
Notes
Article history
The research reported in this issue of the journal was commissioned by the HTA programme as project number 05/11/02. The contractual start date was in December 2005. The draft report began editorial review in November 2009 and was accepted for publication in May 2010. As the funder, by devising a commissioning brief, the HTA programme specified the research question and study design. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the referees for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
None
Permissions
Copyright statement
© 2010 Queen’s Printer and Controller of HMSO. This journal is a member of and subscribes to the principles of the Committee on Publication Ethics (COPE) (http://www.publicationethics.org/). This journal may be freely reproduced for the purposes of private research and study and may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NETSCC, Health Technology Assessment, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2010 Queen’s Printer and Controller of HMSO
Chapter 1 Introduction
Introduction
Anal cancer is an uncommon cancer. It is a disease in which cancer (malignant) cells are found in the anus. Like most cancers, anal cancer is best treated when it is diagnosed soon after it develops. Primary treatment is generally concomitant radiotherapy (RT) and chemotherapy (if tolerated) to preserve the anal sphincter, but, despite these approaches, local disease failure is considerable, and requires salvage radical surgery with associated high morbidity and mortality. Anal cancer is predominantly a disease of the elderly and is near to zero in early life. The human papillomavirus (HPV), has been implicated as a causal agent of anal cancer. HPV infection, for the majority of cases, is transmitted sexually. The vulnerability of individuals with human immunodeficiency virus (HIV) to HPV infections has seen an increase in the number of cases from this population presenting with anal cancer.
To decide whether the screening of groups of people for a specific condition is suitable, there are well-defined criteria that can be used to aid the decision process. 1 The condition should be an important health problem, and the natural history and epidemiology must be understood. The test itself should be safe, simple, accurate and acceptable to the general population.
Aim of the review
The aim of this review is to estimate the cost-effectiveness of screening for anal cancer in men and women who are HIV positive, and, in particular, men who have sex with men (MSM), who have been identified as being at greater risk of the disease, by developing a model that incorporates all of the above criteria.
Epidemiology
Cancer is predominantly a disease of the elderly, with overall crude rates of cancer registrations of 462 per 100,000 of the population for males and 451 per 100,000 of the population for females in England for 2003,2 with anal cancer being no exception. Anal cancer is a rare disease; in 2003 there were 722 registrations of newly diagnosed malignant neoplasm of anus and anal canal in England, with 291 of registrations being male and 431 female. 2 Anal cancer is also very much a cancer of the elderly, with 37% (108) of males with newly diagnosed anal cancer being aged 65 or over and 56% (241) of females with newly diagnosed anal cancer being aged 65 or over. 2 For anal cancer, the rate per 100,000 of the general population in England 2003 was 1.2 per 100,000 for males and 1.7 per 100,000 for females (Table 1). 2
| Rate per 100,000 | Total new cases | Percentage aged 65 years or over | |
|---|---|---|---|
| Males | 1.2 | 291 | 37 |
| Females | 1.7 | 431 | 56 |
Incidence of anal cancer
Johnson et al. 3 reported that the incidence rate for anal cancer in the USA was 2.04 per 100,000 for men and 2.06 per 100,000 women, based on data collected between 1973 and 2000 on diagnosis and outcomes of invasive and in situ anal cancer. The data came from the Surveillance Epidemiology and End Results (SEER) programme (see Appendix 1), a system of population-based tumour registries in the USA. The rate for US males is almost double the rate of English males, whereas the rate for US females is slightly higher than that of English females.
Karandikar et al. 4 undertook a retrospective audit of the squamous (epidermoid) type of anal cancer diagnosed and treated in the principality of Wales over a 5-year period (1995–99), with follow-up until 2005. Patients diagnosed with anal cancer were identified from the Welsh Cancer Registry, Welsh Cancer Intelligence and Surveillance Unit (WCISU) database, and pathology records from 17 hospitals and five oncology units. Overall, 149 patients with anal cancer were identified from the WCISU and hospital pathology databases. Thirteen patients with adenocarcinoma involving the anal canal with or without involvement of the rectum, two patients with melanoma and one with a neuroendocrine tumour of the anal canal were excluded, leaving a cohort of 133 patients. The annual incidence rate of anal cancer from this audit of the principality of Wales was 1.3 per 100,000.
In 1990, Scholefield et al. 5 reported that anal cancer was a rare tumour in Britain, with no published epidemiology studies from this country. Scholefield et al. 5 reported 1988 statistics showing 250–300 cases of anal cancer per year. Scholefield et al. 5 undertook a retrospective study of anal cancer registrations, with colon cancer as controls, from Thames, West of Scotland and West Midlands Cancer Registries. Colorectal cancer was chosen as a control as there was no evidence that a sexual transmission agent is involved in its aetiology. Anonymous details for all anal and colorectal cancers for a 13-year period (1975–87) were obtained from the previously mentioned registries. Scholefield et al. 5 collected information on gender, marital status and 5-year age group.
Scholefield et al. 5 reported that from the Thames Cancer Registry (TCR) there were 846 cases of anal cancer and 26,359 cases of colon cancer, 182 cases of anal cancer and 9613 cases of colon cancer from the West of Scotland Registry and 288 cases of anal cancer and 11,905 cases of colon cancer from the West Midlands Cancer Registry. This gave a total of 1316 cases of anal cancer and 47,877 cases of colon cancer for the 13-year period.
In 1993, Frisch et al. 6 reported the findings of a descriptive epidemiological study based on data from the Danish Cancer Registry. The aim of the study was to examine long-term trends in incidence of anal cancer in a well-monitored, unselected population. The Danish Cancer Registry has recorded all cases of cancer in Denmark since 1943 (only invasive non-adenocarcinoma and non-melanoma anorectal cancers were included in the study) and 888 cases of anal cancers (303 men and 585 women) were identified.
Frisch et al. 6 reported that since around 1960 the incidence rates had nearly doubled in men and tripled in women. Data for 1983–7 gave incidence rates of 0.38 per 100,000 for men and 0.74 per 100,000 for women (world standardised).
Gatta et al. 7 gave details on survival and incidence from rare cancers (defined as those with an annual crude incidence rate of less than 2 per 100,000 for both sexes combined) in 2006, based on data of 39 adult cancer registries for 59,021 patients aged 15–99 years, diagnosed with a selected rare cancer between 1983 and 1994. Data were collected from 18 European countries. Gatta et al. 7 reported that for the UK (England, Scotland and Wales) there was a crude incidence rate of anal squamous cell carcinoma (SCC) of 0.73 per 100,000 and a world-standardised incidence rate of 0.51 per 100,000.
Table 2 displays the available evidence over the years of reported anal cancer incidence rates, and number of new cases. Care needs to be taken in evaluating the table as data are drawn from different sources and presented in different formats, for example age-standardised rates and non-standardised rates. Given that anal cancer is a rare disease, it would indicate that anal cancer is not a significant burden of disease in the population. The criteria for appraising screening programmes1 (Appendix 2) identify that the first criterion to be satisfied before screening for a specific condition is that the condition should be an important health problem. Screening for anal cancer would identify only a low number of cases.
| Study details | Study type | Country | New cases per year | Annual incidence per 100,000 population | ||
|---|---|---|---|---|---|---|
| General | Males | Females | ||||
| Scholefield et al. 19905 | Retrospective cohort study | Britain | 250–300 | – | – | – |
| Frisch et al. 19936 | Descriptive epidemiological study | World | – | – | 0.38a | 0.74a |
| Chiao et al. 20058 | Population-based analysis | USA, 1973–81 | – | 0.60b | – | – |
| USA, 1982–95 | – | 0.80b | – | – | ||
| USA, 1996–2001 | – | 1.00b | – | – | ||
| Office of National Statistics2 | Registry data | England, 2003 | 722 | 1.20 | 1.10b | 1.30b |
| Johnson et al. 20043 | Population-based analysis | USA, 1973–2001 | – | – | 2.04b | 2.06b |
| Karandikar et al. 20064 | Registry data | Wales, 1995–99 | – | 1.30 | – | – |
| Gatta et al. 20067 | Registry data | UK, 1983–94 | – | 0.51a | – | – |
Incidence rate by age and gender
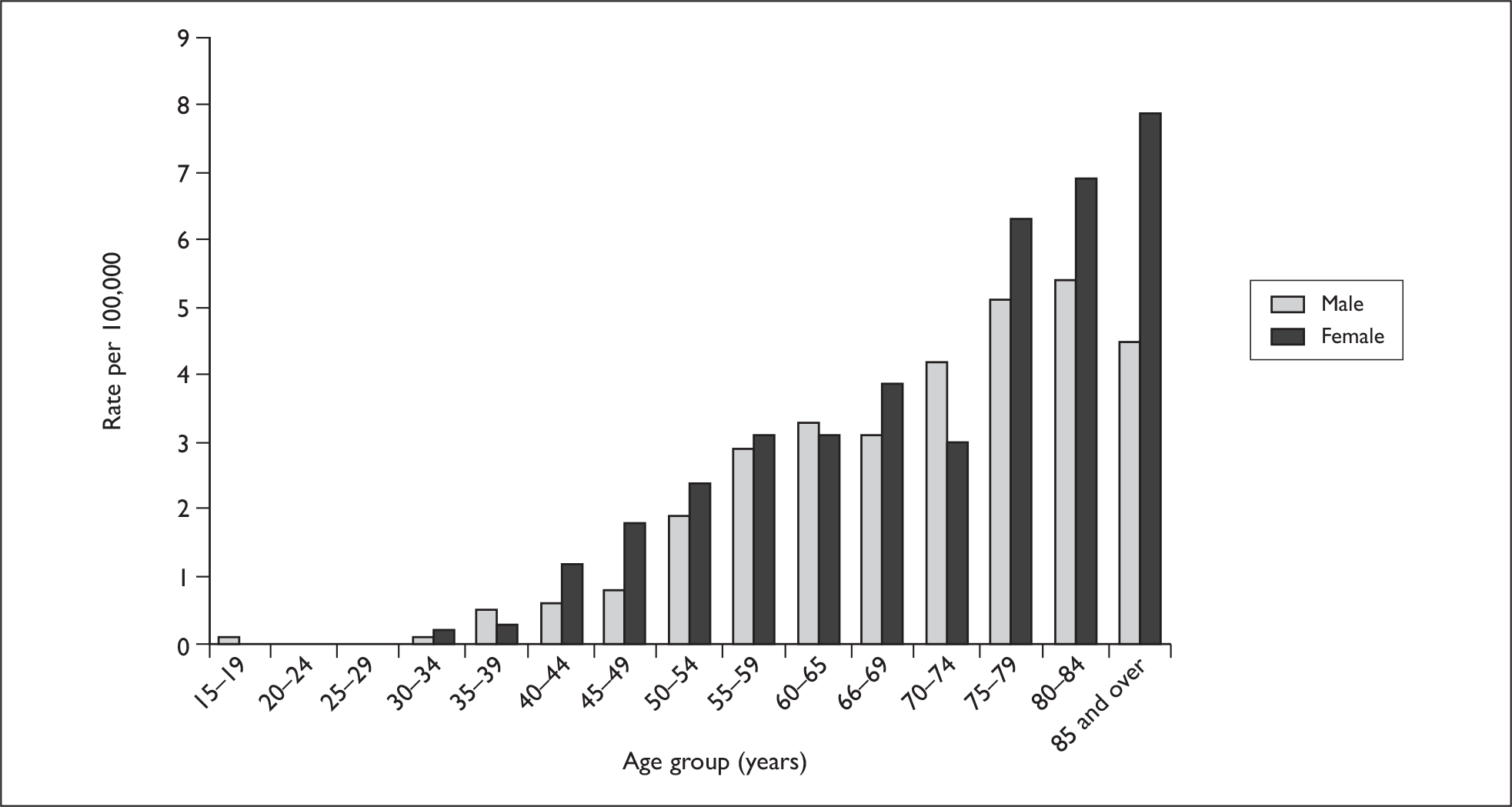
The probability of developing anal cancer rises sharply with age and the UK population is ageing. In young people, the risk is very low, but between the ages of 55 and 65 the annual incidence rate is approximately 3 per 100,000 for both males and females. Amongst those aged between 75 and 84 years, the annual incidence rate is over 5 per 100,000 and over 6 per 100,000 per year for males and females, respectively. Figure 1 shows the age-specific incidence rate for anal cancer, based on data from the Office of National Statistics. 2
FIGURE 1.
Annual incidence rate per 100,000 for newly diagnosed anal cancer by gender and age in England 2003. Compiled from data from the Office for National Statistics. 2
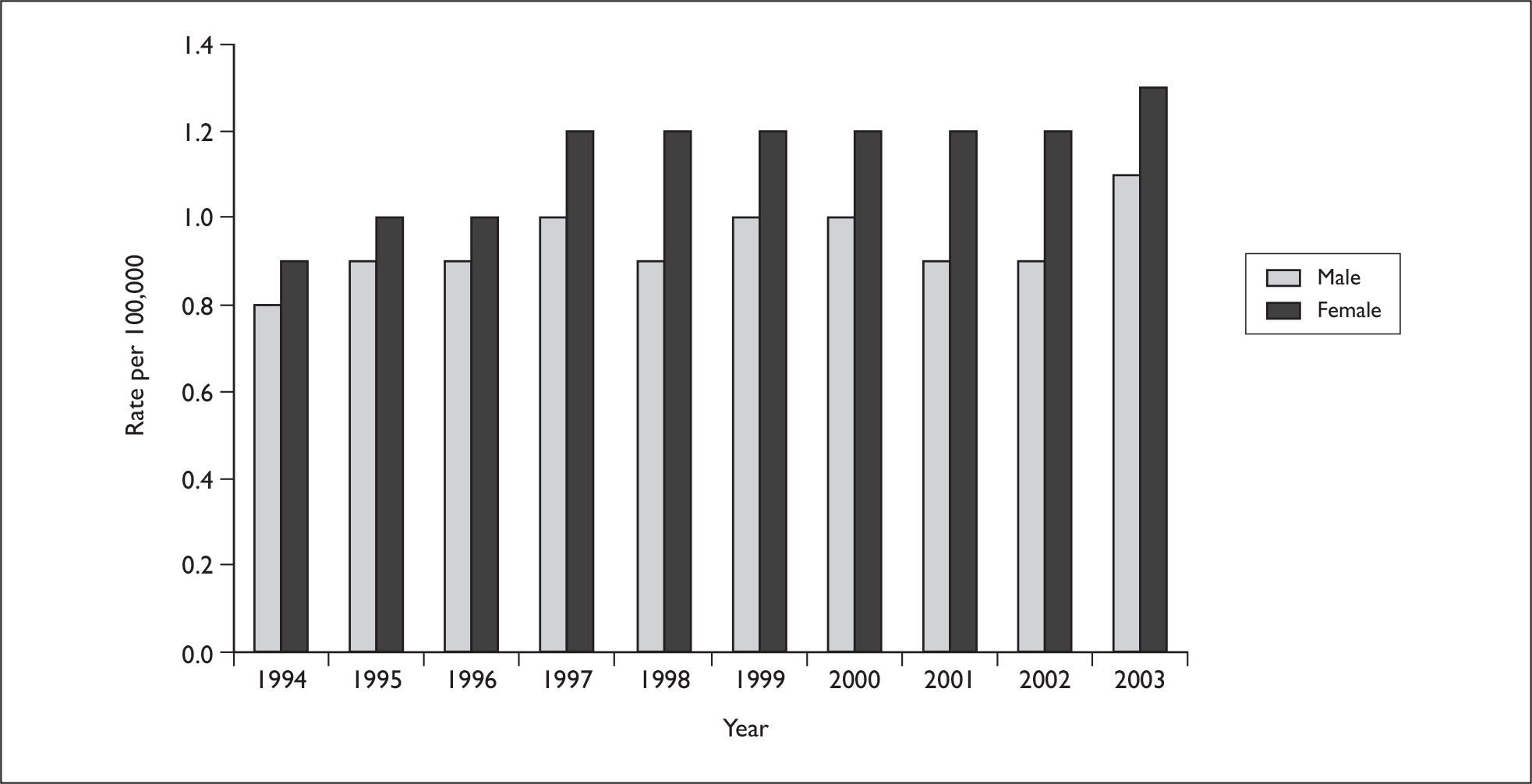
The annual incidence rate (directly age-standardised rates) has remained constant over the last decade, remaining at around 1.0 per 100,000 for males. For females, there has been a slight rise in directly age-standardised rates from the late 1990s, rising from around 1.0 per 100,000 to around 1.2 per 100,000 (Figure 2).
FIGURE 2.
Directly age-standardised rate per 100,000 for newly diagnosed anal cancer by gender in England 1994–2003. Compiled from data from the Office for National Statistics. 2
In 2006, Brewster and Bhatti9 publicised the findings of their study describing secular trends in incidence of SCC of the anus in Scotland, before and during the HIV epidemic. Incidence cases of malignant neoplasms of the anus and anal canal were extracted from the Scottish Cancer Registry for the years 1975–2002. Brewster and Bhatti9 identified 757 cases of SCC (278 males and 479 females) registered, with an incident date falling within the 28-year period of the study. The authors found that in males the standardised incidence rate per 100,000 increased from 0.14 to 0.17 in the late 1970s to around 0.37 in the late 1990s, with a peak of 0.44 in the period 1993–7. For females, the incidence rate was generally higher, increasing from 0.23–0.27 in the late 1970s to a peak of 0.55 in the period 1998–2002.
Incidence by marital status
Scholefield et al. 5 reported that the odds ratio (OR) for never-married men compared with ever-married men was 2.2 [95% confidence interval (CI) 1.8 to 2.8] and the OR for never-married women compared with ever-married women was 0.6 (95% CI 0.5 to 0.8). The authors concluded that there is a clear increase in the risk of anal cancer among never-married men.
Frisch et al. 6 examined incidence according to marital status, using a nested case-controlled design in which all anal cancer patients (n = 888) served as cases and all patients with colon cancer (n = 54,207) and stomach cancer (n = 58,198) were used as controls. The authors found that 17% (53 of 303) of men with anal cancer had never married, compared with 7% (1790 of 24,420) of never-married men with colon cancer and 9% (2877 of 33,248) of never-married men with stomach cancer. Among women the figures were 11% (64 of 585) anal cancer, 13% (3898 of 30,787) colon cancer, and 12% (2859 of 24,062) stomach cancer. The adjusted ORs were 2.7 (95% CI 2.0 to 3.6) for men and 1.0 (95% CI 0.8 to 1.3) for women, with colon cancer as control, and 2.1 (95% CI 1.5 to 2.8) for men and 1.2 (95% CI to 0.9–1.6) for women with stomach cancer as control. The authors of this study6 concluded that men who had never married were found at increased risk since the 1940s, indicating a potential association with male homosexuality.
Rabkin and Yellin10 reported in 1994 the results of a study to determine the types and rates of cancers occurring in excess in the presence of HIV-1 infection. The National Cancer Institute’s (NCI) SEER registry data (Appendix 1) was used to identify never-married men aged 25–54 years living in the San Francisco area and whom were HIV-1 seropositive as of late 1984. Age-, race- and sex-specific populations of San Francisco for the years 1973 to 1990 were obtained from Census data and for the period between Census dates they were estimated. For the study period of interest, there were 1,390,000 person-years of observation of the never-married men, 25–54 years of age, living in the San Francisco population. Expected cancers were calculated from age-, race- and period-specific cancer incidence rates of the entire male SEER population for the periods 1973–9 [defined as the pre-acquired immune deficiency syndrome (AIDS) period], 1980–4, 1985–7 and 1988–90.
Rabkin and Yellin10 study showed that in the pre-AIDS period, the incidence of anal cancer in the never-married, 25- to 54-aged San Francisco men group was 3.5 per 100,000. This was 9.9 (95% CI 4.5 to 18.7) times the expected rate of the total male SEER population for that period. By 1988–90, the standardised incidence had increased to 5.9 per 100,000 for the never-married 25- to 54-aged San Francisco men group. The SEER population rates, however, had similarly increased and the observed–expected ratio remained almost unchanged at 10.1 (95% CI 5.0 to 18.0). The authors concluded that HIV-1 is not related to the increase risk of anal cancer in homosexual men that antedated the AIDS epidemic.
Anal cancer and HIV/AIDS
In 2005, Diamond et al. 11 reported on a study that linked cancer registry data from 1988 to 2000 and AIDS registry data from 1981 to 2003 for San Diego County, USA. The authors defined 1991–5 as the pre-highly active antiretroviral therapy (HAART) era and 1996 to 2000 as the post-HAART era. The authors identified 42 men with SCC of the anus. The authors found that amongst men aged 25–64 years with AIDS, the average annual incidence of anal cancer pre-HAART was 88 per 100,000 and post-HAART, 190 per 100,000. They further reported that the annual incidence of invasive anal cancer increased from 0 per 100,000 men aged 25–64 years with AIDS in 1991 to 2224 per 100,000 in 2000. Pre-HAART, the average annual incidence of invasive anal cancer was 49 per 100,000 men aged 25–64 years with AIDS, whereas post HAART it was 144 per 100,000. It was also reported that patients diagnosed with anal cancer during the post-HAART era had a longer duration of diagnosed HIV infection (84 months vs 22 months pre-HAART).
For post-HAART anal cancer, both invasive and in situ, Diamond et al. 11 reported an average incidence of 190 per 100,000 men aged 25–64 years with AIDS (95% CI 209 to 646) compared with men without HIV/AIDS. The authors did acknowledge that the numbers of cases in the study were small but that the information had been collected for more than a decade from both registries.
In 2005, Chiao et al. 8 reported a population-based analysis of temporal trends in the incidence of squamous cell cancer of the anus (SCCA) in relation to the HIV epidemic. Chiao et al. 8 obtained data from the SEER programme, from 1973 to 2001 to characterise the primary site, histology [classified according to the International Classification of Diseases for Oncology, version 3 (ICD-O3)], tumour site, stage at diagnosis, initial radiation therapy, patient demographics, age, gender, race and/or ethnicity, and mortality. Tumours with anatomic sites coded C21.0 through to C21.1 and C21.8 (anus, anal canal and anorectum) were included. The analysis was limited to cases with histological types coded as invasive non-in situ epidermoid cancers according to the ICD-O3. In situ cases were included only in the analysis describing stage at diagnosis.
Chiao et al. 8 used three eras to group the years of diagnosis. As the first case definition of AIDS was adopted in 1982, the period 1973–81 was defined as the pre-HIV era. The years 1982–95 were defined as the HIV era. HAART was widely introduced in 1996, and the years 1996–2001 were defined as the HAART era. A total of 4855 cases on invasive SCCA were reported from 1973 to 2001. The overall incidence from 1973 to 2001 was 0.8 per 100,000 population, an increase from 0.6 (95% CI 0.6 to 0.7) in the pre-HIV era to 0.8 (95% CI 0.8 to 0.8) in the HIV era, and to 1.0 (95% CI 1.0 to 1.1) in the HAART era.
The conclusions reached by Chiao et al. 8 were that the incidence of SCCA has increased steadily over the past three decades, and that since the introduction of HAART the incidence of SCCA has risen particularly among men and younger individuals – the groups most affected by HIV.
Grulich et al. 12 undertook a cohort study involving an Australian nationwide linkage of HIV, AIDS and cancer registry data to describe the incidence of non-AIDS-defining cancers in people with HIV infection before and after the occurrence of AIDS, and to examine the association of cancer risk with immune deficiency. In Australia, HIV and AIDS are reported with a name code (first two letters of first and last name), date of birth and sex. The authors attempted linkage for all of those individuals who had complete data for these three fields on either the national HIV or AIDS database. The procedure of linkage with the cancer register was not fully described, but a link to a paper giving details was given. Briefly, linkage was performed using a modified version of the National Cancer Register, with full names converted to name codes. A match was accepted if there was an exact match on all three fields, or there was a near match supported by consistency between the registers in dates of death and area of residence. Linkage was performed separately for the HIV and AIDS databases. HIV and AIDS data were available up to December 1999, and cancer data until 1995–98 depending on jurisdiction.
Grulich et al. 12 reported that 10 cases were observed for cancer of the anus compared with the expected number of cases of 0.27. The standard incidence rate (SIR) was 37.1 (95% CI 17.8 to 68.3), significant at p <0.05. The author’s conclusions were that, in this study, anal cancer rates increased from HIV diagnosis to the time around AIDS diagnosis, but there were no diagnoses more than 6 months after AIDS. Even in people with the mildest degree of immune deficiency the rates of this cancer were increased 20-fold above what was expected. The authors acknowledged that the data did not support an independent association between invasive anal cancer and HIV-associated immune deficiency but it may be that prolonged observation will be necessary.
In 2000, Frisch et al. 13 described a study looking at lifestyle factors associated with HPV-associated malignancies. The authors studied invasive and in situ HPV-associated cancers amongst 309,365 patients with HIV infection/AIDS in the USA, 5 years before the date of AIDS onset and 5 years after. Between 1995 and 1998, data from AIDS and cancer registries in 11 state and metropolitan locations were linked; these states and locations contained approximately one-third of the US population.
Among both male and female patients with AIDS, the majority were aged between 20 and 49 years at AIDS onset (88% and 86%, respectively). Of the males in the study, HIV infection was via homosexual contact (56%), homosexual contact and intravenous drug use (6%), intravenous drug use (26%), heterosexual contact (3%) or unknown/other (9%).
Frisch et al. 13 reported that invasive and in situ anal cancers were present in 360 patients (239 were invasive cancer and 121 in situ), with a mean age at onset of 41 years for invasive anal cancer and 37 years of in situ anal cancer. For invasive anal cancer, the relative risk (RR) was 6.8 (95% CI 2.7 to 14.0) for females and 37.9 (95% CI 33.0 to 43.4) for males. For in situ anal cancer, the RR was 7.8 (95% CI 0.2 to 43.6) for females and 60.1 (95% CI 49.2 to 72.7) for males.
Anal cancer and HPV
Hemminki and Dong14 used the Swedish Family-Cancer Database to analyse the spectrum of cancers diagnosed in husbands of women with in situ or invasive cervical cancer, and compared these to second carcinogenic events in women presenting with these cancers. The author’s hypothesis was that there was increased cancer susceptibility from HPV. The Swedish Family-Cancer Database (which includes all persons born in Sweden after 1934 with their biological parents, some 9.6 million individuals). From this database the authors identified 313,602 men with cancer after the birth of their last child; 6839 were men whose wife was diagnosed with in situ cervical cancer, and 2813 were men whose wife was diagnosed with invasive cervical cancer. Women (117,921 with in situ cervical cancer and 17,579 with invasive cervical cancer) were followed for second events (i.e. first cancer after in situ cancer and second primary cancer after first primary cancer) until the end of 1996, resulting in 7455 women with first cancers (after in situ cervical cancer) and 1990 women with second primaries (after invasive cervical cancer).
Hemminki and Dong14 reported that for wives with in situ cervical cancer, the husbands had an excess of cancer at six sites: upper aerodigestive tract (including mouth, tongue, larynx and pharynx), stomach, anus, lung, kidney and connective tissue, with anal cancer showing the highest SIR of 1.75. Penile cancer showed an SIR of 1.30 (95% CI 0.91 to 1.77). These sites agreed with first cancers of women who had suffered from an in situ cervical cancer. SIRs for female cancers were high for anus (3.60), lung (2.08) and other tobacco-related sites. The authors concluded that the results suggest that female cervical cancer, probably through HPV infection, is associated with anal and, weakly, with penile cancer in husbands. There was a consistency in husbands’ anal cancers irrespective of wives’ in situ or invasive cervical cancer. The authors reported that the findings are consistent with the demonstrated associations between HPV infection, sexual activity and anal cancer in men and women.
In 2002, De Sanjose and Palefsky15 undertook a review to summarise recently published epidemiological information that contributed to understanding the natural history of cervical and HPV infection and their associated lesions among HIV-infected women and men. De Sanjose and Palefsky15 concluded that HIV-positive women and men are more likely to be infected with oncogenic HPV types and to have cervical intraepithelial neoplasia (CIN) or anal intraepithelial neoplasia (AIN) lesions that may lead to invasive cervical and anal cancer, respectively.
Anal cancer and homosexual partnerships
In 2003, Frisch et al. 16 undertook a retrospective cohort study of 1614 women and 3391 men in Denmark for cancer from their first registration for marriage-like homosexual partnership between 1989 and 1997. The authors used data from the population-based Danish Cancer Registry to investigate the cancer profile of all men and women in Denmark who had one or more records of registered homosexual partnership between 1989 and 1997. The Civil Registration System in Denmark has kept continuously updated files on basic demographic variables of its citizens. The system uses a unique 10-digit personal identification number as key – recorded information includes name, date of birth, marital status, emigration and vital status since 1968.
Frisch et al. 16 reported that for women in registered homosexual partnerships, no incidences of anal cancer were identified and that overall cancer incidence among this group differed little from that of Danish women in general (RR = 0.9, 95% CI 0.6 to 1.4, n = 24 cancers). For men, the overall risk of cancer among 3391 men in registered homosexual partnerships increased twofold (RR = 2.1, 95% CI 1.8 to 2.5, n = 139). The authors reported that this excess was almost entirely due to high numbers of Kaposi’s sarcoma (RR = 136, 95% CI 96 to 186, n = 38) and non-Hodgkin’s lymphoma (RR = 15.1, 95% CI 10.4 to 21.4, n = 32) cases. A statistically significant excess was also seen for anal squamous carcinoma (RR = 31.2, 95% CI 8.4 to 79.8, n = 4).
Frisch et al. 16 concluded that apart from HIV/AIDS-associated cancers and anal squamous carcinoma in men, Danish men and women in registered homosexual partnerships appear not to be at any unusual cancer risk compared with the general population.
In 1999, Lacey et al. 17 reported on a prospective cohort study of HIV-positive homosexual men. A total of 57 subjects were recruited from a larger cohort [300 patients, 33% Centre for Disease Control and Prevention (CDC) group C] attending North Manchester General Hospital for their HIV care in January 1994 and were followed for 18 months.
The participants in the Lacey et al. 17 study were interviewed and underwent screening for sexually transmitted diseases (STDs), anal cytology and HPV at enrolment and at subsequent follow-up visits, with anoscopy and biopsy at the final visit. The study end point with anoscopy and biopsy was reached by 38 participants. The average follow-up was 17 months (range 14–21 months, total 650 months); 184 outpatient visits were attended and 184 cytology and HPV specimens were available for analysis.
Lacey et al. 17 concluded that AIN and infection with multiple oncogenic HPV types are very common among immunosuppressed HIV-positive homosexual men. Apparent progression from low to high-grade cytological changes occurred over a short follow-up period, with no cases of carcinoma. All 23 cases of high-grade anal intraepithelial neoplasia (HG-AIN) were predicted by cytology and/or anoscopy. The authors further concluded that it appears that anoscopy and cytology could be a useful screening procedure in the detection of high-grade disease in immunosuppressed HIV-positive homosexual men, but questions remain to be answered about the significance of HG-AIN in this group of patient, it seems wise to urge caution when considering screening programmes until more data about the natural history and efficacy of treatment options are known.
HPV infection
The natural history of HPV infection is complex, and clearance and persistence of viral DNA, along with progression to squamous intraepithelial lesions (SILs), vary depending on the viral type and patient characteristics, such as age and immune status. 18
Palefsky et al. 19 reported in 1998 the findings of a cohort study to characterise the prevalence of 29 different HPV types and the mixture of 10 additional types in the anal canal among HIV-positive and HIV-negative men. Palefsky et al. 19 recruited 346 HIV-positive and 262 HIV-negative men from among homosexual and bisexual men in the San Francisco Men’s Health Study (SFMHS) in the San Francisco General Hospital Cohort Study (SFGH) and the University of California, San Francisco (UCSF), responding to newspaper advertisements. The participants were interviewed regarding their medical history, prescribed drug use, X-ray exposure, hospitalisation, transfusions, history of sexually transmitted diseases, intestinal parasites, hepatitis anal conditions (such as fissures and fistulas) and symptoms related to HIV. The participants were also asked about sexual practices, cigarette smoking, drinking and recreational drug use. Participants also tested underwent HPV testing. Palefsky et al. 19 reported no differences between HIV-positive and HIV-negative men.
Kreuter et al. 20 conducted a prospective cohort study in Germany to determine the clinical spectrum of AIN and lesional HPV colonisation in a cohort of homosexual men who were HIV-positive and had a history of receptive anal intercourse. Between December 2003 and July 2004, 103 homosexual men with a laboratory-confirmed diagnosis of HIV were recruited for a screening programme for AIN. The participants underwent a standardised interview on medical history, STDs, history of HPV-related diseases and tobacco use before screening.
Kreuter et al. 20 reported that of all patients 86% had anal HPV infection at their first visit. AIN was diagnosed in 20 (19.4%) of the 103 participants. The authors concluded that their data confirmed the high incidence and prevalence of inpatients with AIN who are HPV positive with HIV infection. The authors of this paper were of the opinion that standardised screening programmes for anal cancer prevention and treatment protocols for AIN in patients infected with HIV must be implemented.
Watson et al. 21 in 2006 reported on a prospective cohort of 72 patients (52 women, 20 men) who were diagnosed with AIN between January 1996 and December 2004. These 72 patients, from a single institution in New Zealand, were identified from a prospective database. Data collected from the database were supplemented with information from patient chart review, which included data on age, sex, HIV/AIDS infection, chronic immunosuppression, disease presentation, management and follow-up. All patients underwent biopsy or perianal skin excision between January 1996 and July 2005; 17 patients were initially diagnosed with AIN 1, 10 with AIN 2, and 45 with AIN 3 on first biopsy. A total of 42 patients also had pathological changes that were consistent with HPV infection. Seven patients were recipients of renal transplants and were on immunosuppressive therapy. Five patients were HIV positive and 10 others were on long-term immunosuppressive therapy for other causes.
Watson et al. 21 detailed that, during the study period, 193 procedures were carried out (127 were biopsies only and 66 were perianal skin excisions). Eight patients progressed to develop SCC during the study period (median time 42 months). There was histological evidence of progression in 11 patients, with six patients having AIN 3 progressing to have anal SCC. Two patients with AIN 2 developed cancer and 25 patients with AIN had regression of dysplasia. The conclusion reached by Watson et al. 21 was that their study suggested that patients with HG-AIN are at a higher risk of developing anal SCC than previously thought and surveillance is indicated. The authors also concluded that the patients who are particularly at risk are the immunocompromised, and that the treatment available at present does not prevent AIN in some patients from progressing to invasive cancer and carries the associated risk of faecal incontinence. Watson et al. 21 further concluded that as a result of their study they could not recommend screening of asymptomatic high-risk populations, but that there is a need for research into more effective and less morbid treatments for this disease.
Prognosis
The staging system for anal cancer is the TNM (tumour, node, metastasis) staging system. 22 The TNM staging system is useful for surgical purposes, such as providing guidelines on the extent of resection, it is described in more detail below.
The TNM staging system is based on the anatomical extent of spread, where, T refers to the extent of the primary tumour, N refers to the extent of nodal metastases and M refers to the presence or absence of distant metastases. Each of these three factors is given a number: for T, the number indicates how large the tumour is; for N, the number informs which lymph nodes have cancer cells in them; and for M, the number informs as to whether the cancer has spread to other parts of the body – in general, the higher the number, the more serious the cancer. There are five stages of tumour size in the current TNM classification of anal cancer: T1–T4 and a very early stage called Tis or carcinoma in situ. Anal cancers are not usually found at this very early stage, as they do not cause any symptoms when they are so small. Below are descriptions of each T stage for anal cancer:
-
Tis or carcinoma in situ The earliest stage of anal cancer, when the cancer cells are found only inside the lining of the anus and have not spread elsewhere.
-
T1 The tumour measures 2 cm across or less.
-
T2 The tumour is larger than 2 cm but smaller than 5 cm.
-
T3 The tumour is larger than 5 cm.
-
T4 The cancer can be any size, but is growing into the surrounding tissues or organs, such as the urethra, the vagina or bladder.
Staging is a process that tells the clinician how widespread the cancer may be at the time of diagnosis. It will show whether the cancer has spread and how far. The treatment and outlook for anal cancer depends, to a large extent, on its stage.
In 2004, Johnson et al. 3 reported 5-year survival figures of 58% for males and 64% for females, based on data collected between 1973 and 2000 on diagnosis and outcomes of invasive and in situ anal cancer. The data came from the SEER programme in the USA. Lower 5-year survival figures were reported by Bower et al. 23 for a cohort of English patients with HIV (25 MSM and 1 heterosexual woman) with confirmed cases of invasive anal cancer. Bower et al. 23 reported a 5-year overall survival figure of 47%.
In 2006, Karandikar et al. 4 reported a 5-year overall survival figure of 45%, based on a cohort of patients with anal cancer who were identified from a 5-year audit (1995–9) of anal cancer in Wales.
Also in 2006, Jeffreys et al. 24 reported the results of a study that was based on all first, primary, invasive malignant cancers of the rectum and anus – excluding anal margin and skin – that were diagnosed in adults (15–99 years) and registered in the National Cancer Registry for England and Wales between 1986 and 1999. The aims of the study were to investigate the effects of tumour and patient characteristics on trends in the survival of patients with cancer of the anus or rectum in England and Wales. A total of 132,542 adults who were diagnosed during the 14 years were followed up to 2001 through the National Health Service Central Register. Results were given for patients diagnosed during the calendar periods 1986–90, 1991–5 and 1996–9. Relative survival up to 5 years after diagnosis was estimated, using deprivation-specific life tables. Five-year relative survival rose by about 10% overall, from 38% (1986–90) to 48% (1996–9) in men, and 39% (1986–90) to 51% (1986–90) in women.
Gatta et al. 7 gave details on survival and incidence from rare cancers using data collected from 18 European countries. They reported that the overall 5-year relative survival for anal SCC was good at 53.1% (95% CI 51.5 to 54.8); the authors also reported absolute survival figures, with 53.1% (95% CI 51.7% to 54.4%) for 3-year survival and 43.3% (95% CI 41.9% to 44.6%) for 5-year survival.
For the UK, Gatta et al. 7 reported a 5-year relative survival of 51.9% (95% CI 49.7% to 54.2%). Data for the UK (England, Scotland and Wales) came from national cancer registries or from regional cancer registries.
Quality of life
Allal et al. 25 undertook a study to assess long-term quality of life (QoL) in patients treated by RT with or without chemotherapy. The study population was drawn from 165 patients with anal carcinoma who received sphincter-conserving treatment using RT, with or without chemotherapy, between January 1976 and December 1994. Patients were considered for the study’s QoL assessment if they were 80 years old or less and were alive without disease activity at least 3 years after completion of treatment with a functioning anal sphincter. In total, 52 patients satisfied the inclusion criteria – 49 patients were contacted by telephone to request their participation in the study and three were contacted by mail. Of these patients, 46 patients agreed to participate, one refused, two were assessed to be ineligible because of serious comorbidities and the three contacted by mail did not respond. Among the 46 patients who received the two questionnaires, five refused to complete them for different reasons (two ‘unclear’, two ‘number of questions’, one ‘questions relating to sexual aspects’). This left 41 patients for the analysis.
The QoL questionnaires used by Allal et al. 25 were developed by the QoL Study Group of the European Organisation for Research and Treatment of Cancer (EORTC). One was a validated questionnaire assessing cancer-specific QoL (EORTC QLQ-C30) (Aaronson et al. 1993) and one assessing site-specific (colorectal) QoL (EORTC QLQ-CR38), which at the time of the study was in the process of validation.
The EORTC QLQ-C30 is a patient self-rating questionnaire that comprises six multi-item function scales measuring physical, role, social, emotional and cognitive functions, along with overall QoL. Separate symptom scales are included to assess pain, fatigue and emesis, and five single items to measure gastrointestinal symptoms, dyspnoea, appetite loss and sleep disturbances. A final item evaluates the perceived economic consequences of the disease.
The EORTC QLQ-CR38 is a patient self-rating questionnaire that comprises 38 questions, of which 19 are completed by all patients and the remaining by a subset of patients (males or females, patients with or without a stoma). The general structure comprises four multi-item/single-function scales, seven multi-item symptom scales and one single symptom item. The functioning scales assess effects on micturition, chemotherapy, side effects, gastrointestinal general symptoms, defecation problems, stoma-related problems and sexual dysfunction in males or females. The single symptom item assesses weight loss.
The result reported by Allal et al. 25 for the EORTC QLQ-C30 questionnaire was that the physical function scale scores did not differ significantly in the subgroups, although older patients tended to report lower scores (p = 0.08). For the role function scale, while non-significant, the severity of late complications and poor MSK (Memorial Sloan-Kettering Center anal function criteria) anal function appear to have a negative effect (p = 0.08 for both). For the emotional and the social function scales, no significant differences were noted between the different subgroups. However, the overall QoL score was significantly affected by the severity of late complications (p = 0.005) and the anal function score (p = 0.04). This score did not differ with the current age and pain symptom scales, particularly according to the length of follow-up.
The results of the EORTC QLQ-CR38 questionnaire used by Allal et al. 25 were that body image function score was significantly lower only in patients with advanced T stage (p = 0.003). For the future perspective function scale, no significant differences were noted between subgroups, while lower scores were reported in patients with higher grade of late complications (p = 0.1). The sexual functioning score was significantly lower only in the advanced-age subgroup (p = 0.01). None of the function scale scores seemed to be influenced by the length of follow-up. A significantly higher defecation problems score was reported in patients who were treated with brachytherapy for the boost (p = 0.03).
Allal et al. 25 concluded that in patients treated with sphincter conservation for anal carcinomas, long-term QoL, as measured by the EORTC QLQ-C30 and QLQ-CR38, appeared to be acceptable, with the exception of diarrhoea and, perhaps, sexual function. The subset of patients who presented with severe complications and/or anal dysfunction showed poorer scores in most scales.
In 2005, Pachler and Wille-Jorgensen26 reported on a systematic review of QoL after rectal resection for cancer, with or without permanent colostomy. The objective of the review was to evaluate the QoL in patients treated for rectal cancer with either abdominoperineal excision (APE), with a permanent stoma or rectal anastomosis anterior resection (AR) with preservation of the sphincter function.
The criteria for considering studies to use in the review by Pachler and Wille-Jorgensen26 were:
-
All controlled clinical trials and observational controlled studies in which QoL in patients with rectal cancer, having either APE or AR were studied using a multidimensional QoL instrument.
-
The participants were individuals with verified cancer of the rectum, which had been treated with either APE or AR.
-
No discriminatory criteria concerning age, gender, race or social status.
-
Quality-of-life assessments using validated multidimensional questionnaire, self-reported questionnaires completed by the patient – a relative or independent rater was considered eligible for inclusion.
-
Assessments of functional results or one-dimensional aspects of QoL (e.g. sexual function, urinary function, pain) were not included in the review.
Pachler and Wille-Jorgensen26 reported that 30 potential studies were identified, 11 of these, including 1412 participants (range 23–372), met the inclusion criteria. None was randomised, nine were retrospective and two prospective. Overall, six studies found that patients undergoing APE did not have poorer QoL than patients undergoing AR. One study found that a stoma only slightly affected the patient’s QoL; four found that after APE patients had significantly poorer QoL than after AR. The authors concluded that it was not possible to draw conclusions whether the QoL measures of stoma patients are poorer than for non-stoma patients. However, the results challenge the assumption that people with stoma fare less well than non-stoma patients.
Chapter 2 Methods
Systematic reviews were conducted to identify and assess all literature relating to the screening of anal cancer in high-risk groups.
Search strategies
A comprehensive literature search was undertaken in January 2006 (updated in November 2006) to identify relevant literature pertaining to screening high-risk groups for anal cancer. Four major searches were conducted, which were designed to retrieve papers:
-
describing the epidemiology of anal cancer
-
on the effectiveness of screening technologies for anal cancer
-
on the effectiveness of different screening programmes/policies for anal cancer
-
on the cost-effectiveness and comparative costs of candidate technologies/programmes/policies identified from effectiveness searches. Searches were also undertaken to retrieve papers on the effectiveness of different treatments for anal cancer.
The following electronic bibliographic databases were searched:
-
Applied Social Sciences Index and Abstracts (ASSIA)
-
BIOSIS previews (Biological Abstracts)
-
British Nursing Index (BNI)
-
Cumulative Index to Nursing and Allied Health Literature (CINAHL)
-
Cochrane Database of Systematic Reviews (CDSR)
-
Cochrane Central Register of Controlled Trials (CENTRAL)
-
EMBASE
-
MEDLINE
-
MEDLINE In-Process & Other Non-Indexed Citations
-
NHS Database of Abstracts of Reviews of Effects (DARE)
-
NHS Health Technology Assessment (HTA) Database
-
PsycINFO
-
Science Citation Index (SCI)
-
Social Sciences Citation Index (SSCI).
Attempts were also made to identify ‘grey’ literature by searching appropriate databases (e.g. the King’s Fund, DH-Data) current research registers [e.g. National Research Register (NRR), Current Controlled Trials (CCT) register]. A general internet search was also conducted using a standard search engine (Google) and a meta-search engine (Copernic).
The reference lists of included studies and relevant review articles were also checked.
No date or language restrictions were applied to these searches. The search strategies used in MEDLINE (Ovid) are displayed in Appendix 3.
All prospective and retrospective primary studies groups who were at high risk of anal cancer were included in the review. An assessment was conducted of published literature identified by the search strategy by all four reviewers. All publications were divided into the following broad categories based initially on their titles and abstracts (where available): cost-effectiveness, natural history, prevalence, diagnosis, epidemiology, screening, treatment, risk, QoL, and not relevant – excluded. A paper could be included in more than one category. The reviewers then obtained copies of all papers not excluded. Some papers were reclassified after reading the full text, additional papers were subsequently excluded. Each paper not excluded after the initial readings was given a unique identifier. Hand searching of included papers was conducted to identify any relevant papers not detected by the electronic searches. A quality of reporting of meta-analyses (QUOROM) trial flow chart is displayed in Appendix 4.
Inclusion/exclusion criteria
Papers were selected if they met the following inclusion criteria:
-
contained data on population incidence, effectiveness of screening, health outcomes or screening and/or treatment costs of anal cancer
-
described defined suitable screening technologies
-
prospectively evaluated a test, or a combination of tests, to detect anal cancer.
Papers were excluded if they were a foreign language publication.
Data abstraction
Data from all of the studies meeting the inclusion criteria were extracted into data extraction forms by the clinical effectiveness reviewer.
Chapter 3 Results
Screening
This section reviews studies that evaluated screening procedures for the detection of AIN, anal squamous intraepithelial lesion (ASIL) or anal cancer. Ten studies were identified for inclusion on screening; Table 3 shows the studies characteristics and Appendix 5 gives details on study quality. Nine studies were cohort studies27–35 and one was a systematic review. 36
| Study details | Objective | Population | Inclusion/exclusion criteria | Study type | Screening test |
|---|---|---|---|---|---|
| de Ruiter 199427 | To compare anal cytology with histology as a method of detecting AIN | Homosexual or bisexual men (n = 215) | Homosexual and bisexual men attending a central London department of GU medicine for routine follow-up of their HIV infection or with newly diagnosed anal condylomata | Cohort study | Anal cytological smear performed under standard conditions |
| Palefsky et al. 199728 | To assess the sensitivity, specificity, and positive and NPVs of anal cytology | HIV-positive (n = 407) and HIV-negative (n = 251) homosexual and bisexual men | HIV-positive and HIV-negative homosexual and bisexual men, who were participating in a natural history study of ASIL | Cohort study | Anoscopically directed anal biopsy as standard. Anal cytology results were classified using standard Bethesda criteria38 for cervical cytology |
| Mathews et al. 200429 | To estimate agreement between consecutive anal cytological examinations, between concurrent cytological examination and histopathology, and between HRA visual impression and histopathology and to estimate the prevalence of severe dysplasia by concurrent cytological category | Patients with HIV (n = 1864) | HIV-infected patients receiving anal dysplasia screening as part of routine care for HIV at the University of California at San Diego Owen Clinic, with a history of anal receptive intercourse, anogenital warts or anal/cervical dysplasia | Prospective observational cohort study | Anal Pap test with a repeat Pap test and biopsy performed for patients with a screening Pap diagnosis of ASCUS, LSIL or HSIL |
| Panther et al. 200430 | To determine the accuracy of anal Pap smear as a predictor of paired anal histology results, as well as whether HIV serostatus had an impact on findings | MSM (n = 153) | MSM referred to an anal dysplasia clinic | Cohort study | Anal Pap smears |
| Fox et al. 200537 | To establish whether anal cytology has value as a screening tool and to validate the Palefsky method based on a UK population | Homosexual/bisexual males who underwent high-resolution anoscopy (n = 99) | Cohort study | Dacron swab was inserted blindly 3 cm into the anal canal and rotated using a spiral motion | |
| Arain et al. 200531 | To assess the usefulness and limitations of anal smears in screening for ASILs | Males that had anal smears collected in liquid medium (n = 198) | Anal smears retrieved from files of the pathology department at Cedars-Sinai Medical Centre, Los Angeles | Cohort study | Anal smears collected in liquid medium compared with results of surgical biopsies or repeat smears |
| Friedlander et al. 200332 | To evaluate anorectal cytology as a screening tool and to correlate anorectal cytology with anoscopic and histological findings | Patients that had anorectal specimens on file (n = 51) | Anorectal specimens retrieved from the files of the cytology service at Memorial Sloan-Kettering Cancer Center, New York | Cohort study | Retrieved smears stained with Papanicolaou stain |
| Lampinen et al. 200633 | To compare self- vs clinician-collection procedures with respect to specimen adequacy for cytological evaluation | HIV-1 seronegative MSM aged 18–30 years (n = 222) | Men involved in a study of HIV incidence and risk behaviours among young HIV-1 seronegative MSM conducted in Vancouver | Cross-sectional study | Self- and clinician- collected anorectal Dacron swabs for liquid-based cytological evaluation were collected |
| Cranston et al. 200436 | To assess the performance of results collected by study participants at home compared with samples collected by experienced research clinicians in a clinic of MSM with a high prevalence of AIN | HIV-positive and HIV-negative MSM (n = 125) | HIV-positive and HIV-negative MSM, enrolled at the University of California at San Francisco Anal Neoplasia Study; criterion: who previously had an anal cytology sample taken by a practitioner | Cohort study | Self-collection kit and standard clinician-collected samples |
| Varnai et al. 200536 | To examine methods that may enable the routine diagnosis of HPV-induced changes in the anal rim and the consequences of such detection of a more sensitive diagnosis of AIN | Patients that had tissue samples from anal lesions, which had been archived (n = 87) | Patients who had been diagnosed with the following: invasive anal carcinoma, AIN of varying severity and condylomatous lesions | Cohort study | Tissues samples from anal lesions, which had been archived, were retrospectively examined, for histological examination; the tissue was completely embedded in paraffin and processed according to the usual methods of diagnostic histology |
| Chiao et al. 200636 | To evaluate and summarise indirect evidence concerning anal Pap smear screening for HIV-infected patients | HIV-infected individuals | Studies were excluded if they did not include HIV-infected individuals or did not include original data | Systematic review | Anal Pap smear |
The reporting quality of the screening studies is generally poor, making it difficult to assess the true quality of the work undertaken. Only one of the studies is randomised. The remaining studies are cohort studies. The data tend not to be analysed on an intention-to-treat basis and assessors are not blinded.
Anal cytology
De Ruiter et al. 27 reported on a cohort study that recruited 215 homosexual/bisexual men. The perianal area and anal canal were then examined using a colposcope, and areas macroscopically suggestive of intraepithelial neoplasia were biopsied.
The anal cytology and histology methods used by De Ruiter et al. 27 were:
-
Cytology Patients were examined in the lithotomy position. Anal smears were obtained by blindly inserting a cytobrush 1.5–2.0 cm into the anal canal, rotating through 360°, transferring to a glass slide and fixing with 96% ethanol.
-
Histology An oblique-viewing Graeme Anderson proctoscope was inserted into the anal canal.
The findings from De Ruiter et al. 27 were:
-
Cytology A total of 126 (81.8%) of the 154 patients had macroscopic anal condylomata and 28 (18.2%) had no macroscopic evidence of anal condylomata; 46 patients were found to have features of both HPV and AIN, 85 (55.2%) had evidence of HPV alone and 23 (14.9%) were found to be negative.
-
Histology A total of 169 (78.6%) had macroscopic anal condylomata, 46 (21.4%) did not have macroscopic anal condylomata and 176 (81.9%) were biopsied; 76 patients (35.4%) had histological evidence of both HPV and AIN, 91 (42.3%) had features suggestive of HPV alone and 9 (4.2%) were normal.
-
Comparison between anal cytology and histology Of the 154 patients with an adequate anal smear, 56 (36.4%) had both HPV and AIN on histology; 67 (43.5%) had evidence of HPV alone; and 31 (20.1%) were negative.
The conclusions reached by De Ruiter et al. 27 were that anal cytology is a sensitive but non-specific method of identifying patients with biopsy-proven AIN if cytological features of HPV alone are included as abnormal smears. The authors reported that specificity is improved by restricting abnormal smears to those with features of both HPV and AIN but it markedly lowers the sensitivity of the test. The authors further concluded that at the time of the study, anoscopy and histology are required in addition to anal cytology to differentiate between patients who simply have anal condylomata and those who also have AIN.
The cohort members of the 1997 cohort study by Palefsky et al. 28 were participating in a natural history study of ASIL, using anoscopically directed anal biopsy as the standard. Overall, 658 homosexual or bisexual male subjects were studied: 407 (62%) were HIV positive and 251 were HIV negative. The mean age of HIV-positive men was 41 years, range 21–66 years, whereas for HIV-negative men the mean was 44 years with a range of 25–73 years.
Palefsky et al. 28 reported that, defining abnormal cytology as including atypical squamous cells of undetermined significance (ASCUS) and ASIL, the sensitivity of anal cytology for detection of biopsy-proven ASIL in HIV-positive subjects was 69% (95% CI 60 to 78), specificity 59% (95% CI 53 to 65), the positive predictive value (PPV) was 38% (95% CI 31–45) and the negative predictive value (NPV) was 84% (95% CI 79–89). A PPV is the proportion of those with a positive test who actually have the disease, whereas a NPV is the proportion of those with a negative test who actually do not have the disease.
For HIV-negative subjects, Palefsky et al. 28 reported that, using the previous definition, the sensitivity of anal cytology for detection of biopsy-proven ASIL was 47% (95% CI 26–68), specificity 92% (95% CI 89–95), the PPV 35% (95% CI 15–54) and the NPV was 95% (95% CI 93–98). The authors concluded that anal cytology may be a useful screening tool to detect ASIL, particularly in HIV-positive men. The grade of disease on anal cytology did not always correspond to the histological grade, and anal cytology should be used in conjunction with histopathological confirmation.
Between July 2000 and September 2003, Mathews et al. 29 identified 1864 patients who underwent 2918 Pap tests: 8.4% were female, 11.5% were black, 21.5% were Hispanic, 60.4% were white and 6.6% from other ethnic groups; 68.4% were MSM, 15.4% related to injection drug abuse, 9.4% were related to heterosexual transmission and 6.8% were related to other risk factors. Median age was 39 years (35–45 interquartile range). The authors suggested that the reproducibility of key screening measures is moderate at best but of similar magnitude to that of other studies of anal and cervical dysplasia screening.
Panther et al. 30 accounted the results of a study that looked at comparing the pathological diagnoses obtained by anal Pap smear with those obtained by anal biopsy or by surgical excision for 153 MSM. The medical histories, high-resolution anoscopy (HRA) findings and pathology reports of these MSM were recorded. Of the 153 MSM, 100 (65%) were HIV positive and 53 (35%) were HIV-negative. The basis for referral was an abnormal screening anal Pap smear finding [24 (24%) of 100 HIV-positive and 22 (42%) of 53 HIV-negative subjects], HG-AIN on pathological examination of surgically removed anogenital condylomata [19 HIV-positive subjects (19%) and six HIV-negative subjects (11%)], or a history of internal and/or external anal condylomata for 40 HIV-positive subjects (40%) and 14 HIV-negative subjects (26%). The remainder of the cohort was referred for anal bleeding, palpable internal and/or external anal mass, or screening.
