

Notes
Article history
The research reported in this issue of the journal was funded by the HTA programme as project number 11/01/04. The contractual start date was in November 2012. The draft report began editorial review in October 2020 and was accepted for publication in April 2021. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Permissions
Copyright statement
Copyright © 2021 Roberts et al. This work was produced by Roberts et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaption in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2021 Roberts et al.
Chapter 1 Introduction
Some of the text in this chapter is reproduced with permission from Roberts et al. ,1 Brenner et al. 2 and the HALT-IT (Haemorrhage ALleviation with Tranexamic acid – Intestinal system) Trial Collaborators. 3 These are Open Access articles distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon these works, for commercial use, provided the original works are properly cited. See: https://creativecommons.org/licenses/by/4.0/. The text below includes minor additions and formatting changes to the original text.
Acute gastrointestinal bleeding (AGIB) is a common emergency and an important cause of death worldwide. 4 Bleeding can occur from the upper or lower gastrointestinal (GI) tract, but upper GI bleeding is more common. Symptoms of GI bleeding include haematemesis and coffee ground vomitus, melaena and the passage of fresh red blood in the stool, and clinical signs of shock, such as hypotension and tachycardia. Despite evidence suggesting improvements in survival in recent decades, the case fatality rate is about 10% for upper GI bleeding and 3% for lower GI bleeding. 5,6 However, mortality in patients with lower GI bleeding increases to about 20% in patients who are admitted to hospital for other reasons and have a GI bleed. 7 Most cases occur in the elderly and many are associated with the use of non-steroidal anti-inflammatory drugs (NSAIDs). 8,9
Prevalence of gastrointestinal bleeding
The incidence of GI bleeding varies widely between countries, depending on the population prevalence of risk factors, with a reported incidence of upper GI bleeding of 50–140 per 100,000 people across the USA, Europe and Scandinavia. 10–18 In the UK, acute upper GI bleeding accounts for about 60,000 hospital admissions each year and causes the death of about 10% of these patients. 5,10 Lower GI bleeding accounts for a further 15,000 UK admissions each year, with a case fatality of about 15%. GI bleeding is also common in low- and middle-income countries, where patients are usually young and poor.
Causes of gastrointestinal bleeding
The leading causes of upper GI bleeding are peptic ulcer, oesophageal varices and erosive mucosal disease. Peptic ulcer disease and erosions due to Helicobacter pylori infection and NSAID use are common causes of GI bleeding worldwide. 4,5,10,15,19–24 Leading causes of lower GI bleeding are diverticular disease, colitis and cancer. 25 Common causes of acute upper GI bleeding in high-income countries are ulcers (40%) and oesophageal varices (11%). 5 Although gastro-oesophageal varices due to liver cirrhosis are an increasingly common cause of bleeding in the West, they are also a major cause of bleeding in parts of South America, Asia, Africa and the Middle East, where there is high prevalence of hepatitis or schistosomiasis. 26–33 In low- and middle-income countries, variceal bleeding is particularly common (45%), with peptic ulcers accounting for about 30% of cases. In sub-Saharan Africa, schistosomiasis is an important cause of portal hypertension, responsible for about 130,000 deaths from haematemesis each year. 34 Despite advances in the management of upper GI bleeding in the past two decades, mortality remains high. In a nationwide UK study, the case fatality for new presentations to hospital was 7%, rising to > 26% in patients already hospitalised for another condition. 5,35 In addition to cause of bleeding, other factors associated with mortality include older age, signs of shock, severe bleeding, active bleeding, rebleeding and extent of comorbid disease. 4,36–39
Rebleeding
Some patients with GI bleeding initially stop bleeding and have a brief period of haemodynamic stability before starting to bleed again. This phenomenon, known as rebleeding, is common and can affect between 5% and 40% of patients with acute GI bleeding. Rebleeding is a strong predictor of mortality in patients with GI bleeding and is associated with a four-fold increased risk of death. 5,6,36,37,40 The risk of rebleeding is highest in the days immediately after the index bleed and declines rapidly with time. 41–43 A study in patients with bleeding peptic ulcers44 found that more than half of the rebleeds occurred in the 24 hours after initial treatment. Rebleeding rates have not changed significantly over the past 15 years,5,45,46 and ongoing research should focus on improving this outcome. 45
Existing treatment options for gastrointestinal bleeding
Patients with acute severe GI bleeding usually present with hematemesis or melaena. Patients are often haemodynamically unstable and in need of urgent resuscitation. Acute management of GI bleeding includes blood product transfusion, medical or endoscopic therapy and surgery.
For patients with massive acute upper GI bleeding, the National Institute for Health and Care Excellence (NICE) guidelines recommend transfusing patients with blood, platelets and clotting factors in line with local protocols for managing massive bleeding. 47 Patients with severe acute upper GI bleeding are usually referred for endoscopy immediately after resuscitation. For the endoscopic treatment of non-variceal upper GI bleeding, one of the following is recommended: a mechanical method (e.g. clips) with or without adrenaline, thermal coagulation with adrenaline, or fibrin or thrombin with adrenaline. 47 If endoscopy in such patients also reveals stigmata of recent haemorrhage, then proton pump inhibitors are recommended. 47 Interventional radiology is used in unstable patients who rebleed after endoscopic treatment and these patients are urgently referred for surgery if interventional radiology is not immediately available. Terlipressin is recommended for patients with suspected variceal bleeding at presentation. For oesophageal varices, band ligation is often used, and transjugular intrahepatic portosystemic shunts may be considered if the bleeding is not controlled by band ligation. 47 For upper GI bleeding from gastric varices, the NICE guidelines recommend endoscopic injection of N-butyl-2-cyanoacrylate and then, if that fails to control the bleeding, transjugular intrahepatic portosystemic shunts. 47
For patients with lower GI bleeding, the most common intervention is red blood cell (RBC) transfusion. 48 Flexible sigmoidoscopy and colonoscopy can be used to provide endoscopic treatment, although this is not commonly used in the UK. 6 Radiological investigations are used in > 25% of cases. 6 If extravasation of contrast is shown on computed tomography angiography, formal, invasive angiography with the option of mesenteric embolisation can be undertaken, although, in practice, embolisation is used in < 1% of all cases. 49
Tranexamic acid and gastrointestinal bleeding
In normal haemostasis, coagulation occurs rapidly at the site of a damaged blood vessel, forming a stable fibrin blood clot. However, fibrinolytic enzymes in the blood can impair clot stability through the process of clot breakdown, known as fibrinolysis. 50 Fibrinolysis may play an important role in GI bleeding and rebleeding because blood clots at the bleeding site may break down prematurely,51,52 which may worsen the bleeding. Tranexamic acid (TXA) reduces bleeding by inhibiting fibrinolysis through the inhibition of fibrin degradation by plasmin. It can, therefore, enhance the ability to form stable blood clots.
Tranexamic acid is commonly given to patients either before or during surgery to reduce bleeding and the need for blood transfusion. It has been shown to decrease bleeding and the need for blood transfusion in surgery and to reduce death due to bleeding in patients with traumatic and post-partum haemorrhage. 53–55 The knowledge that TXA reduces blood loss in surgery and reduces mortality in traumatic bleeding raises the possibility that it might also be effective for GI bleeding.
Studies have shown that many patients with acute upper GI bleeding have elevated levels of fibrin degradation products (a surrogate marker for fibrinolysis) and that this is associated with worse outcomes. 51,52 Fibrinolysis may also increase the risk of rebleeding. TXA reduces blood loss and the need for transfusion when administered before and during surgery and increases survival in traumatic bleeding, especially when given soon after injury. Early administration in patients with acute GI bleeding could possibly reduce the duration and amount of bleeding at presentation and the risk of rebleeding by stabilising blood clots at the bleeding site. This could reduce mortality and the need for blood transfusion.
Existing research on tranexamic acid
Tranexamic acid is commonly given to surgical patients to reduce bleeding and the need for blood transfusion. A systematic review of the effect of TXA in surgical patients showed that it reduces the probability of blood transfusion by about one-third [risk ratio (RR) 0.62, 95% confidence interval (CI) 0.58 to 0.65], with no evidence of any increase in risk of thromboembolic events. 53
Tranexamic acid decreases surgical bleeding and reduces death due to bleeding in patients with traumatic and post-partum haemorrhage. 54–57 The Clinical Randomisation of an Antifibrinolytic in Significant Haemorrhage 2 (CRASH-2)54 trial showed that early administration of TXA reduces deaths due to bleeding (RR 0.85, 95% CI 0.76 to 0.96) and all-cause mortality (RR 0.91, 95% CI 0.85 to 0.97) in trauma patients, without increasing thromboembolic events. Among patients treated soon after injury, the reduction in mortality with TXA is even greater. 58 The Clinical Randomisation of an Antifibrinolytic in Significant Head Injury 3 (CRASH-3)57 trial showed that early TXA treatment reduces head injury deaths. Cost-effectiveness analysis reveals that the administration of TXA to bleeding trauma patients is highly cost-effective. 59 Based on these results, TXA was included in guidelines for the pre-hospital care of trauma patients.
A systematic review and meta-analysis60 of TXA in patients with upper GI bleeding found a significant reduction in all-cause mortality with TXA (RR 0.60, 95% CI 0.42 to 0.87; p = 0.007) and a non-significant reduction in rebleeding (RR 0.72, 95% CI 0.50 to 1.03). However, the quality of the included trials was poor and, therefore, this estimate is imprecise. Moreover, the included trials were too small to assess the effect of TXA on thromboembolic events. Therefore, the effectiveness and safety of TXA in GI bleeding remains uncertain. 60
Rationale for trial
A meta-analysis60 of clinical trials on TXA in patients with upper GI bleeding found a significant reduction in all-cause mortality with TXA (RR 0.60, 95% CI 0.42 to 0.87; p = 0.007). However, all but one of the trials were conducted before the use of endoscopy and proton pump inhibitors and were too small to assess the effect of TXA on thromboembolic events. The HALT-IT trial aims to provide reliable evidence about the effects of TXA on death and thromboembolic events in acute GI bleeding. 1 If TXA reduces mortality in patients with GI bleeding, this would be of considerable significance worldwide.
Chapter 2 Methods
Some of the text in this chapter is reproduced with permission from Roberts et al. ,1 Brenner et al. 2 and the HALT-IT Trial Collaborators. 3 These are Open Access articles distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon these works, for commercial use, provided the original works are properly cited. See: https://creativecommons.org/licenses/by/4.0/. The text below includes minor additions and formatting changes to the original text.
Trial design
The HALT-IT trial was a large, international, pragmatic, randomised, double-blind, placebo-controlled trial to quantify the effects of TXA (Cyklokapron® injection, Pfizer, Inc., New York, NY, USA) on mortality and morbidity in adults with significant acute upper or lower GI bleeding. 1 The trial protocol was peer reviewed and published in BioMed Central’s Trials as an open access article in 2014. 1 [See the trial protocol at the National Institute for Health Research (NIHR) Journals Library web page; www.journalslibrary.nihr.ac.uk/programmes/hta/110104/#/documentation; accessed October 2021.]
The HALT-IT trial was the fourth international, multicentre, randomised, placebo-controlled trial in significant haemorrhagic conditions conducted by the London School of Hygiene & Tropical Medicine (LSHTM) Trial Co-ordinating Centre (TCC). CRASH-254 examined the effects of early administration of a short course of TXA in trauma patients. The trial recruited 20,211 patients from 274 hospitals in 40 countries. The World Maternal Antifibrinolytic (WOMAN)55 trial assessed the effects of early administration of TXA on death, hysterectomy and other relevant outcomes in women with post-partum haemorrhage. The WOMAN55 trial recruited 20,060 women from 193 hospitals in 21 countries. CRASH-357 investigated the effects of TXA on death and disability in patients with traumatic brain injury and recruited 12,737 patients from 175 hospitals in 29 countries.
The HALT-IT trial recruited patients from 164 hospitals in 15 countries. Suitable collaborating sites and investigators were assessed on the number of potentially eligible patients and their ability to conduct the trial. In advance of the trial starting at a site, all potential principal investigators had to agree to follow good clinical practice guidelines and all relevant regulations in their country. All relevant regulatory and ethics approvals were in place before the trial started at a site. See Appendix 1 for a list of the trial collaborators by country.
Various treatments are used for GI bleeding and, as the trial was conducted worldwide, each participating site was instructed to follow its own clinical guidelines for the treatment of patients with GI bleeding. No clinically indicated treatment needed to be withheld for the trial. TXA or placebo was provided as a treatment in addition to the usual management of GI haemorrhage.
Approvals
The Medical Research and Ethics Committee and Health Research Authority reviewed the HALT-IT trial protocol and supporting documents and gave a favourable opinion on 13 March 2013 (Research Ethics Committee reference 13/EE/0038). The Medicines and Healthcare products Regulatory Agency (MHRA) granted authorisation for the HALT-IT trial on 12 February 2013 (reference 17072/0008/001-0001). A favourable ethics opinion was received from the Observational/Interventions Research Ethics Committee at LSHTM on 19 December 2012 (reference 6328). Protocol amendments and their approval dates are listed in Amendments to the trial.
All relevant approvals were also obtained from national and local research ethics committees and national regulatory authorities, where applicable, in all participating non-UK countries.
Participants (inclusion and exclusion)
All adults with significant acute upper or lower GI bleeding were eligible for the trial. The diagnosis of significant bleeding was clinical, but significant implies a risk of bleeding to death, and patients with significant bleeding may include those with hypotension, tachycardia or signs of shock, as well as those needing urgent transfusion, endoscopy or surgery. Patients were randomised once consent had been obtained in accordance with the approved procedures.
The fundamental eligibility criterion was the responsible clinician’s ‘uncertainty’ as to whether or not to use TXA in a particular patient with GI bleeding. The eligibility criteria were based on the uncertainty principle, which is a well-established approach to trial eligibility. 61 A patient could be enrolled if, and only if, the responsible clinician was substantially uncertain as to which trial treatment would be the most appropriate for that particular patient. A patient was not to be enrolled if the responsible clinician or the patient (or his/her representative) were for any medical or non-medical reasons reasonably certain that one of the two allocated treatments (TXA or placebo) would not be appropriate for this particular individual (in comparison with either no treatment or some other treatment that could be offered). In other words, patients in whom the responsible clinician considered there to be a clear indication for TXA (e.g. traumatic haemorrhage) or contraindication to TXA (e.g. history of convulsions, thromboembolic disease) were excluded.
The pragmatic design allowed us to find out how effective the treatment actually is in routine practice. Clinicians, patients and their representatives were provided with information about the trial treatment to assist them in their judgement. The TXA summary of product characteristics62 and an investigator’s brochure were provided to investigators to ensure that they had adequate information when considering the risk–benefit ratio and the appropriateness of the trial for each patient.
Consent
Significant acute GI bleeding is an emergency, and the priority is to provide appropriate emergency care. Eligible patients have a life-threatening condition. Their physical, mental and emotional state may be affected by their blood loss. This may impair their decision-making and affect their ability to give prior informed consent to participate in the trial. Because randomisation and administration of the trial treatment should be undertaken as early as possible once significant GI bleeding is suspected, the consent process in this situation required careful consideration, bearing in mind the applicable regulatory requirements, adherence to the International Council for Harmonisation – Good Clinical Practice63 and the requirements in the Declaration of Helsinki. 64 As acknowledged in the Declaration of Helsinki, patients who are incapable of giving consent are an exception to the general rule of informed consent in clinical trials. 64
In the HALT-IT trial, bearing in mind the clinical situation and the patient’s level of distress, the patient and, if present, the patient’s relative were provided with brief information about the trial (see the brief information sheet in Appendix 2). If the patient was fully competent, written consent was sought. If the patient’s capacity was impaired and a personal or professional representative was available, consent was sought from the patient’s representative. If the patient or their representative objected to the inclusion of the patient in the trial, their views were respected and the patient was not enrolled.
If neither was able to provide informed consent, the need for consent was waived. This process involved the investigator and one independent person who was not participating in the trial enrolling the patient. They were required to confirm that the patient had significant GI bleeding and was unable to give consent because of their condition, that it was not feasible to contact a representative for the patient to obtain consent, and that they were not aware of any objections to the patient participating in the trial. The patient, or their representative, was then informed about the trial and asked for consent for ongoing data collection as soon as possible afterwards. If the patient or their representative declined consent, participation stopped.
The approach that allowed the patient to have the most input into the decision-making process without endangering their life was utilised. If the person giving consent was unable to read or write, the information sheet was read to them and they then marked the consent form with either a cross or a thumbprint. In this event, a witness not associated with the trial was required to provide a full signature confirming the mark.
All requirements of local and national ethics committees were adhered to (see Appendix 3 for an overview of the consent procedure).
Randomisation and blinding
Patient eligibility was determined from routinely collected clinical information and recorded on the trial entry form (see Appendix 4). No trial-specific tests were required. Sites were advised to randomise eligible patients as soon as possible. Following confirmation of eligibility, patients were randomly allocated to receive TXA or matching placebo (sodium chloride 0.9%) by intravenous injection in the case of the loading dose and by intravenous infusion in the case of the maintenance dose. Block randomisation was used but randomisation was not stratified. Randomisation codes were generated and secured by an independent statistician from Sealed Envelope Ltd (London, UK). The codes were then given to Sharp Clinical Services, UK (Crickhowell, UK), a good manufacturing practice (GMP)-certified clinical trial service provider, to make the treatment packs in accordance with the randomisation list.
After baseline information was collected on the entry form, patients were randomised by taking the next lowest consecutively numbered pack from a box of eight treatment packs. At the point when all of the treatment ampoules were confirmed as being intact, the patient was considered to be randomised to the trial. The trial treatment was then started immediately. Once a patient was randomised, the entry form data were sent to the TCC as soon as possible. This was carried out by trial team members entering the data into a secure online database.
Both participants and study staff (site investigators and TCC staff) were masked to treatment allocation. An emergency unblinding service was available for use in the rare situations when the clinician believed that clinical management depended on the knowledge of whether the patient had received TXA or placebo.
Pfizer Manufacturing (Sandwich, UK) (marketing authorisation number PL 00057/0952) manufactured the TXA (cyklokapron injection) and Torbay and South Devon NHS Foundation Trust [manufacturing authorisation number (investigational medicinal product) 13079] manufactured the sodium chloride 0.9% placebo. The ampoules and packaging were identical in appearance.
Sharp Clinical Services, UK (Crickhowell, UK) [manufacturing authorisation number (investigational medicinal product) 10284], was responsible for masking, manufacturing the study drug treatment packs, which contained either the active drug TXA or placebo and the first-stage qualified person (QP) release. This involved removing the original manufacturer’s label and replacing it with the clinical trial label and treatment pack number. Apart from the randomisation number, the pack label text was identical for TXA and placebo. Sharp Clinical Services, UK, was also responsible for maintaining the product specification file until final database lock and unblinding of the trial data.
The coding of the blinded ampoules was checked by testing random samples of final QP-released drug packs from each batch with high-performance liquid chromatography to determine the contents. The tested samples were unblinded to assure accuracy of blinding.
Trial intervention
Eligible patients were randomised to TXA or placebo as soon as possible and the treatment was started immediately. Patients received a loading dose of 1 g of TXA or placebo (sodium chloride 0.9%), which was added to a 100-ml infusion bag of 0.9% sodium chloride and infused by slow intravenous injection over 10 minutes. This was followed by a maintenance dose of 3 g of TXA or placebo added to 1 litre of any isotonic intravenous solution and infused at 125 mg/hour for 24 hours. The maintenance dose was started as soon as the loading dose was completed. Where fluid restriction was required, the volume used to administer the maintenance dose could be reduced to 500 ml.
Every patient was assigned a uniquely numbered treatment pack, each of which contained eight ampoules of TXA 500 mg or placebo, one 100-ml bag of 0.9% sodium chloride (to use with the loading dose), two sterile 10-ml syringes and needles, stickers with the trial details and randomisation number (for attaching to infusion bags, forms and the medical records), and instructions. The lowest-numbered treatment pack was taken from a box of eight packs. We separately provided information for patients and representatives, consent forms and data collection forms. The stickers, instructions, leaflets and forms were in local languages.
The TCC was responsible for ensuring that all relevant approvals were available at the TCC before release of the trial treatment to a site. A separate manual of operating procedures detailed the drug accountability system. The investigator’s brochure and investigational medicinal product dossier provided detail about the labelling of the trial treatment and other processes for ensuring adherence to GMP.
Dose selection
Tranexamic acid has been used to reduce bleeding in elective surgery for many years. In randomised trials in cardiac surgery, TXA dose regimens vary widely. Loading doses range from 2.5 to 100 mg/kg and maintenance doses range from 0.25 to 4 mg/kg/hour, which are given over periods of 1–12 hours. 65 A loading dose of 10 mg/kg of TXA followed by an infusion of 1 mg/kg/hour has been shown to produce plasma concentrations sufficient to inhibit fibrinolysis in vitro. 66 In emergency situations, the administration of a fixed dose is more practicable, given that weighing patients is difficult. In the CRASH-2 trial, a fixed dose of a 1-g loading dose of TXA followed by a 1-g maintenance dose over 8 hours was found to reduce mortality in bleeding trauma patients, with no evidence of significant adverse effects. 54,58 In the HALT-IT trial, a fixed dosage of a 1-g loading dose of TXA followed by 3 g infused over 24 hours was selected. This dosage is within the range that has been shown to inhibit fibrinolysis. 66 It was efficacious for larger patients (> 100 kg) but was also safe for smaller patients (< 50 kg), given that the estimated dose per kilogram that the patients in the latter group would receive has been applied in other trials without significant adverse effects. 65,66 The loading dose (1 g) is the same as was used in the CRASH-254 and CRASH-357 trials. A maintenance dose is provided but over a longer duration (24 hours) than in the CRASH-254 and CRASH-357 trials to cover the period when the patient is at greatest risk of rebleeding.
Sites
We recruited patients with significant acute upper or lower GI bleeding from 164 hospitals in 15 countries. We enrolled the first patient on 4 July 2013 and the last patient on 21 June 2019. We stopped recruiting when the planned sample size was reached. A total of 12,009 patients were enrolled worldwide. See Appendix 5 for the total number of randomised patients by geographical region.
Data collection
Data were collected at each site by local investigators and transmitted to the TCC. Only data outlined on the entry, outcome and adverse event forms were collected for this trial.
To allow for variation in available technology for data transfer, a variety of methods were used. Data were collected by the investigator on paper case report forms and transmitted to the TCC by fax or e-mail, or by entering the data directly into the trial database. The data were used in accordance with local laws and ethics committee approval.
Baseline data
The trial entry form (see Appendix 4) was used to collect the following baseline characteristics: age, biological sex, time from onset of GI bleeding symptoms to randomisation, suspected location of bleeding, clinical symptoms (e.g. haematemesis and melaena), suspected variceal bleeding, systolic blood pressure (SBP), heart rate, signs of shock, suspected active bleeding, major comorbidities, anticoagulation therapy and type of admission. Relevant data were recorded on the entry form to assess the patient’s eligibility before randomisation and the form was completed if the patient was randomised.
Outcome data
The trial protocol required the outcome form (see Appendix 6) to be completed at death, discharge from the randomising hospital or 28 days after randomisation, whichever occurred first. These data were collected from the patients’ routine medical records because no special tests were required. Any adverse events that became known to the investigator were reported up to 28 days after randomisation. Once patients were randomised, outcome data were collected even if the treatment was interrupted or was not actually given. Specific patient-orientated outcomes were assessed.
Initially, the collection of patient-identifiable information, including a patient’s name, date of birth, NHS number and postcode, was planned to allow trial staff based at LSHTM to follow up the patients’ status at 12 months after randomisation. Follow-up was planned by linking this personal information to Hospital Episode Statistics through the Trusted Data Linkage Service of the NHS Information Centre for England and to the Patient Episode Database for Wales through the Secure Anonymised Information Linkage Databank.
In July 2018, the outcome form was modified to allow the collection of the date or dates on which the patients experienced rebleeding.
Monitoring
The trial was assessed as low risk, because TXA is widely used; the trial collected adverse event data, which were then reviewed routinely by the independent Data Monitoring Committee (DMC), and all treatment apart from the study drug was given as per usual practice. Therefore, central trial monitoring and central statistical monitoring were used in conjunction with investigators’ training and meetings, and extensive written guidance, to make sure that the trial was carried out properly. Trial investigators and their institutions provided direct access to the source data for trial-related monitoring, audits and regulatory inspections. Monitoring was carried out in accordance with the sponsor’s standard operating procedure and the trial protocol. Formal inspections were carried out by the relevant regulatory agencies including the UK MHRA, Irish Health Products Regulatory Authority and Nigeria’s National Agency for Food and Drug Administration and Control. The adherence to allocation sequence was monitored throughout the trial and any out-of-sequence pack use was automatically flagged in the trial database and the investigators were retrained.
