
Notes
Article history
The research reported in this issue of the journal was commissioned by the HTA programme as project number 05/43/01. The contractual start date was in January 2007. The draft report began editorial review in June 2009 and was accepted for publication in January 2010. As the funder, by devising a commissioning brief, the HTA programme specified the research question and study design. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the referees for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
None
Permissions
Copyright statement
© 2010 Queen’s Printer and Controller of HMSO. This journal is a member of and subscribes to the principles of the Committee on Publication Ethics (COPE) (http://www.publicationethics.org/). This journal may be freely reproduced for the purposes of private research and study and may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NETSCC, Health Technology Assessment, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2010 Queen’s Printer and Controller of HMSO
Chapter 1 Background and project design
Introduction
In vitro fertilisation (IVF) treatments for infertility involve the collection of eggs from the woman, usually after hormonal stimulation, and the fertilisation of those eggs in the laboratory using sperm from the partner or other donor. Fertilisation is achieved either by incubation in a dish (standard IVF) or by injecting the sperm directly into the egg (intracytoplasmic sperm injection, ICSI). The resultant fertilised eggs are cultured in the laboratory for 2–3 days to form embryos typically containing between two and eight cells. If fertilisation and culture are successful, then one or more embryos will be transferred to the woman (fresh embryo transfer cycle) and the remainder may be frozen for future use in subsequent frozen embryo transfer cycles. If, for some reason, it is not appropriate to transfer any fresh embryos, they may all be frozen. In any one attempt to become pregnant a woman may have several egg retrieval cycles, each with a fresh transfer and potentially several frozen transfers. In order to increase the success rate, embryo transfer cycles historically have involved the transfer of multiple embryos, leading to high rates of multiple pregnancies. In recent years UK clinics have been restricted to a maximum of two embryos, or three in exceptional circumstances, which has almost eliminated triplets and higher-order multiple births. However, the standard practice of transferring two embryos does lead to a high twin incidence, and twin births do carry a higher risk of maternal and infant morbidity. Thus, many advocate a policy of single embryo transfer (SET) to reduce this burden. In the UK the regulatory authority, the Human Fertilisation and Embryology Authority (HFEA), has now implemented a multiple birth minimisation policy aimed at reducing the twin birth rate to 10% over a number of years.
The Manchester IVF centres (St Mary’s Hospital and Manchester Fertility Services) have had a long-standing interest in reducing the incidence of twins and increasing the use of SET. The towardSET? project described here was conceived in 2006 both as a continuation of statistical modelling work we had begun on a Manchester patient cohort1,2 and as a response to a specific call from the UK National Institute for Health Research (NIHR) Health Technology Assessment (HTA) programme. HTA funding was obtained and the project was undertaken between January 2007 and April 2009. At that time it was clear that patients might be sceptical of any move towards increased use of SET. In conceiving this project, we were very aware that patient perspectives were crucial to the implementation of any twin-reduction policy and indeed that patients might not be persuadable. Thus, we emphasised the movement towards SET, rather than presuming that it was the destination, and maintained a small question mark to demonstrate this doubt – see Figure 1.
FIGURE 1.
The project logo.
The concept was to combine complex statistical modelling of currently available data with in-depth considerations of patient perspectives and allow the two strands to each impact on the other.
The time period in which we undertook this project was one of very active developments in UK policy towards reducing the twin rates associated with IVF and SET. These developments are discussed below (see Research context).There was significant interaction between that policy development and this project, and much of the emphasis of this work was changed by policy developments, even though the formal protocol remained unchanged.
Structure of this report
This chapter gives the background to, and motivation for, the project then outlines the project design, informally reviews the relevant literature, and finally introduces some of the methodology used. Subsequent chapters describe the project components, with detailed methodology and results along with discussion. Chapter 2 describes the work on patient perspectives. Chapters 3 and 4 develop predictive models based on two large datasets, and then Chapter 5 uses these models to predict and simulate elective single embryo transfer (eSET) policies. In Chapter 6 we describe patient reactions to the policy options. Chapter 7 discusses specific issues around the use of routine data for studies such as this one, and the final chapter attempts to synthesise the components and draw out the important conclusions, implications for practice and needs for further research.
Throughout this report, additional material giving details of the methodology is provided that is not necessary in order to understand the results and conclusions. The sections containing such material are indicated with an asterisk and can be omitted by the reader without losing any of the cohesiveness of the report.
The towardSET? project design
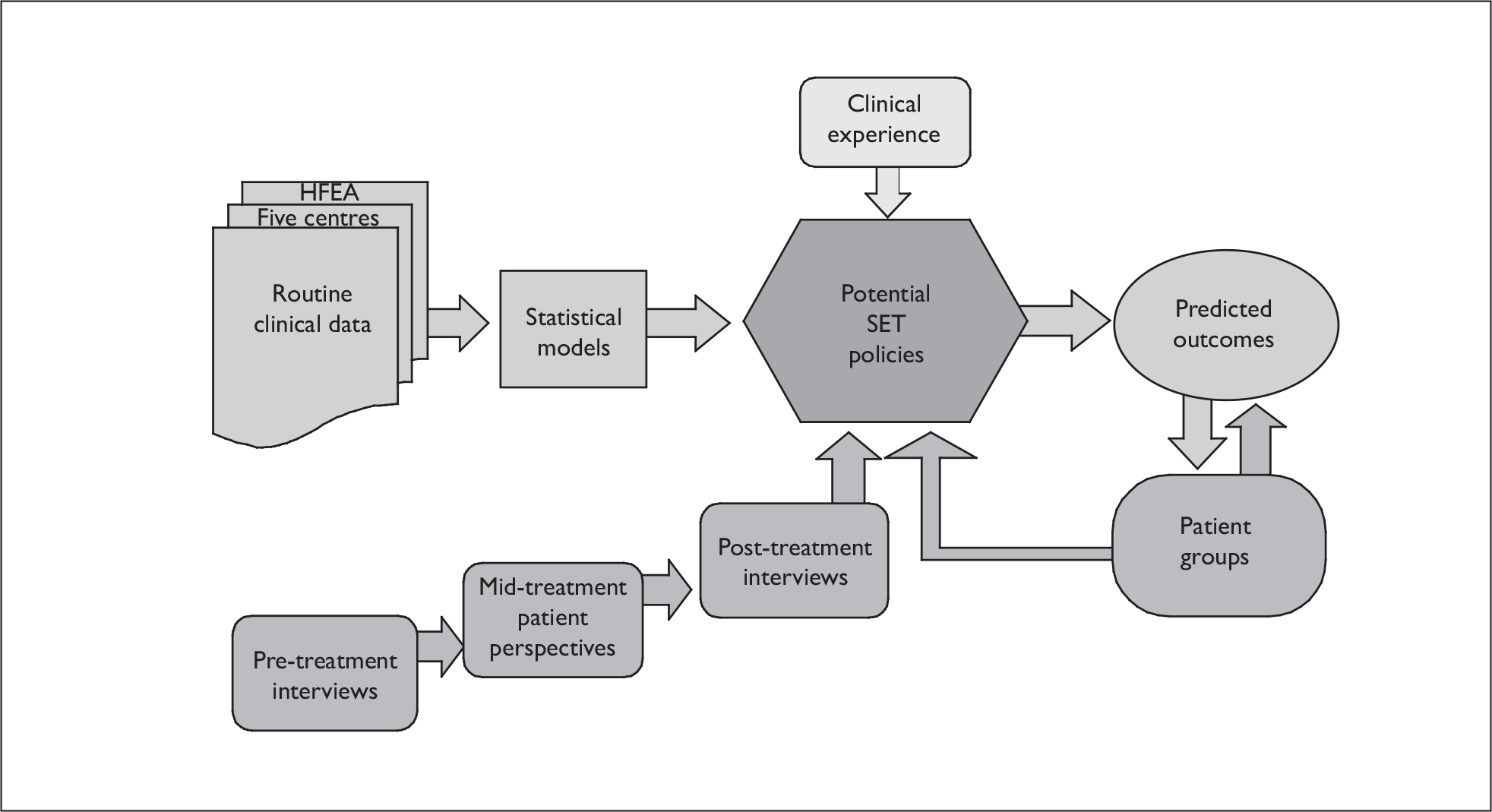
Figure 2 shows, in schematic form, the structure of the project. The major elements were statistical modelling of routine data to obtain information on factors affecting twin rates and predictive models, alongside work with patients at various stages of treatment to understand their perspectives. Following this work, we considered various policy options informed by the modelling, patient perspectives, clinical opinion and (crucially) the policy environment and estimated their effects. The project outcomes were then fed back to patient groups and their views incorporated into our assessments.
FIGURE 2.
Schematic of project structure.
Research objectives
The project objectives as defined in the protocol were:
-
To collate high-quality cohort data from a series of individual treatment centres to be considered alongside HFEA data.
-
To develop predictive models from each of the data sources for (a) twinning probabilities in patients treated with double embryo transfer (DET) from fresh or frozen embryos, (b) success probabilities in couples receiving SET, and (c) potential singleton and twin rates if couples had been offered SET. In each case, to consider the full range of potentially prognostic factors associated with the couple and the available embryos, including age, fertility history, cause of infertility and embryo quality (the last is not available for the HFEA data).
-
To understand, through qualitative work, the patients’ perspective on these choices as they travel through the treatment process.
-
To involve couples in developing patient-relevant outcome measures for IVF treatment programmes and a range of potential choices and treatment options for consideration.
-
To consider a number of potential outcomes and denominators (including, but not limited to, per couple, per embryo transfer cycle, per stimulated cycle started, per completed cycle) from a clinical and patient perspective, and to predict these for potential treatment scenarios based on proposals in the literature and developed with patients and clinicians.
-
To use the modelling results to investigate with patients the acceptability of the scenarios and the changes in public policy required to make SET acceptable.
-
To suggest appropriate randomised controlled trials (RCTs) to test the effectiveness of the most favourable policies.
Research context
At the time this study was designed (early 2006) there was growing awareness that the high twin birth rate from IVF-treated couples was potentially a significant public health issue and a burden on health-care resources. Standard care was to transfer two embryos if available, in all but exceptional cases. Although a few individuals and centres were advocating SET in order to reduce the chances of twin births, it was rare in practice. The decision whether to have SET or DET was made by the individual couple following advice and counselling from the clinical staff. Thus, it was important to understand the patient perspective on twins and SET. Even if one were to advocate a policy of compulsory SET, in formulating such a policy the patients’ views would need to be considered.
After the start of this project the HFEA commissioned an expert group to consider the incidence and consequences of multiple births3 and undertook a consultation exercise leading to a policy decision in 2008 requiring clinics to reduce their twin rate, incrementally with a target rate reducing to 10% twins per live birth event (LBE) over a number of years. Rather than restrict DET to certain groups of patients, or mandate SET for other groups, the UK policy is based around target twin rates for individual clinics, with each clinic needing to develop its own policy (known as a Multiple Birth Minimisation Plan) to meet the target. This target started at 24% (approximately the national average in 2007) twins per LBE for the reporting year of 2009, with a series of interim targets. The emphasis of this project was therefore centred around the implications of this specific UK policy and the need for clinics to be able to develop strategies to meet the targets, and this formed the basis of discussion with patients and simulations of policy.
Research methods
We undertook an interdisciplinary approach in which quantitative retrospective cohort studies and predictive modelling were embedded within qualitative studies of patient perspectives in an integrated manner. The various components are described below.
Literature review
We informally reviewed the literature to (1) identify studies where SET has been compared to DET, both randomised trials and cohort studies, (2) identify prognostic factors to be included in the models, (3) identify series in which published data are available with sufficient detail to be used in model verification, and (4) identify strategies for the use of SET in clinical practice and the obstacles to their adoption. The results of this review are incorporated into the background section below (Informal review of the relevant literature).
Retrospective cohort studies (objectives 1 and 2)
We undertook two linked cohort studies to determine factors associated with success and twin rates in SET and DET. The sample was designed to include the full spectrum of patient settings, including NHS-funded patients attending a centre offering only NHS treatment, private patients attending a fully private clinic, and NHS-funded, fee-paying NHS patients and self-funded (private) patients all treated within NHS clinics. The centres included cover a range of policies on SET, embryo selection and freezing.
Specifically we collated data from the following sources:
-
Data from the national HFEA register covering 2000–5. This provides outcome data on each embryo replacement cycle conducted in the UK, with a useful, but not exhaustive, set of patient, partner and cycle factors. However, this dataset contains no embryo-level data. The data are anonymised, but records relating to the same couples are linked. There are issues about data quality in such databases (and these are assessed in Chapter 7), but the HFEA Historic Audit project at least validates the quality of the data in cycles that generated a clinical pregnancy or live birth.
-
A collection of single-centre, information-rich datasets with embryo quality measures on all transferred embryos. We extracted a cohort with full outcome data for treatments completed in the 2000–5 time frame. Six centres agreed to take part in the study and provide data, giving an estimated 13,000 cycles. In practice, two of the centres failed to supply data owing to changes in local circumstances, but one additional centre was recruited. The number of patients in the existing centres was significantly larger than originally estimated and these centres gave us a database with 23,582 cycles, which was considered more than sufficient to achieve the stated aims.
-
During the period of the cohorts, two Manchester centres (one NHS only, one private patients only) had a day 1 embryo freezing policy, which means that a maximum of four embryos were available on day 2 for selection of one (SET) or two (DET) for transfer. The other collaborating centres were all NHS centres of excellence with a mixture of NHS and fee-paying patients. They all had an embryo freezing policy that allowed all embryos to be available for selection on the day of transfer, with freezing taking place after selection of embryos for fresh transfer, in contrast to the Manchester centres.
-
We also intended to utilise a dataset from a prospective study of the use of amino acid profiles for the prediction of embryo viability. Unfortunately this study failed to complete owing to technical issues and so could not be used formally, although the project did contribute informally. However, we did utilise the embryo grading data from that study to inform the simulation studies of Chapter 5.
Formal sample size computations were not appropriate here as the aim was to develop predictive models, not to formally test hypotheses. Experience and heuristic arguments suggest that datasets in excess of 10,000 cycles are required for this exercise. Rules of thumb for reliable predictive modelling suggest 10–20 events per considered variable. We expected to have around 40 potential variables, which, with a success rate of 20%, would imply a minimum dataset of 4000 independent cycles, around 8000 patients, given that many patients have multiple cycles and we wished to look at multicycle end points. The sample size was, in practice, determined by the need to have a representative set of centres and a sufficiently long time span to capture treatment histories along with computational feasibility, and the numbers analysed were well in excess of the minimum numbers above.
From these data we developed a series of statistical models for the per-embryo replacement outcomes as a function of the patient, embryo and treatment characteristics.
The aim of this phase of the study was to produce a series of statistical models relating outcome (singleton, twins) to prognostic indicators for fresh and frozen embryo transfer across multiple egg retrieval and embryo replacement cycles. These models identify prognostic factors leading to high risk of twins and high chance of success, and provide the basis for the consideration of the role of SET.
The analysis of the HFEA data is described in detail in Chapter 3 and the individual centre cohorts in Chapter 4.
Patient perspectives (objectives 3 and 4)
In this phase of the study we undertook qualitative interviews with couples who were in the process of undergoing IVF treatment. The aim was to explore the patient perspective of treatment choices as they travel through the treatment process. Therefore interviews covered a range of decision-making stages: (1) waiting list; (2) after the first information meeting and clinic appointment (pre-treatment); and (3) after the second cycle of treatment. This last group allowed for views to be assessed once the outcome of an initial treatment cycle was known and after having the opportunity to reflect on the choices through a second treatment cycle. It was planned that 5–10 couples per stage would be invited to take part in this study. Purposive sampling techniques were employed to ensure maximum diversity of sample including different female ages, parity, duration of infertility and source of funding (which is related to the number of treatment cycles that the couple receive).
Specifically we planned:
-
To assess couples’ knowledge and views on embryo transfer and twin birth prior to treatment, after provision of information and post treatment.
-
To explore the potential facilitators and barriers to eSET.
-
To evaluate the patient perspectives on the decision-making process during key stages of the treatment journey, including consideration of measures of success and attitudes to twin births.
-
To determine the level of involvement couples would prefer in the decision-making process regarding treatment choices.
-
To establish at what stage (pre-treatment) information regarding treatment choices about eSET should be presented, and in what format.
-
To explore couples’ attitudes to research, in particular their understanding of randomisation into a clinical trial.
Predictive modelling (objectives 5 and 6)
Based on our survey of the literature and the qualitative work above, we aimed to identify a limited number of potential treatment policies and choices involving the use of SET, based on a patient perspective of the whole treatment course. These were to include, but not be limited to, SET cycle choices, single DET versus two cycles of SET (with the second fresh or frozen), and include a range of couple prognoses. We used the models developed above to predict the outcomes of the various scenarios for the whole range of prognostic factors, with estimates of their reliability. This predictive modelling encompassed both direct prediction from the models and the use of model parameters (and their associated uncertainties) to make predictions for treatment policies not contained within the source datasets. In developing the models we took care to consider the correlations between cycles, and to assess the errors in the prediction, validating against both internal and external data where these existed. This simulation work is described in Chapter 5.
We planned to establish three focus groups (two NHS, one private sector) of patients and partners who had been through the IVF process to present to them the results from the modelling process. This methodology has been successfully employed to explore sensitive issues. 4,5 A convenience sample of couples who had undergone IVF treatment were to be invited to participate in a structured focus group. Following a general discussion about the various treatment options, a selection of scenarios from the statistical modelling were presented to the groups in a user-friendly format. The groups were asked to rate and discuss the scenarios. This allowed us to explore the responses to the results and determine potential barriers to the proposed solutions and could have led to alternative strategies to be investigated. Owing to changes in circumstances and availability, the composition and conduct of these focus groups was somewhat different from that originally planned and is described in detail in Chapter 6.
Economics
It was planned to synthesise the results of this study with ongoing economic analyses being conducted elsewhere. Unfortunately these studies did not report during the time frame of this study; however, the data generated here have been supplied to one of the groups undertaking economic analysis of SET, and that work will be conducted outside the scope of this project.
Towards randomised controlled trials (objective 7)
Ultimately any proposed treatment strategies would need to be tested in rigorous RCTs. Based on the knowledge gained from these studies we planned to suggest a design for such a trial or trials, defining patient populations, treatments and end points. Such a trial should also include a rigorous health economic assessment. However the failure of the ECOSSE trial (see below), and the fact that, in the UK, policy has now been decided, suggest that any such trial may well be infeasible, and so, although such trials are still needed, we confined ourselves to a general discussion of principles rather than detailed designs (see Chapter 8, Implications for research).
Ethical approval and governance
Ethical approval was obtained from the South Manchester Research Ethics Committee (06/Q1403/254 and 06/Q1403/255). Sponsorship was from the University of Manchester (PS120906). A Project Management Group, consisting of the named investigators, met regularly to oversee the day-to-day running of the project. An Advisory Group consisting of representatives of the centres contributing data, the HFEA and a patient group (Table 1) was established to provide oversight of the study.
| Jenny Dunlop | IVF counsellor | St Mary’s Hospital, Manchester, and Manchester Fertility Services |
| Tony Rutherford | Consultant obstetrician and gynaecologist and Chair of the BFS Policy and Practice Committee | The Leeds Reproductive Medicine Unit |
| Jan Hogg | Lead embryologist | |
| Steve Troup | Scientific director and member of ACE executive | The Hewitt Centre for Reproductive Medicine, Liverpool |
| Natalie Scott | Embryologist | |
| Jane Saxton | Senior embryologist | Centre for Reproductive Medicine and Fertility, Sheffield Teaching Hospitals NHS Trust |
| Juliet Tizzard, then Jessica Watkin | Policy manager | HFEA |
| Cheryl Fitzgerald | Consultant gynaecologist | St Mary’s Hospital, Manchester |
| Karen Arnold | Fertility nurse practitioner | |
| Debbie Falconer, Louise Warner | Principal clinical embryologists | Manchester Fertility Services |
| Clare Lewis-Jones | Chief executive | Infertility Network UK |
Informal review of the relevant literature
We undertook a narrative literature review. Given the nature of the project we did not attempt a systematic review (a Cochrane review6 of the trials has already been undertaken and recently revised), rather we sought to set the context of the project, identify relevant methodology and identify putative prognostic factors to inform the modelling.
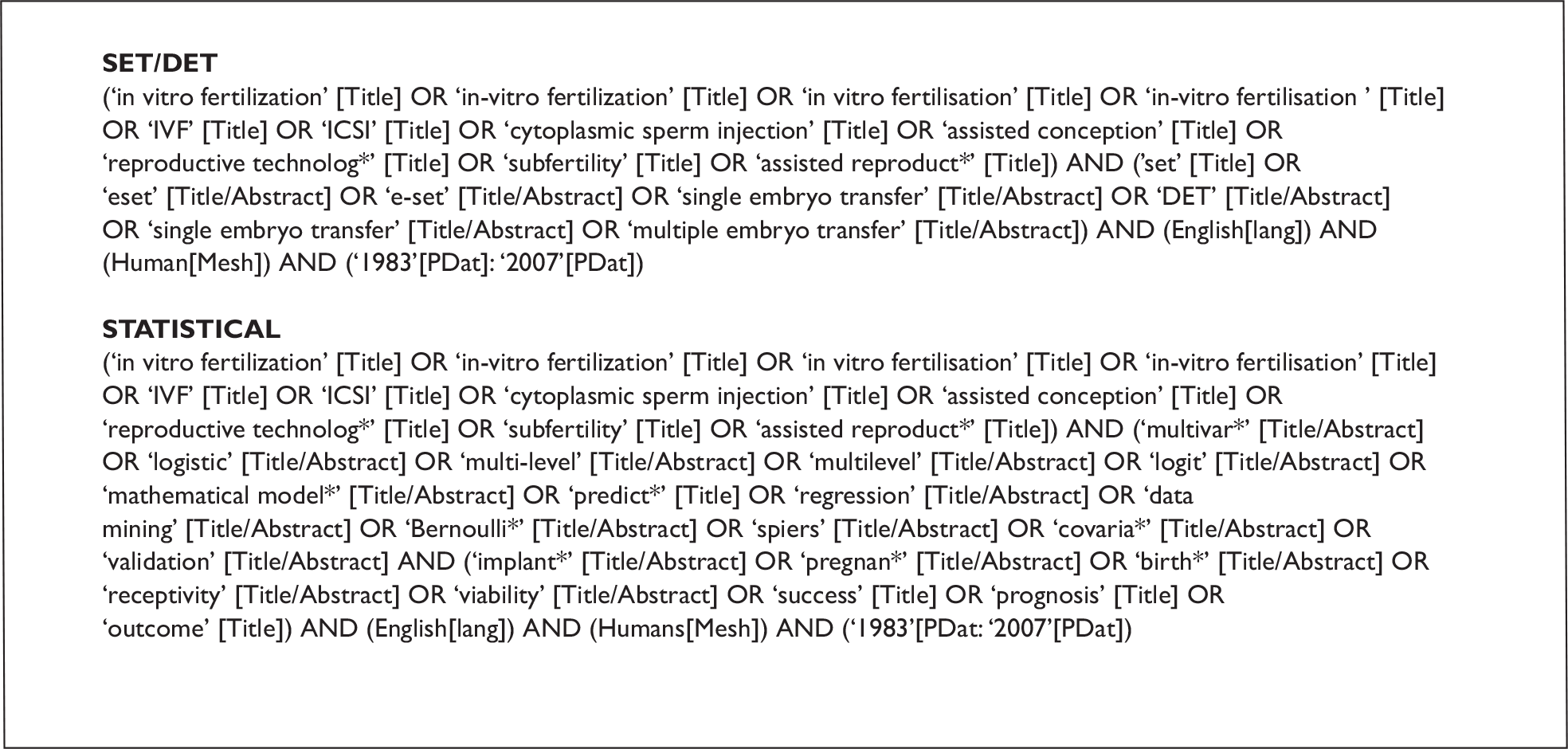
Literature was identified from expert knowledge within and without the study team and Advisory Group, from tracking the references therein, and from a formal search of the Web of Science (see Figure 3 for search terms) and PubMed (Figure 4) databases.
FIGURE 3.
Search strategy for Web of Science.
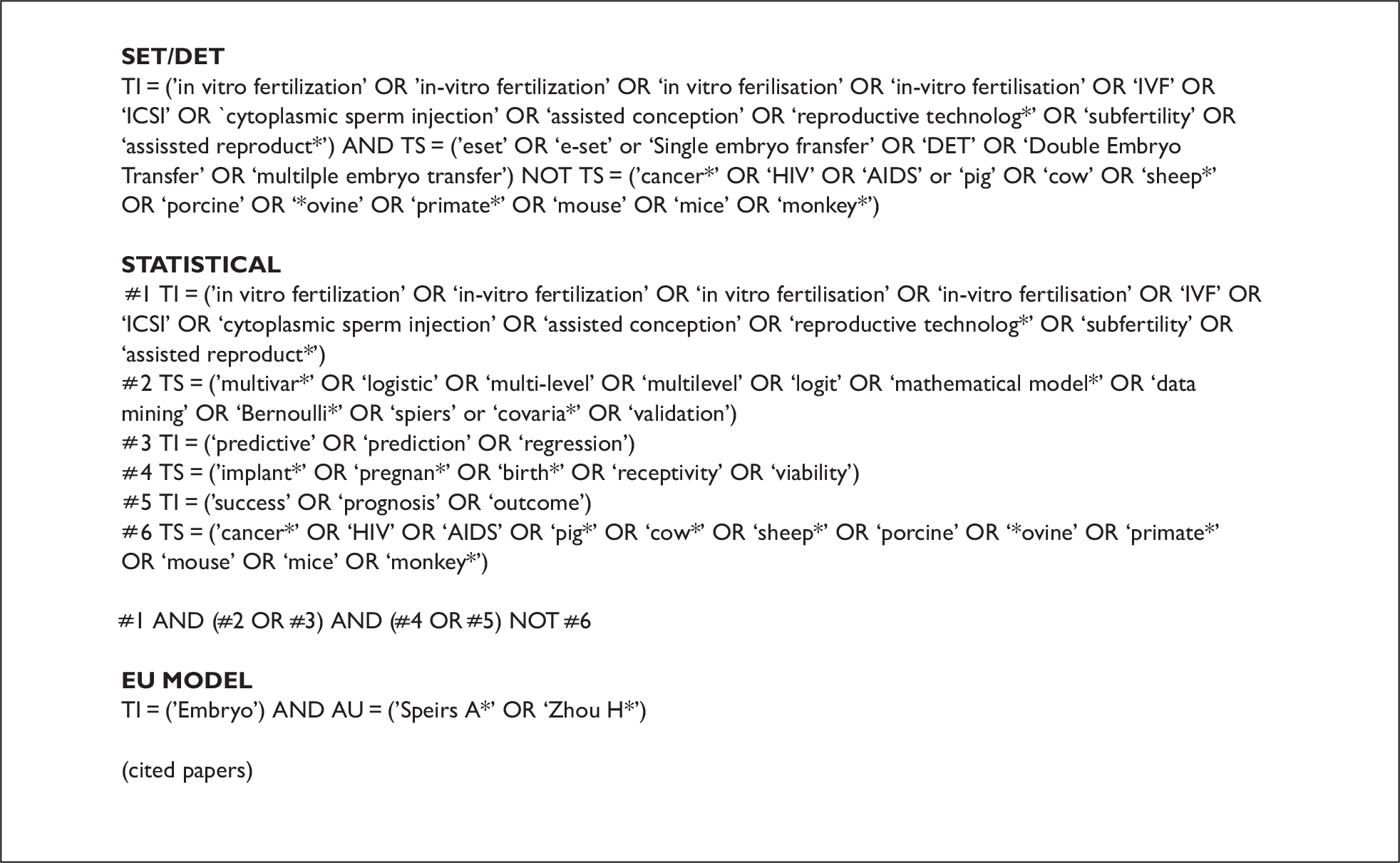
FIGURE 4.
Search strategy for MEDLINE/PubMed.
Single embryo transfer
Elective single embryo transfer has been widely advocated on the basis that it reduces the number of multiple pregnancies, and the consequent risk to the mother and offspring (e.g. see Pinborg7). Many cohort studies (reviewed in references 8 and 9) suggest that, on a per-transfer cycle basis, SET does indeed reduce twinning rates compared with DET but that this is associated with a reduced success (live birth) rate. This has been confirmed in a limited number of relatively small randomised trials7, although no good-quality randomised data are yet available. 6 The subsequent replacement of single thawed embryos increases the pregnancy rate per episode of IVF on a cumulative basis (e.g. Lukassen et al. 10). Strategies to implement SET are likely to require evaluation across multiple cycles of embryo transfer: in the UK a trial was organised comparing a single fresh cycle of DET with two cycles of SET, one fresh and one utilising a frozen embryo from the first cycle. This trial (the ECOSSE trial, led by Dr Bhattacharya, Aberdeen) was subsequently suspended apparently because of patient reluctance to enter the study (Dr S Bhattacharya, Aberdeen Maternity Hospital, 2009, personal communication).
Subsequent to the start of this project, in 2008 the UK HFEA, after a review and consultation process,3 adopted a policy requiring clinics to reduce the number of twin births as a proportion of live births to 10% over a 3-year period from 2009. The British Fertility Society (BFS) and Association of Clinical Embryologists (ACE) have produced clinical guidelines, with input from the towardSET? project team, reviewing the evidence and supporting this policy change. 11
Elective single embryo transfer trials
Six RCTs, comparing forms of SET with DET in, generally, patients with a good prognosis,10,12–18 and a Cochrane review6 have been undertaken. SET alone gave poorer outcomes in terms of live birth rate per embryo transfer cycle but reduced the incidence of twins to a rate comparable with natural pregnancies. In two small randomised trials, SET with two episodes of embryo replacement was associated with a similar live birth rate as DET but with a significant reduction in the number of multiple births (Lukassen et al. 10 and Thurin et al. 15). There is a lack of large, good-quality trials comparing practical policies with appropriate end points. Cohort studies8,9 show similar conclusions, but these are harder to interpret as the patients undergoing SET are selected by a combination of the clinician and the couple. Most of these analyses used simple per-transfer end points and failed to account for the correlations between cycles from the same patients. Clinical experience in Sweden and elsewhere8 suggests that a legal prescription towards eSET has led to an increased use of SET while maintaining success rates and dramatically reducing twin rates, but these comparisons suffer from the use of historic control data and the use of per-transfer outcomes.
Clinician and regulatory perspectives on eSET
There is widespread agreement among IVF clinicians that, at least in patients with good prognosis, policies to prevent multiple pregnancies, including twin pregnancies, are to be preferred. Although there are counter-arguments, for example Gleicher and Barad,19 claiming that if one assumes that the majority of patients want two babies, a comparison of risk between a single event of IVF twins and two separate IVF singleton pregnancies can be in favour of twins. Many recommendations have been made to increase the proportion of eSET and this is now legally prescribed in Sweden (reviewed in Bergh8). However many centres in the UK are reluctant to adopt policies that might lead to a reduction in pregnancy rates, particularly in the format published by the HFEA, and particularly where patients pay directly for the treatment. The format of outcome data published by the HFEA allows centres to be rated in ‘league tables’. This is widely seen as being of commercial value to centres in the top echelons; SET is more popular where the treatments are publicly funded, as in northern Europe. For example, in 2005 in Manchester within the NHS at St Mary’s Hospital the SET rate was 30%, while in the private sector at Manchester Fertility Services it was 10%. The definition of treatment success rate is crucial here20 but, as yet, there is no consensus on a measure that takes the whole treatment programme, including embryo freezing, into account.
Patient perspectives on SET
Opinions on SET may differ between health professionals/policy makers and patients undergoing treatment; patients often view twins as a positive and not a negative outcome. Blennborn et al. 21 interviewed 272 patients undergoing IVF (males and females) using a semistructured questionnaire to investigate the couple’s decision-making in IVF treatment. Factors associated with opting for SET were previous childbirth and the availability of spare embryos to freeze. DET was more likely in couples who had undergone previous IVF treatment, and in those who held the belief that transferring two embryos would increase their chances of becoming pregnant. They also noted that, in spite of receiving good information on the associated risks, most couples preferred to have two embryos transferred. Pinborg et al. 22 conducted a national survey in Denmark to explore the attitudes of IVF/ICSI twin mothers towards twins and SET. They found that this group of mothers was more likely to desire twins as a first child than either a singleton or a non-twin mother group. This group appeared to accept the known clinical risks of twins, as well as the associated social and physical outcomes of caring for two babies. Acceptance of SET was influenced by the experience of a very low birthweight baby; this presumably heightened awareness of morbidity and mortality outcomes in multiple birth. Many other studies have supported the view that patients undergoing IVF show a preference for twin pregnancies. 23–25
In view of the evidence of patient preference for having two embryos transferred, Murray et al. 26 sought to investigate methods that might improve the acceptability of SET. Couples undergoing IVF treatment were randomised to one of three groups: group 1 (control) received the standard clinic information pack; group 2 received the standard pack plus an extra information sheet outlining the possible adverse outcomes of twin pregnancy; group 3 received the same as groups 1 and 2 with an added 10-minute discussion with a member of staff, focused on the information on twin pregnancy. No new information was given, although couples could ask specific questions. The results revealed that neither method increased couples’ knowledge of the risk of twins or changed their attitudes towards SET. This is perhaps not surprising as attitudes and beliefs develop over extended periods of time and can be resistant to change. 27 This particular intervention was not specifically targeted and did not allow for the member of staff to explore and work with the couple’s belief systems.
The clinical effectiveness and cost-effectiveness of SET cannot be fully assessed without conducting an RCT. Given the strength of feeling concerning choosing between SET and DET, and the emotional effects of treatment, the design and conduct of an RCT with this patient group would require careful consideration. Porter and Battacharya25 undertook an exploration of the opinions of patients undergoing IVF and the views of staff of a proposed trial of eSET. They found that patients lacked awareness of the risks of multiple births. Opinions of the proposed RCT were largely adverse, except in younger women. Although staff appreciated the need for a thorough evaluation of SET, the notion of a double-blind RCT raised both practical and ethical concerns, which often conflicted with their caring role.
Research that has emerged during the conduct of this study has continued to reinforce the strong patient preference for twins, while exploring methods of understanding the complex decision-making process of women and couples in treatment. Twisk et al. 28 presented a range of scenarios to women (in the stimulation phase of IVF or ICSI plus thawed/frozen embryos if available) to assess whether they would be willing to accept a lowered probability of pregnancy from SET in order to reduce twin pregnancies. When women were presented with a scenario in which the pregnancy rate of SET and DET were equal, 46% chose SET. However, once the pregnancy rates were adjusted to show that SET was 1%, 3% and 5% less effective than DET, the preference for SET fell to 36%, 24% and 15% respectively. Similarly, when women were asked to consider additional cycles of SET to optimise pregnancy rates, preference rates began to decline after three treatment cycles. The findings show that the strong desire for a pregnancy outweighed the need to avoid a multiple pregnancy. They also note that treatment preferences may be different in couples who are self-funding.
van Peperstraten et al. 29 used in-depth interviews with 20 patients and 19 IVF health professionals in the Netherlands to explore in more detail the factors that may influence treatment decisions. They found that couples and professionals lacked understanding about SET, and both groups were not clear about the advantages of performing SET in practice. There was concern about the lowered chances of success when using frozen embryos. Furthermore, in order to improve the uptake of SET both groups discussed the need for a positive reimbursement system for this treatment option.
The higher-risk profile associated with multiple pregnancies is not always recognised or acknowledged by couples undergoing treatment. One recent study investigated women’s and men’s understanding of information and the decision-making process in SET. 30 They found that, although women were aware of fetal risks associated with a twin pregnancy, they were less well informed about maternal risks. In this small sample of 54 couples, acceptance of SET was associated with previous pregnancy, younger age and duration of infertility. One interesting study investigated whether the strength of the preferences for twins would be mitigated by providing knowledge of the more severe adverse outcomes. 31 This was compared with the outcome of not achieving a pregnancy. A standard gamble method was used to explore preferences in 74 women waiting for IVF treatment. Scenarios included giving birth to a child with physical or cognitive or visual impairments and experiencing a perinatal death, without a subsequent pregnancy. A further scenario considered another birth outcome, that of a very preterm birth with morbidity and mortality left unspecified. The findings revealed that some women found the risk of severe child disability associated with DET to be more desirable than not having a child at all. The authors note that this construction of ‘treatment success’ is not in line with that of clinicians. They speculate that this may go some way to explain why couples continue to request DET, whether or not they have a good understanding of the associated risks of twin pregnancy.
In order for patients to make informed choices, accurate and relevant information is essential to this process. 32 However, studies in subfertile couples undergoing IVF treatment have shown that information to date has either not been adequate or not been presented in a relevant and targeted way. 26,30 The work of Scotland et al. 31 has crystallised the strength and magnitude of the preference to achieve a pregnancy at all costs. This suggests that for many couples there is a need for a more in-depth information-giving process, which takes into account attitude and belief systems and allows patients to make their own informed decisions. Therefore, further research is required to understand the specific information needs of this patient group and the presentation and timing of this information.
Embryo selection for eSET
The ability to select a ‘top-quality’ embryo for transfer is crucial to the success of eSET (see, for example, De Neubourg et al. 33). Selection is normally made on morphological grounds, with different scoring systems in use in different centres, based predominantly on embryo developmental stage (i.e. cell number, and morphological appearance including cell size, regularity, fragmentation, etc.). There is considerable interest in selection criteria34 and in alternative markers to morphology. 35,36 Selection of embryos by extended in vitro culture to the blastocyst stage has received much attention,37–39 and a Cochrane review,39 and was one approach suggested in the ACE/BFS guidelines. 11 Invasive pre-implantation genetic screening has been advocated as a potential approach and is available clinically. 40 However, there is little evidence for its effectiveness in increasing treatment outcomes and, in contrast, recent prospective RCTs have provided evidence that the invasive nature of the embryo biopsy procedure may be detrimental. 41,42 Treatment policies on the length of time for which embryos are cultured before transfer or freezing and the use of cryopreservation differ between centres; thus, different centres will have differing numbers of embryos at different stages from which to select. To our knowledge, no comparative or modelling studies have been undertaken that consider the impact of different cryopreservation/selection policies, and it is crucial to capture this in any assessment of the impact of SET. Horne et al. 43 prospectively compared day 1 freezing with day 2, with transfer of fresh embryos on day 2 in both arms of the study. They found that the day 2 freezing strategy led to a higher live birth rate from the fresh cycle, presumably as a result of enhanced embryo selection because all embryos were available for selection for fresh transfer, but a lower pregnancy rate per frozen embryo cycle. Both strategies yielded similar final cumulative pregnancy rates.
Economics of eSET
Few studies looking specifically at eSET from the economic perspective have been reported (reviewed in Bergh8 and Fiddelers et al. 44). From a societal perspective, these indicate that the savings in health costs associated with twin pregnancies may offset the direct additional costs of the repeat SET cycles required to maintain the same take-home baby rate. However, in many cases the direct costs of treatment are borne by the patients, while the costs associated with multiple births are (in the UK) met within the NHS. A recent publication45 studied the impact of multiple births from a UK perspective. In addition, there are less readily quantifiable costs associated with a potential requirement for extra treatment cycles per baby in eSET.
Inference from patient cohorts
Three approaches have been used to extract information from retrospective data from patient cohorts:
-
Estimation of pregnancy or live birth rates arising from SET versus DET, with a range of outcome definitions and patient subsets. 46–51 These suffer from inbuilt biases in the selection of patients for SET. In many retrospective datasets it is difficult to know the true reason for SET, unless only one embryo is available. In some studies this is ‘patient choice’, in others it is perceived clinical need (patients for whom twin pregnancies are contraindicated) or some combination of the two.
-
Logistic regression of success rates and twin rates in DET have been commonly used to determine factors that predict a high twinning probability (e.g. Strandell et al. 52). These methods potentially identify high-risk groups but give no information on the potential outcomes if SET were used.
-
Explicit modelling of embryo and recipient (uterine) effects. Within this framework, models derived from DET data can be used to predict SET outcomes. The first published example utilising this embryo–uterus (EU) approach, Hunault et al. ,53 uses the Zhou and Weinberg model,54 but attributes all the prognostic parameters to the embryo, fitting a constant uterine receptivity (U). Analysis of a Manchester series2 also used the EU approach and considered the possibility that factors may influence both the E and U components, but there was insufficient data to identify which of the submodels (E or U) was appropriate for each parameter. A Bayesian approach with the possibility of incorporating a hierarchical structure was examined by Dukic and Hogan,55 although issues surrounding prior distributions and parameter identifiably were observed. These models have the advantage that they allow predictions of SET outcomes from multiple embryo transfer data, avoiding the selection issues in the retrospective comparative studies. The models make other assumptions, particularly around the independence of the embryo and uterine effects, although there is no evidence that these assumptions are inappropriate.
Other methodological approaches that have received attention are case-based reasoning algorithms,56 causal models57 and Markov chain models. 58 The last study provided an alternative to time-to-event analysis for multiple cycles where in each cycle a patient can move across outcome states. These methods are not readily applicable to the questions posed by this study, so are not considered further. They may or may not have advantages in other situations.
In all these types of analysis considerable care and expertise is required in conducting and interpreting the analyses, not only because of the inbuilt biases of the observational data but also to account appropriately for the non-trivial correlation structures between multiple egg-collection and replacement cycles from the same individuals and from centre and cohort effects. Such considerations are rare in the analyses published to date.
Prognostic factors for IVF success
Retrospective studies have identified a number of patient, embryo and treatment factors that are associated with treatment success. In order to derive a list of factors that should be considered in any modelling exercise, a review of the literature was undertaken in May 2007 and updated in November 2008. Searching electronic databases identified 51 papers in which potential prognostic factors were analysed for their influence on an IVF-related response. The tables below were collated for each type of risk (broadly categorised as age, diagnosis, egg and embryo numbers, embryo quality, biological, treatment, and other factors). These show studies where an association between the risk factor and the response was found, but do not include studies where a risk factor was tested but not found to be of significant interest. The results also indicate the nature of the observed effect, the size of the dataset and the methodology employed. There was no attempt made to synthesise this evidence or to assess the quality of the studies and their relevance to the general population of patients undergoing IVF.
As expected, age appears to be the variable with the greatest body of evidence to support an impact on IVF response (Table 2). Though many studies include age as a continuous variable in the linear predictors and universally observe a decline in success as patients get older, studies that allowed more complex representations of age tended to find the greatest success rate for patients in their twenties. There is also strong evidence that various measures of embryo quality can impact on success rates (Table 3). This is despite the fact that most studies adopted an aggregated approach in taking a measure to represent all embryos. This is often taken with a measure of egg or embryo number, such as the number of retrieved oocytes or fertilised embryos (Table 4). Both studies adopting the EU approach, which avoids the necessity for aggregation, found embryo quality measures to be strongly prognostic.
| Study | Nature of effect | Dataset size | Model type – response |
|---|---|---|---|
| Akande et al. 200260 | Cubic (peak mid-20s) | 2684 embryos, 977 transfers | Logistic regression – pregnancy and birth |
| Alsalili et al. 199561 | Age (decline in success as older) | 5209 cycles (2391 couples) | Time-to-event (Cox) – pregnancy |
| Chuang et al. 200362 | Age (decline in success as older) | 1405 (1st cycle) | Logistic regression – pregnancy and cancellation |
| Commengues-Ducos et al. 199863 | Poorer prognosis ≥ 38 years | 923 transfers | Logistic regression (with REs) – pregnancy and implantation |
| Croucher et al. 199864 | Age (five bands) | 5073 (1st cycle) | Significance tests – number of oocytes, pregnancy |
| Elizur et al. 200565 | Age (banded – 26–30 years best) | 5310 cycles (with transfer) | Survival analysis (discrete) – live birth |
| Engmann et al. 200166 | Age (decline in success as older) | 7700 cycles (4417 women) | Logistic regression (robust) – birth |
| Haan et al. 199167 | Age (> 36 poorer) | 3392 cycles | Logistic regression – pregnancy |
| Haggarty et al. 200668 | Age (decline in success as older) | 602 women (1st cycle) | Logistic/ordinal – birth |
| Hunault et al. 200253 | Age | 642 women (1st cycle) | Logistic/EU model – pregnancy + twin pregnancy |
| Kupka et al. 200369 | Age (banded – peak mid–20s) | 174,909 treatments | Logistic – pregnancy |
| Lee et al. 200670 | Age (decline in success as older) | 584 transfers | Logistic – pregnancy |
| Minaretzis et al. 199871 | Age (decline in success as older) | 544 cycles | Logistic – pregnancy, birth and multiples |
| Ottosen et al. 200772 | Age | 2193 DET cycles | Logistic (robust) – pregnant vs not pregnant, twin vs not twin |
| Rhodes et al. 200573 | Age (decline in success as older) | 205 (1st cycle) | Logistic – pregnancy |
| Roberts et al. 20092 | Age (spline – cubic) | 1198 | EU model – multinomial response (live birth) |
| Roseboom et al. 199574 | Age (decline in success as older) | 222 transfers | Logistic – pregnancy |
| Sabatin et al. 200875 | Age (interaction with FSH) | 1589 | Significance tests (various outcomes), logistic regression (live births) |
| Sharif et al. 199876 | Age | 344 (1st cycle) | Logistic – pregnancy |
| Stolwijk et al. 199677 | Age (decline in success) | 757 (1st cycle) 454 (2nd cycle) | Logistic – pregnancy (1st and 2nd given first) |
| Strandell et al. 200052 | Age (decline in success) | 2107 cycles | Logistic (robust) – birth and multiple birth |
| Tan et al. 199278 | Age (decline) | 5055 cycles | Survival analysis and logistic – pregnancy + live birth + failure of pregnancy |
| Templeton et al. 199679 | Age (polynomial – cubic – peak 25–30) | 36,961 cycles (2893 women) | Logistic (robust) – birth |
| Terriou et al. 200180 | Age (decline in success as older) | 10,000 transfers (5000 build model and 5000 test) | Logistic – pregnancy |
| Tsafrir et al. 200781 | Age | 381 (over 40 year olds) | Logistic – pregnancy |
| van der Gaast et al. 200682 | Age (in relation to number of oocytes) | 7422 (1st cycle) | Not clear – multivariable – number of oocytes, pregnancy |
| Wald et al. 200583 | Age | 113 cycles (85 patients) | Neural networks, discriminant analysis, logistic – pregnancy |
| Weigert et al. 200184 | Age (grouped 26–30 best) | 8185 cycles | Logistic – pregnancy |
| Wheeler et al. 199885 | Age (decline in success) | 795 cycles | Logistic/conditional logistic – implantation |
| Zhou and Weinberg 199854 | Age (decline in success) | 161 patients | EU model |
| Study | Nature of effect | Dataset size | Model type – response |
|---|---|---|---|
| Commengues-Ducos et al. 199863 | Aggregated approach (e.g. one bad and two good) | 923 transfers | Logistic regression (with REs) – pregnancy and implantation |
| Hunault et al. 200253 | Development stage, morphology score | 642 women (1st cycle) | Logistic/EU model – pregnancy and twin pregnancy |
| Lee et al. 200670 | Cumulative embryo score (top three) | 584 transfers | Logistic – pregnancy |
| Minaretzis et al. 199871 | Embryo cell/quality | 544 cycles | Logistic – pregnancy, birth and multiples |
| Ottosen et al. 200772 | Embryo quality of best and second best | 2193 DET cycles | Logistic (robust) – pregnant vs not pregnant, twin vs not twin |
| Roberts et al. 20092 | Embryos score (spline) | 1198 | EU model – multinomial response (live birth) |
| Roseboom et al. 199574 | Average morphology score | 222 transfers | Logistic – pregnancy |
| Stolwijk et al. 199677 | Number transferred embryos of good quality | 757 (1st cycle), 454 (2nd cycle) | Logistic – pregnancy (1st and 2nd given first) |
| Strandell et al. 200052 | Number transferred embryos of good quality | 2107 cycles | Logistic (robust) – birth and multiple birth |
| Terriou et al. 200180 | Cumulative score/mean score | 10,000 transfers (5000 build model and 5000 test) | Logistic – pregnancy |
| Wheeler et al. 199885 | Total embryo score | 795 cycles | Logistic/conditional logistic – implantation |
| Wilding et al. 200787 | Oocyte score | 822 | Significance tests, linear regression (fertilisation outcome) |
| Zhou et al. 199854 | Number cells (embryo level) | 161 patients | EU model |
| Study | Nature of effect | Dataset size | Model type – response |
|---|---|---|---|
| Elizur et al. 200565 | Two embryos doubles live birth | 5310 cycles (with transfer) | Survival analysis (discrete) – live birth |
| Hunault et al. 200253 | Number of oocytes | 642 women (1st cycle) | Logistic/EU model – pregnancy and twin pregnancy |
| Rhodes et al. 200573 | Number of oocytes, % fertilised | 205 (1st cycle) | Logistic – pregnancy |
| Roseboom et al. 199574 | Number embryos | 222 transfers | Logistic – pregnancy |
| Stolwijk et al. 199677 | Number fertilised oocytes, number transferred embryos | 757 (1st cycle) 454 (2nd cycle) | Logistic – pregnancy (1st and 2nd given first) |
| Terriou et al. 200180 | Number oocytes retrieved, number transferred | 10,000 transfers (5000 build model and 5000 test) | Logistic – pregnancy |
| Tsafrir et al. 200781 | Number transferred | 381 (over 40-year-olds) | Logistic – pregnancy |
| van der Gaast et al. 200686 | Number retrieved oocytes | 7422 (1st cycle) | Not clear – multivariable – number of oocytes, pregnancy |
| Weigert et al. 200184 | Number transferred | 8185 cycles | Logistic – pregnancy |
Many studies suggested that diagnosis (Table 5), treatment (Table 6) and biological (Table 7) variables can impact on the success of IVF. Previous success or pregnancy/live birth appear to have an impact (Table 6). The evidence for an impact of biological variables such as follicle-stimulating hormone (FSH) is less clear, and the results of the meta-analysis59 were equivocal. There is some weak evidence for an impact of lifestyle factors such as smoking, alcohol consumption and body mass index (BMI) on outcome (Table 8), but there is a dearth of lifestyle studies with objective measures.
| Study | Nature of effect | Dataset size | Model type – response |
|---|---|---|---|
| Alsalili et al. 199561 | Male infertility (worse) | 5209 cycles (2391 couples) | Time-to-event (Cox) – pregnancy |
| Engmann et al. 200166 | Diagnosis | 7700 cycles (4417 women) | Logistic regression (robust) – birth |
| Haan et al. 199167 | Male factor (worse), one ovary (worse) | 3392 cycles | Logistic regression – pregnancy |
| Minaretzis et al. 199871 | Diagnosis | 544 cycles | Logistic – pregnancy, birth and multiples |
| Roberts et al. 20092 | Diagnosis (idiopathic – better) | 1198 | EU model – multinomial response (live birth) |
| Roseboom et al. 199574 | Age–diagnosis interaction | 222 transfers | Logistic – pregnancy |
| Stolwijk et al. 199677 | Idiopathic (worse) | 757 (1st cycle), 454 (2nd cycle) | Logistic – pregnancy (1st and 2nd given first) |
| Strandell et al. 200052 | Diagnosis (tubal worse) | 2107 cycles | Logistic (robust) – birth and multiple birth |
| Tan et al. 199278 | Diagnosis (male factor worse) | 5055 cycles | Survival analysis and logistic – pregnancy + live birth + failure of pregnancy |
| Templeton et al. 199679 | Diagnosis (unexplained better) | 36,961 cycles (2893 women) | Logistic (robust) – birth |
| Wald et al. 200583 | Male infertility/sperm | 113 cycles (85 patients) | Neural networks, discriminant analysis, logistic – pregnancy |
| Study | Nature of effect | Dataset size | Model type – response |
|---|---|---|---|
| Commengues-Ducos et al. 199863 | Number of ampoules of gonadotrophins, use of donor sperm, previous treatment | 923 transfers | Logistic regression (with REs) – pregnancy and implantation |
| Croucher et al. 199864 | Previous pregnancy (1st cycle) – increase | 2396 (2nd cycle) | Significance tests |
| de Klerk et al. 200892 | Treatment regime | 289 | Logistic – live birth |
| Elizur et al. 200565 | ICSI – increase | 5310 cycles (with transfer) | Survival analysis (discrete) – live birth |
| Engmann et al. 200166 | Previous live birth (IVF) – increase; number of previous failures – decrease | 7700 cycles (4417 women) | Logistic regression (robust) – birth |
| Haan et al. 199167 | Duration of infertility (≥ 6 years worse); treatment number – decrease | 3392 cycles | Logistic regression – pregnancy |
| Hunault et al. 200253 | Day of transfer | 642 women (1st cycle) | Logistic/EU model – pregnancy and twin pregnancy |
| Kupka et al. 200369 | Previous ART success – increase | 174,909 treatments | Logistic – pregnancy |
| Rhodes et al. 200573 | ICSI – increase; Cook catheter – decrease; Catheter blood – decrease; embryologist | 205 (1st cycle) | Logistic – pregnancy |
| Roberts et al. 20092 | Attempt number (> 2 = worse) | 1198 | EU model – multinomial response (live birth) |
| Stolwijk et al. 199677 | Previous pregnancy – increase; previous 1st cycle embryo transfer (increase) | 757 (1st cycle) 454 (2nd cycle) | Logistic – pregnancy (1st and 2nd given first) |
| Strandell et al. 200052 | No. of previous cycles – decrease | 2107 cycles | Logistic (robust) – birth and multiple birth |
| Tan et al. 199278 | Decrease over cycles | 5055 cycles | Survival analysis and logistic – pregnancy + live birth + failure of pregnancy |
| Tan et al. 199493 | Treatment regime | 2893 women | Life-table/logistic |
| Templeton et al. 199679 |
Use of donor eggs improves response Previous pregnancy (stronger effect for live birth and previous IVF) Duration of infertility – longer = worse |
36,961 cycles (2893 women) | Logistic (robust) – birth |
| Tsafrir et al. 200781 | Drug dose | 381 (over 40-year-olds) | Logistic – pregnancy |
| Wald et al. 200583 | Duration of infertility | 113 cycles (85 patients) | Neural networks, discriminant analysis, logistic – pregnancy |
| Study | Nature of effect | Dataset size | Model type – response |
|---|---|---|---|
| Akande et al. 200260 | FSH linear/non-linear decline | 2684 embryos, 977 transfers | Logistic regression – pregnancy and birth |
| Alsalili et al. 199561 | Serum estradiol (positive) | 5209 cycles (2391 couples) | Time-to-event (Cox)/pregnancy |
| Bancsi et al. 200359 | FSH (of limited value) | 21 studies | Meta-analysis |
| Chuang et al. 200362 | FSH | 1405 (1st cycle) | Significance test, ANOVA – number of oocytes retrieved and fertilised |
| Dafopoulos et al. 200588 | Sperm motility (ICSI patients) | 165 (1st cycle) | Logistic regression – pregnancy |
| Ferlitsch et al. 200489 | FSH (lower = better) | 171 (1st cycle) | Logistic regression – pregnancy |
| Fujimoto et al. 200790 | FSH (lower = better), normal menstrual cycle = better | 112 (age over 40) | Significance tests – live births |
| Ottosen et al. 200772 | FSH | 2193 DET cycles | Logistic (robust) – pregnant vs not pregnant, twin vs not twin |
| Roberts et al. 20092 | FSH, sperm count, previous pregnancy = better | 1198 | EU model – multinomial response (live birth) |
| Sabatin et al. 200875 | Age (interaction with FSH) | 1589 | Significance tests (various outcomes), logistic regression (live births) |
| Yanushpolsky et al. 200391 | FSH (day 3 and day 10) | 483 retrievals (353 patients) | Logistic – pregnancy and live birth |
| Study | Nature of effect | Dataset size | Model type – response |
|---|---|---|---|
| de Klerk et al. 200892 | Anxiety/depression (mild does worse – but small effect) | 289 | Logistic – live birth |
| Haan et al. 199167 | Treatment centre | 3392 cycles | Logistic regression – pregnancy |
| Haggarty et al. 200668 | Genetic, nutritional | 602 women (1st cycle) | Logistic/ordinal – birth, logistic/ordinal – multiples |
| Ferlitsch et al. 200489 | BMI (lower = better) | 171 (1st cycle) | Logistic regression – pregnancy |
| Morris et al. 200694 | Exercise (> 4 hours/week may reduce live births/increase cancellation of cycle and cardiovascular work may reduce live births) | 2232 | Logistic (live births vs four separate failure outcomes) |
| Purcell et al. 200795 | Ethnicity (Asian origin poorer) | 23,772 (1st cycle) | Logistic – pregnancy and live birth |
| Roberts et al. 20092 | Smoking (worse) and alcohol | 1198 | EU model – multinomial response (live birth) |
| Sneed et al. 200896 | BMI (interaction with age – high BMI in young patients = poor response) | 1273 | Logistic and linear regression (various responses) |
| Weigert et al. 200184 | Seasonality (December optimal) | 8185 cycles | Logistic – pregnancy |
The published results give us a good indication of what variables should be included (where available) in analyses for this study. If confirmed they could provide a basis for selection by showing which characteristics are likely to produce a live birth, and furthermore show which are most likely to differentiate cycles with a singleton live birth versus multiple live births.
Statistical modelling approaches
Logistic regression models
Most work on prognostic factors has utilised standard logistic regression in one form or another with IVF outcome being modelled as a function of patient and cycle characteristics. Some of this work is reviewed above (see Prognostic factors for IVF success). Utilising standard logistic regression (LR) models using patient-level covariates poses two problems: firstly the nature of the outcome, and secondly the handling of embryo-level covariates.
The usual measure of IVF outcome is the number of live babies produced in some unit of treatment, which may be a singleton, twin or a higher-order multiple birth. Most work in the field uses a binary LBE – one or more babies, but this is clearly not very useful if we wish to look at twin incidence. Some workers have created separate models for live birth and for multiple births. 53,72 Another approach, and the one we adopt here, is to model LBE and then multiple births in those who have an LBE. 85
Characteristics, such as morphological grade, measured on the transferred embryos are difficult to incorporate into a patient/cycle LR model, not least as it is in many cases unknown which of the embryos led to a successful outcome. The usual approach is to create some aggregate embryo covariate using either an average of the embryo parameters or the ‘best’ embryo. The approach here follows that of Roberts1 and uses a simple mean of the parameters across all transferred embryos.
A third issue is the non-independence of multiple cycles from the same couples. Although this can in principle be very complex,97 for most realistic scenarios these can be handled by the addition of standard random effects representing levels in the hierarchy above the cycle. In the work considered here there are couple effects (repeat egg collections from the same couple) and egg collection effect (multiple transfer cycles of fresh or cryopreserved eggs collected in a single procedure).
The EU model
Full details of the approach used here are given in the papers by Roberts1 and Roberts et al. 2 The EU approach was first introduced by Speirs et al. 98 In the EU model the success of an embryo transfer is portioned into two components: the embryo implantation probability, E, and the uterine receptivity, U. For a successful transfer at least one embryo has to implant and the uterus has to be receptive. The E and U parameters give the probabilities of each of these events, and simple probability calculations can then give the probabilities of success (one or more embryos implanting in a receptive uterus), failure (no embryos or a non-receptive uterus) or multiple pregnancies. The Speirs model assumes a constant E and U across all embryos and uteri. The model has been extended to model separately the E and U components using logistic regression models. 1,54
It is to be noted that this formulation explicitly excludes monozygous twins, and such events would be considered single successful embryos within the context of the model. Generally monozygous twins are not identified in the available data, but the incidence is low and not a major bias in the analysis. 99
There is an explicit assumption that the embryos and uterine probabilities are independent (after conditioning on the covariates). There are some claims that embryos exert a ‘helper effect’ on each other,100 but the evidence is weak and compromised by incomplete consideration of covariates and patient selection biases.
The interpretation of the uterine component, U, has broadened since its inception by Speirs et al. 98 In analyses such as these it encompasses a wider range of influences that act on any potentially implanting embryos and includes a range of cycle-specific as well as parental factors that may affect the ability of the mother to carry the pregnancy to term.
*Fitting the EU model
Given the model defined in the section above, we can construct an observed data likelihood function, and obtain parameter estimates for the covariates by direct maximisation of this likelihood. Full details are given in Roberts. 1 For this study the optimisation is performed used custom-developed code in the statistical programming language R101 using a quasi-Newton method. 102
Models are formally compared using standard likelihood ratio tests (LRTs), and these are used to derive significance levels for parameters. Standard errors of parameter estimates are derived using a Wald-style approximation based on the inverse of the Hessian of the log-likelihood function. Profile likelihood limits as used in, for example Roberts et al. 2 are computationally infeasible in datasets of the size being analysed here.
The EU model has two submodels, one for characteristics affecting the embryos, E, and one for ‘uterine’ characteristics, U. It is not clear a priori whether factors such as age should be entered into the E, the U or both submodels. Although patient characteristics such as age are measured at the patient (U) level, they may act through embryo characteristics. In some cases there is a natural level at which a clinical observation should be added: for example, a tubal diagnosis is unlikely to affect embryo quality or the use of donor sperm uterine receptivity. However, even in these cases it is feasible that in observational data effects in submodels that would be considered clinically unreasonable may be mediated through patient selection and treatment effects. In principle, the appropriate submodel can be identified from the data, where there are multiple embryo transfers, as it affects the twin rates differently from success rates, but such identification is weak. 1 Additionally the models being compared are not nested, so no inferential test exists and we have to use model selection criteria such as Akaike’s information criterion (AIC, see below).
*Extending the EU model to include between-cycle correlations
The EU model can be relatively easily extended to include a single random effect in the U submodel. This exploits the fact that the observed data likelihood can be factorised into a product of individual cycle components, and the multidimensional integral necessary to allow for the random effects then becomes a product of one-dimensional integrals, and therefore computationally feasible. Even so, given the sizes of datasets in this project, computationally it is only possible to look at a few restricted models in this way. Extensions to allow for random effects in E or multilevel random effects are not yet feasible.
Presentation of model fits
Tables of the parameter estimates are shown together with their estimated standard errors (derived from a standard Wald approach). Depending on the context these are presented with LRT-derived p-values for removal of each variable from the model. Note that each variable in the model may include a number of model parameters: we generally present significance tests for the removal of these as a set.
Sets of plots such as those shown in Figure 5 are used to visualise the fits. In these plots predicted (fitted) probabilities are shown against selected variables, in this example year of treatment. Panel (a) shows the probability of an LBE, panel (b) that of a multiple birth event, and panel (c) the ratios of multiple births to LBE. Box and whisker plots show the range of predicted probabilities across all the individuals in the dataset with the given values of the selected variable, with a horizontal line for the median value, a shaded box covering the interquartile range and whiskers extending to the full range of values seen in the data. These show the actual values in the full population, allowing for any differences in other variables that may be associated with the given variable. For example, the distribution of patient ages may vary between years, and this will be reflected in the predictions shown. To visualise the pure effect of the selected variable a line is added showing the prediction for a ‘typical’ patient where all other variables are held constant and only the variable in question varied. This typical patient has mean or modal values for the parameters as shown in Table 9. As can be seen in Figure 5, this typical patient may have success or twin probabilities that appear somewhat different than the median of patients; setting each individual parameter to a typical value does not necessarily produce a patient with a totally typical prognosis.
FIGURE 5.
Example plots showing a fit and its predicted values for an EU model. (a) Live births; (b) multiple births; (c) multiple birth rate; (d) U; (e) E.
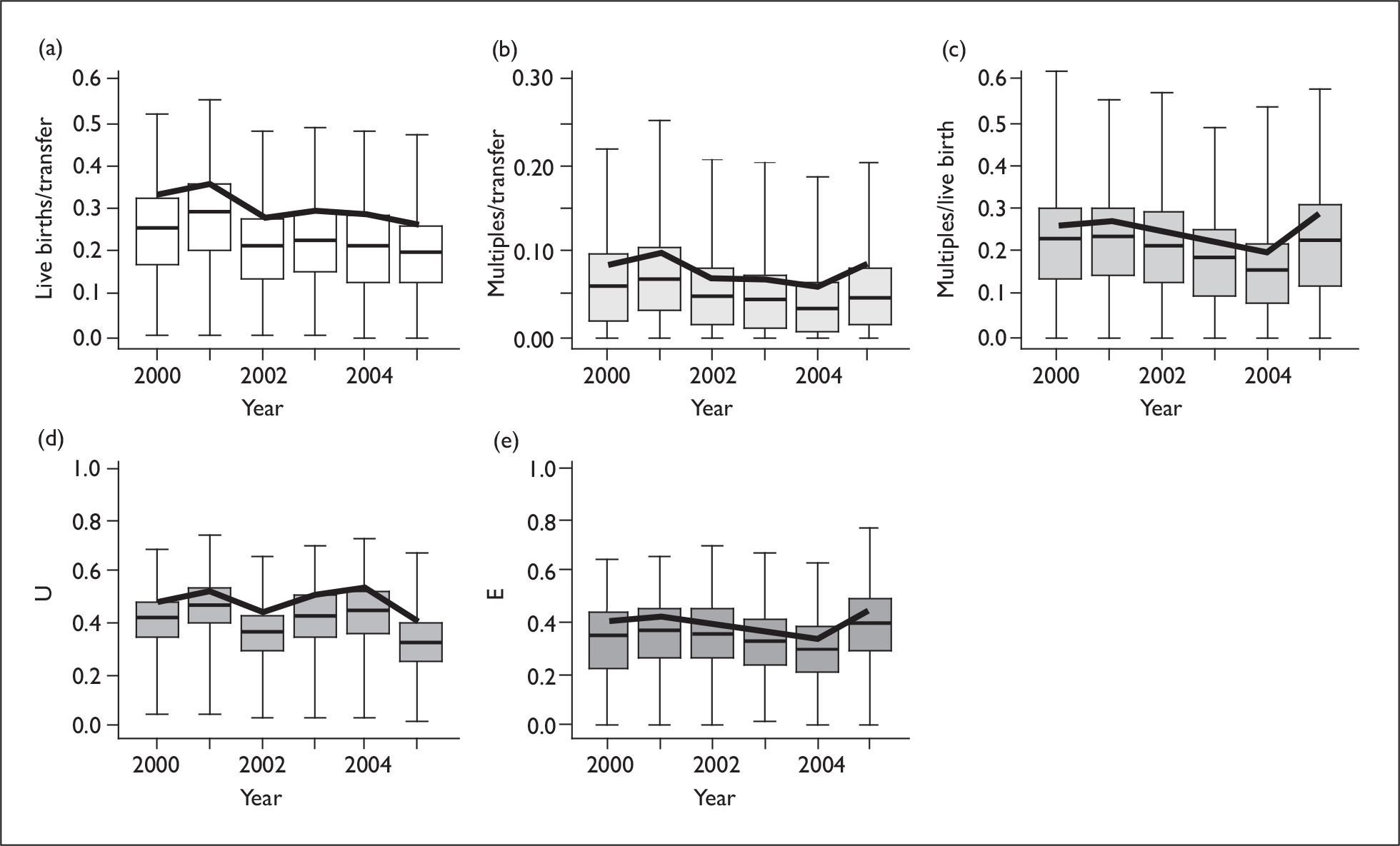
| Variable | Value |
|---|---|
| Age | 34 |
| Embryos created | 6 |
| Previous treatments | 0 |
| Pregnancy history | Never pregnant |
| Duration of infertility | 4 years |
| Diagnosis | Idiopathic |
| Type of fertilisation | IVF |
| Sperm source | Partner |
| Day of transfer | 2 |
| Year of treatment | 2003 |
For an EU model we can produce similar plots for the E and U probabilities as shown in panels (d) and (e) of Figure 5.
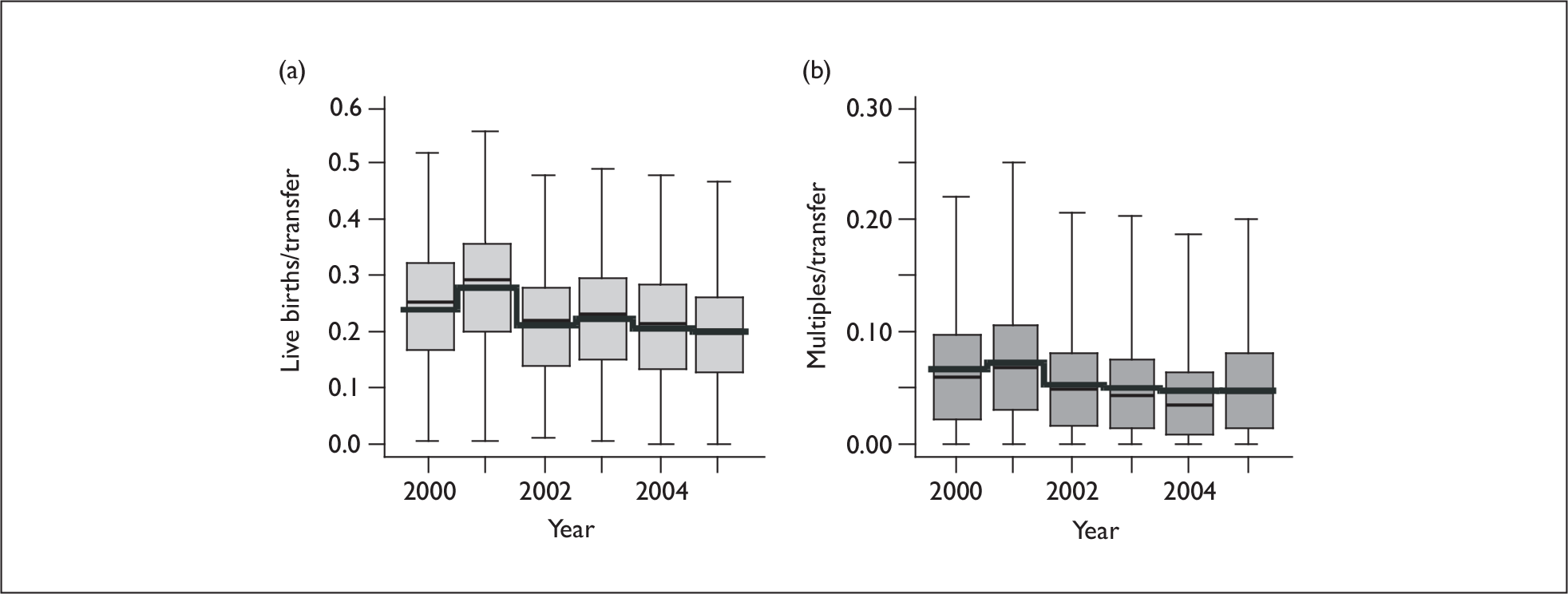
Similar plots can be produced showing the spread of predicted values and the observed values, and an example is show in Figure 6, in which the thick line shows the actual probabilities in the dataset used to derive the fit.
FIGURE 6.
Example fitted value plot showing addition of actual probabilities from the dataset. (a) Live births; (b) multiple births.
Assessment of model fits
With any statistical model it is important to assess how closely it fits the observed values in the dataset. Our models have binary (yes/no) outcomes such as LBE and twins. One useful measure of goodness of fit is the predictive accuracy, measured by the area under the receiver operating characteristic (ROC) curve, which in practice takes values from 0.5 (useless) to 1.0 (perfect). Simple visual methods, such as the examination of observed versus predicted outcomes for groups of patients (as in Figure 6), are often informative, along with systematic testing of additional model complexity.
As a model becomes more complicated with additional terms it can only fit more and more closely to the observed data. There is then a danger of ‘overfitting’, in that the model is so specific to the observed dataset that it loses generalisability. The aim of our modelling is parsimony – to include only the important terms so as to find a relatively simple model that describes the observed data. For logistic regression this is often addressed by likelihood ratio testing – formal tests of statistical significance. The addition of each term is assessed by comparison of the goodness of fit with and without that term, and only terms that justify their inclusion (statistically significant) are retained. However statistical significance is not the best indicator of the ‘best’ model, as factors that would not be considered significant (using, say, the usual p = 0.05 criterion) can be useful predictors. Moreover, for some of the more sophisticated models presented here likelihood ratio testing is not always possible.
Thus ‘information criteria’ are used to choose between models. The AIC is the most widely used to trade model complexity against goodness of fit. We use this and the Bayesian information criterion (BIC), the latter having the advantage in large datasets of also accounting for the influence of sample size in determining statistical significance (in large datasets almost any effect is ‘significant’).
For estimating sampling errors in the model parameters and predicted outcomes we have used bootstrapping,103 a relatively recent but increasingly standard method for complex end points. We have also utilised a bootstrap-based calibration procedure104 to assess whether the fitted model displays characteristics of overfitting. A well-fitting model should give a calibration intercept close to 0 and slope close to 1.
Chapter 2 Patients’ perspectives on twins and single embryo transfer
Patients’ perspectives on twins and SET
This chapter describes the methodology and results from the in-depth qualitative interviews that were conducted in order to access patient perspectives with couples who were undergoing IVF treatment.
Interview conduct and analysis methods
The aim was to explore the patients’ perspective of treatment choices as they travel through the treatment process. Therefore, interviews were conducted at three key decision-making phases:
-
pre-treatment – patients on the waiting list for IVF (NHS only)
-
in treatment – after the first information meeting and clinical appointment or receiving active treatment
-
post treatment – after the second cycle of treatment or treatment completed – this last group was included as it allowed for views to be assessed once the outcome of an initial treatment cycle was known and after having had the opportunity to reflect on the choices through a second treatment cycle.
The interviews were semistructured and designed to be conversational in style. An interview schedule was designed in response to the aims of the project and the existing research literature. This schedule was refined and adapted over the first few interviews. Each interview began by explaining the purpose of the study and by asking a few short demographic questions relevant to the study. As the interviews were conducted with women and couples at varying treatment stages, the interviewer used hypothetical questions to access opinions on key issues or where couples lacked direct experience. The interview enquired about the general experience and impact of treatment to date, and perceptions of what constitutes a ‘good’ outcome were explored. The second focus of the interview concentrated on the move towards SET. Current knowledge of the difference between SET and DET was explored, and attitudes and beliefs towards multiple births were sought. A particular emphasis was placed on the patients’ understanding of the risks associated with multiple pregnancies. Facilitators and barriers to potential changes in SET policy were investigated. Other areas covered included preferences about involvement in treatment decision-making, current sources of information and information needs and views on RCTs of eSET.
Setting and sample
A purposive sampling technique was employed to ensure maximum diversity of sample to include different female ages, parity, duration of infertility and source of funding (which is also related to the number of treatment cycles that the couple receive). Couples and women were recruited from two assisted conception centres (one NHS and one private hospital). Three recruitment strategies were used, one facilitated by the NHS clinic research nurse:
-
Patients were selected by a research nurse from the clinic waiting/appointments list. The research nurse was briefed on the selection criteria for the interviews. The nurse then mailed a letter of invitation and provided information about the study to the patients. Those who expressed a wish to be contacted were then followed up by the researcher. Patients were contacted by telephone or email (LMcG) to discuss the study and answer any queries or concerns. In total 80 patients were mailed. Forty-six couples did not respond to the initial mail request. Owing to ethical and time constraints we were not able to do a follow-up mailing or use other reminders that may have improved the response rate. Seventeen replied stating that they were not willing to be contacted. Of those who agreed to be contacted one declined to take part as she had recently experienced a failed cycle, and three did not respond to telephone calls and/or emails. In total this approach yielded 13 interviews.
-
The qualitative researcher (LMcG) attended one meeting held at the NHS hospital for patients on the waiting list. The purpose of these meetings was to brief patients about the treatment process. At the end of the session the researcher described the study briefly. Those who expressed an interest were given a study pack. This approach resulted in eight positive enquires and four interviews were subsequently conducted.
-
A poster was placed in the waiting room of the private hospitals. Patients who were interested in the study were asked to request an information pack from the nurses in the clinic. They then took this home and replied to the researcher using the invitation slip if they wished to be contacted. It is not possible to gauge an accurate response rate with this approach. However, all the private clinic patients (n = 10) were recruited by this means.
The first two strategies were exclusively used in the NHS setting, and proved to be of limited value. In particular, the mail shot was the least successful method of recruiting patients. The use of a poster (option 3) proved to be a successful mode of recruitment in the private clinic (i.e. more patients recruited in shortest amount of time). The use of a study poster was first suggested by the manager of the private clinic and this was the most successful method.
The final number of interviews conducted was 27. The sample consisted of 14 couples and 13 women (who attended the interview without their partner); 17 were funded by the NHS and 10 were self-funded. Seven were interviewed pre-treatment, 13 during treatment and seven post treatment. It should be noted that three of the women interviewed under the classification post treatment were not pregnant at the time of being approached to do the interview; however, by the time the interview was conducted these women were approximately 5 weeks pregnant. This was because these women initially did not know that they were pregnant following a cycle or they had undertaken a new cycle before agreeing to be interviewed. All these women were receiving treatment from the private clinic.
Characteristics of the sample are displayed in Table 10a and 10b.
| Mean (range) | ||
|---|---|---|
| Time seeking treatment (reported by participants) | 40 months (18–180) | |
| n | (%) | |
| Funding (total) | ||
| Private | 10 | (37) |
| NHS | 17 | (63) |
| Funding (NHS only) | ||
| Three cycles funded by PCT | 16 | (94) |
| Woman did not know | 1 | (6) |
| Stage of treatment | ||
| Pre-treatment | 7 | (26) |
| In treatment | 13 | (48) |
| Post treatment | 7 | (26) |
| Types of treatment | ||
| IVF only | 22 | (81) |
| IVF + ICSI | 3 | (11) |
| IVF + surgical sperm retrieval | 2 | (7) |
| IVF + donor insemination | 1 | (4) |
| IVF + egg donation | 1 | (4) |
| Reason for infertility/IVFa | ||
| Female (n = 27) | ||
| Unexplained | 8 | (30) |
| Blocked fallopian tube | 7 | (26) |
| Endometriosis + blocked fallopian tube | 2 | (7) |
| PCOS | 2 | (7) |
| Previous kidney transplant | 1 | (4) |
| Low ovulation | 1 | (4) |
| Turner syndrome | 1 | (4) |
| No problem | 5 | (19) |
| Partner (n = 26 male, n = 1 female) | ||
| No problem | 22 | (81) |
| Failed vasectomy reversal | 2 | (7) |
| Absence of vas deferens | 1 | (4) |
| Low semen count | 1 | (4) |
| Operation affected fertility | 1 | (4) |
| Female | 1 | (4) |
| Age | Mean (range) | |
|---|---|---|
| Female (n = 27) | 34 (24–42) | |
| Partner (n = 26 male, n = 1 female) | 38 (28–46) | |
| n | (%) | |
| Ethnicity | ||
| Female (n = 27) | ||
| White British | 22 | (80) |
| South African | 2 | (7) |
| Pakistani | 1 | (4) |
| Somalian | 1 | (4) |
| Bangladeshi | 1 | (4) |
| Partner (n = 26 male, n = 1 female) | ||
| White British | 20 | (72) |
| Pakistani | 1 | (4) |
| Somalian | 1 | (4) |
| Bangladeshi | 1 | (4) |
| Turkish | 1 | (4) |
| New Zealand | 1 | (4) |
| Chinese | 1 | (4) |
| South African | 1 | (4) |
| Number of children in family | ||
| None (includes single woman and same sex couple) | 20 | (74) |
| One | 5 | (19) |
| Two (males previous relationship) | 1 | (4) |
| Four (males previous relationship) | 1 | (4) |
Data collection
Data were collected by in-depth semistructured interviews. All interviews were digitally recorded, with permission, and transcribed verbatim. Codes were used to conceal participants’ identity and anonymity and confidentiality were assured. Participants were reassured that the digital recordings would be destroyed after transcription, and that all names referred to in the recordings would be replaced with pseudonyms. Interviews were conducted in a place of the participants choosing, usually at home (eight interviews in a hospital setting). The length of the interviews ranged from 40 minutes to 3.5 hours.
Data were managed using the qualitative software package nvivo 7. 105
Data analysis
The 27 interviews were analysed following the principles of framework analysis. 106 This method was designed to facilitate the systematic analysis of qualitative data, which summarises and classifies data within a thematic framework. The analysis can be based in original accounts of those studied (inductive), or be derived from a priori hypotheses (deductive), or both. Framework analysis was chosen for the following reasons:
It provides coherence and structure to otherwise cumbersome, qualitative data (i.e. interview transcripts).
-
It facilitates systematic analysis, thus allowing the research process to be explicit and replicable.
-
Despite the inherent structure, the process of abstraction and conceptualisation allow the researcher to be creative with the data.
Framework analysis involves a number of stages, but this does not imply linearity, as these stages are highly interconnected. There are five key stages involved in the analysis:
-
Familiarisation The transcripts are read thoroughly by the researcher, so that he or she becomes immersed in the data.
-
Developing a thematic framework The process of familiarisation leads to the development of broad key themes. This initial framework was then taken and applied to the interview transcripts. A numeric colour coding system was developed and applied to this thematic framework. In addition, subthemes were beginning to emerge, which were noted in memos. Thus, the framework was expanded and refined accordingly.
-
Indexing The identification of a thematic framework begins the process of abstraction and conceptualisation, which is further developed by indexing and charting the data. Themes and emerging subthemes are subsequently labelled and indexed.
-
Charting Framework analysis involves devising a series of thematic charts or matrices. The indexed data is entered into the appropriate cell. Charts were constructed using a thematic approach, by which cases were drawn up for each key subject area and entries were made from each respondent (case). This process allows for the checking of emergent themes and cross-referencing to the original data. The researchers’ intention was to keep the original exploratory nature of the study in mind as data was ‘lifted’ from the original context and placed in to the appropriate theme/subtheme. These data were not necessarily direct quotes but notes that captured the context of the discourse. Thus, the charts allowed for the full pattern of views, perceptions and attitudes to be reviewed. ‘Charting’ is an evolving process, the end result being that data are grounded in the respondents own accounts.
-
Mapping and interpretation The aim is to bring out the key characteristics and map and interpret the data as a whole (Ritchie and Spencer,106 p. 186). This process can take several forms in order to define concepts and map the phenomena under consideration. The end point is to provide explanation and meaning, some of which may relate to the initial research aims or emerge directly from the dataset. This is not a purely mechanical process; indeed Ritchie and Spencer106 suggest that each step requires ‘leaps of intuition and imagination’ (p. 186). In order to achieve this aim several strategies were utilised. These included continuous reviewing of transcripts, charts and field notes searching for patterns, interconnections, similarities and dissimilarities. ‘Running ideas’ past those with direct clinical experience in the area of assisted conception proved useful. A benefit of using framework analysis is that strategies and recommendations for policy may be elicited at this stage.
For the purpose of the analysis the interview transcripts were allocated into one of three groups: (1) pre-treatment; (2) in treatment; and (3) post treatment so that any effect of stage of treatment could be more easily identified. During the analytical process the researcher (LMcG) remained cognisant of other potential external factors that may have influenced the couples’ and women’s views on SET (e.g. female ages, parity, duration of infertility and source of funding). The process of analysis was verified by a second external qualitative researcher Lynne Austin at the charting phase to verify the principal researchers’ interpretation (all charts were cross-checked with the original interview transcripts and thematic chart). Any discrepancies were resolved by discussion.
Findings
The above process resulted in a final framework which incorporated seven main themes and several subthemes (see Table 11). The findings will be presented in line with the thematic framework described above. Where patterns and cross-cutting themes emerge across the data these will be discussed.
| Main theme | Subtheme |
|---|---|
| 1. Sources of information | 1.1 General |
| 1.2 Medical/nursing staff | |
| 1.3 Infertility websites | |
| 1.4 Internet | |
| 2. Views on policy | 2.1 Views on introducing a SET policy |
| 2.2 Personal choice regarding SET | |
| 2.3 Improve your odds | |
| 2.4 Maternal age as a selection factor | |
| 2.5 Source of funding | |
| 2.6 Policy drivers | |
| 3. Views on multiple birth | 3.1 Attitudes/beliefs towards multiple birth |
| 3.2 Risk perception from multiple birth | |
| 4. Views on frozen embryos | 4.1 Costs and benefits of embryo freezing |
| 4.2 Ownership of embryos | |
| 5. Experience of treatment | 5.1 Treatment journey to IVF |
| 5.2 Emotional effects of treatment | |
| 6. Consultation process | 6.1 Consultation style – general |
| 6.2 Consultation experience – SET vs DET | |
| 7. Views on RCTs of eSET | 7.1 Views on RCTs – general |
| 7.2. Negative views |
Theme 1: Sources of information
Sources of information included general, medical and specific fertility websites and the internet (see Table 12). It appears that the main sources of information were gained outside formal clinic consultations.
| Sources of Information | Pre-treatment (n = 7) | In treatment (n = 13) | Post treatment (n = 7) |
|---|---|---|---|
| 1.1. General |
2 (29%) [103, 106] |
11 (85%) [108, 109, 110, 111, 112, 113, 115, 117, 118, 119, 120, 121] |
4 (57%) [122, 123, 124, 126] |
| 1.2 Medical/nursing staff |
1 (14%) [101] |
3 (23%) [109, 112, 113] |
2 (29%) [125, 116] |
| 1.3 Fertility websites |
3 (43%) [104, 106, 107] |
9 (69%) [110, 111, 112, 113, 114, 115, (117), 118, 120] |
4 (57%) [122, 123, 125, 126] |
| 1.4 Internet |
7 (100%) [101, 102, 103, 104, 105, 106, 107] |
12 (92%) [108, 109, 110, 111, 112, 113, 114, 117, 118, (119), 120, 121] |
7 (100%) [122, 123, 124, 125, 126, 127, 116] |
General sources of information included booklets, leaflets concerning fertility as well as books, novels and newspapers. A thirst for knowledge was described for those who had not yet started treatment. The process of obtaining information was likened to studying for a medical degree. However, the majority of persons seeking information were those in treatment. Some had received the HFEA booklet at the waiting list meeting or had contacted HFEA direct. Others described receiving the information packs from the clinics. Descriptions of the packs ranged from basic and just ‘shoved together’ to useful and informative or simply being daunted by a ‘whopping great pack of stuff’. Some described already having a general knowledge in this area, while others noted feeling desperate to know what everything means and needing to have more information.
For those in treatment, views on the information given by medical and nursing staff varied. These ranged from feeling that patients know as much as the doctors to finding the clinic information good and trusting the information given. One woman felt that information is not always given as it may frighten people.
Specific websites for women undergoing fertility treatment were also used to combat feelings of being overwhelmed and to buddy up with like-minded people and make friends as often existing friends were not ‘in the same boat’. Negative thoughts regarding websites included getting confused with the wealth of information, the number of sites and badly designed sites.
Theme 2: Views on policy
Not surprisingly, this was the topic which prompted the most discourse. Five subthemes were identified which related to the potential change in policy to limit the number of embryos from two to one. These are listed below.
Subtheme 2.1: Views on introducing a SET policy
There was a range of awareness of the debates surrounding SET, from no understanding prior to entering this study to those who had more detailed knowledge and opinions:
Were you aware of this before, you know, you came into the study, were you aware of this policy shift that might be coming in?
No.
Right. So you’d not picked up in the media or anything.
No.
(Couple, in treatment, NHS 108)
There was limited awareness of the proposed policy change particularly within the pre-treatment group, although some had seen reports in the media.
They had discussed this on the news … I was aware they were wanting to go that way [one embryo] they say due to health issues.
(Woman, in treatment, private 109)
Others had a good understanding of SET. However, several women and couples perceived the move towards SET to be inextricably linked with the need to control NHS resources:
My understanding is that you can have one embryo put back, or you can have two embryos put back, and obviously that might result in one baby, or it might result in two babies, possibly at least, but you know, there’s a strong possibility you could end up with two.
(Woman, in treatment, private 110)
As far as I’m concerned if I’d paid in the legitimate way, I should be able to get something out of it, regardless of whether I’ve had IVF to get my children, which in my instance I actually funded myself. Because I knew my age limit was coming up, thank you very much, stick another label on my head, write me off! No, I don’t see what the issue is. I don’t think.. … well I don’t know the full statistics on how many babies … IVF babies end up in Neonatal Units, but how many under age mothers’ children end up in Neonatal Units?
(Woman, in treatment, post baby, private, 115)
Subtheme 2.2: Personal choice regarding SET
Several factors influenced couples decision to transfer one or two embryos. These included previous experience of treatment, length of treatment, maternal age and perceptions of which method would be most successful. Previous experience of a failed cycle prompted this couple to opt for two:
What do you think the main things are that influence your decision to favour two embryos?
Success rate. It’s as simple as that. Success rate. I’m not the only woman that would sit here and go ‘oh well perhaps’. If you’ve got the chance of having two, if I’d have had two first time around I wouldn’t be sitting here today.
