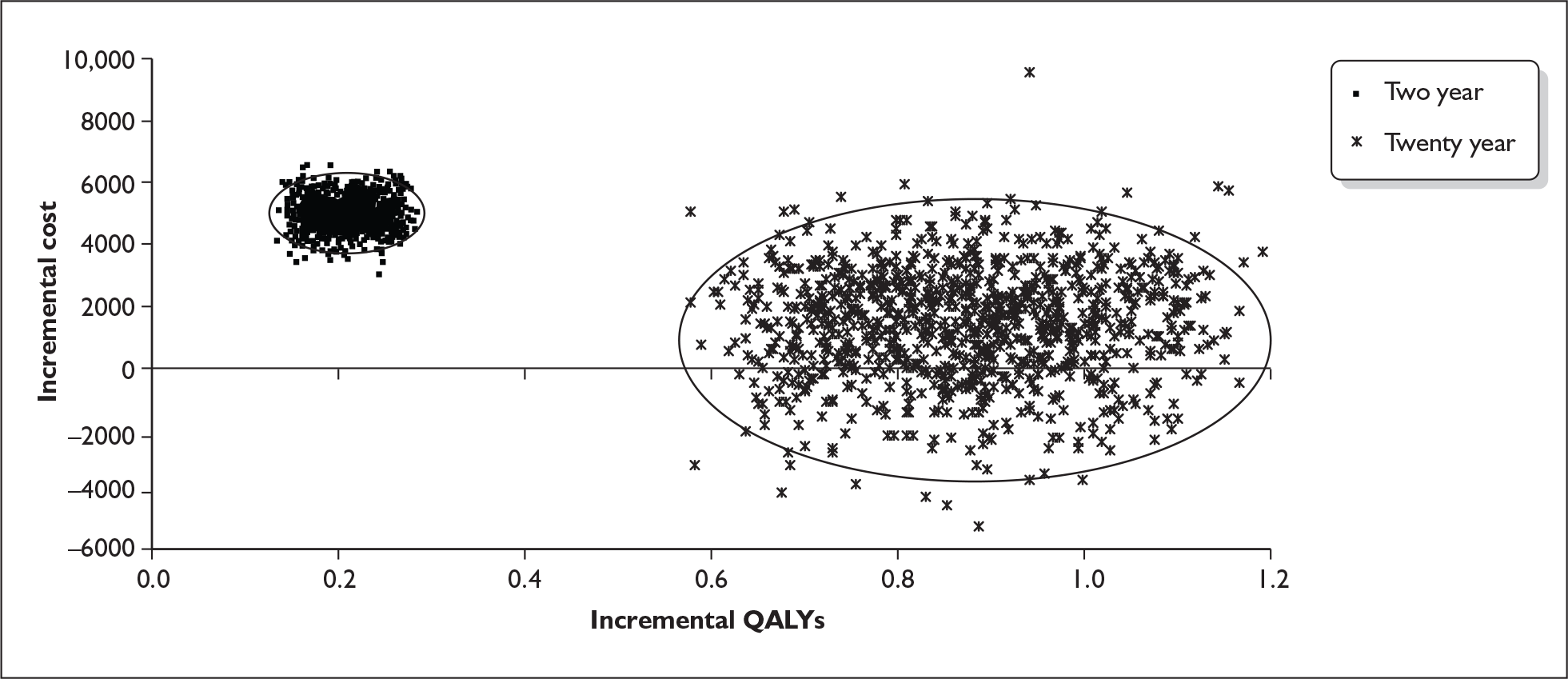
In this analysis surgical management with adjustable gastric banding had a probability of being cost-effective (compared with non-surgical management) of 17.5% at a willingness-to-pay threshold of £20,000 per QALY and 83.8% at a willingness-to-pay threshold of £30,000 per QALY for a time horizon of two years when assuming weight loss observed at two years occurs immediately after surgery (Figure 6). If the simulations are rerun assuming a gradual reduction in weight following surgery the probability of being cost-effective, with a two-year time horizon falls to 2.5% at a willingness-to-pay threshold of £20,000 per QALY and 50.6% at a willingness-to-pay threshold of £30,000 per QALY. In contrast, for a 20-year time horizon, the probability of surgical management being cost-effective is 100% at both willingness-to-pay thresholds, irrespective of assumptions regarding the pattern of early weight loss (see Figure 6).
FIGURE 6.
Cost-effectiveness acceptability curves for adjustable gastric banding in patients with moderate to severe obesity (BMI ≥ 30 and < 40), with Type 2 diabetes.
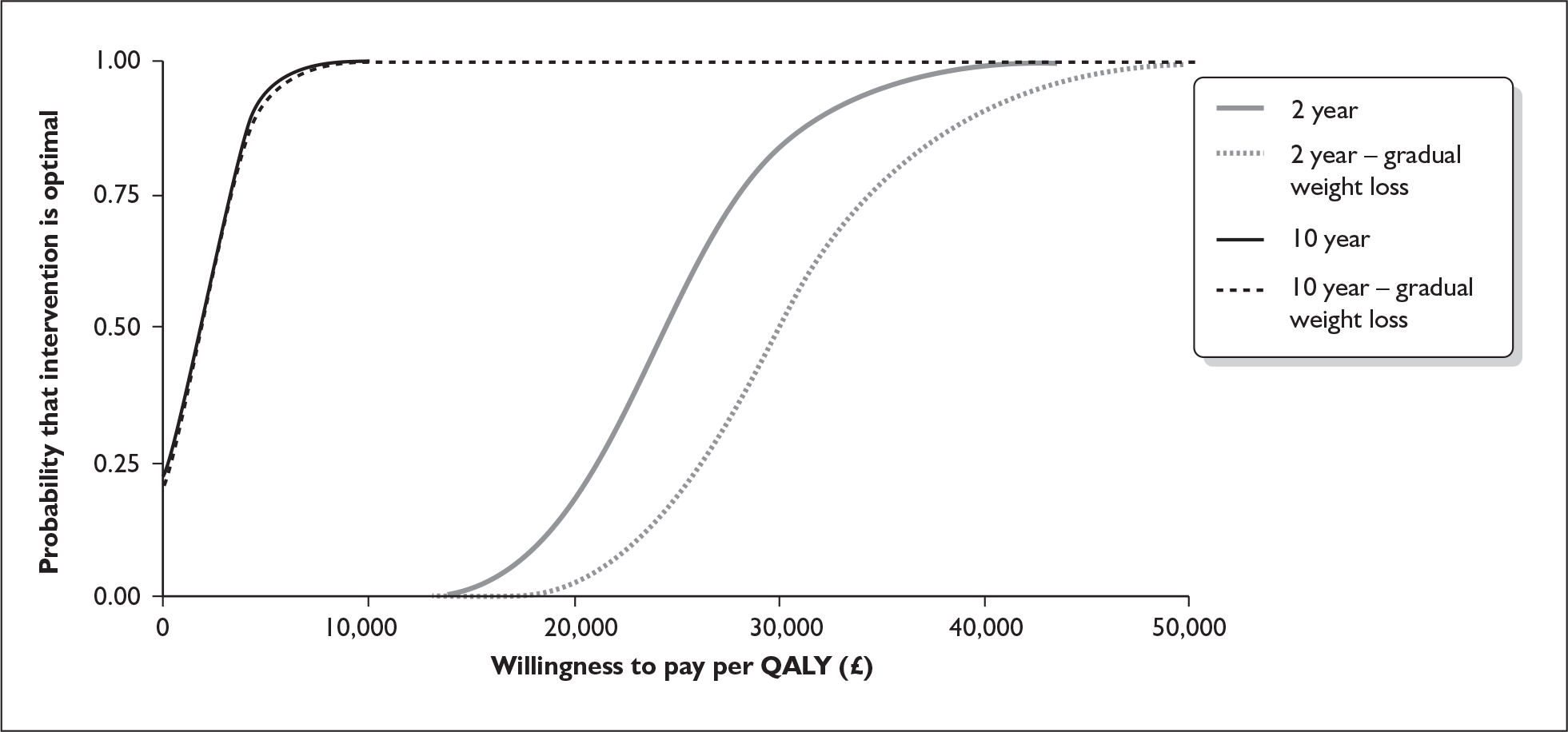
Cost-effectiveness of bariatric surgery (adjustable gastric banding) for moderate obesity (BMI ≥ 30 and < 35) – base-case analysis
Table 72 reports the total costs and total QALYs for the baseline cohort of moderately obese (BMI ≥ 30 and < 35) patients undergoing adjustable gastric banding and non-surgical management – see section Baseline cohort of patients with morbid obesity, this chapter, for assumptions on this cohort. All costs and outcomes are discounted at 3.5%. The estimated cost of surgery is based on assumptions outlined in Table 61, with regard to operating time, length of stay and costs of consumables. Costs associated with reoperations because of failure of the initial surgery or reoperation as the result of late complications were based on complication rates reported for the trial population [0 reoperations for initial failures and 10% (4/39, three in year 1 and one in year 2) reoperation rate because of late complications in the first and second year following surgery]. 115 In addition, one patient had an elective laparoscopic cholecystectomy in the second year following initial surgery.
| Model time horizon | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 2 years | 5 years | 20 years | |||||||
| Non-surgical | Surgical | Difference | Non-surgical | Surgical | Difference | Non-surgical | Surgical | Difference | |
| Cost (£) | 3484 | 8403 | 4919 | 4503 | 9393 | 4890 | 9311 | 14,398 | 5087 |
| QALY | 1.62 | 1.70 | 0.08 | 3.74 | 4.03 | 0.30 | 11.12 | 11.52 | 0.40 |
| ICER (£) | 60,754 | 16,381 | 12,763 | ||||||
Costs for the intensive medical programme were based on the trial report,115 which stated that patients were seen in outpatient setting by a physician every two weeks for the intensive phase (first six months) of the programme and every six weeks for the remainder of the two-year intervention period. During the intensive phase patients initiated a VLCD for the first 12 weeks, combined VLCD with initiation of pharmacotherapy with orlistat over the next four weeks, before transitioning to pharmacotherapy only (see Table 64 for costing assumptions). It was reported that eight patients could not tolerate orlistat and three others chose not to use it – the costs of pharmacotherapy in the postintensive management phase of the programme have been adjusted to take account of this. The principal cost relating to adverse events in the non-surgical cohort relate to surgical procedures related to cholecystitis. The trial report stated that four non-surgical patients developed acute cholecystitis and underwent elective laparoscopic cholecystectomy (three in year one, and one in year two, corresponding to surgical rates of 10% and 3.7% respectively). It was assumed that non-surgical patients reverted to standard non-surgical management (see Table 63) after two years on the weight loss programme.
Table 72 reports results for three time horizons:
-
two years, which corresponds to the duration of clinical trial report115
-
five years, where outcomes reported in the clinical trial have been extrapolated beyond two years, based on data on the trend in weight reduction observed in the non-surgical cohort, where BMI was tending to revert to the baseline value (see Figure 3)
-
20 years, where outcomes reported in the clinical trial have been extrapolated using methods discussed above. By the 20-year time horizon all patients are assumed to have reverted to baseline weight and those patients who achieved remission of Type 2 diabetes will have relapsed.
Surgical management of moderately obese patients with adjustable gastric banding is estimated to be more costly, but also results in improved outcomes (in terms of QALYs) over each of the modelled time horizons. Adopting a two-year time horizon costs for the surgical cohort are more than double the costs for the non-surgical cohort. However, as the time horizon increases, the absolute difference in costs between the surgical and non-surgical cohorts remains more or less constant, and the proportionate difference reduces. Costs for the two cohorts increase, as the result of the need to maintain follow-up of both surgically and non-surgically treated patients and also because of the increasing proportion of each cohort with Type 2 diabetes. This was assumed to be approximately 5%, based on BMI-specific prevalence of Type 2 diabetes reported in the Health Survey for England 2003,17 where diabetes prevalence in the population with a BMI between 30 and 35 was 7.21% for males and 4.71% for females. By the end of the 20-year time horizon prevalence of Type 2 diabetes was estimated at 15.4% in the non-surgical cohort and 13.8% in the surgical cohort.
The total discounted QALYs with surgical management are greater than with non-surgical management for each of the time horizons modelled, with the incremental gain increasing with increasing time horizon. For the longest time horizon (20 years) the majority of the QALY gains for the surgical cohort are realised in the first 10 years – these are the utility gains from reduced weight. In the base-case weight in the surgical cohort is assumed to revert to baseline level at around eight years following surgery – utility gains following this are the result of the lower proportion of patients with Type 2 diabetes and a lower proportion with CVD.
Cost-effectiveness of bariatric surgery (adjustable gastric banding) for moderate obesity (BMI ≥ 30 and < 35) – deterministic sensitivity analysis
A series of one-way sensitivity analyses were conducted for each time horizon. These are reported in Table 73. Scenarios considered in the sensitivity analysis include:
-
reducing the change in utility associated with a unit change in BMI (from 0.0166 to 0.0075)
-
including a low operative mortality for surgery (rather than zero, as applied in the base case)
-
allowing band adjustments in the second and/or third year rather than four only in year one
-
considering the impact of surgeon inexperience – on duration of surgery, on revision rates and on outcome (in terms of weight reduction)
-
increasing elements of surgical cost by 20%
-
varying costs of health-service contacts for patients on the intensive programme
-
considering the impact on reducing health-state costs for diabetes.
| Model time horizon | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| 2 years | 5 years | 20 years | |||||||
| Incr. cost (£) | Incr. QALYs | ICER (£) | Incr. cost (£) | Incr. QALYs | ICER (£) | Incr.cost (£) | Incr. QALYs | ICER (£) | |
| Base case | 4919 | 0.08 | 60,754 | 4890 | 0.30 | 16,381 | 5087 | 0.40 | 12,763 |
| Health state utility (0.0075 gain per unit reduction in BMI) | 4919 | 0.04 | 131,229 | 4890 | 0.14 | 35,322 | 5087 | 0.20 | 25,247 |
| Operative mortality (0.1%) | 4917 | 0.08 | 62,012 | 4887 | 0.29 | 16,595 | 5079 | 0.39 | 13,122 |
| Operative mortality (0.05%) | |||||||||
| Band adjustments in second year (4) | 4919 | 0.08 | 60,754 | 4890 | 0.30 | 16,381 | 5087 | 0.40 | 12,763 |
| Band adjustments third year (2) | 5532 | 0.08 | 68,329 | 5503 | 0.30 | 18,436 | 5700 | 0.40 | 14,302 |
| Surgeon experience: increase duration of surgery (50%) and double revision rates | 6993 | 0.08 | 86,370 | 6964 | 0.30 | 23,329 | 7161 | 0.40 | 17,967 |
| Surgeon experience: reduce estimated weight loss by 25% | 6996 | 0.04 | 188,545 | 6986 | 0.17 | 40,016 | 7346 | 0.22 | 33,058 |
| Increase cost of preoperative assessment by 20% | 5142 | 0.08 | 63,505 | 5113 | 0.30 | 17,128 | 5310 | 0.40 | 13,322 |
| Increase operative cost by 20% | 5890 | 0.08 | 72,745 | 5861 | 0.30 | 19,634 | 6058 | 0.40 | 15,199 |
| Increase postoperative costs by 20% | 5266 | 0.08 | 65,040 | 5408 | 0.30 | 18,117 | 6205 | 0.40 | 15,569 |
| Increase all costs by 20% | 6460 | 0.08 | 79,783 | 6602 | 0.30 | 22,115 | 7399 | 0.40 | 18,563 |
| Reduction in SBP (increase by 50% for surgical patients) | 4919 | 0.08 | 60,694 | 4889 | 0.30 | 16,340 | 5087 | 0.40 | 12,570 |
| Reduction in TC : HDL ratio (increase by 50% for surgical patients) | 4919 | 0.08 | 60,673 | 4890 | 0.30 | 16,329 | 5090 | 0.41 | 12,530 |
| Reduction in SBP and TC : HDL ratio (increase by 50% for surgical patients) | 4919 | 0.08 | 60,627 | 4889 | 0.30 | 16,296 | 5089 | 0.41 | 12,368 |
| Reduce diabetes health state cost by 50% | 4965 | 0.08 | 61,319 | 5032 | 0.30 | 16,856 | 5461 | 0.40 | 13,701 |
| Reduce costs of health-service contacts for patients on intensive programme by 50% | 6174 | 0.08 | 76,254 | 6162 | 0.30 | 20,643 | 6359 | 0.40 | 15,955 |
| Increase costs of health service contacts for patients on intensive programme by 50% | 3664 | 0.08 | 45,255 | 3618 | 0.30 | 12,120 | 3815 | 0.40 | 9571 |
In all cases the least favourable ICERs are associated with a short model time horizon, ranging from around £45,000 per QALY gained up to £190,000 per QALY gained. More favourable ICERs are found for the five-year and 20-year time horizons, ranging from around £16,000 per QALY gained up to £40,000 per QALY gained for five-year time horizon and from around £12,500 per QALY gained up to £33,000 per QALY gained for the 20-year time horizon. In some scenarios, even for longer time horizons, the ICERs are above the range conventionally deemed as cost-effective from an NHS decision-making perspective.
In general the results are robust to changes in assumptions. However, changes in some key assumptions produce less favourable cost-effectiveness estimates than the base case adopted for this analysis.
-
Applying a lower utility gain for reduction in BMI has a large impact on the QALY gain associated with surgery, reducing from 0.08 to 0.04 at two years (applying a utility gain per unit BMI reduction of 0.0075, the value adopted in the previous review). This effect is maintained over the varying time horizons of the model, with the QALY gain being reduced by between 49% and 54%. The effect of this is to raise the ICER substantially so that it remains above conventionally acceptable cost-effectiveness thresholds until the time horizon extends to 20 years.
-
Repeating the scenario analysis, described earlier, for surgical experience leads to increased costs (because of increased duration in surgery and increases in the rate of revision) and poorer outcomes (i.e. reduced QALYs as the result of lower weight reduction). The effect of these altered assumptions is shown cumulatively, with the effects on costs considered first. Increasing duration of surgery and revision rates leads to an increase in incremental costs of approximately £2000. The ICER increases to £86,370 at two years and £17,967 at 20 years. Reducing estimated weight loss by 25% reduces the QALY for surgical management by around 0.04 QALYs at two years and 0.18 QALYs at 20 years (approximately 54% and 44% reduction respectively) resulting in an ICER of £188,545 at two years and £33,058 at 20 years.
-
Increasing operative costs by 20% increases incremental costs for surgery by approximately £1000, increasing the ICER at two years to £72,745 (£15,199 at 20 years). Increasing postoperative costs by 20% increases incremental costs by approximately £350, increasing the ICER to £65,040 at two years and £15,569 at 20 years. Increasing all surgery-related costs by 20% leads to an increase in incremental costs increasing by approximately £1500, increasing the ICER to £79,783 at two years and £18,563 at 20 years.
-
Variation in the cost of health service contacts for patients on the intensive medical programme has a relatively large impact on incremental costs as these comprise a substantial proportion of the total costs of the intensive medical programme. Reducing costs of contacts by 50% increases incremental costs by approximately £1300 and increases the ICER at two years to £76,254 (£15,955 at 20 years). Conversely, increasing costs of contacts by 50% reduces incremental costs by approximately £1300 and reduces the ICER at two years to £45,255 (£9571 at 20 years).
Cost-effectiveness of bariatric surgery (adjustable gastric banding) for moderate obesity (BMI ≥ 30 and < 35) – probabilistic sensitivity analysis
In a probabilistic sensitivity analysis, where percentage weight loss, reduction in systolic blood pressure and TC : HDL ratio, proportion of patients with remission of Type 2 diabetes, health-state utility, health-state costs and costs of health service contacts for non-surgical patients during the intensive medical programme were sampled probabilistically, all simulations produced incremental cost-effectiveness estimates that were in the north-east quadrant of the cost-effectiveness map (Figure 7, which also shows the 95% confidence ellipses for the ICER).
FIGURE 7.
Cost-effectiveness plane – incremental costs and incremental QALYs for patients with moderate obesity (BMI ≥ 30 and < 35), undergoing adjustable gastric banding compared with an intensive medical programme. QALYs, quality-adjusted life-years.
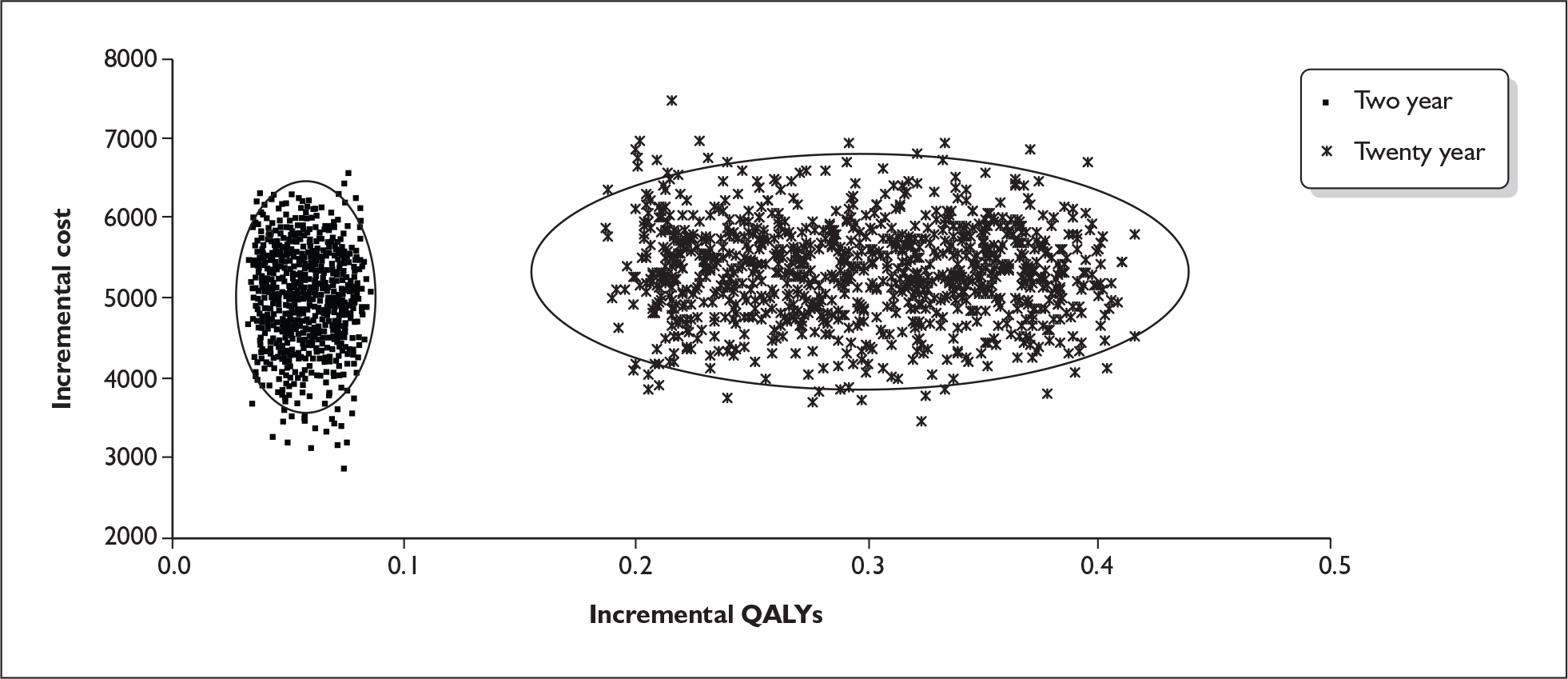
In this analysis, surgical management with adjustable gastric banding had a probability of being cost-effective (compared with the intensive medical programme) of 64% at a willingness-to-pay threshold of £20,000 per QALY and 98% at a willingness-to-pay threshold of £30,000 per QALY for a time horizon of 20 years (Figure 8). In contrast the probability of surgical management being cost-effective was zero at both willingness-to-pay thresholds, when adopting a time horizon of two years (i.e. when using data from the clinical trial report115 with no extrapolation of outcomes).
FIGURE 8.
Cost-effectiveness acceptability curve for adjustable gastric banding in patients with moderate obesity (BMI ≥ 30 and < 35) using a 20-year time horizon. QALY, quality-adjusted life-year.
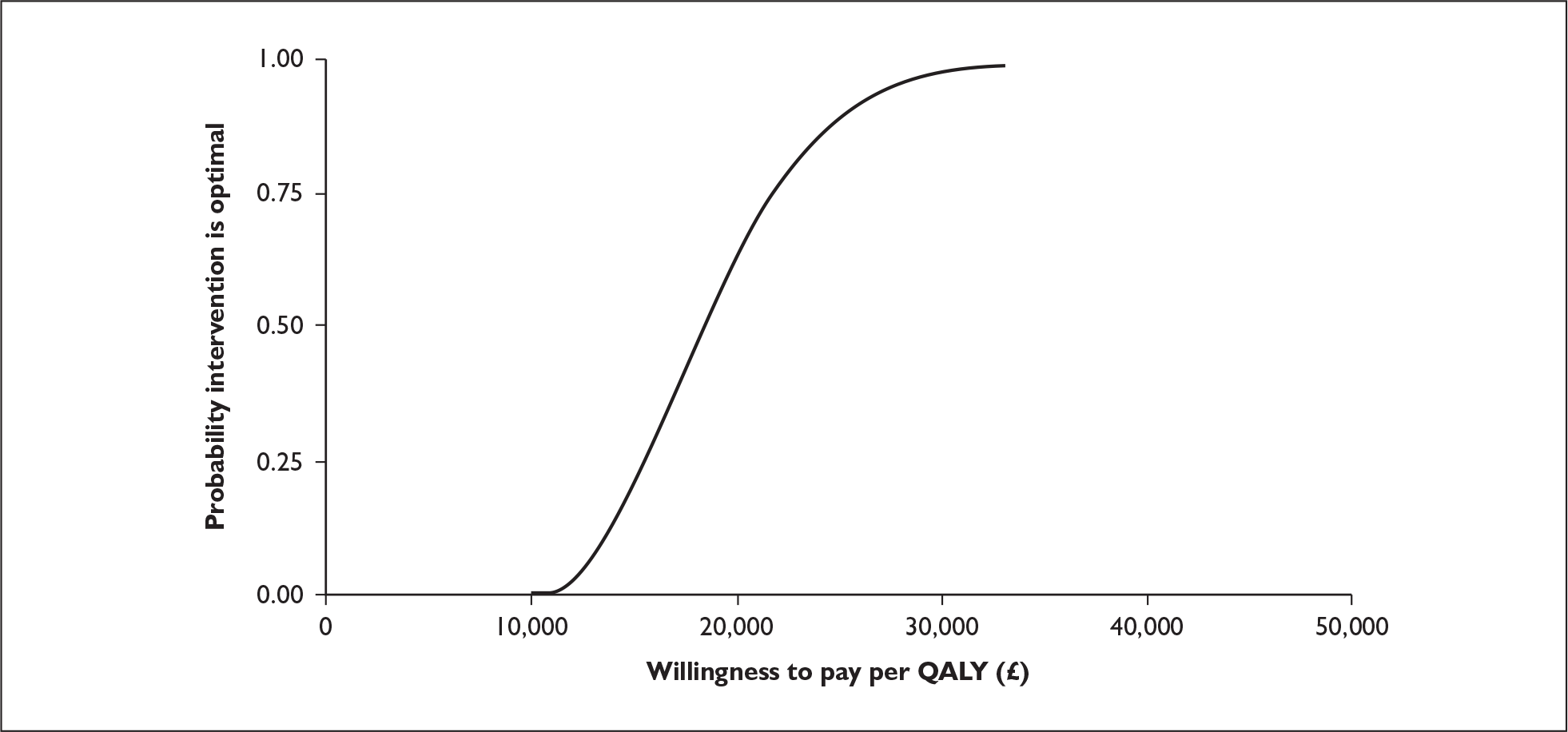
Discussion of cost-effectiveness
Summary of key results
-
We reviewed the economic model developed for the previous assessment report and identified a number of potential updates that could be applied in this report:
-
– The conceptual model (including health states for non-diabetic, postdiabetic and diabetic patients as well as death) was extended to include CHD and stroke. Methods relevant to modelling the incidence of CHD and stroke in obese and Type 2 diabetes populations were investigated.
-
– Updated estimates of the utility impact of weight reduction were incorporated, including estimates of the impact of comorbidity.
-
– BMI-specific diabetes incidence estimates were incorporated into the model as well as estimates of the impact of weight reduction on the development of cardiovascular comorbidities.
-
– Expert opinion suggested that resource use assumptions adopted in the previous report, for costing bariatric surgery, did not reflect current practice in the UK. Updated resource use assumptions were developed, based on review of the literature, discussion with surgical specialists and a costing developed by a specialist service.
-
– While the conceptual model was extended to include CHD and stroke, it was recognised that appropriate parameter inputs to include these comorbidities may not be available for all modelled populations. In this situation an updated version of the model used in the previous assessment report (updated for cost and utility estimates) would be adopted.
-
-
The analysis was developed for three patient populations covered by studies included in the clinical effectiveness review:
-
– patients with morbid (Class III, BMI ≥ 40) obesity – as in the previous review;
-
– patients with moderate to severe (Class I to Class II, BMI > 30 and < 40) obesity with significant comorbidity at baseline (Type 2 diabetes) undergoing laparoscopic adjustable gastric banding or receiving conventional therapy, based on data from a single trial117
-
– patients with moderate (Class I, BMI ≥ 30 and < 35) obesity undergoing laparoscopic adjustable gastric banding or an intensive medical programme, based on data from a single trial. 115
-
-
Included trials for patients with morbid obesity did not report measures of cardiovascular risks that were suitable for our new model. Hence the model developed for the previous assessment report was used for this population. The economic model adopted ‘optimistic’ estimates (based on the previous assessment report) and an alternative ‘pessimistic’ estimate (based on a recently published trial107 comparing gastric bypass and gastric banding), as the clinical effectiveness review concluded that meta-analysis was not appropriate. Weight loss outcomes were extrapolated to 10 years following surgery based on long-term outcomes reported for the SOS study. 97 In the absence of a robust, pooled estimate of treatment effect (with associated estimate of variability) we felt it was inappropriate to undertake probabilistic sensitivity analysis for the model applied to patients with morbid obesity.
-
The clinical trials reporting the use of adjustable gastric banding for moderate-to-severely obese (BMI ≥ 30 and < 40) patients with Type 2 diabetes and for moderately obese (BMI ≥ 30 and < 35) patients reported sufficient information, up to two years of follow-up, to apply the new model. The time horizon for these analyses was initially for the period of the trial follow-up only. However, extrapolations based on data from the SOS study (where relevant) or on the basis of data reported in the trial were undertaken.
Cost-effectiveness of bariatric surgery (gastric bypass or adjustable gastric banding) for morbid obesity (BMI ≥ 40)
-
Surgical management of morbid obesity with gastric bypass or adjustable gastric banding is estimated to be more costly than non-surgical management, but results in improved outcomes (in terms of QALYs) over the modelled 20-year time horizon. Using the optimistic assumption on weight reduction up to five years following surgery the QALY gain for adjustable gastric banding is 1.88, while using the pessimistic assumption the QALY gain is 0.92. The equivalent values for gastric bypass are 1.98 and 1.52 QALYs. These QALY gains are larger than those estimated in the previous report, because of extrapolation of effects over 10 years (rather than the assumption of immediate reversion to baseline weight at five years) and updated assumptions on the utility gain associated with a unit reduction in BMI. The ICERs range between £1897 and £4127 per QALY gained.
-
The results were generally robust to changes in assumptions in the deterministic sensitivity analysis, and in all cases the ICERs remained within the range conventionally regarded as cost-effective from an NHS decision-making perspective. Some key assumptions produced less favourable cost-effectiveness estimates – in particular reducing the utility gain associated with a weight loss to the value used in the previous review, and adopting alternative, less favourable assumptions (longer duration of surgery, higher revision rates and lower weight loss) that might be associated with less experienced surgical operators.
Cost-effectiveness of bariatric surgery (adjustable gastric banding) for moderate to severe obesity (BMI ≥ 30 and < 40) in patients with Type 2 diabetes
-
Results were reported for three time horizons: two years (corresponding to the duration of the clinical trial report), five years and 20 years [by which time it was assumed all patients had reverted to baseline weight, systolic blood pressure and TC : HDL ratio, and that all patients who resolved Type 2 diabetes (following surgery or through conventional treatment) had relapsed]. For each time horizon, surgical management of moderate to severe obesity in patients with Type 2 diabetes is estimated to be more costly than non-surgical management, but results in improved outcomes. The QALY gain of 0.27 at two years, increases to 1.10 for the 20-year time horizon. Incremental costs reduced from £5032 at two years to £1500 for the 20-year time horizon. The reduction in incremental cost arises from the difference in Type 2 diabetes resolution between the two modelled cohorts, with 73% of surgically treated patients resolving Type 2 diabetes at two years of follow-up (relative risk, compared with non-surgical patients, of 5.5, 95% CI 2.2 to 14.0). 117 The ICER reduced with longer time horizon from £18,930 at two years to £1367 at 20 years.
-
The results were generally robust to changes in assumptions in the deterministic sensitivity analysis. However, some key assumptions produced less favourable cost-effectiveness estimates – in particular reducing the diabetes health-state cost, assuming a gradual (rather than immediate) reduction in weight following surgery, reducing the utility gain associated with weight loss to the value used in the previous review, and adopting alternative, less favourable assumptions (longer duration of surgery, higher revision rates and lower weight loss) that might be associated with less-experienced surgeons. The impact of these changed assumptions was particularly marked for the two-year time horizon.
-
In the probabilistic sensitivity analysis all simulations were associated not only with increased QALYs, but also increased costs, when adopting a two-year time horizon. However, when the time horizon was extended to 20-years, while all simulations showed increased QALYs a proportion had negative incremental costs (total discounted costs for the surgical cohort were lower than for the non-surgical cohort). These occurred in simulations where surgical treatment was associated with high proportions of patients with remission of Type 2 diabetes. With a two-year time horizon the probability of surgical management being cost-effective (compared with non-surgical management) was 2.5% at a willingness-to-pay threshold of £20,000 per QALY and 50.6% at a willingness-to-pay threshold of £30,000 per QALY, assuming a gradual reduction in weight following surgery. In contrast the probability of surgical management being cost-effective was 100% at both willingness-to-pay thresholds, for a 20-year time horizon.
Cost-effectiveness of bariatric surgery (adjustable gastric banding) for moderate (BMI ≥ 30 and < 35) obesity
-
Results were reported for three time horizons: two years (corresponding to the duration of the clinical trial report), five years and 20 years. For each time horizon, surgical management of moderate obesity is estimated to be more costly than non-surgical management, but results in improved outcomes. The QALY gain of 0.08 at two years, increases to 0.40 for the 20-year time horizon. Incremental costs are approximately £5000 for each time horizon. The ICER reduced with longer time horizon – from £60,754 at two years to £12,763 at 20 years.
-
In the deterministic sensitivity analysis the least favourable ICERs were associated with short model time horizon, ranging from around £60,000 per QALY gained up to £190,000 per QALY gained. More favourable ICERs were found for the five and 20-year time horizons, ranging from around £16,000 per QALY gained up to £40,000 per QALY gained for the five-year time horizon and from around £12,500 per QALY gained up to £33,000 per QALY gained for the 20-year time horizon. In some scenarios, even for longer time horizons, the ICERs are above the range conventionally deemed as cost-effective from an NHS decision-making perspective – in particular reducing the utility gain associated with a weight loss to the value used in the previous review, and adopting assumptions that might be associated with less experienced surgeons were associated with high ICERs for all time horizons.
-
In the probabilistic sensitivity analysis all simulations were associated with increased QALYs but also increased costs, for all time horizons. With a 20-year time horizon the probability of surgical management being cost-effective (compared with an intensive medical programme) was 64% at a willingness-to-pay threshold of £20,000 per QALY and 98% at a willingness-to-pay threshold of £30,000 per QALY. In contrast, the probability of surgical management being cost-effective was zero at both willingness-to-pay thresholds, for a two-year time horizon.
Generalisability
-
In general, the clinical trials used to model the effectiveness of bariatric surgery for morbidly obese (BMI ≥ 40) patients reflect the key characteristics of the population discussed in Chapter 1, Description of Health problem, with the majority of patients recruited to the trials being female. These trials also generally recruit patients meeting the eligibility specified by current NICE guidance, with inclusion criteria specifying a BMI > 40, or a BMI > 35 for patients with significant comorbidity. An exception to this, is the trial reported by O’Brien and colleagues,115 which recruited patients with moderate obesity (BMI ≥ 30 and < 35), below the threshold for weight loss surgery adopted in current clinical guidelines. 9,146 The majority of patients recruited to the trial also seemed to be free of major comorbidities associated with obesity. In addition, in those trials recruiting patients meeting current clinical criteria for weight loss surgery (in terms of BMI) it is not always clear from the trial reports, what previous weight loss regimes the patients have undergone and whether they failed to achieve and maintain weight loss with non-surgical management (as specified in the NIH146 and NICE guidance9).
-
Some of the included trials specified inclusion criteria in relation to patient age – for example Angrisani and colleagues107 recruited patients between the ages of 16 and 50 years, van Dielen and colleagues127 recruited patients between 18 and 60 years, Lee and colleagues124 recruited patients between 18 and 59 years, while Howard and colleagues120 recruited patients below 50 years of age. The lower age criteria relate to distinctions between adult and adolescent/paediatric services. However, it is more likely that the upper age limits reflect issues in the design of the clinical trials (for example, to recruit patients whose comorbidities are more likely to be obesity-related rather than age-related) rather than the expected patient group for bariatric surgery.
-
The patient population in the trial reported by Angrisani and colleagues107 was 83% female with a BMI between 35 and 50, without specifying the presence of comorbidities and therefore had inclusion criteria wider than the current NICE guidance, whereas in the trial reported by Nilsell and colleagues126 the inclusion criteria specified a BMI of greater than 40, or greater than 37 with an obesity-related comorbidity. Inclusion criteria for the trial reported by Dixon and colleagues117 were also wider than the current NICE guidance with moderate to severely obese patients with Type 2 diabetes – patients were included if their BMI was greater than 30 but less than 40.
-
Clinical trials providing data used in the economic model were conducted in a variety of countries (Italy, Sweden and Australia). It is not clear how differences in clinical practice between countries are likely to influence the outcomes of procedures, nor the extent to which the results obtained in specialist centres conducting clinical trials can be generalised to other settings. Some of the included clinical trials (for example, Angrisani and colleagues107) refer directly to the impact of surgeon experience and the learning curve on patient outcomes – particularly with respect to the frequency of operative complications. To some extent this uncertainty is addressed in the analysis by considering a scenario where less-experienced surgeons are characterised by longer operative duration, higher operative mortality rates, higher rates of non-fatal complications and poorer outcomes (in terms of average weight loss).
-
Expert opinion suggested that resource use estimates (in terms of duration of surgery and length of stay) extracted from included clinical trials were likely to overestimate resource use in the UK setting. Updated estimates were developed based on expert clinical opinion. However, these have not been validated against any external standard. Discussion with clinical experts suggested that there was likely to be considerable variation in surgical practice (for example, some centres may undertake prophylactic cholecystectomy on all patients, while others would not perform any cholecystectomies on bariatric surgery patients at the time of the initial operation) and in the involvement of clinical psychology (for example, some services may limit involvement to patients with documented psychological illness). The costings in the report are based, as far as possible, on implementation of NICE guidance and therefore assume that all patients have a psychological evaluation and continuing psychological support following surgery.
-
As far as possible the economic analyses have used routinely available unit cost estimates – NHS Reference Costs185 and Unit costs of health and social care. 177 As no appropriate reference cost exists for bariatric surgery we developed a resource use protocol, which was refined by clinical experts (as discussed above) and costed in consultation with the costing unit at Southampton University Hospitals NHS Trust. Similarly, as no cost estimates existed for non-surgical management, protocols were developed – based on the previous assessment report, for morbidly obese patients, and on details in the clinical trial reports115,117 – and costed using appropriate UK unit costs. Details of the costing protocols are presented in the Data sources, Cost data section in this chapter. The accuracy and comprehensiveness of costing for non-surgical management in the trials reported by Dixon and colleagues117 and O’Brien and colleagues115 is dependent on the reporting of the interventions in the clinical trial reports.
Strengths and limitations
-
– The model adopted for the economic evaluation in this review is based upon a previously published model, developed for assessing the cost-effectiveness of bariatric surgery in a UK setting. The model has been extended, where possible, to include cardiovascular comorbidity, and has been updated with respect to duration of weight loss following bariatric surgery, the estimated utility gain associated with reduction in BMI, remission (and durability of remission) of Type 2 diabetes, resource use and health-care costs.
-
– Clinical evidence, in terms of weight reduction, revision rates and operative complications, were extracted from the RCTs included, and critically appraised in the clinical effectiveness review. Where necessary, these sources were supplemented with data from long-term cohort studies within the scope of the review. These were also critically appraised in the clinical effectiveness review. The main effectiveness parameter in the model, weight reduction, is an accepted primary aim of bariatric surgery, although not all included trials were powered on a measure of weight loss (where sample size calculations were reported). For example, the trial reported by Dixon and colleagues117 was powered to detect a 1% difference in HbA1c and also powered for diabetes remission rates (expected values 60% in the surgical group and 20% in conventional therapy).
-
– The majority of the data included in the model are in the public domain. Where updated assumptions have been developed in the course of this review (for example, resource use assumptions) these have been clearly documented and are presented in the body of this report. The model structure, assumptions and data inputs are clearly presented in this report. This should facilitate replication and testing of model assumptions and analyses.
-
– Patient utility was related to the main effectiveness parameter in the model using a published estimate of the change in utility associated with a unit change in BMI. The utility model was based on health-state preferences expressed by subjects in an RCT of pharmacotherapy and dietary modification for the treatment of obesity. Subjects covered a wide range of BMI, including 76 (of 621) categorised as morbidly (Class III) obese. Health-state preferences were assessed using a visual analogue scale (VAS; anchored at 0 for death and 100 for perfect health) to rank participants’ current health states. VAS scores were transformed to their equivalent time trade-off values using a published conversion method. 189 These time trade-off values were included in a multiple regression model to derive an estimate of the change in utility associated with a unit change in BMI, controlling for baseline utility age and sex. A review of health-state preference values, related to changes in BMI, concluded that these were the most methodologically sound published estimates to include in the model. The robustness of the results to assumptions regarding utility were addressed in a sensitivity analysis.
-
– Published economic evaluations of bariatric surgery for morbid obesity were reviewed to develop estimates of resource use associated with bariatric surgery. Duration of surgery, length of stay, ITU and/or HDU admissions were extracted from identified reports and compared with assumptions developed for the previous report. Updated assumptions were discussed with clinical experts who felt that these overestimated the duration of surgery and length of stay in comparison with current UK practice. New resource use estimates were developed, based on expert opinion, and were costed in consultation with the costing unit at Southampton University Hospitals Trust.
-
– A review of previous economic evaluations of surgery for morbid obesity identified factors that were likely to be particularly influential on cost and outcome estimates. The impact of these factors was tested in deterministic sensitivity analyses.
-
– A weakness in the economic model is that we were not able to conduct a robust meta-analysis on outcomes. For the morbidly obese population the clinical effectiveness review concluded that meta-analysis was inappropriate because, for comparison of certain surgical procedures there was only one study, and where there was more than one RCT there was heterogeneity in patient groups, comparator treatments and in outcomes reported. An additional practical limitation was the fact that standard deviations (or data to calculate them) were not reported in the majority of studies. For moderate-to-severely obese (BMI ≥ 30 and < 40) patients with Type 2 diabetes and moderately obese (BMI ≥ 30 and < 35) patients there was only one included trial each, comparing adjustable gastric banding with non-surgical management. These trials had limited follow-up periods – two years each, with some loss to follow-up [12.5% (5/40) of patients in the non-surgical group were reported as lost to follow-up at two years in the trial reported by O’Brien and colleagues115]. For the morbidly obese (BMI > 40) population the analysis is primarily based on three trials (for surgery outcomes, in terms of weight loss, the ‘optimistic’ assumption uses data from one trial for adjustable gastric banding126 and another for gastric bypass,120 while the pessimistic assumption uses both arms of the trial reported by Angrisani and colleagues107), whereas the effectiveness of non-surgical management is modelled through assumption based on the control cohort reported in the SOS study. 97 In all cases the comprehensiveness of the analysis (for effects such as reoperation or complications) is dependent on quality and completeness of reporting. A similar caveat applies to the resource assumptions and costings based on clinical trial reports.
-
– The cost-effectiveness model applies utility values for reduction in BMI associated with surgical or non-surgical management of obesity, but takes no account of any utility impact of side effects or complications of interventions. The cost impact of complications resulting in admission to ITU or reoperation are estimated based on proportions reported in included trials – although, as noted in the clinical effectiveness review, reporting of adverse events and complications is variable between studies. Similarly, in the analysis of surgery versus non-surgical management of moderate obesity (BMI ≥ 30 and < 35), the impact of approximately 30% of non-surgical patients being intolerant to VLCD or orlistat (reported by O’Brien and colleagues115) is included in cost calculations, but there is no assessment of the impact of side effects on utility. Reporting of long-term adverse effects – such as frequent vomiting or flatulence – following surgery is variable and of limited duration in included trials (up to three years postsurgery). However, where reported, the proportion of patients reporting such effects are non-trivial (28.5% frequent vomiting,129 13–25% emesis and 13–22% flatulence118). The likely duration of the side effects is not clear nor is it apparent how far the impact of these effects may offset any utility gains from reduction in BMI alone.
-
– A potentially serious weakness in published utility models is an assumption of linear additivity, with respect to BMI or change in BMI – the effect of reduction in BMI (or absolute value of BMI in the model applied in the previous review) is assumed to be constant over the range of BMI values. Hakim and colleagues152 reported investigating more complex functional forms, but opted for a simple model on the grounds of parsimony and that the more complex specifications failed to add significant explanatory power (assessed using the adjusted R2). However, the simple linear model cannot exclude the possibility of estimating utility values outside the logical range (in particular estimating values greater than one, where a large change in BMI is observed). An additional, implicit, assumption is that the utility change is independent of initial BMI or that it is independent of proximity to an ‘ideal’ or target BMI. Hakim and colleagues152 conducted a subgroup analysis re-estimating the regression on patients with a BMI greater than or equal to 30, but did not report any analysis of potential interactions between utility gain from reduction in BMI and baseline BMI, proximity to the non-obese range (i.e. to BMI below 30) or to a target or ‘ideal’ value (such as BMI of 25).
-
– There is uncertainty over resource use and costs associated with surgical management. Costs associated with the surgical admission, used in the economic model, are based on resource use protocols developed using expert opinion. Published resource use protocols were regarded as overestimates, in terms of duration of surgery and length of stay, and as poor predictors of cost in the UK. However, it has not been possible to validate the updated cost assumptions against external standards, reflecting current UK practice. Similarly, assumptions over preoperative assessments and postsurgical follow-up have been based on protocols, informed by expert opinion. Costs for non-surgical comparators were based on brief resource use protocols included in clinical trial reports – as such, they are dependent on the comprehensiveness of coverage in the clinical trial reports.
-
– A major source of uncertainty in the economic model relates to the absence of reliable, long-term data on the effectiveness (in terms of sustained weight loss) and the need for operative revision and conversion to alternative weight-loss methods. Data on long-term outcomes from the SOS study were used to extrapolate from clinical trial outcomes to longer term outcomes for patients with morbid obesity (BMI > 40) and also for patients with moderate-to-severe obesity (BMI ≥ 30 and < 40) and Type 2 diabetes. However, the validity of applying these data may be questioned – for example, in the clinical trial reported by Dixon and colleagues117 surgical patients were treated with adjustable gastric bands, while an unknown proportion of patients in the SOS study were treated with non-adjustable bands. It is not clear how changes in surgical techniques (or indeed in non-surgical management of obese patients) occurring over the duration of long-term cohort studies may affect the outcomes observed. On the other hand, it is unlikely that clinical trials – powered to detect differences in outcomes within two years – will be able to provide robust data on longer-term outcomes, even assuming complete follow-up. Surgical experts providing advice during this review have been particularly concerned about the absence of data on the proportion of patients who initially undergo adjustable gastric banding, but who will require reoperation and ultimately undergo conversion to gastric bypass in the longer term – estimated at approximately 30%. This has not been included in the economic evaluation because, while it would be relatively straightforward to include a range of possible costs for reoperation and conversion in the economic model, there are no data to model the effect on outcome of patients who undergo late conversion to gastric bypass following initial adjustable gastric banding.
Chapter 6 Assessment of factors relevant to the NHS and other parties
The prevalence of obesity is rising and the NICE commissioning guide for the bariatric surgical service68 has suggested that the average number of people receiving bariatric surgery (in line with NICE guidance) for a standard PCT population of 250,000 should be 25 per year in five years time, which equates to more than a threefold increase compared with estimated levels in 2006. Expert opinion has suggested that this may be too low. Such increases may necessitate a step change in service provision.
It is likely that greater resources will be required in primary care because for people to meet NICE criteria for surgery they must first have tried all appropriate non-surgical measures, unless they have a BMI of 50 or over in which case surgery may be considered as a first-line option. Following surgery the management of any minor adverse events will also occur within primary care and GPs and practice nurses may need more training to recognise and manage some of these events appropriately.
Greater resources may be required to provide band adjustment services for people who have received a gastric band. At present, expert opinion suggests that the pattern of follow-up care is variable both in quality and quantity. Appropriate band adjustment may improve weight loss outcomes and have effects on utility and costs.
Chapter 7 Discussion
Statement of principal findings
Clinical effectiveness
Surgery versus non-surgical interventions
Weight loss
The surgical option has been shown to be the more effective intervention for weight loss in obese people in each RCT115–117,119 and cohort study102–104 comparing gastric bypass, adjustable gastric banding and biliopancreatic diversion with a non-surgical intervention, and in each cohort study82–101,105 where participants received a different mix of surgical options. A variety of measures were used to report weight outcomes over different time spans. One RCT117 reports a statistically significant difference in per cent initial weight lost after two years (laparoscopic adjustable gastric banding 20.0% (± 9.4) versus 1.4% (± 4.9) in the conservative therapy group, p < 0.001) and in kg of weight lost at two years. The statistical significance of the reported reduction in BMI and per cent excess weight loss at two years is not reported. Another RCT with a maximum follow-up of two years115,116 reports statistically significant differences between the laparoscopic adjustable gastric banding and non-surgical group using four different outcome measures (weight in kg, BMI, per cent initial weight lost and per cent excess weight lost). In contrast, the third RCT119 did not report a statistical comparison between biliopancreatic diversion and a dietary intervention but instead reported separately for men and women statistically significant reductions from baseline to one year for measures of weight, BMI, fat-free mass and fat mass in the biliopancreatic diversion group that were not apparent in the dietary group. The cohort study102–104 that compared adjustable gastric banding and gastric bypass with a non-surgical intervention reported that BMI was statistically significantly lower two years after surgery [laparoscopic adjustable gastric banding 33.2 (± 4.7) or open Roux-en-Y gastric bypass 32.9 (± 6.7) versus control 41.0 (± 3.4), p < 0.001]. Weight and total fat mass were also statistically significantly reduced in comparison to baseline in the laparoscopic adjustable gastric banding group whereas the reductions that occurred in the Roux-en-Y gastric bypass group were not statistically significantly different. In the control group small increases that were not statistically significant occurred in both these measures after two years. The remaining two studies both compared a cohort that received different surgical interventions with a no surgery cohort97,99,100,105 and reported a greater change in BMI after a mean of 3.2 years105 and 10 years97,99,100 following surgery. Absolute mean BMI values, although lower in the surgical cohorts, were not reported to be statistically significantly different in one study105 and in the other a statistical comparison was not reported. 97,99,100 One study105 reported one further weight loss outcome, finding that surgery led to a statistically significantly greater per cent excess weight loss after 3.2 years of follow-up. The other study97,99,100 provides five further weight loss outcomes for this review update; surgery led to statistically significantly better outcomes in terms of per cent weight change and per cent BMI change after two years, and also weight and per cent weight change at 10 years. The difference in per cent weight change at 10 years was greater following surgery, but a statistical comparison with the control group is not reported.
HRQoL
There is evidence for improvement in some measures of HRQoL, particularly in the first couple of years following surgery. One RCT115,116 provided evidence for a statistically significant improvement in five of the eight domains of the SF-36 (physical function, physical role, general health, vitality and emotional role) two years after laparoscopic adjustable gastric banding. Over longer time periods (up to 10 years) there is mixed evidence from a large cohort study100 with statistically significantly greater change following surgery after 10 years observed in some HRQoL measures but not others.
Comorbidities
Surgical interventions led to greater improvements in comorbidities than non-surgical interventions. One RCT117 specifically enrolled people with Type 2 diabetes and after two years found statistically significantly higher remission of the disease following laparoscopic adjustable gastric banding than conventional therapy (laparoscopic adjustable gastric banding: 73% of participants with remission versus 13% in the conventional therapy group, p < 0.001) and statistically significantly fewer people with the metabolic syndrome. A large cohort study96,97,136 has reported that after 10 years a statistically significantly greater proportion of people who had received surgery had recovered from diabetes, hypertension, hypertriglyceridaemia, low HDL-cholesterol and hyperuricaemia. Furthermore, in those without the relevant comorbidities at baseline, the incidence of diabetes, hypertriglyceridaemia and hyperuricaemia (but not hypercholesterolaemia) was statistically significantly lower in the surgical cohort than the control cohort.
Mortality, adverse events and complications
The commonly reported adverse events associated with the non-surgical interventions were intolerance to prescribed medications such as orlistat and metformin, or intolerance to a VLCD or meal replacement. These events can be resolved by discontinuing treatment. A further complication of rapid weight loss, which is also observed following surgical interventions, is cholecystitis which occurred in a greater proportion of people receiving conventional therapy than those receiving laparoscopic adjustable gastric banding in the single RCT that reported this outcome. However, a cohort study96 reported that after two years obesity surgery statistically significantly increased the incidence of cholelithiasis and cholecystectomies in men, but that there was no difference in the incidence of these events among women.
Surgery versus other surgical interventions
Gastric bypass
Gastric bypass has been compared with four other surgical options and is reported to be more effective than adjustable gastric banding (one trial107), and more effective than vertical banded gastroplasty (statistically significant difference in three trials,108,109,120,123 greater weight loss in the remaining four trials either not statistically significantly different106,121,122 or no statistical comparison reported73,124). At five years, laparoscopic Roux-en-Y gastric bypass was statistically significantly better than adjustable gastric banding in terms of per cent excess weight loss, mean weight and mean BMI. 107 There were also statistically significantly fewer weight loss failures and more participants with a BMI < 30 following laparoscopic Roux-en-Y gastric bypass than adjustable gastric banding. 107 In the seven trials that assessed gastric bypass and vertical banded gastroplasty surgery, greater weight loss was observed following gastric bypass using a variety of different measures. However, statistically significant differences in favour of gastric bypass were only reported by three trials,108,109,120,123 and in two of these trials the statistically significant difference only applied to the per cent excess weight loss outcomes. 108,109,120 Statistical comparisons for the other weight loss outcomes were not reported. The trial comparing gastric bypass with laparoscopic sleeve gastrectomy125 was inconclusive. Adjustable gastric banding, vertical banded gastroplasty and laparoscopic isolated sleeve gastrectomy are restrictive procedures. Weight loss with gastric bypass was not significantly different to that with banded gastric bypass (one trial118). There were no differences in weight loss in the four trials reporting on the open and laparoscopic approaches to gastric bypass surgery (four trials112–114,130,131).
HRQoL
The HRQoL of people with gastric bypass has been compared with that of people with vertical banded gastroplasty (one trial124). Twelve months after surgery HRQoL as measured by the GIQLI had significantly improved for all patients but gastric bypass patients scored significantly better than vertical banded gastroplasty patients on 14 of the 36 individual items that make up the GIQLI. Vertical banded gastroplasty patients scored significantly better than gastric bypass patients on only one item. HRQoL following either open or laparoscopic gastric bypass has also been reported (1 trial113,114) and after three years there were no significant differences in MAQoL or BAROS outcome scores.
Two studies comparing gastric bypass with adjustable gastric banding (one trial107) and banded gastric bypass (one trial118) reported comorbidities. The numbers of participants with comorbidities were low and unevenly dispersed between the groups in the small trial that compared gastric bypass and adjustable gastric banding. Therefore it is not possible to determine whether one procedure has a greater impact on comorbidities than the other. After gastric bypass and banded gastric bypass there was no statistically significant difference in the proportion of patients experiencing resolution of the six reported comorbidities. There was no statistically significant difference in the improvement or resolution of eight out of 10 comorbidities that were reported on following either open or laparoscopic gastric bypass (one trial113,114). For the other two comorbidities a statistically significant difference was found in improvement/resolution of dyslipidaemia in favour of open gastric bypass, and in improvement/resolution of osteoarthritis symptoms in favour of laparoscopic gastric bypass.
Of the 10 studies comparing gastric bypass to another surgical option eight reported no deaths in either trial arm. 106–109,118,120–122,124,125 In one study123 two deaths occurred among the 20 patients in the Roux-en-Y gastric bypass group (10%) and none in the vertical banded gastroplasty group. In one trial73 one death occurred among the 77 patients enrolled in the study (1.3%), but the trial arm in which this death occurred is not stated (gastric bypass, or loop gastric bypass or gastric banding, the latter trial arm has not been reported in this review). Gastric bypass was associated with more early complications than laparoscopic adjustable gastric banding and vertical banded gastroplasty, but a level of late complications similar to vertical banded gastroplasty and similar or reduced reoperation rates compared to laparoscopic adjustable gastric banding or vertical banded gastroplasty respectively. There were no differences in complications between gastric bypass and banded gastric bypass. In the four trials that compared the open and laparoscopic approaches to gastric bypass surgery, two reported no deaths,112–114 but deaths occurred in both the open (1/51, 2%) and laparoscopic (2/53, 3.8% although one reported to be unrelated to surgery) groups in one trial,130 and in the laparoscopic arm of the fourth trial (1/30, 3%). 131 Conversion to open surgery ranged from 0 to 23%. Anastomotic stricture and reoperations were more frequent following the laparoscopic approach, but wound infections and hernias were more common after open surgery.
Vertical banded gastroplasty
Vertical banded gastroplasty has been compared with two other surgical options and found to be less effective than gastric bypass as discussed above. The results from the trials comparing vertical banded gastroplasty to adjustable gastric banding (three trials110,126–128) do not enable a conclusion to be drawn regarding which procedure leads to greater weight loss. One year after surgery greater improvements in weight (reported by one trial126), per cent excess weight loss (reported by two trials110,127,128) and BMI (reported by two trials110,127,128) were evident for vertical banded gastroplasty. However, a statistical comparison was not presented for the one-year weight outcome126 nor for one of the trials reporting one-year BMI outcomes. 127,128 A statistically significant difference at one year was reported by both trials reporting per cent excess weight loss110,127,128 and one of the trials reporting one-year BMI. 110 After two years statistically significant differences in BMI and per cent excess weight loss were only apparent in one of the two trials reporting these outcomes. 127,128 There were no differences in weight loss between the open and laparoscopic approaches to vertical banded gastroplasty surgery (one trial111).
The HRQoL of people with a vertical banded gastroplasty has been compared with that of people with a gastric bypass (one trial) as discussed above.
Vertical banded gastroplasty has been compared with one other surgical option, adjustable gastric banding (one trial127,128). Although the overall number of patients with comorbidity significantly decreased following both vertical banded gastroplasty and adjustable gastric banding there were no significant differences in improvements in comorbidities between the groups.
Of the 10 trials comparing vertical banded gastroplasty to another surgical option six reported no deaths106,108–110,120–122,124 and one reported no immediate deaths related to surgery. 126 Deaths occurred in two trials comparing vertical banded gastroplasty with gastric bypass as discussed above, and in one trial comparing vertical banded gastroplasty to adjustable gastric banding where two of the 50 participants undergoing vertical banded gastroplasty died (4%), whereas there were no deaths in the adjustable gastric banding group. 123,124 Vertical banded gastroplasty was associated with fewer early complications than gastric bypass and a similar or reduced level of late complications than gastric bypass and laparoscopic adjustable gastric banding respectively. There were fewer reoperations following vertical banded gastroplasty than with gastric bypass and adjustable gastric banding. GERD occurred more often after vertical banded gastroplasty than adjustable gastric banding. In the trial that compared the open and laparoscopic approaches to vertical banded gastroplasty there were no deaths. Surgery wound problems, pathological scars and hernias were more common following open surgery.
Adjustable gastric banding
Adjustable gastric banding has been compared with three other surgical options and found to be less effective than gastric bypass (one trial) as discussed above, and less effective than laparoscopic isolated sleeve gastrectomy (one trial129) for the three weight loss outcomes reported: per cent excess weight loss, weight loss and BMI decrease. In the comparison of adjustable gastric banding with vertical banded gastroplasty (three trials) the results were equivocal as already stated above. There were no differences in weight loss between the open and laparoscopic approaches to adjustable gastric banding surgery (one trial132).
None of the studies reporting on adjustable gastric banding included an assessment of HRQoL.
Adjustable gastric banding has been compared with three other surgical options. Comorbidity outcomes in comparison with gastric bypass (one trial) and vertical banded gastroplasty (one trial) are discussed above. Only one comorbidity, GERD, was reported on in comparison to laparoscopic isolated sleeve gastrectomy (one trial129). At one year, GERD had resolved in a greater percentage of participants in the laparoscopic adjustable gastric banding group than the laparoscopic isolated sleeve gastrectomy group, but statistical significance was not reported.
Of the five trials comparing adjustable gastric banding to another surgical option three reported no deaths and one reported no immediate deaths related to surgery. The only deaths reported occurred in one trial comparing adjustable gastric banding to vertical banded gastroplasty and these did not occur in the adjustable gastric banding group as noted above. Adjustable gastric banding was associated with more late complications and a greater level of revisional surgery than vertical banded gastroplasty. Adjustable gastric banding was also associated with gastrointestinal effects such as more frequent vomiting than in laparoscopic isolated sleeve gastrectomy. In the trial that compared the open and laparoscopic approaches to adjustable gastric banding there were no deaths. Open surgery for adjustable gastric banding involved a longer hospital stay and more readmissions than laparoscopic adjustable gastric banding. Incisional hernia also occurred following open adjustable gastric banding.
Laparoscopic sleeve gastrectomy
Laparoscopic sleeve gastrectomy was superior to adjustable gastric banding (one trial129), but similar to gastric bypass (one trial125), as noted above.
The studies reporting on laparoscopic sleeve gastrectomy did not include an assessment of HRQoL.
Resolution of GERD following laparoscopic isolated sleeve gastrectomy was compared with adjustable gastric banding (one trial129) as reported above. Comorbidity was not fully assessed in the trial comparing laparoscopic sleeve gastrectomy with gastric bypass,125 although diabetes resolved in both the patients who had this comorbidity at baseline (both were in the gastric bypass group).
Laparoscopic isolated sleeve gastrectomy led to generally fewer gastrointestinal effects than laparoscopic adjustable gastric banding and no deaths were reported. Similarly, the trial reporting on the comparison between laparoscopic sleeve gastrectomy and LGBP reported no conversions to open surgery and no intraoperative or postoperative complications.
Banded gastric bypass
Banded gastric bypass did not result in a significantly different weight loss to gastric bypass (one trial).
The study reporting on banded gastric bypass did not include an assessment of HRQoL.
After gastric bypass and banded gastric bypass there was no statistically significant difference in the proportion of patients experiencing resolution of the six reported comorbidities.
No deaths were reported. The only gastrointestinal symptom score that was statistically different between the groups was the score for emesis, which was statistically significantly better in the non-banded gastric bypass group. However, the proportion of participants with food intolerance was statistically significantly higher in this group.
Cost-effectiveness
Published economic evaluations
Five original economic evaluations were assessed in this report. Four of these compared different types of bariatric surgeries with a non-surgical treatment 138,140–142 and one was an economic evaluation alongside a clinical trial. 139 All modelled economic evaluations138–142 found the evaluated bariatric surgeries to be cost-effective in comparison to non-surgical treatment although the variability in estimates of costs and outcomes is large. The results of the economic evaluation alongside a clinical trial139 were inconclusive.
The choice and the range of model parameter estimates used in sensitivity analyses were not justified. Nevertheless, with respect to the limited number of parameters used in the sensitivity analyses the results appear to be robust to parameter variations. However, Craig and Tseng140 identified some subgroups of older and less obese men for whom an open gastric bypass may exceed the threshold of US$50,000 per QALY depending on the value of clinical effectiveness parameters.
The reported results should be interpreted with care:
-
because the natural disease progression was not explicitly modelled in terms of probabilities of obesity-related diseases in any of the identified modelled economic evaluations
-
because of the various methodological shortcomings in modelled economic evaluations138,140–142 identified and explained in the relevant sections of Chapter 5.
-
because of some of the assumptions used in modelled economic evaluations.
The most important concerns are summarised below:
-
Clinical evidence used to obtain the primary outcomes (weight reduction). In all four studies with modelled economic evaluations138,140–142 the BMI values were taken from the published evidence; however, it does not appear that any study conducted a systematic literature search and evidence analysis. Two studies, Craig and Tseng140 and Jensen and Flum,141 used the outcomes from a single published source of evidence, which may affect the validity of the estimate of the differential weight loss in the alternative treatments and the generalisability of results. Generalisability of results is also impaired by the choice of evidence that applies only to a subgroup of the obese population: the population of obese patients with Type 2 diabetes as in Ackroyd and colleagues138 and white female patients who were obese at the age of 18 as in Jensen and Flum. 141
-
Assumptions about the target population. Craig and Tseng140 and Salem and colleagues142 have assumed that the cohort of obese patients with BMI > 40 have no comorbidities at the baseline, which may not be a realistic assumption.
-
Assumptions about the outcomes of bariatric surgeries. Ackroyd and colleagues138 implicitly assumed that there is no differential operative mortality and postoperative morbidity between the two surgeries and the non-surgical treatment comparator. This is not likely to be a realistic assumption. The same is also true with respect to the assumption of a zero weight gain over the modelled time horizon in patients in the non-surgical treatment arm in Ackroyd and colleagues,138 Craig and Tseng140 and Salem and colleagues. 142
-
Utility estimates. Utility estimates reported in Ackroyd and colleagues,138 were also used in Craig and Tseng140 and Salem and colleagues. 142 However, these are not likely to be unbiased estimates of the HRQoL because of the multiple methodological shortcomings in the way they were derived from the available data. In addition the source data relate to the general population whose health-related preferences may differ from those of the obese population.
In summary, it appears that the identified studies have not provided reliable and generalisable estimates of the incremental cost-effectiveness of bariatric surgeries in comparison to non-surgical treatment.
SHTAC economic model
-
The model developed for the previous assessment report was assessed against other published models for completeness and relevance, and the conceptual model was extended to include CHD and stroke. Cardiovascular risks are typically estimated using variables other than body weight or BMI (such as blood pressure and cholesterol measurements, as well as patients’ age, sex, smoking status), so the inclusion of these additional health states in the economic model depends on the methods adopted to estimate transitions to these states and the extent to which appropriate measurements are reported in clinical studies.
-
The analysis was developed for three patient populations covered by studies included in the clinical effectiveness review:
-
– patients with morbid (Class III, BMI > 40) obesity – as in the previous review
-
– patients with moderate to severe (Class I to Class II, BMI > 30 and < 40) obesity with significant comorbidity at baseline (Type 2 diabetes), based on data from a single trial117
-
– patients with moderate (Class I, BMI ≥ 30 and < 35) obesity, based on data from a single trial. 115
-
-
All surgical patients in the latter two groups above underwent laparoscopic adjustable gastric banding. Therefore gastric bypass was only included in the economic model for patients with morbid obesity (BMI > 40).
-
The relevance of the three populations to current clinical guidelines was considered. Patients in the first group (with morbid obesity) and a subgroup of the second group (those with BMI greater than 35 and significant comorbidity) are considered appropriate for weight loss surgery under current clinical guidelines9,146 if they have failed to achieve sustained weight loss using other methods. Some clinical opinion suggests that patients with less severe obesity (BMI between 30 and 35) who have significant comorbidity that may respond to surgically induced weight loss (such as Type 2 diabetes), may be potential candidates for weight loss surgery. However, they emphasise that further research is required, with a clearer indication of the patient’s overall cardiovascular risk rather than relying on BMI. 190 In all cases the clinical consensus seems to suggest that weight loss surgery would not be an appropriate option for patients with mild obesity in the absence of evidence of cardiovascular risk or other significant comorbidity (which appears to be the majority of the patient population in the trial reported by O’Brien and colleagues,115 where, at baseline, no patients had coronary artery disease, 38% had metabolic syndrome and 20% had hypertension).
-
Meta-analysis of included clinical data was considered inappropriate. This has implications for the economic model. We adopted two estimates of the effect of gastric bypass and gastric banding on weight loss for the morbidly obese population. The first was an ‘optimistic’ scenario (based on the previous assessment report) and the second a ‘pessimistic’ scenario (based on a recently published trial107 comparing gastric bypass and gastric banding). Outcomes, in terms of weight loss at five years following surgery, were extrapolated using data from the SOS study. 97
-
Effectiveness data, in terms of weight loss, from the clinical trials reporting the use of adjustable gastric banding for severely obese patients with Type 2 diabetes and for moderately obese patients were used directly in the model. The analysis was initially undertaken for the period of the trial follow-up only. Extrapolations of longer-term weight loss were undertaken based on data from the SOS study, where relevant, or on the basis of data reported in the trial.
-
We reviewed recently published studies reporting estimates of change in utility associated with change in weight or change in BMI. There is large variation in the estimated change in utility associated with a unit change in BMI, which relates to differences in the characteristics of the populations studied, and may also relate to the number of covariates included in the analysis. For the base case in the economic model we adopted values estimated by Hakim and colleagues152 as these were derived from an obese (rather than an overweight) population, attempted to derive appropriate time trade-off values, and explicitly controlled for baseline utility. However, one potential problem with adopting this model is the assumption of a linear relationship between change in utility and change in BMI, that may produce biased or unfeasible estimates for large changes in BMI or at the extremes of the BMI range. The economic model does not include any utility adjustments for patients experiencing adverse effects associated with surgical or non-surgical management, nor are any adjustments included for patients undergoing surgical revision of their initial procedure. A scenario is included in the deterministic sensitivity analysis to reduce the utility gain associated with reduction in BMI to the value adopted in the previous assessment report.
-
Updated resource use assumptions, to reflect current UK practice, were developed, based on discussion with surgical specialists and a costing developed by a specialist service. These were costed in consultation with a local NHS costing unit, based within the Trust Finance Department.
Cost-effectiveness of bariatric surgery for morbid obesity (BMI > 40)
-
Surgical management with gastric bypass or adjustable gastric banding of morbid obesity was more costly than non-surgical management, but resulted in improved outcomes (in terms of QALYs) over the modelled 20-year time horizon. Differences between the optimistic and pessimistic scenarios were greater for adjustable gastric banding than for gastric bypass. Using the optimistic assumption on weight reduction up to five years following surgery the QALY gain for adjustable gastric banding is 1.88, while using the pessimistic assumption the QALY gain is 0.92. The equivalent values for gastric bypass are 1.98 and 1.52 QALYs. These QALY gains are larger than those estimated in the previous report, because of extrapolation of effects over 10 years (rather than the assumption of immediate reversion to baseline weight at five years) and updated assumptions on the utility gain associated with a unit reduction in BMI. The ICERs ranged between £1897 and £4127 per QALY gained.
