

Notes
Article history
The research reported in this issue of the journal was commissioned and funded by the HTA programme on behalf of NICE as project number 14/66/01. The protocol was agreed in August 2018. The assessment report began editorial review in July 2019 and was accepted for publication in February 2020. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Neil Gittoes reports personal fees for being a member of the advisory board to Union Chimique Belge (UCB) S.A. (Brussels, Belgium) and personal fees for contributing to educational meeting sponsored by Eli Lilly and Company (Indianapolis, IN, USA), outside the submitted work. He is also a trustee of the National Osteoporosis Society, a member of the advisory board of the National Osteoporosis Guideline Group and Deputy Chairperson of the Specialised Endocrinology Clinical Reference Group, NHS England.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2020. This work was produced by Davis et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2020 Queen’s Printer and Controller of HMSO
Chapter 1 Background
Description of the health problem
Osteoporosis is a disease characterised by low bone mass and structural deterioration of bone tissue, with a consequent increase in susceptibility to fragility fracture (a broken bone as a result of a fall from standing height or lower). The definition provided by the World Health Organization (WHO)1 defines the condition as bone mineral density (BMD) that is 2.5 standard deviations (SDs) below the average peak bone mass of healthy females aged 20–29 years, as measured by dual-energy X-ray absorptiometry (DXA). The WHO operational definition is updated to refer specifically to DXA at the femoral neck. 2 The term ‘established osteoporosis’ includes the presence of a fragility fracture. 1 Primary osteoporosis can occur in both men and women, but is most common in women after menopause, when it is termed postmenopausal osteoporosis. In contrast, secondary osteoporosis may occur in anyone as a result of medications, specifically glucocorticoids, or in the presence of particular hormonal disorders and other chronic diseases. 3
Fragility fractures are fractures that result from mechanical forces that would not ordinarily result in fracture, known as low-level (or ‘low-energy’) trauma, quantified as forces equivalent to a fall from a standing height or lower. 1 Although osteoporosis is an important predictor of the risk of fragility fracture, 70% of fragility fractures in postmenopausal women occur in those who do not meet the criteria for osteoporosis. 4
The prevalence of osteoporosis in the EU has been estimated at 22 million women and 5.5 million men. 5 In the UK, the number of women and men aged > 50 years with osteoporosis has been estimated as 2,527,331 women and 679,424 men, with approximately 536,000 new fragility fractures, comprising 79,000 hip fractures, 66,000 vertebral fractures, 69,000 forearm fractures and 322,000 other fractures (i.e. fractures of the pelvis, rib, humerus, tibia, fibula, clavicle, scapula, sternum and other femoral fractures). 6
In 2010, the number of postmenopausal women living with osteoporosis in the UK, based on the definition of a BMD at least 2.5 SDs lower than a young healthy woman (T-score of ≤ –2.5 SDs), was predicted to increase to 2.1 million in 2020 (+ 16.5%). 7 The prevalence of osteoporosis in the general population of women aged ≥ 50 years in the UK was assumed to remain stable over time, at approximately 15.5%.
Current service provision
Clinical guidelines
Currently, related National Institute for Health and Care Excellence (NICE) guidance includes a clinical guideline (CG) for identifying women and men at risk of fracture (CG1468) and four technology appraisals (TAs) of treatments for osteoporosis (TA464,9 TA204,10 TA16111 and TA16012).
Current National Institute for Health and Care Excellence technology appraisal guidance
The NICE guidance TA4649 recommends oral bisphosphonates [alendronate (ALN), ibandronate (IBN) and risedronate (RIS)] and intravenous (i.v.) bisphosphonates [IBN and zoledronic acid (ZOL)] as options for treating osteoporosis in people who are eligible for risk assessment, as defined in NICE’s CG146 on osteoporosis,8 depending on the person’s risk of fragility fracture. 9 However, the risk level at which oral bisphosphonates are cost-effective is not a clinical intervention threshold. NICE guidance TA4649 should be applied clinically in conjunction with the NICE quality standard (QS) 149 on osteoporosis,13 which defines the clinical intervention thresholds. These thresholds are based on the NICE-accredited National Osteoporosis Guideline Group (NOGG) guideline. 14
The NICE guidance TA20410 recommends denosumab (DEN) (Prolia®; Amgen Inc., Thousand Oaks, CA, USA) for the primary prevention of fragility fractures in postmenopausal women at specified fracture risks, defined by age, T-score and number of independent clinical risk factors for fracture, who have osteoporosis and who are unable to comply with the special instructions for administering ALN and either RIS or etidronate (which is no longer marketed in the UK), or have an intolerance of, or a contraindication to, those treatments. TA20410 also recommends DEN for the secondary prevention of osteoporotic fragility fractures in postmenopausal women who are at an increased risk of fractures and who are unable to comply with the special instructions for administering ALN and either RIS or etidronate, or have an intolerance of, or a contraindication to, ALN and either RIS or etidronate.
The NICE guidance TA16111 recommends raloxifene (RLX) (Evista®; Daiichi Sankyo Company, Ltd, Tokyo, Japan) and strontium ranelate (discontinued at the time this research was conducted), and teriparatide (TPTD) (Forsteo®; Eli Lilly and Company, Indianapolis, IN, USA) at specified fracture risks, defined by age, T-score and number of independent clinical risk factors for fracture, for women who have already sustained a fracture and who cannot take ALN. 11 NICE guidance TA16012 does not recommend RLX as a treatment option for the primary prevention of osteoporotic fragility fractures in postmenopausal women. 12
Current service cost
Hernlund et al. 5 reviewed the literature on fracture incidence and costs of fractures in the 27 EU countries and incorporated data into a model estimating the clinical and economic burden of osteoporotic fractures in 2010. The cost of osteoporosis, including pharmacological intervention in the EU in 2010 was estimated at €37B. Costs of treating incident fractures represented 66% of this cost, pharmacological prevention represented 5% and long-term fracture care represented 29%. Excluding the costs of pharmacological prevention, hip fractures represented 54% of the costs, vertebral and forearm fractures represented 5% and 1%, respectively, of the costs and ‘other fractures’ represented 39%. The estimated number of life-years lost in the EU as a result of incident fractures was approximately 26,300 in 2010. The total health burden, measured in terms of lost quality-adjusted life-years (QALYs), was estimated at 1,180,000 QALYs for the EU.
In the UK, the cost of osteoporosis (excluding the value of QALYs lost) in 2010 was estimated by Hernlund et al. 5 at €103M (£91.8M in 2017 prices) for pharmacological fracture prevention, €3977M (£3546M in 2017 prices) for cost of fractures, and €1328M (£1185M in 2017 prices) for cost of long-term disability. The 2010 cost of UK osteoporosis fracture in relation to population and health-care spending was €5408M (£4822M in 2017 prices). The 2010 prices reported by Hernlund et al. 5 in euros were converted back to Great British pounds (2006 prices). The conversion ratio from 2006 prices to 2010 prices used by Hernlund et al. 5 was estimated by the School of Health and Related Research (ScHARR) as 1.4065 by comparing the unit cost for nursing home stay against the cited UK-specific source data from 2006. 15 Costs were then uplifted to 2017 prices using the Hospital and Community Health Service inflation indices from the Personal Social Services Research Unit (PSSRU)16 (302.3 for 2016/17 vs. 240.9 for 2005/6).
Current treatment pathway
The NICE 2018 osteoporosis overview pathway17 and fragility fracture risk assessment pathway18 cover NICE guidance on osteoporosis in adults (aged ≥ 18 years), including assessing the risk of fragility fracture and drug treatment for the primary and secondary prevention of osteoporotic fragility fractures. (The recommendations on assessment of fracture risk in CG1468 are summarised in Measurement of disease.)
Description of the technology under assessment
Interventions considered in the scope of this report
Four interventions are considered in this assessment: DEN, RLX, romosozumab (ROMO) [Evenity®; Union Chimique Belge (UCB) S.A. (Brussels, Belgium) and Amgen Inc.] and TPTD.
Mode of action
Treatments for osteoporosis generally fall into two classes: bone-forming agents (ROMO and TPTD) and anti-resorptive agents (bisphosphonates, DEN and RLX). Bone-forming agents are used for shorter durations of treatment, often in patients at very high risk of fracture, whereas anti-resorptive agents are used as long-term treatments and sometimes after bone-forming agents. 19 It should be noted that the company submission by UCB S.A. states that ROMO leads to ‘an increase in bone formation and reduction in bone resorption’, suggesting that it has both bone-forming and anti-resportive properties. 20
Marketing licence and administration method
Denosumab is a monoclonal antibody that reduces osteoclast activity, and so reduces bone breakdown. It is administered as a single 60-mg subcutaneous (s.c.) injection once every 6 months. DEN has a marketing authorisation in the UK for the treatment of osteoporosis in postmenopausal women and in men at increased risk of fractures. 19 DEN also has a marketing authorisation for the treatment of bone loss associated with long-term systemic glucocorticoid therapy in adult patients at increased risk of fracture. 21
Raloxifene is a selective oestrogen receptor modulator. It is administered orally at a dose of 60 mg daily. RLX has a marketing authorisation in the UK for the treatment and prevention of osteoporosis in postmenopausal women. Non-proprietary RLX [Sandoz International GmBH (Holzkirchen, Germany), Consilient Health Ltd (Dublin, Ireland), Actavis UK (now Accord-UK Ltd, Barnstaple, UK), Mylan Pharma UK Ltd (Sandwich, UK)] is also available for the same indication. 19
Romosozumab is a monoclonal antibody that inhibits the protein sclerostin, increasing bone formation and decreasing bone breakdown. It has been studied in clinical trials as 12 months of ROMO followed by at least 12 months of ALN, compared with at least 24 months of ALN alone, in postmenopausal women. It has also been studied in a randomised, placebo-controlled clinical trial for treating osteoporosis in men. 19 This report was prepared while ROMO was still being assessed by the European Medicines Agency; therefore, it was based on the anticipated licensed indication for ROMO. A marketing authorisation was issued in December 2019; the recommended dose is 210 mg (administered as two s.c. injections of 105 mg each) once monthly for 12 months. This is consistent with the anticipated licensed indication used in preparation of this report.
Teriparatide is a recombinant fragment of human parathyroid hormone and, as an anabolic agent, it stimulates formation of new bone and increases resistance to fracture. It is administered subcutaneously at a dose of 20 µg daily for up to 24 months. TPTD has a marketing authorisation in the UK for treatment of osteoporosis in postmenopausal women and in men at increased risk of fracture. It also has a marketing authorisation in the UK for treatment of osteoporosis associated with sustained systemic glucocorticoid therapy in women and men at increased risk of fracture. Biosimilar versions of TPTD [Movymia, Internis Pharmaceuticals Ltd (Huddersfield, UK);22 Terrosa, Gedeon Richter plc (Budapest, Hungary)23] have been licensed for the same indications. 19
Contraindications, special warnings and precautions
The Summary of Product Characteristics (SmPC) for each intervention describes the contraindications and special warnings for bisphosphonates. 20,24,25
A s.c. injection of 60 mg of DEN once every 6 months is contraindicated in patients with hypocalcaemia or hypersensitivity to the active substance or to any of its excipients. Adequate intake of calcium and vitamin D is important in all patients. 24 Special warnings and precautions include hypocalcaemia, renal impairment, skin infections, osteonecrosis of the jaw (ONJ) and atypical femoral fracture. 24
A 60-mg daily oral dose of RLX is contraindicated in women with child-bearing potential and in patients with an active or past history of venous thromboembolism (VTE), including deep-vein thrombosis (DVT), pulmonary embolism (PE) and retinal vein thrombosis; hepatic impairment including cholestasis; severe renal impairment; unexplained uterine bleeding; signs or symptoms of endometrial cancer; or hypersensitivity to the active substance or to any of the excipients. 25
The draft SmPC for ROMO notes special precautions in patients (confidential information has been removed). Special warnings and precautions include (confidential information has been removed). 20
Teriparatide administered subcutaneously at a dose of 20 µg daily is contraindicated in women who are pregnant or breastfeeding and in patients with pre-existing hypercalcaemia, severe renal impairment, metabolic bone diseases (including hyperparathyroidism and Paget’s disease of bone) (other than primary osteoporosis or glucocorticoid-induced osteoporosis), unexplained elevations of alkaline phosphatase, prior external beam or implant radiation therapy to the skeleton, skeletal malignancies or bone metastases, or hypersensitivity to the active substance or to any of the excipients. 25 Precautions include elevations of serum calcium concentrations, active or recent urolithiasis, orthostatic hypotension and renal impairment. 25
Place in treatment pathway
Denosumab is recommended as a treatment option for the primary prevention of osteoporotic fragility fractures only in postmenopausal women at increased risk of fracture who are unable to comply with the special instructions for administering ALN and either RIS or etidronate, or have an intolerance of, or a contraindication to, those treatments and who have a sufficiently high risk of fracture as determined by a combination of T-score, age and number of independent clinical risk factors for fracture. 10 DEN is also recommended ‘as a treatment option for the secondary prevention of osteoporotic fragility fractures in postmenopausal women at increased risk of fractures who are unable to comply with the special instructions for administering alendronate and either risedronate or etidronate, or have an intolerance of, or a contraindication to, those treatments’ (TA204)10 (© NICE 2010 Denosumab for the Prevention of Osteoporotic Fractures in Postmenopausal Women. Technology Appraisal Guidance [TA204]. Available from www.nice.org.uk/guidance/ta204. All rights reserved. Subject to Notice of rights. NICE guidance is prepared for the National Health Service in England. All NICE guidance is subject to regular review and may be updated or withdrawn. NICE accepts no responsibility for the use of its content in this product/publication.). DEN has a marketing authorisation in the UK for the treatment of osteoporosis in postmenopausal women and in men at increased risk of fractures, and for the treatment of bone loss associated with long-term systemic glucocorticoid therapy in adult patients at increased risk of fracture. 21
Raloxifene is recommended as an alternative treatment option for the secondary prevention of osteoporotic fragility fractures in postmenopausal women who are unable to comply with the special instructions for the administration of ALN and RIS, or have a contraindication to, or are intolerant of, ALN and RIS and who also are at a sufficiently high risk of fracture as determined by a combination of T-score, age and number of independent clinical risk factors for fracture.
Romosozumab is not currently part of any NICE osteoporosis treatment pathway.
Teriparatide is recommended as an alternative treatment option for the secondary prevention of osteoporotic fragility fractures in postmenopausal women who are unable to take ALN and RIS, or who have a contraindication to or are intolerant of ALN and RIS, or who have had an unsatisfactory response to treatment with ALN or RIS, and who are aged ≥ 65 years and have a T-score of ≤ –4.0 SD, or a T-score of ≤ –3.5 SD plus more than two fractures, or who are aged 55–64 years and have a T-score of ≤ –4 SD plus more than two fractures. 12
Identification of important subgroups
The final NICE scope specified subgroups based on patient characteristics that increase the risk of fracture (those specified in NICE CG1468) or that affect the impact of fracture on lifetime costs and outcomes. 19
Current usage in the NHS
Data from the 2017 Prescription Cost Analysis26 were analysed to determine the level of non-bisphosphonate usage in primary care across England in 2017. It can be seen from the data summarised in Table 1 that generic RLX was the most commonly prescribed preparation in primary care. The prescribing costs in hospitals and the community in England in 2016/17 for treatment of osteoporosis was £11,930,475 for DEN, £355,530 for RLX and £4,409,696 for TPTD. 27
| Drug | Generic or branded | Dosing schedule | Prescriptions in thousandsa | Description of preparations |
|---|---|---|---|---|
| DEN | Branded | Once every 6 months | 43.063 | Prolia injection, 60 mg/1 ml pre-filled syringe |
| RLX | Branded | Daily | 1.738 | Evista tablet, 60 mg |
| Generic | Daily | 57.301 | RLX hydrochloride tablet, 60 mg | |
| TPTD | Branded | Daily | 0.964 | Forsteo injection, 250 µg/ml, 2.4 ml pre-filled pen |
Anticipated costs associated with interventions
Table 2 summarises the 2018 net costs associated with the interventions, based on their list prices. 28
| Drug | Generic or branded | Unit type and dose | Price per unit28 |
|---|---|---|---|
| DEN | Branded | Prolia injection, 60 mg/1 ml, one pre-filled disposable injection |
|
| RLX | Branded | Evista tablet, 60 mg, 28 tablets |
|
| Generic | RLX HCl tablet, 60 mg, 28 tablets | Activis UK:
|
|
| TPTD | Branded | Forsteo injection, 250 µg/ml 2.4 ml pre-filled pen, one pre-filled disposable injection (i.e. 30 daily doses) |
|
Impact of health problem
Significance for patients
Fractures cause significant pain, disability and loss of independence and can be fatal. 1 In the UK, the number of fracture-related deaths in 2010 was estimated at 6059. 6 Hip, vertebral and other fractures accounted for 2764, 1795 and 1500 deaths, respectively. 6
Significance for the NHS
The cost of osteoporosis in the UK in 2010 was estimated at £4.4B. First-year costs, subsequent-year costs and pharmacological fracture prevention costs amounted to £3.2B, £1.1B and £84M, respectively. 6
Measurement of disease
Quantitative diagnosis in the UK relies on the assessment of BMD, usually by central DXA. BMD at the femoral neck provides the reference site. It is defined as a value for BMD of ≥ 2.5 SDs below the young female adult mean (i.e. a T-score of ≤ –2.5 SDs). Severe osteoporosis (established osteoporosis) describes osteoporosis in the presence of one or more fragility fractures. 29
The NICE CG1468 recommends the estimation of absolute risk of fragility fracture when assessing risk of fracture and recommends the use either FRAX® (web version 3.9, University of Sheffield, Sheffield, UK)30 (without a BMD value if DXA has not previously been undertaken) or QFracture® (QFracture-2012 open source revision 38, Clinrisk Ltd, Leeds, UK),31 within their allowed age ranges, to estimate the 10-year predicted absolute fracture risk when assessing risk of fracture. 8 Above the upper age limits defined by the tools, people are considered to be at high risk. 8
The guideline8 recommends that assessment is indicated in all women aged ≥ 65 years and all men aged ≥ 75 years and in women aged < 65 years and men aged < 75 years in the presence of risk factors (i.e. previous fragility fracture, current use or frequent recent use of oral or systemic glucocorticoids, history of falls, family history of hip fracture, other causes of secondary osteoporosis, low body mass index, smoking and alcohol intake of > 14 units per week for women and of > 21 units per week for men). The guideline8 recommends not routinely assessing fracture risk in people aged < 50 years unless they have major risk factors (i.e. current or frequent recent use of systemic corticosteroids, untreated premature menopause or previous fragility fracture). The guideline8 also recommends interpretation with caution of the estimated absolute risk of fracture in people aged > 80 years, because predicted 10-year fracture risk may underestimate their short-term fracture risk.
Chapter 2 Definition of the decision problem
Decision problem
This assessment addresses the following question: what is the clinical effectiveness and cost-effectiveness of DEN, RLX, ROMO and TPTD, within their licensed indications, for the prevention of osteoporotic fragility fractures, as compared with each other, bisphosphonates or a non-active treatment?
Overall aims and objectives of the assessment
-
To evaluate the clinical effectiveness of each intervention in terms of osteoporotic fragility fractures, and femoral neck BMD.
-
Population: adults assessed for risk of osteoporotic fragility fracture, according to the recommendations in NICE CG146. 8
-
Interventions: DEN, RLX, ROMO and TPTD.
-
Comparators: placebo or no active treatment control; interventions compared with each other; the bisphosphonates ALN, RIS, IBN (oral or i.v.) and ZOL.
-
Outcomes: osteoporotic fragility fracture, BMD at the femoral neck, adverse events (AEs) and health-related quality of life (HRQoL).
-
-
To evaluate the incremental cost-effectiveness of each intervention compared with (1) each other, (2) the bisphosphonates ALN, IBN (oral or i.v.), RIS and ZOL and (3) no active treatment.
From here on, the term bisphosphonates will be used to refer only to those bisphosphonates included as comparators in this assessment, namely ALN, RIS, IBN (oral or i.v.) and ZOL.
Chapter 3 Assessment of clinical effectiveness
This report contains reference to confidential information provided as part of the NICE appraisal process. This information has been removed from the report and the results, discussions and conclusions of the report do not include the confidential information. These sections are clearly marked in the report.
A systematic review of the literature and network meta-analyses (NMAs) were conducted to evaluate the clinical effectiveness of DEN, RLX, ROMO and TPTD in the treatment of adults with osteoporosis in terms of preventing osteoporotic fragility fractures.
The systematic review of the evidence was undertaken in accordance with the general principles recommended in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 32,33
Methods for reviewing effectiveness
Search strategy
A comprehensive search was undertaken to systematically identify clinical effectiveness literature relating to the bisphosphonates ALN, IBN, RIS and ZOL, and the non-bisphosphonates DEN, RLX, ROMO and TPTD, within their licensed indications, for the prevention of fragility fractures.
The search strategy comprised the following main elements:
-
searching of electronic databases
-
contact with experts in the field
-
scrutiny of bibliographies of retrieved papers.
The following database and trials registries were searched on 11 July 2018:
-
MEDLINE and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and MEDLINE (via Ovid), searched from 1946 to 2018
-
EMBASE (via Ovid), searched from 1974 to 2018
-
Cochrane Database of Systematic Reviews (via Wiley Online Library), searched from 1996 to 2018
-
Database of Abstracts of Reviews of Effects (via Wiley Online Library), searched from 1995 to 2015
-
Cochrane Central Register of Controlled Trials (via Wiley Online Library), searched from 1898 to 2018
-
Health Technology Assessment Database (via Wiley Online Library), searched from 1995 to 2016
-
Science Citation Index Expanded (via Web of Science), searched from 1900 to 2018
-
Conference Proceedings Citation Index – Science (via Web of Science), searched from 1990 to 2018
-
WHO International Clinical Trials Registry Platform.
Existing evidence reviews commissioned by NICE, which included literature published up to September 2014, were assumed to have identified all papers published prior to 2014 that were relevant to this review.
Searches were not restricted by language or publication type. Subject headings and keywords for ‘osteoporosis’ were combined with each of the named drug interventions. The MEDLINE search strategy is presented in Appendix 1. The search was adapted across the other databases. Highly sensitive study design filters were used to retrieve clinical trials and systematic reviews on MEDLINE and other databases, when appropriate. Industry submissions and relevant systematic reviews were also hand-searched to identify any further relevant clinical trials. The WHO International Clinical Trials Registry Platform was searched for ongoing and recently completed research projects. Citation searches of key included studies were also undertaken using the Web of Science database. All potentially relevant citations were downloaded to the bibliographic software EndNote version X9.1 [Clarivate Analytics (formerly Thomson Reuters), Philadelphia, PA, USA] and deduplication of citation records undertaken.
Other resources
In addition to database searches, the reference lists of relevant studies were checked. Identified systematic reviews were checked to identify any additional trials meeting the inclusion criteria.
Bisphosphonate studies were identified from the assessment report34 used to inform the development of NICE TA464. 9 As the searches for this TA were last updated in September 2014, more recent studies were sought from the database searches.
When data from included trials were missing, the company submissions were checked. Any academic or commercial-in-confidence data taken from a company submission were underlined and highlighted in the assessment report.
Study selection
All titles and abstracts identified by the searches were screened by one reviewer, and 10% were screened by a second reviewer. Full-text articles were assessed by one reviewer, with queries addressed by a second reviewer; discrepancies were resolved by discussion.
Inclusion and exclusion criteria for the selection of clinical effectiveness evidence were defined according to the decision problem outlined in the NICE scope. 19
Inclusion criteria
Population
Adults at risk of osteoporotic fragility fracture, according to the recommendations in NICE CG1468 (see Chapter 1, Measurement of disease).
Interventions
Four interventions are considered in this assessment: DEN, RLX, ROMO and TPTD. These four interventions were assessed in accordance with their licensed indications, at licensed doses. At the time that searches were conducted, ROMO did not have a marketing authorisation in the UK for treating osteoporosis, but had been submitted to the European Medicines Agency, given as monthly 210-mg s.c. injections (draft SmPC, as provided in the company submission). 20
Comparators
Interventions may be compared with placebo, no active treatment control, each other or the bisphosphonates ALN, RIS, IBN (oral or i.v.) and ZOL, within their licensed indications (including s.c. and i.v. where licensed).
Studies that allowed concomitant treatment with calcium and/or vitamin D for patients in both the intervention and comparator arms were included.
Studies that planned treatment sequences or open-label extensions with participants in allocated randomised groups were included.
Outcomes
The main outcome sought was osteoporotic fragility fracture. Vertebral fractures, when data allowed, were considered separately for clinical/symptomatic fractures and morphometric/radiographic fractures. Radiographic fractures, defined according to Genant et al. ,35 were those resulting in a ≥ 20% reduction in vertebral height; however, if a study did not specify that the Genant et al. 35 definition was used, morphometric/radiographic fracture data were still included. Non-vertebral fracture data were sought, and, when reported, hip, wrist and proximal humerus fractures were considered separately. Although planned, data on concordance were not extracted owing to time constraints.
In addition, BMD at the femoral neck (assessed by DXA) data were sought. Only femoral neck BMD data were included in the NMA; however, when trials did not report these data, BMD measured at the lumbar spine was tabulated.
The following outcome measures were also included: mortality (overall or following fracture), AEs of treatment, and HRQoL.
Study design
Randomised controlled trials (RCTs) were included. Studies published as abstracts or conference presentations were included only if sufficient details were presented to allow both an appraisal of the methodology and an assessment of the results to be undertaken. Systematic reviews and CGs were used only as potential sources of additional RCTs of efficacy evidence.
Exclusion criteria
-
Studies with patients with normal or unspecified BMD.
-
Studies with patients with other indications for the same drugs. Cancer populations at risk of osteoporosis that are covered by NICE guideline (NG) 10136 and NICE CG175. 37
-
Studies in which interventions were administered not in accordance with licensed indications.
-
Studies in which interventions were co-administered with any other therapy with the potential to augment bone, unless concomitant treatments are specified in the SmPC.
-
Studies that were considered methodologically unsound in terms of study design or the method used to assess outcomes.
-
Reports published as abstracts or conference presentations only, for which insufficient details are reported to allow an assessment of study quality or results.
-
Studies that were published in languages other than English.
-
Studies based on animal models, and pre-clinical and biological studies.
-
Narrative reviews, editorials, opinions.
Data extraction and critical appraisal
Data relevant to the decision problem were extracted by one reviewer and checked by a second reviewer. Discrepancies were resolved by discussion. Data were extracted without blinding to authors or journal. Data from study arms for which intervention treatments were administered in line with licensed indications were extracted; data from unlicensed treatment arms were not extracted.
For studies included in NICE TA464, the data used were those previously extracted. 34
Methodological quality of RCTs identified for inclusion were assessed using the Cochrane Collaboration risk-of-bias assessment criteria. 38 Two independent reviewers undertook quality assessment. Risk-of-bias plots were produced using Cochrane Review Manager (RevMan) version 5.3 (The Cochrane Collaboration, The Nordic Cochrane Centre, Copenhagen, Denmark).
The revised tool (RoB 2.0)39 to assess the risk of bias in randomised trials,39 published in September 2018, was not applied as this review commenced prior to the publication of the revised risk-of-bias tool.
Randomised controlled trials were classified as being at high risk of attrition bias when the dropout rate in any treatment arm was ≥ 10%. 40
Data synthesis
The extracted data and quality assessment variables were presented for each study, both in structured tables and as a narrative description. Information on between-group differences extracted from included studies were presented. When these were not reported by included studies, these were estimated using Cochrane RevMan version 5.3, as either risk ratio (RR) or mean difference (MD).
Data were pooled across studies in NMAs, the methods of which are described in Methods for the network meta-analysis.
Results
Quantity of research available
Study selection is shown in Figure 1. As a result of the searches described in Search strategy, a total of 7898 citations were identified for the clinical review. At abstract sift, 7792 were excluded. At full-text sift, 34 records were excluded. These are listed in Appendix 2, along with reasons for exclusion. Fifty-two RCTs of the interventions of interest were included (published in 69 articles; see Table 3).
FIGURE 1.
The PRISMA flow diagram of study selection.
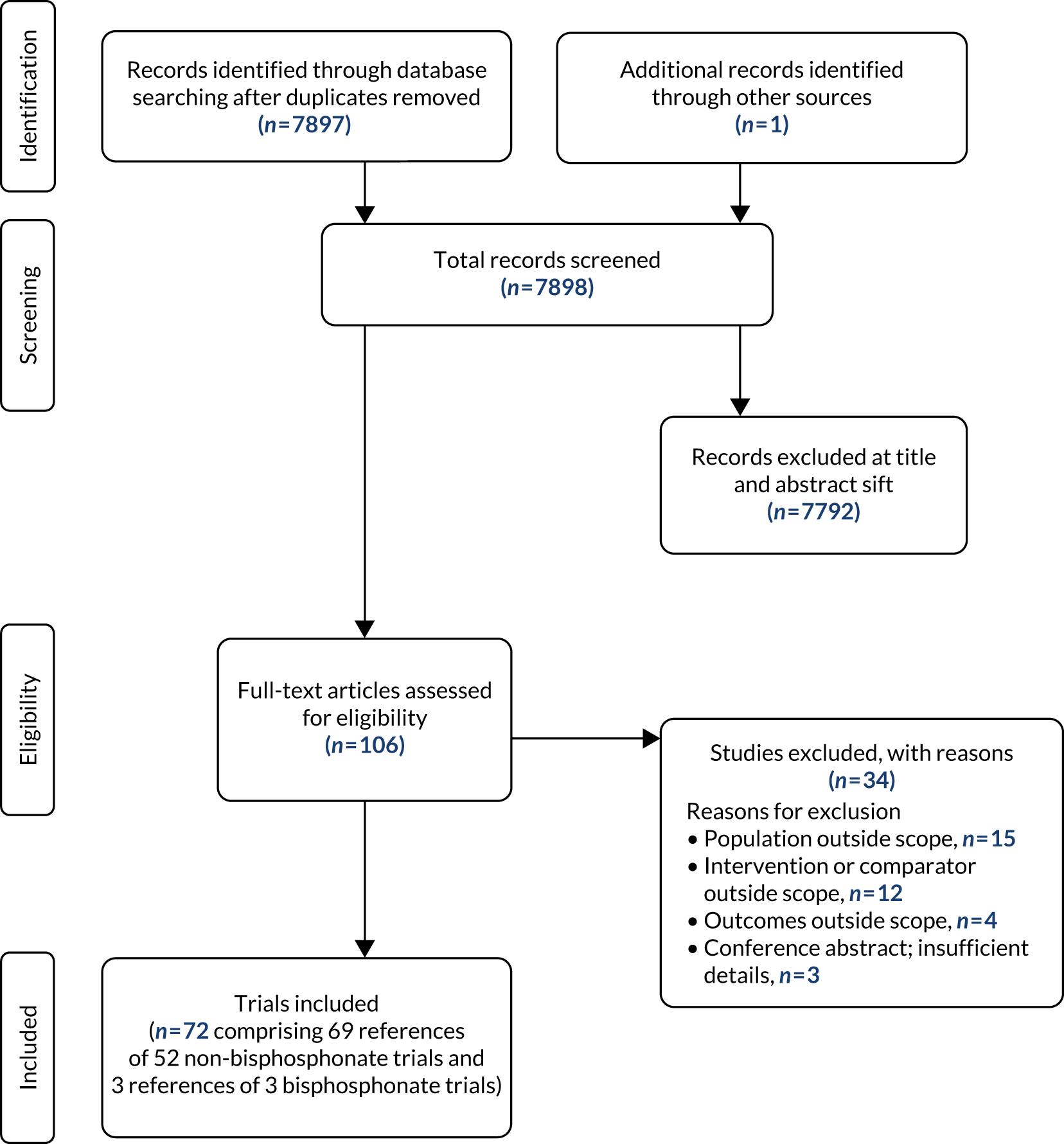
In addition, three bisphosphonate RCTs were identified and added to the 48 RCTs of bisphosphonates identified from TA46434 (see Appendix 3).
Randomised controlled trials included in the systematic review of clinical effectiveness of fracture and femoral neck BMD are presented in Table 3; data from licensed dose arms only for DEN, RLX, ROMO and TPTD were extracted and presented in this assessment report.
| Trial | Intervention and comparators | Population | Reported vertebral fracture data | Reported femoral neck BMD data |
|---|---|---|---|---|
| DEN vs. placebo | ||||
| FREEDOM41 |
|
Postmenopausal women with osteoporosis | Yes | Yes |
| ADAMO (Orwoll 2012)42 |
|
Men with osteoporosis | Yes | Yes |
| DIRECT43 |
|
Postmenopausal women with osteoporosis and men with osteoporosis | Yes | Yes |
| Nakamura 201244 |
|
Postmenopausal women with osteoporosis | Yes | No |
| Koh 201645 |
|
Postmenopausal women with osteoporosis | No | Yes |
| RLX vs. placebo | ||||
| Adami 200846 |
|
Postmenopausal women with osteoporosis | No | Yes |
| Morii 200347 |
|
Postmenopausal women with osteoporosis | Yes | No |
| Liu 200448 |
|
Postmenopausal women with osteoporosis | Yes | Yes |
| Gorai 201249 |
|
Postmenopausal women with osteoporosis | No | No, lumbar spine BMD |
| Silverman 200850 |
|
Postmenopausal women with osteoporosis | Yes | Yes |
| MORE51 |
|
Postmenopausal women with osteoporosis | Yes | Yes |
| Lufkin 199852 |
|
Postmenopausal women with osteoporosis | Yes | No |
| Mok 201153 |
|
Postmenopausal women with osteoporosis | Yes | Yes |
| ROMO vs. placebo | ||||
| FRAME54 |
|
Postmenopausal women with osteoporosis | Yes | Yes |
| Ishibashi 201755 |
|
Postmenopausal women with osteoporosis | No | Yes |
| BRIDGE56 |
|
Men with osteoporosis | No | Yes |
| TPTD vs. placebo | ||||
| Orwoll 200357 |
|
Men with osteoporosis | No | Yes |
| Miyauchi 201058 |
|
Women and men with osteoporosis | Yes | Yes |
| Miyauchi 200859 |
|
Women with osteoporosis | No | Yes |
| ACTIVE60 |
|
Postmenopausal women with osteoporosis | Yes | Yes |
| Leder 201561 |
|
Postmenopausal women with osteoporosis | No | Yes |
| FPT62 |
|
Postmenopausal women with prior fractures | Yes | Yes |
| Sethi 200863 |
|
Postmenopausal women with osteoporosis | No | Yes |
| Head-to-head non-bisphosphonates | ||||
|
Postmenopausal women with osteoporosis | No | Yes | |
| EUROFORS66 |
|
Postmenopausal women with osteoporosis | Yes | Yes |
| STRUCTURE67 |
|
Postmenopausal women with osteoporosis | Yes | Yes |
| McClung 201468 (also bisphosphonate comparator) |
|
Postmenopausal women with osteoporosis | No | Yes |
| DEN vs. bisphosphonates | ||||
| DECIDE69 |
|
Postmenopausal women with osteoporosis | No | Yes |
| STAND70 |
|
Postmenopausal women with osteoporosis | No | Yes |
| DAPS71 |
|
Postmenopausal women with osteoporosis | No | Yes |
| AMG 162 Bone Loss study72 |
|
Postmenopausal women with osteoporosis | No | Yes |
| Recknor 201373 |
|
Postmenopausal women with osteoporosis | No | Yes |
| Saag 201874 |
|
Glucocorticoid-induced osteoporosis (men and women) | No | Yes |
| Miller 201675 |
|
Postmenopausal women with osteoporosis | No | Yes |
| RLX vs. bisphosphonates | ||||
| EFFECT (international)76 |
|
Postmenopausal women with osteoporosis | Yes | Yes |
| EFFECT (USA)77 |
|
Postmenopausal women with osteoporosis | No | Yes |
| Johnell 200278 |
|
Postmenopausal women with osteoporosis | No | Yes |
| Muscoso 200479 |
|
Postmenopausal women with osteoporosis | Yes | No |
| EVA80 |
|
Postmenopausal women with osteoporosis | Yes | Yes |
| Sanad 201181 |
|
Postmenopausal women with osteoporosis | No | Yes |
| Michalská 200682 |
|
Postmenopausal women with osteoporosis | No | Yes |
| ROMO vs. bisphosphonates | ||||
| ARCH83 |
|
Postmenopausal women with osteoporosis | Yes | Yes |
| TPTD vs. bisphosphonates | ||||
| FACT84 |
|
Postmenopausal women with osteoporosis | No | Yes |
| Saag 200985 |
|
Glucocorticoid-induced osteoporosis (men and women) | Yes | Yes |
| Panico 201186 |
|
Postmenopausal women with osteoporosis | Yes | Yes |
| EuroGIOPs87 |
|
Glucocorticoid-induced osteoporosis (men) | No | Yes |
| Anastasilakis 200888 |
|
Postmenopausal women with osteoporosis | No | No, lumbar spine BMD |
| Walker 201389 |
|
Glucocorticoid-induced osteoporosis (men) | Yes | Yes |
| VERO90 |
|
Postmenopausal women with osteoporosis | Yes | No |
| Hadji 201291 |
|
Postmenopausal women with osteoporosis | Yes | Yes |
| MOVE92 |
|
Post surgery for osteoporotic hip fracture | Yes | Yes |
| Cosman 201193 |
|
Postmenopausal women with osteoporosis | Yes | Yes |
Of the 52 RCTs included, 23 compared non-bisphosphonates with placebo, four were head-to-head comparisons of non-bisphosphonates (of which one RCT also included a bisphosphonate arm) and 25 RCTs compared a non-bisphosphonate with a bisphosphonate.
Listed treatment arms were all at licensed doses.
Trial characteristics are shown in Appendix 4. All 52 included trials were RCTs, with the majority being multicentre studies. All trials providing data for the NMAs involved concomitant treatment with calcium and vitamin D. The most common primary outcome measure was percentage change in BMD from baseline.
The majority of RCTs had populations of postmenopausal women. Population baseline characteristics of RCTs are shown in Appendix 4. There was some variation between trials in baseline BMD T-scores and the percentage of participants with fractures at baseline. In the RCTs, population baseline characteristics were balanced between treatment arms.
Quality of research available
Results of the risk-of-bias assessment
Non-bisphosphonates versus placebo
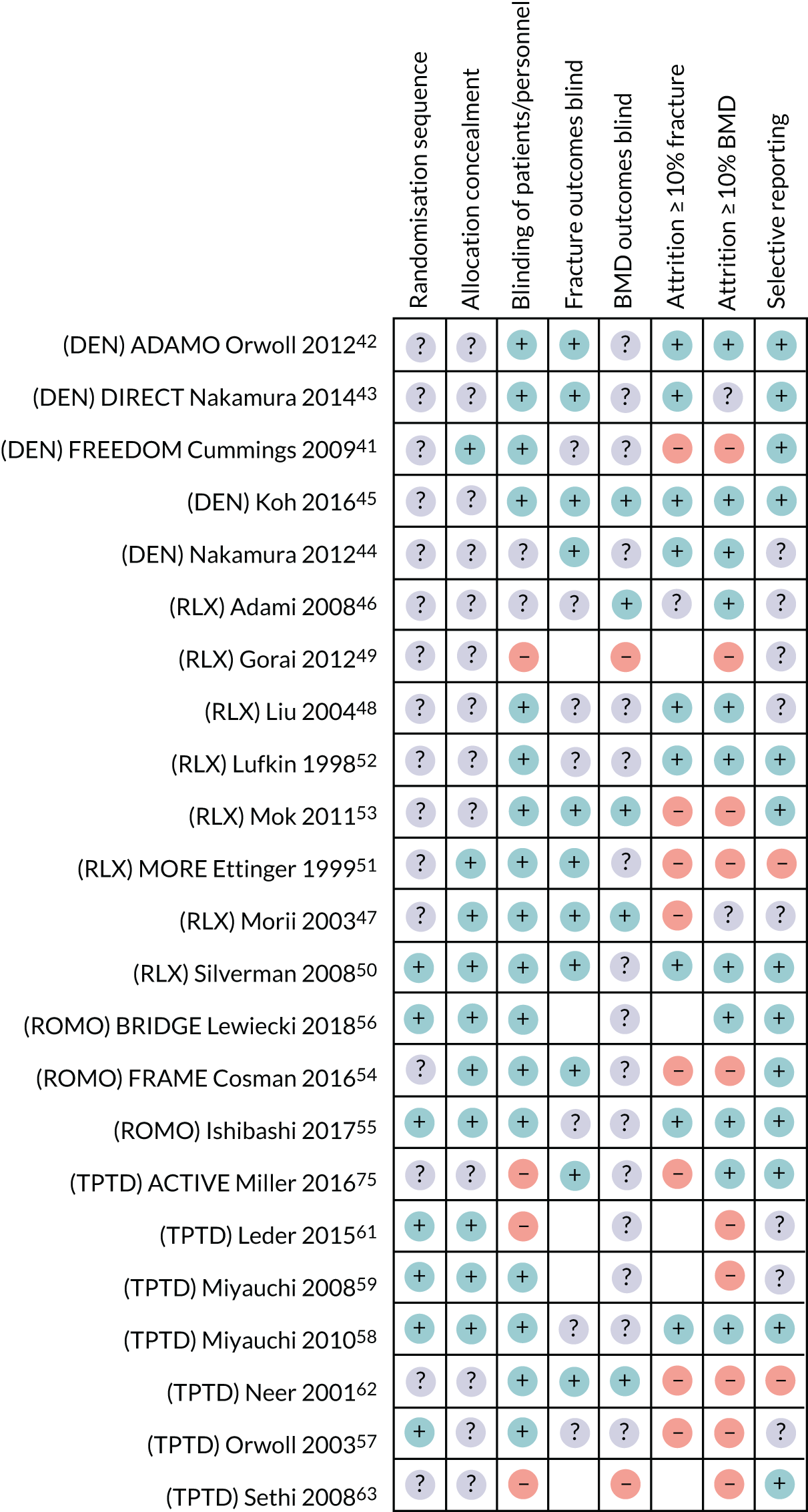
A summary of the Cochrane risk-of-bias assessment across the placebo-controlled non-bisphosphonate studies is presented in Figure 2.
FIGURE 2.
Cochrane risk-of-bias summary across placebo-controlled non-bisphosphonate studies. ?, Unclear-risk of bias; +, low-risk of bias; –, high-risk of bias; blank cells, not a study outcome. ACTIVE, Abaloparatide Comparator Trial In Vertebral Endpoints; ADAMO, A multicenter, randomized, double-blind, placebo-controlled study to compare the efficacy and safety DenosumAb versus placebo in Males with Osteoporosis; BRIDGE, phase III randomized placeBo-contRolled double-blind study evaluatIng the efficacy and safety of Romosozumab in treatinG mEn with osteoporosis; DIRECT Denosumab fracture Intervention RandomizEd placebo Controlled Trial; FRAME, Fracture Study in Postmenopausal Women with Osteoporosis; FREEDOM, Fracture REduction Evaluation of Denosumab in Osteoporosis every 6 Months; MORE, Multiple Outcomes for Raloxifene Evaluation.
Denosumab versus placebo
None of the five studies comparing DEN with placebo41–45 reported how the random sequence was generated, and only two reported that allocation to treatment groups was concealed. 41,42
Four of the five studies reported that participants and personnel were blinded to treatment allocation. 41–43,45 Four studies reported that fracture assessment was blinded to treatment allocation. 42–45 However, only one reported that BMD assessment was blinded to treatment allocation. 42
One study was considered to have a high risk of attrition bias for both fracture and BMD outcomes as ≥ 10% of participants in both treatment groups did not complete the study. 41
Only one study did not report the location of a study protocol, against which the reported outcomes could be checked for selective reporting. 44 The remaining four studies of DEN vs. placebo were all considered to have a low risk of bias for this domain. 41–43,45
Raloxifene versus placebo
Of the eight studies comparing RLX with placebo,46–48,50–53,94 only one reported how the random sequence was generated (it was computer generated), and was considered to have a low risk of bias for this domain. 50 Only three of the eight studies reported that allocation to treatment groups was concealed. 47,50,51
Six of the studies reported that participants and personnel were blinded to treatment allocation. 47,48,50–53 One study was considered to have a high risk of bias for this domain as it was described as open label. 94
Four of the studies comparing RLX with placebo reported that fracture assessment was blinded to treatment allocation,47,50,51,53 and three reported that BMD assessment was blinded to treatment allocation. 46,47,53 One study reported that BMD assessment was not blinded to treatment allocation;94 this study was therefore considered to have a high risk of bias for this domain.
Four studies were considered to have a high risk of attrition bias for fracture and/or BMD outcomes, as ≥ 10% of participants did not complete the study. 47,51,53,94
Only three studies reported the location of a protocol, against which outcomes could be checked;50,52,53 these studies were considered to have a low risk of bias, as all outcomes in the protocol had been reported. 50,52,53
In one study, which did not report a protocol location, BMD was reported for only a subset of participants and AEs were not reported by the different RLX doses. 51 This study was considered to have a high risk of bias for selective reporting.
Romosozumab versus placebo
All three of the studies comparing ROMO with placebo reported that allocation to treatment groups was concealed,54–56 and two reported how the random sequence was generated (all adequate methods). 55,56 All three reported that participants and personnel were blinded to treatment allocation. 54–56
All three studies assessed BMD,54–56 but none reported whether or not the assessment was blinded. Only one54 of the two studies54,55 assessing fracture reported that this outcome was blinded to treatment allocation.
One study was considered to have a high risk of attrition bias (≥ 10% participants did not complete the study) for both BMD and fracture outcomes,54 and one study was considered to have a low risk of bias for BMD and fracture outcomes,55 as was one study that assessed only BMD. 56
All three studies reported the location of the protocol and all items in the protocol were reported in all three study publications. 54–56
Teriparatide versus placebo
Across the seven studies comparing TPTD with placebo,57–59,61–63,95 four reported a method for the random sequence generation (all adequate)57–59,61 and three reported that allocation to treatment groups was concealed. 58,59,61
Three of the studies were described as open label and were considered to have a high risk of bias for blinding of participants and study personnel. 63,65,95 The other four trials were considered to have a low risk of bias for this domain. 57–59,62
When fractures and/or BMD were outcomes, only two of the studies reported that fracture assessment was blinded62,95 and only one reported that BMD assessment was blinded to treatment allocation. 62 One study that reported that BMD assessment was unblinded (fractures were not an outcome) was considered to have a high risk of bias for this domain. 63
Attrition bias of ≥ 10% was evident for reporting of fracture outcomes in three studies,57,62,95 and evident for five studies reporting BMD outcomes, all of which were judged to be at high risk of attrition bias. 57,59,62,63,65
Three studies reporting the location of a protocol were judged to be at low risk of selective reporting bias. 58,63,95 One study was judged to be at high risk of selective reporting bias62 as safety outcomes were not clearly reported in the publication and, although the online protocol described safety as a planned outcome, no results for any outcome had been posted. 96
When considering studies of non-bisphosphonates compared with placebo, those reporting fracture data had a similar risk of bias to those reporting BMD data, although a higher percentage of studies reporting fracture data reported blinding of outcome assessors than did those reporting BMD data. 97
Head-to-head non-bisphosphonates
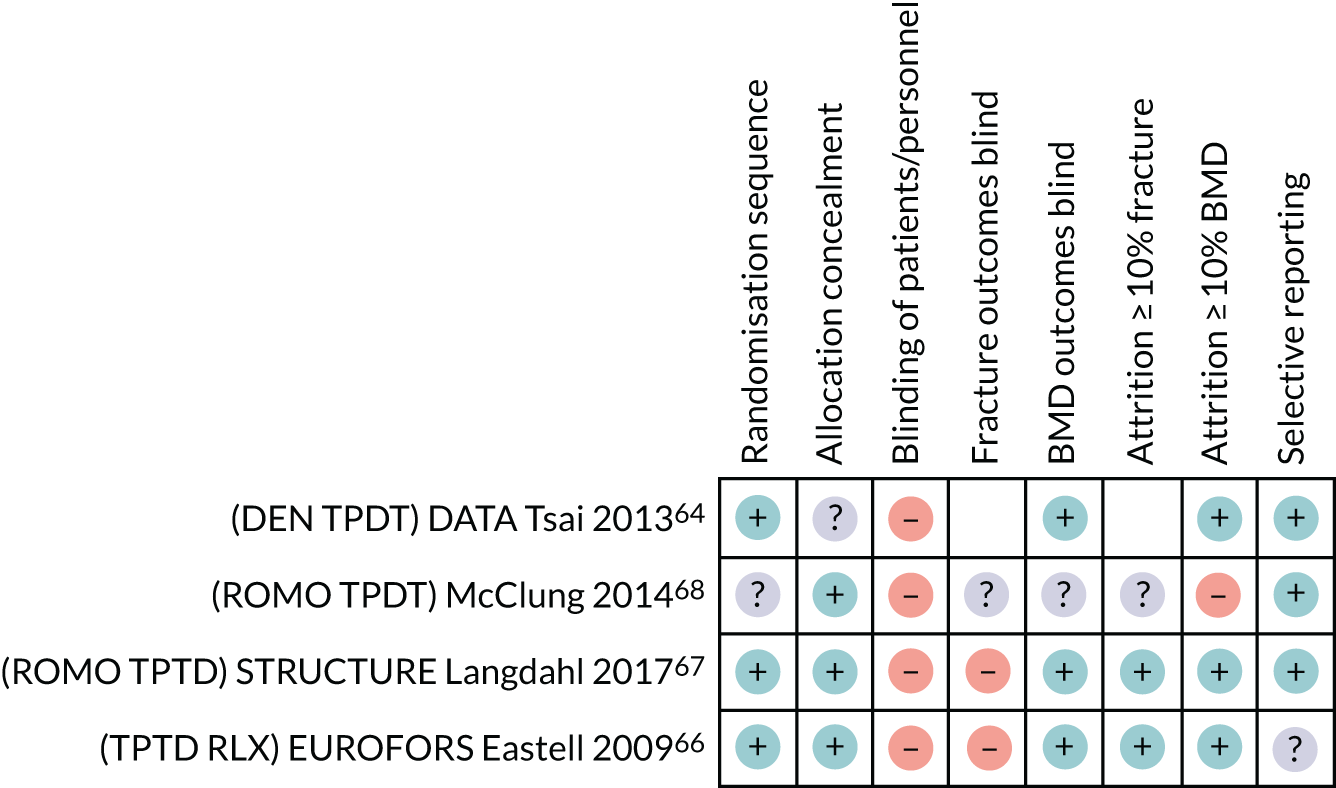
The summary of the Cochrane risk-of-bias assessment across the head-to-head non-bisphosphonate studies is presented in Figure 3.
FIGURE 3.
Cochrane risk-of-bias summary across head-to-head non-bisphosphonate studies. ?, Unclear-risk of bias; +, low-risk of bias; –, high-risk of bias; blank cells, not a study outcome. DATA, Denosumab and Teriparatide Administration; DIRECT, Denosumab fracture Intervention RandomizEd placebo Controlled Trial; EUROFORS, European Study of Forsteo; EVA, EVista Alendronate comparison; STRUCTURE, STudy evaluating effect of RomosozUmab Compared with Teriparatide in postmenopaUsal women with osteoporosis at high risk for fracture pReviously treated with bisphosphonatE therapy.
Of the four head-to-head studies,64,66–68 three reported the method for the random sequence generation,64,66,67 and three reported that allocation was concealed. 66–68
All four studies were reported as open label and were considered to have a high risk of bias for blinding of participants and personnel. 64,66–68
All four studies reported fractures as an outcome;64,66–68 of these, two studies reported that fracture assessment was not blinded to treatment allocation. 66,67 All four studies assessed BMD and three were considered to have a low risk of bias for the blinding of BMD assessments. 64,66,67
Two66,67 of the three studies assessing fracture were considered to have a low risk of attrition bias (< 10% of participants withdrew/were not included in the analysis). 64,66,67 All four studies reported BMD outcomes;64,66–68 one of these was considered to have a high risk of attrition bias (≥ 10% of participants in both treatment groups did not complete the study) for this domain. 68 All other studies were considered to have a low risk of bias.
Three studies reporting the location of a protocol were judged to be at low risk of selective reporting bias. 64,67,68
Non-bisphosphonates versus bisphosphonates
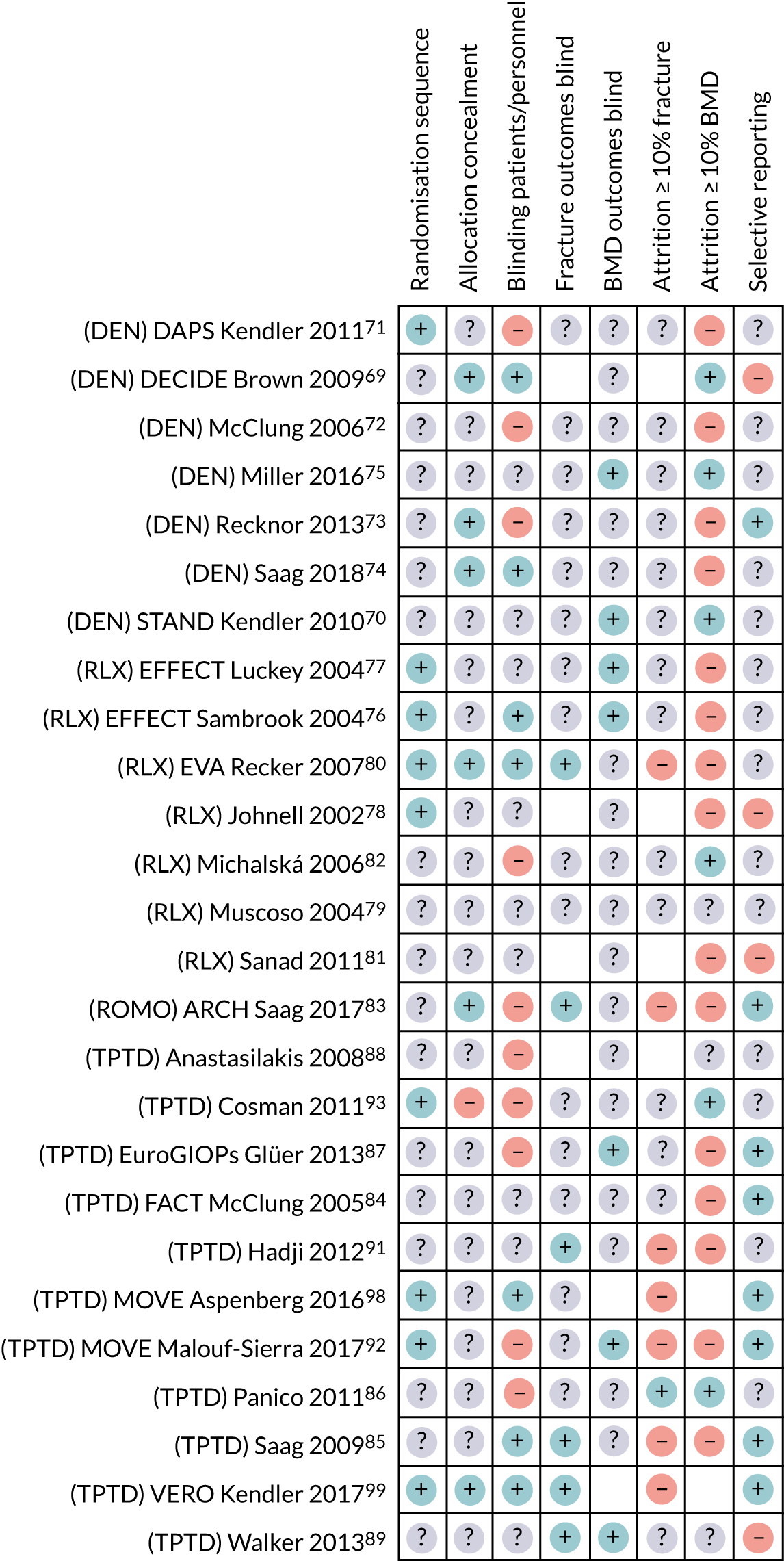
The summary of the Cochrane risk-of-bias assessment across the non-bisphosphonate versus bisphosphonate studies is presented in Figure 4.
FIGURE 4.
Cochrane risk-of-bias summary across non-bisphosphonate vs. bisphosphonate studies. ?, Unclear-risk of bias; +, low-risk of bias; –, high-risk of bias; blank cells, not a study outcome. ARCH, Active-controlled fracture study in postmenopausal women with osteoporosis at high risk; DAPS, Denosumab Adherence Preference Satisfaction; DECIDE, Determining Efficacy: Comparison of Initiating Denosumab versus alEndronate; EFFECT, EFficacy of Fosamax versus Evista Comparison Trial; EVA, EVista Alendronate comparison; FACT, Forteo Alendronate Comparator Trial; STAND, Study of Transitioning from Alendronate to Denosumab; VERO, VERtebral fracture treatment comparisons in Osteoporotic women.
Denosumab versus bisphosphonates
Of the seven studies comparing DEN with a bisphosphonate,69–75 only one reported the method for the random sequence generation,71 and only three reported the method of treatment allocation concealment. 69,73,74
Three studies comparing DEN with a bisphosphonate were reported as open label and were considered to have a high risk of bias for blinding of participants and personnel. 71–73
All seven studies assessed BMD as an outcome, but only one reported that the assessment was blinded to treatment allocation. 75 The remaining six studies were considered to have an unclear risk of bias for this domain. 69–74 Four of these studies were also considered to have a high risk of attrition bias (≥ 10% of participants in both treatment groups did not complete the study) for BMD outcomes. 71–74
The six studies that assessed fracture as an outcome were all considered at unclear-risk of bias for blinded assessment. 70–75 All six studies were also considered at unclear risk of attrition bias (≥ 10% of participants in both treatment groups did not complete the study) for BMD outcomes.
Only one of the studies comparing DEN with a bisphosphonate reported the location of a protocol against which to check outcomes; this study was considered to have a low risk of bias for selective reporting. 73
For one study,69 HRQoL was reported as an outcome in the manufacturer’s company submission. 100 However, this outcome was not reported in the published study, which was considered to have a high risk of bias for selective reporting. 69
Raloxifene versus bisphosphonates
Of the seven studies comparing RLX with a bisphosphonate,76–82 four reported the method for the random sequence generation (all adequate). 76–78,80 However, only one reported a method of treatment allocation concealment. 80
Two of the studies comparing RLX with a bisphosphonate reported that participants and personnel were blinded to treatment allocation (low risk of bias)76,80 and one study reported an open-label design (high risk of bias). 82 All other studies comparing RLX with a bisphosphonate were considered to have an unclear risk of bias for blinding of participants and study personnel. 77–79,81
Across studies comparing RLX with a bisphosphonate that assessed fracture and/or BMD,76–82 only one study reported that the fracture assessment was blinded to treatment allocation,80 and only two reported that fracture assessment was blinded to treatment allocation. 76,77
One study comparing RLX with a bisphosphonate that reported fracture outcomes was considered to have a high risk of attrition bias (≥ 10% of participants in both treatment groups did not complete the study),80 and four studies assessing BMD were considered to have a high risk of attrition bias (≥ 10% of participants in both treatment groups did not complete the study). 76–78,80
No study comparing RLX with a bisphosphonate reported the location of a study protocol. In one of the studies, AEs were not fully reported in the study publication,78 and one study reported that fracture was an assessed outcome, but did not report any results in the study publication. 81 These two studies were considered to have a high risk of selective reporting.
Romosozumab versus bisphosphonates
In the one study that compared ROMO with a bisphosphonate,83 the method for the sequence generation was not reported, although the method for allocation concealment was. This study was described as open label and was considered to have a high risk of bias for blinding of participants and study personnel. Blinding of fracture outcome assessment was reported; however, blinding of BMD assessment was not. Both fracture and BMD outcomes were considered to have a high risk of attrition bias (≥ 10% of participants in both treatment groups did not complete the study). All outcomes in the study protocol were reported.
Teriparatide versus bisphosphonates
Across the 11 studies that compared TPTD with a bisphosphonate,84–89,91–93,99,101 four92,93,99,101 reported an adequate method of random sequence generation and only one study reported an adequate method of treatment allocation concealment. 99 One study reported that unblinded pharmacists distributed the study drug, and was considered to have a high risk of bias for allocation concealment. 93
Three of the studies comparing TPTD with a bisphosphonate reported that participants and personnel were blinded to treatment allocation (low risk of bias),85,99,101 and five studies reported an open-label design (high risk of bias). 86–88,92,93 The other three studies comparing TPTD with a bisphosphonate were considered to have an unclear risk of bias for blinding of participants and study personnel. 84,89,91
Four of the studies comparing TPTD with a bisphosphonate reported that fracture assessment was blinded to treatment allocation,85,89,91,99 and three reported that BMD assessment was blinded to treatment allocation. 87,89,92
Five of the studies (comparing TPTD with a bisphosphonate) that reported fracture outcomes were considered to have a high risk of attrition bias (≥ 10% of participants in both treatment groups did not complete the study),85,91,92,99,101 and five studies assessing BMD were considered to have a high risk of attrition bias (≥ 10% of participants in both treatment groups did not complete the study). 84,85,87,91,92
Six studies (comparing TPTD with a bisphosphonate) that reported the location of a protocol against which to check outcomes were considered to have a low risk of selective reporting bias. 84,85,87,92,99,101 One study reporting an intention-to-treat and a per-protocol analysis stated in the study publication that the data from the per-protocol analysis were not reported. 89 This study was considered to have a high risk of selective reporting. 89
Assessment of effectiveness: fractures
Here we summarise the fracture results for the individual non-bisphosphonate RCTs included in the review. The results of the NMAs, which include both the bisphosphonate and non-bisphosphonate studies, are summarised in Results of the network meta-analysis.
Vertebral fractures
Results for vertebral fractures reported in the included studies are presented in Appendix 5, Table 17, for the non-bisphosphonate treatments compared with placebo, non-bisphosphonate treatments compared head to head, and non-bisphosphonate treatments compared with bisphosphonates. Fracture data used in the NMAs are shown in Appendix 9.
Clinical vertebral fractures: efficacy
One study comparing DEN with placebo reported a statistically significant between-group difference in clinical vertebral fractures at 36 months in favour of DEN in postmenopausal women with osteoporosis (p < 0.001). 41
Three of the studies comparing RLX with placebo in postmenopausal women with osteoporosis reported on clinical vertebral fractures. 48,50,102 One of these reported a statistically significant between-group difference in favour of RLX at 12 months in postmenopausal women with osteoporosis (p < 0.001). 102 In the other two studies comparing RLX with placebo,48,50 the between-group difference was not statistically significant (RLX, 0% vs. placebo, 4.90%; p > 0.05;48 and RLX, 2.36% vs. placebo, 4.10%; p = 0.8950).
None of the studies comparing ROMO with placebo reported on clinical vertebral fractures.
Only one study comparing TPTD (prescribed open label) with placebo reported on clinical vertebral fractures at 18 months in postmenopausal women with osteoporosis. 95 The estimated between-group difference was not statistically significant (TPTD, 0.40% vs. placebo, 1.10%; p = 0.10).
One study comparing TPTD with RLX in an open-label design, in postmenopausal women with severe osteoporosis who were all pre-treated with TPTD for 12 months prior to randomisation, reported that there was no statistically significant between-group difference in clinical vertebral fractures at 12 months following randomisation (TPTD, 1.32% vs. RLX, 0%; p-value not reported). 66
The estimated between-group difference in clinical vertebral fractures for one study comparing DEN with RIS in women and men receiving glucocorticoids was not statistically significant at 12 months (DEN, 3.00% vs. RIS, 4.00%; p = 0.34). 74
The estimated between-group difference in clinical vertebral fractures for one study comparing RLX with ALN in postmenopausal women with osteoporosis was not statistically significant after approximately 45 weeks of treatment (study stopped early owing to difficulty in finding treatment-naive women) (ALN, 3.14% vs. RLX, 1.93%; p = 0.20). 80
The reported between-group difference in clinical vertebral fractures for one study comparing ROMO with ALN in postmenopausal women with osteoporosis was not statistically significant at 12 months (ALN, 0.9% vs. ROMO, 0.50%; p = 0.14). 83
The reported between-group difference in clinical vertebral fractures for one study comparing TPTD with ALN in women and men receiving glucocorticoids was not statistically significant at 18 months (p = 0.07). 103 However, the between-group difference at 36 months was statistically significant, in favour of TPTD (p = 0.037). 103
Morphometric assessment was not always defined, but for studies that assessed vertebral fracture as an efficacy measure, this was most often reported as using the method described by Genant et al. 35
One study comparing DEN with placebo in postmenopausal women with osteoporosis reported a statistically significant between-group difference at 36 months in new morphometric vertebral fractures in favour of DEN (p < 0.001). 41 The estimated between-group differences for this study over 0-12, 12-24 and 24-36 months were also statistically significant in favour of DEN (p < 0.05). 104 However, the estimated between-group difference at the end of the 7-year open-label extension to this study following treatment-switching (all participants received DEN) was not statistically significant (placebo switched to DEN, 7.30% vs. continued DEN, 7.04%; p = 0.76). 105
In a single study comparing DEN with placebo in women and men with osteoporosis, the reported between-group difference in new morphometric vertebral fractures at 24 months was statistically significant in favour of DEN (p < 0.0001). 43 The estimated between-group difference was also statistically significant in favour of DEN at 36 months, including a 12-month open-label extension following treatment-switching (all participants received DEN) (p < 0.0001). 106 The estimated between-group difference for the 12-month open-label extension alone was p = 0.05 (placebo switched to DEN, 2.00% vs. continued DEN, 0.25%). 106
Across two studies comparing RLX with placebo in postmenopausal women with osteoporosis, at 36 months the reported or estimated between-group differences were statistically significant in favour of RLX in reducing new morphometric vertebral fractures (p < 0.05). 50,51 However, the between-group difference was not statistically significant in two studies of postmenopausal women with osteoporosis that reported this outcome at 12 months (placebo, 2.30% vs. RLX, 0%; estimated p = 0.3347 and placebo, 40.00% vs. RLX, 48.84%; estimated p = 0.4152) and in one study of postmenopausal women on long-term glucocorticoids that reported this outcome at 12 months (placebo, 5.36% vs. RLX, 0%; reported p = 0.24). 53
In the one study that compared ROMO with placebo in postmenopausal women with osteoporosis, statistically significant between-group differences in new morphometric vertebral fractures in favour of ROMO were reported at 12 months (p < 0.001) and 24 months (p < 0.001). 54 Following treatment-switching to DEN (all participants), (confidential information has been removed) between-group differences in new vertebral fracture (confidential information has been removed) group were reported at 36 months (confidential information has been removed). 20
In one study comparing TPTD with placebo in postmenopausal women with osteoporosis, the reported between-group difference at 18 months was statistically significant in favour of TPTD in reducing new morphometric vertebral fractures (p < 0.001). 95 However, the estimated between-group difference was not statistically significant in one study in postmenopausal women with osteoporosis that reported this outcome at 12 months (placebo, 5.97% vs. TPTD, 3.68%; p = 0.46). 58
New morphometric vertebral fracture was not an outcome in the study comparing TPTD with RLX in postmenopausal women with osteoporosis. 66
The estimated between-group difference in new morphometric vertebral fractures after approximately 45 weeks of treatment in one study comparing RLX with ALN in postmenopausal women with osteoporosis (study stopped early owing to difficulty in finding treatment-naive women) was not statistically significant (ALN, 3.14% vs. RLX, 1.93%; p = 0.39). 80
The reported between-group difference between new morphometric vertebral fractures for one study comparing ROMO with ALN in postmenopausal women with osteoporosis was statistically significant at 12 months [modified intent to treat (mITT), p = 0.003; last observation carried forward (LOCF), p = 0.008] and 24 months following treatment-switching to ALN, in favour of the group that switched from ROMO to ALN (mITT and LOCF, p < 0.001). 83
The reported between-group difference in new morphometric vertebral fractures for one study comparing TPTD with ALN in women and men receiving glucocorticoids was statistically significant at 18 months (p = 0.004) and 36 months (p = 0.007) in favour of TPTD. 103 However, the estimated between-group difference at 18 months for men and women separately was not statistically significant (men: ALN, 4.48% vs. TPTD, 0.72%; p = 0.09; women: ALN, 12.90% vs. TPTD, 0%; p = 0.13). 107 One open-label study of postmenopausal women with severe osteoporosis receiving treatment for osteoporosis reported that there was no statistically significant difference between TPTD and ALN at 18 months (p-value not reported) (ALN, 15.7% vs. TPTD, 2.4%; estimated p = 0.08). 86
Across studies comparing TPTD with RIS, no statistically significant between-group differences in new morphometric vertebral fractures were evident at 18 months in men with osteoporosis (RIS, 10.00% vs. TPTD, 0%; estimated p = 0.52)89 or at 6 months in postmenopausal women with osteoporosis (RIS, 5.10% vs. TPTD, 4.20%; reported p = 0.6). 91 However, statistically significant between-group differences in new morphometric vertebral fractures in postmenopausal women with osteoporosis in favour of TPTD were reported at 18 months (p = 0.01)91 and at 24 months (p < 0.0001). 99
One study comparing DEN with placebo in men with osteoporosis reported that there was no statistically significant between-group difference in clinical fractures assessed as a safety outcome at 12 months (placebo, 0.83% vs. DEN, 0%; p = 0.50). 42
One study comparing RLX with ALN in postmenopausal women with osteoporosis reported vertebral fractures as a safety outcome, but did not report the assessment method. 76 Zero events were reported in both treatment groups in this study. 76 One study comparing RLX, ALN and RIS in postmenopausal women with osteoporosis reported vertebral fractures as an efficacy outcome, but did not report the assessment method. 79 When estimable, the between-group difference was not statistically significant in this study (ALN, 0.2% vs. RLX, 0%; p = 0.66; RIS, 0% vs. RLX, 0%; p-value not estimable). 79
In one study comparing TPTD with RIS in women and men with low BMD following hip fracture surgery, for which clinical vertebral fractures were a safety outcome,108 zero events were reported in both groups at 6 months. The between-group difference at 18 months was not statistically significant (RIS, 1.00% vs. TPTD, 0%; p = 1.00). 92
One study of postmenopausal women with osteoporosis comparing TPTD (plus a placebo for ZOL) with ZOL (without a placebo for TPTD) also reported vertebral fractures as a safety outcome (the assessment method was not reported). 93 The estimated between-group difference at 12 months was not statistically significant (TPTD + placebo, 0.70% vs. ZOL, 3.70%; p = 0.14). 93
There is evidence from a single study41 that DEN is statistically more effective than placebo at reducing clinical vertebral fractures at 36 months in postmenopausal women with osteoporosis. There is also evidence from a single study48 that RLX is statistically more effective than placebo at reducing clinical vertebral fractures at 12 months in postmenopausal women with osteoporosis. Evidence from a single open-label study95 has found no statistical difference between TPTD and placebo on clinical vertebral fractures at 18 months in postmenopausal women with osteoporosis. There are, at present, no placebo-controlled studies of ROMO that evaluate clinical vertebral fractures.
There is evidence from a single study that there is no statistically significant difference between DEN and RIS,74 between RLX and ALN,76 and between ROMO and ALN83 in the reduction of clinical vertebral fractures at up to 12 months in postmenopausal women with osteoporosis.
There is also evidence from a single study103 that there is a statistically significant between-group difference between TPTD and ALN in favour of TPTD in the reduction of clinical vertebral fractures at 36 months in women and men receiving glucocorticoids.
There is evidence from a single study41 that DEN is statistically more effective than placebo at reducing new morphometric vertebral fractures at 24 months and 36 months in postmenopausal women with osteoporosis, and at 24 months in men and women with osteoporosis. There is evidence from two studies50,51 that RLX is statistically more effective than placebo at reducing new morphometric vertebral fractures at 36 months in postmenopausal women with osteoporosis. There is evidence from a single study54 that ROMO is statistically more effective than placebo at reducing new morphometric vertebral fractures at 12 and 24 months in postmenopausal women with osteoporosis. There is also evidence from a single study95 that TPTD is statistically more effective than placebo at reducing new morphometric vertebral fractures at 18 months in postmenopausal women with osteoporosis.
There is evidence from a single study that there is no statistically significant difference in new morphometric vertebral fractures between RLX and ALN at approximately 45 weeks (study stopped early owing to difficulty in finding treatment-naive women) in postmenopausal women with osteoporosis,80 between TPTD and ALN at 18 months in women with severe osteoporosis receiving treatment for osteoporosis,103 and between TPTD and RIS at 18 months in men with osteoporosis. 89 However, there is evidence from a single study that ROMO is significantly more effective than ALN at reducing new morphometric vertebral fractures at 12 months in postmenopausal women with osteoporosis,83 and that TPTD is significantly more effective than ALN at reducing new morphometric vertebral fractures at 18 and 36 months in women and men receiving glucocorticoids. 103 There is also evidence from two studies89,99 that TPTD is significantly more effective than RIS at reducing new morphometric vertebral fractures at 18 and 24 months in postmenopausal women with osteoporosis.
Non-vertebral fractures
Non-vertebral fracture outcomes were reported in 28 RCTs and are shown in Appendix 5, Table 18. Hip, wrist and proximal humerus fracture outcomes were reported separately in 22 RCTS; these are shown in Appendix 5, Table 19. These fractures are also counted among the non-vertebral fracture total. Results of the NMAs for these outcomes are shown in Results of the network meta-analysis. Fracture data used in the NMAs are shown in Appendix 9.
Non-bisphosphonates versus placebo
The Fracture REduction Evaluation of Denosumab in Osteoporosis every 6 Months (FREEDOM) trial41 reported a significant (p = 0.01) advantage in non-vertebral fractures for DEN (6.1%) over placebo (7.5%) at 36 months for postmenopausal women. The FREEDOM trial41 also had a lower rate of non-vertebral fractures for DEN (7.3%) than for placebo/DEN (9.9%) (significance not reported; estimated in RevMan as p = 0.01) 84 months into the open-label extension. At 36 months, the FREEDOM trial41 reported a significantly (p = 0.04) lower rate of hip fracture for DEN (0.7%) than for placebo (1.2%) (see Appendix 5, Table 19). The Denosumab fracture Intervention RandomizEd placebo Controlled Trial (DIRECT),43 a RCT of postmenopausal women and of men, did not find a difference in the number of non-vertebral fractures at 24 months between the DEN and placebo groups (both 4.1%), although there was a trend (p = 0.0577) towards fewer major non-vertebral fractures in the DEN group (1.6%) than in the placebo group (3.7%). The rate of non-vertebral fractures in the DEN group at 24 months of the international population of FREEDOM41 was similar to that of the Japanese population of DIRECT. 43 Following a further year during which all participants received DEN, DIRECT106 reported non-vertebral fracture rates of 6.7% for placebo/DEN and 5.2% for DEN, with rates of major non-vertebral fractures of 5.4% and 2.0%, respectively. At 24 months, DIRECT43 reported 0% hip fractures for DEN and 0.4% for placebo.
Of the RLX versus placebo RCTs, the Morii et al. 47 and Lufkin et al. 52 studies were not powered to detect a difference between groups; however, both studies had a 0% rate of non-vertebral fractures in the RLX group at 12 months. In the Silverman et al. 50 RCT, there was no significant difference (estimated in RevMan as p = 0.6409) in non-vertebral fractures at 36 months between the RLX (6.3%) and placebo (5.7%) groups (see Appendix 5, Table 18), with rates of hip fracture of 0.3% in both groups (see Appendix 5, Table 19).
The Fracture Study in Postmenopausal Women with Osteoporosis (FRAME)54 reported a non-significant (p = 0.096) difference between ROMO (1.6%) and placebo (2.1%) at 12 months for non-vertebral fractures. At 24 months, FRAME54 reported a significant advantage for ROMO/DEN over placebo/DEN in non-vertebral fractures (2.7% vs. 3.6%; p = 0.029), with a trend (p = 0.059) favouring ROMO/DEN for hip fractures (0.3%) over placebo/DEN (0.6%).
The Miyauchi et al. 58 trial, which included women and men, reported a lower (significance not reported; estimated in RevMan as p = 0.1838) rate of non-vertebral fractures for TPTD (2.2%) than for placebo (6.0%) at 12 months. In postmenopausal women, the Abaloparatide Comparator Trial In Vertebral Endpoints (ACTIVE)95 did not find a significant difference (p = 0.22) between TPTD (3.3%) and placebo (4.7%) in the prevention of non-vertebral fractures at 18 months. In ACTIVE,95 no hip fractures were reported in the TPTD group, whereas 0.2% of participants in the placebo group reported hip fractures. The Fracture Prevention Trial (FPT)62 found a significant (p = 0.04) advantage of TPTD (6.3%) over placebo (9.7%) in the prevention of non-vertebral fractures. The FPT62 reported hip fracture rates of 0.4% in the TPTD group and of 0.7% in the placebo group. The population in the FPT62 all had vertebral fractures at baseline, in contrast to ACTIVE,95 in which two-thirds had prior fractures at baseline. The FPT62 was blinded, whereas the TPTD arm in ACTIVE95 was open label, as the trial was designed compare abaloparatide with placebo.
Studies reporting non-vertebral fracture rates as safety data reported, for postmenopausal women, the 6-month non-vertebral fracture rates for DEN (1.5%) and placebo (1.5%)45 and the 12-month rates for ROMO (3.2%) and placebo 1.6%,55 and, for men, the 12-month rates of DEN (0.8%) and placebo (1.7%). 42
Head-to-head non-bisphosphonates
The European Study of Forsteo (EUROFORS)66 reported fractures as an efficacy outcome, and found no significant difference between TPTD (2.96%) and RLX (2.06%) in non-vertebral fractures at 12 months’ follow-up in postmenopausal women with prior TPTD treatment. Rates of hip fracture were 0.3% for TPTD and 0% for RLX.
The STudy evaluating effect of RomosozUmab Compared with Teriparatide in postmenopaUsal women with osteoporosis at high risk for fracture pReviously treated with bisphosphonatE therapy (STRUCTURE)67 reported fractures as a safety outcome in postmenopausal women. The rates of non-vertebral fractures at 12 months were 3.21% for ROMO and 3.67% for TPTD. Rates of hip fracture were 0.5% for ROMO and 0% for TPTD. 67
Non-bisphosphonates versus bisphosphonates
Saag et al. 74 reported rates (no significance reported; estimated in RevMan as p = 0.1781) of non-vertebral fractures of 4.0% for DEN and 3.0% for RIS at 12 months’ follow-up, and hip fracture rates of 0.3% for both groups.
Muscoso et al. 79 reported rates of non-vertebral fractures of 0% in both the RLX and RIS groups and of 0.2% in the ALN group in both the first and second years of the RCT. The EVista Alendronate comparison (EVA)80 RCT found no significant difference (estimated in RevMan as p = 0.8092) between rates of non-vertebral fracture in the RLX (2.2%) and ALN (2.0%) groups. The EVA80 RCT reported hip fracture rates of 0.3% for RLX and 0.1% for ALN.
The Active-controlled fracture study in postmenopausal women with osteoporosis at high risk (ARCH)83 reported a trend (p = 0.057) favouring ROMO (3.4%) over ALN (4.6%) for the prevention of non-vertebral fractures at 12 months; for the prevention of major non-vertebral fractures (pelvis, distal femur, proximal tibia, ribs, proximal humerus, forearm and hip), there was a significant (p = 0.019) difference between the groups (2.9% for ROMO and 4.3% for ALN). There was no significant (p = 0.19) difference in hip fracture rates at 12 months. 83 The results of the primary analysis show that there was a significant (p = 0.037) advantage of ROMO/ALN (8.7%) over ALN (10.6%) in the prevention of non-vertebral fractures, as well as the prevention of major non-vertebral fractures (p = 0.004) and hip fractures (p = 0.015).
Saag et al. 103 found no significant (p = 0.6) difference between rates of non-vertebral fractures for TPTD (5.6%) and ALN (3.7%) at 18 months, and also no significant treatment difference for subgroups of men (p = 0.6) or women (p = 0.3). Two RCTs of postmenopausal women comparing TPTD with RIS found no significant treatment difference for the prevention of non-vertebral fractures: VERtebral fracture treatment comparisons in Osteoporotic women (VERO) (Kendler et al. )99 at 24 months (TPTD, 4.0% and RIS, 6.0%; p = 0.10) and Hadji et al. 91 at 6 months (TPTD, 7.8% and RIS, 8.3%; p = 0.89). The population in the Hadji et al. 91 study were selected because they had back pain due to vertebral fracture, which may explain why the rates were higher in both these groups than they were in VERO. 99 The rates of hip fracture were 0.3% for TPTD and 0.7% for RIS in VERO,99 and 1.4% for TPTD and 0.6% for RIS in Hadji et al. 91
For studies reporting fractures as safety data, non-vertebral fracture rates for postmenopausal women at 12 months were 0.8% for DEN and 0.9% for ALN,109 3.9% for RLX and 2.5% for ALN,77 5.1% for TPTD,93 5.8% for ZOL93 and, for women pre treated (with ALN), 3.2% for DEN and 1.6% for ALN. 70 At 24 months, non-vertebral fracture rates were 3.0% for RLX, 3.0% for ALN and 6.0% for placebo for women pre treated (with ALN). 82 Hip fracture rates at 12 months were reported as 0.4% for RLX and 0.0% for ALN. 76 For men with glucocorticoid-induced osteoporosis, non-vertebral fracture rates of 0.0% for TPTD and 10.6% for RIS (trend p = 0.056) were reported at 18 months. 87 In a population that had had hip surgery, at 18 months’ follow-up reported non-vertebral fracture rates were 4.7% for TPTD and 9.1% for RIS; hip fracture rates were 1.9% for TPTD and 6.4% for RIS. 92
Across placebo-controlled trials and trials with comparators of non-bisphosphonates or bisphosphonates, when reported, non-bisphosphonates had wrist fracture rates of no more than 2.5% and proximal humerus fracture rates of no more than 1.1%.
Assessment of effectiveness: bone mineral density
Here we summarise the BMD results of the individual non-bisphosphonate RCTs included in the review. The results of the NMAs, which include both the bisphosphonate and non-bisphosphonate studies, are summarised in Results of the network meta-analysis. Given the multiple time points often reported for BMD, we decided to focus on annual or final follow-up.
Femoral neck bone mineral density
Results for femoral neck BMD reported by the included studies are presented in Appendix 5, Table 20, for the non-bisphosphonate treatments compared with placebo, non-bisphosphonate treatments compared head to head, and non-bisphosphonate treatments compared with bisphosphonates.
Non-bisphosphonates versus placebo: femoral neck bone mineral density
Three studies comparing DEN with placebo reported a statistically significant between-group difference in femoral neck BMD in favour of DEN: at 6 months in postmenopausal women with osteoporosis (p = 0.0042),45 at 12 months in men with osteoporosis (p < 0.0001)42 and at 24 months in women and men with osteoporosis (p < 0.0001). 43 The estimated between-group differences were also statistically significant in favour of DEN in the open-label extensions to these studies. However, the open-label extension estimates were all reliant on data extracted from graphs.
Statistically significant between-group differences in femoral neck BMD in favour of RLX over placebo were evident at 36 months for two studies of postmenopausal women with osteoporosis (p < 0.0000150 and p < 0.00151) and at 12 months for one study of postmenopausal women with osteoporosis who were pre treated with TPTD (p < 0.001). 46 However, the between-group difference in the open-label extensions to the study of postmenopausal women with osteoporosis pre treated with TPTD was not statistically significant (see Appendix 5, Table 20). 46 The estimated between-group difference at 12 months in one study of postmenopausal women with osteoporosis was not statistically significant,48 nor was the between-group difference at 12 months in one study of postmenopausal women receiving long-term glucocorticoids (data estimated from graph). 53
Statistically significant between-group differences in femoral neck BMD in favour of ROMO over placebo were reported at 12 months for two studies of postmenopausal women with osteoporosis (p < 0.00154 and p < 0.0000155), and at 12 months in one study of men with osteoporosis (p < 0.001). 56 The reported between-group difference was also statistically significant at 24 months in one study following an open-label treatment-switching extension, favouring switching from ROMO to DEN over switching from placebo to DEN (p < 0.001)54 (see Appendix 5, Table 20). A study of postmenopausal women with osteoporosis reported statistically significant between-group differences in femoral neck BMD in favour of ROMO over ALN at 12 months (p < 0.001), and in favour of ROMO/ALN over ALN/ALN at 24 and 36 months (p < 0.001).
Four studies comparing TPTD with placebo reported a statistically significant between-group difference in femoral neck BMD in favour of TPTD at 6 months in postmenopausal women with osteoporosis (p < 0.01). 61 Statistically significant between-group differences in favour of TPTD at 12 months were also reported by one study (p = 0.015),58 at 18 months by one study (p < 0.0001)95 and at 24 months by one study (p < 0.001). 62 The estimated between-group difference was also statistically significant in favour of continued TPTD in the open-label extension in one of these studies, compared with switching from placebo to TPTD at 18 months (p = 0.03), but not at 24 months (see Appendix 5, Table 20). 58 The estimated between-group difference at 6 months for one study comparing TPTD with placebo in postmenopausal women with osteoporosis was not statistically significant,59 nor was the estimated between-group difference at 6 months of one study comparing TPTD plus calcium and vitamin D with calcium and vitamin D alone. 63
Non-bisphosphonates compared head to head: femoral neck bone mineral density
One study comparing TPTD with DEN in postmenopausal women with osteoporosis reported no statistically significant between-group difference in femoral neck BMD at either 1264 or 24 months. 110 However, statistically significant differences were reported in the open-label extension following treatment-switching, in favour of the group switching from TPTD to DEN, at 24 and 48 months following switching. 65
A statistically significant between-group difference in femoral neck BMD at 12 months in postmenopausal women with osteoporosis, who were pre treated with ALN prior to randomisation, was reported by one study comparing TPTD with ROMO, in favour of ROMO (p < 0.0001). 67
One study comparing TPTD, RLX and a non-active control in postmenopausal women with osteoporosis who were pre treated with ALN reported on the between-group difference in femoral neck BMD for TPTD compared with control only; the result was statistically significantly in favour of the non-active treatment (p < 0.05). 66 No variance estimates were reported by this study. Therefore, the other between-group comparisons could not be estimated.
