
Notes
Article history
The research reported in this issue of the journal was commissioned and funded by the HTA programme on behalf of NICE as project number 08/36/01. The protocol was agreed in September 2008. The assessment report began editorial review in May 2009 and was accepted for publication in August 2009. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and would like to thank the referees for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
None
Permissions
Copyright statement
© 2010 Queen’s Printer and Controller of HMSO. This journal may be freely reproduced for the purposes of private research and study and may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NETSCC, Health Technology Assessment, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2010 Queen’s Printer and Controller of HMSO
Chapter 1 Background
Description of underlying health problem
Lung cancer can be categorised into four major cell types: small cell lung cancer (SCLC), squamous cell carcinoma (SCC), adenocarcinoma (AC) and large cell carcinoma. 1 The last three cell types are most often described as ‘non-small cell lung cancer’ (NSCLC). SCLCs are usually centrally located, with extensive mediastinal involvement, tend to grow rapidly and spread quickly to distant sites (metastases). 2 SCLC is typically classified using a two-stage system: limited-stage disease and extensive-stage disease, according to the level of progression of the disease. Limited-stage disease is generally confined to one hemithorax and its regional lymph nodes, in the absence of malignant effusion, and can be encompassed in one radiotherapy port. Extensive-stage disease is disease beyond the confines of the thorax at diagnosis, with the presence of systemic metastases, and cannot be encompassed safely in one radiotherapy port. 3 The prognosis for patients with extensive-stage disease is much poorer than for those with limited-stage disease. Most SCLCs present with metastases – a recent review found that two-thirds of patients have extensive disease on presentation. 4
In most patients the disease is symptomatic on presentation. In some, there are non-specific symptoms such as fatigue, anorexia, and weight loss, whereas in others there are more direct signs and symptoms, such as breathlessness, chest discomfort and haemoptysis (blood-stained sputum). 2 SCLC is also associated with systemic symptoms that are related to paraneoplastic syndromes. 5 These are caused by the release of bioactive substances produced by the tumour, or in response to the tumour,2 and include endocrine syndromes and neurological syndromes. 5 The most common endocrine syndrome in SCLC is inappropriate secretion of antidiuretic hormone (leading to water retention), hyponatraemia (low sodium), and hypotension (low blood pressure). Digital clubbing and hypertrophic pulmonary osteoarthropathy are common skeletal manifestations. 2
Small cell lung cancer is initially very sensitive to chemotherapy, with 60–90% of patients with limited-stage disease responding to first-line therapy, and 40–70% of patients achieving a complete response (CR) (no further evidence of disease). 6 For extensive-stage disease, approximately 50–85% of patients respond to first-line therapy. 7
Aetiology
Risk factors for lung cancer include tobacco exposure, occupational exposure, gender, diet and chronic lung disease. Smoking is the leading cause of lung cancer, accounting for approximately 80–90% of cases,8,9 although it is likely that the cause of lung cancer is multifactorial and involves more than a simple association with smoking. 10 When compared with people who have never smoked, those who have smoked without quitting successfully have a 20-fold increase in lung cancer risk. 11 The risk for lung cancer among cigarette smokers increases with the duration of smoking and the number of cigarettes smoked per day. 11 The association with smoking has been shown to be much stronger in SCLC than NSCLCs in a meta-analysis. 12 Passive smoking [referred to as environmental tobacco smoke (ETS)] is also associated with lung cancer, albeit more weakly than active smoking. 8
Lung cancer was initially seen at higher rates in males, being associated with an earlier start of smoking tobacco and the higher quantities of tobacco smoked. 8,10 However, the disease has been declining in recent years in males, but increasing in women, most likely due to changes in smoking practices. 10,12 Whether men and women differ in their susceptibility to the carcinogens in tobacco smoke remains the focus of controversy. Some studies report that women who smoke have a significantly larger relative increase in lung cancer risk than men. 13 Other studies, however, have found that there do not appear to be differences between men and women in their susceptibility to lung cancer, given comparable smoking histories. 12,14 A recent cohort study13 of 279,214 men and 184,623 women, for example, suggests that women are not more susceptible than men to the carcinogenic effects of cigarette smoking.
Occupational exposure to compounds such as asbestos, radon, chromium and nickel has also been recognised to be a risk factor for lung cancer. 15 A diet that is rich in fruits and vegetables is associated with a reduced risk of lung cancer in smokers, ex-smokers and those who have never smoked. 8,16 Some studies have also shown an association between dietary beta-carotene intake and a lower risk of lung cancer. 8 However, intervention trials of beta-carotene supplementation have either shown no effect, or an increased risk of lung cancer. 16 Other dietary factors that may have an association with a higher risk of lung cancer are high fat and cholesterol content, meat consumption, high intakes of dairy products and high consumption of alcohol. 16 However, because tobacco smoking has such an overwhelming contribution to the risk of lung cancer, it is often difficult to assess whether dietary factors independently are risk factors for lung cancer. 8,16
An increased susceptibility to lung cancer may also result from the presence of previous lung disease. 10 Associations have been noted in the literature, but, as with the association with dietary factors, these are also possibly confounded by tobacco smoking and therefore findings are contestable. 8 Chronic obstructive pulmonary disease (COPD) has been shown to be an independent predictor of lung cancer risk in some studies, however. 10
Diagnosis and staging
Lung cancer is usually suspected on the basis of an initial clinical assessment – taking into account the patients’ symptoms, history and a physical examination – in addition to an abnormal chest radiograph. Confirmation of the diagnosis is then achieved using histological and cytological tests. Patients with SCLC are generally staged by clinical evaluation and computerised tomography (CT) scan of the chest and abdomen. 3,17 The TNM (tumour, node, metastases) stage scores are not usually relevant in SCLC due to the high proportion of patients presenting with metastases and its poor prediction of survival. 4,17 As previously mentioned, SCLC is classified as limited-stage disease or extensive-stage disease, classified according to the level of progression of disease. Selection of the most appropriate treatment is determined primarily by the stage of disease (see Current service provision).
Performance status
Measurement of the functional status of a patient is often described in terms of the World Health Organization/Eastern Cooperative Oncology Group (WHO/ECOG) performance status scores. 18 This scale rates the effect on daily living on a scale of 0–5, where 0 is ‘fully active, able to carry on all pre-disease performance without restriction’, 4 is ‘completely disabled, cannot carry out any self-care, totally confined to bed or chair’ and 5 is ‘dead’ (see Appendix 1). The Karnofsky performance status scale, can also be used to measure functional status in SCLC. This is a 100-point scale, rating performance from death (0), through inability to care for self, to able to carry on normal activity with no evidence of disease (100)19 (for full details, see Appendix 1).
Epidemiology
Lung cancer is one of the most common cancers in England, accounting for some 15% of all malignancies in males and 11% in females in 2005. 20 Lung cancer is the most common cause of death from cancer worldwide. 21–23 The proportion of lung cancer cases classified as small cell type has been steadily falling over the years. The reasons for this are unclear, but it has been attributed to changing smoking habits. 8,12,24 Cancer statistics do not appear to distinguish between the different histological types of lung cancer in their rates. However, estimates suggest that small cell lung cancers account for approximately 10–20% of lung cancers, with rates in more recent estimates reflecting the lower end of this range. 3,25,26 Therefore, crude estimates of the epidemiology of SCLC can be generated from the overall rates of lung cancer.
There were 33,181 new cases of lung cancer in England and Wales in 2005,20,27 with more cases in males than in females (19,261 males, 13,920 females). European age-standardised incidence rates of lung cancer in England in 2005 were 72.9 per 100,000 in males and 50.6 per 100,000 in females. 20 The corresponding rates in Wales in 2005 were 62.5 per 100,000 (males) and 39.5 per 100,000 (females). 27 In 2006, estimates of the age-standardised incidence rates of lung cancer in the UK were lower than estimates for all European Union countries for males (57.1 per 100,000 compared with 71.8 per 100,000), but higher for females (34.6 per 100,000 versus 21.7 per 100,000). 21 Taking a range of 10–20% for SCLC, an estimate of the number of new cases of SCLC per year (using 2005 estimates for England and Wales20,27) would be in the region of 3300–6600 for England and Wales.
The incidence of lung cancer rises with increasing age. Very few people are diagnosed under the age of 40 years, and the incidence shows a peak in rates around ages 75–84 years. Most cases occur in people over the age of 60 years. 28 Time trends in the incidence of lung cancer show an overall decline in rates between 1995 and 2004. 28 Recently, the National Lung Cancer Audit was set up in England and Wales to collect information on lung cancer, with the aim of understanding incidence, treatments, and outcomes and to explore regional variations. The report for the period 2006–726 presents data derived from the National Lung Cancer Data Audit (LUCADA) database in England and via the Cancer Network Information System Cymru (CANISC) in Wales, and includes data from 93% of trusts from these countries. This showed that the incidence of lung cancer is clearly associated with the degree of deprivation; there was more than a twofold difference in incidence between the most affluent groups and the most deprived groups. 26 The report confirms the positive association between deprivation and levels of smoking, which may account for much of this difference.