-
Some alternative scenarios considered in the deterministic sensitivity analysis produced less favourable cost-effectiveness estimates – in particular reducing the utility gain associated with a weight loss to the value used in the previous review, and adopting less favourable assumptions (in terms of duration of surgery, revision rates and weight loss) that might be associated with less experienced surgical operators. However, the results were generally robust to changes in assumptions in the deterministic sensitivity analysis, and in all cases the ICERs remained within the range conventionally regarded as cost-effective from an NHS decision-making perspective.
Cost-effectiveness of adjustable gastric banding for moderate to severe obesity (BMI ≥ 30 and < 35) in patients with Type 2 diabetes
-
Results were reported for time horizons of two years (corresponding to the duration of the clinical trial report), five years and 20 years. For each time horizon, surgical management of moderate to severe obesity in patients with Type 2 diabetes was more costly than non-surgical management, but resulted in improved outcomes. The QALY gain of 0.27 at two years, increased to 1.10 for the 20-year time horizon. Incremental costs reduced from £5032 at two years to £1500 for the 20-year time horizon, because of the difference in Type 2 diabetes resolution between the two modelled cohorts. The ICER reduced with longer time horizon – from £18,930 at two years to £1367 at 20 years.
-
The results were generally robust to changes in assumptions in the deterministic sensitivity analysis. However, reducing the diabetes health-state cost, assuming a gradual (rather than immediate) reduction in weight following surgery, reducing the utility gain associated with weight loss to the value used in the previous review, and adopting less favourable assumptions (in terms of duration of surgery, revision rates and weight loss) that might be associated with less-experienced surgeons, produced less favourable cost-effectiveness estimates. The impact of these changed assumptions was particularly marked for the two-year time horizon.
-
In the probabilistic sensitivity analysis all simulations were associated with increased QALYs, but also increased costs when adopting a two-year time horizon. However, when the time horizon was extended to 20 years a proportion of simulations had negative incremental costs (total discounted costs for the surgical cohort were lower than for the non-surgical cohort). These occurred in simulations where surgical treatment was associated with high proportions of patients with remission of Type 2 diabetes. With a two-year time horizon the probability of surgical management being cost-effective (compared with non-surgical management) was 2.5% at a willingness-to-pay threshold of £20,000 per QALY and 50.6% at a willingness-to-pay threshold of £30,000 per QALY, assuming a gradual reduction in weight following surgery. In contrast, for a 20-year time horizon, the probability of surgical management being cost-effective was 100% at both thresholds.
Cost-effectiveness of adjustable gastric banding for moderate obesity (BMI ≥ 30 and < 35)
-
Results were reported for time horizons of two years, five years and 20 years. For each time horizon, surgical management was estimated to be more costly than non-surgical management, but resulted in improved outcomes. The QALY gain of 0.08 at two years, increased to 0.40 for the 20-year time horizon. Incremental costs were approximately £5000 for each time horizon. The ICER reduced with longer time horizon – from £60,754 at two years to £12,763 at 20 years.
-
In the deterministic sensitivity analysis the least favourable ICERs were associated with short model time horizon, ranging from around £60,000 per QALY gained up to £190,000 per QALY gained. More favourable ICERs were found for the five and 20-year time horizons, ranging from around £16,000 per QALY gained up to £40,000 per QALY gained for the five-year time horizon and from around £12,500 per QALY gained up to £33,000 per QALY gained for the 20-year time horizon. In some scenarios, even for longer time horizons, the ICERs are above the range conventionally deemed acceptable from an NHS decision-making perspective – in particular, reducing the utility gain associated with a weight loss to the value used in the previous review and adopting assumptions that might be associated with less-experienced surgeons were associated with high ICERs for all time horizons.
-
In the probabilistic sensitivity analysis all simulations were associated not only with increased QALYs but also increased costs, for all time horizons. With a 20-year time horizon the probability of surgical management being cost-effective (compared with an intensive medical programme) was 64% at a willingness-to-pay threshold of £20,000 per QALY and 98% at a willingness-to-pay threshold of £30,000 per QALY. In contrast, for a two-year time horizon, the probability of surgical management being cost-effective was zero at both thresholds.
Strengths and limitations of the assessment
This review has the following strengths.
-
It is independent of any vested interest.
-
It has been undertaken following the principles for conducting a systematic review. The methods were set out in a research protocol (Appendix 1), which defined the research question, inclusion criteria, quality criteria, data extraction process and methods to be employed at different stages of the review.
-
An advisory group has informed the review from its initiation. The research protocol was informed by comments received from the advisory group and the advisory group has reviewed and commented on the final report.
-
The review brings together the evidence for the clinical effectiveness and cost-effectiveness of bariatric surgery for obese people. This evidence has been critically appraised and presented in a consistent and transparent manner.
-
An economic model has been developed de novo following recognised guidelines and systematic searches have been conducted to identify data for the economic model. The main results have been summarised and presented.
In contrast, this review also has certain limitations:
-
Synthesis of the included studies was through narrative review. Although 26 eligible studies were identified either comparing surgery with no surgery or comparing different surgical procedures, in several cases only one study assessed a particular pair of interventions, for example gastric bypass versus adjustable gastric banding, or gastric bypass versus biliopancreatic diversion.
-
Meta-analysis was deemed inappropriate. In cases where the same procedures are compared by several studies, limitations in the literature prevented us from proceeding with meta-analysis. The most common limitation in the literature is that SDs are not reported by the majority of studies. In addition, data such as exact p-values or CIs, which might have been used to calculate a standard deviation, are also not reported. Furthermore, there are often differences in the outcome measures reported by the studies, or differences in the patient groups. If these limitations had applied to a minority of the studies available for meta-analysis we would have considered using a standard technique to impute the missing standard deviations. For example, the comparison assessed by the greatest number of studies was gastric bypass versus vertical banded gastroplasty, which was assessed by seven RCTs. Five of these RCTs reported similar outcomes that could be combined in a meta-analysis, but only two reported any measure of variance. All five trials found greater weight loss with gastric bypass. Notably, the two studies that reported different outcome measures both found no statistically significant difference. To combine these five RCTs in a meta-analysis (if SDs could be obtained from the authors) would be inappropriate not only because a proportion of the evidence would be ignored, but also because it would give undue weight to these procedures relative to other different surgical procedures that could not be combined in a meta-analysis.
-
Despite conducting a wide ranging and systematic search of the literature we did not identify any studies that met the inclusion criteria and assessed bariatric surgery in young people. There were also only two studies that included adults with either Class I or Class II obesity (BMI ranges 30–34.99 and 35–39.99 respectively).
-
Deaths, adverse events and some complications are generally rare events and therefore it is not likely that evidence presented here provides reliable estimates of the incidence of these rare events because most of the studies, particularly the RCTs, were of a limited size and duration. The proportion of deaths reported by the included studies within surgical cohorts or single surgical trial arms ranged from 0.25 to 10%. A recent systematic review and meta-analysis of mortality in bariatric surgery reports meta-analysis of total mortality at 30 days or less was 0.28% (95% CI 0.22 to 0.34) with restrictive operations having the lowest mortality. 191 The limited size and duration of the RCTs may have led to an underestimate of some of the more frequently encountered complications such as failure of gastric bands, e.g. due to band slip or erosion, complications that usually necessitate band removal. The SOS cohort study which has been ongoing for over a decade provides data for greater numbers of participants but is vulnerable to various kinds of bias. In addition, some RCTs compared different procedures with open surgery being undertaken for one intervention, and laparoscopic surgery for the other.
-
The included studies provided insufficient information on surgeon experience for learning curve effects to be assessed in the comparisons of open versus laparoscopic surgeries.
-
Owing to the time constraints of this review we were unable to contact the authors of the primary studies to request additional data. Although this might have provided some additional useful information, we cannot be certain that sufficient data would have been forthcoming to enable a meta-analysis, and it is unlikely that further details would have changed our conclusions.
-
The utility model adopted for the base case maybe an over-simplification by assuming linear additivity, with respect to change in BMI. The utility gain associated with a reduction in BMI (or conversely the utility loss associated with an increase in BMI) is assumed to be constant over the range of BMI values and therefore cannot exclude the possibility of estimating utility values outside the logical range. Moreover, the model does not allow for interactions between baseline BMI or proximity to a target or ‘ideal’ value, that may modify the effect of change in BMI on utility.
-
The economic model applies utility values to the reduction in BMI associated with surgical or non-surgical management of obesity, but takes no account of any utility impact of side effects or complications of interventions. Reporting of long-term adverse effects following surgery is variable and of limited duration in included trials. However, where reported, the proportion of patients reporting such effects is non-trivial. The likely duration of the side effects is not clear, nor is it apparent how far the impact of these effects may offset any utility gains from reduction in BMI alone.
-
Costs associated with the surgical admission in the economic model are based on resource use protocols developed using expert opinion. Published resource use protocols were regarded as overestimates, in terms of duration of surgery and LOS, and as poor predictors of cost in the UK. However, it has not been possible to validate the updated cost assumptions against external standards, reflecting current UK practice. Similarly, assumptions over preoperative assessments and postsurgical follow-up have been based on protocols, informed by expert opinion. Costs for non-surgical comparators were based on brief resource use protocols included in clinical trial reports – as such, they are dependent on the comprehensiveness of coverage in the clinical trial reports.
-
A major source of uncertainty in the economic model relates to the absence of reliable, long-term data on the effectiveness (in terms of sustained weight loss) and the need for operative revision and conversion to alternative weight loss methods. Data on long-term outcomes from the SOS study were used to extrapolate from clinical trial outcomes to longer-term outcomes. However, the validity of applying these data may be questioned – for example, a proportion of patients in the SOS study were treated with non-adjustable bands, which would not be considered an acceptable strategy in current practice. It is not clear how changes in surgical techniques (or indeed in non-surgical management of obese patients) occurring over the duration of long-term cohort studies may affect the outcomes observed.
Other relevant factors
-
This review updates a previous Technology Assessment Report15 and Cochrane review. 70,71 The criteria for this updated review were broadened to include adults and young people with Class I and Class II obesity, as well as those considered to be morbidly obese (Class III obesity). To maintain the relevance of the review to current practice the historical procedures of horizontal gastroplasty and jejunoileal bypass have been excluded from this updated review.
-
The duration of the majority of the studies included in this review lay between one and three years with, in general, very few dropouts reported or apparent from the shortest studies. However, it was reported or apparent from the results of the few studies with durations of four to six years that only a half to one-quarter of the study population contributed outcome data at the final time points.
-
Only five (three RCTs, two cohort studies) of the studies included in this review reported any assessment of QoL issues. It is therefore difficult to make any judgement about the impact of weight loss interventions on the quality of an obese person’s daily life.
-
It was beyond the remit of this research to assess the impact of preintervention and postintervention education, counselling and support on the outcomes of the interventions. However, the majority of the studies included in this review did not provide such details, which may be important for understanding patient compliance with the lifestyle and diet modifications that are necessary for successful weight loss maintenance.
-
Few studies included participants aged over 60 years, so it is uncertain how generalisable these results are to older adults.
-
Most study participants were women, so it is uncertain how generalisable the results are to men.
-
All the studies included in this review were conducted in countries other than the UK. It is difficult to determine how generalisable the results of the included studies are to the ethnically diverse population within the UK.
-
Only two RCTs assessed sleeve gastrectomy and none of the included studies assessed a two-stage approach to gastric surgery for obesity using sleeve gastrectomy before another bariatric procedure. We are therefore not able to draw any conclusion regarding the use of a two-stage approach.
-
The relatively short duration of the majority of the RCTs available for inclusion in this review may mean that the impact of late complications (such as gastric ulcers, stomal stenosis and erosions, and band slippage) and the need for revisional surgery are underestimated.
-
Expert opinion indicates that vertical banded gastroplasty is almost never undertaken now. However, this procedure forms the bulk of the evidence base, reported by 11 of 20 comparisons of surgical procedures and one of the six comparisons with non-surgical interventions. Similarly, the bariatric procedures in common use are mainly undertaken laparoscopically now, but the available evidence includes a number of trials that include open procedures.
-
In common with earlier versions15,70,71 of this review, bariatric surgery interventions were found to be more effective than any of the non-surgical interventions in terms of weight loss and improvements in comorbidities. The longer-term information from one cohort study that is now available on quality of life (up to 10 years) provides mixed evidence with some HRQoL measures showing significantly greater change after surgery, but not others. Only two comparisons, gastric bypass versus vertical banded gastroplasty, and vertical banded gastroplasty versus adjustable gastric banding, are common to both our previous reviews15,70,71 and this review. Gastric bypass continues to appear more effective for weight loss than vertical banded gastroplasty because three trials report statistically significant greater weight loss and greater weight loss is apparent in the remaining four trials although this loss is either not statistically different or no statistical comparison is reported. Data on comorbidities were not assessed in these trials. Three trials contributed evidence to the comparison of vertical banded gastroplasty versus adjustable gastric banding and the results continue to be conflicting regarding which procedure leads to greater weight loss. There was no new information to include on comorbidities for this comparison. There was no new information to include on QoL for either the gastric bypass versus vertical banded gastroplasty or the vertical banded gastroplasty versus adjustable gastric banding comparisons.
-
It has not been possible for us to determine how similar the results of this review are to the results of reviews of bariatric surgery undertaken by other authors because these have generally focused on one particular surgical intervention, and/or have included study types other than RCTs and/or have included interventions that are no longer in current use. Therefore the results are not directly comparable.
Chapter 8 Conclusions
Implications for service provision
A NICE commissioning guide for the bariatric surgical service was produced alongside the NICE obesity guideline. The commissioning guide has estimated that the benchmark rate at five years for a bariatric surgical service is 0.01% per year (or 10 per 100,000 population). 68 This means that for a standard PCT population of 250,000, the average number of people receiving bariatric surgery (in line with NICE guidance) would be 25 per year in five years time. The commissioning guide indicates that this equates to more than a threefold increase compared with the current estimated rate of bariatric surgery commissioned by the NHS in 2006.
Suggested research priorities
-
There continues to be a need for good-quality, long-term RCTs comparing different operative techniques for obesity that include an assessment of patient QoL. To enable future meta-analysis, RCT data should be comprehensively reported, ideally including more than one widely used outcome measure such as weight, per cent excess weight loss or BMI, and details of the standard deviation about the mean for each outcome reported.
-
A comparison of procedures which combine restrictive and malabsorption components such as gastric bypass with the purely restrictive procedures in current use, particularly adjustable gastric banding, would be desirable as only two small RCTs contribute evidence on these comparisons. However, this may not be possible because expert opinion suggests that in practice severity of obesity and the presence of comorbid conditions determines which procedure is suitable for an individual patient.
-
The evidence base for the clinical effectiveness of bariatric surgery for adults with Class I or Class II obesity is very limited. Similarly, no evidence to inform on the clinical effectiveness of surgical intervention for obesity in young people was found that met our inclusion criteria. Further good-quality RCTs are required to provide clinical effectiveness and QoL evidence for these two groups. In addition, it is essential that any new research reports on the resolution and/or development of comorbidities such as Type 2 diabetes and hypertension so that the potential benefits of early intervention can be assessed.
-
Assessing the risks of different bariatric procedures is hampered by a lack of consistency in the reporting of adverse outcomes. A core set of important adverse outcomes should be identified so that a standardised approach to describing adverse outcomes can be developed.
-
It was beyond the remit of this review to assess the impact of preintervention and postintervention education, counselling and support on patients’ understanding of the procedures and the consequences of undergoing surgery. The provision of postsurgical care, e.g. frequency and amount of band adjustment, was also beyond the remit of this review. As all of these aspects have the potential to affect the outcome of the intervention they should be reviewed. The impact that these aspects have on outcomes should be reviewed.
-
In addition to good-quality, long-term RCTs, there is a need for good-quality, long-term cohort studies to:
-
– identify reoperation for late complications following all bariatric procedures and conversion to gastric bypass for patients initially managed with gastric banding
-
– identify the duration of remission, following surgical or non-surgical management, of comorbidities associated with obesity to determine whether this is primarily associated with durability of weight loss or with other prognostic factors
-
– identify providers at different stages of the learning curve and to document the impact of experience on the safety, effectiveness and efficiency of surgery
-
– identify resource use for patients during preoperative assessment, surgical admissions and postoperative management to develop robust costings for bariatric procedures.
-
-
Current utility models indicate that reduction in BMI is associated with gains in utility. However, there is uncertainty over the magnitude of this gain. Further research is required to establish the utility gain associated with reduction in BMI, to establish the most appropriate functional forms (current models tend to assume linear additivity which may lead to infeasible values) and to investigate interactions between utility gain from reduction in BMI and baseline BMI, proximity to the non-obese range or to a target ‘ideal’ value. The research should also consider whether utility gains from reduction in BMI that are observed over the short-term, are maintained over the longer term.
-
Current utility models relate gains in utility to change in BMI. Further research is required to investigate whether there are additional utility gains associated with the resolution of comorbidity following surgical or non-surgical management of obesity. Similarly, economic models of surgical or non-surgical management of obesity would be improved by including estimates of the QoL impact of the side effects of treatment. This would require more systematic recording and reporting of adverse effects, as well as additional research on their impact on patients’ QoL and the extent to which these may offset quality of life gains associated with reduction in BMI.
Acknowledgements
We would like to thank members of our advisory group panel who provided expert advice and comments on the protocol and/or a draft of this report: Professor John Baxter, Consultant in General Surgery, Morriston Hospital, Swansea [J.B. is president of the British Obesity Surgery Society (BOSS)]; Mr Ken Clare, Service User (K.C. has been paid for presenting at conferences by the National Obesity Forum and the Association for the Study of Obesity. He has been supported to attend IFSO 2006 by Covidien. He is a Trustee of weight loss surgery information and support, a registered charity. He is employed as a bariatric specialist nurse by Gravitas Bariatric Surgery Limited); Dr Richard Fordham, Director, Health Economics Support Programme NHS and Senior Lecturer in Health Economics, University of East Anglia, Norwich; Ms Jane Munro, Bariatric Research Nurse, Glasgow University, Glasgow; Professor John Wilding, Professor of Medicine and Honorary Consultant Physician, University Hospital Aintree, Liverpool [J.W. has acted as an advisor to, and is currently an investigator for, companies who currently market drugs for the treatment of obesity, including Roche (orlistat), Abbott (sibutramine) and Sanofi-Aventis (rimonabant), and for several companies who have such products in development]. In addition, we also acknowledge advice provided by Mr Ian Bailey, Consultant Surgeon, Southampton General Hospital; Dr Utkarsh Kulkarni, NHS Grampian; Fiona Boyle, Finance Manager – Costing, Southampton University Hospitals NHS Trust; Mrs Bryre Butcher, Senior Costing Accountant, Southampton University Hospitals NHS Trust.
We are also grateful to Karen Welch, Information Specialist (SHTAC, University of Southampton), for conducting the searches; Elizabeth Hodson, Information Assistant (WIHRD, University of Southampton) for retrieving references and Andrea Takeda, Senior Research Fellow (SHTAC, University of Southampton) for reviewing a draft of this report.
Contributions of authors
J. Picot (Research Fellow) developed the research protocol, drafted the background section, assisted in the development of the search strategy, assessed studies for inclusion, extracted data from and quality-assessed the included studies, synthesised evidence, drafted and edited the final report, and project managed the study; J. Jones (Principal Research Fellow) developed the research protocol, assisted with drafting the background section, assessed studies for inclusion, extracted data from and quality-assessed the included studies, synthesised evidence, developed the economic evaluation, and drafted the report; J.L. Colquitt (Senior Research Fellow) developed the research protocol, drafted the background section, assisted in the development of the search strategy, assessed studies for inclusion, extracted data from and quality-assessed the included studies, synthesised evidence, and drafted the report; E. Gospodarevskaya (Senior Research Fellow) developed the research protocol, assisted with drafting the background section, assessed studies for inclusion, extracted data from and quality-assessed the included studies, synthesised evidence, developed the economic evaluation, and drafted the report; E. Loveman (Senior Research Fellow) developed the research protocol, drafted the background section, assessed studies for inclusion, extracted data from and quality-assessed the included studies, synthesised evidence, and drafted the report; L. Baxter (Research Fellow) assessed studies for inclusion, extracted data from and quality-assessed the included studies, synthesised evidence, and drafted the report; A.J. Clegg (Professor/Director of SHTAC) developed the research protocol, drafted the background section, assessed studies for inclusion, extracted data from and quality-assessed the included studies, synthesised evidence, and drafted the report.
Associated Cochrane Review
The systematic review of clinical effectiveness is published as a Cochrane Review in the Cochrane Database of Systematic Reviews 2009, Issue 2 Cochrane Reviews are regularly updated as new evidence emerges and in response to comments and criticisms, and the Cochrane Database of Systematic Reviews should be consulted for the most recent version of the Review.
Disclaimers
The views expressed in this publication are those of the authors and not necessarily those of the HTA programme or the Department of Health.
References
- Walley AJ, Blakemore AIF, Froguel P. Genetics of obesity and the prediction of risk for health. Hum Mol Genet 2006;15:R124-R130.
- Wilding JPH. Pathophysiology and aetiology of obesity. Medicine 2006;34:501-5.
- Rissanen A, Heliovaara M, Aromaa A. Overweight and anthropometric changes in adulthood: a prospective study of 17,000 Finns. Int J Obes 1988;12:391-40.
- McTigue KM, Garrett JM, Popkin BM. The natural history of the development of obesity in a cohort of young U.S. adults between 1981 and 1998. Ann Intern Med 2002;136:857-64.
- Kahn HS, Cheng YJ. Longitudinal changes in BMI and in an index estimating excess lipids among white and black adults in the United States. Int J Obes (Lond) 2008;32:136-43.
- Gordon-Larsen P, Adair LS, Nelson MC, Popkin BM. Five-year obesity incidence in the transition period between adolescence and adulthood: the National Longitudinal Study of Adolescent Health. Am J Clin Nutr 2004;80:569-75.
- World Health Organization . Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser 1995;854:1-452.
- World Health Organization . Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser 2000;894:i-253.
- National Institute for Health and Clinical Excellence . Obesity – Guidance on the Prevention, Identification, Assessment and Management of Overweight and Obesity in Adults and Children 2006.
- Parikh NI, Pencina MJ, Wang TJ, Lanier KJ, Fox CS, D’Agostino RB, et al. Increasing trends in incidence of overweight and obesity over 5 decades. Am J Med 2007;120:242-50.
- Nafziger AN, Stenlund H, Wall S, Jenkins PL, Lundberg V, Pearson TA, et al. High obesity incidence in northern Sweden: how will Sweden look by 2009?. Eur J Epidemiol 2006;21:377-82.
- World Health Organization . Overweight and Obesity 2006.
- Craig R, Mindell J. Health survey for England 2006. Latest trends. A survey carried out for NHS The Information Centre; 2006.
- Issued by Statistical Directorate WAG . Welsh Health Survey 2007 2008.
- Clegg AJ, Colquitt J, Sidhu MK, Royle P, Loveman E, Walker A. The clinical effectiveness and cost-effectiveness of surgery for people with morbid obesity: a systematic review and economic evaluation. Health Technol Assess 2002;6:1-153.
- National Statistics TIC . Statistics on Obesity, Physical Activity and Diet: England, January 2008 2008.
- National Centre for Social Research . Health Survey for England, 2003 n.d. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsStatistics/DH_4098712.
- Zaninotto P, Wardle H, Stamatakis E, Mindell J, Head J. Forecasting obesity to 2010. Joint Health Surveys Unit, National Centre for Social Research, Department of Epidemiology and Public Health at the Royal Free and University College Medical School; 2006.
- Welsh Assembly Government . Health Statistics Wales, 2008 2008.
- McPherson K, Marsh T, Brown M. Foresight. Tackling obesities: future choices – modelling future trends in obesity and the impact on health. London: Government Office for Science; 2007.
- Lobstein T, Leach R. Foresight. Tackling obesities: future choices – international comparisons of obesity trends, determinants and responses – evidence review. London: Government Office for Science; 2007.
- Boddy LM, Hackett AF, Stratton G, Taylor SR. Effect on prevalence rates of using three different definitions of obesity in 9–10 year old children. Int J Hlth Promotion Educ 2007;45:11-6.
- Frost GS, Lyons GF. Counterweight Project Team . Obesity impacts on general practice appointments. Obes Res 2005;13:1442-9.
- Report By The Comptroller and Auditor General. Tackling Obesity in England 2001.
- Peeters A, Barendregt JJ, Willekens F, Mackenbach JP, Al MA, Bonneux L. Obesity in adulthood and its consequences for life expectancy: a life-table analysis. Ann Intern Med 2003;138:24-32.
- House of Commons Health Committee . Obesity 2004 n.d.
- Craig R, Mindell J. Health survey for England 2005: health of older people. London: National Centre for Social Research; 2007.
- Brown CD, Higgins M, Donato KA, Rohde FC, Garrison R, Obarzanek E, et al. Body mass index and the prevalence of hypertension and dyslipidemia. Obes Res 2000;8:605-19.
- Peytremann-Bridevaux I, Santos-Eggimann B. Health correlates of overweight and obesity in adults aged 50 years and over: results from the Survey of Health, Ageing and Retirement in Europe (SHARE). Swiss Med Wkly 2008;138:261-6.
- Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M. Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet 2008;371:569-78.
- Allender S, Rayner M. The burden of overweight and obesity-related ill health in the UK. Obes Rev 2007;8:467-73.
- Rojas-Rodriguez J, Escobar-Linares LE, Garcia-Carrasco M, Escarcega RO, Fuentes-Alexandro S, Zamora-Ustaran A. The relationship between the metabolic syndrome and energy-utilization deficit in the pathogenesis of obesity-induced osteoarthritis. Med Hypotheses 2007;69:860-8.
- Teichtahl AJ, Wluka AE, Proietto J, Cicuttini FM. Obesity and the female sex, risk factors for knee osteoarthritis that may be attributable to systemic or local leptin biosynthesis and its cellular effects. Med Hypotheses 2005;65:312-15.
- Liu B, Balkwill A, Banks E, Cooper C, Green J, Beral V. Relationship of height, weight and body mass index to the risk of hip and knee replacements in middle-aged women. Rheumatology (Oxford) 2007;46:861-7.
- Young T, Peppard PE, Taheri S. Excess weight and sleep-disordered breathing. J Appl Physiol 2005;99:1592-9.
- Bhattacharya S, Campbell DM, Liston WA, Bhattacharya S. Effect of body mass index on pregnancy outcomes in nulliparous women delivering singleton babies. BMC Public Health 2007;7.
- Robinson HE, O’Connell CM, Joseph KS, McLeod NL. Maternal outcomes in pregnancies complicated by obesity. Obstet Gynecol 2005;106:1357-64.
- Rode L, Nilas L, Wojdemann K, Tabor A. Obesity-related complications in Danish single cephalic term pregnancies. Obstet Gynecol 2005;105:537-42.
- Driul L, Cacciaguerra G, Citossi A, Martina MD, Peressini L, Marchesoni D. Prepregnancy body mass index and adverse pregnancy outcomes. Arch Gynecol Obstet 2008;278:23-6.
- Chu SY, Callaghan WM, Kim SY, Schmid CH, Lau J, England LJ, et al. Maternal obesity and risk of gestational diabetes mellitus. Diabetes Care 2007;30:2070-6.
- Raatikainen K, Heiskanen N, Heinonen S. Transition from overweight to obesity worsens pregnancy outcome in a BMI-dependent manner. Obesity (Silver Spring) 2006;14:165-71.
- De Ferranti SD, Osganian SK. Epidemiology of paediatric metabolic syndrome and type 2 diabetes mellitus. Diab Vasc Dis Res 2007;4:285-96.
- Din-Dzietham R, Liu Y, Bielo MV, Shamsa F. High blood pressure trends in children and adolescents in national surveys, 1963 to 2002. Circulation 2007;116:1488-96.
- Schiel R, Beltschikow W, Kramer G, Stein G. Overweight, obesity and elevated blood pressure in children and adolescents. Eur J Med Res 2006;11:97-101.
- Helmrath MA. Adolescent obesity and bariatric surgery. Surg Clin North Am 2006;86:441-54.
- Leigh-Hunt N, Rudolf M. A review of local practice regarding investigations in children attending obesity clinics and a comparison of the results with other studies. Child Care, Health Dev 2008;34:55-8.
- Falagas ME. Obesity and infection. Lancet Infect Dis 2006;6:438-46.
- Kral JG. Management: Part III – Surgery. BMJ 2006;333:900-3.
- Lean M, Finer N. Management: Part II – Drugs. BMJ 2006;333:794-7.
- Avenell A, Sattar N, Lean M. Management: Part I – Behaviour change, diet, and activity. BMJ 2006;333:740-3.
- Avenell A, Broom J, Brown TJ, Poobalan A, Aucott L, Stearns SC, et al. Systematic review of the long-term effects and economic consequences of treatments for obesity and implications for health improvement. Health Technol Assess 2004;8:1-194.
- Levy P, Fried M, Santini F, Finer N. The comparative effects of bariatric surgery on weight and type 2 diabetes. Obes Surg 2007;17:1248-56.
- Poobalan AS. Long-term weight loss effects on all cause mortality in overweight/obese populations. Obes Rev 2007;8:503-13.
- Christensen R, Bartels EM, Astrup A, Bliddal H. Effect of weight reduction in obese patients diagnosed with knee osteoarthritis: a systematic review and meta-analysis. Ann Rheum Dis 2007;66:433-9.
- Curioni C, Andre C, Veras R. Weight reduction for primary prevention of stroke in adults with overweight or obesity. Cochrane Database Syst Rev 2006.
- Kral JG. Management: Part III – Surgery. BMJ 2006;333:900-3.
- Weinsier RL, Wilson LJ, Lee J. Medically safe rate of weight loss for the treatment of obesity: a guideline based on risk of gallstone formation. Am J Med 1995;98:115-17.
- Nutrition Committee of the Royal College of Physicians . Anti-Obesity Drugs. Guidance on Appropriate Prescribing and Management 2003.
- National Institute for Health and Clinical Excellence . Rimonabant for the Treatment of Overweight and Obese Patients 2008.
- Lee CW, Kelly JJ, Wassef WY. Complications of bariatric surgery. Curr Opin Gastroenterol 2007;23:636-43.
- Suter M, Calmes JM, Paroz A, Giusti V. A 10-year experience with laparoscopic gastric banding for morbid obesity: high long-term complication and failure rates. Obes Surg 2006;16:829-35.
- Bueter M, Maroske J, Thalheimer A, Gasser M, Stingl T, Heimbucher J, et al. Short- and long-term results of laparoscopic gastric banding for morbid obesity. Langenbeck’s Archiv Surg 2008;393:199-205.
- Scopinaro N, Gianetta E, Civalleri D, Bonalumi U, Bachi V. Bilio-pancreatic bypass for obesity: II. Initial experience in man. Br J Surg 1979;66:618-20.
- Buchwald H. Consensus conference statement bariatric surgery for morbid obesity: health implications for patients, health professionals, and third-party payers. Surg Obes Relat Dis 2005;1:371-81.
- Jung RT, Cuschieri A, Cuschieri A, Steele RJC, Moosa AR. Essential surgical practice – Volume 1. Oxford: Butterworth Heinemann; 2000.
- Scopinaro N, Adami GF, Marinari GM, Traverso E, Camerini G, Baschieri G, et al. Long-term results of biliopancreatic diversion in the treatment of morbid obesity. Acta Chir Austr 1998;30:166-71.
- Ells L, Macknight N, Wilkinson J. Obesity Ssrgery in England: an examination of the health episode statistics 1996–2005. Obes Surg 2007;17:400-5.
- National Institute for Health and Clinical Excellence . Assumptions Used in Estimating a Population Benchmark. n.d. http://www.nice.org.uk/usingguidance/commissioningguides/bariatric/determininglocalservicelevels/Assumptions.jsp (accessed 23 July 8 A.D.).
- British Obesity Patient Association n.d. http://www.bospa.org/information.aspx?page=46 (accessed 23 July 8 A.D.).
- Colquitt J, Clegg A, Sidhu M, Royle P. Surgery for morbid obesity. Cochrane Database Syst Rev 2003. 10.1002/14651858.CD003641.
- Colquitt J, Clegg A, Loveman E, Royle P, Sidhu MK. Surgery for morbid obesity. Cochrane Database Syst Rev 2005. 10.1002/14651858.CD003641.pub2.
- Walker O, Strong M, Atchinson R, Saunders J, Abbott J. A qualitative study of primary care clinicians’ views of treating childhood obesity. BMC Fam Pract 2007;8.
- Agren G, Naslund I. A prospective randomized comparison of vertical banded gastroplasty (VBG), loop gastric bypass (GBY) and gastric banding (GB). Int J Obes 1989;13.
- CRD . Undertaking Systematic Reviews of Research on Effectiveness 2001.
- Higgins J, Altman D. Cochrane Handbook for Systematic Reviews of Interventions. 2007.
- Drummond MF, Jefferson TO. Guidelines for authors and peer reviewers of economic submissions to the BMJ. The BMJ Economic Evaluation Working Party. BMJ 1996;313:275-83.
- Phillips Z, Ginnelly L, Sculpher M, Claxton K, Golder S, Riemsma R, et al. Review of guidelines for good practice in decision-analytic modelling in health technology assessment. Health Technol Assess 2004;8:1-172.
- Ansay J. Vertical banded gastroplasty for morbid obesity. Laparotomy or coelioscopy? A randomized study. Obes Surg 1996;6.
- Axagra JS, Goergen M, Ansay J, Bialek D, De Simone P. Intervention of Mason: laparoscopy versus laparotomy. Preliminary results of a randomized prospective series. Obes Surg 1997;7.
- Miller K, Mayer E, Pichler M, Hell E. Quality-of-life outcomes of patients with the Lap-Band registered versus non-operative treatment of obesity. Preliminary results of an ongoing long-term follow-up study. Obes Surg 1997;7.
- Wolf S. Gastric pacing for morbid obesity – the Magdeburg SPACE-BAND study. Int J Obes 2001;25.
- Karason K, Wallentin I, Larsson B, Sjostrom L. Effects of obesity and weight loss on left ventricular mass and relative wall thickness: survey and intervention study. BMJ 1997;315:912-16.
- Karason K, Wikstrand J, Sjostrom L, Wendelhag I. Weight loss and progression of early atherosclerosis in the carotid artery: a four-year controlled study of obese subjects. Int J Obes Relat Metab Disord 1999;23:948-56.
- Karason K, Molgaard H, Wikstrand J, Sjostrom L. Heart rate variability in obesity and the effect of weight loss. Am J Cardiol 1999;83:1242-7.
- Karason K, Lindroos AK, Stenlof K, Sjostrom L. Relief of cardiorespiratory symptoms and increased physical activity after surgically induced weight loss: results from the Swedish Obese Subjects study. Arch Intern Med 2000;160:1797-802.
- Karlsson J, Sjostrom L, Sullivan M. Swedish obese subjects (SOS) – an intervention study of obesity. Two-year follow-up of health-related quality of life (HRQL) and eating behavior after gastric surgery for severe obesity. Int J Obes Relat Metab Disord 1998;22:113-26.
- Narbro K, Agren G, Jonsson E, Larsson B, Naslund I, Wedel H, et al. Sick leave and disability pension before and after treatment for obesity: a report from the Swedish Obese Subjects (SOS) study. Int J Obes Relat Metab Disord 1999;23:619-24.
- Sjostrom CD, Lissner L, Wedel H, Sjostrom L. Reduction in incidence of diabetes, hypertension and lipid disturbances after intentional weight loss induced by bariatric surgery: the SOS Intervention Study. Obes Res 1999;7:477-84.
- Sjostrom CD, Peltonen M, Wedel H, Sjostrom L. Differentiated long-term effects of intentional weight loss on diabetes and hypertension. Hypertension 2000;36:20-5.
- Sjostrom CD, Peltonen M, Sjostrom L. Blood pressure and pulse pressure during long-term weight loss in the obese: the Swedish obese subjects (sos) intervention study. Obes Res 2001;9:188-95.
- Agren G, Narbro K, Jonsson E, Naslund I, Sjostrom L, Peltonen M. Cost of in-patient care over 7 years among surgically and conventionally treated obese patients. Obes Res 2002;10:1276-83.
- Agren G, Narbro K, Naslund I, Sjostrom L, Peltonen M. Long-term effects of weight loss on pharmaceutical costs in obese subjects. A report from the SOS intervention study. Int J Obes Relat Metab Disord 2002;26:184-92.
- Ryden A, Karlsson J, Sullivan M, Torgerson JS, Taft C. Coping and distress: what happens after intervention? A 2-year follow-up from the Swedish Obese Subjects (SOS) study. Psychosom Med 2003;65:435-42.
- Ryden A, Sullivan M, Torgerson JS, Karlsson J, Lindroos AK, Taft C. A comparative controlled study of personality in severe obesity: a 2-y follow-up after intervention. Int J Obes 2004;28:1485-93.
- Sjostrom CD. Surgery as an intervention for obesity. Results from the Swedish obese subjects study. Growth Horm IGF Res 2003:S22-S26.
- Torgerson JS, Lindroos AK, Naslund I, Peltonen M. Gallstones, gallbladder disease, and pancreatitis: cross-sectional and 2-year data from the Swedish Obese Subjects (SOS) and SOS reference studies. Am J Gastroenterol 2003;98:1032-41.
- Sjostrom L, Lindroos AK, Peltonen M, Torgerson J, Bouchard C, Carlsson B, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med 2004;351:2683-93.
- Sjostrom L, Narbro K, Sjostrom CD. Bariatric surgery lowers all-cause mortality in the morbidly obese. J Fam Pract 2007;56.
- Sjostrom L, Narbro K, Sjostrom CD, Karason K, Larsson B, Wedel H, et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med 2007;357:741-52.
- Karlsson J, Taft C, Ryden A, Sjostrom L, Sullivan M. Ten-year trends in health-related quality of life after surgical and conventional treatment for severe obesity: the SOS intervention study. Int J Obes 2007;31:1248-61.
- Gummesson A, Sjostrom L, Lystig T, Carlsson L. Effects of bariatric surgery on cancer incidence in Swedish obese subjects. Int J Obes 2008;32.
- Stoeckli R, Chanda R, Langer I, Keller U. Changes of body weight and plasma ghrelin levels after gastric banding and gastric bypass. Obes Res 2004;12:346-50.
- Von Mach MA, Stoeckli R, Bilz S, Kraenzlin M, Langer I, Keller U. Changes in bone mineral content after surgical treatment of morbid obesity. Metabolism: Clin Exp 2004;53:918-21.
- Christ-Crain M, Stoeckli R, Ernst A, Morgenthaler NG, Bilz S, Korbonits M, et al. Effect of gastric bypass and gastric banding on proneurotensin levels in morbidly obese patients. J Clin Endocrinol Metab 2006;91:3544-7.
- Buddeberg-Fischer B, Klaghofer R, Krug L, Buddeberg C, Muller MK, Schoeb O, et al. Physical and psychosocial outcome in morbidly obese patients with and without bariatric surgery: a 4½-year follow-up. Obes Surg 2006;16:321-30.
- Vanwoert J, Michalek A, Alger S, Carter J, Howard L. A prospective randomized trial (PRT) of gastric bypass (GB) versus vertical banded gastroplasty (VBG) for morbid obesity (MO). Clin Res 1992;40.
- Angrisani L, Lorenzo M, Borrelli V. Laparoscopic adjustable gastric banding versus Roux-en-Y gastric bypass: 5-year results of a prospective randomized trial. Surg Obes Related Dis 2007;3:127-32.
- Olbers T, Fagevik-Olsen M, Maleckas A, Lonroth H. Randomized clinical trial of laparoscopic Roux-en-Y gastric bypass versus laparoscopic vertical banded gastroplasty for obesity. Br J Surg 2005;92:557-62.
- Olbers T, Bjorkman S, Lindroos A, Maleckas A, Lonn L, Sjostrom L, et al. Body composition, dietary intake, and energy expenditure after laparoscopic Roux-en-Y gastric bypass and laparoscopic vertical banded gastroplasty: a randomized clinical trial. Ann Surg 2006;244:715-22.
- Morino M, Toppino M, Bonnet G, del Genio G. Laparoscopic adjustable silicone gastric banding versus vertical banded gastroplasty in morbidly obese patients: a prospective randomized controlled clinical trial. Ann Surg 2003;238:835-41.
- Davila-Cervantes A, Borunda D, Dominguez-Cherit G, Gamino R, Vargas-Vorackova F, Gonzalez-Barranco J, et al. Open versus laparoscopic vertical banded gastroplasty: a randomized controlled double blind trial. Obes Surg 2002;12:812-18.
- Sundbom M, Gustavsson S. Randomized clinical trial of hand-assisted laparoscopic versus open Roux-en-Y gastric bypass for the treatment of morbid obesity. Br J Surg 2004;91:418-23.
- Nguyen NT, Goldman C, Rosenquist CJ, Arango A, Cole CJ, Lee SJ, et al. Laparoscopic versus open gastric bypass: a randomized study of outcomes, quality of life, and costs. Ann Surg 2001;234:279-89.
- Puzziferri N, ustrheim-Smith IT, Wolfe BM, Wilson SE, Nguyen NT. Three-year follow-up of a prospective randomized trial comparing laparoscopic versus open gastric bypass. Ann Surg 2006;243:181-8.
- O’Brien PE, Dixon JB, Laurie C, Skinner S, Proietto J, McNeil J, et al. Treatment of mild to moderate obesity with laparoscopic adjustable gastric banding or an intensive medical program: a randomized trial.[summary for patients in Ann Intern Med. 2006 May 2;144(9): I12; PMID: 16670127]. Ann Intern Med 2006;144:625-33.
- Dixon JB, Strauss BJ, Laurie C, O’Brien PE. Changes in body composition with weight loss: obese subjects randomized to surgical and medical programs. Obesity (Silver Spring, Md) 2007;15:1187-98.
- Dixon JB, O’Brien PE, Playfair J, Chapman L, Schachter LM, Skinner S, et al. Adjustable gastric banding and conventional therapy for type 2 diabetes: a randomized controlled trial. JAMA 2008;299:316-23.
- Bessler M, Daud A, Kim T, DiGiorgi M. Prospective randomized trial of banded versus nonbanded gastric bypass for the super obese: early results. Surg Obes Related Dis 2007;3:480-4.
- Mingrone G, Greco AV, Giancaterini A, Scarfone A, Castagneto M, Pugeat M. Sex hormone-binding globulin levels and cardiovascular risk factors in morbidly obese subjects before and after weight reduction induced by diet or malabsorptive surgery. Athersclerosis 2002;161:455-62.
- Howard L, Malone M, Michalek A, Carter J, Alger S, Van Woert J. Gastric bypass and vertical banded gastroplasty – a prospective randomized comparison and 5-year follow-up. Obes Surg 1995;5:55-60.
- MacLean LD, Rhode BM, Forse RA, Nohr C. Surgery for obesity – an update of a randomized trial. Obes Surg 1995;5:145-53.
- MacLean LD, Rhode BM, Sampalis J, Forse RA. Results of the surgical treatment of obesity. Am J Surg 1993;165:155-60.
- Sugerman HJ, Starkey JV, Birkenhauer R. A randomized prospective trial of gastric bypass versus vertical banded gastroplasty for morbid obesity and their effects on sweets versus non-sweets eaters. Ann Surg 1987;205:613-24.
- Lee WJ, Huang MT, Yu PJ, Wang W, Chen TC. Laparoscopic vertical banded gastroplasty and laparoscopic gastric bypass: a comparison. Obes Surg 2004;14:626-34.
- Karamanakos SN, Vagenas K, Kalfarentzos F, Alexandrides TK. Weight loss, appetite suppression, and changes in fasting and postprandial ghrelin and peptide-YY levels after Roux-en-Y gastric bypass and sleeve gastrectomy: a prospective, double blind study. Ann Surg 2008;247:401-7.
- Nilsell K, Thorne A, Sjostedt S, Apelman J, Pettersson N. Prospective randomised comparison of adjustable gastric banding and vertical banded gastroplasty for morbid obesity. Eur J Surg 2001;167:504-9.
- van Dielen FM, Soeters PB, de Brauw LM, Greve JW. Laparoscopic adjustable gastric banding versus open vertical banded gastroplasty: a prospective randomized trial. Obes Surg 2005;15:1292-8.
- Schouten R, Wiryasaputra D, van Dielen F, Greve J. Laparoscopic adjustable gastric banding (LAGB) versus open vertical banded gastroplasty (VBG): long-term results of a prospective randomized trial. Obes Surg 2008;18.
- Himpens J, Dapri G, Cadiere GB. A prospective randomized study between laparoscopic gastric banding and laparoscopic isolated sleeve gastrectomy: results after 1 and 3 years. Obes Surg 2006;16:1450-6.
- Lujan JA, Frutos MD, Hernandez Q, Liron R, Cuenca JR, Valero G, et al. Laparoscopic versus open gastric bypass in the treatment of morbid obesity: a randomized prospective study. Ann Surg 2004;239:433-7.
- Westling A, Gustavsson S. Laparoscopic vs open Roux-en-Y gastric bypass: a prospective, randomized trial. Obes Surg 2001;11:284-92.
- de Wit LT, Mathus-Vliegen L, Hey C, Rademaker B, Gouma DJ, Obertop H. Open versus laparoscopic adjustable silicone gastric banding – A prospective randomized trial for treatment of morbid obesity. Ann Surg 1999;230:800-5.
- Buddeberg-Fischer B, Klaghofer R, Sigrist S, Buddeberg C. Impact of psychosocial stress and symptoms on indication for bariatric surgery and outcome in morbidly obese patients. Obes Surg 2004;14:361-9.
- Pocard M, Treich G, Boige V, Jayr C, Terrier-Lacombe MJ, Fournier S, et al. Panniculectomy as first part of colorectal resection for cancer in a morbidly obese patient. Ann Chirurg 2006;131:556-8.
- Mortori VM, Devereaux PJ, Adhikari NK, Burns KE, Eggert CH, Briel M, et al. Randomized trials stopped early for benefit: a systematic review. JAMA 2005;294:2203-9.
- Consten EC, Gagner M. Perioperative outcome of laparoscopic left lateral liver resection is improved by using staple line reinforcement technique: a case report. J Gastrointest Surg 2005;9:360-4.
- Torgerson JS, Sjostrom L. The Swedish Obese Subjects (SOS) study – rationale and results. Int J Obes 2001;25:s2-s4.
- Ackroyd R, Mouiel J, Chevallier JM, Daoud F. Cost-effectiveness and budget impact of obesity surgery in patients with type-2 diabetes in three European countries. Obes Surg 2006;16:1488-503.
- van Mastrigt GA, van Dielen FM, Severens JL, Voss GB, Greve JW. One-year cost-effectiveness of surgical treatment of morbid obesity: vertical banded gastroplasty versus Lap-Band. Obes Surg 2006;16:75-84.
- Craig BM, Tseng DS. Cost-effectiveness of gastric bypass for severe obesity. Am J Med 2002;113:491-8.
- Jensen C, Flum DR. ABS Consensus Conference . The costs of nonsurgical and surgical weight loss interventions: is an ounce of prevention really worth a pound of cure?. Surg Obes Related Dis 2005;1:353-7.
- Salem L, Devlin A, Sullivan SD, Flum DR. Cost-effectiveness analysis of laparoscopic gastric bypass, adjustable gastric banding, and nonoperative weight loss interventions. Surg Obes Related Dis 2008;4:26-32.
- Salem L, Jensen CC, Flum DR. Are bariatric surgical outcomes worth their cost? A systematic review. J Am Coll Surgeons 2005;200:270-8.
- Thompson D, Edelsberg J, Colditz GA. Lifetime health and economic consequenses of obesity. Arch Intern Med 1999;159:2177-83.
- The Swedish Council on Technology Assessment in Health Care . Obesity, Problems and Interventions – a Systematic Review 2002.
- National Institutes of Health . Clinical Guidelines on the Identification, Evaluation and Treatment of Overweight and Obesity in Adults. The Evidence Report 1998.
- Van Dielen FMH, Severens JS, Voss GBWE, Greve JWM. One-year cost-effectiveness of surgical treatment of morbid obesity: vertical banded gastroplasty versus Lap-Band. Obes Surg 2005;15.
- Pories WJ, Swanson MS, MacDonald KG. Who would have thought it? An operation proves to be the most effective therapy for adult-onset diabetes mellitus. Ann Surg 1995;222:339-50.
- Hall JC, Watts JM, O’Brien PE, Dunstan RE, Walsh JF, Slavotinek AH, et al. Gastric surgery for morbid obesity. The Adelaide Study. Ann Surg 1990;211:419-27.
- Heshka S, Greenway F, Anderson JW, Atkinson RL, Hill JO, Phinney SD, et al. Self-help weight loss versus a structured commercial program after 26 weeks: a randomized controlled study. Am J Med 2000;109:282-7.
- Chapman A, Kiroff G, Game P. Laparascopic adjustable gastric banding in the treatment of obesity: a systematic literature review. Surgery 2004;135:326-51.
- Hakim Z, Wolf A, Garrison LP. Estimating the effect of changes in body mass index on health state preferences. Pharmacoeconomics 2008;20:393-404.
- Kral JG, Christou NV, Flum DR, Wolfe BM, Schauer PR, Gagner M, et al. Medicare and bariatric surgery. Surg Obes Related Dis 2005;1:35-63.
- Caro JJ, Stillman IO, Danel A, Getsios D, McEwan P. Cost effectiveness of rimonabant use in patients at increased cardiometabolic risk: estimates from a Markov model. J Med Econ 2007;10:239-54.
- Erickson P, Wislon R, Shannon I. Years of healthy life. Statistical notes. Washington DC: US Department of Health and Human Services; 1995.
- Cardiff Research Consortium . Health Outcomes Data Repository 2008.
- Data on the US Population Distribution of BMI for White Women 2008. www.soph.uab.edu/statgenetics/Research/Tables/YLL.htm.
- Agency for Healthcare Research and Quality . HCUPnet, Healthcare Cost and Utilisation Project 2008.
- Jonsson B. Revealing the cost of type-2 diabetes in Europe. Diabetologia 2002;45:S5-S12.
- Williams R, Baxter H, Bottomley J, Bibby J, Burns E, Harvey J, et al. CODE-2 UK: our contribution to a European study of the costs of type 2 diabetes. Pract Diabet Int 2001;18:235-8.
- Pories WJ, Flickinger EG, Meelheim D, Van Rij AM, Thomas FT. The effectiveness of gastric bypass over gastric partition in morbid obesity: consequence of distal gastric and duodenal exclusion. Ann Surg 1982;196:389-99.
- Beck JR, Kassirer JP, Pauker SG. A convenient Approximation of Life Expectancy (The “DEALE”) I. Validation of the Method. Am J Med 1982;73:883-8.
- Warren E, Brennan A, Akehurst R. Cost-effectiveness of sibutramine in the treatment of obesity. Med Decis Making 2004;24:9-19.
- Colditz GA, Willett WC, Rotzinsky A, Manson JE. Weight gain as a risk factor for clinical diabetes mellitus in women. Ann Intern Med 1995;122:481-6.
- Jousilahti P, Tuomilehto J, Vartiainen E, Pekkanen J, Puska P. Body weight, cardiovascular risk factors, and coronary mortality: 15-year follow-up of middle-aged men and women in Eastern Finland. Circulation 1996;93:1372-9.
- Calle EE, Thun MJ, Petrelli JM, Rodriguez C, Heath CW. Body-mass index and mortality in a prospective cohort of U.S. adults. N Engl J Med 1999;341:1097-105.
- Stevens J, Cai J, Pamuk ER, Williamson DF, Thun MJ, Wood JL. The effect of age on the association between body-mass index and mortality. N Engl J Med 1998;338:1-7.
- Andersen KM, Odell PM, Wilson WF, Kannel WB. Cardiovascular disease risk profiles. Am Heart J 1991;121:2-293.
- Caro JJ, O’Brien JA, Hollenbeak CS, Spackman E, Ben-Joseph R, Okamoto LJ, et al. Economic burden and risk of cardiovascular disease and diabetes in patients with different cardiometabolic risk profiles. Value Hlth 2007;10:S12-S20.
- Jones DW, Chambless LE, Folsom AR, Heiss G, Hutchinson RG, Sharrett AR, et al. Risk factors for coronary heart disease in African Americans: the atherosclerosis risk in communities study, 1987–1997. Archiv Intern Med 2002;162:2565-71.
- Rexrode KM, Hennekens CH, Willett WC, Colditz GA, Stampfer MJ, Rich-Edwards JW, et al. A prospective study of body mass index, weight change, and risk of stroke in women. JAMA 1997;277:1539-45.
- Dennett SL, Boye KS, Yurgin NR. The impact of body weight on patient utilities with or without type 2 diabetes: a review of the medical literature. Value Hlth 2008;11:478-86.
- Dixon S, Currie CJ, McEwan P. Utility values for obesity and preliminary analysis of the health outcomes data repository. Exp Rev Pharmacoecon Outcomes Res 2004;4:657-65.
- Bagust A, Beale S. Modelling EuroQol health-related utility values for diabetic complications from CODE-2 data. Hlth Econ 2005;14:217-30.
- Kortt MA, Clarke PM. Estimating utility values for health states of overweight and obese individuals using the SF-36. QoL Res 2005;14:2177-85.
- Tucker D, Palmer A, Valentine W, Roze S, Ray J. Counting the costs of overweight and obesity: modeling clinical and cost outcome. Curr Med Res 2006;22:575-86.
- Curtis L. Unit costs of health and social care. Canterbury: PSSRU, University of Kent; 2007.
- Currie C, Pool C, Woehl A, Morgan CL, Cawley S, Rousculp MD, et al. The health-related utility and health-related quality of life of hospital-treated subjects with Type I and Type 2 diabetes with particular reference to differing severity of peripheral neuropathy. Diabetologia 2006;49:2272-80.
- Lee AJ, Morgan CL, Morrissey M, Wittrup-Jensen KU, Kennedy-Martin T, Currie CJ. Evaluation of the association between the EQ-5D index (health related utility) and body mass index (obesity) in hospital-treated people with type 1 diabetes, type 2 diabetes and with no diagnosed diabetes. Diabet Med 2005;22:1482-6.
- Andersen T, Backer OG, Astrup A, Quaade F. Horizontal or vertical banded gastroplasty after pretreatment with very-low-calorie formula diet: a randomized trial. Int J Obes 1987;11:295-304.
- Amaral JF, Thompson WR. Gallbladder disease in morbidly obese. Am J Surg 1985;149:551-7.
- Deitel M, Petrov I. Incidence of symptomatic gallstones after bariatric operations. Surg Gynecol Obstet 1987;164:549-52.
- Shiffman ML, Sugerman HJ, Kellum JM. Changes in gallbladder bile composition following gallstone formation and weight reduction. Gastroenterology 1992;103:214-21.
- Miller K, Hell E, Lang B, Lengauer E. Gallstone formation prophylaxis after gastric restrictive procedures for weight loss. a randomized double-blind placebo-controlled trial. Ann Surg 2003;238:697-702.
- Department of Health . NHS Reference Costs 2006–2007 2008.
- Ward S, Lloyd Jones M, Pandor A, Holmes M, Ara R, Ryan A, et al. A systematic review and economic evaluation of statins for the prevention of coronary events. Health Technol Assess 2007.
- Youman P, Wilson K, Harraf F, Kalra L. The economic burden of stroke in the United Kingdom. Pharmacoeconomics 2003;21:43-50.
- Clegg A, Colquitt J, Sidhu M, Royle P, Walker A. Clinical and cost effectiveness of surgery for morbid obesity: a systematic review and economic evaluation. Int J Obes Related Metabol Disord: J Int Assoc Study Obes 2003;27:1167-77.
- Stiggelbout AM, Eijkemans MJC, Kiebert GM. The ‘Utility’ of the visual analog scale in medical decision making and technology assessment: is it an alternative to the time tradeoff?. Int J Technol Assessment Hlthcare 1996;12:291-8.
- Wadden TA, Tsai AG. Bariatric surgery: crossing a body mass index threshold. Ann Intern Med 2006;144:689-91.
- Buchwald H, Estok R, Fahrbach K, Banel D, Sledge I. Trends in mortality in bariatric surgery: a systematic review and meta-analysis. Surgery 2007;142:621-32.
- Van Rij AM. Gastric bypass and gastric partitioning in morbid obesity: results of a controlled trial [abstract]. Aust NZ J Med Suppl 1984;14.
- Mason EE, Tang S, Renquist KE, Barnes DT, Cullen JJ, Doherty C, et al. A decade of change in obesity surgery. National Bariatric Surgery Registry (NBSR) Contributors. Obes Surg 1997;7:189-97.
- Wu EC, Barba CA. Current practices in the prophylaxis of venous thromboembolisms in bariatric surgery. Obes Surg 2000;10:7-13.
- 2000 Drug topics Red Book. Montvale, NJ: Medical Economics Company; 2000.
- Heshka S, Anderson, JW, Atkinson RL, Greenway FL, Hill JO, Phinney SD, et al. Weight loss with self-help compared with a structured commercial program: a randomised trial. JAMA 2003;289:1792-8.
- Hakim Z, Wolf A, Garrison LP. Estimating the effect of change in body mass index on health state preference. Pharmacoeconomics 2002;20:392-404.
Appendix 1 Protocol methods
Report methods for synthesis of evidence of clinical effectiveness
A review of the evidence for clinical effectiveness and cost-effectiveness will be undertaken systematically following the general principles outlined in CRD Report Number 4 (2nd edition) ‘Undertaking Systematic Reviews of Research on Effectiveness’. 74
Search strategy
The search strategies will be devised and tested by an experienced information scientist. The strategies will be designed to identify: (1) clinical effectiveness studies reporting on comparisons between different bariatric surgical techniques, and comparisons between bariatric surgery and non-surgical interventions for obesity; and (2) studies reporting on the cost-effectiveness of different bariatric surgical techniques, and comparisons between bariatric surgery and non-surgical interventions for obesity.
The search strategy will involve searching the following electronic databases: MEDLINE; EMBASE; PreMedline In-Process & Other Non-Indexed Citations; The Cochrane Library including the Cochrane Systematic Reviews Database, Cochrane Controlled Trials Register, DARE, NHS EED and HTA databases; Web of Knowledge Science Citation Index (SCI); Web of Knowledge ISI Proceedings; PsycInfo; CRD; and Biosis.
This work will update a previous assessment,15 but the updated work will include obese people as well as morbidly obese people. The searches for the previous assessment were carried out in 2001. Clinical effectiveness searches were then carried out again in 2004 to inform the Cochrane review which was updated in 2005. The results of these searches will help to inform our review. In particular we will check the 2001–2004 search results for studies that were excluded because the patients were not morbidly obese, but which would meet the criteria for this updated review that will include obese people. New searches will be conducted for clinical effectiveness evidence published since 2004. For the cost-effectiveness section searches will be carried out from 2001. Searches for other evidence to inform cost-effectiveness modelling will be conducted as required and may include a wider range of study types (including non-randomised studies and cost-effectiveness analyses of pharmaceuticals for weight reduction).
All searches will be updated when the draft report is under review, before submission of the final report.
Bibliographies of related papers will be assessed for relevant studies.
Members of the Expert Advisory Group will be asked to review the adequacy of the searches and to indicate whether they are aware of any additional published or unpublished evidence.
Inclusion and exclusion criteria
Patients
Inclusion criteria
-
Adult patients fulfilling the standard definition of obese, i.e. people with a BMI of 30 kg/m2 or over.
-
Young people who fulfil the definition of obesity for their age, sex and height.
-
Where data are available clinical effectiveness and cost-effectiveness will be reported separately for patients who meet current NICE guidelines for bariatric surgery, those with a lower BMI who would not currently meet the NICE criteria for bariatric surgery, and young people.
Exclusion criteria
-
Adults with a BMI under 30 kg/m2.
Interventions
Inclusion criteria
-
Open and laparoscopic bariatric surgical procedures in current use. The procedures likely to be included are vertical banded gastroplasty, gastric banding (including adjustable gastric banding), biliopancreatic diversion (including biliopancreatic diversion with duodenal switch), gastric bypass and sleeve gastrectomy.
Comparators
Inclusion criteria
-
Surgical procedures in current use will be compared with one another.
-
Open surgery will be compared with laparoscopic surgery for the same procedure.
-
Surgical procedures in current use will be compared to non-surgical interventions. These non-surgical interventions may include drugs such as orlistat, sibutramine and rimonabant, dietary interventions, exercise and combinations of non-surgical interventions such as diet and exercise.
Exclusion criteria
-
Comparisons of variations in technique for a single type of surgical procedure.
Outcomes
Inclusion criteria
-
Studies must have reported on at least one of the following outcomes following a minimum of 12 months of follow-up: weight change; quality of life; or change in obesity-related comorbidities.
-
Data will also be extracted on perioperative and postoperative mortality and morbidity, revision rates for surgical procedures, change in obesity-related comorbidities and cost-effectiveness.
Exclusion criteria
-
Studies will not be included if they have only reported short-term outcomes (less than 12 months).
Types of studies
Inclusion criteria
-
RCTs will be included. For the comparisons of surgical procedures with non-surgical procedures it is likely that few or no RCTs will be found, controlled clinical trials and prospective cohort studies (with a control cohort) will therefore also be eligible for inclusion.
-
For the systematic review of cost-effectiveness study types will include full cost-effectiveness analyses, cost–utility analyses, cost–benefit analyses and cost–consequence analyses.
-
Studies published as abstracts or conference presentations will only be included if sufficient details are presented to allow an appraisal of the methodology and the assessment of results to be undertaken.
Exclusion criteria
-
Case series and case studies.
-
Narrative reviews, editorials and opinions.
Inclusion and data extraction process
Reference screening strategy
-
Titles and abstracts identified by searching will be examined for inclusion, according to the inclusion/exclusion criteria detailed above, by two reviewers independently. Disagreements will be resolved by consensus or by recourse to a third reviewer where necessary.
-
For studies which appear potentially relevant on title or abstract, full papers will be requested for further assessment. All full papers will be screened independently by two reviewers and a final decision regarding inclusion will be agreed. Any disagreements will be resolved by discussion, with involvement of the third reviewer where necessary.
Data extraction strategy
-
Data will be extracted by one reviewer using a standardised data extraction form. Extracted data will be independently checked by a second reviewer. Discrepancies will be resolved by discussion, with involvement of another reviewer when necessary.
Quality assessment
-
Cohort studies will be assessed using criteria recommended by the NHS CRD (University of York). 74
-
RCTs will be assessed using the Cochrane criteria for judging risk of bias. 75 These criteria include consideration of the following factors:
-
– sequence generation
-
– allocation concealment
-
– blinding of participants, personnel and outcome assessors
-
– incomplete outcome data
-
– selective outcome reporting
-
– topic-specific, design-specific or other potential threats to validity.
-
-
Economic evaluations will be assessed using the critical appraisal checklist for economic evaluations proposed by Drummond and Jefferson. 76
-
The checklist for assessing good practice in decision analytic modelling will be used for critically appraising any decision models identified. 77
Methods of analysis/synthesis
-
Clinical effectiveness and cost-effectiveness data will be tabulated and discussed in a narrative review.
If clinical effectiveness data are of sufficient quantity, quality and homogeneity, a meta-analysis will be performed to estimate a summary measure of effect on relevant outcomes based on ITT analyses. If a meta-analysis is appropriate it will be performed using [sc]review manager[/sc] ([sc]revman[/sc]) software.
Methods for synthesising evidence of cost-effectiveness
The inclusion and exclusion criteria for evidence required to inform the economic model will be identical to the criteria for the systematic review of clinical effectiveness, with the following exceptions:
-
The cost-effectiveness model will focus on the surgical procedures identified in the clinical effectiveness review as being those that are clinically effective and in current use. These will be further restricted to those that are in widespread current use within the UK NHS if necessary.
-
Searches for other evidence to inform cost-effectiveness modelling [for example long-term cohort studies to obtain parameter estimates for the comparator arm of the model (non-surgical treatment), studies assessing HRQoL in obese people, studies estimating the relationship between improvements in obesity-related risk factors and the associated potential changes in morbidity and mortality], will be conducted as required and may be drawn from the wide range of sources (such as non-randomised studies and the cost-effectiveness analyses of pharmaceuticals for weight reduction).
A new economic evaluation will be carried out, from the perspective of the UK NHS and Personal Social Services (PSS), using a decision analytic modelling approach. Model structure will be determined on the basis of research evidence and clinical expert opinion of:
-
the biological disease process (i.e. knowledge of the natural history of the disease)
-
the main diagnostic and care pathways for patients in the UK NHS context [both with and without the intervention(s) of interest]
-
the disease states or events that are most important in determining patients’ clinical outcomes, quality of life and consumption of NHS or PSS resources.
Where possible, the incremental cost-effectiveness of each intervention will be estimated in comparison with other surgical procedures, as well as the non-surgical comparator(s) for adults meeting the current NICE criteria for bariatric surgery. Cost-effectiveness will be estimated in terms of incremental cost per QALY gained. Cost-effectiveness modelling of bariatric surgery for adults with a lower BMI than suggested by current NICE criteria, and bariatric surgery for obese young people will only be considered if sufficient data to inform the cost-effectiveness model are available.
Parameter values will be obtained from relevant research literature, including the systematic review of clinical and cost-effectiveness. Where parameter estimates are not available from good-quality published studies data may be obtained from lower quality evidence sources or expert clinical opinion. Sources for parameters will be stated clearly. A specific systematic literature search will be conducted for publications reporting health-related quality of life and/or health state utility associated with obesity.
Resource use will be specified from the perspective of the NHS and PSS and will be valued using appropriate NHS185 and PSS177 reference costs. Where national reference costs are not appropriate, unit cost estimates will be extracted from published work. If insufficient data are retrieved from published sources, costs may be obtained from individual NHS Trusts or groups of Trusts.
The simulated population will be defined on the basis of evidence about the characteristics of the UK adult population undergoing bariatric surgery. Simulated populations of (1) adult patients with a lower BMI who do not meet NICE criteria for bariatric surgery, and (2) young people will only be defined separately if good-quality effectiveness, resource use, and cost data are available for these groups.
If data allow, the time horizon of our analysis will be a patient’s lifetime in order to reflect the chronic nature of the disease. Alternatively, the base-case analysis will be based on best available data, with lifetime horizon explored in a scenario analysis. Both cost and QALY will be discounted at 3.5%.
Analysis of uncertainty will focus on cost–utility. Uncertainty will be explored through both one-way sensitivity analysis and probabilistic sensitivity analysis (PSA) if the modelling approach permits this. If PSA is undertaken the outputs will be presented both as plots on the cost-effectiveness plane and cost-effectiveness acceptability curves.
Appendix 2 Literature search strategies
The databases searched for the 2008 update of this review are listed below, together with the full search strategies employed. Further information regarding the searches undertaken for the identification of studies in the original review and earlier updates is provided in Appendix 3
| Database searched | Clinical effectiveness searches | Cost-effectiveness and QoL searches |
|---|---|---|
| Medline: 1996–2008 | Restricted to 2004–2008 | 2001–2008 |
| EMBASE | 2004–2008 | 2001–2008 |
| PreMEDLINE: In-Process & Other Non-Indexed Citations | 2004–2008 | 2001–2008 |
| Cochrane: includes Central, Dare, CDSR, and HTA databases | 2004–2008 | 2001–2008 |
| Web of Knowledge: Science Citation Index (SCI) | 2004–2008 | 2001–2008 |
| Web of Knowledge: ISI Proceedings | 2004–2008 | 2004–2008 |
| PsycInfo | 2004–2008 | 2001–2008 |
| CRD | 2004–2008 | 2001–2008 |
| BIOSIS | 2008 | 2008 |
| CINAHL | 2004–2008 | 2001–2008 |
| AMED | 2004–2008 | 2001–2008 |
| BNI | 2004–2008 | 2001–2008 |
| Searched for Ongoing Trials |
|---|
| UKCRN |
| National Research Register |
| Clinicaltrials.gov |
| Controlled clinical trials |
| Australian New Zealand Clinical Trials Registry |
Clinical effectiveness
The MEDLINE search strategy for the clinical effectiveness section of the review is reproduced below. This was adjusted as necessary for cost-effectiveness searches and for searching the other electronic databases listed in the table above for both clinical effectiveness and cost-effectiveness literature (including quality of life information). Search strategies are available from the report authors on request. The MEDLINE database search was restricted to 2004–08. Citations identified by the search were added to a [sc]reference manager[/sc] database on 6 February 2008.
| Search strategy | |
|---|---|
| 1 | exp obesity/(44949) |
| 2 | Overweight/(1562) |
| 3 | over?weight.ti,ab. (11311) |
| 4 | over weight.ti,ab. (106) |
| 5 | overeating.ti,ab. (440) |
| 6 | over?eating.ti,ab. (626) |
| 7 | exp Weight Loss/(11322) |
| 8 | weight loss.ti,ab. (18540) |
| 9 | weight reduc$.ti,ab. (2722) |
| 10 | or/1–9 (66439) |
| 11 | bariatric surg$.ti,ab. (1788) |
| 12 | exp bariatric surgery/(5414) |
| 13 | (surg$adj5 bariatric).ti,ab. (1825) |
| 14 | anti?obesity surg$.ti,ab. (6) |
| 15 | antiobesity surg$.ti,ab. (6) |
| 16 | (obesity adj5 surgery).ti,ab. (842) |
| 17 | (obesity adj5 surgical).ti,ab. (503) |
| 18 | (gastroplasty or gastro?gastostomy or “gastric bypass” or “gastric surgery” or “restrictive surgery”).ti,ab. (2723) |
| 19 | exp gastric bypass/(2110) |
| 20 | exp jejunoileal bypass/(159) |
| 21 | jejuno?ileal bypass.ti,ab. (75) |
| 22 | jejunoileal bypass.ti,ab. (75) |
| 23 | gastrointestinal surg$.ti,ab. (524) |
| 24 | gastrointestinal diversion$.ti,ab. (1) |
| 25 | exp biliopancreatic diversion/(405) |
| 26 | biliopancreatic diversion.ti,ab. (304) |
| 27 | bilio?pancreatic diversion.ti,ab. (304) |
| 28 | biliopancreatic bypass.ti,ab. (14) |
| 29 | bilio?pancreatic bypass.ti,ab. (14) |
| 30 | gastric band$.ti,ab. (1033) |
| 31 | silicon band$.ti,ab. (5) |
| 32 | exp gastroenterostomy/(2415) |
| 33 | gastrectomy.ti,ab. (4171) |
| 34 | gastrectomy.ti,ab. (4171) |
| 35 | gastroplasty/(1745) |
| 36 | LAGB.ti,ab. (236) |
| 37 | stomach stapl$.ti,ab. (7) |
| 38 | lap band$.ti,ab. (165) |
| 39 | lap-band$.ti,ab. (165) |
| 40 | malabsorptive surg$.ti,ab. (7) |
| 41 | mason$procedure.ti,ab. (9) |
| 42 | Roux-en-Y”.ti,ab. (1930) |
| 43 | anastomosis, Roux-en-Y/(1338) |
| 44 | malabsorptive procedure$.ti,ab. (34) |
| 45 | duodenal switch$.ti,ab. (177) |
| 46 | stomach stapl$.ti,ab. (7) |
| 47 | obesity/su (746) |
| 48 | exp Obesity, Morbid/su [Surgery] (2991) |
| 49 | or/11–46 (12551) |
| 50 | 10 and 49 (4612) |
| 51 | 47 or 48 or 50 (4902) |
| 52 | limit 51 to yr=“2001 – 2008” (4023) |
| 53 | limit 52 to humans (3963) |
| 54 | limit 53 to yr=“2004 – 2008” (2914) |
| 55 | limit 54 to (clinical trial, phase iii or clinical trial, phase iv or clinical trial or comparative study or controlled clinical trial or evaluation studies or guideline or meta analysis or multicenter study or practice guideline or randomized controlled trial or “scientific integrity review” or technical report or twin study or validation studies) (555) |
| 56 | Cohort Studies/(66145) |
| 57 | Randomized Controlled Trial/(150030) |
| 58 | Prospective Studies/(156648) |
| 59 | Evaluation Studies/(96370) |
| 60 | Follow-Up Studies/(185572) |
| 61 | (control$or prospectiv$or volunteer$or placebo$or random$).ti,ab. (1202900) |
| 62 | ((single$or doubl$or trebl$or tripl$) adj (mask$or blind$)).ti,ab. (47022) |
| 63 | or/56–62 (1477917) |
| 64 | 54 and 63 (1130) |
| 65 | 55 or 64 (1284) |
Reference lists
The reference lists of relevant trials and reviews identified were examined.
