

Notes
Article history
The research reported in this issue of the journal was funded by the HTA programme as project number 15/118/01. The contractual start date was in March 2017. The draft report began editorial review in March 2020 and was accepted for publication in December 2020. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Permissions
Copyright statement
Copyright © 2022 Oliveira et al. This work was produced by Oliveira et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaption in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2022 Oliveira et al.
Chapter 1 Background
Background
Looked-after children are a very vulnerable group who are at greatly increased risk of experiencing mental health problems and poor long-term social, emotional and educational outcomes. 1,2 Despite this, remarkably few interventions exist that have proven efficacy for intervening in the case of or preventing poor outcomes for these children. 3 Accordingly, there is an urgent need to develop new and effective interventions to improve the outcomes of children in care. In particular, looked-after children are at a fivefold increased risk of all childhood mental, emotional and behavioural problems, and are six to seven times more likely to have conduct disorders. In adulthood, they are between four and five times more likely to self-harm. 1
Critically, the number of children in care has risen steadily in the UK in recent years. Figures from the Department for Education show that, in 2019, the number of children looked after by local authorities in England increased by 4% since 2018, to 78,150. 4 Although the number of children entering care during the year decreased by 2% (to 31,680), the number of children leaving care during the year also decreased 2% (to 29,460), suggesting that some children are spending longer in care. Children ceasing to be looked after during 2018–19 as a result of adoption, in particular, fell by 7% (to 3570), a continuing drop seen since 2015. On the other hand, children who ceased to be looked after as a result of a special guardianship order (SGO) increased by 11% to 3830. There has been a slight decrease in the proportion of looked-after children who are placed in foster care, but foster care remains the most common type of placement. In 2019, 72% of looked-after children were in foster care; the great majority were placed with a foster carer who was not a relative or friend.
Given the size and disproportionately at-risk nature of this group, and the level of responsibility borne by foster carers, there is great need for evidence-based foster carer-led interventions to support them in improving the short- and long-term outcomes of looked-after children.
The most common primary reason for children becoming looked after is abuse or neglect (63%), followed by family disfunction (14%); other parenting difficulties account for the majority of the remaining cases, with child factors (e.g. child disability) identified in a minority of cases as the primary reason. 4 Thus, children who are looked after have typically been exposed to harmful experiences; abuse, neglect and major disruptions in parent–child bonds are prominent. 5 Although these experiences almost certainly affect child development in a number of ways, one very well-documented and important area is in the development of attachment. 6 Attachment is a critical early-appearing developmental phenomenon that is observable from the first year of life, in which children maintain proximity to and selectively seek comfort from their carers when they are worried, anxious or distressed, and attachment is thought to be critical for their optimal long-term development. Attachment is believed to be largely instinctive, but the way in which a child’s attachment behaviour is manifested or organised is dependent on the environment and, particularly, on the quality of care. 7 A large body of research has demonstrated that suboptimal and disordered patterns of attachment behaviour can arise when children experience insensitive, frightening, neglectful or abusive care, or frequent change of carers. 7,8 These early difficulties in attachment leave a child at risk of poor social and emotional outcomes. 9,10 In contrast, a secure attachment, whereby a child is able to openly communicate their attachment needs and be readily comforted by contact, is consistently associated with better developmental outcomes across a range of areas7,9–12
Following an extensive review of the literature, a recent National Institute for Health and Care Excellence (NICE) guideline13 identified three clinically important forms of suboptimal attachment patterns that should be considered important targets for intervention among children in care. These patterns, referred to collectively as ‘attachment problems’ by the guideline group, are reactive attachment disorder (RAD), disinhibited social engagement disorder (DSED) and disorganised attachment. RAD and DSED are observed almost exclusively among children who have been subjected to extreme neglect and/or repeated changes in caregivers, whereas disorganised attachment may arise in the context of abuse, neglect or highly insensitive/atypical parenting. 10
Reactive attachment disorder is considered an attachment disorder in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition14 (DSM-5) (previously referred to as the RAD-inhibited subtype in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition), and refers to a pervasive absence of attachment behaviour by young children towards their carers, combined with highly withdrawn and fearful behaviour and emotional volatility. RAD is observed at relatively high rates among children raised in institutions (43% in Zeanah et al. 5), but there is considerable uncertainty regarding its prevalence among children in UK foster care (Zeanah et al. 5 reported 35% RAD in a US foster care sample).
Although DSED has traditionally been defined as an attachment disorder (previously referred to as RAD-disinhibited subtype), it has been reclassified as a disorder of social behaviour in the DSM-5. These children show a striking lack of reticence with strangers, are prone to engaging in inappropriately intimate social (including physical) contact with strangers, and may wander off with strangers. Despite this behaviour with strangers, they show attachment behaviour, sometimes even of the secure type, to their primary caregivers in standard separation–reunion procedures such as the Strange Situation Procedure. 8 The evidence is quite clear that RAD and DSED are different disorders, showing distinct characteristics, aetiologies and courses. 10 Although the precise relation between DSED and the attachment construct is controversial, it is generally accepted that it reflects a lack of selectivity in social approach, which is at least closely related to attachment. 15
Disorganised attachment is observed in around 3–15% of normative populations, and it is much more prevalent among children raised in highly deprived circumstances or those exposed to abuse (48% of abused pre-schoolers are disorganised according to meta-analytic work; see van IJzendoorn et al. 16). Disorganised attachment is also observed at elevated rates in children in foster care compared with controls (d = 0.41; see van den Dries et al. 17). Disorganised attachment is not a disorder and is arguably more accurately described as a relational or developmental vulnerability factor that increases the likelihood of adjustment difficulties in the future.
A large number of intervention studies have shown that it is possible to increase the rate of secure attachment and reduce rates of disorganised attachment in a range of normative, at-risk and clinical populations by improving the sensitive responsiveness of parental care. 13,18,19 Such interventions often combine a number of treatment elements, but share the common objective of helping parents to become sensitively attuned to a child’s attachment cues, and to respond to them consistently and appropriately.
Video-feedback techniques are a commonly used and effective strategy for helping parents to increase their sensitivity to attachment cues and video-feedback-based interventions reliably increase rates of secure attachment and reduce rates of disorganised attachment (d = 0.44, k = 5). 19 Indeed, video-feedback interventions may be particularly helpful for high-risk children who have experienced significant disruptions in care. Three trials have used video-feedback interventions focused on improving caregiver sensitivity as a means of reducing attachment difficulties (specifically disorganised attachment) among children who had been adopted or maltreated, and all reported positive, significant and sizeable treatment effects (Bernard et al. :20 d = 0.72; Juffer et al. :21 d = 0.80; and Moss et al. :22 d = 0.90).
Two independent and wide-ranging reviews, one commissioned by the National Institute for Health and Care Research (NIHR) Health Technology Assessment (HTA) programme19 and the other conducted by NICE,13 concluded that interventions promoting sensitivity had the best evidence of effectiveness for reducing attachment problems among children in care. The NICE guidance13 specifically recommended video-feedback methods because of their good clinical efficacy and cost-effectiveness profiles.
The Video-feedback Intervention to promote Positive Parenting and Sensitive Discipline (VIPP-SD)23 is the most rigorously tested sensitivity-focused video-feedback intervention; it has repeatedly been shown to improve parental sensitivity to attachment cues (d = 0.47, k = 12)24 and has been used in a broad range of contexts and age ranges (up to the age of 5–6 years), making it an attractive choice for a brief and cost-effective treatment for children in foster care.
It is critical to note, however, that the HTA programme review19 also highlighted the fact that no study had yet tested whether or not any intervention can effectively treat RAD. Given the likely high prevalence of RAD in the foster care population, this is a serious research gap. 8 It is also noteworthy that no studies have tested the effectiveness of the VIPP-SD for improving attachment security and reducing attachment problems in a UK health-care setting for any target group, although a trial for children at risk of behavioural problems is due to report its findings imminently (UK Clinical Research Network identifier: 18423). 25 However, that trial does not target children in care and will not include children with RAD. Finally, although the VIPP-SD has been trialled for children who have been adopted, (see Juffer et al. 24 and van den Dries et al. 17) no studies, to our knowledge, have tested the effectiveness of the VIPP-SD for children in foster care at the time of the current study (but see Schoemaker et al. ,26 who have recently published the findings from their study with foster children in the Netherlands).
Although we currently lack evidence regarding the most effective treatments for RAD, the most promising approach for young children with difficulties falling under this rubric (primarily, failing to show attachment behaviour when distressed) is to focus on improving parental awareness and understanding of the child’s distress, and encouraging comfort-seeking by supporting what contemporary attachment theory and research indicates is the central driver of secure attachment: parental sensitive responsiveness. Such an intervention would also benefit from incorporating support for carers in managing challenging behaviour. 27 The VIPP-SD represents the most thoroughly tested video-feedback intervention for promoting sensitive responsiveness, includes techniques for behaviour management and is specifically recommended by NICE for treating attachment problems for children in care. It is, therefore, a strong candidate for the treatment of RAD symptoms in the foster care context.
Correctly reading and being consistently sensitive and attuned to a child’s attachment cues may be maximally difficult; therefore, enhanced support and training may be necessary when a child has attachment problems and a complex and traumatic history. A recent modified VIPP-SD programme designed for children in foster care [the Video-feedback Intervention to promote Positive Parenting and Sensitive Discipline, Foster Care (VIPP[SD]-Foster Care or VIPP-FC for short)]28 pays particular attention to the need to help carers recognise signals, which may be quite challenging and difficult to understand, that are more commonly observed in children in foster care, so that the carers are better equipped to respond sensitively and to support the child’s secure attachment to them as their carer. In particular, children in foster care tend to demonstrate attachment signals that are very subtle, highly distorted or absent, for example not crying when hurt because they are not used to being comforted, or becoming angry or fearful when comforted. By helping foster carers become aware of these subtle, distorted or absent signals and training them to respond appropriately, it is hoped that the child can learn that foster carers can be relied on in times of need and that it is safe to show their distress and seek comfort. For many children in foster care, their experience of physical interactions with carers has been extremely negative; hence, the VIPP-FC also specifically addresses how to gently and sensitively support a child’s needs for physical contact and comfort. 28
Rationale for the study
There is an urgent need to address the lack of evidence underpinning prevention and intervention work for young children in foster care with attachment needs. 13 The current report presents the results of a feasibility study investigating the acceptability of the VIPP-FC and the practical feasibility of implementing a randomised study of its efficacy. As part of this feasibility work, we explore the views of foster carers and professionals about the challenges of and barriers to supporting children with attachment needs in the foster care context, and the challenges of and potential solutions to running a research trial in this context. We undertook a small-scale trial to test a range of critical feasibility questions and conducted qualitative interviews with recipients of the VIPP-FC to better understand its strengths and limitations and foster carers’ experiences of the process of change. The present study represents an important step towards addressing a serious gap in the capacity of the NHS and social care services to meet the needs of looked-after children, in a context in which comparatively few research trials of therapeutic interventions have been undertaken.
Overview of study aims and design
In this study, we aimed to conduct a series of studies that represent key preparatory steps necessary to pave the way for a full-scale randomised trial of the VIPP-FC for children in foster care, who are at risk of attachment difficulties. This study comprised the following:
-
Modifying the existing VIPP-FC clinical manual to be suitable for the UK foster care context and to meet the requirements of children with attachment difficulties commonly presenting among children in foster care, such as those under the rubric of the RAD label.
-
Testing the acceptability of the intervention from the point of view of practitioners and foster carers, and working with local authorities, foster carers, parents and young people to establish the optimal systems, procedures and ethics considerations required to identify and support children with attachment difficulties in UK foster care populations.
-
Investigating the feasibility of a randomised controlled trial (RCT) of the modified intervention.
The study was divided into three phases. Phase 1 involved the refinement of the VIPP-FC manual through iterative consultation with an expert advisory group (including the developers, expert clinicians and foster carers), leading to the production of an initial, revised treatment manual. Phase 2a involved the initial testing of the treatment (no random allocation) with a small series of children with RAD-type difficulties and their foster carers, the results of which informed a further revision of the VIPP-FC clinical manual; in parallel with this, phase 2b involved a scoping study of the organisational, ethics and practical landscape within which a trial of VIPP-FC for foster children would need to operate. Phases 1 and 2 informed the final research protocol for the feasibility trial conducted in phase 3. Phase 3 involved recruiting a new group of children in foster care and undertaking a pilot RCT of VIPP-FC (with random allocation). This last phase also included a series of qualitative interviews with the recipients of the VIPP-FC to illuminate feasibility and acceptability questions.
As a treatment development and feasibility study, we adopted a mixed-methods approach, in which quantitative and qualitative data were collected sequentially and integrated at the analysis stage to obtain a better understanding of the treatment development process; the organisational and professional context that will constrain the operation of a future trial; and carers’, practitioners’ and care managers’ experiences and views of the programme, as well as evaluating the feasibility of a randomised trial using a small-scale pilot. In doing so, we adopted a pragmatic implementation-focused approach to establishing the initial feasibility of evaluating a complex intervention such as this, in line with the approach advocated in the Medical Research Council’s guidance. 29
The clinical intervention and the assessment framework were grounded in attachment theory and methods, which conceive of attachment as a critical biobehavioural process that develops in the context of routine caregiving interactions, serving to support children’s needs for comfort when they are anxious or feel vulnerable. 21 In addition to providing a rich and evidence-based account of the environmental mechanisms that shape the development of attachment (mechanisms which are the targets of attachment-focused interventions), attachment research provides a well-developed set of systematic and rigorously evaluated tools for measuring attachment at different ages. In the current study, we used gold-standard instruments for evaluating attachment difficulties [the Disturbances of Attachment Interview (DAI) and the Strange Situation Procedure] to show that their use is feasible in a clinical trial in this context, which will ensure confidence in the findings of any future full-scale trial.
Data management
The data in all phases of this study were collected and processed in accordance with the Data Protection Act (1998)30 and the General Data Protection Regulation (2018). 31 Management of the data was overseen by the chief investigator with support from the Trial Co-ordinating Team. Study data were collected by an experienced research assistant who had been trained to work with high-risk populations, with support from one or two other research assistants. Regular supervision by the chief investigator, Trial Co-ordinating Team and research assistants ensured the reliability of data collection. When necessary, the research assistants were fully trained and certified in administering all research measures. For data that required coding using standardised measures, we employed trained reliable coders, ensuring sufficient inter-rater reliability among coders. Although a number of NHS trusts and higher education institutions were involved in this study, all data were collected, collated and stored at University College London (UCL).
All data collected containing non-identifiable information were entered into a Research Electronic Data Capture (REDCap) database (Vanderbilt University, Nashville, TN, USA), a secure web application for building and managing online surveys and databases. 32,33 A master log of participants who were randomised was kept in the trial master file, detailing names and randomisation codes. Paper forms were kept in a locked filing cabinet, and electronic files were kept in an encrypted hard drive and on the UCL Data Safe Haven platform. Screening data and consent forms signed online were completed in REDCap within the UCL Data Safe Haven, as they contained identifiable information. Video- and audio-recordings were stored in the UCL Data Safe Haven or Citrix (Citrix Systems, Inc., Fort Lauderdale, FL, and Santa Clara, CA, USA), two secure and accredited technical solutions for storing, handling and analysing identifiable data.
Study management
Structured oversight of the project was undertaken by a Trial Steering Committee (TSC) and a Data Monitoring and Ethics Committee (DMEC). Both had an independent chairperson and the recommended proportion of independent members (subject experts and a public member), and were convened in accordance with guidelines for the NIHR HTA programme. The TSC and DMEC met regularly to guide the conduct of the study and agreed the details of project set-up, initiation and changes to the design and supervision of the study.
Ethics amendments and protocol modifications
During the study, we submitted three substantial amendments and five non-substantial amendments. See Appendix 1 for an outline of the reasons for the amendments.
The protocol went through six versions. The key changes introduced in the earlier stages of the study were (1) a mechanism to facilitate access to participants (to avoid the team being dependent on the return of paper questionnares to contact foster carers) by adding the possibility of social workers obtaining verbal consent from foster carers for their contact details to be passed on to the research team, and (2) allowing the possibility for the RCT to begin before the case series ended to avoid delaying the start of the RCT owing to difficulties in recruiting to the case series. After the RCT began, the key changes to the protocol were as follows: (1) adding online screening to aid recruitment; (2) the introduction of a reward for participants returning screening questionnaires (either on paper or online) to aid recruitment; (3) a change in target population – opening up the eligibility criteria to allow children who did not meet the criteria for RAD as defined by the DSM-5; this was a solution agreed with the TSC to allow thorough testing of the intervention; (4) allowing practitioners other than Child and Adolescent Mental Health Services (CAMHS) professionals to deliver the intervention to increase clinical capacity; (5) the addition of new sites; and (6) an extension of study dates. See Appendix 1 for an outline and dates of approval of these changes.
Patient and public involvement
Involvement of foster and kinship carers was integral to this study: in its preparation, in the refinement of methods and procedures throughout, and in the dissemination of the findings and discussions regarding a future trial.
The research team included an experienced foster carer who was closely involved, particularly in the early stages of the study, in setting up and refining the procedures. For example, this foster carer team member recommended that carers be offered the possibility of completing screening online and that a contact sheet should be the first step in the online screening to allow us to contact foster carers even if they did not complete all of the steps of the online screening. They also supported the introduction of a voucher to encourage and thank participants for completing the screening questionnaires (until this point, participants were rewarded after baseline and follow-up assessments only). This foster carer team member was also involved in the development of the modified treatment manual. In addition, we recruited one foster carer to sit on the DMEC and another to sit on the TSC.
We established a foster carers advisory group composed of three members, which contributed to several aspects of study design, implementation and dissemination. The foster carers advisory group members were appropriately supported by the study team and remunerated for their time in accordance with INVOLVE guidelines. 34 Owing to ongoing difficulties in scheduling face-to-face meetings at times that worked for all three members, this group provided their input remotely. One of the key aspects of the study about which we consulted this group was the screening packs; specifically, in the face of the low return rate in the case series (see Chapter 3), we intended to rethink the packs, fine-tune their contents and make them more attractive. Carer feedback was incorporated into the substantial amendment, such as the introduction of a colourful front sheet with a summary of what is required and rewording the participant information sheet to make it clearer that we were interested in hearing from everyone, even if they thought that the social and emotional problems described did not apply to the child in their care. They were also consulted for their opinions on the usefulness of adding the online screening and to get their feedback on the qualitative interview schedules.
We also consulted the Parent and Young People Panel from the Anna Freud National Centre for Children and Families about the screening packs and its feedback was incorporated in the packs, specifically, changing the order of the questionnaires in the pack to have the ‘friendlier’ one first and rewording instructions to avoid missing data, which initially occurred with one of the questionnaires (on which it was not clear that a respondent was required to answer all questions).
It is also important to note that, in the context of the feasibility nature of the case series and pilot RCT, we continuously asked participating foster carers for their views regarding the study procedures and measures. For example, as a result of this feedback, we offered participants the possibility of completing the screening questionnaires during a home visit; we kept the out-of-home research visits short and in locations that were easy for participants to get to; we provided extra instructions and support to complete the outcome measure that carers had more difficulty with (the computer-based questionnaire); and we introduced communications by text message, as this was a preferred method for many foster carers. It was clear that most foster carers had a preference for face-to-face contact with the research team and that they often experienced what one of them called ‘questionnaire fatigue’. This is an obstacle for a recruitment system that relies on questionnaire return, as the questionnaires often get ‘thrown onto the pile’ without being given appropriate consideration. We introduced several changes (the key changes are outlined in Ethics amendments and protocol modifications) to deal with this frequently reported obstacle.
A crucial patient and public involvement part of this study was the running of two conferences/seminars for all stakeholders: one mid-study, in September 2018, and another near the end of the study, in December 2019. Both were half-day, free events, during which we presented the project and preliminary findings and heard from world-renowned guest speakers, who were all experts in attachment and development of looked-after children. The events were very well received, with an audience that included foster carers, social workers, service managers and VIPP-SD/VIPP-FC interveners. The second event included a foster carers’ forum, where carers who had participated in the study discussed their experiences and insights and offered feedback to the study team. A key learning point from these events was that foster carers enjoyed contributing to the research, both those who received the intervention and those who did not, once they were ‘in’. This reinforces our conclusion from the conversion numbers in earlier stages versus later stages of the study (discussed in more detail in Chapter 5) that, once in direct contact with the team, foster carers tended to find the study very acceptable. Foster carers who could not attend the events were very pleased to receive the final study newsletter with a summary of the findings.
Feedback from the foster carers at all stages of the study was invaluable. In future studies involving this population, foster carer involvement should be sought at all stages of the project, bearing in mind that flexibility is needed to accommodate their busy schedules and child-care commitments.
Timeline
The study began in May 2017 and the final outcome assessments from the feasibility RCT were completed in January 2020. As outlined in Chapter 5, Results and Discussion there were numerous challenges in identifying and recruiting foster carers to the trial, which meant that, among other significant adjustments to the initial design, the timeline for recruitment was extended considerably: originally planned to cover March 2018–March 2019, recruitment to the feasibility and pilot trial began in May 2018 and ended in September 2019.
The methods, the results and an interim discussion for each study phase are presented separately in the following chapters, followed by a general discussion and conclusions.
Chapter 2 Manual development and programme modification
Phase 1 of the study aimed to refine the Video-feedback Intervention to promote Positive Parenting and Sensitive Discipline (VIPP-SD) programme (which has previously been adapted for foster care in the Netherlands) for the context of children in foster care in the UK. This intervention is named the Video-feedback Intervention to promote Positive Parenting and Sensitive Discipline, Foster Care [VIPP-FC (UK)]. In this chapter, we provide a succinct description of VIPP-SD and summarise the adaption process.
The VIPP-SD is a brief home-based attachment and parenting intervention. It is highly acceptable to families, has a clear and empirically supported model of change and has good evidence of efficacy with families of young children in many settings. 21 Practitioners who are trained and accredited to deliver the intervention visit families at home for six 90-minute sessions. Sessions 1–5 take place biweekly and focus on improving the carer’s sensitivity to the child. Session 6 is a booster session; it can take place approximately 1 month after session 5 and focuses on consolidating the information provided in sessions 1–5 and teaching carers sensitive discipline skills. In the original intervention programme, there is usually an additional booster session.
Sessions involve both the carer and the child, and start by video-recording carer–child interactions, following specific intructions that are given to the parent/carer (e.g. to play with a certain toy, to read a book together, to share a meal). The intervener films clips that provide the basis for themed discussions in the next session, when the intervener plays the clips back to the carer and discusses what they are observing. Themes include recognising the child’s attachment signals and expressions, providing prompt and adequate responses to them, promoting empathy for the child, praising positive behaviour and appropriate ignoring of negative behaviour. Carers are also given exercises and tips. Session content is consistent across families, although its presentation and the video feedback are tailored to the specific needs of each family. This description of the VIPP-SD also applies to the modified VIPP-FC. A summary of the VIPP-FC adaptation process follows.
Methods
Prior to this study, the intervention manual for the VIPP-SD had been modified for a foster care population, resulting from pilot clinical work conducted in the Netherlands. 28 We proposed to further modify this revised intervention (VIPP-FC) to specifically account for the clinical features of RAD, as well as to incorporate local (UK) health and social care policies and practices. In addition, given the differences between foster care in the Netherlands and foster care in the UK, other potential differences between the two groups of children and carers had to be considered.
An expert advisory group of the programme developers, UK clinicians (including colleagues in CAMHS, social care and the third sector) and foster carers was set up to review the existing VIPP-FC manual and advise the Manual Development Working Group (composed of members of the study team), which implemented the recommended changes. The consultation and revision processes were iterative, consisting of three advisory meetings and three rounds of manual revision. The Manual Development Working Group made an initial adaptation of the existing VIPP-FC manual for the context of children in foster and kinship care in the UK; this draft version of the manual was used in a small case series (phase 2a). After the completion of the intervention programme with participants in the case series, the Manual Development Working Group met again and further modified the manual. This modified manual was then used in the feasibility RCT (phase 3) of the research project and was reviewed once the RCT was completed.
Results
Although the adaptation process was planned to primarily focus on adapting the VIPP-SD/Dutch VIPP-FC for use in a population of children with high levels of difficulty in the domain of RAD symptoms, the Manual Development Working Group decided early on that the existing (Dutch) VIPP-FC manual was already constructed to handle clinical issues linked to RAD presentations. Therefore, the modifications that resulted from the work of the Manual Development Working Group dealt primarily with either contextual characteristics of the UK foster care population or more general needs that many children in this setting may present with, rather than RAD symptoms per se. These are described in more detail in the next two sections.
Initial adaptation of the VIPP-SD programme for the foster care population
Although the Leiden group’s original version of VIPP-SD for foster care was tailored to be appropriate for children in foster care,28 the adaptation undertaken in the Dutch context did not reflect the UK setting; as previously noted, the majority of changes recommended by the Manual Development Working Group reflect these differences in context and practice between the UK and the Netherlands. Before outlining the second phase of adaptation for the UK context, we summarise the main differences between the original VIPP-SD manual and the adapted VIPP-FC manual, as adapted by the Leiden group for the Dutch foster care context.
On the whole, the original VIPP-SD manual and the VIPP-FC manual were very similar, with similar tasks, visits and messages. However, the VIPP-FC manual included some extra key themes introduced in the manual specifically for foster children:
-
Additional content highlighting that foster children do not always show what they are feeling, as they may not be used to having their needs met, hence the need to address the more subtle signals of the child.
-
Additional content about not asking for help – children in foster care do not always behave in the ways that carers would expect them to, hence the need to react to the absence of attachment behaviour as well (e.g. if they do not cry when they hurt themselves, the carer should show them attention anyway to demonstrate that they can be trusted when something is wrong). These were added by the Leiden developers to encourage children to learn that they can rely on their carers. These modifications, in particular, relate to difficulties in the domain of RAD symptoms.
-
Additional content regarding the importance of physical contact – how it can cause anxiety for children who have experienced maltreatment and how gently encouraging it can help them overcome these anxieties, particularly if it is done in a structured and sensitive way (such as a song involving touch).
-
Additional content encouraging carers to compliment/praise small steps in the right direction – this is even more important for allowing foster children to know that they are doing something right.
-
Additional content about strategies to manage indiscriminate friendliness.
-
Alternative tasks to those in the original manual; for example, some short extra tasks were added that involve physical touch in a game/song to introduce physical touch in a safe way for the child.
-
‘Don’t touch’ task puts more emphasis on maintaining eye contact with the child than in the original VIPP-SD version, and also a suggestion of naming a book or toy to play with after they have calmed down so that they can more easily imagine the reward they will receive if they are able to wait.
Revisions to the VIPP-FC manual: the work of the manual development group
The modifications made to the VIPP-FC manual for this study were based on discussions within and feedback from the Manual Development Working Group, as well as on learning acquired during the case series, feedback from which was also reviewed by the Manual Development Working Group (see Chapter 3). Some modifications reflect changes to the manual itself, such as the wording of certain messages or tasks, whereas others have to do with the broader context for delivery of the intervention, such as introduction of forms and letters to aid in the delivery of the VIPP-FC in UK mental health services. There follows a summary of all of these modifications:
-
An additional guidance document was written to be used alongside the manual for interveners working with specific types of carers/children. This document aimed to guide interveners on where they should adapt their wording to ensure that the language they use is sensitive and tailored to the circumstances of a child and their foster carer; for example, the VIPP-FC manual regularly asks the intervener to refer to the child having had ‘previous adverse experiences’, but this was considered not always appropriate for some carers, such as when the carer is a relative of the birth parent or when the carer has had the child since birth. The four main groups that required the modified wording were (1) a child in a SGO, (2) a child in kinship care, (3) a child who has been with the family since birth and (4) a child who is likely to stay with the family on a long-term basis. As an example, for the fourth group of children, we removed a paragraph that referred to the importance of the carer’s relationship with the child even if they were not going to remain with them long term.
-
Following feedback from the Manual Development Working Group, we changed the word ‘obey’ to ‘do what you ask them to do’ throughout the manual as it was felt to be a little outdated and because it has negative connotations that contrast with the sensitive parenting that the VIPP-SD is trying to encourage.
-
We shortened the manual to from seven to six visits as it was deemed more suitable for the sometimes short-term nature of placements within the population of foster children and to minimise the chances that the intervention work would be disrupted by a change in placement. The timing of the last two visits was also changed so that there was only a 2-week gap instead of a gap of 3 or 4 weeks, again to ensure that the programme could be finished relatively swiftly.
-
A games booklet was introduced to the manual (adapted from a version created by the Tavistock and Portman NHS Foundation Trust for use with adopted families) to give to the carer in visit 4, which includes numerous songs involving actions and touch for the carer to use as a resource with the child (and with other children they may care for currently or in the future).
-
The Goal-Based Outcome form was incorporated into the manual. This change reflects a standard requirement in CAMHS in the UK, where this form is used as a routine outcome measure and has also been incorporated more generally into clinical practice. The Goal-Based Outcome form is completed during a discussion with the carer in visit 1, to gauge and manage their expectations and goals for the programme, and to reframe or find common ground from which to work if their aims are out of the scope of the programme. The intervener also completes a final Goal-Based Outcome form with the carer at the end of the programme in visit 6 to assess if and how the goals were met, and if not, why not.
-
Some extra guidance was added for the intervener supporting them in explaining or framing the importance of the work, even if the placement is expected to be short. The guidance helps the practitioner to explain that research supports the view that responsive and sensitive care is important for children even when relationships do not last, and that the relationship they build with them in this early stage of life can act as a foundation for the child’s future relationships and well-being. This was to counter beliefs that foster carers might have that it is best not to ‘bond’ with the child if they are not likely to be with them long term, and to help them understand how important it is for the child to experience warm and supportive care, regardless of the length of the placement.
-
In keeping with the need for close communication between members of a child’s professional team, a closing letter was introduced in which interveners are instructed to write a letter about how the programme went, what improved and what issues may still require support at the end of the programme, which is sent to the social worker, copying in the foster/kinship carer.
-
All names of Dutch games/songs were changed to English ones and additional instructions were added to explain how they worked, in case carers were not familiar with them.
-
Photograph booklets were provided for the carer and child at the end of the programme with stills from their VIPP-FC/research videos depicting memorable moments of shared sensitive interaction. It was decided that this booklet with stills was a more acceptable option than providing the video clips themselves, owing to the complexities of consent and data protection of video material in this population.
As previously mentioned, the majority of these modifications were introduced during the initial phase of the work of the Manual Development Working Group, and some were added after the Manual Development Working Group considered feedback from practitioners and supervisors after the case series cases were completed. Although the manual was open to further modifications on review of the RCT cases, no additional changes were deemed necessary to the manual and programme themselves. Nevertheless, challenges with interveners’ capacity and availability, as well as interveners having dual roles in some cases (e.g. interveners who also worked in other roles in the local authority or mental health service provider), throughout the RCT led to discussion of the best model for the delivery of the VIPP-FC, which we return to in Chapter 8.
Discussion
The VIPP-SD is a well-evidenced parenting intervention informed by both attachment and social learning models. It uses video feedback as the primary means of introducing change by focusing the caregiver’s attention on moments of connection and examples of sensitive care highlighted by a trained intervener, who uses their knowledge and skills to frame their feedback into a coherent, attachment-informed message, drawing attention to the child’s cues and communications, the carer’s sensitive response and the positive effect that this has on the child. Despite its extensive track record for promoting sensitivity in parenting in a range of populations, VIPP-SD has not been used before in the context of UK foster care and has only recently been adapted for the foster care context in its country of origin, the Netherlands. Transporting the VIPP-FC to the context of UK foster care requires careful attention to the particular needs and ways of communicating and interacting that children in foster care may present with, as well as the professional context and systems around the child, so that it can be used efficiently by practitioners in CAMHS and other related sectors. Our initial appraisal and adaptation of the VIPP-FC treatment manual suggests that it is well suited to the needs of children in foster care and the Manual Development Working Group’s suggested modifications should make it suitable and appropriate for the UK CAMHS context. The acceptability of the intervention from the point of view of foster carers is considered in greater depth in Chapter 7.