The estimated between-group difference in femoral neck BMD at 12 months for one study comparing TPTD with ROMO in postmenopausal women was not statistically significant. 68 In this study, the estimated between-group differences for both non-bisphosphonates compared with placebo were statistically significant in favour of the active treatment (TPTD, p = 0.0007; ROMO, p = 0.0002). However, when comparing ROMO with ALN and TPTD with ALN, the results were not statistically significant.
Non-bisphosphonates versus bisphosphonates: femoral neck bone mineral density
Across two open-label studies comparing DEN with ALN, statistically significant between-group differences in femoral neck BMD in favour of DEN were reported at 12 months in one study of postmenopausal women with osteoporosis (p = 0.0001),69 and at 12 months in one study of postmenopausal women with osteoporosis already receiving ALN (p < 0.0121). 70 The estimated between-group difference for one study comparing DEN with ALN in postmenopausal women with osteoporosis, which was not powered for femoral neck BMD, was not statistically significant (see Appendix 5, Table 20). 71
In one open-label study comparing DEN with IBN (oral) in postmenopausal women with osteoporosis, at 12 months the between-group difference in femoral neck BMD was statistically significant in favour of DEN (p < 0.001). 73
Statistically significant between-group differences in femoral neck BMD in favour of DEN at 12 months were also reported by one study comparing DEN with RIS in women and men with osteoporosis who were continuing or initiating glucocorticoids (continuing: p = 0.004; initiating: p = 0.020),74 and at 12 months by one study comparing DEN with ZOL in postmenopausal women with osteoporosis previously treated with bisphosphonates (p < 0.0001). 75
Two studies comparing RLX with ALN in postmenopausal women with osteoporosis reported statistically significant between-group differences in femoral neck BMD in favour of RLX at 12 months (p = 0.0001)76 and 24 months (p = 0.002). 80 However, one study comparing RLX with ALN in postmenopausal women with osteoporosis,77 and one study comparing RLX with ALN in postmenopausal women with osteoporosis who were previously treated with bisphosphonates,82 reported that the between-group difference at 12 months was not statistically significant. In one of these studies,82 the estimated between-group difference following a 12-month open-label extension to 24 months (data estimated from graph) was statistically significant in favour of ALN (p = 0.03). One other study comparing RLX with ALN in postmenopausal women with osteoporosis also reported a statistically significant between-group difference in favour of ALN at 12 months (p < 0.05). 78
One study comparing TPTD with ALN in women and men with osteoporosis receiving glucocorticoids reported a statistically significant between-group difference in femoral neck BMD at 36 months (p < 0.001). 103 The between-group difference reported by one study comparing TPTD with ALN at 18 months in postmenopausal women with osteoporosis was p = 0.05. 84
Across three studies comparing TPTD with RIS, statistically significant between-group differences in femoral neck BMD in favour of TPTD were reported at 18 months: in men with osteoporosis receiving glucocorticoids (p = 0.026),87 in postmenopausal women with osteoporosis (p = 0.02)91 and in women and men with low BMD following hip fracture surgery (p = 0.003). 92 However, one of these studies91 reported an imbalance in femoral neck BMD across study groups at baseline. One study comparing TPTD with RIS in men with osteoporosis reported that the between-group difference at 18 months was not statistically significant. 89
One study comparing TPTD (plus a placebo for ZOL) with ZOL (without a placebo for TPTD) reported a statistically significant between-group difference in femoral neck BMD in favour of ZOL at 12 months in postmenopausal women with osteoporosis (p < 0.05). 93
Summary: femoral neck bone mineral density
There is evidence that DEN is statistically more effective than placebo at increasing femoral neck BMD at 6 months in postmenopausal women with osteoporosis,45 at 12 months in men with osteoporosis42 and at 24 months in women and men with osteoporosis. 43
The evidence is mixed for RLX increasing femoral neck BMD, compared with placebo. There is evidence from a single study that RLX is statistically more effective than placebo at 36 months in postmenopausal women with osteoporosis50,51 and at 12 months in postmenopausal women with osteoporosis who were pre treated with TPTD. 46 However, there is evidence from a single study that the between-group difference between RLX and placebo is not statistically significantly different at 12 months in postmenopausal women with osteoporosis46 or at 12 months in postmenopausal women receiving long-term glucocorticoids (data estimated from graph). 53
There is evidence from two studies that ROMO is statistically more effective than placebo at increasing femoral neck BMD at 12 months in postmenopausal women with osteoporosis. 54,55 and at 12 months in men with osteoporosis. 56
The evidence is mixed for TPTD increasing femoral neck BMD, compared with placebo. There is evidence from a single study that TPTD is statistically more effective than placebo at 6,61 1258 and 18 months95 in postmenopausal women with osteoporosis. However, there is evidence from a single study that the between-group difference in TPTD compared with placebo,59 or TPTD plus calcium and vitamin D compared with calcium or vitamin D alone,63 is not statistically significantly different at 6 months in postmenopausal women with osteoporosis.
There is evidence from a single study that, although TPTD is not statistically more effective than placebo at increasing femoral neck BMD at 12 or 24 months in postmenopausal women with osteoporosis, treatment-switching from TPTD to DEN is significantly more effective than continued DEN at a further 24 and 48 months (open label). 65
There is evidence from a single study that ROMO is statistically more effective than TPTD at increasing femoral neck BMD at 12 months in postmenopausal women with osteoporosis who were pre treated with ALN. 67
There is evidence from a single study that DEN is statistically more effective than ALN at increasing femoral neck BMD at 12 months in postmenopausal women with osteoporosis69 and at 12 months in postmenopausal women with osteoporosis already receiving ALN. 70 There is also evidence from a single study that DEN is statistically more effective than oral IBN at 12 months in postmenopausal women with osteoporosis,73 that DEN is statistically more effective than RIS at 12 months in women and men with osteoporosis continuing or initiating glucocorticoids,74 and that DEN is statistically more effective than ZOL at 12 months in postmenopausal women with osteoporosis who were previously treated with bisphosphonates. 75
The evidence for RLX compared with ALN is mixed. There is evidence from a single study that RLX is statistically more effective than ALN at increasing femoral neck BMD at 12 months in postmenopausal women with osteoporosis. 76 However, there is evidence that the between-group difference between RLX and placebo is not statistically significantly different at 12 months in postmenopausal women with osteoporosis (two studies). 77,82 There is also evidence that ALN is statistically more effective than RLX at increasing femoral neck BMD at 12 months in postmenopausal women with osteoporosis (two studies). 78,82
There is evidence from a single study that ROMO is statistically more effective than ALN at increasing femoral neck BMD at 12 months in postmenopausal women with osteoporosis and that switching from ROMO to ALN is statistically more effective than continued ALN at 24 and 36 months (open label). 83
The evidence is mixed for TPTD increasing femoral neck BMD, compared with placebo. There is evidence that TPTD is statistically more effective than RIS at increasing femoral neck BMD at 12 months in postmenopausal women with osteoporosis (two studies). There is also evidence from a single study that TPTD is statistically more effective than RIS at increasing femoral neck BMD at 18 months in women and men with osteoporosis receiving glucocorticoids, in men with osteoporosis receiving glucocorticoids and in women and men with low BMD following hip fracture surgery. However, there is evidence from a single study that the between-group difference for TPTD and RIS is not statistically significantly different at 18 months in men with osteoporosis.
There is evidence from a single study that ZOL without placebo is statistically more effective than TPTD with placebo at increasing femoral neck BMD at 12 months in postmenopausal women with osteoporosis. 93
Lumbar spine bone mineral density
Six RCTs did not report femoral neck BMD, but did report lumbar spine BMD (see Appendix 5, Table 23). One RCT reported a significant increase in lumbar spine BMD for DEN, compared with placebo. 44 A placebo-controlled trial reported a significant increase in lumbar spine BMD for RLX,47 and a small RCT reported an advantage for RLX plus alfacalcidol (n = 31), compared with alfacalcidol alone (n = 34),49 whereas another small trial found no significant difference for RLX (n = 48) compared with a non-active treatment control (n = 48). 52 One RCT of RLX versus bisphosphonates reported that ALN and RIS had a higher percentage increase in lumbar spine BMD at 24 months than RLX (estimated in RevMan as p < 0.001). 79 One small RCT did not find a significant difference between TPTD (n = 22) and RIS (n = 22) in the improvement of lumbar spine BMD. 88
Assessment of effectiveness: adverse events
Mortality
Mortality across the included studies is presented in Appendix 5, Table 21, for the non-bisphosphonate treatments compared with placebo, non-bisphosphonate treatments compared head to head and non-bisphosphonate treatments compared with bisphosphonates. None of the included studies reported on mortality following hip fracture, mortality following vertebral fracture or mortality following any other type of fracture.
Non-bisphosphonates versus placebo: mortality
Of the studies comparing DEN with placebo, six reported on mortality;41–43,45,106,111 of the studies comparing RLX with placebo, two reported on mortality;48,50 and of studies comparing ROMO with placebo, three reported on mortality. 54–56 Six studies comparing TPTD with placebo reported on numbers of mortality;57–59,61,63,95 one reported that there was no statistically significant between-group difference (data were not reported). 62
When mortality was reported in studies comparing non-bisphosphonates with placebo, event rates were low with active treatment (0.0–1.8%). Only one study reported a between-group difference,41 which was not statistically significant (p = 0.08). For the studies for which between-group differences were not reported, the estimated between-group differences were not statistically significant (p > 0.05).
Non-bisphosphonates compared head to head: mortality
The Denosumab and Teriparatide Administration (DATA)64 and DATA-Switch studies,65 that compared DEN with TPTD, did not report on mortality; neither did the EUROFORS,66 which compared TPTD with RLX. In the two studies that compared ROMO with TPTD and reported on mortality,67,68 event rates for mortality were low with either treatment (0–2%). The estimated between-group differences were not statistically significant (p > 0.05).
Non-bisphosphonates versus bisphosphonates: mortality
Of the studies comparing DEN with bisphosphonates and reporting on mortality, three studies compared DEN with ALN;69,70,72 one compared DEN with oral IBN,73 one compared DEN with RIS74 and one compared DEN with ZOL. 75 Across these studies event rates for mortality were low across treatments (< 1%) and the estimated between-group differences were not statistically significant (p > 0.05).
Of the studies comparing RLX with bisphosphonates, two studies comparing RLX with ALN reported on mortality. 76,80 Of these two studies,76,80 event rates for mortality were low across treatments (< 1%) and the estimated between-group differences were not statistically significant (p > 0.05).
One study comparing ROMO with ALN reported mortality rates of < 2% with either treatment at 12 months prior to treatment-switching and of < 5% at 24 months following treatment-switching. 83 The estimated between-group differences were not statistically significant (p > 0.05).
Of the studies of TPTD compared with bisphosphonates, one study comparing TPTD with ALN;74 four comparing TPTD with RIS,87,91,99,101 and one comparing TPTD with ZOL93 reported on mortality. Across these studies, event rates ranged from 0% to 4.4% with TPTD and from < 1% to 6.4% with bisphosphonates. The estimated between-group differences were not statistically significant (p > 0.05).
Adverse events and serious adverse events
Adverse events and serious adverse events (SAEs) reported across the included studies are presented in Appendix 5, Table 22, for the non-bisphosphonate treatments compared with placebo, non-bisphosphonate treatments compared head to head and non-bisphosphonate treatments compared with bisphosphonates.
Non-bisphosphonates versus placebo: adverse events
Five studies comparing DEN with placebo,41–45,106,111 three studies comparing RLX with placebo,47,50,94 three studies comparing ROMO with placebo54–56 and five studies comparing TPTD with placebo,57–59,61,63,95 reported on AEs. Event rates ranged from 37% to 94.3% with DEN, from 27.1% to 96% with RLX, from 12.9% to 78.4% with ROMO and from 21.9% to 91.9% with TPTD. The between-group differences that were reported were not statistically significant, nor were those that were estimated by ScHARR (p > 0.05).
Non-bisphosphonates versus placebo: serious adverse events
Five studies comparing DEN with placebo,41–45,106,111 three studies comparing RLX with placebo,47,48,50,94 three studies comparing ROMO with placebo54–56 and six studies comparing TPTD with placebo57–59,61–63,95 reported on SAEs. Event rates ranged from 2.0% to 25.8% with DEN, from 2.0% to 18.6% with RLX, from 3.2% to 12.9% with ROMO and from 0% to 10.0% with TPTD. The between-group differences that were reported were not statistically significant, nor were those that were estimated (p > 0.05).
Non-bisphosphonates compared head to head: adverse events
One study that compared TPTD with DEN,64 one study that compared TPTD with RLX66 and two studies that compared TPTD with ROMO67,68 reported on AEs. Across these studies, event rates for TPTD ranged from 16.1%64 to 90%,68 and from 75.0%67 to 82.0%68 for ROMO; event rates were 12.1%64 for DEN and 54.6%66 for RLX. The reported and estimated between-group differences were not statistically significant (p > 0.05).
Non-bisphosphonates compared head to head: serious adverse events
The DATA64 and DATA-Switch65 studies, which compared TPTD with DEN before and after treatment-switching,64 and two studies that compared TPTD with ROMO,67,68 reported on SAEs. Across these studies, event rates for TPTD ranged from 6.5%64 to 11.0%95 (22.0% following treatment-switching to DEN64) and from 8.0%67 to 10.0%68 for ROMO; the event rate for DEN was 3%. 64 The estimated between-group differences were not statistically significant (p > 0.05).
Non-bisphosphonates versus bisphosphonates: adverse events
Of the studies of DEN compared with bisphosphonates, three studies comparing DEN with ALN,69,71,72,109 one comparing DEN with oral IBN,73 one comparing DEN with RIS74 and one comparing DEN with ZOL75 reported on AEs. Across these studies, event rates for DEN ranged from 59.6%73 to 80.9%;69 event rates for bisphosphonates ranged from 64.1%71 to 91.3%72 for ALN, and were 56.1%73 for IBN, 69.0%74 for RIS and 62.2%75 for ZOL. Across these studies, both the reported and estimated between-group differences were not statistically significant (p > 0.05).
Of the studies of RLX compared with bisphosphonates, four studies comparing RLX with ALN reported on AEs. 76,77,80,82 Across these studies,76,77,80,82 event rates ranged from 24% to 75.2% for RLX and from 12.0% to 74.2% for ALN. Across these studies, both the reported and estimated between-group differences were not statistically significant (p > 0.05).
One study comparing ROMO with ALN reported AEs at 12 months prior to treatment-switching (75.7% vs. 78.6%) and at 24 months following treatment-switching to ALN (86.6% vs. 88.6%). 83 The estimated between-group difference was p = 0.02 at 12 months in favour of ROMO and was p = 0.05 at 24 months in favour of switching from ROMO to ALN.
Of the studies comparing TPTD with bisphosphonates, one study comparing TPTD with ALN,74 six comparing TPTD with RIS87,88,91,92,99,101 and one comparing TPTD with ZOL93 reported on AEs. Across these studies, event rates ranged from 31.9% to 79.1% for TPTD and from 33.3% to 81.4% for RIS; the event rate was 86% for ALN and 70.1% for ZOL. 93 The estimated between-group difference for the study comparing TPTD with ZOL93 was statistically significantly in favour of TPTD (p = 0.006). All other reported or estimated between-group differences were not statistically significant (p > 0.05).
Non-bisphosphonates versus bisphosphonates: serious adverse events
Of the studies comparing DEN with bisphosphonates, three studies comparing DEN with ALN,69,71,72,109 one comparing DEN with oral IBN,73 one comparing DEN with RIS74 and one comparing DEN with ZOL75 reported on SAEs. Across these studies, event rates for DEN ranged from 2.4% to 16.0%. Event rates for bisphosphonates ranged from 2.2% to 6.4% for ALN, and were 5.4% for IBN, 17% for RIS and 9.1% for ZOL. The study comparing DEN with IBN73 reported a between-group difference in favour of IBN of p = 0.046. Across all other studies, both the reported and estimated between-group differences were not statistically significant (p > 0.05).
Of the studies comparing RLX with bisphosphonates, four studies comparing RLX with ALN reported on SAEs. 76,77,82 Across these studies, event rates ranged from 24% to 75.2% for RLX and from 12% to 74.2% for ALN. Across these studies, both the reported and estimated between-group differences were not statistically significant (p > 0.05).
One study comparing ROMO with ALN reported on SAEs at 12 months prior to treatment-switching (ROMO, 12.8% vs. ALN, 13.8%) and 24 months following treatment-switching to ALN (ROMO switched to ALN, 28.7% vs. continued ALN, 30.0%). 83 The estimated between-group differences were not statistically significant (p > 0.05).
Of the studies comparing TPTD with bisphosphonates, one study comparing TPTD with ALN74 four comparing TPTD with RIS87,91,92,99,101 and one comparing TPTD with ZOL93 reported on SAEs. Across these studies, event rates ranged from 11% to 28.9% for TPTD and from 16.6% to 46.8% for RIS, and were 30% for ALN and 14.6% for ZOL. The estimated between-group difference for the study comparing TPTD with ZOL93 was statistically in favour of TPTD (p = 0.006). All other reported or estimated between-group differences were not statistically significant (p > 0.05).
Specific adverse events
Details of VTE, stroke, ONJ and atypical femoral fractures reported by the included studies are presented in Appendix 7.
Other evidence on adverse events
The NICE TA20410 found that, although the SmPC indicates that conditions associated with DEN include urinary tract infection, upper respiratory tract infection, sciatica, cataracts, constipation, rash, pain in extremity and skin infections, there is no evidence of increased incidence of cataracts or diverticulitis in postmenopausal women with osteoporosis and that cataracts and diverticulitis occur only in patients with prostate cancer. 21 The SmPC also states that ONJ has been reported in patients receiving DEN or bisphosphonates, with most cases occurring in people with cancer, but that some occurred in people with osteoporosis. 21
The NICE TA20410 for DEN also found that studies of DEN for other indications have shown that treatment may be associated with ONJ, but that there is no evidence of this from the clinical studies of DEN in women with osteoporosis and that that the available clinical evidence indicates that DEN is a well-tolerated treatment for the prevention of osteoporotic fragility fractures in postmenopausal women.
The European Medicines Agency assessment report for DEN112 found that no cases of ONJ were seen in the clinical studies it summarised and that there was no increased frequency of cardiovascular events or abnormal electrocardiographs in DEN-treated patients. The report112 found that, in one study in postmenopausal women, more subjects receiving DEN than those receiving placebo developed an infection that necessitated hospitalisation. The report112 found that infections reported among DEN-treated subjects were characterised by common infections (e.g. pneumonia, urinary tract infection, cellulitis, appendicitis and diverticulitis) and were not distinguishable as opportunistic infections, and that serious infection events tended to occur 6–12 months after the initial administration of DEN.
The report112 found that, in the combined safety analysis across the four pivotal trials, the small differences noted in individual studies in the number of certain SAEs were not evident across the postmenopausal women and hormone ablation therapy populations. For other SAEs, the report found that fatalities in DEN and placebo groups occurred with the same frequencies. In one study of postmenopausal women, the report observed that significantly more patients in the DEN group than in the placebo group reported SAEs, particularly osteoarthritis and pneumonia. However, in another study of postmenopausal women, the report observed that there were no significant differences in SAEs between treatment groups.
The report112 also found that no single type of malignancy was reported at an increased frequency in any trial of DEN. However, a significantly greater incidence of cataracts was evident in males receiving hormone ablation therapy treated with DEN than in males receiving the control.
The NICE TA161,11 which included RLX for the secondary prevention of osteoporotic fragility fractures in postmenopausal women, found that VTE is the most SAE reported with RLX, with an approximate threefold increased risk of VTE. The incidence of hot flushes, arthralgia, dizziness, leg cramps, influenza-like symptoms, endometrial cavity fluid, peripheral oedema and worsening diabetes is also statistically significantly greater with RLX than with placebo. The report also found that, although the impact that RLX had on cardiovascular disease is unclear, there is evidence that it lowers serum concentrations of fibrinogen, as well as total and low-density lipoprotein cholesterol levels, without increasing high-density lipoprotein cholesterol.
The European Medicines Agency SmPC for RLX24 states that RLX is associated with an increased risk of venous thromboembolic events in postmenopausal women, which occurred in < 1.1% of treated patients.
The European Medicines Agency public assessment report for RLX113 states that the most common side effects (seen in more than one patient in 10) are vasodilation and influenza-like symptoms.
The draft SmPC for ROMO12 notes under special precautions that (confidential information has been removed).
The NICE TA161,11 which included TPTD for the secondary prevention of osteoporotic fragility fractures in postmenopausal women, reported only on AEs associated with TPTD administered at 40 µg per day compared with placebo, which were nausea and headache.
The European Medicines Agency’s initial marketing scientific discussion for TPTD114 reported that, in the clinical pharmacology studies, orthostatic hypotension was observed in healthy subjects following administration of TPTD at doses of more than 20 µg per day; at the proposed therapeutic dose of 20 µg per day, the most frequently reported AEs were leg cramps, nausea and headache. The more recent European Medicines Agency variation on the scientific discussion115 concluded that no further safety issues had been identified from further studies. The European Medicines Agency SmPC115 states that the most commonly reported adverse reactions in patients treated with TPTD are nausea, pain in limb, headache and dizziness.
Health-related quality of life
Five studies86,90,101,116,117 published results of reported HRQoL, measured by a validated assessment tool (see Appendix 6).
Non-bisphosphonates versus placebo: health-related quality of life
Health-related quality of life was reported as part of the FREEDOM trial. 116,118 At 3 years’ follow-up, there were no significant differences between DEN and placebo groups on the physical function, emotional status or back-pain dimension of the Osteoporosis Assessment Questionnaire-Short Version (OPAQ-SV) (see Appendix 6). 116
The HRQoL of the RLX and placebo groups did not change significantly from baseline, as measured by the Women’s Health Questionnaire, the Quality of Life Questionnaire of the European Foundation for Osteoporosis-41 items (QUALEFFO-41), the EuroQol - Visual Analogue Scale (EQ-VAS) or the EuroQol-5 Dimensions (EQ-5D) Health State Profile Utility Score (see Appendix 6) at 36 months’ follow-up in the Silverman et al. 50 RCT.
Non-bisphosphonates versus bisphosphonates: health-related quality of life
In the Panico et al. 86 RCT, both the ALN and TPTD groups improved significantly at 18 months on the QUALEFFO-41 domains of pain, everyday activities, domestic job, locomotor function, social activities and health perception, with more improvement (p-value not reported) for TPTD. In the mood domain, only the TPTD group improved significantly (see Appendix 6).
In the VERO RCT,90 there was no significant difference between the TPTD and RIS groups: both showed significant improvement in the EQ-VAS. The MOVE RCT101 also reported no significant difference between the TPTD and RIS groups, which both showed significant improvement in the physical component of the Short Form questionnaire-36 items.
Network meta-analysis
Methods for the network meta-analysis
A network meta-analysis was conducted for each of the five main fracture types (vertebral, non-vertebral, hip, wrist and proximal humerus) and for femoral neck BMD.
For consistency with NICE TA464,34 the model for the NMA assumed exchangeable treatment effects (i.e. a class effect) for bisphosphonate treatments, whereby individual treatment effects are estimated for each bisphosphonate treatment, but these are assumed to arise from a common distribution (or class). Unrelated treatment effects were assumed for all non-bisphosphonate interventions. For comparison, sensitivity analyses were also conducted using a standard random effects model with unrelated treatment effects for all interventions. Further details of the statistical models are provided in Appendix 8.
For fracture outcomes, treatment effects are presented as hazard ratios (HRs) relative to placebo, with a HR of < 1 reflecting a reduced risk of fracture relative to the comparator treatment. To account for different durations of follow-up across the trials, the model assumed an underlying Poisson process for each trial arm, with constant event rate. 119 For femoral neck BMD, the model for the NMA included a covariate for the duration of follow-up in each study, and treatment effects are presented as the difference in mean percentage change from baseline in BMD relative to placebo after 1.6 years of follow-up (which was the average duration of follow-up in these studies).
For fracture outcomes (i.e. binomial data), heterogeneity in treatments effects was characterised as being mild (SD < 0.1), moderate (0.1 ≤ SD < 0.5), high (0.5 ≤ SD < 1) or extremely high (SD ≥ 1); for femoral neck BMD, characterisation was based on a conversion as described in Ren et al. 120 When appropriate, heterogeneity in treatment effects was explored by considering potential treatment effect modifiers using meta-regression. 121 Baseline risk/response can be used as a proxy for differences in participant characteristics across trials that may be modifiers of treatment effect. Adjustment for baseline risk/response was assessed using the method of Achana et al. 122
Potential inconsistency between direct and indirect evidence was assessed using node-splitting. 123
All analyses were conducted in the freely available software package WinBUGS (MRC Biostatistics Unit, Cambridge, UK)124 and R (The R Foundation for Statistical Computing, Vienna, Austria), using the R2Winbugs125 interface package. Convergence to the target posterior distributions was assessed using the Gelman–Rubin statistic, as modified by Brooks and Gelman,126 for two chains with different initial values. For all outcomes, a burn-in of 75,000 iterations of the Markov chain was used, with a further 20,000 iterations retained to estimate parameters. Samples from the posterior distributions exhibited moderate correlation between successive iterations of the Markov chain, so were thinned by retaining every 15th sample.
The absolute goodness of fit was checked by comparing the total residual deviance with the total number of data points included in an analysis. The deviance information criterion (DIC) provides a relative measure of goodness of fit that penalises complexity and was used to compare different models for the same likelihood and data. 127 Lower values of DIC are favourable, suggesting a more parsimonious model.
Results are presented using the posterior median treatment effects, 95% credible intervals (CrIs) and 95% prediction intervals (PrIs). The probability of each intervention ranking was computed by counting the proportion of iterations of the Markov chain in which each intervention had each rank. The treatment effects of each intervention compared with placebo, together with the median rank and the probability of being the highest-ranking treatment, are displayed in forest plots (see Figures 6, 8, 13 and 14).
Selection of evidence contributing to the network meta-analysis
Studies included in the systematic literature review were eligible to be included in the NMA. Characteristics of the studies are summarised in Appendix 4, Table 15, and vertebral fractures are summarised in Appendix 5, Table 17.
Vertebral fractures may be assessed using either clinical methods or radiographic techniques. For studies that reported outcomes using multiple methods/definitions, radiographical assessment was selected for the main analysis, as this was the most widely reported outcome. If radiographical assessment was not available for a given study, then clinically assessed outcomes were included. Studies that did not state the assessment method were also included. A sensitivity analysis was performed (SA2) to assess the impact of including only those RCTs with clinical assessment of fractures.
Outcomes may be reported at different time points across studies. For the primary analysis data set, the longest reported time point was selected for each study and the difference in trial durations is accounted for in the statistical model, under the assumption that the fracture event rate in each study arm is constant over time. To assess this assumption, a sensitivity analysis (SA1) was conducted that restricted the analysis to studies that reported outcomes at 12 months.
To contribute to the NMA, studies were required to provide the number of events and the analysed sample size in each arm. When not reported, these quantities were estimated from other information (e.g. reported percentages, figures); however, the exact numbers are subject to uncertainty. Sensitivity was therefore assessed (SA3) by excluding these studies, along with other studies that raised concerns regarding risk of bias due to blinding issues and early study termination.
A sensitivity analysis was also conducted that excluded studies for which prior treatment with bisphosphonates was permitted (SA4).
In summary, the following four sensitivity analyses were conducted for vertebral fracture outcomes:
-
SA1 – 12-month data
-
SA2 – clinical assessment
-
SA3 – exclusion for quality issues
-
SA4 – exclusion for prior bisphosphonate treatment.
For each of the sensitivity analyses, results were compared with the main analysis to assess the impact of the NMA inclusion criteria.
Data for femoral neck BMD outcomes were presented in two different formats: as the percentage change in femoral neck BMD for each treatment group or as the MD in the percentage change between treatment groups. In addition, data were presented either numerically or in graphical format.
When available, numerical estimates for each treatment group were selected as the most accurate summaries of means and variances. For RCTs that presented results for each treatment group in graphical format, although presenting MDs numerically in the text, MDs were selected. Six RCTs51,81,82,86,92,104 that did not provide variance estimates (in any format) were excluded.
Results of the network meta-analysis
Network diagrams for fracture outcomes and femoral neck BMD are presented in Figures 5 and 6, respectively.
FIGURE 5.
Network diagrams for fracture outcomes. (a) Vertebral; (b) non-vertebral; (c) hip; (d) wrist; and (e) proximal humerus fracture outcomes.
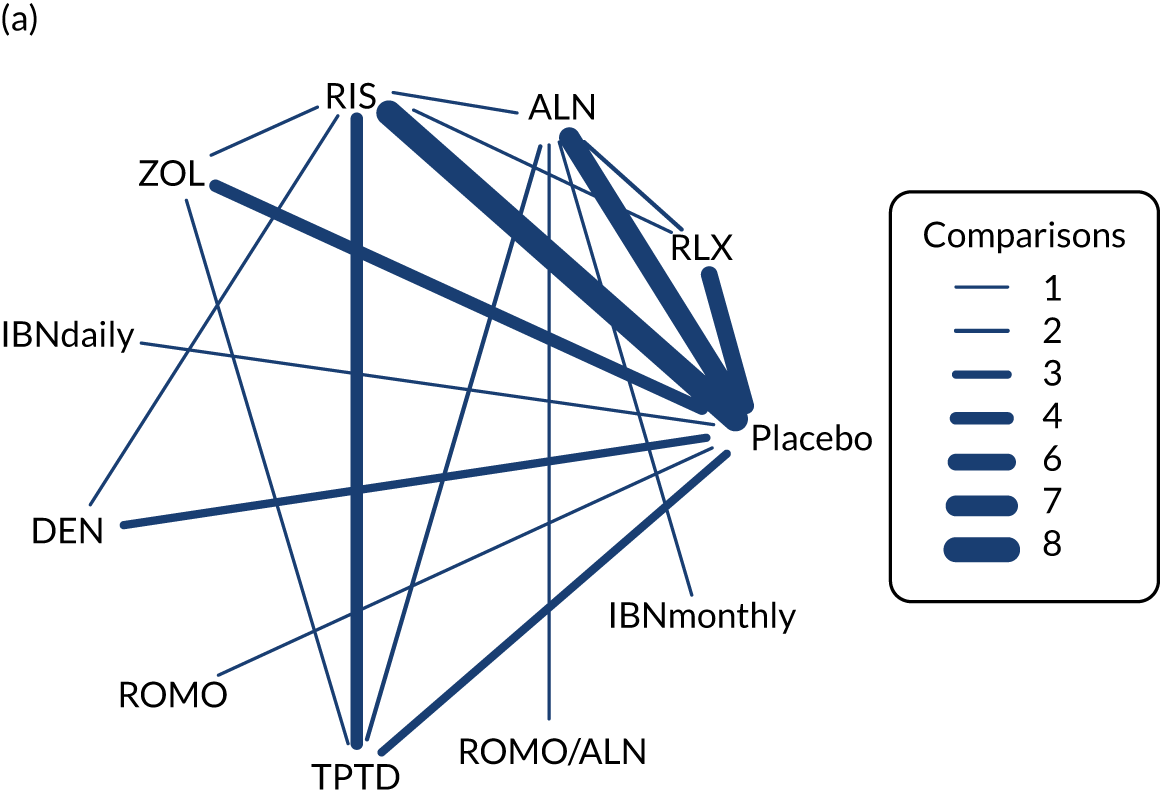
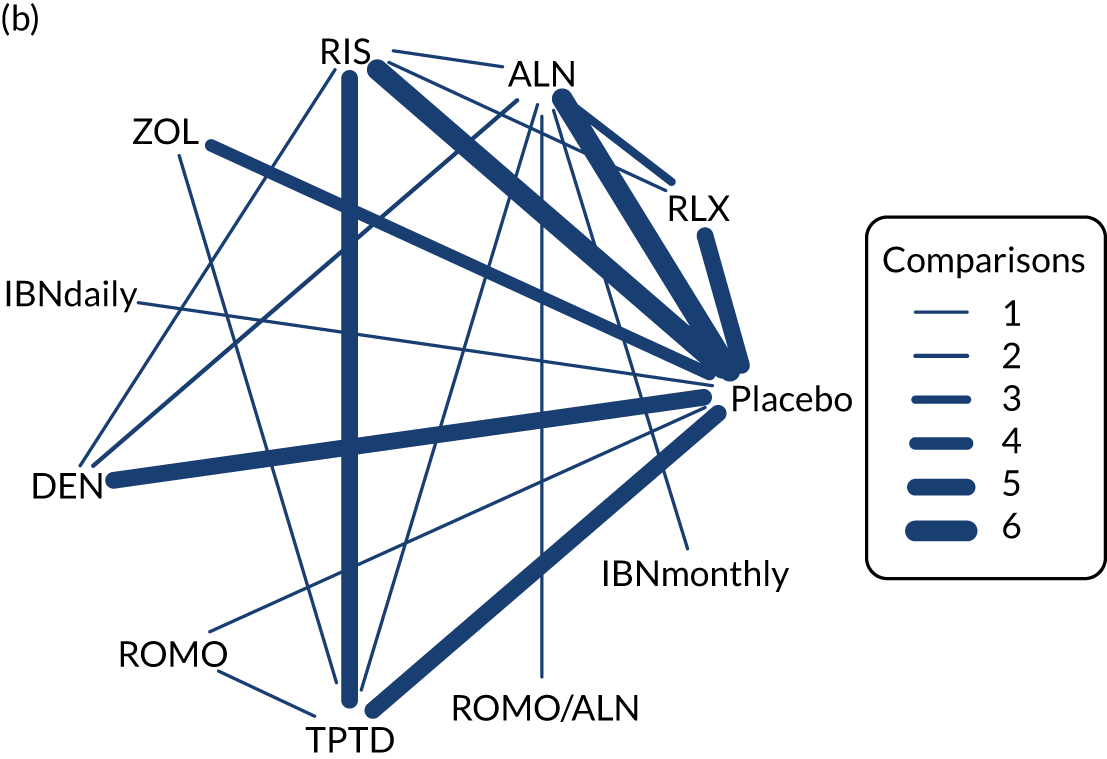
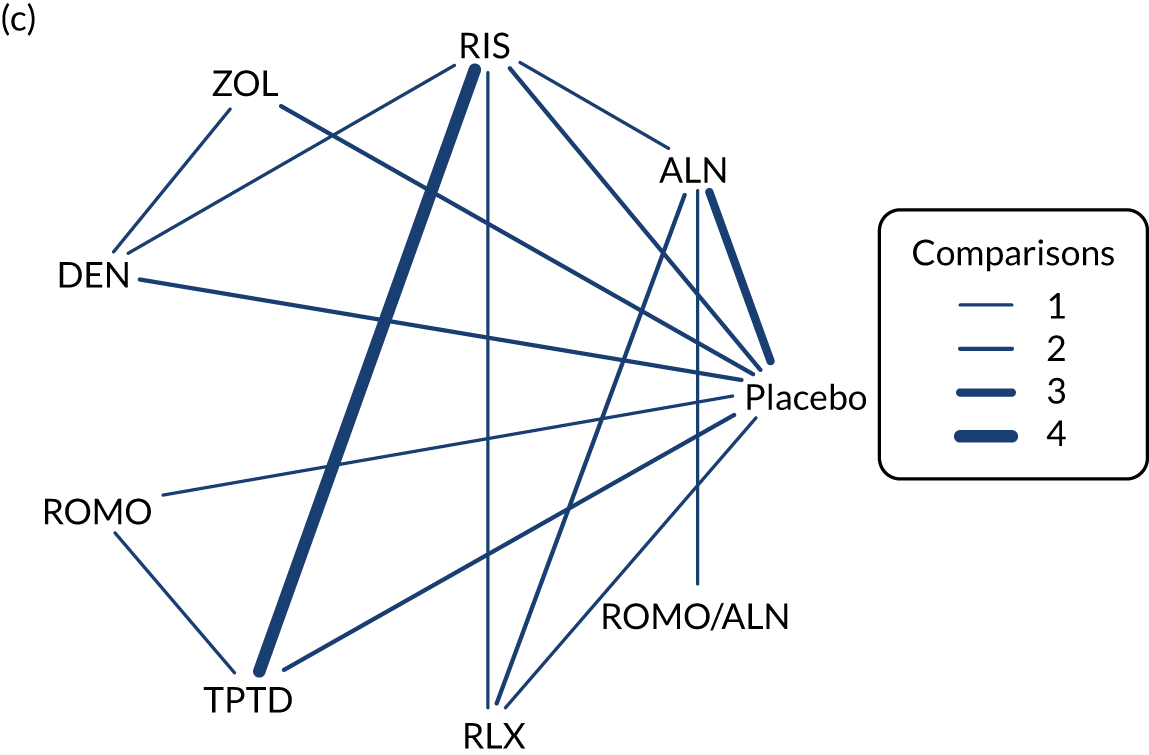
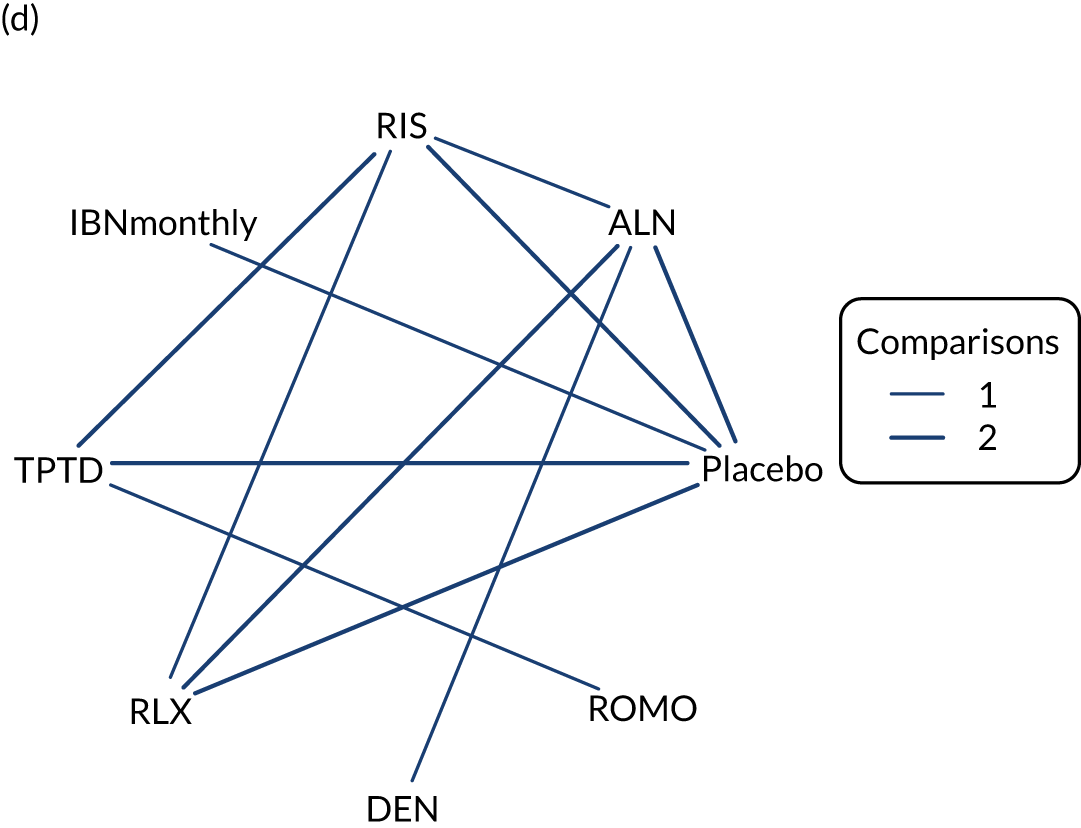
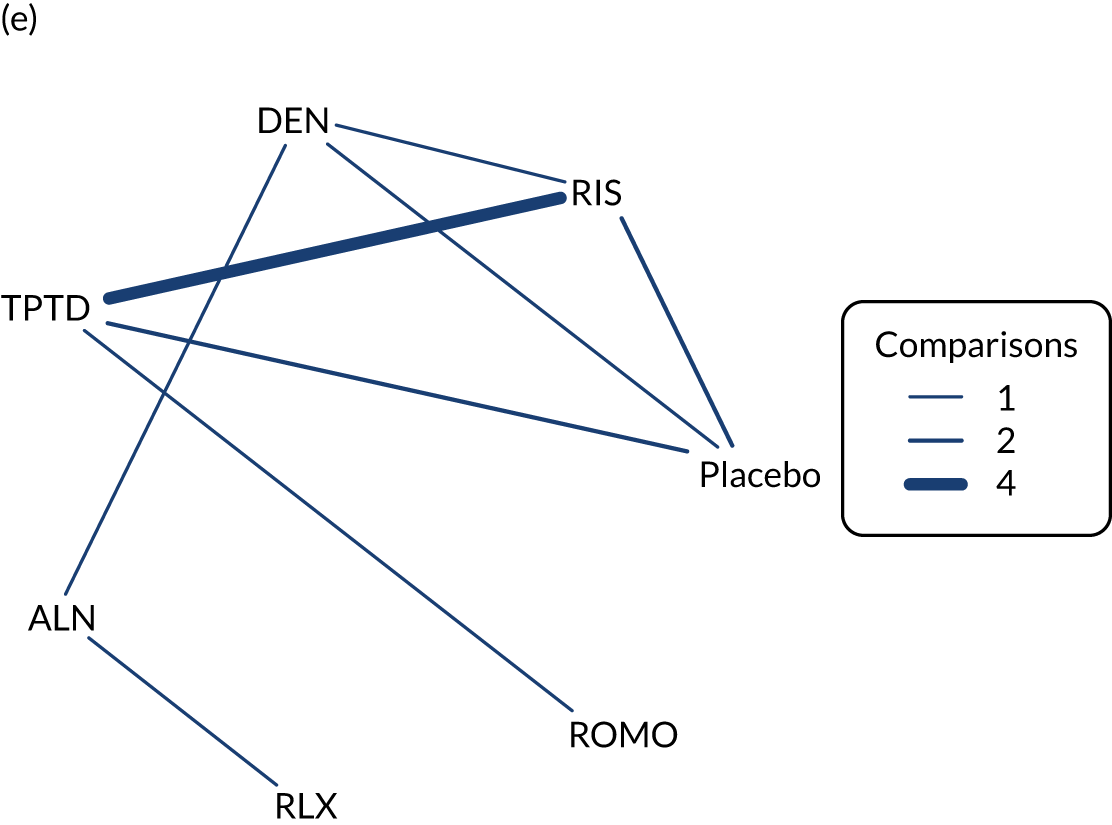
FIGURE 6.
Network diagram for percentage change in femoral neck BMD.
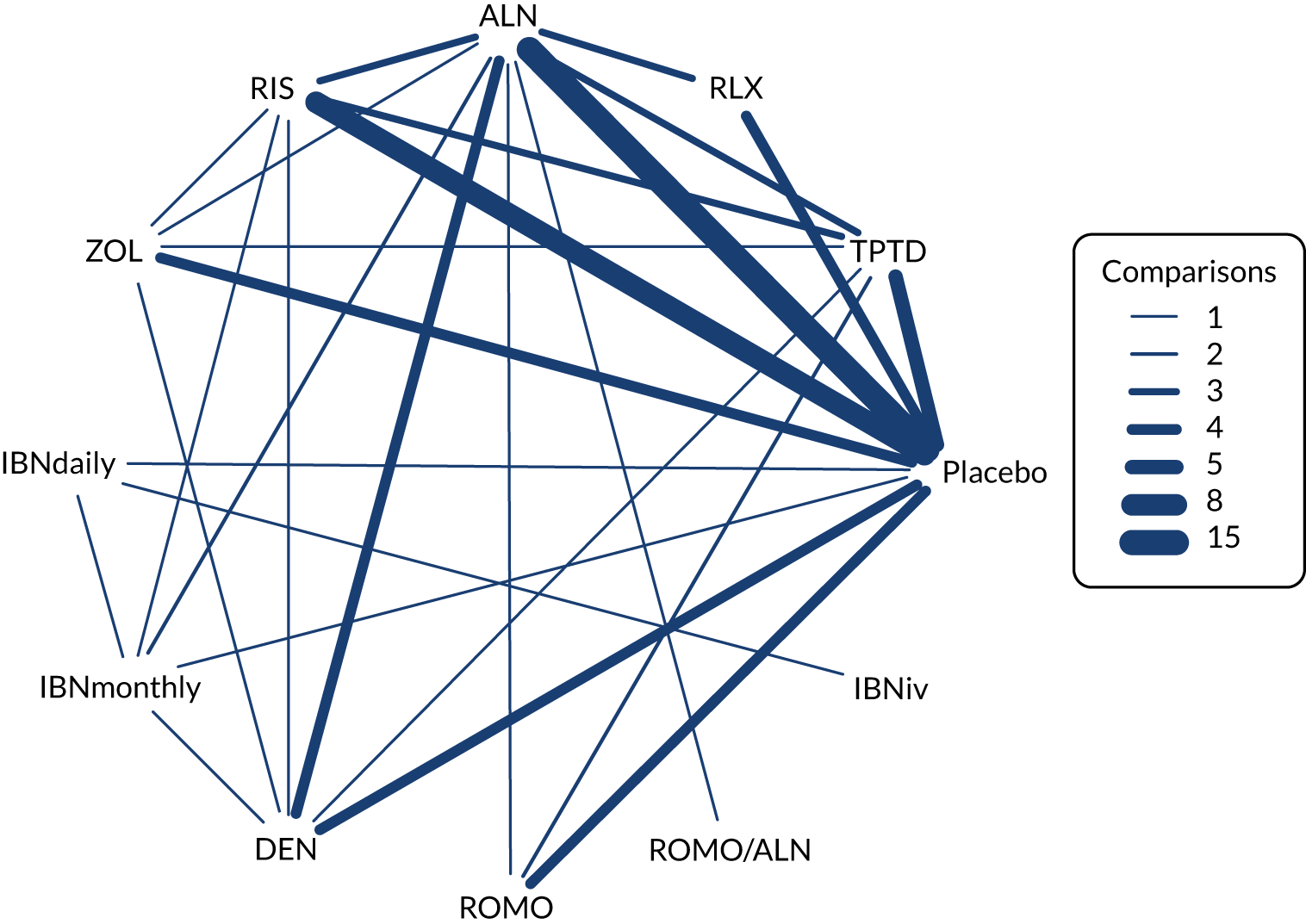
The effects of each treatment relative to placebo are presented in Figure 7 for all fracture outcomes based on the primary model, with class effect for bisphosphonate treatments, and unrelated treatment effects for all other interventions. Model fit is summarised in Table 4. For all outcomes, the model fitted the data well, with total residual deviance close to the number of data points in the network.
FIGURE 7.
Forest plot for all fracture outcomes, main analysis. PB, probability of being the best-ranking treatment.
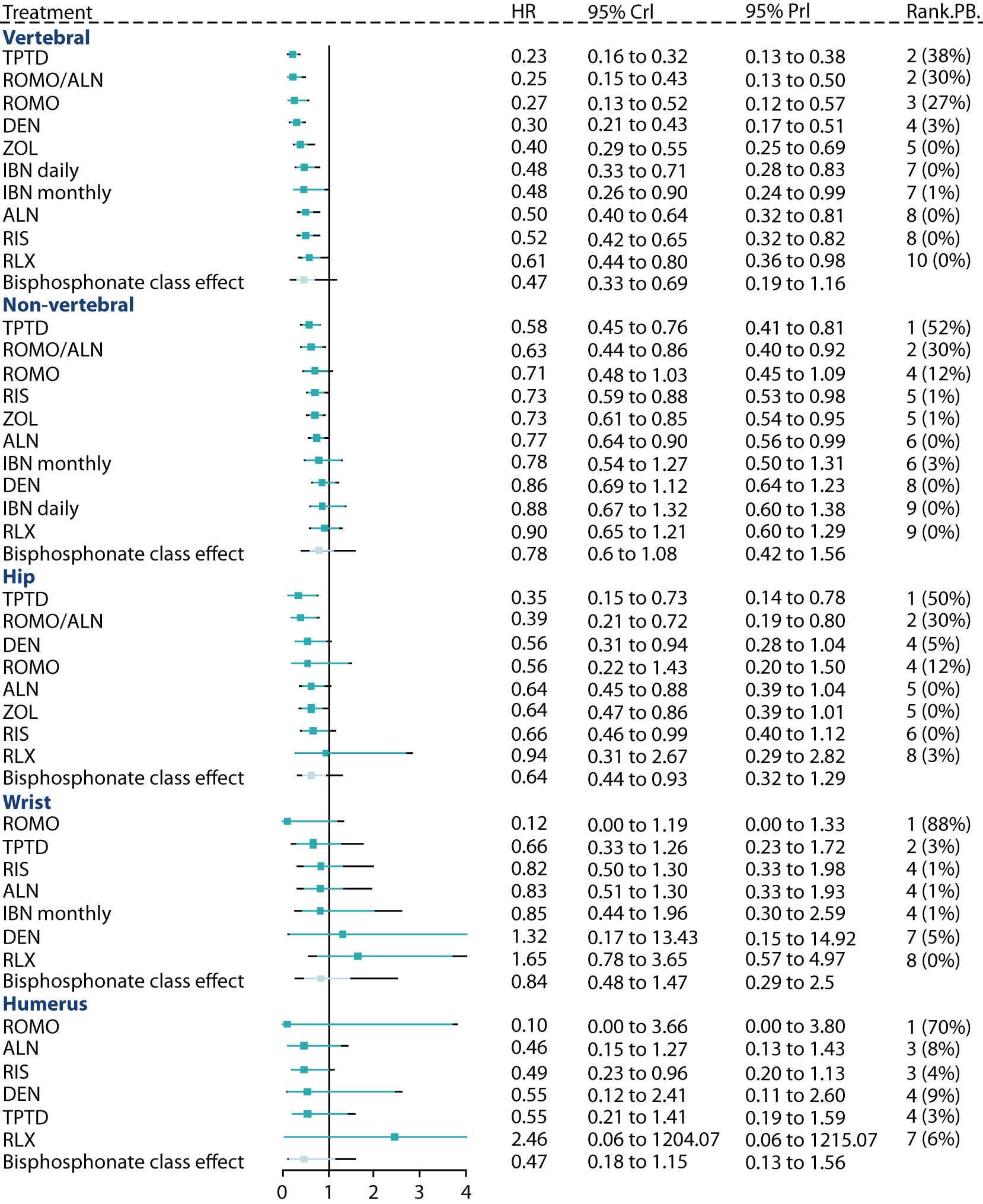
| Outcome | Absolute model fit | DIC | Heterogeneity | ||
|---|---|---|---|---|---|
| D res | Data points (n) | SDa (95% CrI) | SDtb (95% CrI) | ||
| Vertebral | 91.21 | 93 | 153.31 | 0.17 (0.02 to 0.37) | 0.21 (0.01 to 0.90) |
| Non-vertebral | 74.05 | 86 | 128.40 | 0.08 (0 to 0.24) | 0.15 (0.01 to 0.73) |
| Hipc | 38.63 | 47 | 70.23 | 0.12 (0.01 to 0.4) | 0.13 (0.01 to 0.53) |
| Wristc | 30.38 | 31 | 54.64 | 0.32 (0.04 to 0.67) | 0.17 (0.01 to 0.62) |
| Proximal humerusc | 21.99 | 26 | 41.83 | 0.17 (0.01 to 0.57) | 0.21 (0.01 to 0.7) |
| Femoral neck BMD | 144.70 | 137 | 258.86 | 0.85 (0.64 to 1.12) | 0.74 (0.25 to 2.26) |
For comparison, results using a standard random effects model with unrelated treatment effects for all interventions are provided in Appendix 10. Results from the two models were found to be consistent, with a better fit (as indicated by a lower DIC) provided by the primary model.
Vertebral fractures
Vertebral fracture data were available from 46 RCTs; 45 of these compared two treatments and one was a three-arm study. 79 Nineteen of these studies were included in TA46434 (including one study79 for which an additional non-bisphosphonate treatment arm was added for the current review). Two further bisphosphonate studies129,130 not already in TA464,34 and 24 non-bisphosphonate studies were included from the current review. A total of 11 interventions were assessed, including five non-bisphosphonate treatments.
The effects of each treatment relative to placebo are presented in Figure 7, and pairwise comparisons between treatments are provided in Appendix 12, Table 34. All treatments were associated with statistically significant beneficial treatment effects relative to placebo. TPTD was associated with the greatest effect (HR 0.23, 95% CrI 0.16 to 0.32), with the highest probability of being the best-ranking treatment (PB) (0.38), and was statistically significantly more effective than all active treatments apart from DEN, ROMO and ROMO/ALN (see Appendix 12, Table 34). The HR for a randomly chosen study for a new bisphosphonate is 0.47 (95% PrI 0.19 to 1.16), with the reported prediction interval allowing for both between-study and between-treatment heterogeneity.
In the network, both direct and indirect comparisons were available for 12 treatment pairs. None of the comparisons showed significant evidence of inconsistency (see Appendix 13, Table 40).
Four sensitivity analyses were conducted for the main vertebral fracture network. Treatment effects are provided in Appendix 11, Figure 14, and a summary of model fit and heterogeneity is shown in Appendix 11, Table 33.
Sensitivity analysis 1 included data reported at 12 months only. Data were available from 29 RCTs, which assessed a total of 10 interventions, including four non-bisphosphonate treatments. The main difference in the results is that RIS has a more beneficial treatment effect in the 12-month sensitivity (HR 0.44, 95% CrI 0.32 to 0.60) than in the primary analysis (HR 0.52, 95% CrI 0.42 to 0.65). In both analyses, RIS has zero probability of being the best-ranking treatment. It was concluded that the results are generally consistent with those of the primary analysis, which included the longest duration of follow-up for each study, and therefore supports the use of a constant HR.
Sensitivity analysis 2 included outcomes assessed by clinical methods only. Data were available from 20 RCTs, which assessed a total of 11 interventions, including five non-bisphosphonate treatments. It was concluded that the results are generally consistent with those of the primary analysis, which includes both clinical and morphometric/radiographic outcomes. This supports the assumption that the treatment effect is not highly influenced by assessment method.
Sensitivity analysis 3 excluded studies for which there was a risk of bias in the reported outcomes. Four studies86,92,93,95 were excluded owing to blinding issues, two studies62,80 were terminated early and, for 10 studies,42,43,50,129,131–136 the number of events or analysis sample size was estimated from other information. Data were available from 30 RCTs, which assessed a total of 10 interventions, including five non-bisphosphonate treatments. It was concluded that the results are consistent with those of the primary analysis, which includes all studies, and therefore supports the use of the full network of 46 studies to improve the strength of the network.
Sensitivity analysis 4 excluded studies for which prior treatment with bisphosphonates was permitted. The proportion of individuals receiving prior treatment ranged from 8–73% across the studies. Data were available from 36 RCTs, which assessed a total of 11 interventions, including five non-bisphosphonate treatments. It was concluded that the results were consistent with those of the primary analysis.
Non-vertebral fractures
Non-vertebral fracture data were available from 42 RCTs; 40 of these compared two treatments, and two were three-arm studies. 79,82 Fifteen of these studies were included in TA46434 (including one study79 for which an additional non-bisphosphonate treatment arm was added for the current review), and 27 non-bisphosphonate studies from the current review were included. A total of 11 interventions were assessed, including four non-bisphosphonate treatments.
Pairwise comparisons between treatments are provided in Appendix 12, Table 35. All treatments were associated with beneficial treatment effects relative to placebo, although the results were not statistically significant for all treatments. TPTD was associated with the greatest effect (HR 0.58, 95% CrI 0.45 to 0.76), with the highest PB (0.52), although there was insufficient evidence to differentiate between TPTD and the other active treatments apart from IBN daily, DEN and RLX (see Appendix 12, Table 35). The HR for a randomly chosen study for a new bisphosphonate is 0.78 (95% CrI 0.60 to 1.08), with the reported prediction interval allowing for both between-study and between-treatment heterogeneity.
In the network, both direct and indirect comparisons were available for 14 treatment pairs. None of the comparisons showed significant evidence of inconsistency (see Appendix 12, Table 35).
Hip fractures
Hip fracture data were available from 23 RCTs; 22 of these studies compared two treatments and one was a three-arm study. 79 Eight of these studies were included in TA46434 (including one study79 for which an additional non-bisphosphonate treatment arm was added for the current review), and 15 non-bisphosphonate studies from the current review were included. A total of nine interventions were assessed, including five non-bisphosphonate treatments.
Pairwise comparisons between treatments are provided in Appendix 12, Table 36. All treatments were associated with beneficial treatment effects relative to placebo, although the comparison with placebo was not statistically significant for RLX. TPTD was associated with the greatest effect (HR 0.35, 95% CrI 0.15 to 0.73), with the highest PB (0.50), although there was insufficient evidence to differentiate between TPTD and the other active treatments (see Appendix 12, Table 36). The HR for a randomly chosen study for a new bisphosphonate is 0.64 (95% PrI 0.32 to 1.29), with the reported PrI allowing for both between-study and between-treatment heterogeneity.
In the network, both direct and indirect comparisons were available for 14 treatment pairs. None of the comparisons showed significant evidence of inconsistency (see Appendix 13, Table 42).
Wrist fractures
Wrist fracture data were available from 15 RCTs; 14 of these compared two treatments and one was a three-arm study. 79 Six of these studies were included in TA46434 (including one study79 for which an additional non-bisphosphonate treatment arm was added for the current review), and eight non-bisphosphonate studies from the current review were included. A total of eight interventions were assessed, including four non-bisphosphonate treatments.
Pairwise comparisons between treatments are provided in Appendix 12, Table 37. All treatments were associated with beneficial treatment effects relative to placebo, apart from DEN and RLX. Treatment effects for DEN are based only on one small study with two events in the ALN arm and three events in the DEN arm. 70 Treatment effects for these interventions are therefore highly uncertain.
Romosozumab was associated with the greatest effect (HR 0.12, 95% CrI 0.00 to 1.19), with the highest PB (0.88), although there was insufficient evidence to differentiate between ROMO and the other active treatments (see Appendix 12, Table 37). The HR for a randomly chosen study for a new bisphosphonate is 0.84 (95% PrI 0.29 to 2.50), with the reported PrI allowing for both between-study and between-treatment heterogeneity.
In the network, both direct and indirect comparisons were available for eight treatment pairs. None of the comparisons showed significant evidence of inconsistency (see Appendix 13, Table 43).
Proximal humerus fractures
Proximal humerus fracture data were available from 13 RCTs, each comparing two treatments. Two of these studies were included in TA46434 and 11 non-bisphosphonate studies from the current review were included. A total of eight interventions were assessed, including two bisphosphonate treatments.
Pairwise comparisons between treatments are provided in Appendix 12, Table 38. All treatments were associated with beneficial treatment effects relative to placebo, apart from RLX. Treatment effects for RLX are based on one small study77 only, with zero events in the ALN arm and one event in the RLX arm, and so treatment effects are highly uncertain. Event numbers were generally low in this network and five of the 13 included RCTs had zero counts in one of the treatments arms.
Romosozumab was associated with the greatest effect (HR 0.10, 95% CrI 0.0 to 3.66), with the highest PB (0.77), although the treatment effect was highly uncertain and there was insufficient evidence to differentiate between ROMO and the other active treatments (see Appendix 12, Table 38). Only RIS was associated with a HR that was statistically significant compared with placebo (HR 0.49, 95% CrI 0.23 to 0.96). The HR for a randomly chosen study for a new bisphosphonate is 0.47 (95% CrI 0.18 to 1.15), with the reported PrI allowing for both between-study and between-treatment heterogeneity.
In the network, both direct and indirect comparisons were available for five treatment pairs. None of the comparisons showed significant evidence of inconsistency (see Appendix 12, Table 38).
Heterogeneity in treatment effects between studies, and between bisphosphonates, is summarised in Table 4. The estimates of between-study SD suggest mild (non-vertebral) and moderate (vertebral, hip, wrist, proximal humerus, femoral neck BMD) heterogeneity in treatment effects between RCTs. The estimates of between-treatment SD indicate moderate heterogeneity in effects between treatments for all outcomes (i.e. the effects of the bisphosphonates are relatively similar).
Meta-regressions were conducted to test for different treatment effects separately, according to the mean age of participants in each study and the proportion of female participants. A common meta-regression coefficient was assumed for all treatments. 121 Based on comparison of models with and without a covariate for mean age or mean percentage of females, there was no evidence that treatment effect varied with age or sex. Meta-regression coefficients were not statistically significantly different from zero, and DIC estimates were higher, implying a less favourable model. A summary of the results is provided in Appendix 14, Table 45.
Baseline fracture risk can be used as a proxy for differences in participant characteristics across trials that may be modifiers of treatment effect, and so introduce a potential source of heterogeneity in the NMA. The effect of baseline fracture risk as a potential treatment-effect modifier was explored using the method of Achana et al. ,122 assuming a common meta-regression coefficient for all treatments (as for age and sex), and assuming that the baselines of each study follow a normal distribution with common mean and between-study variance. Based on a comparison of models with and without an adjustment for baseline risk, and inspection of the regression coefficients, there was no evidence that treatment effect varied with baseline risk for any of the fracture outcomes (see Appendix 14, Table 45).
Femoral neck bone mineral density
Femoral neck BMD data were available from 73 RCTs; 69 of these each compared two treatments, one was a four-arm study68 and three were three-arm studies. 72,78,137 Thirty-two of these studies were included in TA464. 34 Three further bisphosphonate studies129,137,138 not already in TA464,34 and 38 non-bisphosphonate studies, were included from the current review. A total of 12 interventions were assessed, including five non-bisphosphonate treatments. The network is shown in Figure 6.
The effects of each treatment relative to placebo are presented in Figure 8. Pairwise comparisons between treatments are provided in Appendix 12, Table 39. All treatments were associated with statistically significant beneficial treatment effects relative to placebo. ROMO/ALN was associated with the greatest treatment effect (MD 6.08, 95% CrI 4.25 to 7.91), with the highest PB (0.96), and was statistically significantly more effective than all active treatments apart from ROMO (see Appendix 12, Table 39). The treatment effect for a randomly chosen study for a new bisphosphonate is 2.34 (95% PrI 1.26 to 3.28), with the reported PrI allowing for both between-study and between-treatment heterogeneity.
FIGURE 8.
Forest plot for percentage change in femoral neck BMD.
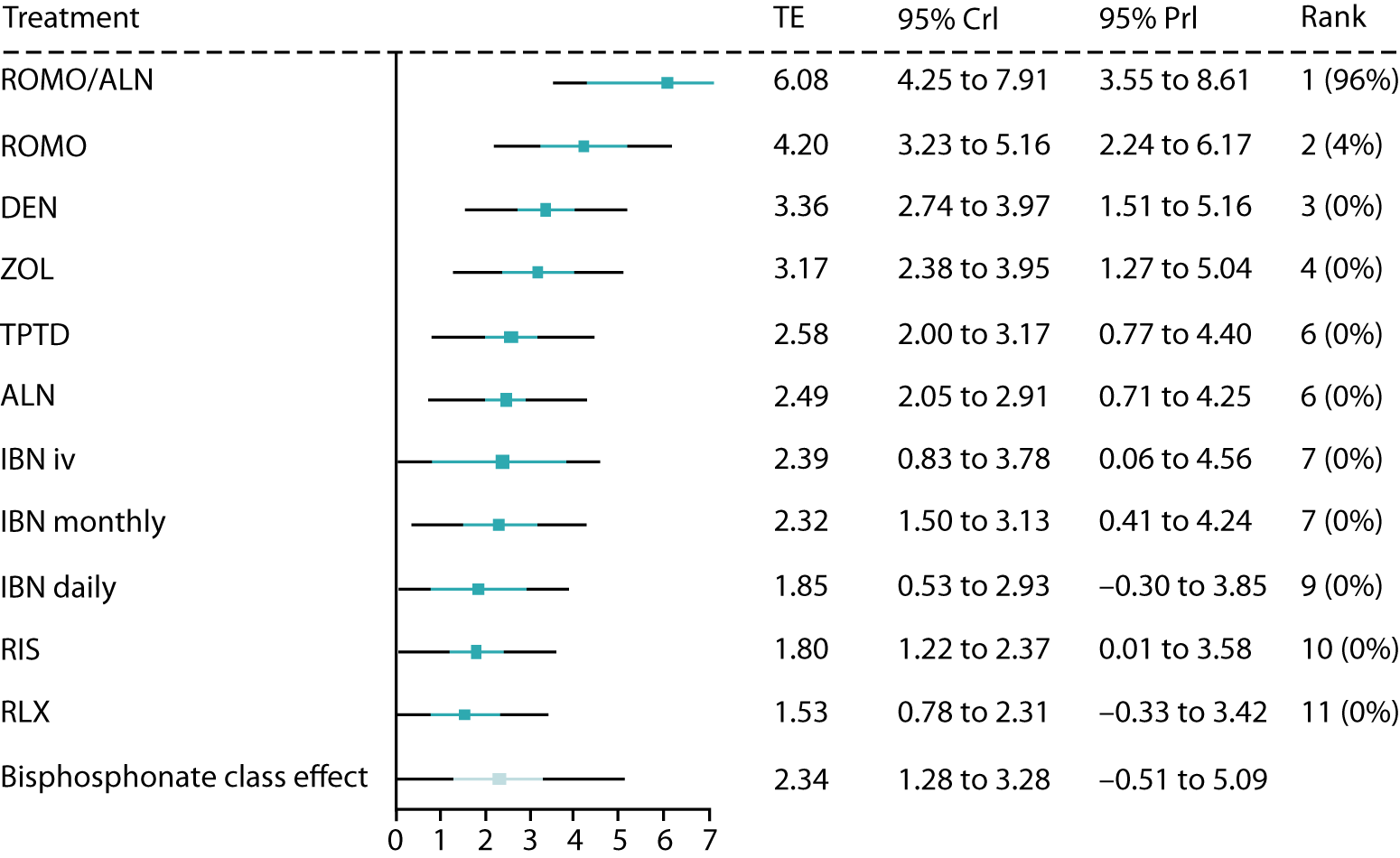
To account for differing trial durations, study duration was included as a trial-level covariate. The estimated impact on treatment effect of study duration, assuming a common relationship for each treatment, was 1.09 (95% CrI 0.73 to 1.45), indicating an increase in treatment effect with increasing duration of study, as expected.
As for fracture outcomes, there was no evidence that treatment effect varied with age, sex or baseline response (see Appendix 14, Table 45).
Discussion
Quantity and quality of randomised controlled trial evidence
A systematic literature search identified 7898 records. Fifty-two RCTs of non-bisphosphonates were included (published in 69 references). Of the 52 RCTs included, 23 were RCTs comparing non-bisphosphonates with placebo, four were head-to-head comparisons of non-bisphosphonates (of which one RCT also included a bisphosphonate arm) and 25 were RCTs comparing a non-bisphosphonate with a bisphosphonate.
Studies varied in quality according to blinding and attrition. However, a sensitivity analysis removing lower-quality studies from the NMA gave results consistent with those of the main analysis. Most of the included RCTs were conducted with postmenopausal women, although there were some trials of men and steroid-induced osteoporosis for interventions for which these were licensed indications. The majority of included trials typically excluded people with underlying conditions that influence bone metabolism or people taking medications that influence bone metabolism.
Quality assessment of other domains, particularly methods for randomisation and allocation concealment, indicated a lack of reporting of the methods used by the included studies to minimise selection bias, detection bias, attrition bias and reporting bias, resulting in a judgement of ‘unclear risk of bias’ for many of the domains across the included studies. As a result, we were unable to identify those studies that were deemed to be at either high or low risk for all quality assessment domains. Therefore, the degree that methodological biases contributed to study results, and thus the findings of this assessment report, is unknown for some studies, meaning that the findings of this assessment report should be interpreted with caution.
Adverse events and health-related quality of life
Across studies reporting on overall mortality, event rates ranged from 0% to 6.4% across non-bisphosphonates and comparators, and between-group differences were not statistically significant. None of the included studies reported on mortality following hip fracture, mortality following vertebral fracture or mortality following any other type of fracture.
Adverse event rates ranged from 12.1% to 94.3% for DEN, from 24.0% to 96% for RLX and from 74.6% to 82% for ROMO across non-treatment-switch studies; AE rates were 86.6% in one study in which ROMO was switched to ALN, and ranged from 16.1% to 91.9% for TPTD. The majority of reported and estimated between-group differences were not statistically significant for comparisons with placebo/no active treatment, head-to-head non-bisphosphonate comparisons or comparisons with bisphosphonates. This was with the exception of one study reporting a comparison of ROMO with ALN, for which the estimated between-group difference was p = 0.02 at 12 months in favour of ROMO and p = 0.05 at 24 months in favour of ROMO switched to ALN, and one study comparing TPTD with ZOL for which the between-group difference was statistically in favour of TPTD (p = 0.006).
Serious adverse event rates ranged from 2% to 25.8% for DEN, from 2% to 18.6% for RLX, from 3.2% to 12.9% for ROMO and from 0% to 33% for TPTD. The majority of reported and estimated between-group differences were not statistically significant for comparisons with placebo/no active treatment, head-to-head non-bisphosphonate comparisons or comparisons with bisphosphonates. This was with the exception of one study that compared DEN with oral IBN, for which the between-group difference was statistically in favour of IBN (p = 0.046).
Disease-specific measures of HRQoL were reported as showing no treatment difference between DEN and placebo, or between RLX and placebo, but more improvement with TPTD than with ALN, suggested by one RCT for each comparison. On generic measures of HRQoL, there was similarity for RLX and placebo (one RCT), and TPTD and RIS (two RCTs).
Discussion of network meta-analysis results
Network meta-analyses were conducted for vertebral fractures (46 RCTs, 11 interventions), non-vertebral fractures (42 RCTs, 11 interventions), hip fractures (23 RCTs, nine interventions), wrist fractures (15 RCTs, eight interventions), proximal humerus fractures (13 RCTs, eight interventions) and femoral neck BMD (73 RCTs, 12 interventions).
For vertebral, non-vertebral and hip fractures and for femoral neck BMD, all treatments were associated with beneficial effects, relative to placebo. For both vertebral fractures and percentage change in femoral neck BMD, the treatment effects were statistically significant at a conventional 5% level for all treatments. TPTD was associated with the greatest effect for vertebral (HR 0.23, 95% CrI 0.16 to 0.32, PB 0.38), non-vertebral (HR 0.58, 95% CrI 0.45 to 0.76, PB 0.52) and hip fractures (HR 0.35, 95% CrI 0.15 to 0.73, PB 0.50), whereas ROMO was the most effective for wrist (HR 0.12, 95% CrI 0.00 to 1.19) and proximal humerus fractures (HR 0.10, 95% CrI 0.00 to 3.66), and ROMO/ALN (HR 0.10, 95% CrI 0 to 3.66, PB 0.77) was the most effective for percentage change in femoral neck BMD. For wrist and proximal humerus fractures networks, there was less RCT evidence, with treatment effects for non-bisphosphonate treatments often contributed by single studies with low event numbers, and so there is considerable uncertainty in treatment effects for certain interventions in these networks.
The reported primary analyses used outcomes reported at the longest available time point for each study and assume that the fracture event rate is constant over time. Inclusion of studies reporting vertebral fractures at 12 months only did not provide any evidence to suggest different treatment effects when the analysis is limited to specific outcome measurement times. Assessment within the studies of vertebral fractures was based on both clinical and morphometric fractures. Consideration of the studies reporting clinical fractures did not provide any evidence to suggest different treatment effects according to assessment method. Similarly, sensitivity analyses conducted to assess the impact of study quality and prior bisphosphonate treatment did not suggest different treatment effects when the affected studies were excluded.
The primary analysis model for the NMA assumed exchangeable treatment effects (i.e. a class effect) for bisphosphonate treatments and unrelated treatment effects are assumed for all non-bisphosphonate interventions. The treatment effects estimated using the primary model were broadly similar qualitatively (i.e. direction of effect) and quantitatively (i.e. magnitude of effect) to those estimated using the standard random-effects model with unrelated treatment effects for all interventions. The estimates of treatment effects for bisphosphonate interventions from the primary model are slightly closer together than those from the unrelated treatment effect model (as would be expected); however, the difference is small.
Chapter 4 Assessment of cost-effectiveness
Systematic review of existing cost-effectiveness evidence
Methods
A comprehensive search was undertaken, with a cut-off date of 16 July 2018, to identify papers published in 2006 or later that evaluated the cost-effectiveness of DEN, RLX, ROMO or TPTD in any of the patient groups eligible for risk assessment within CG146. 8 Subject headings and keywords for ‘osteoporosis’ were combined with an economic filter without named interventions from 2014 to 2018 to update the searches conducted for TA464. 34 In addition, for records between 2006 and 2013, each of the named non-bisphosphonate interventions (RLX, DEN, ROMO and TPTD) was combined with an economics search filter to cover the years between 2006 and 2013, as studies for interventions would not have been retrieved in the review for TA464. The search strategy is provided in Appendix 1. The searches were limited to those published since the start of 2006 because studies reporting cost-effectiveness estimates for RLX, DEN and TPTD are assumed to have been captured in the searches and reviews that informed TA160,12 TA16111 and TA20410 and studies reporting the cost-effectiveness of ROMO are not expected prior to 2006. However, any relevant studies published prior to 2006 that were identified in these previous appraisals or in published systematic reviews were included.
The following databases were searched:
-
MEDLINE(R) In-Process & Other Non-Indexed Citations and MEDLINE(R) (via Ovid), 1946–2018
-
EMBASE (via Ovid), 1974–2018
-
Database of Abstract of Reviews of Effects [via Centre for Reviews and Dissemination (CRD) database], 1995–2015
-
Health Technology Assessment Database (via CRD database), 1995–2016
-
NHS Economic Evaluation Database (via CRD database), 1995–2015.
Published economic evaluations cited in the consultee submissions were cross-checked with those identified from the search. Searches of key included studies were undertaken using the Web of Science.
Inclusion/exclusion criteria
Studies were included in the review if they reported full economic evaluations comparing DEN, RLX, ROMO or TPTD with each other, with bisphosphonates or with no treatment. Studies were included if any of the population considered would be eligible for risk assessment as per CG146. 8 For example, studies of postmenopausal women were included whether or not they specified that the women had risk factors, as those aged > 65 years would be eligible for risk assessment under CG1468 even without risk factors being present. 8 Studies that did not assess outcomes using QALYs or that did not report the incremental cost per QALY of alternative treatment strategies were excluded. Studies that did not assess the cost-effectiveness in a UK setting were excluded, to ensure consistency with the NICE reference case. 139 Studies that assessed the cost-effectiveness of treatment at non-licensed doses were also excluded, as were studies that used treatments for other indications such as the treatment of Paget’s disease or metastatic bone disease. Studies published prior to 2006 were included when identified in existing NICE appraisals or published systematic reviews, as described previously. Studies were included only if they were reported as full papers; conference abstracts were excluded from the review as they present insufficient detail to allow for a rigorous assessment of study quality. Studies not reported in the English language were also excluded. De novo economic analyses reported in the consultee submissions were included if they met the inclusion criteria of the review.
Review methods
The results of the economic searches described above were combined with the results of the searches conducted for the HRQoL review (see Appendix 11) and a combined sift was conducted to pick up any cross-relevant papers. The combined database was sifted by title and abstract by one reviewer. The full papers of studies that potentially met the inclusion criteria were retrieved for further inspection by the same reviewer. Studies included in the systematic review were examined to determine whether or not they met the NICE reference case. 139 We stated in our protocol that we would critically appraise the included cost-effectiveness analyses using the checklist published by Philips et al. ,140 but this was not done owing to time constraints.
Results
The study selection process is summarised in the form of a PRISMA flow diagram32 in Figure 9, with the most common reason for exclusion being that they were non-UK studies.
FIGURE 9.
The PRISMA flow diagram of the study selection process: cost-effectiveness review.
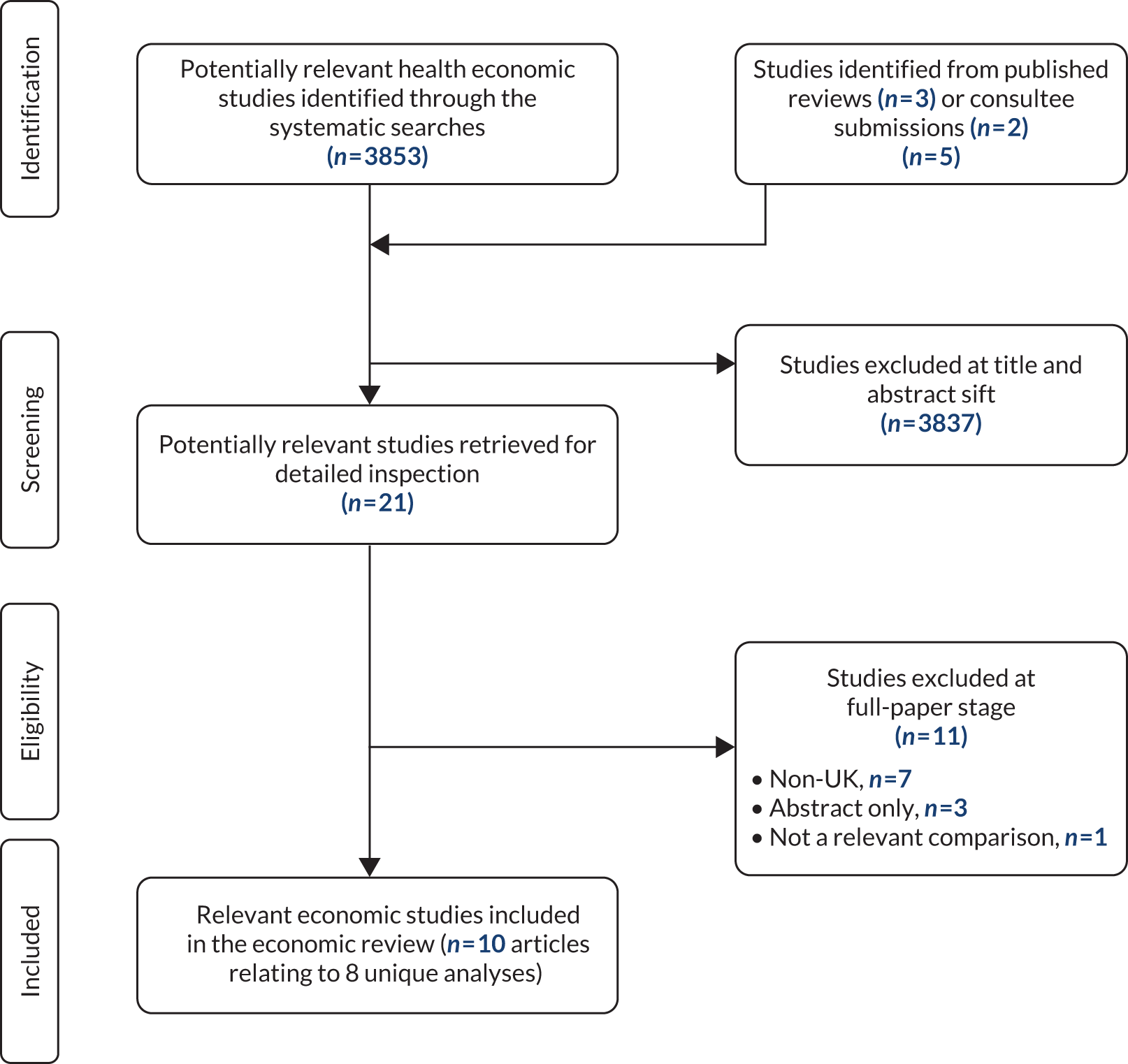
Quantity of evidence identified
The database search identified 3853 citations across the combined cost-effectiveness and HRQoL searches. Three additional articles141–143 were identified from the reference list of published reviews. None of the consultee submissions identified any published analyses not already picked up by the systematic search, but two reported de novo economic analyses, which were included, giving a total of 3858 citations. Of these, 3837 were excluded at the title and abstract stage and a further 11 were excluded at the full-paper stage; the most common reasons for exclusion were that they were non-UK studies or conference abstracts with limited data presented. Appendix 15 provides the reasons for exclusion for those papers that were included during the title and abstract sift, but were later excluded after considering the full paper.
A total of 10 articles20,34,100,141–147 were included; however, one paper, Kanis et al. ,142 reported a previous version of the model reported by Stevenson et al. ,143 and was therefore not separately extracted, and two articles provided the Evidence Review Group’s summary of the company submission for TA204. 145,147 Therefore, the review included eight unique cost-effectiveness analyses. Additional documents related to TA20410 were downloaded from the NICE website to allow a full examination of this model [note that this model is referred to as ‘Waugh et al. 147’ to avoid confusion with the Amgen submission for the current multiple technology appraisal (MTA)]. The model described in the Amgen submission for the current MTA100 was an adaptation of the model described in the company submission for TA204,145,147 but these were separately extracted owing to differences between the decision problems.
Although the assessment report for TA464 by Davis et al. 34 did not strictly meet the inclusion criteria for this review, as it did not include any non-bisphosphonate interventions, it has been included as it was stated in the protocol for this MTA that, to ensure consistency across related appraisals, the economic analysis conducted to inform TA464 was intended to be used as the starting point for any cost-effectiveness analysis conducted by the assessment group (AG). Therefore, it was necessary to compare this model with the relevant published analyses to identify any significant areas of difference.
Study characteristics
The characteristics of the included studies are summarised in Table 5. Here we describe the key differences between the models in terms of their population, structure and assumptions.
| First author | Population and interventions | Type of evaluation | Perspective | Time horizon | Cost year and cost discount rate | Cost source | Benefits population and benefits discount rate | Benefits source and benefits instrument | Effectiveness data |
|---|---|---|---|---|---|---|---|---|---|
| Kanis 2005141 (MORE) |
|
Cohort Markov model | UK NHS | Not stated |
|
Published estimates and reference costs |
|
EQ-5D in Swedish patients using UK valuation set | Single study estimate (MORE). In addition to fracture outcomes, includes beneficial effect on breast cancer and heart disease and adverse effect on VTE |
| Stevenson 2005143 |
|
Patient-level Markov model | UK NHS and PSS | Lifetime |
|
Fracture costs were based on published estimates that were uplifted |
|
|
Systematic review and meta-analysis conducted by authors |
| Kanis 2008144 (BONE) |
|
Cohort Markov model | UK NHS (includes nursing home admission) | Lifetime |
|
Published literature (UK estimates of length of stay and cost per bed-day and Swedish estimates of ratio of outpatient to inpatient costs) | 3.5% | EQ-5D in Swedish patients using UK tariff | Published systematic review and meta-analysis including breast cancer reduction for RLX |
| Scotland145/Waugh 2011147/Amgen submission for TA204147 |
|
Cohort Markov model | UK NHS and PSS | Lifetime |
|
HRG costs and BNF drug prices |
|
EQ-5D using UK tariff | Company’s systematic review and meta-analysis with indirect comparison (Bucher method148) |
| Strom 2013146 |
|
Cohort Markov model | UK NHS | Lifetime |
|
Published literature (UK estimates of length of stay and cost per bed-day and Swedish estimates of ratio of outpatient to inpatient costs) |
|
EQ-5D in Swedish patients using UK tariff | Systematic review and meta-analysis |
| Davis 201634 |
|
Discrete event simulation (patient-level model to capture individual’s history) | UK NHS and PSS | Lifetime |
|
NHS reference costs, PSSRU unit costs, national drug tariff and database of generic drug costs |
|
EQ-5D using UK tariff from published studies identified by systematic review | Author’s systematic review and NMA |
| UCB S.A. 201820 |
|
Patient-level Markov model | UK NHS and PSS | Lifetime |
|
NHS reference costs, PSSRU unit costs, national drug tariff (same source cited for fracture costs but different figures provided) |
|
|
Company’s systematic review and NMA |
| Amgen Inc. 2018100 |
|
Cohort Markov model | UK NHS and PSS | Lifetime |
|
NHS reference costs, PSSRU unit costs, national drug tariff and database of generic drug costs (costs as for TA46434 except changes in monitoring and administration costs) |
|
|
Company’s review and NMA |
Population and subgroups
Six of the included studies20,141,143,144,146,147 were of postmenopausal women. The company submission by UCB S.A. restricted the population modelled to postmenopausal women at imminent risk of fracture, which it characterised as those with a recent major osteoporotic fracture. 20 Although no results were presented for men, UCB S.A. 20 argued that the results would also be applicable to men, as it is assumed that men will not respond differently to postmenopausal women. The AG model for TA464 (Davis et al. 34) included all patients eligible for risk assessment under CG146,8 thereby including both men and women, those with steroid-induced osteoporosis and those with and those without a prior fracture. However, Davis et al. 34 examined subgroups according to absolute fracture risk rather than according to any of these specific patient characteristics. The submission by Amgen Inc. 100 did not restrict the population to postmenopausal women; instead, it included people eligible for risk assessment under CG1468 at varying levels of absolute fracture risk. This was similar to the approach taken in TA464,34 except that the only risk cut-off points examined in the Amgen Inc. 100 submission were 10-year risks of 10% and 20%, whereas Davis et al. 34 reported outcomes for 10 risk deciles and also used regression to estimate thresholds for cost-effective intervention when treating risk as a continuous variable.
Several of the analyses presented results separately for those with and those without a prior fracture141,143,144,147 or presented separate estimates for subgroups defined by combinations of age and T-Score,147 age and number of risk factors146 or T-Score and risk factors. 147 Two studies34,146 estimated the threshold for cost-effective intervention and expressed this using 10-year risk of fracture. Two studies20,100 provided results for patients with a specific level of absolute fracture risk, but explored alternative specified levels of absolute fracture risk in scenario analyses.