Prognosis
Lung cancer is the most common cause of death from cancer in both men and women. 22,23 The survival rate has improved in recent years,29 although deaths from lung cancer remain high (5-year age-standardised survival rate of 5.8% and 6.4% in males and females, respectively, from 1996–9) in the UK. 29 This is partly owing to diagnosis often being at a late stage, when curative treatments are not possible. 30 SCLCs tend to grow rapidly and have a greater tendency to widely metastasise. 10 An important predictor of prognosis in SCLC is the extent of disease progression. Without treatment, SCLC has an aggressive clinical course, with life expectancy of about 3.5 months for limited-stage disease and 6 weeks for extensive-stage disease. 31 With treatment, median survival for patients with limited-stage disease is 16 to 22 months; for those with extensive-stage disease median survival is 10 months. 32 Approximately 20–40% of patients with limited-stage SCLC and fewer than 5% of patients with extensive-stage SCLC survive for 2 years. 33 Survivors often continue to relapse up to, and occasionally after, 5 years. However, for those surviving long term, relapse after 5–6 years appears to be a rare event,34 although in one study, longer-term survivors appeared to be at high risk of a second primary cancer. 34
Prognostic factors have been reported by a number of studies in the literature and while comparisons are not necessarily easy to make between these different studies, a number of key variables do appear to be consistently identified as having an effect on prognosis. In a review for the Lung Cancer Subcommittee of the United Kingdom Coordinating Committee on Cancer Research (UKCCCR) in 1990, Rawson and Peto35 identified a number of variables which contributed significantly to the prediction of likely survival over the 6 months after starting treatment. They demonstrated that performance status, alkaline phosphatase and disease stage were the most important prognostic factors. More recent epidemiological studies show similar results. Lassen and colleagues36 studied prognostic factors that correlated with survival after 18-months in a retrospective review of 1714 patients with SCLC. The extent of disease and the performance status were found to be of prognostic significance. In limited-stage disease, an elevated lactate dehydrogenase (LDH) (an enzyme that is often raised in cancers and can be used as a marker of disease) was considered unfavourable. In this study, gender appeared to have no significant influence on survival. 36 Similar findings were observed in an analysis by the Southwest Oncology Group in the USA, although in this study female gender was seen to be an additional independent favourable predictor. 37 In this latter study, predictors of survival in those with extensive-stage SCLC were the number of metastatic sites, with lower numbers of sites being related to better prognosis. In an exploratory analysis of patients from four European clinical trials, characteristics that were associated with a higher objective response rate included higher performance status, limited-stage disease, and absence of brain metastases. 38 This study also found that women fared better than men,38 as did an analysis of prognostic factors from a 5-year randomised controlled trial (RCT). 39 Prominent prognostic factors among all patients with SCLC in this latter study were also extent of disease, LDH levels and weight loss. 39 SCLC is frequently associated with paraneoplastic syndromes (above), which can be caused by either ectopic hormone production or antibody-mediated tissue destruction. 33 Ectopic hormone production is the synthesis and secretion of a hormone by a tumour of a tissue that does not normally produce the particular hormone, and it has been associated with extensive-stage SCLC and a poorer outcome. 40 Antibody-mediated paraneoplastic syndromes are, however, associated with more favourable outcomes. 33,40
Current service provision
Selection of the most appropriate first-line treatment for SCLC is determined primarily by the stage of disease. Treatments include chemotherapy, radiotherapy or a combination of these treatments, with increased survival attributed to combination therapy. 41 The majority of patients with SCLC are inoperable,42 as the disease is often widespread at the time of diagnosis. 5
The current National Institute for Health and Clinical Excellence (NICE) guidelines3 recommend that patients with SCLC should be offered a multidrug platinum-based chemotherapy as first-line therapy. Those with limited-stage disease should be offered radiation concurrently with the first or second cycle, or following completion if a good partial response (PR) is seen within the thorax. Their initial treatment is usually followed by prophylactic cranial irradiation, in order to reduce the risk of cerebral metastases. 26 For those with extensive-stage disease, prophylactic cranial radiation should be considered following chemotherapy if there has been a CR at distant sites and at least a good PR in the thorax. 43
The platinum-based treatment combinations for first-line therapy that are offered (and recommended by NICE) are either cisplatin or carboplatin with etoposide. Other active agents include anthracyclines (doxorubicin, epirubicin), alkylating agents (cyclophosphamide, ifosfamide), vinca alkaloids (vindesine, vincristine) and taxanes (paclitaxel).
While guidelines for rapid referral of patients exist, there are many routes of patient referral. 26 Only 48% of patients are directly referred to specialist lung cancer teams via their GP, possibly due to the non-specific nature of lung cancer symptoms. 26 The majority of trusts in England and Wales now have rapid access clinics, managed by a multidisciplinary team (MDT). 26 The national lung cancer audit report 2006–7 asserts that outcomes for patients with lung cancer in the UK vary widely across the country and are poor when compared to many other countries. 26 The specialist nature of cancer treatments means that patients are often treated by more than one trust. 26 Despite NICE’s recommendation that all patients are reviewed, figures suggest that this occurs in only 86% of cases. 26 Specific anticancer treatment – such as chemotherapy and radiotherapy – as first-line treatment are suggested to remain low by international standards. 26 In addition, the likelihood of receiving chemotherapy in the UK declines rapidly for anyone over 75 years of age. 26 The report suggests that while prognosis for patients with lung cancer has remained poor with little improvement in long-term survival, applying best practice could provide a considerate improvement in outcomes. 26
Objective tumour response is assessed by radiograph or CT scan. A response requires the tumour to reduce by at least 30% using a unidimensional measure such as the Response Evaluation Criteria In Solid Tumors (RECIST) or 50% using a bidimensional measure (WHO), with reduction maintained for at least 4 weeks (see Appendix 1). Response to first-line therapy for SCLC can be categorised as ‘sensitive’, ‘resistant’ or ‘refractory’. 6 ‘Sensitive’ refers to a tumour response of more than 90 days, ‘resistant’ to tumour recurrence within 90 days and ‘refractory’ to tumours that either never responded or progressed during first-line therapy. It is generally thought that those with a sensitive response will have the greatest potential for second-line therapy. 6
Second-line treatment decisions depend on the response to first-line therapy and the duration of that response. 3,44 Evidence suggests that the best results from second-line chemotherapy are achieved in those with at least 3 months between response and progression. 4 On relapse, re-treatment with the same chemotherapy regimen is reasonable if a durable first-line response is achieved. For other patients, this may not be appropriate due to a short duration of response, the development of resistance or other contraindications. 45 In these patients, alternative chemotherapy regimens can be used. 46
Intravenous topotecan has been assessed by the Scottish Medicines Consortium (SMC) [which makes recommendations to the National Health Service (NHS) in Scotland], but was not recommended for the treatment of patients with relapsed SCLC, ‘for whom re-treatment with the first-line regimen is not considered appropriate’. 47 In contrast, the All Wales Medicines Strategy Group (AWMSG) has recommended i.v. topotecan for ‘use within NHS Wales for the treatment of patients with relapsed small SCLC for whom re-treatment with the first-line regimen is not considered appropriate’. 48 However, the AWMSG also noted that topotecan should be initiated only by specialists who are experienced in the treatment of SCLC and it was not recommended for shared care.
UK research, using a 4-year retrospective patient-chart analysis, determined the average cost for the treatment of patients with SCLC using a variety of sources. 49 The calculated cost per patient from a cohort of 109 patients was £11,556, with the most expensive element through all phases of the disease being hospitalisation. 49 The average patient cost for first-line treatment was estimated at £6128 (48.7% of total costs), with 28% of the total costs down to recurrence of the disease until death. The average cost per patient for second-line treatment was around £5008. 49
Description of new intervention
Topotecan is an anticancer treatment that acts by the inhibiting the enzyme topoisomerase I, which is required for DNA replication. This leads to cell death.
Topotecan is indicated for patients as a second-line therapy in those patients with relapsed SCLC for whom re-treatment with the first-line regimen is not considered appropriate. The marketing authorisation for i.v. therapy was granted in the UK in 2006, and, more recently, a licence was granted for oral therapy (2008). The recommended dose for i.v. treatment is 1.5 mg/m2 of body surface area/day in a 30-minute infusion for 5 consecutive days, in a 21-day cycle. The cost of i.v. topotecan is £97.65 per milligram, which equates to £147.47 m2/day. 50 For oral treatment the recommended dose is 2.3 mg/m2/day, administered for 5 consecutive days, in 21-day cycles. The cost of oral topotecan is £30 per milligram, which equates to £69 m2/day. 51 Each oral capsule contains topotecan hydrochloride equivalent to 0.25 mg or 1 mg of topotecan. The advantage of the oral form of topotecan is that it does not need specialist preparation and administration, and can therefore be self-administered. 52 However, no guidance advising which form may provide the better treatment has been identified.
Treatment may continue until disease progression if the treatment is well tolerated. Oral topotecan can be self-administered on an outpatient basis. Intravenous topotecan is administered in secondary or tertiary care settings, usually on a day-case basis.
Topotecan is contraindicated in patients who have a history of hypersensitivity to the active substance, are breastfeeding or already have severe bone marrow depression prior to starting the first course. Haematological toxicity may occur, and a full blood count (FBC) including platelets should be monitored regularly. As with other anticancer therapies, topotecan can cause severe myelosuppression, which can lead to sepsis. Other potential adverse effects include nausea and vomiting, diarrhoea, alopecia and fatigue. Topotecan rarely causes life-threatening neutropenic colitis. Topotecan is produced by GlaxoSmithKline (GSK) and trades under the name ‘Hycamtin’.
Chapter 2 Methods
The a priori methods for systematically reviewing the evidence of clinical and cost-effectiveness are described in the research protocol (Appendix 2), which was sent to experts for comment. No comments were received which identified specific problems with the methods of the review. The methods outlined in the protocol are briefly summarised below. The methods of the SHTAC (Southampton Health Technology Assessments Centre) economic evaluation can be seen in Chapter 4 (Methods for economic analysis).
Search strategy
The search strategy was developed, tested and refined by an experienced information scientist. Separate searches were conducted to identify studies of clinical effectiveness, cost-effectiveness, quality of life (QoL), resource use/costs and epidemiology/natural history. Sources of information and search terms are provided in Appendix 3.
Searches for clinical and cost-effectiveness literature were undertaken from 1990 to August 2008. Given that marketing authorisation for topotecan was first granted in 1996, it was deemed unlikely that there would be any trials before 1990 for topotecan for any indication. Electronic databases searched included the Cochrane Database of Systematic Reviews (CDSR), the Cochrane Central Register of Controlled Trials, CRD (University of York) Database of Abstracts of Reviews of Effectiveness (DARE), the NHS Economic Evaluation Database (NHS EED) and the Health Technology Assessment (HTA) database, MEDLINE (OVID), EMBASE (OVID), PREMEDLINE In-Process & Other Non-Indexed Citations; Web of Knowledge Science Citation Index (SCI); Web of Knowledge ISI Proceedings; PsycInfo (EBSCO), Biosis, CINAHL (EBSCO), NIHR Clinical Research Network Portfolio, Current Controlled Trials, ClinicalTrials.gov and Cancer Research UK trials. Key cancer resources including the American Society of Clinical Oncology (ASCO) and relevant cancer symposia, including the 12th World Lung Cancer Conference, were also searched. Updated searches were carried out in February 2009.