The progress of the HALT-IT trial, including recruitment, data quality, outcomes and safety data, was reviewed by an independent DMC. Four interim analyses were conducted by the DMC in total.
Outcome measures
Primary outcome
The primary outcome was death due to bleeding within 5 days of randomisation. The primary end point was originally death due to bleeding within 28 days of randomisation, but the protocol was changed in March 2019. Cause of death was assigned by local principal investigators, who provided a narrative of the events leading to death. These were reviewed by the chief investigator (blind to treatment allocation) and queried if more information was needed to confirm whether death was due to bleeding or another cause.
Secondary outcome
Secondary outcomes were death due to bleeding within 24 hours and within 28 days of randomisation, all-cause and cause-specific mortality at 28 days, rebleeding within 24 hours, within 5 days and within 28 days of randomisation, surgery or radiological intervention, blood product transfusion, thromboembolic events (i.e. deep-vein thrombosis, pulmonary embolism, stroke and myocardial infarction), seizures, other complications (including other significant cardiac event, sepsis, pneumonia, respiratory failure, renal failure and liver failure), days in an intensive care unit (ICU), and functional status.
Death due to bleeding within 28 days was changed to a secondary outcome in March 2019. The diagnosis of rebleeding was made by the clinician based on established criteria. A diagnosis of thromboembolic events was made using strict definitions and diagnostic criteria, including a clinical assessment, diagnostic imaging, biomarker tests and post-mortem examination. Seizures were diagnosed by clinical assessment. Functional status was measured with the Katz Index of Independence in Activities of Daily Living either at hospital discharge or in hospital at 28 days.
Adverse events
Tranexamic acid is not a new drug and has a well-documented safety profile. Although the Summary of Product Characteristics62 suggests that rare cases of thromboembolic events and seizures might be associated with TXA administration, there is no evidence that the TXA treatment regimen used in this trial is associated with an increased risk of thromboembolic events or seizures.
Nevertheless, data on thromboembolic events (e.g. deep-vein thrombosis, pulmonary embolism, myocardial infarction and stroke), seizures, other significant cardiac event, and respiratory, liver and renal failure were collected as secondary outcomes up to day 28 after randomisation and were presented to the independent DMC for unblinded review.
Amendments to the trial
Various amendments were made to the HALT-IT trial throughout the time that it was being conducted. The main amendments and the rationale for them are summarised below.
Substantial amendment to the protocol from version 1.0 to version 1.1 (UK), August 2014
The UK protocol was amended to clarify that clinicians in participating hospitals would at all times retain the freedom to act in the patient’s best interest, and that each participating site should follow its own clinical practice for the treatment of GI bleeding. Centres in which TXA is in routine use (including those where it is either specifically mandated or recommended for GI bleeding in a massive haemorrhage treatment protocol) were excluded from taking part in the trial. This amendment included monitoring the use of open-label TXA for the treatment of GI bleeding at collaborating sites and the procedure to be followed at sites where this is common.
Rationale
These changes were made in line with the recommendations of the Research Ethics Committee. The Data Access Advisory Group, Health and Social Care Information Centre also requested an amendment to the information sheet and consent form to allow data on patient status in England and Wales to be shared with us at 1 year.
This amendment was approved by the Multicentre Research Ethics Committee (MREC) on 12 August 2014 and by the MHRA on 21 August 2014.
Non-substantial amendment to the protocol from UK version 1.1 to version 1.2 and international protocol version 1.0 to version 1.1, October 2016
The protocol was updated to version 1.2 to extend the planned date of last patient enrolment by 1 year, from 30 November 2016 to 30 November 2017.
Rationale
A delay in the issue of the funding contract had led to recruitment starting late. The recruitment extension was necessary to ensure that the target number of patients were recruited.
Substantial amendment to increase the number of patients from the UK and European Economic Area, February 2017
A substantial amendment was submitted to increase the UK sample size from 4000 to 5000 patients, and to increase the European Economic Area sample size from 5000 to 6000 patients. The total international sample size remained as 8000 patients. The protocol was not updated as a result of this amendment.
Rationale
When the original trial application was submitted, there were no reliable data on which to base recruitment in the UK. We, therefore, originally planned for a more conservative number. However, recruitment in the UK was much higher than anticipated.
This amendment was approved by the MREC on 27 February 2017.
Substantial amendment to the protocol from version 1.2 (UK) and version 1.1 (international) to version 2.0, November 2017
This amendment increased the sample size from 8000 to 12,000 patients and added death from haemorrhage as the main secondary outcome. The recruitment period was also extended by 18 months from 30 November 2017 to 31 May 2019.
Rationale
Accumulating evidence of the effect of TXA on traumatic bleeding (CRASH-2 trial54) and post-partum haemorrhage (the WOMAN trial55) showed that TXA reduces deaths from haemorrhage with no apparent effect on any other cause of death. The reductions in bleeding deaths in trauma and obstetric patients provided good reason to anticipate that TXA may reduce bleeding deaths (but not other causes of death) in patients with GI haemorrhage. The primary outcome in the HALT-IT trial was all-cause mortality within 28 days of randomisation. This was based on the assumption that most deaths in the trial would be from bleeding. However, the accumulated (blinded) data showed that a substantial proportion of deaths are not bleeding related (e.g. cancer, pneumonia and liver failure). Given that the effect of TXA was likely to be on death from haemorrhage, with the original sample size of 8000 patients there was a risk that the trial might fail to detect a clinically relevant treatment benefit, leaving the therapeutic question unresolved. The sample size was, therefore, increased from 8000 to 12,000 patients and death from haemorrhage was added as the main secondary outcome. The recruitment period was also extended by 18 months. The increase in the sample size meant that the trial should have enough power to detect a reduction in death from haemorrhage, and there would be a smaller chance of missing a clinically important reduction in all-cause mortality. This amendment was given a favourable opinion by the MREC on 23 October 2017 and was approved by the MHRA on 14 November 2017.
Substantial amendment to the protocol from version 2.0 to version 2.1 (UK), May 2018
An amendment to the UK protocol was made to provide clarification on the definition of ‘significant bleeding’, stating that ‘the diagnosis of significant bleeding is clinical but significant implies a risk of bleeding to death and may include patients with hypotension, tachycardia, signs of shock, or those needing urgent transfusion, endoscopy or surgery’.
Rationale
This amendment was submitted following the recommendation of MHRA. This amendment was given a favourable opinion by the MREC on 1 May 2018 and was approved by the MHRA on 25 May 2018.
Substantial amendment to the outcome form from version 1.0 to version 2.0, September 2018
This amendment was submitted to retrospectively collect the date when patients experienced rebleeding. The outcome form was modified to allow the collection of the date when any rebleeding took place. Rebleeding was a secondary outcome of the HALT-IT trial, and if patients experienced rebleeds this was captured in the outcome form as a complication. The outcome form was completed 28 days after randomisation, at discharge from the randomising hospital or at death, whichever occurred first.
Rationale
In addition to reducing the duration and amount of bleeding, early administration of TXA could reduce the risk of rebleeding. However, a patient may experience a rebleed long after having received the trial treatment, and this would be recorded if it occurred up to 28 days post randomisation. In some cases, even if a patient received TXA, this may have little or no biological effect if the rebleed occurred outside the TXA therapeutic window. The amendment was given a favourable opinion by the MREC on 24 August 2018 and was approved by the MHRA on 9 September 2018.
Substantial amendment to the protocol from version 2.1 (UK) and version 2.0 (international) to version 3.0, November 2018
The decision to refine the primary outcome was made by the Trial Steering Committee in November 2018. The primary outcome was changed from death from all causes within 28 days of randomisation to death from haemorrhage within 5 days of randomisation. Death from haemorrhage within 28 days of randomisation, all-cause and cause-specific mortality within 28 days of randomisation and need for endoscopy were added as secondary outcomes. The recruitment period was extended by 4 months from 31 May 2019 to 30 September 2019.
Rationale
Tranexamic acid is an antifibrinolytic drug that helps to stop bleeding by inhibiting the breakdown of fibrin blood clots. Combined data from large randomised controlled trials (RCTs) using TXA in acute severe haemorrhage have shown that TXA reduces deaths from haemorrhage with no apparent effect on other causes of death. The original primary outcome in the HALT-IT trial (all-cause mortality within 28 days) was based on the assumption that most deaths in the trial would be due to bleeding. However, an analysis of blinded data shows that over half (55%) of patients died from non-bleeding causes, such as cancer, pneumonia and liver failure. Because all-cause mortality is a composite of different causes of death, the treatment effect on all-cause mortality is a weighted average of the cause-specific effects. For example, assuming that 45% of deaths are due to bleeding and that TXA reduces deaths by 25% but has no effect on other causes of death, the treatment effect on all-cause mortality would be:
The inclusion of non-bleeding causes of death, which are unlikely to be affected by TXA, would dilute the treatment effect towards the null, reducing the power to detect an effect if one exists. Although the original sample size of 8000 patients was increased to 12,000, if non-bleeding deaths are unaffected by TXA, even with 12,000 patients, the trial would have low power to detect an effect on all-cause mortality. For example, a trial with a 10% event rate would have just 54% power to detect an 11% reduction in all-cause mortality. By contrast, a trial with a 4% event rate would have 85% power to detect a 25% reduction in death from haemorrhage. By changing the primary outcome, the power of the trial was substantially increased. In addition, because the relative contributions of different causes of death vary within and between patient populations, all-cause mortality is not a generalisable outcome measure. Finally, around 10% of patients with acute GI bleeding experience rebleeding, which affects > 50% of those with variceal bleeding and is associated with increased mortality. These rebleeding episodes can occur several days or weeks after the index bleed. Patients receive TXA (or placebo) for their index bleed but not for rebleeding episodes. TXA has a half-life of around 3 hours and, therefore, is unlikely to affect the risk of late death due to bleeding that occurs after it has been excreted. Therefore, we chose to restrict the primary outcome to early deaths from haemorrhage, defined as those occurring within 5 days of randomisation. In summary, changing the primary outcome to death from haemorrhage within 5 days of randomisation should have provided adequate power to detect a plausible reduction in death due to bleeding.
This amendment received a favourable opinion from the MREC on 10 April 2019 and MHRA approval on 25 April 2019.
Sample size
The original sample size estimate assumed a control group all-cause mortality risk of 10%. It was, therefore, originally estimated that a trial with 8000 patients would have > 90% power (two-sided alpha of 5%) to detect a 25% reduction (RR 0.75) in all-cause mortality. The sample size calculation was initially based on all-cause mortality as the primary outcome because we expected that most deaths would be due to bleeding. 1 However, while the trial was under way, we observed that over half of all deaths were due to non-bleeding causes. Accumulating evidence from other large trials of TXA found no apparent effect on non-bleeding deaths. 67 The sample size was, therefore, increased to 12,000 patients to provide adequate power to detect a plausible reduction in death from haemorrhage and all-cause mortality. The trial was then estimated to have > 80% power to detect a 15% (RR 0.85) reduction in all-cause mortality. In 2019, the primary outcome was changed to death due to bleeding within 5 days of randomisation. Based on the amended primary outcome, and assuming a risk of death due to bleeding of 4%, a study with 12,000 patients would have about 85% power (two-sided alpha = 5%) to detect a clinically important 25% relative reduction in death due to bleeding from 4% to 3%.
Statistical methods and analysis plan
The statistical analysis plan was published before unblinding. 2 The plan gave our reasons for amending the primary outcome measure and for increasing the sample size. The main analyses compared those patients allocated to TXA with those allocated to placebo on a modified intention-to-treat basis, excluding patients who received neither dose of the allocated treatment. Effect estimates (RRs) were calculated with a measure of precision (95% CIs). The safety of participants was overseen by an independent DMC, which reviewed four unblinded interim analyses.
Subgroup analysis
Four subgroup analyses were planned to examine the effects of TXA on the primary outcome stratified by the following baseline characteristics: time to treatment (≤ 3 vs. > 3 hours), site of bleeding (upper vs. lower GI), cause of bleeding (suspected variceal bleeding and/or comorbid liver disease vs. other or unknown causes) and clinical Rockall score. We fitted an interaction term between treatment group and each of the subgroup factors in a Poisson regression model. We used a test for interaction to explore whether or not the treatment effect (if any) varied across the subgroups. Time to treatment was analysed as both a categorical and a continuous variable. Post hoc subgroup analyses were conducted to examine the effects of TXA on the primary outcome stratified by World Bank classification of country income level (high vs. low or middle income), anticoagulant use and SBP.
Economic evaluation methods
An economic analysis was conducted to evaluate the cost-effectiveness of the current standard of care for people with AGIB with and without the administration of TXA. The evaluated TXA regimen mirrored that used in the HALT-IT trial. The analysis followed the NICE technology appraisal guidelines for conducting economic evaluations. 68 The evaluation used a decision model to combine the clinical results from the HALT-IT trial with evidence from other sources to estimate costs and outcomes over a lifetime horizon for the two treatment options. The analysis adopts a UK NHS cost perspective and expresses health outcomes in terms of life-years (LYs) and quality-adjusted life-years (QALYs). Full details of the methods and results are provided in Chapter 5.
Patient and public involvement
Patient and public involvement (PPI) that was previously conducted by the TCC team was used to inform the HALT-IT trial procedures and to achieve the following objectives:
-
to gain lay perspectives on PPI involvement in the design and management of emergency care clinical trials
-
to identify an appropriate consent procedure for entering critically ill trauma patients into emergency clinical trials that could be used for the HALT-IT trial
-
to ensure that patient-facing documents for the trial were appropriate and clear
-
to provide a lay perspective on the management of the trial and interpretation of the results.
We included PPI groups’ input into different stages of the trial; this included people who suffered severe haemorrhage. Formative research and research with a PPI group had previously been carried out to guide the PPI activities for our programme of emergency care research. The outcome of much of this PPI engagement was used to inform the HALT-IT trial procedures. This is summarised below.
Formative research method
A qualitative study was conducted to elicit views on how best to involve patients and the public in the design, conduct and reporting of clinical trials involving people in emergency situations, gathering perspectives on which areas of the research programme they believed that public contribution would be most appropriate. Approaches to designing a consent process to enter patients into emergency clinical trials were also explored.
Specifically for the HALT-IT trial, two focus group discussions were carried out involving a group of older men belonging to a social club and a group of older women who were involved in a continuing education project and crafts-based activities.
The sessions included a PowerPoint® (Microsoft Corporation, Redmond, WA, USA) presentation detailing why clinical trials are conducted in emergency medicine, how they are conducted and the key principles, including issues of consent, randomisation and the use of placebos. This was followed by three exercises using group work and discussion techniques.
Two key areas of inquiry emerged from these discussions: public involvement in the design and management of clinical trials and decisions about entering patients into clinical trials in an emergency.
Formative research outcome: involvement in clinical trial design and management
Participants were highly supportive of clinical medical research, seeing it as essential for the progress of medical science. They also had a sense that the public should be consulted in principle. However, they struggled to identify how they might usefully contribute to the design and management of clinical trials in practice, seeing this as the province of highly skilled and qualified experts. Although there were individuals who could envisage a role for themselves with appropriate information and preparation, it was important to acknowledge that others felt that they had neither the inclination nor the aptitude to become involved, trusting the expertise and competence of clinical researchers. Participants did have strong opinions in one area, namely that decision-making about the outcomes of clinical research should not be confined to treatment efficacy or safety but must take account of quality-of-life issues, which they considered patients and the public to be well placed to comment on.
Formative research outcome: consent process for involving patients in clinical trials in an emergency
Initially, a minority opposed entering patients into trials without their consent, but these views tended be modified as participants considered the comments of others about the incapacitation of patients, the time-critical nature of emergency medicine and the necessity of clinical trials for medical progress.
Overall, among both groups there was a very high regard for the medical profession and a strong faith in the skills and competence of medics, as well as a belief that clinicians would always act in the best interest of the patient. This was reflected in a sense that clinicians should be allowed to exercise their clinical judgement without undue burden to seek consent from next of kin when patients could not consent for themselves. However, moderating this perspective for some was a belief in the principle that, where practicable, next of kin should be consulted; others argued that this might place a heavy burden of responsibility on families and that the clinician’s greater expertise may in fact render better decisions.
Interestingly, when the participants were asked what they would want for themselves, all the participants expressed a desire for the clinician (or their own family) to enter them into the trial.
Patient and public involvement for the HALT-IT trial
Drafts of the brief information sheet, full information sheet and consent form were reviewed by PPI representatives.
A PPI representative who had experience of severe gastrointestinal haemorrhage provided a lay perspective on the management of the trial as part of the Trial Steering Committee. They also provided a lay perspective on the trial results and dissemination as part of the Writing Committee for the trial.
Outcome of patient and public involvement
Patient and public involvement contributed to the success of the trial. The consent process that was developed with PPI groups was used in all countries that took part in the trial, and was accepted by all ethics committees and regulatory agencies, with only local modifications needed.
Chapter 3 Baseline results
The first patient was enrolled on 4 July 2013 and the last patient was enrolled on 21 June 2019. Recruitment ended when the planned sample size of 12,000 patients had been reached. When the decision to refine the primary outcome was made in November 2018, we had recruited 10,190 patients. This decision was made blind to the accumulating trial data.
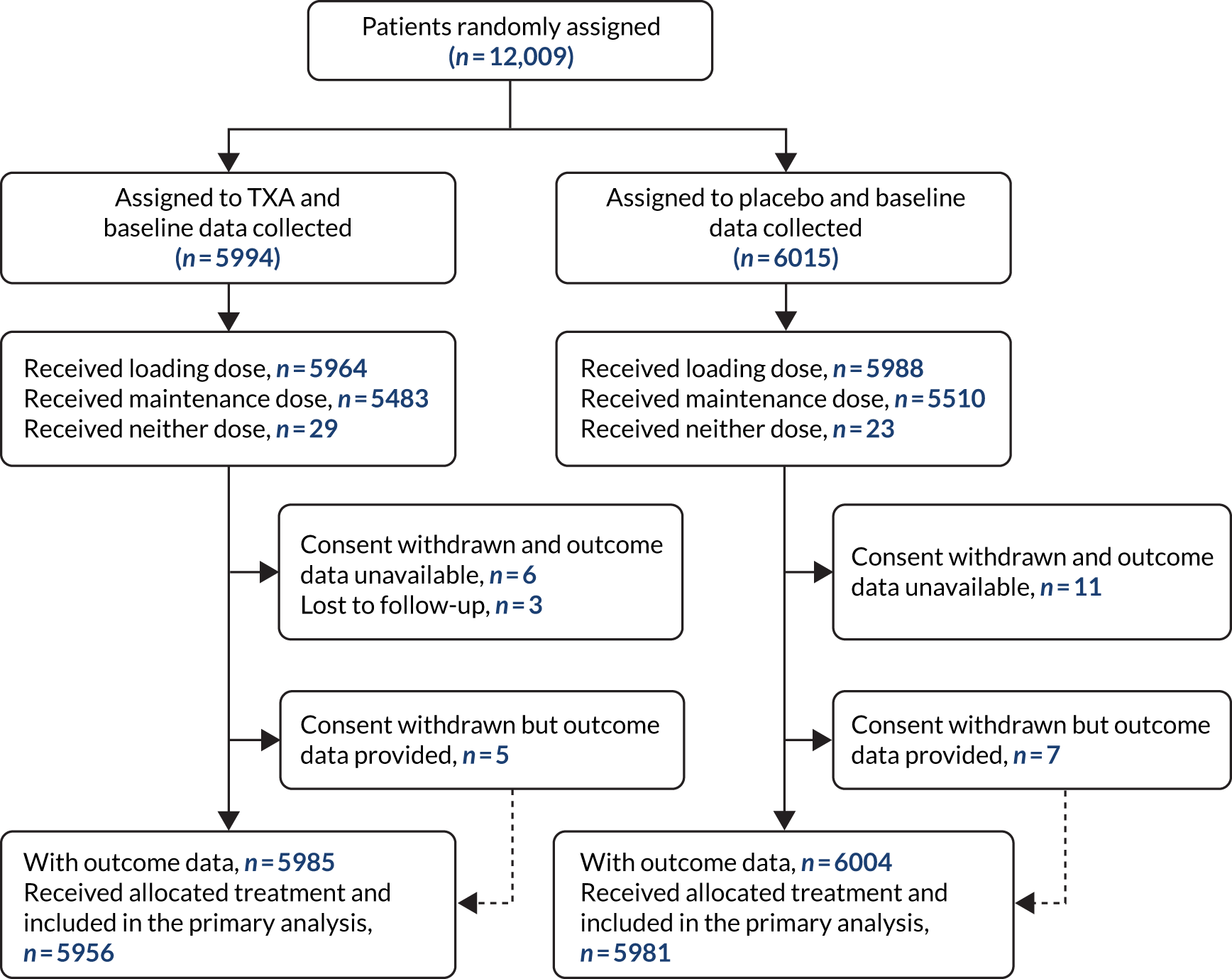
A total of 12,009 patients were enrolled and randomly assigned to received either TXA (n = 5994, 49.9%) or matching placebo (n = 6015, 50.1%), of whom 11,952 (99.5%) received the first dose of the allocated treatment (Figure 1). A total of 29 patients (11 in the TXA group and 18 in the placebo group) withdrew consent after randomisation, but, of those, 12 (five in the TXA group and seven in the placebo group) agreed to provide outcome data or had outcome data collected as part of adverse event reporting. We obtained primary outcome data for all but three patients in the TXA group. There were 14 protocol violations (seven in the TXA group and seven in the placebo group). Eleven patients did not meet the inclusion criteria [10 received TXA prior to randomisation (six in the TXA group and four in the placebo group) and one patient in the placebo group was aged < 16 years] and there were three consent protocol violations (one in the TXA group and two in the placebo group). A total of 28 patients were unmasked to treatment [17 because the hospital team wanted to administer TXA, six because of adverse events, three because of clinical concerns and two as part of post-mortem investigations (13 in the TXA group and 15 in the placebo group)]. Fifty-two patients received neither dose of the allocated trial treatment (29 patients in the TXA group and 23 patients in the placebo group). A total of 223 patients received antifibrinolytic drugs as part of their clinical care, outside the trial protocol (105 patients in the TXA group and 118 patients in the placebo group). Baseline characteristics were similar in both groups (Table 1).
FIGURE 1.
Trial profile.
| Baseline characteristic | Treatment group, n (%) | |
|---|---|---|
| TXA (N = 5994) | Placebo (N = 6015) | |
| Age at randomisation (years) | ||
| Mean (SD) | 58.1 (17.0) | 58.1 (17.0) |
| < 40 | 791 (13) | 779 (13) |
| 40–59 | 2356 (39) | 2333 (39) |
| 60–79 | 2078 (35) | 2130 (35) |
| ≥ 80 | 769 (13) | 773 (13) |
| Sex | ||
| Female | 2142 (36) | 2124 (35) |
| Male | 3852 (64) | 3891 (65) |
| Time from onset to randomisation (hours) | ||
| Mean (SD) | 21.4 (36.4) | 22.5 (37.8) |
| ≤ 3 | 960 (16) | 975 (16) |
| > 3 to ≤ 8 | 1607 (27) | 1551 (26) |
| > 8 | 3427 (57) | 3488 (58) |
| Missing | 0 | 1 (< 1) |
| Suspected location of bleeding | ||
| Lower GI tract | 674 (11) | 654 (11) |
| Upper GI tract | 5320 (89) | 5361 (89) |
| Haematemesis | ||
| Yes | 4285 (72) | 4240 (71) |
| No | 1709 (29) | 1775 (30) |
| Melaena or fresh blood per rectum | ||
| Yes | 4573 (76) | 4626 (77) |
| No | 1421 (24) | 1389 (23) |
| Suspected variceal bleeding | ||
| Yes | 2694 (45) | 2739 (46) |
| No | 3300 (55) | 3276 (54) |
| Suspected active bleeding | ||
| Yes | 5247 (88) | 5226 (87) |
| No | 747 (12) | 789 (13) |
| SBP (mmHg) | ||
| ≥ 90 | 5222 (87) | 5216 (87) |
| 76–89 | 577 (10) | 577 (10) |
| ≤ 75 | 181 (3) | 201 (3) |
| Missing | 14 (< 1) | 21 (< 1) |
| Heart rate (beats per minute) | ||
| < 77 | 812 (14) | 756 (13) |
| 77–91 | 1546 (26) | 1644 (27) |
| 92–107 | 1760 (29) | 1720 (29) |
| > 107 | 1864 (31) | 1885 (31) |
| Missing | 12 (< 1) | 10 (< 1) |
| Signs of shock | ||
| Yes | 2574 (43) | 2648 (44) |
| No | 3420 (57) | 3367 (56) |
| Rockall score | ||
| 1–2 | 1419 (24) | 1395 (23) |
| 3–4 | 2306 (38) | 2332 (39) |
| 5–7 | 2269 (38) | 2288 (38) |
| Taking anticoagulants | ||
| Yes | 528 (9) | 500 (8) |
| No | 5422 (90) | 5466 (91) |
| Unknown | 44 (1) | 49 (1) |
| Emergency admission | ||
| Yes | 5673 (95) | 5687 (94) |
| No | 321 (5) | 328 (6) |
| Major comorbidities | ||
| Cardiovascular | 1108 (18) | 1132 (19) |
| Respiratory | 337 (6) | 324 (5) |
| Liver | 2432 (41) | 2532 (42) |
| Renal | 325 (5) | 310 (5) |
| Malignancy | 417 (7) | 382 (6) |
| Other | 999 (17) | 968 (16) |
| Any comorbidity | 4308 (72) | 4329 (72) |
Chapter 4 Outcome and results
Outcome data were available for 11,989 randomised patients (5985 patients allocated to the TXA group and 6004 patients allocated to the placebo group). A total of 11,952 (99.5%) patients received the loading dose of the allocated treatment and 10,993 (91.5%) received the 24-hour maintenance dose.