None of the included economic evaluations provided an incremental analysis across all of the interventions and comparators identified in the scope of this appraisal. Two141,144 provided comparisons of RLX versus no treatment. Strom et al. 146 compared DEN with bisphosphonates (ALN and RIS) and no treatment. Stevenson et al. 143 conducted an incremental analysis across multiple technologies, but did not include DEN or ROMO. The submission by UCB S.A. 20 did not provide a comparison with oral or i.v. IBN, but included all other comparators. The Amgen Inc. submission100 stated that DEN was primarily used in primary care by patients unable to take an oral bisphosphonate; therefore, the main comparator was RLX or no treatment. However, secondary analyses were provided comparing DEN with i.v. ZOL and oral bisphosphonates. The company submission for TA204, described by Waugh et al. ,147 also restricted the decision problem to patients unable to take bisphosphonates. Their primary analysis compared DEN with RLX and no treatment, but they also included comparisons with i.v. IBN, i.v. ZOL, TPTD and oral bisphosphonates in secondary analyses. Davis et al. included only bisphosphonates and no treatment in their incremental analysis, which was consistent with the scope of TA464. 34
Model structure and outcomes modelled
Seven studies20,100,141,143,144,146,147 used a Markov model framework: five used a cohort-level modelling approach and two20,143 used a patient-level Markov simulation. Four20,100,146,147 of the Markov models employed a 6-monthly cycle length, whereas the other three141,143,144 used an annual cycle length. The AG for TA464 used a discrete event framework, which is a patient-level simulation that does not require the use of fixed time cycles. All of the studies included separate health states for hip fracture and vertebral fracture, and all of the studies incorporated long-term consequences for these two fracture sites either by incorporating post-hip and post-vertebral fracture health states in a cohort-level model or by tracking patient’s prior fracture status in a patient-level simulation. All studies included wrist fracture. All but one study141 included fractures at sites other than the hip, wrist and vertebrae, but some34,100,141,143,147 modelled wrist fractures separately to other fracture sites. One study20 bundled wrist fracture together in a health state with fractures at other sites. Davis et al. 34 incorporated separate health states for wrist and proximal humerus fracture; fractures at additional sites (femoral shaft, humeral shaft, pelvis, scapula, clavicle, sternum, ribs, tibia and fibula) were incorporated by increasing the incidence of fractures at the four main sites (hip, wrist, vertebral and proximal humerus), with the allocation of these additional fractures to the main fracture type expected to have similar costs and utilities. The majority of the other studies included fractures at additional sites in a single health state, with the costs, mortality and utility estimates being based on either a weighted mean across the included sites or an assumption that the consequences would be consistent with those for a known fracture site such as the wrist.
The use of a cohort-level approach meant that, in four models,141,144,146,147 future fractures were restricted for a patient experiencing a hip or vertebral fracture to ensure that patients did not transition to a health state with lower costs or better quality of life when experiencing a subsequent fracture that was less severe than the initial fracture experienced. In general, the approach taken was that patients experiencing a hip fracture were only at risk of subsequent hip fractures and patients experiencing a vertebral fracture were only at risk of hip or subsequent vertebral fractures. One model,100 which used a similar hierarchical Markov structure, adjusted for the missing fracture outcomes in patients having hip and vertebral fractures by estimating the ‘downstream’ costs of subsequent fractures that were prevented by the hierarchical Markov structure. It was not necessary to restrict the sequence of fractures experienced in either of the patient-level simulations, as costs and utilities can be made dependent on an individual’s entire history. However, Davis et al. 34 restricted the number of fractures possible for each fracture type to one per bone, with an additional limit of four vertebral fractures, four rib fractures and two pelvic fractures.
Three studies included non-skeletal health outcomes, with three141,143,144 including breast cancer, two141,144 including coronary heart disease (CHD) and two141,144 including either stroke or VTE. All except one study141 reported including an increased risk of nursing home admission after hip fracture. 20,34,100,143,144,146,147 None of the studies included an increased risk of nursing home admission following fractures at other sites, but Davis et al. 34 presented a sensitivity analysis in which an equivalent rate of nursing home admission occurred for both vertebral fracture and hip fracture.
Treatment duration
Four of the studies modelled a maximum treatment duration of 5 years for all treatments. 141,144,146,147 Davis et al. 34 assumed a 5-year intended treatment duration for all bisphosphonates except i.v. ZOL, for which a 3-year intended treatment duration was assumed. Stevenson et al. 143 assumed a 5-year treatment duration for all treatments except TPTD, for which the treatment duration was assumed to be 18 months. One study (Amgen Inc. 100) assumed a treatment duration of 10 years for DEN, 3 years for ZOL and 5 years for RLX. Another study assumed a 4-year treatment duration for all interventions except DEN, which was assumed to be given lifelong (UCB S.A. 20) (although it was noted that, in the actual model, persistence data were set to zero from 5 years, so it is unclear what treatment duration was actually implemented).
Treatment initiation, monitoring, and administration
All but one of the studies (Davis et al. 34) incorporated resource use for the monitoring of treatment. None of the studies included any costs for the administration of oral therapies. However, there was inconsistency across the studies for the administration costs for s.c. and i.v. therapies. The exact costs for administration and monitoring are discussed further in Treatment initiation, administration and monitoring, where we also describe the approach taken in the AG analysis.
Persistence
Persistence was included in either the base-case or sensitivity analysis in six of the models. 20,34,100,144,146,147 In Davis et al. ,34 the persistence data applied in the model were identified from a review of systematic reviews. In the other models, one146 used published estimates but did not describe how they were identified, one20 used a mixture of published and unpublished data, two100,147 used data on file from an unpublished study and one applied the assumption made in the model that informed TA160 and TA161. 149 Many of the estimates came from analyses of real-world data sources, such as administrative databases, with three models incorporating estimates from a large UK primary care database [Clinical Practice Research Datalink (CPRD)/General Practice Research Database (GPRD)]. 20,100,147 A full discussion of the data sources used in these models and the choice of data source for the AG model is provided in Treatment persistence.
Treatment effectiveness beyond the treatment period
All of the studies assumed that treatment effectiveness falls linearly over time after patients discontinue treatment. The period between treatment discontinuation and when the treatment effect has fallen to zero is known as the offset period. Three studies assumed an offset period equal to the treatment duration for all interventions. 141,144,146 Davis et al. 34 and Stevenson et al. 143 made the same assumption for all but one intervention. Owing to the shorter treatment period for TPTD (18 months), Stevenson et al. 143 applied the full treatment effect for 3.5 years after the end of treatment, and this was noted as a very favourable assumption. Davis et al. 34 assumed a longer offset (7 years) for ZOL, such that the treatment effect fell to zero by 10 years, despite the shorter treatment duration of 3 years. In the base-case analysis, in which the treatment persistence was < 3 years, the same ratio of offset period to treatment duration was applied by Davis et al. 34 (i.e. offset = 7/3 × treatment persistence). Two studies assumed a 1-year offset for all treatments,100,147 and one study20 assumed an offset equal to treatment duration for all interventions except DEN, for which it was set to 1 year. The evidence regarding offset periods and the choice of offset period assumed in the AG model is discussed further in Offset period.
Adverse events
All of the studies included some AEs in either their base-case or their sensitivity analyses, but there was considerable inconsistency between the studies in terms of the AEs included. Three papers included gastrointestinal (GI) AEs in their base-case analysis20,34,147 and two included them in a sensitivity analysis. 144,146 The model reported in the company submission by Amgen Inc. for TA204 (Waugh et al. 147), included GI AEs for oral bisphosphonates, but these were not included in the updated version of this model reported in the company submission by Amgen Inc. for the current appraisal. 100 Stevenson et al. 143 did not include any GI AEs for bisphosphonates in their analysis, but their model was later adapted to include GI AEs for bisphosphonates in an analysis by Stevenson and Davis149 conducted to inform TA160 and TA161. There was some consistency in the assumptions regarding GI AEs across the various models, with three models144,146,147 using the assumptions from TA160 and TA161 and one20 using assumptions consistent with those applied in TA464 (Davis et al. 34), which themselves were very similar to those applied by Stevenson and Davis. 149 Davis et al. 34 included a one-off QALY loss to account for influenza-like symptoms following administration of i.v. bisphosphonates. None of the other studies included any AEs for i.v. bisphosphonates. Two studies included VTE as a side effect of RLX. 141,144 Amgen Inc. included cellulitis (a common bacterial skin infection) as an AE of DEN in the model reported in the company submission for TA204,147 but did not include any AEs for DEN in the model reported in the company submission for the current appraisal. 100 Strom et al. 146 did note that skin infections are more frequently reported for DEN, but did not include cellulitis in their model. No studies reported including AEs for ROMO or TPTD. None of the studies included atypical femoral fracture or ONJ as AEs.
Mortality following fracture
Davis et al. 34 incorporated post-hip fracture mortality by assuming that a fixed proportion (which was sex and age specific) of patients experiencing hip fracture would die 3 months after fracture. This was based on evidence from a study by Tosteson et al. ,150 which found that the excess risk of mortality was limited to the first 6 months after fracture when adjusting for a number of prognostic factors including pre-fracture health status, and evidence from a study by Abrahamsen et al. ,151 which found that approximately half of all excess mortality had occurred at 3 months. Davis et al. 34 incorporated an increased risk of death following hip and vertebral fracture and assumed no increased risk for fractures at other sites. The same temporal pattern of risk was assumed for vertebral fractures.
Four of the other models identified in the review20,100,146,147 applied HRs to the general population mortality rate, with the HRs for hip and vertebral fracture applied for 8 years following fracture and the HRs for non-hip non-vertebral fractures applied for 1 year following fracture. The data inputs appear to be consistent across these four models, with the primary source cited being Johnell et al. 152 for clinical vertebral fractures, Jönsson et al. 153 for hip fractures and Barrett et al. 154 for ‘other fractures’. These four models all assumed that only 30% of the increased risk was attributable to the fracture itself and downweighted the additional mortality risks accordingly. Kanis et al. 141 cited the same data source152 for mortality after vertebral fracture, but details are not provided on the duration over which the HR is applied or the proportion of excess risk that is considered attributable to fracture. Kanis et al. 144 cited alternative sources155–157 and stated that 30% was assumed to be causally related, but does not describe the duration over which the HRs are applied. Stevenson et al. 143 used unpublished estimates from the Anglian audit of hip fracture,158 which reported mortality risk for several different age bands, and adjusted these to remove those deaths not causally related to hip fracture using the data from Parker and Anand. 157 Stevenson et al. 143 based their risk of death following vertebral fracture on a study by Center et al. 159 Stevenson et al. 143 included a twofold increase in mortality following proximal humerus fracture, citing Johnell et al. ,152 but assumed no increased risk of mortality following wrist fractures. None of the published models identified sources of data that were more recent than those identified by the AG during TA464. 34
Consistency with the National Institute for Health and Care Excellence reference case
All of the included studies measured direct health effects for patients, and none included any benefits for carers. All of the studies reported using published estimates of utility following fracture from studies that had measured utility using the EQ-5D using the UK general population valuation set. There was some inconsistency in the approach taken to estimating utility following nursing home admission, with one study147 reporting no additional disutility, one study143 reporting using a value based on an expert panel, one study34 reporting a value based on the EQ-5D and several studies not reporting the approach taken to estimating utility values for nursing home admission. 20,100,141,144,146
One study141 based its effectiveness estimate on a single RCT and reported a comparison only between the interventions included in the RCT (RLX vs. no treatment). The other studies all sourced their effectiveness estimates from a systematic review and meta-analysis, although only the three most recent models20,34,100 used NMA to estimate the relative treatment between active comparators. One study147 used the method published by Bucher et al. 148 to conduct an indirect comparison. Two studies143,146 present incremental analyses that appear to be based on naive indirect comparisons based on equivalent outcomes for patients receiving placebo. The remaining study144 provided comparisons only against no treatment.
Five studies explicitly reported using an NHS and Personal Social Services (PSS) perspective. 20,34,100,143,147 Three studies reported taking a health-care perspective,141,144,146 but two of these144,146 also included nursing home costs, which are likely to fall under PSS rather than NHS in a UK context, although some may also fall under societal costs if families pay privately for nursing home care. Discounting consistent with the current NICE reference case (3.5% for both costs and QALYs)139 was applied in all but two studies,141,143 in which discounting was applied at rates consistent with previous NICE methods guidance (6% for costs and 1.5% for QALYs). The time horizon is not explicitly stated for the 2005 publication by Kanis et al. ,141 but, otherwise, all of the included economic evaluations incorporated a lifetime horizon, although, in the analysis by Stevenson et al. ,143 the Markov model was used for the first 10 years and then additional calculations were used to estimate QALYs gained over the remaining lifetime.
Quality and applicability of studies
The only analyses considered to be broadly consistent with the NICE reference case were the models described in the submissions by UCB S.A. 20 and Amgen Inc. 100 and the analysis by Davis et al. ,34 which informed TA464. 9 None of the other models provided an incremental analysis informed by a systematic review and NMA, which is a significant deviation from the NICE reference case, and may be a potential source of bias. However, it is noted that the analysis by Davis et al. 34 was not relevant to the decision problem; it was included purely to allow comparisons to be made between the published models and the model we intended to adapt for this appraisal.
Study conclusions
Owing to the concerns regarding applicability to the decision problem and consistency with the NICE reference case, for several of the studies34,141,144–147 included in the review, results are summarised here only for the UCB S.A. 20 and Amgen Inc. 100 submissions.
In the Amgen Inc. company submission,100 which investigated the cost-effectiveness of DEN in a population of patients with a 10-year fracture risk of 20%, DEN was found to be associated with an incremental cost-effectiveness ratio (ICER) of £27,792 per QALY, compared with RLX, and an ICER of £27,363 per QALY compared with no treatment. At the same risk of facture, DEN was also found to dominate ZOL.
In the UCB S.A. submission,20 which investigated the cost-effectiveness of a treatment sequence of 1 year of ROMO followed by 4 years of ALN (ROMO/ALN), in a population of postmenopausal women with a 10-year fracture risk of 30%, ROMO/ALN was found to be associated with an ICER of (confidential information has been removed) per QALY compared with ALN alone, and (confidential information has been removed) per QALY compared with no treatment. The UCB S.A. submission20 also presented scenario analyses comparing ROMO/ALN with RIS, ZOL, RLX, DEN and TPTD (administered for 18 months and 24 months). The ICERs for ROMO/ALN when compared with these alternative comparators were (confidential information has been removed) and dominating (ROMO/ALN had more QALYs and a lower cost than TPTD for both the 18- and 24-month treatment durations), respectively, when using the Patient Access Scheme (PAS) price for ROMO.
Review conclusions
The review has identified that there are no published cost-effectiveness studies that compare all of the interventions and comparators specified in the scope of this appraisal across the broad population specified in the scope, which is patients eligible for risk assessment under CG146. 8 Although the Amgen Inc. 100 and UCB S.A. 20 submissions provide an incremental analysis for the majority of the interventions and comparators specified in the scope (neither compared with i.v. IBN), their analyses are restricted to high-risk subgroups of the population. However, this review was useful in identifying areas where the model used in TA46434 differed from the models included in the review. These are discussed further in Independent economic assessment, where we describe the changes made to the model reported by Davis et al. 34
Independent economic assessment
Methods
Having considered the review of published models and the models included in the company submissions, the AG decided to adapt the model used to inform TA464 (Davis et al. 34) rather than developing a de novo model for this assessment. However, based on the review of models, the AG recognised that there were several areas where it would be useful to consider whether or not the model should be updated or adapted. The areas identified for consideration were as follows:
-
treatment persistence – the duration of time the patient persists with treatment
-
offset period – the period between when treatment ends and the treatment effect reaches zero
-
incorporation of AEs specific to non-bisphosphonates
-
resource use associated with monitoring and administration of treatments
-
utility values following fracture
-
drug prices
-
disease costs (i.e. fracture, nursing home admission).
It was not feasible to conduct a full systematic review of the literature to inform each of these updates to the model. Instead, the AG considered any additional sources of evidence provided in the company submission or cited in the published cost-effectiveness studies. This was supplemented by ad hoc searches using Google Scholar (Google Inc., Mountain View, CA, USA) to identify any recent systematic reviews. A more rigorous approach was taken to identifying updated estimates of utility following fracture. For this, we conducted a full systematic search for studies reporting utility pre and post fracture, as measured by the EQ-5D. The aim of this review was to update the review conducted for TA464 by Davis et al. 34
In addition to these updates, the AG also identified that changes to the Visual Basic for Applications (VBA) code would be needed to (1) increase the number of treatment strategies that can be modelled, (2) allow for drug-specific offset periods and (3) allow for sequences of treatments to be modelled.
Unless otherwise stated, all other aspects of the model remain unchanged from the model used to inform TA464,9 as described in the Assessment Report for TA464 (Davis et al. 34), with the additional change regarding nursing and residential care home costs described in the addendum provided before the second committee meeting. 160 The other changes documented in the addendum are superseded by the updated NMA reported in Chapter 3, Network meta-analysis, and the need to update drug costs to reflect current prices.
Model structure
The ScHARR osteoporosis model (used in TA46434) is a discrete event simulation (DES), which simulates the clinical events occurring over the lifetimes of individual patients with heterogeneous characteristics. A patient-level simulation approach was chosen to allow the future events experienced by patients to be affected by prior events such as incident fractures. We chose to model a heterogeneous population because we anticipated that certain patient characteristics, such as age, would be non-linearly related to cost-effectiveness. For example, older patients are more likely to have experienced a prior fracture, and may therefore have a lower quality of life at baseline, and they are also more likely than younger patients to be admitted to a long-term nursing or residential care home following a hip fracture. Both of these factors will influence the costs and QALYs that can be gained from avoiding a fracture. In this situation, the cost-effectiveness for a patient with average characteristics is not the same as the average cost-effectiveness when taking into account the distribution of that characteristic across the population.
In general, in a DES model, a patient’s progression through the model is determined by the events that occur, rather than by the health states they occupy. Figure 10 shows the clinical events that can occur during a patient’s lifetime, with the arrows showing which events can occur following other events (note that this is not a state-transition diagram, as patients do not reside in the state defined by the most recent event until the next event is experienced). In the ScHARR osteoporosis model, the main clinical events were fracture, death and new admission to residential care. Fractures at different sites were processed using separate fracture events for hip; wrist; vertebral and proximal humerus. These are the sites most strongly associated with osteoporosis and these are the fracture sites included by both the QFracture and FRAX risk calculators. Fractures at additional sites (e.g. femoral shaft, humeral shaft, pelvis, scapula, clavicle, sternum, ribs, tibia and fibula) have been incorporated by increasing the incidence of these four event types, rather than by adding additional competing events.
FIGURE 10.
Clinical events that can occur during a patient’s lifetime in the DES.
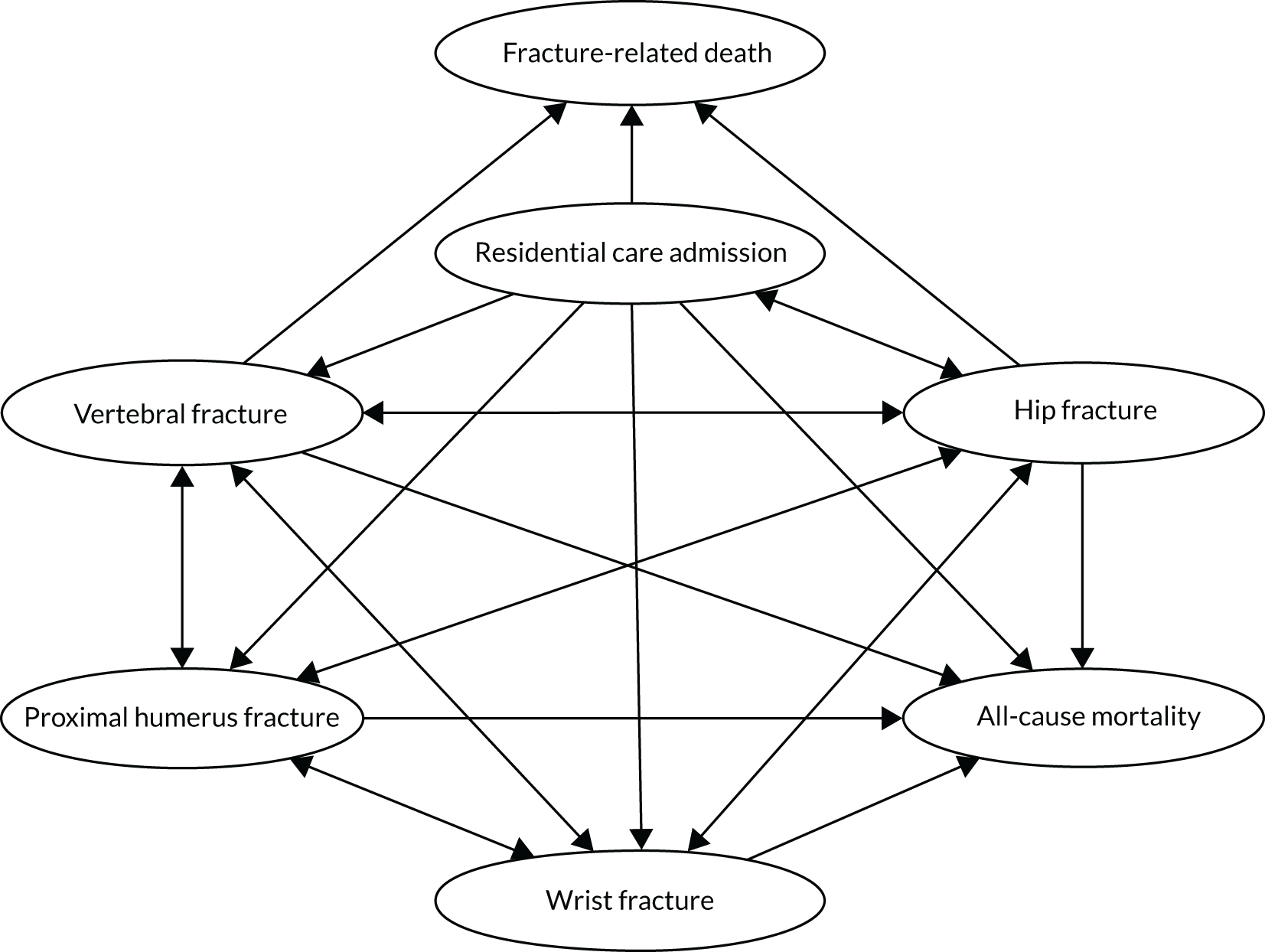
In a DES, no changes are made to a patient’s attributes between events, but the event list that determines the future events experienced can be resampled each time an event occurs to incorporate any changes in patient characteristics. Dummy events were included in the model to ensure that patient attributes were updated at 1 year after the start of the model, at the end of treatment, at the end of the offset period, at 5 years, at 10 years and 1 year after each incident fracture. Linear approximation is used to adjust for age-related changes in utilty between events.
Utility in the model is based on a combination of sex, age, fracture history and residential status (community dwelling or institutionalised). Separate utility multipliers and costs are applied to the first and subsequent years after fracture to reflect the differences between the acute and chronic impact of fracture. The chronic cost is set to the maximum chronic cost for all fracture events experienced so far. Therefore, the maximum chronic cost for any individual is the cost for institutionalised patients. Drug costs are applied from the start of the simulation until the end of the treatment period and are assumed to accrue at a constant rate across time. Death does not incur any additional costs in the model, but the acute cost of fracture is incurred for both fatal and non-fatal fractures.
The model also incorporates the following structural assumptions:
-
There are no restrictions on the sequence of fractures that can be experienced.
-
The maximum number of fractures that can be experienced is limited to one per bone (i.e. two hip fractures), with an additional limit of four vertebral fractures, four rib fractures and two pelvic fractures.
-
Death attributable to fracture occurs 3 months after fracture, with other fracture events possible during this period, but no mortality from non-fracture-related causes.
-
Incident fractures increase the risk of future fractures.
-
A fracture event occurring < 1 year after a previous event supersedes the dummy event used to update patient attributes 1 year after fracture, thus reducing the acute period for the earlier fracture.
-
Nursing home admission can occur only following fracture; therefore, patients who are community dwelling at the start of the simulation do not transfer to nursing home care as they age unless this is simulated to occur following a fracture.
A brief overview of the key features of the ScHARR osteoporosis model used in TA46434 is provided in Table 6, alongside a description of the key changes to the model since TA464. The only deviation from the NICE reference case to note is that the utility estimates for ONJ have been valued using the US rather than the UK valuation set for the EQ-5D.
| Model feature | Description of model in TA46434 | Description of revised model |
|---|---|---|
| Decision problem | To assess the cost-effectiveness of bisphosphonates compared with no treatment at varying levels of absolute fracture risk as defined by the FRAX and QFracture risk assessment tools | To assess the cost-effectiveness of non-bisphosphonates compared with bisphosphonates and no treatment at varying levels of absolute fracture risk as defined by the FRAX and QFracture risk assessment tools |
| Type of economic evaluation | Cost-effectiveness analysis with benefits expressed as QALYs | No change |
| Population/subgroups |
|
No change (see Population) |
| Interventions |
|
|
| Comparators | No treatment | No treatment and the bisphosphonates listed as comparators for TA464 (see Interventions and comparators) |
| Perspective | NHS and PSS | No change |
| Model type | DES with heterogeneous patient population | No change |
| Model events |
Clinical events are fracture, death (all-cause mortality and fracture-related mortality) and nursing home admission. There are four possible fracture events (hip, wrist, vertebral and proximal humerus), with fracture at other sites included by increasing the incidence of these events Dummy events are used to update attributes 1 year after fracture and to update the fracture risks once treatment finishes |
No change (see description of model events in Model structure) |
| Time horizon | Lifetime (up to the age of 100 years) | No change |
| Duration of treatment | Mean duration of persistence with treatment from observational studies | Data sources for persistence with oral bisphosphonates have been updated. Additional persistence data have been identified for non-bisphosphonates (see Treatment persistence) |
| Natural history | Time to fracture is based on the estimate of absolute fracture risk for major osteoporotic fractures (hip, wrist, proximal humerus and vertebral) provided by either QFracture or FRAX, which is uplifted to include fractures at additional sites. The distribution of fractures across different sites is based on incidence data from Sweden. The increased risks of fracture following incident fracture are based on a published systematic review | No change |
| Effectiveness | The HRs from the systematic review and NMA are applied for the duration of treatment. Some effectiveness is assumed to persist beyond treatment during the ‘offset period’. A linear decline in treatment effect is assumed during this time |
|
| AEs | Upper GI side effects for oral bisphosphonates and influenza-like symptoms for i.v. bisphosphonates are included by applying one-off cost and QALY deductions in the first month of treatment | Additional AEs have been incorporated for the following (see Adverse events):
|
| Mortality | No change | |
| Utility data | Utility decrements based on EQ-5D scores pre and post fracture were obtained from a systematic review. Utility decrement for nursing home admission was based on a single study, identified from the literature, that used EQ-5D. Variation in baseline utility by age and sex was based on UK EQ-5D population estimates |
|
| Resource use and unit costs |
|
|
| Discounting | 3.5% per annum for both costs and QALYs | No change |
| Sensitivity analysis |
Probabilistic sensitivity analysis was undertaken for the base-case scenario to estimate the mean costs and benefits when taking into account parameter uncertainty Structural uncertainty was assessed through scenario analysis in which parameters were set to their mid-point values |
No change |
Population
The population is patients eligible for risk assessment under CG146,8 as per the final NICE scope (see Chapter 1, Measurement of disease). It should be noted that this includes both men and women, those with and those without a prior fracture, those with steroid-induced osteoporosis, those with secondary osteoporosis and those with other risk factors for fragility fracture. CG146 recommends that either FRAX30 or QFracture31,163,164 be used to assess the absolute risk of fracture. To explore whether or not the most cost-effective treatment varies for patients at different levels of absolute fracture risk, we report the variation in incremental net monetary benefit (INMB) across risk using two approaches. First, we report outcomes for 10 risk categories, based on deciles of absolute fracture risk. Second, we use regression to determine the relationship between INMB and absolute risk as a continuous variable. These steps are undertaken for absolute risk assessed by FRAX and for absolute risk assessed by QFracture.
Interventions and comparators
The treatment strategies modelled (and the intended treatment durations) were as follows:
-
oral ALN (5 years)
-
oral RIS (5 years)
-
oral IBN (5 years)
-
i.v. IBN (5 years)
-
i.v. ZOL (3 years)
-
RLX (5 years)
-
DEN (10 years)
-
TPTD (2 years)
-
ROMO (1 year) followed by ALN (4 years).
These were all compared with a strategy of no treatment to estimate the incremental costs, incremental QALYs and INMB relative to no treatment. We note that, in the base-case analysis, the actual treatment duration modelled is determined by the duration of treatment persistence rather than the intended treatment duration, but it is necessary to specify the intended treatment duration for the scenario analysis assuming full persistence.
The intended treatment durations for bisphosphonates (3 years for ZOL and 5 years for all others) are based on the assumption made in TA464. 34 For the sequence of ROMO followed by ALN, the 1-year treatment duration for ROMO is based on the anticipated marketing authorisation. However, the anticipated marketing authorisation also states that ROMO should be followed by an anti-resorptive agent, but does not specify the duration for anti-resportive treatment. In the ARCH trial,83 patients in both arms received open-label ALN after the 1-year double-blind phase. In the clinical study report20 for the ARCH trial, the mean duration of ALN exposure after the 1-year double-blind phase is (confidential information has been removed) in both arms, but the maximum treatment exposure is between (confidential information has been removed) years across the two trial arms. To have the same overall intended treatment duration as the ALN strategy, we decided to model the ROMO/ALN strategy as including 4 years of ALN. For DEN, we have assumed an intended treatment duration of 10 years, as this is what was assumed in the Amgen Inc. submission,100 in which it was argued that there are data from the FREEDOM study104 on the efficacy and safety of up to 10 years of DEN treatment.
Treatment persistence
In the AG model, we have assumed that costs and benefits are linearly related to the duration of treatment persistence; therefore, the individual-level variation in persistence does not need to be modelled. The assumption was found to be reasonable in sensitivity anslyses reported by Davis et al. 34 Therefore, the variable that needs estimating to inform the model is the mean treatment persistence and standard error of the mean, which describes the uncertainty around the mean for the probabilistic sensitivity analysis (PSA).
In the model that informed TA464, Davis et al. 34 used published estimates of treatment persistence from observational cohort studies, with separate estimates applied for oral bisphosphonates, based on a systematic review by Imaz et al. ,165 and for i.v. bisphosphonates, based on a US study of Medicare patients (Curtis et al. 166). Davis et al. 34 applied the mean persistence reported in these studies to all patients receiving treatment, rather than modelling individual-level heterogeneity in treatment persistence. The model in the Amgen Inc. submission100 used persistence data from a retrospective analysis of a large UK primary care database (the CPRD) (Amgen Inc.,100 data on file). The proportion persisting with treatment over 5 years was estimated from these data and extrapolated beyond 5 years in the model based on the last year of data. The model in the UCB S.A. submission20 used published estimates for treatment persistence for bisphosphonates and RLX from a UK GPRD study and data from a non-UK registry study for DEN. Unpublished data were cited by UCB S.A. 20 as the source for TPTD and ZOL persistence. For the sequence of ROMO followed by ALN, the model submitted by UCB S.A. 20 assumed that 90% of patients would persist with ROMO up to 1 year, based on experience from clinical trials, and that, once patients switched to ALN, the treatment persistence would be 85% of that observed for DEN – the treatment with the highest persistence rate, based on the published estimates. Strom et al. 146 used persistence data for oral bisphosphonates from a UK CPRD study (Li et al.;167 similarities suggest that this is the same study cited by UCB S.A.) to model persistence over time for the first 3 years and then assumed that all patients reaching 3 years would continue on oral bisphosphonates. Strom et al. 146 used a non-UK randomised crossover comparison study109 to model treatment persistence with DEN. Kanis et al. 144 assumed that 50% of patients receiving oral bisphosphonates persist up to 3 months and the rest persist up to the intended treatment duration, based on the assumption used in the analysis that informed TA160 and TA161. It is not clear what assumption was made by Kanis et al. 144 regarding treatment persistence for RLX. In the model based on the MORE study,141 patient compliance was not taken into account, but it was noted in the discussion that 92% of patients took > 80% of their study medication. In the model submitted by Amgen Inc. for TA204,147 treatment persistence was assumed to be 100% for all treatments in the base-case analysis, but a lower rate of treatment persistence for oral bisphosphonates was applied in a sensitivity analysis based on data from the GPRD (GPRD is the previous name of the CPRD, but the data used here appear to be from a different study to that used in the current Amgen Inc. submission100).
Both of the company submissions used data from the same large UK primary care database (GPRD/CPRD). The published analysis by Li et al. 168 gave median durations of persistence for oral bisphosphonates ranging from 5 to 7 months across the more commonly used weekly and monthly preparations, whereas the more recent, but unpublished, analysis cited in the Amgen Inc. submission100 had a lower median persistence of (confidential information has been removed) months for all oral bisphoshonates. However, the AG notes that the data from Li et al. 168 suggest that the time-to-discontinuation curve has a long tail, so mean persistence will be longer than median persistence.
The AG estimated mean time on treatment from the Kaplan–Meier estimates published by Li et al. 168 by crudely estimating the area under tha Kaplan–Meier curve, assuming linear changes between the estimates reported. The data from the more recent analysis presented in the Amgen Inc. submission100 were considered less mature than the data presented by Li et al. 168 Mean durations of persistence in the first 5 years after starting treatment were estimated to be 1.7 years, 1.5 years and 1.4 years for ALN, RIS and RLX, respectively. Estimates for oral IBN were not possible owing to missing data at 5 years. Although separate estimates of persistence are provided for ALN and RIS, in the absence of any data demonstrating that treatment persistence differs significantly between different oral bisphosphonates, we decided to apply the average persistence data from ALN and RIS to all oral bisphosphonates. We note that mean treatment persistence is approximately three times longer under this assumption than assumed previously in the model that informed TA464. 34
The AG was not convinced that data from a primary care database, as used in the Amgen Inc. model,100 would be generalisable to i.v. bisphosphonates (and likewise TPTD) as these are usually prescribed in secondary care. Given this concern, and in the absence of any other alternative data sources, the AG decided to use the same estimates of treatment persistence for i.v. bisphosphonates as assumed in the model that informed TA464. 34
The evidence on the long-term persistence with DEN appears to be very limited, with most studies reporting a maximum of 24 months’ follow-up. 109,169–171 It is difficult to estimate the mean or median duration of treatment from studies that are limited to 2 years when persistence is high at 2 years and it is possible for DEN to be given long term. The analysis of CPRD data presented in the Amgen Inc. submission100 presents data beyond 2 years, but these were described as exploratory analyses only. The AG were concerned about whether or not the analysis of CPRD data presented by Amgen Inc. would accurately capture DEN persistence as, although DEN may sometimes be administered in primary care, treatment is usually initiated in secondary care. Therefore, any estimate of persistence derived solely from primary care records may fail to accurately capture treatment discontinuation in the transition between secondary and primary care. The persistence data used for DEN in the UCB S.A. submission20 match the cited source (Karlsson et al. 170) up to 24 months, but beyond that they have simply assumed a fixed proportional decrease in the numbers that are persistent, based on a comparison between the 18-month and 24-month persistence rates. The AG decided to estimate the mean treatment persistence from the CRPD data presented by Amgen Inc. in their model. The estimates of persistence appear to be very uncertain beyond 4 years, but there appears to be a constant risk of discontinuation from years 2 to 4. The AG decided to use the rate of discontinuation between years 2 and 4 to estimate the proportionate decrease in persistence experienced thereafter. From this, the mean treatment persistence over 10 years was estimated to be (confidential information has been removed). The AG notes that these estimates are uncertain owing to the exclusive use of primary care records and the need for an assumption to be made to extrapolate persistence up to 10 years because of the low proportion of patients captured in the analysis beyond 2 years (confidential information has been removed).
Several sources of persistence data were identified for TPTD. As stated above, the estimates based on UK primary care databases were discounted based on the fact that TPTD is usually prescribed in secondary care. However, two published articles172,173 were identified from ad hoc literature searches that described persistence in UK patients in real clinical practice based on data from the main home care provider of TPTD in the UK. Both these studies were conducted before the maximum duration of treatment in the marketing authorisation was extended from 18 to 24 months, but they show high levels of persistence at 18 months of 79%172 and 74%173 for women and men, respectively. However, these estimates were based on Kaplan–Meier data taking into account the censoring of patients who were still on treatment at the longest follow-up. Data from the European Extended Forsteo Observational Study (ExFOS),174 which was a large European real-life clinical practice study of TPTD use after the licence was extended to 24 months, showed a mean treatment duration of 20.7 months, despite 29% of patients residing in countries where the licence remained restricted to 18 months. All three papers show a fairly linear fall-off in persistence, although a more rapid fall in persistence was seen in the ExFOS study at 18 months in the countries with 24-month reimbursement, which could be explained by a lack of uptake of the longer dosing schedule. We decided to use the data from UK women to estimate the average duration of treatment. To do this, we assumed a constant rate of discontinuation from 0 to 24 months, based on the rate observed over 18 months by Arden et al. ,172 giving an estimated mean persistence time of 1.72 years (20.6 months), which is reasonably consistent with the estimate from ExFOS, which had a mean treatment duration of 20.7 months. We decided to take the standard error of the mean (0.14 months) from the ExFOS study as the measure of uncertainty for the estimate applied in the model. When sampling this parameter in the PSA, the maximum number of doses was capped at 24, as per the SmPC for TPTD. 25
For ROMO, the manufacturer claimed that 90% of patients persisted to 12 months, based on data from the clinical trials. The AG used data on doses received in the ARCH study83 to estimate mean persistence with treatment, and found that this agreed with patients being treated for a mean of (confidential information has been removed), although it noted that only (confidential information has been removed) of patients received all 12 doses of ROMO. When sampling this parameter in the PSA, the maximum number of doses was capped at 12, as per the draft SmPC for ROMO provided in the UCB S.A. submission. 12 For the sequence of ROMO followed by ALN, we have assumed that treatment persistence with ALN is the same as for the ALN-only strategy.
Effectiveness data
The HRs estimated in the NMA (see Figure 6) were applied in the model for the duration of treatment, with a linear increase to a HR of 1 (i.e. no treatment effect) during the offset period. For the treatment sequence of ROMO followed by ALN, the HR for ROMO followed by ALN was applied during both the ROMO and the ALN treatment periods, as the HR estimate in the NMA was based on fractures occurring during both treatment phases. The NMA requires a single estimate of treatment effect for each study; therefore, it would not have been possible to generate separate estimates of treatment efficacy for the ROMO and ALN parts of the treatment sequence.
When data on fracture outcomes were lacking for i.v. IBN, the AG used the NMA estimate for daily oral IBN, as the marketing authorisation for i.v. IBN was based on studies demonstrating that i.v. IBN had superior BMD outcomes compared with daily oral IBN. It is noted that this is potentially unfavourable to i.v. IBN if superior BMD outcomes translate into superior fracture prevention outcomes. However, this is consistent with the approach taken in TA464. 34
For vertebral fracture, we have used the outputs of the base-case NMA, which included studies reporting morphometric fractures. This is because the outcome of morphometric fracture was more widely reported, and the NMA sensitivity analysis that excluded studies that reported only morphometric fractures, leaving just those studies reporting clinical vertebral fracture, was found to produce results that were consistent with the base-case analysis.
In the model that informed TA464,34 it was possible to use the bisphosphonate class effect estimate when data on individual bisphosphonates were lacking. In the updated networks described in Chapter 3, Network meta-analysis, no hip fracture data were available for i.v. IBN and monthly oral IBN, but data were available for all non-bisphosphonates. We decided to apply the bisphosphonate class effect estimate for i.v. IBN and monthly oral IBN when data were lacking for hip fracture. We note that the class effect for bisphosphonates was very similar to the estimates for ALN, RIS and ZOL, and so this was not considered to unfairly bias the cost-effectiveness analysis.
In the analysis that informed TA464,34 the data were considered too sparse for the outcome of proximal humerus fracture, so the non-vertebral NMA estimates were used instead. In the NMAs conducted for the current MTA, the networks were sparsely populated for non-bisphosphonates for the outcomes of both wrist fracture and proximal humerus fracture. The AG decided to use the NMA estimates from the non-vertebral fracture NMA for both wrist and proximal humerus fractures as this allowed a single network to be used to estimate HRs for all interventions. This was considered preferable to using data from different networks for bisphosphonates and non-bisphosphonates, as the wrist and proximal humerus fracture estimates would be more uncertain than the non-vertebral fracture estimates.
In the base-case analysis, the convergence diagnosis and output analysis (CODA) samples from the NMA were used, as these preserve the underlying joint distribution of the HRs, but, in the deterministic analyses, the median HR was used.
Offset period
The AG used a review by Idolazzi et al. 175 and papers cited in the company submission to identify relevant studies that could be used to inform the assumptions regarding the appropriate offset periods for the different treatments modelled.
For ALN, the key study was considered to be the Fracture Intervention Trial Long-term Extension (FLEX),176,177 as this provided comparative data on both fracture risk and BMD for patients remaining on, or stopping treatment with, ALN after 5 years of treatment. This study found that it took 5 years for total hip BMD to return to pre-treatment levels when treatment with ALN was discontinued after 5 years. This was supported by no separation of the time-to-event curves for non-vertebral fractures for patients remaining on treatment compared with those stopping treatment. There was some evidence of a continued treatment effect for lumbar spine BMD, and a continued reduction in vertebral fracture risk was observed (RR 0.45, 95% CI 0.24 to 0.88) for patients who continued ALN compared with those who discontinued ALN.
For RIS, two studies were identified. 178,179 Watts et al. 179 reported the outcomes of patients randomised to either placebo or RIS in the year after discontinuing the study drug. Eastell et al. 178 reported the outcomes of patients in the year after completing the Vertebral Efficacy with Risedronate Therapy-Multinational (VERT-MN) study, in which patients were randomised to either RIS or placebo for 3 years, followed by a 2-year open-label extension on the allocated study drug, followed by 2 years of open-label RIS in both groups. Both studies reported that BMD gains at the hip were lost in the 1 year following treatment discontinuation, although Watts et al. 179 observed smaller losses in lumbar spine BMD and reported a statistically significant reduction in vertebral fracture incidence between those previously treated with RIS and those previously treated with placebo, in the year after treatment discontinuation.
The data identified for oral IBN were limited to those from 1-year post-trial follow-up from an early dose-finding study,180 which included the 2.5-mg daily dose that has been shown in non-inferiority bridging studies to be equivalent to the 150-mg monthly dose that is now licensed. 181 This study180 appears to show a similar pattern to that seen for RIS, in that hip BMD appears to return to pre-treatment levels in the year after treatment, with a slightly slower return for lumbar spine BMD. However, as the duration of treatment was only 1 year, it is not clear whether the offset time is 1 year regardless of treatment duration, or whether it would increase in proportion to treatment duration.
For oral bisphosphonates, the AG decided to keep the assumption made previously in the model that informed TA464,34 which was that treatment effect falls to zero over a period equal to the initial treatment duration for all oral bisphosphonates, as this was accepted previously by the NICE Appraisal Committee. However, in a sensitivity analysis, we have also explored the possibility of a fixed 1-year offset time for RIS and oral IBN.
For i.v IBN, no studies were identified that explored BMD or fracture outcomes following treatment discontinuation. Therefore, we assumed that the offset period would be the same as for oral IBN and set it equal to treatment duration, with a fixed 1-year offset explored in a sensitivity analysis.
For i.v. ZOL, data from the Health Outcomes and Reduced Incidence with Zoledronic Acid Once Yearly (HORIZON) – Pivotal Fracture Trial extension study are provided by Black et al. 182 In the extension study, patients who had received 3 years of ZOL were randomised to receive either ZOL or placebo for a further 3 years. At the end of the study, femoral neck BMD had declined in those who switched to placebo, but not to baseline levels, suggesting an offset period that is longer than the treatment duration when measured based on BMD changes. This suggests a slightly longer tailing-off of treatment effect than observed for ALN in the FLEX study. There was, however, no statistically significant difference in non-vertebral fractures between placebo and ZOL in the extension phase. Similar to the results from the FLEX study, further gains were made in lumbar spine BMD after discontinuation, and there was a statistically significant difference in new vertebral fractures in the extension stage of HORIZON.
For i.v. ZOL, the AG decided to keep the assumption made previously in the model that informed TA464,34 which was that treatment effect falls to zero 10 years after the start of a 3-year treatment period. For patients stopping treatment early, the offset duration was assumed to decrease proportionately. A sensitivity analysis assuming an offset period equal to treatment duration was also conducted.
For TPTD, data on treatment in women were identified from the FPT follow-up study,183,184 which followed up patients for a median duration of 30 months after the RCT phase of the study. The RCT phase was terminated early (owing to concerns regarding the safety of long-term use); the median treatment duration was 20 months. During the follow-up study, patients were treated according to local standards and a high proportion (i.e. 56.9% of those randomised to the licensed dose of TPTD in the RCT phase) received other osteoporosis interventions. To account for this, results were presented for the subgroup with no further osteoporosis intervention, in addition to the analysis for all patients. Statistically significant reductions in vertebral fractures were reported by Lindsay et al. 183 in the 18 months following discontinuations, and not all of the lumbar spine BMD gained during treatment had been lost by 18 months. For non-vertebral fractures, statistically significant differences were not found for the licensed dose compared with placebo at the longer follow-up point of 30 months post discontinuation when adjusting for usage of other osteoporosis medications. Furthermore, the gains in femoral neck and total hip BMD appeared to be lost by 18 months in the group not receiving other osteoporosis interventions. A second smaller study185 in men with a shorter follow-up time had similar findings. Based on these two studies, we decided to assume an offset period equal to the treatment duration.
For RLX, two relevant studies were identified. One compared continuation with RLX with discontinuation in patients previously treated for 96 weeks. 186 Although there were some baseline differences in BMD, the percentage change in lumbar spine BMD from baseline was no longer statistically significant at 144 weeks in the group that had discontinued at 96 weeks, whereas the benefit in lumbar spine BMD was maintained in those continuing RLX up to 192 weeks from baseline. A second RCT extension study,187 which examined 1-year outcomes in patients discontinuing after 5 years of RLX, oestrogen or placebo, found that BMD values were significantly lower 1 year after discontinuing than at the end of treatment therapy for both lumbar spine and femoral neck BMD. Although these data are from a small study, they support a rapid loss of efficacy in the year after treatment even for patients treated for > 2 years. Based on these two studies,186,187 we decided to apply a 1-year offset period for RLX.
For DEN, two papers188,189 reporting outcomes from a single study were identified. The paper reporting 2 years’ follow-up post discontinuation in patients allocated to either 2 years of DEN or 2 years of placebo found that gains in both lumbar spine BMD and total hip BMD were lost in the first year after discontinuation, suggesting that an offset period of 1 year would be reasonable for DEN. A third paper,190 presenting an analysis of post-trial outcomes of patients from the FREEDOM study, was also identified, which described a rapid fall in BMD in the first year after discontinuation, even after treatment lasting 10 years. Although this analysis was limited to 12 women from a single site, and can therefore be considered as only weak evidence, this analysis is supportive of a fixed offset period of 1 year, rather than one that varies with treatment duration. Therefore, for DEN we have assumed a fixed offset period equal to 1 year (or, when this is < 1 year, the treatment duration).
For ROMO, no data were identified in the published literature on the treatment effect following discontinuation. In sequences in which ROMO is followed by ALN, we have assumed an offset period equal to the total duration of the treatment sequence, with efficacy during the offset linearly declining from the efficacy observed across the treatment sequence. This is consistent with the assumption applied by UCB S.A. 20
Drug costs
For drugs with multiple preparations, the cost was based on the lowest cost preparation available. For drugs administered in primary care, the costs were taken from the NHS drug tariff. 191 For drugs administered in secondary care, the electronic market information tool (eMIT) database192 was used for generic preparations (i.v. bisphosphonates) and the NHS drug tariff191 price was used when no generic preparation was listed as being available (i.e. for TPTD and DEN). For ROMO, the annual costs for both the list price and the PAS price were taken from the company submission. The PAS price was used in the AG’s base-case analysis. The price used for TPTD was based on the branded formulation (Forsteo), as no prices were available for the biosimilar versions (Movymia and Terrosa)22,23 when this report was prepared.
The dosing, cost per item and annual cost for each treatment strategy are summarised in Table 7.
| ALN/RIS/IBN (oral) | IBN i.v. | ZOL i.v. | RLX | DEN | TPTD | ROMO/ALNa | |
|---|---|---|---|---|---|---|---|
| Intended treatment duration (years) | 5 | 5 | 3 | 5 | 10 | 2 | 1 |
| Mean persistence (years) | 1.60 | 1.1 | 1.7 | 1.38 | Confidential information has been removed | 1.72 | Confidential information has been removed |
| Offset | 1.60 | 1.10 | 3.96 | 1.00 | 1.00 | 1.72 | N/Ab |
| Drug acquisition costs | |||||||
| Dosing unit | 70 mg/35 mg/150 mg | 3 mg in 3 ml | 5 mg/100 ml | 60 mg | 60 mg | 20 µg | 210 mg |
| Dosing frequency | Weekly/weekly/monthly | Quarterly | Annual | Daily | Biannual | Daily | Monthly |
| Unit cost | £0.76 per 4/£0.76 per 4/£0.99 per 1 | £7.89 per 1 | £13.24 per 1 | £3.27 per 28 | £183.00 per 1 | £271.88 per 30 | Not provided |
| Total cost per year (£) | 9.91/9.91/11.88 | 31.56 | 13.24 | 42.63 | 366.00 | 3307.87 | Confidential information has been removed |
| Administration costs | |||||||
| Route of administration | Oral | i.v. | i.v. | Oral | s.c. injection | s.c. injection | s.c. injection |
| Resource use for administrations | N/A | Outpatient | Day case | N/A | Two as outpatient, then general practice nurse | Self-administered | Self-administered |
| Cost per administration (£) | N/A | 150.38 | 253.32 | N/A | 10.85 (150.38 first year) | N/A | 0.00 |
| Number of administrations per year | N/A | 4 | 1 | N/A | 2 | N/A | 12 |
| Total cost per year (£) | 0.00 | 601.52 | 253.32 | 0.00 | 21.70 (300.76 first year) | N/A | 0.00 |
| Monitoring costs | |||||||
| Type of follow-up visit | GP | Outpatient | Outpatient | GP | GP, with one in four as outpatient | Outpatient | Outpatient |
| Cost (£) per follow-up visit (one per annum) | 38.00 | 150.38 | 150.38 | 38.00 | 66.09 (average) | 150.38 | 150.38 |
| Years between DXA | 5 | 5 | 3 | 5 | 5 | 2 | 1 |
| Annualised BMD measurement costs (£) | 13.66 | 13.66 | 13.66 | 13.66 | 13.66 | 34.14 | 68.29 |
| Total monitoring costs per year (£) | 51.66 | 165.04 | 173.14 | 51.66 | 79.75 | 184.52 | 218.67 |
| Total annual costs (£) | 61.57/61.57/63.54 | 797.11 | 439.71 | 94.29 | 467.45 (746.51 in first year) | 3492.40 | Confidential information has been removed |
Treatment initiation, administration and monitoring
Six of the studies assumed that patients would undergo DXA every other year while on treatment. 20,100,141,144,146,147 Stevenson et al. 143 assumed that patients would undergo DXA at years 2 and 5. Davis et al. 34 did not include any DXA to monitor treatment with bisphosphonates. Not all of the papers were explicit about whether or not patients were assumed to have undergone DXA before starting treatment, but, in Davis et al. ,34 all costs that related to risk assessment, which may include DXA for some patients, were considered to have been already inccurred prior to treatment choice, as these were included in the cost-effectiveness analysis for risk assessment in CG146. 8 The AG considered that the inclusion of routine DXA in the model was problematic as the approach taken may differ depending on the baseline risk of the patient and the treatment being administered. For example, CG146 does not recommend that DXA is performed routinely as part of the risk assessment of patients. 8 Therefore, it is reasonable to assume that many patients may be started on the current first-line therapy, which is oral bisphosphonates, without DXA, and this is consistent with the approach recommended in the NICE-accredited NOGG guideline. 14 However, the NOGG also recommends that FRAX with BMD is used to reassess patients at the end of 5 years of bisphosphonate therapy (3 years for ZOL). On this basis, we decided to assume that patients undergo DXA when they reach the end of the intended treatment duration. We made an exception for DEN, as the intended treatment duration is much longer than for other therapies, so we assumed that DXA is undertaken every 5 years. This was based on advice from one of our clinical experts that patients receiving DEN in primary care would be likely to be reviewed in specialist care at 3 or 5 years. For the treatment sequence of ROMO followed by ALN, we assumed that a patient would undergo DXA once at the end of the 1 year of ROMO and once at the end of the 4 years of ALN. Because treatment duration in the model is based on average treatment persistence rather than the distribution of persistence across the population, the AG incorporated the cost of DXA as an annualised cost; otherwise, no DXA costs would be applied, as the average patient never reaches the intended treatment duration. This is consistent with the assumption that costs and benefits are linearly related to the duration of treatment persistence and, therefore, the individual-level variation in persistence does not need to be modelled. The cost applied for DXA is based on the NHS reference cost for direct-access DXA (£68.29 for RD50Z). 193
Four of the studies assumed that patients would attend annual general practitioner (GP) appointments to monitor treatment. 20,141,146,147 Amgen Inc. 100 assumed the same for treatments given in primary care (which included oral bisphosphonates and DEN), but assumed secondary care follow-up appointments for i.v. bisphosphonates. Kanis et al. 144 assumed one GP appointment to initiate treatment. Stevenson et al. 143 assumed two GP appointments per annum, whereas Davis et al. 34 did not include any GP appointments for monitoring. There is now a NICE QS13 that states that patients having bone-sparing treatments should have medication reviews to discuss AEs and adherence, but the frequency of the reviews is not specified. We have assumed that patients will have annual reviews and that those reviews will occur in primary care for oral bisphosphonates and RLX. For this, we applied the cost per average GP patient contact (£38.00 per 9.22 minutes). 16 For DEN, we were advised that patients would be reviewed in secondary care every 3–5 years, so we have assumed that one in four annual reviews will occur in secondary care. For i.v. bisphosphonates, ROMO and TPTD, we have assumed that the annual review occurs in secondary care as an outpatient endocrinology appointment. The cost (£150.38) for a consultant-led, non-admitted, face-to-face follow-up attendance at endocrinology outpatient has been applied [Healthcare Resource Group (HRG) currency code WF01A, service code 302]. 193
As noted previously, none of the studies identified in the review included any costs for the administration of oral therapies; this was the assumption applied in our model. UCB S.A. 20 also assumed no administration costs for s.c. therapies (i.e. DEN, TPTD and ROMO). In the Amgen Inc. submission for this MTA,100 it was assumed that DEN would be given by a general practice nurse, whereas, in the Amgen Inc. submission for TA204,147 they assumed that one injection would be administered during the annual GP visit, and therefore one additional GP appointment was required per annum for the second injection. For DEN, we assumed that patients would initiate treatment in secondary care, with the first two doses being given as an outpatient procedure using the same HRG codes as applied for i.v. IBN. Thereafter, it was assumed that DEN would be administered under a shared care agreement, with a primary care nurse providing future doses during a 15.5-minute appointment at a cost of £10.85 (based on £42.00 per hour for general practice nurse contact time). 16 This was based on advice from our clinical experts that, ideally, only the first one or two doses would be given in secondary care, although they also noted that there is significant variation in practice surrounding shared care agreements, with some local areas having a poor uptake of primary care administration.
Stevenson et al. 143 do not describe any additional administration costs for TPTD. Waugh et al. 147 included one additional GP appointment for initiation of TPTD. The AG did not consider that any additional costs were necessary for the administration of TPTD, given that it is self-administered, and an annual secondary care review has already been included for TPTD, as described previously.
Davis et al. 34 assumed that i.v. IBN is delivered during an outpatient endocrinology appointment and that i.v. ZOL is delivered as a day-case procedure using the HRG code for administration of a simple parenteral chemotherapy (SB12Z). UCB S.A. 20 assumed that administration of i.v. ZOL occurred in secondary care, but the exact source of the cost applied is unclear. In the Amgen Inc. submission for TA204, administration of i.v. bisphosphonates was assumed to occur in secondary care under the same HRG code as used by Davis et al. 34 for i.v. ZOL. However, in the Amgen Inc. submission for the current MTA,100 it was argued that the use of an oncology HRG was inappropriate; instead, the cost was based on day case and elective inpatient spells averaged over nine HRG codes related to non-inflammatory bone and joint disorders and pathological fractures. The AG was already aware of a study that compared the cost of secondary care infusion of ZOL with a home-care delivery model in a UK NHS setting. 194 In correspondence with the study author (Opinder Sahota, Nottingham University Hospitals NHS Trust, 2018, personal communication), it was stated that the reference cost, including the drug costs, for this activity was £300 per patient (£14,980 per 50 patients), and this included acquisition of the drug at a discounted (undisclosed) cost from the manufacturer. However, the income for the activity based on the tariff was much lower, at £143 per patient, which also includes the cost of drug acquisition. Based on these figures, we felt that the estimates provided by Amgen Inc. were probably too high and we decided to use the HRG codes applied in the model that informed TA464,34 but updated to the latest reference costs,193 giving a cost of £253 for day-case infusion of i.v. ZOL (day case, SB12Z delivery of simple parenteral chemotherapy at first attendance).
For i.v. IBN, no alternative estimates of administration costs were identified from the studies included in the review. Therefore, we decided to assume the same resource use as in the model used to inform TA46434 (one outpatient endocrinology follow-up appointment), but we updated the unit cost to reflect the latest reference costs,193 giving a cost of £150.
Adverse events
For oral and i.v. bisphosphonates, the AG decided not to change the approach to modelling AEs that was adopted in TA464,34 as there was no new evidence on which to base alternative assumptions identified from the review of cost-effectiveness studies.
The AG decided to include serious (i.e. leading to hospitalisation) cellulitis as an AE for DEN because it had been included in the model that informed TA204,147 although it was noted that the 10-year results of the FREEDOM study41,104 suggest that the incidence rate of cellulitis is low, at ≤ 0.2% in each of the study years. The HRG cost for a non-elective inpatient spell for minor skin conditions with interventions ranges from £2588 to £7764, depending on the level of complications and comorbidities, with a weighted average of £4467. 193 Assuming an incidence rate of 0.2% per annum and applying this weighted cost to the incident population would increase the cost of DEN by £8.93 per annum. The AG identified a paper that had estimated the QALY loss of cellulitis as 0.005 QALYs (reduction in EQ-5D score by 26.3% for 7 days), based on a comparison of EQ-5D scores in a prospective RCT of antibiotics versus placebo to prevent recurrent cellulitis. 195 This is equivalent to a loss in INMB of £0.20 per annum. As the duration of treatment persistence with DEN in the model is (confidential information has been removed) years, this would suggest that the total impact of cellulitis is a reduction in INMB for DEN of the order of (confidential information has been removed). Costs and QALY losses for cellulitis per year of exposure to DEN have been included in the base-case model.
The AG notes that the Medicines and Healthcare products Regulatory Agency (MHRA)/Commission on Human Medicines (CHM) has issued advice regarding the risk of atypical femoral fractures for both DEN and bisphosphonates,28 but this advice states that these events are rare and that they are primarily related to long-term use. The AG decided not to include atypical femoral fractures as a separate AE in the model. This was, first, because the HRs for fractures estimated from the clinical trials would already include any impact of the drug on atypical femoral fractures, and including them as a separate event may result in these outcomes being double-counted in the model. The AG accepts that atypical femoral fractures may not have been captured in the trials if they occur only after long-term use of osteoporosis treatment. However, the AG notes that the base-case scenario incorporates real-world treatment persistence, which is much shorter than the intended treatment duration for both bisphosphonates and DEN, making these AEs that occur with long-term use less relevant to these treatments as they are modelled.
The AG notes the MHRA/CHM advice regarding the risk of ONJ in patients receiving bisphosphonates. 28 The advice states that the risk is considered to be substantially higher in those receiving i.v. bisphosphonates in the treatment of cancer than in those receiving i.v. bisphosphonates for the treatment of osteoporosis, and the risk is said to be related to cumulative dose. Similarly, the MHRA/CHM advice on DEN states that it is a common side effect for those patients receiving DEN for the treatment of cancer and recommends dental examination and preventative dentistry treatment in all patients starting DEN for cancer. 28 It should be noted that the dose for cancer is 120 mg monthly, rather than 60 mg every 6 months, and, in the context of using DEN to prevent osteoporotic fracture, such precautions are recommended by the MHRA/CHM only for those with risk factors. 28 The AG also notes that a systematic review by Boquete-Castro et al. 196 states ‘it should be stressed that most of the adverse effects of DEN appear with doses of 120 mg. Adverse effects with doses of 60 mg are directly related to the duration of treatment.’. Although there appears to be less concern regarding ONJ in patients receiving anti-resportive agents for osteoporosis than for ONJ in patients receiving anti-resportive agents for cancer, the AG decided to incorporate this AE in the model to establish the likely impact on the cost-effectiveness estimates.
The AG examined a systematic review reported by Khan et al. ,197 which was conducted to inform an international consensus statement on ONJ. Khan et al. 197 conclude from their review that ‘the incidence of ONJ in the osteoporosis patient population appears to be very low, ranging from 0.15% to < 0.001% person-years of exposure and may be only slightly higher than the frequency observed in the general population’. For oral bisphosphonates, the review by Khan et al. 197 identified a UK (Scottish) prospective case series that reported an incidence for ONJ of one case per 4545 drug patient-years (0.022%) for patients exposed to ALN. 198 This was within the incidence range of 1.04–69 cases per 100,000 patient-years reported by the other studies identified in the review by Khan et al. 197 It should be noted that Lo et al. 199 found, in a cross-sectional survey conducted in the USA, that prevalence of ONJ was related to duration of exposure, with estimated prevalences of 0%, 0.05% and 0.21% in patients exposed for < 2 years, 2 to just under 4 years and ≥ 4 years. For i.v. bisphosphonates, Khan et al. 197 reported an incidence range of 0–90 per 100,000 patient-years. The incidence estimated across five RCTs is given by Khan et al. 197 as < 1 in 14,200 patient-years of exposure (< 0.007%). For DEN, Khan et al. 197 reported that the estimates of incidence ranged from 0 to 30.2 per 100,000 patient-years. However, more recent data from the 10-year follow-up of the FREEDOM trial41,104 gave an exposure-adjusted incidence of ONJ of 5.2 per 10,000 participant-years (0.052%). The SmPC for DEN states that the incidence is related to the duration of exposure. 200 Given that there is a lack of comparative data on the incidence of ONJ across the different forms of anti-resportives, and that the estimates for the different anti-resportive drugs all relate to different periods of exposure, we have decided to assume the same incidence per year of drug exposure across all anti-resportives. This was based on the estimate from the prospective case series in Scotland. 198 This was because this estimate fell within the range provided by Kahn et al. 197 for each type of anti-resportive (oral bisphosphonates, i.v. bisphosphonates and DEN) and was based on the average duration of use in clinical practice; therefore, it would be more applicable to the duration of treatment persistence modelled in this analysis.
A paper201 measuring health utility in patients with ONJ was identied using ad hoc searches of Google Scholar. It reported utility measured by the EQ-5D in 34 cancer patients with bisphosphonate-associated ONJ. However, it should be noted that it was not compliant with the reference case in several ways. First, although the pateints had all themselves experienced ONJ, they were asked to value clinical vignettes describing different stages of ONJ in patients who also have cancer, rather than being asked to value their own health state. Second, the utilty weights applied were from the US, rather than the UK, valuation set. However, given the lack of alternative estimates, we calculated the average utility decrement based on the utility decrements (relative to patients with cancer but without ONJ) for stages 2 and 3 (–0.33 and –0.61, respectively) and the distribution of ONJ stages (two were stage 3 and nine were stage 2) across the UK prospective case series reported by Malden and Lopes. 198 This gave an average utility decrement of –0.38. The mean time from diagnosis to healing (6.5 months) was taken from the same study198 to give an average QALY loss of 0.206 per case of ONJ. The NHS reference cost for a minor outpatient oral surgical procedure was applied (HRG code CD03A, £166)193 to account for the cost of surgical management, as most patients in the Malden and Lopes198 case series had some form of surgical management, with debridement being the most common procedure. We note that the Malden and Lopes198 case series may have missed less severe cases of ONJ, which would be classed as stage 1. However, as cancer pateints with stage 1 ONJ were found not to have EQ-5D values significantly different from those of cancer patients without ONJ (Miksad et al. 201), and patients with stage 1 would be more likely to be managed conservatively,197 we felt that exclusion of this group was unlikely to significantly bias the estimates of costs and QALYs resulting from ONJ, provided they are excluded from both the incidence estimates and the estimates of costs and QALYs per case. Costs and QALY losses per year of exposure to DEN, oral bisphosphoantes and i.v. bisphosphonates have been included in the base-case analysis, but we note that their impact is very small owing to the extremely low incidence.
Kanis et al. 141 applied HRG costs and a utility loss in the year after VTE, but not beyond. The utility decrement was based on an assumption, as no estimate was identified from the literature. No other models identified in the literature review included VTE as an adverse outcome. Rather than extend the AG model to incorporate the competing risk of VTE in patients at risk of fracture, the AG decided to estimate the average discounted lifetime cost and QALY loss attributable to VTE using a published model (Pandor et al. 202). As this model was constructed to estimate the costs and benefits of thromboprophylaxis, the AG removed all costs and QALY losses attributable to the thromboprophylaxis itself, including the increased risks of bleeding during the prophylaxis, thereby reducing the model to a comparison of two groups whereby the only difference between them is their risk of VTE. All conseqeunces related to asymptomatic VTE were removed from the model as these were not considered relevant, as it is only symptomatic VTE that has been recorded as an adverse outcome. The AG then compared costs, QALYs and the number of symptomatic VTEs for the strategies of prophyalixs for all and prophyalixs for none. These figures were used to estimate the average discounted lifetime cost and QALY loss per symptomatic VTE, which were estimated to be £1890 and 0.77 QALYs for a patient with a starting age of 50 years.
The largest RCT reporting VTE as an adverse outcome for RLX was the MORE study,51,102 which reported that 25 out of 2557 patients receiving RLX experienced VTE, whereas eight out of 2576 patients receiving placebo experienced VTE. Based on the increased incidence observed in the MORE study, the excess rate of VTE attributable to RLX was estimated to be 0.67% over the 3-year study period. Ettinger et al. 51 did not report the proportion of these events that were PEs, but did say that a mixture of PE and DVT events were observed. The study by Silverman et al. 50 did report the breakdown by type of VTE: four of the 12 VTE events in the RLX-treated arm were PEs. It should be noted that, in the model by Pandor et al. ,202 30% of symptomatic VTE events are PEs, which is reasonably consistent with the ratio of PE to DVT observed in the RLX arm of the study by Silverman et al. 50
By applying the estimates of costs and QALYs per symptomatic VTE derived from Pandor et al. 202 to the excess incidence observed in the MORE study, we estimated a reduction in INMB of £116 per patient enrolled in the MORE study when valuing a QALY at £20,000 (and assuming that VTE occurred at 50 years of age). Given that the average duration of persistence in the model for treatment with RLX is 1.38 years, if we assume that the absolute risk is proportional to the time spent on treatment, the INMB loss attributable to VTE would be of the order of £53 per patient started on treatment (cost of £5.80, QALY loss of 0.00237). It should be noted that the QALY losses would be fewer for older patients experiencing VTE, as much of the QALY loss is attributed to long-term sequelae that have a greater impact on patients with a higher life expectancy. However, when assuming a start age of 75 years, the INMB loss attributable to VTE per patient started on RLX was estimated to be £47 (compared with £53 for patients aged 50 years), so the error associated with applying costs and QALYs as estimated for a patient aged 50 years was not considered likely to have resulted in a large bias. The average cost and QALY loss attributable to excess VTE were applied to each patient initiating treatment with RLX, with the risk proportional to time spent on treatment, such that they have a bigger impact in the sensitivity analysis assuming full treatment persistence.
Disease costs
The costs of fracture in the TA46434 model were based on a UK resource use study reported in two papers by Gutiérrez et al. ,203,204 which used a general practice database (The Health Improvement Network) to estimate resource use for those who fractured compared with matched controls. Unit costs from the 2013/14 reference costs205 and the 2014 PSSRU unit costs206 were then applied to this resource use to estimate the total cost in the year of fracture and in the subsequent years following fracture. None of the studies included in the review provided a more recent source of resource use. Two studies20,100 reported using costs based on Gutiérrez et al. ,203,204 and five141,143,144,146,147 used estimates from the literature from less recent publications.
The AG identified two additional relevant UK studies in the systematic database search conducted to identify published cost-effectiveness analyses. Lambrelli et al. 207 used a methodology similar to that employed by Gutiérrez et al. , but using an alternative primary care database (the CPRD), with linkage to a secondary care database [Hospital Episode Statistics (HES)]. Lambrelli et al. 207 reported costs in the year following hip fracture of £7359. Leal et al. 208 reported higher costs, of £14,163, based on an analysis of HES data alone. This analysis excluded activity in primary care and was focused solely on patients admitted to hospital following fracture. For comparison, the estimate used in TA464,34 based on the data from Gutiérrez et al. ,203,204 when excluding the costs of home help, was £6274. The AG decided to use the data from TA464,34 and to adjust it using 2017 PSSRU inflation indices,16 as the two studies by Gutiérrez et al. 203,204 provided a consistent methodology for estimating both hip and non-hip fractures, included activity in both primary and secondary care settings and incorporated prescription costs.
Costs for home help and residential care/nursing home admission were estimated by uplifting the estimates used in TA46434 using PSSRU inflation indices. 16
The costs applied in the first and subsequent years following fracture are summarised in Table 8.
| Parameter | Fracture | New admission to residential care | |||
|---|---|---|---|---|---|
| Hip | Vertebrae | Proximal humerus | Wrist | ||
| Costs in year of fracturea (£) | 8568 | 4342 | 1358 | 896 | 24,519 |
| Costs in subsequent yearsa (£) | 110 | 345 | 73 | 73 | 24,519 |
| Utility multiplier in year of fracture | 0.55b | 0.68b | 0.78c | 0.83b | 0.625d |
| Utility in subsequent years | 0.86b | 0.85b | 1.00c | 0.99b | 0.625d |
Health-related quality of life
We conducted a rapid update of the systematic review of HRQoL studies conducted for TA464. 34 This comprised a systematic serach for studies reporting EQ-5D utility data for the year post fracture. Further details on the review methods and findings can be found in Appendix 16. In summary, the review identified four papers all reporting outcomes from the International Costs and Utilities Related to Osteoporotic Fractures Study (ICUROS). 209,210,212,213 This study was previously identified in the review conducted for TA464. 34 However, the four new papers identified reported additional data. ICUROS was an international multicentre study; two of the papers210,212 reported outcomes from specific countries that formed subgroups of the overall ICUROS population. The other two papers reported longer-term follow-up from the overall international data set. One of these papers213 restricted its analysis to those patients with complete follow-up on both the EQ-5D and the EQ-VAS, which resulted in a smaller population available for analysis. The paper reporting outcomes from the international cohort without restricting to patients who also reported EQ-VAS was chosen, as it was the larger data set. 209 This paper reported utility multipliers for the year following fracture and subsequent years for hip, wrist and vertebral fractures. The multipliers presented in the paper were applied directly in the model. However, no data were presented in this paper for proximal humerus fractures. The only paper reporting outcomes following proximal humerus fracture was the one reporting outcomes for the Australian subpopulation of ICUROS. 210 Although these data were specific to a different country, results were presented in an appendix using the UK time trade-off tariff for the EQ-5D. From these data, we calculated utility multipliers for the year following humerus fracture and subsequent years, using the same methodology as employed in the international paper for the other fracture types. The utility values applied are summarised in Table 8.
Model validation
The model is designed to operate in several different modes, which facilitates debugging and validation. A description of the general validation methods used, and the specific methods used to validate each structural change to the model, is provided in Appendix 17.
Approach to sensitivity analysis
A PSA has been conducted to estimate the mean costs and QALYs gained when taking into account the uncertainty in the parameter values used in the model. In general, parameters were estimated using the following distributions: gamma distributions for costs, log-normal distributions for HRs (except the efficacy estimates, which were based on the CODA samples from the NMA) and beta distributions for utility values and probabilities. The treatment persistence estimates were assumed to be normally distributed, but maximum and minimum values were applied to ensure that they did not fall below zero or exceed the intended treatment duration. None of the parameters used to estimate fracture risk, in the absence of treatment, was varied in the PSA. This was to ensure that a specific set of patient characteristics was consistently mapped to the same survival curve for fracture-free survival without any parameter uncertainty. The following additional parameters were not varied in the PSA: drug prices; discount rates; unit costs sourced from the PSSRU; utility in the second year after proximal humerus fracture; life expectancy after fracture associated with excess mortality; unit costs for prescriptions after fracture; the proportion of self-funders for residential care; and costs and QALY decrements for AEs.
Structural sensitivity analyses were conducted to explore whether or not the results were sensitive to different model assumptions. To reduce model computation time, the structural sensitivity analyses were conducted using mid-point parameter inputs, rather than using the full PSA version of the model. Any structural sensitivity analyses conducted during TA464 that showed minimal impact were not repeated here. The structural sensitivity analyses that were found to have the biggest impact in TA464 were those related to treatment perisistence and AEs.
We conducted the following structural sensitivity analyses:
-
assuming full persistence with treatment up to the intended treatment duration
-
alternative assumptions for offset periods [1-year offset periods for RIS, IBN (oral and i.v.) and TPTD, and an offset period equal to treatment duration for ZOL, DEN and RLX]
-
HRs for bisphosphonates based on class effect estimate (the predicted HR for a new drug in the same class).
We noted that both the Amgen Inc. 100 and UCB S.A. 20 submissions focused on high-risk subgroups. To generate some comparable results, we conducted an exploratory scenario analysis in which we fixed the patient characteristics to obtain an estimate of the cost-effectiveness for an example high-risk patient. The patient characteristics were chosen to match those used in the UCB S.A. model20 as closely as possible, although an exact match was not possible as the AG model uses FRAX for unknown BMD whereas the UCB S.A. model20 specifies the T-score of the patient. The patient characteristics selected were female, aged 75 years, had a history of fracture, a body mass index of 21 kg/m2 and one additional risk factor, which was chosen to be moderate alcohol consumption (3–6 units per day) to give a FRAX risk that was similar to the FRAX risk of 30% reported for the patient population in the UCB S.A. economic model. This example patient had a FRAX score of 31.6%. The model was then run for 500,000 PSA samples with these patient characteristics fixed, but allowing life expectancy to be sampled.
Base-case results
The base-case results are based on model outcomes for 2 million patients from the PSA version of the model. For each individual patient, a unique set of PSA parameter inputs was sampled (see Approach to the sensitivity analysis). As the cost-effectivenss is dependent on absolute risk of fracture, results are provided for 10 risk categories, each containing approximately 200,000 patients. The results presented for each risk category are based on the average costs and QALYs across the simulated patients falling into that risk category. It should be noted that the patients in the risk categories differ for QFracture and FRAX, as each risk category is based on a decile of risk scores across the population modelled to ensure that each risk category contains approximately the same number of patients and is not underpowered relative to the other risk categories.
The adverse clinical outcomes avoided (i.e. fractures, fatal fractures and new admissions to nursing/residential care) compared with no treatment, when using QFracture to estimate fracture risk, are summarised in Table 9, along with the life-years gained (the equivalent data when using FRAX to estimate fracture risk can be found in Appendix 18). It should be noted that, as these are based on the mean outcomes from the PSA, which incorporates estimates of efficacy based on the CODA samples from the NMA, it is possible for a drug with a mid-point HR close to 1 and a broad CrI to have an adverse impact on fracture, on average, across the PSA samples. This is the case for RLX, for which the HR for hip fracture was 0.93 (95% CrI 0.30 to 2.76), resulting in a predicted small increase in hip fractures, on average, across the PSA samples. This was not observed when running the model using the mid-point HRs; therefore, it clear that it is being caused by the distribution of CODA samples for the hip fracture HR for RLX.
| Drug | Number of adverse clinical outcomes avoided per 100,000 patients treated, when compared with no treatment | Total life-years gained per patient vs. no treatment | ||||||
|---|---|---|---|---|---|---|---|---|
| Total fractures | Hip fracture | Vertebral fracture | Proximal humerus fracture | Wrist fracture | Nursing home/residential care admission | Fatal fracture | ||
| ALN | 353 | 93 | 85 | 45 | 130 | 16 | 14 | 0.0011 |
| RIS | 366 | 83 | 85 | 52 | 147 | 15 | 13 | 0.0010 |
| IBN (oral) | 295 | 81 | 85 | 35 | 94 | 13 | 13 | 0.0010 |
| IBN (i.v.) | 147 | 52 | 55 | 9 | 31 | 8 | 9 | 0.0007 |
| ZOL | 617 | 145 | 161 | 80 | 231 | 25 | 26 | 0.0020 |
| RLX | 37 | –16 | 27 | 17 | 9 | 5 | –1 | 0.0005 |
| DEN | 507 | 172 | 182 | 42 | 110 | 41 | 30 | 0.0029 |
| TPTD | 660 | 176 | 147 | 91 | 247 | 31 | 27 | 0.0020 |
| ROMO/ALN | 833 | 248 | 158 | 129 | 298 | 56 | 34 | 0.0030 |
It can be seen from Table 9 that ROMO/ALN results in the largest number of fractures avoided, followed by TPTD. DEN has fewer fractures avoided in total than TPTD, but a higher number of life-years gained. This is because the life-years gained are dependent on both the number and the type of fractures avoided, as only hip and vertebral fractures have an excess mortality risk. It can be seen that DEN avoids a similar number of hip fractures as TPTD, but DEN avoids more vertebral fractures than TPTD, meaning that there are fewer fatal fractures for DEN, which results in a greater number of life-years gained.
The ICERs for non-bisphosphonates versus no treatment and the treatment with maximum INMB (when valuing a QALY at either £20,000 or £30,000) for each risk category are summarised in Table 10. We used a regression using a generalised additive model to estimate the relationship between INMB and absolute risk as a continuous variable for both QFracture and FRAX. Plots of the predicted INMBs when valuing a QALY at £20,000 for each non-bisphosphonate treatment are summarised in Figure 11 for QFracture and in Figure 12 for FRAX (results for ROMO/ALN are confidential and have been removed). A negative INMB in Figures 11 and 12 indicates an ICER of > £20,000 per QALY compared with no treatment. It can be seen that the INMB relative to no treatment increases with increasing baseline risk for both QFracture and FRAX for DEN, TPTD and ROMO/ALN, but the INMBs remain under zero across the range of fracture risk observed in the population eligible for risk assessment. For RLX, the relationship between fracture risk and INMB is less clear, particularly when using FRAX to estimate fracture risk. The INMB of RLX versus no treatment predicted by the regression does go above zero from a FRAX score of 32.6–37.8%, but it should be noted that the predictions become more uncertain as the risk scores increase, as they are informed by estimates from fewer simulated patients. For example, only 2% of patients have a FRAX score of > 30% and 0.2% of patients have a FRAX score of > 40%, which is why we do not present the INMB plots for FRAX scores of > 40%. The risks of fracture predicted by QFracture are generally lower than the risks predicted by FRAX, meaning that only 0.3% have a risk score of > 30% when using QFracture. The plot of INMB versus risk for RLX may also be less well defined for RLX than for the other non-bisphosphonates, as RLX resulted in the fewest number of fractures being prevented, making the estimates of average INMB gains from prevented fractures more uncertain.
| Drug | ICERs by risk decile | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | All | |
| Qfracture score (%) | 0.5 | 0.7 | 1.0 | 1.4 | 2.0 | 2.7 | 3.9 | 5.5 | 8.4 | 16.0 | NA |
| ALN | £675,004 | £290,229 | £125,805 | £126,025 | £77,059 | £65,281 | £30,452 | £14,820 | £5622 | Dominates | £31,200 |
| RIS | £829,832 | £319,027 | £129,889 | £100,618 | £81,404 | £64,979 | £32,482 | £17,119 | £7235 | Dominates | £33,840 |
| IBN (oral) | £948,571 | £301,165 | £119,370 | £137,375 | £93,736 | £68,805 | £34,713 | £21,840 | £9443 | Dominates | £38,321 |
| IBN (i.v.) | Dominated | Dominated | Dominated | Dominated | Dominated | £4,373,315 | £1,250,818 | £564,407 | £398,475 | £266,492 | £1,442,071 |
| ZOL | Dominated | £2,984,339 | £808,583 | £723,860 | £442,296 | £353,780 | £210,441 | £127,491 | £93,903 | £60,300 | £236,247 |
| RLX | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated |
| DEN | £1,794,421 | £1,092,301 | £1,868,896 | £632,830 | £523,142 | £502,655 | £462,072 | £250,729 | £166,441 | £126,392 | £388,796 |
| TPTD | £8,610,782 | £5,871,874 | £3,731,997 | £3,083,847 | £2,356,350 | £1,964,475 | £1,366,400 | £971,695 | £671,001 | £457,894 | £1,419,377 |
| ROMO/ALN | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| Which treatment has maximum INMB at £20,000 per QALY | No treatment | No treatment | No treatment | No treatment | No treatment | No treatment | No treatment | ALN | ALN | ALN | No treatment |
| Which treatment has maximum INMB at £30,000 per QALY | No treatment | No treatment | No treatment | No treatment | No treatment | No treatment | No treatment | ALN | ALN | ALN | No treatment |
| FRAX score (%) | 3.1 | 4.3 | 5.0 | 5.6 | 6.2 | 7.3 | 8.8 | 10.7 | 14.9 | 25.1 | NA |
| ALN | £28,541 | £27,325 | £16,808 | £15,524 | £11,362 | £8951 | £3791 | Dominates | Dominates | Dominates | £3659 |
| RIS | £32,429 | £27,654 | £15,575 | £17,389 | £11,265 | £8736 | £4572 | Dominates | Dominates | Dominates | £4181 |
| IBN (oral) | £34,519 | £27,349 | £17,728 | £16,459 | £12,209 | £12,389 | £6035 | £734 | Dominates | Dominates | £5333 |
| IBN (i.v.) | £1,214,068 | £853,480 | £443,563 | £430,771 | £342,182 | £362,332 | £367,423 | £215,680 | £163,225 | £111,944 | £299,662 |
| ZOL | £170,998 | £145,587 | £110,846 | £96,012 | £82,355 | £82,446 | £63,432 | £51,057 | £37,737 | £20,257 | £68,512 |
| RLX | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | £57,050 | Dominated | Dominated | Dominated |
| DEN | £398,751 | £250,782 | £195,106 | £220,601 | £184,386 | £193,385 | £140,582 | £95,158 | £89,300 | £58,730 | £145,830 |
| TPTD | £1,254,448 | £1,115,769 | £832,835 | £745,024 | £632,511 | £622,664 | £542,248 | £439,478 | £343,693 | £244,558 | £549,324 |
| ROMO/ALN | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| Which treatment has maximum INMB at £20,000 per QALY | No treatment | No treatment | RIS | ALN | RIS | ALN | ALN | ALN | ALN | ALN | ALN |
| Which treatment has maximum INMB at £30,000 per QALY | ALN | ALN | RIS | ALN | RIS | ALN | ALN | ALN | ALN | ALN | ALN |
FIGURE 11.
The INMB as a function of absolute fracture risk, as determined by QFracture.
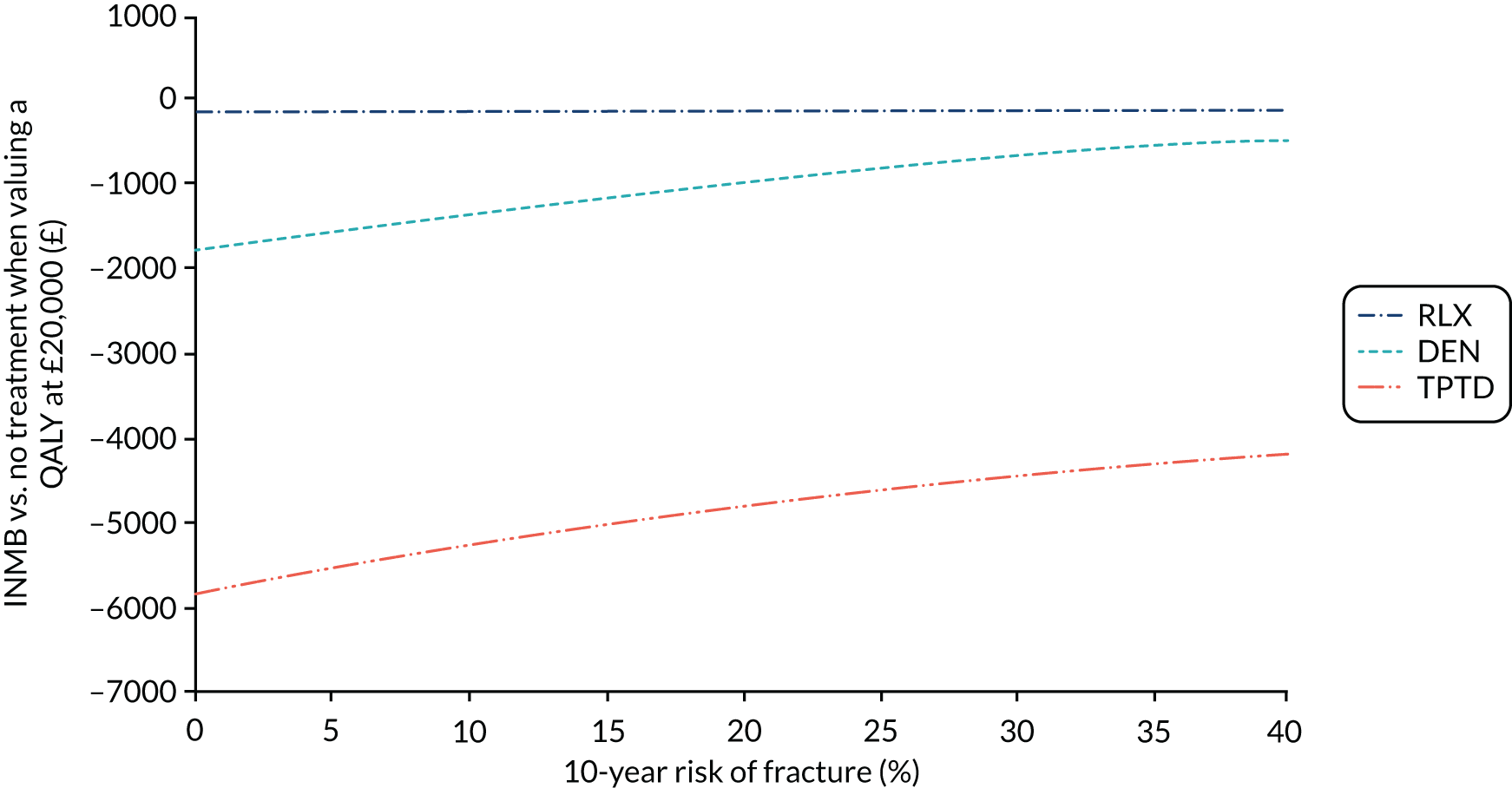
FIGURE 12.