The searches were restricted to English language. Bibliographies of related papers were screened for relevant studies, and the manufacturer’s submission (MS) to NICE was assessed for any additional studies [see Appendix 4 for a critique of the clinical effectiveness section of the MS, and Chapter 4 (Methods for economic analysis) for further discussion of the cost-effectiveness section]. Experts who were contacted for advice and peer review were also asked to identify additional published and unpublished references. The authors of the five included studies were contacted to establish whether the patient populations in the trials met the review inclusion criteria with regard to being inappropriate for re-treatment with first-line therapy.
Inclusion and data extraction process
Titles and abstracts identified by the search strategy for the clinical effectiveness section of the review were assessed for possible eligibility by two independent reviewers. The full texts of relevant papers were then obtained, and inclusion criteria were applied by one reviewer and checked by a second reviewer. Any disagreements over eligibility were resolved by consensus or by recourse to a third reviewer. Data were extracted by one reviewer using a standardised data extraction form and checked by a second reviewer.
Titles and abstracts identified by the search strategy for the cost-effectiveness section of the review were assessed for potential eligibility by two health economists. Economic evaluations were considered for inclusion if they reported both health service costs and effectiveness, or presented a systematic review of such evaluations. Full papers were formally assessed for inclusion by one health economist.
Quality assessment
The quality of included RCTs and systematic reviews was assessed using criteria recommended by the Centre for Reviews and Dissemination (CRD)53 (Appendix 5). Quality criteria were applied by one reviewer and checked by a second reviewer. At each stage, any differences in opinion were resolved through discussion or consultation with a third reviewer.
Inclusion criteria
Population
-
Adults (≥ 18 years) with relapsed SCLC who responded to first-line treatment and for whom re-treatment with first-line therapy is not considered appropriate (due to contraindications, adverse effects).
-
Patients may have had limited-stage disease or extensive-stage disease.
-
Response to initial treatment may have been either CR or PR.
-
Patients who did not respond to first-line therapy (including patients whose tumours did not respond, or who progressed, during first-line treatment) were not included.
-
Studies with a mix of untreated and previously treated patients (or responders and non-responders) were not included unless the groups were reported separately.
Intervention
-
Intravenous topotecan (administered as second-line treatment).
-
Oral topotecan (administered as second-line treatment).
-
Studies with a focus on first-line treatment were not included.
-
Effectiveness data for oral and i.v. topotecan were not combined.
Comparators
-
Intravenous and oral topotecan compared with each other.
-
Best supportive care (BSC) (including radiotherapy).
-
CAV (cyclophosphamide, doxorubicin, vincristine).
-
Other chemotherapy regimens.
Outcomes
Studies reporting one or more of the following outcomes were included:
-
time to disease progression (TTP)
-
progression-free survival (PFS)
-
response rate (see below)
-
response duration
-
overall survival (OS)
-
symptom control
-
health-related QoL (using a validated measure)
-
cost-effectiveness (incremental cost per life-year gained) or cost–utility [incremental cost per quality-adjusted life-year (QALY) gained].
Adverse effects of treatments were reported if available within trials that met the prespecified inclusion criteria above.
Understanding the definition of treatment ‘response’ used within the studies is important. Two criteria have been identified, which appear to be widely reported in oncology research – the WHO criteria54 and the RECIST guidelines. 55 These are summarised in Appendix 1. Where a clinical trial documents which criteria were used to define treatment response and related outcomes, this is reported in the current review. Where it is not certain what the definition of response was, this is similarly noted.
Types of studies
RCTs were included. Studies published as abstracts or conference presentations were included only if sufficient details were presented to allow an appraisal of the methodology and the assessment of results to be undertaken. Systematic reviews were used only as a source of references.
For the systematic review of cost-effectiveness, studies were only eligible for inclusion if they reported the results of full economic evaluations [cost-effectiveness analyses (reporting cost per life-year gained), cost–utility analyses or cost–benefit analyses].
Data synthesis
Data were synthesised through a narrative review, with tabulation of results of all included studies. Full data extraction forms are presented in Appendix 6. It was not considered appropriate to combine the included RCTs in a meta-analysis due to clinical heterogeneity in the patient groups and comparator treatments.
Chapter 3 Clinical effectiveness
Quantity and quality of research available
Included studies
Searches identified 395 references, after removal of duplicates. After initial screening of titles and abstracts, 385 references were excluded. Ten full copies of articles were retrieved, with four excluded on further inspection. In addition, 22 abstracts were identified on searches of the proceedings of ASCO, with 21 of these being excluded during the screening process. The included ASCO abstract later became available as a fully published article. Two (out of nine) abstracts were also identified from the 12th World Lung Cancer Conference 2007, which were linked to one of the included studies. Eight studies were identified in the updated searches, but none were included. The total number of published papers included at each stage of the systematic review is shown in the flow chart in Figure 1, and the list of excluded studies can be seen in Appendix 7. The level of agreement between reviewers assessing study eligibility was high.
FIGURE 1.
Flow chart of identification of studies for inclusion in the review. a Includes total number of studies identified in searches of ASCO, 12th World Lung Cancer Conference and updated search in addition to main search. b One identified ASCO abstract subsequently published as a full publication.
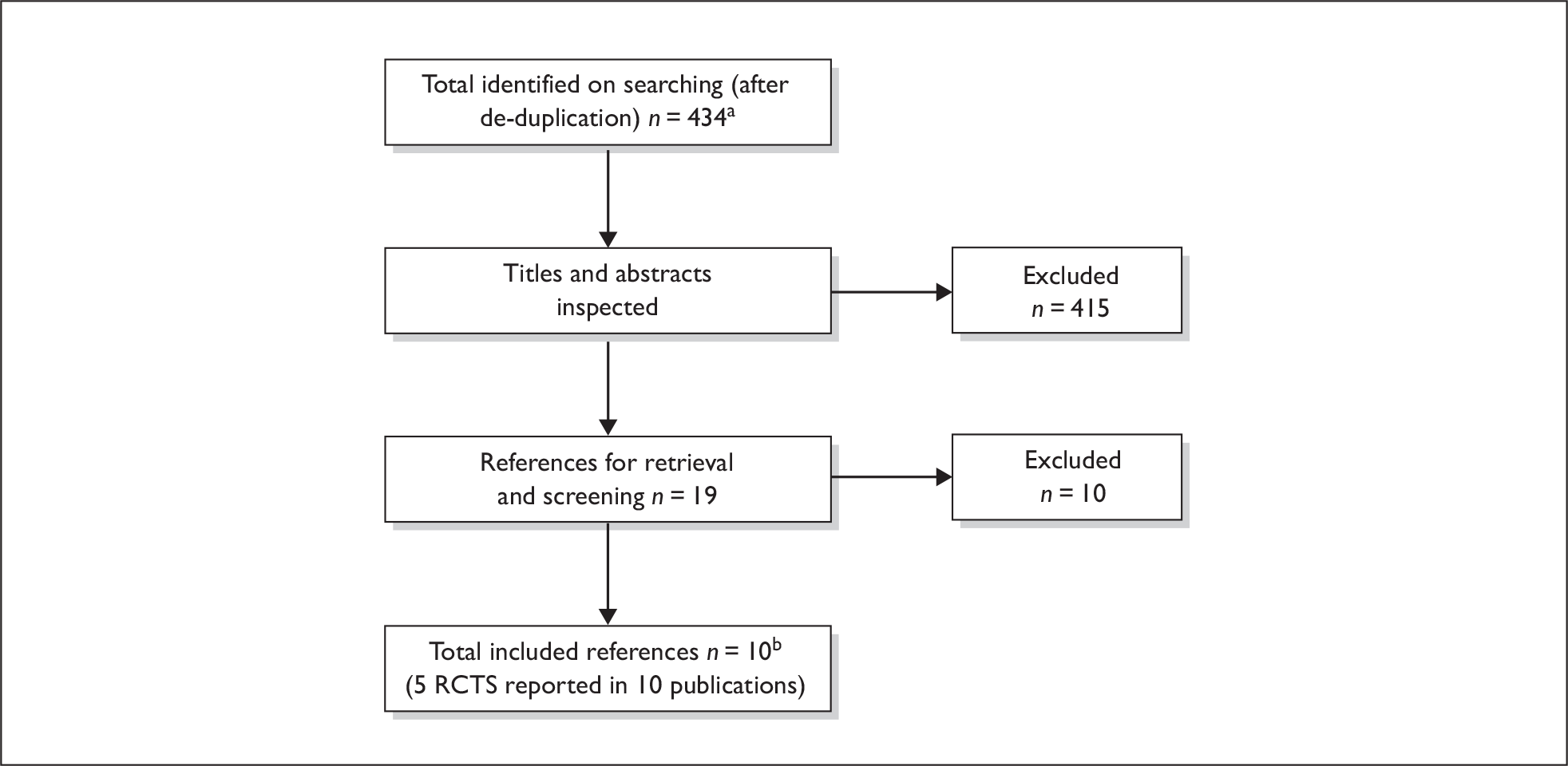
Ten publications describing five RCTs appeared to meet the inclusion criteria of the review. 56–65 Five of the articles were either earlier abstracts60–62 or abstracts presenting additional results64,65 linked to full publications,56,57,59,63 leaving five RCTs to be evaluated. Only one trial appeared to fully meet the inclusion criteria of the review on inspection of the published article,57 and this was confirmed in correspondence with the author (participants were inappropriate for re-treatment with their original first-line chemotherapy for reasons such as contraindication, toxicity and refusal). The remaining four RCTs did not appear to fully meet the inclusion criteria of having participants for whom re-treatment with their first-line chemotherapy regimen was not appropriate, as per the licensed indication for topotecan. Authors of all of these publications were contacted to clarify this aspect of our inclusion criteria. Response from one author established that two of the included trials58,59 did meet this aspect of the inclusion criteria. In the correspondence with the author from a third trial,63 it was reported that participants were not required to have a ‘contraindication’ to re-treatment with their first-line therapy to meet the study protocol. Whether there were other reasons that would have deemed participants as being inappropriate for re-treatment, or whether all participants could have been appropriate for re-treatment, however, is not clear. No reply was received from the author of one other study,56 so it remains unclear whether the included participants fully met the licensed indication for topotecan. Despite these uncertainties, these last two studies were included, although we emphasise the need for caution in the interpretation of results, as the population groups may be slightly different than those eligible for topotecan according to the marketing authorisation. In summary, five trials were included in this review (Table 1).