(Woman, in treatment, post baby, private 115)
Advancing maternal age was also a factor:
Plus age is such a huge factor for me now as well because I’m 39, you know, I don’t want to be doing this when I’m 40 so I, you know, I’ve only got, you know, this year to hopefully get pregnant. You don’t need any other children do you? No, because let’s say if you’re like 38 years and then you have twins, those twins, when they are 9 months you’re going to be like 38 something, when they’re being born it’s like you’re 39 something, so you don’t have any chance to do a further cycle, so I think I’d just go for it.
(Woman, in treatment, post baby, private 113)
There was considerable evidence of joint decision-making within the interviews. When interviewing couples the interviewer often attempted to assess the congruence of decision-making as illustrated by the following quote:
So did you agree with [woman] then, when, when it came to the decision to transfer one or two embryos, how did … ?
I’d, I’d have planted more. No, I was looking at [his wife] saying, oh, well what if we have more children? I mean it’s not as though they wouldn’t be loved and cared for the, the point is I so desperately, desperately wanted her to have a child, you know, because it’s …
It’s got to bring the level down if they only start putting one back surely.
(Couple, post treatment, pregnant, NHS 125)
For some, the move towards a SET policy was seen as a direct affront to personal choice:
They’re just trying to cut down on multiple births, to an extent, and, but, I think, I think that choice should still be there, because I mean we know that a lot of people would rather have that choice and be able to have twins if possible, or I more. I mean it’s only a minute chance of having more than two anyway. But, for ourselves, we’d rather do that, wouldn’t we, we’d rather have twins in one go if we could do.
(Couple, post treatment, pregnant, NHS 125)
So, we would definitely want more than one child, and I think if somebody turned around to me and said, you can only have one embryo replaced, I’d be really angry about it, and that’s, that’s, that’s not a dramatic reaction, I would be very angry that somebody had taken away my choice because …
It’s your liberty …
… it’s actually …
… it’s your freedom of choice …
(Couple, post treatment, private 127)
During several interviews women and couples asked the interviewer specific questions about the rationale for SET, for example:
The argument they would say is that spontaneous twins happen and they can’t control it. Whereas in IVF they can control it. I’m not saying it’s right or wrong …
If I lived in China, fine. You tell that to one of those mothers who’s just lost their children there [in a recent earthquake]. And I’m like no, sorry, I don’t live in that environment. I had the freedom of choice. I chose … well I didn’t actually have the choice, I was dealt a hand where I couldn’t have, and I went the best way to help my partner and I have a family.
(Woman, in treatment, post baby, private 115)
This couple felt that the discussions regarding the risks of treatment dominated the consultation they had undergone, but that their reasons for their own personal treatment choice had been overlooked:
We’ve obviously had the risks explained to us from the double embryo, uhm, twins, triplets, quadruplets and things like that. Uhm, we obviously had questions when that came up in so much as, what are the risks? And where’s the choice? I mean for our choice it was quite simple, we want more than one child anyway, so if we had two or three …
(Couple, in treatment, NHS 118)
Subtheme 2.3: Improve your odds
The belief that having two embryos transferred would improve couples’ chances of getting pregnant, and having at least one baby, was prevalent in this set of interviews. Therefore, although couples and women would accept that there were risks with twin pregnancies, their individual risk assessment was tempered by the desire for a pregnancy. Most couples and women interviewed felt that having DET would give them ‘better odds’ of achieving a pregnancy:
And it is a numbers game, it really is, and so, you know, now my thinking, when they asked me how many I wanted transferred this time, you know, I’d no hesitation of saying two, because I don’t want to, you know, I don’t, I don’t even know if it is true, but it’s got, in my own mind, you’ve got to have a better chance if two have been put back than one.
(Woman, in treatment, private 113)
Women and couples had often thought carefully about the decision to opt for SET or DET. As here, many had gone over the scenario of having twins, including the practical implications:
Just for the, the best possible chance really, I mean, you know, we read all the time that the, the uhm, the success rates aren’t that great, we know now the trauma of not having the success, uhm, and uhm, yeh, we just wanted to give ourselves the best possible chance really, and we knew that there was a possibility of twins, and that’s something we did think about very closely, very strong, you know, very, we thought about it a lot, I can’t think of the right words, but we did think about it a lot and talk about it a lot really and even practically how, if we had twins, how would we cope, and also the fact that I understand that there is a, uhm, a higher risk of miscarriage if you had twins, or if you were pregnant with twins, and we discussed that as well, but we, we just came to the decision that we just wanted to give ourselves the best possible chance really.
(Woman, in treatment, private 110)
Subtheme 2.4: Maternal age as selection factor
The interviewer introduced the view that maternal age could be used as a factor to select women who were offered SET. Thus, women under 35 years of age would be offered SET and women over 35 years DET. Some women and couples were amenable to this strategy:
Uhm, I guess, in my own mind I think, well, you should have the choice, you should be able to make your own choice, uhm, and it’s my decision to take, but I can see that there’s the safety aspect of this and protecting people, uhm, and I guess thinking about it, the younger women would be more likely to have higher success rates, uhm, so you could maybe afford more to let them just have one embryo implanted, but if you’ve got women over 35 that have got less of a chance, then give them a better chance with the two embryos, so I think that’s quite, in my mind, quite a sensible idea
(Woman, in treatment, private 110)
Several others thought that such a cut-off was arbitrary and felt that this type of policy decision would be unfair to women of a younger age:
Obviously being nearly 35 and knowing where I am on the waiting list, but I wouldn’t want anybody who was 25 to endure the amount of pain and the waiting and suffering and doing multiple IVF treatments, you know, and obviously you don’t get the NHS funding for a second treatment anyway. So the cost is to, to myself at the moment, no matter what age I would be, extreme. I mean my house is for sale because of it.
(Woman, pre-treatment, NHS 106)
Subtheme 2.5: Source of funding
Women and couples interviewed in this study were receiving treatment either in an NHS or private setting. In IVF treatment many move between these settings in the pursuit of a successful outcome. Therefore, the effects of the source of funding on decision-making were explored:
We all work hard to earn the money we’ve got and to complete my family it’s going to cost me another £5000–£6000. Well £5000–£6000 a throw doesn’t take long before it puts you into a difficult situation. Now if that’s not dedication to actually want a family, what is?
(Woman, in treatment, post baby, private 115)
Opting for private treatment for some women and couples was seen as a necessity which meant that savings would be made elsewhere to fund IVF treatment:
I mean, as I say, we don’t smoke or drink, we don’t get to go out very often ‘cos of baby sitters, so someone else who might have a really busy hectic social life and, you know, things like that who smokes and drinks a lot will spend that in a year probably on – that really goes down the drain as well, but uhm, we, I couldn’t say that, you know, we could afford to do it again. So soon anyway, you know, maybe it could be considered in the future cos I’ve got age on my side, cos I’m doing it so young you know.
(Woman, in treatment, post baby, private 111)
As with other areas, source of funding was one of several factors which influenced the preference for DET. For the following two women it was an interaction between funding, limited availability of treatment cycles and burden of treatment:
Uhm, I think if I wasn’t self-funding and there wasn’t a limit on the amount of times you could have a go, that, that would, then I, then twins wouldn’t be, you know, you know, I know, I know people with twins and I know how hard it can be and stuff, and I know there can be more complications and stuff, but I think [pause] if I wasn’t self-funding and there wasn’t a limit and then I think one would be absolutely fine, if I knew I could come back and do it again and stuff, uhm, but that said, the only thing that would stop me saying that would be the – I hadn’t appreciated when I started out on this, and I know people say how stressful the whole process is. And you don’t realise how much it takes over your whole life, it’s just all encompassing, so …
(Woman, in treatment, private 109)
I think this is the difference again between private and NHS. If they said that were free then potentially, but you’re probably talking over a thousand pounds through private for that difference, uhm, in fact I think more than that, probably about up to fifteen hundred, so I think again, it comes down to almost to finance, as well as the mental strain of that, because while you’re working as well …
(Woman, in treatment, post baby, private 114)
Subtheme 2.6: Policy drivers
Several participants attributed the move towards SET as being driven by external factors, for example the government, and related to NHS resource issues rather than clinical considerations:
Uh, I, I, I feel like the choice would have been taken away from me personally, I can see why it is done, and I know they’re try- but, maybe, I don’t know, you think cynically and you think they’re just thinking about financial reasons for the hospitals and things, which is fair enough, because we know what the NHS is suffering at the minute, staff and finance etcetera, but I don’t think they’re taking into account people’s wishes personally.
(Couple, in treatment, NHS 118)
This view also raised the issue of fairness when allocating resources to various groups of patients. The following interviews show that some participants felt that other groups of patients were being prioritised over those seeking assisted conception:
I think that’s swings and roundabouts because at the end of the day people choose to smoke, I don’t smoke, and they cost the health service millions in cancer treatment and liver disease and, you know, all things like that for alcoholics, so, uhm, if I chose to have two embryos put in, and I don’t smoke, I’m definitely a non-smoker, and I very rarely drink, so, you know, they choose to do that in life, so if I chose to have two children, two embryos put in, the cost of that might, uhm, balance out what they’re draining off the health services as well, so that’s how I look at it.
(Woman, in treatment, private 111)
… these people that just throw kids out willy nilly to different fathers, you know, and all these foreigners that are coming in with four, five, six kids and they – they’re still throwing kids out, and British citizens who’ve paid taxes, or even people who’ve not paid taxes, but British citizens are being told by the government, because of the financial situation, sorry, that, that they can’t, you know, they’re being limited to how many children they can have, the governments saying, well, you can have one, you can’t have two because we can’t fund it.
(Couple, in treatment, NHS 119)
The wider public health perspective of multiple pregnancies being a drain on the NHS was also questioned by this couple:
Because we [the government] can’t afford to put two in intensive care, I think that’s a bit, uhm …
Yeh.
So no, we’re not for it [SET] at all.
(Couple, in treatment, NHS 119)
Theme 3: Views on multiple birth
Subtheme 3.1: Attitudes and beliefs towards multiple births
The view that twins would be a positive outcome from IVF treatment reflected the majority opinion of most women and couples interviewed in this study. The stage of treatment did not appear to affect this viewpoint:
I just, I just loved the idea of twins because I think, uh, it’s so cute, I know it sounds silly, I just think it’s so cute [both laughing] I mean it’s lovely to have a baby, but if you’ve got two, I know there’s the flip side to it and it’s not as easy and all that, but I feel as if I’m young enough to cope with it.
(Woman, in treatment, post baby, private 111)
Twins were seen as providing a ‘ready-made’ family after treatment that was at times lengthy, emotionally, physically and, for some, financially draining:
Get it all over and done with, because I’d be scared, not, I’m not saying that I wouldn’t, if I had one obviously I’d be thrilled to bits, but I don’t want – and I might just be happy with one, but I always thought, like, we’d like have two.
Yeh, I wouldn’t like to go through it all again.
I don’t want to have to go through it again. And I’m not sure that I would go through it again. If I had a healthy baby, one healthy baby, I think I’d be happy with that, and I’m not sure …
(Couple, in treatment, NHS 119)
Subtheme 3.2: Risk perception from multiple birth
When couples and women were asked what they knew about the risks associated with multiple birth, they mainly referred to those factors that affect the baby and not the mother. They also tended to minimise the associated risk, particularly if they knew of someone who had given birth to twins:
Yeh, we’ve decided to have two in yeh. Uhm, you know, that’s just, something both, we’ve both said from the beginning that we’ll, we will do that, so fingers crossed … ‘cos one of my brother’s girlfriend’s sisters just had ICSI and she’s got twins from that and she’s been fine so, you know, you kind of want what they have.
(Woman, in treatment, post baby, private 111)
As the interview progressed the researcher probed more to enquire about the extent of their knowledge of the risks associated with multiple birth. This was mainly limited to the risks of premature birth and the likelihood of having a caesarean section, both of which were perceived as acceptable risks:
What about the risk of premature birth?
I do have a success story about that. My husband was born at 28 weeks so, I know that’s like these days they can be born before then, but he’s absolutely nothing wrong with him, he’s a strapping guy, bloke, you know, he’s, there’s nothing premature to look at him now, about him, so, I believe that they, they can, it can happen, but it can also be successful and the child grows up to just be as normal as anybody else. So, unfortunate as it is it can, it can be bad, but it can also be, uhm, a good outcome.
(Woman, in treatment, private 111)
Even when women and couples had been given a range of adverse outcomes regarding twins, they tended minimise the risks and regard this as an acceptable ‘trade-off’ for a successful pregnancy:
When you said about twin pregnancies then, you knew about the risk. What risks are you aware of with twin pregnancies?
That they are likely to happen, there can be complications, you can have early births, you can lose one, you can lose both. Basically anything and everything that you could be told, we were told.
Yes.
But that’s the chance you take.
(Woman, in treatment, post baby, private 115)
Twins were perceived by many as a normal event, an acceptable risk in pregnancy, whereas the higher risks associated with triplets and above were acknowledged. This appeared to be because most people knew someone who had had twins, or was a twin themselves:
I know there’s risks to me in carrying them and risks to the babies as well, isn’t there? But, I don’t know that it’s that bad, because loads of people have twins, don’t they? I know with more like triplets or quads it’s more, then obviously, and obviously that wouldn’t be ideal, but I mean there’s obviously there’s risk with any pregnancy isn’t there, so that’s all I know really.
(Couple, in treatment, NHS 119)
For those who expressed the view that twins were the ‘norm’, there appeared to more resistance to the counter-argument provided by clinicians:
I think, I get the personal feeling that there’s some scaremongering going on, I really do. Because everybody knows that there are twins and we know couples that have got twins and we know it’s harder to look after them and we also know, you know, this is previous information that we’ve had, but that uhm, there’s a chance, there’s a higher chance of the pregnancy not going full term for at least one of them … when we went for the consultation at [hospital], he was doing his absolute level best to persuade us not to have twins and the things he was saying is, half of all people who, who, who are pregnant with twins, they end up, he says, he says, they end up in hospital, these twins end up being born and they’re deformed and they’re in hospital. Well I’m sorry, but if the situation was that bad we’d know about it because it’d be, there’d be, there’d be trusts and charities and stuff asking for the problem about twins and it’s, it’s, I think suddenly they’ve tried to make out that having twins is, is worse than what is, because they want us to go away from this idea of having twins, this is what it feels like …
(Couple, in treatment, NHS 112)
When couples and women personally knew someone who had had an adverse outcome during a twin pregnancy or at birth, this raised their awareness of the risks and appeared to influence their decision to opt for SET:
Yeh, you’ve got, I mean, I actually have another friend, it’s well known twin pregnancies don’t go full term so that sort of does, you know, add to the risk, and, you know, because there’s less room in there, there’s more chance of having twin to twin transfusion and things, I just thought well, I want a baby, but I don’t want a baby that desperate I’m going to risk my own life and risk their life and, you know, increase the risk of a handicapped because I mean, you know, nobody really wants a less than perfect baby do they? So you’re not going to put yourself up there with the risk.
(Couple, post treatment, pregnant, NHS 126)
Theme 4: Views on frozen embryos
Subtheme 4.1: Costs and benefits of embryo freezing
The interviews revealed that couples and women, while on the whole accepting, were somewhat sceptical about the process, and success rates, of treatments that used frozen embryos:
It’s like cryogenics and things that you just see on some sci-fi movie or something.
(Woman, in treatment, post baby, private 111)
Uhm, I think that’s a good idea, but I understood from the research that I was given, the chances of it then succeeding then reduce (because of the of thawing out) to sort of 20% or whatever it is and, and for me it’s very much a numbers game I think.
(Woman, in treatment, private 109)
I think it would if they could provide the reassurance that, uhm, you know, the chances are equal to that frozen one embryo, I think if they were, if they were taking that chance away, not taking the chance away, you know, if they couldn’t provide the, uhm, confidence and evidence that actually you would get as much chance from the frozen ones as the fresh ones then again I think you’d feel a bit, well I’d feel a bit, you know, not fair type thing …
(Woman, post treatment, post baby, private 116)
Another woman, in private treatment, viewed the extra cost and treatment time as being one of the major differences between being a self-funding or an NHS patient:
I think this is the difference again between private and NHS. If they said that were free then potentially, but you’re probably talking over a thousand pounds through private for that difference, uhm, in fact I think more than that, probably about up to fifteen hundred, so I think again, it comes down to almost to finance, as well as the mental strain of that, because while you’re working as well, I suppose I work in [states employers name] as well so an employer only has a certain level of tolerance as, ‘cos this isn’t seen as a sickness, as to how much time you can have off …
(Woman, in treatment, post baby, private 114)
However, some people were more open to the option of embryo freezing. It became apparent that participants would be more amenable to choosing a frozen cycle if certain ‘trade-offs’, such as free cycle, were offered:
Well it depends whether they were saying we’ll freeze it at your costs as well, you know, I mean if it was like we’ll freeze it and you’ll get the opportunity to use it again as part of this treatment then that would – that would be acceptable in my mind.
(Couple, in treatment, post baby, private 111)
It was also noted that one of the major advantages of having a frozen cycle was the lack of intensive treatment process that was associated with a fresh cycle:
I do agree with it because, uhm, it’s giving, it is giving another opportunity, you know, and the, and the going through all the drugs part of it is an intrusive kind of part of your life, you know, and you do it, you just get on with it, but it is like, seven o’clock every night we’re out with the needles and we can’t, and it feels quite uncomfortable when your ovaries are, you know, can get a bit like, get a bit of a dull ache and what not, uhm, so you’re not doing anything, you’re just focusing on that all the time, uhm, so if you’ve got the chance of having eggs available without having to do that part of it and perhaps just the other part of getting your womb ready, uhm, and then defrosting [laughing] and then just put them in!
(Woman, in treatment, post baby, private 111)
This woman discussed the influence of being self-funded on her decision to choose SET and then freeze any spare embryos. The cost implications clearly impacted on her decision-making process:
Because I compare myself to my friend who’s had twins through IVF and they, uh, were on the NHS, but the decisions of to freeze or not to freeze, again, if it was NHS, I wouldn’t have thought twice about it probably, because there’s one side which is the risk of damage to the embryo, but the other side is the financial one versus the risk, and if you don’t have that financial argument, you’re more likely to say, well I’ll chance it, all you actually lose is time, you lose, I don’t know what that would be, but a month or two, by going for an extra replacement. Whereas when they start to talk to you about, well it’s a thousand pounds plus, plus, plus, you think, well for that percentage chance, am I better to just say, invest my full amount of money and go for the whole lot again. And so the financial just adds an extra sort of dimension to it all really.
(Woman, in treatment, post baby, private 114)
Subtheme 4.2: Ownership of embryos
Discussion surrounding the freezing of embryos sometimes provoked strong reactions and concerns about ownership of embryos. In the following sequence the interviewer discusses a hypothetical example to explain how the offer of another cycle of treatment using a frozen embryo could be used to encourage SET. Where treatment was self-funded this cycle would be free of charge. Previous experience of a failed treatment appears to have influenced the views of this particular woman:
And in order to, say, persuade you to have a single embryo, I would say that we’ll implant one embryo now and freeze the other one for later, and that would be a free treatment.
Have you ever frozen meat? [raised voice]
Yes.
Do you know what happens to meat when it defrosts? Why would I give you the authority to do that to my embryo? Been down that road, no chance. No chance.
What happened when you went down that road, Amanda?
It didn’t work.
(Woman, in treatment, post baby, private, 115)
She raised concerns that emotional feelings towards embryos as human beings are often overlooked, her feelings towards her embryos had made the decision to freeze particularly difficult for her:
And you are fiercely protective of it. And it is the most peculiar sensation when you see two embryos that are only six to eight cells you know they are a living being, and I know for a fact that one of those turned into a child … who’s got the right to say you can’t do that? I am fiercely protective about it, and you suddenly become it like instant, it’s a switch that goes on …
(Woman, in treatment, post baby, private 115)
Theme 5: Experience of treatment
Subtheme 5.1: Treatment journey to IVF
For many women and couples the treatment journey to IVF had been a long and arduous one. This was particularly the case for those women and couples seeking treatment in NHS settings, who could wait several years before a referral was made to an IVF centre. The journey typically started with a consultation with a GP, then investigations at a local district hospital before being referred to a specialist assisted reproduction centre. Some couples reported that communication between services before they reached an IVF centre was inadequate and they found that distressing. One particular couple had to follow up on several appointments due to lack of communication between services:
This time we were thinking we might give up to be honest, because as much as we want children I was thinking is this going to be too much really for us; we got to nearly forty and we’re quite happy. We’ve got other interests, we are quite happy in our little set up and we do other things and I thought is this really what we want. And we did have times where we thought let’s just forget it and carry on as normal. But, anyway, we decided to carry on. Anyway, unfortunately, the information from our appointment in May hadn’t been sent to the hospital [IVF centre], so only for me ringing up in September, they didn’t know anything about us, so that was another …
… knock back.
(Couple, in treatment, NHS 121)
Many women had complicated gynaecological and obstetric histories, and, as this woman adds, the social pressure from relatives and friends also has an impact:
Yeh, it was a lot to deal with, ‘cos they were quite close how it had happened where there was the miscarriage and then there was the ectopic pregnancy and obviously, also knowing it was a struggle just to get pregnant, because I’d not used contraception all the way through our relationship completely, I mean we’ve been together 8 years now so like we’ve never needed to buy condoms or even go on the pill so, you know, that’s always in the back of your mind ‘cos you know how hard it is, I mean there’s people popping up everywhere with kids and ‘I’m pregnant’ and I’m like you know, and mum’s like, it might be you next time, and stuff like that, and, and it isn’t, so …
(Woman, in treatment, private, 111)
For the following couple the length of time they had been waiting for treatment had impacted on their desire for two babies:
I mean for me it’s not just we want, you know, we want to two and we’ve been trying dead long, we want twins and that’s it, you know …
(Couple, pre-treatment, NHS 104)
Subtheme 5.2: Emotional and physical effects of treatment
The emotional, physical and, for some, financial, burden of undergoing IVF treatment was a dominant theme throughout the interviews. This was one of the factors that impacted on the decision in the majority of women and couples interviewed to prefer DET as twins were perceived as a ‘ready-made’ family and further treatment would not be necessary:
It does take a lot out of you, the whole thing, I mean it’s not just the IVF, it’s the whole, it’s leading up to it, it’s the whole 2 years of trying to, trying to have a baby, uhm, and then we’ve got the miscarriages story which just, I mean that just takes everything out of you when that happens …
(Couple, post treatment, NHS 127)
For the following woman obtaining a diagnosis of infertility had taken some time – she was feeling very frustrated and was keen to start treatment as soon as possible:
It’s just taken so many years, it’s taken a heck of a long time from going to have, you know, really, really bad problems with my own health to getting to a point where I fully understood that I’m infertile. It’s probably taken around three, three and a half years. So I’ve just expressed to my doctor that, you know, I’m very, very frustrated, and I understand that there probably would be some panic, ‘oh, let’s get the IVF going’ and you know and ‘let’s research into treatments’, ‘cos that’s how you do feel, when you find out that you do need treatment, you go into a blind panic, you get on the internet, start researching absolutely everything as if you’re, you know, studying for a medical degree, and there is a thirst for it, so I think maybe the reaction was to prevent panic a little bit, but I wish they had told me sooner [that she had infertility].
(Woman, pre-treatment, NHS 106)
For those women and couples who required more than one treatment cycle the effect of an unsuccessful treatment was emotionally draining. For this woman the effect was compounded by the fact that the couple had self-funded their treatment:
And at the end of the day, being brutal, it’s a lot of money to throw away, because that’s what happens basically. And there isn’t a bottomless pit of funding.
No.
You have to be a bit … I don’t know … I don’t know if I’m … it’s something we [woman and her partner] haven’t spoken about really since March, because it just devastated us that it didn’t work. And things got a bit … you get a bit ostrich-like about it …
(Woman, post treatment, post baby, private, 115)
Theme 6: Consultation process
Women and couples were asked to reflect on their experience of consultations with doctors, nurses and other relevant health professionals. The aim was to explore what style of consultation people preferred and to explore their experience of consultations that had focused on the decision to choose either SET or DET.
Subtheme 6.1: Consultation style – general
Most women and couples expressed a preference for a collaborative style of consultation, whereby they were allowed to express their views and concerns. However, when it came to the decision to opt for SET or DET several people preferred the consultation to be more medically led and guided by the expertise of the doctor:
I think at the end it’s just uh the doctor’s decision because whatever they decide is just good for the patient, because I might say I want like two back in, and then they’ll tell me, two back in is going to be like risky, and stuff, going to have like miscarriage or going to have … I think they just think what the risks are.
(Woman, in treatment, NHS 117)
I think, I guess, the doctor to lead really if there were options available, then I think to have them explain and give the patient the opportunity to make a decision. Uhm obviously a doctor’s the expert in treatment, there’s no doubt about that, and I guess you’ve got to put trust in them to be able to make the right decision as well.
Yeh. I’d go with that.
(Couple, in treatment, NHS 108)
This woman felt that she was more in control in her consultation when she entered IVF treatment for the second time:
Uhm, I think first time round I didn’t really feel that I had a lot of control, uhm, and I was going on whatever the consultant said … whereas after that [slight interruption], once I’d, once I’d been through it once then, then I did feel that I was kind of in control in terms of when I would do it and what I would do.
(Woman, in treatment, private 113)
Subtheme 6.2: Consultation experience – SET vs DET
The initial consultation prior to IVF treatment offers an opportunity to ensure that patients have an understanding of the differences between SET and DET, and to improve their knowledge regarding the risks associated with multiple birth. Women and couples were asked to recall whether any of these issues were addressed in their consultation.
Did anybody discuss with you when you came with your partner about whether you would have one or two embryos transferred?
Yes I did discuss it with Dr A, and I obviously chose this week to have two put back and discussed it with my partner as well, but yeh, I mean it was, it wasn’t really discussed on, uhm, kind of medical risks to me, it was more just about it being my personal choice and he just sort of said most people put two back. I don’t know if that’s true.
(Woman, in treatment, private 109)
Did he address, did he say about the risks of twins and …
Yeh, he did yeh he said the risks and stuff like that, yeh, he did explain the risks … he didn’t quite say that it was a drain on the economy or anything like that … [both laughing]
(Woman, in treatment, post baby, private 111)
Consultations appeared to be more directive where there was a known risk factor (e.g. medical condition) to a woman having a twin pregnancy and birth:
We’ve sort of been told that we will only have one.
Because of [woman’s] specific situation. But the risk, the risk, initial risk of having more than one, uhm, one baby is, is detrimental to the fact that she’s got this [medical condition] so it was just not an option.
(Couple, in treatment, NHS 108)
Not surprisingly, many women and couples made an ‘a priori’ decision about how many embryos they would like to be transferred prior to their consultation:
And from the beginning I’d had, I’d had it in my head that I wanted two embryos anyway, and I’d discussed it with my husband, we’d discussed it together, and if he’d have said, well I think one, then we’d have had that discussion, but he didn’t he said two from, like me, from the beginning so we did agree it before we even came for our consultation really, so as long as the, the doctor was happy to do it, we were happy to do it, and they didn’t say otherwise, so it was just sort of, well we’re having two, that’s it, you know, we’re having two, he’s said we’re having two, we’ve said we’re having two, so that’s what we’re having.
(Woman, post treatment, pregnant, private 116)
Following this consultation this woman did reflect on her initial preference for DET, and this appeared to be mediated by the number of cycles she could obtain:
I think Dr M she explained it very well, she said obviously people go for twin embryos to increase their chances, but the chances of miscarriage later on, or other complications are obviously increased as well she said obviously, like she said, you’re not designed to uh, carry two babies at once, not like sheep, so other animals do. Uh, I was concerned thinking like there was only three chances you’d get, so that’s why you would want to maximise your chances. Uhm, but the fact that you can actually have three chances….
(Woman, pre-treatment, NHS 101)
One couple who had undergone IVF treatment in the past noted the change in the advice from clinicians had changed over time. In their first round of treatment they had been encouraged to have two embryos transferred:
There was, yeh, there was a lot of discussion about that, but at that time, and it’s interesting, probably get on to it, we’ve just gone through it again and the advice we’ve been given has changed a lot in that, what, two and a half years. Uhm, and at the time we were basically encouraged to go for two embryos because there was a higher chance of, of outcome, and the chance of multiple birth, we were explained, was incredibly low, uhm, so yeh, we were basically encouraged to go for two. So we didn’t know any otherwise so we went for it.
(Couple, post treatment, private 116)
Theme 7: Views on randomised controlled trials of eSET
The majority of women and couples interviewed had limited knowledge about RCTs. When the interviewer explained this research design many could see the value of such a design but did not think it was feasible for those undergoing IVF treatment.
Subtheme 7.1: Views on RCTs – general
For this woman entering a trial had the potential to threaten her treatment ‘success’, therefore she would not consider this option:
I wouldn’t want to do it, I wouldn’t want to be a guinea pig for something that I’m putting everything into, uhm, and I’m so desperate for this [a pregnancy] to happen, you know, if it was, you know, if it was research into something else that was less important to me, then no problem. But not like, not where I potentially am reducing the risk of success.
(Woman, in treatment, post baby, private 113)
Others could see that this might appeal to some couples if there was an inbuilt reward, for example treatment costs were waived for those in the trial or extra cycles were offered. The following woman also raised the issue of the juxtaposition of science and emotion in IVF treatment:
You know, if the NHS was paying for it, I don’t know, because, God, if I was in the NHS and I had my one go, you know, I might just want to maximise what chances I have. I think that, you know, that the issues are scientific, but for most, the lay person, it’s more of an emotional thing and the science is kind of, you could tell them that, anything, and I think that most people would still choose two. Just ‘cos in their head that just feels like more success I think.
(Woman, in treatment, private 109)
This couple were more open to this design as they felt that it would be a good way of accurately determining success rates as long as informed consent was obtained:
If you just said I want one … so it’s tossing a coin whether you had one or two embryos implanted.
Right. It’s probably a good idea. I think it would be interesting don’t you, to see how affected … I think it’s a good thing.
That would be the best thing. But in terms of the other bits, the emotion of you going through treatment …
As long as you’ve agreed to that.
You’d have to sign …
Yes, it would have to be with your full consent.
That’s fair enough, yes.
(Couple, in treatment, NHS 120)
Subtheme 7.2: Views on randomised controlled trials – negative
Some of those interviewed were opposed to RCTs in this area, and expressed negative views. Funding source was also a factor in rejecting this type of research design:
Ohhhh!!! Shine a light. No bloody way!
How would you feel about that?
No way. Not if I’m paying for it. No chance. End of conversation. No.
(Woman, in treatment, post baby, private 115)
The following woman thought that RCTs would be useful for other conditions (e.g. heart disease) but not for couples with infertility problems. Again, the emotional impact of the expected ‘outcome’ (live birth) was emphasised:
I don’t think that would be, I wouldn’t agree with that because it wouldn’t be fair to someone, well, you might end up with twins, but you know, it’s possible that we didn’t put one embryo back, because your hopes and dreams of having a family are so important, you know, so none of us want the IVF, we only want a family, so, you know, you will get people dreaming that they’re going to have twins and then they can get on with their lives and it’s a little bit different from having, you know, a heart condition [pause]. I’m sure there’s people with heart conditions would like an operation that get rid of, or something that would ultimately get rid of the problem, I mean infertility, the problems not going to be solved without having the family, I’m not, I’m not sure. I think that’s playing God a little bit too much with people’s bodies.
(Woman, pre-treatment, NHS 106)
Discussion
The findings reveal that most of the women and couples undergoing IVF treatment who were interviewed in this study show a preference for DET over SET. The interviews were conducted to assess the views of patients as they travelled through the treatment journey of IVF. More specifically, interviews were conducted at three key treatment phases (pre-treatment; in treatment; post treatment) to assess whether treatment stage had an effect on decision-making. They also included interviews with couples who self-funded their treatment. In addition, five women were interviewed who already had a baby and were seeking treatment for the second time. The interviews captured the richness and diversity of experience and views from a wide range of selected women and couples in the IVF process. The interviews were conducted over a 2-year period, during which time the momentum towards a SET policy has gained in strength and publicity. However, despite some women and couples showing increased awareness of this policy over time, its effect on the decision to opt for SET appears minimal.
The reasons for this preference for DET are complex and multifaceted, and not just simply related to the desire for twins. Several factors appear to impinge on the decision-making process, including enhancing treatment success, length of infertility, treatment experience, desire for a baby, lack of information and uncertainty about using frozen embryos, advancing maternal age and the emotional, physical and sometimes financial burden of IVF treatment. For individual women and couples several distinct factors may combine which can ultimately influence treatment decisions.
The strong preference for DET found here is of interest because the sample of women and couples seeking treatment via the NHS were attending a centre in which the uptake of SET was higher than average. This particular centre reports a 35% SET rate, with an accompanying twin rate of above 20%. Despite being in this pro-SET environment, there was limited knowledge of SET and the risks associated with twin pregnancies in this sample. This could be explained by the highly selective sampling strategy used in this study. However, it appears that both local clinic policy and wider publicity campaigns (e.g. Braude3) have had little effect in increasing understanding and knowledge. Some of the factors influencing women and couples to favour SET were consistent with past research, for example having a pre-existing medical condition, advancing maternal age (for some), e.g. Pinborg et al. ,22 Blennborn et al. , 30 van Peperstraten et al. 29
The finding that subfertile couples prefer twins is not new and has been well documented in the literature. 23,24,107 This appears to be a strong and enduring preference that is resistant to change, even when the associated risks are fully explained. 26,31 In this study women’s and couples’ knowledge of the associated risks of multiple birth were mainly confined to fetal outcomes, as previously described by Blennborn et al. 30 The interviewees consistently minimised their personal risk profile of twins, even when the interviewer discussed the maternal, fetal and societal risk in more detail. This can be explained, in part, by the finding that most women and couples thought that twins were a normal event in society, both in IVF treatment and in naturally conceived pregnancies. They did not perceive that they had a greater risk profile than women who achieve a pregnancy through natural conception. This finding can be compared with that of Scotland et al. 31 who found that the concept of ‘treatment success’ took priority over future concerns about the risks to babies in twin pregnancy and birth. In this sample, it can be argued that the risk of twins was minimised in comparison with the perceived greater risks associated with not having children at all.
It is known that people in general often provide an inaccurate judgement of personal risk, with a tendency to downplay the associated risks across a range of events. 108 This process of risk minimisation can be further contextualised in a psychological framework provided by Schwarzer. 109 He argues that optimism is a cognitive construct that plays a part in influencing behaviour change. He describes two forms of optimism: functional and defensive. Functional optimism is a facilitative concept that is likely to enhance positive health behaviours, whereas defensive optimism acts to reduce risk perception and this could encourage people to ignore risk profiles as being relevant to others but not to them. It could be argued that many of the women and couples interviewed in this study displayed this form of defensive optimism, and, given the complexity of the emotional and physical aspects of IVF treatment, this could be as a protective mechanism. What was apparent in the interviews is that women and couples generated their own subjective risk factor theories which were personalised to their own experiences. Future interventions designed to influence the decision-making process regarding the choice of SET or DET would need to address these subjective beliefs that have developed over time.
In this study the drive to encourage SET in couples undergoing IVF was viewed by many as a ‘smoke screen’ to cover the need for the NHS to ration limited resources. Several participants thought that the move towards SET was more of a government initiative, rather than being part of the remit of IVF clinicians, clinics and policy advisors. Women and couples found it difficult to engage with the wider public health concerns about the cost of twins on health and social-care resources. They compared this with the ‘hidden’ costs associated with infertility, for example, the emotional, physical and often financial burden associated with treatment. Women also expressed a concern that employers viewed infertility as a lifestyle choice and not a genuine medical condition, thus taking time off work to access treatment could be difficult. These comparisons appeared to cancel out any wider societal costs.
Furthermore, where the introduction of SET was viewed as the government’s way of limiting resources, this created a sense of injustice in the system. Several interviewees commented that they did not drink or smoke and viewed having children as contributing to society as a whole. In some cases this caused resentment towards other groups of individuals (e.g. teenage mothers, alcoholics, etc.) who were perceived as having an unfair claim on such resources. This perception, while unhelpful in the long term, can be understood in the context of those seeking IVF treatment who may have already encountered inequity of resource allocation. This can be seen in the postcode lottery associated with individual PCTs, and how many cycles they are prepared to fund. For some the drive towards SET was seen as an affront to personal treatment choice, which is at odds with the Department of Health’s ‘patient choice’ agenda. 110 This policy initiative focuses on enabling patient choice across a variety of conditions to encourage a greater sense of control and provide more personalised services. For patients undergoing IVF who express a preference for DET, the sense of being steered towards SET could be viewed as way of curtailing patient choice.
As far as we are aware this is the first study to specifically target the views of women and couples undergoing private treatment, as well as that in the NHS. This is an important aspect as, within IVF, the need to access private treatment can be related to lack of access to NHS funding, rather than an option for those who are financially able to pay for treatment. The interviews in this study revealed that, not surprisingly, funding did impact on the decision to opt for SET. For those who self-funded their treatment this added an extra layer to their decision-making process. The high cost of private treatment enhanced the view that it was better to opt for DET, in order to negate the need for further treatment, increase success rates, and achieve a ‘ready-made’ family rather than pay for subsequent cycles. This view was also prevalent in those women who already had a child (via either IVF or natural conception). This shows that, for a subset of women, preference for twins is not mitigated by a previous successful live birth. This finding differs from that of Glazebrook et al. 111 who found that having a child mitigated the desire for twins however, their sample were not self-funding. Opinions on frozen embryos revealed a mixed profile from both NHS and private patients: some found the option of SET followed by a frozen cycle as unacceptable, and viewed this as a threat to success rates. Concerns about ownership of embryos were also raised. Others were more amenable to this form of treatment; however, several self-funding participants felt that this should be offered as a free cycle if the uptake of SET was to be encouraged.
There are several limitations to this study. As this was a small qualitative study, the findings cannot be viewed as generalisable to all women and couples undergoing IVF treatment. The initial mail shot at the NHS clinic yielded a low response rate, and unfortunately ethical and time restraints did not allow for repeated mailings. Patients undergoing IVF treatment reported a considerable treatment burden over a concentrated timeframe, and as such it is possible that the timing of the request is crucial. Future studies would benefit from a longer recruitment period, more innovative recruitment strategies and additional reminder systems. In addition, the selectiveness of the sample may have attracted only those people who held particular views about SET. Clinicians’ views were not accessed in this study, but we know from previous work that clinicians display a range of views regarding SET and that this can have an effect on the consultation. 29,112 The clinician/patient interaction in the decision-making process to choose SET or DET can be inferred only from the data collected in the interviews. However, despite these limitations, rich data were obtained from a wide variety of women and couples undergoing IVF which would not have been possible within the confines of a routine clinical treatment consultation. The interviewer was independent of the treatment process, and the majority of the interviewers were conducted in the participants’ own home at their convenience with no time limit on the interview, which potentially could have increased the couple’s feelings of control and empowerment. The men interviewed in this study contributed equally in the interviews, and this may not always be the case in a clinical setting.
In conclusion, the findings show that the strong desire to maximise treatment success (in terms of achieving a pregnancy) and the emotional, physical and, for some, financial burden of IVF treatment appear to negate the argument for offering more treatment cycles with SET in order to bring success rates in line with DET. Furthermore, offering a treatment plan of SET plus embryo freezing would not be acceptable to some groups of patients. There is a lack of accurate information regarding the freezing of embryos, and any policy would need to take into account the emotional feelings towards embryos expressed by some women in this study. In addition, whereas a frozen cycle may not have the same treatment burden as a fresh cycle, the accompanying emotional burden is not necessarily reduced. There is need to verify the findings of this study with a larger national survey sample to assess how representative the views expressed in this study are of the wider population undergoing IVF.
This study has shown that the decision-making process surrounding the choice of SET versus DET is complex, multifaceted and dependent on a number of factors. In order to promote SET, clinicians, clinics and policy-makers need to be aware of the strength of women’s and couples’ beliefs. Such belief systems have been formed over time, and are unlikely to be significantly altered in a routine clinic consultation. As Bergh et al. 112 comment, although legislation has been highly effective in reducing multiple births in Sweden, changing attitudes is an equally important goal. More work is needed, focused on helping women and couples undergoing IVF make treatment choices that are tailored to them as individuals, particularly as past interventions have met with limited success. 26 It is apparent that information needs to be tailored and targeted to the various subgroups of patients undergoing IVF treatment. The view that twins are a normal event was prevalent in this sample, and this normalisation process requires acknowledgement. The perception that twins could have negative outcomes was only really addressed by those who had experience of these outcomes in their own social networks. There is a possible role for counsellors, who specialise in subfertility, and psychologists in the development of such interventions, to help guide clinicians in the identification and modification of unhelpful attitudes and beliefs. The move towards a SET policy for women and couples undergoing IVF treatment faces many challenges; however, these are perhaps more heightened in the private sector where financial outlay by patients may affect their acceptance of SET.
Summary
The interviews indicate that, despite having had the risks explained, for many patients a twin birth is the ideal outcome. There is scepticism concerning the motivation to reduce twin numbers.
Many equate this to saving money and a lack of due priority for fertility treatments. Potential restrictions on DET are seen to conflict with the NHS patient choice agenda. Scepticism also exists over the use of cryopreservation and frozen transfers.
Chapter 3 Modelling the national data
Introduction
The HFEA, which regulates IVF treatment, maintains a register of all such treatments performed in the UK. All treatments must be registered with the HFEA by law. Clinic returns contain details of the treatments and the numbers of embryos generated and their fates and basic patient data, along with minimal outcome data, are recorded. However there are no data on embryo quality. These data collected by the HFEA are used for regulatory purposes, to monitor clinics’ performance and to provide basic information about clinics to patients. Here we have analysed a cohort of IVF treatments from 2000–5 inclusive.
In the next section we describe the data extraction and cleaning necessary to enable a meaningful analysis, and then go on to present the characteristics of the resultant dataset, describe how the LR models were developed, present the models, along with some model validation work, including the extension to include frozen cycles, discuss the implications for eSET, and conclude with a discussion. There are a number of sections which are of more technical interest and do not contain information necessary to understand the rest of the material: these are indicated with an asterisk against the title.
Data extraction and cleaning
This section outlines the process by which the dataset provided was processed to give the data analysed.
Data source
The original data provided from the HFEA registry had 232,990 treatment cycles covering the period 2000–5. These included a variety of treatments not appropriate to this study. Of the 232,990 cycles, 128,139 were recorded as IVF (with 102,152 of these having one to three embryos transferred) and 91,262 as ICSI (with 84,761 of these having one to three embryos transferred).
Data selection
Cycles were included if they met the following inclusion criteria:
-
treatment type: ICSI or IVF
-
cycles with one, two, or three embryos transferred
-
age 19–54
-
patient’s own eggs
-
date started trying to conceive or last pregnant after start of 1980.
Cycles were excluded if they met any of the following exclusion criteria:
-
donor eggs
-
frozen/thawed eggs
-
natural or hormone replacement therapy (HRT) induction
-
cases with rare, non-standard, ovulation induction regimes (defined as induction types recorded for fewer than 150 cycles in the database)
-
cycles not fully identifiable as either fresh or frozen cycles (no mixed cycles), i.e. fresh cycles with frozen embryos and frozen cycles with fresh eggs mixed or cycles classified as fresh and frozen.
After selecting the relevant data we had 172,189 embryo transfers from 104,610 patients in 84 treatment centres.
*Data cleaning and exploration of missing data
Table 13 lists some of the integrity checks made on the database and the number of cycles that failed each test. A number of tests that never failed are not listed. In this table we give the total failing the test, the breakdown by outcome, the mean age of those failing the test and the proportion failing in fresh cycles. Cycles could fail multiple tests so there are more failures noted than cycles excluded.
| Reason for exclusion | Number failing | Number of births | Mean age (SD) | Number of fresh cycles (%) | ||
|---|---|---|---|---|---|---|
| 0 (%) | 1 (%) | 2+ (%) | ||||
| Age (missing) | 2496 | 2027 (81%) | 341 (14%) | 128 (5%) | 2206 (88%) | |
| Duration (missing or impossible value due to input errors) | 15,679 | 12,084 (77%) | 2739 (17%) | 856 (6%) | 35.1 (4.3) | 12,557 (80%) |
| Previous assisted pregnancies > total previous pregnancies | 226 | 162 (72%) | 52 (23%) | 12 (5%) | 34.6 (4.5) | 174 (77%) |
| Previous births > total previous pregnancies | 234 | 162 (69%) | 60 (26%) | 12 (5%) | 35.0 (4.2) | 179 (76%) |
| Previous IVF treatments = 0 (or missing) and previous assisted pregnancies > 0 | 3640 | 2685 (74%) | 724 (20%) | 231 (6%) | 35.1 (4.4) | 3025 (83%) |
| Primary/secondary diagnosis conflicts (female) | 5306 | 3886 (73%) | 1068 (20%) | 352 (7%) | 34.8 (4.4) | 4432 (84%) |
| Primary/secondary diagnosis conflicts (male) | 7817 | 6107 (78%) | 1314 (17%) | 396 (5%) | 35.4 (4.6) | 6732 (86%) |
| Primary/secondary diagnosis conflicts (couple) | 4926 | 3789 (77%) | 893 (18%) | 244 (5%) | 35.6 (4.5) | 4167 (85%) |
| Total eggs mixed > total mixed with partners sperm + total mixed with donor sperm | 22 | 16 (73%) | 5 (23%) | 1 (5%) | 34 (3.7) | |
| Embryos created > eggs mixed (fresh cycles) | 66 | 56 (85%) | 9 (14%) | 1 (2%) | 34.7 (4.3) | |
| Embryos created > embryos created with partner + embryos created with donor (fresh cycles) | 16 | 12 (75%) | 4 (25%) | 0 (0%) | 33.9 (4.2) | |
| Embryos created < embryos transferred (fresh cycles) | 95 | 83 (87%) | 11 (12%) | 1 (1%) | 34.7 (4.4) | |
| Embryos thawed + viable > embryos thawed (frozen cycles) | 4 | 3 (75%) | 1 (25%) | 0 (0%) | 34.2 (3.8) | |
| Embryos thawed + viable < embryos transferred (frozen cycles) | 231 | 209 (90%) | 18 (8%) | 4 (2%) | 34.2 (4.3) | |
| Source of sperm is partner but embryos transferred field not flagged as partner | 1938 | 1603 (83%) | 269 (14%) | 66 (3%) | 34.4 (4.4) | 519 (27%) |
| Cycle recorded as having embryo transfer but a reason for not transferring embryos given | 87 | 82 (94%) | 5 (6%) | 0 (0%) | 34.7 (4.4) | 75 (86%) |
| Egg collection date missing (fresh) or present (frozen) | 694 | 548 (79%) | 111 (16%) | 35 (5%) | 34.2 (4.3) | 547 (79%) |
| Date egg thawed present | 31 | 31 (100%) | 0 (0%) | 0 (0%) | 33.8 (4.1) | 11 (35%) |
After data failing these checks had been removed, we were left with 139,848 transfers from 85,349 patients in 84 treatment centres. 19% of the cycles contained some missing or invalid data. The biggest problem was in the recording of the duration of infertility, with significant loss also due to conflicts in the definitions of primary and secondary infertility.
Reassuringly there is no indication that there was differential loss of data according to any of the characteristics we have explored, except that more frozen cycles were lost. Figure 7 shows the values of outcome, age and transfer type (fresh/frozen) for the removed and included cases. It is of note that we can detect no difference in data quality between cycles leading to a pregnancy and those that did not (as demonstrated in the figure); we would expect such a difference owing to the extra data checking that was instituted in the HFEA historic data project.
FIGURE 7.
Cases included and removed from the analysis. Pairs of panels show excluded and included cases, upper panels show percentages by outcome, middle panels the age distributions as a box and whisker plot and lower panels percentages of fresh and frozen cycles.
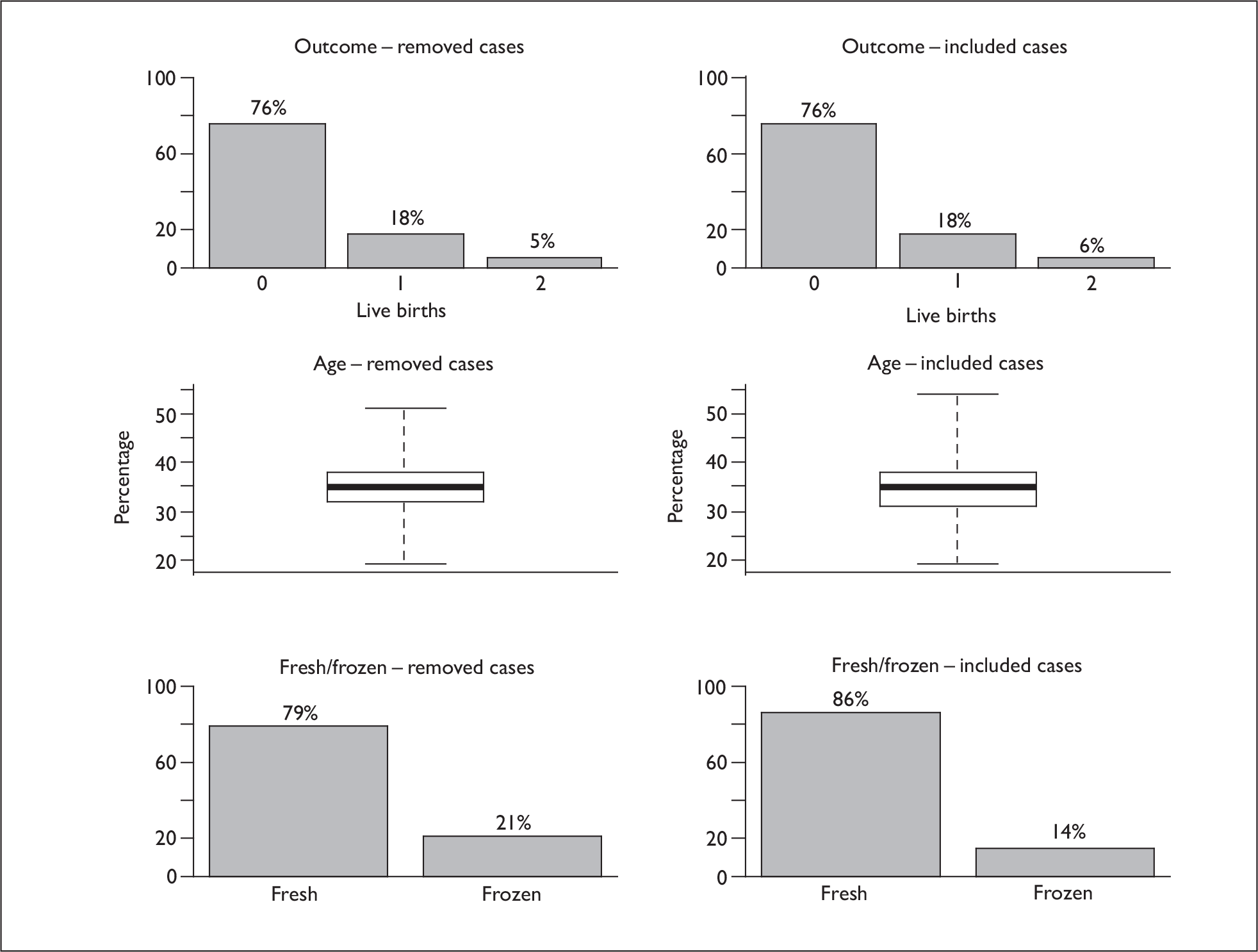
*Patient history in the HFEA data
One specific issue with the HFEA data is updating of patient history. For individuals with several cycles it has been confirmed by the HFEA that variables such as previous pregnancies, infertility status and previous treatments are not updated from cycle to cycle. In other words, the history recorded on the database is always that at the time the couple first attended for treatment. We have updated the dataset where possible to adjust for this but obviously there may be further errors in the dataset arising from this issue. Attempt number, as defined by the HFEA, includes all previous treatments with and without embryo transfer, being derived from the number of registered cycles.
Characteristics of the dataset
After cleaning, the total number of transfer cycles available for analysis was 139,848: 119,930 fresh and 19,918 frozen, from 85,349 couples (Table 14).
| Couples | Cycles | Cycles with one embryo transferred (%) | Cycles with two embryos transferred (%) | Cycles with three embryos transferred (%) | |
|---|---|---|---|---|---|
| All | 85,349 | 139,848 | 13,285 (9.5%) | 106,143 (75.9%) | 20,420 (14.6%) |
| Fresh | 81,965 | 119,930 | 10,139 (8.5%) | 92,271 (76.9%) | 17,520 (14.6%) |
| Frozen | 14,884 | 19,918 | 3146 (15.8%) | 13,872 (69.6%) | 2900 (14.6%) |
Table 15 summarises the characteristics of the patients in the dataset for the variables available and considered for the modelling process, while Table 16 summarises the outcomes on a per-embryo transfer basis. In Table 15 we see that around 1000 (5%) frozen transfers were recorded as first attempts, which must reflect incorrect recording or inconsistent definition of attempt number, possibly reflecting egg retrievals with no transfer being omitted from the attempt count.
| Parameter | Categoriesa | Fresh cycles (%) | Frozen cycles (%) |
|---|---|---|---|
| Numbers of transfers | 119,930 (86%) | 19,918 (14%) | |
| Number of embryos transferred | 1 | 10,139 (8%) | 3146 (16%) |
| 2 | 92,271 (77%) | 13,872 (70%) | |
| 3 | 17,520 (15%) | 2900 (15%) | |
| Age | Mean (SD) [range] | 34.4 (4.4) [19–50] | 34.5 (4.4) [19–54] |
| Number of eggs collected | Mean (SD) [range] | 10.5 (5.9) [1–85] | |
| Number of eggs inseminated | Mean (SD) [range] | 9.4 (5.4) [1–65] | |
| Number of embryos created/recovered | Mean (SD) [range] | 6.5 (4.2) [1–45] | 3.7 (2) [1–22] |
| Treatment attempt | 1st | 69,123 (58%) | 1073 (5%) |
| 2nd | 27,354 (23%) | 8835 (44%) | |
| 3rd | 12,835 (11%) | 4826 (24%) | |
| > 3rd | 10,618 (9%) | 5184 (26%) | |
| IVF or ICSI | IVF | 63,182 (53%) | 11,461 (58%) |
| ICSI | 56,748 (47%) | 8457 (42%) | |
| Total previous pregnancies/births | Never pregnant | 69,681 (58%) | 8835 (44%) |
| Previously pregnant | 29,919 (25%) | 5872 (29%) | |
| 1 previous live birth | 16,315 (14%) | 4469 (22%) | |
| ≥2 previous live births | 4015 (3%) | 742 (4%) | |
| Years infertile | Mean (SD) [range] | 5.1 (3.9) [0–25] | 4.8 (4) [0–25] |
| Tubal diagnosis | Yes | 29,108 (24%) | 5446 (27%) |
| Diagnosis of PCOS | Yes | 15,116 (13%) | 2927 (15%) |
| Endometriosis | Yes | 8567 (7%) | 1105 (6%) |
| Male factor diagnosis | Yes | 52,300 (44%) | 8380 (58%) |
| Idiopathic diagnosis | Yes | 25,305 (21%) | 3877 (19%) |
| Donor sperm | Yes | 2681 (2%) | 495 (2%) |
| Day of transfer | < 2 | 1386 (1%) | NA |
| 2 | 82,299 (69%) | ||
| 3 | 31,560 (26%) | ||
| > 3 | 4685 (4%) | ||
| Year | 2000 | 17,338 (14%) | 1478 (7%) |
| 2001 | 18,834 (16%) | 2694 (14%) | |
| 2002 | 19,195 (16%) | 3235 (16%) | |
| 2003 | 19,864 (17%) | 4003 (20%) | |
| 2004 | 22,031 (18%) | 4066 (20%) | |
| 2005 | 22,668 (19%) | 4442 (22%) | |
| Transfers per couple | 1 | 55,020 (67%) | 11,228 (75%) |
| 2 | 19,083 (23%) | 2709 (18%) | |
| > 2 | 7862 (10%) | 947 (7%) |
| Cycle | Embro transfer | 0 live births (%) | 1 live birth (%) | ≥ 2 live births (%) | LBEs (%) | Twin ratea |
|---|---|---|---|---|---|---|
| All | 1 | 12,039 (91%) | 1233 (9%) | 13 (0%) | 1246 (9%) | 1% |
| 2 | 77,809 (73%) | 21,168 (20%) | 7166 (7%) | 28,334 (27%) | 25% | |
| 3 | 16,107 (79%) | 3085 (15%) | 1228 (6%) | 4313 (21%) | 28% | |
| Fresh | 1 | 9163 (90%) | 964 (10%) | 12 (0%) | 976 (10%) | 1% |
| 2 | 66,421 (72%) | 19,117 (21%) | 6733 (7%) | 25,850 (28%) | 26% | |
| 3 | 13,732 (78%) | 2676 (15%) | 1112 (7%) | 3788 (22%) | 29% | |
| Frozen | 1 | 2876 (91%) | 269 (9%) | 1 (0%) | 270 (9%) | 0% |
| 2 | 11,388 (82%) | 2051 (15%) | 433 (3%) | 2480 (18%) | 17% | |
| 3 | 2375 (82%) | 409 (14%) | 116 (4%) | 514 (18%) | 20% |
Developing a logistic regression model
This section describes the development of the LR models. The basic approach and presentation of the results was described in Chapter 1, Statistical modelling approaches. The basic models include random effect terms (simple random intercepts) to allow for correlations between transfers in the same patients and for centre differences, with models without these effects also fitted for comparison.
LR model development for fresh cycles
We adopted a strategy whereby the variables to be included in the model were pre-specified and included as main effects regardless of statistical considerations. As there was an excess of data, rather than assume a functional form for numerical variables such as age and numbers of embryos, these were fitted as categorical variables with a large number of groups. The relationships were expected to be highly non-linear. Preliminary exploratory analysis of the variable distribution was performed to select appropriate categorisation suitable across all the subsets of data to be used, avoiding groups with small numbers of observations. Three of the potential variables were very similar measures of the success of the stimulation and fertilisation process and were highly correlated: eggs collected, eggs mixed and embryos created. Owing to concerns over co-linearity, the most predictive of these variables was considered for the model: each was added individually to a model with number transferred and age group, and embryos created selected as having the lowest AIC.
The variables included in the models with their categorisation are shown in Table 17.
| Parameter | Categoriesa | Comments |
|---|---|---|
| Numbers of embryos transferred | 1, 2 or 3 | This is included to allow for the possibility that the clinical decision may select different patient populations |
| Age | ≤ 26, 27–29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40–42, ≥ 43 | Well-documented predictor (see Chapter 1, Informal review of the relevant literature) |
| Number of embryos createdb | 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11–12, 13–16, ≥ 17 | Well-documented predictor (see Chapter 1, Informal review of the relevant literature) |
| Number of embryos thawed and viablec | 1, 2, 3, 4, ≥5 | |
| Treatment attempt | 1st, 2nd, 3rd, 4th, 5th, ≥ 6th |
Well-documented predictor (see Chapter 1, Informal review of the relevant literature) Note: attempt is defined as total fresh and frozen cycles with or without transfer |
| IVF or ICSI | IVF, ICSI | |
| Birth history | 0 previous pregnancies, previously pregnant, 1 live birth, ≥ 2 live births | |
| Years infertile | 0–1, 2, 3, 4, 5, 6, 7, 8, 9, 10–11, ≥ 12 | |
| Tubal diagnosis | No, yes | Previous studies are conflicting in the role of diagnosis (see Chapter 1, Informal review of the relevant literature). It was decided to include diagnosis as a set covering the main recorded diagnoses |
| Diagnosis of PCOS | No, yes | |
| Endometriosis | No, yes | |
| Male factor diagnosis | No, yes | |
| Idiopathic diagnosis | No, yes | |
| Donor sperm | No, yes | |
| Day of transfer | < 2, 2, 3, > 3 | |
| Year | 2001, 2002, 2003, 2004, 2005 | Trends over time are expected |
*Interactions
Interactions were added to the model with all variables according to the BIC. The reason for choosing the BIC was to prevent overcomplicated terms being included purely as a result of the size of the dataset. Whereas the AIC penalises according to the number of parameters in the model only, the BIC also penalises on the size of the dataset. We considered interactions of each variable with each of the three most important variables (number transferred, age and embryos created). Thus there were 14 + 13 + 12 = 39 interactions tested. No interactions met the inclusion criteria for the model for all fresh cycles and so these were not considered further.
LR models including frozen cycles
In order to compare the outcomes of fresh and frozen cycles the full model for all cycles was refitted to the combined fresh and frozen cycle data. The number of embryos created was not available for the frozen cycles; for these cycles, this was set to a new category ‘frozen’. Thus, the coefficient for ‘frozen’ is comparable to a fresh cycle with six embryos created. Transfer day was also removed from the model as it does not have a simple interpretation for frozen data.
A nested random effects model to allow for clustering at the centre and patient levels was used, as with the fresh cycles. It would have been desirable to include each egg collection as a clustering variable but this information was not present in the HFEA dataset owing to a lack of linkage between the frozen cycles and the fresh cycle in which the embryos were created.
Each variable was tested for an interaction with a fresh/frozen binary variable (using the fixed model for computational reasons), allowing us to see if individual variables behave differently in frozen cycles. These interactions were added sequentially, with the variable with the most significant value for the LRT being included first. As there was some evidence of different behaviour in frozen cycles for some variables (in particular, age), to enable comparison a model for frozen cycles alone was fitted. This was equivalent to the model for fresh cycles, apart from the number of embryos created which was not present, but a new variable, number of embryos thawed and viable, was included instead. This enables direct comparison of the effects of variables on the fresh and frozen cycles.
The logistic regression models
Here we present the LR models for the HFEA dataset. We first present a model for LBEs in the total dataset. We then present a model for twins given an LBE. For this model we consider only patients with DET, as it clearly does not make sense in patients undergoing SET, and cycles with more than two embryos transferred are not relevant to the SET/DET decision. We therefore additionally present a model for LBEs in the DET patients. Finally, we present the model for LBEs in frozen transfers. Some details of the model validation work are presented but can be omitted (see section LR model validation).
Model for LBEs in all fresh cycles
The model parameters are shown in Table 18 and the fitted LBE rates are shown in Figures 8 and 9. Table 18 shows the coefficients for the LR model for a successful treatment outcome from a single fresh cycle. The left-hand columns give the estimates for a fixed effect model – i.e. without any allowance for intercouple correlations – while the right hand columns show the estimates for the model which includes a couple random effect. There is a strong dependence with age as expected (see, for example, Templeton et al. 79), with a steep decline in success rates after around age 32. The number of embryos created is a strong prognostic factor – more embryos created gives more from which the embryos to be transferred can be selected – and so acts as a surrogate indicator of embryo quality. It is likely that the embryo number also acts as a surrogate for hormonal status as this is correlated with the number of eggs collected. 2,113
| Variablea | Fixed effects only | Including REs | |||||
|---|---|---|---|---|---|---|---|
| β | SE | p b | OR | 95% CI | β | SE | |
| Intercept | –0.69 | 0.04 | 0.50 | 0.46 to 0.54 | –0.81 | 0.05 | |
| Number of embryos transferred | < 0.001 | ||||||
| 1 | –0.66 | 0.05 | 0.52 | 0.47 to 0.57 | –0.66 | 0.05 | |
| 3 | 0.03 | 0.02 | 1.03 | 0.99 to 1.07 | –0.02 | 0.02 | |
| Age (years) | < 0.001 | ||||||
| ≤ 26 | 0.10 | 0.04 | 1.11 | 1.02 to 1.20 | 0.14 | 0.04 | |
| 27–29 | 0.15 | 0.03 | 1.16 | 1.10 to 1.23 | 0.17 | 0.03 | |
| 30 | 0.19 | 0.03 | 1.21 | 1.14 to 1.28 | 0.22 | 0.04 | |
| 31 | 0.13 | 0.03 | 1.14 | 1.07 to 1.21 | 0.15 | 0.03 | |
| 32 | 0.16 | 0.03 | 1.18 | 1.11 to 1.24 | 0.18 | 0.03 | |
| 33 | 0.12 | 0.03 | 1.12 | 1.06 to 1.20 | 0.14 | 0.03 | |
| 34 | 0.06 | 0.03 | 1.06 | 1.00 to 1.13 | 0.07 | 0.03 | |
| 36 | –0.12 | 0.03 | 0.89 | 0.84 to 0.94 | –0.13 | 0.03 | |
| 37 | –0.26 | 0.03 | 0.77 | 0.73 to 0.82 | –0.27 | 0.03 | |
| 38 | –0.31 | 0.03 | 0.74 | 0.69 to 0.78 | –0.32 | 0.04 | |
| 39 | –0.53 | 0.04 | 0.59 | 0.54 to 0.64 | –0.55 | 0.04 | |
| 40–42 | –0.99 | 0.04 | 0.37 | 0.34 to 0.40 | –1.03 | 0.04 | |
| ≥ 43 | –2.21 | 0.10 | 0.11 | 0.09 to 0.13 | –2.26 | 0.10 | |
| Number of embryos created | < 0.001 | ||||||
| 1 | –0.70 | 0.07 | 0.50 | 0.43 to 0.57 | –0.72 | 0.07 | |
| 2 | –0.61 | 0.03 | 0.54 | 0.51 to 0.58 | –0.63 | 0.04 | |
| 3 | –0.36 | 0.03 | 0.70 | 0.66 to 0.74 | –0.37 | 0.03 | |
| 4 | –0.21 | 0.03 | 0.81 | 0.76 to 0.86 | –0.21 | 0.03 | |
| 5 | –0.10 | 0.03 | 0.90 | 0.85 to 0.96 | –0.10 | 0.03 | |
| 7 | 0.01 | 0.03 | 1.01 | 0.95 to 1.07 | 0.01 | 0.03 | |
| 8 | 0.11 | 0.03 | 1.12 | 1.05 to 1.18 | 0.11 | 0.03 | |
| 9 | 0.09 | 0.03 | 1.09 | 1.03 to 1.16 | 0.09 | 0.03 | |
| 10 | 0.17 | 0.04 | 1.18 | 1.10 to 1.28 | 0.17 | 0.04 | |
| 11–12 | 0.17 | 0.03 | 1.19 | 1.12 to 1.26 | 0.17 | 0.03 | |
| 13–16 | 0.20 | 0.03 | 1.22 | 1.15 to 1.30 | 0.20 | 0.03 | |
| ≥ 17 | 0.17 | 0.04 | 1.18 | 1.10 to 1.28 | 0.18 | 0.04 | |
| Cycle | < 0.001 | ||||||
| 2nd | –0.21 | 0.02 | 0.81 | 0.78 to 0.84 | –0.18 | 0.02 | |
| 3rd | –0.24 | 0.02 | 0.78 | 0.76 to 0.82 | –0.20 | 0.02 | |
| 4th | –0.32 | 0.03 | 0.73 | 0.68 to 0.77 | –0.26 | 0.04 | |
| 5th | –0.26 | 0.05 | 0.77 | 0.70 to 0.85 | –0.19 | 0.05 | |
| 6th ≥ | –0.42 | 0.05 | 0.66 | 0.60 to 0.72 | –0.35 | 0.06 | |
| ICSI | –0.05 | 0.02 | 0.02 | 0.96 | 0.91 to 0.99 | –0.06 | 0.02 |
| Previous history | < 0.001 | ||||||
| Previous pregnancy | 0.02 | 0.02 | 1.02 | 0.98 to 1.06 | 0.02 | 0.02 | |
| Previous live birth | 0.32 | 0.02 | 1.38 | 1.32 to 1.43 | 0.31 | 0.02 | |
| Two or more previous live births | 0.25 | 0.04 | 1.29 | 1.19 to 1.39 | 0.27 | 0.04 | |
| Duration of infertility (years) | < 0.001 | ||||||
| 0–1 | 0.17 | 0.03 | 1.19 | 1.12 to 1.26 | 0.17 | 0.03 | |
| 2 | 0.09 | 0.03 | 1.09 | 1.03 to 1.16 | 0.08 | 0.03 | |
| 3 | 0.04 | 0.02 | 1.05 | 1.00 to 1.08 | 0.04 | 0.02 | |
| 5 | –0.05 | 0.03 | 0.95 | 0.90 to 1.01 | –0.05 | 0.03 | |
| 6 | –0.08 | 0.03 | 0.92 | 0.87 to 0.98 | –0.07 | 0.03 | |
| 7 | –0.11 | 0.03 | 0.89 | 0.84 to 0.95 | –0.10 | 0.04 | |
| 8 | –0.13 | 0.04 | 0.88 | 0.81 to 0.95 | –0.11 | 0.04 | |
| 9 | –0.12 | 0.05 | 0.89 | 0.80 to 0.98 | –0.09 | 0.05 | |
| 10–11 | –0.13 | 0.04 | 0.87 | 0.81 to 0.95 | –0.11 | 0.04 | |
| ≥ 12 | –0.19 | 0.03 | 0.82 | 0.78 to 0.88 | –0.17 | 0.03 | |
| Cause of infertility | < 0.001 | ||||||
| Tubal diagnosis | –0.21 | 0.02 | 0.81 | 0.78 to 0.84 | –0.22 | 0.02 | |
| Diagnosis of PCOS | 0.04 | 0.02 | 0.07 | 1.04 | 1.00 to 1.08 | 0.03 | 0.02 |
| Endometriosis | 0.00 | 0.03 | 0.94 | 1.00 | 0.94 to 1.06 | –0.03 | 0.03 |
| Idiopathic diagnosis | 0.05 | 0.03 | 0.05 | 1.05 | 0.99 to 1.11 | 0.06 | 0.03 |
| Male factor diagnosis | 0.09 | 0.02 | < 0.001 | 1.10 | 1.05 to 1.14 | 0.08 | 0.02 |
| Donor sperm | 0.29 | 0.05 | < 0.001 | 1.34 | 1.21 to 1.47 | 0.31 | 0.05 |
| Day of transfer | |||||||
| 3 | 0.00 | 0.02 | < 0.001 | 1.00 | 0.96 to 1.04 | –0.07 | 0.02 |
| ≤ 2 | –0.07 | 0.07 | 0.93 | 0.81 to 1.07 | –0.01 | 0.07 | |
| > 3 | 0.42 | 0.03 | 1.52 | 1.44 to 1.61 | 0.28 | 0.04 | |
| Year | < 0.001 | ||||||
| 2004 | –0.09 | 0.02 | 0.92 | 0.88 to 0.95 | –0.09 | 0.02 | |
| 2003 | –0.08 | 0.02 | 0.92 | 0.89 to 0.96 | –0.08 | 0.02 | |
| 2002 | –0.09 | 0.02 | 0.91 | 0.88 to 0.95 | –0.10 | 0.02 | |
| 2001 | –0.20 | 0.02 | 0.82 | 0.79 to 0.85 | –0.19 | 0.02 | |
| 2000 | –0.21 | 0.03 | 0.81 | 0.76 to 0.86 | –0.19 | 0.03 | |
FIGURE 8.
LBE rates from the LR model fitted to the HFEA dataset.
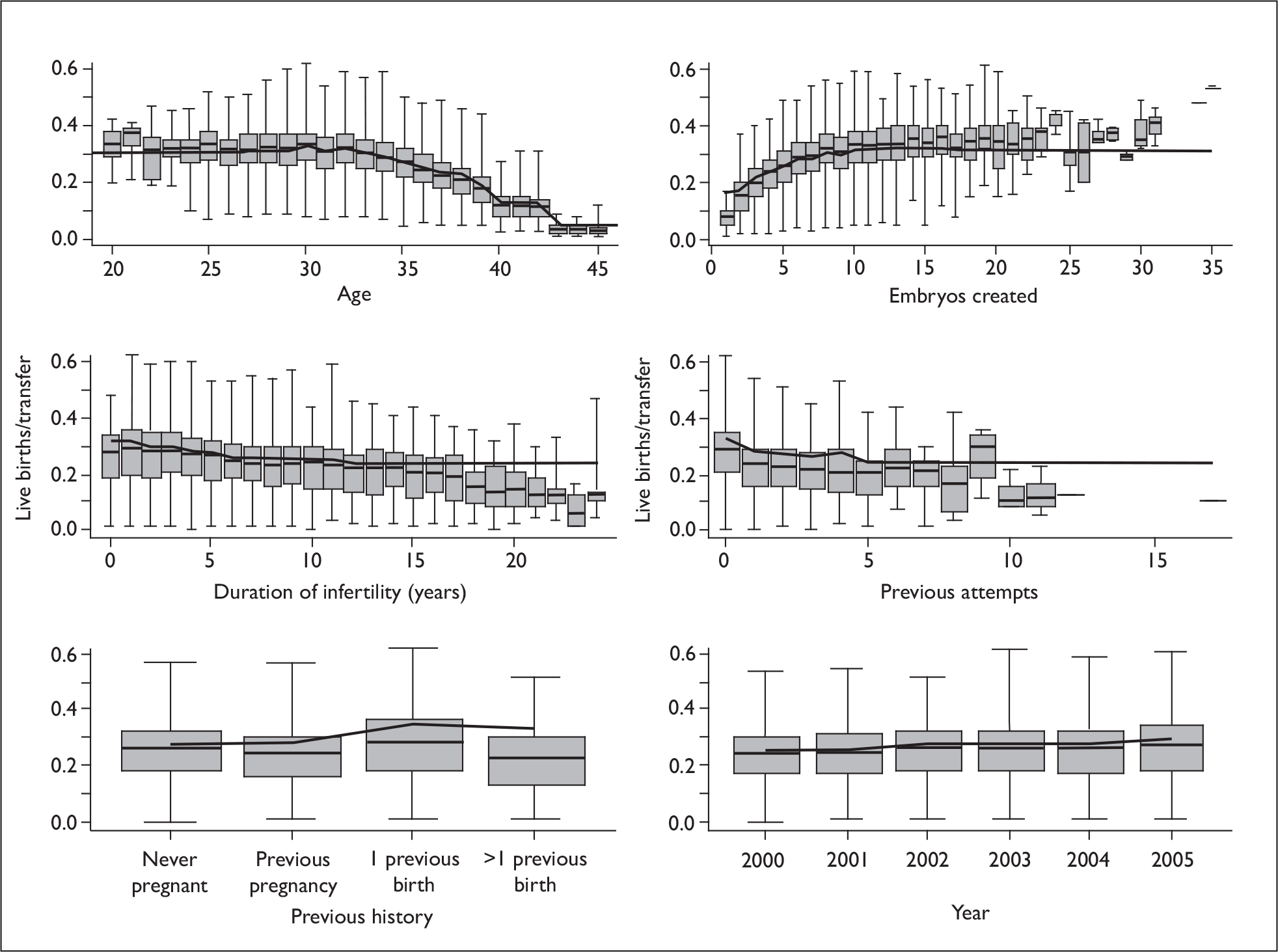
FIGURE 9.
LBE rates from the LR model fitted to the HFEA dataset.
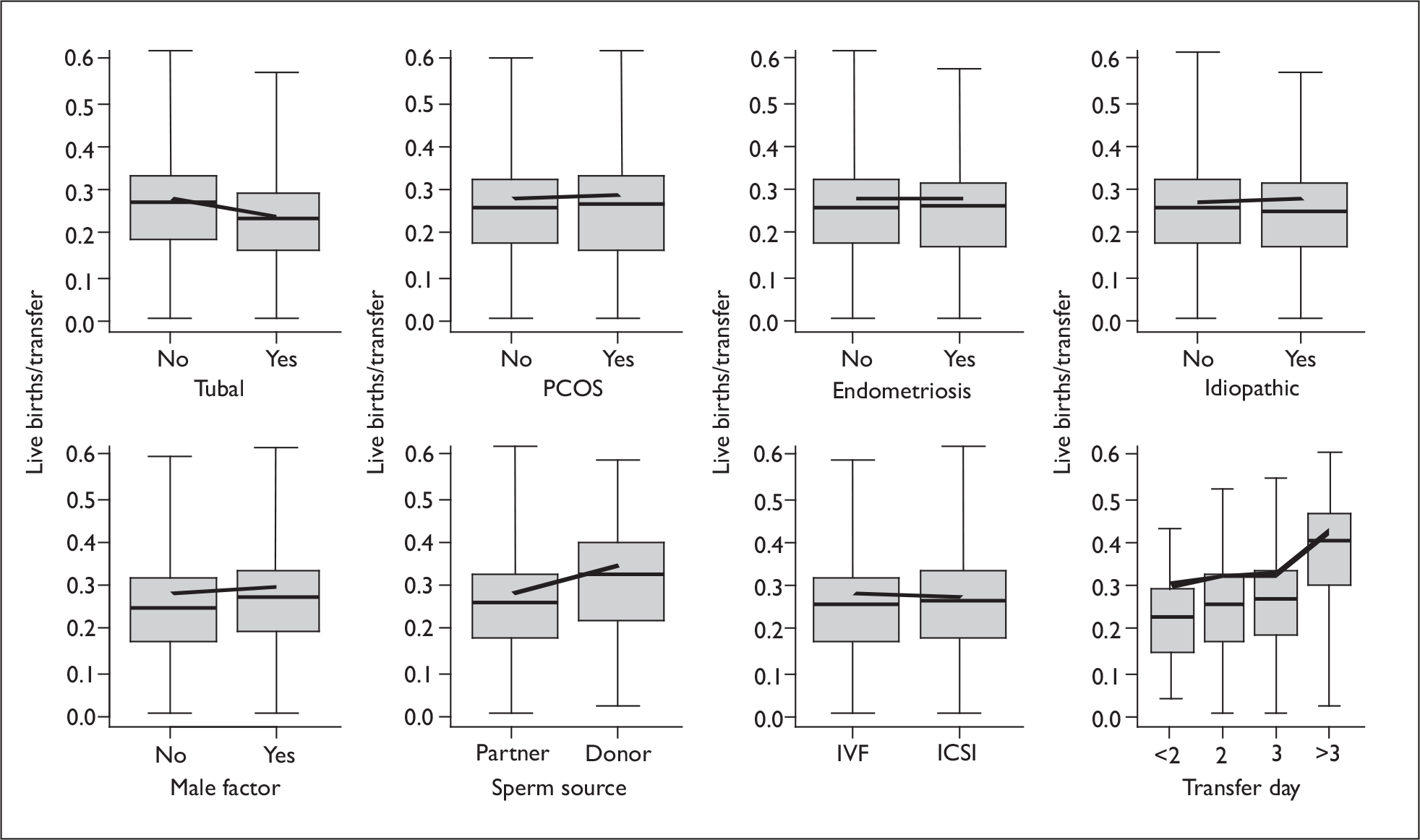
We note that although there are strong dependencies on age (and the other covariates), there is a wide variation between individuals of any given age, with young patients with poor prognosis and old patients with relatively good prognosis.
Cycles with a single embryo transferred did worse, with an odds ratio for LBEs of about 0.5 compared with DET. This would be expected as a consequence of fewer embryos but also reflects patient selection as the patients who received SET in this series would have different characteristics. In particular, many of these would have clinical conditions contraindicative of multiple pregnancies. Many would have had only a single embryo available: although this is allowed for in the model, embryo quality is not, and patients with few embryos would be likely also to have poorer-quality embryos transferred. Three embryo transfer does not improve LBEs as might be expected; this reflects the restriction on its use to only poor prognosis situations – again the likelihood that these cycles have only poor-quality embryos is not accounted for in the model.
Day 2 and 3 transfers have similar outcomes, and longer culture times do lead to a higher per transfer LBE rate. However the data do not include information on the numbers of cycles in which no embryos survive for transfer, so we cannot conclude from this analysis that the overall success rate per full cycle is improved.
The number of previous attempts is only weakly prognostic, and might be expected to be larger. 114 However, as noted above, the data on attempt number are not totally reliable and so there may be some attenuation of this effect due to measurement error. Additionally, there are strong and complex selection effects due to treatment policies, availability of funding and patient choice, which means that the patient populations who receive more treatments are not the same as those who receive less. The weak effect of duration of infertility is subject to the same caveats. A positive birth history is unsurprisingly associated with better outcomes. 69,79
There are three related variables associated with male infertility. ICSI is associated with marginally worse outcomes. A male cause of infertility is associated with better outcome, as is the use of donor sperm, these two variables being strongly related to each other. Given the strong relationships between these three variables, it is difficult to assign direct causal effects to any specific variable.
A tubal diagnosis is associated with worse outcomes, as has been noted in other work. 52 An idiopathic diagnosis shows a weak association with better outcomes, which is of borderline statistical significance. Even in this very large dataset the effects of other diagnoses did not reach statistical significance once the associated factors were accounted for.
There was a small, but significant, improvement in outcome over the period of the cohort.
Models for LBE and twin rates in fresh DET cycles
Tables 19 and 20 give the parameter estimates for LBEs and twins, given an LBE for fresh DET cycles, and the predicted outcomes for selected variables are plotted in Figure 10. Results for LBEs are consistent with the full dataset. The parameters of the twin model are generally similar to that of the LBE DET model, indicating little differential effect of prognostic parameters for twins, as for LBEs.
| Variablea | Fixed effects only | Including REs | |||||
|---|---|---|---|---|---|---|---|
| β | SE | p b | OR | 95% CI | β | SE | |
| Intercept | –0.67 | 0.05 | 0.51 | 0.46 to 0.56 | –0.79 | 0.06 | |
| Age (years) | < 0.001 | ||||||
| ≤ 26 | 0.10 | 0.04 | 1.11 | 1.02 to 1.20 | 0.14 | 0.04 | |
| 27–29 | 0.14 | 0.03 | 1.16 | 1.08 to 1.22 | 0.17 | 0.03 | |
| 30 | 0.21 | 0.04 | 1.23 | 1.14 to 1.33 | 0.23 | 0.04 | |
| 31 | 0.14 | 0.04 | 1.15 | 1.06 to 1.24 | 0.16 | 0.04 | |
| 32 | 0.16 | 0.03 | 1.18 | 1.11 to 1.24 | 0.18 | 0.04 | |
| 33 | 0.12 | 0.03 | 1.13 | 1.06 to 1.20 | 0.14 | 0.03 | |
| 34 | 0.07 | 0.03 | 1.07 | 1.01 to 1.14 | 0.08 | 0.03 | |
| 36 | –0.11 | 0.04 | 0.89 | 0.83 to 0.97 | –0.12 | 0.04 | |
| 37 | –0.26 | 0.04 | 0.77 | 0.71 to 0.83 | –0.27 | 0.04 | |
| 38 | –0.33 | 0.04 | 0.72 | 0.66 to 0.78 | –0.34 | 0.04 | |
| 39 | –0.55 | 0.04 | 0.58 | 0.53 to 0.62 | –0.57 | 0.04 | |
| 40–42 | –1.05 | 0.05 | 0.35 | 0.32 to 0.39 | –1.07 | 0.05 | |
| ≥ 43 | –2.16 | 0.15 | 0.12 | 0.09 to 0.15 | –2.21 | 0.15 | |
| Number of embryos created | < 0.001 | ||||||
| 2 | –0.61 | 0.04 | 0.54 | 0.50 to 0.59 | –0.63 | 0.04 | |
| 3 | –0.37 | 0.03 | 0.69 | 0.65 to 0.73 | –0.38 | 0.03 | |
| 4 | –0.21 | 0.03 | 0.81 | 0.76 to 0.86 | –0.22 | 0.03 | |
| 5 | –0.11 | 0.03 | 0.90 | 0.84 to 0.95 | –0.11 | 0.03 | |
| 7 | 0.01 | 0.03 | 1.01 | 0.95 to 1.07 | 0.01 | 0.03 | |
| 8 | 0.09 | 0.03 | 1.10 | 1.03 to 1.16 | 0.09 | 0.03 | |
| 9 | 0.08 | 0.04 | 1.09 | 1.00 to 1.17 | 0.08 | 0.04 | |
| 10 | 0.16 | 0.04 | 1.17 | 1.09 to 1.27 | 0.16 | 0.04 | |
| 11–12 | 0.17 | 0.03 | 1.19 | 1.12 to 1.26 | 0.18 | 0.04 | |
| 13–16 | 0.18 | 0.04 | 1.19 | 1.11 to 1.29 | 0.18 | 0.04 | |
| ≥ 17 | 0.14 | 0.05 | 1.15 | 1.04 to 1.27 | 0.16 | 0.05 | |
| Cycle | < 0.001 | ||||||
| 2nd | –0.23 | 0.02 | 0.79 | 0.76 to 0.83 | –0.21 | 0.02 | |
| 3rd | –0.27 | 0.03 | 0.76 | 0.72 to 0.81 | –0.25 | 0.03 | |
| 4th | –0.33 | 0.04 | 0.72 | 0.66 to 0.78 | –0.30 | 0.04 | |
| 5th | –0.28 | 0.06 | 0.75 | 0.67 to 0.85 | –0.24 | 0.06 | |
| 6th ≥ | –0.42 | 0.07 | 0.65 | 0.57 to 0.75 | –0.37 | 0.07 | |
| ICSI | –0.06 | 0.02 | < 0.001 | 0.94 | 0.91 to 0.98 | –0.06 | 0.02 |
| Previous history | < 0.001 | ||||||
| Previous pregnancy | 0.03 | 0.02 | 1.03 | 0.99 to 1.07 | 0.03 | 0.02 | |
| Previous live birth | 0.32 | 0.02 | 1.38 | 1.32 to 1.43 | 0.32 | 0.02 | |
| Two or more previous live births | 0.27 | 0.05 | 1.31 | 1.19 to 1.44 | 0.29 | 0.05 | |
| Duration of infertility (years) | < 0.001 | ||||||
| 0–1 | 0.15 | 0.03 | 1.16 | 1.10 to 1.23 | 0.15 | 0.03 | |
| 2 | 0.08 | 0.03 | 1.08 | 1.02 to 1.15 | 0.07 | 0.03 | |
| 3 | 0.05 | 0.03 | 1.05 | 0.99 to 1.11 | 0.05 | 0.03 | |
| 5 | –0.04 | 0.03 | 0.96 | 0.91 to 1.02 | –0.04 | 0.03 | |
| 6 | –0.09 | 0.03 | 0.92 | 0.86 to 0.97 | –0.08 | 0.03 | |
| 7 | –0.11 | 0.04 | 0.90 | 0.83 to 0.97 | –0.09 | 0.04 | |
| 8 | –0.13 | 0.04 | 0.87 | 0.81 to 0.95 | –0.11 | 0.04 | |
| 9 | –0.11 | 0.05 | 0.89 | 0.81 to 0.99 | –0.09 | 0.05 | |
| 10–11 | –0.12 | 0.04 | 0.88 | 0.82 to 0.96 | –0.10 | 0.04 | |
| ≥ 12 | –0.19 | 0.04 | 0.83 | 0.76 to 0.89 | –0.17 | 0.04 | |
| Cause of infertility | |||||||
| Tubal diagnosis | –0.23 | 0.03 | < 0.001 | 0.80 | 0.75 to 0.84 | –0.24 | 0.03 |
| Diagnosis of PCOS | 0.04 | 0.03 | 0.14 | 1.04 | 0.98 to 1.10 | 0.04 | 0.03 |
| Endometriosis | –0.03 | 0.03 | 0.37 | 0.97 | 0.92 to 1.03 | –0.05 | 0.03 |
| Idiopathic diagnosis | 0.05 | 0.03 | 0.10 | 1.05 | 0.99 to 1.11 | 0.06 | 0.03 |
| Male factor diagnosis | 0.10 | 0.03 | < 0.001 | 1.10 | 1.04 to 1.17 | 0.08 | 0.03 |
| Donor sperm | 0.31 | 0.05 | < 0.001 | 1.36 | 1.24 to 1.5 | 0.33 | 0.05 |
| Day of transfer | < 0.001 | ||||||
| 3 | 0.01 | 0.02 | 1.01 | 0.97 to 1.05 | –0.04 | 0.02 | |
| < 2 | –0.05 | 0.07 | 0.95 | 0.83 to 1.09 | –0.01 | 0.08 | |
| > 3 | 0.49 | 0.04 | 1.63 | 1.51 to 1.77 | 0.34 | 0.04 | |
| Year | < 0.001 | ||||||
| 2004 | –0.09 | 0.02 | 0.91 | 0.88 to 0.95 | –0.09 | 0.02 | |
| 2003 | –0.07 | 0.02 | 0.93 | 0.90 to 0.97 | –0.07 | 0.02 | |
| 2002 | –0.10 | 0.02 | 0.90 | 0.87 to 0.94 | –0.10 | 0.03 | |
| 2001 | –0.19 | 0.03 | 0.83 | 0.78 to 0.88 | –0.18 | 0.03 | |
| 2000 | –0.21 | 0.03 | 0.81 | 0.76 to 0.86 | –0.21 | 0.03 | |
| Variablea | Fixed effects only | Including REs | |||||
|---|---|---|---|---|---|---|---|
| β | SE | p b | OR | 95% CI | β | SE | |
| Intercept | –0.87 | 0.09 | 0.42 | 0.35 to 0.50 | –0.87 | 0.09 | |
| Age (years) | < 0.001 | ||||||
| ≤ 26 | 0.39 | 0.07 | 1.48 | 1.29 to 1.69 | 0.40 | 0.07 | |
| 27–29 | 0.26 | 0.06 | 1.30 | 1.15 to 1.46 | 0.27 | 0.06 | |
| 30 | 0.34 | 0.07 | 1.41 | 1.22 to 1.61 | 0.35 | 0.07 | |
| 31 | 0.29 | 0.07 | 1.33 | 1.17 to 1.53 | 0.29 | 0.07 | |
| 32 | 0.27 | 0.06 | 1.30 | 1.16 to 1.47 | 0.27 | 0.06 | |
| 33 | 0.12 | 0.06 | 1.12 | 1.00 to 1.27 | 0.12 | 0.06 | |
| 34 | 0.11 | 0.06 | 1.11 | 0.99 to 1.26 | 0.11 | 0.06 | |
| 36 | –0.10 | 0.07 | 0.91 | 0.79 to 1.04 | –0.10 | 0.07 | |
| 37 | –0.24 | 0.08 | 0.78 | 0.67 to 0.92 | –0.25 | 0.08 | |
| 38 | –0.49 | 0.09 | 0.61 | 0.51 to 0.73 | –0.49 | 0.09 | |
| 39 | –0.57 | 0.10 | 0.57 | 0.46 to 0.69 | –0.57 | 0.10 | |
| 40–42 | –1.02 | 0.14 | 0.36 | 0.27 to 0.47 | –1.02 | 0.14 | |
| ≥ 43 | –1.16 | 0.53 | 0.31 | 0.11 to 0.89 | –1.17 | 0.53 | |
| Number of embryos created | < 0.001 | ||||||
| 2 | –0.63 | 0.08 | 0.53 | 0.46 to 0.62 | –0.64 | 0.08 | |
| 3 | –0.31 | 0.07 | 0.73 | 0.64 to 0.84 | –0.32 | 0.07 | |
| 4 | –0.18 | 0.06 | 0.83 | 0.74 to 0.94 | –0.19 | 0.06 | |
| 5 | –0.08 | 0.06 | 0.92 | 0.82 to 1.04 | –0.08 | 0.06 | |
| 7 | –0.05 | 0.06 | 0.96 | 0.85 to 1.07 | –0.05 | 0.06 | |
| 8 | 0.00 | 0.06 | 1.00 | 0.89 to 1.12 | 0.00 | 0.06 | |
| 9 | 0.01 | 0.07 | 1.01 | 0.88 to 1.16 | 0.00 | 0.07 | |
| 10 | 0.01 | 0.07 | 1.01 | 0.88 to 1.16 | 0.01 | 0.07 | |
| 11–12 | 0.04 | 0.06 | 1.04 | 0.93 to 1.17 | 0.04 | 0.06 | |
| 13–16 | 0.03 | 0.06 | 1.03 | 0.92 to 1.16 | 0.02 | 0.06 | |
| ≥ 17 | 0.09 | 0.08 | 1.10 | 0.94 to 1.28 | 0.10 | 0.08 | |
| Cycle | 0.04 | ||||||
| 2nd | –0.11 | 0.04 | 0.90 | 0.83 to 0.97 | –0.11 | 0.04 | |
| 3rd | –0.02 | 0.05 | 0.98 | 0.89 to 1.08 | –0.02 | 0.05 | |
| 4th | –0.01 | 0.08 | 0.99 | 0.85 to 1.16 | –0.01 | 0.08 | |
| 5th | –0.02 | 0.12 | 0.98 | 0.77 to 1.24 | –0.02 | 0.12 | |
| 6th ≥ | –0.29 | 0.14 | 0.75 | 0.57 to 0.98 | –0.29 | 0.14 | |
| ICSI | –0.06 | 0.04 | 0.11 | 0.94 | 0.87 to 1.02 | –0.07 | 0.04 |
| Previous history | < 0.001 | ||||||
| Previous pregnancy | 0.05 | 0.04 | 1.05 | 0.97 to 1.14 | 0.05 | 0.04 | |
| Previous live birth | 0.17 | 0.04 | 1.19 | 1.10 to 1.28 | 0.17 | 0.04 | |
| Two or more previous live births | 0.26 | 0.09 | 1.30 | 1.09 to 1.55 | 0.27 | 0.09 | |
| Duration of infertility (years) | 0.08 | ||||||
| 0–1 | –0.13 | 0.06 | 0.88 | 0.78 to 0.99 | –0.13 | 0.06 | |
| 2 | –0.10 | 0.05 | 0.91 | 0.82 to 1.00 | –0.10 | 0.05 | |
| 3 | –0.04 | 0.05 | 0.96 | 0.87 to 1.06 | –0.04 | 0.05 | |
| 5 | –0.04 | 0.06 | 0.96 | 0.85 to 1.08 | –0.04 | 0.06 | |
| 6 | 0.01 | 0.06 | 1.01 | 0.90 to 1.14 | 0.01 | 0.06 | |
| 7 | –0.14 | 0.07 | 0.87 | 0.76 to 1.00 | –0.13 | 0.07 | |
| 8 | 0.01 | 0.08 | 1.01 | 0.86 to 1.18 | 0.01 | 0.09 | |
| 9 | –0.17 | 0.1 | 0.85 | 0.69 to 1.03 | –0.16 | 0.10 | |
| 10–11 | –0.24 | 0.09 | 0.79 | 0.66 to 0.94 | –0.24 | 0.09 | |
| ≥ 12 | –0.05 | 0.07 | 0.95 | 0.83 to 1.09 | –0.05 | 0.07 | |
| Cause of infertility | |||||||
| Tubal diagnosis | –0.08 | 0.05 | 0.09 | 0.92 | 0.84 to 1.02 | –0.09 | 0.05 |
| Diagnosis of PCOS | –0.06 | 0.05 | 0.25 | 0.94 | 0.85 to 1.04 | –0.06 | 0.05 |
| Endometriosis | 0.00 | 0.06 | 0.98 | 1.00 | 0.89 to 1.12 | 0.00 | 0.06 |
| Idiopathic diagnosis | –0.04 | 0.06 | 0.50 | 0.96 | 0.85 to 1.08 | –0.04 | 0.06 |
| Male factor diagnosis | –0.07 | 0.05 | 0.15 | 0.93 | 0.85 to 1.03 | –0.08 | 0.05 |
| Donor sperm | 0.09 | 0.10 | 0.35 | 1.09 | 0.90 to 1.33 | 0.09 | 0.10 |
| Day of transfer | < 0.001 | ||||||
| 3 | –0.06 | 0.03 | 0.94 | 0.89 to 1.00 | –0.08 | 0.04 | |
| < 2 | 0.16 | 0.14 | 1.17 | 0.89 to 1.54 | 0.15 | 0.15 | |
| > 3 | 0.48 | 0.06 | 1.62 | 1.44 to 1.82 | 0.43 | 0.06 | |
| Year | 0.40 | ||||||
| 2004 | –0.09 | 0.04 | 0.91 | 0.85 to 0.99 | –0.09 | 0.04 | |
| 2003 | –0.04 | 0.05 | 0.96 | 0.87 to 1.06 | –0.04 | 0.05 | |
| 2002 | –0.06 | 0.05 | 0.94 | 0.85 to 1.04 | –0.06 | 0.05 | |
| 2001 | –0.08 | 0.05 | 0.92 | 0.84 to 1.02 | –0.08 | 0.05 | |
| 2000 | –0.07 | 0.05 | 0.93 | 0.85 to 1.03 | –0.08 | 0.05 | |
FIGURE 10.