Other searches
Authors of included studies and relevant experts were contacted where possible in order to obtain additional references, missing data, unpublished trials and any ongoing trials.The authors of a systematic review of treatments for obesity51 provided the results of hand searches of the following journals:
-
International Journal of Obesity (1977 to 2000, volume 24, part 12);
-
Obesity Research (1993 to 2001, volume 9, part 2);
-
Obesity Surgery (1991 to 2001, volume 11, part 2);
-
American Journal of Clinical Nutrition (1966 to 2000, volume 72, part 6);
-
Proceedings of the Nutrition Society (1960 to 2000, volume 59, part 4);
-
Journal of Human Nutrition and Dietetics (1988 to 2001, volume 14, part 1);
-
Journal of the American Dietetic Association (1980 to 1990, volume 90, part 12)
Appendix 3 Identification of studies in the original review and updates
There are three previously published versions of this systematic review of bariatric surgery;15,70,71 each differs slightly in the studies included as the review has evolved. This section explains how the review has evolved and notes the main differences between the reviews. A flow chart of the identification of studies at each stage can be seen in Figure 9.
FIGURE 9.
Flow chart of inclusion through the review updates. SOS, Swedish Obese Subjects.
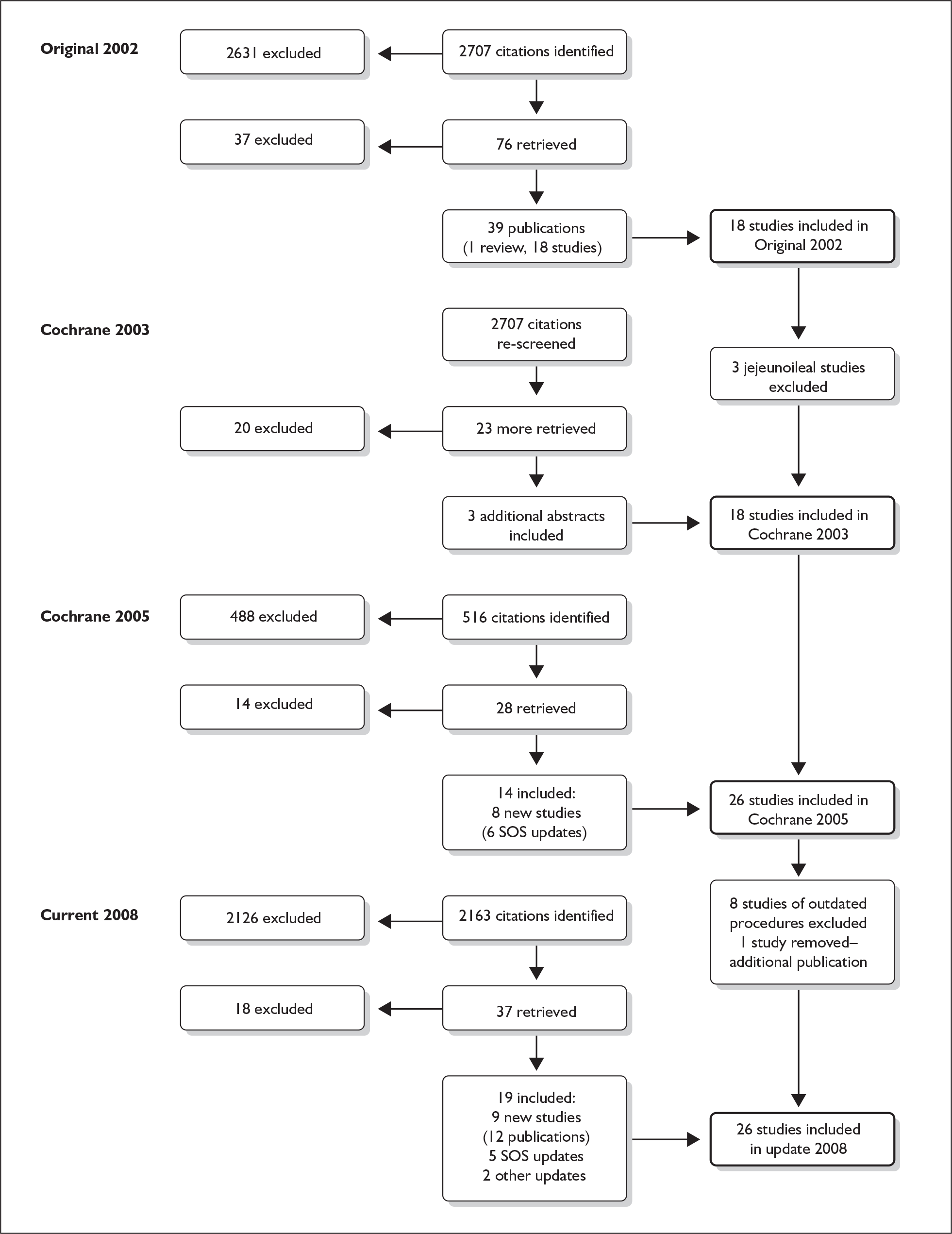
Original review 200215
For the first edition of this review 2707 citations were identified by the searches, of which 2631 were excluded and 76 were retrieved for detailed examination. Thirty-seven studies were then excluded. 15 Eighteen studies and one systematic review were included (reported in 39 publications). This version included jejunoileal bypass (an intervention that is no longer practised and is not included in subsequent versions of this review), and excluded abstracts and non-English language publications.
Cochrane 200370
The 2003 Cochrane review was conducted using the same 2707 citations obtained from the 2002 report. 15 The citations were rescreened to identify non-English language publications and studies published only as abstracts for inclusion in the Cochrane review. Three additional studies published as abstracts only were included and three studies (seven publications) of jejunoileal bypass were excluded from the Cochrane review (Appendix 16). Eighteen trials reported in 33 publications therefore met the inclusion criteria.
The three additional studies included in the 2003 Cochrane review were:
Cochrane 2005 update71
The updated searches in 2005 identified 516 citations, of which 488 were excluded and 28 were retrieved for detailed examination. Thirteen studies were then excluded, and authors of one study were contacted as the eligibility was unclear, but no response was received so this was also excluded (Appendix 16). Fourteen new studies therefore met the inclusion criteria; eight of these were primary studies and six were additional publications of the SOS study included in the first edition of the review. 91–96
The eight additional primary studies included in the 2005 Cochrane update were:
Current update 2008
The updated searches in 2008 identified 2163 citations, of which 2126 were excluded and 37 were retrieved for detailed examination. Eighteen studies were then excluded (Appendix 16). Nineteen publications therefore met the inclusion criteria; nine of these were new primary studies (three studies each had two publications), two were updates of studies included in previous versions of the review102,113 and five were additional publications of the SOS study included in all versions of this review. 97–101
The nine additional primary studies included in this update are:
Studies in original review that were excluded from 2008 update
As a result of the changes in the eligibility criteria for the 2008 update (Chapter 2, Decision problem), a further eight studies (in 14 publications) that were included in previous versions of this review have now been excluded as the surgical procedures assessed (horizontal gastroplasty and vertical gastroplasty without banding) are not in current use (Appendix 16).
A total of 11 studies (in 21 publications) of jejunoileal bypass, horizontal gastroplasty and vertical gastroplasty without banding have therefore been excluded from this update. These are listed in Appendix 16.
In addition, two studies that were included in the 2005 update (Stoeckli et al. 102 and von Mach et al. 103) were later identified to be two publications of the same study (this was confirmed by the authors), and have therefore been combined in this update.
Summary of included studies
In summary, a total of 5386 references were identified through the original and updated searches. Twenty-six studies reported in 52 publications met the current inclusion criteria (Figure 9).
Appendix 4 Quality assessment
Risk of bias table for included RCTs
| Item | Judgementa | Description |
|---|---|---|
|
Adequate sequence generation? (Describe the method used to generate the allocation sequence in sufficient detail to allow an assessment of whether it should produce comparable groups.) |
||
|
Allocation concealment? (Describe the method used to conceal the allocation sequence in sufficient detail to determine whether intervention allocations could have been foreseen in advance of, or during, recruitment.) |
||
|
Blinding of outcome assessors?a (Describe all measures used, if any, to blind study participants and personnel from knowledge of which intervention a participant received. Provide any information relating to whether the intended blinding was effective.) |
||
| Blinding of participants on self-reported outcomes? | ||
|
Incomplete outcome data addressed?a Weight loss [Describe the completeness of outcome data for each main outcome, including attrition and exclusions from the analysis. State whether attrition and exclusions were reported, the numbers (compared with total randomised participants), reasons for attrition/exclusions where reported, and any reinclusions in analyses performed by the review authors.] |
||
| Incomplete outcome data addressed?a QoL | ||
| Incomplete outcome data addressed?a Comorbidity | ||
|
Free of selective outcome reporting? (State how the possibility of selective outcome reporting was examined by the review authors, and what was found.) |
||
|
Free of other sources of bias? (State any important concerns about bias not addressed in the other items in the tool. If particular questions/items were prespecified in the review’s protocol, responses should be provided for each question/item.) |
Quality assessment criteria for cohort studies
| Quality item | Yes/No/Uncertain | |
|---|---|---|
| 1. | Is there sufficient description of the groups and the distribution of prognostic factors? | |
| 2. | Are the groups assembled at a similar point in their disease progression? | |
| 3. | Is the intervention/treatment reliably ascertained? | |
| 4. | Were the groups comparable on all important confounding factors? | |
| 5. | Was there adequate adjustment for the effects of these confounding variables? | |
| 6. | Was outcome assessment blind to exposure status? | |
| 7. | Was follow-up long enough for the outcomes to occur? | |
Appendix 5 Data extraction tables: surgery versus non-surgical interventions
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Dixon et al. (2008)117 Design: single centre, RCT Follow-up: 24 months |
Country: Australia Number: Total 60, LAGB 30, Conventional (Con) therapy 30 Age (mean ± SD): LAGB 46.6 (7.4); Con therapy 47.1 (8.7) years Sex (male): LAGB 15 (50%), Con therapy 13 (43%) BMI (mean ± SD): LAGB 37.0 (2.7); Con therapy 37.2 (2.5) Weight, kg (mean ± SD): LAGB 105.6 (13.8); Con therapy 105.9 (14.2) Hypertension, no (%): LAGB 28 (93); Con therapy 27 (90) Metabolic syndrome, no (%): LAGB 29 (97%); Con therapy 29 (97%) Coronary artery disease, no (%): LAGB 0; Con therapy 1 (3) Neck circumference, cm (mean ± SD): LAGB 41.8 (4.0); Con therapy 42.4 (4.5) p = ns for all baseline characteristics Other baseline characteristics linked to outcomes noted in results below Characteristics of target population: aged 20–60 years, BMI of 30–40, diagnosed with clearly documented Type 2 diabetes within the previous 2 years, had no evidence of renal impairment or diabetic retinopathy, and were able to understand and comply with the study process Exclusion criteria: history of type 1 diabetes, diabetes secondary to a specific disease, previous bariatric surgery, history of medical problems such as mental impairment, drug or alcohol addiction, recent major vascular event, internal malignancy, or portal hypertension; or a contraindication for either study group. Also excluded if did not attend two initial information visits |
1. LAGB in addition to the conventional-therapy programme 2. Conventional therapy. Best medical practice for treatment, education and follow-up of Type 2 diabetes. Visits at least every 6 weeks throughout the 2 years. Lifestyle modification programmes individually structured to reduce energy intake, fat (< 30%) and saturated fats, to encourage low glycaemic index and high-fibre foods. Physical activity advice to encourage 10,000 steps per day and 200 minutes per week of structured activity. Low-calorie diets and medications discussed with all participants and used in some cases |
Primary outcome: Proportion of patients achieving remission of Type 2 diabetes (fasting plasma glucose < 126 mg/dl and HbA1c < 6.2% without the use of oral hypoglycaemic agents or insulin) Secondary outcomes: % change in HbA1c Weight loss Blood pressure Waist circumference Fasting lipids (including total cholesterol, triglycerides, and high-density lipoprotein cholesterol) Changes in medication use Changes in proportion with metabolic syndrome (as defined by the National Cholesterol Education Program Adult Treatment Panel III criteria) Changes in indirect measures of insulin resistance (using homeostatic model assessment method) Adverse events |
Method of data analysis: states data analysed using an ITT analysis. Data expressed as mean (SD) and differences with 95% confidence intervals given Sample size/power calculation: selected to provide power of 80% to detect a 1% difference in HbA1c at 2 years and for diabetes remission rates to be approximately 60% in the surgical group and 20% in the conventional-therapy group. This required a minimum of 27 patients in each study group. Paper states caution required as not powered for multiple outcome measures Conflict of interests: study funded by manufacturers of the technologies involved. Paper states they had no role in the design or conduct, data collection, analysis or interpretation of the study Other: 16/26 Con therapy participants who completed the 2 years elected to use a very-low-calorie diet (n = 11) or sibutramine (n = 7) at some stage |
Table of results
| Weight change | QoL/comorbidity | Events/procedures (complications, reoperations) |
|---|---|---|
|
Percentage weight loss (mean ± SD): LAGB 20.0% (9.4) at 2 years; Con therapy 1.4% (4.9), p < 0.001. Using BMI of 25 as ideal weight this represents a loss of 62.5% of excess weight in the LAGB group compared with 4.3% in the Con therapy group and a reduction in BMI from 36.9 to 29.5 compared with 37.1 to 36.6 in the two groups respectively Weight loss, kg (mean ± SD): LAGB 84.6 (15.8) [change – 21.1 (10.5)]; Con therapy 104.8 (15.3) [change – 1.5 (5.4)], difference (in change) between groups: – 19.6 (95% CI – 23.8 to – 15.2), p < 0.001 Reported change in self-reported rates of physical activity and relationship with weight loss, but not data extracted Waist circumference (mean ± SD cm) at baseline: LAGB 114.1 (10.2); Con therapy 116.0 (10.0). At end point LAGB 95.8 (10.3) [change – 17.9 (10.8)], Con therapy 112.7 (10.3) [change – 4.0 (9.1)], difference (in change) between groups: – 13.9 (95% CI – 19.0 to – 8.7), p < 0.001 Waist to hip ratio (mean ± SD cm) at baseline: LAGB 0.96 (0.09); Con therapy 0.96 (0.10). At end point LAGB 0.90 (0.06) [change – 0.06 (0.06)], Con therapy 0.95 (0.08) [change – 0.01 (0.06)]. Difference (in change) between groups: – 0.05 (95% CI – 0.07 to – 0.007), p = 0.02 |
Remission of Type 2 diabetes at 2 years: LAGB 22/30 (73%); Con therapy 4/30 (13%), p < 0.001. Relative risk of remission for LAGB 5.5 (95% CI 2.2 to 14.0), p < 0.001. (ITT analysis). Text states this represented 76% and 15% remission rates among completers in the LAGB and conventional therapy groups respectively Data on the association between weight loss and lower HbA1c/remission reported but not data extracted Metabolic syndrome (NOT meeting criteria): Baseline LAGB 1 (3%), Con therapy 1 (3%) 2 years LAGB 21 (70%), Con 4 (13%), p < 0.001 HbA1c (mean ± SD%) at baseline: LAGB 7.8 (1.2); Con therapy 7.6 (1.4). At end point LAGB 6.00 (0.82) [change – 1.81 (1.24)]; Con therapy 7.21 (1.39) [change – 0.38 (1.26)], difference (in change) between groups – 1.43 [95% CI – 2.1 to – 0.80], p < 0.001 Proportion with HbA1c < 6.2% at baseline: LAGB 2 (7%), Con therapy 4 (13%). At 2 years LAGB 24 (80%), Con therapy 6 (20%). Statistical analysis within group comparison only reported Systolic blood pressure (mean ± SD mmHg) at baseline: LAGB 136.4 (15.6); Con therapy 135.3 (14.4). At end point LAGB 130.4 [19.0) (change – 6.0 (17.9)]; Con therapy 132.6 (17.7) [change – 1.7 (14.2)], difference (in change) between groups: – 4.3 (95% CI – 13.6 to 5.1), p = 0.37 Diastolic blood pressure (mean ± SD mmHg) at baseline: LAGB 86.6 (9.4); Con therapy 84.5 (9.8). At end point LAGB 85.4 (7.0) [change – 0.7 (11.1)], Con therapy 83.1 (8.5) [change – 0.9 (11.1)], difference (in change) between groups: 0.2 (95% CI – 5.4 to 6.0), p = 0.92 Plasma glucose (mean ± SD mg/dl) at baseline: LAGB 156.7 (38.5); Con therapy 158.0 (48.7). At end point LAGB 105.6 (30.3) [change – 51.2 (37.6)]; Con therapy 139.6 (38.1) [change – 18.4 (41.2)], difference (in change) between groups: – 32.8 (95% CI – 53.1 to – 12.3), p = 0.002 Plasma insulin (median + IQR μIU/ml) at baseline: LAGB 19.7 (16.5–27.5); Con therapy 18.7 (13.7–30.7). At end point: LAGB 9.8 (4.7) [change – 12.4 (8.4)]; Con therapy 24.1 (13.6) [change 1.0 (14.8)], difference (in change) between groups: – 13.4 (95% CI – 19.6 to – 7.3), p < 0.001 Total cholesterol (mean ± SD mg/dl) at baseline: LAGB 201.8 (32.7); Con therapy 198.2 (56.7). At end point: LAGB 205.4 (46.6) [change 3.6 (51.6)]; Con therapy 197.8 (59.3) [change -0.4 (31.4)], difference (in change) between groups: 4.0 (95% CI – 18.8 to 26.0), p = 0.72 |
Adverse events LAGB: one superficial wound infection, two gastric pouch enlargement at 10 months (both had revisional surgery to replace band), one band removal after 15 days because of eating difficulties and regurgitation, one patient febrile episodes, one minor hypoglycaemic episode, one gastrointestinal tract intolerance to metformin Con therapy: two minor gastrointestinal tract adverse events (not defined), one persistent diarrhoea with metformin, one vasculitic rash (possibly due to rosiglitazone), one multiple hypoglycaemic episodes, one angina and transient cerebral ischaemic episode, two intolerant to very low-calorie meal replacement Mean procedure time 54 minutes (SD 10.8, range 40–74 minutes) Hospital admissions for LAGB: 23 (80%) stayed in for 1 day; five (17%) for 2 days; one (3%) for 4 days (band was removed on day 15 due to intolerance) |
|
Triglycerides (mean ± SD mg/dl) at baseline: LAGB 190.6 (106.6); Con therapy 188.7 (111.8). At end point: LAGB 118.9 (79.7) [change – 71.7 (92.9)]; Con therapy 186.7 (127.2) [change – 2.1 (120.6)], difference (in change) between groups: – 69.6 (95% CI – 125.3 to – 13.6), p = 0.02 HDL-C (mean ± SD mg/dl) at baseline: LAGB 47.1 (10.1); Con therapy 48.1 (11.1). At end point: LAGB 59.7 (13.6) [change 12.6 (9.8)]; Con therapy 50.7 (12.1) [change 2.6 (6.1)], difference (in change) between groups: 10.0 (95% CI 5.8 to 14.2), p < 0.001 Total cholesterol to HDL-cholesterol ratio (mean ± SD mg/dl) at baseline: LAGB 4.41 (0.87); Con therapy 4.23 (1.11). At end point: LAGB 3.58 (1.00) [change – 0.82 (1.9)]; Con therapy 4.1 (1.4) [change – 0.14 (1.04)], difference (in change) between groups: – 0.68 (– 1.24 to – 0.14), p = 0.02 Use of diabetes medication (numbers): No medication. At baseline: LAGB 2, Con therapy 4. At 2 years LAGB 26, Con therapy 8 Metformin use. At baseline: LAGB 28, Con therapy 26. At 2 years LAGB 3, Con therapy 18. Statistical analysis within group comparison only reported Other hypoglycaemic use. At baseline: LAGB 9, Con therapy 8. At 2 years LAGB 1, Con therapy 7. Statistical analysis within group comparison only reported Insulin use. At baseline: LAGB 1, Con therapy 0. At 2 years LAGB 0, Con therapy 3 Use of non-diabetes medication (numbers): Antihypertensive agents. At baseline LAGB 20/29, Con therapy 15/26. At 2 years LAGB 6/29, Con therapy 15/26. Statistical analysis within group comparison only reported Lipid-lowering agents. At baseline LAGB 12/29, Con therapy 8/26. At 2 years LAGB 4/29, Con therapy 7/26. Statistical analysis within group comparison only reported HOMA IR (insulin resistance by homeostatic model assessment) also reported at end point but not reported here |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Yes | Randomisation was computer derived, with blocking into three groups to allow for orderly recruitment into both study groups and to reduce the risk of uneven recruitment late in the series |
| Allocation concealment? | Unclear | Not reported |
| Blinding of outcome assessors? | No | States study not blinded |
| Blinding of participants on self-reported outcomes? | n/a | Not blinded, but no self-reported measures |
| Incomplete outcome data addressed? Weight loss | Yes | Of the 30 randomised to LAGB one withdrew preoperatively. Of the 30 randomised to conventional therapy, four withdrew after randomisation. Reasons not given |
| Incomplete outcome data addressed? QoL | n/a | |
| Incomplete outcome data addressed? Comorbidity | Yes | As above |
| Free of selective outcome reporting? | Unclear | All the outcomes mentioned in the methods section seem to be reported as results, although ‘physical activity’ is not mentioned in the methods but results are reported. Protocol not available |
| Free of other sources of bias? | No |
Participants took part in at least 3 months of run-in where alterations to eating, exercise, glucose self-monitoring and medications were suggested. Compliance was measured during this time. The endocrinologist then independently determined when a participant was ready for randomisation Of 158 potentially eligible participants only 60 were randomised. Reasons for exclusions before randomisation were noted No statistically significant differences in baseline characteristics Block randomisation used in an unblinded trial, which may be possible to predict assignments |
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Mingrone et al. 2002119 Design: RCT, single centre Follow-up: 1 year |
Country: Italy Number: Total 79, BPD 46, Diet 33 Age: 30–45 years Sex: 27 men (BPD 15, Diet 12), 52 women (BPD 31, Diet 21) BMI: Women, Diet 48.4 (8.9), BPD 48.3 (6.3). Men, Diet 47.8 (8.8), BPD 48.0 (5.4) Mean weight (SD), kg: women, diet 121.6 kg (24.1), BPD 125.3 kg (12.8). Men, diet 147.3 kg (26.8), BPD 151.8 kg (17.1) Characteristics of target population: Morbidly obese. Non smoking, normal electrocardiogram at rest and during exercise test Exclusion criteria: Pregnancy, history or diagnosis of diabetes, heart disease, hypertension or other chronic diseases, hormone replacement therapy, chronic steroid therapy, history of alcohol or drug abuse, glucose intolerance (2 hour glucose level > 140 mg/dl after 75 g oral glucose load and of stable weight, within ± 2 kg, 6 months before testing) |
1. Biliopancreatic diversion (BPD) 2. Diet (20 kcal/kg fat-free mass, 55% carbohydrates, 30% fat, 15% proteins). Modified every 6 months according to analysis of fat-free mass |
Mean weight BMI Fat-free mass Fat mass Metabolic variables reported but not extracted |
Allocation to treatment groups: Randomised, method not reported Blinding of outcome assessors: Not reported Comparability of treatment groups: Baseline weight, BMI, fat-free mass, fat mass presented, no statistical comparisons made. Groups appear to be similar Method of data analysis: Means and SD presented. Student’s t test used to compare the same groups before and after BPD or diet Sample size/power calculation: Not reported Attrition/dropout: None |
Table of results
| Weight change | QoL/comorbidity | Events/procedures (complications, reoperations) |
|---|---|---|
|
Mean weight (SD): Women. Baseline: Diet 121.6 kg (24.1), BPD 125.3 kg (12.8); 1 year: Diet 114.5 kg (24.5), BPD 90.2 kg (15.0)a Men. Baseline: Diet 147.3 kg (26.8), BPD 151.8 kg (17.1); 1 year: Diet 138.2 kg (27.1), BPD 99.7 kg (7.0)a Mean BMI (SD): Women. Baseline: Diet 48.4 (8.9), BPD 48.3 (6.3); 1 year: Diet 43.8 (7.7), BPD 35.2 (7.6)a Men. Baseline: Diet 47.8 (8.8), BPD 48.0 (5.4); 1 year: Diet 44.8 (8.4), BPD 30.4 (3.5)a Fat-free mass (SD) Women. Baseline: Diet 58.3 kg (8.8), BPD 59.3 kg (5.6); 1 year: Diet 56.7 kg (8.8), BPD 50.5 kg (4.7)a Men. Baseline: Diet 87.3 kg (11.4), BPD 88.7 kg (8.1); 1 year: Diet 83.7 kg (11.8) BPD 74.2 kg (5.4)a Fat mass (SD) Women. Baseline: Diet 63.3 kg (16.2), BPD 65.9 kg (10.2); 1 year: Diet 57.8 kg (16.5), BPD 39.8 kg (12.7)a Men. Baseline: Diet 60.0 kg (15.6), BPD 63.1 kg (10.2); 1 year: Diet 54.6 kg (15.6), BPD 25.5 kg (2.7)a |
Not reported | Not reported |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Unclear | Not reported |
| Allocation concealment? | Unclear | Not reported |
| Blinding of outcome assessors? | Unclear | Not reported |
| Blinding of participants on self-reported outcomes? | n/a | |
| Incomplete outcome data addressed? Weight loss | Yes | No losses |
| Incomplete outcome data addressed? QoL | n/a | |
| Incomplete outcome data addressed? Comorbidity | n/a | |
| Free of selective outcome reporting? | Unclear | Adverse effects not reported |
| Free of other sources of bias? | Unclear |
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Design: single centre, RCT Follow-up: 24 months |
Country: Australia Number: total 80, LAGB n = 40, non-surgical n = 40. One patient assigned to LAGB withdrew from the study before surgery and declined to be followed further LAGB n = 40, non-surgical n = 40 Age [mean (SD)]: LAGB 41.8 (6.4) years; non-surgical 40.7 (7.0) Sex (male%): LAGB 25; non-surgical 22.5 BMI [mean (SD)]: LAGB 33.7 (1.8), 95% CI 32.9 to 34.4; non-surgical 33.5 (1.4) 95% CI 32.7 to 34.3, p = 0.71 Weight [mean (SD) kg]: LAGB 96.1 (11.2); non-surgical 93.6 (11.9) Different baseline weight data are given in Table 2 of O'Brian115 [mean (95% CI) kg]: LAGB 95.0 (94.1–95.9); non-surgical 94.8 (93.9–95.7) p = 0.88 Mean Short Form-36 QoL domain scores below estimated from figure by reviewer (note 95% CIs presented in figure but not possible to extract accurately) Physical function: LAGB 65; non-surgical 74 Physical role: LAGB 63; non-surgical 70 Pain: LAGB 68; non-surgical 76 General health: LAGB 52; non-surgical 59 Energy: LAGB 42; non-surgical 42 Social functioning: LAGB 65; non-surgical 72 Emotional role: LAGB 63; non-surgical 65 Mental health: LAGB 65; non-surgical 65 |
1. Laparoscopic adjustable gastric band (Lap-Band system) (LAGB) 2. Intensive non-surgical programme (Non-surgical) The non-surgical programme centred on the use of behavioural modification, very-low-calorie diet (VLCD), and pharmacotherapy with education and professional support on appropriate eating and exercise behaviour. The programme began with a 6-month VLCD (500–550 kcal/day) which used Optifast for 12 weeks, then over 4 weeks some VLC meals with 120 mg orlistat before the non-VLC meals, and then 120 mg orlistat before all meals. The 6-month intensive phase was followed by further courses of VLCD or orlistat as tolerated, as well as continuous behavioural, dietary and exercise advice. Physician saw each patient every 2 weeks during the VLCD programme, and every 4–6 weeks during the rest of the study |
Primary end points related to weight change: change in absolute weight (kg), body mass index, percentage of initial weight lost and excess weight lost, and the percentage of patients who lost more than 50% of excess weight at 2 years Secondary end points were health, quality of life and side effects of treatment (adverse drug reactions, protocol violations, perioperative problems, need for revisional surgery) Health status was also documented at baseline and reassessed at later time points Related paper116 reports on body composition measurements for those participants who completed all of the body composition studies (voluntary aspect of the study) |
Method of data analysis: States an intention-to-treat analysis was used Continuous data expressed as means (SDs). p < 0.05 considered statistically significant Sample size/power calculation: set on the basis of weight loss, expressed as percentage of excess weight lost, at 2 years after entry into the study. From existing data, it was expected that the mean excess weight lost for the surgical programme would be 54%. A difference of at least 20% (either < 44% or > 64%) would be clinically significant. To achieve 80% power of detecting this 20% difference (at a two-sided significance level of 5%), 72 patients in total would be required. A total initial recruitment of 80 patients was planned Potential conflict of interests: stated (consultancies and grants received) |
|
States no significant differences between the groups at baseline, but p values not shown Recruitment took place between May 2000 and November 2001. Final patient follow-up at 2 years after entry complete by November 2003 Characteristics of target population: age between 20 and 50 years, BMI 30 to 35 with identifiable problems, including an obesity-related comorbid condition (such as hypertension, dyslipidaemia, diabetes, obstructive sleep apnoea, or gastro-oesophageal reflux disease), severe physical limitations, or clinically significant psychosocial problems associated with their obesity; had attempted to reduce weight over at least the previous 5 years; could understand the options offered and the randomisation process; and were willing to comply with the requirements of each programme Exclusion criteria: candidates with a history of bariatric surgery or medical problems that contraindicated treatment in either study group, such as impaired mental status, drug or alcohol addiction, or portal hypertension. Participants were also excluded if they had undergone an intensive, physician-supervised programme that used very-low-calorie diets or pharmacotherapy or if they did not attend the two initial patient information visits |
Common programme: All patients were instructed and encouraged to follow appropriate lifestyle behaviour of good eating practices and increased exercise and activity. All participants were encouraged to exercise for at least 200 minutes a week | Supported by a grant from the Department of Surgery, Monash University. Equipment devices and products supplied by IN-AMED health (manufacturer of the Lap-Band system); Novartis (manufacturer of Optifast); and US Surgical Corp (manufacturer of disposable laparoscopic instruments) |
Table of results
| Weight change | QoL/comorbidity | Events/procedures (complications, reoperations) |
|---|---|---|
|
Weight at 12 months [mean (95% CI) kg]: LAGB 76.3 (74.1–78.5), non-surgical 85.3 (83.0–87.5). p < 0.001 Weight at 18 months [mean (95% CI) kg]: LAGB 75.2 (73.1–77.4), non-surgical 87.7 (79.9–83.0). p < 0.001 Weight at 24 months [mean (95% CI) kg]: LAGB 74.5 (72.4–76.7), non-surgical 89.5 (80.5–83.6). p < 0.001 BMI at 12 months [mean (95% CI)]: LAGB 27.0 (26.2–27.8), non-surgical 29.9 (29.1–30.8). p < 0.001 BMI at 18 months [mean (95% CI)]: LAGB 26.7 (25.9–27.5), non-surgical 30.9 (30.0–31.8). p < 0.001 BMI at 24 months [mean (95% CI)]: LAGB 26.4 (25.6–27.2), non-surgical 31.5 (30.6–32.4). p < 0.001 Percentage of initial weight lost at 2 years (95% CI): LAGB 21.6% (19.3 % to 23.9%); non-surgical 5.5% (3.2% to 7.9%) Percentage of excess weight lost at 12 months [mean (95% CI)]: LAGB 78.6 (69.2–88.1); non-surgical 41.1 (31.2–50.9). p < 0.001 Percentage of excess weight lost at 18 months [mean (95% CI)]: LAGB 83.6 (74.2–93.1); non-surgical 29.01 (19.0–38.9). p < 0.001 Percentage of excess weight lost at 2 years [mean (95% CI)]: LAGB 87.2 (77.7–96.6); non-surgical 21.8 (11.9–31.6) (p < 0.001) Proportion achieving excess weight loss greater than 50% at 2 years: 33/39 (85%) LAGB, 8/31 (26%); non-surgical (chi-square; p < 0.001) Proportion achieving satisfactory weight loss (greater than 25% of excess weight lost): 39/40 (98%) LAGB, 14/40 (35%); non-surgical (p < 0.001) 39 (98%) of LAGB participants, and 33 (83%) of non-surgical participants completed the 2-year follow-up programme |
SF-36 QoL domain scores At 2 years the non-surgical group had statistically significant improvements in three domain scores: physical function, vitality and mental health. The LAGB group had statistically significant improvements in all eight domain scores. The change in domain scores between baseline and 2 years shows a statistically significantly greater improvement in five of the eight domains in the LAGB group than in the non-surgical group Mean SF-36 QoL domain scores below estimated from figure by reviewer (note 95% CIs presented in figure) at 2 years Physical function: LAGB 90; non-surgical 87* Physical role: LAGB 92; non-surgical 70* Pain: LAGB 83; non-surgical 78 General health: LAGB 73; non-surgical 68* Vitality (note this is ‘Energy’ on the figure): LAGB 66; non-surgical 57* Social functioning: LAGB 85; non-surgical 81 Emotional role: LAGB 92; non-surgical 72* Mental health: LAGB 76; non-surgical 72 *Statistically significantly greater improvement in LAGB vs non-surgical group (p < 0.05) Comorbidity outcomes Metabolic syndrome: LAGB before treatment n = 15/40 (37.5%), 2 years after treatment n = 1/39 (2.7%). non-surgical before treatment n = 15/40 (37.5%), 2 years after treatment n = 8/33 (24%). (Difference between groups at end point p = 0.006.) Reduction within group p < 0.001 for surgical group, p = 0.22 for non-surgical group Paper also reports data on BP, cholesterol, data not extracted |
Total of adverse events [Value (%)]: LAGB 7/39 (18); non-surgical 18/31 (58) 5-mm port site infection [Value (%)]: LAGB 1/39 (2.6); non-surgical n/a Acute cholecystitis [Value (%)]: LAGB 1/39 (2.6); non-surgical 4/31 (13) Prolapse, posterior (laparoscopic revision) [Value (%)]: LAGB 4/39 (10); non-surgical n/a Loss to follow-up [Value (%)]: LAGB 1/39 (2.6); non-surgical 5/31 (12.5) Operative interventions [Value (%)]: LAGB 5/39 (13); non-surgical 4/31 (13) Intolerance to very-low-calorie diet [Value (%)]: LAGB n/a; non-surgical 1/31 (3) Intolerance to orlistat [Value (%)] LAGB n/a; non-surgical 8/31 (26) |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Yes | Computer-derived random allocation sequence prepared at the trial office. No blocking or stratification |
| Allocation concealment? | Yes | Trial co-ordinator contacted the trial office by telephone to obtain the allocation |
| Blinding of outcome assessors? | No | States that the study was not blinded (outcomes assessors not specified but assume not blinded) |
| Blinding of participants on self-reported outcomes? | No | Participants could not have been blinded to treatment. |
| Incomplete outcome data addressed? Weight loss | Unclear | Withdrawals noted in both groups: one LAGB participant withdrew preoperatively, five non-surgical participants withdrew (weeks 4, 6, 8, 10 and 52), and two non-surgical participants moved overseas. Uneven withdrawals between groups but as reasons not provided for all withdrawals it is unclear whether withdrawals were related to the outcome. States intention-to-treat analysis conducted but in the surgical group the one patient who withdrew preoperatively was not included in the analysis |
| Incomplete outcome data addressed? QoL | Unclear | As above, however for QoL data were analysed only for those who completed the study (case analysis, LAGB n = 39/40, non-surgical n = 33/40) |
| Incomplete outcome data addressed? Comorbidity | Unclear | As above with a case analysis |
| Free of selective outcome reporting? | Unclear | Study protocol not available. Outcomes listed in the methods reported on |
| Free of other sources of bias? | Unclear | Study appears free of other sources of bias |
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Buddeberg-Fischer et al. (2006)105,133 DESIGN: Prospective cohort study with subjects recruited from specialised surgical units (one paper32 states three units, the other paper105 states two units) INTERVALS [mean (SD)]: Baseline to first follow-up 25 months (6.19) Surgery to first follow-up 10 months (5.67) (less than 12 months so not data extracted) Surgery to second follow-up 3.2 years (1.3), range 0.28–5.8 years Interval Recruitment took place from 1998 to 2000 |
Country: Switzerland Number: Total n = 93. Surgery n = 63, no surgery n = 30 [131 approached, a total of 119 at first follow-up (Surgery = 9, no surgery = 50, not extracted), 93 at second follow-up] Total = 93 BMI [mean (SD)]: Surgery (n = 63), 44.7 (6.1) [LGBP (n = 23), 47.3 (7.8); LAGB (n = 40), 43.4 (4.5)]; no surgery (n = 30) 42.9 (5.5) Sex (M : F) 23 : 70 Mean age 43.5 years (SD 9.8, range 21.65) States no difference in age and gender Weight: not reported Duration of morbid obesity n = 119 [mean, (range)]: 20 years (4–45 years) Medication for weight loss: 96/119 (81%) Medication for obesity-related comorbidity: 50/119 (42%) Antidepressants: 21/119 (18%) (Data above not reported for each group) HADS – Anxiety [Mean (SD)]: surgery 5.86 (4.14); no surgery 7.10 (3.99) HADS – Depression [Mean (SD)]: surgery 6.62 (4.56); no surgery 6.23 (3.62) BSQ (Mean (SD)): surgery 12.11 (9.10); no surgery 12.47 (9.61) PAssQ [Mean (SD)]: surgery 1.92 (1.86); no surgery 2.17 (2.17) Characteristics of target population: Patients applying for Surgery. Patient has already tried to lose weight by strict dieting for 2 years, and has a BMI > 40, or > 35 with substantial comorbidity Exclusion criteria: Being over 60 years of age105 |
|
BMI,% BMI change between time points,% EWL. Medication use for weight reduction, physical comorbidity or psychiatric comorbidity, Physical and psychological health, HADS anxiety and HADS depression scores, BSQ scores and PAssQ scores Also reported but not data extracted are outcomes on Doctor consultations,105,133 employability,105 Time off work in last 3 months,105 Nutritional habits,105 Attitude toward the decision to have surgery,105 and Reasons against opting to have surgery105 Psychosocial Stress and Symptom Questionnaire (PSSQ): this consisted of three validated instruments. The Hospital Anxiety and Depression Scale (HADS), the Binge Scale Questionnaire (BSQ), and the Psychosocial Assessment Questionnaire (PAssQ). HADS contains 14 items on a four-point response scale, summed up to separate scores on anxiety and depression; scale scores of less than 8 are in the normal range, 8–10 indicates possible psychiatric morbidity, and scores over 10 probable mood disorder. The BSQ consists of nine items. A sum score which is an indicator of the severity of binge eating is computed from the nine items. The PAssQ consists of 11 dichotomous items which are not specifically obesity-related. A sum score which is an indicator of psychosocial stress is computed from the 11 items |
Method of data analysis: Descriptive statistics by means and standard deviations, and by sample sizes and percentages. ITT not used where there are missing data. p-value that would be considered statistically significant not noted. Sample size/power calculation: not reported Conflict of interests: not reported Patient flow is described in a figure105 which indicates that patients at the second follow-up are different to those at the first follow-up as 16 patients changed group (two Surgery group to no Surgery (debanded), nine no Surgery to Surgery (RYGBP), and five Surgery LAGB to RYGBP) One study reports133 that all patients included in the study met the criteria of having already tried to lose weight by strict dieting for 2 years, and having a BMI > 40, or > 35 with substantial comorbidity. The same reference later states that of the 13 male subjects and 37 female subjects who did not receive surgery, 23.1% males and 16.2% females gave the reason against surgical treatment that their BMI was under the limit for morbid obesity. However, the second study report105 states that all but three included patients met the criteria: one had a BMI of 31.6, and two were over 60 years of age. In all three cases there were special indications for Surgery. |
Table of results
| Weight change | QoL/comorbidity | Events/procedures (complications, reoperations) |
|---|---|---|
|
BMI [mean (SD)] n = 93 Surgery (n = 63): 34.9 (5.5); no surgery (n = 30): 40.6 (7.4). Between-group comparison p = 0.09 Group × time interaction p < 0.001 BMI change [mean (SD)]: Surgery (n = 63): – 21.0 (13.4); no surgery (n = 30): – 5.5 (11.1). Between-group comparison p < 0.001 % EWL [mean (SD)]: Surgery (n = 63): 42.2 (23.4); no surgery (n = 30): 11.5 (25.8). Between-group comparison p < 0.001 BMI [mean (SD)] n = 63 LGBP (n = 23): 32.9 (3.7); LAGB (n = 40): 35.8 (6.1). Between-group comparison p = 0.68 Group × time interaction p < 0.001 BMI change [mean (SD)]: LGBP (n = 23): – 27.7 (12.6); LAGB (n = 40): – 17.2 (12.5). Between-group comparison p = 0.002 % EWL [mean (SD)]: LGBP (n = 23): 52.8 (17.0); LAGB (n = 40): 36.0 (24.5). Between-group comparison p = 0.005 |
Medication for obesity (number of different drugs) in the last 3 months [mean, median (range)]: Surgery (n = 59/63): 0.03, 0 (0–1); no surgery (n = 30/30): 0.32, 0 (0–2). Between-group comparison p < 0.001 Medication for somatic comorbidity (number of different drugs) in the last 3 months [mean, median (range)]: Surgery (n = 59/63): 2.29, 2 (0–15); no surgery (n = 30/30): 2.10, 1 (0–9). Between-group comparison p = 0.98 Medication for psychiatric comorbidity (number of different drugs) in the last 3 months [mean, median (range)]: Surgery (n = 59/63): 0.17, 0 (0–3); no surgery (n = 30/30): 0.6, 0 (0–2). Between-group comparison p = 0.25 Assessment of overall physical health (good) [n (%)]: Surgery (n = 59/63): 46 (79.3); no surgery (n = 30/30): 20 (64.5). Between-group comparison p = 0.10 Assessment of overall mental health (good) [n (%)]: Surgery (n = 59/63): 45 (77.6); no surgery (n = 30/30): 21 (67.7). Between-group comparison p = 0.22 HADS – Anxiety Score [mean (SD)] Surgery (n = 63): 5.76 (4.27); no surgery (n = 30): 6.53 (4.29). Between-group comparison p = 0.21 HADS – Depression Score [mean (SD)] Surgery (n = 63): 4.67 (4.58); no surgery (n = 30): 4.33 (3.01). Between-group comparison p = 0.65 BSQ Score [mean (SD)] Surgery (n = 63): 7.16 (9.68); no surgery (n = 30): 8.87 (9.52). Between-group comparison p = 0.55 PAssQ Score [mean (SD)] Surgery (n = 63): 2.11 (2.04); no surgery (n = 30):1.87 (2.08). Between-group comparison p = 0.99 |
n = 119. Reoperations 7/69 (LAGB to RYGBP = 5, LAGB to debanding = 2) |
Quality criteria (CRD Report 4)
| Quality item | Yes/No/Uncertain | Methodological comments |
|---|---|---|
| Cohort studies | ||
| 1. Is there sufficient description of the groups and distribution of prognostic factors? | No | The characteristics of the whole sample are described, but the characteristics of each group are only reported separately for BMI and psychosocial stress and symptoms |
| 2. Are the groups assembled at a similar point in their disease progression? | Uncertain | For the study sample as a whole subjects mean duration of morbid obesity was 20 years (range 4–45 years). However, this was not reported for each group separately |
| 3. Is the intervention/treatment reliably ascertained? | Yes | Although there may be minor reporting errors, on the whole it is clear how many people received which intervention |
| 4. Were the groups comparable on all important confounding factors? | Uncertain | Not reported |
| 5. Was there adequate adjustment for the effects of these confounding variables? | No | |
| 6. Was outcome assessment blind to exposure status? | No | All measures, including BMI, were self-reported |
| 7. Was follow-up long enough for the outcomes to occur? | Yes | |
| 8. What proportion of the cohort was followed-up? | Yes | Proportion of cohorts followed up reported. 119/131 at first follow-up, 93/131 at second follow-up. Dropouts noted but reasons not always reported |
| 9. Were dropout rates and reasons for dropout similar across intervention and unexposed groups? | No | Baseline (n = 131), 12 dropouts before first follow-up (n = 119) not reported separately for each group. After first follow-up (n = 119) a further 26 dropouts: surgery 13/69 (19%) (RYGBP 3/12, LAGB 10/57), no surgery 13/50 (26%), occurred before the second follow-up (n = 93). In addition, of the n = 93 assessed at the second follow-up, some had switched status: surgery LAGB reoperation to RYGBP n = 5, surgery LAGB to debanding (joined no surgery group) n = 2, no surgery to surgery (RYGBP) n = 9. Reasons for dropouts from each group not reported. In addition to the dropouts, data on four patients were missing from the surgery group for some outcomes (doctor consultations, etc.) |
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
SOS Design: Multicentre, cohort study with matched controls Follow-up: (Length of follow-up and sample size varies with publication of different outcomes) Weight loss 10 years Diabetes 8 years Blood pressure 8 years HRQoL 10 years Lipid disturbances 2 years Comorbidities 10 years Medication use 6 years Cancer incidence average 11 years |
Country: Sweden Baseline characteristics, mean (SD) unless stated Karason 2000,85 weight loss outcomes at 2 years: Number: total 2620. After mortality, dropouts and data pending: Surgical 1210; controls 1099 Age: surgical 47 years (SD 6), control: 49 years (SD 6) Sex: surgical 67% women, control 67% women Weight: surgical 121 kg (SD 17), control 114 kg (SD 16) BMI: surgical 42.2 (SD 4.4); control 39.7 (SD 4.4) Sjostrom 2000,89 weight loss/diabetes/blood pressure outcomes: Number: total 483, surgical 251, control 232 Age (mean): surgical 46 yrs (6), control 47 years (6) Sex: surgical 65.9% female, control 65.9% female Weight: surgical 119.7 kg (15.6), control 117.4 kg (16.6) BMI: surgical 41.6 (3.9), control 41 (4.7) Karlsson 1998,86 HRQoL at 2 years: Number: total 974, surgical 487, control 487 Age (mean): surgical 46.6 years (95% CI 46.1 to 47.1), control 47.7 years (95% CI 47.2 to 48.3) Sex: surgical 67% female, control 67% female. Sjostrom 1999,88 lipid disturbances: Number: total 1479, surgical 767, control 712 Age: surgical 47 years (5.8), control 48.6 years (6.3) Sex: surgical 69% female, control 68% female Weight: surgical 120.5 kg (16), control 114.1 kg (17) BMI: surgical 42.1 (4.3), control 39.8 (4.6) Togerson 2003,96 gallstones, gall bladder disease and pancreatitis: Number: total 2682, surgical 1422, control 1260 Age, years, Men: surgical 47.3 (5.7), controls 48.4 (6.1), p = 0.005. Women: surgical 47.1 (5.9), controls 48.3 (6.3), p < 0.001 Sex (M : F): surgical 468 : 954, controls 418 : 842. |
|
Weight loss (kg) BMI Blood pressure, systolic and diastolic Health-related quality of life (HRQoL) Diabetes Lipid disturbances Gallstones, Gall bladder disease, pancreatitis Medication for CVD and diabetes Pharmaceutical costs (not extracted) Cancer incidence |
Allocation to treatment groups: Patients could volunteer for conventional or surgical treatment. For each surgical case a computerised matching procedure selects the optimal control from a registry taking 18 different variables into account [inc. gender (absolute match) age, weight, height, waist and hip circumferences, systolic blood pressure, serum cholesterol and triglyceride concentrations, smoking, diabetes, pre/postmenopausal, four psychosocial variables with known associations with mortality, two personality traits related to treatment preferences] Blinding: Not applicable Comparability of treatment groups: Average interval between matching of controls and inclusion into study (surgery) was 0.8 years (SD 7). During this period, surgical group gained weight and control group lost weight, resulting in average difference of 6.4 kg (p < 0.001). At inclusion, surgical group were younger than controls (p < 0.001), had a higher prevalence of hypertension (p < 0.05) and were more often smokers (not significant). Also reports higher BMI (p < 0.001), blood pressure (p < 0.001) and energy intake (p < 0.001) in surgical patients |
|
Height, m, men: surgery 1.79 (0.07), controls 1.80 (0.07), p = 0.263. Women: surgery 1.64 (0.06), controls 1.65 (0.06), p = 0.207. Weight, kg, men: surgery 132.4 (16.9), controls 125.3 (16.6), p < 0.001. Women: surgery 115.7 (13.4), controls 110.4 (14.3), p < 0.001. BMI, men: surgery 41.2 (4.7), control 38.8 (4.7), p < 0.001. Women: surgery 42.8 (4.1), controls 40.6 (4.4), p < 0.001. Agren 2002,136 medication use Number: total 965, surgery 510, control 455. Mean age, yrs: surgery 47.1 (5.8), control 48.6 (6.1). Sex,% of men: surgery 31.0, control 31.0. Mean BMI: surgery 41.8 (4.1), control 39.9 (4.6). % on medication for CVD: surgery 29.4, control 27.5 Diabetes: surgery 6.3, control 4.6. Sjostrom 2007,99 mean follow-up of 10.9 (3.5) years. Number: total 4047, surgery 2010, control 2037 Mean age, yrs: surgery 47.2 (5.9), control 48.7 (6.3), p < 0.001 Sex (M:F): surgery 590/1420, control 590/1447, p = 0.79 Weight: surgery 121.0 (16.6), control 114.7 (16.5), p < 0.001 Height: surgery 1.69 (0.09), control 1.69 (0.09), p = 0.68 Mean BMI: surgery 42.4 (4.5), control 40.1 (4.7), p < 0.001 Other baseline measures reported, but not extracted. Karlson 2007,100 HRQoL at 10 years: Number: total 1703, of these 1276 (74.9%) were available for analysis. surgery 655 (of 851), control 621 (of 852) Mean age: surgery 47.0 (5.7), control 48.4 (6.7) years Weight: surgery 120.1 (16.5) kg, control 113.9 (16.8) kg BMI: surgery 41.9 (4.2), control 39.9 (4.6) HRQoL (all measures validated): Current health perceptions (scale 0–100, high score = well-being): surgery 51.8 (24.1), control 58.8 (24.8) Social interaction (scale 0–100, high score = dysfunction): surgery 11.7 (11.0), control 7.2 (9.7) |
Method of data analysis: Analysis on completers except where ITT specified. When all included patients were analysed, missing data handled by last-value imputation according to ITT principles. Completer and ITT analysis resulted in almost identical results. Dissimilarities between groups at inclusion were adjusted for in calculations. t tests, paired t tests and anova used according to the general linear model used. anova used to test differences between surgical procedure. For comparisons of changes in proportions between two groups, a two-sample McNemar test was used. Unconditional logistic regression was used for comparing incidences in the two treatment groups, because these were matched on a group level and not on an individual level. HRQoL: 15 reversals and eight controls who demanded and received surgery were considered as belonging to their original treatment groups according to ITT principles. Differences between groups were analysed by Fisher’s permutation test and Kruskal–Wallis anova of mean ranks and Tukeys range test Sample size/power calculation: Study aimed to recruit 2000 surgical cases and 2000 matched controls over approx. 4 years, which they report to suffice for the detection of a 10-year excess mortality risk that is 50% higher in the non-surgically treated group. No calculation given for other outcomes |
|||
|
Obesity-related problems (scale 0–100, high score = dysfunction): surgery 58.0 (27.0), control 40.9 (26.8) Overall mood (scale 1–4, high score = well-being): surgery 2.93 (0.59), control 3.06 (0.60) Depression (scale 0–21, high score = symptoms): surgery 5.1 (3.6), control 4.2 (3.3) Anxiety (scale 0–21, high score = symptoms): surgery 6.1 (4.6), control 5.4 (4.5) N.B.: Statistical analysis for differences in baseline undertaken on those completing and those not completing, or between these two groups and a third ‘reference group’, so not reported here Sjostrom 2004,97 comorbidity data at 2 and 10 years Those completing 2 years: Number: total 3505, surgery 1845, control 1660 Mean age: surgery 47.4 (5.9), control 48.8 (6.2), p < 0.001 Sex (% male): surgery 29.3%, control 29.7%, p = ns Weight: surgery 120.6 (16.4) kg; control 114.6 (16.4) kg, p < 0.001 Height: surgery 1.69 (0.09), control 1.69 (0.09), p = ns BMI: surgery 42.3 (4.4), control 40.0 (4.6), p < 0.001 Those completing 10 years: Number: total 1268, surgery 641, control 627 Mean age: surgery 47.0 (5.6), control 48.4 (6.3), p < 0.001 Sex (% male): surgery 30.6%, control 31.4%, p = ns Weight: surgery 120.0 (16.4) kg; control 113.9 (16.7) kg, p < 0.001 Height: surgery 1.69 (0.09), control 1.69 (0.09), p = ns BMI: surgery 41.9 (4.2), control 39.9 (4.6), p < 0.001 Gummesson 2008,101 cancer incidence (abstract only) Number: total 4047, surgery 2010, control 2037. No further details although note that participant numbers are the same as those reported by Sjostrom 200799 Characteristics of target population: between 37 and 60 years, BMI of ≥ 34 for men and ≥ 38 for women |
Attrition/dropout: As a result of mortality, dropouts and data pending (numbers not specified), data reported on 73% of surgical and 67% of control patients in study with 8-year follow-up. In controls, future dropouts higher prevalence of diabetes (22%, 8%, p = 0.002) and smoking (40%, 24%, p = 0.002) than completers at inclusion. In surgical, future dropouts had higher body weight (125 kg vs 120 kg, p = 0.02) and alcohol consumption (7.0 g/day vs 4.8 g/day p = 0.01) than completers at inclusion Of 965 patients who completed 6 years follow-up on medication use, five had missing data on weight, and four had missing data on medication use at 2 years follow-up, group not specified Sjostrom 2007:99 At follow-up examinations at 2, 10 and 15 years (from substudy with mean of 10.9 years follow-up) participation rates in the surgery group were 94%, 84% and 66% respectively. For the control groups these rates were 83%, 75%, and 87% Karlsson 2007:100 Of the 1703 patients in the 10-year HRQoL substudy, 77% of the surgery group and 72.9% of the control group were followed up Sjostrom 2004:97 Losses to follow-up Patients followed for 10 years: |
|||
|
Exclusion criteria: Previous bariatric surgery, gastric surgery for other causes in last 6 years, serious health problems including active malignancy and recent myocardial infarction, bulimic eating pattern, drug or alcohol abuse, psychological problems likely to lead to poor co-operation, regular use of cortisone or non-steroidal anti-inflammatory drugs |
Surgery 210/851 (24.7%), controls 225/852 (26.4%) Patients followed for 2 years: Surgery 165/2010 (8.2%), controls 377/2037 (18.5%) |
Table of results
| Weight change | QoL/comorbidity | Events/procedures (complications, reoperations) |
|---|---|---|
|
Karason 200085 Weight loss at 2 years Weight (kg) surgical (n = 1210) vs control (n = 1099): Baseline: difference 7 kg (95% CI 5.7 to 8.3) 24 months: difference – 21 kg (95% CI – 23 to – 19) Weight loss after 24 months: surgical: 28 kg (23%); control: unchanged, p < 0.001 Sjostrom 200089 Weight changes at 8 years:(surgical n = 232, control n = 251) Baseline: surgical 120.4 kg (16.0), control 114.7 kg (17.8) 8 years: surgical 100.3 kg (17.8), control 115.4 kg (19.2) Difference In weight change between groups at 8 years: 20.7 kg (p < 0.001) Relative weight change at 8 years: surgical – 16.3% (12.3%); control 0.9% (10.8%) Weight at 8 years: GBP 92 kg vs VBG 100 kg (p = ns) vs GBand 103 kg (p < 0.05). All had a larger weight reduction than controls (p < 0.01) Togerson 200396 Weight loss at 2 years: Men: surgery 29.4 kg (15.3), 21.9% (10.0), controls 0.3 kg (9.5), 0.1% (7.4), p < 0.001 Women: surgery 28.0 kg (13.8), 23.9% (10.7), controls 0.6 kg (8.6), 0.3% (7.9), p < 0.001 |
Karlsson 199886 Health Related QoL Current health perception GHRI/CH (mean; 95% CI): Baseline – surgery 26.9 (26.1 to 27.7); control 29.4 (28.5 to 30.2). 2 years – surgery 34.3 (33.4 to 35.1); control 30.2 (29.4 to 31.1) Psychosocial functioning OP change by 2 years (mean, 95% CI): surgery – males – 1.01 (– 1.14 to – 0.87), females – 1.10 (– 1.19 to – 1.00); Control – males – 0.07 (– 0.17 to 0.03) (p = 0.001); females – 0.16 (– 0.22 to – 0.09) (p = 0.001) SIP/SI change by 2 years (mean, 95% CI): surgery – males – 3.3 (– 5.0 to – 1.5), females – 5.2 (– 6.5 to – 4.0); control – males 1.5 (0.2 to 3.2) (p = 0.001); females 1.2 (0.2 to 2.2) (p = 0.0001) Mental well-being scales MACL change by 2 years (mean, 95% CI): pleasantness/unpleasantness Surgery 0.21 (0.16 to 0.26); control – 0.04 (– 0.09 to 0.01) (p = 0.001); activation/deactivation Surgery 0.32 (0.27 to 0.37); control 0.00 (– 0.04 to 0.05) (p = 0.001); calmness/tension Surgery 0.20 (0.15 to 0.26); control – 0.01 (– 0.06 to 0.04) (p = 0.001) HADs change by 2 years (mean, 95% CI): Anxiety: surgery – 1.7 (– 2.0 to – 1.4); control – 0.6 (– 0.9 to – 0.2) (p = 0.0001); Depression: surgery – 2.2 (– 2.5 to – 1.9); control – 0.4 (– 0.6 to – 0.1) (p = 0.0001); At 24 months: improvement in surgical vs controls on all HQRL measures (p < 0.0001) Changes in all HRQoL measures significantly related to magnitude of weight loss Sjostrom 200089 Diabetes and Hypertension Diabetes: 2-year unadjusted incidence: controls 4.7%, surgical 0.0% (p = 0.0012) 8-year unadjusted incidence: controls 18.5%, surgical 3.6% (p = 0.0001) Adjusted odds ratios of developing diabetes, 8 years: Completers (n = 437) 0.17 (95% CI 0.08 to 0.38) All (ITT) (n = 611) 0.16 (95% CI 0.07 to 0.36) |
Sjostrom 199988 (lipid disturbances data) 15 surgical operations reversed during first 2 years. Five GBand were converted to GBP, one GBand converted to VBG, seven VBG converted to GBP Togerson 2001137 (overview paper) Postoperative mortality: Four (0.2%) deaths, three due to leakage detected too late and one due to a technical laparoscopic mistake Perioperative complications (n = 1164): 151 patients (13%) experienced 193 complications. Bleeding 0.9%, thromboembolic events 0.8%, wound complications 1.8%, abdominal infection 2.1%, pulmonary symptoms 6.2%, miscellaneous 4.8% Complications requiring reoperation: 26 patients (2.2%) Sjostrom 2007,99 mean 10.9 years follow-up Cumulative overall mortality during a period of up to 16 years: Surgery group hazard ratio compared with control group: 0.76 (95% CI 0.59 to 0.99), p = 0.04 Deaths, n(%) Surgery: 101/2010 (5.0%), control: 129/2037 (6.3%) Cause of death: Cardiovascular condition: Any event: surgery 43, control 53 of which: Cardiac: surgery 35 (myocardial infarction 13, heart failure 2, sudden death 20); control 44 (myocardial infarction 25, heart failure 5, sudden death 14) |
|
Agren 2002136 Relative weight change, mean (SD): 2 years: surgery – 22.6% (10.6), control – 0.3% (7.9) 6 years: surgery – 16.2% (11.5), control 0.8% (9.6) Sjostrom 200799 Mean % weight loss, mean 10.9 years follow-up (reported 10 and 15 years only here, note different values of n) Control group, weight remained within ± 2% at 10 years (886/2037 followed up) and 15 years (190/2037 followed up) Surgery, mean % weight losses were 25 ± 11% for GBP, 16 ± 11% for VBG, 14 ± 14% for banding at 10 years. The numbers followed up for each of the three procedures were 58/265, 746/1369 and 237/376 for the three groups, respectively After 15 years, weight losses were 27 ± 12% for GBP, 18 ± 11% for VBG and 13 ± 14% for banding (corresponding numbers followed up were: 10/265, 108/1369, 52/376) Karlsson 2007100 At 10 years follow-up Weight at 10 years: surgery 100.5 kg (17.7), change – 19.7 kg (15.8); control 115.2 kg (19.9), change 1.3 kg (13.8). Surgery vs control p < 0.0001 Weight loss between surgical subgroups at 10 years: 13.2% (SD 13) banding (n = 161); 16.5% (SD 11) VBG (n = 457); 25.1% (SD 11) GBP (n = 37) Weight change at 10 years: Surgery (loss of weight): 16% (12.1), men 15.8% (12.3), women 16.1% (12.1) Controls (gain of weight): 1.5% (9.9), men 1.9% (12.8), women 1.4% (12.1) |
Hypertension: 2-year unadjusted incidence: controls 9.9%, surgical 3.2% (p = 0.032) 8 year unadjusted incidence: controls 25.8%, surgical 26.4% (p = 0.91) Adjusted odds ratios of developing hypertension, 24 months: Completers (n = 257) 0.27 (95% CI 0.07 to 0.99). All (ITT) (n = 377) 0.27 (95% CI 0.09 to 0.76) Adjusted odds ratios of developing hypertension, 8 years: Completers (n = 257) 1.05 (95% CI 0.58 to 1.89) All (ITT) (n = 377) 1.01 (95% CI 0.61 to 1.67) Sjostrom 199988 Lipid disturbances: Lipids: Adjusted odds ratios at 24 months (95% CI): Hypertriglyceridaemia 0.10 (95% CI 0.04 to 0.25) p < 0.001 Hypo HDL-cholesterolaemia 0.28 (95% CI 0.16 to 0.49) p < 0.001 Hypercholesterolaemia 1.24 (95% CI 0.84 to 1.8) p = ns Relative risks for recovery from disease: Hyperinsulinaemia (n = 221) 1.4 (95% CI 1.2 to 1.7) p < 0.00001 Hypertriglyceridaemia (n = 314) 1.9 (95% CI 1.5 to 2.4) p < 0.00001 Hypo HDL-cholesterolaemia (n = 216) 1.7 (95% CI 1.4 to 2.1) p < 0.00001 Hypercholesterolaemia (n = 531) 1.2 (95% CI 0.95 to 1.5) p = ns Togerson 200396 Biliary disease: Biliary disease and pancreatitis; frequencies over 2 years (%), Fisher’s exact test and OR (95% CI) adjusted for age and BMI at baseline Cholelithiasis, men: surgery 4.0, controls 1.2, p = 0.011, OR 4.2 (1.5 to 12.0). Women: surgery 5.5, controls 4.5, p = 0.328, OR 1.1 (0.7 to 1.8) Cholecystitis, men: surgery 2.5, controls 0.7, p = 0.058, OR 4.5 (1.2 to 17.1). Women: surgery 3.3, controls 2.5, p = 0.379, OR 1.4 (0.7 to 2.5) Cholecystectomy, men: surgery 3.4, controls 0.7, p = 0.008, OR 5.4 (1.5 to 19.6). Women: surgery 3.5, controls 2.3, p = 0.191, OR 1.6 (0.9 to 3.0) Total biliary disease, men: surgery 4.1, controls 1.5, p = 0.024, OR 3.5 (1.3 to 9.2). Women: surgery 6.8, controls 5.3, p = 0.223, OR 1.2 (0.8 to 1.9) Pancreatitis, men: surgery 1.1, controls 0.2, p = 0.219, OR 3.6 (0.4 to 31.2). Women: surgery 0.7, controls 0.4, p = 0.514, OR 1.8 (0.4 to 7.6) |
Stroke: surgery six (intracerebral haemorrhage two, infarction one, subarachnoid bleeding three); control six (intracerebral haemorrhage four, infarction two) Other: surgery two (aortic aneurysm one, diabetic gangrene one); control three (aortic aneurysm two, aortic thrombosis one) Non-cardiovascular condition: Any event: surgery 58, control 76, of which: Tumour: surgery 29 (Cancer 29); control 48 (cancer 47, meningioma one) Infection: surgery 12, control three Thromboembolic disease: surgery five (pulmonary embolism four, vena caval thrombosis one); control seven (pulmonary embolism 7) Other: surgery 12, control 18 Deaths within 90 days of surgery: Five in surgery group (0.25%)(four from peritonitis with organ failure, one sudden death) and two in control group (0.10%) (one from pancreatic cancer, one from alcohol-related causes) surgical reoperations or conversions (excluding operations caused by postoperative complications) in those followed up for at least 10 years (n = 1338): banding 31%, VBG 21%, GBP 17% |
|
BMI at 10 years: Surgery 35.3 (5.4), change -6.7 (5.4); control 40.6 (5.9), change 0.7 (4.9). Surgery vs control p < 0.0001 Sjostrom 200497 At 2 and 10 years follow-up (N.B. different cohort numbers for each). At 2 years: Weight,% change: Surgery – 23.4, control 0.1, difference 22.2 (95% CI 21.6 to 22.8), p < 0.001 BMI,% change: Surgery –23.3, control 0.1, difference 22.1 (95% CI 21.5 to 22.7), p < 0.001 At 10 years: Weight,% change: Surgery – 16.1, control 1.6 (12), difference 16.3 (95% CI 14.9 to 17.6), p < 0.001 BMI,% change: Surgery – 15.7, control 2.3, difference 16.5 (95% CI 15.1 to 17.8), p < 0.001 |
Agren 2002,136 medication use: Proportion on CVD medication, risk ratio (95% CI adjusted to mean values of sex, age, and BMI at baseline): Subjects on medication at baseline, surgery n = 150, control n = 125 Proportion on medication at: 2 years,%: surgery 61.7, control 91.2, RR 0.69 (0.60 to 0.80), p < 0.05 6 years,%: surgery 64.7, control 86.4, RR 0.77 (0.67 to 0.88), p < 0.05 Subjects not on medication at baseline, surgery n = 360, control n = 330 Proportion on medication at: 2 years,%: surgery 3.1, control 10.1, RR 0.28 (0.14 to 0.56), p < 0.05 6 years,%: surgery 13.3, control 16.7, RR 0.80 (0.56 to 1.16) Proportion on diabetes medication, risk ratio (95% CI adjusted to mean values of sex, age and BMI at baseline): Subjects on medication at baseline, surgery n = 32, control n = 21 Proportion on medication at: 2 years,%: surgery 56.2, control 100.0, RR 0.56 (0.41 to 0.76), p < 0.05 6 years,%: surgery 68.8, control 100.0, RR 0.71 (0.56 to 0.89), p < 0.05 Subjects not on medication at baseline, surgery n = 478, control n = 434 Proportion on medication at: 2 years,%: surgery 0.2, control 3.7, RR 0.08 (0.01 to 0.58), p < 0.05 6 years,%: surgery 2.1, control 11.3, RR 0.20 (0.10 to 0.38), p < 0.05 Karlsson 2007100 HRQoL at 10 years Current health perceptions: 1-year follow-up: surgery 48% improvement, control 7% improvement 10-year follow up: surgery 57.5 (26.8), change 5.8 (27.6) (11% improvement); control 55.4 (25.1), change – 3.4 (25.2), p = ns difference between groups, p < 0.0001 difference in change. Effect size (ES) of change calculated (where 0 to < 0.20 trivial, 0.20 to < 0.50 small, 0.50 to < 0.80 moderate, ≥ 0.80 large) reported to be 0.21 for surgery and -0.13 for control groups Social interaction: 1-year follow-up: surgery ~ 60% improvement, control 7% 10-year follow-up: surgery 8.4 (12.4), change – 3.2 (13.0); control 7.7 (11.1), change 0.5 (10.0), p = ns difference between groups, p < 0.01 difference in change. Effect size (ES) of change surgery 0.25, control – 0.05 Obesity-related problems: 1-year follow-up: surgery ~ 63% improvement, control 7% 10-year follow-up: surgery 29.7(27.3), change 28.3 (28.3); control 31.3 (25.5), change 9.6 (22.6), p = ns difference between groups, p < 0.0001 difference in change. Effect size (ES) of change surgery 1.00, control 0.42 |
|
|
Overall mood 10-year follow-up: surgery 3.06 (0.59), change 0.14 (0.56); control 3.11 (0.56), change 0.05 (0.51), p = ns (between groups and change between groups). Effect size (ES) of change surgery 0.25, control 0.10 Depression 10-year follow-up: surgery 3.7 (3.7), change – 1.4 (3.9); control 3.7 (3.5), change – 0.5 (3.4), p = ns difference between groups, p < 0.05 difference in change. Effect size (ES) of change surgery 0.35, control 0.14 Anxiety 10-year follow-up: surgery 4.6 (4.4), change – 1.4 (4.3); control 4.0 (4.2), change – 1.4 (3.9), p < 0.01 difference between groups, p = ns difference in change. Effect size (ES) of change surgery 0.33, control 0.35 HRQoL at 10 years in surgically treated patients by weight change, and 10-year trends in weight loss and HRQoL in surgically treated patients with weight loss ≥ 10% vs < 10% after 10 years reported but not extracted Sjostrom 200497 comorbidity at 2 and 10 years (N.B. different cohort numbers for each) 2-year outcomes: Systolic blood pressure at baseline: surgery 143.5 (18.8), control 137.5 (17.9), p < 0.001. Change at end point: surgery – 4.4, control 0.5, difference 2.8 (95% CI 2.1 to 3.6), p < 0.001 Diastolic blood pressure at baseline: surgery 88.7 (11.2), control 84.7 (10.5), p < 0.001. Change at end point: surgery – 5.2, control 0.3, difference 3.2 (95% CI 2.4 to 3.9), p < 0.001 Glucose (mmol/l) at baseline: surgery 5.4 (2.1), control 5.2 (1.9), p < 0.001. Change at end point: surgery -13.6, control 5.1, difference 16.6 (95% CI 15.0 to 18.3) p < 0.001 Insulin (mU/l) at baseline: surgery 21.2 (12.6), control 18.0 (11.5), p < 0.001. Change at end point: surgery – 46.2, control 10.3, difference 51.4 (95% CI 48.0 to 54.8), p < 0.001 Uric acid (μmol/L) at baseline: surgery 359.4 (80.1), control 353.3 (79.3), p < 0.05. Change at end point: surgery – 14.9, control – 0.4, difference 13.5 (95% CI 12.5 to 14.6), p < 0.001 Triglycerides (mmol/l) at baseline: surgery 2.23 (1.52), control 2.01 (1.35), p < 0.001. Change at end point: surgery – 27.2, control 6.3, difference 29.9 (95% CI 27.4 to 32.5), p < 0.001 HDL cholesterol (mmol/L) at baseline: surgery 1.20 (0.28), control 1.19 (0.29), p < 0.001. Change at end point: surgery 22.0, control 3.5, difference – 18.7 (95% CI – 20.1 to – 17.3) Total cholesterol (mmol/l) at baseline: surgery 5.85 (1.12), control 5.60 (1.06), p < 0.001. Change at end point: surgery – 2.9, control 0.1, difference 1.0 (95% CI 0.1 to 1.9), p < 0.05 |
||
|
10-year outcomes: Systolic blood pressure at baseline: surgery 143.8 (19.3), control 138.4 (17.6), p < 0.001. Change at end point: surgery 0.5, control 4.4, difference 1.1 (95% CI – 0.3 to 2.6) Diastolic blood pressure at baseline: surgery 89.6 (11.3), control 85.8 (10.6), p < 0.001. Change at end point: surgery – 2.6, control – 2.0, difference – 2.3 (95% CI – 3.5 to – 1.0), p < 0.001 Glucose (mmol/l) at baseline: surgery 5.5 (2.1), control 5.1 (1.7), p < 0.001. Change at end point: surgery – 2.5, control 18.7, difference 18.4 (95% CI 14.7 to 22.1) p < 0.001 Insulin (mU/l) at baseline: surgery 21.2 (11.4), control 18.3 (11.2), p < 0.001. Change at end point: surgery – 28.2, control 12.3, difference 30.3 (95% CI 23.9 to 36.6), p < 0.001 Uric acid (μmol/l) at baseline: surgery 366.2 (84.2), control 357.7 (78.9), p = ns. Change at end point: surgery – 6.2, control 3.9, difference 8.8 (95% CI 6.4 to 11.1), p < 0.001 Triglycerides (mmol/l) at baseline: surgery 2.30 (1.56), control 2.12 (1.49), p < 0.05. Change at end point: surgery – 16.3, control 2.2, difference 14.8 (95% CI 10.4 to 19.1) p < 0.001 HDL-cholesterol (mmol/l) at baseline: surgery 1.19 (0.28), control 1.18 (0.29), p = ns. Change at end point: surgery 24.0, control 10.8, difference – 13.6 (95% CI – 16.5 to – 10.6), p < 0.001 Total cholesterol (mmol/l) at baseline: surgery 6.02 (1.13), control 5.76 (1.10), p < 0.001. Change at end point: surgery – 5.4, control – 6.0, difference – 2.0 (95% CI – 0.2 to – 3.8), p < 0.05 Incidence of comorbidities after 2 and 10 years in those without disease at baseline (n values for numerators calculated by reviewer and rounded): Hypertriglyceridaemia at 2 years: surgery 58/731 (8%), control 176/801 (22%), odds ratio 0.29 (95% CI 0.21 to 0.41), p < 0.001 Hypertriglyceridaemia at 10 years: surgery 38/225 (17%), control 75/281 (27%), odds ratio 0.61 (95% CI 0.39 to 0.95), p = 0.03 Low HDL-cholesterol at 2 years: surgery 25/1293 (2%), control 117/1174 (10%), odds ratio 0.21 (95% CI 0.14 to 0.32), p < 0.001 Low HDL-cholesterol at 10 years: surgery 13/431 (3%), control 26/440 (6%), odds ratio 0.57 (95% CI 0.29 to 1.15), p = 0.12 Hypercholesterolaemia at 2 years: surgery 136/504 (27%), control 143/596 (24%), odds ratio 1.27 (95% CI 0.95 to 1.69), p = 0.11 Hypercholesterolaemia at 10 years: surgery 40/135 (30%), control 51/188 (27%), odds ratio 1.16 (95% CI 0.69 to 1.95), p = 0.57 Diabetes at 2 years: surgery 15/1489 (1%), control 112/1402 (8%), odds ratio 0.14 (95% CI 0.08 to 0.24), p < 0.001 Diabetes at 10 years: surgery 36/517 (7%), control 129/539 (24%), odds ratio 0.25 (95% CI 0.17 to 0.38), p < 0.001 Hypertension at 2 years: surgery 149/623 (24%), control 223/770 (29%), odds ratio 0.78 (95% CI 0.60 to 1.01), p = 0.06 |
||
|