Panther et al. 30 stated that the detection of high-grade squamous intraepithelial lesion (HSIL) on an anal Pap smear had a sensitivity of 47% (95% CI 35–59) and specificity of 90% (95% CI 81–96) for detection of a high-grade histological finding (AIN level 2, AIN level 3 or SCC) in the paired specimen. Panther et al. 30 believe that the cross-sectional data presented in their article independently confirmed a substantial incidence of histologically proven high-grade anal dysplasia in MSM who present with minimally abnormal anal Pap smear findings. The authors also stated that their study independently confirmed that a substantial proportion of low-grade dysplasia on anal Pap smears occurs with HG-AIN in MSM, and that it confirmed that abnormal anal cytological findings of any grade should suggest the possibility of high-grade histological findings.
Fox et al. 37 prospectively collected data from 99 consecutive homosexual/bisexual male patients who underwent HRA at the Chelsea and Westminster Hospital anoscopy clinic. Data from follow-up visits on this group of patients were also included in the study. The anoscopy procedure used by Fox et al. 37 utilised the cytology method developed by Palefsky, whereby a Dacron swab was inserted blindly 3 cm into the anal canal and rotated, using a spiral motion, outward pressure was applied on the anal canal and the swab was gradually withdrawn. They reported that 160 anoscopic procedures were reviewed from 99 homosexual or bisexual men in whom both cytological and histological examinations were planned. Eighty-nine (90%) patients were HIV positive and 10 were known to be HIV negative. They concluded that anal cytology by the Palefsky method is simple to undertake, and can therefore be used as the basis of a pilot screening project in centres with large cohorts of HIV-positive homosexual men who have a high risk of developing anal carcinoma. HPV genotyping is not a useful adjunct to cytological screening.
Arain et al. 31 studied the cytomorphological features of 200 consecutive anal smears collected in liquid medium from 198 patients, and the findings were correlated with results of surgical biopsies and/or repeat smears that became available for 71 patients within 6 months. They concluded that liquid based anal smears had a high sensitivity (98%) for detection of ASIL but a low specificity (50%) for predicting the severity of the abnormality in subsequent biopsy, and suggested that all patients with a diagnosis of ASCUS should be recommended for HRA with biopsy.
Anorectal cytology
Friedlander et al. 32 collected 78 consecutive anorectal specimens representing 51 patients: 33 patients were HIV positive (27 males, six females). All HIV-positive females also had a history of gynaecological (vulvar, vaginal or cervical) intraepithelial neoplasia. The mean age of the patients was 43 years (range 26–74 years). The results from this study were that with histology as the gold standard, the sensitivity of cytology to distinguish benign from dysplasic or malignant lesions was 92% but the specificity was only 50%. Friedlander et al. 32 concluded that anorectal cytology is an accurate method for screening patients for anal squamous lesions. Atypical parakeratotic cells represent a potential pitfall. Anoscopy is important in confirming the presence of a lesion, but only a biopsy can accurately determine the grade of a lesion.
Self-screening
In 2006, Lampinen et al. 33 evaluated self-screening for anal cancer by MSM. Paired self- and clinician-collected anorectal Dacron swabs for liquid-based cytological evaluation were collected in random sequence from this cohort of young MSM. Each participant provided at the same study visit two anorectal swab specimens: one self-collected and one collected by the study clinician. Specimens collected by clinicians were more adequate than those collected by men who were wholly naive to the procedure; however, it was found that the vast majority of self-collected anorectal swab specimens from MSM were adequate for cytological evaluation. The conclusion reached by Lampinen et al. 33 was that self-collection of anorectal swab specimens for cytological screening in research and possibly clinical settings appears feasible, particularly if specimen adequacy can be further improved. The severity of biopsy-confirmed anorectal disease is seriously underestimated by cytological screening, regardless of collector.
A total of 125 MSM were invited to take part in the study by Cranston et al. ,34 and 102 were included in the analysis: 82 were HIV positive and 20 HIV negative. The participants in the study by Cranston et al. 34 were given a cytology self-collection kit, with written instructions for use, and requested to collect the sample 1 month after the clinic visit. Cranston et al. 34 reported that the sensitivity of any grade of anal cytology abnormality for detection of AIN 1, AIN 2, or AIN 3 was comparable between clinician-collected (70%) and self-collected (68%) samples. The sensitivity of any grade of anal cytology abnormality for detection of a high-grade lesion (AIN 2 or 3) was also comparable between clinician-collected (74%) and self-collected (71%) samples. The sensitivity of anal cytology to detect AIN in self-collected samples was higher among HIV-positive men than among HIV-negative men. Among the 57 HIV-positive men, anal cytology to detect AIN overall or AIN 2 or 3 specifically was also higher for HIV-positive men in the clinician-collected samples, and the magnitude of these differences in sensitivity was similar to those seen in self-collected samples (p = 0.15 for AIN overall; p = 1.0 for AIN 2 or 3). The conclusions reached by Cranston et al. 34 were that MSM with biopsy-proven AIN can self-collect anal cytology samples with sensitivity comparable with that of experienced clinicians, and that this may facilitate screening for AIN.
Histological markers
Varnai et al. 35 retrospectively examined biopsy samples from 87 patients for microscopic indications of HPV infection. After microdissection, additional HPV analysis via polymerase chain reaction (PCR) was carried out. Varnai et al. 35 reported that in 38 of 47 cases of anal carcinoma, HPV DNA could be detected via PCR (80.9%), the majority of which were HPV 16 (33 out of 38 = 86.8%). In 29 of the 33 cases of AIN, HPV DNA was detected (87.9%), most of these in AIN 3 (15 out of 16 = 93.8%). Histological markers of HPV infection were detected in all 87 cases. The authors recommended any histological reports on excision of anal lesions to include a statement as to whether histological markers of HPV infection were detected. In individual cases, that, validation via HPV PCR must be considered.
Anal Pap smear screening for HIV-infected patients
Chiao et al. 36 systematic review of the English-language literature published from July 1996 through to July 2005 noted that the natural history of progression from anal intraepithelial neoplasia to anal cancer is unknown, and although low-grade anal dysplasia has been shown to progress to high-grade dysplasia (HGD) in a majority of HIV-infected men within 2 years after initial diagnosis, the true rate of progression from HGD to invasive anal cancer remains unclear.
Chiao et al. 36 commented that the data published to date highlight limitations to current anal Pap smear screening-related research, no randomised or cohort studies exist to determine if there are improved survival or outcomes for those who have been screened with anal Pap smears, and that there have been no ecological studies to correlate use of screening and the incidence or outcomes of SCCA.
Screening summary/discussion
The sensitivity, specificity, PPV and NPV (where given) of the studies reported in Chapter 3 (see Screening) are displayed in Table 4. The PPV will depend on the prevalence rate of the disease: if the disease (such as anal cancer) has a low prevalence rate then we would expect to have a low PPV. Where reported, 95% CIs are included.
| Study details | Screening test | n | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|---|---|
| de Ruiter et al. 199427 | Anal cytology | 154 | 88 | 16 | 37 | 70 |
| Histology | 215 | 34 | 73 | 41 | 66 | |
| Palefsky et al. 199728 | Anal cytology (ASCUS and above) HIV-positive patients | 407 | 69 (95% CI 60 to 78) | 59 (95% CI 53 to 65) | 38 (95% CI 31 to 45) | 84 (95% CI 79 to 89) |
| Anal cytology (ASCUS and ASIL) HIV-negative patients | 251 | 47 (95% CI 26 to 68) | 92 (95% CI 89 to 95) | 35 (95% CI 15 to 54) | 95 (95% CI 93 to 98) | |
| Anal cytology ASIL, HIV-positive patients | 407 | 46 (95% CI 36 to 56) | 81 (95% CI 76 to 85) | 46 (95% CI 36 to 57) | 80 (95% CI 76 to 85) | |
| Anal cytology ASIL, HIV-negative patients | 251 | 26 (95% CI 5 to 47) | 98 (95% CI 96 to 100) | 56 (95% CI 22 to 89) | 94 (95% CI 91 to 97) | |
| Fox et al. 200437 | Anal cytology | 99 | 83 | 38 | 86 (95% CI 78 to 91) | 33 (95% CI 19 to 51) |
| Cranston et al. 200434 | Self-collected anal cytology samples | 102 | 68 | Not reported | Not reported | Not reported |
| Clinician-collected anal cytology samples | 102 | 70 | Not reported | Not reported | Not reported | |
| Panther et al. 200430 | Anal Pap smear (HG-AIN) | 153 | 47 (95% CI 35 to 59) | 90 (95% CI 81 to 96) | 81 (95% CI 66 to 92) | 65 (95% CI 55 to 74) |
| Anal Pap smear (LSIL) | 68 (95% CI 56 to 78) | 48 (95% CI 36 to 59) | 59 (95% CI 48 to 69) | 57 (95% CI 44 to 70) | ||
| Arain et al. 200531 | Anal Pap smear | 71 | 98 | 50 | Not reported | Not reported |
|
Varnai et al. 200635 |
Histology | 87 | 94 | 80 | 85 | 91 |
Since the late 1990s, the sensitivity and specificity of reported screening tests for anal cancer appear to have improved (Table 4). Within recent years, sensitivity values of 70–98% have been reported,31,34,35 which would highly suggest that screening techniques have improved. However, the reported PPVs are mixed while a number of studies fail to report these values (Table 4). This reflects the relative rarity of anal cancer. Large numbers would need to be screened to identify a relatively small number of affected individuals. Table 4 allows comparisons to be made between the historical data and the positive and NPVs. ROC (receiver operating characteristic) curves have not been generated for this review.
The two studies by Lampinen et al. 33 and Cranston et al. 34 reported that self-collected samples (anorectal swabs or anal cytology) are adequate for interpretation, although further research is needed before using self-collected samples in a screening programme. However, both the De Ruiter et al. 27 and Palefsky et al. 28 studies put forward that anal cytology should be used in conjunction with histopathological confirmation.
Treatment
Six studies40–45 were identified and included in this review: Table 5 displays characteristics of the studies and Appendix 6 gives details on study quality. The criteria of the National Screening Committee (NSC) for appraising the viability, effectiveness and appropriateness of a screening programme (Appendix 2) states that there should be an effective treatment or intervention for patients identified through early detection, with evidence of early treatment leading to better outcomes than late treatment. Therefore, survival from treatment options is of interest. For completeness, comments from an editorial38 and Effective Health Care bulletin issued in March 200439 are included at the end of this section.
| Study details | Study type | Design | Patient group | Study objectives |
|---|---|---|---|---|
| UKCCCR Anal Cancer Working Party 199640 | RCT |
Multicentre RCT with a main end point of local failure whether due to disease or complications of treatment, as indicated by the need for major surgical intervention. Five-year survival was a secondary end point. Eligible patients had epidermoid carcinoma (squamous, basaloid or cloacogenic) of the anal canal or margin, no evidence of major hepatic or renal dysfunction, and normal blood counts From 856 patients considered for entry to the multicentre trial, 585 patients were randomised to receive initially either 45-gray (Gy) RT in 20 or 25 fractions over 4–5 weeks (290 patients) or the same regimen of RT combined with 5-FU by continuous infusion during the first and final weeks of RT and mitomycin (12 mg/m2) on day 1 of the first course (295 patients). Clinical response was assessed 6 weeks after initial treatment: good responders were recommended for boost RT and poor responders for salvage surgery. The main end point was local failure rate (≥ 6 weeks after initial treatment); secondary end points were overall and cause-specific survival. Analysis was by intention to treat |
Any patient with anal cancer | To compare the most promising regimens of RT alone with CMT |
| Cummings et al. 198441 | Case series | A subset (25 patients) of 51 anal canal carcinoma patients treated by radical external beam radiation alone (RT) between 1958 and 1978, were compared with 30 patients with anal canal carcinoma treated by combined 5-FU, mitomycin C and radical radiation therapy (FUMIR) between 1978 and 1982 | Any patient with anal cancer | The results and toxicity of treatment of anal canal carcinoma by radiation therapy or radiation therapy and chemotherapy in a single centre |
| Doniec et al. 200642 | Case series | From 1993 to 2001, 50 patients with histologically confirmed primary cancer of the anal canal (n = 38) and the anal margin (n = 12) without evidence of distant metastases were treated at the University Clinic Kiel with curative intention. Prior to treatment, all patients underwent staging, consisting of digital and EUS investigation of the anus and the rectum (7-MHz transducer, BandK Medical), sphincter manometry, total colonoscopy, ultrasound of the abdomen and the inguinal region, and CT scan of the pelvis. Forty-five patients were admitted and examined | Any patient with anal cancer | To optimise local tumour control by TRUS-guided brachytherapy and thereby minimise the risk of local recurrence, resulting in a reduced rate of salvage abdominoperineal resection |
| Brown et al. 199943 | Between 1989 and 1996, 46 patients were identified with HG-AIN; 34 underwent local excision of all macroscopically abnormal disease and the resulting defect was left open, closed primarily or skin grafted. Regular follow-up subsequently included anoscopy and biopsy of any suspicious lesions. All patients diagnosed in one hospital with HG-AIN between 1989 and 1996 were included | Any patient with anal cancer | ||
| Edelman and Johnstone 200644 | Case series | Retrospective review of the records of 17 HIV-positive patients with anal SCC treated with CMT of RT and concurrent chemotherapy, between 1991 and 2004, at a single institution | HIV-positive patients | To report the toxicity and survival data of HIV-positive patients with anal SCC treated with CMT of RT and concurrent chemotherapy |
| Place et al. 200145 | Case series | This was a retrospective cohort study, which identified 73 patients with anal SCC, treated at the University of Texas Southwestern Medical Center-affiliated hospitals; 23 were HIV positive. In the HW-positive group, nine had in situ squamous carcinomas and 14 had invasive SCCs. Data collected included age, CD4 count, treatment, complications and survival | HIV-positive patients | To determine the outcome of HIV-positive patients with anal SCCs |
RT alone vs a combination of RT/chemotherapy
Two studies reported on the treatment of anal cancer by RT alone or a versus combination of RT/chemotherapy: there was one randomised controlled trial (RCT)40 and one cohort study. 41
In 1996, the United Kingdom Co-ordinating Committee for Cancer Research (UKCCCR) Anal Cancer Working Party40 reported on a trial to compare combined modality therapy (CMT) with RT alone in patients with epidermoid anal cancer. The aim was to compare the most promising regimens of RT alone with CMT, within a multicentre RCT. The main end point of the trial was local failure whether due to disease or complications of treatment, as indicated by the need for major surgical intervention, with 5-year survival as a secondary end point. Patients were eligible if they had epidermoid carcinoma (squamous, basaloid or cloacogenic) of the anal canal or margin, no evidence of major hepatic or renal dysfunction, and normal blood counts. The Working Party40 reported that from 856 patients considered for entry to the multicentre trial, 585 patients were randomised to receive initially either 45 Gy RT in 20 or 25 fractions over 4–5 weeks (290 patients) or the same regimen of RT combined with 5-fluorouracil (5-FU) (1000 mg/m2 for 4 days or 750 mg/m2 for 5 days) by continuous infusion during the first and the final weeks of RT and mitomycin (12 mg/m2) on day 1 of the first course (295 patients). Clinical response was assessed 6 weeks after initial treatment: good responders were recommended for boost RT and poor responders for salvage surgery.
The UKCCCR Anal Cancer Working Party40 findings were that, after a median follow-up of 42 months (interquartile range 28–62), 164 of 279 (59%) patients receiving RT had a local failure compared with 101 of 283 (36%) of patients receiving CMT. This gave a 46% reduction in the risk of local failure in the patients receiving CMT (RR 0.54, 95% CI 0.42 to 0.69, p < 0.0001). The risk of death from anal cancer was also reduced in the CMT arm (0.71, 95% 0.53 to 0.95, p = 0.02). There was no overall survival advantage (0.86, 95% CI 0.67 to 1.11, p = 0.25). Early morbidity was significantly more frequent in the CMT arm (p = 0.03), but late morbidity occurred at similar rates. There was no statistically significant difference in overall survival between the two groups, with a 58% 3-year survival rate for the RT arm and 65% for the CMT arm.
The authors reported that the UKCCCR Anal Cancer Working Party trial40 showed that the standard treatment for most patients with epidermoid anal cancer should be a combination of RT and infused 5-FU and mitomycin, with surgery reserved for those who fail on this regimen.
In 1984, Cummings et al. 41 reported on the results and toxicity of treatment of anal canal carcinoma by radiation therapy or radiation therapy and chemotherapy in a single centre. In this study, a subset (25 patients) of 51 patients with anal canal carcinoma, treated by radical external beam radiation alone between 1958 and 1978, were compared with 30 patients with anal canal carcinoma treated by combined 5-FU, mitomycin C and radical radiation therapy (FUMIR) between 1978 and 1982.
Cummings et al. 41 reported that the uncorrected 5-year survival rate in each group was approximately 70%, but primary tumour control was achieved in 93% (28 of 30 patients) in the FUMIR group compared with 60% (15 of 25 patients) treated with RT. The authors further reported that colostomies were needed as part of treatment for residual carcinoma or for the management of treatment-related toxicities in 11 of the 25 patients treated by radiation alone, and required (at the date of the study) in 4 out of the 30 patients treated by FUMIR.
The conclusion reached by Cummings et al. 41 was that the improvement in the primary tumour control rate, and the reduction in the number of patients requiring colostomy when compared with the results of RT, favour combined chemotherapy and radiation as the initial treatment for anal canal carcinoma.
RT combined with chemotherapy
One prospective cohort study42 and two retrospective cohort studies44,45 reported on patients treated with RT combined with chemotherapy.
Doniec et al. 42 reported using CMT of anal cancer and transrectal ultrasound (TRUS)-guided high dose rate (HDR) after-loading therapy on 50 patients with histologically confirmed primary cancer of the anal canal (n = 38) and the anal margin (n = 12) with curative intention. Prior to treatment, all patients underwent staging consisting of digital and endosonographic ultrasonography (EUS) investigation of the anus and the rectum (7-MHz transducer, BandK Medical), sphincter manometry, total colonoscopy, ultrasound of the abdomen and the inguinal region, and CT scan of the pelvis. All patients underwent follow-up examination 3 months after completion of brachytherapy, including clinical examination and TRUS. This was repeated at 3-month intervals for 1 year, followed by 6-month intervals during the second year, and annually thereafter. The median follow-up was 34 months (range 6–96). Relapse rates, disease-specific survival and overall survival were calculated according to the Kaplan–Meier method.
Doniec et al. 42 reported a 5-year overall survival rate of 74% for 50 patients with anal cancer and treated by combination radiochemotherapy; the specific disease-related 5-year survival rate was 82%. The conclusion reached by Doniec et al. 42 was that EUS-guided brachytherapy for anal cancer may decrease the side effects of conventional brachytherapy.
Edelman and Johnstone44 conducted a retrospective review of the records of 17 HIV-positive patients with anal SCC who were treated with CMT of RT and concurrent chemotherapy at a single institution. The objective of the study was to report the toxicity and survival data of these patients. For these patients the actuarial 18-month survival was 67%.
Place et al. 45 conducted a retrospective analysis of 73 patients with anal SCC of these 73 patients, 23 were HIV-positive and included in the study. Of these 23 patients, 9 had SCC in situ (SCCIS) and 14 had SCCA. All 23 were homosexual men. Mean age was 40 (range 28–58) years, with a mean age of 42 years for the patients with SCCA and 36 years for the patients with SCCIS (p = 0.05). The 1- and 5-year mortality rates of HIV-positive patients with SCCA with follow-up of at least 1 year (which excluded all new patients receiving HAART) were 40% and 80%, respectively. The 1- and 5-year mortality rates of HIV-positive patients with SCCIS were 17% and 50%, respectively.
Radiation therapy and chemotherapy were offered to 13 of the 14 patients with SCCA. The remaining patient had a T2 margin tumour and was offered wide local excision with radiation therapy. For the 13 patients who were offered chemotherapy, 11 received 5-FU and cisplatinum, one received 5-FU and mitomycin C, and one declined therapy. Standard fraction external beam radiation therapy was given to 12, with two declining therapy. Six of 14 patients with SCCA and 8 of 9 patients with SCCIS received antiretroviral therapy before their anal malignancy diagnosis, and all continued it during treatment. The nine patients with SCCIS received local excision only.
Place et al. 45 concluded that HIV-positive patients with in situ carcinomas present at an earlier age than those with infiltrating lesions. The authors also concluded that because these patients appear to succumb to their HIV status and not the anal disease, anal SCC should be included with cervical SCC as an AIDS-defining illness. HIV-positive patients, particularly patients with AIDS, with invasive anal cancers and without effective antiretroviral therapy obtain little benefit and significant toxicity from current radiation therapy and chemotherapy.
Surgery
Brown et al. 43 reported in 1999 on a study that looked at intermediate and long-term follow-up of these patients, with particular reference to the incidence of recurrent disease and the associated surgical morbidity. Patients diagnosed in one hospital with HG-AIN between 1989 and 1996 were included in the study. 43 Thirty-four underwent local excision of all macroscopically abnormal disease and the resulting defect was left open, closed primarily or skin grafted. Regular follow-up subsequently included anoscopy and biopsy of any suspicious lesions.
The median follow-up reported by Brown et al. 43 was 41 months (range 12–104); 19 patients had histological evidence of incomplete excision at the time of initial resection. Some 12 of the 19 had histologically proven recurrent HG-AIN within 1 year. Even with microscopically complete excision, 2 of 15 patients subsequently developed recurrent HG-AIN at 6 and 32 months after operation. It was reported that no patient developed invasive anal cancer, although it was not clear whether this was due to surgery and intensive follow-up or because of the low risk of anal cancer.
Brown et al. 43 concluded that although no definite recommendations can be made for the treatment of HG-AIN, the results illustrated some potential drawbacks of surgical excision with a high potential for incomplete excision and persistent disease, even after complete excision in some patients and a high morbidity rate.
Treatment summary/discussion
Anal cancer is usually treated aggressively with a combination of chemotherapy and RT (chemoradiation), but the treatment can have very unpleasant side-effects. Surgery can be used to remove precancerous and cancerous cells from the anus; however, the precancerous or cancerous cells may recur. Surgery is more likely if the cancer is small and near the anal margin. The chemotherapy treatment will be a combination of mitomycin C and 5-FU during the first and final weeks of the RT course.
Table 6 shows the survival results from the above studies; for completeness, survival data from cohort studies and registry data are also present in the table, although treatment given is not known. The study by Cummings et al. 41 reports only an approximation of the uncorrected 5-year survival rate. The UKCCCR Anal Cancer Working Party reports only a 3-year survival rate. Johnson et al. 3 reported 5-year survival figures of 58% for males and 64% for females, based on data collected between 1973 and 2000 on diagnosis and outcomes of invasive and in situ anal cancer. The data came from the SEER programme in the USA. Lower 5-year survival figures were reported by Bower et al. 23 for a cohort of English HIV-positive patients (25 MSM and one heterosexual woman) with confirmed cases of invasive anal cancer. Bower et al. 23 reported a 5-year overall survival figure of 47%.
| Study details | Study type | Treatment | 5-year survival rate (%) | 3-year survival rate (%) |
|---|---|---|---|---|
| Hospital-based studies | ||||
| Cummings et al. 198441 | Cohort study | RT alone, n = 25 | ≈ 70a | Unknown |
| CMT, n = 30 | ≈ 70a | Unknown | ||
| UKCCCR Anal Cancer Working Party 199640 | RCT | RT alone, n = 285 | Unknown | 58b |
| CMT, n = 292 | Unknown | 65b | ||
| Bower et al. 200423 | Prospective cohort study | Unknown | 47b | Unknown |
| Doniec et al. 200642 | Cohort study | Combined radiochemotherapy | 74b | Unknown |
| Population-based studies | ||||
| Johnson et al. 20043 | Registry data, 1973–2000 | Unknown | 58b (men), 64b (women) | Unknown |
| Karandikar et al. 20064 | Registry data, 1995–9 | Unknown | 45b | Unknown |
| Jeffreys et al. 200624 | England and Wales Registry data, 1986–99 | Unknown | 48%b (men), 51%b (women) | Unknown |
| Gatta et al. 20067 | European Registry data, 1983–94 | Unknown | 43b | 53b |
In 1997, Myerson et al. 46 reported on a study to review the patterns of presentation, care and outcome reflected in data from the National Cancer Data Base, which represented a broad range of medical centres. Data on patients with anal carcinoma (on 1050 patients from 1988 and 1289 patients from 1993) were reviewed for patterns of care and presentation. The 1988 cases were also reviewed for outcome data. Records of patients with anal carcinoma were extracted on basis of anatomic site (ICD-O2 site code of C21) and histology (ICD-O2 histology codes of M801–67 and M894). Other eligibility criteria included an accession year of 1988 or 1993, and diagnosis and/or treatment having taken place at the reporting hospital.
Myerson et al. 46 reported that the mean age at diagnosis decreased slightly between 1988 and 1993 – from 62.8 years to 61.8 years. The gender distribution of patients changed little, with 64.3% being female in 1988 compared with 62.5% in 1993. It was also reported that there was an increase in the use of chemotherapy between 1988 and 1993 (from 61.6% to 67.2%) and that substantial differences were observed in the management of epidermoid carcinomas and adenocarcinomas. The majority of epidermoid carcinomas were managed non-surgically, principally with combined chemotherapy and radiation, whereas three-quarters of patients with adenocarcinoma underwent surgery. The authors reported that the most important factors for favourable 5-year survival were early stage (ranging from 71.3% for stage 1 to 23.1% for stage 4), epidermoid carcinoma histology (57.6%, compared with 41.3% for adenocarcinoma), and female gender (56.2%, compared with 49.6% for males).
The conclusion reached by Myerson et al. 46 was that their study confirmed a trend in patterns of care favouring non-surgical management with radiochemotherapy for epidermoid carcinomas of the anus. For adenocarcinomas, there had been a trend towards increasing use of multimodality therapy with surgery and adjuvant radiochemotherapy. Survival data from the 1988 cases confirm the efficacy of conservative treatment with radiation plus chemotherapy for epidermoid carcinomas.
The Effective Health Care bulletin39 issued in March 2004 reported that two large RCTs comparing RT alone with chemoradiotherapy (CRT) have demonstrated a highly statistically significant reduction in local failure. Both saw improvements in colostomy-free survival and reduction in deaths from anal cancer with CRT. Neither showed any significant effect on overall survival. A third RCT tested the benefit of adding mitomycin C to 5-FU and RT. This also demonstrated statistically significant improvements in colostomy-free and disease-free survival. Other forms of treatment, such as surgical excision, may be considered by anal cancer multidisciplinary teams, but surgery is usually reserved for salvage.
In 2005, James et al. 38 presented an editorial on the current status of the Second UK Phase III Anal Cancer Trial, the ACT II study. The RT schedule in the ACT II trial is a continuous schedule of 50.4 Gy in 28 fractions with either 5-FU and mitomycin C (5-FU/MMC) or 5-fluoroacil and cisplatin (5-FU/CDDP). The authors reported that analysis on early trial data were highly encouraging, and showed that the chemoradiation regimen and maintenance chemotherapy could be given without interruption and had acceptable toxicity.
A study by Adjani et al. 47 reported in 2008, while this review was in completion, giving results from the USA. The large trial of 682 patients compared two chemoradiation therapies: the first, fluorouracil plus mitomycin and RT; the second, fluorouracil plus cisplatin and RT. The primary end point was 5-year disease-free survival; the secondary end point was the overall survival and time to relapse. The 5-year local recurrence for mitomycin-based treatment was 25% (95% CI 20 to 30) and 33% (95% CI 27 to 40). The 5-year overall survival rate was 75% (95% CI 67 to 81) in the mitomycin arm and 70% (95% CI 63 to 76) in the cisplatin arm. In their report it was noted that there was an increased colostomy rate in the cisplatin group and it was recommended that this combination should be avoided in the treatment of localised anal cancer. They also note that there has been little improvement in the survival outcomes for patients since the 1990s. Of interest to this current review is the finding that the mitomycin group of patients suffered a higher degree of haematological toxicity. Although this is the treatment modality used in the model it is worth noting that this study specifically excluded patients with HIV. These patients do present a problem, as they often have increased toxicity to chemotherapy.
Treatment summary/discussion
Published studies of treatment can be helpful in developing estimates of effect as part of a screening model. However, not all treatment studies give the information in such a way that it can be used for modelling. For example, reporting that an intention to treat analysis was undertaken but not reporting fully on these results makes it more difficult to incorporate the results into the model. Some studies were excluded for this reason.
The ideal treatment study for a screening evaluation would take patients identified through screening and randomise them into treatment and watchful waiting groups. This could then be used to estimate the true benefits of treatment in patients otherwise not presenting with disease.
A study that looks at patients that present with symptoms may have useful information regarding the effect of treatment at different stages of disease but will be biased towards patients with overt symptoms.
When considering including a treatment study in evaluating screening for use in the UK, consideration should be given to the population under investigation, how they were identified for randomisation, and how the control group were monitored. Whereas the biological level of differences between populations may be small when comparing outcomes, the structural differences in health-care systems can greatly affect the use of data from other settings.
The construction of an evaluation of a screening programme makes little use of the specifics of treatment. In effect, the evaluation is concerned with the outcome (good or bad) of treatment for those identified as having the disease.
Some of the treatment studies are used to estimate the natural history of the disease process. This is an important first step in evaluating the effect of screening, as those not diagnosed through the usual clinical pathway will have the outcomes of natural history (no treatment) unless screening identifies them.
In the following model, we have used broad estimates of the effects of treatment, based on a selection of studies that cover a range of treatment variations. In fact, it is the relative benefit of treatment over the health state that would have been experienced if the treatment had not been initiated that gives the benefit of the screen detection.
By not linking the screening evaluation too closely to a particular treatment modality the evaluation can be considered robust even if the treatment of choice changes, provided that the sensitivity analysis applied covers the range of outcomes expected.
In this specific case, the effect of systematic screening the at-risk population would be expected to bring forward the start of treatment, rather than expose cases to treatment they would not otherwise have had. As such, this means the effect of screening is measured in the effect of the earlier treatment. In this study we have included some papers that cite local recurrence rates from the reported treatment modalities. The emphasis in this model was, as previously stated, to look at bringing forward the start of treatment rather than wait until individuals were symptomatic. The assumption being that early treatment following screening would prevent the problems found in treating symptomatic patients.
The following model considers several scenarios for the effect of this change, with the noted above trials falling within these parameters.
Chapter 4 Risk of anal cancer
In Chapters 1 and 3 risk is used in a descriptive and general sense; in this chapter, risk is used in the context of modelling and does not necessarily draw upon the same evidence.
Anal cancer is a rare neoplasm that affects the epithelium of the anal canal. The increased incidence in men, particularly in the USA is etiologically related to a sexually transmitted agent. 48 HPV has been implicated as a causal agent of anal cancer.
Risk of anal cancer is near to zero in early life. Sexual activity is virtually essential for transmission of HPV. Multiple partners bring the risk of a greater variety of strains, and, in turn, a greater chance of a more dangerous strain (with regard to anal cancer). Other genitourinary (GU) infections may be a marker of multiple sexual partners, sex with infected individuals and high-risk behaviour. There may be some potential of HPV infection with some other GU infections. The criteria for appraising screening programmes1 list the importance of there being a detectable risk factor when considering implementing a screening programme.
Once HPV infection occurs, the dysplastic process at the anal margin follows more frequently with certain types of HPV, and appears to be seen more frequently where receptive anal intercourse occurs.
Infection with HIV has a profound effect on the immune system. It is the immune system that fights infection but also this same system guards against dysplastic changes. It is this latter role that explains much of the increased cancer risk in patients with HIV and AIDS.
Kim et al. 49 undertook a retrospective cohort study, comparing HIV-positive and HIV-negative patients with respect to treatment tolerance and outcome. HIV-positive and HIV-negative patients were compared by age, gender, sexual orientation, stage at diagnosis, treatment provided, response to treatment, tolerance and survival.
Kim et al. 49 reviewed the records of 98 patients with anal neoplasms. Seventy-three patients had invasive anal epidermoid (squamous or cloacogenic) carcinoma and formed the study group.
Of the 73 patients, 13 were HIV-positive and 60 were HIV-negative. Biopsies were performed on all primary tumours. Preoperative staging was performed using examination, anal ultrasound, chest X-rays and computerised tomography (CT) scanning. After completion of primary therapy, patients were seen every 2–3 months for 3 years, every 6 months until the end of the fifth year, and then annually. Post-treatment evaluation included a careful clinical examination with digital palpation and anoscopy at each visit.
The findings by Kim et al. 49 were that the HIV-positive and HIV-negative groups differed significantly by age (42 vs 62 years, p < 0.001), male gender (92% vs 42%, p < 0.001) and homosexuality (46% vs 15%, p < 0.05). The authors found that there were no differences by stage at diagnosis or radiation dose received. Acute treatment major toxicity differed significantly (HIV-positive 80% vs HIV-negative 30%, p < 0.005). Kim et al. 49 reported that only 62% of HIV-positive patients were rendered disease free after initial therapy versus 85% of HIV-negative patients (p = 0.11), and that the median time to cancer-related death was 1.4 vs 5.3 years (p < 0.05). A survival model did not show age, gender, stage or treatment to be independent predictors.
Kim et al. 49 found that HIV-positive patients with anal carcinoma seemed to be a different population from HIV-negative patients by age, gender and sexual orientation. They have a poorer tolerance for combined therapy and a shorter time to cancer-related death. A strong trend to poorer initial response rate was also seen.
Once dysplasia has occurred, progression to higher levels of dysplasia [from low-grade squamous intraepithelial lesions (LSILs) to HSILs] takes place over time. This progression is seen at an increased rate in persons with HIV (regardless of how contracted).
Once anal cancer is present, prognosis is better in patients with an intact immune system. Patients with HIV and AIDS have a poorer prognosis despite having developed the cancer at a younger age.
The first diagram in Appendix 7 summarises the life course model for this condition. The second diagram shows how this model is modified for HIV-negative women.
Model parameters
There are four groups that can possibly be modelled:
-
A men with HIV
-
B men who have sex with men (without HIV)
-
C women with HIV
-
D women with high risk of anal cancer.
A Men with HIV
After onset of HIV, incidence of HPV infection, dysplasia and cancer will be greater than in the general population. There may be differences between men with HIV who acquired HIV through anal intercourse compared with others. This is a closed group in that there is no transition to any other group. Prognosis once cancer has developed is likely to be the same regardless of mode of acquisition of HIV. HAART can be seen to increase life expectancy over those not treated.
B Men who have sex with men (without HIV)
Incidence of HPV infection, dysplasia and cancer will be greater than the general population but less than that for group A. Risk will increase with time, as risk of contracting a more oncogenic strain will be increased (through repeated exposure and multiple partners). Persons in this group can move to group A if HIV is acquired.
C Women with HIV
After onset of HIV, incidence of HPV infection, dysplasia and cancer will be greater than in the general population. There may be differences between women with HIV acquired through sexual exposure compared with others. This is a closed group. Prognosis once cancer develops is likely to be the same regardless of mode of acquisition of HIV. HAART can be seen to increase life expectancy over those not treated.
D Women with high risk of anal cancer
For example, women with known cervical cancer. Incidence of HPV infection, dysplasia and cancer will be greater than the general population, but less than that for group C. Evidence suggests risk does not increase greatly with time, as new sexual partners are less frequently acquired after 30 years of age. Persons in this group can move to group C if HIV is acquired.
For each of the previous defined groups, the available literature and findings are present in the following sections.
High-risk groups
Men who have sex with men may identify themselves as homosexual or bisexual, and these men are at increased risk for STDs such as HIV infection, HPV and anal cancer. Knight50 reported that many men are engaging in dangerous sexual practices that may jeopardise their health. These sexual practices include anal sex without a condom (‘bare backing’), oral sex without a condom, oral stimulation of the anus (‘rimming’) without protection, multiple sex partners at one time and use of illicit drugs.
Halperin51 reported in 1999 the results of a review examining the practice of anal sex among heterosexual population, related sociocultural factors and risk of associated health problems. Halperin51 stated that heterosexual anal sex remained understudied, but that analysis of available evidence suggesting that this stigmatised behaviour is not so rarely practised among heterosexuals. The review reported that surveys from North America, Europe and Australia suggest that between 7% and 25% of the population reported practising heterosexual anal intercourse. For men, surveys from the late 1980s and early/mid 1990s suggest that approximately 2–5% of men reported having a same-sex experience, although only a small proportion of these engage in receptive anal intercourse.
Dodds et al. 52 reported the findings of an annual behavioural survey of homosexual men (from 1996 to 2000) who socialised in gay venues across London. Participants completed a short anonymous self-completion questionnaire covering demographic details, sexual health service use, HIV testing history, self-perceived HIV status and sexual behaviour. The authors found that the proportion of men having unprotected anal intercourse (UAI) increased significantly each year from 30% in 1996 to 42% in 2000 (p < 0.001).
In 1997, Frisch et al. 53 reported on a population-based case–control study, undertaken in Denmark and Sweden to examine if the incidence of anal cancer had increased, particularly amongst women. The authors conducted telephone interviews with 324 women and 93 men in whom invasive or in situ anal cancer was diagnosed between 1991 and 1994, 534 controls with adenocarcinoma of the rectum and 554 population controls. The interviews covered a wide spectrum of possible risk factors for anal cancer. ORs were calculated by logistic regression. Specimens of anal cancer tissue and samples of rectal adenocarcinomas were tested for HPV DNA using PCR.
Frisch et al. 53 searched national cancer registries in Denmark and Sweden to identify all incident cases of histologically verified invasive or in situ anal or rectal epidermoid carcinoma (anal cancer) reported during the period from 1991 to 1994. Danish patients were considered eligible for the study if the tumour was rectum, anal canal, anus, anorectum or perianal skin. Swedish patients were eligible if the topography was anus or rectum. The authors also included two control groups, with one group consisting of patients with adenocarcinoma of the rectum, who were chosen as controls to minimise any possible bias due to differential recall between patients with anal cancer and controls. The other control group consisted of persons from the general population. For the men, we tried to match two patients with rectal adenocarcinoma and two population controls to each patient with anal cancer, and for the women, a 1 : 1 : 1 match was sought. Controls were frequency matched within each country for sex and age (in 5-year intervals, except for the youngest patients in the cancer control group, because of the rarity of rectal cancer in young persons), and the patients with rectal adenocarcinoma were matched for the year of the diagnosis.
Overall, 417 patients with anal cancer (93 men and 324 women), 534 controls with adenocarcinoma of the rectum (191 men and 343 women), and 554 population controls (205 men and 349 women) were interviewed. The participation rate was 78–79% among female patients (cases and cancer controls) and 71–73% among male patients. Participation rates were 60–61% among population controls of both sexes.
Frisch et al. 53 found that, for men, indicators of sexual promiscuity were positively correlated with the risk of anal cancer. Among men who reported ever having had heterosexual intercourse, there was a statistically significant trend towards an association between the lifetime number of female sexual partners and the risk of anal cancer, with men reporting a total of two or three partners at lowest risk (p-value for trend = 0.004). Men with 10 or more female partners had 2.8 times the risk of those with two or three partners. Twenty-three per cent of patients with anal cancer, compared with 15% of controls, reported having visited a prostitute [OR 1.8 (95% CI 0.99 to 3.2)]. Unmarried men were at high risk for anal cancer: among those who did not report a current heterosexual relationship, the OR was 3.3 (95% CI 1.5 to 7.3), and among those who lived with a female partner, the OR was 8.7 (95% CI 3.1 to 25.0).
Men with HIV
Increased risk of HPV and other infections
Bjorge et al. 54 in 2004 reported on a case–cohort study examining the relationship between HPV infection and the subsequent risk of anal and perianal skin cancer, using Finnish and Norwegian cancer registries. The Finnish and Norwegian cancer registries are nationwide and population based. The data files of the serum banks and cancer registries were linked on the basis of the personal identification number to identify anal, perianal, and head and neck cancers.
Bjorge et al. 54 identified 28 anal and perianal cancer cases [25 anal cancer (20 in Norway, five in Finland); three perianal cancer, all in Norway]. These 28 cases and 1500 controls were analysed for the presence of immunoglobin G (IgG) antibodies to HPV types 16, 18, 33 or 73, and ORs of developing anal and perianal skin cancer were calculated. The authors reported ORs that showed an increased risk of developing anal and perianal skin cancer among subjects who were seropositive for HPV 16 (OR 3.0, 95% CI 1.1 to 8.2) and HPV 18 (OR 4.4, 95% CI 1.1 to 17). In total, 29% of anal and perianal cancer cases were positive for HPV 16 compared with 8% of controls.
In 2005, Van Der Snoek et al. 55 undertook a study to establish the prevalence of HPV infection in relation to being HIV-positive in a group of Dutch MSM; 286 MSM were recruited between February 1999 to February 2003. The cohort participants were tested for STDs and HIV every 6 months over a period of 3 years. HPV specimens were taken on the third and sixth visits only. At the sixth visit, 213 MSM were tested: 17 were HIV positive and 196 HIV negative. Van Der Snoek et al. 55 found that persistence of HPV 31 at the perianal region was significantly more often seen in HIV-positive MSM (p = 0.036), whereas the incidence of HPV 16 may be associated with HIV positivity (p = 0.059).
In 2004, Sobhani et al. 56 reported on a cohort study of 228 patients with anal cancer condylomas the incidence of HGD. Patients referred to a department of coloproctology in Paris between June 1993 and June 2002 were recruited for a prospective cohort study. Patients with invasive anal cancer at baseline were excluded. A total of 228 consecutive patients (164 HIV positive) were included, after curing of their lesions. Patients were interviewed using a standardised questionnaire and underwent proctological examination at baseline, 1 month later and every 3–6 months thereafter. Overall, 199 patients underwent all of the examinations required and were included in the analysis.
Sobhani et al. 56 reported that HGD was detected in 38 (19%) patients: 32 HIV-positive patients and six HIV-negative patients in at least one examination. A positive HIV test at baseline was identified as an independent risk factor for cancer and HGD. In HPV-infected patients, the incidence of HGD was 15.5% and for invasive carcinoma was 3.5%.
Palefsky et al. 57 reported in 1998 on the incidence of anal cancer amongst HIV-positive and HIV-negative homosexual and bisexual men: 346 HIV-positive and 262 HIV-negative men were enrolled in this prospective cohort study. Participants were interviewed and asked about their current status regarding HIV-related diseases and conditions, medications, sexually transmitted diseases, anal conditions and behavioural topics – such as smoking, drinking, substance use and sexual practices – that might be associated with anal disease. HIV-positive subjects were interviewed every 6 months and HIV-negative subjects every year. Subjects were followed for 4 years. Anal swabs for cytology and HPV studies were obtained, followed by biopsies of visible lesions.
Palefsky et al. 57 found that HIV-positive men were more likely to develop HSIL than HIV-negative men with a RR of 3.7 (95% CI 2.6 to 5.7). The authors concluded that HIV infection and HPV infection were associated with high rates of incident HSIL among homosexual men.
Time with HIV
Fagan et al. 58 in 2005 reported on a retrospective cohort study of 14 HIV-positive patients diagnosed with anal neoplasms. These patients were identified from the records of all HIV-positive patients diagnosed with either AINs (group 1) or anal carcinoma (group 2), between January 1998 and November 2004 at a veteran medical centre in Texas, USA. Seven patients in each group were included in the analysis. The authors concluded that the most significant factor for the development of invasive anal carcinoma in patients with HIV is duration of disease. The authors reported that with the advent of HAART, HIV has changed from a terminal illness to a chronic disease, and as a result of improved long-term survival secondary to new HIV therapy, anal invasive carcinoma will become an increasing problem.
Effect of HAART
In 2005, Palefsky et al. 59 reported the findings of a point-prevalence analysis in a prospective cohort study, in which 357 HIV-positive MSM with no history of anal cancer completed a questionnaire detailing behaviours and medical history, anal cytology and HPV testing, and HRA with biopsy for detection of AIN. Participants had a clinical examination, consisting of an anal swab for cytology and another anal swab for anal HPV testing. The participants were interviewed and asked about lifetime history of medical conditions, common HIV conditions, lifetime use of antiretroviral medication, cigarette use, alcohol consumption, recreational drug use and sexual behaviour factors (receptive/insertive anal intercourse, rimming and use of objects in the anus).
The findings from this study by Palefsky et al. 59 was that prevalence of AIN remained high among this cohort of HIV-positive MSM since the introduction of HAART therapy in 1996, indicating that HAART is not associated with a reduced prevalence of AIN. However, the study was carried out on a group of men with a high proportion that had been HIV-positive for a number of years, and may not be generalisable to people who have only been HIV-positive for a few years.
In 2001, Palefsky et al. 60 reported the findings of an analysis of study participants who were HIV-positive MSM, enrolled in two anal neoplasia cohort studies61,62 and treated with HAART continuously for at least 3 months, while participating in the studies, between the years 1991 and 1994. A total of 98 HIV-positive MSM were followed for at least 6 months before initiation of HAART, and results confirmed with data collected during follow-up, 6 months after HAART initiation.
Of the 98 MSM included in the analysis by Palefsky et al. ,60 the mean age at HAART initiation was 46 years (range 30–69). The conclusions by the authors were that 6 months’ treatment with HAART had relatively little impact on the natural history of ASIL and anal HPV infection. In the absence of screening and treatment of anal HSIL, the longer survival owing to HAART may increase the risk of progression to cancer as most of these lesions persist after HAART initiation.
The findings from Palefsky et al. 59,60 were supported by another study conducted by Piketty and Kazatchkine63 in 2005. In a review of published studies that assessed the impact of HAART on cervical and anal disease, Piketty and Kazatchkine63 suggest that HAART has little impact on the incidence of HPV-related cervical and anal cancer.
A study was undertaken by Oehler-Janne et al. 64 to investigate the outcome of HIV-seropositive patients, under HAART, with anal cancer treated with RT alone or in combination with standard chemotherapy. Overall, 81 HIV-seronegative patients and 10 consecutive HIV-seropositive patients under HAART that were treated with RT were retrospectively analysed. Ten TNM stage- and age-matched HIV-seronegative patients were compared with the 10 HIV-seropositive patients. The main findings from Oehler-Janne et al. 64 were that despite high response rates to organ-preserving treatment with RT with or without chemotherapy, local tumour failure seems to be high in HIV-positive patients receiving HAART.
Proportion affected
Palefsky et al. 65 in 1990 reported the findings of a cohort study of male homosexuals with AIDs and HIV. Each participant was asked about anal symptoms and history of receptive anal intercourse. A smear for anal cytology was obtained using a Dacron swab inserted into the anorectal junction. The conclusions reached by the authors indicated that immunosuppressed male homosexuals have a high prevalence of anal HPV infection and AIN, and that this population may be at significant risk for the development of anal cancer. However, it should be noted that these conclusions were based on the results of 97 participants of a highly selected population.
Palefsky et al. 66 in 1992 reported the findings of a study on 37 homosexual men with group IV HIV, who were attending an outpatient clinic. These 37 men were originally in the earlier study by Palefsky et al. 65 and received a 17-month follow-up visit. This subsample of the original study may not be a very representative sample of homosexual men. The authors of the 1992 study66 found that during the 17-month period, the proportion of subjects with abnormal anal cytology increased from 27% to 65% from the original findings, and that the proportion with AIN increased from 8% to 32%. It was also found that the proportion of the group with anal HPV infection also increased from 58% to 89%. The authors concluded that the results indicated that this particular population may be at significant risk of developing anal cancer. Both of the above studies were carried out in San Francisco, which has a high population of homosexuals.
In 1998, Critchlow et al. 67 reported on a longitudinal study of 287 HIV-seronegative and 322 HIV-seropositive men attending a community-based clinic in the USA. The study objective was to identify risk factors for the detection of prevalent and incident of HPV infection, and HPV persistence among HIV-seropositive and seronegative homosexual men.
To be eligible for the study by Critchlow et al. ,67 subjects had to be men reporting having sex with other men and were at least 18 years of age. Of the 910 men enrolled, 287 HIV-seronegative and 322 HIV-seropositive men were seen for at least two visits, at which specimens adequate for the detection of anal HPV DNA were obtained. At enrolment, subjects underwent a standardised interview and were asked questions concerning demographic characteristics, sexual behaviour, other behavioural characteristics and health status. Self-administered questionnaires were completed at each return visit, with information obtained regarding recent sexual behaviour, use of antiretroviral therapies, and occurrence of symptoms associated with AIDS, anal disease or other STDs. At enrolment, and at each subsequent visit, participants underwent a standardised physical examination, and a standardised unaided and colposcopic anal examination.
Critchlow et al. 67 reported that HIV seropositivity was associated with increased levels of high risk, but not low or intermediate risk HPV types. The authors wrote that risk of anal HPV infection appears to increase with sexual exposure, epithelial trauma, HIV infection and immune deficiency. Incident infection may result from recent sexual exposure or reactivation of latent infection.
In 2003, Piketty et al. 68 reported on a cross-sectional study that compared the prevalence of and risk factors for abnormal anal histological or cytological findings in HIV-positive men who had sex with men with male HIV-positive injection drug users who reported no history of anal intercourse. Participants in the study by Piketty et al. 68 were interviewed by using a standardised, comprehensive, self-administered questionnaire that included questions on age, education status, professional activity, tobacco use, route of HIV infection, medical history, history of sexually transmitted diseases, history of HPV-related disease, history of treatment for anal disease, drug use, age at first intercourse, total number of sexual partners, total number of receptive and insertive anal intercourse, and history of commercial sex work with men. The questionnaires were self-administered, and the investigators were blinded to the results to better ensure patient privacy and accuracy of the data. Participants had a thorough anal examination that included insertion of a Dacron swab for anal cytological and HPV testing.
The study by Piketty et al. 68 included 50 male HIV-1 positive injection drug users and 67 HIV-1 positive men who had sex with men. Human papillomavirus 16 was the most common high-risk genotype found in the two groups (30% in the men who had sex with men and 22% in the injection drug users; p > 0.2). Human papillomavirus 18 was found in 16% of the men who had sex with men and 4% of the injection drug users; p > 0.2.
The findings from Piketty et al. 68 were that anal HPV infection and ASIL may be acquired in the absence of anal intercourse in HIV-positive men, and that prevalence of HSIL is high among HIV-positive injection drug users.
Forty-five HIV-infection MSM from the previous study68 were analysed in a later study by Piketty et al. 69 and the results reported in 2004. These 45 MSM had previously received HAART treatment and protease inhibitors for at least 6 months. Anal cytology was abnormal in 32 (72%) of the cohort, which included four participants with ASCUS, 22 with LSIL and six with HSIL; HPV DNA was detected in 36 (80%) of the cohort. The authors concluded that their results demonstrated a high prevalence of ASIL, including high-grade SIL, and anal HPV infection in HIV-infected MSM, despite immune restoration under HAART. The authors speculated that if HAART exhibits little or no effect on the restoration of specific immunity against HPV, there would be more time for HSIL to progress to cancer. That could lead, in turn, to an increase in anogenital cancer among patients receiving HAART because they are living longer.
In 1998, Palefsky et al. 70 reported on the parameters of incidence and progression of ASIL in HIV-positive and HIV-negative homosexual men, with the same population from another of their studies. 57 They found that the incidence of HSIL within 2 years was 20% in HIV-positive men and 8% in HIV-negative men, for ASIL the incidence was 52% in HIV-positive men and 17% in HIV-negative men who had no evidence of lesions at baseline. However, the Palefsky70 data only included 2 years of follow-up. As progression from HSIL to anal cancer may take several years, HIV-positive individuals on HAART may be at increased risk of progression to anal cancer if HAART prolongs their lifespan but does not lead to HSIL regression.
Summary
The available evidence has been carried out mainly on HIV-positive males who are homosexual or bisexual, indicating that this is a particular high risk group of interest. Table 7 shows the results of some studies examining the risk to HIV-positive males of HPV infection. An indirect comparison to the sample of HIV-positive heterosexual males in the study by Piketty et al. 68 shows that HIV-positive homosexuals/MSM have a high rate of HPV infection. The majority of studies also have a higher rate of HPV infection when an indirect comparison is made to the group of HIV-negative MSM in the study by Critchlow et al. 67
| Study details | Population | n | Proportion (%) with: | |||
|---|---|---|---|---|---|---|
| AIN | HPV | LSIL | HSIL | |||
| Palefsky et al. 199065 | HIV-positive homosexual men | 97 | 15 | 54 | ||
| Palefsky et al. 199266 | HIV-positive homosexual men (subgroup of the above study, followed up after 17 months) | 37 | 32 | 89 | ||
| Critchlow et al. 199867 | HIV-positive MSM | 322 | 92 | |||
| HIV-negative MSM | 287 | 66 | ||||
| Palefsky et al. 199870 | HIV-positive homosexual men | 346 | 20 | |||
| HIV-negative homosexual men | 262 | 8 | ||||
| Piketty et al. 200368 | HIV-positive heterosexual males | 67 | 46 | 16 | 18 | |
| HIV-infected MSM | 50 | 85 | 49 | 18 | ||
| Piketty et al. 200469 | HIV-infected MSM | 45 | 80 | 42 | 22 | |
MSM (without HIV)
In 1982, Daling et al. 71 reported on a study looking at whether characteristics that are correlated with male homosexual behaviour are associated with the incidence of cancer. The authors linked patients’ names on a population-based cancer reporting system covering 13 Washington counties in the USA, with names on the Washington State Department of Social and Health Services syphilis registry, as syphilis was believed to be correlated with homosexual activity. Of 47 men identified to have anal cancer, eight were considered to have syphilis, when the authors expected 0.4, based on the proportion of syphilis cases among men with other sites of cancer, thus suggesting that anal intercourse may be a risk factor for anal cancer.
Daling et al. 71 did state that the incidence of anal cancer was not high, either in men in general (approximately 1.1 per 100,000) or in homosexual men (the rate of which was unknown). The report authors, assuming that homosexual men have an anal cancer risk of 25–50 times that of heterosexual men, believed the annual incidence of anal cancer in homosexual men would be only between 12.5 and 36.9 per 100,000.
Chin-Hong et al. 72 reported findings from the EXPLORE study on age-related prevalence of HPV infection in HIV-negative MSM in 2004 and 2005. The authors reported on age-related prevalence of anal cancer precursors in HIV-negative MSM. The EXPLORE study, a randomised clinical trial of the efficacy of a behavioural intervention to reduce the risk of HIV acquisition in sexually active HIV-negative MSM, recruited participants from four cities in America (Boston, Denver, New York and San Francisco). Males were eligible for inclusion into the study if aged 16 years or older and reported as having receptive or insertive anal intercourse with one or more men within the preceding year. The study recruited 1409 men, with a median age of 37 years (interquartile range 31–43) and the median age at first receptive anal intercourse was 20 years (interquartile range 17–24). During the 6 months preceding entry into the study, the participants reported a median of eight sexual partners (range 4–20) and 77% reported having receptive anal intercourse.
In 2004, Chin-Hong et al. 72 reported on 1218 participants of the EXPLORE study: 8% reported a history of injection drug use and 49% were current smokers or had smoked in the past. Using PCR testing, the authors found that 57% of the HIV-negative MSM were HPV positive, and that 26% were infected with a high-risk HPV type, indicating that a high proportion of HIV-negative MSM may be at risk for developing anal cancer.
In 2005, Chin-Hong et al. 73 reported on a cross-sectional analysis of prevalence and determinants of ASIL in 1262 of 1409 HIV-negative MSM recruited to the EXPLORE study, for whom anal cytology and behavioural data were obtained. From an earlier analysis of participants of the EXPLORE study, it was believed that HIV-negative MSM are a population that is at an increased risk for the development of invasive anal cancer compared to the general population. It was reported that factors statistically significantly associated with ASIL were having more than five receptive anal sex partners compared with fewer than two receptive anal sex partners during the previous 6 months [OR 1.8 (95% CI 1.1 to 2.8), p = 0.018], older age at first receptive anal intercourse [OR 1.3 per 10-year increase in age (95% CI, 1.0 to 1.7), p = 0.045], injected drug use two or more times per month compared with no use in the previous 6 months [OR 17 (95% CI 1.2 to 223), p = 0.035], PCR evidence of an anal HPV infection [OR 2.5 (95% CI 1.3 to 4.9), p = 0.008] and anal HPV infection with increasing numbers of HPV type (p < 0.001 for linear trend). Although neither age nor smoking status were statistically significantly associated with ASILs in univariate analysis, the authors included both factors in the final multivariate model because previous studies had indicated that they are important risk factors for anal cancer.