Fitted success (LBEs) and twin rates for fresh DET transfers in the HFEA dataset. Live births (left); twins per LBE (right).
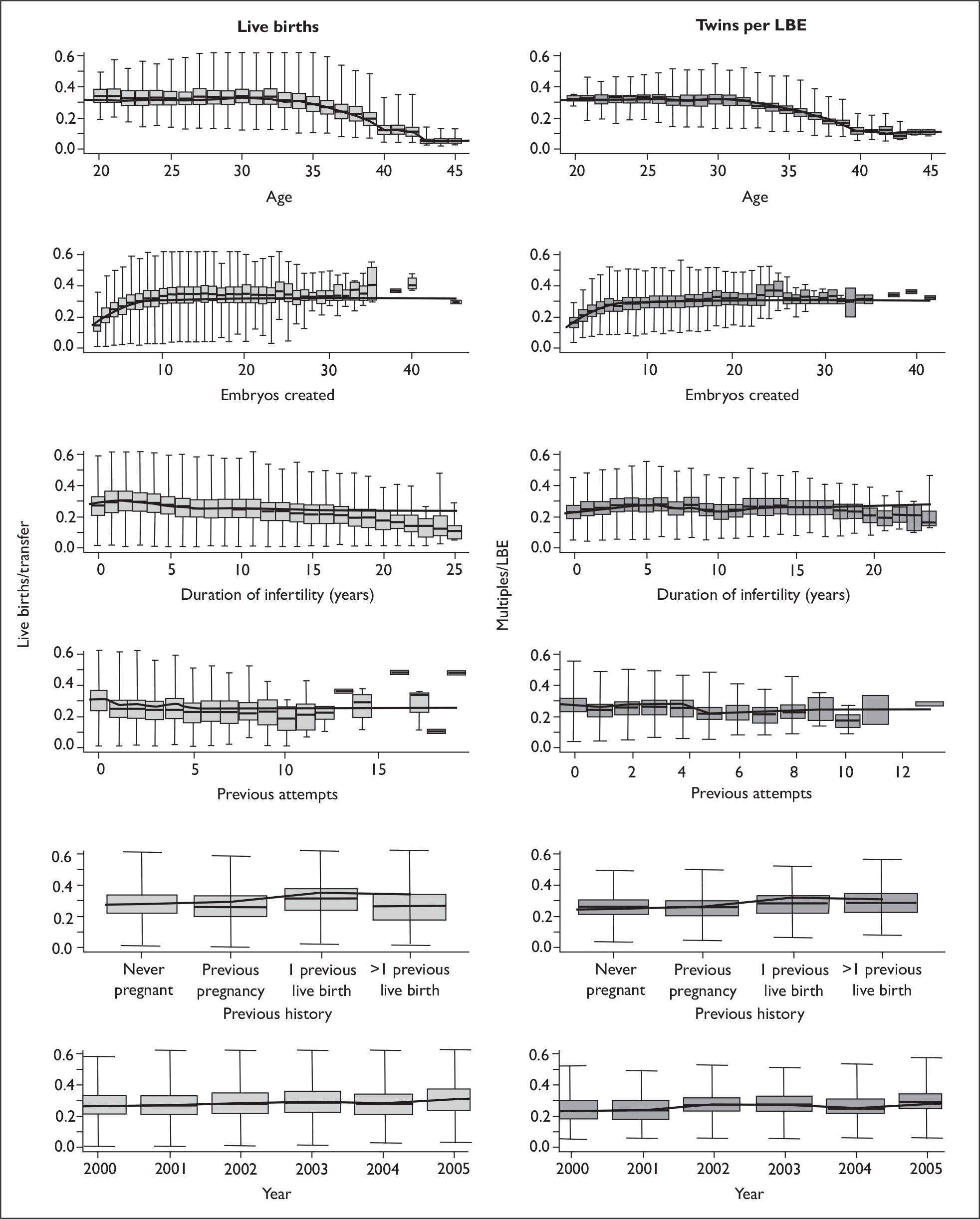
*Random effects estimates from the mixed logistic regression models
In order to account for the correlations between multiple cycles from the same patients, and between patients from the same clinics (treatment centre effects), we included patient and centre effects as random effects in the LR models. Inclusion of these random effects did not affect the estimates of the other model parameters. Such models are computationally expensive to fit, and a number of approximations have been developed to speed up the computation. However these approximations are known to perform badly in logistic models: although the fixed effect estimates are reliable, the estimates of the random effects are often biased. 115 Thus, there is a pay-off between accuracy in estimation of random effects and practical fitting of the models. In this dataset it was not practical to fit the full dataset with a reliably accurate method [adaptive quadrature (AQ)] and a Laplace approximation had to be used to make the fitting feasible. Therefore, we derived a smaller dataset of approximately 10% the size by sampling 100 patients from each treatment centre (or all patients if the number was less than 100). Even this relatively small sample of the HFEA dataset took a couple of days to fit via adaptive quadrature, using the stata glamm procedure. 116 In this dataset the Laplace approximation gave a reasonable fitting time but appeared to underestimate the random effects at the patient level.
Table 21 shows the random effect estimates, expressed as the standard deviation of the distribution of effects between centres and patients (within centre). The Laplace approximation does underestimate the magnitude of the effects, particularly the lower-level patient effects. There are reasonably large intrapatient effects, with the standard deviation being equivalent to the difference between a 35- and a 39-year-old patient. There are differences between centres that are of a magnitude to be clinically relevant: the standard deviation of 0.35 on the log-odds scale is equivalent to an odds ratio of 1.4. The random effect for the twin model is small, reflecting the fact that once LBEs are accounted for, the twin rates do not vary much.
| Dataset | Number of transfers | Number of centres | Number of patients | Random effect SD (estimate SEa) | |
|---|---|---|---|---|---|
| Centre | Patient | ||||
| All cycles LBE (full – Laplace) | 119,930 | 84 | 81,965 | 0.28 | 0.30 |
| All cycles LBE (sample – Laplace) | 11,875 | 84 | 8280 | 0.32 | 0.23 |
| All cycles LBE (sample – AQ) | 11,875 | 84 | 8280 | 0.35 (0.04) | 0.56 (0.16) |
| DET cycles LBE (full – Laplace) | 92,271 | 84 | 67,657 | 0.27 | 0.27 |
| DET cycles LBE (sample – Laplace) | 10,632 | 84 | 8009 | 0.27 | 0.23 |
| DET cycles LBE (sample – AQ) | 10,632 | 84 | 8009 | 0.29 (0.04) | 0.56 (0.16) |
| DET cycles twins given LBE (full – Laplace) | 25,850 | 84 | 25,158 | 0.09 | NAb |
| DET cycles twins given LBE (full – AQ) | 25,850 | 84 | 25,158 | 0.09 (0.02) | NAb |
*LR model validation
Figure 11 shows the observed and fitted data plotted against age and number of embryos created, showing that, overall, the models were a good fit to the dataset. There is no evidence of any systematic lack of fit in the model, but there is some evidence of overfitting and a somewhat coarser categorisation of the continuous variable might be more realistic.
FIGURE 11.
Fitted and observed outcomes for the LR models for the two most predictive variables in the HFEA dataset. Live births (left); twins per LBE (right).
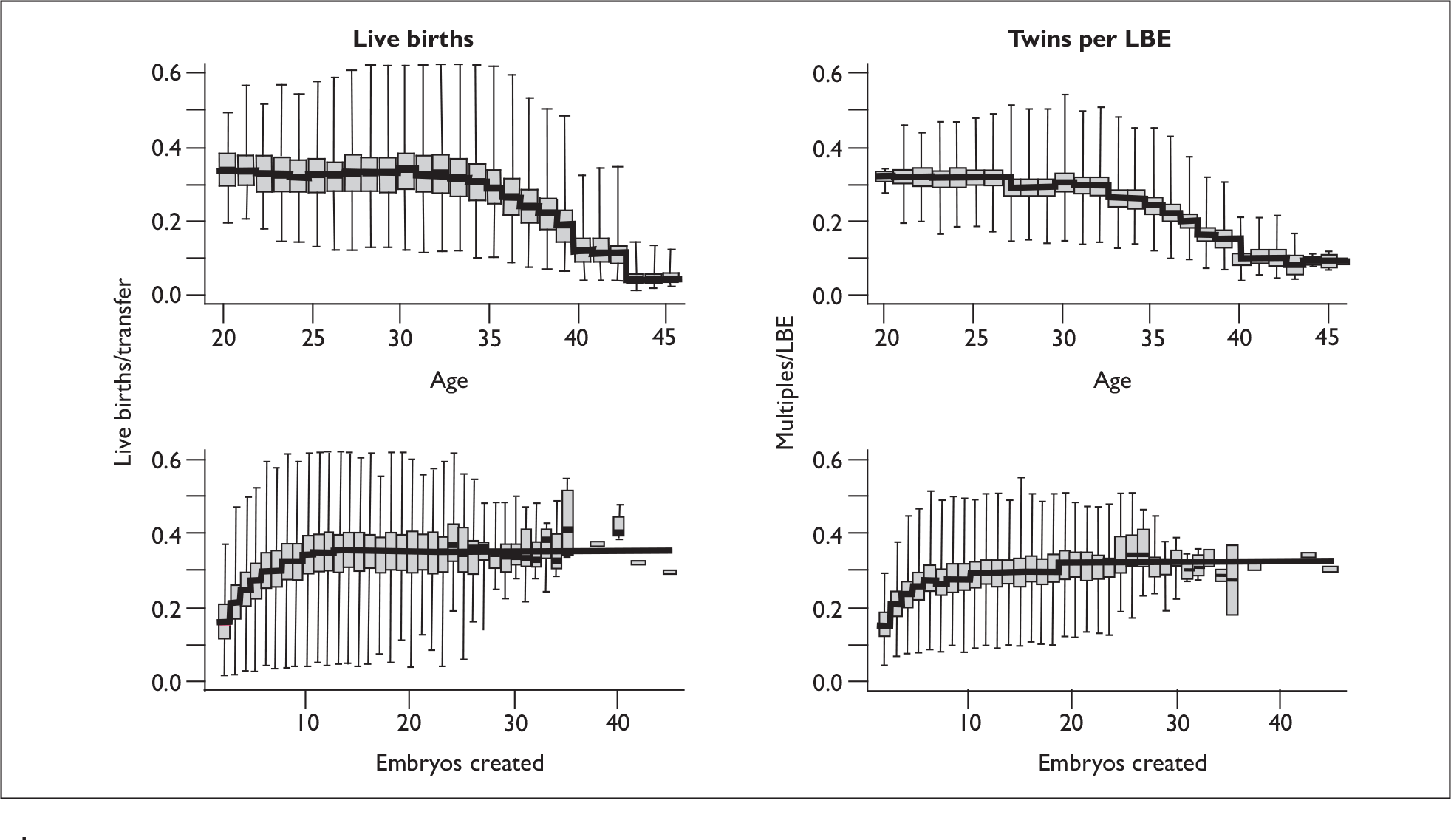
Table 22 gives the area under the receiver operating characteristic (ROC) curve (AUC) for the various LR models, a measure of the goodness of fit; a value of 0.5 implies that the model prediction is essentially random while a value of 1 gives perfect classification. The fits are reasonable; with the random effect increasing the AUC fit by a modest amount. Clearly the models would not be useful for predicting individual outcomes, but this does not preclude their usefulness for predicting population outcomes. The fitted AUC values are in line with those found by Hunault et al. ,53 who observed AUC values of 0.68 with a logistic regression to model pregnancy and 0.71 when modelling a twin versus no-twin outcome (as opposed to the conditional model used here).
| Dataset | AUC | |
|---|---|---|
| Fixed effects only | With REs | |
| All cycles LBE | 0.66 | 0.71 |
| DET cycles LBE | 0.63 | 0.69 |
| DET cycles twins given LBE | 0.60 | 0.61 |
Table 23 shows the results of a bootstrap-based calibration procedure. 104 This procedure is designed to assess whether the fitted model displays characteristics of overfitting, with a well-fitting model giving a calibration intercept close to 0 and slope close to 1. There is no evidence of serious overfitting, despite the large number of parameters included in the model.
| Dataset | Bootstraps (n = 100) | ||
|---|---|---|---|
| Calibration intercept | Calibration slope | AUC | |
| All cycles LBE | –0.01 | 0.99 | 0.66 |
| DET cycles LBE | –0.01 | 0.98 | 0.63 |
| DET cycles twins given LBE | –0.08 | 0.92 | 0.61 |
It is possible that observations with several previous cycles may not behave the same in the model as those from earlier cycles. Therefore, as a sensitivity analysis, the model was fitted to first cycles only and the parameter estimates compared with the model above (Table 24). No differences were observed, and there was no evidence that variables behave differently in models for all cycles or of an interaction between cycle number and other effects (based on the BIC).
| Variable | All cycles [OR (95% CI)] | First cycles only [OR (95% CI)] | ||
|---|---|---|---|---|
| Number of embryos transferred | ||||
| 1 | 0.52 | 0.47 to 0.57 | 0.47 | 0.41 to 0.55 |
| 3 | 1.03 | 0.98 to 1.08 | 1.03 | 0.96 to 1.12 |
| Age (years) | ||||
| ≤ 26 | 1.11 | 1.03 to 1.20 | 1.16 | 1.05 to 1.27 |
| 27–29 | 1.16 | 1.09 to 1.23 | 1.19 | 1.10 to 1.29 |
| 30 | 1.21 | 1.13 to 1.30 | 1.31 | 1.19 to 1.44 |
| 31 | 1.14 | 1.07 to 1.22 | 1.21 | 1.10 to 1.32 |
| 32 | 1.18 | 1.10 to 1.25 | 1.19 | 1.09 to 1.30 |
| 33 | 1.12 | 1.05 to 1.19 | 1.13 | 1.04 to 1.24 |
| 34 | 1.06 | 1.00 to 1.13 | 1.10 | 1.01 to 1.20 |
| 36 | 0.89 | 0.83 to 0.95 | 0.89 | 0.81 to 0.98 |
| 37 | 0.77 | 0.72 to 0.83 | 0.77 | 0.70 to 0.85 |
| 38 | 0.74 | 0.69 to 0.79 | 0.75 | 0.68 to 0.83 |
| 39 | 0.59 | 0.55 to 0.64 | 0.59 | 0.53 to 0.66 |
| 40–42 | 0.37 | 0.34 to 0.40 | 0.33 | 0.30 to 0.37 |
| ≥ 43 | 0.11 | 0.09 to 0.13 | 0.09 | 0.07 to 0.13 |
| Number of embryos created | ||||
| 1 | 0.50 | 0.43 to 0.58 | 0.50 | 0.41 to 0.61 |
| 2 | 0.54 | 0.51 to 0.58 | 0.57 | 0.52 to 0.63 |
| 3 | 0.70 | 0.65 to 0.74 | 0.74 | 0.68 to 0.80 |
| 4 | 0.81 | 0.76 to 0.86 | 0.79 | 0.73 to 0.85 |
| 5 | 0.90 | 0.85 to 0.96 | 0.91 | 0.84 to 0.99 |
| 7 | 1.01 | 0.95 to 1.08 | 1.07 | 0.98 to 1.17 |
| 8 | 1.12 | 1.05 to 1.19 | 1.13 | 1.04 to 1.23 |
| 9 | 1.09 | 1.02 to 1.17 | 1.15 | 1.05 to 1.25 |
| 10 | 1.18 | 1.10 to 1.27 | 1.19 | 1.08 to 1.31 |
| 11–12 | 1.19 | 1.11 to 1.26 | 1.19 | 1.09 to 1.30 |
| 13–16 | 1.22 | 1.15 to 1.30 | 1.23 | 1.12 to 1.34 |
| ≥ 17 | 1.18 | 1.08 to 1.29 | 1.11 | 0.98 to 1.24 |
| ICSI | 0.96 | 0.92 to 0.99 | 0.94 | 0.89 to 0.99 |
| Previous history | ||||
| Previous pregnancy | 1.02 | 0.99 to 1.06 | 1.06 | 1.01 to 1.12 |
| Previous live birth | 1.38 | 1.32 to 1.44 | 1.25 | 1.17 to 1.34 |
| Two or more previous live births | 1.29 | 1.18 to 1.40 | 1.25 | 1.12 to 1.40 |
| Duration of infertility (years) | ||||
| 0–1 | 1.19 | 1.12 to 1.26 | 1.19 | 1.09 to 1.29 |
| 2 | 1.09 | 1.04 to 1.15 | 1.12 | 1.05 to 1.20 |
| 3 | 1.05 | 1.00 to 1.10 | 1.08 | 1.01 to 1.15 |
| 5 | 0.95 | 0.90 to 1.01 | 0.99 | 0.92 to 1.07 |
| 6 | 0.92 | 0.87 to 0.98 | 0.97 | 0.89 to 1.05 |
| 7 | 0.89 | 0.83 to 0.96 | 0.92 | 0.83 to 1.01 |
| 8 | 0.88 | 0.81 to 0.95 | 0.94 | 0.85 to 1.05 |
| 9 | 0.89 | 0.81 to 0.97 | 0.89 | 0.78 to 1.01 |
| 10–11 | 0.87 | 0.81 to 0.94 | 0.90 | 0.82 to 1.00 |
| ≥ 12 | 0.82 | 0.77 to 0.88 | 0.87 | 0.79 to 0.95 |
| Cause of infertility | ||||
| Tubal diagnosis | 0.81 | 0.78 to 0.85 | 0.78 | 0.73 to 0.83 |
| Diagnosis of PCOS | 1.04 | 1.00 to 1.09 | 1.04 | 0.98 to 1.11 |
| Endometriosis | 1.00 | 0.94 to 1.06 | 1.02 | 0.94 to 1.10 |
| Idiopathic diagnosis | 1.05 | 1.00 to 1.11 | 1.06 | 0.99 to 1.14 |
| Male factor diagnosis | 1.10 | 1.05 to 1.15 | 1.08 | 1.01 to 1.16 |
| Donor sperm | 1.34 | 1.22 to 1.48 | 1.33 | 1.16 to 1.53 |
| Day of transfer | ||||
| 3 | 1.00 | 0.97 to 1.03 | 1.01 | 0.96 to 1.05 |
| < 2 | 0.93 | 0.82 to 1.07 | 0.88 | 0.73 to 1.06 |
| > 3 | 1.52 | 1.43 to 1.63 | 1.61 | 1.45 to 1.79 |
| Year | ||||
| 2004 | 0.92 | 0.88 to 0.96 | 0.91 | 0.86 to 0.97 |
| 2003 | 0.92 | 0.88 to 0.97 | 0.91 | 0.86 to 0.97 |
| 2002 | 0.91 | 0.87 to 0.95 | 0.90 | 0.84 to 0.96 |
| 2001 | 0.82 | 0.78 to 0.86 | 0.82 | 0.76 to 0.87 |
| 2000 | 0.81 | 0.77 to 0.85 | 0.81 | 0.75 to 0.86 |
LR models including frozen cycles
If we fit the fresh and frozen data to the same model, allowing for an overall (intercept) difference in LBEs due to freezing, we obtain an estimate of b = –0.52 (SE 0.03) for the freezing effect compared with a fresh cycle with six embryos created. This translates to an odds ratio of 0.6 (95% CI 0.57 to 0.64). It would not be unexpected to see an odds ratio a little less than 1 for frozen embryo transfer as the majority of patients will have already undergone an unsuccessful fresh cycle; however, this result does indicate that frozen cycles are less successful.
There is evidence that the effect of freezing varies according to some of the clinical characteristics, and Table 25 shows the results of the tests for interaction that proved to be statistically significant (with each variable added sequentially – no further variables were significant).
| Interaction term | Model AIC | Interaction df | LRT p-value |
|---|---|---|---|
| None | 146,291 | ||
| Age group | 146,243 | 13 | < 0.0001 |
| Number transferred | 146,234 | 2 | 0.0001 |
| Attempt number | 146,226 | 5 | 0.003 |
The fit to the frozen data is shown in Table 26, which should be compared with the fresh cycles in Table 18. Figure 12 compares the predicted outcomes for the fresh and frozen transfers. Success rates in frozen transfers are similarly lower for all patient characteristics. Overall, the effects of the clinical characteristics are very similar between fresh and frozen transfers once the much lower overall success rate is taken into account.
| Variablea | Fixed effects only | Including REs | |||||
|---|---|---|---|---|---|---|---|
| β | SE | p b | OR | 95% CI | β | SE | |
| Intercept | –1.54 | 0.14 | 0.21 | 0.16 to 0.28 | –1.57 | 0.15 | |
| Number of embryos transferred | < 0.001 | ||||||
| 1 | –0.74 | 0.12 | 0.48 | 0.38 to 0.60 | –0.75 | 0.12 | |
| 3 | 0.08 | 0.07 | 1.09 | 0.94 to 1.24 | 0.07 | 0.07 | |
| Age (years) | < 0.001 | ||||||
| ≤ 26 | 0.04 | 0.12 | 1.05 | 0.82 to 1.32 | 0.06 | 0.12 | |
| 27–29 | 0.13 | 0.09 | 1.14 | 0.95 to 1.36 | 0.14 | 0.09 | |
| 30 | 0.18 | 0.10 | 1.20 | 0.98 to 1.46 | 0.20 | 0.10 | |
| 31 | 0.09 | 0.10 | 1.10 | 0.90 to 1.33 | 0.10 | 0.10 | |
| 32 | 0.17 | 0.10 | 1.19 | 0.97 to 1.44 | 0.17 | 0.10 | |
| 33 | 0.20 | 0.09 | 1.22 | 1.02 to 1.46 | 0.21 | 0.09 | |
| 34 | 0.05 | 0.09 | 1.05 | 0.88 to 1.25 | 0.05 | 0.09 | |
| 36 | –0.02 | 0.09 | 0.98 | 0.82 to 1.17 | –0.01 | 0.09 | |
| 37 | 0.03 | 0.09 | 1.03 | 0.86 to 1.23 | 0.03 | 0.10 | |
| 38 | –0.25 | 0.10 | 0.78 | 0.64 to 0.95 | –0.25 | 0.11 | |
| 39 | –0.21 | 0.11 | 0.81 | 0.65 to 1.01 | –0.21 | 0.11 | |
| 40–42 | –0.45 | 0.10 | 0.64 | 0.52 to 0.78 | –0.46 | 0.10 | |
| ≥ 43 | –1.16 | 0.20 | 0.31 | 0.21 to 0.46 | –1.17 | 0.20 | |
| Number of embryos thawed and viable | < 0.001 | ||||||
| 1 | 0.04 | 0.14 | 1.04 | 0.79 to 1.37 | 0.04 | 0.14 | |
| 3 | 0.19 | 0.05 | 1.21 | 1.10 to 1.33 | 0.18 | 0.06 | |
| 4 | 0.24 | 0.06 | 1.27 | 1.13 to 1.43 | 0.22 | 0.07 | |
| 5+ | 0.46 | 0.06 | 1.59 | 1.41 to 1.78 | 0.45 | 0.07 | |
| Cycle | < 0.001 | ||||||
| 2nd | 0.08 | 0.09 | 1.08 | 0.91 to 1.29 | 0.02 | 0.10 | |
| 3rd | –0.02 | 0.10 | 0.98 | 0.81 to 1.19 | –0.08 | 0.10 | |
| 4th | 0.02 | 0.10 | 1.02 | 0.84 to 1.24 | –0.04 | 0.11 | |
| 5th | –0.18 | 0.12 | 0.84 | 0.66 to 1.06 | –0.25 | 0.12 | |
| ≥ 6th | –0.22 | 0.12 | 0.80 | 0.63 to 1.02 | –0.28 | 0.13 | |
| ICSI | –0.17 | 0.05 | < 0.001 | 0.84 | 0.76 to 0.93 | –0.15 | 0.06 |
| Previous history | < 0.001 | ||||||
| Previous pregnancy | –0.04 | 0.06 | 0.96 | 0.85 to 1.08 | –0.05 | 0.06 | |
| Previous live birth | 0.32 | 0.05 | 1.37 | 1.25 to 1.52 | 0.30 | 0.06 | |
| Two or more previous live births | 0.28 | 0.11 | 1.32 | 1.07 to 1.64 | 0.26 | 0.11 | |
| Duration of infertility (years) | < 0.001 | ||||||
| 0–1 | 0.19 | 0.08 | 1.20 | 1.03 to 1.41 | 0.19 | 0.08 | |
| 2 | 0.01 | 0.08 | 1.01 | 0.86 to 1.18 | 0.00 | 0.08 | |
| 3 | 0.02 | 0.07 | 1.02 | 0.89 to 1.17 | 0.01 | 0.08 | |
| 5 | –0.14 | 0.08 | 0.87 | 0.74 to 1.02 | –0.14 | 0.09 | |
| 6 | –0.27 | 0.09 | 0.77 | 0.64 to 0.91 | –0.26 | 0.10 | |
| 7 | –0.21 | 0.10 | 0.81 | 0.67 to 0.99 | –0.20 | 0.10 | |
| 8 | –0.19 | 0.12 | 0.83 | 0.65 to 1.05 | –0.18 | 0.12 | |
| 9 | –0.04 | 0.12 | 0.96 | 0.76 to 1.22 | –0.02 | 0.13 | |
| 10–11 | –0.19 | 0.12 | 0.83 | 0.65 to 1.05 | –0.17 | 0.12 | |
| ≥ 12 | –0.32 | 0.10 | 0.73 | 0.60 to 0.88 | –0.31 | 0.10 | |
| Cause of infertility | |||||||
| Tubal diagnosis | –0.23 | 0.06 | < 0.001 | 0.79 | 0.71 to 0.89 | –0.24 | 0.06 |
| Diagnosis of PCOS | –0.03 | 0.06 | 0.66 | 0.97 | 0.86 to 1.09 | –0.04 | 0.06 |
| Endometriosis | 0.15 | 0.09 | 0.08 | 1.16 | 0.97 to 1.39 | 0.11 | 0.09 |
| Idiopathic diagnosis | 0.03 | 0.08 | 0.68 | 1.03 | 0.88 to 1.21 | 0.02 | 0.08 |
| Male factor diagnosis | 0.20 | 0.07 | <0.001 | 1.22 | 1.06 to 1.40 | 0.18 | 0.07 |
| Donor sperm | 0.21 | 0.13 | 0.09 | 1.24 | 0.96 to 1.59 | 0.24 | 0.13 |
| Year | <0.001 | ||||||
| 2004 | –0.16 | 0.06 | 0.85 | 0.76 to 0.96 | –0.15 | 0.06 | |
| 2003 | –0.07 | 0.06 | 0.93 | 0.83 to 1.05 | –0.06 | 0.06 | |
| 2002 | –0.22 | 0.06 | 0.80 | 0.71 to 0.90 | –0.22 | 0.07 | |
| 2001 | –0.28 | 0.07 | 0.75 | 0.66 to 0.87 | –0.25 | 0.07 | |
| 2000 | –0.26 | 0.09 | 0.77 | 0.65 to 0.92 | –0.24 | 0.09 | |
FIGURE 12.
Fitted success (LBE) rates for fresh and frozen transfers in the HFEA dataset. Fresh transfers (left); frozen transfers (right).
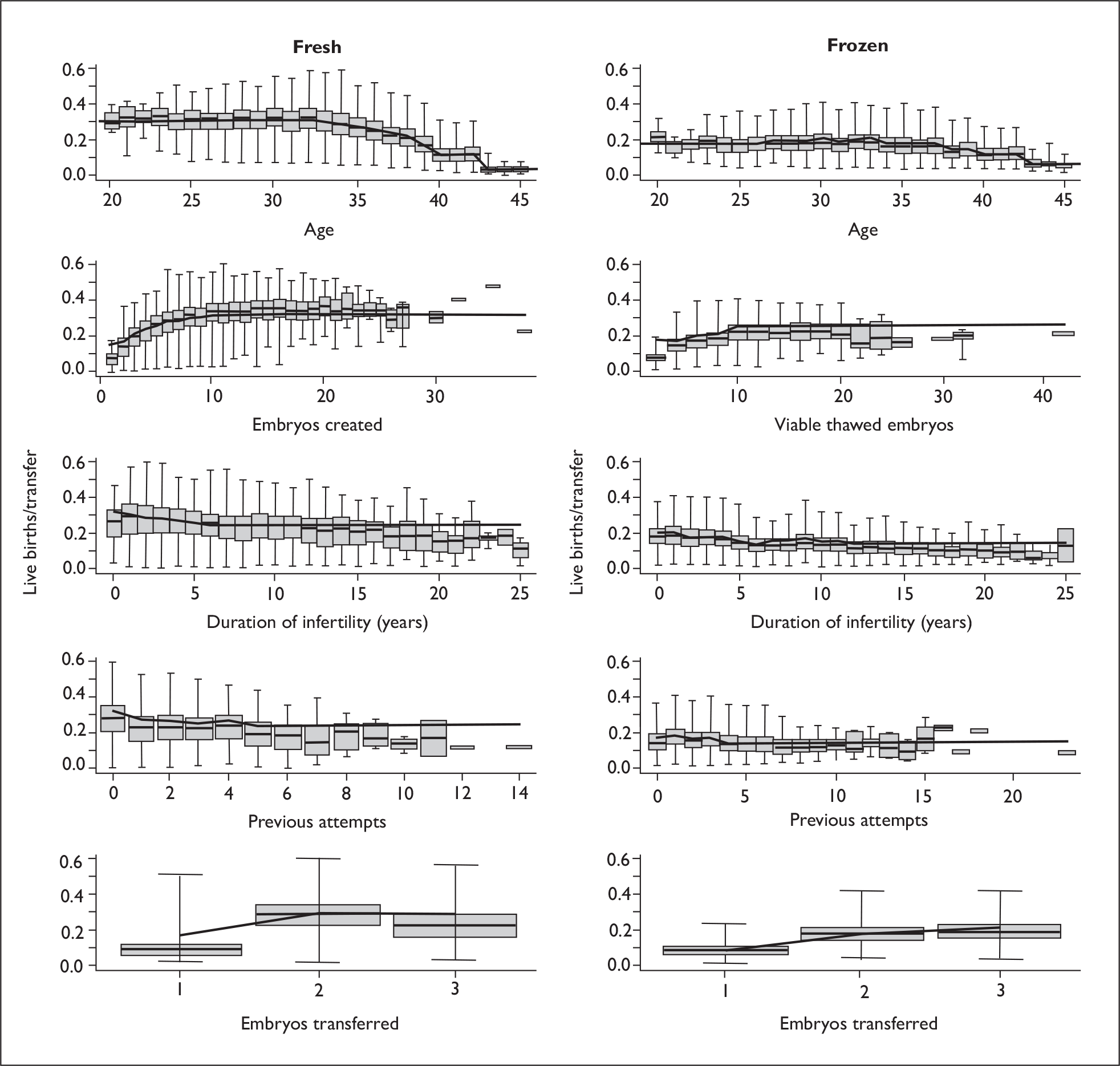
The decline in success with age appears to be somewhat less in frozen transfers, reflecting the statistically significant interaction. In this data we did not have the age at which the embryos were created (there is no link to the fresh cycle), so it is possible that this is due to the fact that transfers in older patients utilise embryos created when the patients were younger. Three-embryo transfers did relatively better in frozen cycles compared with fresh cycles. During this period three-embryo transfers should have been undertaken only in exceptional circumstances, and it is likely that this effect reflects different selection criteria for fresh and frozen transfers and therefore different patient populations. Also, without a measure of embryo quality, it is not possible to ascertain whether this difference reflects different quality embryos in the three-embryo transfers between fresh and frozen transfers. The third characteristic that showed a difference between fresh and frozen transfers was the attempt number. The effect of attempt number was attenuated in frozen cycles compared with fresh. Attempt number contains a mixture of fresh and frozen transfers. Many clinics and patients do not undertake frozen transfers, so the population of patients who have these will differ from those who do not. Additionally, as the success rate of frozen transfers is low, patients who have these will have a larger number of failed transfers. These biases are likely to be sufficient to explain the differential effect of attempt number seen here.
The interaction effects are all small in nature and, while potentially of interest mechanistically, probably reflect issues in the data structure and are of little practical significance.
Implications for eSET
Figure 13 compares the predicted twin rates and LBE rates derived from the two LR models. The twin rate is highly correlated with the LBE rate, with no evidence of subsets of patients with particularly high or low twin rates given their overall prognosis. Patients with a poor prognosis produce relatively fewer twins if successful, while patients with a good prognosis are at high risk of twin outcomes if given DET.
FIGURE 13.
Predicted twin rates versus live birth rates in fresh DET from the LR models in the HFEA dataset. For clarity only a random sample of 3000 points is shown.
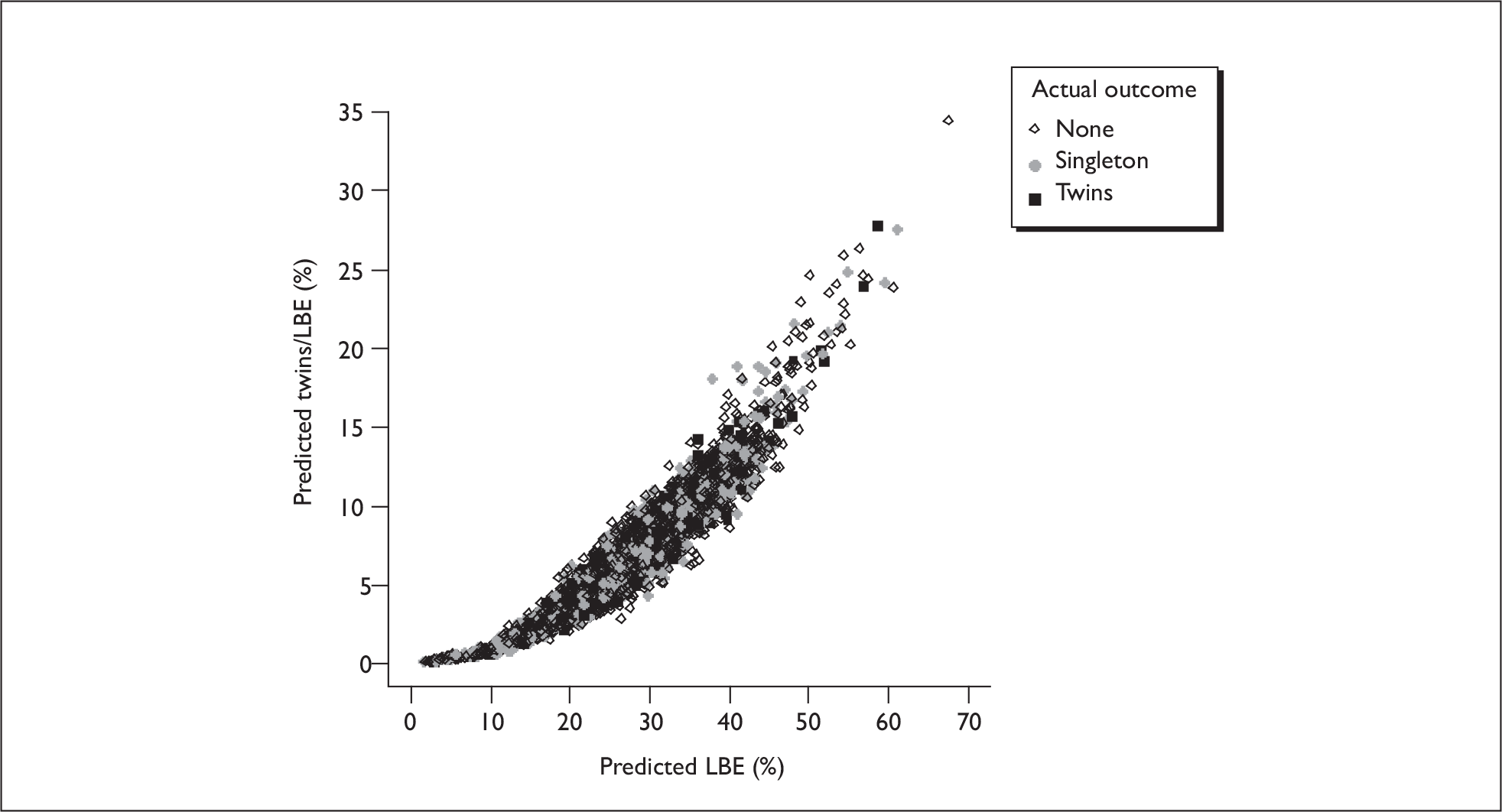
Discussion
This analysis of the national data is, as far as we are aware, the largest series of UK data analysed to date. The limitations of the data mean that any conclusions can only be tentative. In the context of this study the data and analysis serve largely to form a reference point and context for the more detailed analysis of the towardSET? collaborative data.
Limitations and caveats
The data do contain a large number of errors, and we must assume that there are many we cannot detect by simple consistency checks. There is no evidence that these errors are anything other than apparently random data entry errors, but we cannot rule out appreciable bias. In particular the measurement error will attenuate the effects of covariates. Attempt number is particularly problematic in this context, particularly with respect to frozen cycle attempt numbers, which appear to be incorrectly coded in some cycles (see Characteristics of the dataset). The lack of linkage of frozen cycles to their parent fresh cycle is a major limitation in the use of these data.
There are only a limited number of variables available, but these do include most of the relevant prognostic factors. The major exception to this is the lack of any measure of embryo quality, other than the number of embryos created.
The size of the dataset, with over 100,000 cycles and a large number of covariates, imposes limits on the computational feasibility of the analyses, particularly when we include random effects in the models. Due to these computational constraints and the limited linkage in the data, only simple correlation structures have been considered, and we cannot rule out more complex correlations as might, for example, be represented by random coefficient rather than random intercept models. Models can take many hours to run and, as such, preclude some of the computer-intensive methods that we might otherwise employ.
The data reflect the 2000–5 time period – the data that were available at the start of the project. Practice and success rates are continually improving and the absolute success rates may not apply to current patients; however, it is unlikely that for fresh cycles the differential between patients with different prognoses has changed appreciably in this time period. However, for frozen cycles there have been some additional changes in practice, so some caution is required in applying these results to current patients.
Impact of cryopreservation
The outcomes from frozen transfers in this dataset were generally poor compared with current best practice, and many centres performed few or no such treatments. Thus, it is very likely that the results here provide a lower bound on the success rates that can be achieved with best current practice. The odds ratio for frozen versus fresh transfers of 0.6 reflects a significant loss in viability due to the freezing and thawing processes, although of course selection effects will contribute to this loss. Although there are caveats around the quality of the cryopreservation techniques, there was no evidence of any substantive influence of patient factors on the loss in success due to freezing.
Conclusions
The analyses presented here refer to individual embryo transfer procedures, the data not allowing any meaningful analyses of cumulative outcome beyond the estimation of simple intercycle correlations. We can however demonstrate that there are correlations between outcomes from repeat cycles from the same couples; although these effects do not materially affect estimates of the influence of covariates, they will be important in predicting more relevant outcomes that span multiple transfers across a treatment course. These effects may reflect unmeasured (or inaccurately measured) prognostic factors.
The results for prognostic factors are consistent with other studies, but are estimated here with greater precision due to the large cohort. These factors are similar for live birth outcomes and twin outcomes, with no factors or combinations of factors being identified that specifically predict twin outcomes.
The data on frozen cycles is of poorer quality but does suggest that predictors of success are similar to those in fresh cycles.
Summary
The statistical analysis of the national dataset revealed no characteristics that specifically predicted multiple birth outcomes beyond those that predicted treatment success. A number of prognostic factors were confirmed, with age and the number of embryos created being the major predictors. The limited data on the transfer of frozen embryos suggests that the prognostic factors behave similarly for these cycles.
Chapter 4 The towardSET? collaborative data
Introduction
This chapter describes the development of predictive models for the data collated from five centres as part of the towardSET? collaboration. First the data collation is described, then models are developed using both the LR and EU modelling approaches, allowing where appropriate and possible for correlations between transfers in the same individuals. The two resultant sets of models are presented and the roles of the various prognostic factors are explored. The models are then extended to look at the effects of embryo cryopreservation. Finally, a number of validation analyses are performed to ascertain the validity and uncertainty in the EU model which will be used in later simulation studies (Chapter 5).
Data extraction and cleaning
Data were extracted from the clinic databases in five UK assisted conception units for the 2000–5 period. The time period was chosen so that live birth outcomes were available at the time the project commenced. Cycles using donor eggs or sperm were excluded, the only other exclusions being for atypical treatments or patients. 23,582 cycles (17,857 fresh, 5725 frozen) from 11,767 patients were available for analysis. The sections marked with an asterisk below give technical details of the extraction and data cleaning methodology: these sections are not essential to the understanding of the project outcomes, but are provided for readers interested in the methodology.
Data sources
Data were obtained from five centres (Table 27). Each centre has a database on to which details of every assisted conception treatment are entered, and these data are used as the basis for statutory returns to the HFEA as well as for internal monitoring, audit and, in some cases, costing. Data were requested from 2000 to 2005, this representing a 5-year cohort with full pregnancy outcome at the start of the project.
| Site | Database system | Type of embryo transfer | Cycles with embryo transfer before clean-up | Cycles with embryo transfer after clean-upa |
|---|---|---|---|---|
| Clarendon Wing, Leeds General Infirmary | acusys | All | 6828 | 6799 |
| Fresh | 5660 | 5632 | ||
| Frozen | 1168 | 1167 | ||
| Hewitt Centre for Reproductive Medicine, Liverpool Women’s Hospital | ideas | All | 4639 | 2257 |
| Fresh | 3497 | 2257 | ||
| Frozenb | 1142 | 0 | ||
| Manchester Fertility Services | acusys | All | 2296 | 2291 |
| Fresh | 1641 | 1636 | ||
| Frozen | 655 | 655 | ||
| St Mary’s Hospital, Manchester | acusys | All | 4222 | 4200 |
| Fresh | 2433 | 2413 | ||
| Frozen | 1789 | 1787 | ||
| Centre for Reproductive Medicine and Fertility (Jessop Wing), Sheffield | ideas | All | 1388 | 549 |
| Fresh | 1142 | 549 | ||
| Frozenb | 246 | 0 | ||
| All | – | All | 19,373 | 16,096 |
| Fresh | 14,373 | 12,487 | ||
| Frozen | 5000 | 3609 |
Centres provided either reports from the databases or raw database tables. Any identifying information was removed by local centre staff and the database/report files transferred electronically to Manchester, where they were assembled into a common format as detailed below.
Data selection
Cycles were included if they met all the following inclusion criteria:
-
treatment type: ICSI or IVF
-
cycles with one, two, or three embryos transferred
-
age 19–54
-
patient’s own eggs
-
date started trying or last pregnant after 1980.
Cycles were excluded if they met any of the following exclusion criteria:
-
donor eggs
-
frozen/thawed eggs
-
natural or HRT induction.
Additionally we defined a core set of covariates, and cycles were excluded if any of these variables were missing:
-
embryo cell number and grade
-
age
-
number of previous attempts
-
number of previous pregnancies and live births
-
diagnosis
-
duration of infertility
-
number of eggs collected in fresh cycles
-
number of embryos created in fresh cycles or thawed in frozen cycles
-
transfer day (for fresh cycles)
-
treatment centre
-
year of treatment.
*Data cleaning
*Patient history
The acusys database holds only a single set of records for patient history, which are updated each time the patient presents for treatment. Thus it is necessary to ‘unwind’ the history to obtain the values that appertained for earlier cycles in the database. For one centre this was done manually (in itself potentially error prone), while for the other two sites a computer algorithm was used. Table 28 shows the concordance (exact agreement) between the manually and algorithmically corrected data for the manually corrected centre, indicating that this procedure was reasonably successful.
| Variable | % Agreement | |
|---|---|---|
| Uncorrected vs manual | Manual vs algorithm | |
| Gravida | 65 | 86 |
| Parity | 73 | 91 |
| Primary infertility (female) | 78 | 90 |
| Primary infertility (male) | 76 | 90 |
| Primary infertility (couple) | 73 | 90 |
| Male previous pregnancies | 65 | 85 |
*Zero/null entries
For a number of variables there was ambiguity in that variables were recorded as zero or null and these entries could be interpreted as either zero or missing. For sperm quality measures these were assumed to be zero, if single values were zero, but to be missing if the whole set of measurements on a given sample were zero. Variables relating to time periods, height and weight, drug doses, hormone levels and embryo grading were assumed to be missing if recorded as zero.
*Previous treatments, duration of infertility, gravida, parity and diagnosis
The datasets from Liverpool and Sheffield were abstracted from the ideas database, and attempt number, duration of infertility (for Liverpool), diagnosis (for Sheffield) and pregnancy/birth history were either incomplete or not available from the supplied data. Data for the same period, originally derived from the same source, were available in the HFEA database, and similar variables were available in that dataset, although both datasets were anonymised and so could not be directly matched. By matching the two datasets on egg collection date, age and number of eggs available it was possible to identify the cycles in 91% of fresh cycles for Liverpool and 78% of fresh cycles for Sheffield, and therefore infer the values of these parameters for the majority of cycles (although some variables such as duration of infertility were incomplete in the HFEA data also). It should be noted that for the three sites where this data was available in both the HFEA dataset and the raw data supplied by the sites, the accuracy in matching for attempt number was 93% for an exact match and 98% for a match within one attempt. Considering that attempt number itself for these sites had to be redefined to match the HFEA definition of total fresh and frozen cycles with or without transfer, and this match was obtained for over 95% of all cycles for these three sites, we can be reasonably confident in the data obtained using this procedure.
*Normalisation of embryo grading across sites
All sites nominally used similar embryo grading criteria, modified from Steer et al. 117 (although the labelling was reversed in some sites relative to the others – here we adopt the convention that increasing score implies increasing quality). However, preliminary exploratory analysis suggested that the grading schemes were not consistent between the sites: the proportions given each grade differed substantially between sites, and preliminary models incorporating grade showed a significant grade by site interaction. We therefore normalised the grades: we based the normalisation on an assumption that the underlying embryo grade distribution was the same across sites and computed a site-specific score for each site to maintain this condition. This normalisation method was justified post hoc by the lack of site by grade interaction in the fitted models.
Embryo cell number (stage) was transformed to log2(cells)/(days in culture), using the recorded time in culture. Where culture time was unavailable, a mean value, given the transfer day, was used. Thus we represent embryo growth by the number of cell doublings per day, allowing day 2 and day 3 embryos to be assessed on the same scale.
The analysis datasets
The dataset as obtained contained 19,373 embryo transfers, 14,373 fresh and 5000 frozen from five centres as shown in Table 27. After cleaning the total number of cycles available for analysis was 16,096: 12,487 fresh and 3609 frozen, from 9040 couples (Table 29).
| Couples | Cycles | Cycles with one embryo transfer, no. (%) | Cycles with two embryo transfers, no. (%) | Cycles with three embryo transfers, no. (%) | |
|---|---|---|---|---|---|
| All | 9040 | 16,096 | 2472 (15.4) | 12,644 (78.6) | 980 (6.1) |
| Fresh | 8775 | 12,487 | 1330 (10.7) | 10,418 (83.4) | 739 (5.9) |
| Frozen | 2088 | 3609 | 1142 (31.6) | 2226 (61.7) | 241 (6.7) |
Variables included in the models
The variables for inclusion in the model were pre-selected on the basis of previous knowledge (see Chapter 1, Informal review of the relevant literature) and the data available and are listed in Table 30 along with the chosen representation (categories or splines). Cervical diagnosis was not considered as there were so few observations with this diagnosis. After normalisation the grade variable has a distribution that clusters around the original values. In order to capture the underlying continuum and so as not to overfit the data, a smooth curve was fitted (based on a cubic spline representation with three degrees of freedom) representing the underlying four-point scale. A similar representation was used for the cell number (doublings). These choices was justified post hoc, as increasing the spline degrees of freedom did not improve the fit as assessed by the AIC.
| Parameter | Categoriesa | Comments |
|---|---|---|
| Numbers of embryos transferred | 1, 2 or 3 | This is included to allow for the possibility that the clinical decision might select different patient populations |
| Age | ≤ 26, 27–29, 30–31, 32–33, 34–35, 36–37, 38–39, 40–42, ≥ 43 | Well-documented predictor (see Chapter 1, Informal review of the relevant literature) |
| Number of embryos created | 1, 2, 3, 4, 5, 6, 7–8, 9–12, ≥ 13 | Well-documented predictor (see Chapter 1, Informal review of the relevant literature) |
| Treatment attempt | 1st, 2nd, 3rd, > 3rd | Well-documented predictor (see Chapter 1, Informal review of the relevant literature). Following the HFEA data, attempt is defined as total previous fresh and frozen cycles with or without transfer |
| IVF or ICSI | IVF, ICSI | |
| Total previous pregnancies/births | 0 previous pregnancies, previously pregnant, 1 live birth, ≥ 2 live births | |
| Years infertile | 0–2, 3, 4, 5, 6, 7–8, ≥9 | |
| Tubal diagnosis | No, yes | Previous studies are conflicting in the role of diagnosis (see Chapter 1, Informal review of the relevant literature). It was decided to include diagnosis as a set covering the main recorded diagnoses |
| Diagnosis of PCOS | No, yes | |
| Endometriosis | No, yes | |
| Male factor diagnosis | No, yes | |
| Idiopathic diagnosis | No, yes | |
| Donor sperm | No, yes | |
| Day of transfer | 2, 3 | |
| Year | 2001, 2002, 2003, 2004, 2005 | Trends over time are expected |
| Centre | 1, 2, 3, 4, 5 | |
| Embryo growth rate | Spline | Fitted as a cubic spline with 3 df |
| Embryo grade | Spline | Fitted as a cubic spline with 3 df |
Given the issues in recording of patient histories and having to match cycles with those in the HFEA data, rather than including separate variables representing whether a patient had previous pregnancies or live births, a simplified variable denoted as ‘birth history’ was defined with four levels, namely never pregnant, previously pregnant, one previous live birth and more than one previous live birth.
In presenting the models the data are referred to a reference category indicated in bold text in the second column of Table 30. In general the reference categories represent medial or modal values.
Characteristics of the dataset
Table 31 summarises the characteristics of the 16,096 cycles from 9040 patients in the dataset, while Table 32 summarises the outcomes on a per-embryo-transfer basis. The characteristics, success and twin rates are similar to the national cohort, other than there being fewer day 3 transfers and transfers with three embryos transferred. Thus, we concluded that this cohort is a representative sample of UK IVF treatment during the study period.
| Parameter | Categories | Fresh cycles | Frozen cycles |
|---|---|---|---|
| Number of embryo transfers | 12,487 | 3609 | |
| Number of patients | 8775 | 2088 | |
| Numbers of embryos transferred | 1 | 1330 (11%) | 1142 (32%) |
| 2 | 10,418 (83%) | 2226 (62%) | |
| 3 | 739 (6%) | 241 (7%) | |
| Age | Mean (SD) [range] | 33.8 (4.2) [19–47] | 33.8 (4.1) [19–47] |
| Number of embryos created/recovered | Mean (SD) [range] | 6 (3.7) [1–26] | 2.9 (1.5) [1–21] |
| Treatment attempt | 1st | 6797 (54%) | 0 |
| 2nd | 2904 (23%) | 1399 (39%) | |
| 3rd | 1426 (11%) | 945 (26%) | |
| > 3rd | 1360 (12%) | 1265 (35%) | |
| IVF or ICSI | IVF | 6470 (52%) | 2188 (61%) |
| ICSI | 6017 (48%) | 1421 (39%) | |
| Total previous pregnancies/births | No previous pregnancies | 6788 (54%) | 1556 (43%) |
| Previously pregnant | 3481 (28%) | 1259 (35%) | |
| 1 previous live birth | 1769 (14%) | 675 (19%) | |
| ≥ 2 previous live births | 449 (4%) | 119 (3%) | |
| Years infertile | Mean (SD) [range] | 5.2 (3.5) [0–24] | 5.1 (3.6) [0–21] |
| Tubal diagnosis | Yes | 3133 (25%) | 1203 (33%) |
| Diagnosis of PCOS | Yes | 1298 (10%) | 512 (14%) |
| Endometriosis | Yes | 1144 (9%) | 284 (8%) |
| Male factor diagnosis | Yes | 4667 (37%) | 1158 (32%) |
| Idiopathic diagnosis | Yes | 3348 (27%) | 849 (24%) |
| Donor sperm | Yes | 354 (3%) | 117 (3%) |
| Day of transfer | 2 | 11,671 (93%) | NA |
| 3 | 816 (7%) | NA | |
| Year | 2000 | 1494 (12%) | 220 (6%) |
| 2001 | 1682 (13%) | 465 (13%) | |
| 2002 | 2307 (18%) | 577 (16%) | |
| 2003 | 2208 (18%) | 670 (19%) | |
| 2004 | 2472 (20%) | 812 (22%) | |
| 2005 | 2324 (19%) | 865 (24%) | |
| Embryo growth rate | Mean (SD) [range] | 1 (0.2) [0–2.5] | NA |
| Embryo grade | Mean (SD) [range] | 3.2 (0.5) [1–4] | 3 (0.6) [1–4] |
| Transfers per couple | 1 | 6086 (69%) | 1223 (59%) |
| 2 | 1935 (22%) | 497 (24%) | |
| > 2 | 754 (9%) | 368 (17%) |
| Cycle | Embryos transferred | No live births (%) | 1 live birth (%) | ≥ 2 live births (%) | LBEs (%) | Twin ratea |
|---|---|---|---|---|---|---|
| All | 1 | 2247 (91%) | 221 (9%) | 4 (0%) | 225 (9%) | 2% |
| 2 | 9774 (77%) | 2177 (17%) | 693 (6%) | 2870 (23%) | 24% | |
| 3 | 791 (81%) | 138 (14%) | 51 (5%) | 189 (19%) | 27% | |
| Fresh | 1 | 1195 (90%) | 133 (10%) | 2 (0%) | 135 (10%) | 1% |
| 2 | 7898 (76%) | 1874 (18%) | 646 (6%) | 2520 (24%) | 26% | |
| 3 | 587 (79%) | 107 (14%) | 45 (7%) | 152 (21%) | 30% | |
| Frozen | 1 | 1052 (92%) | 88 (8%) | 2 (0%) | 90 (8%) | 2% |
| 2 | 1876 (84%) | 303 (14%) | 47 (2%) | 350 (16%) | 13% | |
| 3 | 204 (85%) | 31 (13%) | 6 (2%) | 37 (15%) | 16% |
Logistic regression models
We present models for LBE outcomes and multiple births in those with an LBE. As, in this context, multiple births are only relevant in those having multiple embryos transferred, and as UK policy allows more than two embryos only in exceptional cases, the multiple birth models are developed in those patients receiving DET only. A comparable LBE model is derived for the DET patients for comparison. All the variables in Table 30 were included in the model, regardless of statistical significance. Following previous work1 we included the mean values of embryo growth rate and grade of the transferred embryos. Centre differences were included as a specific fixed effect. A random effect for couple was included to allow for correlations between successive transfers from the same patients.
After fitting a model with all parameters entered as main effects, all two-way interactions between number transferred, age, previous cycles, embryos created, site, stage and grade were considered. No such interactions reached statistical significance so a model with main effects only was adopted.
For each model we present first a table giving the raw coefficients, odds ratios and their 95% confidence interval. The sizes of the random effects are presented in terms of their standard deviations (SD), which is a measure on the same scale as the parameter estimates and gives some idea as to how important the differences between patients are. Plots are then shown as described in Chapter 1, Statistical modelling approaches.
Logistic regression models for success (all data)
Table 33 shows the coefficients for the LR model for successful treatment outcome from a single fresh cycle. The left-hand columns give the estimates for a fixed effect model – that is without any allowance for intercouple correlations – while the right-hand columns show the estimates for a model which includes a couple random effect. The parameter estimates are almost identical for the two models. The coefficients for the cubic spline functions are not shown as they have no ready interpretation, but plots of the stage and grade functions are shown in Figure 14. The patient random effect has a variance of 0.28 corresponding to a standard deviation of 0.54 on the log-odds scale. The correspondence in parameter estimates of the fixed effect and random effect models suggests that the simpler fixed effect model would be adequate for prediction for individual cycles.
| Variablea | Fixed effects only | Including couple REs | |||||
|---|---|---|---|---|---|---|---|
| β | SE | p b | OR | 95%CI | β | SE | |
| Intercept | –3.88 | 0.95 | –3.98 | 0.98 | |||
| Number of embryos transferred | < 0.001 | ||||||
| 1 | –0.39 | 0.15 | 0.68 | 0.50 to 0.91 | –0.41 | 0.15 | |
| 3 | 0.27 | 0.11 | 1.30 | 1.06 to 1.63 | 0.28 | 0.11 | |
| Age (years) | < 0.001 | ||||||
| ≤ 26 | 0.14 | 0.11 | 1.15 | 0.93 to 1.43 | 0.14 | 0.11 | |
| 27–29 | 0.15 | 0.08 | 1.16 | 0.99 to 1.36 | 0.15 | 0.09 | |
| 30–31 | 0.24 | 0.08 | 1.28 | 1.09 to 1.49 | 0.25 | 0.08 | |
| 32–33 | 0.14 | 0.07 | 1.15 | 1.00 to 1.32 | 0.15 | 0.08 | |
| 36–37 | –0.18 | 0.08 | 0.84 | 0.71 to 0.98 | –0.19 | 0.08 | |
| 38–39 | –0.34 | 0.09 | 0.71 | 0.60 to 0.85 | –0.36 | 0.09 | |
| 40–42 | –1.01 | 0.13 | 0.36 | 0.28 to 0.47 | –1.06 | 0.14 | |
| ≥ 43 | –2.09 | 0.42 | 0.12 | 0.05 to 0.28 | –2.17 | 0.43 | |
| Number of embryos created | < 0.001 | ||||||
| 1 | –0.46 | 0.20 | 0.63 | 0.43 to 0.93 | –0.48 | 0.21 | |
| 2 | –0.19 | 0.11 | 0.83 | 0.67 to 1.03 | –0.20 | 0.11 | |
| 3 | –0.16 | 0.10 | 0.85 | 0.70 to 1.04 | –0.17 | 0.10 | |
| 4 | –0.10 | 0.09 | 0.91 | 0.76 to 1.08 | –0.11 | 0.10 | |
| 5 | 0.00 | 0.09 | 1.00 | 0.84 to 1.19 | 0.00 | 0.10 | |
| 7–8 | 0.08 | 0.09 | 1.08 | 0.91 to 1.29 | 0.08 | 0.09 | |
| 9–12 | 0.14 | 0.08 | 1.15 | 0.98 to 1.35 | 0.15 | 0.09 | |
| ≥ 13 | 0.19 | 0.10 | 1.21 | 0.99 to 1.47 | 0.20 | 0.11 | |
| Cycle | < 0.001 | ||||||
| 2nd | –0.15 | 0.06 | 0.86 | 0.77 to 0.97 | –0.13 | 0.06 | |
| 3rd | –0.14 | 0.08 | 0.87 | 0.74 to 1.02 | –0.09 | 0.08 | |
| ≥ 4th | –0.25 | 0.08 | 0.78 | 0.67 to 0.91 | –0.18 | 0.10 | |
| ICSI | –0.05 | 0.06 | 0.40 | 0.95 | 0.85 to 1.07 | –0.06 | 0.07 |
| Previous history | < 0.001 | ||||||
| Previous pregnancy | –0.06 | 0.06 | 0.94 | 0.84 to 1.06 | –0.06 | 0.06 | |
| Previous live birth | 0.19 | 0.07 | 1.21 | 1.05 to 1.39 | 0.18 | 0.07 | |
| Two or more previous live births | 0.20 | 0.13 | 1.22 | 0.95 to 1.58 | 0.19 | 0.13 | |
| Duration of infertility (years) | < 0.001 | ||||||
| 0–2 | 0.19 | 0.08 | 1.21 | 1.03 to 1.41 | 0.21 | 0.08 | |
| 3 | 0.03 | 0.08 | 1.03 | 0.88 to 1.21 | 0.03 | 0.08 | |
| 5 | –0.08 | 0.08 | 0.92 | 0.79 to 1.08 | –0.08 | 0.09 | |
| 6 | –0.05 | 0.09 | 0.95 | 0.80 to 1.13 | –0.05 | 0.10 | |
| 7–8 | –0.13 | 0.09 | 0.88 | 0.74 to 1.05 | –0.14 | 0.09 | |
| ≥ 9 | –0.10 | 0.09 | 0.90 | 0.76 to 1.08 | –0.11 | 0.09 | |
| Cause of infertility | |||||||
| Tubal diagnosis | –0.22 | 0.08 | < 0.001 | 0.80 | 0.69 to 0.94 | –0.24 | 0.08 |
| Diagnosis of PCOS | 0.04 | 0.08 | 0.66 | 1.04 | 0.89 to 1.22 | 0.03 | 0.09 |
| Endometriosis | 0.18 | 0.08 | 0.03 | 1.20 | 1.02 to 1.40 | 0.19 | 0.09 |
| Idiopathic diagnosis | 0.01 | 0.09 | 0.94 | 1.01 | 0.85 to 1.20 | 0.00 | 0.09 |
| Male factor diagnosis | 0.10 | 0.08 | 0.22 | 1.11 | 0.94 to 1.29 | 0.10 | 0.09 |
| Donor sperm | 0.17 | 0.14 | 0.25 | 1.18 | 0.90 to 1.56 | 0.17 | 0.15 |
| Day 3 transfer | –0.22 | 0.12 | 0.05 | 0.80 | 0.63 to 1.02 | –0.23 | 0.12 |
| Year | < 0.001 | ||||||
| 2004 | 0.02 | 0.07 | 1.02 | 0.89 to 1.17 | 0.02 | 0.08 | |
| 2003 | 0.05 | 0.08 | 1.05 | 0.90 to 1.23 | 0.05 | 0.08 | |
| 2002 | –0.08 | 0.08 | 0.92 | 0.79 to 1.08 | –0.09 | 0.08 | |
| 2001 | 0.25 | 0.08 | 1.29 | 1.1 to 1.5 | 0.26 | 0.09 | |
| 2000 | 0.10 | 0.09 | 1.10 | 0.93 to 1.32 | 0.08 | 0.09 | |
| Centre | < 0.001 | ||||||
| 2 | –0.16 | 0.07 | 0.85 | 0.74 to 0.98 | –0.19 | 0.08 | |
| 3 | –0.04 | 0.07 | 0.96 | 0.84 to 1.10 | –0.05 | 0.08 | |
| 4 | –0.20 | 0.07 | 0.82 | 0.71 to 0.94 | –0.22 | 0.08 | |
| 5 | 0.26 | 0.13 | 1.30 | 1.01 to 1.67 | 0.26 | 0.14 | |
| Stage (3 df for spline) | See Figure 14 | < 0.001 | See Figure 14 | ||||
| Grade (3 df for spline) | See Figure 14 | < 0.001 | See Figure 14 | ||||
FIGURE 14.
Spline functions for embryo growth rate and grade in the LR model for the full towardSET? dataset. Grade is shown on the normalised scale with 0 being poorest- and 1 best-quality embryos; the vertical lines indicate the mean normalised grade for embryos graded 1:4 as indicated. Note: in the left-hand panel the curve without REs is obscured behind that with REs.
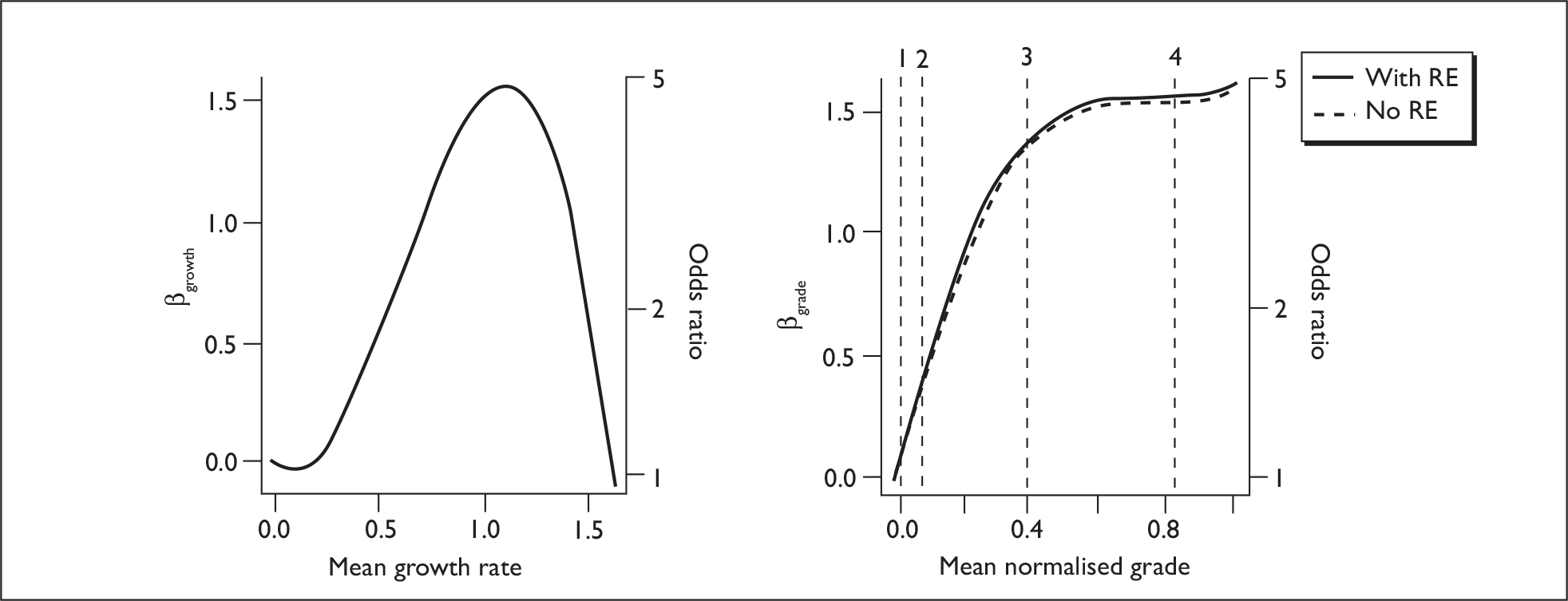
In Figure 15 we show the fitted LBE probabilities plotted against the major prognostic factors. As would be expected, age is the major predictor of success, with an accelerating decline from around age 32 and very low success rates by age 43–45. The number of embryos created is a moderately strong predictor of success: here we note that for any given treatment (solid line in Figure 15) the success rate was lower if only small numbers of embryos were available, but the predicted rate across cycles (boxes) with low numbers of embryos was a lot lower. This reflects the fact that where there are small numbers of embryos to select from, the resultant quality of the transferred embryos is likely to be lower. Couples who have been infertile for a longer time are less likely to have a successful outcome, although this may in part reflect a patient selection effect as patients funded by the NHS will generally only be treated after a longer period of infertility compared with privately funded patients. There was a small decrease in success with later attempts, but it is important to note that the vast majority of later attempts will be from patients with previous failures, so patients having later cycles will be more likely to have a poor prognosis. Having had a previous successful pregnancy (but not an unsuccessful one) is associated with better outcomes. Diagnosis generally only had a small impact on success outcome, with a tubal diagnosis and endometriosis being the only ones that reach statistical significance. A tubal diagnosis led to a poorer prognosis (as seen in other studies such as Strandell et al. 52), while endometriosis was associated with slightly better outcomes.
FIGURE 15.
LBE probabilities from LR model for principal variables.
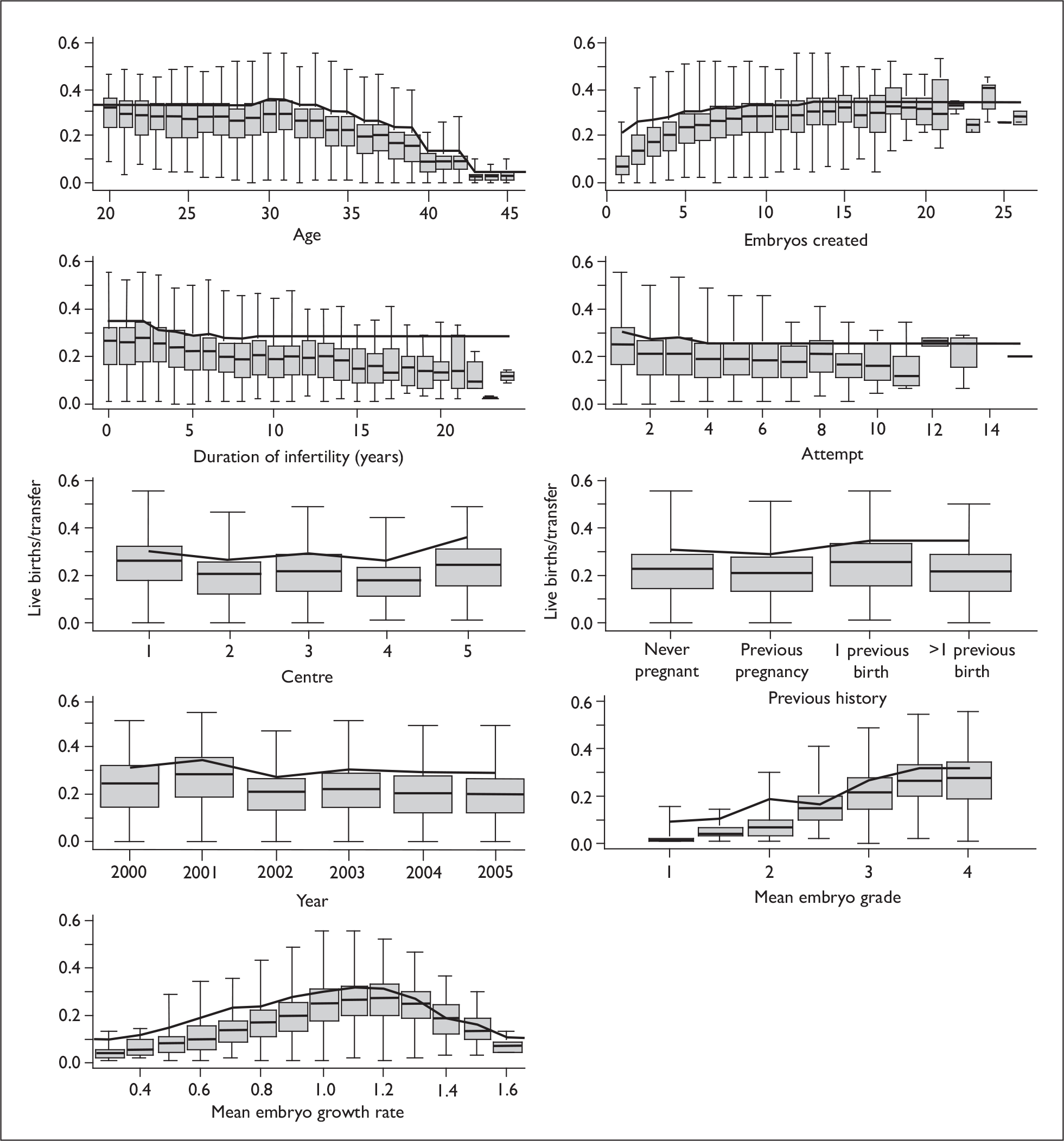
There were highly significant associations between treatment success and centre and year which are difficult to interpret. There was little evidence of a consistent improvement over time in this cohort. The differences between patients treated in the various centres is not explained by the covariates in the model, but may still reflect patient selection effects and not differences in treatment quality.
As noted by others,2,118,119 successful transfers are associated with embryo cell numbers close to one doubling per day and slow- and fast-growing embryos both do poorly. Embryo grade is consistent with the need for one grade 3 or 4 embryo to have a good chance of success. However embryo quality is hard to assess reliably in a model that requires the aggregation of the transferred embryos.
LR models for success and twins in DET
Here we consider only those patients who had DET. The fixed and random effect models for success had again almost identical parameter estimates (Table 34, Figure 16), and the estimate of the within-patient standard deviation for LBE was 0.53.
| Variablea | Fixed effects only | Including couple REs | |||||
|---|---|---|---|---|---|---|---|
| β | SE | p b | OR | 95% CI | β | SE | |
| Intercept | –2.89 | 1.11 | –2.99 | 1.14 | |||
| Age (years) | < 0.001 | ||||||
| ≤ 26 | 0.10 | 1.11 | 1.11 | 0.89 to 1.37 | 0.10 | 0.12 | |
| 27–29 | 0.13 | 0.09 | 1.14 | 0.95 to 1.36 | 0.13 | 0.09 | |
| 30–31 | 0.26 | 0.08 | 1.30 | 1.11 to 1.52 | 0.27 | 0.08 | |
| 32–33 | 0.17 | 0.08 | 1.18 | 1.01 to 1.39 | 0.17 | 0.08 | |
| 36–37 | –0.17 | 0.08 | 0.84 | 0.72 to 0.99 | –0.18 | 0.09 | |
| 38–39 | –0.27 | 0.10 | 0.76 | 0.63 to 0.93 | –0.29 | 0.10 | |
| 40–42 | –0.96 | 0.15 | 0.38 | 0.29 to 0.51 | –1.01 | 0.16 | |
| ≥ 43 | –1.50 | 0.47 | 0.22 | 0.09 to 0.56 | –1.56 | 0.48 | |
| Number of embryos created | < 0.001 | ||||||
| 2 | –0.26 | 0.11 | 0.77 | 0.62 to 0.96 | –0.27 | 0.12 | |
| 3 | –0.22 | 0.10 | 0.80 | 0.66 to 0.98 | –0.23 | 0.11 | |
| 4 | –0.14 | 0.10 | 0.87 | 0.71 to 1.06 | –0.15 | 0.10 | |
| 5 | –0.02 | 0.10 | 0.98 | 0.81 to 1.19 | –0.03 | 0.10 | |
| 7–8 | 0.03 | 0.09 | 1.03 | 0.86 to 1.23 | 0.03 | 0.09 | |
| 9–12 | 0.11 | 0.09 | 1.11 | 0.94 to 1.33 | 0.11 | 0.09 | |
| ≥ 13 | 0.14 | 0.11 | 1.15 | 0.93 to 1.43 | 0.14 | 0.11 | |
| Cycle | < 0.001 | ||||||
| 2nd | –0.16 | 0.06 | 0.85 | 0.76 to 0.96 | –0.14 | 0.06 | |
| 3rd | –0.20 | 0.08 | 0.82 | 0.70 to 0.96 | –0.16 | 0.09 | |
| ≥ 4th | –0.27 | 0.09 | 0.76 | 0.64 to 0.91 | –0.20 | 0.10 | |
| ICSI | –0.04 | 0.06 | 0.54 | 0.96 | 0.85 to 1.08 | –0.05 | 0.07 |
| Previous history | < 0.001 | ||||||
| Previous pregnancy | –0.10 | 0.06 | 0.90 | 0.80 to 1.02 | –0.10 | 0.06 | |
| Previous live birth | 0.18 | 0.07 | 1.19 | 1.04 to 1.37 | 0.17 | 0.08 | |
| Two or more previous live births | 0.22 | 0.13 | 1.25 | 0.97 to 1.61 | 0.22 | 0.14 | |
| Duration of infertility (years) | < 0.001 | ||||||
| 0–2 years | 0.24 | 0.08 | 1.27 | 1.09 to 1.49 | 0.25 | 0.09 | |
| 3 years | 0.04 | 0.08 | 1.04 | 0.89 to 1.22 | 0.04 | 0.09 | |
| 5 years | –0.06 | 0.09 | 0.95 | 0.79 to 1.12 | –0.05 | 0.09 | |
| 6 years | –0.07 | 0.10 | 0.93 | 0.77 to 1.13 | –0.07 | 0.10 | |
| 7–8 years | –0.12 | 0.09 | 0.89 | 0.74 to 1.06 | –0.12 | 0.10 | |
| ≥ 9 years | –0.08 | 0.09 | 0.92 | 0.77 to 1.10 | –0.09 | 0.10 | |
| Cause of infertility | |||||||
| Tubal diagnosis | –0.22 | 0.08 | 0.01 | 0.80 | 0.69 to 0.94 | –0.24 | 0.09 |
| Diagnosis of PCOS | 0.03 | 0.09 | 0.75 | 1.03 | 0.86 to 1.23 | 0.02 | 0.09 |
| Endometriosis | 0.14 | 0.09 | 0.13 | 1.15 | 0.96 to 1.37 | 0.14 | 0.09 |
| Idiopathic diagnosis | 0.01 | 0.09 | 0.94 | 1.01 | 0.85 to 1.20 | 0.00 | 0.10 |
| Male factor diagnosis | 0.09 | 0.09 | 0.31 | 1.09 | 0.92 to 1.31 | 0.09 | 0.09 |
| Donor sperm | 0.16 | 0.15 | 0.29 | 1.18 | 0.87 to 1.57 | 0.17 | 0.16 |
| Day 3 transfer | –0.28 | 0.13 | 0.03 | 0.75 | 0.59 to 0.98 | –0.30 | 0.14 |
| Year | < 0.001 | ||||||
| 2004 | 0.01 | 0.08 | 1.01 | 0.86 to 1.18 | 0.01 | 0.08 | |
| 2003 | 0.08 | 0.08 | 1.08 | 0.93 to 1.27 | 0.08 | 0.08 | |
| 2002 | –0.07 | 0.08 | 0.94 | 0.80 to 1.09 | –0.07 | 0.08 | |
| 2001 | 0.27 | 0.09 | 1.31 | 1.10 to 1.56 | 0.28 | 0.09 | |
| 2000 | 0.06 | 0.09 | 1.06 | 0.89 to 1.27 | 0.05 | 0.10 | |
| Centre | < 0.001 | ||||||
| 2 | –0.18 | 0.07 | 0.84 | 0.73 to 0.96 | –0.20 | 0.08 | |
| 3 | –0.09 | 0.08 | 0.91 | 0.78 to 1.07 | –0.11 | 0.08 | |
| 4 | –0.21 | 0.08 | 0.81 | 0.69 to 0.95 | –0.24 | 0.08 | |
| 5 | 0.31 | 0.14 | 1.37 | 1.04 to 1.79 | 0.31 | 0.15 | |
| Stage (3 df for spline) | See Figure 16 | < 0.001 | See Figure 16 | ||||
| Grade (3 df for spline) | See Figure 16 | < 0.001 | See Figure 16 | ||||
FIGURE 16.
Spline functions for embryo growth rate and grade in the LR model for DET. Grade is shown on the normalised scale with 0 being poorest- and 1 best-quality embryos; the vertical lines indicate the mean normalised grade for embryos graded 1:4 as indicated. The arbitrary intercepts have been set to enable comparison between LBE and twin models.