Chapter 3 Case series
Overview
Phase 2a of the study consisted of a small case series. Using a preliminary version of the treatment manual, resulting from the work of the Manual Development Working Group, we trained a group of practitioners in the modified Video-feedback Intervention to promote Positive Parenting and Sensitive Discipline, Foster Care (VIPP-FC) to work with a target of six children in foster care and their carers. We proposed to purposively recruit a sample reflecting variations in age and presentation of RAD symptoms, to road-test the modified VIPP-FC treatment manual and examine its clinical suitability for these children in real-world clinical practice. During this phase of the study, we recruited from a single local authority and identified a small number of cases using screening measures of RAD with the help of the children’s services. The case series also allowed us to undertake preliminary tests of the feasibility and acceptability of the screening process and the proposed research assessments. The case series was originally planned to run in two local authorities. However, shortly before we were due to begin work, the partner trust in one site lost their contract to deliver CAMHS locally, which meant that we were unable to proceed with that site for the case series.
Methods
Ethics considerations
Two key ethics issues required careful consideration in this study: consent and the RAD label/diagnosis. The determination of who must provide consent for a child in foster care to take part in a research study and how this should be done is recognised in the literature as a complex problem. 35 An important aim of the current study was to investigate the range of views on how this should be achieved, from local authorities in different regions and from parents and carers. However, the starting point for the purposes of this study was to follow a procedure used in another NIHR pilot trial being conducted by our group for older children in foster care [aged 6–16 years; NHS Research Ethics Committee reference number 15/EE/0032; award ID: PB-PG-0614-34079 (https://fundingawards.nihr.ac.uk/award/PB-PG-0614-34079)]. The consent protocol for that study was developed from a review of the literature and consultation with a local authority director of social care and their legal department. The general principle informing the protocol was that written, informed consent to take part in the study must be received from all parents and from the local authority when holding parental responsibility, and that every effort should be made to secure the consent of parents when they do not have sole legal parental responsibility.
On the basis of these considerations, to take part in the intervention phase of the study (i.e. after initial screening), parents of children on full care orders were sent information sheets and an opt-out letter (with a 14-day period for opting out) in all but exceptional circumstances. Specifically, children on a full care order could enter the study without parental consent if the local authority [which shares parental responsibility with the birth parent(s)] deemed it not in the child’s best interests to seek it, or when every attempt had been made to inform parents of the study and to secure consent, but this had failed. For all other children, full written consent was obtained from the child’s parent(s). The child’s social worker initially made contact with the parent(s) and provided parents with the information sheets. It was at the discretion of the social worker whether to seek verbal consent for parents’ contact details to be passed on to the research team so that a meeting could be arranged to sign the full written consent or to seek the full signed consent from the parents themselves. In either case, the research team’s contact details were always provided to parents in case they wished to ask more in-depth questions. Active refusal of consent by a parent was always respected, regardless of the care order. Furthermore, a parent’s decision to withdraw their child once the child had started in the study was always respected, regardless of the care order.
Full informed consent was obtained from all participating foster carers and from the local authority. As the children were all aged ≤ 6 years, they did not provide written consent, but the researchers were trained to obtain verbal assent in an age-appropriate fashion for children old enough to do so (age ≥ 4 years).
Throughout our discussions with colleagues in the local authorities, a recurrent theme was professionals’ concerns regarding the diagnostic term ‘RAD’. In particular, professionals expressed conerns that if this diagnosis became a part of a child’s social work record, this may have direct implications for the child’s subsequent care, including their likelihood of being adopted. For a more in-depth discussion of this issue, see Chapter 4: stakeholder interviews drew attention to the potential difficulties associated with using diagnostic terms and a diagnostic criterion as part of the eligibility criteria for entry to the study, as well as the complications associated with information-sharing regarding diagnoses.
Because we included children presenting with varying degrees of RAD-type behaviour and as our assessments were based on research instruments rather than full clinical assessments, we did not use the term ‘RAD’ in our communications with participating families (e.g. in participant information sheets or verbally) to refer to the set of behaviours the study was focused on. Instead, we described the specific behaviours that are considered under the rubric of RAD, which tend to carry fewer unhelpful connotations (e.g. difficulties in seeking comfort from available caregivers). The same avoidance of diagnoses applied to written correspondence with foster carers and social workers about each child.
Target population
The target population was children in foster care aged between 11 months and 6 years, and their foster or kinship carer(s).
Eligibility criteria
Inclusion criteria
Families recruited to the study were eligible if the following criteria were met:
-
parental figure –
-
foster carer(s) who is (are) primary carer(s) for the child
-
aged ≥ 18 years
-
proficient in English
-
-
child –
-
living with foster carer(s) in a placement planned to last at least 4 months
-
has lived with foster carer for at least 4 weeks
-
presence of RAD symptom(s) as defined by the DSM-5
-
aged between 11 months and 6 years.
-
Exclusion criteria
-
Parental figure: already engaged in a similar parenting intervention.
-
Child: severe developmental disability.
As a pragmatic study, we deliberately minimised exclusion criteria; this was to enable the later feasibility trial to reach a participant population that is broad and reasonably representative so that we could address the clinical suitability of VIPP-FC for a wide range of children in foster care. We did, however, collect detailed information about factors that might be relevant to the suitability of the VIPP-FC intervention for children with RAD, such as co-occurring conditions, placement variables and care order.
It is a pragmatic requirement of this form of intervention that the foster carer has some proficiency in English language because of the reliance of this programme on dialogue between the carer and practitioner as part of the video-feedback procedure. Thus far, the Video-feedback Intervention to promote Positive Parenting and Sensitive Discipline (VIPP-SD) has not been tested using interpreters, and we considered that this project was not the appropriate context in which to do such testing. Furthermore, on the basis of consultation with colleagues in the local authorities, we determined that comparatively few foster carers would not have adequate command of English language to participate in the programme. The research assistant in contact with the foster carer made a judgement regarding the suitability of their English-language proficiency, making sure that they met the minimal requirements necessary to take part in the study.
Although the programme is suitable for children with a range of levels of cognitive ability, and would be appropriate for children with physical and mild to moderate disabilities, it has not been used before among children with very severe global delay; such global delay would also substantially complicate, if not preclude, a reliable RAD assessment. Therefore, children with global developmental delay would need to be excluded from the study. This exclusion criterion was assessed by asking carers if the child had any medical diagnoses relating to severe developmental delays.
Owing to the risk of participant overburden and the contamination/confounding of treatment effects, it would be problematic for families to be engaged in similar parenting interventions simultaneously; hence, this was also an exclusion criterion. We did not consider it to be problematic that families were involved in other forms of social, psychological or medical treatment; therefore, no such exclusion criteria were applied. Furthermore, we explicitly assessed the presence or absence of comorbid psychiatric conditions in the child because these may be important factors influencing both clinical management and outcome, and are also likely to be quite prevalent. Exclusion on that basis would therefore be inappropriate. However, when other diagnoses were identified that warranted intervention (e.g. attention deficit hyperactivity disorder), we notified the child’s social worker and foster carer and recommended a referral.
Extensive consideration was given to the range of care arrangements that should be eligible for this pilot project. Children in foster care can be subject to a range of different care orders and placement arrangements (e.g. interim care order, full care order, section 20 voluntary placement36). Children placed in family and friends care may be placed under a SGO, a residence order or a care order and, rarely, as an informal placement. These issues are primarily relevant to the feasibility of intervention delivery, rather than child mental health need (as children in all of these circumstances are likely to present with raised rates of attachment problems and RAD). In consultation with colleagues in the local authorities, we decided that this is an important feasibility question and exclusion on the basis of placement setting or type of order would unhelpfully limit the learning that the feasibility study could produce. Regarding family and friends care in particular, there was a clear view from our consultation, which was highly consistent with recommendations made by NICE, that family and friends care, which is increasingly common, should be within the scope of this study. 13 Children placed under a section 2036 (a voluntary placement, whereby the parents retain full parental responsibility) or on an interim care order may present the most difficulties from a practical point of view because the duration of the placement will be uncertain. Nevertheless, it is not uncommon for such placements to last at least 6 months (i.e. long enough for an intervention to be put in place) and duration cannot be predicted in advance. Therefore, our view, which was supported by our discussions with local authorities, was that an inclusive strategy should be taken.
One critical point to emerge from these discussions was that there may be great value in considering adaptations to the intervention that allow for the programme to ‘follow the child’ when there is a transition in the placement arrangements (e.g. to adoption, to a more permanent foster care placement or back to the child’s parents). A lack of continuity in care is a problem highlighted by many in the field and by children in care themselves. 13,27 We planned to discuss this process carefully with the study advisory groups and we proposed to test, in a small number of cases as they arose, the workability of the plan they recommended. In such cases, we anticipated that the work would not begin again, but would focus on transferring what had been learnt during treatment to the subsequent placement and supporting a smooth transition.
Recruitment
Screening and identification stage
The screening process involved close collaboration with the partner local authority, which sent out information sheets, initial consent forms and screening measures to the foster carers in the study locality. In addition, as noted previously, the local authority sent out a letter to all parents explaining the study and the opting-out process, including the contact details of the research team. They communicated to their staff members within the children’s social care team to raise awareness of the study and draw attention to the support required from children’s social workers. We originally planned to invite all foster carers or special guardians registered with the local authority caring for children aged ≤ 6 years. In practice, the local authority applied its own exclusion criteria at this point (e.g. excluding highly complex cases undergoing assessments for court or cases with restricted files), as we note in Results and Conclusion.
We also contacted and sent leaflets to several foster care agencies inviting them to take part in the study. When direct self-referrals or clinician referrals were received by the research team, foster carers/clinicians were asked for the child’s social worker’s contact details in order for the local authority to initiate the screening process, including contacting the birth parents. Regardless of the route of recruitment to screening, a minimum 2-week period was given between sending out the letter to parents and initiating the child’s participation in the study.
Once initial consent forms and screening measures had been received by the research team, research assistants contacted participants, thanking them for their response and reiterating the research process. Invitations and follow-up telephone calls were made to all foster carers to take part in a face-to-face interview assessment to confirm eligibility, unless it was clear from the information provided at that point that they would not be eligible (e.g. the child had already left placement or the placement was very far from the borough). Owing to the comparatively small number of carers who could be invited to take part, we opted to invite all foster carers who returned the questionnaires to take part in the DAI so that we gained experience of the acceptability of the interview and a reasonable level of initial data on the performance of the screening questionnaires. As the screening/identification stage involved no direct contact with the child and involved minimal burden or risk, we obtained active consent from the foster carer only. However, a letter was sent to all birth parents with an explanation of the study and the process of opting out (except in circumstances in which the local authority deemed it inappropriate to inform the parents). If, after the 2-week period for opting out, the local authority or the research team had not been contacted by the parent to opt out, the screening process was initiated. Foster carers received an information sheet explaining the study fully and a contact telephone number of a member of the research team in case they had any questions. The information sheet explained that completing the screening measures did not entail any obligation to participate in the subsequent stages of the study (i.e. the baseline research assessments, treatment and follow-up assessments).
Post-screening stage
If eligibility was confirmed, foster carers were invited to the next stage of the study, involving baseline assessments, receiving the VIPP-FC and completing follow-up (i.e. post-treatment) assessments. The baseline assessment took place as soon as possible after all consents had been obtained (the target was within 4 weeks). At this point, we initiated the more comprehensive consent process (i.e. consent to baseline/follow-up assessments and treatment). Consent from birth parents (if applicable) and consent from the social worker or team manager were obtained before the baseline study visit. At the baseline study visit, we obtained the foster/kinship carer’s consent, as well as the child’s assent, if they were aged > 4 years.
The baseline assessment took place in our partner CAMHS, in the local authorities’ premises, or at UCL, depending on the preference of the foster carer. Carers were paid £30 at both the baseline and follow-up (i.e. post-treatment) outcome assessments to thank them for their time, and were reimbursed any travel expenses. Children were given a sticker after each visit.
Sample
For this (non-randomised) case series, we aimed to recruit six cases for piloting the clinical intervention, and testing screening and assessment procedures. As noted previously, we proposed to include a mixture of cases obtaining high RAD scores on the screening measures and cases falling below this threshold to explore whether or not the intervention required adjustment for these groups of children, and to maintain the pace of manual development in the event that prevalence was lower than expected.
Screening measures
There is no pre-existing established tool to screen for RAD. This is a significant gap in health technology in this field, as early detection may be critical for improving outcomes for children in care. In this study, we used two different instruments that each have their individual limitations, but may be useful in combination for screening for symptoms of RAD. The Attachment Screening Assessment (ASA) (Danya Glaser, Saul Hillman, Yael Shmueli-Goetz and Vivian Prior, the Anna Freud National Centre for Children and Families and UCL, 2013, personal communication) is a new instrument designed specifically to capture behaviours reflective of the DSM-5 symptoms of RAD and DSED, as well as standard Ainsworth-type attachment classifications. 37 In pilot work (Ching Yiu Ng and Saul Hillman, the Anna Freud National Centre for Children and Families and UCL, 2015, personal communication), the RAD items in particular have been found to discriminate well between children in care and those from the community, as well as children with greater overall psychopathology on the Strengths and Difficulties Questionnaire (SDQ). However, the ASA has thus far not been validated against formal diagnostic assessments, which limits the extent to which it can be used alone as a screening measure. The Development and Well-Being Assessment (DAWBA) includes a recently revised set of items for DSM-5 RAD. 38 We proposed to use these two instruments so that we could test the optimal configuration of measures for case identification.
Primary outcome: attachment measure
The DAI is a semistructured interview to evaluate the presence of signs of disordered attachment. 39 For each of 12 sections, the interviewer asks multiple questions and follows up with probes sufficient to yield a rating reflecting the degree of evidence of disturbed or disordered attachment: 0 = none/never, 1 = somewhat/sometimes and 2 = considerable/frequently. The first five sections of the interview address signs of emotionally withdrawn/inhibited attachment disturbance (i.e. RAD), yielding total scores ranging from 0 to 10 points. The inhibited attachment disturbance items are 1 – does not differentiate among adults, 2 – does not actively seek comfort when hurt/upset or does not seek comfort preferentially, 3 – does not respond to comfort when hurt/frightened, 4 – does not respond reciprocally with familiar caregivers and 5 – does not regulate emotions well. The next three sections address signs of indiscriminate behaviour and the last four sections address other signs of disturbances in attachment behaviour (known as ‘secure base distortions’). There is sound evidence for the validity of this measurement system. First, it distinguishes between institutionalised and non-institutionalised children, reliably identifies signs of attachment disturbance in maltreated children and validly distinguishes RAD from DSED. 5,39–41 Second, it has shown very good inter-rater reliability and high levels of internal consistency. 39,40,42 Third, criterion validity has been demonstrated through the convergence of attachment disorder diagnosis by different measurements. Construct validity has also been demonstrated by the association of DAI ratings with quality of care. 43
Secondary outcome measures
Attachment insecurity and disorganisation
Strange Situation Procedure
Participants were observed with their foster carer while in an unfamiliar room for the Strange Situation Procedure. The Strange Situation is a standardised procedure lasting a maximum of 21 minutes. It is divided into a series of episodes involving brief separations and reunions with the parent/caregiver; exposure to an unfamiliar, but friendly, female adult; and a period of time alone. These episodes are video-recorded for subsequent rating by trained coders, resulting in a classification of the infant–caregiver dyad into one of the four attachment categories: secure, insecure-avoidant, insecure-resistant or disorganised. For children aged > 24 months, an adaptation of the administration of the Strange Situation (mainly concerning the timing of each episode) and the respective coding system for the pre-school years was implemented (Jude Cassidy, Pennsylvania State University, 1992, personal communication; Robert Marvin, University of Virginia, 1992, personal communication; and the MacArthur Working Group on Attachment, University of Virginia, 1992, personal communication). Even though the pre-school rating system was originally created for children up to the age of 54 months, we did not anticipate problems in extending it to the 6-year-old participants. Indeed, the pre-school system was created based on the assumption that the ‘strategies’ associated with each one of the three organised attachment categories remain the same throughout development.
Co-occurring disorders/difficulties
The DAWBA was used to assess the presence of psychiatric symptomatology co-occurring with RAD through the foster carer interviews. The DAWBA is a well-validated diagnostic interview schedule that has been recently extended to children as young as aged 2 years and has been updated for the DSM-5. The DAWBA has been used extensively in clinical trials and epidemiological studies. The system has high levels of inter-rater reliability and provides automated algorithms for scoring and assigning diagnoses. It should be noted that, owing to some limitations in the validity of the DAWBA for assessing RAD, we relied on the DAI as the main instrument to identify RAD symptoms.
The Child Behavior Checklist (CBCL) is a very widely used carer-reported questionnaire for assessing children’s emotional and behavioural problems, and yields well-validated continuous measures of internalising problems, externalising problems, total problems and specific ‘syndrome’ scales for narrow-band symptom areas (such as attention problems, aggression, social problems). 44 It is valid for children from the age of 1.5 years and has age-appropriate forms for children aged 1.5–5 years and ≥ 5 years.
Broader impact measures
To assess quality of caregiving, we rated the observed carer sensitivity and other related parameters of parenting (e.g. co-operation, positive regard for the child). We used standardised observational procedures for assessing carer sensitivity during free play and routine caregiving interactions. Specifically, we video-recorded an interaction between carer and child for 10 minutes (excluding instructions), during which a set of structured instructions given to the carer were followed: (1) to teach the child how to play with a challenging toy for their age, (2) to then play with the child using no toys, (3) free play with the toys and (4) to help the child tidy up the toys. These video-recordings were subsequently scored blind to treatment condition and status (pre vs. post) by trained and reliable coders. The scoring system used was the National Institute of Child Health and Human Development (NICHD) sensitivity scales, which have been validated in numerous studies. 45
We also administered two parenting-related questionnaires. The Parenting Stress Index-Short Form was used to assess carer well-being, carer strain and the carer–child relationship. 46 The Brief Parental Self-Efficacy Scale is a measure of beliefs and confidence about parenting skills. 47
The Child and Adolescent Service Use Schedule (CA-SUS) assesses resource use for health economic evaluation. 48 Previous versions of the CA-SUS measuring service use by pre-school children with autism and young looked-after children formed the basis of a modified version suitable for the current population, with modifications being determined, initially, by expertise in the research group and, subsequently, by testing for acceptability and comprehensiveness. Specifically, this initial draft version was tested and modified in two ways. First, after a sufficient number of cases, the interviewers and the CA-SUS authors discussed necessary amendments and clarifications that were incorporated into the previous (draft) version. Second, the measure’s comprehensiveness in capturing all relevant services was assessed. Testing was important to identify items that were redundant or important services that had been omitted.
The proposed battery of outcome assessments was similar to those we have used in other trials and cohort studies,25,49,50 and our previous experience was that it would not be excessively burdensome. However, we planned consultation with foster carers (through the foster carers advisory group), as well as with those taking part in the study, regarding the level of acceptability and burden. Establishing the optimal balance between participant time/burden and the robustness of the outcome assessments was an important aim of this project as preparation for a full-scale trial.
The research team attempted to follow-up all families involved in the study, including children who moved to a different placement during the time of the research. Any additional relevant consent that was required as a result of placement changes was obtained (e.g. consent from the new carer).
One of the aims of the case series was to establish initial feasibility of the intervention protocol and the acceptability of the programme and outcome assessments to foster carers. Accordingly, research assistants closely monitored the recruitment and assessment processes and requested continuous feedback from carers to make any necessary adjustments to the protocol for the feasibility RCT (phase 3). In addition, treatment progress and process were closely monitored, and feedback was presented and discussed by the Manual Development Working Group (from phase 1) to allow consideration of further appropriate manual modifications. Practitioner feedback forms were used to provide additional qualitative feedback about the experience of using the VIPP-FC in practice. The results of the case series also informed revision of the research protocol in preparation for phase 3.
Intervention
Intervention description
The VIPP-SD is a brief home-based attachment and parenting intervention. It is highly acceptable to families, has a clear and empirically supported model of change and has strong evidence of efficacy with families of young children in many settings. 21 We proposed to have staff who had received training in the intervention visit families at home for six 90-minute sessions over 4 months. Sessions 1–5 take place biweekly and focus on improving carer sensitivity to the child. Session 6 is a booster session; it can take place approximately 1 month after the fifth session and focuses on consolidating the information provided in sessions 1–5 and teaching carers sensitive discipline skills.
Sessions involve both the carer and child, and start by video-recording carer–child interactions, which provides the basis for themed discussion in the next session when the intervener feeds back the clips, pausing the video at certain moments to highlight and provide messages according to manualised themes. Themes include recognising the child’s attachment signals and expressions, providing prompt and adequate responses to them, promoting empathy for the child, praising positive behaviour and appropriate ignoring of negative behaviour. Carers are also given exercises and tips. Session content is consistent across families, although its presentation and the video feedback are tailored to the specific needs of each family.
The VIPP-SD has recently been modified specifically for the Dutch foster care context by the developers of the programme in the Netherlands. This modified programme (VIPP-FC) pays particular attention to the need to help carers recognise signals that are specific to foster children, which may be quite challenging and difficult to understand, so that they are better equipped to respond sensitively and to support the child’s secure attachment to them as their carer. The VIPP-FC is thus designed to specifically address the attachment difficulties often shown by children in foster care. In particular, these children tend to demonstrate attachment signals that are very subtle, highly distorted or absent, for example not crying when hurt because they are not used to being comforted, or becoming angry or fearful when comforted. By helping foster carers become aware of these subtle, distorted or absent signals and training them to respond appropriately, the child can learn that foster carers can be relied on in times of need and that it is safe to show their distress and seek comfort.
Many children in foster care have extremely negative experience of physical interactions with carers; hence, the VIPP-SD modified for foster care also specifically addresses how to gently and sensitively support a child’s needs for physical contact and comfort. 28
The intervention manual and delivery were further modified for this study to meet the systems and circumstances of the UK foster care context, as described in Chapter 2. We will refer to the modified intervention as VIPP-FC.
Training of interveners
We trained a group of individuals from an NHS Specialist Looked-after Children’s CAMHS team in the delivery of the VIPP-FC modified intervention. The interveners of the case series were already VIPP-SD trained, experienced practitioners. Each intervener was trained by an accredited VIPP-SD trainer and was required to undertake supervised practice before becoming a study therapist. Accredited supervision face to face, by telephone and by e-mail was provided to all practitioners.
Treatment fidelity
We ensured fidelity through supervision of three visits per case. All interveners completed logbooks for each visit, outlining how closely they followed the manual, if they completed all the filming tasks and if they included key messages in their feedback to the carer; logbooks were required for each different visit. They were also required to audio record at least one of their feedback sessions per case.
Results
Screening response rates
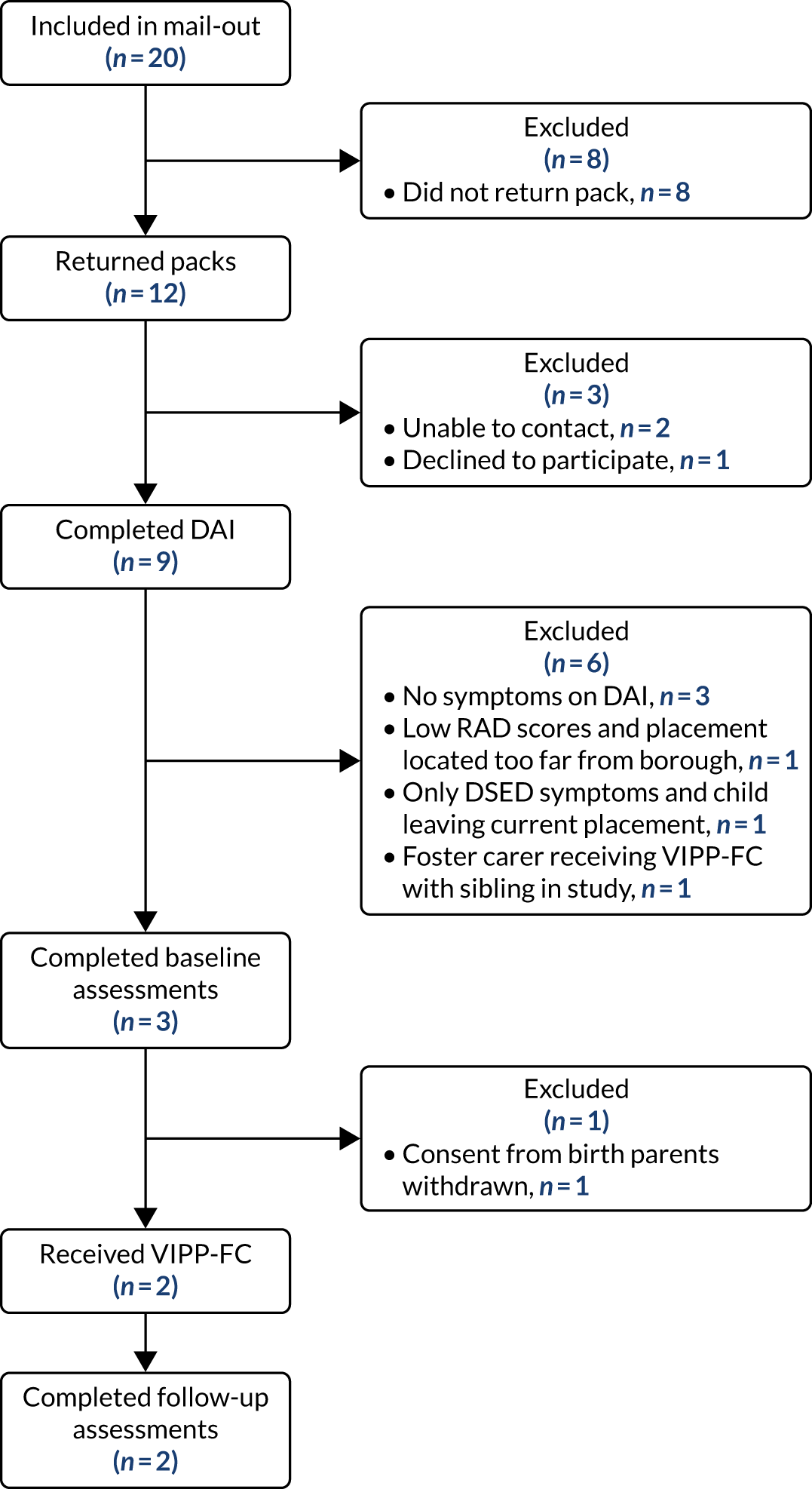
We present the overall response and retention rates in the form of a Consolidated Standards of Reporting Trials (CONSORT) flow diagram in Figure 1. As is evident from the diagram, we achieved a relatively good response rate of 60%, or 12 out of 20 carers.
FIGURE 1.
The CONSORT flow diagram for the case series.
Performance of the screening questionnaires
We found a moderate prevalence of RAD symptoms in this sample. Specifically, five out of the nine completing the DAI scored positive for at least one RAD symptom/sign, and four scored positive for more than one. It is unclear, of course, if the prevalence in this small sample is representative of the population of children in foster and kinship care or placed with guardians in the UK, and, with such a small sample size and low sample rate, the estimate has a very high degree of uncertainty attached to it.
Treated cases
Of the nine children whose carers completed the DAI, only three were eligible to proceed to treatment (see the reasons for exclusion in Figure 1). These three children underwent all baseline assessments with their carer. After the assessments were completed, one of them left the study because the child’s birth parents (who had received opt-out letters) contacted the social worker to refuse the child’s participation.
Hence, two children went on to receive the VIPP-FC, each provided VIPP-FC by a different CAMHS practitioner. They both completed all six sessions and all of the follow-up (i.e. post-treatment) research assessments.
Process observations: recruitment and consent
It is important to note that the 60% return rate was achieved only after substantial effort, which involved the study team calling social workers multiple times and asking them to encourage carers to return questionnaires, which, in turn, often required social workers speaking to carers several times. Another key learning point from the case series was that only a very small proportion (15%) of those potentially eligible (i.e. the 20 included in the mail-out) were eligible and willing to consent to the second stage of the study, during which they would receive the intervention.
Although return of the questionnaires was challenging, once we were in direct contact with the foster carers, they were generally very willing to hear more about the study and to take part in the subsequent stages. In spite of that, six out of the nine who completed the post-screening interview were, for various reasons, ineligible to take part in the baseline/follow-up assessments and receive the intervention. The feedback of those who took part in the more comprehensive assessments (i.e. at baseline and follow-up) was that these were acceptable and not overly tiresome.
Before and during the recruitment period, a member of the research team attended social worker and supervising social worker meetings to disseminate the study and encourage their involvement. Social workers appeared interested in the research and, in some instances, were able to identify cases that were potentially appropriate for taking part. On the other hand, some negative reactions were also experienced, such as disappointment regarding the limited age range of the target population and some confusion regarding the nature of the clincal presentation we were focusing on. Attempts to join foster carer groups were not successful.
The research team was able to explore and record the reasons for refusal from the birth parents who withdrew consent for their child’s participation, because the father consented to a member of the research team contacting him. The reasons for refusal provided by the father can be summarised as (1) frustration and anger at the local authority for having removed the child from his care; (2) an unwillingness to ‘help’ the local authority and what was seen as one of its partners (the research team); and (3) an unwillingness to allow a service to be offered to the child in the context of his relationship with his current (foster) carers, which was seen as contributing to the quality of the placement. The local authority and the TSC, in response to this, raised the more general question of whether or not there were circumstances in which parents may be considered to be not acting in the best interests of the child, for example when there has been limited contact and there are fraught relationships with the local authority. The TSC recommended that this issue be raised with the Research Ethics Committee. On discussion with the chairperson of the Research Ethics Committee, we agreed a revision of the initial consent procedure for cases on a full care order. Specifically, for the subsequent rounds of recruitment, local authorities were instructed to consider carefully if any birth parents with a child on a full care order might not be in a position to act in the child’s best interests. In such circumstances, the local authority could be permitted to give consent unilaterally.
Process observations: joint working with the local authority
This project involved working closely with the children’s services within a local authority; indeed, the initial step of making contact with foster carers and parents could be completed by the local authority only. Therefore, the study team needed to establish a strong partnership with the local authority, and considerable effort was focused on working and continuously improving the collaboration with the local authority to support the smooth running of the study.
Although the case series involved a single local authority only, a number of key practical implementation issues arose that were critical to consider in preparing the subsequent pilot RCT in other sites. Here we summarise the main findings regarding implementation with respect to the screening process and joint working with the local authority:
-
The importance of social worker involvement and agreement – social workers play a central role in implementing a workable screening system in this context. At least two key issues arose in this respect. First, information in local authority digital records was not always up to date, and social workers sometimes held the most up-to-date information about children and their situations, including details and nuances about children’s placements and plans that might not be possible to gather from their electronic files. Because children’s circumstances can change quite often and quickly, close liaison with a child’s social worker was critical. This was not always easy, as social workers were generally very busy and were not always able to return telephone calls or reply to e-mails. This link to social workers for rapid communication of important case information or updates regarding location or suitability of cases is a critical potential vulnerability and a considerable amount of study team time/resourcing was required to make this work. Under-resourcing this aspect of project infrastructure could jeopardise a trial. Second, as representatives of the child’s interests, individual social workers’ agreement or ‘approval’ for a child’s participation in the study was generally expected (by the social workers themselves and, often, by the foster carers), even if someone with the relevant authority had granted permission already. This reinforces the importance of close working relationships with the children’s social workers, as well as the wider team within the local authority.
-
Importance of the role of a ‘link’ member of staff – it was clear during this work that it is essential to have a contact person at the local authority who links the study team to the rest of the children’s services team. In the first study site, an internal member of staff at the local authority (initially, a senior social worker and, at a later stage, an administrative support worker) fulfilled this role of connecting the study team and the children’s services. Owing to the changing and somewhat unpredictable environment of these settings, it may not always be realistic to maintain a continuous dialogue with a large number of members of staff working directly with children. Therefore, this ‘link person’ is crucial to make communication effective and not diffuse responsibility for taking the project forward within the local authority. It is likely to be helpful if this is the same person who is designated to undertake the administrative tasks required for recruitment of participants to the study, namely obtaining a list of potential participants, mailing out letters and screening packs, and contacting carers.