| Study | Intervention | Comparator |
|---|---|---|
| O’Brien et al. 200657,64,65 | Oral topotecan + BSC | BSC alone |
| von Pawel et al. 199959,61 | Intravenous topotecan | CAV |
| Eckardt et al. 200756,60a | Oral topotecan | Intravenous topotecan |
| von Pawel et al. 200158 | Oral topotecan | Intravenous topotecan |
| Inoue et al. 200862,63a | Intravenous topotecan | Intravenous amrubicin |
Description of the included studies
Four56–59 of the included studies were international, multicentre RCTs, varying between 31 and 83 centres (numbers not reported in one59). The fifth study63 was a multicentre RCT carried out in 12 centres in Japan. Two of the studies were phase II trials. 58,63 Four of the trials were sponsored by the drug manufacturers,56–59 whereas financial support was reported to be provided by two of the authors in the trial by Inoue and colleagues. 63
The study of O’Brien and colleagues (2006)57 investigated oral topotecan plus BSC versus BSC alone in a population of participants who were considered to be unsuitable for further i.v. chemotherapy. The study initially excluded participants with a treatment-free interval (TFI) of > 90 days for whom treatment with BSC was not acceptable. This changed during the trial and some participants with sensitive SCLC, who were unsuitable for standard i.v. chemotherapy due to co-morbidities or who had refused i.v. chemotherapy due to the risk of toxicity, became eligible for inclusion in the study. The study protocol was amended to allow the inclusion of such patients. In the topotecan plus BSC group, participants received 2.3 mg/m2 of oral topotecan on days 1–5 every 21 days. A minimum of four treatment cycles were recommended, but delays and dose adjustments were anticipated in the study protocol. BSC was defined as including measures such as ‘analgesics, antibiotics, corticosteroids, appetite stimulants, antidepressants, red blood cell transfusions, deep relaxation therapy, and palliative radiotherapy or surgical procedures’. Both treatment groups had equal access to these treatments.
A study by von Pawel and colleagues (1999)59 compared i.v. topotecan with CAV in a population of participants with limited- or extensive-stage SCLC, with a CR or PR to first-line chemotherapy and who had relapsed ≥ 60 days after cessation of first-line therapy. Participants who were contraindicated to re-treatment with CAV were specifically excluded from this study and therefore the participants may not be those that would normally be eligible for topotecan. The i.v. topotecan group received 1.5 mg/m2 as a 30-minute infusion for 5 days every 21 days, whereas the CAV group received an infusion of 1000 mg/m2 (maximum 2000 mg) of cyclophosphamide, 45 mg/m2 (maximum 100 mg) of doxorubicin and 2 mg of vincristine, all on day 1 of each 21-day course. Second-line treatment duration was dependent on response to second-line treatment. Participants with stable disease received a minimum of four treatment cycles, whereas patients with a CR or PR received at least six.
Two studies56,58 compared oral topotecan with i.v. topotecan, in a population of participants with limited- or extensive-stage relapsed SCLC who had CR or PR to first-line therapy with disease recurrence after ≥ 90 days. In both studies, participants received 2.3 mg/m2 of oral topotecan compared with 1.5 mg/m2 of i.v. topotecan for 5 days every 21 days. Treatment duration depended on response, but in both studies participants with stable disease received at least four treatment cycles. Protocol-specified dose adjustments were permitted in both trials.
The trial by Inoue and colleagues63 compared i.v. topotecan with i.v. amrubicin (an anthracycline) in a population of participants with SCLC, who were previously treated with platinum-containing chemotherapy and who had either sensitive (relapse ≥ 90 days after cessation of first-line therapy) or refractory relapse (defined as no response to first-line chemotherapy or relapse within 90 days after cessation of first-line therapy). The study suggested that the latter category may also include participants who never responded to first-line treatment, although whether this is the case or what proportion this includes is unknown. The majority of participants were sensitive to the first-line therapy. Participants received 40 mg/m2 of amrubicin as a 5-minute infusion on days 1–3 every 3 weeks. Topotecan was administered as a 30-minute infusion on days 1–5 every 3 weeks at a dose of 1.0 mg/m2, which is the approved dosage in Japan. This is lower than the UK recommended dose (1.5 mg/m2/day) given in the other studies. 56,58,59
The key characteristics of the RCTs are shown in Table 2. The numbers of participants ranged from 59 in the Inoue and colleagues trial63 to 309 in the Eckardt and colleagues trial. 56 The age ranges of the participants in four of the studies was similar (the mean ages were not reported consistently across studies), whereas the fifth study provided no information about the age of the participants. 59 All studies had a higher percentage of male participants in both treatment arms (male range 57–83%, female range 17–43%). Where reported, studies had a higher proportion of participants with extensive-stage disease and these were similar across treatment groups. The percentage of participants with extensive disease was similar in three studies,56–58 at 61–72%, higher in a fourth study59 at 83–85%, and not reported by the fifth study. 63
| Study details | Interventions | Key inclusion criteria and patient characteristics | Outcomes |
|---|---|---|---|
|
O’Brien et al. 2006,57 Chen et al. 200764 (abstract) and O’Brien et al. 200765 (abstract) Study design: RCT Countries: Europe, Canada and Russia Number of centres: 40 Sponsor: GlaxoSmithKline Follow-up: Median time on study 7.8 weeks in the BSC group and 12.3 weeks in the topotecan group |
1. Oral topotecan + BSC, 2.3 mg/m2/day on days 1 to 5 every 21 days (n = 71). 2. BSC (n = 70) |
Target population: Only those considered unsuitable for further i.v. chemotherapy were recruited Inclusion criteria: Extensive or limited-stage SCLC, resistant or sensitive disease, one prior chemotherapy regimen, age ≥ 18 years, ECOG PS of 0, 1 or 2, at least 24 hours since last radiotherapy, at least 3 months since last immunotherapy Gender (M/F), n (%): topotecan 52/19 (73/27), BSC 51/19 (73/27) Mean age (SD), range, years: topotecan 59.8 (9.0) 37–76, BSC 58.6 (8.2), 43–79 Performance status, n (%): 0: topotecan 8 (11), BSC 6 (9) 1: topotecan 44 (62), BSC 41 (59) 2: topotecan 19 (27), BSC 23 (33) Disease stage, n (%): Limited: topotecan 23 (32), BSC 27 (39) Extensive: topotecan 48 (68), BSC 43 (61) Previous treatment, n (%): Any prior treatment: topotecan 46 (65), BSC 48 (69) Radiotherapy: topotecan 38 (54), BSC 34 (49) Surgery: topotecan 18 (25), BSC 20 (29) Immunotherapy: topotecan 0, BSC 4 (6) Cisplatin or carboplatin: topotecan 80%, BSC 77% Etoposide: topotecan 76%, BSC 74% Duration of response to first-line chemotherapy (TTP since completion of first-line therapy) [days, n (%)]: ≤ 60: topotecan 22 (31), BSC 20 (29) > 60: topotecan 49 (69), BSC 50 (71) ≤ 90: topotecan 41 (58), BSC 35 (50) > 90: topotecan 30 (42), BSC 35 (50) Presence of liver metastases, n (%): Present: topotecan 20 (28), BSC 14 (20) Absent: topotecan 51 (72), BSC 56 (80) |
Primary outcomes: OS Secondary outcomes: Response rate, TTP, patient symptom assessment (PSA), QoL and safety |
|
von Pawel et al. 199959 and Schiller et al. 199861 (abstract) Study design: RCT Countries: Germany, Canada, France, UK and USA Number of centres: Not reported Sponsor: SmithKline Beecham Follow-up: Unclear, although the range for TTP was 75 weeks and for survival up to 101 weeks |
1. Topotecan, 1.5 mg/m2/day as 30-minute infusion for 5 days every 21 days (n = 107) 2. CAV, C 1000 mg/m2 (maximum 2000 mg), D 45 mg/m2 (maximum 100 mg), and V 2-mg infusion all on day 1 of each 21-day course (n = 104) Minimum of four courses of treatment for patients with stable disease, ≥ 6 courses for patients with CR or PR |
Target population: Patients with progressive, limited or extensive-stage SCLC, with date of progression ≥ 60 days after completion of first-line therapy Inclusion criteria: One previous chemotherapy regimen, at least one lesion bidimensionally measurable; ≥ 4 weeks between prior surgery or immunotherapy and study entry; ≥ 24 hours between radiotherapy and initiation of study drugs; ECOG PS ≤ 2 Gender (M/F), n (%): topotecan 61/46 (57/43), CAV 71/33 (68/32) Mean age: not reported Performance status, n (%): 0: topotecan 18 (16.8), CAV 20 (19.2) 1: topotecan 64 (59.8), CAV 64 (61.5) 2: topotecan 25 (23.4), CAV 20 (19.2) Disease stage, n (%): Limited: topotecan 18 (16.8), CAV 16 (15.4) Extensive: topotecan 89 (83.2), CAV 88 (84.6) Duration of response to first-line chemotherapy, median weeks (range): topotecan 24.4 (7.6–430.6), CAV 22.9 (8.7–156.7) Presence of liver metastases, n (%): Present: topotecan 43 (40.2), CAV 42 (40.4) Absent: topotecan 64 (59.8), CAV 62 (59.6) |
Primary outcomes: Response rate and duration to response Secondary outcomes: TTP, time to response, survival and improvement of disease-related symptoms |
|
Eckardt et al. 200756 and Eckardt et al. 200360 (abstract) Study design: Open-label RCT Countries: Europe, N America, SE Asia and Australia Number of centres: 83 Sponsor: GlaxoSmithKline Follow-up: Median of four courses (i.e. 12 weeks); at least 40% of patients in each group received treatment beyond course 4 |
Oral topotecan, 2.3 mg/m2/day on days 1–5 every 21 days (n = 155) Intravenous topotecan, 1.5 mg/m2/day, on days 1–5 every 21 days (n = 154) Duration depended on response but those with stable disease recommended to have at least four cycles Note: baseline characteristics and results based on n = 153 oral and n = 151 i.v. participants who received at least one treatment |