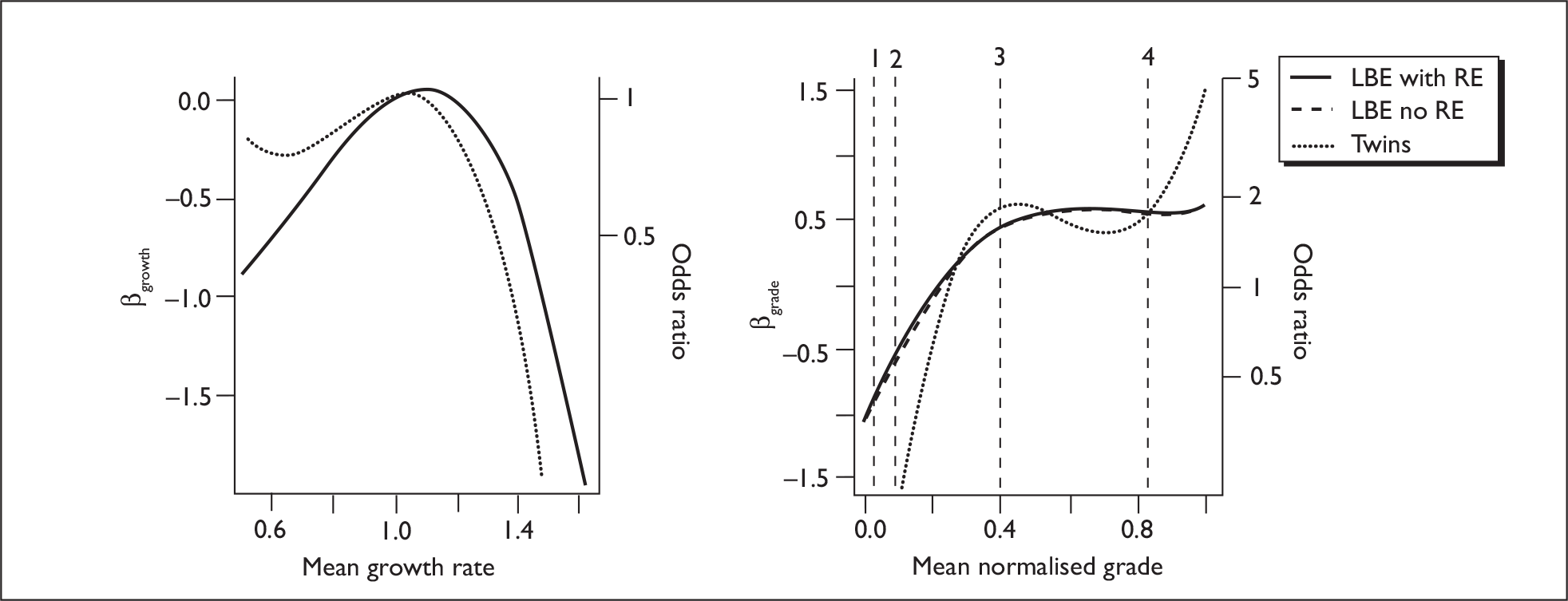
Very few patients had more than one twin birth, so it was not possible to estimate a random effect for the twin model. The parameter estimates for twins, given an LBE, are shown in Table 35 and Figure 16. Figure 17 shows both the fitted models graphically according to patient characteristics, with Figure 18 showing predictions as a function of the averaged embryo characteristics.
| Variablea | Fixed effects only | ||||
|---|---|---|---|---|---|
| β | SE | p b | OR | 95% CI | |
| Intercept | –3.76 | 1.81 | |||
| Age (years) | < 0.001 | ||||
| ≤ 26 | 0.54 | 0.21 | 1.72 | 1.14 to 2.59 | |
| 27–29 | 0.37 | 0.17 | 1.44 | 1.04 to 2.02 | |
| 30–31 | 0.43 | 0.15 | 1.54 | 1.15 to 2.06 | |
| 32–33 | 0.03 | 0.15 | 1.03 | 0.77 to 1.38 | |
| 36–37 | –0.04 | 0.17 | 0.96 | 0.69 to 1.34 | |
| 38–39 | –0.38 | 0.22 | 0.69 | 0.44 to 1.05 | |
| 40–42 | –0.82 | 0.45 | 0.44 | 0.18 to 1.06 | |
| ≥ 43 | 0.09 | 1.14 | 1.09 | 0.12 to 10.22 | |
| Number of embryos created | 0.04 | ||||
| 2 | –0.87 | 0.27 | 0.42 | 0.25 to 0.71 | |
| 3 | –0.14 | 0.21 | 0.87 | 0.58 to 1.31 | |
| 4 | –0.33 | 0.20 | 0.72 | 0.49 to 1.06 | |
| 5 | 0.00 | 0.19 | 1.00 | 0.69 to 1.45 | |
| 7–8 | –0.22 | 0.17 | 0.80 | 0.58 to 1.12 | |
| 9–12 | –0.19 | 0.17 | 0.83 | 0.59 to 1.15 | |
| ≥ 13 | –0.09 | 0.20 | 0.92 | 0.62 to 1.35 | |
| Cycle | 0.89 | ||||
| 2nd | –0.01 | 0.12 | 0.99 | 0.78 to 1.25 | |
| 3rd | 0.00 | 0.17 | 1.00 | 0.72 to 1.40 | |
| ≥ 4th | –0.15 | 0.19 | 0.86 | 0.59 to 1.25 | |
| ICSI | –0.06 | 0.13 | 0.64 | 0.94 | 0.73 to 1.22 |
| Previous history | 0.82 | ||||
| Previous pregnancy | 0.07 | 0.12 | 1.07 | 0.85 to 1.36 | |
| Previous live birth | 0.08 | 0.14 | 1.08 | 0.82 to 1.43 | |
| Two or more previous live births | –0.13 | 0.28 | 0.88 | 0.51 to 1.52 | |
| Duration of infertility (years) | 0.71 | ||||
| 0–2 | 0.12 | 0.16 | 1.13 | 0.82 to 1.54 | |
| 3 | 0.03 | 0.17 | 1.03 | 0.74 to 1.44 | |
| 5 | 0.19 | 0.18 | 1.21 | 0.85 to 1.72 | |
| 6 | 0.28 | 0.19 | 1.32 | 0.91 to 1.92 | |
| 7–8 | 0.04 | 0.19 | 1.04 | 0.72 to 1.51 | |
| ≥ 9 | –0.02 | 0.19 | 0.98 | 0.68 to 1.42 | |
| Cause of infertility | |||||
| Tubal diagnosis | –0.10 | 0.17 | 0.54 | 0.90 | 0.65 to 1.26 |
| Diagnosis of PCOS | –0.11 | 0.17 | 0.51 | 0.89 | 0.64 to 1.25 |
| Endometriosis | 0.00 | 0.18 | 0.99 | 1.00 | 0.70 to 1.42 |
| Idiopathic diagnosis | –0.02 | 0.19 | 0.90 | 0.98 | 0.68 to 1.42 |
| Male factor diagnosis | 0.09 | 0.18 | 0.61 | 1.09 | 0.77 to 1.56 |
| Donor sperm | –0.24 | 0.32 | 0.45 | 0.79 | 0.42 to 1.47 |
| Day 3 transfer | –0.27 | 0.27 | 0.32 | 0.76 | 0.45 to 1.30 |
| Year | 0.33 | ||||
| 2004 | –0.17 | 0.16 | 0.84 | 0.62 to 1.15 | |
| 2003 | –0.16 | 0.16 | 0.86 | 0.62 to 1.17 | |
| 2002 | –0.02 | 0.16 | 0.98 | 0.72 to 1.34 | |
| 2001 | 0.11 | 0.17 | 1.12 | 0.80 to 1.56 | |
| 2000 | 0.17 | 0.19 | 1.18 | 0.82 to 1.72 | |
| Centre | 0.01 | ||||
| 2 | 0.34 | 0.15 | 1.40 | 1.05 to 1.89 | |
| 3 | 0.18 | 0.15 | 1.19 | 0.89 to 1.61 | |
| 4 | –0.24 | 0.16 | 0.79 | 0.57 to 1.08 | |
| 5 | 0.47 | 0.29 | 1.60 | 0.91 to 2.82 | |
| Stage (3 df for spline) | See Figure 16 | 0.02 | See Figure 16 | ||
| Grade (3 df for spline) | See Figure 16 | < 0.001 | See Figure 16 | ||
FIGURE 17.
Success and twin predicted probabilities for LR models in fresh DET transfers in the towardSET? dataset. Live births (left); twins per LBE (right).
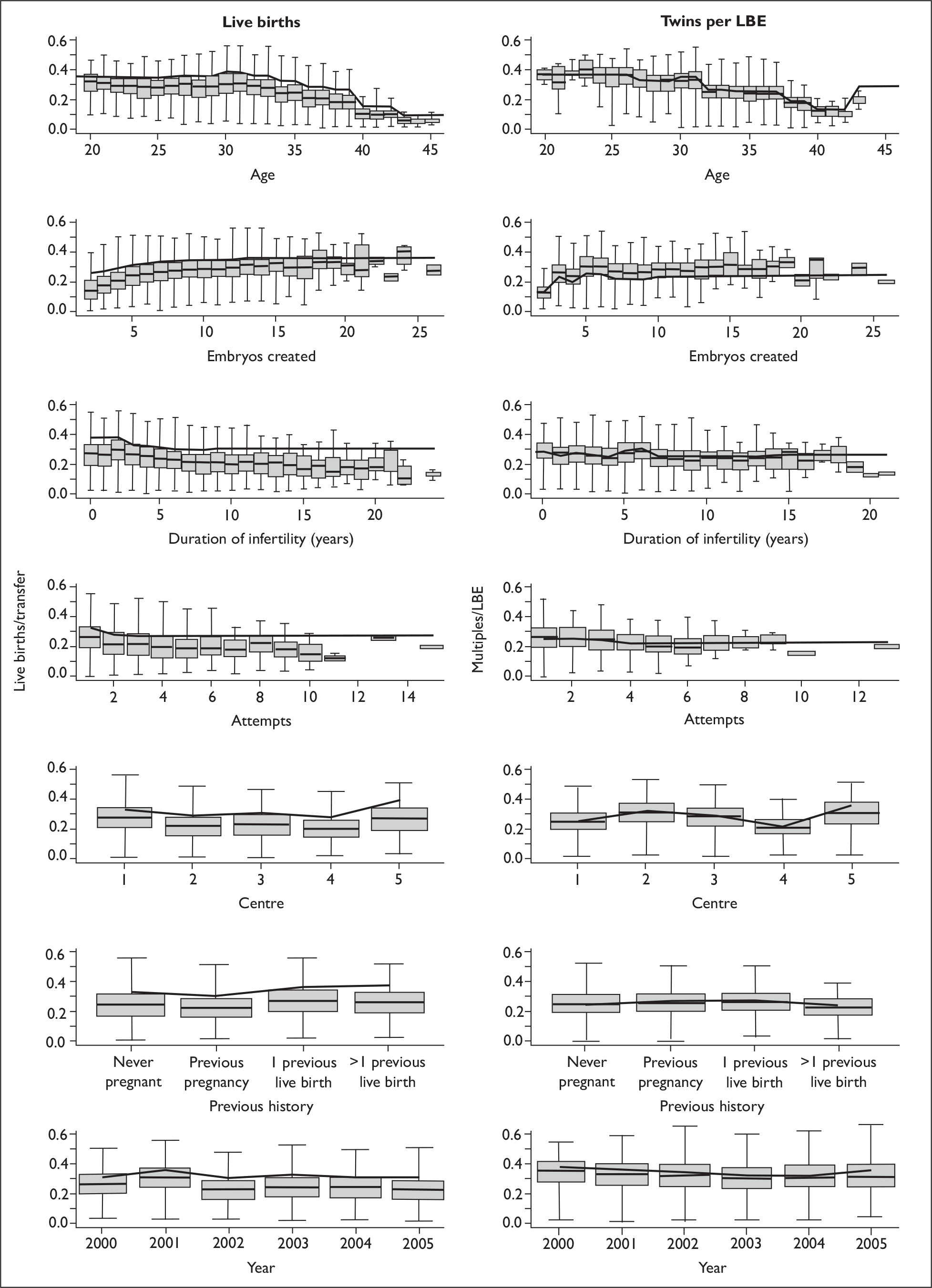
FIGURE 18.
LBE and twin rates from LR model in fresh DET transfers as a function of embryo growth rate and grade in the towardSET? dataset. Live births (left); twins per LBE (right).
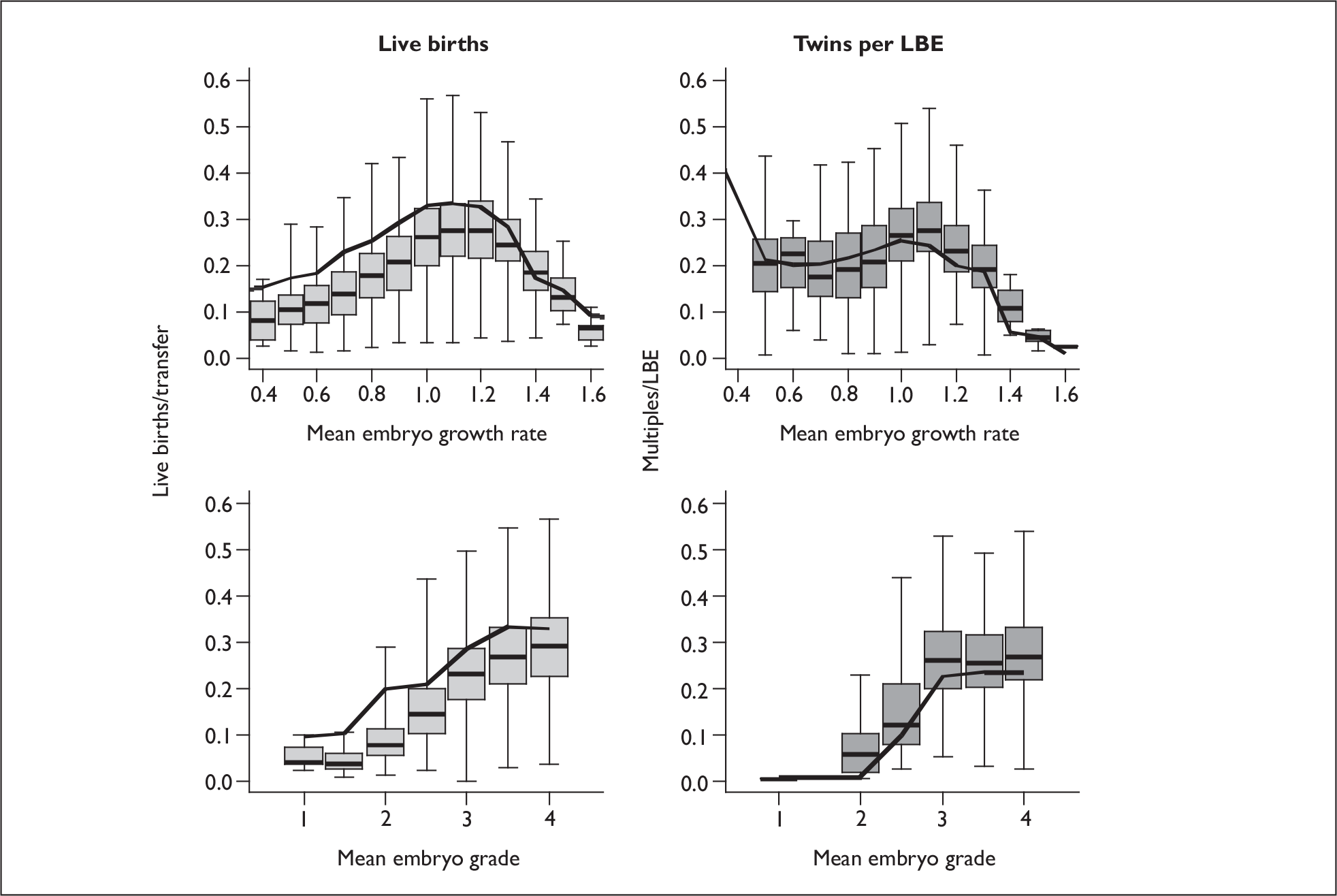
In general the relationships between twin rates and covariates are similar to those for live birth. There is no evidence that there are any patient subgroups (as defined by the available covariates) that are at a higher risk of twins beyond that due to a higher success rate. The exception to this is the centre effects which do show some heterogeneity, with centre 1 in particular having a lower twin rate and centre 2 a relatively higher twin rate than would be expected from the LBE rates (Figure 17). There is also an indication that those with previous births have a higher success rate but not a higher twin rate, but this may be an artefact of the relatively small numbers of such patients or patient selection effects due to differing policies between privately and publicly funded treatments.
*Random effects estimates from the mixed LR models
Here we were able to use the more accurate adaptive quadrature method to obtain the estimates of the patient random effects in contrast to the analysis of the HFEA data (see Chapter 3, The logistic regression models). Table 36 summarises the random effect estimates for the LR LBE model on the log-odds scale (i.e. the same scale as the parameter estimates, b). The random effect estimates the differences between individuals that are not accounted for by the known covariates, and the standard deviation approximately corresponds to a difference between the reference 35-year-old and a patient in the 38- to 39-year-old group. The estimate is slightly lower if only DET cycles are included, which is consistent with this being a more homogeneous population.
| Dataset | Number of transfers | Number of patients | RE standard deviation (standard error of RE) |
|---|---|---|---|
| All cycles LBE | 12,487 | 8775 | 0.54 (0.16) |
| DET cycles LBE | 10,418 | 7661 | 0.53 (0.18) |
*LR model validation
Figure 19 shows the fitted and predicted values (see Chapter 1, Statistical modelling approaches, for details) for the two most prognostic patient factors, showing a good fit to the data across all patients.
FIGURE 19.
Fitted and observed outcomes for the LR model for the two most predictive variables. Live births (left); twins per LBE (right).
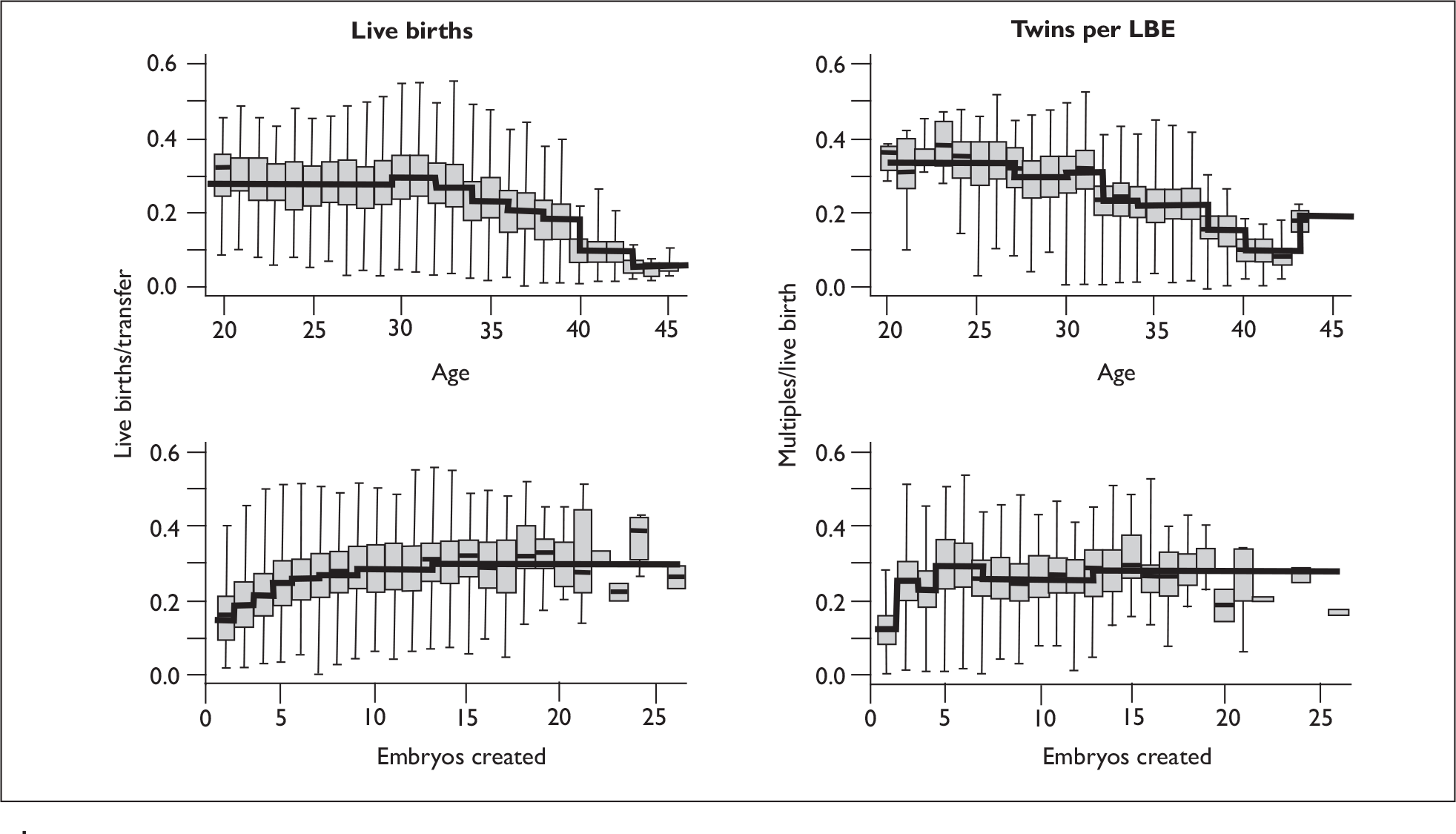
Table 37 gives AUC for the various LR models, a measure of the goodness of fit. The fits are reasonable, with the random effects increasing the AUC value. The towardSET? data give a slightly better fit than the HFEA data (after the inclusion of patient-level random effects), which we can attribute to the availability of embryo grade data. However, as would be expected, the models do not provide useful predictions for individuals, as opposed to population groups.
| Dataset | AUC | |
|---|---|---|
| Fixed effects only | With REs | |
| All cycles LBE | 0.67 | 0.78 |
| DET cycles LBE | 0.65 | 0.77 |
| DET cycles twins given LBE | 0.64 | NAa |
Table 38 gives the results of a bootstrap-based recalibration of the model, showing that the LBE models perform well but that the twins model may be overfitted and unreliable (we would desire the calibration slope to be much nearer 1).
| Dataset | Bootstraps (n = 100) | ||
|---|---|---|---|
| Calibration intercept | Calibration slope | AUC | |
| All cycles LBE | –0.09 | 0.92 | 0.67 |
| DET cycles LBE | –0.10 | 0.91 | 0.65 |
| DET cycles twins given LBE | –0.37 | 0.64 | 0.62 |
LR modelling of the effect of frozen cycles
Here we consider statistical models that include the frozen transfers. We were able to match frozen cycles with the fresh cycle only where the embryos were created in three of the centres (see Chapter 4, Data extraction and cleaning). There were therefore a total of 9681 fresh and 3609 frozen transfers available for this analysis. There were difficulties in developing models that include both the fresh and frozen cycles as the embryo morphological measurements were not recorded in a compatible way, and this led to a rather non-intuitive parameterisation of the frozen effects.
As the exact time of transfer for frozen cycles is more difficult to define, embryo cell number data (as defined by growth rate in the fresh cycle analysis) was not a feasible variable to include in this analysis, and in any case time of transfer was not available for these data. We therefore defined mean growth rate as being ‘slow’, ‘normal’ or ‘fast’ for fresh cycles (based on the 33rd and 66th percentiles of growth rate, defining a ‘slow’ growth rate as less and 0.99 and ‘fast’ as greater than 1.07). Cell number was also not recorded for the frozen data, and, in any event, it is difficult to include without detailed data on the time in culture both before and after cryopreservation. Preliminary exploration indicated that the decrement due to freezing may differ between centres. To avoid identifiability problems while including an interaction between site and fresh and frozen cycles, a new factor was created with six levels as shown in Table 39.
| Fresh | Frozen | |||||
|---|---|---|---|---|---|---|
| Normal growtha | Slow growth | Fast growth | Centre 1 | Centre 3 | Centre 4 | |
| Number of cycles | 3096 | 3373 | 3212 | 1167 | 655 | 1787 |
This combined variable was added to those included in the LR model for fresh cycles, replacing the cell growth spline function, and fitted to the full (fresh and frozen) dataset. As centre is also in the model as a variable in itself (not shown here), the new variable shown in Table 39 provides an interaction test for frozen cycles and site.
The data contains 10,071 egg collections for 6926 patients. Ideally we would have fitted the model with a nested random effect for egg collection within patient. However this proved to be computationally impossible: the average number of egg collections per patient was approximately 1.1. Thus, we included just a single random effect for egg retrieval. Including this random effect led to virtually identical parameter estimates (Table 40). The estimate of the standard deviation of the random effect was 0.64, which is slightly larger than that estimated between repeat cycles from the same individuals.
| Variable | Fixed effects only | Including egg-retrieval REs | |||||
|---|---|---|---|---|---|---|---|
| β | SE | p b | OR | 95% CI | β | SE | |
| Fresh cycle, ‘normal’ growtha | 0 | < 0.001 | 1 | – | 0 | – | |
| Fresh cycle, ‘fast’ growth | –0.10 | 0.06 | 0.9 | 0.80 to 1.02 | –0.11 | 0.06 | |
| Fresh cycle, ‘slow’ growth | –0.59 | 0.07 | 0.56 | 0.48 to 0.64 | –0.63 | 0.08 | |
| Frozen cycle, Centre 1 | –0.79 | 0.10 | 0.46 | 0.37 to 0.55 | –0.77 | 0.11 | |
| Frozen cycle, Centre 3 | –0.79 | 0.15 | 0.45 | 0.34 to 0.61 | –0.75 | 0.16 | |
| Frozen cycle, Centre 4 | –0.49 | 0.11 | 0.61 | 0.49 to 0.76 | –0.45 | 0.12 | |
The parameter estimates for this combined growth/freezing variable are shown in Table 40. The other parameters are comparable in terms of direction and magnitude to those of the fresh model, so are not shown.
For each site, frozen cycles performed significantly poorer than fresh cycles – their success rate being in the region of half that of fresh cycles with ‘normal’ growing embryos – with odds ratios for LBEs of 0.45 to 0.61.
Predictive models using the EU approach
In this section we describe the development of a predictive model using the EU framework (see Chapter 1, Statistical modelling approaches), whereby we explicitly model the outcomes in terms of embryo viability and maternal receptivity, and can explicitly include the individual embryo measurements. These models allow, under assumptions about the model applicability, predictions to be made for outcomes when different numbers of embryos are transferred and thus allow the ‘what if’ questions to be asked, specifically the question ‘What would the outcomes have been if patients who received DET had received SET?’ The next two sections give technical details of the model development and describe the final model used for prediction. Its implications for eSET are described towards the end of this chapter. An interesting interaction effect was observed and that model is described below but was not used in prediction. Some model validation and comparison is given in the section EU model validation, which can be omitted. We then show that the model predictions for eSET are consistent with the trial data. The final sections estimate the effects of intracouple correlations and freezing, which are needed for the more detailed simulation work of Chapter 5.
*Building the models
All the variables listed in Table 30 were included regardless of statistical significance.
Each of the variables can, in principle, be included in either or both the E and U models, i.e. they can affect the embryo viability or the uterine receptivity. This gives 183 = 5832 possible models, and hence an exhaustive search would be computationally infeasible. We therefore adopted a multistage procedure to determine the appropriate levels (E or U) at which to include each variable:
-
First, the embryo parameters were included in the E submodel and not the U. As site reflected potential population differences, this was always included in both submodels. With embryo quality and site in the model, the three models with age in the E, U and both submodels were fitted, and, based on the AIC, the best fit (age in both components) was selected.
-
Second, a forward selection model was developed. Each variable was tested as an addition in each of the three submodels (E, U, and E&U) in a base model including age (E&U), embryo quality (E) and site (E&U), and the model with lowest AIC selected. The final forward model included each variable at its optimal submodel(s) based on the age/embryo/site base.
-
Third, a backward selection model was developed. Here we took a base model with all variables fitted in both the E and U components. Then, for each variable in turn, models were considered with that variable in either just the E or just the U submodel, and the position with lowest AIC selected. The final backward model included each variable at its optimal position with respect to a full model base.
-
The results of the forward and backward selection processes yielded clear positions for some variables, but left a degree of ambiguity around others. The selected components are shown in Table 41.
-
The IVF/ICSI variable and use of donor sperm were considered to naturally fall in the E model, although there was no evidence either way from the model fitting. It was considered important to represent any temporal changes in prognosis, therefore year was included in both components, despite the ambiguous statistical evidence. This left three variables (transfer day and male and idiopathic diagnoses) which still could not be assigned to an appropriate component, although the statistical evidence did not favour inclusion in both component models. Therefore we ran all eight possible combinations and selected the one with the lowest AIC.
-
As a final step we considered potential interactions between the major prognostic variables. Given knowledge gained from the logistic regression where no interactions were observed, a small subset of important variables (namely age, embryos created, site, grade and growth rate) was considered. Models were fitted with the additional interaction terms and the change in AIC computed. Table 42 shows the results of these tests. Most interactions tested led to a worse fit to the data (as quantified by the AIC). Only the age by grade interaction improved the fit, and this only by a small amount. Following inspection of the magnitude and nature of this interaction, it was decided that the interaction might be of biological interest but was not of practical relevance for prediction, and therefore the interaction was not included it in the final model for prediction, but is discussed separately (see An interaction model below).
| Optimal selection | ||||||
|---|---|---|---|---|---|---|
| Forward | Backward | Selected submodel | ||||
| Submodel | AIC differencea | Submodel | AIC differenceb | Chosen | Reason for choice | |
| No. embryos transferred | E | 2.6 | E | 1.8 | E | AIC |
| Embryos created | U | 7.7 | U | 6.3 | U | AIC |
| Attempt | U | 3.9 | U | 4.0 | U | AIC |
| IVF/ICSI | U | 0.0 | E | 1.3 | E | Prior beliefc |
| Sperm source | U | 0.2 | E&U | 0.5 | E | Prior beliefc |
| Birth history | U | 4.1 | U | 4.5 | U | AIC |
| Duration | U | 7.0 | U | 7.8 | U | AIC |
| Diagnosis | ||||||
| Tubal | U | 0.8 | E | 0.5 | U | Maternal diagnosis as a set of variables favour U |
| PCOS | U | 0.4 | U | 0.2 | U | |
| Endometriosis | U | 1.8 | U | 1.7 | U | |
| Idiopathic | E | 0.1 | U | 0.0 | ? | Undecided: test eight possibilities |
| Male factor | E | 0.3 | U | 0.4 | ? | |
| Transfer day | U | 1.0 | E | 0.7 | ? | |
| Year | U | 0.4 | E&U | 1.3 | E&U | |
| Final model AIC | 15597.96 | 15596.27 | ||||
| Interaction added | AIC |
|---|---|
| No interaction | 15596.62 |
| U interactions | |
| Age group:site | 15635.40 |
| Age group:embryos created | 15661.76 |
| Site:embryos created | 15632.29 |
| E interactions | |
| Age group:growth rate | 15607.17 |
| Age group:grade | 15595.10 |
| Age group:site | 15596.62 |
| Growth rate:grade | 15598.00 |
| Growth rate:site | 15601.00 |
| Grade:site | 15605.24 |
We note that the model selection process yielded a large number of fits that were close to the optimal fit in terms of AIC. These fits were saved and are utilised to explore the influence of model selection on predicted outcomes (see EU model validation).
The predictive EU model
The process outlined above leads to a statistical model which is utilised in the predictive and simulation work. In this section we describe the resultant model, then we look specifically at the strength of the statistical evidence around specific embryo (E) or uterine (U) effects. There was some weak evidence for an interaction between grade and age, but discussion of this is deferred to the next section.
Table 43 and Figure 20 give the parameter estimates of the final selected model. The covariate effects are similar to those seen in the LR model (see Logistic regression models above) and so need no discussion here. The EU model, being based on the actual cell number and grades of each embryo, rather than their means, gives a more reliable indication of the role of embryo quality. We see that there is a strong relationship with embryo growth, with both slow- and fast-growing embryos having a poor implantation probability compared with those with a normal growth of around one doubling per day. This has been observed previously. 2,118,119 The morphological grade shows the expected relationships, with grades 1 and 2 having very poor prognosis and grades 3 and 4 similar, but good, prognosis.
| Variablea | U submodel | E submodel | p b | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | SE | OR | 95% CI | β | SE | OR | 95% CI | ||
| Intercept | –0.26 | 0.19 | –3.71 | 0.84 | |||||
| Number of embryos transferred | 0.10 | ||||||||
| 1 | 0.19 | 0.18 | 1.21 | 0.84 to 1.74 | |||||
| 3 | –0.22 | 0.12 | 0.80 | 0.63 to 1.01 | |||||
| Age (years) | < 0.001 | ||||||||
| < 26 | –0.19 | 0.19 | 0.82 | 0.57 to 1.20 | 0.51 | 0.20 | 1.66 | 1.13 to 2.44 | |
| 27–29 | –0.19 | 0.15 | 0.83 | 0.62 to 1.12 | 0.48 | 0.15 | 1.62 | 1.20 to 2.19 | |
| 30–31 | 0.07 | 0.15 | 1.07 | 0.80 to 1.44 | 0.33 | 0.14 | 1.39 | 1.06 to 1.82 | |
| 32–33 | 0.14 | 0.15 | 1.15 | 0.85 to 1.55 | 0.07 | 0.14 | 1.07 | 0.82 to 1.40 | |
| 36–37 | –0.19 | 0.16 | 0.83 | 0.60 to 1.14 | –0.05 | 0.15 | 0.95 | 0.71 to 1.28 | |
| 38–39 | –0.12 | 0.22 | 0.89 | 0.58 to 1.37 | –0.34 | 0.19 | 0.71 | 0.49 to 1.03 | |
| 40–42 | –0.66 | 0.37 | 0.52 | 0.25 to 1.07 | –0.69 | 0.36 | 0.50 | 0.25 to 1.01 | |
| ≥ 43 | –2.13 | 0.79 | 0.12 | 0.03 to 0.56 | –0.30 | 1.04 | 0.74 | 0.10 to 5.67 | |
| Number of embryos created | < 0.001 | ||||||||
| 1 | –0.62 | 0.24 | 0.54 | 0.34 to 0.86 | |||||
| 2 | –0.32 | 0.14 | 0.72 | 0.55 to 0.95 | |||||
| 3 | –0.22 | 0.12 | 0.80 | 0.63 to 1.02 | |||||
| 4 | –0.14 | 0.12 | 0.87 | 0.69 to 1.11 | |||||
| 5 | –0.02 | 0.12 | 0.98 | 0.77 to 1.25 | |||||
| 7–8 | 0.11 | 0.11 | 1.11 | 0.89 to 1.39 | |||||
| 9–12 | 0.16 | 0.11 | 1.18 | 0.95 to 1.46 | |||||
| ≥ 13 | 0.24 | 0.14 | 1.27 | 0.97 to 1.67 | |||||
| Attempt | < 0.001 | ||||||||
| 2nd | –0.20 | 0.07 | 0.82 | 0.71 to 0.94 | |||||
| 3rd | –0.16 | 0.10 | 0.85 | 0.70 to 1.03 | |||||
| ≥ 4th | –0.32 | 0.10 | 0.73 | 0.59 to 0.89 | |||||
| ICSI cycle | –0.09 | 0.07 | 0.91 | 0.79 to 1.06 | 0.22 | ||||
| Previous history | < 0.001 | ||||||||
| Previous pregnancy | –0.08 | 0.07 | 0.92 | 0.80 to 1.06 | |||||
| 1 previous birth | 0.25 | 0.09 | 1.29 | 1.08 to 1.54 | |||||
| ≥ 2 previous births | 0.28 | 0.17 | 1.32 | 0.95 to 1.84 | |||||
| Duration of infertility (years) | < 0.001 | ||||||||
| 0–2 | 0.27 | 0.10 | 1.31 | 1.07 to 1.60 | |||||
| 3 | 0.05 | 0.10 | 1.05 | 0.86 to 1.29 | |||||
| 5 | –0.10 | 0.11 | 0.91 | 0.73 to 1.12 | |||||
| 6 | –0.07 | 0.12 | 0.94 | 0.74 to 1.18 | |||||
| 7–8 | –0.15 | 0.11 | 0.86 | 0.69 to 1.07 | |||||
| ≥ 9 | –0.12 | 0.11 | 0.89 | 0.72 to 1.10 | |||||
| Cause of infertility | |||||||||
| Tubal diagnosis | –0.34 | 0.08 | 0.71 | 0.60 to 0.84 | < 0.001 | ||||
| Diagnosis of PCOS | 0.01 | 0.10 | 1.01 | 0.82 to 1.23 | 0.94 | ||||
| Diagnosis of endometriosis | 0.19 | 0.11 | 1.21 | 0.98 to 1.49 | 0.07 | ||||
| Idiopathic diagnosis | –0.06 | 0.09 | 0.94 | 0.79 to 1.13 | 0.52 | ||||
| Male factor diagnosis | 0.10 | 0.09 | 1.11 | 0.94 to 1.31 | 0.24 | ||||
| Donor sperm | –0.01 | 0.16 | 0.99 | 0.72 to 1.35 | 0.93 | ||||
| Transfer day 3 | –0.34 | 0.14 | 0.71 | 0.54 to 0.95 | 0.02 | ||||
| Year | < 0.001 | ||||||||
| 2004 | 0.47 | 0.17 | 1.60 | 1.15 to 2.25 | –0.50 | 0.16 | 0.61 | 0.45 to 0.83 | |
| 2003 | 0.38 | 0.16 | 1.46 | 1.06 to 1.99 | –0.36 | 0.16 | 0.69 | 0.51 to 0.95 | |
| 2002 | 0.10 | 0.15 | 1.11 | 0.82 to 1.49 | –0.22 | 0.17 | 0.80 | 0.57 to 1.11 | |
| 2001 | 0.43 | 0.17 | 1.53 | 1.09 to 2.16 | –0.10 | 0.18 | 0.90 | 0.64 to 1.28 | |
| 2000 | 0.28 | 0.17 | 1.32 | 0.94 to 1.86 | –0.14 | 0.18 | 0.87 | 0.61 to 1.24 | |
| Centre | < 0.001 | ||||||||
| 2 | –0.55 | 0.12 | 0.58 | 0.45 to 0.73 | 0.47 | 0.13 | 1.60 | 1.24 to 2.07 | |
| 3 | –0.13 | 0.19 | 0.88 | 0.60 to 1.28 | 0.11 | 0.18 | 1.11 | 0.78 to 1.59 | |
| 4 | 0.08 | 0.18 | 1.08 | 0.76 to 1.54 | –0.35 | 0.15 | 0.70 | 0.52 to 0.95 | |
| 5 | –0.03 | 0.21 | 0.97 | 0.64 to 1.48 | 0.43 | 0.23 | 1.53 | 0.99 to 2.38 | |
| Growth rate | See Figure 20 | See Figure 20 | < 0.001 | ||||||
| Embryo grade | See Figure 20 | See Figure 20 | < 0.001 | ||||||
FIGURE 20.
Spline functions for embryo parameters for the EU model fit to the towardSET? dataset. Grade is shown on the normalised scale, with 0 being poorest and 1 best quality embryos; the vertical lines indicate the mean normalised grade for embryosgraded 1–4 as indicated.
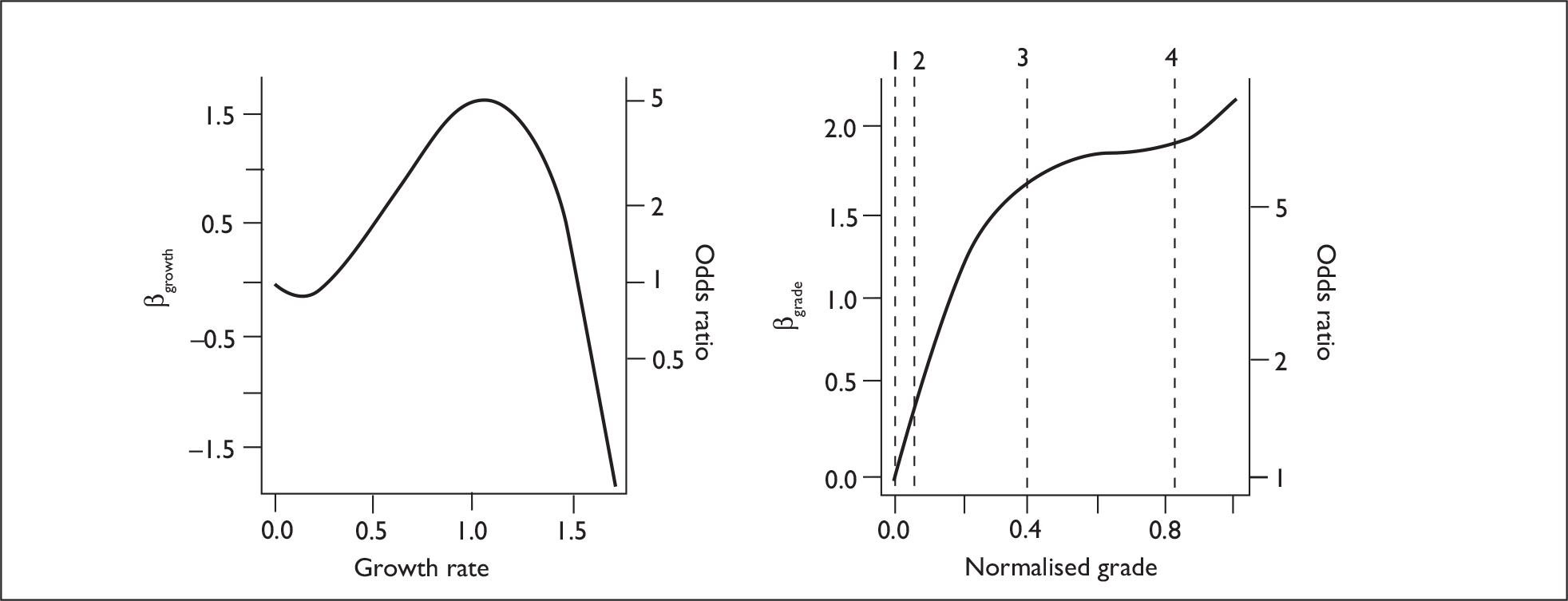
Figures 21 and 22 show the predicted LBE and twin rates for the EU model for the population and for a typical patient as a function of the covariates in the model. These are very similar to the equivalent plots for the LR model (Figure 17), as would be expected. It is pertinent to note how the centre effects show differential differences between the centres in the LBE and twin rates; this may simply reflect differences in patient characteristics that are not represented by the available covariates, or may reflect differences in treatment practice.
FIGURE 21.
Predicted outcomes for EU model fit to the towardSET? dataset, plotted for major predictors. Live births (left); multiplebirth rate (right).
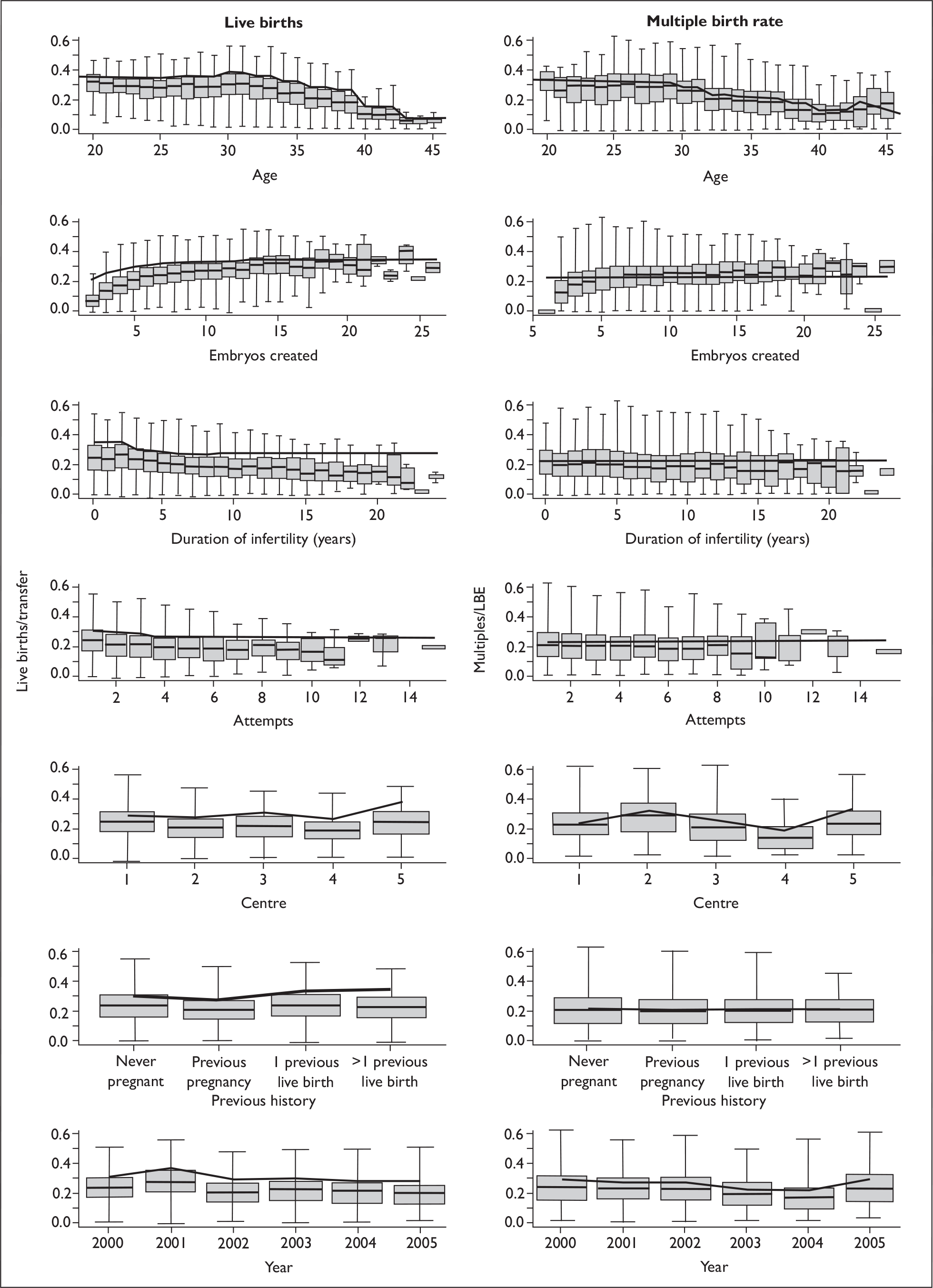
FIGURE 22.
Predicted outcomes for EU model fit to the towardSET? dataset plotted for less important predictors. Live births (columns 1 and 3); multiple birth rate (columns 2 and 4).
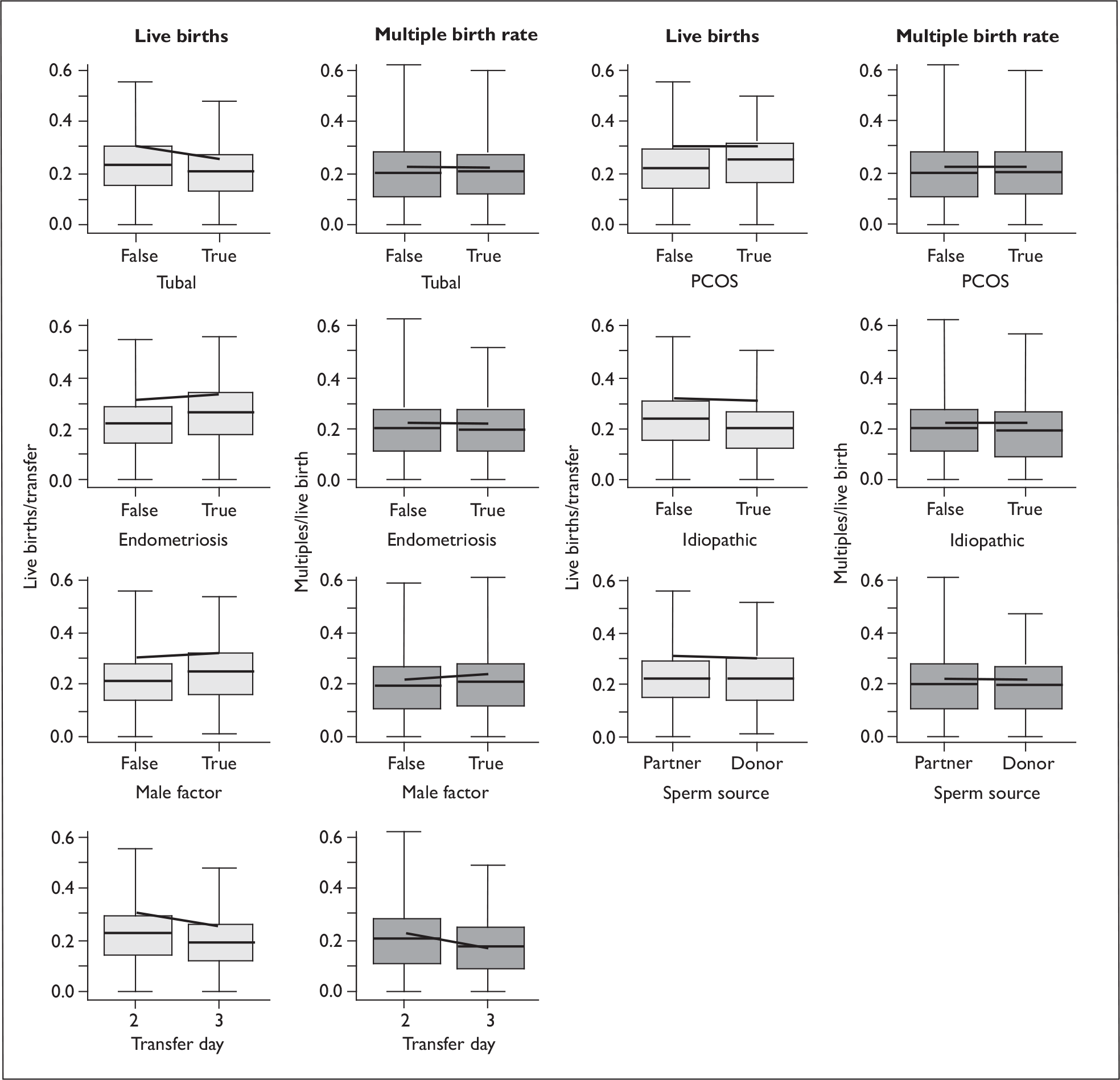
Figure 23 shows the E and U submodels for the primary variables. Except for the very oldest patients, of whom there are only small numbers, there is only a very weak age effect in the U submodel. Most of the age effect is in the E component, and a formal significance test shows that age is not statistically significant in the U submodel (p = 0.11). The centre differences are marked: for example, centre 2 has a low U and a high E compared with the other centres, and this results in a high twin rate for a relatively low success rate (compare Figure 21), while centre 4 has a low E and a higher U, giving a low twin rate. The E components here relate to factors that directly affect the embryo viability and embryo fertilisation, handling and culture processes, and there are many such factors that are not measured, relating to laboratory practice, which can potentially differ between centres. Similarly, U relates to the condition of the potential mother and factors around the drug regimens and implantation procedures, and even the clinical environment and psychological factors can similarly differ between centres and lead to intercentre heterogeneity in U. The fact that a group of centres show this degree of variability suggests that, were these factors controlled to match the best practice, there could be significant improvements in success rates, although a component of these differences will be due to unchangeable differences in population characteristics which are not contained in the measured covariates (including the funding mechanism).
FIGURE 23.
towardSET? dataset: predictions of uterine viability (U) and embryo implantation probability (E) for selected predictors.
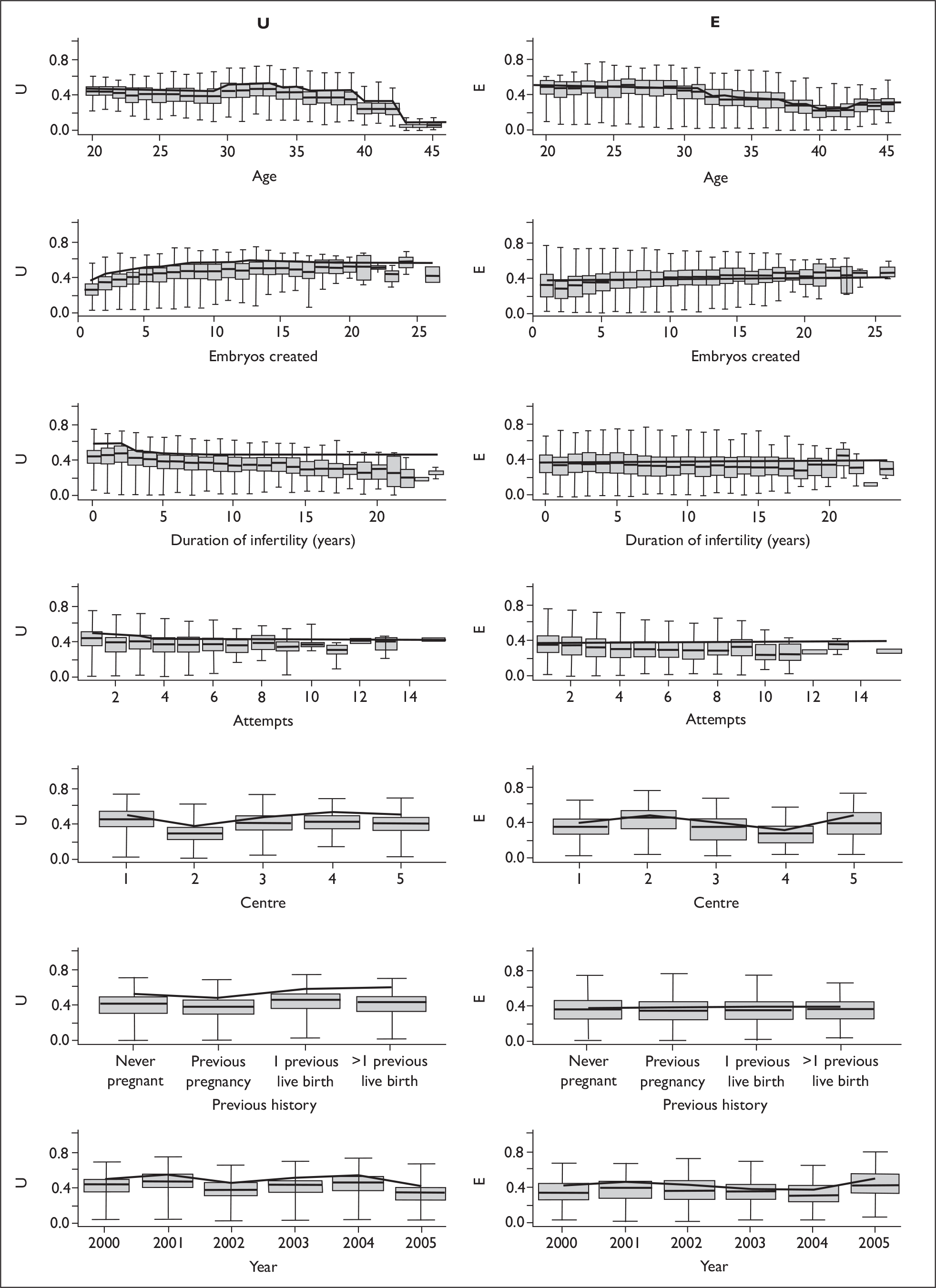
Indeed practice is evolving in all the centres and success rates are slowly improving. In Figure 24 we show the embryo viability as a function of embryo growth and stage, showing the range of values in the population alongside the estimates for a typical patient.
FIGURE 24.
towardSET? dataset: predicted probabilities of an embryo being viable as a function of embryo stage (doublings per day) and grade. Zero growth rate represents single-cell embryos.
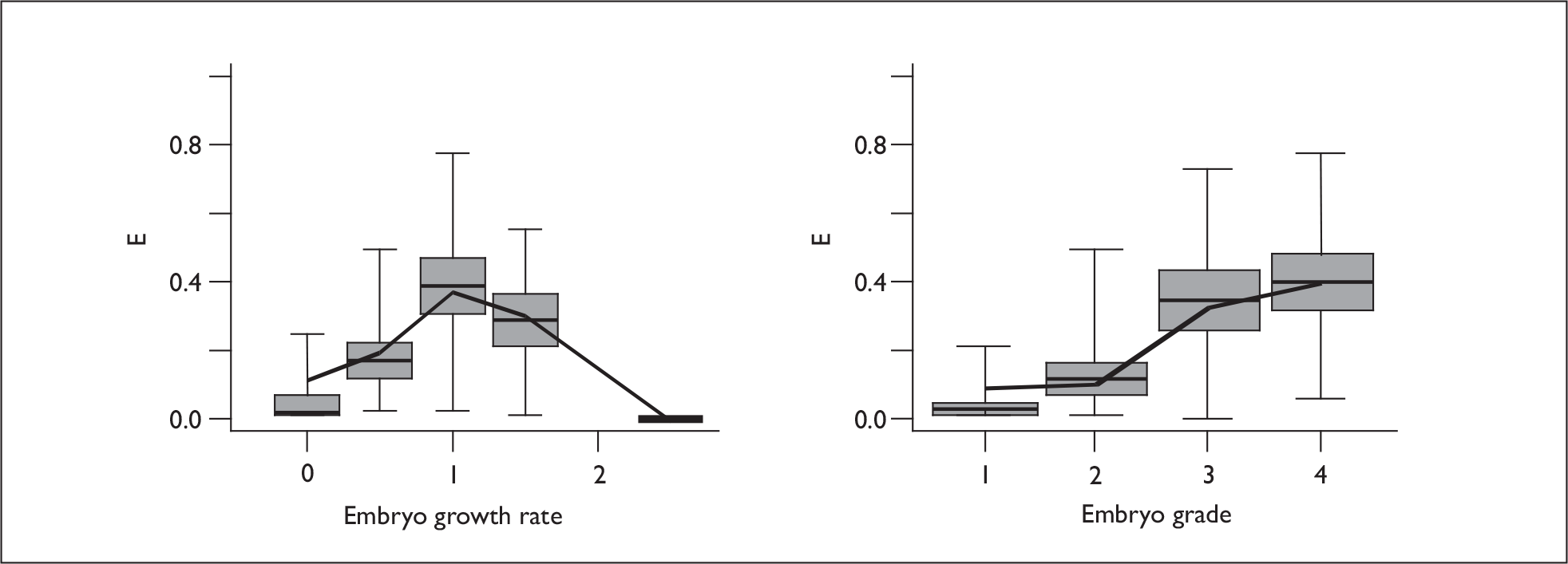
Do prognostic factors act on embryo or uterus?
The EU model has the potential to provide evidence about which submodel each prognostic factor should be included in, i.e. whether a variable acts primarily via the embryo or via the maternal environment. As noted previously, two such distinctions are only weakly identified through the differential effect of covariates on the twin rates, and large datasets are needed to enable any discrimination, but here we do have a large dataset. The various models are not completely nested and therefore standard inference is not possible, so we compared models using the AIC. We consider an AIC difference > 2 as providing evidence that one model is to be preferred, this being the criterion by which an additional model parameter would be justified. Starting from the final model, each variable was refitted at all four possible positions (E, U, both E and U, neither E nor U) and the differences in AIC from the final model are shown in Table 44. In this table the zeros indicate the position in the final model and positive values indicate worse fits to the data. The few negative values indicate better fits than the final model and such fits could be considered alternative models that are in some sense better than our selected model. A statistically better fit to the data would have been obtained if age had been omitted from the U model, but we considered that it was important to understand the age effect as it is the most important patient characteristic determining outcome. We note that in the model with few other covariates the AIC suggested that age should be in both submodels (see above, step 1). In this case the large number of parameters associated with age would have increased the AIC and a simpler age function may well have warranted inclusion. The number of embryos created shows good evidence of contributing through U, suggesting that it may be a surrogate marker for hormonal factors. 113 Attempt number, though a weak effect, acts through U also, suggesting that the systematic decline in success with later attempts reflects poorer uterine or hormonal environments in these patients. However, interpretation of multiple attempts is difficult in these data as the later attempts are predominantly from patients who have failed earlier attempts but have funding for more, so there were large selection effects. Birth and infertility history both seem to reflect uterine environment rather than embryo factors. Most of the diagnoses have little impact on outcome, but a tubal diagnosis was significantly associated with poorer outcome, as noted previously52 (see also Chapter 3, The logistic regression models), and unsurprisingly acts through the uterine component. Site and year of treatment both contribute strongly to both components, indicative of variations in both clinical and embryological practice between centres and over time. There is weak evidence that the use of donor sperm should be included in the U rather than the E submodel, but stronger evidence that it could be excluded entirely. Although, at face value, donor sperm can only affect embryos, it does reflect a male cause for the infertility and may therefore be a surrogate marker for better maternal factors, so either is plausible, but the data provide no strong evidence for either.
| Variable | Difference in AIC from final fit | |||
|---|---|---|---|---|
| Omit | E only | U only | E&U | |
| Age group | 175.06 | –3.05 | 21.25 | 0 |
| Number of embryos transferred | 0.55 | 0 | 1.69 | 0.53 |
| Number of embryos created | 19.33 | 5.57 | 0 | 10.04 |
| Attempt number | 8.05 | 3.82 | 0 | 5.54 |
| ICSI | –0.50 | 0 | 1.06 | 1.94 |
| Birth history | 8.48 | 5.90 | 0 | 5.41 |
| Duration of infertility | 10.44 | 8.67 | 0 | 7.37 |
| Diagnosis | ||||
| Tubal | 14.21 | 4.32 | 0 | 1.35 |
| PCOS | –1.99 | –0.04 | 0 | 1.85 |
| Endometriosis | 1.18 | 1.26 | 0 | 1.98 |
| Idiopathic | –1.58 | 0.22 | 0 | 0.82 |
| Male factor | –0.63 | 0 | 0.74 | 1.96 |
| Donor sperm | –1.99 | 0 | –1.15 | –0.89 |
| Transfer day | 3.47 | 0 | 1.59 | 1.94 |
| Year | 13.04 | 5.03 | 1.83 | 0 |
| Site | 24.74 | 13.49 | 15.50 | 0 |
| Growth rate | 105.66 | 0 | – | – |
| Grade | 92.57 | 0 | – | – |
An interaction model
The model with an age by embryo grade interaction was a slightly better fit to the data than the selected model. An LRT gives p = 0.020, which would not be considered statistically significant if we allowed for the fact that a number of interactions were tested.
Figure 25 shows the embryo implantation probabilities for the interaction model alongside those of the main-effects model. This shows that the effect of grade is somewhat weaker in the older patients – grade is not as good a predictor of success above ∼35 as it is in younger patients. While this could be an artefact of the grading systems or the normalisation procedure required to unify data between centres, it is biologically plausible if there are important age-related components of embryo viability that are not detectable by the morphological systems employed here. Genetic abnormalities such as aneuploidy are an obvious candidate here, as the incidence of these increases strongly with maternal age, but the correlation between aneuploidy and embryo morphology is less strong. 120
FIGURE 25.
Plots of embryo success probabilities against age and grade for the interaction model (solid lines) compared with the main-effects model (broken lines).
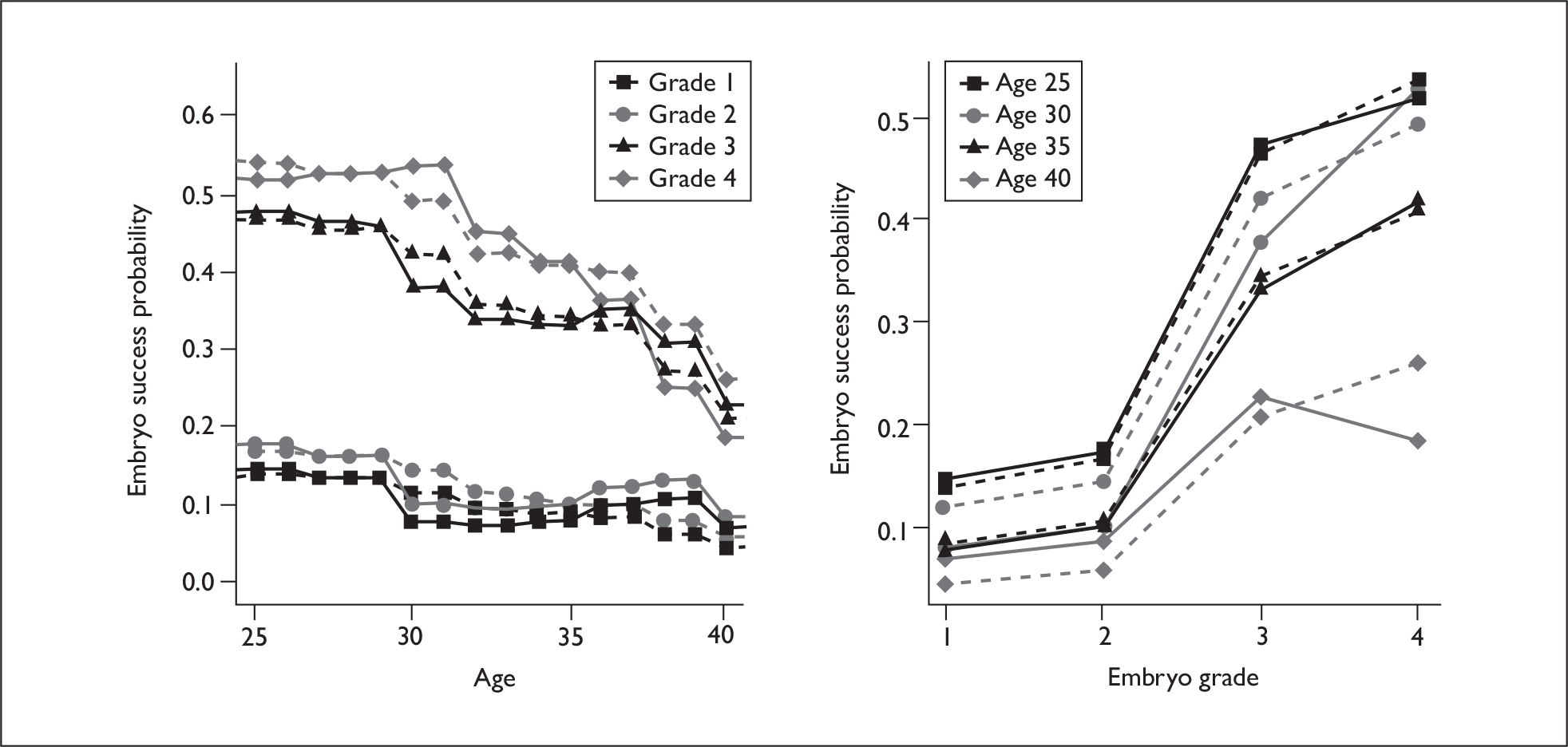
*EU model validation
Figure 26 shows the observed versus fitted values (see Chapter 1, Statistical modelling approaches) for the main-effects model as a function of the two most predictive covariates. There is no evidence of any systematic lack of fit.
FIGURE 26.
Fitted and observed outcomes for the EU model for the two most predictive variables. Live births (left); multiple birth rate (right).
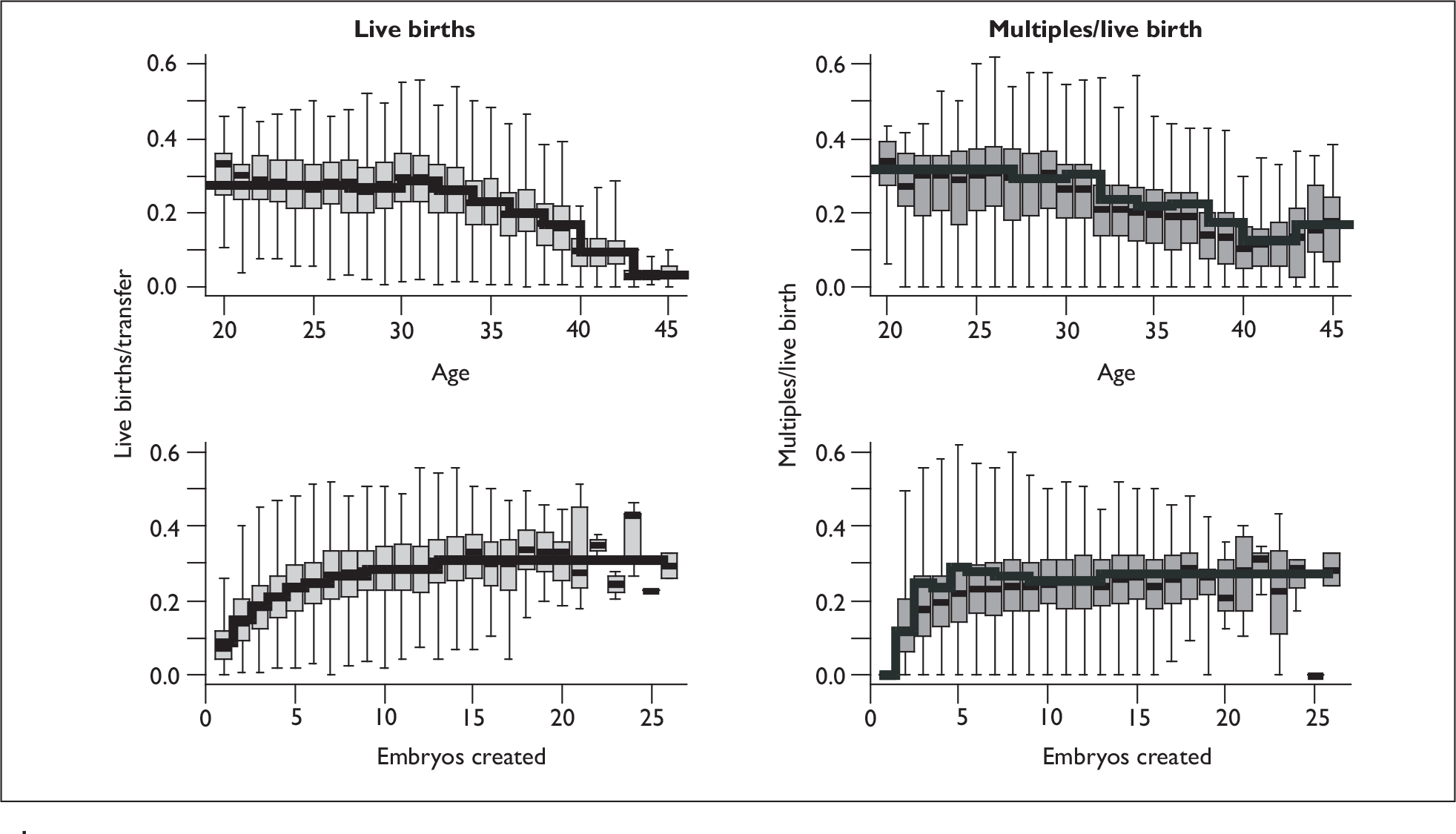
A formal measure of the goodness of fits is given by the AUC. As we have a multinomial outcome there are three AUC parameters, one for each of treatment failure and singleton and twin outcomes. These are shown in Table 45, and the estimates are similar to those seen in the LR model. The two models show equally good fits to the data. As observed in another study,53 the EU model produces a similar AUC to the fixed-effects logistic model for singleton success. Although not directly comparable it would appear that the EU model is better able to classify twin events than the conditional logistic model for twins. The values are also similar to those published by Roberts et al. 2 (0.70, 0.67 and 0.78 for not pregnant, singleton and twin outcomes respectively), although other variables were available for use in that single site analysis that are not available in this analysis of data from several sites (such as FSH and lifestyle indicators).
| AUC | ||
|---|---|---|
| Main effects | Interaction | |
| No live birth | 0.67 | 0.67 |
| Singleton | 0.63 | 0.64 |
| Twins | 0.73 | 0.73 |
In order to assess the uncertainty in the predicted values, the data were refitted using bootstrap resampling and the predicted values computed. The results of 150 bootstrap samples are shown in Figure 27. The model selection process (see above) yielded a number of models that were close to optimal, and consideration of the variability in predicted values between these allows us to make an assessment of the uncertainty owing to model selection. In Figure 28 we show the standard deviation of predictions for all 77 models that had an AIC of < 15,600, i.e. within 3.4 of the final model. Models with an AIC of more than 3 different from the optimum would be considered to be poorer fits with good evidence against them and favouring the optimal fit. Even with this generous inclusion criterion, the model variability is clearly much less than the variability owing to the data. This indicates that the model selection process (here concerned only with identifying the appropriate submodel) and uncertainty in the final choice does not contribute appreciably to the uncertainty in the model predictions.
FIGURE 27.
Variation in predicted estimates from bootstrap resampling. Data shows mean and standard deviation of 150 estimates for individual embryo transfers, ordered by the estimate in the original dataset.
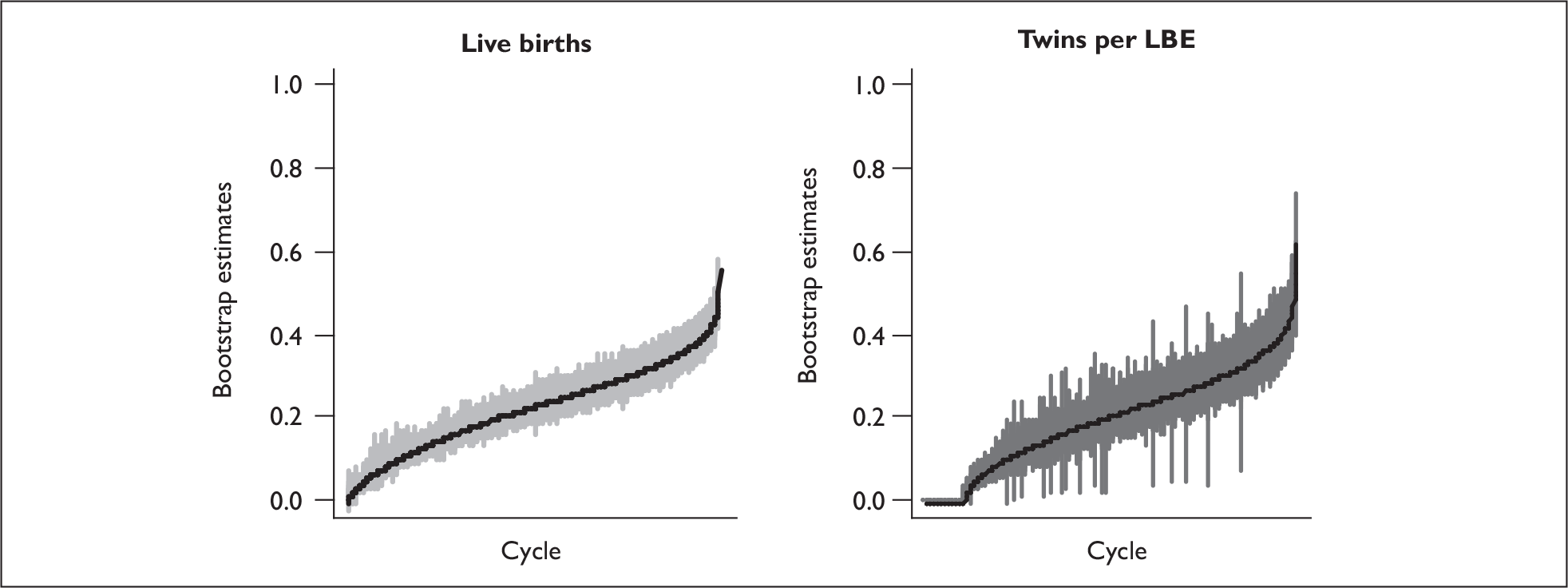
FIGURE 28.
Variation in predicted estimates across 72 models. Data shows mean and standard deviation of estimates for individual embryo transfers, ordered by the estimate in the selected model.
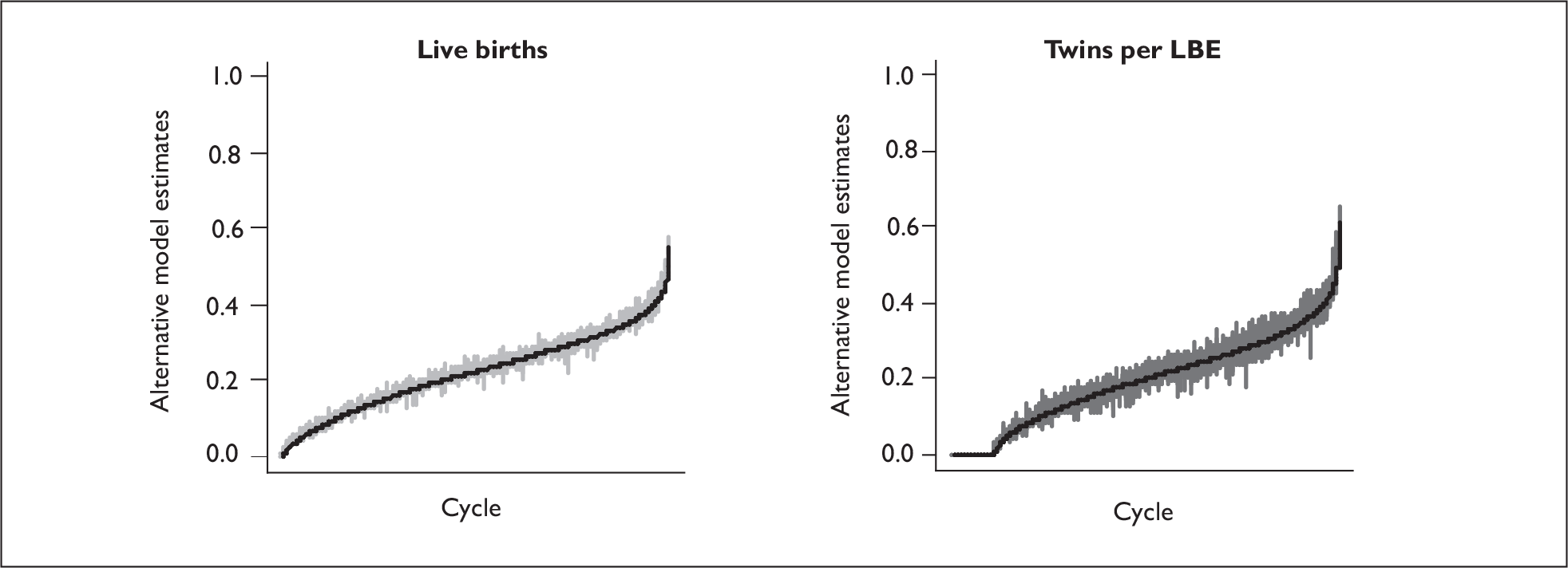
The bootstrap samples give a standard error of prediction between replicates of 3.1% for LBE rate and 4.7% for twin rate, expressed as absolute percentages, while the sample of close to optimum models gives a standard error of prediction of 0.8% for LBE rate and 1.5% for twin rate.
Comparison with data from randomised trials
There have been a number of clinical trials that have randomised patients to receive SET or DET as cleavage stage embryos. These are listed in Table 46 and reviewed in detail in a Cochrane review. 6 These trials were mostly small and of variable quality. Most of the trials explicitly included only good prognosis patients, and beyond this it is to be expected that better prognosis patients would be more likely to consent to participate in a trial, as shown by comparisons between those who consented and those who refused in two of the trials. 14,18 It is also generally accepted that patients in clinical trials have better outcomes than is routine.
| Trial | Population | Number of cycles |
|---|---|---|
| Moustafa et al. 200817 | ≥ 1 good embryo; age ≤ 30 | 81 |
| van Montfoort et al. 200618 | > 1 embryo; ‘unselected’ | 308 |
| Lukassen et al. 200510 | 1st treatment; age ≤ 35; > 1 good embryo | 107 |
| Thurin et al. 200415 | Age < 36; < 2 previous cycles; > 1 good embryo | 661a |
| Martikainen et al. 200114 | > 3 good embryos; some age selection; < 2 previous cycles | |
| Gerris et al. 199913 | 1st treatment; age < 34; > 1 good embryo | 53 |
Thus, we expect that overall success rates will be higher in the trials than in those undergoing routine care. In Figure 29 panels (a) and (b) show the LBE rates for SET and DET from the trials, with 95% confidence intervals along with the model predictions, showing an overall higher success rate in the trial series. Of more relevance is panel (c) which shows the ratio of success rates for SET:DET. Both the total sample and the patients with good prognosis are predicted to have a success rate in SET which is 67% of that in DET, and this is consistent with that observed in all the trials, and indeed is close to an ideal pooled estimate of the ratio in the trials. Similarly, the twin rate [panel (d)] fits the trial data reasonably well once we allow for patient selection. These comparisons give us confidence that the predictions from the EU model are indeed applicable to what is observed in SET treatments in practice.
FIGURE 29.
A comparison of outcomes from trials (estimate with 95% CI) and predicted outcomes from the EU model developed in unselected patients. The two vertical lines indicate the predictions from the EU model for patients who underwent DET, selecting either all patients (solid line) or patients under age 35 (broken line). See text for a detailed description. (a) LBE rate for SET. (b) LBE rate for DET. (c) LBE ratio for SET:DET. (d) Twin rate for DET.
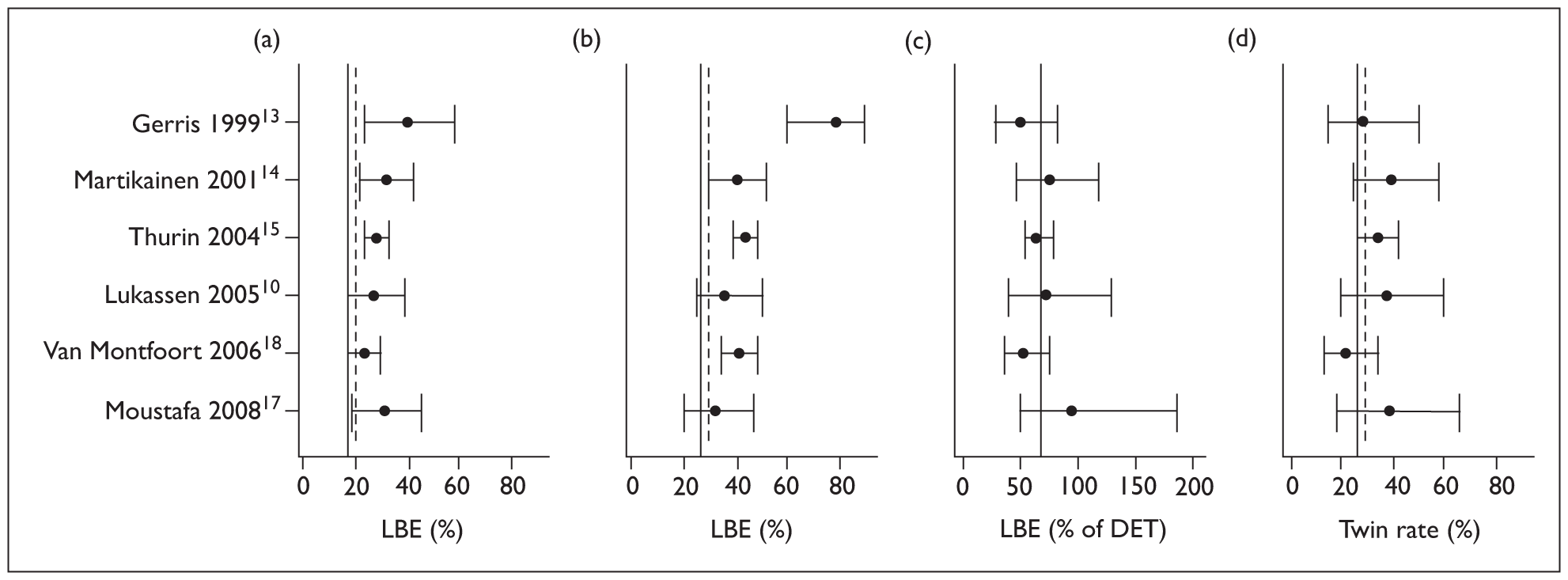
EU modelling of the effect of frozen cycles
Following the approach used for the LR model (see above), we modelled the fresh and frozen cycles together with a six-level factor combining fresh cell growth and freezing, combining the latter with centre as defined in Table 39. This factor was tested in the E submodel. The age of the mother at egg retrieval was used in the E submodel and that of the mother at the time of transfer in the U submodel. We also considered a simple fresh/frozen parameter in the U component, but the fitted estimate (–0.2) was negligible and did not reach statistical significance (p = 0.3). The parameter estimates are shown in Table 47.
| Variable | E submodel | |||
|---|---|---|---|---|
| β | SE | OR | 95% CI | |
| Fresh ‘normal’ growtha | 0 | – | 1 | – |
| Fresh ‘fast’ growth | –0.74 | 0.09 | 0.48 | 0.40 to 0.57 |
| Fresh ‘slow’ growth | –0.22 | 0.08 | 0.80 | 0.68 to 0.93 |
| Frozen cycle (Centre 1) | –1.12 | 0.12 | 0.33 | 0.26 to 0.41 |
| Frozen cycle (Centre 3) | –1.09 | 0.17 | 0.34 | 0.24 to 0.47 |
| Frozen cycle (Centre 4) | –0.63 | 0.13 | 0.53 | 0.41 to 0.69 |
The loss due to freezing is large, with embryo implantation odds ratios between one-third and one-half, with quite large differences between centres.
*Intercycle correlations in the EU model
All the work above ignores the correlations between cycles from the same couple. This was owing to the computational infeasibility of fitting such models to the size of datasets and number of parameters involved. The omission can be justified from observations in the LR model formulation that inclusion of patient random effects had only negligible effects on the parameter estimates. It is possible within the EU model framework to fit a single random effect in the U component (see Chapter 1, Statistical modelling approaches), but this is only computationally feasible if there are a small number of covariates. Therefore, to obtain an estimate of the magnitude of the interpatient correlation we refitted a model derived from the final models described above with the inclusion of an interpatient random effect. In order to reduce the model complexity we computed the linear predictors of the E and U submodels and fitted these as single covariates in E and U. To allow a direct comparison, both models were fitted to the three centre data used to develop the frozen models.
Table 48 shows the random effect estimates for the two models. A naive LRT showed that these effects are of borderline statistical significance, but these tests are known to be inaccurate for testing whether a random effect is zero. 104 Although there is no strong statistical evidence for non-zero correlations between cycles in this dataset, and the magnitude of these intrapatient correlations is not precisely determined, the correlation estimates are of a magnitude that is clinically relevant. The estimates are standard deviations of patient- (or egg-collection)-specific effects on the same linear predictor scale as the model parameter estimates (b), and thus these effects are smaller than the differences due to age and embryo quality but larger than (for example) the effects of patient history or diagnosis.
Implications for eSET
The EU model allows us to predict the potential outcomes for DET cycles were they to have received SET. Assuming that the better-quality embryo of the two is transferred (based on the predicted success probabilities given growth rate and grade) the overall LBE rate in fresh DET cycles in this cohort of 24.4% would be reduced to 16.5% if these cycles had been SET, a reduction of 32%. This compares to a fitted overall success rate of 13.2% (and an observed rate of 13.7%) in those who actually received SET and had two or more embryos available. This group is an undefined mixture of a small number of true eSET cycles and cycles in which DET was contraindicated. Cycles in which only a single embryo was available gave a much lower LBE rate of 8.3%.
Figure 30 [panel (a)] shows that there is a weak age dependence of the proportion of birth events lost in moving from DET to SET in the initial fresh cycle, with the loss being a little greater in older patients. This is true both for the patients in the population (box plots) with their varying characteristics, and as a conditional effect with the other characteristics being held constant (broken line). Most of the variation between individual patients is due to the embryo quality, as illustrated in panel (b), which shows the SET:DET LBE ratio as a function of the difference in embryo grade between the two DET embryos. If the difference was large, i.e. the embryo that was not transferred in the SET treatment was of poor quality, there is only a small loss in LBE rate as the poor embryo contributed little to the success (and incidentally was unlikely to produce a twin pregnancy). Where there were two good embryos (and a higher chance of twins) the loss in eSET was larger.
FIGURE 30.
Loss in fresh cycle success rate in DET cycles had they received SET. Loss is expressed as the ratio of SET:DET LBE rate and plotted against (a) age and (b) the difference in grade between the two embryos (best–worst). The box plots show the range of predictions. The thin horizontal lines indicate the population average of 68%. In panel (a) the broken horizontal line shows the ratio for a ‘typical’ patient (i.e. all parameters other than age held constant) with two top-quality embryos.
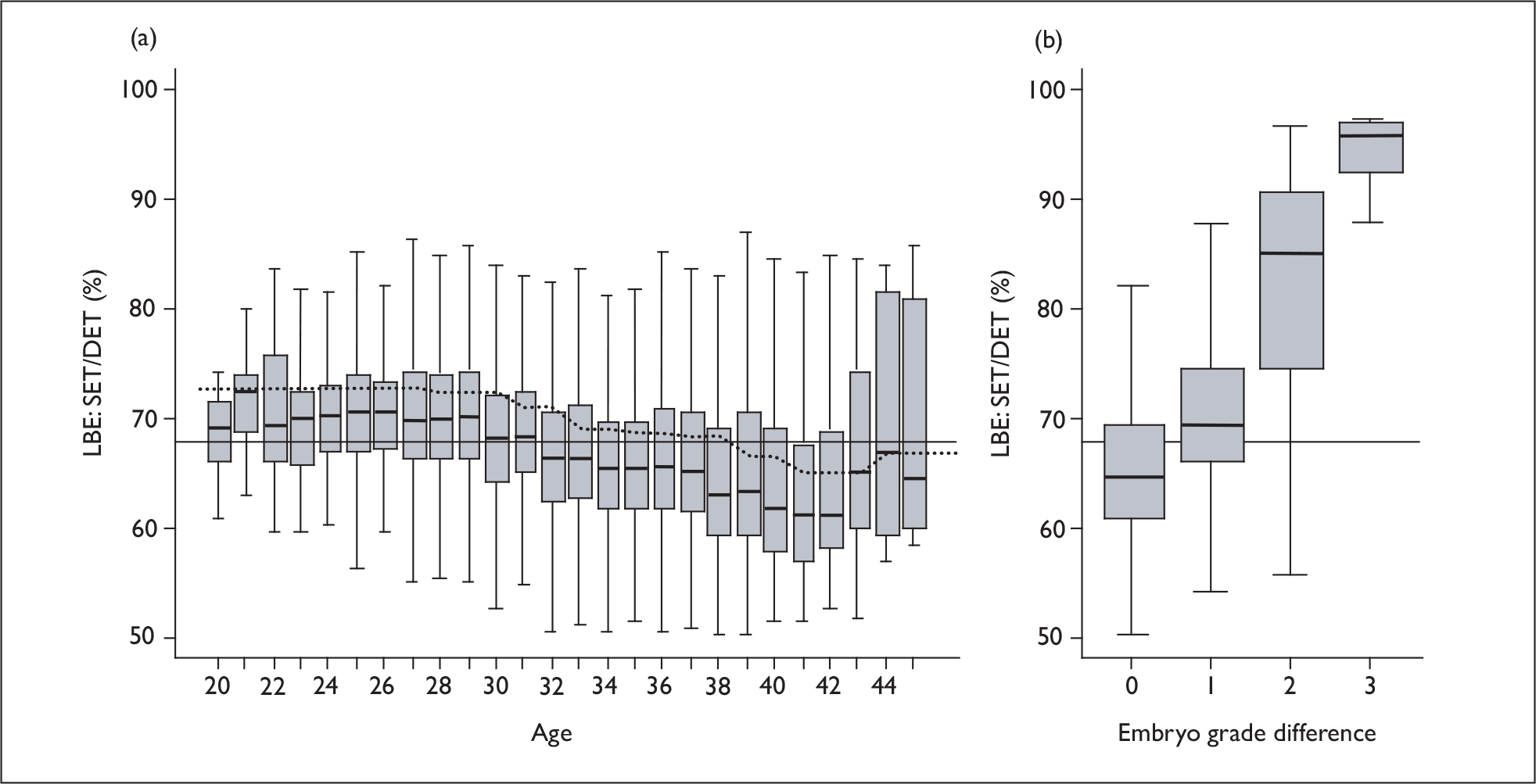
In Figure 31 this loss in initial fresh transfer success is plotted against the predicted twin rate under DET. In panel (a) we see that those with only a small reduction in success from SET were those with poor-quality second embryos and a low chance of twins. In these plots the data all lie above a diagonal line, which is a consequence of selecting the better of the two embryos for putative eSET. Patients would be clearly indicated for eSET (high twin rate and low loss in LBEs) if they were in the top right quadrant of this plot – there are no such patients! In panel (b) we see that it is the younger patients who had the highest twin rates with somewhat less loss due to eSET, but the loss was still substantial in nearly all patients – and those in which it was not were those with a very low success rate.