Primary outcome
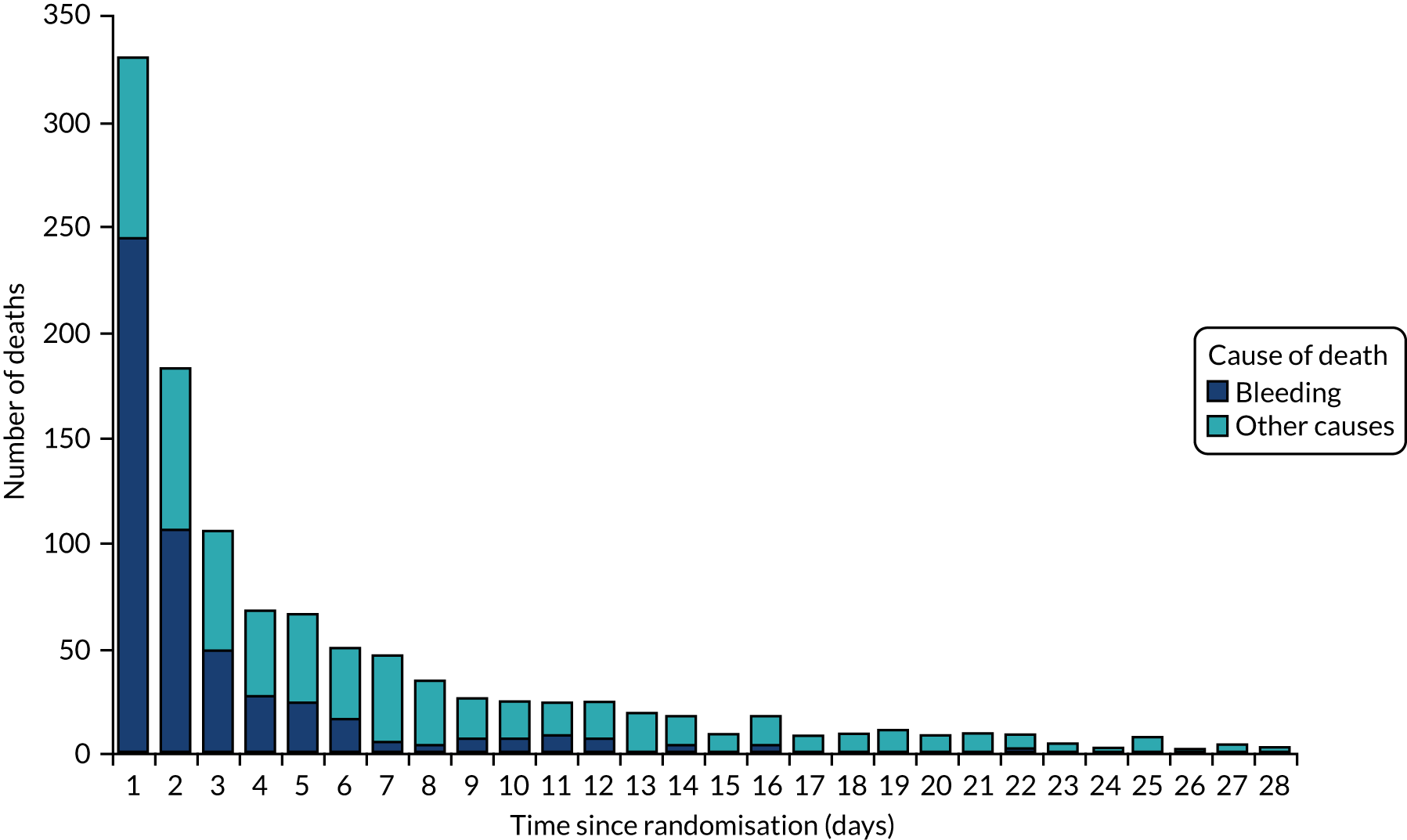
Figure 2 shows the number of deaths and cause of death by days since randomisation. There were 1121 deaths in total. The median time to death was 55 hours after randomisation (interquartile range 18.2–161.8 hours).
FIGURE 2.
Mortality by days from randomisation.
Death due to bleeding within 5 days of randomisation (Table 2) occurred in 222 patients (3.7%) in the TXA group and in 226 patients (3.8%) in the placebo group (RR 0.99, 95% CI 0.82 to 1.18). Similar results were obtained after adjusting for baseline covariates (RR 0.98, 95% CI 0.82 to 1.17) and in a per-protocol analysis (RR 0.94, 95% CI 0.71 to 1.23). When the 223 patients who received open-label antifibrinolytics were removed from the analysis, the results were similar (RR 0.97, 95% CI 0.81 to 1.17) (Table 3).
| Treatment group, n (%) | RR (95% CI) | ||
|---|---|---|---|
| TXA (N = 5956) | Placebo (N = 5981) | ||
| Death due to bleeding within 24 hours | 124 (2.1) | 120 (2.0) | 1.04 (0.81 to 1.33) |
| Death due to bleeding within 5 days | 222 (3.7) | 226 (3.8) | 0.99 (0.82 to 1.18) |
| Death due to bleeding within 28 days | 253 (4.2) | 262 (4.4) | 0.97 (0.82 to 1.15) |
| Rebleeding within 24 hoursa | 41 (0.7) | 41 (0.7) | 1.00 (0.65 to 1.55) |
| Rebleeding within 5 daysa | 287 (4.8) | 315 (5.3) | 0.91 (0.78 to 1.07) |
| Rebleeding within 28 daysa | 410 (6.8) | 448 (7.5) | 0.92 (0.81 to 1.05) |
| Treatment group, n/N (%) | RR (95% CI) | ||
|---|---|---|---|
| TXA | Placebo | ||
| No antifibrinolytics | 214/5854 (3.66) | 220/5867 (3.75) | 0.97 (0.81 to 1.17) |
| No vasopressin | 76/3608 (2.11) | 77/3554 (2.17) | 0.97 (0.71 to 1.33) |
| No proton pump inhibitor | 23/647 (3.55) | 20/588 (3.4) | 1.05 (0.58 to 1.88) |
Subgroup analysis
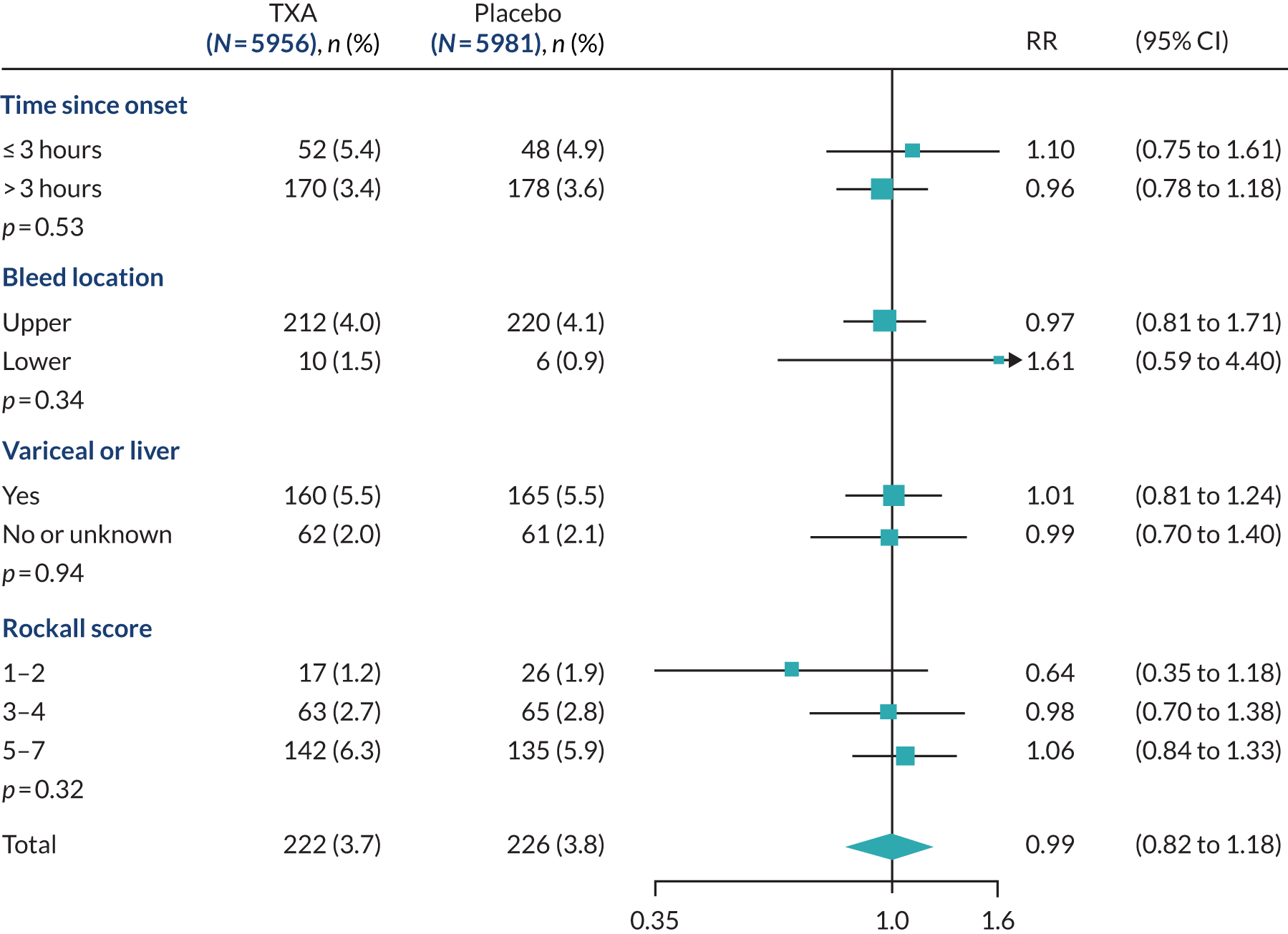
We examined the effect of TXA on death due to bleeding within 5 days of randomisation in prespecified subgroup analyses stratified by time to treatment (heterogeneity p = 0.53), location of bleeding (p = 0.34), cause of bleeding (p = 0.94) and clinical Rockall score (p = 0.32), but recorded no evidence of heterogeneity for these factors (Figure 3). When time since bleeding onset was modelled as a continuous variable, there was no evidence of an interaction (heterogeneity p = 0.53).
FIGURE 3.
Effect of TXA on death due to bleeding within 5 days. Analysis stratified by time since bleeding onset, suspected bleed location, suspected variceal bleeding or comorbid liver disease, and Rockall score.
We examined the effect of TXA on death due to bleeding within 5 days of randomisation, stratified by the World Bank’s classification of country income level (high vs. low or middle income), anticoagulant use and SBP. These exploratory analyses were not prespecified. The RRs did not appear to vary by country income, anticoagulant use or SBP.
Secondary outcome
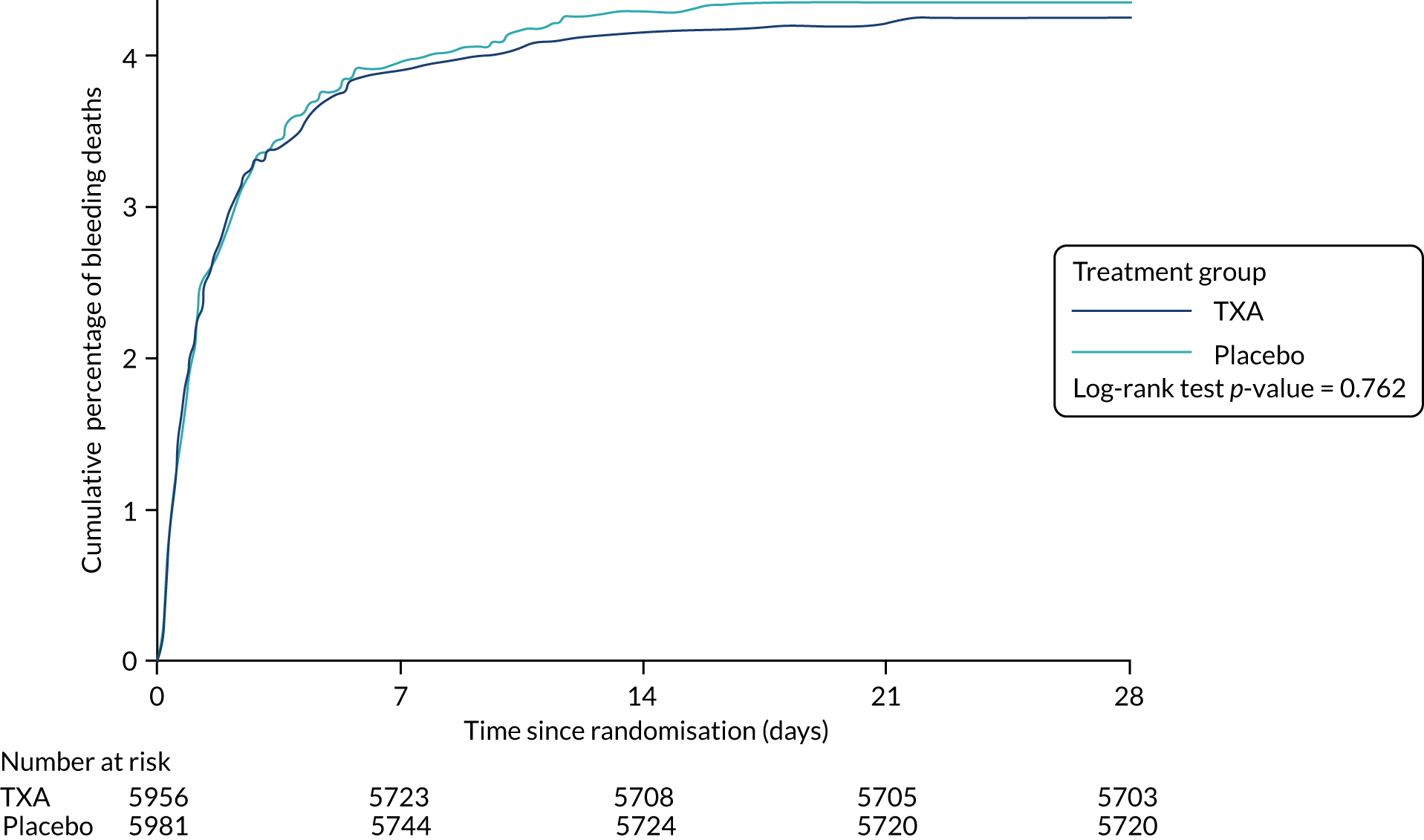
Death due to bleeding within 24 hours of randomisation occurred in 124 (2.1%) patients in the TXA group and 120 (2.0%) patients in the placebo group. Death due to bleeding within 28 days of randomisation occurred in 253 (4.2%) patients in the TXA group and 262 (4.4%) patients in the placebo group (RR 1.04, 95% CI 0.81 to 1.33) (Figure 4). Death due to bleeding within 28 days of randomisation occurred in 253 (4.2%) patients in the TXA group and 262 (4.4%) patients in the placebo group (0.97, 95% CI 0.82 to 1.15). Death from all causes within 28 days of randomisation (Table 4) occurred in 564 patients (9.5%) in the TXA group and in 548 patients (9.2%) in the placebo group (RR 1.03, 95% CI 0.92 to 1.16).
FIGURE 4.
Cumulative incidence plot of death due to bleeding. Hazard ratio 0.97, 95% CI 0.82 to 1.16.
| Cause of death | Treatment group, n (%) | RR (95% CI) | |
|---|---|---|---|
| TXA (N = 5956) | Placebo (N = 5981) | ||
| Bleeding | 253 (4.2) | 262 (4.4) | 0.97 (0.82 to 1.15) |
| Thromboembolic event | 26 (0.4) | 17 (0.3) | 1.54 (0.83 to 2.83) |
| Organ failure | 109 (1.8) | 114 (1.9) | 0.96 (0.74 to 1.25) |
| Pneumonia | 57 (1.0) | 42 (0.7) | 1.36 (0.92 to 2.03) |
| Sepsis | 33 (0.6) | 49 (0.8) | 0.68 (0.44 to 1.05) |
| Malignancy | 65 (1.1) | 40 (0.7) | 1.63 (1.10 to 2.42) |
| Other | 21 (0.4) | 24 (0.4) | 0.88 (0.49 to 1.58) |
| All cause | 564 (9.5) | 548 (9.2) | 1.03 (0.92 to 1.16) |
The proportion of patients with rebleeding was similar in both groups at 24 hours, 5 days and 28 days after randomisation (see Table 2). The proportion of patients who had surgery, radiological intervention and blood product transfusion was also similar in both groups (Table 5).
| Treatment group | Effect size (95% CI) | ||
|---|---|---|---|
| TXA | Placebo | ||
| Interventions, n/N (%) | |||
| Diagnostic endoscopy | 4781/5953 (80.3) | 4729/5978 (79.1) | 1.02 (1.00 to 1.03)a |
| Therapeutic endoscopy | 2542/5952 (42.7) | 2658/5978 (44.5) | 0.96 (0.92 to 1.00)a |
| Diagnostic radiological procedure | 1704/5953 (28.6) | 1744/5978 (29.2) | 0.98 (0.93 to 1.04)a |
| Therapeutic radiological procedure | 74/5953 (1.2) | 89/5978 (1.5) | 0.83 (0.61 to 1.13)a |
| Surgical intervention | 146/5953 (2.5) | 158/5978 (2.6) | 0.93 (0.74 to 1.16)a |
| Any surgical, endoscopic or radiological intervention | 5216/5956 (87.6) | 5236/5981 (87.5) | 1.00 (0.99 to 1.01)a |
| Any transfusion | 4076/5951 (68.5) | 4129/5978 (69.1) | 0.99 (0.97 to 1.02)a |
| Whole blood or red cells | 3984/4076 (97.7) | 4018/4129 (97.3) | 1.00 (1.00 to 1.01)a |
| Frozen plasma | 910/4076 (22.3) | 993/4129 (24.0) | 0.93 (0.86 to 1.00)a |
| Any platelets | 219/4076 (5.4) | 255/4129 (6.2) | 0.87 (0.73 to 1.04)a |
| Blood product transfusions, mean (SD) | |||
| Units of whole blood or red cells | 2.8 (2.4) | 2.9 (2.7) | –0.06 (0.05 to –0.18)b |
| Units of frozen plasma | 0.9 (2.4) | 1.0 (2.6) | –0.05 (–0.01 to –0.23)b |
| Units of any platelets | 0.2 (0.9) | 0.2 (1.0) | –0.02 (0.02 to –0.06)b |
The mean number of days spent in intensive care was similar in both groups (Table 6). The mean score on the Katz Index of Independence in Activities of Daily Living was also similar in both groups (see Table 6).
| Treatment group | Effect size (95% CI) | ||
|---|---|---|---|
| TXA | Placebo | ||
| Complications, n/N (%) | |||
| Any thromboembolic event | 86/5952 (1.4) | 72/5977 (1.2) | 1.20 (0.88 to 1.64)a |
| Venous events (deep-vein thrombosis, pulmonary embolism) | 48/5952 (0.8) | 26/5977 (0.4) | 1.85 (1.15 to 2.98)a |
| Deep-vein thrombosis | 23/5952 (0.4) | 12/5977 (0.2) | 1.92 (0.96 to 3.86)a |
| Pulmonary embolism | 28/5952 (0.5) | 16/5977 (0.3) | 1.76 (0.95 to 3.24)a |
| Arterial events (myocardial infarction, stroke) | 42/5952 (0.7) | 46/5977 (0.8) | 0.92 (0.60 to 1.39)a |
| Myocardial infarction | 24/5952 (0.4) | 28/5977 (0.5) | 0.86 (0.50 to 1.48)a |
| Stroke | 19/5952 (0.3) | 18/5977 (0.3) | 1.06 (0.56 to 2.02)a |
| Renal failure | 142/5951 (2.4) | 157/5978 (2.6) | 0.91 (0.73 to 1.14)a |
| Liver failure | 196/5952 (3.3) | 184/5977 (3.1) | 1.07 (0.88 to 1.30)a |
| Respiratory failure | 105/5952 (1.8) | 131/5978 (2.2) | 0.81 (0.62 to 1.04)a |
| Cardiac event | 100/5952 (1.7) | 89/5977 (1.5) | 1.13 (0.85 to 1.50)a |
| Sepsis | 210/5952 (3.5) | 216/5977 (3.6) | 0.98 (0.81 to 1.18)a |
| Pneumonia | 193/5952 (3.2) | 174/5978 (2.9) | 1.11 (0.91 to 1.36)a |
| Seizure | 38/5952 (0.6) | 22/5977 (0.4) | 1.73 (1.03 to 2.93)a |
| Self-care capacity, mean (SD) | |||
| Days in ICU | 0.4 (1.8) | 0.4 (2.0) | –0.06 (0.01 to –0.13)b |
| Katz score | 5.5 (1.5) | 5.5 (1.4) | –0.03 (0.02 to –0.09)b |
Adverse events
The risk of fatal or non-fatal thromboembolic events and arterial thromboembolic events (myocardial infarction or stroke) was similar in the TXA group and the placebo group (see Table 6). The risk of venous thromboembolic events (deep-vein thrombosis or pulmonary embolus) was higher in the TXA group than in the placebo group (see Table 6), and similar risk was observed after excluding patients who did not receive the maintenance dose (42 events with TXA compared with 20 events with placebo) (RR 2.11, 95% CI 1.24 to 3.59). In an exploratory subgroup analysis, the risk of venous thromboembolic events was higher in patients with suspected variceal bleeding or liver disease (14 vs. 2 events; RR 7.26, 95% CI 1.65 to 31.90) than in patients with other causes of bleeding (34 vs. 24 events; RR 1.38, 95% CI 0.82 to 2.32; p = 0.035 for heterogeneity). The risk of renal, hepatic and respiratory failure, cardiac events, sepsis and pneumonia was similar in TXA- and placebo-treated patients (see Table 6). Seizures occurred in 38 patients in the TXA group and in 22 patients in the placebo group (0.6% vs. 0.4%; RR 1.73, 95% CI 1.03 to 2.93) (see Table 6); after excluding patients who did not receive the maintenance dose the corresponding numbers were 33, compared with 17 events (RR 1.95, 95% CI 1.09 to 3.50). See Appendix 7 for a list of all adverse events.
Analyses that are specified in the statistical analysis plan, but not reported above, will be reported in separate publications.
Chapter 5 Economic evaluation results
The HALT-IT trial did not demonstrate that TXA significantly reduces key outcome measures, such as death due to bleeding within 5 days of randomisation (RR 0.99, 95% CI 0.82 to 1.18) or all-cause mortality (RR 1.03, 95% CI 0.92 to 1.16), when administered to people with AGIB. This means by default that, even if it is relatively inexpensive, TXA is unlikely to represent value for money in this indication. However, we have proceeded with the economic evaluation on the basis that it is important to assess the level of uncertainty around the cost-effectiveness of TXA based on the data available.
Methods
Decision problem
The analysis evaluates the cost-effectiveness of the current standard of care for people with AGIB with and without the administration of TXA. The evaluated TXA regimen mirrors that used in the HALT-IT trial, specifically a TXA loading dose (1 g) added to a 100-ml infusion bag of 0.9% sodium chloride, infused by slow intravenous injection over 10 minutes, and a TXA maintenance dose (3 g) added to 1 litre of an isotonic intravenous solution, infused over 24 hours.