In summary, the findings of these three studies indicate that HIV-negative MSM are at an increased risk of anal cancer due to receptive anal intercourse.
Females with HIV
In 1999, Hankins et al. 74 reported on a study undertaken to explore risk factors for HPV infection in HIV-positive women using data from the Canadian Women’s HIV Study, a prospective open cohort study that recruited HIV-positive women at 28 sites across Canada. HPV test results were available for 375 women, with a median age of 32.5 (range 16.5–77.3) years. It was reported that sexual transmission was the most frequent source of HIV infection (69.9%, n = 262); 14.1% (n = 53) were infected through injection drug use and 9.1% (n = 34) through the receipt of infected blood or blood products. Overall, two-thirds (67.2%, 252 out of 375) of the women were positive for HPV, with 28.8% having more than one HPV type. The global prevalence of high-risk oncogenic HPV types (16, 18, 45 and 56) and of intermediate-risk oncogenic HPV types (31, 33, 35, 39, 51, 52 and 58) in the cohort was 32.3%.
The findings from this study74 indicated, when HPV prevalence was examined by age, a consistent inverse relation between the presence of HPV and age (p = 0.006). HPV infection was found in 74.6% (141 out of 189) of women under the median age of 32.5 years, as compared with 59.7% (111 out of 186) of older women (p = 0.002).
In 2001, Holly et al. 75 reported on a study that evaluated HPV-related abnormalities in 251 HIV-positive women and 68 HIV-negative women from the San Francisco Bay Area site of the multicentre Women’s Interagency HIV study between the years 1995 and 1997. Questionnaire data on medical history and relevant sexual practices was obtained and study participants underwent a physical examination. The study was conducted before HAART therapy became widely available.
Holly et al. 75 found that their study indicated that HIV-positive women were at higher risk of abnormal anal cytology than high-risk HIV-negative women. Risk factors for abnormal cytology in HIV-positive women included detection of anal HPV DNA, a lower number of CD4 cells, a higher plasma level of HIV ribonucleic acid (RNA), a history of receptive anal intercourse and concurrent abnormal cervical cytology.
The two studies in this section suggest that that women who are HIV-positive, particularly younger HIV-positive women, are of high risk of HPV infection.
Females with higher risk of anal cancer
Sexual behaviour
In 1997, Frisch et al. 53 reported on a population-based case–control study (undertaken in Denmark and Sweden) on factors positively correlated with the risk of anal cancer. Telephone interviews were conducted with 324 women in whom invasive or in situ anal cancer was diagnosed and 343 controls with adenocarcinoma of the rectum and 349 population controls.
Of the women participating in the survey,53 approximately 1 out of 10 reported having had anal intercourse at least once. This practice was more common in the group of women with anal cancer than in either control group [OR 2.2 (95% CI 1.4 to 3.4)]. Having had anal intercourse for the first time at or after the age of 30 years was not associated with an increased risk of anal cancer. In contrast, women who had experienced anal intercourse before the age of 30 were clearly at increased risk of anal cancer (OR 4.4), lifetime number of anal-sex partners was positively correlated with the risk of venereal diseases. Women with anal cancer were also significantly more likely than controls to have had gonorrhoea (OR 4.4), trichomoniasis (OR 2.2) and prior cervical neoplasia (OR 2.6). No other venereal disease occurred significantly more frequently among women with anal cancer, but they had been tested for HIV more often than controls (OR 2.0).
Frisch et al. 53 also reported that fewer female patients with anal cancer (70%) than controls (82%) were married or widowed, and female patients with anal cancer reported more sexual promiscuity among their partners. The risk of anal cancer among women whose partners had experienced three or more other sexual partners was twice as high as the risk among women whose partners had experienced no other sexual partners. The significant trend towards an association between the number of male partners and the risk of anal cancer persisted after adjustment for differences in smoking status and education. Anal intercourse remained associated with an elevated risk, but the OR was reduced from 2.2 to 1.6 after adjustment for differences in the lifetime number of male partners, smoking status and education. Female subjects who had a history of anogenital warts, gonorrhoea or cervical neoplasia, those who had been tested for HIV, and those whose partners had experienced sexually transmitted infections (STIs) remained at significantly increased risk.
HPV infection
Moscicki et al. 76 reported in 1999 on a cohort study undertaken in March 1994, recruiting women who were participating in an ongoing natural history study of HPV. Women aged 13–20 years were screened for cervical HPV DNA detection, those women who tested positive for cervical HPV DNA were recruited. Women who consented had samples obtained for anal HPV DNA and anal cytology. The study reported the prevalence and risks for anal cytological abnormalities over a 1-year period.
The study76 group comprised 442 women, with an average age of 22.5 years (± 2.3 years), with 49.3% of women in the study reported ever having had anal intercourse. A total of 269 samples were analysed for HPV DNA status: 66.7% were positive for HPV within 1 year prior to the visit at which they were diagnosed. The factors the authors found to be significantly associated with abnormal anal cytology were a history of anal sex [OR 6.90 (95% CI 1.7 to 47.2)], a history of cervical SILs [OR 4.13 (95% CI 1.3 to 14.9)] and a current anal HPV infection [OR 12.28 (95% CI 3.9 to 43.5)]. There was a strong association between anal intercourse and the development of HPV-induced SILs, which supports the role of sexual transmission of HPV in ASILs.
In 2001, Palefsky et al. 77 presented results from the same study as Holly et al. ,75 which showed that anal HPV infection is under-recognised in HIV-positive and HIV-negative women. The study found that 76% (170 out of 223) HIV-positive women and 42% (24 out of 57) HIV-negative women had anal HPV infection.
In 2003 Chan et al. 78 reported on a study that evaluated factors that predict regression of untreated CIN2 and CIN3. A cohort of 93 women with untreated CIN2 or CIN3, from a prospective, double-blinded, randomised, placebo-controlled trial of -carotene, were prospectively analysed. The cohort was analysed by age, race, parity, smoking history, oral contraceptive use, marital status, lesion grade, sexual history and HPV status. At enrolment into the study, HPV infection was detected in 84% (78 out of 93) women and most patients had HPV types that were considered high risk for progressing to cancer. Chan et al. 78 reported that in multivariate analysis, HPV status and the number of sexual partners remained as significant independent predictors of regression of untreated CIN2 and CIN3.
In 2005, Hernandez et al. 79 reported on the findings of a cohort study which sought to characterise anal HPV infection in a cohort of Hawaiian women. Women were eligible to take part if they were ≥ 18 years of age; women were ineligible if they had been pregnant within the past year, had blood-clotting disorders or could not speak/understand English. A total of 2392 ethnically diverse women were recruited from five clinic sites in Honolulu, Hawaii, and followed with repeat visits at 4-monthly intervals. Of these 2392 women, 88% (1378) agreed to provide anal specimens and had sufficient specimens. Overall, 27% (372 out of 1378) of women were positive for anal HPV DNA.
Of the 2392 participants in this study,79 826 did not have an anal specimen collected and 1566 did. When asked about anal intercourse, women providing anal specimens were more likely to have engaged in anal intercourse compared with women who did not provided anal specimens (21% compared with 11.6%).
Other factors
In 2003, Evans et al. 80 reported the findings of a retrospective cohort study that examined the occurrence of second primary cancers in women in the area covered by the TCR, who had been diagnosed with either CIN3 or invasive cervical cancer, compared with the expected cancer incidence derived from registered age- and period-specific incidence rates for all women in the same population. The TCR is a population-based cancer registry that started in 1960 and, at the time of the study by Evans et al. ,80 covered a population of 14 million in South East England.
Evans et al. 80 identified a cohort of women with CIN3 (ICD-10 D06) who were diagnosed prior to any invasive cancer between 1960 and 1999, and, in addition, a second cohort of women with a first cancer diagnosed in the uterine cervix (ICD-10 C53) between 1960 and 1999 was also identified. A total of 21,703 women were identified with an initial cervical cancer diagnosed between 1960 and 1999, and 98 of these were excluded because they had a different cancer diagnosed on the same day. Approximately 5% of the remaining 21,605 women had a further cancer diagnosed (1055 women had two cancers, 51 had three, and four women had four cancers each).
Evans et al. 80 calculated SIRs for subsequent cancer sites after CIN3 and invasive cervical cancer. Women who were diagnosed with CIN3 had a significantly increased risk of developing subsequent cancer at the following six sites: anus (SIR 5.9, 95% CI 3.7 to 8.8), lung (SIR 1.8, 95% CI 1.5 to 2.1), cervix uteri (SIR 2.8, 95% CI 2.4 to 3.2), vulva (SIR 4.4, 95% CI 2.8 to 6.6), vagina (SIR 18.5, 95% CI, 13.0 to 25.5) and kidney (SIR 1.6, 95% 1.0 to 2.4). None of the cancer sites had a significantly decreased incidence. The increase in anal cancer was only significant 10 or more years after the initial diagnosis of CIN3. Women who were diagnosed with cancer of the cervix uteri had a significantly increased risk of developing subsequent cancer at the following eight sites: rectum (SIR 1.4, 95% CI 1.1 to 1.9), anus (SIR 6.3, 95% CI 3.7 to 10.0), lung (SIR 2.5, 95% CI 2.2 to 2.8), connective tissue (SIR 2.7, 95% CI 1.2 to 5.3), vulva (SIR 1.9, 95% CI 1.0 to 3.3), vagina (SIR 8.0, 95% CI 4.4 to 13.5), bladder (SIR 1.7, 95% CI 1.3 to 2.3) and kidney (SIR 1.9, 95% CI 1.2 to 2.8). Cancers of the rectum and anus were significantly raised within 4 years of the initial diagnosis and then again after 15 years. The results of this study supported the hypothesis that cancers of the cervix, anus, vulva and vagina share common risk factors, such as HPV and smoking.
In summary, there is little available research on women with anal cancer, and while HIV-positive women were at higher risk than HIV-negative women, the current available evidence points to women being at significantly less risk of anal cancer than MSM in general, and HIV-positive MSM are the group with the greatest risk of developing anal cancer.
Chapter 5 Modelling methods for the cost-effectiveness analysis of screening for anal cancer
This section reports the decision modelling methods that informed the cost-effectiveness analysis of multiple alternative screening programmes for the early detection of anal cancer and precancerous AIN lesions. The analysis focuses on MSM as an aggregate group of individuals who are at significantly increased risk of developing anal cancer. However, the analysis separates this aggregate group into MSM with diagnosed HIV infection, and MSM who are HIV negative or have undiagnosed HIV infection. Alternative screening programmes target at the former group, and at both groups of MSM are analysed. As MSM have been identified at the group at greatest risk the cost-effectiveness analysis focuses on this group. If cost-effectiveness of a screening programme is not cost-effective in the highest-risk group then it will not be cost-effective in groups with a far lower risk of disease.
The analysis is undertaken from the perspective of the UK National Health Service (NHS), and presents the results of the analysis with respect to the health service costs incurred and quality-adjusted life-years (QALYs) gained as a result of the implementation of each screening programme, as well as a ‘no screening’ option. Costs and QALYs are discounted at 3.5%.
Only two previous papers describing cost-effectiveness analyses of screening for anal cancer were identified. 81,82 Both were undertaken by the same set of authors and used a cohort Markov model to assess screening for anal cancer in HIV-negative and HIV-positive MSM, respectively. These studies are not reviewed explicitly, rather specific issues and approaches adopted by Goldie et al. 81,82 are critiqued at relevant points in the description of the methods used to develop and populate the model used in the current analysis. The following section describes the model structure used to evaluate screening for anal cancer. The subsequent sections describe the data, analyses and assumptions used to populate the model.
Anal cancer screening model structure
The anal cancer model structure develops the published models used by Goldie et al. 81,82 to evaluate anal cancer screening in HIV-negative and HIV-positive MSM. The model describes progression of anal cancer from no AIN lesions, to either low or HG-AIN lesions, and from HG-AIN lesions to anal cancer. Individuals’ low-grade anal intraepithelial neoplasia (LG-AIN) lesions may either regress to a healthy state or progress to the high-grade lesion state.
Figure 3 presents the structure of the model used in the current analysis. The major difference to the Goldie model81,82 is that the current model structure combines HIV-negative, undiagnosed HIV-positive, and diagnosed HIV-positive MSM in the same model. Goldie et al. 81,82 modelled HIV-negative and HIV-positive MSM separately so that their model did not allow for the transition from HIV negative to HIV positive, and it was not clear how undiagnosed HIV-positive MSM were modelled (the implicit assumption was that all HIV-positive MSM were diagnosed).
FIGURE 3.
Anal cancer model structure.
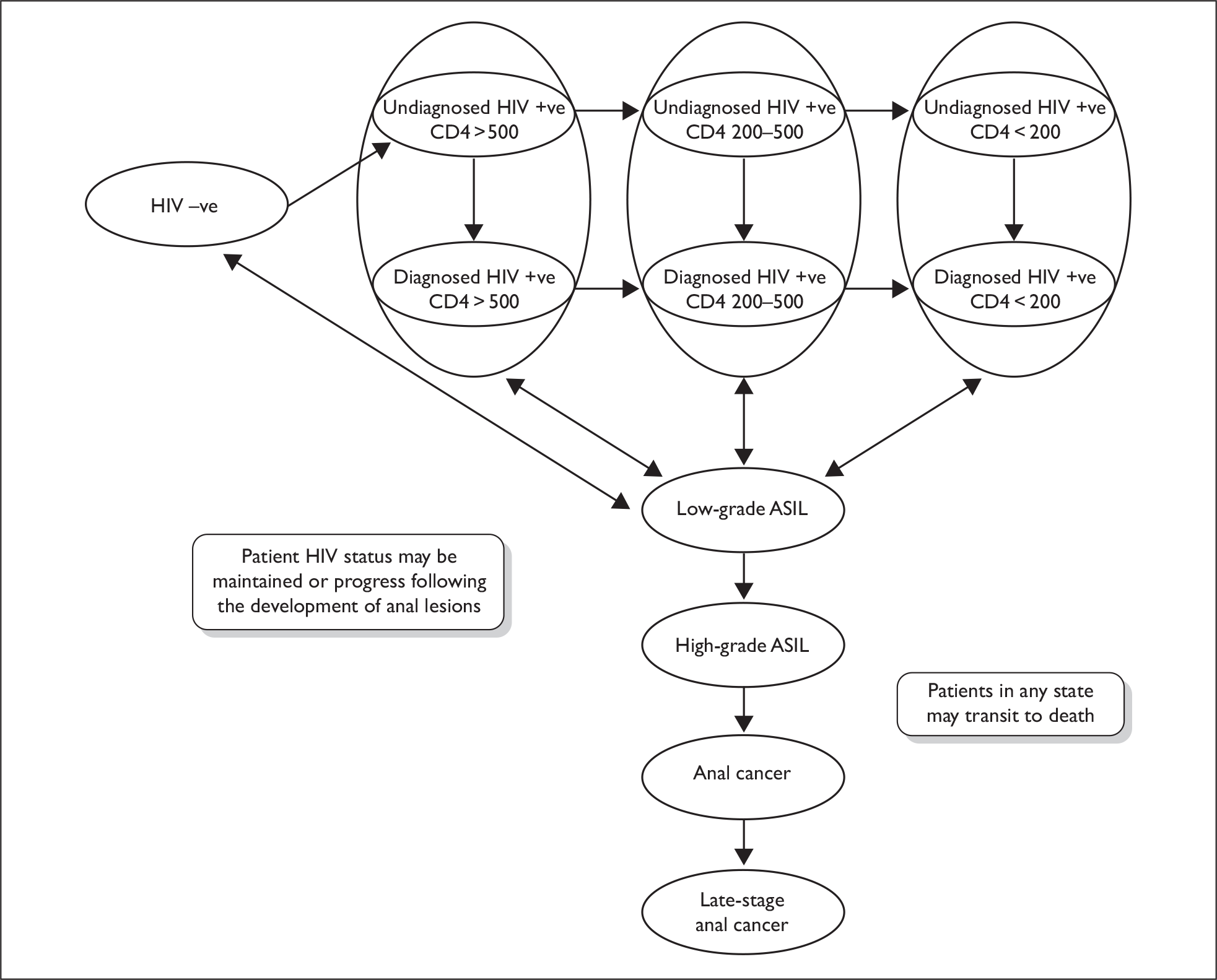
Thus, the baseline (natural history) model allows for the parallel description of the incidence and progression of HIV infection (through three decreasing CD4 count categories), the incidence and progression of anal cancer and its precursors (including the regression of LG-AIN), the diagnosis of HIV infection and the diagnosis of anal cancer and its precursors.
Another difference is that Goldie et al. 81,82 described the existence of ASCUS as a separate state that was handled by assuming that 24% of men in this state had underlying LSILs and 18% had underlying HSILs. It was not clear how this aspect was handled practically, for example did these proportions move to these states and the others to a normal state? In the current model, it is assumed that an ASCUS screening results is a positive test results, and screening test characteristics (i.e. sensitivity and specificity) are estimated accordingly. The resource implications of the differential processing of ASCUS and more definitive positive test results are assumed to be minor.
Alternative screening programmes are overlaid on the natural history, which act to increase the likelihood of detection of anal cancer in individuals eligible for screening in the years in which screening is offered.
The main screening model was developed as a cohort Markov model, so exact estimates of costs and benefits were estimated for each set of input parameters analysed. It was implemented in Microsoft excel spreadsheets, with associated macros. Submodels (as described below) were also developed as cohort Markov models in Microsoft excel.
The model moved forward in cycles of 1 year. It is recognised that disease may progress through multiple stages within a single year, but, as an annual screening programme was the shortest interval tested, the improvements in accuracy from reducing the cycle length were not considered to justify the necessary increase in model complexity. The time horizon of the model followed MSM to a maximum age of 100 years. The starting age of the model was varied to reflect the current distribution of MSM (this aspect is explained in more detail in the following section).
Model population
The subsequent sections describe the data, analyses and assumptions used to populate the model. The separate sections describe the estimation of the age-specific size of the MSM population; the incidence and progression of HIV infection; the incidence and progression of AIN lesions; the effects of treatment of precancerous and cancerous AIN lesions; the model’s screening-related parameters (screening attendance, as well as test sensitivity and specificity); and costs and utility weights associated with different events and states included in the model.
Age-specific prevalence of MSM
The prevalence of MSMs within each age range was estimated using UK life table data to estimate the mean annual prevalence of men in each age range over the period 1990–2005, and data from the National Survey of Sexual Attitudes and Lifestyles (NATSAL) II. 83 NATSAL II was a cross-sectional study of a multistage stratified random sample of 12,110 men and women, aged 16–44 years, living in private households in Great Britain in 2000–1. A range for the proportion of men who are MSM was based on answers to the questions about whether male respondents had experienced sex with a man in the last year (upper estimate) and in the last 3 months (lower estimate). Rates in the 46–55, 56–65, 66–75 and 76+ age ranges were not informed by the NATSAL and so were assumed to be 95%, 75%, 5% and 0% of the rates estimated for the 35–44 age range.
Age-specific MSM prevalence was then calculated by multiplying the estimated prevalence proportions by the mean male population size in each age range. The resulting ranges are presented in Table 8.
| Age (years) | n | Proportion of MSM | Male population | No. of MSM | ||
|---|---|---|---|---|---|---|
| Lower bound | Upper bound | Lower bound | Upper bound | |||
| 16–17 | 372 | 0.005 | 0.009 | – | – | – |
| 18–19 | 312 | 0.000 | 0.004 | – | – | – |
| 20–24 | 826 | 0.016 | 0.018 | – | – | – |
| 16–24 | 1510 | 0.010 | 0.013 | 3,019,907 | 30,151 | 38,927 |
| 25–34 | 2132 | 0.026 | 0.027 | 3,460,727 | 89,979 | 93,440 |
| 35–44 | 2033 | 0.017 | 0.020 | 3,635,349 | 61,801 | 72,707 |
| 46–55a | 0.016 | 0.019 | 3,219,359 | 51,993 | 61,168 | |
| 56–65a | 0.013 | 0.015 | 2,553,926 | 32,563 | 38,309 | |
| 66–75a | 0.00085 | 0.001 | 1,921,442 | 1633 | 1921 | |
| > 75a | 0 | 0 | 1,361,287 | 0 | 0 | |
HIV incidence and progression in MSM
The following sections describe the estimation of the HIV-related parameters included in the anal cancer screening model. The analysis of the HIV parameters used the common categorisation of HIV as CD4 counts of ‘> 500’, ‘200–500’ and ‘< 200’.
Age-specific prevalence of diagnosed and undiagnosed HIV (by CD4 count) in MSM
Data describing the number of diagnosed HIV-positive MSM (in 2005) were directly informed by data provided by the Survey Of Prevalent HIV Infections Diagnosed (SOPHID) team at the HPA, with only minor adjustments required to assign those cases for which CD4 count was not reported.
The SOPHID team did not have quantitative information on the age or CD4 distribution of undiagnosed HIV-infected MSM, although they estimated the number of MSM aged 15–59 living in the UK with undiagnosed HIV-infection to be 9000 (range 6600–12,400). A log-normal distribution was used to represent the uncertainty in this aggregate figure. Qualitatively, the SOPHID team stated that it is likely that the proportion of undiagnosed cases decreases with age, as men are increasingly likely to develop symptoms or attend a genitourinary medicine clinic.
To allocate the estimated number of undiagnosed HIV-positive MSM by age and stage, relative likelihoods of remaining undiagnosed were assigned to individuals of different ages, based on clinical opinion. Individuals in the youngest age groups (15- to 25- and 26- to 35-year-olds) were assigned a relative value of 1; 36- to 45- and 46- to 55-year-olds, 0.5; and 56- to 65-year-olds, 0.25. An aggregate undiagnosed HIV-positive MSM population and a set of age-specific diagnosed HIV-positive MSM populations were sampled from relevant Poisson distributions. For each iteration, the non-adjusted numbers of undiagnosed HIV-positive MSM (aggregate undiagnosed cases multiplied by proportion of diagnosed cases in each age group) in each age group were multiplied by the relative likelihood weights, which were then adjusted proportionately so that the aggregate number of undiagnosed individuals equalled the sampled value from the range estimated by the SOPHID team.
The stage distribution was estimated by applying clinical opinion-based relative likelihoods that individuals in each of the three CD4 stages would remain undiagnosed (< 200 CD4, 0.05; 200–500 CD4, 0.1; > 500 CD4, 1), and then adjusting to equal the estimated aggregate number of undiagnosed HIV cases.
Finally, the estimated numbers of diagnosed and undiagnosed HIV-positive MSMs were converted to prevalence rate ranges by dividing the lower and upper estimates of the numbers by the upper and lower estimates of the relevant age-specific numbers of MSM in the general population, respectively. The resulting figures and presented in Table 9.
| CD4 count | Age group (years) | Diagnosed | Undiagnosed | ||
|---|---|---|---|---|---|
| Lower est. | Upper est. | Lower est. | Upper est. | ||
| < 200 CD4 count | 15–25 | 0.0010 | 0.0023 | 0.0001 | 0.0002 |
| 26–35 | 0.0034 | 0.0044 | 0.0002 | 0.0005 | |
| 36–45 | 0.0090 | 0.0122 | 0.0003 | 0.0007 | |
| 46–55 | 0.0060 | 0.0088 | 0.0002 | 0.0005 | |
| 56–65 | 0.0045 | 0.0074 | 0.0001 | 0.0002 | |
| 66–75 | 0.0052 | 0.0126 | 0.0000 | 0.0000 | |
| 200–500 CD4 count | 15–25 | 0.0090 | 0.0142 | 0.0013 | 0.0032 |
| 26–35 | 0.0244 | 0.0275 | 0.0033 | 0.0066 | |
| 36–45 | 0.0555 | 0.0695 | 0.0038 | 0.0084 | |
| 46–55 | 0.0364 | 0.0470 | 0.0025 | 0.0056 | |
| 56–65 | 0.0242 | 0.0333 | 0.0009 | 0.0019 | |
| 66–75 | 0.0346 | 0.0557 | 0.0000 | 0.0000 | |
| > 500 CD4 count | 15–25 | 0.0053 | 0.0089 | 0.0080 | 0.0194 |
| 26–35 | 0.0169 | 0.0193 | 0.0234 | 0.0458 | |
| 36–45 | 0.0440 | 0.0554 | 0.0299 | 0.0664 | |
| 46–55 | 0.0269 | 0.0352 | 0.0187 | 0.0415 | |
| 56–65 | 0.0158 | 0.0224 | 0.0057 | 0.0127 | |
| 66–75 | 0.0148 | 0.0282 | 0.0000 | 0.0000 | |
Transition probabilities for movement between the HIV states
Separate sets of transition probabilities were required for diagnosed and undiagnosed individuals. For undiagnosed individuals, mean estimates of the transition probabilities between the three defined states have been reported by Sweeting et al. 84 Goldie et al. 82 report transition data that aim to reflect the impact of HAART. The reported transition times from the two sources are similar for the highest CD4 count state, with a small difference estimated for the mean time spent in the intermediate CD4 state (4 years vs 3.63 years by Sweeting et al. 84 and Goldie et al. ,82 respectively). The transition probabilities used in the model are presented in Table 10; the lower and upper CIs are informed by multiplying the mean duration in each state by 1.25 and 0.75, respectively.
| Mean | 95% CI | ||
|---|---|---|---|
| Lower | Upper | ||
| Undiagnosed | |||
| > 500 to 200–500 CD4 count | 0.166 | 0.135 | 0.215 |
| 200–500 to < 200 CD4 count | 0.221 | 0.181 | 0.283 |
| Diagnosed | |||
| > 500 to 200–500 CD4 count | 0.166 | 0.135 | 0.215 |
| 200–500 to < 200 CD4 count | 0.241 | 0.198 | 0.307 |
Clinical presentation rates by CD4 count state
Sweeting et al. 84 present an application of Bayesian back-calculation to estimate median estimates of the quarterly probabilities of diagnosis (with 95% credibility intervals) for each of the three CD4 count states for homosexual men between 1984 and 2002. These data are assumed to inform clinical presentation rates in MSM. Table 11 presents the estimated ranges of the annual probabilities of clinical presentation, which were based on lowest and highest intervals between 1991 and 2002 as estimated by Sweeting et al. 84 These ranges were presented by uniform distributions in the calibration analysis.
| HIV category | Lower bound | Upper bound |
|---|---|---|
| CD4 count > 500 | 0.060 | 0.091 |
| CD4 count 200–500 | 0.189 | 0.381 |
| CD4 count < 200 | 0.570 | 0.984 |
Age-specific clinical presentation rates were estimated by applying subjectively defined weights that increased the likelihood of older MSM presenting clinically and reduced the probabilities in younger MSM.
Age-specific incidence rates of HIV
Sweeting et al. 84 also present aggregate annual estimates of the incidence of HIV in homosexual men from 1981 to 2002. A separate Markov model was developed in order to estimate age-specific HIV incidence rates using a range of alternative data sources.
The HIV incidence submodel assumes that:
-
all individuals developing an HIV infection start in the ‘> 500’ CD4 count category
-
all individuals who developed HIV prior to 1990 were dead by the year 2005
-
age-specific incidence rates of HIV have remained constant since 1990
-
HIV progression from the ‘> 500’ CD4 count category is not affected by treatment.
The estimation process involves the following stages. For individuals entering the ‘> 500’ CD4 count state at every age between 15 and 84 years, the submodel estimates the probability that individuals remain in the ‘> 500’ state at each subsequent age. Individuals may leave the ‘> 500’ state due to transition to another CD4 state (informed by transition probabilities described above) or death (informed by UK male life tables as a CD4 count > 500) has been shown to have little effect on mortality. 85 The mean duration in the ‘> 500’ state prior to transition to another CD4 state for both diagnosed and undiagnosed cases was estimated to be 5.5 years (transition probability = 0.166). 82,84 In the absence of empirical estimates, duration in the ‘> 500’ state was assumed to be normally distributed with a subjective standard deviation of 1 year.
A simulation exercise was undertaken to identify the combinations of input parameter values (including age-specific HIV incidence rates) that best predicted the estimated age-specific prevalence of diagnosed and undiagnosed HIV-infected MSM with a CD4 count of > 500. Outputs from each iteration of the submodel were inputted to the following equation, which was solved for ages 15–84 years and combined into the seven age categories used by the HPA,
where:
-
x = 2005 minus current year of incidence (1990–2005)
-
I(age–x) = incidence of HIV infected individuals with a CD4 > 500 at ‘age in 2005–x’ years
-
P(age–x) = probability of incident cases at ‘age in 2005–x’ years remaining in the ‘> 500’ state at ‘age in 2005’ years.
The calibration process identified 2451 of the 5000 eligible iterations that predicted aggregate numbers of HIV-infected MSM within the 95% CI estimated from the HPA data (11,722–15,718). Probabilities representing the likelihood that each of the 2451 parameter sets was the most relevant set were estimated using the following process:
-
For each model iteration, the sum of differences between the age-specific incidence estimates informed by the submodel and the bounds of the respective HPA-based 95% CIs were estimated.
-
The proportion of the sum of differences contributed by each iteration were estimated.
-
The reciprocals of the proportions of the sum of differences contributed by each iteration were estimated (no iterations had a sum of differences of zero).
-
The reciprocals were divided by the sum of the reciprocals to estimate the probability that each of the 2451 parameter sets was the most relevant set.
The calibrated age-specific annual incidence of HIV-infected MSMs were converted to incidence rates based on the number of MSM at risk of HIV infection within each age range. These parameters were estimated as the prevalence estimate of all MSM (in each age range) minus the sum of prevalent HIV-infected MSMs at the start of each age range and one-half of all incident cases across each age range. The prevalence of HIV infected MSMs at the start of each age range was estimated by assuming that 90%, 85%, 80%, 75%, 70% and 65% of incident cases in the previous two age ranges (i.e. the previous 20 years) remain alive at the start and throughout the 15–25, 26–35, 36–45, 46–55, 56–65, 66–75 and 76+ age ranges, respectively.
This process was undertaken for each set of HIV incidence parameters that were included following the calibration of the HIV incidence model (as described above). The estimates for age groups over 66 years using the above process were unstable due to small numbers (e.g. estimated incidence probabilities ranged from negative values to 6.51). As the incident numbers were so small for these age groups, incidence rates of zero are assumed.
Mortality rates in HIV-positive individuals
Two studies were identified that assessed the RR of death in HIV-positive cohorts compared to mortality in the general population. 86,87 A third study presented quantitative estimates of the effects of CD4 count on the incidence of AIDS and non-AIDS related serious illnesses. 88
Ormaasen et al. 86 evaluated HIV related and non-HIV related mortality compared with the general population before and after introduction of HAART. Median follow-up for 398 patients with HIV who were receiving HAART was 38 months. The RR for 5-year mortality compared with an age-matched Norwegian general population was 3.96 (95% CI 2.25 to 6.97) in the post-HAART era.
Martínez et al. 87 prospectively followed-up consecutive HIV-infected adults who were prescribed HAART in a Catalonian hospital between January 1997 and December 2004 or until death, loss to follow-up or discontinuation of HAART. RRs for all-cause mortality compared with an age-matched Catalonian general population were estimated from the figures presented by Martínez et al. , and are shown in Table 12. Mortality rates decreased over time in HIV-infected patients (p < 0.001, chi-squared test for trend), although the rate remained between four and seven times higher than that for the age-matched general population. The proportion of AIDS-related deaths decreased significantly over time – from 84% in 1997 to 7% in 2004.
| Year | Mortality rate per 100 person-years | RR | |
|---|---|---|---|
| HIV positive | General population | ||
| 1997 | 4.497 | 0.200 | 22.49 |
| 1998 | 2.694 | 0.200 | 13.47 |
| 1999 | 1.618 | 0.200 | 8.09 |
| 2000 | 0.895 | 0.200 | 4.47 |
| 2001 | 0.925 | 0.200 | 4.62 |
| 2002 | 1.030 | 0.200 | 5.15 |
| 2003 | 1.236 | 0.200 | 6.18 |
| 2004 | 1.317 | 0.200 | 6.58 |
Baker et al. 88 found that the risk of non-AIDS defining illnesses decreased by around 16% for every 100 cell increment in CD4 cell count (hazard ratio 0.84, p <0.01), while the risk of AIDS-defining events fell by 43% for every 100 cell increment in CD4 cell count (hazard ratio 0.57, p < 0.01). They calculated the risk of these events through a multivariate analysis, which adjusted for the latest viral load and CD4 cell count, age, gender, prior AIDS diagnosis, hepatitis co-infection and injecting-drug use.
Based on the above studies, the following parameter estimates were derived:
-
relative risk for death of HIV patients compared with the general population = 4–7 (uniform distribution)
-
proportion AIDS-related deaths = 0.07
-
relative risk of AIDS for 100 CD count increment = 0.57 (subjective 95% CI 0.46 to 0.68)
-
proportion non-AIDS-related deaths = 0.93
-
relative risk of non-AIDS illness for 100 CD count increment = 0.84 (subjective 95% CI 0.73 to 0.95)
-
distribution of CD4 < 200, 200–500, > 500 categories = 0.25, 0.5, 0.25, respectively.
A simulation process was applied to estimate the distributions of the RRs of death compared with the general population for patients in each of the three defined CD4 count categories (Table 13). First, RRs for mortality for the 200–500 and > 500 CD4 count categories, relative to the < 200 category, were informed by sampled values of the RRs for AIDS and non-AIDS-related illnesses. Second, the Solver function in excel was used to fit the RR of death in patients with a CD4 count of < 200 to a sampled value for the overall RR of death for patients with HIV. This process was repeated 1000 times to obtain a joint distribution of the RRs for the three CD4 count categories.
| CD4 count | Mean | Percentile | |
|---|---|---|---|
| 2.5th | 97.5th | ||
| Treated | |||
| < 200 | 8.56 | 5.89 | 11.62 |
| 200–500 | 5.24 | 3.57 | 7.16 |
| > 500 | 3.01 | 1.49 | 5.41 |
| Untreated | |||
| < 200 | 53.37 | 39.51 | 69.88 |
| 200–500 | 16.07 | 10.65 | 22.64 |
| > 500 | 4.35 | 1.36 | 10.52 |
A similar process was undertaken for non-diagnosed HIV patients based on the combined RR for death observed in 1997 (uniform distribution 17.5–27.5) and the proportion of AIDS-related deaths in 1997 (84%), which was assumed to be representative of the pre-HAART era.
Anal cancer epidemiology and natural history
Values for the following anal cancer transition probabilities were required:
-
no AIN to LG-AIN
-
no AIN to HG-AIN
-
progression from LG-AIN to HG-AIN
-
progression from HG-AIN to early stage invasive cancer
-
progression from early stage invasive cancer to late stage invasive cancer
-
regression from LG-AIN to no AIN
-
regression from high-grade to LG-AIN.
The estimation of these parameters is discussed in the following sections, as well as in the model calibration section.
Data sources for incidence and progression up to HG-AIN
Two studies, published in the mid- to late 1990s, inform parameter estimates of the natural history of anal cancer in HIV-negative and positive homosexual men. 57,61,70,89 Other studies were excluded on account of the absence of any histological follow-up, for example Sayers et al. 90 report a study based in Edinburgh, which followed up 20 HIV-positive men with dyskaryosis that was suggestive of AIN.
Critchlow et al. 89 undertook a prospective study beginning in January 1991, which followed 158 HIV-positive and 147 HIV-negative men in Seattle, Washington. This study excluded men with any positive cytology at baseline. Figure 4 describes the pathway to the final study sample. The mean follow-ups were 20.2 and 22.1 months for HIV-negative and positive men, respectively.
FIGURE 4.
Seattle study: pathway to study sample.
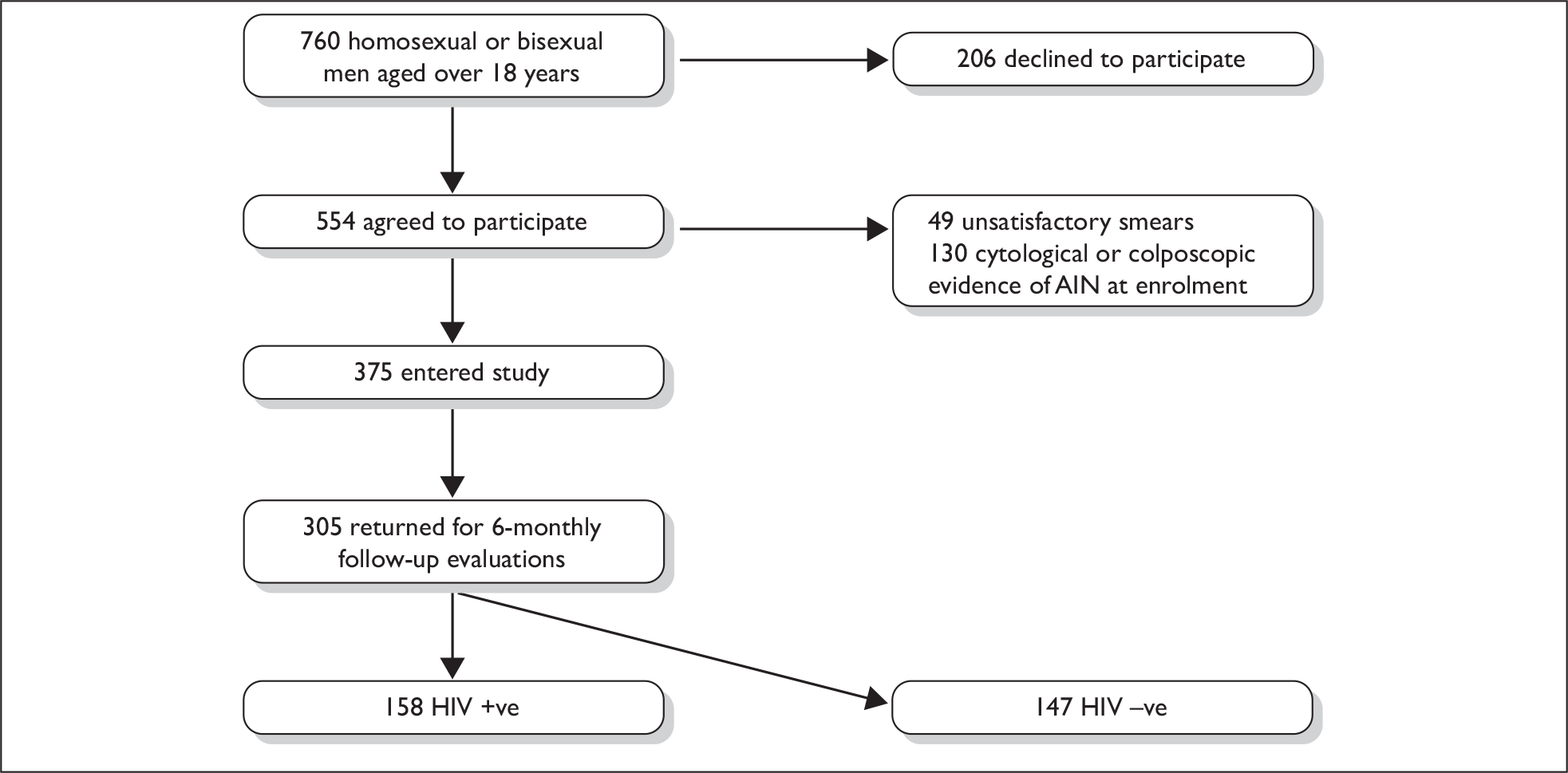
The other main study recruited a prospective cohort of homosexual and bisexual men in San Francisco between November 1991 and March 1994. 57,61 Analyses from the study are presented after 2-year70 and 4-year follow-up57 periods. The pathways to inclusion for these two analyses are presented in Figures 5 and 6.
FIGURE 5.
San Francisco study, 2-year analysis: pathway to study sample.
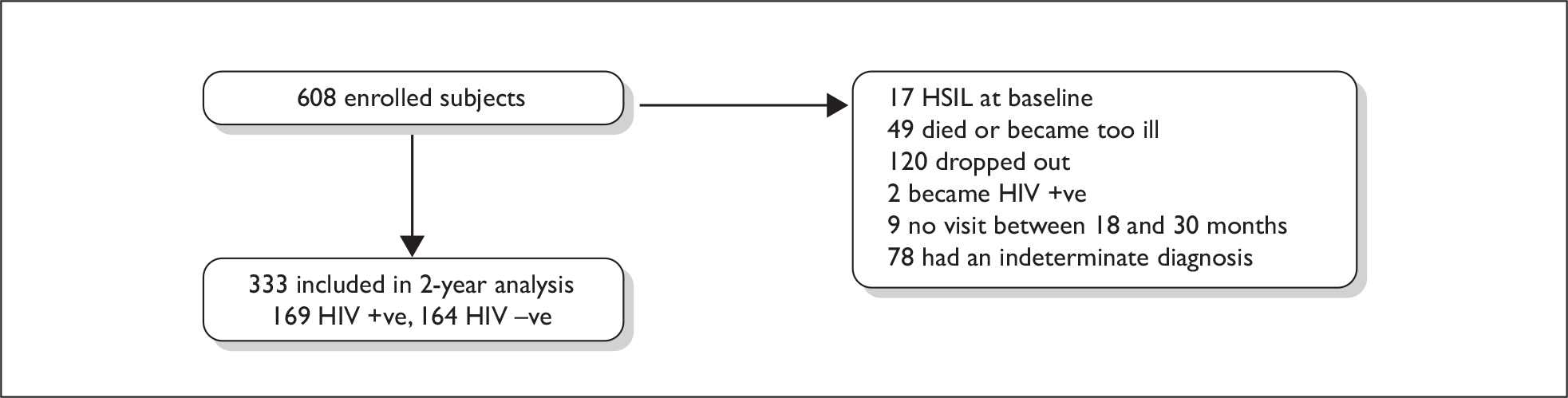
FIGURE 6.
San Francisco study, 4-year analysis: pathway to study sample.
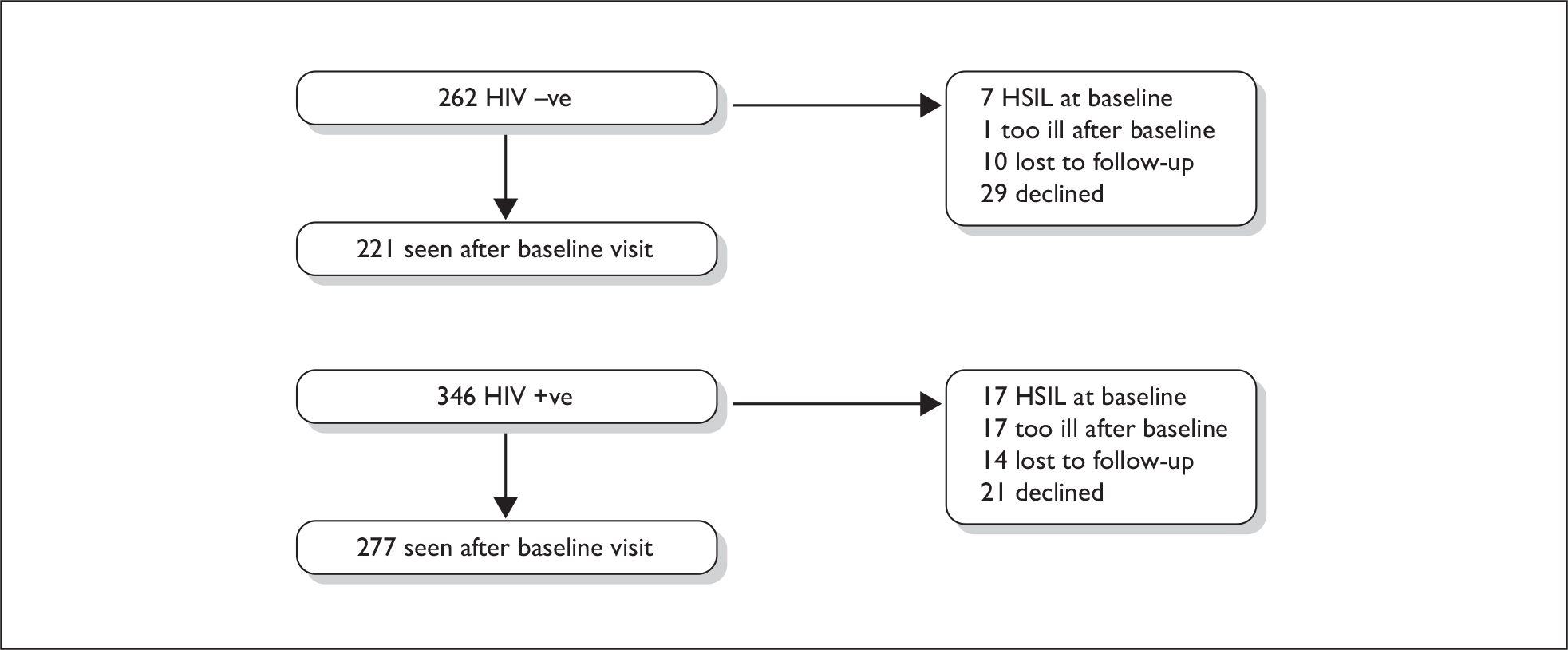
Analyses of the Seattle and San Francisco cohort studies
The data from the two natural history studies were analysed using methods that are categorised as either complex or simple. The complex analysis used literature-based sources to control for false-negative and false-positive results in ‘cytology alone’-detected cases, the unobserved development of low-grade disease prior to high-grade disease, the timing of events and incomplete follow-up. The simple analyses treat the data ‘as is’ and restrict the application of assumptions to a minimum. The complex analyses are described first, followed by the simple analyses.
Table 14 presents the relevant results from the Seattle study.
| HIV status | n | Mean follow-up | HG-AIN incidence | LG-AIN prior to HG-AIN | HG-AIN diagnosis | |
|---|---|---|---|---|---|---|
| Histology | Cytology | |||||
| HIV positive | 158 | 20.2 | 24 | 14 | 13 | 11 |
| HIV negative | 147 | 22.1 | 8 | 4 | 4 | 4 |
To estimate the direct transition probability from normal to HG-AIN, the numbers of incident HG-AIN cases (direct from no AIN) were adjusted to account for the sensitivity and specificity of cytology. The follow-up times were adjusted to account for the cases developing LG-AIN prior to HG-AIN. The following assumptions and analyses were undertaken:
-
Of the 15 cytologically detected cases, nine did not undergo biopsy and six did receive biopsy but could not locate areas of high-grade disease. In eight of the nine cases without biopsy, the cytological findings did not return to normal over a mean 16.5 additional months; in five of the six cases with biopsy, the cytological findings did not return to normal over a mean 23.8 additional months. The implication that the number of true-positives is between 9 and 13 (60–87% specificity). Palefsky et al. 57 state that they found that 70% of cytologically identified HG-AIN cases were confirmed histologically when a lesion was seen (for HIV-positive men), although the data reported in the referenced paper indicate that the rate is between 57% and 60%. 28 No cytological high-grade cases were reported in HIV-negative men in the screening study paper. 28
-
Based only on high-grade cytological screen results, the data presented by Palefsky et al. 57 indicate a sensitivity rate for the detection of histologically defined HG-AIN of 27% (3 out of 11) in HIV-positive men, and 0% (0 out of 1) in HIV-negative men. Panther et al. 30 stated that the detection of HSILs on an anal Pap smear had a sensitivity of 47% (95% CI 35 to 59) and specificity of 90% (95% CI 81 to 96%) for detection of a high-grade histological finding.
-
In the Seattle study, subjects with cytological evidence of HG-AIN or visible evidence of abnormalities of the internal anal canal were referred for biopsy. Thus, sensitivity is likely to be markedly increased compared with the use of cytology alone, while specificity may be reduced. Based on the above data describing test characteristics, a range of 60–87% was assumed for specificity, and a range of 80–90% was assumed for sensitivity for the Seattle study observations of HG-AIN that were not detected histologically.
-
Based on the Palefsky et al. screening study,28 sensitivity rates of 48.5% and 27.8% were defined for the detection of LG-AIN for HIV-positive and negative men, respectively. Specificity rates of 43.8% and 55.6% were defined for LG-AIN for HIV-positive and negative men, respectively. These estimates were used to adjust the numbers of HG-AIN cases detected in the absence of prior low-grade disease.
-
The mean follow-up time was re-estimated to exclude the time post development of LG-AIN (LG-AIN was assumed to occur at the mid-point of the mean follow-up). This will still overestimate the mean follow-up time, as it was not possible to exclude follow-up time in men developing LG-AIN who did not subsequently develop HG-AIN.
Observed transition matrices for HIV-negative and positive men between baseline and 2 years in the San Francisco study are presented in Table 15. Table 16 presents the relevant data published from the 4-year analysis:
-
The San Francisco data were simplified by assuming that the ASCUS cases were normal. The numbers of high-grade cases were re-estimated using the same methodology and sensitivity and specificity rates as used for the analysis of the Seattle data (including the number of normal to high-grade cases that passed through LG-AIN based on the Seattle data, by HIV status). In the 2-year analysis, the proportions of normal to HSIL, and LSIL to HSIL cases detected histologically were assumed to be the same as reported for the 4-year analysis. 57
-
The 2-year data included only men who were observed over the full 2-year study period, and it was assumed events occurred at the mid-point.
-
The 4-year data presented in Table 16 report the numbers of observed cases of HG-AIN over the 4-year follow-up period, but do not indicate the mean follow-up time, assuming a 4-year follow-up period would underestimate the incidence figures. Total person-years at risk are presented for HIV-negative and HIV-positive men for the estimation of RRs of developing HG-AIN. 57 Dividing the person-years by the respective numbers of HIV-negative and HIV-positive men estimates mean follow-up times of 2.4 and 2.7 years, respectively.
-
Presented life table analysis of the 4-year data predicted that 49% of HIV-positive men would develop HG-AIN at 4 years’ follow-up57 compared with the 38% estimated from the data reported in Table 16. Applying the monthly progression rate implied by the 49% event rate at 4 years (1.4%), the mean follow-up time at which 38% progression would be expected to be observed is 34 months (2.8 years). This analysis provides some evidence that the progression rate is approximately stable.
-
The 2-year data indicates zero regression from LG-AIN to no AIN in HIV-positive men, and a 36% LG-AIN regression rate in HIV-negative men. Other observations may have passed through two states prior to their status at 2 years, for example a case in LSIL at baseline and 2 years may have regressed to normal and then progressed back to LSIL.
| Status at baselinea | Status at 2 yearsa | |||
|---|---|---|---|---|
| Normal | ASCUS | LSIL | HSIL | |
| HIV positive | ||||
| Normal | 28 | 14 | 28 | 17 |
| ASCUS | 5 | 3 | 10 | 9 |
| LSIL | 0 | 0 | 21 | 34 |
| HIV negative | ||||
| Normal | 101 | 13 | 12 | 11 |
| ASCUS | 6 | 3 | 3 | 1 |
| LSIL | 4 | 1 | 4 | 5 |
| Status at baseline | n | Incident HSIL during 4-year follow-up | ||
|---|---|---|---|---|
| Cytological | Histological | Either | ||
| HIV positive | ||||
| Benign | 115 | 20 | 28 | 34 |
| Indeterminate | 27 | 4 | 8 | 10 |
| ASCUS | 45 | 8 | 15 | 15 |
| LSIL | 90 | 27 | 43 | 47 |
| Total | 277 | 59 | 94 | 106 |
| HIV negative | ||||
| Benign | 173 | 9 | 16 | 20 |
| Indeterminate | 14 | 0 | 3 | 3 |
| ASCUS | 17 | 2 | 4 | 4 |
| LSIL | 17 | 6 | 6 | 7 |
| Total | 221 | 17 | 29 | 34 |
Separate sets of simpler analyses were also undertaken that did not adjust for test sensitivity and specificity, that estimated person-years at risk assuming individuals experiencing an AIN event had one-half of the follow-up of those not experiencing an event, and that one-half of the observed cases of HG-AIN (in individuals with no AIN at baseline) experienced prior LG-AIN.
Outputs from the Seattle and San Francisco cohort studies analyses
The results of the complex data analyses are presented in Table 17. Transition probabilities from no AIN to LG-AIN show that HIV-positive men are significantly more likely to develop LG-AIN, whereas HIV-negative men are more likely to regress back to a normal state once they have developed LG-AIN.
| Transition | HIV positive | HIV negative | ||||
|---|---|---|---|---|---|---|
| Seattle | San Francisco | Seattle | San Francisco | |||
| 2-year data | 4-year data | 2-year data | 4-year data | |||
| Normal to LG-AIN | – | 0.523 (0.413 to 0.632) | – | – | 0.072 (0.034 to 0.122) | – |
| Normal to HG-AIN | 0.027 (0.004 to 0.056) | 0.069 (0.008 to 0.152) | 0.041 (0.005 to 0.085) | 0.021 (0.008 to 0.040) | 0.057 (0.024 to 0.103) | 0.037 (0.019 to 0.058) |
| LG-AIN to normal | – | 0.017 (0.000 to 0.063) | – | – | 0.071 (0.002 to 0.236) | – |
| LG-AIN to HG-AIN | – | 0.595 (0.464 to 0.716) | 0.260 (0.197 to 0.331) | – | 0.350 (0.129 to 0.599) | 0.180 (0.075 to 0.322) |
The CIs from all three analyses of the direct transition probabilities from no AIN to HG-AIN overlap in both HIV-positive and HIV-negative men. No significant difference is observed between HIV-positive and HIV-negative men.
More divergence is noted in the transition probabilities between LG-AIN and HG-AIN that were based on the 2- and 4-year San Francisco data. The 2-year data lead to a significantly higher estimate of the transition probabilities, which may be partially explained by differential disease severity profiles in the two cohorts. Higher proportions of men in the 4-year analysis had CD4 counts of < 200 (29% vs 19%) and < 500 (71% vs 66%). Thus, the higher estimated transition probabilities in the 2-year data are unlikely to be due to increased disease severity. Indeed, regarding the 2-year analysis, Palefsky et al. 70 state that ‘the true incidence in HIV-positive men may have been underestimated, because subjects with the most advanced immunosuppression were less likely to have been included in the 2 year analysis’ (p. 318).
Uncertainty around the follow-up times may also affect the comparison. For example, although the 4-year data analysis is informed by a clearer aggregate estimate of the timing of events, it was not possible to define separate follow-up intervals by baseline AIN status. In HIV-positive men, the mean follow-up to detection of HG-AIN (or the end of the study follow-up period) was 2.4 years, but the mean follow-up in men with LG-AIN at baseline would likely be significantly less. If follow-up in this cohort was reduced by one-third to 1.6 years, the resulting transition probabilities would have been 0.366 (original value 0.595) and 0.281 (original value 0.35) in HIV-positive and HIV-negative men, respectively.