Target population: Patients with limited- or extensive-stage relapsed SCLC, who had CR or PR to first-line therapy with disease recurrence after ≥ 90 days. Inclusion criteria: ≥ 18 years, only one prior chemotherapy regimen, bidimensionally measurable disease (according to WHO criteria), ECOG PS ≤ 2, prior surgery was allowed if ≥ 4 weeks had passed, as were immunotherapy (≥ 3 months) and radiotherapy (≥ 24 hours) Gender (M/F), n (%): oral 98/55 (64.1/35.9), i.v. 96/55 (63.6/36.4) Mean age (range), years: oral 62.5 (41–82), i.v. 62.0 (35–82) Performance status, n (%): 0: oral 48 (31.4), i.v. 35 (23.2) 1: oral 85 (55.6), i.v. 98 (64.9) 2: oral 20 (13.1), i.v. 18 (11.9) Disease stage, n (%): Limited: oral 51 (33.3), i.v. 45 (29.8) Extensive: oral 102 (66.7), i.v. 106 (70.2) Previous treatment: platinum- and anthracycline-based combination regimens Duration of response to first-line chemotherapy, n (%) (data missing for four patients in the oral group and one patient in the i.v. group): < 3 months: oral 15 (9.8), i.v. 13 (8.6) 3–6 months: oral 50 (32.7), i.v. 54 (35.8) > 6 months: oral 84 (54.9), i.v. 83 (55.0) Presence of liver metastases, n (%): Present: oral 44 (28.8), i.v. 43 (28.5) Absent: oral 109 (71.2), i.v. 108 (71.5) |
Primary outcomes: Response rate Secondary outcomes: Time to response, response duration, TTP, OS, toxicities and health-related quality of life (HRQoL) |
|
von Pawel et al. 200158 Study design: RCT (phase II) Countries: Europe, S Africa and Australia Number of centres: 31 Sponsor: SmithKline Beecham Follow-up: Unclear, although progression was assessed up to 54 weeks and survival up to 64 weeks |
1. Oral topotecan, 2.3 mg/m2/day for 5 days every 21 days (n = 52) 2. i.v. topotecan, 1.5 mg/m2/day, 30-minute infusion for 5 days every 21 days (n = 54) Duration depended on response but those with stable disease recommended to have at least four cycles |
Target population: Patients with limited- or extensive-stage SCLC, with a CR or PR to first-line chemotherapy and who had relapsed ≥ 3 months after cessation of first-line therapy Inclusion criteria: ≥ 18 years, only one prior chemotherapy regimen, measurable disease of ≥ 2cm in diameter, WHO performance status of ≤ 2, life expectancy of at least 2 months, ≥ 4 weeks since previous surgery and ≥ 24 hours since last radiotherapy Gender (M/F), n (%): oral 39/13 (75/25), i.v. 43/11 (79.6/20.4) Mean age (range), years: oral 59.9 (38–79), i.v. 58.2 (35–74) Performance status, n (%): 0: oral 10 (19.2), i.v. 18 (33.3) 1: oral 34 (65.4), i.v. 21 (38.9) 2: oral 8 (15.4), i.v. 15 (27.8) Disease stage, n (%) (data missing for one participant in each group): Limited: oral 14 (26.9), i.v. 14 (25.9) Extensive: oral 37 (71.2), i.v. 39 (72.2) Previous treatment: previous radiotherapy (%): oral 71.2, i.v. 72.2 Duration of response to first-line chemotherapy, n (%): TTP since completion of first-line therapy: < 3 monthsa: oral 1 (1.9), i.v. 1 (1.8) 3–6 months: oral 19 (36.5), i.v. 19 (35.2) > 6 months: oral 32 (61.5), i.v. 34 (63.0) Presence of liver metastases, n (%): Present: oral 16 (30.8), i.v. 17 (31.5) Absent: oral 36 (69.2), i.v. 37 (68.5) |
Primary outcomes: Response, response duration, TTP Secondary outcomes: Time to response, survival, symptoms and toxicities |
|
Inoue et al. 200863 and Sugawara et al. 200862 (abstract and presentation) Study design: RCT (phase II) Countries: Japan Number of centres: 12 Sponsor: Two authors provided financial support Follow-up: Not stated |
1. Intravenous amrubicin, 40 mg/m2/day on days 1–3 every 3 weeks (n = 29b) 2. Intravenous topotecan, 1.0 mg/m2/day on days 1–5 every 3 weeks (n = 30) At least three cycles (amrubicin: median 3, range 1–7; topotecan: median 2, range 1–4) |
Target population: Previously platinum-treated patients with SCLC who relapsed within 90 days or ≥ 90 days after cessation of first-line treatment. (Note: some participants may have never responded to first-line therapy.) Inclusion criteria: age ≥ 20 years, one platinum-containing previous chemotherapy regimen, measurable disease with RECIST criteria, no chemotherapy or chest radiotherapy within 4 weeks prior to enrolment, ECOG PS of 0–2 Gender (M/F), n (%): amrubicin 24/5 (83/17), topotecan 25/5 (83/17), p = 1.000 Age (years), median (range): amrubicin 70 (54–77), topotecan 64 (32–78), p = 0.195 Performance status, n (%): 0: amrubicin 14 (48); topotecan 17 (57) 1: amrubicin 10 (34); topotecan 9 (30) 2: amrubicin: 5 (17); topotecan 4 (13), p = 0.731 Disease stage: not reported Duration of response to first-line chemotherapy: not reported Presence of liver metastases, n (%): not reported Previous treatment, n (%): Radiotherapy: amrubicin 15 (52); topotecan 16 (53) Chemotherapy: Platinum + etoposide: amrubicin 22 (76), topotecan 20c (67) Platinum + irinotecan: amrubicin 7 (24), topotecan 11c (37) Response type, n (%): Sensitive: amrubicin 17 (59), topotecan 19 (63) Refractory: amrubicin 12 (41), topotecan 11 (37), p = 0.793 |
Primary outcomes: Overall response rate (ORR) Secondary outcomes: PFS, OS and toxicity profile Also reports disease control rates, but data not extracted |
The proportion of participants with a performance status of zero was lowest in the O’Brien and colleagues study57 (∼10%), higher in three trials,56,58,59 ranging from 17% to 33%, whereas the trial by Inoue and colleagues63 had a much higher proportion (48–57%). Four trials had similar proportions of participants (55–65%) with a performance status of one,56–59 with the exception of the i.v. topotecan group in the von Pawel and colleagues (2001) trial58, which was lower (39%). This was similar to the proportions in both treatment groups (30–34%) in the study by Inoue and colleagues (2008). 63 When grouping together performance status zero and one, all trials had similar numbers of good performance status participants (70–80%). The percentage of participants with a performance status of two were mixed between studies. Within two studies,56,63 the proportion was low and similar across arms (12–17%). In a third study,59 percentages were slightly higher (19–24%), and in a fourth trial57 percentages were higher still (27–33%), but similar across treatment arms. In the trial by von Pawel and colleagues (2001),58 there were almost twice as many participants with a performance status of two in the i.v. topotecan group (28%) compared with the oral topotecan group (15%).
Liver metastases were present in around 30% of participants in two studies,56,58 but higher in both treatment groups (∼40%) in the study by von Pawel and colleagues (1999). 59 In the O’Brien and colleagues’ study,57 liver metastases were present in a greater proportion of topotecan participants (28%) compared to BSC (20%), although the authors do not report that this is a statistically significant difference. Presence of liver metastases was not reported in the trial by Inoue and colleagues. 63 Duration of response to first-line chemotherapy was 6 months or more for the majority of patients in both treatment groups for two studies,56,58 and around a median of 23–24 weeks in another study. 59 Inoue and colleagues63 did not report these data. In the study by O’Brien and colleagues,57 this was reported as median TTP after first-line chemotherapy, and was 84 days in the topotecan arm and 90 days in the BSC arm.
Four RCTs56,58,59,63 reported response rate as the primary outcome measure, with the two trials by von Pawel and colleagues also reporting duration of response58,59 and TTP. 58 OS and toxicities/symptoms were reported as secondary outcomes in these four studies. O’Brien and colleagues57 reported OS as the primary outcome and response rate, TTP and adverse effects/toxicities as secondary outcome measures. Two trials56,57 reported health-related QoL.
Quality assessment of included studies
The methodological quality of reporting in the included studies was assessed using criteria set by the CRD at the University of York,53 and varied across studies (Table 3). Two trials57,59 described an adequate randomisation procedure that ensured both true random assignment to treatment groups and adequate concealment of allocation. The other three studies56,58,63 provided no details of the methods of generating the randomisation sequence, nor the allocation procedure used, and, consequently, are rated as unknown on these quality factors. Without adequate published information it is not possible to assess whether there is a risk of selection bias in these studies, with the allocation sequence being open to possible manipulation.
| Study | Randomisation | Allocation concealment | Baseline characteristics | Eligibility | Blinding of assessors | Blinding of care providers | Patient blinding | Reporting outcomes | ITT analysis | Withdrawals explained |
|---|---|---|---|---|---|---|---|---|---|---|
| Eckardt et al. 200756,60 | Un | Un | Rep | Ad | Par | Un | Un | Ad | In | Ad |
| Inoue et al. 200862,63 | Un | Un | Rep | Ad | Un | Un | Un | Par | In | Ad |
| O’Brien et al. 200657 | Ad | Ad | Rep | Ad | In | Un | Un | Ad | Ad | Ad |
| von Pawel et al.199959,61 | Ad | Ad | Rep | Ad | Par | Un | Un | Ad | Ad | Par |
| von Pawel et al. 200158 | Un | Un | Rep | Ad | Par | Un | Un | Ad | Ad | In |
All the trials reported eligibility criteria adequately and participants appeared similar at baseline on key demographic and prognostic characteristics, although in some cases supporting statistical comparisons were not provided. None of the RCTs reported if either the caregivers or participants were blinded to the treatment. However, given the disparity in the treatment interventions, blinding of participants or care providers may have not been possible in some trials, but the studies did not discuss this. Details of blinding for outcome assessors were partially reported by three trials,56,58,59 inadequately reported in one trial57 and unknown in one trial. 63 This may lead to detection bias, particularly for subjective outcomes such as QoL assessments. Outcomes were reported adequately in four trials,56–59 and partially in one. 63 An appropriate intention-to-treat (ITT) data analysis was reported to be undertaken and assessed as adequate in only three trials. 57–59 In two trials,56,63 the analysis was not true ITT, as it was based on all of those who received treatment, not on all of those who were randomised. Reasons for withdrawals were adequately explained by three trials,56,57,63 partially reported by one,59 and classed as inadequate for another trial, as there was no discussion of numbers or reasons for any attrition. 58 Overall, methodological quality was judged to be reasonably good in two trials, and unknown in three trials.