We followed the NICE technology appraisal guidelines for conducting economic evaluations. 68 The evaluation uses a decision model to combine the clinical results from the HALT-IT trial with evidence from other sources to estimate costs and outcomes over a lifetime horizon for the two treatment options. The analysis adopts a UK NHS cost perspective and expresses health outcomes in terms of LYs and QALYs. Costs are reported in 2017/18 Great British pounds. All future costs and QALYs have been discounted at an annual rate of 3.5%.
Decision model
We have based our analysis on an existing Markov model of TXA following AGIB to estimate its cost-effectiveness in the AGIB setting. 69 The model consists of two health states, alive and dead, as shown in Figure 5. People with AGIB enter the model in the alive health state. People in the no-TXA group progress to the dead health state over the initial 28-day period (the HALT-IT trial period) using daily data taken directly from the trial on all-cause deaths from the placebo group of the HALT-IT trial; this includes data for all UK and non-UK participants. For the remaining 337 days of the first year, the daily probability of death in the no-TXA group was estimated using UK general population age-related mortality statistics,70 adjusted using a standardised mortality ratio (SMR) to reflect the long-term risk of excess death associated with surviving an AGIB episode. 71 In the base case, this SMR is applied for the entire time horizon. After this initial 1-year period, the model cycles yearly, applying the same probability function of death adjusted for the yearly rather than the daily cycle period. In line with the HALT-IT trial, the mean age of people entering the model was assumed to be 58.1 years.
FIGURE 5.
Markov model structure showing both health states in the model.

The SMR associated with the risk of death following an AGIB episode compared with that of the general population was derived from a study by Crooks et al. ,71 in which longitudinal data from the UK’s Hospital Episodes Statistics data set, the General Practice Research Database and the Office for National Statistics death register between 1997 and 2010 were linked to define a cohort of people with non-variceal bleeds. Controls were matched at the start of the study by age, sex, practice and year. Given that the study showed that the risk of death was highest in the first year following an AGIB episode, separate SMRs were derived for year 1 (SMR 5.21, 95% CI 4.25 to 6.38) and year 2 onwards (SMR 1.74, 95% CI 1.42 to 2.13). In the deterministic sensitivity analysis, excess mortality was excluded after 1 year.
Treatment effect
The base-case cycle probabilities of death in the TXA group were calculated in exactly the same manner as in the placebo group, but a relative treatment effect was also applied using a RR of all-cause death of 1.03 (95% CI 0.92 to 1.16); this RR is based on all trial participants and is not UK specific given that the subgroup analysis did not reveal any differences in treatment effect by country income level. Note that the HALT-IT trial results for the primary outcome measure, death due to bleeding within 5 days from randomisation, were similar in both treatment groups (RR 0.99, 95% CI 0.82 to 1.18), although the mean estimate slightly favoured TXA. However, given that the risks of venous thromboembolic events (deep-vein thrombosis or pulmonary embolus) and death from malignancy (RR 1.63, 95% CI 1.10 to 2.42) were higher in the TXA group than in the placebo group (RR 1.85, 95% CI 1.15 to 2.98), the RR of all-cause mortality was used as the estimate of effect, as it reflects the overall observed relative impact of TXA treatment on survival.
Utilities
Utility data were not collected as part of the HALT-IT trial; therefore, values were sourced from the existing literature. Only one directly relevant study could be identified: the relatively recent TRIGGER (Transfusion in Gastrointestinal Bleeding) RCT. 72 This trial evaluated the feasibility and safety of a restrictive compared with liberal RBC transfusion policy for adults admitted to UK hospitals with AGIB. Between August 2012 and March 2013, almost 950 people were randomised. Similar to the HALT-IT trial, the trial time horizon was 28 days. Of note, the EuroQol-5 Dimensions, three-level version, questionnaire73 was administered in the study, and the utility values have been reported in a separate publication. 74
We have taken a relatively simple approach to applying the utility values within the model base case, although this approach mirrors that used in a previous economic evaluation of TXA. 69 Specifically, individuals who died within the first 28 days were all assigned a utility of 0 over the entirety of this 28-day period. Campbell et al. 74 report a mean utility value of 0.735 (95% CI 0.70 to 0.77) for AGIB survivors on day 28 in the TRIGGER trial. In the base-case analysis, this value was applied to all participants in both treatment groups, who were alive at day 28, both during the initial 28-day period and at all times thereafter until death. Note that functional status was measured in the HALT-IT trial using the Katz Index of Independence in Activities of Daily Living75 either at hospital discharge or in hospital at day 28; the scores in both groups were similar. An age adjustment was also applied to the utility value in each cycle using the decrements reported by Kind et al. ,76 so that overall utility declined with age. In a sensitivity analysis, the utility value of 0.735 after 1 year was replaced with age-adjusted population values, also reported by Kind et al. ,76 whereby the utility values after the first year increased in line with the utility values of the UK’s general population. The latter approach mimics survivors of AGIB returning to ‘full health’ after 1 year; however, given the high prevalence of comorbidities in this population, which are themselves risk factors for an AGIB episode, it is unclear whether or not this is a realistic scenario.
Costs
Tranexamic acid treatment
The resources associated with providing TXA treatment were derived from the HALT-IT trial and by making a number of assumptions. The total TXA dose (4 g) included the loading and maintenance dose, for which the total cost was derived from the British National Formulary77 (£12 per patient). The cost of the equipment for treatment was assumed to include a needle (£0.04), syringe (£0.06), sodium chloride infusion bag (£0.55) and isotonic intravenous solution (£3.77). To account for the administration time of TXA, hourly staff costs were calculated from the Personal Social Services Research Unit costs for 2018. 78 The model assumed that a band 5 nurse would take 21 minutes to administer TXA (£12.95), following the treatment administration and expert guidance used within the economic evaluations of the CRASH59,69 and WOMAN trials. 79 This led to a total TXA treatment and administration cost of £29.37 per person (Table 7).
| Parameter | Value | 95% CIs | Distribution | Source |
|---|---|---|---|---|
| Age at model start (years) | 58.1 | – | – | HALT-IT |
| SMR year 1 | 5.21 | 4.25 to 6.38 | Log-normal | Crooks et al.71 |
| SMR year 2 | 1.74 | 1.42 to 2.13 | Log-normal | Crooks et al.71 |
| RR of all-cause mortality | 1.03 | 0.92 to 1.16 | Log-normal | HALT-IT |
| 28-day probability of deatha | 0.092 | 0.084 to 0.099 | Beta | HALT-IT |
| Utility AGIB survivor | 0.735 | 0.70 to 0.77 | Beta | Campbell et al.74 |
| Utility decrements by age (years) | Kind et al.76 | |||
| 55–64 | 0 | – | – | |
| 65–74 | 0.02 | – | – | |
| ≥ 75 | 0.07 | – | – | |
| Utility UK general population | By age | – | – | Kind et al.76 |
| All–cause mortality | By age | – | – | ONS70 |
| Discount rate costs | 3.5% | – | – | NICE68 |
| Discount rate QALYs | 3.5% | – | – | NICE68 |
Inpatient stay costs during the initial 28 days
Information from the HALT-IT trial was used to derive the costs of inpatient stays during this period. The total mean length of stay recorded by people receiving TXA was 5.83 days, and by those receiving placebo it was 5.80 days (Table 8). In both treatment groups, 0.4 of these days were spent in the ICU. These lengths of stay were multiplied by NHS reference costs for 2017/1880 for non-elective stays to derive mean hospital costs of £2292 per person for TXA and £2284 per person for no TXA.
| Parameter | Value | Standard error or proportion | Distribution | Source |
|---|---|---|---|---|
| TXA administration | £29.37 | – | – | British National Formulary,77 assumptions |
| Inpatient stays to day 28 | ||||
| Total length of stay (days) | ||||
| TXA | 5.83 | 1.46 | Gamma | HALT-IT |
| No TXA | 5.80 | 1.47 | Gamma | HALT-IT |
| Days in ICU | ||||
| TXA | 0.4 | 0.46 | Gamma | HALT-IT |
| No TXA | 0.4 | 0.51 | Gamma | HALT-IT |
| Unit cost per day in non-ICU | £313 | – | – | NHS reference costs80 |
| Unit cost per day in ICU | £1479 | – | – | NHS reference costs80 |
| Procedures to day 28 | ||||
| Probability endoscopy: diagnostic | ||||
| TXA | 0.8 | 4781/5953 | Beta | HALT-IT |
| No TXA | 0.79 | 4729/5978 | Beta | HALT-IT |
| Unit cost | £617 | – | – | NHS reference costs80 |
| Probability endoscopy therapeutic | ||||
| TXA | 0.43 | 2542/5953 | Beta | HALT-IT |
| No TXA | 0.44 | 2658/5978 | Beta | HALT-IT |
| Unit cost | £721 | – | – | NHS reference costs80 |
| Probability surgical intervention | ||||
| TXA | 0.02 | 146/5953 | Beta | HALT-IT |
| No TXA | 0.03 | 158/5978 | Beta | HALT-IT |
| Unit cost | £1065 | – | – | NHS reference costs80 |
| Probability radiological diagnostic | ||||
| TXA | 0.29 | 1704/5953 | Beta | HALT-IT |
| No TXA | 0.29 | 1744/5978 | Beta | HALT-IT |
| Unit cost | £4625 | – | – | NHS reference costs80 |
| Probability radiological therapeutic | ||||
| TXA | 0.01 | 74/5953 | Beta | HALT-IT |
| No TXA | 0.01 | 89/5978 | Beta | HALT-IT |
| Unit cost | £4625 | – | – | NHS reference costs80 |
| Transfusions | ||||
| Probability blood or red cells | ||||
| TXA | 0.67 | 3984/5951 | Beta | HALT-IT |
| No TXA | 0.67 | 4018/5978 | Beta | HALT-IT |
| Mean units of blood or red cells | ||||
| TXA | 2.80 | 0.61 | Gamma | HALT-IT |
| No TXA | 2.90 | 0.69 | Gamma | HALT-IT |
| Unit cost | £122 | – | – | NHS Blood and Transplant Price List 81 |
| Probability fresh-frozen plasma | ||||
| TXA | 0.15 | 910/5951 | Beta | HALT-IT |
| No TXA | 0.16 | 993/5978 | Beta | HALT-IT |
| Mean units of fresh-frozen plasma | ||||
| TXA | 0.90 | 0.61 | Gamma | HALT-IT |
| No TXA | 1.0 | 0.66 | Gamma | HALT-IT |
| Unit cost | £28 | – | – | NHS Blood and Transplant Price List 81 |
| Probability platelets | ||||
| TXA | 0.04 | 219/5951 | Beta | HALT-IT |
| No TXA | 0.04 | 255/5978 | Beta | HALT-IT |
| Mean units of platelets | ||||
| TXA | 0.20 | 0.23 | Gamma | HALT-IT |
| No TXA | 0.20 | 0.26 | Gamma | HALT-IT |
| Unit cost | £178 | – | – | NHS Blood and Transplant Price List 81 |
| Post-discharge costs | ||||
| Year 1 | £3989 | £1995a | Gamma | Ramagopalan et al.82 |
| Year 2 | £1816 | £908a | Gamma | Ramagopalan et al.82 |
| Year 3 | £1777 | £889a | Gamma | Ramagopalan et al.82 |
Procedures
While in hospital during the 28-day trial period, participants underwent a number of procedures, including endoscopies, surgery and radiological interventions (see Table 8). The cost of these procedures by treatment group was calculated using information from the HALT-IT trial, multiplying the probability that of each procedure being required by the NHS reference cost for 2017/18. 80 The mean per-person procedural cost was £2216 in the TXA group and £2260 in the placebo group.
Transfusions
While in hospital during the initial 28 days, some participants received transfusions of blood/RBCs, fresh-frozen plasma and platelets (see Table 8). Information from the HALT-IT trial on the frequency and the mean number of units for each transfusion type were combined with unit costs from the NHS Blood and Transplant Price List81 to generate overall costs. The mean per-person transfusion cost was £234 in the TXA group and £245 in the placebo group.
Post-discharge costs
The HALT-IT and TRIGGER trials observed participants for a maximum of 28 days; therefore, longer-term care costs were sourced from the literature. A specific study related to AGIB could not be identified. However, a recent UK study by Ramagopalan et al. 82 estimated the costs of GI bleeding among people with non-valvular atrial fibrillation by comparing the costs in people who were and those who were not experiencing a bleed, and used a difference-in-difference approach to calculate the costs attributable to a GI bleed (cases, n = 7753; controls, n = 7753). The controls were matched to cases on a 1 : 1 basis using a propensity scoring approach and nearest neighbour matching with replacement. Information on resource use was derived from the Clinical Practice Research Data link and Hospital Episode Statistics, and included information on primary care, procedures, prescriptions, inpatient stays and outpatient visits. A matching study used a variety of sources to estimate unit costs in this study, including the 2017/18 NHS reference costs. 80
The study allows the annual costs of caring for people with a bleed to be calculated for 3 years after the date of the bleeding event (see Table 8). In the absence of other information, the reported year 3 costs were inputted to the model for year 4 onwards, although they were assumed to be one-third of the original amount. The standard errors that the costing study reports could not be easily incorporated into our analysis (the statistical approach used allowed costs to be negative) and, therefore, were assumed to be 50% of the mean value in all instances, which is considered to reflect a relatively large degree of uncertainty in the mean estimates. The importance of these assumptions was assessed in the sensitivity analysis.
Subgroup analysis
The HALT-IT trial protocol2 specifies subgroup analyses to examine the effects of TXA on death due to bleeding within 5 days of randomisation based on time to treatment (≤ 3 vs. > 3 hours), site of bleeding (upper vs. lower GI), cause of bleeding (suspected variceal bleeding or comorbid liver disease vs. other or unknown causes) and clinical Rockall score. Post hoc subgroup analyses stratified by World Bank classification of country income level (high vs. low or middle income), anticoagulant use and SBP were also undertaken. However, no evidence of heterogeneity was recorded. For this reason, we do not report any cost-effectiveness results for different AGIB subgroups.
Sensitivity analysis
Various one-way deterministic sensitivity analyses were undertaken to assess the robustness of the results to alternative assumptions. A probabilistic sensitivity analysis (PSA) was also undertaken using 10,000 Monte Carlo simulations; the parameter distributions are specified in Tables 7 and 8. Risk ratios were specified as log-normal distributions, utilities and other proportions as beta-distributions and costs as gamma-distributions. Parameters that were excluded from the PSA are not assigned a distribution type in the tables.
We report the results as incremental cost-effectiveness ratios (ICERs), incremental net monetary benefits (INMBs), cost-effectiveness planes and cost-effectiveness acceptability curves (CEACs). A threshold of willingness to pay for an additional QALY of £20,000–30,000 was used to determine cost-effectiveness, in line with the NICE technology appraisal recommendations. 68
Results
The base-case results are shown in Table 9. In both the deterministic and the probabilistic analyses TXA was associated with marginally smaller gains in LYs and QALYs, and lower costs, than treatment without TXA. For example, the deterministic QALYs and costs associated with TXA and no TXA were 8.58 and 8.61, and £16,706 and £16,764, respectively. The associated ICERs are £1413 per LY gained and £1981 per QALY gained if no TXA is used instead of TXA (i.e. at NICE-recommended threshold willingness-to-pay values, no TXA is the preferred option). The deterministic and mean probabilistic results are almost identical (see Table 9).
| Analysis | Costs (£) | LYs | QALYs | ICER LYs (£) | ICER QALYs (£) |
|---|---|---|---|---|---|
| Deterministic | |||||
| No TXA | 16,764 | 12.08 | 8.61 | 1413 | 1981 |
| TXA | 16,706 | 12.04 | 8.58 | – | – |
| Probabilistic (PSA) | |||||
| No TXA | 16,895 | 12.21 | 8.70 | 1419 | 1988 |
| TXA | 16,840 | 12.17 | 8.67 | – | – |
The lower mean health outcomes for TXA are driven by the fact that the mean RR for all-cause mortality (i.e. the relative treatment effect inputted to the model) slightly favours the no-TXA treatment group (RR 1.03). The higher incremental costs associated with no TXA are largely driven by the fact that people who did not receive TXA live for marginally longer than those who received TXA; thus, patients who are not treated with TXA incur slightly higher post-discharge costs and marginally higher intervention and transfusion costs than those who are treated with TXA, and these costs more than outweigh the additional cost of TXA administration.
Various deterministic one-way sensitivity analyses are shown Table 10. In all but one instance the results show that the base-case ICER was very robust to alternative model parameter and structural assumptions. The exception is when the RR of all-cause mortality is reduced to 0.92 (the lower bound of the 95% CI). In this instance, TXA produces marginally better health outcomes at slightly higher costs than no TXA, producing an ICER of £1144 per QALY gained if TXA is used instead of no TXA. Note that, even when the cost of TXA and its administration was set to £0 instead of the base-case value of £29.37, the ICER per QALY gained remained under £3000, favouring no TXA.
| Parameter | Incremental costs (£) | Incremental LYs | Incremental QALYs | ICER LYs (£) | ICER QALYs (£) | INMB (QALY) (£) |
|---|---|---|---|---|---|---|
| Base case | –58 | –0.04 | –0.03 | 1413 | 1981 | –524 |
| Excess mortality excluded after first year | –62 | –0.05 | –0.03 | 1306 | 1843 | –611 |
| Monitoring costs (full monitoring costs for year 4 onwards) | –96 | –0.04 | –0.03 | 2357 | 3304 | –486 |
| Monitoring costs not included beyond 3 years | –38 | –0.04 | –0.03 | 941 | 1319 | –544 |
| 0% discount rate | –70 | –0.06 | –0.04 | 1162 | 1646 | –783 |
| 6% discount rate | –52 | –0.03 | –0.02 | 1609 | 2243 | –412 |
| Utility: general population utility after first year | –58 | –0.04 | –0.03 | 1413 | 1826 | –574 |
| Monitoring costs: inpatient costs excluded in year 1 | –49 | –0.04 | –0.03 | 1204 | 1688 | –533 |
| TXA all-cause mortality RR (0.92) | 79 | 0.10 | 0.07 | 816a | 1144a | 1310 |
| TXA all-cause mortality RR (1.16) | –210 | –0.19 | –0.14 | 1080 | 1514 | –2568 |
| Total TXA administration at £0 | –87 | –0.04 | –0.03 | 2133 | 2990 | –600 |
The base-case cost-effectiveness plane and CEAC for the probabilistic costs and QALYs are shown in Figures 6 and 7, respectively. The cost-effectiveness plane shows that the simulations are clustered around the origin and distributed relatively evenly across all four cost-effectiveness quadrants. This is because the point estimate for the RR of all-cause mortality is only slightly above 1, and is included within its CI (RR 1.03, 95% CI 0.92 to 1.16); therefore, there is little to choose between the two treatment options in terms of outcomes. The same is also true of the relatively low cost of TXA administration (£29.37 per person), meaning that the majority of the costs incurred are the hospital costs (hospital stay, interventions and transfusions) and post-discharge costs. The CEAC summarises the cost-effectiveness plane and shows that at any willingness to pay for an additional QALY above £2000, no TXA is likely to be the more cost-effective option. For example, at the NICE-specified willingness-to-pay threshold levels of £20,000 and £30,000 per additional QALY, TXA has a 34% and 33% probability of being the most cost-effective option, respectively. Note that the base-case CEAC does not indicate that there is a 0% probability that TXA is the most cost-effective treatment option, irrespective of the willingness-to-pay value. The lowest that this value can reduce to is 15% because TXA treatment produced more QALYs at lower cost in this proportion of simulations (i.e. it was the ‘dominant’ treatment option in this proportion of simulations). Re-running the PSA assuming the standard error of the post-discharge costs to be 20%, instead of 50%, of their mean value had a negligible impact on the probability of TXA being cost-effective.
FIGURE 6.
Base-case cost-effectiveness plane. The north-east quadrant contains 15% of simulations, the south-west quadrant 37%, the south-east quadrant 14% and the north-west quadrant 34%.
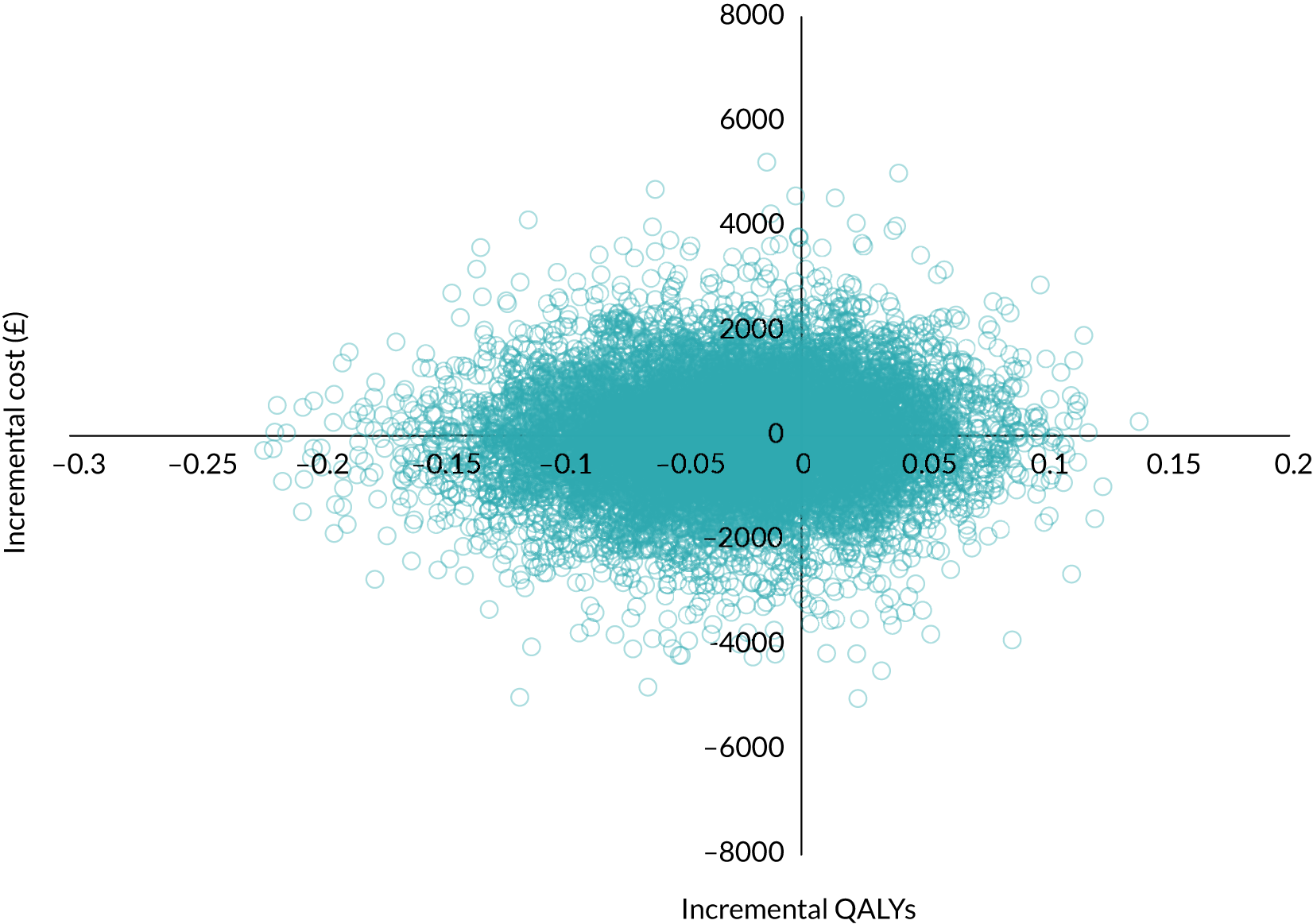
FIGURE 7.
Base-case CEAC. The north-east quadrant contains 27% of simulations, the south-west quadrant 25%, the south-east quadrant 24% and the north-west quadrant 24%.