-
Limited resourcing – it was clear from the first phase of work that local authorities’ resources are limited and that social workers and support staff tend to be under considerable pressure and have little time available to dedicate to a research project, despite their willingness in principle. We made extensive efforts to make sure that the study was ‘on the radar’ of colleagues in the local authority, but the sheer volume of work they face often slowed study procedures significantly (obtaining up-to-date lists of potential recruits, gaining local authority consents, sending out letters, speaking to foster carers on behalf of the study team, etc.). We explored the possibility of bringing a member of the research team into the local authority to support these administrative activities and to lessen the impact on core staff (e.g. from within our team or a clinical support officer from the Clinical Research Network). However, we faced some anxiety from the local authority about allowing an external person into the authority (with an appropriate honorary contract/appointment in place) to support its participation in the study. The reluctance to pursue this possibility appeared to be partly apprehension about governance and training issues, but was also related to an unwillingness to invest the time required to set up such a contract, which was perceived to be an arduous bureaucratic process.
-
Lengthy delays in obtaining data from the local authority – gathering information and, particularly, obtaining a list of potential participants (even with relatively simple criteria, such as children aged ≤ 6 years in certain types of placement) took longer than anticipated, usually at least several weeks after all the agreements had been put in place and the go-ahead had been given by a relevant senior manager to generate a list. Therefore, recruitment needs to be planned well in advance and with this time frame in mind. Because children’s circumstances can change quite rapidly, this can also mean that the list becomes out of date by the time it is acted on and may need updating.
-
Researcher presence at social workers meetings – we expected that it would be important for the research team to attend social workers’ team meetings to disseminate the study and engage social workers and supervising social workers. It was clear that it would not be enough to go to a single meeting as the study could quickly become forgotten and we would not be able to meet all staff in a single meeting. However, we found that getting invited to these meetings was a challenge in itself, despite the local authority’s willingness to invite the team in principle. Our impression was that this largely reflected the very busy working environment and the stretched resources within local authorities.
-
Lack of availability of social workers – social workers (particularly children’s social workers) tended to be extremely busy and were often away from their desks on home visits. They were, in the majority of cases, difficult to reach by e-mail or telephone. It was clear that the study would work best if it relied on them as little as possible and used what little time they had available for the most critical functions. For example, it did not appear to be feasible to ask individual social workers to mail out screening packs or to ask foster carers to return the packs via the social worker. Furthermore, although relying on individual social workers to follow up on questionnaire completion from carers is often necessary, it is important to also have alternative strategies in place to supplement that work (e.g. having an administrator in the local authority to make direct telephone calls to carers).
-
We tended to find that supervising social workers were easier to get a hold of and could be very helpful in following up foster carers about screening questionnaires. They were also interested in promoting the study as an aspect of improved foster carer training.
-
Social workers appreciated receiving feedback from the research assessments, which, in some cases, could be incorporated into relevant clinical reports about the child.
-
Finally, we had no success recruiting from foster care agencies, partly because we would still be dependent on the local authorities to obtain consent to screen specific cases and partly because they were difficult to engage. Therefore, we were not able to recruit any cases through these agencies, despite contacting > 40 of them.
Process observations: working with foster carers
-
Foster carers tended to be very busy, often caring for more than one child, and were responsible for completing a great deal of paperwork for the local authority as part of their formal role responsibilities. This was a challenge for the completion of the screening questionnaires and some foster carers fed back to us that if there is no one specifically highlighting the study, then questionnaires may just be ‘thrown on the pile’. The feedback reinforced the importance of promoting the study at multiple levels and in multiple forums, and, in particular, the importance of finding ways to encourage social workers (supervising social workers and children’s social workers) to promote the study directly to foster carers.
-
Foster carers tended not to take the initiative to contact the research team if they had questions. In several instances, foster carers had queries about the questionnaires or about whether or not they were allowed to take part [i.e. whether or not the local authority had approved it (even though the cover letter indicated that it had)], but did not use the contact details provided to ask them. Follow-up telephone calls from the local authority on behalf of the research team were very important in these cases.
-
Virtually no foster carers completed the research questionnaires without some chasing from the children’s social worker or the supervising social worker (or both), often on several occasions.
-
Social workers’ encouragement of foster carers to complete the questionnaires was vital, but, given that it was very challenging to get social workers to do that, we proposed a protocol amendment to the Research Ethics Committee to allow us to contact foster carers directly if they gave the local authority/social worker verbal consent for us to do so. This was very helpful as it gave the research team the opportunity to follow up on the questionnaires, clarify any doubts and show that they were available to help, and to do so without depending on a social worker to make several calls on their behalf. We suspect that making direct personal contact in this way was also reassuring to foster carers and helped build a direct relationship with the study team.
-
Some foster carers did not complete the questionnaires because they thought that the child would not be eligible for several reasons. This would tend to mean that non-completion could be non-random and selectively over-represented by low-scoring cases. This may be less of a problem for simply identifying cases, but is problematic for estimating the proportions of cases meeting RAD criteria. We tried to mitigate this in preparation for the RCT by emphasising in the information sheet that we were keen to hear from all foster carers, including those caring for children who did not have any emotional difficulties, but it was unclear how much impact this information had.
-
We concluded in discussions with our foster carer team member that an incentive to return questionnaires, in the form of a voucher offered to the carer, might help with return rates; although we could not implement this in time for the case series, we were able to introduce this change to the feasibility RCT.
-
Research assessments – the baseline and follow-up assessments took longer to complete than initially expected. To manage this, we implemented a number of strategies that generally worked well. Specifically, to make the study visit of a manageable duration, we offered flexible options for completing any assessments that did not require a formal assessment/laboratory context to complete (i.e. all but the Strange Situation Procedure and interaction observation). Thus, we offered families the opportunity to complete paper questionnaires before the visit and to complete the DAWBA online at home, as well as the opportunity to pay a second visit to a carer’s home to complete these, if needed. We explored the possibility of doing the DAWBA or the DAI over the telephone, but concluded that this was not feasible, as reading aloud the questions and options for the former took too long, and being unable to see and establish rapport with the interviewee made the latter more challenging.
-
Foster carers appreciated receiving feedback about the assessments and found it helpful. This also proved to be very valuable for social workers, both for their own use and because they appreciated the support it offered foster carers.
-
Although based on a very small number of cases, we found that, once initial contact was established and the team met foster carers in person, foster carers tended to remain engaged with the study and complete all of the assessments and all VIPP-FC sessions.
Process observations: working with parents
-
Parents often did not live at the same address; thus, the decision of whom to send the information letter to (i.e. one or both parents) was made by the local authority.
-
Even though the research team was available to seek consent from birth parents directly and in person, social workers preferred to be the ones requesting consent from parents in person, usually when they were meeting them for other reasons. However, this meant that obtaining written consent from parents could take a long time, as we had to wait for the social workers to obtain this.
-
Although parents have a right to refuse consent for their child to take part in the study, we encountered an example in which the local authority considered that the parents were refusing for reasons that the authority deemed were not in the child’s best interest. Clearly, in some cases, relationships between parents and the local authority can become strained and parents may have limited involvement in their child’s life. After discussion with the local authority and the TSC, we met with the chairperson of the NHS Research Ethics Committee, who advised us that the protocol provided scope, when a child is subject to a full care order, for local authorities to exercise discretion about whether or not the parent is in a position to give consent in the best interests of the child. Thus, on the recommendation of the TSC, we moved to asking local authorities to verify, case by case, which parents should be notified about the study before seeking their consent (both at the screening stage and at the baseline stage).
Process observations: working with children
-
In this young cohort (i.e. aged ≤ 6 years) placements are often short term and there is some unpredictability in terms of the duration of placements. A key question we needed to consider was when a child should be considered eligible for the study, which involves a minimum 4-month intervention, when the likely duration of placement is difficult to predict. Through discussions with social workers and direct experience through the case series, we concluded that the best approach is to contact as many foster carers as possible at the screening stage (i.e. not limit screening based on expected placement length initially) and to have discussions on a case-by-case basis regarding potential progression to the intervention stage. Maintaining ongoing communication with those cases for whom there was uncertainty about placement length was important (e.g. if a final hearing was scheduled during the early phases of engagement or screening). Allowing flexibility and individualised decision-making would be beneficial for a future study, given that such cases are unlikely to be rare.
-
Research assessments: we found, albeit in a small set of cases, that the children were happy to come to the study visits and do the assessments. It was also clear that it was important to keep the visits relatively short, as children could become impatient or tired after a while, particularly when they were not involved directly (i.e. when the carer was being interviewed).
-
When the carer needs to bring siblings along to the study visit, it is crucial to have at least a second member of the research team to help.
Conclusion
The reason for including a testing phase, in the form of a series of case studies, was to road-test the mechanisms of a study that we predicted to be challenging. Specifically, this phase aimed to pilot the recruitment and screening procedures, as well as the modified VIPP-FC, and to examine its clinical suitability for children with RAD symptoms in real-world clinical practice. The implementation of the case series was indeed challenging, but highlighted many crucial practical issues about what works and what does not, allowing us to introduce important modifications to the research protocol for the feasibility RCT.
The most important learning points from this first stage of the study were as follows:
-
Staff in local authority children’s services are extremely busy and find it difficult to effectively support research; therefore, when possible, researchers need to minimise the burden on social work staff, and local authorities more generally, to allow them to participate and focus exclusively on aspects of the study that are most important or ‘mission critical’ and cannot be done by others.
-
Foster carers are also very busy and ‘desensitised’ to requests for completing paperwork, thus they need encouragement and support to complete research forms and questionnaires.
-
The adaptations of the VIPP-FC manual for this study were mainly concerned with specificities of the population (i.e. looked-after children in the UK), and not, for the most part, in the fundamental intervention approach, including whether or not it is suitable for children with RAD in particular. The VIPP-FC was generally considered to be suitable and appropriate, and the intervention was considered helpful and acceptable by the foster carers who received it. A substantial number of adaptations to the VIPP-FC programme concerned the practicalities of the implementation and surrounding context.
-
The percentage of conversion from numbers approached to numbers recruited to the intervention was low (15%).
We faced unexpected delays and challenges to recruitment from using a single mail-out in a single recruitment site. A key issue was that the initially lengthy list of potential participants was substantially reduced after the social work teams removed inappropriate cases or cases expected to be very short placements. As a result, we could not easily recruit further cases from this site to continue to the case series. The data we obtained suggested comparatively good return rates for the screening measures from foster carers (60%), and we encountered no difficulties with the data quality or in the administration of the baseline and follow-up research instruments. In addition, the Manual Development Working Group took the view that the manual was working smoothly and was unlikely to require further changes. On that basis, and with the agreement of the TSC, it was concluded that we should expand the number of recruitment sites and proceed to the main pilot trial.
To conclude, the case series highlighted some significant challenges to recruitment and organisational complexities, but, at the same time, it gave a promising indication for the application of this intervention to improve mental health outcomes among looked-after children in the UK.
Chapter 4 A qualitative study of barriers to and facilitators of implementation of a video-feedback intervention in a Child and Adolescent Mental Health Services and social care setting
Overview
Implementation science suggests that barriers to promoting evidence-based practice occur at multiple levels, spanning factors at the individual, organisational, intervention and systems levels. 51 As the proposed feasibility trial was designed to work with children involved in the social care system, we expected the process of recruitment and engagement to be more complex than that for a trial based in the health-care environment, as more professionals tend to be involved in the former, there are complex regulatory constraints, resources are tight and this setting is less used to being involved in research. 35 Recruiting children in foster care and their foster carers was expected to be significantly dependent on the support of their social workers, who act as gatekeepers in these children’s care. 52 Social workers tend to view their role as to protect the vulnerable children in their care; therefore, a social worker’s beliefs about a child’s vulnerability, the potential benefits of the study and the timing (i.e. engaging in research after a recent placement transition) may affect their willingness to refer families to a study. 53
The process of consent in the context of children who are looked after also poses numerous challenges, as it can be particularly difficult to determine from whom consent must be obtained and how this should be done. 35 Beyond this, there may be a reluctance among social workers to consent to engage in research as many social workers do not identify their profession as a scientific discipline; therefore, they may be unaware of the methodological processes involved in a RCT. 54
Dixon et al. ’s53 RCT of Multi-dimensional Treatment Foster Care for Adolescents (MTFC-A) highlighted that social workers’ understandings of randomisation affected recruitment, with many social workers adopting their own clinical judgement when selecting children to enrol in the study, rather than relying on the formal eligibility criteria. Later research by Mezey et al. ,55 involving a peer mentoring intervention to reduce the incidence of teenage pregnancy among children and young people who are looked after in the UK, also highlighted misconceptions among stakeholders about recruitment criteria and the purpose of randomisation as key barriers to implementation. Although there was often a theoretical acceptance of the need for randomisation, in practice this rarely occurred. 56 Similarly, Dale and Watson52 noted that, if key stakeholders do not fully believe that an intervention is of tangible benefit, their engagement and acceptance of the research project can be compromised. Although these studies highlight interesting dilemmas for conducting a RCT with looked-after children, their populations largely focused on adolescents. There has been little research to date on the potential barriers to and their impact on implementing a RCT with younger children in foster care.
We expected that the climate of financial constraints and changes in organisational policy and structure within local authorities may affect our study. As many others have found in their research involving children’s services, social workers often have very large case loads, which affects their ability to engage in research tasks. 57 Efforts to engage children’s social care in outcome research have encountered challenges associated with competing demands, staff turnover and financial strain. 51 Other studies involving local authorities have found that the reorganisation of services and a general lack of research infrastructure and support affected services’ abilities to engage in research studies. 52,55
Many of the studies that have documented challenges of implementing evidence-based programmes in a local authority context also discuss potential facilitators of the process. These have included access and support from the development team;51 face-to-face meetings and having a research ‘champion’ within a team;52 continual dialogue to address divergent perspectives; 58 social workers acknowledging the importance of strong links between research and practice;59 and contractual agreements, incentives and greater acknowledgement of ethical dilemmas. 53
Studies that attempt to implement evidence-based programmes often focus on knowledge development, with little information about strategies to prepare people and organisations for this new knowledge. 60 However, without this, it is likely that progress will be slow at best. The Medical Research Council has emphasised the importance of including stakeholders in complex intervention planning,61 as it allows the research team to gain insights into the processes that may contribute to positive or negative study outcomes.
Aims of the current study
This chapter presents the results of a scoping study using qualitative methodology to understand the impact, acceptability and feasibility of implementing a trial of the Video-feedback Intervention to promote Positive Parenting and Sensitive Discipline, Foster Care (VIPP-FC) in a CAMHS and local authority context. To understand the facilitators of and barriers to the implementation of the VIPP-FC, the current study adopts a qualitative approach to exploring stakeholders’ experiences of and views on the general and specific research challenges posed by a clinical trial of an attachment intervention for young children in foster care. The primary aims were to further our understanding of the intervention–setting fit, the perceived usefulness and effectiveness of the intervention for this population, the facilitators of and barriers to implementation specific to local authorities’ children services and to identify stakeholders’ main concerns and key areas for future study development. 62 The qualitative data gathered from stakeholders can then be utilised to establish optimal systems and procedures for a future trial of the VIPP-FC.
This study ran in parallel with and after the case series, so that the participating stakeholders had acquired experience of the intervention (including training), the recruitment process and the challenges involved in preparing the partner sites to take part in the RCT. The majority of stakeholders involved in this initial phase (qualitative work) were selected from the research site participating in the case series project, as they had already experienced all phases of the research process, from initial engagement, planning, recruitment, obtaining consent and screening to treatment delivery. To maximise learning from this process and to gain the perspectives of other sites not involved in the case series, we also interviewed a small number of stakeholders during the early set-up phases of the feasibility RCT, whose input is also incorporated into this report.
Methods
Participants
Stakeholders involved in the early phases of the organisation and implementation of the VIPP-FC were invited to take part in the study. In total, 26 stakeholders were contacted. Of the 26 invited to interview, 15 responded and 13 agreed to be interviewed. One dropped out because of poor health, another had left their post and one had yet to begin work on the project locally as a result of delays in site set-up. Consequently, 10 stakeholders were interviewed.
Participants comprised six children’s social workers, three of whom were either service managers or deputy managers; two clinical psychologists, both of whom were service leads; one local authority commissioner; and one CAMHS practitioner. One participant worked in a CAMHS service, four worked in specialist adoption and fostering CAMHS teams, and the remaining participants were employed by local authorities. In terms of their roles in the VIPP-FC study, three participants held a strategic role (i.e. involvement in study design), five participants were involved in service delivery (i.e. offering the VIPP-FC in their service or being a trained VIPP-FC practitioner) and two participants were involved in both aspects. Two male participants and eight female participants were interviewed, with clinical experience ranging from approximately 3–20 years.
Procedure
To gather information on the facilitators and barriers that may affect the acceptability and feasibility of the intervention, stakeholders who were involved in the set-up and delivery of the VIPP-FC study in local authorities and CAMHS were invited to be interviewed. Participants who expressed initial interest were then contacted by a researcher and sent information about the study, as well as consent forms. Two of the interviews were carried out by telephone because of a lack of availability for face-to-face meetings.
Interviews
A semistructured interview schedule was developed based on Smith’s63 established guidelines. As the research involved stakeholders from various roles and professional backgrounds, four different interview schedules were drafted to suit these different positions held by the stakeholders in the study. The interview schedules addressed four general themes: (1) engagement of participants in the study, (2) supervision and training, (3) obstacles to and challenges of implementation and (4) acceptability of the VIPP-FC. The interview schedules were applied flexibly and the order in which these topics were explored was dependent on the material the participants brought. This helped to ensure that the interview flowed naturally and that spontaneous information could emerge. 64 Throughout the interview, participants were encouraged to elaborate on their answers by giving specific examples. The interviews lasted 50–70 minutes and were audio-recorded. Participants were invited to add additional comments or discuss topics that the interview schedule may not have captured at the end of the interview.
Qualitative analysis
Thematic analysis was applied to the interview transcriptions to understand the key patterns arising from the data. This approach was deemed suitable for the research objectives as it allowed the researcher to capture both similarities and differences among participants’ perspectives. 64 The process followed the general protocol outlined by Braun and Clarke;65 there were five phases of the analysis. NVivo 12 (QSR International, Warrington, UK) was used for data management. In the first phase, the qualitative researcher began by reading through the transcripts and familiarising themselves with their content. Once transcripts had been read through in their entirety, the researcher read the transcripts in a more active manner, taking notes of ideas, phrases or topics of interest. Phase 2 involved the initial generation of thematic codes. This involved the researcher working systematically through the transcripts, semantically identifying different features of the data. 65 The researcher also took note of data that did not fit the more common narratives during this process. Following this, in phase three, the researcher analysed these codes to consider how they could be combined to form broader themes and how they might be organised hierarchically. In phase four, each of the extracts that were coded for a theme were reviewed and examined to identify an overarching, coherent thematic framework. Themes were refined and divided into subthemes or merged together to form a larger theme. Once completed, these themes were then placed in the context of the entire data set to examine whether or not they reflect the meanings that were evident in the data. 65 The fifth phase involved the researcher trying to capture the essence of each theme and its application to the original narratives. This involved a final examination of each transcript to allow for theme refinement and ensuring that all nuances, contradictions and exceptions had been captured.
Credibility checks
Although thematic analysis includes some intrinsic quality-verifying procedures (e.g. checking of themes against coded data, the reviewing of themes against the entire data set), the qualitative researcher also undertook several credibility checks following good-practice guidelines developed by Barker and Pistrang,66 as well as those set forth by Elliot et al. ,67 to enhance the quality and validity of their analysis and subsequent conclusions. 65
In the initial stages of analysis, the researcher involved a second qualitative researcher and provided them with two transcripts to code. They then checked their coding of the two interviews against those coded by the second researcher to identify overstatements, discrepancies and potential errors. 67 Following this, a consensus approach was adopted to the development of the thematic framework. The researcher also involved a third member of the research team to review a selection of the data, compare ideas and discuss the best ways to represent the data.
Results
The analysis generated three overarching themes, which comprised eight subthemes. The first overarching theme, ‘challenges of implementation’, addressed the difficulties and barriers perceived by respondents in setting up and delivering the study. The second main theme addressed ‘benefits and impact of the VIPP-FC’, which captures respondents’ feelings about the potential value for foster children, foster carers and the professional network in engaging in the study. The final overarching theme focused on ‘key initial learning’ and reflected stakeholders’ ideas about how to overcome some of the barriers that might arise during implementation, or barriers that had already arisen during the case series work or early set-up phase of the feasibility RCT.
Overarching theme 1: challenges of implementation
Box 1 presents the theme and subthemes of ‘challenges of implementation’. Throughout the interview process, participants reflected on the barriers to implementing the study, both from their direct experience of having been involved in the early stages of the project and their wider knowledge of the system. It was evident that there were three main areas that posed challenges: ‘chaos in the system’, ‘conducting a RCT in a local authority context’ and ‘elements of the VIPP-FC’. These subthemes operated on varying levels from a more macro systems, cultural level, to specific aspects of the intervention itself.
Challenges of implementation.
Subthemes-
Chaos in the system.
-
Priorities.
-
Additional work.
-
Capacity.
-
-
System structures.
-
Structural issues.
-
Organisational inertia.
-
-
Conducting a RCT in a children in care context.
-
Consent.
-
Ethical dilemmas of a RCT.
-
Information sharing.
-
-
Elements of the VIPP-FC.
-
Manualisation.
-
Logistics.
-
-
Chaos in the system
All of the participants in the study spoke about the struggles of implementing a RCT in a setting that can feel quite disordered and in which there is a lot of disruption. They mentioned difficulties within the professional network such as managing multiple priorities and the often-changing structures within local authorities as key potential barriers to successful study implementation.
Priorities
Considerable emphasis was placed on the idea that being involved in the VIPP-FC study was something ‘additional’ to many professionals’ everyday work. It was commonly noted that social workers were often not consistently engaged in supporting the study; the study was not a mandatory activity and therefore could be easily placed on the ‘backburner’:
. . . because social workers are so busy and so stressed and have such a high demand to deal with whatever is the most crisis situation, that research, however much they support it, it’s kind of on the bottom of their list.
One of the social workers mentioned that perhaps as the study was more of a ‘mental health’ intervention, rather than a social care construct, this may have also contributed to the study being viewed as an add-on and not wholly relevant to their work. Several participants echoed this sentiment, questioning where the ‘incentive’ for social workers to engage in the research would be, as it involves extra work and they may not perceive many potential gains for them as social care professionals.
Although the ‘key learnings’ theme captures participants’ views about potential solutions to challenges in greater detail, the discussion around the ‘additional work’ theme often generated ideas about how to overcome the specific challenges within the system, such as the social workers having to juggle and manage the priorities of the local authority, on top of those presented by the VIPP-FC study. Three of the participants felt that in some way making the study an intrinsic part of one’s role (e.g. making it effectively ‘part of their job description’) would be helpful in giving them organisational permission to allocate time to and prioritise the VIPP-FC work. This underscores the need for buy-in at a relatively high level within the local authority, as well as specific discussion and organisational planning to cascade these high-level priorities down to social work teams.
Linking to the previous subtheme, capacity and lack of resources, primarily in the local authorities, was highlighted as a challenge by all participants. Many of the participants, whether or not they were social workers by profession, were able to empathise with how ‘incredibly busy’ social workers were and recognised that research, albeit with an intervention component, would not necessarily be a priority for them. Interviewees often expressed concerns that what the study needed from the local authorities, in terms of participation, may be unrealistic given the hectic environment of many local authorities, which often do not represent ‘research-friendly environments’. Several participants expressed feelings of frustration with the system not being able to support the research processes more, while also showing awareness of why this may be the case:
. . . they have got no manpower, they’ve got no spare capacity to support the research process . . .
System structures
Participants spoke of the structural changes and organisational issues that local authorities often face as a significant hindrance to the smooth running of a trial. There was a distinct feeling among stakeholders that conducting research within local authorities is a uniquely ‘complex’ and demanding process. One cause of this, identified by several interviewees, was the lack of standardised organisational structures across different local authorities:
There’s so many layers, and every local authority is different, every local authority has a different structure and a different attitude . . . corporate structure and management structure about who you need to speak to, you cannot generalise information.
Not only was variability in organisational structures identified as a challenge, but many of the participants also spoke of the struggles within the network to bring people together. They commented that, in looked-after children’s services specifically, there was often a ‘fragmentation’ within the network and that perhaps if this could be overcome or avoided, then local authorities could provide a more ‘benign environment’ for research to take place. Participants also spoke of the regularity of change and the impact that this can have on study momentum. They discussed difficulties encountered in the setting up of the study because key stakeholders had moved positions, ‘lost jobs’ or became invested in something else. Alongside these issues, participants identified the ‘churn within social care’ as an important potential barrier to successful implementation of the study:
We have a huge problem with turnover and I think all of these things make a kind of perfect storm really and set up a context where it’s really easy to disengage with anything else other than the basic work that you’re meant to do.
A few of the social workers spoke directly about the ‘internal politics’ that went alongside these structural obstacles. They voiced some frustration at the system being unwilling or unable to create space for research within its organisational structures, despite, in principle, willingness. In some instances, interviewees felt that this may create unhelpful pressure on certain members of staff to try to implement the VIPP-FC without being fully supported by senior managers. An additional structural challenge that participants referred to regularly related to positioning, both in terms of who to target in the system to gain support for the study, and also more generally about the challenges of being an outside body coming into an organisation where they are not necessarily known. A few participants spoke of how difficult it can be to work in such a complex system, let alone trying to ‘infiltrate’ it as an outsider:
. . . it’s quite hard for you to know where to press on the system to get things to happen . . .
Another interesting subtheme that was primarily endorsed by the social workers who were interviewed was focused on the challenges of change and the organisational inertia that one often faces when introducing something new within local authorities. Some participants spoke of how local authorities sometimes adopt a somewhat defensive position to the prospect of change and new studies/interventions. They reasoned that this may be as a result of the system undergoing so much structural change already:
There’s been so much change in terms of policy and direction and government interference and regulatory bodies, you know, in the last 10 years it’s really ridiculous the amount of change.
Many of the participants were able to empathise with this scepticism of change, describing local authorities as being under significant pressure and constantly having things ‘coming at you from all directions’. One participant highlighted that change, in general, is difficult on an individual level, but trying to mobilise change in a system that is used to and ‘comfortable with’ doing things in a particular way is ‘almost impossible’.
Several participants spoke specifically about how this reluctance to engage in something new and innovative is perhaps reflective of a wider organisational culture. They recognised that local authorities can be quite ‘a hostile place’ to work, as employees often have to deal with difficult dynamics and real or potential criticism from external sources. They hypothesised that external researchers could be perceived as another external actor judging or interfering with their work, without understanding the struggles and pressures they face:
Of course, I mean, from the social workers’ point of view, you know, these are ivory tower people . . . you need to get down a bit.
Conducting a randomised controlled trial in a foster care context
Thinking about offering an intervention such as the VIPP-FC evoked some concerns among stakeholders; one of the key worries centred on the process of consent. Several of the participants highlighted that the foster care population poses additional challenges to the usual consenting process. Questions emerged over who to obtain consent from, legalities around parental responsibilities, and ‘best interest decisions’. Similar to other themes, a few of the participants reflected on the fact that the complex and sometimes chaotic nature of the children’s social care system meant that obtaining consent for this population was not as straightforward a process as it would be for other populations of children:
. . . there’s layers of consent, it’s just . . . they’re there to protect children, but they’re horrendous to navigate.
Respondents discussed the fact that, for this population, consent is not only multifaceted, but also distributed throughout the network, with different people holding more or less influential roles in the process. Linking with this, several of the participants spoke about the dilemma of whether or not consent would be needed from birth parents. Some social work interviewees in particular felt unsure over whether or not this might, in fact, be harmful to the child and their relationships, as they felt that the child had been removed from the family home ‘for a reason’, and, as social workers, they needed to protect the child and do what is in the child’s best interests, which might conflict with what parents would want. Other participants felt that asking the parents could also complicate the consent process, as parents may be irritated that foster carers were being offered support that they might perceive as helping the foster carer to ‘bond’ with their child, while they may not have been offered anything to help their relationship with their child. One participant role-played how they envisaged some parents to respond to this:
Well why does the foster carer get offered that intervention? Why didn’t I get offered it as part of the package to support me in my parenting, so I could become a better parent and keep my child?
Participants also provided several examples of how shared parental responsibility and whether or not court proceedings were ongoing could make consenting to research difficult and be a possible reason why recruitment rates in the case series were low. In general, the respondents reflected on the tensions between the rights of parents to be consulted and involved in decision-making, the possible conflicts of interests and complex relationships parents may have with the local authority, and the best interests of the child.
Participants highlighted a number of different causes for concern in conducting a RCT with foster children, which left them pondering whether or not it felt ethical to conduct a RCT with foster children. A significant proportion of the stakeholders felt that there was a ‘diagnostic’ element to the inclusion criteria of the RCT. They raised concerns related to the potential pathologising impact that a ‘diagnosis’ can have, especially on a young child, as well as fears as to what it may mean for a child’s prospects (e.g. for adoption) if the ‘diagnostic report’ was available to non-research staff:
Yeah you don’t want to thwart their chances of being seen as a child, an adoptable child . . .
Participants also expressed discomfort with specific elements of the exclusion criteria and with some children not receiving the intervention, a process that is expected in a RCT model. Specifically, several participants felt that the age range and focus on RAD meant that children who they felt could have benefited from being involved in the study did not meet inclusion criteria. Likewise, participants described concerns that, if a child was randomised to treatment as usual, with this population that ‘could mean [they receive] nothing’. All the participants who thought that this was an issue also felt that perhaps this could be a barrier to people’s engagement with the study, as they reasoned:
. . . it would be easier to get families to put themselves forward if they know that they would get something, whereas with this they may get something or they may not.
In this way, participants began noticing that perhaps there is a conflict between their way of looking at things as clinicians and the needs of a research study. Although the majority of the participants who noted this dilemma were able to appreciate that the study needed to have certain guidelines to ensure ‘fidelity’ and ‘study efficacy’, they sometimes found it difficult to switch from their clinical mindset and step into that of a partner in a research study.
Participants provided many examples of how information-sharing with this population, particularly in a research study, can be challenging to manage. Most participants felt concerned about how and what information would be shared. They emphasised the need for researchers and those involved in the study to ensure that they took the necessary precautions to safeguard these ‘vulnerable children’. The social workers interviewed felt particularly strongly that their role is to protect the children in their care, and so they expressed the most concern about how the team as an external body would manage the data and the video-recording element of the intervention:
. . . you are, you know, a third party to these children’s lives, not directly involved in their care or offering day-to-day therapy, so, for me, there’s a little bit of that sharing information and then you step out, so I think it’s about the confidentiality . . .
However, a number of participants then also wanted information gathered in the study to be shared within their network. They felt that it would be a shame for the potential learnings and information collected about both the child’s needs and the foster carers’ skills to be lost to the wider professional network, as it could benefit future placements and planning. This, they recognised, posed a dilemma as to how much, when and with whom this information should be shared; participants feared that a report that was less positive could be misconstrued by some actors in a child’s professional network, now or in the future.
Elements of the VIPP-FC
Opinion among those using the model was somewhat divided on the benefits and drawbacks of the structured and manualised nature of the VIPP-FC. Many of the VIPP-FC interveners felt that having to follow a more ‘rigid’ protocol than they were used to meant that they often found themselves having to say things that did not feel fully applicable to the families with which they were working. This left some practitioners feeling ‘stuck’ and unsatisfied on occasion. Some participants shared that, although the manual was thorough, it would have been helpful if it allowed more flexibility and greater use of ‘clinical judgement’:
. . . it would just be really helpful to have the flexibility to adapt the message . . . certain messages you really, very strongly felt didn’t apply to that family, you didn’t have to read them out.
Some of the participants reflected that perhaps the VIPP-FC is a ‘different way of working’ that may not suit everyone’s style, including that of foster carers, as different foster carers may hold different beliefs about ‘how to discipline their child’.
Although many of the participants felt that the VIPP-FC could be improved by allowing some deviations from the manual, a few participants praised the manual for being mindful of these children and their contexts. Specifically, they felt that the ‘language’ was appropriate and helpful in reflecting the ‘experience of children who perhaps are in transition’.