Table 18 presents the results of the simplified analyses of HG-AIN incidence by HIV status and AIN at baseline status, based on the 4-year San Francisco data. Table 19 presents incidence rates of LG-AIN by HIV status, based on the 2-year San Francisco data. The simplified analyses generally produce lower progression estimates than the more complicated analyses presented in Table 17.
| n | No HG-AIN | HG-AIN | Person-years | Person-years at riska | ||
|---|---|---|---|---|---|---|
| Per non-HG-AIN case | Per HG-AIN case | |||||
| Summary data | ||||||
| HIV negative | 221 | 188 | 33 | 671 | 3.3 | 1.65 |
| HIV positive | 277 | 170 | 107 | 593 | 2.7 | 1.35 |
| LG-AIN to HG-AIN annual transition probabilities | ||||||
| LSIL at baseline | n | No HG-AIN | HG-AIN | Total person-years at risk | Mean (95% CIs) | |
| HIV negative | 17 | 10 | 7 | 44.3 | 0.158 (0.068 to 0.278) | |
| HIV positive | 90 | 43 | 47 | 218.2 | 0.215 (0.164 to 0.272) | |
| Normal to HG-AIN annual transition probabilities | ||||||
| Normal at baseline | n | No HG-AIN | HG-AIN | HG-AIN without prior LG-AIN | Total person-years at risk | Mean (95% CIs) |
| HIV negative | 204 | 178 | 26 | 13 | 626.7 | 0.021 (0.011 to 0.033) |
| HIV positive | 187 | 127 | 60 | 30 | 515.1 | 0.058 (0.040 to 0.080) |
| Status at baseline | Status at 2 years | Revised status at 2 yearsa | Pysb | Normal to LG-AIN annual transition probabilities: mean (95% CIs) | |||
|---|---|---|---|---|---|---|---|
| Normal (+ ASCUS) | LSIL | HSIL | Normal (+ ASCUS) | LSIL | |||
| HIV positive | |||||||
| Normal | 28 | 28 | 17 | 28 | 36.5 | 92.5 | 0.395 (0.298 to 0.496) |
| Normal + ASCUS | 50 | 38 | 26 | 50 | 51 | 151 | 0.338 (0.265 to 0.415) |
| HIV negative | |||||||
| Normal | 101 | 12 | 11 | 101 | 17.5 | 219.5 | 0.080 (0.048 to 0.119) |
| Normal + ASCUS | 123 | 15 | 12 | 123 | 21 | 267 | 0.079 (0.050 to 0.114) |
As a result of the uncertainties and assumptions involved in the above analyses, it was decided to base the initial calibration analyses on the relevant estimates produced by the simplified analyses of the 2- and 4-year San Francisco data, as presented in Tables 18 and 19. Estimates of the regression rates from LG-AIN were informed by the complex analysis of the 2-year San Francisco data, as presented in Table 17.
AIN progression by HIV status
The 2- and 4-year analyses of the San Francisco study both present estimates of the RRs for anal lesion progression (including progression from normal to any grade AIN, and from LG-AIN to HG-AIN) for HIV-positive men with differing CD4 counts (> 500, 200–500, < 200) compared with HIV-negative men. The RRs are presented in Table 20. The results show that HIV status and CD4 count are significant predictors of anal cancer progression (the p-value test for trend was < 0.0005).
| HIV status | RRs (95% CIs) | ||
|---|---|---|---|
| 2-year follow-up | 4-year follow-up | Model inputs | |
| HIV negative | 1 | 1 | 1 |
| HIV positive CD4 > 500 | 1.8 (1.2 to 2.6) | 2.1 (1.1 to 3.5) | 2.1 (1.1 to 3.5) |
| HIV positive CD4 200–500 | 2.7 (2.0 to 3.6) | 3.3 (2.1 to 5.3) | 3.3 (2.0 to 5.3) |
| HIV positive CD4 < 200 | 3.1 (2.3 to 4.1) | 5.8 (3.7 to 9.3) | 5.8 (2.3 to 9.3) |
None of the observed increases in RR between the 2- and 4-year follow-up was statistically significant, although the increase in CD4 < 200 approached significance. As it is not possible to disentangle the specific effects, if the observed increase is a true result it may be an indication that incidence increases with age (within the age range of the study cohort) and/or AIN progresses at an increasing rate in HIV-positive MSM. It is also noted that the analysis of the 4-year cohort was not an extension of the 2-year analysis – different inclusion criteria led to significant differences in the disease severity profiles of the two cohorts.
Given the uncertainty around the time dependence of the AIN progression parameters in HIV-positive MSM, the model did not incorporate this aspect. The RRs (and CIs as presented in Table 20) were used to adjust aggregate transition probabilities to HG-AIN for HIV-positive patients by CD4 count.
Progression from HG-AIN to invasive anal cancer
Marchesa et al. 91 report on 47 patients with HG-AIN treated surgically between 1972 and 1993 (retrospectively followed up). Three cases of invasive anal cancer were observed in the conservatively treated group (20 patients). The duration of follow-up in the radical and conservative groups is not stated, although the overall median duration was 104 months (range 16–273). In addition, 35 patients who were symptomatic at the time of detection of HG-AIN had experienced symptoms for a mean duration of 19 months (range 1–120).
Other relevant studies reported no incidence of anal cancer, including the Seattle and San Francisco studies and prospective studies of patients treated for HG-AIN. 43,92
Given the limited data informing progression from HG-AIN to anal cancer, alternative uniform distributions for this transition probability were tested during the full model calibration process.
No evidence of increased progression rates in HIV-positive MSM was identified and so separate transition probabilities for HIV-negative and HIV-positive MSM were not estimated. However, the probability of transition to anal cancer was assumed to increase with age. The rationale behind the use of age-specific transition probabilities was that an increasing likelihood of transition with increased lesion duration has been observed in other cancer models (e.g. colorectal cancer93). Infeasible increases in model complexity prevented the direct modelling of time dependent transition probabilities, so the use of age increasing transition probabilities acted as a proxy for this potential relationship.
Aggregate transition probabilities (sampled from a uniform distribution) were converted to age-specific probabilities assuming RRs of transition (compared with age group 15–25 years) of 1, 1.5 and 5 for ages 26–35, 36–45 and over 45 years. Weighted aggregate RRs (estimated using the estimated numbers of MSM in each age category) were fitted to sampled aggregate transition probabilities. The reference case transition probabilities are presented in Table 21 (the calibration process is described in Chapter 6).
| Age (years) | Mean (95% CIs) |
|---|---|
| 15–35 | 0.0009 (0.0006 to 0.0012) |
| 36–45 | 0.0014 (0.0009 to 0.0018) |
| 45+ | 0.0045 (0.0032 to 0.0060) |
In the earlier cost-effectiveness analysis of anal cancer, Goldie et al. 81,82 fitted an annual transition probability of approximately 5% in HIV-positive MSM and 3.6% (range 0.36% to 6%) in HIV-negative MSM. This is a major area of difference in the current study and potential reasons are explored in the model sensitivity analyses.
Treatment of AIN lesions
Chin-Hong and Palefsky94 state that AIN 1 (LG-AIN) is treated to reduce risk of further spread or enlargement to the point at which topical therapy is no longer possible. They also present treatment algorithms describing treatment pathways for AIN 1 and AIN 2 or 3. In both cases, small lesions are treated topically (common therapies are liquid nitrogen and 80% trichloroacetic acid). Medium or large AIN 1 lesions are surgically removed only if symptomatic. AIN 2 or 3 lesions are treated whenever possible. They also state that treatment of HIV-positive patients with AIN is more challenging as lesions are often larger and recur at a higher rate or are never eliminated at all.
We contacted Dr Chin-Hong to try to ascertain the proportion of AIN 2 or 3 lesions that present as small lesions that may be treated topically, as no indication of the proportion of AIN 2 or 3 lesions that are amenable to topical treatment was identified in the literature. He responded that parameter estimates will depend on whether the patient is HIV positive or negative. In general, for AIN 2/3, only about 10–20% present as small lesions and the rest (80–90%) have to be referred to surgery. If small enough, topical therapy will be effective in about 65–75% of cases.
Dr Chin-Hong pointed out that his experience is based on a clinic population that probably has a higher proportion of more complex cases. It is possible that a general clinic-based population will have a higher proportion of men with smaller lesions. He also talked about the use of an outpatient method called infrared coagulator (IRC), where many of these lesions can be treated very effectively as outpatients (regardless of size). The impact of this change could lead to only 10% of these lesions being referred to surgery. However, the extent to which this technology is being used in the UK is unclear.
Chang et al. 92 undertook a prospective study of 37 patients treated surgically for large-volume HSILs. Eight HIV-negative patients were followed up for a mean period of 32.3 ± 20.6 months, during which time zero recurrences were observed. Twenty-nine HIV-positive patients were followed up (28.6 ± 12.9 months) with 23 recurrences occurring. Mean time to recurrence was 12 months. The Kaplan–Meier analysis demonstrates that risk of recurrence approaches 100% by 50 months. However, recurrent HSIL can be retreated and no cases of anal cancer were reported in this cohort. In a survey of side effects, 16 out of 29 reported uncontrolled pain for a mean of 2.9 weeks (range 1 day to 4 months).
Brown et al. 43 followed up 34 patients who received surgical intervention for HG-AIN. The paper implies that 24 patients underwent a local excision, while the remaining 10 patients received a complete excision ± grafting. After a median follow-up of 41 (range 12–104) months, 14 patients (41%) developed recurrent HG-AIN; 13 of the 14 recurred within 1 year, while 4 of the 14 patients experienced more than one excision of recurrent disease – two in one patient, four in two patients and seven in one patient. No patient developed carcinoma but five had complications of anal stenosis or faecal incontinence.
Marchesa et al. 91 report on 47 patients with HG-AIN, who were treated between 1972 and 1993 (retrospectively followed up). Patients receiving radical operations (27 patients) (wide local excision/abdominoperineal resection) had a statistically significantly lower recurrence rate than those receiving conservative operations (20 patients) (local excision/laser vaporisation): Kaplan–Meier 7-year recurrence rates of approximately 23% versus 70%.
On the basis of these data, treatment of LG-AIN was not modelled because treatment effectiveness is not established and the proportion of potentially treatable LG-AIN is unknown.
All detected HG-AIN lesions are assumed to receive treatment. It is assumed that 20–30% of detected HG-AIN is small enough to be treated non-surgically. The remainder was assumed to receive the seemingly more effective radical surgery, defined as wide local excision. The effectiveness of both forms of treatment was assumed to be similar, with a RR of between 0.2 and 0.4 for progression to anal cancer. The high rate of effectiveness incorporates the treatment of recurrences, with the average HIV-positive patient assumed to receive treatment for recurrence every 2 years. Recurrences in HIV-negative patients were assumed to be less common, occurring once every 10 years.
Progression of treated and non-treated anal cancer
The anal cancer model was initially specified to differentiate between early-stage (primary) and late-stage (metastatic) anal cancer. Evidence informing the progression of early-stage anal cancer following treatment was identified from selected treatment papers. Only two studies42,96 presented any information regarding progression from early- to late-stage disease, and these data were of limited value, as the absolute rate of progression was unclear and no information on the timing of progression was presented. No data describing prognosis in patients with metastatic anal cancer were identified.
Assumptions of similar progression rates, and effects of metastatic disease, to those reported for other cancer locations (e.g. breast or cervical cancer) were considered. However, similar data limitations and/or significant additional assumptions and uncertainties precluded this approach.
As most studies presented survival rates following treatment of early-stage anal cancer, the model structure was adapted and the distinction between early-stage and late-stage anal cancer was removed. The final model structure described transition to death from a single anal cancer state.
The review section presented the reported mortality rates in treatment studies of early stage anal cancer, from which relevant studies were selected to populate the model. Most studies included patient populations that are unlikely to be representative of the population of MSMs with anal cancer.
Survival is therefore estimated in two parts. First, non-anal cancer-related mortality rates are estimated separately for HIV-positive and HIV-negative patients. HIV-negative patients were assumed to have the same mortality rate as the general population, while an additional cause of mortality (RR between 4 and 7) was assumed in HIV-positive patients (see Chapter 5, Mortality rates in HIV-positive individuals).
Second, anal cancer-specific mortality was estimated from the reviewed papers. Table 22 summarises the study characteristics and relevant survival estimates. Disease-specific survival (DSS) in treated patients was informed by the more effective chemoradiation (CMT) arm of the UKCCCR trial. The UKCCCR trial included patients with metastatic disease, although only 15 out of 585 patients were identified as having metastases at trial entry. 40 In the chemoradiation arm, 77 out of 111 (69%) deaths were related to anal cancer or treatment for anal cancer (7 out of 77). The presented Kaplan–Meier analyses for deaths from anal cancer show 5-year survival of 52% and 64% in the RT and CMT arms, respectively. A subjective 95% CI of 0.54 to 0.74 was assumed around the mean 5-year DSS of 0.64.
| Stage | UKCCR | Doniec | Wong | Edelman | Place | Stadler | Oehler-Janne | |||
|---|---|---|---|---|---|---|---|---|---|---|
| CMT | RT | HIV– | Matched HIV– | HIV+ | ||||||
| Country | UK | UK | Germany | Australia | USA | USA | USA | Switzerland | ||
| No. | 292 | 50 | 38 | 17 | 14 | 8 | 81 | 10 | 10 | |
| Age | 63 (26–85) | 65 (26–88) | 64 ± 15 | 62 | 38 (31–47) | 42 ± 9 | 44 (34–61) | 62 ± 13 | 45.2 ± 7 | 44.5 ± 10 |
| T1 | 0.13 | 0.13 | 0.20 | 0.33 | 0.38 | 0.21 | – | 0.15 | 0.2 | 0.2 |
| T2 | 0.32 | 0.37 | 0.57 | 0.29 | 0.38 | 0.36 | – | 0.43 | 0.6 | 0.6 |
| T3 | 0.40 | 0.39 | 0.20 | 0.27 | 0.25 | 0.43 | – | 0.31 | 0.2 | 0.2 |
| T4 | 0.15 | 0.11 | 0.03 | 0.10 | 0.00 | 0.00 | – | 0.11 | 0 | 0 |
| Node positive | 0.23 | 0.18 | 0.30 | 0.18 | 0.31 | 0.43 | – | 0.605 | 0.1 | 0.1 |
| Metastatic | 0.03 | 0.02 | 0.00 | 0.08 | 0.12 | 0 | – | – | 0 | 0 |
| HIV positive | – | – | – | 0.17 | 1 | 1 | 1 | 0 | 0 | 1 |
| HAART | N/A | N/A | N/A | – | – | 0 | 1 | N/A | N/A | 1 |
| 5-year OS | 0.49 | 0.4 | 0.74 | 0.63 | 0.33 | 0.2 | 0.43a | 0.69a | 0.69a | 0.7a |
| 5-year DSS | 0.64 | 0.52 | 0.82 | 0.67a | – | – | 0.43b | 0.87a | 1a | 0.82a |
Oehler-Janne et al. 64 matched 10 HIV-positive patients treated with HAART with 10 HIV-negative patients based on TNM stage (80% T1/2), age (44.5 years) and grading (80% G1/2). Overall survival at 1 year was 90% and 100% in the HIV-positive and negative groups, respectively. At 5 years, survival was 70% and 69%, respectively. Although based on a very small sample, in the current era of HAART, these data were used to inform an assumption of equal anal cancer-related mortality in HIV-positive and HIV-negative patients with early-stage anal cancer.
To estimate survival probabilities in individuals with untreated anal cancer, the mean 5-year DSS in the RT arm of the UKCCCR trial was defined as the upper 95% CI interval. The mean was subjectively estimated to be 0.42, and the lower CI interval to be 0.32.
Anal screening test and clinical presentation parameters
Parameters associated with the process of clinical diagnosis, leading to potential treatment are described in the following sections.
Clinical presentation
To estimate clinical presentation probabilities in individuals with undiagnosed anal cancer, reference was made to Wong et al. ,95 who reported on their local experience between 1991 and 2001. In the absence of screening they found that of 50 presenting patients, only four presented with metastatic disease. This implies that most patients present prior to the distant spread of disease. The parameter values remains highly uncertain, although it is assumed that diagnosed HIV-positive patients are more likely to be diagnosed with anal cancer due to their higher contact rate with the health service.
Table 23 presents the ranges that were included in the final calibration analysis for the annual clinical presentation probabilities for HIV negative or undiagnosed HIV positive, and diagnosed HIV-positive individuals. Alternative probabilities were specified for HG-AIN, and for anal cancer. The values were sampled from uniform distributions.
| AIN and HIV status | Range (%) |
|---|---|
| HIV negative, HG-AIN | 1–3 |
| HIV positive, HG-AIN | 5–10 |
| HIV negative, anal cancer | 3–8 |
| HIV positive, anal cancer | 10–15 |
Screening test characteristics
A recent published systematic review of six eligible screening studies (two studies with methodological issues were excluded) found the sensitivity of anal Pap smear evaluation compared with HRA-directed biopsies to be between 69% and 93%, with specificity being between 32% and 59%. 36 The ranges reported by the published review are similar to those found by the current review reported in the section on screening.
Variation in the results of the screening studies may be due to differences in the extent to which screen results were histologically confirmed, positive test definitions (i.e. whether an ASCUS result is defined as a positive screen), as well as the characteristics of the included individuals (e.g. Palefsky et al. 28 and Cranston et al. 34 reported different test characteristics in HIV-positive and HIV-negative MSM). These potential sources of variation precluded the application of meta-analytical methods to estimate screening test characteristics, and so the parameter values are informed by the presented ranges, with adjustment for differential rates in HIV-positive and HIV-negative MSM.
Table 24 presents analyses of test characteristics based on screening data for HIV-positive and HIV-negative MSM under alternative assumptions. 28 The results show that anal cytology is predicted to be a highly specific test in HIV-negative MSM, although sensitivity is low. Sensitivity is improved in HIV-positive MSM, particularly when ASCUS is defined as a positive test.
| Normal | ASIL | Sensitivity | Specificity | |
|---|---|---|---|---|
| Palefsky, HIV-negative MSM (assuming lesions seen, but not biopsied, were ASILs) | ||||
| Normal | 204 | 21 | ||
| ASCUS | 13 | 4 | 0.30 (0.15 to 0.5)a | 0.92 (0.88 to 0.95)a |
| ASIL | 4 | 5 | 0.17 (0.06 to 0.35)b | 0.98 (0.95 to 0.995)b |
| Palefsky, HIV-negative MSM (assuming lesions seen, but not biopsied, were not ASILs) | ||||
| Normal | 215 | 10 | ||
| ASCUS | 13 | 4 | 0.47 (0.25 to 0.705)a | 0.93 (0.88 to 0.955)a |
| ASIL | 4 | 5 | 0.26 (0.1 to 0.51)b | 0.98 (0.95 to 0.995)b |
| Palefsky, HIV-positive MSM (assuming lesions seen, but not biopsied, were ASILs) | ||||
| Normal | 163 | 43 | ||
| ASCUS | 59 | 33 | 0.67 (0.58 to 0.75)a | 0.59 (0.53 to 0.65)a |
| ASIL | 53 | 55 | 0.42 (0.335 to 0.51)b | 0.81 (0.75 to 0.85)b |
| Palefsky, HIV-positive MSM (assuming lesions seen, but not biopsied, were not ASILs) | ||||
| Normal | 175 | 31 | ||
| ASCUS | 69 | 23 | 0.69 (0.59 to 0.78)a | 0.57 (0.51 to 0.63)a |
| ASIL | 62 | 46 | 0.46 (0.36 to 0.56)b | 0.80 (0.75 to 0.84)b |
The studies include very few cases of HG-AIN and so the assumption of differential test characteristics based on lesion type is not included in the model. The model does differentiate between test characteristics in HIV-negative and positive MSM, and assumes that an ASCUS test result would be considered a positive test.
Table 25 presents the screening test parameter values, which were based on the reported aggregate ranges,36 subjectively adjusted for the differences between HIV-positive and HIV-negative patients (based on the rates presented in Table 23). The presented data were represented as triangular distributions in the screening model.
| HIV status | Sensitivity (range) | Specificity (range) |
|---|---|---|
| HIV negative | 0.6 (0.45 to 0.75) | 0.5 (0.3 to 0.7) |
| HIV positive | 0.85 (0.65 to 0.95) | 0.3 (0.15 to 0.45) |
The second category of screening parameters describes the likelihood that individuals eligible for screening will attend for screening. Cranston et al. 34 reported that around 10% of 125 MSM who were invited to take part in a screening study refused. However, as Knight50 suggests, the more limiting factor is likely to be the identification of MSM to whom screening can be offered.
Men who have sex with men indicate that their preferred sources of safer sex support are predominantly friends, the gay press and sexual peers rather than formal HIV services. 96 A corresponding literature review concerning MSM in Public Sex Environments distinguishes between MSMs who identify as being either gay men or bisexual men, and MSM who do not identify as either. 97 The authors found that MSM who do not identify as gay or bisexual have not been reached in significant numbers.
Without direct quantitative estimates of the effectiveness of the identification of MSM from the literature, it was assumed that screening would be offered to 40–60% of HIV negative or undiagnosed HIV-positive MSM, and 80–90% of diagnosed HIV-positive MSM. It is further assumed that 5–20% of all MSMs offered screening will refuse.
Costs
Cost inputs to the anal cancer screening model include the cost of screening, costs of diagnosis of precancerous AIN lesions, costs of diagnosis of anal cancer, and costs of treating diagnosed anal cancer. The estimation of these parameters is described in the following sections.
Costs of screening for anal cancer
Goldie et al. 82 present estimates of the cost of anal cytology screening in the USA, using Medicare average allowed charges. In the earlier paper, screening costs are based solely on the cost of an anal Papanicolaou smear (cost US$26), whereas the later paper includes also the cost of a ‘brief office visit’ at an apparent additional cost of US$50.
In preference to using US costs, we have based our screening cost estimates on detailed costs estimated for the provision of cervical cancer screening in the UK. 98 The estimated cost per screen in this report was estimated to be £22.99 (range £20.52–28.17).
Costs of diagnosis and treatment of precancerous AIN lesions
Goldie et al. 82 applied Medicare average allowed charges clinical care algorithms, developed by the University of California at San Francisco Faculty Practice, to estimate the cost of diagnosis and treatment of precancerous lesions. Low-grade ASIL required a diagnostic anoscopy and biopsy of any abnormal lesion but no treatment. High-grade ASIL required referral to a surgeon, one preoperative office visit with anoscopy, electrocautery or excisional biopsy through a colposcope with anaesthesia in an outpatient surgical setting, postoperative oral analgesia for 2 weeks, one postoperative visit at 30 days, and subsequent follow-up every 6 months with anoscopy.
UK-relevant unit costs were attached to the resource use described above for the diagnosis, treatment and follow-up of LG-AIN and HG-AIN. In the absence of unit costs for procedures specific to anal cancer, unit costs reported for similar procedures for the diagnosis and treatment cervical cancer were applied. The resulting cost estimates are presented in Table 26.
| Resource | Mean cost (£) (range) | Cost sourcea |
|---|---|---|
| AIN diagnosis (anascopy and biopsy) | 403 (310 to 503) | Colposcopy, biopsy of cervix uteri |
| Follow-up (anascopy) | 215 (165 to 250) | Colposcopy |
| Treatment of detected HG-AIN lesions | 1041 (722 to 1308) | Lower genital tract minor procedures |
The AIN diagnosis cost is applied to all individuals at the point at which they are either clinically diagnosed with AIN or they are subject to a false-positive screening test. It is assumed that patients diagnosed with LG-AIN will receive two follow-up anascopies per year while they remain in the LG-AIN state.
High-grade AIN treatment and follow-up costs are differentially applied to HIV-positive and HIV-negative patients, based on the finding in the treatment review that HIV-positive patients have a substantially higher rate of recurrence of HG-AIN. All individuals with diagnosed HG-AIN are assumed to have repeat anascopy and biopsy every 6 months. As reported in the modelling review of treatment strategies, HIV-negative and positive patients were assumed to experience recurrences every 10 and 2 years, respectively.
Costs of treating diagnosed anal cancer
Ideally, the anal cancer model would specify stage-specific treatment costs for anal cancer, and model progression of disease to death (from anal cancer or other causes). This would allow differentiation between the (presumably) lower costs incurred by screen-detected cases who are more likely to be diagnosed with an earlier stage of disease than clinically presenting patients.
Unfortunately, as discussed in the anal cancer treatment section, limited data were available to describe the progression of anal cancer. The screening model simply describes the duration of DSS for treated and untreated individuals with anal cancer. This means that only the mean cost of treating anal cancer can be applied to the model. Goldie et al. 81 seemingly estimated the lifetime costs of treating anal cancer, based on the costs of initial treatment, continuing care and terminal care for colorectal cancer, which were similar to costs reported for a discharge diagnosis of anal cancer from the Healthcare Cost and Utilization Project. 99
No UK relevant anal cancer treatment costs were identified, although a recent relevant study of screening for colorectal cancer provided UK-specific lifetime cost estimates of treatment for colorectal cancer by stage at diagnosis. 100 The uprated lifetime costs associated with cancer diagnosed at Dukes stage A (£8895) and at Dukes stage B (£13,334) were assumed to represent the costs of screen-detected and clinically presenting anal cancers, respectively. No ranges were presented around the published cost estimates and so 95% CIs ranging from 75% to 125% of the estimated mean costs were assumed (represented as log-normal distributions). The sensitivity analysis assessed the impact of assuming equal lifetime costs for screen detected and clinically presenting anal cancers.
Costs of treating diagnosed HIV infection
Relevant UK-based costs of treating HIV infection by CD4 count were reported by Miners et al. ,101 which were derived from the National Prospective Monitoring System HIV Health Economics Consortium (NPMS HHC) study. These costs were uprated to 2007 values, and are reported in Table 27.
| CD4 count | Mean (£) (95% CI) |
|---|---|
| > 200 | 9655 (8630 to 10,938) |
| < 200 | 10,598 (9362 to 11,810) |
Utility values
In their study of screening for HIV-positive MSM, Goldie et al. 82 estimated a constant utility weight of 0.56 for individuals with AIDS and AIDS-related cancer. These estimates were derived from a rating scale valuation undertaken by patients (sample not given), and the subsequent Torrance transformation of rating scale valuations.
In the study of HIV-negative men, Goldie et al. 81 applied a quality adjustment weight of 0.60 (range 0.17 to 0.79) for individuals with anal cancer, which was based on utility weights reported for gastrointestinal cancer.
The utility weights applied by Goldie et al. 81 for anal cancer are comparable with utility estimates for metastatic disease in other cancers (e.g. breast cancer102), and so applying these weights to all cancer patients may overestimate the utility effects of anal cancer. However, in the absence of alternative data sources, a same approach to representing the utility effects of anal cancer in HIV-positive and HIV-negative men was used in the current study.
The utility decrements were applied to both diagnosed and undiagnosed individuals. This application accounts for the likelihood that undiagnosed patients may have slightly higher utility than diagnosed patients, but that later diagnosed patients may have lower utility during their treatment period due to less later treatment being less effective in reducing symptoms (or increased symptoms due to more aggressive treatment).
Estimates of the utility impact of HIV infection were sourced from a number of studies that reported patient-based elicitation of utility values, as presented in Table 28. The weights reported by Mauskopf et al. 103 are lower than the other three studies, which all present similar weights by CD4 count category. To maintain comparability, the utility weights reported by Goldie et al. 81 were used in the current model.
| Study | Country | Instrument | Sample | HIV health state | Value |
|---|---|---|---|---|---|
| Mauskopf103 | USA | QWB Scale | 139 HIV patients | CD4 100–199 | 0.66 |
| CD4 200–349 | 0.69 | ||||
| CD4 350–500 | 0.72 | ||||
| CD4 > 500 | 0.72 | ||||
| Trueman104 | Canada | Standard gamble | 249 HIV patients | CD4 < 200 | 0.79 |
| CD4 200–500 | 0.82 | ||||
| Goldie81 | USA | QWB Scale | 139 HIV patients | CD4 < 200 | 0.8 |
| CD4 200–500 | 0.88 | ||||
| CD4 > 500 | 0.94 | ||||
| Goldie105 | USA | Rating scale | HIV patients | CD4 < 200 | 0.84 |
| CD4 > 200 | 0.94 |
Goldie et al. 81 used the same process to estimate a utility value for patients receiving treatment for HG-AIN lesions of 0.98. In the current study, a utility multiplier was specified for the HG-AIN state, which was applied to relevant HIV-negative and HIV-positive states in cycles where patients received treatment for HG-AIN. The final parameter values for the utility parameters are presented in Table 29, which were represented as triangular distributions in the model.
| Health state | Utility weight (range) |
|---|---|
| HIV negative, no anal cancer | 1 |
| HG-AIN (utility multiplier)a | 0.98 (0.95 to 0.99) |
| Anal cancer | 0.58 (0.5 to 0.7) |
| HIV positive, CD4 > 500 | 0.94 (0.9 to 0.98) |
| HIV positive, CD4 200–500 | 0.87 (0.84 to 0.9) |
| HIV positive, CD4 < 200 | 0.80 (0.76 to 0.84) |
Chapter 6 Anal cancer screening model calibration
Calibration of the anal cancer model was undertaken due to the extreme uncertainty in a number of the input parameters, but also to represent the joint parameter uncertainty. Parameters that were particularly uncertain include transition probabilities from HG-AIN to anal cancer, and clinical presentation rates for MSM (by HIV status) with precancerous and cancerous AIN lesions. Joint parameter uncertainty refers to the uncertainty around feasible combinations of values for different parameters, for example, combing values from the upper intervals of both the ‘transition to anal cancer’ and ‘clinical presentation rate’ parameters may predict unfeasible anal cancer incidence rates.
The general calibration process involves sampling 5000 sets of input parameters from the probability distributions defined for each parameter in Chapter 5, running the model for each set and comparing the predicted model outputs with observed output values.
Calibration outputs
The anal cancer screening model was calibrated to age-specific estimates of the incidence of anal cancer in the year 2003 as reported by the Cancer Registries,2 which should reflect the impact of HAART on incidence rates in HIV-positive individuals. Some adjustments were made to the presented incidence estimates to account for the completeness of the registry data.
Forman106 investigated the completeness of incident cases of skin cancer in Yorkshire recorded by the regional cancer registry in 1994. Patients diagnosed with skin cancer were identified from four independent information sources (pathology laboratories, outpatient clinics, general practices and the NHS Trust’s Information Services for information on patients who received inpatient care), which were then cross-checked against the regional cancer register. In total, the cancer registry registered 83.5% of all patients with skin cancer identified across the region.
Silcocks and Waterhouse107 applied the Flow method to patients diagnosed with cancer in 1996. For all cancers, completeness was 87.2% by 1 year and 92.3% by 5 years. Completeness was greater, and increased more quickly, for rapidly fatal cancers, with 1- and 5-year values of 96.4% and 97.3% (lung), and 95.3% and 96.5% (stomach) compared with 77.3% and 89.1% (female breast) and 76.9% and 88.8% (prostate). Colorectal cancers were an intermediate case (86.3% and 91.8%).
Based on the findings of the above two studies, and the fact that anal cancer appears to be a relatively slow progressing cancer, it was assumed that the cancer registry estimates for anal cancer had 77% completeness. The estimated numbers of cancers in each age group were, therefore, multiplied by 1.3 (1/0.77) to account for the missing cases.
The reported age-specific incidence rates were represented by beta distributions informed by the adjusted number of observed cases and the respective populations at risk, as presented in Table 30.
| Age group | Population at riska | Observed | Adjustedb |
|---|---|---|---|
| 15–24 | 3,019,907 | 1.64 | 2.13 |
| 25–34 | 3,460,727 | 1.97 | 2.56 |
| 35–44 | 3,635,349 | 20.46 | 26.60 |
| 45–54 | 3,219,359 | 45.08 | 58.60 |
| 55–64 | 2,553,926 | 79.37 | 103.19 |
| 65–74 | 1,921,442 | 69.75 | 90.67 |
| 75–84 | 1,096,245 | 57.64 | 74.94 |
| 85+ | 265,042 | 8.76 | 11.39 |
To estimate anal cancer incidence rates in the MSM population, it was necessary to define RRs of anal cancer for HIV-positive and HIV-negative MSM (compared with non-MSM). Age-specific anal cancer incidence rates in the non-MSM, and HIV-negative and HIV-positive MSM populations were then fitted to the observed aggregate anal cancer incidence rates for iteratively sampled RRs for each group, and the sizes of the respective groups.
Lampinen et al. 33 reference RRs of anal cancer among HIV-negative and HIV-positive MSM of 35 and 70, respectively. They also state that recent studies suggest that incidence rates among HIV-positive MSM may have further doubled, owing to increased survival since 1996 among men receiving potent antiretroviral treatment. A UK cohort study of 8640 HIV-positive individuals found the incidence of invasive anal cancer (diagnosed in 26 patients) to be 92 (95% CI 52 to 149) per 100,000 patient-years of follow-up in the post-HAART era (1996–2003),23 a mean RR of 176 compared with the general population.
Based on these studies, the calibration process assumed a mean RR for HIV-negative MSM of 35 (with a subjectively defined 95% CI 25 to 45). The RR for HIV-positive men was taken directly from the UK study (mean 176, 95% CI 99 to 285). Random values for these parameters were sampled from log-normal distributions.
Frisch et al. 13 estimated RRs for the incidence of invasive anal cancers in AIDS patients by age. They found elevated risks, particularly among patients under the age of 30 years, as shown in Table 31. Age-specific RRs for HIV-negative and HIV-positive MSMs were fitted to the respective sampled aggregate values, and the age-specific RRs (i.e. the age-specific RRs were fitted such that the relationship between the age-specific RRs was as estimated by Frisch, and the weighted aggregate RR equalled the sampled aggregate RR).
| Age group (years) | RR |
|---|---|
| < 30 | 163 |
| 30–39 | 40 |
| 40–49 | 39 |
| > 50 | 23 |
Age-specific estimates of the size of the MSM HIV-positive population were sampled from Poisson distributions informed by the data provided by the HPA, which were used to estimate the incidence of HIV in the MSM population (as described in Chapter 5, HIV incidence and progression in MSM). The sizes of the HIV-negative MSM populations were estimated by subtracting the sampled HIV-positive MSM population sizes from age-specific estimates of the MSM populations (as described in Chapter 5, HIV incidence and progression in MSM). The size of the non-MSM population at risk was estimated by subtracting the estimated numbers of MSM from age-specific estimates of the male population, informed by UK life tables.
For a sampled set of RRs and age-specific population sizes (non-MSM, HIV-positive MSM and HIV-negative MSM), a calibration outputs model defined the relationship between the anal cancer incidence rates in the different populations. The model then fitted the incidence rate in the non-MSM populations so that the weighted incidence rates matched the sampled aggregate incidence rates. This process was repeated for 5000 iterations in order to represent the correlated uncertainty around the age-specific incidence rates in HIV-negative and positive MSMs. The resulting estimates are presented in Table 32.
| Mean | 95% CI | ||
|---|---|---|---|
| Lower | Upper | ||
| Observed (estimated) | |||
| Aggregate | 37.4 | 22.7 | 57.6 |
| HIV positive | 9.1 | 4.0 | 23.0 |
| HIV negative | 28.3 | 15.9 | 48.8 |
| Predicted | |||
| Aggregate | 40.8 | 27.0 | 54.8 |
| HIV positive | 11.3 | 7.6 | 15.5 |
| HIV negative | 29.5 | 18.8 | 40.9 |
The model was also calibrated against the observed estimates of the prevalence of HIV-positive MSMs, as provided by the HPA and described in the HIV modelling section.
The calibration model
A separate model was developed to estimate model outputs for the year 2003 in the format of the calibration outputs described in the previous section. The calibration model commences in the year 1990, and runs separate analyses for individuals at the mid-point age of the six relevant age groups (15–25, 26–35, 36–45, 46–55, 56–65 and 66–75) from either the year in which they became 15 years old (i.e. 1998 for individuals aged 20 in the year 2003) or from 1990 at the age they were at the start of 1990 (e.g. 16 years for 30-year-olds in 2003).
Age groups aged over 15 years in 1990 were distributed between the ‘HIV negative, no anal lesions’ and the ‘HIV negative, undiagnosed HG-AIN’ states in the year 1990. The probability of having HG-AIN was informed by a simple submodel that estimated the progression of HIV-negative MSM from normal to HG-AIN (either directly or via LG-AIN) from an assumed incident MSM age of 26 years (using the transition probabilities for HIV-negative MSM described in Chapter 1, Incidence rate by age and gender).
Thus, the calibration model makes the following assumptions:
-
No MSMs who were HIV positive prior to 1990 remain alive in 2003.
-
Transition probabilities have remained constant between 1990 and 2003 (i.e. probabilities vary by age but not by calendar year)
It is recognised that neither of the above assumptions are likely to be true, although they bias the model in opposite directions. Assumption 1 decreases estimated cases of anal cancer, while the introduction of HAART in the mid-1990s is likely to have increased the incidence of anal cancer, so assuming that HAART influenced transition probabilities in the early 1990s will compensate the impact of assumption 1 to some degree.
For each of 2000 sets of input parameter values, the calibration model collected the age-specific incident rates of anal cancer in HIV-negative, and HIV-positive MSMs in 2003.
To account for slight bias due to the use of the mid-point age of each age group, the mean MSM rate was estimated as the mean proportion of each age group (in 2003) that were MSM during the preceding 13 years. In each age group, the mean MSM rate is compared with the proportion of MSM in the mid-point age for the age group, as those were the ages on which the calibration model is based. The ratio of the mean MSM rate to the MSM rate in the mid-point age for each age group was used to adjust the calibration estimates by multiplying the respective model outputs by this ratio.
Calibration data analysis
A two-stage calibration process was adopted. The first stage applied a threshold in which the predicted aggregate incidence rate of anal cancer was compared with the 95% CI for the aggregate incidence rate as estimated using the Cancer Registry data (described in Chapter 5, Anal cancer screening model structure).
The corresponding predicted estimates of the aggregate incidence of anal cancer in MSM, and in MSM by HIV status are presented in Table 32. The calibration threshold analysis found that 1719 of the 2000 input parameter sets estimated aggregate incidence rates within the 95% CIs. The comparison of the observed and predicted incidence rates (and 95% CIs) shows a close relationship.
The second stage of the calibration analysis involved estimating the sum of differences between the 1719 predicted output parameter values and the anal cancer incidence rate 95% CIs, by age group and HIV status. Table 33 presents the observed and predicted ranges for each incidence category. The results show that extremely small numbers are expected in the early age groups, such that the differences between the observed and predicted incidence in these groups had minimal impact on the cost-effectiveness results. The overlap between the predicted and observed incidence in the other age categories is encouraging.
| Age range (years) | ||||||
|---|---|---|---|---|---|---|
| 15–24 | 25–34 | 35–44 | 45–54 | 55–64 | 65–74 | |
| HIV positive | ||||||
| Observed | ||||||
| Lower | 0.018 | 0.087 | 3.100 | 3.667 | 1.869 | 0.382 |
| Upper | 0.495 | 1.783 | 9.495 | 10.265 | 5.591 | 1.162 |
| Predicted | ||||||
| Lower | 0.002 | 0.643 | 1.431 | 4.142 | 0.299 | 0.006 |
| Upper | 0.015 | 2.083 | 4.364 | 15.997 | 1.773 | 0.061 |
| HIV negative | ||||||
| Observed | ||||||
| Lower | 0.096 | 0.174 | 2.394 | 6.943 | 7.430 | 0.922 |
| Upper | 2.210 | 3.067 | 6.036 | 13.996 | 14.223 | 1.865 |
| Predicted | ||||||
| Lower | 0.069 | 2.344 | 2.051 | 6.587 | 5.248 | 0.550 |
| Upper | 0.438 | 7.645 | 7.010 | 22.330 | 17.108 | 1.785 |
The following stages informed the assignment of sampling probabilities to each of the eligible input parameters:
-
Sum of differences between each age- and HIV status-specific incidence estimate and the bounds of the respective observed 95% CIs were calculated for each iteration.
-
Proportions of the sum of differences contributed by each input parameter set were estimated.
-
Reciprocals of the proportions of the sum of differences contributed by each iteration were estimated (no iterations had a sum of differences of zero).
-
Reciprocals were divided by the sum of the reciprocals to estimate the probability that each of the 1719 parameter sets was the most relevant set.
Anal cancer screening model analysis
Following the calibration process, and the identification and ranking of eligible input parameter sets, the model was analysed to estimate the costs and QALYs associated with 10 alternative screening programmes as well as a no screening option. The 10 programmes included five programmes for HIV-positive MSM only, and five programmes for all MSM. Screening intervals of 1, 2, 3, 4 and 5 years were analysed for both eligible populations.
The starting states for each age group (i.e. the distribution of each population across model’s states in 2003) were informed by the calibration model that recorded the finishing states of each population for each input parameter set at the end of the calibration period (i.e. the year 2003). The model analysed each age group to a maximum age of 100 years and then combined the discounted (at 3.5% per annum) costs and effects for each age group on the basis of the respective proportions of the total person-years represented within the full model time horizon.
The reference case analysis involved the random sampling of 2000 sets of input parameter sets based on the ranking probabilities estimated as part of the calibration process. Additional analyses were undertaken in which the following assumptions were tested:
-
no utility effects associated with false-positives or treatment for HG-AIN
-
increasing the regression rates for individuals with LG-AIN lesions returning to having no AIN lesion.
Chapter 7 Screening for anal cancer in MSM: cost-effectiveness results
The section presents the results of the cost-effectiveness model built to analyse the cost-effectiveness of 10 alternative screening programmes for anal cancer compared with a no-screening option. The following discussion section provides a discussion and interpretation of the results in the context of decisions regarding the implementation of an anal cancer screening programme by the NHS.
Reference case cost-effectiveness results
The mean results from the reference case analysis of the model are presented in Table 34, which show that screening is actually more costly and less effective than providing no screening, i.e. no screening dominates screening for either HIV-positive MSM alone or all MSM. The reduced number of QALYs gained is due to the utility decrements associated with false-positive screening results, and the treatment effects of HG-AIN.
| Model | Costs (£) | QALYs: aggregate | ICER compared with no screening | |||||
|---|---|---|---|---|---|---|---|---|
| Aggregate | Screening | False-positives | Treatment | |||||
| AIN and monitoring | Cancer | HIV | ||||||
| No screening | ||||||||
| 32,250 | 0.00 | 0.00 | 2554 | 69.04 | 29,627 | 18.0197 | ||
| HIV positive | ||||||||
| Annual | 32,800 | 3.71 | 3.02 | 3021 | 66.13 | 29,707 | 18.0136 | Dominated |
| 2 yearly | 32,830 | 3.93 | 3.22 | 3046 | 65.17 | 29,711 | 18.0133 | |
| 3 yearly | 32,899 | 4.50 | 4.12 | 3106 | 62.57 | 29,722 | 18.0125 | |
| 4 yearly | 32,999 | 5.53 | 6.51 | 3192 | 60.56 | 29,734 | 18.0112 | |
| 5 yearly | 33,094 | 7.28 | 12.35 | 3280 | 47.51 | 29,747 | 18.0099 | |
| All MSM | ||||||||
| Annual | 37,201 | 71.13 | 36.93 | 5057 | 85.07 | 31,951 | 18.0041 | Dominated |
| 2 yearly | 37,425 | 76.46 | 38.96 | 5190 | 85.61 | 32,034 | 18.0034 | |
| 3 yearly | 38,148 | 92.35 | 48.25 | 5540 | 85.57 | 32,382 | 18.0014 | |
| 4 yearly | 39,841 | 112.28 | 77.11 | 6238 | 86.78 | 33,327 | 17.9992 | |
| 5 yearly | 41,764 | 168.82 | 144.85 | 6972 | 70.99 | 34,408 | 17.9980 | |
Calculations were undertaken to inform the cost-effectiveness acceptability frontier, which describes the probability that the screening option with the highest expected net benefits is the most cost-effective option. These estimates show that no screening has the highest expected net benefits and is 100% certain (given the reference case model, inputs and assumptions) to be the most cost-effective option, to a value of a QALY of £50,000.
Sensitivity analyses
In addition to the probabilistic sensitivity analysis reported above, additional sensitivity analyses were undertaken around the most uncertain input parameters. The estimates of anal cancer incidence used to calibrate the model were not excessively uncertain, and conservative assumptions had been implemented, for example a low completeness rate was assumed for the cancer registry data, and high estimates of the RRs for HIV-positive and HIV-negative MSM developing anal cancer were specified. Thus, anal cancer incidence in high-risk groups was not a key parameter for investigation.
Additional sensitivity analyses tested the impact of assuming that the effects of investigation following false-positive screen results and treatment for HG-AIN incurred no utility decrements. The mean results of this analysis are presented in Table 35, which show that the screening programmes for diagnosed HIV-positive individuals are now shown to be more effective than no screening, although the minimum incremental cost per QALY gained (ICQ) is almost £66,000. The ICQs for screening for all MSM drop to £50,000, but remain well above accepted cost-effectiveness thresholds. The related cost-effectiveness acceptability frontier is presented in Figure 7. This shows that no screening retains a very high probability of being the most cost-effective option, with the highest mean net benefits to a QALY value of £50,000.
| Screening option | Costs (£) | QALYs: aggregate | ICER compared to no screening (£) | |||||
|---|---|---|---|---|---|---|---|---|
| Aggregate | Screening | False-positives | Treatment | |||||
| AIN and monitoring | Cancer | HIV | ||||||
| No screening | ||||||||
| 32,250 | 0.00 | 0.00 | 2554 | 69.04 | 29,627 | 18.1294 | ||
| HIV positive | ||||||||
| Annual | 32,799 | 1.86 | 3.02 | 3021 | 66.13 | 29,707 | 18.1364 | 77,984 |
| 2 yearly | 32,828 | 1.97 | 3.22 | 3046 | 65.17 | 29,711 | 18.1368 | 77,502 |
| 3 yearly | 32,896 | 2.25 | 4.12 | 3106 | 62.57 | 29,722 | 18.1378 | 76,946 |
| 4 yearly | 32,997 | 2.77 | 6.51 | 3192 | 60.56 | 29,734 | 18.1389 | 78,421 |
| 5 yearly | 33,091 | 3.64 | 12.35 | 3280 | 47.51 | 29,747 | 18.1401 | 78,628 |
| All MSM | ||||||||
| Annual | 37,165 | 35.57 | 36.93 | 5057 | 85.07 | 31,951 | 18.2259 | 50,907 |
| 2 yearly | 37,387 | 38.23 | 38.96 | 5190 | 85.61 | 32,034 | 18.2316 | 50,280 |
| 3 yearly | 38,102 | 46.18 | 48.25 | 5540 | 85.57 | 32,382 | 18.2457 | 50,299 |
| 4 yearly | 39,784 | 56.14 | 77.11 | 6238 | 86.78 | 33,327 | 18.2754 | 51,585 |
| 5 yearly | 41,680 | 84.41 | 144.85 | 6972 | 70.99 | 34,408 | 18.3080 | 52,787 |
FIGURE 7.
Cost-effectiveness acceptability frontier assuming no utility decrement from false-positive screen results or treatment for high-grade anal intraepithelial neoplasia. NB, net benefit.
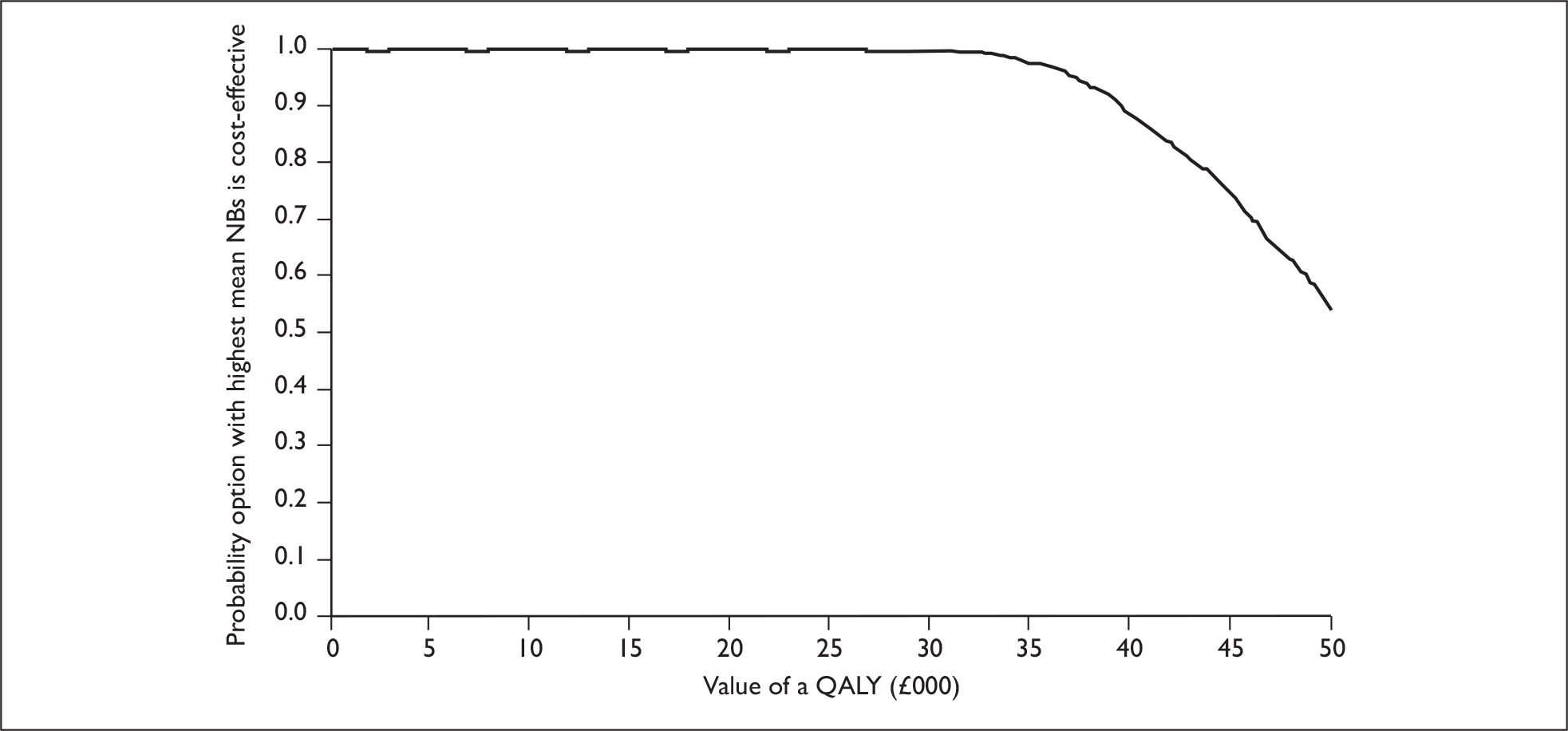
Another uncertain parameter was the rate of regression of LG-AIN, which had been informed by the two main cohort studies of MSM and anal cancer. 57,61,70,89 However, Goldie et al. 81 had estimated higher regression rates, which may impact on cost-effectiveness by increasing the likelihood of progression from HG-AIN to anal cancer. The calibration model was re-run incorporating revised annual probabilities of regression from LG-AIN to no AIN (30% in HIV-negative MSM, 15% in HIV-positive MSM with CD4 count > 500, 10% with CD4 count 200–500, and 5% with CD4 count < 200), which were fitted to observed anal cancer incidence rates by altering the transition probability between HG-AIN and anal cancer. Recalibrating the model required increasing the HG-AIN to anal cancer rates by 22%.
Table 36 presents the mean results from the combining increased AIN regression rates with no utility decrements from screening, which show that the minimum ICQ from implementing any of the screening programmes for MSM is reduced to £44,656. Screening all MSM is shown to be more effective than screening HIV-positive MSM due to gains from the early detection of undiagnosed HIV-positive MSM as a result of screening for anal cancer.
| Screening option | Costs (£) | QALYs: aggregate | ICER compared to no screening (£) | |||||
|---|---|---|---|---|---|---|---|---|
| Aggregate | Screening | False-positives | Treatment | |||||
| AIN and monitoring | Cancer | HIV | ||||||
| No screening | ||||||||
| 31,339 | 0.00 | 0.00 | 2079 | 69.98 | 29,190 | 18.1174 | ||
| HIV positive | ||||||||
| Annual | 31,890 | 2.21 | 8.70 | 2528 | 67.21 | 29,284 | 18.1257 | 66,407 |
| 2 yearly | 31,926 | 2.38 | 9.70 | 2557 | 66.22 | 29,290 | 18.1263 | 66,173 |
| 3 yearly | 32,000 | 2.81 | 12.60 | 2617 | 63.57 | 29,303 | 18.1274 | 65,923 |
| 4 yearly | 32,108 | 3.61 | 19.56 | 2705 | 61.53 | 29,318 | 18.1288 | 67,457 |
| 5 yearly | 32,221 | 5.19 | 37.71 | 2796 | 48.15 | 29,334 | 18.1303 | 68,675 |
| All MSM | ||||||||
| Annual | 35,079 | 45.97 | 79.35 | 3969 | 85.15 | 30,899 | 18.1917 | 50,328 |
| 2 yearly | 35,336 | 51.34 | 87.34 | 4103 | 85.83 | 31,008 | 18.2069 | 44,656 |
| 3 yearly | 35,957 | 64.56 | 110.57 | 4394 | 85.90 | 31,302 | 18.2205 | 44,810 |
| 4 yearly | 37,335 | 86.70 | 174.65 | 4937 | 87.34 | 32,050 | 18.2472 | 46,182 |
| 5 yearly | 39,143 | 149.23 | 334.40 | 5557 | 71.45 | 33,032 | 18.2799 | 48,040 |
The cost-effectiveness acceptability frontier (Figure 8) shows that no screening has the highest mean net benefits to a value of a QALY of £45,000 with the probability of no screening being the most cost-effective option remaining above 50%. At higher QALY values, screening programmes for all MSM have higher expected net benefits, although no screening retains a probability of cost-effectiveness of over 50% to a QALY value of £50,000.
FIGURE 8.
Cost-effectiveness acceptability frontier assuming increased anal intraepithelial neoplasia (AIN) regression and no utility decrement from false-positive screen results or treatment for high-grade AIN. NB, net benefit.
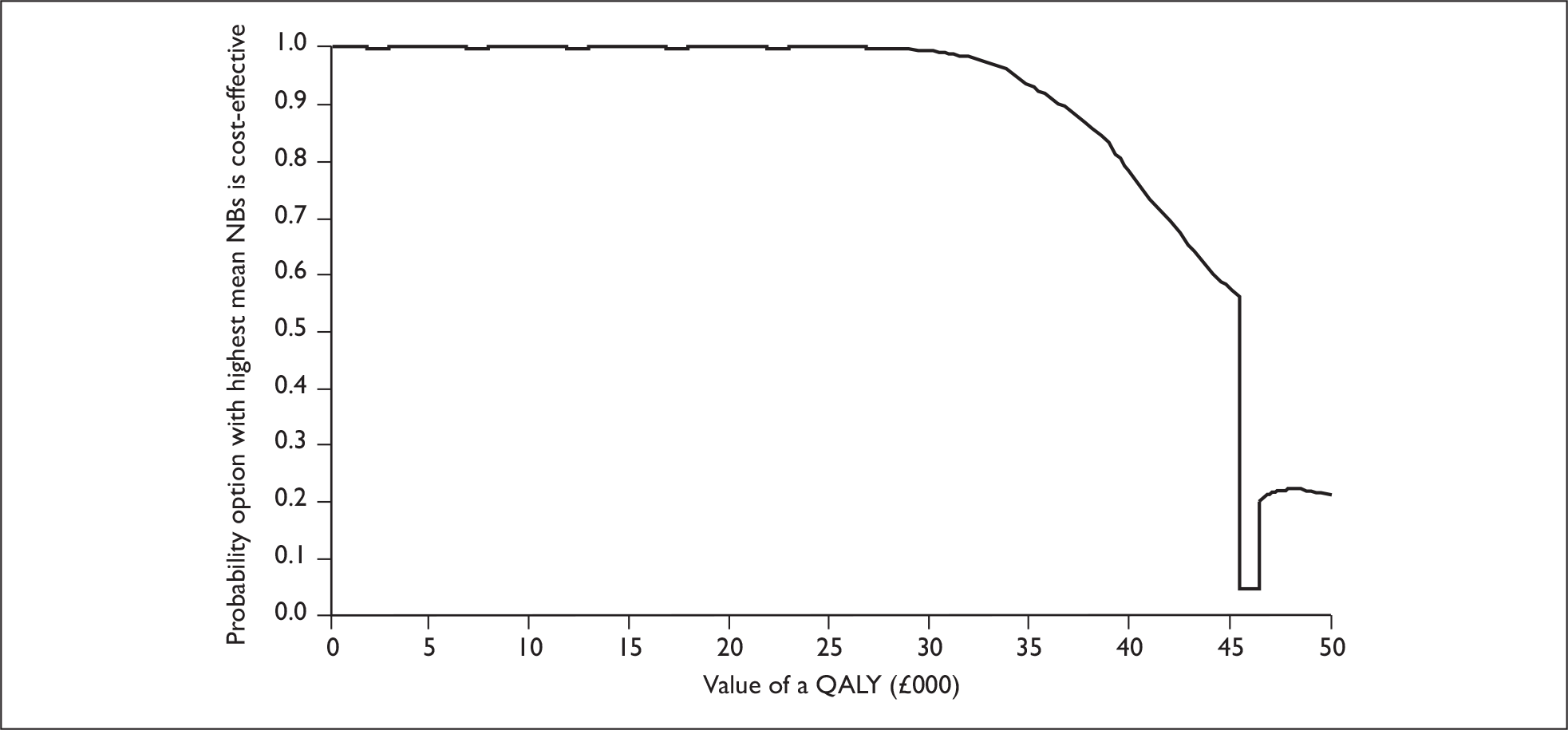
Chapter 8 HIV-positive women: anal cancer screening analysis
The anal cancer screening model developed to evaluate screening options for MSM was adapted to evaluate screening programmes for high-risk women. Initial analyses focused on HIV-positive women, as cross-sectional data has shown that 26% of 251 HIV-positive women had AIN, compared with 8% of the high-risk HIV-negative women. 15 If screening is shown to be cost-effective in HIV-positive women then screening of other high-risk groups will then be explored.