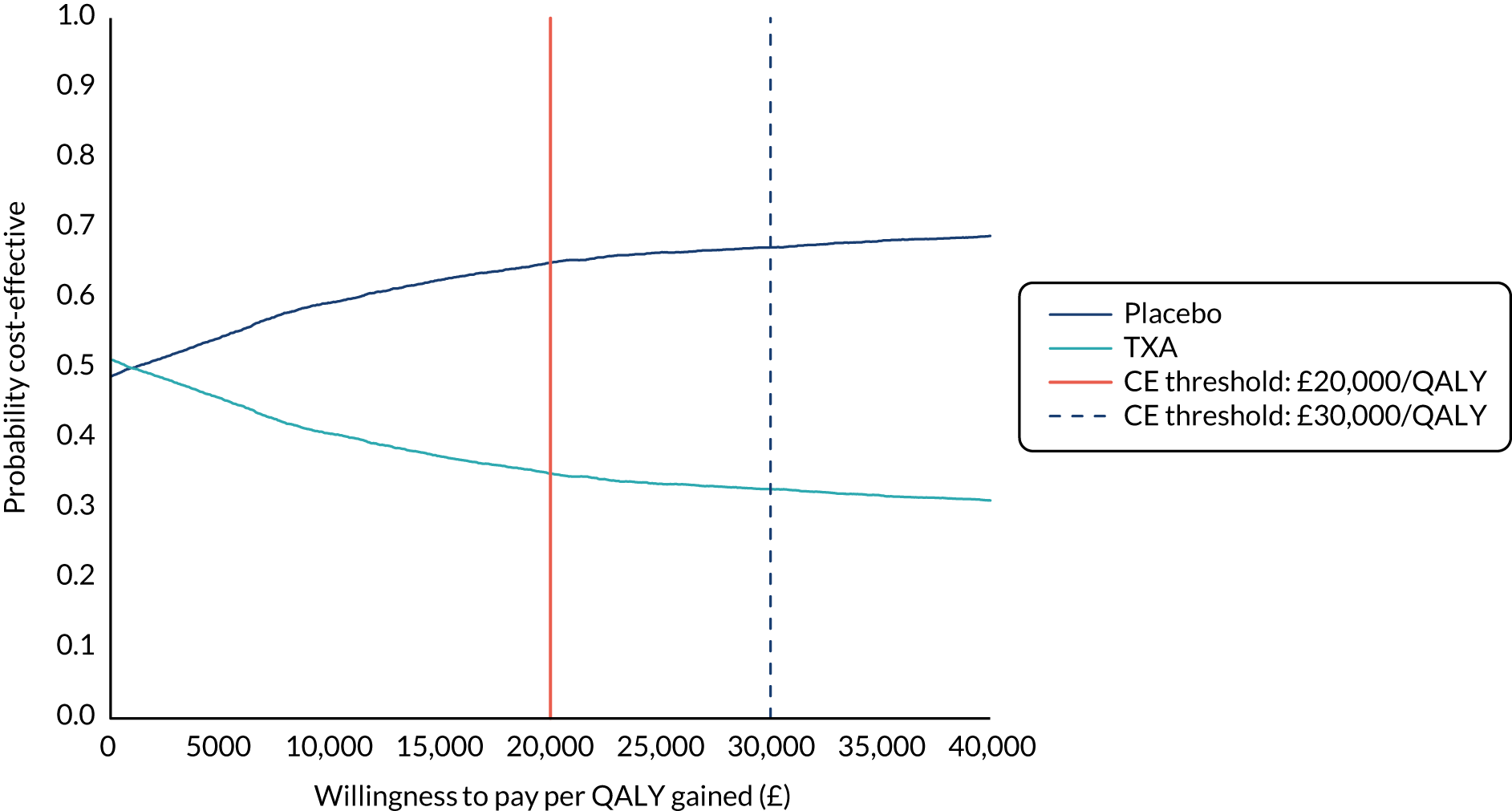
To demonstrate the sensitivity of the results to alternative parameter values for the RR for all-cause mortality, the PSA was re-run assuming a RR of 1.00 (95% CI 0.88 to 1.10). These values are somewhat arbitrary/hypothetical, but include a point estimate that does not favour either treatment, with a wide CI that still includes a value of 1. Irrespective of the threshold willingness-to-pay level, the probability of TXA being the most cost-effective option is approximately 50% (Figure 8), demonstrating its low administration cost.
FIGURE 8.
Cost-effectiveness acceptability curve assuming a hypothetical RR of all-cause mortality of 1.00 (95% CI 0.88 to 1.10).
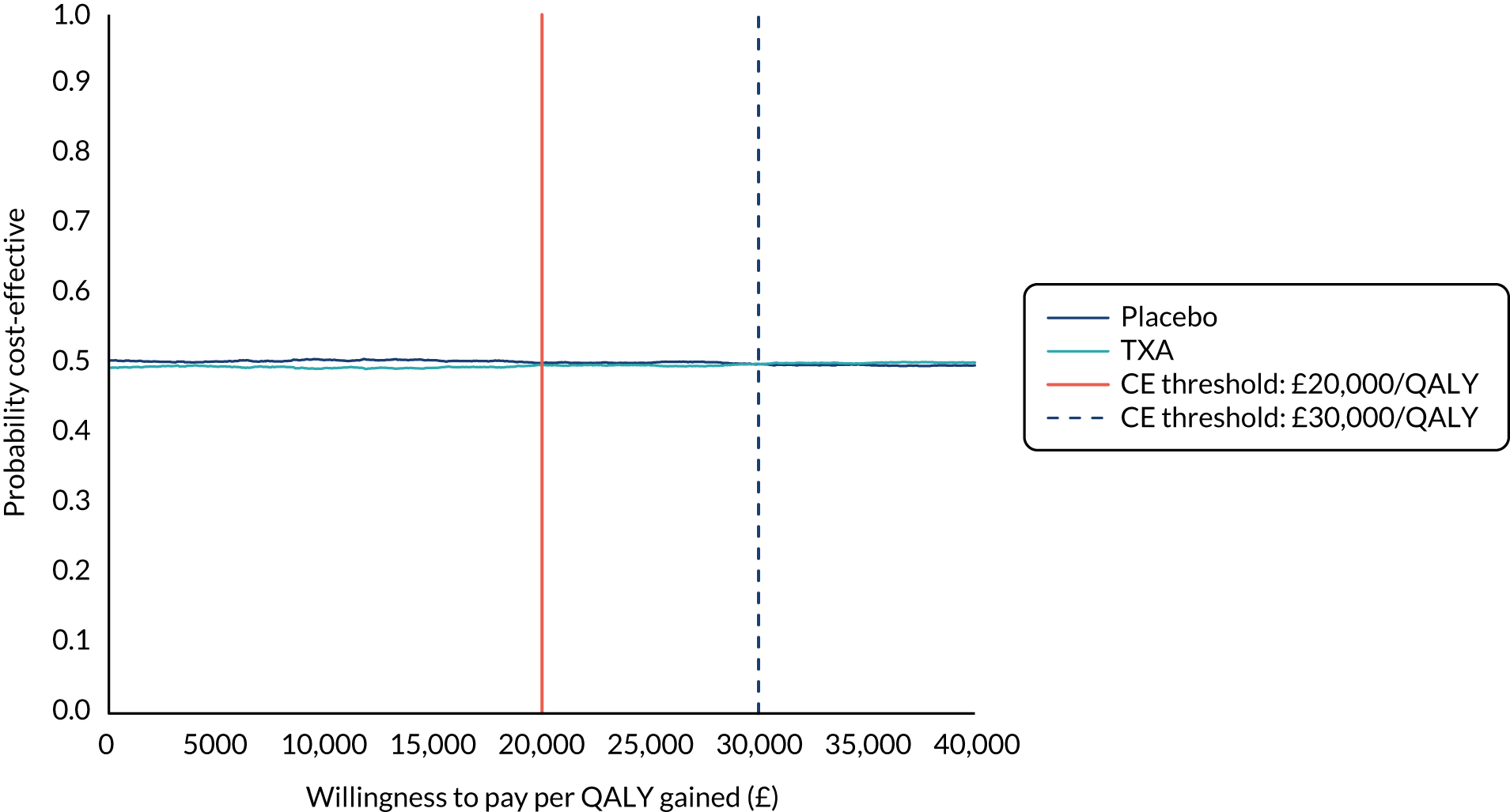
Chapter 6 Discussion
In this trial, TXA did not reduce death from GI bleeding but was associated with an increased risk of venous thromboembolic events and seizures. The proportion of patients experiencing rebleeding was similar in the TXA and placebo groups.
Administration of TXA within 3 hours of bleeding onset reduces death due to bleeding in patients with trauma or post-partum haemorrhage without increasing the risk of thromboembolic events. In these bleeding scenarios, the timing of onset is easy to determine: most patients present early and there are well-documented changes in fibrinolysis that provide a biological rationale for TXA treatment. 83,84 However, in the case of GI bleeding it is difficult to determine the time of bleeding onset, presentation is often delayed (> 80% of patients present > 3 hours after bleeding onset) and the contribution of increased fibrinolysis to bleeding is less clear.
Almost half of the patients included in our trial had suspected variceal bleeding due to liver disease, and because these patients have a greater risk of death they accounted for nearly three-quarters of deaths. Recent research shows that acutely ill patients with cirrhosis have a mixed fibrinolytic phenotype. 85 Some have increased fibrinolysis but others have profound hypofibrinolysis. The prevalence of hypofibrinolysis appears to be greatest in the most critically ill patients. Using the same clot lysis assay, reduced fibrinolysis has been shown to be associated with a small increased risk of venous thrombosis. 86 In our trial, the increased risk of venous thromboembolic events with TXA appeared to be more marked in patients with liver disease, although this was an exploratory subgroup analysis and there was no strong evidence of heterogeneity. Nevertheless, reduced fibrinolysis in patients with liver disease might explain the lack of any reduction in bleeding deaths with TXA and the increased risk of venous thromboembolic events.
The dose of TXA used in this trial was higher and the duration of treatment was longer (4 g over 24 hours) than that in randomised trials of TXA in trauma54,57 (2 g over 8 hours) or post-partum haemorrhage55 (1-g bolus with a repeat 1-g dose if bleeding continued), which did not record any increase in adverse events with TXA. Patients with GI bleeding often rebleed after initial haemostasis, particularly within the first 24 hours. Because TXA has a short half-life, we used a longer treatment duration to cover this high-risk period. Furthermore, previous trials in GI bleeding that appeared to show a large mortality reduction with TXA used a high dose and a longer duration of treatment than trials in trauma and post-partum haemorrhage. 87 The longer duration of TXA treatment in this trial may explain the increased risk of venous thromboembolic events, and the higher dose may explain the increased risk of seizures. 88
In summary, we found no evidence that TXA decreases the risk of death in patients with GI bleeding. Our results caution against a uniform approach to the management of patients with major haemorrhage and highlight the need for randomised trials targeted at specific pathophysiological processes. Given that GI bleeding is a licensed indication for TXA, our results may have regulatory implications.
Strengths and limitations
Our trial had several strengths but also some limitations. The randomisation method ensured that participating clinicians had no foreknowledge of the treatment allocation and the placebo control ensured that the outcome assessment was blind to treatment group. The inclusion criteria were clinical, reflecting the full range of GI bleeding presentations that doctors face in day-to-day practice. Baseline prognostic factors were well balanced and almost all randomly assigned patients were followed up. The primary outcome was death due to bleeding within 5 days of randomisation. Our scientific reasons for prespecifying death due to bleeding as the primary outcome in the statistical analysis plan are presented in detail elsewhere. 67 Although some misclassification of cause of death is possible, the assessment was blind to the treatment group. However, as there was no evidence of a treatment effect for the prespecified primary end point (death due to bleeding at 5 days) or for death from any cause at 28 days, the choice of end point does not influence the interpretation of the results. Misclassification might also have affected our subgroup analyses because at the time of recruitment the site and cause of bleeding could not be known with certainty. Our use of the pre-endoscopy Rockall score may have misclassified the baseline risk. 89 To minimise the risk of false positives, we used strict criteria to diagnose thromboembolic events, including a positive result on imaging (e.g. ultrasound) or at post-mortem examination. Although this may have led to some under-reporting because the diagnostic tests have high specificity, the RR estimates should be unbiased. Although some patients received antifibrinolytics outside the protocol, the treatment effect was the same when these patients were excluded. Although this is one of the largest randomised trials in GI bleeding, we cannot rule out a modest increase or decrease in death due to bleeding with TXA. However, we can rule out the large mortality reduction suggested by the Cochrane systematic review and meta-analysis of previous small trials. 87
Cost-effectiveness
The results of the analysis suggest that the costs and outcomes of treating people with AGIB with and without TXA, as enrolled and treated in the HALT-IT trial, are very similar. However, the base-case probabilistic analysis showed that the probability that TXA is the most cost-effective option is 34% and 33% at thresholds of willingness to pay for an additional QALY of £20,000 and £30,000, respectively. This means that, on balance, no TXA is more likely to be the most cost-effective option. The deterministic sensitivity analyses confirmed the robustness of this finding. These results are in line with our prior expectations given the additional, albeit modest cost (£29.37), of providing TXA and the knowledge that it was not associated with a statistically significantly reduction in all-cause mortality (RR 1.03, 95% CI 0.92 to 1.16), as reported by the HALT-IT trial.
As with all decision models, our analysis includes a number of parameter and structural assumptions. For example, assumptions were made regarding the longer-term costs of caring for people who recover from an initial episode of AGIB, and the utility values were sourced from outside the HALT-IT study and were assumed to be equal for both treatment groups. Moreover, unlike previous economic evaluations of TXA, we estimated the impact of treatment based on a RR of all-cause mortality rather than death due to bleeding, given that TXA was associated with a higher risk of death due to thromboembolic events and malignancies. However, only the scenarios that included a point RR of all-cause mortality favouring TXA over no TXA resulted in TXA being considered the most cost-effective option. We therefore do not believe that any of the assumptions that have been made, or the use of alternative measure of treatment effect, are of particular importance in terms of affecting the overall conclusions regarding cost-effectiveness.
To the best of our knowledge, no other cost-effectiveness analyses of TXA for people with AGIB have been reported. However, economic evaluations based on the series of CRASH RCTs57 and the WOMAN RCT55 concluded that TXA is highly cost-effective in other indications, specifically following trauma injury69 and post-partum haemorrhage. 79 The dose of TXA used in the HALT-IT trial is higher than that used in the previous studies. However, the increased cost of treatment is negligible and does not explain the clearly different cost-effectiveness results. The basic reason for the difference is that the HALT-IT trial did not provide any evidence to support a statistically significant improvement in health outcomes from using TXA, whereas evidence of benefit was much stronger in the other indications. However, 80% of participants in the HALT-IT trial received treatment > 3 hours after the suspected onset of bleeding. This is important because there is reason to believe from the RCTs of TXA in trauma and post-partum haemorrhage that earlier treatment is associated with improved outcomes. Our cost-effectiveness results reflect the timing of treatment as given in the HALT-IT trial, meaning that we cannot rule out the possibility of TXA being the most cost-effective option if treatment is more promptly administered.
Findings in context
Evidence before this study
Before this study, a Cochrane systematic review and meta-analysis87 of randomised trials of TXA for upper GI bleeding included seven trials with a total of 1654 patients. There was a large reduction in mortality with TXA (pooled RR 0.61, 95% CI 0.42 to 0.89; p = 0.01). 87 However, given the small size of the included trials and the potential for selection and other biases, we considered this evidence to be hypothesis-generating, requiring confirmation in larger trials. Furthermore, there was substantial uncertainty about the risk of thromboembolic events with TXA (pooled RR 1.86, 95% CI 0.66 to 5.24).
Added value of this study
The HALT-IT trial included 12,009 patients from 164 hospitals in 15 countries. Adult patients with significant upper or lower GI bleeding were randomly assigned to receive TXA (a 1-g loading dose followed by a 3-g maintenance dose over 24 hours) or matching placebo. TXA did not reduce death from GI bleeding (RR 0.99, 95% CI 0.82 to 1.18) but was associated with an increased risk of venous thromboembolic events (RR 1.85, 95% CI 1.15 to 2.98) and seizures (RR 1.73, 95% CI 1.03 to 2.93).
Implications of all the available evidence
The most recent update of the Cochrane review included eight small randomised trials with 1701 participants and showed a reduction in mortality with TXA (RR 0.60, 95% CI 0.42 to 0.87). Although we cannot entirely rule out a modest increase or decrease in death due to bleeding with TXA, we can rule out the large mortality reduction suggested by the Cochrane review. 60 Furthermore, TXA appears to increase the risk of venous thromboembolic events in patients with GI bleeding. On the basis of our results, TXA should not be used for the treatment of GI bleeding outside the context of a randomised trial. Our results highlight the unreliability of meta-analyses of small trials.
Implications for practice in the NHS
Many emergency physicians and surgeons believe that TXA improves outcomes in patients with acute severe GI bleeding. Emergency physicians and surgeons are familiar with TXA, which is widely used in trauma and elective surgery based on compelling evidence from large, high-quality, randomised trials. The promotion of ‘major haemorrhage protocols’ in UK hospitals encourages the notion that all bleeding is fundamentally the same and can be treated in a similar way. Furthermore, the Cochrane systematic review and meta-analysis87 of previous trials of TXA in GI bleeding shows a large reduction in mortality with TXA (pooled RR 0.61, 95% CI 0.42 to 0.89; p = 0.01). Despite the small size of the included trials, the potential for selection and other biases and the lack of data on adverse effects suggest that these results should be seen as hypothesis-generating rather than confirmatory; these methodological caveats can be lost on a doctor struggling to control a life-threatening GI bleed. Indeed, even the methodologically sophisticated NIHR Health Technology Assessment (HTA) Commissioning Board questioned the need for the HALT-IT trial given the evidence from the Cochrane review.
‘The Board expressed significant concerns about the need of this trial in the light of current evidence for benefit for TXA in GI bleeding and other conditions. Therefore, the applicants should argue the case for this trial very thoroughly in their full application.’ (NIHR, 2011, personal communication).
The results of the HALT-IT trial showed that TXA did not reduce death from GI bleeding but was associated with an increased risk of venous thromboembolic events and seizures. The proportion of patients with rebleeding was similar in the TXA and placebo groups. These results caution against a ‘one size fits all’ approach to the management of patients with major haemorrhage and highlight the need for randomised trials targeted at specific pathophysiological processes. In traumatic bleeding, the timing of bleeding onset is easy to determine: most patients present early and there are well-documented changes in fibrinolysis that provide a biological rationale for TXA treatment. However, in the case of GI bleeding, it is difficult to determine the time of bleeding onset, presentation is often delayed (> 80% of patients present more than 3 hours after bleeding onset) and the contribution of increased fibrinolysis to bleeding is less clear. Based on the HALT-IT trial results, TXA should not be used for the treatment of GI bleeding outside the context of a randomised trial.
Implications for research in the NHS
Although we cannot rule out a modest increase or decrease in the risk of death due to bleeding with TXA, we can rule out the large mortality reduction suggested by the Cochrane systematic review and meta-analysis87 of previous small trials. In this respect, the HALT-IT trial highlights the dangers of overinterpreting results from systematic reviews of small trials. Although the review authors emphasised the methodological weakness of the included trials, pointing out the ‘limitations in their internal and external validity’, the large, statistically significant reduction in all-cause mortality is hard to ignore and has had a considerable impact on research on this topic. As previously stated, the HTA Board questioned the need for a trial given the systematic review evidence. The large mortality reduction also made it harder to justify a large randomised trial. The investigators sent the trial protocol to The Lancet for peer review. The Lancet reviewers’ main concern was that the HALT-IT trial was unnecessarily large. The possibility that systematic reviews of small trials could cause research waste by encouraging underpowered trials was raised by the chief investigator in 2015:90
Systematic reviews of small trials increase waste by advertising to the scientific community inflated, often significant treatment effects that become smaller or absent when large, high-quality trials are done. Effect estimates from systematic reviews often inform sample size calculations. However, because most reviews provide exaggerated estimates of treatment effects due to inclusion of small, poor-quality trials, new trials will be underpowered to detect modest but potentially important effects.
Although it is hard to quantify the impact of the Cochrane review on clinical equipoise on this topic, open-label use of TXA was a recurrent problem in the UK and led to the closure of recruitment to the HALT-IT trial at many UK hospitals. Had it not been for brisk recruitment in the non-UK hospitals, the HALT-IT trial may not have achieved its recruitment target. The large discrepancy between the results of the Cochrane review and the results of the HALT-IT trial should encourage a reconsideration of the role of systematic reviews of small trials in informing health care and health research. Most meta-analyses are dominated by small trials. The median number of trials in Cochrane reviews is six, and the median number of patients per trial is approximately 80. 91 In most cases, the results of such reviews should be considered hypothesis-generating, requiring confirmation in adequately powered randomised trials.
Despite that, with 12,000 patients, the HALT-IT trial is, to the best of our knowledge, the largest randomised trial of TXA in GI bleeding, we cannot rule out a modest treatment benefit. Because there is strong evidence that TXA reduces bleeding deaths in patients with traumatic and post-partum haemorrhage, individual patient data meta-analyses should assess the strength of the evidence that the effectiveness and safety of TXA vary by the site and cause of bleeding. Basic research could also inform this question by examining the role of fibrinolysis in patients with GI bleeding and whether or not this varies depending on the aetiology of the bleeding.
Chapter 7 Dissemination
A dissemination plan (see Appendix 8) was written to guide the dissemination of the study results. This document outlined the background to the trial, objectives of the dissemination strategy and planned specific outputs of dissemination.
Objectives
A key objective of the dissemination plan was to inform the trial collaborators of the HALT-IT trial results and to help them to disseminate the results in their countries. The successful completion of the trial was entirely dependent on the work of collaborators in the participating hospitals. Hence, the results of the trial were reported first to trial collaborators.
Developing dissemination tools that collaborators could use for national and international audiences helped to achieve this. The various dissemination documents were uploaded onto the trial website to allow collaborators to download these resources and use them locally. Further dissemination tools for collaborating investigators were created to help them raise awareness of the trial results.
Dissemination of the results to all trial participants, particularly those who asked to be informed of the trial results, was also a vital objective. A lay summary of the results was sent to sites to communicate the results to their participants directly, and wider dissemination to participants took place via the media and the trial website (URL: https://haltit.lshtm.ac.uk/). The dissemination plan also aimed to make the results accessible to the public by using social media [including Twitter (Twitter, Inc., San Francisco, CA, USA; www.twitter.com), Facebook (Facebook, Inc., Menlo Park, CA, USA; www.facebook.com) and WhatsApp (Facebook, Inc.; www.whatsapp.com), the trial website (https://haltit.lshtm.ac.uk/), the LSHTM Clinical Trial Unit (CTU) website (https://ctu.lshtm.ac.uk/) and by broadcasting the results in The Resus Room podcast.
In terms of the scientific and medical community, the objective was to disseminate the results as widely as possible through publication of the results in a peer-reviewed medical journal, through conference presentations, by sharing the link to the publication in all applicable trial registers and by posting the dissemination materials on the HALT-IT website, on the LSHTM CTU website and on social media. Following completion of all prespecified analyses, another key dissemination objective was to share individual de-identified patient data, including data dictionary via the LSHTM CTU data-sharing platform, The Free Bank of Injury and Emergency Research Data (freeBIRD) at https://freebird.lshtm.ac.uk. The purpose of this was to allow maximum utilisation of the data to improve patient care and advance medical knowledge.
Outputs
-
The trial results were published in The Lancet on 20 June 2020. 3
-
All trial collaborators, regardless of whether or not their site recruited participants, were sent a copy of the publication in The Lancet, a PowerPoint presentation containing the trial results and the social media dissemination pack, enabling them to disseminate the trial results in their own hospitals and countries.
-
Links to The Lancet publication were made available in all applicable trial registers, the HALT-IT trial website and the LSHTM CTU website.
-
A PowerPoint presentation of the results was made available for use by doctors and other health-care professionals.
-
The results were disseminated to patients via social media (LSHTM CTU Twitter account @CTU_LSHTM and the LSHTM CTU Facebook page) and the trial website (URL: haltit.lshtm.ac.uk).
-
A lay summary of the results was provided to sites to be shared with trial participants.
-
A social media dissemination pack was created for dissemination of the trial results and other dissemination tools on social media.
-
The trial website was upgraded to ensure that trial-related dissemination materials could be downloaded by investigators and others and used for dissemination.
-
A podcast with the breakdown of the trial results and an interview with Professor Ian Roberts was recoded with The Resus Room (@TheResusRoom).
-
The trial protocol, statistical analysis plan and trial publication are all freely available online.
-
Following completion of all prespecified analyses, totally anonymised trial data will be shared via the LSHTM CTU data-sharing platform at freebird.lshtm.ac.uk. This will allow for maximum utilisation of the data to improve patient care and advance medical knowledge.
The impact of COVID-19
It is important to note that the trial results were published during the COVID-19 pandemic, and this limited the impact of our dissemination plan. As a result of the pandemic, both printed and broadcast media were, justifiably, almost entirely focused on COVID-19 and, therefore, there was no room for reporting non-COVID-related research. Unfortunately, this resulted in less coverage than was expected in the general media and we were unable to use the media to reach a wider audience with these important results.