Participants with experience of offering the VIPP-FC or working with children in foster care provided an abundance of examples of practical and logistical obstacles they faced in trying to deliver the intervention according to protocol. One of the most significant difficulties faced was the available time of the foster carers. They detailed struggles in getting foster carers to commit to the programme and in trying to manage a clinician’s time while fitting in birth parent visits, court dates and various appointments:
. . . so, there were four children in the placement of different ages with different contact arrangements and different needs, and a single carer.
Another key challenge centred on both the practical and ethical issues of other children being in the home. Nearly all of the participants who mentioned logistics highlighted this dilemma, detailing how sometimes it felt as though foster carers’ attention was divided by other children ‘running around’, which made the feedback process challenging:
It would be easier if the child wasn’t there during the feedback, so yourself and the parent could have a proper conversation, without the parent being distracted by trying to manage the child’s behaviour all the time . . .
Others felt that their visits were quite time-consuming; they did not want other children to feel left out, so they felt that they had to spend time interacting with them as well. Some participants questioned the timings of the VIPP-FC and spoke of concerns relating to placement timings. They explained that it can sometimes feel uncomfortable offering an intervention that may increase attachment when there was uncertainty over whether or not the child would remain with that foster carer for long.
Overarching theme 2: benefits and impact of the VIPP-FC
Box 2 presents the theme and subthemes of ‘benefits and impact of the VIPP-FC’. The likely benefits and impact of being involved in the VIPP-FC study were separated into three distinct subthemes, each relating to a different layer within the ecological system. 68 The first, ‘creating an evidence base’, explores the wider system-level benefits that the study could have for developing the evidence base for support for children in foster care. The second relates to service-level benefits for engaging in the research and the impact the study could have on the practices of services. Finally, participants highlighted the potential positive benefits for the child and for the wider caregiving system around the child.
Benefits and impact of the VIPP-FC.
Subthemes-
Creating an evidence base.
-
Benefits to services.
-
Benefits to families.
Creating an evidence base
There was a unanimous feeling among stakeholders that creating an evidence base for children in care was hugely important. The current ‘lack of evidence’ was highlighted as being ‘problematic’. Several of the participants mentioned their ‘excitement’ and eagerness to be involved in research that could potentially ameliorate this issue. Many participants elaborated on this by explaining that, even when services are following what is commonly agreed on as good-practice guidelines, they still lack high-quality, scientific evidence to support their work, and are therefore keen to work to change this. This included consideration not only of direct therapeutic interventions, but also of methods for assessing children’s needs:
I think the SDQ is poor, which is nationally what is used for foster children for outcome measures. It is not the most sophisticated tool. It doesn’t really work for some children because it doesn’t really pick up any of the nuances . . . it doesn’t capture exactly what they go through.
Stakeholders who held more strategic roles, such as managers, identified the building of an evidence base as an essential component for commissioning of services. They spoke of how research could potentially aid future decision-making, contribute to developing NICE guidelines for this population and allow services for children in care to ‘negotiate money differently’.
Benefits to services
Generally, participants expressed positive views about the VIPP-FC from a service-level perspective. Many of them referenced the benefits of being able to offer something additional that was ‘free’ to vulnerable children and families who receive ‘little support’. A few participants held the realistic standpoint that, although the VIPP-FC is not the ‘panacea that means all placements are great’, they felt hopeful that it would add to the repertoire of interventions offered, and thus give both families and clinicians more choice regarding treatment. A couple of participants also highlighted the benefits of being an organisation engaging in research, particularly when undergoing inspections or scrutiny from external bodies.
Participants whose services were actively involved in delivering the VIPP-FC spoke of how their service had developed as a result of engaging in the RCT. Service managers spoke about it being ‘nice’ to be able to offer staff new opportunities for continuing professional development that may not have been available otherwise. They also reflected that their teams had been able to share some of the learning from the VIPP-FC training, which brought new perspectives to their work.
Several participants expressed the view that, through engagement in the study, services would benefit not only from having clinicians with additional skills, but also by providing foster carers with more resources and strategies, which, in turn, may improve the quality of foster care and even potentially lead to cost savings for services:
. . . if there are less placement breakdowns and more placement stability, that’s going to save the local authority money . . .
There were mixed comments in relation to the impact on time and workload that came with study involvement. A handful of participants felt that being involved was not ‘overly onerous’, and therefore could easily fit in with the service’s usual day to day. However, some raised that the training and the intervention itself were more ‘time-consuming’ and ‘intensive’ than they had expected, which meant that there was ‘a limit to the amount of it people can do, along with their day job’.
Benefits to the families
Nearly all of the participants with experience of the VIPP-FC described it as a positive and ‘enjoyable’ intervention for both families and practitioners. The strengths-based nature of the programme was highlighted as a core feature of its positive reception. There was a sense among the stakeholders that the VIPP-FC was more ‘therapeutic’ and ‘holistic’ than many other approaches currently offered, and that it was less likely to have any aversive or ‘harmful’ effects.
Participants spoke of how the visual aspect of the intervention is empowering, as it goes beyond praise or verbal feedback and allows foster carers to see for themselves what they are doing well:
. . . things which usually stick in your mind may be the more difficult moments, whereas, when you watch it back on video, you can’t escape those positive moments, especially with the way that VIPP[-FC] really highlights them.
Several of the VIPP-FC interveners also emphasised the power that video has in building foster carers’ insight and ability to be more mindfully present. They referred to the ‘slowing down’ during the video feedback as being a key moment for foster carers, allowing the moments of sensitivity and attunement to be ‘magnified’ and further reinforced. Alongside this, participants thought that this gave them and the families an opportunity to spot things that may otherwise have been missed.
Practitioners also felt that the intervention carved out valuable time to focus on important aspects of a child’s development that are crucial for relationship-building, specifically noting the importance that the VIPP-FC attaches to ‘play’. They reflected on their experiences of seeing the children engage in games and playful interactions and how ‘special’ the experience of those minutes of interaction were for the child.
Several participants spoke of how engaging in the VIPP-FC study could have a lasting impact on families. They shared that, even if the VIPP-FC had not been completed in its entirety, families could still benefit from its core messages of sensitive responsiveness, sensitive discipline and attunement. Nearly all of the participants felt that the intervention would stand to benefit both children and families in the long term by building children’s resilience and foster carers’ understanding, regardless of whether or not they were still placed together:
. . . they’re going to be able to use those skills, not just with this one child, but with all the children who go through to stay with this particular foster carer.
All of the participants were hopeful that the VIPP-FC intervention would allow foster carers to feel better skilled and supported for working with these vulnerable children.
Overarching theme 3: key learnings
Box 3 presents the theme and subthemes of ‘key learnings’. This overarching theme consisted of two main subthemes: ‘importance of relationships’ and ‘recruitment fundamentals’. The latter comprised three subthemes, which addressed barriers to and facilitators of the recruitment process.
Key learnings.
Subthemes-
Importance of relationships.
-
Recruitment fundamentals.
-
Lack of understanding.
-
Contextual issues.
-
Presence.
-
Importance of relationships
Nearly all of the participants mentioned the importance of adopting a relational approach to this type of study. Several of the participants spoke of the confusion they encountered at various points, both in the set-up and delivery of the VIPP-FC. Some participants felt that they were not always clear who was responsible for which aspects of recruitment:
‘Oh, I thought you were doing that’, ‘no I thought you were doing that’, ‘oh you mean we must do that?’, and so that sort of is problematic.
These participants felt that it was important to ensure that there was ‘clarity’ regarding responsibilities and expectations of the various professionals involved in the study, and widespread engagement of all of the relevant parties. It was generally felt by respondents working with local authorities that having an identified ‘key person’ in each team who takes ‘ownership’ and is the service’s first port of call for everything VIPP-FC related is enormously important. For those in sites where this was clearly in place, it allowed them to avoid falling ‘at the first hurdle’. When responsibility was more diffuse or had changed, there was a perception that this was because teams were overburdened with mandatory tasks and no one was willing to volunteer to sign up and take on this added responsibility.
Many emphasised the importance of the sharing of information and learning between the research team and local authorities. Some respondents expressed the view that it was crucial to engage the entire network and to share their findings from individual interventions with local authorities so that they could see the study as beneficial to their care-planning and place greater emphasis on supporting foster carers to take part. However, participants also noted that information-sharing in a research study, compared with routine practice, may be complicated owing to data protection considerations.
Participants noted that, even after establishing an initial agreement and plan with a local authority, there also needed to be considerable resourcing dedicated to maintaining those relationships across the lifetime of the study. One learning point that participants highlighted was that, although it is necessary to obtain support from ‘the top’, it is just as important to engage key stakeholders ‘on the ground’, as these people act as the ‘gatekeepers’ for this type of intervention, even if engaging them is very difficult and time-consuming because of social workers’ lack of availability. Some suggestions were put forward by several of the participants with regard to how to overcome some of these difficulties. A number of them discussed the idea of holding a ‘network meeting’ to share the learning from the VIPP-FC with those involved in the child’s care. However, one participant felt that:
You couldn’t include the intervener into a network meeting or something because it’s just not catered for as part of the research.
Recruitment fundamentals
Lack of understanding
One of the major areas of learning that participants identified related to the (lack of) understanding around the recruitment process. They suggested a number of reasons why uptake to the case series was low and were able to think about potential solutions to these issues.
There was a distinct view among many participants that one of the major barriers was linked to a lack of understanding of the study aims and approach at the ground level, namely children’s social workers and foster carers. Some participants questioned how well the children’s social workers understood the VIPP-FC study and the potential benefits that might be accrued if families engaged. They felt that social workers could become more engaged in the recruitment process if they could see more clearly that the screening process could provide them with valuable information about the child and, furthermore, that the intervention could help the foster carer to be better able to manage potential challenging behaviours:
Perhaps they could complete the questionnaire with the social worker and foster carer together? What might they [the social worker] glean about the foster carer that they don’t already know?
Another issue, also linked to a lack of understanding, concerned the dynamics that sometimes play out between the social worker and the foster carer. Some of the participants noted that foster carers can sometimes feel ‘judged’ by professionals, so they emphasised the importance of being clear about the potential benefits to foster carers and specifically emphasising its strengths-based approach. Communication, particularly with social workers and indirectly to foster carers, was therefore highlighted as critical.
Contextual issues
Opinions were quite consistent in relation to the contextual issues that affect recruitment. Participants felt that although they, as stakeholders, could see benefits to engaging in the study, they also understood social workers’ and foster carers’ apprehensions, as ‘foster care is not a permanent solution’. They felt that the issue of placement instability and unpredictability may block recruitment and may be a barrier to engagement:
Looked-after children, it’s just chaotic, you know, there’s no point in investing in now because who knows what is going to happen in 6 months’ time?
A few participants spoke of the fact that the framing of the intervention as ‘attachment based’ could be off-putting to foster carers, as they may be fearful of forming relationships when the child is likely to move on. They explained that it may be helpful to frame the study as a ‘training opportunity’, which may increase foster carers’ understanding and develop their resources and skills.
Presence
Linking with the earlier theme of ‘importance of relationships’, the presence and approach of the research team was stressed as being important. Several participants felt that the research team would need to be a continuous physical presence within teams and with foster carers, although they recognised the numerous barriers to that, including the lack of access to foster carers prior to obtaining consent and the heavy workloads of social workers. Nevertheless, ‘face-to-face’ communication was considered crucial:
. . . you know you can send e-mails until you’re blue in the face, but until you actually make eye contact with someone and see them, it’s a different thing.
Participants felt that it was important to be visible within the network: attending meetings and making introductions in person. It was acknowledged that this would require a lot of ‘perseverance’ and human resources, but many participants felt strongly that ‘a physical presence and a relationship’ would be crucial.
Discussion
The interviews with stakeholders highlighted the complexity of conducting a RCT in the context of foster care. Although challenges were noted in relation to the involvement of CAMHS in treatment delivery, these were not strongly emphasised in the interviews. The focus was primarily on the context of local authorities, who are a key bridge to foster carers, and on the relationship between the local authorities and the research team.
In keeping with the principles of implementation science, the themes arising from this study could be placed in a multilevel framework, with factors relevant at individual, organisational and cultural/system levels. 51 A key focus, however, was on the organisational level. The qualitative interviews highlighted challenges to working in such a complex, and sometimes chaotic, set of systems. Unsurprisingly, difficulties were encountered by stakeholders attempting to secure research involvement and ongoing engagement when it may be viewed by ‘front-line staff’ as a non-statutory and additional task. Stakeholders hypothesised that this may be due to competing demands and heavy case loads, which echoes previous findings by Gilbertson and Barber. 57 The implication would appear to be that it could be highly beneficial to find ways to support the local authorities in taking full ownership of the research, perhaps through co-production and joint management. Alternatively, having research members embedded within the local authorities (e.g. through honorary contracts and relevant organisational agreements) may also be a useful strategy for increasing awareness, contact and trust between the two teams.
One of the most significant challenges, as perceived by the stakeholders, was the complexity of the organisational structures within local authorities. As also noted by Mezey et al. ,55 we found that the lack of an embedded research infrastructure was a significant hurdle. The stakeholder interviews also highlighted the significance of staff turnover within children’s social care teams, perhaps exacerbated by recent policy changes and budget pressures. The high staff turnover, combined with a fatigued and overstretched system, produced a challenging environment for external researchers to operate in. This echoed some of the contextual issues that Dale and Watson52 encountered in their attempts to recruit looked-after children for health research and the barriers they encountered when approaching stakeholders about their research.
Linking with this, stakeholders reflected on the readiness and preparedness of local authorities to adapt to a new initiative such as a research project. Thinking about the acceptability of the VIPP-FC in this context, participants highlighted the struggles encountered in trying to implement a study in a system that undergoes frequent change and restructuring. Although many other studies have addressed intraorganisational issues affecting the implementation of evidence-based interventions,51,69 few have discussed the defensive mechanisms that organisations may adopt when faced with new demands, which may reflect a form of organisational homeostasis at times of uncertainty, as touched on by some of the participants in this study. Stakeholders noted that holding such a position, although entirely natural, stifles innovation and, in the longer term, hinders innovation.
The study identified several key elements of a RCT that social workers considered potential roadblocks to study engagement. Randomisation was highlighted as an issue that some stakeholders found difficult. However, unlike previous studies, which suggested that this dilemma arises from social workers’ lack of understanding of the importance of randomisation in research, the social workers in this study spoke very positively about the need for bias-free research evaluation. It appeared that their difficulties were more ethically grounded, related to concerns about children not receiving treatment, which matches Dixon et al. ’s53 findings, and also finding it challenging to maintain the boundaries between their role in facilitating research and having a clinical responsibility to the children.
Participants drew attention to the potential difficulties associated with using diagnostic terms and a diagnostic criterion as part of the eligibility criteria for entry to the study. Relatedly, information-sharing was also brought up by participants as a potential complicating factor. Although other researchers have encountered social workers’ wariness of engaging in RCTs, few have specifically spoken about the potential effects of sharing information within the network. 55 This could be linked to the ages of the children in the current project, as, generally, younger children are more likely to be adopted than their older counterparts; thus, stakeholders may have been concerned about the impact that diagnostic information may have for the children’s adoptability. 4
As recognised by Bogolub and Thomas,35 consent was viewed by stakeholders as a complex problem. It appears that there is still confusion in the children’s social care context about who must provide consent and how the process should be conducted. Indeed, this reflected our experience when we sought ethics approval for the study, whereby significant disagreement was encountered between stakeholders more closely aligned with the rights of parents versus those with responsibilities primarily to the child. Although our stakeholder interviews raised this as an issue, there was still uncertainty about how this could be overcome. This uncertainty may be quite widespread in the field and may explain apparent inconsistency in practice in different localities or ethics committees.
The interviews with stakeholders highlighted the potential benefits of the proposed research, alongside challenges they encountered or anticipated. From an organisational and systems level, it was viewed as beneficial to engage in research and contribute to developing an evidence base for children in foster care. The majority of research to date on implementing evidence-based practice has tended to focus on stakeholders as sometimes being sceptical of engaging in health and mental health research;59 however, in this study, participants were excited to be contributing to scientific research and intervention development. Considerable value was placed on developing evidence-based interventions and participants spoke of sometimes feeling frustrated when others did not understand the potential benefits of doing so.
Stakeholders were largely positive about the VIPP-FC as an intervention. It was felt that this adapted version of the Video-feedback Intervention to promote Positive Parenting and Sensitive Discipline (VIPP-SD) has great potential to be beneficial to the families with whom our stakeholders worked. They highlighted how helpful its strengths-based nature was and emphasised the importance of play. 21 However, the VIPP-FC programme did elicit some questions and potential difficulties in the minds of our stakeholders. The manualised approach posed some difficulties for some interveners, relating to its perceived lack of flexibility, which could constrain the role of clinical judgement and limit scope for personalising the intervention. Greater flexibility in delivery and, especially, timing was considered worthy of further exploration.
Stakeholders generated several ideas for tackling some of the barriers to implementing a RCT. A key message was the importance of taking a relational approach, giving time and resources to building relationships with all the key players in the system, especially at the ‘front-line’. As Beidas et al. 51 emphasised, implementation of evidence-based practice requires three core components: co-ordination, co-operation and communication. Stakeholders highlighted the importance of role clarity, leadership, persistence and physical presence for successful implementation. A key suggestion was to consider involving service users (foster carers) as study champions, and even to use video to disseminate people’s experiences of receiving the VIPP-FC, to build confidence and interest in the project in the wider community of foster carers and social workers.
Chapter 5 Feasibility and pilot randomised controlled trial
Overview
The final phase (phase 3) of the study consisted of a pilot RCT of the modified Video-feedback Intervention to promote Positive Parenting and Sensitive Discipline (VIPP-SD) programme [i.e. the Video-feedback Intervention to promote Positive Parenting and Sensitive Discipline, Foster Care (VIPP-FC)]. A new group of children was randomised to receive the VIPP-FC plus care as usual (CAU), versus CAU only. The VIPP-FC was delivered in-home by trained CAMHS practitioners or other appropriately qualified VIPP-trained interveners. Baseline and end-of-treatment measures included validated assessments of RAD and co-occurring conditions, security of attachment (including disorganised attachment), sensitivity of parenting, child adjustment, carer well-being, and the CA-SUS measure of service use. In addition to these outcome measurements, we also conducted qualitative interviews regarding carers’ experiences of the programme, the results of which are presented in Chapter 7. The specific aims of the pilot RCT were to:
-
test the feasibility of identifying sufficient numbers of appropriate cases through social care using appropriate screening instruments across several local authorities and locales (rural and urban)
-
test the feasibility of recruiting and consenting foster families with young children (including those with RAD symptoms) to a RCT (numbers contacted and consented)
-
conduct an initial evaluation of the feasibility of randomising to the VIPP-FC or CAU (numbers refusing randomisation)
-
document study throughput – uptake, numbers of sessions attended and numbers completing treatment, rate and stage of dropout, and acceptability of the treatment
-
establish the feasibility and acceptability of baseline and outcome assessments and level of data completeness
-
modify and test a version of the CA-SUS measure of service use to ensure suitability for pre-school/primary school aged fostered children
-
identify the most appropriate primary outcome
-
obtain initial estimates of variance of key outcome measures
-
explore the appropriateness of exclusion criteria, particularly concerning co-occurring conditions
-
establish the optimal and most acceptable screening tools for RAD, as recently redefined in the DSM-5.
Methods
Setting
The study was a multisite RCT involving eight NHS trusts and nine linked local authorities, and took place across four large and distinctive regions in England: Greater London (North, South, East and West), Hertfordshire, Peterborough, and the Yorkshire and Humber region. As noted previously, a substantial number of local authorities was necessary to ensure adequate recruitment and to capture important variability in organisational contexts that may be important to understand when preparing a future larger-scale clinical trial.
Recruitment
Participants were identified initially through a large community screening process in the nine local authorities, with a view to identifying ‘at source’ (rather than through referrals or CAMHS; however, these were also accepted as a recruitment route) children experiencing high levels of behavioural signs of RAD on the screening questionnaires. Positively screened cases were assessed using the DAI to establish, using a validated and rigorous investigator-led diagnostic schedule, whether or not children showed evidence of RAD. Serious challenges to recruitment mid-way through the study led to a decision, supported by the TSC and funder, to remove the RAD eligibility criterion so that there was greater opportunity to run a reasonable number of cases through the research and intervention protocol. The decision to remove the RAD eligibility criterion also reflected a view shared by the research team and TSC that children in foster care are at substantially heightened risk of not only RAD, but a range of attachment difficulties and behavioural and emotional problems, and may therefore benefit, as a group, from the VIPP-FC. The outcome measures continued to track impact on RAD symptoms as well as these other clinical domains. The number of participants and their characteristics are described in Results, as they represent important feasibility-related outcomes.
Changes to protocol between the case series and the pilot randomised controlled trial
For the most part, the research protocol proceeded smoothly during the case series, so no changes were made to the assessment battery. The primary challenges were the somewhat lower than hoped for return rates of the screening questionnaires and the modest numbers of cases meeting criteria for RAD on the DAI. A key challenge was the lack of capacity within the local authority to undertake follow-up telephone calls to foster carers to encourage return of the screening instruments. In response to this, and in discussion with the TSC, we revised the protocol to allow members of the social work team to obtain verbal consent from foster carers for the research team to contact them directly by telephone. In consultation with our foster carer advisory group, we also substantially revised the study leaflets and information sheets to make them clearer and more appealing. We also introduced an alternative online screening/agreement to be contacted form following recommendations from our foster carer study member and advisory group. The study team received e-mail notifications from the study database when a participant gave consent and completed questionnaires online. Both the paper and online consent forms required the carer to provide their contact details (including the child’s initials) so that the research team could contact them to thank them and invite them to the interview stage. As these changes generally did not affect the overall research protocol, the methods are presented succinctly here; see Chapter 3 for detailed information about the research instruments.
Consent
No changes were made to the consent process from that used in the case series. During screening, active consent was required from the foster carer only. Passive consent was obtained from parents. After screening, if the child met the eligibility criteria to take part in the trial, full written consent was obtained from all those holding parental responsibility and from the foster carer, as well as assent from the child.
Measures
No changes were made to the assessment battery between the case series and pilot trial. The assessments consisted of the following:
-
screening – the DAWBA Relationships with Adults scale, the ASA and the DAI
-
baseline and post treatment – the Strange Situation Procedure, the DAWBA (full instrument), the CBCL, the Parenting Stress Index and the Parental Self-efficacy Scale, the CA-SUS and a carer–child interaction task (for coding of parental sensitivity with the NICHD scales).
Process data and qualitative outcomes
Process data were collected during the pilot RCT to document the uptake, numbers completing treatment, rate and stage of dropout, and acceptability of the treatment to participating families. Records were kept of the number of families approached that refused to take part in the study; data were also obtained on the range of care pathways observed (for example distribution of care orders and placement types, e.g. family and friends care, long-term foster care), the numbers moving placements before or after treatment commenced, and the destinations and timing of any movements out of placement. Records were also kept of essential information on a child’s previous history, such as number and type of previous placements. These data were obtained from a child’s social worker and/or foster carer. Reasons for refusing to take part in the study and for dropping out were also recorded.
The acceptability data gathered through the conduct of qualitative in-depth interviews with all consenting families that received the intervention as part of the pilot RCT.
Randomisation
Participants were individually randomised in a 1 : 1 ratio to one of the two treatment arms: the VIPP-FC plus CAU or CAU only. Randomisation with minimisation was employed, with minimisation factors age (≤ 4 vs. > 4 years), sex and site. Minimisation included a random factor, as implemented in the minimisation program SiMin. 70 Randomisation was requested by the research assistant using a standardised form following completion of all necessary screening and consent procedures, and was performed by an unblinded member of the trial co-ordination team. The allocation list was held in the Trial Master File. A member of the trial co-ordination team contacted the child’s social worker and VIPP-FC intervener (the latter for those allocated to VIPP-FC). The foster carer and the individual(s) giving consent on behalf of the child (the parent and/or local authority social worker with parental responsibility, as appropriate, see Chapter 5, Consent) were notified of the outcome by letter/e-mail by the unblinded member of the trial co-ordination team. The foster carer was also contacted by telephone to ensure a timely initiation of the intervention.
Blinding
All outcome assessments were performed by research assistants blind to trial arm allocation. All data handling and communication regarding unblinded information was undertaken by the Trial Co-ordinating Team. Prior to all research visits, the trial co-ordinator briefed the foster carer(s) about the importance of assessor blindness and any cases of inadvertent unblinding were recorded by the research assistant(s). By definition, foster families were not blind to the treatment arm to which they had been randomised.
Intervention
The VIPP-FC
The VIPP-FC is described in detail in Chapter 3 and the clinical protocol was not changed after the first phase of manual development and modification, as described in Chapter 2.
Care as usual
The VIPP-FC was compared with CAU, as there is no pre-existing integrated care pathway for children in foster care. Usual care varies widely between localities and good-quality data were not recorded that would allow precise specification of CAU prior to undertaking the study. Systematically documenting CAU was therefore a key objective of this study. Initial consultations with CAMHS teams in our study sites identified several potential treatments that may be offered within CAU: (1) Theraplay, (2) one to three sessions of foster carer consultation, (3) network consultation, (4) The Incredible Years® (The Incredible Years, Inc., Seattle, WA, USA), (5) foster carer support, (6) 6–12 sessions of psychotherapy, (7) behaviour support and (8) foster parent groups.
As assessments of attachment disorders are rarely undertaken, it is not possible to determine the extent to which the type and intensity of services offered to this particular group are different from those offered to other young children in foster care referred to CAMHS. We used the CA-SUS to systematically describe and quantify the services received by children and carers in the comparator arm of the pilot RCT. The CA-SUS asks participants to confirm whether or not they have attended any health services, mental health services, support services or child-care services, and if so, how many times they have attended these services in a defined period of time.
Sample size considerations
The planned sample size of 40 participants (20 per arm) was based on common recommendations for feasibility studies, in which the aim is to test practical implementation parameters, rather than to test treatment effects. Using data obtained from the Department for Education from 201471 (which we have corroborated against a selection of figures obtained in 201671 from our participating local authorities), we expected the full population of children in foster care in our target age groups across our sites to be in the region of 700. Previous screening work with this population led us to aim for 70–80% of foster carers to return the initial screening questionnaires; on that basis, and bearing in mind cost implications, we aimed for a sample size for the screening stage of 500 participants. To identify cases likely to present RAD, we planned to choose cases above the highest 66th percentile for symptoms of RAD, leading to a sample size of 150 who would be invited to take part in the more in-depth assessment of RAD symptoms using the DAI. Based on the previous RCT of the Fostering Changes programme,72 we expected two-thirds of those to agree to take part and complete the assessment. From this pool of 100 children, we expected to have scope to identify the target 40 cases who would be eligible for treatment, as long as the prevalence of RAD in the high-scoring screened group was ≥ 50% (allowing for a further 10% dropout at this stage).
It is important to note that, at the planning stage of this study, two key pieces of information were subject to considerable uncertainty. First, although clinical screening work within routine services locally were able to obtain 70–80% return rates, these were not obtained in the context of a research trial and had not been tested in all sites. In the case series, we obtained a screening questionnaire return rate of 60% (based on 20 cases), which, although lower, was not drastically out of line with expectations. However, this was from a single site only. Second, we lacked reliable information concerning the prevalence of RAD in UK foster care; thus, the 50% prevalence within the population of children exceeding the symptom threshold was subject to considerable uncertainty. Consequently, we planned for an interim analysis after 15 cases had been assessed to establish whether or not the proportion of RAD cases was below this expected proportion. The lower bound of the 95% confidence interval (CI) around a proportion of 0.50 is 0.22 with a sample size of 15. Thus, identification of fewer than three cases out of 15 would suggest that the prevalence was lower than 0.50. In this event, we planned to widen the eligibility criteria to include children not meeting full RAD diagnostic criteria, subject to approval from the TSC.
A sample size of 40 participants provides a reasonable balance between precision and cost. Assuming that the proportion of participants successfully completing the key outcome assessment is 75%, this yields a 95% CI of 59% to 87%. The consent/uptake rates could be estimated at two stages: for consent to take part in the eligibility assessment, and, following eligibility, the proportion entering treatment/being randomised. The former rates would be estimated with higher precision as they are based on larger samples. Assuming 67% (100/150) of participants take part in the eligibility assessment, this yields a 95% CI of 59% to 74%. Similarly, assuming that 80% of cases identified with RAD (40/50 participants) go on to be randomised, we would obtain CIs around that proportion of 66% to 90%.
Data analysis
Point estimates and 95% CIs were calculated for the key feasibility parameters based on proportions (proportions of cases identified, consented, randomised, completing treatment and completing outcome measures). Approximate variance estimates were obtained for the main outcome measures using the upper 80th percentile of the relevant CI. Specifically, we tested the following feasibility parameters:
-
Test the feasibility of identifying sufficient numbers of appropriate cases using screening instruments.
-
Target n for screening tests returned, n = 500. Test a.1 = proportion and 95% CI of those returning screening instruments from total sent out.
-
Target n of diagnostic assessments, n = 100. Test a.2 = proportion and 95% CI of positively screened cases (above upper 66th percentile) agreeing to full assessment.
-
Target n for positive diagnosis from upper 66th percentile of screened cases, n = 50. Test a.3 = proportion and 95% CI of cases for whom diagnosis is confirmed.
-
Test a.4 – initial test of false negative rate = proportion (of 25 cases) and 95% CI of detected diagnoses in random sample of cases not meeting screening threshold.
-
Test a.5 – initial non-parametric receiver operating characteristic (ROC) curve analysis (target n = 125), based on assumption that the DAI diagnosis is gold standard.
-
-
Test the feasibility of recruiting/consenting foster families with children with RAD to a RCT.
-
Target n of consented cases, n = 40. Test b.1 = proportion and 95% CI of cases consenting to enter pilot trial from those meeting entry criteria.
-
-
Investigate feasibility of randomising to the VIPP-FC or CAU.
-
Test c.1 – proportion and 95% CI of cases accepting randomisation.
-
-
Document study throughput.
-
Test d.1 – proportion and 95% CI of cases who are randomised completing treatment (definition of completing = 80% of offered sessions).
-
Test d.2 – proportion of cases attending each session (six proportions and 95% CIs).
-
Acceptability of treatment – qualitative methods for client experience of treatment interviews (see Chapter 7).
-
-
Establish the feasibility and acceptability of baseline and outcome assessments.
-
Test e.1 – proportion and 95% CI of cases with complete data. See also qualitative methods for client feedback regarding measures.
-
-
Identify the most appropriate primary outcome. Key assessment was participant feedback from qualitative interviews. However, preliminary tests from tests a.3, a.4 and a.5, were also considered.
-
Obtain initial estimates of variance of key outcome measures for future power analyses. Test – standard deviation (SD) of RAD symptom counts and 95% CI.
-
Establish the optimal and most acceptable screening tools for RAD, as recently redefined in the DSM-5. Tested with qualitative interviews and tests a.4 and a.5.
Results
Recruitment sites and flow
The pilot RCT commenced in February 2018; recruitment ended in September 2019. All follow-up assessments were completed by the end of January 2020. Recruitment was attempted from a total of nine local authority children’s services and eight linked NHS trusts. The first site to open to recruitment was the site that took part in the case series. The second site opened in January 2018 and the remaining sites opened throughout 2018 and 2019, with the last site opening in April 2019. The first participant was recruited to the screening stage of the study in May 2018 and the first participant was recruited to the second-stage RCT in July 2018. Owing to serious challenges with recruitment and some delays in site initiations, recruitment was extended from the originally planned period of 12 months to 17 months.
Of the nine sites, we were able to recruit successfully from seven. Even with considerable effort, we were not able to progress with two London local authorities, despite their initial agreement and support. Throughout the recruitment period, we implemented several adjustments to the protocol to aid recruitment (see Chapter 1, Ethics amendments and protocol modifications and Appendix 1). The key changes that were implemented during the RCT period included the inclusion of additional sites and the dropping of the RAD-related eligibility criterion in March 2019. We illustrate the timeline and key events against progress on recruitment in Figure 2.
FIGURE 2.
Recruitment rate over time. Reproduced with permission from Oliveira et al. 73 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/. The figure includes minor additions and formatting changes to the original figure.