The INMB as a function of absolute fracture risk, as determined by FRAX.
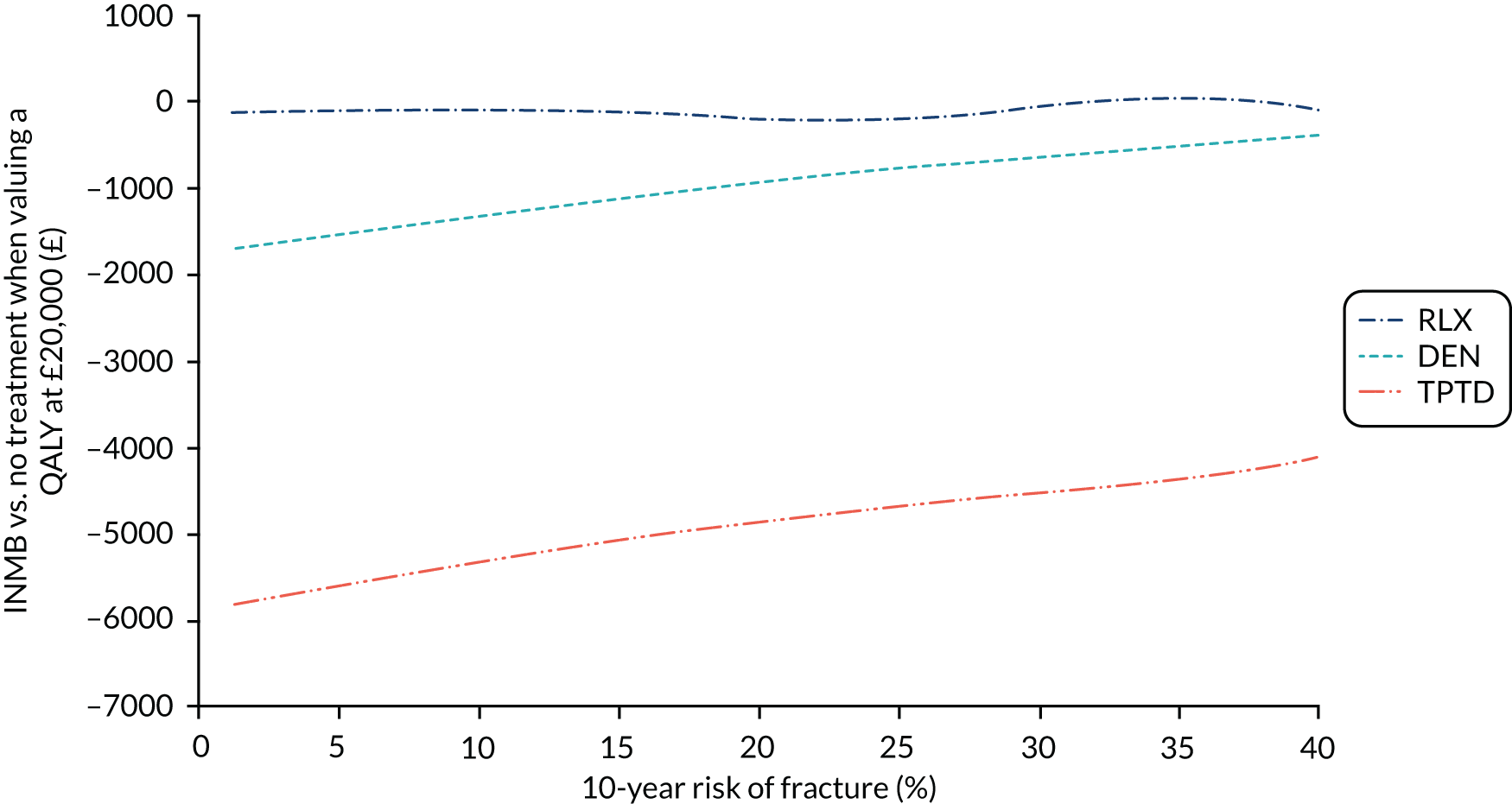
The AG also ran the regression of INMB against QFracture and FRAX when assuming that a QALY is valued at £30,000. The predicted INMBs remained under zero across the full range of risk scores observed for RLX, TPTD and ROMO/ALN for both QFracture and FRAX. For DEN, the predicted INMB was above zero, indicating that DEN has an ICER of < £30,000 compared with no treatment for FRAX scores of > 45%; it remained under zero for the full range of QFracture scores. However, the AG notes that the estimates of INMB at these very high levels of risk are uncertain as they are informed by < 0.05% of the simulated population.
A full incremental analysis for each risk category is presented in Appendix 19 for QFracture and in Appendix 20 for FRAX. The optimal treatment (i.e. the one with the maximum INMB) when valuing a QALY at either £20,000 or £30,000 is summarised in Table 10 for easy reference. It can be seen that the optimal treatment when valuing a QALY at £20,000 is no treatment for patients in the lower-risk categories and oral bisphosphonates for patients in the higher-risk categories. When valuing a QALY at £30,000, oral bisphosphonates have the maximum INMB even in the lowest-risk category when using FRAX to estimate fracture risk (average risk of 3.1%), but no treatment is still the optimal strategy in the lowest-risk category when using QFracture to estimate fracture risk. Using the predicted INMBs from the regression we can say that oral bisphosphonates have maximum INMB from a FRAX score of 4.5% and from a QFracture score of 5.2% when valuing a QALY at £20,000.
The i.v. bisphosphonates never have a higher INMB than the oral bisphosphonates. However, ZOL has a positive INMB compared with no treatment for a fracture risk of 31.1% for Qfracture and of 22.5% for FRAX. Conversely, i.v. IBN is always dominated by i.v. ZOL because of the higher costs associated with quarterly administration and the poorer efficacy estimates.
Raloxifene is dominated by no treatment (higher costs and fewer QALYs gained) across all QFracture risk categories and across all but one FRAX risk category (category 8, with an average risk of 10.7%). This is explained by the few numbers of fracture prevented and the VTE risk associated with RLX.
Teriparatide is consistently dominated by ROMO/ALN across all risk categories for both QFracture and FRAX, despite having similar efficacy estiamtes. This is because the treatment duration and offset period for the ROMO/ALN sequence, which determine how long the efficacy estimates are appied in the model, are based on the combined duration of the treatment sequence but the cost for the ALN part of the sequence is much lower than the cost of TPTD.
Sensitivity analyses results
The results for the structural sensitivity analyses (conducted using mid-point parameter estimates) are presented in Appendix 21. In broad terms, the results for non-bisphosphonates were consistent with the base-case analysis in that none of the non-bisphosphonates had an ICER of < £30,000 per QALY when compared with no treatment in any of the QFracture or FRAX risk categories across any of the sensitivity analyses examined.
The exploratory scenario analysis examining a population with fixed patient characteristics, chosen to give a FRAX score of approximately 30%, resulted in an ICER of £13,544 for DEN compared with no treatment (see Appendix 21, Table 74). The ICER for ZOL compared with no treatment was £11,427, but ZOL was extendedly dominated, leaving ALN, DEN and ROMO/ALN on the cost-effectiveness frontier. ALN remained the optimal treatment when valuing a QALY at £20,000, as DEN compared with ALN had an ICER of £26,977. However, this scenario analysis shows that the results may be more favourable when considering specific high-risk groups, even though the ICER for DEN compared with no treatment in the highest decile of FRAX risk scores, in which the average risk score was 25%, was > £30,000 per QALY. However, the AG believes that this exploratory scenario analysis should be interpreted cautiously, given that it is based on a single example set of patient characteristics and the cost-effectiveness may differ for patients with different characteristics but the same FRAX score. It is also noted that the results for the same patient were qualitatively different when using QFracture to estimate fracture risk, as the risk was much lower (13.3%) than the fracture risk obtained when using FRAX. In this scenario, none of the non-bisphosphonates had an ICER of < £30,000 when compared with no treatment (see Appendix 21, Table 75) and using QFracture to estimate absolute fracture risk.
Discussion
A key strength of the approach we have taken is that we have been able to adapt the model used in TA464 to allow the cost-effectiveness of non-bisphosphonates to be assessed in a manner consistent with the approach used previously to assess the cost-effectiveness of bisphosphonates. However, although the overall model structure and many of the data inputs have remained unchanged to maintain consistency, there are several differences that should be noted. We have updated the estimates of treatment persistence used for oral bisphosphonates to incorporate a new data source identified in the UCB S.A. company submission. 20 This has increased the duration of treatment persistence for oral bisphosphonates threefold. We have incorporated monitoring costs for bisphosphonates consisting of annual follow-up appointments to encourage persistence and manage AEs and DXA when completing treatment to assess the need for continued treatment. We have applied the HRs from the NMA for each individual bisphosphonate, as per the original AG report for TA464,34 rather than the estimates based on the bisphosphonate class effect as presented in the addendum160 that followed the original assessment report. However, this only affects the incremental cost-effectiveness of non-bisphosphonates relative to bisphosphonates. We have incorporated ONJ, VTE and cellulitis as AEs in the model. The utility values applied following fracture in the revised model are based on an updated systematic review of utility estimates. The costs following fracture have been uplifted to reflect price changes over time, and the drug costs were updated to reflect current prices. For consistency, we have used non-vertebral fracture HRs for wrist fractures for all interventions owing to few data on this outcome for non-bisphosphonates, whereas previously we used wrist fracture-specific outcomes for the bisphosphonates, as the data were less sparse when considering only the bisphosphonate interventions.
Although assessing the cost-effectiveness of non-bisphosphonates was the objective of this analysis, it is noted that the level of fracture risk at which the oral and i.v. bisphosphonates become cost-effective is higher than in the analysis that informed TA464. 34 This is due to the inclusion of monitoring costs, which add an additional £52 per annum to the drug costs, which are around £10 per annum. However, these revised estimates of cost-effectiveness for oral bisphosphonates appear to be reasonably consistent with the intervention thresholds specified in the NICE QS149,13 which provide age-related intervention thresholds varying from a 10-year absolute risk level of 5.9% in patients aged 40 years to 20% in patients aged ≥ 70 years. In addition, it is noted that TA4649 recommends i.v. bisphosphonates for patients with a fracture risk of ≥ 10%, but i.v. IBN and ZOL had ICERs of > £30,000 at this risk level in the revised analysis. Again, this is likely to be as a result of the incorporation of additional costs for monitoring in secondary care and the correction to the administration costs for i.v. IBN.
The models in the UCB S.A. 20 and Amgen Inc. 100 submissions both focused their analysis only on higher-risk subgroups of the population specified in the scope, whereas the AG model provides cost-effectiveness estimates for 10 risk categories covering the whole population eligible for risk assessment under CG146. 8 It is therefore difficult to compare the results directly. However, the AG model provides much higher ICERs than those provided by the analyses described in the UCB S.A. 20 and Amgen Inc. 100 submissions, even for the highest FRAX and QFracture risk categories, although an exploratory scenario analysis examining an example high-risk patient with a FRAX score of approximately 30% resulted in an ICER for DEN compared with no treatment that was < £30,000 per QALY. This finding suggests that the cost-effectiveness estimates for some non-bisphosphonates may be more favourable for specific high-risk patients, although the AG notes that this scenario analysis should be interpreted somewhat cautiously, as cost-effectiveness may differ for patients with a similar FRAX score.
There are several key differences between the AG analysis and the analyses presented in the UCB S.A. 20 and Amgen Inc. 100 submissions that should also be noted when interpreting these differences. The model in the Amgen Inc. submission100 incorporated a much higher cost of administration for i.v. ZOL than the AG model (£559 vs. £253), which resulted in a more favourable comparison of DEN with ZOL. The model in the Amgen Inc. submission100 assumed that all DEN treatments would be administered in primary care, whereas the AG model assumed that the first two DEN treatments would be given in secondary care, which substantially increases the administration costs for DEN. The model in the Amgen Inc. submission100 applied a 1-year offset to all drugs, which is unfavourable compared with what the AG assumed for all drugs except DEN and RLX. The approach taken to model mortality following fracture differed in the models in the Amgen Inc. 100 and UCB S.A. 20 submissions, which allowed for an increased risk of mortality that persisted beyond the 6-month time frame assumed by the AG for excess mortality attributable to fracture. However, it was not possible to assess the impact of the different assumptions on mortality attributable to fracture in the AG model because of the different model structures employed. The model in the UCB S.A. submission20 applied different efficacy estimates at different time points (different estimates every 6 months, up to 4 years). The AG found that restricting the NMA to studies reporting vertebral fractures at 12 months did not provide any evidence to suggest different treatment effects when the analysis is limited to specific outcome measurement times. Based on this, the NMA used to inform the AG model incorporated outcomes reported at the longest available time point for each study, and assumed that the fracture event rate is constant over time. UCB S.A. applied the maximum of a time-dependent RR for recent fracture and the RR of having had a prior fracture according to FRAX. In contrast to this, the AG model included HRs that increase the risk of fracture following an incident fracture, which are applied for the remainder of the model. However, in the AG model, the increased risk incoporated in the QFracture and FRAX scores is removed at the time of the incident fracture. It is unclear what effect these different approaches have had on the estimates of future fracture risk following an incident fracture. UCB S.A. applied different persistence assumptions for patients receiving ALN following ROMO than for patients receiving ALN from the start of the model, whereas the AG assumed that a patient’s persistence with ALN treatment woud be independent of whether or not they had previously received ROMO.
One of the key limitations of the AG analysis is that we have assumed that all of the treatment strategies modelled are viable options for all patients in the population. This allowed us to run the model once for the whole population eligible for risk assessment and to determine a single absolute risk threshold for cost-effective intervention for each treatment. Applying a strict interpretation of the licensed indications for each treatment would have required running the analysis multiple times for different groups that have different treatment options, which was not feasible. Although incremental analyses are usually conducted over a set of potentially interchangeable treatments, in reality, it is often the case that some of the cohort of patients who are eligible for one treatment would be contraindicated for another, and allowances are made for this when interpreting the cost-effectiveness results. For example, it is possible to rank the treatments in order of decreasing INMB and treat with the next most cost-effective treatment when the optimal treatment is contraindicated.
Similarly, although we have not explicitly conducted separate analyses within and between particular drug classes, it is possible to use the INMB estimates provided to identify the optimal treatment in a particular class. For example, deleting the RLX, TPTD and ROMO/ALN rows from the results tables shown in Appendices 14 and 15 and examining the INMBs estimates for the remaining interventions would allow the optimal treatment to be identified within the class of anti-resportives (ALN, RIS, IBN, ZOL and DEN). Alternatively, deleting the bisphosphonate rows from the tables would allow the optimal treatment to be identified for patients for whom bisphosphonates are contraindicated.
The AG economic model assumes that the relative treatment effect (i.e. HR) is consistent across all populations included in the scope, despite there being heterogeneity in terms of sex, risk factors (e.g. prior fracture and steroid use) and baseline risk across studies included in the NMA. However, there was no evidence that treatment effect varied with age, sex or baseline risk, based on the meta-regression conducted for the NMA outcomes of fracture and BMD.
We note that there are limited data on the long-term persistence for all treatments, but particularly for the non-bisphosphonates, and the estimates of treatment persistence for TPTD and DEN, in particular, are based on a fairly crude extrapolation of Kaplan–Meier plots for treatment discontinuation. However, the sensitivity analyses in which patients were assumed to persist for the full intended treatment duration did not result in ICERs falling under £30,000 per QALY for any of the non-bisphosphonate treatments.
The economic analysis of ROMO is based on the assumption that it will be used in sequence with 4 years of ALN and that the efficacy observed during the 24 months of the ARCH83 RCT will continue during the full 4 years of ALN. This results in the treatment effect being extrapolated beyond the trial period in the analysis, assuming full persistence with treatment. However, the overall duration of treatment is < 4 years in the base-case model because of the application of real-world persistence data for ALN; therefore, the need for extrapolation is minimised.
Adverse events have been incorporated in a fairly crude manner by applying an average cost and QALY decrement to every individual treated, based on the average incidence, rather than including the AEs as separate competing events in the model. The benefit of doing this is that it avoids the impact of very rare AEs, such as ONJ, being missed because they do not occur often in the simulated population. The estimates of costs and QALY decrements attributable to AEs were also not included in the PSA, which may mean that the decision uncertainty associted with AEs will be underestimated. However, this is unlikely to be a significant limitation for cellulitis and ONJ, for which the AE event rates were very low and the average costs and QALY decrements per treated patient were small and are therefore unlikely to be significant drivers of cost-effectiveness. However, the average loss of INMB attributable to the AE of VTE for RLX was relatively large in comparison to the cost of treatment (discounted INMB decrement of £53 per patient started on treatment vs. an annual drug cost of £43), meaning that this is likely to be a significant driver of cost-effectiveness for RLX. (Although an explicit scenario analysis has not been conducted, the AG expects that, for the majority of the risk categories, the INMBs would be unlikely to be above zero when removing the impact of VTE, based on the results presented.)
We note that the cost-effectiveness analysis is based on current prices for each intervention and, when there is more than one preparation, we have assumed that the lowest-cost preparation is used, which is often the generic form, when one is available. We also note that prices for the two biosimilar versions of TPTD (Movymia and Terrosa)22,23 were not available when this report was prepared. It is likely that these biosimilar preparations will have a lower cost; therefore, the estimates of cost-effectiveness for TPTD may be overly pessimistic compared with what may be achieved in practice in future years if there is widespread uptake of these biosimilars and they are made available at a substantially lower cost than TPTD.
The scope19 of the MTA stated that treatment sequences would be considered if the evidence allowed. The only treatment sequence modelled by the AG is ROMO/ALN, as no other treatment sequences were included in the NMA for fracture outcomes. The AG notes that the UCB S.A. submission20 also contained cost-effectiveness estimates for the sequence of ALN/ROMO, but it appears that this was based on an assumption of clinical equivalence for ROMO/ALN and ALN/ROMO and assumptions regarding the appropriate offset period. Although there was RCT evidence comparing the sequence of ROMO/DEN with placebo followed by DEN from the FRAME54 RCT, it was not possible to include this RCT in the NMAs (as neither study arm connected with any other studies included in the networks); therefore, we have not been able to estimate the cost-effectiveness of the ROMO/DEN sequence.
One of the strengths of this analysis is that we have been able to estimate the cost-effectiveness of each intervention across the broad range of absolute fracture risk observed in the population eligible for risk assessment under CG146. 8 However, the downside of the approach we have taken is that the estimates of cost-effectiveness are uncertain in patients at high risk of fracture (e.g. > 30%) as they are informed by fewer simulated patients. We tried to address this by conducting an exploratory sensitivity analysis for an example high-risk patient; however, we note that the cost-effectiveness of other patients with similar FRAX scores may differ and that the regression of INMB across the full range of risk scores observed in the population eligible for fracture risk assessment did not identify a risk at which the ICER fell under £20,000 for any of the non-bisphosphonates.
Chapter 5 Assessment of factors relevant to the NHS and other parties
The only non-bisphosphonate not currently in use in the NHS in England is ROMO. The UCB S.A. submission20 states that ‘there is likely no administration costs or initiation costs associated with romosozumab as the training of injection techniques will be provided as part of the patient support program provided by UCB’. The AG believes that the impact on NHS services of introducing ROMO to the NHS in England is anticipated to be small, as the needs of patients on ROMO are likely to be simlar to those on TPTD, which is already an established treatment.
Chapter 6 Discussion
Statement of principal findings
Fifty-two RCTs of non-bisphosphonates were included in the review. An additional 51 RCTs of bisphosphonates were included for the NMAs.
Across studies reporting overall mortality, there were no significant differences between non-bisphosphonate treatment arms and their comparators of placebo, other non-bisphosphonates or bisphosphonates. The ranges of SAE rates were as follows: DEN, 2–25.8%; RLX, 2–18.6%; ROMO, 3.2–12.9%; and TPTD, 0–33%.
In NMAs for vertebral, non-vertebral and hip fractures, and for femoral neck BMD, all treatments were associated with beneficial effects relative to placebo. For both vertebral fractures and percentage change in femoral neck BMD, the treatment effects were statistically significant at a conventional 5% level for all treatments. TPTD was associated with the greatest effect for vertebral (HR 0.23, 95% CrI 0.16 to 0.32, PB 0.38), non-vertebral (HR 0.58, 95% CrI 0.45 to 0.76, PB 0.52) and hip fractures (HR 0.35, 95% CrI 0.15 to 0.73, PB 0.50), whereas ROMO was the most effective for wrist fractures (HR 0.12, 95% CrI 0.00 to 1.19) and proximal humerus fractures (HR 0.10, 95% CrI 0.00 to 3.66), and ROMO/ALN was the most effective for percentage change in femoral neck BMD (HR 0.10, 95% CrI 0 to 3.66, PB 0.77). In general, the ranking of treatments varied for the different outcomes.
The cost-effectiveness review found that there are no published studies that compare all of the interventions and comparators specified in the scope of this appraisal across the broad population specified in the scope. The models described in the UCB S.A. 20 and Amgen Inc. 100 submissions focused on high-risk poulations and a subset of comparators.
The ICERs are > £20,000 per QALY for all non-bisphosphonate interventions compared with no treatment across the range of QFracture and FRAX scores expected in the population eligible for fracture risk assessment. The ICER for DEN was predicted by the regression analysis to fall below £30,000 at very high levels of risk (FRAX score of > 45%), but the estimates of cost-effectiveness are very uncertain at this level of risk. An exploratory scenario analysis examining an example high-risk patient also suggested that the cost-effectiveness of DEN may be more favourable for high-risk patients with specific characteristics.
The incremental analysis found that the intervention with maximum INMB (when valuing a QALY at either £20,000 or £30,000) was either no treatment or oral bisphosphonates across all 10 risk categories for both QFracture and FRAX scores.
Strengths and limitations of the assessment
Strengths
A comprehensive search for RCTs was undertaken. RCTs were available for all treatments of interest, reporting fracture data and femoral neck BMD data. NMAs were used to synthesise the evidence, permitting a coherent comparison of the efficacy of interventions in terms of fracture and femoral neck BMD. Although studies varied in quality, a sensitivity analysis removing lower-quality studies from the NMA gave results consistent with the main analysis.
A key strength of the approach we have taken in the economic evaluation is that we have been able to adapt the model used in TA464 to allow the cost-effectiveness of non-bisphosphonates to be assessed in a manner consistent with the approach used previously to assess the cost-effectiveness of bisphosphonates.
Limitations
Evidence was restricted to English-language publications. Most RCTs had a primary end point of BMD, which is a surrogate end point, rather than fractures, which are of clinical importance to patients. Studies varied in quality, particularly on the domains of blinding and attrition, and were not all well reported. For wrist and proximal humerus fractures, there was less RCT evidence. Although NMAs were conducted, there is considerable uncertainty in treatment effects for certain interventions in these networks. However, for the economic analysis, we were able to use the non-vertebral fracture NMA outcomes for wrist and proximal humerus fracture, as the evidence in this network was less sparse.
Owing to the limitations of the evidence available, we were able to model only one treatment sequence in the economic analysis. Although we were able to estimate the INMB as a function of absolute risk across the full range of risk scores expected among the population eligible for risk assessment, the estimates of INMB in patients at very high risk of fracture (e.g. > 30%) are uncertain as they are based on a small proportion of the simulated population (< 2% for FRAX and < 0.2% for QFracture).
Uncertainties
Although statistically significant treatment effects were found when comparing interventions with placebo, the effects of non-bisphosphonates were generally similar (with non-statistically significant pairwise HRs). There was evidence of moderate heterogeneity in treatment effects between studies.
Other relevant factors
Any future introduction of biosimilar treatments for TPTD or DEN would be likely to change the cost-effectiveness of these treatments. This assessment report was prepared while ROMO was still being assessed by the European Medicines Agency; therefore, it is based on the anticipated rather than the final licensed indication for ROMO.
Chapter 7 Conclusions
Randomised controlled trials, of varying quality, were available for all non-bisphosphonate treatments of interest, reporting fracture data and femoral neck BMD data. Domains regarding methodological quality were not consistently reported across trials. All treatments were associated with beneficial effects, relative to placebo. For each intervention, reported SAEs varied across trials, with the majority of between-group differences not being statistically significant for comparisons with placebo/no active treatment, head-to-head non-bisphosphonate comparisons or comparisons with bisphosphonates.
The ICERs are > £20,000 per QALY for all non-bisphosphonate interventions compared with no treatment across the range of QFracture and FRAX scores expected in the population eligible for fracture risk assessment. The ICER for DEN was predicted by the regression analysis to fall below £30,000 at very high levels of risk (FRAX score of > 45%), but the estimates of cost-effectiveness are very uncertain at this level of risk. An exploratory scenario analysis examining an example high-risk patient also suggested that the cost-effectiveness of DEN may be more favourable for high-risk patients with specific characteristics.
Implications for service provision
As the majority of the non-bisphosphonate interventions are already part of current practice, and the additional treatment of ROMO is likely to be delivered in a similar manner to TPTD, we do not anticipate any significant implications for service provision associated with these treatments.
Suggested research priorities
Additional head-to-head studies, of good methodological quality, comparing non-bisphosphonates would be beneficial, as few of the RCTs identified in the systematic review were head-to-head comparisons. In particular, it would be useful to know whether or not a treatment sequence of TPTD followed by ALN provides similar efficacy to the ROMO/ALN sequence. RCTs with a primary end point of fractures, rather than BMD, are preferable, as fractures are of clinical relevance to patients.
There were not many trials with a follow-up of > 36 months. The reporting of long-term outcomes from the ARCH83 and FRAME54 studies for ROMO, in particular, would be useful, to see if the treatment effectiveness persists during the following years of anti-resportive treatment.
Although there were few data on wrist and humerus fractures for non-bisphosphonates, further research to gather these is unlikely to be useful, as we were able to use the outcomes from the non-vertebral fracture network. Similarly, although there were few RCTs with men or of steroid-induced osteoporosis, these showed similar treatment effect patterns to postmenopausal women, and so further research in these populations is not considered a research priority.
Acknowledgements
We would like to thank Matt Stevenson (ScHARR) for providing comments on the draft report, and Andrea Shippam (Programme Manager, ScHARR) for providing administrative support and for preparing and formatting the report.
Contributions of authors
Sarah Davis (https://orcid.org/0000-0002-6609-4287) (Senior Lecturer in Health Economics) acted as the overall project lead and conducted the review of published cost-effectiveness studies and the economic evaluation.
Emma Simpson (https://orcid.org/0000-0001-7353-5979) (Senior Research Fellow) conducted the systematic review of clinical effectiveness studies.
Jean Hamilton (https://orcid.org/0000-0003-3326-9842) (Research Fellow in Statistics) conducted the NMAs.
Marrissa Martyn-St James (https://orcid.org/0000-0002-4679-7831) (Research Fellow) conducted the systematic review of clinical effectiveness studies.
Andrew Rawdin (https://orcid.org/0000-0002-1944-458X) (Research Assistant) conducted the review of published cost-effectiveness studies and the review of HRQoL following fracture.
Ruth Wong (https://orcid.org/0000-0002-4536-4794) (Information Specialist) conducted the searches.
Edward Goka (https://orcid.org/0000-0002-6754-3312) (Research Assistant) quality assured some of the fracture data extraction.
Neil Gittoes (https://orcid.org/0000-0001-5963-214X) (Consultant and Honorary Professor of Endocrinology) and Peter Selby (https://orcid.org/0000-0001-9465-9268) (Consultant Physician and Honorary Clinical Professor of Metabolic Bone Disease) provided clinical advice.
All authors were involved in drafting and commenting on the final report.
Publication
Simpson EL, Martyn-St James M, Hamilton J, Wong R, Gittoes N, Selby P, Davis S. Clinical effectiveness of denosumab, raloxifene, romosozumab, and teriparatide for the prevention of osteoporotic fragility fractures: a systematic review and network meta-analysis. Bone 2020;130:115081.
Data-sharing statement
Data can be obtained from the corresponding author, subject to their being non-confidential.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health and Social Care.
References
- World Health Organization . Assessment of Fracture Risk and Its Application to Screening for Postmenopausal Osteoporosis: Report of a WHO Study Group 1994.
- Kanis JA, Burlet N, Cooper C, Delmas PD, Reginster JY, Borgstrom F, et al. European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO) . European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int 2008;19:399-428. https://doi.org/10.1007/s00198-008-0560-z.
- NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy . Osteoporosis prevention, diagnosis, and therapy. JAMA 2001;285:785-95. https://doi.org/10.1001/jama.285.6.785.
- Pasco JA, Seeman E, Henry MJ, Merriman EN, Nicholson GC, Kotowicz MA. The population burden of fractures originates in women with osteopenia, not osteoporosis. Osteoporos Int 2006;17:1404-9. https://doi.org/10.1007/s00198-006-0135-9.
- Hernlund E, Svedbom A, Ivergård M, Compston J, Cooper C, Stenmark J, et al. Osteoporosis in the European Union: medical management, epidemiology and economic burden . A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch Osteoporos 2013;8. https://doi.org/10.1007/s11657-013-0136-1.
- Svedbom A, Hernlund E, Ivergård M, Compston J, Cooper C, Stenmark J, et al. Osteoporosis in the European Union: a compendium of country-specific reports. Arch Osteoporos 2013;8. https://doi.org/10.1007/s11657-013-0137-0.
- Gauthier A, Kanis JA, Jiang Y, Martin M, Compston JE, Borgström F, et al. Epidemiological burden of postmenopausal osteoporosis in the UK from 2010 to 2021: estimations from a disease model. Arch Osteoporos 2011;6:179-88. https://doi.org/10.1007/s11657-011-0063-y.
- National Institute for Health and Care Excellence . Osteoporosis: Assessing the Risk of Fragility Fracture. Clinical Guideline [CG146] 2012. www.nice.org.uk/guidance/cg146/resources/osteoporosis-assessing-the-risk-of-fragility-fracture-pdf-35109574194373 (accessed 20 November 2018).
- National Institute for Health and Care Excellence . Bisphosphonates for Treating Osteoporosis. Technology Appraisal Guidance [TA464] 2017. www.nice.org.uk/guidance/ta464/resources/bisphosphonates-for-treating-osteoporosis-pdf-82604905556677 (accessed 20 November 2018).
- National Institute for Health and Care Excellence . Denosumab for the Prevention of Osteoporotic Fractures in Postmenopausal Women. Technology Appraisal Guidance [TA204] 2010. www.nice.org.uk/Guidance/TA204 (accessed 31 October 2018).
- National Institute for Heath and Care Excellence . Raloxifene and Teriparatide for the Secondary Prevention of Osteoporotic Fragility Fractures in Postmenopausal Women [TA161] 2008. www.nice.org.uk/Guidance/TA161 (accessed 2 November 2018).
- National Institute for Heath and Care Excellence . Alendronate, Etidronate, Risedronate, Raloxifene and Strontium Ranelate for the Primary Prevention of Osteoporotic Fragility Fractures in Postmenopausal Women (Amended) [TA160] 2011. www.laalamedilla.org/GUIAS/Guia%20NICE%20osteoporosis%20P12011.pdf (accessed 31 October 2018).
- National Institute for Health and Care Excellence . NICE Quality Standard 149 on Osteoporosis 2017. www.nice.org.uk/guidance/qs149/resources/osteoporosis-pdf-75545487906757 (accessed 20 November 2018).
- National Osteoporosis Guideline Group . NOGG 2017: Clinical Guideline for the Prevention and Treatment of Osteoporosis 2017. www.sheffield.ac.uk/NOGG/NOGG%20Guideline%202017.pdf (accessed 20 November 2018).
- Stevenson M, Davis S. Analyses of the Cost-Effectiveness of Pooled Alendronate and Risedronate, Compared With Strontium Ranelate, Raloxifene, Etidronate and Teriparatide 2006. www.nice.org.uk/guidance/TA160/documents/dsu-economic-evaluation-of-pooled-alendronate-and-risedronate-compared-with-strontium-ranelate-raloxifene-etidronate-and-teriparatide2 (accessed 30 November 2018).
- Curtis L, Burns A. Unit Costs of Health and Social Care 2017. Canterbury: Personal Social Services Research Unit, University of Kent; 2017.
- National Institute for Health and Care Excellence . Osteoporosis Overview – NICE Pathway 2018. https://pathways.nice.org.uk/pathways/osteoporosis#content = view-index (accessed 20 November 2018).
- National Institute for Health and Care Excellence . Fragility Fracture Risk Assessment – NICE Pathway 2018. https://pathways.nice.org.uk/pathways/osteoporosis#path%20=%20view%3A/pathways/osteoporosis/fragility-fracture-risk-assessment.xml%26content%20=%20view-index (accessed 30 November 2018).
- National Institute for Health and Care Excellence . Non-Bisphosphonates for Treating Osteoporosis: Final Scope 2018.
- Union Chimique Belge (UCB) S.A . Company Evidence Submission for Romosozumab n.d.
- Amgen Ltd . Summary of Product Characteristics for Prolia 60 Mg Solution for Injection in Pre-Filled Syringe 2015. www.medicines.org.uk/emc/product/568/smpc (accessed 31 October 2018).
- European Medicines Agency . Summary of Opinion 1 (Initial Authorisation) – Movymia 2016. www.ema.europa.eu/en/documents/product-information/movymia-epar-product-information_en.pdf (accessed 6 April 2020).
- European Medicines Agency . Summary of Opinion 1 (Initial Authorisation) – Terrosa 2016. www.ema.europa.eu/en/documents/product-information/terrosa-epar-product-information_en.pdf (accessed 6 April 2020).
- Daiichi Sankyo UK Ltd . Summary of Product Characteristics for Evista 60 Mg Film-Coated Tablets 2018. www.medicines.org.uk/emc/product/3778/smpc (accessed 20 November 2018).
- Eli Lilly and Company Ltd . Summary of Product Characteristics for Forsteo 20 Micrograms 80 Microlitres Solution for Injection in Pre-Filled Pen 2018. www.medicines.org.uk/emc/product/2215 (accessed 20 November 2018).
- NHS Digital . Prescription Cost Analysis – England, 2017 [PAS] 2017. https://digital.nhs.uk/data-and-information/publications/statistical/prescription-cost-analysis/prescription-cost-analysis-england-2017 (accessed 21 November 2018).
- NHS Digital . Prescribing Costs in Hospitals and the Community, England 2016 17 2017. https://digital.nhs.uk/data-and-information/publications/statistical/prescribing-costs-in-hospitals-and-the-community/2016-17 (accessed 21 November 2018).
- Joint Formulary Committee . British National Formulary n.d. www.medicinescomplete.com (accessed 21 November 2018).
- Compston J, Cooper A, Cooper C, Francis R, Kanis JA, Marsh D, et al. Guidelines for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK. Maturitas 2009;62:105-8. https://doi.org/10.1016/j.maturitas.2008.11.022.
- Centre for Metabolic Bone Diseases, University of Sheffield . Welcome to FRAX® 2014. www.shef.ac.uk/FRAX/ (accessed 11 December 2014).
- ClinRisk Ltd . Welcome to the QFracture® – 2012 Risk Calculator 2012. https://qfracture.org (accessed 11 December 2014).
- Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group . Preferred reporting items for systematic reviews and meta-analyses: the PRISMA Statement. Open Med 2009;3:e123-30. https://doi.org/10.1371/journal.pmed.1000097.
- Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med 2015;162:777-84. https://doi.org/10.7326/M14-2385.
- Davis S, Martyn-St James M, Sanderson J, Stevens J, Goka E, Rawdin A, et al. A systematic review and economic evaluation of bisphosphonates for the prevention of fragility fractures. Health Technol Assess 2016;20. https://doi.org/10.3310/hta20780.
- Genant HK, Wu CY, van Kuijk C, Nevitt MC. Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res 1993;8:1137-48. https://doi.org/10.1002/jbmr.5650080915.
- National Institute for Health and Care Excellence . Early and Locally Advanced Breast Cancer: Diagnosis and Management 2018. www.nice.org.uk/guidance/ng101 (accessed 21 August 2018).
- National Institute for Health and Care Excellence . Prostate Cancer: Diagnosis and Management 2014. www.nice.org.uk/Guidance/CG175 (accessed 21 August 2018).
- Higgins J, Altman A, Sterne J, Higgins J, Churchill R, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions version 5. 2. 0 (updated June 2017). London: The Cochrane Collaboration; 2017.
- The Cochrane Collaboration . Current Version of RoB 2 n.d. https://sites.google.com/site/riskofbiastool/welcome/rob-2-0-tool/current-version-of-rob-2 (accessed 21 November 2018).
- Wright CC, Sim J. Intention-to-treat approach to data from randomized controlled trials: a sensitivity analysis. J Clin Epidemiol 2003;56:833-42. https://doi.org/10.1016/S0895-4356(03)00155-0.
- Cummings SR, San Martin J, McClung MR, Siris ES, Eastell R, Reid IR, et al. Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N Engl J Med 2009;361:756-65. https://doi.org/10.1056/NEJMoa0809493.
- Orwoll E, Teglbjærg CS, Langdahl BL, Chapurlat R, Czerwinski E, Kendler DL, et al. A randomized, placebo-controlled study of the effects of denosumab for the treatment of men with low bone mineral density. J Clin Endocrinol Metab 2012;97:3161-9. https://doi.org/10.1210/jc.2012-1569.
- Nakamura T, Matsumoto T, Sugimoto T, Hosoi T, Miki T, Gorai I, et al. Clinical Trials Express: fracture risk reduction with denosumab in Japanese postmenopausal women and men with osteoporosis: denosumab fracture intervention randomized placebo controlled trial (DIRECT). J Clin Endocrinol Metab 2014;99:2599-607. https://doi.org/10.1210/jc.2013-4175.
- Nakamura T, Matsumoto T, Sugimoto T, Shiraki M. Dose-response study of denosumab on bone mineral density and bone turnover markers in Japanese postmenopausal women with osteoporosis. Osteoporos Int 2012;23:1131-40. https://doi.org/10.1007/s00198-011-1786-8.
- Koh JM, Chung DJ, Chung YS, Kang MI, Kim IJ, Min YK, et al. Assessment of denosumab in Korean postmenopausal women with osteoporosis: randomized, double-blind, placebo-controlled trial with open-label extension. Yonsei Med J 2016;57:905-14. https://doi.org/10.3349/ymj.2016.57.4.905.
- Adami S, San Martin J, Muñoz-Torres M, Econs MJ, Xie L, Dalsky GP, et al. Effect of raloxifene after recombinant teriparatide [hPTH(1-34)] treatment in postmenopausal women with osteoporosis. Osteoporos Int 2008;19:87-94. https://doi.org/10.1007/s00198-007-0485-y.
- Morii H, Ohashi Y, Taketani Y, Fukunaga M, Nakamura T, Itabashi A, et al. Effect of raloxifene on bone mineral density and biochemical markers of bone turnover in Japanese postmenopausal women with osteoporosis: results from a randomized placebo-controlled trial. Osteoporos Int 2003;14:793-800. https://doi.org/10.1007/s00198-003-1424-1.
- Liu JL, Zhu HM, Huang QR, Zhang ZL, Li HL, Qin YJ, et al. Effects of raloxifene hydrochloride on bone mineral density, bone metabolism and serum lipids in Chinese postmenopausal women with osteoporosis: a multi-center, randomized, placebo-controlled clinical trial. Chin Med J 2004;117:1029-35.
- Gorai I, Hattori S, Tanaka Y, Iwaoki Y. Alfacalcidol-supplemented raloxifene therapy has greater bone-sparing effect than raloxifene-alone therapy in postmenopausal Japanese women with osteoporosis or osteopenia. J Bone Miner Metab 2012;30:349-58. https://doi.org/10.1007/s00774-011-0325-1.
- Silverman SL, Christiansen C, Genant HK, Vukicevic S, Zanchetta JR, de Villiers TJ, et al. Efficacy of bazedoxifene in reducing new vertebral fracture risk in postmenopausal women with osteoporosis: results from a 3-year, randomized, placebo-, and active-controlled clinical trial. J Bone Miner Res 2008;23:1923-34. https://doi.org/10.1359/jbmr.080710.
- Ettinger B, Black DM, Mitlak BH, Knickerbocker RK, Nickelsen T, Genant HK, et al. Reduction of vertebral fracture risk in postmenopausal women with osteoporosis treated with raloxifene: results from a 3-year randomized clinical trial. Multiple Outcomes of Raloxifene Evaluation (MORE) Investigators. JAMA 1999;282:637-45. https://doi.org/10.1001/jama.282.7.637.
- Lufkin EG, Whitaker MD, Nickelsen T, Argueta R, Caplan RH, Knickerbocker RK, et al. Treatment of established postmenopausal osteoporosis with raloxifene: a randomized trial. J Bone Miner Res 1998;13:1747-54. https://doi.org/10.1359/jbmr.1998.13.11.1747.
- Mok CC, Ying KY, To CH, Ho LY, Yu KL, Lee HK, et al. Raloxifene for prevention of glucocorticoid-induced bone loss: a 12-month randomised double-blinded placebo-controlled trial. Ann Rheum Dis 2011;70:778-84. https://doi.org/10.1136/ard.2010.143453.
- Cosman F, Crittenden DB, Adachi JD, Binkley N, Czerwinski E, Ferrari S, et al. Romosozumab treatment in postmenopausal women with osteoporosis. N Engl J Med 2016;375:1532-43. https://doi.org/10.1056/NEJMoa1607948.
- Ishibashi H, Crittenden DB, Miyauchi A, Libanati C, Maddox J, Fan M, et al. Romosozumab increases bone mineral density in postmenopausal Japanese women with osteoporosis: a phase 2 study. Bone 2017;103:209-15. https://doi.org/10.1016/j.bone.2017.07.005.
- Lewiecki EM, Blicharski T, Goemaere S, Lippuner K, Meisner PD, Miller PD, et al. A Phase III randomized placebo-controlled trial to evaluate efficacy and safety of romosozumab in men with osteoporosis. J Clin Endocrinol Metab 2018;103:3183-93. https://doi.org/10.1210/jc.2017-02163.
- Orwoll ES, Scheele WH, Paul S, Adami S, Syversen U, Diez-Perez A, et al. The effect of teriparatide [human parathyroid hormone (1-34)] therapy on bone density in men with osteoporosis. J Bone Miner Res 2003;18:9-17. https://doi.org/10.1359/jbmr.2003.18.1.9.
- Miyauchi A, Matsumoto T, Sugimoto T, Tsujimoto M, Warner MR, Nakamura T. Effects of teriparatide on bone mineral density and bone turnover markers in Japanese subjects with osteoporosis at high risk of fracture in a 24-month clinical study: 12-month, randomized, placebo-controlled, double-blind and 12-month open-label phases. Bone 2010;47:493-502. https://doi.org/10.1016/j.bone.2010.05.022.
- Miyauchi A, Matsumoto T, Shigeta H, Tsujimoto M, Thiebaud D, Nakamura T. Effect of teriparatide on bone mineral density and biochemical markers in Japanese women with postmenopausal osteoporosis: a 6-month dose-response study. J Bone Miner Metab 2008;26:624-34. https://doi.org/10.1007/s00774-008-0871-3.
- Miller PD, Leder BZ, Hattersley G, Lau E, Alexandersen P, Hala T, et al. Effects of abaloparatide on vertebral and non-vertebral fracture incidence in postmenopausal women with osteoporosis-results of the phase 3 active trial. Endocrine 2015;36.
- Leder BZ, O’Dea LS, Zanchetta JR, Kumar P, Banks K, McKay K, et al. Effects of abaloparatide, a human parathyroid hormone-related peptide analog, on bone mineral density in postmenopausal women with osteoporosis. J Clin Endocrinol Metab 2015;100:697-706. https://doi.org/10.1210/jc.2014-3718.
- Neer RM, Arnaud CD, Zanchetta JR, Prince R, Gaich GA, Reginster JY, et al. Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med 2001;344:1434-41. https://doi.org/10.1056/NEJM200105103441904.
- Sethi BK, Chadha M, Modi KD, Kumar KM, Mehrotra R, Sriram U. Efficacy of teriparatide in increasing bone mineral density in postmenopausal women with osteoporosis – an Indian experience. J Assoc Physicians India 2008;56:418-24.
- Tsai JN, Uihlein AV, Lee H, Kumbhani R, Siwila-Sackman E, McKay EA, et al. Teriparatide and denosumab, alone or combined, in women with postmenopausal osteoporosis: the DATA study randomised trial. Lancet 2013;382:50-6. https://doi.org/10.1016/S0140-6736(13)60856-9.
- Leder BZ, Tsai JN, Uihlein AV, Wallace PM, Lee H, Neer RM, et al. Denosumab and teriparatide transitions in postmenopausal osteoporosis (the DATA-Switch study): extension of a randomised controlled trial. Lancet 2015;386:1147-55. https://doi.org/10.1016/S0140-6736(15)61120-5.
- Eastell R, Nickelsen T, Marin F, Barker C, Hadji P, Farrerons J, et al. Sequential treatment of severe postmenopausal osteoporosis after teriparatide: final results of the randomized, controlled European Study of Forsteo (EUROFORS). J Bone Miner Res 2009;24:726-36. https://doi.org/10.1359/jbmr.081215.
- Langdahl BL, Libanati C, Crittenden DB, Bolognese MA, Brown JP, Daizadeh NS, et al. Romosozumab (sclerostin monoclonal antibody) versus teriparatide in postmenopausal women with osteoporosis transitioning from oral bisphosphonate therapy: a randomised, open-label, phase 3 trial. Lancet 2017;390:1585-94. https://doi.org/10.1016/S0140-6736(17)31613-6.
- McClung MR, Grauer A, Boonen S, Bolognese MA, Brown JP, Diez-Perez A, et al. Romosozumab in postmenopausal women with low bone mineral density. N Engl J Med 2014;370:412-20. https://doi.org/10.1056/NEJMoa1305224.
- Brown JP, Prince RL, Deal C, Recker RR, Kiel DP, de Gregorio LH, et al. Comparison of the effect of denosumab and alendronate on BMD and biochemical markers of bone turnover in postmenopausal women with low bone mass: a randomized, blinded, phase 3 trial. J Bone Miner Res 2009;24:153-61.
- Kendler DL, Roux C, Benhamou CL, Brown JP, Lillestol M, Siddhanti S, et al. Effects of denosumab on bone mineral density and bone turnover in postmenopausal women transitioning from alendronate therapy. J Bone Miner Res 2010;25:72-81. https://doi.org/10.1359/jbmr.090716.
- Kendler DL, McClung MR, Freemantle N, Lillestol M, Moffett AH, Borenstein J, et al. Adherence, preference, and satisfaction of postmenopausal women taking denosumab or alendronate. Osteoporos Int 2011;22:1725-35. https://doi.org/10.1007/s00198-010-1378-z.
- McClung MR, Lewiecki EM, Cohen SB, Bolognese MA, Woodson GC, Moffett AH, et al. Denosumab in postmenopausal women with low bone mineral density. N Engl J Med 2006;354:821-31. https://doi.org/10.1056/NEJMoa044459.
- Recknor C, Czerwinski E, Bone HG, Bonnick SL, Binkley N, Palacios S, et al. Denosumab compared with ibandronate in postmenopausal women previously treated with bisphosphonate therapy: a randomized open-label trial. Obstet Gynecol 2013;121:1291-9. https://doi.org/10.1097/AOG.0b013e318291718c.
- Saag KG, Wagman RB, Geusens P, Adachi JD, Messina OD, Emkey R, et al. Denosumab versus risedronate in glucocorticoid-induced osteoporosis: a multicentre, randomised, double-blind, active-controlled, double-dummy, non-inferiority study. Lancet Diabetes Endocrinol 2018;6:445-54. https://doi.org/10.1016/S2213-8587(18)30075-5.
- Miller PD, Pannacciulli N, Brown JP, Czerwinski E, Nedergaard BS, Bolognese MA, et al. Denosumab or zoledronic acid in postmenopausal women with osteoporosis previously treated with oral bisphosphonates. J Clin Endocrinol Metab 2016;101:3163-70. https://doi.org/10.1210/jc.2016-1801.
- Sambrook PN, Geusens P, Ribot C, Solimano JA, Ferrer-Barriendos J, Gaines K, et al. Alendronate produces greater effects than raloxifene on bone density and bone turnover in postmenopausal women with low bone density: results of EFFECT (Efficacy of FOSAMAX versus EVISTA Comparison Trial) International. J Intern Med 2004;255:503-11. https://doi.org/10.1111/j.1365-2796.2004.01317.x.
- Luckey M, Kagan R, Greenspan S, Bone H, Kiel RD, Simon J, et al. Once-weekly alendronate 70 mg and raloxifene 60 mg daily in the treatment of postmenopausal osteoporosis. Menopause 2004;11:405-15. https://doi.org/10.1097/01.GME.0000119981.77837.1F.
- Johnell O, Scheele WH, Lu Y, Reginster JY, Need AG, Seeman E. Additive effects of raloxifene and alendronate on bone density and biochemical markers of bone remodeling in postmenopausal women with osteoporosis. J Clin Endocrinol Metab 2002;87:985-92. https://doi.org/10.1210/jcem.87.3.8325.
- Muscoso E, Puglisi N, Mamazza C, Lo Giudice F, Testai M, Abbate S, et al. Antiresorption therapy and reduction in fracture susceptibility in the osteoporotic elderly patient: open study. Eur Rev Med Pharmacol Sci 2004;8:97-102.
- Recker RR, Kendler D, Recknor CP, Rooney TW, Lewiecki EM, Utian WH, et al. Comparative effects of raloxifene and alendronate on fracture outcomes in postmenopausal women with low bone mass. Bone 2007;40:843-51. https://doi.org/10.1016/j.bone.2006.11.001.
- Sanad Z, Ellakwa H, Desouky B. Comparison of alendronate and raloxifene in postmenopausal women with osteoporosis. Climacteric 2011;14:369-77. https://doi.org/10.3109/13697137.2010.537408.
- Michalská D, Stepan JJ, Basson BR, Pavo I. The effect of raloxifene after discontinuation of long-term alendronate treatment of postmenopausal osteoporosis. J Clin Endocrinol Metab 2006;91:870-7. https://doi.org/10.1210/jc.2004-2212.
- Saag KG, Petersen J, Brandi ML, Karaplis AC, Lorentzon M, Thomas T, et al. Romosozumab or alendronate for fracture prevention in women with osteoporosis. N Engl J Med 2017;377:1417-27. https://doi.org/10.1056/NEJMoa1708322.
- McClung MR, San Martin J, Miller PD, Civitelli R, Bandeira F, Omizo M, et al. Opposite bone remodeling effects of teriparatide and alendronate in increasing bone mass. Arch Intern Med 2005;165:1762-8. https://doi.org/10.1001/archinte.165.15.1762.
- Saag KG, Zanchetta JR, Devogelaer JP, Adler RA, Eastell R, See K, et al. Effects of teriparatide versus alendronate for treating glucocorticoid-induced osteoporosis: thirty-six-month results of a randomized, double-blind, controlled trial. Arthritis Rheum 2009;60:3346-55. https://doi.org/10.1002/art.24879.
- Panico A, Lupoli GA, Marciello F, Lupoli R, Cacciapuoti M, Martinelli A, et al. Teriparatide vs. alendronate as a treatment for osteoporosis: changes in biochemical markers of bone turnover, BMD and quality of life. Med Sci Monit 2011;17:CR442-448. https://doi.org/10.12659/MSM.881905.
- Glüer CC, Marin F, Ringe JD, Hawkins F, Möricke R, Papaioannu N, et al. Comparative effects of teriparatide and risedronate in glucocorticoid-induced osteoporosis in men: 18-month results of the EuroGIOPs trial. J Bone Miner Res 2013;28:1355-68. https://doi.org/10.1002/jbmr.1870.
- Anastasilakis AD, Goulis DG, Polyzos SA, Gerou S, Koukoulis GN, Efstathiadou Z, et al. Head-to-head comparison of risedronate vs. teriparatide on bone turnover markers in women with postmenopausal osteoporosis: a randomised trial. Int J Clin Pract 2008;62:919-24. https://doi.org/10.1111/j.1742-1241.2008.01768.x.
- Walker MD, Cusano NE, Sliney J, Romano M, Zhang C, McMahon DJ, et al. Combination therapy with risedronate and teriparatide in male osteoporosis. Endocrine 2013;44:237-46. https://doi.org/10.1007/s12020-012-9819-4.
- Geusens P, Marin F, Kendler DL, Russo LA, Zerbini CA, Minisola S, et al. Effects of teriparatide compared with risedronate on the risk of fractures in subgroups of postmenopausal women with severe osteoporosis: the VERO trial. J Bone Miner Res 2018;33:783-94. https://doi.org/10.1002/jbmr.3384.
- Hadji P, Zanchetta JR, Russo L, Recknor CP, Saag KG, McKiernan FE, et al. The effect of teriparatide compared with risedronate on reduction of back pain in postmenopausal women with osteoporotic vertebral fractures. Osteoporos Int 2012;23:2141-50. https://doi.org/10.1007/s00198-011-1856-y.
- Malouf-Sierra J, Tarantino U, García-Hernández PA, Corradini C, Overgaard S, Stepan JJ, et al. Effect of teriparatide or risedronate in elderly patients with a recent pertrochanteric hip fracture: final results of a 78-week randomized clinical trial. J Bone Miner Res 2017;32:1040-51. https://doi.org/10.1002/jbmr.3067.
- Cosman F, Eriksen EF, Recknor C, Miller PD, Guañabens N, Kasperk C, et al. Effects of intravenous zoledronic acid plus subcutaneous teriparatide [rhPTH(1-34)] in postmenopausal osteoporosis. J Bone Miner Res 2011;26:503-11. https://doi.org/10.1002/jbmr.238.
- Gorai I, Tanaka Y, Hattori S, Iwaoki Y. Assessment of adherence to treatment of postmenopausal osteoporosis with raloxifene and/or alfacalcidol in postmenopausal Japanese women. J Bone Miner Metab 2010;28:176-84. https://doi.org/10.1007/s00774-009-0112-4.
- Miller PD, Hattersley G, Riis BJ, Williams GC, Lau E, Russo LA, et al. Effect of abaloparatide vs placebo on new vertebral fractures in postmenopausal women with osteoporosis: a randomized clinical trial. JAMA 2016;316:722-33. https://doi.org/10.1001/jama.2016.11136.
- ClinicalTrials.gov . Effects of Teriparatide in the Treatment of Postmenopausal Women With Osteoporosis 2008. http://clinicaltrials.gov/show/NCT00670501 (accessed 6 November 2018).
- Simpson EL, Martyn-St James M, Hamilton J, Wong R, Gittoes N, Selby P, et al. Clinical effectiveness of denosumab, raloxifene, romosozumab, and teriparatide for the prevention of osteoporotic fragility fractures: a systematic review and network meta-analysis. Bone 2020;130. https://doi.org/10.1016/j.bone.2019.115081.
- Aspenberg P, Malouf J, Tarantino U, García-Hernández PA, Corradini C, Overgaard S, et al. Effects of teriparatide compared with risedronate on recovery after pertrochanteric hip fracture: results of a randomized, active-controlled, double-blind clinical trial at 26 weeks. J Bone Joint Surg Am 2016;98:1868-78. https://doi.org/10.2106/JBJS.15.01217.
- Kendler DL, Marin F, Zerbini CAF, Russo LA, Greenspan SL, Zikan V, et al. Effects of teriparatide and risedronate on new fractures in post-menopausal women with severe osteoporosis (VERO): a multicentre, double-blind, double-dummy, randomised controlled trial. Lancet 2017;391:230-40. https://doi.org/10.1016/S0140-6736(17)32137-2.
- Amgen Inc . Company Evidence Submission for Denosumab n.d.
- Abtahi J, Henefalk G, Aspenberg P. Randomised trial of bisphosphonate-coated dental implants: radiographic follow-up after five years of loading. Int J Oral Maxillofac Surg 2016;45:1564-9. https://doi.org/10.1016/j.ijom.2016.09.001.
- Maricic M, Adachi JD, Sarkar S, Wu W, Wong M, Harper KD. Early effects of raloxifene on clinical vertebral fractures at 12 months in postmenopausal women with osteoporosis. Arch Intern Med 2002;162:1140-3. https://doi.org/10.1001/archinte.162.10.1140.
- Saag KG, Shane E, Boonen S, Marín F, Donley DW, Taylor KA, et al. Teriparatide or alendronate in glucocorticoid-induced osteoporosis. N Engl J Med 2007;357:2028-39. https://doi.org/10.1056/NEJMoa071408.
- Bone HG, Wagman RB, Brandi ML, Brown JP, Chapurlat R, Cummings SR, et al. 10 years of denosumab treatment in postmenopausal women with osteoporosis: results from the phase 3 randomised FREEDOM trial and open-label extension. Lancet Diabetes Endocrinol 2017;5:513-23. https://doi.org/10.1016/S2213-8587(17)30138-9.
- ClinicalTrials.gov . Extension Study to Evaluate the Long Term Safety and Efficacy of Denosumab in the Treatment of Osteoporosis 2007. https://clinicaltrials.gov/ct2/show/NCT00523341 (accessed 20 October 2018).
- Sugimoto T, Matsumoto T, Hosoi T, Miki T, Gorai I, Yoshikawa H, et al. Three-year denosumab treatment in postmenopausal Japanese women and men with osteoporosis: results from a 1-year open-label extension of the Denosumab Fracture Intervention Randomized Placebo Controlled Trial (DIRECT). Osteoporos Int 2015;26:765-74. https://doi.org/10.1007/s00198-014-2964-2.
- Langdahl BL, Marin F, Shane E, Dobnig H, Zanchetta JR, Maricic M, et al. Teriparatide versus alendronate for treating glucocorticoid-induced osteoporosis: an analysis by gender and menopausal status. Osteoporos Int 2009;20:2095-104. https://doi.org/10.1007/s00198-009-0917-y.
- Aspenberg P, Tarantino U, Corradini C, Overgaard S, Borris L, Frihagen F, et al. Teriparatide seems to improve recovery after pertrochanteric hip fracture: comparison with risedronate in a randomized, controlled trial. HIP 2016;26.
- Freemantle N, Satram-Hoang S, Tang ET, Kaur P, Macarios D, Siddhanti S, et al. Final results of the DAPS (Denosumab Adherence Preference Satisfaction) study: a 24-month, randomized, crossover comparison with alendronate in postmenopausal women. Osteoporos 2012;23:317-26. https://doi.org/10.1007/s00198-011-1780-1.
- Leder BZ, Tsai JN, Uihlein AV, Burnett-Bowie SA, Zhu Y, Foley K, et al. Two years of Denosumab And Teriparatide Administration in postmenopausal women with osteoporosis (the DATA extension study): a randomized controlled trial. J Clin Endocrinol Metab 2014;99:1694-700. https://doi.org/10.1210/jc.2013-4440.
- Langdahl BL, Teglbjærg CS, Ho PR, Chapurlat R, Czerwinski E, Kendler DL, et al. A 24-month study evaluating the efficacy and safety of denosumab for the treatment of men with low bone mineral density: results from the ADAMO trial. J Clin Endocrinol Metab 2015;100:1335-42. https://doi.org/10.1210/jc.2014-4079.
- European Medicines Agency . CHMP Assessment Report for Prolia 2010. www.ema.europa.eu/documents/assessment-report/prolia-epar-public-assessment-report_en.pdf (accessed 31 October 2018).
- European Medicines Agency . CHMP Assessment Report for Evista 2009. www.ema.europa.eu/en/documents/overview/evista-epar-summary-public_en.pdf (accessed 31 October 2018).
- European Medicines Agency . EPAR Scientific Discussion for Forsteo 2005. www.ema.europa.eu/documents/scientific-discussion/forsteo-epar-scientific-discussion_en.pdf (accessed 2 November 2018).
- European Medicines Agency . Summary of Product Characteristics for Forsteo 2016. www.ema.europa.eu/documents/product-information/forsteo-epar-product-information_en.pdf (accessed 2 November 2018).
- Silverman S, Viswanathan H, Wang A, Ragi-Eis S, Fardellone P, Gilchrist N, et al. Evaluation of health-related quality of life in postmenopausal women with osteoporosis who participated in the freedom trial. Osteoporos 2010;21.
- ClinicalTrials.gov . Study Evaluating Bazedoxifene Acetate In Osteoporosis In Postmenopausal Women 2005. https://clinicaltrials.gov/ct2/show/NCT00205777 (accessed 20 October 2018).
- Silverman S, Viswanathan HN, Yang YC, Wang A, Boonen S, Ragi-Eis S, et al. Impact of clinical fractures on health-related quality of life is dependent on time of assessment since fracture: results from the FREEDOM trial. Osteoporos Int 2012;23:1361-9. https://doi.org/10.1007/s00198-011-1720-0.
- Dias S, Sutton AJ, Ades AE, Welton NJ. Evidence synthesis for decision making 2: a generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med Decis Making 2013;33:607-17. https://doi.org/10.1177/0272989X12458724.
- Ren S, Oakley JE, Stevens JW. Incorporating genuine prior information about between-study heterogeneity in random effects pairwise and network meta-analyses. Med Decis Making 2018;38:531-42. https://doi.org/10.1177/0272989X18759488.
- Dias S, Sutton AJ, Welton NJ, Ades AE. Evidence synthesis for decision making 3: heterogeneity – subgroups, meta-regression, bias, and bias-adjustment. Med Decis Making 2013;33:618-40. https://doi.org/10.1177/0272989X13485157.
- Achana FA, Cooper NJ, Dias S, Lu G, Rice SJ, Kendrick D, et al. Extending methods for investigating the relationship between treatment effect and baseline risk from pairwise meta-analysis to network meta-analysis. Stat Med 2013;32:752-71. https://doi.org/10.1002/sim.5539.
- Dias S, Welton NJ, Caldwell DM, Ades AE. Checking consistency in mixed treatment comparison meta-analysis. Stat Med 2010;29:932-44. https://doi.org/10.1002/sim.3767.
- Lunn DJ, Thomas A, Best N, Spiegelhalter D. WinBUGS – a Bayesian modelling framework: concepts, structure, and extensibility. Stat Computing 2000;10:325-37. https://doi.org/10.1023/A:1008929526011.
- Sturtz S, Ligges U, Gelman A. R2WinBUGS: a package for running WinBUGS from R. J Stat 2005;12:1-16. https://doi.org/10.18637/jss.v012.i03.
- Brooks SP, Gelman A. General methods for monitoring convergence of iterative simulations. J Comput Graph Stat 1998;7:434-55. https://doi.org/10.1080/10618600.1998.10474787.
- Spiegelhalter DJ, Best NG, Carlin BR, Van Der Linde A. Bayesian measures of model complexity and fit. J Royal Stat Soc 2002;64:583-616. https://doi.org/10.1111/1467-9868.00353.
- ClinicalTrials.gov . A Study That Will Compare the Effect of Two Drugs on Participants With Low Bone Mass and a Recent Hip Fracture (MOVE) 2015. https://clinicaltrials.gov/ct2/show/NCT00887354 (accessed 28 November 2018).
- Miller PD, Schnitzer T, Emkey R, Orwoll E, Rosen C, Ettinger M, et al. Weekly oral alendronic Acid in male osteoporosis. Clin Drug Investig 2004;24:333-41. https://doi.org/10.2165/00044011-200424060-00003.
- Nakamura T, Fukunaga M, Nakano T, Kishimoto H, Ito M, Hagino H, et al. Efficacy and safety of once-yearly zoledronic acid in Japanese patients with primary osteoporosis: two-year results from a randomized placebo-controlled double-blind study (ZOledroNate treatment in Efficacy to osteoporosis; ZONE study). Osteoporos Int 2017;28:389-98. https://doi.org/10.1007/s00198-016-3736-y.
- Dursun N, Dursun E, Yalçin S. Comparison of alendronate, calcitonin and calcium treatments in postmenopausal osteoporosis. Int J Clin Pract 2001;55:505-9.
- Hooper MJ, Ebeling PR, Roberts AP, Graham JJ, Nicholson GC, D’Emden M, et al. Risedronate prevents bone loss in early postmenopausal women: a prospective randomized, placebo-controlled trial. Climacteric 2005;8:251-62. https://doi.org/10.1080/13697130500118126.
- Black DM, Delmas PD, Eastell R, Reid IR, Boonen S, Cauley JA, et al. Once-yearly zoledronic acid for treatment of postmenopausal osteoporosis. N Engl J Med 2007;356:1809-22. https://doi.org/10.1056/NEJMoa067312.
- Liberman UA, Weiss SR, Bröll J, Minne HW, Quan H, Bell NH, et al. Effect of oral alendronate on bone mineral density and the incidence of fractures in postmenopausal osteoporosis. N Engl J Med 1995;333:1437-44. https://doi.org/10.1056/NEJM199511303332201.
- Carfora E, Sergio F, Bellini P. Effect of treatment of postmenopausal osteoporosis with continuous daily oral alendronate and the incidence of fractures. Gazzetta Medica Ital Arch Per Le Sci Mediche 1998;157:106-9.
- Chesnut CH, Skag A, Christiansen C, Recker R, Stakkestad JA, Hoiseth A, et al. Effects of oral ibandronate administered daily or intermittently on fracture risk in postmenopausal osteoporosis. J Bone Miner Res 2004;19:1241-9. https://doi.org/10.1359/JBMR.040325.
- Paggiosi MA, Peel N, McCloskey E, Walsh JS, Eastell R. Comparison of the effects of three oral bisphosphonate therapies on the peripheral skeleton in postmenopausal osteoporosis: the TRIO study. Osteoporos Int 2014;25:2729-41. https://doi.org/10.1007/s00198-014-2817-z.
- Tan W, Sun J, Zhou L, Li Y, Wu X. Randomized trial comparing efficacies of zoledronate and alendronate for improving bone mineral density and inhibiting bone remodelling in women with post-menopausal osteoporosis. J Clin Pharm Ther 2016;41:519-23. https://doi.org/10.1111/jcpt.12429.
- National Institute for Health and Care Excellence . Guide to the Methods of Technology Appraisal 2013 2013.
- Philips Z, Ginnelly L, Sculpher M, Claxton K, Golder S, Riemsma R, et al. Review of guidelines for good practice in decision-analytic modelling in health technology assessment. Health Technol Assess 2004;8. https://doi.org/10.3310/hta8360.
- Kanis JA, Borgström F, Johnell O, Oden A, Sykes D, Jönsson B. Cost-effectiveness of raloxifene in the UK: an economic evaluation based on the MORE study. Osteoporos Int 2005;16:15-2. https://doi.org/10.1007/s00198-004-1688-0.
- Kanis JA, Brazier JE, Stevenson M, Calvert NW, Lloyd Jones M. Treatment of established osteoporosis: a systematic review and cost-utility analysis. Health Technol Assess 2002;6. https://doi.org/10.3310/hta6290.
- Stevenson M, Jones ML, De Nigris E, Brewer N, Davis S, Oakley J. A systematic review and economic evaluation of alendronate, etidronate, risedronate, raloxifene and teriparatide for the prevention and treatment of postmenopausal osteoporosis. Health Technol Assess 2005;9. https://doi.org/10.3310/hta9220.
- Kanis JA, Adams J, Borgström F, Cooper C, Jönsson B, Preedy D, et al. The cost-effectiveness of alendronate in the management of osteoporosis. Bone 2008;42:4-15. https://doi.org/10.1016/j.bone.2007.10.019.
- Scotland G, Waugh N, Royle P, McNamee P, Henderson R, Hollick R. Denosumab for the prevention of osteoporotic fractures in post-menopausal women: a NICE single technology appraisal. PharmacoEconomics 2011;29:951-61. https://doi.org/10.2165/11589310-000000000-00000.
- Strom O, Jonsson B, Kanis JA. Intervention thresholds for denosumab in the UK using a FRAX-based cost-effectiveness analysis. Osteoporos 2013;24:1491-502. https://doi.org/10.1007/s00198-012-2115-6.
- Waugh N, Royle P, Scotland G, Henderson R, Hollick R, McNamee P. Denosumab for the prevention of osteoporotic fractures in postmenopausal women. Health Technol Assess 2011;15. https://doi.org/10.3310/hta15suppl1/06.
- Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J Clin Epidemiol 1997;50:683-91. https://doi.org/10.1016/S0895-4356(97)00049-8.
- Stevenson M, Davis S. Analyses of the Cost Effectiveness of Pooled Alendronate and Risedronate, Compared with Strontium Ranelate, Raloxifene, Etidronate and Teriparatide. Sheffield: University of Sheffield; 2006.
- Tosteson AN, Gottlieb DJ, Radley DC, Fisher ES, Melton LJ. Excess mortality following hip fracture: the role of underlying health status. Osteoporos Int 2007;18:1463-72. https://doi.org/10.1007/s00198-007-0429-6.
- Abrahamsen B, van Staa T, Ariely R, Olson M, Cooper C. Excess mortality following hip fracture: a systematic epidemiological review. Osteoporos Int 2009;20:1633-50. https://doi.org/10.1007/s00198-009-0920-3.
- Johnell O, Kanis JA, Odén A, Sernbo I, Redlund-Johnell I, Petterson C, et al. Mortality after osteoporotic fractures. Osteoporos Int 2004;15:38-42. https://doi.org/10.1007/s00198-003-1490-4.
- Jönsson B, Ström O, Eisman JA, Papaioannou A, Siris ES, Tosteson A, et al. Cost-effectiveness of denosumab for the treatment of postmenopausal osteoporosis. Osteoporos Int 2011;22:967-82. https://doi.org/10.1007/s00198-010-1424-x.
- Barrett JA, Baron JA, Beach ML. Mortality and pulmonary embolism after fracture in the elderly. Osteoporos Int 2003;14:889-94. https://doi.org/10.1007/s00198-003-1494-0.
- Kanis JA, Oden A, Johnell O, De Laet C, Jonsson B. Excess mortality after hospitalisation for vertebral fracture. Osteoporos Int 2004;15:108-12. https://doi.org/10.1007/s00198-003-1516-y.
- Kanis JA, Oden A, Johnell O, De Laet C, Jonsson B, Oglesby AK. The components of excess mortality after hip fracture. Bone 2003;32:468-73. https://doi.org/10.1016/S8756-3282(03)00061-9.
- Parker MJ, Anand JK. What is the true mortality of hip fractures?. Public Health 1991;105:443-6. https://doi.org/10.1016/S0033-3506(05)80614-6.
- Todd CJ, Freeman C, Camilleri-Ferrante C, Laxton C, Murrell P, Palmer C, et al. Anglian Audit of Hip Fracture 2. Cambridge: Unviersity of Cambridge; 1999.
- Center JR, Nguyen TV, Schneider D, Sambrook PN, Eisman JA. Mortality after all major types of osteoporotic fracture in men and women: an observational study. Lancet 1999;353:878-82. https://doi.org/10.1016/S0140-6736(98)09075-8.
- Davis S, Sanderson J, Stevenson M, Strong M. Bisphosphonates for Preventing Osteoporotic Fragility Fractures (Including a Partial Update of NICE Technology Appraisal Guidance 160 and 161). Addendum 2017. www.nice.org.uk/guidance/ta464/documents/committee-papers (accessed 15 November 2018).
- Office for National Statistics . National Life Tables, England 2011–2013 2014. www. ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/lifeexpectancies/bulletins/ nationallifetablesunitedkingdom/2014-09-25 (accessed 11 November 2014).
- van Staa TP, Kanis JA, Geusens P, Boonen A, Leufkens HGM, Cooper C. The cost-effectiveness of bisphosphonates in postmenopausal women based on individual long-term fracture risks. Value Health 2007;10:348-57. https://doi.org/10.1111/j.1524-4733.2007.00188.x.
- Hippisley-Cox J, Coupland C. Predicting risk of osteoporotic fracture in men and women in England and Wales: prospective derivation and validation of QFractureScores. BMJ 2009;339. https://doi.org/10.1136/bmj.b4229.
- Hippisley-Cox J, Coupland C. Derivation and validation of updated QFracture algorithm to predict risk of osteoporotic fracture in primary care in the United Kingdom: prospective open cohort study. BMJ 2012;344. https://doi.org/10.1136/bmj.e3427.
- Imaz I, Zegarra P, González-Enríquez J, Rubio B, Alcazar R, Amate JM. Poor bisphosphonate adherence for treatment of osteoporosis increases fracture risk: systematic review and meta-analysis. Osteoporos Int 2010;21:1943-51. https://doi.org/10.1007/s00198-009-1134-4.
- Curtis JR, Yun H, Matthews R, Saag KG, Delzell E. Adherence with intravenous zoledronate and intravenous ibandronate in the United States Medicare population. Arthritis Care Res 2012;64:1054-60. https://doi.org/10.1002/acr.21638.
- Li L, Roddam A, Gitlin M, Taylor A, Shepherd S, Jick S. Non-persistence to anti-osteoporosis medications in the UK using the General Practice Research Database (GPRD). Rheumatology 2010;49:i23-5. https://doi.org/10.1093/rheumatology/keq708.
- Li L, Roddam A, Gitlin M, Taylor A, Shepherd S, Shearer A, et al. Persistence with osteoporosis medications among postmenopausal women in the UK General Practice Research Database. Menopause 2012;19:33-40. https://doi.org/10.1097/gme.0b013e318221bacd.
- Hadji P, Papaioannou N, Gielen E, Feudjo Tepie M, Zhang E, Frieling I, et al. Persistence, adherence, and medication-taking behavior in women with postmenopausal osteoporosis receiving denosumab in routine practice in Germany, Austria, Greece, and Belgium: 12-month results from a European non-interventional study. Osteoporos Int 2015;26:2479-89. https://doi.org/10.1007/s00198-015-3164-4.
- Karlsson L, Lundkvist J, Psachoulia E, Intorcia M, Ström O. Persistence with denosumab and persistence with oral bisphosphonates for the treatment of postmenopausal osteoporosis: a retrospective, observational study, and a meta-analysis. Osteoporos Int 2015;26:2401-11. https://doi.org/10.1007/s00198-015-3253-4.
- Silverman SL, Siris E, Belazi D, Recknor C, Papaioannou A, Brown JP, et al. Persistence at 24 months with denosumab among postmenopausal women with osteoporosis: results of a prospective cohort study. Arch Osteoporos 2018;13. https://doi.org/10.1007/s11657-018-0491-z.
- Arden NK, Earl S, Fisher DJ, Cooper C, Carruthers S, Goater M. Persistence with teriparatide in patients with osteoporosis: the UK experience. Osteoporos Int 2006;17:1626-9. https://doi.org/10.1007/s00198-006-0171-5.
- Abhishek A, Pande I. Teriparatide in men: persistence and geographical variation in the UK. Osteoporos Int 2009;20:1453-4. https://doi.org/10.1007/s00198-008-0788-7.
- Napoli N, Langdahl BL, Ljunggren Ö, Lespessailles E, Kapetanos G, Kocjan T, . Effects of teriparatide in patients with osteoporosis in clinical practice: 42-month results during and after discontinuation of treatment from the European Extended Forsteo® Observational Study (ExFOS). Calcif Tissue Int 2018;103:359-71. https://doi.org/10.1007/s00223-018-0437-x.
- Idolazzi L, Fassio A, Gatti D, Tamanini S, Viapiana O, Rossini M, et al. Duration of treatment for osteoporosis. Reumatismo 2013;65:22-35. https://doi.org/10.4081/reumatismo.2013.22.
- Schwartz AV, Bauer DC, Cummings SR, Cauley JA, Ensrud KE, Palermo L, et al. Efficacy of continued alendronate for fractures in women with and without prevalent vertebral fracture: the FLEX trial. J Bone Miner Res 2010;25:976-82. https://doi.org/10.1002/jbmr.11.
- Black DM, Schwartz AV, Ensrud KE, Cauley JA, Levis S, Quandt SA, et al. Effects of continuing or stopping alendronate after 5 years of treatment: the Fracture Intervention Trial Long-term Extension (FLEX): a randomized trial. JAMA 2006;296:2927-38. https://doi.org/10.1001/jama.296.24.2927.
- Eastell R, Hannon RA, Wenderoth D, Rodriguez-Moreno J, Sawicki A. Effect of stopping risedronate after long-term treatment on bone turnover. J Clin Endocrinol Metab 2011;96:3367-73. https://doi.org/10.1210/jc.2011-0412.
- Watts NB, Chines A, Olszynski WP, McKeever CD, McClung MR, Zhou X, et al. Fracture risk remains reduced one year after discontinuation of risedronate. Osteoporos Int 2008;19:365-72. https://doi.org/10.1007/s00198-007-0460-7.
- Ravn P, Christensen JO, Baumann M, Clemmesen B. Changes in biochemical markers and bone mass after withdrawal of ibandronate treatment: prediction of bone mass changes during treatment. Bone 1998;22:559-64. https://doi.org/10.1016/S8756-3282(98)00044-1.
- Reginster JY, Adami S, Lakatos P, Greenwald M, Stepan JJ, Silverman SL, et al. Efficacy and tolerability of once-monthly oral ibandronate in postmenopausal osteoporosis: 2 year results from the MOBILE study. Ann Rheum Dis 2006;65:654-61. https://doi.org/10.1136/ard.2005.044958.
- Black DM, Reid IR, Boonen S, Bucci-Rechtweg C, Cauley JA, Cosman F, et al. The effect of 3 versus 6 years of zoledronic acid treatment of osteoporosis: a randomized extension to the HORIZON-Pivotal Fracture Trial (PFT). J Bone Miner Res 2012;27:243-54. https://doi.org/10.1002/jbmr.1494.
- Lindsay R, Scheele WH, Neer R, Pohl G, Adami S, Mautalen C, et al. Sustained vertebral fracture risk reduction after withdrawal of teriparatide in postmenopausal women with osteoporosis. Arch Intern Med 2004;164:2024-30. https://doi.org/10.1001/archinte.164.18.2024.
- Prince R, Sipos A, Hossain A, Syversen U, Ish-Shalom S, Marcinowska E, et al. Sustained nonvertebral fragility fracture risk reduction after discontinuation of teriparatide treatment. J Bone Miner Res 2005;20:1507-13. https://doi.org/10.1359/JBMR.050501.
- Kaufman JM, Orwoll E, Goemaere S, San Martin J, Hossain A, Dalsky GP, et al. Teriparatide effects on vertebral fractures and bone mineral density in men with osteoporosis: treatment and discontinuation of therapy. Osteoporos Int 2005;16:510-6. https://doi.org/10.1007/s00198-004-1713-3.
- Naylor KE, Clowes JA, Finigan J, Paggiosi MA, Peel NF, Eastell R. The effect of cessation of raloxifene treatment on bone turnover in postmenopausal women. Bone 2010;46:592-7. https://doi.org/10.1016/j.bone.2009.10.043.
- Neele SJ, Evertz R, De Valk-De Roo G, Roos JC, Netelenbos JC. Effect of 1 year of discontinuation of raloxifene or estrogen therapy on bone mineral density after 5 years of treatment in healthy postmenopausal women. Bone 2002;30:599-603. https://doi.org/10.1016/S8756-3282(01)00706-2.
- Bone HG, Bolognese MA, Yuen CK, Kendler DL, Wang H, Liu Y, et al. Effects of denosumab on bone mineral density and bone turnover in postmenopausal women. J Clin Endocrinol Metab 2008;93:2149-57. https://doi.org/10.1210/jc.2007-2814.
- Bone HG, Bolognese MA, Yuen CK, Kendler DL, Miller PD, Yang YC, et al. Effects of denosumab treatment and discontinuation on bone mineral density and bone turnover markers in postmenopausal women with low bone mass. J Clin Endocrinol Metab 2011;96:972-80. https://doi.org/10.1210/jc.2010-1502.
- Popp AW, Varathan N, Buffat H, Senn C, Perrelet R, Lippuner K. Bone mineral density changes after 1 year of denosumab discontinuation in postmenopausal women with long-term denosumab treatment for osteoporosis. Calcif Tissue Int 2018;103:50-4. https://doi.org/10.1007/s00223-018-0394-4.
- NHS Prescription Services . The Electronic Drug Tariff 2018. www.drugtariff.nhsbsa.nhs.uk/#/00446515-DC_2/DC00446511/Home (accessed 6 November 2018).
- Commercial Medicines Unit . EMit National Database 2017. www.gov.uk/government/publications/drugs-and-pharmaceutical-electronic-market-information-emit (accessed 6 November 2018).
- Department of Health and Social Care . National Schedule of Reference Costs – Year 2015 16 – NHS Trusts and NHS Foundation Trusts 2016.
- Wong SM, Pacey S, Sahota O. Setting up a homecare service for zoledronic acid treatment of osteoporosis. Eur J Hosp Pharm 2016;23:364-5. https://doi.org/10.1136/ejhpharm-2015-000742.
- Mason JM, Thomas KS, Crook AM, Foster KA, Chalmers JR, Nunn AJ, et al. Prophylactic antibiotics to prevent cellulitis of the leg: economic analysis of the PATCH I. II trials. PLOS ONE 2014;9. https://doi.org/10.1371/journal.pone.0082694.
- Boquete-Castro A, Gómez-Moreno G, Calvo-Guirado JL, Aguilar-Salvatierra A, Delgado-Ruiz RA. Denosumab and osteonecrosis of the jaw. A systematic analysis of events reported in clinical trials. Clin Oral Implants Res 2016;27:367-75. https://doi.org/10.1111/clr.12556.
- Khan AA, Morrison A, Hanley DA, Felsenberg D, McCauley LK, O’Ryan F, et al. Diagnosis and management of osteonecrosis of the jaw: a systematic review and international consensus. J Bone Miner Res 2015;30:3-23. https://doi.org/10.1002/jbmr.2405.
- Malden N, Lopes V. An epidemiological study of alendronate-related osteonecrosis of the jaws. A case series from the south-east of Scotland with attention given to case definition and prevalence. J Bone Miner Metab 2012;30:171-82. https://doi.org/10.1007/s00774-011-0299-z.
- Lo JC, O’Ryan FS, Gordon NP, Yang J, Hui RL, Martin D, et al. Prevalence of osteonecrosis of the jaw in patients with oral bisphosphonate exposure. J Oral Maxillofac Surg 2010;68:243-53. https://doi.org/10.1016/j.joms.2009.03.050.
- Compston J, Bowring C, Cooper A, Cooper C, Davies C, Francis R, et al. Diagnosis and management of osteoporosis in postmenopausal women and older men in the UK: National Osteoporosis Guideline Group (NOGG) update 2013. Maturitas 2013;75:392-6. https://doi.org/10.1016/j.maturitas.2013.05.013.
- Miksad RA, Lai KC, Dodson TB, Woo SB, Treister NS, Akinyemi O, et al. Quality of life implications of bisphosphonate-associated osteonecrosis of the jaw. Oncologist 2011;16:121-32. https://doi.org/10.1634/theoncologist.2010-0183.
- Pandor A, Horner D, Davis S, Goodacre S, Stevens JW, Clowes M, et al. Different strategies for pharmacological thromboprophylaxis for lower-limb immobilisation after injury: systematic review and economic evaluation. Health Technol Assess 2019;23. https://doi.org/10.3310/hta23630.
- Gutiérrez L, Roskell N, Castellsague J, Beard S, Rycroft C, Abeysinghe S, et al. Study of the incremental cost and clinical burden of hip fractures in postmenopausal women in the United Kingdom. J Med Econ 2011;14:99-107. https://doi.org/10.3111/13696998.2010.547967.
- Gutiérrez L, Roskell N, Castellsague J, Beard S, Rycroft C, Abeysinghe S, et al. Clinical burden and incremental cost of fractures in postmenopausal women in the United Kingdom. Bone 2012;51:324-31. https://doi.org/10.1016/j.bone.2012.05.020.
- Department of Health and Social Care . National Schedule of Reference Costs – Year 2013 14 2015.
- Curtis L. Unit Costs of Health and Social Care 2014. Canterbury: PSSRU, University of Kent; 2014.
- Lambrelli D, Burge R, Raluy-Callado M, Chen SY, Wu N, Schoenfeld MJ. Retrospective database study to assess the economic impact of hip fracture in the United Kingdom. J Med Econ 2014;17:817-25. https://doi.org/10.3111/13696998.2014.959588.
- Leal J, Gray AM, Prieto-Alhambra D, Arden NK, Cooper C, Javaid MK, et al. REFReSH study group . Impact of hip fracture on hospital care costs: a population-based study. Osteoporos Int 2016;27:549-58. https://doi.org/10.1007/s00198-015-3277-9.
- Svedbom A, Borgstöm F, Hernlund E, Ström O, Alekna V, Bianchi ML, et al. Quality of life for up to 18 months after low-energy hip, vertebral, and distal forearm fractures-results from the ICUROS. Osteoporos Int 2018;29:557-66. https://doi.org/10.1007/s00198-017-4317-4.
- Abimanyi-Ochom J, Watts JJ, Borgström F, Nicholson GC, Shore-Lorenti C, Stuart AL, et al. Changes in quality of life associated with fragility fractures: Australian arm of the International Cost and Utility Related to Osteoporotic Fractures Study (AusICUROS). Osteoporos Int 2015;26:1781-90. https://doi.org/10.1007/s00198-015-3088-z.
- Tidermark J, Zethraeus N, Svensson O, Törnkvist H, Ponzer S. Femoral neck fractures in the elderly: functional outcome and quality of life according to EuroQol. Qual Life Res 2002;11:473-81. https://doi.org/10.1023/a: 1015632114068.
- Jürisson M, Pisarev H, Kanis J, Borgström F, Svedbom A, Kallikorm R, et al. Quality of life, resource use, and costs related to hip fracture in Estonia. Osteoporos Int 2016;27:2555-66. https://doi.org/10.1007/s00198-016-3544-4.
- Svedbom A, Borgström F, Hernlund E, Ström O, Alekna V, Bianchi ML, et al. Quality of life after hip, vertebral, and distal forearm fragility fractures measured using the EQ-5D-3L, EQ-VAS, and time-trade-off: results from the ICUROS. Qual Life Res 2018;27:707-16. https://doi.org/10.1007/s11136-017-1748-5.