Assessment of clinical effectiveness
Oral topotecan plus BSC versus BSC alone
Survival
One trial (O’Brien and colleagues57) was included, which compared oral topotecan plus BSC with BSC alone. Overall survival was the primary outcome in this study. The median survival was reported to be 25.9 [95% confidence interval (CI) 18.3 to 31.6] weeks in the oral topotecan plus BSC-treated participants and 13.9 (95% CI 11.1 to 18.6) weeks in those with BSC alone. This was not tested for statistical significance. Six-month survival rates were 49% versus 26% for the oral topotecan plus BSC, and BSC groups, respectively (Table 4). Using Kaplan–Meier analysis, the hazard ratio (HR) for OS was 0.64 (95% CI 0.45 to 0.90) in favour of oral topotecan. With adjustment for covariates, the HR was reported to be 0.61 (95% CI 0.43 to 0.87). This showed a statistically significant benefit for the oral topotecan plus BSC group, compared with BSC alone (log-rank p = 0.01).
| Study: O’Brien et al. 200657 | Treatment arms | p-value | |
|---|---|---|---|
| Oral topotecan + BSC (n = 71) | BSC (n = 70) | ||
| OS, median (weeks) | 25.9 (95% CI 18.3 to 31.6) | 13.9 (95% CI 11.1 to 18.6) | Not reported |
| 6-month survival rate (%) | 49 | 26 | Not reported |
Data were presented on subgroup analyses of survival according to the various stratification factors (gender, performance status, TTP, presence of liver metastases). However, the HRs and 95% CI were only presented in a figure and hence are not reported in detail here. Estimates of these rates can be seen, however, in Appendix 6. Overall, the data indicate a survival trend favouring oral topotecan plus BSC for all subgroups analysed. However, the 95% CI cross 1.0 for TTP > 60 days, male gender, PS 0/1, and liver metastases on the figures presented in the paper. It is also not clear whether the study was powered for these analyses.
Participant dropout rates differed between the study arms (30% topotecan plus BSC, 47% BSC), although the study reports that an ITT principle to the analyses of data were applied. No participants crossed over, although there were a number of participants in both groups who received additional chemotherapy and/or radiotherapy post-study. It is not clear whether this may have had an impact on the OS rates shown, but the proportions receiving post-study chemotherapy are observed to be similar between treatment arms (18.6% and 18.3% for the topotecan plus BSC and BSC arms, respectively).
Progression-free survival was not reported in the O’Brien and colleagues57 study.
Response
The overall response rate (ORR) (classified as either CR or PR, although only PRs were seen) was measured in 60 out of the 71 participants randomised to oral topotecan plus BSC. This was measured using WHO criteria and was reported to be 7% (95% CI 2.33 to 15.67). The study also reports a subgroup analysis according to one stratification factor (TTP) for response, but these data are not reported here, as they were only for the oral topotecan plus BSC group.
Duration of response
The median time to progressive disease in the oral topotecan plus BSC group was 16.3 weeks (95% CI 12.9 to 20.0). Those in the BSC group were already in a progressive disease state and hence no comparison was made in the study report. It was also reported that 83% (n = 59) of the oral topotecan plus BSC group experienced progression and 34% (n = 24) reached progressive disease (by WHO criteria). Some 44% (n = 31) of participants had achieved stable disease. It is unclear in the study report at what point these data were collected.
Quality of life
The study of O’Brien and colleagues57 reports the rate of deterioration of QoL (per 3-month period) as measured by the EuroQol 5 dimension health questionnaire (EQ-5D) (lower score indicates worse QoL). Baseline EQ-5Ds were completed by 68 (96%) participants in the oral topotecan plus BSC group and 65 (93%) participants in the BSC group. At least one postbaseline questionnaire was completed by 63 (89%) participants in the oral topotecan plus BSC group and 49 (70%) participants in the BSC group. No baseline scores were presented (see Appendix 11). The results showed a difference between treatment arms, favouring the oral topotecan plus BSC arm (topotecan + BSC: –0.05, 95% CI –0.11 to 0.02; BSC: –0.20, 95% CI –0.27 to –0.12, difference 0.15, 95% CI 0.05 to 0.25).
The Chen and colleagues (2007)64 abstract reported additional QoL data on the EQ-5D index as well as the visual analogue scale [(VAS) – lower score indicates poorer imaginable health state]. The mean change from baseline in both the EQ-5D index and VAS for the pooled and last evaluation analyses was statistically significantly different between groups (Table 5), indicating a smaller decline in health status for those receiving oral topotecan plus BSC. It should be noted that the high proportion of participants reported to have completed at least one postbaseline questionnaire does not necessarily reflect the number of participants in the pooled and last evaluation analyses. In the pooled estimate, there will be a number of participants who were tested a number of times (depending on, for example, survival, inability or refusal to complete the questionnaire) with the results of multiple assessments averaged; in the last evaluation analysis, it is possible that results from some participants were missing for the same reasons, but these numbers are not known. Also caution should be taken in interpreting the results as the data are reported in abstract form only.
| Study: O’Brien et al. 200657,64 | Treatment arms | p-value | |
|---|---|---|---|
| Oral topotecan + BSC (n = 71) | BSC (n = 70) | ||
| EQ-5D, rate of deterioration per 3-month interval |
–0.05 (95% CI –0.11 to 0.02) |
–0.20 (95% CI –0.27 to –0.12) |
Difference 0.15 (95% CI 0.05 to 0.25) |
| EQ-5D index (pooled analysisa), mean change from baseline | –0.03 | –0.12 |
Difference 0.09 (p = 0.0036) |
| EQ-5D index (changeb), mean change from baseline | –0.10 | –0.30 |
Difference 0.2 (p = 0.0034) |
| EQ-5D VAS (pooled analysisa), mean change from baseline | 0.30 | –7.41 |
Difference 7.71 (p < 0.0001) |
| EQ-5D VAS (changeb), mean change from baseline | –3.98 | –14.46 |
Difference 10.48 (p = 0.0025) |
Symptoms
O’Brien and colleagues57 also report participant symptoms based on a self-reported measure, the patient symptom assessment (PSA) scale, which evaluates the degree to which participants experience nine symptoms, rating from 1 (no symptom) to 4 (very severe symptoms). The results are presented as odds ratios (ORs) of the likelihood of symptom improvement with oral topotecan plus BSC relative to BSC alone. The ORs presented for each individual symptom suggest that shortness of breath (OR 2.18, 95% CI 1.09 to 4.38), sleep disturbance (OR 2.16, 95% CI 1.15 to 4.06) and fatigue (OR 2.29, 95% CI 1.25 to 4.19) may be improved in those with oral topotecan plus BSC (all p < 0.05). The other symptoms were not found to be statistically significantly different between the two treatment arms (individual symptoms can be seen in Table 6). For this measure, baseline questionnaires were completed by 70 participants in the topotecan plus BSC group and 67 participants in the BSC group. The numbers of participants with sufficient data to be included in the analyses varied for the symptom scores between 47 and 48 for the BSC group, and between 60 and 61 for the topotecan plus BSC group. In addition, although this scale is reported to resemble a well-validated lung cancer symptom scale (LCSS), it is unclear whether the PSA scale has been validated, therefore the outcomes should be cautiously interpreted. A more recent abstract (2007) by O’Brien and colleagues65 presents a subgroup analysis of the association between baseline PSA total scores and performance status according to PR or stable disease for the oral topotecan plus BSC group only, but the data have neither been extracted nor reported here.
| Study: O’Brien et al. 200657 | Odds ratio: oral topotecan–BSC | 95% CI | p-value |
|---|---|---|---|
| Improvement in PSA scores | |||
| Shortness of breath | 2.18 | 1.09 to 4.38 | p < 0.05 |
| Cough | 1.35 | 0.68 to 2.66 | NS |
| Chest pain | 2.07 | 1.00 to 4.28 | NS |
| Coughing blood | 1.95 | 0.46 to 8.27 | NS |
| Loss of appetite | 1.02 | 0.57 to 1.84 | NS |
| Interference of sleep | 2.16 | 1.15 to 4.06 | p < 0.05 |
| Hoarseness | 1.35 | 0.63 to 2.87 | NS |
| Fatigue | 2.29 | 1.25 to 4.19 | p < 0.05 |
| Interference with daily activity | 1.70 | 0.95 to 3.03 | NS |
Adverse events and toxicity
Rates of adverse events between those in the oral topotecan plus BSC arm and those in the BSC alone arm were reported for non-sepsis infection, sepsis, diarrhoea, fatigue, vomiting, dyspnoea and cough in the O’Brien and colleagues study,57 and can be seen in Table 7. From this it can be observed that rates were generally low and similar across groups, with the exception of diarrhoea and dyspnoea, which are slightly different between the groups. None of these was tested for statistical significance, and it is not clear whether the definitions of these symptoms differ from those used in the PSA as reported above. All-cause mortality within 30 days of randomisation was 7% in the oral topotecan plus BSC arm and 13% in the BSC alone arm.
| Study: O’Brien et al. 200657 | Treatment arms: | |
|---|---|---|
| Oral topotecan + BSC (n = 71) | BSC (n = 70) | |
| Non-sepsis infection ≥ grade 2 | 10 (14%) | 8 (12%) |
| Sepsis | 3 (4%) | 1 (1%) |
| Diarrhoea | 6% | 0 |
| Fatigue | 4% | 4% |
| Vomiting | 3% | 0 |
| Dyspnoea | 3% | 9% |
| Cough | 0 | 2% |
Treatment-related toxicity was also presented for the oral topotecan-treated group and is shown in Table 8. From this it can be seen that 61% had grade 3 or 4 neutropenia, with 3% of participants (n = 2) observed to have febrile neutropenia. Grade 3 or 4 thrombocytopenia was seen in 38% of participants, and anaemia in 25%. It is unclear, because of the nature of the study, what the impact of these rates of toxicities may be taken to mean as there can be no comparator data. Toxic deaths occurred in 4 (6%) participants, three of which were due to haematological toxicity.
| Study: O’Brien et al. 200657 | Topotecan + BSC (n = 71) |
|---|---|
| Treatment-related toxicity (%) | |
| Grade 3/4 neutropenia | 61 |
| Grade 3/4 thrombocytopenia | 38 |
| Grade 3/4 anaemia | 25 |
| Febrile neutropenia | 3 |
Summary of effectiveness of oral topotecan plus BSC versus BSC alone
In this one RCT of reasonable quality, there appears to be an OS benefit to having oral topotecan in addition to BSC. The HR, adjusted for baseline covariates, was favourable to oral topotecan. OS was the primary outcome in this study. Response was measured in only those in the oral topotecan group, as no comparator was appropriate. In those who were assessed, QoL was better in those who were given oral topotecan in addition to BSC. Rates of adverse events appeared to be similar between the two groups. Toxicities were reported, but, due to the nature of the comparator intervention, cannot be placed into context in this study alone.