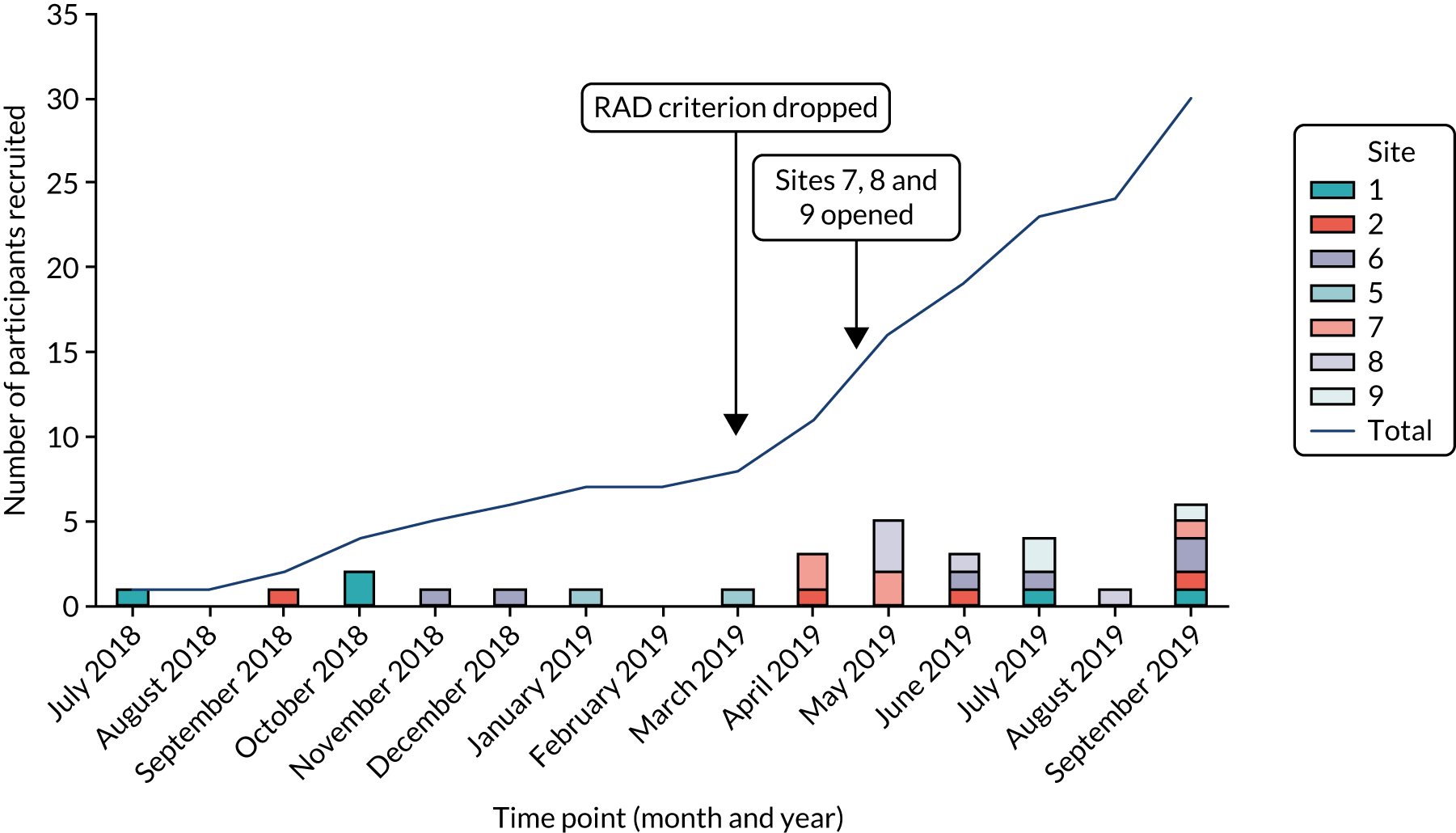
Recruitment flow increased substantially in the last period of the study, as can be seen in Figure 2. It is not possible to precisely determine the reasons for the improved recruitment rates, but the improved rates largely coincided with the removal of the RAD criterion, the addition of three new and engaged sites (notably, all of which were outside London), and our success in one site in obtaining an honorary contract for a member of the research team to work within the local authority children’s services to directly support recruitment. The rate of recruitment in this final phase was four cases per month. Most of the other sites were unable to maintain their recruitment efforts in the final stages of the study. Therefore, this final phase primarily reflected recruitment from four sites. By the end of the recruitment period, we were able to recruit and randomise 30 cases to the trial, which was 10 cases below the original target.
Screening response rates and recruitment
The screening process involved close collaboration with partner local authorities, which sent out information sheets, initial consent forms and screening measures to the foster carers in the study localities. In addition, local authorities sent out a letter to all parents explaining the study and the opting-out process, and the letter included the contact details of the research team. They all communicated to their staff members within the children’s social care teams to raise awareness of the study and draw attention to the support required from children’s social workers. For this screening phase, we aimed to invite all foster carers or special guardians registered with the local authority caring for children aged ≤ 6 years. In practice, different local authorities applied their own exclusion criteria at this point (e.g. excluding highly complex cases undergoing assessments for court or cases with restricted files), as we note in Discussion.
The overall response and retention rates are shown as a CONSORT flow diagram in Figure 3. As is evident from the figure, the overall response rate to the screening questionnaire was 29% (95% CI 24% to 34%), which is substantially below the original target of 80% and below the rate achieved in the case series (60%). Specifically, of the 336 foster carers invited to complete the screening, 96 returned completed questionnaires. The overall number of mailed-out questionnaires was also smaller than the original target (n = 500), largely due to significant numbers of children registered with the local authorities being considered inappropriate or ineligible for the study (e.g. very short placements, placed out of borough). It is important to note that the return rate varied substantially per site, ranging from 3% to 63% (median 30%).
FIGURE 3.
The CONSORT flow diagram for the VIPP-FC pilot trial. LA, local authority. Reproduced with permission from Oliveira et al. 73 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: https://creativecommons.org/licenses/by/4.0/. The figure includes minor additions and formatting changes to the original figure.
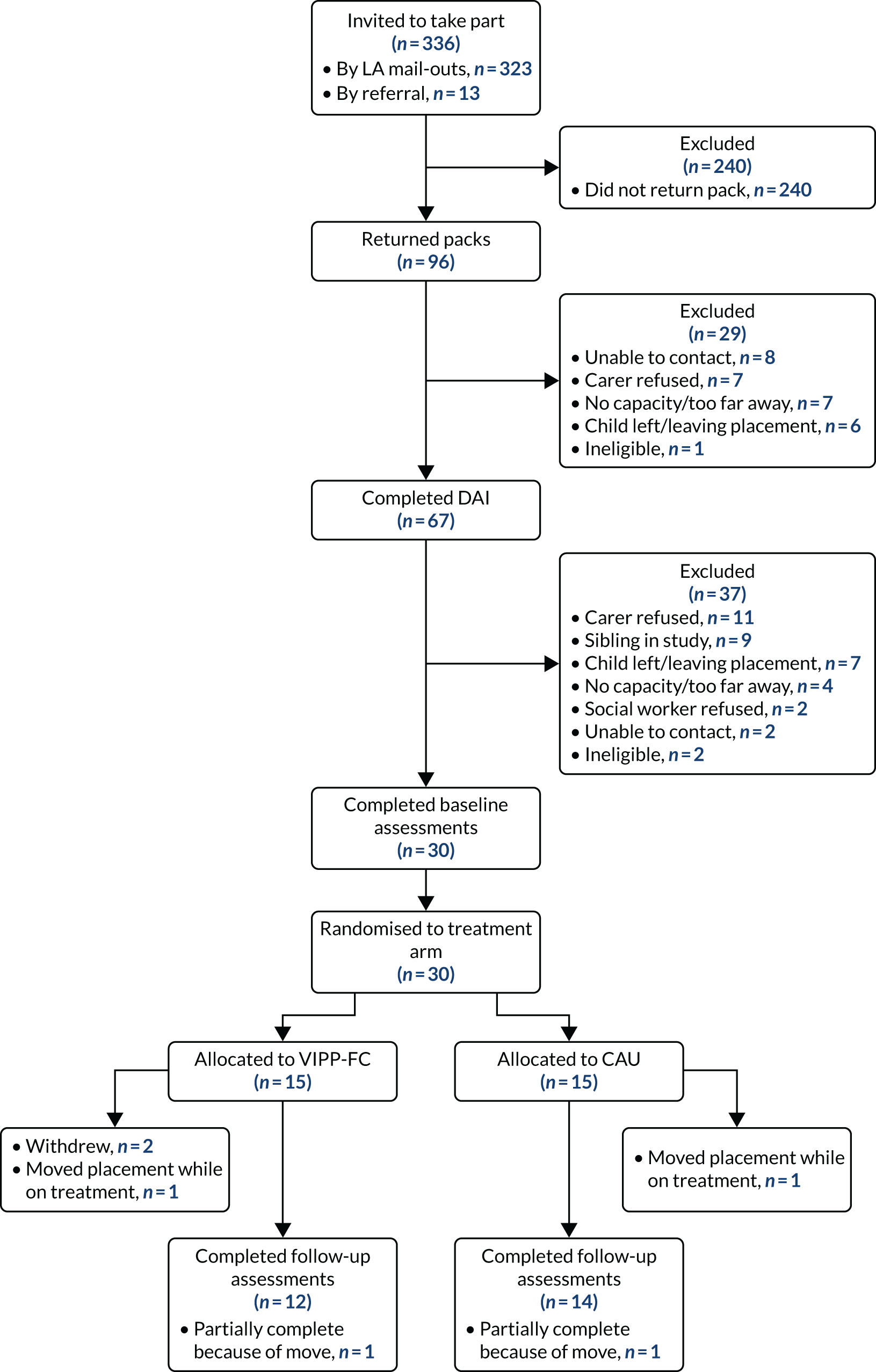
Approximate prevalence of reactive attachment disorder
The results of the DAI indicated an approximate prevalence of significant RAD symptoms in this sample of 33% (22/67 children assessed, 95% CI 22% to 44%). This proportion is based on cases scoring ≥ 3 points on the total RAD score, which indicates clinically significant difficulties (Charles Zeanah, Tulane University, 2015, personal communication). Furthermore, 41 out of the 67 foster carers’ DAIs received a score of at least 1 point (scores can range from 0 to 2 points for each item) on at least one RAD item, and of these participants, 33 received a total RAD score of ≥ 2 points (51%, 95% CI 37% to 61%). These can be seen as cases who show some difficulties in the areas of development tapped by the DAI-RAD items.
Participant characteristics
As demographic data were collected both at initial screening and at entry to the RCT, it is possible to compare the composition of the trial sample with that of the larger group of screened cases for indications of sampling bias. Table 1 shows the key demographic data for the larger and the smaller subsamples; as can be seen in the table, children and carers that took part in the trial (n = 30) did not appear to be different from the overall group of children who took part in the screening, except for legal status: a larger proportion of children on a full care orders were in the sample taking part in the trial. This is likely to be related to the fact that these children tend to remain in their current placement for longer and to the simpler consent process for these children, as their parents were not required to provide active written consent.
| Characteristic | Participants | |
|---|---|---|
| Screening (N = 96) | RCT (N = 30) | |
| Child’s sex, n (%) | ||
| Male | 58 (60) | 17 (57) |
| Female | 38 (40) | 13 (43) |
| Child’s age (months), mean (SD) | 47.92 (24.01) | 47.37 (21.20) |
| Child’s legal status, n (%) | ||
| Full care order | 57 (61) | 24 (80) |
| Interim care order | 22 (24) | 4 (13) |
| SGO | 11 (12) | 2 (7) |
| Voluntary agreement | 3 (3) | 0 (0) |
| Unknown | 3 (3) | 0 (0) |
| Total time in foster care (months), mean (SD) | 17.32 (14.06) | 18.13 (15.03) |
| Carer’s sex: female, n (%) | 86 (90) | 29 (97) |
| Carer type, n (% or minimum–maximum %) | ||
| Foster carer | – (74–81) | 24 (80%) |
| Family and friends carer | – (19–26) | 6 (20%) |
| Child’s ethnicity,a n (%) | ||
| White British | 35 (52) | 14 (47) |
| Caribbean | 6 (9) | 2 (7) |
| White/Caribbean mixed | 5 (8) | 3 (10) |
| Other ethnicities | 21 (31) | 11 (36) |
| Child’s first placement?,a n (%) | ||
| Yes | 35 (52) | 15 (50) |
| No | 32 (48) | 15 (50) |
| Carer’s agea (years), mean (SD) | 51.86 (8.32) | 49.87 (9.66) |
| Carer support,a n (%) | ||
| Shared carer | 42 (63) | 20 (67) |
| Single carer | 25 (37) | 10 (33) |
| Carer’s ethnicity,a n (%) | ||
| White British | 50 (75) | 22 (73) |
| Caribbean | 8 (12) | 3 (10) |
| Other ethnicities | 9 (13) | 5 (17) |
| Carer’s number of years of experience,a mean (SD) | 6.59 (6.35) | 5.97 (5.91) |
Timing of randomisation, baseline and follow-up assessments
The original study design aimed to allocate cases quickly after baseline assessments had been completed and ideally within 48 hours. The period between baseline and follow-up was expected to be approximately 4 months, which was the expected duration of the intervention. However, we expected this to be potentially quite variable in practice and so allowed the outcome assessments to be undertaken after treatment had ended for all cases in the treatment arm. To balance duration of follow-up across the arms of the trial and reduce the risk of unblinding, we trialled a procedure in which the follow-up period in the CAU arm was yoked to a case in the treatment arm. Matching was undertaken with a relatively wide window (up to 1 month) to not excessively constrain scheduling of follow-ups. The resulting timing of follow-ups is presented in Table 2.
| Time period | Trial arm | |||||||
|---|---|---|---|---|---|---|---|---|
| CAU | VIPP-FC | |||||||
| Mean | SD | Minimum | Maximum | Mean | SD | Minimum | Maximum | |
| Baseline to randomisation | 6.13 | 6.07 | 0 | 17 | 7.87 | 13.21 | 0 | 50 |
| Baseline to follow-up | 159.67 | 56.42 | 65 | 278 | 184.92 | 67.16 | 94 | 343a |
| Randomisation to follow-up | 153.53 | 55.27 | 51 | 261 | 176.25 | 67.44 | 94 | 343a |
As Table 2 indicates, in general, the time period between baseline and randomisation was comparatively short, but some delays occurred in a number of cases, with one very lengthy delay, which was due to a lack of availability of a VIPP-FC intervener in the relevant site. On average, the actual period between baseline and follow-up was 6.4 months. The duration of the follow-up period was relatively balanced between the two arms of the trial, although the small number of cases with long delays shifted the mean time period in the VIPP-FC arm to more than that of the CAU arm, despite the pairwise matching.
Evaluation of feasibility parameters
In this section, we summarise the data on the key feasibility questions we set out to address in the pilot trial, as detailed in Methods. Each question is presented in the order described in that section.
A. Feasibility of identifying sufficient numbers of appropriate cases using screening instruments
-
The proportion of screening questionnaires returned from the total sent out was 0.29 (95% CI 0.24 to 0.34).
-
The proportion of positively screened cases (above the upper 66th percentile) agreeing to full assessment on the DAI was 0.73 (95% CI 0.60 to 0.86). Scoring high on the screening questionnaires did not seem to make a significant difference to whether or not carers accepted the DAI. Specifically, the proportion of cases scoring below the 66th percentile on the screening questionnaires that agreed to participate in the DAI was 68%.
-
The proportion of cases scoring above the 66th percentile on either screening questionnaire that scored ≥ 3 points on the DAI was 0.86 (95% CI 0.71 to 1.0). The proportion of cases scoring ≥ 2 points on the DAI (the less stringent threshold) that were above the 66th percentile on either questionnaire was 0.76 (95% CI 0.61 to 0.91).
We conducted a more fine-grained analysis of the detection rates for each questionnaire. Of the cases confirmed as presenting a RAD score on the DAI of ≥ 3 points, 77% were detected by the DAWBA alone and 68% were detected by the ASA alone, with each case again using the 66th percentile threshold.
-
The false-negative rate, that is the proportion of cases with a DAI RAD score of ≥ 3 points but not meeting the screening threshold on either questionnaire, was 0.09 (95% CI 0.00 to 0.21). If we use the less stringent DAI RAD threshold, the false-negative rate was 0.24 (95% CI 0.09 to 0.39).
Considering each questionnaire separately, the false-negative rate (based on the 66th percentile threshold) was 0.23 for the DAWBA and 0.32 for the ASA. Using the less stringent DAI criterion, the corresponding rates were 0.36 and 0.45.
-
Initial non-parametric ROC curve analysis was undertaken based on the assumption that DAI diagnosis is gold standard. We used non-parametric ROC curve analysis to investigate the overall performance of the two screening questionnaires against the DAI. Considering the DAWBA first, non-parametric ROC analysis estimated an area under the curve (AUC) of 0.84 (95% CI 0.74 to 0.92). The ROC curve is shown in Figure 4a. In general, the DAWBA showed good sensitivity, with a raw score threshold of ≥ 2 points, yielding an estimated sensitivity of 0.96 and specificity of 0.48. At this cut-off point, the positive predictive value was 49% (95% CI 35% to 63%), the negative predictive value was 96% (95% CI 77% to 99%), the positive likelihood ratio was 1.74 (95% CI 1.33 to 2.27) and the negative likelihood ratio was 0.09 (95% CI 0.01 to 0.60). A threshold of ≥ 3 points (which is the 66th percentile in our sample) yielded a sensitivity of 0.77 and a specificity of 0.80. With a cut-off point of 3 points, the positive predictive value was 63% (95% CI 44% to 79%), the negative predictive value was 85% (95% CI 71% to 94%), the positive likelihood ratio was 3.01 (95% CI 1.77 to 5.13) and the negative likelihood ratio was 0.31 (95% CI 0.15 to 0.64). Depending on the objectives and, therefore, the preferred balance of false negatives and false positives, a threshold score of 2 or 3 points would seem appropriate using this instrument.
The ASA scored similarly well, with an estimated AUC of 0.83 (95% CI 0.71 to 0.91). The ROC curve is shown in Figure 4b. Inspection of the graph suggests that after (1 – specificity) rises to around 0.26–0.30, improvements in performance level off. A threshold score on the ASA of ≥ 24 points yields an estimated sensitivity of 0.74 and specificity of 0.78. For this cut-off point, the positive predictive value was 57% (95% CI 39% to 74%), the negative predictive value was 84% (95% CI 68% to 94%), the positive likelihood ratio was 2.41 (95% CI 1.51 to 3.85) and the negative likelihood ratio was 0.34 (95% CI 0.16 to 0.70). A lower threshold of ≥ 21 points yields sensitivity of 0.91 and specificity of 0.66. A cut-off point of 21 points yielded a positive predictive value of 55% (95% CI 39% to 70%), a negative predictive value of 93% (95% CI 77% to 99%), a positive likelihood ratio of 2.17 (95% CI 1.53 to 3.08) and a negative likelihood ratio of 0.13 (95% CI 0.03 to 0.52). In our sample, a score of 21 points reflects the 51st percentile, which is considerably lower than our original screening cut-off point. Overall, there is indication in these data that the ASA may be marginally superior to the DAWBA for identifying cases, possibly reflecting its greater variability. Across all cases in the study, the DAWBA yielded 10 different recorded scores (reflecting the number of items), whereas the ASA showed a considerably wider range of scores (26 different values, 12–47 points).
-
Combining and standardising both questionnaires yielded an estimate of the AUC of 0.87 (95% CI 0.78 to 0.94). The ROC curve is shown in Figure 4c. An averaged z-score on this composite measure of –0.036 (close to the sample mean) yielded a sensitivity of 0.92 and a specificity of 0.78. For this cut-off point, the positive predictive value was 66% (95% CI 47% to 81%), the negative predictive value was 88% (95% CI 74% to 96%), the positive likelihood ratio was 3.45 (95% CI 1.99 to 5.98) and the negative likelihood ratio was 0.25 (95% CI 0.11 to 0.56). A z-score of –0.26 gave a sensitivity of 0.96, while retaining a comparatively good specificity of 0.65. In this case, the positive predictive value was 60% (95% CI 43% to 74%), the negative predictive value was 97% (95% CI 83% to 99%), the positive likelihood ratio was 2.66 (95% CI 1.80 to 3.92) and the negative likelihood ratio was 0.06 (95% CI 0.01 to 0.42). These results suggest that combining the DAWBA with the ASA is preferable if time and considerations of burden allow for this. Consistent with that inference, a logistic regression, based on z-standardised scores, showed that both the DAWBA and the ASA RAD scales independently contributed to the prediction of RAD diagnosis based on the DAI (DAWBA odds ratio 5.0; p = 0.003; ASA odds ratio 3.6; p = 0.004).
FIGURE 4.
The ROC curves for screening questionnaires against the DAI, with 95% CIs. (a) DAWBA; (b) ASA; and (c) DAWBA and ASA combined.
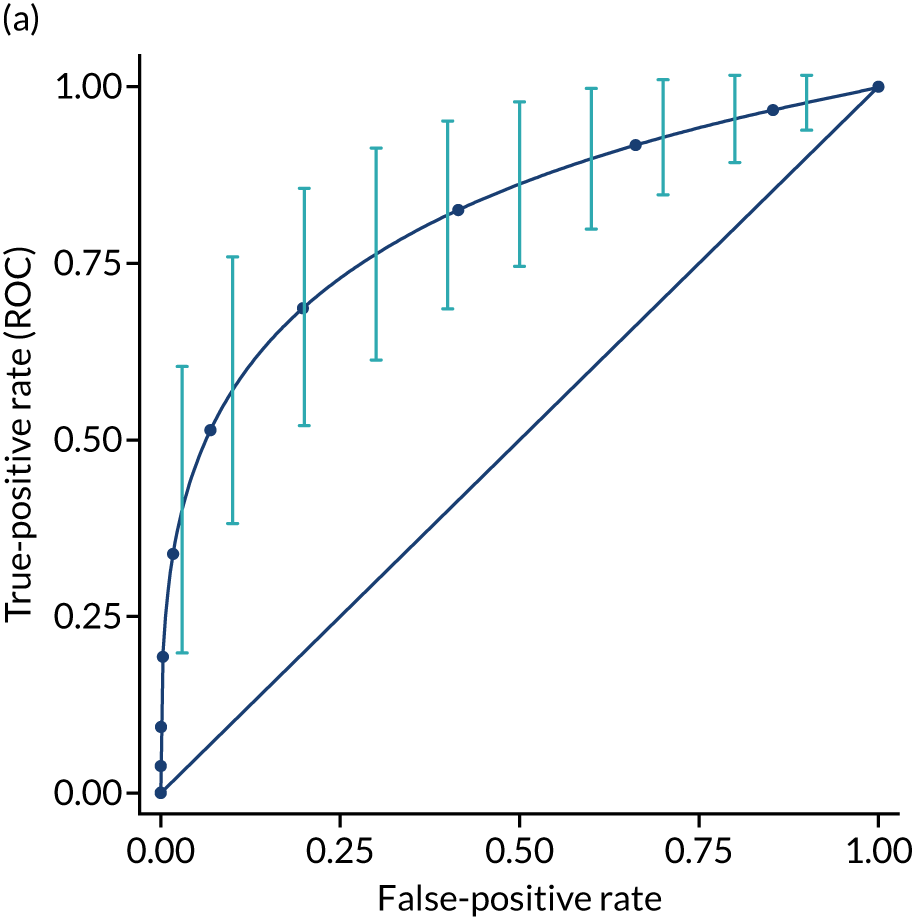
B. Feasibility of recruiting/consenting foster families with children aged ≤ 6 years presenting with reactive attachment disorder symptoms
The proportion and 95% CI of cases consenting to enter the pilot trial from those meeting entry criteria are as follows. For the cases who completed screening (including the DAI assessment) prior to the dropping of the RAD eligibility criterion, 56% went on to take part in the trial (23/41, 95% CI 41% to 71%). Of these, 11 (27%) declined to participate in the trial stage of the project and the remainder could not participate for other practical reasons. If we ignore the RAD eligibility criterion, then the proportion of the whole sample is 45% (30/67, 95% CI 33% to 57%). As a percentage of the total cases invited to take part (prior to screening), the conversion rate was 9% (95% CI 6% to 12%).
C. Feasibility of randomising to the VIPP-FC or care as usual
No cases refused randomisation.
D. Document intervention throughput and acceptability
-
The proportion and 95% CI of cases who were randomised and completed treatment (definition of completion = 80% of offered sessions). Four cases who had been randomised to the VIPP-FC did not proceed to receive it. Two failed to receive it because of a lack of clinical capacity in the study site and two because of social worker concerns about competing interventions that had begun since initial contact. All other cases completed 100% of the planned sessions.
-
Acceptability of treatment: this is addressed in Chapter 7 using qualitative interviews with recipients of the VIPP-FC.
E. Establish the feasibility and acceptability of baseline and outcome assessments
The proportion of participants who completed post-treatment outcome assessments was 0.93 (95% CI 0.84 to 1.0); missing outcome assessments post treatment were due to two families dropping out from the trial after randomisation (these were two children who had the same social worker who decided to withdraw these two families from the study). In two other cases, the children moved to a new placement; thus, only some of the outcome assessments were possible; taking this into account lowers the completion of outcome assessments to 0.87 (95% CI 0.75 to 0.99]). Finally, it is also important to consider the proportion of cases with complete data, defined as having completed all of the assessments; Table 3 details the number of missing data in the baseline and follow-up assessments. In general, there were few missing data. However, some difficulties were encountered with the post-treatment DAWBA (when we use the entire questionnaire), which was completed online. Several participants did not manage to complete this measure, owing to its length and some technical difficulties experienced by several participants in using the website.
| Data | Completed, n (%) |
|---|---|
| Screening | |
| Basic demographics | 30 (100) |
| ASA | 30 (100) |
| DAWBA: relationship with adults | 30 (100) |
| Post-screening interview | |
| DAI | 30 (100) |
| Further demographics | 30 (100) |
| Baseline assessments | |
| Strange Situation Procedure | 30 (100) |
| Interaction task: NICHD scales | 30 (100) |
| CA-SUS | 30 (100) |
| CBCL | 28 (93) |
| Parenting Stress Index | 28 (93) |
| (Brief) Parental Self-Efficacy Scale | 28 (93) |
| Full DAWBA | 26 (87) |
| Follow-up assessments | |
| ASA | 25 (83) |
| DAI | 28 (93) |
| Strange Situation Procedure | 27 (90) |
| Interaction task: NICHD scales | 26 (87) |
| CA-SUS | 28 (93) |
| CBCL | 25 (83) |
| Parenting Stress Index | 25 (83) |
| (Brief) Parental Self-Efficacy Scale | 25 (83) |
| Full DAWBA | 15 (50) |
| DAWBA: relationship with adults | 23 (77) |
F. Identify the most appropriate primary outcome
The primary basis for deciding on the most appropriate outcome measure was consideration of acceptability. The feedback (reported in detail in Chapter 7) generally supported the use of the DAI, as foster carers tended to prefer in-person assessments and found the interview format helpful. Although the sample size was too small to complete formal estimates of the sensitivity of these measures for detecting change, it was notable that the DAWBA (RAD scale) and the DAI showed an overall trend for reductions from pre treatment to post treatment (across both arms of the trial, including all participants with follow-up data; DAWBA, t = 2.35; p = 0.03; DAI, t = 1.95; p = 0.06), whereas the ASA did not (t = –0.07; p = 0.95). On balance, we judge that the DAI should be the preferred tool for assessing RAD symptoms for a trial of this nature.
G. Obtain initial estimates of the variance of key outcome measures
Table 4 summarises the pre-treatment and post-treatment descriptive statistics for the main outcome variables. To obtain an approximate estimate of the SD of the RAD symptom measures for future trial planning, we relied on the screening data, for which the sample size was largest. For the DAWBA-RAD subscale, the variance was 5.0 points, with an upper 80% confidence limit of 6.07 points (based on 101 screening cases). For the ASA-RAD subscale, the variance was 52.3 points, with an upper 80% confidence limit of 64.8 points. Finally, for the DAI-RAD subscale, the variance was 4.16 points (based on 73 interviews), with an upper 80% confidence limit of 5.2 points. We do not report tests of group difference, as these would not be meaningful given the very small sample size.
| Outcome measure | Trial arm (score/points) | |||||||
|---|---|---|---|---|---|---|---|---|
| CAU | VIPP-FC | |||||||
| Mean | SD | Minimum | Maximum | Mean | SD | Minimum | Maximum | |
| Baseline | ||||||||
| DAI-RAD subscale | 2.40 | 1.72 | 0 | 5 | 2.73 | 2.02 | 0 | 6 |
| DAWBA-RAD subscale | 3.13 | 1.41 | 1 | 5 | 2.36 | 2.21 | 0 | 8 |
| ASA-RAD subscale | 23.86 | 6.32 | 12 | 34 | 23.54 | 8.50 | 13 | 35 |
| CBCL-total problems subscale | 53.69 | 33.09 | 12 | 96 | 55.67 | 39.33 | 3 | 113 |
| Parenting Stress Index total | 135.36 | 21.19 | 98 | 167 | 145.00 | 21.89 | 106 | 177 |
| Parental Self-Efficacy Scale total | 21.92 | 2.66 | 17 | 25 | 21.80 | 2.78 | 16 | 25 |
| NICHD-sensitivity composite | 3.26 | 0.42 | 2.31 | 3.88 | 3.24 | 0.36 | 2.56 | 3.94 |
| Post treatment | ||||||||
| DAI-RAD subscale | 1.87 | 1.64 | 0 | 5 | 2.23 | 2.28 | 0 | 6 |
| DAWBA-RAD subscale | 1.92 | 1.89 | 0 | 5 | 2.10 | 1.66 | 0 | 5 |
| ASA-RAD subscale | 23.58 | 6.92 | 13 | 32 | 23.00 | 6.70 | 15 | 34 |
| CBCL-total problems subscale | 50.92 | 29.82 | 15 | 98 | 57.18 | 40.93 | 0 | 118 |
| Parenting Stress Index total | 134.00 | 20.41 | 104 | 1.69 | 144.90 | 23.96 | 104 | 174 |
| Parental Self-Efficacy Scale total | 22.36 | 2.50 | 18 | 25 | 22.27 | 3.50 | 15 | 25 |
| NICHD-sensitivity composite | 3.12 | 0.37 | 2.44 | 3.69 | 3.15 | 0.47 | 2.31 | 3.88 |
H. Establish the optimal and most acceptable screening tools for reactive attachment disorder as defined in the DSM-5
The analyses of screening test performance indicated that both the DAWBA-RAD and the ASA-RAD scales were adequate as potential screening instruments. Although feedback during the case series did not indicate difficulties with either of these measures, in the pilot trial some participants reported difficulties with the response format of the ASA and this also appeared to lead to a few missing data. The DAWBA-RAD subscale is also considerably shorter. From that point of view, we would recommend the DAWBA as a screening instrument. However, we would also note that we lost considerable numbers of DAWBA data when it was collected online at the post-treatment phase; therefore, we would not recommend this mode of data collection for this population. It is also worth noting that feedback from foster carers indicated that they preferred in-person interviews to questionnaires in general, and, in that regard, the DAI had a high level of acceptability. Thus, under some scenarios (e.g. when screening can be undertaken at a face-to-face meeting), the DAI may be preferable, as not only is it a rigorous and in-depth assessment procedure, but it is also preferred by foster carers and can help to build rapport and engagement.