FIGURE 31.
Plot of predicted loss of success rate by use of eSET against predicted twin rate for DET for 1000 randomly selected fresh cycles. Panel (a) highlights good- (grade 3/4) and poor- (grade 1/2) quality embryos, while panel (b) indicates the younger and older patients.
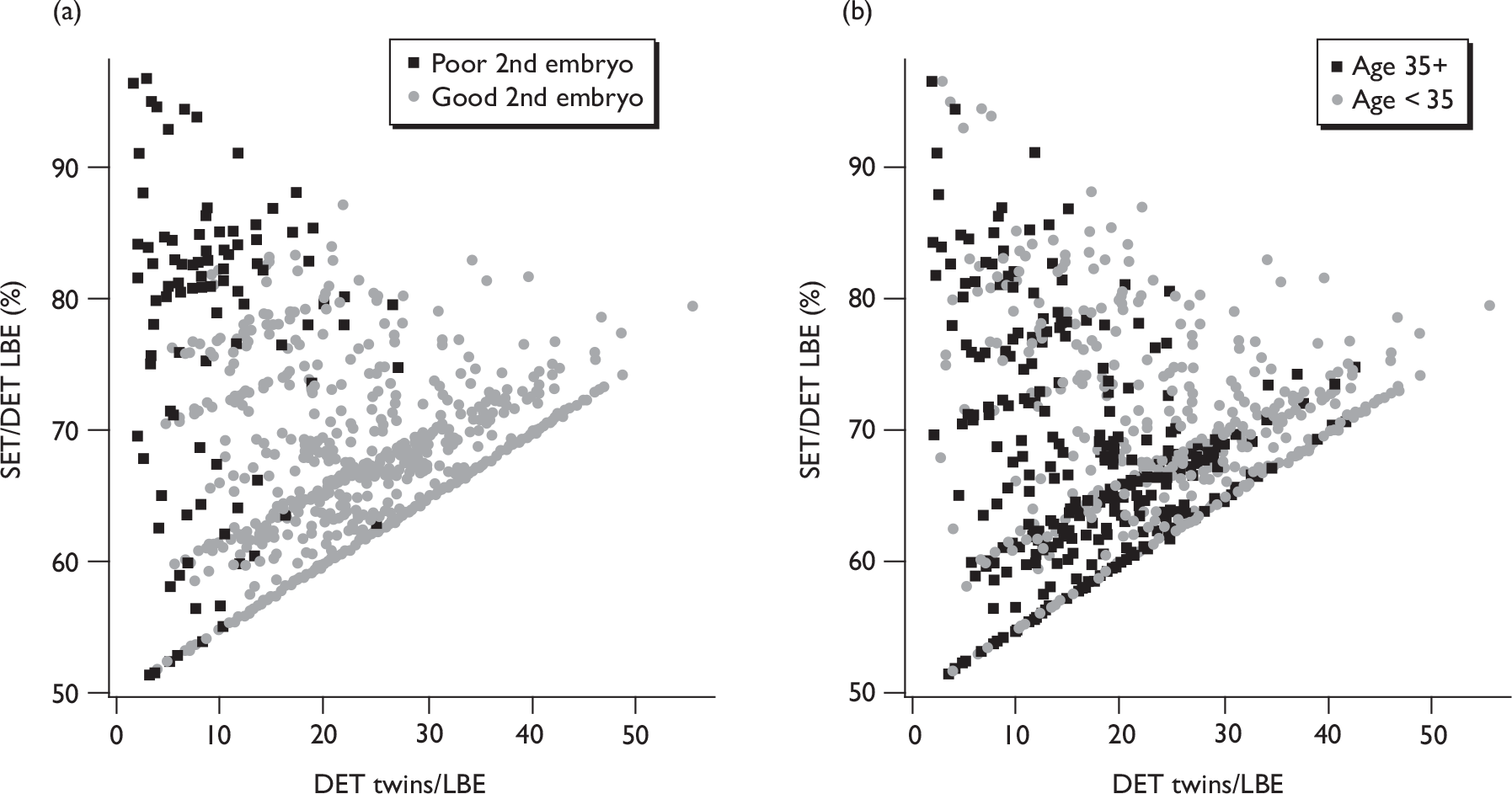
Discussion
Limitations and caveats
The models developed in this chapter give predictions for outcomes of individual embryo transfer procedures, and therefore do not directly predict the more relevant clinical outcomes across a treatment course that may include several egg retrieval and transfer procedures involving both fresh and frozen embryos.
The study was designed to use routinely collected data which was recorded into commercially developed clinical databases, and, as such, was believed to be robust and accurate. However, we discovered that the database design of these systems was flawed, as was their usage. Moreover, the data were not as accurately recorded as we might have believed. These issues are discussed further in Chapter 7. Here we note that there was a non-trivial amount of missing and invalid data, and that we were not able to extract as many potential covariates as we would have wished (for example: sperm quality, hormone levels and source of funding). However, we have found no evidence that the missing data will have biased the results: as far as we can determine it was missing effectively at random. More covariates may have improved the predictive power of the models, and further work is required to test any additional covariates.
The centres recruited all used nominally similar embryo grading schemes, based on the same criteria – although the numerical scores were inverted in some sites relative to the rest. However, it was clear that the implementations were not identical, and a normalisation had to be employed with a strong assumption that the underlying embryo grade distributions were similar between sites. Although post hoc tests did not show any site differences in grading after the normalisation, this nonetheless may have introduced subtle biases, in particular to the intercentre comparisons.
We used two different, but related, modelling approaches. The LR models can be readily fitted to datasets of this size, with some practical restrictions on the estimation of random effects. For the EU model the sample size and number of covariates is about the limit of computational feasibility, with each fit taking several hours. Fitting of random effects in this framework is not possible, and computationally intensive methods such as bootstrapping and profile likelihoods are not in general feasible, although we did run a series of bootstrapped fits, a process which took several weeks of computing time. We were able gain an estimate of the random effect by utilising a two-step fitting process.
The data on frozen embryo transfers were generally of poorer quality, and in attempting to model such transfers we uncovered a number of shortcomings in the data recording. These are again discussed in some detail in Chapter 7.
As discussed previously (see Chapter 3, The logistic regression models), attempt number was not well recorded and these effects need to be treated with caution.
The EU model allowed us to identify the level at which a number of the covariates act – embryo or recipient. While this gives results that appear reasonable and have some statistical support, more methodological work is required to understand this and validate whether the identification is real and its sensitivity to the model assumptions and data structures. The EU model has itself a number of assumptions that it is not possible to test, although there is no evidence of any systematic lack of fit to indicate that the model is not valid. Monozygotic twins are not included in the model and are not considered.
Finally we note that these data were derived from the 2000–5 time period. The data and results are generally consistent with that from the national database from the same period, but clinical practice and success rates have improved since that time period. Further work is required to validate these models with more recent data as it becomes available.
Impact of cryopreservation
The impact of cryopreservation is not reliably determined from this dataset. First, there are weaknesses in the data which mean that it is not possible to fully model frozen cycles: factors such as pre- and post-freezing culture times were not recorded. Second, freezing practices may have changed since the time the data were collected, when most centres were not doing much embryo freezing. We therefore only attempted to estimate a simple loss factor for frozen cycles, although we were able to see that the prognostic factors behaved similarly to those in fresh cycles. Because of the strong caveats, we believe that the estimates here form a lower bound on the success of frozen cycles, and that much better results will be attainable where freezing is routinely performed and optimised. Furthermore, any rigorous analysis of freezing policies must take into account the whole treatment course with an appropriate cumulative outcome measure.
Conclusions
The analysis here confirms the role of the prognostic factors seen in the national dataset (Chapter 3). Again, the factors that predict twin rates are essentially the same as those that predict treatment success. We have been able to provide statistical evidence that some prognostic factors, including age, act primarily through the embryo viability, whereas others, including the number of embryos created and patient history, principally act through the uterine receptivity.
There were quite large differences between the five centres included in the dataset, and it is interesting that treatment centre affects both the embryo and uterine components. Centres with high E relative to U will produce more twins per live birth, as was observed. We do see some evidence of higher twin rates in fresh DET in some centres compared with others, although the overall LBE rates are quite similar. This may suggest that centres may have preferentially optimised either the embryology or the clinical components of treatment to achieve acceptable success rates, and, if both could be optimised, further gains in treatment outcomes could be achieved. It is noteworthy that efforts to optimise embryo quality will lead to higher twin rates.
It is a simply demonstrable mathematical truth that any individual patient will have a lower chance of a successful outcome in a given transfer cycle from SET compared with DET, and the EU model allows us to estimate the magnitude of this loss in the initial fresh cycle. For all patients there will be a loss of approximately one-third in the chances of a live birth from the initial fresh cycle if they receive SET rather than DET, with only very weak differences in this loss with differing patient characteristics, a result that is consistent with the limited trial data. This loss is less than the 50% that might naively be expected. This is intuitively obvious as some of the treatment failures will be due to maternal characteristics.
The data from frozen cycles are of limited quality, but, as with the HFEA data (Chapter 3), the analyses do indicate a significant loss in success rates associated with freezing, with no dependence on treatment or patient characteristics being observed.
Summary
The statistical analysis of the towardSET? dataset again revealed no characteristics that specifically predicted multiple birth outcomes beyond those that predicted treatment success. A number of prognostic factors were confirmed and it was possible to identify some acting specifically through the embryo viability or uterine receptivity. In the fresh transfer following egg retrieval, SET would lead to a reduction of approximately one-third in the live birth probability compared to DET, a result consistent with the limited data from clinical trials. Furthermore, this reduction showed only weak dependence on patient characteristics. The limited data from frozen cycles indicate a significant loss in success rates associated with freezing, with no major dependence on treatment or patient characteristics being observed.
Chapter 5 Predictions and simulations of eSET policies
Introduction
The HFEA policy on reducing multiple births puts the onus on individual clinics to reduce their multiple birth rate, defined as the number of multiple births per LBE. This has led to an emphasis in discussions with clinical teams and with patients around the selection of patients and treatment cycles for SET. A number of clinicians have communicated to us the belief that if they can select the right subset of patients/cycles for SET, then they can reduce the twin rate with little or no impact on overall success rates. Patients are concerned about the loss of choice over their treatment and over the perceived fairness of any imposed policies. The first part of the simulation work described below focuses on the choice around how many embryos to transfer in the initial fresh embryo transfer following an egg retrieval, i.e. we address the question of whether we can effectively select patients/cycles for SET or DET based on their characteristics.
It is clear from the limited trial data, the fresh cycle computations above (see Chapter 4, Implications for eSET) and the computations below that in the initial fresh cycle, SET will lead to lower per-transfer success rates in the fresh transfers, and that multiple transfers, including cryopreservation, need to be considered as part of any policy. Here we define a ‘complete’ or ‘full’ treatment cycle as a transfer of all the good-quality embryos created and including transfers of frozen embryos. Predictions of multiple fresh or frozen transfer outcomes requires further assumptions as the data do not allow us to develop statistical models of the complete treatment programmes. First, we have to assume that the models developed for single fresh cycle prediction apply across the range of multiple transfers, both fresh and frozen; this is not unreasonable as the data include fresh and frozen transfers across the full range of attempt numbers, but subtle biases cannot be excluded. Second, we need to allow for correlations between multiple treatments from the same couples: we have estimates of the couple-level random effects which provide an estimate of these correlations, albeit with uncertainty around the magnitude and structure of these effects. With these assumptions we can simulate multiple fresh transfers (see Simulations of multiple fresh embryo cycles).
Computing the outcomes from frozen transfers is more problematic. As noted in Chapters 3 and 4 the available data on success after cryopreservation is poor and does not yield reliable numerical estimates that can be used directly in simulation studies. Thus we use the data as a guide and make what we believe are plausible estimates of the loss in treatment success from freezing. The analyses did not provide any evidence that the loss due to freezing, when appropriately expressed, differed appreciably across patient groups, so in these simulations we assume a constant (odds ratio) loss. Finally, the data did not contain data on the quality of the non-transferred embryos, so data from another source is needed to enable consideration of subsequent transfers. Recognising these uncertainties, we present indicative simulations of various policies involving fresh and frozen transfers (‘complete cycles’), showing likely trends and highlighting the uncertainties (see Simulation of ‘complete’ cycles).
A number of proposed methods for increasing SET success rates using embryo selection – particularly extended in vitro (blastocyst) culture and pre-implantation genetic screening, result in a loss of embryos and leave fewer for cryopreservation or later transfer. As it is not clear whether the increased success rate in the fresh cycle is sufficient to offset the loss of further attempts, such techniques need to be considered in a multitransfer context across a whole treatment programme. However, we do not have any data on these treatments, so we do not consider such approaches in this simulation work, but offer some comments in the discussion below.
Predictions for fresh embryo replacements
It has been shown that, with care, the EU model can be used for prediction purposes outside the observed data and also in strategies for selecting patients for SET. 2,121 Using the EU models developed in Chapter 4 we can predict the outcomes for DET cycles were they to have received SET, as well as for the DET that they in fact received. SET predictions assume that the embryo with the greatest viability is selected for transfer. We compute the outcome probabilities for all the fresh DET cycles in the dataset for both DET and SET transfers. These estimates explicitly exclude monozygotic twins, which, although not common, are increased in number in IVF-conceived pregnancies compared with the general population. 99
These model-derived estimates can then be utilised to test various scenarios for patient/cycle selection for eSET at the point of a fresh cleavage-stage embryo transfer decision. It should be emphasised that these analyses consider only part of the overall treatment policy, and do not take into account additional retrieval cycles (see Simulations of multiple fresh embryo replacement cycles), cryopreservation strategies (see Simulations of ‘complete’ cycles) or the use of alternative selection methodologies such as extended in vitro culture or embryo diagnostics.
Some selected eSET policies
Based on a reading of the literature, discussions with clinical collaborators and the patient interviews described in Chapter 2 we determined a series of representative potential policies for the selection of patients for eSET in the fresh transfer cycle. These are not exhaustive, nor are they all meant to represent practical policies but rather are intended to cover the range of potential treatment policies, including inappropriate selection. It should be understood that ‘selection’ refers to those who actually get eSET as the result of any given policy (which may be persuasive or prescriptive) and does not necessarily imply that the patients have no choice. The specific scenarios investigated were:
RANDOM Select patients for eSET purely at random to achieve a given proportion of SET, ρ. This is not proposed as a potential policy, but forms a baseline for policy comparison, approximating the haphazard selection of patients that may occur if no specific selection policy were in place.
AGE Select patients under a given age, Ac, to have SET.
AGE + GOOD Select patients under a given age, Ac, who have a top-quality embryo (grade 3 or 4, growth rate 0.95–1.15 doublings per day) to have SET. (The range for doublings per day was chosen to represent the best-quality embryos based on the spline function shown in Figure 20.)
EMBRYO NUMBER Select patients with more than Ec embryos created to have SET. This is based on two concepts: (1) patients with greater embryo numbers have a better prognosis and a higher twin risk; (2) treatment cycles with more embryos are likely to have embryos to freeze for a later frozen transfer. The data do not include embryo grades of non-transferred embryos, but supplementary data (see Simulations of ‘complete’ cycles) indicates that around three-quarters of created embryos will be of sufficient quality to consider freezing and therefore a criterion of three to five embryos created will correspond to having enough embryos to enable cryopreservation, depending on clinic policy.
EMBRYO NUMBER + GOOD Select patients with more than Ec embryos created, including at least one top-quality (grade 3 or 4, growth rate 0.95–1.15 doublings per day) embryo to have SET. This selection method has the advantage, from the patient perspective, that it can be seen as based on the success probabilities of the individual cycle and related to the potential for further frozen cycles. It can be considered as a multitransfer SET policy with DET if there is not the potential for frozen transfers. The use of the potential for frozen transfers as a method for patient selection has been adopted as part of the SET policy in at least one UK centre (Drs G Horne, D Brison and C Fitzgerrald, St Mary’s Hospital, Manchester, 24 September 2008 personal communication).
AGE + EMBRYO NUMBER + GOOD Select patients with age < Ac and at least one top-quality (grade 3 or 4, growth rate 0.95–1.15 doublings per day) embryo to have SET, with the additional requirement that at least Ec embryos are available for selection and hence potentially Ec – 1 for cryopreservation if selected for eSET. These selection criteria capture most of the twin risk predictors.
FULL MODEL Patients where the full EU model predicts a twin/LBE rate > Tc are selected for SET. The predictions here are based on a standard site to reflect the reality that decisions have to be made within each centre, and similarly transfer day and year are held constant. This scenario reflects the maximum that can be achieved with the present set of predictors. We also considered variants of this approach using selection based on predicted absolute success or twin probabilities, and these gave almost identical results, so are not presented here.
REVERSE AGE In patient interviews the view was expressed that younger couples may be those best able to cope with the demands of twins, both through pregnancy and in terms of coping with the demands of infants. Thus, for illustrative purposes we consider a policy whereby the youngest couples are given DET and the older couples SET, i.e. patients with age > Ac are selected for SET.
REVERSE AGE + GOOD Patients with age > Ac are selected for SET providing they have at least one good-quality (grade 3 or 4, growth rate 0.95–1.15 doublings per day) embryo.
*Predictions of fresh cycle eSET selection policies
Using the main-effects model of Chapter 4 (Predictive models using the EU approach) we computed for each patient that received DET in the towardSET? collaborative dataset the predicted outcome under DET and SET. For the SET predictions we selected the embryo with the highest embryo success probability (E). Although the interaction model was a marginally better fit to the data, we considered that the extra complexity was not justified for the purposes here. This was justified post hoc by considering the uncertainties in the predictions in Chapter 4.
Using custom-written code in R,101 we selected patients for DET and SET according to a particular policy. Given the individual success and twin probabilities with SET and DET, the population LBE rate and twin probabilities can be readily computed, and from these the twin rate (twins/LBE).
These computations focus on the DET cycles in the dataset and thus implicitly excluded those patients with only a single embryo available for transfer (∼ 7% of cycles in this cohort) and those who have a clinical contraindication or preference for SET (∼ 2% of cycles); for both these groups DET was not an option. Thus, the quoted twin rates for the whole patient population may be slightly lower than those presented here.
Results for selected eSET policies – fresh cycles
In this section we show predicted outcomes from applying the selection policies above to all the fresh DET cycles in the towardSET? dataset. For most of the policies considered there is an adjustable ‘cut-off’ parameter (e.g. age). In order to present all policies in a consistent way, outcomes are plotted against the proportion receiving SET as the cut-off is adjusted across its available range. Tables then give estimates of the cut-off and proportion of SET required to achieve specific twin rate targets (20%, 15%, 10%). We first show the results of selecting patients at random, then show the full model – the best that can be achieved with the data available. Following this, we look at simpler selection algorithms based on patients and embryo characteristics. Finally, we consider the effect of inappropriate selection.
Random selection
Figure 32 shows the predicted fresh transfer LBE and twin rates based on selecting patients for DET randomly. As shown in the left-hand panel, random selection reduces the live birth rate in a linear manner as the proportion receiving SET increases. The number of twin births per transfer (not shown) is reduced in a similar linear manner, but, as the right-hand panel shows, the twin/LBE rate is slightly non-linear as both the numerator and denominator vary with the proportion of SET. Reading off the right-hand panel we see that for a 10% twin rate (per LBE), we would require 68% SET, and from the left-hand panel this would lead to a decline in success rate compared with DET from 24% to 19%.
FIGURE 32.
Predicted live birth and twin rates for single fresh transfer cycles with patients randomly selected for SET or DET.
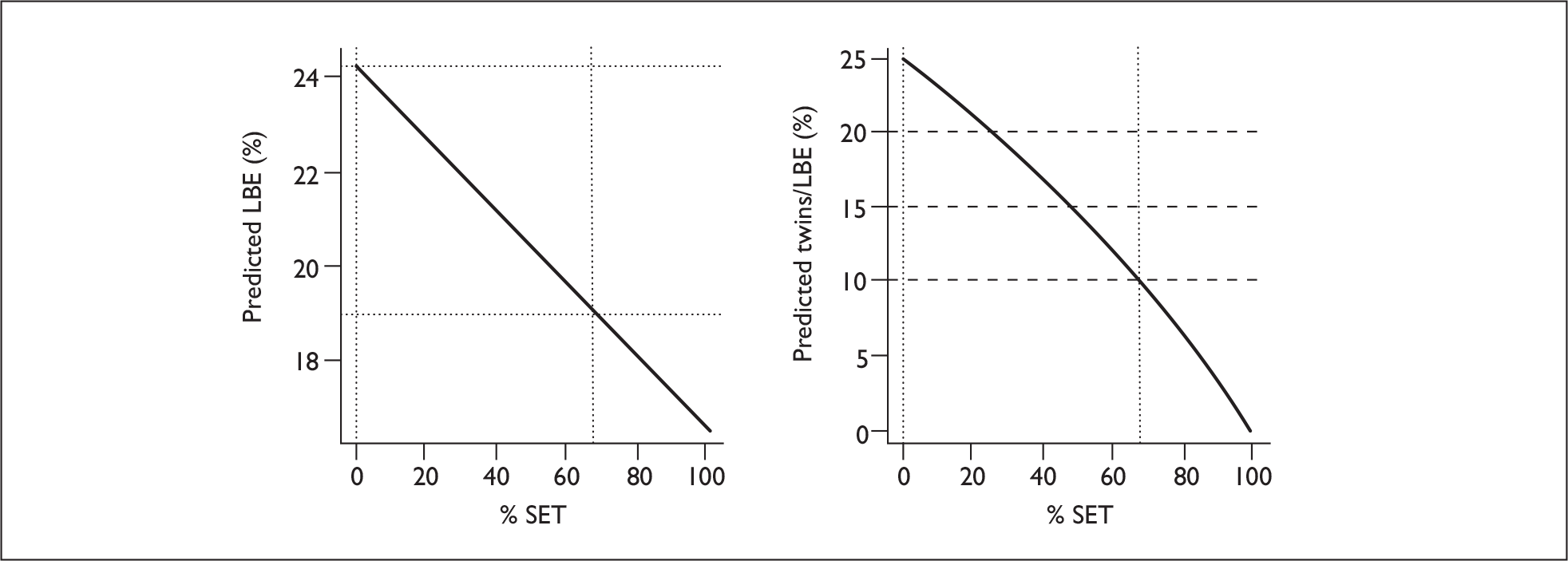
Selection using full model
Figure 33 shows the predicted fresh transfer LBE and twin rates based on selecting patients using the full predictive model, along with simple random selection for comparison.
FIGURE 33.
Predicted live birth and twin rates for single fresh transfer cycles with patients selected for SET using the full model probabilities.
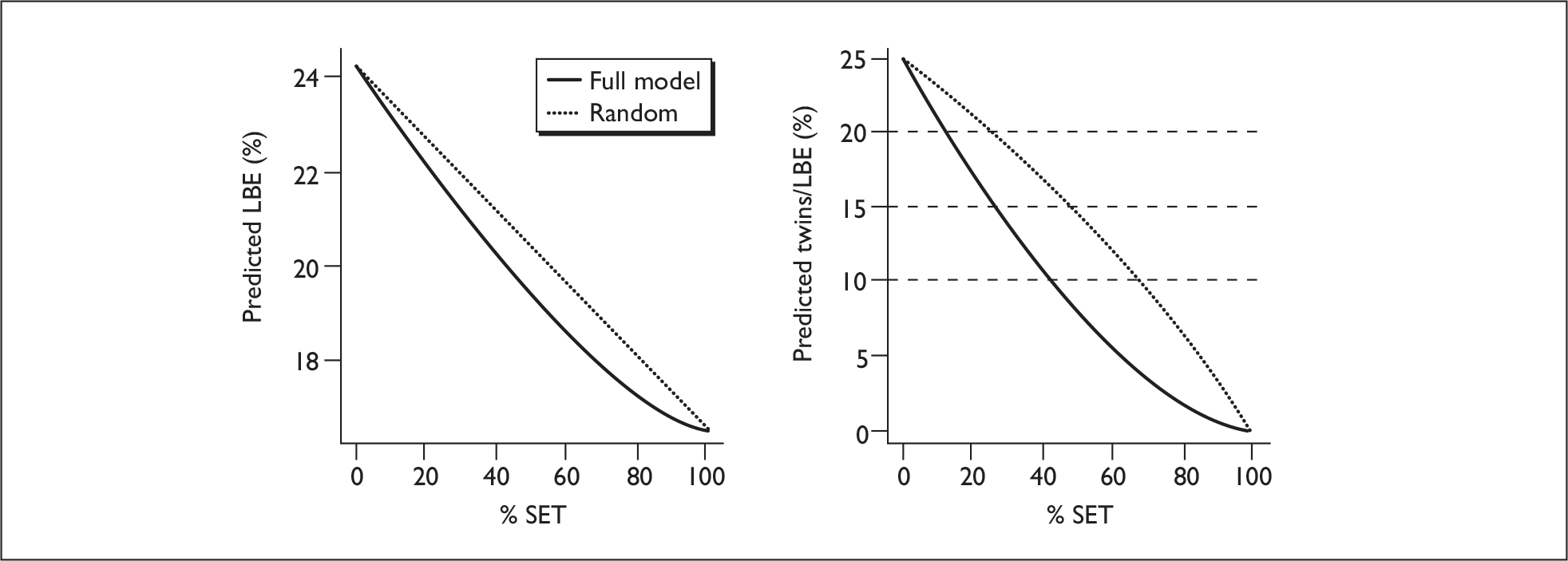
In Table 49 we show the proportion of SET and resultant success rates for selection using the full model, again compared with random selection. This clearly performs better than simple random selection, in terms of requiring fewer patients to undergo SET. The benefit of selection in terms of LBEs is not very large compared with unselected patients, and the 41% SET required to achieve a 10% twin rate reduces the LBE rate from 24% to 20% – i.e. an 18% drop in fresh cycle, per transfer, success rate. Pure SET would give an LBE rate of 16.5% in this population, thus around 60% of the loss can be mitigated at a patient population level, although of course each individual patient at the time of transfer suffers either all or none of the loss in success chances.
| Twin rate | Variant | % SET | Live births (%) |
|---|---|---|---|
| 25% | All DET | 0 | 24.3 |
| 20% | Random selection | 25.9 | 22.3 |
| Model-based selection | 11.7 | 23.2 | |
| 15% | Random selection | 48.9 | 20.5 |
| Model-based selection | 26.2 | 21.6 | |
| 10% | Random selection | 68.3 | 19.0 |
| Model-based selection | 42.5 | 20.1 | |
| 0% | All SET | 100 | 16.5 |
Selection on patient characteristics
The predicted fresh cycle outcomes for the towardSET? cohort with eSET selection using patient characteristics are shown in Figure 34 and Table 50. Of the single parameters, age alone is a better selection criterion than embryo number. The stipulation that a cycle has at least one good-quality embryo does improve the selection process. Note that not all cycles have a good-quality embryo, so policies with an embryo quality threshold have an implicit a maximum possible eSET rate and the curves in Figure 34 do not cover the whole range of SET proportions.
FIGURE 34.
Predicted live birth and twin rates for single fresh transfer cycles with patients selected for SET using patient characteristics. The predictions for selection using random selection are also shown for comparison.
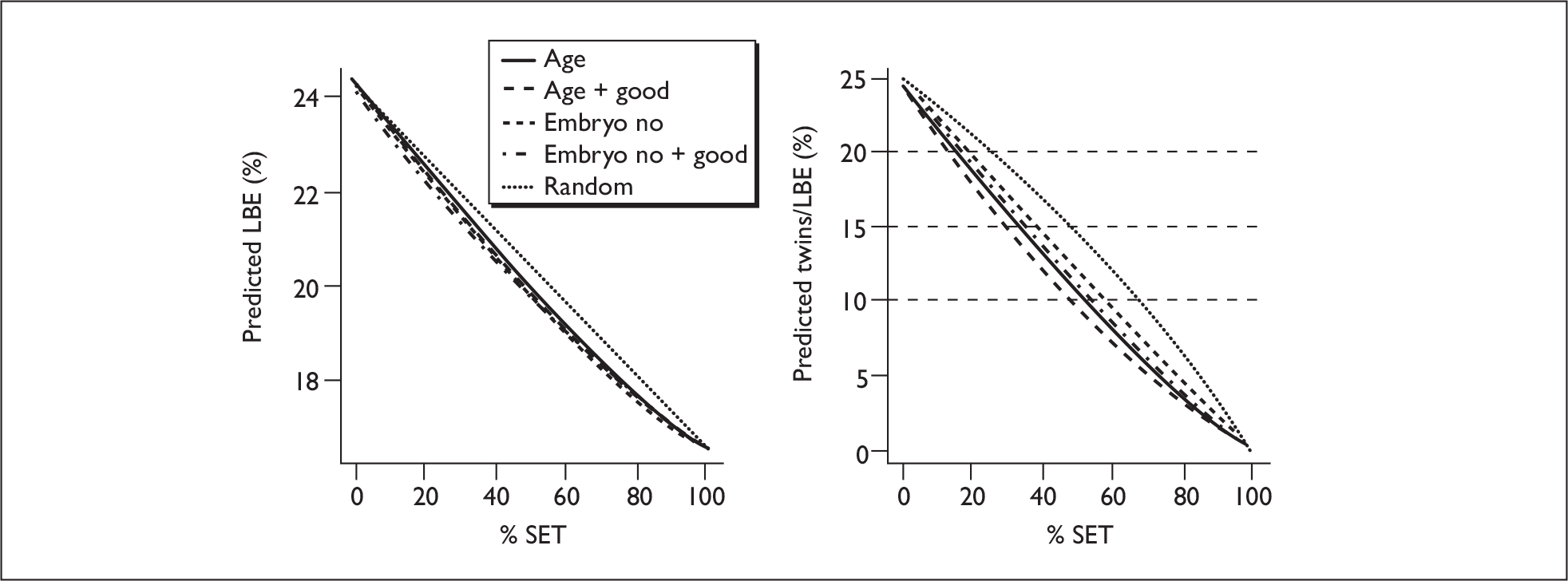
| Twin rate | Cut-off a | Policy | %SET | Live births (%) |
|---|---|---|---|---|
| 25% | – | All DET | 0 | 24.3 |
| 20% | – | Random | 25.9 | 22.3 |
| Age < 28.9 | Age | 15.8 | 23.0 | |
| Age < 29.2 | Age + good | 14.1 | 23.1 | |
| > 9.0 embryos | Embryo number | 19.2 | 22.5 | |
| > 8.7 embryos | Embryo number + good | 17.6 | 22.6 | |
| 15% | – | Random | 48.9 | 20.5 |
| Age < 31.1 | Age | 32.1 | 21.5 | |
| Age < 31.8 | Age + good | 29.7 | 21.6 | |
| > 6.4 embryos | Embryo number | 38.2 | 20.8 | |
| > 6.0 embryos | Embryo number + good | 35.3 | 20.9 | |
| 10% | – | Random | 68.3 | 19.0 |
| Age < 33.3 | Age | 51.8 | 19.8 | |
| Age < 34.3 | Age + good | 48.2 | 19.9 | |
| > 4.7 embryos | Embryo number | 56.6 | 19.2 | |
| > 4.0 embryos | Embryo number + good | 52.7 | 19.4 | |
| 0% | – | All SET | 100 | 16.5 |
Although the SET rates of around 50% needed to achieve a 10% twin rate are somewhat higher than the 41% using the full model (Table 49), the LBE rates are only marginally worse (19.9% cf. 20.1%).
We extend this by considering a policy selecting on age where there is a good embryo and sufficient embryos to enable freezing. The data does not contain data on the quality of non-transferred embryos, but a surrogate might be patients having more than, say, four embryos created. In Figure 35 and Table 51 we show the predicted outcomes with thresholds of minimum numbers of four or five embryos created.
FIGURE 35.
Predicted live birth and twin rates for single fresh transfer cycles with patients selected for SET using age, conditional on having a good-quality embryo and four or five embryos created. The predictions for selection using the full model and random selection are also shown for comparison.
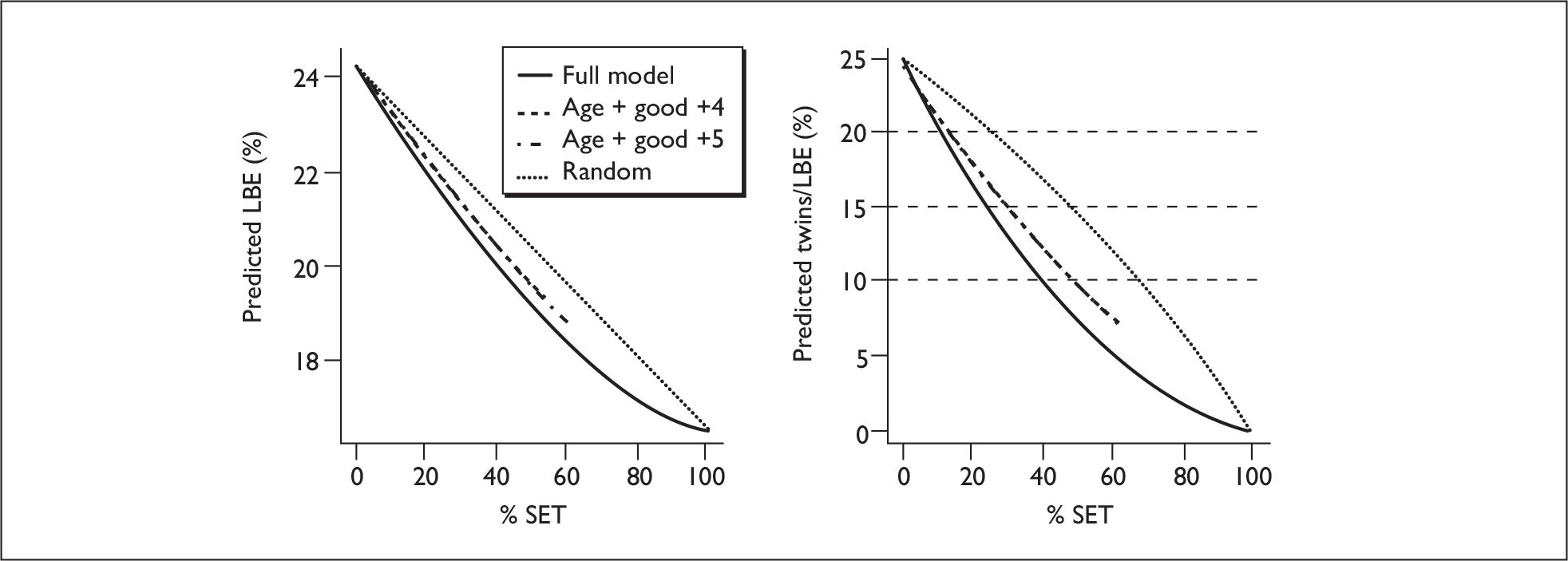
| Twin rate | Cut-offa | Policy | % SET | Live births (%) |
|---|---|---|---|---|
| 25% | – | All DET | 0 | 24.3 |
| 20% | – | Random | 25.9 | 22.3 |
| Age < 30.0 | Age + good + four embryos | 13.3 | 23.1 | |
| Age < 30.5 | Age + good + five embryos | 13.2 | 23.0 | |
| – | Full model | 10.9 | 23.1 | |
| 15% | – | Random | 48.9 | 20.5 |
| Age < 33.4 | Age + good + four embryos | 29.9 | 21.4 | |
| Age < 34.8 | Age + good + five embryos | 31.3 | 21.2 | |
| – | Full model | 24.9 | 21.6 | |
| 10% | – | Random | 68.3 | 19.0 |
| Age < 40.5 | Age + good + four embryos | 52.0 | 19.5 | |
| NAb | Age + good + five embryos | NAb | NAb | |
| – | Full model | 41.2 | 20.0 | |
| 0% | – | All SET | 100 | 16.5 |
Note in Table 51 that if we use a criterion of five embryos created, including one top-quality embryo, to indicate SET, then there are insufficient patients meeting this criterion to achieve a 10% twin rate (although in fact the minimum twin rate is very close to 10%). The SET rates of 52% needed to achieve a 10% twin rate is still somewhat higher than the 41% using the full model; the LBE rates are a little worse (19.5% cf. 20.1%).
Figure 36 shows the age distributions of the patients receiving SET and DET under the various selection procedures. The full model and schemes requiring at least one good-quality embryo for SET all have significant numbers of younger patients receiving DET. This further illustrates that age alone is not a particularly good selection criterion.
FIGURE 36.
Maternal age distributions of couples receiving DET and SET under various polices to achieve a 10% twin rate. Selection procedures: (a) random; (b) full model; (c) age; (d) age + good; (e) four embryos + good; (f) age + four embryos + good.
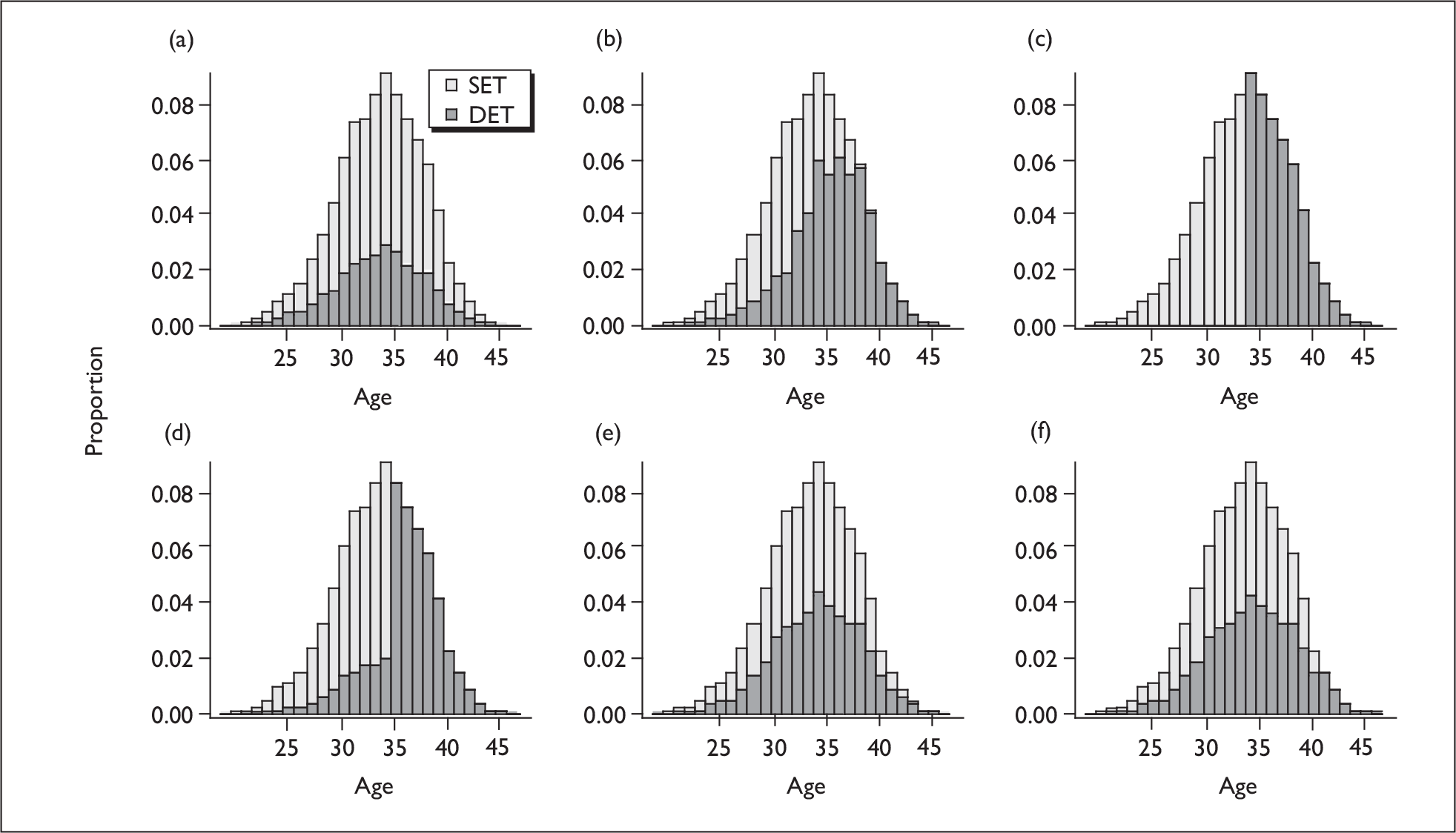
Selecting younger patients for DET
The outcomes if the older patients are given SET are shown in Figure 37 and Table 52. Both require high SET rates to achieve 10% twin rates, although giving DET to the 20% youngest patients (under 30) could be attractive to some. However, a success rate of 18.3% represents a 10% loss of treatment success compared with DET. Including a requirement that at least one good embryo is available improves the success rates, but these are still lower than if SET were used for younger patients.
FIGURE 37.
Predicted live birth and twin rates for single fresh transfer cycles with younger patients selected for DET. Results for random selection are shown for comparison.
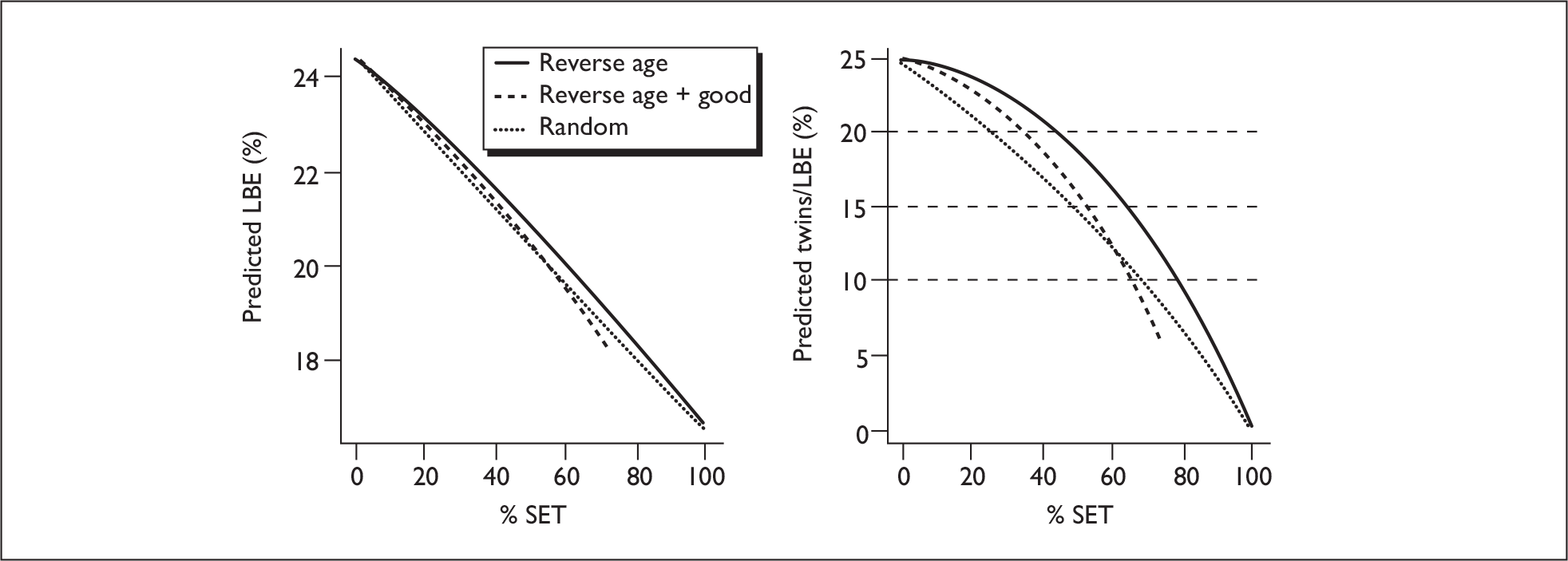
| Twin rate | Cut-offa | Policy | % SET | Live births (%) |
|---|---|---|---|---|
| 25% | – | All DET | 0 | 24.3 |
| 20% | – | Random | 25.9 | 22.3 |
| Age > 33.8 | Reverse age | 43.8 | 21.4 | |
| Age > 33.3 | Reverse age + good | 35.4 | 21.7 | |
| 15% | – | Random | 48.9 | 20.5 |
| Age> 31.4 | Reverse age | 65.9 | 19.5 | |
| Age > 30.8 | Reverse age + good | 54.0 | 20.0 | |
| 10% | – | Random | 68.3 | 19.0 |
| Age > 29.6 | Reverse age | 79.4 | 18.3 | |
| Age > 38.7 | Reverse age + good | 65.6 | 18.8 | |
| 0% | – | All SET | 100 | 16.5 |
Clearly in the fresh transfer the use of an appropriate selection policy can have a modest impact on clinic success rates. In order to assess the potential impact of inappropriate selection we consider the extreme case in which we use the full model to determine SET or DET but then invert the selection. This does not represent a realistic scenario, but serves to provide an upper limit on the potential impact of a poor selection policy. The results are shown in Figure 38. These results demonstrate that, while the gains from appropriate selection seem modest, the losses from inappropriate selection can potentially be significant. It is possible to have a SET rate > 80% and fail to meet a 10% twin target.
FIGURE 38.
Impact of inappropriate selection, inverting the selection choice from the full model.
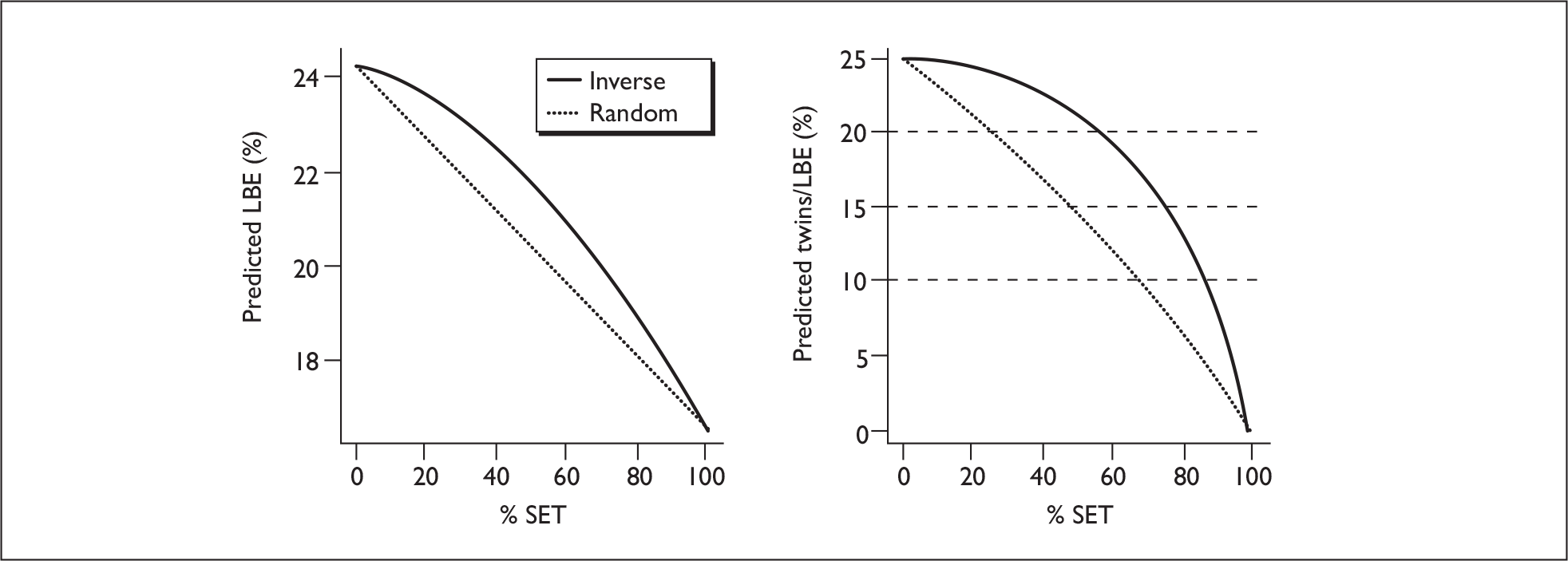
Precision of policy predictions
In order to estimate the precision of the policy predictions the estimates have been recomputed using 100 bootstrap samples of the data, refitting the model and recomputing the outcomes with the new data and model. The results of this exercise are illustrated in Figure 39. The outcomes (LBE and twins/LBE) are expressed as a percentage difference from the estimate for all DET in the bootstrap sample, as the absolute rates will differ between samples of the data. The errors are rather small. In practice, errors in differences between policies will be strongly correlated, so these plots overestimate the errors when comparing policies.
FIGURE 39.
Precision of estimates of selection policies based on bootstrap resampling of the data. Shaded areas indicate the 95% CI around the estimates indicated by the lines. Data are shown for two policies, random selection (broken line) and selection using the full model (solid line), and normalised by the LBE and twin rates where all patients receive DET.
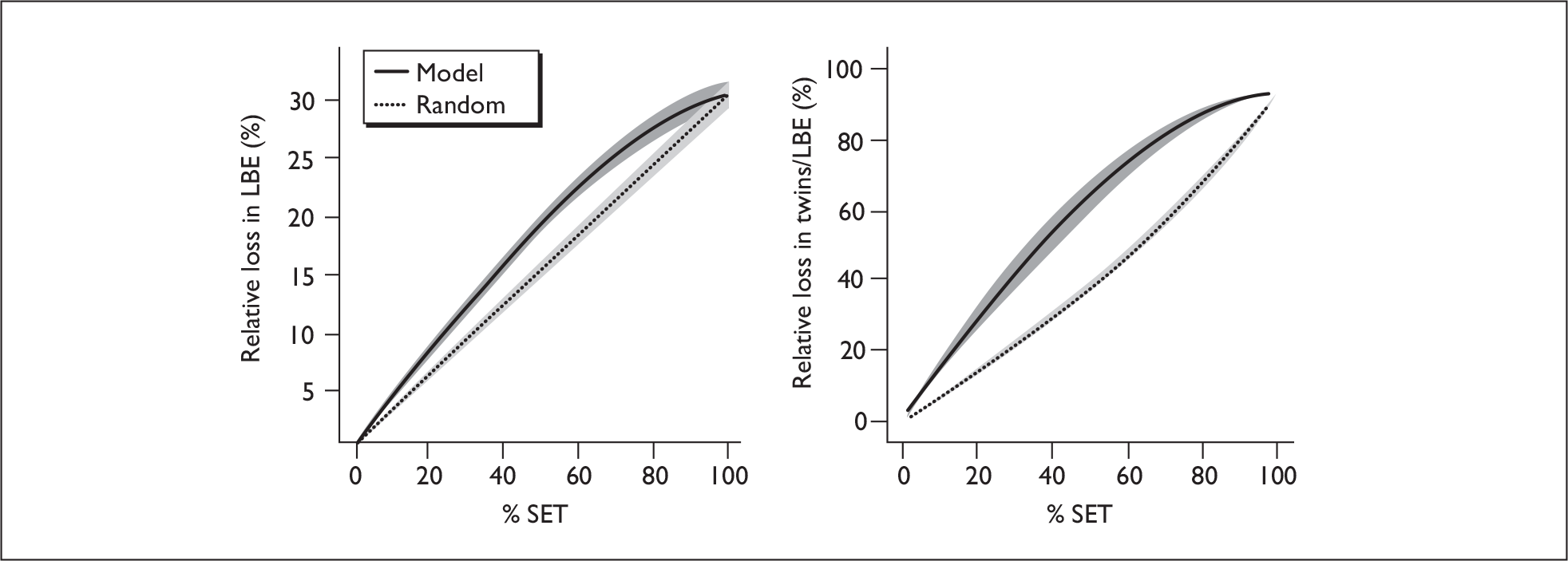
Simulations of multiple fresh embryo replacement cycles
Given the statistical model developed in Chapter 4, we can readily compute the outcomes of multiple fresh transfers (i.e. with ovarian stimulation, egg retrieval and transfer). In this exercise we are not considering frozen transfers. In doing these calculations we need to allow for intra-patient correlations beyond those induced by the covariates, which can readily be achieved using the estimates of the random effects obtained in Chapter 4 (see Intercycle correlations in the EU model). As this estimate is uncertain, we allow for values between zero and twice the observed value.
*Details of simulation method
Outcomes were computed using the main effects EU model developed in Chapter 4. For each simulation run we computed the outcome probabilities for 5000 patients, selected at random from the dataset, ensuring that couples were sampled only once. All clinical parameters were held constant over the multiple cycles, including embryo number and quality. We did consider allowing for variation in embryo yields between cycles, but this added complexity and did not materially alter the results. SET outcomes were based on the better of the two embryos. Prior to computing the probabilities a random effect was sampled from a normal distribution with standard deviation σ for each patient and added to the U submodel for each cycle for that patient. Simulated outcomes were realised by sampling from binomial distributions with the predicted probabilities from the EU model.
Predicted outcomes
We can compute the number of LBEs and twins for each cycle and hence the overall LBE rate and number of babies produced from a series of several egg retrievals plus fresh replacement – i.e. without freezing. This reflects the current UK situation in which some centres do very little or no embryo freezing. Because for many patients two children is seen as the ideal outcome from an IVF treatment, we also computed the number of couples with two or more babies assuming that couples who are successful have a full number of cycles subsequent to the first LBE – this may not be realistic under current funding arrangements. Here we show outcomes for fresh transfers from a series of one to four SET cycles and one or two fresh DET transfers. We consider two variants of eSET: first, we considered eSET for all patients, and, second, we considered SET if there is at least one good-quality embryo (grade 3 or 4) and the patient is aged under 35, a selection policy that produces a low twin rate of 8% in this sample. These simulations included a range of estimates for the correlations between patients, with the random effect standard deviation taking values for 0 to 1.6; this made little difference, so we present the results for the observed standard deviation of 0.8 only. The results are illustrated in Figure 40, where we see that two fresh SET cycles have better LBE outcomes than a single fresh DET cycle, and three SET cycles are roughly equivalent to two DET cycles in terms of live births. We do note that if all patients are given the full number of cycles, i.e. successful patients receive further cycles, then slightly more SET cycles are needed to get a ‘complete family’.
FIGURE 40.
LBE and proportion of treatments yielding two babies in total for multiple fresh SET transfers compared with one and two fresh DET transfers (horizontal dashed lines). Simulations are shown for pure SET (all patients, solid line) and DET for patients over 35 with at least one good embryo (dashed line).
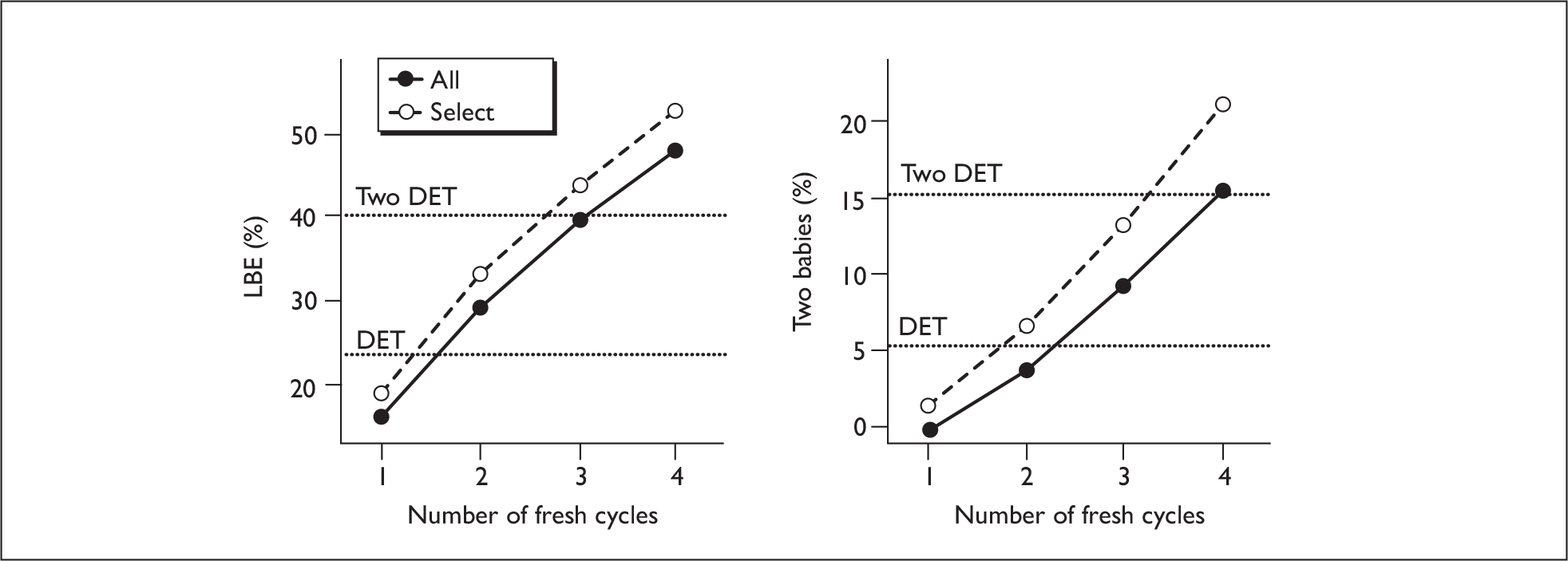
The LBE rate is not linear in the number of SET cycles owing to selection effects; patients who have an LBE are not considered (in the computation of LBE) in subsequent cycles, which are consequently enriched with patients with a poorer prognosis. 114 The magnitude of the intracouple correlation does not have a great effect on the results here.
Simulations of ‘complete cycles’
In assessing any IVF treatment policy it is necessary to take into account the whole treatment course, including transfers of cryopreserved embryos. A treatment course of stimulation, egg recovery and replacement of all embryos created, fresh and frozen, is termed a ‘complete’ treatment cycle, and couples may undertake more than one such complete cycle in any attempt to produce a baby. Here we consider predicting outcomes of a single such ‘complete’ cycle.
The data provide reasonably reliable estimates of the success and twin probabilities, with some quantification of the uncertainty, and the EU models allow the estimation of outcomes for both SET and DET treatments in each individual. We are also able to extract information on the intercycle correlations (see Chapter 4, Intercycle correlations in the EU model). As noted in Chapters 3 (see The logistic regression models) and 4 (see EU modelling of the effect of frozen cycles) the routine data does not provide robust estimates of the effect of freezing embryos, and embryo-freezing policies and techniques are improving rapidly. In addition, data are only available for the embryos that were transferred; there is very little data on the embryos that were frozen or discarded, and any such information is seriously confounded by selection and freezing policies in different clinics. Additional information on the characteristics of all embryos created is needed from a different source.
Thus, to develop simulations across multiple cycles we combined the predictive models with a range of reasonable assumptions about freezing/thawing success and the loss in success due to freezing and additional data to estimate the distribution of embryo parameters.
The simulation model
We consider an idealised strategy for utilising all the embryos created in a given egg collection cycle:
-
First all embryos are graded and the best one or two are transferred as fresh embryos. We consider policies of SET, DET and selection for DET based on embryo and patient characteristics.
-
Then all remaining embryos above a certain quality threshold (embryo grade ≥ min.grade) are frozen for subsequent use, providing there are sufficient embryos (≥ min.freeze) for freezing (many centres will not freeze single embryos).
-
For subsequent replacement cycles, batches of a fixed size (nthaw embryos per batch) are thawed at random (embryos are not always stored individually) for replacement. A proportion fail to thaw successfully (probability of successful thawing: pthaw). The best one or two are replaced under a SET policy or a DET policy or one based on patient and embryo characteristics.
-
There is no refreezing of thawed embryos.
*Simulation parameters
The EU model (main effects model of Chapter 4, Predictive models using the EU approach) gives predicted probabilities for a fresh replacement. In Chapters 3 and 4 we showed that frozen cycles have very similar predictors to fresh cycles but with an overall lower success rate. In the EU context this can be represented by a reduction (–Δf) in the linear predictor for the E component. The fits of Chapter 4 (EU modelling of the effects of frozen cycles) indicate that a reduction of around 1 is possible (corresponding to an odds ratio for embryo implantation of 0.37). We also consider a smaller offsets of Δf = –0.7 (the smallest decrement across the centres in the dataset) and –0.25 corresponding to odds ratios of 0.5 and 0.78, which represent values that may be achieved with improvements in freezing practice. For comparison we also consider Δf = 0, no loss in viability due to the freezing process.
The fits of Chapter 4 (Intercycle correlations in the EU model) allow us to estimate the correlations between multiple cycles from a single egg collection, giving a standard deviation of 0.8 on the linear predictor scale. We consider values spanning zero to twice this value.
The data provide grading only for the embryos transferred. As part of another project35 we have a series of 266 unselected embryos (all embryos created from 61 egg retrieval cycles) with grading information using the same grading scheme. Exploratory analyses indicate that the embryo cell numbers and grades are largely independent of patient characteristics, thus we can use the distribution of grading parameters from this series to simulate the grades of the whole embryo cohort.
Overview of simulation process
-
First we sample a number of fresh cycles from the full dataset (ensuring no couple is sampled twice).
-
We then sample a number of embryos, as given by the number in the sampled cycle, from the set of embryo-grading data.
-
We select the best embryo(s) for transfer, based on the probabilities of success from the EU model. If a DET transfer is being indicated and only one embryo is available, a SET transfer is performed. Any embryos not meeting the freezing criteria (grade < min.grade) are discarded.
-
The EU model then gives the predicted outcome probabilities for the fresh cycle.
-
For the remaining embryos we select random batches (of size nthaw), remove a proportion (1– pthaw) at random to allow for failed thawing and select the best one or two for transfer. In the absence of relevant data, we assume that failure to thaw is independent of patient and embryo characteristics.
-
If there are no embryos for replacement, a cancelled cycle is recorded. Similarly, if DET is indicated, but only one embryo is available, then a SET cycle is simulated.
-
We predict the outcome probabilities for the frozen cycles using the EU model with an adjustment for freezing and allowing for the intercycle correlation.
-
This process continues (from step 4) until either there is a successful outcome or there are no more frozen embryos remaining.
*Some technical details of the simulation process
Random effects are sampled from a normal distribution with zero mean and variance ω2, which is added to the linear predictor of U in each fresh and frozen transfer from that couple. This particular representation matches the computationally feasible model fitted to the EU model for which we have data – other alternative random effects could have been considered, but there were no data on which to base these.
The model gives probabilities for each replacement cycle. We compute the probabilities of success for all the cycles until there are no more embryos remaining. We then realise the probabilities using a multinomial distribution on a series of (typically five) replicate cycles and, for each replicate, truncate the series on successful outcomes.
Five thousand cycles with five replicates give an expected 95% CI on an estimate of 20% of ± 0.5%
Adding a single frozen transfer to a fresh SET cycle
Figure 41 shows the simulated LBE rate across the towardSET? population for a fresh plus a single frozen transfer. Results are shown for a range of decrements in success for frozen embryo transfers (Δf, where zero represents no loss in viability owing to freezing, and the average in the 2000–5 data was around 1), and we also consider two estimates of the proportions of embryos that fail to survive the freeze/thaw process (10% and 25%). Providing freezing quality is reasonable in terms of loss of implantation and recovery rate, one additional frozen SET can more than compensate for the loss in success owing to a fresh SET.
FIGURE 41.
Simulation results for success rate from one fresh SET plus one frozen SET as a function of embryo freezing quality (Δf). The freezing quality relates to the loss in viability owing to the freeze/thaw process. Horizontal lines indicate success rates from single SET and DET fresh transfers. Min.grade = 3, min.freeze = 1, thaw number to be transferred, σ = 0.8. The two panels show data assuming different values for the proportions that fail to recover from the freeze/thaw process and are unable to be transferred: (a) 10% fail freeze/thaw; (b) 25% fail freeze/thaw.
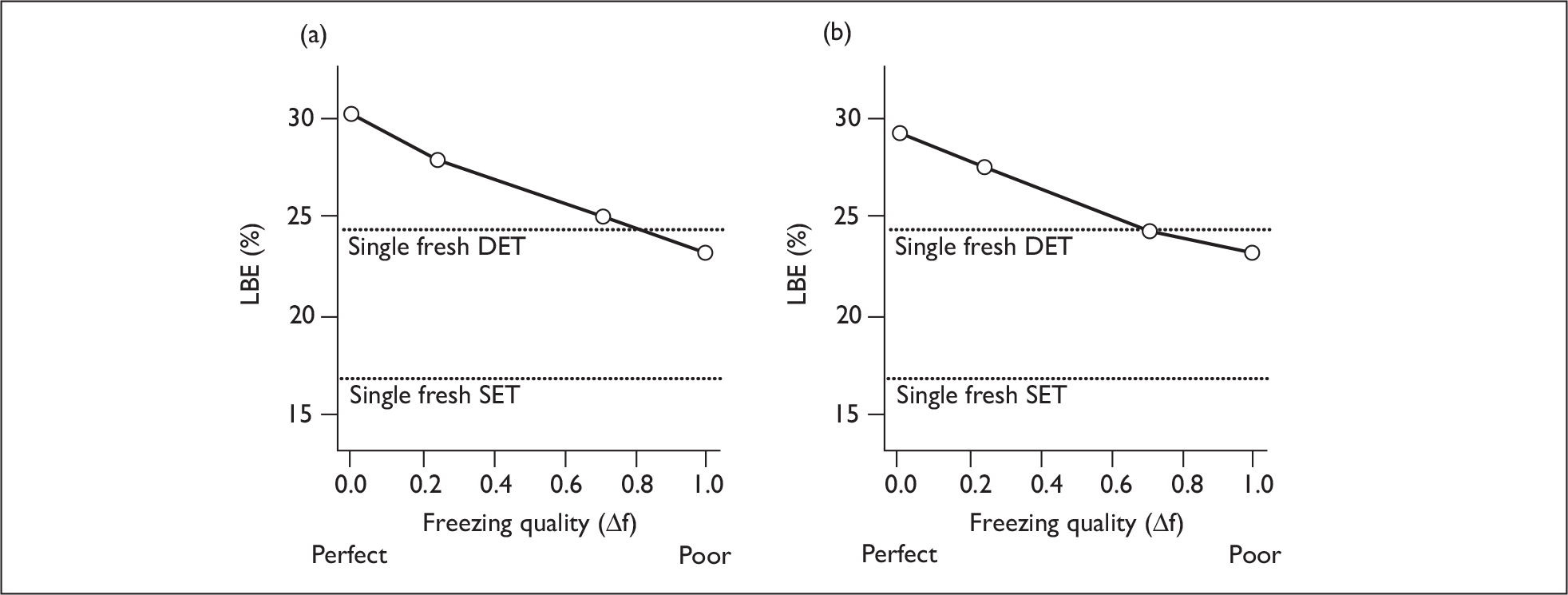
Complete treatment cycles
It is now recommended that a treatment cycle comprises the fresh transfer plus the freezing and transfer of all remaining good-quality embryos. Here we compare outcomes of complete treatment cycles in which we freeze all good-quality (grade 3 or 4) embryos not transferred in the fresh cycle and thaw the number to be transferred with or without a spare for subsequent cycles. We compare policies of (1) SET throughout (SET + SET); (2) DET throughout (providing there are two embryos remaining) (DET + DET) and (3) SET for the fresh cycle with DET for the frozen cycles (SET + DET). Here we assume that there is no selection of patients for SET. The results are shown in Table 53 and Figure 42, where we consider a range of freezing qualities and estimate success, twin rates, and the number of embryo transfer cycles required to achieve a live birth. As DET produces some twins, we also consider the number of treatments that would produce two or more babies if all embryos are eventually transferred.
| Min.grade = 3 Min.freeze = 1 σ = 0.8 |
SET + SET nthaw = 1 | SET + SET nthaw = 2 | SET + DET nthaw = 2 | SET + DET nthaw = 3 | DET + DET nthaw = 2 | DET + DET nthaw = 3 | |
|---|---|---|---|---|---|---|---|
| 10% freezing failure: pthaw = 0.9 | |||||||
| Data estimates Δf = 1 | Success (%)a | 29.4 | 26.6 | 29.5 | 27.9 | 32.5 | 31.1 |
| Twin rate (%)a | 0 | 0 | 3.2 | 3.0 | 20.7 | 20.3 | |
| ET cyclesa | 2.3 | 1.7 | 1.8 | 1.6 | 1.4 | 1.3 | |
| 2+ babies (%)b | 6.1 | 3.8 | 6.5 | 5.4 | 10.5 | 9.5 | |
|
Better freezing Δf = 0.7 |
Success (%)a | 32.6 | 28.5 | 32.0 | 30.5 | 33.3 | 32.0 |
| Twin rate (%)a | 0 | 0 | 4.3 | 5.1 | 19.8 | 19.9 | |
| ET cyclesa | 2.4 | 1.8 | 1.9 | 1.6 | 1.5 | 1.4 | |
| 2+ babies (%)b | 8.1 | 5.0 | 8.4 | 7.0 | 11.4 | 10.4 | |
|
Much better freezing Δf = 0.25 |
Success (%)a | 37.2 | 32.7 | 36.0 | 33.6 | 37.0 | 35.5 |
| Twin rate (%)a | 0 | 0 | 6.0 | 7.8 | 20.0 | 21.8 | |
| ET cyclesa | 2.5 | 1.9 | 1.9 | 1.7 | 1.6 | 1.4 | |
| 2+ babies (%)b | 11.6 | 7.5 | 11.5 | 9.8 | 14.0 | 13.1 | |
|
Perfect freezing Δf = 0 |
Success (%)a | 41.1 | 34.6 | 39.6 | 37.0 | 38.4 | 36.4 |
| Twin rate (%)a | 0 | 0 | 8.0 | 9.4 | 20.9 | 22.0 | |
| ET cyclesa | 2.5 | 2.0 | 2.0 | 1.8 | 1.6 | 1.5 | |
| 2+ babies (%)b | 14.3 | 8.9 | 14.3 | 12.4 | 15.9 | 14.4 | |
| 25% freezing failure: pthaw = 0.75 | |||||||
|
Data estimates Δf = 1 |
Success (%)a | 27.8 | 25.7 | 27.7 | 26.3 | 30.8 | 30.4 |
| Twin ratea | 0 | 0 | 2.1 | 2.8 | 21.4 | 20.8 | |
| ET cyclesa | 2.0 | 1.7 | 1.7 | 1.5 | 1.4 | 1.3 | |
| 2+ babiesb | 4.9 | 3.5 | 5.2 | 4.7 | 9.8 | 8.9 | |
|
Better freezing Δf = 0.7 |
Success (%)a | 30.7 | 27.0 | 30.2 | 28.5 | 32.1 | 31.9 |
| Twin rate (%)a | 0 | 0 | 3.1 | 3.4 | 20.6 | 20.9 | |
| ET cyclesa | 2.1 | 1.7 | 1.8 | 1.6 | 1.4 | 1.3 | |
| 2+ babies (%)b | 6.5 | 4.5 | 6.8 | 5.7 | 10.9 | 10.1 | |
|
Much better freezing Δf = 0.25 |
Success (%)a | 35.0 | 30.9 | 33.7 | 32.1 | 34.3 | 34.8 |
| Twin rate (%)a | 0 | 0 | 4.9 | 6.2 | 19.0 | 20.6 | |
| ET cyclesa | 2.3 | 1.8 | 1.9 | 1.7 | 1.5 | 1.4 | |
| 2+ babies (%)b | 9.8 | 6.5 | 9.4 | 8.5 | 12.1 | 12.2 | |
|
Perfect freezing Δf = 0 |
Success (%)a | 37.1 | 32.9 | 36.9 | 34.8 | 36.0 | 35.3 |
| Twin rate (%)a | 0 | 0 | 5.8 | 8.2 | 20.5 | 21.3 | |
| ET cyclesa | 2.3 | 1.9 | 1.9 | 1.7 | 1.6 | 1.4 | |
| 2+ babies (%)b | 11.4 | 7.7 | 11.7 | 10.6 | 13.8 | 13.1 | |
FIGURE 42.
Comparison of outcomes of complete cycles with SET (SET + SET) with complete cycles with DET (DET + DET) as a function of the loss in viability owing to freezing (Δf). Upper panels show predictions if 10% of embryos are lost in the freezing process (pthaw = 0.9) and the lower panels if 25% are lost (pthaw = 0.75). Simulation parameters: min.grade = 3, min.freeze = 1, thaw number to be transferred, σ = 0.8; 5000 simulated treatments. Upper panels: 10% fail freeze/thaw (a) LBE per egg retrieval; (b) transfers per egg retrieval; (c) two or more babies per egg retrieval if all embryos transferred. Lower panels: 25% fail freeze/thaw (d) LBE per egg retrieval; (e) transfers per egg retrieval; (f) two or more babies per egg retrieval if all embryos transferred.
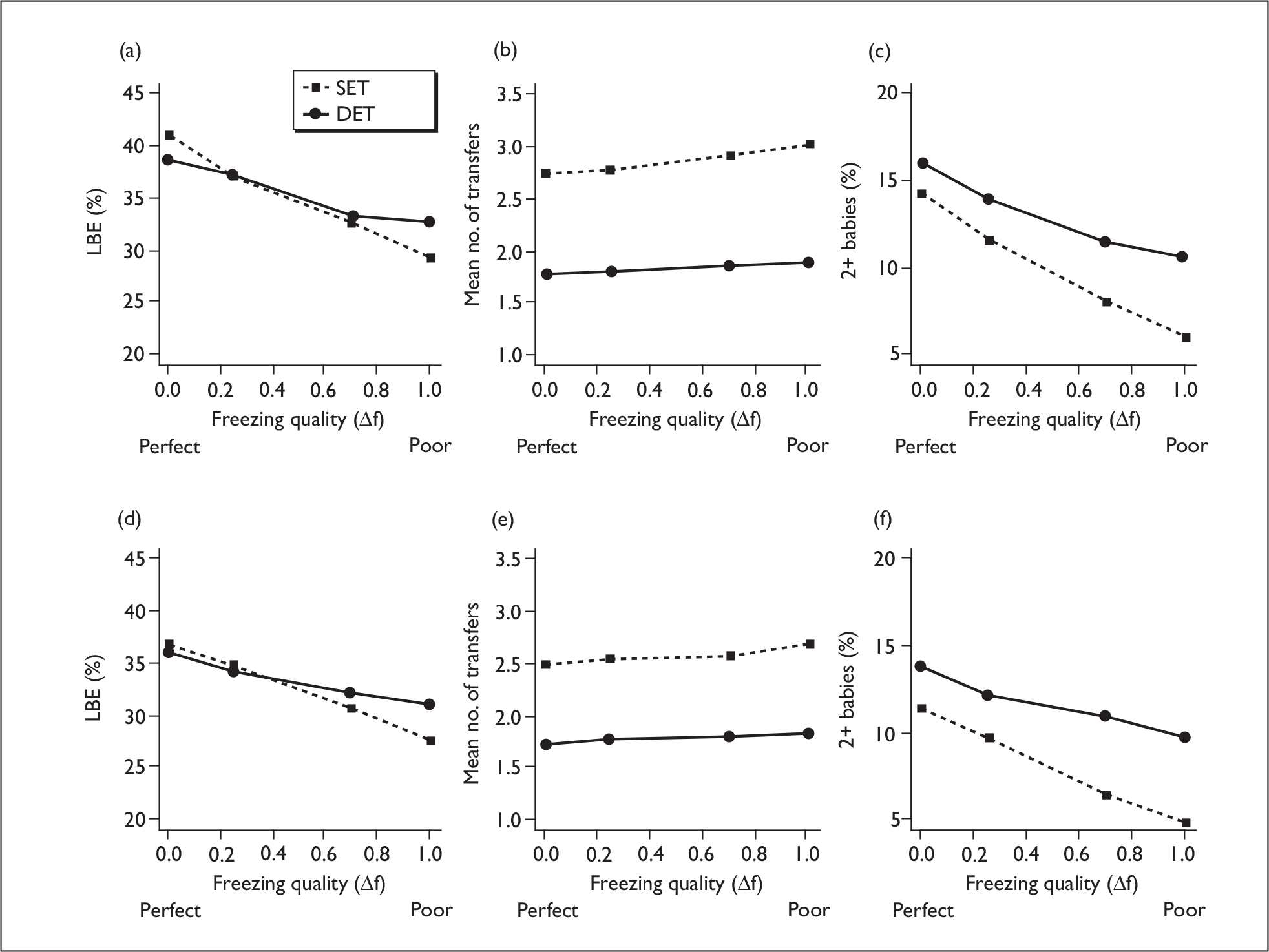
Using the estimates of success following freezing given by the data, the overall success rate per egg collection is slightly lower for SET compared with DET. If, however, the loss owing to freezing were somewhat better – around the best seen in the data, DET and SET could give very similar per-egg collection outcomes, providing embryos were thawed one at a time. If one is prepared to thaw individual embryos, frozen DET is not advantageous as it requires the thawing of more embryos per transfer and therefore reduces the number of transfers available. Thawing individual embryos for SET does incur a penalty in cancelled cycles in those cases in which thawing is unsuccessful. The number of couples having two babies if all embryos are transferred is somewhat lower for SET unless freezing is very efficient.
The equality between SET and DET is maintained across the whole age range as shown in Figure 43. If freezing preserves sufficient of the embryo viability and not too many embryos are lost during the freeze/thaw process, then complete cycle DET and SET are approximately equivalent across the whole of the age range. In Figure 43, the small differences between age groups are smaller than the simulation errors and should not be interpreted as having any meaning.
FIGURE 43.
LBE for complete cycles with SET and DET as a function of maternal age. Panels show outcomes for different assumptions for the freezing quality as measured by the parameter Df. Here we assume a low loss of embryos owing to freezing (10%, pthaw = 0.9) and that one spare embryo is thawed. 5000 simulated patients with min.grade = 3, min.freeze = 1 and σ = 0.8. (a) Poor freezing: Δf = 1. (b) Better freezing: Δf = 0.7. (c) Good freezing Δf = 0.25.
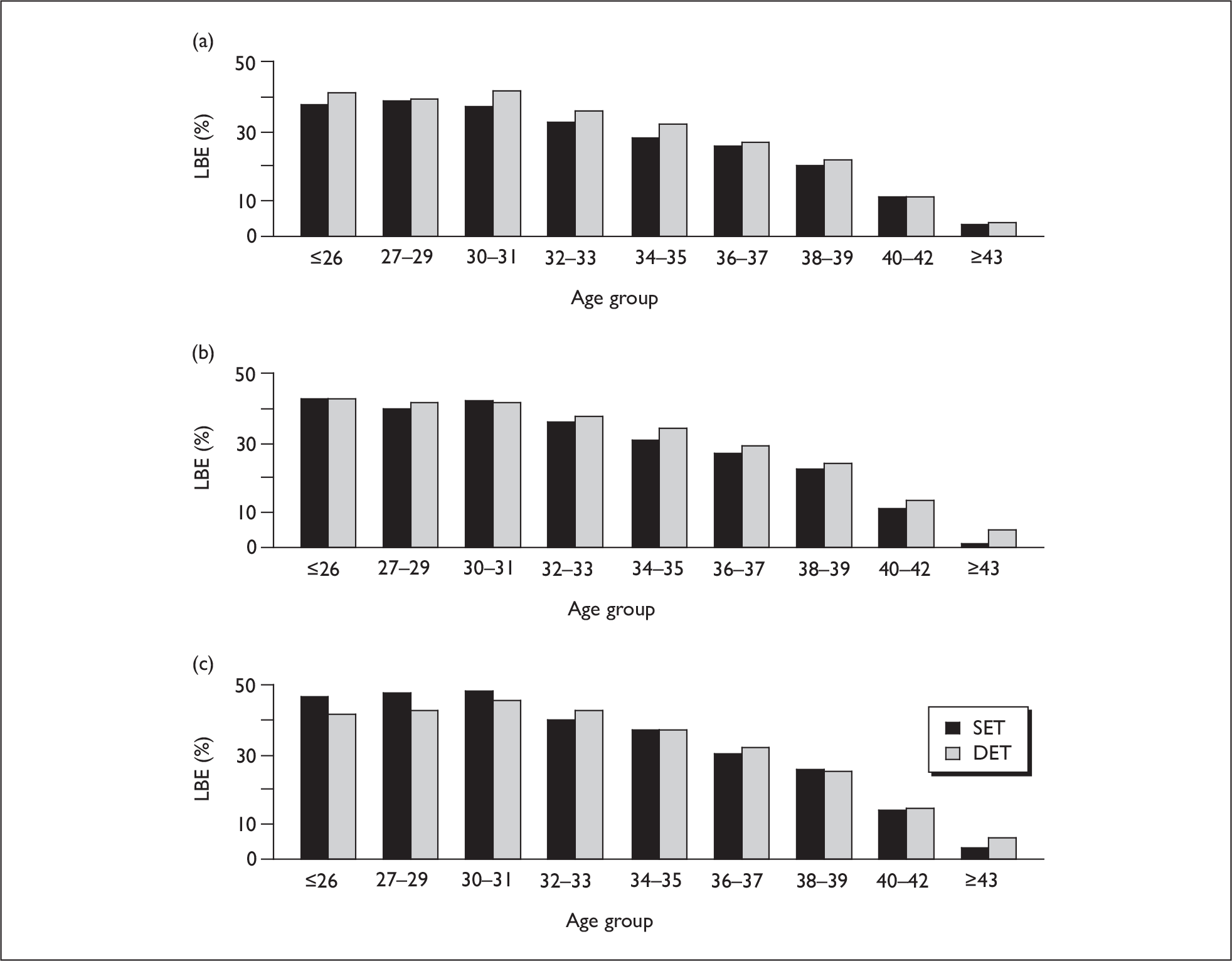
This equality of complete cycle DET and SET can also be shown across the range of patient prognoses. In Figure 44 we divide the patients into five groups according to their predicted LBE rate. There is no evidence of differential benefit of SET or DET across the prognosis groups. The same trends are seen if the loss in thawing is somewhat greater, except that a slightly lesser loss in success rate is required to achieve equality.
FIGURE 44.
LBE for complete cycles with SET and DET as a function of patient prognosis. Data is plotted for five prognosis groups as defined by the quintiles of the predicted LBE probability. Panels show outcomes for different assumptions for the freezing quality as measured by the parameter Δf. Here we assume a low loss of embryos owing to freezing (10%, pthaw = 0.9) and that one spare embryo is thawed. 5000 simulated patients with min.grade = 3, min.freeze = 1 and σ = 0.8. (a) Poor freezing: Δf = 1. (b) Better freezing: Δf = 0.7. (c) Good freezing Δf = 0.25.
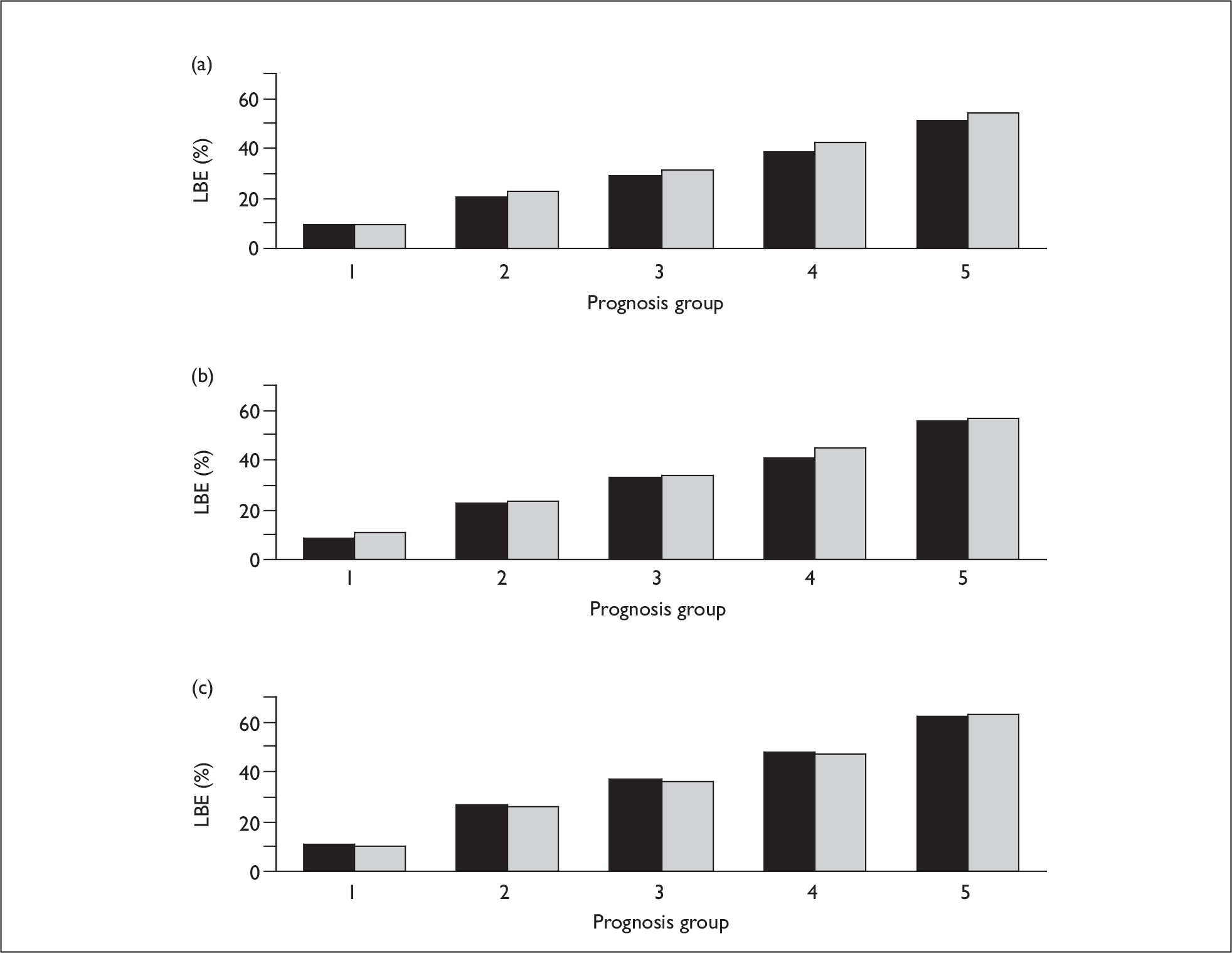
These results, although somewhat tentative given the assumptions required in the simulation process, do suggest, from the point of view of a complete cycle, that SET may be applicable to all patients and selection on patient characteristics is not necessary. This is investigated further in the next section.
Complete cycle treatments with patient selection
In this section we consider potential treatment policies that combine selection for SET using patient characteristics with complete cycle treatments. We consider a representative programme in which patients are selected for eSET providing they have at least three embryos of sufficient quality to allow freezing (grade 3 or 4), i.e. poor-quality embryos are not frozen. In addition, we consider selection of older patients to have DET regardless of the potential for further frozen transfers. In this example we assume that grade 1 and 2 embryos are too poor quality to freeze and just the number of embryos required for transfer are thawed for each frozen transfer, with the best one being transferred in patients below the age cut-off and two transferred in women above that age.The results are shown in Figure 45, which shows the outcomes for differing values of the freezing loss, Δf. As can be seen, the effect of selection is rather small, which would be expected from the results above which show equivalence between complete cycle SET and DET across patient prognosis groups. In fact, in some circumstances the simulations indicate that patient selection (beyond that forced by circumstances) can lead to lower overall success rates, although the uncertainties inherent in this exercise would not allow us to say conclusively if or under what circumstances this occurs. What selection does achieve, in allowing DET for some cycles, is a shorter time to success and fewer cycles overall, but this is at the expense of an increased twin rate.