Intravenous topotecan versus CAV
Survival
The von Pawel and colleagues (1999) trial59 was the only trial that compared i.v. topotecan with CAV. The median OS was reported to be 25.0 weeks (range 0.4–90.7) for participants who were given topotecan and 24.7 weeks (range 1.3–101.3) for participants given CAV (Table 9). The Cox regression model for survival showed no statistically significant difference between treatment groups (p = 0.795), with a risk ratio (RR) of topotecan–CAV of 1.039. At the time of analysis, 11.2% and 12.5% of topotecan and CAV participants, respectively, were censored for survival. The 6- and 12-month survival rates, calculated using Kaplan–Meier analysis, were similar between treatment groups and can be seen in Table 9.
| Study: von Pawel et al. 199959 | Treatment arms | p-value | |
|---|---|---|---|
| Intravenous topotecan (n = 107) | CAV (n = 104) | ||
| OS (weeks), median (range) | 25 (0.4–90.7)a | 24.7 (1.3–101.3) | p = 0.795 |
| Survival rate (%) | |||
| 6 months | 46.7 | 45.2 | Not reported |
| 12 months | 14.2 | 14.4 | Not reported |
Subgroup analyses (see Appendix 6 for full data) of the two stratification factors, baseline performance status and extent of disease, found that these were statistically significant prognostic factors for survival (p < 0.001). In addition to the stratification factors, gender, baseline liver metastases and baseline brain metastases were also found to be significant factors for survival (p < 0.05). However, after adjustment for the covariates, the effect of treatment was still not statistically significant (RR 1.17, p = 0.322). It should be noted that it is unclear if the study was powered for the subgroup analyses and results should be interpreted with caution.
Progression-free survival was not reported in the von Pawel and colleagues (1999) study. 59
Response
Response rate and duration of response were the primary outcomes in this study, and response rates were determined using the WHO criteria. The ORR was 24.3% (95% CI 16.2 to 32.4) for participants who received topotecan compared with 18.3% (95% CI 10.8 to 25.7) for participants who received CAV (p = 0.285), with a difference in the rates of response of 6.0% (95% CI 6 to 18) (Table 10). A CR was achieved in only one participant (CAV); 24.3% and 17.3% of topotecan and CAV participants, respectively, achieved a PR. A logistic regression model (evaluating the effect of baseline characteristics) identified presence of baseline liver metastases and gender as significant factors in determining response (p = 0.043 and p = 0.008, respectively – see Appendix 6). It should be noted that the authors only presented data for the factors that were shown to be statistically significant. After adjusting for the covariates, it is reported that those treated with topotecan showed a greater propensity to respond than did those treated with CAV, although the result was not statistically significant (OR 1.24, p = 0.557). Subgroup analyses for males and females, and for those experiencing relapse 60–90 days after completion of first-line chemotherapy, were reported, but not tested, for statistical significance (see Appendix 6).
| Study: von Pawel et al. 199959 | Treatment arms | p-value, 95% CI | |
|---|---|---|---|
| Intravenous topotecan (n = 107) | CAV (n = 104) | ||
| ORR, n (%) | 26 (24.3), 95% CI 16.2 to 32.4 | 19 (18.3), 95% CI 10.8 to 25.7 | p = 0.285, difference 6.0% (95% CI 6 to 18a) |
| – CR | 0 | 1 (1) | |
| – PR | 26 (24.3) | 18 (17.3) | |
| Response duration (weeks), median (range) |
n = 26 14.4 (9.4–50.1) |
n = 19 15.3 (8.6–69.9)b |
p = 0.300 |
| Time to response (weeks), median (range) |
n = 26 6 (2.4–15.7) |
n = 19 6.1 (5.4–18.1) |
p = 0.953 |
| Non-responders, n (%) | |||
| – overall | 81 (75.7) | 85 (81.7) | Not reported |
| – stable disease | 21 (19.6) | 12 (11.5) | Not reported |
| – progressive disease | 49 (45.8) | 55 (52.9) | Not reported |
| – not assessable | 11 (10.3) | 18 (17.3) | Not reported |
Duration of response and time to response
High proportions of participants in each treatment group did not respond to treatment. The proportion of non-responders reported to have stable or progressive disease (according to WHO criteria) or who were not assessable are shown in Table 10. On the whole, the proportions appear similar between treatment groups, although slightly more in the topotecan arm were classed as having stable disease. However, no statistical comparison was reported. The median duration of response was 14.4 weeks (range 9.4–50.1) in the topotecan group and 15.3 weeks (range 8.6–69.9) in the CAV group, with no statistically significant difference between groups (p = 0.300). Similarly, the median time to response was not statistically different between treatments (p = 0.953) and was approximately 6 weeks in each arm.
Time to progression
No statistically significant difference was found between topotecan and CAV for median TTP (13.3 weeks versus 12.3 weeks, respectively, p = 0.552) (Table 11).
Quality of life
Quality of life was not reported in the von Pawel and colleagues (1999) study. 59
Symptoms
von Pawel and colleagues (1999)59 used a symptom-specific SCLC questionnaire to measure participant symptoms. Patient symptom assessments were scored on a four-point ordinal scale (1, not at all; 2, a little bit; 3, quite a bit; 4, very much), and improvement had to be sustained for two consecutive courses. Symptom evaluation also included the time to symptom worsening as defined by the interval from the first dose of study medication until the first evidence of worsening in the postbaseline assessment.
Using Pearson’s uncorrected chi-squared statistic to compare treatment groups, greater symptomatic improvement was seen in participants who received topotecan for symptoms of dyspnoea (p = 0.002), anorexia (p = 0.042), hoarseness (p = 0.043) and fatigue (p = 0.032), as well as for interference with daily activity (p = 0.023). The other symptoms (Table 12) were not found to be statistically significantly different between the two treatment arms. For this measure, the number of participants with sufficient data to be included in the analyses (i.e. baseline and at least one postbaseline assessment) varied for the symptom scores between 15 and 70 for topotecan, and between 12 and 65 for CAV. The study also reported significant differences in the length of time to worsening of dyspnoea (p = 0.046) and anorexia (p = 0.003), with symptoms progressing more slowly in the topotecan group. However, data were not presented for any symptom for this latter outcome. It should also be noted that the symptom-specific questionnaire used in this study was not a validated instrument, and it is therefore unclear how reliable the results are.
| Study: von Pawel et al. 199959 | Treatment arms: | p-value | |
|---|---|---|---|
| Intravenous topotecan (n = 107) | CAV (n = 104) | ||
| Improvement in disease-related symptoms, n/Na (%) | |||
| Dyspnoea | 19/68 (27.9) | 4/61 (6.6) | 0.002b |
| Cough | 17/69 (24.6) | 9/61 (14.8) | 0.160 |
| Chest pain | 11/44 (25.0) | 7/41 (17.1) | 0.371 |
| Haemoptysis | 4/15 (26.7) | 4/12 (33.3) | 0.706 |
| Anorexia | 18/56 (32.1) | 9/57 (15.8) | 0.042b |
| Insomnia | 19/57 (33.3) | 10/53 (18.9) | 0.085 |
| Hoarseness | 13/40 (32.5) | 5/38 (13.2) | 0.043b |
| Fatigue | 16/70 (22.9) | 6/65 (9.2) | 0.032b |
| Interference with daily activity | 18/67 (26.9) | 7/63 (11.1) | 0.023b |
Toxicity and adverse events
Adverse events of all grades, which were related, or possibly related, to treatment, and which occurred in more than 10% of participants, were reported for the two treatment groups, and can be seen in Table 13 (see Appendix 6 for rates of adverse events of grades 1/2 and 3/4). The most frequently reported adverse events were nausea, fatigue, vomiting, anorexia and alopecia. Overall, the groups appeared comparable for all reported adverse events, although in participants receiving topotecan the incidence of fatigue was lower and the incidence of alopecia was higher than in those receiving CAV. The trial did not report a statistical comparison between treatment groups. Six deaths (5.6%) in the topotecan group and four deaths (3.8%) in the CAV group were related, or possibly related, to treatment. Of the 10 deaths, seven (four topotecan, three CAV) were associated with therapy-induced myelosuppression with sepsis/infection.
| Study: von Pawel et al. 199959 | Treatment arms | |
|---|---|---|
| Intravenous topotecan (n = 107) | CAV (n = 104) | |
| Adverse events (all grades) occurring in > 10% of patients, n (%) | ||
| Nausea | 42 (39.3) | 42 (40.4) |
| Alopeciaa | 38 (35.5) | 23 (22.1) |
| Fatigue | 28 (26.2) | 35 (33.7) |
| Vomiting | 26 (24.3) | 25 (24.0) |
| Anorexia | 20 (18.7) | 23 (22.1) |
| Stomatitis | 15 (14.0) | 13 (12.5) |
| Diarrhoea | 13 (12.1) | 13 (12.5) |
| Feverb | 13 (12.1) | – |
| Constipation | – | 16 (15.4) |
| Asthenia | – | 14 (13.5) |
| Treatment-related deaths | 4 | 3 |
| Deaths possibly related or related to therapy | 2 | 1 |
The incidence of haematological toxicities are presented in Table 14. Grade 4 neutropenia occurred significantly more frequently in the topotecan group than CAV (p < 0.001) for treatment courses (see Appendix 6), but this was not statistically significant for the participant analysis. In addition, the incidence of grade 4 thrombocytopenia (p < 0.001) and grade 3/4 anaemia (p < 0.001) was significantly higher in participants receiving topotecan. Infectious complications were reported to be similar between treatment groups.