Adverse and significant events
No adverse events were recorded during the course of the trial, but substantial numbers of significant events were noted. The significant events recording was designed to capture pertinent changes in a child’s health and circumstances tailored for children in foster care. At baseline, foster carers were asked whether or not any significant events had occurred to the child in terms of their health, their schooling (if applicable), their care order or contact arrangements (Table 5 shows all of the categories). In general, the most common significant events were changes in foster placement, contact arrangements with parents, schooling and care order. Table 5 shows the number of individual events recorded for each category for the two arms of the trial.
| Trial arm | Events (n) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Change of foster placement | Significant change in foster placement | Change of school | Identification of learning difficulties | Change of social worker | Change in contact arrangement | Return to birth family | Other change in care order | Allegation (e.g. of maltreatment) | Other key transition/loss | Other | Total | |
| Baseline (previous 4 weeks) | ||||||||||||
| CAU (n = 15) | 0 | 2 | 0 | 2 | 1 | 3 | 0 | 1 | 0 | 0 | 2 | 11 |
| VIPP-FC (n = 15) | 0 | 3 | 2 | 1 | 2 | 2 | 0 | 0 | 0 | 1 | 0 | 11 |
| Follow-up (since baseline) | ||||||||||||
| CAU (n = 15) | 0 | 4 | 4 | 0 | 1 | 4 | 0 | 3 | 0 | 3 | 4 | 23 |
| VIPP-FC (n = 15) | 1 | 0 | 1 | 0 | 2 | 1 | 0 | 2 | 0 | 1 | 0 | 8 |
We did not plan any statistical analysis of the significant events data. Nevertheless, we note that there was indication of possible differences in the rates of significant events between the two arms of the trial at follow-up, which was not apparent at baseline. The mean number of events at baseline was 0.73 for both groups (VIPP-FC, SD 1.02; CAU, SD 0.96). At follow-up, the mean number of events was 0.61 (SD 1.12) for the VIPP-FC group and 1.5 (SD 1.25) for the CAU group. The mean difference at follow-up adjusted for baseline was 0.95 (95% CI 0.04 to 1.9). The apparent difference in rates largely concerns significant events linked to changes in the placement and care order, with fewer of these events reported for the children receiving the VIPP-FC. It is not possible to determine in all cases whether or not these were planned changes, or, indeed, whether they are positive or negative outcomes. Nevertheless, given the negative impact of placement instability, the smaller number of placement-related changes in the VIPP-FC group is quite notable, if very tentative, given the small number of cases involved.
Description of care as usual
One aim of this feasibility study was to find out which services are typically used by the target population. Given that difficulties in the realm of attachment problems in this younger cohort of looked-after children are often not assessed or treated, we anticipated that most children would not be receiving targeted psychological therapeutic interventions. On the other hand, emotional–behavioural difficulties often result in children and their families being offered other support services; therefore, it was important to take a broad perspective when asking about service usage to capture any kind of health, educational and community service (see Chapter 6 for a detailed analysis of all these types of services). In addition, given the multilevel difficulties often associated with being looked after, as well as the complex system involved in caring for these children, we expected that they would be involved with a large number of services and professionals.
The findings were in line with these expectations. We report details of the services that the whole group of 30 children were reported to use during the 4 weeks prior to being interviewed. Carers reported that children were seen by a general practitioner (GP) (n = 3 at surgery and n = 1 by telephone consultation); a nurse at the surgery (n = 2); a health visitor, district nurse or school nurse (n = 11); and a family partnership nurse (n = 1). A small number of children had been seen by a care co-ordinator or case manager (n = 2), and the same number had been seen by a family support worker (n = 2). The majority of children had seen their social worker in the previous 4 weeks (n = 22). Other related services that families had used were a foster support worker (n = 1) and an adoption social worker (n = 1). Seven children had received speech and language therapy in the previous 4 weeks. One child had been seen by a community paediatrician for their health and care plan. In terms of psychological services accessed in the previous 4 weeks, a few children had seen an art/drama/music/occupational therapist (n = 3), and others had seen a CAMHS worker (n = 3), a counsellor (n = 2) or a clinical psychologist (n = 2).
New service types that children received between baseline and follow-up were (1) a psychiatrist, (2) a community psychiatric nurse, (3) an educational psychologist and (4) a play therapist.
Children aged ≤ 6 years in foster or kinship care clearly receive a diverse set of services related to their development and well-being. The services that are offered can include universal services related to being in care (e.g. social worker visits), services for children identified as requiring additional support (e.g. carer consultation or one-to-one support at school), or services offered for reasons other than being identified as requiring additional support; our aim was not to determine whether or not the services related specifically to RAD, but to describe which services participants were using and how frequently. This will be important information to consider when planning a larger trial, as it will allow careful consideration of the comparator arm.
Intervention delivery process
Prior to conducting baseline assessments, a careful process of capacity-checking had to take place, considering participants’ and interveners’ locations and availability, so that, as far as possible, if a case was randomised to the VIPP-FC an intervener would be available to take on the case. As we had only one or two interveners in any one locality, small runs of cases randomised to the VIPP-FC or changes in staff availability (e.g. when staff move jobs) could lead to an inability to allocate or to lengthy delays. In the following sections, we summarise observations of the process of intervener training, the allocation process and the treatment delivery itself.
Training of interveners
We trained a group of practitioners from NHS CAMHS teams, clinical study officers, psychologists and social workers, as well as other appropriately qualified practitioners, in the delivery of the VIPP-FC. Each intervener was trained by an accredited VIPP trainer and was required to undertake supervised practice before becoming a study therapist. Accredited supervision face to face, by telephone and by e-mail was provided to all practitioners during the pilot case series and feasibility trial.
The VIPP-FC interveners
We engaged a total of 23 interveners. Of these, we provided the full training to nine professionals, that is we offered the VIPP-SD training (4 days plus practice families) and a VIPP-FC adaptation half-day training. These practitioners were from across CAMHS and local authorities. In addition, 14 practitioners who were already trained VIPP-SD interveners were then trained in the VIPP-FC adaptation for this study (half a day’s training). Out of our pool of 23 interveners, only 12 delivered a case (this includes the case series; only two interveners saw more than one case). Of the 11 who did not deliver a case, this was for the following reasons:
-
Two left CAMHS before being allocated a case.
-
One left CAMHS during a case.
-
Two left the study because of heavy workload.
-
Six could not be allocated cases that matched their locations/availability.
Intervention fidelity
We supported fidelity to the VIPP-FC model through supervision of three visits per case or all visits per case when the intervener was training. All interveners completed logbooks for each visit, outlining how closely they followed the manual, if they completed all of the filming tasks, and if they included key messages in their feedback to the carer, which was required for each different visit. They were also required to audio-record at least one of their feedback sessions per case.
Intervention delivery
Of the 30 randomised cases, 15 (50%) were randomised to receive the VIPP-FC. Of these, 11 received the VIPP-FC, but four did not. There were different reasons why each of these four families did not receive the intervention. In one case, the child left the placement straight after randomisation. Although the team took great care to invite to the trial only those children who were expected to remain in placement for the duration of the programme (approximately 4 months), this was sometimes difficult to predict and changes in circumstances could occur suddenly. For another two cases, professionals involved with the families decided, after randomisation, that it was not appropriate for the child to receive the intervention at that moment in time. For one child, the social worker considered that engaging in another intervention programme was too much for the child, who was already also receiving Theraplay. Similarly, for another, the child’s CAMHS worker felt that the foster carer and child were already engaged with too many services. The fourth case could not be allocated because of a lack of VIPP-FC intervener capacity.
Process observations regarding intervention delivery
The modifications introduced to the manual and delivery of the programme, including shortening the gaps between sessions, were received well. We received positive feedback from both interveners and foster carers about the programme overall. We also collected feedback about the VIPP-FC from the interveners’ logbooks, which they completed after every session. The key points that interveners noted were as follows:
-
Foster carers enjoyed watching the videos and engaged with them.
-
The programme helped them to notice, interpret and react to behaviours and signals of their child that they had not seen before.
-
The programme helped carers notice changes and improvements in the child’s behaviour over time that they would not otherwise have noticed.
-
The programme enabled carers to recognise how they can more sensitively respond to the child.
-
It helped carers to see how strong their bond was with their child.
See Chapter 7 for the detailed impressions of foster carers.
The main challenges with the delivery of the intervention were the changing capacity of interveners, the small numbers of interveners in any one site (despite the large number overall) and, relatedly, difficulties in matching incoming cases to interveners’ locations and availability. This meant that, in addition to one child not being allocated to the intervention, six interveners whom we had trained were not allocated to any cases.
Challenges to clinical process
One common problem to emerge was that, because we were working with older children (up to aged 7 years) than is usually the case with the VIPP-SD, the older children often listened to the instructions the intervener was giving or to the feedback; this meant that interveners had to be sensitive to the wording and language used in front of the child. Accordingly, a recommendation for the future is that it would be ideal to plan for older children not to be present for the delivery of feedback. Another recommendation is to plan to have someone present to look after the other children at home when watching the clips. Sometimes foster carers said that the other foster child(ren) might be distressed by the target child having the programme and them not, or they would require their attention too much throughout the visit.
Relatedly, a frequent experience of interveners was a greater need to think ‘on their feet’ as the children could be particularly challenging and the carer was sometimes very busy/distracted by what else was going on for the child that day, or by other children, both when filming and during the feedback. It also became apparent how important it was for interveners to fully understand the stress that a lot of foster carers are under and the types of concerns they have. An issue raised by some interveners was that foster carers noted that some VIPP-FC tips can appear to contradict advice given by social workers, for example about whether or not to use physical touch with the child. In future, this could be incorporated into the intervener training so that they are more prepared to handle this sort of situation.
An important issue that emerged in this study related to the fact that some interveners had a dual role, both study intervener and holding another position within the local authority or CAMHS. It was reported to be difficult for some interveners to keep their VIPP-FC role separate from their main role, especially if the case was also being seen by their team independently of the VIPP-FC work. For example, sometimes the carers wanted to talk about non-VIPP-related issues, such as network meetings, in the visits, which then led to much longer visits. This also raises the question of who is best placed to deliver the VIPP-FC with this population. For a future trial, the advantages and disadvantages of different models of delivery need to be considered. Some advantages and disadvantages of having the VIPP-FC embedded in CAMHS, rather than delivered by, for example, external trial therapists, were noted.
Discussion
In this study, we ran a pilot RCT to test a number of key feasibility questions facing any future trial of VIPP-FC in a UK foster care context. Key issues to be addressed include the identification and recruitment process, retention rates in the research protocol and the intervention, and the quality and completeness of data collection. Issues of acceptability of the intervention and of the research are primarily dealt with in Chapter 7.
Overall, the screening tools performed well, demonstrating good convergence and sensitivity against the DAI, which is generally considered a gold-standard assessment. We concluded that, on balance, the DAWBA-RAD subscale is the most suitable screening instrument if a short questionnaire is required, but noted that the DAI itself was often preferred by foster carers. Given that in-person contact may be extremely important in engaging foster carers, home-based recruitment and initial screening using the DAI may even be preferable to a postal or online mail-out system for this population.
The return rate for the screening questionnaires was disappointing and, unfortunately, much lower than our first pilot run during the case series. Overall, the return rate was 30%, which meant that the total number of potential recruits in any one site was quite low from the outset. One possible reason for this is that, despite considerable effort, we were rarely able to effectively join social worker team meetings or foster carer meetings, and we lacked a mode of direct contact with foster carers. In several sites, it was not possible to find a person who could consistently act as the study champion. Relatedly, in only one of our study sites was a member of the research team granted access to the local authority through an honorary contract, despite efforts to achieve this in all sites. Crucially, the effectiveness with which we were able to implement processes to support the follow-up and encouragement of carers to return the questionnaires in each site was a major determinant of the return rate. When this went comparatively well, return rates were between 40% and 60%.
Our preliminary data suggest that approximately one-third of children in the sample meet the criteria for RAD, according to the DAI. However it is unclear, of course, if the prevalence in this sample is representative of the population of children in foster and kinship care or placed with guardians in the UK, as non-responses may not be random and our sample may selectively over-represent low- or high-scoring cases. This rate was close to our initial projections, albeit based on very limited epidemiological data. In that sense, the primary reasons for low recruitment rates concerned the smaller than expected number of cases deemed suitable (by the local authority) prior to screening and the relatively low return rate for the screening questionnaires [as well as impacts caused by delays, sometimes related to Office for Standards in Education, Children’s Services and Skills (Ofsted) inspection processes, and two sites becoming unworkable]. It was not possible for us to access data on the children who were excluded from the initial screening lists, so we lack vital information on the validity of this initial triaging process undertaken by the local authorities (which no doubt varied across sites). Nevertheless, anecdotally, a considerable number of cases were excluded from the screening lists for valid reasons, often related to the short-term nature of the placement or complex upcoming court hearings.
Even though the prevalence of RAD symptoms was not substantially below our expectations, it nevertheless meant that two-thirds of foster families who were engaged in the screening process could not take part in the trial. The poor recruitment rate threatened our ability to run a sufficient number of cases through the intervention and research process and jeopardised our ability to study a number of other key feasibility questions. In the light of these issues, and in view of the high level of vulnerability to more broadly defined attachment and emotional difficulties of children in foster care, we chose to remove the RAD criterion and widen the group of children allowed to take part in the trial. This, combined with the inclusion of three additional sites, led to a substantial improvement in recruitment rates. Notably, the majority of children who entered the trial who would not have qualified according to the RAD criterion presented with other (non-RAD-related) significant concerns regarding their emotional development.
It is also critical to note that the inclusion of the three additional sites probably made a significant contribution to the later improvements in recruitment. Our informal observations suggest several characteristics of successful sites. First, we generally had greater success in sites outside of London. Second, sites tended to be more successful when we were able to identify a single energetic individual in the local authority who could take responsibility for moving the project forward and who had strong support from their management team. Third, sites tended to work well when CAMHS colleagues worked very closely with the local authority and/or when a member of the research team held a local authority honorary contract. Having all of these factors in place consistently is likely to be essential for a successful larger-scale trial.
Other factors that had a negative impact on recruitment in the local authorities were significant changes in the senior management teams, Ofsted inspections and high levels of staff turnover. Indeed, organisational changes and frequent staff turnover also had a negative impact on the delivery of the intervention. In the course of the study, we trained a large number of interveners to replace those who became unavailable as a result of changes in their availability or because they moved jobs. Simultaneously, the very limited time that interveners were able to dedicate to the study in each site meant that sites could easily run out of capacity to deliver the VIPP-FC; in two instances, this meant that cases randomised to the VIPP-FC were not actually provided with the intervention. Our reliance on the goodwill of CAMHS staff to dedicate their unfunded time to deliver the VIPP-FC was a limiting factor, leading services to offer very small numbers of practitioners and limiting their involvement to a very small number of cases (usually only one case at a time). All of these observations speak to the value of having a comparatively small number of large and well-functioning sites, and finding mechanisms to adequately support clinical services in providing the intervention (or having university-based trial therapists). The new NIHR funding formula for treatment costs, which came into effect after this study, may make this more feasible in the future.
The research protocol itself proved to be feasible, with no refusals of randomisation and high levels of data completeness. Missing data were more of an issue for the post-intervention DAWBA, which was conducted online; for this population, this is not an approach we would recommend. Retention in the intervention was very high; indeed, in all cases the reason for not proceeding with the intervention was resolvable process issues, rather than dropout or refusal. The study visits were relatively straightforward to arrange, although it was notable that an essential ingredient in this was the research team’s flexibility regarding the location, date and time of day for the research visits. Children who attended primary school (as opposed to nursery) or who had contact with the birth family several times per week tended to be more difficult to schedule. Overall, carers’ feedback regarding the assessments was positive, particularly regarding interviews and observational measurements. In addition, carers often commented on how the children enjoyed coming to the study assessments. However, a common piece of negative feedback was that carers felt that they completed many questionnaires and forms as part of their role, and so the study measures represented a tiresome additional burden. Keeping questionnaires, and forms more generally, to a minimum is recommended.
In conclusion, the pilot trial demonstrated that many aspects of a trial for the VIPP-FC in the foster care context were feasible, but fundamental questions arose about the feasibility of recruitment.
Chapter 6 Testing and adapting health economic measures for young children in foster care
Overview and aims
The health economic component of this feasibility study had two main aims. The first involved the modification and testing of an appropriate version of the CA-SUS, for the collection of service use data in this population. The second aim was to explore recent literature to assess how realistic it might be to include a measure of health-related quality of life (HRQoL) capable of generating quality-adjusted life-years (QALYs), for use in a cost–utility analysis, in this very young age group.
Part 1: modification and testing of the Child and Adolescent Service Use Schedule
Methods
The CA-SUS is a service use schedule that was developed originally for use in economic evaluations of mental health services for children and adolescents. It is generally completed in interview with parents, although it can be completed in interview with older children (i.e. adolescent populations). The CA-SUS is a retrospective measure that asks respondents to report use of various services over a specific period, for example over the previous 3 months. The CA-SUS contains a number of sections that can be included or excluded dependent on the economic perspective of the study, for example hospital services, community health and social care services, medication, accommodation and education.
The CA-SUS has been successfully applied in a number of populations similar to the Video-feedback Intervention to promote Positive Parenting and Sensitive Discipline, Foster Care (VIPP-FC) population, including looked-after populations and pre-school populations. 50,74,75 Because study participants, economic perspective, and duration and timing of follow-up vary by study, the CA-SUS must be adapted for the purpose of each new study. These earlier versions of the CA-SUS formed the basis of a modified version suitable for the current population,50,74,75 with modifications being determined, initially, by expertise in the research group and, subsequently, by testing the acceptability and comprehensiveness of the VIPP-FC CA-SUS in the feasibility study.
The VIPP-FC CA-SUS was administered in interview with foster carers during the baseline interview, covering service use over the previous 4 weeks, and at the 4-month follow-up, covering service use in the period between the baseline assessment and the follow-up interview date. The economic perspective was the NHS and social services perspective, preferred by NICE, plus education sector resources (support services provided in schools and education facilities attended), given the age of the population.
The initial draft version of the VIPP-FC CA-SUS was tested and modified in two ways. First, using feedback from research assessors who supported participants to complete the CA-SUS in interviews, we assessed research assessors’ and respondents’ understanding of the questions and modified the wording or added an explanation when anything was unclear. Second, we assessed the measure’s comprehensiveness in capturing all relevant services by identifying services used by young participants but not included in the draft CA-SUS (missing items), and any items included in the draft CA-SUS but not used by the young participants (redundant items). To assess missing items, research assessors probed for and recorded any services used by young participants that had not been covered during the course of the CA-SUS interview.
Amendments to the CA-SUS were made during the data collection period to provide an opportunity to test an improved version during the feasibility study and at the end of data collection. Initial amendments were made after 12 interviews had been completed (n = 9 at baseline and n = 3 at the 4-month follow-up) and involved discussions between the research assessors and CA-SUS designers to explore the findings so far. Research assessors highlighted any difficulties with clarity and any missing items that were being reported by a number of participants, and necessary adjustments were made. The new version of the CA-SUS was then used for all subsequent baseline and follow-up interviews. At the end of the study, all hard-copies of completed CA-SUS questionnaires (n = 58) and the CA-SUS data contained in the study database were checked for errors, redundant items (no recorded use), missing items (recorded under ‘any other service use’) and any additional feedback from research assessor notes on the hard copies of the CA-SUS.
Results
Feedback from research assessors suggested that the CA-SUS was easy to use, taking between 5 and 10 minutes to complete, and was acceptable to both interviewers and interviewees. Interviewers found that foster carers were able to answer all of the questions and there was no need to interview social workers to fill any gaps.
A summary of CA-SUS item completeness, including percentage of missing data (no response provided), redundant items (no use recorded) and missing items (additional service use recorded under ‘any other service use’) is provided in Table 6; for reference, the adjusted version of the CA-SUS is presented in Appendix 2. Some items contained in the CA-SUS are excluded from Table 6; these were not intended to be costed and included in the economic evaluation, but were of interest to the research group (e.g. statement of special education needs, days of school missed).
| CA-SUS section | Service use item | Missing data (%) | Redundant items (no use recorded) | Number of missing items (‘other’ items reported) |
|---|---|---|---|---|
| A: accommodation | A1 Type of accommodation | 0 | Items 01 and 05–13a | 0 |
| B: education | B1 Type of education | 0 | Items 03 and 04a | 8 |
| C: hospital services | C1 Hospital admission | 0 | N/A | N/A |
| C2 Inpatient specialty | 0 | N/A | 3 | |
| C3 Outpatient/day-patient appointment | 0 | N/A | N/A | |
| C4 Outpatient/day-patient specialty | 0 | N/A | 8 | |
| C5 Accident and emergency attendance | 0 | N/A | N/A | |
| D: community services | D1 Service type | 0 | Items 01, 03, 12, 18, 19 and 20a | 12 |
| D1 Number of contacts | 0 | N/A | N/A | |
| D1 Average duration of contacts | 16 | N/A | N/A | |
| E: medication | E1 Any medication? | 0 | N/A | N/A |
| E2 Name and dose | 0 | N/A | N/A |
Overall, almost all of the questions in each section of the CA-SUS were completed appropriately and almost all of the questions contained a response; therefore, the issue of missing data was not identified as a problem, which suggests that participants were able to understand the questions and found them acceptable.
The accommodation section (A1) was 100% completed, with no implausible values. The only accommodation types reported were formal foster care, provided by local authorities or private agencies, and formal kinship care. All other accommodation types were reported as zero use (redundant items), including domestic accommodation with parents/adoptive parents, informal foster care including informal kinship care, residential care provided by a local authority or private agency, residential mother and baby facility, bed and breakfast, boarding house or hotel, refuge, supported housing and short break/respite care. No ‘other’ accommodation was reported; thus, there were no missing items.
Type of education (B1) was 100% completed, with no implausible values. No children received home tuition or were in residential schools (redundant items). Additional schooling types recorded under ‘other’ included portage (n = 2), special needs school (n = 2), speech and language therapy at school (n = 1), early risers (n = 1), breakfast club (n = 1), small support group (n = 1) and booster classes (n = 1). A number of responses appear to relate to school-based services, rather than education types, and thus can be excluded from this section (e.g. breakfast club, small support group, booster classes). However, it may be appropriate to consider them for inclusion in the community service section of the VIPP-FC CA-SUS, with some rewording. For example, ‘speech and language therapy at school’ can be classified alongside other community speech and language contacts. Most of the remaining responses lacked enough detail to determine what exactly was being reported and thus were ignored (e.g. early risers, small support group and booster classes). One service was reported that the team felt could potentially be relevant to the population (portage: a home-visiting educational service for pre-school children with special educational needs and disabilities), and thus should be added to the community services section of the VIPP-FC CA-SUS. The only responses focused on education types (e.g. education facilities) were for special needs schools; again, the team felt that this could potentially be relevant for this population and so should be added to a the VIPP-FC CA-SUS.
In terms of hospital services, use of inpatient, outpatient/day-patient and accident and emergency services (C1, C3 and C5; yes/no response required) was 100% completed. Number of inpatient nights, number of outpatient/day-patient appointments and details of any accident and emergency attendances were all 100% completed (C2, C4 and C6). However, a number of additional responses were recorded under ‘other’, where specialty was unknown (C2 and C4). These responses are used to help identify the appropriate specialty. Responses for inpatient specialty included bronchoscopy, magnetic resonance imaging and sleep study. Responses for outpatient/day-patient specialty included bronchoscopy, eye appointment, immunology, blood test, heart screen, sleep test, physiotherapy and genetic test.
The community services section (D1) was 100% completed, with zeros recorded to indicate no service use. No service use was recorded for GP home visits, GP telephone contact, family therapist, education welfare officer, advice service or helpline. Some feedback was received from research assessors. First, they suggest a need to distinguish between a child’s social worker and a foster carer’s supervising social worker. Second, they reported that item 19, ‘advice service’, did not seem to apply to this population, perhaps because foster carers instead turn to their supervising social worker. In terms of number of contacts with each service accessed, these sections were 100% complete. Average duration of contacts with community services, however, was missing for a number of services, including community psychiatric nurses (missing for one out of one contact reported), counsellors (missing for two out of three contacts reported), social worker (missing for 1/48 contacts reported), educational psychologists (missing for one out of one contact reported), speech and language therapist (missing for 4/15 contacts reported).
Additional community services reported under ‘other’ included physiotherapist (n = 2), community paediatrician (n = 1), personal education plan (n = 1), family partnership nurse (n = 1), adoption social worker (n = 1), play therapist (n = 1), community nurse (n = 1), foster support worker (n = 1), dietitian (n = 1), occupational therapist (n = 1) and audiologist (n = 1). Some of these services can be reclassified within the existing list of services. For example, ‘adoption social worker’ can be included under ‘social worker’. ‘Community nurse’ and ‘family partnership nurse’ are community nurses, and can be classified alongside ‘school/college nurse, health visitor, midwife or district nurse’, suggesting the need to reword this item to make clear that this should include all nurses working in the community. ‘Foster support worker’ could be classified alongside ‘family support worker’, again suggesting the need to reword this item to make clear that this should include any support workers. All but one of the remaining services were reported by only one respondent. However, categories emerged that could be useful to add, for example there were a range of different ‘therapists’ (physiotherapist, occupational therapist, play therapist) that may usefully be added to the VIPP-FC CA-SUS.
The medication section was 100% completed, with 15 out of 58 respondents reporting use of prescribed medication.
Conclusions and recommendations
Items to be removed
Items for which no use was reported and for which the research team did not feel strongly that the item may be important for a larger sample include the following:
-
accommodation – ‘residential mother/baby facility’; ‘bed and breakfast’, ‘boarding house’ or ‘hotel’; ‘refuge’; ‘supported housing’
-
education – ‘residential school’, ‘home tuition’
-
community services – ‘family therapist’, ‘advice services’, ‘helplines’.
Items to be added
Items reported under ‘other’ sections in the CA-SUS that were reported by a number of respondents that may thus be important to the population, and so should be added to the CA-SUS, include the following:
-
education – ‘specialist school [e.g. specialist schools for children with emotional and behavioural disorders (EBD) school, special needs school]’
-
community services – ‘portage’, ‘physiotherapist/occupational therapist/play therapist’.
Items requiring rewording
Feedback from research assessors and responses given under ‘other’ in the community services section of the CA-SUS suggest that the following should be reworded:
-
replace ‘general practitioner – home’, ‘general practitioner – surgery’ and ‘general practitioner – telephone’ with ‘general practitioner (in surgery, by telephone or at home)’
-
change ‘school/college nurse, health visitor, midwife or district’ to ‘nurse in school/college or in the community (e.g. health visitor, midwife, district nurse)’
-
change ‘social worker’ to ‘social worker focused on the child (including adoption social worker)’
-
change ‘family support worker’ to ‘support worker (e.g. family support worker, foster support worker)’
-
change ‘speech and language therapist’ to ‘speech and language therapist in the community or in school/college’.
Part 2: measurement of health-related quality of life in young children (aged ≤ 6 years)
Methods
The second aim involved exploration of recent literature to assess how realistic it might be to include a measure of HRQoL capable of generating QALYs in this young age group. QALYs are a generic, preference-based measure of HRQoL that are used in cost–utility analysis and allow comparison across different disorders for resource allocation purposes. Without such a measure, it is difficult to make clear resource allocation decisions through the application of the NICE threshold of £20,000–30,000 per QALY. However, when the VIPP-FC feasibility study was proposed, no validated measure existed for children aged ≤ 6 years and methodological guidance for alternative approaches was limited. We therefore proposed exploring any developments in the literature that occured during the course of the feasibility study that might provide better guidance.
We searched various databases and websites for guidance in very young children, including the NIHR website, the NICE website, clinical trial registries (ClinicalTrials.gov, the EU Clinical Trials Register) and websites for instruments known to be used to derive child health utilities in the UK. We contacted experts in child health utilities asking for their insights, any new evidence and if they were aware of any ongoing work developing or testing child health utility measures in children aged ≤ 6 years.
Results
Current literature
A review of current literature identified few publications focused on the measurement and valuation of utilities in children. One 2020 review explored valuation methods of preference-based measures of health for economic evaluation in child and adolescent populations,76 one explored agreement between self-reported versus proxy-reported utility values77 and a third reported a systematic review and meta-analysis of childhood health utilities. 78 None of these reviews considered methods for children aged ≤ 6 years.
The consensus from the literature seems to be that it is still too difficult to measure self-reported health in very young children, even with a well-designed patient outcome measure. 79 Very young children and children with developmental or cognitive impairments are likely to be less able than older children and adolescents to perceive, understand and value their subjective experience of health. 76,77
In these situations, proxy reports could be completed by parents, caregivers or health-care professionals. This does, however, rely on the proxies accurately perceiving and understanding a child’s subjective experience of their health. For older children, studies that have compared child report with proxy report have generally found that agreement was poorer on subjective attributes (e.g. cognition, emotion, pain) than on physical attributes (e.g. mobility, self-care, speech, vision) of HRQoL. 77 The situation for very young and infant children is often complicated by the severity and intensity of the conditions they are suffering from and the treatments they are receiving in response,77 in this population, proxy-reporting of HRQoL, which focuses on symptoms and physical aspects of the condition, may have more validity. For example, the Infant Health-Related Quality of Life instrument, a mobile-based generic measure for infants aged < 12 months, covers seven items including sleeping, feeding, stooling, mood, skin and interaction. 80
Developments in progress
Current NICE guidance states that:
When necessary, consideration should be given to alternative standardised and validated preference-based measures of health-related quality of life that have been designed specifically for use in children. The standard version of the EQ-5D [EuroQol-5 Dimensions] has not been designed for use in children. An alternative version for children aged 7–12 years is available, but a validated UK valuation set is not yet available.
A recent report by the Office of Health Economics notes that NICE is reviewing its recommendations on child utilities and QALYs and will make recommendations as part of the current NICE review of its methods for technology appraisals, which will publish a final programme manual in December 2020 after a public consultation in the summer of 2020. 79,82 A search of the NICE website on 2 March 2021 did not produce any further information on this review.
Review of known child health utility measures
There are two main instruments used in the UK to measure child health utilities, the Child Health Utility Index-9 Dimensions (CHU-9D) and the EuroQol-5 Dimensions-Youth version (EQ-5D-Y).
The CHU-9D website, hosted by the University of Sheffield, states that studies are under way trialling a proxy version with children aged 5–7 years and a proxy version with guidance notes for children aged < 5 years [www.sheffield.ac.uk/scharr/sections/heds/mvh/paediatric/about-chu9d (accessed 25 March 2020)]. To our knowledge, these studies are, at the time of writing, still ‘work in progress’ (Oliver Rivero Arias, University of Oxford, February 2020, personal communication; and Donna Rowen, University of Oxford, February 2020, personal communication). Interestingly, a 2020 review of valuation methods of child health utilities reported the appropriate age range for the CHU-9D as aged 4–17 years, rather than the aged 7–17 years age range stated on the CHU-9D website. 76 The aged < 7 years age range refers to the proxy version, although the authors acknowledge that there is no published evidence to support the validity of this version (Donna Rowen, personal communication). The CHU-9D is currently being revalued in the UK using discrete choice experiments with adult responders (Donna Rowen, personal communication).
The EQ-5D-Y is a ‘child-friendly’ version of the EuroQol-5 Dimensions, three-level version (EQ-5D-3L); it contains the same questions and levels, but with more comprehensible wording for young people. The EQ-5D-Y covers young people aged 8–15 years, with a proxy version available for children aged 4–7 years. 83 The EuroQol Group is currently developing an international valuation protocol for the EQ-5D-Y. In a forthcoming review of the psychometric performance of the EQ-5D-Y, CHU-9D, Health Utilities Index Mark 2 (HUI2) and Health Utilities Index Mark 3 (HUI3), the EQ-5D-Y performed best in terms of psychometric properties, followed by the CHU-9D, with the HUI2 and HUI3 being used in more studies, but with more mixed evidence (Donna Rowen, personal communication).
Conclusions and recommendations
In summary, although proxy versions for children aged ≤ 6 years are available for both the CHU-9D and EQ-5D-Y, there is no evidence currently to support the validity or reliability of these proxy versions. In addition, the EQ-5D-Y proxy measure is for use with children aged 4–7 years and, although no minimum is stated for the CHU-9D, it is possible that neither measure is suitable for children aged 0–3 years. Given these findings, it is not currently possible to recommend any specific measures for inclusion in a future trial of VIPP-FC; thus, the primary economic evaluation should be a cost-effectiveness analysis using the primary clinical outcome measure or using an assessment of meaningful change on the primary clinical outcome measure. However, neither option is ideal, given the limitations of cost-effectiveness analysis using clinical measures, compared with cost–utility analysis using QALYs, for which the results can be assessed against a national threshold, such as the cost per QALY threshold preferred by NICE. We therefore additionally recommend that a future trial of the VIPP-FC may be a good opportunity to compare the construct validity and sensitivity to change of the proxy versions of the CHU-9D and/or the EQ-5D-Y by exploring the relationship of these measures with clinical outcomes such as the SDQ and CBCL.