Chapter 8 Reflections and concluding remarks
The HALT-IT trial was one of the largest clinical trials in GI bleeding ever conducted. It found no evidence that TXA reduces deaths from stomach bleeding, but there was evidence that TXA may increase the risk of thromboembolic events (deep-vein thrombosis or pulmonary embolism). There were also more seizures with TXA and rebleeding was similar in both groups.
In 2010, the CRASH-2 trial,54 a large multicentre randomised trial of TXA in trauma patients, found that this inexpensive, generic drug reduces the number of deaths by one-sixth. Following these results, the team at LSHTM CTU wondered whether or not TXA could have a similar effect in GI bleeding. The Cochrane review found a surprisingly large (40%) reduction in gastric bleeding deaths; however, this review was based on the results of a number of smaller trials. To determine whether or not TXA cuts gastric bleeding deaths, a large trial was needed, and the LSHTM CTU team began work on the HALT-IT trial.
Initially, NIHR questioned the need for a trial because of the Cochrane review. Even during the trial, many UK doctors would recruit bleeding patients, randomly allocate them to TXA or placebo but, if they continued bleeding, would give them TXA regardless. As a result, many UK hospitals were closed to recruitment owing to lack of clinical equipoise; without strong recruitment from non-UK hospitals, particularly in Pakistan, we would have failed to reach our recruitment target. The discrepancy between the results of the Cochrane review and the results of the HALT-IT trial is alarming, but not unusual. It should prompt a reconsideration of the role of systematic reviews in informing UK health care.
The funders originally requested a 1-year follow-up on the patients randomised in the UK; however, the follow-up period for these patients was 28 days. The LSHTM CTU team requested access to 1-year follow-up data from the NHS Health and Social Care Information Centre (now NHS Digital). After the protocol was finalised in 2014, the NHS Health and Social Care Information Centre requested changes in the patient information sheet and consent form as a condition of sharing its data. This allowed the data to be released in 2015. However, in 2016 the policy changed again, and data-sharing was refused.
These results also demonstrate that TXA should not be used for the treatment of GI bleeding outside the context of a randomised trial, and caution against the use of generic ‘major haemorrhage protocols’ in the UK. Although it is often assumed that a treatment that works in one bleeding situation, such as traumatic bleeding or post-partum haemorrhage, will probably work in another, these results highlight the need for clinical trials that target specific causes of bleeding. Patients with GI bleeding may respond differently to those with traumatic and post-partum bleeding. In particular, patients with underlying liver disease may be more prone to side effects from unwanted clotting. GI bleeding is currently a licensed indication for TXA and, therefore, our results could have regulatory implications.
Acknowledgements
All authors made substantial contributions to the conception and design, or acquisition of data, analysis and interpretation of data, all were involved in the drafting of the manuscript or revising it critically for important intellectual content, and all authors approved the final version to be published.
Role of funding source
The HALT-IT trial was funded by the NIHR HTA programme. The funders of the trial had no role in study design, data collection, data analysis, data interpretation, or report writing. The corresponding author and Writing Committee members had full access to all the study data and had final responsibility for the decision to submit for publication.
Contributions of authors
Ian Roberts (https://orcid.org/0000-0003-1596-6054) (Professor of Epidemiology and Public Heath) was involved in the design, conduct, analysis and reporting phases.
Haleema Shakur-Still (https://orcid.org/0000-0002-6511-109X) (Professor of Global Health Clinical Trials) was involved in the design, conduct, analysis and reporting phases.
Adefemi Afolabi (https://orcid.org/0000-0002-6195-6669) (Senior Lecturer and Consultant Surgeon) was involved in the conduct and reporting phases.
Adegboyega Akere (https://orcid.org/0000-0002-9596-3998) (Lecturer and Consultant Physician and Gastroenterologist) was involved in the conduct and reporting phases.
Monica Arribas (https://orcid.org/0000-0002-1405-9391) (Trial Manager/Research Assistant) was involved in the design, conduct and reporting phases.
Emma Austin (https://orcid.org/0000-0003-2817-5534) (Assistant Trial Manager) was involved in the conduct phase.
Kiran Bal (https://orcid.org/0000-0003-0242-8660) (Assistant Trial Manager) was involved in the conduct phase.
Nuha Bazeer (https://orcid.org/0000-0002-4851-8402) (MSc Student in Health Policy, Planning and Financing) was involved in the economic analyses included in this report.
Danielle Beaumont (https://orcid.org/0000-0002-2530-9608) (Senior Trial Manager/Research Fellow) was involved in the conduct phase.
Amy Brenner (https://orcid.org/0000-0003-2017-5994) (Research Fellow in Epidemiology) was involved in the analysis and reporting phases.
Laura Carrington (https://orcid.org/0000-0002-8322-2092) (Assistant Trial Administrator) was involved in the conduct phase.
Rizwana Chaudhri (https://orcid.org/0000-0002-5428-3988) (Dean and Professor of Obstetrics and Gynaecology) was involved in the conduct and reporting phases.
Timothy Coats (https://orcid.org/0000-0003-2736-2784) (Professor of Emergency Medicine) was involved in the design, conduct and reporting phases.
Ian Gilmore (https://orcid.org/0000-0003-0720-3612) (Professor of Hepatology) was involved in the design and reporting phases.
Kenneth Halligan (https://orcid.org/0000-0002-0762-9958) (Patient Representative) was involved in the design, conduct and reporting phases.
Irshad Hussain (https://orcid.org/0000-0002-5342-0530) (Dean of Faculty of Medicine and Allied Specialties and Professor of Medicine) was involved in the conduct and reporting phases.
Vipul Jairath (https://orcid.org/0000-0002-1092-0033) (Professor of Medicine) was involved in the design, conduct and reporting phases.
Kiran Javaid (https://orcid.org/0000-0001-6260-0552) (Assistant Research Co-ordinator) was involved in the conduct and reporting phases.
Aasia Kayani (https://orcid.org/0000-0003-2782-9508) (Research Co-ordinator) was involved in the conduct and reporting phases.
Ton Lisman (https://orcid.org/0000-0002-3503-7140) (Professor of Experimental Surgery) was involved in the reporting phase.
Raoul Mansukhani (https://orcid.org/0000-0002-9456-5859) (Research Fellow in Medical Statistics) was involved in the analysis and reporting phases.
Alec Miners (https://orcid.org/0000-0003-1850-1463) (Associate Professor in Health Economics) was involved in the economic analyses included in this report.
Muttiullah Mutti (https://orcid.org/0000-0002-9338-962X) (Dean and Professor of Medicine) was involved in the conduct and reporting phases.
Muhammad Arif Nadeem (https://orcid.org/0000-0002-6984-5330) (Professor of Medicine) was involved in the conduct and reporting phases.
Richard Pollok (https://orcid.org/0000-0001-6452-6763) (Consultant Physician and Reader in Gastroenterology) was involved in the conduct and reporting phases.
Danielle Prowse (https://orcid.org/0000-0002-7470-4823) (Data Manager) was involved in the conduct phase.
Jonathan Simmons (https://orcid.org/0000-0002-6339-4110) (Gastroenterology Consultant) was involved in the conduct and reporting phases.
Simon Stanworth (https://orcid.org/0000-0002-7414-4950) (Associate Professor of Haematology and Transfusion Medicine) was involved in the design and reporting phases.
Andrew Veitch (https://orcid.org/0000-0001-5418-2370) (Consultant Gastroenterologist) was involved in the design, conduct and reporting phases.
Jack Williams (https://orcid.org/0000-0002-1331-387X) (Research Fellow in Health Economics) was involved in the economic analyses included in this report.
Publications
Manno D, Ker K, Roberts I. How effective is tranexamic acid for acute gastrointestinal bleeding? BMJ 2014;348:g1421.
Brenner A, Afolabi A, Ahmad SM, Arribas M, Chaudhri R, Coats T, et al. Tranexamic acid for acute gastrointestinal bleeding (the HALT-IT trial): statistical analysis plan for an international, randomised, double-blind, placebo-controlled trial. Trials 2019;20:467.
Roberts I, Shakur-Still H, Afolabi A, Akere A, Arribas M, Brenner A, et al. Effects of a high-dose 24-h infusion of tranexamic acid on death and thromboembolic events in patients with acute gastrointestinal bleeding (HALT-IT): an international randomised, double-blind, placebo-controlled trial. Lancet 2020;395:1927–36.
Related publications
The HALT-IT trial protocol is available here: https://trialsjournal.biomedcentral.com/articles/10.1186/1745-6215-15-450.
The Statistical Analysis Plan for the HALT-IT trial is available here: https://trialsjournal.biomedcentral.com/articles/10.1186/s13063-019-3561-7.
The HALT-IT trial results publication is available here: www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30848-5/fulltext.
Data-sharing statement
Individual de-identified patient data, including data dictionary, will be made available via our data-sharing portal, The Free Bank of Injury and Emergency Research Data (freeBIRD) website, indefinitely (URL: http://freebird.Lshtm.ac.uk). This will allow for maximum utilisation of the data to improve patient care and advance medical knowledge. Requests for access to the data should be addressed to the corresponding author or through the data-sharing portal.
Patient data
This work uses data provided by patients and collected by the NHS as part of their care and support. Using patient data is vital to improve health and care for everyone. There is huge potential to make better use of information from people’s patient records, to understand more about disease, develop new treatments, monitor safety, and plan NHS services. Patient data should be kept safe and secure, to protect everyone’s privacy, and it’s important that there are safeguards to make sure that it is stored and used responsibly. Everyone should be able to find out about how patient data are used. #datasaveslives You can find out more about the background to this citation here https://understandingpatientdata.org.uk/data-citation.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HTA programme or the Department of Health and Social Care.
References
- Roberts I, Coats T, Edwards P, Gilmore I, Jairath V, Ker K, et al. HALT-IT – tranexamic acid for the treatment of gastrointestinal bleeding: study protocol for a randomised controlled trial. Trials 2014;15. https://doi.org/10.1186/1745-6215-15-450.
- Brenner A, Afolabi A, Ahmad SM, Arribas M, Chaudhri R, Coats T, et al. Tranexamic acid for acute gastrointestinal bleeding (the HALT-IT trial): statistical analysis plan for an international, randomised, double-blind, placebo-controlled trial. Trials 2019;20. https://doi.org/10.1186/s13063-019-3561-7.
- HALT-IT Trial Collaborators . Effects of a high-dose 24-h infusion of tranexamic acid on death and thromboembolic events in patients with acute gastrointestinal bleeding (HALT-IT): an international randomised, double-blind, placebo-controlled trial. Lancet 2020;395:1927-36. https://doi.org/10.1016/S0140-6736(20)30848-5.
- van Leerdam ME. Epidemiology of acute upper gastrointestinal bleeding. Best Pract Res Clin Gastroenterol 2008;22:209-24. https://doi.org/10.1016/j.bpg.2007.10.011.
- Hearnshaw SA, Logan RF, Lowe D, Travis SP, Murphy MF, Palmer KR. Acute upper gastrointestinal bleeding in the UK: patient characteristics, diagnoses and outcomes in the 2007 UK audit. Gut 2011;60:1327-35. https://doi.org/10.1136/gut.2010.228437.
- Oakland K, Guy R, Uberoi R, Hogg R, Mortensen N, Murphy MF, et al. UK Lower GI Bleeding Collaborative . Acute lower GI bleeding in the UK: patient characteristics, interventions and outcomes in the first nationwide audit. Gut 2018;67:654-62. https://doi.org/10.1136/gutjnl-2016-313428.
- Farrell JJ, Friedman LS. Review article: the management of lower gastrointestinal bleeding. Aliment Pharmacol Ther 2005;21:1281-98. https://doi.org/10.1111/j.1365-2036.2005.02485.x.
- Williams JG, Roberts SE, Ali MF, Cheung WY, Cohen DR, Demery G, et al. Gastroenterology services in the UK. The burden of disease, and the organisation and delivery of services for gastrointestinal and liver disorders: a review of the evidence. Gut 2007;56:1-113. https://doi.org/10.1136/gut.2006.117598.
- Longstreth GF. Epidemiology and outcome of patients hospitalized with acute lower gastrointestinal hemorrhage: a population-based study. Am J Gastroenterol 1997;92:419-24.
- Button LA, Roberts SE, Evans PA, Goldacre MJ, Akbari A, Dsilva R, et al. Hospitalized incidence and case fatality for upper gastrointestinal bleeding from 1999 to 2007: a record linkage study. Aliment Pharmacol Ther 2011;33:64-76. https://doi.org/10.1111/j.1365-2036.2010.04495.x.
- Hippisley-Cox J, Coupland C. Predicting risk of upper gastrointestinal bleed and intracranial bleed with anticoagulants: cohort study to derive and validate the QBleed scores. BMJ 2014;349. https://doi.org/10.1136/bmj.g4606.
- Theocharis GJ, Thomopoulos KC, Sakellaropoulos G, Katsakoulis E, Nikolopoulou V. Changing trends in the epidemiology and clinical outcome of acute upper gastrointestinal bleeding in a defined geographical area in Greece. J Clin Gastroenterol 2008;42:128-33. https://doi.org/10.1097/01.mcg.0000248004.73075.ad.
- Czernichow P, Hochain P, Nousbaum JB, Raymond JM, Rudelli A, Dupas JL, et al. Epidemiology and course of acute upper gastro-intestinal haemorrhage in four French geographical areas. Eur J Gastroenterol Hepatol 2000;12:175-81. https://doi.org/10.1097/00042737-200012020-00007.
- van Leerdam ME, Vreeburg EM, Rauws EA, Geraedts AA, Tijssen JG, Reitsma JB, et al. Acute upper GI bleeding: did anything change? Time trend analysis of incidence and outcome of acute upper GI bleeding between 1993/1994 and 2000. Am J Gastroenterol 2003;98:1494-9. https://doi.org/10.1111/j.1572-0241.2003.07517.x.
- Hreinsson JP, Kalaitzakis E, Gudmundsson S, Björnsson ES. Upper gastrointestinal bleeding: incidence, etiology and outcomes in a population-based setting. Scand J Gastroenterol 2013;48:439-47. https://doi.org/10.3109/00365521.2012.763174.
- Laine L, Yang H, Chang SC, Datto C. Trends for incidence of hospitalization and death due to GI complications in the United States from 2001 to 2009. Am J Gastroenterol 2012;107:1190-5. https://doi.org/10.1038/ajg.2012.168.
- Wuerth BA, Rockey DC. Changing Epidemiology of upper gastrointestinal hemorrhage in the last decade: a nationwide analysis. Dig Dis Sci 2018;63:1286-93. https://doi.org/10.1007/s10620-017-4882-6.
- Abougergi MS, Travis AC, Saltzman JR. The in-hospital mortality rate for upper GI hemorrhage has decreased over 2 decades in the United States: a nationwide analysis. Gastrointest Endosc 2015;81:882-8.e1. https://doi.org/10.1016/j.gie.2014.09.027.
- Di Fiore F, Lecleire S, Merle V, Hervé S, Duhamel C, Dupas JL, et al. Changes in characteristics and outcome of acute upper gastrointestinal haemorrhage: a comparison of epidemiology and practices between 1996 and 2000 in a multicentre French study. Eur J Gastroenterol Hepatol 2005;17:641-7. https://doi.org/10.1097/00042737-200506000-00008.
- Kaviani MJ, Pirastehfar M, Azari A, Saberifiroozi M. Etiology and outcome of patients with upper gastrointestinal bleeding: a study from South of Iran. Saudi J Gastroenterol 2010;16:253-9. https://doi.org/10.4103/1319-3767.70608.
- Ugiagbe R, Omuemu C. Etiology of upper gastrointestinal bleeding in the University of Benin Teaching Hospital, South-Southern Nigeria. Niger J Surg Sci 2016;26:29-32. https://doi.org/10.4103/njss.njss_7_15.
- Wang J, Cui Y, Wang J, Chen B, He Y, Chen M. Clinical epidemiological characteristics and change trend of upper gastrointestinal bleeding over the past 15 years. Zhonghua Wei Chang Wai Ke Za Zhi 2017;20:425-31.
- Minakari M, Badihian S, Jalalpour P, Sebghatollahi V. Etiology and outcome in patients with upper gastrointestinal bleeding: study on 4747 patients in the central region of Iran. J Gastroenterol Hepatol 2017;32:789-96. https://doi.org/10.1111/jgh.13617.
- Kim JJ, Sheibani S, Park S, Buxbaum J, Laine L. Causes of bleeding and outcomes in patients hospitalized with upper gastrointestinal bleeding. J Clin Gastroenterol 2014;48:113-18. https://doi.org/10.1097/MCG.0b013e318297fb40.
- Barnert J, Messmann H. Diagnosis and management of lower gastrointestinal bleeding. Nat Rev Gastroenterol Hepatol 2009;6:637-46. https://doi.org/10.1038/nrgastro.2009.167.
- Hassan Al-Dholea MHH, Mohsen Mohammed Al-Makdad ASM, Mohammed Al-Haimi MA. Determinants and outcome of acute upper gastrointestinal bleeding in Yemen. J Gastrointest Dig Syst 2014;4. https://doi.org/10.4172/2161-069x.1000235.
- Elwakil R, Reda MA, Abdelhakam SM, Ghoraba DM, Ibrahim WA. Causes and outcome of upper gastrointestinal bleeding in Emergency Endoscopy Unit of Ain Shams University Hospital. J Egypt Soc Parasitol 2011;41:455-67.
- Alema ON, Martin DO, Okello TR. Endoscopic findings in upper gastrointestinal bleeding patients at Lacor hospital, northern Uganda. Afr Health Sci 2012;12:518-21. https://doi.org/10.4314/ahs.v12i4.19.
- Jiang Y, Li Y, Xu H, Shi Y, Song Y, Li Y. Risk factors for upper gastrointestinal bleeding requiring hospitalization. Int J Clin Exp Med 2016;9:4539-44.
- Gado AS, Ebeid BA, Abdelmohsen AM, Axon AT. Clinical outcome of acute upper gastrointestinal hemorrhage among patients admitted to a government hospital in Egypt. Saudi J Gastroenterol 2012;18:34-9. https://doi.org/10.4103/1319-3767.91737.
- Zaltman C, Souza HS, Castro ME, Sobral Mde F, Dias PC, Lemos V. Upper gastrointestinal bleeding in a Brazilian hospital: a retrospective study of endoscopic records. Arq Gastroenterol 2002;39:74-80. https://doi.org/10.1590/S0004-28032002000200002.
- Kayamba V, Sinkala E, Mwanamakondo S, Soko R, Kawimbe B, Amadi B, et al. Trends in upper gastrointestinal diagnosis over four decades in Lusaka, Zambia: a retrospective analysis of endoscopic findings. BMC Gastroenterol 2015;15. https://doi.org/10.1186/s12876-015-0353-8.
- Sher F, Ullah RS, Khan J, Mansoor SN, Ahmed N. Frequency of different causes of upper gastrointestinal bleeding using endoscopic procedure at a tertiary care hospital. Pak Armed Forces Med J 2014;64:410-3.
- van der Werf MJ, de Vlas SJ, Brooker S, Looman CW, Nagelkerke NJ, Habbema JD, et al. Quantification of clinical morbidity associated with schistosome infection in sub-Saharan Africa. Acta Trop 2003;86:125-39. https://doi.org/10.1016/S0001-706X(03)00029-9.
- British Society of Gastroenterology . UK Comparative Audit of Upper Gastrointestinal Bleeding and the Use of Blood 2007. www.bsg.org.ukpdf_word_docsblood_audit_report_07.pdf (accessed 13 October 2020).
- Lanas A, Aabakken L, Fonseca J, Mungan ZA, Papatheodoridis GV, Piessevaux H, et al. Clinical predictors of poor outcomes among patients with nonvariceal upper gastrointestinal bleeding in Europe. Aliment Pharmacol Ther 2011;33:1225-33. https://doi.org/10.1111/j.1365-2036.2011.04651.x.
- Rockall TA, Logan RF, Devlin HB, Northfield TC. Risk assessment after acute upper gastrointestinal haemorrhage. Gut 1996;38:316-21. https://doi.org/10.1136/gut.38.3.316.
- Roberts SE, Button LA, Williams JG. Prognosis following upper gastrointestinal bleeding. PLOS ONE 2012;7. https://doi.org/10.1371/journal.pone.0049507.
- Jairath V, Thompson J, Kahan BC, Daniel R, Hearnshaw SA, Travis SP, et al. Poor outcomes in hospitalized patients with gastrointestinal bleeding: impact of baseline risk, bleeding severity, and process of care. Am J Gastroenterol 2014;109:1603-12. https://doi.org/10.1038/ajg.2014.263.
- Kwak MS, Cha JM, Han YJ, Yoon JY, Jeon JW, Shin HP, et al. The clinical outcomes of lower gastrointestinal bleeding are not better than those of upper gastrointestinal bleeding. J Korean Med Sci 2016;31:1611-6. https://doi.org/10.3346/jkms.2016.31.10.1611.
- Hsu PI, Lin XZ, Chan SH, Lin CY, Chang TT, Shin JS, et al. Bleeding peptic ulcer – risk factors for rebleeding and sequential changes in endoscopic findings. Gut 1994;35:746-9. https://doi.org/10.1136/gut.35.6.746.
- Northfield TC. Factors predisposing to recurrent haemorrhage after acute gastrointestinal bleeding. Br Med J 1971;1:26-8. https://doi.org/10.1136/bmj.1.5739.26.
- Smith JL, Graham DY. Variceal hemorrhage: a critical evaluation of survival analysis. Gastroenterology 1982;82:968-73. https://doi.org/10.1016/S0016-5085(82)80264-3.
- Lau JY, Sung JJ, Lee KK, Yung MY, Wong SK, Wu JC, et al. Effect of intravenous omeprazole on recurrent bleeding after endoscopic treatment of bleeding peptic ulcers. N Engl J Med 2000;343:310-16. https://doi.org/10.1056/NEJM200008033430501.
- Jairath V, Barkun AN. Improving outcomes from acute upper gastrointestinal bleeding. Gut 2012;61:1246-9. https://doi.org/10.1136/gutjnl-2011-300019.
- Rockall TA, Logan RF, Devlin HB, Northfield TC. Incidence of and mortality from acute upper gastrointestinal haemorrhage in the United Kingdom. Steering Committee and members of the National Audit of Acute Upper Gastrointestinal Haemorrhage. BMJ 1995;311:222-6. https://doi.org/10.1136/bmj.311.6999.222.
- National Institute for Health and Care Excellence (NICE) (UK) . Acute Upper Gastrointestinal Bleeding in Over 16s: Management 2016. www.nice.org.uk/guidance/cg141 (accessed 13 October 2020).
- National Comparative Audit of Blood Transfusion . Results from a National Audit National Comparative Audit of Lower Gastrointestinal Bleeding and the Use of Blood 2016. www.acpgbi.org.uk/content/uploads/2016/07/National-Lower-Gastrointestinal-Bleed-Audit-Results-2016.pdf (accessed 13 October 2020).
- Oakland K, Chadwick G, East JE, Guy R, Humphries A, Jairath V, et al. Diagnosis and management of acute lower gastrointestinal bleeding: guidelines from the British Society of Gastroenterology. Gut 2019;68:776-89. https://doi.org/10.1136/gutjnl-2018-317807.
- Prentice CR. Basis of antifibrinolytic therapy. J Clin Pathol Suppl 1980;14:35-40. https://doi.org/10.1136/jcp.33.Suppl_14.35.
- al-Mohana JM, Lowe GD, Murray GD, Burns HG. Association of fibrinolytic tests with outcome of acute upper-gastrointestinal-tract bleeding. Lancet 1993;341:518-21. https://doi.org/10.1016/0140-6736(93)90278-O.
- Poller L, Thomson J. Evidence for a relationship between fibrinolysis and haematemesis. Br J Haematol 1973;24.
- Ker K, Edwards P, Perel P, Shakur H, Roberts I. Effect of tranexamic acid on surgical bleeding: systematic review and cumulative meta-analysis. BMJ 2012;344. https://doi.org/10.1136/bmj.e3054.
- The CRASH-2 Trial Collaborators . Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet 2010;376:23-32. https://doi.org/10.1016/S0140-6736(10)60835-5.
- The WOMAN Trial Collaborators . Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial. Lancet 2017;389. https://doi.org/10.1016/S0140-6736(17)30638-4.
- Myles PS, Smith JA, Forbes A, Silbert B, Jayarajah M, Painter T, et al. Tranexamic acid in patients undergoing coronary-artery surgery. N Engl J Med 2017;376:136-48. https://doi.org/10.1056/NEJMoa1606424.
- The CRASH-3 Trial Collaborators . Effects of tranexamic acid on death, disability, vascular occlusive events and other morbidities in patients with acute traumatic brain injury (CRASH-3): a randomised, placebo-controlled trial. Lancet 2019;394:1713-23. https://doi.org/10.1016/S0140-6736(19)32233-0.