Model population and calibration
A key aspect of the female HIV-positive screening model was that incidence of AIN in HIV-negative women is negligible, and assumed to be zero. As in the MSM model, the women’s model includes HIV-negative individuals in order to describe the incidence of HIV-positive women over time, but all incident HIV-positive women enter the ‘CD4 count > 500’ state without AIN.
Fewer data were available from the literature to populate parameters for the HIV-positive women screening model, for example no longitudinal data describing AIN progression in HIV-positive women were identified. Indeed, the only female-specific data included estimates of age-specific HIV incidence, and the data required to estimate the calibration output parameters (age-specific anal cancer incidence). All other parameters were informed by data collected to populate the MSM screening model, although a separate calibration process was undertaken for the female screening model.
Unlike men, incidence rates of HIV infection in women have varied significantly over time, with low rates in the early 1990s (around 500 per year), rising to a peak in 2003 (3251) and then falling back to 2283 in 2007. 108 Thus, separate HIV incidence rates were defined for the years 1992–2000 and 2002–7 for the calibration model, while the latter incidence rates were used in the main analysis model.
The model was calibrated to age-specific numbers of anal cancers occurring in HIV-positive women (the calibration outputs), which were estimated using the following data:
-
age-specific estimates of anal cancer incidence in women in 2005 (uprated to allow for under registration)2
-
relative risk of anal cancer in HIV-positive women (6.8, 95% CI 2.7 to 14)13
-
age-related RRs of anal cancer in HIV-positive women (e.g. RR of anal cancer in HIV women aged under 30 years, 30–39 years, etc.), informed by a study of HIV-associated anogenital cancers by age at onset of AIDS13
-
prevalence of diagnosed HIV women in 2005 (converted to age-specific numbers assuming a similar proportional split to HIV-positive males)109
-
prevalence of undiagnosed HIV women, based on observation that 33.7% of all HIV-positive individuals in the UK were undiagnosed in 2004 (assumed to have the same age distribution as diagnosed HIV women). 110
Age-specific anal cancer incidence in HIV-positive women in 2005 was estimated using an adjusted version of the calibration outputs model described for MSM in Chapter 6. The model estimated the incidence rates in the HIV-positive female populations by sampling a set of parameter values describing the aggregate age-specific incidence of anal cancer in women, the aggregate RR of anal cancer in HIV-positive women, age-related RRs of anal cancer, and the size of the HIV-positive female population. For a sampled set of values, the model defined the relationship between the incidence rates for the HIV-positive and HIV-negative populations using the sampled RRs. The model then fitted the incidence rate in the HIV-negative population so that the weighted age-specific anal cancer incidence rates (based on the sampled sizes of the respective populations) matched the sampled aggregate incidence rate. This process was repeated for 2000 iterations in order to represent the correlated uncertainty around the age-specific incidence rates in HIV-negative and HIV-positive women. The resulting estimates are presented in Table 37.
| Mean | 95% CI | |
|---|---|---|
| Lower | Upper | |
| Observed (estimated) | ||
| 1.1 | 0.3 | 3.9 |
| Predicted (applying calibrated disease progression parameters from the MSM analysis) | ||
| 2.03 | 1.16 | 3.28 |
| Predicted (applying calibrated disease progression parameters from the MSM analysis, but decreasing AIN incidence rates by 67%) | ||
| 1.10 | 0.61 | 1.77 |
Table 37 shows that the calibration results obtained from applying the same AIN incidence and progression parameter values, as fitted for the MSM model, overestimated the rate of anal cancer in HIV-positive women. To the clinical authors’ knowledge, there is no known biological reason that AIN would progress differently in HIV-positive men and HIV-positive women, but one might expect AIN incidence to be lower in HIV-positive women than in HIV-positive MSM. Therefore, the model was recalibrated, keeping the same AIN progression parameters as estimated for the MSM model, but lowering AIN incidence until a good fit was achieved with the estimated anal cancer incidence rates (in HIV-positive women). This was achieved when HIV-positive MSM AIN incidence rates were reduced by 67%, and all 2000 iterations estimated rates within the 95% CI for the observed rates. Estimated AIN incidence rates across the eligible populations are compared in Table 38.
| AIN incidence | Mean | 95% CI | ||
|---|---|---|---|---|
| Lower | Upper | |||
| HIV-negative MSM | ||||
| Low grade | 0.074 | 0.048 | 0.106 | |
| High grade | 0.019 | 0.011 | 0.031 | |
| HIV-positive MSM | ||||
| > 500 CD4 count | Low grade | 0.165 | 0.051 | 0.314 |
| High grade | 0.028 | 0.009 | 0.057 | |
| 200–500 CD4 count | Low grade | 0.246 | 0.151 | 0.346 |
| High grade | 0.043 | 0.025 | 0.063 | |
| < 200 CD4 count | Low grade | 0.681 | 0.401 | 0.885 |
| High grade | 0.118 | 0.065 | 0.177 | |
| HIV-positive women | ||||
| > 500 CD4 count | Low grade | 0.054 | 0.017 | 0.104 |
| High grade | 0.009 | 0.003 | 0.019 | |
| 200–500 CD4 count | Low grade | 0.081 | 0.050 | 0.114 |
| High grade | 0.014 | 0.008 | 0.021 | |
| < 200 CD4 count | Low grade | 0.226 | 0.133 | 0.292 |
| High grade | 0.039 | 0.021 | 0.058 | |
The second stage of the calibration analysis involved estimating the sum of differences between the 2000 predicted output parameter values and the anal cancer incidence rate (95% CIs) by age group. Table 39 presents the observed and predicted ranges for each incidence category. The results show that the ranges for the observed and expected data are an extremely good fit, which is encouraging.
| Age range (years) | ||||||
|---|---|---|---|---|---|---|
| 15–24 | 25–34 | 35–44 | 45–54 | 55–64 | 65–74 | |
| Observed | ||||||
| Lower | 0 | 0.046 | 0.146 | 0.154 | 0.058 | 0.009 |
| Upper | 0.019 | 0.446 | 0.834 | 0.832 | 0.303 | 0.045 |
| Predicted | ||||||
| Lower | 0.000 | 0.018 | 0.163 | 0.249 | 0.061 | 0.009 |
| Upper | 0.003 | 0.120 | 0.896 | 1.454 | 0.340 | 0.058 |
Anal cancer screening model analysis
The model was analysed to estimate the costs and QALYs associated with programmes for HIV-positive women with screening intervals of 1, 2, 3, 4 and 5 years. The starting states for each age group (i.e. the distribution of each population across model’s states in 2003) were informed by the calibration model that recorded the finishing states of each population for each input parameter set at the end of the calibration period (i.e. the year 2003). The model analysed each age group to a maximum age of 100 years, and then combined the discounted costs and effects (at 3.5% per annum) for each age group on the basis of the respective proportions of the total person-years represented within the full model time horizon.
The reference case analysis involved the random sampling of 2000 sets of input parameter sets, based on the ranking probabilities estimated as part of the calibration process. Additional analyses were undertaken in which the following assumptions were tested:
-
no utility effects associated with false-positives or treatment for HG-AIN
-
increasing the regression rates for individuals with LG-AIN lesions and returning to having no AIN lesion.
Results
The mean results from the reference case analysis of the model are presented in Table 40. As for MSM, screening HIV-positive women is more costly and less effective than providing no screening, i.e. no screening dominates screening. The reduced number of QALYs gained is due to the utility decrements associated with false-positive screening results, and the treatment effects of HG-AIN.
| Model | Costs (£) | QALYs: aggregate | ICER compared with no screening | |||||
|---|---|---|---|---|---|---|---|---|
| Aggregate | Screening | False-positives | Treatment | |||||
| AIN, plus monitoring | Cancer | HIV | ||||||
| No screening | ||||||||
| 234 | 0.00 | 0.00 | 5 | 0.09 | 228 | 20.49186 | ||
| HIV positive | ||||||||
| 5 yearly | 238 | 0.05 | 0.21 | 8 | 0.08 | 229 | 20.49181 | Dominated |
| 4 yearly | 238 | 0.06 | 0.24 | 9 | 0.08 | 229 | 20.49181 | Dominated |
| 3 yearly | 239 | 0.07 | 0.31 | 9 | 0.08 | 229 | 20.49180 | Dominated |
| 2 yearly | 240 | 0.09 | 0.49 | 10 | 0.07 | 229 | 20.49179 | Dominated |
| Annual | 241 | 0.15 | 0.95 | 10 | 0.06 | 229 | 20.49178 | Dominated |
Calculations were undertaken to inform the cost-effectiveness acceptability frontier, which describes the probability that the screening option with the highest expected net benefits is the most cost-effective option. These estimates show that no screening has the highest expected net benefits and is 100% certain (given the reference case model, inputs and assumptions) to be the most cost-effective option, to a value of a QALY of £50,000.
Sensitivity analyses
Additional sensitivity analyses tested the impact of assuming that the effects of investigation following false-positive screen results and treatment for HG-AIN incurred no utility decrements. The mean results of this analysis are presented in Table 41, which show that the screening programmes for diagnosed HIV-positive women are now shown to be more effective than no screening, although the minimum ICQ is £88,247. Data to inform the related cost-effectiveness acceptability frontier shows that no screening retains a 100% probability of being the most cost-effective option, with the highest expected net benefits to a QALY value of £50,000. Increasing regression rates from LG-AIN had little further effect on the ICQs for screening HIV-positive women.
| Screening option | Costs (£) | QALYs: aggregate | ICER compared with no screening (£) | |||||
|---|---|---|---|---|---|---|---|---|
| Aggregate | Screening | False-positives | Treatment | |||||
| AIN, plus monitoring | Cancer | HIV | ||||||
| No screening | ||||||||
| 234 | 0.00 | 0.00 | 5 | 0.09 | 228 | 20.49200 | ||
| HIV positive | ||||||||
| 5 yearly | 238 | 0.02 | 0.21 | 8 | 0.08 | 229 | 20.49205 | 88,247 |
| 4 yearly | 238 | 0.03 | 0.24 | 9 | 0.08 | 229 | 20.49205 | 88,403 |
| 3 yearly | 239 | 0.03 | 0.31 | 9 | 0.08 | 229 | 20.49206 | 89,837 |
| 2 yearly | 240 | 0.05 | 0.49 | 10 | 0.07 | 229 | 20.49207 | 94,372 |
| Annual | 241 | 0.08 | 0.95 | 10 | 0.06 | 229 | 20.49207 | 102,878 |
Chapter 9 Discussion
The discussion of the findings of this report on the cost-effectiveness of screening anal cancer in high-risk groups is presented in two parts. The first section concerns the findings of the systematic review of all aspects of screening for anal cancer. The second section describes the outputs, interpretations, and limitations of the presented model-based cost-effectiveness analysis of screening for anal cancer.
The systematic review
Limited information is available from published research about the potential impact of anal cancer screening of high-risk groups. The limitations are from the study designs used, as well as the quality of reporting of the studies.
The main role of the screening studies27,28,30,31,34,35 included in the report is in assessing whether the screening test performance is adequate to justify the establishment of an anal cancer screening programme. Not all the studies gave completeness of the information.
In their systematic review of anal Pap smear screening for HIV-infected patients, Chiao et al. 36 reported that the data published highlight limitations to current anal Pap smear screening-related research, with no randomised or cohort studies existing to determine if there are improved survival or outcomes for those who have been screened.
The NSC1 has produced a modified version of the World Health Organization (WHO) screening criteria to take into account the more rigorous standards of evidence, as well as to increase the weight given to the potential negative effects of screening. The document states that all the criteria should be satisfied before a screening programme is introduced.
The NSC1 criteria (where applicable) are outlined below, and are commented on with reference to anal cancer screening.
The condition
-
The condition should be an important health problem.
As mentioned in the background section, anal cancer in the general population is a rare disease. However, in high-risk groups it is more prevalent, but identifying and accessing these high-risk groups could be problematic.
-
The epidemiology and natural history of the condition, including development from latent to declared diseases, should be adequately understood and there should be a detectable risk factor, or disease marker and a latent period or early symptomatic stage.
The natural history of anal cancer is not well understood.
-
All of the cost-effective primary prevention interventions should have been implemented as far as practicable.
If primary prevention is taken as identification of risk factors then some risk factors are known. HIV and receptive anal intercourse are two of the risk factors identified with anal cancer. It is possible that some prevention of anal cancer could be achieved by the modification of risk factors, but high-risk groups would need to be notified of their risk of anal cancer.
The test
-
There should be a simple, safe, precise and validated screening test.
All types of screening included in this report appear to meet the above criterion.
-
The test should be acceptable to the population.
Anal cancer screening may be undertaken by using anal cytology or anal pap smears. Self-collected anal cytology specimens has been evaluated in two studies33,34 and self-collected specimens seem to be comparable with clinician collect specimens. However, neither study reported on how acceptable the population thought the test was.
The treatment
-
There should be an effective treatment or intervention for patients identified through early detection, with evidence of early treatment leading to better outcomes than later treatment.
The treatment and outlook for anal cancer will depend, to a large extent, on its stage. Treatment options such as RT and combined RT plus chemotherapy are available.
The screening programme
-
There must be evidence from high-quality randomised controlled trials that the screening programme is cost-effective in reducing mortality or morbidity.
No such RCTs were identified.
-
There should be evidence that the complete screening programme (test, diagnostic procedures, treatment/intervention) is clinically, socially and ethically acceptable to health professionals and the public.
No evidence has been identified by this review that answers this question.
-
The benefit from the screening programme should outweigh the physical and psychological harm (caused by the test, diagnostic procedures and treatment).
The screening process does not appear to present any physical harm; however, any psychological effects of anal cytology screening or pap smears have not been evaluated in the studies included in this review.
-
The opportunity cost of the screening programme (including testing, diagnosis, treatment, administration, training and quality assurance) should be economically balanced in relation to expenditure on medical care as a whole (i.e. value for money).
See following section.
Other criteria from the NSC1 are not discussed further as they do not have a direct relevance to this review.
The cost-effectiveness model
Parameter uncertainty
The reference case cost-effectiveness model found that screening for anal cancer is very unlikely to be cost-effective. A key determinant of this finding was the low observed incidence of anal cancer in the UK population. Estimated anal cancer incidence in the MSM population (by HIV status) was not conservative, incorporating upper ranges of the RRs of anal cancer in HIV-negative and HIV-positive MSM compared with the general population of 45 and 272, respectively. The analysis also used a low estimate of completeness in the observation of cases of anal cancer by the Cancer registries (assuming 30% of cases were not recorded). The assumed low completeness rate may occur due to the higher likelihood of comorbidities in HIV-positive patients, although based on the available evidence, the analysis allowed for high estimates of anal cancer incidence.
The dominance of the no screening option for HIV-positive women was driven by the estimated RR of HIV-positive women developing anal cancer compared with the general population (mean 6.8, 95% CI 2.7 to 14). This is compared to an estimated RR of 176 for HIV-positive MSM.
Confidence in the results of the anal cancer screening model would be further increased, however, with an audit of the accuracy of the cancer registries’ identification of cases of anal cancer. A linked activity that would also help justify the observed results would be an audit of the proportion of cancer cases that occurred in HIV-positive men and women, and/or MSM.
Sensitivity analyses showed that the reference case results were most sensitive to alternative assumptions around the utility effects of false-positive results and treatment of HG-AIN. It is unlikely that a false-positive screening result, and in particular, treatment of HG-AIN, have no utility effects, but direct estimation of these effects would further increase the confidence in the results of the cost-effectiveness model.
Alternative estimates of the probability of regression from LG-AIN altered the reference case results, although not as significantly. The reference case regression rates were informed by published data from two cohort studies of AIN incidence and progression in MSM. These data were not presented in the best format to inform regression rates, and so assumptions were required to estimate the regression parameters. A next step might be to request access to the primary data from these studies to enable analyses more appropriate to populating the anal cancer screening model reported in this study.
A value of information (VoI) analysis could have been undertaken, but this study provides an example of the possible limitations of VoI analyses. It is clear that the reference case model would attach a zero value to the collection of further information (as all iterations to a QALY value of £50,000 showed no screening to be cost-effective), whereas the sensitivity analyses around utility decrements and AIN regression would only show a positive VoI at high values of a QALY (i.e. over £40,000). Thus, a VoI analysis was not conducted.
Structural uncertainty
In the HIV-positive screening programmes, costs associated with treating HIV infection are increased slightly, as would be expected due to the small increase in survival of HIV-positive individuals due to the detection of some additional cases of anal cancer. In the screening programmes for all MSM, HIV treatment costs increase more substantially. This is a consequence of the assumptions in the model around the detection of HIV infection as a result of detecting AIN lesions. The model assumed that individuals with undiagnosed HIV infection, in whom an AIN lesion was detected, would receive a diagnostic test for HIV infection and subsequently receive treatment for HIV. Treatment for HIV infection also leads to improved outcomes, which is a potential by-product of the anal cancer screening programme.
The issue of screening for anal cancer leading to the detection of additional HIV-positive MSM is a moot point, as undiagnosed HIV infected individuals may be more or less likely to attend a screening programme. It is unknown whether undiagnosed HIV-positive individuals are undiagnosed because they avoid contact with the health service and, therefore, would be unlikely to attend an anal cancer screening programme, or whether they are hesitant to directly ask for an HIV test but would view the opportunity to be screened for anal cancer as an indirect (and possibly preferred) approach to ascertaining their HIV status. The model assumes undiagnosed HIV-positive MSM are equally likely to be screened as HIV-negative MSM, although all of the screening attendance parameters are subject to significant uncertainty.
To identify and screen individuals at high risk of anal cancer would be a difficult task. A specific mode of operation for a screening programme was not defined due to the unique issues around identifying and inviting different categories of MSM to a screening programme. Based on published qualitative data, it was assumed that screening would be offered to 40–60% of HIV-negative or undiagnosed HIV-positive MSM, and 80–90% of diagnosed HIV-positive MSM. Quantitative data informed an estimate that 5–20% of all MSMs offered screening will refuse. If further research on the natural history of anal cancer identifies screening as potentially cost-effective then pilot screening studies could usefully inform screening attendance and acceptance parameters.
The anal cancer screening model was complicated, jointly modelling HIV and AIN progression. Due to previous experience in the development of complex screening models with limited data, every effort was made to apply the model as a cohort-based model rather than as an individual sampling model (ISM). To apply the probabilistic calibration methods described in this report, ISMs require model running times several orders of magnitude higher than cohort models.
The main limiting assumptions of the applied cohort model included the use of non-time-dependent transition probabilities. This meant that the probability of individuals with, for example, HG-AIN, progressing to anal cancer was not described as a function of the time with HG-AIN. However, the model did incorporate a proxy for time-dependent progression by assuming that transition probability increased with age.
The model did not represent the impact of repeat episodes; for example, it did not differentiate between individuals with no evidence of AIN who had previously regressed from LG-AIN and those who had never had AIN. It also did not separately categorise patients by the numbers of recurrences experienced following treatment for HG-AIN.
Our decision was to include the costs associated with antiretroviral treatment for those individuals who are HIV positive. We did this specifically as screening would lead to the identification of HIV-positive MSMs, with associated treatment costs, and the lifetime costs of care for HIV-positive individuals will be determined, in part, by life expectancy. These are legitimate factors to consider in assessing the overall costs and benefits of introducing a screening programme in these high-risk groups.
Finally, the model adopted a simplistic representation of the postdiagnosis phase of the disease, primarily due to data inadequacies. The model represented only a single anal cancer state that did not allow for the explicit differentiation between stages of presentation for screen-detected and clinically presenting cases of anal cancer. The reference cases analysis incorporated a cost differentiation proxy by assuming greater lifetime treatment costs for clinically presenting cancers. The impact on survival was handled by assuming a high annual mortality rate in undiagnosed cancers, based on the lowest survival rates in relevant clinical trials.
The influence of the above model limitations is difficult to predict, although it is likely that they have only a minor impact on the cost-effectiveness results given the extent to which no screening has been shown to generate the highest net benefits.
Other possible limitations of the analysis include the lack of relevant data to inform anal cancer natural history transition probabilities from a UK MSM population. The San Francisco study states that ‘results should be interpreted with caution since they were performed in highly sexually active populations with a mean age of over 40 years’57 (p. 501), although no data on sexual activity levels were presented. The Seattle study showed that the study population had provided a mean of between four and five sexual partners in the past year; over 50% had experienced over 51 lifetime sexual partners; 15% (HIV negative) and 29% (HIV positive) had receptive anal intercourse more than three times per month. The Seattle study also presented data describing the RR of HG-AIN for men engaging in receptive anal intercourse more than three times per month. The RR of 2.2 (95% CI 0.9 to 5.5) indicates that this may well be a significant risk factor.
No data to inform the level of sexual activity in MSM living in the UK were identified and so the USA-based transition probabilities were not adjusted. If UK MSM are less sexually active, transition probabilities to HG-AIN may be reduced. This would mean that fewer MSM would develop HG-AIN (the screening programme would detect fewer positive cases) and that the calibrated rates of progression from HG-AIN to anal cancer would increase (detected cases would have been more likely to progress to cancer).
Chapter 10 Conclusions
From the review sections of this report, it is clear that many of the criteria for assessing the need for a population screening programme1 have not been met for anal cancer. There is limited knowledge about the epidemiology and natural history of the disease, along with a paucity of good-quality evidence concerning the effectiveness of screening for anal cancer. The absence of such data, combined with the possible reluctance of high-risk groups to attend an anal cancer screening programme, makes introduction of population-based screening for anal cancer difficult.
The reported cost-effectiveness analyses of screening for anal cancer emphasise this conclusion. The results show little likelihood that screening any of the identified high-risk groups will generate health improvements at reasonable cost. These results could be further confirmed by updating some key parameters at little additional cost. The most efficient way to proceed would be audit the accuracy of the cancer registries identification of cases of anal cancer, as well as audit the proportion of cancer cases that occur in HIV-positive men and women, and/or MSM. If these data show the screening model has underestimated the impact of anal cancer in any of the populations evaluated, a utility study of the effects of treatment for HG-AIN may be justified.
The findings of this review and model are consistent with the available evidence. However, the advice not to initiate a large-scale screening programme weighs heavily on those clinicians who are only too aware of the increasing risk of anal cancer in their HIV-positive patients. 111 Concerned clinicians will be proactive in undertaking awareness raising with their patients and undertaking anal examination when they present in clinic.
Chapter 11 Recommendations
-
Based on the available evidence, an organised screening programme for anal cancer is unlikely to be cost-effective in any of the proposed eligible populations.
-
The existing cancer registries should be audited to further inform estimates of the incidence of anal cancer in high-risk groups.
-
Consideration of (1) the feasibility, (2) effectiveness and (3) the cost-effectiveness of routine testing of high-risk populations attending NHS services for other purposes would be valuable.
-
Further research into the likely adherence and compliance of high-risk populations with (1) opportunistic testing and (2) preventative treatment strategies is also required.
-
Research to further clarify the risk contribution of HPV infection, and, by extension, the potential value of HPV vaccination in HIV-negative and HIV-positive high-risk populations would also be justified.
Acknowledgements
Contribution of the authors
Jon Karnon undertook the cost-effectiveness reviewing, constructed the model and prepared those sections of the draft report. Carolyn Czoski-Murray undertook sections of the reviewing and preparation of the draft report. Roy Jones was the main reviewer and prepared sections of the draft report. Kevin Smith assisted with the selection of papers relevant to a screening model, and provided expert advice on the appropriate assumptions of the screening model and preparation of the draft report. George Kinghorn assisted with the selection of papers and the impact on the genitourinary medicine services, and contributed to the draft report.
Ed Levine, although not listed as a co-author, was a clinician at the Christie Hospital, Manchester, and provided clinical advice on the population of interest to the review and advised on the selection of clinical trials of relevance to the screening model.
Marc Chattle, School of Health and Related Research, University of Sheffield, provided administrative and clerical support in the formatting of the draft report.
Disclaimers
The views expressed in this publication are those of the authors and not necessarily those of the HTA programme or the Department of Health.
References
- UK National Screening Committee (UK NSC) . Criteria for Appraising the Viability, Effectiveness and Appropriateness of a Screening Programme 2006.
- Office for National Statistics . Cancer Statistics Registrations 2005.
- Johnson LG, Madeleine MM, Newcomer LM, Schwartz SM, Daling JR. Anal cancer incidence and survival: the surveillance, epidemiology, and end results experience, 1973–2000. Cancer 2004;101:281-8.
- Karandikar SS, Borley A, Crosby T, Williams G, Reynolds S, Radcliffe AG. A five-year audit of anal cancer in Wales. Colorectal Dis 2006;8:266-72.
- Scholefield JH, Jones HT, Cuzick J, Northover JMA. Anal cancer and marital status. Br J Cancer 1990;62:286-8.
- Frisch M, Melbye M, Moller H. Trends in incidence of anal cancer in Denmark. BMJ 1993;306:419-22.
- Gatta G, Ciccolallo L, Kunkler I, Capocaccia R, Berrino F, Coleman MP, et al. Survival from rare cancer in adults: a population-based study. Lancet Oncol 2006;7:132-40.
- Chiao EY, Krown SE, Stier EA, Schrag D. A population-based analysis of temporal trends in the incidence of squamous anal canal cancer in relation to the HIV epidemic. J Acquir Immune Defic Syndr 2005;40:451-5.
- Brewster DH, Bhatti LA. Increasing incidence of squamous cell carcinoma of the anus in Scotland, 1975–2002. Br J Cancer 2006;95:87-90.
- Rabkin CS, Yellin F. Cancer incidence in a population with a high prevalence of infection with human immunodeficiency virus type 1. J Natl Cancer Inst 1994;86:1711-16.
- Diamond C, Taylor TH, Aboumrad T, Bringman D, Anton-Culver H. Increased incidence of squamous cell anal cancer among men with AIDS in the era of highly active antiretroviral therapy. Sex Transm Dis 2005;32:314-20.
- Grulich AE, Li Y, McDonald A, Correll PKL, Law MG, Kaldor JM. Rates of non-AIDS-defining cancers in people with HIV infection before and after AIDS diagnosis. Aids 2002;16:1155-61.
- Frisch M, Biggar RJ, Goedert JJ. Human papillomavirus-associated cancers in patients with human immunodeficiency virus infection and acquired immunodeficiency syndrome. J Natl Cancer Inst 2000;92:1500-10.
- Hemminki K, Dong C. Cancer in husbands of cervical cancer patients. Epidemiology 2000;11:347-9.
- De Sanjose S, Palefsky J. Cervical and anal HPV infections in HIV positive women and men. Virus Res 2002;89:201-11.
- Frisch M, Smith E, Grulich A, Johansen C. Cancer in a population-based cohort of men and women in registered homosexual partnerships. Am J Epidemiol 2003;157:966-72.
- Lacey HB, Wilson GE, Tilston P, Wilkins EG, Bailey AS, Corbitt G, et al. A study of anal intraepithelial neoplasia in HIV positive homosexual men. Sex Transm Infect 1999;75:172-7.
- Myers ER, McCrory DC, Nanda K, Bastian L, Matchar DB. Mathematical model for the natural history of human papillomavirus infection and cervical carcinogenesis. Am J Epidemiol 2000;151:1158-71.
- Palefsky JM, Holly EA, Ralston ML, Jay N. Prevalence and risk factors for human papillomavirus infection of the anal canal in human immunodeficiency virus (HIV)-positive and HIV-negative homosexual men. J Infect Dis 1998;177:361-7.
- Kreuter A, Brockmeyer NH, Hochdorfer B, Weissenborn SJ, Stucker M, Swoboda J, et al. Clinical spectrum and virologic characteristics of anal intraepithelial neoplasia in HIV infection. J Am Acad Dermatol 2005;52:603-8.
- Watson AJ, Smith BB, Whitehead MR, Sykes PH, Frizelle FA, Watson AJM, et al. Malignant progression of anal intra-epithelial neoplasia. ANZ J Surg 2006;76:715-17.
- American Joint Committee on Cancer (AJCC) . Collaborative Staging Manual and Coding Instructions 2004.
- Bower M, Powles T, Newsom-Davis T, Thirlwell C, Stebbing J, Mandalia S, et al. HIV-associated anal cancer: has highly active antiretroviral therapy reduced the incidence or improved the outcome?. J Acquir Immune Defic Syndr 2004;37:1563-5.
- Jeffreys M, Rachet B, McDowell S, Habib AG, Lepage C, Coleman MP. Survival from rectal and anal cancers in England and Wales, 1986–2001. Eur J Cancer 2006;42:1434-40.
- Allal AS, Sprangers MA, Laurencet F, Reymond MA, Kurtz JM. Assessment of long-term quality of life in patients with anal carcinomas treated by radiotherapy with or without chemotherapy. Br J Cancer 1999;80:1588-94.
- Pachler J, Wille-Jorgensen P. Quality of life after rectal resection for cancer, with or without permanent colostomy. Cochrane Database Syst Rev 2005;2.
- de Ruiter A, Carter P, Katz DR, Kocjan G, Whatrup C, Northover J, et al. A comparison between cytology and histology to detect anal intraepithelial neoplasia. Genitourin Med 1994;70:22-5.
- Palefsky JM, Holly EA, Hogeboom CJ, Berry JM, Jay N, Darragh TM. Anal cytology as a screening tool for anal squamous intraepithelial lesions. JAIDS 1997;14:415-22.
- Mathews WC, Sitapati A, Caperna JC, Barber RE, Tugend A, Go U. Measurement characteristics of anal cytology, histopathology, and high-resolution anoscopic visual impression in an anal dysplasia screening program. JAIDS 2004;37:1610-15.
- Panther LA, Wagner K, Proper J, Fugelso DK, Chatis PA, Weeden W, et al. High resolution anoscopy findings for men who have sex with men: inaccuracy of anal cytology as a predictor of histologic high-grade anal intraepithelial neoplasia and the impact of HIV serostatus. Clin Infect Dis 2003;38:1490-2.
- Arain S, Walts AE, Thomas P, Bose S. The anal pap smear: cytomorphology of squamous intraepithelial lesions. Cytojournal 2005;2.
- Friedlander MA, Stier E, Lin O. Anorectal cytology as a screening tool for anal squamous lesions: cytologic, anoscopic, and histologic correlation. Cancer 2004;102:19-26.
- Lampinen TM, Miller ML, Chan K, Anema A, van ND, Schilder AJ, et al. Randomized clinical evaluation of self-screening for anal cancer precursors in men who have sex with men. Cytojournal 2006;3.
- Cranston RD, Darragh TM, Holly EA, Jay N, Berry JM, Da CM, et al. Self-collected versus clinician-collected anal cytology specimens to diagnose anal intraepithelial neoplasia in HIV-positive men. JAIDS 2004;36:915-20.
- Varnai AD, Bollmann M, Griefingholt H, Speich N, Schmitt C, Bollmann R, et al. HPV in anal squamous cell carcinoma and anal intraepithelial neoplasia (AIN): impact of HPV analysis of anal lesions on diagnosis and prognosis. Int J Colorectal Dis 2006;21:135-42.
- Chiao EY, Giordano TP, Palefsky JM, Tyring S, El Serag H. Screening HIV-infected individuals for anal cancer precursor lesions: A systematic review. Clin Infect Dis 2006;43:223-33.
- Fox PA, Seet JE, Stebbing J, Francis N, Barton SE, Strauss S, et al. The value of anal cytology and human papillomavirus typing in the detection of anal intraepithelial neoplasia: a review of cases from an anoscopy clinic. Sex Transm Infect 2005;81:142-6.
- James R, Meadows H, Wan S. ACT II: the second UK phase III anal cancer trial. Clin Oncol (R Coll Radiol) 2005;17:364-6.
- University of York, Centre for Reviews and Dissemination . The management of colorectal cancer. Eff Health Care 2004;8.
- Arnott SJ, Cunningham D, Gallagher J, Gray R, Hardcastle J, Houghton J, et al. Epidermoid anal cancer: results from the UKCCCR randomised trial of radiotherapy alone versus radiotherapy, 5-fluorouracil, and mitomycin. Lancet 1996;348:1049-54.
- Cummings B, Keane T, Thomas G. Results and toxicity of the treatment of anal canal carcinoma by radiation therapy or radiation therapy and chemotherapy. Cancer 1984;54:2062-8.
- Doniec JM, Schniewind B, Kovacs G, Kahlke V, Loehnert M, Kremer B. Multimodal therapy of anal cancer added by new endosonographic-guided brachytherapy. Surg Endosc 2006;20:673-8.
- Brown SR, Skinner P, Tidy J, Smith JH, Sharp F, Hosie KB. Outcome after surgical resection for high-grade anal intraepithelial neoplasia (Bowen’s disease). Br J Surg 1999;86:1063-6.
- Edelman S, Johnstone PAS. Combined modality therapy for HIV-infected patients with squamous cell carcinoma of the anus: outcomes and toxicities. Int J Radiat Oncol Biol Phys 2006;66:206-11.
- Place RJ, Gregorcyk SG, Huber PJ, Simmang CL. Outcome analysis of HIV-positive patients with anal squamous cell carcinoma. Dis Colon Rectum 2001;44:506-12.
- Myerson RJ, Karnell LH, Menck HR. The National Cancer Data Base report on carcinoma of the anus. Cancer 1997;80:805-15.
- Ajani JA, Winter KA, Gunderson LL, Pedersen J, Benson AB, Thomas CR, et al. Fluorouracil, mitomycin, and radiotherapy vs fluorouracil, cisplatin, and radiotherapy for carcinoma of the anal canal: a randomized controlled trial. JAMA 2008;299:1914-21.
- Spence AR, Franco EL, Ferenczy A. The role of human papillomaviruses in cancer: evidence to date. Am J Cancer 2005;4:49-64.
- Kim JH, Sarani B, Orkin BA, Young HA, White J, Tannebaum I, et al. HIV-positive patients with anal carcinoma have poorer treatment tolerance and outcome than HIV-negative patients. Dis Colon Rectum 2001;44:1496-502.
- Knight D. Health care screening for men who have sex with men. Am Fam Physician 2004;69:2149-56.
- Halperin DT. Heterosexual anal intercourse: prevalence, cultural factors, and HIV infection and other health risks, part I. AIDS Patient Care STDS 1999;13:717-30.
- Dodds JP, Mercey DE, Parry JV, Johnson AM. Increasing risk behaviour and high levels of undiagnosed HIV infection in a community sample of homosexual men. Sex Transm Infect 2004;80:236-40.
- Frisch M, Glimelius B, van den Brule AJC, Wohlfahrt J, Meijer JLM, Walboomers JMM, et al. Sexually transmitted infection as a cause of anal cancer. N Engl J Med 1997;337:1350-8.
- Bjorge T, Engeland A, Luostarinen T, Mork J, Gislefoss RE, Jellum E, et al. Human papillomavirus infection as a risk factor for anal and perianal skin cancer in a prospective study. Br J Cancer 2002;87:61-4.
- Van Der Snoek EM, Niesters HGM, Van Doornum GJJ, Mulder PGH, Osterhaus ADME, Van Der Meijden WI. Acquisition and clearance of perianal human papillomavirus infection in relation to HIV-positivity in men who have sex with men in the Netherlands. Acta Derm Venereol 2005;85:437-43.
- Sobhani I, Walker F, Roudot-Thoraval F, Abramowitz L, Johanet H, Henin D, et al. Anal carcinoma: incidence and effect of cumulative infections. Aids 2004;18:1561-9.
- Palefsky JM, Holly EA, Ralston ML, Jay N, Berry JM, Darragh TM. High incidence of anal high-grade squamous intra-epithelial lesions among HIV-positive and HIV-negative homosexual and bisexual men. Aids 1998;12:495-503.
- Fagan SP, Bellows CF, Albo D, Rodriquez-Barradas M, Feanny M, Awad SS, et al. Length of human immunodeficiency virus disease and not immune status is a risk factor for development of anal carcinoma. Am J Surg 2005;190:732-5.
- Palefsky JM, Holly EA, Efirdc JT, Da Costa M, Jay N, Berry JM, et al. Anal intraepithelial neoplasia in the highly active antiretroviral therapy era among HIV-positive men who have sex with men. Aids 2005;19:1407-14.
- Palefsky JM, Holly EA, Ralston ML, Da CM, Bonner H, Jay N, et al. Effect of highly active antiretroviral therapy on the natural history of anal squamous intraepithelial lesions and anal human papillomavirus infection. JAIDS 2001;28:422-8.
- Palefsky JM, Holly EA, Ralston ML, Arthur SP, Jay N, Berry JM, et al. Anal squamous intraepithelial lesions in HIV-positive and HIV-negative homosexual and bisexual men prevalence and risk factors. JAIDS 1998;17:320-6.
- Palefsky JM, Holly EA, Ralston ML, Arthur SP, Hogeboom CJ, Darragh TM. Anal cytological abnormalities and anal HPV infection in men with centers for disease control group IV HIV disease. Genitourin Med 1997;73:174-80.
- Piketty C, Kazatchkine MD. Human papillomavirus-related cervical and anal disease in HIV-infected individuals in the era of highly active antiretroviral therapy. Curr HIV AIDS Rep 2005;2:140-5.
- Oehler-Janne C, Seifert B, Lutolf UM, Ciernik IF. Local tumor control and toxicity in HIV-associated anal carcinoma treated with radiotherapy in the era of antiretroviral therapy. Radiat Oncol 2006;1.
- Palefsky JM, Gonzales J, Greenblatt RM, Ahn DK, Hollander H. Anal intraepithelial neoplasia and anal papillomavirus infection among homosexual males with group IV HIV disease. JAMA 1990;263:2911-16.
- Palefsky JM, Holly EA, Gonzales J, Lamborn K, Hollander H. Natural history of anal cytologic abnormalities and papillomavirus infection among homosexual men with group IV HIV disease. JAIDS 1992;5:1258-65.
- Critchlow CW, Hawes SE, Kuypers JM, Goldbaum GM, Holmes KK, Surawicz CM, et al. Effect of HIV infection on the natural history of anal human papillomavirus infection. Aids 1998;12:1177-84.
- Piketty C, Darragh TM, Da CM, Bruneval P, Heard I, Kazatchkine MD, et al. High prevalence of anal human papillomavirus infection and anal cancer precursors among HIV-infected persons in the absence of anal intercourse. Ann Intern Med 2003;138:453-9.
- Piketty C, Darragh TM, Heard I, Da CM, Bruneval P, Kazatchkine MD, et al. High prevalence of anal squamous intraepithelial lesions in HIV-positive men despite the use of highly active antiretroviral therapy. Sex Transm Dis 2004;31:96-9.
- Palefsky JM, Holly EA, Hogeboom CJ, Ralston ML, DaCosta MM, Botts R, et al. Virologic, immunologic, and clinical parameters in the incidence and progression of anal squamous intraepithelial lesions in HIV-positive and HIV- negative homosexual men. JAIDS 1998;17:314-19.
- Daling JR, Weiss NS, Klopfenstein LL. Correlates of homosexual behavior and the incidence of anal cancer. JAMA 1982;247:1988-90.
- Chin-Hong PV, Vittinghoff E, Cranston RD, Buchbinder S, Cohen D, Colfax G, et al. Age-specific prevalence of anal human papillomavirus infection in HIV-negative sexually active men who have sex with men: The EXPLORE study. J Infect Dis 2004;190:2070-6.
- Chin-Hong PV, Vittinghoff E, Cranston RD, Browne L, Buchbinder S, Colfax G, et al. Age-related prevalence of anal cancer precursors in homosexual men: The EXPLORE study. J Natl Cancer Inst 2005;97:896-905.
- Hankins C, Coutlee F, Lapointe N, Simard P, Tran T, Samson J, et al. Prevalence of risk factors associated with human papillomavirus infection in women living with HIV. CMAJ 1999;160:185-91.
- Holly EA, Ralston ML, Darragh TM, Greenblatt RM, Jay N, Palefsky JM. Prevalence and risk factors for anal squamous intraepithelial lesions in women. J Natl Cancer Inst 2001;93:843-9.
- Moscicki AB, Hills NK, Shiboski S, Darragh TM, Jay N, Powell K, et al. Risk factors for abnormal anal cytology in young heterosexual women. Cancer Epidemiol Biomarkers Prev 1999;8:173-8.
- Palefsky JM, Holly EA, Ralston ML, Da-Costa M, Greenblatt RM. Prevalence and risk factors for anal human papillomavirus infection in human immunodeficiency virus (HIV)-positive and high-risk HIV-negative women. J Infect Dis 2001;183:383-91.
- Chan JK, Monk BJ, Brewer C, Keefe KA, Osann K, McMeekin S, et al. HPV infection and number of lifetime sexual partners are strong predictors for ‘natural’ regression of CIN2 and 3. Br J Cancer 2003;89:1062-6.
- Hernandez BY, McDuffie K, Zhu X, Wilkens LR, Killeen J, Kessel B, et al. Anal human papillomavirus infection in women and its relationship with cervical infection. Cancer Epidemiol Biomarkers Prev 2005;14:2550-6.
- Evans HS, Newnham A, Hodgson SV, Moller H. Second primary cancers after cervical intraepithelial neoplasia III and invasive cervical cancer in Southeast England. Gynecol Oncol 2003;90:131-36.
- Goldie SJ, Kuntz KM, Weinstein MC, Freedberg KA, Palefsky JM. Cost-effectiveness of screening for anal squamous intraepithelial lesions and anal cancer in human immunodeficiency virus-negative homosexual and bisexual men. Am J Med 2000;108:634-41.
- Goldie SJ, Kuntz KM, Weinstein MC, Freedberg KA, Welton ML, Palefsky JM. The clinical effectiveness and cost-effectiveness of screening for anal squamous intraepithelial lesions in homosexual and bisexual HIV-positive men. JAMA 1999;281:1822-9.
- Erens B, McManus S, Field J, Korovessis C, Johnson A, Fenton K, et al. National Survey of Sexual Attitudes and Lifestyles II 2001.
- Sweeting MJ, De Angelis D, Aalen OO. Bayesian back-calculation using a multi-state model with application to HIV. Stat Med 2005;24:3991-4007.
- Responders to Antiretroviral Treatment over 500 CD4 Mm3 Reach Same Mortality Rates As General Population: APROCO and Aquitaine Cohorts n.d.
- Ormaasen V, Sandvik L, Gjeruldsen Dudman S, Bruun JN, . HIV Related and Non-HIV Related Mortality Compared to the General Population before and After the Introduction of Highly Active Antiretroviral Therapy (HAART) in Norway n.d.
- Martínez E, Milinkovic A, Buira E. Incidence and causes of death in HIV-infected persons receiving highly active antiretroviral therapy compared with estimates for the general population of similar age and from the same geographical area. HIV Med 2007;8:251-8.
- Baker J. HIV-Related Immune Suppression After ART Predicts Risk of Non-Opportunistic Diseases: Results from the FIRST Study n.d.
- Critchlow CW, Surawicz CM, Holmes KK, Kuypers J, Daling JR, Hawes SE, et al. Prospective study of high grade anal squamous intraepithelial neoplasia in a cohort of homosexual men: influence of HIV infection, immunosuppression and human papillomavirus infection. Aids 1995;9:1255-62.
- Sayers SJ, McMillan A, McGoogan E. Anal cytological abnormalities in HIV-infected homosexual men. Int J STD AIDS 1998;9:37-40.
- Marchesa P, Fazio VW, Oliart S, Goldblum JR, Lavery IC. Perianal Bowen’s disease: a clinicopathologic study of 47 patients. Dis Colon Rectum 1997;40:1286-93.
- Chang GJ, Berry JM, Jay N, Palefsky JM, Welton ML. Surgical treatment of high-grade anal squamous intraepithelial lesions: a prospective study. Dis Colon Rectum 2002;45:453-8.
- Ness RM, Holmes AM, Klein R. Cost-utility of colonoscopic screening for colorectal cancer at various ages. Am J Gastroenterol 2000;97:1800-11.
- Chin-Hong PV, Palefsky JM. Natural history and clinical management of anal human papillomavirus disease in men and women infected with human immunodeficiency virus. Clin Infect Dis 2002;35:1127-34.
- Wong S, Gibbs P, Chao M, Jones I, McLaughlin S, Tjandra J, et al. Carcinoma of the anal canal: a local experience and review of the literature. ANZ J Surg 2004;74:541-6.
- Scott P, Coxon T, Kirk M, Pinson D. Cottaging and Cruising in Barnet, Brent and Harrow: Final Project Report n.d. http://racoon.dircon.co.uk/bbh/cot.htm (accessed 2 July 2007).
- Scott P, Coxon T, Kirk M, Pinson D. MSM in Public Sex Environments n.d. http://racoon.dircon.co.uk/spots.41.htm.
- Moss SM, Gray A, Legood R, Henstock E. Evaluation of HPV LBC Cervical Screening Pilot Studies. First Report to the Department of Health on Evaluation of LBC 2002.
- Agency for Health Care Policy and Research . Statistics from the Healthcare Cost and Utilization Project (HCUP-3): Nationwide Inpatient Sample for 1994. Principal Diagnoses 1994.
- Tappenden P, Chilcott J, Eggington S, Sakai H, Karnon J, Patnick J. Option appraisal of population-based colorectal cancer screening programmes in England. Gut 2007;56:677-84.
- Miners AH, Sabin CA, Trueman P, Youle M, Mocroft A, Johnson M, et al. Assessing the cost-effectiveness of HAART for adults with HIV in England. HIV Med 2001;2:52-8.
- Sorensen S, Brown R, Benedict A, Flood E, Revicki D. Patient-Rated Utilities in Postmenopausal Early Breast Cancer: A Cross Country Comparison n.d.
- Mauskopf J, Lacey L, Kempel A, Simpson K. The cost-effectiveness of treatment with lamivudine and zidovudine compared with zidovudine alone: a comparison of Markov model and trial data estimates. Am J Manag Care 1998;4:1004-12.
- Trueman P, Youle M, Sabin CA, Miners AH, Beck EJ. The cost-effectiveness of triple nucleoside analogue therapy antiretroviral regimens in the treatment of HIV in the United Kingdom. HIV Clin Trials. HIV Clin Trials 2000;1:27-35.
- Goldie SJ, Weinstein MC, Kuntz KM, Freedberg KA. The costs, clinical benefits, and cost-effectiveness of screening for cervical cancer in HIV-infected women. Ann Intern Med 1999;130:97-107.
- Forman D. Effective Registration of Skin Cancer in Yorkshire n.d. http://ReFeR.nhs.uk/ViewRecord.asp?ID=682 (accessed 22 June 2007).
- Silcocks PB, Waterhouse A. How Good Are Our Data? Initial Studies of Completeness n.d. www.trentcancer.nhs.uk/publications/02iacrpbs1.html.
- Health Protection Agency (HPA) . New HIV Diagnoses Surveillance Tables, No. 77 2007.
- Goubar A, . Multi-Parameter Evidence Synthesis Method n.d. http://sepho.org.uk/Download/Public/10761/1/Prev_Modelling_Presentation_v1.ppt#7.
- The UK Collaborative Group for HIV and STI surveillance . HIV and Other Sexually Transmitted Infections in the United Kingdom 2005.
- Fox P. Anal cancer screening in men who have sex with men. Curr Opin HIV AIDS 2009;4:64-7.
Appendix 1 Surveillance Epidemiology and End Results (SEER)
The Surveillance Epidemiology and End Results (SEER) programme of the National Cancer Institute (NCI) is an authoritative source of information on cancer incidence and survival in the USA. SEER currently collects and publishes cancer incidence and survival data from population-based cancer registries covering approximately 26% of the US population. SEER coverage includes 23% of African Americans, 40% of the Hispanic population, 42% of American Indians and Alaska Natives, 53% of Asians and 70% of Hawaiian/Pacific Islanders.
The SEER programme registries routinely collect data on patient demographics, primary tumour site, tumour morphology and stage at diagnosis, first course of treatment, and follow-up for vital status. The SEER programme is the only comprehensive source of population-based information in the USA that includes stage of cancer at the time of diagnosis and patient survival data.
Appendix 2 NSC criteria for appraising the viability, effectiveness and appropriateness of a screening programme
Ideally, all of the following criteria should be met before screening for a condition is initiated.
The condition
-
1. The condition should be an important health problem.
-
2. The epidemiology and natural history of the condition, including development from latent to declared disease, should be adequately understood and there should be a detectable risk factor, disease marker, latent period or early symptomatic stage.
-
3. All of the cost-effective primary prevention interventions should have been implemented as far as practicable.
-
4. If the carriers of a mutation are identified as a result of screening the natural history of people with this status should be understood, including the psychological implications.
The test
-
5. There should be a simple, safe, precise and validated screening test.
-
6. The distribution of test values in the target population should be known, and a suitable cut-off level defined and agreed.
-
7. The test should be acceptable to the population.
-
8. There should be an agreed policy on the further diagnostic investigation of individuals with a positive test result, and on the choices available to those individuals.
-
9. When testing for mutations, if all possible mutations are not being tested then the criteria used to select the subset of mutations to be covered by screening should be clearly set out.
The treatment
-
10. There should be an effective treatment or intervention for patients identified through early detection, with evidence of early treatment leading to better outcomes than late treatment.
-
11. There should be agreed evidence-based policies covering which individuals should be offered treatment and the appropriate treatment to be offered.
-
12. Clinical management of the condition and patient outcomes should be optimised in all health-care providers prior to participation in a screening programme.
The screening programme
-
13. There should be evidence from high-quality RCTs to show that the screening programme is effective in reducing mortality or morbidity. Where screening is aimed solely at providing information to allow the person being screened to make an ‘informed choice’ (e.g. Down’s syndrome, cystic fibrosis carrier screening), there must be evidence from high-quality trials that the test accurately measures risk. The information that is provided about the test and its outcome must be of value and readily understood by the individual being screened.
-
14. There should be evidence that the complete screening programme (test, diagnostic procedures, treatment/intervention) is clinically, socially and ethically acceptable to health professionals and the public.
-
15. The benefit from the screening programme should outweigh the physical and psychological harm (caused by the test, diagnostic procedures and treatment).
-
16. The opportunity cost of the screening programme (including testing, diagnosis and treatment, administration, training and quality assurance) should be economically balanced in relation to expenditure on medical care as a whole (i.e. value for money).
-
17. There should be a plan for managing and monitoring the screening programme, and an agreed set of quality assurance standards.
-
18. Adequate staffing and facilities for testing, diagnosis, treatment and programme management should be available prior to the commencement of the screening programme.
-
19. All other options for managing the condition should have been considered (e.g. improving treatment, providing other services) to ensure that no further cost-effective intervention could be introduced or current interventions increased within the resources available.
-
20. Evidence-based information, explaining the consequences of testing, investigation and treatment, should be made available to potential participants to assist them in making an informed choice.
-
21. Public pressure for widening the eligibility criteria for reducing the screening interval, and for increasing the sensitivity of the testing process, should be anticipated. Decisions about these parameters should be scientifically justifiable to the public.
-
22. If screening is for a mutation then the programme should be acceptable to people who are identified as carriers and to other family members.
Appendix 3 Search strategies
Epidemiology search strategy
Database: Ovid MEDLINE (1966 to January week 1 2006).
Search strategy
-
exp Anus Neoplasms/
-
anus neoplasm$.tw.
-
neoplasm$, anus.tw.
-
anal neoplasm$.tw.
-
neoplasm$, anal.tw.
-
anal cancer$.tw.
-
cancer$, anal.tw.
-
cancer of anus.tw.
-
anus cancer$.tw.
-
cancer of the anus.tw.
-
anal squamous carcinoma.tw.
-
circumanal gland neoplasm$.tw.
-
exp Anal Gland Neoplasms/
-
neoplasm$, anal gland.tw.
-
anal gland neoplasm$.tw.
-
neoplam$, circumanal gland.tw.
-
neoplasm$, perianal gland.tw.
-
perianal gland neoplasm$.tw.
-
or/1–18
-
exp Epidemiology/
-
exp Natural History/
-
epidemiolog$.ti.
-
inciden$.ti.
-
prevalen$.ti.
-
Incidence/
-
Prevalence/
-
or/20–26
-
19 and 27
Search terms for the disease (anal cancer) (1–18) were combined with ‘epidemiology’ search terms (20–26).
Screening technologies search strategy
Database: Ovid MEDLINE (1966 to January week 1 2006).
Search strategy
-
anal cytologic screening.tw.
-
anoscopy.tw.
-
anal cytology.tw.
-
liquid based cytology.tw.
-
Mass Screening/
-
Occult Blood/
-
Sigmoidoscopy/
-
Colonoscopy/
-
mass screening.tw
-
occult blood.tw.
-
Diagnostic Tests, Routine/
-
diagnos$.tw.
-
diagnosis/
-
diagnostic us$.tw.
-
“reproducibility of results”/
-
Observer Variation/
-
di.fs.
-
sigmoidoscop$.ti,ab.
-
colonoscop$.ti,ab.
-
reproducibility of results.ti,ab.
-
observer variation$.ti,ab.
-
Diagnosis/
-
or/1–22
-
exp Anus Neoplasms/
-
anus neoplasm$.tw.
-
neoplasm$, anus.tw.
-
anal neoplasm$.tw.
-
neoplasm$, anal.tw.
-
anal cancer$.tw.
-
cancer$, anal.tw.
-
cancer of anus.tw.
-
anus cancer$.tw.
-
cancer of the anus.tw.
-
anal squamous carcinoma.tw.
-
circumanal gland neoplasm$.tw.
-
exp Anal Gland Neoplasms/
-
neoplasm$, anal gland.tw.
-
anal gland neoplasm$.tw.
-
neoplam$, circumanal gland.tw.
-
neoplasm$, perianal gland.tw.
-
perianal gland neoplasm$.tw.
-
exp Precancerous Conditions/
-
preneoplastic condition$.tw.
-
exp *Papillomavirus, Human/
-
human papillomavirus$.ti,ab.
-
infectious human wart virus$.ti,ab.
-
human wart virus, infectious.ti,ab.
-
papilloma virus, human.ti,ab.
-
anal cytological abnormalit$.ti,ab.
-
anal human papillomavirus disease$.ti,ab.
-
anal squamous intraepithelial neoplasia.ti,ab.
-
anal high grade squamous intraepithelial lesion$.ti,ab.
-
high-grade anal squamous intraepithelial lesion$.ti,ab.
-
or/24–53
-
exp Cohort Studies/
-
Prognosis/
-
exp Mortality/
-
exp morbidity/
-
morbidity.ti,ab.
-
mortality.ti,ab.
-
(natural adj history).ti,ab.
-
prognos$.ti,ab.
-
course.ti,ab.
-
predict$.ti,ab.