Chapter 7 A qualitative study of foster carers’ experiences of a video-feedback intervention to promote sensitive caregiving
Overview
In this chapter, we present the results of qualitative interviews conducted with foster carers who had received the modified Video-feedback Intervention to promote Positive Parenting and Sensitive Discipline, Foster Care (VIPP-FC), which focused on the practical experience of engaging with the intervention and the foster carers’ perceptions of the key processes that supported change.
Methods
Recruitment
All participants who received the VIPP-FC as part of the case series or feasibility RCT were eligible and were invited to take part in this study. Interviews were completed with 11 foster carers (nine from the RCT and two from the case series). Reasons for not interviewing eligible foster carers were as follows: two foster carers who were randomised to the VIPP-FC did not receive the intervention; in addition, one carer dropped out of the RCT prior to the intervention taking place, one child was moved before the VIPP-FC work started, one carer declined to be interviewed and we were unable to contact one foster carer.
Data collection
Interviews were conducted face to face in foster carers’ homes between January and March 2020. After addressing any questions and obtaining written consent, the interviews were audio-recorded. An interview schedule was developed in consultation with the study team and through discussion with and feedback from the study’s foster carer advisors. The interview focused on all stages of the trial process, from initial contact and screening to receiving the intervention and completing the research assessments.
Data analysis
The audio-recordings were transcribed verbatim and anonymised by a member of the research team. We adopted the same analytic approach as in the previous qualitative study, presented in Chapter 4. Thematic analysis is well suited to implementation research and provides a helpful framework for drawing out both similarities and differences among participants’ perspectives and conceptually organising emergent themes. 64 This involved the researcher working systematically through the transcripts, identifying notable features of the narratives and coding/labelling them using NVivo. 65 These lower-level codes were then combined to form broader themes and subthemes, and initial drafts of emergent overarching themes were teased out. The overarching themes and subthemes were then reviewed again in relation to their fit with the original narratives and were adjusted when necessary. 65
Results
A summary of the key themes and subthemes is presented in Table 7.
| Theme | Subtheme |
|---|---|
| 1. Motivation | 1.1 Helping research |
| 1.2 Helping the child in my care | |
| 1.3 Learning new skills | |
| 2. Experience of the VIPP-FC | 2.1 Practicalities |
| 2.2 Relationship with interveners | |
| 2.3 Being videoed | |
| 3. Learnings from the VIPP-FC | 3.1 Learnt new skills |
| 3.2 Reassurance and confirmation | |
| 3.3 Learning about the child in my care | |
| 3.4 Seeing something I would not have noticed otherwise | |
| 3.5 Seeing my attachment/bond/connection with the child | |
| 4. Future improvements | 4.1 Targeted (who should receive the intervention) |
| 4.2 Time between sessions | |
| 4.3 The intervention as training |
Theme 1: motivation for taking part in the study
Participants expressed a range of reasons for taking an interest in the study; indeed, many could not confidently enough to state precisely what had led them to agree in the first place. For some of them, this may have been partly related to the somewhat lengthy process between initial contact at the screening stage to completing the intervention and feedback interviews. Participants’ expectations of the VIPP-FC varied greatly, with some clearly hopeful about the difference it might make, for example to ‘try something new’ [participant (P) 3] and ‘gain knowledge’ (P8), whereas one felt that ‘[given my experience of] things that I had done with the children before, . . . I didn’t really hold out much hope if I’m going to be totally honest’ (P1). Foster carers’ motivation and expectations about receiving the VIPP-FC responses could be divided into three subthemes: to help research, to help the child or to learn new skills.
Helping research
In many of the interviews, participants commented on the significance of this being a research trial. This was emphasised when, for example, they described their experiences of completing the screening questionnaires and research assessments:
. . . the questionnaires are important because you need them to get an idea of where the child is and where the child is going to end up at the end of it, so you need those.
P6
Participants referred to taking part and helping with research as a key part of their motivation and described research as ‘a good way of finding out things’. Many participants seemed to have a clear understanding of the role of research in increasing knowledge and improving care, which underpinned their desire to help:
We agreed to it because I’m a great fan of studies, otherwise you don’t learn to improve and get on.
P6
And also, if it helps other foster carers, or new foster carers in particular, yeah, I think, for young children, then that’s all brilliant.
P2
I just hope it helps, you know if it helps you guys and your research.
P4
One foster carer who was asked to take part after the eligibility criteria had changed owing to low initial recruitment rates explained that this was a factor that persuaded her to take part:
I thought ‘how can anything ever get better if people don’t take part?’, so that kind of swayed me, and I thought ‘you know what, I am going to do it’.
P9
Participants’ knowledge and support for research trials was also evident when they discussed the randomisation process. All of the participants agreed that the randomisation process was not a significant barrier to them; indeed, some carers commented that they were ‘not worried’, ‘not bothered’ and ‘didn’t mind’. The participants seemed to understand that their involvement in the study and the randomisation process was crucial to the research element of the study:
I don’t think it would have worried me whichever group because I knew whichever group, whether you were in the group that was taking part and was going to be used for the study or not, it would benefit.
P6
Overall, the majority of participants described the research assessment process as ‘interesting’. Most participants and carers had positive views of the questionnaires in terms of ease of completion and understanding. A number of participants found the questions straightforward to complete. The only negative comments about the screening process was that the questionnaires were ‘repetitive’ (P9) or, in one case, a carer felt that they were ‘not relevant’ (P7) to their child.
Helping the child in their care
Participants consistently emphasised that a key part of their motivation to take part came from a desire to help the child in their care. Two participants mentioned behaviours of the child in their care that worried them and how they had taken part in the hope that the programme would help them specifically with those concerns:
I just done it for [child’s name] really, I thought that he would get something out of it as well.
P5
I realised that this child really needed some help with his play and getting close with trust and things, so I thought that was really important for him.
P3
When asked what they considered when deciding whether or not to be involved, one carer said:
What benefits could come out of it for [child’s name] because obviously she needs as much help as she can get, it’s very few and far between.
P7
Learn new skills
A number of foster carers mentioned that they had seen their involvement in the study as an opportunity to learn new skills:
Just to learn something new, tactics of what I may and not try, what may or may not work over a length of time . . . Just some insight really, some new tips and to see if any of us together could come up with something that would help in the long-term, not just the short-term.
P1
Is it the right thing? Can we improve, what else can we do to make it better for them, their experiences, that sort of thing.
P6
I thought it was quite a good idea to be honest, em, you know some child . . . some children are sort of struggling a little bit and you could get help from someone and they would give you advice how to do it, I think it’s worth it.
P5
. . . because children who come into foster care, very often they have come from a difficult background, and they can’t attach to you and you end up with a child with difficult behaviour and you don’t know how to cope with it or what you can do to help them and you can be a little bit lost and it can sort of make the situation more volatile, when you are trying to do something with the child and they really don’t want to do it and you can’t think – ‘why don’t they want me to do it?!’.
P8
Well, I just thought it would be interesting, and learning something new is always a good thing.
P10
Theme 2: experience of the VIPP-FC intervention
In general, all participants spoke very positively of their experience of the VIPP-FC. There were three subthemes that articulated how the participants felt about their involvement in the intervention. These themes are practicalities, the relationship with the intervener and being video-recorded.
Practicalities
Foster carers’ working and family lives can present significant challenges for participating in research or indeed in any ‘additional activities’. Foster carers’ busy schedule of meetings, family contacts and paperwork all presented obstacles to be navigated when scheduling the six sessions of the VIPP-FC. However, all of the participants interviewed agreed that setting aside time for the intervener to come to them was manageable, as the intervener was able to be flexible around the child and their timetable:
. . . she came at different times, she would always text me and ask me, say she had to come at lunchtime one day to video us having lunch which wasn’t a problem and we managed that, and we managed the right time.
P6
Not a problem at all. We arranged it around [child’s name]’s nursery.
P8
Even when the child was at school, foster carers and the interveners were generally able to find suitable times to do the work, although this required flexibility on both sides:
We booked it in advance, so we knew, so that was, yeah, it was OK if we booked it with school and with me. We had it all worked out, so it was fine.
P1
It was fine because we done it after school . . . Yeah so it was a lot easier. Taking him out of school ruins his routine. He wouldn’t like it.
P5
Furthermore, the intervention took place at the foster carer and child’s home, a factor about which foster carers were very positive. They emphasised that this was preferable:
Oh no, that was brilliant, I much preferred her coming here than having to go somewhere else to have it done.
P2
Not only did it make the intervention more convenient, some of the foster carers mentioned that they felt that it helped the child as well:
I think [child’s name] felt more at home being at home and then she could just have her lunch and pop to nursery and we could watch the videos, so I think it worked.
P2
Many foster carers mentioned that the interveners were able to arrange sessions at their convenience and that even when there were unusual circumstances, the interveners could be flexible around it:
She fitted in very nicely and, in fact, I had builders here then and she fitted in around that and was really very, you know, great.
P3
One foster carer mentioned a specific difficulty she had when looking after a baby at the same time as caring for the index child. The baby cried in the next-door room, but the intervener reassured the foster carer that this was OK for the intervention and, in fact, it could be important and helpful to have the child in the environment if this was how life tended to be day to day:
And she just fitted in with what we were doing and because that’s part of [child’s name]’s life as well and she said it was important to get all that as well . . . so yeah we managed.
P6
The interview responses emphasised that practicalities were generally not significant challenges, as long as the interveners were willing and able to be flexible and understanding. With that in place, the foster carers reported that they generally found that it was easy to plan the sessions around their timetables and that the interveners were extremely flexible.
Relationship with interveners
The relationship with the intervener was consistently emphasised as a key aspect of foster carers’ experiences of the VIPP-FC. All of the interviewed participants said they had a good relationship with their intervener; they described some of them as ‘perfect’ (P5), ‘brilliant, absolutely brilliant’ (P2) and ‘lovely’ (P6).
Several foster carers described how the intervener would help them to feel at ease during the sessions:
Yeah very good, she was very relaxed, very comfortable to be around. Sort of her mannerisms and the way she spoke, how she interacted with [child’s name]. It just made you very comfortable. So, it was very comfortable to do the sessions because she made you feel comfortable.
P8
She was really friendly, very warm, she came into the home always at a time that’s convenient for us and she never felt intrusive at all, you know she always was very calm and a great tone in the house so that was really good.
P3
I just found her lovely and she just came in and it felt like she was part of the family really, just sat down and . . . yeah natural, natural.
P9
She was amazing, I think she is absolutely lovely. She will try and work with you . . . nothing was a problem.
P11
Linking to the subtheme of flexibility, foster carers also commented on how helpful it was that interveners were able to fit in with whatever the situation happened to be when they arrived, including the presence of other children in the home:
Lovely. She was really friendly, really warm. You know, really accepting of the situation here, of [child’s name], and me and his sister and just giving really good practical tips. Nah, she was fine, [child’s name] really got on well with her and thought she was great.
P1
So, she was always very sweet with them [the other siblings] as well and, in fact, some of the activities, she did include the others, like the sandwich-making – she had them involved.
P3
When asked, all participants said that they felt understood by their intervener and emphasised how important that was:
I think sometimes you wouldn’t understand how much that is important to a foster carer to have somebody to speak to about these kind of things and actually wants to give the time to talk about your child in that kind of level because there is a lot of tick-boxing going on with them, some people, because nobody really wants to discuss in such detail your child’s emotional needs, and that’s really good.
P3
Being video-recorded
A majority of foster carers expressed their initial dislike of being filmed. Several participants said they felt self-conscious or embarrassed, aware of being watched, or possibly judged, or aware of how they sounded or looked:
I don’t like being videoed, I can’t stand it! No one likes it but I can’t bear it. I sound awful on it! . . . I can’t imagine a lot of people would want to be videoed! . . . I hated it, but I done it, [child’s name] wasn’t even deterred by it. He was alright, it didn’t bother him . . .. By the end I did get quite used to it, you know what I think when they video, what I don’t like, they video and you can’t speak to them. That is a bit off-putting.
P5
No not really – just the videos! Yeah, you think ‘oh god, I’m being videoed’. But you get used to it actually, you do get better as it goes along. But you are conscious to start with. It gets better as it goes along . . .. The first one was quite, for me I was thinking ‘oh no, someone is watching me’ and that sort of thing, especially when you’re not used to it, but I think as the more videoing happened, the more you got used to it and just ignored it really once, you got used to it, you forgot, but yeah, it is just that initial getting used to.
P6
I had to forget it was there because otherwise it would just be like ‘oh gosh, we are being watched’ and you’d be more conscious of what you were doing and saying then so just forget it was there.
P1
One foster carer thought the videoing could be something that would put other foster carers off as they might be ‘intimidated’ (P5). However, all of the foster carers we interviewed said that, even if they had found the video-recording, or the prospect of it, difficult initially, by the end they had become used to it or tended to forget it was there, and so ultimately being filmed was not a serious problem and felt worthwhile.
Theme 3: learnings from the VIPP-FC intervention
The theme that occupied the largest portion of the narratives revolved around the positive things that foster carers felt they had learned or gained from the VIPP-FC sessions. This theme could be divided into several subthemes: strategies, techniques and tips, learning about the children in my care, noticing things I would not have noticed before, and confirmation or confidence in what I am already doing.
Learnt new skills: tips, techniques and strategies
An important aspect of the VIPP-FC intervention from the foster carers’ points of view was that they learnt new tips and techniques to help with some of the more challenging behaviours that the foster children they cared for could sometimes display:
. . . as we got further into doing the sessions, there was some useful advice on how to manage [child’s name] and his behaviours when I’m trying to do something else. So yeah, some good advice and good strategies came out of it.
P8
Yes, because normally I would get wrapped up, got to feed the baby, ‘you play with our toys’ and then he would start throwing his toys, but now if we spend just 5 minutes – not even 5 minutes – playing pat-a-cake or singing a song, he is quite happy then just to let me feed the baby without trying to pull the bottle out of the baby’s mouth. So yeah, that has helped.
P8
Several participants discussed how the VIPP-FC had helped them to realise how important playing with the children is for their development and their relationship, and it encouraged them to set aside time for the child:
I do give them more – even if, like, I said its 5/10 minutes more, doesn’t matter what it is that they want to do, but that’s just their 5/10 minutes . . . the only thing that I can say that has changed in relation to that is the fact they now get their own specific time every day and so they know that they are getting it, so that’s what’s special to them.
P1
I just, I think differently when I am playing with her and it makes me think back when I looked at the videos and saw how she really, really enjoyed it, so I’d probably make a little more time to sit and play a game with her than I did before.
P2
Some participants mentioned how the VIPP-FC changed the way in which they play with their child. One carer realised that she had been leading the play and needing the child to do things in a certain way. By watching the videos, she could see the child’s reaction when she allowed him to play in the way he would like to:
. . . how to let him lead play because that’s one thing that, watching the videos back, I didn’t do, I was always ‘no you put the cup in the saucer and the tea in the cup’, that’s how you play with it, rather than letting him play with it how he wanted, I wanted him to conform to how I thought or how things are done properly. [Laughs.] Whereas [child’s name] was better when I left him to it and let him do what he wanted, and then I praised him for doing what he wanted rather than what I wanted. So, I learnt that, I learnt to step back and not direct his play, but just join in and let him play.
P8
Finally, foster carers also mentioned the potential scope of these skills, as they may be transferable to other children in their care. Some stated that, even if they could not use the techniques for the children they presently care for, they could understand how they would be useful in the future:
So, for me it was really interesting, possibly not in relation to [child’s name] but in relation, I could relate it to children I had in the past and then I can use everything I’ve learnt for any potential children I get in the future . . . how some children, they don’t want you to physically touch them or go near them and how you can get over that if you do have a child like that . . . I can use everything I have learnt for any future placements that we do have difficulties with.
P8
One carer described that they already transfer the skills to another child in their care:
Yeah I think it does, it makes you notice more about how she is and how she is reacting to things from watching the videos of when you are doing things, so yeah, it does.
P6
Reassurance and confirmation
Not only did the foster carers say that they learnt new skills, they also mentioned the benefits of having the videos to confirm and reassure them that what they already do is on the right track:
There are lots of little strategies that I was using before, that have been reinforced now, to the point of doing all of this and how they react to how I would parent.
P1
It was good to know, you know, that the things I’m doing are correct, it’s nice to be reassured that you’re doing the right things and stuff, so yeah it was good.
P7
. . . actually confirms what you are doing is right and how important it is for that child.
P6
I think it would be good to do that with quite a lot of foster carers, just to reinforce what they are doing, and ‘yeah you are doing the right thing’ and even they might not realise.
P6
Two foster carers mentioned that the intervention helped them to look at and appreciate what they had been doing as foster carers:
Yeah I think it has made me sit up and think ‘wow, look what you’ve done!’.
P2
I watched myself do that and I said to [intervener’s name], ‘wow, I didn’t know I could do that!’.
P4
Learning about the child in my care
Carers also expressed that they felt that the VIPP-FC had provided them with insights and helped them learn about the child in their care:
I mean, I knew that [child’s name] was quite ahead of his age and it’s reinforced that, that he is quite advanced for his age, you know he is 2 and he is counting and colours and all of that and he is quite emotionally, quite stable.
P6
. . . how his smile got bigger when I left him to do his own things and praise him for doing his own thing, rather than me wanting to direct his play, that just sticks in my mind.
P8
Yeah, I realised that she really enjoys reading books a lot more than I thought, because we were reading a book together in the videos and looking at her properly concentrating and you don’t see it when you’re doing it.
P10
Another carer said that the videos helped them to notice more about their foster child’s character:
No, it was interesting to see, like the things she did surprised me in a lot of the ways. And like, she’s quite, like you can see in some of the videos she is quite, thinking about things and then deciding how she is going to react. She’s a lot more switched on than perhaps you might think.
P9
One carer mentioned that the videos showed them that their foster child had perhaps missed out on playing. The carer described it as a ‘massive eye opener to see that he couldn’t sing Row, Row, Row Your Boat’ (P11) and they said that, since the intervention, they have ‘brought out some of the younger toys and we’ve seen he’s interacting better’ (P11).
Seeing something that I would not have noticed otherwise
Closely related to the previous theme, the majority of carers described the video feedback as helping them to see things that they would not otherwise have seen and explained that by watching the videos with the intervener they gained new insights into the child in their care:
you can really pick up things that you are doing that you don’t even realise you are doing, so that’s really . . . I thought that was really good.
P6
There were things that were pointed out to me that I would never, ever have noticed.
P8
It is quite interesting when you watch back, what you can see that you ordinarily wouldn’t . . . And they are the things that you wouldn’t normally see on a day-to-day basis. Yeah, because, I mean, the difference in size; he’s down here and I’m up there and when he’s looking at you or if he’s behind you, you don’t see the expression on his face, you don’t see the little touches that he does or, you know, the extended arm because he wants to have a cuddle, you don’t see that ordinarily. Sometimes you could miss those things.
P1
Two carers mentioned that they noticed that more was happening for the child when they were playing that they had seen before:
I just thought that I was just playing with him [laughs], so yeah I didn’t take, yeah you don’t take those little things, you don’t take notice of them in the day to day . . . so that was really nice.
P8
When you are playing with a child, doing stuff and then when you go through that and talk about it, afterwards you’re noticing things that you don’t notice when you’re playing. You’re noticing the child’s expression, which you might have noticed all the time, you notice when they are happy and when they are pleased, but there are other expressions in there when you are playing that you don’t notice.
P6
One carer described a moment when the intervener helped them to notice and interpret their child’s behaviour in a very different and important way:
I learnt, to be honest with you, I know when, sometimes I don’t always know when [child’s name] is quite nervous, quite stressed a little bit, but we learnt through the sessions, little signs that he gets that I know now, when he does certain things he is going to get stressed and he is going to get worried, like he shakes his leg and I never noticed that before . . . Yeah, I still think about it now because I never picked up on it before, but I do now.
P5
When discussing seeing the connection between the two of them, one carer was asked whether or not they felt that it was the videos that helped them see that and they responded:
Yeah definitely. Definitely, definitely. Yeah, I would never have seen it otherwise.
P2
Seeing the attachment/bond/connection with my child
A number of carers reported that the intervention helped them to realise or become more aware of the special connection or bond that they had with the child in their care. Two carers in particular felt that, through the VIPP-FC, they came to realise how close their relationship was:
And I just thought oh yeah, I didn’t realise I had that effect on her really. It was really lovely to see that she’s made good secure attachment and yeah it was really lovely to see, really lovely.
P2
It’s definitely helped me to look at how I manage [child’s name], and how we’ve grown to love each other and have a really good connection, and, as I said, I didn’t see that, as I said, until I saw the videos, so it was worth it for that.
P2
You know when you sit and see her playing with me, it’s almost like I’m her mum and that she has built such a good relationship and you sort of kind of know it but you don’t really, until you see it . . . but looking back on the videos, every time I thought ‘oh god, she really does like love me’ and I can see that and she loves everything that I do with her and . . . she would look back at me and listen to me differently and she loves me interacting with her and I didn’t realise how much until you saw the videos.
P2
I found them rewarding because I got to see the bond we had rather than, you know, just feel it, so I find it quite rewarding myself.
P7
I knew we had a strong bond because I could feel it, but I hadn’t seen it, and, seeing the videos back, I could actually see the bond being there.
P7
Probably on the first video, when we watched it back, when she actually looked up into my eyes and smiled, that was quite a warm feeling, yeah.
P7
Theme 4: future improvements
The foster carers who received the VIPP-FC as part of the study had a number of thoughts and suggestions for improvements to the project for a study. A number of the foster carers felt that the intervention should be more targeted to carers and children who need it the most. These reflected suggestions about targeting, timing and the need for local authorities to make training such as this part of routine support for foster carers and their foster children.
Targeting (who should receive the intervention)
For some carers who had looked after their child for a long time, there was sometimes a sense that, although the experience of the VIPP-FC had been very positive, their relationship was already well established and it felt less crucial:
I don’t know if it helped because we have got a good one anyway because he has been with us for 6 months anyway so . . . em . . . but I think it would help with a child that has not been with you very long, you know.
P6
One carer described how they perceived two somewhat distinct ways in which the VIPP-FC can be helpful, reflecting earlier themes: first, even in a relationship that is going well, the carer can learn a lot that they can then apply with other children; and, second, there may be relationships in which there is real difficulty present, and the support may be more urgent and more directly helpful to the child. When asked if they would recommend the VIPP-FC, this foster carer said:
Absolutely! Personally, I think it should be rolled out to all foster carers. Probably more focused on the foster carers you pick up, foster carers that do have attachment issues with the child that they have got in placement. Absolutely brilliant for them! For me and [child’s name] yeah I’ve learnt loads and it’s been really good, but for us personally our attachment is already there and I don’t really have to build on an attachment, but I can use everything I have learnt for any future placements that we do have difficulties with. So that has been great for me, but I think a focused approach and rolling it out and going to foster carers would be a huge benefit. I think it would help a lot of placements not break down because once you understand why a child is doing it, then your whole mindset will change and you will look to manage that child in a totally different way. And I think that would be really helpful . . . I think it should be more focused, so you are not using resources when you don’t need to and I think that would be a better use of everything you’ve got in place.
P8
Another foster carer emphasised that they had enjoyed the VIPP-FC process, but it may have been more helpful for a carer who had not had the child as long as she had:
You know, what I did think to myself, I thought for me and my little foster child, it might have been better when she was here before, when she first came into care or a couple of months in, because then her behaviours and the way she managed things were very difficult, whereas she has settled now so I do think there would have been a real big difference in the beginning, even though there was some things we saw in the videos was lovely.
P2
Time between sessions
According to the manual, the period between the VIPP-FC sessions should be 2 weeks; however, owing to a wide variety of factors, this could sometimes be longer or, rarely, shorter. One carer felt that there had been too long between the sessions and that they would have preferred weekly sessions:
That’s the only thing I would say – I’d do it quicker . . . Yeah I think once a week maybe because it’s only an hour, but I know how children do after-school activities, do you know what I mean. So, once a week might be good or probably would have been fine.
P5
Another carer who had received the sessions a week apart described this as a positive:
. . . for her to know that [intervener’s name] is coming the next week is better than leaving it for 2 weeks. So, no I think it worked well.
P2
The intervention should be training
When asked, all foster carers said that they would recommend the VIPP-FC to other carers. There was a general feeling that it should be rolled out; two carers also added that it should be offered in place of training and one even suggested that it should be mandatory:
I don’t know if they should [be] made to do it to be honest, to be honest. It makes you a better foster carer and the child happier, it should be, I don’t know if it can be compulsory, I don’t know, it probably can’t.
P5
Another carer described the training she already had in place:
It’s a 3-month, nurturing attachment course and you go once a week for 3 months, and it’s a classroom environment, and there are psychologists there, and they go through everything that pertains to attachments about, you know, these children with some of the vital building blocks and how to build attachments, and that’s great and you learn a lot, but when you come down to watching these videos back, seeing that put into practice, it all clicks into place and once that has clicked into place you can then approach that child in a totally different manner and it is . . . it is just that, it clicks in your head and you then, you see that child for what they are doing and what they have been through, rather than they are just misbehaving, so the classroom is great, but this is much, much better because you are physically there and you can see it’s relevant to you, it’s you and your child working together with somebody from the outside and they can pick things up where you can’t.
P8
Conclusion
This qualitative study explored the experiences of foster carers taking part in a feasibility study of a modified video-feedback intervention for foster carers, the VIPP-FC. The interviews explored foster carers’ views and thoughts on all stages of the project from initial contact and screening through to engaging with the intervention itself and completing the research outcome assessments. The feedback in general was very positive. The majority of carers spoke about the importance of research and endorsed its valuable contribution towards promoting best practice in the foster care context. Foster carers were generally motivated to join the study because they wished to help the child in their care, to help research and to learn new skills.
When describing their personal experience of the intervention work, foster carers explained that it had a range of benefits. In particular, many carers felt that they had learnt new strategies that were helpful in the here and now, as well as strategies that could be transferable to other children in the future. They felt that the video feedback helped them notice behaviours and signals in the child that they would not have seen otherwise, as well as raising their awareness of their own behaviour and improving the relationship between the carer and child. They greatly valued their relationship with the interveners and were highly positive about how the intervention focuses on the relationship and on what is going well. One foster carer fed back to the study through their intervener that taking part had led them to decide to move towards permanence for the child in their care, having only taken on comparatively short-term placements in the past. When asked, all carers said that they would recommend the intervention and many took the view that the VIPP-FC could, and perhaps should, be used as universal training in the context of foster care. It is critical to note, of course, that the foster carers whom we were able to interview were a small subset of the larger group of foster carers in the study and the views of those with whom we were not able to engage may be quite different from the views presented here. Throughout the project as a whole, a key challenge was recruitment, and so understanding the barriers to engagement for the wider population of foster carers continues to be an important goal for future research.
Chapter 8 General discussion
It is widely recognised that children in foster care are at very heightened risk of poor outcomes, and there are major gaps in the evidence base regarding intervention and prevention strategies to reduce that risk and promote children’s well-being and development. Thus, there is an urgent need for rigorous research to support the provision of effective interventions to improve outcomes for children in foster care. A key domain that is particularly relevant and important in the foster care context is the quality of caregiving and the security of attachment, which is a logical target when attempting to promote foster children’s outcomes and reduce the risk of emotional and behavioural problems. 13 Currently, there is very limited evidence regarding effective programmes for specifically addressing the attachment needs of young children in foster care. At the same time, many researchers working in this field have noted the serious challenges to outcome research inherent in the systems around children in care, which no doubt explains, in part, the relatively scant and methodologically weak evidence base. 53 This feasibility study focused on adapting a parenting intervention designed to improve attachment security to meet the needs and contexts of children in foster care with symptoms of RAD, and conducting initial feasibility work to assess the extent to which a full-scale RCT might be possible. In this chapter, we summarise the main findings and consider the prospect of a definitive trial.
Summary of findings
Phase 1 of the study aimed to refine the Video-feedback Intervention to promote Positive Parenting and Sensitive Discipline, Foster Care (VIPP-FC) programme to the context of children in foster care in the UK. The Manual Development Working Group implemented a series of quite minor changes to the intervention protocol that focused on improving the suitability of the video-feedback intervention for the UK foster care context, and endorsed the content and approach of the intervention. In general, the expert group considered the VIPP-FC to be highly appropriate for use with foster carers and foster children. The enhancements suggested by the expert reference group included changes to the wording of the manual to reflect the fact that some children were cared for by special guardians and kinship carers, adjustments to the use of language to reflect the British context, reduction in the total number of visits from seven to six and a shorter gap between the sessions, adding a games booklet to help carers engage in play, inclusion of a goal-based outcome measure in the intervention to mirror processes routinely used in UK CAMHS and changes in the manual to acknowledge the sometimes time-limited nature of foster care.
Phase 2a of the study consisted of a small case series to road-test the recruitment and screening procedures, as well as the modified VIPP-FC, and to examine its clinical suitability for children with RAD symptoms in real-world clinical practice. The implementation of the case series was challenging, but highlighted many crucial practical issues that needed resolving prior to proceeding to the feasibility trial. A key issue arising from this initial work was that the return rate of screening questionnaires was comparatively low, which was compounded by the fact that a significant proportion of cases could not be approached, as they were deemed inappropriate by the local authority. This is an important consideration for future work because initial estimates of potential samples based on cases held by the local authority may significantly overestimate the effective recruitment pool. Nevertheless, at this stage in the study, the proportion of foster carers returning screening questionnaires was not below the original target, even though the amount of follow-up and support required to achieve this proportion was greater than we had expected. The process observations during this phase highlighted the critical importance of social worker involvement and engagement in the project, which is not easy to achieve because of their heavy case loads. Having a ‘champion’ of the study within the local authority, a high level of visibility of the research team, and additional administrative support to help local authorities contact foster carers and identify cases were noted as important potential solutions to problems with identification and engagement of eligible families.
To further enhance our understanding of the barriers to and constraints of recruitment and intervention, the learning from the case series was complemented by qualitative interviews with stakeholders. These qualitative interviews highlighted the complexity of conducting a RCT in the context of foster care. On the other hand, stakeholders also emphasised the potential benefits of the proposed research, particularly in bringing an effective intervention to this vulnerable population and the potential of the approach to increase foster carer skill and confidence. Stakeholders were generally positive about the VIPP-FC as an intervention: it was felt that this adapted version of the Video-feedback Intervention to promote Positive Parenting and Sensitive Discipline (VIPP-SD) had great potential to be beneficial to the families with whom stakeholders worked. However, greater flexibility in delivery, and especially timing, was considered worthy of further exploration. Stakeholders generated several ideas for tackling some of the barriers to implementing a RCT. A key message was the importance of taking a relational approach, giving time and resources to building relationships with all the key players in the system, especially those at the ‘frontline’.
The final phase (phase 3) of the study consisted of a pilot RCT of the modified VIPP-FC programme. A new group of children was randomised to receive either the VIPP-FC plus CAU or CAU only. The VIPP-FC was delivered in-home by trained CAMHS practitioners or other appropriately qualified VIPP-trained interveners. Baseline and end-of-treatment measures included validated assessments of RAD and co-occurring conditions, security of attachment (including disorganised attachment), sensitivity of parenting, child adjustment, carer well-being and the CA-SUS measure of service use.
Despite implementating a range of changes to the protocol in the light of learning from the case series and stakeholder interviews, the pilot trial encountered significant challenges to recruitment that mirrored our experiences during the case series. The most significant barriers were encountered during the initial stages of contact with foster carers. The overall number of mailed-out questionnaires, n = 336, was smaller than the original target of 500, largely due to significant numbers of children registered with the local authorities being considered inappropriate or ineligible for the study. The overall response rate to the screening questionnaires was low (indeed, considerably lower than in the case series), at 29%, and varied substantially by site. We were unable to recruit the target sample size of 40, even after numerous initiatives were introduced to increase recruitment, including, in stages, allowing online screening, engaging additional sites and, finally, allowing all children in foster care to enter the study even if RAD diagnostic criteria were not met. By the end of the study, we were able to recruit three-quarters of the target sample size to the feasibility trial. Of the randomised families, 15 were allocated to the VIPP-FC and 15 continued to receive usual care.