- Roberts I, Shakur H, Afolabi A, Brohi K, Coats T, . The CRASH-2 Trial Collaborators . The importance of early treatment with tranexamic acid in bleeding trauma patients: an exploratory analysis of the CRASH-2 randomised controlled trial. Lancet 2011;377:1096-101. https://doi.org/10.1016/S0140-6736(11)60278-X.
- Guerriero C, Cairns J, Perel P, Shakur H, Roberts I. CRASH 2 trial collaborators . Cost-effectiveness analysis of administering tranexamic acid to bleeding trauma patients using evidence from the CRASH-2 trial. PLOS ONE 2011;6. https://doi.org/10.1371/journal.pone.0018987.
- Bennett C, Klingenberg SL, Langholz E, Gluud LL. Tranexamic acid for upper gastrointestinal bleeding. Cochrane Database Syst Rev 2014;11. https://doi.org/10.1002/14651858.CD006640.pub3.
- Straube S, Tramèr MR, Moore RA, Derry S, McQuay HJ. Mortality with upper gastrointestinal bleeding and perforation: effects of time and NSAID use. BMC Gastroenterol 2009;9. https://doi.org/10.1186/1471-230X-9-41.
- Electronic medicines compendium (emc) . Cyklokapron Tablets – Summary of Product Characteristics (SmPC) n.d. www.medicines.org.uk/emc/medicine/16512/SPC/Cyklokapron+Tablets/ (accessed 15 May 2020).
- Committee for Human Medicinal Products . Guideline for Good Clinical Practice E6(R2) 2016. www.ema.europa.eu/en/documents/scientific-guideline/ich-e-6-r2-guideline-good-clinical-practice-step-5_en.pdf (accessed 1 September 2021).
- World Medical Association . World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA 2013;310:2191-4. https://doi.org/10.1001/jama.2013.281053.
- Henry DA, Carless PA, Moxey AJ, O’Connell D, Stokes BJ, Fergusson DA, et al. Anti-fibrinolytic use for minimising perioperative allogeneic blood transfusion. Cochrane Database Syst Rev 2011;1. https://doi.org/10.1002/14651858.CD001886.pub3.
- Horrow JC, Van Riper DF, Strong MD, Grunewald KE, Parmet JL. The dose-response relationship of tranexamic acid. Anesthesiology 1995;82:383-92. https://doi.org/10.1097/00000542-199502000-00009.
- Brenner A, Arribas M, Cuzick J, Jairath V, Stanworth S, Ker K, et al. Outcome measures in clinical trials of treatments for acute severe haemorrhage. Trials 2018;19. https://doi.org/10.1186/s13063-018-2900-4.
- National Institute for Health and Care Excellence . Guide to the Methods of Technology Appraisal 2013 n.d. https://doi.org/10.2165/00019053-200826090-00002 (accessed 2 October 2020).
- Williams J, Roberts I, Shakur-Still H, Lecky FE, Chaudhri R, Miners A. Cost-effectiveness analysis of tranexamic acid for the treatment of traumatic brain injury, based on the results of the CRASH-3 randomised trial: a decision modelling approach. BMJ Glob Health 2020;5. https://doi.org/10.1136/bmjgh-2020-002716.
- Morgan E. National Life Tables, UK: 2016 to 2018. Newport: Office for National Statistics; 2019.
- Crooks CJ, Card TR, West J. Excess long-term mortality following non-variceal upper gastrointestinal bleeding: a population-based cohort study. PLOS Med 2013;10. https://doi.org/10.1371/journal.pmed.1001437.
- Jairath V, Kahan BC, Gray A, Doré CJ, Mora A, James MW, et al. Restrictive versus liberal blood transfusion for acute upper gastrointestinal bleeding (TRIGGER): a pragmatic, open-label, cluster randomised feasibility trial. Lancet 2015;386:137-44. https://doi.org/10.1016/S0140-6736(14)61999-1.
- The EuroQol Group . EuroQol – a new facility for the measurement of health-related quality of life. Health Policy 1990;16:199-208. https://doi.org/10.1016/0168-8510(90)90421-9.
- Campbell HE, Stokes EA, Bargo D, Logan RF, Mora A, Hodge R, et al. Costs and quality of life associated with acute upper gastrointestinal bleeding in the UK: cohort analysis of patients in a cluster randomised trial. BMJ Open 2015;5. https://doi.org/10.1136/bmjopen-2014-007230.
- Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA 1963;185:914-19. https://doi.org/10.1001/jama.1963.03060120024016.
- Kind P, Dolan P, Gudex C, Williams A. Variations in population health status: results from a United Kingdom national questionnaire survey. BMJ 1998;316:736-41. https://doi.org/10.1136/bmj.316.7133.736.
- Joint Formulary Committee . British National Formulary 2019.
- Curtis L, Burns A. Unit Costs of Health and Social Care 2018. Canterbury: Personal Social Services Research Unit, University of Kent; 2018.
- Li B, Miners A, Shakur H, Roberts I. WOMAN Trial Collaborators . Tranexamic acid for treatment of women with post-partum haemorrhage in Nigeria and Pakistan: a cost-effectiveness analysis of data from the WOMAN trial. Lancet Glob Health 2018;6:e222-e228. https://doi.org/10.1016/S2214-109X(17)30467-9.
- NHS Improvement . National Schedule of Reference Costs 2017 18 n.d. https://webarchive.nationalarchives.gov.uk/20200501111106/https://improvement.nhs.uk/resources/reference-costs/ (accessed 2 October 2020).
- NHS Blood and Transplant . NHS Blood and Transplant Price List 2018 2019 n.d. https://nhsbtdbe.blob.core.windows.net/umbraco-assets-corp/14810/price_list_bc_nhs_2018-19.pdf (accessed 2 October 2020).
- Ramagopalan SV, Samnaliev M, Weir S, Sammon CJ, Carroll R, Alikhan R. Costs of gastrointestinal bleeding events in atrial fibrillation: a UK Clinical Practice Research Datalink study. Future Cardiol 2019;15:367-75. https://doi.org/10.2217/fca-2019-0033.
- Coats TJ, Morsy M. Biological mechanisms and individual variation in fibrinolysis after major trauma. Emerg Med J 2020;37:135-40. https://doi.org/10.1136/emermed-2019-209181.
- Roberts I, Shakur H, Fawole B, Kuti M, Olayemi O, Bello A, et al. Haematological and fibrinolytic status of Nigerian women with post-partum haemorrhage. BMC Pregnancy Childbirth 2018;18. https://doi.org/10.1186/s12884-018-1794-1.
- Blasi A, Patel VC, Adelmeijer J, Azarian S, Hernandez Tejero M, Calvo A, et al. Mixed fibrinolytic phenotypes in decompensated cirrhosis and acute-on-chronic liver failure with hypofibrinolysis in those with complications and poor survival. Hepatology 2020;71:1381-90. https://doi.org/10.1002/hep.30915.
- Lisman T. Decreased plasma fibrinolytic potential as a risk for venous and arterial thrombosis. Semin Thromb Hemost 2017;43:178-84. https://doi.org/10.1055/s-0036-1585081.
- Gluud LL, Klingenberg SL, Langholz E. Tranexamic acid for upper gastrointestinal bleeding. Cochrane Database Syst Rev 2012;1. https://doi.org/10.1002/14651858.CD006640.pub2.
- Lecker I, Wang DS, Whissell PD, Avramescu S, Mazer CD, Orser BA. Tranexamic acid-associated seizures: causes and treatment. Ann Neurol 2016;79:18-26. https://doi.org/10.1002/ana.24558.
- Stanley AJ, Laine L, Dalton HR, Ngu JH, Schultz M, Abazi R, et al. Comparison of risk scoring systems for patients presenting with upper gastrointestinal bleeding: international multicentre prospective study. BMJ 2017;356. https://doi.org/10.1136/bmj.i6432.
- Roberts I, Ker K. How systematic reviews cause research waste. Lancet 2015;386. https://doi.org/10.1016/S0140-6736(15)00489-4.
- Mallett S, Clarke M. The typical Cochrane review: how many trials? How many participants?. Int J Technol Asses Health Care 2002;18:820-3. https://doi.org/10.1017/S0266462302000624.
Appendix 1 HALT-IT trial organisation
Trial Steering Committee
Christopher Hawkey (chairperson), Adefemi Afolabi, Jack Cuzick, Kenneth Halligan (patient representative), David Henry, Chris Metcalfe and Ian Roberts.
Data Monitoring and Ethics Committee
Richard Gray (chairperson), Alan Barkun, Suresh David, Philip Devereaux and Tony Brady (independent statistician).
Protocol Committee
Ian Roberts, Haleema Shakur-Still, Timothy Coats, Phil Edwards, Ian Gilmore, Vipul Jairath, Katharine Ker, Daniela Manno, Simon Stanworth and Andrew Veitch.
Trial Co-ordinating Centre Team
Clinical Trials Unit
Monica Arribas (trial manager/research assistant), Emma Austin (assistant trial manager), Kiran Bal (assistant trial manager), Eni Balogun (trial manager), Collette Barrow (trial administrator), Danielle Beaumont (senior trial manager/research fellow), Myriam Benyahia (CTU administrator), Amy Brenner (research fellow), Imogen Brooks (trial assistant 2016–18), Madeleine Cargill (data assistant), Laura Carrington (trial administrator), Phil Edwards (statistician 2012–16), Lauren Frimley (trial manager/research assistant), Amber Geer (assistant data manager), Daniel Gilbert (data assistant 2012–13), Catherine Gilliam (trial administrator), Julio Gil Onandia (clerical assistant), Nayia Golfi (trial manager 2013–15), Daniel Hetherington (trial assistant 2012–15), Courtenay Howe (CTU administrator 2015–17), Carolyn Hughes (data assistant 2016–17), David I’anson (assistant trial manager 2016–17), Rob Jackson (data manager 2012–15), Miland Joshi (statistician 2016–17), Sneha Kansagra (assistant trial manager 2016–18), Taemi Kawahara (senior trial manager 2012–15), Katharine Ker (lecturer), Sergey Kostrov (systems officer 2015–19), Daniela Manno (clinical lecturer 2012–15), Raoul Mansukhani (medical statistician 2019–20), Hakim Miah (IT systems manager 2013–19), Bernard Ndungu (assistant trial manager 2016–17), Kelly Needham (statistician 2018–20), Aroudra Outtandy (trial assistant 2013–15), Daniel Pearson (data assistant 2018–19), Tracey Pepple (acting senior data manager 2014–19), Danielle Prowse (assistant data manager), Nigel Quashi (data manager 2013–16), Anna Quinn (data assistant 2013–15), Maria Ramos (senior project administrator 2012–15), Laura Ranopa (trial assistant 2015–20), Mia Reid (clerical assistant 2016–18), Ian Roberts (chief investigator/CTU co-director), Chris Roukas (trial administrator 2013–15), Haleema Shakur-Still (project director/CTU co-director), Chelci Squires (trial assistant 2014–16), Jemma Tanner (clinical trials associate 2013–16), Andrew Thayne (data assistant) and Ruhama Uddin (trial assistant 2018–19).
Rawalpindi Medical University Pakistan National Co-ordinating Centre Team
Rizwana Chaudhri (co-ordinating centre director), Muttiullah Mutti (clinical lead), Kiran Javaid (assistant research co-ordinator) and Aasia Kayani (research co-ordinator).
Nigeria Co-ordinating Team, University College Hospital Ibadan
Bukola Fawole (co-ordinating centre director), Folasade Adenike Bello (co-ordinating centre director), Oladapo Olayemi (co-ordinating centre director), Adefemi Afolabi (national principal investigator), Olujide Okunade (assistant trial co-ordinator) and Olusade Adetayo (assistant trial co-ordinator).
National Co-ordinators
Rizwana Chaudhri (Pakistan), Muttiullah Mutti (Pakistan), Adefemi Afolabi (Nigeria), Folasade Adenike Bello (Nigeria), Bukola Fawole (Nigeria), Oladapo Olayemi (Nigeria), Hussein Khamis (Egypt), Mohammad Shukri Bin Jahit (Malaysia), Tamar Gogichaishvili (Georgia), Radu Bogdan Mateescu (Romania), Ajay Adhikaree (Nepal), Abdelmounem Eltayeib Abdo (Sudan), Mohammad Zaher (Saudi Arabia), Conor Deasy (Ireland), Joaquin Alvarez Gregori (Spain), Bobby Wellsh (Papua New Guinea) and Luke Lawton (Australia).
HALT-IT Trial Collaborators by country
UK (n = 4751)
Royal Stoke University Hospital (n = 303)
Raghavendra Kamath, Adrian Barry, Racquel Carpio, Kay Finney and Holly Maguire.
Queen’s Medical Centre Campus Nottingham (n = 208)
Martin James, Frank Coffey, Chris Gough, Lisa Sawers and Aye-Aye Thi.
Royal Berkshire Hospital (n = 191)
Jonathan Simmons, Claire Burnett, Nicola Jacques and Victoria Murray.
St George’s Hospital (n = 173)
Richard Pollok, Heather Jarman, Christine Lambe and Sarah Rounding.
Blackpool Victoria Hospital (n = 166)
Simon Tucker, Romaih Al-Idari, Samuel Guest and Emma Stoddard.
Queen Elizabeth Hospital Birmingham (n = 150)
David Yeo, Colin Bergin, Elaine Hardy and Joanne Thunder.
University Hospital Coventry (n = 128)
Paul Jhalli, Edward Hartley, Catherine Jarvis and Carly Swann.
Royal Infirmary of Edinburgh (n = 125)
Matthew Reed, Bernadette Gallagher, Julia Grahamslaw and Rachel O’Brien.
Royal London Hospital (n = 125)
Timothy Harris, Geoffrey Bellhouse, Olivia Boulton and Imogen Skene.
Glasgow Royal Infirmary (n = 120)
Adrian Stanley, Janet Johnstone, Donogh Maguire and Susan Thornton.
University College London Hospital (n = 113)
Matthew Banks, Georgia Bercades, Daniel Marks and Jung Ryu.
Whipps Cross University Hospital (n = 108)
Timothy Harris, Claire Dowty, Jason Pott and Imogen Skene.
John Radcliffe Hospital (n = 107)
James East, Adam Bailey, Sally Beer and Sian Davies.
Royal Devon & Exeter Hospital (n = 97)
Andrew Appelboam, Daisy Mackle and Jennifer Small.
Queen Alexandra Hospital Portsmouth (n = 88)
Christiane Vorwerk, Rachel Atkins and Isobel Bradbury.
Leicester Royal Infirmary (n = 84)
Timothy Coats, Catriona Bryceland and Lisa McClelland.
Salford Royal Hospital (n = 83)
Martin Thomas, Kate Clayton and Angiy Michael.
Great Western Hospital (n = 80)
Stephen Haig, Saif Al-Nahhas and Tim Godfrey.
Southampton General Hospital (n = 80)
Philip Boger, Rachel Comer and Barbara Watkins.
Darlington Memorial Hospital (n = 79)
Ola Afolabi, Shazad Afzal and Amanda Cowton.
St James University Hospital Leeds (n = 79)
Simon Everett, Ruth Fazakerley and Felicia Onoviran.
Poole Hospital (n = 77)
Jonathon Snook, Jackie Berry and Diane Simpson.
King’s College Hospital (n = 73)
Jeff Keep, Hannah Cotton and Sinead Helyar.
University Hospital of North Tees (n = 73)
Matthew Rutter, Tracey Johnston and Laura O’Rourke.
Basingstoke and North Hampshire Hospital (n = 72)
Louisa Chan, Joanna Tambellini and Dawn Trodd.
Dorset County Hospital (n = 68)
James Shutt, Sarah Moreton and Abby Oglesby.
Addenbrooke’s Hospital (n = 67)
Adrian Boyle, Nicola Haeger and Susie Hardwick.
Southmead Hospital (n = 67)
Jason Kendall, Beverley Faulkner and Ruth Worner.
Royal Victoria Infirmary (n = 64)
Sarah Hearnshaw, Mary Doona and Maria Price.
St Thomas’ Hospital (n = 64)
Laura Hunter, Maggie Bell and Vania Loureiro.
Derriford Hospital (n = 61)
Anthony Kehoe, Alison Jefferey and Rosalyn Squire.
Ipswich Hospital (n = 60)
David Hartin, Stephanie Bell and Alexandra Newman.
Musgrove Park Hospital (n = 59)
James Gagg, Jayne Foot and Sue Wakeford.
Royal Oldham Hospital (n = 58)
Gabrielle May, Thomas Bartram and Paul Cumpstay.
Whittington Hospital (n = 58)
Lucy Parker, Rita Das and Sheik Pahary.
Basildon University Hospital (n = 57)
Gavin Wright, Georgina Butt and Natasha Christmas.
Wexham Park Hospital (n = 56)
Sarah Wilson, Mohammed Ashfaq and Louise Chandler.
Royal United Hospital Bath (n = 50)
Saif Al-Nahhas, Carrie Demetriou and Philip Kaye.
Manchester Royal Infirmary (n = 48)
Simon Carley and Andrew Brown.
Chesterfield Royal Hospital (n = 44)
Lucy Jones and Amanda Whileman.
James Cook University Hospital (n = 44)
John Greenaway and Julie Tregonning.
Newham University Hospital (n = 44)
Timothy Harris and Geoffrey Bellhouse.
Northern General Hospital (n = 44)
Avril Kuhrt and Steve Goodacre.
Royal Shrewsbury Hospital (n = 43)
John Jones and Charlotte Owen.
Charing Cross Hospital (n = 41)
Anu Mitra and Abby Harper-Payne.
Sandwell General Hospital (n = 37)
Nigel Trudgill and Anne Hayes.
South Tyneside District Hospital (n = 36)
Faheem Butt and Gayle Clifford.
Victoria Hospital, Fife (n = 35)
Andrew Kinnon and Susan Fowler.
Chelsea and Westminster Hospital (n = 34)
Kris Pillay and Shweta Gidwani.
Queen Elizabeth Hospital Woolwich (n = 34)
Alistair McNair and Omer Omer.
Gloucestershire Royal Hospital (n = 31)
Tanya de Weymarn and Adnan Amin.
Royal Hampshire County Hospital (n = 31)
Louisa Chan and Jane Martin.
Torbay Hospital (n = 31)
Nick Mathieu and Simon Barnes.
York Hospital (n = 31)
James Turvill and Helen Sweeting.
University Hospital Crosshouse (n = 29)
Morten Draegebo and Marion McNaught.
Worthing Hospital (n = 29)
Mandy Grocutt and Jordi Margalef.
Barnsley Hospital (n = 27)
Julia Humphrey and Richard Jackson.
North Devon District Hospital (n = 27)
Fionn Bellis and Jane Hunt.
St Mary’s Hospital (n = 24)
Anu Mitra.
University Hospital Ayr (n = 22)
Alastair Stevenson.
King’s Mill Hospital (n = 19)
Nicholas Watson.
Royal Sussex County Hospital (n = 19)
Steven Barden.
Forth Valley Royal Hospital (n = 16)
Stuart Paterson.
New Cross Hospital (n = 16)
Andrew Veitch.
Cumberland Infirmary Hospital (n = 14)
Chris Macdonald.
Sunderland Royal Hospital (n = 14)
David Hobday.
West Cumberland Hospital (n = 13)
Olu Orugun.
Yeovil District Hospital (n = 13)
Andrew Allison.
Northampton General Hospital (n = 12)
Tristan Dyer.
Royal Lancaster Infirmary (n = 12)
Samuel McBride.
Royal Liverpool University Hospital (n = 12)
Wojciech Sawicki.
Hull Royal Infirmary (n = 10)
Ben Rayner.
Frimley Park Hospital (n = 8)
Lynsey Flowerdew.
Queen Elizabeth Hospital – Gateshead (n = 7)
Jamie Barbour.
Salisbury District Hospital (n = 7)
Jason Klein.
Aintree University Hospital (n = 6)
Stephen Hood.
University Hospital of Wales (n = 5)
Nicola Palmer.
Northwick Park Hospital (n = 4)
Jacob de Wolff.
Colchester General Hospital (n = 3)
Achuth Shenoy.
Birmingham City Hospital (n = 2)
Nigel Trudgill.
Royal Bournemouth Hospital (n = 1)
Peter Swallow.
University Hospital Lewisham (n = 1)
Rajaventhan Srirajaskanthan.
Pakistan (n = 4420)
King Edward Medical University, Mayo Hospital Lahore (n = 539)
Irshad Hussain, Hamza Arshad, Naeem Aslam, Anam Bangash, Muhammad Qamar and Haroon Zahoor.
Rawalpindi Medical University Pakistan, Holy Family Hospital, Unit II (n = 501)
Muttiullah Mutti, Saba Arshad, Quratul ain Ghalib, Tehseen Hameed, Tayyaba Saif and Wajahat Shafi.
Services Institute of Medical Sciences/Services Hospital GI/Medical Unit III Lahore (n = 443)
Muhammad Arif Nadeem, Abid Ali, Shehroze Khan, Muhammad Muaaz and Ahmad Taj.
Lady Reading Hospital (n = 386)
Aamir Ghafoor, Aamir Afridi, Mansoor Ahmad, Mujahid Aslam and Sandeep Kumar.
Asian Institute of Medical Sciences (n = 360)
Majid Soomro, Mohsin Ali, Ubedullah Bughio, Adil Chang and Sana Shaikh.
Jinnah Postgraduate Medical Centre Karachi (n = 296)
Syed Ahmad, Zeeshan Ali, Marium Waqar, Aiman Mushir and Sadaf Sattar.
DHQ Teaching Hospital Sargodha (n = 207)
Saifullah Goraya, Sharmeen Aslam, Nighat Fatima, Saadia Noreen and Sheraz Saleem.
Rawalpindi Medical University Pakistan, Benazir Bhutto Hospital Unit I (n = 196)
Fazal Rahman, Nadeem Iqbal, Mohammad Khalid and Umar Riaz.
Rawalpindi Medical University Pakistan, Holy Family Hospital, Unit I (n = 169)
Muhammad Umar, Tayyab Akhter, Javaria Khan and Noureen Misbah.
Aziz Bhatti Shaheed Teaching Hospital (n = 160)
Muhammad Afzal, Mobeen Kayani, Syed Shah and Shahida Tarar.
Bolan Medical Complex Hospital (n = 149)
Sherbat Khan, Yasir Iqbal, Essa Khan and Maqbool Reki.
Rawalpindi Medical University Pakistan, Benazir Bhutto Hospital Unit II (n = 120)
Tanveer Hussain, Shafqat Iqbal, Muhammad Khurram and Muhammad Shafi.
Ghulam Muhammad Mahar Medical College and Teaching Hospital Unit I (n = 120)
Abrar Shaikh, Aijaz Ahmed, Ameet Kumar and Pinkey Sachdev.
Jinnah Hospital Unit I (n = 88)
Khalid Mahmood Nasir, Zafar Iqbal Chaudhry and Muhammad Zubair.
Lahore General Hospital Medical Unit I (n = 84)
Ghias Tayyab, Junaid Mushtaq and Muhammad Nasir.
Mardan Medical Complex and Teaching Hospital (n = 80)
Amir Khan, Amjad Ali and Sajjad Ali.
POF Hospital (n = 76)
Wasim Uddin, Sohaib Ahmed and Tazaeen Kazmi.
Ghulam Muhammad Mahar Medical College Teaching Hospital (n = 58)
Saleh Channa, Adeeqa Aman and Mouzam Shaikh.
DHQ Hospital Faisalabad (n = 47)
Tahir Rizvi and Amjad Hussain.
Rawalpindi Medical University Pakistan, DHQ Hospital Rawalpindi (n = 47)
Haider Zaigham Baqai and Zakawat Rasheed.
Shifa International Hospital (n = 41)
Abdus Khan and Adeela Irfan.
Allied Hospital Faisalabad Medical Unit III (n = 38)
Aamir Husain and Asifa Aslam.
Madinah Teaching Hospital Faisalabad (n = 34)
Khalid Yahya and Salman Azhar.
Liaquat National Hospital and Postgraduate Medical Centre (n = 33)
Mansoor Ul Haq and Adeel Afzal.
Services Institute of Medical Sciences/Services Hospital GI/Medical Unit II Lahore (n = 33)
Muhammad Imran and Iram Saeed.
Shaukat Khanum Memorial Hospital and Research Centre (n = 29)
Aasim Yusuf and Mariam Hassan.
Hayatabad Medical Complex (n = 25)
Mumtaz Marwat and Muhammad Ishfaq.
Sir Ganga Ram Hospital Medical Unit III (n = 20)
Tahir Bashir.