- Tsourdi E, Langdahl B, Cohen-Solal M, Aubry-Rozier B, Eriksen EF, Guañabens N, et al. Discontinuation of Denosumab therapy for osteoporosis: a systematic review and position statement by ECTS. Bone 2017;105:11-7. https://doi.org/10.1016/j.bone.2017.08.003.
- Nayak S, Greenspan SL. Osteoporosis treatment efficacy for men: a systematic review and meta-analysis. J Am Geriatr Soc 2017;65:490-5. https://doi.org/10.1111/jgs.14668.
- Kim SM, Kang KC, Kim JW, Lim SJ, Hahn MH. Current role and application of teriparatide in fracture healing of osteoporotic patients: a systematic review. J Bone Metab 2017;24:65-73. https://doi.org/10.11005/jbm.2017.24.1.65.
- Shi Z, Zhou H, Pan B, Lu L, Liu J, Kang Y, et al. Effectiveness of teriparatide on fracture healing: a systematic review and meta-analysis. PLOS ONE 2016;11. https://doi.org/10.1371/journal.pone.0168691.
- Beaudoin C, Jean S, Bessette L, Ste-Marie LG, Moore L, Brown JP. Denosumab compared to other treatments to prevent or treat osteoporosis in individuals at risk of fracture: a systematic review and meta-analysis. Osteoporos Int 2016;27:2835-44. https://doi.org/10.1007/s00198-016-3607-6.
- Chen JF, Yang KH, Zhang ZL, Chang HC, Chen Y, Sowa H, et al. A systematic review on the use of daily subcutaneous administration of teriparatide for treatment of patients with osteoporosis at high risk for fracture in Asia. Osteoporos Int 2015;26:11-28. https://doi.org/10.1007/s00198-014-2838-7.
- Diédhiou D, Cuny T, Sarr A, Norou Diop S, Klein M, Weryha G. Efficacy and safety of denosumab for the treatment of osteoporosis: a systematic review. Ann Endocrinol 2015;76:650-7. https://doi.org/10.1016/j.ando.2015.10.009.
- Fujiwara S, Hamaya E, Sato M, Graham-Clarke P, Flynn JA, Burge R. Systematic review of raloxifene in postmenopausal Japanese women with osteoporosis or low bone mass (osteopenia). Clin Interv Aging 2014;9:1879-93. https://doi.org/10.2147/CIA.S70307.
- Trevisani VF, Riera R, Imoto AM, Saconato H, Atallah AN. Teriparatide (recombinant human parathyroid hormone 1-34) in postmenopausal women with osteoporosis: systematic review. Sao Paulo Med J 2008;126:279-84. https://doi.org/10.1590/S1516-31802008000500007.
- Brandão CM, Lima MG, Silva AL, Silva GD, Guerra AA, Acúrcio Fde A. Treatment of postmenopausal osteoporosis in women: a systematic review. Cad Saude Publica 2008;24:s592-606. https://doi.org/10.1590/S0102-311X2008001600011.
- Gallacher SJ, Dixon T. Impact of treatments for postmenopausal osteoporosis (bisphosphonates, parathyroid hormone, strontium ranelate, and denosumab) on bone quality: a systematic review. Calcif Tissue Int 2010;87:469-84. https://doi.org/10.1007/s00223-010-9420-x.
- Lin T, Yan SG, Cai XZ, Ying ZM, Yuan FZ, Zuo X. Alendronate versus raloxifene for postmenopausal women: a meta-analysis of seven head-to-head randomized controlled trials. Int J Endocrinol 2014;2014. https://doi.org/10.1155/2014/796510.
- MacLean C, Newberry S, Maglione M, McMahon M, Ranganath V, Suttorp M, et al. Systematic review: comparative effectiveness of treatments to prevent fractures in men and women with low bone density or osteoporosis. Ann Intern Med 2008;148:197-213. https://doi.org/10.7326/0003-4819-148-3-200802050-00198.
- Liu CL, Lee HC, Chen CC, Cho DY. Head-to-head comparisons of bisphosphonates and teriparatide in osteoporosis: a meta-analysis. Clin Invest Med 2017;40:E146-E157. https://doi.org/10.25011/cim.v40i3.28394.
- Liu GF, Wang ZQ, Liu L, Zhang BT, Miao YY, Yu SN. A network meta-analysis on the short-term efficacy and adverse events of different anti-osteoporosis drugs for the treatment of postmenopausal osteoporosis. J Cell Biochem 2018;119:4469-81. https://doi.org/10.1002/jcb.26550.
- Murad MH, Drake MT, Mullan RJ, Mauck KF, Stuart LM, Lane MA, et al. Clinical review. Comparative effectiveness of drug treatments to prevent fragility fractures: a systematic review and network meta-analysis. J Clin Endocrinol Metab 2012;97:1871-80. https://doi.org/10.1210/jc.2011-3060.
- Saito T, Sterbenz JM, Malay S, Zhong L, MacEachern MP, Chung KC. Effectiveness of anti-osteoporotic drugs to prevent secondary fragility fractures: systematic review and meta-analysis. Osteoporos Int 2017;28:3289-300. https://doi.org/10.1007/s00198-017-4175-0.
- Liu Y, Cao Y, Zhang S, Zhang W, Zhang B, Tang Q, et al. Romosozumab treatment in postmenopausal women with osteoporosis: a meta-analysis of randomized controlled trials. Climacteric 2018;21:189-95. https://doi.org/10.1080/13697137.2018.1433655.
- Wang YK, Qin SQ, Ma T, Song W, Jiang RQ, Guo JB, et al. Effects of teriparatide versus alendronate for treatment of postmenopausal osteoporosis: a meta-analysis of randomized controlled trials. Medicine 2017;96. https://doi.org/10.1097/MD.0000000000006970.
- Wang G, Sui L, Gai P, Li G, Qi X, Jiang X. The efficacy and safety of vertebral fracture prevention therapies in post-menopausal osteoporosis treatment: Which therapies work best? a network meta-analysis. Bone Joint Res 2017;6:452-63. https://doi.org/10.1302/2046-3758.67.BJR-2016-0292.R1.
- Lou S, Lv H, Wang G, Li Z, Li M, Zhang L, et al. The effect of sequential therapy for postmenopausal women with osteoporosis: a PRISMA-compliant meta-analysis of randomized controlled trials. Medicine 2016;95. https://doi.org/10.1097/MD.0000000000005496.
- Amiche MA, Albaum JM, Tadrous M, Pechlivanoglou P, Lévesque LE, Adachi JD, et al. Efficacy of osteoporosis pharmacotherapies in preventing fracture among oral glucocorticoid users: a network meta-analysis. Osteoporos Int 2016;27:1989-98. https://doi.org/10.1007/s00198-015-3476-4.
- Chen LX, Zhou ZR, Li YL, Ning GZ, Zhang TS, Zhang D, et al. Comparison of bone mineral density in lumbar spine and fracture rate among eight drugs in treatments of osteoporosis in men: a network meta-analysis. PLOS ONE 2015;10. https://doi.org/10.1371/journal.pone.0128032.
- Freemantle N, Cooper C, Diez-Perez A, Gitlin M, Radcliffe H, Shepherd S, et al. Results of indirect and mixed treatment comparison of fracture efficacy for osteoporosis treatments: a meta-analysis. Osteoporos Int 2013;24:209-17. https://doi.org/10.1007/s00198-012-2068-9.
- Bolland MJ, Grey AB, Gamble GD, Reid IR. Effect of osteoporosis treatment on mortality: a meta-analysis. J Clin Endocrinol Metab 2010;95:1174-81. https://doi.org/10.1210/jc.2009-0852.
- Gu HF, Gu LJ, Wu Y, Zhao XH, Zhang Q, Xu ZR, et al. Efficacy and safety of denosumab in postmenopausal women with osteoporosis: a meta-analysis. Medicine 2015;94. https://doi.org/10.1097/MD.0000000000001674.
- Han SL, Wan SL. Effect of teriparatide on bone mineral density and fracture in postmenopausal osteoporosis: meta-analysis of randomised controlled trials. Int J Clin Pract 2012;66:199-20. https://doi.org/10.1111/j.1742-1241.2011.02837.x.
- Lin T, Wang C, Cai XZ, Zhao X, Shi MM, Ying ZM, et al. Comparison of clinical efficacy and safety between denosumab and alendronate in postmenopausal women with osteoporosis: a meta-analysis. Int J Clin Pract 2012;66:399-408. https://doi.org/10.1111/j.1742-1241.2011.02806.x.
- Nakamura T, Tsujimoto M, Hamaya E, Sowa H, Chen P. Consistency of fracture risk reduction in Japanese and Caucasian osteoporosis patients treated with teriparatide: a meta-analysis. J Bone Miner Metab 2012;30:321-5. https://doi.org/10.1007/s00774-011-0313-5.
- Schwarz P, Jorgensen NR, Mosekilde L, Vestergaard P. Effects of increasing age, dosage, and duration of PTH treatment on BMD increase – a meta-analysis. Calcif Tissue Int 2012;90:165-73. https://doi.org/10.1007/s00223-011-9564-3.
- von Keyserlingk C, Hopkins R, Anastasilakis A, Toulis K, Goeree R, Tarride JE, et al. Clinical efficacy and safety of denosumab in postmenopausal women with low bone mineral density and osteoporosis: a meta-analysis. Semin Arthritis Rheum 2011;41:178-86. https://doi.org/10.1016/j.semarthrit.2011.03.005.
- Benjamin B, Benjamin MA, Swe M, Sugathan S. Review on the comparison of effectiveness between denosumab and bisphosphonates in post-menopausal osteoporosis. Osteoporos Sarcopenia 2016;2:77-81. https://doi.org/10.1016/j.afos.2016.03.003.
- Sutton EE, Riche DM. Denosumab, a RANK ligand inhibitor, for postmenopausal women with osteoporosis. Ann Pharmacother 2012;46:1000-9. https://doi.org/10.1345/aph.1Q543.
- Whelan AM, Raman-Wilms L. Denosumab: a new injectable treatment for postmenopausal osteoporosis. Can Pharm J 2011;144:72-8. https://doi.org/10.3821/1913-701X-144.2.72.
- Dore RK, Cohen SB, Lane NE, Palmer W, Shergy W, Zhou L, et al. Effects of denosumab on bone mineral density and bone turnover in patients with rheumatoid arthritis receiving concurrent glucocorticoids or bisphosphonates. Ann Rheum Dis 2010;69:872-5. https://doi.org/10.1136/ard.2009.112920.
- Cosman F, Wermers RA, Recknor C, Mauck KF, Xie L, Glass EV, et al. Effects of teriparatide in postmenopausal women with osteoporosis on prior alendronate or raloxifene: differences between stopping and continuing the antiresorptive agent. J Clin Endocrinol Metab 2009;94:3772-80. https://doi.org/10.1210/jc.2008-2719.
- Smith MR, Egerdie B, Hernández Toriz N, Feldman R, Tammela TL, Saad F, et al. Denosumab in men receiving androgen-deprivation therapy for prostate cancer. N Engl J Med 2009;361:745-55. https://doi.org/10.1056/NEJMoa0809003.
- Ellis GK, Bone HG, Chlebowski R, Paul D, Spadafora S, Smith J, et al. Randomized trial of denosumab in patients receiving adjuvant aromatase inhibitors for nonmetastatic breast cancer. J Clin Oncol 2008;26:4875-82. https://doi.org/10.1200/JCO.2008.16.3832.
- Gnant M, Pfeiler G, Dubsky PC, Hubalek M, Greil R, Jakesz R, et al. Adjuvant denosumab in breast cancer (ABCSG-18): a multicentre, randomised, double-blind, placebo-controlled trial. Lancet 2015;386:433-43. https://doi.org/10.1016/S0140-6736(15)60995-3.
- Klotz L, Smith MR, Coleman RE, Pittman KB, Milecki P, Wei R, et al. Symptomatic skeletal events (SSE) in patients with advanced prostate cancer: results from a Phase III trial of denosumab for the prevention of skeletal-related events. J Clin 2014;32. https://doi.org/10.1200/jco.2014.32.15_suppl.5075.
- Raje N, Terpos E, Willenbacher W, Shimizu K, García-Sanz R, Durie B, et al. Denosumab versus zoledronic acid in bone disease treatment of newly diagnosed multiple myeloma: an international, double-blind, double-dummy, randomised, controlled, phase 3 study. Lancet Oncol 2018;19:370-81. https://doi.org/10.1016/S1470-2045(18)30072-X.
- Henry DH, Von Moos R, Hungria V, Costa L, Woll PJ, Scagliotti G, et al. Delaying skeletal-related events in a randomized Phase III study of denosumab versus zoledronic acid in patients with advanced cancer. J Clin Oncol 2010;28. https://doi.org/10.1200/jco.2010.28.15_suppl.9133.
- Fazeli PK, Wang IS, Miller KK, Herzog DB, Misra M, Lee H, et al. Teriparatide increases bone formation and bone mineral density in adult women with anorexia nervosa. J Clin Endocrinol Metab 2014;99:1322-9. https://doi.org/10.1210/jc.2013-4105.
- Ensrud KE, Stock JL, Barrett-Connor E, Grady D, Mosca L, Khaw KT, et al. Effects of raloxifene on fracture risk in postmenopausal women: the Raloxifene Use for the Heart Trial. J Bone Miner Res 2008;23:112-20. https://doi.org/10.1359/jbmr.070904.
- Bonani M, Brockmann J, Cohen CD, Fehr T, Nocito A, Schiesser M, et al. FP668A randomized open-label clinical trial examining the effect of denosumab on the prevention of 1st-year bone mineral density loss after renal transplantation (POSTOP study; NCT01377467). Nephrology Dialysis Transplantation 2012;27:ii304-ii316.
- Haghverdi F, Farbodara T, Mortaji S, Soltani P, Saidi N. Effect of raloxifene on parathyroid hormone in osteopenic and osteoporotic postmenopausal women with chronic kidney disease stage 5. Iran J Kidney Dis 2014;8:461-6.
- Szczepanek K, Pedziwiatr M, Klek S. Denosumab improves bone mineral density in patients with intestinal failure receiving home parenteral nutrition: results from a randomized, controlled clinical trial. JPEN J Parenter Enter Nutr 2017;42:652-7. https://doi.org/10.1177/0148607117695247.
- Zhu H, Tang H, Cheng Q, He L, Li P, Xue Q, et al. Efficacy and safety of denosumab in Chinese postmenopausal women with osteoporosis at increased risk of fracture: results from a 12-month, randomized, double-blind, placebo-controlled phase III study. J Bone Miner Res 2017;31.
- Thomas T, Cheung AM, Shane E, Zanchetta JR, Kearns A, Hans D, et al. Changes in lumbar spine QCT, DXA and TBS following treatment with denosumab (DMAB), alendronate (ALN), or placebo (PBO) in postmenopausal women with low bone mass. Osteoporos Int 2014;25. https://doi.org/10.1530/boneabs.3.PP356.
- Galesanu C, Lisnic N, Moisii L. Denosumab significantly increases BMD compared with alendronate in postmenopausal women. Osteoporos Int 2015;26.
- Nakano T, Shiraki M, Sugimoto T, Kishimoto H, Ito M, Fukunaga M, et al. Once-weekly teriparatide reduces the risk of vertebral fracture in patients with various fracture risks: subgroup analysis of the Teriparatide Once-Weekly Efficacy Research (TOWER) trial. J Bone Miner Metab 2014;32:441-6. https://doi.org/10.1007/s00774-013-0505-2.
- Cosman F, Nieves JW, Zion M, Barbuto N, Lindsay R. Effect of prior and ongoing raloxifene therapy on response to PTH and maintenance of BMD after PTH therapy. Osteoporos Int 2008;19:529-35. https://doi.org/10.1007/s00198-007-0475-0.
- Body JJ, Gaich GA, Scheele WH, Kulkarni PM, Miller PD, Peretz A, et al. A randomized double-blind trial to compare the efficacy of teriparatide [recombinant human parathyroid hormone (1-34)] with alendronate in postmenopausal women with osteoporosis. J Clin Endocrinol Metab 2002;87:4528-35. https://doi.org/10.1210/jc.2002-020334.
- Finkelstein JS, Wyland JJ, Lee H, Neer RM. Effects of teriparatide, alendronate, or both in women with postmenopausal osteoporosis. J Clin Endocrinol Metab 2010;95:1838-45. https://doi.org/10.1210/jc.2009-1703.
- Iseri K, Iyoda M, Watanabe M, Matsumoto K, Sanada D, Inoue T, et al. Comparison of the efficacy of denosumab and alendronate in glucocorticoid-induced osteoporosis. Nephrol Dialy Transplant 2017;32. https://doi.org/10.1093/ndt/gfx147.SP365.
- Iwamoto J, Sato Y, Uzawa M, Takeda T, Matsumoto H. Comparison of effects of alendronate and raloxifene on lumbar bone mineral density, bone turnover, and lipid metabolism in elderly women with osteoporosis. Yonsei Med J 2008;49:119-28. https://doi.org/10.3349/ymj.2008.49.1.119.
- Roux C, Hofbauer LC, Ho PR, Wark JD, Zillikens MC, Fahrleitner-Pammer A, et al. Denosumab compared with risedronate in postmenopausal women suboptimally adherent to alendronate therapy: efficacy and safety results from a randomized open-label study. Bone 2014;58:48-54. https://doi.org/10.1016/j.bone.2013.10.006.
- Mok CC, Ho LY, Ma KM. Denosumab for patients receiving long-term glucocorticoids who do not have adequate response to bisphosphonate treatment: a randomized controlled trial. Ann Rheum Dis 2014;73. https://doi.org/10.1136/annrheumdis-2014-eular.3767.
- Gonnelli S, Martini G, Caffarelli C, Salvadori S, Cadirni A, Montagnani A, et al. Teriparatide’s effects on quantitative ultrasound parameters and bone density in women with established osteoporosis. Osteoporos Int 2006;17:1524-31. https://doi.org/10.1007/s00198-006-0157-3.
- Siris ES, Harris ST, Eastell R, Zanchetta JR, Goemaere S, Diez-Perez A, et al. Skeletal effects of raloxifene after 8 years: results from the Continuing Outcomes Relevant to Evista (CORE) study. J Bone Miner Res 2005;20:1514-24. https://doi.org/10.1359/JBMR.050509.
- Majima T, Komatsu Y, Shimatsu A, Satoh N, Fukao A, Ninomiya K, et al. Efficacy of combined treatment with raloxifene and alfacalcidol on bone density and biochemical markers of bone turnover in postmenopausal osteoporosis. Endocr J 2008;55:127-34. https://doi.org/10.1507/endocrj.K07E-027.
- Seeman E, Delmas PD, Hanley DA, Sellmeyer D, Cheung AM, Shane E, et al. Microarchitectural deterioration of cortical and trabecular bone: differing effects of denosumab and alendronate. J Bone Miner Res 2010;25:1886-94. https://doi.org/10.1002/jbmr.81.
- Dempster DW, Zhou H, Recker RR, Brown JP, Bolognese MA, Recknor CP, et al. Skeletal Histomorphometry in subjects On Teriparatide or Zoledronic acid therapy (SHOTZ) study: a randomized controlled trial. J Clin Endocrinol Metab 2012;97:2799-808. https://doi.org/10.1210/jc.2012-1262.
- Bai H, Jing D, Guo A, Yin S. Randomized controlled trial of zoledronic acid for treatment of osteoporosis in women. J Int Med Res 2013;41:697-704. https://doi.org/10.1177/0300060513480917.
- Dempster DW, Zhou H, Recker RR, Brown JP, Recknor CP, Lewiecki EM, et al. Differential effects of teriparatide and denosumab on intact PTH and bone formation indices: AVA osteoporosis study. J Clin Endocrinol Metab 2016;101:1353-63. https://doi.org/10.1210/jc.2015-4181.
- Adami S, Passeri M, Ortolani S, Broggini M, Carratelli L, Caruso I, et al. Effects of oral alendronate and intranasal salmon calcitonin on bone mass and biochemical markers of bone turnover in postmenopausal women with osteoporosis. Bone 1995;17:383-90. https://doi.org/10.1016/S8756-3282(95)00262-6.
- Black DM, Cummings SR, Karpf DB, Cauley JA, Thompson DE, Nevitt MC, et al. Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Fracture Intervention Trial Research Group. Lancet 1996;348:1535-41. https://doi.org/10.1016/S0140-6736(96)07088-2.
- Cummings SR, Black DM, Thompson DE, Applegate WB, Barrett-Connor E, Musliner TA, et al. Effect of alendronate on risk of fracture in women with low bone density but without vertebral fractures: results from the Fracture Intervention Trial. JAMA 1998;280:2077-82. https://doi.org/10.1001/jama.280.24.2077.
- Bone HG, Greenspan SL, McKeever C, Bell N, Davidson M, Downs RW, et al. Alendronate and estrogen effects in postmenopausal women with low bone mineral density. Alendronate/Estrogen Study Group. J Clin Endocrinol Metab 2000;85:720-6. https://doi.org/10.1210/jcem.85.2.6393.
- Greenspan SL, Schneider DL, McClung MR, Miller PD, Schnitzer TJ, Bonin R, et al. Alendronate improves bone mineral density in elderly women with osteoporosis residing in long-term care facilities. A randomized, double-blind, placebo-controlled trial. Ann Intern Med 2002;136:742-6. https://doi.org/10.7326/0003-4819-136-10-200205210-00009.
- Greenspan SL, Resnick NM, Parker RA. Combination therapy with hormone replacement and alendronate for prevention of bone loss in elderly women: a randomized controlled trial. JAMA 2003;289:2525-33. https://doi.org/10.1001/jama.289.19.2525.
- Ho AY, Kung AW. Efficacy and tolerability of alendronate once weekly in Asian postmenopausal osteoporotic women. Ann Pharmacother 2005;39:1428-33. https://doi.org/10.1345/aph.1E580.
- Orwoll E, Ettinger M, Weiss S, Miller P, Kendler D, Graham J, et al. Alendronate for the treatment of osteoporosis in men. N Engl J Med 2000;343:604-10. https://doi.org/10.1056/NEJM200008313430902.
- Pols HA, Felsenberg D, Hanley DA, Stepán J, Muñoz-Torres M, Wilkin TJ, et al. Multinational, placebo-controlled, randomized trial of the effects of alendronate on bone density and fracture risk in postmenopausal women with low bone mass: results of the FOSIT study. Fosamax International Trial Study Group. Osteoporos Int 1999;9:461-8. https://doi.org/10.1007/PL00004171.
- Saag KG, Emkey R, Schnitzer TJ, Brown JP, Hawkins F, Goemaere S, et al. Alendronate for the prevention and treatment of glucocorticoid-induced osteoporosis. Glucocorticoid-Induced Osteoporosis Intervention Study Group. N Engl J Med 1998;339:292-9. https://doi.org/10.1056/NEJM199807303390502.
- Adachi JD, Saag KG, Delmas PD, Liberman UA, Emkey RD, Seeman E, et al. Two-year effects of alendronate on bone mineral density and vertebral fracture in patients receiving glucocorticoids: a randomized, double-blind, placebo-controlled extension trial. Arthritis Rheum 2001;44:202-11. https://doi.org/10.1002/1529-0131(200101)44: 1<202::AID-ANR27>3.0.CO;2-W.
- Chesnut CH, Ettinger MP, Miller PD, Baylink DJ, Emkey R, Harris ST, et al. Ibandronate produces significant, similar antifracture efficacy in North American and European women: new clinical findings from BONE. Curr Med Res Opin 2005;21:391-40. https://doi.org/10.1185/030079905X30752.
- McClung MR, Bolognese MA, Sedarati F, Recker RR, Miller PD. Efficacy and safety of monthly oral ibandronate in the prevention of postmenopausal bone loss. Bone 2009;44:418-22. https://doi.org/10.1016/j.bone.2008.09.011.
- Delmas PD, Adami S, Strugala C, Stakkestad JA, Reginster JY, Felsenberg D, et al. Intravenous ibandronate injections in postmenopausal women with osteoporosis: one-year results from the dosing intravenous administration study. Arthritis Rheum 2006;54:1838-46. https://doi.org/10.1002/art.21918.
- Eisman JA, Civitelli R, Adami S, Czerwinski E, Recknor C, Prince R, et al. Efficacy and tolerability of intravenous ibandronate injections in postmenopausal osteoporosis: 2-year results from the DIVA study. J Rheumatol 2008;35:488-97.
- Miller PD, McClung MR, Macovei L, Stakkestad JA, Luckey M, Bonvoisin B, et al. Monthly oral ibandronate therapy in postmenopausal osteoporosis: 1-year results from the MOBILE study. J Bone Miner Res 2005;20:1315-22. https://doi.org/10.1359/JBMR.050313.
- Boonen S, Orwoll ES, Wenderoth D, Stoner KJ, Eusebio R, Delmas PD. Once-weekly risedronate in men with osteoporosis: results of a 2-year, placebo-controlled, double-blind, multicenter study. J Bone Miner Res 2009;24:719-25. https://doi.org/10.1359/jbmr.081214.
- Cohen S, Levy RM, Keller M, Boling E, Emkey RD, Greenwald M, et al. Risedronate therapy prevents corticosteroid-induced bone loss: a twelve-month, multicenter, randomized, double-blind, placebo-controlled, parallel-group study. Arthritis Rheum 1999;42:2309-18. https://doi.org/10.1002/1529-0131(199911)42:11<2309::AID-ANR8>3.0.CO;2-K.
- Fogelman I, Ribot C, Smith R, Ethgen D, Sod E, Reginster JY. Risedronate reverses bone loss in postmenopausal women with low bone mass: results from a multinational, double-blind, placebo-controlled trial. BMD-MN Study Group. J Clin Endocrinol Metab 2000;85:1895-900. https://doi.org/10.1210/jcem.85.5.6603.
- Harris ST, Watts NB, Genant HK, McKeever CD, Hangartner T, Keller M, et al. Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis: a randomized controlled trial. Vertebral Efficacy With Risedronate Therapy (VERT) Study Group. JAMA 1999;282:1344-52. https://doi.org/10.1001/jama.282.14.1344.
- Ste-Marie LG, Sod E, Johnson T, Chines A. Five years of treatment with risedronate and its effects on bone safety in women with postmenopausal osteoporosis. Calcif Tissue Int 2004;75:469-76. https://doi.org/10.1007/s00223-004-0039-7.
- Reginster J, Minne HW, Sorensen OH, Hooper M, Roux C, Brandi ML, et al. Randomized trial of the effects of risedronate on vertebral fractures in women with established postmenopausal osteoporosis. Vertebral Efficacy with Risedronate Therapy (VERT) Study Group. Osteoporos Int 2000;11:83-91. https://doi.org/10.1007/s001980050010.
- Sorensen OH, Crawford GM, Mulder H, Hosking DJ, Gennari C, Mellstrom D, et al. Long-term efficacy of risedronate: a 5-year placebo-controlled clinical experience. Bone 2003;32:120-6. https://doi.org/10.1016/S8756-3282(02)00946-8.
- Leung JY, Ho AY, Ip TP, Lee G, Kung AW. The efficacy and tolerability of risedronate on bone mineral density and bone turnover markers in osteoporotic Chinese women: a randomized placebo-controlled study. Bone 2005;36:358-64. https://doi.org/10.1016/j.bone.2004.10.014.
- Reid DM, Hughes RA, Laan RF, Sacco-Gibson NA, Wenderoth DH, Adami S, et al. Efficacy and safety of daily risedronate in the treatment of corticosteroid-induced osteoporosis in men and women: a randomized trial. European Corticosteroid-Induced Osteoporosis Treatment Study. J Bone Miner Res 2000;15:1006-13. https://doi.org/10.1359/jbmr.2000.15.6.1006.
- Ringe JD, Faber H, Farahmand P, Dorst A. Efficacy of risedronate in men with primary and secondary osteoporosis: results of a 1-year study. Rheumatol Int 2006;26:427-31. https://doi.org/10.1007/s00296-005-0004-4.
- Ringe JD, Farahmand P, Faber H, Dorst A. Sustained efficacy of risedronate in men with primary and secondary osteoporosis: results of a 2-year study. Rheumatol Int 2009;29:311-15. https://doi.org/10.1007/s00296-008-0689-2.
- Reid IR, Gamble GD, Mesenbrink P, Lakatos P, Black DM. Characterization of and risk factors for the acute-phase response after zoledronic acid. J Clin Endocrinol Metab 2010;95:4380-7. https://doi.org/10.1210/jc.2010-0597.
- Lyles KW, Colón-Emeric CS, Magaziner JS, Adachi JD, Pieper CF, Mautalen C, et al. Zoledronic acid and clinical fractures and mortality after hip fracture. N Engl J Med 2007;357:1799-809. https://doi.org/10.1056/NEJMoa074941.
- Adachi JD, Lyles KW, Colón-Emeric CS, Boonen S, Pieper CF, Mautalen C, et al. Zoledronic acid results in better health-related quality of life following hip fracture: the HORIZON-Recurrent Fracture Trial. Osteoporos Int 2011;22:2539-49. https://doi.org/10.1007/s00198-010-1514-9.
- Boonen S, Eastell R, Su G, Mesenbrink P, Cosman F, Cauley JA, et al. Time to onset of antifracture efficacy and year-by-year persistence of effect of zoledronic acid in women with osteoporosis. J Bone Miner Res 2012;27:1487-93. https://doi.org/10.1002/jbmr.1605.
- McClung M, Miller P, Recknor C, Mesenbrink P, Bucci-Rechtweg C, Benhamou CL. Zoledronic acid for the prevention of bone loss in postmenopausal women with low bone mass: a randomized controlled trial. Obstet Gynecol 2009;114:999-1007. https://doi.org/10.1097/AOG.0b013e3181bdce0a.
- Miller PD, Epstein S, Sedarati F, Reginster JY. Once-monthly oral ibandronate compared with weekly oral alendronate in postmenopausal osteoporosis: results from the head-to-head MOTION study. Curr Med Res Opin 2008;24:207-13. https://doi.org/10.1185/030079908x253889.
- Sarioglu M, Tuzun C, Unlu Z, Tikiz C, Taneli F, Uyanik BS. Comparison of the effects of alendronate and risedronate on bone mineral density and bone turnover markers in postmenopausal osteoporosis. Rheumatol Int 2006;26:195-200. https://doi.org/10.1007/s00296-004-0544-z.
- Rosen CJ, Hochberg MC, Bonnick SL, McClung M, Miller P, Broy S, et al. Treatment with once-weekly alendronate 70 mg compared with once-weekly risedronate 35 mg in women with postmenopausal osteoporosis: a randomized double-blind study. J Bone Miner Res 2005;20:141-51. https://doi.org/10.1359/JBMR.040920.
- Bonnick S, Saag KG, Kiel DP, McClung M, Hochberg M, Burnett SM, et al. Comparison of weekly treatment of postmenopausal osteoporosis with alendronate versus risedronate over two years. J Clin Endocrinol Metab 2006;91:2631-7. https://doi.org/10.1210/jc.2005-2602.
- Reid DM, Hosking D, Kendler D, Brandi ML, Wark JD, Weryha G, et al. Alendronic acid produces greater effects than risedronic acid on bone density and turnover in postmenopausal women with osteoporosis: results of FACTS-international. Clinical Drug Investigation 2006;26:63-74. https://doi.org/10.2165/00044011-200626020-00002.
- Reid DM, Hosking D, Kendler D, Brandi ML, Wark JD, Marques-Neto JF, et al. A comparison of the effect of alendronate and risedronate on bone mineral density in postmenopausal women with osteoporosis: 24-month results from FACTS-International. Int J Clin Pract 2008;62:575-84. https://doi.org/10.1111/j.1742-1241.2008.01704.x.
- Reid I, Boonen S, Black DM, Colon-Emeric C, Eastell R, Magaziner J, et al. Once-yearly treatment with zoledronic acid continues to be effective in old age. Bone 2009;44. https://doi.org/10.1016/j.bone.2009.01.212.
- Chesnut CH, McClung MR, Ensrud KE, Bell NH, Genant HK, Harris ST, et al. Alendronate treatment of the postmenopausal osteoporotic woman: effect of multiple dosages on bone mass and bone remodeling. Am J Med 1995;99:144-52. https://doi.org/10.1016/S0002-9343(99)80134-X.
- Klotz LH, McNeill IY, Kebabdjian M, Zhang L, Chin JL. Canadian Urology Research Consortium. A phase 3, double-blind, randomised, parallel-group, placebo-controlled study of oral weekly alendronate for the prevention of androgen deprivation bone loss in nonmetastatic prostate cancer: the Cancer and Osteoporosis Research with Alendronate and Leuprolide (CORAL) study. Eur Urol 2013;63:927-35. https://doi.org/10.1016/j.eururo.2012.09.007.
- Shilbayeh S, S-Zumeili A, Hilow HM. The efficacy and safety of Calidron tablets for management of osteoporosis in Jordanian women: a randomised clinical trial. Saudi Pharm J 2004;12:86-95.
- Smith BJ, Laslett LL, Pile KD, Phillips PJ, Phillipov G, Evans SM, et al. Randomized controlled trial of alendronate in airways disease and low bone mineral density. Chron Respir Dis 2004;1:131-7. https://doi.org/10.1191/1479972304cd025oa.
- Lester JE, Dodwell D, Purohit OP, Gutcher SA, Ellis SP, Thorpe R, et al. Prevention of anastrozole-induced bone loss with monthly oral ibandronate during adjuvant aromatase inhibitor therapy for breast cancer. Clin Cancer Res 2008;14:6336-42. https://doi.org/10.1158/1078-0432.CCR-07-5101.
- Choo C, Lukka H, Kiss A, Danjoux C. Double-blinded, placebo-controlled randomized study evaluating the efficacy of risedronate to prevent the loss of bone mineral density in non-metastatic prostate cancer patients undergoing radiotherapy plus 2–3 years of androgen ablation therapy. Int J Radiat Oncol Biol Phys 2011;81. https://doi.org/10.1016/j.ijrobp.2011.06.086.
- McClung MR, Geusens P, Miller PD, Zippel H, Bensen WG, Roux C, et al. Effect of risedronate on the risk of hip fracture in elderly women. N Engl J Med 2001;344:333-40. https://doi.org/10.1056/NEJM200102013440503.
- Taxel P, Dowsett R, Richter L, Fall P, Klepinger A, Albertsen P. Risedronate prevents early bone loss and increased bone turnover in the first 6 months of luteinizing hormone-releasing hormone-agonist therapy for prostate cancer. BJU Int 2010;106:1473-6. https://doi.org/10.1111/j.1464-410X.2010.09329.x.
- Atmaca A, Gedik O. Effects of alendronate and risedronate on bone mineral density and bone turnover markers in late postmenopausal women with osteoporosis. Adv Ther 2006;23:842-53. https://doi.org/10.1007/BF02850205.
- Hadji P, Gamerdinger D, Spieler W, Kann P, Loeffler H, Articus K, et al. The Rapid Onset and Sustained Efficacy (ROSE) study: zoledronic acid vs. alendronate. Osteoporos Int 2010;21:S192-3.
- Hadji P, Gamerdinger D, Spieler W, Kann PH, Loeffler H, Articus K, et al. Rapid Onset and Sustained Efficacy (ROSE) study: results of a randomised, multicentre trial comparing the effect of zoledronic acid or alendronate on bone metabolism in postmenopausal women with low bone mass. Osteoporos Int 2012;23:625-33. https://doi.org/10.1007/s00198-011-1583-4.
- Silverman SL. The Osteoporosis Assessment Questionnaire (OPAQ): a reliable and valid disease-targeted measure of health-related quality of life (HRQOL) in osteoporosis. Qual Life Res 2000;9:767-74. https://doi.org/10.1023/A:1008934208764.
- Hunter MS. The Women’s Health Questionnaire (WHQ): Frequently Asked Questions (FAQ). Health Qual Life Outcomes 2003;1. https://doi.org/10.1186/1477-7525-1-41.
- Lips P, Cooper C, Agnusdei D, Caulin F, Egger P, Johnell O, et al. Quality of life in patients with vertebral fractures: validation of the Quality of Life Questionnaire of the European Foundation for Osteoporosis (QUALEFFO). Working Party for Quality of Life of the European Foundation for Osteoporosis. Osteoporos Int 1999;10:150-60. https://doi.org/10.1007/s001980050210.
- EuroQol Group . EuroQol – a new facility for the measurement of health-related quality of life. Health Policy 1990;16:199-208. https://doi.org/10.1016/0168-8510(90)90421-9.
- Brazier JE, Harper R, Jones NM, O’Cathain A, Thomas KJ, Usherwood T, et al. Validating the SF-36 health survey questionnaire: new outcome measure for primary care. BMJ 1992;305:160-4. https://doi.org/10.1136/bmj.305.6846.160.
- ClinicalTrials.gov . Denosumab Fracture Intervention Randomized Placebo Controlled Trial in Japanese Patients With Osteoporosis (DIRECT) 2008. www.clinicaltrials.gov/ct2/show/NCT00680953 (accessed November 2018).
- Chapurlat R, Papapoulos S, Brown JP, Franchimont N, Brandi ML, Czerwinski E, et al. Treatment of postmenopausal women with osteoporosis for six years with denosumab: three-year results from the freedom extension. Ann Rheum Dis 2012;71. https://doi.org/10.1136/annrheumdis-2012-eular.3288.
- ClinicalTrials.gov . Phase 2 Dose-Finding Study to Evaluate the Effects of BA058 in the Treatment of Postmenopausal Women With Osteoporosis 2007. https://clinicaltrials.gov/ct2/show/NCT00542425 (accessed November 2018).
- ClinicalTrials.gov . Determine the Efficacy, Safety and Tolerability of Denosumab (AMG 162) in the Treatment of Postmenopausal Women With Low Bone Mineral Density 2007. https://clinicaltrials.gov/ct2/show/NCT00043186 (accessed November 2018).
- ClinicalTrials.gov . Efficacy and Safety of Denosumab Compared With Risedronate in Individuals Taking Glucocorticoids (GIOP) 2012. https://clinicaltrials.gov/ct2/show/NCT01575873 (accessed 28 November 2018).
- ClinicalTrials.gov . Safety and Efficacy Study to Evaluate Denosumab Compared With Zoledronic Acid in Postmenopausal Women With Osteoporosis 2012. https://clinicaltrials.gov/ct2/show/NCT01732770 (accessed 20 October 2018).
- ClinialTrials.gov . Comparison of Teriparatide With Alendronate for Treating Glucocorticoid-Induced Osteoporosis 2003. https://clinicaltrials.gov/ct2/show/NCT00051558 (accessed November 2018).
- Saag KG, Shane E, Boonen S, Marin F, Donley DW, Taylor KA, et al. Teriparatide or alendronate in glucocorticoid-induced osteoporosis. Obstetrical Gynecological Survey 2008;63:232-3. https://doi.org/10.1097/01.ogx.0000310357.43258.f1.
- Griffin XL, Parsons N, Achten J, Fernandez M, Costa ML. Recovery of health-related quality of life in a United Kingdom hip fracture population. The Warwick Hip Trauma Evaluation – a prospective cohort study. Bone Joint J 2015;97:372-82. https://doi.org/10.1302/0301-620X.97B3.35738.
Appendix 1 Literature search strategies
Clinical effectiveness
Ovid MEDLINE(R) Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Ovid MEDLINE(R) Daily, Ovid MEDLINE and Versions(R), 1946–2018
Searched: 11 July 2018.
| # | Searches |
|---|---|
| 1 | exp osteoporosis/ |
| 2 | osteoporo*.tw. |
| 3 | bone diseases, metabolic/ |
| 4 | exp Bone Density/ |
| 5 | (bone adj3 densit*).tw. |
| 6 | exp fractures, bone/ |
| 7 | fractures, cartilage/ |
| 8 | fracture*.tw. |
| 9 | (bone* adj2 fragil*).tw. |
| 10 | bone mineral densit*.tw. |
| 11 | bone loss.tw. |
| 12 | bmd.tw. |
| 13 | or/1-12 |
| 14 | (alendron* or fosomax or fosavance or 121268-17-5).mp. |
| 15 | (ibandron* or boniva or bondronat or bonviva or adronil or 114084-78-5).mp. |
| 16 | (risedron* or actonel or atelvia or benet or 105462-24-6).mp. |
| 17 | (zoledron* or zometa or zomera or aclasta or reclast or 118072-93-8).mp. |
| 18 | or/14-17 |
| 19 | limit 18 to yr = “2014 -Current” |
| 20 | (abaloparatide or eladynos or 247062-33-5).mp. |
| 21 | (DEN or prolia or xgeva or 615258-40-7).mp. |
| 22 | (RLX or evista or keoxifene or 84449-90-1).mp. |
| 23 | (ROMO or evenity or 909395-70-6).mp. |
| 24 | (TPTD or forsteo or 52232-67-4 or movymia or terrosa).mp. |
| 25 | or/20-24 |
| 26 | 13 and (19 or 25) |
| 27 | meta-analysis as topic/ |
| 28 | (meta analy* or metaanaly*).tw. |
| 29 | Meta-Analysis/ |
| 30 | (systematic adj (review*1 or overview*1)).tw. |
| 31 | ‘Review Literature as Topic’/ |
| 32 | or/27-31 |
| 33 | (cochrane or embase or psychlit or psyclit or psychinfo or psycinfo or cinahl or cinhal or science citation index or bids or cancerlit).ab. |
| 34 | ((reference adj list*) or bibliograph* or hand-search* or (relevant adj journals) or (manual adj search*)).ab. |
| 35 | ((selection adj criteria) or (data adj extraction)).ab. |
| 36 | “review”/ |
| 37 | 35 and 36 |
| 38 | comment/or editorial/or letter/ |
| 39 | Animals/ |
| 40 | Humans/ |
| 41 | 39 not (39 and 40) |
| 42 | 38 or 41 |
| 43 | 32 or 33 or 34 or 37 |
| 44 | 43 not 42 |
| 45 | 26 and 44 |
| 46 | Randomized controlled trials as Topic/ |
| 47 | Randomized controlled trial/ |
| 48 | Random allocation/ |
| 49 | randomized controlled trial.pt. |
| 50 | Double blind method/ |
| 51 | Single blind method/ |
| 52 | Clinical trial/ |
| 53 | exp Clinical Trials as Topic/ |
| 54 | controlled clinical trial.pt. |
| 55 | clinical trial*.pt. |
| 56 | multicenter study.pt. |
| 57 | or/46-56 |
| 58 | (clinic* adj25 trial*).ti,ab. |
| 59 | ((singl* or doubl* or treb* or tripl*) adj (blind* or mask*)).tw. |
| 60 | Placebos/ |
| 61 | Placebo*.tw. |
| 62 | (allocated adj2 random).tw. |
| 63 | or/58-62 |
| 64 | 57 or 63 |
| 65 | Case report.tw. |
| 66 | Letter/ |
| 67 | Historical article/ |
| 68 | 65 or 66 or 67 |
| 69 | exp Animals/ |
| 70 | Humans/ |
| 71 | 69 not (69 and 70) |
| 72 | 68 or 71 |
| 73 | 64 not 72 |
| 74 | 26 and 73 |
| 75 | 45 or 74 |
EMBASE, 1974–2018
Searched: 11 July 2018.
| # | Searches |
|---|---|
| 1 | exp osteoporosis/ |
| 2 | osteoporo*.tw. |
| 3 | metabolic bone disease/ |
| 4 | exp bone density/ |
| 5 | (bone adj3 densit*).tw. |
| 6 | exp fracture/ |
| 7 | cartilage fracture/ |
| 8 | fracture*.ti,ab. |
| 9 | (bone* adj2 fragil*).tw. |
| 10 | bone mineral densit*.tw. |
| 11 | bone loss.tw. |
| 12 | bmd.tw. |
| 13 | or/1-12 |
| 14 | (alendron* or fosomax or fosavance or 121268-17-5).mp. |
| 15 | (ibandron* or boniva or bondronat or bonviva or adronil or 114084-78-5).mp. |
| 16 | (risedron* or actonel or atelvia or benet or 105462-24-6).mp. |
| 17 | (zoledron* or zometa or zomera or aclasta or reclast or 118072-93-8).mp. |
| 18 | or/14-17 |
| 19 | limit 18 to yr = “2014 -Current” |
| 20 | (abaloparatide or eladynos or 247062-33-5).mp. |
| 21 | (DEN or prolia or xgeva or 615258-40-7).mp. |
| 22 | (RLX or evista or keoxifene or 84449-90-1).mp. |
| 23 | (ROMO or evenity or 909395-70-6).mp. |
| 24 | (TPTD or forsteo or 52232-67-4 or movymia or terrosa).mp. |
| 25 | or/20-24 |
| 26 | 13 and (19 or 25) |
| 27 | exp Meta Analysis/ |
| 28 | ((meta adj analy*) or metaanalys*).tw. |
| 29 | (systematic adj (review*1 or overview*1)).tw. |
| 30 | or/27-29 |
| 31 | cancerlit.ab. |
| 32 | cochrane.ab. |
| 33 | embase.ab. |
| 34 | (psychlit or psyclit).ab. |
| 35 | (psychinfo or psycinfo).ab. |
| 36 | (cinahl or cinhal).ab. |
| 37 | science citation index.ab. |
| 38 | bids.ab. |
| 39 | or/31-38 |
| 40 | reference lists.ab. |
| 41 | bibliograph*.ab. |
| 42 | hand-search*.ab. |
| 43 | manual search*.ab. |
| 44 | relevant journals.ab. |
| 45 | or/40-44 |
| 46 | data extraction.ab. |
| 47 | selection criteria.ab. |
| 48 | 46 or 47 |
| 49 | review.pt. |
| 50 | 48 and 49 |
| 51 | letter.pt. |
| 52 | editorial.pt. |
| 53 | animal/ |
| 54 | human/ |
| 55 | 53 not (53 and 54) |
| 56 | or/51-52,55 |
| 57 | 30 or 39 or 45 or 50 |
| 58 | 57 not 56 |
| 59 | 26 and 58 |
| 60 | Clinical trial/ |
| 61 | Randomized controlled trial/ |
| 62 | Randomization/ |
| 63 | Single blind procedure/ |
| 64 | Double blind procedure/ |
| 65 | Crossover procedure/ |
| 66 | Placebo/ |
| 67 | Randomi?ed controlled trial*.tw. |
| 68 | Rct.tw. |
| 69 | Random allocation.tw. |
| 70 | Randomly allocated.tw. |
| 71 | Allocated randomly.tw. |
| 72 | (allocated adj2 random).tw. |
| 73 | Single blind*.tw. |
| 74 | Double blind*.tw. |
| 75 | ((treble or triple) adj blind*).tw. |
| 76 | Placebo*.tw. |
| 77 | Prospective study/ |
| 78 | or/60-77 |
| 79 | Case study/ |
| 80 | Case report.tw. |
| 81 | Abstract report/or letter/ |
| 82 | or/79-81 |
| 83 | animal/ |
| 84 | human/ |
| 85 | 83 not (83 and 84) |
| 86 | or/79-81,85 |
| 87 | 78 not 86 |
| 88 | 26 and 87 |
| 89 | 59 or 88 |
Web of Science® Core Collection
Science Citation Index Expanded (1900–2018); Conference Proceedings Citation Index – Science (1990–2018)
Searched: 11 July 2018.
| # | Searches |
|---|---|
| # 1 | TOPIC: (osteoporo*) |
| # 2 | TOPIC: ((bone NEAR/3 densit*)) |
| # 3 | TOPIC: (fracture*) |
| # 4 | TOPIC: (bone mineral densit*) |
| # 5 | TOPIC: (bone loss) |
| # 6 | TOPIC: (bmd) |
| # 7 | #6 OR #5 OR #4 OR #3 OR #2 OR #1 |
| # 8 | TOPIC: ((alendron* or fosomax or fosavance or 121268-17-5)) |
| # 9 | TOPIC: ((ibandron* or boniva or bondronat or bonviva or adronil or 114084-78-5)) |
| # 10 | TOPIC: ((risedron* or actonel or atelvia or benet or 105462-24-6)) |
| # 11 | TOPIC: ((zoledron* or zometa or zomera or aclasta or reclast or 118072-93-8)) |
| # 12 | #11 OR #10 OR #9 OR #8 |
| Timespan = 2014-2018 | |
| # 13 | TS = ((abaloparatide or eladynos or 247062-33-5)) |
| # 14 | TS = ((DEN or prolia or xgeva or 615258-40-7)) |
| # 15 | TS = ((RLX or evista or keoxifene or 84449-90-1)) |
| # 16 | TS = ((ROMO or evenity or 909395-70-6)) |
| # 17 | TS = ((TPTD or forsteo or 52232-67-4 or movymia or terrosa)) |
| # 18 | #17 OR #16 OR #15 OR #14 OR #13 |
| # 19 | #7 and (#12 or #18) |
| # 20 | TS = ((meta-analysis or meta analy* or metaanaly*)) OR TS = ((“review literature” or “literature review”)) OR TS = ((“systematic review*” or “systematic overview*”)) OR TS = ((cochrane or embase or psychlit or psyclit or psychinfo or psycinfo or cinahl or cinhal or science citation index or bids or cancerlit)) OR TS = ((“reference list*” or bibliograph* or hand-search* or “relevant journals” or “manual search*”)) OR TS = (((“selection criteria” or “data extraction”) and review)) |
| # 21 | #20 AND #19 |
| # 22 | TS = ((“clinic* trial*” or “randomi* controlled trial*”)) OR TS = (((singl* or doubl* or treb* or tripl*) and (blind* or mask*))) OR TS = ((placebo*)) OR TS = ((allocat* and random*)) |
| # 23 | #22 AND #19 |
Cochrane Database of Systematic Reviews: Wiley Online Library, 1996–2018; Cochrane Central Register of Controlled Trials (CENTRAL): Wiley Online Library, 1898–2018; Health Technology Assessment Database: Wiley Online Library, 1995–2016; Database of Abstracts of Reviews of Effects (DARE): Wiley Online Library, 1995–2015
Searched: 11 July 2018.
| # | Searches |
|---|---|
| #1 | MeSH descriptor: [Osteoporosis] explode all trees |
| #2 | osteoporo*:ti,ab,kw |
| #3 | MeSH descriptor: [Bone Diseases, Metabolic] this term only |
| #4 | MeSH descriptor: [Bone Density] this term only |
| #5 | (bone next/3 densit*):ti,ab,kw |
| #6 | MeSH descriptor: [Fractures, Bone] explode all trees |
| #7 | MeSH descriptor: [Fractures, Cartilage] explode all trees |
| #8 | fracture*:ti,ab |
| #9 | (bone* next/2 fragil*):ti,ab,kw |
| #10 | bone mineral densit*:ti,ab,kw |
| #11 | bone loss:ti,ab,kw |
| #12 | bmd:ti,ab,kw |
| #13 | #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or #9 or #10 or #11 or #12 |
| #14 | (alendron* or fosomax or fosavance or 121268-17-5):ti,ab,kw |
| #15 | (ibandron* or boniva or bondronat or bonviva or adronil or 114084-78-5):ti,ab,kw |
| #16 | (risedron* or actonel or atelvia or benet or 105462-24-6):ti,ab,kw |
| #17 | (zoledron* or zometa or zomera or aclasta or reclast or 118072-93-8):ti,ab,kw |
| #18 | (or #14-#17) |
| #19 | #13 and #18 Publication Year from 2014 to 2018 |
| #20 | (abaloparatide or eladynos or 247062-33-5):ti,ab,kw |
| #21 | (DEN or prolia or xgeva or 615258-40-7):ti,ab,kw |
| #22 | (RLX or evista or keoxifene or 84449-90-1):ti,ab,kw |
| #23 | (ROMO or evenity or 909395-70-6):ti,ab,kw |
| #24 | (TPTD or forsteo or 52232-67-4 or movymia or terrosa):ti,ab,kw |
| #25 | (or #20-#24) |
| #26 | #19 or #25 |
World Health Organization International Clinical Trials Registry Platform
Searched: 11 July 2018.
| # | Searches |
|---|---|
| 1 | (alendron* or fosomax or fosavance or 121268-17-5).mp. |
| 2 | (ibandron* or boniva or bondronat or bonviva or adronil or 114084-78-5).mp. |
| 3 | (risedron* or actonel or atelvia or benet or 105462-24-6).mp. |
| 4 | (zoledron* or zometa or zomera or aclasta or reclast or 118072-93-8).mp. |
| 5 | (abaloparatide or eladynos or 247062-33-5).mp. |
| 6 | (DEN or prolia or xgeva or 615258-40-7).mp. |
| 7 | (RLX or evista or keoxifene or 84449-90-1).mp. |
| 8 | (ROMO or evenity or 909395-70-6).mp. |
| 9 | (TPTD or forsteo or 52232-67-4 or movymia or terrosa).mp. |
Thirty-four systematic reviews were checked for RCTs meeting the inclusion criteria. 214–247
Cost-effectiveness studies of osteoporosis
Ovid MEDLINE(R) and Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Daily, and Versions(R), 1946–2018
Searched: 16 July 2018.
| # | Searches |
|---|---|
| 1 | exp osteoporosis/ |
| 2 | osteoporo*.tw. |
| 3 | bone diseases, metabolic/ |
| 4 | exp Bone Density/ |
| 5 | (bone adj3 densit*).tw. |
| 6 | exp fractures, bone/ |
| 7 | fractures, cartilage/ |
| 8 | fracture*.tw. |
| 9 | (bone* adj2 fragil*).tw. |
| 10 | bone mineral densit*.tw. |
| 11 | bone loss.tw. |
| 12 | bmd.tw. |
| 13 | or/1-12 |
| 14 | exp “Costs and Cost Analysis”/ |
| 15 | Economics/ |
| 16 | exp Economics, Hospital/ |
| 17 | exp Economics, Medical/ |
| 18 | Economics, Nursing/ |
| 19 | exp models, economic/ |
| 20 | Economics, Pharmaceutical/ |
| 21 | exp “Fees and Charges”/ |
| 22 | exp Budgets/ |
| 23 | budget*.tw. |
| 24 | ec.fs. |
| 25 | cost*.ti. |
| 26 | (cost* adj2 (effective* or utilit* or benefit* or minimi*)).ab. |
| 27 | (economic* or pharmacoeconomic* or pharmaco-economic*).ti. |
| 28 | (price* or pricing*).tw. |
| 29 | (financial or finance or finances or financed).tw. |
| 30 | (fee or fees).tw. |
| 31 | (value adj2 (money or monetary)).tw. |
| 32 | quality-adjusted life years/ |
| 33 | (qaly or qalys).af. |
| 34 | (quality adjusted life year or quality adjusted life years).af. |
| 35 | or/14-34 |
| 36 | 13 and 35 |
| 37 | limit 36 to yr = “2014 -Current” |
EMBASE, 1974–2018
Searched: 16 July 2018.
| # | Searches |
|---|---|
| 1 | exp osteoporosis/ |
| 2 | osteoporo*.tw. |
| 3 | metabolic bone disease/ |
| 4 | exp bone density/ |
| 5 | (bone adj3 densit*).tw. |
| 6 | exp fracture/ |
| 7 | cartilage fracture/ |
| 8 | fracture*.ti,ab. |
| 9 | (bone* adj2 fragil*).tw. |
| 10 | bone mineral densit*.tw. |
| 11 | bone loss.tw. |
| 12 | bmd.tw. |
| 13 | or/1-12 |
| 14 | *economics/ |
| 15 | (economic adj2 model*).mp. |
| 16 | (cost minimi* or cost-utilit* or health utilit* or economic evaluation* or economic review* or cost outcome or cost analys?s or economic analys?s or budget* impact analys?s).ti,ab,hw,kw. |
| 17 | (cost-effective* or pharmacoeconomic* or pharmaco-economic* or cost-benefit or costs).ti,hw,kw. |
| 18 | (life year or life years or qaly* or cost-benefit analys?s or cost-effectiveness analys?s).ab,hw,kw. |
| 19 | (cost or economic*).ti,hw,kw. and (costs or cost-effectiveness or markov).ab. |
| 20 | or/14-19 |
| 21 | 13 and 20 |
| 22 | limit 21 to yr = “2014 -Current” |
Health Technology Assessment Database: Centre for Reviews and Dissemination, 1995–2016; NHS Economic Evaluation Database: Centre for Reviews and Dissemination, 1995–2015; Database of Abstracts of Reviews of Effects: Centre for Reviews and Dissemination, 1995–2015
Searched: 16 July 2018.
| # | Searches |
|---|---|
| 1 | MeSH DESCRIPTOR Osteoporosis EXPLODE ALL TREES |
| 2 | (osteoporo*) |
| 3 | MeSH DESCRIPTOR Bone Diseases, Metabolic |
| 4 | MeSH DESCRIPTOR Bone Diseases |
| 5 | (bone adj3 densit*) |
| 6 | MeSH DESCRIPTOR Fractures, Bone EXPLODE ALL TREES |
| 7 | MeSH DESCRIPTOR Fractures, Cartilage EXPLODE ALL TREES |
| 8 | (fracture*) |
| 9 | (bone* adj2 fragil*) |
| 10 | (bone mineral densit*) |
| 11 | (bone loss) |
| 12 | (bmd) |
| 13 | #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 |
| 14 | (#14) FROM 2014 TO 2018 |
| 15 | (#15) IN HTA FROM 2014 TO 2018 |
| 16 | (#15) IN NHSEED FROM 2014 TO 2018 |
| 17 | (#15) IN DARE FROM 2014 TO 2018 |
The EuroQol-5 Dimensions and osteoporosis
Ovid MEDLINE(R) and Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Daily, and Versions(R), 1946–2018
Searched: 19 July 2018.
| # | Searches |
|---|---|
| 1 | exp osteoporosis/ |
| 2 | bone diseases, metabolic/ |
| 3 | osteoporo*.tw. |
| 4 | or/1-3 |
| 5 | (bone adj6 densit*).tw. |
| 6 | bone density/ |
| 7 | bmd.ti,ab. |
| 8 | (bone or bones).mp. |
| 9 | exp densitometry/ |
| 10 | tomography, x-ray computed/ |
| 11 | densit*.tw. |
| 12 | 10 and 11 |
| 13 | 9 or 12 |
| 14 | 8 and 13 |
| 15 | 5 or 6 or 7 or 14 |
| 16 | exp fractures, bone/ |
| 17 | fractures, cartilage/ |
| 18 | fracture*.ti,ab. |
| 19 | or/16-18 |
| 20 | 15 or 19 |
| 21 | 4 and 20 |
| 22 | (euroqol or euro qol or eq5d or eq 5d).mp. |
| 23 | 21 and 22 |
| 24 | limit 23 to yr = “2014 -Current” |
EMBASE, 1974–2018
Searched: 19 July 2018.
| # | Searches |
|---|---|
| 1 | exp osteoporosis/ |
| 2 | osteoporo*.tw. |
| 3 | metabolic bone disease/ |
| 4 | or/1-3 |
| 5 | (bone adj6 densit*).tw. |
| 6 | bone density/ |
| 7 | bmd.ti,ab. |
| 8 | (bone or bones).mp. |
| 9 | exp densitometry/ |
| 10 | tomography/ |
| 11 | densit*.tw. |
| 12 | 10 and 11 |
| 13 | 9 or 12 |
| 14 | 8 and 13 |
| 15 | 5 or 6 or 7 or 14 |
| 16 | exp fracture/ |
| 17 | cartilage fracture/ |
| 18 | fracture*.ti,ab. |
| 19 | 16 or 17 or 18 |
| 20 | 15 or 19 |
| 21 | 4 and 20 |
| 22 | (euroqol or euro qol or eq5d or eq 5d).mp. |
| 23 | 21 and 22 |
| 24 | limit 23 to yr = “2014 -Current” |
Appendix 2 Excluded studies
Thirty-four studies of non-bisphosphonates were excluded.
| Trial | Reason for exclusion |
|---|---|
| Bone 2008188 and extension (Bone 2011)189 |
|
| Naylor 2010186 |
|
| Dore 2010248 |
|
| Cosman 2009249 |
|
| Smith 2009250 |
|
| Ellis 2008251 |
|
| Gnant 2015252 |
|
| Klotz 2014253 |
|
| Raje 2018254 |
|
| Henry 2010255 |
|
| Fazeli 2014256 |
|
| RUTH257 |
|
| Bonani 2012258 |
|
| Haghverdi 2014259 |
|
| Szczepanek 2017260 |
|
| Zhu 2017261 |
|
| Thomas 2014262 |
|
| Galesanu 2015263 |
|
| TOWER264 |
|
| Cosman 2008265 |
|
| Body 2002266 |
|
| Finkelstein 2010267 |
|
| Iseri 2017268 |
|
| Iwamoto 2008269 |
|
| Roux 2014270 |
|
| Mok 2014271 |
|
| Gonnelli 2006272 |
|
| CORE (extension of MORE)273 |
|
| Majima 2008274 |
|
| Seeman 2010275 |
|
| SHOTZ276 |
|
| Bai 2013277 |
|
| AVA osteoporosis278 |
|
Appendix 3 Bisphosphonate studies
Of 48 RCTs (reported in 59 references) included in TA464,9,34 38 RCTs (reported in 48 references) were included in the NMAs of fracture and/or femoral neck BMD data in this report.
Three additional bisphosphonate RCTs were identified by the searches in this report (see Appendix 1) to update the review of TA464. These were included in the NMAs.
Seven RCTs from TA464 were excluded for not reporting either fracture or femoral neck BMD data. In addition, three RCTs of bisphosphonates from TA464 were excluded for being conducted in a cancer population.