Notwithstanding the difficulties with recruitment, many other features of the pilot trial design worked well. The screening tools performed well in identifying potentially eligible participants, demonstrating good convergence and sensitivity against the research diagnostic interview. We achieved good outcome data completeness and all of the participants who received the treatment completed all sessions. The implications were quite clear: the intervention itself and the research protocol for evaluating its impact were robust and implementable to a high degree of rigour, but recruitment problems could not be fully surmounted.
In addition to the questions regarding the feasibility of implementation of a RCT of the VIPP-FC, we undertook important feasibility work linked to health economic evaluation. This had two main aims. The first involved the modification and testing of an appropriate version of the CA-SUS for the collection of service use data in this population. The results showed that the modified CA-SUS, after some adjustments, worked well and was acceptable to both interviewers and interviewees. The second aim was to explore the recent literature to assess how realistic it might be to include a measure of HRQoL capable of generating QALYs, for use in a cost–utility analysis, in this very young age group. Results indicated that it is not currently possible to recommend any specific measures for inclusion in a future trial of the VIPP-FC; thus, the primary economic evaluation should be a cost-effectiveness analysis using the primary clinical outcome measure or using an assessment of meaningful change on the primary clinical outcome measure. It was further recommended that a future trial of the VIPP-FC may be a good opportunity to compare the construct validity and sensitivity to change of the proxy versions of existing instruments by exploring the relationship of these measures with clinical outcomes.
In the final stage of the study, foster carers who had received the modified VIPP-FC took part in qualitative interviews to explore their experiences of the intervention. In general, foster carers’ experiences of the VIPP-FC were very positive. Foster carers endorsed the importance of the research and its valuable contribution towards promoting best practice in the foster care context. Foster carers described a range of benefits associated with receiving the intervention programme, from enhanced skills to improved relationship with their child, and found it acceptable and helpful.
Considerations regarding progression to a full trial
Within the TSC and among stakeholders, there was a clear steer that progressing this work is important and should be considered seriously, despite the challenges of recruitment. The results of the feasibility trial indicated very strongly that the research protocol itself was feasible. In the course of the study, we developed a robust protocol for managing consent, for intervention delivery and for assessing outcomes. We did not encounter any difficulties with randomisation. We were able to identify good candidate measures for screening and for outcome evaluation, and were able to recommend the DAI as a robust primary outcome measure, as it showed high levels of acceptability, adequate range and indications of sensitivity to change (significant reductions overall from pre treatment to follow-up). The rate of follow-up to post treatment was high and engagement in treatment was good. The fundamental barrier to progression to a full-scale trial is recruitment. As noted in Chapter 5, there are clear indications about the most important ingredients that make up a successful site and knowing those could allow the active identification and selection of such sites from the outset. Doing so ought to make consistent recruitment at the rate we observed in the final stages of the pilot study feasible. In that regard, one strategy to consider for a future trial is careful selection of sites based on research capability. However, we note a clear downside of such an approach, which is that it may bias both the populations of foster families included in the trial and the service contexts in which trial delivery would take place, thereby limiting generalisability. With that in mind, we also identified a range of factors that could significantly enhance recruitment and could provide routes to more effective recruitment in the future. Owing to a lack of resource, we could not easily implement all of these adjustments during the course of the study. Most important among these is the provision of administrative capacity in local authorities to manage and support recruitment, as well as additional capacity in the research team to allow researchers to be present in each recruitment site to a greater degree. Given the highly vulnerable nature of this population, the feasibility of most elements of the trial protocol, the high levels of acceptability of the VIPP-FC and the good evidence of its efficacy in other broadly similar populations, we believe that it is imperative to find ways to resolve these systemic problems with recruitment.
Research recommendations
On the basis of the above considerations, we make the following recommendations:
-
A RCT is an appropriate design to evaluate the VIPP-FC in the foster care context.
-
Drawing on evidence from this study and a number of other sources, we consider the DAI symptom count to be an appropriate primary outcome for such a trial.
-
A range of other measures, including continuous RAD symptom questionnaires, the Strange Situation Procedure, measures of child adjustment, parenting sensitivity and carer burden, are feasible and appropriate secondary outcomes in a randomised trial.
-
We are not able to recommend online data collection as a method for obtaining baseline and follow-up assessments.
-
The primary economic evaluation of such a trial should be a cost-effectiveness analysis using the DAI or using an assessment of meaningful change in the DAI.
-
In the light of the large proportion of children in foster care showing RAD symptoms and the challenging nature of recruitment, a future trial should not select participants on the basis of RAD diagnosis, but instead address the efficacy of the VIPP-FC for children in foster care in general, measuring RAD symptoms as the primary outcome.
-
We obtained an estimate of the SD of the DAI of 4.16 points in the foster care population, with an upper 80% confidence limit of 5.2 points. We suggest that a difference of 2 points on the DAI is a minimum clinically significant difference, which equates to a standardised effect size of approximately d = 0.40. To detect such an effect size with 80% power at α = 0.05 and an equal allocation ratio would require a minimum sample size of 200 participants. A sample size of 266 would be required for 90% power.
-
A randomised trial should not proceed until more robust recruitment procedures can be established. Recruitment should be supported by adequate resourcing within local authorities, high levels of engagement of social work teams and should involve direct contact between the research team and all eligible foster carers (e.g. during joint home visits with social workers).
As recruitment was by far the most significant barrier to a robust trial, researchers may wish to consider a range of alternative recruitment and sampling strategies. One alternative strategy suggested by our research team is to consider extending recruitment to children who have been adopted, who present with similar rates of attachment difficulties to those of children in foster care and whose adoptive parents are typically highly motivated to receive support. 17 It is also noteworthy that, although we encouraged local authorities to consider recruiting special guardians and friends and family carers to take part in the trial, many did not, largely because SGOs tended to be managed by different teams. More active engagement of these groups of carers in a future trial may also markedly increase the total pool from which recruits can be drawn. We also take the view that it may be worth considering implementing a trial of the VIPP-FC as part of universal foster carer training, which would largely remove most barriers to recruitment. Feedback we received during the study from stakeholders and foster carers provided considerable initial support for this suggestion, as both groups noted that ‘live’ training in attachment principles may be more effective as a means of enhancing foster carers’ professional skills than more pedagogical approaches commonly used in the foster care sector, while also providing more immediate and direct benefit to children.
Acknowledgements
First and foremost, we would like to thank and acknowledge the foster and kinship carers, the children who participated in this study, and the parents and social workers who consented to their participation. We acknowledge the support and collaboration of the children’s services from all of the participating local authorities, the practitioners from involved CAMHS and all other VIPP interveners. We would like to thank the patient and public involvement group members for their input at all stages of the study. We would also like to acknowledge the students and research assistants who contributed to data collection and coding. Finally, we would like to acknowledge the contribution of the clinical trials co-ordinators at Imperial College London.
Contributions of authors
Paula Oliveira (https://orcid.org/0000-0003-1523-8225) (Senior Research Fellow) was responsible for the day-to-day running of the project and data collection and analysis, and co-wrote the final report.
Eloise Stevens (https://orcid.org/0000-0001-7671-3670) (Trial Co-ordinator and Early Years Therapist and Trainer) led the treatment allocation and clinical delivery, as well as supervision of treatments.
Lydia Barge (https://orcid.org/0000-0001-9568-5417) (Doctoral Student) contributed to data collection and the day-to-day running of the project, conducted the qualitative study presented in Chapter 7 and wrote Chapter 7.
Julie Comyn (https://orcid.org/0000-0001-8143-8394) (Doctoral Student) and Kirsty Langley (https://orcid.org/0000-0002-8997-5060) (Doctoral Student) collected and analysed the qualitative data in Chapter 4 and drafted Chapter 4.
Paul Ramchandani (https://orcid.org/0000-0003-3646-2410) (LEGO Professor of Play in Education, Development and Learning), Barry Wright (https://orcid.org/0000-0002-8692-6001) (Professor of Child Mental Health), Matt Woolgar (https://orcid.org/0000-0002-3618-0395) (Consultant Clinical Psychologist and Senior Researcher) and Eilis Kennedy (https://orcid.org/0000-0002-4162-4974) (Consultant Child and Adolescent Psychiatrist and Trust Director of Research and Development) contributed to the study design and delivery and commented on early versions of the final report.
Sarah Byford (https://orcid.org/0000-0001-7084-1495) (Professor of Health Economics) planned, analysed and wrote Chapter 6 and commented on early versions of the final report.
James Shearer (https://orcid.org/0000-0002-1658-9767) (Lecturer in Health Economics) planned, analysed and wrote Chapter 6.
Stephen Scott (https://orcid.org/0000-0003-4680-6213) (Professor of Child Health and Behaviour), Jane Barlow (https://orcid.org/0000-0001-8418-4270) (Professor of Evidence Based Intervention and Policy Evaluation), Danya Glaser (https://orcid.org/0000-0002-8786-1377) (Visiting Professor and Honorary Consultant Child and Adolescent Psychiatrist), Rob Senior (https://orcid.org/0000-0003-3282-0428) (Medical Director and Consultant Child and Adolescent Psychiatrist) and Peter Fonagy (https://orcid.org/0000-0003-0229-0091) (Head of the Division of Psychology and Language Sciences at UCL and Chief Executive at the Anna Freud National Centre for Children and Families) contributed to the study design and delivery and commented on early versions of the final report.
Pasco Fearon (https://orcid.org/0000-0003-1847-8443) (Chair in Developmental Psychopathology) managed the study overall, supervised the research team, liaised with trusts and local authorities, designed the study and co-wrote the final report.
Publication
Oliveira P, Barge L, Stevens E, Byford S, Shearer J, Spies R, et al. Children in foster care with symptoms of reactive attachment disorder: feasibility randomised controlled trial of a modified video-feedback parenting intervention. BJPsych Open 2022;8:e134.
Data-sharing statement
All data requests should be submitted to the corresponding author for consideration.
Patient data
This work uses data provided by patients and collected by the NHS as part of their care and support. Using patient data is vital to improve health and care for everyone. There is huge potential to make better use of information from people’s patient records, to understand more about disease, develop new treatments, monitor safety, and plan NHS services. Patient data should be kept safe and secure, to protect everyone’s privacy, and it’s important that there are safeguards to make sure that it is stored and used responsibly. Everyone should be able to find out about how patient data are used. #datasaveslives You can find out more about the background to this citation here: https://understandingpatientdata.org.uk/data-citation.
Disclaimers
This report presents independent research funded by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the HTA programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, the HTA programme or the Department of Health and Social Care.
References
- Ford T, Vostanis P, Meltzer H, Goodman R. Psychiatric disorder among British children looked after by local authorities: comparison with children living in private households. Br J Psychiatry 2007;190:319-25. https://doi.org/10.1192/bjp.bp.106.025023.
- Tarren-Sweeney M, Hazell P. Mental health of children in foster and kinship care in New South Wales, Australia. J Paediatr Child Health 2006;42:89-97. https://doi.org/10.1111/j.1440-1754.2006.00804.x.
- Luke N, Sinclair I, Woolgar M, Sebba J. What Works in Preventing and Treating Poor Mental Health in Looked After Children? 2014. https://mhinnovation.net/sites/default/files/downloads/resource/What%20works%20in%20preventing%20treating%20mental%20health%20looked%20after%20children%20report.pdf (accessed 25 March 2020).
- Department for Education . Children Looked After in England (Including Adoption) 2018–2019 2019. https://gov.uk/government/statistics/children-looked-after-in-england-including-adoption-2018-to-2019 (accessed 25 March 2020).
- Zeanah CH, Scheeringa M, Boris NW, Heller SS, Smyke AT, Trapani J. Reactive attachment disorder in maltreated toddlers. Child Abuse Negl 2004;28:877-88. https://doi.org/10.1016/j.chiabu.2004.01.010.
- Bowlby J. Attachment and Loss, Volume I: Attachment. New York, NY: Basic Books; 1969.
- Fearon RMP, Groh AM, Bakermans-Kranenburg MJ, van IJzendoorn MH, Roisman GI, Cicchetti D. Developmental Psychopathology, Volume One: Theory and Method. New York, NY: John Wiley & Sons, Inc.; 2016.
- Zeanah CH, Gleason MM. Annual research review: attachment disorders in early childhood – clinical presentation, causes, correlates, and treatment. J Child Psychol Psychiatry 2015;56:207-22. https://doi.org/10.1111/jcpp.12347.
- Fearon RP, Bakermans-Kranenburg MJ, van Ijzendoorn MH, Lapsley AM, Roisman GI. The significance of insecure attachment and disorganization in the development of children’s externalizing behavior: a meta-analytic study. Child Dev 2010;81:435-56. https://doi.org/10.1111/j.1467-8624.2009.01405.x.
- Rutter M, Kreppner J, Sonuga-Barke E. Emanuel Miller lecture: attachment insecurity, disinhibited attachment, and attachment disorders: where do research findings leave the concepts?. J Child Psychol Psychiatry 2009;50:529-43. https://doi.org/10.1111/j.1469-7610.2009.02042.x.
- Groh AM, Fearon RP, Bakermans-Kranenburg MJ, van Ijzendoorn MH, Steele RD, Roisman GI. The significance of attachment security for children’s social competence with peers: a meta-analytic study. Attach Hum Dev 2014;16:103-36. https://doi.org/10.1080/14616734.2014.883636.
- Groh AM, Roisman GI, van Ijzendoorn MH, Bakermans-Kranenburg MJ, Fearon RP. The significance of insecure and disorganized attachment for children’s internalizing symptoms: a meta-analytic study. Child Dev 2012;83:591-610. https://doi.org/10.1111/j.1467-8624.2011.01711.x.
- National Institute for Health and Care Excellence (NICE) . Children’s Attachment: Attachment in Children and Young People Who Are Adopted from Care, in Care or at High Risk of Going into Care. NICE Guideline [NG26] 2015. https://nice.org.uk/guidance/ng26 (accessed 25 March 2020).
- Diagnostic and Statistical Manual of Mental Disorders. Arlington, VA: American Psychiatric Association; 2013.
- Lyons-Ruth K. Commentary: should we move away from an attachment framework for understanding disinhibited social engagement disorder (DSED)? A commentary on Zeanah and Gleason (2015). J Child Psychol Psychiatry 2015;56:223-7. https://doi.org/10.1111/jcpp.12373.
- van Ijzendoorn MH, Schuengel C, Bakermans-Kranenburg MJ. Disorganized attachment in early childhood: meta-analysis of precursors, concomitants, and sequelae. Dev Psychopathol 1999;11:225-49. https://doi.org/10.1017/s0954579499002035.
- van den Dries L, Juffer F, van IJzendoorn MH, Bakermans-Kranenburg MJ. Fostering security? A meta-analysis of attachment in adopted children. Child Youth Serv Rev 2009;31:410-21. https://doi.org/10.1016/j.childyouth.2008.09.008.
- Bakermans-Kranenburg MJ, van IJzendoorn MH, Juffer F. Less is more: meta-analyses of sensitivity and attachment interventions in early childhood. Psychol Bull 2003;129:195-21. https://doi.org/10.1037/0033-2909.129.2.195.
- Wright B, Barry M, Hughes E, Trépel D, Ali S, Allgar V, et al. Clinical effectiveness and cost-effectiveness of parenting interventions for children with severe attachment problems: a systematic review and meta-analysis. Health Technol Assess 2015;19. https://doi.org/10.3310/hta19520.
- Bernard K, Dozier M, Bick J, Lewis-Morrarty E, Lindhiem O, Carlson E. Enhancing attachment organization among maltreated children: results of a randomized clinical trial. Child Dev 2012;83:623-36. https://doi.org/10.1111/j.1467-8624.2011.01712.x.
- Juffer F, Bakermans-Kranenburg MJ, van IJzendoorn MH. Promoting Positive Parenting: An Attachment-Based Intervention. New York, NY: Taylor & Francis Group/Lawrence Erlbaum Associates Routledge; 2008.
- Moss E, Dubois-Comtois K, Cyr C, Tarabulsy GM, St-Laurent D, Bernier A. Efficacy of a home-visiting intervention aimed at improving maternal sensitivity, child attachment, and behavioral outcomes for maltreated children: a randomized control trial. Dev Psychopathol 2011;23:195-210. https://doi.org/10.1017/S0954579410000738.
- Juffer F, Bakermans-Kranenburg MJ, van IJzendoorn MH. Pairing attachment theory and social learning theory in video-feedback intervention to promote positive parenting. Curr Opin Psychol 2017;15:189-94. https://doi.org/10.1016/j.copsyc.2017.03.012.
- Juffer F, Bakermans-Kranenburg MJ, van IJzendoorn MH, Steele H, Steele M. Handbook of Attachment-Based Interventions. New York, NY: Guilford Press; 2018.
- Ramchandani PG, O’Farrelly C, Babalis D, Bakermans-Kranenburg MJ, Byford S, Grimas ESR, et al. Preventing enduring behavioural problems in young children through early psychological intervention (Healthy Start, Happy Start): study protocol for a randomized controlled trial. Trials 2017;18. https://doi.org/10.1186/s13063-017-2293-9.
- Schoemaker NK, Juffer F, Rippe RC, Vermeer HJ, Stoltenborgh M, Jagersma GJ, et al. Positive parenting in foster care: testing the effectiveness of a video-feedback intervention program on foster parents’ behavior and attitudes. Child Youth Serv Rev 2020;110. https://doi.org/10.1016/j.childyouth.2020.104779.
- National Institute for Health and Care Excellence (NICE) . Looked-After Children and Young People. Public Health Guideline [PH28] 2010. https://nice.org.uk/guidance/ph28 (accessed 25 March 2020).
- Schoemaker NK, Jagersma G, Stoltenborgh M, Maras A, Vermeer HJ, Juffer F, et al. The effectiveness of Video-feedback Intervention to promote Positive Parenting for Foster Care (VIPP-FC): study protocol for a randomized controlled trial. BMC Psychol 2018;6. https://doi.org/10.1186/s40359-018-0246-z.
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Medical Research Council Guidance . Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ 2008;337. https://doi.org/10.1136/bmj.a1655.
- Great Britain . Data Protection Act 1998 1998.
- European Parliament, Council of the European Union . Regulation on the Protection of Natural Persons With Regard to the Processing of Personal Data and on the Free Movement of Such Data, and Repealing Directive 95 46 EC (Data Protection Directive) 2018.
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009;42:377-81. https://doi.org/10.1016/j.jbi.2008.08.010.
- Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O’Neal L, et al. The REDCap consortium: building an international community of software partners. J Biomed Inform 2019;95. https://doi.org/10.1016/j.jbi.2019.103208.
- National Institute for Health and Care Research (NIHR) . INVOLVE: Payment and Recognition for Public Involvement n.d. https://invo.org.uk/resource-centre/payment-and-recognition-for-public-involvement/ (accessed 5 July 2018).
- Bogolub EB, Thomas N. Parental consent and the ethics of research with foster children: beginning a cross-cultural dialogue. Qual Soc Work 2005;4:271-92. https://doi.org/10.1177/1473325005055592.
- Great Britain . Children Act 1989 1989.
- Ainsworth MDS, Blehar MC, Waters E, Wall S. Patterns of Attachment: A Psychological Study of the Strange Situation. Hillsdale, NJ: Lawrence Erlbaum; 1978.
- Goodman R, Ford T, Richards H, Gatward R, Meltzer H. The development and well‐being assessment: description and initial validation of an integrated assessment of child and adolescent psychopathology. J Child Psychol 2000;41:645-55. https://doi.org/10.1111/j.1469-7610.2000.tb02345.x.
- Smyke AT, Dumitrescu A, Zeanah CH. Attachment disturbances in young children. I: the continuum of caretaking casualty. J Am Acad Child Adolesc Psychiatry 2002;41:972-82. https://doi.org/10.1097/00004583-200208000-00016.
- Zeanah CH, Smyke AT, Dumitrescu A. Attachment disturbances in young children. II: indiscriminate behavior and institutional care. J Am Acad Child Adolesc Psychiatry 2002;41:983-9. https://doi.org/10.1097/00004583-200208000-00017.
- Oosterman M, Schuengel C. Physiological effects of separation and reunion in relation to attachment and temperament in young children. Dev Psychobiol 2007;49:119-28. https://doi.org/10.1002/dev.20207.
- Oliveira PS, Fearon RMP, Belsky J, Fachada I, Soares I. Quality of institutional care and early childhood development. Int J Behav Dev 2015;39:161-70. https://doi.org/10.1177/0165025414552302.
- Soares I, Belsky J, Oliveira P, Silva J, Marques S, Baptista J, et al. Does early family risk and current quality of care predict indiscriminate social behavior in institutionalized Portuguese children?. Attach Hum Dev 2014;16:137-48. https://doi.org/10.1080/14616734.2013.869237.
- Achenbach TM, Rescorla LA. Manual for the ASEBA Preschool Forms and Profiles. Burlington, VT: University of Vermont Department of Psychiatry; 2000.
- National Institute of Child Health and Human Development (NICHD) Early Child Care Network . The NICHD Study of Early Child Care and Youth Development: Findings for Children up to Age 4 1 2 Years 2006. https://nichd.nih.gov/sites/default/files/publications/pubs/documents/seccyd_06.pdf (accessed 25 March 2020).
- Abidin RR. Parenting Stress Index: (Short Form). Charlottesville, VA: Pediatric Psychology Press; 1990.
- Woolgar M, Beckett C, Falconer S, Humayun S, Marsden A, Scott S, et al. A New Brief Measure of Parental Efficacy for Parenting Practitioners. London: Department of Child and Adolescent Psychiatry/National Academy of Parenting Practitioners; 2012.
- Barrett B, Byford S, Chitsabesan P, Kenning C. Mental health provision for young offenders: service use and cost. Br J Psychiatry 2006;188:541-6. https://doi.org/10.1192/bjp.bp.105.010108.
- Longhi E, Murray L, Hunter R, Wellsted D, Taylor-Colls S, MacKenzie K, et al. The NSPCC UK Minding the Baby® (MTB) home-visiting programme, supporting young mothers (aged 14–25) in the first 2 years of their baby’s life: study protocol for a randomised controlled trial. Trials 2016;17. https://doi.org/10.1186/s13063-016-1618-4.
- Midgley N, Besser SJ, Fearon P, Wyatt S, Byford S, Wellsted D. The Herts and Minds study: feasibility of a randomised controlled trial of mentalization-based treatment versus usual care to support the wellbeing of children in foster care. BMC Psychiatry 2019;19. https://doi.org/10.1186/s12888-019-2196-2.
- Beidas RS, Stewart RE, Adams DR, Fernandez T, Lustbader S, Powell BJ, et al. A multi-level examination of stakeholder perspectives of implementation of evidence-based practices in a large urban publicly-funded mental health system. Adm Policy Ment Health 2016;43:893-908. https://doi.org/10.1007/s10488-015-0705-2.
- Dale H, Watson L. Exploring the barriers and facilitators to health research with children and young people who are looked after. Scott J Resid Child Care 2010;9:37-43.
- Dixon J, Biehal N, Green J, Sinclair I, Kay C, Parry E. Trials and tribulations: challenges and prospects for randomised controlled trials of social work with children. Br J Soc Work 2014;44:1563-81. https://doi.org/10.1093/bjsw/bct035.
- Murphy A, McDonald J. Power, status and marginalisation: rural social workers and evidence-based practice in multidisciplinary teams. Aust Soc Work 2004;57:127-36. https://doi.org/10.1111/j.1447-0748.2004.00127.x.
- Mezey G, Robinson F, Campbell R, Gillard S, Macdonald G, Meyer D, et al. Challenges to undertaking randomised trials with looked after children in social care settings. Trials 2015;16. https://doi.org/10.1186/s13063-015-0708-z.
- Macdonald G, Davies H, Nutley S, Smith P. What Works? Evidence-Based Policy and Practice in Public Service. Bristol: Policy Press; 2000.
- Gilbertson R, Barber JG. Obstacles to involving children and young people in foster care research. Child Fam Soc Work 2002;7:253-8. https://doi.org/10.1046/j.1365-2206.2002.00251.x.
- Goodkind JR, Amer S, Christian C, Hess JM, Bybee D, Isakson BL, et al. Challenges and innovations in a community-based participatory randomized controlled trial. Health Educ Behav 2017;44:123-30. https://doi.org/10.1177/1090198116639243.
- Gray M, Joy E, Plath D, Webb SA. Opinions about evidence: a study of social workers’ attitudes towards evidence-based practice. J Soc Work 2014;14:23-40. https://doi.org/10.1177/1468017313475555.
- Flynn PM, Brown BS. Implementation research: issues and prospects. Addict Behav 2011;36:566-9. https://doi.org/10.1016/j.addbeh.2010.12.020.
- Medical Research Council . Developing and Evaluating Complex Interventions: New Guidance 2006. www.mrc.ac.uk/complexinterventionsguidance (accessed 25 March 2020).
- Hickey G, McGilloway S, O’Brien M, Leckey Y, Devlin M, Donnelly M. Strengthening stakeholder buy-in and engagement for successful exploration and installation: a case study of the development of an area-wide, evidence-based prevention and early intervention strategy. Child Youth Serv Rev 2018;91:185-95. https://doi.org/10.1016/j.childyouth.2018.06.008.
- Smith JA, Smith JA, Harre R, van Langenhove L. Rethinking Methods in Psychology. London: SAGE Publications Ltd; 1995.
- Breakwell G, Smith JA, Wright DB. Research Methods in Psychology. London: SAGE Publications Ltd; 2012.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol 2006;3:77-101. https://doi.org/10.1191/1478088706qp063oa.
- Barker C, Pistrang N. Quality criteria under methodological pluralism: implications for conducting and evaluating research. Am J Community Psychol 2005;35:201-12. https://doi.org/10.1007/s10464-005-3398-y.
- Elliott R, Fischer CT, Rennie DL. Evolving guidelines for publication of qualitative research studies in psychology and related fields. Br J Clin Psychol 1999;38:215-29. https://doi.org/10.1348/014466599162782.
- Bronfenbrenner U. The Ecology of Human Development: Experiments by Nature and Design. Cambridge, MA: Harvard University Press; 1979.
- Langley AK, Nadeem E, Kataoka SH, Stein BD, Jaycox LH. Evidence-based mental health programs in schools: barriers and facilitators of successful implementation. School Ment Health 2010;2:105-13. https://doi.org/10.1007/s12310-010-9038-1.
- Wade A, Pan H, Eaton S, Pierro A, Ong E. An investigation of minimisation criteria. BMC Med Res Methodol 2006;6. https://doi.org/10.1186/1471-2288-6-11.
- Department for Education . Statistics: Looked-After Children n.d. https://gov.uk/government/collections/statistics-looked-after-children (accessed 25 March 2020).
- Briskman J, Castle J, Blackeby K, Bengo C, Slack K, Stebbens C, et al. Randomised Controlled Trial of the Fostering Changes Programme 2012. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/183398/DFE-RR237.pdf (accessed 25 March 2020).
- Oliveira P, Barge L, Stevens E, Byford S, Shearer J, Spies R, et al. Children in foster care with symptoms of reactive attachment disorder: feasibility randomised controlled trial of a modified video-feedback parenting intervention. BJPsych Open 2022;8. https://doi.org/10.1192/bjo.2022.538.
- Murphy E. Social-Emotional Under 4’s Screening &Amp; Intervention S.U.S.I. (SUSI) 2016. https://clinicaltrials.gov/ct2/show/NCT02151955 (accessed 25 March 2020).
- Byford S, Cary M, Barrett B, Aldred CR, Charman T, Howlin P, et al. Cost-effectiveness analysis of a communication-focused therapy for pre-school children with autism: results from a randomised controlled trial. BMC Psychiatry 2015;15. https://doi.org/10.1186/s12888-015-0700-x.
- Rowen D, Rivero-Arias O, Devlin N, Ratcliffe J. Review of valuation methods of preference-based measures of health for economic evaluation in child and adolescent populations: where are we now and where are we going?. Pharmacoeconomics 2020;38:325-40. https://doi.org/10.1007/s40273-019-00873-7.
- Khadka J, Kwon J, Petrou S, Lancsar E, Ratcliffe J. Mind the (inter-rater) gap. An investigation of self-reported versus proxy-reported assessments in the derivation of childhood utility values for economic evaluation: a systematic review. Soc Sci Med 2019;240. https://doi.org/10.1016/j.socscimed.2019.112543.
- Kwon J, Kim SW, Ungar WJ, Tsiplova K, Madan J, Petrou S. A systematic review and meta-analysis of childhood health utilities. Med Decis Making 2018;38:277-305. https://doi.org/10.1177/0272989X17732990.
- Devlin N, Norman R, Ratcliffe J, Mulhern B, Dalziel K, Chen G, et al. Do Child QALYs = Adult QALYs? Five Reasons Why They Might Not 2020. https://ohe.org/news/do-child-qalys-adult-qalys-five-reasons-why-they-might-not (accessed 25 March 2020).
- Jabrayilov R, Vermeulen KM, Detzel P, Dainelli L, van Asselt ADI, Krabbe PFM. Valuing health status in the first year of life: the Infant Health-Related Quality of Life instrument. Value Health 2019;22:721-7. https://doi.org/10.1016/j.jval.2018.12.009.
- National Institute for Health and Care Excellence (NICE) . Guide to the Methods of Technology Appraisal 2013 n.d. www.nice.org.uk/process/pmg9/ (accessed 25 March 2020).
- National Institute for Health and Care Excellence (NICE) . Changes to Health Technology Evaluation 2020. https://nice.org.uk/about/what-we-do/our-programmes/nice-guidance/nice-technology-appraisal-guidance/changes-to-health-technology-evaluation (accessed 25 March 2020).
- van Reenen M, Janssen B, Oppe M, Kreimeier S, Greiner W. EQ-5D-Y User Guide 2014. https://euroqol.org/eq-5d-instruments/eq-5d-y-about/valuation/ (accessed 25 March 2020).
Appendix 1 Ethics amendments
| Amendment | Date approved | Reasons |
|---|---|---|
| SA1 | February 2018 |
|
| SA2 | September 2018 |
|
| SA3 | March 2019 |
|
| NSA1 | December 2017 | Addition of site 7 |
| NSA2 | March 2018 | Addition of site 6 |
| NSA3 | May 2018 |
|
| NSA4 | December 2018 |
|
| NSA5 | August 2019 | Extension of study dates |
Appendix 2 Child and Adolescent Service Use Schedule
List of abbreviations
- ASA
- Attachment Screening Assessment
- AUC
- area under the curve
- CA-SUS
- Child and Adolescent Service Use Schedule
- CAMHS
- Child and Adolescent Mental Health Services
- CAU
- care as usual
- CBCL
- Child Behavior Checklist
- CHU-9D
- Child Health Utility Index-9 Dimensions
- CI
- confidence interval
- CONSORT
- Consolidated Standards of Reporting Trials
- DAI
- Disturbances of Attachment Interview
- DAWBA
- Development and Well-Being Assessment
- DMEC
- Data Monitoring and Ethics Committee
- DSED
- disinhibited social engagement disorder
- DSM-5
- Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition
- EQ-5D-Y
- EuroQol-5 Dimensions-Youth version
- GP
- general practitioner
- HRQoL
- health-related quality of life
- HTA
- Health Technology Assessment
- NICE
- National Institute for Health and Care Excellence
- NICHD
- National Institute of Child Health and Human Development
- NIHR
- National Institute for Health and Care Research
- Ofsted
- Office for Standards in Education, Children’s Services and Skills
- QALY
- quality-adjusted life-year
- RAD
- reactive attachment disorder
- RCT
- randomised controlled trial
- ROC
- receiver operating characteristic
- SD
- standard deviation
- SDQ
- Strengths and Difficulties Questionnaire
- SGO
- special guardianship order
- TSC
- Trial Steering Committee
- UCL
- University College London
- VIPP-FC
- Video-feedback Intervention to promote Positive Parenting and Sensitive Discipline, Foster Care
- VIPP-SD
- Video-feedback Intervention to promote Positive Parenting and Sensitive Discipline