Liaquat University of Medical and Health Sciences Medical Unit II (n = 17)
Santosh Kumar.
DHQ Hospital, Narowal (n = 16)
Sajjad Yaqoob.
DHQ Hospital Khuzdar (n = 8)
Abdul Wahid.
Nigeria (n = 770)
University College Hospital Ibadan (n = 143)
Adegboyega Akere, Tinuola Fakoya, Temitope Oke and Edries Tejan.
National Hospital Abuja (n = 109)
Oluwole Olaomi, Olawale Badejo, Okafor Nnaemaka and Nancy Ukwu.
Obafemi Awolowo University Teaching Hospital, Ile-Ife (n = 99)
Olukayode Arowolo, Adewale Aderounmu and Funmilola Wuraola.
University of Benin Teaching Hospital (n = 74)
Rose Ugiagbe, Alexander Atiri and Enadeghe Eghaghe.
Olabisi Onabanjo University Teaching Hospital (n = 49)
Adeleke Adekoya, Adedayo Oluyomi Tade and Olatunji Shonoiki.
University of Ilorin Teaching Hospital (n = 49)
Samuel Olatoke and Toafiq Raji.
Federal Medical Centre, Owerri (n = 46)
Christopher Ekwunife and Chigozirim Onyekpere.
Ahmadu Bello University Teaching Hospital (n = 40)
Adamu Ahmed and Daniyan Muhammad.
Lagos University Teaching Hospital (n = 37)
Emuobor Odeghe, Olufunmilayo Lesi and Azeberoje Osueni.
Aminu Kano Teaching Hospital (n = 25)
Adamu Samaila and Aminu Nahuche.
Ekiti State University Teaching Hospital (n = 24)
Akande Ajayi.
Irrua Specialist Teaching Hospital (n = 24)
Andrew Dongo.
University of Nigeria Teaching Hospital, Enugu (n = 18)
Uchenna Ijoma.
Federal Medical Centre, Abeokuta (n = 8)
Ademola Tolulope Adebanjo.
Lagos State University Teaching Hospital (n = 7)
Rufina Igetei.
University of Abuja Teaching Hospital (n = 7)
Monday Yilkudi.
Maitama District Hospital (n = 6)
Kehinde Osisanya.
Jos University Teaching Hospital (n = 3)
Edith Nonyelum Okeke.
Imo State University Teaching Hospital (n = 2)
Oguamanam Okezie Enwere.
Egypt (n = 709)
Kasr Al Aini Internal Medicine Hospital, Cairo University (n = 641)
Serag Esmat, Omar Ashoush, Mazen Naga, Fady Nagy, Mostafa Saiid and Ahmed Shaker.
Mataria Teaching Hospital (n = 60)
Hussein Khamis, Ashraf Helmy and Saafan Saafan.
Badr Hospital, Helwan University (n = 8)
Mohammed Abdel Monem.
Malaysia (n = 464)
Hospital Tengku Ampuan Afzan (n = 123)
Jiffre Din, Khairul Azis, Muhyuddin Brukan and Sanjay Singh.
Hospital Universiti Sains Malaysia (n = 110)
Andee Zakaria, Shaik Farid, Nizam Hashim and Masykurin Mafauzy.
Hospital Sultanah Bahiyah (n = 71)
Wan Najmi, Nil Amri and Xin Yi.
Hospital Raja Permaisuri Bainun (n = 63)
Mohammad Hisyam, Elaine Ng and Zuhrirahimi Ramli.
Pulau Pinang General Hospital (n = 55)
Shyang Yee Lim, Kelvin Voon and Sir Young Yam.
Sungai Buloh Hospital (n = 42)
Mohammad Jahit and Lee Joon.
Georgia (n = 425)
High Technology Medical Centre, University Clinic (n = 364)
Besik Melikidze, Davit Kazaishvili, Tamar Gogichaishvili, Nino Grubelashvili and Baadur Mosidze.
Centre of Emergency Surgery and Traumatology (n = 61)
Gia Tomadze and Avto Megreladze.
Romania (n = 287)
Clinical Emergency Hospital Bucharest – SCUB Floreasca (n = 128)
Ruxandra Oprita, Dorina Pestroiu Calescu, Camèlia Chioncel and Andrei Ragea.
Colentina Clinical Hospital (n = 58)
Bogdan Mateescu, Bogdan Busuioc and Andrei Voiosu.
Municipal Emergency Hospital Moinesti (n = 45)
Adrian Cotirlet and Iulia Pintilie.
Central University Emergency Military Hospital, ‘Carol Davila’ University of Medicine and Pharmacy, Bucharest (n = 38)
Mariana Jinga and Daniel Balaban.
Regional Institute of Gastroenterology and Hepatology ‘Prof Dr Octavian Fodor’ (n = 11)
Marcel Tanţău.
University Hospital of Emergency Bucharest (n = 5)
Lucian Negreanu.
Emergency County Hospital Mures (n = 2)
Simona Bataga.
Nepal (n = 50)
Lifeline Hospital (n = 16)
Khushboo Priya.
Gandaki Medical College and Teaching Hospital (n = 12)
Shankar Baral.
Nepal Medical College and Teaching Hospital (n = 12)
Anuj KC.
Janaki Medical College (n = 4)
Vijay Sah.
National Medical College and Teaching Hospital (n = 4)
Vijay Yadav.
Lumbini Medical College and Teaching Hospital (n = 2)
Ajay Adhikaree.
Sudan (n = 40)
Ibn Sina Hospital (n = 40)
Abdelmounem Abdo and Dalia Ahmed.
Saudi Arabia (n = 19)
Prince Mohammed Bin Abdulaziz Hospital (n = 19)
Marzouqah Al Anazi and Areej Al Balkhi.
Ireland (n = 17)
Cork University Hospital (n = 17)
Conor Deasy.
Spain (n = 17)
Hospital Nuestra Señora del Prado (n = 9)
Joaquín Álvarez Gregori.
Torrecardenas Hospital (n = 8)
Helio Fornieles Pérez.
Albania (n = 16)
University Hospital Centre ‘Mother Teresa’ (n = 16)
Arben Beqiri.
Papua New Guinea (n = 13)
Port Moresby General Hospital (n = 13)
Bobby Wellsh.
Australia (n = 11)
The Townsville Hospital (n = 11)
Luke Lawton.
Appendix 2 Brief information sheet
Appendix 3 Consent procedure overview
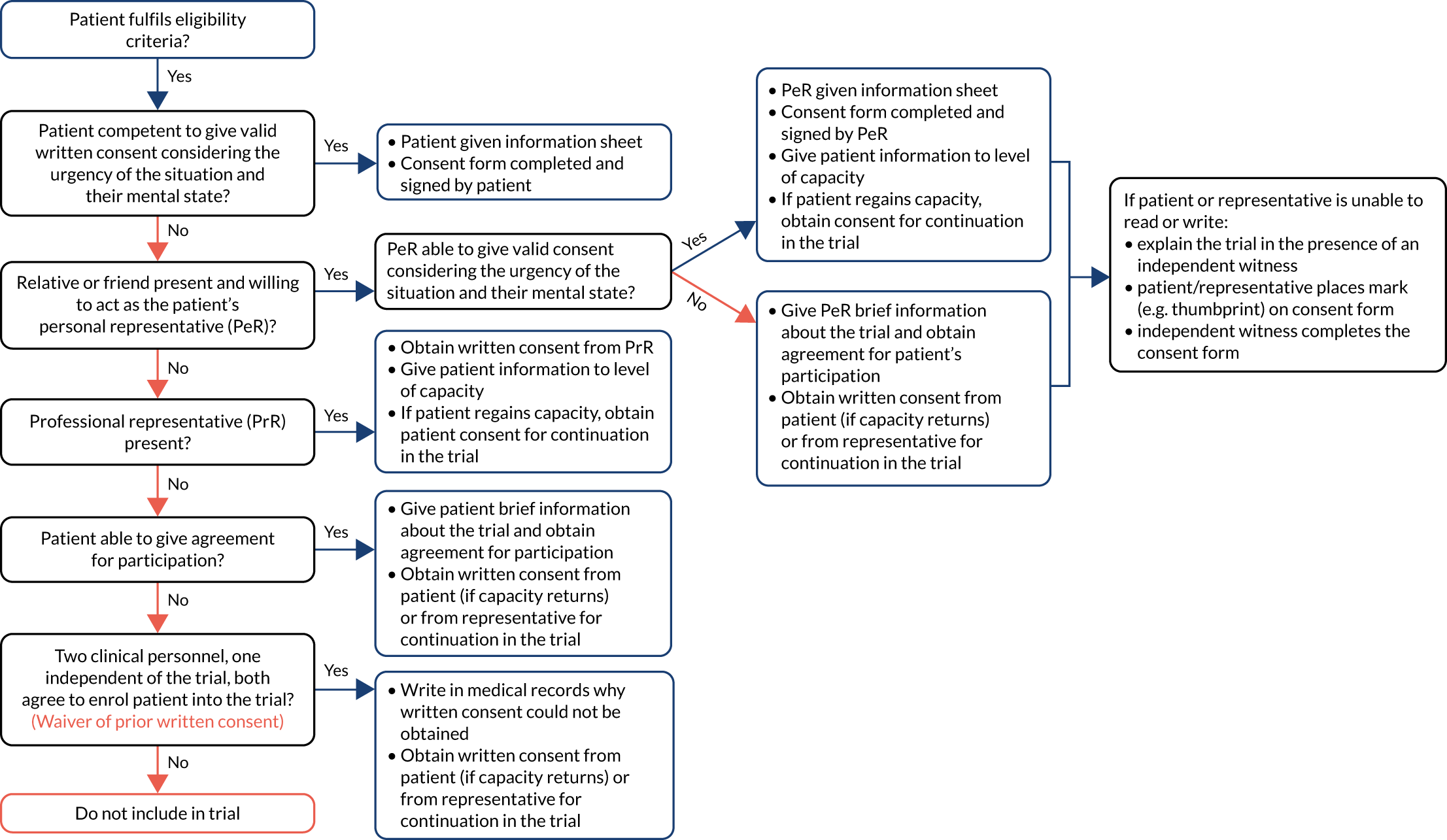
Appendix 4 Entry form
Appendix 5 Total number of randomisations by geographical region and treatment group
| Geographical region | Treatment group (n) | Total (N) | |
|---|---|---|---|
| TXA | Placebo | ||
| Africa | 756 | 763 | 1519 |
| Asia | 2479 | 2474 | 4953 |
| Europe, Australia and North America | 2752 | 2772 | 5524 |
| Caribbean, Central and South America | 0 | 0 | 0 |
| Oceania | 7 | 6 | 13 |
| Total | 5994 | 6015 | 12,009 |
Appendix 6 Outcome form
Appendix 7 Adverse events between groups
| Adverse event | TXA group | Placebo group | Total |
|---|---|---|---|
| Abdominal distension | 0 | 1 | 1 |
| Abdominal pain | 2 | 3 | 5 |
| Abscess | 1 | 1 | 2 |
| Acute confusion state | 3 | 1 | 4 |
| Acute enterocolitis | 1 | 0 | 1 |
| Adenocarcinoma | 0 | 1 | 1 |
| Alcohol intoxication | 1 | 0 | 1 |
| Alcoholic withdrawal symptoms | 1 | 2 | 3 |
| Allergic reaction | 5 | 6 | 11 |
| Anaemia | 5 | 13 | 18 |
| Angina pectoris | 2 | 0 | 2 |
| Angiodysplasia | 1 | 0 | 1 |
| Appendicitis | 1 | 0 | 1 |
| Arterioenteric fistula | 1 | 0 | 1 |
| Ascites | 2 | 4 | 6 |
| Aspiration | 0 | 1 | 1 |
| Atrial fibrillation | 0 | 2 | 2 |
| Bowel infarction | 0 | 1 | 1 |
| Bowel perforation | 0 | 1 | 1 |
| Brain lesion | 0 | 1 | 1 |
| COPD exacerbation | 3 | 2 | 5 |
| Calculus biliary | 1 | 0 | 1 |
| Cardiac arrest | 0 | 1 | 1 |
| Cardiac failure congestive | 0 | 3 | 3 |
| Cellulitis | 3 | 4 | 7 |
| Cerebral infarction | 1 | 0 | 1 |
| Chemotherapy NOS | 0 | 2 | 2 |
| Chest pain | 2 | 2 | 4 |
| Cholangiocarcinoma | 0 | 1 | 1 |
| Cholangitis | 1 | 0 | 1 |
| Cholecystitis | 0 | 1 | 1 |
| Chronic venous insufficiency | 0 | 1 | 1 |
| Clostridium difficile infection | 2 | 6 | 8 |
| Coagulopathy | 1 | 0 | 1 |
| Colorectal cancer | 0 | 1 | 1 |
| Conjunctivitis | 1 | 0 | 1 |
| Constipation | 5 | 3 | 8 |
| Contusion | 1 | 0 | 1 |
| Crohn’s disease | 0 | 1 | 1 |
| Crystal arthropathy | 0 | 1 | 1 |
| Cyanosis | 0 | 1 | 1 |
| Deep-vein thrombosis | 4 | 1 | 5 |
| Dehydration | 0 | 1 | 1 |
| Delirium | 1 | 2 | 3 |
| Diarrhoea | 3 | 2 | 5 |
| Diverticular disease | 3 | 1 | 4 |
| Duodenal perforation | 1 | 0 | 1 |
| Dyspepsia | 0 | 1 | 1 |
| Embolus in foot | 1 | 0 | 1 |
| Encephalopathy | 2 | 2 | 4 |
| Enterocutaneous fistula | 1 | 0 | 1 |
| Epistaxis | 1 | 1 | 2 |
| Erythema | 1 | 1 | 2 |
| Fall | 6 | 9 | 15 |
| Febrile neutropenia | 2 | 0 | 2 |
| Fluid overload | 1 | 1 | 2 |
| Fluid retention | 1 | 0 | 1 |
| Fracture of unspecified intracapsular femur | 0 | 1 | 1 |
| Frailty | 1 | 0 | 1 |
| Gallbladder polyp | 1 | 0 | 1 |
| Gastric cancer | 1 | 0 | 1 |
| Gastric ulcer | 1 | 0 | 1 |
| Gastritis | 1 | 4 | 5 |
| Gastroenteritis | 1 | 1 | 2 |
| GI haemorrhage | 66 | 80 | 146 |
| Gout | 3 | 1 | 4 |
| Groin pain | 1 | 0 | 1 |
| Haematoma | 1 | 0 | 1 |
| Haematuria traumatic | 0 | 1 | 1 |
| Haemodilution | 1 | 0 | 1 |
| Haemorrhoids | 2 | 2 | 4 |
| Head injury | 1 | 0 | 1 |
| Heart failure | 0 | 1 | 1 |
| Hemicolectomy | 0 | 1 | 1 |
| Hepatic cirrhosis | 6 | 3 | 9 |
| Hepatic encephalopathy | 0 | 1 | 1 |
| Hepatitis | 0 | 1 | 1 |
| Hepatocellular carcinoma | 0 | 1 | 1 |
| Hepatorenal syndrome | 1 | 0 | 1 |
| Humerus fracture | 0 | 1 | 1 |
| Hydrocele | 0 | 1 | 1 |
| Hypernatraemia | 0 | 1 | 1 |
| Hypoglycaemia | 2 | 2 | 4 |
| Hypokalaemia | 2 | 1 | 3 |
| Hypomagnesaemia | 1 | 0 | 1 |
| Hyponatraemia | 1 | 2 | 3 |
| Hypotension | 1 | 0 | 1 |
| Hypoxia | 0 | 1 | 1 |
| Infected skin ulcer | 0 | 1 | 1 |
| International normalised ratio abnormal | 1 | 0 | 1 |
| Intestinal stoma leak | 0 | 1 | 1 |
| Ischaemic heart disease | 0 | 1 | 1 |
| Ischaemic hepatitis | 0 | 1 | 1 |
| Ischaemic stroke | 3 | 3 | 6 |
| Jaundice | 0 | 1 | 1 |
| Large bowel obstruction | 1 | 0 | 1 |
| Leg ischaemia | 0 | 1 | 1 |
| Liver abscess | 0 | 1 | 1 |
| Liver carcinoma ruptured | 1 | 0 | 1 |
| Liver cirrhosis | 1 | 0 | 1 |
| Lower respiratory tract infection | 1 | 1 | 2 |
| Lung cancer | 1 | 0 | 1 |
| Mallory–Weiss tear | 0 | 1 | 1 |
| Mastoid effusion | 0 | 1 | 1 |
| Meningioma | 1 | 0 | 1 |
| Multiorgan failure | 2 | 0 | 2 |
| Myocardial infarction | 2 | 1 | 3 |
| Nasogastric tube irritation | 1 | 0 | 1 |
| Necrotising otitis externa | 0 | 1 | 1 |
| Neuropathy peripheral | 0 | 1 | 1 |
| Obstructive jaundice | 0 | 1 | 1 |
| Oedema | 1 | 3 | 4 |
| Oesophageal cancer | 1 | 1 | 2 |
| Oesophageal candida | 0 | 3 | 3 |
| Oesophagitis | 0 | 3 | 3 |
| Overdose | 1 | 1 | 2 |
| Pain | 1 | 0 | 1 |
| Palpitations | 1 | 0 | 1 |
| Pancreatitis | 1 | 0 | 1 |
| Panic attack | 1 | 0 | 1 |
| Perforated gastric ulcer | 1 | 0 | 1 |
| Pericardial effusion | 1 | 0 | 1 |
| Peritonitis | 4 | 0 | 4 |
| Pharyngitis | 1 | 0 | 1 |
| Phlebitis | 2 | 0 | 2 |
| Pleural effusion | 0 | 2 | 2 |
| Pneumonia | 9 | 3 | 12 |
| Portal vein thrombosis | 1 | 1 | 2 |
| Postural hypotension | 1 | 2 | 3 |
| Pressure sore | 1 | 1 | 2 |
| Pulmonary embolism | 3 | 3 | 6 |
| Pulmonary haemorrhage | 1 | 0 | 1 |
| Pulmonary oedema | 1 | 0 | 1 |
| Pyelonephritis | 0 | 1 | 1 |
| Pyrexia | 3 | 3 | 6 |
| Rash | 1 | 0 | 1 |
| Refeeding syndrome | 0 | 2 | 2 |
| Renal failure | 2 | 1 | 3 |
| Respiratory infection | 12 | 1 | 13 |
| Seizure | 3 | 1 | 4 |
| Sepsis | 6 | 7 | 13 |
| Shingles | 0 | 1 | 1 |
| Shortness of breath | 1 | 0 | 1 |
| Small bowel obstruction | 2 | 2 | 4 |
| Staphylococcal bacteraemia | 1 | 0 | 1 |
| Stoma site bleeding | 1 | 0 | 1 |
| Suicidal ideation | 0 | 1 | 1 |
| Supraventricular tachycardia | 0 | 1 | 1 |
| Swollen lips | 1 | 0 | 1 |
| Syncope | 1 | 1 | 2 |
| Thoracic aneurysm, ruptured | 0 | 1 | 1 |
| Thrombocytopenia | 1 | 1 | 2 |
| Thrombosis | 2 | 1 | 3 |
| Transfusion reaction | 0 | 1 | 1 |
| Transient ischaemic attack | 1 | 2 | 3 |
| Type 2 diabetes mellitus | 1 | 0 | 1 |
| Upper GI haemorrhage | 1 | 0 | 1 |
| Urinary incontinence | 0 | 1 | 1 |
| Urinary retention | 1 | 1 | 2 |
| Urinary tract infection | 12 | 12 | 24 |
| Ventricular tachycardia | 1 | 0 | 1 |
| Vomiting | 1 | 2 | 3 |
| Total | 273 | 281 | 554 |
Appendix 8 Dissemination plan
Background
Gastrointestinal bleeding, from peptic ulcers, dilated gullet veins and cancer, is a common medical emergency that causes hundreds of thousands of deaths worldwide. Patients can either vomit blood or pass blood in the stools, and up to 10% of affected patients die. Some patients stop bleeding only to start bleeding again a short time later, and these patients have particularly high death rates. Treatment includes blood transfusion and emergency surgery to tie off the bleeding vessels.
Tranexamic acid reduces bleeding in surgery and reduces deaths from bleeding after serious injury and childbirth, in both cases without increasing side effects. TXA is licensed for the treatment of GI bleeding. Only a few small trials have looked at the effect of TXA in stomach bleeding but, when these trials were added together, there appeared to be a large reduction in deaths with TXA. For many doctors, this evidence was conclusive; indeed, many were so convinced that they refused to take part in the trial given that this would mean that half of their patients would receive a placebo. However, doctors at LSHTM were sceptical and decided to carry out a large international clinical trial.
The HALT-IT trial
The HALT-IT trial is a randomised, blinded, placebo-controlled trial in 12,009 patients with severe GI bleeding. Patients were recruited from 164 hospitals across 15 countries. The aim was to assess the effects of TXA in patients with GI bleeding. The primary outcome was death due to bleeding within 5 days of randomisation.
Objectives of dissemination
The results showed that TXA does not reduce deaths from stomach bleeding but increases the risk of thromboembolic events (clots in the veins of the legs that can move to the lungs). There were also more seizures with TXA. Rebleeding was similar in both groups.
Although it is often assumed that a treatment that works in one bleeding situation will probably work in another, these results highlight the need for clinical trials that target specific causes of bleeding. Stomach bleeding may respond differently, particularly in patients with underlying liver disease, who may be more prone to side effects from unwanted clotting.
Given that TXA is already in use for the treatment of GI bleeding, these results have the potential to change medical practice.
Help our collaborators to disseminate the results in their respective countries
Dissemination tools will be developed that collaborators can use for national and international audiences. We need to upgrade our trial website and make sure that it hosts all of the trial dissemination materials that can be downloaded and used locally. Dissemination tools for collaborating investigators will be created so they can raise awareness about the trial results. Collaborating investigators will play a vital role in disseminating the results to colleagues and patients in their countries.
Specific outputs
-
Main publication of the trial results in The Lancet is expected on 20 June 2020.
-
Links to the publication will be made available in all applicable trial registers, the trial and CTU websites.
-
A PowerPoint presentation of the results will be prepared and made available for use by doctors and other health-care professionals.
-
Dissemination of results to patients will take place via the media and the trial website (haltit.lshtm.ac.uk).
-
A lay result summary is being prepared for sharing with trial participants.
-
A social media strategy is being prepared. However, it is important to note that the trial results are being published during the COVID-19 pandemic and this may limit the impact of our dissemination plan.
-
Upgrade the trial website: make sure that it hosts trial-related materials that can be downloaded by investigators and others and used for dissemination.
-
A podcast with the breakdown of the trial results and interview with Professor Ian Roberts will be broadcasted at The Resus Room (@TheResusRoom).
-
Once all prespecified analyses are completed, totally anonymised data will be shared via the LSHTM CTU data-sharing platform at freebird.lshtm.ac.uk. This will allow for maximum utilisation of the data to improve patient care and advance medical knowledge. The trial protocol, statistical analysis plan and trial publications will be freely available online.
List of abbreviations
- AGIB
- acute gastrointestinal bleeding
- CEAC
- cost-effectiveness acceptability curve
- CI
- confidence interval
- CRASH-2
- Clinical Randomisation of an Antifibrinolytic in Significant Haemorrhage 2
- CRASH-3
- Clinical Randomisation of an Antifibrinolytic in Significant Head Injury 3
- CTU
- Clinical Trial Unit
- DMC
- Data Monitoring Committee
- GI
- gastrointestinal
- GMP
- good manufacturing practice
- HALT-IT
- Haemorrhage ALleviation with Tranexamic acid – Intestinal system
- HTA
- Health Technology Assessment
- ICER
- incremental cost-effectiveness ratio
- ICU
- intensive care unit
- INMB
- incremental net monetary benefit
- LSHTM
- London School of Hygiene & Tropical Medicine
- LY
- life-year
- MHRA
- Medicines and Healthcare products Regulatory Agency
- MREC
- Multicentre Research Ethics Committee
- NICE
- National Institute for Health and Care Excellence
- NIHR
- National Institute for Health Research
- NSAID
- non-steroidal anti-inflammatory drug
- PPI
- patient and public involvement
- PSA
- probabilistic sensitivity analysis
- QALY
- quality-adjusted life-year
- QP
- qualified person
- RBC
- red blood cell
- RCT
- randomised controlled trial
- RR
- risk ratio
- SBP
- systolic blood pressure
- SMR
- standardised mortality ratio
- TCC
- Trial Co-ordinating Centre
- TRIGGER
- Transfusion in Gastrointestinal Bleeding
- TXA
- tranexamic acid
- WOMAN
- World Maternal Antifibrinolytic