Hypertension at 10 years: surgery 88/215 (41%), control 137/279 (49%), odds ratio 0.75 (95% CI 0.52 to 1.08), p = 0.13 Hyperuricaemia at 2 years: surgery 42/1044 (4%), control 163/1017 (16%), odds ratio 0.22 (95% CI 0.15 to 0.31), p < 0.001 Hyperuricaemia at 10 years: surgery 58/342 (17%), control 107/382 (28%), odds ratio 0.49 (95% CI 0.34 to 0.71), p < 0.001 Recovery From comorbidities after 2 and 10 years in those with disease at baseline (n values for numerators calculated by reviewer and rounded): Hypertriglyceridaemia at 2 years: surgery 683/1102 (62%), control 187/850 (22%), odds ratio 5.28 (95% CI 4.29 to 6.49), p < 0.001 Hypertriglyceridaemia at 10 years: surgery 185/402 (46%), control 79/331 (24%), odds ratio 2.57 (95% CI 1.85 to 3.57), p < 0.001 Low HDL-cholesterol at 2 years: surgery 338/445 (76%), control 154/396 (39%), odds ratio 5.28 (95% CI 3.85 to 7.23), p < 0.001 Low HDL-cholesterol at 10 years: surgery 123/169 (73%), control 88/166 (53%), odds ratio 2.35 (95% CI 1.44 to 3.84), p < 0.001 Hypercholesterolaemia at 2 years: surgery 292/1327 (22%), control 178/1048 (17%), odds ratio 1.22 (95% CI 0.98 to 1.51), p = 0.07 Hypercholesterolaemia at 10 years: surgery 105/498 (21%), control 74/435 (17%), odds ratio 1.30 (95% CI 0.92 to 1.83), p = 0.14 Diabetes at 2 years: surgery 246/342 (72%), control 52/248 (21%), odds ratio 8.42 (95% CI 5.68 to 12.5), p < 0.001 Diabetes at 10 years: surgery 42/118 (36%), control 11/84 (13%), odds ratio 3.45 (95% CI 1.64 to 7.28), p < 0.001 Hypertension at 2 years: surgery 409/1204 (34%), control 185/880 (21%), odds ratio 1.72 (95% CI 1.40 to 2.12), p < 0.001 Hypertension at 10 years: surgery 81/424 (19%), control 38/342 (11%), odds ratio 1.68 (95% CI 1.09 to 2.58), p = 0.02 Hyperuricaemia at 2-years: surgery 562/792 (71%), control 197/637 (31%), odds ratio 5.36 (95% CI 4.23 to 6.78), p < 0.001 Hyperuricaemia at 10-years: surgery 140/292 (48%), control 66/243 (27%), odds ratio 2.37 (95% CI 1.61 to 3.47), p < 0.001 |
||
|
Gummesson 2008,101 cancer incidence, average 11 years follow-up Cancer status not known for 3/4047 (follow-up rate 99.9%), group not specified Cases of first-time cancers: surgery 126/2010, control 173/2037 Unadjusted hazard ratio for overall cancer incidence: 0.71 (p = 0.003) for surgery group compared with control group. Hazard ratio adjusted for risk factors: 0.74 (p = 0.011). 95% CIs not reported. Unadjusted hazard ratio for: Men (n = 1178): 0.98 (95% CI 0.63 to 1.51, p = 0.91) Women (n = 2867): 0.63 (95% CI 0.48 to 0.82), p = 0.001) Hazard ratios using specific cancer types as outcomes did not reach statistical significance |
Quality criteria (CRD Report 4)
| Quality item | Yes/No/Uncertain | Methodological comments | |
|---|---|---|---|
| Cohort studies | |||
| 1. | Is there sufficient description of the groups and the distribution of prognostic factors? | Yes | Differences between groups |
| 2. | Are the groups assembled at a similar point in their disease progression? | Unclear | |
| 3. | Is the intervention/treatment reliably ascertained? | Yes | |
| 4. | Were the groups comparable on all important confounding factors? | No | Significant differences between groups |
| 5. | Was there adequate adjustment for the effects of these confounding variables? | Yes | States adjustments made where appropriate |
| 6. | Was outcome assessment blind to exposure status? | No | |
| 7. | Was follow-up long enough for the outcomes to occur? | Yes | |
| 8. | What proportion of the cohort was followed-up? |
At 2 years: 84% surgical, 93% control At 8 years: 73% of surgical, 67% control At 10 years: varies between the different substudies |
|
| 9. | Were dropout rates and reasons for dropout similar across intervention and unexposed groups? | Unclear | Numbers and reasons not given |
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Stoeckli, 2004102 Von Mach 2004103 Christ-Crain 2006104 Design: prospective cohort study, single centre Follow-up: 24 months |
Country: Switzerland Stoeckli 2004 and Christ-Crain 2006: Number: total 20, LAGB 8, RYGBP 5, controls 7 Mean age, years (SE): LAGB 41.1 (2.6), RYGBP 43.8 (4.4), controls 49.9 (2.6) Sex (F : M): LAGB (6 : 2), RYGBP (5 : 0), controls (5 : 2). Mean BMI (SE): LAGB 41.7 (1.0), RYGBP 43.6 (2.0), controls 41.1 (1.0) Von Mach 2004 Number: total 19, LAGB 9, RYGBP 4, controls 6 Mean age (SEM), years: LAGB 41.1 (2.2), RYGBP 44.5 (4.8), controls 49 (2.9) Sex (F : M): LAGB 6 : 3, RYGBP 4 : 0, controls 4 : 2 BMI (SEM): LAGB 41.0 (1.1), RYGBP 42.7 (2.2), controls 41.2 (1.2) Characteristics of target population: Patients with morbid obesity (BMI > 37) undergoing bariatric surgery. Controls were obese subjects who did not receive operations Exclusion criteria: not reported |
|
Plasma ghrelin concentration (data not extracted) BMI Fat mass Bone mineral content (data not extracted) |
Allocation to treatment groups: Observational study. Patients opting for surgical treatment chose LAGB or RYGBP after detailed discussion of the individual situation. Patients who attended a diet consultation served as controls. Reasons for control group not undergoing surgery are not given in Stoeckli 2004 Blinding of outcome assessors: Not reported Comparability of treatment groups: No significant differences between groups for age, BMI and laboratory parameters Method of data analysis: Data expressed as means (SE). Spearman correlation tests, unpaired Student’s t tests (two-sided) and Mann–Whitney U tests used for comparison of single time points among groups, depending on whether data showed a normal distribution. Repeated measures anova performed for serial measurements. Bonferroni correction applied when multiple comparisons made among groups Sample size/power calculation: Not reported Attrition/dropout: Not reported. Additional information from the author: ‘the papers are from the same study, and depending on the available samples, the n of patients may have been slightly different’ |
Table of results
| Weight change | QoL/comorbidity | Events/procedures (complications, reoperations) |
|---|---|---|
|
Stoeckli 2004 and Christ-Crain 2006: MEAN BMI (SE, SD) Baseline: LAGB 41.7 (1.0, SD 2.8), RYGBP 43.6 (2.0, SD 4.4), controls 41.1 (1.0, SD 2.6) 24 months: LAGB 33.2 (1.7, SD 4.7), RYGBP 32.9 (3.0, SD 6.7), controls 41.0 (1.4, SD 3.4) (p < 0.001 controls vs LAGB, and controls vs RYGBP) Stoeckli 2004 Change in BMI (majority estimated from figure) 3 months: LAGB – 5, RYGBP – 6.5*#, controls – 1.5 6 months: LAGB – 6**, RYGBP – 9*##, controls – 1.7 12 months: LAGB – 8**, RYGBP – 11.2*, controls – 0.3 24 months: LAGB – 8**, RYGBP – 10.8*, controls – 0.3 (0.4) *p < 0.01 vs controls, **p < 0.001 vs controls (Note: these p-values seem incorrect) #p < 0.05 RYGBP vs LAGB, ##p < 0.01 RYGBP vs LAGB Von Mach 2004 BMI Baseline: LAGB 41.0, RYGBP 42.7, control 41.2 3 months: LAGB 36, RYGBP 36, control 40. (Estimated from figure). 6 months: LAGB 35, RYGBP 33, control 39, p < 0.05 LAGB and RYGBP vs controls. (Estimated from figure.) 12 months: LAGB 34, RYGBP 30, control 41, LAGB and RYGBP p < 0.05 vs controls. (Estimated from figure.) 24 months: LAGB 34.0, RYGBP 30.5, control 41.4, LAGB and RYGBP p < 0.05 vs controls Mean body weight, kg (SEM). Baseline: LAGB 117.2 (2.5), RYGBP 113.3 (4.9), control 113.5 (4.9).% change: LAGB – 16.0 (3.2)*, RYGBP – 28.6 (3.6)*, control + 0.5 (1.2). *p < 0.01 Total fat mass, kg (SEM). Baseline: LAGB 63.7 (2.2), RYGBP 63.6 (2.2), control 64.8 (4.7).% change: LAGB – 33.9 (5.3)*, RYGBP – 51.0 (5.2)*, control + 2.5 (3.3). *p < 0.001 |
Not reported | Not reported |
Quality criteria (CRD Report 4)
| Quality item | Yes/No/Uncertain | Methodological comments |
|---|---|---|
| Cohort studies | ||
| 1. Is there sufficient description of the groups and the distribution of prognostic factors? | Yes | |
| 2. Are the groups assembled at a similar point in their disease progression? | Unclear | |
| 3. Is the intervention/treatment reliably ascertained? | Yes | |
| 4. Were the groups comparable on all important confounding factors? | Yes | |
| 5. Was there adequate adjustment for the effects of these confounding variables? | Not applicable | |
| 6. Was outcome assessment blind to exposure status? | Uncertain | |
| 7. Was follow-up long enough for the outcomes to occur? | Yes | |
| 8. What proportion of the cohort was followed-up? | Uncertain | |
| 9. Were dropout rates and reasons for dropout similar across intervention and unexposed groups? | Uncertain |
Appendix 6 Data extraction tables: gastric bypass versus vertical banded gastroplasty (versus gastric banding)
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Agren 198973 (abstract only) Sweden Single-centre, RCT |
Total: 77 Characteristics of target population: Morbidly obese Exclusion criteria: Not reported Participants: Mean preoperative weight 123.6, BMI 42.8 |
Treatment arms:
|
Primary and secondary outcome measures used: mortality, morbidity, excess weight loss Method of assessing outcomes: not stated Length of follow-up: 12 and 18 months |
Allocation to treatment groups: randomised, but method not stated Blinding of outcome assessors: not reported Comparability of treatment groups: states groups comparable in age, sex, preoperative weight and ideal body weight. Data not presented Method of data analysis: standard deviation or CI not reported Sample size/power calculation: not reported Attrition/dropout: not reported Generalisability: eligibility criteria not reported Outcome measures: per cent excess weight loss Intercentre variability: single centre study Conflict of interests: funding support not mentioned |
Table of results
| Weight change | QoL and comorbidities | Events/procedures (complications, reoperations) |
|---|---|---|
|
Mean excess weight loss: 12 months: loop GBP 76.6%; VBG 58.3%, GBand 62.2% 18 months: loop GBP 76.6%; VBG 59.8%, GBand 62.5%. p not reported |
Not assessed |
Mortality: one patient (group not specified) Morbidity: states low and not significantly different, but data not presented One VBG: reoperation for staple-line disruption 11 (44%) GBand: reoperation, mainly for inadequate weight loss or nutritional disorder and increased vomiting which commonly occurred without stomal stenosis |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Unclear | Randomised, but method not stated |
| Allocation concealment? | Unclear | |
| Blinding of outcome assessors? | Unclear | |
| Blinding of participants on self-reported outcomes? | n/a | |
| Incomplete outcome data addressed? Weight loss | Unclear | Not reported |
| Incomplete outcome data addressed? QoL | n/a | |
| Incomplete outcome data addressed? Comorbidity | n/a | |
| Free of selective outcome reporting? | Unclear | Limited information as reported in abstract only. Reports % excess weight loss; SD or CI not reported |
| Free of other sources of bias? | Unclear | Limited information as reported in abstract only. |
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Howard 1995120 Design: single centre, RCT Follow-up: 12 to 78 months. |
Country: USA Number: Total 42, GBP 20, VBG 22 Age (mean): GBP 38.1 years (SE 1.9), VBG 36.5 years (SE 2.3) Sex: GBP 75% female, VBG 22% female Mean Max. weight: GBP 154 kg (SE 26), VBG 142 kg (SE 17) p = 0.09 Mean excess preoperative weight: GBP 71 kg (SE 19), VBG 67 kg (SE 15) p = 0.41 Characteristics of target population: Class IV obesity (BMI > 40); < 50 years; attempts at non-operative weight loss; realistic view of operation and likely impact on life Exclusion criteria: BMI < 40, 50 years or older, psychiatrically unstable |
|
Weight change (preoperative and postoperative) % excess weight loss compared to maximum excess weight % lost > 50% and > 75% of excess weight Early postoperative complications (wound dehiscence, infection and thromboembolism) |
Allocation to treatment groups: randomised, method not stated Blinding: not stated Comparability of treatment groups: no significant difference (p > 0.05) between the groups with respect to age, gender, maximum or preoperative weight. Both groups equal with respect to proportion of super-obese (BMI > 50) Method of data analysis: not ITT. Statistical comparison between the groups made using Student’s t test and a p-value of less than 0.05 was considered significant Sample size/power calculation: not stated Attrition/dropout: two of 44 (5%) patients withdrew from study within 4 weeks of surgery, and only 12 patients followed up for 60 months [GBP 6/20 (30%), VBG 6/22 (28%)] Generalisability: excluded patients with BMI < 40, and age ≥ 50 years, and those psychiatrically unstable Outcome measures: mean weight loss as a percentage of weight loss relative to patients’ maximum excess weight, and percentage of excess weight lost Intercentre variability: setting not known Conflict of interests: not mentioned |
Table of results
| Weight change | QoL/comorbidities | Events/procedures (complications, reoperations) |
|---|---|---|
|
% excess weight loss compared to maximum excess weight (data from figure): 12 months GBP 78%, VBG 52%, p < 0.05 60 months GBP (n = 6) 70%, VBG (n = 6) 37%, p < 0.05 % patients with at least 50% of excess weight loss (data from figure): 12 months GBP 100% (20/20), VBG 55% (12/22) (p not stated) 60 months GBP 100% (6/6), VBG 0% (0/6) (p not stated) % patients with more than 75% of excess weight loss: 12 months GBP 60% (12/20), VBG 18% (4/22) (p not stated) 60 months GBP 50% (3/6), VBG 0% (0/6) (p not stated) Data from figure |
Not assessed |
Early complications: Deaths GBP 0, VBG 0; wound infection one (2%) super-obese patient. Late complications: Symptomatic ulcer disease GBP 25% (50% further surgery), VBG 0%; intraoperative cholecystectomy GBP 20%, VBG 14%; postoperative cholecystectomy VBG 29%; GBP 29% |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Unclear | Randomised, method not stated |
| Allocation concealment? | Unclear | |
| Blinding of outcome assessors? | Unclear | Not stated |
| Blinding of participants on self-reported outcomes? | n/a | |
| Incomplete outcome data addressed? Weight loss | Yes | Two of 44 (5%) patients withdrew from study within 4 weeks of surgery, and only 12 patients followed up for 60 months. Numbers at each follow-up are given. Reasons not given |
| Incomplete outcome data addressed? QoL | n/a | |
| Incomplete outcome data addressed? Comorbidity | n/a | |
| Free of selective outcome reporting? | Unclear | |
| Free of other sources of bias? | Unclear |
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Lee, 2004115 Design: RCT, single centre Follow-up: Mean 20 months (range 18 to 30) |
Country: Taiwan Number: total 80, LVBG 40, LBG 40 Mean age (SD): LVBG 32.5 years (7.8), LRYGBP 31.6 years (8.6) Sex (F : M): LVBG 29 : 11, LRYGBP 27 : 13 Mean weight: LVBG 119.0 kg (21.4), LRYGBP 120.7 kg (26.3) BMI: LVBG 43.14 (6.1), LRYGBP 43.18 (7.5) Previous abdominal surgery: LVBG 3, LRYGBP 5 Waist circumference: LVBG 123.7 cm (16.7), LRYGBP 123.3 cm (18.5) Systolic bp: LVBG 136 mmHg (16), LGB 136 mmHg (17) Diastolic bp: LVBG 87 mmHg (14), LRYGBP 86 mmHg (13) Blood glucose: LVBG 117 mg/dl (56), LRYGBP 106 mg/dl (35) Cholesterol: LVBG 207 mg/dl (34), LRYGBP 191 mg/dl (43) Triglyceride: LVBG 179 mg/dl (121), LRYGBP 171 mg/dl (128) GOT: LVBG 32 IU/l (22), LRYGBP 29 IU/l (19) GPT: LVBG 41 IU/l (33), LRYGBP 43 IU/l (29) Uric acid: LVBG 7.5 mg/dl (1.8), LRYGBP 7.1 mg/dl (1.8) Albumin: LVBG 4.5 mg/dl (0.3), LRYGBP 4.5 mg/dl (0.5) WBC: LVBG 8.3 (2.1), LRYGBP 8.9 (3.2) Haemoglobin: LVBG 13.8 g/dl (1.5), LRYGBP 13.6 g/dl (1.2) MCV: LVBG 87.6 fl (6.2), LRYGBP 87.7 fl (6.8) Characteristics of target population: Significant obesity > 5 years, BMI > 40 or BMI > 35 with comorbidities, documented past weight loss attempts, good motivation for surgery, age 18–59 years Exclusion criteria: Previous bariatric surgery, previous gastric surgery, large abdominal ventral hernia, pregnancy, psychiatric disease or BMI > 60 |
|
Perioperative clinical parameters: operative time, estimated blood loss, dosages required during hospital stay, length to postoperative flatus passage, hospital stay, early complications (occurring within 30 postoperative days), major complications (required interventional management and hospitalisation > 14 days), late complications (related to operation occurring after 30 days and requiring readmission) BMI % excess weight loss 36-item gastrointestinal quality of life index (GIQLI). Scored 0–4 (worst-best), max score 144. 4 domains |
Allocation to treatment groups: randomised using sealed envelopes Blinding of outcome assessors: not reported comparability of treatment groups: comparable in sex, age, mean weight, BMI and laboratory tests, differences all statistically non-significant Method of data analysis: ITT analysis. Expressed as mean (SD) or median (range). Analyses of differences between groups for demographic and operative data were performed using two-sample t tests or Fisher exact test for categorical data. Mann–Whitney U tests were performed for non-parametric data. Paired Student’s t test used to compare each item before and after surgery. Two-tailed t test used for comparison of total scores and scores in each subgroup, before operation and at follow-up Sample size/power calculation: not reported Attrition/dropout: not reported |
Table of results
| Weight change | QoL/comorbidity | Events/procedures (complications, reoperations) |
|---|---|---|
|
Mean BMI Baseline: LVBG 43.14, LRYGBP 43.18 3 months: LVBG 36.7, LRYGBP 35.6 6 months: LVBG 33.3, LRYGBP 31.8 9 months: LVBG 32.2, LRYGBP 30.7 12 months: LVBG 31.1, LRYGBP 29.6 24 months: LVBG 31.9, LRYGBP 28.5 Numbers of participants providing data for BMI outcome at different time points not reported Percentage excess weight loss 12 months: LRYGBP 62.9% (n = 40), LVBG 55.4% (n = 40) 24 months: LRYGBP 71.4% (n = 26), LVBG 53.1% (n = 27) |
Note: baseline data presented for both groups combined only GIQLI at 12 months Overall: preoperative 106.9, LVBG 106.4, LRYGBP 121 Symptoms domain: preoperative 63.7, LVBG 54.3, LRYGBP 60.9 Physical domain: preoperative 16.1, LVBG 20.9, LRYGBP 24 Emotional domain: preoperative 12.8, LVBG 14.7, LRYGBP 17.7 Social domain: preoperative 14.3, LVBG 16.5, LRYGBP 18.4 Significantly higher subtotals at follow-up were found for physical function, social function and emotional function domains in both groups. LVBG patients had a significant decrease in domain of symptoms, resulting in no improvement in total score LRYGBP scored better (p = 0.04 to p < 0.001) than LVBG in 7/19 symptom items, 4/5 emotional items, 1/7 physical items, 2/5 social items. LVBG scored better than LRYGBP in symptom of abdominal flatulence (p = 0.02) GIQLI score for each item (preoperative, follow-up LVBG, follow-up LRYGBP, p value LVBG vs LRYGBP) Abdominal pain: 3.3, 3.1, 3.4, p = ns Abdominal fullness: 2.7, 2.7, 2.7, p = ns Abdominal bloating: 3.2, 2.2**, 3.5, p = 0.02 Flatulence: 3.1, 2.4**, 1.8**, p = 0.02 Belching: 3.5, 2.7**, 3.2, p = 0.04 Abdominal noises: 3.6, 2.8**, 2.7**, p = ns Bowel frequency: 3.4, 3.1, 3.5, p = ns Enjoyed eating: 2.2, 2.1, 2.8, p = 0.01 Restricted eating: 2.8, 1.5***, 2.5, p = 0.001 Regurgitation: 3.6, 3.0*, 2.8**, p = ns Dysphagia: 3.9, 2.9**, 3.9, p = 0.001 |
Perioperative parameters Mean operative time, minutes: LVBG 126 (38), LRYGBP 209 (50), p < 0.001 Mortality: LVBG 0, LRYGBP 0, p = ns Conversion rate: LVBG 0, LRYGBP 1 (2.5%), p = ns Intraoperative blood loss, ml: LVBG 31 (77), LRYGBP 35 (26), p = ns Early postoperative complication: LVBG 1 (2.5%), LRYGBP 7 (17.5%), p < 0.05 Early complication – major: LVBG 0, LRYGBP 3 (7.5%) Early complication – minor: LVBG 1 (2.5%), LRYGBP 4 (10%) Postoperative flatus passage, days: LVBG 1.9 (0.6), LRYGBP 2.5 (1.2), p < 0.01 Analgesic use, units: LVBG 1.4 (1.5), LRYGBP 2.4 (3.0), p < 0.05 Postoperative stay, days: LVBG 3.5 (0.9), LRYGBP 5.7 (2.2), p < 0.001 Late complication (readmission): LVBG 2 (5%), LRYGBP 4 (10%), p = ns Complications details LRYGBP Major complications (three): two anastomotic leakage (5%), requiring reoperation by laparoscopy and open laparotomy, one abdominal abscess requiring percutaneous drainage and total parenteral nutrition Minor complications (four): upper gastrointestinal bleeding, sutured nasogastric tube, minor leakage from drainage tube |
|
Eating speed: 3.7, 2.3***, 3.7, p < 0.001 Nausea: 3.5, 3.1, 3.3, p = ns Diarrhoea: 3.2, 3.4, 3.1, p = ns Bowel urgency: 3.7, 3.7, 3.7, p = ns Constipation: 3.1, 2.3**, 3.7*, p < 0.001 Blood in stool: 3.7, 3.8, 3.8, p = ns Heartburn: 3.6, 3.4, 3.8, p = ns Incontinence: 3.9, 3.8, 4.0, p = ns Emotional items Coping with stress: 2.5, 2.7, 2.6, p = ns Sadness: 2.4, 2.9*, 3.7***, p = 0.01 Nervousness: 2.9, 2.9, 3.6**, p = 0.02 Frustration: 2.6, 3.1*, 3.9**, p = 0.01 Happiness: 2.4, 3.1**, 3.9***, p = 0.01 Physical items Fatigue: 2.6, 2.8, 3.4**, p = 0.05 Feeling unwell: 2.6, 2.8, 3.1*, p = ns Wake-up at night: 3.2, 3.4, 3.4, p = ns Appearance: 2.0, 3.6**, 4.0***, p = ns Physical strength: 1.9**, 2.9***, 3.1, p = ns Endurance: 1.7, 2.7**, 2.9**, p = ns Feeling unfit: 2.1, 2.7*, 3.1**, p = ns Social items Daily activities: 2.9, 3.1, 3.6*, p = 0.05 Leisure activities: 2.7, 3.5*, 3.9**, p = ns Bothered by treatment: 2.8, 3.2, 3.8**, p = 0.03 Personal relationship: 3.1, 3.4, 3.6, p = ns Sexual life: 2.8, 3.2, 3.5*, p = ns Compared with preoperative data, *p < 0.05, **p < 0.01, ***p < 0.001 |
Late complications (four, 10%): one anastomotic stricture requiring endoscopic dilatation, two marginal ulcer requiring blood transfusion and prolonged medication, one pyothorax 2 months postoperatively requiring percutaneous drainage LVBG Minor complication (one): wound infection related to a minimal staple-line leakage, healed within 14 days Late complications (two, 5%): reflux oesophagitis requiring medication with one case receiving laparoscopic revision surgery |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Unclear | Randomised using sealed envelopes |
| Allocation concealment? | Unclear | Not reported |
| Blinding of outcome assessors? | Unclear | Not reported |
| Blinding of participants on self-reported outcomes? | Unclear | Not reported |
| Incomplete outcome data addressed? Weight loss | Unclear | Not reported |
| Incomplete outcome data addressed? QoL | Unclear | Not reported |
| Incomplete outcome data addressed? Comorbidity | n/a | |
| Free of selective outcome reporting? | Unclear | |
| Free of other sources of bias? | Unclear |
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Design: single centre, RCT Follow-up: 3–6.5 years |
Country: Canada Number: total 106, VBG 54, RYGBP 52 Age (mean): VBG 38.8 years (SD 9.5), RYGBP 40.1 years (SD 7.7) Sex: not reported Weight (mean): VBG 278 lb (SD 41) (126 kg; SD 19), RYGBP 295 lb (SD 53) (134 kg; SD 24) BMI (mean): VBG 48.2 (SD 6.5), RYGBP 49.9 (SD 7.4) Characteristics of target population: Not stated Exclusion criteria: Not stated |
1. Vertical banded gastroplasty (VBG) (with a division between staple lines) 2. Roux-en-Y gastric bypass (RYGBP) (staple lines not divided) |
Success: BMI < 35 or < 50% excess weight and reoperation not required Reoperation defined as failure, regardless of ultimate outcome Mean length of follow-up Reoperation rates |
Allocation to treatment groups: randomisation took place at time of surgery. No other details Blinding: not stated Comparability of treatment groups: no significant differences in baseline characteristics (age, BMI and mean weight) Method of data analysis: differences in continuous variables evaluated using Student’s t test (two groups) or anova (more than two groups). Chi-squared used for categorical variables. Multiple linear regression and anova used to test differences with respect to change in BMI from baseline Sample size/power calculation: not stated Attrition/dropout: one patient possibly lost to follow-up after conversion to IGBP, but information contradictory Generalisability: inclusion/exclusion criteria not defined Outcome measures: mean BMI or weight loss after surgery not reported Intercentre variability: not mentioned Conflict of interests: funding information not given |
Table of results
| Weight change | QoL/comorbidities | Events/procedures (complications, reoperations) |
|---|---|---|
|
∼ 36 months Mean follow-up: VBG 38.6 months (SD 8.5); RYGBP 33.1 months (SD 12.4) Success rate (BMI < 35 or < 50% excess weight and no reoperation) VBG (31 remained with op) success rate 21 (39%) RYGBP (40 remained with op) success rate 30 (58%) VBG vs RYGBP p = 0.08 up to 78 months: Mean follow-up: VBG 70.9 months (SD 5.8); RYGB 66.5 months (SD 9.1) Success rate (BMI < 35 or < 50% excess weight and no reoperation) VBG (25 remained with operation) Success rate 9 (16%) RYGBP (32 remained with operation) Success rate 16 (34%) VBG vs RYGBP p = 0.112 |
Not assessed. |
Deaths: VBG 0, RYGBP 0 Conversions, Approx. 36 months: VBG 5 (9%) to normal, 18 (33%) to isolated gastric bypass (IGBP) RYGBP 0 to normal, 12 (23%) to IGBP Up To 6.5 years: VBG 5 (9%) to normal, 24 (44%) to IGBP RYGBP 1 (2%) to normal, 19 (37%) to IGBP Reoperation: total VBG 43% (23 patients), RYGBP 23% (12 patients); stenosis VBG 20% (11 patients), RYGBP 0%; enlarged orifice VBG 13% (7 patients), RYGBP 0%; staple-line fistula VBG 4% (2 patients), RYGBP 23% (12 patients); clinical failure VBG 4% (2 patients), RYGBP 0%; abscess VBG 2% (1 patient), RYGBP 0%; stomal ulcer VBG 0%, RYGBP 13% (7 patients, these were 7 of the 12 patients with staple-line fistula) |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Unclear | Randomisation took place at time of surgery. No other details |
| Allocation concealment? | Unclear | |
| Blinding of outcome assessors? | Unclear | Not stated |
| Blinding of participants on self-reported outcomes? | n/a | |
| Incomplete outcome data addressed? Weight loss | Unclear | One patient possibly lost to follow-up after conversion to IGBP, but information contradictory |
| Incomplete outcome data addressed? QoL | n/a | |
| Incomplete outcome data addressed? Comorbidity | n/a | |
| Free of selective outcome reporting? | Unclear | Reported success (BMI < 35 or < 50% excess weight and reoperation not required), did not report BMI or weight loss |
| Free of other sources of bias? | Unclear |
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Design: single centre, RCT Follow-up: 24 months |
Country: Sweden Number: total originally 100, but after randomisation 13 participants expressed a preference (nine for LRYGBP, four for LVBG) and were excluded. A further four participants were found to have a BMI > 50 and were also excluded. Therefore 83 remained, 37 randomised to LRYGBP, 46 to LVBG Note: in related paper109 baseline weight, BMI and age data are very slightly different to those reported below. For weight and BMI the re ason for the discrepancy is unclear, but maybe the result of a reporting error, or rounding error. For age the related paper reports mean (SD) whereas median and range is reported below Age (median, range): LRYGBP 37 years, 34–61 years; LVBG 34 years, 26–60 years Sex (M : F): LRYGBP 12 : 25; LVBG 10 : 36 BMI [mean (SD)]: LRYGBP 42.7 (4.0); LVBG 42.1 (4.2) Weight [mean (SD) kg]: LRYGBP 123.9 (16.4) LVBG 123.3 (15.0) States no statistically significant differences between groups at baseline Recruitment: March 2000 to April 2001 Characteristics of target population: BMI > 40 or > 35 with obesity-associated morbidity, and BMI < 50 Exclusion criteria: BMI > 50 |
|
Perioperative complications Change in BMI (states primary outcome) Excess body weight loss Remedial surgical intervention (states primary outcome) Oxygen saturation, forced vital capacity, peak expiratory flow, grip force and time to mobilisation after surgery (these results not data extracted) Related paper109 reports on body composition, energy expenditure and dietary intake (not extracted) |
Method of data analysis: the results for the 17 excluded participants were analysed separately Data given as median with range, or mean with 95% confidence intervals. p < 0.05 considered statistically significant Sample size/power calculation: reported that sample size was determined by calculations based on previous data on weight change and postoperative pulmonary complications, which indicated the need for about 80 patients (40 per group) to give sufficient power to demonstrate a difference at the 95% significance level (group sizes were 37 and 46) Conflict of interests: not stated Supported in part by a grant from the Research Council of the Västra Götaland Region, Sweden |
Table of results
| Weight change | QoL/comorbidity | Events/procedures (complications, reoperations) |
|---|---|---|
|
Mean BMI at 1 and 2 years: Results [mean (SD)] presented in a figure only, mean values below estimated by researcher. Text states weight loss significantly better after LRYGP but p-values not reported for the BMI outcome Mean BMI at 1 year: LRYGBP 29 (n = 36/37); LVBG 32 (n = 39/46). p-value not reported Mean BMI at 2 years: LRYGBP 28 (n = 36/37); LVBG 32 (n = 35/46). p-value not reported % excess weight loss at 1-year (mean (SD)): LRYGBP 78.3 (20.0)%; LVBG 62.9 (28.4)%, p = 0.009 % excess weight loss at 2 years [mean (SD)]: LRYGBP 84.4 (22.1)%; LVBG 59.8 (29.6)%, p < 0.001 Proportion achieving excess weight loss of at least 50% without remedial surgery after 2 years: 34/36 LRYGBP, 21/35 LVBG |
Conversions to open surgery perioperatively: None Operating time [mean (SD)]: 138 (41) minutes LRYGBP; 105 (35) minutes LVBG, p < 0.001 Early reoperations: five LRYGBP (three haemorrhage, one for stenosis, one suspected leak); 1 LVBG (suspected leak), not significantly different between groups p = 0.080 Perioperative complications (in addition to conversion to open surgery and reoperations above): LRYGBP two minor bleeding, one deep infection; LVBG four minor bleeding, one deep infection Thrombotic complications – none Pulmonary complications – no difference between groups, p = 0.888 Median hospital stay: LRYGBP 3 days (range 2–15 days), LVBG 3 days (range 1–16 days) Remedial surgical intervention: 0 LRYGBP; eight LVBG (four in the first year, four in the second. Conversion to RYGBP. Due to one migration of outlet restricting band, five vomiting and insufficient weight loss, two vomiting and excessive weight loss) One LRYGBP had an intra-abdominal abscess after discharge Results (perioperative complications, postoperative respiratory function, time to mobilisation, weight change over 2 years,% excess weight loss) also presented for the 17 excluded patients |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Yes | Randomisation by a computer program that stratified for weight, BMI, age and associated morbidity |
| Allocation concealment? | Unclear | Not described |
| Blinding of outcome assessors? | Unclear | Not described |
| Blinding of participants on self-reported outcomes? | n/a | No participant self-reported outcomes |
| Incomplete outcome data addressed? Weight loss | Yes |
Reasons for missing outcome data given and unlikely to be related to true outcome. Missing data for similar reasons across groups (other than the four LVBG participants reoperated on) Follow-up rate was 97.6%. One paper108 states that one patient in each group was lost to follow-up 1 year after surgery and two patients who had undergone LVBG could not be contacted at the 2-year follow-up. Two women were pregnant at the 1-year follow-up and another two were pregnant at the 2-year follow-up. Their weights were excluded from the analysis. Figure 1 in reference 108 indicates 36/37 LRYGBP and 39/46 LVBG at 1-year follow-up, and 36/37 LRYGBP and 35/46 LVBG at 2-year follow-up. This statement is in agreement with that in the second paper:109 At the 1-year follow-up four patients randomised and operated on with LVBG had been reoperated on (conversion to GBP), and two women were pregnant. These patients were excluded from the analysis. In addition, one patient from each group was lost to follow-up therefore 1-year follow-up was for 36 LRYGBP and 39 LVBG At the 1-year follow-up there was a tolerance of ± 6 weeks |
| Incomplete outcome data addressed? QoL | n/a | |
| Incomplete outcome data addressed? Comorbidity | n/a | |
| Free of selective outcome reporting? | Unclear | Primary outcomes not prespecified. Some outcomes listed in the methods but unclear whether these match some of the outcomes reported because different terminology is used, e.g. methods lists Major haemorrhage and Minor haemorrhage with definitions for both, whereas results reports on Bleeding and Minor bleeding with no definitions provided |
| Free of other sources of bias? | Unclear | Uncertainty around the effect of the 17 patients who were excluded after randomisation either because they expressed a preference about the surgery they received, or were found to have a BMI > 50 |
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Sugerman 1987123 Design: single centre, RCT Follow-up: 3 years |
Country: USA Number: total 40, RYGBP 20, VBG 20 Age: RYGBP 38 years (± 11), VBG 38 years (± 9) Sex: RYGBP 90% female, VBG 90% female % ideal weight: RYGBP 213% (± 49), VBG 225% (± 41) Characteristics of target population: More than 100 lb (45 kg) above ideal weight, 1959 Metropolitan Life Insurance tables. Failed to lose weight by supervised dietary programme(s) or had a significant medical problem related to obesity (respiratory insufficiency, insulin-dependent adult-onset diabetes, pseudo-tumour cerebri, etc.) Exclusion criteria: none reported |
|
Weight loss Percentage weight lost Percentage excess weight lost Percentage ideal body weight achieved Mortality Complications |
Allocation to treatment groups: feasibility of performing either procedure determined at laparotomy. Cards designating each operation were combined in groups of five, shuffled, and a card selected ‘blindly’. Blinding: not stated Comparability of treatment groups: No differences in baseline characteristics of groups (age, sex, ideal body weight, percentage of ideal body weight) Method of data analysis: not ITT. Analysis of covariance or Student’s t test for unpaired data Sample size/power calculation: not stated Attrition/dropout: VBG: one patient lost to follow-up immediately after surgery, one patient fatally stabbed at 25 months. Two patients converted to RYGBP, within 1 year and at 18 months and excluded from further analysis. Number of patients analysed were: 1 year, 19 RYGBP, 18 VBG; 2 year, 18 RYGBP, 17 VBG; 3 year, 18 RYGBP, 16 VBG Generalisability: Inclusion criteria described Outcome measures: appropriate outcome measures used Intercentre variability: not applicable Conflict of interests: No funding information provided Other: Study stopped after 9 months when a difference (p < 0.05) noted in favour of RYGBP |
Table of results
| Weight change | QoL/comorbidities | Events/procedures (complications, reoperations) |
|---|---|---|
|
Percentage ideal body weight (SD): 12 months RYGBP 138% ± 32; VBG 176% ± 41 (p < 0.01) 24 months RYGBP 139% ± 32; VBG 178% ± 41 (p < 0.01) 36 months RYGBP 142% ± 37; VBG 180% ± 44 (p < 0.01) Weight loss (SD) ( kg ): 12 months RYGBP 43.5 kg ± 11.3; VBG 32.2 kg ± 10.9 (p < 0.001) 24 months RYGBP 43.5 kg ± 15.4; VBG 30.4 kg ± 12.2 (p < 0.001) 36 months RYGBP 41.3 kg ± 12.7; VBG 27.2 kg ± 14.5 (p < 0.01) per cent weight lost: 12 months RYGBP 33% ± 7; VBG 22% ± 8 (p < 0.001) 24 months RYGBP 33% ± 9; VBG 22% ± 9 (p < 0.001) 36 months RYGBP 32% ± 9; VBG 20% ± 10 (p < 0.01) per cent excess weight lost: 12 months RYGBP 68% ± 17; VBG 43% ± 18 (p < 0.001) 24 months RYGBP 66% ± 29; VBG 39%± 24 (p < 0.001). (From figure) 36 months RYGBP 62% ± 18; VBG 37% ± 19 (p < 0.001). (From figure) per cent decrease in excess weight (SD) (n) for sweets eaters vs non-sweets eaters: RYGBP 12 months: sweet eaters 69% ± 12 (n = 12), non-sweet eaters 67% ± 17 (n = 7), p = ns 24 months: sweet eaters 62% ± 11 (n = 11), non-sweet eaters 75% ± 19 (n = 7), p = ns 36 months: sweet eaters 59% ± 11 (n = 11), non-sweet eaters 71% ± 21 (n = 7), p = ns VBG 12 months: sweet eaters 36% ± 13 (n = 12), non-sweet eaters 57% ± 18 (n = 6), p < 0.05 24 months: sweet eaters 35% ± 14 (n = 11), non-sweet eaters 53% ± 22 (n = 6), p < 0.05 36 months: sweet eaters 32% ± 18 (n = 11), non-sweet eaters 50% ± 21 (n = 5), p < 0.05 |
Not assessed |
Mortality: RYGBP two (10%), 3 days and 12 months (both assumed arrhythmia) No significant deficiencies in most vitamins, electrolytes, renal or liver function tests. RYGBP lower vitamin B12 levels (286 ± 149 pg/ml) than VBG (461 ± 226) at 24 months (p < 0.05) RYGBP: 25% intractable vomiting and stomal stenosis, 5% marginal ulcer of jejunal side of gastrojejunostomy VBG: 5% superficial stomal erosions Conversions from VBG to RYGBP: 5% at 1 month (one patient disrupted vertical staple line), 5% at 18 months (one patient failed to lose weight because of eating sweets and high starch foods), 10% at 38 months (two patients failed to lose weight) |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Yes | Feasibility of performing either procedure determined at laparotomy. Cards designating each operation were combined in groups of five, shuffled, and a card selected ‘blindly’ |
| Allocation concealment? | Unclear | |
| Blinding of outcome assessors? | Unclear | Not stated |
| Blinding of participants on self-reported outcomes? | n/a | |
| Incomplete outcome data addressed? Weight loss | Yes | One patient lost to follow-up immediately after surgery, one patient fatally stabbed at 25 months. Two patients converted to RYGBP, within 1 year and at 18 months and excluded from further analysis. Number of patients analysed were: 1 year 19 RYGBP, 18 VBG; 2 years 18 RYGBP, 17 VBG; 3 years 18 RYGBP, 16 VBG |
|
Incomplete outcome data addressed? QoL |
n/a | |
| Incomplete outcome data addressed? Comorbidity | n/a | |
| Free of selective outcome reporting? | Unclear | |
| Free of other sources of bias? | No | Groups of five cards used, unclear exactly what this means but may refer to blocked randomisation |
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
VanWoert 1992106 (abstract only) USA Single-centre, RCT Length of follow-up: 36 months |
Total: 32 Characteristics of target population: BMI > 40 Exclusion criteria: Not reported Participants (mean ± SD): GBP: Max weight % IBW 228 ± 55, BMI 52 ± 10, age 38 ± 8, M : F 4 : 11 VBG: Max weight % IBW 222 ± 27, BMI 51 ± 6, age 38 ± 10, M : F 3 : 14 |
Treatment arms: 1. Gastric bypass (GBP) 2. Vertical banded gastroplasty (VBG) |
Primary and secondary outcome measures used: % of IBW, mortality, major operative complications Method of assessing outcomes: not stated |
Allocation to treatment groups: randomised, but method not stated Blinding of outcome assessors: not reported Comparability of treatment groups: similar reported characteristics Method of data analysis: mean % IBW reported, no standard deviation or CI reported Sample size/power calculation: not reported Attrition/dropout: not reported General comments Generalisability: eligibility criteria not reported Outcome measures: % IBW reported Intercentre variability: single centre study Conflict of interests: funding support not mentioned |
Table of results
| Weight change | QoL/comorbidities | Events/procedures (complications, reoperations) |
|---|---|---|
|
% IBW at 36 months: GBP 121%, VBg 123%, p = ns |
Not assessed |
Mortality: no deaths Major late operative complications: Cholelithiasis: GBP 13%, VBG 24% Peptic gastro-oesophagitis: GBP 33%, VBG 18% |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Unclear | Not reported |
| Allocation concealment? | Unclear | |
| Blinding of outcome assessors? | Unclear | |
| Blinding of participants on self-reported outcomes? | n/a | |
| Incomplete outcome data addressed? Weight loss | Unclear | Not reported |
| Incomplete outcome data addressed? QoL | n/a | |
| Incomplete outcome data addressed? Comorbidity | n/a | |
| Free of selective outcome reporting? | Unclear | Limited data as reported in abstract only. Reports % ideal body weight, no SD or CI |
| Free of other sources of bias? | Unclear | Limited information as reported in abstract only |
Appendix 7 Data extraction tables: gastric bypass (non-banded) versus banded gastric bypass
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Bessler et al. 2007118 Design: single centre, RCT Follow-up: up to 36 months |
Country: USA Number: total 90 (out of 278 patients who underwent surgery during the recruitment period) Banded GBP n = 46 Non-banded GBP n = 44 Age (years): banded GBP 40.6 ± 7.4; non-banded GBP 42.6 ± 7.2. p = ns Sex (% women): banded GBP 56.5; non-banded GBP 73.8. p = 0.09 BMI: Banded GBP 59.4 ± 7.3; non-banded GBP 59.7 ± 7.1. p = ns Weight: not reported Hypertension (%): banded GBP 50; non-banded GBP 46. p = ns Diabetes mellitus (%): banded GBP 26; non-banded GBP 26. p = ns Hyperlipidaemia (%): banded GBP 31; non-banded GBP 30. p = ns Arthritis (%): banded GBP 91; non-banded GBP 72. p < 0.05 Gastro-oesophageal reflux disease (GERD) (%): banded GBP 39; non-banded GBP 43. p = ns Stress urinary incontinence (%): banded GBP 27; non-banded GBP 36. p = ns Characteristics of target population: BMI > 50 Exclusion criteria: Patients who had undergone previous gastric surgery. Minors |
Surgery took place from June 2001 and July 2005 by one surgeon |
% excess weight lost, improvement or resolution of comorbidities; incidence of complications Assessments at 6, 12, 24 and 36 months postoperatively Postoperative gastrointestinal symptoms were scored according to a subjective scale where 0 = none, 1 = mild, 2 = moderate, 3 = severe |
Method of data analysis: where point estimates are provided the paper does not state which measure is being presented. However, it is presumed that the data presented are means. A measure of variability around the point estimate (presumed to be ± SD although not stated) is provided for baseline data. No measure of variability is provided for outcome measures. p < 0.05 was considered significant Sample size/power calculation: not reported Conflict of interests: reported, the primary author is a consultant to, and has received research support from Ethicon Endo-Surgery. This author is also a consultant to, and receives marketing support from Inamed (LabBand) and is a consultant to USGI, Intrapace, Metacure, and Bard/Davol |
Table of results
| Weight change | QoL/comorbidity | Events/procedures (complications, reoperations) |
|---|---|---|
|
% EWL at 12 months: banded GBP 64; non-banded GBP 57.4. p = ns % EWL at 24 months: banded GBP 64.2; non-banded GBP 57.2. p = ns % EWL at 36 months: banded GBP 73.4; non-banded GBP 57.7. p < 0.05 Achieving a BMI of < 35 at 12 months (%): banded GBP 47.8; non-banded GBP 41.0. p not reported Achieving a BMI of < 35 at 24 months (%): banded GBP 52.9; non-banded GBP 37.5. p not reported |
Resolution of comorbidities: study does not state which follow-up period is being reported, or numerators and denominators Hypertension (%): banded GBP 79; non-banded GBP 90. p = ns Resolution of diabetes mellitus (%): banded GBP 92; non-banded GBP 98. p = ns Hyperlipidaemia (%): banded GBP 50; non-banded GBP 62. p = ns Arthritis (%): banded GBP 76; non-banded GBP 91. p = ns Gastro-oesophageal reflux disease (GERD) (%): banded GBP 94; non-banded GBP 83. p = ns Stress urinary incontinence (%): banded GBP 83; non-banded GBP 93. p = ns |
Mortality: 0 Total complications [n (%)]: banded GBP 12 (26); non-banded GBP 13 (29.5). p = ns Wound infection [n (%)]: banded GBP 7 (15.2); non-banded GBP 5 (11). p = ns Anastomotic leak [n (%)]: banded GBP 0; non-banded GBP 2 (4.8). p = ns Pneumonia (n (%)): banded GBP 1 (2.1); non-banded GBP 1 (2.2). p = ns Pulmonary embolism [n (%)]: banded GBP 0; non-banded GBP 0. Small bowel obstruction [n (%)]: banded GBP 1 (2.1); non-banded GBP 1 (2.2). p = ns Band erosion/slippage/removal [n (%)]: banded GBP 0; non-banded GBP N/A. Other [n (%)]: banded GBP 3 (6.5); non-banded GBP 4 (9.0). p = ns Gastrointestinal symptoms (average scores) Dumping: banded GBP 0.12; non-banded GBP 0.05. p = ns (p = 0.06) Emesis: banded GBP 0.35; non-banded GBP 0.13. p = 0.0002 Diarrhoea: banded GBP 0.11; non-banded GBP 0.13. p = ns Constipation: banded GBP 0.07; non-banded GBP 0.08. p = ns Flatulence: banded GBP 0.22; non-banded GBP 0.13. p = ns Abdominal pain: banded GBP 0.04; non-banded GBP 0.06. p = ns Food intolerance (%): banded GBP 79; non-banded GBP 33. p < 0.05 (Study does not state which follow-up period is being reported or n-values) |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Unclear | Sequence generation not reported. Paper states ‘Randomisation was performed by opening 1 of 100 sequentially numbered sealed envelopes’ but it is not clear whether any process was used to generate the sequence of items contained within these envelopes |
| Allocation concealment? | Yes | Group allocation was concealed within 100 sequentially numbered sealed envelopes containing the words ‘banded’ or ‘non-banded; (50 each in random order) on a folded piece of paper. However, it is not clear whether the envelopes were opaque |
| Blinding of outcome assessors? | Unclear | Not reported. Assume no blinding (although it would have been possible to blind patients and outcome assessors in this study) |
| Blinding of participants on self-reported outcomes? | Unclear | Uncertain how gastrointestinal symptom scores were ascertained. Methods imply that these were scored by the study authors ‘We scored…’ but presumably participants would have reported on these outcomes to the study investigators. Presume participants were not blinded |
| Incomplete outcome data addressed? Weight loss | Unclear | Ninety randomised out of 278. Reasons not given. Numbers not reported. % EWL at 36 months – the paper reports a significant difference between groups but states ‘However, this was calculated from the small number of patients reaching the 36-month follow-up period.’ The number of participants at the 36-month follow-up is not stated. There were no significant differences between the groups for this outcome at earlier time points. Sample sizes not reported for any outcome measures. In the discussion the authors state ‘our total rate of follow-up was close to 90%’, but goes on to say ‘the follow-up at 36 months included a limited number of patients’ |
| Incomplete outcome data addressed? QoL | n/a | |
| Incomplete outcome data addressed? Comorbidity | Unclear | As above |
| Free of selective outcome reporting? | No | % EWL reported at 6, 12, 24 and 36 months (significant difference at 36 months). BMI reported at 12 and 24 months only, p values not reported. SDs not reported |
| Free of other sources of bias? | Unclear |
Appendix 8 Data extraction tables: laparoscopic gastric bypass versus laparoscopic adjustable gastric banding
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Angrisani et al (2007)107 Design: single centre, RCT Follow-up: 60 months |
Country: Italy Number: total 51, LRYGBP 24, LAGB 27 Age [mean ± SD (range)]: LRYGBP 34.1 ± 8.9 (21–50) years; LAGB 33.8 ± 9.1 (21–50) years Sex (M : F): LRYGBP 4 : 20; LAGB 5 : 22 BMI [mean ± SD (range)]: LRYGBP 43.8 ± 4.1 (38.9–48.9); LAGB 43.4 ± 4.2 (38.1–49.2) Weight [mean ± SD (range) kg]: LRYGBP 118.2 ± 13.2 (92–152); LAGB 117.1 ± 12.8 (95–147) Comorbidities reported below Characteristics of target population: BMI > 35 to < 50, age > 16 years, but < 50 years Exclusion criteria: history of hiatal hernia, previous major abdominal surgery |
|
Mortality Conversion to open procedure Postoperative complications leading to reoperation Hospital stay Weight loss and percentage of excess weight loss BMI and decrease in BMI Comorbidities Operative time |
Method of data analysis: states not an ITT analysis Sample size/power calculation: not reported Conflict of interests: states none |
Table of results
| Weight change | QoL/comorbidity | Events/procedures (complications, reoperations) |
|---|---|---|
|
Mean weight at 5 years (range 60–66 months): LRYGBP 84 kg, LAGB 97.9 kg, p < 0.001 Mean weight at 12 months: LRYGBP 92.8 kg; LAGB 102.4 kg Mean weight at 36 months: LRYGBP 83.5 kg; LAGB 98.7 kg Mean BMI at 5 years (range 60–66 months): LRYGBP 29.8; LAGB 34.9, p < 0.001 Mean BMI at 12 months: LRYGBP 35.4; LAGB 38.7 Mean BMI at 36 months: LRYGBP 29.1; LAGB 35.6 % Excess weight loss at 12 months: LAGB 34.7, LRYGBP 51.3 % Excess weight loss at 36 months: LAGB 47.3, LRYGBP 67.3 % Excess weight loss at 5-years (range 60–66 months): LRYGBP 66.6%; LAGB 47.5%, p < 0.001 Weight loss failure (BMI > 35 at 5 years): LRYGBP 1/24 (4.2%); LAGB 9/26 (34.6%), p < 0.001 BMI < 30 at 5 years: LRYGBP 15/24 (62.5%); LAGB 3/26 (11.5%), p < 0.001 |
Comorbidities. Baseline: LRYGBP two hyperlipaemia, one hypertension, one Type 2 diabetes; LAGB three hypertension, one sleep apnoea At 5-year reports diabetes, sleep apnoea and hyperlipaemia resolved |
Mortality: none Reoperation: LRYGBP 3/24 (12.5%) (each for a potentially lethal complication); LAGB 4/26 (15.2%) (two pouch dilatation, two band removal because of inadequate weight loss: one of these was converted to biliopancreatic diversion, three waiting list for LRYGBP) Early complications (occurring < 30 days postoperatively): LRYGBP 1/24 (4.2%) posterior pouch leak intraoperatively causing conversion to open surgery, one (4.2%) sepsis caused by jejunal perforation (sutured and intestine resected). LAGB: none Late complications: LRYGBP one internal hernia/small bowel obstruction at 15 months; LAGB 2/26 (7.6%) gastric pouch dilatation (treated by band removal) Mean operative time: LRYGBP 220 ± 100 minutes; LAGB 60 ± 20 minutes, p < 0.001 Mean hospital stay: LRYGBP 4 ± 2 days, LAGB 2 ± 1 days, p < 0.05. One LRYGBP required intensive care stay of 40 days |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Unclear | Described as randomised but no detail of the method used to generate the randomisation sequence |
| Allocation concealment? | Unclear | Randomisation by sealed envelopes but no further details |
| Blinding of outcome assessors? | Unclear | Blinding of outcome assessors not reported |
| Blinding of participants on self-reported outcomes? | n/a | Patients were informed of the operation to which they had been randomised preoperatively, but no self-reported outcomes |
| Incomplete outcome data addressed? Weight loss | Yes | Eight patients were excluded after randomisation because they refused to undergo the procedure to which they had been assigned (five LRYGBP, three LAGB); one LAGB reported to be lost to follow-up |
| Incomplete outcome data addressed? QoL | n/a | |
| Incomplete outcome data addressed? Comorbidity | Yes | |
| Free of selective outcome reporting? | Unclear | Outcomes listed in methods section all reported in results but no way to check if all results reported in protocol are reported in paper |
| Free of other sources of bias? | Unclear | Authors state that for LRYGBP they were in the early phase of the learning curve, whereas for LAGB approximately 150 people had been operated by the senior author |
Appendix 9 Data extraction tables: laparoscopic Roux-en-Y gastric bypass versus laparoscopic sleeve gastrectomy
Characteristics of included study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Karamanakos 2008125 Design: single centre, RCT Follow-up: 12 months |
Country: Greece Number: total 32, LRYGBP 16, LSG 16 Age, years [mean (SD, range)]: LRYGBP 37 (8.25, 21–55), LSG 30.6 (7.8, 19–50), p = 0.023 Sex (M : F): LRYGBP 4 : 12, LSG 1 : 15 BMI [mean (SD, range)]: LRYGBP 46.6 (3.7, 40.2–51.9), LSG 45.1 (3.6, 36.8–51.1) Weight, kg [mean (SD, range)]: LRYGBP 125.2 (14.7, 100–150), LSG 122.1 (18.1, 96–160) LRYGBP: two diabetes mellitus, one anaemia, five hypercholesterolaemia, five hypertriglyceridaemia LSG: one glucose intolerance, three anaemia, three hypercholesterolaemia, three hypertriglyceridaemia Characteristics of target population: not reported Exclusion criteria: chronic medical or psychiatric illness, substance abuse, previous gastrointestinal surgery |
Gastric sleeve tube 40–60 ml remained, 85% of stomach excised |
BMI % EWL The following not data extracted: Ghrelin levels Peptide-YY levels Appetite |
Method of data analysis: data expressed as mean (SD). Differences between means evaluated using analysis of variance or Student’s t test. Significance at p < 0.05 Sample size/power calculation: not reported Conflict of interests: not reported |
Table of results
| Weight change | QoL/comorbidity | Events/procedures (complications, reoperations) |
|---|---|---|
|
BMI at 12 months [mean (SD)]: LRYGBP: 31.5 (3.4) LSG: 28.9 (3.6), p = 0.41 % EWL at 12 months [mean (SD)]: LRYGBP: 60.5 (10.7) LSG: 69.7 (14.6), p = 0.05 Weight loss at 12 months [mean (SD)], kg: LRYGBP: 40.0 (8.3) LSG: 43.6 (11.7), p = 0.322 |
Diabetes resolved in both LRYGBP patients |
Conversions to open surgery = 0. Intraoperative and postoperative complications = 0 |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Yes | Computer-generated numbers were used to assign the type of surgery |
| Allocation concealment? | Unclear | Type of surgery was written on a card sealed in a completely opaque envelope. Not stated if sequentially numbered |
| Blinding of outcome assessors?* | Yes | States that ‘blinding as to the type of the procedure involved the patient and the medical staff, and the independent data collector’ |
| Blinding of participants on self-reported outcomes? | n/a | |
| Incomplete outcome data addressed?* Weight loss | Yes | States that all patients had a complete evaluation at all time points of the follow-up |
| Incomplete outcome data addressed?* QoL | n/a | |
| Incomplete outcome data addressed?* Comorbidity | n/a | |
| Free of selective outcome reporting? | Unclear | |
| Free of other sources of bias? | Unclear |
Appendix 10 Data extraction tables: vertical banded gastroplasty versus adjustable gastric banding
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Morino, 2003110 Design: RCT, single centre. Follow-up: minimum 2 years, mean 33.1 months (range 24–46 months) LAGB: 1 year 98% 2 years 94% 3 years 90% LVBG 1 year 90% 2 years 88% 3 years 95% |
Country: Italy Number: total 100, LAGB 49, LVBG 51 Age, years: LAGB 37.2 (20–55), LVBG 38.2 (21–58) Sex (F : M): LAGB 38 : 11, LVBG 43 : 8 BMI: LAGB 44.7 (40.1–50.0), LVBG 44.2 (40.0–50.0) Weight, kg: LAGB 121.5 (90–175), LVBG 118.7 (90–160) Percentage excess weight: LAGB 106.5 (79.3–142.6), LVBG 104.8 (79.4–136.0) Characteristics of target population: history of obesity at least 5 years, documented weight loss attempts in the past, BMI 40–50, aged 18–60 years Exclusion criteria: contraindications to creation of pneumoperitoneum (e.g. glaucoma), large oesophageal hiatal hernias (> 3 cm), symptomatic gastro-oesophageal reflux disease, pregnancy, drug or alcohol abuse, psychological disorders (e.g. bulimia, depression), hormonal or genetic obesity-related disease, previous gastric surgery. Evaluated by a dietitian to exclude concentrated sweet eaters and binge eaters 175 submitted to surgery, 75 excluded from study: BMI > 50 (35), BMI < 40 with comorbidities (5), specific contraindication to pneumoperitoneum (4), previous gastric surgery (6), severe reflux disease (14), refused (11) |
|
Primary end point: reoperation rate Secondary end points: early and late complication rates,% excess weight loss at 1, 2, 3 years Surgical time (skin incision to wound closure) Anaesthesiology time (global time in operative room) Conversion rate Intraoperative and postoperative morbidity 60-day mortality Length of hospital stay Residual BMI Percentage of excess weight loss Reinhold classification: Excellent 0–25% excess weight, Good 26–50%, Fair 51–75%, Poor 76–100%, Failure > 100% excess weight at time of evaluation |
Allocation to treatment groups: randomisation performed 1 day before surgery by means of sealed opaque envelopes containing computer-generated numbers Blinding of outcome assessors: not reported Comparability of treatment groups: comparable in sex, age, mean weight, BMI, % excess weight, laboratory test results Method of data analysis: categorical variables compared by chi-squared test, with Yates correction and the Fisher exact test (two-tailed) when necessary. Continuous variables compared by Student’s t test or the Mann–Whitney U test, depending on distribution. All p values were two-sided. p < 0.05 indicated statistical significance Sample size/power calculation: calculated based on assumption of a difference of 5% in the reoperation rate between LAGB and LVBG, a difference of 5% in early and late complications, and a difference of 10% in % excess weight loss. These differences were considered clinically significant, and a sample size of 100 (50 in each group) was needed Attrition/dropout: per cent present at 1-, 2- and 3-year follow-up reported for each group |
Table of results
| Weight change | QoL/comorbidity | Events/procedures (complications, reoperations) |
|---|---|---|
|
BMI 1 year: LAGB 35.5, LVBG 30.1, p < 0.05 2 years: LAGB 34.8, LVBG 29.7, p = ns 3 years: LAGB 35.7, LVBG 30.7, p = ns Percentage of excess weight loss 1 year: LAGB 39.2, LVBG 62.3, p < 0.05 2 years: LAGB 41.4, LVBG 63.5, p = ns 3 years: LAGB 39.0, LVBG 58.9, p = ns Reinhold classification Patients with an excellent or good result (residual excess weight < 50%) 2 years: LAGB 35%, LVBG 74%, p < 0.001 3 years: LAGB 25%, LVBG 63%, p = 0.056 Patients with procedural failure resulting from insufficient weight loss (residual excess weight > 100%) 2 years: LAGB 5%, LVBG 0 3 years: LAGB 6%, LVBG 0 |
Not assessed. |
Mortality, %: LAGB 0, LVBG 0 Operative time, min: LAGB 65.4 (35–120), LVBG 94.2 (40–270), p < 0.05 Hospital stay, days: LAGB 3.7 (2–6), LVBG 6.6 (3–58), p < 0.05 Conversion to open surgery, %: LAGB 0, LVBG 0 Early morbidity, %: LAGB 6.1, LVBG 9.8, p = 0.754 Late complications, %: LAGB 32.7, LVBG 14, p < 0.05 Late reoperations, %: LAGB 24.5, LVBG 0, p < 0.001 Associated procedures (10% of both groups) LAGB: four cholecystectomies, one lymph node biopsy LVBG: five cholecystectomies LAGB: One early postoperative band slippage on day 7, treated with laparoscopic repositioning, one port infection, one haematoma at port site LVBG: One fistula at staple line day 2, treated with open gastric bypass; two prolonged postoperative pyrexia, non-operative treatment; two respiratory failures without evidence of pulmonary embolism, conservative therapy Late complications: LAGB 32.7% (16/49), LVBG 14% (7/50), p < 0.05 LAGB: Nine gastric band slippage, three symptomatic reflux disease, one complete food intolerance, one poor compliance, one infected port, one port twisted LVBG: One pouch dilatation, one asymptomatic pouch-to-fundus fistula, four symptomatic reflux diseases, one gastric bezoar Late reoperations: LAGB: 24.5% (12/49), LVBG 0/50, p < 0.001 LAGB: Eight bands removed (six for slipping, one for severe reflux oesophagitis, one for poor compliance), one slipped band replaced laparoscopically, one gastric bypass due to food intolerance without complications related to the band, one port repositioned, one port removed |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Yes | Randomisation performed 1 day before surgery by means of sealed opaque envelopes containing computer-generated numbers |
| Allocation concealment? | Yes | Sealed opaque envelopes |
| Blinding of outcome assessors? | Unclear | Not reported |
| Blinding of participants on self-reported outcomes? | n/a | |
| Incomplete outcome data addressed? Weight loss | Yes | per cent present at 1-, 2- and 3-year follow-up reported for each group. Reasons for losses not given |
| Incomplete outcome data addressed? QoL | n/a | |
| Incomplete outcome data addressed? Comorbidity | n/a | |
| Free of selective outcome reporting? | Unclear | |
| Free of other sources of bias? | Unclear |
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Nilsell 2001126 Design: single centre, RCT Follow-up: 4–5 years |
Country: Sweden Number: total 59, AGB 29, VBG 30 Age: AGB 38 years (20–58), VBG 39 years (19–59) Sex: AGB 72% female, VBG 80% female Weight: AGB 124 kg (24.0), VBG 123 kg (11.4) BMI: AGB 42.8 (5.4), VBG 43.9 (3.8) Characteristics of target population: people with BMI > 40 or BMI > 37 with obesity-associated comorbidity Exclusion criteria: age > 60 years, severe psychiatric disorders or alcoholism |
|
Complications Late reoperations Weight change Patient satisfaction Reflux symptoms |
Allocation to treatment groups: randomised using sealed envelopes the day before surgery Blinding: staff and patients were not blinded to treatment Comparability of treatment groups: groups similar in age, height, weight, diabetes, asthma, joint pain, hypertension Method of data analysis: mean (SEM) with Fisher’s exact test at p = 0.05 level Sample size/power calculation: none stated Attrition/dropout: two died from causes unrelated to bariatric operation. three AGB and two VBG were lost to follow-up Generalisability: predominantly limited to females, aged in mid- to late 30s who are morbidly obese Intercentre variability: single centre Conflict of interests: none stated |
Table of results
| Weight change | QoL/comorbidities | Events/procedures (complications, reoperations) |
|---|---|---|
|
Weight [Mean (SEM)]: Baseline AGB 124 kg (29); VBG 123 kg (30) 1 year AGB 98 kg (28); VBG 82 kg (25) 2 years AGB 88 kg (23); VBG 85 kg (29) 3 years AGB 85 kg (13); VBG 90 kg (15) 4 years AGB 86 kg (17); VBG 95 kg (15) 5 years AGB 81 kg (16); VBG 88 kg (16) (Data for years 1 to 4 are estimated from graph) |
Patient satisfaction: Patients satisfied: AGB 21/26 (81%); VBG 15/27 (56%) |
Complications: Deaths: one patient per arm died of causes unrelated to surgery. No postoperative deaths Gastro-oesophageal reflux disease: AGB 3/26 (11.5%); VBG 4/27 (14.8%) Anastomotic leak: AGB 0, VBG 1 (reoperation third postoperative day) Late reoperations: 3/26 AGB reoperated (two due to dilatation of gastric pouch (band replaced), one removed at patient’s request) 10/27 VBG reoperated (due to strictures of stoma with vomiting or intolerance of solid food or to staple-line disruption leading to regain of weight). Types of operation: removal of band (four), gastrogastrostomy (three), longer band (one), gastric banding (two) Three VBG with staple-line disruption were not reoperated. Total incidence of staple-line disruption 18.5% (5/27) |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Unclear | Randomised using sealed envelopes the day before surgery |
| Allocation concealment? | Unclear | As above |
| Blinding of outcome assessors? | No | States that staff and patients not blinded (outcome assessors not specified, but assume not blinded) |
| Blinding of participants on self-reported outcomes? | No | Staff and patients were not blinded to treatment |
| Incomplete outcome data addressed? Weight loss | Yes | Two died from causes unrelated to bariatric operation. Three AGB and two VBG were lost to follow-up |
| Incomplete outcome data addressed? QoL | n/a | |
| Incomplete outcome data addressed? Comorbidity | n/a | |
| Free of selective outcome reporting? | Unclear | |
| Free of other sources of bias? | Unclear |
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Design: single centre, RCT Follow-up: 24 months 84 months follow-up reported in abstract only128 |
Country: Netherlands Number: total 100, open VBG 50, LAGB 50 (but one converted to GBP during surgery) Age (mean ± SD) Open VBG 39 ± 8.5 years; LAGB 37.2 ± 9.7 years, p = ns Sex (M : F): open VBG 10 : 40; LAGB 10 : 40, p = ns BMI (mean ± SD): open VBG 46.6 ± 6.4; LAGB 46.7 ± 6.1, p = ns Number of comorbidities per patient (mean ± SD): open VBG 1.3 ± 1.1; LAGB 1.3 ± 1.0, p = ns Recruitment: May 1999 to December 2001 Characteristics of target population: BMI > 40 or > 35 with comorbidities; age between 18 and 60 years; had failed previous non-surgical attempts at weight loss Exclusion criteria: previous obesity surgery or gastric surgery; patients with severe psychological disorders |
|
Mortality Conversion to open procedure Immediate postoperative complications, late complications Hospital length of stay per cent excess weight loss BMI Reduction in comorbidities |
Method of data analysis: whether ITT not stated, but does state follow-up of 100% achieved for both groups. Data given as mean ± SD. p < 0.5 denoted as statistically significant Sample size/power calculation: not reported Conflict of interests: not stated Supported by AGIKO-stipendium of the Netherlands Organisation of Scientific Research |
Table of results
| Weight change | QoL/comorbidity | Events/procedures (complications, reoperations) |
|---|---|---|
|
Mean BMI at 1 year: Open VBG 31.1 ± 6.2; LAGB 35.0 ± 6.3 Mean BMI at 2 years: Open VBG 31.0 ± 6.0; LAGB 34.6 ± 6.5, p ≤ 0.002 (in favour of VBG) |
Comorbidities. Preoperative: open VBG 41 (82%) patients with comorbidity – 29 (58%) joint problems, 8 (16%) pulmonary problems, 10 (20%) hypertension, 7 (14%) diabetes mellitus, 3 (6%) cardiovascular problems, 2 (4%) hypercholesterolaemia, 2 (4%) reflux disease, 1 (2%) sleep apnoea, 0 (0%) neurological problems LAGB 39 (78%) patients with comorbidity – 28 (56%) joint problems, 9 (18%) pulmonary problems, 7 (14%) hypertension, 5 (10%) diabetes mellitus, 2 (4%) cardiovascular problems, 2 (4%) hypercholesterolaemia, 3 (6%) reflux disease, 1 (2%) sleep apnoea, 1 (2%) neurological problems |
Mortality: open VBG 2 (4%) one due to sepsis, one due to pneumonia. LAGB none Immediate postoperative complications: open VBG: complications occurred in nine patients: three (6%) leakage, requiring reoperation, two (4%) splenectomy (intraoperative due to iatrogenic injury), two (4%) obstruction (gastroscopy necessary), with seven infections in five (10%) patients [sepsis three (6%) one of these patients died, urinary tract infection one (2%], pneumonia three (6%) one of these patients died), wound infection one (2%). LABG two (4%) conversion to open LABG due to technical problems, one (2%) conversion to gastric bypass as a result of perforation during retro-gastric tunnelling. There were no infections |
|
% Excess weight loss at 1-year: Open VBG 71.1 ± 24.0%; LAGB 53.3 ± 21.2%, p ≤ 0.001 (in favour of VBG) % Excess weight loss at 2 years: Open VBG 70.1 ± 25.5%; LAGB 54.9 ± 23.3%, p ≤ 0.001 (in favour of VBG) At mean 84 months follow-up:128 % excess BMI loss: VBG 68.8%, LAGB 56.9%. States significant, but statistics not reported |
At 1 year: Open VBG 14 (30.4%)a patients with comorbidity – 7 (15.2%)a joint problems, 3 (6.5%)b pulmonary problems, 8 (17.4%) hypertension, 1 (2.2%)b diabetes mellitus, 2 (4.3%) cardiovascular problems, 1 (2.2%) hypercholesterolaemia, 0 (0%) reflux disease, 0 (0%) sleep apnoea, 0 (0%) neurological problems LAGB 18 (37.5%)a patients with comorbidity – 10 (20.8%)a joint problems, 3 (6.3%)b pulmonary problems, 5 (10.4%) hypertension, 1 (2.1%)b diabetes mellitus, 2 (4.2%) cardiovascular problems, 2 (4.2%) hypercholesterolaemia, 0 (0%) reflux disease, 0 (0%) sleep apnoea, 1 (2.1%) neurological problems At 2 years: Open VBG 23 (47.9%)a patients with comorbidity – 13 (27.1%)a joint problems, 3 (6.3%)b pulmonary problems, 7 (14.6%) hypertension, 1 (2.1%)b diabetes mellitus, 1 (2.1%) cardiovascular problems, 1 (2.1%) hypercholesterolaemia, 0 (0%) reflux disease, 0 (0%) sleep apnoea, 1 (2.1%) neurological problems LAGB 20 (40%)a patients with comorbidity – 12 (24%)a joint problems, 1 (2%)b pulmonary problems, 5 (10%) hypertension, 1 (2%)b diabetes mellitus, 3 (6%) cardiovascular problems, 1 (2%) hypercholesterolaemia, 0 (0%) reflux disease, 0 (0%) sleep apnoea, 1 (2%) neurological problems Although the number of comorbidities in both groups decreased following surgery no differences in comorbidities were observed between groups |