FIGURE 45.
Simulations of complete cycles with selection for eSET by patient characteristics. Simulation parameters: min.grade = 3, min.freeze = 1, thaw number to be transferred, σ = 0.8; Two simulation runs of 5000 simulated treatments are shown with a quadratic regression line.
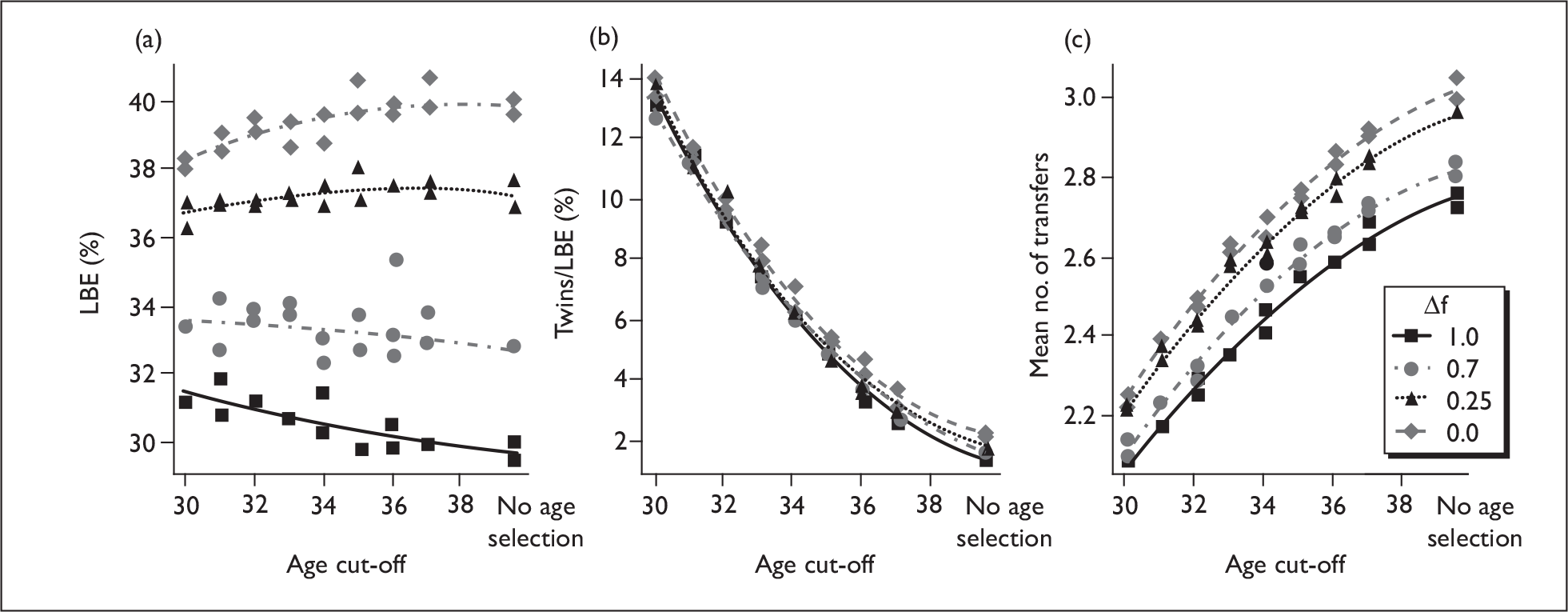
How many to thaw?
Embryos are typically not thawed out individually, but in batches. There is a trade-off between the number of embryos available to select the best from and the number of frozen cycles that one can have. Also, if only one embryo is thawed, there are potentially a significant number of replacements that have to be abandoned as the thawing process is not 100% efficient.
Based on a pure SET policy Figure 46 shows simulated outcome measures as a function of the number of embryos thawed per batch. In this simulation we assume that only good-quality embryos are frozen (grade 3 and 4) and that single embryos will be frozen. The optimum in terms of overall success rate in SET is to thaw individual embryos, but this does lead to a proportion of cancelled cycles, which is virtually eliminated if two embryos are thawed. With one thawed embryo the average number of replacement cycles is around three. Thawing two embryos at a time reduces the per-egg retrieval success rate appreciably as fewer transfers can be performed – the average number of cycles is around two.
FIGURE 46.
Simulation of the effect of varying the number thawed prior to each frozen transfer in a compete SET policy setting. Upper panels assume that 10% of embryos fail to thaw (pthaw = 0.9) and the lower panels 25% (pthaw = 0.75). 5000 simulated patients, simulation parameters: min.grade = 3, min.freeze = 1, σ = 0.8. Top panels: 10% fail freeze/thaw. Lower panels: 25% fail freeze/thaw.
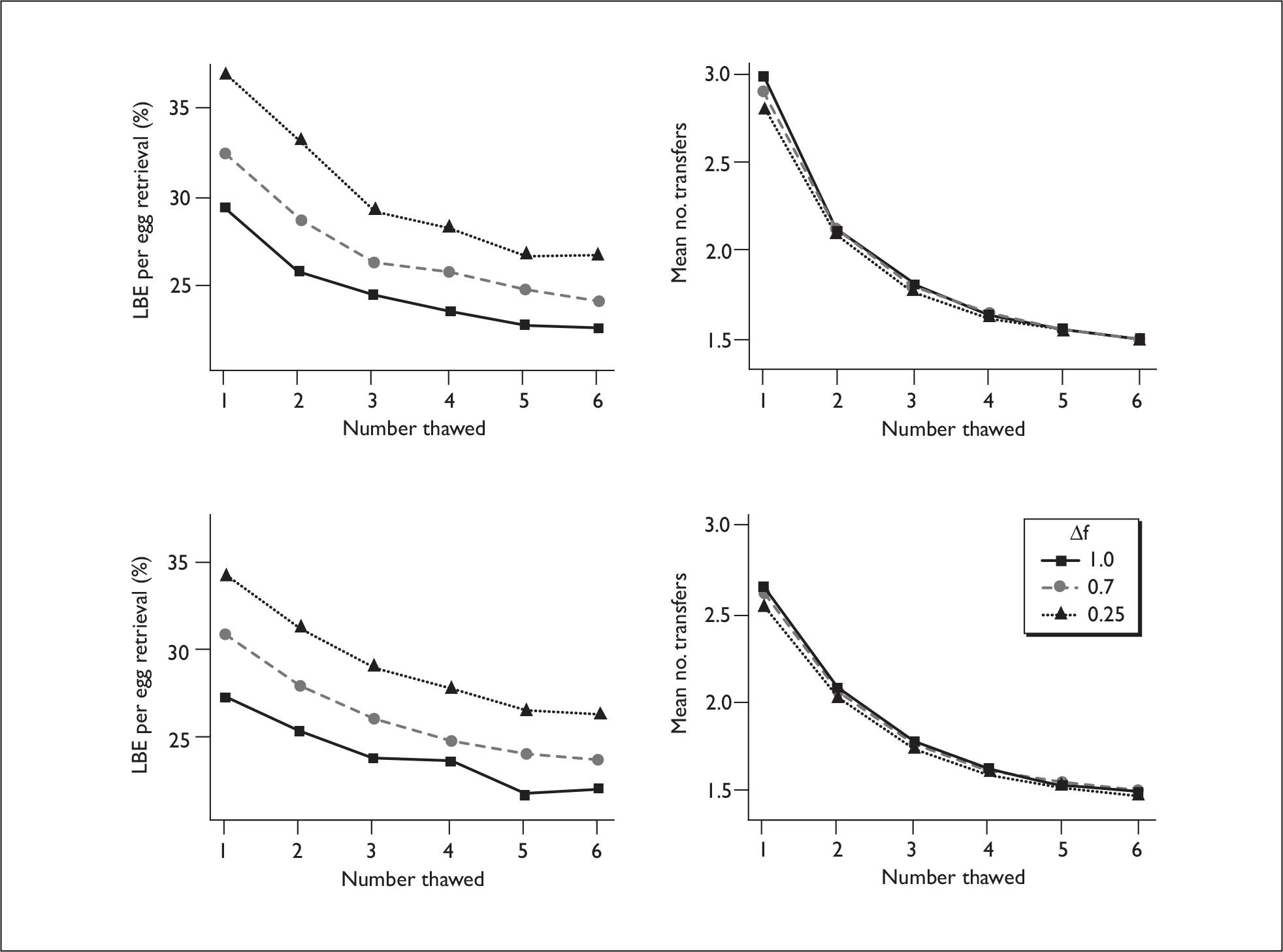
Which embryos should be frozen?
Due to reasons of cost-effectiveness and the risk of a failed frozen embryo replacement cycle, many clinics will not freeze single embryos. Here we take a standard complete SET policy with a minimum freezing grade of 3, thawing in batches of two (or single embryos if only one available). The results are shown in Figure 47 for a range of freezing quality (Δf). Not freezing single embryos has a marginal effect on overall success (<1%), but if larger numbers than two are required to enable freezing then the loss is more substantial.
FIGURE 47.
Simulation of the effect on success (per egg retrieval) and number of transfers of varying the minimum number of embryos that are frozen. 5000 simulated patients. (min.grade = 3, nthaw = 2, σ = 0.8). Results are shown for 10% (pthaw = 0.9, upper panels) and 25% (pthaw = 0.75, lower panels) freezing loss (embryos non-viable after thawing). Top panels: 10% fail freeze/thaw. Lower panels: 25% fail freeze/thaw.
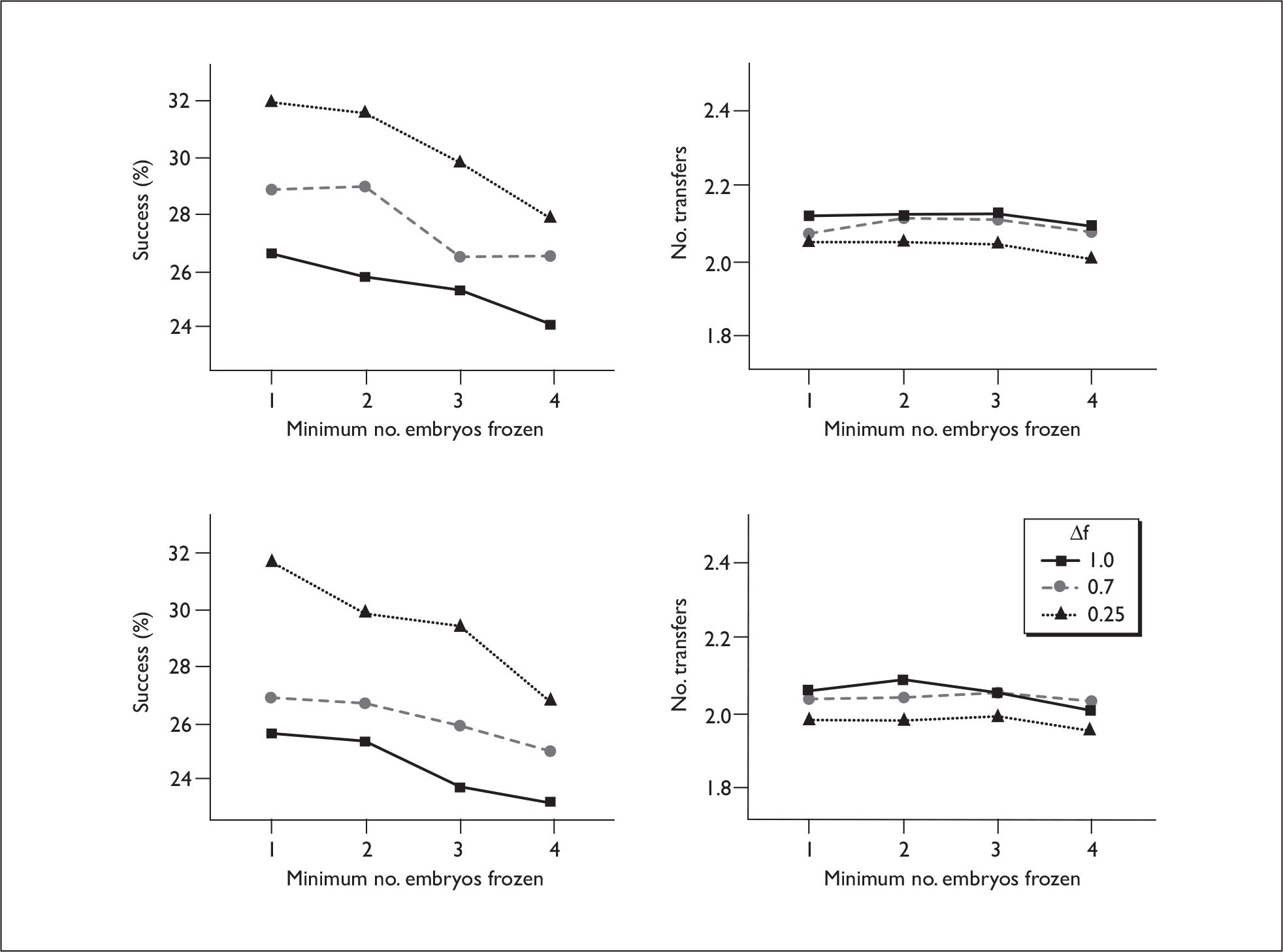
Most centres do not freeze poor-quality embryos. There is a trade-off between the increased success rate from the few of these extra transfers enabled by preserving these embryos and the additional number of cycles with a very low probability of success. Figure 48 shows the success rate as the grade threshold for freezing is increased.
FIGURE 48.
Simulation of the effect on success (per egg retrieval) and number of transfers of varying the minimum grade of embryo that will be frozen. 5000 simulated patients. (min.freeze = 1, nthaw = 2, pthaw = 0.9, σ = 0.8). Top panels: 10% fail freeze/thaw. Lower panels: 25% fail freeze/thaw.
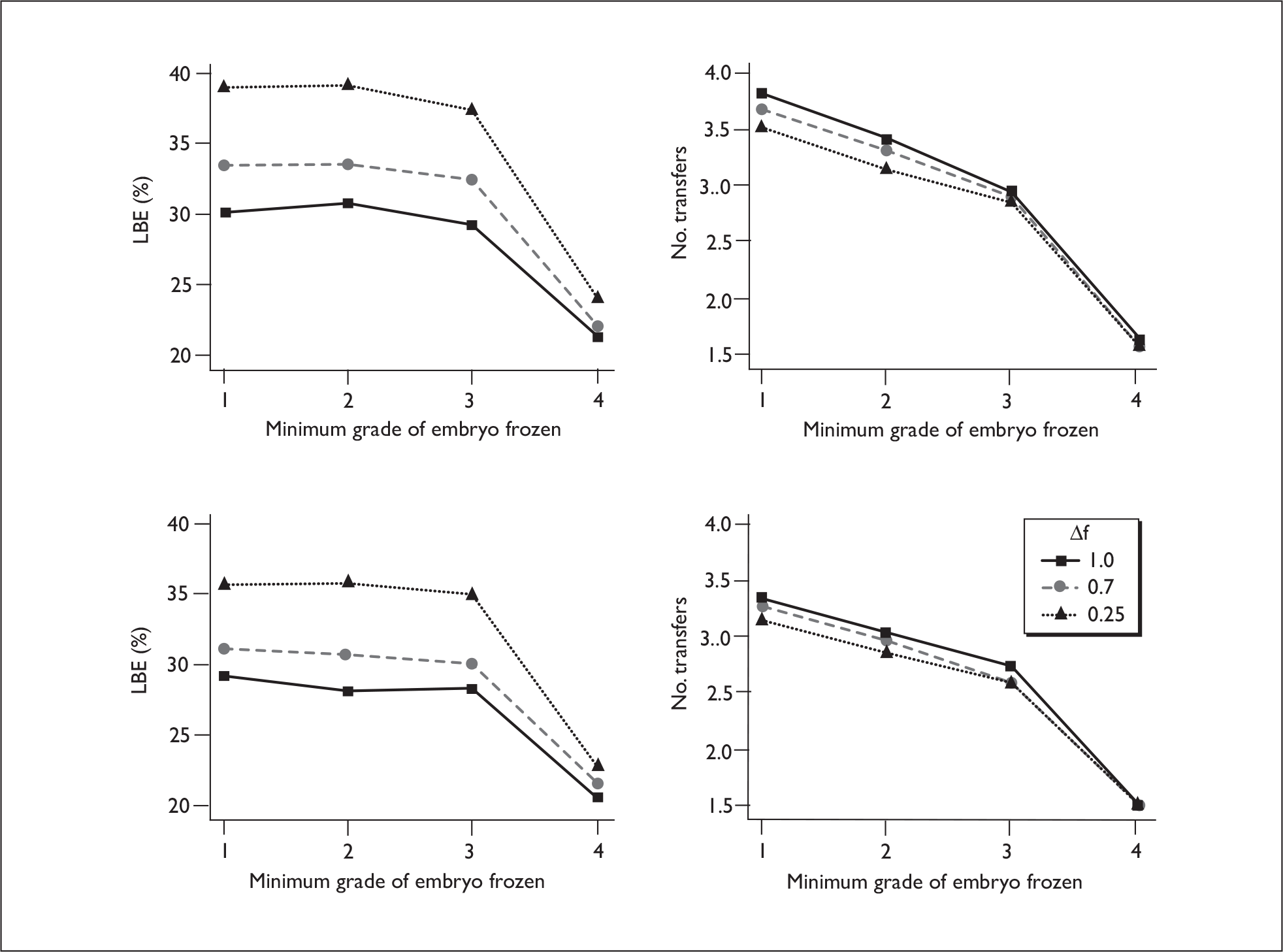
There is very little increase in success rate to be gained by freezing poor-quality (grade 1 or 2) embryos and a big increase in the number of transfer cycles. This would be highly disadvantageous in terms of cost-effective treatment within the NHS and direct cost to the patient in the private or fee-paying sectors, and in terms of expenditure of time and emotion by patients. As would be expected, there is only real value in freezing grade 3 and 4 embryos.
Sensitivity to intrapatient correlations
The simulations above all assume a value of ω = 0.8 for the standard deviation of the patient random effect, based on the model fits (Chapter 4, Intercycle correlations in the EU model). This parameter captures the correlation between repeat cycles for the same patients, and was not well determined by the data with wide confidence intervals which included zero. We have repeated the simulations of complete cycle SET and DET with a range of values of σ from zero to twice the best estimate to determine the sensitivity of the results to this parameter. The results are shown in Figure 49. There are no strong trends over the wide range of σ considered and none of the conclusions are affected by the choice of s. There is some reduction in benefit of multiple cycles as correlation increases, but the ordering of the various treatments remains the same.
FIGURE 49.
Sensitivity to the random effect parameter, σ, which controls the correlation between treatments in the same patients. LBE for complete cycle SET and DET, where either the number of embryos thawed is the number being transferred, or one more to allow a spare in case of freezing loss. Lines are linear regression plots to the simulation data, with two to three simulation runs per parameter set. Simulations are shown for a range of loss in viability (Df). In this example only grade 3 and above embryos are frozen but single embryos will be frozen. 5000 simulated patients. (a) SET thaw number needed. (b) SET thaw number needed plus spare. (c) DET thaw number needed. (d) DET thaw number needed plus spare.
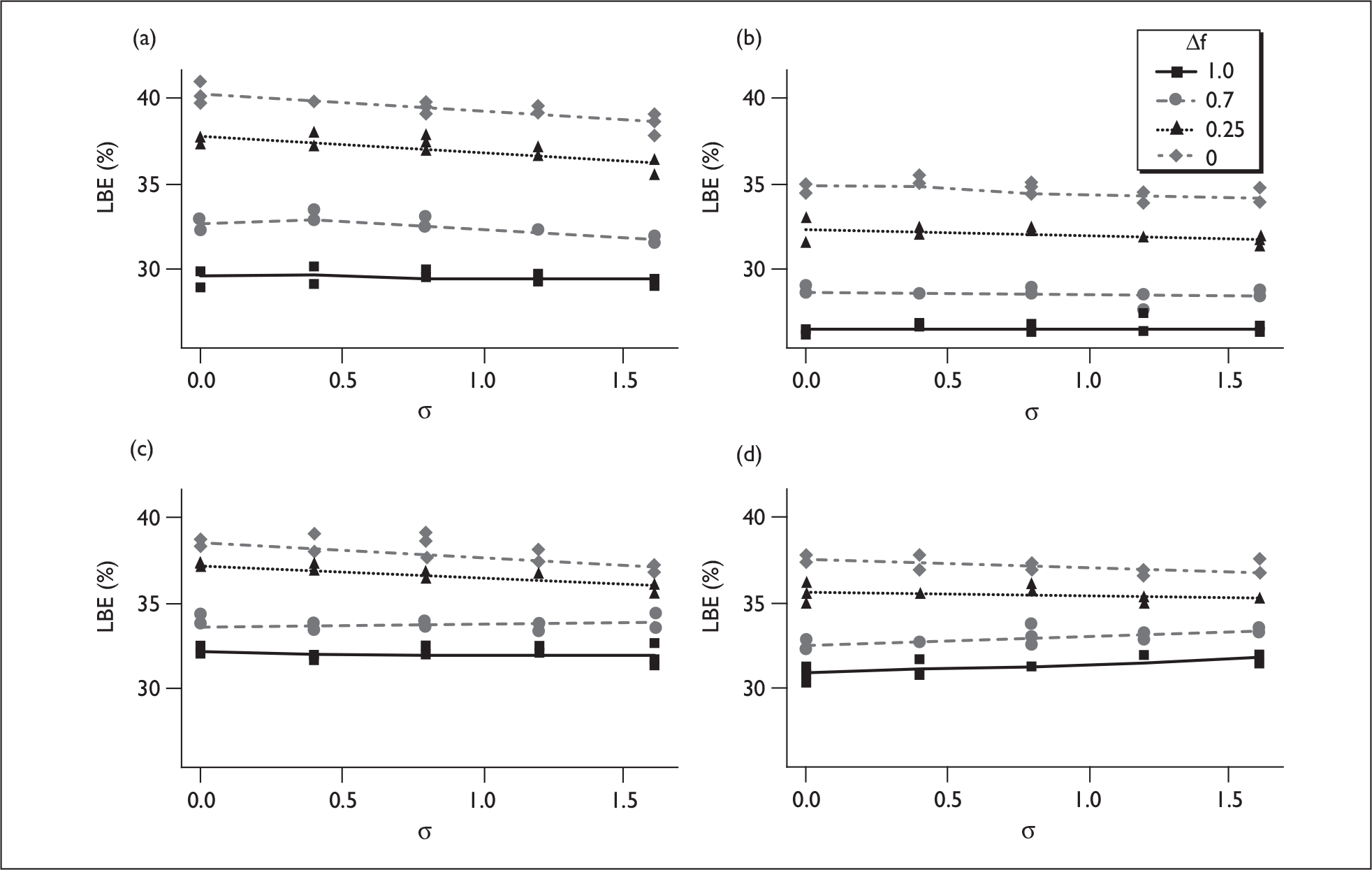
Comparison with data from randomised trials
There are three randomised trials that have reported outcomes of multiple SET and DET transfer and the details of these are summarised in Table 54. One very small study17 gave similar outcomes for multiple SET and DET transfers in a population with good prognosis, although the confidence intervals do not exclude a twofold difference. Two trials10,15 compared a single fresh DET with two cycles of SET (one fresh, one frozen) in selected patients and showed roughly equivalent LBEs between arms, although neither trial was powered to detect anything but very large differences. SET reassuringly did reduce the twin rate to zero or close to zero – although even here the small trials do not eliminate the possibility of significant twin rates.
| Trial | Treatment | LBEs | Twins per transfer | ||
|---|---|---|---|---|---|
| n | % (95% CI) | n | % (95% CI) | ||
| Moustafa et al. 200817 | DET cumulative | 19/40 | 48 (33 to 63) | 8/19 | 42 (23 to 64) |
| SET cumulative | 18/40 | 45 (31 to 60) | 0/18 | 0 (0 to 18) | |
| Lukassen et al. 200510 | DET fresh | 19/53 | 36 (24 to 49) | 7/19 | 37 (19 to 59) |
| SET + 1 frozen SET | 22/54 | 41 (29 to 54) | 0/22 | 0 (0 to 15) | |
| Thurin et al. 200415 | DET fresh | 142/331 | 43 (38 to 48) | 47/142 | 33 (26 to 41) |
| SET + 1 frozen SET | 128/330 | 39 (34 to 44) | 1/128 | 1 (0 to 4) | |
The simulation studies presented here indicate that for the two scenarios tested in the trials there should be close to equivalence between the treatments, as is observed, depending on the quality of cryopreservation and its implementation. Although the trial data provide only very weak evidence, it is consistent with the simulated results.
Discussion
The EU model allows direct predictions of outcomes of fresh DET and SET within the same patients. These predictions are dependent on the assumptions of the EU model, specifically the conditional independence of the embryo and uterine components given the measured covariates. There is no evidence that these assumptions are unwarranted, and the conformity of the model predictions with those of the clinical trials (see Chapter 4 and above) gives confidence in them. The other major caveat is that the predictions are based on data from the 2000–5 period, and certain elements of clinical practice may have changed since then and success rates improved somewhat. Further work is required to confirm the validity of the models used in more recent datasets.
Monozygous twins are not considered in these simulations as the policies being investigated have no effect on the monozygous twin rate and currently monozygous twins are a small proportion of IVF twins. Some proposed and more invasive techniques, such as blastocyst transfer, have the potential to increase the monozygous twin rate and this may need to be considered more seriously when overall twin rates are lower.
The direct predictions of ‘what if’ scenarios for single fresh transfers allocating patients to DET or SET by a number of different algorithms suggest that the large (> 30%) relative loss in LBEs incurred in an eSET transfer can be somewhat ameliorated by appropriate selection of patients and treatment cycles (e.g. based on embryo number and quality) but not eliminated: the loss even with the best patient selection will still be significant. Age selection is attractive to clinics but is perceived as unfair by many patients (see Chapter 2). The work here suggests that from the point of view of the fresh cycle, selection by characteristics of the embryos available in the particular treatment cycle may be nearly as effective, although this too has problems with the lateness of the decision in the treatment process. One thing that is very clear is that inappropriate selection of patients can lead to high SET rates with high twin rates and still with a loss in headline live birth rates compared with DET. It will be important that clinics monitor carefully how their eSET policy works out in practice and that patient or clinical decision-making does not lead to such inappropriate selection.
Success and twin rates are patient population and clinic dependent. Some of these differences may be due to unmeasured, or imprecisely measured, population differences, and in the future these differences may be lessened by better data recording, the identification of better prognostic factors such as hormone levels, and, particularly, the adoption of uniform, quality-controlled embryo-grading systems. Nevertheless, it is likely that real centre differences in population and practice will remain. Therefore, we believe that it is not appropriate to adopt specific criteria based on this or any other work, rather the general principles need to be applied in an iterative manner to determine the appropriate criteria for each clinic and patient population.
When we come to consider multiple embryo transfers we have to rely on Monte Carlo simulations, and some of the required data are not well determined, so we have to consider a range of possible values. Nonetheless, the general trends are quite clear and not dependent on the parameter uncertainty, even if the actual estimates of outcome are. Providing the viability of frozen embryos is not too much reduced from the fresh embryo, a series of SET transfers from a single egg collection would be predicted to have very similar outcomes to a series of DET transfers. This result is consistent with the very limited trial data. The simulation data suggest that this may be true for all patients, not just those with good prognosis. Although this result may be sensitive to the assumptions around the distributions of embryo quality, it does suggest that if one takes a complete cycle perspective, SET might be advocated for everyone, and the issues over patient selection become redundant. Indeed in some scenarios patient selection may actually reduce the overall success rate over a complete cycle compared with SET for all. In this light the trade-off between DET and SET becomes a balance between the number of twin births and the number of transfers it takes to get pregnant, not overall success.
A complete SET policy would require more transfers, which would place a greater burden on the patients. Although, with intelligent NHS commissioning and private practice financial models basing funding on ‘complete’ cycles, the financial burden could be controlled, the emotional burden and time commitment would still be increased. Patients will need persuading that this burden is reasonable. In addition, even if the remaining embryos were transferred subsequent to a successful treatment, it is unlikely that the number of babies produced per egg retrieval (as opposed to LBEs) will be maintained, unless freezing techniques are greatly improved. This might disadvantage those patients who would like more than one child.
The present data do not allow any assessment as to the comparative burden on the NHS of complete SET; this requires a full economic analysis in the context of the full patient treatment in an attempt to have a baby. It may also be crucially dependent on the configuration of service provision and organisation, which may make frozen transfers more cost-effective.
The simulations suggest that a complete cycle approach has the potential to eliminate the loss in success rate owing to eSET, with the extra transfers available by using one embryo at a time compensating for the loss owing to the initial fresh SET cycle. However, this is dependent on good-quality cryopreservation, both from the measures of success and from the point of view of patient credibility. Some work has been undertaken on the technical freezing techniques. 122 The work reported here suggests that the policy concerning which embryos are frozen and thawed can have a significant impact; in particular, the willingness and ability to thaw single good-quality embryos can be advantageous, albeit at the expense of some cancelled transfers. Conversely, there is little value in freezing poor-quality embryos. Although thawing single embryos is optimal in terms of success rates, the burden of cancelled cycles (both emotional and financial) needs to be considered. Single thawing is only likely to be acceptable if the loss rates are low and the number of cancelled cycles small. Careful economic analyses are required here that consider not just financial costs but also the patient’s trade-off between cancelled cycles and success chances.
Although the simulations can only be considered indicative rather than definitive, they do suggest that providing there is a good-quality cryopreservation programme, complete cycle SET can match or even outperform DET over a complete egg retrieval plus replacement cycle. If one takes this complete cycle perspective, then the selection of patients for DET may become less relevant, with the trade-off being the number of twins versus the number of frozen transfers and time to get a successful outcome, rather than the overall success rate. The issues around funding for the freezing, storage and extra cycles does of course remain, as does the additional burden on patients of longer treatment courses. In terms of developing eSET policies it may be more important to focus on freezing issues rather than patient selection. But this would require a strong refocusing of attention away from the fresh transfer and towards cumulative outcomes.
This simulation work has not considered the potential for embryo selection, by either invasive (genetic screening) or non-invasive (metabolomic) procedures or by extended culture (blastocyst transfer). Although the methods used here could be extended to cover such possibilities, the data on which to base such simulations are not available. It will be important to consider such approaches in future simulation work. For invasive techniques, it is not clear whether the increase in success rate in the fresh cycle will exceed the losses incurred and the consequent lack of embryos for frozen transfer. Although non-invasive methods may not increase the overall success rates they may effectively bring forward successes, requiring fewer treatments and saving both cost and patient burden.
Summary
In the fresh transfer following egg retrieval a SET would lead to a reduction of approximately one-third in the live birth probability compared with a DET. From the population or clinic perspective, selection of patients based on prognostic indicators might mitigate about half of the loss in live births associated with SET in the initial fresh transfer while achieving a twin rate of 10% or less. A number of strategies based on the woman’s age and the number and quality of available embryos perform broadly similarly.
Any meaningful comparison of IVF treatments must take a complete treatment perspective, comparing success rates after use of all available frozen embryos from an egg-retrieval procedure. Our data-based simulations suggest that if all good-quality embryos are replaced over multiple frozen embryo transfers, then repeated SET has the potential to produce similar or even more LBEs than repeated DET, and this is likely to be true for all patients. This critically depends on optimising cryopreservation procedures. Universal SET could potentially both reduce the number of twin births and lead to more couples having a child, but at an average cost of one more embryo transfer procedure per egg retrieval.
Although the detailed results provide indicators as to appropriate policies, it is likely that the detailed algorithms will be treatment and centre specific, and an iterative development of centre policies will be required, which could be based on those developed in this project.
Chapter 6 Patients’ reactions to policy options: focus groups
This chapter describes the methodology and results from two focus groups that were conducted in order to access patients’ views on the results of the statistical modelling and potential approaches to twin reduction policies. The aim was to use the modelling results to investigate with patients the acceptability of SET in the context of specific treatment scenarios within the current regulatory, funding and clinical environment.
Focus group conduct and analysis methods
Focus groups
Focus groups were chosen as a suitable method as they have been successfully employed to assess a range of views in health-care settings;123 they are also a format whereby it is possible to explore sensitive issues. 4,5 In order to facilitate maximum face-to-face group interaction, groups consisting of between six to eight couples were sought. This group size is considered ideal when dealing with knowledgeable participants. 124 More recently, online focus groups/forums have gained in popularity and acceptance. These ‘virtual’ groups have the advantage of being accessible to people across a large geographical area, they reduce the influence of the facilitator and they allow people to interact in a comfortable and familiar setting. 125
Development of the focus group presentation
The focus group had the specific aim of informing patients of the study in general and feeding back the results of the statistical modelling, thus the groups were structured to achieve these goals. In order to achieve this brief a powerpoint presentation was developed in conjunction with the principal investigator (SR), who is also a statistician. That presentation is available as an appendix to this report (Appendix 2) and reflects the state of the modelling and interim conclusions at the time of writing. The presentation raised issues about proposed policy changes and displayed the preliminary findings from the statistical modelling studies in a user-friendly format. This was designed to stimulate discussion and debate and to provide information on potential treatment choices. Questions were embedded within the presentation, but participants were actively encouraged to state their own opinions and generate questions for the researcher to answer. The intention was that the presentation addressed the following three objectives, each with time allocated specifically for questions (see Appendix 2):
-
To give an overview of the project
-
– opportunity for open questions.
-
-
To discuss draft guidelines regarding single embryo transfer
-
– structured questions.
-
-
To show statistical analysis of datasets and treatment options
-
– structured questions
-
– opportunity for open questions.
-
The presentation was slightly modified for the patient organisation participants, guided by the Director of Infertility Network UK, as this group accessed the material directly in an online forum on the organisation’s website. An additional slide was included to address any distress that the presentation might evoke, and relevant contact details included.
Setting and sample
The initial study design outlined a plan to recruit two focus groups (one NHS, one private) then to validate the findings with a third NHS group. However, recruitment at the private clinic was not successful, so the research team made the decision to access a patient organisation group (Infertility Network UK) and to run the ‘focus group’ or consultation within the context of an online forum.
Recruitment
A sample of convenience was sought in order to access participants. It was envisaged that this would result in a diverse sample. It was not possible to purposively sample patients on specific characteristics as the recruitment method of open advertising did not allow for this. Sample characteristics, for example age, stage of treatment, funding source, etc., cannot be identified unless specified by the participants in their responses. Thus, the groups were self-selecting from a cohort of patients either undergoing, or who had recent experience of, IVF treatment.
Sample 1 – NHS Patients were invited to participate in a structured focus group by means of a poster placed in the clinic waiting room. Patients who were interested in the study were asked to request an information pack from the nurses in the clinic. They then took this home with them and replied to the researcher using the invitation slip if they wished to be contacted. In total 40 packs were given to the clinic, 30 packs were taken away (although it is not possible to certain that these were read) and the researcher had 10 positive responses. Following telephone conversations with the researcher, three couples and two women agreed to participate (n = 8). However, on the evening the focus group was held, one couple phoned to say that they were delayed by heavy traffic and would not be able to get to the hospital on time, and one woman did not attend. Thus, the final sample consisted of two couples and one woman (n = 5).
Sample 2 – private clinic The same recruitment procedure was used as that outlined for the NHS clinic above. Twenty packs were placed in the clinic, and, although 10 were taken away, no volunteers emerged at this site. In discussion with the clinic staff this was thought be owing, at least in part, to the distance patients would need to travel to the clinic for a specific time and date which might not have fitted with their treatment schedules. It was decided that recruitment was likely to be unsuccessful and so no further attempts were made at this centre.
Sample 3 – patient organisation The recruitment for the online forum group was conducted with the help of two key staff members [the director and the IT (information technology) officer]. A similar format to that used in the NHS setting was adapted for the online environment. Thus, the poster and information sheet were posted online. In addition, the researcher produced a short biography with a photograph in order to introduce herself to the audience. A brief outline of the project was also available. The IT officer announced the project online and a dedicated forum space was allocated where participants could either post to a shared forum or post privately directly to the researcher. The forum was opened for 1 month for the purpose of this study. During this time 622 viewings of the site were recorded, and this resulted in 10 online forum postings and one private response to the researcher. Further data have been accumulated since this study period and will be added at a later date.
Conduct of the focus groups
NHS group
Patients who consented to take part were sent a formal invitation stating the time, date and location of the focus group. This pack also contained patient information and a consent form (which participants were advised to return by stamped addressed envelope). This group was held in the NHS clinic. Arrangements were made for the group to run in an evening for approximately one and half hours.
The group was conducted by two facilitators, one to present the findings and answer questions and queries (LMcG), and the other to maintain the recording equipment and take fieldnotes (Diane Escott).Participants were greeted warmly on arrival and refreshments were freely available. Initial introductions were made and the consent process was outlined, which included group consent to digitally record the session. Consent forms were available for those participants who had not returned their initial forms. Prior to the powerpoint presentation ground rules were established with the group. Anonymity and confidentiality were assured, and participants agreed that everything that was said in the room should remain confidential. Participants were informed that anonymised quotes might be used in future reports and publications, but that they would not be identifiable in any way. The timing of a mid-point break was also agreed. Although the presentation had ‘built in’ questions, participants were encouraged to ask questions and discuss concerns at any point.
Online group
Many of the principles of a face-to-face focus group are applicable to the online environment (as outlined above). Key differences included the fact that the online participants were not required to give formal consent as they were ‘volunteers’ within the context of a patient organisation. However, a patient information sheet was posted online, as well as information about the researcher, the study in general, and any relevant contact details. Although, confidentiality and anonymity were assured, it should be noted that participants within all the forums and chat rooms had been already anonymised according to Infertility Network UK policy and the research team had no access to any individual’s identity. The researcher (LMcG) was also guided by the rules of Netiquette, as described by Virginia Shea,126 in order to facilitate productive, safe and ethical interactions within the online environment.
Data analysis
The findings from the transcribed verbatim data of the NHS group and the transcripts from the online group were integrated with the original thematic framework from the patient interview data where themes and subthemes were repeated. Emergent themes and subthemes were added to this framework and redundant themes removed. This process was guided by framework analysis (Ritchie and Lewis,127 Ritchie and Spencer106). Analysis involved three main stages of data management, providing descriptive analysis of the data then explanatory accounts. This analysis was co-conducted by two researchers (LMcG; Diane Escott). The data were first collated in a matrix. The next stage concerned a descriptive analysis of the charted data. Further synthesis of the data involved the researcher interpreting the data in a more conceptual way by studying the charted data and abstracting further descriptions and categories. The final stage comprised an explanation of the data as a coherent whole by establishing patterns and applying the data to wider policy.
Findings
The above process resulted in a final framework which incorporated four main themes and several subthemes (Table 55). The majority of the data fitted well into the original thematic framework developed from the patient interview data (see Chapter 2). To allow for cross-comparisons the original numbers applied to this framework have been used. New and emergent themes which were identified in the focus group data are displayed in italics. Quotes are identified by line number and group (e.g. focus group or online).
| Main theme | Subthemea |
|---|---|
| 2. Views on policy | 2.1 Views on introducing a SET policy |
| 2.2 Personal choice regarding SET | |
| 2.4 Source of funding | |
| 2.5 Policy drivers | |
| 2.6 How can we encourage the uptake of SET? | |
| 3. Views on multiple birth | 3.1 Attitudes/beliefs towards multiple birth |
| 3.2 Perception of risk from multiple birth | |
| 5. Experience of treatment | 5.2 Emotional effects of treatment |
| 7. Reaction to the presentation of statistical modelling results | 7.1 Calculating the odds |
| 7.2 No change of opinion | |
| 7.3 What happens next? |
Theme 2: Views on policy
Subtheme 2.1: Views on introducing a SET policy
Views and opinions towards a SET policy generated a lot of discussion in both the face-to-face and online groups. On the whole, participants did not favour a change in policy, and questioned the need for this change. Several reasons were given to support this opposition. Some participants were not convinced by the risk profile they had been given:
Erm, yes and no, I mean, I don’t … personally I don’t even remember what the risks are from natural, IVF, you know, overall (L1380–1). I know that there are risks, I’ve been told about premature risks and that but so far, there doesn’t seem, I can’t see how, you know, what justifies such a drastic move as to say, right okay we’ve got to go for a single (L1385–7). And I’ve seen nothing so far that’s convinced me it’s necessary at all (L1393).
(Focus group)
Many participants suggested that the physical and emotional burden of treatment was being marginalised by policy-makers:
I strongly urge anyone making decisions on the patients behalf, to consider the impacts of SET on the emotional mindset of those patients – desperate for their chance to conceive and have a take-home baby – as well as the physical ones it takes to put oneself through the turmoil of further treatment. It is all very well to be in that position of trust, with letters after one’s name but it’s vital you do speak for the patient with the views of a patient at the heart of this matter.
(L70–5, online forum)
Later in the posting she states:
Sounds simple to do SET but for those for whom it doesn’t work, it elongates the misery.
(L98–9, online forum)
However, one participant did favour SET, as long as pregnancy rates were not reduced:
I noted that the HFEA have set a target to reduce the multiple birth rate from IVF/ICSI treatment down to 10%. This is a commendable target to achieve, as long as clinical pregnancy rates are not affected overall. As far as I can see, this would mean targeting patients perceived to be at higher risk of twin pregnancy and offering them SET.
(L223–7, online forum)
Subtheme 2.2: Personal choice regarding SET
Personal choice regarding the decision to opt for SET or DET was often influenced by previous experience. For this woman, post miscarriage, DET was deemed to be the only option:
One final point, I had actually intended a path for myself of two SETs then a third DET as final go. I got pregnant with my first SET but miscarried at 12 weeks. I was by then another year older and given a 20% chance of pregnancy with DET. All I wanted was to be pregnant again, so I went for a DET and maximising my chances. What I am getting at is I would have needed some pretty intense and effective counselling to change that mindset post miscarriage … I am not sure if that even exists.
(L90–5, online forum)
Another participant had opted for SET because it was the clinic preference, and particularly her personal choice:
I think we’ll be having just one put back because our clinic is SET all the way. But if they gave me a free choice then I would risk it and put two back.
(L397–9, online forum)
The following woman felt that imposing SET was a direct threat to personal choice:
But to … to have that choice taken away it’s just … it’s very, very difficult and that final … that last bit there about what sort of education that I should need (L466–7). I think you’d need a hell of a lot more than what we’ve got now (L471).
(Focus group)
Subtheme 2.3: Improve your odds
For many participants choosing DET was associated with improving their chances of a successful outcome, and, when this was related to other factors such as treatment experience, DET became the obvious choice:
You can’t take the emotion out of this. I’ve just had a SET – not through choice, but because there was only one embryo to transfer. And if last week, someone had offered me the choice of another embryo being transferred or another cycle, I would have leapt at the chance of that second embryo, no hesitation. 25% or 16% chance of success for 35 and over? Another egg collection and more injections, more drugs or that extra transfer? There’s no contest.
(L204–9, online forum)
The following participant chose DET because she rationalised that, despite the associated risks, DET would improve her chances of pregnancy and a live birth of at least one child:
There’s a risk of losing, erm, one of the babies, but that there’s a risk and there’s up to one in three miscarriages anyway with a singleton (L1347–9). Then you can almost think if you’re going to be real cold and think, I want a baby, well okay them, if I’m having twins and I lose one, I’ve still got one (L1355–6). You know, like, if I’m pregnant and I lose the one, then I’ve got to start all over again and you … things like that … (L1360–1)
(Focus group)
Subtheme 2.4: Source of funding
One participant noted that the same policy should apply to self-funding patients, if the reason for the policy was related to reducing risk rather than cost:
But the reason for them saying this about the NHS that, is the fact that there could be problems, risks for the mother, etc. … (L667–8) … that would be nothing to do with cost, would it? (L672) So it would have to be the same in private as in the NHS … (L676) … because they haven’t [voices overlap 28:11] a risk of a premature birth … (L680) … and you could lose one baby or … (L684) So you would have to be the same for them as well.
(Focus group)
Again, as sense of unfairness regarding the timing of the proposed policy change was raised:
… but then for a couple that’s paid four thousand pounds are able to have two and end up with twins just like, somebody that goes, you know, six months later… (L694–6) … and only had one but pays the same amount of money (L700). But then again, you don’t know when they’re going to change the rules, but it would have to be the same for both (L704–5).
(Focus group)
The costs associated with private treatment were a driving factor for some when choosing between SET or DET, particularly when this was added to the burden of treatment:
We had already made the decision that there would be no further treatment for us due to the impact it was having on my health, and because financially we have exhausted all of our resources after spending in excess of £15,000.
(L134–6, online forum)
Subtheme 2.5: Policy drivers
As with the patient interviews, some participants felt that those undergoing IVF treatment were being unfairly targeted when compared with other groups, and that SET was principally being promoted to reduce NHS costs:
When you’ve got … you can see all these, like, sixteen-year-olds [inaudible 56:44] and they say, they tell you shouldn’t drink and you shouldn’t smoke but you see people that are having babies that are drinking and smoking … (L1451–3) Drinking and smoking! (L1455) … and then you come to have IVF and it’s like, they want to know, like, fine details about your personal life… (L1457–8) … and on top of that, they seem to be trying to take it away from you even more (L1462). Yeah (L1464).
(Focus group)
However, another woman could see value in encouraging patients to choose SET:
I’ve just had a read through this [presentation] … all very interesting and I can see what they’re trying to do; twin pregnancies are more risky to both mum and babies – and I suspect also more expensive to the NHS … ? So it does make sense in one way – keep people safer and reduce the financial burden on the NHS.
(L365–8, online forum)
Subtheme 2.6: How can we encourage the uptake of SET?
As part of the consultation process the researcher asked both groups how the uptake of SET could be encouraged, given that this policy was likely to be implemented. The following participant identified funding and service issues as significant barriers:
The funding issues and the waiting lists need to be sorted out before you will get many people signing up for SET in my opinion. The idea that some PCTs require people to have been trying for 5 years before they can get IVF is awful – and then the NHS wonders why people want to give themselves every possible chance? And why so many of us would consider twins as a perfect outcome? Hmmm!
(L391–4, online forum)
Another participant felt that blastocyst transfer should be encouraged as she had read a research paper which stated that this form of treatment had higher rates of success:
… to encourage SET I think that the NHS should include funding of blastocyst culture (where funding is offered). We have just had our one and only funded ICSI cycle and yet still had to pay £800 for blastocyst culture. Even in non-NHS funded cycles, perhaps the NHS would consider at least funding the blastocyst culture fee and possibly also the freezing of any spare embryos.
(L232–7, online forum)
Theme 3: Views on multiple birth
Subtheme 3.1: Attitudes/beliefs towards multiple birth
In line with the data from the patient interviews (see Chapter 2), twins were seen as a positive outcome and any associated risks were viewed as acceptable. In the focus group all three women were in agreement that twins constituted a good outcome, for example:
And you know when you get to that point you just think, yeah, give me two, its fine! I’m happy with that (L326–7). So, I … yeah, that’s my opinion (L331). I think that would be absolutely great, I would be happy with that to be honest (L335–6).
(Focus group)
Participants expressed doubt that the ‘experts’ themselves were not sure about the absolute risk values:
I don’t know whether you, whether you, might just end up being a little bit cynical if you think about it like that but, you’re absolutely right, they can’t tell you, 24% is multiple births but only 2% of that 24% results in something going wrong (L619–22). If that’s the case, again, it’s not a lot is it? (L626). Is it a risk that people are worth taking? (L630).
(Focus group)
One woman referred to a recent media report where an ‘expert’ had compared the risk of multiple birth to that of undergoing repeated IVF cycles. This was met with approval from the group:
I would [have DET]. Also, I read something when, erm, there was talk of this on the news [inaudible 47:31], erm, there was a doctor and I can’t remember his name, [inaudible 47:38] he said, erm, that he thought that, erm, it should be taken … if you’re going to say, if you’re going to go and compare the risk of multiple births for people that are having IVF treatment, then you want to compare with, erm, you need to compare it with having two pregnancies because people generally do want more than one child.
(L1171–6, focus group)
Subtheme 3.2: Risk perception from multiple birth
Several participants showed awareness of the increased risks associated with multiple births, but deemed these risks as acceptable given the context. For the following woman, in private treatment, costs were also a consideration:
Last week my clinic asked me for my views on the subject and in no uncertain terms we told the clinic that we were aware and accept the risks of a multiple birth, indeed we would welcome it. The reasons are many: after waiting this long the arrival of two babies would be a double blessing; my chances of having one healthy baby are doubled; I am 33, healthy and I don’t smoke; if I wait for the NHS to start my treatment it will be at least 2 years so we need to self-fund. I am sorry but the sheer cost has to be a consideration also. At our clinic the rate of survival for twins born in the higher end of the 24–28 weeks is good, though at the lower end of this scale the chances of disability are 80%. A scary statistic but one I am willing to take.
(L421–3, online forum)
This was a particularly emotional issue for one woman who had lost one embryo following DET, but went on to have a live birth:
I’m against SET. We finally had a beautiful baby [identifier removed] when I had two embryos put back nearly 4 years ago now. Obviously one failed – and if that had been the only one we’d had then of course she wouldn’t be here now (L157–9). This is such an emotional issue. I understand all the logic involved, but sometimes you need to ‘feel’ an argument (which obviously won’t happen). But we all want to be given the best chance of success. Even with the pre-eclampsia, I would still happily have borne the risk of twins as this was my last shot at being a mummy. And if I’d had SET my beautiful baby might not even be here, and that thought is completely unimaginable (L166–9).
(Online forum)
As with the patient interviews (Chapter 2), many participants viewed twins as ‘normal’ and had experience of interacting with twins in everyday life. This further normalised twin pregnancy and birth, thus minimising the risk profile:
It’s just, sort of, like, you know, yes you might have to be monitored a bit more than … and yes your baby might be little at birth. I’m Godmother to twin boys and they are, you know, fantastic when they were born, fine, healthy, erm, she said she didn’t want to push out the second one because she got too tired! [Laughs]. But, you know, that type of thing, that’s the only risk that she had. So you see that and you see something else and, like I say, you’d turn around and say well if you get pregnant with twins you’re [voices overlap 50:32].
(L1244–9, focus group)
Theme 5: Experience of treatment
Subtheme 5.2: Emotional effects of treatment
It was clear from the patient interviews and the focus groups that the emotional effects of IVF treatment play a large role in the decision-making process. While this was a distinct subtheme, discourse surrounding the emotional issues associated with treatment pervaded most of the other themes. This is illustrated by the quote below:
It’s like, you don’t want to be here [voices overlap 1:05:49] (L1719). And you’re always going to have, I think you’re always going to have the emotional side that far outweighs the facts and figures … (L1721–2) … they need to be there and yeah, it’s good that they can give it to you, I think you’re always … just the fact that we’ve got to this stage, means you’ve had some period of wait, and some period of trying, so that says it all really doesn’t it? (L1726–8). All that time, your emotion’s built up and, you know, you’re going to have a lot of points to make! [laughing] (L1732–3).
(Focus group)
Theme 7: Reaction to the presentation of statistical modelling results
One of the main aims of this part of the study was to present the modelling results to patients in a user-friendly format, to assess the acceptability of the various treatment scenarios. The presentation (see Appendix 2) was used to convey fairly complex information from the statistical analysis. The researcher was on hand, either physically in the focus group or online, to provide added information and answer questions and queries as required. This presentation was well received by both the face-to-face and online groups. Participants were happy that their views were being sought, and were keen to have an influence on policy implementation.
Theme 7.1: Calculating the odds
The presentation of the treatment scenarios prompted participants to weigh up the probabilities of their own treatment success. There was a sense that they were attempting to work out which combination of treatment had the highest success rate. The following quote was in response to the researcher explaining that SET followed by a frozen embryo cycle had approximately equivalent outcomes to that of a DET:
Can I ask … what the basis are for them saying it’s, err, a single embryo transfer plus a frozen one is the equivalent of a double one … (L989–90) … so what about, like you said before, if you have your double embryo transferred and that doesn’t work and then you have the frozen embryo transferred then surely your chances are even higher (L1002–4) … so surely then, if in the first place you have a double embryo transferred but you’re not successful then you go on and have a frozen embryo transferred, surely the chances are higher because you can put your two back in the first place if that doesn’t succeed then you go on the frozen … (L1029–32) … if the chances are low with a single one, I don’t know, I’m not sure I’m making sense … (L1036).
(Focus group)
The following woman had contextualised the treatment scenarios in terms of how these would affect her chances of treatment success:
In terms of the success rate going down, it is such a big drop for me when I see it like that [in the presentation]. I think it is from a one in four success rate to a one in six – that is quite a drop. When you find yourself in this position, you don’t tend to think that the odds are in your favour anyway, so we definitely want to do all we can to increase those odds. We are doing so many things already on a daily basis – both of us – just for that hope that it might help, it then seems almost foolish to knock our chances by such a degree.
(L333–40, online forum)
Several participants raised the point that the presentation had not directly addressed the risks associated with IVF treatment when discussing treatment options. The following woman noted that the health risks for women having repeated IVF cycles could be compared with the risk to mothers and babies in multiple births:
Have the implications for the woman’s health been considered of having greater numbers of cycles? IVF in itself isn’t without its risks. There’s nothing in your presentation to weigh the risks of IVF against the health risks to mother and child/children (sorry if I’ve missed it) of DET. From a personal perspective (and I know this may be limited to me), four IVF cycles have not had a good effect on my overall health.
(L196–200, online forum)
An active conversation ensued surrounding the pros and cons of using frozen embryos. The researcher noted that there was a lack of knowledge and understanding of frozen embryo transfer, in terms of treatment process and relationship to success rates. The researcher then explained:
This is where, yeah, the thing about frozen embryos is, this is where the research is really changing a lot, and, like I said, there’s actually been new data come out recently to say that because the environment isn’t stimulated, frozen embryos actually do better when they’re implanted back in. But, like you say, there’s a certain amount of loss still at thawing, the thawing process.
(L1095–9, researcher)
And so that has a good success rate … (L1110) … erm, telling that to somebody who’s, you know, percentages are a bit higher, then they might opt for SET knowing that the frozen egg has a better chance of taking than putting two back in when the odds aren’t great (L1114–16).
(Focus group)
Subtheme 7.2: No change of opinion
Although the presentation was not designed to change opinions, it was of interest to see if presenting the modelling results and treatment scenarios had influenced the patients’ perspectives in any way. However, there was no evidence of this in the discussion with either the focus group or the online forum participants. However, many participants commented that the extra information was helpful, particularly in terms of treatment decisions. For some the results appeared to reinforce their original viewpoints:
I just think they seem to give you the data and it is as near to damn it as, you know, you can get …( L1549–50) … but I don’t know, I personally, seeing that, that’s great because you’ve explained it all very, very well, but I’d still have the same opinion … (L1554–5) … and I don’t know whether giving people that kind of information, it helps them, you know, they can have more, you’ve got more knowledge about it now, I suppose, but I still don’t think it will change the decision and how do you make sure they do [laughing] (L1559–62). I’ve looked for more information and I’m assuming that we’ll get it tonight so my initial thoughts were before we came here definitely, you know, given [coughing] [inaudible 1:01:04] … (L1564–6) … but I thought maybe I’ll go and see them tonight but all I feel now is that I’ll still go for double but I’m making an even more informed decision than I was before … (L1570–2).
(Focus group)
For this woman the sheer burden of treatment cancelled out any of the proposed benefits associated with the multiple cycle treatment option:
Although the presentation talks about offering an additional cycle to couples, the stress of having a cycle shouldn’t be underestimated. Personally, I would rather have DET than another cycle (L201–3). From my perspective there is nothing in your presentation that would make me change my mind about multiple embryo transfers (L412–3).
(Online forum)
Subtheme 7.3: What happens next?
A few participants expressed concern about when the SET policy would be implemented in their immediate clinical setting, as they were concerned about how this would affect their treatment:
Can it be made public [the guidelines for the local hospital]? (L1824) … this hospital, say, for instance, and they put down to us, the guidelines that they’re going to try and enforce … we should be able to ask, we should be able to know, shouldn’t we, what their intentions are? (L1834–5).
(Focus group)
The participants in both groups said it was important to listen to the patient perspective and valued the opportunity to express their opinions. However, one woman questioned whether the ‘experts’, governing bodies and policy-makers would actually listen to the patient ‘voice’:
I just wondered whether, you know, whether or not they do actually read the stuff (L1781) … just think, I mean, in some ways I’m going to say it sounds like, you know, you will go back to them and say, look, you know, it’s probably not such a good idea, I’ve got all this stuff, they might just say, oh we don’t want to listen to what they’ve got to say, I mean … (L1796–8)
(Focus group)
Discussion
The aim of this patient consultation study was to access patients’ views on the results of the statistical modelling element of the main study, gauge reactions to the proposed policy change towards SET, and explore treatment options. Consistent with the findings from the interview study (Chapter 2), the majority of participants from both the face-to-face focus groups and the online forum showed a preference for DET. The reasons for this preference were broadly in line with the patient interviews. Participants felt that SET would lower their chances of success and could potentially expose them to more prolonged treatment. Twins were seen as a positive and not a negative outcome of treatment. The emotional, physical and, in some cases, financial burden of the IVF treatment journey was highly prevalent in both groups. These findings are in line with the wider research literature (e.g. Porter and Bhattacharya,25 Blennborn et al. , 21 Glazebrook et al. 111).
This study has shown that patients undergoing IVF treatment are amenable to voicing their views and opinions in an open forum (either focus group or online forum). The participants welcomed the opportunity to comment on policy initiatives. Furthermore, participants liked the presentation and, on the whole, understood the content. They were able to digest quite complex statistical information in a relatively short space of time. They also found it useful to have the researcher on hand to answer any queries or concerns. Although the presentation was not designed to change views and opinions, the researcher did ask all participants whether the extra information regarding SET had any effect. The majority of those taking part indicated that the presentation and question and answer session with the researcher had reinforced their original views; however, they felt that they would now be able to make more informed choices. In contrast to the interviews, a few participants displayed more favourable opinions towards SET in the light of the new information they had received. This raises the possibility that future group sessions could be designed that were more targeted to the specific concerns raised by participants, and delivered in a format that acknowledged individual views, attitudes and beliefs.
During the presentation, a range of treatment scenarios was presented. The scenario that provoked the most discussion was related to multiple cycles of treatment. Data were presented to show that the slightly reduced success of SET compared with DET could be mitigated by certain treatment options, for example further full treatment cycles, SET with an additional frozen embryo cycle, and the use of extended embryo culture (blastocyst transfer). Most participants were resistant to the idea of compensatory cycles as this incurred further treatment. Many felt that the researcher had failed to address the enormous burden of treatment associated with additional IVF cycles. The researcher tried several modes of delivery of this information during the focus group and attempted to further explain that SET was preferable to a twin pregnancy in terms of risk reduction for birth mother and baby. However, participants reiterated that the psychological and physical effects of IVF treatment were extremely high and posed a significant barrier to the acceptance of SET. Many commented on the general lack of resources (e.g. funding issues, number of cycles funded by the PCT, etc.) for assisted conception, which further influenced the decision to have two embryos transferred in an attempt to maximise their chances of success. This is in contrast to Twisk et al. ,28 who found that additional IVF cycles were acceptable, if the pregnancy rates were not significantly reduced. However, unlike the present study, the various treatment scenarios were adjusted to show varying success rates. 28 When the success rates were equivocal between SET and DET, about half of the women interviewed would accept SET. As the pregnancy rates of subsequent scenarios began to decline, the preference towards DET began to increase. The modelling data produced in this study are more in line with outcomes one would expect in an everyday clinical situation. As such, it is important that clinicians are aware of how patients might respond to this data.
As with the interview study, group participants in this consultation exercise minimised the risk of twin pregnancy and birth. It is known that people tend to downplay the associated risks across a range of events, and often provide an inaccurate judgement of personal risk. 108 In this study participants talked frequently about improving their odds in any given treatment scenario. When represented with ‘real’ data they attempted to recalculate this data to suit their own case scenario. Not only did they downplay their personal risk profile regarding twins, they also compared that risk to the risk of repeated treatment cycles to the woman’s psychological and physical health status. Thus, there was a ‘trade-off’ between twin pregnancy and multiple cycles, with the former being viewed as the more positive outcome. This way of cognitively appraising their own personal situation provided one of the rationales for opting for DET.
There was limited knowledge and understanding regarding the use of frozen embryos. This was particularly noticeable in the focus group. When the researcher explained more about frozen embryo cycles, participants appeared more amenable to that option. However, there were concerns about the effects of the thawing process on embryos and how many would survive the process. Opposition to the use of frozen embryos per se appeared to be less than in the interview sample; within the group consultation the main focus was on the need to reduce multiple cycles. There is a need to greatly improve knowledge and understanding regarding the use of frozen embryos, as SET plus a frozen cycle is comparable in success rates to DET. If patients are to be encouraged in the uptake of SET to reduce multiple pregnancies and births, a more comprehensive understanding of frozen embryo transfer may help make SET plus frozen embryo transfer a more attractive option.
This part of the study has several limitations. The findings are based on a small convenience sample, accessed from a single NHS clinic and an online patient organisation. The sample is not representative, and, as such, the findings should be interpreted with caution. Focus group methodology was chosen to enable the researcher to feed back the results of statistical modelling via a presentation. This would have been difficult to achieve in face-to-face interviews.
Recruitment issues in the NHS and private clinics led the research team to develop the online groups with Infertility Network UK. The use of a different patient population was very informative and provided useful validation data for the previous in-depth interviews. It is possible that those who viewed the responses to the online presentation and information did not have anything further to add. Another method the team did consider using, in partnership with Infertility Network UK, was an online ‘live’ forum, in which the researcher could present the material then answer questions and concerns in a given time frame. Unfortunately, time restraints prevented the uptake of this strategy. This might have yielded a higher number of postings, and it is something that should be considered for future studies. Furthermore, the full characteristics of the sample could not be ascertained. However, it does add to other arenas where patient views on SET policy have been encouraged, such as the HFEA and patient organisations which represent patients who are subfertile (e.g. Infertility Network UK). There is a need to quantify the extent of the attitudes revealed in this consultation in a carefully designed patient survey.
In conclusion, this focused consultation exercise has given participants the opportunity to comment on SET policy as it evolves. UK clinics are now charged with the responsibility of reducing their twin rates in order to meet HFEA targets. In order to achieve these targets, clinics need to be able to persuade their patients that SET is an acceptable treatment option. To do this clinicians need to be aware of patients’ views and beliefs so that they can work with patients collaboratively when they are making treatment choices. Participants in this study emphasised the need for researchers, clinicians and policy-makers to take into account the enormous emotional, physical and, often, financial burden of IVF treatment. This must be acknowledged if negative views and opinions about SET are to be challenged and modified. This study showed that a single presentation was able to raise awareness about key issues, even though core opinions remained unchanged. The findings indicate that patients are more than able to deal with complex information, as long as it is delivered in the right way, with an opportunity to ask questions and raise concerns. In future, more targeted educational interventions could be designed to increase patient knowledge, or work with their existing knowledge base. Patients need to be reassured that the move towards a SET policy is for both their and their babies’ benefit, and not driven by external factors such as resource rationing or financial considerations.
Summary
The focus group data suggest that: despite the potential to maintain overall success rates over a complete cycle with SET, patients would prefer DET; the potential for twins is seen as positive; and additional transfer procedures are emotionally, physically and financially draining.
Chapter 7 Issues in the use of routine clinical data for modelling studies
Introduction
The collation and analysis of the two datasets in Chapters 3 and 4 raise a number of issues relating to the use of routine clinical data for investigation of prognostic factors, the development of predictive models and for the use of such data to monitor and audit clinic performance. The issues encountered are collated here along with discussion of some potential implications for future work. This project utilised data from three different database systems: the HFEA provided data from their UK national registry, three centres used the acusys system (developed at the Lister Hospital, London) and two used the ideas database application. 128 Other centres outside this project use different recording systems, commercial or bespoke, and some of the centres involved in this project have changed systems since providing data to the project. The observations here reflect the use of the database systems in practice in the centres studied at that time. We have not studied the specification or design capability of the systems or what may be achievable with optimal use.
We identified three main sets of issues: first, issues around standardisation between data from different sources; second, issues around data quality; and, third, and most importantly, some fundamental issues around the way databases are structured. These sets of issues are discussed in each of the sections below, and followed by a more general discussion of data issues.
Data standardisation
In attempting to analyse data from several sources we observed that there are ambiguities in definition, design or implementation that make use of current databases difficult and which in the future will hamper the use of clinical data for monitoring of practice.
Attempt number
In vitro fertilisation treatment attempt number is often considered an important prognostic indicator. For the analyses in this project we adopted the HFEA definition ‘treatment cycle at clinic – as calculated’. This incorporates all fresh and frozen cycles available to the HFEA for that patient. Another variable provided in the HFEA dataset was ‘total number of previous IVF treatments’. Although missing in many cases, this did not change across cycles for a given patient (see Chapter 3, Data extraction and cleaning) and bore little correlation with the calculated value for treatment cycle used in the analysis. This example demonstrates the importance of clarity and strict definition of variables in this type of study. This is further demonstrated by the fact that the definition of attempt number was different again in the clinical databases. The acusys database system counts fresh and frozen cycles separately. Hence, a patient with three fresh and two subsequent frozen cycles would have attempt numbers of 1, 2, 3, 4, 5 in the HFEA database and 1, 2, 3, 1, 2 according to the acusys definition.
In the HFEA database, treatment attempt number is calculated based on cycles that are registered with the HFEA. In contrast, clinic databases rely on patient history-taking, and treatments in other clinics may not be fully ascertained or recorded. In some cases it is the number of attempts at the same clinic that is recorded. Increasingly couples are having IVF treatment in other countries, and clinics are treating patients resident abroad, but cycles outside the UK are not captured by the HFEA. Patients presenting for treatment in the UK may not disclose full details of treatments received elsewhere, particularly given the restricted access to treatment in the NHS.
In the data analysed here there are relatively few frozen transfers and most transfers are DET. Therefore, there is little difference between attempt numbers based on registered cycles, egg collections or embryo transfers. In an environment with increased use of eSET and cryopreservation, couples might have very different numbers of egg collections and transfers and not all transfers would be equivalent (SET or DET, fresh or frozen). In order to understand the role (if any) of previous treatment as a prognostic factor it will be necessary to treat separately the various previous treatments and a much richer ascertainment and recording of treatment history will be required. Multiple definitions of previous attempts may well be needed (egg collection, fresh transfers, frozen transfers – total or within this attempt to produce a child, etc.).
Embryo assessments
The clinic databases all record a morphological assessment of all embryos that are transferred. Grading systems differ between centres and there is a clear need for a unified, quality-assessed scoring system to allow intercentre collation of data. 11 In the present dataset, with nominally equivalent grading schemes across the centres (see Chapter 4, Data extraction and cleaning), it was necessary to normalise the grades between centres. This process is non-trivial and inexact, requiring rather strong assumptions.
The increased use of eSET and the need to optimise such treatment policies increases the need for good embryo quality assessment, and good recording of such data. Use of a common and quality-controlled grading system should be strongly encouraged,11 but assessment of additional measures of quality should also be supported. Selection policies for eSET are likely to depend on an assessment of the quality of embryos available. 11 Therefore, in order to assess and audit eSET policies it will be necessary to consider embryo quality for both transferred and non-transferred embryos. The HFEA database does not include any data on embryo quality, an omission that considerably weakens its utility for research purposes and in the future for realistic assessment of centres’ performance.
Further, some proposed schemes rely on extended embryo culture and multiple assessments of embryo quality. Current databases do not allow for multiple assessments of embryo grade. Ideally, each embryo should be identifiable and its grade history obtainable, but this may be impractical given laboratory practice and the burden of data entry.
Prognostic factors
Given the increasing diversity of treatments, it is likely that some form of prognosis-adjusted comparison between centres will be needed in order to compare outcomes and evaluate treatments. Thus, there is a need to record accurately these known prognostic factors, with uniform definitions and quality control checks. This requirement is common in other fields of medicine and the principles are well established. 129
Levels of hormones such as FSH and anti-müllerian hormone are now being shown to be useful predictors of treatment outcome. 2,60,113 With the explosion of ‘omic’ technologies it is likely that a large number of potential markers will become available, and flexibility in database design will be needed to rapidly accommodate new markers as they become available, allowing first their evaluation and potentially their use in monitoring outcomes.
Single-centre studies of putative prognostic markers are relatively straightforward to undertake, requiring simple linkage of prognostic data to existing databases, or even manual extraction from paper records. However, such studies have limited statistical power and multicentre studies are usually required. This applies particularly to studies around strategies for reducing multiple births, in which the number of multiple birth events in any centre is too low to draw any statistically reliable conclusions. Multicentre studies are difficult, requiring collation of data from different database structures with different variable definitions, and more consistency would assist such studies.
Lifestyle variables
As part of standard history-taking and patient advice, most clinics ask couples about their lifestyle, in particular smoking and alcohol consumption. Increasingly, treatment is refused to couples who are, for example, unwilling to give up smoking or lose weight. Although the clinical databases have fields for limited recording of lifestyle data, these fields are not consistently utilised. In any case such self-reported data are unlikely to be reliable. Other studies in more favourable circumstances have found significant under-reporting. 130 Here, where treatment availability may depend (actually or in the couple’s perception) on what is revealed, it is even less likely to provide good data. In this case it is unlikely that routine clinical data will provide a useful research tool, and any such data collection can only serve immediate clinical purposes. Any studies of the effects of lifestyle parameters will require dedicated data collection, probably backed up by biochemical assessments. 130
Data quality issues
Data accuracy
In assembling the data for analysis we found many inconsistencies between data recorded in different fields. Examples from the HFEA database include:
-
number of previous births greater than previous pregnancies
-
number of embryos created greater than number of eggs
-
fewer embryos created than transferred
-
more embryos thawed and viable than thawed (for frozen cycles).
Many of these errors could have easily been detected at the time of entry by applying simple consistency checks. Simple range checks also showed values that were at least implausible, if not impossible. Examples include:
-
duration of infertility several hundred years
-
date of transfer prior to date of egg collection.
Beyond simple within-record checks, data quality could simply be improved by cross-checks of data against previous treatments of the same couple, implemented on data entry so that inconsistent data is not entered.
We note that the HFEA database for the period concerned was based on re-entry of paper-based returns. Nineteen per cent of the cycles in that database were excluded as containing some missing or invalid data (see Chapter 3, Data extraction and cleaning), and presumably there were also errors that were not detected as the values were plausible. This level of data error is not unexpected with manually entered data (particularly here where the data have been manually entered twice) where there are no validity checks or verification. The HFEA has now introduced electronic data interchange, eliminating manual re-entry, so, in principal at least, the accuracy should improve. However, if the clinic databases do not include these simple, but important, checks the data will remain inaccurate.
The HFEA policy requirement that clinics meet targets for twin rates will mean that clinics require more accurate and timely data. Monitoring and audit of policies and protocols will require accurate clinical, embryological and outcome data. Traditionally the entering of data on to electronic databases has had low priority, and this is reflected in the quality of the data. The entered data are seen as having little value to the individuals and organisations responsible for data entry; the data quality is sufficient for their needs in clinical management and administrative returns to regulators.
One approach that would improve data quality would be a move to make the electronic record the primary source. Using fully electronic records has significant benefits in terms of the availability of records across multiple locations. Such systems could, in principle at least, be linked to quality control and safety monitoring procedures within the embryology laboratories. However, such a system requires a high-quality and robust computer and network infrastructure, which cannot be assumed to be available.
The HFEA could encourage better data-keeping by making it part of their regulation and inspection criteria.
Handling of missing data
We have encountered many instances in which there was no clear distinction made between zero and missing values. In the case of the HFEA data, in a number of places it could not be determined whether a recording of NULL truly indicated a zero or that a value was not recorded. As an example, the original HFEA dataset (as provided to this project) the variable containing the number of previous pregnancies had 145,969 NULL values and only 1207 zeros, with 85,834 values > 0. Clearly we have to assume that the vast majority of the cases recorded as NULL to be zero. But this is a strong assumption that would not be required if data were recorded more accurately.
Conversely, for several variables from the treatment centre databases it was not clear whether the presence of a zero was a genuine observation or an indication of a missing value (for example, recording of lifestyle indicators such as smoking and alcohol consumption), making the use of such variables impossible. In other cases of variables with values recorded as zero a judgement had to be made as to the correct interpretation (following advice from the data providers). For example, in the case of sperm counts a set of values can be inferred as missing if all the related entries are zero, but individual zero counts can be assumed to be genuinely zero.
In general, the reasons for data being missing are not recorded and clinical databases do not provide fields where the reason for missing values can be documented.
Issues arising from data structures
Databases developed for clinical or regulatory purposes are not always structured in ways that allow the data needed for research questions to be extracted.
Record linkage
In the HFEA and ideas databases it proved impossible to identify for a frozen transfer cycle the cycle in which the eggs were collected. Such linkage is required, for example, to look at cumulative pregnancy rates and for accurate modelling of the inter cycle correlations and therefore the outcomes of multi cycle protocols. This is a critical weakness if SET policies catalyse a move towards some form of cumulative outcome rate as a primary outcome measure. This weakness reflects a fundamental weakness in database design and/or usage.
The current use of ‘cycle’ is ambiguous and not a good basis for data storage. Embryo transfer cycles are naturally nested within egg collection cycles (although there can be exceptions if frozen embryos from more than one cycle are transferred together), and multiple cycles of both types will be associated with an attempt to have a child. With greater diversity of treatments and approaches a more flexible approach is likely to be needed. One possibility would be that data be stored on the basis of procedures and their direct outcomes. Data would then be held for parents, donors and the resultant embryos. Each procedure should be identified by separate male and female donors and the procedures that provided material (e.g. embryo transfer should link to the egg collection procedure, donor eggs to the egg retrieval procedure, embryos to their egg and sperm collection, etc.). Freezing and thawing would be separate procedures.
As discussed above there are problems with the definition of previous attempt number. This is symptomatic of a lack of linkage in the databases between multiple treatments for the same patients. Good database design would make the computation of any number of such variables trivial, although there would always be an issue with treatments outside the authority of the recording centre.
Outcomes
Outcomes proved difficult to extract from current databases, often requiring parsing of free text fields. For instance, a live birth was defined for the analyses presented here from the HFEA dataset using text fields for the status of up to four ‘heart birth’ outcomes. While the acusys systems have a specific (albeit rather complex) code for outcome, sites using ideas had to have outcome extracted from text fields. The treatment centre database designs seen in this study have a single outcome variable, when in reality outcome is multidimensional. The HFEA database has records on total fetal sacs as well as gestation, birth outcome, weight, sex, delivery date, delivery method and congenital abnormalities for up to four babies. Explicit coding of relevant variables (where an individual value represents an outcome rather than a free text field) would make usage simpler. Of relevance to the eSET question is the recording of twin births, and, in particular, zygosity. This is not explicitly or systematically recorded in any of the databases we have utilised, although some information may be available in textual form.
It is unlikely that in the future with a greater variety of treatments that a single outcome measure will be appropriate. Although arguments can be made for a cumulative per-egg collection outcome (maybe number of live births within 18 or 24 months of egg collection), multiple outcomes will be needed to gain a rounded picture of a clinic’s performance. Thus, data will need be collected and stored in a way that allows easy collation of multiple outcomes, each of which in turn may be multidimensional.
Patient histories
Clinical databases are oriented towards the present condition of the patient. As such they may not retain details of the status at previous times. The acusys database records patient history as a single table which is updated at each clinical presentation. For any analysis of historic data, it is the patient status at the time of treatment that is required. As detailed in Chapter 4 (Data extraction and cleaning), for the purposes of the analyses in the towardSET? study, we have had to ‘unwind’ the patient history for variables such as primary/secondary infertility, previous pregnancies, duration of infertility and attempt numbers, taking the latest cycle and subtracting appropriately for each previous cycle in turn – a potentially error-prone process and one that is reliant on an assumption that there is complete information on all cycles within the databases. In the HFEA database, rather that having to ‘unwind’ the patient’s history it was necessary to update variables that changed between cycles for a given patient, the assumption here being that the observed value of variables is correct for the first cycle observed and all intermediate cycles are in the database.
For audit and analysis complete and concurrent patient history thus needs to be stored with each procedure, allowing analysis of the patient state at the time of the procedure. Historically, there was a need to economise on data storage requirements, making such designs appropriate. Data storage requirements are no longer a practical limitation and the need for proper audit trails and clinical monitoring to optimise treatments suggests that this is no longer an appropriate way to structure data.
Novel treatments
The move towards eSET is driving innovation in IVF treatments with developments in, for example, embryo selection by non-invasive measurement35 or extended culture,39 alternative stimulation regimens and enhanced cryopreservation. 122 Current clinical databases are built around a conventional IVF cycle, and the HFEA database is also very limited in its ability to store treatment variables. Embryo selection techniques need at least to be recorded, and any assessment of their utility will require significant extension of existing databases, or linkage to additional datasets.
Discussion
The HFEA twin policy increases the onus on individual centres to monitor their outcomes and justify their SET policy. Good recording of clinical parameters, including patient characteristics and embryo grades, is essential to this effort. It is the data at the time of treatment decision that are required, not present or initial values. The needs for such monitoring needs to be factored in to the database design, and robust systems of data entry and checking will be required. The availability of good-quality data will become a vital part of treatment quality improvement and regulatory control.
Individual clinic databases vary in the quality of the database design and its implementation and in the quality of data entry. There is an urgent need to define minimum standards for clinic databases to enable quality control and audit of clinics’ performance. As outlined above, basic data linkage and checking are not properly implemented, and personal communications with users of other packages suggests that this problem is not restricted to the systems investigated here. There may be a role for the HFEA or the professional bodies either to facilitate a set of guidelines for database designers or to commission the production of a database that would meet the needs of clinics, the regulatory authorities and research. The UK transplant service has a similar role to the HFEA and has developed robust systems for handling the data structures with multiple donors, multiple recipients and multiple treatments, along with the statistical infrastructure to utilise these data effectively. This service may provide a useful source of experience and a model that can be followed.
The HFEA register is potentially a useful source of data for research purposes, but the large amount of data requested at present is burdensome to clinics and the resulting data quality is low. For regulatory purposes some prognostic information is required to assess a clinic’s performance and, now, to monitor its twin reduction policies. Changes in database structure to allow more appropriate outcome measures to be constructed is necessary, linkage between egg recovery and transfer as well as between treatments on the same individuals and donors is essential. Researchers would like to have access to a wide range of established and potential markers, but it is questionable whether this is appropriate for a regulatory authority to collect, given the burden on clinics. In any case, a small set of reliable and well-linked data is more useful for both regulatory and research purposes than a larger set of unreliable data. It is probably inappropriate for the HFEA to request data beyond that needed for regulatory purposes, but these purposes do require the collection of prognostic measures. Prognostic measures requested by regulators should probably be restricted to those which are routinely available and for which there is a good evidence base, with the flexibility in the system and databases to allow these to be modified as more evidence accumulates.
Research into other factors will probably have to utilise individual clinic databases, which need to be of better quality. Multicentre studies will be necessary and greater standardisation with consistent data structures and good quality control will greatly facilitate such research. The HFEA database imposes a common, if limited, dataset. One possibility for the HFEA to consider would be to facilitate optional additional data collation for consortia of centres interested in particular prognostic markers, either through enhanced returns or through the encouragement of better database design as discussed above.
Although current clinical databases may be fit for the purpose of assisting treatment delivery and administrative returns, they are unlikely to remain adequate even for their existing uses in an environment where more complex outcome measures are required for a wider range of treatments. The need to audit and monitor and develop twin policies suggests that there is an urgent need to develop more appropriately structured database systems. This requirement is more crucial for the HFEA where the need to monitor clinic performance and twin policies will require good-quality data with a good set of ‘case mix’ variables and the ability to link treatment programmes together to enable a range of outcome measures. The current database does not meet these needs. The HFEA has improved its data collection, especially through the introduction of electronic data interchange and has recently undertaken consultations on the use of its data registry and on data reporting, although the policy outcomes are not yet finalised.
Summary
In attempting to analyse data from several sources we have observed that there are ambiguities in definition, design or implementation which make the use of current databases difficult and which in the future will hamper the use of clinical data for monitoring of practice. Particularly difficult is the definition and recording of previous treatment history and the use of multiple embryo-grading schemes without any standardisation. There are significant issues with the quality of the data recording, much of which could easily be improved by better database design, including appropriate cross-validation, and rigorous handling of missing data, but also reflects the low priority given to data recording for non-clinical purposes. There are major shortcomings in the ability to link together treatment histories, so making it difficult to consider more relevant outcomes of complete treatment cycles (linking frozen cycles to the fresh cycle in which the embryos were created) or cumulative outcomes over a single attempt to produce a baby.
Chapter 8 Conclusions and implications for practice
General discussion
The benefits of a mixed-methods approach
We adopted a multidisciplinary approach, combining state-of-the-art statistical modelling with in-depth qualitative exploration of patient perspectives. The components were integrated formally through input from patients into the scenarios considered for modelling and feedback of the modelling results to patient groups, and informally through cross-disciplinary discussions within the research team. The work with patients is fundamental to the analysis and interpretation presented throughout this report. The experience of the study team was that this mixed approach was very fruitful in this particular project, possibly owing to the complex interactions between treatment choices and patient wishes and perceptions that are central to the research questions. Although we had valuable input from patient representatives it was, in this case, the direct involvement with patients mediated through a qualitative researcher that provided the insight and grounding that the study required. It was particularly valuable that the qualitative and quantitative studies were taking place in parallel with regular feedback across the research team, allowing the quantitative understanding and issues raised to feed directly into the qualitative interview and focus group schedules, and conversely for questions and issues raised in these in-depth discussions to inform the thinking of the quantitative researchers. This followed the complementarity approach of Teddlie and Tashakkori:131 the data from each method were analysed separately but the inferences from each were integrated to inform the final report. This complementarity type of mixed method study is defined as when at least two phases (qualitative then quantitative or vice versa) are carried out chronologically and each phase complements the other. 131 According to O’Cathain et al. 132 the yield from a mixed-methods study has two key indicators: first, that the potential for the integration between the quantitative and qualitative components of the study have been fully exploited, and, second, that the results of this integration are reported. The experience from this project would suggest that it is the composition, integration and dynamics of the research team that leads to a successful implementation of a mixed-methods approach such as we have adopted here.
Predictors of IVF success and twin rates
The analysis of the HFEA data and the towardSET? collaborative data both show that similar factors are predictive of outcome, factors that are consistent with other studies. There are significant data structure and accuracy problems with both sets of data. The lack of full linkage of treatment courses restricts the modelling of multiple transfers and restricts much of the analysis to embryo transfer end points rather than complete treatment course end points. Data errors may lead to the attenuation of real effects. The strong patient selection effects in the observational data, with treatment being dependent on prognosis (often in unrecorded ways), means that these effects need to be interpreted cautiously.
Other than the availability of good-quality embryos, we have been unable to identify any factors that specifically predict twin birth, and patients who have a good probability of success will have a high chance of twins if they receive two embryos. Thus, twins are produced predominantly from patients and cycles with a good prognosis, although even 40-year-old patients have a 10% twin rate (twins per LBE) for fresh DET.
One novel feature of the analysis and dataset is that we have been able to identify a number of patient and treatment characteristics as acting specifically on the embryo viability or uterine receptivity. Age seems to act predominantly as an embryo effect. Embryo number, attempt, duration of infertility and tubal diagnoses act through the uterine factors. Treatment year and centre seem to act on both components. While it is possible that this identification is model dependent or a consequence of data biases, the assignments do make clinical sense and suggest reasonable biological mechanisms.
Patient views on twins and eSET
The patient interviews and focus group consultation showed that patients undergoing IVF treatment have a preference for twins, confirming earlier reports in the literature. This is perhaps not surprising given the reported physical, emotional, and, often, financial burden associated with treatment. Twins were seen as an ideal outcome, in which the need for prolonged treatment is negated. Several participants in this study found it difficult to understand the rationale for SET, as they believed that this option would lower their chances of achieving a pregnancy and live birth. Thus, participants were sceptical about the motives behind the move towards SET and attributed this to the need for the government and regulatory bodies to control NHS funding and resources. Interestingly, many did not see this as being promoted directly by their doctors and individual clinics. Several participants felt that the introduction of a SET policy was an affront to their own personal choice, and that this policy does not sit well with the NHS Patient Choice agenda. The use of frozen embryos produced a mixed response, with participants showing limited knowledge of this treatment choice. They also expressed concerns about the ownership of embryos and the emotional attachment that an embryo can evoke. More education is required to help patients to fully understand options involving embryo freezing. If patients are to accept SET, their views and beliefs need to be incorporated into clinical consultations and they need to be reassured that this will provide the best outcome for them and their babies, and is not driven by other external factors. For those who self-fund, the rationale for SET is even less appealing as each cycle comes at a cost.
Implications for practice
Developing an eSET policy
eSET in fresh cycles
The available data only allow predictive models to be developed for the outcomes of individual embryo transfer procedures. As the frozen transfer data is of limited quality and completeness, we can only develop models with any reliability for the initial fresh cycle following egg retrieval. While it is common clinical practice to quote and compare such outcomes, these may not be the most relevant outcomes for the comparison of SET and DET treatments, which need to take a whole treatment perspective. Nevertheless, such outcomes are of importance to the patients (see Chapter 2) and form a basis from which outcomes of complete treatment programmes may be simulated.
The EU models provide a statistical model for assessing prognostic factors but also allow the ‘what if’ computation of potential outcomes for different numbers of transferred embryos. The models then predict that in this initial fresh transfer there will be a significant reduction in live births if patients receive SET rather than DET. If SET is applied to the whole patient population for whom DET is potentially possible, then the overall success rate in that fresh transfer would be reduced by around one-third, a result that is consistent with the limited data from clinical trials. It is important to appreciate that for every patient in every transfer their chances of a successful treatment are reduced by having SET rather than DET. This is an obvious statement, with intuitive appeal, given that the second embryo must have some chance of developing. Equally, it is intuitively obvious that in any one transfer a patient may or may not be in optimal condition to receive an embryo in any particular transfer cycle, and therefore spreading the embryos over a larger number of transfers could well be advantageous, providing of course that the losses due to freezing are sufficiently small.
The analysis suggests that the relative loss of around one-third in LBEs for this fresh cycle as a result of SET is similar across all patient groups, with only weak dependence on patient characteristics, although the absolute loss is greater in patients with a good prognosis.
There are three approaches to ameliorating or compensating for this loss, which are discussed in the following subsections.
Patient selection in the fresh cycle
Considerable emphasis has been placed in the SET literature over selection of the appropriate patients for eSET. Much of this literature places undue emphasis on the initial fresh transfer, rather than taking a complete treatment perspective, and careful interpretation is needed to put such schemes into their full perspective.
Computations based on the EU model show that, at a population level, in the fresh cycle about half the loss in success owing to SET can be mitigated by selecting appropriate patients for DET. Although there are small differences between them, most suggested strategies selecting older patients and those with few good-quality embryos for DET perform similarly, with around 50% SET being needed to achieve a 10% twin rate. Although the detailed results provide indicators as to appropriate policies, it is likely that the detailed algorithms will be treatment and centre specific, and an iterative development of centre policies will be required, which could be based on those developed in this project. Selection for DET by age is perceived by some patients as unfair (see Chapter 2): a strategy of SET if there are embryos available for freezing and therefore another attempt, and DET if there can be only a single cycle, may be more attractive. However, additional treatment cycles are burdensome, and the work with patients suggests that they are reluctant to accept additional cycles and would still prefer DET. Such a policy also requires that the decision over the number to transfer occurs late in the treatment process, usually on the day of embryo transfer and with little time for consideration, which can be difficult for the patient unless standardised protocols are used and agreed beforehand. Also such policies rely heavily on standardised embryo-grading schemes to ensure generalisability of policy across all clinics.
It should be stressed that, although from this limited single fresh cycle perspective, patient selection may allow clinics to meet twin rate targets, each individual patient would have a greater chance of a successful outcome in that fresh cycle if she had DET rather than SET.
Complete cycle treatments
The available datasets do not provide good-quality data to allow direct prediction of outcomes beyond the initial fresh cycle. However, they do provide reasonable estimates of that fresh cycle outcome and allow estimation of the intercycle correlations. The limited frozen data indicate that it is not unreasonable to assume that the fresh cycle outcome estimates can be applied to frozen cycles with a simple adjustment for an overall lower success rate. Under these assumptions, and utilising data from another study to estimate the distribution of embryo quality, we have been able to undertake simulations of treatment courses. The caveats and uncertainties mean that these should be treated as indicative rather than definitive.