| Trial | Population | Intervention and comparator(s) | Vertebral fracture NMA | Femoral neck BMD NMA |
|---|---|---|---|---|
| Adami 1995279 | Postmenopausal women with osteoporosis |
|
Yes | |
| FIT I (Black 1996)280 | Postmenopausal women with osteoporosis |
|
Yes | Yes |
| FIT II (Cummings 1998)281 | Postmenopausal women with osteoporosis |
|
Yes | Yes |
| Bone 2000282 | Postmenopausal women with osteoporosis |
|
Yes | |
| Carfora 1998135 | Postmenopausal women with osteoporosis |
|
Yes | |
| Dursun 2001131 | Postmenopausal women with osteoporosis |
|
Yes | Yes |
| Greenspan 2002283 | Postmenopausal women with osteoporosis |
|
Yes | |
| Greenspan 2003284 | Postmenopausal women aged ≥ 65 years |
|
Yes | |
| Ho 2005285 | Postmenopausal women with osteoporosis |
|
Yes | |
| Liberman 1995134 | Postmenopausal women with osteoporosis |
|
Yes | Yes |
| Orwoll 2000286 | Men with osteoporosis |
|
Yes | Yes |
| Miller 2004129 | Men with osteoporosis |
|
Yes | |
| FOSIT (Pols 1999)287 | Postmenopausal women with osteoporosis |
|
Yes | |
| Saag 1998;288 Adachi 2001289 | Men and women with glucocorticoid-induced osteoporosis |
|
Yes | |
| BONE (Chesnut 2004);136 Chesnut 2005290 | Postmenopausal women with osteoporosis |
|
Yes | Yes |
| McClung 2009291 | Postmenopausal women with osteoporosis |
|
Yes | |
| DIVA (Delmas 2006);292 Eisman 2008293 | Postmenopausal women with osteoporosis |
|
Yes | |
| MOBILE (Miller 2005);294 Reginster 2006181 | Postmenopausal women with osteoporosis |
|
Yes | |
| Boonen 2009295 | Men with osteoporosis |
|
Yes | Yes |
| Cohen 1999296 | Men and women aged 18–85 years receiving glucocorticoids |
|
Yes | Yes |
| BMD-MN (Fogelman 2000)297 | Postmenopausal women with osteoporosis |
|
Yes | Yes |
| Hooper 2005132 | Postmenopausal women with osteoporosis |
|
Yes | Yes |
| VERT-NA (Harris 1999);298 Ste-Marie (2004)299 | Postmenopausal women with osteoporosis |
|
Yes | Yes |
| VERT-MN (Reginster 2000);300 Sorensen 2003301 | Postmenopausal women with osteoporosis |
|
Yes | Yes |
| Leung 2005302 | Postmenopausal women with osteoporosis |
|
Yes | |
| Reid 2000303 | Men and women taking glucocorticoids for ≥ 6 months |
|
Yes | Yes |
| Ringe 2006;304 Ringe 2009305 | Men with osteoporosis |
|
Yes | |
| HORIZON-PFT (Black 2007);133 Reid 2010306 | Postmenopausal women with osteoporosis |
|
Yes | Yes |
| HORIZON-RFT (Lyles 2007);307 Adachi 2011308 | Men and women aged ≥ 50 years within 90 days after surgical repair of a hip fracture |
|
Yes | Yes |
| Boonen 2012309 | Men with osteoporosis |
|
Yes | Yes |
| McClung 2009310 | Postmenopausal women with osteoporosis |
|
Yes | |
| MOTION (Miller 2008)311 | Postmenopausal women with osteoporosis |
|
Yes | Yes |
| Muscoso 200479 | Postmenopausal women with osteoporosis |
|
Yes | |
| Sarioglu 2006312 | Postmenopausal women with osteoporosis |
|
Yes | |
| FACT (Rosen 2005);313 Bonnick 2006314 | Postmenopausal women with osteoporosis |
|
Yes | |
| FACTS (Reid 2006;315 Reid 2008316) | Postmenopausal women with osteoporosis |
|
Yes | |
| HORIZON (Reid 2009)317 | Men and women taking glucocorticoids for < 3 months or ≥ 3 months |
|
Yes | Yes |
| Trial | Population | Intervention and comparators | Included in fracture rate NMA? | Included in femoral neck BMD NMA? |
|---|---|---|---|---|
| TRIO137 | Postmenopausal women with osteoporosis |
|
No | Yes |
| Tan 2016138 | Postmenopausal women with osteoporosis |
|
No | Yes |
| ZONE130 | Women and men with osteoporosis |
|
Yes | No |
| Trial | Population | Intervention and comparators | Reason for exclusion |
|---|---|---|---|
| Chesnut 1995318 | Postmenopausal women with osteoporosis |
|
Outcome outside scope |
| CORAL (Klotz 2013)319 | Men with androgen deprivation bone loss in non-metastatic prostate cancer |
|
Population outside scope, cancer |
| Shilbayeh 2004320 | Postmenopausal women with osteoporosis |
|
Outcome outside scope |
| Smith 2004321 | Men and women with asthma and/or chronic obstructive airways disease |
|
Outcome outside scope |
| ARIBON (Lester 2008)322 | Postmenopausal women with breast cancer |
|
Outcome outside scope |
| Choo 2011323 | Men with androgen deprivation bone loss in non-metastatic prostate cancer |
|
Population outside scope; cancer |
| McClung 2001324 | Postmenopausal women with osteoporosis |
|
Outcome outside scope |
| Taxel 2010325 | Men aged > 55 years and within 1 month of receiving an initial injection of androgen deprivation therapy for prostate cancer |
|
Population outside scope; cancer |
| Atmaca 2006326 | Postmenopausal women with osteoporosis |
|
Outcome outside scope |
| ROSE (Hadji 2010;327 Hadji 2012328) | Postmenopausal women with osteoporosis |
|
Outcome outside scope |
Appendix 4 Trial and population characteristics
| Trial name: first author and year | Trial design | Population eligibility | Intervention and comparators, number randomised to each group | Concomitant treatment | Follow-up duration | Primary outcome |
|---|---|---|---|---|---|---|
| DEN vs. placebo | ||||||
| FREEDOM: Cummings 2009;41 Bone 2017104 | International, randomised, placebo-controlled trial – 21 centres in USA and Canada | Women between the ages of 60 and 90 years with a lumbar spine or total hip T-score of < –2.5 |
|
All women received daily supplements containing at least 1000 mg of calcium | 36 months and OLE to 84 months | New vertebral fracture |
| Excluded if they had conditions that influence bone metabolism or had taken oral bisphosphonates for > 3 years | ||||||
| ADAMO (NCT00980174): Orwoll 201242 | Randomised placebo-controlled Phase III trial; international, multicentre (Belgium, Canada, Denmark, France, Poland, Sweden, the USA) | Men with low BMD, lumbar spine or femoral neck BMD T-score of ≤ –2.0 or ≥ –3.5, or previous major osteoporotic fracture and BMD-score of ≤ –1.0 or ≥ –3.5 |
|
Daily calcium (≥ 1000 mg) and vitamin D (≥ 800 IU) | 24 months | Lumbar spine BMD percentage change from baseline at 12 months |
| Excluded if severe, or multiple, vertebral fracture(s), conditions that influence bone metabolism or prior bisphosphonate treatment (≥ 3 months in previous 2 years or ≥ 1 month in prevous year or within 3 months of randomisation | ||||||
| DIRECT (NCT00680953): Nakamura 201443 | Randomised placebo-controlled Phase III trial, multicentre, Japan, OLE | Postmenopausal women and men aged ≥ 50 with osteoporosis; 1–4 vertebral fractures and lumbar spine BMD T-score of < –1.7 (YAM in Japan 80%), or total hip BMD T-score of < –1.6 |
|
Daily calcium (≥ 600 mg) and vitamin D (≥ 400 IU) | 36 months | Incidence of new or worsening vertebral fracture by X-ray at 24 months |
| Excluded if severe, or two or more moderate, vertebral fractures, conditions that influence bone metabolism, or prior bisphosphonate treatment (≥ 3 years, or with 6 months of randomisation), prior hormonal treatments, calcitonin or TPTD within 6 weeks of enrolment | ||||||
| Nakamura 201244 | Randomised placebo-controlled Phase II trial, multicentre, Japan | Postmenopausal women aged ≤ 80 years, ambulatory, osteoporosis, lumbar spine BMD T-score (for Japanese subjects) of ≤ –2.5 or ≥ –4.0 or femoral neck or total hip BMD of ≤ –2.5 or ≥ –3.5 |
|
Daily calcium (≥ 600 mg) and vitamin D (≥ 400 IU) | 12 months | Lumbar spine BMD percentage change from baseline at 12 months |
| Excluded if any severe or two or more moderate vertebral fracture, hypocalcaemia, prior bisphosphonates or parathyroid hormone within 12 months, or hormonal or calcium treatment within 3 months prior to randomisation | ||||||
| Koh 201645 (NCT01457950) | Randomised placebo-controlled Phase III trial, multicentre, Korea, OLE | Postmenopausal women aged 60–90 years, Korean-born, lumbar spine or total hip BMD of < –2.5 or ≥ –4.0 |
|
Daily calcium (≥ 1000 mg) and vitamin D (≥ 400 IU) | 12 months | Lumbar spine BMD percentage change from baseline at 6 months |
| Excluded if conditions that influence bone metabolism, increased risk of ONJ, hypo- or hypercalcaemic, vitamin D deficiency, prior treatment with bone metabolism drugs | ||||||
| RLX vs. placebo | ||||||
| Adami 200846 | International, randomised-controlled trial – 32 clinical centres in seven countries (the USA, France, Germany, Spain, Italy, Canada and Australia) | Postmenopausal women aged 50–80 years, BMD T-score of < –2.5 at the lumbar spine |
|
All participants received oral supplements of at least 500 mg per day of elemental calcium and 400–800 IU per day of vitamin D | 12 months from randomisation | Lumbar spine BMD |
| Exclude if had condition or receiving treatment affecting BMD | ||||||
| Morii 2003;47 Japan; Clinical Trial Research Group | Randomised placebo-controlled, multicentre; Japan | Postmenopausal (≥ 2 years) women, aged ≤ 80 years, lumbar spine BMD of ≤ –2.5 YAM |
|
Daily calcium (500 mg) and vitamin D (200 IU) | 12 months | Lumbar spine BMD percentage change from baseline at 12 months |
| Excluded if conditions that influence bone metabolism, hormonal therapy, pathologic fractures or lumbar spine BMD unevaluable, bisphosphonates within 6 months | ||||||
| Liu 200448 | Randomised placebo-controlled, multicentre; China | Postmenopausal (≥ 2 years) women, aged 50–80 years, lumbar spine or femoral neck BMD T-score of ≤ –2.5 |
|
Daily calcium (500 mg) and vitamin D (200 IU) | 12 months | Lumbar spine BMD percentage change from baseline at 12 months |
| Excluded if conditions or treatments that influence bone metabolism | ||||||
| Gorai 201249 | Randomised controlled trial, open-label, two centres, Japan | Postmenopausal (≥ 2 years) women, lumbar spine BMD of ≤ –2.0 YAM |
|
NA | 24 months | Lumbar spine BMD percentage change from baseline and bone turnover |
| Excluded if conditions or treatments that influence bone metabolism, bisphosphonates within 18 months | ||||||
| Silverman 200850 (NCT00205777) | Randomised controlled trial, Phase III, multicentre, Argentina, Australia, Austria, Belgium, Brazil, Bulgaria, Canada, Chile, Croatia, Denmark, Estonia, Finland, France, Germany, Greece, Hong Kong, Hungary, Italy, Lithuania, Mexico, the Netherlands, New Zealand, Norway, Poland, Romania, Russian Federation, Slovakia, South Africa, Spain, the USA | Postmenopausal (≥ 2 years) women, aged 55–85 years, lumbar spine or femoral neck BMD T-score of ≤ –2.0 or ≥ –4.0, or one or more mild vertebral fracture and lumbar spine or femoral neck BMD T-score of ≥ –4.0 |
|
Daily calcium (≤ 1200 mg) and vitamin D (400–800 IU) | 36 months | Percentage of new vertebral fractures, as determined by X-ray, at 36 months |
| Excluded if conditions that influence bone metabolism, history of thrombosis, hormonal or bisphosphonate treatment within 6 months | ||||||
| MORE51,102 | Randomised controlled trial, multicentre, Canada, Europe, South America, USA | Postmenopausal (≥ 2 years) women, femoral neck or lumbar spine BMD T-score of < –2.5; or one or more moderate or severe, or two or more mild or moderate, vertebral fractures |
|
Daily calcium (500 mg) and vitamin D (400–600 IU) | 36 months | Incident vertebral fractures and BMD |
| Excluded if conditions that influence bone metabolism, history of thrombosis, hormonal therapy 2 months, bisphosphonates with 6 months, pathologic fractures, unevaluable by thoracic/lumbar X-ray | ||||||
| Lufkin 199852 | Randomised controlled trial, two centres, USA | Postmenopausal (≥ 5 years) women, aged 45–75 years, ambulatory, lumbar spine or femoral neck BMD ≤ 10th percentile of normal and one or more non-traumatic vertebral fracture |
|
Daily calcium (750 mg) and vitamin D (800 IU) | 12 months | Biochemical markers of bone turnover |
| Excluded if conditions that influence bone metabolism, history of thrombosis, prior bisphosphonates, hormonal therapy within 6 months | ||||||
| Mok 201153 (NCT00371956) | Randomised placebo-controlled trial, Phase IV, two sites, China | Postmenopausal (≥ 1 year) women receiving long-term glucocorticoid treatment (prednisone, ≤ 10 mg per day or equivalent) for ≥ 6 months |
|
Daily calcium (1000 mg) and calcitrol (0.25 µg) | 12 months | Lumbar spine and hip BMD percentage change from baseline at 12 months |
| Excluded if history of thrombosis or hypercoagulability, prior bisphosphonates or PTH | ||||||
| ROMO vs. placebo | ||||||
| FRAME: Cosman 201654 | International, randomised controlled trial – 25 countries across Latin America, Central and Eastern Europe, Western Europe, Australia or New Zealand, Asia Pacific and the USA | Women aged 55–90 years with a T-score of –2.5 to –3.5 at the total hip or femoral neck |
|
|
12 months from randomisation then a further 12 months open label following treatment-switching | New vertebral fractures |
| Excluded if had a history of hip or severe vertebral fracture, conditions or treatment affecting BMD, ONJ and low 25-hydroxyvitamin D level | ||||||
| Ishibashi 201755 (NCT01992159) | Randomised placebo-controlled trial, Phase II, multicentre, Japan | Postmenopausal women aged 55–85 years, ambulatory, lumbar spine, femoral neck or total hip BMD T-score of ≤ –2.5, lumbar spine BMD of > –4.0, femoral neck or total hip BMD of > –3.5 |
|
Daily calcium (≥ 500 mg) and vitamin D (≥ 600 IU) | 15 months | Lumbar spine BMD percentagte change from baseline at 12 months |
| Excluded if condition or prior treatment influencing bone metabolism, including i.v. bisphosphonates within 5 years, oral bisphosphonates within 6 months or for ≥ 1 months within 1 year, or > 3 years, or prior DEN within 18 months, or PTH within 1 year, history of vertebral or hip fracture | ||||||
| BRIDGE: (NCT02186171)56 | Randomised placebo-controlled trial, Phase III, multicentre, Europe, Latin America, Japan, North America | Men aged 55–90 years, lumbar spine, total hip or femoral neck BMD T-score of ≤ –2.5, or ≤ –1.5 with fragility fracture, evaluable for lumbar spine and hip DXA |
|
Daily calcium (500–1000 mg) and vitamin D (600–800 IU) | 15 months | Lumbar spine BMD percentage change from baseline at 12 months |
| Excluded if condition or current treatment influencing bone metabolism, hip or femoral neck T-score of ≤ –3.5, hip fracture | ||||||
| TPTD vs. placebo | ||||||
| Orwoll 200357 | International, randomised, placebo-controlled trial – 37 centres in 11 countries (countries NR) | Men aged 30–85 years with lumbar spine or proximal femur (neck or total hip) BMD at least 2 SD below the average for young, healthy men |
|
All subjects also received supplemental calcium and vitamin D | The study was stopped after a median duration of 11 months | Lumbar spine BMD percentage change from baseline |
| Secondary causes of metabolic bone disease, were excluded | ||||||
| Miyauchi 201058 (NCT00433160) | Randomised placebo-controlled Phase III trial, multicentre, Japan | Postmenopausal (≥ 5 years) women and men, ambulatory, aged ≥ 55 years, lumbar spine BMD of < 80% YAM for Japanese subjects (approximate T-score –2.6) and one or more vertebral fragility fracture; or aged ≥ 65 years approximate lumbar spine BMD T-score of –1.7; or aged ≥ 55 years with lumbar spine BMD of < 65% YAM |
|
Daily calcium (610 mg) and vitamin D (400 IU) | 24 months | Lumbar spine BMD percentage change from baseline at 12 months |
| Miyauchi 200859 | Randomised placebo-controlled Phase II trial, multicentre, Japan | Postmenopausal (≥ 5 years) women, ambulatory, aged ≥ 55 years, lumbar spine BMD of < 80% YAM for Japanese subjects (approximate T-score of –2.6) and one or more moderate, or two or more mild, vertebral fragility fracture; or aged ≥ 65 years and < 70% YAM; or lumbar spine BMD of < 60% YAM |
|
Daily calcium (610 mg) and vitamin D (400 IU) | 6 months | Lumbar spine BMD percentage change from baseline at 24 weeks |
| Excluded if conditions that influence bone metabolism, treatment influencing bone metabolism within 24 months of randomisation | ||||||
| ACTIVE95 (NCT01343004) | Randomised placebo-controlled Phase III trial, multicentre, Argentina, Brazil, Czech Republic, Denmark, Estonia, Hong Kong, Lithuania, Poland, Romania, the USA | Postmenopausal women, age 49–86 years, femoral neck or lumbar spine BMD T-score of ≤ –2.5 or > –5.0 and two or more mild or one or more moderate vertebral fractures, or other low-trauma fracture within 5 years; or age ≥ 65 years and T-score of ≤ –2.0 or > –5.0; or age ≥ 65 years without fracture and T-score of ≤ –3.0 or > –5.0 |
|
Adequate calcium and vitamin D (25-hydroxyvitamin D concentrations in serum > 37.5 nmol/l) | 18 months | Percentage with one or more new vertebral fracture (as determined by X-ray) |
| Excluded if severe, or four or more mild/moderate, vertebral fractures, < 2 evaluable lumbar vertebrae, hip BMD unevaluable, conditions that influence bone metabolism, treatment influencing bone metabolism, bisphosphonates (≥ 3 months) within 5 years, DEN within 1 year | ||||||
| Leder 201561 | Randomised, parallel-group, multicentre, dose-finding, double-blind, placebo-controlled trial – 30 centres in the USA, Argentina, India and the UK | Postmenopausal women aged 55–85 years with a T-score of ≤ –2.5 at the lumbar spine or femoral neck or total hip, or T-score of ≤ –2.0 plus low-trauma fracture, or T-score of ≤ –2.0 plus risk factor for osteoporosis |
|
All subjects received supplemental calcium (500–1000 mg) and vitamin D (400–800 IU) | 6 months plus a further 6-month extension to 12 months | BMD percentage change from baseline and bone turnover markers |
| Treatments and conditions affecting BMD were excluded | ||||||
| FPT62 (NCT00670501) | Randomised placebo-controlled Phase III trial, multicentre, Argentina, Australia, Austria, Belgium, Canada, Czech Republic, Denmark, Finland, Hungary, Israel, Italy, the Netherlands, New Zealand, Norway, Poland, Sweden, the USA | Postmenopausal (≥ 5 years) women, ambulatory, one or more moderate or two or more mild atraumatic vertebral fractures; or fewer than two moderate fractures, T-score BMD hip or lumbar spine of ≤ –1 |
|
Daily calcium 1000 mg and vitamin D 400–1200IU | Trial stopped early. Maximum follow-up 24 months. Median follow-up of 21 months for radiographic outcomes and 19 for other outcomes | Percentage with 1 + new vertebral fracture (X-ray) |
| Excluded if conditions that influence bone metabolism, bisphosphonates within 3 months before randomisation or for ≥ 60 days in the 24 months before randomisation, other prior treatment that influenced bone metabolism within 6 months | ||||||
| Sethi 200863 (NCT00500409) | Randomised placebo-controlled, open-label, Phase III trial, multicentre, India | Postmenopausal (≥ 3 years) women, aged 45–75 years, lumbar spine or femoral neck BMD T-score of ≤ –2.5 |
|
Daily calcium (1000 mg) and vitamin D | 180 days | Lumbar spine BMD percentage change from baseline at 6 months |
| Excluded if conditions that influence bone metabolism, lumbar spine BMD unevaluable, prior treatment that influenced bone metabolism within 6 months, current steroids, anticoagulants or anticonvulsants | ||||||
| Head-to-head non-bisphosphonates | ||||||
| DATA64 (NCT00926380); DATA-Switch65 | Randomised controlled Phase II trial, open-label single centre, the USA | Postmenopausal women, aged ≥ 45 years, lumbar spine, femoral neck or hip T-score of ≤ –2.5; or T-score of ≤ –2.5 plus risk factor for fracture; or T-score of ≤ –1.0 plus fragility fracture |
|
Daily calcium (1200 mg) and vitamin D (25-hydroxyvitamin D concentrations in serum > 50 nmol/l) | 24 months | Lumbar spine BMD percentage change from baseline at 12 months |
| Excluded if conditions that influence bone metabolism, history of i.v. bisphosphonates or strontium ranelate; glucocorticoids or oral bisphosphonates within 6 months; hormonal or calcium therapy with 3 months of randomisation | ||||||
| EUROFORS66 | Randomised controlled open-label trial, multicentre, Austria, Belgium, Denmark, France, Germany, Greece, Iceland, Portugal, Spain, the UK | Postmenopausal (≥ 2 years) women, aged ≥ 55 years, lumbar spine or femoral neck or total hip BMD T-score of ≤ –2.5, one or more vertebral or non-vertebral fragility fracture within 3 years, ≥ 2 BMD evaluable lumbar vertebrae |
|
Daily calcium (≥ 500 mg) and vitamin D (400–800 IU) | 12 months post randomisation (24 months total) | Lumbar spine BMD percentage change from baseline at 24 months |
| Excluded if conditions or treatments that influence bone metabolism | ||||||
| STRUCTURE67 (NCT01796301) | Randomised controlled trial, open-label, Phase III, multicentre, North America, Latin America, Europe | Postmenopausal osteoporosis (≥ 3 years); aged 55–90 years; vertebral fracture or non-vertebral after age 50; lumbar spine, femoral neck or total hip BMD T-score of ≤ –2.5; ≥ 3 years of bisphosphonate therapy; evaluable for hip and lumbar spine BMD |
|
Daily calcium (500–1000 mg) and vitamin D (600–800 IU) | 12 months | Hip BMD percentage change from baseline at 12 months |
| Excluded if condition, or non-bisphosphonate treatment, influencing bone metabolism | ||||||
| McClung 201468 | Phase III, multicentre, international, randomised, placebo-controlled, parallel-group, eight-group study – 28 centres in Argentina, Austria, Belgium, Canada, Denmark, Spain, and the USA | Postmenopausal women aged 55–85 years with a T-score of ≤ –2.0 at the lumbar spine, total hip or femoral neck and ≥ –3.5 at each of these sites |
|
All the participants were required to take at least 1000 mg of elemental calcium and 800 IU of vitamin D daily | 12 months | Lumbar spine BMD percentage change from baseline |
| Treatments and conditions affecting BMD were excluded | ||||||
| DEN vs. bisphosphonates | ||||||
| DECIDE69 | Randomised controlled trial, Phase III, non-inferiority, multicentre, Australia, Europe, North America, South America | Postmenopausal women, ambulatory, lumbar spine or total hip BMD T-score of ≤ –2.0, evaluable for hip and lumbar spine BMD |
|
Daily calcium (≥ 500 mg) and vitamin D (400–800 IU) | 12 months | Lumbar spine BMD percentage change from baseline at 12 months |
| Excluded if condition influencing bone metabolism, prior i.v. bisphosphonates, other treatments influencing bone metabolism within 3 months | ||||||
| STAND: Kendler 201070 | Phase III international, multicentre, randomised, double-blind, double-dummy, parallel-group. Countries NR | Women aged ≥ 55 years with a lumbar spine or total hip T-score of between –4.0 and –2.0, receiving ALN equivalent to 70 mg per week for at least 6 months | Open-label ALN, 70 mg weekly for 1 month then one of the following:
|
Daily calcium (1000 mg) and at least 400 IU of vitamin D | 12 months | Total hip BMD percentage change from baseline |
| Treatments and conditions affecting BMD were excluded | ||||||
| DAPS: Kendler 201171 and 2012109 | Multicentre, randomised, open-label, 2-year, crossover – 20 centres in the USA and five centres in Canada | Postmenopausal women with low BMD who had not received prior bisphosphonate or DEN therapy, with T-scores of between –4.0 and –2.0 at the lumbar spine, total hip or femoral neck |
|
Daily calcium (1000 mg) and vitamin D (≥ 400 IU) supplementation | 12 months prior to crossover | Treatment adherence in the first 12 months |
| Treatments and conditions affecting BMD were excluded | ||||||
| AMG 162 Bone Loss study: McClung 200672 | Randomised, placebo-controlled, dose-ranging study – 29 study centres in the USA | Osteopenic and osteoporotic postmenopausal women ages ≤ 80 years with a T-score of –1.8 to –4.0 at the lumbar spine or –1.8 to –3.5 at either the femoral neck or total hip |
|
Daily calcium (1 g) and vitamin D (400 IU) | 12 months | Lumbar spine BMD percentage change from baseline |
| Treatments and conditions affecting BMD were excluded | ||||||
| Recknor 201373 | Randomised, open-label, parallel-group study – 74 centres in the USA and Europe | Postmenopausal women aged ≥ 55 years with T-score of ≤ –2 or ≥ –4 at the total hip who had either discontinued or had insufficient adherence to bisphosphonates for ≥ 1 month before screening |
|
Daily calcium (≥ 500 mg) and vitamin D (≥800 IU) | 12 months | Total hip BMD percentage change from baseline |
| Treatments and conditions affecting BMD were excluded | ||||||
| Saag 201874 | Phase II, international, randomised, double-blind, double-dummy, active-controlled, non-inferiority study – 79 centres in 16 countries in Europe, Latin America, Asia and the USA | Women and men aged ≥ 18 years who were either continuing or initiating glucocorticoids (≥ 7.5 mg prednisone, or its equivalent, daily). Patients aged < 50 years had to have a history of osteoporosis-related fracture. Continuing patients had to have total hip, femoral neck or lumbar spine T-score of ≤ 2.0 or ≤ 1.0 with a history of fracture |
|
At least 1000 mg of calcium and at least 800 IU of vitamin D daily | 12 months | Lumbar spine BMD percentage change from baseline |
| Miller 201675 | International, multicentre, randomised, double-blind, double-dummy, active-controlled, parallel-group study – 37 study centres in Belgium, Denmark, Poland, Spain, Canada, the USA and Australia | Postmenopausal women aged ≥ 55 years who received oral bisphosphonate therapy for ≥ 2 years with a T-score of ≤ 2.5 at the lumbar spine, total hip or femoral neck |
|
≥ 1000 mg of elemental calcium and ≥ 800 IU of vitamin D daily | 12 months | Lumbar spine BMD percentage change from baseline |
| Treatments and conditions affecting BMD were excluded | ||||||
| RLX vs. bisphosphonates | ||||||
| EFFECT (International): Sambrook 200476 | Randomised, double-masked, double-dummy, multinational study – 50 centres in 16 countries throughout Europe, South America and Asia-Pacific | Postmenopausal women with low BMD at least 2.0 SD below the young normal mean at either the total hip or lumbar spine |
|
Calcium and vitamin D | 12 months | Lumbar spine BMD percentage change from baseline |
| Treatments and conditions affecting BMD were excluded | ||||||
| EFFECT (USA): Luckey 200477 | Double-blind, randomised, active-controlled, multicentre study – 52 centres in the USA | Postmenopausal women aged > 40 years with low BMD at least 2.0 SD below the young normal mean at either the total hip or lumbar spine |
|
500–1000 mg of calcium and 200 IU of vitamin D daily | 12 months | Lumbar spine BMD percentage change from baseline |
| Treatments and conditions affecting BMD were excluded | ||||||
| Johnell 200278 | Phase III, randomised, double-blind study – 30 centres in Australia, Belgium, Canada, Italy, Mexico, South Africa, Spain and Sweden | Postmenopausal women aged ≥ 75 years, femoral neck BMD ≥ 2.0 SD below peak bone mass for healthy premenopausal women |
|
Daily elemental calcium (500 mg) and vitamin D (400–600 IU) | 12 months | Lumbar spine BMD and femoral neck BMD percentage change from baseline |
| Treatments and conditions affecting BMD were excluded | ||||||
| Muscoso 200479 | Randomised trial – centres and countries NR | Women with osteoporosis. No further details of inclusion or exclusion criteria reported |
|
1000 mg of calcium and 800 IU of vitamin D daily | 24 months |
|
| EVA: Recker 200780 | Randomised double-blind study – 13 centres in Canada and the USA (NCT00035971) | Postmenopausal women aged 50–80 years with femoral neck T-score of –2.5 to –4.0 and no prevalent vertebral fractures |
|
Calcium (500 mg per day) and vitamin D (400 IU per day) |
|
Number of women with one or more new osteoporotic vertebral or non-vertebral fractures |
| Treatments and conditions affecting BMD were excluded | ||||||
| Sanad 201181 | Randomised clinical study – single centre, Egypt | Postmenopausal women aged 50–70 years with BMD at lumbar spine or femoral neck of –2.5 SDs below a reference population of young postmenopausal women |
|
1500 mg of calcium carbonate and 400 IU of vitamin D3 | 12 months |
|
| Treatments and conditions affecting BMD were excluded | ||||||
| Michalska 200682 | Placebo-controlled, randomised trial – single centre, Austria | Postmenopausal women aged 50–80 years with previous treatment with ALN (10 mg per day) for > 3 years and lumbar spine or femoral neck T-score of < –2.5 |
|
Calcium (500 mg per day) and vitamin D (800 IU per day) | 12 months followed by 12 months open-label extension | Lumbar spine BMD percentage change from baseline |
| ROMO vs. bisphosphonates | ||||||
| ARCH: Saag 201783 | Phase III, multicentre, international, randomised, double-blind trial – 137 centres (NCT01631214) | Postmenopausal women aged 55–90 years with either T-score of ≤ –2.5 at the total hip or femoral neck plus one or more moderate/severe or two or more mild vertebral fractures; or T-score of ≤ –2.0 with two or more moderate/severe vertebral or proximal femur fractures |
|
Daily calcium and vitamin D | 12 months from randomisation then a further 12 months open label following treatment-switching | Vertebral fractures and clinical fracture (non-vertebral and symptomatic vertebral fracture) at 24 months |
| TPTD vs. bisphosphonates | ||||||
| FACT: McClung 200584 | Randomised, double-blind, active comparator study – 19 clinical sites globally | Postmenopausal women aged 45–84 years, with lumbar spine or femoral neck T-score of between –2.5 and –4.0 |
|
Daily supplementation of calcium (1000 mg) and vitamin D (400–800 IU) | 18 months | Lumbar spine and hip BMD percentage change from baseline |
| Treatments and conditions affecting BMD were excluded | ||||||
| Saag 200985 | Randomised, double-blind, double-dummy, active comparator–controlled –13 countries at 76 centres | Women aged ≥ 21 years who had taken prednisone or its equivalent at a dosage of ≥ 5 mg per day for ≥ 3 months with lumbar spine, femoral neck, or total hip BMD T-score of ≤ –2 or of ≤ –1 plus a prevalent fracture |
|
Calcium (1000 mg per day) and vitamin D (800 IU per day) were provided | 36 months | Lumbar spine BMD percentage change from baseline |
| Panico 201186 | Randomised controlled trial, single centre, Italy | Postmenopausal women, lumbar spine or femoral neck BMD T-score of ≤ –2.5, two or more fractures, back pain, prior treatment for osteoporosis |
|
Daily calcium (1000 mg) and vitamin D (800 IU) | 18 months | Percentage change from baseline in biochemical markers of bone turnover |
| Excluded if condition influencing bone metabolism, increased risk of osteosarcoma | ||||||
| EuroGIOPs: Glüer 201387 | Phase III, randomised, open-label, active comparator-controlled study – 16 centres in Germany, Greece, Italy and Spain | Men aged ≥ 25 years with a lumbar spine, femoral neck or total hip T-score ≤ 1.5 SDs below normal young adult male taking glucocorticoids (≥ 5.0 mg of prednisone, or its equivalent, daily) for ≥ 3 months |
|
1000 mg of calcium and 800–1200 IU of vitamin D per day | 18 months | Lumbar spine BMD percentage change from baseline, measured by QCT |
| Treatments and conditions affecting BMD were excluded | ||||||
| Anastasilakis 200888 | Randomised, open-label trial – Greece | Postmenopausal women with osteoporosis and T-score of < –2.5 (site NR) |
|
500 mg of elemental calcium and 400 IU of vitamin D daily | 12 months | Bone turnover markers |
| Treatments and conditions affecting BMD were excluded | ||||||
| Walker 201389 | Randomised, double-blind, placebo-controlled trial – USA | Men aged 30–85 years with low BMD secondary to idiopathic osteoporosis, and lumbar spine, femoral neck or total hip T-score of < –2.0 |
|
500 mg of calcium and 400 IU of vitamin D daily | 18 months | Lumbar spine BMD percentage change from baseline |
| Treatments and conditions affecting BMD were excluded | ||||||
| VERO: Kendler 201899 | Randomised, double-blind, active-controlled, parallel-group trial – 123 centres 14 countries in Europe, South America and the USA | Postmenopausal women aged > 45 years with a lumbar spine, femoral neck or total hip T-score of ≥ –1.50 with prevalent vertebral fragility fracture |
|
Daily supplements of 500–1000 mg of calcium and 400–800 IU of vitamin D3 or D2, or 2000 IU per day, if baseline serum 25-hydroxyvitamin D levels were ≤ 40 ng/ml | 24 months | New radiographic vertebral fractures |
| Treatments and conditions affecting BMD were excluded | ||||||
| Hadji 201291 | Randomised, parallel, double-blind, double-dummy, active-controlled trial – 72 international study locations (NCT00343252) | Postmenopausal women aged ≥ 45 years with a history of back pain likely to be caused by osteoporotic vertebral fracture, with lumbar spine, femoral neck or total hip T-score of ≤ –2; and a minimum of one moderate vertebral fracture |
|
1000 mg per day of calcium and 800 IU per day of vitamin D | 18 months | Proportion of patients experiencing ≥ 30% reduction in worst back pain at 6 months |
| Treatments and conditions affecting BMD were excluded | ||||||
| MOVE: Abtahi 2016101 and Malouf-Sierra 201792 | Multinational, multicentre, prospective, randomised, active-controlled study – 17 countries including the USA and Mexico, and countries in Europe | Men and postmenopausal women with low bone mass (T-score of < –2.0 s at the total hip, femoral neck or lumbar spine who had sustained a recent unilateral pertrochanteric fracture |
|
Calcium (500–1000 mg per day) and vitamin D (800 IU per day). For patients with a baseline serum 25-hydroxyvitamin D level of ≤ 40 ng/ml, loading dose of 100,000 IU of vitamin D2 or D3 | Lumbar spine BMD percentage change from baseline | |
| Cosman 201193 | Partial double-blinded, randomised, multicentre, multinational – centres and countries NR | Women aged 45–89 years with BMD T-scores of ≤ –2.5 at the femoral neck, total hip or lumbar spine or a BMD T-score of ≤ –2.0 at any site plus one or more documented vertebral or non-vertebral fractures |
|
Daily calcium (1000–1200 mg) and vitamin D (400–800 IU) | 12 months | Lumbar spine BMD percentage change from baseline |
| Treatments and conditions affecting BMD were excluded | ||||||
| Trial name: first author and year | Treatment arms (n) | Age (years), mean (SD) | Sex (% female) | T-score femoral neck (or lumbar spine if femoral neck not reported), mean (SD) | BMD at femoral neck (or lumbar spine if femoral neck not reported) (g/cm2), mean (SD) | Fractures (at baseline), n (%) | Prior treatment for osteoporosis (%) |
|---|---|---|---|---|---|---|---|
| DEN vs. placebo | |||||||
| FREEDOM41,104 | Placebo, n = 3906 | 72.3 (5.2) | 100 | –2.17 (0.71) | NR | 915 (23.4) | 0 |
| DEN, 60 mg s.c. every 6 months, n = 3902 | 72.3 (5.2) | 100 | –2.15 (0.72) | NR | 929 (23.8) | 0 | |
| ADAMO42 | Placebo for 1 year, then open-label DEN for 1 year, n = 121 | 65.0 (SD 9.1) | 0 | –1.9 (0.6) | NR | 48 (39.7) | NR |
| DEN: 60 mg of DEN every 6 months for 2 years (1 year blinded, then 1 year open label), n = 121 | 64.9 (SD 10.5) | 0 | –1.9 (0.6) | NR | 47 (38.8) | NR | |
| DIRECT: Nakamura 201443 | Placebo, n = 480 | 69.0 (7.67) | 95.0 | –2.29 (0.71) | NR | 471 (98.1) | NR |
| DEN, 60 mg every 6 months, n = 472 | 69.9 (7.36) | 95.1 | –2.38 (0.70) | NR | 466 (98.7) | NR | |
| Nakamura 201244 | Placebo, n = 55 | 64.6 (7.0) | 100 | Lumbar spine: –3.02 (0.34) | Lumbar spine: 0.652 (0.040) | 7 (12.7) | NR |
| DEN, 60 mg every 6 months, n = 54 | 65.1 (6.3) | 100 | Lumbar spine: –3.10 (0.44) | Lumbar spine: 0.642 (0.051) | 7 (13.0) | NR | |
| Koh 201645 (NCT01457950) | Placebo for 6 months then open-label DEN for 6 months, n = 66 | 66.0 (4.77) | 100 | –2.4 (0.61) | NR | 15 (23) | NR |
| DEN, 60 mg for 6 months then open-label DEN for 6 months, n = 69 | 67.0 (4.86) | 100 | –2.5 (0.56) | NR | 21 (30) | NR | |
| RLX vs. placebo | |||||||
| Adami 200846 | Placebo, n = 172 | 67.1 (6.5) | 100 | NR | 0.62 (0.10) | NR | 0 |
| RLX, 60 mg daily, n = 157 | 66.7 (6.4) | 100 | NR | 0.64 (0.10) | NR | 0 | |
| Morii 200347 | Placebo, n = 97 | 64.3 (6.5) | 100 | NR | 0.64 (0.05) | 26 (26.8) | NR |
| RLX, 60 mg per day, n = 90 | 65.2 (6.2) | 100 | NR | 0.66 (0.5) | 22 (24.4) | NR | |
| Liu 200448 | Placebo, n = 102 | 65.1 (5.4) | 100 | NR | NR |
|
0 |
| RLX, n = 102 | 165.5 (6.5) | 100 | NR | NR |
|
0 | |
| Gorai 201249 | Alfacalcidol, n = 46 | 165.2 (6.5) | 100 | NR | Lumbar spine: 0.663 (0.082) | NR | NR |
| RLX, n = 42 | 164.4 (6.6) | 100 | NR | Lumbar spine: 0.678 (0.083) | NR | NR | |
| Alfacalcidol plus RLX, n = 45 | 65.1 (7.6) | 100 | NR | Lumbar spine: 0.670 (0.067) | NR | NR | |
| Silverman 200850 (NCT00205777) | Placebo, n = 1885 | 66.5 (6.8) | 100 | –1.8 (0.9) | NR | 981 (56.4) | NR |
| RLX, n = 1849 | 66.4 (6.7) | 100 | 1–1.7 (0.9) | NR | 954 (56.3) | NR | |
| MORE51,102 | Placebo, n = 2576 | 66.6 (7.1) | 100 | NR |
|
(36.4) | NR |
| RLX, n = 2557 | 66.5 (7.0) | 100 | NR |
|
(38.1) | NR | |
| Lufkin 199852 | Control, n = 48 | 68.2 (0.7) | 100 | NR | LS 0.54 (0.01) | NR | NR |
| RLX, n = 48 | 69.9 (0.5) | 100 | NR | LS 0.52 (0.01) | NR | NR | |
| Mok 201153 (NCT00371956) | Placebo, n = 57 | 55.2 (7.6) | 100 | NR | 0.683 (0.126) | 2 (4) | 5 |
| RLX, n = 57 | 55.4 (7.8) | 100 | NR | 0.647 (0.117) | 4 (7) | 11 | |
| ROMO vs. placebo | |||||||
| FRAME: Cosman 201654 |
|
70.8 (6.9) | 100 | –2.74 (0.29) | NR | 496 (13.8) | 0 |
|
70.9 (7.0) | 100 | –2.76 (0.28) | NR | 506 (14.1) | 0 | |
| Ishibashi 201755 (NCT01992159) | Placebo, n = 63 | 67.8 (7.2) | 100 | –2.31 (0.47) | NR | 0 | NR |
| RLX, n = 63 | 68.3 (5.9) | 100 | –2.32 (0.59) | NR | 0 | NR | |
| BRIDGE56 (NCT02186171) | Placebo, n = 82 | 71.5 (6.9) | 0 | –2.3 (0.52) | NR | 46 (56.1) |
|
| ROMO, n = 163 | 72.4 (7.4) | 0 | –2.34 (0.52) | NR | 86 (52.8) |
|
|
| TPTD vs. placebo | |||||||
| Orwoll 200357 | Placebo, n = 147 | 59 (13) | 0 | –2.7 (0.8) | Lumber spine BMD: 0.85 (0.14) | NR | 8.16 |
| TPTD, 20 µg s.c. daily, n = 151 | 59 (13) | 0 | –2.6 (0.8) | 0.89 (0.15) | NR | 7.95 | |
| Miyauchi 201058 | Placebo for 12 months and then option of open-label TPTD for 12 months, n = 67 | 70.4 (5.4) | 92.5 | NR | Lumbar spine: 0.638 (0.079) | 29 (43.3) | 34.3 |
| TPTD for 12 months and then open-label TPTD for 12 months, n = 136 | 69.2 (6.3) | 93.4 | NR | Lumbar spine: 0.639 (0.069) | 54 (39.7) | 36.8 | |
| Miyauchi 200859 | Placebo, n = 38 | 69.9 (3.6) | 100 | NR | 0.5068 (0.0802) | 17 (44.7) | 21.1 |
| TPTD, 20 µg daily, n = 39 | 71.5 (5.1) | 100 | NR | 0.5168 (0.0927) (n = 38) | 16 (41.0) | 25.6 | |
| ACTIVE95 (NCT01343004) | Placebo, n = 821 | 68.7 (6.5) | 100 | –2.2 (0.7) | 0.732 (0.099) | 514 (62.6) | NR |
| TPTD, 20 µg daily, n = 818 | 68.8 (6.6) | 100 | –2.1 (0.7) | 0.737 (0.096) | 510 (62.3) | NR | |
| Leder 201561 | Placebo, n = 45 | 65.0 (7.1) | 100 | –2.26 (0.72) | 0.65 (0.11) | NR | 0 |
| TPTD, 20 µg daily, n = 45 | 64.5 (7.5) | 100 | –2.09 (0.75) | 0.66 (0.11) | NR | 0 | |
| FPT62 (NCT00670501) | Placebo, n = 448 | 69 (7) | 100 | NR | Lumbar spine: 0.82 (0.17) | 448 (100) | 15 |
| TPTD, 20 µg daily, n = 444 | 69 (7) | 100 | NR | Lumbar spine: 0.82 (0.17) | 444 (100) | 16 | |
| Sethi 200863 (NCT00500409) | Control, n = 41 | 63.0 (6.3) | 100 | –2.34 (0.73) | 0.62 (0.09) | NR | NR |
| TPTD, 20 µg daily, n = 41 | 61.0 (6.3) | 100 | –2.49 (0.55) | 0.62 (0.08) | NR | NR | |
| Head-to-head non-bisphosphonates | |||||||
| DATA64 | TPTD, 20 µg daily, n = 36 | 65.5 (7.9) | 100 | –1.9 (0.5) | 0.643 (0.061) | 16 (52) | Bisphosphonates: 42 |
| DEN, 60 mg every 6 months, n = 34 | 66.3 (8.3) | 100 | –1.9 (0.8) | 0.641 (0.086) | 12 (36) | Bisphosphonates: 36 | |
| EUROFORS66 |
|
69.1 (8.6) | 100 | Lumbar spine: –3.1 (0.89) | Lumbar spine: 0.75 (0.11) | 102 (100) | Antiresorptive: 62.7 |
|
69.4 (7.0) | 100 | Lumbar spine: –3.2 (0.85) | Lumbar spine: 0.75 (0.12) | 97 (100) | Antiresorptive: 64.9 | |
|
69.2 (7.2) | 100 | Lumbar spine: –3.2 (0.87) | Lumbar spine: 0.74 (0.11) | 304 (100) | Antiresorptive: 72.4 | |
| STRUCTURE67 | TPTD, n = 218 | 71.2 (7.7) | 100 | –2.43 (0.66) | NR | (99.5) | Bisphosphonates: 100 |
| ROMO, n = 218 | 71.8 (7.4) | 100 | –2.49 (0.67) | NR | (100) | Bisphosphonates: 100 | |
| McClung 201468 | Pooled placebo (mix of administrations), n = 52 | 67.0 (6.5) | 100 | –1.76 (0.56) | NR | NR | 0 |
| Open-label ALN, 70 mg weekly, n = 51 | 67.1 (5.8) | 100 | –1.91 (0.61) | NR | NR | 0 | |
| TPTD, 20 µg daily, n = 54 | 66.8 (5.7) | 100 | –1.79 (0.67) | NR | NR | 0 | |
| ROMO 210 mg s.c. monthly, 55 | 66.3 (6.5) | 100 | –1.87 (0.58) | NR | NR | 0 | |
| DEN vs. bisphosphonates | |||||||
| DECIDE69 | DEN plus placebo, n = 594 | 64.1 (8.6) | 100 | Lumbar spine: –2.57 (0.75) | NR | (40) |
|
| ALN plus placebo, n = 595 | 64.6 (8.3) | 100 | Lumbar spine: –2.57 (0.75) | NR | (41) |
|
|
| STAND: Kendler 201070 | ALN, 70 mg per week plus placebo, n = 251 | 68.2 (7.7) | 100 | Lumbar spine T-score: –2.62 (0.79) | NR | NR | 0 |
| DEN, 60 mg s.c., every 6 months plus placebo, n = 253 | 66.9 (7.8) | 100 | –2.64 (0.75) | NR | NR | 0 | |
| DAPS: Kendler 201171 and 2012109 | ALN, 70 mg per week, n = 124 | 65.3 (7.7) | 100 | –2.03 (0.62) | NR | NR | 0 |
| DEN, 60 mg s.c., every 6 months, n = 126 | 65.1 (7.6) | 100 | –2.01 (0.55) | NR | NR | 0 | |
| AMG 162 Bone Loss study72 | Placebo, s.c. every 3 months, n = 46 | 63.7 (9.1) | 100 | –1.9 (0.6) | NR | 0 | 0 |
| ALN, 70 mg per week, n = 47 (open label) | 62.8 (8.2) | 100 | –1.9 (0.7) | NR | 0 | 0 | |
| DEN, 60 mg s.c., every 6 months, n = 47 | 63.1 (8.1) | 100 | –1.9 (0.7) | NR | 0 | 0 | |
| Recknor 201373 | IBN, 150 mg every month, n = 416 | 66.2 (7.8) | 100 | –2.1 (0.7) | NR | NR | Prior bisphosphonate: 374 (89.9) |
| DEN, 60 mg s.c., every 6 months, n = 417 | 67.2 (8.1) | 100 | –2.1 (0.7) | NR | NR | Prior bisphosphonate: 377 (90.4) | |
| Saag 201874 | RIS, 5 mg daily plus placebo, n = 39 |
|
|
Lumbar spine T-score:
|
NR |
|
0 |
| DEN, 60 mg s.c., every 6 months plus placebo, n = 398 |
|
|
Lumbar spine T-score:
|
NR |
|
0 | |
| Miller 201675 | ZOL, 5 mg i.v. annually plus placebo, n = 322 | 69.5 (7.7) | 100 | Lumbar spine T-score: –2.64 (0.86) | NR | 159 (49.4) | Prior oral bisphosphonates (years), mean (SD): 6.4 (3.7) |
| DEN, 60 mg s.c., every 6 months plus placebo, n = 321 | 68.5 (7.1) | 100 | –2.74 (0.83) | NR | 169 (52.6) | Prior oral bisphosphonates, (years), mean (SD): 6.2 (3.8) | |
| RLX vs. bisphosphonates | |||||||
| EFFECT: Sambrook 200476 | ALN, 10 mg plus placebo, n = 246 | 61.5 (8.2) | 100 | Lumbar spine T-score: –2.89 (0.78) | NR | NR | 0 |
| RLX, 60 mg daily plus placebo, n = 241 | 61.8 (7.7) | 100 | Lumbar spine T-score: –2.86 (0.76) | NR | NR | 0 | |
| EFFECT: Luckey 200477 | ALN, 70 mg weekly plus placebo, n = 223 | 63.8 (9.9) | 100 | Lumbar spine T-score: –2.43 (0.78) | NR | NR | 0 |
| RLX, 60 mg daily plus placebo, n = 233 | 64.7 (9.8) | 100 | Lumbar spine T-score: –2.5 (0.69) | NR | NR | 0 | |
| Johnell 200278 | Placebo (ALN and RLX), n = 82 | 63.8 (5.3) | 100 | NR | 0.62 (0.09) | NR | 0 |
| ALN, 10 mg daily, and RLX placebo, n = 83 | 63.7 (6.0) | 100 | NR | 0.62 (0.08) | NR | 0 | |
| RLX, 60 mg daily, and ALN placebo, n = 82 | 63.4 (6.3) | 100 | NR | 0.62 (0.07) | NR | 0 | |
| Muscoso 200479 | ALN, 10 mg daily, n = 1000 | 71 (8) | 100 | NR | NR | NR | NR |
| RIS, 5 mg daily, n = 100 | 66 (9) | 100 | NR | NR | NR | NR | |
| RLX, 60 mg daily, n = 100 | 64 (3) | 100 | NR | NR | NR | NR | |
| EVA: Recker 200780 | ALN, 10 mg daily, n = 716 | 65.7 (7.8) | 100 | –2.39 (0.56) | 0.61 (0.09) | 0 | 0 |
| RLX, 60 mg daily, n = 717 | 65.5 (7.7) | 100 | –2.39 (0.54) | 0.61 (0.09) | 0 | 0 | |
| Sanad 201181 | ALN, 10 mg daily, n = 31 | 61.7 (4.3 | 100 | NR | 0.63 (0.03) | NR | 0 |
| RLX, 60 mg daily, n = 35 | 62.5 (3.9) | 100 | NR | 0.63 (0.05); | NR | 0 | |
| Michalska 200682 | Blind placebo, n = 33 | 64.5 (6.3) | 100 | NR | 0.616 (0.075) | Non-vertebral, 18/33 (54.5) | 100 (≥ 3 years ALN) |
| Open-label ALN, 10 mg daily, n = 33 | 65.4 (6.8) | 100 | NR | 0.609 (0.063) | 9/33 (27.3) | 100 (≥ 3 years ALN) | |
| RLX, 60 mg daily, n = 33 | 65.6 (7.1) | 100 | NR | 0.633 (0.087) | 16/33 (48.5) | 100 (≥ 3 years ALN) | |
| ROMO vs. bisphosphonates | |||||||
| ARCH: Saag 201783 | ALN, 70 mg weekly (n = 2047) for 12 months then ALN 70 mg weekly open label, for 12 months | 74.2 (7.5) | 100 | –2.90 (0.50) | NR | 1964/2047 (95.9) | 0 |
| ROMO, 210 mg s.c. monthly (n = 2046) for 12 months then ALN, 70 mg weekly open label, for 12 months | 74.4 (7.5) | 100 | 1–2.89 (0.49) | NR | 1969/2046 (96.2) | 0 | |
| TPTD vs. bisphosphonates | |||||||
| FACT: McClung 200584 | ALN, 10 mg daily plus placebo, n = 101 | 66.6 (8.5) | 100 | –2.3 (0.8) | NR | NR | 0 |
| TPTD, 20 µg s.c. daily plus placebo, n = 102 | 65.3 (8.4) | 100 | –2.3 (0.6) | NR | NR | 0 | |
| Saag 200985 and 2007103 | ALN, 10 mg daily plus placebo, n = 214 | 57.3 (14.0) | 100 | –2.1 (0.10) | 0.721 (0.013) | X-ray confirmed, 53/214 (25) | 0 |
| TPTD, 20 µg s.c. daily plus placebo, n = 214 | 56.1 (13.4) | 100 | –2.2 (0.10) | 0.705 (0.013) | X-ray confirmed, 63/214 (30) | 0 | |
| Panico 201186 | TPTD, n = 42 | 65 (9.0) | 100 | –3.07 (0.60) | NR | 42 (100) | 100 |
| ALN, n = 39 | 60 (14.4) | 100 | –3.02 (0.61) | NR | 38 (97) | 97 | |
| EuroGIOPs: Glüer 201387 | Open-label RIS, 35 mg weekly, n = 47 | 55.1 (15.5) | 0 | –1.82 (0.91) | NR | 17/47 (36.2) | 0 |
| TPTD, 20 µg s.c. daily, n = 45 | 57.5 (12.8) | 0 | –1.95 (0.78) | NR | 19/45 (42.2) | 0 | |
| Anastasilakis 200888 | Open-label RIS, 35 mg weekly, n = 22 | 64.7 (7.0) | 100 | NR | Lumbar spine BMD: 0.757 (0.08) | NR | 0 |
| TPTD, 20 µg s.c. daily, n = 22 | 65.4 (7.5) | 100 | NR | Lumbar spine BMD: 0.764 (0.11) | NR | 0 | |
| Walker 201389 | RIS, 35 mg weekly plus placebo, n = 10 | 54.0 (6.3) | 100 | –2.1 (0.63) | 0.669 (0.09) | 0 | Bisphosphonates: 20 |
| TPTD, 20 µg s.c. daily plus placebo, n = 9 | 51.6 (11.7) | 100 | –2.0 (0.9) | 0.659 (0.12) | 33 | Bisphosphonates: 33 | |
| VERO: Kendler 201899 | RIS, 35 mg weekly plus placebo, n = 680 | 71.6 (8.58) | 100 | –2.24 (0.74) | 0.67 (0.11) | (100) | 71 |
| TPTD, 20 µg s.c. daily plus placebo, n = 680 | 72.6 (8.77) | 100 | –2.27 (0.76) | 0.66 (0.11) | (100) | 73 | |
| Hadji 201291 | RIS, 35 mg weekly plus placebo, n = 350 | 71.6 (8.1) | 100 | –2.44 (0.67) | NR | 90% confirmed by X-ray (all back pain likely to be due to vertebral fracture) | 73.7 |
| TPTD, 20 µg s.c. daily plus placebo, n = 360 | 70.5 (8.8) | 100 | –2.32 (0.75) | NR | 89.7% confirmed by X-ray (all back pain likely to be due to vertebral fracture) | 74.2 | |
| MOVE: Abtahi 2016101 and Malouf-Sierra 201792 | RIS, 35 mg weekly plus placebo, n = 85 | 76.4 (7.5) | 77.6 | –2.63 (0.657) | 0.602 (0.116) | (100) | 12.9 |
| TPTD, 20 µg s.c. daily plus placebo, n = 86 | 77.2 (8.0) | 76.7 | –2.63 (0.519) | 0.603 (0.098) | (100) | 14.0 | |
| Cosman 201193 | ZOL, 5 mg i.v. annually, n = 137 | 66.1 (9.0) | 100 | Lumbar spine T-score: –2.88 (0.883) | NR | 21 (15.3) | 0 |
| TPTD, 20 µg s.c. daily plus placebo, n = 138 | 63.8 (9.1) | 100 | Lumbar spine T-score: –2.87 (0.807) | NR | 22 (15.9) | 0 | |
Appendix 5 Clinical effectiveness results
| Trial name: first author and year; population | Efficacy or safety outcome | Method of vertebral fracture assessment (clinical/morphometric) | Treatments, n randomised | Treatments, n analysed | Follow-up (months) | Vertebral fracture outcomes n/N (%) (reported between-group difference) |
|---|---|---|---|---|---|---|
| DEN vs. placebo | ||||||
| FREEDOM: Cummings 2009;41 postmenopausal women with osteoporosis | Efficacy |
|
|
|
36 |
|
| FREEDOM: Cummings 2009;41 postmenopausal women with osteoporosis | Efficacy | Clinical |
|
|
36 |
|
| FREEDOM: Cummings 2009;41 postmenopausal women with osteoporosis | Efficacy | Morphometric, multiple (> 2) |
|
|
36 |
|
| FREEDOM: Bone 2017104 postmenopausal women with osteoporosis | Efficacy | Morphometric, new |
|
|
0–12 |
|
| FREEDOM: Bone 2017104 postmenopausal women with osteoporosis | Efficacy | Morphometric, new | As above |
|
12–24 |
|
| FREEDOM: Bone 2017104 postmenopausal women with osteoporosis | Efficacy | Morphometric, new | As above |
|
24–36 |
|
| FREEDOM Bone 2017105 OLE; postmenopausal women with osteoporosis | Efficacy | Morphometric, new |
|
|
84 from OLE |
|
| ADAMO: Orwoll 2012;42 men with osteoporosis | Safety | Clinical |
|
|
12 |
|
| DIRECT: Nakamura 2014;43 women and men with osteoporosis | Efficacy |
|
|
|
24 |
|
| DIRECT: Nakamura 2014;43 women and men with osteoporosis | Efficacy | Morphometric, new or worsening | As above |
|
24 |
|
| DIRECT: Sugimoto 2015;106 women and men with osteoporosis | Efficacy | Morphometric, new |
|
|
36 including 12 OLE |
|
| DIRECT: Sugimoto 2015;106 women and men with osteoporosis | Efficacy | Morphometric, new or worsening | As above |
|
36 including 12 OLE |
|
| DIRECT: Sugimoto 2015;106 women and men with osteoporosis | Efficacy | Morphometric, new | As above |
|
12 OLE |
|
| DIRECT: Sugimoto 2015;106 women and men with osteoporosis | Efficacy | Morphometric, new or worsening | As above |
|
12 OLE |
|
| Nakamura 2012;44 postmenopausal women with osteoporosis | Efficacy | Morphometric, new or worsening |
|
|
12 |
|
| RLX vs. placebo | ||||||
| Morii 2003;47 postmenopausal women with osteoporosis | Efficacy |
|
|
|
12 |
|
| Liu 2004;48 postmenopausal women with osteoporosis | Efficacy | Clinical |
|
|
12 |
|
| Silverman 2008;50 postmenopausal women with osteoporosis | Efficacy |
|
|
|
36 |
|
| Silverman 200850 and NCT00205777;117 postmenopausal women with osteoporosis | Efficacy | Clinical | As above |
|
36 |
|
| MORE: Ettinger 1999;51 women with osteoporosis | Efficacy |
|
|
|
36 |
|
| MORE: Ettinger 1999;51 women with low BMD + fracture | Efficacy | Morphometric, new |
|
|
36 |
|
| MORE: Maricic 2002;102 postmenopausal women with osteoporosis | Efficacy | Clinical |
|
|
0–12 |
|
| MORE: Maricic 2002;102 postmenopausal women with osteoporosis | Efficacy | Clinical | As above |
|
12–24 |
|
| MORE: Maricic 2002;102 postmenopausal women with osteoporosis | Efficacy | Clinical | As above |
|
24–36 |
|
| MORE: Maricic 2002;102 postmenopausal women with osteoporosis | Efficacy | Clinical | As above |
|
36 |
|
| MORE: Maricic 2002;102 postmenopausal women with osteoporosis | Efficacy | Clinical | As above |
|
24 |
|
| Lufkin 1998;52 postmenopausal women with osteoporosis | Efficacy |
|
|
|
12 |
|
| Mok 2011;53 postmenopausal women on long-term GCCs | Efficacy |
|
|
|
12 |
|
| ROMO vs. placebo | ||||||
| FRAME: Cosman 2016;54 postmenopausal women with osteoporosis | Efficacy |
|
|
|
12 |
|
| FRAME: Cosman 2016;54 postmenopausal women with osteoporosis | Efficacy | Morphometric, multiple or worsening | As above |
|
12 |
|
| FRAME: Cosman 2016;54 postmenopausal women with osteoporosis | Efficacy | Morphometric, new |
|
|
24 |
|
| FRAME: Cosman 2016;54 postmenopausal women with osteoporosis | Efficacy | Morphometric, multiple or worsening | As above |
|
24 |
|
| FRAME: Cosman 2016;20 postmenopausal women with osteoporosis | Efficacy | Morphometric, new |
|
|
36 |
|
| FRAME: Cosman 2016;20 postmenopausal women with osteoporosis | Efficacy | Morphometric, multiple or worsening | As above |
|
36 |
|
| TPTD vs. placebo | ||||||
| ACTIVE: Miller 2016;95 postmenopausal women with osteoporosis | Efficacy |
|
|
|
18 |
|
| ACTIVE: Miller 2016;95 postmenopausal women with osteoporosis | Efficacy | Clinical | As above |
|
18 |
|
| Miyauchi 2010;58 women and men with osteoporosis | Efficacy | Morphometric, any |
|
|
12 |
|
| Miyauchi 2010;58 women and men with osteoporosis | Efficacy |
|
As above |
|
12 |
|
| Miyauchi 2010;58 women and men with osteoporosis | Efficacy |
|
As above |
|
12 |
|
| FPT: Neer 2001;62 postmenopausal women with osteoporosis | Efficacy |
|
|
|
24 (trial stopped early; mean time to last radiograph was 21 months) |
|
| FPT: Neer 2001;62 postmenopausal women with osteoporosis | Efficacy | Morphometric, one or more fractures | As above | As above | 24 (trial stopped early; mean time to last radiograph was 21 months) |
|
| FPT: Neer 2001;62 postmenopausal women with osteoporosis | Efficacy | Morphometric, one or more moderate or severe fractures | As above | As above | 24 (trial stopped early; mean time to last radiograph was 21 months) |
|
| Head-to-head non-bisphosphonates | ||||||
| EUROFORS: Eastell 2009;66 postmenopausal women with osteoporosis pre treated with TPTD | Efficacy | Clinical |
|
|
12 |
|
| DEN vs. bisphosphonates | ||||||
| Saag 2018;74 women and men on GCCs with osteoporosis or low BMD + fracture | Efficacy | Clinical |
|
|
12 |
|
| Miller 201675 | Safety | NR |
|
|
12 |
|
| RLX vs. bisphosphonates | ||||||
| EFFECT: Sambrook 200476 (international not including USA); postmenopausal women with osteoporosis | Safety | NR |
|
|
12 |
|
| Muscoso 2004;79 postmenopausal women with osteoporosis | Efficacy | NR |
|
|
0–12 |
|
| Muscoso 2004;79 postmenopausal women with osteoporosis | Efficacy | NR | As above |
|
12–24 |
|
| EVA: Recker 2007;80 postmenopausal women with osteoporosis | Efficacy |
|
|
|
Mean 312 (SD 252) days |
|
| EVA: Recker 2007;80 postmenopausal women with osteoporosis | Efficacy |
|
|
|
Mean 312 (SD 252) days |
|
| EVA: Recker 2007;80 postmenopausal women with osteoporosis | Efficacy | Clinical | As above |
|
Mean 312 (SD 252) days |
|
| ROMO vs. bisphosphonates | ||||||
| ARCH: Saag 2017;83 postmenopausal women with osteoporosis | Efficacy |
|
|
|
12 |
|
| ARCH: Saag 2017;83 postmenopausal women with osteoporosis | Efficacy | Morphometric, new, ITT LOCF | As above |
|
12 |
|
| ARCH: Saag 2017;83 postmenopausal women with osteoporosis | Efficacy | Morphometric new or worsening | As above |
|
12 |
|
| ARCH: Saag 2017;83 postmenopausal women with osteoporosis | Efficacy | Clinical | As above |
|
12 |
|
| ARCH: Saag 2017;83 postmenopausal women with osteoporosis | Efficacy | Morphometric, new, ITT MI |
|
|
24 |
|
| ARCH: Saag 2017;83 postmenopausal women with osteoporosis | Efficacy | Morphometric, new, ITT LOCF | As above |
|
24 |
|
| ARCH: Saag 2017;83 postmenopausal women with osteoporosis | Efficacy | Morphometric, new or worsening | As above |
|
24 |
|
| TPTD vs. bisphosphonates | ||||||
| Saag 2009;103 women and men on GCCs with osteoporosis or low BMD + fracture | Efficacy |
|
|
|
18 |
|
| Saag 2009;103 women and men on GCCs with osteoporosis or low BMD + fracture | Efficacy | Clinical | As above |
|
18 |
|
| Saag 2009;103 women and men on GCCs with osteoporosis or low BMD + fracture | Efficacy | Morphometric, new | As above |
|
36 |
|
| Saag 200985 | Efficacy | Clinical | As above |
|
36 |
|
| Langdahl 2009;107 women and men on GCCs with osteoporosis or low BMD + fracture | Efficacy | Morphometric, new |
|
|
18 |
|
| Langdahl 2009;107 women and men on GCCs with osteoporosis or low BMD + fracture | Efficacy | Morphometric, new |
|
|
18 |
|
| Panico 2011;86 postmenopausal women with severe osteoporosis + fracture and on treatment for osteoporosis | Efficacy | Morphometric, new |
|
|
18 |
|
| Walker 2013;89 men with osteoporosis | Efficacy |
|
|
|
18 |
|
| Hadji 2012;91 postmenopausal women with osteoporosis | Efficacy |
|
|
|
6 |
|
| Hadji 2012;91 postmenopausal women with osteoporosis | Efficacy | Morphometric, new or worsening | As above |
|
6 |
|
| Hadji 2012;91 postmenopausal women with osteoporosis | Efficacy | Morphometric, new | As above |
|
18 |
|
| Hadji 2012;91 postmenopausal women with osteoporosis | Efficacy | Morphometric, new or worsening | As above |
|
18 |
|
| VERO: Kendler 2018;99 postmenopausal women with osteoporosis | Efficacy |
|
|
|
24 |
|
| VERO: Kendler 2018;99 postmenopausal women with osteoporosis | Efficacy | Morphometric, new and worsening | As above |
|
24 |
|
| VERO: Kendler 2018;99 postmenopausal women with osteoporosis | Efficacy | Morphometric, multiple | As above |
|
24 |
|
| VERO: Kendler 2018;99 postmenopausal women with osteoporosis | Efficacy | Morphometric, multiple | As above |
|
12 |
|
| MOVE: Aspenberg 2016;108 women and men with low BMD + recent hip fracture surgery | Safety | Clinical |
|
|
6 |
|
| MOVE: Malouf-Sierra 2017;92 women and men with low BMD + recent hip fracture surgery | Safety | Clinical | As above |
|
18 |
|
| Cosman 2011;93 postmenopausal women with osteoporosis | Safety | AE |
|
|
12 |
|
| Trial name or first author and year | Efficacy or safety outcome | Treatments, n randomised | Follow-up (months) | Non-vertebral fractures, n/N (%) (reported between-group difference) |
|---|---|---|---|---|
| DEN vs. placebo | ||||
| FREEDOM41 | Efficacy |
|
36 |
|
| FREEDOM104 | Efficacy |
|
0–12 |
|
| FREEDOM104 | Efficacy |
|
12–24 |
|
| FREEDOM104 | Efficacy |
|
24–36 |
|
| FREEDOM OLE105 | Efficacy |
|
84 from OLE |
|
| ADAMO42 | Safety |
|
12 |
|
| DIRECT43 | Efficacy |
|
24 | All:
|
| DIRECT106 | Efficacy |
|
36 including 12 OLE | All:
|
| Koh 201645 | Safety |
|
6 |
|
| Koh 2016 OLE45 | Safety |
|
6–12 OLE |
|
| RLX vs. placebo | ||||
| Morii 200347 | Efficacy |
|
12 |
|
| Silverman 200850 (NCT00205777) | Efficacy |
|
36 |
|
| Lufkin 199852 | Efficacy |
|
12 |
|
| ROMO vs. placebo | ||||
| FRAME54 | Efficacy |
|
12 |
|
| FRAME54 | Efficacy |
|
24 |
|
| Ishibashi 201755 | Safety |
|
12 |
|
| TPTD vs. placebo | ||||
| Miyauchi 201058 | Efficacy |
|
12 |
|
| Miyauchi 201058 | Efficacy |
|
12–18 OLE |
|
| Miyauchi 201058 | Efficacy |
|
18–24 OLE |
|
| ACTIVE95 | Efficacy |
|
18 |
|
| FPT62 | Efficacy |
|
24 (trial stopped early; mean time to last visit was 19 months) |
|
| Head-to-head non-bisphosphonates | ||||
| EUROFORS66 | Efficacy |
|
12 |
|
| STRUCTURE67 | Safety |
|
12 |
|
| Non-bisphosphonates vs. bisphosphonates | ||||
| STAND70 | Safety |
|
12 |
|
| DAPS109 | Safety |
|
12 |
|
| DAPS109 | Safety |
|
12–24 |
|
| Saag 201874 | Efficacy |
|
12 |
|
| EFFECT (USA)77 | Safety |
|
12 |
|
| Muscoso 200479 | Efficacy |
|
0–12 |
|
| Muscoso 200479 | Efficacy |
|
12–24 |
|
| EVA80 | Efficacy |
|
Mean 312 (SD 252) days |
|
| Michalska 200682 | Safety |
|
24 |
|
| ARCH83 | Efficacy |
|
12 |
|
| ARCH83 | Efficacy |
|
12 | Major (pelvis, distal femur, proximal tibia, ribs, proximal humerus, forearm and hip):
|
| ARCH83 | Efficacy |
|
24 |
|
| ARCH83 | Efficacy |
|
24 | Major (pelvis, distal femur, proximal tibia, ribs, proximal humerus, forearm and hip):
|
| Saag 2009103 | Efficacy | Men and women
|
18 |
|
| Saag 2009103 | Efficacy | Men and women
|
36 |
|
| Saag 2009107 | Efficacy | Men
|
18 |
|
| Saag 2009107 | Efficacy | Women
|
18 |
|
| EuroGIOPs87 | Safety |
|
18 |
|
| VERO99 | Efficacy |
|
24 |
|
| VERO99 | Efficacy |
|
12 |
|
| Hadji 201291 | Efficacy |
|
6 |
|
| MOVE92 | Safety |
|
18 |
|
| Cosman 201193 | Safety |
|
12 |
|
| Trial name or first author and year | Treatment arms | Follow-up (months) | Fracture, n/N (%) (reported between-group difference) | ||
|---|---|---|---|---|---|
| Hip | Wrist | Proximal humerus | |||
| DEN vs. placebo | |||||
| FREEDOM41 | Placebo | 0–36 | 43/3906 (1.2) | NR | NR |
| DEN |
|
NR | NR | ||
| FREEDOM104 | Placebo | 1–12 | 21/3906 (0.55) | NR | NR |
| DEN |
|
NR | NR | ||
| Placebo | 12–24 | 14/3906 (0.36) | NR | NR | |
| DEN |
|
NR | NR | ||
| Placebo | 24–36 | 11/3906 (0.27) | NR | NR | |
| DEN |
|
NR | NR | ||
| ADAMO42 | Placebo | 12 | NR | NR | 1/120 (0.8) |
| DEN | NR | NR | 0/120 (0) | ||
| DIRECT43 | Placebo | 24 | 2/480 (0.4) | NR | NR |
| DEN | 0/472 (0) | NR | NR | ||
| RLX vs. placebo | |||||
| Silverman 2008;50 NCT00205777117 | Placebo | 36 | 6/1885 (0.3) | 31/1885 (1.6) | NR |
| RLX | 5/1849 (0.3) | 46/1849 (2.5)117 | NR | ||
| Lufkin 199852 | Placebo | 12 | 0/45 (0) | 0/45 (0) | NR |
| RLX | 0/43 (0) | 0/43 (0) | NR | ||
| ROMO vs. placebo | |||||
| FRAME54 | Placebo | 12 | 13/3591 (0.4) | NR | NR |
| ROMO |
|
NR | NR | ||
| FRAME54 | Placebo followed by DEN | 24 | 22/3591 (0.6) | NR | NR |
| ROMO followed by DEN |
|
NR | NR | ||
| Ishibashi 201755 | Placebo | 12 | NR | 0/63 (0) | NR |
| ROMO | NR | 1/63 (1.6) | NR | ||
| TPTD vs. placebo | |||||
| ACTIVE95 | Placebo | 18 | 2/821 (0.2) | 15/821 (1.8) | 3/821 (0.4) |
| TPTD |
|
|
|
||
| FPT62 | Placebo | 24 (trial stopped early; mean time to last visit was 19 months) | All:
|
All:
|
All:
|
| TPTD | All:
|
All:
|
All:
|
||
| Head-to-head non-bisphosphonates | |||||
| EUROFORS66 | No active treatment (for 12 months) (following pre-randomisation TPTD for 12 months) | 24 | 0/102 (0) | 0/102 (0) | 0/102 (0) |
| RLX (following TPTD) | 0/97 (0) | 0/97 (0) | 1/97 (1.0) | ||
| TPTD (for 12 months) (following 12 months of pre-randomisation TPTD) | 1/304 (0.3) | 3/304 (1.0) | 0/304 (0) | ||
| STRUCTURE67 | TPTD | 12 | 0/218 (0) | 4/218 (1.8) | 1/218 (0.5) |
| ROMO | 1/218 (0.5) | 1/218 (0.5) | 0/218 (0) | ||
| Non-bisphosphonates vs. bisphosphonates | |||||
| STAND70 | ALN | 12 | NR | 2/249 (0.8) | 0/249 (0) |
| DEN | NR | 3/253 (1.2) | 1/253 (0.4) | ||
| Saag 201874 | RIS | 12 | 1/397 (0.3) | NR | 3/397 (0.8) |
| DEN | 1/398 (0.3) | NR | 3/398 (0.8) | ||
| EFFECT (International)76 | RLX plus placebo | 12 | 1/241 (0.4) | NR | NR |
| ALN plus placebo | 0/246 (0) | NR | NR | ||
| EFFECT (USA)77 | RLX plus placebo | 12 | NR | 1/206 (0.5) | 1/206 (0.5) |
| ALN plus placebo | NR | 0/199 (0) | 0/199 (0) | ||
| Muscoso 200479 | ALN | 12 | 1/1000 (0.1) | 1/1000 (0.1) | NR |
| RLX | 10/100 (0) | 0/100 (0) | NR | ||
| RIS | 0/100 (0) | 0/100 (0) | NR | ||
| ALN | 12–24 | 2/1000 (0.2) | 0/1000 (0) | NR | |
| RLX | 0/100 (0) | 0/100 (0) | NR | ||
| RIS | 0/100 (0) | 0/100 (0) | NR | ||
| EVA80 | RLX | 24 | 2/699 (0.3) | 8/699 (1.1) | NR |
| ALN |
|
|
NR | ||
| ARCH83 | ROMO | 12 | 14/2046 (0.7) | NR | NR |
| ALN |
|
NR | NR | ||
| ROMO followed by ALN | Median 2.7 years | 41/2046 (2.0) | NR | NR | |
| ALN followed by ALN |
|
NR | NR | ||
| EUROGIOPs87 | RIS | 18 | 1/47 (2.1) | NR | 1/47 (2.1) |
| TPTD | 0/45 (0) | NR | 0/45(0) | ||
| VERO99 | RIS | 24 | 5/680 (0.7) | 15/680 (2.2) | 2/680 (0.3) |
| TPTD | 2/680 (0.3) | 6/680 (0.9) | 14/680 (0.6) | ||
| Hadji 201291 | RIS | 18 | 2/350 (0.6) | 2/350 (0.6) | 5/350 (1.4) |
| TPTD | 5/360 (1.4) | 4/360 (1.1) | 4/360 (1.1) | ||
| MOVE101 | RIS | 6 | 5/110 (4.5) | NR | 1/110 (0.9) |
| TPTD | 2/106 (1.9) | NR | 1/106 (0.9) | ||
| MOVE92 | RIS | 18 | 7/110 (6.4) | NR | 1/110 (0.9) |
| TPTD | 2/106 (1.9) | NR | 1/106 (0.9) | ||
| Trial name: first author and year; population | Treatments, n randomised | Treatments, n analysed | Follow-up (months) | Femoral neck BMD, percentage change from baseline, mean (SD) | Which data were estimated from graph? | Femoral neck BMD, reported (estimated) between-group difference |
|---|---|---|---|---|---|---|
| DEN vs. placebo | ||||||
| FREEDOM: Bone 2017;104 postmenopausal women with osteoporosis |
|
|
36 |
|
Nothing |
|
| FREEDOM: Bone 2017 OLE;105 postmenopausal women with osteoporosis |
|
|
84 from OLE |
|
Nothing |
|
| ADAMO: Orwoll 2012;42 men with osteoporosis |
|
|
12 | 95% CIs | p < 0.0001 | |
| DIRECT: Nakamura 2014;43 women and men with osteoporosis |
|
|
24 | 95% CIs | p < 0.0001 | |
| DIRECT: Sugimoto 2015;106 women and men with osteoporosis |
|
|
36 including 12 OLE | 95% CIs |
|
|
| DIRECT: Sugimoto 2015;106 women and men with osteoporosis |
|
|
24–36 OLE |
|
Nothing |
|
| Koh 2016;45 postmenopausal women with osteoporosis |
|
|
6 | Means and 95% CIs | MD between groups in percentage change: 1.4% (95% CI 0.4% to 2.3%; p = 0.0042 | |
| Koh 2016;45 postmenopausal women with osteoporosis |
|
|
6–12 OLE | Means and 95% CIs |
|
|
| RLX vs. placebo | ||||||
| Adami 2008;46 postmenopausal women with osteoporosis pre treated with TPTD |
|
|
12 | Nothing | p < 0.001 | |
| Adami 2008;46 postmenopausal women with osteoporosis pre treated with TPTD |
|
|
36 including 24 OLE | Nothing |
|
|
| Liu 2004;48 postmenopausal women with osteoporosis |
|
|
12 |
|
Nothing |
|
| Silverman 2008;50 postmenopausal women with osteoporosis |
|
|
36 | Nothing |
|
|
| MORE: Ettinger 1999;51 women with osteoporosis |
|
|
36 | NR | Nothing | RLX group increased by 2.1% compared with placebo, p < 0.001 |
| Mok 2011;53 postmenopausal women on long-term GCCs |
|
|
12 | Mean and SEMs |
|
|
| ROMO vs. placebo | ||||||
| FRAME: Cosman 2016;54 postmenopausal women with osteoporosis |
|
Substudy
|
12 | 95% CIs | ROMO group compared with placebo: 5.9% (95% CI 4.3 to 7.4); p < 0.001 | |
| FRAME: Cosman 2016;54 postmenopausal women with osteoporosis |
|
|
24 | 95% CIs | ROMO group compared with placebo: 6.0% (95% CI 4.4 to 7.7); p < 0.001 | |
| Ishibashi 2017;55 postmenopausal women with osteoporosis |
|
|
12 | Nothing | ROMO group compared with placebo: 3.5% (one-sided 95% CI 2.3%, NA); (p < 0.00001) | |
| BRIDGE;56 men with osteoporosis |
|
|
12 | 95% CIs | p < 0.001 | |
| TPTD vs. placebo | ||||||
| ACTIVE: Miller 2016;95 postmenopausal women with osteoporosis |
|
|
18 |
|
Nothing | p < 0.0001 |
| Orwoll 2003;57 men with osteoporosis |
|
|
12 |
|
Nothing | p = 0.029 |
| Miyauchi 2010;58 women and men with osteoporosis |
|
|
12 |
|
Nothing | p = 0.015 |
| Miyauchi 2010;58 women and men with osteoporosis |
|
|
12–18 OLE |
|
Nothing |
|
| Miyauchi 2010;58 women and men with osteoporosis |
|
|
18–24 OLE |
|
Nothing |
|
| Miyauchi 2008;59 postmenopausal women with osteoporosis |
|
|
6 |
|
Nothing |
|
| Leder 2015;61 postmenopausal women with osteoporosis |
|
|
6 |
|
Nothing | p < 0.01 |
| Leder 2015;61 postmenopausal women with osteoporosis |
|
|
12 |
|
Nothing |
|
| Neer 2001;62 postmenopausal women with osteoporosis |
|
|
24 (trial stopped early; mean time to last visit was 19) |
|
Nothing | p < 0.001 |
| Sethi 2008;63 postmenopausal women with osteoporosis |
|
|
6 |
|
Nothing |
|
| Head-to-head non-bisphosphonates | ||||||
| DATA: Tsai 2013;64 postmenopausal women with osteoporosis |
|
|
12 |
|
Nothing | p = 0.1939 |
| DATA: Leder 2014;110 postmenopausal women with osteoporosis | As above |
|
24 |
|
Nothing | p = 0.23 |
| DATA-Switch65 |
|
|
0–24 | Nothing | p < 0.0005 | |
| DATA-Switch65 |
|
|
24–48 | Nothing | p < 0.0005 | |
| EUROFORS: Eastell 2009;66 postmenopausal women with osteoporosis pre treated with TPTD |
|
|
24 |
|
Nothing |
|
| STRUCTURE;67 postmenopausal women with osteoporosis pre treated with ALN |
|
|
12 | Nothing | p < 0.0001 | |
| McClung 2014;68 postmenopausal women with osteoporosis |
|
|
12 | Nothing |
|
|
| DEN vs. bisphosphonates | ||||||
| DECIDE;69 postmenopausal women with osteoporosis |
|
|
12 | 95% CIs | Absolute treatment difference 0.6% (95% CI 0.3 to 1.0); p = 0.0001 | |
| STAND;70 postmenopausal women with osteoporosis already on ALN |
|
|
12 | Means and 95% CIs | p < 0.0121 | |
| DAPS;71 postmenopausal women with osteoporosis |
|
|
12 |
|
Nothing |
|
| DAPS:109 postmenopausal women with osteoporosis |
|
|
12–24 (post cross-over) |
|
Nothing |
|
| McClung 2006;72 postmenopausal women with osteoporosis or osteopenia |
|
|
12 | Nothing |
ALN and DEN vs. placebo, both p < 0.001 (ALN vs. DEN MD 0.00, 95% CI –1.38 to 1.38; p = 1.00) |
|
| Recknor 2013;73 postmenopausal women with osteoporosis |
|
|
12 | 95% CIs | p < 0.001 | |
| Saag 2018;74 women and men continuing GCCs with osteoporosis or low BMD + fracture |
|
|
12 | 95% CIs | p = 0.004 | |
| Saag 2018;74 women and men initiating GCCs with osteoporosis or low BMD + fracture |
|
|
12 | 95% CIs | p = 0.020 | |
| Miller 2016;75 postmenopausal women with osteoporosis previously treated with bisphosphonates |
|
|
12 | Nothing | p < 0.0001 | |
| RLX vs. bisphosphonates | ||||||
| EFFECT: Sambrook 200476 (international not including USA); postmenopausal women with osteoporosis |
|
|
12 | SEMs | 1.3%, 95% CI 0.5 to 2.1; p = 0.0001 | |
| EFFECT (USA);77 postmenopausal women with osteoporosis |
|
|
12 | Means and SEMs | p = 0.396 | |
| Johnell 2002;78 postmenopausal women with osteoporosis |
|
|
12 | Nothing |
|
|
| EVA: Recker 2007;80 postmenopausal women with osteoporosis |
|
|
24 | SEMs | p = 0.002 | |
| Sanad 2011;81 postmenopausal women with osteoporosis |
|
|
12 |
|
Means |
|
| Michalska 2006;82 postmenopausal women with osteoporosis previously treated with bisphosphonates |
|
|
12 |
|
Means (SEMs in graph overlap – unable to extract) |
|
| Michalska 2006;82 postmenopausal women with osteoporosis previously treated with bisphosphonates |
|
|
24 including 12 OLE | Means and SEMs |
|
|
| ROMO vs. bisphosphonates | ||||||
| ARCH: Saag 2017;83 postmenopausal women with osteoporosis |
|
|
12 | Nothing | p < 0.001 | |
| ARCH: Saag 2017;83 postmenopausal women with osteoporosis |
|
|
24 | Nothing | p < 0.001 | |
| ARCH: Saag 2017;83 postmenopausal women with osteoporosis | As above |
|
36 | Nothing | p < 0.001 | |
| TPTD vs. bisphosphonates | ||||||
| FACT;84 postmenopausal women with osteoporosis |
|
|
18 | 95% CIs | p = 0.05 | |
| Saag 2009;103 women and men on GCCs with osteoporosis or low BMD + fracture |
|
|
36 | 95% CIs | p < 0.001 | |
| EUROGIOPs;87 men on GCCs with osteoporosis |
|
|
18 | SEMs | p = 0.026 | |
| Walker 2013;89 men with osteoporosis |
|
|
18 | Nothing | p ≥ 0.05 | |
| Hadji 2012;91 postmenopausal women with osteoporosis |
|
|
18 | Nothing | p = 0.02 | |
| MOVE: Malouf-Sierra 2017;92 women and men with low BMD + recent hip fracture surgery |
|
|
18 |
|
Nothing | p = 0.003 |
| Cosman 2011;93 postmenopausal women with osteoporosis |
|
|
12 | Nothing | p < 0.05 | |
| Trial name: first author and year | Treatment arm (n participants) | Follow-up (months) | Overall mortality, n/N (%) | Reported between-group difference |
|---|---|---|---|---|
| DEN vs. placebo | ||||
| FREEDOM: Cummings 200941 and Bone 2017104 |
|
36 |
|
p = 0.08 |
| ADAMO: Orwoll 201242 |
|
12 |
|
NR |
| ADAMO: Langdahl 2015111 |
|
12–24 |
|
NR |
| DIRECT: Nakamura 201443 |
|
24 |
|
NR |
| DIRECT: Sugimoto 2015106 |
|
24–36 |
|
NR |
| Nakamura 201244 |
|
12 |
|
NR |
| Koh 201645 (NCT01457950) |
|
6 |
|
NR |
| Koh 201645 (NCT01457950) |
|
6–12 |
|
NR |
| RLX vs. placebo | ||||
| Adami 200846 | All TPTD for 12 months then:
|
12 | NR | NR |
| Morii 200347 |
|
12 | NR | NR |
| Liu 200448 |
|
12 |
|
NR |
| Gorai 201294 |
|
12 | NR | NR |
| Silverman 200850 (NCT00205777) |
|
36 |
|
NR |
| MORE: Ettinger 199951 and Maricic 2002102 |
|
36 | NR | NR |
| Lufkin 199852 |
|
12 | NR | NR |
| Mok 201153 (NCT00371956) |
|
12 | NR | NR |
| ROMO vs. placebo | ||||
| BRIDGE: Lewiecki 2018;56 (NCT02186171) |
|
12 |
|
NR |
| FRAME: Cosman 201654 |
|
12 and 24 | 12 months:
|
NR |
| Ishibashi 201755 (NCT01992159) |
|
12 |
|
NR |
| TPTD vs. placebo | ||||
| Orwoll 200357 |
|
Median 11 |
|
NR |
| Miyauchi 201058 |
|
24 |
|
NR |
| Miyauchi 200859 |
|
6 |
|
NR |
| ACTIVE95 (NCT01343004) |
|
18 |
|
NR |
| Leder 201561 |
|
6, plus a further 6-month extension to 12 months | 6 months:
|
NR |
| Neer 200162 (NCT00670501) |
|
24 (stopped early; mean time to last visit was 19 months) | NR | Reports no significant difference. Data NR |
| Sethi 200863 (NCT00500409) |
|
6 |
|
Reports no significant difference |
| Head-to-head non-bisphosphonates | ||||
| DATA64 |
|
12 | NR | NR |
| DATA64 (NCT00926380) |
|
24 | NR | NR |
| DATA-Switch65 |
|
24–48 | NR | NR |
| EUROFORS: Eastell 200966 |
|
24 | NR | NR |
| STRUCTURE67 |
|
12 |
|
NR |
| McClung 201468 |
|
12 |
|
NR |
| DEN vs. bisphosphonates | ||||
| DECIDE69 |
|
12 |
|
|
| STAND: Kendler 201070 |
|
12 |
|
p = 1.0000 |
| DAPS: Kendler 201171 and Freemantle 2012109 |
|
12 | NR | NR |
| McClung 200672 |
|
12 |
|
NR |
| Recknor 201373 |
|
12 |
|
p = 0.299 |
| Saag 201874 (NCT01575873) |
|
12 |
|
NR |
| Miller 201675 |
|
12 | Fatal AEs:
|
NR |
| RLX vs. bisphosphonates | ||||
| EFFECT (international, excluding USA): Sambrook 200476 |
|
12 |
|
|
| EFFECT (USA): Luckey 200477 |
|
12 | NR | NR |
| Johnell 200278 |
|
12 | NR | NR |
| Muscoso 200479 |
|
24 | NR | NR |
| EVA: Recker 200780 |
|
24 |
|
|
| Sanad 201181 |
|
12 | NR | NR |
| Michalska 200682 | Open label:
|
12, followed by 12 months’ open-label extension | NR | NR |
| ROMO vs. bisphosphonates | ||||
| ARCH: Saag 201783 |
|
12 from randomisation, then a further 12 open label, following treatment-switching | 0–12 months:
|
NR |
| TPTD vs. bisphosphonates | ||||
| FACT: McClung 200584 |
|
18 | NR | NR |
| Saag 200985 (NCT01575873) |
|
36 |
|
|
| Panico 201186 |
|
18 | NR | NR |
| EuroGIOPs: Glüer 201387 |
|
18 |
|
p = 0.613 |
| Anastasilakis 200888 |
|
12 | NR | NR |
| Walker 201389 |
|
18 | NR | NR |
| Hadji 201291 |
|
18 |
|
p = 0.75 |
| VERO: Kendler 201899 |
|
24 |
|
p = 0.13 |
| MOVE: Abtahi 2016101 |
|
6 |
|
p = 0.446 |
| MOVE: Malouf-Sierra 201792 | 24 |
|
p = 0.171 | |
| Cosman 201193 |
|
12 |
|
NR |
| Trial name: first author and year | Treatment arm (n participants) | Follow-up (months) | One or more SAE(s), n/N (%) | Reported between-group difference | One or more AE(s), n/N (%) | Reported between-group difference |
|---|---|---|---|---|---|---|
| DEN vs. placebo | ||||||
| FREEDOM: Cummings 200941 and Bone 2017104 |
|
36 |
|
p = 0.61 |
|
p = 0.91 |
| ADAMO: Orwoll 201242 |
|
12 |
|
NR |
|
NR |
| ADAMO: Langdahl 2015111 |
|
12–24 |
|
NR |
|
NR |
| DIRECT: Nakamura 201443 |
|
24 |
|
NR |
|
NR |
| DIRECT106 |
|
24–36 |
|
NR |
|
NR |
| Nakamura 201244 |
|
12 |
|
NR |
|
NR |
| Koh 201645 (NCT01457950) |
|
6 |
|
NR |
|
NR |
| Koh 201645 (NCT01457950) |
|
6–12 |
|
NR |
|
NR |
| RLX vs. placebo | ||||||
| Adami 200846 | All TPTD for 12 months then:
|
12 | NR | NR | NR | NR |
| Morii 200347 |
|
12 |
|
p = 0.452 |
|
|
| Liu 200448 |
|
12 |
|
Not significant at p < 0.05 | NR | |
| Gorai 201294 |
|
12 | NR | NR |
|
NR |
| Silverman 200850 (NCT00205777) |
|
36 |
|
NR |
|
NR |
| MORE: Ettinger 199951 and Maricic 2002102 |
|
36 | NR | NR | NR | NR |
| Lufkin 199852 |
|
12 | NR | NR | NR | NR |
| Mok 201153 (NCT00371956) |
|
12 | NR | NR | NR | NR |
| ROMO vs. placebo | ||||||
| BRIDGE56 (NCT02186171) |
|
12 |
|
NR |
|
NR |
| FRAME: Cosman 201654 |
|
12 from randomisation, then a further 12 following treatment-switching | 12 months:
|
NR | 12 months:
|
NR |
| Ishibashi 201755 (NCT01992159) |
|
12 |
|
NR |
|
NR |
| TPTD vs. placebo | ||||||
| Orwoll 200357 |
|
Median 11 | NR | NR | Reports that the overall incidence of AEs was similar across groups. No data | NR |
| Miyauchi 201058 |
|
24 |
|
Reported as not significant. p-value NR |
|
Reported as not significant. p-value NR |
| Miyauchi 200859 |
|
6 | NR as number of participants with SAE |
|
NR | |
| ACTIVE95 (NCT01343004) |
|
18 |
|
NR |
|
NR |
| Leder 201561 |
|
6, plus a further 6-month extension to 12 months | 6 months:
|
NR | 6 months:
|
NR |
| Neer 200162 (NCT00670501) |
|
24 (stopped early; mean time to last visit was 19 months) |
|
NR | NR | NR |
| Sethi 200863 (NCT00500409) |
|
6 |
|
Reported as not significant. p-value NR |
|
Reported as not significant. p-value NR |
| Head-to-head non-bisphosphonates | ||||||
| DATA64 |
|
12 |
|
NR | NR | NR |
| DATA64 (NCT00926380) |
|
24 |
|
NR |
|
NR |
| DATA-Switch65 |
|
24–48 |
|
NR | NR | NR |
| STRUCTURE67 |
|
12 |
|
NR |
|
NR |
| EUROFORS66 | All TPDT for 12 months then:
|
24 | NR | NR |
|
Not significant at p < 0.05 |
| McClung 201468 |
|
12 |
|
NR |
|
NR |
| DEN vs. bisphosphonates | ||||||
| DECIDE69 |
|
12 |
|
0.71 |
|
Non-significant p = 0.60 |
| STAND: Kendler 201070 |
|
12 |
|
p = 0.8546 |
|
p = 0.8294 |
| DAPS: Kendler 201171 and 2012109 |
|
12 |
|
NR |
|
p = 0.403 |
| McClung 200672 |
|
12 |
|
NR |
|
NR |
| Recknor 201373 |
|
12 |
|
p = 0.046 |
|
p = 0.635 |
| Saag 201874 |
|
12 |
|
NR |
|
NR |
| Miller 201675 |
|
12 |
|
NR |
|
NR |
| RLX vs. bisphosphonates | ||||||
| EFFECT (international excluding USA); Sambrook 200476 |
|
12 |
|
p = 0.543 |
|
p = 0.573 |
| EFFECT (USA); Luckey 200477 |
|
12 |
|
p = 0.43 |
|
p = 0.83 |
| Johnell 200278 |
|
12 | NR | NR | NR | NR |
| Muscoso 200479 |
|
24 | NR | NR | NR | NR |
| EVA: Recker 200780 |
|
24 | NR | NR |
|
p = 0.92 |
| Sanad 201181 |
|
12 | NR | NR | NR | NR |
| Michalska 200682 | Open label:
|
12, followed by 12 months’ open-label extension | NR | NR |
|
p = 0.126 |
| ROMO vs. bisphosphonates | ||||||
| ARCH: Saag 201783 |
|
12 from randomisation, then a further 12 open label, following treatment-switching | 0–12 months:
|
NR | 0–12 months:
|
NR |
| TPTD vs. bisphosphonates | ||||||
| FACT: McClung 200584 |
|
18 | NR | NR | NR | NR |
| Saag 200985 |
|
36 |
|
p = 0.518 |
|
p = 0.116 |
| Panico 201186 |
|
18 | NR | NR | NR | NR |
| EuroGIOPs: Glüer 201387 |
|
12 |
|
p = 0.089 |
|
p = 0.080 |
| Anastasilakis 200888 |
|
12 | NR | NR |
|
Not significant at p < 0.05 |
| Walker 201389 |
|
18 | NR | NR | NR | NR |
| Hadji 201291 |
|
18 |
|
p = 0.27 |
|
p = 0.45 |
| VERO: Kendler 201899 |
|
24 |
|
p = 0.13 |
|
p = 0.76 |
| MOVE: Abtahi 2016101 |
|
6 |
|
p = 0.271 |
|
p = 0.683 |
| MOVE: Malouf-Sierra 201792 | 24 |
|
p = 0.418 |
|
p = 0.684 | |
| Cosman 201193 (NCT00439244) |
|
12 |
|
NR |
|
NR |
| Trial | Intervention and comparators (n) | Follow-up duration (months) | Lumbar spine BMD percentage change from baseline, mean (SD) (reported between-group difference) |
|---|---|---|---|
| Nakamura 201244 | Placebo, n = 55 | 12 |
|
| DEN, n = 54 | 16.73 (NR) | ||
| Morii 200347 | Placebo, n = 97 | 12 |
|
| RLX, n = 90 |
|
||
| Gorai 201249 | Alfacalcidol, n = 34 | 24 | –0.8 (4.6) |
| RLX, n = 33 |
|
||
| Alfacalcidol plus RLX, n = 31 |
|
||
| Lufkin 199852 | Control, n = 48 | 12 |
|
| RLX, n = 48 | 1.34 (1.02) | ||
| Muscoso 200479 | ALN, n = 1000 | 24 | 7.2 (1.9) |
| RIS, n = 100 | 6.2 (2.0) | ||
| RLX, n = 100 | 2.4 (1.1) | ||
| Anastasilakis 200888 | RIS, n = 22 | 12 |
|
| TPTD, n = 22 |
|
Appendix 6 Health-related quality of life
| Trial | Measure | Follow-up | Treatment group | Results (change from baseline) |
|---|---|---|---|---|
| FREEDOM116,118 | OPAQ-SV329 | 36 months | Placebo, n = NR | Mean:
|
|
DEN, n = NR (n across both groups: |
|
|||
| Silverman 200850 (NCT00205777) | Women’s Health Questionnaire330 | 36 months | Placebo, n = 1179 | Least squares, mean (SE): 0.005 (0.005) |
| RLX, n = 1168 |
|
|||
| QUALEFFO-41331 | 36 months | Placebo, n = 1176 | Least squares, mean (SE): –0.35 (0.3) | |
| RLX, n = 1168 |
|
|||
| EQ-VAS332 | 36 months | Placebo, n = 1120 | Least squares, mean (SE): 4.66 (1.70) | |
| RLX, n = 1092 |
|
|||
| EQ-5D Health State Profile Utility Score332 | 36 months | Placebo, n = 1128 | Least squares, mean (SE): –0.00 (0.01) | |
| RLX, n = 1111 |
|
|||
| Panico 201186 | QUALEFFO-41331 | 18 months | ALN, n = 39 |
|
| TPTD, n = 42 |
|
|||
| VERO90 | EQ-VAS UK332 | 24 months | RIS plus placebo |
|
| TPTD plus placebo |
|
|||
| MOVE101 | SF-36 Physical Function Component (post surgery)333 | 26 weeks | RIS plus placebo | Mean (SD):
|
| TPTD plus placebo | Mean (SD):
|
The UCB S.A. company submission20 reported that, in both the FRAME54 (ROMO vs. PBO) and the ARCH83 (ROMO vs. ALN) studies, there was (confidential information has been removed) between treatment groups in HRQoL, (confidential information has been removed).
The Amgen Inc. company submission100 reported that the Determining Efficacy: Comparison of Initiating Denosumab versus alendronate (DECIDE)69 study found (confidential information has been removed) difference between DEN and ALN, as measured by the EQ-5D.
Appendix 7 Specific adverse events
Bisphosphonate studies: specific adverse events
Three additional bisphosphonate RCTs130,137,138 were identified by the search (Table 25). Of these, two RCTs assessed atypical femoral fractures and found no incidences of atypical femoral fractures in participants treated with ZOL compared with those treated with ALN,138 or those treated with ZOL compared with those treated with placebo. 130 One study assessed ONJ and found no incidences in participants treated with ZOL or placebo. 130
| Trial name: first author and year | Treatment arms (n) | Follow-up (months) | AE | |||
|---|---|---|---|---|---|---|
| VTE(s), n/N (%) | Stroke, n/N (%) | ONJ, n/N (%) | Atypical femoral fractures, n/N (%) | |||
| TRIO: Paggiosi 2014137 |
|
24 | NR | NR | NR | NR |
| Tan 2016138 |
|
36 | NR | NR | NR |
|
| ZONE130 |
|
24 | NR | NR |
|
|
Non-bisphosphonate studies: specific adverse events
Venous thromboembolism
Across the studies comparing a non-bisphosphonate with placebo, five reported thrombotic events of venous origin,43,46,47,50,51 and one study reported on arterial limb thrombosis. 42 Across these studies, event rates were ≤ 1%. The estimated between-group differences were not statistically significant at p < 0.05 (p-values not presented), with the exception of one study comparing RLX with placebo at 36 months in postmenopausal women with osteoporosis, which was statistically significantly in favour of placebo (estimated p = 0.005). 51
None of the studies that compared bisphosphonates with non-bisphosphonates head-to-head reported on VTE.
Across the studies comparing a non-bisphosphonate with a bisphosphonate, two studies reported on thrombosis but did not specify whether this was venous or arterial in origin,72,74 eight reported on thrombotic events of venous origin,74,77,80,81,91,98,99,103 and one reported on peripheral artery thrombosis. 75 Across these studies, event rates were ≤ 3%. The estimated between-group differences were not statistically significant at p < 0.05 (p-values not presented).
Stroke
Across the studies comparing a non-bisphosphonate with placebo, four reported on stroke. 41,50,56,111 Across these studies, event rates were ≤ 2% and no statistically significant between-group differences were evident (reported or estimated).
None of the studies that compared bisphosphonates with non-bisphosphonates head-to-head reported on stroke.
Across the studies comparing a non-bisphosphonate with placebo, eight reported on stroke. 72,74,83,91,93,98,99,103 Across these studies, event rates were ≤ 2%. The estimated between-group differences were not statistically significant at p < 0.05 (p-values not presented). However, the estimated between-group difference in stoke for one of these studies comparing ROMO with ALN in postmenopausal women with osteoporosis was statistically significant at 24 months following treatment-switching to ALN, in favour of the continued ALN group (p = 0.004). 83
Osteonecrosis of the jaw
Osteonecrosis of the jaw was reported by nine studies comparing a non-bisphosphonate with placebo,41,42,44,45,54–56,111 one study comparing non-bisphosphonates head to head67 and three studies comparing a non-bisphosphonate with a bisphosphonate. 71,74,83 Across these studies, event rates were ≤ 1% and no statistically significant between-group differences were evident (reported or estimated).
Atypical femoral fracture
Atypical femoral fracture was reported by nine studies comparing a non-bisphosphonate with placebo,41,42,45,54–56,106,111,334 one study comparing non-bisphosphonates head to head67 and three studies comparing a non-bisphosphonate with a bisphosphonate. 74,75,83,109 Across these studies, event rates were ≤ 1% and no statistically significant between-group differences were evident (reported or estimated).
| Trial name: first author and year; population | Treatment arms (n) | Follow-up (months) | AE | |||
|---|---|---|---|---|---|---|
| VTE(s), n/N (%) | Stroke, n/N (%) | ONJ, n/N (%) | Atypical femoral fractures, n/N (%) | |||
| DEN vs. placebo | ||||||
| FREEDOM: Cummings 2009;41 postmenopausal women with osteoporosis |
|
36 | NR |
|
|
|
| ADAMO: Orwoll 2012;42 men with osteoporosis |
|
12 | Arterial limb thrombosis
|
NR |
|
|
| ADAMO: Langdahl 2015;111 men with osteoporosis |
|
24, including 12 OLE | NR | Transient ischaemic attack
|
|
|
| DIRECT: Nakamura 2014;334 women and men with osteoporosis (NCT00680953) |
|
24 |
|
NR |
|
|
| DIRECT: Sugimoto 2015;106 women and men with osteoporosis |
|
24–36 | NR | NR |
|
|
| Nakamura 2012;44 postmenopausal women with osteoporosis |
|
12 | NR | NR |
|
NR |
| Koh 2016;45 postmenopausal women with osteoporosis |
|
6 | NR | NR |
|
|
| Koh 2016;45 postmenopausal women with osteoporosis |
|
6–12 OLE | NR | NR |
|
|
| RLX vs. placebo | ||||||
| Adami 2008;46 postmenopausal women with osteoporosis pre treated with TPTD |
|
12 months |
|
NR | NR | NR |
| Morii 2003;47 postmenopausal women with osteoporosis |
|
12 |
|
NR | NR | NR |
| Liu 2004;48 postmenopausal women with osteoporosis |
|
12 |
|
NR | NR | NR |
| Gorai 2012;94 postmenopausal women with low osteopenia |
|
12 | NR | NR | NR | NR |
| Silverman 2008;50,117 postmenopausal women with osteoporosis |
|
36 |
|
|
NR | NR |
| MORE: Ettinger 1999;51 women with osteoporosis |
|
36 |
|
NR | NR | NR |
| Lufkin 1998;52 postmenopausal women with osteoporosis |
|
12 |
|
NR | NR | NR |
| Mok 2011;53 postmenopausal women on long-term GCCs |
|
12 |
|
NR | NR | NR |
| ROMO vs. placebo | ||||||
| FRAME: Cosman 2016;54 postmenopausal women with osteoporosis |
|
12 | NR | NR |
|
|
| FRAME: Cosman 2016;54 postmenopausal women with osteoporosis |
|
24 | NR | NR |
|
|
| Ishibashi 2017;55 postmenopausal women with osteoporosis |
|
12 | NR | NR |
|
|
| BRIDGE;56 men with osteoporosis |
|
12 | NR |
|
|
|
| TPTD vs. placebo | ||||||
| ACTIVE: Miller 2016;95 postmenopausal women with osteoporosis |
|
18 | NR | NR | NR | NR |
| Orwoll 2003;57 men with osteoporosis |
|
The study was stopped after a median duration of 11 months | NR | NR | NR | NR |
| Miyauchi 2010;58 women and men with osteoporosis |
|
12 | NR | NR | NR | NR |
| Miyauchi 2010;58 women and men with osteoporosis |
|
24, including 12 OLE | NR | NR | NR | NR |
| Miyauchi 2008;59 postmenopausal women with osteoporosis |
|
6 | NR | NR | NR | NR |
| Leder 2015;61,336 postmenopausal women with osteoporosis |
|
6 | NR | NR | NR | NR |
| Neer 2001;62 postmenopausal women with osteoporosis |
|
24 (stopped early; mean time to last visit was 19 months) | NR | NR | NR | NR |
| Sethi 2008;63 postmenopausal women with osteoporosis |
|
6 | NR | NR | NR | NR |
| Head-to-head non-bisphosphonates | ||||||
| DATA: Tsai 2013;64 postmenopausal women with osteoporosis |
|
12 | NR | NR | NR | NR |
| DATA: Leder 2014;110 postmenopausal women with osteoporosis |
|
24 | NR | NR | NR | NR |
| EUROFORS: Eastell 2009;66 postmenopausal women with osteoporosis pre treated with TPTD |
|
24 | NR | NR | NR | NR |
| STRUCTURE;67 postmenopausal women with osteoporosis pre treated with ALN |
|
12 | NR | NR |
|
|
| McClung 2014;68 postmenopausal women with osteoporosis |
|
12 | NR | NR | NR | NR |
| DEN vs. bisphosphonates | ||||||
| DECIDE;69 postmenopausal women with osteoporosis |
|
12 | NR | NR | NR | NR |
| STAND;70 postmenopausal women with osteoporosis already on ALN |
|
12 | NR | NR | NR | NR |
| DAPS;71 postmenopausal women with osteoporosis |
|
12 | NR | NR |
|
NR |
| DAPS;109 postmenopausal women with osteoporosis |
|
24 | NR | NR |
|
|
| McClung 2006;72,337 postmenopausal women with osteoporosis or osteopenia |
|
12 | Thrombosis
|
|
NR | NR |
| Recknor 2013;73 postmenopausal women with osteoporosis |
|
12 | NR | NR | NR | NR |
| Saag 2018;74,338 women and men on GCCs with osteoporosis or low BMD + fracture (NCT01575873) |
|
12 | DVT
|
|
|
|
| Miller 2016;75,339 postmenopausal women with osteoporosis previously treated with bisphosphonates (NCT01732770) |
|
12 | Peripheral artery thrombosis
|
NR | NR |
|
| RLX vs. bisphosphonates | ||||||
| EFFECT: Sambrook 200476 (international not including USA); postmenopausal women with osteoporosis |
|
12 | NR | NR | NR | NR |
| EFFECT (USA);77 postmenopausal women with osteoporosis |
|
12 |
|
NR | NR | NR |
| Johnell 2002;78 postmenopausal women with osteoporosis |
|
12 | NR | NR | NR | NR |
| Muscoso 2004;79 postmenopausal women with osteoporosis |
|
24 | NR | NR | NR | NR |
| EVA: Recker 2007;80 postmenopausal women with osteoporosis |
|
24 | DVT:
|
NR | NR | NR |
| Sanad 2011;81 postmenopausal women with osteoporosis |
|
12 |
|
NR | NR | NR |
| Michalska 2006;82 postmenopausal women with osteoporosis previously treated with bisphosphonates |
|
12 | NR | NR | NR | NR |
| ROMO vs. bisphosphonates | ||||||
| ARCH: Saag 2017;83 postmenopausal women with osteoporosis |
|
12 | NR |
|
|
|
| ARCH: Saag 2017;83 postmenopausal women with osteoporosis |
|
24, including 12 months’ OLE | NR |
|
|
|
| TPTD vs. bisphosphonates | ||||||
| FACT;84 postmenopausal women with osteoporosis |
|
18 | NR | NR | NR | NR |
| Saag 2009,103 Langdahl 2009107 and Lips 1999;340 women and men on GCCs with osteoporosis or low BMD + fracture (NCT01732770) |
|
36 | DVT:
|
|
NR | NR |
| Panico 2011;86 postmenopausal women with severe osteoporosis +fracture and on treatment for osteoporosis |
|
18 | NR | NR | NR | NR |
| Anastasilakis 200888 |
|
12 | NR | NR | NR | NR |
| EUROGIOPs;87 men with osteoporosis on GCCs |
|
18 | NR | NR | NR | NR |
| Walker 2013;89 men with osteoporosis |
|
18 | NR | NR | NR | NR |
| Hadji 2012;91 postmenopausal women with osteoporosis (NCT00343252) |
|
18 | DVT
|
|
NR | NR |
| VERO: Kendler 2018;99 postmenopausal women with osteoporosis (NCT01709110) |
|
24 | DVT
|
|
NR | NR |
| MOVE: Aspenberg 201698 and Malouf-Sierra 201792,128 (NCT00887354) |
|
NR | Venous thrombosis
|
|
NR | NR |
| Cosman 2011;93 postmenopausal women with osteoporosis (NCT00439244) |
|
12 | NR |
|
NR | NR |
Appendix 8 Statistical methods for the network meta-analysis
Statistical model for the network meta-analysis of fracture outcomes
The RCTs presented data in terms of the number of individuals experiencing at least one fracture. For each fracture type, rik is defined as the number of events out of the total number of participants, nik, where the participants are receiving treatment tik in arm k of trial i. The data generation process is assumed to follow a binomial likelihood such that:
where pik represents the probability of an event in arm k of trial i (i = 1, . . . ns, k = 1 . . . na) after follow-up time fi. For all RCTs, the number of arms included in the analysis is two (i.e. na = 2) and the number of RCTs, ns, varies according to fracture type.