Mean length of hospital stay: Open VBG 6.8 ± 10.4 days (range 2–56 days), LAGB 3.5 ± 1.5 days (range 2–9 days), p < 0.001 Late complications: Open VBG: revisional surgery (conversion to gastric bypass) 18 (36%) (due to vertical staple-line disruption 15 (30%), Narrow outlet two (4%), Insufficient weight loss one (2%). A further eight (16%) patients developed an incisional hernia for which surgical repair was needed. Outlet stenosis or obstruction in six (12%) patients required gastroscopy. Two patients developed peroneal nerve paralysis associated with rapid weight loss [table records neurological problems for only one patient (2%)]. LAGB: 20 reoperations (40%) took place, 16 were major reoperations (pouch dilatation/pouch slippage 12 (24%), band leakage 2 (4%), band erosion 2 (4%)). Four were minor operations [painful access-port 2 (4%), infection around access-port 1 (2%), port leakage 1 (2%)]. Of the 12 (24%) patients reoperated on for pouch dilatation/pouch slippage, the band was repositioned in eight cases, reduction and refixation of the pouch was performed in three cases and one new LAGB was placed At mean 84 months follow-up:128 States that long-term complications ‘were mainly’ (assume all not reported): VBG: staple-line disruption 51%, incisional hernia 27% LAGB: pouch dilatation 24%, anterior slippage 15% Major reoperation: VBG: conversion to gastric bypass 59% LAGB: total 46%, refixation or band replacement 35%, conversion to another procedure in 11% Major complications after reoperation that necessitated reintervention: VBG 4% LAGB 2% |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Yes | Computer-generated randomisation list, made before the start of the study, used for randomisation |
| Allocation concealment? | Unclear | Not described |
| Blinding of outcome assessors? | Unclear | Not described, assume no blinding |
| Blinding of participants on self-reported outcomes? | n/a | No self-reported outcomes. Patients were informed about their surgical treatment group during administration to hospital |
| Incomplete outcome data addressed? Weight loss | Yes | The authors state that 100% follow-up in both groups was achieved at 2 years. One LAGB converted to open GBP during procedure. At mean 84 months, follow-up was 91%. No further details given |
| Incomplete outcome data addressed? QoL | n/a | |
| Incomplete outcome data addressed? Comorbidity | Yes | |
| Free of selective outcome reporting? | Unclear | Outcomes not-prespecified |
| Free of other sources of bias? | Unclear | No other obvious sources of bias |
Appendix 11 Data extraction tables: laparoscopic adjustable gastric banding versus laparoscopic isolated sleeve gastrectomy
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Himpens et al. 2006129 Design: single centre, RCT Follow-up: 36 months |
Country: Belgium Number: total 80, LAGB 40, LISG 40 Age (median, range) years: LAGB 36 (20–61); LISG 40 (22–65), p = ns Sex: LAGB ratio M : F: 7 : 33; LISG 9 : 31, p = ns BMI (median, range): LAGB 37 (30–47); LISG 39 (30–53), p = ns Weight: baseline not reported Gastro-oesophageal reflux disease (GERD) requiring drug therapy with proton pump inhibitors (PPI): LAGB 6/40 (15%); LISG 8/40 (20%) Characteristics of target population: only inclusion criteria are candidates for laparoscopic restrictive operation Exclusion criteria: none reported |
|
Primary: relative weight loss Other outcomes: BMI, GERD (number on PPI medication), complications and reoperations. Also feeling of hunger, craving for eating sweets as assessed by questionnaire (latter two not extracted here) |
Method of data analysis: not reported if ITT analysis, median values used for analyses of outcomes, p values < 0.05 were statistically significant Sample size/power calculation: text refers to the statistical test used depending on the requirements by sample size but no details of the sample size calculation reported Conflict of interests: none reported |
Table of results
| Weight change | QoL/comorbidity | Events/procedures (complications, reoperations) |
|---|---|---|
|
Weight loss (median and range): After 1 year: LAGB 14 kg (– 5 to 38); LISG 26 kg (0 to 46), p < 0.0001 After 3 years: LAGB 17 kg (0 to 40); LISG 29.5 kg (1 to 48), p < 0.0001 Excess weight loss (median%, range): At 1 year: LAGB 41.4% (– 11.8 to 130.5); LISG 57.7% (0 to 125.5), p = 0.0004 At 3 years: LAGB 48% (0 to 124.8); LISG 66% (– 3.1 to 152.4), p = 0.0025 BMI (decrease, median and range): After 1 year: LAGB 15.5 (5 to 39); LISG 25 (0 to 45), p < 0.0001 After 3 years: LAGB 18 (0 to 39); LISG 27.5 (0 to 48), p = 0.0004 |
GERD Appeared by 1 year in 3/34 (8.8%) LAGB and 7/32 (21.8%) LISG, p = ns Appeared by 3 years in 7/34 (20.5%) LAGB and 1/32 (3.1%) LISG, p = ns Numbers for denominator are those without GERD at baseline, although figure 3 (Himpens et al. , 2006)129 notes these as those who had GERD at baseline. Disappeared by 1 year in 5/6 (83.3%) LAGB and 6/8 (75%) LISG. This remained the same at 3 years. |
Complications (not requiring surgery): At 1 year: LAGB shoulder pain three (7.5%); frequent vomiting six (15%), poor choice of alimentation two (5%); LISG gastric pain two (5%), frequent vomiting one (2.5%), mineral deficiency two (5%). At 3 years: LAGB shoulder pain three (8.5%); frequent vomiting ten (28.5%), poor choice of alimentation 17 (48.5%), gastric ulcer one (2.8%); LISG frequent vomiting five (16.6%), poor choice of alimentation eight (26.6%), mineral deficiency three (10%) Complications (requiring surgery): LAGB: no early postoperative complications, seven late complications of which: three pouch dilatation (treated with band removal in two, and conversion to RYGBP in one); one gastric erosion (treated by conversion to RYGBP); three disconnections of the port (treated by reconnection). In addition, two patients presented insufficient weight loss and treated by conversion to RYGBP. LISG: two early postoperative complications of which: one was an intraperitoneal bleed requiring laparoscopy and one gastric ischaemia requiring laparoscopic total gastrectomy. No late complications were recorded. Two patients presented insufficient weight loss and were converted to laparoscopic duodenal switch |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Unclear | States patients ‘…operated consecutively and randomly assigned…’. No details of randomisation sequence reported |
| Allocation concealment? | Unclear | No details reported |
| Blinding of outcome assessors? | Unclear | No details reported |
| Blinding of participants on self-reported outcomes? | n/a | |
| Incomplete outcome data addressed? Weight loss | Unclear | States that 80 randomised, 40 in each group. No discussion of any attrition or exclusions, appears to be no losses at 3 years but unable to check as numbers not presented in any details of weight loss results |
| Incomplete outcome data addressed? QoL | n/a | |
| Incomplete outcome data addressed? Comorbidity | Unclear | GERD outcomes: all numbers were reported, but data were statistically analysed by subgroup for this outcome – those without GERD at baseline to see if it appeared, those with it at baseline to see if it disappeared |
| Free of selective outcome reporting? | Unclear | Reports data on outcomes listed in methods, but study protocol not available, only reports mean change and range, not standard deviations |
| Free of other sources of bias? | Unclear | The characteristics of the patients were reported to be similar for the two groups, although states medians and ranges were performed unclear what the reason is for this. Insufficient information to assess whether an important risk of bias exists |
Appendix 12 Data extraction tables: open versus laparoscopic gastric bypass
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Luján, 2004130 DESIGN: RCT, single centre FOLLOW-UP: mean 23 months |
Country: Spain Number: total 104, LGBP 53, open GBP 51 Age, years: LGBP 37 (18–64), open GBP 38 (20–63), p = ns Sex (M : F): LGBP 10 : 43, open GBP 13 : 38, p = ns. BMI: LGBP 48.53 (36–78), open GBP 52.20 (37–80), p = ns WEIGHT: LGBP 130.70 (92–208), open GBP 137.57 (96–214), p = ns Characteristics of target population: BMI > 40 without coexisting pathological disorders or BMI > 35 with coexisting pathological disorders Exclusion criteria: patients evaluated by the Psychiatry, Endocrinology, Anaesthesia and Surgery units to rule out significant contraindications for surgery |
|
Operating time Intraoperative complications Early (< 30 days) postoperative complications Late (> 30 days) postoperative complications Hospital stay Short-term evolution of BMI |
Allocation to treatment groups: randomisation performed before assessment by computer generated numbers, concealed in sequentially numbered sealed opaque envelopes Blinding of outcome assessors: not reported Comparability of treatment groups: similar age, gender, preoperative weight and BMI, no statistically significant differences Method of data analysis: mean, SD, medians and range calculated, Comparisons between groups performed with Student’s t test for quantitative variables and chi-squared Pearson test for qualitative variables Sample size/power calculation: not reported Attrition/dropout: 100% follow-up. States mean follow-up is 23 months, but range not given. Not clear how many patients are included at each follow-up point |
Table of results
| Weight change | QoL/comorbidity | Events/procedures (complications, reoperations) |
|---|---|---|
|
BMI (estimated from figure), p = ns 3 months: LGBP 41, open GBP 47 6 months: LGBP 36, open GBP 41 12 months: LGBP 33, open GBP 37 18 months: LGBP 31, open GBP 36 24 months: LGBP 32, open GBP 35 36 months: LGBP 31, open GBP 35.5 |
Postoperative mortality: LGBP two (one unrelated to surgery), open GBP one Mean operating time, minutes: LGBP 186.4 (125–290), open GBP 201.7 (129–310), p < 0.05 LGBP Conversions to laparotomy: four (8%), due to extreme hepatomegaly, portal hypertension secondary to hepatic cirrhosis discovered in the course of the operation, anaesthetic problems (hypercapnia), and splenic lesion during dissection of the angle of His. All occurred in the first 20 patients Open GBP Intraoperative complications four (8%): three splenectomies, one splenic vein tear requiring suture Early complications (< 30 days): LGBP 12 (22.6%), open GBP 15 (29.4%), p = ns LGBP: three intestinal subocclusions, two asymptomatic leaks, two intra-abdominal bleeding, two upper gastrointestinal haemorrhage (one requiring blood transfusion), one lower gastrointestinal haemorrhage, one thromophlebitis, one stenosis of gastro-entero-anastomosis Open GBP: four subphrenic abscesses, three upper gastrointestinal haemorrhage, four wound infections, three respiratory infections, one evisceration (death) Late complications (> 30 days): LGBP 6 (11%), open GBP 12 (24%), p < 0.05 LGBP: three intestinal obstructions (conservative, death, reoperation), two pancreatitis/cholecystectomy, one sudden death (possible pulmonary thromboembolism) Open GBP: 10 eventrations, one subphrenic abscess, one intestinal constriction (reoperation) Mean hospital stay: LGBP 5.2 days (1–13), open GBP 7.9 days (2–28), p < 0.05 |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Yes | Randomisation performed before assessment by computer-generated numbers |
| Allocation concealment? | Yes | Concealed in sequentially numbered sealed opaque envelopes |
| Blinding of outcome assessors? | Unclear | Not reported |
| Blinding of participants on self-reported outcomes? | n/a | |
| Incomplete outcome data addressed? Weight loss | Unclear | 100% follow-up. States mean follow-up is 23 months, but range not given. Not clear how many patients are included at each follow-up point |
| Incomplete outcome data addressed? QoL | n/a | |
| Incomplete outcome data addressed? Comorbidity | n/a | |
| Free of selective outcome reporting? | Unclear | BMI reported in figure only, with no exact data reported and no measure of variance |
| Free of other sources of bias? | Unclear |
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Nguyen et al 2001113 Puzziferri et al 2006114 Design: single centre, RCT Follow-up: 36 months. Mean 39 ± 8 months (range 24–58) |
Country: USA Original publication: Number: total 155, LGBP 79, open 76 Age: LGBP 40 years (± 8), open 42 years (± 9) Sex: LRYGBP 91% female, RYGBP 88% female Weight: LGBP 289 lb (± 38) (131 ± 17 kg), open 296lb (± 44) (135 ± 20 kg) BMI: LGBP 47.6 (± 4.7), open 48.4 (± 5.4) Updated publication: Number: total 116, RYGBP 57, LRYGBP 59 Age [mean (SD)]: LRYGBP 47 (± 7) years: RYGBP 50 (± 8) years Sex: LRYGBP female 56; male 3: RYGBP female 51, male 6 BMI (mean SD): LRYGBP 48 (± 5): RYGBP 49(± 6) Weight: not reported History cholecystectomy: LRYGBP 16 (27%): RYGBP 17 (30%) Comorbidities (see results section) Characteristics of target population: BMI 40–60; 21–60 years of age, failed previous medical interventions for weight loss Exclusion criteria: those with previous bariatric surgery, previous gastric surgery, large abdominal ventral hernia, history of deep vein thrombosis or pulmonary embolism, and severe cardiovascular, respiratory, hepatic or renal disease |
Cholecystectomy undertaken concomitantly with the procedures in some cases |
Length of time for return to activities of daily living Operative time, length of skin incision, estimated blood loss, number of patients requiring intensive-care unit stay, length of hospital stay, early and late (> 30 days) complications, early reoperation (< 30 days), weight loss (mean % of excess body weight loss), time to return to work, quality of life (SF-36 and BAROS) and costs Weight loss, Changes in comorbidities, QoL [Moorehead-Ardelt Quality of Life Questionnaire (MAQoL)] The Bariatric Analysis and Reporting Outcome System (BAROS) Late complications (occurring > 3 months after surgery) The Moorehead-Ardelt QoL questionnaire assesses five categories; self-esteem, physical activity, social life, work conditions, sexual interest/activity. Points are added for positive changes and deducted for negative changes The BAROS takes into account three outcomes: % excess body weight loss, changes in comorbidities, the MAQoL. A maximum of three points are given for each category. Points are deducted for complications and reoperations. The scale is rated as excellent (> 7–9); very good (> 5–7); good (> 3–5); fair (> 1–3); failure (≤ 1) |
Method of data analysis: states ITT analysis and LRYGBP converted to RYGBP were analysed as laparoscopic. However, two patients initially allocated to RYGBP were excluded after randomisation (one withdrew consent; one had an intraoperative splenic injury) and unclear if included in analysis. Differences between groups were assessed using two-sample t tests or Fisher exact tests. Mann–Whitney U-test was used for non-parametric data. Repeated measures of variance and unpaired t test were used. p < 0.05 was considered significant Sample size/power calculation: mean time to return to activities of daily living was 20 ± 17 days in open GBP – with difference of 7 days between procedures clinically significant – 73 patients per group necessary to detect difference using two tailed test type 1 error of 0.05 and Type 2 error 0.2 Conflict of interests: not stated |
Table of results
| Weight change | QoL/comorbidity | Events/procedures (complications, reoperations) |
|---|---|---|
|
Nguyen et al. 2001: Percentage excess body weight loss (SD): 12 months: LGBP (n = 29) 68% (± 15); open (n = 25) 62% (± 14) (p = 0.07) Puzziferri et al. 2006: (for 116 participants) % Excess body weight lost at 3 years (mean SD): LRYGBP (n = 30) 77% ± 22%; RYGBP (n = 33) 67% ± 21%, p = ns % Excess body weight lost at 4 years (mean SD) LRYGBP (n = 22) 76% ± 19%; RYGBP (n = 18) 71% ± 25%, p = ns |
Nguyen et al. 2001: Quality of Life SF-36 Scores [mean (± SD)] (preoperative LRYGBP n = 70, RYGBP n = 73; 3 months LRYGBP n = 54, RYGBP n = 42) Physical functioning: preoperative LRYGBP 46.5 (21.3), RYGBP 40.0 (24.4), p = ns; 1 month LRYGBP 60.9 (24.7), RYGBP 46.3 (24.7), p < 0.05; 3 months LRYGBP 80.2 (19.1), RYGBP 67.8 (26.6), p = ns; US norms 84.2 (23.3) Role-physical: preoperative LRYGBP 47.2 (40.2), RYGBP 37.5 (37.9), p = ns; 1 month LRYGBP 29.7 (39.2), RYGBP 18.5 (32.3), p = ns; 3 months LRYGBP 80.7 (32.5), RYGBP 76.8 (33.3), p = ns; US norms 81.0 (34.0) Bodily pain: preoperative LRYGBP 51.0 (22.7), RYGBP 48.7 (24.1), p = ns; 1 month LRYGBP 59.2 (21.5), RYGBP 45.1 (24.4), p < 0.05; 3 months LRYGBP 75.1 (24.7), RYGBP 68.1 (25.6), p = ns; US norms 75.2 (23.7) General health: preoperative LRYGBP 54.5 (21.6), RYGBP 52.9 (22.3), p = ns; 1 month LRYGBP 71.3 (18.0), RYGBP 64.0 (18.1), p < 0.05; 3 months LRYGBP 77.2 (15.7), RYGBP 72.4 (16.5), p = ns; US norms 72.0 (20.3) Vitality: preoperative LRYGBP 38.5 (20.0), RYGBP 36.6 (19.9), p = ns; 1 month LRYGBP 45.4 (20.5), RYGBP 39.1 (18.9), p = ns; 3 months LRYGBP 65.8 (17.7), RYGBP 73.1 (95.2), p = ns; US norms 60.9 (21.0) Social functioning: preoperative LRYGBP 64.4 (26.3), RYGBP 61.6 (29.5), p = ns; 1 month LRYGBP 67.6 (24.5), RYGBP 51.9 (29.1), p < 0.05; 3 months LRYGBP 87.3 (17.9), RYGBP 74.1 (30.0), p = ns; US norms 83.3 (22.7) Role-emotional: preoperative LRYGBP 49.1 (24.4), RYGBP 45.5 (27.2), p = ns; 1 month LRYGBP 78.5 (28.2), RYGBP 69.5 (33.5), p = ns; 3 months LRYGBP 83.0 (29.6), RYGBP 74.6 (40.7), p = ns; US norms 81.3 (33.0) Mental health: preoperative LRYGBP 73.0 (15.1), RYGBP 71.9 (17.3), p = ns; 1 month LRYGBP 76.8 (17.4), RYGBP 70.8 (19.4), p = ns; 3 months LRYGBP 82.9 (14.2), RYGBP 75.0 (19.2), p = ns; US norms 74.7 (18.1) Moorehead-Ardelt QoL scores (3 months LRYGBP n = 47, RYGBP n = 36; 6 months LRYGBP n = 34, RYGBP n = 28) Self-esteem: 3 months LRYGBP 0.81 (0.3), RYGBP 0.73 (0.32) (p = ns); 6 months LRYGBP 0.84 (0.27), RYGBP 0.80 (0.28) (p = ns) |
Nguyen et al. 2001 Operative outcomes Operative time (minutes): LRYGBP 225 (± 40), RYGBP 195 (± 41) p < 0.001 Estimated blood loss (ml); LRYGBP 137 (± 79), RYGBP 395 (± 284) p < 0.001 Proportion requiring intensive-care unit stay: LRYGBP 7.6%, RYGBP 21.1% p = 0.03 Median length of hospital stay (days): LRYGBP 3 (IQR 1), RYGBP 4 (IQR 2) p < 0.001 Proportion requiring reoperation: LRYGBP 7.6%, RYGBP 6.6% p = ns Return to activities of daily living (days): LRYGBP 8.4 (± 8.6), RYGBP 17.7 (± 19.1) p < 0.001 Return to work (days): LRYGBP 32.2 (± 19.8), RYGBP 46.1 (± 20.6) p = 0.02 Intraoperative transfusion: LRYGBP 0, RYGBP 3.9% Conversion from LRYGBP to RYGBP: 2.5% due to failure of circular stapler; inability to insufflate abdomen safely Complications Major complications: total LRYGBP 7.6%, RYGBP 9.2% (p = 0.78); anastomotic leak LRYGBP 1, RYGBP 1; gastric pouch outlet obstruction LRYGBP 0, RYGBP 1; hypopharyngeal perforation LRYGBP 1, RYGBP 0; jejunojejunostomy obstruction LRYGBP 3, RYGBP 0; pulmonary embolism LRYGBP 0, RYGBP 1; respiratory failure LRYGBP 0, RYGBP 1; gastrointestinal bleeding LRYGBP 1, RYGBP 0; wound infection LRYGBP 0, RYGBP 2; retained laparotomy sponge LRYGBP 0, RYGBP 1 |
|
Physical: 3 months LRYGBP 0.48 (0.40), RYGBP 0.46 (0.44) (p = ns); 6 months LRYGBP 0.37 (0.17), RYGBP 0.34 (0.18) (p = ns) Social: 3 months LRYGBP 0.31 (0.19), RYGBP 0.24 (0.21) (p = ns); 6 months LRYGBP 0.33 (0.19), RYGBP 0.29 (0.21) (p = ns) Labour: 3 months LRYGBP 0.24 (0.19), RYGBP 0.13 (0.29) (p < 0.05); 6 months LRYGBP 0.28 (0.21), RYGBP 0.21 (0.27) (p = ns) Sexual: 3 months LRYGBP 0.20 (0.21), RYGBP 0.09 (0.24) (p < 0.05); 6 months LRYGBP 0.26 (0.20), RYGBP 0.19 (0.26) (p = ns) Puzziferri et al. 2006: MAQoL scores [LRYGBP (n = 22) RYGBP (n = 22)] Self-esteem: 3 years LRYGBP 0.89, RYGBP 0.88, p = ns Physical activity: 3 years LRYGBP 0.40, RYGBP 0.36, p = ns Social life: LRYGBP 0.34, RYGBP 0.33, p = ns Labour or work conditions: LRYGBP 0.33, RYGBP 0.25, p = ns Sexual interest/activity: LRYGBP 0.20, RYGBP 0.24, p = ns Puzziferri et al. 2006: BAROS scores [LRYGBP (n = 22) RYGBP (n = 22)] Rates as % Fair: 3 years LRYGBP 4.5%, RYGBP 9.1% Good, very good or excellent: LRYGBP 95.5%; RYGBP 86.4%, p = ns Failure: text states for LRYGBP and RYGBP overall failure rate, 2.3%; figure suggests failures in RYGBP group only Scores on BAROS (estimated from graph, unsure if mean) Excellent: LRYGBP 3, RYGBP 5 Very good: LRYGBP 14, RYGBP 11 Good: LRYGBP 4, RYGBP 3 Fair: LRYGBP 1, RYGBP 2 Failure: LRYGBP 0, RYGBP 1 |
Minor complications: total LRYGBP 7.6%, RYGBP 11.8% (p = 0.42); gastrointestinal Ileus LRYGBP 1, RYGBP 0; Clostridium difficile colitis LRYGBP 1, RYGBP 0; gastrogastric fistula LRYGBP 0, RYGBP 1; asymptomatic leak LRYGBP 0, RYGBP 1; gastrointestinal bleeding LRYGBP 2, RYGBP 0; wound infection LRYGBP 1, RYGBP 6; deep venous thrombosis LRYGBP 1, RYGBP 1 Late complications: total LRYGBP 18.9%, RYGBP 15.8% (p = 0.52); anastomotic stricture LRYGBP 9/79 (11.4%), RYGBP 2/76 (2.6%) p = 0.06; prolonged nausea/vomiting LRYGBP 1, RYGBP 2; small bowel obstruction LRYGBP 1, RYGBP 0; cholelithiasis LRYGBP 3, RYGBP 0; ventral hernia LRYGBP 0, RYGBP 6 (p = 0.01); anaemia LRYGBP 0, RYGBP 2; protein-calorie malnutrition LRYGBP 1, RYGBP 0 Puzziferri et al. 2006, late complications at 3 years (LRYGBP n = 59, RYGBP n = 57) Incisional hernia: LRYGBP 3 (5%), RYGBP 22 (39%), p < 0.01 Anaemia: LRYGBP 8 (14%), RYGBP 3 (5%), p = ns Vitamin B12 deficiency: LRYGBP 3 (5%), RYGBP 6 (11%), p = ns Chronic nausea/vomiting: LRYGBP 3 (5%), RYGBP 2 (4%), p = ns Chronic abdominal pain: LRYGBP 2 (3%), RYGBP 1 (2%), p = ns Marginal ulcer: LRYGBP 0, RYGBP 1 (2%), p = ns Small bowel obstruction: LRYGBP 2 (3%), RYGBP 1 (2%), p = ns Cholecystectomy (excludes those with previous cholecystectomy): LRYGBP 12/43 (28%), RYGBP 2/40 (5%), p = 0.03 No perioperative deaths No late deaths |
|
|
Puzziferri et al. 2006: (for 116 participants) Osteoarthritis: baseline LRYGBP 30 (51%), RYGBP 31 (54%) (p = ns); improvement/resolution at 3 years LRYGBP 24 (80%), RYGBP 19 (61%) (p < 0.05) Hypertension: baseline LRYGBP 18 (31%), RYGBP 28 (49%) (p = ns); improvement/resolution at 3 years LRYGBP 15 (83%), RYGBP 28 (100%) (p = ns) Depression: baseline LRYGBP 17 (29%), RYGBP 17 (30%) (p = ns); improvement/resolution at 3 years LRYGBP 13 (76%), RYGBP 12 (71%) (p = ns) Gastro-oesophageal reflux: baseline LRYGBP 14 (24%), RYGBP 21 (37%) (p = ns); improvement/resolution at 3 years LRYGBP 14 (100%), RYGBP 21 (100%) (p = ns) Dyslipidaemia: baseline LRYGBP 8 (14%), RYGBP 14 (25%) (p = ns); improvement/resolution at 3 years LRYGBP 7 (88%), RYGBP 17a (100%) (p < 0.01). Sleep apnoea: baseline LRYGBP 5 (8%), RYGBP 15 (26%) (p < 0.05); improvement/resolution at 3 years LRYGBP 5 (100%), 12 (86%) (p = ns) Diabetes mellitus: baseline LRYGBP 5 (8%), RYGBP 8 (14%) (p = ns); improvement/resolution at 3 years LRYGBP 5 (100%), RYGBP 7 (88%) (p = ns) Infertility: baseline LRYGBP 7 (12%), RYGBP 5 (9%) (p = ns); improvement/resolution at 3 years LRYGBP 2 (29%), RYGBP 2 (40%) (p = ns) Urinary incontinence: baseline LRYGBP 8 (14%), RYGBP 4 (7%) (p = ns); improvement/resolution at 3 years LRYGBP 7 (88%), RYGBP 4 (100%) (p = ns) Lower extremity oedema: baseline LRYGBP 2 (3%), RYGBP 3 (5%) (p = ns); improvement/resolution at 3 years LRYGBP 1 (50%); RYGBP 3 (100%) (p = ns) |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Unclear | Randomisation was performed by the use of sealed envelopes, stratified by BMI (< 50; ≥ 50) and in blocks of six patients however method of sequence generation not reported |
| Allocation concealment? | Unclear | Sealed envelopes but no further details |
| Blinding of outcome assessors? | Unclear | Not described |
| Blinding of participants on self-reported outcomes? | No | Patients were informed of their treatment during preoperative clinic visit |
| Incomplete outcome data addressed? Weight loss | Unclear |
Patients who withdrew consent or did not undergo GBP were excluded from the analysis; 19 eligible patients did not undergo randomisation; 13 requested laparoscopic GBP and 6 requested open GBP; 2 randomised to GBP were excluded after randomisation (1 withdrew consent, 1 needed splenectomy) Second publication reports data for 117 of the original 155 participants for weight loss and comorbidities. No reasons for missing data are given |
| Incomplete outcome data addressed? QoL | Unclear | Only 44 participants were reported for QoL |
| Incomplete outcome data addressed? Comorbidity | Unclear | Second publication reports data for 117 of the original 155 participants for weight loss and comorbidities. No reasons for missing data are given |
| Free of selective outcome reporting? | Unclear | % EBW reported but data are integers and appear to have been rounded. Weight loss or BMI not reported. Some listed outcomes have not been reported on |
| Free of other sources of bias? | No | Baseline characteristics in second publication (Puzziferri et al.) were reanalysed for those who had the 3-year follow-up only. Block randomisation used in an unblinded trial therefore may be possible to predict assignment to groups |
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Sundbom, 2004112 Design: RCT, single centre. Follow-up: 12 months |
Country: Sweden Number: total 50, hand 25, open 25 Median age (range), years: hand 37 (19–54), Open 38 (24–54) Sex (M : f): hand 2 : 23, open 3 : 22 BMI: hand 44 (36–54), open 45 (34–54) Previous abdominal surgery: hand 11, open 11 Comorbidity requiring medication: hand 14, open 21 Characteristics of target population: Patients who had not undergone previous bariatric surgery. All had undergone thorough medical investigation in the hospital metabolic unit and had failed conservative treatment, including dietary advice and pharmacological treatment. Fully informed and motivated to undergo gastric bypass Exclusion criteria: BMI > 55, simultaneous cholecystectomy One eligible patient refused to participate, one could not be randomised because of availability of techniques, five were excluded because of BMI > 55, one excluded as the result of planned simultaneous cholecystectomy |
|
Length of postoperative hospital stay Morphine requirement Sick leave Weight reduction BMI Blood transfusion Duration of surgery Peroperative bleeding Abdominal wall thickness |
Allocation to treatment groups: randomised by sealed envelope after induction of anaesthesia. Stratified by sex Blinding of outcome assessors: identical dressings were used so that nursing staff and patients were blinded to the treatment received. Patients informed of procedure at discharge Comparability of treatment groups: states well matched for age, sex, BMI, previous abdominal surgery and comorbid conditions. Data presented, no statistics reported. Appears to be higher comorbidity in the Open group Method of data analysis: ITT analysis. Presented as median (range). p < 0.050 considered statistically significant. anova and Mann–Whitney U test used Sample size/power calculation: sample size was calculated at 21 patients in each group when using a power of 90%, a standard deviation of 1 (as in the pilot study) and an expected difference in postoperative hospital stay of 1 day or more Attrition/dropout: no patient dropped out after randomisation and follow-up data were available for all patients Protocol violated in two patients in hand group – cholecystectomy performed through slightly enlarged incision for the hand-assisted device, and fenestration of incidentally discovered large liver cyst. Both remained in study analysis, but exclusion did not alter results substantially |
Table of results
| Weight change | QoL/comorbidity | Events/procedures (complications, reoperations) |
|---|---|---|
|
Median weight reduction (range): 4–6 weeks: hand 13 kg, open 13 kg 1 year: hand 39 kg (23–57), open 41 kg (26–57) Median BMI: 1 year: hand 29, open 30 Reduction in BMI was 15 units in both groups |
Hand Laparoscopic conversions to laparotomy: 0 Oozing intra-abdominal bleeding: three (two developed arterial bleeding after removing the left 12-mm epigastric trocar, stopped by compression in one, and in one the retracted traumatised epigastric artery was ligated after a fascial incision has been made) Open Two intense intraluminal bleeding from the gastrojejunostomy, managed by digital compression through the jejunotomy Peroperative and postoperative data, median (range) Abdominal wall thickness, cm: hand 6 (3–9), open 6 (5–7) Peroperative bleeding, ml: hand 250 (0–1300), open 250 (0–900) Duration of surgery, minutes: hand 150 (110–265), open 85 (60–150), p < 0.001 Reoperation: hand 1a, open 0 Patients requiring blood transfusion: hand 1 (2 units)b, open 1 (2 units)b Morphine requirement, mg: Day 1: hand (n = 25) 48 (12–148), open (n = 25) 32 (6–150) Day 2: hand (n = 20) 36 (14–123), open (n = 22) 30 (12–118) Day 3: hand (n = 16) 28 (12–99), open (n = 11) 25 (10–62) Total days 1–3: Hand 98 (12–370), open 66 (6–318) Length of hospital stay, days: hand 6 (4–14), open 6 (3–7) Deaths within 30 days postoperation: hand 0, open 0 Respiratory systems requiring prolonged antibiotic treatment and physiotherapy treatment: hand 8, open 5 Clinical deep vein thrombosis, pulmonary embolism, or wound dehiscence: hand 0, open 0 |
|
|
One month follow-up: Various grades of dysphagia: 18 (group not stated) Narrow anastomosis revealed by gastroscopy, with successful balloon dilatation (no stomal ulcers seen): Hand 2, Open 4 Wound infection with pus: hand 1, open 1 Abnormal secretions: 4 (group not stated) Total sick leave, days (n = 40), median (range): hand 30 (15–59), open 37 (19–95) 10 patients retired or on long-term sick leave One year follow-up Anaemic requiring intensive treatment: two women Symptomatic incisional hernia: hand 0, open 1 Short-term treatment with a proton pump inhibitor: hand 3, open 3 Small stomal ulcer revealed by gastroscopy: hand 0, open 1 One patient died 11 months after operation from metastatic breast cancer. Treatment not affected by gastric bypass |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Unclear | Randomised by sealed envelope after induction of anaesthesia. Stratified by sex |
| Allocation concealment? | Unclear | |
| Blinding of outcome assessors? | Unclear | Identical dressings were used so that nursing staff and patients were blinded to the treatment received. Patients informed of procedure at discharge |
| Blinding of participants on self-reported outcomes? | n/a | |
| Incomplete outcome data addressed? Weight loss | Yes | No patient dropped out after randomisation and follow-up data were available for all patients. Protocol violated in two patients in Hand group – cholecystectomy performed through slightly enlarged incision for the hand-assisted device, and fenestration of incidentally discovered large liver cyst. Both remained in study analysis, but exclusion did not alter results substantially |
| Incomplete outcome data addressed? QoL | n/a | |
| Incomplete outcome data addressed? Comorbidity | n/a | |
| Free of selective outcome reporting? | Unclear | Median BMI reported at 12 months. No measures of variance reported |
| Free of other sources of bias? | No | Appears to be higher co morbidity in the Open group |
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Westling and Gustavsson 2001131 Design: single centre, RCT Follow-up: 1 year |
Country: Sweden Number: total 51, LRYGBP 30, open 21 Age: 36 years (± 9) Sex: 94% female BMI: LRYGBP 41 (± 4), open 44 (± 4) Characteristics of target population: people with BMI > 40 or BMI > 35 with significant comorbidity; failed in various supervised non-surgical long-term weight loss programmes within hospital; fully informed of operation and consequences Exclusion criteria: 70 patients were excluded before randomisation because they were unsuitable for laparoscopy (n = 21), had gallstones (n = 7), or were scheduled for RYGBP as a revisional procedure (n = 42) |
|
Complications from standard questionnaire on stomach pain, vomiting, dysphagia, nausea, diarrhoea, excessive dumping, general well-being, need for sick leave Body weight Incisional hernias |
Allocation to treatment groups: blocked randomisation 60% laparoscopic and 40% open due to presupposed need for conversion. Stratified for gender, not BMI. Used sealed envelopes in theatre Blinding: patients and ward staff were blinded to procedure with the use of sham bandages. Patients were informed on discharge Comparability of treatment groups: mean preoperative BMI was lower in the laparoscopy group (p < 0.05). Well balanced for concomitant medications. No other comparative information provided Method of data analysis: mean and standard deviation, median and range, Student’s t test, chi-squared, rank sum test and linear regression. Significance at p < 0.05 Sample size/power calculation: none stated Attrition/dropout: no patients were lost to follow-up Generalisability: predominantly limited to females, aged in mid- to late 30s who are morbidly obese Intercentre variability: single centre Conflict of interests: none stated |
Table of results
| Weight change | QoL/comorbidity | Events/procedures (complications, reoperations) |
|---|---|---|
|
Mean BMI 1 year: LRYGBP 27 (± 4); open 30.6 (± 4) Mean change in BMI 1 year: LRYGBP 14 (± 3); open 13 (± 3) (p = ns) |
Patient satisfaction All patients: 92% very satisfied, 8% satisfied. No difference between groups (no data reported) |
Complications Deaths: one LRYGBP from malignant hyperthermia (family history) Gastrointestinal symptoms (dumping/vomiting/diarrhoea): 5% of all patients Incisional hernia one LRYGBP; small embolus one LRYGBP; colicky pain and vomiting because of narrow stricture of tunnel through mesocolon five LRYGBP, and to herniated Roux limb one LRYGBP; leakage because of failure of hand sewn part, one open (reoperated); jejunal ulcers three LRYGBP, two open (p = ns); stricture in gastrojejunostomy: one LRYGBP treated by endoscopic dilatation; superficial wound infection: three open Readmission: LRYGBP one (for unexplained fever); open: three [pneumonia (one), epigastric pain and/or vomiting with normal gastroscopy (two)] Surgical outcomes Conversions: seven (23%) LRYGBP patients converted to open (due to either bleeding (four) or other operative concerns). Duration (minutes): LRYGBP(n = 30) 245 (135–390); open (n = 21) 100 (70–150) Preoperative bleeding (ml): LRYGBP(n = 30) 250 (50–1500); open (n = 21) 300 (200–500) Six (20%) LRYGBP patients without conversion reoperated (these were the 6 LRYGBP above with colicky pain and vomiting) Early postoperative outcomes Pain – morphine dose (mg): LRYGBP (n = 29) 98 (± 71.5) (p = ns); LRYGBP: conversions excluded (n = 22) 69 (± 46.4) (p < 0.005); open (n = 21) 140 (± 90) Hospital stay (days): LRYGBP (n = 29) 4.5 (± 1.2) (p = ns); LRYGBP: conversions excluded (n = 22) 4 (± 0.8) (p = 0.025); open (n = 21) 6 (± 3.8) Sick leave (weeks): LRYGBP (n = 24) 3.9 (± 2.1) (p = ns); LRYGBP: conversions excluded (n = 18) 2.8 (± 1.8) (p = 0.025); open (n = 14) 5 (± 3.3) |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Unclear | Blocked randomisation 60% laparoscopic and 40% open due to presupposed need for conversion. Stratified for gender, not BMI |
| Allocation concealment? | Unclear | Used sealed envelopes in theatre |
| Blinding of outcome assessors? | Unclear | Patients and ward staff were blinded to procedure with the use of sham bandages. Patients were informed on discharge. No description of blinding of outcome assessors |
| Blinding of participants on self-reported outcomes? | No | Patient satisfaction at 1 year reported (patients were informed on discharge) |
| Incomplete outcome data addressed? Weight loss | Yes | No patients were lost to follow-up |
| Incomplete outcome data addressed? QoL | n/a | |
| Incomplete outcome data addressed? Comorbidity | n/a | |
| Free of selective outcome reporting? | Unclear | |
| Free of other sources of bias? | No | Mean preoperative BMI was lower in the laparoscopy group (p < 0.05). Well balanced for concomitant medications. No other comparative information provided. Blocked randomisation in an unblinded study |
Appendix 13 Data extraction tables: open versus laparoscopic vertical banded gastroplasty
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
Davila-Cervantes 2002111 Design: RCT, single centre Follow-up: 1 year |
Country: Mexico Number: total 30, open 14, LVBP 16 Age median: open 36.5 years (22–56), LVBP 34.5 years (24–46) Sex, F : M: open 13 : 1, LVBP 14 : 2 BMI median: open 43 (37–50), LVBP 45 (38–50) Excess body weight: open 91%, LVBP 100% Comorbid, n: open 8, LVBP 9 Characteristics of target population: all morbidly obese patients seen at the Obesity Clinic between 1999 and 2000 who were considered candidates for bariatric surgery Inclusion criteria: BMI 40–50, no previous surgery in upper abdomen, no formal contraindication for laparoscopic surgery Exclusion criteria: active peptic ulcer disease, history of high carbohydrate intake |
|
Surgical time Blood transfusions Conversions Length of stay BMI % excess body weight Analgesic requirements Spirometric parameters postoperatively (not extracted) Mobilisation postoperatively (not extracted) Daily activities (not extracted) |
Allocation to treatment groups: randomised on morning of operation using sealed envelopes Blinding of outcome assessors: identical dressings were used in all patients to avoid bias of the patient or evaluator. All dressings removed after 72 postoperative hours or before if complication occurred (therefore unblinding) Comparability of treatment groups: states that groups were highly comparable in terms of general characteristics, no statistically significant differences. Baseline data for age, sex, BMI, % excess body weight and number of comorbid diseases presented Method of data analysis: frequencies or medians and minimum and maximum values presented. Groups compared using Pearson’s chi-square, Fisher’s exact test or Mann-Whitney U test Sample size/power calculation: not reported Attrition/dropout: states that the surgical procedure was completed in all patients and none were lost during follow-up |
Table of results
| Weight change | QoL/comorbidity | Events/procedures (complications, reoperations) |
|---|---|---|
|
Excess body weight loss at 12 months: Open 55% (30–88), LVBP 47% (22–97) BMI at 12 months (estimated from figure): open 33, LVBP 33 |
Surgical details (median, min–max) Surgical time: open 1.45 hours (1.1–2.5), LVBP 2.1 hours (1.5–4.0), p < 0.002 Blood transfusions: open 0, LVBP 0 Conversion: LVBP 0 Hospitalisation: open 4 days (3–42a), LVBP 4 days (3–97a), p = ns Complications Open: six wound problems (seroma, dehiscence or infection) LVBP: one pulmonary atelectasis requiring physical therapy, one wound infection No significant difference in pain intensity Number of extra doses of analgesics: 1st postoperative day: open 2 (0–3), LVBP 1 (0–2), p = 0.04 2nd postoperative day: open 1 (0–1), LVBP 2 (0–2), p = 0.78 3rd postoperative day: open 1 (0–1), LVBP 0 (0), p = 0.46 12 months follow-up (median, range): Patient satisfaction: open 1 (0–2), LVBP 2 (0–2), p = 0.006. (0 = dislike, 1 = neutral, 2 = satisfied) Number with pathological scar: open 12, LVBP 5, p = 0.002 Open: two patients developed abdominal wall hernias |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Unclear | Randomised on morning of operation using sealed envelopes |
| Allocation concealment? | Unclear | No details |
| Blinding of outcome assessors? | Unclear | Identical dressings used in all patients to avoid bias of the patient or evaluator. All dressings removed after 72 hours or before if complication occurred (therefore unblinding) |
| Blinding of participants on self-reported outcomes? | n/a | |
| Incomplete outcome data addressed? Weight loss | Yes | States that the surgical procedure was completed in all patients and none were lost during follow-up |
| Incomplete outcome data addressed? QoL | n/a | |
| Incomplete outcome data addressed? Comorbidity | n/a | |
| Free of selective outcome reporting? | Unclear | |
| Free of other sources of bias? | Unclear |
Appendix 14 Data extraction tables: open versus laparoscopic adjustable silicone gastric banding
Characteristics of study
| Study | Participants | Interventions | Outcomes | Notes |
|---|---|---|---|---|
|
de Wit 1999132 Design: single centre, RCT Follow-up: 1 year |
Country: Netherlands Number: total 50, LAGB 25, open AGB 25 Age: not reported Sex: LAGB 68% female, open AGB 68% female Weight (mean): LAGB 152.2kg (SD 31.4), open AGB 146.4kg (SD 19.9) BMI: LAGB 51.3 (SD 10.4), open AGB 49.7 (SD 5.6) Characteristics of target population: history of obesity > 5 years, BMI > 40, documented attempts at weight loss in past, good motivation for surgery, aged 18–55 years Exclusion criteria: Previous gastric surgery, large hiatal hernias, alcohol abuse, pregnancy, psychiatric disease or treatment, hormonal or genetic obesity related diseases Considered ineligible by gastroenterologist after evaluation. High risk for anaesthesia |
|
Surgical complications Length of hospital stay Difficulty of procedure Surgical time In-hospital deaths Long-term complications Additional procedures Readmissions Mean weight loss Reduction of BMI |
Allocation to treatment groups: randomised after stratification into gender and BMI 40–45, 45–50, and greater, by computer generated randomisation by separate group Blinding: outcome assessments not stated Comparability of treatment groups: two groups were comparable in sex, age, mean weight, BMI and laboratory test results. No significant differences between groups Method of data analysis: although results appeared to be ITT, two LAGB patients were converted to open AGB. Mann–Whitney U test used to compare data. Means, SD and p values given Sample size/power calculation: for weight loss assumed that no differences in weight loss will be found between groups, considered 10% difference of weight acceptable and clinically unimportant (significance 95%, power 80%). For hospital stay assumed a reduction in hospital stay could be expected from 8 days after open AGB to 4 days after LAGB (significance 95%, power 90%) Attrition/dropout: one patient in group 2 lost to follow-up after 1 year Generalisability: inclusion/exclusion criteria defined, unclear what cut-offs were to be used for various investigations, or if any were excluded Outcome measures: weight loss yes, unclear how objective other measures are. Only 1 year follow-up Intercentre variability: all one surgeon and one of two anaesthetists Conflict of interests: not mentioned Other: significant weight lost but BMI remained around 40 |
Table of results
| Weight change | QoL/comorbidities | Events/procedures (complications, reoperations) |
|---|---|---|
|
Mean weight loss (12 months): LAGB 35kg, open AGB 34.4 kg (p = ns) Reduction from baseline p < 0.05 for LAGB and open AGB BMI reduction (12 months): LAGB 11.6, open AGB 10.6 (p = ns) Reduction from baseline p < 0.05 for LAGB and open AGB |
Not assessed |
Early postoperative complications (LAGB vs open AGB): cholecystectomy (8% vs 20%); adhesiolysios (4% vs 0%); gall bladder puncture (to obtain samples for study purposes): (0% vs 28%); pulmonary complications (8% vs 8%); urinary infection (8% vs 0%); rhabdomyolysis (4% vs 0%); neurological complication (neuropraxis) (4% vs 4%); perforation pouch (0% vs 4%); wound abscess (0% vs 4%); fever (0% vs 8%); gout (0% vs 4%) First year surgical complications (LAGB vs open AGB): incisional hernia [0% vs 28% (seven hernias in three (12%) patients; p = ns]; migration band (0% vs 4%, p = ns); umbilical hernia (4% vs 0%, p = ns) First year access port complications: total 28% (20% patients) vs 24% (20% patients), p = ns; dislocation (8% vs 4%, p = ns); dislodgement (20% vs 16%, p = ns); infection (0% vs 4%, p = ns); replacement (20% vs 16%, p = ns) Mean days in hospital: LAGB 5.9 (range 4–10); open AGB 7.2 (range 5–13) p < 0.05 Readmissions (LAGB vs open AGB): patients 20% vs 28%, p = ns; total readmissions: 24% vs 60%, p < 0.05 Mean overall length of hospital stay (LAGB vs open AGB): 7.8 days (SD 6) vs 11.8 days (SD 10.5), p < 0.05 Conversions: LAGB to open AGB procedure: 8% Surgical time: LAGB 150 minutes (SD 48), open AGB 76 minutes (SD 20) p < 0.05 Mean rating of difficulty of procedure on 1–10 scale (1 = easy, 10 = could not be performed or had to be converted: LAGB 4.7 (SD 2.1, range 3–10), open AGB 3.8 (SD 1.1, range 3–7) p < 0.05 |
Risk of bias
| Item | Judgement | Description |
|---|---|---|
| Adequate sequence generation? | Yes | Randomised after stratification into gender and BMI 40–45, 45–50, and greater, by computer-generated randomisation by separate group |
| Allocation concealment? | Yes | Central allocation – patients randomly allocated by computer on day of surgery |
| Blinding of outcome assessors? | Unclear | Not stated |
| Blinding of participants on self-reported outcomes? | n/a | |
| Incomplete outcome data addressed? Weight loss | Yes | One patient in group 2 lost to follow-up after 1 year. No reasons documented |
| Incomplete outcome data addressed? QoL | n/a | |
| Incomplete outcome data addressed? Comorbidity | n/a | |
| Free of selective outcome reporting? | Unclear | |
| Free of other sources of bias? | Unclear |
Appendix 15 Data extraction tables: systematic review of cost-effectiveness studies
Reference
|
Ackroyd, R. Mouiel, J. Chevallier J.-M. Daoud F. 138 Cost-effectiveness and budget impact of obesity surgery in patients with Type 2 diabetes in three European countries |
Study characteristics
Research question
What are the stated objectives of the evaluation?
| To establish a payer-perspective cost-effectiveness and budget impact model of adjustable gastric banding (AGB) and gastric bypass (GBP) versus conventional treatment (CT) in patients with BMI ≥ 35 kg/m2 and Type 2 diabetes (T2DM) in Germany, UK and France. |
Study population
What definition was used for obesity?
| BMI ≥ 35 kg/m2, i.e. eligibility for bariatric surgery |
What are the characteristics of the baseline cohort for the evaluation?
| Age | Not reported |
| Sex | Not reported |
| Race (if appropriate) | Not reported |
| Comorbidities | Type 2 diabetes |
| Other characteristics | The population in the cost-effectiveness analysis consists of obese T2DM patients who failed at least one previous year of well-conducted medical treatment (not elaborated) |
Interventions and comparators
What number of interventions/strategies were included?
| Two |
Was a no treatment/supportive care strategy included?
| Yes – the conventional treatment (CT) although no single standard was identified across the countries. Therefore CT was identified as either ‘annual follow-up watchful waiting’ or ‘continuation of the second year of a medically guided dieting’. In the latter case it was assumed to take place for the first year followed by conventional treatment of T2DM and no weight-reducing interventions over the remaining 4 years assumed in an economic evaluation. |
Describe interventions/strategies
|
Intervention/strategy 1: adjustable gastric banding (AGB) Intervention/strategy 2: [laparoscopic] gastric bypass (GBP) Pair-wise comparisons were performed, i.e. AGB versus CT and GBP versus CT; AGB was not compared to GBP in cost-effectiveness analysis. |
Analytical perspective
What is the perspective adopted for the evaluation [health service, health and personal social services, third party payer, societal (i.e. including costs borne by individuals and lost productivity)]?
|
The payers’ perspective (in case of the UK this is the National Health Service) |
Study type
Cost-effectiveness/cost–utility/cost–benefit analysis?
|
CEA (incremental cost per BMI × year; incremental cost per T2DM-free year) CUA (Incremental cost per QALY) |
Institutional setting
Where is/are the intervention(s) being evaluated usually provided?
| Not indicated, but presumably hospitals for AGB and GBP and predominately ambulatory care for CT |
Country/currency
Has a country setting been provided for the evaluation? In what currency are the costs expressed and does the publication give the base year to which those costs relate?
| Currency is a 2005 euro (€) in the case of Germany and France and a 2005 British Pound (£) in surgical interventions. The cost of comparator treatment is expressed in 1998 prices (according to the source – CODE-2 data) |
Data sources
Effectiveness
Were the effectiveness data derived from:
| Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? | |
| A single study | ||
| A review/synthesis or combination of previous studies | ✓ |
It does not seem that a systematic review was undertaken, clinical data were obtained from the HTA reports (Clegg, 2002, NICE guidelines) and their analogues in EU countries. These data were complemented by the search in June 2005 of PubMed for the RCT and non-comparative prospective series of consecutive surgery patients that were published after the HTA reports. For AGB the data on BMI reduction and T2DM prevalence (and the rates of complications though these are not effectiveness outcomes) were taken from 13 publications (ref 46–58 in Ackroyd et al. 138). For GBP the data on BMI reduction and T2DM prevalence were extracted from (ref 59–69 in Ackroyd et al. 138) the rate of complications from one systematic literature review (24) and a single cohort study of 400 patients (70). Effectiveness of the comparator CT in terms of BMI and T2DM over 3 years was taken from the Swedish HTA systematic review (2002) and the US Clinical guidelines (1998) (ref 23, 25 in Ackroyd et al. 138) and extrapolated for years 4 and 5. |
| Expert opinion | ✓ | In particular in estimating the frequency of complications, where experts opinion took priority over the published data (p. 1489) |
Give the definitions of treatment effect used in the evaluation
|
In each year over the period of 5 years (the time interval used in cost-effectiveness analysis) the outcome is defined as a change in BMI from the baseline multiplied by 1 year. This is called annual marginal effectiveness and expressed in kg/m2 × year. The aggregate outcome is a cumulative reduction in BMI over the specified period (e.g. 5 years). In each year over the period of 5 years the effectiveness with respect to the T2DM status is assessed in an incremental change in proportion of patients free of T2DM from the baseline. This is called an ‘annual marginal T2DM-free year gained at a particular year’. The average cumulative T2DM-free years are calculated by aggregating T2DM-free years over the specified period (e.g. 5 years). |
Give the size of treatment effect used in the evaluation
|
The authors did not elaborate on the clinical meaning of the reduction in BMI which varied across the interventions |
include values used for subgroups (if applicable). Indicate the source for individual treatment effects (if appropriate)
Intervention costs
Were the cost data derived from:
| Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? | |
| A single (observational) study | ||
| A review/synthesis or combination of previous studies | ✓ | Some cost inputs were taken from the literature, e.g. annual cost of diabetes treatment (Jonsson, 2002)159. The complete list of references was not provided. |
| Expert opinion | ✓ | Resource use for (alternative interventions?) in natural units was obtained from the literature (no references were provided). Clinicians were asked to provide their opinion on the plausibility of the amount of resources (lowest in the range, average, highest number) |
List the direct intervention costs used in the evaluation – include resource estimates (and sources for these estimates, if appropriate) as well as sources for unit costs used
| Resource category | Type of resources | Unit cost estimate (UK data) | Source | |
|---|---|---|---|---|
| Intervention costs (laparoscopic GBP and AGB) | It seems that for each type of surgical intervention the range of resource items was identified, checked with experts and multiplied by the corresponding unit costs | Not reported in detail |
Not elaborated ‘Ranges and unit costs were collected using applicable national tariffs, registries, publications and interviews when no other source was available’ (p. 1489). Usual resource use for initial admission was confirmed by two NHS hospitals (p. 1492) See tables 6–8 in Ackroyd et al. 138 In Germany and France the DRG-type tariffs were used to estimate the cost of initial admission |
|
| In UK the costs of initial admission was based on ‘micro-costing’ (p. 1491) and seems to include: | AGB | GBP | ||
| aggregated cost of preoperative assessment | £610 | £610 | ||
| hospital staff costs (surgeons, physicians, nurses, nutritionists) | Not indicated | |||
| implants | £1175 | £2591 | ||
| imaging and laboratory tests | Not indicated | |||
| operating room overheads (in proportion to hours); | £492 hours = 1.9 | £186.71 hours = 3.84 | ||
| postsurgical recovery room [per diem × length of stay (LOS)] | £241, LOS = 5 | £235, LOS = 4.88 | ||
| [other?] consultations | Not indicated | |||
| average annual cost of follow-up | £439 | £312 | ||
|
£492 £186.71 hours=1.9 hours=3.84 £241 £235 LOS=5 LOS=4.88 Not indicated £439 £312 |
||||
Comparator conventional treatment (1999 prices)
| Cost of treating T2DM applies to all patients in the comparator and patients from intervention groups who did not achieve a remission | First year |
CODE-2 survey published in Jonsson159 Original estimates are reported in euros Conversion rate is not reported but it seems to be £1 = 1.54 € |
|
| GP consultations n = 4 | £14 | ||
| District nurse consultations n = 2 | £20.50 | ||
| Practice nurse consultations n = 2 | £5.50 | ||
| Dietician consultations n = 2 | £23 | ||
| Laboratory assessments | £150 | ||
| Food substitutes n = 56 | £1 | ||
| Ambulatory care | £543 | ||
| Anti-diabetic drugs | £44 | ||
| Other drugs | £337 | ||
| Hospital care | £500 | ||
| The cost of years 2–5 does not include district nurse and practice nurse consultations, food substitutes or dietitian consultations |
Other direct costs
(Cost of postsurgical complications)
Were the cost data derived from:
| Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? | |
| A single (observational) study | ||
| A review/synthesis or combination of previous studies | ✓ | The ranges and averages reported in the literature (no references were provided) served as a reference base. |
| Expert opinion | ✓ | Authors’ expert opinion was used instead when published data appeared obsolete. |
List the costs used in the evaluation – if quantities of resource use are reported separately from cost values, show sources for the resource estimates as well as sources for unit costs used.
| Cost of complications (not clear whether the resource items were collected by the type of complication, specific to each intervention, and then aggregated as a weighted sum where weights are the frequency of each complication Tables 3–4. Alternatively average cost across all complication was attributed to each intervention in some way) | ||
| Tables 6, 7 | AGB | GBP |
| Preoperative assessment | £610 | £610 |
| Initial hospital admission for surgery | £3314.80 | £4455.64 |
| Annual follow-up | £439 | £312 |
| indicate the source for individual cost values (if appropriate) | ||
Indirect costs
(costs due to lost productivity, unpaid inputs to patient care)
Were indirect costs included:
| Not applicable |
Describe how indirect costs were estimated (e.g. how days of lost productivity were estimated and how those days were valued)
| Not applicable |
indicate the source for individual cost values (if appropriate)
Health state valuations/utilities (if study uses quality of life adjustments to outcomes)
Were the utility data derived from:
| Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? | |
| The EQ-5D utility estimates were derived from a database of 13,547 individuals according to their BMI and T2DM status. | ✓ | The methods for deriving utility estimates were not clearly described. The source of the estimates is empirical data from the Health Outcomes Data Repository. HODaR Cardiff Research Consortium. www.crc-limited.co.uk |
| A review/synthesis or combination of previous studies | ||
| Expert opinion |
List the utility values used in the evaluation
|
Although the methods for deriving utility estimates were not clearly explained, it seems that initially the utility weights for T2DM and non-T2DM subgroups were estimated from two separate regression equations derived from the empirical data (HODaR). for T2DM: u = – 0.0108 BMI + 0.8654 for non-T2DM: u = – 0.0128 BMI + 1.0254 The authors reasonably assumed that there might not be a statistically significant difference in the estimates of regression coefficients (slope) between T2DM and non-T2DM subgroups. Therefore alternative (not specified) regression equations were used to estimate utility values in both subgroups. It seems that the modified regression equations for T2DM and non-T2DM subgroups have different constant terms (from the original regression equations) but the same slope, equal to the weighted average of the slopes in regression equations for two separate subgroups. |
indicate the source for individual utility values (if appropriate)
Modelling
|
The authors used a ‘deterministic linear algorithm’ which can be interpreted as a simple decision analytic model. The cumulative outcomes with respect to BMI and T2DM over the 5-year period were obtained by multiplying the probability of reduction in BMI from the baseline and reduction in% of patients with T2DM from the baseline (100% of patients with T2DM) in each year and aggregating across the time interval. It was assumed that the probability of obtaining a particular value of the outcome in each year was independent of the value of this or another outcome in the previous year (i.e. the implicit assumption is that the BMI reduction occurs independently of the T2DM status). No discounting was used with respect to these outcomes. The outcome expressed in QALYs was obtained by combining separate utility estimates in proportion to T2DM and non-T2DM prevalence and according to the BMI reduction observed in any particular year and aggregating the calculated values over the 5 year period. The cost was calculated by combining the resources (multiplied by the corresponding unit prices) used in any particular year over the 5-year period. The 3.5% discounting rate was used. |
Was this a newly developed model or was it adapted from a previously reported model? If an adaptation, give the source of the original.
| The authors are aware of the more advanced modelling techniques but stated that ‘deterministic models prove reasonably accurate and more intuitive for stakeholders’ (p. 1496) |
What was the purpose of the model (i.e. why was a model required in this evaluation)?
| How do the surgery and continued conventional treatment compare in terms of outcomes, costs and value for money in patients in whom conventional treatment has already been proven to fail (p. 1496) |
What are the main components of the model (e.g. health states within a Markov model)? Are sources for assumptions over model structure (e.g. allowable transitions) reported – list them if reported.
| The health state to which utility weights are applied is solely determined by the combination of BMI and the T2DM status. No other obesity related comorbidity was included. The postsurgery complications are not considered to be a differential clinical outcome in comparing different types of interventions therefore no corresponding health state was identified in the calculation. This is inconsistent with the differential accounting of the cost of complications associated with GBP and AGB. Also, an implicit assumption in cost-effectiveness calculations is that no patient dies over the 5-year period (i.e. a health state associated with ‘death’ was not included). |
Extract effectiveness data for [natural history/disease progression] model and show sources (refer to table 1 and table 5, p. 1492, p. 1494, sources are not clearly indicated)
| Comparator | ||
|---|---|---|
| Change from the baseline status: 100%T2DM and BMI ≥ 35 kg/m2 prevalence | Change in BMI | Change in T2DM |
| Year 1 | – 2.0 | 20% |
| Year 2 | 0 | 0% |
| Year 3 | 0 | 0% |
| Year 4 | 0 | 0% |
| Year 5 | 0 | 0% |
| AGB | ||
| Change from baseline status: T2DM and BMI ≥ 35 kg/m2 | Change in BMI (SD or range?) | Change in T2DM prevalence |
| Year 1 | – 9.2 (6.6–13.9) | 64% |
| Year 2 | – 11.2 (9.0–17.9) | 45% |
| Year 3 | – 12.3 (8.5–19.0) | 56% |
| Year 4 | – 14.9 (14.9–19.1) | 50% |
| Year 5 | – 13.2 (12.3–15.0) | 50% |
| GBP | ||
| Change from baseline status: T2DM and BMI ≥ 35 kg/m2 | Change in BMI (SD or range?) | Change in T2DM prevalence |
| Year 1 | – 17.7 (13.0–20.0) | 82% |
| Year 2 | – 16.9 (13.0–18.0) | 50% |
| Year 3 | – 16.9 (13.0–18.0) | 75% |
| Year 4 | – 16.2 (10.0–18.0) | 50% |
| Year 5 | – 16.1 (8.0–18.0) | 50% |
What is the model time horizon? Duration of the cycle?
| The time interval in cost-effectiveness analysis is 5 years. The authors stated that this time interval was recommended by Clegg et al. (2002).15 |
What, if any, discount rates have been applied in the model? Same rate for costs and outcomes?
| All costs and QALYs were discounted at a 3.5% annual rate. The BMI × year and T2DM-free years were not discounted. It is not clear whether discounted or undiscounted incremental cost was used in calculating cost-effectiveness ratios with respect to these outcomes. |
Results/analysis
What measure(s) of benefit were reported in the evaluation?
| BMI × year; T2DM-free year; QALY |
Provide a summary of the clinical outcome/benefits estimated for each intervention/strategy assessed in the evaluation (UK data only. See table 10, p. 1496)
|
Over 5-year time interval LAGB as compared to CT is associated with incremental undiscounted 57.8 kg/m2 × year; incremental undiscounted 2.5 years free of T2DM incremental discounted 1.0 QALY LGBP as compared to CT is associated with incremental undiscounted 80.8 kg/m2 × year; incremental undiscounted 2.6 years free of T2DM incremental discounted 1.3 QALY |
Provide a summary of the costs estimated for each intervention/strategy assessed in the evaluation (table 13, p. 1498)
|
Over the 5-year time interval ABG as compared to CT is associated with incremental £1984 per patient GBP as compared to CT is associated with incremental £2033 per patient It is not clear whether the costs reported in table 13 were discounted or not as there is no correspondence with the discounted cumulative costs reported in tables 6–9. |
Synthesis of costs and benefits – are the costs and outcomes reported together (e.g. as cost-effectiveness ratios)? If so, provide a summary of the results.
|
The comparative performance of alternative treatment strategies was measured by the incremental cost-effectiveness ratio (ICER), defined as the incremental cost of a surgery, divided by the incremental outcome. (p. 1494) AGB as compared to CT ICER = £34.3 per kg/m2 year ICER = £810 per T2DM-free year ICER is equal to £1929 per QALY gained, costs and outcomes are discounted at 3.5% GBP as compared to CT ICER = £25.2 per kg/m2 year ICER = £776 per T2DM-free year ICER is equal to £1517 per QALY gained, costs and outcomes are discounted at 3.5% |
Give results of any statistical analysis of the results of the evaluation.
| None provided |
Was any sensitivity analysis performed – if yes, what type(s) (i.e. deterministic (one-way, two-way etc) or probabilistic).
|
The authors conducted analysis called ‘worst case scenario’. In this analysis the clinical effectiveness of AGB and GBP is said to be reduced by 20% with respect to both BMI reduction and T2DM prevalence in interventions and no temporary benefits from CT assumed in the first year. No change in cost estimate was assumed. The figures reported in table 14 (p. 1500) that were allegedly used in the sensitivity analysis do not seem to correspond to the 20% reduction in BMI and T2DM prevalence. Because removal of the small benefits of CT assumed in the first year in the base-case scenario are unlikely to have a significant contribution to the change in the ICER estimated in the ‘worst-case scenario’, it may be considered as a two-way sensitivity analysis with respect to the outcome expressed in QALYs and one-way sensitivity analysis with respect to the ICER expressed in terms of BMI reduction and T2DM prevalence. UK data only The ICER for AGB compared to CT changed from £1929 to £3251 per QALY and almost doubled with respect to T2DM-free years. The ICER for GBP compared to CT changed from £1517 to £2599 per QALY and almost doubled with respect to T2DM-free years |
What scenarios were tested in the sensitivity analysis? How do these relate to structural uncertainty (testing assumptions over model structure such as relationships between health states), methodological uncertainty (such as choices of discount rate or inclusion of indirect costs) or parameter uncertainty (assumptions over values of parameters in the model, such as costs, quality of life or disease progression rates)?
| Assuming that patients in CT do not continue receiving any active medical treatment that they have failed in Year 1 can be considered an equivalent to scenario analysis. However, this was not conducted independently of the sensitivity analysis which varied the estimates of clinical effectiveness. |
Give a summary of the results of the sensitivity analysis – did they differ substantially from the base-case analysis. If so, what were the suggested causes?
|
The ICER (regardless of the choice of the outcome) is very sensitive to the assumptions about clinical effectiveness. The sensitivity of results to the variations in utility estimates was not tested. The authors concluded that ‘The level of reaction displayed by the model… suggests that the model is a relatively reliable instrument to address the questions for which it has been designed with real life inputs. Moreover, the ability to BMI × years and T2DM-free years as an alternative to QALY removes the inevitable uncertainty related to interpretation of outcomes as patient-interpreted utility.” |
Conclusions/implications
Give a brief summary of the author’s conclusions from their analysis
| Authors suggested that in patients with BMI ≥ 35 kg/m2 and T2DM in AGB and GBP (in comparison to CT) are effective at 5 year follow-up in cost-savings in Germany and France, and are cost-effective in UK (p.1488 –abstract). |
What are the implications of the evaluation for practice?
|
The authors stated (p. 1495–6) that the budget impact over 5 years of treating a cohort of 1000 in Germany with bariatric surgery instead of conventional treatment is a net saving of 5.03 million euros in the case of GBP and 3.6 million euros in the case of AGB. In France a net savings of 5.88 million euros in the case of GBP and 4.48 million euros in the case of AGB. In the UK it is a net cost increase of 2.03 million pounds in the case of GBP and 1.98 million pounds in the case of AGB. The authors do not comment on the reversal in the results with respect to the UK but it seems that this can be explained by the difference in the cost of CT, which is estimated as more expensive in Germany and in France than in UK (approximately by €6000 and €4000, respectively). This difference in estimates of the cost of CT may relate to the difference in methodological approach to cost data collection or the differences in the resource use associated with comparator treatment or a combination of both. In either case, the results are not strictly comparable across the countries. |
Reference
|
van Mastrigt, G.A.; van Dielen, F.M.; Severens, J.L.; Voss, G.B.; Greve,J.W. 139 One-year cost-effectiveness of surgical treatment of morbid obesity: vertical banded gastroplasty versus Lap-Band® |
Study characteristics
Research question
What are the stated objectives of the evaluation?
| To evaluate the 1-year cost-effectiveness of surgical treatment of morbid obesity comparing two strategies: [open] Vertical Banded Gastroplasty (VBG) versus Lap-Band® (Laparoscopic Adjustable Gastric Banding System – AGB) by conducting an economic evaluation alongside a randomised clinical trial (n = 100, split equally between the arms nVBG = 50; nAGB = 50) |
Study population
What definition was used for obesity?