Two fresh SET cycles outperformed a single DET cycle in terms of outcomes, although the burden on patients of two egg retrievals and embryo replacements should not be underestimated. Similarly, providing that the cryopreservation is of sufficiently high quality, a treatment programme of one fresh plus one frozen SET transfer had similar outcomes to a single fresh DET transfer. These results are in line with the observational and limited trial data. Although the data do not provide any strong evidence on what is achievable in terms of freezing quality, the break-even point is around the levels found in the best of the centres studied here, although there are large uncertainties in the data underlying the estimates of freezing loss. There have also been advances in techniques and practice since the time of the data analysed here so there is reason to believe that the necessary freezing quality is achievable, although careful evaluation will be required.
Taking a ‘complete cycle’ perspective, the simulations indicate that, if all the embryos created from an ovarian stimulation procedure are transferred in a series of embryo transfers, then transferring the embryos one at a time can have similar, or even better, success rates to transferring them two at a time, although this does require good freezing procedures. Interestingly, in these simulations this remained true for patients with poor as well as good prognosis. Although this result may be sensitive to the assumptions around the distributions of embryo quality, it does suggest that, if one takes a complete cycle perspective, SET can be advocated for everyone, and the issues over patient selection become redundant. Indeed, in some scenarios patient selection can actually reduce the overall success rate over a complete cycle compared with SET for all. In this light the trade-off between DET and SET becomes a balance between the number of twin births and the number of transfers it takes to get pregnant, not overall success. The burden on patients of additional transfers is not trivial and patients will still need persuading, despite the maintenance of success rates.
Maintaining a complete cycle success rate will require good freezing procedures, somewhat better than that seen in the best centre over the study period. Technical developments in the period since the cohort analysed here make this seem achievable. For SET, the willingness to thaw single embryos may be crucial to the maintenance of success rates. Such a policy implies a number of cancelled transfers, another burden on patients that should not be ignored. Although thawing more than one embryo is suboptimal in terms of success rates this will need to be balanced against the costs (emotional and financial) of cancelled cycles. There is little to be gained from freezing poor-quality embryos, unless they can be stored separately and retained for final attempts after the good-quality embryos have been used. However, in these circumstances the low chances of success would probably indicate a new egg retrieval, as the low success probabilities mean that such treatments are burdensome to patients.
Embryo selection
If we focus on the initial fresh cycle, then there is considerable scope for improving the success rates for SET by optimal selection of embryos, perhaps using biomarkers35 or by extended culture. 39 If we take a complete cycle perspective, with cumulative pregnancy outcomes, then selection will at best only improve the time to achieve pregnancy as all embryos will be transferred later (although knowledge of the potential of all the embryos will enable optimisation across multiple egg retrievals). If the assessment of embryo quality carries a non-zero embryo mortality rate, as in extended culture or pre-implantation genetic screening, then these methods may well improve the initial transfer success at the expense of later (frozen) transfers and lead to a lower overall success rate.
Such methods may well be useful, but reliable data do not exist. There is a need for rigorous evaluation of such techniques in a realistic clinical setting that takes into account the whole patient treatment course until a live birth is achieved or the patient ceases to try for a baby. Some insights could be gained from simulations, such as performed in this work, although it may be difficult to get good estimates of the parameters required.
Data collection and auditing
As discussed in some detail in Chapter 7, there are significant shortcomings in the existing data sources, both as a research tool and for use in the audit and monitoring of twin reduction policies. Databases need to be capable of linking treatments across patient treatment programmes and producing a variety of appropriate outcomes beyond the often misleading per-transfer outcomes. There is a need to record embryo quality, preferably using a quality-assured methodology. The HFEA is reviewing its registry data and the way in which it reports outcomes. Clinics need to look at their future information needs and develop appropriate data storage systems to enable reliable treatment monitoring. Crucially, in our view, data entry and quality need to be given a higher priority in IVF clinics.
Patient information needs
For many well-informed patients, the ideal outcome of an IVF treatment remains twins. For some this is because of incomplete information on the risks, but well-informed and rational patients also accede to this view, balancing the risks of twins against the emotional and financial costs of failed treatments. While better information on twin risks may help some to accept SET, many will not be convinced. It is important that accurate and relevant information about twin risks is available. Many of the figures quoted refer to all twins – including monozygotic twins, which are at a much higher risk, and non-IVF twins, which include a broader population. Patients need information on the risks specific to IVF twins and their parents, information that is difficult to obtain at present in a UK setting as information on the mechanism of conception is not available to obstetric services. It needs to be accepted that, for any individual couple, the desire for twins may result from a rational assessment of their personal risks, needs and values. Although the need to reduce twins may be valid from a societal and public health perspective, this may well conflict with the unconstrained choices of individual women.
The patient interviews and focus groups revealed significant scepticism over the motivation for a twin reduction policy, with many patients believing that it is in some way financially rather than clinically driven. This may be inevitable in an area of medicine where funded treatment is very restricted, and it is true that financial arguments were well used in justifying and developing the UK policy. However, the public health argument for reducing unnecessary twins is strong. Patients need to be reassured that a move towards SET is clinically motivated, and that any financial gain from savings in obstetric care and other areas is not the principal motivator.
While many patients accept embryo freezing, appreciating the ‘second chance’, there is a subset (of unknown size) for whom the idea seems unnatural and dangerous. These feelings are strongly held and arise from an invalid (but reasonable) extrapolation from everyday experience. A more detailed understanding of these attitudes could well lead to targeted information that will increase the acceptance of embryo cryopreservation. This is a rapidly developing area in clinical practice and clear, up-to-date and specific information is required on the success rates from frozen transfers, both in terms of IVF outcomes and the long-term health of the babies.
Implications for research
The need for better data
As summarised in Chapter 7, there is an urgent need for better quality data that permit the evaluation of complete treatments (fresh plus frozen transfers) and link multiple treatments of the same couples. Existing clinical and regulatory database systems do not in practice provide data that can robustly and directly answer the key questions. Proposed developments in the HFEA register may help towards this, but there is a real need for good, reliable data collection within treatment centres. It will be important to update the work done here with more recent data that include a greater proportion of SET to validate and extend the findings and to include other covariates. Analyses including more centres are required to gain greater understanding of the centre effects and identify the potential to improve practice and hence outcomes.
Policy implementation
The present UK policy of requiring clinics to reduce their own twin rates requires a degree of sophistication in the monitoring process, and the numbers of patients treated in any given centre do not allow for robust auditing or evaluation of policy changes. Research is needed to adapt existing data monitoring tools to this application and provide usable evaluation tools to clinics and regulators. This suggests that future studies could be based around the implementation and monitoring of twin reduction policies across a number of centres.
Although much of the patient antipathy to SET is related to the burden of treatment and the desire for a complete family while minimising the treatment burden, some of the resistance arises from a failure to appreciate the clinical reasons behind the policy and a mistrust of embryo freezing. These considerations may be amenable to carefully tailored and accurate information, which takes account of patients’ beliefs and previous experiences. Further work to develop such targeted interventions is called for, along with an assessment of the training needs of staff to enable the delivery of such information.
Although there is a growing body of qualitative data on patient views on SET and twins, there is a need for more studies to quantify the extent to which these attitudes are held across the patient population and differ according to circumstances. Similarly, more data are needed on clinical attitudes, particularly in the private sector.
The present methodology can readily be extended to consider various embryo selection policies, based either on biomarkers or on extended culture. As data become available on these methods, further simulation studies would be informative in determining their optimal use.
Future clinical trials of eSET
The limited existing trial data, observational data and the modelling studies presented here all suggest that, in the context of a complete cycle (egg retrieval plus transfer of all embryos created) a policy of SET throughout the treatment course could be broadly equivalent, or potentially better, in terms of cumulative live birth rates than the previously accepted practice of replacing two embryos. If a rigorous RCT along these lines were conducted, it could provide very strong evidence in favour of a SET policy. We would advocate a pragmatic trial, allowing centres to adopt their own freezing policies, and thus test treatment policy. If the trial were large enough, properly constructed subgroup analyses would provide information on the relative efficacy of different freezing policies. Inclusion criteria should be broad, excluding only patients for whom DET is contraindicated, or where the clinic freezing policy would preclude either arm (e.g. not freezing single embryos). The primary end point would be a cumulative live birth rate, such as the number of live births within 18 months of egg retrieval, with twin numbers and obstetric adverse events being important secondary end points.
As the trial would be looking for equivalence, or non-inferiority rather than superiority, the sample size would be large. For example, if the success rate was 35% and we were looking for a 5% equivalence margin, a sample size of ∼1500 per arm would be required for 80% power (based on a 95% two-sided confidence interval). Larger numbers again would be needed for subgroup analysis or if a smaller non-inferiority margin were required. This would be large but feasible over a 2-year period with a few centres, as virtually all patients undergoing IVF would be eligible. However, given the current state of policy development in the UK, it would be difficult to conduct such a trial where a national policy has been agreed and clinics have specific twin targets, and exceptions for trial centres would be required. More importantly, a similar trial in Scotland failed to recruit as patients were unwilling to be randomised. Informal soundings suggest that there is little enthusiasm for SET trials in the UK at the present time, and such a trial would not be likely to be prioritised by the relevant Comprehensive Research Networks.
Although a specific trial of SET versus DET may not be practical (at least in the UK) it is important that the range of techniques being considered as part of an eSET policy are rigorously assessed in a realistic clinical setting, i.e. in unselected patients over a complete treatment programme.
Methodological issues
The EU models are useful and allow prediction of DET and SET outcomes in the same patients. However these predictions rely on assumptions (particularly the conditional independence of the E and U components after allowing for covariates). These assumptions cannot currently be tested or relaxed.
Current implementations of the EU model are very computationally intensive and better implementations or alternative models are required to allow full consideration of random effects and more accurate statistical inference (e.g. profile likelihood or bootstrap methods for obtaining confidence intervals).
Further methodological work is needed to clarify these issues, and one such programme of work is currently being undertaken in the University of Manchester Health Methodology Research Group.
Key messages
-
For any one transfer, SET has about a one-third loss of success rate relative to DET.
-
The loss can be only partially mitigated by patient and treatment cycle selection, and criteria may be criticised as unfair: all patients receiving SET will have a lower chance of success than they would have with DET.
-
If we consider complete cycles (fresh plus frozen transfers), it is possible for repeat SET to produce more live births than repeat DET.
-
Then, for all patients, it is possible for repeat SET to outperform DET in terms of cumulative outcomes.
-
Such a strategy would require support from funders and acceptance by patients of both cryopreservation and the burden of additional transfer cycles.
Acknowledgements
We thank the members of the towardSET? Advisory Group (see Table 1) for their help and support throughout this project. We gratefully acknowledge the members of the towardSET? collaboration who provided data for this study:
Tony Rutherford and Jan Hogg (The Leeds Reproductive Medicine Unit)
Steve Troup and Natalie Scott (The Hewitt Centre for Reproductive Medicine, Liverpool)
Helen Hunter (St Mary’s Hospital, Manchester)
Debbie Falconer and Louise Warner (Manchester Fertility Services)
Jane Saxton (Centre for Reproductive Medicine and Fertility, Sheffield)
We wish to thank the staff at St Mary’s Hospital and Manchester Fertility Services for their support and assistance in recruitment for the qualitative work. We are grateful to Infertility Network UK for helpful contributions throughout and particularly for facilitating the online focus group.
Diane Escott and Lynn Austin assisted in the analysis of the qualitative work. The work was supported by the Manchester Biomedical Research Centre.
Contribution of authors
Stephen Roberts (Senior Lecturer in Medical Statistics) designed the overall project and oversaw the data modelling components of the project and conducted the simulations. Linda McGowan (Lecturer in Women’s Health) designed and conducted the qualitative components of the project. Mark Hirst (Research Associate Statistician) collated the datasets and undertook the statistical modelling. Daniel Brison (Consultant Embryologist) was involved in the design of the project and provided clinical expertise throughout. Andy Vail (Senior Lecturer in Medical Statistics) was involved in the design of the project and provided statistical expertise throughout. Brian Lieberman (Retired consultant obstetrician) was involved in the design of the project.
Disclaimers
The views expressed in this publication are those of the authors and not necessarily those of the HTA programme or the Department of Health.
References
- Roberts SA. Models for assisted conception data with embryo-specific covariates. Stat Med 2007;26:156-70.
- Roberts SA, Fitzgerald CT, Brison DR. Modelling the impact of single embryo transfer in a national health service IVF programme. Hum Reprod 2009;24:122-31.
- Braude P. One child at a time. Reducing multiple births after IVF. London: HFEA; 2006.
- Kitzinger J. Recalling the pain. Nurs Times 1990;86:38-40.
- Kitzinger J. Qualitative research. Introducing focus groups. BMJ 1995;311:299-302.
- Pandian Z, Templeton A, Serour G, Bhattacharya S. Number of embryos for transfer after IVF and ICSI: a Cochrane review. Hum Reprod 2005;20:2681-7.
- Pinborg A. IVF/ICSI twin pregnancies: risks and prevention. Hum Reprod Update 2005;11:575-93.
- Bergh C. Single embryo transfer: a mini-review. Hum Reprod 2005;20:323-7.
- Gerris JMR. Single embryo transfer and IVF/ICSI outcome: a balanced appraisal. Hum Reprod Update 2005;11:105-21.
- Lukassen HG, Braat DD, Wetzels AM, Zielhuis GA, Adang EM, Scheenjes E, et al. Two cycles with single embryo transfer versus one cycle with double embryo transfer: a randomized controlled trial. Hum Reprod 2005;20:702-8.
- Cutting R, Morroll D, Roberts SA, Pickering S, Rutherford A. Elective single embryo transfer: guidelines for practice British Fertility Society and Association of Clinical Embryologists. Hum Fertil (Camb) 2008;11:1-16.
- Gardner DK, Surrey E, Minjarez D, Leitz A, Stevens J, Schoolcraft WB. Single blastocyst transfer: a prospective randomized trial. Fertil Steril 2004;81:551-5.
- Gerris J, De Neubourg D, Mangelschots K, Van Royen E, Van de Meerssche M, Valkenburg M. Prevention of twin pregnancy after in-vitro fertilization or intracytoplasmic sperm injection based on strict embryo criteria: a prospective randomized clinical trial. Hum Reprod 1999;14:2581-7.
- Martikainen H, Tiitinen A, Tomas C, Tapanainen J, Orava M, Tuomivaara L, et al. One versus two embryo transfer after IVF and ICSI: a randomized study. Hum Reprod 2001;16:1900-3.
- Thurin A, Hausken J, Hillensjo T, Jablonowska B, Pinborg A, Strandell A, et al. Elective single-embryo transfer versus double-embryo transfer in in vitro fertilization. N Engl J Med 2004;351:2392-402.
- van Montfoort APA, Janssen JM, Fiddelers AAA, Derhaag JG, Dirksen CD, Evers JLH, et al. Single versus double embryo transfer: a randomised study. Hum Reprod 2005;19.
- Moustafa MK, Sheded SA, Mousta MAEA. Elective single embryo transfer versus double embryo transfer in assisted reproduction. Reprod Biomed Online 2008;17:82-7.
- van Montfoort AP, Fiddelers AA, Janssen JM, Derhaag JG, Dirksen CD, Dunselman GA, et al. In unselected patients, elective single embryo transfer prevents all multiples, but results in significantly lower pregnancy rates compared with double embryo transfer: a randomized controlled trial. Hum Reprod 2006;21:338-43.
- Gleicher N, Barad D. Twin pregnancy, contrary to consensus, is a desirable outcome in infertility. Fertil Steril 2009;91:2426-31.
- Bhattacharya S, Templeton A. What is the most relevant standard of success in assisted reproduction? Redefining success in the context of elective single embryo transfer: evidence, intuition and financial reality. Hum Reprod 2004;19:1939-42.
- Blennborn M, Nilsson S, Hillervik C, Hellberg D. The couple’s decision-making in IVF: one or two embryos at transfer?. Hum Reprod 2005;20:1292-7.
- Pinborg A, Loft A, Schmidt L, Andersen AN. Attitudes of IVF/ICSI-twin mothers towards twins and single embryo transfer. Hum Reprod 2003;18:621-7.
- Gleicher N, Campbell DP, Chan CL, Karande V, Rao R, Balin M, et al. The desire for multiple births in couples with infertility problems contradicts present practice patterns. Hum Reprod 1995;10:1079-84.
- Goldfarb J, Kinzer DJ, Boyle M, Kurit D. Attitudes of in vitro fertilization and intrauterine insemination couples toward multiple gestation pregnancy and multifetal pregnancy reduction. Fertil Steril 1996;65:815-20.
- Porter M, Bhattacharya S. Investigation of staff and patients’ opinions of a proposed trial of elective single embryo transfer. Hum Reprod 2005;20:2523-30.
- Murray S, Shetty A, Rattray A, Taylor V, Bhattacharya S. A randomized comparison of alternative methods of information provision on the acceptability of elective single embryo transfer. Hum Reprod 2004;19:911-16.
- Ajzen I. Attitudes, personality and behaviour. Milton Keynes: Open University Press; 2005.
- Twisk M, van der Veen F, Repping S, Heineman MJ, Korevaar JC, Bossuyt PM. Preferences of subfertile women regarding elective single embryo transfer: additional in vitro fertilization cycles are acceptable, lower pregnancy rates are not. Fertil Steril 2007;88:1006-9.
- van Peperstraten AM, Nelen WLDM, Hermens RPMG, Jansen L, Scheenje E, Braat DDM, et al. Why don’t we perform elective single embryo transfer? A qualitative study among IVF patients and professionals. Hum Reprod 2008;23:2036-42.
- Blennborn M, Hellberg D, Nilsson S. Differences in female and male perception of information and decision-making in single-embryo transfer in in vitro fertilization in Sweden. J Assist Reprod Genet 2007;24:337-42.
- Scotland GS, McNamee P, Peddie VL, Bhattacharya S. Safety versus success in elective single embryo transfer: women’s preferences for outcomes of in vitro fertilisation. BJOG 2007;114:977-83.
- Deyo RA. A key medical decision maker: the patient. BMJ 2001;323:466-7.
- De Neubourg D, Gerris J, Mangelschots K, Van RE, Vercruyssen M, Elseviers M. Single top quality embryo transfer as a model for prediction of early pregnancy outcome. Hum Reprod 2004;19:1476-9.
- Ebner T, Moser M, Sommergruber M, Tews G. Selection based on morphological assessment of oocytes and embryos at different stages of preimplantation development: a review. Hum Reprod Update 2003;9:251-62.
- Brison DR, Houghton FD, Falconer D, Roberts SA, Hawkhead J, Humpherson PG, et al. Identification of viable embryos in IVF by non-invasive measurement of amino acid turnover. Hum Reprod 2004;19:2319-24.
- Brison DR, Hollywood K, Arnesen R, Goodacre R. Predicting human embryo viability: the road to non-invasive analysis of the secretome using metabolic footprinting. Reprod Biomed Online 2007;15:296-302.
- El-Toukhy T, Khalaf Y, Braude P. IVF results: Optimize not maximize. Am J Obstet Gynecol 2006;194:322-31.
- Khalaf Y, El-Toukhy T, Coomarasamy A, Kamal A, Bolton V, Braude P. Selective single blastocyst transfer reduces the multiple pregnancy rate and increases pregnancy rates: a pre- and postintervention study. BJOG 2008;115:385-90.
- Blake D, Proctor M, Johnson N, Olive D. Cleavage stage versus blastocyst stage embryo transfer in assisted conception. Cochrane Database Syst Rev 2005;4.
- Munne S, Chen S, Fischer J, Colls P, Zheng XZ, Stevens J, et al. Preimplantation genetic diagnosis reduces pregnancy loss in women aged 35 years and older with a history of recurrent miscarriages. Fertil Steril 2005;84:331-5.
- Hardarson T, Hanson C, Lundin K, Hillensjo T, Nilsson L, Stevic J, et al. Preimplantation genetic screening in women of advanced maternal age caused a decrease in clinical pregnancy rate: a randomized controlled trial. Hum Reprod 2008;23:2806-12.
- Mastenbroek S, Twisk M, van Echten-Arends J, Sikkema-Raddatz B, Korevaar JC, Verhoeve HR, et al. In vitro fertilization with preimplantation genetic screening. N Engl J Med 2007;357:9-17.
- Horne G, Critchlow JD, Newman MC, Edozien L, Matson PL, Lieberman BA. A prospective evaluation of cryopreservation strategies in a two-embryo transfer programme. Hum Reprod 1997;12:542-7.
- Fiddelers AAA, Severens JL, Dirksen CD, Dumoulin JCM, Land JA, Evers JLH. Economic evaluations of single- versus double-embryo transfer in IVF. Hum Reprod Update 2007;13:5-13.
- Ledger WL, Anumba D, Marlow N, Thomas CM, Wilson EC. The costs to the NHS of multiple births after IVF treatment in the UK. BJOG 2006;113:21-5.
- Gerris J, De Neubourg D, Mangelschots K, Van Royen E, Vercruyssen M, Barudy-Vasquez J, et al. Elective single day 3 embryo transfer halves the twinning rate without decrease in the ongoing pregnancy rate of an IVF/ICSI programme. Hum Reprod 2002;17:2626-31.
- Martikainen H, Orava M, Lakkakorpi J, Tuomivaara L. Day 2 elective single embryo transfer in clinical practice: better outcome in ICSI cycles. Hum Reprod 2004;19:1364-6.
- De Neubourg D, Mangelschots K, Van Royen E, Vercruyssen M, Ryckaert G, Valkenburg M, et al. Impact of patients’ choice for single embryo transfer of a top quality embryo versus double embryo transfer in the first IVF/ICSI cycle. Hum Reprod 2002;17:2621-5.
- Tiitinen A, Unkila-Kallio L, Halttunen M, Hyden-Granskog C. Impact of elective single embryo transfer on the twin pregnancy rate. Hum Reprod 2003;18:1449-53.
- van Montfoort AP, Dumoulin JC, Land JA, Coonen E, Derhaag JG, Evers JL. Elective single embryo transfer (eSET) policy in the first three IVF/ICSI treatment cycles. Hum Reprod 2005;20:433-6.
- Vilska S, Tiitinen A, Hyden-Granskog C, Hovatta O. Elective transfer of one embryo results in an acceptable pregnancy rate and eliminates the risk of multiple birth. Hum Reprod 1999;14:2392-5.
- Strandell A, Bergh C, Lundin K. Selection of patients suitable for one-embryo transfer may reduce the rate of multiple births by half without impairment of overall birth rates. Hum Reprod 2000;15:2520-5.
- Hunault CC, Eijkemans MJC, Pieters MHEC, Velde ERT, Habbema JDF, Fauser BCJM, et al. A prediction model for selecting patients undergoing in vitro fertilization for elective single embryo transfer. Fertil Steril 2002;77:725-32.
- Zhou HB, Weinberg CR. Evaluating effects of exposures on embryo viability and uterine receptivity in in vitro fertilization. Stat Med 1998;17:1601-12.
- Dukic V, Hogan JW. A hierarchical Bayesian approach to modeling embryo implantation following in vitro fertilization. Biostatistics 2002;3:361-77.
- Jurisica I, Mylopoulos J, Glasgow J, Shapiro H, Casper RF. Case-based reasoning in IVF: prediction and knowledge mining. Artif Intell Med 1998;12:1-24.
- Hogan JW, Scharfstein DO. Estimating causal effects from multiple cycle data in studies of in vitro fertilization. Stat Meth Med Res 2006;15:195-209.
- McDonnell J, Goverde AJ, Rutten FFH, Vermeiden JPW. Multivariate Markov chain analysis of the probability of pregnancy in infertile couples undergoing assisted reproduction. Hum Reprod 2002;17:103-6.
- Bancsi LFJM, Broekmans FJM, Mol BWJ, Habbema JDF, Velde ERT. Performance of basal follicle-stimulating hormone in the prediction of poor ovarian response and failure to become pregnant after in vitro fertilization: a meta-analysis. Fertil Steril 2003;79:1091-100.
- Akande VA, Fleming CF, Hunt LP, Keay SD, Jenkins JM. Biological versus chronological ageing of oocytes, distinguishable by raised FSH levels in relation to the success of IVF treatment. Hum Reprod 2002;17:2003-8.
- Alsalili M, Yuzpe AA, Tummon IS, Parker J, Martin JSB, Nisker JA, et al. Confounding variables affecting in-vitro fertilization success – a decade of experience. J Assist Reprod Genet 1995;12:88-92.
- Chuang CC, Chen CD, Chao KH, Chen SU, Ho HN, Yang YS. Age is a better predictor of pregnancy potential than basal follicle-stimulating hormone levels in women undergoing in vitro fertilization. Fertil Steril 2003;79:63-8.
- Commenges-Ducos M, Tricaud S, Papaxanthos-Roche A, Dallay D, Horovitz J, Commenges D. Modelling of the probability of success of the stages of in-vitro fertilization and embryo transfer: stimulation, fertilization and implantation. Hum Reprod 1998;13:78-83.
- Croucher CA, Lass A, Margara R, Winston RM. Predictive value of the results of a first in-vitro fertilization cycle on the outcome of subsequent cycles. Hum Reprod 1998;13:403-8.
- Elizur SE, Lerner-Geva L, Levron J, Shulman A, Bider D, Dor J. Factors predicting IVF treatment outcome: a multivariate analysis of 5310 cycles. Reprod Biomed Online 2005;10:645-9.
- Engmann L, Maconochie N, Tan SL, Bekir J. Trends in the incidence of births and multiple births and the factors that determine the probability of multiple birth after IVF treatment. Hum Reprod 2001;16:2598-605.
- Haan G, Bernardus RE, Hollanders JMG, Leerentveld RA, Prak FM, Naaktgeboren N. Results of IVF from a prospective multicenter study. Hum Reprod 1991;6:805-10.
- Haggarty P, McCallum H, McBain H, Andrews K, Duthie S, McNeill G, et al. Effect of B vitamins and genetics on success of in-vitro fertilisation: prospective cohort study. Lancet 2006;367:1513-19.
- Kupka MS, Dorn C, Richter O, Felberbaum R, van der Ven H C. Impact of reproductive history on in vitro fertilization and intracytoplasmic sperm injection outcome: evidence from the German IVF Registry. Fertil Steril 2003;80:508-16.
- Lee TH, Chen CD, Tsai YY, Chang LJ, Ho HN, Yang YS. Embryo quality is more important for younger women whereas age is more important for older women with regard to in vitro fertilization outcome and multiple pregnancy. Fertil Steril 2006;86:64-9.
- Minaretzis D, Harris D, Alper MM, Mortola JF, Berger MJ, Power D. Multivariate analysis of factors predictive of successful live births in in vitro fertilization (IVF) suggests strategies to improve IVF outcome. J Assist Reprod Genet 1998;15:365-71.
- Ottosen LDM, Kesmodel U, Hindkjaer J, Ingerslev HJ. Pregnancy prediction models and eSET criteria for IVF patients – do we need more information?. J Assist Reprod Genet 2007;24:29-36.
- Rhodes TL, Mccoy TP, Higdon HL, Boone WR. Factors affecting assisted reproductive technology (ART) pregnancy rates: a multivariate analysis. J Assist Reprod Genet 2005;22:335-46.
- Roseboom TJ, Vermeiden JPW, Schoute E, Lens JW, Schats R. The probability of pregnancy after embryo transfer is affected by the age of the patient, cause of infertility, number of embryos transferred and the average morphology score, as revealed by multiple logistic regression analysis. Hum Reprod 1995;10:3035-41.
- Sabatin L, Zosmer A, Hennessy EM, Tozer A, Al-Shawaf T. Relevance of basal serum FSH to IVF outcome varies with patient age. Reprod Biomed Online 2008;17:10-9.
- Sharif K, Elgendy M, Lashen H, Afnan M. Age and basal follicle stimulating hormone as predictors of in vitro fertilisation outcome. Br J Obstet Gynaecol 1998;105:107-12.
- Stolwijk AM, Zielhuis GA, Hamilton CJCM, Straatman H, Hollanders JMG, Goverde HJM, et al. Prognostic models for the probability of achieving an ongoing pregnancy after in-vitro fertilization and the importance of testing their predictive value. Hum Reprod 1996;11:2298-303.
- Tan SL, Royston P, Campbell S, Jacobs HS, Betts J, Mason B, et al. Cumulative conception and live birth rates after in vitro fertilization. Lancet 1992;339:1390-4.
- Templeton A, Morris JK, Parslow W. Factors that affect outcome of in-vitro fertilisation treatment. Lancet 1996;348:1402-6.
- Terriou P, Sapin C, Giorgetti C, Hans E, Spach JL, Roulier R. Embryo score is a better predictor of pregnancy than the number of transferred embryos or female age. Fertil Steril 2001;75:525-31.
- Tsafrir A, Simon A, Revel A, Reubinoff B, Lewin A, Laufer N. Retrospective analysis of 1217 IVF cycles in women aged 40 years and older. Reprod Biomed Online 2007;14:348-55.
- van der Gaast MH, Eijkemans MJC, van der Net JB, de Boer EJ, Burger CW, van Leeuwen FE, et al. Optimum number of oocytes for a successful first IVF treatment cycle. Reprod Biomed Online 2006;13:476-80.
- Wald M, Sparks AET, Sandlow J, Van-Voorhis B, Syrop CH, Niederberger CS. Computational models for prediction of IVF/ICSI outcomes with surgically retrieved spermatozoa. Reprod Biomed Online 2005;11:325-31.
- Weigert M, Feichtinger W, Kulin S, Kaali SG, Dorau P, Bauer P. Seasonal influences on in vitro fertilization and embryo transfer. J Assist Reprod Genet 2001;18:598-602.
- Wheeler CA, Cole BF, Frishman GN, Seifer DB, Lovegreen SB, Hackett RJ. Predicting probabilities of pregnancy and multiple gestation from in vitro fertilization – a new model. Obstet Gynecol 1998;91:696-700.
- van der Gaast MH, Eijkemans MJC, van der Net JB, de Boer EJ, Burger CW, van Leeuwen FE, et al. Optimum number of oocytes for a successful first IVF treatment cycle. Reprod Biomed Online 2006;13:476-80.
- Wilding M, Di Matteo L, D’Andretti S, Montanaro N, Capobianco C, Dale B. An oocyte score for use in assisted reproduction. J Assist Reprod Genet 2007;24:350-8.
- Dafopoulos K, Griesinger G, Schultze-Mosgau A, Orief Y, Schopper B, Nikolettos N, et al. Factors affecting outcome after ICSI with spermatozoa retrieved from cryopreserved testicular tissue in non-obstructive azoospermia. Reprod Biomed Online 2005;10:455-60.
- Ferlitsch K, Sator MO, Gruber DM, Rucklinger E, Gruber CJ, Huber JC. Body mass index, follicle-stimulating hormone and their predictive value in in vitro fertilization. J Assist Reprod Genet 2004;21:431-6.
- Fujimoto A, Fujiwara T, Osuga Y, Yano T, Tsutsumi O, Taketani Y. Predictive factors of assisted reproductive technology outcome in women over the age of 40. Fertil Steril 2007;88.
- Yanushpolsky EH, Hurwitz S, Tikh E, Racowsky C. Predictive usefulness of cycle day 10 follicle-stimulating hormone level in a clomiphene citrate challenge test for in vitro fertilization outcome in women younger than 40 years of age. Fertil Steril 2003;80:111-15.
- de Klerk C, Hunfeld JAM, Heijnen EMEW, Eijkemans MJC, Fauser BCJM, Passchier J, et al. Low negative affect prior to treatment is associated with a decreased chance of live birth from a first IVF cycle. Hum Reprod 2008;23:112-16.
- Tan SL, Maconochie N, Doyle P, Campbell S, Balen A, Bekir J, et al. Cumulative conception and live-birth rates after in-vitro fertilization with and without the use of long, short, and ultrashort regimens of the gonadotropin-releasing-hormone agonist buserelin. Am J Obstet Gynecol 1994;171:513-20.
- Morris SN, Missmer SA, Cramer DW, Powers RD, McShane PM, Hornstein MD. Effects of lifetime exercise on the outcome of in vitro fertilization. Obstet Gynecol 2006;108:938-45.
- Purcell K, Schembri M, Frazier LM, Rall MJ, Shen SH, Croughan M, et al. Asian ethnicity is associated with reduced pregnancy outcomes after assisted reproductive technology. Fertil Steril 2007;87:297-302.
- Sneed ML, Uhler ML, Grotjan HE, Rapisarda JJ, Lederer KJ, Beltsos AN. Body mass index: impact on IVF success appears age-related. Hum Reprod 2008;23:1835-9.
- Ecochard R, Clayton DG. Multi-level modelling of conception in artificial insemination by donor. Stat Med 1998;17:1137-56.
- Speirs AL, Lopata A, Gronow MJ, Kellow GN, Johnston WIH. Analysis of the benefits and risks of multiple embryo transfer. Fertil Steril 1983;39:468-71.
- Vitthala S, Gelbaya T, Brison D, Fitzgerald C, Nardo L. The risk of monozygotic twins after assisted reproductive technology: a systematic review and meta-analysis. Hum Reprod Update 2009;15:45-5.
- Matorras R, Matorras F, Mendoza R, Rodriguez M, Remohi J, Rodriguez-Escudero FJ, et al. The implantation of every embryo facilitates the chances of the remaining embryos to implant in an IVF programme: a mathematical model to predict pregnancy and multiple pregnancy rates. Hum Reprod 2005;20:2923-31.
- R Development Core Team . R: a Language and Environment for Statistical Computing 2008.
- Nocedal J, Wright SJ. Numerical optimization. New York: Springer; 2006.
- Efron B, Tibshirani R. An introduction to the bootstrap. Boca Raton, FL: Chapman & Hall/CRC; 1993.
- Harrell FE. Regression modeling strategies: with applications to linear models, logistic regression, and survival analysis. New York: Springer-Verlag; 2001.
- QSR International . NVivo Qualitative Data Analysis Software 2006.
- Ritchie J, Spencer L, Bryman A, Burgess RG. Analysing qualitative data. London: Routledge; 1994.
- Austin CM, Stewart SP, Goldfarb JM, Sheean LA, Gindlesperger VR, Duchon MA. Limiting multiple pregnancy in in vitro fertilization embryo transfer (IVF-ET) cycles. J Assist Reprod Genet 1996;13:540-5.
- Lek YY, Bishop GD. Perceived vulnerability to illness threats – the role of disease type, risk factor perception and attributions. Psychology Health 1995;10:205-17.
- Schwarzer R. Optimism, Vulnerability, and self-beliefs as health-related cognitions – a systematic overview. Psychology Health 1994;9:161-80.
- Department of Health . Patient Choice 2009. www.dh.gov.uk/en/Healthcare/PatientChoice/DH_469 (accessed March 2009).
- Glazebrook C, Sheard C, Winstanley L, Ndukwe G. Attitudes of infertile couples to a multiple birth: A review of the literature and results from a survey. Curr Issues Womens Health 2007;3:43-8.
- Bergh C, Soderstrom-Anttila V, Selbing A, Aittomaki K, Hazekamp J, Loft A, et al. Attitudes towards and management of single embryo transfer among Nordic IVF doctors. Acta Obstet Gynecol Scandinavica 2007;86:1222-30.
- Nardo LG, Gelbaya TA, Wilkinson H, Roberts SA, Yates A, Pemberton P, et al. Circulating basal anti-Müllerian hormone levels as predictor of ovarian response in women undergoing ovarian stimulation for in vitro fertilization. Fertil Steril 2009;92:1586-93.
- Dias S, McNamee R, Vail A. Bias in frequently reported analyses of subfertility trials. Stat Med 2008;27:5605-19.
- Agresti A. Categorical data analysis. Hoboken, NJ: John Wiley & Sons; 2002.
- Rabe-Hesketh S, Skrondal A, Pickles A. Maximum likelihood estimation of limited and discrete dependent variable models with nested random effects. J Econometrics 2005;128:301-23.
- Steer CV, Mills CL, Tan SL, Campbell S, Edwards RG. The cumulative embryo score: a predictive embryo scoring technique to select the optimal number of embryos to transfer in an in-vitro fertilization and embryo transfer programme. Hum Reprod 1992;7:117-19.
- Testart J. Cleavage state of human-embryos 2 days after fertilization in vitro and their developmental ability after transfer into the uterus. Hum Reprod 1986;1:29-31.
- Giorgetti C, Terriou P, Auquier P, Hans E, Spach JL, Salzmann J, et al. embryo score to predict implantation after in-vitro fertilization – based on 957 single embryo transfers. Hum Reprod 1995;10:2427-31.
- Munne S, Chen S, Colls P, Garrisi J, Zheng X, Cekleniak N, et al. Maternal age, morphology, development and chromosome abnormalities in over 6000 cleavage-stage embryos. Reprod Biomed Online 2007;14:628-34.
- Hunault CC, te Velde ER, Weima SM, Macklon NS, Eijkemans MJ, Klinkert ER, et al. A case study of the applicability of a prediction model for the selection of patients undergoing in vitro fertilization for single embryo transfer in another center. Fertil Steril 2007;87:1314-21.
- Granne I, Child T, Hartshorne G. Embryo cryopreservation: evidence for practice. Hum Fertil (Camb) 2008;11:159-72.
- Parahoo K. Nursing research: principles, process and issues. London: Macmillan; 1997.
- Kruegar RA. Focus groups: a practical guide for applied research. London: Sage; 1994.
- Sweet C. Anatomy of an Online Focus Group 1999. www.quirks.com/articles/a1999/19991213.aspx?searchID=29309232 (accessed March 2009).
- Shea V. The Core Rules of Netiquette 2005. www.albion.com/netiquette/corerules.html (accessed March 2009).
- Ritchie J, Lewis J. Qualitative research practice: a guide for social science students and researchers. Thousand Oaks, CA: Sage; 2003.
- Mellowood Medical . IDEAS – Fertility Clinic Management Software 2009. www.mellowoodmedical.com (accessed March 2009).
- Bird SM, Cox D, Farewell VT, Goldstein H, Holt T, Smith PC. Performance indicators: good, bad, and ugly. J R Stat Soc Series A Stat Soc 2005;168:1-27.
- Gorber SC, Schofield-Hurwitz S, Hardt J, Levasseur G, Tremblay M. The accuracy of self-reported smoking: a systematic review of the relationship between self-reported and cotinine-assessed smoking status. Nicotine Tobacco Res 2009;11:12-24.
- Teddlie C, Tashakkori A. Foundations of mixed methods research: integrating quantitative and qualitative approaches in the social and behavioral sciences. Thousand Oaks, CA: Sage; 2009.
- O’Cathain A, Murphy E, Nicholl J. Integration and publications as indicators of ‘yield’ from mixed methods studies. J Mixed Methods Res 2007;1:147-63.
Appendix 1 Original protocol
Appendix 2 Focus group presentation
List of abbreviations
- b
- model coefficient
- AQ
- adaptive quadrature – an optimal method for fitting random effects in the statistical models
- ACE
- [UK] Association of Clinical Embryologists
- AIC
- Akaike’s information criterion
- AUC
- area under [ROC] curve
- BIC
- Bayesian information criterion
- BFS
- British Fertility Society
- CI
- confidence interval
- DET
- double embryo transfer
- df
- degrees of freedom
- eSET
- elective single embryo transfer
- ET
- embryo transfer
- EU [model]
- embryo–uterus [model] (see Chapter 1, Statistical modelling approaches)
- FSH
- follicle-stimulating hormone
- HFEA
- [UK] Human Fertilisation and Embryology Authority
- HRT
- hormone replacement therapy
- HTA
- [UK National Institute for Health Research] Health Technology Assessment programme
- ICSI
- intracytoplasmic sperm injection
- IVF
- in vitro fertilisation
- LBE
- live birth event – treatment outcome one or more live babies
- LR [model]
- logistic regression [model] (see Chapter 1, Statistical modelling approaches)
- LRT
- likelihood ratio test
- OR
- odds ratio
- PCOS
- polycystic ovary syndrome
- PCT
- primary care trust
- RCT
- randomised controlled trial
- RE
- random effect
- ROC [curve]
- receiver operating characteristic [curve]
- SD
- standard deviation
- SE
- standard error [of parameter estimate]
- SET
- single embryo transfer
Notes
Health Technology Assessment reports published to date
-
Home parenteral nutrition: a systematic review.
By Richards DM, Deeks JJ, Sheldon TA, Shaffer JL.
-
Diagnosis, management and screening of early localised prostate cancer.
A review by Selley S, Donovan J, Faulkner A, Coast J, Gillatt D.
-
The diagnosis, management, treatment and costs of prostate cancer in England and Wales.
A review by Chamberlain J, Melia J, Moss S, Brown J.
-
Screening for fragile X syndrome.
A review by Murray J, Cuckle H, Taylor G, Hewison J.
-
A review of near patient testing in primary care.
By Hobbs FDR, Delaney BC, Fitzmaurice DA, Wilson S, Hyde CJ, Thorpe GH, et al.
-
Systematic review of outpatient services for chronic pain control.
By McQuay HJ, Moore RA, Eccleston C, Morley S, de C Williams AC.
-
Neonatal screening for inborn errors of metabolism: cost, yield and outcome.
A review by Pollitt RJ, Green A, McCabe CJ, Booth A, Cooper NJ, Leonard JV, et al.
-
Preschool vision screening.
A review by Snowdon SK, Stewart-Brown SL.
-
Implications of socio-cultural contexts for the ethics of clinical trials.
A review by Ashcroft RE, Chadwick DW, Clark SRL, Edwards RHT, Frith L, Hutton JL.
-
A critical review of the role of neonatal hearing screening in the detection of congenital hearing impairment.
By Davis A, Bamford J, Wilson I, Ramkalawan T, Forshaw M, Wright S.
-
Newborn screening for inborn errors of metabolism: a systematic review.
By Seymour CA, Thomason MJ, Chalmers RA, Addison GM, Bain MD, Cockburn F, et al.
-
Routine preoperative testing: a systematic review of the evidence.
By Munro J, Booth A, Nicholl J.
-
Systematic review of the effectiveness of laxatives in the elderly.
By Petticrew M, Watt I, Sheldon T.
-
When and how to assess fast-changing technologies: a comparative study of medical applications of four generic technologies.
A review by Mowatt G, Bower DJ, Brebner JA, Cairns JA, Grant AM, McKee L.
-
Antenatal screening for Down’s syndrome.
A review by Wald NJ, Kennard A, Hackshaw A, McGuire A.
-
Screening for ovarian cancer: a systematic review.
By Bell R, Petticrew M, Luengo S, Sheldon TA.
-
Consensus development methods, and their use in clinical guideline development.
A review by Murphy MK, Black NA, Lamping DL, McKee CM, Sanderson CFB, Askham J, et al.
-
A cost–utility analysis of interferon beta for multiple sclerosis.
By Parkin D, McNamee P, Jacoby A, Miller P, Thomas S, Bates D.
-
Effectiveness and efficiency of methods of dialysis therapy for end-stage renal disease: systematic reviews.
By MacLeod A, Grant A, Donaldson C, Khan I, Campbell M, Daly C, et al.
-
Effectiveness of hip prostheses in primary total hip replacement: a critical review of evidence and an economic model.
By Faulkner A, Kennedy LG, Baxter K, Donovan J, Wilkinson M, Bevan G.
-
Antimicrobial prophylaxis in colorectal surgery: a systematic review of randomised controlled trials.
By Song F, Glenny AM.
-
Bone marrow and peripheral blood stem cell transplantation for malignancy.
A review by Johnson PWM, Simnett SJ, Sweetenham JW, Morgan GJ, Stewart LA.
-
Screening for speech and language delay: a systematic review of the literature.
By Law J, Boyle J, Harris F, Harkness A, Nye C.
-
Resource allocation for chronic stable angina: a systematic review of effectiveness, costs and cost-effectiveness of alternative interventions.
By Sculpher MJ, Petticrew M, Kelland JL, Elliott RA, Holdright DR, Buxton MJ.
-
Detection, adherence and control of hypertension for the prevention of stroke: a systematic review.
By Ebrahim S.
-
Postoperative analgesia and vomiting, with special reference to day-case surgery: a systematic review.
By McQuay HJ, Moore RA.
-
Choosing between randomised and nonrandomised studies: a systematic review.
By Britton A, McKee M, Black N, McPherson K, Sanderson C, Bain C.
-
Evaluating patient-based outcome measures for use in clinical trials.
A review by Fitzpatrick R, Davey C, Buxton MJ, Jones DR.
-
Ethical issues in the design and conduct of randomised controlled trials.
A review by Edwards SJL, Lilford RJ, Braunholtz DA, Jackson JC, Hewison J, Thornton J.
-
Qualitative research methods in health technology assessment: a review of the literature.
By Murphy E, Dingwall R, Greatbatch D, Parker S, Watson P.
-
The costs and benefits of paramedic skills in pre-hospital trauma care.
By Nicholl J, Hughes S, Dixon S, Turner J, Yates D.
-
Systematic review of endoscopic ultrasound in gastro-oesophageal cancer.
By Harris KM, Kelly S, Berry E, Hutton J, Roderick P, Cullingworth J, et al.
-
Systematic reviews of trials and other studies.
By Sutton AJ, Abrams KR, Jones DR, Sheldon TA, Song F.
-
Primary total hip replacement surgery: a systematic review of outcomes and modelling of cost-effectiveness associated with different prostheses.
A review by Fitzpatrick R, Shortall E, Sculpher M, Murray D, Morris R, Lodge M, et al.
-
Informed decision making: an annotated bibliography and systematic review.
By Bekker H, Thornton JG, Airey CM, Connelly JB, Hewison J, Robinson MB, et al.
-
Handling uncertainty when performing economic evaluation of healthcare interventions.
A review by Briggs AH, Gray AM.
-
The role of expectancies in the placebo effect and their use in the delivery of health care: a systematic review.
By Crow R, Gage H, Hampson S, Hart J, Kimber A, Thomas H.
-
A randomised controlled trial of different approaches to universal antenatal HIV testing: uptake and acceptability. Annex: Antenatal HIV testing – assessment of a routine voluntary approach.
By Simpson WM, Johnstone FD, Boyd FM, Goldberg DJ, Hart GJ, Gormley SM, et al.
-
Methods for evaluating area-wide and organisation-based interventions in health and health care: a systematic review.
By Ukoumunne OC, Gulliford MC, Chinn S, Sterne JAC, Burney PGJ.
-
Assessing the costs of healthcare technologies in clinical trials.
A review by Johnston K, Buxton MJ, Jones DR, Fitzpatrick R.
-
Cooperatives and their primary care emergency centres: organisation and impact.
By Hallam L, Henthorne K.
-
Screening for cystic fibrosis.
A review by Murray J, Cuckle H, Taylor G, Littlewood J, Hewison J.
-
A review of the use of health status measures in economic evaluation.
By Brazier J, Deverill M, Green C, Harper R, Booth A.
-
Methods for the analysis of quality-of-life and survival data in health technology assessment.
A review by Billingham LJ, Abrams KR, Jones DR.
-
Antenatal and neonatal haemoglobinopathy screening in the UK: review and economic analysis.
By Zeuner D, Ades AE, Karnon J, Brown J, Dezateux C, Anionwu EN.
-
Assessing the quality of reports of randomised trials: implications for the conduct of meta-analyses.
A review by Moher D, Cook DJ, Jadad AR, Tugwell P, Moher M, Jones A, et al.
-
‘Early warning systems’ for identifying new healthcare technologies.
By Robert G, Stevens A, Gabbay J.
-
A systematic review of the role of human papillomavirus testing within a cervical screening programme.
By Cuzick J, Sasieni P, Davies P, Adams J, Normand C, Frater A, et al.
-
Near patient testing in diabetes clinics: appraising the costs and outcomes.
By Grieve R, Beech R, Vincent J, Mazurkiewicz J.
-
Positron emission tomography: establishing priorities for health technology assessment.
A review by Robert G, Milne R.
-
The debridement of chronic wounds: a systematic review.
By Bradley M, Cullum N, Sheldon T.
-
Systematic reviews of wound care management: (2) Dressings and topical agents used in the healing of chronic wounds.
By Bradley M, Cullum N, Nelson EA, Petticrew M, Sheldon T, Torgerson D.
-
A systematic literature review of spiral and electron beam computed tomography: with particular reference to clinical applications in hepatic lesions, pulmonary embolus and coronary artery disease.
By Berry E, Kelly S, Hutton J, Harris KM, Roderick P, Boyce JC, et al.
-
What role for statins? A review and economic model.
By Ebrahim S, Davey Smith G, McCabe C, Payne N, Pickin M, Sheldon TA, et al.
-
Factors that limit the quality, number and progress of randomised controlled trials.
A review by Prescott RJ, Counsell CE, Gillespie WJ, Grant AM, Russell IT, Kiauka S, et al.
-
Antimicrobial prophylaxis in total hip replacement: a systematic review.
By Glenny AM, Song F.
-
Health promoting schools and health promotion in schools: two systematic reviews.
By Lister-Sharp D, Chapman S, Stewart-Brown S, Sowden A.
-
Economic evaluation of a primary care-based education programme for patients with osteoarthritis of the knee.
A review by Lord J, Victor C, Littlejohns P, Ross FM, Axford JS.
-
The estimation of marginal time preference in a UK-wide sample (TEMPUS) project.
A review by Cairns JA, van der Pol MM.
-
Geriatric rehabilitation following fractures in older people: a systematic review.
By Cameron I, Crotty M, Currie C, Finnegan T, Gillespie L, Gillespie W, et al.
-
Screening for sickle cell disease and thalassaemia: a systematic review with supplementary research.
By Davies SC, Cronin E, Gill M, Greengross P, Hickman M, Normand C.
-
Community provision of hearing aids and related audiology services.
A review by Reeves DJ, Alborz A, Hickson FS, Bamford JM.
-
False-negative results in screening programmes: systematic review of impact and implications.
By Petticrew MP, Sowden AJ, Lister-Sharp D, Wright K.
-
Costs and benefits of community postnatal support workers: a randomised controlled trial.
By Morrell CJ, Spiby H, Stewart P, Walters S, Morgan A.
-
Implantable contraceptives (subdermal implants and hormonally impregnated intrauterine systems) versus other forms of reversible contraceptives: two systematic reviews to assess relative effectiveness, acceptability, tolerability and cost-effectiveness.
By French RS, Cowan FM, Mansour DJA, Morris S, Procter T, Hughes D, et al.
-
An introduction to statistical methods for health technology assessment.
A review by White SJ, Ashby D, Brown PJ.
-
Disease-modifying drugs for multiple sclerosis: a rapid and systematic review.
By Clegg A, Bryant J, Milne R.
-
Publication and related biases.
A review by Song F, Eastwood AJ, Gilbody S, Duley L, Sutton AJ.
-
Cost and outcome implications of the organisation of vascular services.
By Michaels J, Brazier J, Palfreyman S, Shackley P, Slack R.
-
Monitoring blood glucose control in diabetes mellitus: a systematic review.
By Coster S, Gulliford MC, Seed PT, Powrie JK, Swaminathan R.
-
The effectiveness of domiciliary health visiting: a systematic review of international studies and a selective review of the British literature.
By Elkan R, Kendrick D, Hewitt M, Robinson JJA, Tolley K, Blair M, et al.
-
The determinants of screening uptake and interventions for increasing uptake: a systematic review.
By Jepson R, Clegg A, Forbes C, Lewis R, Sowden A, Kleijnen J.
-
The effectiveness and cost-effectiveness of prophylactic removal of wisdom teeth.
A rapid review by Song F, O’Meara S, Wilson P, Golder S, Kleijnen J.
-
Ultrasound screening in pregnancy: a systematic review of the clinical effectiveness, cost-effectiveness and women’s views.
By Bricker L, Garcia J, Henderson J, Mugford M, Neilson J, Roberts T, et al.
-
A rapid and systematic review of the effectiveness and cost-effectiveness of the taxanes used in the treatment of advanced breast and ovarian cancer.
By Lister-Sharp D, McDonagh MS, Khan KS, Kleijnen J.
-
Liquid-based cytology in cervical screening: a rapid and systematic review.
By Payne N, Chilcott J, McGoogan E.
-
Randomised controlled trial of non-directive counselling, cognitive–behaviour therapy and usual general practitioner care in the management of depression as well as mixed anxiety and depression in primary care.
By King M, Sibbald B, Ward E, Bower P, Lloyd M, Gabbay M, et al.
-
Routine referral for radiography of patients presenting with low back pain: is patients’ outcome influenced by GPs’ referral for plain radiography?
By Kerry S, Hilton S, Patel S, Dundas D, Rink E, Lord J.
-
Systematic reviews of wound care management: (3) antimicrobial agents for chronic wounds; (4) diabetic foot ulceration.
By O’Meara S, Cullum N, Majid M, Sheldon T.
-
Using routine data to complement and enhance the results of randomised controlled trials.
By Lewsey JD, Leyland AH, Murray GD, Boddy FA.
-
Coronary artery stents in the treatment of ischaemic heart disease: a rapid and systematic review.
By Meads C, Cummins C, Jolly K, Stevens A, Burls A, Hyde C.
-
Outcome measures for adult critical care: a systematic review.
By Hayes JA, Black NA, Jenkinson C, Young JD, Rowan KM, Daly K, et al.
-
A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding.
By Fairbank L, O’Meara S, Renfrew MJ, Woolridge M, Sowden AJ, Lister-Sharp D.
-
Implantable cardioverter defibrillators: arrhythmias. A rapid and systematic review.
By Parkes J, Bryant J, Milne R.
-
Treatments for fatigue in multiple sclerosis: a rapid and systematic review.
By Brañas P, Jordan R, Fry-Smith A, Burls A, Hyde C.
-
Early asthma prophylaxis, natural history, skeletal development and economy (EASE): a pilot randomised controlled trial.
By Baxter-Jones ADG, Helms PJ, Russell G, Grant A, Ross S, Cairns JA, et al.
-
Screening for hypercholesterolaemia versus case finding for familial hypercholesterolaemia: a systematic review and cost-effectiveness analysis.
By Marks D, Wonderling D, Thorogood M, Lambert H, Humphries SE, Neil HAW.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of glycoprotein IIb/IIIa antagonists in the medical management of unstable angina.
By McDonagh MS, Bachmann LM, Golder S, Kleijnen J, ter Riet G.
-
A randomised controlled trial of prehospital intravenous fluid replacement therapy in serious trauma.
By Turner J, Nicholl J, Webber L, Cox H, Dixon S, Yates D.
-
Intrathecal pumps for giving opioids in chronic pain: a systematic review.
By Williams JE, Louw G, Towlerton G.
-
Combination therapy (interferon alfa and ribavirin) in the treatment of chronic hepatitis C: a rapid and systematic review.
By Shepherd J, Waugh N, Hewitson P.
-
A systematic review of comparisons of effect sizes derived from randomised and non-randomised studies.
By MacLehose RR, Reeves BC, Harvey IM, Sheldon TA, Russell IT, Black AMS.
-
Intravascular ultrasound-guided interventions in coronary artery disease: a systematic literature review, with decision-analytic modelling, of outcomes and cost-effectiveness.
By Berry E, Kelly S, Hutton J, Lindsay HSJ, Blaxill JM, Evans JA, et al.
-
A randomised controlled trial to evaluate the effectiveness and cost-effectiveness of counselling patients with chronic depression.
By Simpson S, Corney R, Fitzgerald P, Beecham J.
-
Systematic review of treatments for atopic eczema.
By Hoare C, Li Wan Po A, Williams H.
-
Bayesian methods in health technology assessment: a review.
By Spiegelhalter DJ, Myles JP, Jones DR, Abrams KR.
-
The management of dyspepsia: a systematic review.
By Delaney B, Moayyedi P, Deeks J, Innes M, Soo S, Barton P, et al.
-
A systematic review of treatments for severe psoriasis.
By Griffiths CEM, Clark CM, Chalmers RJG, Li Wan Po A, Williams HC.
-
Clinical and cost-effectiveness of donepezil, rivastigmine and galantamine for Alzheimer’s disease: a rapid and systematic review.
By Clegg A, Bryant J, Nicholson T, McIntyre L, De Broe S, Gerard K, et al.
-
The clinical effectiveness and cost-effectiveness of riluzole for motor neurone disease: a rapid and systematic review.
By Stewart A, Sandercock J, Bryan S, Hyde C, Barton PM, Fry-Smith A, et al.
-
Equity and the economic evaluation of healthcare.
By Sassi F, Archard L, Le Grand J.
-
Quality-of-life measures in chronic diseases of childhood.
By Eiser C, Morse R.
-
Eliciting public preferences for healthcare: a systematic review of techniques.
By Ryan M, Scott DA, Reeves C, Bate A, van Teijlingen ER, Russell EM, et al.
-
General health status measures for people with cognitive impairment: learning disability and acquired brain injury.
By Riemsma RP, Forbes CA, Glanville JM, Eastwood AJ, Kleijnen J.
-
An assessment of screening strategies for fragile X syndrome in the UK.
By Pembrey ME, Barnicoat AJ, Carmichael B, Bobrow M, Turner G.
-
Issues in methodological research: perspectives from researchers and commissioners.
By Lilford RJ, Richardson A, Stevens A, Fitzpatrick R, Edwards S, Rock F, et al.
-
Systematic reviews of wound care management: (5) beds; (6) compression; (7) laser therapy, therapeutic ultrasound, electrotherapy and electromagnetic therapy.
By Cullum N, Nelson EA, Flemming K, Sheldon T.
-
Effects of educational and psychosocial interventions for adolescents with diabetes mellitus: a systematic review.
By Hampson SE, Skinner TC, Hart J, Storey L, Gage H, Foxcroft D, et al.
-
Effectiveness of autologous chondrocyte transplantation for hyaline cartilage defects in knees: a rapid and systematic review.
By Jobanputra P, Parry D, Fry-Smith A, Burls A.
-
Statistical assessment of the learning curves of health technologies.
By Ramsay CR, Grant AM, Wallace SA, Garthwaite PH, Monk AF, Russell IT.
-
The effectiveness and cost-effectiveness of temozolomide for the treatment of recurrent malignant glioma: a rapid and systematic review.
By Dinnes J, Cave C, Huang S, Major K, Milne R.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of debriding agents in treating surgical wounds healing by secondary intention.
By Lewis R, Whiting P, ter Riet G, O’Meara S, Glanville J.
-
Home treatment for mental health problems: a systematic review.
By Burns T, Knapp M, Catty J, Healey A, Henderson J, Watt H, et al.
-
How to develop cost-conscious guidelines.
By Eccles M, Mason J.
-
The role of specialist nurses in multiple sclerosis: a rapid and systematic review.
By De Broe S, Christopher F, Waugh N.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of orlistat in the management of obesity.
By O’Meara S, Riemsma R, Shirran L, Mather L, ter Riet G.
-
The clinical effectiveness and cost-effectiveness of pioglitazone for type 2 diabetes mellitus: a rapid and systematic review.
By Chilcott J, Wight J, Lloyd Jones M, Tappenden P.
-
Extended scope of nursing practice: a multicentre randomised controlled trial of appropriately trained nurses and preregistration house officers in preoperative assessment in elective general surgery.
By Kinley H, Czoski-Murray C, George S, McCabe C, Primrose J, Reilly C, et al.
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) Acute day hospital versus admission; (2) Vocational rehabilitation; (3) Day hospital versus outpatient care.
By Marshall M, Crowther R, Almaraz- Serrano A, Creed F, Sledge W, Kluiter H, et al.
-
The measurement and monitoring of surgical adverse events.
By Bruce J, Russell EM, Mollison J, Krukowski ZH.
-
Action research: a systematic review and guidance for assessment.
By Waterman H, Tillen D, Dickson R, de Koning K.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of gemcitabine for the treatment of pancreatic cancer.
By Ward S, Morris E, Bansback N, Calvert N, Crellin A, Forman D, et al.
-
A rapid and systematic review of the evidence for the clinical effectiveness and cost-effectiveness of irinotecan, oxaliplatin and raltitrexed for the treatment of advanced colorectal cancer.
By Lloyd Jones M, Hummel S, Bansback N, Orr B, Seymour M.
-
Comparison of the effectiveness of inhaler devices in asthma and chronic obstructive airways disease: a systematic review of the literature.
By Brocklebank D, Ram F, Wright J, Barry P, Cates C, Davies L, et al.
-
The cost-effectiveness of magnetic resonance imaging for investigation of the knee joint.
By Bryan S, Weatherburn G, Bungay H, Hatrick C, Salas C, Parry D, et al.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.
By Forbes C, Shirran L, Bagnall A-M, Duffy S, ter Riet G.
-
Superseded by a report published in a later volume.
-
The role of radiography in primary care patients with low back pain of at least 6 weeks duration: a randomised (unblinded) controlled trial.
By Kendrick D, Fielding K, Bentley E, Miller P, Kerslake R, Pringle M.
-
Design and use of questionnaires: a review of best practice applicable to surveys of health service staff and patients.
By McColl E, Jacoby A, Thomas L, Soutter J, Bamford C, Steen N, et al.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.
By Clegg A, Scott DA, Sidhu M, Hewitson P, Waugh N.
-
Subgroup analyses in randomised controlled trials: quantifying the risks of false-positives and false-negatives.
By Brookes ST, Whitley E, Peters TJ, Mulheran PA, Egger M, Davey Smith G.
-
Depot antipsychotic medication in the treatment of patients with schizophrenia: (1) Meta-review; (2) Patient and nurse attitudes.
By David AS, Adams C.
-
A systematic review of controlled trials of the effectiveness and cost-effectiveness of brief psychological treatments for depression.
By Churchill R, Hunot V, Corney R, Knapp M, McGuire H, Tylee A, et al.
-
Cost analysis of child health surveillance.
By Sanderson D, Wright D, Acton C, Duree D.
-
A study of the methods used to select review criteria for clinical audit.
By Hearnshaw H, Harker R, Cheater F, Baker R, Grimshaw G.
-
Fludarabine as second-line therapy for B cell chronic lymphocytic leukaemia: a technology assessment.
By Hyde C, Wake B, Bryan S, Barton P, Fry-Smith A, Davenport C, et al.
-
Rituximab as third-line treatment for refractory or recurrent Stage III or IV follicular non-Hodgkin’s lymphoma: a systematic review and economic evaluation.
By Wake B, Hyde C, Bryan S, Barton P, Song F, Fry-Smith A, et al.
-
A systematic review of discharge arrangements for older people.
By Parker SG, Peet SM, McPherson A, Cannaby AM, Baker R, Wilson A, et al.
-
The clinical effectiveness and cost-effectiveness of inhaler devices used in the routine management of chronic asthma in older children: a systematic review and economic evaluation.
By Peters J, Stevenson M, Beverley C, Lim J, Smith S.
-
The clinical effectiveness and cost-effectiveness of sibutramine in the management of obesity: a technology assessment.
By O’Meara S, Riemsma R, Shirran L, Mather L, ter Riet G.
-
The cost-effectiveness of magnetic resonance angiography for carotid artery stenosis and peripheral vascular disease: a systematic review.
By Berry E, Kelly S, Westwood ME, Davies LM, Gough MJ, Bamford JM, et al.
-
Promoting physical activity in South Asian Muslim women through ‘exercise on prescription’.
By Carroll B, Ali N, Azam N.
-
Zanamivir for the treatment of influenza in adults: a systematic review and economic evaluation.
By Burls A, Clark W, Stewart T, Preston C, Bryan S, Jefferson T, et al.
-
A review of the natural history and epidemiology of multiple sclerosis: implications for resource allocation and health economic models.
By Richards RG, Sampson FC, Beard SM, Tappenden P.
-
Screening for gestational diabetes: a systematic review and economic evaluation.
By Scott DA, Loveman E, McIntyre L, Waugh N.
-
The clinical effectiveness and cost-effectiveness of surgery for people with morbid obesity: a systematic review and economic evaluation.
By Clegg AJ, Colquitt J, Sidhu MK, Royle P, Loveman E, Walker A.
-
The clinical effectiveness of trastuzumab for breast cancer: a systematic review.
By Lewis R, Bagnall A-M, Forbes C, Shirran E, Duffy S, Kleijnen J, et al.
-
The clinical effectiveness and cost-effectiveness of vinorelbine for breast cancer: a systematic review and economic evaluation.
By Lewis R, Bagnall A-M, King S, Woolacott N, Forbes C, Shirran L, et al.
-
A systematic review of the effectiveness and cost-effectiveness of metal-on-metal hip resurfacing arthroplasty for treatment of hip disease.
By Vale L, Wyness L, McCormack K, McKenzie L, Brazzelli M, Stearns SC.
-
The clinical effectiveness and cost-effectiveness of bupropion and nicotine replacement therapy for smoking cessation: a systematic review and economic evaluation.
By Woolacott NF, Jones L, Forbes CA, Mather LC, Sowden AJ, Song FJ, et al.
-
A systematic review of effectiveness and economic evaluation of new drug treatments for juvenile idiopathic arthritis: etanercept.
By Cummins C, Connock M, Fry-Smith A, Burls A.
-
Clinical effectiveness and cost-effectiveness of growth hormone in children: a systematic review and economic evaluation.
By Bryant J, Cave C, Mihaylova B, Chase D, McIntyre L, Gerard K, et al.
-
Clinical effectiveness and cost-effectiveness of growth hormone in adults in relation to impact on quality of life: a systematic review and economic evaluation.
By Bryant J, Loveman E, Chase D, Mihaylova B, Cave C, Gerard K, et al.
-
Clinical medication review by a pharmacist of patients on repeat prescriptions in general practice: a randomised controlled trial.
By Zermansky AG, Petty DR, Raynor DK, Lowe CJ, Freementle N, Vail A.
-
The effectiveness of infliximab and etanercept for the treatment of rheumatoid arthritis: a systematic review and economic evaluation.
By Jobanputra P, Barton P, Bryan S, Burls A.
-
A systematic review and economic evaluation of computerised cognitive behaviour therapy for depression and anxiety.
By Kaltenthaler E, Shackley P, Stevens K, Beverley C, Parry G, Chilcott J.
-
A systematic review and economic evaluation of pegylated liposomal doxorubicin hydrochloride for ovarian cancer.
By Forbes C, Wilby J, Richardson G, Sculpher M, Mather L, Riemsma R.
-
A systematic review of the effectiveness of interventions based on a stages-of-change approach to promote individual behaviour change.
By Riemsma RP, Pattenden J, Bridle C, Sowden AJ, Mather L, Watt IS, et al.
-
A systematic review update of the clinical effectiveness and cost-effectiveness of glycoprotein IIb/IIIa antagonists.
By Robinson M, Ginnelly L, Sculpher M, Jones L, Riemsma R, Palmer S, et al.
-
A systematic review of the effectiveness, cost-effectiveness and barriers to implementation of thrombolytic and neuroprotective therapy for acute ischaemic stroke in the NHS.
By Sandercock P, Berge E, Dennis M, Forbes J, Hand P, Kwan J, et al.
-
A randomised controlled crossover trial of nurse practitioner versus doctor-led outpatient care in a bronchiectasis clinic.
By Caine N, Sharples LD, Hollingworth W, French J, Keogan M, Exley A, et al.
-
Clinical effectiveness and cost – consequences of selective serotonin reuptake inhibitors in the treatment of sex offenders.
By Adi Y, Ashcroft D, Browne K, Beech A, Fry-Smith A, Hyde C.
-
Treatment of established osteoporosis: a systematic review and cost–utility analysis.
By Kanis JA, Brazier JE, Stevenson M, Calvert NW, Lloyd Jones M.
-
Which anaesthetic agents are cost-effective in day surgery? Literature review, national survey of practice and randomised controlled trial.
By Elliott RA, Payne K, Moore JK, Davies LM, Harper NJN, St Leger AS, et al.
-
Screening for hepatitis C among injecting drug users and in genitourinary medicine clinics: systematic reviews of effectiveness, modelling study and national survey of current practice.
By Stein K, Dalziel K, Walker A, McIntyre L, Jenkins B, Horne J, et al.
-
The measurement of satisfaction with healthcare: implications for practice from a systematic review of the literature.
By Crow R, Gage H, Hampson S, Hart J, Kimber A, Storey L, et al.
-
The effectiveness and cost-effectiveness of imatinib in chronic myeloid leukaemia: a systematic review.
By Garside R, Round A, Dalziel K, Stein K, Royle R.
-
A comparative study of hypertonic saline, daily and alternate-day rhDNase in children with cystic fibrosis.
By Suri R, Wallis C, Bush A, Thompson S, Normand C, Flather M, et al.
-
A systematic review of the costs and effectiveness of different models of paediatric home care.
By Parker G, Bhakta P, Lovett CA, Paisley S, Olsen R, Turner D, et al.
-
How important are comprehensive literature searches and the assessment of trial quality in systematic reviews? Empirical study.
By Egger M, Jüni P, Bartlett C, Holenstein F, Sterne J.
-
Systematic review of the effectiveness and cost-effectiveness, and economic evaluation, of home versus hospital or satellite unit haemodialysis for people with end-stage renal failure.
By Mowatt G, Vale L, Perez J, Wyness L, Fraser C, MacLeod A, et al.
-
Systematic review and economic evaluation of the effectiveness of infliximab for the treatment of Crohn’s disease.
By Clark W, Raftery J, Barton P, Song F, Fry-Smith A, Burls A.
-
A review of the clinical effectiveness and cost-effectiveness of routine anti-D prophylaxis for pregnant women who are rhesus negative.
By Chilcott J, Lloyd Jones M, Wight J, Forman K, Wray J, Beverley C, et al.
-
Systematic review and evaluation of the use of tumour markers in paediatric oncology: Ewing’s sarcoma and neuroblastoma.
By Riley RD, Burchill SA, Abrams KR, Heney D, Lambert PC, Jones DR, et al.
-
The cost-effectiveness of screening for Helicobacter pylori to reduce mortality and morbidity from gastric cancer and peptic ulcer disease: a discrete-event simulation model.
By Roderick P, Davies R, Raftery J, Crabbe D, Pearce R, Bhandari P, et al.
-
The clinical effectiveness and cost-effectiveness of routine dental checks: a systematic review and economic evaluation.
By Davenport C, Elley K, Salas C, Taylor-Weetman CL, Fry-Smith A, Bryan S, et al.
-
A multicentre randomised controlled trial assessing the costs and benefits of using structured information and analysis of women’s preferences in the management of menorrhagia.
By Kennedy ADM, Sculpher MJ, Coulter A, Dwyer N, Rees M, Horsley S, et al.
-
Clinical effectiveness and cost–utility of photodynamic therapy for wet age-related macular degeneration: a systematic review and economic evaluation.
By Meads C, Salas C, Roberts T, Moore D, Fry-Smith A, Hyde C.
-
Evaluation of molecular tests for prenatal diagnosis of chromosome abnormalities.
By Grimshaw GM, Szczepura A, Hultén M, MacDonald F, Nevin NC, Sutton F, et al.
-
First and second trimester antenatal screening for Down’s syndrome: the results of the Serum, Urine and Ultrasound Screening Study (SURUSS).
By Wald NJ, Rodeck C, Hackshaw AK, Walters J, Chitty L, Mackinson AM.
-
The effectiveness and cost-effectiveness of ultrasound locating devices for central venous access: a systematic review and economic evaluation.
By Calvert N, Hind D, McWilliams RG, Thomas SM, Beverley C, Davidson A.
-
A systematic review of atypical antipsychotics in schizophrenia.
By Bagnall A-M, Jones L, Lewis R, Ginnelly L, Glanville J, Torgerson D, et al.
-
Prostate Testing for Cancer and Treatment (ProtecT) feasibility study.
By Donovan J, Hamdy F, Neal D, Peters T, Oliver S, Brindle L, et al.
-
Early thrombolysis for the treatment of acute myocardial infarction: a systematic review and economic evaluation.
By Boland A, Dundar Y, Bagust A, Haycox A, Hill R, Mujica Mota R, et al.
-
Screening for fragile X syndrome: a literature review and modelling.
By Song FJ, Barton P, Sleightholme V, Yao GL, Fry-Smith A.
-
Systematic review of endoscopic sinus surgery for nasal polyps.
By Dalziel K, Stein K, Round A, Garside R, Royle P.
-
Towards efficient guidelines: how to monitor guideline use in primary care.
By Hutchinson A, McIntosh A, Cox S, Gilbert C.
-
Effectiveness and cost-effectiveness of acute hospital-based spinal cord injuries services: systematic review.
By Bagnall A-M, Jones L, Richardson G, Duffy S, Riemsma R.
-
Prioritisation of health technology assessment. The PATHS model: methods and case studies.
By Townsend J, Buxton M, Harper G.
-
Systematic review of the clinical effectiveness and cost-effectiveness of tension-free vaginal tape for treatment of urinary stress incontinence.
By Cody J, Wyness L, Wallace S, Glazener C, Kilonzo M, Stearns S, et al.
-
The clinical and cost-effectiveness of patient education models for diabetes: a systematic review and economic evaluation.
By Loveman E, Cave C, Green C, Royle P, Dunn N, Waugh N.
-
The role of modelling in prioritising and planning clinical trials.
By Chilcott J, Brennan A, Booth A, Karnon J, Tappenden P.
-
Cost–benefit evaluation of routine influenza immunisation in people 65–74 years of age.
By Allsup S, Gosney M, Haycox A, Regan M.
-
The clinical and cost-effectiveness of pulsatile machine perfusion versus cold storage of kidneys for transplantation retrieved from heart-beating and non-heart-beating donors.
By Wight J, Chilcott J, Holmes M, Brewer N.
-
Can randomised trials rely on existing electronic data? A feasibility study to explore the value of routine data in health technology assessment.
By Williams JG, Cheung WY, Cohen DR, Hutchings HA, Longo MF, Russell IT.
-
Evaluating non-randomised intervention studies.
By Deeks JJ, Dinnes J, D’Amico R, Sowden AJ, Sakarovitch C, Song F, et al.
-
A randomised controlled trial to assess the impact of a package comprising a patient-orientated, evidence-based self- help guidebook and patient-centred consultations on disease management and satisfaction in inflammatory bowel disease.
By Kennedy A, Nelson E, Reeves D, Richardson G, Roberts C, Robinson A, et al.
-
The effectiveness of diagnostic tests for the assessment of shoulder pain due to soft tissue disorders: a systematic review.
By Dinnes J, Loveman E, McIntyre L, Waugh N.
-
The value of digital imaging in diabetic retinopathy.
By Sharp PF, Olson J, Strachan F, Hipwell J, Ludbrook A, O’Donnell M, et al.
-
Lowering blood pressure to prevent myocardial infarction and stroke: a new preventive strategy.
By Law M, Wald N, Morris J.
-
Clinical and cost-effectiveness of capecitabine and tegafur with uracil for the treatment of metastatic colorectal cancer: systematic review and economic evaluation.
By Ward S, Kaltenthaler E, Cowan J, Brewer N.
-
Clinical and cost-effectiveness of new and emerging technologies for early localised prostate cancer: a systematic review.
By Hummel S, Paisley S, Morgan A, Currie E, Brewer N.
-
Literature searching for clinical and cost-effectiveness studies used in health technology assessment reports carried out for the National Institute for Clinical Excellence appraisal system.
By Royle P, Waugh N.
-
Systematic review and economic decision modelling for the prevention and treatment of influenza A and B.
By Turner D, Wailoo A, Nicholson K, Cooper N, Sutton A, Abrams K.
-
A randomised controlled trial to evaluate the clinical and cost-effectiveness of Hickman line insertions in adult cancer patients by nurses.
By Boland A, Haycox A, Bagust A, Fitzsimmons L.
-
Redesigning postnatal care: a randomised controlled trial of protocol-based midwifery-led care focused on individual women’s physical and psychological health needs.
By MacArthur C, Winter HR, Bick DE, Lilford RJ, Lancashire RJ, Knowles H, et al.
-
Estimating implied rates of discount in healthcare decision-making.
By West RR, McNabb R, Thompson AGH, Sheldon TA, Grimley Evans J.
-
Systematic review of isolation policies in the hospital management of methicillin-resistant Staphylococcus aureus: a review of the literature with epidemiological and economic modelling.
By Cooper BS, Stone SP, Kibbler CC, Cookson BD, Roberts JA, Medley GF, et al.
-
Treatments for spasticity and pain in multiple sclerosis: a systematic review.
By Beard S, Hunn A, Wight J.
-
The inclusion of reports of randomised trials published in languages other than English in systematic reviews.
By Moher D, Pham B, Lawson ML, Klassen TP.
-
The impact of screening on future health-promoting behaviours and health beliefs: a systematic review.
By Bankhead CR, Brett J, Bukach C, Webster P, Stewart-Brown S, Munafo M, et al.
-
What is the best imaging strategy for acute stroke?
By Wardlaw JM, Keir SL, Seymour J, Lewis S, Sandercock PAG, Dennis MS, et al.
-
Systematic review and modelling of the investigation of acute and chronic chest pain presenting in primary care.
By Mant J, McManus RJ, Oakes RAL, Delaney BC, Barton PM, Deeks JJ, et al.
-
The effectiveness and cost-effectiveness of microwave and thermal balloon endometrial ablation for heavy menstrual bleeding: a systematic review and economic modelling.
By Garside R, Stein K, Wyatt K, Round A, Price A.
-
A systematic review of the role of bisphosphonates in metastatic disease.
By Ross JR, Saunders Y, Edmonds PM, Patel S, Wonderling D, Normand C, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of capecitabine (Xeloda®) for locally advanced and/or metastatic breast cancer.
By Jones L, Hawkins N, Westwood M, Wright K, Richardson G, Riemsma R.
-
Effectiveness and efficiency of guideline dissemination and implementation strategies.
By Grimshaw JM, Thomas RE, MacLennan G, Fraser C, Ramsay CR, Vale L, et al.
-
Clinical effectiveness and costs of the Sugarbaker procedure for the treatment of pseudomyxoma peritonei.
By Bryant J, Clegg AJ, Sidhu MK, Brodin H, Royle P, Davidson P.
-
Psychological treatment for insomnia in the regulation of long-term hypnotic drug use.
By Morgan K, Dixon S, Mathers N, Thompson J, Tomeny M.
-
Improving the evaluation of therapeutic interventions in multiple sclerosis: development of a patient-based measure of outcome.
By Hobart JC, Riazi A, Lamping DL, Fitzpatrick R, Thompson AJ.
-
A systematic review and economic evaluation of magnetic resonance cholangiopancreatography compared with diagnostic endoscopic retrograde cholangiopancreatography.
By Kaltenthaler E, Bravo Vergel Y, Chilcott J, Thomas S, Blakeborough T, Walters SJ, et al.
-
The use of modelling to evaluate new drugs for patients with a chronic condition: the case of antibodies against tumour necrosis factor in rheumatoid arthritis.
By Barton P, Jobanputra P, Wilson J, Bryan S, Burls A.
-
Clinical effectiveness and cost-effectiveness of neonatal screening for inborn errors of metabolism using tandem mass spectrometry: a systematic review.
By Pandor A, Eastham J, Beverley C, Chilcott J, Paisley S.
-
Clinical effectiveness and cost-effectiveness of pioglitazone and rosiglitazone in the treatment of type 2 diabetes: a systematic review and economic evaluation.
By Czoski-Murray C, Warren E, Chilcott J, Beverley C, Psyllaki MA, Cowan J.
-
Routine examination of the newborn: the EMREN study. Evaluation of an extension of the midwife role including a randomised controlled trial of appropriately trained midwives and paediatric senior house officers.
By Townsend J, Wolke D, Hayes J, Davé S, Rogers C, Bloomfield L, et al.
-
Involving consumers in research and development agenda setting for the NHS: developing an evidence-based approach.
By Oliver S, Clarke-Jones L, Rees R, Milne R, Buchanan P, Gabbay J, et al.
-
A multi-centre randomised controlled trial of minimally invasive direct coronary bypass grafting versus percutaneous transluminal coronary angioplasty with stenting for proximal stenosis of the left anterior descending coronary artery.
By Reeves BC, Angelini GD, Bryan AJ, Taylor FC, Cripps T, Spyt TJ, et al.
-
Does early magnetic resonance imaging influence management or improve outcome in patients referred to secondary care with low back pain? A pragmatic randomised controlled trial.
By Gilbert FJ, Grant AM, Gillan MGC, Vale L, Scott NW, Campbell MK, et al.
-
The clinical and cost-effectiveness of anakinra for the treatment of rheumatoid arthritis in adults: a systematic review and economic analysis.
By Clark W, Jobanputra P, Barton P, Burls A.
-
A rapid and systematic review and economic evaluation of the clinical and cost-effectiveness of newer drugs for treatment of mania associated with bipolar affective disorder.
By Bridle C, Palmer S, Bagnall A-M, Darba J, Duffy S, Sculpher M, et al.
-
Liquid-based cytology in cervical screening: an updated rapid and systematic review and economic analysis.
By Karnon J, Peters J, Platt J, Chilcott J, McGoogan E, Brewer N.
-
Systematic review of the long-term effects and economic consequences of treatments for obesity and implications for health improvement.
By Avenell A, Broom J, Brown TJ, Poobalan A, Aucott L, Stearns SC, et al.
-
Autoantibody testing in children with newly diagnosed type 1 diabetes mellitus.
By Dretzke J, Cummins C, Sandercock J, Fry-Smith A, Barrett T, Burls A.
-
Clinical effectiveness and cost-effectiveness of prehospital intravenous fluids in trauma patients.
By Dretzke J, Sandercock J, Bayliss S, Burls A.
-
Newer hypnotic drugs for the short-term management of insomnia: a systematic review and economic evaluation.
By Dündar Y, Boland A, Strobl J, Dodd S, Haycox A, Bagust A, et al.
-
Development and validation of methods for assessing the quality of diagnostic accuracy studies.
By Whiting P, Rutjes AWS, Dinnes J, Reitsma JB, Bossuyt PMM, Kleijnen J.
-
EVALUATE hysterectomy trial: a multicentre randomised trial comparing abdominal, vaginal and laparoscopic methods of hysterectomy.
By Garry R, Fountain J, Brown J, Manca A, Mason S, Sculpher M, et al.
-
Methods for expected value of information analysis in complex health economic models: developments on the health economics of interferon-β and glatiramer acetate for multiple sclerosis.
By Tappenden P, Chilcott JB, Eggington S, Oakley J, McCabe C.
-
Effectiveness and cost-effectiveness of imatinib for first-line treatment of chronic myeloid leukaemia in chronic phase: a systematic review and economic analysis.
By Dalziel K, Round A, Stein K, Garside R, Price A.
-
VenUS I: a randomised controlled trial of two types of bandage for treating venous leg ulcers.
By Iglesias C, Nelson EA, Cullum NA, Torgerson DJ, on behalf of the VenUS Team.
-
Systematic review of the effectiveness and cost-effectiveness, and economic evaluation, of myocardial perfusion scintigraphy for the diagnosis and management of angina and myocardial infarction.
By Mowatt G, Vale L, Brazzelli M, Hernandez R, Murray A, Scott N, et al.
-
A pilot study on the use of decision theory and value of information analysis as part of the NHS Health Technology Assessment programme.
By Claxton K, Ginnelly L, Sculpher M, Philips Z, Palmer S.
-
The Social Support and Family Health Study: a randomised controlled trial and economic evaluation of two alternative forms of postnatal support for mothers living in disadvantaged inner-city areas.
By Wiggins M, Oakley A, Roberts I, Turner H, Rajan L, Austerberry H, et al.
-
Psychosocial aspects of genetic screening of pregnant women and newborns: a systematic review.
By Green JM, Hewison J, Bekker HL, Bryant LD, Cuckle HS.
-
Evaluation of abnormal uterine bleeding: comparison of three outpatient procedures within cohorts defined by age and menopausal status.
By Critchley HOD, Warner P, Lee AJ, Brechin S, Guise J, Graham B.
-
Coronary artery stents: a rapid systematic review and economic evaluation.
By Hill R, Bagust A, Bakhai A, Dickson R, Dündar Y, Haycox A, et al.
-
Review of guidelines for good practice in decision-analytic modelling in health technology assessment.
By Philips Z, Ginnelly L, Sculpher M, Claxton K, Golder S, Riemsma R, et al.
-
Rituximab (MabThera®) for aggressive non-Hodgkin’s lymphoma: systematic review and economic evaluation.
By Knight C, Hind D, Brewer N, Abbott V.
-
Clinical effectiveness and cost-effectiveness of clopidogrel and modified-release dipyridamole in the secondary prevention of occlusive vascular events: a systematic review and economic evaluation.
By Jones L, Griffin S, Palmer S, Main C, Orton V, Sculpher M, et al.
-
Pegylated interferon α-2a and -2b in combination with ribavirin in the treatment of chronic hepatitis C: a systematic review and economic evaluation.
By Shepherd J, Brodin H, Cave C, Waugh N, Price A, Gabbay J.
-
Clopidogrel used in combination with aspirin compared with aspirin alone in the treatment of non-ST-segment- elevation acute coronary syndromes: a systematic review and economic evaluation.
By Main C, Palmer S, Griffin S, Jones L, Orton V, Sculpher M, et al.
-
Provision, uptake and cost of cardiac rehabilitation programmes: improving services to under-represented groups.
By Beswick AD, Rees K, Griebsch I, Taylor FC, Burke M, West RR, et al.
-
Involving South Asian patients in clinical trials.
By Hussain-Gambles M, Leese B, Atkin K, Brown J, Mason S, Tovey P.
-
Clinical and cost-effectiveness of continuous subcutaneous insulin infusion for diabetes.
By Colquitt JL, Green C, Sidhu MK, Hartwell D, Waugh N.
-
Identification and assessment of ongoing trials in health technology assessment reviews.
By Song FJ, Fry-Smith A, Davenport C, Bayliss S, Adi Y, Wilson JS, et al.
-
Systematic review and economic evaluation of a long-acting insulin analogue, insulin glargine
By Warren E, Weatherley-Jones E, Chilcott J, Beverley C.
-
Supplementation of a home-based exercise programme with a class-based programme for people with osteoarthritis of the knees: a randomised controlled trial and health economic analysis.
By McCarthy CJ, Mills PM, Pullen R, Richardson G, Hawkins N, Roberts CR, et al.
-
Clinical and cost-effectiveness of once-daily versus more frequent use of same potency topical corticosteroids for atopic eczema: a systematic review and economic evaluation.
By Green C, Colquitt JL, Kirby J, Davidson P, Payne E.
-
Acupuncture of chronic headache disorders in primary care: randomised controlled trial and economic analysis.
By Vickers AJ, Rees RW, Zollman CE, McCarney R, Smith CM, Ellis N, et al.
-
Generalisability in economic evaluation studies in healthcare: a review and case studies.
By Sculpher MJ, Pang FS, Manca A, Drummond MF, Golder S, Urdahl H, et al.
-
Virtual outreach: a randomised controlled trial and economic evaluation of joint teleconferenced medical consultations.
By Wallace P, Barber J, Clayton W, Currell R, Fleming K, Garner P, et al.
-
Randomised controlled multiple treatment comparison to provide a cost-effectiveness rationale for the selection of antimicrobial therapy in acne.
By Ozolins M, Eady EA, Avery A, Cunliffe WJ, O’Neill C, Simpson NB, et al.
-
Do the findings of case series studies vary significantly according to methodological characteristics?
By Dalziel K, Round A, Stein K, Garside R, Castelnuovo E, Payne L.
-
Improving the referral process for familial breast cancer genetic counselling: findings of three randomised controlled trials of two interventions.
By Wilson BJ, Torrance N, Mollison J, Wordsworth S, Gray JR, Haites NE, et al.
-
Randomised evaluation of alternative electrosurgical modalities to treat bladder outflow obstruction in men with benign prostatic hyperplasia.
By Fowler C, McAllister W, Plail R, Karim O, Yang Q.
-
A pragmatic randomised controlled trial of the cost-effectiveness of palliative therapies for patients with inoperable oesophageal cancer.
By Shenfine J, McNamee P, Steen N, Bond J, Griffin SM.
-
Impact of computer-aided detection prompts on the sensitivity and specificity of screening mammography.
By Taylor P, Champness J, Given- Wilson R, Johnston K, Potts H.
-
Issues in data monitoring and interim analysis of trials.
By Grant AM, Altman DG, Babiker AB, Campbell MK, Clemens FJ, Darbyshire JH, et al.
-
Lay public’s understanding of equipoise and randomisation in randomised controlled trials.
By Robinson EJ, Kerr CEP, Stevens AJ, Lilford RJ, Braunholtz DA, Edwards SJ, et al.
-
Clinical and cost-effectiveness of electroconvulsive therapy for depressive illness, schizophrenia, catatonia and mania: systematic reviews and economic modelling studies.
By Greenhalgh J, Knight C, Hind D, Beverley C, Walters S.
-
Measurement of health-related quality of life for people with dementia: development of a new instrument (DEMQOL) and an evaluation of current methodology.
By Smith SC, Lamping DL, Banerjee S, Harwood R, Foley B, Smith P, et al.
-
Clinical effectiveness and cost-effectiveness of drotrecogin alfa (activated) (Xigris®) for the treatment of severe sepsis in adults: a systematic review and economic evaluation.