To account for different trial durations, an underlying Poisson process is assumed for each trial arm, so that tik (the time until a fracture occurs in arm k of study i) follows an exponential distribution, tik ∼ exp(λik), where λik is the event rate in arm k of study i, assumed constant over time. The probability that there are no events at time fi is given by the survivor function P(Tik > fi) = exp(–λikfi). For each study, i, the probability of an event in arm k after follow-up time fi can be written as:
which is dependent on follow-up time. The probabilities of fracture are non-linear functions of event rates, and so were modelled using the complementary log–log link function:
Here, the µi are trial-specific baselines, representing the log-hazards of fracture in the baseline treatment, which is assumed to be arm k = 1 for all trials. Note that, for some trials, the baseline may be an active treatment rather than placebo. The trial-specific treatment effects, δi,1k, are log-hazard ratios of fracture for the treatment in arm k, relative to the baseline treatment.
As described later, two different modelling strategies were considered for the treatment effects: (1) standard independent random (treatment) effects model and (2) exchangeable treatment effects (i.e. a class effect) for bisphosphonate treatments with unrelated treatment effects for all other interventions. The main results are based on model 2, and the results for the standard independent random-effects model are provided here for comparison.
Standard independent random-effects model
The trial-specific treatment effects, δi,1k, were assumed to arise from a common population distribution with mean treatment effect relative to the reference treatment, which was defined as placebo for this analysis, such that:
where dti1tik represents the mean effect of the treatment in arm k of study i (tik) compared with the treatment in arm 1 of study i (ti1) and τ2 represents the between-study variance in treatment effects (heterogeneity), which is assumed to be the same for all treatments.
The model was completed by specifying prior distributions for the parameters. When there were sufficient sample data, conventional reference prior distributions were used:
-
trial-specific baseline, µi ∼ N(0,1002)
-
treatment effects relative to reference treatment, d1k ∼ N(0,1002)
-
between-study SD of treatment effects, τ ∼ U(0,2).
For hip, wrist and proximal humerus fracture outcomes, there were relatively few RCTs to allow Bayesian updating (i.e. estimation of parameters from the sample data alone) of the reference prior distribution for the between-study SD. When prior distributions do not represent reasonable prior beliefs, then, in the absence of sufficient sample data, posterior distributions will not represent reasonable posterior beliefs. Therefore, rather than using a reference prior distribution, a weakly informative prior distribution was used for the between-study SD, such that τ ∼ HN(0,0.322).
Primary analysis model
In the previous NICE assessment for bisphosphonates, a class-effects model was used. Not all RCTs contributing wrist fracture data provide evidence about all bisphosphonates; in particular, there was no evidence about ZOL. To allow an assessment of the uncertainty associated with ZOL for inclusion in the economic model, a class-effects model was fitted, from which the predictive distribution of a new intervention in the same class can be generated. This modelling approach also has the benefit of addressing data sparsity in the hip network.
For the primary analysis model, a class effects was assumed for bisphosphonate treatments only. Under a class-effects model, the trial-specific treatment effects are again assumed to be normally distributed as in equation (3), but the mean effects of each treatment are assumed to be exchangeable and assumed to arise from a normal distribution with mean, D, with variance τD2:
The model was completed by specifying prior distributions for the parameters:
-
mean bisphosphonate effect, D ∼ N(0,1002)
-
between-treatment SD, τD ∼ U(0,2).
For hip, wrist and proximal humerus outcomes, a weakly informative prior was used for the between-treatment SD, such that: σD2∼HN(0,0.322).
Predicting effects in new randomised controlled trials
To account for heterogeneity in the effect of treatments between RCTs, results are also presented for the predictive distributions of the effect of treatment in a new (randomly chosen) study.
From equation (4), it follows that the study-specific population log-hazard ratio, δi,j, for study i, evaluating any given treatment j in reference to the control treatment can be written as:
where εij ∼ N(0,τ2). The predictive distribution for the effect of a particular treatment δi,j in a new study is as follows:
The class-effects model also allows generation of the predictive distribution of a new, randomly chosen bisphosphonate treatment from the same class. From Equation 5, it follows that the population log-hazard ratio for each treatment can be written as:
where ξ∼N(0,τD2). Therefore, combining Equations 6 and 8, the study-specific population log-hazard ratio, δi,j, for study i evaluating bisphosphonate j is:
For a new, randomly chosen bisphosphonate, the expectation is E[δij]=E[D+ζj+εij]=D, with variance:
Therefore, the predictive distribution for the effect of a new, randomly chosen, study from the same class is:
which accounts for both between-study, τ2, and between-treatment within class, τD2, heterogeneity for any (including a new) treatment.
It is the predictive distribution of a new treatment within the class and the predictive distribution of a new study for a new treatment within the class that we use to characterise the uncertainty about the effect of ZOL for hip fractures.
Statistical model for the network meta-analysis of femoral neck bone mineral density
Data for femoral neck BMD outcomes were presented in two different formats: either as the percentage change in femoral neck BMD for each treatment group or as the mean difference in the percentage change between treatment groups. Two different data generation (i.e. likelihood) models are therefore required.
Percentage change in femoral neck bone mineral density
The majority of RCTs presented data as the percentage change in femoral neck BMD, yik, and associated standard errors, seik, for arm k of trial i with study duration fi years. The data generation process is assumed to follow a normal likelihood, such that:
where the population variance of the mean, seik2, is assumed to be known and equal to the sample estimate. The parameters of interest, θik, are modelled using the identity link function and, to account for differing trial durations, study duration was included as a trial-level covariate. The link function is given by:
Where β11 = 0, and β1k(k = 2, . . . na) are the treatment-specific interactions, describing the relationship between the effect of treatment on percentage change in femoral neck BMD and duration of study. The trial baselines, µi, represent the percentage change in femoral neck BMD from baseline in the reference arm. The treatment effects, δi,1k, represent the difference between the percentage change in the treatment group and the reference group. Assumptions about the relationship between the interaction terms are described further in the meta-regression section.
Difference between treatments in mean change in femoral neck bone mineral density
Some RCTs provided data in terms of the mean difference in percentage change in femoral neck BMD between two treatments, defined as:
together with the associated standard errors of the mean difference, νi,1k, rather than the percentage change in femoral neck BMD for individual treatments. The difference between treatments in the mean change are also assumed to be normally distributed, such that:
where the population standard error of the difference, vi1k2, is assumed to be known and equal to the sample estimate. From the mean differences, no trial-specific effects of the baseline treatment can be estimated. The linear predictor is then given by:
The study-specific treatment effects, δi,1k, have the same interpretation as those from Equation 13; thus, they can be combined to estimate the mean effects for each treatment, regardless of the way the data were reported.
A class-effects model was assumed such that the treatment effects of the individual bisphosphonates were assumed to be exchangeable and to arise from a normal distribution with mean, D, with variance τD2:
The model was completed by specifying prior distributions for the parameters, using conventional reference prior distributions:
-
trial-specific baseline, µi ∼ N(0,1002)
-
treatment effects relative to reference treatment, d1k ∼ N(1,1002)
-
between-study SD of treatment effects, τ ∼ U(0,100).
-
mean of related treatment effects, D ∼ N(0,1002)
-
between-treatment SD, τD ∼ U(0,100).
Meta-regression
When appropriate, heterogeneity in treatment effects was explored by considering potential treatment effect modifiers. Meta-regression was used to test for interactions between the treatment effects and trial-level covariates, as described in Dias et al. :121
An interaction term, β, is introduced on the treatment effect by replacing:
Where xi is the trial-level covariate for trial i and may represent a subgroup, continuous covariate or baseline risk (as described in more detail later), and β11 = 0. The regression is centred at the mean value of the covariate across the RCTs so that the interpretation of the treatment effect is as the effect at the average value of the covariate.
Different assumptions can be made about the relationship between the interaction terms for each treatment. For the main analysis, we assume a common interaction for each treatment relative to treatment 1, such that:
for k = 2, . . . , na. We also considered a model in which the interaction terms for each treatment were considered to be related but not identical (i.e. exchangeable), such that:
Meta-regression on baseline risk/response
Baseline risk/response can be used as a proxy for differences in patient characteristics across trials that may be modifiers of treatment effect, and so introduce a potential source of heterogeneity in the NMA. Adjustment for baseline risk/response was assessed using the method of Achana et al. 122
Dependence on baseline risk is introduced through an interaction term, so that:
where εi,ti1tik∼N(0,τ2) The updated study-specific treatment effects, δ˜i,1k, are now adjusted using the ‘true’ but unobserved baseline risk/response in the placebo arm of trial i, µiP. The coefficient, βti1tik, represents the change in the treatment effect (e.g. log HR or difference between treatments in mean change) per unit change in the baseline risk/response. The baseline risk/response is centred on µ¯P, the observed mean (e.g. log HR or difference between treatments in mean change) in the placebo group, and β11 = 0.
For RCTs with an active treatment control, (t11 ≠ P), there is no direct estimate of the placebo baseline risk/response. Under the consistency of evidence arising from the exchangeability assumption, the substitution dti1tik=dPtik–dPti1 can be made, allowing Equation 21 to be expressed as:
Although a placebo treatment may not be included in all RCTs, the assumption of exchangeability means that the treatment arms can be assumed missing at random without loss to efficacy, and the baseline risk/response in RCTs without a placebo arm can be estimated, borrowing strength from other RCTs.
As previously described, some RCTs report data on the mean differences in percentage change between two treatments. Under the model described in Equations 15 and 16, study-specific effects of the baseline treatment cannot be estimated. These RCTs still contribute to the model through estimation of the treatment effects, but do not directly contribute to estimation of the slope in the meta-regression.
Appendix 9 Data contributing to the network meta-analysis
| Study | Treatment | Assessment time point | Number of participants in study arm | Number of events in study arm | Main analysis | SA1 | SA2 | SA3 | SA4 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | |||||||
| Liberman 1995134 | Placebo | ALN | – | 36 | 355 | 175 | – | 22 | 5 | – | 1 | 0 | 0 | 0 | 1 |
| Orwoll 2000286 | Placebo | ALN | – | 24 | 94 | 146 | – | 7 | 1 | – | 1 | 0 | 0 | 0 | 1 |
| FIT I: Black 1996280 | Placebo | ALN | – | 36 | 965 | 981 | – | 192 | 83 | – | 1 | 0 | 0 | 1 | 1 |
| FIT I: Black 1996280 | Placebo | ALN | – | 36 | 1000 | 1000 | – | 50 | 23 | – | 0 | 0 | 1 | 0 | 0 |
| FIT II: Cummings 1998281 | Placebo | ALN | – | 48 | 2077 | 2057 | – | 78 | 43 | – | 1 | 0 | 0 | 1 | 1 |
| Dursun 2001131 | Placebo | ALN | – | 12 | 35 | 38 | – | 14 | 12 | – | 1 | 1 | 0 | 0 | 1 |
| Carfora 1998134 | Placebo | ALN | – | 30 | 34 | 34 | – | 4 | 1 | – | 1 | 0 | 0 | 0 | 0 |
| Cohen 1999296 | Placebo | RIS | – | 12 | 35 | 34 | – | 5 | 2 | – | 1 | 1 | 0 | 1 | 1 |
| Fogelman 2000297 | Placebo | RIS | – | 24 | 125 | 112 | – | 17 | 8 | – | 1 | 0 | 0 | 1 | 1 |
| VERT-USA: Harris 1999298 | Placebo | RIS | – | 36 | 678 | 696 | – | 93 | 61 | – | 1 | 0 | 0 | 1 | 1 |
| VERT-USA: Harris 1999298 | Placebo | RIS | – | 12 | 660 | 669 | – | 42 | 16 | – | 0 | 1 | 0 | 0 | 0 |
| VERT-EU: Reginster 2000300 | Placebo | RIS | – | 36 | 346 | 344 | – | 89 | 53 | – | 1 | 0 | 0 | 1 | 1 |
| VERT-EU: Reginster 2000300 | Placebo | RIS | – | 12 | 334 | 333 | – | 45 | 19 | – | 0 | 1 | 0 | 0 | 0 |
| Hooper 2005132 | Placebo | RIS | – | 24 | 125 | 129 | – | 10 | 10 | – | 1 | 0 | 0 | 0 | 1 |
| Reid 2000303 | Placebo | RIS | – | 12 | 60 | 60 | – | 9 | 3 | – | 1 | 1 | 0 | 1 | 1 |
| Boonen 2009295 | Placebo | RIS | – | 24 | 80 | 179 | – | 0 | 2 | – | 1 | 0 | 0 | 1 | 0 |
| Ringe 2006304 | Placebo | RIS | – | 12 | 158 | 158 | – | 20 | 8 | – | 1 | 1 | 1 | 1 | 1 |
| Boonen 2012309 | Placebo | ZOL | – | 24 | 574 | 533 | – | 28 | 9 | – | 1 | 0 | 0 | 1 | 1 |
| Boonen 2012309 | Placebo | ZOL | – | 12 | 574 | 553 | – | 16 | 5 | – | 0 | 1 | 0 | 0 | 0 |
| HORIZON-PFT: Black 2007133 | Placebo | ZOL | – | 36 | 3861 | 3875 | – | 84 | 19 | – | 0 | 0 | 1 | 0 | 0 |
| HORIZON-PFT: Black 2007133 | Placebo | ZOL | – | 12 | 3861 | 3875 | – | 143 | 58 | – | 0 | 1 | 0 | 0 | 0 |
| HORIZON-PFT: Black 2007133 | Placebo | ZOL | – | 36 | 3861 | 3875 | – | 310 | 92 | – | 1 | 0 | 0 | 0 | 0 |
| HORIZON-RFT: Lyles 2007307 | Placebo | ZOL | – | 36 | 1062 | 1065 | – | 39 | 21 | – | 1 | 0 | 1 | 1 | 0 |
| HORIZON-RFT: Lyles 2007307 | Placebo | ZOL | – | 12 | 1057 | 1054 | – | 21 | 13 | – | 0 | 1 | 0 | 0 | 0 |
| BONE: Chesnut 2004136 | Placebo | IBN daily | – | 36 | 975 | 977 | – | 73 | 37 | – | 1 | 0 | 0 | 0 | 1 |
| BONE: Chesnut 2004136 | Placebo | IBN daily | – | 12 | 889 | 929 | – | 24 | 13 | – | 0 | 1 | 0 | 0 | 0 |
| BONE: Chesnut 2004136 | Placebo | IBN daily | – | 36 | 975 | 977 | – | 41 | 22 | – | 0 | 0 | 1 | 0 | 0 |
| HORIZON-SIO Reid 2009317 | RIS | ZOL | – | 12 | 381 | 378 | – | 3 | 5 | – | 1 | 1 | 0 | 1 | 1 |
| MOTION: Miller 2008308 | ALN | IBN monthly | – | 12 | 859 | 874 | – | 5 | 5 | – | 1 | 1 | 1 | 1 | 1 |
| ZONE: Nakamura 2017130 | Placebo | ZOL | – | 24 | 327 | 330 | – | 29 | 10 | – | 1 | 0 | 0 | 1 | 1 |
| ZONE: Nakamura 2017130 | Placebo | ZOL | – | 24 | 331 | 330 | – | 17 | 5 | – | 0 | 0 | 1 | 0 | 0 |
| ZONE: Nakamura 2017130 | Placebo | ZOL | – | 12 | 331 | 330 | – | 6 | 4 | – | 0 | 1 | 0 | 0 | 0 |
| FREEDOM: Bone 2017104 | Placebo | DEN | – | 36 | 3691 | 3702 | – | 264 | 86 | – | 1 | 0 | 0 | 1 | 1 |
| FREEDOM: Bone 2017104 | Placebo | DEN | – | 36 | 3906 | 3902 | – | 92 | 29 | – | 0 | 0 | 1 | 0 | 0 |
| FREEDOM: Bone 2017104 | Placebo | DEN | – | 12 | 3691 | 3702 | – | 82 | 32 | – | 0 | 1 | 0 | 0 | 0 |
| FRAME: Cosman 201654 | Placebo | ROMO | – | 12 | 3322 | 3321 | – | 59 | 16 | – | 1 | 1 | 0 | 1 | 1 |
| FRAME: Cosman 201654 | Placebo | ROMO | – | 12 | 3591 | 3589 | – | 17 | 3 | – | 0 | 0 | 0 | 0 | 0 |
| ADAMO: Orwoll 201242 | Placebo | DEN | – | 12 | 120 | 120 | – | 1 | 0 | – | 1 | 1 | 1 | 1 | 1 |
| DIRECT: Nakamura 201443 | Placebo | DEN | – | 24 | 480 | 472 | – | 41 | 10 | – | 1 | 0 | 0 | 0 | 1 |
| DIRECT: Nakamura 201443 | Placebo | DEN | – | 12 | 480 | 472 | – | 9 | 6 | – | 0 | 1 | 0 | 0 | 0 |
| Miyauchi 201058 | Placebo | TPTD | – | 12 | 67 | 136 | – | 4 | 5 | – | 1 | 1 | 0 | 1 | 0 |
| ACTIVE: Miller 201675 | Placebo | TPTD | – | 18 | 711 | 717 | – | 30 | 6 | – | 1 | 0 | 0 | 0 | 1 |
| ACTIVE: Miller 201675 | Placebo | TPTD | – | 18 | 821 | 818 | – | 9 | 3 | – | 0 | 0 | 1 | 0 | 0 |
| Neer 200162 | Placebo | TPTD | – | 24 | 448 | 444 | – | 64 | 22 | – | 1 | 0 | 0 | 0 | 0 |
| Morii 200347 | Placebo | RLX | – | 12 | 87 | 79 | – | 2 | 0 | – | 1 | 1 | 0 | 1 | 1 |
| Liu 200448 | Placebo | RLX | – | 12 | 102 | 102 | – | 5 | 0 | – | 1 | 1 | 1 | 1 | 1 |
| Silverman 200850 | Placebo | RLX | – | 36 | 1741 | 1696 | – | 71 | 40 | – | 1 | 0 | 0 | 0 | 1 |
| Silverman 200850 | Placebo | RLX | – | 36 | 1741 | 1696 | – | 16 | 15 | – | 0 | 0 | 1 | 0 | 0 |
| MORE: Maricic 2002102 | Placebo | RLX | – | 12 | 2292 | 2259 | – | 19 | 6 | – | 0 | 1 | 0 | 0 | 0 |
| MORE: Maricic 2002102 | Placebo | RLX | – | 36 | 2292 | 2259 | – | 81 | 47 | – | 0 | 0 | 1 | 0 | 0 |
| MORE: Maricic 2002102 | Placebo | RLX | – | 36 | 2292 | 2259 | – | 231 | 148 | – | 1 | 0 | 0 | 1 | 1 |
| Lufkin 199852 | Placebo | RLX | – | 12 | 45 | 43 | – | 18 | 21 | – | 1 | 1 | 0 | 1 | 1 |
| Saag 2007103 | ALN | TPTD | – | 36 | 169 | 173 | – | 13 | 3 | – | 1 | 0 | 0 | 1 | 1 |
| Saag 2007103 | ALN | TPTD | – | 36 | 169 | 173 | – | 4 | 0 | – | 0 | 0 | 1 | 0 | 0 |
| Walker 201389 | RIS | TPTD | – | 18 | 10 | 9 | – | 1 | 0 | – | 1 | 0 | 0 | 1 | 1 |
| VERO: Kendler 201799 | RIS | TPTD | – | 24 | 533 | 516 | – | 64 | 28 | – | 1 | 0 | 0 | 1 | 0 |
| VERO: Kendler 201799 | RIS | TPTD | – | 12 | 533 | 516 | – | 11 | 4 | – | 0 | 1 | 1 | 0 | 0 |
| Hadji 201291 | RIS | TPTD | – | 18 | 309 | 317 | – | 33 | 16 | – | 1 | 0 | 0 | 1 | 0 |
| MOVE: Malouf-Sierra 201792 | RIS | TPTD | – | 18 | 106 | 116 | – | 1 | 0 | – | 1 | 0 | 1 | 0 | 1 |
| Cosman 201193 | ZOL | TPTD | – | 12 | 137 | 137 | – | 5 | 1 | – | 1 | 1 | 0 | 0 | 1 |
| EVA: Recker 200780 | ALN | RLX | – | 10.26 | 255 | 259 | – | 8 | 5 | – | 1 | 0 | 0 | 0 | 1 |
| EVA: Recker 200780 | ALN | RLX | – | 10.26 | 713 | 699 | – | 3 | 0 | – | 0 | 0 | 1 | 0 | 0 |
| Muscoso 200479 | ALN | RLX | RIS | 12 | 1000 | 100 | 100 | 2 | 0 | 0 | 0 | 1 | 0 | 0 | 0 |
| Muscoso 200479 | ALN | RLX | RIS | 24 | 1000 | 100 | 100 | 6 | 0 | 0 | 1 | 0 | 0 | 1 | 0 |
| ARCH: Saag 201783 | ALN | ROMO | – | 12 | 1703 | 1696 | – | 85 | 55 | – | 0 | 1 | 0 | 0 | 0 |
| ARCH: Saag 201783 | ALN | ROMO/ALN | – | 24 | 1834 | 1825 | – | 147 | 74 | – | 1 | 0 | 0 | 1 | 1 |
| ARCH: Saag 201783 | ALN | ROMO/ALN | – | 24 | 2047 | 2046 | – | 18 | 10 | – | 0 | 0 | 1 | 0 | 0 |
| Panico 201186 | ALN | TPTD | – | 18 | 39 | 42 | – | 6 | 1 | – | 1 | 0 | 0 | 0 | 1 |
| Saag 201874 | RIS | DEN | – | 12 | 342 | 333 | – | 15 | 10 | – | 1 | 1 | 0 | 1 | 1 |
| Mok 201153 | Placebo | RLX | – | 12 | 56 | 51 | – | 3 | 0 | – | 1 | 1 | 0 | 1 | 0 |
| Miller 2004129 | Placebo | ALN | – | 12 | 41 | 80 | – | 3 | 6 | – | 1 | 1 | 0 | 0 | 1 |
| Miller 2004129 | Placebo | ALN | – | 12 | 58 | 109 | – | 3 | 5 | – | 0 | 0 | 1 | 0 | 0 |
| Study | Treatment | Assessment time point | Number of participants in study arm | Number of events in study arm | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | ||
| FREEDOM: Cummings 200941 | Placebo | DEN | – | 36 | 3906 | 3902 | – | 293 | 238 | – |
| FRAME: Cosman 201654 | Placebo | ROMO | – | 12 | 3591 | 3589 | – | 75 | 56 | – |
| Orwoll 200357 | Placebo | TPTD | – | 12 | 147 | 151 | – | 3 | 2 | – |
| ADAMO: Orwoll 201242 | Placebo | DEN | – | 12 | 120 | 120 | – | 2 | 1 | – |
| DIRECT: Nakamura 201443 | Placebo | DEN | – | 24 | 480 | 472 | – | 20 | 19 | – |
| Koh 201645 | Placebo | DEN | – | 6 | 66 | 69 | – | 1 | 1 | – |
| Miyauchi 201058 | Placebo | TPTD | – | 12 | 67 | 136 | – | 1 | 1 | – |
| ACTIVE: Miller 201695 | Placebo | TPTD | – | 18 | 821 | 818 | – | 33 | 24 | – |
| Neer 200162 | Placebo | TPTD | – | 24 | 544 | 541 | – | 30 | 14 | – |
| Silverman 200850 | Placebo | RLX | – | 36 | 1885 | 1849 | – | 118 | 109 | – |
| Ishibashi 201755 | Placebo | RLX | – | 12 | 63 | 63 | – | 1 | 2 | – |
| STRUCTURE: Langdahl 201767 | ROMO | TPTD | – | 12 | 218 | 214 | – | 7 | 8 | – |
| STAND: Kendler 201070 | ALN | DEN | – | 12 | 249 | 253 | – | 4 | 8 | – |
| DAPS: Freemantle 2012109 | ALN | DEN | – | 12 | 118 | 125 | – | 1 | 1 | – |
| Saag 200985 | ALN | TPTD | – | 36 | 214 | 214 | – | 15 | 16 | – |
| EuroGIOPs: Glüer 201387 | RIS | TPTD | – | 18 | 47 | 45 | – | 5 | 0 | – |
| VERO: Kendler 201799 | RIS | TPTD | – | 24 | 680 | 680 | – | 38 | 25 | – |
| Hadji 201291 | RIS | TPTD | – | 18 | 350 | 360 | – | 29 | 28 | – |
| Malouf-Sierra 201792 | RIS | TPTD | – | 18 | 110 | 106 | – | 10 | 5 | – |
| Cosman 201193 | ZOL | TPTD | – | 12 | 137 | 137 | – | 8 | 7 | – |
| Muscoso 200479 | ALN | RLX | RIS | 24 | 1000 | 100 | 100 | 4 | 0 | 0 |
| ARCH: Saag 201783 | ALN | ROMO/ALN | – | 32.4 | 2047 | 2046 | – | 217 | 178 | – |
| EFFECT (USA): Luckey 200477 | ALN | RLX | – | 12 | 199 | 206 | – | 5 | 8 | – |
| ZONE: Nakamura 2017130 | Placebo | ZOL | – | 24 | 331 | 330 | – | 37 | 20 | – |
| Lufkin 199852 | Placebo | RLX | – | 12 | 45 | 43 | – | 3 | 0 | – |
| Saag 201874 | RIS | DEN | – | 12 | 397 | 398 | – | 10 | 17 | – |
| Michalská 200682 | Placebo | ALN | RLX | 24 | 33 | 33 | 33 | 2 | 1 | 1 |
| Fogelman 2000297 | Placebo | RIS | – | 36 | 125 | 112 | – | 13 | 7 | – |
| VERT-USA: Harris 1999298 | Placebo | RIS | – | 36 | 815 | 812 | – | 52 | 33 | – |
| VERT-EU: Reginster 2000300 | Placebo | RIS | – | 24 | 406 | 406 | – | 51 | 36 | – |
| Hooper 2005132 | Placebo | RIS | – | 12 | 125 | 129 | – | 6 | 5 | – |
| Ringe 2006304 | Placebo | RIS | – | 48 | 158 | 158 | – | 17 | 10 | – |
| FIT I: Black 1996280 | Placebo | ALN | – | 36 | 1005 | 1022 | – | 148 | 122 | – |
| FIT II: Cummings 1998281 | Placebo | ALN | – | 48 | 2218 | 2214 | – | 294 | 261 | – |
| Orwoll 2000286 | Placebo | ALN | – | 24 | 94 | 146 | – | 5 | 6 | – |
| FOSIT: Pols 1999287 | Placebo | ALN | – | 12 | 958 | 950 | – | 37 | 19 | – |
| Bone 2000282 | Placebo | ALN | – | 24 | 50 | 92 | – | 4 | 5 | – |
| HORIZON-PFT: Black 2007133 | Placebo | ZOL | – | 11 | 3861 | 3875 | – | 388 | 292 | – |
| HORIZON-RFT: Lyles 2007307 | Placebo | ZOL | – | 36 | 1062 | 1065 | – | 107 | 79 | – |
| BONE: Chesnut 2004136 | Placebo | IBN daily | – | 36 | 975 | 977 | – | 80 | 89 | – |
| MOTION: Miller 2008311 | ALN | IBN monthly | – | 12 | 859 | 874 | – | 12 | 14 | – |
| Morii 200347 | Placebo | RLX | – | 12 | 97 | 88 | – | 4 | 1 | – |
| Study | Treatment | Assessment time point | Number of participants in study arm | Number of events in study arm | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | ||
| FREEDOM: Cummings 200941 | Placebo | DEN | – | 36 | 3906 | 3902 | – | 43 | 26 | – |
| FRAME: Cosman 201654 | Placebo | ROMO | – | 12 | 3591 | 3589 | – | 13 | 7 | – |
| DIRECT: Nakamura 201443 | Placebo | DEN | – | 24 | 480 | 472 | – | 2 | 0 | – |
| ACTIVE: Miller 201675 | Placebo | TPTD | – | 18 | 821 | 818 | – | 2 | 0 | – |
| Neer 200162 | Placebo | TPTD | – | 24 | 544 | 541 | – | 4 | 1 | – |
| STRUCTURE: Langdahl 201767 | ROMO | TPTD | – | 12 | 218 | 218 | – | 1 | 0 | – |
| Miller 201675 | ZOL | DEN | – | 12 | 320 | 320 | – | 2 | 1 | – |
| EuroGIOPs: Glüer 201387 | RIS | TPTD | – | 18 | 47 | 45 | – | 1 | 0 | – |
| VERO: Kendler 201799 | RIS | TPTD | – | 24 | 680 | 680 | – | 5 | 2 | – |
| Hadji 201291 | RIS | TPTD | – | 18 | 350 | 360 | – | 2 | 5 | – |
| EFFECT: Sambrook 200476 | ALN | RLX | – | 12 | 246 | 241 | – | 0 | 1 | – |
| MOVE: Malouf-Sierra 201792 | RIS | TPTD | – | 18 | 110 | 106 | – | 7 | 2 | – |
| Muscoso 200479 | ALN | RLX | RIS | 24 | 1000 | 100 | 100 | 3 | 0 | 0 |
| ARCH: Saag 201783 | ALN | ROMO/ALN | – | 32.4 | 2047 | 2046 | – | 66 | 41 | – |
| Saag 201874 | RIS | DEN | – | 12 | 397 | 398 | – | 1 | 1 | – |
| Silverman 200850 | Placebo | RLX | – | 36 | 1885 | 1849 | – | 6 | 5 | – |
| VERT-USA: Harris 1999298 | Placebo | RIS | – | 36 | 815 | 812 | – | 15 | 12 | – |
| VERT-EU: Reginster 2000300 | Placebo | RIS | – | 36 | 406 | 406 | – | 11 | 9 | – |
| FIT I: Black 1996280 | Placebo | ALN | – | 36 | 1005 | 1022 | – | 22 | 11 | – |
| FIT II: Cummings 1998281 | Placebo | ALN | – | 48 | 2218 | 2214 | – | 24 | 19 | – |
| Greenspan 2002283 | Placebo | ALN | – | 24 | 164 | 163 | – | 4 | 2 | – |
| HORIZON-PFT: Black 2007133 | Placebo | ZOL | – | 36 | 3861 | 3875 | – | 88 | 52 | – |
| HORIZON-RFT: Lyles 2007307 | Placebo | ZOL | – | 36 | 1062 | 1065 | – | 33 | 23 | – |
| Study | Treatment | Assessment time point | Number of participants in study arm | Number of events in study arm | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | ||
| ACTIVE: Miller 201695 | Placebo | TPTD | – | 18 | 821 | 818 | – | 15 | 17 | – |
| Neer 200162 | Placebo | TPTD | – | 24 | 544 | 541 | – | 7 | 2 | – |
| Ishibashi 201755 | Placebo | RLX | – | 12 | 63 | 63 | – | 0 | 1 | – |
| STRUCTURE: Langdahl 201767 | ROMO | TPTD | – | 12 | 218 | 218 | – | 1 | 4 | – |
| STAND: Kendler 201070 | ALN | DEN | – | 12 | 249 | 253 | – | 2 | 3 | – |
| VERO: Kendler 201799 | RIS | TPTD | – | 24 | 680 | 680 | – | 15 | 6 | – |
| Hadji 201291 | RIS | TPTD | – | 18 | 350 | 360 | – | 2 | 4 | – |
| Muscoso 200479 | ALN | RLX | RIS | 24 | 1000 | 100 | 100 | 1 | 0 | 0 |
| EFFECT (USA): Luckey 200477 | ALN | RLX | – | 12 | 199 | 206 | – | 0 | 1 | – |
| Silverman 200850 | Placebo | RLX | – | 36 | 1885 | 1849 | – | 31 | 46 | – |
| VERT-USA: Harris 1999298 | Placebo | RIS | – | 36 | 815 | 812 | – | 22 | 14 | – |
| VERT-EU: Reginster 2000300 | Placebo | RIS | – | 36 | 406 | 406 | – | 21 | 15 | – |
| FIT I: Black 1996280 | Placebo | ALN | – | 36 | 1005 | 1022 | – | 41 | 22 | – |
| FIT II: Cummings 1998281 | Placebo | ALN | – | 48 | 2218 | 2214 | – | 70 | 83 | – |
| McClung 2009291 | Placebo | IBN monthly | – | 12 | 83 | 77 | – | 0 | 1 | – |
| Study | Treatment | Assessment time point | Number of participants in study arm | Number of events in study arm | |||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 1 | 2 | 1 | 2 | ||
| ADAMO: Orwoll 201242 | Placebo | DEN | 12 | 120 | 120 | 1 | 0 |
| ACTIVE: Miller 201695 | Placebo | TPTD | 18 | 821 | 818 | 3 | 2 |
| Neer 200162 | Placebo | TPTD | 24 | 544 | 541 | 2 | 2 |
| STRUCTURE: Langdahl 201767 | ROMO | TPTD | 12 | 218 | 218 | 0 | 1 |
| STAND: Kendler 201070 | ALN | DEN | 12 | 249 | 253 | 0 | 1 |
| EuroGIOPs: Glüer 201387 | RIS | TPTD | 18 | 47 | 45 | 1 | 0 |
| VERO: Kendler 201799 | RIS | TPTD | 24 | 680 | 680 | 2 | 4 |
| Hadji 201291 | RIS | TPTD | 18 | 350 | 360 | 5 | 4 |
| MOVE: Malouf-Sierra 201792 | RIS | TPTD | 18 | 110 | 106 | 1 | 1 |
| EFFECT (USA): Luckey 200477 | ALN | RLX | 12 | 199 | 206 | 0 | 1 |
| Saag 201874 | RIS | DEN | 12 | 391 | 398 | 3 | 3 |
| VERT-MN Harris 1999298 | Placebo | RIS | 36 | 815 | 812 | 10 | 4 |
| VERT-MN Reginster 2000300 | Placebo | RIS | 36 | 406 | 406 | 14 | 7 |
Appendix 10 Network meta-analysis results from random-effects model
Treatment effects versus placebo from the random-effects model is shown in Figure 13, and a summary of model fit and heterogeneity is shown in Table 32. For all outcomes the DIC was larger for the random-effects model, implying that the primary model (class effect for bisphosphonate treatments, and unrelated treatment effects for all other interventions) provides a better fit to the data. Treatment effects from the random-effects model are generally consistent with primary model.
FIGURE 13.
Forest plot of HRs for all fracture outcomes using a random-effects model.
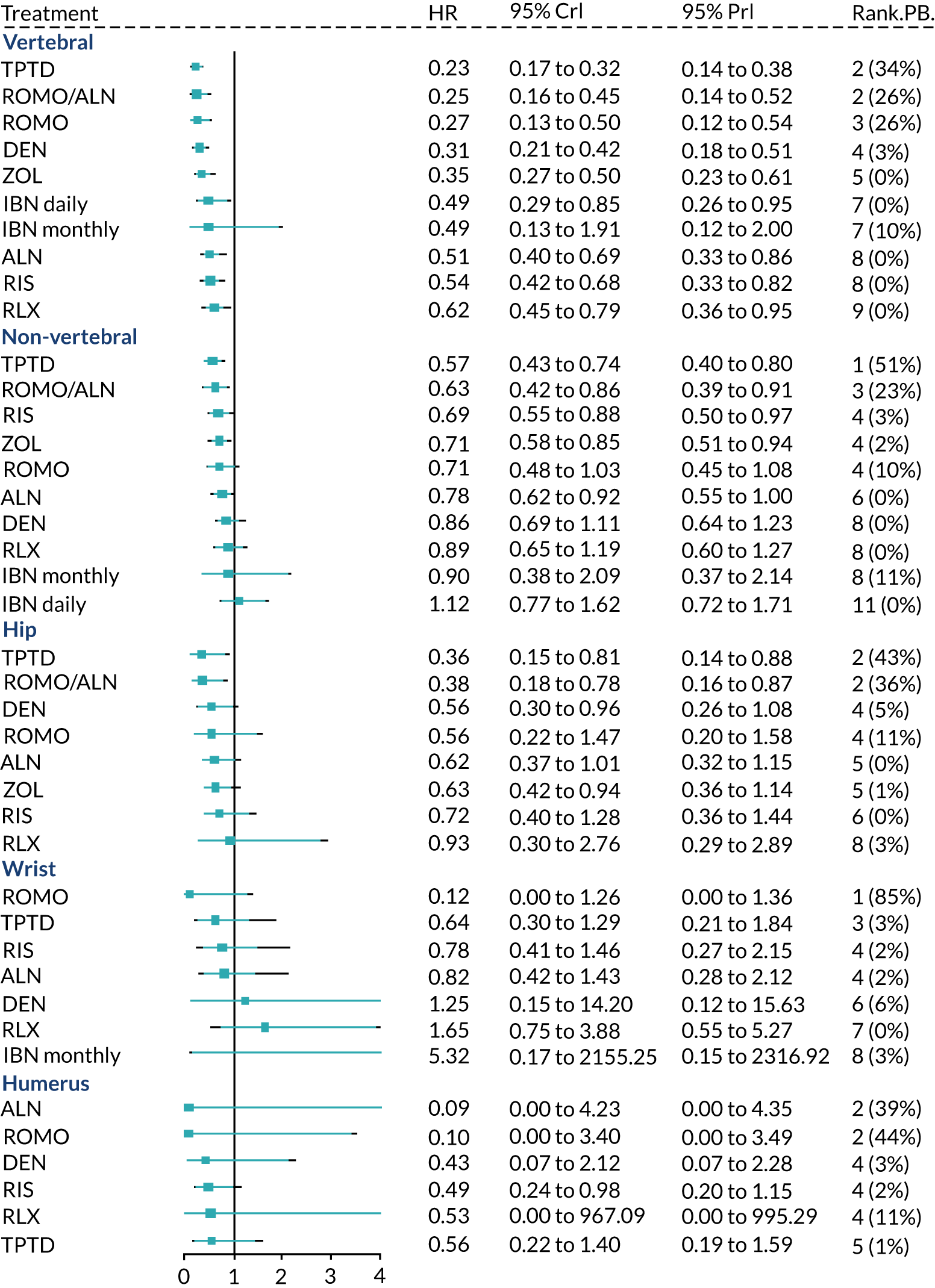
| Outcome | Absolute model fit | DIC | SDb (95% CI) | |
|---|---|---|---|---|
| D res a | Data points | |||
| Vertebral fractures | 93.42 | 93 | 156.43 | 0.15 (0.01 to 0.37) |
| Non-vertebral fractures | 73.93 | 86 | 129.50 | 0.08 (0.01 to 0.24) |
| Hipc | 39.58 | 47 | 72.37 | 0.13 (0.01 to 0.45) |
| Wristc | 30.76 | 31 | 56.63 | 0.34 (0.05 to 0.71) |
| Proximal humerusc | 22.87 | 26 | 44.02 | 0.17 (0.01 to 0.58) |
| Femoral neck BMD | ||||
Treatment effects from the two models appear most different for proximal humerus fractures. Using a random-effects model, ALN has a highly beneficial HR (0.09, 95% CrI 0 to 4.23) and PB of 0.39. Under the class-effects model, the HR for ALN is less extreme (0.46, 95% CrI 0.15 to 1.27) as it is also influenced by the estimate for RIS (the only other bisphosphonate included in the network). The estimate for ALN is only contributed by one study77 with zero events in the ALN arm and one event in the RLX arm, and so is highly uncertain.
Appendix 11 Vertebral fracture sensitivity analyses
Four sensitivity analyses were conducted for the vertebral fracture network:
-
SA1: 12-month data only
-
SA2: clinically assessed fractures only
-
SA3: exclusion of studies with quality issues
-
SA4: exclusion of studies in which prior bisphosphonate treatment had been received.
Treatment effects versus placebo is summarised in Figure 14, and a summary of model fit and heterogeneity is shown in Table 33.
FIGURE 14.
Forest plot of vertebral fracture network sensitivity analyses.
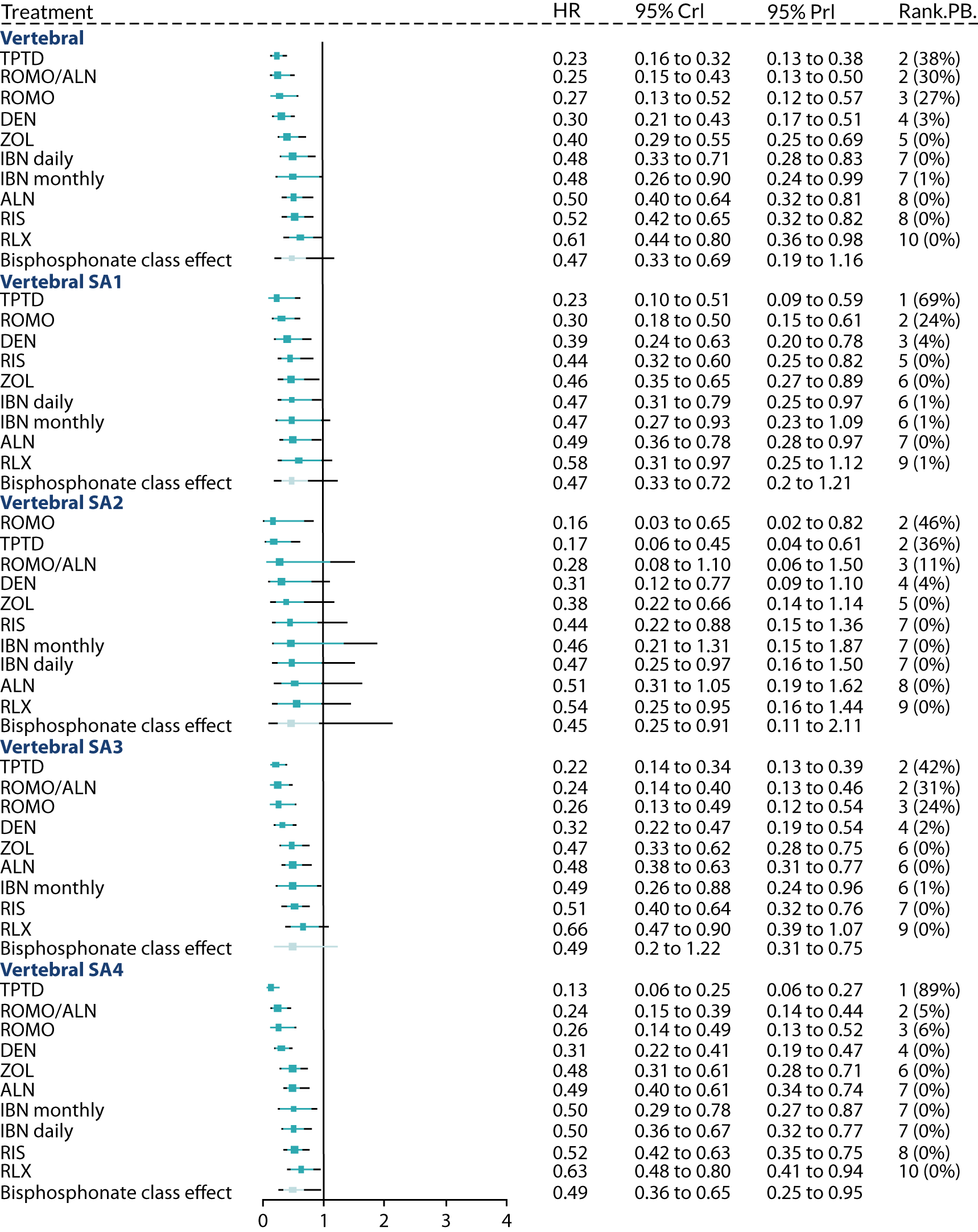
| Outcome | Absolute model fit | DIC | Heterogeneity, SD (95% CrI) | ||
|---|---|---|---|---|---|
| D res a | Data points | Between study | Between treatment | ||
| Vertebral fractures | 91.21 | 93 | 153.31 | 0.17 (0.02 to 0.37) | 0.21 (0.01 to 0.90) |
| SA1: 12-month data | 56.17 | 59 | 95.94 | 0.17 (0.01 to 0.51) | 0.15 (0.01 to 0.86) |
| SA2: clinical fractures | 40.14 | 40 | 72.49 | 0.32 (0.02 to 0.89) | 0.29 (0.02 to 1.33) |
| SA3: excluding studies with quality issues | 58.27 | 61 | 99.4 | 0.13 (0.01 to 0.38) | 0.149 (0.01 to 1.04) |
| SA4: excluding studies with prior treatment | 69.83 | 72 | 117.47 | 0.11 (0.01 to 0.34) | 0.117 (0.01 to 0.69) |
Appendix 12 Pairwise summary tables
Pairwise summary tables for all outcomes are shown in this appendix. Median HR and 95% CrIs are presented below the diagonal, median HR and 95% PrI are shown above the diagonal.
| Placebo | ALN | RIS | ZOL | IBN daily | IBN monthly | DEN | ROMO | TPTD | RLX | ROMO/ALN | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Placebo | 0.50 (0.32 to 0.81) | 0.52 (0.32 to 0.82) | 0.39 (0.25 to 0.69) | 0.48 (0.28 to 0.83) | 0.48 (0.24 to 0.99) | 0.31 (0.17 to 0.51) | 0.27 (0.12 to 0.57) | 0.23 (0.13 to 0.38) | 0.62 (0.36 to 0.98) | 0.25 (0.13 to 0.50) | |
| ALN | 0.50 (0.40 to 0.64) | 1.06 (0.53 to 1.90) | 0.78 (0.42 to 1.61) | 0.98 (0.47 to 1.87) | 0.96 (0.42 to 2.16) | 0.61 (0.29 to 1.20) | 0.53 (0.21 to 1.28) | 0.47 (0.23 to 0.88) | 1.24 (0.60 to 2.29) | 0.49 (0.23 to 1.06) | |
| RIS | 0.52 (0.42 to 0.65) | 1.03 (0.77 to 1.39) | 0.74 (0.42 to 1.63) | 0.93 (0.47 to 1.86) | 0.92 (0.41 to 2.17) | 0.58 (0.29 to 1.19) | 0.51 (0.20 to 1.25) | 0.44 (0.23 to 0.85) | 1.17 (0.59 to 2.28) | 0.47 (0.22 to 1.09) | |
| ZOL | 0.40 (0.29 to 0.55) | 0.81 (0.54 to 1.08) | 0.77 (0.52 to 1.08) | 1.23 (0.57 to 2.43) | 1.19 (0.53 to 2.91) | 0.79 (0.34 to 1.50) | 0.68 (0.24 to 1.60) | 0.60 (0.26 to 1.11) | 1.58 (0.68 to 2.90) | 0.63 (0.26 to 1.37) | |
| IBN daily | 0.48 (0.33 to 0.71) | 0.98 (0.63 to 1.43) | 0.95 (0.61 to 1.37) | 1.18 (0.82 to 1.99) | 0.99 (0.42 to 2.40) | 0.63 (0.29 to 1.32) | 0.55 (0.21 to 1.40) | 0.48 (0.23 to 0.99) | 1.27 (0.59 to 2.56) | 0.51 (0.22 to 1.21) | |
| IBN monthly | 0.48 (0.26 to 0.90) | 0.98 (0.51 to 1.75) | 0.95 (0.47 to 1.71) | 1.14 (0.68 to 2.50) | 1.00 (0.49 to 1.98) | 0.64 (0.25 to 1.52) | 0.55 (0.19 to 1.56) | 0.48 (0.19 to 1.13) | 1.28 (0.52 to 2.91) | 0.51 (0.20 to 1.34) | |
| DEN | 0.30 (0.21 to 0.43) | 0.61 (0.39 to 0.91) | 0.58 (0.40 to 0.88) | 0.77 (0.46 to 1.19) | 0.63 (0.38 to 1.03) | 0.64 (0.31 to 1.26) | 0.87 (0.33 to 2.23) | 0.76 (0.36 to 1.57) | 2.01 (0.95 to 4.14) | 0.81 (0.35 to 1.97) | |
| ROMO | 0.27 (0.13 to 0.52) | 0.53 (0.25 to 1.06) | 0.51 (0.25 to 1.03) | 0.67 (0.30 to 1.35) | 0.55 (0.25 to 1.16) | 0.55 (0.22 to 1.36) | 0.87 (0.40 to 1.86) | 0.87 (0.34 to 2.22) | 2.31 (0.89 to 5.79) | 0.93 (0.33 to 2.71) | |
| TPTD | 0.23 (0.16 to 0.32) | 0.46 (0.31 to 0.66) | 0.44 (0.32 to 0.61) | 0.58 (0.36 to 0.90) | 0.47 (0.29 to 0.77) | 0.48 (0.25 to 0.95) | 0.76 (0.46 to 1.20) | 0.87 (0.41 to 1.87) | 2.65 (1.28 to 5.45) | 1.06 (0.48 to 2.61) | |
| RLX | 0.61 (0.44 to 0.80) | 1.23 (0.82 to 1.71) | 1.17 (0.82 to 1.68) | 1.54 (0.94 to 2.32) | 1.26 (0.78 to 1.97) | 1.27 (0.65 to 2.47) | 2.01 (1.25 to 3.13) | 2.30 (1.09 to 4.83) | 2.66 (1.72 to 4.11) | 0.40 (0.18 to 0.98) | |
| ROMO/ALN | 0.25 (0.15 to 0.43) | 0.50 (0.30 to 0.80) | 0.47 (0.28 to 0.86) | 0.62 (0.33 to 1.11) | 0.51 (0.28 to 0.98) | 0.51 (0.24 to 1.12) | 0.81 (0.44 to 1.59) | 0.93 (0.40 to 2.29) | 1.06 (0.60 to 2.06) | 0.40 (0.23 to 0.78) |
| Placebo | ALN | RIS | ZOL | IBN daily | IBN monthly | DEN | ROMO | TPTD | RLX | ROMO/ALN | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Placebo | 0.78 (0.56 to 0.99) | 0.73 (0.53 to 0.98) | 0.73 (0.54 to 0.95) | 0.89 (0.60 to 1.38) | 0.79 (0.50 to 1.31) | 0.86 (0.64 to 1.23) | 0.71 (0.45 to 1.09) | 0.58 (0.41 to 0.81) | 0.90 (0.60 to 1.29) | 0.63 (0.40 to 0.92) | |
| ALN | 0.77 (0.64 to 0.90) | 0.95 (0.65 to 1.43) | 0.94 (0.65 to 1.42) | 1.15 (0.75 to 1.91) | 1.02 (0.63 to 1.78) | 1.10 (0.76 to 1.84) | 0.92 (0.56 to 1.56) | 0.75 (0.51 to 1.18) | 1.16 (0.74 to 1.87) | 0.81 (0.52 to 1.27) | |
| RIS | 0.73 (0.59 to 0.88) | 0.96 (0.73 to 1.19) | 1.00 (0.66 to 1.48) | 1.22 (0.76 to 2.11) | 1.07 (0.65 to 1.96) | 1.18 (0.79 to 1.91) | 0.97 (0.57 to 1.65) | 0.80 (0.52 to 1.20) | 1.23 (0.76 to 1.97) | 0.86 (0.51 to 1.38) | |
| ZOL | 0.73 (0.61 to 0.85) | 0.96 (0.76 to 1.17) | 1.00 (0.79 to 1.28) | 1.23 (0.77 to 2.08) | 1.07 (0.65 to 1.93) | 1.18 (0.79 to 1.90) | 0.97 (0.58 to 1.63) | 0.80 (0.52 to 1.24) | 1.24 (0.76 to 1.94) | 0.86 (0.52 to 1.37) | |
| IBN daily | 0.88 (0.67 to 1.32) | 1.13 (0.91 to 1.76) | 1.20 (0.93 to 1.98) | 1.20 (0.93 to 1.91) | 0.91 (0.47 to 1.49) | 0.95 (0.57 to 1.69) | 0.79 (0.43 to 1.43) | 0.65 (0.38 to 1.09) | 1.00 (0.57 to 1.71) | 0.70 (0.39 to 1.19) | |
| IBN monthly | 0.78 (0.54 to 1.27) | 1.01 (0.70 to 1.66) | 1.05 (0.74 to 1.84) | 1.05 (0.74 to 1.83) | 0.93 (0.50 to 1.32) | 1.08 (0.61 to 1.98) | 0.90 (0.47 to 1.68) | 0.74 (0.40 to 1.28) | 1.14 (0.61 to 2.00) | 0.79 (0.43 to 1.38) | |
| DEN | 0.86 (0.69 to 1.12) | 1.12 (0.87 to 1.57) | 1.18 (0.90 to 1.63) | 1.18 (0.91 to 1.63) | 0.97 (0.62 to 1.46) | 1.09 (0.65 to 1.73) | 0.83 (0.46 to 1.38) | 0.68 (0.41 to 1.05) | 1.05 (0.60 to 1.65) | 0.74 (0.40 to 1.16) | |
| ROMO | 0.71 (0.48 to 1.03) | 0.92 (0.62 to 1.39) | 0.97 (0.64 to 1.49) | 0.97 (0.64 to 1.47) | 0.79 (0.47 to 1.28) | 0.90 (0.50 to 1.53) | 0.82 (0.51 to 1.26) | 0.82 (0.48 to 1.41) | 1.27 (0.71 to 2.25) | 0.88 (0.48 to 1.57) | |
| TPTD | 0.58 (0.45 to 0.76) | 0.76 (0.57 to 1.02) | 0.80 (0.61 to 1.04) | 0.80 (0.60 to 1.08) | 0.66 (0.40 to 0.96) | 0.74 (0.42 to 1.14) | 0.68 (0.47 to 0.94) | 0.82 (0.53 to 1.28) | 1.55 (0.93 to 2.53) | 1.08 (0.62 to 1.79) | |
| RLX | 0.90 (0.65 to 1.21) | 1.17 (0.84 to 1.63) | 1.23 (0.85 to 1.77) | 1.23 (0.87 to 1.74) | 1.01 (0.62 to 1.53) | 1.14 (0.66 to 1.83) | 1.05 (0.68 to 1.49) | 1.27 (0.78 to 2.05) | 1.55 (1.03 to 2.28) | 0.70 (0.40 to 1.19) | |
| ROMO/ALN | 0.63 (0.44 to 0.86) | 0.81 (0.61 to 1.09) | 0.86 (0.58 to 1.25) | 0.86 (0.59 to 1.23) | 0.70 (0.42 to 1.06) | 0.79 (0.46 to 1.26) | 0.73 (0.46 to 1.06) | 0.88 (0.53 to 1.44) | 1.08 (0.70 to 1.62) | 0.70 (0.44 to 1.08) |
| Placebo | ALN | RIS | ZOL | DEN | ROMO | TPTD | RLX | ROMO/ALN | |
|---|---|---|---|---|---|---|---|---|---|
| Placebo | 0.64 (0.39 to 1.04) | 0.66 (0.40 to 1.12) | 0.63 (0.39 to 1.01) | 0.56 (0.28 to 1.04) | 0.56 (0.20 to 1.50) | 0.34 (0.14 to 0.78) | 0.93 (0.29 to 2.82) | 0.39 (0.19 to 0.80) | |
| ALN | 0.64 (0.45 to 0.88) | 1.03 (0.56 to 2.01) | 1.00 (0.54 to 1.85) | 0.88 (0.38 to 1.94) | 0.88 (0.29 to 2.64) | 0.54 (0.20 to 1.37) | 1.48 (0.44 to 4.81) | 0.62 (0.29 to 1.28) | |
| RIS | 0.66 (0.46 to 0.99) | 1.02 (0.71 to 1.63) | 0.97 (0.51 to 1.79) | 0.85 (0.36 to 1.84) | 0.85 (0.27 to 2.63) | 0.52 (0.21 to 1.23) | 1.41 (0.42 to 4.71) | 0.59 (0.26 to 1.32) | |
| ZOL | 0.64 (0.47 to 0.86) | 1.00 (0.70 to 1.44) | 0.99 (0.62 to 1.38) | 0.88 (0.39 to 1.91) | 0.88 (0.29 to 2.65) | 0.54 (0.20 to 1.34) | 1.48 (0.44 to 4.82) | 0.62 (0.27 to 1.37) | |
| DEN | 0.56 (0.31 to 0.94) | 0.88 (0.45 to 1.63) | 0.85 (0.43 to 1.57) | 0.88 (0.46 to 1.59) | 1.00 (0.31 to 3.31) | 0.61 (0.21 to 1.77) | 1.68 (0.47 to 5.95) | 0.70 (0.28 to 1.89) | |
| ROMO | 0.56 (0.22 to 1.43) | 0.88 (0.33 to 2.41) | 0.85 (0.31 to 2.33) | 0.88 (0.33 to 2.36) | 1.01 (0.33 to 3.04) | 0.61 (0.17 to 2.19) | 1.65 (0.37 to 7.39) | 0.70 (0.21 to 2.41) | |
| TPTD | 0.35 (0.15 to 0.73) | 0.54 (0.23 to 1.19) | 0.52 (0.23 to 1.06) | 0.54 (0.23 to 1.18) | 0.62 (0.24 to 1.58) | 0.61 (0.19 to 1.97) | 2.74 (0.68 to 11.24) | 1.14 (0.40 to 3.51) | |
| RLX | 0.94 (0.31 to 2.67) | 1.48 (0.49 to 4.20) | 1.42 (0.45 to 4.21) | 1.47 (0.48 to 4.27) | 1.69 (0.50 to 5.45) | 1.64 (0.41 to 6.67) | 2.73 (0.73 to 10.19) | 0.42 (0.12 to 1.52) | |
| ROMO/ALN | 0.39 (0.21 to 0.72) | 0.62 (0.36 to 1.03) | 0.59 (0.31 to 1.12) | 0.61 (0.32 to 1.13) | 0.70 (0.32 to 1.62) | 0.70 (0.22 to 2.14) | 1.14 (0.44 to 3.09) | 0.42 (0.13 to 1.39) |
| Placebo | ALN | RIS | IBN monthly | DEN | ROMO | TPTD | RLX | |
|---|---|---|---|---|---|---|---|---|
| Placebo | 0.82 (0.28 to 2.12) | 0.78 (0.27 to 2.15) | 5.34 (0.15 to 2316.92) | 1.24 (0.12 to 15.63) | 0.12 (0.00 to 1.36) | 0.64 (0.21 to 1.84) | 1.64 (0.55 to 5.27) | |
| ALN | 0.82 (0.42 to 1.43) | 0.96 (0.24 to 4.30) | 6.77 (0.16 to 3022.57) | 1.55 (0.15 to 20.29) | 0.14 (0.00 to 2.15) | 0.79 (0.18 to 3.59) | 2.01 (0.50 to 9.64) | |
| RIS | 0.78 (0.41 to 1.46) | 0.96 (0.42 to 2.43) | 6.89 (0.16 to 3288.50) | 1.59 (0.13 to 23.95) | 0.15 (0.00 to 2.04) | 0.83 (0.21 to 3.19) | 2.10 (0.47 to 10.22) | |
| IBN monthly | 5.32 (0.17 to 2155.25) | 6.60 (0.20 to 2849.07) | 6.89 (0.19 to 2995.07) | 0.22 (0.00 to 18.93) | 0.02 (0.00 to 1.60) | 0.12 (0.00 to 5.15) | 0.31 (0.00 to 13.60) | |
| DEN | 1.25 (0.15 to 14.20) | 1.54 (0.20 to 16.36) | 1.60 (0.17 to 18.83) | 0.23 (0.00 to 15.84) | 0.08 (0.00 to 2.91) | 0.52 (0.03 to 6.41) | 1.31 (0.09 to 17.37) | |
| ROMO | 0.12 (0.00 to 1.26) | 0.14 (0.00 to 1.72) | 0.15 (0.00 to 1.62) | 0.02 (0.00 to 1.42) | 0.09 (0.00 to 2.37) | 5.57 (0.46 to 188.50) | 14.49 (0.99 to 574.10) | |
| TPTD | 0.64 (0.30 to 1.29) | 0.79 (0.32 to 2.08) | 0.82 (0.39 to 1.70) | 0.12 (0.00 to 4.25) | 0.51 (0.04 to 4.92) | 5.44 (0.57 to 159.42) | 2.55 (0.57 to 12.79) | |
| RLX | 1.65 (0.75 to 3.88) | 2.02 (0.82 to 5.87) | 2.12 (0.79 to 6.12) | 0.31 (0.00 to 11.44) | 1.32 (0.11 to 13.41) | 14.42 (1.17 to 500.04) | 2.57 (0.92 to 7.92) |
| Placebo | ALN | RIS | DEN | ROMO | TPTD | RLX | |
|---|---|---|---|---|---|---|---|
| Placebo | 0.46 (0.13 to 1.43) | 0.48 (0.20 to 1.13) | 0.55 (0.11 to 2.60) | 0.10 (0.00 to 3.80) | 0.55 (0.19 to 1.59) | 2.48 (0.06 to 1215.07) | |
| ALN | 0.46 (0.15 to 1.27) | 1.03 (0.36 to 3.52) | 1.21 (0.24 to 6.59) | 0.23 (0.00 to 10.16) | 1.22 (0.32 to 4.89) | 5.48 (0.16 to 2806.02) | |
| RIS | 0.49 (0.23 to 0.96) | 1.01 (0.47 to 2.78) | 1.13 (0.24 to 5.46) | 0.22 (0.00 to 8.19) | 1.15 (0.38 to 3.48) | 5.27 (0.14 to 2596.20) | |
| DEN | 0.55 (0.12 to 2.41) | 1.21 (0.26 to 5.68) | 1.14 (0.28 to 4.57) | 0.19 (0.00 to 9.50) | 1.00 (0.18 to 5.72) | 4.63 (0.09 to 2621.17) | |
| ROMO | 0.10 (0.00 to 3.66) | 0.23 (0.00 to 9.49) | 0.22 (0.00 to 7.54) | 0.19 (0.00 to 8.82) | 5.11 (0.16 to 2773.07) | 34.06 (0.14 to 132817.46) | |
| TPTD | 0.55 (0.21 to 1.41) | 1.22 (0.39 to 4.05) | 1.15 (0.50 to 2.63) | 1.00 (0.20 to 5.02) | 5.10 (0.17 to 2692.22) | 4.63 (0.11 to 2511.00) | |
| RLX | 2.46 (0.06 to 1204.07) | 5.43 (0.17 to 2598.02) | 5.19 (0.15 to 2496.67) | 4.64 (0.10 to 2526.10) | 33.91 (0.15 to 126105.00) | 4.58 (0.12 to 2345.00) |
| Placebo | ALN | RIS | ZOL | IBN daily | IBN monthly | IBN i.v. | DEN | ROMO | TPTD | RLX | ROMO/ALN | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Placebo | 2.48 (0.71 to 4.25) | 1.80 (0.01 to 3.58) | 3.16 (1.27 to 5.04) | 1.84 (–0.30 to 3.85) | 2.30 (0.41 to 4.24) | 2.38 (0.06 to 4.56) | 3.35 (1.51 to 5.16) | 4.20 (2.24 to 6.17) | 2.58 (0.77 to 4.40) | 1.52 (–0.33 to 3.42) | 6.09 (3.55 to 8.61) | |
| ALN | 2.49 (2.05 to 2.91) | –0.70 (–3.20 to 1.78) | 0.68 (–1.91 to 3.19) | –0.65 (–3.37 to 1.98) | –0.19 (–2.74 to 2.37) | –0.12 (–2.97 to 2.66) | 0.87 (–1.69 to 3.36) | 1.71 (–0.94 to 4.34) | 0.10 (–2.41 to 2.57) | –0.97 (–3.49 to 1.60) | 3.60 (0.57 to 6.64) | |
| RIS | 1.80 (1.22 to 2.37) | –0.69 (–1.29 to –0.09) | 1.36 (–1.22 to 3.95) | 0.03 (–2.66 to 2.70) | 0.51 (–2.03 to 3.10) | 0.58 (–2.30 to 3.37) | 1.56 (–0.95 to 4.08) | 2.40 (–0.25 to 5.10) | 0.79 (–1.70 to 3.30) | –0.26 (–2.84 to 2.35) | 4.27 (1.25 to 7.38) | |
| ZOL | 3.17 (2.38 to 3.95) | 0.68 (–0.09 to 1.49) | 1.37 (0.41 to 2.28) | –1.32 (–4.14 to 1.41) | –0.86 (–3.48 to 1.85) | –0.77 (–3.72 to 2.08) | 0.18 (–2.39 to 2.77) | 1.04 (–1.67 to 3.76) | –0.58 (–3.21 to 2.06) | –1.63 (–4.24 to 1.02) | 2.92 (–0.15 to 5.99) | |
| IBN daily | 1.85 (0.53 to 2.93) | –0.63 (–1.97 to 0.41) | 0.05 (–1.24 to 1.15) | –1.31 (–2.86 to –0.06) | 0.48 (–2.17 to 3.17) | 0.54 (–2.18 to 3.28) | 1.52 (–1.20 to 4.27) | 2.39 (–0.52 to 5.22) | 0.75 (–1.94 to 3.51) | –0.29 (–3.05 to 2.52) | 4.25 (1.07 to 7.52) | |
| IBN monthly | 2.32 (1.50 to 3.13) | –0.16 (–0.99 to 0.63) | 0.51 (–0.33 to 1.41) | –0.83 (–1.95 to 0.15) | 0.47 (–0.56 to 1.73) | 0.07 (–2.80 to 2.88) | 1.04 (–1.55 to 3.64) | 1.91 (–0.87 to 4.59) | 0.29 (–2.38 to 2.87) | –0.78 (–3.47 to 1.87) | 3.78 (0.64 to 6.90) | |
| IBN i.v. | 2.39 (0.83 to 3.78) | –0.10 (–1.66 to 1.32) | 0.56 (–0.92 to 2.09) | –0.73 (–2.53 to 0.64) | 0.52 (–0.69 to 1.92) | 0.06 (–1.47 to 1.54) | 0.97 (–1.90 to 3.87) | 1.82 (–1.16 to 4.85) | 0.21 (–2.62 to 3.15) | –0.86 (–3.69 to 2.15) | 3.72 (0.33 to 7.10) | |
| DEN | 3.36 (2.74 to 3.97) | 0.87 (0.24 to 1.49) | 1.56 (0.83 to 2.30) | 0.19 (–0.70 to 1.09) | 1.52 (0.33 to 2.91) | 1.04 (0.16 to 1.95) | 0.97 (–0.50 to 2.60) | 0.85 (–1.79 to 3.53) | –0.78 (–3.31 to 1.80) | –1.82 (–4.36 to 0.80) | 2.73 (–0.36 to 5.83) | |
| ROMO | 4.20 (3.23 to 5.16) | 1.71 (0.67 to 2.75) | 2.40 (1.28 to 3.51) | 1.03 (–0.22 to 2.28) | 2.36 (0.88 to 3.95) | 1.88 (0.65 to 3.12) | 1.82 (0.10 to 3.65) | 0.84 (–0.30 to 1.96) | –1.63 (–4.27 to 1.00) | –2.66 (–5.40 to 0.03) | 1.88 (–1.33 to 5.12) | |
| TPTD | 2.58 (2.00 to 3.17) | 0.09 (–0.56 to 0.75) | 0.78 (0.02 to 1.54) | –0.59 (–1.52 to 0.35) | 0.73 (–0.47 to 2.14) | 0.25 (–0.68 to 1.22) | 0.19 (–1.30 to 1.85) | –0.78 (–1.57 to 0.01) | –1.62 (–2.63 to –0.60) | –1.04 (–3.65 to 1.56) | 3.51 (0.41 to 6.59) | |
| RLX | 1.53 (0.78 to 2.31) | –0.95 (–1.74 to –0.14) | –0.26 (–1.19 to 0.66) | –1.63 (–2.70 to –0.56) | –0.30 (–1.64 to 1.17) | –0.79 (–1.86 to 0.31) | –0.85 (–2.42 to 0.87) | –1.82 (–2.77 to –0.86) | –2.66 (–3.89 to –1.42) | –1.04 (–1.98 to –0.09) | 4.55 (1.42 to 7.67) | |
| ROMO/ALN | 6.08 (4.25 to 7.91) | 3.59 (1.81 to 5.37) | 4.29 (2.40 to 6.14) | 2.92 (0.93 to 4.86) | 4.26 (2.14 to 6.42) | 3.76 (1.79 to 5.73) | 3.70 (1.41 to 6.03) | 2.72 (0.83 to 4.61) | 1.89 (–0.22 to 3.98) | 3.50 (1.57 to 5.41) | 4.55 (2.57 to 6.50) |
Appendix 13 Assessment of inconsistency
Vertebral fractures
Twelve treatment contrasts have both direct and indirect evidence; however, only 10 of these were assessed for consistency. RIS–ALN was not assessed because the direct comparison is contributed by one small study79 with a zero count in the control arm. ZOL–TPTD was not assessed because the direct comparison is contributed by one small study,93 with only one event in the TPTD arm. Multiple testing should be taken into account when considering p-values.
Comparing the DIC for the different node-splits with that of the full consistency NMA model, only the placebo–ZOL comparison provides a lower DIC when the node is split. However, the difference is small (–0.7); therefore, there is not a clear advantage of one model over the other. The HRs from both the direct and indirect evidence favour ZOL and the combined estimate is more heavily influenced by the direct studies. It was concluded that there is no strong evidence for inconsistency in the network.
| Treatment 1 | Treatment 2 | Heterogeneity | Model fit | HRs (95% CrI) | p-valued | ||||
|---|---|---|---|---|---|---|---|---|---|
| SDa (95% CrI) | SDtb (95% CrI) | D res c | DIC | All evidence | Direct | Indirect | |||
| Placebo | ALN | 0.14 (0.01 to 0.34) | 0.42 (0.05 to 1.48) | 90.4 | 152.7 | 0.50 (0.40 to 0.64) | 0.46 (0.36 to 0.62) | 0.76 (0.43 to 1.68) | 0.18 |
| Placebo | RIS | 0.16 (0.01 to 0.37) | 0.19 (0.01 to 0.86) | 92.31 | 155 | 0.52 (0.41 to 0.65) | 0.57 (0.42 to 0.74) | 0.45 (0.32 to 0.65) | 0.31 |
| Placebo | ZOL | 0.12 (0.01 to 0.31) | 0.13 (0.00 to 0.92) | 91.29 | 151.6 | 0.40 (0.29 to 0.55) | 0.33 (0.25 to 0.45) | 0.56 (0.38 to 1.25) | 0.03 |
| Placebo | TPTD | 0.17 (0.02 to 0.37) | 0.19 (0.01 to 0.89) | 90.18 | 153.33 | 0.23 (0.16 to 0.32) | 0.30 (0.19 to 0.49) | 0.18 (0.11 to 0.28) | 0.12 |
| RIS | ZOL | 0.16 (0.01 to 0.35) | 0.23 (0.02 to 0.97) | 92.07 | 155.02 | 0.78 (0.52 to 1.08) | 1.78 (0.40 to 9.98) | 0.73 (0.49 to 1.05) | 0.26 |
| RIS | DEN | 0.18 (0.01 to 0.38) | 0.21 (0.01 to 0.91) | 91.95 | 155.44 | 0.59 (0.39 to 0.88) | 0.67 (0.26 to 1.65) | 0.56 (0.35 to 0.90) | 0.72 |
| RIS | TPTD | 0.18 (0.02 to 0.39) | 0.20 (0.01 to 0.90) | 91.82 | 155.24 | 0.44 (0.32 to 0.61) | 0.44 (0.27 to 0.68) | 0.45 (0.27 to 0.72) | 0.94 |
| Placebo | RLX | 0.16 (0.01 to 0.36) | 0.20 (0.01 to 0.90) | 91.58 | 154.34 | 0.61 (0.44 to 0.80) | 0.64 (0.47 to 0.85) | 0.30 (0.09 to 0.90) | 0.19 |
| Placebo | DEN | 0.18 (0.02 to 0.38) | 0.21 (0.01 to 0.90) | 91.97 | 155.54 | 0.30 (0.21 to 0.43) | 0.29 (0.19 to 0.43) | 0.35 (0.14 to 0.90) | 0.72 |
| ALN | TPTD | 0.15 (0.01 to 0.35) | 0.22 (0.02 to 0.92) | 90.5 | 153.26 | 0.46 (0.31 to 0.66) | 0.18 (0.04 to 0.51) | 0.53 (0.35 to 0.77) | 0.06 |
| Consistency model | |||||||||
| 0.17 (0.02 to 0.37) | 0.20 (0.01 to 0.91) | 91.24 | 152.34 | ||||||
Non-vertebral fractures
Fourteen treatment contrasts have both direct and indirect evidence; however, only 13 of these were assessed for consistency. RIS–ALN was not assessed because the direct comparison is contributed by one small study79 with a zero count in the RIS arm. Multiple testing should be taken into account when considering p-values.
Comparing the DIC for the different node-splits with that of the full consistency NMA model, only the placebo–ALN comparison provides a lower DIC when the node is split. However, the difference is small; therefore, there is not a clear advantage of one model over the other, and the p-values are large for all comparisons. It was concluded that there is no strong evidence for inconsistency in the network.
| Treatment 1 | Treatment 2 | Heterogeneity | Model fit | HRs (95% CrI) | p-valued | ||||
|---|---|---|---|---|---|---|---|---|---|
| SDa (95% CrI) | SDtb (95% CrI) | D res c | DIC | All evidence | Direct | Indirect | |||
| Placebo | RLX | 0.88 (0.62 to 1.19) | 1.14 (0.39 to 3.23) | 74.61 | 129.85 | 0.90 (0.65 to 1.21) | 0.88 (0.62 to 1.19) | 1.14 (0.39 to 3.23) | 0.65 |
| Placebo | ALN | 0.81 (0.65 to 0.95) | 0.66 (0.39 to 0.91) | 73.06 | 127.94 | 0.77 (0.64 to 0.90) | 0.81 (0.65 to 0.95) | 0.66 (0.39 to 0.91) | 0.31 |
| Placebo | RIS | 0.65 (0.48 to 0.86) | 0.80 (0.59 to 1.12) | 73.8 | 128.78 | 0.73 (0.59 to 0.88) | 0.65 (0.48 to 0.86) | 0.80 (0.59 to 1.12) | 0.28 |
| Placebo | ZOL | 0.71 (0.57 to 0.86) | 0.78 (0.42 to 1.33) | 74.3 | 129.46 | 0.73 (0.61 to 0.85) | 0.71 (0.57 to 0.86) | 0.78 (0.42 to 1.33) | 0.65 |
| Placebo | DEN | 0.82 (0.65 to 1.05) | 1.34 (0.69 to 2.61) | 73.41 | 128.2 | 0.86 (0.69 to 1.12) | 0.82 (0.65 to 1.05) | 1.34 (0.69 to 2.61) | 0.19 |
| Placebo | ROMO | 0.75 (0.49 to 1.14) | 0.50 (0.16 to 1.46) | 74.45 | 129.95 | 0.71 (0.48 to 1.03) | 0.75 (0.49 to 1.14) | 0.50 (0.16 to 1.46) | 0.49 |
| Placebo | TPTD | 0.60 (0.39 to 0.89) | 0.57 (0.40 to 0.80) | 74.6 | 129.91 | 0.58 (0.45 to 0.76) | 0.60 (0.39 to 0.89) | 0.57 (0.40 to 0.80) | 0.88 |
| ALN | TPTD | 1.06 (0.52 to 2.23) | 0.71 (0.52 to 0.96) | 73.84 | 128.86 | 0.76 (0.57 to 1.02) | 1.06 (0.52 to 2.23) | 0.71 (0.52 to 0.96) | 0.3 |
| RIS | DEN | 1.75 (0.78 to 4.16) | 1.12 (0.85 to 1.57) | 74.15 | 129.18 | 1.18 (0.90 to 1.63) | 1.75 (0.78 to 4.16) | 1.12 (0.85 to 1.57) | 0.33 |
| RIS | TPTD | 0.69 (0.47 to 0.99) | 0.97 (0.66 to 1.46) | 72.89 | 128.22 | 0.80 (0.61 to 1.04) | 0.69 (0.47 to 0.99) | 0.97 (0.66 to 1.46) | 0.22 |
| ZOL | TPTD | 0.85 (0.29 to 2.51) | 0.79 (0.58 to 1.07) | 74.84 | 130.26 | 0.80 (0.60 to 1.08) | 0.85 (0.29 to 2.51) | 0.79 (0.58 to 1.07) | 0.89 |
| ROMO | TPTD | 1.15 (0.37 to 3.53) | 0.77 (0.46 to 1.24) | 74.43 | 129.92 | 0.82 (0.53 to 1.28) | 1.15 (0.37 to 3.53) | 0.77 (0.46 to 1.24) | 0.49 |
| ALN | DEN | 0.07 (0.00 to 0.23) | 0.16 (0.01 to 0.74) | 74.49 | 129.77 | 1.12 (0.87 to 1.57) | 1.83 (0.58 to 6.33) | 1.09 (0.84 to 1.52) | 0.39 |
| Consistency model | |||||||||
| 0.08 (0 to 0.24) | 0.15 (0.01 to 0.73) | 74.047 | 128.4 | ||||||
Hip fractures
Fourteen treatment contrasts have both direct and indirect evidence; however, only nine of these were assessed for consistency. For five of these (RIS–ALN, RIS–DEN, RIS–RLX, ZOL–DEN, ROMO–TPTD), the direct comparison is contributed by small studies. 67,79,341 Multiple testing should be taken into account when considering p-values.
Comparing the DIC for the different node-splits with that of the full consistency NMA model, for all comparisons there is a higher DIC (indicating a less favourable model) when the node is split and the p-values are large. It was concluded that there is no strong evidence for inconsistency in the network.
| Treatment 1 | Treatment 2 | Heterogeneity | Model Fit | HRs (95% CrI) | p-valued | ||||
|---|---|---|---|---|---|---|---|---|---|
| SDa (95% CrI) | SDtb (95% CrI) | D res c | DIC | All evidence | Direct | Indirect | |||
| Placebo | ALN | 0.16 (0.01 to 0.63) | 0.38 (0.02 to 1.77) | 39.72 | 73.1 | 0.64 (0.41 to 0.94) | 0.62 (0.35 to 1.07) | 0.62 (0.16 to 1.92) | 0.98 |
| Placebo | RIS | 0.15 (0.00 to 0.61) | 0.32 (0.01 to 1.70) | 39.32 | 72.68 | 0.67 (0.43 to 1.10) | 0.80 (0.40 to 1.58) | 0.57 (0.19 to 1.22) | 0.45 |
| Placebo | ZOL | 0.16 (0.01 to 0.63) | 0.43 (0.02 to 1.81) | 39.58 | 72.92 | 0.64 (0.44 to 0.92) | 0.62 (0.39 to 1.02) | 0.72 (0.20 to 4.39) | 0.76 |
| Placebo | DEN | 0.15 (0.01 to 0.59) | 0.24 (0.01 to 1.59) | 39.76 | 73.08 | 0.56 (0.29 to 0.99) | 0.57 (0.28 to 1.05) | 0.41 (0.04 to 2.75) | 0.73 |
| Placebo | ROMO | 0.14 (0.01 to 0.58) | 0.23 (0.01 to 1.60) | 40.01 | 73.68 | 0.56 (0.20 to 1.48) | 0.52 (0.17 to 1.48) | 1.97 (0.05 to 642.60) | 0.49 |
| Placebo | TPTD | 0.15 (0.01 to 0.59) | 0.25 (0.01 to 1.60) | 39.75 | 73.33 | 0.34 (0.15 to 0.77) | 0.19 (0.02 to 1.03) | 0.39 (0.14 to 0.98) | 0.49 |
| Placebo | RLX | 0.14 (0.01 to 0.58) | 0.23 (0.01 to 1.57) | 39.91 | 73.18 | 0.94 (0.31 to 2.85) | 0.83 (0.22 to 3.08) | 1.10 (0.10 to 7.81) | 0.84 |
| ALN | RLX | 0.15 (0.01 to 0.58) | 0.23 (0.01 to 1.57) | 40.03 | 73.46 | 1.49 (0.47 to 4.66) | 1.73 (0.16 to 11.56) | 1.31 (0.31 to 5.34) | 0.83 |
| RIS | TPTD | 0.15 (0.01 to 0.58) | 0.25 (0.01 to 1.58) | 39.42 | 72.97 | 0.51 (0.23 to 1.07) | 0.59 (0.24 to 1.41) | 0.27 (0.04 to 1.33) | 0.42 |
| Consistency model | |||||||||
| 0.14 (0.01 to 0.56) | 0.23 (0.01 to 1.54) | 39.0876 | 71.572 | ||||||
Wrist
Eight treatment contrasts have both direct and indirect evidence; however, only five of these were assessed for consistency. For three of these (RIS–ALN, ALN–RLX, RIS–RLX), the direct comparison is contributed by small studies. 77,79 Multiple testing should be taken into account when considering p-values.
Comparing the DIC for the different node-splits with that of the full consistency NMA model, for all comparisons there is a higher DIC (indicating a less favourable model) when the node is split and the p-values are large. It was concluded that there is no strong evidence for inconsistency in the network.
| Treatment 1 | Treatment 2 | Heterogeneity | Model Fit | HR’s (95% CrI) | p-valued | ||||
|---|---|---|---|---|---|---|---|---|---|
| SDa (95% CrI) | SDtb (95% CrI) | D res c | DIC | All evidence | Direct | Indirect | |||
| Placebo | ALN | 0.34 (0.06 to 0.71) | 0.20 (0.01 to 0.69) | 30.48 | 55.35 | 0.83 (0.51 to 1.30) | 0.85 (0.43 to 1.52) | 0.77 (0.29 to 1.86) | 0.85 |
| Placebo | RIS | 0.31 (0.04 to 0.68) | 0.20 (0.01 to 0.68) | 30.44 | 55.17 | 0.82 (0.50 to 1.30) | 0.79 (0.32 to 1.79) | 0.99 (0.49 to 2.24) | 0.40 |
| Placebo | TPTD | 0.31 (0.04 to 0.68) | 0.17 (0.01 to 0.62) | 30.80 | 55.57 | 0.66 (0.33 to 1.26) | 0.79 (0.32 to 1.79) | 0.47 (0.15 to 1.43) | 0.45 |
| Placebo | RLX | 0.32 (0.05 to 0.68) | 0.17 (0.01 to 0.61) | 31.21 | 56.44 | 1.65 (0.78 to 3.65) | 1.59 (0.70 to 3.75) | 2.29 (0.18 to 24.15) | 0.79 |
| RIS | TPTD | 0.31 (0.04 to 0.67) | 0.17 (0.01 to 0.62) | 30.83 | 55.65 | 0.81 (0.40 to 1.58) | 0.62 (0.24 to 1.65) | 1.05 (0.37 to 2.68) | 0.45 |
| Consistency model | |||||||||
| 0.32 (0.04 to 0.67) | 0.17 (0.01 to 0.62) | 30.38 | 54.64 | ||||||
Humerus
Five treatment contrasts have both direct and indirect evidence; however, only four of these were assessed for consistency. For the placebo–DEN comparison, the direct comparison is contributed by one small study42 with zero events in the DEN arm. Multiple testing should be taken into account when considering p-values.