| BMI > 40 kg/m2 or between 35 and 40 if significant comorbidity is present. |
What are the characteristics of the baseline cohort for the evaluation?
| Age | In VBG arm mean age was 38.9 (SD = 8.53) |
| In AGB arm mean age was 37.2 (SD = 9.64) | |
| Sex | In VBG arm female patients = 80% |
| In AGB arm female patients = 78% | |
| Race (if appropriate) | Not reported |
| Comorbidities | 14% in VBG arm and 10% in AGB arm had Type 2 diabetes |
| 20% in VBG arm and 14% in AGB arm had hypertension | |
| For the full list of comorbidities see table 1 p. 78 | |
| Other characteristics | In VBG arm the mean BMI was 46.5 (SD = 6.42) |
| In AGB arm the mean BMI was 46.5 (SD = 6.42) | |
| Occupational status was recorded (to conduct CEA from the societal perspective) |
Interventions and comparators
What number of interventions/strategies were included?
| Two |
Was a no treatment/supportive care strategy included?
| No |
Describe interventions/strategies
|
Intervention/strategy 1: Vertical banded gastroplasty (VBG) Intervention/strategy 2: Laparoscopic adjustable gastric banding (AGB) |
Analytical perspective
What is the perspective adopted for the evaluation [health service, health and personal social services, third-party payer, societal (i.e. including costs borne by individuals and lost productivity)]?
| A societal perspective (including non-health-care system costs, e.g. the costs of informal care and lost productivity) |
Study type
Cost-effectiveness/cost–utility/cost–benefit analysis?
|
CEA (incremental cost per 1% of extra weight loss – EWL) CUA (Incremental cost per QALY) |
Institutional setting
Where is/are the intervention(s) being evaluated usually provided?
| Apparently a single Netherlands hospital. The randomised patients undertook either VBG or AGB from April 1999 to December 2002 |
Country/currency
Has a country setting been provided for the evaluation? In what currency are costs expressed and does the publication give the base year to which those costs relate?
| The resource use was originally assessed in Netherlands 1999 guilders and then converted to euros the conversion rate and a year to which it applied was not reported (2002?) |
Data sources
Effectiveness
Were the effectiveness data derived from:
| Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? | |
| A single study | ✓ | The clinical effectiveness data are reported in van Dielen et al.123 |
| A review/synthesis or combination of previous studies | ||
| Expert opinion |
Give the definitions of treatment effect used in the evaluation
| Percentage of excess weight loss. Clinical effect is not expressed in terms of BMI and is not easy to convert because the average height of the patients in each arm was not reported (maybe in the clinical paper?). |
Give the size of treatment effect used in the evaluation
| The percentage of excess weight loss (% EWL) at 12 months. The authors did not elaborate on the effect size that would be meaningful in clinical and economic senses (i.e. sufficient to detect a change in utility weights) |
include values used for subgroups (if applicable). Indicate the source for individual treatment effects (if appropriate)
Intervention costs
Were the cost data derived from:
| Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? | |
| A single (observational) study | ✓ |
Quantity of resource use in natural units with respect to surgery costs were obtained from the observational study for 10 surgical procedures of both types of surgery (p. 79). Other hospital costs were obtained from the hospital billing system. Other medical resource items (e.g. medications) were obtained from patients’ cost-diaries. |
| A review/synthesis or combination of previous studies | ||
| Expert opinion |
List the direct intervention costs used in the evaluation – include resource estimates (and sources for these estimates, if appropriate) as well as sources for unit costs used
| Resource category | Type of resources | Unit cost estimate | Source |
|---|---|---|---|
| Intervention costs (open VBG and laparoscopic AGB) |
Medical cost components: Inpatient days Clinical procedures Surgery Outpatient clinics Dietitian consults GP consultations prescribed medications |
The only unit costs that were reported were those that were subjected to the deterministic sensitivity analysis (see below). The unit cost of ‘time of the personnel’ involved in surgical procedures used in the base-case analysis was €2.96 per minute (p. 79) The inpatient cost per day (per diem) used in the base-case analysis was € 332 (p. 81) |
Quantity of resource use in natural units with respect to surgery costs was obtained from the (observational) study. Other hospital costs were obtained from the hospital billing system |
Other direct costs
(cost of postsurgical complications)
Were the cost data derived from:
| Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? | |
| A single (observational) study | ✓ | Out-of-pocket medical and non-medical expenses were obtained from patients’ cost-diaries. |
| A review/synthesis or combination of previous studies | ||
| Expert opinion |
List the costs used in the evaluation – if quantities of resource use are reported separately from cost values, show sources for the resource estimates as well as sources for unit costs used.
|
Out-of-pocket medical and non-medical expenses (not reported as a comprehensive list of items, no unit costs were not provided). Examples: cost of paid help over-the-counter medications |
| indicate the source for individual cost values (if appropriate) |
Indirect costs
(costs due to lost productivity, unpaid inputs to patient care)
Were indirect costs included:
|
Unpaid help was included Productivity loss was included |
| Describe how indirect costs were estimated (e.g. how days of lost productivity were estimated and how those days were valued) |
|
Quantity of unpaid help was apparently obtained from patients’ cost-diaries kept for the first 3 months after the surgery. How the change in occupational status and change in the sick leave days were collected is not clear Productivity loss was estimated by the friction cost method (not elaborated) |
indicate the source for individual cost values (if appropriate)
Health state valuations/utilities
(if study uses quality of life adjustments to outcomes)
Were the utility data derived from:
| Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? | |
| The EQ-5D utility estimates were derived from a database of 13,547 individuals according to their BMI and T2DM status. | ✓ | Yes. The EQ-5D data were collected from the trial participants at the baseline and at 3, 6 and 12 months of follow-up. (p. 77) |
| A review/synthesis or combination of previous studies | ||
| Expert opinion |
List the utility values used in the evaluation
| The utility values were collected observed at baseline, 3, 6 and 12 months using the EQ-5D. To obtain a QALY the EQ-5D scores were multiplied by the duration of time to which these scores related (p. 77). The mean utility values observed at each observation point were reported in the graphical format in figure 3 p. 79. There is a possibly statistically significant difference in utility values at the baseline (absolute baseline difference was not reported). At 3 and 6 months the utility scores in the comparator arm (VBG), which is associated with the higher values of%EWL are nevertheless lower than the utility scores in the AGB arm that correspond to the lesser%EWL. |
indicate the source for individual utility values (if appropriate)
Modelling
If a model was used, describe the type of model used (e.g. Markov state transition model, discrete event simulation)
| Model was not required for the economic evaluation alongside a clinical trial |
Was this a newly developed model or was it adapted from a previously reported model? If an adaptation, give the source of the original.
| Not applicable |
What was the purpose of the model (i.e. why was a model required in this evaluation)?
| Not applicable |
What are the main components of the model (e.g. health states within a Markov model)? Are sources for assumptions over model structure (e.g. allowable transitions) reported – list them if reported.
| The economic evaluation is not model-based. A ‘health state’ was not defined in terms of the disease progression. |
Extract effectiveness data for (natural history/disease progression) model and show sources
| The economic evaluation is not model-based. The intermediate outcome of %EWL was not converted in the final outcomes. See the observed clinical effectiveness results below |
What is the model time horizon? Duration of the cycle?
| One year |
What, if any, discount rates have been applied in the model? Same rate for costs and outcomes?
| Given the one-year time horizon discounting rates were appropriately not applied |
Results/analysis
What measure(s) of benefit were reported in the evaluation?
| %EWL; EQ-5D utility scores |
Provide a summary of the clinical outcome/benefits estimated for each intervention/strategy assessed in the evaluation
|
Statistical methods and assumptions in relation to comparing clinical effectiveness between the two arms were reported elsewhere (see van Dielen et al. 123) At 12 months in the VBG arm the mean loss of excess weight was 71.69% (SD = 20.79) In the AGB arm the mean loss of excess weight was 53.87% (SD = 20.64) The mean difference in %EWL of 17.82% was statistically significant (p < 0.001) At 12 months in the VBG arm the mean EQ-5D scores (weighted according to the time interval to which the observed values relate) was 0.76 (SD = 0.2) At 12 months in the AGB arm the mean EQ-5D scores (weighted according to the time interval to which the observed values relate) was 0.81 (SD = 0.13) The mean difference of 0.05 utility scores is not statistically significant (p = 0.138) Two patients from the VBG arm died within 30 days after surgery. EQ-5D data were missing in 8% of observations. Missing observations were substituted with mean values (calculated across the entire sample?). |
Provide a summary of the costs estimated for each intervention/strategy assessed in the evaluation (table 13, p. 1498)
| Cost components | VBG | AGB |
| Cost of surgery (p.79) | ||
| ‘Capacity’ cost | €67 | €158 |
| Material cost (including medication) | €691 | €2,143 |
| Overheads | €87 | €87 |
| Personnel (minutes x €2.96 -cost per minute) | 2.50 × 2.96 = €444 | 3.26 × 2.96 = €579 |
| Reported subtotal (not equal to the sum of the above) | €1676 | €3861 |
| Other costs of initial hospitalisation | ||
| Cost of inpatient days, including intensive care (length of stay by per diem specific to the type of care?) | not reported | not reported |
| Total cost of initial hospitalisation | €5954 | €5258 |
| Total cost of rehospitalisation (surgical department) | €599 | €724 |
| Reported total hospitalisation (≠ to the sum of the above) | €6679 | €5857 |
| Outpatient care | €869 | €1214 |
| Prescribed medications | €218 | €193 |
| Primary care | €339 | €71 |
| Cost of follow-up | €1426 | €1479 |
| Non-medical costs (change in productivity, paid help?) | €5080 | €3963 |
| Total direct and indirect costs (≠ to the sum of the above) | €13,185 (€ 14,611) | €11,299 (€12,777) |
|
In addition, the difference in length of stay was reported: AGB was associated with the mean stay of 5.56 (median 4) days and VBG was associated with the mean stay of 6.78 (median 4) days. Five patients from the VBG arm were admitted to the intensive-care unit and none from the AGB arm. In the AGB arm nine (18%) were readmitted to the hospital department and in the VBG arm five (10%) were readmitted (p. 80) Cost data from the patients’ diaries were missing in three cases (6%) in the VBG arm and in two cases (4%) in the AGB arm. Missing observations were substituted with mean values (calculated across the entire sample?). |
||
Synthesis of costs and benefits – are the costs and outcomes reported together (e.g. as cost-effectiveness ratios)? If so, provide a summary of the results.
|
On the basis of the observational data collected alongside an RCT involving 100 patients it appears that at 12 months the LAGB is both less expensive and less effective than VBG in terms of %EWL. The authors erroneously claimed that moving from VBG (comparator) to LAGB would involve an additional amount of €105.80 per each additional %EWL (– €1885.91/– €17.82) (p. 80). In fact, this amount is what society would be spending for choosing not to switch from VBG to LAGB. Moving from VBG to AGB would involve a saving of €105.80 per each % extra weight retained. With respect to the outcome expressed in QALYs a different (and somewhat contradictory) result was reported: LAGB appears to be both less expensive and more effective than VBG (i.e. a dominant strategy). In QALY calculations the utility values were adjusted for the duration of the time interval to which they relate (therefore the values reported on p. 79 do not correspond to the values in figure 3). The procedure is likely to have reduced the bias in the estimate of the utility gain that comes from the difference in utility scores observed at the baseline. |
Give results of any statistical analysis of the results of the evaluation.
|
Incremental costs and effects were analysed using bootstrap sampling method to estimate the joint distribution of incremental costs and outcomes. In the bootstrap analysis with respect to %EWL outcome was conducted and involved 1000 replications. In this analysis LAGB in comparison to VBG was both less effective and less costly in 86% of trials; in 14% of trials it was less effective and more expensive (i.e. dominated by VBG). With respect to the outcomes expressed in QALYs a different (and somewhat contradictory) result was reported: LAGB appears to be both less expensive and more effective than VBG (i.e. a dominant strategy). A bootstrap analysis with respect to a QALY showed that in 79% of trials LAGB was both more effective and less expensive in comparison to VBG (i.e. dominant); and in 14% of trials it was more effective but also more expensive. There was a negligible probability of VBG being dominant (3%) or being both less effective and less expensive (4%). |
Was any sensitivity analysis performed – if yes, what type(s) (i.e. deterministic (one-way, two-way etc) or probabilistic).
|
The results of eight one-way sensitivity analyses (in terms of the outcomes of a bootstrapping analysis of joint distribution of incremental costs and outcomes) were reported in table 3 (p. 82). The cost of personnel time (€2.96 per minute) was substituted in turn for the maximum and minimum values of €3.56 and €2.66 per minute, respectively and the joint distribution of costs and outcomes (%EWL and QALY in turn) was investigated. The per diem cost (€332 per day in hospital) was substituted in turn for the maximum and minimum values of €432 and €232 per day, respectively. Also the joint distribution of costs and outcomes (%EWL and QALY in turn) was investigated. |
What scenarios were tested in the sensitivity analysis? How do these relate to structural uncertainty (testing assumptions over model structure such as relationships between health states), methodological uncertainty (such as choices of discount rate or inclusion of indirect costs) or parameter uncertainty (assumptions over values of parameters in the model, such as costs, quality of life or disease progression rates)?
| An alternative perspective for an economic evaluation that excluded non-medical costs (paid and unpaid help + productivity change, presumably) was tested in the scenario analysis. Exclusion of non-medical costs that constitute 39% and 35% in VBG and AGB, respectively, has not altered the overall results; however, the certainty about the AGB being less costly than VBG has been reduced. For example, a bootstrapping analysis with respect to a QALY showed that VBG in comparison to AGB was both more effective and less costly in 68% (instead of 79% in the base-case analysis) of trials (i.e. dominant); and in 27% (instead of 14% in the base-case analysis) of trials it was more effective but also more costly. |
Give a summary of the results of the sensitivity analysis – did they differ substantially from the base-case analysis. If so, what were the suggested causes?
| The joint distribution of incremental costs and outcomes (regardless of the choice of the outcome) varied very little with respect to the variables tested in the one-way sensitivity analyses. |
Conclusions/implications
Give a brief summary of the author’s conclusions from their analysis
| The study estimated the cost-effectiveness of VBG versus AGB (using Lap-Band® as opposed to other types of gastric banding, e.g. Swedish Adjustable Gastric band). The authors (somewhat inconsistently with the results of the CEA) concluded that at 12 months after surgery the costs and outcomes (in terms of QALYs) of the two alternative technologies were found to be equal (p. 75; abstract). Therefore the selection of the procedure can be based on the clinical aspects, efficacy and safety at one year. |
What are the implications of the evaluation for practice?
| Assuming that the conclusions are valid (see below) replacing VBG with LAGB is associated with the considerable savings to the society (with respect to QALY gained). Although the authors do not seem to realise that in such cases comparisons with haemodialysis and artery bypass are not appropriate as these technologies are associated with additional resource use rather than savings |
Reference
|
Craig, B.M.; Tseng, D.S. 140 Cost-effectiveness of gastric bypass for severe obesity |
Study characteristics
Research question
| What are the stated objectives of the evaluation? |
| To estimate the cost-effectiveness of (open) gastric bypass (versus no treatment) in the treatment of severe obesity |
To estimate the cost-effectiveness of (open) gastric bypass (versus no treatment) in the treatment of severe obesity
Study population
What definition was used for obesity?
|
Stated BMI > 40 kg/m2 and BMI < 50 kg/m2 However, Pories et al. 148 (see below) reported data on 608 obese patients who were eligible for GBP if BMI ≥ 40 kg/m2 or BMI ≥ 35 kg/m2 with comorbidities such as diabetes, arthritis or cardiopulmonary failure |
|
What are the characteristics of the baseline cohort for the evaluation? From Pories et al. 148 cohort study used for clinical effectiveness inputs |
What are the characteristics of the baseline cohort for the evaluation?
From Pories et al.148 cohort study used for clinical effectiveness inputs
| Age | Stated as 35 to 55 years old; however, Pories et al. reported data on 608 obese patients with age range 14 to 64 years (average age at the time of surgery was 37.3) |
| Sex | Separate analysis is conducted by male/female subgroups |
| Race (if appropriate) | Not reported [in Pories et al. cohort of 608 patients 506 were women (66.4% were white and 16.8% were African-American) and 102 were men (14.3% were white and 2.5% were African-American)] |
| Comorbidities | In Pories et al. cohort of 608 patients 27% of the patients had non-insulin-dependent diabetes and 27% had impaired glucose tolerance; 58.1% had hypertension at the baseline. |
| Other characteristics | All patients were assumed non-smoking without a cardiovascular disease (CVD), drug addiction or major psychological disorder who failed conservative therapies consisting of dieting, exercise, behaviour therapy and pharmacotherapy. However, this is not consistent with characteristics of the population from whom utility values and life expectancy data were derived |
Interventions and comparators
What number of interventions/strategies were included?
| One |
Was a no treatment/supportive care strategy included?
| Yes |
Describe interventions/strategies
|
Intervention/strategy 1: [open?] gastric bypass Comparator: not specified, ‘no-treatment’, it is not clear whether dieting, exercise, behaviour therapy and pharmacotherapy are assumed to continue |
Analytical perspective
What is the perspective adopted for the evaluation [health service, health and personal social services, third-party payer, societal (i.e. including costs borne by individuals and lost productivity)]?
| The authors stated that the perspective is a payer’s one. However, this can be interpreted as either the health-care system perspective as in the base-case scenario or as a perspective of an insured individual whose out of pocket expenses are only a part of the total medical cost (as in the scenario analysis). |
Study type
Cost-effectiveness/cost–utility/cost–benefit analysis?
|
CEA cost per additional LY CUA (Incremental cost per incremental QALY) |
Institutional setting
Where is/are the intervention(s) being evaluated usually provided?
| Hospitals |
Country/currency
Has a country setting been provided for the evaluation? In what currency are costs expressed and does the publication give the base year to which those costs relate?
| Medical costs are reported in 2001 US$ |
Data sources
Effectiveness
Were the effectiveness data derived from:
| Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? | |
| A number of single studies for the short-term (1–5 years) clinical effectiveness inputs (weight loss; postsurgery complications; rates of revision; rates of reversal) were used | ✓ |
1. Weight loss (and some complication rates – included only on the cost side) were taken from the case series study (Pories et al. 148) n = 608 follow-up was 14 years with 96.3% of follow-up rate (47% were interviewed by phone). 2. Complication rates were taken from Pories et al. ,148 and the International Bariatric surgery registry (Mason et al. 193; Wu et al. 194) 3. Rates of revision surgery were also taken from Pories et al. 148 and Hall et al. 149 (abdominoplasty) 4. Rates of reversal surgeries were taken from RCT of GBP versus VBG Hall et al. 149 Different lengths of hospital stay and post-hospital recovery attract different utility weights. Length of hospital stay associated with initial surgery (by gender) was apparently obtained from the Healthcare Cost and Utilisation project database (1997)195 |
| A review/synthesis or combination of previous studies | ||
| Expert opinion | ✓ | The length of post-hospital recovery associated with initial surgery, revision and reversal surgeries and various complications was obtained from experts’ opinion |
Give the definitions of treatment effect used in the evaluation
| Pories et al. reported weight loss in BMI over the period of 14 years. The weight loss is stabilised and even slightly reversed after 5 years (figure 3B, p. 344) |
Give the size of treatment effect used in the evaluation
| Although the size of treatment effect is not explicitly identified, utility weights are assumed to be different for the patients with different BMI (in increments of 5 kg/m2) which is probably assumed to be the least clinically meaningful weight loss |
include values used for subgroups (if applicable). Indicate the source for individual treatment effects (if appropriate)
Intervention costs
Were the cost data derived from:
| Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? | |
|
Cost components of the intervention and its short-term (1–5 years) consequences (postsurgery complications; cost of revision surgery; cost of reversal surgery) Use of medications |
✓ |
Aggregated cost categories (ICD-9-CM code charges) for the GBP and, complications, revision and reversal surgeries were obtained from the Healthcare Cost and Utilisation project database (1997)158 and adjusted for inflation using medical care component of the consumer price index. Unit costs were obtained from the 2000 Drug topics Red Book, Montvale, NJ: Medical Economics Company. 2000 |
| A review/synthesis or combination of previous studies | ||
| Expert opinion |
List the direct intervention costs used in the evaluation – include resource estimates (and sources for these estimates, if appropriate) as well as sources for unit costs used. Quantity of resource use in natural units are not reported.
| Resource category | Type of resources (not elaborated by cost components) | Cost estimate (US$2001 prices) | Source | |
|---|---|---|---|---|
| Men | Women | Aggregated cost categories (ICD-9-CM code charges) for the GBP and, complications, revision and reversal surgeries were obtained from the Healthcare Cost and Utilisation project database (1997)158 and adjusted for inflation using the medical care component of the consumer price index | ||
| Cost of surgery | Gastric bypass | 26,100 | 20,500 | |
| Cost of complications | Minor wound infection | 192 | 192 | |
| Major wound infection | 20,600 | 19,200 | ||
| Deep vein thrombosis | 8700 | 8100 | ||
| Pulmonary embolism | 14,700 | 13,900 | ||
| Cholelithiasis | 27,100 | 22,700 | ||
| Incisional hernia | 13,200 | 12,500 | ||
| Abdominoplasty | 13,600 | 12,200 | ||
| Rrvision surgey | 38,500 | 25,600 | ||
| Reversal surgery | 38,500 | 25,600 | ||
| Perioperative death | 27,600 | 29,000 | ||
Other direct costs
(Cost of postsurgical complications)
Were the cost data derived from:
| Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? | |
| A single data source was used for the estimates of the expected lifetime medical cost [of selected obesity-related diseases] reported by age/gender/BMI in Thompson et al.144 | ✓ | Not clear how the estimates reported in Thompson et al.144 were used to obtain the expected lifetime medical cost for the BMI values other than reported. |
| A review/synthesis or combination of previous studies | ||
| Expert opinion | ✓ |
Cost of follow-up visits and was obtained from written personal communication It is not clear from where the quantities and types of supplements (vitamins, minerals, etc.) used by postsurgical patients for the duration of their life time were obtained. Unit costs were obtained from the 2000 Drug topics Red Book, Montvale, NJ: Medical Economics company. 195 |
List the costs used in the evaluation – if quantities of resource use are reported separately from cost values, show sources for the resource estimates as well as sources for unit costs used.
| Follow-up costs (annual?) | Follow-up visits | $150 (both genders) |
| Pharmaceuticals | $68 (both genders) | |
| Expected lifetime cost medical cost estimates of selected obesity-related diseases | See Results section below for the cost values associated with selected age/gender/BMI baseline characteristics | Taken from Thompson et al.144 and extrapolated to include expected lifetime medical cost for the BMI values other than reported |
indicate the source for individual cost values (if appropriate)
Indirect costs
(costs due to lost productivity, unpaid inputs to patient care)
Were indirect costs included:
| Not included |
Describe how indirect costs were estimated (e.g. how days of lost productivity were estimated and how those days were valued)
| Not applicable |
indicate the source for individual cost values (if appropriate)
Health-state valuations/utilities
(if study uses quality of life adjustments to outcomes)
Were the utility data derived from:
| Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? | |
| Not clear. Utilities might have been elicited from two questions (activity limitations and perceived health status) that were included in the 1997 USA National Health Interview Survey and interpreted as attributes of the (non-existent) QoL generic instrument | ✓ |
A reference to methodology for eliciting utilities using the data from the 1997 USA National Health Interview Survey was provided (Erickson et al. 155). It is not clear whether the complex modelled calculations reported in Erickson et al. 155 were fully replicated with respect to the data from the US population which participated in the 1997 National Health Survey stratified by gender. It does not seem that the 1997 National Health Survey data were also adjusted for BMI values. |
List the utility values used in the evaluation
|
These are reported in table 2 (p. 493), by age, gender and BMI categories. The utility values vary from 0.93 in a 35-year-old male with BMI of 25 kg/m2 to 0.58 in a 75-year-old female with BMI of 50 kg/m2 In addition arbitrary utility values are applied to the period of time spent in hospital and in postsurgery recovery. In the first instance the age/gender/BMI-specific utility value is reduced by 200% (assuming that being in hospital is equivalent to the health state which is ‘worse than death’). The utility value associated with the recovery time was 50% of the applicable age/gender/BMI-specific utility value. No justification for the choice of these values was provided. Reduced (by 50% apparently) utility weights also apply to the patients during their postreversal surgery years of life. |
indicate the source for individual utility values (if appropriate)
Modelling
If a model was used, describe the type of model used (e.g. Markov state transition model, discrete event simulation)
| A deterministic decision model (a decision tree) |
Was this a newly developed model or was it adapted from a previously reported model? If an adaptation, give the source of the original.
| Newly developed model |
What was the purpose of the model (i.e. why was a model required in this evaluation)?
| To compare the lifetime expected costs and outcomes between [open] gastric bypass and no treatment of severe obesity from a payer’s perspective (p. 491) |
What are the main components of the model (e.g. health states within a Markov model)? Are sources for assumptions over model structure (e.g. allowable transitions) reported – list them if reported.
|
The no-treatment arm of the decision tree model assumes that the patients do not lose or gain weight and their QALY depends on the initial BMI, gender and the baseline age. The open gastric bypass arm of the decision tree model assumes four surgery outcomes that occur in the first instance: successful surgery, revision surgery, reversal surgery and death. Revision surgery and reversal surgery are in turn associated with probability of a postsurgical death, while the former may be followed (in 4% of the cases) by the subsequent reversal surgery, which is also associated with the probability of death (figure 1 p. 492). The life expectancy depends on the eventual BMI, gender and the age at which the surgery was undertaken. Life expectancy was adjusted for the estimated perioperative mortality (assumed at 1.5% for the original and 3% for the revisional and reversal surgeries). Utility values (differentiated by gender, age and BMI) are applied to the estimated life-years spent with the eventual BMI to obtain QALYs. The arbitrary assigned utility values are applied to the period of time spent in the hospital and in recovering (presumably after the hospital stay). It was also assumed that the patients who underwent the reversal surgery have ‘never recovered completely’ (p. 493). A 50% reduction in utility weights was applied to these patients for the rest of their lives. |
Extract effectiveness data for [natural history/disease progression] model and show sources
|
Short-term (1–5 years apparently) effectiveness data for the open gastric bypass comprised the following Long-term outcomes (QALYs) were obtained from combining QALYs were also adjusted for the arbitrary utility estimates that applied to the time spent in hospital and in post-hospital recovery |
What is the model time horizon? Duration of the cycle?
| Lifetime |
What, if any, discount rates have been applied in the model? Same rate for costs and outcomes?
| 3% discounting rates applied to both costs and outcomes (QALYs) |
Results/analysis
What measure(s) of benefit were reported in the evaluation?
| Life expectancy and QALYs |
Provide a summary of the costs estimated for each intervention/strategy assessed in the evaluation (table 13, p. 1498)
|
Results are reported for the four ‘risk subgroups’ identified by gender and the age at which the surgery is undertaken (35 years or 55 years). Results in a numerical format for men and women in the lower (40 kg/m2) and the upper (50 kg/m2) BMI limits are reported in tables 3 and 4. Results in graphical format for the range of other baseline BMI values for men and women of either 35 or 55 years at the baseline is presented in figure 2, p. 496. For the risk subgroup of the adults of 35 years of age who had BMI of 40 kg/m2 at the baseline the outcomes are as follows: |
|||||||
| Life expectancy | QALY | ||||||
|---|---|---|---|---|---|---|---|
| Gastric bypass | No treatment | Gastric bypass | No treatment | ||||
| Men | Women | Men | Women | Men | Women | Men | Women |
| 23.00 | 24.63 | 22.97 | 24.72 | 19.56 | 19.82 | 18.51 | 18.21 |
| For the risk subgroup of the adults of 35 years of age who had BMI of 50 kg/m2 at the baseline the outcomes are as follows: | |||||||
| Life expectancy | QALY | ||||||
| Gastric bypass | No treatment | Gastric bypass | No treatment | ||||
| Men | Women | Men | Women | Men | Women | Men | Women |
| 22.83 | 24.46 | 22.52 | 24.46 | 18.87 | 18.88 | 16.83 | 16.03 |
| For the risk subgroup of the adults of 55 years of age who had BMI of 40 kg/m2 at the baseline the outcomes are as follows: | |||||||
| Life expectancy | QALY | ||||||
| Gastric bypass | No treatment | Gastric bypass | No treatment | ||||
| Men | Women | Men | Women | Men | Women | Men | Women |
| 16.44 | 18.58 | 16.15 | 18.49 | 13.32 | 13.94 | 12.48 | 12.62 |
| For the risk subgroup of the adults of 55 years of age who had BMI of 50 kg/m2 at the baseline the outcomes are as follows: | |||||||
| Life expectancy | QALY | ||||||
| Gastric bypass | No treatment | Gastric bypass | No treatment | ||||
| Men | Women | Men | Women | Men | Women | Men | Women |
| 16.22 | 18.41 | 15.51 | 18.08 | 12.81 | 13.23 | 11.17 | 10.88 |
| Provide a summary of the costs estimated for each intervention/strategy assessed in the evaluation (table 13, p. 1498) | |||||||
| For the risk subgroup of the adults of 35 years of age the costs (US$) are as follows: | |||||||
| Life expectancy | QALY | ||||||
| Gastric bypass | No treatment | Gastric bypass | No treatment | ||||
| Men | Women | Men | Women | Men | Women | Men | Women |
| 68,600 | 59,000 | 38,500 | 35,300 | 75,000 | 54,800 | 53,200 | 48,500 |
| For the risk subgroup of the adults of 55 years of age the costs (US$) are as follows: | |||||||
| Life expectancy | QALY | ||||||
| Gastric bypass | No treatment | Gastric bypass | No treatment | ||||
| Men | Women | Men | Women | Men | Women | Men | Women |
| 77,600 | 69,600 | 47,900 | 48,200 | 85,300 | 77,000 | 63,500 | 64,100 |
Synthesis of costs and benefits – are the costs and outcomes reported together (e.g. as cost-effectiveness ratios)? If so, provide a summary of the results.
| For the risk subgroup of the adults of 35 years of age the baseline costs (US$) per life-year saved and cost per QALY are reported below | |||||||
| Incremental cost per extra life-year saved | Incremental cost per additional QALY | ||||||
|---|---|---|---|---|---|---|---|
| BMI of 40 kg/m2 | BMI of 50 kg/m2 | BMI of 40 kg/m2 | BMI of 50 kg/m2 | ||||
| Men | Women | Men | Women | Men | Women | Men | Women |
| 844,700 | No treatment strategy is dominant | 70,300 | 9,130,000 | 28,600 | 14,700 | 10,700 | 5700 |
| For the risk subgroup of the adults of 55 years of age the costs are reported below | |||||||
| Incremental cost per extra life-year saved | Incremental cost per additional QALY | ||||||
| BMI of 40 kg/m2 | BMI of 50 kg/m2 | BMI of 40 kg/m2 | BMI of 50 kg/m2 | ||||
| Men | Women | Men | Women | Men | Women | Men | Women |
| 100,200 | 248,500 | 30,700 | 38,900 | 35,600 | 16,100 | 13,300 | 5400 |
Give results of any statistical analysis of the results of the evaluation.
| None provided |
Was any sensitivity analysis performed – if yes, what type(s) [i.e. deterministic (one-way, two-way etc) or probabilistic].
|
A series of one-way sensitivity analyses were performed that varied the estimated loss of excess weight, mortality rates and complication rates (clinical effectiveness parameters). A sensitivity analysis was conducted to assess the impact of the variation in utility estimates. However, instead of varying the utility values used in calculation of QALYs, the regression coefficients in the (unreported) multiple regression equation used to obtain utility values were decreased by 25%. It is not clear how this affected the actual utility values used to estimate QALYs. A sensitivity analysis was conducted to test the various assumptions about incremental (from 0% to 100%) loss of life-years as a result of the elevated BMI. The two-way sensitivity analysis varying both the lifetime medical cost and the discount rate was undertaken. Another two-way sensitivity analysis varied the estimated of loss of weight and the medical cost adjusted for the different reimbursement rate (see below), which was used a threshold analysis for the subgroup of 55-year-old men with BMI of 40 kg/m2. |
What scenarios were tested in the sensitivity analysis? How do these relate to structural uncertainty (testing assumptions over model structure such as relationships between health states), methodological uncertainty (such as choices of discount rate or inclusion of indirect costs) or parameter uncertainty (assumptions over values of parameters in the model, such as costs, quality of life or disease progression rates)?
| Cost incurred by the payer was also reduced by the median reimbursement rate, which is effectively an equivalent to the change of the perspective of economic evaluation from the one of the health-care system (regardless of who is paying) to the perspective of the individual insured patient. |
Give a summary of the results of the sensitivity analysis – did they differ substantially from the base-case analysis. If so, what were the suggested causes?
|
The cost-effectiveness ratios appear to be sensitive to the change in clinical effectiveness parameters (in particular, to the excess weight loss), assumptions about additional loss of life as the result of the elevated BMI, lifetime medical-care cost, values of regression coefficients used to estimate utility values. However, according to figure 3, which presents the results of the one-way sensitivity analysis with respect to the above parameters for the 45-year-old men and women with BMI 40 kg/m2, the threshold of $50,000 per QALY was breached when the base-case value of excess weight loss of 58% was reduced to 38%. When the rate of gastric bypass mortality was changed from 0.015% to 0.03%, the complication rates were increased by 25% and the procedure remained cost-effective except in some older less obese men (not specified). The threshold analysis for the subgroup of 55-year-old men with BMI of 40 kg/m2 where both loss of weight and the different reimbursement rate were varied indicated that under the base-case assumptions about the 67% reimbursement rate, the loss of excess weight greater than 46% is sufficient for the incremental cost per incremental QALY to be below $50,000. |
Conclusions/implications
Give a brief summary of the authors’ conclusions from their analysis
| Although an open gastric bypass is not a cost-saving strategy from the payer’s perspective, it is cost-effective among all categories of patients under the base-case assumptions. The results appear to be robust to parameter variations with respect to women and younger more obese men. An open gastric bypass may not be cost-effective for some subgroups of older and less obese men, i.e. exceeding $50,000 per QALY when the base-case assumptions about some clinical effectiveness parameters are varied. |
What are the implications of the evaluation for practice?
| Although an open gastric bypass is a cost-effective strategy, the decision to undergo a procedure must be individualised because of the associated risks, and patients should understand the long-term commitment that the treatment entails |
Reference
|
Jensen C, Flum D R141 The costs of nonsurgical and surgical weight loss interventions: is an ounce of prevention really worth a pound of cure? |
Study characteristics
Research question
What are the stated objectives of the evaluation?
| The study was intended to answer the hypothetical question of which of the two interventions for the treatment of obesity, was more cost-effective from a societal perspective: open gastric bypass surgery (GBP) implemented at the age of 40 or diet and exercise implemented at the age of 18. |
Study population
What definition was used for morbid obesity/eligibility for bariatric surgery?
| BMI > 40 kg/m2 |
What are the characteristics of the clinical trial population used in economic evaluation?
| Age |
Intervention group: white 18-year-old females who undergo a bariatric surgery at the age of 40 years and BMI > 40 kg/m2 The patients from the study (Sjostrom et al. 89) used to obtain parameters of the model were on average more than 40 years old Not clear. Comparator group: white 18-year-old female with BMI > 33 kg/m2 (as stated on p. 353) or white 18-year-old female with BMI ≥ 35 kg/m2 (as stated in the diagram of the model, p. 354) The average weight of the participants of the weight loss programme used to obtained parameters of the model was 33.8 kg/m2 (Heshka et al. 196). The participants were older (age was not indicated) than the 18-year-old population in the comparator arm. |
| Sex | Female |
| Race (if appropriate) | White |
| Comorbidities | Not indicated |
| Other characteristics | The weight in the comparator group was derived from the cut-off BMI value for the upper 4.4% in the distribution of the 18-year-old white female obese population in the USA. (http://www.soph.uab.edu/statgenetics/Research/Tables/YLL.htm) |
Interventions and comparators
What number of interventions/strategies were included?
| One |
Was a no treatment/supportive care strategy included?
| Yes; a commercial programme of diet and exercise |
Describe interventions/strategies
|
Intervention/strategy 1: open gastric bypass Comparator: dieting and exercise |
Analytical perspective
What is the perspective adopted for the evaluation [(health service, health and personal social services, third-party payer, societal (i.e. including costs borne by individuals and lost productivity)]?
| A societal perspective |
Study type
Cost-effectiveness/cost–utility/cost–benefit analysis?
| CUA (Incremental cost per incremental QALY) |
Institutional setting
Where is/are the intervention(s) being evaluated usually provided?
| Hospitals |
Country/currency
Has a country setting been provided for the evaluation? In what currency are costs expressed and does the publication give the base year to which those costs relate?
| All costs are reported in 2004 US$. |
Data sources
Effectiveness
Were the effectiveness data derived from:
| Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? | |
|
Intervention (GBP). Clinical effectiveness data assessed in the weight loss (in BMIs) were taken from a single study for the mid-term (8 years) Control. Diet and exercise. Clinical effectiveness data assessed in the weight loss (in BMIs) were taken from a single study for the short-term (2 years) |
✓ |
Weight loss and complication rates are taken from the Swedish case–control longitudinal study by Sjostrom et al. 89 346 GBP patients were matched with 346 non-surgical controls and followed up for 8 years. Weight loss is taken from the USA case–control longitudinal study by Heshka et al. 196 211 patients undergoing a commercial programme were matched with 212 controls undergoing a self-help programme and followed up for 2 years. |
| A review/synthesis or combination of previous studies | ||
| Expert opinion |
Give the definitions of treatment effect used in the evaluation
| Weight loss in BMI was converted into the differential years of life that applied to the patients from the different arms. |
Give the size of treatment effect used in the evaluation
| Although the size of treatment effect is not explicitly identified, both longevity and utility weights are assumed to be different for the patients with different BMI (in increments of 1 kg/m2) |
include values used for subgroups (if applicable). Indicate the source for individual treatment effects (if appropriate)
Intervention costs
Were the cost data derived from:
| Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? | |
|
Intervention (GBP). Cost data were taken from a single study comparing open with laparoscopic GBP. Control. Diet and exercise. Cost data were taken from a single study |
✓ |
Nguyen et al. 113 (n = 68 in each arm) The costs were inflated to 2004 US prices using the Bureau of Labor statistics Inflation calculator (rather than the health-care-specific inflator) Costs (including the unit costs) were taken from the USA case–control longitudinal study by Heshka et al. 196 |
| A review/synthesis or combination of previous studies | ||
| An educated guess in relation to the cost of GBP-related complications | ✓ | No |
List the direct intervention costs used in the evaluation – include resource estimates (and sources for these estimates, if appropriate) as well as sources for unit costs used.
| Resource category | Type of resources | Unit cost estimate (UK data) | Source |
|---|---|---|---|
| Cost of surgery | Operative costs | Nguyen et al.113 | |
| Gastric bypass | Operative time and supplies | 4,098 ± 1,538 | |
| Postanaesthesia | 504 ± 487 | ||
| Hopsital service cost | |||
| diagnostic | 467 ± 170 | ||
| nursing | 1,201 ± 821 | ||
| pharmaceutical | 418 ± 232 | ||
| therapeutic | 97 ± 249 | ||
| other | 268 ± 213 | ||
| Indirect costs | 6,645 ± 2,437 | ||
| Total | 14,087 ± 5,237 | ||
| Cost of complications | Not specified | $5,000 | An educated guess |
| Cost of diet and exercise | 1 hour weekly weight loss program | Annual cost $9 cost per session × 52 × 2 years | Heshka et al.196 |
Other direct costs
(Cost of postsurgical complications)
Were the cost data derived from:
| Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? | |
| A single data source was used for the estimates of the expected lifetime medical cost (of selected obesity-related diseases) reported by age/gender/BMI in Thompson et al.144 | ✓ |
As only the limited (up to 37.5 BMIs by increments of 5 BMIs) cost data were reported in Thompson et al. 144 the authors undertook a linear regression analysis to obtain estimates of costs for each value of BMI within the studied range (figure 3, p. 356) The cost was based on the patient at age 49 and divided by the remaining years of life to achieve a yearly cost |
| A review/synthesis or combination of previous studies | ||
| Expert opinion |
List the costs used in the evaluation – if quantities of resource use are reported separately from cost values, show sources for the resource estimates as well as sources for unit costs used.
| The aggregated costs associated with obesity-related diseases (hypertension hypercholesterolemia, Type 2 diabetes, coronary heart disease and stroke) | Using a linear regression equation the authors estimated that with each additional kg/m2 the aggregated cost increases by US$1100. The regression equation is Lifetime cost US$ = 1100(BMI in kg/m2) –6500) |
indicate the source for individual cost values (if appropriate)
Indirect costs
(costs due to lost productivity, unpaid inputs to patient care)
Were indirect costs included:
|
Cost of patient time in the GBP arm is assumed to be zero to the society (a transfer) as most of the patients are on disability benefits (Narbro et al. 87) Caregiver time in the GBP arm (Nguyen et al. 113) Cost of patient time in the diet and exercise arm was inconsistently assumed not to be zero |
Describe how indirect costs were estimated (e.g. how days of lost productivity were estimated and how those days were valued)
|
Caregiver time in the GBP arm was calculated as follows: US average hourly wage × 4 hours/day × 18 days (the average period for which the GBP patients were unable to complete the daily activities; Nguyen et al. 113) Cost of patient time in the diet and exercise arm was calculated as follows: (1 hour to attend the programme + ½ hours to travel) × US average hourly wage × 52 weeks × 2 years Note: The US average hourly wage was obtained from the bureau of Labour statistics |
indicate the source for individual cost values (if appropriate)
Health state valuations/utilities
(if study uses quality of life adjustments to outcomes)
Were the utility data derived from:
| Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? | |
| A single study | ✓ | Hakim et al.197 used time trade-off techniques to estimate utility for persons for the range of BMI values. They also investigated the relationship between utility weights and kg/m2 |
| A review/synthesis or combination of previous studies | ||
| Expert opinion |
List the utility values used in the evaluation
| Using the estimate reported in Hakim et al.197 a utility gain of 0.017 is associated with each BMI reduction of 1 kg/m2 |
indicate the source for individual utility values (if appropriate)
Modelling
If a model was used, describe the type of model used (e.g. Markov state transition model, discrete event simulation)
| A deterministic decision model (a decision tree) |
Was this a newly developed model or was it adapted from a previously reported model? If an adaptation, give the source of the original.
| A newly developed model |
What was the purpose of the model (i.e. why was a model required in this evaluation)?
| To compare the lifetime expected costs and outcomes between open gastric bypass and diet and exercise programme from the societal perspective. |
What are the main components of the model (e.g. health states within a Markov model)? Are sources for assumptions over model structure (e.g. allowable transitions) reported – list them if reported.
|
The decision tree model has the following options (1) ‘Intervention (a reduced BMI) without immediate complications’, (2) ‘Intervention (a reduced BMI) with immediate complications’; (3) Death; (4) ‘Alive with reduced BMI’ and ‘Alive with baseline BMI’. The diet and exercise arm of the decision tree model reasonably assumes that no patient experiences complications associated with GBP. The surviving patients from the control arm follow the pathway corresponding to the no-complication branch in the GBP arm of the decision tree. The open gastric bypass arm of the decision tree model assumes two outcomes: surgery resulting in immediate complications and surgery without immediate complications. In both cases patients face the probability of death. The surviving patients may have a reduced BMI or remain with their initial BMI. Life expectancy depends on the BMI. The starting age of patients is 18 years in both arms (although this can be confusing and could only be deduced from the commentaries on scenario analyses, p. 356) the GBP takes place when the GBP cohort exceeds 40 kg/m2 which happens when they are 40 years old. In the base-case scenario BMI values increase from one year to another at the rate observed in general USA population in the 95.6th percentile for weight (a cut-off point for the BMI of > 40 kg/m2 which corresponds to 4.4% of the population at age 40). In the base case this rate is applied to all surviving patients in each branch of the decision tree. However, the BMI reduction obtained as a result of the GBP or a diet and exercise programme is retained for life. As a result the BMI in such patients, although increasing at the above rate, is always reduced by the incremental BMI value observed after the intervention. Utility values corresponding to the BMI observed in each year (Hakim et al. 197) were applied to obtain QALYs. |
Extract effectiveness data for (natural history/disease progression) model and show sources
|
Control group (diet and exercise) has apparently attained some weight loss achieving 31.8 kg/m2 at the age of 19 starting from either > 33 kg/m2 or > 35 kg/m2 (Heshka et al. 196) The open gastric bypass group has achieved a larger weight loss of 29.93 kg/m2 at the age of 48 starting from > 40 kg/m2 (Sjostrom et al. 89) Long-term outcomes (QALYs) were obtained from combining life-years (as a function of age, and BMI) reported in Thompson et al. 144 that were extrapolated by linear approximation to obtain life expectancy for each BMI category with utility weights reported in Hakim et al. 197 |
What is the model time horizon? Duration of the cycle?
| Lifetime |
Lifetime
What, if any, discount rates have been applied in the model? Same rate for costs and outcomes?
| Discounting seems to have been conducted however the discounting rates were not reported. |
Results/analysis
What measure(s) of benefit were reported in the evaluation?
| QALYs |
Provide a summary of the clinical outcome/benefits estimated for each intervention/strategy assessed in the evaluation
| Not reported. GBP is associated with additional 0.61of life expectancy (not adjusted for quality of life) |
Provide a summary of the costs estimated for each intervention/strategy assessed in the evaluation
| Not reported. GBP is associated with additional cost of $4600 |
Synthesis of costs and benefits – are the costs and outcomes reported together (e.g. as cost-effectiveness ratios)? If so, provide a summary of the results.
|
It appears that the cost-effectiveness was determined using an ICER, but this was not entirely clear (NHS EED) ICER = $7126/QALY gained |
Give results of any statistical analysis of the results of the evaluation.
| None provided |
Was any sensitivity analysis performed – if yes, what type(s) [i.e. deterministic (one-way, two-way etc) or probabilistic].
| The authors investigated uncertainty in the model parameters, but the parameters included and the ranges, and methods used to derive them, were not clear. However, the authors did not report the results satisfactorily. A series of one-way sensitivity analyses were performed that proved to be sensitive to the estimated cost of complications (although the range was not reported) and the discount rate (neither the value nor the range were reported). |
What scenarios were tested in the sensitivity analysis? How do these relate to structural uncertainty (testing assumptions over model structure such as relationships between health states), methodological uncertainty (such as choices of discount rate or inclusion of indirect costs) or parameter uncertainty (assumptions over values of parameters in the model, such as costs, quality of life or disease progression rates)?
|
Worst-case and best-case scenarios for the assumption of the weight trajectory after the intervention were also investigated. In the worst-case scenario all weight lost through the interventions was regained within 3 years and the patients followed the trajectory of the 95.6th percentile. In the best-case scenario the BMIs were unchanged at the postintervention levels in both groups for the remaining duration of their life. |
Give a summary of the results of the sensitivity analysis – did they differ substantially from the base-case analysis. If so, what were the suggested causes?
| In both worst-case and best-case scenarios the results were higher than in the base case but still cost-effective at < $35,000 per QALY |
Conclusions/implications
Give a brief summary of the author’s conclusions from their analysis
| Gastric bypass (GBP) surgery is a worthwhile investment that provides the greatest amount of QALYs for the invested dollar |
What are the implications of the evaluation for practice?
| When it come to the obesity ‘an ounce of prevention does not appear to be worth a pound of cure’ |
Reference
| Salem, L.; Devlin, A.; Sullivan, S.D.; Flum, D.R.142 | Cost-effectiveness analysis of laparoscopic gastric bypass, adjustable gastric banding, and non-operative weight loss interventions |
Study characteristics
Research question
What are the stated objectives of the evaluation?
| Given the differential risk and effectiveness of the laparoscopic gastric bypass (LGBP) and laparoscopic adjustable gastric banding (LAGB), the aim of the study was to evaluate the incremental cost-effectiveness of these two surgical procedures compared with non-operative weight loss interventions and with each other |
Study population
What definition was used for obesity?
| By implication, BMI > 40 kg/m2 |
What are the characteristics of the baseline cohort for the evaluation?
| Age |
1. Aged 35 with BMI = 40 kg/m2 2. Aged 45 with BMI = 50 kg/m2 3. Aged 55 with BMI = 60 kg/m2 |
| Sex | Separate analysis is conducted by male/female subgroups |
| Race (if appropriate) | Not specified |
| Comorbidities | Patients are assumed to have no obesity-related comorbidities at the baseline |
| Other characteristics | None specified |
Interventions and comparators
What number of interventions/strategies were included?
| Two |
Was a no treatment/supportive care strategy included?
| Yes |
Describe interventions/strategies
|
Intervention/strategy 1: Laparoscopic gastric bypass Intervention/strategy 2: Laparoscopic adjustable gastric banding Comparator: non-operative treatment of obesity |
Analytical perspective
What is the perspective adopted for the evaluation [(health service, health and personal social services, third-party payer, societal (i.e. including costs borne by individuals and lost productivity)]?
| The perspective of an economic analysis is that of a USA payer’s. |
Study type
Cost-effectiveness/cost–utility/cost–benefit analysis?
| CUA (Incremental cost per incremental QALY) |
Institutional setting
Where is/are the intervention(s) being evaluated usually provided?
| Hospitals |
Country/currency
Has a country setting been provided for the evaluation? In what currency are costs expressed and does the publication give the base year to which those costs relate?
| All costs are reported in US$2004. |
Data sources
Effectiveness
Were the effectiveness data derived from:
| Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? | |
| A single study | ||
| A review/synthesis or combination of previous studies | ✓ |
Operative mortality was taken from the systematic literature review of LAGB by Chapman et al. 151 Primary clinical effectiveness outcomes (excess body weight loss) were taken from the range of studies including cohort and case series studies. It does not seem that the systematic review of the data obtained from the various sources was conducted. Base-case estimates were derived by averaging the reported values. |
|
Expert opinion was sought on the following clinical outcomes: % of patients needing band removal Perioperative mortality after revision surgery % of patients with leak non-operative for LGBP |
Not explained |
Give the definitions of treatment effect used in the evaluation
|
The authors indicated that the major clinical end points were (surgery-related) survival and weight loss (in excess body weight loss converted to BMI). Other clinical effectiveness end points are the rates of revisional and reversal surgeries. Surgery-related complications for each intervention were included only on the cost side of the equation. These intermediate outcomes were converted into the differential years of life that applied to the patients from different arms of the model. |
Give the size of treatment effect used in the evaluation
| The primary clinical end point was measured in excess body weight loss converted to BMI. The conversion rule was not reported. |
include values used for subgroups (if applicable). Indicate the source for individual treatment effects (if appropriate)
Intervention costs
Were the cost data derived from:
| Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? | |
| For both interventions (LAGB and LGBP). Cost data were taken from the published data source | ✓ |
Aggregated cost categories for both interventions and some surgery-related complications, were obtained from the Healthcare Cost and Utilisation project database (1997) and adjusted for inflation using the medical-care component of the consumer price index. There are no corresponding costs for non-surgery treatment. |
| A review/synthesis or combination of previous studies | ||
|
Expert opinion was sought on the following cost components: Band adjustment (LAGB) Band removal (LAGB) Cost of revision surgery both (LAGB and LGBP) Number of follow-up visits for both interventions |
✓ | Not explained |
List the direct intervention costs used in the evaluation – include resource estimates (and sources for these estimates, if appropriate) as well as sources for unit costs used (table 1, p. 28).
| Resource category | Type of resources – not elaborated by cost components | LAGB – cost estimates (US$2004 prices) | LGBP – cost estimates (US$2004 prices) |
|---|---|---|---|
| Cost of surgery | 16,200 | 27,560 | |
| Band adjustment | 150 (10 visits) [per visit?] | not applicable | |
| Revision surgery | 5000 | 10,000 | |
| Reversal surgery (band removal) | 6000 | not applicable | |
| Reversal srugery LGBP | not specified | ||
| Cost of complications | Minor wound infection | 204 | 204 |
| Major wound infection | 11,236 | 11,236 | |
| Deep venous thrombosis | 9222 | 9222 | |
| Pulmonary embolism | 15,582 | 15,582 | |
| Leak non-operative | not applicable | 50,000 | |
| Laparoscopic cholecystectomy | 16,000 | 16,000 | |
| Incisional hernia | 14,416 | 14,416 | |
| Abdominoplasty | 13,992 | 13,992 |
Other direct costs
(Cost of postsurgical complications)
Were the cost data derived from:
| Lifetime medical costs associated with obesity | Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? |
| A single data source was used for the estimates of the expected lifetime medical cost reported by age/gender/BMI in Thompson et al.144 | ✓ | Not clear how the estimates reported in Thompson et al.144 were used to obtain the expected lifetime medical cost for the BMI values other than reported. |
| A review/synthesis or combination of previous studies | ||
| Expert opinion | ✓ |
Cost of follow-up visits It is not clear from where the quantities and type of supplements (vitamins, minerals, etc.) used by postsurgical patients for the duration of their life time were obtained. Unit costs were obtained from the 2000 Drug topics Red Book, Montvale, NJ: Medical Economics company. 2000. 195 |
List the costs used in the evaluation – if quantities of resource use are reported separately from cost values, show sources for the resource estimates as well as sources for unit costs used.
| Lifetime medical costs associated with obesity | Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? |
| A single data source was used for the estimates of the expected lifetime medical cost reported by age/gender/BMI in Thompson et al.144 | ✓ | Not clear how the estimates reported in Thompson et al.144 were used to obtain the expected lifetime medical cost for the BMI values other than reported. |
| A review/synthesis or combination of previous studies | ||
| Expert opinion | ✓ |
Cost of follow-up visits It is not clear from where the quantities and type of supplements (vitamins, minerals, etc.) used by postsurgical patients for the duration of their life time were obtained. Unit costs were obtained from the 2000 Drug topics Red Book, Montvale, NJ: Medical Economics company. 2000. 195 |
indicate the source for individual cost values (if appropriate)
Indirect costs
(costs due to lost productivity, unpaid inputs to patient care)
Were indirect costs included:
| Not applicable |
Describe how indirect costs were estimated (e.g. how days of lost productivity were estimated and how those days were valued)
| Not applicable |
indicate the source for individual cost values (if appropriate)
Health state valuations/utilities
(if study uses quality of life adjustments to outcomes)
Were the utility data derived from:
| Tick | Were the methods for deriving these data adequately described (give sources if using data from other published studies)? | |
| A single study by Craig and Tseng140 that reported utility values that were elicited from the general population | ✓ | Not explained. See comments to Craig and Tseng140 for methodology used in eliciting utilities |
| A review/synthesis or combination of previous studies | ||
| Expert opinion |
List the utility values used in the evaluation
| See comments to Craig and Tseng140 |
indicate the source for individual utility values (if appropriate)
Modelling
If a model was used, describe the type of model used (e.g. Markov state transition model, discrete event simulation)
| A deterministic decision model (a decision tree) |
Was this a newly developed model or was it adapted from a previously reported model? If an adaptation, give the source of the original.
| An adjusted model published in Craig and Tseng140 |
What was the purpose of the model (i.e. why was a model required in this evaluation)?
| We designed a model to evaluate the incremental cost-effectiveness of LGBP and LAGB compared with non-operative weight loss interventions and with each other |
What are the main components of the model (e.g. health states within a Markov model)? Are sources for assumptions over model structure (e.g. allowable transitions) reported – list them if reported.
|
The no-treatment arm of the decision tree model assumes that the patients do not lose or gain weight and that their QALYs depend on the initial BMI, gender and the baseline age. Both arms of the decision tree model assume two surgery outcomes that occur in the first instance: successful surgery and death. In the LGBP arm the surviving patients may need to undergo a revisional surgery, which can be successful or result in the death of a patient. In the LAGB arm the surviving patients may need to undergo a reversal surgery (band removal), which is not associated with the risk of death. All surviving patients in both arms (except those who underwent a reversal surgery) achieve weight loss specific to the type of surgery (figure 1, p. 27). It is not clear how the probability of revisional surgery for LAGB (5%) was incorporated into the model. The remaining life-years and lifetime costs for the population in the surgical and non-surgical treatment alternatives depend on the gender; baseline age and the eventual BMI (Thompson et al. 144). The BMI is determined by the decision analytic model with the horizon of 3 years. The utility values published in Craig and Tseng140 (2002) and differentiated by gender, age and BMI are applied to remaining life-years to obtain QALYs. |
Extract effectiveness data for [natural history/disease progression] model and show sources
|
Short term (1–3 years) effectiveness data for the open gastric bypass comprised the following 1. Weight loss (in percentage of excess body weight) for LGBP and LAGB was apparently taken from the range of studies (see table 1 for the references), averaged across them and converted into BMI (the formula is not provided so the actual values used in the model are not known). 2. Perioperative mortality (1% for LGBP and 0.05% for LAGB) and deep venous thrombosis rates were taken from the 2004 systematic literature review (Chapman et al. 151). 3. Rates of revisional surgery (5% for LGBP and 5% for LAGB) were taken from the range of studies (see table 1 for the references) 4. Perioperative mortality rates for revisional surgery (1% for LGBP and 0.05% for LAGB) were taken from the experts’ opinion 5. Other complication rates were taken from the US Health Cost and Utilization Project and the experts’ opinion. 6. The rate of a reversal surgery (band removal – 5%) was taken from the experts’ opinion The clinical outcomes in terms of differential complication rates included only in the cost side of the incremental C : E ratio and are not reported here Utility weights for men and women (for a specific values of BMI and age variables) were obtained from Craig and Tseng140 (see relevant comments in the review of their paper). |
Utility weights for men and women (for a specific values of BMI and age variables) were obtained from Craig and Tseng140 (see relevant comments in the review of their paper).
What is the model time horizon? Duration of the cycle?
| Although the decision analytic model covers costs and outcomes over the initial 3 years involving a surgical intervention in two out of three arms of the model, the economic evaluation extends to the lifetime due to the nature of the data on the life expectancy and lifetime costs available from Thompson et al.144 |
What, if any, discount rates have been applied in the model? Same rate for costs and outcomes?
| Cost and QALYs were discounted at 3% |
Results/analysis
What measure(s) of benefit were reported in the evaluation?
| QALYs |
Provide a summary of the clinical outcome/benefits estimated for each intervention/strategy assessed in the evaluation
| Not reported |
Provide a summary of the costs estimated for each intervention/strategy assessed in the evaluation (table 13, p. 1498)
| Not reported |
Synthesis of costs and benefits – are the costs and outcomes reported together (e.g. as cost-effectiveness ratios)? If so, provide a summary of the results.
|
Although the objective of the study was to evaluate the incremental cost-effectiveness of LGBP and LAGB compared with non-operative weight loss interventions and with each other it does not seem that the ICER of LGBP versus LAGB was calculated. The results are presented in terms of an incremental cost per additional QALY comparing LGBP with non-surgical treatment and LAGB with non-surgical treatment. A set of ICERs was produced for different combinations of gender, the baseline age and BMI. The results are only available for men and women at 35 years of age and 40 kg/m2 at the baseline. |
|
| LGBP versus non-surgical treatment | |
| Incremental cost per additional QALY | |
| Baseline age 35 years; BMI 40 kg/m2 | |
| Men | Women |
| 18,543 | 14,680 |
| LAGB versus non-surgical treatment | |
| Incremental cost per additional QALY | |
| Baseline age 35 years; BMI 40 kg/m2 | |
| Men | Women |
| 11,604 | 8878 |
| Although no other results are reported, the authors commented that for other baseline ages (35-, 45- and 55-year-old) and BMI categories (40, 50, 60 kg/m2) the ICER comparing LGBP with no-treatment strategy is consistently higher than the ICER comparing LAGB with no-treatment strategy. | |
Give results of any statistical analysis of the results of the evaluation.
| None provided |
Was any sensitivity analysis performed – if yes, what type(s) [i.e. deterministic (one-way, two-way etc) or probabilistic].
|
The authors investigated uncertainty associated with parameter estimates in the model, but the source of the ranges in parameter estimates, and methods used to derive them, were not clear. A series of one-way sensitivity analyses were performed and results proved to be sensitive to the value of the primary clinical outcome (weight loss measured in the% of excess weight loss), cost of the surgical procedure, number of times the band adjustment was required for the LAGB procedure and the estimated rate of perioperative mortality for LGBP procedure (figure 2, p. 29). A two-way sensitivity analysis was conducted where clinical effect (weight reduction measured in the% of excess weight loss) was varied simultaneously over the range of 0–100% in both arms. The results for a 45-year-old female with the baseline BMI of 40 kg/m2 were presented in figure 3, p. 30. the authors concluded that for this subgroup of patients the ‘difference in cost-effectiveness’ mostly favours LAGB and that included the base-case point observations of 55% of excess weight loss in LAGB patients versus 71% of excess weight loss in LGBP patients. However, the ‘difference in cost-effectiveness’ apparently refers to the difference in cost-effectiveness ratios calculated in two arms of the model rather than the ICER. Therefore, the authors’ conclusion of the likely superiority of the LAGB procedure over the LGBP procedure is not supported by the means of this particular two-way sensitivity analysis. |
What scenarios were tested in the sensitivity analysis? How do these relate to structural uncertainty (testing assumptions over model structure such as relationships between health states), methodological uncertainty (such as choices of discount rate or inclusion of indirect costs) or parameter uncertainty (assumptions over values of parameters in the model, such as costs, quality of life or disease progression rates)?
| None |
Give a summary of the results of the sensitivity analysis – did they differ substantially from the base-case analysis. If so, what were the suggested causes?
| In this study the authors found that both bariatric procedures were cost-effective at < $25,000 per QALY for all base-case scenarios (i.e. the combinations of baseline ages of 35, 45 or 55 years and BMI of either 40, 50, 60 kg/m2). |
Conclusions/implications
Give a brief summary of the author’s conclusions from their analysis
| The authors also concluded that LAGB is more cost-effective than LGBP for all base-case scenarios. However, because the ICER directly comparing these two surgical interventions was not calculated this conclusion may not be true across the range of combinations of the baseline age and BMI values. |
What are the implications of the evaluation for practice?
Appendix 16 List of studies excluded from review of clinical effectiveness
Studies included in previous publications of the systematic review but excluded from 2008 update
The following 11 trials (21 publications) that were included in previous publications15,70,71 of the systematic review have been excluded from the 2008 update.
Andersen 1984/88
Andersen T, Backer OG, Stokholm KH, Quaade F. Randomized trial of diet and gastroplasty compared with diet alone in morbid obesity. N Engl J Med 1984;310:352–6.
Andersen T, Stokholm KH, Backer OG, Quaade F. Long-term (5-year) results after either horizontal gastroplasty or very-low-calorie diet for morbid obesity. Int J Obes 1988;12:277–84.
Andersen 1987
Andersen T, Backer OG, Astrup A, Quaade F. Horizontal or vertical banded gastroplasty after pretreatment with very-low-calorie formula diet: a randomized trial. Int J Obes 1987;11:295–304.
Buckwalter
Buckwalter JA, Mason EE, Payne JH. A prospective comparison of the jejunoileal and gastric bypass operations for morbid obesity. World J Surg 1977;1:757–68.
Buckwalter JA. Clinical trial of jejunoileal and gastric bypass for the treatment of morbid obesity: four-year progress report. Am Surg 1980;46:377–81.
Buckwalter JA. Clinical trial of surgery for morbid obesity. South Med J 1978;71:1370–1.
Danish Obesity Project
Backer O, Gudmand HE, Andersen B, Baden H, Martiny P, Juhl E, et al. Randomised trial of jejunoileal bypass versus medical treatment in morbid obesity. The Danish Obesity Project. Lancet 1979;2:1255–8.
Quaade F. Studies of operated and nonoperated obese patients. An interim report on the Scandinavian Obesity Project. Am J Clin Nutr 1977;30:16–20.
Stokholm KH, Nielsen PE, Quaade F. Correlation between initial blood pressure and blood pressure decrease after weight loss: A study in patients with jejunoileal bypass versus medical treatment for morbid obesity. Int J Obes 1982;6:307–12.
Griffen 1977
Griffen WOJ, Young VL, Stevenson CC. A prospective comparison of gastric and jejunoileal bypass procedures for morbid obesity. Ann Surg 1977;186:500–9.
Hall 1990
Hall JC, Watts JM, O’Brien PE, Dunstan RE, Walsh JF, Slavotinek Ae. Gastric surgery for morbid obesity. The Adelaide Study. Ann Surg 1990;211:419–27.
Laws 1981
Laws HL, Piantadosi S. Superior gastric reduction procedure for morbid obesity: a prospective, randomized trial. Ann Surg 1981;193:334–40.
Lechner 1981
Lechner GW, Callender AK. Subtotal gastric exclusion and gastric partitioning: a randomized prospective comparison of one hundred patients. Surgery 1981;90:637–44.
Naslund 1988
Naslund I. The size of the gastric outlet and the outcome of surgery for obesity. Acta Chirurg Scand 1986;152:205–10.
Naslund I, Wickbom G, Christoffersson E, Agren G. A prospective randomized comparison of gastric bypass and gastroplasty. Complications and early results. Acta Chirurg Scand 1986;152:681–9.
Naslund I. Gastric bypass versus gastroplasty. A prospective study of differences in two surgical procedures for morbid obesity. Acta Chirurg Scand Suppl 1987;536:1–60.
Naslund I, Beckman KW. Gastric emptying rate after gastric bypass and gastroplasty. Scand J Gastroenterol 1987;22:193–201.
Naslund I, Hallgren P, Sjostrom L. Fat cell weight and number before and after gastric surgery for morbid obesity in women. Int J Obes 1988;12:191–7.
Naslund I, Jarnmark I, Andersson H. Dietary intake before and after gastric bypass and gastroplasty for morbid obesity in women. Int J Obes 1988;12:503–13.
Pories 1982
Pories WJ, Flickinger EG, Meelheim D, Van Rij AM, Thomas FT. The effectiveness of gastric bypass over gastric partition in morbid obesity: consequence of distal gastric and duodenal exclusion. Ann Surg 1982;196:389–99.
Van Rij 1984
Van Rij AM. Gastric bypass and gastric partitioning in morbid obesity: results of a controlled trial [abstract]. Aust N Z J Med 1984;14(Suppl. 1):340.
Studies excluded from updated searches
Adams TD, Avelar E, Cloward T, Crosby RD, Farney RJ, Gress R et al. Design and rationale of the Utah obesity study. A study to assess morbidity following gastric bypass surgery. Contemp Clin Trials 2005;26:534–51. [Twelve-month results not reported, reports design and baseline only.]
Andersson I, Adolfsson B, Apelman J, Bengtsson B, Rossner S, Thorne A. Prospective randomised controlled study with a 3 year follow-up-behaviour modification + adjustable gastric banding (AGB) vs AGB. Int J Obes 2001;25(Suppl. 2):S27. [Intervention – behaviour modification, length of follow-up.]
Arcila D, Velazquez D, Gamino R, Sierra M, Salin-Pascual R, Gonzalez-Barranco J et al. Quality of life in bariatric surgery. Obes Surg 2002;12:661–5. [Study design – cross-sectional study.]
Batsis JA, Romero-Corral A, Collazo-Clavell M, Sarr MG, Somers V, Lopez-Jimenez F. The effect of bariatric surgery on metabolic syndrome: a population based, long-term controlled study. Diabetes 2008;57:A484–A485. [Study design.]
Blanco-Engert R, Weiner S, Pomhoff I, Matkowitz R, Weiner RA. Outcome after laparoscopic adjustable gastric banding, using the Lap-Band and the Heliogast band: a prospective randomized study. Obesity Surgery 2003;13:776–9. [Interventions – comparison of techniques rather than different procedures.]
Bouillot JL, Servajean S, Coupaye M, Berger N, Veyrie N, Poitou C et al. Laparoscopic surgery for morbid obesity: Results of a comparative study: Gastric banding vs gastric bypass. Obes Surg 2006;16:416. [Study design not an RCT for comparison of surgical procedures.]
Busetto L, Mirabelli D, Petroni ML, Mazza M, Favretti F, Segato G et al. Comparative long-term mortality after laparoscopic adjustable gastric banding versus nonsurgical controls. Surg Obes Related Dis 2007;3:496–502. [Study design, not concurrent controls.]
Christou NV, Sampalis JS, Liberman M, Look D, Auger S, McLean AP et al. Surgery decreases long-term mortality, morbidity, and health care use in morbidly obese patients. Ann Surg 2004;240:416–23. [Study design – retrospective cohort study.]
Cummings DE, Weigle DS, Frayo RS, Breen PA, Ma MK, Dellinger EP et al. Plasma ghrelin levels after diet-induced weight loss or gastric bypass surgery. N Engl J Med 2002;346:1623–30. [Patients, study design, length of follow-up.]
DeMaria EJ. Bariatric surgery for morbid obesity. N Engl J Med 2007;356:2176–83. [Study design.]
Deveney CW, MacCabee D, Marlink K, Welker K, Davis J, McConnell DB. Roux-en-Y divided gastric bypass results in the same weight loss as duodenal switch for morbid obesity. Am J Surg 2004;187:655–9. [Study design.]
Dittmar M, Heintz A, Hardt J, Egle UT, Kahaly GJ. Metabolic and psychosocial effects of minimal invasive gastric banding for morbid obesity. Metab Clin Exp 2003;52:1551–7. [Unclear length of follow-up, no reply from authors.]
Dixon AFR, Dixon JB, O’Brien PE. Laparoscopic adjustable gastric banding induces satiety: a randomized crossover study. Int J Obes 2004;28:S39. [Patients, study design.]
Gravante G, Araco A, Araco F, Delogu D, De LA, Cervelli V. Laparoscopic adjustable gastric bandings: a prospective randomized study of 400 operations performed with 2 different devices. Archiv Surg 2007;142:958–961. [Intervention – comparison of devices rather than different procedures.]
Griffen WO, Jr., Young VL, Stevenson CC. A prospective comparison of gastric and jejunoileal bypass procedures for morbid obesity. 1977. Surg Obes Related Dis 2005;1:163–72. [Reprint of 1977 paper – excluded for intervention – jejunoileal bypass.]
Herron DM. Biliopancreatic diversion with duodenal switch vs. gastric bypass for severe obesity. J Gastrointest Surg 2004;8:406–7. [Overview.]
Holeczy P, Bolek M, Sevcikova J. Comparison of first 25 laparoscopic gastric banding and gastric sleeve resections with 1 year follow-up. Obes Surg 2008;18:482. [Study design.]
Keating C, Moodie M, O’Brien P, Peeters A, Dixon J. Cost-effectiveness of surgically induced weight loss for the management of type-2 diabetes: randomised trial. Int J Obes 2008;32(Suppl. 1). [Outcomes.]
Lawson ML, Kirk S, Mitchell T, Chen MK, Loux TJ, Daniels SR et al. One-year outcomes of Roux-en-Y gastric bypass for morbidly obese adolescents: a multicenter study from the Pediatric Bariatric Study Group. J Pediatr Surg 2006;41:137–43. [Study design – retrospective.]
Lee W-J. Laparoscopic Roux-en-Y versus mini-gastric bypass for the treatment of morbid obesity: a prospective randomized controlled clinical trial. Ann Surg 2005;242:20–8. [Comparison of surgical technique (gastric bypass vs mini gastric bypass).]
Lee WJ, Wang W, Huang MT. Laparoscopic adjustable silicone gastric banding versus vertical banded gastroplasty in morbidly obese patients. Ann Surg 2004;240:391–2. [Letter – overview.]
Liorci MP, Ilias EJ, Kassab P, Castro OA. [Roux en Y gastric bypass surgery or gastric band to the treatment of the morbid obesity?.]. [In Portuguese.]. Rev Assoc Med Brasil 1900;52:195-Aug. [Overview.]