-
exp “Outcome Assessment (Health Care)”/
-
outcomes$1.ti,ab.
-
(inception adj cohort$1).ti,ab.
-
disease progression/
-
exp survival analysis/
-
or/55–69
-
23 and 54 and 70
Search terms for specific diagnostic test and diagnosis terms (1–22) were combined with search terms for anal cancer (24–41) and premalignant indicators of disease (42–53) and search terms for morbidity and mortality (55–69) the primary outcome that diagnosis is trying to prevent.
Screening policies/programmes search strategy
Database: Ovid MEDLINE (2004 to November week 3 2006).
Search strategy
-
screening program$.ti,ab.
-
Mass Screening/
-
mass screening$.ti,ab.
-
cancer screening$.ti,ab.
-
screening programme$.ti,ab.
-
screening polic$.ti,ab.
-
screening$.ti,ab.
-
screening campaign$.ti,ab.
-
or/1–8
-
exp Anus Neoplasms/
-
anus neoplasm$.tw.
-
neoplasm$, anus.tw.
-
anal neoplasm$.tw.
-
neoplasm$, anal.tw.
-
anal cancer$.tw.
-
cancer$, anal.tw.
-
cancer of anus.tw.
-
anus cancer$.tw.
-
cancer of the anus.tw.
-
anal squamous carcinoma.tw.
-
circumanal gland neoplasm$.tw.
-
exp Anal Gland Neoplasms/
-
neoplasm$, anal gland.tw.
-
anal gland neoplasm$.tw.
-
neoplam$, circumanal gland.tw.
-
neoplasm$, perianal gland.tw.
-
perianal gland neoplasm$.tw.
-
or/10–27
-
9 and 28
Search terms for screening policies and programmes (1–8) were combined with search terms for anal cancer (10–27).
The screening policies/programmes and screening technologies effectiveness searches was combined with methodological search filters designed to retrieve the highest levels of evidence.
Guidelines
-
guideline.pt.
-
Health Planning Guidelines/
-
practice guideline.pt.
-
or/1–3
Systematic reviews
-
meta-analysis/
-
exp review literature/
-
(meta-analy$ or meta analy$ or metaanaly$).tw.
-
meta analysis.pt.
-
review academic.pt.
-
review literature.pt.
-
(systematic$ adj3 (review$ or overview$)).tw.
-
or/1–7
RCTs
-
clinical trial.pt
The screening police/programmes and screening technologies search strategies were also combined with search terms for high-risk groups:
-
Sexual Behavior/
-
anal intercourse.ti,ab.
-
anal sex.ti,ab.
-
at-risk sexual behaviour$.ti,ab.
-
at-risk sexual behavior$.ti,ab.
-
Bisexuality/
-
bisexual$.ti,ab.
-
gay$.ti,ab.
-
hiv-negative.ti,ab.
-
human immunodeficiency virus-negative.ti,ab.
-
hiv-positive.ti,ab.
-
hiv-infected person$.ti,ab.
-
human immunodeficiency virus-positive.ti,ab.
-
exp HIV/
-
homosexual$.ti,ab.
-
exp Homosexuality/
-
male-male sex.ti,ab.
-
men who have sex with men.ti,ab.
-
unprotected anal intercourse.ti,ab.
-
or/1–19
Cost-effectiveness searches
To retrieve papers on cost-effectiveness and comparative costs of candidate technologies/programmes/policies, searches were conducted in MEDLINE, EMBASE, NHS Economic Evaluation Database (EED) and Office of Health Economics (OHE) Health Economic Evaluations Database (HEED). Search terms for screening technologies and programmes/policies given above were utilised. Search filters designed to retrieve economic evaluations, economic models and QoL literature were applied to the MEDLINE and EMBASE searches. An example of the MEDLINE (Ovid) search filter is provided below:
-
exp “Patient Acceptance of Health Care”/
-
exp “Costs and Cost Analysis”/
-
cost$.ti.
-
(cost$ adj2 (effective$ or util$ or benefit$ or minimi$)).ab.
-
(economic$ or pharmaco economic$ or pharmoco-economic$).tw.
-
Quality-Adjusted Life Years/
-
quality adjusted life.tw.
-
(qaly$ or qald$ or qale$ or qtime$).tw.
-
disability adjusted life.tw.
-
daly$.tw.
-
Health Status Indicators/
-
(sf36 or sf 36 or short form 36 or shortform 36 or sf thirtysix or sf thirty six or shortform thirtysix or shortform thirty six or short from thirtysix or short form thirty six).tw.
-
(sf6 or sf 6 or short form 6 or shortform 6 or sf six or sfsix or shortform six or short form six).tw.
-
(sf12 or sf 12 or short from 12 or shortform 12 or sf twelve or sftwelve or shortform twelve or short form twelve).tw.
-
(sf16 or sf 16 or short form 16 or shortform 16 or sf sixteen or sfsixteen or shortform sixteen or short form sixteen).tw.
-
(sf20 or sf 20 or short form 20 or shortform 20 or sf twenty or sftwenty or shortform twnety or short from twenty).tw.
-
(euroqol or euro qol or eq5d or eq 5d).tw.
-
(hql or hqol or h qol or hrqol or hr qol).tw.
-
(hye or hyes).tw.
-
health$ year$ equivalent$.tw.
-
health utilit$.tw.
-
(hui or hui1 or hui2 or hui3).tw.
-
disutil$.tw.
-
rosser.tw.
-
quality of wellbeing.tw.
-
qwb.tw.
-
willingness to pay.tw.
-
standard gamble$.tw.
-
time trade off.tw.
-
time tradeoff.tw.
-
tto.tw.
-
exp Models, Economic/
-
*Models, Theoretical/
-
*Models, Organizational/
-
economic model$.tw.
-
Markov Chains/
-
markov$.tw.
-
Monte Carlo Method/
-
monte carlo.tw.
-
exp Decision Theory/
-
(decision$ adj2 (tree$ or analy$ or model$)).tw.
-
or/1–41
Treatment search strategy
Searches on the high-risk groups search terms combined with the treatment search terms below were also conducted.
-
exp Therapeutics/
-
treatment$.ti,ab.
-
therap$.ti,ab.
-
exp Radiotherapy/
-
radiotherap$.ti,ab.
-
chemotherap$.ti,ab.
-
surger$.ti,ab.
-
or/1–7
Appendix 4 QUOROM trial flow chart
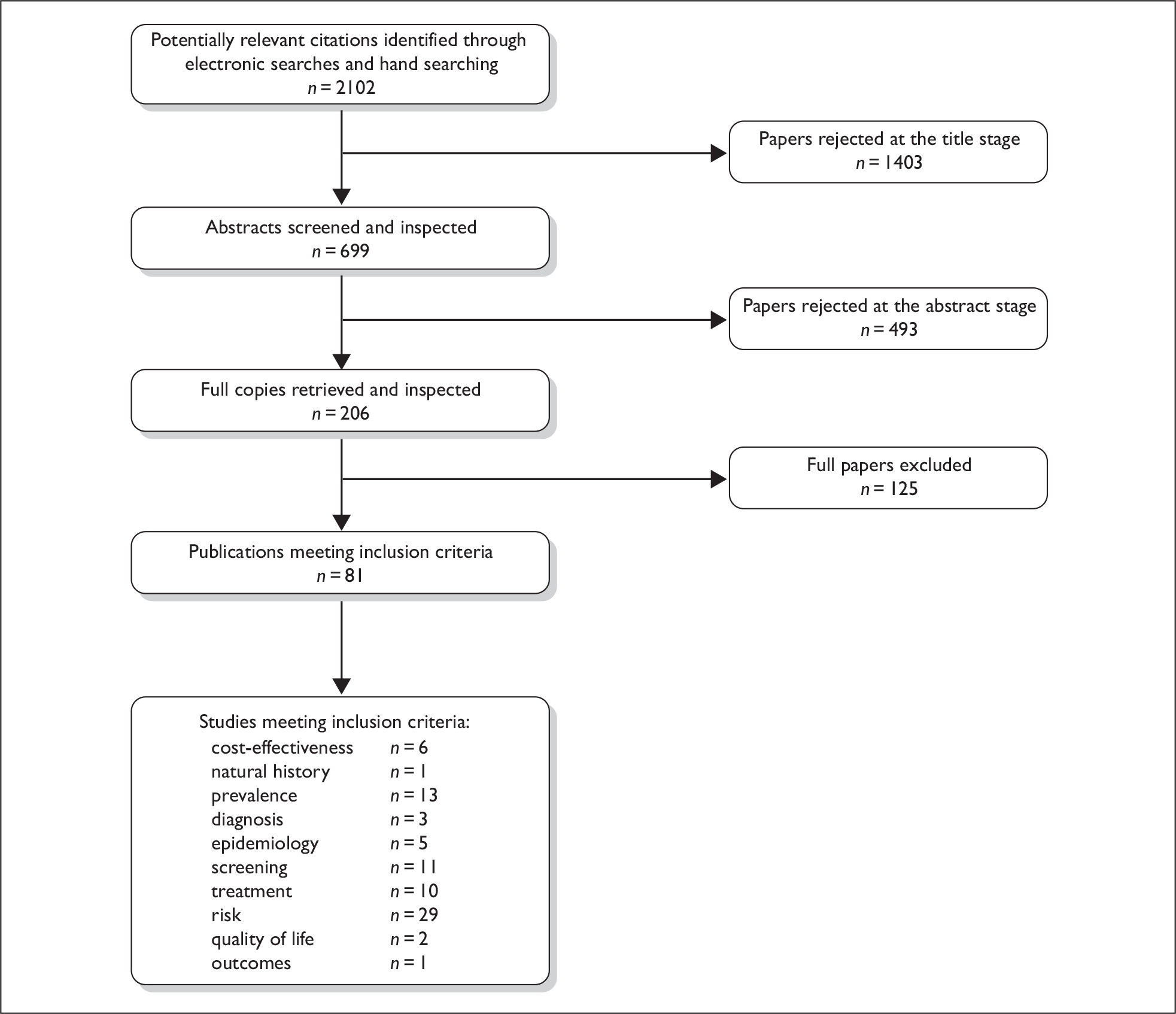
Appendix 5 Quality of screening studies
| Study | Randomisation | Blinding | Patient dropouts/exclusions | Intention-to-treat analysis |
|---|---|---|---|---|
| de Ruiter 199427 | N/A | None reported | 61 patients did not have an adequate anal smear, excluding them from comparison between anal cytology and histology | No |
| Palefsky et al. 199728 | N/A | Analyst (pathologist) | None reported | Yes |
| Mathews et al. 200429 | N/A | None reported | Repeat evaluable anal cytological results were available only for 642 patients, and concurrent anal cytological testing and HRA biopsy were performed in 154 patients who underwent HRA | No |
| Panther et al. 200430 | N/A | None reported | None reported | Yes |
| Fox et al. 200537 | N/A | Analyst (pathologist) | None reported | Yes |
| Arain et al. 200531 | N/A | None reported | 127 patients did not have surgical biopsies and/or repeat smears within 6 months, leaving 71 patients who did so | No |
| Friedlander et al. 200332 | N/A | Analyst (cytotechnologist) | None reported | Yes |
| Lampinen et al. 200633 | Yes, each individual randomly assigned the order in which their paired swabs (self vs clinician) were to be collected using a sealed-envelope method | Analyst (cytopathologist) | None reported | Yes |
| Cranston et al. 200434 | None | None reported | Approximately 10% of those invited to participate refused; of those that agreed, 20% did not return the required materials in a timely fashion. Of the remaining 106 participants, four were excluded because of incomplete collected samples. 102 were included in the analysis | No |
| Varnai et al. 200635 | N/A | None reported | None reported | Yes |
Appendix 6 Quality of treatment studies
| Study | Randomisation | Blinding | Patient dropouts/exclusions | Intention-to-treat analysis |
|---|---|---|---|---|
| UKCCCR Anal Cancer Working Party 199640 | Yes, centre block randomisation | Not reported |
RT group, five classed as ineligible due to inappropriate randomisation, and six deaths RT/chemotherapy group, three classed as ineligible due to inappropriate randomisation, and nine deaths |
Yes |
| Cummings et al. 198441 | None | Analyst | None reported | Yes |
| Doniec et al. 200642 | N/A | Not reported | None reported | Yes |
| Edelman and Johnstone 200644 | N/A | Not reported | None reported | Yes |
| Place et al. 200145 | N/A | Not reported | None reported | Yes |
| Brown et al. 199943 | N/A | Not reported | Of the 46 identified patients, six excluded for HG-AIN, and six excluded from further analysis | No |
Appendix 7 Life course models
Life course model (with HIV)
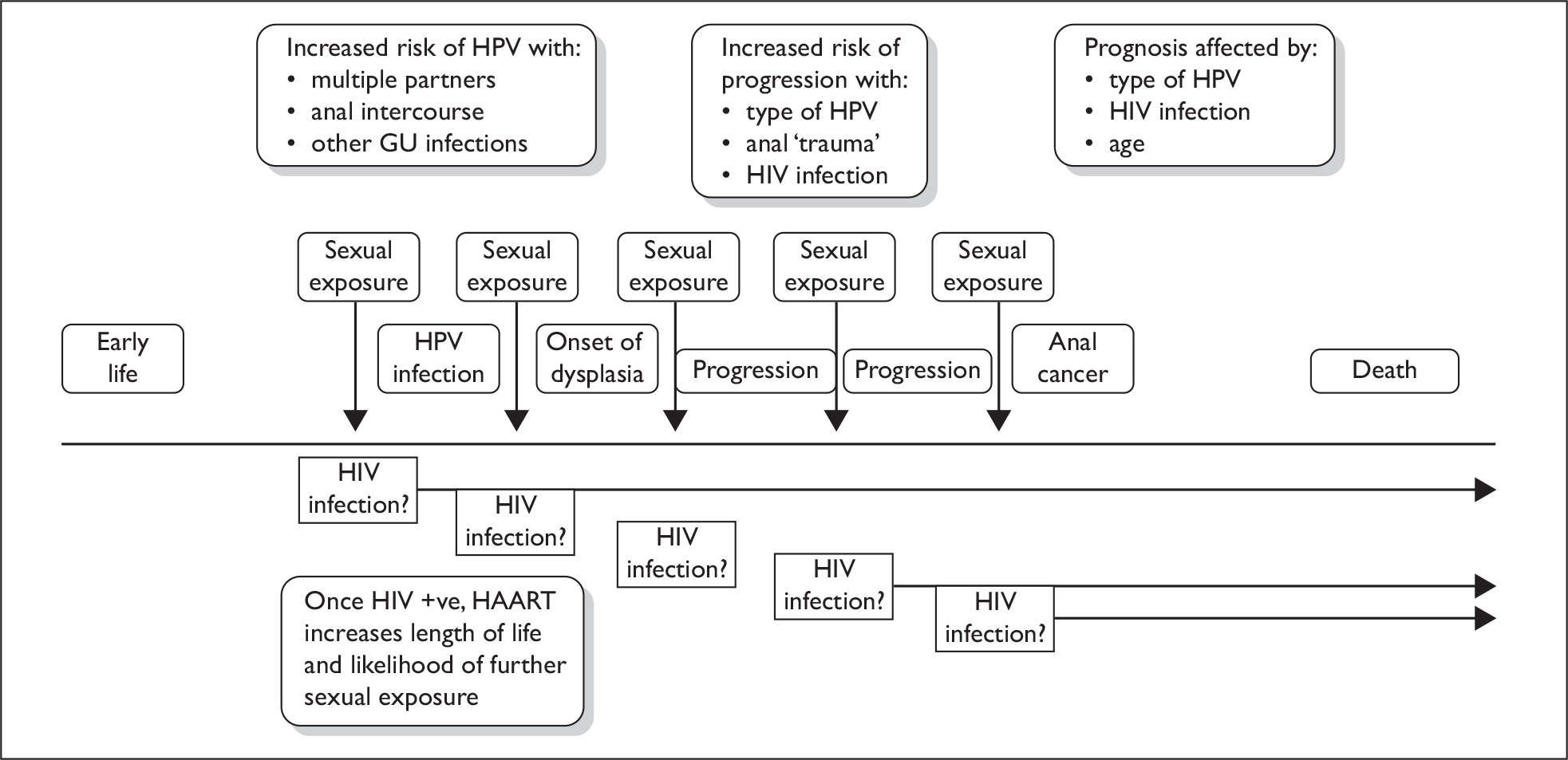
Life course model modified for HIV-negative women
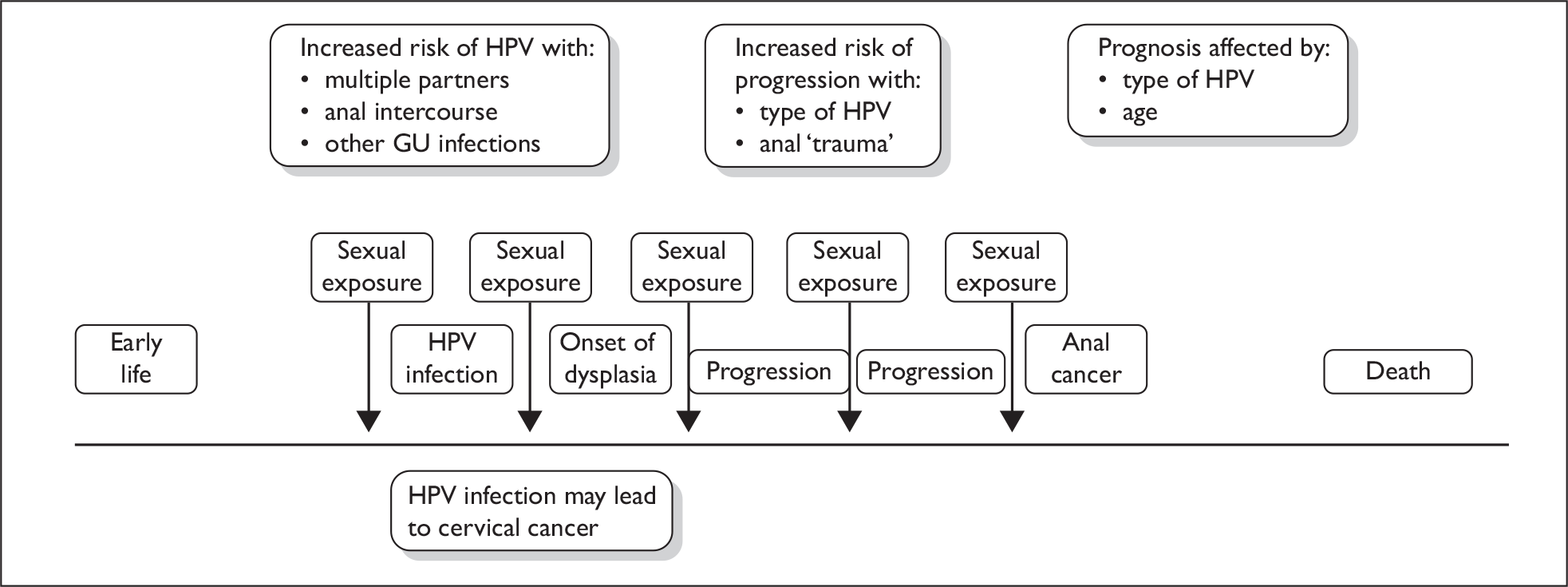
Appendix 8 Updated searches
We carried out the updated full searches in January 2010. After duplicates had been removed, 843 papers were identified. As with the original searches the titles and abstracts were read (where available) to identify any papers which fell into the categories of interest in a screening study, e.g. natural history, epidemiology, screening, diagnostics and treatment. We were particularly looking for any studies that added new and important data which would enhance our current knowledge of screening for anal cancer and in particular any new evidence in the condition in HIV-positive women.
We selected 92 papers for full review.
From these 11 were found to be opinion articles not reporting any data.
Fourteen papers from the title and abstract appeared to report on anal cancer but were actually reporting on other cancers.
Three were letters commenting on previous studies and ordered in error.
Treatment studies fell into two categories, those treating anal cancer and those treating anal warts, and made up the greatest number of studies at 13. These studies reported results very similar to those used in the model for the treatment of anal cancer. The treatment of warts was beyond the scope of the study.
Six studies described the possible impact of vaccination programmes on the future of the disease but these were mostly confined to the impact of cervical cancer.
Six studies described the risk factors in developing anal cancer but reported no new data to that already included in the review.
Nine studies reported on the epidemiology of anal cancer but did not report any new data that would change the parameters used in the model. These papers mostly confirmed that individuals with HIV were at risk of developing anal cancer.
A number of papers (8) reported on HIV-positive women and the increased risk for this group. The evidence reported supported the data used in the model. However, some authors predicted an upward trend in the number of affected individuals.
Four studies reported on the test. They were divided between acceptability, self-administered and new technology such as biomarkers which are at the early stages of development.
Five described screening programmes for anal cancer in non-UK health-care settings.
Two papers came from the economic searches. One of those was on the possible impact of a vaccination programme which included boys, which is currently not judged cost-effective. The second reported on the cost of non-HIV-associated cancers, including anal cancer, in the USA.
Eight reported on HIV and anal cancer in terms of antiretroviral therapies. The case for any link between HAART and the prevention of anal cancer was not made.
One study reported on guidelines for treating anal cancer.
One study reported a survey of current practice in treatment of anal warts in genitourinary clinics in the UK.
One study reported on screening MSM for anal cancer in a UK setting. This has been included in the updated review.
List of abbreviations
- AIDS
- acquired immune deficiency syndrome
- AIN
- anal intraepithelial neoplasia
- APE
- abdominoperineal excision
- AR
- anterior resection
- ASCUS
- atypical squamous cells of undetermined significance
- ASIL
- anal squamous intraepithelial lesion
- CIN
- cervical intraepithelial neoplasia
- CMT
- combined modality therapy
- DSS
- disease-specific survival
- EORTC
- European Organisation for Research and Treatment of Cancer
- EUS
- endosonographic ultrasonography
- FUMIR
- 5-fluorouracil, mitomycin C and radical radiation therapy
- GU
- genitourinary
- HAART
- highly active antiretroviral therapy
- HDR
- high dose rate
- HG-AIN
- high-grade anal intraepithelial neoplasia
- HGD
- high-grade dysplasia
- HIV
- human immunodeficiency virus
- HPA
- Health Protection Agency
- HPV
- human papillomavirus
- HRA
- high-resolution anoscopy
- HSIL
- high-grade squamous intraepithelial lesion
- ICD-O
- International Classification of Diseases for Oncology
- ICQ
- incremental cost per QALY gained
- LG-AIN
- low-grade anal intraepithelial neoplasia
- LSIL
- low-grade squamous intraepithelial lesion
- MSM
- men who have sex with men
- NCI
- National Cancer Institute
- NPV
- negative predictive value
- NSC
- National Screening Committee
- OR
- odds ratio
- PCR
- polymerase chain reaction
- PPV
- positive predictive value
- QALY
- quality-adjusted life-year
- QoL
- quality of life
- RCT
- randomised controlled trial
- RR
- relative risk
- RT
- radiotherapy
- SCC
- squamous cell carcinoma
- SCCA
- squamous cell cancer of the anus
- SCCIS
- squamous cell carcinoma in situ
- SEER
- Surveillance Epidemiology and End Results
- SFGH
- San Francisco General Hospital Cohort Study
- SFMHS
- San Francisco Men’s Health Study
- SIL
- squamous intraepithelial lesion
- SIR
- standard incidence rate
- STD
- sexually transmitted disease
- STI
- sexually transmitted infection
- TCR
- Thames Cancer Registry
- TNM
- tumour, node, metastasis [staging system]
- TRUS
- transrectal ultrasound
- UAI
- unprotected anal intercourse
- UCSF
- University of California, San Francisco
- UKCCCR
- United Kingdom Co-ordinating Committee for Cancer Research
- VOI
- value of information
- WCISU
- Welsh Cancer Intelligence and Surveillance Unit
All abbreviations that have been used in this report are listed here unless the abbreviation is well known (e.g. NHS), or it has been used only once, or it is a non-standard abbreviation used only in figures/tables/appendices, in which case the abbreviation is defined in the figure legend or in the notes at the end of the table.
Notes
Health Technology Assessment reports published to date
-
Home parenteral nutrition: a systematic review.
By Richards DM, Deeks JJ, Sheldon TA, Shaffer JL.
-
Diagnosis, management and screening of early localised prostate cancer.
A review by Selley S, Donovan J, Faulkner A, Coast J, Gillatt D.
-
The diagnosis, management, treatment and costs of prostate cancer in England and Wales.
A review by Chamberlain J, Melia J, Moss S, Brown J.
-
Screening for fragile X syndrome.
A review by Murray J, Cuckle H, Taylor G, Hewison J.
-
A review of near patient testing in primary care.
By Hobbs FDR, Delaney BC, Fitzmaurice DA, Wilson S, Hyde CJ, Thorpe GH, et al.
-
Systematic review of outpatient services for chronic pain control.
By McQuay HJ, Moore RA, Eccleston C, Morley S, de C Williams AC.
-
Neonatal screening for inborn errors of metabolism: cost, yield and outcome.
A review by Pollitt RJ, Green A, McCabe CJ, Booth A, Cooper NJ, Leonard JV, et al.
-
Preschool vision screening.
A review by Snowdon SK, Stewart-Brown SL.
-
Implications of socio-cultural contexts for the ethics of clinical trials.
A review by Ashcroft RE, Chadwick DW, Clark SRL, Edwards RHT, Frith L, Hutton JL.
-
A critical review of the role of neonatal hearing screening in the detection of congenital hearing impairment.
By Davis A, Bamford J, Wilson I, Ramkalawan T, Forshaw M, Wright S.
-
Newborn screening for inborn errors of metabolism: a systematic review.
By Seymour CA, Thomason MJ, Chalmers RA, Addison GM, Bain MD, Cockburn F, et al.
-
Routine preoperative testing: a systematic review of the evidence.
By Munro J, Booth A, Nicholl J.
-
Systematic review of the effectiveness of laxatives in the elderly.
By Petticrew M, Watt I, Sheldon T.
-
When and how to assess fast-changing technologies: a comparative study of medical applications of four generic technologies.
A review by Mowatt G, Bower DJ, Brebner JA, Cairns JA, Grant AM, McKee L.
-
Antenatal screening for Down’s syndrome.
A review by Wald NJ, Kennard A, Hackshaw A, McGuire A.
-
Screening for ovarian cancer: a systematic review.
By Bell R, Petticrew M, Luengo S, Sheldon TA.
-
Consensus development methods, and their use in clinical guideline development.
A review by Murphy MK, Black NA, Lamping DL, McKee CM, Sanderson CFB, Askham J, et al.
-
A cost–utility analysis of interferon beta for multiple sclerosis.
By Parkin D, McNamee P, Jacoby A, Miller P, Thomas S, Bates D.
-
Effectiveness and efficiency of methods of dialysis therapy for end-stage renal disease: systematic reviews.
By MacLeod A, Grant A, Donaldson C, Khan I, Campbell M, Daly C, et al.
-
Effectiveness of hip prostheses in primary total hip replacement: a critical review of evidence and an economic model.
By Faulkner A, Kennedy LG, Baxter K, Donovan J, Wilkinson M, Bevan G.
-
Antimicrobial prophylaxis in colorectal surgery: a systematic review of randomised controlled trials.
By Song F, Glenny AM.
-
Bone marrow and peripheral blood stem cell transplantation for malignancy.
A review by Johnson PWM, Simnett SJ, Sweetenham JW, Morgan GJ, Stewart LA.
-
Screening for speech and language delay: a systematic review of the literature.
By Law J, Boyle J, Harris F, Harkness A, Nye C.
-
Resource allocation for chronic stable angina: a systematic review of effectiveness, costs and cost-effectiveness of alternative interventions.
By Sculpher MJ, Petticrew M, Kelland JL, Elliott RA, Holdright DR, Buxton MJ.
-
Detection, adherence and control of hypertension for the prevention of stroke: a systematic review.
By Ebrahim S.
-
Postoperative analgesia and vomiting, with special reference to day-case surgery: a systematic review.
By McQuay HJ, Moore RA.
-
Choosing between randomised and nonrandomised studies: a systematic review.
By Britton A, McKee M, Black N, McPherson K, Sanderson C, Bain C.
-
Evaluating patient-based outcome measures for use in clinical trials.
A review by Fitzpatrick R, Davey C, Buxton MJ, Jones DR.
-
Ethical issues in the design and conduct of randomised controlled trials.
A review by Edwards SJL, Lilford RJ, Braunholtz DA, Jackson JC, Hewison J, Thornton J.
-
Qualitative research methods in health technology assessment: a review of the literature.
By Murphy E, Dingwall R, Greatbatch D, Parker S, Watson P.
-
The costs and benefits of paramedic skills in pre-hospital trauma care.
By Nicholl J, Hughes S, Dixon S, Turner J, Yates D.
-
Systematic review of endoscopic ultrasound in gastro-oesophageal cancer.
By Harris KM, Kelly S, Berry E, Hutton J, Roderick P, Cullingworth J, et al.
-
Systematic reviews of trials and other studies.
By Sutton AJ, Abrams KR, Jones DR, Sheldon TA, Song F.
-
Primary total hip replacement surgery: a systematic review of outcomes and modelling of cost-effectiveness associated with different prostheses.
A review by Fitzpatrick R, Shortall E, Sculpher M, Murray D, Morris R, Lodge M, et al.
-
Informed decision making: an annotated bibliography and systematic review.
By Bekker H, Thornton JG, Airey CM, Connelly JB, Hewison J, Robinson MB, et al.
-
Handling uncertainty when performing economic evaluation of healthcare interventions.
A review by Briggs AH, Gray AM.
-
The role of expectancies in the placebo effect and their use in the delivery of health care: a systematic review.
By Crow R, Gage H, Hampson S, Hart J, Kimber A, Thomas H.
-
A randomised controlled trial of different approaches to universal antenatal HIV testing: uptake and acceptability. Annex: Antenatal HIV testing – assessment of a routine voluntary approach.
By Simpson WM, Johnstone FD, Boyd FM, Goldberg DJ, Hart GJ, Gormley SM, et al.
-
Methods for evaluating area-wide and organisation-based interventions in health and health care: a systematic review.
By Ukoumunne OC, Gulliford MC, Chinn S, Sterne JAC, Burney PGJ.
-
Assessing the costs of healthcare technologies in clinical trials.
A review by Johnston K, Buxton MJ, Jones DR, Fitzpatrick R.
-
Cooperatives and their primary care emergency centres: organisation and impact.
By Hallam L, Henthorne K.
-
Screening for cystic fibrosis.
A review by Murray J, Cuckle H, Taylor G, Littlewood J, Hewison J.
-
A review of the use of health status measures in economic evaluation.
By Brazier J, Deverill M, Green C, Harper R, Booth A.
-
Methods for the analysis of quality-of-life and survival data in health technology assessment.
A review by Billingham LJ, Abrams KR, Jones DR.
-
Antenatal and neonatal haemoglobinopathy screening in the UK: review and economic analysis.
By Zeuner D, Ades AE, Karnon J, Brown J, Dezateux C, Anionwu EN.
-
Assessing the quality of reports of randomised trials: implications for the conduct of meta-analyses.
A review by Moher D, Cook DJ, Jadad AR, Tugwell P, Moher M, Jones A, et al.
-
‘Early warning systems’ for identifying new healthcare technologies.
By Robert G, Stevens A, Gabbay J.
-
A systematic review of the role of human papillomavirus testing within a cervical screening programme.
By Cuzick J, Sasieni P, Davies P, Adams J, Normand C, Frater A, et al.
-
Near patient testing in diabetes clinics: appraising the costs and outcomes.
By Grieve R, Beech R, Vincent J, Mazurkiewicz J.
-
Positron emission tomography: establishing priorities for health technology assessment.
A review by Robert G, Milne R.
-
The debridement of chronic wounds: a systematic review.
By Bradley M, Cullum N, Sheldon T.
-
Systematic reviews of wound care management: (2) Dressings and topical agents used in the healing of chronic wounds.
By Bradley M, Cullum N, Nelson EA, Petticrew M, Sheldon T, Torgerson D.
-
A systematic literature review of spiral and electron beam computed tomography: with particular reference to clinical applications in hepatic lesions, pulmonary embolus and coronary artery disease.
By Berry E, Kelly S, Hutton J, Harris KM, Roderick P, Boyce JC, et al.
-
What role for statins? A review and economic model.
By Ebrahim S, Davey Smith G, McCabe C, Payne N, Pickin M, Sheldon TA, et al.
-
Factors that limit the quality, number and progress of randomised controlled trials.
A review by Prescott RJ, Counsell CE, Gillespie WJ, Grant AM, Russell IT, Kiauka S, et al.
-
Antimicrobial prophylaxis in total hip replacement: a systematic review.
By Glenny AM, Song F.
-
Health promoting schools and health promotion in schools: two systematic reviews.
By Lister-Sharp D, Chapman S, Stewart-Brown S, Sowden A.
-
Economic evaluation of a primary care-based education programme for patients with osteoarthritis of the knee.
A review by Lord J, Victor C, Littlejohns P, Ross FM, Axford JS.
-
The estimation of marginal time preference in a UK-wide sample (TEMPUS) project.
A review by Cairns JA, van der Pol MM.
-
Geriatric rehabilitation following fractures in older people: a systematic review.
By Cameron I, Crotty M, Currie C, Finnegan T, Gillespie L, Gillespie W, et al.
-
Screening for sickle cell disease and thalassaemia: a systematic review with supplementary research.
By Davies SC, Cronin E, Gill M, Greengross P, Hickman M, Normand C.
-
Community provision of hearing aids and related audiology services.
A review by Reeves DJ, Alborz A, Hickson FS, Bamford JM.
-
False-negative results in screening programmes: systematic review of impact and implications.
By Petticrew MP, Sowden AJ, Lister-Sharp D, Wright K.
-
Costs and benefits of community postnatal support workers: a randomised controlled trial.
By Morrell CJ, Spiby H, Stewart P, Walters S, Morgan A.
-
Implantable contraceptives (subdermal implants and hormonally impregnated intrauterine systems) versus other forms of reversible contraceptives: two systematic reviews to assess relative effectiveness, acceptability, tolerability and cost-effectiveness.
By French RS, Cowan FM, Mansour DJA, Morris S, Procter T, Hughes D, et al.
-
An introduction to statistical methods for health technology assessment.
A review by White SJ, Ashby D, Brown PJ.
-
Disease-modifying drugs for multiple sclerosis: a rapid and systematic review.
By Clegg A, Bryant J, Milne R.
-
Publication and related biases.
A review by Song F, Eastwood AJ, Gilbody S, Duley L, Sutton AJ.
-
Cost and outcome implications of the organisation of vascular services.
By Michaels J, Brazier J, Palfreyman S, Shackley P, Slack R.
-
Monitoring blood glucose control in diabetes mellitus: a systematic review.
By Coster S, Gulliford MC, Seed PT, Powrie JK, Swaminathan R.
-
The effectiveness of domiciliary health visiting: a systematic review of international studies and a selective review of the British literature.
By Elkan R, Kendrick D, Hewitt M, Robinson JJA, Tolley K, Blair M, et al.
-
The determinants of screening uptake and interventions for increasing uptake: a systematic review.
By Jepson R, Clegg A, Forbes C, Lewis R, Sowden A, Kleijnen J.
-
The effectiveness and cost-effectiveness of prophylactic removal of wisdom teeth.
A rapid review by Song F, O’Meara S, Wilson P, Golder S, Kleijnen J.
-
Ultrasound screening in pregnancy: a systematic review of the clinical effectiveness, cost-effectiveness and women’s views.
By Bricker L, Garcia J, Henderson J, Mugford M, Neilson J, Roberts T, et al.
-
A rapid and systematic review of the effectiveness and cost-effectiveness of the taxanes used in the treatment of advanced breast and ovarian cancer.
By Lister-Sharp D, McDonagh MS, Khan KS, Kleijnen J.
-
Liquid-based cytology in cervical screening: a rapid and systematic review.
By Payne N, Chilcott J, McGoogan E.
-
Randomised controlled trial of non-directive counselling, cognitive–behaviour therapy and usual general practitioner care in the management of depression as well as mixed anxiety and depression in primary care.
By King M, Sibbald B, Ward E, Bower P, Lloyd M, Gabbay M, et al.
-
Routine referral for radiography of patients presenting with low back pain: is patients’ outcome influenced by GPs’ referral for plain radiography?
By Kerry S, Hilton S, Patel S, Dundas D, Rink E, Lord J.
-
Systematic reviews of wound care management: (3) antimicrobial agents for chronic wounds; (4) diabetic foot ulceration.
By O’Meara S, Cullum N, Majid M, Sheldon T.
-
Using routine data to complement and enhance the results of randomised controlled trials.
By Lewsey JD, Leyland AH, Murray GD, Boddy FA.
-
Coronary artery stents in the treatment of ischaemic heart disease: a rapid and systematic review.
By Meads C, Cummins C, Jolly K, Stevens A, Burls A, Hyde C.
-
Outcome measures for adult critical care: a systematic review.
By Hayes JA, Black NA, Jenkinson C, Young JD, Rowan KM, Daly K, et al.
-
A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding.
By Fairbank L, O’Meara S, Renfrew MJ, Woolridge M, Sowden AJ, Lister-Sharp D.
-
Implantable cardioverter defibrillators: arrhythmias. A rapid and systematic review.
By Parkes J, Bryant J, Milne R.
-
Treatments for fatigue in multiple sclerosis: a rapid and systematic review.
By Brañas P, Jordan R, Fry-Smith A, Burls A, Hyde C.
-
Early asthma prophylaxis, natural history, skeletal development and economy (EASE): a pilot randomised controlled trial.
By Baxter-Jones ADG, Helms PJ, Russell G, Grant A, Ross S, Cairns JA, et al.
-
Screening for hypercholesterolaemia versus case finding for familial hypercholesterolaemia: a systematic review and cost-effectiveness analysis.
By Marks D, Wonderling D, Thorogood M, Lambert H, Humphries SE, Neil HAW.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of glycoprotein IIb/IIIa antagonists in the medical management of unstable angina.
By McDonagh MS, Bachmann LM, Golder S, Kleijnen J, ter Riet G.
-
A randomised controlled trial of prehospital intravenous fluid replacement therapy in serious trauma.
By Turner J, Nicholl J, Webber L, Cox H, Dixon S, Yates D.
-
Intrathecal pumps for giving opioids in chronic pain: a systematic review.
By Williams JE, Louw G, Towlerton G.
-
Combination therapy (interferon alfa and ribavirin) in the treatment of chronic hepatitis C: a rapid and systematic review.
By Shepherd J, Waugh N, Hewitson P.
-
A systematic review of comparisons of effect sizes derived from randomised and non-randomised studies.
By MacLehose RR, Reeves BC, Harvey IM, Sheldon TA, Russell IT, Black AMS.
-
Intravascular ultrasound-guided interventions in coronary artery disease: a systematic literature review, with decision-analytic modelling, of outcomes and cost-effectiveness.
By Berry E, Kelly S, Hutton J, Lindsay HSJ, Blaxill JM, Evans JA, et al.
-
A randomised controlled trial to evaluate the effectiveness and cost-effectiveness of counselling patients with chronic depression.
By Simpson S, Corney R, Fitzgerald P, Beecham J.
-
Systematic review of treatments for atopic eczema.
By Hoare C, Li Wan Po A, Williams H.
-
Bayesian methods in health technology assessment: a review.
By Spiegelhalter DJ, Myles JP, Jones DR, Abrams KR.
-
The management of dyspepsia: a systematic review.
By Delaney B, Moayyedi P, Deeks J, Innes M, Soo S, Barton P, et al.
-
A systematic review of treatments for severe psoriasis.
By Griffiths CEM, Clark CM, Chalmers RJG, Li Wan Po A, Williams HC.
-
Clinical and cost-effectiveness of donepezil, rivastigmine and galantamine for Alzheimer’s disease: a rapid and systematic review.
By Clegg A, Bryant J, Nicholson T, McIntyre L, De Broe S, Gerard K, et al.
-
The clinical effectiveness and cost-effectiveness of riluzole for motor neurone disease: a rapid and systematic review.
By Stewart A, Sandercock J, Bryan S, Hyde C, Barton PM, Fry-Smith A, et al.
-
Equity and the economic evaluation of healthcare.
By Sassi F, Archard L, Le Grand J.
-
Quality-of-life measures in chronic diseases of childhood.
By Eiser C, Morse R.
-
Eliciting public preferences for healthcare: a systematic review of techniques.
By Ryan M, Scott DA, Reeves C, Bate A, van Teijlingen ER, Russell EM, et al.
-
General health status measures for people with cognitive impairment: learning disability and acquired brain injury.
By Riemsma RP, Forbes CA, Glanville JM, Eastwood AJ, Kleijnen J.
-
An assessment of screening strategies for fragile X syndrome in the UK.
By Pembrey ME, Barnicoat AJ, Carmichael B, Bobrow M, Turner G.
-
Issues in methodological research: perspectives from researchers and commissioners.
By Lilford RJ, Richardson A, Stevens A, Fitzpatrick R, Edwards S, Rock F, et al.
-
Systematic reviews of wound care management: (5) beds; (6) compression; (7) laser therapy, therapeutic ultrasound, electrotherapy and electromagnetic therapy.
By Cullum N, Nelson EA, Flemming K, Sheldon T.
-
Effects of educational and psychosocial interventions for adolescents with diabetes mellitus: a systematic review.
By Hampson SE, Skinner TC, Hart J, Storey L, Gage H, Foxcroft D, et al.
-
Effectiveness of autologous chondrocyte transplantation for hyaline cartilage defects in knees: a rapid and systematic review.
By Jobanputra P, Parry D, Fry-Smith A, Burls A.
-
Statistical assessment of the learning curves of health technologies.
By Ramsay CR, Grant AM, Wallace SA, Garthwaite PH, Monk AF, Russell IT.
-
The effectiveness and cost-effectiveness of temozolomide for the treatment of recurrent malignant glioma: a rapid and systematic review.
By Dinnes J, Cave C, Huang S, Major K, Milne R.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of debriding agents in treating surgical wounds healing by secondary intention.
By Lewis R, Whiting P, ter Riet G, O’Meara S, Glanville J.
-
Home treatment for mental health problems: a systematic review.
By Burns T, Knapp M, Catty J, Healey A, Henderson J, Watt H, et al.
-
How to develop cost-conscious guidelines.
By Eccles M, Mason J.
-
The role of specialist nurses in multiple sclerosis: a rapid and systematic review.
By De Broe S, Christopher F, Waugh N.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of orlistat in the management of obesity.
By O’Meara S, Riemsma R, Shirran L, Mather L, ter Riet G.
-
The clinical effectiveness and cost-effectiveness of pioglitazone for type 2 diabetes mellitus: a rapid and systematic review.
By Chilcott J, Wight J, Lloyd Jones M, Tappenden P.
-
Extended scope of nursing practice: a multicentre randomised controlled trial of appropriately trained nurses and preregistration house officers in preoperative assessment in elective general surgery.
By Kinley H, Czoski-Murray C, George S, McCabe C, Primrose J, Reilly C, et al.
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) Acute day hospital versus admission; (2) Vocational rehabilitation; (3) Day hospital versus outpatient care.
By Marshall M, Crowther R, Almaraz- Serrano A, Creed F, Sledge W, Kluiter H, et al.
-
The measurement and monitoring of surgical adverse events.
By Bruce J, Russell EM, Mollison J, Krukowski ZH.
-
Action research: a systematic review and guidance for assessment.
By Waterman H, Tillen D, Dickson R, de Koning K.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of gemcitabine for the treatment of pancreatic cancer.
By Ward S, Morris E, Bansback N, Calvert N, Crellin A, Forman D, et al.
-
A rapid and systematic review of the evidence for the clinical effectiveness and cost-effectiveness of irinotecan, oxaliplatin and raltitrexed for the treatment of advanced colorectal cancer.
By Lloyd Jones M, Hummel S, Bansback N, Orr B, Seymour M.
-
Comparison of the effectiveness of inhaler devices in asthma and chronic obstructive airways disease: a systematic review of the literature.
By Brocklebank D, Ram F, Wright J, Barry P, Cates C, Davies L, et al.
-
The cost-effectiveness of magnetic resonance imaging for investigation of the knee joint.
By Bryan S, Weatherburn G, Bungay H, Hatrick C, Salas C, Parry D, et al.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.
By Forbes C, Shirran L, Bagnall A-M, Duffy S, ter Riet G.
-
Superseded by a report published in a later volume.
-
The role of radiography in primary care patients with low back pain of at least 6 weeks duration: a randomised (unblinded) controlled trial.
By Kendrick D, Fielding K, Bentley E, Miller P, Kerslake R, Pringle M.
-
Design and use of questionnaires: a review of best practice applicable to surveys of health service staff and patients.
By McColl E, Jacoby A, Thomas L, Soutter J, Bamford C, Steen N, et al.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.
By Clegg A, Scott DA, Sidhu M, Hewitson P, Waugh N.
-
Subgroup analyses in randomised controlled trials: quantifying the risks of false-positives and false-negatives.
By Brookes ST, Whitley E, Peters TJ, Mulheran PA, Egger M, Davey Smith G.
-
Depot antipsychotic medication in the treatment of patients with schizophrenia: (1) Meta-review; (2) Patient and nurse attitudes.
By David AS, Adams C.
-
A systematic review of controlled trials of the effectiveness and cost-effectiveness of brief psychological treatments for depression.
By Churchill R, Hunot V, Corney R, Knapp M, McGuire H, Tylee A, et al.
-
Cost analysis of child health surveillance.
By Sanderson D, Wright D, Acton C, Duree D.
-
A study of the methods used to select review criteria for clinical audit.
By Hearnshaw H, Harker R, Cheater F, Baker R, Grimshaw G.
-
Fludarabine as second-line therapy for B cell chronic lymphocytic leukaemia: a technology assessment.
By Hyde C, Wake B, Bryan S, Barton P, Fry-Smith A, Davenport C, et al.
-
Rituximab as third-line treatment for refractory or recurrent Stage III or IV follicular non-Hodgkin’s lymphoma: a systematic review and economic evaluation.
By Wake B, Hyde C, Bryan S, Barton P, Song F, Fry-Smith A, et al.
-
A systematic review of discharge arrangements for older people.
By Parker SG, Peet SM, McPherson A, Cannaby AM, Baker R, Wilson A, et al.
-
The clinical effectiveness and cost-effectiveness of inhaler devices used in the routine management of chronic asthma in older children: a systematic review and economic evaluation.
By Peters J, Stevenson M, Beverley C, Lim J, Smith S.
-
The clinical effectiveness and cost-effectiveness of sibutramine in the management of obesity: a technology assessment.
By O’Meara S, Riemsma R, Shirran L, Mather L, ter Riet G.
-
The cost-effectiveness of magnetic resonance angiography for carotid artery stenosis and peripheral vascular disease: a systematic review.
By Berry E, Kelly S, Westwood ME, Davies LM, Gough MJ, Bamford JM, et al.
-
Promoting physical activity in South Asian Muslim women through ‘exercise on prescription’.
By Carroll B, Ali N, Azam N.
-
Zanamivir for the treatment of influenza in adults: a systematic review and economic evaluation.
By Burls A, Clark W, Stewart T, Preston C, Bryan S, Jefferson T, et al.
-
A review of the natural history and epidemiology of multiple sclerosis: implications for resource allocation and health economic models.
By Richards RG, Sampson FC, Beard SM, Tappenden P.
-
Screening for gestational diabetes: a systematic review and economic evaluation.
By Scott DA, Loveman E, McIntyre L, Waugh N.
-
The clinical effectiveness and cost-effectiveness of surgery for people with morbid obesity: a systematic review and economic evaluation.
By Clegg AJ, Colquitt J, Sidhu MK, Royle P, Loveman E, Walker A.
-
The clinical effectiveness of trastuzumab for breast cancer: a systematic review.
By Lewis R, Bagnall A-M, Forbes C, Shirran E, Duffy S, Kleijnen J, et al.
-
The clinical effectiveness and cost-effectiveness of vinorelbine for breast cancer: a systematic review and economic evaluation.
By Lewis R, Bagnall A-M, King S, Woolacott N, Forbes C, Shirran L, et al.
-
A systematic review of the effectiveness and cost-effectiveness of metal-on-metal hip resurfacing arthroplasty for treatment of hip disease.
By Vale L, Wyness L, McCormack K, McKenzie L, Brazzelli M, Stearns SC.
-
The clinical effectiveness and cost-effectiveness of bupropion and nicotine replacement therapy for smoking cessation: a systematic review and economic evaluation.
By Woolacott NF, Jones L, Forbes CA, Mather LC, Sowden AJ, Song FJ, et al.
-
A systematic review of effectiveness and economic evaluation of new drug treatments for juvenile idiopathic arthritis: etanercept.
By Cummins C, Connock M, Fry-Smith A, Burls A.
-
Clinical effectiveness and cost-effectiveness of growth hormone in children: a systematic review and economic evaluation.
By Bryant J, Cave C, Mihaylova B, Chase D, McIntyre L, Gerard K, et al.
-
Clinical effectiveness and cost-effectiveness of growth hormone in adults in relation to impact on quality of life: a systematic review and economic evaluation.
By Bryant J, Loveman E, Chase D, Mihaylova B, Cave C, Gerard K, et al.
-
Clinical medication review by a pharmacist of patients on repeat prescriptions in general practice: a randomised controlled trial.
By Zermansky AG, Petty DR, Raynor DK, Lowe CJ, Freementle N, Vail A.
-
The effectiveness of infliximab and etanercept for the treatment of rheumatoid arthritis: a systematic review and economic evaluation.
By Jobanputra P, Barton P, Bryan S, Burls A.
-
A systematic review and economic evaluation of computerised cognitive behaviour therapy for depression and anxiety.
By Kaltenthaler E, Shackley P, Stevens K, Beverley C, Parry G, Chilcott J.
-
A systematic review and economic evaluation of pegylated liposomal doxorubicin hydrochloride for ovarian cancer.
By Forbes C, Wilby J, Richardson G, Sculpher M, Mather L, Riemsma R.
-
A systematic review of the effectiveness of interventions based on a stages-of-change approach to promote individual behaviour change.
By Riemsma RP, Pattenden J, Bridle C, Sowden AJ, Mather L, Watt IS, et al.
-
A systematic review update of the clinical effectiveness and cost-effectiveness of glycoprotein IIb/IIIa antagonists.
By Robinson M, Ginnelly L, Sculpher M, Jones L, Riemsma R, Palmer S, et al.
-
A systematic review of the effectiveness, cost-effectiveness and barriers to implementation of thrombolytic and neuroprotective therapy for acute ischaemic stroke in the NHS.
By Sandercock P, Berge E, Dennis M, Forbes J, Hand P, Kwan J, et al.
-
A randomised controlled crossover trial of nurse practitioner versus doctor-led outpatient care in a bronchiectasis clinic.
By Caine N, Sharples LD, Hollingworth W, French J, Keogan M, Exley A, et al.
-
Clinical effectiveness and cost – consequences of selective serotonin reuptake inhibitors in the treatment of sex offenders.
By Adi Y, Ashcroft D, Browne K, Beech A, Fry-Smith A, Hyde C.
-
Treatment of established osteoporosis: a systematic review and cost–utility analysis.
By Kanis JA, Brazier JE, Stevenson M, Calvert NW, Lloyd Jones M.
-
Which anaesthetic agents are cost-effective in day surgery? Literature review, national survey of practice and randomised controlled trial.
By Elliott RA, Payne K, Moore JK, Davies LM, Harper NJN, St Leger AS, et al.
-
Screening for hepatitis C among injecting drug users and in genitourinary medicine clinics: systematic reviews of effectiveness, modelling study and national survey of current practice.
By Stein K, Dalziel K, Walker A, McIntyre L, Jenkins B, Horne J, et al.
-
The measurement of satisfaction with healthcare: implications for practice from a systematic review of the literature.
By Crow R, Gage H, Hampson S, Hart J, Kimber A, Storey L, et al.
-
The effectiveness and cost-effectiveness of imatinib in chronic myeloid leukaemia: a systematic review.
By Garside R, Round A, Dalziel K, Stein K, Royle R.
-
A comparative study of hypertonic saline, daily and alternate-day rhDNase in children with cystic fibrosis.
By Suri R, Wallis C, Bush A, Thompson S, Normand C, Flather M, et al.
-
A systematic review of the costs and effectiveness of different models of paediatric home care.
By Parker G, Bhakta P, Lovett CA, Paisley S, Olsen R, Turner D, et al.
-
How important are comprehensive literature searches and the assessment of trial quality in systematic reviews? Empirical study.
By Egger M, Jüni P, Bartlett C, Holenstein F, Sterne J.
-
Systematic review of the effectiveness and cost-effectiveness, and economic evaluation, of home versus hospital or satellite unit haemodialysis for people with end-stage renal failure.
By Mowatt G, Vale L, Perez J, Wyness L, Fraser C, MacLeod A, et al.
-
Systematic review and economic evaluation of the effectiveness of infliximab for the treatment of Crohn’s disease.
By Clark W, Raftery J, Barton P, Song F, Fry-Smith A, Burls A.
-
A review of the clinical effectiveness and cost-effectiveness of routine anti-D prophylaxis for pregnant women who are rhesus negative.
By Chilcott J, Lloyd Jones M, Wight J, Forman K, Wray J, Beverley C, et al.
-
Systematic review and evaluation of the use of tumour markers in paediatric oncology: Ewing’s sarcoma and neuroblastoma.
By Riley RD, Burchill SA, Abrams KR, Heney D, Lambert PC, Jones DR, et al.
-
The cost-effectiveness of screening for Helicobacter pylori to reduce mortality and morbidity from gastric cancer and peptic ulcer disease: a discrete-event simulation model.
By Roderick P, Davies R, Raftery J, Crabbe D, Pearce R, Bhandari P, et al.
-
The clinical effectiveness and cost-effectiveness of routine dental checks: a systematic review and economic evaluation.
By Davenport C, Elley K, Salas C, Taylor-Weetman CL, Fry-Smith A, Bryan S, et al.
-
A multicentre randomised controlled trial assessing the costs and benefits of using structured information and analysis of women’s preferences in the management of menorrhagia.
By Kennedy ADM, Sculpher MJ, Coulter A, Dwyer N, Rees M, Horsley S, et al.
-
Clinical effectiveness and cost–utility of photodynamic therapy for wet age-related macular degeneration: a systematic review and economic evaluation.
By Meads C, Salas C, Roberts T, Moore D, Fry-Smith A, Hyde C.
-
Evaluation of molecular tests for prenatal diagnosis of chromosome abnormalities.
By Grimshaw GM, Szczepura A, Hultén M, MacDonald F, Nevin NC, Sutton F, et al.
-
First and second trimester antenatal screening for Down’s syndrome: the results of the Serum, Urine and Ultrasound Screening Study (SURUSS).
By Wald NJ, Rodeck C, Hackshaw AK, Walters J, Chitty L, Mackinson AM.
-
The effectiveness and cost-effectiveness of ultrasound locating devices for central venous access: a systematic review and economic evaluation.
By Calvert N, Hind D, McWilliams RG, Thomas SM, Beverley C, Davidson A.
-
A systematic review of atypical antipsychotics in schizophrenia.
By Bagnall A-M, Jones L, Lewis R, Ginnelly L, Glanville J, Torgerson D, et al.
-
Prostate Testing for Cancer and Treatment (ProtecT) feasibility study.
By Donovan J, Hamdy F, Neal D, Peters T, Oliver S, Brindle L, et al.
-
Early thrombolysis for the treatment of acute myocardial infarction: a systematic review and economic evaluation.
By Boland A, Dundar Y, Bagust A, Haycox A, Hill R, Mujica Mota R, et al.
-
Screening for fragile X syndrome: a literature review and modelling.
By Song FJ, Barton P, Sleightholme V, Yao GL, Fry-Smith A.
-
Systematic review of endoscopic sinus surgery for nasal polyps.
By Dalziel K, Stein K, Round A, Garside R, Royle P.