By Green C, Dinnes J, Takeda A, Shepherd J, Hartwell D, Cave C, et al.
-
A methodological review of how heterogeneity has been examined in systematic reviews of diagnostic test accuracy.
By Dinnes J, Deeks J, Kirby J, Roderick P.
-
Cervical screening programmes: can automation help? Evidence from systematic reviews, an economic analysis and a simulation modelling exercise applied to the UK.
By Willis BH, Barton P, Pearmain P, Bryan S, Hyde C.
-
Laparoscopic surgery for inguinal hernia repair: systematic review of effectiveness and economic evaluation.
By McCormack K, Wake B, Perez J, Fraser C, Cook J, McIntosh E, et al.
-
Clinical effectiveness, tolerability and cost-effectiveness of newer drugs for epilepsy in adults: a systematic review and economic evaluation.
By Wilby J, Kainth A, Hawkins N, Epstein D, McIntosh H, McDaid C, et al.
-
A randomised controlled trial to compare the cost-effectiveness of tricyclic antidepressants, selective serotonin reuptake inhibitors and lofepramine.
By Peveler R, Kendrick T, Buxton M, Longworth L, Baldwin D, Moore M, et al.
-
Clinical effectiveness and cost-effectiveness of immediate angioplasty for acute myocardial infarction: systematic review and economic evaluation.
By Hartwell D, Colquitt J, Loveman E, Clegg AJ, Brodin H, Waugh N, et al.
-
A randomised controlled comparison of alternative strategies in stroke care.
By Kalra L, Evans A, Perez I, Knapp M, Swift C, Donaldson N.
-
The investigation and analysis of critical incidents and adverse events in healthcare.
By Woloshynowych M, Rogers S, Taylor-Adams S, Vincent C.
-
Potential use of routine databases in health technology assessment.
By Raftery J, Roderick P, Stevens A.
-
Clinical and cost-effectiveness of newer immunosuppressive regimens in renal transplantation: a systematic review and modelling study.
By Woodroffe R, Yao GL, Meads C, Bayliss S, Ready A, Raftery J, et al.
-
A systematic review and economic evaluation of alendronate, etidronate, risedronate, raloxifene and teriparatide for the prevention and treatment of postmenopausal osteoporosis.
By Stevenson M, Lloyd Jones M, De Nigris E, Brewer N, Davis S, Oakley J.
-
A systematic review to examine the impact of psycho-educational interventions on health outcomes and costs in adults and children with difficult asthma.
By Smith JR, Mugford M, Holland R, Candy B, Noble MJ, Harrison BDW, et al.
-
An evaluation of the costs, effectiveness and quality of renal replacement therapy provision in renal satellite units in England and Wales.
By Roderick P, Nicholson T, Armitage A, Mehta R, Mullee M, Gerard K, et al.
-
Imatinib for the treatment of patients with unresectable and/or metastatic gastrointestinal stromal tumours: systematic review and economic evaluation.
By Wilson J, Connock M, Song F, Yao G, Fry-Smith A, Raftery J, et al.
-
Indirect comparisons of competing interventions.
By Glenny AM, Altman DG, Song F, Sakarovitch C, Deeks JJ, D’Amico R, et al.
-
Cost-effectiveness of alternative strategies for the initial medical management of non-ST elevation acute coronary syndrome: systematic review and decision-analytical modelling.
By Robinson M, Palmer S, Sculpher M, Philips Z, Ginnelly L, Bowens A, et al.
-
Outcomes of electrically stimulated gracilis neosphincter surgery.
By Tillin T, Chambers M, Feldman R.
-
The effectiveness and cost-effectiveness of pimecrolimus and tacrolimus for atopic eczema: a systematic review and economic evaluation.
By Garside R, Stein K, Castelnuovo E, Pitt M, Ashcroft D, Dimmock P, et al.
-
Systematic review on urine albumin testing for early detection of diabetic complications.
By Newman DJ, Mattock MB, Dawnay ABS, Kerry S, McGuire A, Yaqoob M, et al.
-
Randomised controlled trial of the cost-effectiveness of water-based therapy for lower limb osteoarthritis.
By Cochrane T, Davey RC, Matthes Edwards SM.
-
Longer term clinical and economic benefits of offering acupuncture care to patients with chronic low back pain.
By Thomas KJ, MacPherson H, Ratcliffe J, Thorpe L, Brazier J, Campbell M, et al.
-
Cost-effectiveness and safety of epidural steroids in the management of sciatica.
By Price C, Arden N, Coglan L, Rogers P.
-
The British Rheumatoid Outcome Study Group (BROSG) randomised controlled trial to compare the effectiveness and cost-effectiveness of aggressive versus symptomatic therapy in established rheumatoid arthritis.
By Symmons D, Tricker K, Roberts C, Davies L, Dawes P, Scott DL.
-
Conceptual framework and systematic review of the effects of participants’ and professionals’ preferences in randomised controlled trials.
By King M, Nazareth I, Lampe F, Bower P, Chandler M, Morou M, et al.
-
The clinical and cost-effectiveness of implantable cardioverter defibrillators: a systematic review.
By Bryant J, Brodin H, Loveman E, Payne E, Clegg A.
-
A trial of problem-solving by community mental health nurses for anxiety, depression and life difficulties among general practice patients. The CPN-GP study.
By Kendrick T, Simons L, Mynors-Wallis L, Gray A, Lathlean J, Pickering R, et al.
-
The causes and effects of socio-demographic exclusions from clinical trials.
By Bartlett C, Doyal L, Ebrahim S, Davey P, Bachmann M, Egger M, et al.
-
Is hydrotherapy cost-effective? A randomised controlled trial of combined hydrotherapy programmes compared with physiotherapy land techniques in children with juvenile idiopathic arthritis.
By Epps H, Ginnelly L, Utley M, Southwood T, Gallivan S, Sculpher M, et al.
-
A randomised controlled trial and cost-effectiveness study of systematic screening (targeted and total population screening) versus routine practice for the detection of atrial fibrillation in people aged 65 and over. The SAFE study.
By Hobbs FDR, Fitzmaurice DA, Mant J, Murray E, Jowett S, Bryan S, et al.
-
Displaced intracapsular hip fractures in fit, older people: a randomised comparison of reduction and fixation, bipolar hemiarthroplasty and total hip arthroplasty.
By Keating JF, Grant A, Masson M, Scott NW, Forbes JF.
-
Long-term outcome of cognitive behaviour therapy clinical trials in central Scotland.
By Durham RC, Chambers JA, Power KG, Sharp DM, Macdonald RR, Major KA, et al.
-
The effectiveness and cost-effectiveness of dual-chamber pacemakers compared with single-chamber pacemakers for bradycardia due to atrioventricular block or sick sinus syndrome: systematic review and economic evaluation.
By Castelnuovo E, Stein K, Pitt M, Garside R, Payne E.
-
Newborn screening for congenital heart defects: a systematic review and cost-effectiveness analysis.
By Knowles R, Griebsch I, Dezateux C, Brown J, Bull C, Wren C.
-
The clinical and cost-effectiveness of left ventricular assist devices for end-stage heart failure: a systematic review and economic evaluation.
By Clegg AJ, Scott DA, Loveman E, Colquitt J, Hutchinson J, Royle P, et al.
-
The effectiveness of the Heidelberg Retina Tomograph and laser diagnostic glaucoma scanning system (GDx) in detecting and monitoring glaucoma.
By Kwartz AJ, Henson DB, Harper RA, Spencer AF, McLeod D.
-
Clinical and cost-effectiveness of autologous chondrocyte implantation for cartilage defects in knee joints: systematic review and economic evaluation.
By Clar C, Cummins E, McIntyre L, Thomas S, Lamb J, Bain L, et al.
-
Systematic review of effectiveness of different treatments for childhood retinoblastoma.
By McDaid C, Hartley S, Bagnall A-M, Ritchie G, Light K, Riemsma R.
-
Towards evidence-based guidelines for the prevention of venous thromboembolism: systematic reviews of mechanical methods, oral anticoagulation, dextran and regional anaesthesia as thromboprophylaxis.
By Roderick P, Ferris G, Wilson K, Halls H, Jackson D, Collins R, et al.
-
The effectiveness and cost-effectiveness of parent training/education programmes for the treatment of conduct disorder, including oppositional defiant disorder, in children.
By Dretzke J, Frew E, Davenport C, Barlow J, Stewart-Brown S, Sandercock J, et al.
-
The clinical and cost-effectiveness of donepezil, rivastigmine, galantamine and memantine for Alzheimer’s disease.
By Loveman E, Green C, Kirby J, Takeda A, Picot J, Payne E, et al.
-
FOOD: a multicentre randomised trial evaluating feeding policies in patients admitted to hospital with a recent stroke.
By Dennis M, Lewis S, Cranswick G, Forbes J.
-
The clinical effectiveness and cost-effectiveness of computed tomography screening for lung cancer: systematic reviews.
By Black C, Bagust A, Boland A, Walker S, McLeod C, De Verteuil R, et al.
-
A systematic review of the effectiveness and cost-effectiveness of neuroimaging assessments used to visualise the seizure focus in people with refractory epilepsy being considered for surgery.
By Whiting P, Gupta R, Burch J, Mujica Mota RE, Wright K, Marson A, et al.
-
Comparison of conference abstracts and presentations with full-text articles in the health technology assessments of rapidly evolving technologies.
By Dundar Y, Dodd S, Dickson R, Walley T, Haycox A, Williamson PR.
-
Systematic review and evaluation of methods of assessing urinary incontinence.
By Martin JL, Williams KS, Abrams KR, Turner DA, Sutton AJ, Chapple C, et al.
-
The clinical effectiveness and cost-effectiveness of newer drugs for children with epilepsy. A systematic review.
By Connock M, Frew E, Evans B-W, Bryan S, Cummins C, Fry-Smith A, et al.
-
Surveillance of Barrett’s oesophagus: exploring the uncertainty through systematic review, expert workshop and economic modelling.
By Garside R, Pitt M, Somerville M, Stein K, Price A, Gilbert N.
-
Topotecan, pegylated liposomal doxorubicin hydrochloride and paclitaxel for second-line or subsequent treatment of advanced ovarian cancer: a systematic review and economic evaluation.
By Main C, Bojke L, Griffin S, Norman G, Barbieri M, Mather L, et al.
-
Evaluation of molecular techniques in prediction and diagnosis of cytomegalovirus disease in immunocompromised patients.
By Szczepura A, Westmoreland D, Vinogradova Y, Fox J, Clark M.
-
Screening for thrombophilia in high-risk situations: systematic review and cost-effectiveness analysis. The Thrombosis: Risk and Economic Assessment of Thrombophilia Screening (TREATS) study.
By Wu O, Robertson L, Twaddle S, Lowe GDO, Clark P, Greaves M, et al.
-
A series of systematic reviews to inform a decision analysis for sampling and treating infected diabetic foot ulcers.
By Nelson EA, O’Meara S, Craig D, Iglesias C, Golder S, Dalton J, et al.
-
Randomised clinical trial, observational study and assessment of cost-effectiveness of the treatment of varicose veins (REACTIV trial).
By Michaels JA, Campbell WB, Brazier JE, MacIntyre JB, Palfreyman SJ, Ratcliffe J, et al.
-
The cost-effectiveness of screening for oral cancer in primary care.
By Speight PM, Palmer S, Moles DR, Downer MC, Smith DH, Henriksson M, et al.
-
Measurement of the clinical and cost-effectiveness of non-invasive diagnostic testing strategies for deep vein thrombosis.
By Goodacre S, Sampson F, Stevenson M, Wailoo A, Sutton A, Thomas S, et al.
-
Systematic review of the effectiveness and cost-effectiveness of HealOzone® for the treatment of occlusal pit/fissure caries and root caries.
By Brazzelli M, McKenzie L, Fielding S, Fraser C, Clarkson J, Kilonzo M, et al.
-
Randomised controlled trials of conventional antipsychotic versus new atypical drugs, and new atypical drugs versus clozapine, in people with schizophrenia responding poorly to, or intolerant of, current drug treatment.
By Lewis SW, Davies L, Jones PB, Barnes TRE, Murray RM, Kerwin R, et al.
-
Diagnostic tests and algorithms used in the investigation of haematuria: systematic reviews and economic evaluation.
By Rodgers M, Nixon J, Hempel S, Aho T, Kelly J, Neal D, et al.
-
Cognitive behavioural therapy in addition to antispasmodic therapy for irritable bowel syndrome in primary care: randomised controlled trial.
By Kennedy TM, Chalder T, McCrone P, Darnley S, Knapp M, Jones RH, et al.
-
A systematic review of the clinical effectiveness and cost-effectiveness of enzyme replacement therapies for Fabry’s disease and mucopolysaccharidosis type 1.
By Connock M, Juarez-Garcia A, Frew E, Mans A, Dretzke J, Fry-Smith A, et al.
-
Health benefits of antiviral therapy for mild chronic hepatitis C: randomised controlled trial and economic evaluation.
By Wright M, Grieve R, Roberts J, Main J, Thomas HC, on behalf of the UK Mild Hepatitis C Trial Investigators.
-
Pressure relieving support surfaces: a randomised evaluation.
By Nixon J, Nelson EA, Cranny G, Iglesias CP, Hawkins K, Cullum NA, et al.
-
A systematic review and economic model of the effectiveness and cost-effectiveness of methylphenidate, dexamfetamine and atomoxetine for the treatment of attention deficit hyperactivity disorder in children and adolescents.
By King S, Griffin S, Hodges Z, Weatherly H, Asseburg C, Richardson G, et al.
-
The clinical effectiveness and cost-effectiveness of enzyme replacement therapy for Gaucher’s disease: a systematic review.
By Connock M, Burls A, Frew E, Fry-Smith A, Juarez-Garcia A, McCabe C, et al.
-
Effectiveness and cost-effectiveness of salicylic acid and cryotherapy for cutaneous warts. An economic decision model.
By Thomas KS, Keogh-Brown MR, Chalmers JR, Fordham RJ, Holland RC, Armstrong SJ, et al.
-
A systematic literature review of the effectiveness of non-pharmacological interventions to prevent wandering in dementia and evaluation of the ethical implications and acceptability of their use.
By Robinson L, Hutchings D, Corner L, Beyer F, Dickinson H, Vanoli A, et al.
-
A review of the evidence on the effects and costs of implantable cardioverter defibrillator therapy in different patient groups, and modelling of cost-effectiveness and cost–utility for these groups in a UK context.
By Buxton M, Caine N, Chase D, Connelly D, Grace A, Jackson C, et al.
-
Adefovir dipivoxil and pegylated interferon alfa-2a for the treatment of chronic hepatitis B: a systematic review and economic evaluation.
By Shepherd J, Jones J, Takeda A, Davidson P, Price A.
-
An evaluation of the clinical and cost-effectiveness of pulmonary artery catheters in patient management in intensive care: a systematic review and a randomised controlled trial.
By Harvey S, Stevens K, Harrison D, Young D, Brampton W, McCabe C, et al.
-
Accurate, practical and cost-effective assessment of carotid stenosis in the UK.
By Wardlaw JM, Chappell FM, Stevenson M, De Nigris E, Thomas S, Gillard J, et al.
-
Etanercept and infliximab for the treatment of psoriatic arthritis: a systematic review and economic evaluation.
By Woolacott N, Bravo Vergel Y, Hawkins N, Kainth A, Khadjesari Z, Misso K, et al.
-
The cost-effectiveness of testing for hepatitis C in former injecting drug users.
By Castelnuovo E, Thompson-Coon J, Pitt M, Cramp M, Siebert U, Price A, et al.
-
Computerised cognitive behaviour therapy for depression and anxiety update: a systematic review and economic evaluation.
By Kaltenthaler E, Brazier J, De Nigris E, Tumur I, Ferriter M, Beverley C, et al.
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.
By Williams C, Brunskill S, Altman D, Briggs A, Campbell H, Clarke M, et al.
-
Psychological therapies including dialectical behaviour therapy for borderline personality disorder: a systematic review and preliminary economic evaluation.
By Brazier J, Tumur I, Holmes M, Ferriter M, Parry G, Dent-Brown K, et al.
-
Clinical effectiveness and cost-effectiveness of tests for the diagnosis and investigation of urinary tract infection in children: a systematic review and economic model.
By Whiting P, Westwood M, Bojke L, Palmer S, Richardson G, Cooper J, et al.
-
Cognitive behavioural therapy in chronic fatigue syndrome: a randomised controlled trial of an outpatient group programme.
By O’Dowd H, Gladwell P, Rogers CA, Hollinghurst S, Gregory A.
-
A comparison of the cost-effectiveness of five strategies for the prevention of nonsteroidal anti-inflammatory drug-induced gastrointestinal toxicity: a systematic review with economic modelling.
By Brown TJ, Hooper L, Elliott RA, Payne K, Webb R, Roberts C, et al.
-
The effectiveness and cost-effectiveness of computed tomography screening for coronary artery disease: systematic review.
By Waugh N, Black C, Walker S, McIntyre L, Cummins E, Hillis G.
-
What are the clinical outcome and cost-effectiveness of endoscopy undertaken by nurses when compared with doctors? A Multi-Institution Nurse Endoscopy Trial (MINuET).
By Williams J, Russell I, Durai D, Cheung W-Y, Farrin A, Bloor K, et al.
-
The clinical and cost-effectiveness of oxaliplatin and capecitabine for the adjuvant treatment of colon cancer: systematic review and economic evaluation.
By Pandor A, Eggington S, Paisley S, Tappenden P, Sutcliffe P.
-
A systematic review of the effectiveness of adalimumab, etanercept and infliximab for the treatment of rheumatoid arthritis in adults and an economic evaluation of their cost-effectiveness.
By Chen Y-F, Jobanputra P, Barton P, Jowett S, Bryan S, Clark W, et al.
-
Telemedicine in dermatology: a randomised controlled trial.
By Bowns IR, Collins K, Walters SJ, McDonagh AJG.
-
Cost-effectiveness of cell salvage and alternative methods of minimising perioperative allogeneic blood transfusion: a systematic review and economic model.
By Davies L, Brown TJ, Haynes S, Payne K, Elliott RA, McCollum C.
-
Clinical effectiveness and cost-effectiveness of laparoscopic surgery for colorectal cancer: systematic reviews and economic evaluation.
By Murray A, Lourenco T, de Verteuil R, Hernandez R, Fraser C, McKinley A, et al.
-
Etanercept and efalizumab for the treatment of psoriasis: a systematic review.
By Woolacott N, Hawkins N, Mason A, Kainth A, Khadjesari Z, Bravo Vergel Y, et al.
-
Systematic reviews of clinical decision tools for acute abdominal pain.
By Liu JLY, Wyatt JC, Deeks JJ, Clamp S, Keen J, Verde P, et al.
-
Evaluation of the ventricular assist device programme in the UK.
By Sharples L, Buxton M, Caine N, Cafferty F, Demiris N, Dyer M, et al.
-
A systematic review and economic model of the clinical and cost-effectiveness of immunosuppressive therapy for renal transplantation in children.
By Yao G, Albon E, Adi Y, Milford D, Bayliss S, Ready A, et al.
-
Amniocentesis results: investigation of anxiety. The ARIA trial.
By Hewison J, Nixon J, Fountain J, Cocks K, Jones C, Mason G, et al.
-
Pemetrexed disodium for the treatment of malignant pleural mesothelioma: a systematic review and economic evaluation.
By Dundar Y, Bagust A, Dickson R, Dodd S, Green J, Haycox A, et al.
-
A systematic review and economic model of the clinical effectiveness and cost-effectiveness of docetaxel in combination with prednisone or prednisolone for the treatment of hormone-refractory metastatic prostate cancer.
By Collins R, Fenwick E, Trowman R, Perard R, Norman G, Light K, et al.
-
A systematic review of rapid diagnostic tests for the detection of tuberculosis infection.
By Dinnes J, Deeks J, Kunst H, Gibson A, Cummins E, Waugh N, et al.
-
The clinical effectiveness and cost-effectiveness of strontium ranelate for the prevention of osteoporotic fragility fractures in postmenopausal women.
By Stevenson M, Davis S, Lloyd-Jones M, Beverley C.
-
A systematic review of quantitative and qualitative research on the role and effectiveness of written information available to patients about individual medicines.
By Raynor DK, Blenkinsopp A, Knapp P, Grime J, Nicolson DJ, Pollock K, et al.
-
Oral naltrexone as a treatment for relapse prevention in formerly opioid-dependent drug users: a systematic review and economic evaluation.
By Adi Y, Juarez-Garcia A, Wang D, Jowett S, Frew E, Day E, et al.
-
Glucocorticoid-induced osteoporosis: a systematic review and cost–utility analysis.
By Kanis JA, Stevenson M, McCloskey EV, Davis S, Lloyd-Jones M.
-
Epidemiological, social, diagnostic and economic evaluation of population screening for genital chlamydial infection.
By Low N, McCarthy A, Macleod J, Salisbury C, Campbell R, Roberts TE, et al.
-
Methadone and buprenorphine for the management of opioid dependence: a systematic review and economic evaluation.
By Connock M, Juarez-Garcia A, Jowett S, Frew E, Liu Z, Taylor RJ, et al.
-
Exercise Evaluation Randomised Trial (EXERT): a randomised trial comparing GP referral for leisure centre-based exercise, community-based walking and advice only.
By Isaacs AJ, Critchley JA, See Tai S, Buckingham K, Westley D, Harridge SDR, et al.
-
Interferon alfa (pegylated and non-pegylated) and ribavirin for the treatment of mild chronic hepatitis C: a systematic review and economic evaluation.
By Shepherd J, Jones J, Hartwell D, Davidson P, Price A, Waugh N.
-
Systematic review and economic evaluation of bevacizumab and cetuximab for the treatment of metastatic colorectal cancer.
By Tappenden P, Jones R, Paisley S, Carroll C.
-
A systematic review and economic evaluation of epoetin alfa, epoetin beta and darbepoetin alfa in anaemia associated with cancer, especially that attributable to cancer treatment.
By Wilson J, Yao GL, Raftery J, Bohlius J, Brunskill S, Sandercock J, et al.
-
A systematic review and economic evaluation of statins for the prevention of coronary events.
By Ward S, Lloyd Jones M, Pandor A, Holmes M, Ara R, Ryan A, et al.
-
A systematic review of the effectiveness and cost-effectiveness of different models of community-based respite care for frail older people and their carers.
By Mason A, Weatherly H, Spilsbury K, Arksey H, Golder S, Adamson J, et al.
-
Additional therapy for young children with spastic cerebral palsy: a randomised controlled trial.
By Weindling AM, Cunningham CC, Glenn SM, Edwards RT, Reeves DJ.
-
Screening for type 2 diabetes: literature review and economic modelling.
By Waugh N, Scotland G, McNamee P, Gillett M, Brennan A, Goyder E, et al.
-
The effectiveness and cost-effectiveness of cinacalcet for secondary hyperparathyroidism in end-stage renal disease patients on dialysis: a systematic review and economic evaluation.
By Garside R, Pitt M, Anderson R, Mealing S, Roome C, Snaith A, et al.
-
The clinical effectiveness and cost-effectiveness of gemcitabine for metastatic breast cancer: a systematic review and economic evaluation.
By Takeda AL, Jones J, Loveman E, Tan SC, Clegg AJ.
-
A systematic review of duplex ultrasound, magnetic resonance angiography and computed tomography angiography for the diagnosis and assessment of symptomatic, lower limb peripheral arterial disease.
By Collins R, Cranny G, Burch J, Aguiar-Ibáñez R, Craig D, Wright K, et al.
-
The clinical effectiveness and cost-effectiveness of treatments for children with idiopathic steroid-resistant nephrotic syndrome: a systematic review.
By Colquitt JL, Kirby J, Green C, Cooper K, Trompeter RS.
-
A systematic review of the routine monitoring of growth in children of primary school age to identify growth-related conditions.
By Fayter D, Nixon J, Hartley S, Rithalia A, Butler G, Rudolf M, et al.
-
Systematic review of the effectiveness of preventing and treating Staphylococcus aureus carriage in reducing peritoneal catheter-related infections.
By McCormack K, Rabindranath K, Kilonzo M, Vale L, Fraser C, McIntyre L, et al.
-
The clinical effectiveness and cost of repetitive transcranial magnetic stimulation versus electroconvulsive therapy in severe depression: a multicentre pragmatic randomised controlled trial and economic analysis.
By McLoughlin DM, Mogg A, Eranti S, Pluck G, Purvis R, Edwards D, et al.
-
A randomised controlled trial and economic evaluation of direct versus indirect and individual versus group modes of speech and language therapy for children with primary language impairment.
By Boyle J, McCartney E, Forbes J, O’Hare A.
-
Hormonal therapies for early breast cancer: systematic review and economic evaluation.
By Hind D, Ward S, De Nigris E, Simpson E, Carroll C, Wyld L.
-
Cardioprotection against the toxic effects of anthracyclines given to children with cancer: a systematic review.
By Bryant J, Picot J, Levitt G, Sullivan I, Baxter L, Clegg A.
-
Adalimumab, etanercept and infliximab for the treatment of ankylosing spondylitis: a systematic review and economic evaluation.
By McLeod C, Bagust A, Boland A, Dagenais P, Dickson R, Dundar Y, et al.
-
Prenatal screening and treatment strategies to prevent group B streptococcal and other bacterial infections in early infancy: cost-effectiveness and expected value of information analyses.
By Colbourn T, Asseburg C, Bojke L, Philips Z, Claxton K, Ades AE, et al.
-
Clinical effectiveness and cost-effectiveness of bone morphogenetic proteins in the non-healing of fractures and spinal fusion: a systematic review.
By Garrison KR, Donell S, Ryder J, Shemilt I, Mugford M, Harvey I, et al.
-
A randomised controlled trial of postoperative radiotherapy following breast-conserving surgery in a minimum-risk older population. The PRIME trial.
By Prescott RJ, Kunkler IH, Williams LJ, King CC, Jack W, van der Pol M, et al.
-
Current practice, accuracy, effectiveness and cost-effectiveness of the school entry hearing screen.
By Bamford J, Fortnum H, Bristow K, Smith J, Vamvakas G, Davies L, et al.
-
The clinical effectiveness and cost-effectiveness of inhaled insulin in diabetes mellitus: a systematic review and economic evaluation.
By Black C, Cummins E, Royle P, Philip S, Waugh N.
-
Surveillance of cirrhosis for hepatocellular carcinoma: systematic review and economic analysis.
By Thompson Coon J, Rogers G, Hewson P, Wright D, Anderson R, Cramp M, et al.
-
The Birmingham Rehabilitation Uptake Maximisation Study (BRUM). Homebased compared with hospital-based cardiac rehabilitation in a multi-ethnic population: cost-effectiveness and patient adherence.
By Jolly K, Taylor R, Lip GYH, Greenfield S, Raftery J, Mant J, et al.
-
A systematic review of the clinical, public health and cost-effectiveness of rapid diagnostic tests for the detection and identification of bacterial intestinal pathogens in faeces and food.
By Abubakar I, Irvine L, Aldus CF, Wyatt GM, Fordham R, Schelenz S, et al.
-
A randomised controlled trial examining the longer-term outcomes of standard versus new antiepileptic drugs. The SANAD trial.
By Marson AG, Appleton R, Baker GA, Chadwick DW, Doughty J, Eaton B, et al.
-
Clinical effectiveness and cost-effectiveness of different models of managing long-term oral anti-coagulation therapy: a systematic review and economic modelling.
By Connock M, Stevens C, Fry-Smith A, Jowett S, Fitzmaurice D, Moore D, et al.
-
A systematic review and economic model of the clinical effectiveness and cost-effectiveness of interventions for preventing relapse in people with bipolar disorder.
By Soares-Weiser K, Bravo Vergel Y, Beynon S, Dunn G, Barbieri M, Duffy S, et al.
-
Taxanes for the adjuvant treatment of early breast cancer: systematic review and economic evaluation.
By Ward S, Simpson E, Davis S, Hind D, Rees A, Wilkinson A.
-
The clinical effectiveness and cost-effectiveness of screening for open angle glaucoma: a systematic review and economic evaluation.
By Burr JM, Mowatt G, Hernández R, Siddiqui MAR, Cook J, Lourenco T, et al.
-
Acceptability, benefit and costs of early screening for hearing disability: a study of potential screening tests and models.
By Davis A, Smith P, Ferguson M, Stephens D, Gianopoulos I.
-
Contamination in trials of educational interventions.
By Keogh-Brown MR, Bachmann MO, Shepstone L, Hewitt C, Howe A, Ramsay CR, et al.
-
Overview of the clinical effectiveness of positron emission tomography imaging in selected cancers.
By Facey K, Bradbury I, Laking G, Payne E.
-
The effectiveness and cost-effectiveness of carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma: a systematic review and economic evaluation.
By Garside R, Pitt M, Anderson R, Rogers G, Dyer M, Mealing S, et al.
-
Drug-eluting stents: a systematic review and economic evaluation.
By Hill RA, Boland A, Dickson R, Dündar Y, Haycox A, McLeod C, et al.
-
The clinical effectiveness and cost-effectiveness of cardiac resynchronisation (biventricular pacing) for heart failure: systematic review and economic model.
By Fox M, Mealing S, Anderson R, Dean J, Stein K, Price A, et al.
-
Recruitment to randomised trials: strategies for trial enrolment and participation study. The STEPS study.
By Campbell MK, Snowdon C, Francis D, Elbourne D, McDonald AM, Knight R, et al.
-
Cost-effectiveness of functional cardiac testing in the diagnosis and management of coronary artery disease: a randomised controlled trial. The CECaT trial.
By Sharples L, Hughes V, Crean A, Dyer M, Buxton M, Goldsmith K, et al.
-
Evaluation of diagnostic tests when there is no gold standard. A review of methods.
By Rutjes AWS, Reitsma JB, Coomarasamy A, Khan KS, Bossuyt PMM.
-
Systematic reviews of the clinical effectiveness and cost-effectiveness of proton pump inhibitors in acute upper gastrointestinal bleeding.
By Leontiadis GI, Sreedharan A, Dorward S, Barton P, Delaney B, Howden CW, et al.
-
A review and critique of modelling in prioritising and designing screening programmes.
By Karnon J, Goyder E, Tappenden P, McPhie S, Towers I, Brazier J, et al.
-
An assessment of the impact of the NHS Health Technology Assessment Programme.
By Hanney S, Buxton M, Green C, Coulson D, Raftery J.
-
A systematic review and economic model of switching from nonglycopeptide to glycopeptide antibiotic prophylaxis for surgery.
By Cranny G, Elliott R, Weatherly H, Chambers D, Hawkins N, Myers L, et al.
-
‘Cut down to quit’ with nicotine replacement therapies in smoking cessation: a systematic review of effectiveness and economic analysis.
By Wang D, Connock M, Barton P, Fry-Smith A, Aveyard P, Moore D.
-
A systematic review of the effectiveness of strategies for reducing fracture risk in children with juvenile idiopathic arthritis with additional data on long-term risk of fracture and cost of disease management.
By Thornton J, Ashcroft D, O’Neill T, Elliott R, Adams J, Roberts C, et al.
-
Does befriending by trained lay workers improve psychological well-being and quality of life for carers of people with dementia, and at what cost? A randomised controlled trial.
By Charlesworth G, Shepstone L, Wilson E, Thalanany M, Mugford M, Poland F.
-
A multi-centre retrospective cohort study comparing the efficacy, safety and cost-effectiveness of hysterectomy and uterine artery embolisation for the treatment of symptomatic uterine fibroids. The HOPEFUL study.
By Hirst A, Dutton S, Wu O, Briggs A, Edwards C, Waldenmaier L, et al.
-
Methods of prediction and prevention of pre-eclampsia: systematic reviews of accuracy and effectiveness literature with economic modelling.
By Meads CA, Cnossen JS, Meher S, Juarez-Garcia A, ter Riet G, Duley L, et al.
-
The use of economic evaluations in NHS decision-making: a review and empirical investigation.
By Williams I, McIver S, Moore D, Bryan S.
-
Stapled haemorrhoidectomy (haemorrhoidopexy) for the treatment of haemorrhoids: a systematic review and economic evaluation.
By Burch J, Epstein D, Baba-Akbari A, Weatherly H, Fox D, Golder S, et al.
-
The clinical effectiveness of diabetes education models for Type 2 diabetes: a systematic review.
By Loveman E, Frampton GK, Clegg AJ.
-
Payment to healthcare professionals for patient recruitment to trials: systematic review and qualitative study.
By Raftery J, Bryant J, Powell J, Kerr C, Hawker S.
-
Cyclooxygenase-2 selective non-steroidal anti-inflammatory drugs (etodolac, meloxicam, celecoxib, rofecoxib, etoricoxib, valdecoxib and lumiracoxib) for osteoarthritis and rheumatoid arthritis: a systematic review and economic evaluation.
By Chen Y-F, Jobanputra P, Barton P, Bryan S, Fry-Smith A, Harris G, et al.
-
The clinical effectiveness and cost-effectiveness of central venous catheters treated with anti-infective agents in preventing bloodstream infections: a systematic review and economic evaluation.
By Hockenhull JC, Dwan K, Boland A, Smith G, Bagust A, Dundar Y, et al.
-
Stepped treatment of older adults on laxatives. The STOOL trial.
By Mihaylov S, Stark C, McColl E, Steen N, Vanoli A, Rubin G, et al.
-
A randomised controlled trial of cognitive behaviour therapy in adolescents with major depression treated by selective serotonin reuptake inhibitors. The ADAPT trial.
By Goodyer IM, Dubicka B, Wilkinson P, Kelvin R, Roberts C, Byford S, et al.
-
The use of irinotecan, oxaliplatin and raltitrexed for the treatment of advanced colorectal cancer: systematic review and economic evaluation.
By Hind D, Tappenden P, Tumur I, Eggington E, Sutcliffe P, Ryan A.
-
Ranibizumab and pegaptanib for the treatment of age-related macular degeneration: a systematic review and economic evaluation.
By Colquitt JL, Jones J, Tan SC, Takeda A, Clegg AJ, Price A.
-
Systematic review of the clinical effectiveness and cost-effectiveness of 64-slice or higher computed tomography angiography as an alternative to invasive coronary angiography in the investigation of coronary artery disease.
By Mowatt G, Cummins E, Waugh N, Walker S, Cook J, Jia X, et al.
-
Structural neuroimaging in psychosis: a systematic review and economic evaluation.
By Albon E, Tsourapas A, Frew E, Davenport C, Oyebode F, Bayliss S, et al.
-
Systematic review and economic analysis of the comparative effectiveness of different inhaled corticosteroids and their usage with long-acting beta2 agonists for the treatment of chronic asthma in adults and children aged 12 years and over.
By Shepherd J, Rogers G, Anderson R, Main C, Thompson-Coon J, Hartwell D, et al.
-
Systematic review and economic analysis of the comparative effectiveness of different inhaled corticosteroids and their usage with long-acting beta2 agonists for the treatment of chronic asthma in children under the age of 12 years.
By Main C, Shepherd J, Anderson R, Rogers G, Thompson-Coon J, Liu Z, et al.
-
Ezetimibe for the treatment of hypercholesterolaemia: a systematic review and economic evaluation.
By Ara R, Tumur I, Pandor A, Duenas A, Williams R, Wilkinson A, et al.
-
Topical or oral ibuprofen for chronic knee pain in older people. The TOIB study.
By Underwood M, Ashby D, Carnes D, Castelnuovo E, Cross P, Harding G, et al.
-
A prospective randomised comparison of minor surgery in primary and secondary care. The MiSTIC trial.
By George S, Pockney P, Primrose J, Smith H, Little P, Kinley H, et al.
-
A review and critical appraisal of measures of therapist–patient interactions in mental health settings.
By Cahill J, Barkham M, Hardy G, Gilbody S, Richards D, Bower P, et al.
-
The clinical effectiveness and cost-effectiveness of screening programmes for amblyopia and strabismus in children up to the age of 4–5 years: a systematic review and economic evaluation.
By Carlton J, Karnon J, Czoski-Murray C, Smith KJ, Marr J.
-
A systematic review of the clinical effectiveness and cost-effectiveness and economic modelling of minimal incision total hip replacement approaches in the management of arthritic disease of the hip.
By de Verteuil R, Imamura M, Zhu S, Glazener C, Fraser C, Munro N, et al.
-
A preliminary model-based assessment of the cost–utility of a screening programme for early age-related macular degeneration.
By Karnon J, Czoski-Murray C, Smith K, Brand C, Chakravarthy U, Davis S, et al.
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.
By Shepherd J, Jones J, Frampton GK, Tanajewski L, Turner D, Price A.
-
Absorbent products for urinary/faecal incontinence: a comparative evaluation of key product categories.
By Fader M, Cottenden A, Getliffe K, Gage H, Clarke-O’Neill S, Jamieson K, et al.
-
A systematic review of repetitive functional task practice with modelling of resource use, costs and effectiveness.
By French B, Leathley M, Sutton C, McAdam J, Thomas L, Forster A, et al.
-
The effectiveness and cost-effectivness of minimal access surgery amongst people with gastro-oesophageal reflux disease – a UK collaborative study. The reflux trial.
By Grant A, Wileman S, Ramsay C, Bojke L, Epstein D, Sculpher M, et al.
-
Time to full publication of studies of anti-cancer medicines for breast cancer and the potential for publication bias: a short systematic review.
By Takeda A, Loveman E, Harris P, Hartwell D, Welch K.
-
Performance of screening tests for child physical abuse in accident and emergency departments.
By Woodman J, Pitt M, Wentz R, Taylor B, Hodes D, Gilbert RE.
-
Curative catheter ablation in atrial fibrillation and typical atrial flutter: systematic review and economic evaluation.
By Rodgers M, McKenna C, Palmer S, Chambers D, Van Hout S, Golder S, et al.
-
Systematic review and economic modelling of effectiveness and cost utility of surgical treatments for men with benign prostatic enlargement.
By Lourenco T, Armstrong N, N’Dow J, Nabi G, Deverill M, Pickard R, et al.
-
Immunoprophylaxis against respiratory syncytial virus (RSV) with palivizumab in children: a systematic review and economic evaluation.
By Wang D, Cummins C, Bayliss S, Sandercock J, Burls A.
-
Deferasirox for the treatment of iron overload associated with regular blood transfusions (transfusional haemosiderosis) in patients suffering with chronic anaemia: a systematic review and economic evaluation.
By McLeod C, Fleeman N, Kirkham J, Bagust A, Boland A, Chu P, et al.
-
Thrombophilia testing in people with venous thromboembolism: systematic review and cost-effectiveness analysis.
By Simpson EL, Stevenson MD, Rawdin A, Papaioannou D.
-
Surgical procedures and non-surgical devices for the management of non-apnoeic snoring: a systematic review of clinical effects and associated treatment costs.
By Main C, Liu Z, Welch K, Weiner G, Quentin Jones S, Stein K.
-
Continuous positive airway pressure devices for the treatment of obstructive sleep apnoea–hypopnoea syndrome: a systematic review and economic analysis.
By McDaid C, Griffin S, Weatherly H, Durée K, van der Burgt M, van Hout S, Akers J, et al.
-
Use of classical and novel biomarkers as prognostic risk factors for localised prostate cancer: a systematic review.
By Sutcliffe P, Hummel S, Simpson E, Young T, Rees A, Wilkinson A, et al.
-
The harmful health effects of recreational ecstasy: a systematic review of observational evidence.
By Rogers G, Elston J, Garside R, Roome C, Taylor R, Younger P, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of oesophageal Doppler monitoring in critically ill and high-risk surgical patients.
By Mowatt G, Houston G, Hernández R, de Verteuil R, Fraser C, Cuthbertson B, et al.
-
The use of surrogate outcomes in model-based cost-effectiveness analyses: a survey of UK Health Technology Assessment reports.
By Taylor RS, Elston J.
-
Controlling Hypertension and Hypotension Immediately Post Stroke (CHHIPS) – a randomised controlled trial.
By Potter J, Mistri A, Brodie F, Chernova J, Wilson E, Jagger C, et al.
-
Routine antenatal anti-D prophylaxis for RhD-negative women: a systematic review and economic evaluation.
By Pilgrim H, Lloyd-Jones M, Rees A.
-
Amantadine, oseltamivir and zanamivir for the prophylaxis of influenza (including a review of existing guidance no. 67): a systematic review and economic evaluation.
By Tappenden P, Jackson R, Cooper K, Rees A, Simpson E, Read R, et al.
-
Improving the evaluation of therapeutic interventions in multiple sclerosis: the role of new psychometric methods.
By Hobart J, Cano S.
-
Treatment of severe ankle sprain: a pragmatic randomised controlled trial comparing the clinical effectiveness and cost-effectiveness of three types of mechanical ankle support with tubular bandage. The CAST trial.
By Cooke MW, Marsh JL, Clark M, Nakash R, Jarvis RM, Hutton JL, et al. , on behalf of the CAST trial group.
-
Non-occupational postexposure prophylaxis for HIV: a systematic review.
By Bryant J, Baxter L, Hird S.
-
Blood glucose self-monitoring in type 2 diabetes: a randomised controlled trial.
By Farmer AJ, Wade AN, French DP, Simon J, Yudkin P, Gray A, et al.
-
How far does screening women for domestic (partner) violence in different health-care settings meet criteria for a screening programme? Systematic reviews of nine UK National Screening Committee criteria.
By Feder G, Ramsay J, Dunne D, Rose M, Arsene C, Norman R, et al.
-
Spinal cord stimulation for chronic pain of neuropathic or ischaemic origin: systematic review and economic evaluation.
By Simpson EL, Duenas A, Holmes MW, Papaioannou D, Chilcott J.
-
The role of magnetic resonance imaging in the identification of suspected acoustic neuroma: a systematic review of clinical and cost-effectiveness and natural history.
By Fortnum H, O’Neill C, Taylor R, Lenthall R, Nikolopoulos T, Lightfoot G, et al.
-
Dipsticks and diagnostic algorithms in urinary tract infection: development and validation, randomised trial, economic analysis, observational cohort and qualitative study.
By Little P, Turner S, Rumsby K, Warner G, Moore M, Lowes JA, et al.
-
Systematic review of respite care in the frail elderly.
By Shaw C, McNamara R, Abrams K, Cannings-John R, Hood K, Longo M, et al.
-
Neuroleptics in the treatment of aggressive challenging behaviour for people with intellectual disabilities: a randomised controlled trial (NACHBID).
By Tyrer P, Oliver-Africano P, Romeo R, Knapp M, Dickens S, Bouras N, et al.
-
Randomised controlled trial to determine the clinical effectiveness and cost-effectiveness of selective serotonin reuptake inhibitors plus supportive care, versus supportive care alone, for mild to moderate depression with somatic symptoms in primary care: the THREAD (THREshold for AntiDepressant response) study.
By Kendrick T, Chatwin J, Dowrick C, Tylee A, Morriss R, Peveler R, et al.
-
Diagnostic strategies using DNA testing for hereditary haemochromatosis in at-risk populations: a systematic review and economic evaluation.
By Bryant J, Cooper K, Picot J, Clegg A, Roderick P, Rosenberg W, et al.
-
Enhanced external counterpulsation for the treatment of stable angina and heart failure: a systematic review and economic analysis.
By McKenna C, McDaid C, Suekarran S, Hawkins N, Claxton K, Light K, et al.
-
Development of a decision support tool for primary care management of patients with abnormal liver function tests without clinically apparent liver disease: a record-linkage population cohort study and decision analysis (ALFIE).
By Donnan PT, McLernon D, Dillon JF, Ryder S, Roderick P, Sullivan F, et al.
-
A systematic review of presumed consent systems for deceased organ donation.
By Rithalia A, McDaid C, Suekarran S, Norman G, Myers L, Sowden A.
-
Paracetamol and ibuprofen for the treatment of fever in children: the PITCH randomised controlled trial.
By Hay AD, Redmond NM, Costelloe C, Montgomery AA, Fletcher M, Hollinghurst S, et al.
-
A randomised controlled trial to compare minimally invasive glucose monitoring devices with conventional monitoring in the management of insulin-treated diabetes mellitus (MITRE).
By Newman SP, Cooke D, Casbard A, Walker S, Meredith S, Nunn A, et al.
-
Sensitivity analysis in economic evaluation: an audit of NICE current practice and a review of its use and value in decision-making.
By Andronis L, Barton P, Bryan S.
-
Trastuzumab for the treatment of primary breast cancer in HER2-positive women: a single technology appraisal.
By Ward S, Pilgrim H, Hind D.
-
Docetaxel for the adjuvant treatment of early node-positive breast cancer: a single technology appraisal.
By Chilcott J, Lloyd Jones M, Wilkinson A.
-
The use of paclitaxel in the management of early stage breast cancer.
By Griffin S, Dunn G, Palmer S, Macfarlane K, Brent S, Dyker A, et al.
-
Rituximab for the first-line treatment of stage III/IV follicular non-Hodgkin’s lymphoma.
By Dundar Y, Bagust A, Hounsome J, McLeod C, Boland A, Davis H, et al.
-
Bortezomib for the treatment of multiple myeloma patients.
By Green C, Bryant J, Takeda A, Cooper K, Clegg A, Smith A, et al.
-
Fludarabine phosphate for the firstline treatment of chronic lymphocytic leukaemia.
By Walker S, Palmer S, Erhorn S, Brent S, Dyker A, Ferrie L, et al.
-
Erlotinib for the treatment of relapsed non-small cell lung cancer.
By McLeod C, Bagust A, Boland A, Hockenhull J, Dundar Y, Proudlove C, et al.
-
Cetuximab plus radiotherapy for the treatment of locally advanced squamous cell carcinoma of the head and neck.
By Griffin S, Walker S, Sculpher M, White S, Erhorn S, Brent S, et al.
-
Infliximab for the treatment of adults with psoriasis.
By Loveman E, Turner D, Hartwell D, Cooper K, Clegg A
-
Psychological interventions for postnatal depression: cluster randomised trial and economic evaluation. The PoNDER trial.
By Morrell CJ, Warner R, Slade P, Dixon S, Walters S, Paley G, et al.
-
The effect of different treatment durations of clopidogrel in patients with non-ST-segment elevation acute coronary syndromes: a systematic review and value of information analysis.
By Rogowski R, Burch J, Palmer S, Craigs C, Golder S, Woolacott N.
-
Systematic review and individual patient data meta-analysis of diagnosis of heart failure, with modelling of implications of different diagnostic strategies in primary care.
By Mant J, Doust J, Roalfe A, Barton P, Cowie MR, Glasziou P, et al.
-
A multicentre randomised controlled trial of the use of continuous positive airway pressure and non-invasive positive pressure ventilation in the early treatment of patients presenting to the emergency department with severe acute cardiogenic pulmonary oedema: the 3CPO trial.
By Gray AJ, Goodacre S, Newby DE, Masson MA, Sampson F, Dixon S, et al. , on behalf of the 3CPO study investigators.
-
Early high-dose lipid-lowering therapy to avoid cardiac events: a systematic review and economic evaluation.
By Ara R, Pandor A, Stevens J, Rees A, Rafia R.
-
Adefovir dipivoxil and pegylated interferon alpha for the treatment of chronic hepatitis B: an updated systematic review and economic evaluation.
By Jones J, Shepherd J, Baxter L, Gospodarevskaya E, Hartwell D, Harris P, et al.
-
Methods to identify postnatal depression in primary care: an integrated evidence synthesis and value of information analysis.
By Hewitt CE, Gilbody SM, Brealey S, Paulden M, Palmer S, Mann R, et al.
-
A double-blind randomised placebo-controlled trial of topical intranasal corticosteroids in 4- to 11-year-old children with persistent bilateral otitis media with effusion in primary care.
By Williamson I, Benge S, Barton S, Petrou S, Letley L, Fasey N, et al.
-
The effectiveness and cost-effectiveness of methods of storing donated kidneys from deceased donors: a systematic review and economic model.
By Bond M, Pitt M, Akoh J, Moxham T, Hoyle M, Anderson R.
-
Rehabilitation of older patients: day hospital compared with rehabilitation at home. A randomised controlled trial.
By Parker SG, Oliver P, Pennington M, Bond J, Jagger C, Enderby PM, et al.
-
Breastfeeding promotion for infants in neonatal units: a systematic review and economic analysis.
By Renfrew MJ, Craig D, Dyson L, McCormick F, Rice S, King SE, et al.
-
The clinical effectiveness and cost-effectiveness of bariatric (weight loss) surgery for obesity: a systematic review and economic evaluation.
By Picot J, Jones J, Colquitt JL, Gospodarevskaya E, Loveman E, Baxter L, et al.
-
Rapid testing for group B streptococcus during labour: a test accuracy study with evaluation of acceptability and cost-effectiveness.
By Daniels J, Gray J, Pattison H, Roberts T, Edwards E, Milner P, et al.
-
Screening to prevent spontaneous preterm birth: systematic reviews of accuracy and effectiveness literature with economic modelling.
By Honest H, Forbes CA, Durée KH, Norman G, Duffy SB, Tsourapas A, et al.
-
The effectiveness and cost-effectiveness of cochlear implants for severe to profound deafness in children and adults: a systematic review and economic model.
By Bond M, Mealing S, Anderson R, Elston J, Weiner G, Taylor RS, et al.
-
Gemcitabine for the treatment of metastatic breast cancer.
By Jones J, Takeda A, Tan SC, Cooper K, Loveman E, Clegg A.
-
Varenicline in the management of smoking cessation: a single technology appraisal.
By Hind D, Tappenden P, Peters J, Kenjegalieva K.
-
Alteplase for the treatment of acute ischaemic stroke: a single technology appraisal.
By Lloyd Jones M, Holmes M.
-
Rituximab for the treatment of rheumatoid arthritis.
By Bagust A, Boland A, Hockenhull J, Fleeman N, Greenhalgh J, Dundar Y, et al.
-
Omalizumab for the treatment of severe persistent allergic asthma.
By Jones J, Shepherd J, Hartwell D, Harris P, Cooper K, Takeda A, et al.
-
Rituximab for the treatment of relapsed or refractory stage III or IV follicular non-Hodgkin’s lymphoma.
By Boland A, Bagust A, Hockenhull J, Davis H, Chu P, Dickson R.
-
Adalimumab for the treatment of psoriasis.
By Turner D, Picot J, Cooper K, Loveman E.
-
Dabigatran etexilate for the prevention of venous thromboembolism in patients undergoing elective hip and knee surgery: a single technology appraisal.
By Holmes M, C Carroll C, Papaioannou D.
-
Romiplostim for the treatment of chronic immune or idiopathic thrombocytopenic purpura: a single technology appraisal.
By Mowatt G, Boachie C, Crowther M, Fraser C, Hernández R, Jia X, et al.
-
Sunitinib for the treatment of gastrointestinal stromal tumours: a critique of the submission from Pfizer.
By Bond M, Hoyle M, Moxham T, Napier M, Anderson R.
-
Vitamin K to prevent fractures in older women: systematic review and economic evaluation.
By Stevenson M, Lloyd-Jones M, Papaioannou D.
-
The effects of biofeedback for the treatment of essential hypertension: a systematic review.
By Greenhalgh J, Dickson R, Dundar Y.
-
A randomised controlled trial of the use of aciclovir and/or prednisolone for the early treatment of Bell’s palsy: the BELLS study.
By Sullivan FM, Swan IRC, Donnan PT, Morrison JM, Smith BH, McKinstry B, et al.
-
Lapatinib for the treatment of HER2-overexpressing breast cancer.
By Jones J, Takeda A, Picot J, von Keyserlingk C, Clegg A.
-
Infliximab for the treatment of ulcerative colitis.
By Hyde C, Bryan S, Juarez-Garcia A, Andronis L, Fry-Smith A.
-
Rimonabant for the treatment of overweight and obese people.
By Burch J, McKenna C, Palmer S, Norman G, Glanville J, Sculpher M, et al.
-
Telbivudine for the treatment of chronic hepatitis B infection.
By Hartwell D, Jones J, Harris P, Cooper K.
-
Entecavir for the treatment of chronic hepatitis B infection.
By Shepherd J, Gospodarevskaya E, Frampton G, Cooper K.
-
Febuxostat for the treatment of hyperuricaemia in people with gout: a single technology appraisal.
By Stevenson M, Pandor A.
-
Rivaroxaban for the prevention of venous thromboembolism: a single technology appraisal.
By Stevenson M, Scope A, Holmes M, Rees A, Kaltenthaler E.
-
Cetuximab for the treatment of recurrent and/or metastatic squamous cell carcinoma of the head and neck.
By Greenhalgh J, Bagust A, Boland A, Fleeman N, McLeod C, Dundar Y, et al.
-
Mifamurtide for the treatment of osteosarcoma: a single technology appraisal.
By Pandor A, Fitzgerald P, Stevenson M, Papaioannou D.
-
Ustekinumab for the treatment of moderate to severe psoriasis.
By Gospodarevskaya E, Picot J, Cooper K, Loveman E, Takeda A.
-
Endovascular stents for abdominal aortic aneurysms: a systematic review and economic model.
By Chambers D, Epstein D, Walker S, Fayter D, Paton F, Wright K, et al.
-
Clinical and cost-effectiveness of epoprostenol, iloprost, bosentan, sitaxentan and sildenafil for pulmonary arterial hypertension within their licensed indications: a systematic review and economic evaluation.
By Chen Y-F, Jowett S, Barton P, Malottki K, Hyde C, Gibbs JSR, et al.
-
Cessation of attention deficit hyperactivity disorder drugs in the young (CADDY) – a pharmacoepidemiological and qualitative study.
By Wong ICK, Asherson P, Bilbow A, Clifford S, Coghill D, R DeSoysa R, et al.
-
ARTISTIC: a randomised trial of human papillomavirus (HPV) testing in primary cervical screening.
By Kitchener HC, Almonte M, Gilham C, Dowie R, Stoykova B, Sargent A, et al.
-
The clinical effectiveness of glucosamine and chondroitin supplements in slowing or arresting progression of osteoarthritis of the knee: a systematic review and economic evaluation.
By Black C, Clar C, Henderson R, MacEachern C, McNamee P, Quayyum Z, et al.
-
Randomised preference trial of medical versus surgical termination of pregnancy less than 14 weeks’ gestation (TOPS).
By Robson SC, Kelly T, Howel D, Deverill M, Hewison J, Lie MLS, et al.
-
Randomised controlled trial of the use of three dressing preparations in the management of chronic ulceration of the foot in diabetes.
By Jeffcoate WJ, Price PE, Phillips CJ, Game FL, Mudge E, Davies S, et al.
-
VenUS II: a randomised controlled trial of larval therapy in the management of leg ulcers.
By Dumville JC, Worthy G, Soares MO, Bland JM, Cullum N, Dowson C, et al.
-
A prospective randomised controlled trial and economic modelling of antimicrobial silver dressings versus non-adherent control dressings for venous leg ulcers: the VULCAN trial.
By Michaels JA, Campbell WB, King BM, MacIntyre J, Palfreyman SJ, Shackley P, et al.
-
Communication of carrier status information following universal newborn screening for sickle cell disorders and cystic fibrosis: qualitative study of experience and practice.
By Kai J, Ulph F, Cullinan T, Qureshi N.
-
Antiviral drugs for the treatment of influenza: a systematic review and economic evaluation.
By Burch J, Paulden M, Conti S, Stock C, Corbett M, Welton NJ, et al.
-
Development of a toolkit and glossary to aid in the adaptation of health technology assessment (HTA) reports for use in different contexts.
By Chase D, Rosten C, Turner S, Hicks N, Milne R.
-
Colour vision testing for diabetic retinopathy: a systematic review of diagnostic accuracy and economic evaluation.
By Rodgers M, Hodges R, Hawkins J, Hollingworth W, Duffy S, McKibbin M, et al.
-
Systematic review of the effectiveness and cost-effectiveness of weight management schemes for the under fives: a short report.
By Bond M, Wyatt K, Lloyd J, Welch K, Taylor R.
-
Are adverse effects incorporated in economic models? An initial review of current practice.
By Craig D, McDaid C, Fonseca T, Stock C, Duffy S, Woolacott N.
-
Multicentre randomised controlled trial examining the cost-effectiveness of contrast-enhanced high field magnetic resonance imaging in women with primary breast cancer scheduled for wide local excision (COMICE).
By Turnbull LW, Brown SR, Olivier C, Harvey I, Brown J, Drew P, et al.
-
Bevacizumab, sorafenib tosylate, sunitinib and temsirolimus for renal cell carcinoma: a systematic review and economic evaluation.
By Thompson Coon J, Hoyle M, Green C, Liu Z, Welch K, Moxham T, et al.
-
The clinical effectiveness and cost-effectiveness of testing for cytochrome P450 polymorphisms in patients with schizophrenia treated with antipsychotics: a systematic review and economic evaluation.
By Fleeman N, McLeod C, Bagust A, Beale S, Boland A, Dundar Y, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of photodynamic diagnosis and urine biomarkers (FISH, ImmunoCyt, NMP22) and cytology for the detection and follow-up of bladder cancer.
By Mowatt G, Zhu S, Kilonzo M, Boachie C, Fraser C, Griffiths TRL, et al.
-
Effectiveness and cost-effectiveness of arthroscopic lavage in the treatment of osteoarthritis of the knee: a mixed methods study of the feasibility of conducting a surgical placebo-controlled trial (the KORAL study).
By Campbell MK, Skea ZC, Sutherland AG, Cuthbertson BH, Entwistle VA, McDonald AM, et al.
-
A randomised 2 × 2 trial of community versus hospital pulmonary rehabilitation for chronic obstructive pulmonary disease followed by telephone or conventional follow-up.
By Waterhouse JC, Walters SJ, Oluboyede Y, Lawson RA.
-
The effectiveness and cost-effectiveness of behavioural interventions for the prevention of sexually transmitted infections in young people aged 13–19: a systematic review and economic evaluation.
By Shepherd J, Kavanagh J, Picot J, Cooper K, Harden A, Barnett-Page E, et al.
-
Dissemination and publication of research findings: an updated review of related biases.
By Song F, Parekh S, Hooper L, Loke YK, Ryder J, Sutton AJ, et al.
-
The effectiveness and cost-effectiveness of biomarkers for the prioritisation of patients awaiting coronary revascularisation: a systematic review and decision model.
By Hemingway H, Henriksson M, Chen R, Damant J, Fitzpatrick N, Abrams K, et al.
-
Comparison of case note review methods for evaluating quality and safety in health care.
By Hutchinson A, Coster JE, Cooper KL, McIntosh A, Walters SJ, Bath PA, et al.
-
Clinical effectiveness and cost-effectiveness of continuous subcutaneous insulin infusion for diabetes: systematic review and economic evaluation.
By Cummins E, Royle P, Snaith A, Greene A, Robertson L, McIntyre L, et al.
-
Self-monitoring of blood glucose in type 2 diabetes: systematic review.
By Clar C, Barnard K, Cummins E, Royle P, Waugh N.
-
North of England and Scotland Study of Tonsillectomy and Adeno-tonsillectomy in Children (NESSTAC): a pragmatic randomised controlled trial with a parallel non-randomised preference study.
By Lock C, Wilson J, Steen N, Eccles M, Mason H, Carrie S, et al.
-
Multicentre randomised controlled trial of the clinical and cost-effectiveness of a bypass-surgery-first versus a balloon-angioplasty-first revascularisation strategy for severe limb ischaemia due to infrainguinal disease. The Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) trial.
By Bradbury AW, Adam DJ, Bell J, Forbes JF, Fowkes FGR, Gillespie I, et al.
-
A randomised controlled multicentre trial of treatments for adolescent anorexia nervosa including assessment of cost-effectiveness and patient acceptability – the TOuCAN trial.
By Gowers SG, Clark AF, Roberts C, Byford S, Barrett B, Griffiths A, et al.
-
Randomised controlled trials for policy interventions: a review of reviews and meta-regression.
By Oliver S, Bagnall AM, Thomas J, Shepherd J, Sowden A, White I, et al.
-
Paracetamol and selective and non-selective non-steroidal anti-inflammatory drugs (NSAIDs) for the reduction of morphine-related side effects after major surgery: a systematic review.
By McDaid C, Maund E, Rice S, Wright K, Jenkins B, Woolacott N.
-
A systematic review of outcome measures used in forensic mental health research with consensus panel opinion.
By Fitzpatrick R, Chambers J, Burns T, Doll H, Fazel S, Jenkinson C, et al.
-
The clinical effectiveness and cost-effectiveness of topotecan for small cell lung cancer: a systematic review and economic evaluation.
By Loveman E, Jones J, Hartwell D, Bird A, Harris P, Welch K, et al.
-
Antenatal screening for haemoglobinopathies in primary care: a cohort study and cluster randomised trial to inform a simulation model. The Screening for Haemoglobinopathies in First Trimester (SHIFT) trial.
By Dormandy E, Bryan S, Gulliford MC, Roberts T, Ades T, Calnan M, et al.
-
Early referral strategies for management of people with markers of renal disease: a systematic review of the evidence of clinical effectiveness, cost-effectiveness and economic analysis.
By Black C, Sharma P, Scotland G, McCullough K, McGurn D, Robertson L, et al.
-
A randomised controlled trial of cognitive behaviour therapy and motivational interviewing for people with Type 1 diabetes mellitus with persistent sub-optimal glycaemic control: A Diabetes and Psychological Therapies (ADaPT) study.
By Ismail K, Maissi E, Thomas S, Chalder T, Schmidt U, Bartlett J, et al.
-
A randomised controlled equivalence trial to determine the effectiveness and cost–utility of manual chest physiotherapy techniques in the management of exacerbations of chronic obstructive pulmonary disease (MATREX).
By Cross J, Elender F, Barton G, Clark A, Shepstone L, Blyth A, et al.
-
A systematic review and economic evaluation of the clinical effectiveness and cost-effectiveness of aldosterone antagonists for postmyocardial infarction heart failure.
By McKenna C, Burch J, Suekarran S, Walker S, Bakhai A, Witte K, et al.
-
Avoiding and identifying errors in health technology assessment models: qualitative study and methodological review.
By Chilcott JB, Tappenden P, Rawdin A, Johnson M, Kaltenthaler E, Paisley S, et al.
-
BoTULS: a multicentre randomised controlled trial to evaluate the clinical effectiveness and cost-effectiveness of treating upper limb spasticity due to stroke with botulinum toxin type A.
By Shaw L, Rodgers H, Price C, van Wijck F, Shackley P, Steen N, et al. , on behalf of the BoTULS investigators.
-
Weighting and valuing quality-adjusted life-years using stated preference methods: preliminary results from the Social Value of a QALY Project.
By Baker R, Bateman I, Donaldson C, Jones-Lee M, Lancsar E, Loomes G, et al.
-
Cetuximab for the first-line treatment of metastatic colorectal cancer.
By Meads C, Round J, Tubeuf S, Moore D, Pennant M, Bayliss S.
-
Infliximab for the treatment of acute exacerbations of ulcerative colitis.
By Bryan S, Andronis L, Hyde C, Connock M, Fry-Smith A, Wang D.
-
Sorafenib for the treatment of advanced hepatocellular carcinoma.
By Connock M, Round J, Bayliss S, Tubeuf S, Greenheld W, Moore D.
-
Tenofovir disoproxil fumarate for the treatment of chronic hepatitis B infection.
By Jones J, Colquitt J, Shepherd J, Harris P, Cooper K.
-
Prasugrel for the treatment of acute coronary artery syndromes with percutaneous coronary intervention.
By Greenhalgh J, Bagust A, Boland A, Saborido CM, Fleeman N, McLeod C, et al.
-
Alitretinoin for the treatment of severe chronic hand eczema.
By Paulden M, Rodgers M, Griffin S, Slack R, Duffy S, Ingram JR, et al.
-
Pemetrexed for the first-line treatment of locally advanced or metastatic non-small cell lung cancer.
By Fleeman N, Bagust A, McLeod C, Greenhalgh J, Boland A, Dundar Y, et al.
-
Topotecan for the treatment of recurrent and stage IVB carcinoma of the cervix.
By Paton F, Paulden M, Saramago P, Manca A, Misso K, Palmer S, et al.
-
Trabectedin for the treatment of advanced metastatic soft tissue sarcoma.
By Simpson EL, Rafia R, Stevenson MD, Papaioannou D.
-
Azacitidine for the treatment of myelodysplastic syndrome, chronic myelomonocytic leukaemia and acute myeloid leukaemia.
By Edlin R, Connock M, Tubeuf S, Round J, Fry-Smith A, Hyde C, et al.
-
The safety and effectiveness of different methods of earwax removal: a systematic review and economic evaluation.
By Clegg AJ, Loveman E, Gospodarevskaya E, Harris P, Bird A, Bryant J, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of rapid point-of-care tests for the detection of genital chlamydia infection in women and men.
By Hislop J, Quayyum Z, Flett G, Boachie C, Fraser C, Mowatt G.
-
School-linked sexual health services for young people (SSHYP): a survey and systematic review concerning current models, effectiveness, cost-effectiveness and research opportunities.
By Owen J, Carroll C, Cooke J, Formby E, Hayter M, Hirst J, et al.
-
Systematic review and cost-effectiveness evaluation of ‘pill-in-the-pocket’ strategy for paroxysmal atrial fibrillation compared to episodic in-hospital treatment or continuous antiarrhythmic drug therapy.
By Martin Saborido C, Hockenhull J, Bagust A, Boland A, Dickson R, Todd D.
-
Chemoprevention of colorectal cancer: systematic review and economic evaluation.
By Cooper K, Squires H, Carroll C, Papaioannou D, Booth A, Logan RF, et al.
-
Cross-trimester repeated measures testing for Down’s syndrome screening: an assessment.
By Wright D, Bradbury I, Malone F, D’Alton M, Summers A, Huang T, et al.
-
Exploring the needs, concerns and behaviours of people with existing respiratory conditions in relation to the H1N1 ‘swine influenza’ pandemic: a multicentre survey and qualitative study.
By Caress A-L, Duxbury P, Woodcock A, Luker KA, Ward D, Campbell M, et al.
-
Influenza A/H1N1v in pregnancy: an investigation of the characteristics and management of affected women and the relationship to pregnancy outcomes for mother and infant.
By Yates L, Pierce M, Stephens S, Mill AC, Spark P, Kurinczuk JJ, et al.
-
The impact of communications about swine flu (influenza A H1N1v) on public responses to the outbreak: results from 36 national telephone surveys in the UK.
By Rubin GJ, Potts HWW, Michie S.
-
The impact of illness and the impact of school closure on social contact patterns.
By Eames KTD, Tilston NL, White PJ, Adams E, Edmunds WJ.
-
Vaccine effectiveness in pandemic influenza – primary care reporting (VIPER): an observational study to assess the effectiveness of the pandemic influenza A (H1N1)v vaccine.
By Simpson CR, Ritchie LD, Robertson C, Sheikh A, McMenamin J.
-
Physical interventions to interrupt or reduce the spread of respiratory viruses: a Cochrane review.
By Jefferson T, Del Mar C, Dooley L, Ferroni E, Al-Ansary LA, Bawazeer GA, et al.
-
Randomised controlled trial and parallel economic evaluation of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR).
By Peek GJ, Elbourne D, Mugford M, Tiruvoipati R, Wilson A, Allen E, et al.
-
Newer agents for blood glucose control in type 2 diabetes: systematic review and economic evaluation.
By Waugh N, Cummins E, Royle P, Clar C, Marien M, Richter B, et al.
-
Barrett’s oesophagus and cancers of the biliary tract, brain, head and neck, lung, oesophagus and skin.
By Fayter D, Corbett M, Heirs M, Fox D, Eastwood A.
Health Technology Assessment programme
-
Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Medical Care Research Unit, University of Sheffield
Prioritisation Strategy Group
-
Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Medical Care Research Unit, University of Sheffield
-
Dr Bob Coates, Consultant Advisor, NETSCC, HTA
-
Dr Andrew Cook, Consultant Advisor, NETSCC, HTA
-
Dr Peter Davidson, Director of NETSCC, Health Technology Assessment
-
Professor Robin E Ferner, Consultant Physician and Director, West Midlands Centre for Adverse Drug Reactions, City Hospital NHS Trust, Birmingham
-
Professor Paul Glasziou, Professor of Evidence-Based Medicine, University of Oxford
-
Dr Nick Hicks, Consultant Adviser, NETSCC, HTA
-
Dr Edmund Jessop, Medical Adviser, National Specialist, National Commissioning Group (NCG), Department of Health, London
-
Ms Lynn Kerridge, Chief Executive Officer, NETSCC and NETSCC, HTA
-
Dr Ruairidh Milne, Director of NETSCC External Relations
-
Ms Kay Pattison, Senior NIHR Programme Manager, Department of Health
-
Ms Pamela Young, Specialist Programme Manager, NETSCC, HTA
HTA Commissioning Board
-
Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Warwick Clinical Trials Unit
-
Director, Nottingham Clinical Trials Unit
-
Senior Lecturer in General Practice, Department of Primary Health Care, University of Oxford
-
Professor Ann Ashburn, Professor of Rehabilitation and Head of Research, Southampton General Hospital
-
Professor Deborah Ashby, Professor of Medical Statistics, Queen Mary, University of London
-
Professor John Cairns, Professor of Health Economics, London School of Hygiene and Tropical Medicine
-
Professor Peter Croft, Director of Primary Care Sciences Research Centre, Keele University
-
Professor Nicky Cullum, Director of Centre for Evidence-Based Nursing, University of York
-
Professor Jenny Donovan, Professor of Social Medicine, University of Bristol
-
Professor Steve Halligan, Professor of Gastrointestinal Radiology, University College Hospital, London
-
Professor Freddie Hamdy, Professor of Urology, University of Sheffield
-
Professor Allan House, Professor of Liaison Psychiatry, University of Leeds
-
Dr Martin J Landray, Reader in Epidemiology, Honorary Consultant Physician, Clinical Trial Service Unit, University of Oxford?
-
Professor Stuart Logan, Director of Health & Social Care Research, The Peninsula Medical School, Universities of Exeter and Plymouth
-
Dr Rafael Perera, Lecturer in Medical Statisitics, Department of Primary Health Care, University of Oxford
-
Professor Ian Roberts, Professor of Epidemiology & Public Health, London School of Hygiene and Tropical Medicine
-
Professor Mark Sculpher, Professor of Health Economics, University of York
-
Professor Helen Smith, Professor of Primary Care, University of Brighton
-
Professor Kate Thomas, Professor of Complementary & Alternative Medicine Research, University of Leeds
-
Professor David John Torgerson, Director of York Trials Unit, University of York
-
Ms Kay Pattison, NHS R&D Programme/DH, Leeds
-
Dr Morven Roberts, Clinical Trials Manager, Medical Research Council
Diagnostic Technologies and Screening Panel
-
Professor of Evidence-Based Medicine, University of Oxford
-
Consultant Paediatrician and Honorary Senior Lecturer, Great Ormond Street Hospital, London
-
Professor Judith E Adams, Consultant Radiologist, Manchester Royal Infirmary, Central Manchester & Manchester Children’s University Hospitals NHS Trust, and Professor of Diagnostic Radiology, Imaging Science and Biomedical Engineering, Cancer & Imaging Sciences, University of Manchester
-
Mr A S Arunkalaivanan, Honorary Senior Lecturer, University of Birmingham and Consultant Urogynaecologist and Obstetrician, City Hospital
-
Dr Dianne Baralle, Consultant & Senior Lecturer in Clinical Genetics, Human Genetics Division & Wessex Clinical Genetics Service, Southampton, University of Southampton
-
Dr Stephanie Dancer, Consultant Microbiologist, Hairmyres Hospital, East Kilbride
-
Dr Ron Gray, Consultant, National Perinatal Epidemiology Unit, Institute of Health Sciences, University of Oxford
-
Professor Paul D Griffiths, Professor of Radiology, Academic Unit of Radiology, University of Sheffield
-
Mr Martin Hooper, Service User Representative
-
Professor Anthony Robert Kendrick, Professor of Primary Medical Care, University of Southampton
-
Dr Susanne M Ludgate, Director, Medical Devices Agency, London
-
Dr Anne Mackie, Director of Programmes, UK National Screening Committee
-
Dr David Mathew Service User Representative
-
Dr Michael Millar, Lead Consultant in Microbiology, Department of Pathology & Microbiology, Barts and The London NHS Trust, Royal London Hospital
-
Mr Stephen Pilling, Director, Centre for Outcomes, Research & Effectiveness, University College London
-
Mrs Una Rennard, Service User Representative
-
Ms Jane Smith, Consultant Ultrasound Practitioner, Ultrasound Department, Leeds Teaching Hospital NHS Trust, Leeds
-
Dr W Stuart A Smellie, Consultant, Bishop Auckland General Hospital
-
Professor Lindsay Wilson Turnbull, Scientific Director of the Centre for Magnetic Resonance Investigations and YCR Professor of Radiology, Hull Royal Infirmary
-
Dr Alan J Williams, Consultant in General Medicine, Department of Thoracic Medicine, The Royal Bournemouth Hospital
-
Dr Tim Elliott, Team Leader, Cancer Screening, Department of Health
-
Dr Catherine Moody, Programme Manager, Neuroscience and Mental Health Board
-
Dr Ursula Wells, Principal Research Officer, Department of Health
Disease Prevention Panel
-
Medical Adviser, National Specialist Commissioning Advisory Group (NSCAG), Department of Health
-
Professor of Epidemiology, University of Warwick Medical School, Coventry
-
Dr Robert Cook Clinical Programmes Director, Bazian Ltd, London
-
Dr Elizabeth Fellow-Smith, Medical Director, West London Mental Health Trust, Middlesex
-
Dr Colin Greaves Senior Research Fellow, Peninsular Medical School (Primary Care)
-
Dr John Jackson, General Practitioner, Parkway Medical Centre, Newcastle upon Tyne
-
Dr Russell Jago, Senior Lecturer in Exercise, Nutrition and Health, Centre for Sport, Exercise and Health, University of Bristol
-
Dr Chris McCall, General Practitioner, The Hadleigh Practice, Corfe Mullen, Dorset
-
Miss Nicky Mullany, Service User Representative
-
Dr Julie Mytton, Locum Consultant in Public Health Medicine, Bristol Primary Care Trust
-
Professor Irwin Nazareth, Professor of Primary Care and Director, Department of Primary Care and Population Sciences, University College London
-
Professor Ian Roberts, Professor of Epidemiology and Public Health, London School of Hygiene & Tropical Medicine
-
Professor Carol Tannahill, Glasgow Centre for Population Health
-
Mrs Jean Thurston, Service User Representative
-
Professor David Weller, Head, School of Clinical Science and Community Health, University of Edinburgh
-
Ms Christine McGuire, Research & Development, Department of Health
-
Ms Kay Pattison Senior NIHR Programme Manager, Department of Health
-
Dr Caroline Stone, Programme Manager, Medical Research Council
External Devices and Physical Therapies Panel
-
Consultant Physician North Bristol NHS Trust, Bristol
-
Reader in Wound Healing and Director of Research, University of Leeds, Leeds
-
Professor Bipin Bhakta Charterhouse Professor in Rehabilitation Medicine, University of Leeds, Leeds
-
Mrs Penny Calder Service User Representative
-
Professor Paul Carding, Professor of Voice Pathology, Newcastle Hospital NHS Trust, Newcastle
-
Dr Dawn Carnes, Senior Research Fellow, Barts and the London School of Medicine and Dentistry, London
-
Dr Emma Clark, Clinician Scientist Fellow & Cons. Rheumatologist, University of Bristol, Bristol
-
Mrs Anthea De Barton-Watson, Service User Representative
-
Professor Christopher Griffiths, Professor of Primary Care, Barts and the London School of Medicine and Dentistry, London
-
Dr Shaheen Hamdy, Clinical Senior Lecturer and Consultant Physician, University of Manchester, Manchester
-
Dr Peter Martin, Consultant Neurologist, Addenbrooke’s Hospital, Cambridge
-
Dr Lorraine Pinnigton, Associate Professor in Rehabilitation, University of Nottingham, Nottingham
-
Dr Kate Radford, Division of Rehabilitation and Ageing, School of Community Health Sciences. University of Nottingham, Nottingham
-
Mr Jim Reece, Service User Representative
-
Professor Maria Stokes, Professor of Neuromusculoskeletal Rehabilitation, University of Southampton, Southampton
-
Dr Pippa Tyrrell, Stroke Medicine, Senior Lecturer/Consultant Stroke Physician, Salford Royal Foundation Hospitals’ Trust, Salford
-
Dr Sarah Tyson, Senior Research Fellow & Associate Head of School, University of Salford, Salford
-
Dr Nefyn Williams, Clinical Senior Lecturer, Cardiff University, Cardiff
-
Dr Phillip Leech, Principal Medical Officer for Primary Care, Department of Health, London
-
Ms Kay Pattison Senior NIHR Programme Manager, Department of Health
-
Dr Morven Roberts, Clinical Trials Manager, MRC, London
-
Dr Ursula Wells PRP, DH, London
Interventional Procedures Panel
-
Consultant Surgeon & Honorary Clinical Lecturer, University of Sheffield
-
Mr David P Britt, Service User Representative, Cheshire
-
Mr Sankaran ChandraSekharan, Consultant Surgeon, Colchester Hospital University NHS Foundation Trust
-
Professor Nicholas Clarke, Consultant Orthopaedic Surgeon, Southampton University Hospitals NHS Trust
-
Mr Seamus Eckford, Consultant in Obstetrics & Gynaecology, North Devon District Hospital
-
Professor David Taggart, Consultant Cardiothoracic Surgeon, John Radcliffe Hospital
-
Dr Matthew Hatton, Consultant in Clinical Oncology, Sheffield Teaching Hospital Foundation Trust
-
Dr John Holden, General Practitioner, Garswood Surgery, Wigan
-
Dr Nadim Malik, Consultant Cardiologist/ Honorary Lecturer, University of Manchester
-
Mr Hisham Mehanna, Consultant & Honorary Associate Professor, University Hospitals Coventry & Warwickshire NHS Trust
-
Dr Jane Montgomery, Consultant in Anaesthetics and Critical Care, South Devon Healthcare NHS Foundation Trust
-
Dr Simon Padley, Consultant Radiologist, Chelsea & Westminster Hospital
-
Dr Ashish Paul, Medical Director, Bedfordshire PCT
-
Dr Sarah Purdy, Consultant Senior Lecturer, University of Bristol
-
Mr Michael Thomas, Consultant Colorectal Surgeon, Bristol Royal Infirmary
-
Professor Yit Chiun Yang, Consultant Ophthalmologist, Royal Wolverhampton Hospitals NHS Trust
-
Mrs Isabel Boyer, Service User Representative, London
Pharmaceuticals Panel
-
Professor in Child Health, University of Nottingham
-
Unit Manager, Pharmacoepidemiology Research Unit, VRMM, Medicines & Healthcare Products Regulatory Agency
-
Mrs Nicola Carey, Senior Research Fellow, School of Health and Social Care, The University of Reading
-
Mr John Chapman, Service User Representative
-
Dr Peter Elton, Director of Public Health, Bury Primary Care Trust
-
Professor Robin Ferner, Consultant Physician and Director, West Midlands Centre for Adverse Drug Reactions, City Hospital NHS Trust, Birmingham
-
Dr Ben Goldacre, Research Fellow, Division of Psychological Medicine and Psychiatry, King’s College London
-
Dr Bill Gutteridge, Medical Adviser, London Strategic Health Authority
-
Dr Dyfrig Hughes, Reader in Pharmacoeconomics and Deputy Director, Centre for Economics and Policy in Health, IMSCaR, Bangor University
-
Dr Yoon K Loke, Senior Lecturer in Clinical Pharmacology, University of East Anglia
-
Professor Femi Oyebode, Consultant Psychiatrist and Head of Department, University of Birmingham
-
Dr Andrew Prentice, Senior Lecturer and Consultant Obstetrician and Gynaecologist, The Rosie Hospital, University of Cambridge
-
Dr Martin Shelly, General Practitioner, Leeds, and Associate Director, NHS Clinical Governance Support Team, Leicester
-
Dr Gillian Shepherd, Director, Health and Clinical Excellence, Merck Serono Ltd
-
Mrs Katrina Simister, Assistant Director New Medicines, National Prescribing Centre, Liverpool
-
Mr David Symes, Service User Representative
-
Ms Kay Pattison Senior NIHR Programme Manager, Department of Health
-
Mr Simon Reeve, Head of Clinical and Cost-Effectiveness, Medicines, Pharmacy and Industry Group, Department of Health
-
Dr Heike Weber, Programme Manager, Medical Research Council
-
Dr Ursula Wells, Principal Research Officer, Department of Health
Psychological and Community Therapies Panel
-
Professor of Psychiatry, University of Warwick
-
Professor Jane Barlow, Professor of Public Health in the Early Years, Health Sciences Research Institute, Warwick Medical School
-
Dr Sabyasachi Bhaumik, Consultant Psychiatrist, Leicestershire Partnership NHS Trust
-
Mrs Val Carlill, Service User Representative, Gloucestershire
-
Dr Steve Cunningham, Consultant Respiratory Paediatrician, Lothian Health Board
-
Dr Anne Hesketh, Senior Clinical Lecturer in Speech and Language Therapy, University of Manchester
-
Dr Yann Lefeuvre, GP Partner, Burrage Road Surgery, London
-
Dr Jeremy J Murphy, Consultant Physician & Cardiologist, County Durham & Darlington Foundation Trust
-
Mr John Needham, Service User, Buckingmashire
-
Ms Mary Nettle, Mental Health User Consultant, Gloucestershire
-
Professor John Potter, Professor of Ageing and Stroke Medicine, University of East Anglia
-
Dr Greta Rait, Senior Clinical Lecturer and General Practitioner, University College London
-
Dr Paul Ramchandani, Senior Research Fellow/Cons. Child Psychiatrist, University of Oxford
-
Dr Howard Ring, Consultant & University Lecturer in Psychiatry, University of Cambridge
-
Dr Karen Roberts, Nurse/Consultant, Dunston Hill Hospital, Tyne and Wear
-
Dr Karim Saad, Consultant in Old Age Psychiatry, Coventry & Warwickshire Partnership Trust
-
Dr Alastair Sutcliffe, Senior Lecturer, University College London
-
Dr Simon Wright, GP Partner, Walkden Medical Centre, Manchester
-
Ms Kay Pattison Senior NIHR Programme Manager, Department of Health
-
Dr Morven Roberts, Clinical Trials Manager, MRC, London
-
Professor Tom Walley, HTA Programme Director, Liverpool
-
Dr Ursula Wells, Policy Research Programme, DH, London
Expert Advisory Network
-
Professor Douglas Altman, Professor of Statistics in Medicine, Centre for Statistics in Medicine, University of Oxford
-
Professor John Bond, Professor of Social Gerontology & Health Services Research, University of Newcastle upon Tyne
-
Professor Andrew Bradbury, Professor of Vascular Surgery, Solihull Hospital, Birmingham
-
Mr Shaun Brogan, Chief Executive, Ridgeway Primary Care Group, Aylesbury
-
Mrs Stella Burnside OBE, Chief Executive, Regulation and Improvement Authority, Belfast
-
Ms Tracy Bury, Project Manager, World Confederation for Physical Therapy, London
-
Professor Iain T Cameron, Professor of Obstetrics and Gynaecology and Head of the School of Medicine, University of Southampton
-
Dr Christine Clark, Medical Writer and Consultant Pharmacist, Rossendale
-
Professor Collette Clifford, Professor of Nursing and Head of Research, The Medical School, University of Birmingham
-
Professor Barry Cookson, Director, Laboratory of Hospital Infection, Public Health Laboratory Service, London
-
Dr Carl Counsell, Clinical Senior Lecturer in Neurology, University of Aberdeen
-
Professor Howard Cuckle, Professor of Reproductive Epidemiology, Department of Paediatrics, Obstetrics & Gynaecology, University of Leeds
-
Dr Katherine Darton, Information Unit, MIND – The Mental Health Charity, London
-
Professor Carol Dezateux, Professor of Paediatric Epidemiology, Institute of Child Health, London
-
Mr John Dunning, Consultant Cardiothoracic Surgeon, Papworth Hospital NHS Trust, Cambridge
-
Mr Jonothan Earnshaw, Consultant Vascular Surgeon, Gloucestershire Royal Hospital, Gloucester
-
Professor Martin Eccles, Professor of Clinical Effectiveness, Centre for Health Services Research, University of Newcastle upon Tyne
-
Professor Pam Enderby, Dean of Faculty of Medicine, Institute of General Practice and Primary Care, University of Sheffield
-
Professor Gene Feder, Professor of Primary Care Research & Development, Centre for Health Sciences, Barts and The London School of Medicine and Dentistry
-
Mr Leonard R Fenwick, Chief Executive, Freeman Hospital, Newcastle upon Tyne
-
Mrs Gillian Fletcher, Antenatal Teacher and Tutor and President, National Childbirth Trust, Henfield
-
Professor Jayne Franklyn, Professor of Medicine, University of Birmingham
-
Mr Tam Fry, Honorary Chairman, Child Growth Foundation, London
-
Professor Fiona Gilbert, Consultant Radiologist and NCRN Member, University of Aberdeen
-
Professor Paul Gregg, Professor of Orthopaedic Surgical Science, South Tees Hospital NHS Trust
-
Bec Hanley, Co-director, TwoCan Associates, West Sussex
-
Dr Maryann L Hardy, Senior Lecturer, University of Bradford
-
Mrs Sharon Hart, Healthcare Management Consultant, Reading
-
Professor Robert E Hawkins, CRC Professor and Director of Medical Oncology, Christie CRC Research Centre, Christie Hospital NHS Trust, Manchester
-
Professor Richard Hobbs, Head of Department of Primary Care & General Practice, University of Birmingham
-
Professor Alan Horwich, Dean and Section Chairman, The Institute of Cancer Research, London
-
Professor Allen Hutchinson, Director of Public Health and Deputy Dean of ScHARR, University of Sheffield
-
Professor Peter Jones, Professor of Psychiatry, University of Cambridge, Cambridge
-
Professor Stan Kaye, Cancer Research UK Professor of Medical Oncology, Royal Marsden Hospital and Institute of Cancer Research, Surrey
-
Dr Duncan Keeley, General Practitioner (Dr Burch & Ptnrs), The Health Centre, Thame
-
Dr Donna Lamping, Research Degrees Programme Director and Reader in Psychology, Health Services Research Unit, London School of Hygiene and Tropical Medicine, London
-
Mr George Levvy, Chief Executive, Motor Neurone Disease Association, Northampton
-
Professor James Lindesay, Professor of Psychiatry for the Elderly, University of Leicester
-
Professor Julian Little, Professor of Human Genome Epidemiology, University of Ottawa
-
Professor Alistaire McGuire, Professor of Health Economics, London School of Economics
-
Professor Rajan Madhok, Medical Director and Director of Public Health, Directorate of Clinical Strategy & Public Health, North & East Yorkshire & Northern Lincolnshire Health Authority, York
-
Professor Alexander Markham, Director, Molecular Medicine Unit, St James’s University Hospital, Leeds
-
Dr Peter Moore, Freelance Science Writer, Ashtead
-
Dr Andrew Mortimore, Public Health Director, Southampton City Primary Care Trust
-
Dr Sue Moss, Associate Director, Cancer Screening Evaluation Unit, Institute of Cancer Research, Sutton
-
Professor Miranda Mugford, Professor of Health Economics and Group Co-ordinator, University of East Anglia
-
Professor Jim Neilson, Head of School of Reproductive & Developmental Medicine and Professor of Obstetrics and Gynaecology, University of Liverpool
-
Mrs Julietta Patnick, National Co-ordinator, NHS Cancer Screening Programmes, Sheffield
-
Professor Robert Peveler, Professor of Liaison Psychiatry, Royal South Hants Hospital, Southampton
-
Professor Chris Price, Director of Clinical Research, Bayer Diagnostics Europe, Stoke Poges
-
Professor William Rosenberg, Professor of Hepatology and Consultant Physician, University of Southampton
-
Professor Peter Sandercock, Professor of Medical Neurology, Department of Clinical Neurosciences, University of Edinburgh
-
Dr Susan Schonfield, Consultant in Public Health, Hillingdon Primary Care Trust, Middlesex
-
Dr Eamonn Sheridan, Consultant in Clinical Genetics, St James’s University Hospital, Leeds
-
Dr Margaret Somerville, Director of Public Health Learning, Peninsula Medical School, University of Plymouth
-
Professor Sarah Stewart-Brown, Professor of Public Health, Division of Health in the Community, University of Warwick, Coventry
-
Professor Ala Szczepura, Professor of Health Service Research, Centre for Health Services Studies, University of Warwick, Coventry
-
Mrs Joan Webster, Consumer Member, Southern Derbyshire Community Health Council
-
Professor Martin Whittle, Clinical Co-director, National Co-ordinating Centre for Women’s and Children’s Health, Lymington