Mummadi RR, Kasturi KS, Sood G. Effect of bariatric surgery on nonalcoholic fatty liver disease (NAFLD): a meta-analysis. Hepatology 2007;46(4, Suppl. S). [Before and after studies.]
Naslund I. Lessons from the Swedish Obese Subjects Study: the effects of surgically induced weight loss on obesity comorbidity. Surg Obes Related Dis 2005;1:140–4. [Overview.]
Rabl C, Palazzo F, Rogers S, Posselt A, Cello J, Campos G. Laparoscopic gastric bypass is as safe as laparoscopic gastric banding and provides superior weight loss outcomes. Obes Surg 2008;18:459–60. [Study design.]
Ryan D, Stenlof K, Martin P. Design and methods for a randomized clinical evaluation comparing gastric bypass surgery, an intensive medical intervention and usual care for class III obesity. Obes Res 2004;12:A42. [Abstract – no data. Authors contacted – no surgical arm in trial.]
Sampalis JS, Liberman M, Auger S, Christou NV. The impact of weight reduction surgery on health-care costs in morbidly obese patients. Obes Surg 2004;14:939–47. [Length of follow-up of control group.]
Shikora SA. ‘What are the yanks doing?’ The U.S. experience with Implantable Gastric Stimulation (IGS) for the treatment of obesity – update on the ongoing clinical trials. Obes Surg 2004;14(Suppl. 1):S40–S48.[Intervention – implantable gastric stimulation, length of follow-up.]
Skroubis G, Anesidis S, Kehagias I, Mead N, Vagenas K, Kalfarentzos F. Roux-en-Y gastric bypass versus a variant of biliopancreatic diversion in a non-superobese population: prospective comparison of the efficacy and the incidence of metabolic deficiencies. Obes Surg 2006;16:488–95. [Design – not randomised (confirmed with authors).]
Suter M, Giusti V, Worreth M, Heraief E, Calmes JM. Laparoscopic gastric banding: a prospective, randomized study comparing the Lapband and the SAGB: early results. Ann Surg 2005;241:55–62. [Intervention – comparison of techniques rather than different procedures.]
Thorne A, Lonnqvist F, Apelman J, Hellers G, Arner P. A pilot study of long-term effects of a novel obesity treatment: omentectomy in connection with adjustable gastric banding. Int J Obes Related Metabol Disord: J Int Assoc Study Obes 2002;26:193–9. [Intervention – omenectomy.]
Weiss HG, Nehoda H, Labeck B, Peer-Kuehberger R, Oberwalder M, Aigner F et al. Adjustable gastric and esophagogastric banding: a randomized clinical trial. Obes Surg 2002;12:573–8. [Intervention – comparison of techniques rather than procedures.]
Appendix 17 List of studies excluded from the review of cost-effectiveness
Caro JJ, Ozer Stillman I, Danel A, Getsios D, McEwan P. Cost-effectiveness of rimonabant use in patients at increased cardiometabolic risk: estimates from a Markov model. J Med Economics 2007;10:239–54. [Only non-surgical interventions are evaluated.]
Caro JJ, O’Brien J.A, Hollenbeak CS, Spackman E, Ben-Joseph R, Okamoto LJ, et al. Economic burden and risk of cardiovascular disease and diabetes in patients with different cardiometabolic risk profiles. Value in Health 2007;10(Suppl. 1):S12–S20. [Not an economic evaluation of the alternative therapies.]
Christou NV, Sampalis JS, Liberman M, Look D, Auger S, McLean AP, et al. Surgery decreases long-term mortality, morbidity, and health care use in morbidly obese patients. Ann Surg 2004;240:416–23. [Intermediate outcome (percent excess weight loss) is not converted into the final outcome.]
Clegg AJ, Colquitt J, Sidhu MK, Royle P, Loveman E, Walker A. The clinical effectiveness and cost-effectiveness of surgery for people with morbid obesity: a systematic review and economic evaluation. Health Technol Assess 2002;6:1–153. [The previous report.]
Clegg AJ, Colquitt J, Sidhu MK, Royle P, Loveman E, Walker A. Clinical and cost effectiveness of surgery for morbid obesity: a systematic review and economic evaluation. Int J Obes Related Metabol Disord: J Int Assoc Study Obes 2003;27:1167–77. [Journal publication of the previous report.]
Craig BM, Tseng DS, Fang J. Is bariatric surgery worth its weight in gold (costs)? Evidence-Based Gastroenterol 2003;4:88–9. [Not a complete economic evaluation; cost and outcomes are not reported.]
Encinosa WE, Bernard DM, Chen CC, Steiner CA. Healthcare utilization and outcomes after bariatric surgery. Med Care 2006; 44:706–12. [Intermediate outcomes (complication rates, length of stay) are not converted into the final outcomes.]
Fang J. The cost-effectiveness of bariatric surgery. Am J Gastroenterol 2003;98:2097–8. [Not an economic evaluation. A comment to the included paper by Craig and Tseng, 2002.]
Flum DR. Cost and survival outcomes assessment of gastric bypass surgery. Surg Obes Related Dis 2005;1:41–44. [Not a complete economic evaluation, review.]
Flum DR, Salem L, Elrod JA, Dellinger EP, Cheadle A, Chan L. Early mortality among Medicare beneficiaries undergoing bariatric surgical procedures. JAMA 2005;294:1903–8. [Not a complete economic evaluation. Intermediate outcomes (mortality) are not converted into the final outcomes.]
Gallagher SF, Banasiak M, Gonzalvo JP, Paoli DP, Allwood J, Morris D, et al. The impact of bariatric surgery on the Veterans Administration healthcare system: a cost analysis. Obes Surg 2003;13:245–8. [Not a complete economic evaluation; Costing study; outcomes are not reported.]
Haby MM, Vos T, Carter R, Moodie M, Markwick A, Magnus A, et al. A new approach to assessing the health benefit from obesity interventions in children and adolescents: the assessing cost-effectiveness in obesity project. Int J Obes 2006;30:1463–75. [Not a complete economic evaluation, method only.]
Jones Jr, AJD, Benotti PN, Capella RF, Cooper CG, Flanagan L, et al. Open versus laparoscopic Roux-en-Y gastric bypass: A comparative study of over 25,000 open cases and the major laparoscopic bariatric reported series. Obes Surg 2006;16:721–7. [Not a complete economic evaluation intermediate outcomes (complication rates) are not converted into the final outcomes.]
Katopodi T, Katostaras T. The weight reduction operation of choice: Mason vs gastric bypass. A comparative study. Rev Clin Pharmacol Pharmacokin Int Edn 2005;19:155–8. [Costs and outcomes are not converted into the final outcomes.]
Korenkov M, Sauerland S, Junginger T. Surgery for obesity. Curr Opin Gastroenterol 2005;21:679–83. [Not an economic evaluation. Not a systematic review.]
Kral JG, Christou NV, Flum DR, Wolfe BM, Schauer PR, Gagner M et al. Medicare and bariatric surgery. Surg Obes Related Dis 2005;1:35–63. [Not an economic evaluation. Not a systematic review.]
Lamotte M, Annemans L, Lefever A, Nechelput M, Masure J. A health economic model to assess the long-term effects and cost-effectiveness of orlistat in obese type 2 diabetic patients. Diabetes Care 2002;25:303–8. [Only non-surgical interventions are evaluated.]
Levy P, Fried M, Santini F, Finer N. The comparative effects of bariatric surgery on weight and Type 2 diabetes. Obes Surg 2007;17:1248–56. [Not an economic evaluation. Not a systematic review.]
Livingston EH, Fink AS. Quality of life: cost and future of bariatric surgery. Archiv Surg 2003;138:383–8. [Not an economic evaluation; review of non-utility based HRQoL.]
Monk JS, Nagib ND, Stehr W. Pharmaceutical savings after gastric bypass surgery. Obes Surg 2004;14:13–15. [Not an economic evaluation. Costing study.]
Narbro K, Agren G, Jonsson E, Naslund I, Sjostrom L, Peltonen M. Pharmaceutical costs in obese individuals: comparison with a randomly selected population sample and long-term changes after conventional and surgical treatment: the SOS intervention study. Arch Intern Med 2002;162:2061–9. [Costs and outcomes are not converted into the final outcomes.]
Nguyen NT, Goldman C, Rosenquist CJ, Arango A, Cole CJ, Lee SJ, et al. Laparoscopic versus open gastric bypass: a randomized study of outcomes, quality of life, and costs. Ann Surg 2001;234:279–89. [Costs and outcomes are not converted into the final outcomes.]
Nguyen NT, Varela JE, Sabio A, Naim J, Stamos M, Wilson SE. Reduction in prescription medication costs after laparoscopic gastric bypass. Am Surgeon 2006;72:853–6. [Not an economic evaluation. Costing study.]
Paxton JH, Matthews JB. The cost effectiveness of laparoscopic versus open gastric bypass surgery. Obes Surg 2005;15:24–34. [Costs and outcomes are not converted into the final outcomes.]
Sampalis JS, Liberman M, Auger S, Christou NV. The impact of weight reduction surgery on health-care costs in morbidly obese patients. Obes Surg 2004;14:939–47. [Costs and outcomes are not converted into the final outcomes.]
Sanchez-Santos R, Del Barrio MJ, Gonzalez C, Madico C. Long-term health-related quality of life following gastric bypass: influence of depression. Obes Surg 2006;16:580–5. [Costs are not reported; outcomes are not converted into the final outcomes.]
Siddiqui A, Livingston E, Huerta S. A comparison of open and laparoscopic Roux-en-Y gastric bypass surgery for morbid and super obesity: a decision-analysis model. Am J Surg 2006;192(5):e1–e7. [Costs and outcomes are not converted into the final outcomes.]
Snow LL, Weinstein LS., Hannon JK, Lane DR, Ringold FG, Hansen PA, et al. The effect of Roux-en-Y gastric bypass on prescription drug costs. Obes Surg 2004;14:1031–5. [Not an economic evaluation. Costing study.]
Zlabek JA, Grimm MS, Larson CJ, Mathiason MA, Lambert PJ. Kothari SN. The effect of laparoscopic gastric bypass surgery on dyslipidemia in severely obese patients. Surg Obes Related Dis 2005;1:537–42. [Not a complete economic evaluation. Intermediate outcomes are not converted into the final outcomes.]
Appendix 18 Updating discounting practice for previous assessment report
Table 74 reports the total costs and QALYs for each morbidly obese (BMI > 40) patient undergoing surgical and non-surgical management, as reported in the previous assessment report. Table 75 reports the incremental costs for surgical management, with adjustable gastric banding or gastric bypass, compared with non-surgical management. Both surgical procedures are associated with increased total costs and increased QALYs, with ICERs of £8527 for adjustable gastric banding and £6289 for gastric bypass.
| Total Cost (£) | QALYs | |
|---|---|---|
| Usual care | 6964 | 11.23 |
| SAGB | 10,795 | 11.68 |
| Gastric bypass | 9764 | 11.67 |
| Intervention | Comparator | Additional cost (£) | Additional QALYs | Net cost per QALY gained (£) |
|---|---|---|---|---|
| SAGB | Non-surgical | 3831 | 0.45 | 8527 |
| Gastric bypass | Non-surgical | 2800 | 0.45 | 6289 |
The following two tables (Tables 76 and Table 77) report the same analysis, but applying the same discount rate of 3.5% to both costs and QALYs, as is conventional practice in current health technology assessments. This change in discounting practice leads to higher total costs, and reduces the total QALYs as would be expected. However, this change in discounting practice has very little impact on the ICERs, see the final column of Table 77.
| Total cost (£) | QALYs | |
|---|---|---|
| Usual care | 9044 | 9.22 |
| SAGB | 12,588 | 9.63 |
| Gastric bypass | 11,512 | 9.64 |
| Intervention | Comparator | Additional cost (£) | Additional QALYs | Net cost per QALY gained (£) |
|---|---|---|---|---|
| SAGB | Non-surgical | 3544 | 0.41 | 8553 |
| Gastric bypass | Non-surgical | 2468 | 0.42 | 5822 |
Appendix 19 Caro reparameterisation of Framingham Heart Study accelerated failure time models
Table 78 reports the parameters for the Framingham Heart Study CHD risk equation, as reported by Andersen and colleagues. 168 Andersen and colleagues168 also outline the method used to derive an individual’s risk of a CHD event given their characteristics, in terms of age, sex, systolic blood pressure, smoking status, ratio of total cholesterol to high-density lipoproteins and whether they have developed diabetes.
| Parameter estimate | Untransformed input value | Transformed input value | |
|---|---|---|---|
| θ0 | 0.9145 | ||
| θ1 | – 0.2784 | ||
| Constant | 15.5305 | 1 | 1.0000 |
| Female | 28.4441 | 1 | 1.0000 |
| ln(Age) | – 1.4792 | 55 | 4.0073 |
| ln(Age)*Female | – 14.4588 | 4.0073 | |
| [ln(Age)]2*Female | 1.8515 | 16.0587 | |
| ln(SBP) | – 0.9119 | 135 | 4.9053 |
| Smoker | – 0.2767 | 1 | 1.0000 |
| ln(TC : HDL) | – 0.7181 | 4.79 | 1.5669 |
| Diabetes | – 0.1759 | 1 | 1.0000 |
| Diabetes*Female | – 0.1999 | 1.0000 |
Table 79 reproduces the steps outlined in the original article by Andersen and colleagues168 to derive the 10-year predicted probability of a 55-year-old woman, who is a current smoker, with systolic blood pressure of 135 mmHg, and a TC : HDL ratio of 4.79 and who has developed diabetes. The second column in Table 78 shows the parameter estimates from the Framingham Heart Study CHD equation, while the third column lists the input values as described in the previous sentence. The final column in Table 78 lists these input values as they are entered into the risk equation, with log transformations where required (for age, systolic blood pressure and TC : HDL ratio). The first stage in deriving an individual’s risk is to multiply the transformed input values by the relevant parameter estimate – the result of this is reported in the row labelled μ in Table 79. Following the remaining steps outlined in Table 79, gives an estimated 10-year probability of a CHD event of 22%.
| Calculate example in original paper | |
|---|---|
| µ | 3.58765 |
| log(s) = θ0 + θ1 µ | – 0.08430 |
| s = exp(θ0 + θ1µ) | 0.91915 |
| u = [ln(10) – µ]/s | – 1.39809 |
|
10-year predicted probability {1 – exp[– exp(u)]} |
0.21891 |
Alternatively, reparameterising the equation as suggested by Caro and colleagues169 so that:
allows the use of a more standard Weibull formulation to calculate the hazard in any cycle t:
In the above example, this yields an annual risk (assuming annual cycles) from 0.0217 in year 1 to 0.0265 in year 10. Adopting the DEALE method162 to derive an annual risk from the 10-year risk [– 1/10 * ln(1 – 0.21891)], would yield a constant risk of 0.0247 which would tend to slightly overestimate the risk compared with the method based on the reparameterised FHS equations.
Appendix 20 Variables included in probabilistic sensitivity analyses, distributions and parameters of distributions used
Table 80 and Table 81 provide details of the included variables.
| Variable | Distribution | Parameters |
|---|---|---|
| Weight loss – surgical | Normal | Mean = 21.1; SD = 1.917 |
| Systolic blood pressure – surgical | Normal | Mean = 6.00; SD = 3.268 |
| TC : HDL – surgical | Normal | Mean = 0.82; SD = 0.347 |
| Weight loss – non-surgical | Normal | Mean = 1.5; SD = 0.986 |
| Systolic blood pressure – non-surgical | Normal | Mean = 1.70; SD = 2.593 |
| TC : HDL – non-surgical | Normal | Mean = 0.14; SD = 0.190 |
| Utility change per unit change in BMI | Uniform | Minimum = 0.0075; SD = 0.0166 |
| Diabetes remission – surgical | Beta | Alpha = 22; Beta = 8 |
| Diabetes remission – non-surgical | Beta | Alpha = 4; Beta = 26 |
| Diabetes heath state | Gamma | Alpha = 4394.9051; Beta = 0.5 |
| Acute AMI | Gamma | Alpha = 3226.4959; Beta = 0.5 |
| Chronic AMI | Gamma | Alpha = 1130.3026; Beta = 0.5 |
| Acute stroke | Gamma | Alpha = 19079.7077; Beta = 0.5 |
| Chronic stroke | Gamma | Alpha = 5129.1832; Beta = 0.5 |
| Variable | Distribution | Parameters |
|---|---|---|
| Baseline BMI – surgical | Normal | Mean = 37.7; SD = 0.3827 |
| BMI at 6 months – surgical | Normal | Mean = 28.9; SD = 0.4082 |
| BMI at 12 months – surgical | Normal | Mean = 27; SD = 0.4082 |
| BMI at 18 months – surgical | Normal | Mean = 26.7; SD = 0.4082 |
| BMI at 24 months – surgical | Normal | Mean = 26.4; SD = 0.4082 |
| Systolic blood pressure (% change) – surgical | Beta | Alpha = 4.104; Beta = 33.896 |
| TC : HDL (% change) – surgical | Beta | Alpha = 8.094; Beta = 29.906 |
| Baseline BMI – non-surgical | Normal | Mean = 37.5; SD = 0.4082 |
| BMI at 6 months – non-surgical | Normal | Mean = 28.7; SD = 0.4337 |
| BMI at 12 months – non-surgical | Normal | Mean = 29.9; SD = 0. 4337 |
| BMI at 18 months – non-surgical | Normal | Mean = 30.9; SD = 0. 4337 |
| BMI at 24 months – non-surgical | Normal | Mean = 31.5; SD = 0. 4337 |
| Systolic blood pressure (% change) – non-surgical | Beta | Alpha = 2.160; Beta = 27.840 |
| TC : HDL (% change) – non-surgical | Beta | Alpha = 2.400; Beta = 27.600 |
| Utility change per unit change in BMI | Uniform | Minimum = 0.0075; Maximum = 0.0166 |
| Diabetes remission – surgical | Beta | Alpha = 14; Beta = 1 |
| Diabetes remission – non-surgical | Beta | Alpha = 7; Beta = 8 |
| Diabetes heath state | Gamma | Alpha = 4394.9051; Beta = 0.5 |
| Acute AMI | Gamma | Alpha = 3226.4959; Beta = 0.5 |
| Chronic AMI | Gamma | Alpha = 1130.3026; Beta = 0.5 |
| Acute stroke | Gamma | Alpha = 19079.7077; Beta = 0.5 |
| Chronic stroke | Gamma | Alpha = 5129.1832; Beta = 0.5 |
Appendix 21 List of ongoing studies
Comparison of laparoscopic sleeve gastrectomy and Roux-en-Y-gastric bypass in the treatment of morbid obesity
Laparoscopic sleeve-gastrectomy will be compared to laparoscopic proximal Roux-Y-gastric bypass in a prospective randomised study. Primary outcome measure is effectiveness in terms of weight loss, reduction in comorbidity and quality of life over five years. Secondary outcome measures are: early morbidity, duration and cost of the operation, late morbidity, reoperations (for complications, for insufficient weight loss) and postoperative changes of gastrointestinal hormones.
-
Estimated enrolment: 90 (adults with BMI > 40).
-
Study start date: July 2006.
-
Estimated study completion date: August 2016.
-
Estimated primary completion date: September 2010 (final data collection date for primary outcome measure).
-
Sponsors and collaborators: University Hospital, Basel, Switzerland. Swiss National Science Foundation, Ethicon Endo-Surgery.
Laparoscopic adjustable gastric banding versus sleeve gastrectomy
Official title: Laparoscopic adjustable gastric banding versus laparoscopic sleeve gastrectomy: a prospective randomised trial
The investigators aim to determine the clinical and metabolic outcomes of two available bariatric restrictive procedures: laparoscopic adjustable gastric banding and laparoscopic sleeve gastrectomy for the treatment of morbid obesity in veterans. Primary outcome measures are only described as ‘Short and long term clinical outcomes’ over five years. Secondary outcome measures are: metabolic outcomes, oesophagogastric physiology, hormonal physiology and procedure costs.
-
Estimated enrolment: 40 (veterans with BMI > 35 with comorbidities or BMI > 40).
-
Study start date: January 2008.
-
Estimated study completion date: December 2012.
-
Estimated primary completion date: December 2010 (final data collection date for primary outcome measure).
-
Sponsors and collaborators: North Texas Veterans’ Healthcare System.
Laparoscopic bariatric surgery to treat Type 2 diabetes in obese patients
This pilot research study is being performed to determine whether bariatric surgery can safely provide better control of diabetes symptoms in obese diabetics than continuing medical management (antidiabetic drugs in combination with diet and lifestyle changes). This study will be comparing gastric bypass and adjustable gastric banding to treatment with a combination of drugs, diet and lifestyle changes for control of Type 2 diabetes. Primary outcome measure: diabetic control as assessed by HbA1c. Secondary outcome measures: resolution of diabetes; improvement in diabetic control and cardiometabolic profile; weight loss and decrease in BMI; reduction in the usage of insulin or other diabetic drugs; improvement in diabetic complications and end-organ damage; improvement in health-related quality of life and depression scores; and, utilisation of resources and productivity losses. Duration of study not stated.
-
Estimated enrolment: 72 (BMI 30 to < 40 kg/m2) plus have had Type 2 diabetes mellitus for more than five years and have complications).
-
Study start date: May 2007.
-
Study end date: not stated.
-
Sponsors and collaborators: Hamilton Health Sciences.
Mechanisms of diabetes control after weight loss surgery
The aim of this study is to determine whether the magnitude of the incretin effect on insulin secretion is greater after gastric bypass than after an equivalent diet-induced weight loss. We will compare, in obese patients with diabetes, randomised to VLCD or to gastric bypass, the effect of an equivalent weight loss on the incretin effect (difference in insulin secretion after comparable oral and intravenous glucose loads).
-
Study type: observational.
-
Study design: case–control, prospective.
-
Estimated enrolment: 20.
-
Study start date: September 2005.
-
Estimated study completion date: July 2008.
Longitudinal assessment of bariatric surgery (LABS-1) – completed
The primary objectives of this study are to assess the safety of bariatric surgery by estimating the prevalence of short-term adverse outcomes in a multicentre cohort of patients undergoing bariatric surgical procedures and to determine the associations between short-term adverse outcomes after bariatric surgery and both clinical/demographic patient characteristics and features of operative/perioperative care.
-
Study type: observational.
-
Study design: cohort, prospective.
-
Enrolment: 5102.
-
Study start date: March 2005.
-
Study completion date: December 2007.
-
Primary completion date: December 2007. (Final data collection date for primary outcome measure.)
-
Sponsors and collaborators: National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK).
Long-term effects of bariatric surgery (LABS-2)
The primary objective of LABS-2 is to use standardised techniques and measures to assess the longer-term safety and efficacy of bariatric surgery by: (1) comparing postsurgical outcomes with preoperative status; and (2) examining risks and benefits of surgery. LABS-2 will determine the associations between clinical/demographic patient characteristics, components of the surgical procedure, and perioperative and postoperative care with postoperative risks and changes in patient status.
-
Study type: observational.
-
Study design: cohort, prospective.
-
Estimated enrolment: 2400.
-
Study start date: March 2006.
-
Estimated study completion date: August 2009.
-
Sponsors and collaborators: National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK).
Advanced medical therapy versus advanced medical therapy plus bariatric surgery for the resolution of Type 2 diabetes
The aim of the study is to compare the relative clinical outcomes between advanced medical therapy alone or advanced medical therapy combined with bariatric surgery [either Roux-en-Y gastric bypass or laparoscopic sleeve gastrectomy] in patients with Type 2 diabetes and a BMI between 30 and 40 kg/m2. The study will examine the short- and long-term effects of each intervention on biochemical resolution of diabetes, diabetic complications and end-organ damage.
-
Study type: interventional.
-
Study design: treatment, randomised, open label, parallel assignment, safety/efficacy study.
-
Official title: STAMPEDE: Surgical Therapy And Medications Potentially Eradicate Diabetes Efficiently.
-
Estimated enrolment: 150.
-
Study start date: February 2007.
-
Estimated study completion date: December 2013.
-
Estimated primary completion date: January 2011. (Final data collection date for primary outcome measure.)
-
Sponsors and collaborators: The Cleveland Clinic, Ethicon Endo-Surgery, LifeScan.
A prospective randomised controlled intervention study of conventional management versus the placement of the Lap-Band system in severely obese adolescents in effecting weight loss
A group of 50 severely obese adolescents will be randomised to either a conventional management plan incorporating the Active8 Adolescent Programme with dietary and behavioural modification or surgical management with the Lap-Band system.
-
Open parallel study.
-
Start date: 1 February 2005.
-
Closed, but follow-up is continuing.
-
Funding: NHMRC, Inamed Health, Centre for Obesity Research and Education (CORE).
Double-blind randomised controlled study to compare the outcomes of laparoscopic gastric banding and laparoscopic Roux-en-Y gastric bypass in morbidly obese patients attending the Multidisciplinary Morbid Obesity Clinic at King’s College Hospital
-
Anticipated start date: 1 September 2003.
-
Anticipated end date: 1 September 2009.
-
Status of trial: ongoing.
-
Trial design: double-blind randomised controlled study.
Interventions: To compare the outcomes of laparoscopic gastric banding and laparoscopic Roux-en-Y gastric bypass.
1. To compare the early outcome (first six months postoperatively) of the two operations with that of a matched group of morbidly obese patients who are on a low-calorie diet only (controls).
2. To determine if there is any clinical and statistical difference in the outcomes of the two surgical procedures in the early, medium and long term (up to five years postoperatively).
-
Contact name Mr A. G. Patel, King’s College Hospital, London, UK.
-
ISRCTN Register ISRCTN33929407.
List of abbreviations
- AGB
- adjustable gastric banding
- AMI
- acute myocardial infarction
- BAROS
- Bariatric Analysis and Reporting Outcome System
- BMI
- body mass index (kg/m2)
- BOSPA
- British Obesity Surgery Patient Association
- BPD
- biliopancreatic diversion
- BSQ
- Bing Scale Questionnaire
- CEA
- cost-effectiveness analysis
- CHD
- coronary heart disease
- CI
- confidence interval
- CRD
- NHS Centre for Reviews and Dissemination
- CUA
- cost–utility analysis
- CVD
- cardiovascular disease
- DEALE
- Declining Exponential Approximation to Life Expectancy
- EMEA
- European Medicines Agency
- EQ-5D
- European Quality Of Life-5 Dimensions
- EWL
- excess weight loss
- FHS
- Framingham Heart Study
- GBand
- gastric banding
- GBP
- gastric bypass
- GERD
- gastro-oesophageal reflux disease
- GIQLI
- gastrointestinal quality of life index
- GP
- general practitioner
- HADS
- Hospital Anxiety and Depression Scale
- HbA1c
- glycosylated haemoglobin
- HCHS
- Hospital and Community Health Services
- HDL
- high-density lipoprotein
- HDU
- high-dependency unit
- HRQoL
- health-related quality of life
- HSE
- Health Survey for England
- ICER(s)
- incremental cost-effectiveness ratio(s)
- IGBP
- isolated gastric bypass
- IHD
- ischaemic heart disease
- ITU
- intensive-care unit
- IQR
- inter quartile range
- ITT
- intention to treat
- LAGB
- laparoscopic adjustable gastric banding
- Lap
- laparoscopic surgery
- LDL
- low-density lipoprotein
- LGBP
- laparoscopic gastric bypass
- LISG
- laparoscopic isolated sleeve gastrectomy
- LOS
- length of (hospital) stay
- LRYGBP
- laparoscopic Roux-en-Y gastric bypass
- LSG
- laparoscopic sleeve gastrectomy
- LVBG
- laparoscopic vertical banded gastroplasty
- LY(s)
- Life year(s)
- MACL
- Mood Adjective Check List
- MAQoL
- Moorehead–Ardelt Quality of Life questionnaire
- NAO
- National Audit Office
- NHANES
- National Health and Nutrition Examination survey
- NICE
- National Institute for Health and Clinical Excellence
- ns
- not statistically significant
- Open
- open surgery
- PAssQ
- Psychosocial Assessment Questionnaire
- PSS
- personal social services
- PCT(s)
- primary-care trust(s)
- PSSQ
- Psychosocial Stress and Symptom Questionnaire
- QALY(s)
- quality adjusted life-year(s)
- QoL
- quality of life
- RCT(s)
- randomised controlled trial(s)
- RR
- relative risk
- RYGBP
- Roux-en-Y gastric bypass
- SD
- standard deviation
- SF-36
- short form health survey
- SHARE
- Survey of Health, Ageing and Retirement in Europe
- SIGN
- Scottish Intercollegiate Guidelines Network
- SOS
- Swedish Obese Subjects
- TC:HDL
- total cholesterol to high-density lipoprotein ratio
- VAS
- visual analogue scale
- VBG
- vertical banded gastroplasty
- VLCD(s)
- very-low-calorie diet(s)
- vs
- versus
- WHO
- World Health Organization
Notes
Health Technology Assessment reports published to date
-
Home parenteral nutrition: a systematic review.
By Richards DM, Deeks JJ, Sheldon TA, Shaffer JL.
-
Diagnosis, management and screening of early localised prostate cancer.
A review by Selley S, Donovan J, Faulkner A, Coast J, Gillatt D.
-
The diagnosis, management, treatment and costs of prostate cancer in England and Wales.
A review by Chamberlain J, Melia J, Moss S, Brown J.
-
Screening for fragile X syndrome.
A review by Murray J, Cuckle H, Taylor G, Hewison J.
-
A review of near patient testing in primary care.
By Hobbs FDR, Delaney BC, Fitzmaurice DA, Wilson S, Hyde CJ, Thorpe GH, et al.
-
Systematic review of outpatient services for chronic pain control.
By McQuay HJ, Moore RA, Eccleston C, Morley S, de C Williams AC.
-
Neonatal screening for inborn errors of metabolism: cost, yield and outcome.
A review by Pollitt RJ, Green A, McCabe CJ, Booth A, Cooper NJ, Leonard JV, et al.
-
Preschool vision screening.
A review by Snowdon SK, Stewart-Brown SL.
-
Implications of socio-cultural contexts for the ethics of clinical trials.
A review by Ashcroft RE, Chadwick DW, Clark SRL, Edwards RHT, Frith L, Hutton JL.
-
A critical review of the role of neonatal hearing screening in the detection of congenital hearing impairment.
By Davis A, Bamford J, Wilson I, Ramkalawan T, Forshaw M, Wright S.
-
Newborn screening for inborn errors of metabolism: a systematic review.
By Seymour CA, Thomason MJ, Chalmers RA, Addison GM, Bain MD, Cockburn F, et al.
-
Routine preoperative testing: a systematic review of the evidence.
By Munro J, Booth A, Nicholl J.
-
Systematic review of the effectiveness of laxatives in the elderly.
By Petticrew M, Watt I, Sheldon T.
-
When and how to assess fast-changing technologies: a comparative study of medical applications of four generic technologies.
A review by Mowatt G, Bower DJ, Brebner JA, Cairns JA, Grant AM, McKee L.
-
Antenatal screening for Down’s syndrome.
A review by Wald NJ, Kennard A, Hackshaw A, McGuire A.
-
Screening for ovarian cancer: a systematic review.
By Bell R, Petticrew M, Luengo S, Sheldon TA.
-
Consensus development methods, and their use in clinical guideline development.
A review by Murphy MK, Black NA, Lamping DL, McKee CM, Sanderson CFB, Askham J, et al.
-
A cost–utility analysis of interferon beta for multiple sclerosis.
By Parkin D, McNamee P, Jacoby A, Miller P, Thomas S, Bates D.
-
Effectiveness and efficiency of methods of dialysis therapy for end-stage renal disease: systematic reviews.
By MacLeod A, Grant A, Donaldson C, Khan I, Campbell M, Daly C, et al.
-
Effectiveness of hip prostheses in primary total hip replacement: a critical review of evidence and an economic model.
By Faulkner A, Kennedy LG, Baxter K, Donovan J, Wilkinson M, Bevan G.
-
Antimicrobial prophylaxis in colorectal surgery: a systematic review of randomised controlled trials.
By Song F, Glenny AM.
-
Bone marrow and peripheral blood stem cell transplantation for malignancy.
A review by Johnson PWM, Simnett SJ, Sweetenham JW, Morgan GJ, Stewart LA.
-
Screening for speech and language delay: a systematic review of the literature.
By Law J, Boyle J, Harris F, Harkness A, Nye C.
-
Resource allocation for chronic stable angina: a systematic review of effectiveness, costs and cost-effectiveness of alternative interventions.
By Sculpher MJ, Petticrew M, Kelland JL, Elliott RA, Holdright DR, Buxton MJ.
-
Detection, adherence and control of hypertension for the prevention of stroke: a systematic review.
By Ebrahim S.
-
Postoperative analgesia and vomiting, with special reference to day-case surgery: a systematic review.
By McQuay HJ, Moore RA.
-
Choosing between randomised and nonrandomised studies: a systematic review.
By Britton A, McKee M, Black N, McPherson K, Sanderson C, Bain C.
-
Evaluating patient-based outcome measures for use in clinical trials.
A review by Fitzpatrick R, Davey C, Buxton MJ, Jones DR.
-
Ethical issues in the design and conduct of randomised controlled trials.
A review by Edwards SJL, Lilford RJ, Braunholtz DA, Jackson JC, Hewison J, Thornton J.
-
Qualitative research methods in health technology assessment: a review of the literature.
By Murphy E, Dingwall R, Greatbatch D, Parker S, Watson P.
-
The costs and benefits of paramedic skills in pre-hospital trauma care.
By Nicholl J, Hughes S, Dixon S, Turner J, Yates D.
-
Systematic review of endoscopic ultrasound in gastro-oesophageal cancer.
By Harris KM, Kelly S, Berry E, Hutton J, Roderick P, Cullingworth J, et al.
-
Systematic reviews of trials and other studies.
By Sutton AJ, Abrams KR, Jones DR, Sheldon TA, Song F.
-
Primary total hip replacement surgery: a systematic review of outcomes and modelling of cost-effectiveness associated with different prostheses.
A review by Fitzpatrick R, Shortall E, Sculpher M, Murray D, Morris R, Lodge M, et al.
-
Informed decision making: an annotated bibliography and systematic review.
By Bekker H, Thornton JG, Airey CM, Connelly JB, Hewison J, Robinson MB, et al.
-
Handling uncertainty when performing economic evaluation of healthcare interventions.
A review by Briggs AH, Gray AM.
-
The role of expectancies in the placebo effect and their use in the delivery of health care: a systematic review.
By Crow R, Gage H, Hampson S, Hart J, Kimber A, Thomas H.
-
A randomised controlled trial of different approaches to universal antenatal HIV testing: uptake and acceptability. Annex: Antenatal HIV testing – assessment of a routine voluntary approach.
By Simpson WM, Johnstone FD, Boyd FM, Goldberg DJ, Hart GJ, Gormley SM, et al.
-
Methods for evaluating area-wide and organisation-based interventions in health and health care: a systematic review.
By Ukoumunne OC, Gulliford MC, Chinn S, Sterne JAC, Burney PGJ.
-
Assessing the costs of healthcare technologies in clinical trials.
A review by Johnston K, Buxton MJ, Jones DR, Fitzpatrick R.
-
Cooperatives and their primary care emergency centres: organisation and impact.
By Hallam L, Henthorne K.
-
Screening for cystic fibrosis.
A review by Murray J, Cuckle H, Taylor G, Littlewood J, Hewison J.
-
A review of the use of health status measures in economic evaluation.
By Brazier J, Deverill M, Green C, Harper R, Booth A.
-
Methods for the analysis of quality-of-life and survival data in health technology assessment.
A review by Billingham LJ, Abrams KR, Jones DR.
-
Antenatal and neonatal haemoglobinopathy screening in the UK: review and economic analysis.
By Zeuner D, Ades AE, Karnon J, Brown J, Dezateux C, Anionwu EN.
-
Assessing the quality of reports of randomised trials: implications for the conduct of meta-analyses.
A review by Moher D, Cook DJ, Jadad AR, Tugwell P, Moher M, Jones A, et al.
-
‘Early warning systems’ for identifying new healthcare technologies.
By Robert G, Stevens A, Gabbay J.
-
A systematic review of the role of human papillomavirus testing within a cervical screening programme.
By Cuzick J, Sasieni P, Davies P, Adams J, Normand C, Frater A, et al.
-
Near patient testing in diabetes clinics: appraising the costs and outcomes.
By Grieve R, Beech R, Vincent J, Mazurkiewicz J.
-
Positron emission tomography: establishing priorities for health technology assessment.
A review by Robert G, Milne R.
-
The debridement of chronic wounds: a systematic review.
By Bradley M, Cullum N, Sheldon T.
-
Systematic reviews of wound care management: (2) Dressings and topical agents used in the healing of chronic wounds.
By Bradley M, Cullum N, Nelson EA, Petticrew M, Sheldon T, Torgerson D.
-
A systematic literature review of spiral and electron beam computed tomography: with particular reference to clinical applications in hepatic lesions, pulmonary embolus and coronary artery disease.
By Berry E, Kelly S, Hutton J, Harris KM, Roderick P, Boyce JC, et al.
-
What role for statins? A review and economic model.
By Ebrahim S, Davey Smith G, McCabe C, Payne N, Pickin M, Sheldon TA, et al.
-
Factors that limit the quality, number and progress of randomised controlled trials.
A review by Prescott RJ, Counsell CE, Gillespie WJ, Grant AM, Russell IT, Kiauka S, et al.
-
Antimicrobial prophylaxis in total hip replacement: a systematic review.
By Glenny AM, Song F.
-
Health promoting schools and health promotion in schools: two systematic reviews.
By Lister-Sharp D, Chapman S, Stewart-Brown S, Sowden A.
-
Economic evaluation of a primary care-based education programme for patients with osteoarthritis of the knee.
A review by Lord J, Victor C, Littlejohns P, Ross FM, Axford JS.
-
The estimation of marginal time preference in a UK-wide sample (TEMPUS) project.
A review by Cairns JA, van der Pol MM.
-
Geriatric rehabilitation following fractures in older people: a systematic review.
By Cameron I, Crotty M, Currie C, Finnegan T, Gillespie L, Gillespie W, et al.
-
Screening for sickle cell disease and thalassaemia: a systematic review with supplementary research.
By Davies SC, Cronin E, Gill M, Greengross P, Hickman M, Normand C.
-
Community provision of hearing aids and related audiology services.
A review by Reeves DJ, Alborz A, Hickson FS, Bamford JM.
-
False-negative results in screening programmes: systematic review of impact and implications.
By Petticrew MP, Sowden AJ, Lister-Sharp D, Wright K.
-
Costs and benefits of community postnatal support workers: a randomised controlled trial.
By Morrell CJ, Spiby H, Stewart P, Walters S, Morgan A.
-
Implantable contraceptives (subdermal implants and hormonally impregnated intrauterine systems) versus other forms of reversible contraceptives: two systematic reviews to assess relative effectiveness, acceptability, tolerability and cost-effectiveness.
By French RS, Cowan FM, Mansour DJA, Morris S, Procter T, Hughes D, et al.
-
An introduction to statistical methods for health technology assessment.
A review by White SJ, Ashby D, Brown PJ.
-
Disease-modifying drugs for multiple sclerosis: a rapid and systematic review.
By Clegg A, Bryant J, Milne R.
-
Publication and related biases.
A review by Song F, Eastwood AJ, Gilbody S, Duley L, Sutton AJ.
-
Cost and outcome implications of the organisation of vascular services.
By Michaels J, Brazier J, Palfreyman S, Shackley P, Slack R.
-
Monitoring blood glucose control in diabetes mellitus: a systematic review.
By Coster S, Gulliford MC, Seed PT, Powrie JK, Swaminathan R.
-
The effectiveness of domiciliary health visiting: a systematic review of international studies and a selective review of the British literature.
By Elkan R, Kendrick D, Hewitt M, Robinson JJA, Tolley K, Blair M, et al.
-
The determinants of screening uptake and interventions for increasing uptake: a systematic review.
By Jepson R, Clegg A, Forbes C, Lewis R, Sowden A, Kleijnen J.
-
The effectiveness and cost-effectiveness of prophylactic removal of wisdom teeth.
A rapid review by Song F, O’Meara S, Wilson P, Golder S, Kleijnen J.
-
Ultrasound screening in pregnancy: a systematic review of the clinical effectiveness, cost-effectiveness and women’s views.
By Bricker L, Garcia J, Henderson J, Mugford M, Neilson J, Roberts T, et al.
-
A rapid and systematic review of the effectiveness and cost-effectiveness of the taxanes used in the treatment of advanced breast and ovarian cancer.
By Lister-Sharp D, McDonagh MS, Khan KS, Kleijnen J.
-
Liquid-based cytology in cervical screening: a rapid and systematic review.
By Payne N, Chilcott J, McGoogan E.
-
Randomised controlled trial of non-directive counselling, cognitive–behaviour therapy and usual general practitioner care in the management of depression as well as mixed anxiety and depression in primary care.
By King M, Sibbald B, Ward E, Bower P, Lloyd M, Gabbay M, et al.
-
Routine referral for radiography of patients presenting with low back pain: is patients’ outcome influenced by GPs’ referral for plain radiography?
By Kerry S, Hilton S, Patel S, Dundas D, Rink E, Lord J.
-
Systematic reviews of wound care management: (3) antimicrobial agents for chronic wounds; (4) diabetic foot ulceration.
By O’Meara S, Cullum N, Majid M, Sheldon T.
-
Using routine data to complement and enhance the results of randomised controlled trials.
By Lewsey JD, Leyland AH, Murray GD, Boddy FA.
-
Coronary artery stents in the treatment of ischaemic heart disease: a rapid and systematic review.
By Meads C, Cummins C, Jolly K, Stevens A, Burls A, Hyde C.
-
Outcome measures for adult critical care: a systematic review.
By Hayes JA, Black NA, Jenkinson C, Young JD, Rowan KM, Daly K, et al.
-
A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding.
By Fairbank L, O’Meara S, Renfrew MJ, Woolridge M, Sowden AJ, Lister-Sharp D.
-
Implantable cardioverter defibrillators: arrhythmias. A rapid and systematic review.
By Parkes J, Bryant J, Milne R.
-
Treatments for fatigue in multiple sclerosis: a rapid and systematic review.
By Brañas P, Jordan R, Fry-Smith A, Burls A, Hyde C.
-
Early asthma prophylaxis, natural history, skeletal development and economy (EASE): a pilot randomised controlled trial.
By Baxter-Jones ADG, Helms PJ, Russell G, Grant A, Ross S, Cairns JA, et al.
-
Screening for hypercholesterolaemia versus case finding for familial hypercholesterolaemia: a systematic review and cost-effectiveness analysis.
By Marks D, Wonderling D, Thorogood M, Lambert H, Humphries SE, Neil HAW.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of glycoprotein IIb/IIIa antagonists in the medical management of unstable angina.
By McDonagh MS, Bachmann LM, Golder S, Kleijnen J, ter Riet G.
-
A randomised controlled trial of prehospital intravenous fluid replacement therapy in serious trauma.
By Turner J, Nicholl J, Webber L, Cox H, Dixon S, Yates D.
-
Intrathecal pumps for giving opioids in chronic pain: a systematic review.
By Williams JE, Louw G, Towlerton G.
-
Combination therapy (interferon alfa and ribavirin) in the treatment of chronic hepatitis C: a rapid and systematic review.
By Shepherd J, Waugh N, Hewitson P.
-
A systematic review of comparisons of effect sizes derived from randomised and non-randomised studies.
By MacLehose RR, Reeves BC, Harvey IM, Sheldon TA, Russell IT, Black AMS.
-
Intravascular ultrasound-guided interventions in coronary artery disease: a systematic literature review, with decision-analytic modelling, of outcomes and cost-effectiveness.
By Berry E, Kelly S, Hutton J, Lindsay HSJ, Blaxill JM, Evans JA, et al.
-
A randomised controlled trial to evaluate the effectiveness and cost-effectiveness of counselling patients with chronic depression.
By Simpson S, Corney R, Fitzgerald P, Beecham J.
-
Systematic review of treatments for atopic eczema.
By Hoare C, Li Wan Po A, Williams H.
-
Bayesian methods in health technology assessment: a review.
By Spiegelhalter DJ, Myles JP, Jones DR, Abrams KR.
-
The management of dyspepsia: a systematic review.
By Delaney B, Moayyedi P, Deeks J, Innes M, Soo S, Barton P, et al.
-
A systematic review of treatments for severe psoriasis.
By Griffiths CEM, Clark CM, Chalmers RJG, Li Wan Po A, Williams HC.
-
Clinical and cost-effectiveness of donepezil, rivastigmine and galantamine for Alzheimer’s disease: a rapid and systematic review.
By Clegg A, Bryant J, Nicholson T, McIntyre L, De Broe S, Gerard K, et al.
-
The clinical effectiveness and cost-effectiveness of riluzole for motor neurone disease: a rapid and systematic review.
By Stewart A, Sandercock J, Bryan S, Hyde C, Barton PM, Fry-Smith A, et al.
-
Equity and the economic evaluation of healthcare.
By Sassi F, Archard L, Le Grand J.
-
Quality-of-life measures in chronic diseases of childhood.
By Eiser C, Morse R.
-
Eliciting public preferences for healthcare: a systematic review of techniques.
By Ryan M, Scott DA, Reeves C, Bate A, van Teijlingen ER, Russell EM, et al.
-
General health status measures for people with cognitive impairment: learning disability and acquired brain injury.
By Riemsma RP, Forbes CA, Glanville JM, Eastwood AJ, Kleijnen J.
-
An assessment of screening strategies for fragile X syndrome in the UK.
By Pembrey ME, Barnicoat AJ, Carmichael B, Bobrow M, Turner G.
-
Issues in methodological research: perspectives from researchers and commissioners.
By Lilford RJ, Richardson A, Stevens A, Fitzpatrick R, Edwards S, Rock F, et al.
-
Systematic reviews of wound care management: (5) beds; (6) compression; (7) laser therapy, therapeutic ultrasound, electrotherapy and electromagnetic therapy.
By Cullum N, Nelson EA, Flemming K, Sheldon T.
-
Effects of educational and psychosocial interventions for adolescents with diabetes mellitus: a systematic review.
By Hampson SE, Skinner TC, Hart J, Storey L, Gage H, Foxcroft D, et al.
-
Effectiveness of autologous chondrocyte transplantation for hyaline cartilage defects in knees: a rapid and systematic review.
By Jobanputra P, Parry D, Fry-Smith A, Burls A.
-
Statistical assessment of the learning curves of health technologies.
By Ramsay CR, Grant AM, Wallace SA, Garthwaite PH, Monk AF, Russell IT.
-
The effectiveness and cost-effectiveness of temozolomide for the treatment of recurrent malignant glioma: a rapid and systematic review.
By Dinnes J, Cave C, Huang S, Major K, Milne R.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of debriding agents in treating surgical wounds healing by secondary intention.
By Lewis R, Whiting P, ter Riet G, O’Meara S, Glanville J.
-
Home treatment for mental health problems: a systematic review.
By Burns T, Knapp M, Catty J, Healey A, Henderson J, Watt H, et al.
-
How to develop cost-conscious guidelines.
By Eccles M, Mason J.
-
The role of specialist nurses in multiple sclerosis: a rapid and systematic review.
By De Broe S, Christopher F, Waugh N.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of orlistat in the management of obesity.
By O’Meara S, Riemsma R, Shirran L, Mather L, ter Riet G.
-
The clinical effectiveness and cost-effectiveness of pioglitazone for type 2 diabetes mellitus: a rapid and systematic review.
By Chilcott J, Wight J, Lloyd Jones M, Tappenden P.
-
Extended scope of nursing practice: a multicentre randomised controlled trial of appropriately trained nurses and preregistration house officers in preoperative assessment in elective general surgery.
By Kinley H, Czoski-Murray C, George S, McCabe C, Primrose J, Reilly C, et al.
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) Acute day hospital versus admission; (2) Vocational rehabilitation; (3) Day hospital versus outpatient care.
By Marshall M, Crowther R, Almaraz- Serrano A, Creed F, Sledge W, Kluiter H, et al.
-
The measurement and monitoring of surgical adverse events.
By Bruce J, Russell EM, Mollison J, Krukowski ZH.
-
Action research: a systematic review and guidance for assessment.
By Waterman H, Tillen D, Dickson R, de Koning K.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of gemcitabine for the treatment of pancreatic cancer.
By Ward S, Morris E, Bansback N, Calvert N, Crellin A, Forman D, et al.
-
A rapid and systematic review of the evidence for the clinical effectiveness and cost-effectiveness of irinotecan, oxaliplatin and raltitrexed for the treatment of advanced colorectal cancer.
By Lloyd Jones M, Hummel S, Bansback N, Orr B, Seymour M.
-
Comparison of the effectiveness of inhaler devices in asthma and chronic obstructive airways disease: a systematic review of the literature.
By Brocklebank D, Ram F, Wright J, Barry P, Cates C, Davies L, et al.
-
The cost-effectiveness of magnetic resonance imaging for investigation of the knee joint.
By Bryan S, Weatherburn G, Bungay H, Hatrick C, Salas C, Parry D, et al.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.
By Forbes C, Shirran L, Bagnall A-M, Duffy S, ter Riet G.
-
Superseded by a report published in a later volume.
-
The role of radiography in primary care patients with low back pain of at least 6 weeks duration: a randomised (unblinded) controlled trial.
By Kendrick D, Fielding K, Bentley E, Miller P, Kerslake R, Pringle M.
-
Design and use of questionnaires: a review of best practice applicable to surveys of health service staff and patients.
By McColl E, Jacoby A, Thomas L, Soutter J, Bamford C, Steen N, et al.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.
By Clegg A, Scott DA, Sidhu M, Hewitson P, Waugh N.
-
Subgroup analyses in randomised controlled trials: quantifying the risks of false-positives and false-negatives.
By Brookes ST, Whitley E, Peters TJ, Mulheran PA, Egger M, Davey Smith G.
-
Depot antipsychotic medication in the treatment of patients with schizophrenia: (1) Meta-review; (2) Patient and nurse attitudes.
By David AS, Adams C.
-
A systematic review of controlled trials of the effectiveness and cost-effectiveness of brief psychological treatments for depression.
By Churchill R, Hunot V, Corney R, Knapp M, McGuire H, Tylee A, et al.
-
Cost analysis of child health surveillance.
By Sanderson D, Wright D, Acton C, Duree D.
-
A study of the methods used to select review criteria for clinical audit.
By Hearnshaw H, Harker R, Cheater F, Baker R, Grimshaw G.
-
Fludarabine as second-line therapy for B cell chronic lymphocytic leukaemia: a technology assessment.
By Hyde C, Wake B, Bryan S, Barton P, Fry-Smith A, Davenport C, et al.
-
Rituximab as third-line treatment for refractory or recurrent Stage III or IV follicular non-Hodgkin’s lymphoma: a systematic review and economic evaluation.
By Wake B, Hyde C, Bryan S, Barton P, Song F, Fry-Smith A, et al.
-
A systematic review of discharge arrangements for older people.
By Parker SG, Peet SM, McPherson A, Cannaby AM, Baker R, Wilson A, et al.
-
The clinical effectiveness and cost-effectiveness of inhaler devices used in the routine management of chronic asthma in older children: a systematic review and economic evaluation.
By Peters J, Stevenson M, Beverley C, Lim J, Smith S.
-
The clinical effectiveness and cost-effectiveness of sibutramine in the management of obesity: a technology assessment.
By O’Meara S, Riemsma R, Shirran L, Mather L, ter Riet G.
-
The cost-effectiveness of magnetic resonance angiography for carotid artery stenosis and peripheral vascular disease: a systematic review.
By Berry E, Kelly S, Westwood ME, Davies LM, Gough MJ, Bamford JM, et al.
-
Promoting physical activity in South Asian Muslim women through ‘exercise on prescription’.
By Carroll B, Ali N, Azam N.
-
Zanamivir for the treatment of influenza in adults: a systematic review and economic evaluation.
By Burls A, Clark W, Stewart T, Preston C, Bryan S, Jefferson T, et al.
-
A review of the natural history and epidemiology of multiple sclerosis: implications for resource allocation and health economic models.
By Richards RG, Sampson FC, Beard SM, Tappenden P.
-
Screening for gestational diabetes: a systematic review and economic evaluation.
By Scott DA, Loveman E, McIntyre L, Waugh N.
-
The clinical effectiveness and cost-effectiveness of surgery for people with morbid obesity: a systematic review and economic evaluation.
By Clegg AJ, Colquitt J, Sidhu MK, Royle P, Loveman E, Walker A.
-
The clinical effectiveness of trastuzumab for breast cancer: a systematic review.
By Lewis R, Bagnall A-M, Forbes C, Shirran E, Duffy S, Kleijnen J, et al.
-
The clinical effectiveness and cost-effectiveness of vinorelbine for breast cancer: a systematic review and economic evaluation.
By Lewis R, Bagnall A-M, King S, Woolacott N, Forbes C, Shirran L, et al.
-
A systematic review of the effectiveness and cost-effectiveness of metal-on-metal hip resurfacing arthroplasty for treatment of hip disease.
By Vale L, Wyness L, McCormack K, McKenzie L, Brazzelli M, Stearns SC.
-
The clinical effectiveness and cost-effectiveness of bupropion and nicotine replacement therapy for smoking cessation: a systematic review and economic evaluation.
By Woolacott NF, Jones L, Forbes CA, Mather LC, Sowden AJ, Song FJ, et al.
-
A systematic review of effectiveness and economic evaluation of new drug treatments for juvenile idiopathic arthritis: etanercept.
By Cummins C, Connock M, Fry-Smith A, Burls A.
-
Clinical effectiveness and cost-effectiveness of growth hormone in children: a systematic review and economic evaluation.
By Bryant J, Cave C, Mihaylova B, Chase D, McIntyre L, Gerard K, et al.
-
Clinical effectiveness and cost-effectiveness of growth hormone in adults in relation to impact on quality of life: a systematic review and economic evaluation.
By Bryant J, Loveman E, Chase D, Mihaylova B, Cave C, Gerard K, et al.
-
Clinical medication review by a pharmacist of patients on repeat prescriptions in general practice: a randomised controlled trial.
By Zermansky AG, Petty DR, Raynor DK, Lowe CJ, Freementle N, Vail A.
-
The effectiveness of infliximab and etanercept for the treatment of rheumatoid arthritis: a systematic review and economic evaluation.
By Jobanputra P, Barton P, Bryan S, Burls A.
-
A systematic review and economic evaluation of computerised cognitive behaviour therapy for depression and anxiety.
By Kaltenthaler E, Shackley P, Stevens K, Beverley C, Parry G, Chilcott J.
-
A systematic review and economic evaluation of pegylated liposomal doxorubicin hydrochloride for ovarian cancer.
By Forbes C, Wilby J, Richardson G, Sculpher M, Mather L, Reimsma R.
-
A systematic review of the effectiveness of interventions based on a stages-of-change approach to promote individual behaviour change.
By Riemsma RP, Pattenden J, Bridle C, Sowden AJ, Mather L, Watt IS, et al.
-
A systematic review update of the clinical effectiveness and cost-effectiveness of glycoprotein IIb/IIIa antagonists.
By Robinson M, Ginnelly L, Sculpher M, Jones L, Riemsma R, Palmer S, et al.
-
A systematic review of the effectiveness, cost-effectiveness and barriers to implementation of thrombolytic and neuroprotective therapy for acute ischaemic stroke in the NHS.
By Sandercock P, Berge E, Dennis M, Forbes J, Hand P, Kwan J, et al.
-
A randomised controlled crossover trial of nurse practitioner versus doctor-led outpatient care in a bronchiectasis clinic.
By Caine N, Sharples LD, Hollingworth W, French J, Keogan M, Exley A, et al.
-
Clinical effectiveness and cost – consequences of selective serotonin reuptake inhibitors in the treatment of sex offenders.
By Adi Y, Ashcroft D, Browne K, Beech A, Fry-Smith A, Hyde C.
-
Treatment of established osteoporosis: a systematic review and cost–utility analysis.
By Kanis JA, Brazier JE, Stevenson M, Calvert NW, Lloyd Jones M.
-
Which anaesthetic agents are cost-effective in day surgery? Literature review, national survey of practice and randomised controlled trial.
By Elliott RA Payne K, Moore JK, Davies LM, Harper NJN, St Leger AS, et al.
-
Screening for hepatitis C among injecting drug users and in genitourinary medicine clinics: systematic reviews of effectiveness, modelling study and national survey of current practice.
By Stein K, Dalziel K, Walker A, McIntyre L, Jenkins B, Horne J, et al.
-
The measurement of satisfaction with healthcare: implications for practice from a systematic review of the literature.
By Crow R, Gage H, Hampson S, Hart J, Kimber A, Storey L, et al.
-
The effectiveness and cost-effectiveness of imatinib in chronic myeloid leukaemia: a systematic review.
By Garside R, Round A, Dalziel K, Stein K, Royle R.
-
A comparative study of hypertonic saline, daily and alternate-day rhDNase in children with cystic fibrosis.
By Suri R, Wallis C, Bush A, Thompson S, Normand C, Flather M, et al.
-
A systematic review of the costs and effectiveness of different models of paediatric home care.
By Parker G, Bhakta P, Lovett CA, Paisley S, Olsen R, Turner D, et al.
-
How important are comprehensive literature searches and the assessment of trial quality in systematic reviews? Empirical study.
By Egger M, Jüni P, Bartlett C, Holenstein F, Sterne J.
-
Systematic review of the effectiveness and cost-effectiveness, and economic evaluation, of home versus hospital or satellite unit haemodialysis for people with end-stage renal failure.
By Mowatt G, Vale L, Perez J, Wyness L, Fraser C, MacLeod A, et al.
-
Systematic review and economic evaluation of the effectiveness of infliximab for the treatment of Crohn’s disease.
By Clark W, Raftery J, Barton P, Song F, Fry-Smith A, Burls A.
-
A review of the clinical effectiveness and cost-effectiveness of routine anti-D prophylaxis for pregnant women who are rhesus negative.
By Chilcott J, Lloyd Jones M, Wight J, Forman K, Wray J, Beverley C, et al.
-
Systematic review and evaluation of the use of tumour markers in paediatric oncology: Ewing’s sarcoma and neuroblastoma.
By Riley RD, Burchill SA, Abrams KR, Heney D, Lambert PC, Jones DR, et al.
-
The cost-effectiveness of screening for Helicobacter pylori to reduce mortality and morbidity from gastric cancer and peptic ulcer disease: a discrete-event simulation model.
By Roderick P, Davies R, Raftery J, Crabbe D, Pearce R, Bhandari P, et al.
-
The clinical effectiveness and cost-effectiveness of routine dental checks: a systematic review and economic evaluation.
By Davenport C, Elley K, Salas C, Taylor-Weetman CL, Fry-Smith A, Bryan S, et al.
-
A multicentre randomised controlled trial assessing the costs and benefits of using structured information and analysis of women’s preferences in the management of menorrhagia.
By Kennedy ADM, Sculpher MJ, Coulter A, Dwyer N, Rees M, Horsley S, et al.
-
Clinical effectiveness and cost–utility of photodynamic therapy for wet age-related macular degeneration: a systematic review and economic evaluation.
By Meads C, Salas C, Roberts T, Moore D, Fry-Smith A, Hyde C.
-
Evaluation of molecular tests for prenatal diagnosis of chromosome abnormalities.
By Grimshaw GM, Szczepura A, Hultén M, MacDonald F, Nevin NC, Sutton F, et al.
-
First and second trimester antenatal screening for Down’s syndrome: the results of the Serum, Urine and Ultrasound Screening Study (SURUSS).
By Wald NJ, Rodeck C, Hackshaw AK, Walters J, Chitty L, Mackinson AM.
-
The effectiveness and cost-effectiveness of ultrasound locating devices for central venous access: a systematic review and economic evaluation.
By Calvert N, Hind D, McWilliams RG, Thomas SM, Beverley C, Davidson A.
-
A systematic review of atypical antipsychotics in schizophrenia.
By Bagnall A-M, Jones L, Lewis R, Ginnelly L, Glanville J, Torgerson D, et al.
-
Prostate Testing for Cancer and Treatment (ProtecT) feasibility study.
By Donovan J, Hamdy F, Neal D, Peters T, Oliver S, Brindle L, et al.
-
Early thrombolysis for the treatment of acute myocardial infarction: a systematic review and economic evaluation.
By Boland A, Dundar Y, Bagust A, Haycox A, Hill R, Mujica Mota R, et al.
-
Screening for fragile X syndrome: a literature review and modelling.
By Song FJ, Barton P, Sleightholme V, Yao GL, Fry-Smith A.
-
Systematic review of endoscopic sinus surgery for nasal polyps.
By Dalziel K, Stein K, Round A, Garside R, Royle P.
-
Towards efficient guidelines: how to monitor guideline use in primary care.
By Hutchinson A, McIntosh A, Cox S, Gilbert C.
-
Effectiveness and cost-effectiveness of acute hospital-based spinal cord injuries services: systematic review.
By Bagnall A-M, Jones L, Richardson G, Duffy S, Riemsma R.
-
Prioritisation of health technology assessment. The PATHS model: methods and case studies.
By Townsend J, Buxton M, Harper G.
-
Systematic review of the clinical effectiveness and cost-effectiveness of tension-free vaginal tape for treatment of urinary stress incontinence.
By Cody J, Wyness L, Wallace S, Glazener C, Kilonzo M, Stearns S, et al.
-
The clinical and cost-effectiveness of patient education models for diabetes: a systematic review and economic evaluation.
By Loveman E, Cave C, Green C, Royle P, Dunn N, Waugh N.
-
The role of modelling in prioritising and planning clinical trials.
By Chilcott J, Brennan A, Booth A, Karnon J, Tappenden P.
-
Cost–benefit evaluation of routine influenza immunisation in people 65–74 years of age.
By Allsup S, Gosney M, Haycox A, Regan M.
-
The clinical and cost-effectiveness of pulsatile machine perfusion versus cold storage of kidneys for transplantation retrieved from heart-beating and non-heart-beating donors.
By Wight J, Chilcott J, Holmes M, Brewer N.
-
Can randomised trials rely on existing electronic data? A feasibility study to explore the value of routine data in health technology assessment.
By Williams JG, Cheung WY, Cohen DR, Hutchings HA, Longo MF, Russell IT.
-
Evaluating non-randomised intervention studies.
By Deeks JJ, Dinnes J, D’Amico R, Sowden AJ, Sakarovitch C, Song F, et al.
-
A randomised controlled trial to assess the impact of a package comprising a patient-orientated, evidence-based self- help guidebook and patient-centred consultations on disease management and satisfaction in inflammatory bowel disease.
By Kennedy A, Nelson E, Reeves D, Richardson G, Roberts C, Robinson A, et al.
-
The effectiveness of diagnostic tests for the assessment of shoulder pain due to soft tissue disorders: a systematic review.
By Dinnes J, Loveman E, McIntyre L, Waugh N.
-
The value of digital imaging in diabetic retinopathy.
By Sharp PF, Olson J, Strachan F, Hipwell J, Ludbrook A, O’Donnell M, et al.
-
Lowering blood pressure to prevent myocardial infarction and stroke: a new preventive strategy.
By Law M, Wald N, Morris J.
-
Clinical and cost-effectiveness of capecitabine and tegafur with uracil for the treatment of metastatic colorectal cancer: systematic review and economic evaluation.
By Ward S, Kaltenthaler E, Cowan J, Brewer N.
-
Clinical and cost-effectiveness of new and emerging technologies for early localised prostate cancer: a systematic review.
By Hummel S, Paisley S, Morgan A, Currie E, Brewer N.
-
Literature searching for clinical and cost-effectiveness studies used in health technology assessment reports carried out for the National Institute for Clinical Excellence appraisal system.
By Royle P, Waugh N.
-
Systematic review and economic decision modelling for the prevention and treatment of influenza A and B.
By Turner D, Wailoo A, Nicholson K, Cooper N, Sutton A, Abrams K.
-
A randomised controlled trial to evaluate the clinical and cost-effectiveness of Hickman line insertions in adult cancer patients by nurses.
By Boland A, Haycox A, Bagust A, Fitzsimmons L.
-
Redesigning postnatal care: a randomised controlled trial of protocol-based midwifery-led care focused on individual women’s physical and psychological health needs.
By MacArthur C, Winter HR, Bick DE, Lilford RJ, Lancashire RJ, Knowles H, et al.
-
Estimating implied rates of discount in healthcare decision-making.
By West RR, McNabb R, Thompson AGH, Sheldon TA, Grimley Evans J.
-
Systematic review of isolation policies in the hospital management of methicillin-resistant Staphylococcus aureus: a review of the literature with epidemiological and economic modelling.
By Cooper BS, Stone SP, Kibbler CC, Cookson BD, Roberts JA, Medley GF, et al.
-
Treatments for spasticity and pain in multiple sclerosis: a systematic review.
By Beard S, Hunn A, Wight J.
-
The inclusion of reports of randomised trials published in languages other than English in systematic reviews.
By Moher D, Pham B, Lawson ML, Klassen TP.
-
The impact of screening on future health-promoting behaviours and health beliefs: a systematic review.
By Bankhead CR, Brett J, Bukach C, Webster P, Stewart-Brown S, Munafo M, et al.
-
What is the best imaging strategy for acute stroke?
By Wardlaw JM, Keir SL, Seymour J, Lewis S, Sandercock PAG, Dennis MS, et al.
-
Systematic review and modelling of the investigation of acute and chronic chest pain presenting in primary care.
By Mant J, McManus RJ, Oakes RAL, Delaney BC, Barton PM, Deeks JJ, et al.
-
The effectiveness and cost-effectiveness of microwave and thermal balloon endometrial ablation for heavy menstrual bleeding: a systematic review and economic modelling.
By Garside R, Stein K, Wyatt K, Round A, Price A.
-
A systematic review of the role of bisphosphonates in metastatic disease.
By Ross JR, Saunders Y, Edmonds PM, Patel S, Wonderling D, Normand C, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of capecitabine (Xeloda®) for locally advanced and/or metastatic breast cancer.
By Jones L, Hawkins N, Westwood M, Wright K, Richardson G, Riemsma R.
-
Effectiveness and efficiency of guideline dissemination and implementation strategies.
By Grimshaw JM, Thomas RE, MacLennan G, Fraser C, Ramsay CR, Vale L, et al.
-
Clinical effectiveness and costs of the Sugarbaker procedure for the treatment of pseudomyxoma peritonei.
By Bryant J, Clegg AJ, Sidhu MK, Brodin H, Royle P, Davidson P.
-
Psychological treatment for insomnia in the regulation of long-term hypnotic drug use.
By Morgan K, Dixon S, Mathers N, Thompson J, Tomeny M.
-
Improving the evaluation of therapeutic interventions in multiple sclerosis: development of a patient-based measure of outcome.
By Hobart JC, Riazi A, Lamping DL, Fitzpatrick R, Thompson AJ.
-
A systematic review and economic evaluation of magnetic resonance cholangiopancreatography compared with diagnostic endoscopic retrograde cholangiopancreatography.
By Kaltenthaler E, Bravo Vergel Y, Chilcott J, Thomas S, Blakeborough T, Walters SJ, et al.
-
The use of modelling to evaluate new drugs for patients with a chronic condition: the case of antibodies against tumour necrosis factor in rheumatoid arthritis.
By Barton P, Jobanputra P, Wilson J, Bryan S, Burls A.
-
Clinical effectiveness and cost-effectiveness of neonatal screening for inborn errors of metabolism using tandem mass spectrometry: a systematic review.
By Pandor A, Eastham J, Beverley C, Chilcott J, Paisley S.
-
Clinical effectiveness and cost-effectiveness of pioglitazone and rosiglitazone in the treatment of type 2 diabetes: a systematic review and economic evaluation.
By Czoski-Murray C, Warren E, Chilcott J, Beverley C, Psyllaki MA, Cowan J.
-
Routine examination of the newborn: the EMREN study. Evaluation of an extension of the midwife role including a randomised controlled trial of appropriately trained midwives and paediatric senior house officers.
By Townsend J, Wolke D, Hayes J, Davé S, Rogers C, Bloomfield L, et al.
-
Involving consumers in research and development agenda setting for the NHS: developing an evidence-based approach.
By Oliver S, Clarke-Jones L, Rees R, Milne R, Buchanan P, Gabbay J, et al.
-
A multi-centre randomised controlled trial of minimally invasive direct coronary bypass grafting versus percutaneous transluminal coronary angioplasty with stenting for proximal stenosis of the left anterior descending coronary artery.
By Reeves BC, Angelini GD, Bryan AJ, Taylor FC, Cripps T, Spyt TJ, et al.
-
Does early magnetic resonance imaging influence management or improve outcome in patients referred to secondary care with low back pain? A pragmatic randomised controlled trial.
By Gilbert FJ, Grant AM, Gillan MGC, Vale L, Scott NW, Campbell MK, et al.
-
The clinical and cost-effectiveness of anakinra for the treatment of rheumatoid arthritis in adults: a systematic review and economic analysis.
By Clark W, Jobanputra P, Barton P, Burls A.
-
A rapid and systematic review and economic evaluation of the clinical and cost-effectiveness of newer drugs for treatment of mania associated with bipolar affective disorder.
By Bridle C, Palmer S, Bagnall A-M, Darba J, Duffy S, Sculpher M, et al.
-
Liquid-based cytology in cervical screening: an updated rapid and systematic review and economic analysis.
By Karnon J, Peters J, Platt J, Chilcott J, McGoogan E, Brewer N.
-
Systematic review of the long-term effects and economic consequences of treatments for obesity and implications for health improvement.
By Avenell A, Broom J, Brown TJ, Poobalan A, Aucott L, Stearns SC, et al.
-
Autoantibody testing in children with newly diagnosed type 1 diabetes mellitus.
By Dretzke J, Cummins C, Sandercock J, Fry-Smith A, Barrett T, Burls A.
-
Clinical effectiveness and cost-effectiveness of prehospital intravenous fluids in trauma patients.
By Dretzke J, Sandercock J, Bayliss S, Burls A.
-
Newer hypnotic drugs for the short-term management of insomnia: a systematic review and economic evaluation.
By Dündar Y, Boland A, Strobl J, Dodd S, Haycox A, Bagust A, et al.
-
Development and validation of methods for assessing the quality of diagnostic accuracy studies.
By Whiting P, Rutjes AWS, Dinnes J, Reitsma JB, Bossuyt PMM, Kleijnen J.
-
EVALUATE hysterectomy trial: a multicentre randomised trial comparing abdominal, vaginal and laparoscopic methods of hysterectomy.
By Garry R, Fountain J, Brown J, Manca A, Mason S, Sculpher M, et al.
-
Methods for expected value of information analysis in complex health economic models: developments on the health economics of interferon-β and glatiramer acetate for multiple sclerosis.
By Tappenden P, Chilcott JB, Eggington S, Oakley J, McCabe C.
-
Effectiveness and cost-effectiveness of imatinib for first-line treatment of chronic myeloid leukaemia in chronic phase: a systematic review and economic analysis.
By Dalziel K, Round A, Stein K, Garside R, Price A.
-
VenUS I: a randomised controlled trial of two types of bandage for treating venous leg ulcers.
By Iglesias C, Nelson EA, Cullum NA, Torgerson DJ, on behalf of the VenUS Team.
-
Systematic review of the effectiveness and cost-effectiveness, and economic evaluation, of myocardial perfusion scintigraphy for the diagnosis and management of angina and myocardial infarction.
By Mowatt G, Vale L, Brazzelli M, Hernandez R, Murray A, Scott N, et al.
-
A pilot study on the use of decision theory and value of information analysis as part of the NHS Health Technology Assessment programme.