-
Towards efficient guidelines: how to monitor guideline use in primary care.
By Hutchinson A, McIntosh A, Cox S, Gilbert C.
-
Effectiveness and cost-effectiveness of acute hospital-based spinal cord injuries services: systematic review.
By Bagnall A-M, Jones L, Richardson G, Duffy S, Riemsma R.
-
Prioritisation of health technology assessment. The PATHS model: methods and case studies.
By Townsend J, Buxton M, Harper G.
-
Systematic review of the clinical effectiveness and cost-effectiveness of tension-free vaginal tape for treatment of urinary stress incontinence.
By Cody J, Wyness L, Wallace S, Glazener C, Kilonzo M, Stearns S, et al.
-
The clinical and cost-effectiveness of patient education models for diabetes: a systematic review and economic evaluation.
By Loveman E, Cave C, Green C, Royle P, Dunn N, Waugh N.
-
The role of modelling in prioritising and planning clinical trials.
By Chilcott J, Brennan A, Booth A, Karnon J, Tappenden P.
-
Cost–benefit evaluation of routine influenza immunisation in people 65–74 years of age.
By Allsup S, Gosney M, Haycox A, Regan M.
-
The clinical and cost-effectiveness of pulsatile machine perfusion versus cold storage of kidneys for transplantation retrieved from heart-beating and non-heart-beating donors.
By Wight J, Chilcott J, Holmes M, Brewer N.
-
Can randomised trials rely on existing electronic data? A feasibility study to explore the value of routine data in health technology assessment.
By Williams JG, Cheung WY, Cohen DR, Hutchings HA, Longo MF, Russell IT.
-
Evaluating non-randomised intervention studies.
By Deeks JJ, Dinnes J, D’Amico R, Sowden AJ, Sakarovitch C, Song F, et al.
-
A randomised controlled trial to assess the impact of a package comprising a patient-orientated, evidence-based self- help guidebook and patient-centred consultations on disease management and satisfaction in inflammatory bowel disease.
By Kennedy A, Nelson E, Reeves D, Richardson G, Roberts C, Robinson A, et al.
-
The effectiveness of diagnostic tests for the assessment of shoulder pain due to soft tissue disorders: a systematic review.
By Dinnes J, Loveman E, McIntyre L, Waugh N.
-
The value of digital imaging in diabetic retinopathy.
By Sharp PF, Olson J, Strachan F, Hipwell J, Ludbrook A, O’Donnell M, et al.
-
Lowering blood pressure to prevent myocardial infarction and stroke: a new preventive strategy.
By Law M, Wald N, Morris J.
-
Clinical and cost-effectiveness of capecitabine and tegafur with uracil for the treatment of metastatic colorectal cancer: systematic review and economic evaluation.
By Ward S, Kaltenthaler E, Cowan J, Brewer N.
-
Clinical and cost-effectiveness of new and emerging technologies for early localised prostate cancer: a systematic review.
By Hummel S, Paisley S, Morgan A, Currie E, Brewer N.
-
Literature searching for clinical and cost-effectiveness studies used in health technology assessment reports carried out for the National Institute for Clinical Excellence appraisal system.
By Royle P, Waugh N.
-
Systematic review and economic decision modelling for the prevention and treatment of influenza A and B.
By Turner D, Wailoo A, Nicholson K, Cooper N, Sutton A, Abrams K.
-
A randomised controlled trial to evaluate the clinical and cost-effectiveness of Hickman line insertions in adult cancer patients by nurses.
By Boland A, Haycox A, Bagust A, Fitzsimmons L.
-
Redesigning postnatal care: a randomised controlled trial of protocol-based midwifery-led care focused on individual women’s physical and psychological health needs.
By MacArthur C, Winter HR, Bick DE, Lilford RJ, Lancashire RJ, Knowles H, et al.
-
Estimating implied rates of discount in healthcare decision-making.
By West RR, McNabb R, Thompson AGH, Sheldon TA, Grimley Evans J.
-
Systematic review of isolation policies in the hospital management of methicillin-resistant Staphylococcus aureus: a review of the literature with epidemiological and economic modelling.
By Cooper BS, Stone SP, Kibbler CC, Cookson BD, Roberts JA, Medley GF, et al.
-
Treatments for spasticity and pain in multiple sclerosis: a systematic review.
By Beard S, Hunn A, Wight J.
-
The inclusion of reports of randomised trials published in languages other than English in systematic reviews.
By Moher D, Pham B, Lawson ML, Klassen TP.
-
The impact of screening on future health-promoting behaviours and health beliefs: a systematic review.
By Bankhead CR, Brett J, Bukach C, Webster P, Stewart-Brown S, Munafo M, et al.
-
What is the best imaging strategy for acute stroke?
By Wardlaw JM, Keir SL, Seymour J, Lewis S, Sandercock PAG, Dennis MS, et al.
-
Systematic review and modelling of the investigation of acute and chronic chest pain presenting in primary care.
By Mant J, McManus RJ, Oakes RAL, Delaney BC, Barton PM, Deeks JJ, et al.
-
The effectiveness and cost-effectiveness of microwave and thermal balloon endometrial ablation for heavy menstrual bleeding: a systematic review and economic modelling.
By Garside R, Stein K, Wyatt K, Round A, Price A.
-
A systematic review of the role of bisphosphonates in metastatic disease.
By Ross JR, Saunders Y, Edmonds PM, Patel S, Wonderling D, Normand C, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of capecitabine (Xeloda®) for locally advanced and/or metastatic breast cancer.
By Jones L, Hawkins N, Westwood M, Wright K, Richardson G, Riemsma R.
-
Effectiveness and efficiency of guideline dissemination and implementation strategies.
By Grimshaw JM, Thomas RE, MacLennan G, Fraser C, Ramsay CR, Vale L, et al.
-
Clinical effectiveness and costs of the Sugarbaker procedure for the treatment of pseudomyxoma peritonei.
By Bryant J, Clegg AJ, Sidhu MK, Brodin H, Royle P, Davidson P.
-
Psychological treatment for insomnia in the regulation of long-term hypnotic drug use.
By Morgan K, Dixon S, Mathers N, Thompson J, Tomeny M.
-
Improving the evaluation of therapeutic interventions in multiple sclerosis: development of a patient-based measure of outcome.
By Hobart JC, Riazi A, Lamping DL, Fitzpatrick R, Thompson AJ.
-
A systematic review and economic evaluation of magnetic resonance cholangiopancreatography compared with diagnostic endoscopic retrograde cholangiopancreatography.
By Kaltenthaler E, Bravo Vergel Y, Chilcott J, Thomas S, Blakeborough T, Walters SJ, et al.
-
The use of modelling to evaluate new drugs for patients with a chronic condition: the case of antibodies against tumour necrosis factor in rheumatoid arthritis.
By Barton P, Jobanputra P, Wilson J, Bryan S, Burls A.
-
Clinical effectiveness and cost-effectiveness of neonatal screening for inborn errors of metabolism using tandem mass spectrometry: a systematic review.
By Pandor A, Eastham J, Beverley C, Chilcott J, Paisley S.
-
Clinical effectiveness and cost-effectiveness of pioglitazone and rosiglitazone in the treatment of type 2 diabetes: a systematic review and economic evaluation.
By Czoski-Murray C, Warren E, Chilcott J, Beverley C, Psyllaki MA, Cowan J.
-
Routine examination of the newborn: the EMREN study. Evaluation of an extension of the midwife role including a randomised controlled trial of appropriately trained midwives and paediatric senior house officers.
By Townsend J, Wolke D, Hayes J, Davé S, Rogers C, Bloomfield L, et al.
-
Involving consumers in research and development agenda setting for the NHS: developing an evidence-based approach.
By Oliver S, Clarke-Jones L, Rees R, Milne R, Buchanan P, Gabbay J, et al.
-
A multi-centre randomised controlled trial of minimally invasive direct coronary bypass grafting versus percutaneous transluminal coronary angioplasty with stenting for proximal stenosis of the left anterior descending coronary artery.
By Reeves BC, Angelini GD, Bryan AJ, Taylor FC, Cripps T, Spyt TJ, et al.
-
Does early magnetic resonance imaging influence management or improve outcome in patients referred to secondary care with low back pain? A pragmatic randomised controlled trial.
By Gilbert FJ, Grant AM, Gillan MGC, Vale L, Scott NW, Campbell MK, et al.
-
The clinical and cost-effectiveness of anakinra for the treatment of rheumatoid arthritis in adults: a systematic review and economic analysis.
By Clark W, Jobanputra P, Barton P, Burls A.
-
A rapid and systematic review and economic evaluation of the clinical and cost-effectiveness of newer drugs for treatment of mania associated with bipolar affective disorder.
By Bridle C, Palmer S, Bagnall A-M, Darba J, Duffy S, Sculpher M, et al.
-
Liquid-based cytology in cervical screening: an updated rapid and systematic review and economic analysis.
By Karnon J, Peters J, Platt J, Chilcott J, McGoogan E, Brewer N.
-
Systematic review of the long-term effects and economic consequences of treatments for obesity and implications for health improvement.
By Avenell A, Broom J, Brown TJ, Poobalan A, Aucott L, Stearns SC, et al.
-
Autoantibody testing in children with newly diagnosed type 1 diabetes mellitus.
By Dretzke J, Cummins C, Sandercock J, Fry-Smith A, Barrett T, Burls A.
-
Clinical effectiveness and cost-effectiveness of prehospital intravenous fluids in trauma patients.
By Dretzke J, Sandercock J, Bayliss S, Burls A.
-
Newer hypnotic drugs for the short-term management of insomnia: a systematic review and economic evaluation.
By Dündar Y, Boland A, Strobl J, Dodd S, Haycox A, Bagust A, et al.
-
Development and validation of methods for assessing the quality of diagnostic accuracy studies.
By Whiting P, Rutjes AWS, Dinnes J, Reitsma JB, Bossuyt PMM, Kleijnen J.
-
EVALUATE hysterectomy trial: a multicentre randomised trial comparing abdominal, vaginal and laparoscopic methods of hysterectomy.
By Garry R, Fountain J, Brown J, Manca A, Mason S, Sculpher M, et al.
-
Methods for expected value of information analysis in complex health economic models: developments on the health economics of interferon-β and glatiramer acetate for multiple sclerosis.
By Tappenden P, Chilcott JB, Eggington S, Oakley J, McCabe C.
-
Effectiveness and cost-effectiveness of imatinib for first-line treatment of chronic myeloid leukaemia in chronic phase: a systematic review and economic analysis.
By Dalziel K, Round A, Stein K, Garside R, Price A.
-
VenUS I: a randomised controlled trial of two types of bandage for treating venous leg ulcers.
By Iglesias C, Nelson EA, Cullum NA, Torgerson DJ, on behalf of the VenUS Team.
-
Systematic review of the effectiveness and cost-effectiveness, and economic evaluation, of myocardial perfusion scintigraphy for the diagnosis and management of angina and myocardial infarction.
By Mowatt G, Vale L, Brazzelli M, Hernandez R, Murray A, Scott N, et al.
-
A pilot study on the use of decision theory and value of information analysis as part of the NHS Health Technology Assessment programme.
By Claxton K, Ginnelly L, Sculpher M, Philips Z, Palmer S.
-
The Social Support and Family Health Study: a randomised controlled trial and economic evaluation of two alternative forms of postnatal support for mothers living in disadvantaged inner-city areas.
By Wiggins M, Oakley A, Roberts I, Turner H, Rajan L, Austerberry H, et al.
-
Psychosocial aspects of genetic screening of pregnant women and newborns: a systematic review.
By Green JM, Hewison J, Bekker HL, Bryant LD, Cuckle HS.
-
Evaluation of abnormal uterine bleeding: comparison of three outpatient procedures within cohorts defined by age and menopausal status.
By Critchley HOD, Warner P, Lee AJ, Brechin S, Guise J, Graham B.
-
Coronary artery stents: a rapid systematic review and economic evaluation.
By Hill R, Bagust A, Bakhai A, Dickson R, Dündar Y, Haycox A, et al.
-
Review of guidelines for good practice in decision-analytic modelling in health technology assessment.
By Philips Z, Ginnelly L, Sculpher M, Claxton K, Golder S, Riemsma R, et al.
-
Rituximab (MabThera®) for aggressive non-Hodgkin’s lymphoma: systematic review and economic evaluation.
By Knight C, Hind D, Brewer N, Abbott V.
-
Clinical effectiveness and cost-effectiveness of clopidogrel and modified-release dipyridamole in the secondary prevention of occlusive vascular events: a systematic review and economic evaluation.
By Jones L, Griffin S, Palmer S, Main C, Orton V, Sculpher M, et al.
-
Pegylated interferon α-2a and -2b in combination with ribavirin in the treatment of chronic hepatitis C: a systematic review and economic evaluation.
By Shepherd J, Brodin H, Cave C, Waugh N, Price A, Gabbay J.
-
Clopidogrel used in combination with aspirin compared with aspirin alone in the treatment of non-ST-segment- elevation acute coronary syndromes: a systematic review and economic evaluation.
By Main C, Palmer S, Griffin S, Jones L, Orton V, Sculpher M, et al.
-
Provision, uptake and cost of cardiac rehabilitation programmes: improving services to under-represented groups.
By Beswick AD, Rees K, Griebsch I, Taylor FC, Burke M, West RR, et al.
-
Involving South Asian patients in clinical trials.
By Hussain-Gambles M, Leese B, Atkin K, Brown J, Mason S, Tovey P.
-
Clinical and cost-effectiveness of continuous subcutaneous insulin infusion for diabetes.
By Colquitt JL, Green C, Sidhu MK, Hartwell D, Waugh N.
-
Identification and assessment of ongoing trials in health technology assessment reviews.
By Song FJ, Fry-Smith A, Davenport C, Bayliss S, Adi Y, Wilson JS, et al.
-
Systematic review and economic evaluation of a long-acting insulin analogue, insulin glargine
By Warren E, Weatherley-Jones E, Chilcott J, Beverley C.
-
Supplementation of a home-based exercise programme with a class-based programme for people with osteoarthritis of the knees: a randomised controlled trial and health economic analysis.
By McCarthy CJ, Mills PM, Pullen R, Richardson G, Hawkins N, Roberts CR, et al.
-
Clinical and cost-effectiveness of once-daily versus more frequent use of same potency topical corticosteroids for atopic eczema: a systematic review and economic evaluation.
By Green C, Colquitt JL, Kirby J, Davidson P, Payne E.
-
Acupuncture of chronic headache disorders in primary care: randomised controlled trial and economic analysis.
By Vickers AJ, Rees RW, Zollman CE, McCarney R, Smith CM, Ellis N, et al.
-
Generalisability in economic evaluation studies in healthcare: a review and case studies.
By Sculpher MJ, Pang FS, Manca A, Drummond MF, Golder S, Urdahl H, et al.
-
Virtual outreach: a randomised controlled trial and economic evaluation of joint teleconferenced medical consultations.
By Wallace P, Barber J, Clayton W, Currell R, Fleming K, Garner P, et al.
-
Randomised controlled multiple treatment comparison to provide a cost-effectiveness rationale for the selection of antimicrobial therapy in acne.
By Ozolins M, Eady EA, Avery A, Cunliffe WJ, O’Neill C, Simpson NB, et al.
-
Do the findings of case series studies vary significantly according to methodological characteristics?
By Dalziel K, Round A, Stein K, Garside R, Castelnuovo E, Payne L.
-
Improving the referral process for familial breast cancer genetic counselling: findings of three randomised controlled trials of two interventions.
By Wilson BJ, Torrance N, Mollison J, Wordsworth S, Gray JR, Haites NE, et al.
-
Randomised evaluation of alternative electrosurgical modalities to treat bladder outflow obstruction in men with benign prostatic hyperplasia.
By Fowler C, McAllister W, Plail R, Karim O, Yang Q.
-
A pragmatic randomised controlled trial of the cost-effectiveness of palliative therapies for patients with inoperable oesophageal cancer.
By Shenfine J, McNamee P, Steen N, Bond J, Griffin SM.
-
Impact of computer-aided detection prompts on the sensitivity and specificity of screening mammography.
By Taylor P, Champness J, Given- Wilson R, Johnston K, Potts H.
-
Issues in data monitoring and interim analysis of trials.
By Grant AM, Altman DG, Babiker AB, Campbell MK, Clemens FJ, Darbyshire JH, et al.
-
Lay public’s understanding of equipoise and randomisation in randomised controlled trials.
By Robinson EJ, Kerr CEP, Stevens AJ, Lilford RJ, Braunholtz DA, Edwards SJ, et al.
-
Clinical and cost-effectiveness of electroconvulsive therapy for depressive illness, schizophrenia, catatonia and mania: systematic reviews and economic modelling studies.
By Greenhalgh J, Knight C, Hind D, Beverley C, Walters S.
-
Measurement of health-related quality of life for people with dementia: development of a new instrument (DEMQOL) and an evaluation of current methodology.
By Smith SC, Lamping DL, Banerjee S, Harwood R, Foley B, Smith P, et al.
-
Clinical effectiveness and cost-effectiveness of drotrecogin alfa (activated) (Xigris®) for the treatment of severe sepsis in adults: a systematic review and economic evaluation.
By Green C, Dinnes J, Takeda A, Shepherd J, Hartwell D, Cave C, et al.
-
A methodological review of how heterogeneity has been examined in systematic reviews of diagnostic test accuracy.
By Dinnes J, Deeks J, Kirby J, Roderick P.
-
Cervical screening programmes: can automation help? Evidence from systematic reviews, an economic analysis and a simulation modelling exercise applied to the UK.
By Willis BH, Barton P, Pearmain P, Bryan S, Hyde C.
-
Laparoscopic surgery for inguinal hernia repair: systematic review of effectiveness and economic evaluation.
By McCormack K, Wake B, Perez J, Fraser C, Cook J, McIntosh E, et al.
-
Clinical effectiveness, tolerability and cost-effectiveness of newer drugs for epilepsy in adults: a systematic review and economic evaluation.
By Wilby J, Kainth A, Hawkins N, Epstein D, McIntosh H, McDaid C, et al.
-
A randomised controlled trial to compare the cost-effectiveness of tricyclic antidepressants, selective serotonin reuptake inhibitors and lofepramine.
By Peveler R, Kendrick T, Buxton M, Longworth L, Baldwin D, Moore M, et al.
-
Clinical effectiveness and cost-effectiveness of immediate angioplasty for acute myocardial infarction: systematic review and economic evaluation.
By Hartwell D, Colquitt J, Loveman E, Clegg AJ, Brodin H, Waugh N, et al.
-
A randomised controlled comparison of alternative strategies in stroke care.
By Kalra L, Evans A, Perez I, Knapp M, Swift C, Donaldson N.
-
The investigation and analysis of critical incidents and adverse events in healthcare.
By Woloshynowych M, Rogers S, Taylor-Adams S, Vincent C.
-
Potential use of routine databases in health technology assessment.
By Raftery J, Roderick P, Stevens A.
-
Clinical and cost-effectiveness of newer immunosuppressive regimens in renal transplantation: a systematic review and modelling study.
By Woodroffe R, Yao GL, Meads C, Bayliss S, Ready A, Raftery J, et al.
-
A systematic review and economic evaluation of alendronate, etidronate, risedronate, raloxifene and teriparatide for the prevention and treatment of postmenopausal osteoporosis.
By Stevenson M, Lloyd Jones M, De Nigris E, Brewer N, Davis S, Oakley J.
-
A systematic review to examine the impact of psycho-educational interventions on health outcomes and costs in adults and children with difficult asthma.
By Smith JR, Mugford M, Holland R, Candy B, Noble MJ, Harrison BDW, et al.
-
An evaluation of the costs, effectiveness and quality of renal replacement therapy provision in renal satellite units in England and Wales.
By Roderick P, Nicholson T, Armitage A, Mehta R, Mullee M, Gerard K, et al.
-
Imatinib for the treatment of patients with unresectable and/or metastatic gastrointestinal stromal tumours: systematic review and economic evaluation.
By Wilson J, Connock M, Song F, Yao G, Fry-Smith A, Raftery J, et al.
-
Indirect comparisons of competing interventions.
By Glenny AM, Altman DG, Song F, Sakarovitch C, Deeks JJ, D’Amico R, et al.
-
Cost-effectiveness of alternative strategies for the initial medical management of non-ST elevation acute coronary syndrome: systematic review and decision-analytical modelling.
By Robinson M, Palmer S, Sculpher M, Philips Z, Ginnelly L, Bowens A, et al.
-
Outcomes of electrically stimulated gracilis neosphincter surgery.
By Tillin T, Chambers M, Feldman R.
-
The effectiveness and cost-effectiveness of pimecrolimus and tacrolimus for atopic eczema: a systematic review and economic evaluation.
By Garside R, Stein K, Castelnuovo E, Pitt M, Ashcroft D, Dimmock P, et al.
-
Systematic review on urine albumin testing for early detection of diabetic complications.
By Newman DJ, Mattock MB, Dawnay ABS, Kerry S, McGuire A, Yaqoob M, et al.
-
Randomised controlled trial of the cost-effectiveness of water-based therapy for lower limb osteoarthritis.
By Cochrane T, Davey RC, Matthes Edwards SM.
-
Longer term clinical and economic benefits of offering acupuncture care to patients with chronic low back pain.
By Thomas KJ, MacPherson H, Ratcliffe J, Thorpe L, Brazier J, Campbell M, et al.
-
Cost-effectiveness and safety of epidural steroids in the management of sciatica.
By Price C, Arden N, Coglan L, Rogers P.
-
The British Rheumatoid Outcome Study Group (BROSG) randomised controlled trial to compare the effectiveness and cost-effectiveness of aggressive versus symptomatic therapy in established rheumatoid arthritis.
By Symmons D, Tricker K, Roberts C, Davies L, Dawes P, Scott DL.
-
Conceptual framework and systematic review of the effects of participants’ and professionals’ preferences in randomised controlled trials.
By King M, Nazareth I, Lampe F, Bower P, Chandler M, Morou M, et al.
-
The clinical and cost-effectiveness of implantable cardioverter defibrillators: a systematic review.
By Bryant J, Brodin H, Loveman E, Payne E, Clegg A.
-
A trial of problem-solving by community mental health nurses for anxiety, depression and life difficulties among general practice patients. The CPN-GP study.
By Kendrick T, Simons L, Mynors-Wallis L, Gray A, Lathlean J, Pickering R, et al.
-
The causes and effects of socio-demographic exclusions from clinical trials.
By Bartlett C, Doyal L, Ebrahim S, Davey P, Bachmann M, Egger M, et al.
-
Is hydrotherapy cost-effective? A randomised controlled trial of combined hydrotherapy programmes compared with physiotherapy land techniques in children with juvenile idiopathic arthritis.
By Epps H, Ginnelly L, Utley M, Southwood T, Gallivan S, Sculpher M, et al.
-
A randomised controlled trial and cost-effectiveness study of systematic screening (targeted and total population screening) versus routine practice for the detection of atrial fibrillation in people aged 65 and over. The SAFE study.
By Hobbs FDR, Fitzmaurice DA, Mant J, Murray E, Jowett S, Bryan S, et al.
-
Displaced intracapsular hip fractures in fit, older people: a randomised comparison of reduction and fixation, bipolar hemiarthroplasty and total hip arthroplasty.
By Keating JF, Grant A, Masson M, Scott NW, Forbes JF.
-
Long-term outcome of cognitive behaviour therapy clinical trials in central Scotland.
By Durham RC, Chambers JA, Power KG, Sharp DM, Macdonald RR, Major KA, et al.
-
The effectiveness and cost-effectiveness of dual-chamber pacemakers compared with single-chamber pacemakers for bradycardia due to atrioventricular block or sick sinus syndrome: systematic review and economic evaluation.
By Castelnuovo E, Stein K, Pitt M, Garside R, Payne E.
-
Newborn screening for congenital heart defects: a systematic review and cost-effectiveness analysis.
By Knowles R, Griebsch I, Dezateux C, Brown J, Bull C, Wren C.
-
The clinical and cost-effectiveness of left ventricular assist devices for end-stage heart failure: a systematic review and economic evaluation.
By Clegg AJ, Scott DA, Loveman E, Colquitt J, Hutchinson J, Royle P, et al.
-
The effectiveness of the Heidelberg Retina Tomograph and laser diagnostic glaucoma scanning system (GDx) in detecting and monitoring glaucoma.
By Kwartz AJ, Henson DB, Harper RA, Spencer AF, McLeod D.
-
Clinical and cost-effectiveness of autologous chondrocyte implantation for cartilage defects in knee joints: systematic review and economic evaluation.
By Clar C, Cummins E, McIntyre L, Thomas S, Lamb J, Bain L, et al.
-
Systematic review of effectiveness of different treatments for childhood retinoblastoma.
By McDaid C, Hartley S, Bagnall A-M, Ritchie G, Light K, Riemsma R.
-
Towards evidence-based guidelines for the prevention of venous thromboembolism: systematic reviews of mechanical methods, oral anticoagulation, dextran and regional anaesthesia as thromboprophylaxis.
By Roderick P, Ferris G, Wilson K, Halls H, Jackson D, Collins R, et al.
-
The effectiveness and cost-effectiveness of parent training/education programmes for the treatment of conduct disorder, including oppositional defiant disorder, in children.
By Dretzke J, Frew E, Davenport C, Barlow J, Stewart-Brown S, Sandercock J, et al.
-
The clinical and cost-effectiveness of donepezil, rivastigmine, galantamine and memantine for Alzheimer’s disease.
By Loveman E, Green C, Kirby J, Takeda A, Picot J, Payne E, et al.
-
FOOD: a multicentre randomised trial evaluating feeding policies in patients admitted to hospital with a recent stroke.
By Dennis M, Lewis S, Cranswick G, Forbes J.
-
The clinical effectiveness and cost-effectiveness of computed tomography screening for lung cancer: systematic reviews.
By Black C, Bagust A, Boland A, Walker S, McLeod C, De Verteuil R, et al.
-
A systematic review of the effectiveness and cost-effectiveness of neuroimaging assessments used to visualise the seizure focus in people with refractory epilepsy being considered for surgery.
By Whiting P, Gupta R, Burch J, Mujica Mota RE, Wright K, Marson A, et al.
-
Comparison of conference abstracts and presentations with full-text articles in the health technology assessments of rapidly evolving technologies.
By Dundar Y, Dodd S, Dickson R, Walley T, Haycox A, Williamson PR.
-
Systematic review and evaluation of methods of assessing urinary incontinence.
By Martin JL, Williams KS, Abrams KR, Turner DA, Sutton AJ, Chapple C, et al.
-
The clinical effectiveness and cost-effectiveness of newer drugs for children with epilepsy. A systematic review.
By Connock M, Frew E, Evans B-W, Bryan S, Cummins C, Fry-Smith A, et al.
-
Surveillance of Barrett’s oesophagus: exploring the uncertainty through systematic review, expert workshop and economic modelling.
By Garside R, Pitt M, Somerville M, Stein K, Price A, Gilbert N.
-
Topotecan, pegylated liposomal doxorubicin hydrochloride and paclitaxel for second-line or subsequent treatment of advanced ovarian cancer: a systematic review and economic evaluation.
By Main C, Bojke L, Griffin S, Norman G, Barbieri M, Mather L, et al.
-
Evaluation of molecular techniques in prediction and diagnosis of cytomegalovirus disease in immunocompromised patients.
By Szczepura A, Westmoreland D, Vinogradova Y, Fox J, Clark M.
-
Screening for thrombophilia in high-risk situations: systematic review and cost-effectiveness analysis. The Thrombosis: Risk and Economic Assessment of Thrombophilia Screening (TREATS) study.
By Wu O, Robertson L, Twaddle S, Lowe GDO, Clark P, Greaves M, et al.
-
A series of systematic reviews to inform a decision analysis for sampling and treating infected diabetic foot ulcers.
By Nelson EA, O’Meara S, Craig D, Iglesias C, Golder S, Dalton J, et al.
-
Randomised clinical trial, observational study and assessment of cost-effectiveness of the treatment of varicose veins (REACTIV trial).
By Michaels JA, Campbell WB, Brazier JE, MacIntyre JB, Palfreyman SJ, Ratcliffe J, et al.
-
The cost-effectiveness of screening for oral cancer in primary care.
By Speight PM, Palmer S, Moles DR, Downer MC, Smith DH, Henriksson M, et al.
-
Measurement of the clinical and cost-effectiveness of non-invasive diagnostic testing strategies for deep vein thrombosis.
By Goodacre S, Sampson F, Stevenson M, Wailoo A, Sutton A, Thomas S, et al.
-
Systematic review of the effectiveness and cost-effectiveness of HealOzone® for the treatment of occlusal pit/fissure caries and root caries.
By Brazzelli M, McKenzie L, Fielding S, Fraser C, Clarkson J, Kilonzo M, et al.
-
Randomised controlled trials of conventional antipsychotic versus new atypical drugs, and new atypical drugs versus clozapine, in people with schizophrenia responding poorly to, or intolerant of, current drug treatment.
By Lewis SW, Davies L, Jones PB, Barnes TRE, Murray RM, Kerwin R, et al.
-
Diagnostic tests and algorithms used in the investigation of haematuria: systematic reviews and economic evaluation.
By Rodgers M, Nixon J, Hempel S, Aho T, Kelly J, Neal D, et al.
-
Cognitive behavioural therapy in addition to antispasmodic therapy for irritable bowel syndrome in primary care: randomised controlled trial.
By Kennedy TM, Chalder T, McCrone P, Darnley S, Knapp M, Jones RH, et al.
-
A systematic review of the clinical effectiveness and cost-effectiveness of enzyme replacement therapies for Fabry’s disease and mucopolysaccharidosis type 1.
By Connock M, Juarez-Garcia A, Frew E, Mans A, Dretzke J, Fry-Smith A, et al.
-
Health benefits of antiviral therapy for mild chronic hepatitis C: randomised controlled trial and economic evaluation.
By Wright M, Grieve R, Roberts J, Main J, Thomas HC, on behalf of the UK Mild Hepatitis C Trial Investigators.
-
Pressure relieving support surfaces: a randomised evaluation.
By Nixon J, Nelson EA, Cranny G, Iglesias CP, Hawkins K, Cullum NA, et al.
-
A systematic review and economic model of the effectiveness and cost-effectiveness of methylphenidate, dexamfetamine and atomoxetine for the treatment of attention deficit hyperactivity disorder in children and adolescents.
By King S, Griffin S, Hodges Z, Weatherly H, Asseburg C, Richardson G, et al.
-
The clinical effectiveness and cost-effectiveness of enzyme replacement therapy for Gaucher’s disease: a systematic review.
By Connock M, Burls A, Frew E, Fry-Smith A, Juarez-Garcia A, McCabe C, et al.
-
Effectiveness and cost-effectiveness of salicylic acid and cryotherapy for cutaneous warts. An economic decision model.
By Thomas KS, Keogh-Brown MR, Chalmers JR, Fordham RJ, Holland RC, Armstrong SJ, et al.
-
A systematic literature review of the effectiveness of non-pharmacological interventions to prevent wandering in dementia and evaluation of the ethical implications and acceptability of their use.
By Robinson L, Hutchings D, Corner L, Beyer F, Dickinson H, Vanoli A, et al.
-
A review of the evidence on the effects and costs of implantable cardioverter defibrillator therapy in different patient groups, and modelling of cost-effectiveness and cost–utility for these groups in a UK context.
By Buxton M, Caine N, Chase D, Connelly D, Grace A, Jackson C, et al.
-
Adefovir dipivoxil and pegylated interferon alfa-2a for the treatment of chronic hepatitis B: a systematic review and economic evaluation.
By Shepherd J, Jones J, Takeda A, Davidson P, Price A.
-
An evaluation of the clinical and cost-effectiveness of pulmonary artery catheters in patient management in intensive care: a systematic review and a randomised controlled trial.
By Harvey S, Stevens K, Harrison D, Young D, Brampton W, McCabe C, et al.
-
Accurate, practical and cost-effective assessment of carotid stenosis in the UK.
By Wardlaw JM, Chappell FM, Stevenson M, De Nigris E, Thomas S, Gillard J, et al.
-
Etanercept and infliximab for the treatment of psoriatic arthritis: a systematic review and economic evaluation.
By Woolacott N, Bravo Vergel Y, Hawkins N, Kainth A, Khadjesari Z, Misso K, et al.
-
The cost-effectiveness of testing for hepatitis C in former injecting drug users.
By Castelnuovo E, Thompson-Coon J, Pitt M, Cramp M, Siebert U, Price A, et al.
-
Computerised cognitive behaviour therapy for depression and anxiety update: a systematic review and economic evaluation.
By Kaltenthaler E, Brazier J, De Nigris E, Tumur I, Ferriter M, Beverley C, et al.
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.
By Williams C, Brunskill S, Altman D, Briggs A, Campbell H, Clarke M, et al.
-
Psychological therapies including dialectical behaviour therapy for borderline personality disorder: a systematic review and preliminary economic evaluation.
By Brazier J, Tumur I, Holmes M, Ferriter M, Parry G, Dent-Brown K, et al.
-
Clinical effectiveness and cost-effectiveness of tests for the diagnosis and investigation of urinary tract infection in children: a systematic review and economic model.
By Whiting P, Westwood M, Bojke L, Palmer S, Richardson G, Cooper J, et al.
-
Cognitive behavioural therapy in chronic fatigue syndrome: a randomised controlled trial of an outpatient group programme.
By O’Dowd H, Gladwell P, Rogers CA, Hollinghurst S, Gregory A.
-
A comparison of the cost-effectiveness of five strategies for the prevention of nonsteroidal anti-inflammatory drug-induced gastrointestinal toxicity: a systematic review with economic modelling.
By Brown TJ, Hooper L, Elliott RA, Payne K, Webb R, Roberts C, et al.
-
The effectiveness and cost-effectiveness of computed tomography screening for coronary artery disease: systematic review.
By Waugh N, Black C, Walker S, McIntyre L, Cummins E, Hillis G.
-
What are the clinical outcome and cost-effectiveness of endoscopy undertaken by nurses when compared with doctors? A Multi-Institution Nurse Endoscopy Trial (MINuET).
By Williams J, Russell I, Durai D, Cheung W-Y, Farrin A, Bloor K, et al.
-
The clinical and cost-effectiveness of oxaliplatin and capecitabine for the adjuvant treatment of colon cancer: systematic review and economic evaluation.
By Pandor A, Eggington S, Paisley S, Tappenden P, Sutcliffe P.
-
A systematic review of the effectiveness of adalimumab, etanercept and infliximab for the treatment of rheumatoid arthritis in adults and an economic evaluation of their cost-effectiveness.
By Chen Y-F, Jobanputra P, Barton P, Jowett S, Bryan S, Clark W, et al.
-
Telemedicine in dermatology: a randomised controlled trial.
By Bowns IR, Collins K, Walters SJ, McDonagh AJG.
-
Cost-effectiveness of cell salvage and alternative methods of minimising perioperative allogeneic blood transfusion: a systematic review and economic model.
By Davies L, Brown TJ, Haynes S, Payne K, Elliott RA, McCollum C.
-
Clinical effectiveness and cost-effectiveness of laparoscopic surgery for colorectal cancer: systematic reviews and economic evaluation.
By Murray A, Lourenco T, de Verteuil R, Hernandez R, Fraser C, McKinley A, et al.
-
Etanercept and efalizumab for the treatment of psoriasis: a systematic review.
By Woolacott N, Hawkins N, Mason A, Kainth A, Khadjesari Z, Bravo Vergel Y, et al.
-
Systematic reviews of clinical decision tools for acute abdominal pain.
By Liu JLY, Wyatt JC, Deeks JJ, Clamp S, Keen J, Verde P, et al.
-
Evaluation of the ventricular assist device programme in the UK.
By Sharples L, Buxton M, Caine N, Cafferty F, Demiris N, Dyer M, et al.
-
A systematic review and economic model of the clinical and cost-effectiveness of immunosuppressive therapy for renal transplantation in children.
By Yao G, Albon E, Adi Y, Milford D, Bayliss S, Ready A, et al.
-
Amniocentesis results: investigation of anxiety. The ARIA trial.
By Hewison J, Nixon J, Fountain J, Cocks K, Jones C, Mason G, et al.
-
Pemetrexed disodium for the treatment of malignant pleural mesothelioma: a systematic review and economic evaluation.
By Dundar Y, Bagust A, Dickson R, Dodd S, Green J, Haycox A, et al.
-
A systematic review and economic model of the clinical effectiveness and cost-effectiveness of docetaxel in combination with prednisone or prednisolone for the treatment of hormone-refractory metastatic prostate cancer.
By Collins R, Fenwick E, Trowman R, Perard R, Norman G, Light K, et al.
-
A systematic review of rapid diagnostic tests for the detection of tuberculosis infection.
By Dinnes J, Deeks J, Kunst H, Gibson A, Cummins E, Waugh N, et al.
-
The clinical effectiveness and cost-effectiveness of strontium ranelate for the prevention of osteoporotic fragility fractures in postmenopausal women.
By Stevenson M, Davis S, Lloyd-Jones M, Beverley C.
-
A systematic review of quantitative and qualitative research on the role and effectiveness of written information available to patients about individual medicines.
By Raynor DK, Blenkinsopp A, Knapp P, Grime J, Nicolson DJ, Pollock K, et al.
-
Oral naltrexone as a treatment for relapse prevention in formerly opioid-dependent drug users: a systematic review and economic evaluation.
By Adi Y, Juarez-Garcia A, Wang D, Jowett S, Frew E, Day E, et al.
-
Glucocorticoid-induced osteoporosis: a systematic review and cost–utility analysis.
By Kanis JA, Stevenson M, McCloskey EV, Davis S, Lloyd-Jones M.
-
Epidemiological, social, diagnostic and economic evaluation of population screening for genital chlamydial infection.
By Low N, McCarthy A, Macleod J, Salisbury C, Campbell R, Roberts TE, et al.
-
Methadone and buprenorphine for the management of opioid dependence: a systematic review and economic evaluation.
By Connock M, Juarez-Garcia A, Jowett S, Frew E, Liu Z, Taylor RJ, et al.
-
Exercise Evaluation Randomised Trial (EXERT): a randomised trial comparing GP referral for leisure centre-based exercise, community-based walking and advice only.
By Isaacs AJ, Critchley JA, See Tai S, Buckingham K, Westley D, Harridge SDR, et al.
-
Interferon alfa (pegylated and non-pegylated) and ribavirin for the treatment of mild chronic hepatitis C: a systematic review and economic evaluation.
By Shepherd J, Jones J, Hartwell D, Davidson P, Price A, Waugh N.
-
Systematic review and economic evaluation of bevacizumab and cetuximab for the treatment of metastatic colorectal cancer.
By Tappenden P, Jones R, Paisley S, Carroll C.
-
A systematic review and economic evaluation of epoetin alfa, epoetin beta and darbepoetin alfa in anaemia associated with cancer, especially that attributable to cancer treatment.
By Wilson J, Yao GL, Raftery J, Bohlius J, Brunskill S, Sandercock J, et al.
-
A systematic review and economic evaluation of statins for the prevention of coronary events.
By Ward S, Lloyd Jones M, Pandor A, Holmes M, Ara R, Ryan A, et al.
-
A systematic review of the effectiveness and cost-effectiveness of different models of community-based respite care for frail older people and their carers.
By Mason A, Weatherly H, Spilsbury K, Arksey H, Golder S, Adamson J, et al.
-
Additional therapy for young children with spastic cerebral palsy: a randomised controlled trial.
By Weindling AM, Cunningham CC, Glenn SM, Edwards RT, Reeves DJ.
-
Screening for type 2 diabetes: literature review and economic modelling.
By Waugh N, Scotland G, McNamee P, Gillett M, Brennan A, Goyder E, et al.
-
The effectiveness and cost-effectiveness of cinacalcet for secondary hyperparathyroidism in end-stage renal disease patients on dialysis: a systematic review and economic evaluation.
By Garside R, Pitt M, Anderson R, Mealing S, Roome C, Snaith A, et al.
-
The clinical effectiveness and cost-effectiveness of gemcitabine for metastatic breast cancer: a systematic review and economic evaluation.
By Takeda AL, Jones J, Loveman E, Tan SC, Clegg AJ.
-
A systematic review of duplex ultrasound, magnetic resonance angiography and computed tomography angiography for the diagnosis and assessment of symptomatic, lower limb peripheral arterial disease.
By Collins R, Cranny G, Burch J, Aguiar-Ibáñez R, Craig D, Wright K, et al.
-
The clinical effectiveness and cost-effectiveness of treatments for children with idiopathic steroid-resistant nephrotic syndrome: a systematic review.
By Colquitt JL, Kirby J, Green C, Cooper K, Trompeter RS.
-
A systematic review of the routine monitoring of growth in children of primary school age to identify growth-related conditions.
By Fayter D, Nixon J, Hartley S, Rithalia A, Butler G, Rudolf M, et al.
-
Systematic review of the effectiveness of preventing and treating Staphylococcus aureus carriage in reducing peritoneal catheter-related infections.
By McCormack K, Rabindranath K, Kilonzo M, Vale L, Fraser C, McIntyre L, et al.
-
The clinical effectiveness and cost of repetitive transcranial magnetic stimulation versus electroconvulsive therapy in severe depression: a multicentre pragmatic randomised controlled trial and economic analysis.
By McLoughlin DM, Mogg A, Eranti S, Pluck G, Purvis R, Edwards D, et al.
-
A randomised controlled trial and economic evaluation of direct versus indirect and individual versus group modes of speech and language therapy for children with primary language impairment.
By Boyle J, McCartney E, Forbes J, O’Hare A.
-
Hormonal therapies for early breast cancer: systematic review and economic evaluation.
By Hind D, Ward S, De Nigris E, Simpson E, Carroll C, Wyld L.
-
Cardioprotection against the toxic effects of anthracyclines given to children with cancer: a systematic review.
By Bryant J, Picot J, Levitt G, Sullivan I, Baxter L, Clegg A.
-
Adalimumab, etanercept and infliximab for the treatment of ankylosing spondylitis: a systematic review and economic evaluation.
By McLeod C, Bagust A, Boland A, Dagenais P, Dickson R, Dundar Y, et al.
-
Prenatal screening and treatment strategies to prevent group B streptococcal and other bacterial infections in early infancy: cost-effectiveness and expected value of information analyses.
By Colbourn T, Asseburg C, Bojke L, Philips Z, Claxton K, Ades AE, et al.
-
Clinical effectiveness and cost-effectiveness of bone morphogenetic proteins in the non-healing of fractures and spinal fusion: a systematic review.
By Garrison KR, Donell S, Ryder J, Shemilt I, Mugford M, Harvey I, et al.
-
A randomised controlled trial of postoperative radiotherapy following breast-conserving surgery in a minimum-risk older population. The PRIME trial.
By Prescott RJ, Kunkler IH, Williams LJ, King CC, Jack W, van der Pol M, et al.
-
Current practice, accuracy, effectiveness and cost-effectiveness of the school entry hearing screen.
By Bamford J, Fortnum H, Bristow K, Smith J, Vamvakas G, Davies L, et al.
-
The clinical effectiveness and cost-effectiveness of inhaled insulin in diabetes mellitus: a systematic review and economic evaluation.
By Black C, Cummins E, Royle P, Philip S, Waugh N.
-
Surveillance of cirrhosis for hepatocellular carcinoma: systematic review and economic analysis.
By Thompson Coon J, Rogers G, Hewson P, Wright D, Anderson R, Cramp M, et al.
-
The Birmingham Rehabilitation Uptake Maximisation Study (BRUM). Homebased compared with hospital-based cardiac rehabilitation in a multi-ethnic population: cost-effectiveness and patient adherence.
By Jolly K, Taylor R, Lip GYH, Greenfield S, Raftery J, Mant J, et al.
-
A systematic review of the clinical, public health and cost-effectiveness of rapid diagnostic tests for the detection and identification of bacterial intestinal pathogens in faeces and food.
By Abubakar I, Irvine L, Aldus CF, Wyatt GM, Fordham R, Schelenz S, et al.
-
A randomised controlled trial examining the longer-term outcomes of standard versus new antiepileptic drugs. The SANAD trial.
By Marson AG, Appleton R, Baker GA, Chadwick DW, Doughty J, Eaton B, et al.
-
Clinical effectiveness and cost-effectiveness of different models of managing long-term oral anti-coagulation therapy: a systematic review and economic modelling.
By Connock M, Stevens C, Fry-Smith A, Jowett S, Fitzmaurice D, Moore D, et al.
-
A systematic review and economic model of the clinical effectiveness and cost-effectiveness of interventions for preventing relapse in people with bipolar disorder.
By Soares-Weiser K, Bravo Vergel Y, Beynon S, Dunn G, Barbieri M, Duffy S, et al.
-
Taxanes for the adjuvant treatment of early breast cancer: systematic review and economic evaluation.
By Ward S, Simpson E, Davis S, Hind D, Rees A, Wilkinson A.
-
The clinical effectiveness and cost-effectiveness of screening for open angle glaucoma: a systematic review and economic evaluation.
By Burr JM, Mowatt G, Hernández R, Siddiqui MAR, Cook J, Lourenco T, et al.
-
Acceptability, benefit and costs of early screening for hearing disability: a study of potential screening tests and models.
By Davis A, Smith P, Ferguson M, Stephens D, Gianopoulos I.
-
Contamination in trials of educational interventions.
By Keogh-Brown MR, Bachmann MO, Shepstone L, Hewitt C, Howe A, Ramsay CR, et al.
-
Overview of the clinical effectiveness of positron emission tomography imaging in selected cancers.
By Facey K, Bradbury I, Laking G, Payne E.
-
The effectiveness and cost-effectiveness of carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma: a systematic review and economic evaluation.
By Garside R, Pitt M, Anderson R, Rogers G, Dyer M, Mealing S, et al.
-
Drug-eluting stents: a systematic review and economic evaluation.
By Hill RA, Boland A, Dickson R, Dündar Y, Haycox A, McLeod C, et al.
-
The clinical effectiveness and cost-effectiveness of cardiac resynchronisation (biventricular pacing) for heart failure: systematic review and economic model.
By Fox M, Mealing S, Anderson R, Dean J, Stein K, Price A, et al.
-
Recruitment to randomised trials: strategies for trial enrolment and participation study. The STEPS study.
By Campbell MK, Snowdon C, Francis D, Elbourne D, McDonald AM, Knight R, et al.
-
Cost-effectiveness of functional cardiac testing in the diagnosis and management of coronary artery disease: a randomised controlled trial. The CECaT trial.
By Sharples L, Hughes V, Crean A, Dyer M, Buxton M, Goldsmith K, et al.
-
Evaluation of diagnostic tests when there is no gold standard. A review of methods.
By Rutjes AWS, Reitsma JB, Coomarasamy A, Khan KS, Bossuyt PMM.
-
Systematic reviews of the clinical effectiveness and cost-effectiveness of proton pump inhibitors in acute upper gastrointestinal bleeding.
By Leontiadis GI, Sreedharan A, Dorward S, Barton P, Delaney B, Howden CW, et al.
-
A review and critique of modelling in prioritising and designing screening programmes.
By Karnon J, Goyder E, Tappenden P, McPhie S, Towers I, Brazier J, et al.
-
An assessment of the impact of the NHS Health Technology Assessment Programme.
By Hanney S, Buxton M, Green C, Coulson D, Raftery J.
-
A systematic review and economic model of switching from nonglycopeptide to glycopeptide antibiotic prophylaxis for surgery.
By Cranny G, Elliott R, Weatherly H, Chambers D, Hawkins N, Myers L, et al.
-
‘Cut down to quit’ with nicotine replacement therapies in smoking cessation: a systematic review of effectiveness and economic analysis.
By Wang D, Connock M, Barton P, Fry-Smith A, Aveyard P, Moore D.
-
A systematic review of the effectiveness of strategies for reducing fracture risk in children with juvenile idiopathic arthritis with additional data on long-term risk of fracture and cost of disease management.
By Thornton J, Ashcroft D, O’Neill T, Elliott R, Adams J, Roberts C, et al.
-
Does befriending by trained lay workers improve psychological well-being and quality of life for carers of people with dementia, and at what cost? A randomised controlled trial.
By Charlesworth G, Shepstone L, Wilson E, Thalanany M, Mugford M, Poland F.
-
A multi-centre retrospective cohort study comparing the efficacy, safety and cost-effectiveness of hysterectomy and uterine artery embolisation for the treatment of symptomatic uterine fibroids. The HOPEFUL study.
By Hirst A, Dutton S, Wu O, Briggs A, Edwards C, Waldenmaier L, et al.
-
Methods of prediction and prevention of pre-eclampsia: systematic reviews of accuracy and effectiveness literature with economic modelling.
By Meads CA, Cnossen JS, Meher S, Juarez-Garcia A, ter Riet G, Duley L, et al.
-
The use of economic evaluations in NHS decision-making: a review and empirical investigation.
By Williams I, McIver S, Moore D, Bryan S.
-
Stapled haemorrhoidectomy (haemorrhoidopexy) for the treatment of haemorrhoids: a systematic review and economic evaluation.
By Burch J, Epstein D, Baba-Akbari A, Weatherly H, Fox D, Golder S, et al.
-
The clinical effectiveness of diabetes education models for Type 2 diabetes: a systematic review.
By Loveman E, Frampton GK, Clegg AJ.
-
Payment to healthcare professionals for patient recruitment to trials: systematic review and qualitative study.
By Raftery J, Bryant J, Powell J, Kerr C, Hawker S.
-
Cyclooxygenase-2 selective non-steroidal anti-inflammatory drugs (etodolac, meloxicam, celecoxib, rofecoxib, etoricoxib, valdecoxib and lumiracoxib) for osteoarthritis and rheumatoid arthritis: a systematic review and economic evaluation.
By Chen Y-F, Jobanputra P, Barton P, Bryan S, Fry-Smith A, Harris G, et al.
-
The clinical effectiveness and cost-effectiveness of central venous catheters treated with anti-infective agents in preventing bloodstream infections: a systematic review and economic evaluation.
By Hockenhull JC, Dwan K, Boland A, Smith G, Bagust A, Dundar Y, et al.
-
Stepped treatment of older adults on laxatives. The STOOL trial.
By Mihaylov S, Stark C, McColl E, Steen N, Vanoli A, Rubin G, et al.
-
A randomised controlled trial of cognitive behaviour therapy in adolescents with major depression treated by selective serotonin reuptake inhibitors. The ADAPT trial.
By Goodyer IM, Dubicka B, Wilkinson P, Kelvin R, Roberts C, Byford S, et al.
-
The use of irinotecan, oxaliplatin and raltitrexed for the treatment of advanced colorectal cancer: systematic review and economic evaluation.
By Hind D, Tappenden P, Tumur I, Eggington E, Sutcliffe P, Ryan A.
-
Ranibizumab and pegaptanib for the treatment of age-related macular degeneration: a systematic review and economic evaluation.
By Colquitt JL, Jones J, Tan SC, Takeda A, Clegg AJ, Price A.
-
Systematic review of the clinical effectiveness and cost-effectiveness of 64-slice or higher computed tomography angiography as an alternative to invasive coronary angiography in the investigation of coronary artery disease.
By Mowatt G, Cummins E, Waugh N, Walker S, Cook J, Jia X, et al.
-
Structural neuroimaging in psychosis: a systematic review and economic evaluation.
By Albon E, Tsourapas A, Frew E, Davenport C, Oyebode F, Bayliss S, et al.
-
Systematic review and economic analysis of the comparative effectiveness of different inhaled corticosteroids and their usage with long-acting beta2 agonists for the treatment of chronic asthma in adults and children aged 12 years and over.
By Shepherd J, Rogers G, Anderson R, Main C, Thompson-Coon J, Hartwell D, et al.
-
Systematic review and economic analysis of the comparative effectiveness of different inhaled corticosteroids and their usage with long-acting beta2 agonists for the treatment of chronic asthma in children under the age of 12 years.
By Main C, Shepherd J, Anderson R, Rogers G, Thompson-Coon J, Liu Z, et al.
-
Ezetimibe for the treatment of hypercholesterolaemia: a systematic review and economic evaluation.
By Ara R, Tumur I, Pandor A, Duenas A, Williams R, Wilkinson A, et al.
-
Topical or oral ibuprofen for chronic knee pain in older people. The TOIB study.
By Underwood M, Ashby D, Carnes D, Castelnuovo E, Cross P, Harding G, et al.
-
A prospective randomised comparison of minor surgery in primary and secondary care. The MiSTIC trial.
By George S, Pockney P, Primrose J, Smith H, Little P, Kinley H, et al.
-
A review and critical appraisal of measures of therapist–patient interactions in mental health settings.
By Cahill J, Barkham M, Hardy G, Gilbody S, Richards D, Bower P, et al.
-
The clinical effectiveness and cost-effectiveness of screening programmes for amblyopia and strabismus in children up to the age of 4–5 years: a systematic review and economic evaluation.
By Carlton J, Karnon J, Czoski-Murray C, Smith KJ, Marr J.
-
A systematic review of the clinical effectiveness and cost-effectiveness and economic modelling of minimal incision total hip replacement approaches in the management of arthritic disease of the hip.
By de Verteuil R, Imamura M, Zhu S, Glazener C, Fraser C, Munro N, et al.
-
A preliminary model-based assessment of the cost–utility of a screening programme for early age-related macular degeneration.
By Karnon J, Czoski-Murray C, Smith K, Brand C, Chakravarthy U, Davis S, et al.
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.
By Shepherd J, Jones J, Frampton GK, Tanajewski L, Turner D, Price A.
-
Absorbent products for urinary/faecal incontinence: a comparative evaluation of key product categories.
By Fader M, Cottenden A, Getliffe K, Gage H, Clarke-O’Neill S, Jamieson K, et al.
-
A systematic review of repetitive functional task practice with modelling of resource use, costs and effectiveness.
By French B, Leathley M, Sutton C, McAdam J, Thomas L, Forster A, et al.
-
The effectiveness and cost-effectivness of minimal access surgery amongst people with gastro-oesophageal reflux disease – a UK collaborative study. The reflux trial.
By Grant A, Wileman S, Ramsay C, Bojke L, Epstein D, Sculpher M, et al.
-
Time to full publication of studies of anti-cancer medicines for breast cancer and the potential for publication bias: a short systematic review.
By Takeda A, Loveman E, Harris P, Hartwell D, Welch K.
-
Performance of screening tests for child physical abuse in accident and emergency departments.
By Woodman J, Pitt M, Wentz R, Taylor B, Hodes D, Gilbert RE.
-
Curative catheter ablation in atrial fibrillation and typical atrial flutter: systematic review and economic evaluation.
By Rodgers M, McKenna C, Palmer S, Chambers D, Van Hout S, Golder S, et al.
-
Systematic review and economic modelling of effectiveness and cost utility of surgical treatments for men with benign prostatic enlargement.
By Lourenco T, Armstrong N, N’Dow J, Nabi G, Deverill M, Pickard R, et al.
-
Immunoprophylaxis against respiratory syncytial virus (RSV) with palivizumab in children: a systematic review and economic evaluation.
By Wang D, Cummins C, Bayliss S, Sandercock J, Burls A.
-
Deferasirox for the treatment of iron overload associated with regular blood transfusions (transfusional haemosiderosis) in patients suffering with chronic anaemia: a systematic review and economic evaluation.
By McLeod C, Fleeman N, Kirkham J, Bagust A, Boland A, Chu P, et al.
-
Thrombophilia testing in people with venous thromboembolism: systematic review and cost-effectiveness analysis.
By Simpson EL, Stevenson MD, Rawdin A, Papaioannou D.
-
Surgical procedures and non-surgical devices for the management of non-apnoeic snoring: a systematic review of clinical effects and associated treatment costs.
By Main C, Liu Z, Welch K, Weiner G, Quentin Jones S, Stein K.
-
Continuous positive airway pressure devices for the treatment of obstructive sleep apnoea–hypopnoea syndrome: a systematic review and economic analysis.
By McDaid C, Griffin S, Weatherly H, Durée K, van der Burgt M, van Hout S, Akers J, et al.