Comparing the DIC for the different node-splits with that of the full consistency NMA model, for all comparisons there is a higher DIC (indicating a less favourable model) when the node is split and the p-values are large. It was concluded that there is no strong evidence for inconsistency in the network.
| Treatment 1 | Treatment 2 | Heterogeneity | Model fit | HRs (95% CrI) | p-valued | ||||
|---|---|---|---|---|---|---|---|---|---|
| SDa (95% CrI) | SDtb (95% CrI) | D res c | DIC | All evidence | Direct | Indirect | |||
| Placebo | RIS | 0.18 (0.01 to 0.59) | 0.21 (0.01 to 0.71) | 22.98 | 43.98 | 0.48 (0.24 to 0.96) | 0.45 (0.19 to 0.98) | 0.63 (0.12 to 3.00) | 0.71 |
| Placebo | TPTD | 0.17 (0.01 to 0.60) | 0.21 (0.01 to 0.72) | 22.86 | 43.99 | 0.55 (0.21 to 1.41) | 0.77 (0.17 to 3.30) | 0.42 (0.11 to 1.47) | 0.53 |
| RIS | DEN | 0.17 (0.01 to 0.58) | 0.22 (0.01 to 0.72) | 23.05 | 43.93 | 1.14 (0.28 to 4.57) | 0.97 (0.15 to 5.91) | 1.40 (0.13 to 14.31) | 0.8 |
| RIS | TPTD | 0.17 (0.01 to 0.59) | 0.21 (0.01 to 0.72) | 22.61 | 43.46 | 1.15 (0.50 to 2.63) | 1.00 (0.38 to 2.65) | 1.80 (0.33 to 9.58) | 0.54 |
| Consistency model | |||||||||
| 0.17 (0.01 to 0.57) | 0.21 (0.01 to 0.7) | 21.9908 | 41.832 | ||||||
Appendix 14 Network meta-analysis results of meta-regressions
A summary of meta-regression models (covariate estimate, model fit, heterogeneity) is provided in Table 45 for all outcomes.
| Outcome/model | Absolute model fit | DIC | Heterogeneity, SD (95% CI) | Covariate estimate (95% CI) | Baseline parameters | |||
|---|---|---|---|---|---|---|---|---|
| D res a | Data points | SDb | SDtc | Covariate | SD | |||
| Vertebral | ||||||||
| Age | 92.15 | 93 | 155.19 | 0.176 (0.018 to 0.378) | 0.191 (0.011 to 0.882) | –0.028 (–0.227 to 0.192) | NA | NA |
| Sex | 91.31 | 93 | 154.81 | 0.185 (0.03 to 0.379) | 0.2 (0.01 to 0.939) | 0.06 (–0.117 to 0.263) | NA | NA |
| Baseline response | 88.57 | 93 | 147.16 | 0.18 (0.02 to 0.37) | 0.17 (0.01 to 0.8) | 0.13 (–0.04 to 0.3) | –3.1 (–3.41 to –2.8) | 0.96 (0.76 to 1.23) |
| Non-vertebral | ||||||||
| Age | 74.62 | 86 | 130.01 | 0.08 (0.003 to 0.244) | 0.166 (0.009 to 0.768) | 0.014 (–0.16 to 0.207) | ||
| Sex | 74.75 | 86 | 129.92 | 0.077 (0.004 to 0.236) | 0.14 (0.006 to 0.694) | 0.062 (–0.132 to 0.256) | ||
| Baseline response M2 | 73.44 | 86 | 119.99 | 0.1 (0.01 to 0.28) | 0.15 (0.01 to 0.76) | 0.05 (–0.16 to 0.32) | –3.41 (–3.61 to –3.22) | 0.53 (0.39 to 0.73) |
| Hip | ||||||||
| Age | 39.83 | 47 | 72.83 | 0.12 (0.007 to 0.434) | 0.266 (0.011 to 1.594) | –0.103 (–0.782 to 0.538) | NA | NA |
| Sex | 39.55 | 47 | 72.39 | 0.135 (0.006 to 0.47) | 0.248 (0.01 to 1.6) | –0.118 (–1.048 to 0.845) | NA | NA |
| Baseline response M2 | 39.14 | 47 | 67.24 | 0.13 (0.01 to 0.47) | 0.29 (0.01 to 1.66) | 0.08 (–0.37 to 0.74) | –5.21 (–5.62 to –4.77) | 0.77 (0.48 to 1.29) |
| Wrist | ||||||||
| Age | 30.91 | 31 | 55.58 | 0.24 (0.01 to 0.63) | 0.47 (0.02 to 1.85) | –0.67 (–1.58 to 0.16) | NA | NA |
| Baseline response M2 | 28.82 | 31 | 49.16 | 0.34 (0.03 to 0.70) | 0.46 (0.02 to 1.82) | 0.35 (–1.56 to 3.18) | ||
| Humerus | ||||||||
| Age | 23.92 | 26 | 46.12 | 0.179 (0.008 to 0.619) | 0.998 (0.049 to 1.953) | 0.273 (–2.788 to 3.6) | NA | NA |
| Sex | 24.01 | 26 | 46.38 | 0.171 (0.008 to 0.582) | 0.988 (0.052 to 1.951) | 0.412 (–1.351 to 3.199) | NA | NA |
| Baseline response | 22.17 | 26 | 38.53 | 0.18 (0.01 to 0.59) | 1 (0.05 to 1.95) | –0.26 (–1.36 to 3.04) | –5.15 (–6.03 to –3.73) | 0.72 (0.13 to 3.09) |
| Femoral neck BMD | ||||||||
| Age | 144.5 | 137 | 259.24 | 0.86 (0.65 to 1.14) | 0.76 (0.25 to 2.28) | –0.01 (–0.07 to 0.05) | NA | NA |
| Sex | 145.7 | 137 | 258.73 | 0.80 (0.59 to 1.08) | 0.77 (0.28 to 2.34) | 0.01 (0 to 0.02) | NA | NA |
| Baseline response | NA | 137 | NA | 0.81 (0.61 to 1.08) | 0.67 (0.24 to 1.65) | 0.16 (–0.32 to 0.81) | –0.31 (–0.57 to –0.04) | 1.92 (0.91 to 4.18) |
Note that, for age and sex, a common meta-regression coefficient is assumed for all treatments (see Dias et al. 121 for further details). Alternative models were also considered, but did not improve model fit.
For meta-regressions on baseline response, the results for all outcomes assume a common meta-regression coefficient for all treatments (as for age and sex), and the baselines of each study were assumed to follow a normal distribution with common mean and between-treatment variance (see Achana et al. 122 for further details). Alternative models were also considered, but did not improve model fit. Results are provided in Table 45.
Meta-regression on baseline risk, model selection
For the vertebral fractures network, four different baseline risk models were considered, allowing different assumptions about the model for baseline risk and covariate treatment interaction:
-
A1: unconstrained baseline and common slope
-
A2: normal distribution for baseline risk and common slope
-
B1: unconstrained baseline and common slope
-
B2: normal distribution for baseline risk and common slope.
Alternative models were considered for vertebral fractures only (which provide the largest network of evidence). Models with an unconstrained baseline (A1, B1) had a high DIC. Model A2, with normal distribution for baseline risk and assumption of common slope parameter for treatment–covariate interaction, was chosen for the main meta-regression model because this provided the lowest DIC. The results of using this model are provided in Table 45 for all outcomes.
| Model | Absolute model fit | DIC | Heterogeneity, SD (95% CI) | Covariate treatment interaction | Baseline parameters | ||||
|---|---|---|---|---|---|---|---|---|---|
| D res a | Data points | SDb | SDtc | Estimate (95% CrI) | SD (95% CrI) | Covariate (95% CrI) | SD covariate (95% CrI) | ||
| A1 | 89.91 | 93 | 171.57 | 1.06 (0.06 to 1.4) | 0.31 (0.01 to 1.47) | –1 (–1.01 to 0.09) | NA | NA | NA |
| A2 | 88.57 | 93 | 147.16 | 0.18 (0.02 to 0.37) | 0.17 (0.01 to 0.8) | 0.13 (–0.04 to 0.3) | NA | –3.1 (–3.41 to –2.8) | 0.96 (0.76 to 1.23) |
| B1 | 92.85 | 93 | 157.38 | 0.16 (0.02 to 0.39) | 0.2 (0.01 to 1.11) | 0.03 (–0.16 to 0.22) | 0.13 (0.01 to 0.6) | NA | NA |
| B2 | 89.48 | 93 | 148.39 | 0.17 (0.02 to 0.37) | 0.18 (0.01 to 0.94) | 0.14 (–0.03 to 0.33) | 0.09 (0.01 to 0.47) | –3.11 (–3.41 to –2.81) | 0.96 (0.77 to 1.24) |
Appendix 15 Studies excluded, at full-text sift, from the review of published economic evaluations
| Citation | Reason for exclusion |
|---|---|
| Alexander W, Strom O, Macarios D. American Society for Bone and Mineral Research: DEN (Prolia): a cost-effectiveness model. P T 2009;34:633 | Abstract only |
| Davies A, Compston J, Ferguson S, McClosky E, Shearer A, Taylor A. Cost-effectiveness of DEN in the treatment of postmenopausal osteoporosis in Scotland. Value Health 2011;14:A310 | Abstract only |
| Hagen G. Comparative Effectiveness and Cost-Effectiveness of Generic ALN, RIS, DEN and zolendronic acid for secondary prevention of fragility fractures – perliminay results. Value Health 2015;18:A648 | Abstract only |
| Liu H, Michaud K, Nayak S, Karpf DB, Owens DK, Garber AM. The cost-effectiveness of therapy with TPTD and ALN in women with severe osteoporosis. Arch Intern Med 2006;166:1209–17 | Non-UK |
| Meadows ES, Klein R, Rousculp MD, Smolen L, Ohsfeldt RL, Johnston JA. Cost-effectiveness of preventative therapies for postmenopausal women with osteopenia. BMC Womens Health 2007;7:6 | Non-UK |
| Mobley LR, Hoerger TJ, Wittenborn JS, Galuska DA, Rao JK. Cost-effectiveness of osteoporosis screening and treatment with hormone replacement therapy, RLX, or ALN. Med Decis Making 2006;26:194–206 | Non-UK |
| Murphy DR, Klein RW, Smolen LJ, Klein TM, Roberts SD. Using common random numbers in health care cost-effectiveness simulation modelling. Health Serv Res 2013;48:1508–25 | Non-UK |
| O’Hanlon CE, Parthan A, Kruse M, Cartier S, Stollenwerk B, Jiang Y, et al. A Model for assessing the clinical and economic benefits of bone-forming agents for reducing fractures in postmenopausal women at high, near-term risk of osteoporotic fracture. Clin Ther 2017;39:1276–90 | Non-UK |
| Pfister AK, Welch CA, Lester MD, Emmett MK, Saville PD, Duerring SA. Cost-effectiveness strategies to treat osteoporosis in elderly women. South Med J 2006;99:123–31 | Non-UK |
| Turner DA, Khioe RFS, Shepstone L, Lenaghan E, Cooper C, Gittoes N, et al. The cost-effectiveness of screening in the community to reduce osteoporotic fractures in older women in the UK: economic evaluation of the SCOOP study. J Bone Miner Res 2018;33:845–51 | Not a relevant comparison – compares screening with usual care with treatment after screening directed by clinician |
| Zethraeus N, Borgstrom F, Strom O, Kanis JA, Jonsson B. Cost-effectiveness of the treatment and prevention of osteoporosis – a review of the literature and a reference model. Osteoporos Int 2007;18:9–23 | Non-UK |
Appendix 16 Health-related quality of life: review of utility values following fracture
To inform the model, data were needed on the proportionate decrease in HRQoL that occurs in the year following fracture and in subsequent years. This was then used to calculate a utility multiplier, which was applied to the pre-fracture utility value to calculate the post-fracture utility. For example, a proportionate decrease of 10% would translate into a utility multiplier of 0.9. If a patient’s prior fracture utility is 0.8, then the post-fracture utility would be 0.72. Data on the absolute HRQoL after fracture can be obtained from studies that measure HRQoL of patients who have experienced a recent fracture. However, the proportionate decrease can be obtained only if there is some estimate of pre-fracture utility. Ideally, HRQoL would be measured prospectively in a cohort of patients at risk of fracture and these patients would be followed up with HRQoL re-measured at regular intervals with the time of any incident fracture being recorded so that the correlation between HRQoL and incident fracture can be obtained after adjusting for other confounding factors. However, many studies simply recruit patients at the time of fracture and ask them to recall their pre-fracture health state, which is subject to recall bias. Other studies may compare the HRQoL of individuals who have fractured with that of matched controls or population norms, in which case the estimates may be confounded by differences in other factors between cases and controls.
Our intention was to conduct a rapid update of the systematic review of HRQoL data conducted for TA464. 34 Systematic searches were undertaken to identify studies reporting on health utilities associated with different states for osteoporosis published since 2014. Searches were undertaken in July 2018 in the following electronic databases:
-
MEDLINE Epub Ahead of Print, In-Process & Other Non-Indexed Citations: Ovid, 1946–2018.
-
EMBASE: Ovid, 1974–2018.
In line with the NICE reference case,139 and the approach taken previously for TA464, the searches focused specifically on studies that reported HRQoL estimates for health states that were measured and valued using the EQ-5D. The search strategy comprised sensitive Medical Subject Headings (MeSH) or Emtree Thesauri terms and free-text synonyms for ‘osteoporosis’ combined with free-text synonyms for ‘EQ-5D’. The search strategies are presented in Appendix 1.
This search retrieved 111 unique references. The results of the economic searches described above were combined with the results of the searches conducted for the review of published cost-effectieness studies (see Chapter 4, Systematic review of existing cost-effectiveness evidence, Methods), to give a total of 3853 unique references, and a combined sift was conducted to pick up any cross-relevant papers. This initial sift of paper titles by a first reviewer reduced the number thought to be relevant to the HRQoL review to 131. A further sift of the abstracts by a second reviewer identified 53 citations that could be excluded (48 conference proceedings, three non-English papers and two commentaries), leaving 81 studies reporting health utility in patients with an incident osteoporotic fracture. However, values measured during RCTs were excluded because of the possibility that the study interventions may affect HRQoL independently of their impact on fracture. Studies reporting the quality-of-life impact of prevalent fractures were also excluded on the basis that there is no way of knowing how long ago the prevalent fracture was sustained. Furthermore, studies reporting the HRQoL associated with osteoporotic fractures using instruments other than the EQ-5D, such as the Health Utilities Index or Short Form questionnaire-6 Dimensions, were excluded. A further study342 that fulfilled these inclusion criteria was excluded because resulting EQ-5D utilities at specific time points following fracture were presented only graphically, rather than numerically, which means that accurate estimates of the utility values were impossible. This left four studies. A PRISMA flow diagram representing this process is presented in Figure 15.
FIGURE 15.
The PRISMA flow diagram for study selection for the review of HRQoL.
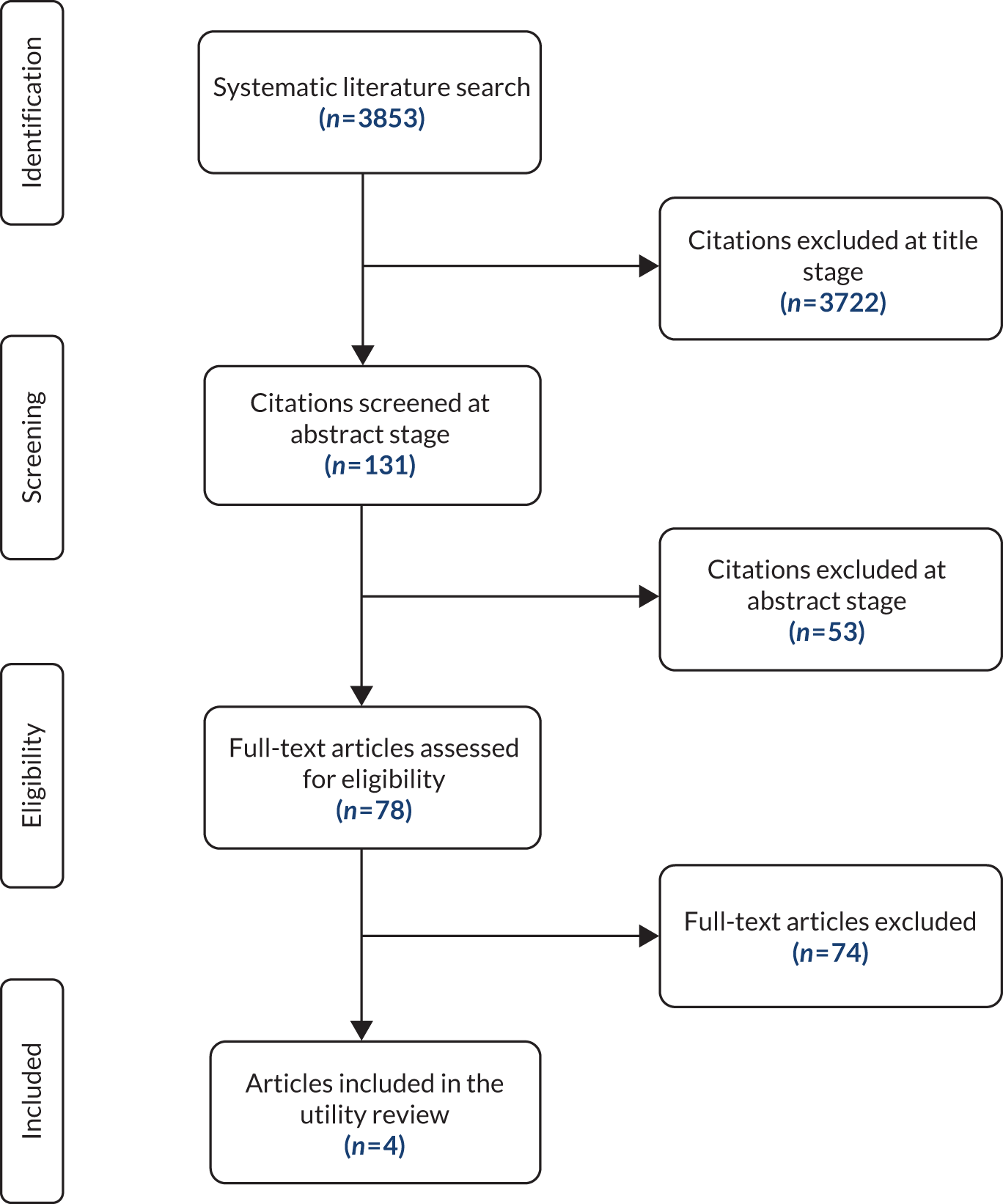
These four remaining studies209,210,212,213 are summarised in Table 47. All four studies reported outcomes from ICUROS. As this study had been previously identified in the review conducted for TA464,34 no new quality appraisal of this study was required. However, the four new papers identified reported additional data. All four provided HRQoL data for hip fracture, three provided it for wrist (distal forearm) fracture,209,210,213 three for vertebral fracture209,210,213 and one for fracture of the proximal humerus (shoulder). 210 One study also reported HRQoL for fracture of the ankle and other fracture. 210
| First author and year of publication | Country | Study design | Cohort description | Sample size at baseline and % of missing data | Valuation set used for EQ-5D |
|---|---|---|---|---|---|
| Svedbom 2018213 | Multicentre (10 countries) | Prospective observational cohort study |
|
|
UK (TTO) |
| Svedbom 2018209 | Multicentre (11 countries) | Prospective observational cohort study |
|
UK (TTO) | |
| Abimanyi-Ochom 2015210 | Australia | Prospective observational cohort study | UK (TTO) | ||
| Jurisson 2016212 | Estonia | Prospective observational cohort study | Hip fracture, n = 205 (18%) | UK (TTO) |
All four studies were based on ICUROS: two of the papers presented values for individual countries in the ICUROS cohort (Australia210 and Estonia212) and two presented values for groups of ICUROS counties. 209,213 One of these papers presented HRQoL utility values for patients in 10 ICUROS countries (Austria, Australia, Estonia, France, Italy, Lithuania, Mexico, Russia, Spain and the UK) who sustained a hip, vertebral and wrist fracture. 213 Utility was measured pre fracture (recall), post fracture (within 2 weeks of the fracture being sustained), 4 months post fracture, 12 months post fracture and 18 months post fracture. However, only data from patients who completed all instruments (not just the EQ-5D) at all time points are included. The second paper presents HRQoL utility values for patients in 11 ICUROS countries (Austria, Australia, Estonia, France, Italy, Lithuania, Mexico, Russia, Spain, the UK and the USA) who sustained a hip, vertebral and wrist fracture. 209 Utility was measured pre fracture (recall), post fracture (within 2 weeks of the fracture being sustained), 4 months post fracture, 12 months post fracture and 18 months post fracture. However, in this analysis, data were included from patients who completed the EQ-5D instrument at all time points. Thus, the HRQoL utility values in the latter of these two studies209 was based on significantly more data (1415 patients for hip fracture, 559 patients for vertebral fracture and 1047 patients for distal forearm (wrist) fracture, compared with 505 patients for hip fracture, 316 patients for vertebral fracture and 589 for distal forearm (wrist) fracture). As a result, the latter of these two studies209 was chosen to provide HRQoL values for hip, vertebral and wrist fracture in the model.
Health-related quality-of-life values associated with proximal humerus fracture were still required by the model, and the only study to provide such values was the study concerned with the Australian ICUROS cohort210 in which the UK value set was used to convert the dimension scores into a utility value. In this study, 65 patients provided HRQoL values at baseline (pre fracture and immediately post fracture), 57 patients provided them at 4 months, 54 patients at 12 months and 34 patients at 18 months. Only 52% of baseline patients survived to 18 months and only 63% of the patients who survived to 12 months survived to 18 months.
Values from four papers209,210,212,213 all came from one study (ICUROS), which included patients aged at least 50 years living in their own home prior to fracture who sustained a low-energy fracture. Initial post-fracture assessment of HRQoL took place within 2 weeks of fracture. Patients who sustained another fracture in the follow-up period were excluded as were people who were lost to follow-up. However, although two of the papers209,213 ensured that data relating to patients excluded at some later point in the study were removed from summary HRQoL utility data at all time points, the remaining two papers 210,212 did not and used all available data at each time point.
The two multicentre papers reported broadly similar values at all time points, except for those recorded at 2 weeks following fracture: those reported in the paper with the larger data set209 were lower than those reported in the paper that excluded more patients for incomplete data213 (hip fracture: –0.11, vertebral fracture: 0.17 and wrist fracture: 0.41, compared with hip fracture: –0.02, vertebral fracture: 0.27 and wrist fracture: 0.47). The study using Australian data but with a UK tariff210 reported values that were, again, higher at 2 weeks following fracture (hip fracture: 0.11, vertebral fracture: 0.32 and wrist fracture: 0.53); these higher values were also reflected at 4 months and 12 months, although by a lessening degree, until the increase had become negligible by 18 months. The Estonian study, which again used the UK tariff,212 also reported higher values at 2 weeks following fracture (0.07). This may raise concerns about the values used in the model, even though they are based on a significantly larger sample size. However, the excluded paper,342 which presented utility values in a graphical rather than a numerical format, suggests similar values to the international ICUROS data set209 for a UK population, with the HRQoL utility value at 2 weeks post fracture being approximately –0.15.
For hip, vertebral and wrist fractures, the utility multipliers for 0–12 months, 12–24 months and > 24 months are presented by Svedbom et al. ,209 together with 95% confidence intervals, enabling SD to be calculated. However, we assume that improvements in utility in the period between 12 and 24 months post fracture are subject to significant uncertainty; thus, we apply the utility values presented for the period > 24 months post fracture in the paper for any period beyond 12 months post fracture in the model. For proximal humerus fracture, we assume that the utility drops at the point of fracture to the value measured in the first 2 weeks post fracture and remains at this value for the first 2 weeks by a gradual linear improvement to 4 months, 12 months and, finally, 18 months. We assume that utility at 18 months is maintained indefinitely. The utility multiplier for the first year post fracture was calculated by dividing the total utility accrued by 12 months by the pre-fracture utility value. The utility value observed at 12 months is assumed to persist in the long term, so the multiplier for the second and subsequent years was calculated by dividing the total utility accrued between month 13 and month 24 again by the pre-fracture utility value. These data are presented in Table 48 and graphically in Figures 16–19.
| Description | Hip fracture | Vertebral fracture | Humerus fracture | Distal forearm fracture | ||||
|---|---|---|---|---|---|---|---|---|
| TA46434 | ICUROS209 | TA46434 | ICUROS209 | TA46434 | ICUROS210 | TA46434 | ICUROS209 | |
| Baseline number of patients | 282 | 1415 | 76 | 559 | 38 | 65 | 325 | 1047 |
| Utility index | ||||||||
| Pre fracture | 0.81 | 0.77 | 0.74 | 0.83 | 0.65 | 0.81 | 0.90 | 0.89 |
| Post fracture | 0.19 | –0.11 | 0.18 | 0.17 | 0.36 | 0.21 | 0.56 | 0.41 |
| 4 months | 0.64 | 0.49 | 0.49 | 0.60 | 0.58 | 0.70 | 0.83 | 0.77 |
| 12 months | 0.69 | 0.59 | 0.49 | 0.70 | 0.65 | 0.77 | 0.88 | 0.85 |
| 18 months | 0.72 | 0.66 | 0.49 | 0.70 | – | 0.83 | 0.90 | 0.88 |
| Utility multiplier | ||||||||
| Year 1 | ||||||||
| Mean | 0.69 | 0.55 | 0.57 | 0.68 | 0.86 | 0.78 | 0.88 | 0.83 |
| SD | 0.02 | 0.01 | 0.03 | 0.01 | 0.08 | 0.03 | 0.02 | 0.01 |
| Subsequently | ||||||||
| Mean | 0.85 | 0.86a | 0.66 | 0.85a | 1.00 | 1.00b | 0.98 | 0.99a |
| SD | NR | 0.01 | NR | 0.01 | NR | 0.04 | NR | 0.01 |
FIGURE 16.
Utility associated with vertebral fracture used in the TA464 Health Technology Assessment report and that chosen from ICUROS.
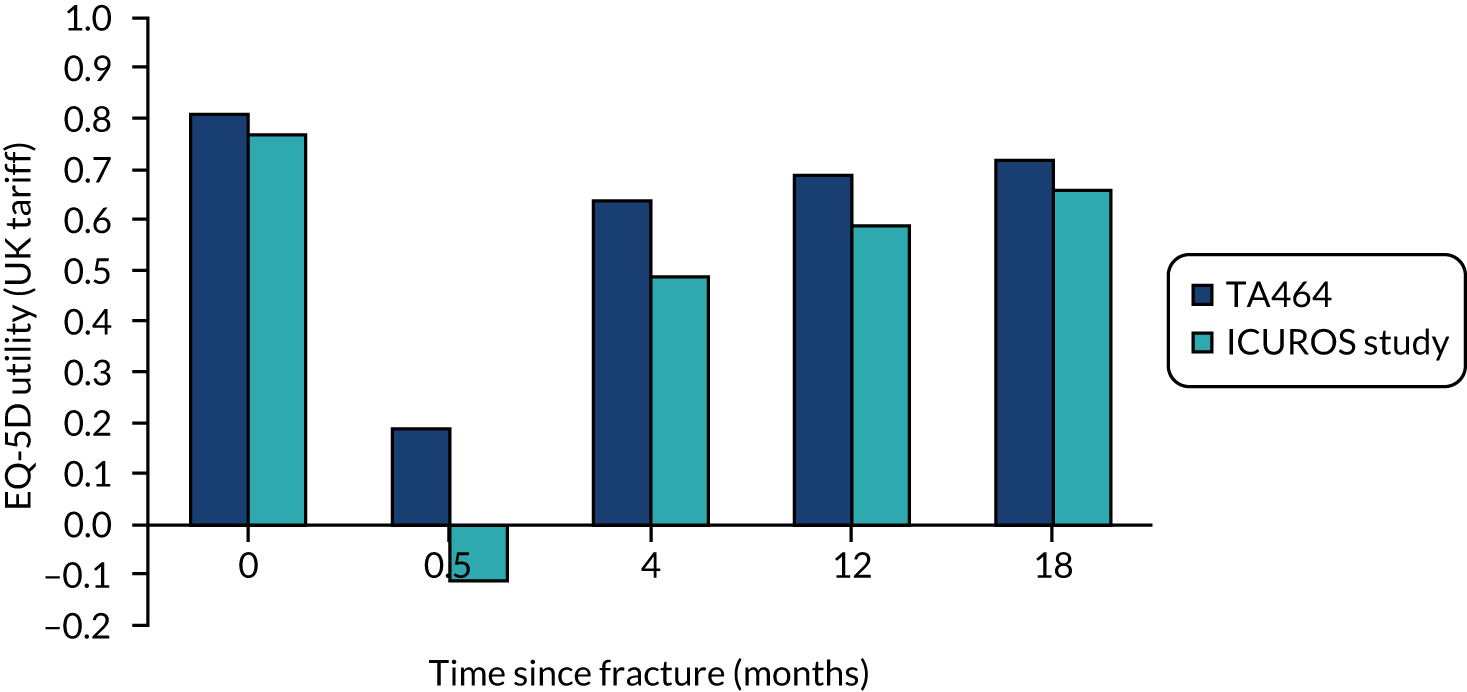
FIGURE 17.
Utility associated with hip fracture used in the TA464 Health Technology Assessment report and that chosen from ICUROS.
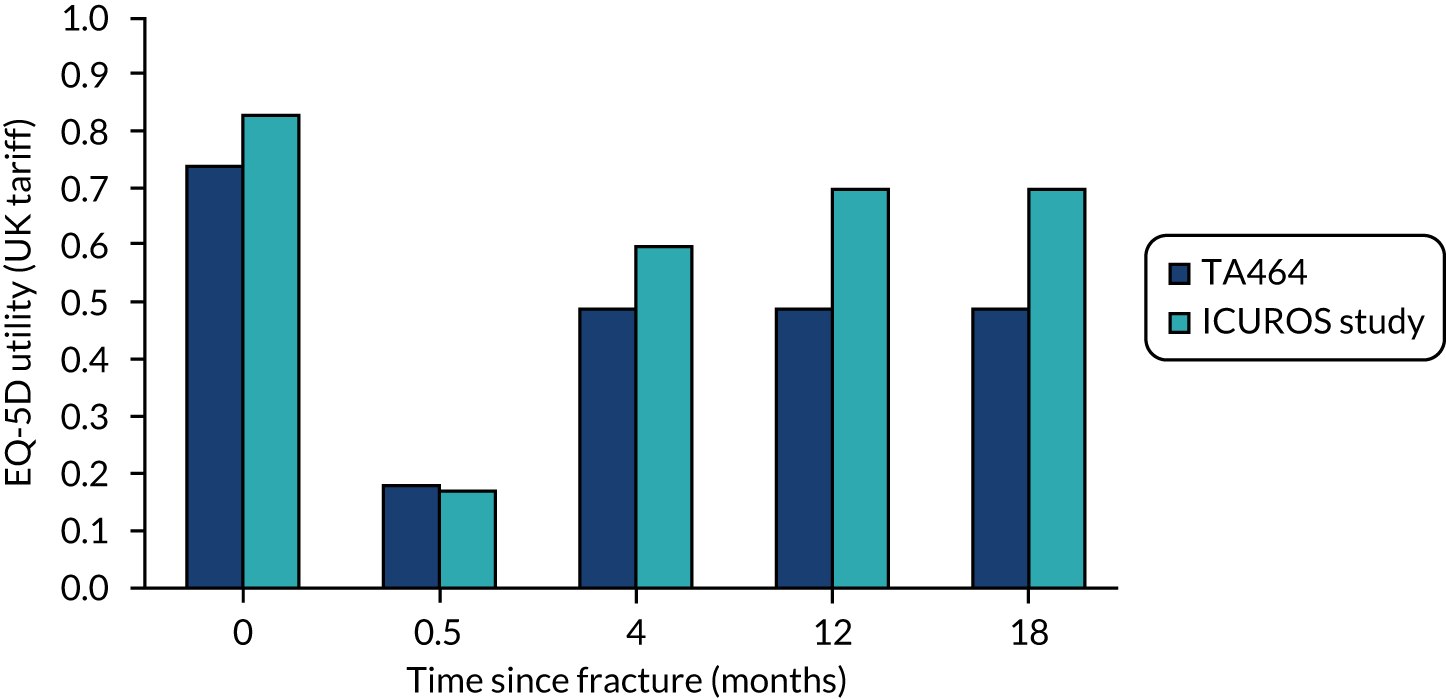
FIGURE 18.
Utility associated with distal forearm (wrist) fracture used in the TA464 Health Technology Assessment report and that chosen from ICUROS.
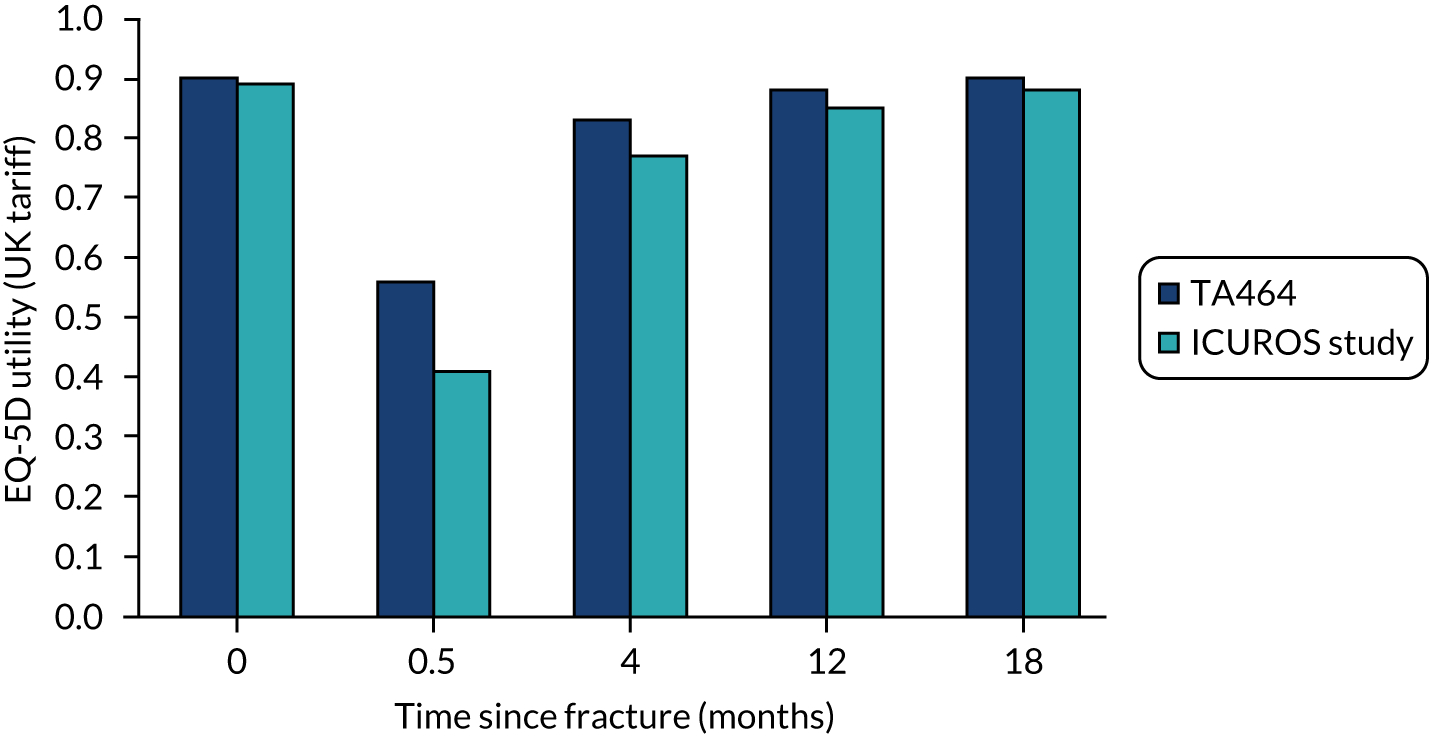
FIGURE 19.
Utility associated with humerus (shoulder) fracture used in the TA464 Health Technology Assessment report and that chosen from ICUROS.
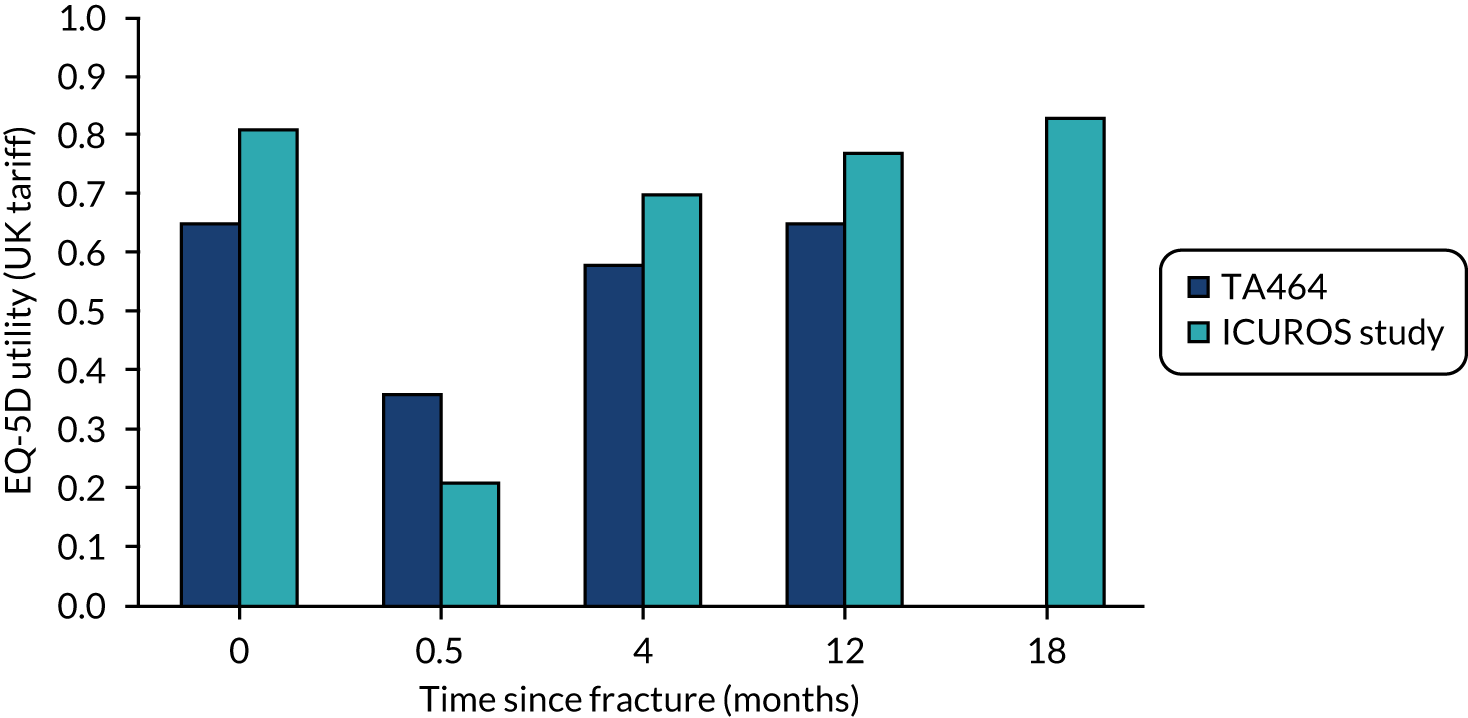
Appendix 17 Model validation methods
The model is designed to operate in several different modes, which facilitates debugging and validation. When running the model with fixed patient chacteristics, using determinisitic inputs and with random number control switched on, the model generates identical results each time it is run. This feature has been used to check that the model continues to operate in a consistent manner when any change is made to the VBA code that aims to restructure the code without altering the basic functioning of the model. The model can also be run in debug mode, whereby it outputs a detailed list of the events experienced and their individual times for each patient. This has been used extensively during model adaptations to check that the model is operating as intended. For example, it was used to check that the additional dummy events required for the new intervention lines were occurring at the correct times.
The code has been extensively commented, with any changes made since T464 identied by the date of change. When making alterations to the VBA code, the developer set up break points where any new code was implemented, allowing the model to be run quickly as far as the new code and then for the new code to be stepped through under observation to check that it behaves as intended. The locals window, within the VBA development environment, which allows the values of any object (variable, array, etc.) to be checked, was used to observe that the various arrays and variables had been filled with the intended data and to see changes to these variables when stepping through the code. The developer also used the immediate window to output specific variables at specific points in the code when trying to verify model behaviour. Error-handling was incorporated to ensure that inputs to functions were within their required ranges and to initiate message boxes describing errors identified and the values of inputs prior to the error.
To assess the face validity of the clinical outcomes predicted by model, the fractures prevented for each treatment (broken down into the four main fractures types) were graphed and compared with the absolute risk reduction for each fracture type multiplied by the ‘effective treatment duration’, which is dependent on both the time on treatment and the offset period (i.e. a drug with a 5-year treatment period and an additional 5-year offset period would have a 7.5-year effective treatment duration). This was done for the outcomes of both the PSA model and the version using mean parameter inputs.
Table 49 lists the main changes to the model made since TA464 and the methods used to validate each adapatation.
| Description of adaptation needed | Description of key changes to model | Validation method |
|---|---|---|
| Increase the number of treatment strategies that can be modelled | The model was already set up to pull in drug-specific inputs as arrays. These arrays were extended to allow for up to 15 lines of treatment to be modelled, with 11 being used in the final analysis (no treatment, nine interventions, with two needed to capture the ROMO/ALN sequence) | The structural changes to the VBA code required to incorporate additional intervention lines were made without any changes to model inputs, allowing outputs to be compared with the TA464 version of the model. New outputs were incoporated only once the model was verified to be equivalent for the additional intervention lines |
| Model inputs for interventions 6–10 and 11–15 were set equal to inputs for interventions 1–5. Model was run in debug mode and patient-level results were checked to ensure that identical outputs were being generated for intervention lines with identical inputs | ||
| Allow for drug-specific offset periods | In the TA464 version, the offset period was twice the treatment period for all drugs except ZOL and specific VBA code was used to adjust the offset period for ZOL. In the revised model, an array of offset inputs were pulled into the model, allowing a unique offset period for each drug | Results were run (with the model set up to produce reproducible outputs) before and after the code for handling the offset period was altered and the outputs were compared |
| Allow for sequences of treatments to be modelled | Two additional input arrays were added: one that says whether or not a treatment switch should occur and one that says which intervention should be swiched to. VBA code for processing the end of treatment event was adapated to reset the treatment period and offset period to the second drug in the sequence. VBA code was adapted to differentiate between the treatment sequence being modelled (drug_index_int) and the current drug, which changes after the swich (person_curr_drug). Costs, efficacy and AEs were made dependent on person_curr_drug | Intervention 6 was set up to have same outcomes as intervention 1, but to achieve this through a treatment switch to intervention 11. To do this, intervention 6 was set to have half the treatment duration of intervention 1, but to switch to intervention 11 on completion. Intervention 11 was set to have half the treatment duration of intervention 1 but the same offset period (as it is the second drug in the sequence that determines the offset period). Costs for intervention 6 and intervention 11 were set equal to the cost for intervention 1 |
| The model was run in debug mode to check that outputs for intervention 6 were identical to outputs for intervention 1 | ||
| Allow resource use for monitoring and administration to be specified for each drug | In TA464, no monitoring costs were included and administration costs were included only for i.v. IBN and i.v. ZOL. Total intervention costs per annum were handled as a single variable. In the revised model, separate arrays are specified for drug costs, resource use and unit costs | Adapatations were made to incorporate the new arrays. The model was run and code was stepped through, with break points placed on the revised code to check that it was performing as expected |
| The model was run in debug mode and patient-level outputs were checked to see if the total undiscounted costs matched the total treatment costs (i.e. drug, administration and monitoring) expected for patients experiencing no fracture events | ||
| Additional inputs required for non-bisphosphonates and new inputs for bisphosphonates | The main changes were to drug costs, efficacy inputs, treatment persistence, teatment offset periods, resource use for administration and monitoring, costs and QALY adjustments for AEs (VTE, ONJ and cellulitis) and post-fracture costs and utilities | Cells that had inputs updated from TA464 were highlighted in orange and were double-checked against the values described in final report |
| Cells that were not marked as changed were double-checked against the model used in TA464 |
Appendix 18 Summary clinical outcomes when using FRAX
| Number of adverse clinical outcomes avoided per 100,000 patients treated, when compared with no treatment | Total life-years gained per patient vs. no treatment | |||||||
|---|---|---|---|---|---|---|---|---|
| Total fractures | Hip fracture | Vertebral fracture | Proximal humerus fracture | Wrist fracture | Nursing home/residential care admission | Fatal fracture | ||
| When using FRAX to estimate risk of fracture | ||||||||
| ALN | 988 | 201 | 245 | 138 | 405 | 33 | 30 | 0.0026 |
| RIS | 1047 | 191 | 239 | 154 | 464 | 33 | 32 | 0.0026 |
| Oral IBN | 847 | 182 | 243 | 107 | 315 | 30 | 30 | 0.0027 |
| i.v. IBN | 419 | 115 | 162 | 38 | 103 | 20 | 18 | 0.0015 |
| ZOL | 1787 | 333 | 467 | 254 | 733 | 53 | 54 | 0.0048 |
| RLX | 336 | –11 | 164 | 95 | 88 | 20 | –35 | –0.0029 |
| DEN | 1611 | 407 | 587 | 212 | 404 | 89 | 29 | 0.0023 |
| TPTD | 1857 | 390 | 414 | 269 | 784 | 64 | 59 | 0.0052 |
| ROMO/ALN | 2589 | 553 | 549 | 400 | 1088 | 106 | 89 | 0.0062 |
Appendix 19 Base-case results from the probabilistic sensitivity analysis for QFracture
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| No treatment | 683 | 16.6049 | 0 | – | 0 | 0 | 0 | |
| ALN | 777 | 16.6050 | 94 | 0.0001 | 675,004 | –91 | –90 | £675,004 |
| RIS | 778 | 16.6050 | 94 | 0.0001 | 829,832 | –92 | –91 | Dominated |
| RLX | 778 | 16.6032 | 95 | –0.0016 | –58,385 | –127 | –143 | Dominated |
| IBN (oral) | 781 | 16.6050 | 97 | 0.0001 | 948,571 | –95 | –94 | Dominated |
| ZOL | 1403 | 16.6048 | 720 | –0.0001 | –9,181,178 | –721 | –722 | Dominated |
| IBN (i.v.) | 1541 | 16.6044 | 858 | –0.0005 | –1,784,152 | –867 | –872 | Dominated |
| DEN | 2454 | 16.6059 | 1770 | 0.0010 | 1,794,421 | –1750 | –1741 | Extendedly dominated |
| ROMO/ALN | Confidential information has been removed | 16.6071 | Confidential information has been removed | 0.0022 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 6502 | 16.6055 | 5819 | 0.0007 | 8,610,782 | –5805 | –5798 | Dominated |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| No treatment | 1152 | 15.3523 | 0 | – | 0 | 0 | 0 | |
| RIS | 1243 | 15.3525 | 91 | 0.0003 | 319,027 | –85 | –82 | Extendedly dominated |
| ALN | 1243 | 15.3526 | 91 | 0.0003 | 290,229 | –85 | –82 | 290,229 |
| IBN (oral) | 1246 | 15.3526 | 94 | 0.0003 | 301,165 | –88 | –85 | Extendedly dominated |
| RLX | 1297 | 15.3507 | 145 | –0.0015 | –96,336 | –175 | –190 | Dominated |
| ZOL | 1864 | 15.3525 | 713 | 0.0002 | 2,984,339 | –708 | –705 | Dominated |
| IBN (i.v.) | 2009 | 15.3518 | 857 | –0.0004 | –1,958,289 | –866 | –870 | Dominated |
| DEN | 2961 | 15.3539 | 1809 | 0.0017 | 1,092,301 | –1776 | –1760 | 1,279,494 |
| ROMO/ALN | Confidential information has been removed | 15.3539 | Confidential information has been removed | 0.0016 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 6961 | 15.3532 | 5809 | 0.0010 | 5,871,874 | –5790 | –5780 | Dominated |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| No treatment | 2260 | 14.0458 | 0 | – | 0 | 0 | 0 | |
| RIS | 2349 | 14.0465 | 89 | 0.0007 | 129,889 | –75 | –68 | Extendedly dominated |
| ALN | 2349 | 14.0465 | 89 | 0.0007 | 125,805 | –75 | –67 | Extendedly dominated |
| IBN (oral) | 2352 | 14.0466 | 92 | 0.0008 | 119,370 | –77 | –69 | £119,370 |
| RLX | 2378 | 14.0436 | 118 | –0.0023 | –52,066 | –163 | –186 | Dominated |
| ZOL | 2968 | 14.0467 | 707 | 0.0009 | 808,583 | –690 | –681 | Extendedly dominated |
| IBN (i.v.) | 3113 | 14.0457 | 853 | –0.0002 | –5,378,179 | –856 | –858 | Dominated |
| DEN | 4041 | 14.0468 | 1781 | 0.0010 | 1,868,896 | –1762 | –1752 | Extendedly dominated |
| ROMO/ALN | Confidential information has been removed | 14.0475 | Confidential information has been removed | 0.0017 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 8059 | 14.0474 | 5799 | 0.0016 | 3,731,997 | –5768 | –5752 | Dominated |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| No treatment | 2722 | 12.6966 | 0 | – | 0 | 0 | 0 | |
| ALN | 2804 | 12.6973 | 82 | 0.0007 | 126,025 | –69 | –63 | Extendedly dominated |
| RIS | 2804 | 12.6974 | 83 | 0.0008 | 100,618 | –66 | –58 | £100,618 |
| IBN (oral) | 2813 | 12.6973 | 91 | 0.0007 | 137,375 | –78 | –71 | Dominated |
| RLX | 2847 | 12.6952 | 126 | –0.0014 | –91,201 | –153 | –167 | Dominated |
| ZOL | 3421 | 12.6976 | 699 | 0.0010 | 723,860 | –680 | –670 | Extendedly dominated |
| IBN (i.v.) | 3572 | 12.6964 | 850 | –0.0002 | –4,066,084 | –854 | –856 | Dominated |
| DEN | 4487 | 12.6994 | 1766 | 0.0028 | 632,830 | –1710 | –1682 | £855,463 |
| ROMO/ALN | Confidential information has been removed | 12.7002 | Confidential information has been removed | 0.0036 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 8497 | 12.6985 | 5776 | 0.0019 | 3,083,847 | –5738 | –5720 | Dominated |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| No treatment | 2936 | 11.6723 | 0 | – | 0 | 0 | 0 | |
| ALN | 3016 | 11.6734 | 80 | 0.0010 | 77,059 | –59 | –49 | £77,059 |
| RIS | 3019 | 11.6733 | 82 | 0.0010 | 81,404 | –62 | –52 | Dominated |
| IBN (oral) | 3021 | 11.6732 | 84 | 0.000 | 93,736 | –66 | –57 | Dominated |
| RLX | 3067 | 11.6712 | 130 | –0.0011 | –118,232 | –153 | –164 | Dominated |
| ZOL | 3625 | 11.6739 | 688 | 0.0016 | 442,296 | –657 | –642 | Extendedly dominated |
| IBN (i.v.) | 3784 | 11.6722 | 848 | –0.0001 | –11,357,805 | –849 | –850 | Dominated |
| DEN | 4695 | 11.6757 | 1759 | 0.0034 | 523,142 | –1692 | –1658 | £721,645 |
| ROMO/ALN | Confidential information has been removed | 11.6763 | Confidential information has been removed | 0.0040 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 8695 | 11.6748 | 5759 | 0.0024 | 2,356,350 | –5710 | –5686 | Dominated |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| No treatment | 3064 | 10.6107 | 0 | – | 0 | 0 | 0 | |
| ALN | 3142 | 10.6119 | 78 | 0.0012 | 65,281 | –54 | –42 | Dominated |
| RIS | 3143 | 10.6119 | 79 | 0.0012 | 64,979 | –55 | –42 | £64,979 |
| IBN (oral) | 3147 | 10.6119 | 83 | 0.0012 | 68,805 | –59 | –47 | Dominated |
| RLX | 3164 | 10.6095 | 100 | –0.0012 | –83,809 | –124 | –136 | Dominated |
| ZOL | 3753 | 10.6126 | 689 | 0.0019 | 353,780 | –650 | –631 | Extendedly dominated |
| IBN (i.v.) | 3908 | 10.6109 | 843 | 0.0002 | 4,373,315 | –840 | –838 | Dominated |
| DEN | 4774 | 10.6141 | 1710 | 0.0034 | 502,655 | –1642 | –1608 | £745,595 |
| ROMO/ALN | Confidential information has been removed | 10.6150 | Confidential information has been removed | 0.0043 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 8798 | 10.6136 | 5733 | 0.0029 | 1,964,475 | –5675 | –5646 | Dominated |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| No treatment | 3277 | 9.5502 | 0 | – | 0 | 0 | 0 | |
| ALN | 3339 | 9.5522 | 62 | 0.0020 | 30,452 | –21 | –1 | £30,452 |
| RIS | 3340 | 9.5521 | 63 | 0.0020 | 32,482 | –24 | –5 | Dominated |
| IBN (oral) | 3345 | 9.5521 | 68 | 0.0020 | 34,713 | –29 | –9 | Dominated |
| RLX | 3448 | 9.5476 | 171 | –0.0026 | –65,412 | –223 | –249 | Dominated |
| ZOL | 3933 | 9.5533 | 656 | 0.0031 | 210,441 | –594 | –562 | £552,756 |
| IBN (i.v.) | 4109 | 9.5509 | 832 | 0.0007 | 1,250,818 | –819 | –812 | Dominated |
| DEN | 5009 | 9.5539 | 1733 | 0.0037 | 462,072 | –1658 | –1620 | Extendedly dominated |
| ROMO/ALN | Confidential information has been removed | 9.5562 | Confidential information has been removed | 0.0060 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 8954 | 9.5544 | 5677 | 0.0042 | 1,366,400 | –5594 | –5553 | Dominated |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| No treatment | 3958 | 8.4539 | 0 | – | 0 | 0 | 0 | |
| ALN | 4001 | 8.4568 | 43 | 0.0029 | 14,820 | 15 | 44 | £14,820 |
| RIS | 4007 | 8.4568 | 48 | 0.0028 | 17,119 | 8 | 36 | Dominated |
| IBN (oral) | 4021 | 8.4568 | 63 | 0.0029 | 21,840 | –5 | 23 | Extendedly dominated |
| RLX | 4081 | 8.4531 | 123 | –0.0008 | –146,142 | –139 | –148 | Dominated |
| ZOL | 4591 | 8.4589 | 633 | 0.0050 | 127,491 | –534 | –484 | £273,143 |
| IBN (i.v.) | 4784 | 8.4554 | 826 | 0.0015 | 564,407 | –796 | –782 | Dominated |
| DEN | 5613 | 8.4605 | 1655 | 0.0066 | 250,729 | –1523 | –1457 | £625,518 |
| ROMO/ALN | Confidential information has been removed | 8.4637 | Confidential information has been removed | 0.0098 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPT | 9593 | 8.4597 | 5635 | 0.0058 | 971,695 | –5519 | –5461 | Dominated |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| No treatment | 6197 | 6.6409 | 0 | – | 0 | 0 | 0 | |
| ALN | 6221 | 6.6451 | 24 | 0.0042 | 5622 | 60 | 102 | £5622 |
| RIS | 6227 | 6.6450 | 30 | 0.0041 | 7235 | 53 | 94 | Dominated |
| IBN (oral) | 6234 | 6.6448 | 37 | 0.0039 | 9443 | 41 | 80 | Dominated |
| RLX | 6308 | 6.6391 | 110 | –0.0017 | –63,265 | –145 | –163 | Dominated |
| ZOL | 6794 | 6.6472 | 597 | 0.0064 | 93,903 | –470 | –406 | £266,114 |
| IBN (i.v.) | 6998 | 6.6429 | 801 | 0.0020 | 398,475 | –761 | –741 | Dominated |
| DEN | 7730 | 6.6501 | 1533 | 0.0092 | 166,441 | –1349 | –1257 | £327,719 |
| ROMO/ALN | Confidential information has been removed | 6.6513 | Confidential information has been removed | 0.0105 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 11,717 | 6.6491 | 5520 | 0.0082 | 671,001 | –5355 | –5273 | Dominated |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| ALN | 13,370 | 4.0837 | –51 | 0.0058 | –8820 | 167 | 225 | |
| RIS | 13,384 | 4.0833 | –37 | 0.0054 | –6896 | 144 | 197 | Dominated |
| IBN (oral) | 13,393 | 4.0831 | –28 | 0.0051 | –5417 | 130 | 181 | Dominated |
| No treatment | 13,421 | 4.0779 | 0 | – | 0 | 0 | 0 | Dominated |
| RLX | 13,524 | 4.0760 | 103 | –0.0019 | –53,780 | –141 | –160 | Dominated |
| ZOL | 13,897 | 4.0858 | 477 | 0.0079 | 60,300 | –318 | –239 | £250,205 |
| IBN (i.v.) | 14,165 | 4.0807 | 744 | 0.0028 | 266,492 | –689 | –661 | Dominated |
| DEN | 14,768 | 4.0886 | 1347 | 0.0107 | 126,392 | –1134 | –1028 | £315,774 |
| ROMO/ALN | Confidential information has been removed | 4.0919 | Confidential information has been removed | 0.0140 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 18,604 | 4.0893 | 5183 | 0.0113 | 457,894 | –4957 | –4844 | Dominated |
Appendix 20 Base-case results from the probabilistic sensitivity analysis for FRAX
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| No treatment | 4241 | 13.6665 | 0 | – | 0 | 0 | 0 | |
| RIS | 4315 | 13.6687 | 73 | 0.0023 | 32,429 | –28 | –5 | Extendedly dominated |
| ALN | 4315 | 13.6690 | 73 | 0.0026 | 28,541 | –22 | 4 | £28,541 |
| IBN (oral) | 4319 | 13.6687 | 78 | 0.0023 | 34,519 | –33 | –10 | Dominated |
| RLX | 4350 | 13.6641 | 109 | –0.0023 | –47,105 | –156 | –179 | Dominated |
| ZOL | 4926 | 13.6705 | 685 | 0.0040 | 170,998 | –605 | –565 | £427,431 |
| IBN (i.v.) | 5088 | 13.6671 | 846 | 0.0007 | 1,214,068 | –832 | –825 | Dominated |
| DEN | 5981 | 13.6708 | 1740 | 0.0044 | 398,751 | –1653 | –1609 | Extendedly dominated |
| ROMO/ALN | Confidential information has been removed | 13.6726 | Confidential information has been removed | 0.0061 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 10,011 | 13.6711 | 5770 | 0.0046 | 1,254,448 | –5678 | –5632 | Dominated |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| No treatment | 4487 | 13.6230 | 0 | – | 0 | 0 | 0 | |
| RLX | 4524 | 13.6228 | 37 | –0.0002 | –199,169 | –41 | –43 | Dominated |
| RIS | 4555 | 13.6255 | 68 | 0.0025 | 27,654 | –19 | 6 | Extendedly dominated |
| ALN | 4556 | 13.6256 | 69 | 0.0025 | 27,325 | –19 | 7 | £27,325 |
| IBN (oral) | 4557 | 13.6256 | 70 | 0.0026 | 27,349 | –19 | 7 | £28,946 |
| ZOL | 5151 | 13.6276 | 664 | 0.0046 | 145,587 | –572 | –527 | £297,575 |
| IBN (i.v.) | 5331 | 13.6240 | 844 | 0.0010 | 853,480 | –825 | –815 | Dominated |
| DEN | 6159 | 13.6297 | 1672 | 0.0067 | 250,782 | –1539 | –1472 | £478,086 |
| ROMO/ALN | Confidential information has been removed | 13.6320 | Confidential information has been removed | 0.0090 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 10,236 | 13.6282 | 5749 | 0.0052 | 1,115,769 | –5646 | –5595 | Dominated |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost | QALY | |||||
| No treatment | 4976 | 13.8999 | 0 | – | 0 | 0 | 0 | |
| RIS | 5033 | 13.9035 | 57 | 0.0037 | 15,575 | 16 | 53 | £15,575 |
| ALN | 5037 | 13.9035 | 61 | 0.0037 | 16,808 | 12 | 48 | Dominated |
| IBN (oral) | 5039 | 13.9034 | 63 | 0.0035 | 17,728 | 8 | 43 | Dominated |
| RLX | 5045 | 13.8992 | 69 | –0.0007 | –105,444 | –83 | –89 | Dominated |
| ZOL | 5635 | 13.9058 | 659 | 0.0059 | 110,846 | –540 | –481 | £263,566 |
| IBN (i.v.) | 5810 | 13.9017 | 834 | 0.0019 | 443,563 | –797 | –778 | Dominated |
| DEN | 6636 | 13.9084 | 1660 | 0.0085 | 195,106 | –1489 | –1404 | £390,788 |
| ROMO/ALN | Confidential information has been removed | 13.9117 | Confidential information has been removed | 0.0118 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 10,708 | 13.9067 | 5732 | 0.0069 | 832,835 | –5594 | –5526 | Dominated |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| No treatment | 5465 | 14.2478 | 0 | – | 0 | 0 | 0 | |
| ALN | 5521 | 14.2515 | 56 | 0.0036 | 15,524 | 16 | 53 | £15,524 |
| IBN (oral) | 5524 | 14.2514 | 59 | 0.0036 | 16,459 | 13 | 49 | Dominated |
| RIS | 5525 | 14.2513 | 60 | 0.0035 | 17,389 | 9 | 44 | Dominated |
| RLX | 5558 | 14.2458 | 94 | –0.0020 | –47,071 | –133 | –153 | Dominated |
| ZOL | 6116 | 14.2546 | 651 | 0.0068 | 96,012 | –516 | –448 | £189,147 |
| IBN (i.v.) | 6295 | 14.2497 | 831 | 0.0019 | 430,771 | –792 | –773 | Dominated |
| DEN | 7152 | 14.2555 | 1687 | 0.0076 | 220,601 | –1534 | –1458 | £1,197,064 |
| ROMO/ALN | Confidential information has been removed | 14.2569 | Confidential information has been removed | 0.0091 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 11,185 | 14.2555 | 5720 | 0.0077 | 745,024 | –5567 | –5490 | Dominated |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| No treatment | 5792 | 12.8154 | 0 | – | 0 | 0 | 0 | |
| ALN | 5845 | 12.8201 | 54 | 0.0047 | 11,362 | 41 | 88 | Extendedly dominated |
| RIS | 5846 | 12.8202 | 54 | 0.0048 | 11,265 | 42 | 90 | £11,265 |
| IBN (oral) | 5849 | 12.8200 | 57 | 0.0047 | 12,209 | 36 | 83 | Dominated |
| RLX | 5873 | 12.8144 | 81 | –0.0010 | –82,569 | –101 | –110 | Dominated |
| ZOL | 6435 | 12.8232 | 644 | 0.0078 | 82,355 | –487 | –409 | £194,815 |
| IBN (i.v.) | 6623 | 12.8178 | 831 | 0.0024 | 342,182 | –783 | –758 | Dominated |
| DEN | 7435 | 12.8243 | 1643 | 0.0089 | 184,386 | –1465 | –1375 | Extendedly dominated |
| ROMO/ALN | Confidential information has been removed | 12.8286 | Confidential information has been removed | 0.0132 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 11,479 | 12.8244 | 5687 | 0.0090 | 632,511 | –5507 | –5417 | Dominated |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| No treatment | 5868 | 11.0066 | 0 | – | 0 | 0 | 0 | |
| RIS | 5906 | 11.0111 | 39 | 0.0044 | 8736 | 50 | 95 | £8736 |
| ALN | 5910 | 11.0114 | 43 | 0.0048 | 8951 | 53 | 101 | £11,817 |
| IBN (oral) | 5922 | 11.0110 | 54 | 0.0044 | 12,389 | 33 | 77 | Dominated |
| RLX | 6012 | 11.0049 | 145 | –0.0018 | –82,686 | –180 | –197 | Dominated |
| ZOL | 6491 | 11.0142 | 623 | 0.0076 | 82,446 | –472 | –396 | £209,233 |
| IBN (i.v.) | 6692 | 11.0089 | 825 | 0.0023 | 362,332 | –779 | –756 | Dominated |
| DEN | 7557 | 11.0154 | 1690 | 0.0087 | 193,385 | –1515 | –1428 | Extendedly dominated |
| ROMO/ALN | Confidential information has been removed | 11.0208 | Confidential information has been removed | 0.0142 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 11,507 | 11.0157 | 5640 | 0.0091 | 622,664 | –5459 | –5368 | Dominated |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| No treatment | 5488 | 9.3617 | 0 | – | 0 | 0 | 0 | |
| ALN | 5508 | 9.3671 | 20 | 0.0054 | 3791 | 87 | 140 | £3,791 |
| RIS | 5511 | 9.3667 | 23 | 0.0050 | 4572 | 77 | 128 | Dominated |
| IBN (oral) | 5518 | 9.3667 | 30 | 0.0050 | 6035 | 70 | 120 | Dominated |
| RLX | 5584 | 9.3615 | 96 | –0.0002 | –455,927 | –100 | –102 | Dominated |
| ZOL | 6070 | 9.3709 | 582 | 0.0092 | 63,432 | –399 | –307 | £147,034 |
| IBN (i.v.) | 6301 | 9.3639 | 813 | 0.0022 | 367,423 | –769 | –747 | Dominated |
| DEN | 7082 | 9.3731 | 1594 | 0.0113 | 140,582 | –1367 | –1254 | Extendedly dominated |
| ROMO/ALN | Confidential information has been removed | 9.3788 | Confidential information has been removed | 0.0170 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 11,069 | 9.3720 | 5581 | 0.0103 | 542,248 | –5375 | –5272 | Dominated |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| ALN | 5754 | 8.1143 | –11 | 0.0066 | –1716 | 142 | 208 | |
| RIS | 5764 | 8.1143 | –2 | 0.0065 | –297 | 132 | 198 | Dominated |
| No treatment | 5766 | 8.1077 | 0 | – | 0 | 0 | 0 | Dominated |
| IBN (oral) | 5770 | 8.1141 | 5 | 0.0064 | 734 | 123 | 187 | Dominated |
| RLX | 5820 | 8.1087 | 54 | 0.0009 | 57,050 | –35 | –26 | Dominated |
| ZOL | 6308 | 8.1184 | 542 | 0.0106 | 51,057 | –330 | –224 | £136,054 |
| IBN (i.v.) | 6556 | 8.1114 | 790 | 0.0037 | 215,680 | –717 | –680 | Dominated |
| DEN | 7247 | 8.1233 | 1482 | 0.0156 | 95,158 | –1170 | –1014 | £189,738 |
| ROMO/ALN | Confidential information has been removed | 8.1266 | Confidential information has been removed | 0.0189 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 11,275 | 8.1203 | 5510 | 0.0125 | 439,478 | –5259 | –5133 | Dominated |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| ALN | 8078 | 7.0926 | –43 | 0.0082 | –5233 | 208 | 290 | |
| RIS | 8082 | 7.0923 | –39 | 0.0080 | –4904 | 200 | 280 | Dominated |
| IBN (oral) | 8085 | 7.0922 | –36 | 0.0079 | –4537 | 194 | 273 | Dominated |
| No treatment | 8121 | 7.0843 | 0 | – | 0 | 0 | 0 | Dominated |
| RLX | 8251 | 7.0837 | 130 | –0.0006 | –206,484 | –142 | –148 | Dominated |
| ZOL | 8615 | 7.0974 | 494 | 0.0131 | 37,737 | –232 | –101 | £110,826 |
| IBN (i.v.) | 8881 | 7.0890 | 760 | 0.0047 | 163,225 | –666 | –620 | Dominated |
| DEN | 9560 | 7.1004 | 1439 | 0.0161 | 89,300 | –1116 | –955 | £312,269 |
| ROMO/ALN | Confidential information has been removed | 7.1056 | Confidential information has been removed | 0.0213 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 13,523 | 7.1000 | 5402 | 0.0157 | 343,693 | –5088 | –4930 | Dominated |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| ALN | 13,031 | 4.7140 | –129 | 0.0110 | –11,748 | 348 | 458 | |
| RIS | 13,040 | 4.7134 | –120 | 0.0104 | –11,572 | 327 | 431 | Dominated |
| IBN (oral) | 13,048 | 4.7130 | –112 | 0.0100 | –11,122 | 312 | 413 | Dominated |
| No treatment | 13,160 | 4.7030 | 0 | – | 0 | 0 | 0 | Dominated |
| RLX | 13,276 | 4.7012 | 116 | –0.0018 | –63,139 | –153 | –172 | Dominated |
| ZOL | 13,487 | 4.7191 | 327 | 0.0161 | 20,257 | –4 | 157 | £88,002 |
| IBN (i.v.) | 13,853 | 4.7092 | 693 | 0.0062 | 111,944 | –569 | –507 | Dominated |
| DEN | 14,370 | 4.7236 | 1210 | 0.0206 | 58,730 | –798 | –592 | £197,979 |
| ROMO/ALN | Confidential information has been removed | 4.7303 | Confidential information has been removed | 0.0273 | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 18,252 | 4.7238 | 5092 | 0.0208 | 244,558 | –4676 | –4468 | Dominated |
Appendix 21 Sensitivity analyses for economic evaluation
Note that these sensitivity analyses are based on the model using mid-point parameter inputs, rather than the average outcomes across the PSA with the exception of Tables 74 and 75, which used 500,000 PSA samples but fixed patient characteristics.
| Drug | ICERs by risk decile (£) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | All | |
| Qfracture score (%) | 0.5 | 0.7 | 1.0 | 1.4 | 2.0 | 2.7 | 3.9 | 5.5 | 8.4 | 16.0 | NA |
| ALN | 498,737 | 412,005 | 157,211 | 149,958 | 68,492 | 44,834 | 37,197 | 16,884 | 745 | Dominates | 29,766 |
| RIS | 565,069 | 441,369 | 160,348 | 158,750 | 69,748 | 47,388 | 38,372 | 16,920 | 2190 | Dominates | 31,628 |
| IBN (oral) | 463,164 | 427,947 | 156,817 | 144,798 | 70,576 | 46,196 | 37,906 | 17,487 | 837 | Dominates | 30,561 |
| IBN (i.v.) | Dominated | Dominated | Dominated | Dominated | 4,767,171 | 1,413,543 | 1,040,966 | 650,661 | 307,706 | 199,398 | 1,066,308 |
| ZOL | 241,951,112 | 21,001,049 | 1,200,415 | 870,723 | 469,207 | 308,198 | 227,473 | 133,550 | 79,528 | 58,085 | 233,405 |
| RLX | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated |
| DEN | 1,998,145 | 1,741,276 | 1,143,632 | 887,398 | 609,344 | 492,380 | 386,626 | 243,281 | 163,466 | 115,933 | 382,864 |
| TPTD | 7,503,596 | 6,096,105 | 4,057,889 | 3,088,025 | 2,244,920 | 1,700,544 | 1,405,530 | 910,295 | 608,736 | 453,776 | 1,361,877 |
| ROMO/ALN | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| FRAX score (%) | 3.1 | 4.3 | 5.0 | 5.6 | 6.2 | 7.3 | 8.8 | 10.7 | 14.9 | 25.1 | NA |
| ALN | 24,918 | 22,192 | 15,189 | 16,287 | 10,585 | 3769 | 1096 | Dominates | Dominates | Dominates | 1350 |
| RIS | 25,690 | 22,982 | 15,820 | 17,515 | 10,337 | 3911 | 1349 | Dominates | Dominates | Dominates | 1814 |
| IBN (oral) | 25,107 | 23,022 | 15,393 | 16,536 | 11,305 | 3733 | 1713 | Dominates | Dominates | Dominates | 1756 |
| IBN (i.v.) | 671,930 | 761,291 | 455,094 | 398,749 | 365,350 | 261,759 | 262,550 | 184,121 | 140,596 | 82,567 | 248,478 |
| ZOL | 152,696 | 146,559 | 111,458 | 96,479 | 78,835 | 66,241 | 57,551 | 48,346 | 33,954 | 18,654 | 63,969 |
| RLX | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | 18,508,020 | 158,275 | 115,977 | 56,599 | Dominated |
| DEN | 325,050 | 281,011 | 205,252 | 190,057 | 166,993 | 147,494 | 130,881 | 106,085 | 81,500 | 52,679 | 137,302 |
| TPTD | 1,123,470 | 983,834 | 869,760 | 767,917 | 670,930 | 601,318 | 482,831 | 444,825 | 330,544 | 232,180 | 532,666 |
| ROMO/ALN | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| Drug | ICERs by risk decile (£) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | All | |
| Qfracture score (%) | 0.5 | 0.7 | 1.0 | 1.4 | 2.0 | 2.7 | 3.9 | 5.5 | 8.4 | 16.0 | NA |
| ALN | 251,941 | 168,092 | 119,902 | 79,284 | 60,970 | 31,766 | 21,485 | 10,432 | 932 | Dominates | 24,274 |
| RIS | 268,409 | 173,111 | 121,180 | 81,223 | 62,848 | 33,001 | 22,356 | 11,356 | 1273 | Dominates | 25,717 |
| IBN (oral) | 249,462 | 167,996 | 116,962 | 80,518 | 62,242 | 32,880 | 21,962 | 10,972 | 1310 | Dominates | 25,052 |
| IBN (i.v.) | 6,829,412 | 3,436,012 | 2,239,222 | 1,466,327 | 1,139,102 | 652,143 | 477,492 | 326,477 | 231,761 | 173,580 | 568,098 |
| ZOL | 1,872,105 | 1,080,025 | 721,322 | 481,417 | 368,038 | 222,443 | 160,376 | 110,764 | 74,556 | 54,055 | 191,981 |
| RLX | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated |
| DEN | 1,961,321 | 1,264,758 | 1,002,128 | 693,856 | 526,207 | 357,560 | 265,653 | 186,577 | 128,911 | 94,665 | 322,714 |
| TPTD | 7,552,870 | 5,127,678 | 4,294,267 | 2,966,878 | 2,601,782 | 1,717,937 | 1,230,354 | 814,753 | 600,894 | 406,640 | 1,288,454 |
| ROMO/ALN | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| FRAX score (%) | 3.1 | 4.3 | 5.0 | 5.6 | 6.2 | 7.3 | 8.8 | 10.7 | 14.9 | 25.1 | NA |
| ALN | 20,826 | 13,265 | 10,205 | 8667 | 7096 | 4570 | Dominates | Dominates | Dominates | Dominates | 629 |
| RIS | 21,225 | 13,435 | 10,374 | 9194 | 7051 | 4739 | Dominates | Dominates | Dominates | Dominates | 1061 |
| IBN (oral) | 21,651 | 13,923 | 10,577 | 9059 | 7570 | 5066 | 26 | Dominates | Dominates | Dominates | 1060 |
| IBN (i.v.) | 424,242 | 313,920 | 269,844 | 243,798 | 238,418 | 216,521 | 174,715 | 133,701 | 114,229 | 84,510 | 187,936 |
| ZOL | 134,229 | 99,921 | 85,457 | 75,996 | 71,730 | 65,020 | 51,386 | 39,131 | 32,428 | 20,158 | 57,147 |
| RLX | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | 697,741 | 196,074 | 107,583 | Dominated |
| DEN | 243,364 | 184,578 | 159,477 | 141,243 | 137,427 | 120,484 | 97,963 | 77,542 | 63,636 | 42,333 | 109,566 |
| TPTD | 1,059,530 | 914,573 | 769,066 | 691,834 | 637,242 | 550,881 | 495,976 | 388,142 | 323,503 | 230,761 | 505,256 |
| ROMO/ALN | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| Drug | ICERs by risk decile (£) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | All | |
| Qfracture score (%) | 0.5 | 0.7 | 1.0 | 1.4 | 2.0 | 2.7 | 3.9 | 5.5 | 8.4 | 16.0 | NA |
| ALN | 799,955 | 486,510 | 172,280 | 106,937 | 85,656 | 59,255 | 27,980 | 12,480 | 5185 | Dominates | 31,647 |
| RIS | 799,955 | 486,510 | 172,280 | 106,937 | 85,656 | 59,255 | 27,980 | 12,480 | 5185 | Dominates | 31,647 |
| IBN (oral) | 826,668 | 502,375 | 178,069 | 110,735 | 88,733 | 61,464 | 29,355 | 13,378 | 5907 | Dominates | 33,205 |
| IBN (i.v.) | Dominated | Dominated | Dominated | Dominated | 7,531,872 | 2,733,301 | 981,482 | 435,481 | 360,520 | 206,403 | 1,086,629 |
| ZOL | Dominated | 10,002,667 | 1,313,565 | 794,622 | 556,859 | 336,315 | 196,111 | 130,628 | 100,210 | 62,599 | 248,980 |
| RLX | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated |
| DEN | 2,346,041 | 1,613,668 | 1,005,637 | 823,644 | 638,855 | 487,738 | 330,852 | 227,692 | 185,220 | 122,045 | 383,999 |
| TPTD | 8,161,900 | 5,841,080 | 4,235,494 | 3,154,275 | 2,175,649 | 1,968,959 | 1,205,259 | 885,276 | 714,965 | 481,048 | 1,415,644 |
| ROMO/ALN | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| FRAX score (%) | 3.1 | 4.3 | 5.0 | 5.6 | 6.2 | 7.3 | 8.8 | 10.7 | 14.9 | 25.1 | NA |
| ALN | 27,834 | 19,286 | 16,881 | 14,023 | 10,907 | 4553 | 1530 | Dominates | Dominates | Dominates | 2591 |
| RIS | 27,834 | 19,286 | 16,881 | 14,023 | 10,907 | 4553 | 1530 | Dominates | Dominates | Dominates | 2591 |
| IBN (oral) | 28,967 | 20,169 | 17,695 | 14,715 | 11,600 | 5160 | 2044 | Dominates | Dominates | Dominates | 3131 |
| IBN (i.v.) | 616,244 | 408,882 | 418,532 | 337,957 | 325,277 | 287,300 | 226,977 | 183,012 | 142,975 | 97,801 | 240,853 |
| ZOL | 178,326 | 130,666 | 122,750 | 96,355 | 106,623 | 78,832 | 63,178 | 54,261 | 38,658 | 24,279 | 72,230 |
| RLX | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | 115,828 | 80,087 | Dominated |
| DEN | 321,955 | 245,827 | 211,101 | 175,962 | 177,597 | 153,423 | 127,213 | 109,102 | 83,514 | 56,914 | 138,658 |
| TPTD | 1,187,281 | 940,410 | 859,389 | 720,901 | 666,582 | 583,940 | 499,370 | 437,612 | 348,992 | 252,450 | 541,645 |
| ROMO/ALN | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| ALN | 7476 | 6.6254 | –235 | 0.0199 | –11,804 | 634 | 834 | |
| RIS | 7479 | 6.6248 | –232 | 0.0193 | –12,014 | 618 | 811 | Dominated |
| IBN (oral) | 7509 | 6.6242 | –202 | 0.0187 | –10,776 | 576 | 764 | Dominated |
| No treatment | 7711 | 6.6055 | 0 | – | 0 | 0 | 0 | Dominated |
| RLX | 7832 | 6.6067 | 121 | 0.0012 | 105,283 | –98 | –87 | Dominated |
| ZOL | 8001 | 6.6308 | 290 | 0.0253 | 11,427 | 217 | 471 | Extendedly dominated |
| IBN (i.v.) | 8329 | 6.6193 | 618 | 0.0138 | 44,785 | –342 | –204 | Dominated |
| DEN | 8491 | 6.6631 | 780 | 0.0576 | 13,544 | 372 | 948 | £26,977 |
| ROMO/ALN | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 12,820 | 6.6418 | 5109 | 0.0363 | 140,684 | –4383 | –4020 | Dominated |
| Treatment strategy | Mean outcomes (discounted) | Incremental outcomes vs. no treatment (discounted) | ICER vs. no treatment (£) | Net benefit at £20,000 per QALY (£) | Net benefit at £30,000 per QALY (£) | Incremental analysisa | ||
|---|---|---|---|---|---|---|---|---|
| Cost (£) | QALY | Cost (£) | QALY | |||||
| ALN | 2782 | 6.8336 | –24 | 0.0071 | –3393 | 167 | 238 | |
| RIS | 2782 | 6.8335 | –24 | 0.0069 | –3463 | 163 | 233 | Dominated |
| IBN (oral) | 2794 | 6.8331 | –12 | 0.0065 | –1819 | 143 | 208 | Dominated |
| No treatment | 2806 | 6.8265 | 0 | – | 0 | 0 | 0 | Dominated |
| RLX | 2947 | 6.8256 | 141 | –0.0009 | –152,373 | –159 | –169 | Dominated |
| ZOL | 3387 | 6.8352 | 581 | 0.0087 | 66,928 | –407 | –321 | Extendedly dominated |
| IBN (i.v.) | 3577 | 6.8307 | 771 | 0.0042 | 183,707 | –687 | –645 | Dominated |
| DEN | 4205 | 6.8478 | 1399 | 0.0212 | 65,851 | –974 | –761 | £100,788 |
| ROMO/ALN | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| TPTD | 8315 | 6.8398 | 5509 | 0.0133 | 414,209 | –5243 | –5110 | Dominated |
| Drug | ICERs by risk decile (£) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | All | |
| Qfracture score (%) | 0.5 | 0.7 | 1.0 | 1.4 | 2.0 | 2.7 | 3.9 | 5.5 | 8.4 | 16.0 | NA |
| ALN | 667,007 | 344,843 | 154,562 | 158,993 | 79,839 | 96,437 | 32,481 | 16,709 | 9373 | Dominating | 37,101 |
| RIS | 833,648 | 378,035 | 155,152 | 176,091 | 87,929 | 98,283 | 33,908 | 19,143 | 9239 | Dominating | 39,904 |
| IBN (oral) | 613,050 | 300,939 | 153,457 | 165,724 | 80,313 | 98,014 | 33,897 | 17,620 | 10,028 | Dominating | 38,227 |
| IBN (i.v.) | Dominated | Dominated | Dominated | Dominated | 6,497,796 | Dominated | 984,778 | 539,348 | 428,815 | 189,330 | 1,167,465 |
| ZOL | Dominated | Dominated | 3,032,964 | 2,134,060 | 694,683 | 813,434 | 266,397 | 215,493 | 141,142 | 79,915 | 359,734 |
| RLX | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated | Dominated |
| DEN | 1,875,580 | 1,067,021 | 725,687 | 574,802 | 412,867 | 409,288 | 226,792 | 186,474 | 119,740 | 84,928 | 277,008 |
| TPTD | 7,103,236 | 5,463,987 | 4,344,868 | 4,130,127 | 2,585,616 | 2,577,445 | 1,336,591 | 1,136,165 | 771,301 | 499,965 | 1,581,013 |
| ROMO/ALN | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
| FRAX score (%) | 3.1 | 4.3 | 5.0 | 5.6 | 6.2 | 7.3 | 8.8 | 10.7 | 14.9 | 25.1 | NA |
| ALN | 43,692 | 29,116 | 20,888 | 16,881 | 14,815 | 10,289 | 6445 | 1671 | Dominating | Dominating | 5789 |
| RIS | 41,868 | 30,603 | 20,138 | 17,014 | 15,644 | 11,783 | 7082 | 2179 | Dominating | Dominating | 6585 |
| IBN (oral) | 43,872 | 29,515 | 21,422 | 17,188 | 15,311 | 10,602 | 7219 | 2062 | Dominating | Dominating | 6353 |
| IBN (i.v.) | 1,135,784 | 620,464 | 432,254 | 341,331 | 362,455 | 346,713 | 338,155 | 209,343 | 172,366 | 96,099 | 280,111 |
| ZOL | 292,309 | 212,340 | 171,060 | 135,810 | 139,460 | 124,920 | 113,027 | 81,472 | 62,310 | 33,641 | 106,395 |
| RLX | Dominated | Dominated | Dominated | 316,965 | Dominated | Dominated | Dominated | 450,493 | 132,412 | 50,539 | 11,272,491 |
| DEN | 228,836 | 180,468 | 152,041 | 132,978 | 126,706 | 114,716 | 105,110 | 74,266 | 59,072 | 38,160 | 101,453 |
| TPTD | 1,492,180 | 1,109,874 | 933,843 | 782,904 | 858,530 | 704,890 | 658,543 | 504,232 | 418,570 | 280,094 | 637,237 |
| ROMO/ALN | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed | Confidential information has been removed |
List of abbreviations
- ACTIVE
- Abaloparatide Comparator Trial In Vertebral Endpoints
- AE
- adverse event
- AG
- assessment group
- ALN
- alendronate
- ARCH
- active-controlled fracture study in postmenopausal women with osteoporosis at high risk
- BMD
- bone mineral density
- CG
- clinical guideline
- CHM
- Commission on Human Medicines
- CODA
- convergence diagnosis and output analysis
- CPRD
- Clinical Practice Research Datalink
- CRD
- Centre for Reviews and Dissemination
- CrI
- credible interval
- DATA
- Denosumab and Teriparatide Administration
- DEN
- denosumab
- DES
- discrete event simulation
- DIC
- deviance information criterion
- DIRECT
- Denosumab fracture Intervention RandomizEd placebo Controlled Trial
- DVT
- deep-vein thrombosis
- DXA
- dual-energy X-ray absorptiometry
- EQ-5D
- EuroQol-5 Dimensions
- EQ-VAS
- EuroQol – Visual Analogue Scale
- EUROFORS
- European Study of Forsteo
- EVA
- EVista Alendronate comparison
- ExFOS
- European Extended Forsteo Observational Study
- FLEX
- Fracture Intervention Trial Long-term Extension
- FPT
- Fracture Prevention Trial
- FRAME
- Fracture Study in Postmenopausal Women with Osteoporosis
- FREEDOM
- Fracture REduction Evaluation of Denosumab in Osteoporosis every 6 Months
- GI
- gastrointestinal
- GP
- general practitioner
- GPRD
- General Practice Research Database
- HES
- Hospital Episode Statistics
- HORIZON
- Health Outcomes and Reduced Incidence with Zoledronic Acid Once Yearly
- HR
- hazard ratio
- HRG
- Healthcare Resource Group
- HRQoL
- health-related quality of life
- ICUROS
- International Costs and Utilities Related to Osteoporotic Fractures Study
- IBN
- ibandronate
- ICER
- incremental cost-effectiveness ratio
- INMB
- incremental net monetary benefit
- i.v.
- intravenous
- LOCF
- last observation carried forward
- MD
- mean difference
- MHRA
- Medicines and Healthcare products Regulatory Agency
- mITT
- modified intent to treat
- MTA
- multiple technology appraisal
- NICE
- National Institute for Health and Care Excellence
- NMA
- network meta-analysis
- NOGG
- National Osteoporosis Guideline Group
- ONJ
- osteonecrosis of the jaw
- PAS
- Patient Access Scheme
- PB
- probability of being the best-ranking treatment
- PE
- pulmonary embolism
- PrI
- prediction interval
- PRISMA
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PSA
- probabilistic sensitivity analysis
- PSS
- Personal Social Services
- PSSRU
- Personal Social Services Research Unit
- QALY
- quality-adjusted life-year
- QS
- quality standard
- QUALEFFO-41
- Quality of Life Questionnaire of the European Foundation for Osteoporosis-41 items
- RCT
- randomised controlled trial
- RevMan
- Review Manager
- RIS
- risedronate
- RLX
- raloxifene
- ROMO
- romosozumab
- RR
- risk ratio
- SA
- sensitivity analysis
- SAE
- serious adverse event
- s.c.
- subcutaneous
- ScHARR
- School of Health and Related Research
- SD
- standard deviation
- SmPC
- Summary of Product Characteristics
- TA
- technology appraisal
- TPTD
- teriparatide
- VBA
- Visual Basic for Applications
- VERO
- VERtebral fracture treatment comparisons in Osteoporotic women
- VTE
- venous thromboembolism
- WHO
- World Health Organization
- ZOL
- zoledronic acid
This monograph is based on the Technology Assessment Report produced for NICE. The full report contained a considerable number of data that were deemed confidential. The full report was used by the Appraisal Committee at NICE in their deliberations. The full report with each piece of confidential data removed and replaced by the statement ‘confidential information (or data) removed’ is available on the NICE website: www.nice.org.uk.
The present monograph presents as full a version of the report as is possible while retaining readability, but some sections, sentences, tables and figures have been removed. Readers should bear in mind that the discussion, conclusions and implications for practice and research are based on all the data considered in the original full NICE report.