By Claxton K, Ginnelly L, Sculpher M, Philips Z, Palmer S.
-
The Social Support and Family Health Study: a randomised controlled trial and economic evaluation of two alternative forms of postnatal support for mothers living in disadvantaged inner-city areas.
By Wiggins M, Oakley A, Roberts I, Turner H, Rajan L, Austerberry H, et al.
-
Psychosocial aspects of genetic screening of pregnant women and newborns: a systematic review.
By Green JM, Hewison J, Bekker HL, Bryant, Cuckle HS.
-
Evaluation of abnormal uterine bleeding: comparison of three outpatient procedures within cohorts defined by age and menopausal status.
By Critchley HOD, Warner P, Lee AJ, Brechin S, Guise J, Graham B.
-
Coronary artery stents: a rapid systematic review and economic evaluation.
By Hill R, Bagust A, Bakhai A, Dickson R, Dündar Y, Haycox A, et al.
-
Review of guidelines for good practice in decision-analytic modelling in health technology assessment.
By Philips Z, Ginnelly L, Sculpher M, Claxton K, Golder S, Riemsma R, et al.
-
Rituximab (MabThera®) for aggressive non-Hodgkin’s lymphoma: systematic review and economic evaluation.
By Knight C, Hind D, Brewer N, Abbott V.
-
Clinical effectiveness and cost-effectiveness of clopidogrel and modified-release dipyridamole in the secondary prevention of occlusive vascular events: a systematic review and economic evaluation.
By Jones L, Griffin S, Palmer S, Main C, Orton V, Sculpher M, et al.
-
Pegylated interferon α-2a and -2b in combination with ribavirin in the treatment of chronic hepatitis C: a systematic review and economic evaluation.
By Shepherd J, Brodin H, Cave C, Waugh N, Price A, Gabbay J.
-
Clopidogrel used in combination with aspirin compared with aspirin alone in the treatment of non-ST-segment- elevation acute coronary syndromes: a systematic review and economic evaluation.
By Main C, Palmer S, Griffin S, Jones L, Orton V, Sculpher M, et al.
-
Provision, uptake and cost of cardiac rehabilitation programmes: improving services to under-represented groups.
By Beswick AD, Rees K, Griebsch I, Taylor FC, Burke M, West RR, et al.
-
Involving South Asian patients in clinical trials.
By Hussain-Gambles M, Leese B, Atkin K, Brown J, Mason S, Tovey P.
-
Clinical and cost-effectiveness of continuous subcutaneous insulin infusion for diabetes.
By Colquitt JL, Green C, Sidhu MK, Hartwell D, Waugh N.
-
Identification and assessment of ongoing trials in health technology assessment reviews.
By Song FJ, Fry-Smith A, Davenport C, Bayliss S, Adi Y, Wilson JS, et al.
-
Systematic review and economic evaluation of a long-acting insulin analogue, insulin glargine
By Warren E, Weatherley-Jones E, Chilcott J, Beverley C.
-
Supplementation of a home-based exercise programme with a class-based programme for people with osteoarthritis of the knees: a randomised controlled trial and health economic analysis.
By McCarthy CJ, Mills PM, Pullen R, Richardson G, Hawkins N, Roberts CR, et al.
-
Clinical and cost-effectiveness of once-daily versus more frequent use of same potency topical corticosteroids for atopic eczema: a systematic review and economic evaluation.
By Green C, Colquitt JL, Kirby J, Davidson P, Payne E.
-
Acupuncture of chronic headache disorders in primary care: randomised controlled trial and economic analysis.
By Vickers AJ, Rees RW, Zollman CE, McCarney R, Smith CM, Ellis N, et al.
-
Generalisability in economic evaluation studies in healthcare: a review and case studies.
By Sculpher MJ, Pang FS, Manca A, Drummond MF, Golder S, Urdahl H, et al.
-
Virtual outreach: a randomised controlled trial and economic evaluation of joint teleconferenced medical consultations.
By Wallace P, Barber J, Clayton W, Currell R, Fleming K, Garner P, et al.
-
Randomised controlled multiple treatment comparison to provide a cost-effectiveness rationale for the selection of antimicrobial therapy in acne.
By Ozolins M, Eady EA, Avery A, Cunliffe WJ, O’Neill C, Simpson NB, et al.
-
Do the findings of case series studies vary significantly according to methodological characteristics?
By Dalziel K, Round A, Stein K, Garside R, Castelnuovo E, Payne L.
-
Improving the referral process for familial breast cancer genetic counselling: findings of three randomised controlled trials of two interventions.
By Wilson BJ, Torrance N, Mollison J, Wordsworth S, Gray JR, Haites NE, et al.
-
Randomised evaluation of alternative electrosurgical modalities to treat bladder outflow obstruction in men with benign prostatic hyperplasia.
By Fowler C, McAllister W, Plail R, Karim O, Yang Q.
-
A pragmatic randomised controlled trial of the cost-effectiveness of palliative therapies for patients with inoperable oesophageal cancer.
By Shenfine J, McNamee P, Steen N, Bond J, Griffin SM.
-
Impact of computer-aided detection prompts on the sensitivity and specificity of screening mammography.
By Taylor P, Champness J, Given- Wilson R, Johnston K, Potts H.
-
Issues in data monitoring and interim analysis of trials.
By Grant AM, Altman DG, Babiker AB, Campbell MK, Clemens FJ, Darbyshire JH, et al.
-
Lay public’s understanding of equipoise and randomisation in randomised controlled trials.
By Robinson EJ, Kerr CEP, Stevens AJ, Lilford RJ, Braunholtz DA, Edwards SJ, et al.
-
Clinical and cost-effectiveness of electroconvulsive therapy for depressive illness, schizophrenia, catatonia and mania: systematic reviews and economic modelling studies.
By Greenhalgh J, Knight C, Hind D, Beverley C, Walters S.
-
Measurement of health-related quality of life for people with dementia: development of a new instrument (DEMQOL) and an evaluation of current methodology.
By Smith SC, Lamping DL, Banerjee S, Harwood R, Foley B, Smith P, et al.
-
Clinical effectiveness and cost-effectiveness of drotrecogin alfa (activated) (Xigris®) for the treatment of severe sepsis in adults: a systematic review and economic evaluation.
By Green C, Dinnes J, Takeda A, Shepherd J, Hartwell D, Cave C, et al.
-
A methodological review of how heterogeneity has been examined in systematic reviews of diagnostic test accuracy.
By Dinnes J, Deeks J, Kirby J, Roderick P.
-
Cervical screening programmes: can automation help? Evidence from systematic reviews, an economic analysis and a simulation modelling exercise applied to the UK.
By Willis BH, Barton P, Pearmain P, Bryan S, Hyde C.
-
Laparoscopic surgery for inguinal hernia repair: systematic review of effectiveness and economic evaluation.
By McCormack K, Wake B, Perez J, Fraser C, Cook J, McIntosh E, et al.
-
Clinical effectiveness, tolerability and cost-effectiveness of newer drugs for epilepsy in adults: a systematic review and economic evaluation.
By Wilby J, Kainth A, Hawkins N, Epstein D, McIntosh H, McDaid C, et al.
-
A randomised controlled trial to compare the cost-effectiveness of tricyclic antidepressants, selective serotonin reuptake inhibitors and lofepramine.
By Peveler R, Kendrick T, Buxton M, Longworth L, Baldwin D, Moore M, et al.
-
Clinical effectiveness and cost-effectiveness of immediate angioplasty for acute myocardial infarction: systematic review and economic evaluation.
By Hartwell D, Colquitt J, Loveman E, Clegg AJ, Brodin H, Waugh N, et al.
-
A randomised controlled comparison of alternative strategies in stroke care.
By Kalra L, Evans A, Perez I, Knapp M, Swift C, Donaldson N.
-
The investigation and analysis of critical incidents and adverse events in healthcare.
By Woloshynowych M, Rogers S, Taylor-Adams S, Vincent C.
-
Potential use of routine databases in health technology assessment.
By Raftery J, Roderick P, Stevens A.
-
Clinical and cost-effectiveness of newer immunosuppressive regimens in renal transplantation: a systematic review and modelling study.
By Woodroffe R, Yao GL, Meads C, Bayliss S, Ready A, Raftery J, et al.
-
A systematic review and economic evaluation of alendronate, etidronate, risedronate, raloxifene and teriparatide for the prevention and treatment of postmenopausal osteoporosis.
By Stevenson M, Lloyd Jones M, De Nigris E, Brewer N, Davis S, Oakley J.
-
A systematic review to examine the impact of psycho-educational interventions on health outcomes and costs in adults and children with difficult asthma.
By Smith JR, Mugford M, Holland R, Candy B, Noble MJ, Harrison BDW, et al.
-
An evaluation of the costs, effectiveness and quality of renal replacement therapy provision in renal satellite units in England and Wales.
By Roderick P, Nicholson T, Armitage A, Mehta R, Mullee M, Gerard K, et al.
-
Imatinib for the treatment of patients with unresectable and/or metastatic gastrointestinal stromal tumours: systematic review and economic evaluation.
By Wilson J, Connock M, Song F, Yao G, Fry-Smith A, Raftery J, et al.
-
Indirect comparisons of competing interventions.
By Glenny AM, Altman DG, Song F, Sakarovitch C, Deeks JJ, D’Amico R, et al.
-
Cost-effectiveness of alternative strategies for the initial medical management of non-ST elevation acute coronary syndrome: systematic review and decision-analytical modelling.
By Robinson M, Palmer S, Sculpher M, Philips Z, Ginnelly L, Bowens A, et al.
-
Outcomes of electrically stimulated gracilis neosphincter surgery.
By Tillin T, Chambers M, Feldman R.
-
The effectiveness and cost-effectiveness of pimecrolimus and tacrolimus for atopic eczema: a systematic review and economic evaluation.
By Garside R, Stein K, Castelnuovo E, Pitt M, Ashcroft D, Dimmock P, et al.
-
Systematic review on urine albumin testing for early detection of diabetic complications.
By Newman DJ, Mattock MB, Dawnay ABS, Kerry S, McGuire A, Yaqoob M, et al.
-
Randomised controlled trial of the cost-effectiveness of water-based therapy for lower limb osteoarthritis.
By Cochrane T, Davey RC, Matthes Edwards SM.
-
Longer term clinical and economic benefits of offering acupuncture care to patients with chronic low back pain.
By Thomas KJ, MacPherson H, Ratcliffe J, Thorpe L, Brazier J, Campbell M, et al.
-
Cost-effectiveness and safety of epidural steroids in the management of sciatica.
By Price C, Arden N, Coglan L, Rogers P.
-
The British Rheumatoid Outcome Study Group (BROSG) randomised controlled trial to compare the effectiveness and cost-effectiveness of aggressive versus symptomatic therapy in established rheumatoid arthritis.
By Symmons D, Tricker K, Roberts C, Davies L, Dawes P, Scott DL.
-
Conceptual framework and systematic review of the effects of participants’ and professionals’ preferences in randomised controlled trials.
By King M, Nazareth I, Lampe F, Bower P, Chandler M, Morou M, et al.
-
The clinical and cost-effectiveness of implantable cardioverter defibrillators: a systematic review.
By Bryant J, Brodin H, Loveman E, Payne E, Clegg A.
-
A trial of problem-solving by community mental health nurses for anxiety, depression and life difficulties among general practice patients. The CPN-GP study.
By Kendrick T, Simons L, Mynors-Wallis L, Gray A, Lathlean J, Pickering R, et al.
-
The causes and effects of socio-demographic exclusions from clinical trials.
By Bartlett C, Doyal L, Ebrahim S, Davey P, Bachmann M, Egger M, et al.
-
Is hydrotherapy cost-effective? A randomised controlled trial of combined hydrotherapy programmes compared with physiotherapy land techniques in children with juvenile idiopathic arthritis.
By Epps H, Ginnelly L, Utley M, Southwood T, Gallivan S, Sculpher M, et al.
-
A randomised controlled trial and cost-effectiveness study of systematic screening (targeted and total population screening) versus routine practice for the detection of atrial fibrillation in people aged 65 and over. The SAFE study.
By Hobbs FDR, Fitzmaurice DA, Mant J, Murray E, Jowett S, Bryan S, et al.
-
Displaced intracapsular hip fractures in fit, older people: a randomised comparison of reduction and fixation, bipolar hemiarthroplasty and total hip arthroplasty.
By Keating JF, Grant A, Masson M, Scott NW, Forbes JF.
-
Long-term outcome of cognitive behaviour therapy clinical trials in central Scotland.
By Durham RC, Chambers JA, Power KG, Sharp DM, Macdonald RR, Major KA, et al.
-
The effectiveness and cost-effectiveness of dual-chamber pacemakers compared with single-chamber pacemakers for bradycardia due to atrioventricular block or sick sinus syndrome: systematic review and economic evaluation.
By Castelnuovo E, Stein K, Pitt M, Garside R, Payne E.
-
Newborn screening for congenital heart defects: a systematic review and cost-effectiveness analysis.
By Knowles R, Griebsch I, Dezateux C, Brown J, Bull C, Wren C.
-
The clinical and cost-effectiveness of left ventricular assist devices for end-stage heart failure: a systematic review and economic evaluation.
By Clegg AJ, Scott DA, Loveman E, Colquitt J, Hutchinson J, Royle P, et al.
-
The effectiveness of the Heidelberg Retina Tomograph and laser diagnostic glaucoma scanning system (GDx) in detecting and monitoring glaucoma.
By Kwartz AJ, Henson DB, Harper RA, Spencer AF, McLeod D.
-
Clinical and cost-effectiveness of autologous chondrocyte implantation for cartilage defects in knee joints: systematic review and economic evaluation.
By Clar C, Cummins E, McIntyre L, Thomas S, Lamb J, Bain L, et al.
-
Systematic review of effectiveness of different treatments for childhood retinoblastoma.
By McDaid C, Hartley S, Bagnall A-M, Ritchie G, Light K, Riemsma R.
-
Towards evidence-based guidelines for the prevention of venous thromboembolism: systematic reviews of mechanical methods, oral anticoagulation, dextran and regional anaesthesia as thromboprophylaxis.
By Roderick P, Ferris G, Wilson K, Halls H, Jackson D, Collins R, et al.
-
The effectiveness and cost-effectiveness of parent training/education programmes for the treatment of conduct disorder, including oppositional defiant disorder, in children.
By Dretzke J, Frew E, Davenport C, Barlow J, Stewart-Brown S, Sandercock J, et al.
-
The clinical and cost-effectiveness of donepezil, rivastigmine, galantamine and memantine for Alzheimer’s disease.
By Loveman E, Green C, Kirby J, Takeda A, Picot J, Payne E, et al.
-
FOOD: a multicentre randomised trial evaluating feeding policies in patients admitted to hospital with a recent stroke.
By Dennis M, Lewis S, Cranswick G, Forbes J.
-
The clinical effectiveness and cost-effectiveness of computed tomography screening for lung cancer: systematic reviews.
By Black C, Bagust A, Boland A, Walker S, McLeod C, De Verteuil R, et al.
-
A systematic review of the effectiveness and cost-effectiveness of neuroimaging assessments used to visualise the seizure focus in people with refractory epilepsy being considered for surgery.
By Whiting P, Gupta R, Burch J, Mujica Mota RE, Wright K, Marson A, et al.
-
Comparison of conference abstracts and presentations with full-text articles in the health technology assessments of rapidly evolving technologies.
By Dundar Y, Dodd S, Dickson R, Walley T, Haycox A, Williamson PR.
-
Systematic review and evaluation of methods of assessing urinary incontinence.
By Martin JL, Williams KS, Abrams KR, Turner DA, Sutton AJ, Chapple C, et al.
-
The clinical effectiveness and cost-effectiveness of newer drugs for children with epilepsy. A systematic review.
By Connock M, Frew E, Evans B-W, Bryan S, Cummins C, Fry-Smith A, et al.
-
Surveillance of Barrett’s oesophagus: exploring the uncertainty through systematic review, expert workshop and economic modelling.
By Garside R, Pitt M, Somerville M, Stein K, Price A, Gilbert N.
-
Topotecan, pegylated liposomal doxorubicin hydrochloride and paclitaxel for second-line or subsequent treatment of advanced ovarian cancer: a systematic review and economic evaluation.
By Main C, Bojke L, Griffin S, Norman G, Barbieri M, Mather L, et al.
-
Evaluation of molecular techniques in prediction and diagnosis of cytomegalovirus disease in immunocompromised patients.
By Szczepura A, Westmoreland D, Vinogradova Y, Fox J, Clark M.
-
Screening for thrombophilia in high-risk situations: systematic review and cost-effectiveness analysis. The Thrombosis: Risk and Economic Assessment of Thrombophilia Screening (TREATS) study.
By Wu O, Robertson L, Twaddle S, Lowe GDO, Clark P, Greaves M, et al.
-
A series of systematic reviews to inform a decision analysis for sampling and treating infected diabetic foot ulcers.
By Nelson EA, O’Meara S, Craig D, Iglesias C, Golder S, Dalton J, et al.
-
Randomised clinical trial, observational study and assessment of cost-effectiveness of the treatment of varicose veins (REACTIV trial).
By Michaels JA, Campbell WB, Brazier JE, MacIntyre JB, Palfreyman SJ, Ratcliffe J, et al.
-
The cost-effectiveness of screening for oral cancer in primary care.
By Speight PM, Palmer S, Moles DR, Downer MC, Smith DH, Henriksson M, et al.
-
Measurement of the clinical and cost-effectiveness of non-invasive diagnostic testing strategies for deep vein thrombosis.
By Goodacre S, Sampson F, Stevenson M, Wailoo A, Sutton A, Thomas S, et al.
-
Systematic review of the effectiveness and cost-effectiveness of HealOzone® for the treatment of occlusal pit/fissure caries and root caries.
By Brazzelli M, McKenzie L, Fielding S, Fraser C, Clarkson J, Kilonzo M, et al.
-
Randomised controlled trials of conventional antipsychotic versus new atypical drugs, and new atypical drugs versus clozapine, in people with schizophrenia responding poorly to, or intolerant of, current drug treatment.
By Lewis SW, Davies L, Jones PB, Barnes TRE, Murray RM, Kerwin R, et al.
-
Diagnostic tests and algorithms used in the investigation of haematuria: systematic reviews and economic evaluation.
By Rodgers M, Nixon J, Hempel S, Aho T, Kelly J, Neal D, et al.
-
Cognitive behavioural therapy in addition to antispasmodic therapy for irritable bowel syndrome in primary care: randomised controlled trial.
By Kennedy TM, Chalder T, McCrone P, Darnley S, Knapp M, Jones RH, et al.
-
A systematic review of the clinical effectiveness and cost-effectiveness of enzyme replacement therapies for Fabry’s disease and mucopolysaccharidosis type 1.
By Connock M, Juarez-Garcia A, Frew E, Mans A, Dretzke J, Fry-Smith A, et al.
-
Health benefits of antiviral therapy for mild chronic hepatitis C: randomised controlled trial and economic evaluation.
By Wright M, Grieve R, Roberts J, Main J, Thomas HC, on behalf of the UK Mild Hepatitis C Trial Investigators.
-
Pressure relieving support surfaces: a randomised evaluation.
By Nixon J, Nelson EA, Cranny G, Iglesias CP, Hawkins K, Cullum NA, et al.
-
A systematic review and economic model of the effectiveness and cost-effectiveness of methylphenidate, dexamfetamine and atomoxetine for the treatment of attention deficit hyperactivity disorder in children and adolescents.
By King S, Griffin S, Hodges Z, Weatherly H, Asseburg C, Richardson G, et al.
-
The clinical effectiveness and cost-effectiveness of enzyme replacement therapy for Gaucher’s disease: a systematic review.
By Connock M, Burls A, Frew E, Fry-Smith A, Juarez-Garcia A, McCabe C, et al.
-
Effectiveness and cost-effectiveness of salicylic acid and cryotherapy for cutaneous warts. An economic decision model.
By Thomas KS, Keogh-Brown MR, Chalmers JR, Fordham RJ, Holland RC, Armstrong SJ, et al.
-
A systematic literature review of the effectiveness of non-pharmacological interventions to prevent wandering in dementia and evaluation of the ethical implications and acceptability of their use.
By Robinson L, Hutchings D, Corner L, Beyer F, Dickinson H, Vanoli A, et al.
-
A review of the evidence on the effects and costs of implantable cardioverter defibrillator therapy in different patient groups, and modelling of cost-effectiveness and cost–utility for these groups in a UK context.
By Buxton M, Caine N, Chase D, Connelly D, Grace A, Jackson C, et al.
-
Adefovir dipivoxil and pegylated interferon alfa-2a for the treatment of chronic hepatitis B: a systematic review and economic evaluation.
By Shepherd J, Jones J, Takeda A, Davidson P, Price A.
-
An evaluation of the clinical and cost-effectiveness of pulmonary artery catheters in patient management in intensive care: a systematic review and a randomised controlled trial.
By Harvey S, Stevens K, Harrison D, Young D, Brampton W, McCabe C, et al.
-
Accurate, practical and cost-effective assessment of carotid stenosis in the UK.
By Wardlaw JM, Chappell FM, Stevenson M, De Nigris E, Thomas S, Gillard J, et al.
-
Etanercept and infliximab for the treatment of psoriatic arthritis: a systematic review and economic evaluation.
By Woolacott N, Bravo Vergel Y, Hawkins N, Kainth A, Khadjesari Z, Misso K, et al.
-
The cost-effectiveness of testing for hepatitis C in former injecting drug users.
By Castelnuovo E, Thompson-Coon J, Pitt M, Cramp M, Siebert U, Price A, et al.
-
Computerised cognitive behaviour therapy for depression and anxiety update: a systematic review and economic evaluation.
By Kaltenthaler E, Brazier J, De Nigris E, Tumur I, Ferriter M, Beverley C, et al.
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.
By Williams C, Brunskill S, Altman D, Briggs A, Campbell H, Clarke M, et al.
-
Psychological therapies including dialectical behaviour therapy for borderline personality disorder: a systematic review and preliminary economic evaluation.
By Brazier J, Tumur I, Holmes M, Ferriter M, Parry G, Dent-Brown K, et al.
-
Clinical effectiveness and cost-effectiveness of tests for the diagnosis and investigation of urinary tract infection in children: a systematic review and economic model.
By Whiting P, Westwood M, Bojke L, Palmer S, Richardson G, Cooper J, et al.
-
Cognitive behavioural therapy in chronic fatigue syndrome: a randomised controlled trial of an outpatient group programme.
By O’Dowd H, Gladwell P, Rogers CA, Hollinghurst S, Gregory A.
-
A comparison of the cost-effectiveness of five strategies for the prevention of nonsteroidal anti-inflammatory drug-induced gastrointestinal toxicity: a systematic review with economic modelling.
By Brown TJ, Hooper L, Elliott RA, Payne K, Webb R, Roberts C, et al.
-
The effectiveness and cost-effectiveness of computed tomography screening for coronary artery disease: systematic review.
By Waugh N, Black C, Walker S, McIntyre L, Cummins E, Hillis G.
-
What are the clinical outcome and cost-effectiveness of endoscopy undertaken by nurses when compared with doctors? A Multi-Institution Nurse Endoscopy Trial (MINuET).
By Williams J, Russell I, Durai D, Cheung W-Y, Farrin A, Bloor K, et al.
-
The clinical and cost-effectiveness of oxaliplatin and capecitabine for the adjuvant treatment of colon cancer: systematic review and economic evaluation.
By Pandor A, Eggington S, Paisley S, Tappenden P, Sutcliffe P.
-
A systematic review of the effectiveness of adalimumab, etanercept and infliximab for the treatment of rheumatoid arthritis in adults and an economic evaluation of their cost-effectiveness.
By Chen Y-F, Jobanputra P, Barton P, Jowett S, Bryan S, Clark W, et al.
-
Telemedicine in dermatology: a randomised controlled trial.
By Bowns IR, Collins K, Walters SJ, McDonagh AJG.
-
Cost-effectiveness of cell salvage and alternative methods of minimising perioperative allogeneic blood transfusion: a systematic review and economic model.
By Davies L, Brown TJ, Haynes S, Payne K, Elliott RA, McCollum C.
-
Clinical effectiveness and cost-effectiveness of laparoscopic surgery for colorectal cancer: systematic reviews and economic evaluation.
By Murray A, Lourenco T, de Verteuil R, Hernandez R, Fraser C, McKinley A, et al.
-
Etanercept and efalizumab for the treatment of psoriasis: a systematic review.
By Woolacott N, Hawkins N, Mason A, Kainth A, Khadjesari Z, Bravo Vergel Y, et al.
-
Systematic reviews of clinical decision tools for acute abdominal pain.
By Liu JLY, Wyatt JC, Deeks JJ, Clamp S, Keen J, Verde P, et al.
-
Evaluation of the ventricular assist device programme in the UK.
By Sharples L, Buxton M, Caine N, Cafferty F, Demiris N, Dyer M, et al.
-
A systematic review and economic model of the clinical and cost-effectiveness of immunosuppressive therapy for renal transplantation in children.
By Yao G, Albon E, Adi Y, Milford D, Bayliss S, Ready A, et al.
-
Amniocentesis results: investigation of anxiety. The ARIA trial.
By Hewison J, Nixon J, Fountain J, Cocks K, Jones C, Mason G, et al.
-
Pemetrexed disodium for the treatment of malignant pleural mesothelioma: a systematic review and economic evaluation.
By Dundar Y, Bagust A, Dickson R, Dodd S, Green J, Haycox A, et al.
-
A systematic review and economic model of the clinical effectiveness and cost-effectiveness of docetaxel in combination with prednisone or prednisolone for the treatment of hormone-refractory metastatic prostate cancer.
By Collins R, Fenwick E, Trowman R, Perard R, Norman G, Light K, et al.
-
A systematic review of rapid diagnostic tests for the detection of tuberculosis infection.
By Dinnes J, Deeks J, Kunst H, Gibson A, Cummins E, Waugh N, et al.
-
The clinical effectiveness and cost-effectiveness of strontium ranelate for the prevention of osteoporotic fragility fractures in postmenopausal women.
By Stevenson M, Davis S, Lloyd-Jones M, Beverley C.
-
A systematic review of quantitative and qualitative research on the role and effectiveness of written information available to patients about individual medicines.
By Raynor DK, Blenkinsopp A, Knapp P, Grime J, Nicolson DJ, Pollock K, et al.
-
Oral naltrexone as a treatment for relapse prevention in formerly opioid-dependent drug users: a systematic review and economic evaluation.
By Adi Y, Juarez-Garcia A, Wang D, Jowett S, Frew E, Day E, et al.
-
Glucocorticoid-induced osteoporosis: a systematic review and cost–utility analysis.
By Kanis JA, Stevenson M, McCloskey EV, Davis S, Lloyd-Jones M.
-
Epidemiological, social, diagnostic and economic evaluation of population screening for genital chlamydial infection.
By Low N, McCarthy A, Macleod J, Salisbury C, Campbell R, Roberts TE, et al.
-
Methadone and buprenorphine for the management of opioid dependence: a systematic review and economic evaluation.
By Connock M, Juarez-Garcia A, Jowett S, Frew E, Liu Z, Taylor RJ, et al.
-
Exercise Evaluation Randomised Trial (EXERT): a randomised trial comparing GP referral for leisure centre-based exercise, community-based walking and advice only.
By Isaacs AJ, Critchley JA, See Tai S, Buckingham K, Westley D, Harridge SDR, et al.
-
Interferon alfa (pegylated and non-pegylated) and ribavirin for the treatment of mild chronic hepatitis C: a systematic review and economic evaluation.
By Shepherd J, Jones J, Hartwell D, Davidson P, Price A, Waugh N.
-
Systematic review and economic evaluation of bevacizumab and cetuximab for the treatment of metastatic colorectal cancer.
By Tappenden P, Jones R, Paisley S, Carroll C.
-
A systematic review and economic evaluation of epoetin alfa, epoetin beta and darbepoetin alfa in anaemia associated with cancer, especially that attributable to cancer treatment.
By Wilson J, Yao GL, Raftery J, Bohlius J, Brunskill S, Sandercock J, et al.
-
A systematic review and economic evaluation of statins for the prevention of coronary events.
By Ward S, Lloyd Jones M, Pandor A, Holmes M, Ara R, Ryan A, et al.
-
A systematic review of the effectiveness and cost-effectiveness of different models of community-based respite care for frail older people and their carers.
By Mason A, Weatherly H, Spilsbury K, Arksey H, Golder S, Adamson J, et al.
-
Additional therapy for young children with spastic cerebral palsy: a randomised controlled trial.
By Weindling AM, Cunningham CC, Glenn SM, Edwards RT, Reeves DJ.
-
Screening for type 2 diabetes: literature review and economic modelling.
By Waugh N, Scotland G, McNamee P, Gillett M, Brennan A, Goyder E, et al.
-
The effectiveness and cost-effectiveness of cinacalcet for secondary hyperparathyroidism in end-stage renal disease patients on dialysis: a systematic review and economic evaluation.
By Garside R, Pitt M, Anderson R, Mealing S, Roome C, Snaith A, et al.
-
The clinical effectiveness and cost-effectiveness of gemcitabine for metastatic breast cancer: a systematic review and economic evaluation.
By Takeda AL, Jones J, Loveman E, Tan SC, Clegg AJ.
-
A systematic review of duplex ultrasound, magnetic resonance angiography and computed tomography angiography for the diagnosis and assessment of symptomatic, lower limb peripheral arterial disease.
By Collins R, Cranny G, Burch J, Aguiar-Ibáñez R, Craig D, Wright K, et al.
-
The clinical effectiveness and cost-effectiveness of treatments for children with idiopathic steroid-resistant nephrotic syndrome: a systematic review.
By Colquitt JL, Kirby J, Green C, Cooper K, Trompeter RS.
-
A systematic review of the routine monitoring of growth in children of primary school age to identify growth-related conditions.
By Fayter D, Nixon J, Hartley S, Rithalia A, Butler G, Rudolf M, et al.
-
Systematic review of the effectiveness of preventing and treating Staphylococcus aureus carriage in reducing peritoneal catheter-related infections.
By McCormack K, Rabindranath K, Kilonzo M, Vale L, Fraser C, McIntyre L, et al.
-
The clinical effectiveness and cost of repetitive transcranial magnetic stimulation versus electroconvulsive therapy in severe depression: a multicentre pragmatic randomised controlled trial and economic analysis.
By McLoughlin DM, Mogg A, Eranti S, Pluck G, Purvis R, Edwards D, et al.
-
A randomised controlled trial and economic evaluation of direct versus indirect and individual versus group modes of speech and language therapy for children with primary language impairment.
By Boyle J, McCartney E, Forbes J, O’Hare A.
-
Hormonal therapies for early breast cancer: systematic review and economic evaluation.
By Hind D, Ward S, De Nigris E, Simpson E, Carroll C, Wyld L.
-
Cardioprotection against the toxic effects of anthracyclines given to children with cancer: a systematic review.
By Bryant J, Picot J, Levitt G, Sullivan I, Baxter L, Clegg A.
-
Adalimumab, etanercept and infliximab for the treatment of ankylosing spondylitis: a systematic review and economic evaluation.
By McLeod C, Bagust A, Boland A, Dagenais P, Dickson R, Dundar Y, et al.
-
Prenatal screening and treatment strategies to prevent group B streptococcal and other bacterial infections in early infancy: cost-effectiveness and expected value of information analyses.
By Colbourn T, Asseburg C, Bojke L, Philips Z, Claxton K, Ades AE, et al.
-
Clinical effectiveness and cost-effectiveness of bone morphogenetic proteins in the non-healing of fractures and spinal fusion: a systematic review.
By Garrison KR, Donell S, Ryder J, Shemilt I, Mugford M, Harvey I, et al.
-
A randomised controlled trial of postoperative radiotherapy following breast-conserving surgery in a minimum-risk older population. The PRIME trial.
By Prescott RJ, Kunkler IH, Williams LJ, King CC, Jack W, van der Pol M, et al.
-
Current practice, accuracy, effectiveness and cost-effectiveness of the school entry hearing screen.
By Bamford J, Fortnum H, Bristow K, Smith J, Vamvakas G, Davies L, et al.
-
The clinical effectiveness and cost-effectiveness of inhaled insulin in diabetes mellitus: a systematic review and economic evaluation.
By Black C, Cummins E, Royle P, Philip S, Waugh N.
-
Surveillance of cirrhosis for hepatocellular carcinoma: systematic review and economic analysis.
By Thompson Coon J, Rogers G, Hewson P, Wright D, Anderson R, Cramp M, et al.
-
The Birmingham Rehabilitation Uptake Maximisation Study (BRUM). Homebased compared with hospital-based cardiac rehabilitation in a multi-ethnic population: cost-effectiveness and patient adherence.
By Jolly K, Taylor R, Lip GYH, Greenfield S, Raftery J, Mant J, et al.
-
A systematic review of the clinical, public health and cost-effectiveness of rapid diagnostic tests for the detection and identification of bacterial intestinal pathogens in faeces and food.
By Abubakar I, Irvine L, Aldus CF, Wyatt GM, Fordham R, Schelenz S, et al.
-
A randomised controlled trial examining the longer-term outcomes of standard versus new antiepileptic drugs. The SANAD trial.
By Marson AG, Appleton R, Baker GA, Chadwick DW, Doughty J, Eaton B, et al.
-
Clinical effectiveness and cost-effectiveness of different models of managing long-term oral anti-coagulation therapy: a systematic review and economic modelling.
By Connock M, Stevens C, Fry-Smith A, Jowett S, Fitzmaurice D, Moore D, et al.
-
A systematic review and economic model of the clinical effectiveness and cost-effectiveness of interventions for preventing relapse in people with bipolar disorder.
By Soares-Weiser K, Bravo Vergel Y, Beynon S, Dunn G, Barbieri M, Duffy S, et al.
-
Taxanes for the adjuvant treatment of early breast cancer: systematic review and economic evaluation.
By Ward S, Simpson E, Davis S, Hind D, Rees A, Wilkinson A.
-
The clinical effectiveness and cost-effectiveness of screening for open angle glaucoma: a systematic review and economic evaluation.
By Burr JM, Mowatt G, Hernández R, Siddiqui MAR, Cook J, Lourenco T, et al.
-
Acceptability, benefit and costs of early screening for hearing disability: a study of potential screening tests and models.
By Davis A, Smith P, Ferguson M, Stephens D, Gianopoulos I.
-
Contamination in trials of educational interventions.
By Keogh-Brown MR, Bachmann MO, Shepstone L, Hewitt C, Howe A, Ramsay CR, et al.
-
Overview of the clinical effectiveness of positron emission tomography imaging in selected cancers.
By Facey K, Bradbury I, Laking G, Payne E.
-
The effectiveness and cost-effectiveness of carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma: a systematic review and economic evaluation.
By Garside R, Pitt M, Anderson R, Rogers G, Dyer M, Mealing S, et al.
-
Drug-eluting stents: a systematic review and economic evaluation.
By Hill RA, Boland A, Dickson R, Dündar Y, Haycox A, McLeod C, et al.
-
The clinical effectiveness and cost-effectiveness of cardiac resynchronisation (biventricular pacing) for heart failure: systematic review and economic model.
By Fox M, Mealing S, Anderson R, Dean J, Stein K, Price A, et al.
-
Recruitment to randomised trials: strategies for trial enrolment and participation study. The STEPS study.
By Campbell MK, Snowdon C, Francis D, Elbourne D, McDonald AM, Knight R, et al.
-
Cost-effectiveness of functional cardiac testing in the diagnosis and management of coronary artery disease: a randomised controlled trial. The CECaT trial.
By Sharples L, Hughes V, Crean A, Dyer M, Buxton M, Goldsmith K, et al.
-
Evaluation of diagnostic tests when there is no gold standard. A review of methods.
By Rutjes AWS, Reitsma JB, Coomarasamy A, Khan KS, Bossuyt PMM.
-
Systematic reviews of the clinical effectiveness and cost-effectiveness of proton pump inhibitors in acute upper gastrointestinal bleeding.
By Leontiadis GI, Sreedharan A, Dorward S, Barton P, Delaney B, Howden CW, et al.
-
A review and critique of modelling in prioritising and designing screening programmes.
By Karnon J, Goyder E, Tappenden P, McPhie S, Towers I, Brazier J, et al.
-
An assessment of the impact of the NHS Health Technology Assessment Programme.
By Hanney S, Buxton M, Green C, Coulson D, Raftery J.
-
A systematic review and economic model of switching from nonglycopeptide to glycopeptide antibiotic prophylaxis for surgery.
By Cranny G, Elliott R, Weatherly H, Chambers D, Hawkins N, Myers L, et al.
-
‘Cut down to quit’ with nicotine replacement therapies in smoking cessation: a systematic review of effectiveness and economic analysis.
By Wang D, Connock M, Barton P, Fry-Smith A, Aveyard P, Moore D.
-
A systematic review of the effectiveness of strategies for reducing fracture risk in children with juvenile idiopathic arthritis with additional data on long-term risk of fracture and cost of disease management.
By Thornton J, Ashcroft D, O’Neill T, Elliott R, Adams J, Roberts C, et al.
-
Does befriending by trained lay workers improve psychological well-being and quality of life for carers of people with dementia, and at what cost? A randomised controlled trial.
By Charlesworth G, Shepstone L, Wilson E, Thalanany M, Mugford M, Poland F.
-
A multi-centre retrospective cohort study comparing the efficacy, safety and cost-effectiveness of hysterectomy and uterine artery embolisation for the treatment of symptomatic uterine fibroids. The HOPEFUL study.
By Hirst A, Dutton S, Wu O, Briggs A, Edwards C, Waldenmaier L, et al.
-
Methods of prediction and prevention of pre-eclampsia: systematic reviews of accuracy and effectiveness literature with economic modelling.
By Meads CA, Cnossen JS, Meher S, Juarez-Garcia A, ter Riet G, Duley L, et al.
-
The use of economic evaluations in NHS decision-making: a review and empirical investigation.
By Williams I, McIver S, Moore D, Bryan S.
-
Stapled haemorrhoidectomy (haemorrhoidopexy) for the treatment of haemorrhoids: a systematic review and economic evaluation.
By Burch J, Epstein D, Baba-Akbari A, Weatherly H, Fox D, Golder S, et al.
-
The clinical effectiveness of diabetes education models for Type 2 diabetes: a systematic review.
By Loveman E, Frampton GK, Clegg AJ.
-
Payment to healthcare professionals for patient recruitment to trials: systematic review and qualitative study.
By Raftery J, Bryant J, Powell J, Kerr C, Hawker S.
-
Cyclooxygenase-2 selective non-steroidal anti-inflammatory drugs (etodolac, meloxicam, celecoxib, rofecoxib, etoricoxib, valdecoxib and lumiracoxib) for osteoarthritis and rheumatoid arthritis: a systematic review and economic evaluation.
By Chen Y-F, Jobanputra P, Barton P, Bryan S, Fry-Smith A, Harris G, et al.
-
The clinical effectiveness and cost-effectiveness of central venous catheters treated with anti-infective agents in preventing bloodstream infections: a systematic review and economic evaluation.
By Hockenhull JC, Dwan K, Boland A, Smith G, Bagust A, Dundar Y, et al.
-
Stepped treatment of older adults on laxatives. The STOOL trial.
By Mihaylov S, Stark C, McColl E, Steen N, Vanoli A, Rubin G, et al.
-
A randomised controlled trial of cognitive behaviour therapy in adolescents with major depression treated by selective serotonin reuptake inhibitors. The ADAPT trial.
By Goodyer IM, Dubicka B, Wilkinson P, Kelvin R, Roberts C, Byford S, et al.
-
The use of irinotecan, oxaliplatin and raltitrexed for the treatment of advanced colorectal cancer: systematic review and economic evaluation.
By Hind D, Tappenden P, Tumur I, Eggington E, Sutcliffe P, Ryan A.
-
Ranibizumab and pegaptanib for the treatment of age-related macular degeneration: a systematic review and economic evaluation.
By Colquitt JL, Jones J, Tan SC, Takeda A, Clegg AJ, Price A.
-
Systematic review of the clinical effectiveness and cost-effectiveness of 64-slice or higher computed tomography angiography as an alternative to invasive coronary angiography in the investigation of coronary artery disease.
By Mowatt G, Cummins E, Waugh N, Walker S, Cook J, Jia X, et al.
-
Structural neuroimaging in psychosis: a systematic review and economic evaluation.
By Albon E, Tsourapas A, Frew E, Davenport C, Oyebode F, Bayliss S, et al.
-
Systematic review and economic analysis of the comparative effectiveness of different inhaled corticosteroids and their usage with long-acting beta2 agonists for the treatment of chronic asthma in adults and children aged 12 years and over.
By Shepherd J, Rogers G, Anderson R, Main C, Thompson-Coon J, Hartwell D, et al.
-
Systematic review and economic analysis of the comparative effectiveness of different inhaled corticosteroids and their usage with long-acting beta2 agonists for the treatment of chronic asthma in children under the age of 12 years.
By Main C, Shepherd J, Anderson R, Rogers G, Thompson-Coon J, Liu Z, et al.
-
Ezetimibe for the treatment of hypercholesterolaemia: a systematic review and economic evaluation.
By Ara R, Tumur I, Pandor A, Duenas A, Williams R, Wilkinson A, et al.
-
Topical or oral ibuprofen for chronic knee pain in older people. The TOIB study.
By Underwood M, Ashby D, Carnes D, Castelnuovo E, Cross P, Harding G, et al.
-
A prospective randomised comparison of minor surgery in primary and secondary care. The MiSTIC trial.
By George S, Pockney P, Primrose J, Smith H, Little P, Kinley H, et al.
-
A review and critical appraisal of measures of therapist–patient interactions in mental health settings.
By Cahill J, Barkham M, Hardy G, Gilbody S, Richards D, Bower P, et al.
-
The clinical effectiveness and cost-effectiveness of screening programmes for amblyopia and strabismus in children up to the age of 4–5 years: a systematic review and economic evaluation.
By Carlton J, Karnon J, Czoski-Murray C, Smith KJ, Marr J.
-
A systematic review of the clinical effectiveness and cost-effectiveness and economic modelling of minimal incision total hip replacement approaches in the management of arthritic disease of the hip.
By de Verteuil R, Imamura M, Zhu S, Glazener C, Fraser C, Munro N, et al.
-
A preliminary model-based assessment of the cost–utility of a screening programme for early age-related macular degeneration.
By Karnon J, Czoski-Murray C, Smith K, Brand C, Chakravarthy U, Davis S, et al.
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.
By Shepherd J, Jones J, Frampton GK, Tanajewski L, Turner D, Price A.
-
Absorbent products for urinary/faecal incontinence: a comparative evaluation of key product categories.
By Fader M, Cottenden A, Getliffe K, Gage H, Clarke-O’Neill S, Jamieson K, et al.
-
A systematic review of repetitive functional task practice with modelling of resource use, costs and effectiveness.
By French B, Leathley M, Sutton C, McAdam J, Thomas L, Forster A, et al.
-
The effectiveness and cost-effectivness of minimal access surgery amongst people with gastro-oesophageal reflux disease – a UK collaborative study. The reflux trial.
By Grant A, Wileman S, Ramsay C, Bojke L, Epstein D, Sculpher M, et al.
-
Time to full publication of studies of anti-cancer medicines for breast cancer and the potential for publication bias: a short systematic review.
By Takeda A, Loveman E, Harris P, Hartwell D, Welch K.
-
Performance of screening tests for child physical abuse in accident and emergency departments.
By Woodman J, Pitt M, Wentz R, Taylor B, Hodes D, Gilbert RE.
-
Curative catheter ablation in atrial fibrillation and typical atrial flutter: systematic review and economic evaluation.
By Rodgers M, McKenna C, Palmer S, Chambers D, Van Hout S, Golder S, et al.
-
Systematic review and economic modelling of effectiveness and cost utility of surgical treatments for men with benign prostatic enlargement.
By Lourenco T, Armstrong N, N’Dow J, Nabi G, Deverill M, Pickard R, et al.
-
Immunoprophylaxis against respiratory syncytial virus (RSV) with palivizumab in children: a systematic review and economic evaluation.
By Wang D, Cummins C, Bayliss S, Sandercock J, Burls A.
-
Deferasirox for the treatment of iron overload associated with regular blood transfusions (transfusional haemosiderosis) in patients suffering with chronic anaemia: a systematic review and economic evaluation.
By McLeod C, Fleeman N, Kirkham J, Bagust A, Boland A, Chu P, et al.
-
Thrombophilia testing in people with venous thromboembolism: systematic review and cost-effectiveness analysis.
By Simpson EL, Stevenson MD, Rawdin A, Papaioannou D.
-
Surgical procedures and non-surgical devices for the management of non-apnoeic snoring: a systematic review of clinical effects and associated treatment costs.
By Main C, Liu Z, Welch K, Weiner G, Quentin Jones S, Stein K.
-
Continuous positive airway pressure devices for the treatment of obstructive sleep apnoea–hypopnoea syndrome: a systematic review and economic analysis.
By McDaid C, Griffin S, Weatherly H, Durée K, van der Burgt M, van Hout S, Akers J, et al.
-
Use of classical and novel biomarkers as prognostic risk factors for localised prostate cancer: a systematic review.
By Sutcliffe P, Hummel S, Simpson E, Young T, Rees A, Wilkinson A, et al.
-
The harmful health effects of recreational ecstasy: a systematic review of observational evidence.
By Rogers G, Elston J, Garside R, Roome C, Taylor R, Younger P, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of oesophageal Doppler monitoring in critically ill and high-risk surgical patients.
By Mowatt G, Houston G, Hernández R, de Verteuil R, Fraser C, Cuthbertson B, et al.
-
The use of surrogate outcomes in model-based cost-effectiveness analyses: a survey of UK Health Technology Assessment reports.
By Taylor RS, Elston J.
-
Controlling Hypertension and Hypotension Immediately Post Stroke (CHHIPS) – a randomised controlled trial.
By Potter J, Mistri A, Brodie F, Chernova J, Wilson E, Jagger C, et al.
-
Routine antenatal anti-D prophylaxis for RhD-negative women: a systematic review and economic evaluation.
By Pilgrim H, Lloyd-Jones M, Rees A.
-
Amantadine, oseltamivir and zanamivir for the prophylaxis of influenza (including a review of existing guidance no. 67): a systematic review and economic evaluation.
By Tappenden P, Jackson R, Cooper K, Rees A, Simpson E, Read R, et al.
-
Improving the evaluation of therapeutic interventions in multiple sclerosis: the role of new psychometric methods.
By Hobart J, Cano S.
-
Treatment of severe ankle sprain: a pragmatic randomised controlled trial comparing the clinical effectiveness and cost-effectiveness of three types of mechanical ankle support with tubular bandage. The CAST trial.
By Cooke MW, Marsh JL, Clark M, Nakash R, Jarvis RM, Hutton JL, et al. , on behalf of the CAST trial group.
-
Non-occupational postexposure prophylaxis for HIV: a systematic review.
By Bryant J, Baxter L, Hird S.
-
Blood glucose self-monitoring in type 2 diabetes: a randomised controlled trial.
By Farmer AJ, Wade AN, French DP, Simon J, Yudkin P, Gray A, et al.
-
How far does screening women for domestic (partner) violence in different health-care settings meet criteria for a screening programme? Systematic reviews of nine UK National Screening Committee criteria.
By Feder G, Ramsay J, Dunne D, Rose M, Arsene C, Norman R, et al.
-
Spinal cord stimulation for chronic pain of neuropathic or ischaemic origin: systematic review and economic evaluation.
By Simpson, EL, Duenas A, Holmes MW, Papaioannou D, Chilcott J.
-
The role of magnetic resonance imaging in the identification of suspected acoustic neuroma: a systematic review of clinical and costeffectiveness and natural history.
By Fortnum H, O’Neill C, Taylor R, Lenthall R, Nikolopoulos T, Lightfoot G, et al.
-
Dipsticks and diagnostic algorithms in urinary tract infection: development and validation, randomised trial, economic analysis, observational cohort and qualitative study.
By Little P, Turner S, Rumsby K, Warner G, Moore M, Lowes JA, et al.
-
Systematic review of respite care in the frail elderly.
By Shaw C, McNamara R, Abrams K, Cannings-John R, Hood K, Longo M, et al.
-
Neuroleptics in the treatment of aggressive challenging behaviour for people with intellectual disabilities: a randomised controlled trial (NACHBID).
By Tyrer P, Oliver-Africano P, Romeo R, Knapp M, Dickens S, Bouras N, et al.
-
Randomised controlled trial to determine the clinical effectiveness and cost-effectiveness of selective serotonin reuptake inhibitors plus supportive care, versus supportive care alone, for mild to moderate depression with somatic symptoms in primary care: the THREAD (THREshold for AntiDepressant response) study.
By Kendrick T, Chatwin J, Dowrick C, Tylee A, Morriss R, Peveler R, et al.
-
Diagnostic strategies using DNA testing for hereditary haemochromatosis in at-risk populations: a systematic review and economic evaluation.
By Bryant J, Cooper K, Picot J, Clegg A, Roderick P, Rosenberg W, et al.
-
Enhanced external counterpulsation for the treatment of stable angina and heart failure: a systematic review and economic analysis.
By McKenna C, McDaid C, Suekarran S, Hawkins N, Claxton K, Light K, et al.
-
Development of a decision support tool for primary care management of patients with abnormal liver function tests without clinically apparent liver disease: a record-linkage population cohort study and decision analysis (ALFIE).
By Donnan PT, McLernon D, Dillon JF, Ryder S, Roderick P, Sullivan F, et al.
-
A systematic review of presumed consent systems for deceased organ donation.
By Rithalia A, McDaid C, Suekarran S, Norman G, Myers L, Sowden A.
-
Paracetamol and ibuprofen for the treatment of fever in children: the PITCH randomised controlled trial.
By Hay AD, Redmond NM, Costelloe C, Montgomery AA, Fletcher M, Hollinghurst S, et al.
-
A randomised controlled trial to compare minimally invasive glucose monitoring devices with conventional monitoring in the management of insulin-treated diabetes mellitus (MITRE).
By Newman SP, Cooke D, Casbard A, Walker S, Meredith S, Nunn A, et al.
-
Sensitivity analysis in economic evaluation: an audit of NICE current practice and a review of its use and value in decision-making.
By Andronis L, Barton P, Bryan S.
-
Trastuzumab for the treatment of primary breast cancer in HER2-positive women: a single technology appraisal.
By Ward S, Pilgrim H, Hind D.
-
Docetaxel for the adjuvant treatment of early node-positive breast cancer: a single technology appraisal.
By Chilcott J, Lloyd Jones M, Wilkinson A.
-
The use of paclitaxel in the management of early stage breast cancer.
By Griffin S, Dunn G, Palmer S, Macfarlane K, Brent S, Dyker A, et al.
-
Rituximab for the first-line treatment of stage III/IV follicular non-Hodgkin’s lymphoma.
By Dundar Y, Bagust A, Hounsome J, McLeod C, Boland A, Davis H, et al.
-
Bortezomib for the treatment of multiple myeloma patients.
By Green C, Bryant J, Takeda A, Cooper K, Clegg A, Smith A, et al.
-
Fludarabine phosphate for the firstline treatment of chronic lymphocytic leukaemia.
By Walker S, Palmer S, Erhorn S, Brent S, Dyker A, Ferrie L, et al.
-
Erlotinib for the treatment of relapsed non-small cell lung cancer.
By McLeod C, Bagust A, Boland A, Hockenhull J, Dundar Y, Proudlove C, et al.
-
Cetuximab plus radiotherapy for the treatment of locally advanced squamous cell carcinoma of the head and neck.
By Griffin S, Walker S, Sculpher M, White S, Erhorn S, Brent S, et al.
-
Infliximab for the treatment of adults with psoriasis.
By Loveman E, Turner D, Hartwell D, Cooper K, Clegg A
-
Psychological interventions for postnatal depression: cluster randomised trial and economic evaluation. The PoNDER trial.
By Morrell CJ, Warner R, Slade P, Dixon S, Walters S, Paley G, et al.
-
The effect of different treatment durations of clopidogrel in patients with non-ST-segment elevation acute coronary syndromes: a systematic review and value of information analysis.
By Rogowski R, Burch J, Palmer S, Craigs C, Golder S, Woolacott N.
-
Systematic review and individual patient data meta-analysis of diagnosis of heart failure, with modelling of implications of different diagnostic strategies in primary care.
By Mant J, Doust J, Roalfe A, Barton P, Cowie MR, Glasziou P, et al.
-
A multicentre randomised controlled trial of the use of continuous positive airway pressure and non-invasive positive pressure ventilation in the early treatment of patients presenting to the emergency department with severe acute cardiogenic pulmonary oedema: the 3CPO trial.
By Gray AJ, Goodacre S, Newby DE, Masson MA, Sampson F, Dixon S, et al. , on behalf of the 3CPO study investigators.
-
Early high-dose lipid-lowering therapy to avoid cardiac events: a systematic review and economic evaluation.
By Ara R, Pandor A, Stevens J, Rees A, Rafia R.
-
Adefovir dipivoxil and pegylated interferon alpha for the treatment of chronic hepatitis B: an updated systematic review and economic evaluation.
By Jones J, Shepherd J, Baxter L, Gospodarevskaya E, Hartwell D, Harris P, et al.
-
Methods to identify postnatal depression in primary care: an integrated evidence synthesis and value of information analysis.
By Hewitt CE, Gilbody SM, Brealey S, Paulden M, Palmer S, Mann R, et al.
-
A double-blind randomised placebocontrolled trial of topical intranasal corticosteroids in 4- to 11-year-old children with persistent bilateral otitis media with effusion in primary care.
By Williamson I, Benge S, Barton S, Petrou S, Letley L, Fasey N, et al.
-
The effectiveness and cost-effectiveness of methods of storing donated kidneys from deceased donors: a systematic review and economic model.
By Bond M, Pitt M, Akoh J, Moxham T, Hoyle M, Anderson R.
-
Rehabilitation of older patients: day hospital compared with rehabilitation at home. A randomised controlled trial.
By Parker SG, Oliver P, Pennington M, Bond J, Jagger C, Enderby PM, et al.
-
Breastfeeding promotion for infants in neonatal units: a systematic review and economic analysis.
By Renfrew MJ, Craig D, Dyson L, McCormick F, Rice S, King SE, et al.
Health Technology Assessment programme
-
Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Medical Care Research Unit, University of Sheffield
Prioritisation Strategy Group
-
Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Medical Care Research Unit, University of Sheffield
-
Dr Bob Coates, Consultant Advisor, NETSCC, HTA
-
Dr Andrew Cook, Consultant Advisor, NETSCC, HTA
-
Dr Peter Davidson, Director of Science Support, NETSCC, HTA
-
Professor Robin E Ferner, Consultant Physician and Director, West Midlands Centre for Adverse Drug Reactions, City Hospital NHS Trust, Birmingham
-
Professor Paul Glasziou, Professor of Evidence-Based Medicine, University of Oxford
-
Dr Nick Hicks, Director of NHS Support, NETSCC, HTA
-
Dr Edmund Jessop, Medical Adviser, National Specialist, National Commissioning Group (NCG), Department of Health, London
-
Ms Lynn Kerridge, Chief Executive Officer, NETSCC and NETSCC, HTA
-
Dr Ruairidh Milne, Director of Strategy and Development, NETSCC
-
Ms Kay Pattison, Section Head, NHS R&D Programme, Department of Health
-
Ms Pamela Young, Specialist Programme Manager, NETSCC, HTA
HTA Commissioning Board
-
Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Medical Care Research Unit, University of Sheffield
-
Senior Lecturer in General Practice, Department of Primary Health Care, University of Oxford
-
Professor Ann Ashburn, Professor of Rehabilitation and Head of Research, Southampton General Hospital
-
Professor Deborah Ashby, Professor of Medical Statistics, Queen Mary, University of London
-
Professor John Cairns, Professor of Health Economics, London School of Hygiene and Tropical Medicine
-
Professor Peter Croft, Director of Primary Care Sciences Research Centre, Keele University
-
Professor Nicky Cullum, Director of Centre for Evidence-Based Nursing, University of York
-
Professor Jenny Donovan, Professor of Social Medicine, University of Bristol
-
Professor Steve Halligan, Professor of Gastrointestinal Radiology, University College Hospital, London
-
Professor Freddie Hamdy, Professor of Urology, University of Sheffield
-
Professor Allan House, Professor of Liaison Psychiatry, University of Leeds
-
Dr Martin J Landray, Reader in Epidemiology, Honorary Consultant Physician, Clinical Trial Service Unit, University of Oxford?
-
Professor Stuart Logan, Director of Health & Social Care Research, The Peninsula Medical School, Universities of Exeter and Plymouth
-
Dr Rafael Perera, Lecturer in Medical Statisitics, Department of Primary Health Care, Univeristy of Oxford
-
Professor Ian Roberts, Professor of Epidemiology & Public Health, London School of Hygiene and Tropical Medicine
-
Professor Mark Sculpher, Professor of Health Economics, University of York
-
Professor Helen Smith, Professor of Primary Care, University of Brighton
-
Professor Kate Thomas, Professor of Complementary & Alternative Medicine Research, University of Leeds
-
Professor David John Torgerson, Director of York Trials Unit, University of York
-
Professor Hywel Williams, Professor of Dermato-Epidemiology, University of Nottingham
-
Ms Kay Pattison, Section Head, NHS R&D Programme, Department of Health
-
Dr Morven Roberts, Clinical Trials Manager, Medical Research Council
Diagnostic Technologies & Screening Panel
-
Professor of Evidence-Based Medicine, University of Oxford
-
Consultant Paediatrician and Honorary Senior Lecturer, Great Ormond Street Hospital, London
-
Professor Judith E Adams, Consultant Radiologist, Manchester Royal Infirmary, Central Manchester & Manchester Children’s University Hospitals NHS Trust, and Professor of Diagnostic Radiology, Imaging Science and Biomedical Engineering, Cancer & Imaging Sciences, University of Manchester
-
Ms Jane Bates, Consultant Ultrasound Practitioner, Ultrasound Department, Leeds Teaching Hospital NHS Trust
-
Dr Stephanie Dancer, Consultant Microbiologist, Hairmyres Hospital, East Kilbride
-
Professor Glyn Elwyn, Primary Medical Care Research Group, Swansea Clinical School, University of Wales
-
Dr Ron Gray, Consultant Clinical Epidemiologist, Department of Public Health, University of Oxford
-
Professor Paul D Griffiths, Professor of Radiology, University of Sheffield
-
Dr Jennifer J Kurinczuk, Consultant Clinical Epidemiologist, National Perinatal Epidemiology Unit, Oxford
-
Dr Susanne M Ludgate, Medical Director, Medicines & Healthcare Products Regulatory Agency, London
-
Dr Anne Mackie, Director of Programmes, UK National Screening Committee
-
Dr Michael Millar, Consultant Senior Lecturer in Microbiology, Barts and The London NHS Trust, Royal London Hospital
-
Mr Stephen Pilling, Director, Centre for Outcomes, Research & Effectiveness, Joint Director, National Collaborating Centre for Mental Health, University College London
-
Mrs Una Rennard, Service User Representative
-
Dr Phil Shackley, Senior Lecturer in Health Economics, School of Population and Health Sciences, University of Newcastle upon Tyne
-
Dr W Stuart A Smellie, Consultant in Chemical Pathology, Bishop Auckland General Hospital
-
Dr Nicholas Summerton, Consultant Clinical and Public Health Advisor, NICE
-
Ms Dawn Talbot, Service User Representative
-
Dr Graham Taylor, Scientific Advisor, Regional DNA Laboratory, St James’s University Hospital, Leeds
-
Professor Lindsay Wilson Turnbull, Scientific Director of the Centre for Magnetic Resonance Investigations and YCR Professor of Radiology, Hull Royal Infirmary
-
Dr Tim Elliott, Team Leader, Cancer Screening, Department of Health
-
Dr Catherine Moody, Programme Manager, Neuroscience and Mental Health Board
-
Dr Ursula Wells, Principal Research Officer, Department of Health
Pharmaceuticals Panel
-
Consultant Physician and Director, West Midlands Centre for Adverse Drug Reactions, City Hospital NHS Trust, Birmingham
-
Professor in Child Health, University of Nottingham
-
Mrs Nicola Carey, Senior Research Fellow, School of Health and Social Care, The University of Reading
-
Mr John Chapman, Service User Representative
-
Dr Peter Elton, Director of Public Health, Bury Primary Care Trust
-
Dr Ben Goldacre, Research Fellow, Division of Psychological Medicine and Psychiatry, King’s College London
-
Mrs Barbara Greggains, Service User Representative
-
Dr Bill Gutteridge, Medical Adviser, London Strategic Health Authority
-
Dr Dyfrig Hughes, Reader in Pharmacoeconomics and Deputy Director, Centre for Economics and Policy in Health, IMSCaR, Bangor University
-
Professor Jonathan Ledermann, Professor of Medical Oncology and Director of the Cancer Research UK and University College London Cancer Trials Centre
-
Dr Yoon K Loke, Senior Lecturer in Clinical Pharmacology, University of East Anglia
-
Professor Femi Oyebode, Consultant Psychiatrist and Head of Department, University of Birmingham
-
Dr Andrew Prentice, Senior Lecturer and Consultant Obstetrician and Gynaecologist, The Rosie Hospital, University of Cambridge
-
Dr Martin Shelly, General Practitioner, Leeds, and Associate Director, NHS Clinical Governance Support Team, Leicester
-
Dr Gillian Shepherd, Director, Health and Clinical Excellence, Merck Serono Ltd
-
Mrs Katrina Simister, Assistant Director New Medicines, National Prescribing Centre, Liverpool
-
Mr David Symes, Service User Representative
-
Dr Lesley Wise, Unit Manager, Pharmacoepidemiology Research Unit, VRMM, Medicines & Healthcare Products Regulatory Agency
-
Ms Kay Pattison, Section Head, NHS R&D Programme, Department of Health
-
Mr Simon Reeve, Head of Clinical and Cost-Effectiveness, Medicines, Pharmacy and Industry Group, Department of Health
-
Dr Heike Weber, Programme Manager, Medical Research Council
-
Dr Ursula Wells, Principal Research Officer, Department of Health
Therapeutic Procedures Panel
-
Consultant Physician, North Bristol NHS Trust
-
Professor of Psychiatry, Division of Health in the Community, University of Warwick, Coventry
-
Professor Jane Barlow, Professor of Public Health in the Early Years, Health Sciences Research Institute, Warwick Medical School, Coventry
-
Ms Maree Barnett, Acting Branch Head of Vascular Programme, Department of Health
-
Mrs Val Carlill, Service User Representative
-
Mrs Anthea De Barton-Watson, Service User Representative
-
Mr Mark Emberton, Senior Lecturer in Oncological Urology, Institute of Urology, University College Hospital, London
-
Professor Steve Goodacre, Professor of Emergency Medicine, University of Sheffield
-
Professor Christopher Griffiths, Professor of Primary Care, Barts and The London School of Medicine and Dentistry
-
Mr Paul Hilton, Consultant Gynaecologist and Urogynaecologist, Royal Victoria Infirmary, Newcastle upon Tyne
-
Professor Nicholas James, Professor of Clinical Oncology, University of Birmingham, and Consultant in Clinical Oncology, Queen Elizabeth Hospital
-
Dr Peter Martin, Consultant Neurologist, Addenbrooke’s Hospital, Cambridge
-
Dr Kate Radford, Senior Lecturer (Research), Clinical Practice Research Unit, University of Central Lancashire, Preston
-
Mr Jim Reece Service User Representative
-
Dr Karen Roberts, Nurse Consultant, Dunston Hill Hospital Cottages
-
Dr Phillip Leech, Principal Medical Officer for Primary Care, Department of Health
-
Ms Kay Pattison, Section Head, NHS R&D Programme, Department of Health
-
Dr Morven Roberts, Clinical Trials Manager, Medical Research Council
-
Professor Tom Walley, Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Dr Ursula Wells, Principal Research Officer, Department of Health
Disease Prevention Panel
-
Medical Adviser, National Specialist, National Commissioning Group (NCG), London
-
Director, NHS Sustainable Development Unit, Cambridge
-
Dr Elizabeth Fellow-Smith, Medical Director, West London Mental Health Trust, Middlesex
-
Dr John Jackson, General Practitioner, Parkway Medical Centre, Newcastle upon Tyne
-
Professor Mike Kelly, Director, Centre for Public Health Excellence, NICE, London
-
Dr Chris McCall, General Practitioner, The Hadleigh Practice, Corfe Mullen, Dorset
-
Ms Jeanett Martin, Director of Nursing, BarnDoc Limited, Lewisham Primary Care Trust
-
Dr Julie Mytton, Locum Consultant in Public Health Medicine, Bristol Primary Care Trust
-
Miss Nicky Mullany, Service User Representative
-
Professor Ian Roberts, Professor of Epidemiology and Public Health, London School of Hygiene & Tropical Medicine
-
Professor Ken Stein, Senior Clinical Lecturer in Public Health, University of Exeter
-
Dr Kieran Sweeney, Honorary Clinical Senior Lecturer, Peninsula College of Medicine and Dentistry, Universities of Exeter and Plymouth
-
Professor Carol Tannahill, Glasgow Centre for Population Health
-
Professor Margaret Thorogood, Professor of Epidemiology, University of Warwick Medical School, Coventry
-
Ms Christine McGuire, Research & Development, Department of Health
-
Dr Caroline Stone, Programme Manager, Medical Research Council
Expert Advisory Network
-
Professor Douglas Altman, Professor of Statistics in Medicine, Centre for Statistics in Medicine, University of Oxford
-
Professor John Bond, Professor of Social Gerontology & Health Services Research, University of Newcastle upon Tyne
-
Professor Andrew Bradbury, Professor of Vascular Surgery, Solihull Hospital, Birmingham
-
Mr Shaun Brogan, Chief Executive, Ridgeway Primary Care Group, Aylesbury
-
Mrs Stella Burnside OBE, Chief Executive, Regulation and Improvement Authority, Belfast
-
Ms Tracy Bury, Project Manager, World Confederation for Physical Therapy, London
-
Professor Iain T Cameron, Professor of Obstetrics and Gynaecology and Head of the School of Medicine, University of Southampton
-
Dr Christine Clark, Medical Writer and Consultant Pharmacist, Rossendale
-
Professor Collette Clifford, Professor of Nursing and Head of Research, The Medical School, University of Birmingham
-
Professor Barry Cookson, Director, Laboratory of Hospital Infection, Public Health Laboratory Service, London
-
Dr Carl Counsell, Clinical Senior Lecturer in Neurology, University of Aberdeen
-
Professor Howard Cuckle, Professor of Reproductive Epidemiology, Department of Paediatrics, Obstetrics & Gynaecology, University of Leeds
-
Dr Katherine Darton, Information Unit, MIND – The Mental Health Charity, London
-
Professor Carol Dezateux, Professor of Paediatric Epidemiology, Institute of Child Health, London
-
Mr John Dunning, Consultant Cardiothoracic Surgeon, Papworth Hospital NHS Trust, Cambridge
-
Mr Jonothan Earnshaw, Consultant Vascular Surgeon, Gloucestershire Royal Hospital, Gloucester
-
Professor Martin Eccles, Professor of Clinical Effectiveness, Centre for Health Services Research, University of Newcastle upon Tyne
-
Professor Pam Enderby, Dean of Faculty of Medicine, Institute of General Practice and Primary Care, University of Sheffield
-
Professor Gene Feder, Professor of Primary Care Research & Development, Centre for Health Sciences, Barts and The London School of Medicine and Dentistry
-
Mr Leonard R Fenwick, Chief Executive, Freeman Hospital, Newcastle upon Tyne
-
Mrs Gillian Fletcher, Antenatal Teacher and Tutor and President, National Childbirth Trust, Henfield
-
Professor Jayne Franklyn, Professor of Medicine, University of Birmingham
-
Mr Tam Fry, Honorary Chairman, Child Growth Foundation, London
-
Professor Fiona Gilbert, Consultant Radiologist and NCRN Member, University of Aberdeen
-
Professor Paul Gregg, Professor of Orthopaedic Surgical Science, South Tees Hospital NHS Trust
-
Bec Hanley, Co-director, TwoCan Associates, West Sussex
-
Dr Maryann L Hardy, Senior Lecturer, University of Bradford
-
Mrs Sharon Hart, Healthcare Management Consultant, Reading
-
Professor Robert E Hawkins, CRC Professor and Director of Medical Oncology, Christie CRC Research Centre, Christie Hospital NHS Trust, Manchester
-
Professor Richard Hobbs, Head of Department of Primary Care & General Practice, University of Birmingham
-
Professor Alan Horwich, Dean and Section Chairman, The Institute of Cancer Research, London
-
Professor Allen Hutchinson, Director of Public Health and Deputy Dean of ScHARR, University of Sheffield
-
Professor Peter Jones, Professor of Psychiatry, University of Cambridge, Cambridge
-
Professor Stan Kaye, Cancer Research UK Professor of Medical Oncology, Royal Marsden Hospital and Institute of Cancer Research, Surrey
-
Dr Duncan Keeley, General Practitioner (Dr Burch & Ptnrs), The Health Centre, Thame
-
Dr Donna Lamping, Research Degrees Programme Director and Reader in Psychology, Health Services Research Unit, London School of Hygiene and Tropical Medicine, London
-
Mr George Levvy, Chief Executive, Motor Neurone Disease Association, Northampton
-
Professor James Lindesay, Professor of Psychiatry for the Elderly, University of Leicester
-
Professor Julian Little, Professor of Human Genome Epidemiology, University of Ottawa
-
Professor Alistaire McGuire, Professor of Health Economics, London School of Economics
-
Professor Rajan Madhok, Medical Director and Director of Public Health, Directorate of Clinical Strategy & Public Health, North & East Yorkshire & Northern Lincolnshire Health Authority, York
-
Professor Alexander Markham, Director, Molecular Medicine Unit, St James’s University Hospital, Leeds
-
Dr Peter Moore, Freelance Science Writer, Ashtead
-
Dr Andrew Mortimore, Public Health Director, Southampton City Primary Care Trust
-
Dr Sue Moss, Associate Director, Cancer Screening Evaluation Unit, Institute of Cancer Research, Sutton
-
Professor Miranda Mugford, Professor of Health Economics and Group Co-ordinator, University of East Anglia
-
Professor Jim Neilson, Head of School of Reproductive & Developmental Medicine and Professor of Obstetrics and Gynaecology, University of Liverpool
-
Mrs Julietta Patnick, National Co-ordinator, NHS Cancer Screening Programmes, Sheffield
-
Professor Robert Peveler, Professor of Liaison Psychiatry, Royal South Hants Hospital, Southampton
-
Professor Chris Price, Director of Clinical Research, Bayer Diagnostics Europe, Stoke Poges
-
Professor William Rosenberg, Professor of Hepatology and Consultant Physician, University of Southampton
-
Professor Peter Sandercock, Professor of Medical Neurology, Department of Clinical Neurosciences, University of Edinburgh
-
Dr Susan Schonfield, Consultant in Public Health, Hillingdon Primary Care Trust, Middlesex
-
Dr Eamonn Sheridan, Consultant in Clinical Genetics, St James’s University Hospital, Leeds
-
Dr Margaret Somerville, Director of Public Health Learning, Peninsula Medical School, University of Plymouth
-
Professor Sarah Stewart-Brown, Professor of Public Health, Division of Health in the Community, University of Warwick, Coventry
-
Professor Ala Szczepura, Professor of Health Service Research, Centre for Health Services Studies, University of Warwick, Coventry
-
Mrs Joan Webster, Consumer Member, Southern Derbyshire Community Health Council
-
Professor Martin Whittle, Clinical Co-director, National Co-ordinating Centre for Women’s and Children’s Health, Lymington