-
Use of classical and novel biomarkers as prognostic risk factors for localised prostate cancer: a systematic review.
By Sutcliffe P, Hummel S, Simpson E, Young T, Rees A, Wilkinson A, et al.
-
The harmful health effects of recreational ecstasy: a systematic review of observational evidence.
By Rogers G, Elston J, Garside R, Roome C, Taylor R, Younger P, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of oesophageal Doppler monitoring in critically ill and high-risk surgical patients.
By Mowatt G, Houston G, Hernández R, de Verteuil R, Fraser C, Cuthbertson B, et al.
-
The use of surrogate outcomes in model-based cost-effectiveness analyses: a survey of UK Health Technology Assessment reports.
By Taylor RS, Elston J.
-
Controlling Hypertension and Hypotension Immediately Post Stroke (CHHIPS) – a randomised controlled trial.
By Potter J, Mistri A, Brodie F, Chernova J, Wilson E, Jagger C, et al.
-
Routine antenatal anti-D prophylaxis for RhD-negative women: a systematic review and economic evaluation.
By Pilgrim H, Lloyd-Jones M, Rees A.
-
Amantadine, oseltamivir and zanamivir for the prophylaxis of influenza (including a review of existing guidance no. 67): a systematic review and economic evaluation.
By Tappenden P, Jackson R, Cooper K, Rees A, Simpson E, Read R, et al.
-
Improving the evaluation of therapeutic interventions in multiple sclerosis: the role of new psychometric methods.
By Hobart J, Cano S.
-
Treatment of severe ankle sprain: a pragmatic randomised controlled trial comparing the clinical effectiveness and cost-effectiveness of three types of mechanical ankle support with tubular bandage. The CAST trial.
By Cooke MW, Marsh JL, Clark M, Nakash R, Jarvis RM, Hutton JL, et al. , on behalf of the CAST trial group.
-
Non-occupational postexposure prophylaxis for HIV: a systematic review.
By Bryant J, Baxter L, Hird S.
-
Blood glucose self-monitoring in type 2 diabetes: a randomised controlled trial.
By Farmer AJ, Wade AN, French DP, Simon J, Yudkin P, Gray A, et al.
-
How far does screening women for domestic (partner) violence in different health-care settings meet criteria for a screening programme? Systematic reviews of nine UK National Screening Committee criteria.
By Feder G, Ramsay J, Dunne D, Rose M, Arsene C, Norman R, et al.
-
Spinal cord stimulation for chronic pain of neuropathic or ischaemic origin: systematic review and economic evaluation.
By Simpson EL, Duenas A, Holmes MW, Papaioannou D, Chilcott J.
-
The role of magnetic resonance imaging in the identification of suspected acoustic neuroma: a systematic review of clinical and cost-effectiveness and natural history.
By Fortnum H, O’Neill C, Taylor R, Lenthall R, Nikolopoulos T, Lightfoot G, et al.
-
Dipsticks and diagnostic algorithms in urinary tract infection: development and validation, randomised trial, economic analysis, observational cohort and qualitative study.
By Little P, Turner S, Rumsby K, Warner G, Moore M, Lowes JA, et al.
-
Systematic review of respite care in the frail elderly.
By Shaw C, McNamara R, Abrams K, Cannings-John R, Hood K, Longo M, et al.
-
Neuroleptics in the treatment of aggressive challenging behaviour for people with intellectual disabilities: a randomised controlled trial (NACHBID).
By Tyrer P, Oliver-Africano P, Romeo R, Knapp M, Dickens S, Bouras N, et al.
-
Randomised controlled trial to determine the clinical effectiveness and cost-effectiveness of selective serotonin reuptake inhibitors plus supportive care, versus supportive care alone, for mild to moderate depression with somatic symptoms in primary care: the THREAD (THREshold for AntiDepressant response) study.
By Kendrick T, Chatwin J, Dowrick C, Tylee A, Morriss R, Peveler R, et al.
-
Diagnostic strategies using DNA testing for hereditary haemochromatosis in at-risk populations: a systematic review and economic evaluation.
By Bryant J, Cooper K, Picot J, Clegg A, Roderick P, Rosenberg W, et al.
-
Enhanced external counterpulsation for the treatment of stable angina and heart failure: a systematic review and economic analysis.
By McKenna C, McDaid C, Suekarran S, Hawkins N, Claxton K, Light K, et al.
-
Development of a decision support tool for primary care management of patients with abnormal liver function tests without clinically apparent liver disease: a record-linkage population cohort study and decision analysis (ALFIE).
By Donnan PT, McLernon D, Dillon JF, Ryder S, Roderick P, Sullivan F, et al.
-
A systematic review of presumed consent systems for deceased organ donation.
By Rithalia A, McDaid C, Suekarran S, Norman G, Myers L, Sowden A.
-
Paracetamol and ibuprofen for the treatment of fever in children: the PITCH randomised controlled trial.
By Hay AD, Redmond NM, Costelloe C, Montgomery AA, Fletcher M, Hollinghurst S, et al.
-
A randomised controlled trial to compare minimally invasive glucose monitoring devices with conventional monitoring in the management of insulin-treated diabetes mellitus (MITRE).
By Newman SP, Cooke D, Casbard A, Walker S, Meredith S, Nunn A, et al.
-
Sensitivity analysis in economic evaluation: an audit of NICE current practice and a review of its use and value in decision-making.
By Andronis L, Barton P, Bryan S.
-
Trastuzumab for the treatment of primary breast cancer in HER2-positive women: a single technology appraisal.
By Ward S, Pilgrim H, Hind D.
-
Docetaxel for the adjuvant treatment of early node-positive breast cancer: a single technology appraisal.
By Chilcott J, Lloyd Jones M, Wilkinson A.
-
The use of paclitaxel in the management of early stage breast cancer.
By Griffin S, Dunn G, Palmer S, Macfarlane K, Brent S, Dyker A, et al.
-
Rituximab for the first-line treatment of stage III/IV follicular non-Hodgkin’s lymphoma.
By Dundar Y, Bagust A, Hounsome J, McLeod C, Boland A, Davis H, et al.
-
Bortezomib for the treatment of multiple myeloma patients.
By Green C, Bryant J, Takeda A, Cooper K, Clegg A, Smith A, et al.
-
Fludarabine phosphate for the firstline treatment of chronic lymphocytic leukaemia.
By Walker S, Palmer S, Erhorn S, Brent S, Dyker A, Ferrie L, et al.
-
Erlotinib for the treatment of relapsed non-small cell lung cancer.
By McLeod C, Bagust A, Boland A, Hockenhull J, Dundar Y, Proudlove C, et al.
-
Cetuximab plus radiotherapy for the treatment of locally advanced squamous cell carcinoma of the head and neck.
By Griffin S, Walker S, Sculpher M, White S, Erhorn S, Brent S, et al.
-
Infliximab for the treatment of adults with psoriasis.
By Loveman E, Turner D, Hartwell D, Cooper K, Clegg A
-
Psychological interventions for postnatal depression: cluster randomised trial and economic evaluation. The PoNDER trial.
By Morrell CJ, Warner R, Slade P, Dixon S, Walters S, Paley G, et al.
-
The effect of different treatment durations of clopidogrel in patients with non-ST-segment elevation acute coronary syndromes: a systematic review and value of information analysis.
By Rogowski R, Burch J, Palmer S, Craigs C, Golder S, Woolacott N.
-
Systematic review and individual patient data meta-analysis of diagnosis of heart failure, with modelling of implications of different diagnostic strategies in primary care.
By Mant J, Doust J, Roalfe A, Barton P, Cowie MR, Glasziou P, et al.
-
A multicentre randomised controlled trial of the use of continuous positive airway pressure and non-invasive positive pressure ventilation in the early treatment of patients presenting to the emergency department with severe acute cardiogenic pulmonary oedema: the 3CPO trial.
By Gray AJ, Goodacre S, Newby DE, Masson MA, Sampson F, Dixon S, et al. , on behalf of the 3CPO study investigators.
-
Early high-dose lipid-lowering therapy to avoid cardiac events: a systematic review and economic evaluation.
By Ara R, Pandor A, Stevens J, Rees A, Rafia R.
-
Adefovir dipivoxil and pegylated interferon alpha for the treatment of chronic hepatitis B: an updated systematic review and economic evaluation.
By Jones J, Shepherd J, Baxter L, Gospodarevskaya E, Hartwell D, Harris P, et al.
-
Methods to identify postnatal depression in primary care: an integrated evidence synthesis and value of information analysis.
By Hewitt CE, Gilbody SM, Brealey S, Paulden M, Palmer S, Mann R, et al.
-
A double-blind randomised placebo-controlled trial of topical intranasal corticosteroids in 4- to 11-year-old children with persistent bilateral otitis media with effusion in primary care.
By Williamson I, Benge S, Barton S, Petrou S, Letley L, Fasey N, et al.
-
The effectiveness and cost-effectiveness of methods of storing donated kidneys from deceased donors: a systematic review and economic model.
By Bond M, Pitt M, Akoh J, Moxham T, Hoyle M, Anderson R.
-
Rehabilitation of older patients: day hospital compared with rehabilitation at home. A randomised controlled trial.
By Parker SG, Oliver P, Pennington M, Bond J, Jagger C, Enderby PM, et al.
-
Breastfeeding promotion for infants in neonatal units: a systematic review and economic analysis.
By Renfrew MJ, Craig D, Dyson L, McCormick F, Rice S, King SE, et al.
-
The clinical effectiveness and cost-effectiveness of bariatric (weight loss) surgery for obesity: a systematic review and economic evaluation.
By Picot J, Jones J, Colquitt JL, Gospodarevskaya E, Loveman E, Baxter L, et al.
-
Rapid testing for group B streptococcus during labour: a test accuracy study with evaluation of acceptability and cost-effectiveness.
By Daniels J, Gray J, Pattison H, Roberts T, Edwards E, Milner P, et al.
-
Screening to prevent spontaneous preterm birth: systematic reviews of accuracy and effectiveness literature with economic modelling.
By Honest H, Forbes CA, Durée KH, Norman G, Duffy SB, Tsourapas A, et al.
-
The effectiveness and cost-effectiveness of cochlear implants for severe to profound deafness in children and adults: a systematic review and economic model.
By Bond M, Mealing S, Anderson R, Elston J, Weiner G, Taylor RS, et al.
-
Gemcitabine for the treatment of metastatic breast cancer.
By Jones J, Takeda A, Tan SC, Cooper K, Loveman E, Clegg A.
-
Varenicline in the management of smoking cessation: a single technology appraisal.
By Hind D, Tappenden P, Peters J, Kenjegalieva K.
-
Alteplase for the treatment of acute ischaemic stroke: a single technology appraisal.
By Lloyd Jones M, Holmes M.
-
Rituximab for the treatment of rheumatoid arthritis.
By Bagust A, Boland A, Hockenhull J, Fleeman N, Greenhalgh J, Dundar Y, et al.
-
Omalizumab for the treatment of severe persistent allergic asthma.
By Jones J, Shepherd J, Hartwell D, Harris P, Cooper K, Takeda A, et al.
-
Rituximab for the treatment of relapsed or refractory stage III or IV follicular non-Hodgkin’s lymphoma.
By Boland A, Bagust A, Hockenhull J, Davis H, Chu P, Dickson R.
-
Adalimumab for the treatment of psoriasis.
By Turner D, Picot J, Cooper K, Loveman E.
-
Dabigatran etexilate for the prevention of venous thromboembolism in patients undergoing elective hip and knee surgery: a single technology appraisal.
By Holmes M, C Carroll C, Papaioannou D.
-
Romiplostim for the treatment of chronic immune or idiopathic thrombocytopenic purpura: a single technology appraisal.
By Mowatt G, Boachie C, Crowther M, Fraser C, Hernández R, Jia X, et al.
-
Sunitinib for the treatment of gastrointestinal stromal tumours: a critique of the submission from Pfizer.
By Bond M, Hoyle M, Moxham T, Napier M, Anderson R.
-
Vitamin K to prevent fractures in older women: systematic review and economic evaluation.
By Stevenson M, Lloyd-Jones M, Papaioannou D.
-
The effects of biofeedback for the treatment of essential hypertension: a systematic review.
By Greenhalgh J, Dickson R, Dundar Y.
-
A randomised controlled trial of the use of aciclovir and/or prednisolone for the early treatment of Bell’s palsy: the BELLS study.
By Sullivan FM, Swan IRC, Donnan PT, Morrison JM, Smith BH, McKinstry B, et al.
-
Lapatinib for the treatment of HER2-overexpressing breast cancer.
By Jones J, Takeda A, Picot J, von Keyserlingk C, Clegg A.
-
Infliximab for the treatment of ulcerative colitis.
By Hyde C, Bryan S, Juarez-Garcia A, Andronis L, Fry-Smith A.
-
Rimonabant for the treatment of overweight and obese people.
By Burch J, McKenna C, Palmer S, Norman G, Glanville J, Sculpher M, et al.
-
Telbivudine for the treatment of chronic hepatitis B infection.
By Hartwell D, Jones J, Harris P, Cooper K.
-
Entecavir for the treatment of chronic hepatitis B infection.
By Shepherd J, Gospodarevskaya E, Frampton G, Cooper K.
-
Febuxostat for the treatment of hyperuricaemia in people with gout: a single technology appraisal.
By Stevenson M, Pandor A.
-
Rivaroxaban for the prevention of venous thromboembolism: a single technology appraisal.
By Stevenson M, Scope A, Holmes M, Rees A, Kaltenthaler E.
-
Cetuximab for the treatment of recurrent and/or metastatic squamous cell carcinoma of the head and neck.
By Greenhalgh J, Bagust A, Boland A, Fleeman N, McLeod C, Dundar Y, et al.
-
Mifamurtide for the treatment of osteosarcoma: a single technology appraisal.
By Pandor A, Fitzgerald P, Stevenson M, Papaioannou D.
-
Ustekinumab for the treatment of moderate to severe psoriasis.
By Gospodarevskaya E, Picot J, Cooper K, Loveman E, Takeda A.
-
Endovascular stents for abdominal aortic aneurysms: a systematic review and economic model.
By Chambers D, Epstein D, Walker S, Fayter D, Paton F, Wright K, et al.
-
Clinical and cost-effectiveness of epoprostenol, iloprost, bosentan, sitaxentan and sildenafil for pulmonary arterial hypertension within their licensed indications: a systematic review and economic evaluation.
By Chen Y-F, Jowett S, Barton P, Malottki K, Hyde C, Gibbs JSR, et al.
-
Cessation of attention deficit hyperactivity disorder drugs in the young (CADDY) – a pharmacoepidemiological and qualitative study.
By Wong ICK, Asherson P, Bilbow A, Clifford S, Coghill D, R DeSoysa R, et al.
-
ARTISTIC: a randomised trial of human papillomavirus (HPV) testing in primary cervical screening.
By Kitchener HC, Almonte M, Gilham C, Dowie R, Stoykova B, Sargent A, et al.
-
The clinical effectiveness of glucosamine and chondroitin supplements in slowing or arresting progression of osteoarthritis of the knee: a systematic review and economic evaluation.
By Black C, Clar C, Henderson R, MacEachern C, McNamee P, Quayyum Z, et al.
-
Randomised preference trial of medical versus surgical termination of pregnancy less than 14 weeks’ gestation (TOPS).
By Robson SC, Kelly T, Howel D, Deverill M, Hewison J, Lie MLS, et al.
-
Randomised controlled trial of the use of three dressing preparations in the management of chronic ulceration of the foot in diabetes.
By Jeffcoate WJ, Price PE, Phillips CJ, Game FL, Mudge E, Davies S, et al.
-
VenUS II: a randomised controlled trial of larval therapy in the management of leg ulcers.
By Dumville JC, Worthy G, Soares MO, Bland JM, Cullum N, Dowson C, et al.
-
A prospective randomised controlled trial and economic modelling of antimicrobial silver dressings versus non-adherent control dressings for venous leg ulcers: the VULCAN trial.
By Michaels JA, Campbell WB, King BM, MacIntyre J, Palfreyman SJ, Shackley P, et al.
-
Communication of carrier status information following universal newborn screening for sickle cell disorders and cystic fibrosis: qualitative study of experience and practice.
By Kai J, Ulph F, Cullinan T, Qureshi N.
-
Antiviral drugs for the treatment of influenza: a systematic review and economic evaluation.
By Burch J, Paulden M, Conti S, Stock C, Corbett M, Welton NJ, et al.
-
Development of a toolkit and glossary to aid in the adaptation of health technology assessment (HTA) reports for use in different contexts.
By Chase D, Rosten C, Turner S, Hicks N, Milne R.
-
Colour vision testing for diabetic retinopathy: a systematic review of diagnostic accuracy and economic evaluation.
By Rodgers M, Hodges R, Hawkins J, Hollingworth W, Duffy S, McKibbin M, et al.
-
Systematic review of the effectiveness and cost-effectiveness of weight management schemes for the under fives: a short report.
By Bond M, Wyatt K, Lloyd J, Welch K, Taylor R.
-
Are adverse effects incorporated in economic models? An initial review of current practice.
By Craig D, McDaid C, Fonseca T, Stock C, Duffy S, Woolacott N.
-
Multicentre randomised controlled trial examining the cost-effectiveness of contrast-enhanced high field magnetic resonance imaging in women with primary breast cancer scheduled for wide local excision (COMICE).
By Turnbull LW, Brown SR, Olivier C, Harvey I, Brown J, Drew P, et al.
-
Bevacizumab, sorafenib tosylate, sunitinib and temsirolimus for renal cell carcinoma: a systematic review and economic evaluation.
By Thompson Coon J, Hoyle M, Green C, Liu Z, Welch K, Moxham T, et al.
-
The clinical effectiveness and cost-effectiveness of testing for cytochrome P450 polymorphisms in patients with schizophrenia treated with antipsychotics: a systematic review and economic evaluation.
By Fleeman N, McLeod C, Bagust A, Beale S, Boland A, Dundar Y, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of photodynamic diagnosis and urine biomarkers (FISH, ImmunoCyt, NMP22) and cytology for the detection and follow-up of bladder cancer.
By Mowatt G, Zhu S, Kilonzo M, Boachie C, Fraser C, Griffiths TRL, et al.
-
Effectiveness and cost-effectiveness of arthroscopic lavage in the treatment of osteoarthritis of the knee: a mixed methods study of the feasibility of conducting a surgical placebo-controlled trial (the KORAL study).
By Campbell MK, Skea ZC, Sutherland AG, Cuthbertson BH, Entwistle VA, McDonald AM, et al.
-
A randomised 2 × 2 trial of community versus hospital pulmonary rehabilitation for chronic obstructive pulmonary disease followed by telephone or conventional follow-up.
By Waterhouse JC, Walters SJ, Oluboyede Y, Lawson RA.
-
The effectiveness and cost-effectiveness of behavioural interventions for the prevention of sexually transmitted infections in young people aged 13–19: a systematic review and economic evaluation.
By Shepherd J, Kavanagh J, Picot J, Cooper K, Harden A, Barnett-Page E, et al.
-
Dissemination and publication of research findings: an updated review of related biases.
By Song F, Parekh S, Hooper L, Loke YK, Ryder J, Sutton AJ, et al.
-
The effectiveness and cost-effectiveness of biomarkers for the prioritisation of patients awaiting coronary revascularisation: a systematic review and decision model.
By Hemingway H, Henriksson M, Chen R, Damant J, Fitzpatrick N, Abrams K, et al.
-
Comparison of case note review methods for evaluating quality and safety in health care.
By Hutchinson A, Coster JE, Cooper KL, McIntosh A, Walters SJ, Bath PA, et al.
-
Clinical effectiveness and cost-effectiveness of continuous subcutaneous insulin infusion for diabetes: systematic review and economic evaluation.
By Cummins E, Royle P, Snaith A, Greene A, Robertson L, McIntyre L, et al.
-
Self-monitoring of blood glucose in type 2 diabetes: systematic review.
By Clar C, Barnard K, Cummins E, Royle P, Waugh N.
-
North of England and Scotland Study of Tonsillectomy and Adeno-tonsillectomy in Children (NESSTAC): a pragmatic randomised controlled trial with a parallel non-randomised preference study.
By Lock C, Wilson J, Steen N, Eccles M, Mason H, Carrie S, et al.
-
Multicentre randomised controlled trial of the clinical and cost-effectiveness of a bypass-surgery-first versus a balloon-angioplasty-first revascularisation strategy for severe limb ischaemia due to infrainguinal disease. The Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) trial.
By Bradbury AW, Adam DJ, Bell J, Forbes JF, Fowkes FGR, Gillespie I, et al.
-
A randomised controlled multicentre trial of treatments for adolescent anorexia nervosa including assessment of cost-effectiveness and patient acceptability – the TOuCAN trial.
By Gowers SG, Clark AF, Roberts C, Byford S, Barrett B, Griffiths A, et al.
-
Randomised controlled trials for policy interventions: a review of reviews and meta-regression.
By Oliver S, Bagnall AM, Thomas J, Shepherd J, Sowden A, White I, et al.
-
Paracetamol and selective and non-selective non-steroidal anti-inflammatory drugs (NSAIDs) for the reduction of morphine-related side effects after major surgery: a systematic review.
By McDaid C, Maund E, Rice S, Wright K, Jenkins B, Woolacott N.
-
A systematic review of outcome measures used in forensic mental health research with consensus panel opinion.
By Fitzpatrick R, Chambers J, Burns T, Doll H, Fazel S, Jenkinson C, et al.
-
The clinical effectiveness and cost-effectiveness of topotecan for small cell lung cancer: a systematic review and economic evaluation.
By Loveman E, Jones J, Hartwell D, Bird A, Harris P, Welch K, et al.
-
Antenatal screening for haemoglobinopathies in primary care: a cohort study and cluster randomised trial to inform a simulation model. The Screening for Haemoglobinopathies in First Trimester (SHIFT) trial.
By Dormandy E, Bryan S, Gulliford MC, Roberts T, Ades T, Calnan M, et al.
-
Early referral strategies for management of people with markers of renal disease: a systematic review of the evidence of clinical effectiveness, cost-effectiveness and economic analysis.
By Black C, Sharma P, Scotland G, McCullough K, McGurn D, Robertson L, et al.
-
A randomised controlled trial of cognitive behaviour therapy and motivational interviewing for people with Type 1 diabetes mellitus with persistent sub-optimal glycaemic control: A Diabetes and Psychological Therapies (ADaPT) study.
By Ismail K, Maissi E, Thomas S, Chalder T, Schmidt U, Bartlett J, et al.
-
A randomised controlled equivalence trial to determine the effectiveness and cost–utility of manual chest physiotherapy techniques in the management of exacerbations of chronic obstructive pulmonary disease (MATREX).
By Cross J, Elender F, Barton G, Clark A, Shepstone L, Blyth A, et al.
-
A systematic review and economic evaluation of the clinical effectiveness and cost-effectiveness of aldosterone antagonists for postmyocardial infarction heart failure.
By McKenna C, Burch J, Suekarran S, Walker S, Bakhai A, Witte K, et al.
-
Avoiding and identifying errors in health technology assessment models: qualitative study and methodological review.
By Chilcott JB, Tappenden P, Rawdin A, Johnson M, Kaltenthaler E, Paisley S, et al.
-
BoTULS: a multicentre randomised controlled trial to evaluate the clinical effectiveness and cost-effectiveness of treating upper limb spasticity due to stroke with botulinum toxin type A.
By Shaw L, Rodgers H, Price C, van Wijck F, Shackley P, Steen N, et al. , on behalf of the BoTULS investigators.
-
Weighting and valuing quality-adjusted life-years using stated preference methods: preliminary results from the Social Value of a QALY Project.
By Baker R, Bateman I, Donaldson C, Jones-Lee M, Lancsar E, Loomes G, et al.
-
Cetuximab for the first-line treatment of metastatic colorectal cancer.
By Meads C, Round J, Tubeuf S, Moore D, Pennant M, Bayliss S.
-
Infliximab for the treatment of acute exacerbations of ulcerative colitis.
By Bryan S, Andronis L, Hyde C, Connock M, Fry-Smith A, Wang D.
-
Sorafenib for the treatment of advanced hepatocellular carcinoma.
By Connock M, Round J, Bayliss S, Tubeuf S, Greenheld W, Moore D.
-
Tenofovir disoproxil fumarate for the treatment of chronic hepatitis B infection.
By Jones J, Colquitt J, Shepherd J, Harris P, Cooper K.
-
Prasugrel for the treatment of acute coronary artery syndromes with percutaneous coronary intervention.
By Greenhalgh J, Bagust A, Boland A, Saborido CM, Fleeman N, McLeod C, et al.
-
Alitretinoin for the treatment of severe chronic hand eczema.
By Paulden M, Rodgers M, Griffin S, Slack R, Duffy S, Ingram JR, et al.
-
Pemetrexed for the first-line treatment of locally advanced or metastatic non-small cell lung cancer.
By Fleeman N, Bagust A, McLeod C, Greenhalgh J, Boland A, Dundar Y, et al.
-
Topotecan for the treatment of recurrent and stage IVB carcinoma of the cervix.
By Paton F, Paulden M, Saramago P, Manca A, Misso K, Palmer S, et al.
-
Trabectedin for the treatment of advanced metastatic soft tissue sarcoma.
By Simpson EL, Rafia R, Stevenson MD, Papaioannou D.
-
Azacitidine for the treatment of myelodysplastic syndrome, chronic myelomonocytic leukaemia and acute myeloid leukaemia.
By Edlin R, Connock M, Tubeuf S, Round J, Fry-Smith A, Hyde C, et al.
-
The safety and effectiveness of different methods of earwax removal: a systematic review and economic evaluation.
By Clegg AJ, Loveman E, Gospodarevskaya E, Harris P, Bird A, Bryant J, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of rapid point-of-care tests for the detection of genital chlamydia infection in women and men.
By Hislop J, Quayyum Z, Flett G, Boachie C, Fraser C, Mowatt G.
-
School-linked sexual health services for young people (SSHYP): a survey and systematic review concerning current models, effectiveness, cost-effectiveness and research opportunities.
By Owen J, Carroll C, Cooke J, Formby E, Hayter M, Hirst J, et al.
-
Systematic review and cost-effectiveness evaluation of ‘pill-in-the-pocket’ strategy for paroxysmal atrial fibrillation compared to episodic in-hospital treatment or continuous antiarrhythmic drug therapy.
By Martin Saborido C, Hockenhull J, Bagust A, Boland A, Dickson R, Todd D.
-
Chemoprevention of colorectal cancer: systematic review and economic evaluation.
By Cooper K, Squires H, Carroll C, Papaioannou D, Booth A, Logan RF, et al.
-
Cross-trimester repeated measures testing for Down’s syndrome screening: an assessment.
By Wright D, Bradbury I, Malone F, D’Alton M, Summers A, Huang T, et al.
-
Exploring the needs, concerns and behaviours of people with existing respiratory conditions in relation to the H1N1 ‘swine influenza’ pandemic: a multicentre survey and qualitative study.
By Caress A-L, Duxbury P, Woodcock A, Luker KA, Ward D, Campbell M, et al.
-
Influenza A/H1N1v in pregnancy: an investigation of the characteristics and management of affected women and the relationship to pregnancy outcomes for mother and infant.
By Yates L, Pierce M, Stephens S, Mill AC, Spark P, Kurinczuk JJ, et al.
-
The impact of communications about swine flu (influenza A H1N1v) on public responses to the outbreak: results from 36 national telephone surveys in the UK.
By Rubin GJ, Potts HWW, Michie S.
-
The impact of illness and the impact of school closure on social contact patterns.
By Eames KTD, Tilston NL, White PJ, Adams E, Edmunds WJ.
-
Vaccine effectiveness in pandemic influenza – primary care reporting (VIPER): an observational study to assess the effectiveness of the pandemic influenza A (H1N1)v vaccine.
By Simpson CR, Ritchie LD, Robertson C, Sheikh A, McMenamin J.
-
Physical interventions to interrupt or reduce the spread of respiratory viruses: a Cochrane review.
By Jefferson T, Del Mar C, Dooley L, Ferroni E, Al-Ansary LA, Bawazeer GA, et al.
-
Randomised controlled trial and parallel economic evaluation of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR).
By Peek GJ, Elbourne D, Mugford M, Tiruvoipati R, Wilson A, Allen E, et al.
-
Newer agents for blood glucose control in type 2 diabetes: systematic review and economic evaluation.
By Waugh N, Cummins E, Royle P, Clar C, Marien M, Richter B, et al.
-
Barrett’s oesophagus and cancers of the biliary tract, brain, head and neck, lung, oesophagus and skin.
By Fayter D, Corbett M, Heirs M, Fox D, Eastwood A.
-
Towards single embryo transfer? Modelling clinical outcomes of potential treatment choices using multiple data sources: predictive models and patient perspectives.
By Roberts SA, McGowan L, Hirst WM, Brison DR, Vail A, Lieberman BA.
-
Sugammadex for the reversal of muscle relaxation in general anaesthesia: a systematic review and economic assessment.
By Chambers D, Paulden M, Paton F, Heirs M, Duffy S, Craig D, et al.
-
Systematic review and economic modelling of the effectiveness and cost-effectiveness of non-surgical treatments for women with stress urinary incontinence.
By Imamura M, Abrams P, Bain C, Buckley B, Cardozo L, Cody J, et al.
-
A multicentred randomised controlled trial of a primary care-based cognitive behavioural programme for low back pain. The Back Skills Training (BeST) trial.
By Lamb SE, Lall R, Hansen Z, Castelnuovo E, Withers EJ, Nichols V, et al.
-
Recombinant human growth hormone for the treatment of growth disorders in children: a systematic review and economic evaluation.
By Takeda A, Cooper K, Bird A, Baxter L, Frampton GK, Gospodarevskaya E, et al.
-
A pragmatic randomised controlled trial to compare antidepressants with a community-based psychosocial intervention for the treatment of women with postnatal depression: the RESPOND trial.
By Sharp DJ, Chew-Graham C, Tylee A, Lewis G, Howard L, Anderson I, et al.
-
Group cognitive behavioural therapy for postnatal depression: a systematic review of clinical effectiveness, cost-effectiveness and value of information analyses.
By Stevenson MD, Scope A, Sutcliffe PA, Booth A, Slade P, Parry G, et al.
-
Screening for hyperglycaemia in pregnancy: a rapid update for the National Screening Committee.
By Waugh N, Royle P, Clar C, Henderson R, Cummins E, Hadden D, et al.
-
Open-label, randomised, parallel-group, multicentre study to evaluate the safety, tolerability and immunogenicity of an AS03B/oil-in-water emulsion-adjuvanted (AS03B) split-virion versus non-adjuvanted wholevirion H1N1 influenza vaccine in UK children 6 months to 12 years of age.
By Waddington CS, Andrews N, Hoschler K, Walker WT, Oeser C, Reiner A, et al.
-
Evaluation of droplet dispersion during non-invasive ventilation, oxygen therapy, nebuliser treatment and chest physiotherapy in clinical practice: implications for management of pandemic influenza and other airborne infections.
By Simonds AK, Hanak A, Chatwin M, Morrell MJ, Hall A, Parker KH, et al.
-
Evaluation of triage methods used to select patients with suspected pandemic influenza for hospital admission: cohort study.
By Goodacre S, Challen, K, Wilson R, Campbell M.
-
Virus shedding and environmental deposition of novel A (H1N1) pandemic influenza virus: interim findings.
By Killingley B, Greatorex J, Cauchemez S, Enstone JE, Curran M, Read R, et al.
-
Neuraminidase inhibitors for preventing and treating influenza in healthy adults: a Cochrane review.
By Jefferson T, Jones M, Doshi P, Del Mar C, Dooley L, Foxlee R.
-
Intensity-modulated radiotherapy for the treatment of prostate cancer: a systematic review and economic evaluation.
By Hummel S, Simpson EL, Hemingway P, Stevenson MD, Rees A.
-
Computerised decision support systems in order communication for diagnostic, screening or monitoring test ordering: systematic reviews of the effects and cost-effectiveness of systems.
By Main C, Moxham T, Wyatt JC, Kay J, Anderson R, Stein K.
-
Relapse prevention in UK Stop Smoking Services: current practice, systematic reviews of effectiveness and cost-effectiveness analysis.
By Coleman T, Agboola S, Leonardi-Bee J, Taylor M, McEwen A, McNeill A.
-
A systematic review of positron emission tomography (PET) and positron emission tomography/computed tomography (PET/CT) for the diagnosis of breast cancer recurrence.
By Pennant M, Takwoingi Y, Pennant L, Davenport C, Fry-Smith A, Eisinga A, et al.
-
Certolizumab pegol (CIMZIA®) for the treatment of rheumatoid arthritis.
By Connock M, Tubeuf S, Malottki K, Uthman A, Round J, Bayliss S, et al.
-
Capecitabine for the treatment of advanced gastric cancer.
By Norman G, Soares M, Peura P, Rice S, Suh D, Wright K, et al.
-
Rituximab for the treatment of relapsed/refractory chronic lymphocytic leukaemia.
By Dretzke J, Barton P, Kaambwa B, Connock M, Uthman O, Bayliss S, et al.
-
The clinical effectiveness and cost-effectiveness of rituximab for the first-line treatment of chronic lymphocytic leukaemia: an evidence review of the submission from Roche.
By Main C, Pitt M, Moxham T, Stein K.
-
Pemetrexed for the maintenance treatment of locally advanced or metastatic non-small cell lung cancer.
By Greenhalgh J, McLeod C, Bagust A, Boland A, Fleeman N, Dundar Y, et al.
-
Everolimus for the second-line treatment of advanced and/or metastatic renal cell cancer: a critique of the submission from Novartis.
By Pitt M, Crathorne L, Moxham T, Bond M, Hyde C.
-
Bevacizumab in combination with fluoropyrimidine-based chemotherapy for the first-line treatment of metastatic colorectal cancer.
By Whyte S, Pandor A, Stevenson M, Rees A.
-
Dronedarone for the treatment of atrial fibrillation and atrial flutter.
By Maund E, McKenna C, Sarowar M, Fox D, Stevenson M, Pepper C, et al.
-
Imatinib as adjuvant treatment following resection of KIT-positive gastrointestinal stromal tumours.
By Dretzke J, Round J, Connock M, Tubeuf S, Pennant M, Fry-Smith A, et al.
-
Gefitinib for the first-line treatment of locally advanced or metastatic non-small cell lung cancer.
By Brown T, Boland A, Bagust A, Oyee J, Hockenhull J, Dundar Y, et al.
-
Systematic review of the links between human resource management practices and performance.
By Patterson M, Rick J, Wood S, Carroll C, Balain S, Booth A.
-
LIFELAX – diet and LIFEstyle versus LAXatives in the management of chronic constipation in older people: randomised controlled trial.
By Speed C, Heaven B, Adamson A, Bond J, Corbett S, Lake AA, et al.
Health Technology Assessment programme
-
Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Medical Care Research Unit, University of Sheffield
Prioritisation Strategy Group
-
Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Medical Care Research Unit, University of Sheffield
-
Dr Bob Coates, Consultant Advisor, NETSCC, HTA
-
Dr Andrew Cook, Consultant Advisor, NETSCC, HTA
-
Dr Peter Davidson, Director of NETSCC, Health Technology Assessment
-
Professor Robin E Ferner, Consultant Physician and Director, West Midlands Centre for Adverse Drug Reactions, City Hospital NHS Trust, Birmingham
-
Professor Paul Glasziou, Professor of Evidence-Based Medicine, University of Oxford
-
Dr Nick Hicks, Consultant Adviser, NETSCC, HTA
-
Dr Edmund Jessop, Medical Adviser, National Specialist, National Commissioning Group (NCG), Department of Health, London
-
Ms Lynn Kerridge, Chief Executive Officer, NETSCC and NETSCC, HTA
-
Professor Ruairidh Milne, Director of NETSCC External Relations
-
Ms Kay Pattison, Senior NIHR Programme Manager, Department of Health
-
Ms Pamela Young, Specialist Programme Manager, NETSCC, HTA
HTA Commissioning Board
-
Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Warwick Clinical Trials Unit
-
Director, Nottingham Clinical Trials Unit
-
Senior Lecturer in General Practice, Department of Primary Health Care, University of Oxford
-
Professor Ann Ashburn, Professor of Rehabilitation and Head of Research, Southampton General Hospital
-
Professor Deborah Ashby, Professor of Medical Statistics, Queen Mary, University of London
-
Professor John Cairns, Professor of Health Economics, London School of Hygiene and Tropical Medicine
-
Professor Peter Croft, Director of Primary Care Sciences Research Centre, Keele University
-
Professor Nicky Cullum, Director of Centre for Evidence-Based Nursing, University of York
-
Professor Jenny Donovan, Professor of Social Medicine, University of Bristol
-
Professor Steve Halligan, Professor of Gastrointestinal Radiology, University College Hospital, London
-
Professor Freddie Hamdy, Professor of Urology, University of Sheffield
-
Professor Allan House, Professor of Liaison Psychiatry, University of Leeds
-
Dr Martin J Landray, Reader in Epidemiology, Honorary Consultant Physician, Clinical Trial Service Unit, University of Oxford?
-
Professor Stuart Logan, Director of Health & Social Care Research, The Peninsula Medical School, Universities of Exeter and Plymouth
-
Dr Rafael Perera, Lecturer in Medical Statisitics, Department of Primary Health Care, University of Oxford
-
Professor Ian Roberts, Professor of Epidemiology & Public Health, London School of Hygiene and Tropical Medicine
-
Professor Mark Sculpher, Professor of Health Economics, University of York
-
Professor Helen Smith, Professor of Primary Care, University of Brighton
-
Professor Kate Thomas, Professor of Complementary & Alternative Medicine Research, University of Leeds
-
Professor David John Torgerson, Director of York Trials Unit, University of York
-
Ms Kay Pattison, NHS R&D Programme/DH, Leeds
-
Dr Morven Roberts, Clinical Trials Manager, Medical Research Council
Diagnostic Technologies and Screening Panel
-
Professor of Evidence-Based Medicine, University of Oxford
-
Consultant Paediatrician and Honorary Senior Lecturer, Great Ormond Street Hospital, London
-
Professor Judith E Adams, Consultant Radiologist, Manchester Royal Infirmary, Central Manchester & Manchester Children’s University Hospitals NHS Trust, and Professor of Diagnostic Radiology, Imaging Science and Biomedical Engineering, Cancer & Imaging Sciences, University of Manchester
-
Mr A S Arunkalaivanan, Honorary Senior Lecturer, University of Birmingham and Consultant Urogynaecologist and Obstetrician, City Hospital
-
Dr Dianne Baralle, Consultant & Senior Lecturer in Clinical Genetics, Human Genetics Division & Wessex Clinical Genetics Service, Southampton, University of Southampton
-
Dr Stephanie Dancer, Consultant Microbiologist, Hairmyres Hospital, East Kilbride
-
Dr Ron Gray, Consultant, National Perinatal Epidemiology Unit, Institute of Health Sciences, University of Oxford
-
Professor Paul D Griffiths, Professor of Radiology, Academic Unit of Radiology, University of Sheffield
-
Mr Martin Hooper, Service User Representative
-
Professor Anthony Robert Kendrick, Professor of Primary Medical Care, University of Southampton
-
Dr Susanne M Ludgate, Director, Medical Devices Agency, London
-
Dr Anne Mackie, Director of Programmes, UK National Screening Committee
-
Dr David Mathew Service User Representative
-
Dr Michael Millar, Lead Consultant in Microbiology, Department of Pathology & Microbiology, Barts and The London NHS Trust, Royal London Hospital
-
Mr Stephen Pilling, Director, Centre for Outcomes, Research & Effectiveness, University College London
-
Mrs Una Rennard, Service User Representative
-
Ms Jane Smith, Consultant Ultrasound Practitioner, Ultrasound Department, Leeds Teaching Hospital NHS Trust, Leeds
-
Dr W Stuart A Smellie, Consultant, Bishop Auckland General Hospital
-
Professor Lindsay Wilson Turnbull, Scientific Director of the Centre for Magnetic Resonance Investigations and YCR Professor of Radiology, Hull Royal Infirmary
-
Dr Alan J Williams, Consultant in General Medicine, Department of Thoracic Medicine, The Royal Bournemouth Hospital
-
Dr Tim Elliott, Team Leader, Cancer Screening, Department of Health
-
Dr Catherine Moody, Programme Manager, Neuroscience and Mental Health Board
-
Dr Ursula Wells, Principal Research Officer, Department of Health
Disease Prevention Panel
-
Medical Adviser, National Specialist Commissioning Advisory Group (NSCAG), Department of Health
-
Professor of Epidemiology, University of Warwick Medical School, Coventry
-
Dr Robert Cook Clinical Programmes Director, Bazian Ltd, London
-
Dr Elizabeth Fellow-Smith, Medical Director, West London Mental Health Trust, Middlesex
-
Dr Colin Greaves Senior Research Fellow, Peninsular Medical School (Primary Care)
-
Dr John Jackson, General Practitioner, Parkway Medical Centre, Newcastle upon Tyne
-
Dr Russell Jago, Senior Lecturer in Exercise, Nutrition and Health, Centre for Sport, Exercise and Health, University of Bristol
-
Dr Chris McCall, General Practitioner, The Hadleigh Practice, Corfe Mullen, Dorset
-
Miss Nicky Mullany, Service User Representative
-
Dr Julie Mytton, Locum Consultant in Public Health Medicine, Bristol Primary Care Trust
-
Professor Irwin Nazareth, Professor of Primary Care and Director, Department of Primary Care and Population Sciences, University College London
-
Professor Ian Roberts, Professor of Epidemiology and Public Health, London School of Hygiene & Tropical Medicine
-
Professor Carol Tannahill, Glasgow Centre for Population Health
-
Mrs Jean Thurston, Service User Representative
-
Professor David Weller, Head, School of Clinical Science and Community Health, University of Edinburgh
-
Ms Christine McGuire, Research & Development, Department of Health
-
Ms Kay Pattison Senior NIHR Programme Manager, Department of Health
-
Dr Caroline Stone, Programme Manager, Medical Research Council
External Devices and Physical Therapies Panel
-
Consultant Physician North Bristol NHS Trust, Bristol
-
Reader in Wound Healing and Director of Research, University of Leeds, Leeds
-
Professor Bipin Bhakta Charterhouse Professor in Rehabilitation Medicine, University of Leeds, Leeds
-
Mrs Penny Calder Service User Representative
-
Professor Paul Carding, Professor of Voice Pathology, Newcastle Hospital NHS Trust, Newcastle
-
Dr Dawn Carnes, Senior Research Fellow, Barts and the London School of Medicine and Dentistry, London
-
Dr Emma Clark, Clinician Scientist Fellow & Cons. Rheumatologist, University of Bristol, Bristol
-
Mrs Anthea De Barton-Watson, Service User Representative
-
Professor Christopher Griffiths, Professor of Primary Care, Barts and the London School of Medicine and Dentistry, London
-
Dr Shaheen Hamdy, Clinical Senior Lecturer and Consultant Physician, University of Manchester, Manchester
-
Dr Peter Martin, Consultant Neurologist, Addenbrooke’s Hospital, Cambridge
-
Dr Lorraine Pinnigton, Associate Professor in Rehabilitation, University of Nottingham, Nottingham
-
Dr Kate Radford, Division of Rehabilitation and Ageing, School of Community Health Sciences. University of Nottingham, Nottingham
-
Mr Jim Reece, Service User Representative
-
Professor Maria Stokes, Professor of Neuromusculoskeletal Rehabilitation, University of Southampton, Southampton
-
Dr Pippa Tyrrell, Stroke Medicine, Senior Lecturer/Consultant Stroke Physician, Salford Royal Foundation Hospitals’ Trust, Salford
-
Dr Sarah Tyson, Senior Research Fellow & Associate Head of School, University of Salford, Salford
-
Dr Nefyn Williams, Clinical Senior Lecturer, Cardiff University, Cardiff
-
Dr Phillip Leech, Principal Medical Officer for Primary Care, Department of Health , London
-
Ms Kay Pattison Senior NIHR Programme Manager, Department of Health
-
Dr Morven Roberts, Clinical Trials Manager, MRC, London
-
Dr Ursula Wells PRP, DH, London
Interventional Procedures Panel
-
Consultant Surgeon & Honorary Clinical Lecturer, University of Sheffield
-
Mr David P Britt, Service User Representative, Cheshire
-
Mr Sankaran ChandraSekharan, Consultant Surgeon, Colchester Hospital University NHS Foundation Trust
-
Professor Nicholas Clarke, Consultant Orthopaedic Surgeon, Southampton University Hospitals NHS Trust
-
Mr Seamus Eckford, Consultant in Obstetrics & Gynaecology, North Devon District Hospital
-
Professor David Taggart, Consultant Cardiothoracic Surgeon, John Radcliffe Hospital
-
Dr Matthew Hatton, Consultant in Clinical Oncology, Sheffield Teaching Hospital Foundation Trust
-
Dr John Holden, General Practitioner, Garswood Surgery, Wigan
-
Dr Nadim Malik, Consultant Cardiologist/ Honorary Lecturer, University of Manchester
-
Mr Hisham Mehanna, Consultant & Honorary Associate Professor, University Hospitals Coventry & Warwickshire NHS Trust
-
Dr Jane Montgomery, Consultant in Anaesthetics and Critical Care, South Devon Healthcare NHS Foundation Trust
-
Dr Simon Padley, Consultant Radiologist, Chelsea & Westminster Hospital
-
Dr Ashish Paul, Medical Director, Bedfordshire PCT
-
Dr Sarah Purdy, Consultant Senior Lecturer, University of Bristol
-
Mr Michael Thomas, Consultant Colorectal Surgeon, Bristol Royal Infirmary
-
Professor Yit Chiun Yang, Consultant Ophthalmologist, Royal Wolverhampton Hospitals NHS Trust
-
Mrs Isabel Boyer, Service User Representative, London
Pharmaceuticals Panel
-
Professor in Child Health, University of Nottingham
-
Unit Manager, Pharmacoepidemiology Research Unit, VRMM, Medicines & Healthcare Products Regulatory Agency
-
Mrs Nicola Carey, Senior Research Fellow, School of Health and Social Care, The University of Reading
-
Mr John Chapman, Service User Representative
-
Dr Peter Elton, Director of Public Health, Bury Primary Care Trust
-
Professor Robin Ferner, Consultant Physician and Director, West Midlands Centre for Adverse Drug Reactions, City Hospital NHS Trust, Birmingham
-
Dr Ben Goldacre, Research Fellow, Division of Psychological Medicine and Psychiatry, King’s College London
-
Dr Bill Gutteridge, Medical Adviser, London Strategic Health Authority
-
Dr Dyfrig Hughes, Reader in Pharmacoeconomics and Deputy Director, Centre for Economics and Policy in Health, IMSCaR, Bangor University
-
Dr Yoon K Loke, Senior Lecturer in Clinical Pharmacology, University of East Anglia
-
Professor Femi Oyebode, Consultant Psychiatrist and Head of Department, University of Birmingham
-
Dr Andrew Prentice, Senior Lecturer and Consultant Obstetrician and Gynaecologist, The Rosie Hospital, University of Cambridge
-
Dr Martin Shelly, General Practitioner, Leeds, and Associate Director, NHS Clinical Governance Support Team, Leicester
-
Dr Gillian Shepherd, Director, Health and Clinical Excellence, Merck Serono Ltd
-
Mrs Katrina Simister, Assistant Director New Medicines, National Prescribing Centre, Liverpool
-
Mr David Symes, Service User Representative
-
Ms Kay Pattison Senior NIHR Programme Manager, Department of Health
-
Mr Simon Reeve, Head of Clinical and Cost-Effectiveness, Medicines, Pharmacy and Industry Group, Department of Health
-
Dr Heike Weber, Programme Manager, Medical Research Council
-
Dr Ursula Wells, Principal Research Officer, Department of Health
Psychological and Community Therapies Panel
-
Professor of Psychiatry, University of Warwick
-
Professor Jane Barlow, Professor of Public Health in the Early Years, Health Sciences Research Institute, Warwick Medical School
-
Dr Sabyasachi Bhaumik, Consultant Psychiatrist, Leicestershire Partnership NHS Trust
-
Mrs Val Carlill, Service User Representative, Gloucestershire
-
Dr Steve Cunningham, Consultant Respiratory Paediatrician, Lothian Health Board
-
Dr Anne Hesketh, Senior Clinical Lecturer in Speech and Language Therapy, University of Manchester
-
Dr Yann Lefeuvre, GP Partner, Burrage Road Surgery, London
-
Dr Jeremy J Murphy, Consultant Physician & Cardiologist, County Durham & Darlington Foundation Trust
-
Mr John Needham, Service User, Buckingmashire
-
Ms Mary Nettle, Mental Health User Consultant, Gloucestershire
-
Professor John Potter, Professor of Ageing and Stroke Medicine, University of East Anglia
-
Dr Greta Rait, Senior Clinical Lecturer and General Practitioner, University College London
-
Dr Paul Ramchandani, Senior Research Fellow/Cons. Child Psychiatrist, University of Oxford
-
Dr Howard Ring, Consultant & University Lecturer in Psychiatry, University of Cambridge
-
Dr Karen Roberts, Nurse/Consultant, Dunston Hill Hospital, Tyne and Wear
-
Dr Karim Saad, Consultant in Old Age Psychiatry, Coventry & Warwickshire Partnership Trust
-
Dr Alastair Sutcliffe, Senior Lecturer, University College London
-
Dr Simon Wright, GP Partner, Walkden Medical Centre, Manchester
-
Ms Kay Pattison Senior NIHR Programme Manager, Department of Health
-
Dr Morven Roberts, Clinical Trials Manager, MRC, London
-
Professor Tom Walley, HTA Programme Director, Liverpool
-
Dr Ursula Wells, Policy Research Programme, DH, London
Expert Advisory Network
-
Professor Douglas Altman, Professor of Statistics in Medicine, Centre for Statistics in Medicine, University of Oxford
-
Professor John Bond, Professor of Social Gerontology & Health Services Research, University of Newcastle upon Tyne
-
Professor Andrew Bradbury, Professor of Vascular Surgery, Solihull Hospital, Birmingham
-
Mr Shaun Brogan, Chief Executive, Ridgeway Primary Care Group, Aylesbury
-
Mrs Stella Burnside OBE, Chief Executive, Regulation and Improvement Authority, Belfast
-
Ms Tracy Bury, Project Manager, World Confederation for Physical Therapy, London
-
Professor Iain T Cameron, Professor of Obstetrics and Gynaecology and Head of the School of Medicine, University of Southampton
-
Dr Christine Clark, Medical Writer and Consultant Pharmacist, Rossendale
-
Professor Collette Clifford, Professor of Nursing and Head of Research, The Medical School, University of Birmingham
-
Professor Barry Cookson, Director, Laboratory of Hospital Infection, Public Health Laboratory Service, London
-
Dr Carl Counsell, Clinical Senior Lecturer in Neurology, University of Aberdeen
-
Professor Howard Cuckle, Professor of Reproductive Epidemiology, Department of Paediatrics, Obstetrics & Gynaecology, University of Leeds
-
Dr Katherine Darton, Information Unit, MIND – The Mental Health Charity, London
-
Professor Carol Dezateux, Professor of Paediatric Epidemiology, Institute of Child Health, London
-
Mr John Dunning, Consultant Cardiothoracic Surgeon, Papworth Hospital NHS Trust, Cambridge
-
Mr Jonothan Earnshaw, Consultant Vascular Surgeon, Gloucestershire Royal Hospital, Gloucester
-
Professor Martin Eccles, Professor of Clinical Effectiveness, Centre for Health Services Research, University of Newcastle upon Tyne
-
Professor Pam Enderby, Dean of Faculty of Medicine, Institute of General Practice and Primary Care, University of Sheffield
-
Professor Gene Feder, Professor of Primary Care Research & Development, Centre for Health Sciences, Barts and The London School of Medicine and Dentistry
-
Mr Leonard R Fenwick, Chief Executive, Freeman Hospital, Newcastle upon Tyne
-
Mrs Gillian Fletcher, Antenatal Teacher and Tutor and President, National Childbirth Trust, Henfield
-
Professor Jayne Franklyn, Professor of Medicine, University of Birmingham
-
Mr Tam Fry, Honorary Chairman, Child Growth Foundation, London
-
Professor Fiona Gilbert, Consultant Radiologist and NCRN Member, University of Aberdeen
-
Professor Paul Gregg, Professor of Orthopaedic Surgical Science, South Tees Hospital NHS Trust
-
Bec Hanley, Co-director, TwoCan Associates, West Sussex
-
Dr Maryann L Hardy, Senior Lecturer, University of Bradford
-
Mrs Sharon Hart, Healthcare Management Consultant, Reading
-
Professor Robert E Hawkins, CRC Professor and Director of Medical Oncology, Christie CRC Research Centre, Christie Hospital NHS Trust, Manchester
-
Professor Richard Hobbs, Head of Department of Primary Care & General Practice, University of Birmingham
-
Professor Alan Horwich, Dean and Section Chairman, The Institute of Cancer Research, London
-
Professor Allen Hutchinson, Director of Public Health and Deputy Dean of ScHARR, University of Sheffield
-
Professor Peter Jones, Professor of Psychiatry, University of Cambridge, Cambridge
-
Professor Stan Kaye, Cancer Research UK Professor of Medical Oncology, Royal Marsden Hospital and Institute of Cancer Research, Surrey
-
Dr Duncan Keeley, General Practitioner (Dr Burch & Ptnrs), The Health Centre, Thame
-
Dr Donna Lamping, Research Degrees Programme Director and Reader in Psychology, Health Services Research Unit, London School of Hygiene and Tropical Medicine, London
-
Mr George Levvy, Chief Executive, Motor Neurone Disease Association, Northampton
-
Professor James Lindesay, Professor of Psychiatry for the Elderly, University of Leicester
-
Professor Julian Little, Professor of Human Genome Epidemiology, University of Ottawa
-
Professor Alistaire McGuire, Professor of Health Economics, London School of Economics
-
Professor Rajan Madhok, Medical Director and Director of Public Health, Directorate of Clinical Strategy & Public Health, North & East Yorkshire & Northern Lincolnshire Health Authority, York
-
Professor Alexander Markham, Director, Molecular Medicine Unit, St James’s University Hospital, Leeds
-
Dr Peter Moore, Freelance Science Writer, Ashtead
-
Dr Andrew Mortimore, Public Health Director, Southampton City Primary Care Trust
-
Dr Sue Moss, Associate Director, Cancer Screening Evaluation Unit, Institute of Cancer Research, Sutton
-
Professor Miranda Mugford, Professor of Health Economics and Group Co-ordinator, University of East Anglia
-
Professor Jim Neilson, Head of School of Reproductive & Developmental Medicine and Professor of Obstetrics and Gynaecology, University of Liverpool
-
Mrs Julietta Patnick, National Co-ordinator, NHS Cancer Screening Programmes, Sheffield
-
Professor Robert Peveler, Professor of Liaison Psychiatry, Royal South Hants Hospital, Southampton
-
Professor Chris Price, Director of Clinical Research, Bayer Diagnostics Europe, Stoke Poges
-
Professor William Rosenberg, Professor of Hepatology and Consultant Physician, University of Southampton
-
Professor Peter Sandercock, Professor of Medical Neurology, Department of Clinical Neurosciences, University of Edinburgh
-
Dr Susan Schonfield, Consultant in Public Health, Hillingdon Primary Care Trust, Middlesex
-
Dr Eamonn Sheridan, Consultant in Clinical Genetics, St James’s University Hospital, Leeds
-
Dr Margaret Somerville, Director of Public Health Learning, Peninsula Medical School, University of Plymouth
-
Professor Sarah Stewart-Brown, Professor of Public Health, Division of Health in the Community, University of Warwick, Coventry
-
Professor Ala Szczepura, Professor of Health Service Research, Centre for Health Services Studies, University of Warwick, Coventry
-
Mrs Joan Webster, Consumer Member, Southern Derbyshire Community Health Council
-
Professor Martin Whittle, Clinical Co-director, National Co-ordinating Centre for Women’s and Children’s Health, Lymington