| Study: von Pawel et al. 1999,59 haematological toxicities, n/Na (%) | Treatment arms | |||
|---|---|---|---|---|
| Intravenous topotecan (n = 107) | CAV (n = 104) | |||
| Grade 3 | Grade 4 | Grade 3 | Grade 4 | |
| Leucopenia | 57/104 (54.8) | 33/104 (31.7) | 38/101 (37.6) | 44/101 (43.6) |
| Neutropenia | 19/104 (18.3) | 73/104 (70.2) | 15/99 (15.2) | 71/99 (71.7) |
| Thrombocytopenia | 30/104 (28.8) | 30/104 (28.8)b | 10/101 (9.9) | 5/101 (5.0)b |
| Anaemia | 41/104 (39.4)c | 3/104 (2.9)c | 18/101 (17.8)c | 2/101 (2.0)c |
Summary of effectiveness of i.v. topotecan versus CAV
In the one RCT identified, topotecan and CAV were not found to be statistically significantly different for the primary outcomes of response and duration of response. Furthermore, there were neither significant differences between groups for OS nor TTP. QoL was not reported. Greater symptomatic improvement was seen in participants who received topotecan for four symptoms as well as interference with daily activity, and symptoms progressed significantly more slowly in the topotecan group for two out of the eight symptoms evaluated. However, the symptom-specific questionnaire used in this study was not a validated instrument. Overall, the treatment groups were comparable for rates of adverse events, although the incidence of some haematological toxicities occurred significantly more frequently in the topotecan group than in the CAV group. The trial was judged to be of reasonable methodological quality.
Oral versus i.v. topotecan
Survival
Two RCTs56,58 compared oral and i.v. topotecan. In both trials, no statistically significant differences in OS were found between treatment groups (Table 15). Eckardt and colleagues56 reported a median survival of 33.0 weeks (range 0.3–185.3) for oral participants and 35.0 weeks (range 0.7–205.3) for i.v. participants (HR 0.98, 95% CI 0.77 to 1.25). At the time of analysis, 13.7% and 10.6% of oral and i.v. topotecan participants, respectively, were censored for survival. The 1- and 2-year survival rates appeared comparable between treatment arms (see Table 15), but a statistical test was not reported. Data collected during poststudy monitoring showed that similar proportions of participants in each group had received third-line chemotherapy (33% and 35% in oral and i.v. groups, respectively). It is not clear whether this may have had an impact on the OS rates presented.
| Study: Eckardt et al. 200756 | Treatment arms | p-value, 95% CI | |
|---|---|---|---|
| Oral topotecan (n = 153) | Intravenous topotecan (n = 151) | ||
| OS (weeks), median (range), 95% CI | 33.0 (0.3 to 185.3),a 29.1 to 42.4 | 35.0 (0.7 to 205.3),a 31.0 to 37.4 | HR = 0.98, 95% CI 0.77 to 1.25, p = ns |
| Survival rate at year 1 (%) | 33 | 29 | Not reported |
| Survival rate at year 2 (%) | 12 | 7 | Not reported |
| von Pawel et al. 200158 | Oral topotecan (n = 52) | i.v. topotecan (n = 54) | |
| OS (weeks) median (range) | 32.3 (0.4–69.1) a | 25.1 (0.6–65.1) a | RR = 0.84, 95% CI 0.53 to 1.32 |
In the study by von Pawel and colleagues (2001),58 median survival was higher in the oral topotecan group (32.3 weeks, range 0.4–69.1) than in the i.v. topotecan group (25.1 weeks, range 0.6–65.1), but this difference was not statistically significant [RR (oral:intravenous) 0.84, 95% CI 0.53 to 1.32]. The study reports that regression modelling identified no baseline liver metastases (p = 0.001) and lower performance status (PS) (p = 0.025), as statistically significantly associated with longer survival. The study presents only the p-values for these two significant factors; no data were presented, neither were there any discussion of the results of the other possible factors tested. This hinders any meaningful interpretation of the results of the modelling and so caution is recommended. After accounting simultaneously for all prognostic factors, the RR (oral:intravenous) of survival was reported to be 0.90 (95% CI 0.55 to 1.47).
Response
Response rate was the primary outcome in both the Eckardt and colleagues study56 and the von Pawel and colleagues58 study, and can be seen in Table 16. The difference in the ORR between those participants treated with oral topotecan and those treated with i.v. topotecan was reported to be –3.6% (95% CI –12.6% to 5.5%) in the Eckardt and colleagues56 study. In contrast, von Pawel and colleagues58 reported a difference in ORR of 8.3% (95% CI –6.6% to 23.1%). Although the overall responses in the two included studies were in different directions, neither was found to be statistically significantly different. The definition of response was not reported in the Eckardt and colleagues56 trial. However, two participants in the oral topotecan group were reported to have a CR, with the remaining 26 having a PR. In the i.v. treatment group, all of those responding were classified as a PR. Response in the von Pawel and colleagues58 study was classified according to the WHO criteria. Of the responders in this study,58 one participant in the oral topotecan group and two in the i.v. topotecan group were classified as complete responders – the remainder were PRs.
| Study | Treatment arms | p-value, 95% CI | |
|---|---|---|---|
| Eckardt et al. 200756 | Oral topotecan (n = 153) | i.v. topotecan (n = 151) | |
| ORR, n (%) | 28 (18.3%) | 33 (21.9%) | Difference (oral – i.v.) 3.6% |
| 95% CI | 12.2% to 24.4% | 15.3% to 28.5% | –12.6% to 5.5% |
| CR | 2 (1.3%) | 0 | |
| PR | 26 (17.0%) | 33 (21.9%) | |
|
Time to response (weeks), median (range) |
n = 28 6.1 (4.4–17.7) |
n = 33 6.1 (2.1–13.9) |
Not reported |
|
Response duration (weeks), median (range) |
n = 28 18.3 (9.0–65.4) |
n = 33 25.4 (8.4–132.1)a |
Not reported |
| Non-responders, n (%)a | |||
| Stable disease | 27 (17.6%) | 35 (23.2%) | Not reported |
| Progressive disease | 78 (51.0%) | 65 (43.0%) | Not reported |
| Not assessable | 20 (13.1%) | 18 (11.9%) | Not reported |
| von Pawel et al. 200158 | Oral topotecan (n = 52) | Intravenous topotecan (n = 54) | |
| ORR, n (%) | 12 (23.1) | 8 (14.8) | Difference 8.3% |
| 95% CI | 11.6 to 34.5 | 5.3 to 24.3 | –6.6% to 23.1% |
| CR | 1 (1.9) | 2 (3.7) | |
| PR | 11 (21.2) | 6 (11.1) | |
| Response duration (weeks), median | n = 12, 18 | n = 8, 14 | Not reported |
| Non-responders, n (%) | |||
| Stable disease | 10 (19.2) | 16 (29.6) | Not reported |
| Progressive disease | 16 (30.8) | 23 (42.6) | Not reported |
| Not assessable | 14 (26.9) | 7 (13.0) | Not reported |
Median time to response was the same (6.1 weeks) for both treatment arms of the Eckardt and colleagues56 study. In the von Pawel and colleagues58 study, there was a median of 18 weeks’ response in the orally treated participants compared with 14 weeks in the intravenously treated participants. This was not tested for statistical significance in the trial. In those responding in the Eckardt and colleagues56 study, the duration of response was longer in the i.v. topotecan arm (median 25.4 weeks) compared with the oral topotecan arm (median 18.3 weeks), but no test of statistical significance was undertaken. In the von Pawel and colleagues58 study, it is reported that regression modelling of response identified two factors that were statistically associated with increased probability of response – female gender (p = 0.021) and no previous radiotherapy (p = 0.015). The study only presented the p-values for these two significant factors, no data were reported. There was also no further discussion of the results of other possible factors, nor any data, so caution is required in interpreting these results of prognostic factors. Accounting simultaneously for all prognostic factors that were identified in the logistic regression analysis, oral topotecan participants were seen to be 1.6 (OR) times more likely to respond than i.v. topotecan participants (95% CI: 0.50 to 5.15).
Of those classified as non-responders in the Eckardt and colleagues56 study, 17.6% of the oral topotecan-treated participants and 23.2% of the i.v. topotecan-treated participants were classified as having stable disease. Progressive disease was reported in 51.0% and 43.0% of participants in the oral topotecan group and i.v. topotecan groups, respectively. The study reported that 38 participants were not assessable for response due to death, withdrawal or completion of treatment after one or two courses (although the study also reports this figure as 32, it is assumed this is an error). Of those classified as non-responders in the von Pawel and colleagues58 study, 19.2% and 29.6% of participants in the oral- and i.v. topotecan groups, respectively, were classified as stable disease. Progressive disease was seen in 30.8% of those treated with oral topotecan compared with 42.6% of those treated with i.v. topotecan. Finally, in this study,58 26.9% and 13.0% of participants in the oral- and i.v. topotecan groups, respectively, were classified as not assessable. No definitions for these classifications were reported in either study, and no statistical analyses of any differences between groups were undertaken.
Time to disease progression
The median TTP in the Eckardt and colleagues56 study was reported to be 11.9 weeks in the oral topotecan group and 14.6 weeks in the i.v. topotecan group (Table 17). The trial publication does not report any statistical analyses of these data between the two groups, but it would appear that i.v. topotecan led to a longer duration before the disease progressed than oral topotecan. Conversely, in the von Pawel and colleagues58 study the median TTP was reported to be 15 weeks in the oral topotecan group and 13 weeks in the i.v. topotecan group. The RR was 0.90 (95% CI 0.59 to 1.39), suggesting no differences between the two treatment options. von Pawel and colleagues58 report that regression modelling of TTP identified female gender (p = 0.041), no liver metastases at baseline (p = 0.020) and lower PS (p = 0.036) as associated with longer TTP. No data were presented for these or any other factors that were tested in the model and therefore caution is recommended when interpreting these results.
| Study | Treatment arms | p-value, 95% CI | |
|---|---|---|---|
| Eckardt et al. 200756 | Oral topotecan (n = 153) | Intravenous topotecan (n = 151) | |
| TTP (weeks), median (range) | 11.9 (0.3 to 149.0)a | 14.6 (0.7 to 177.9)a | Not reported |
| 95% CI | 9.7 to 14.1 | 13.3 to 18.9 | |
| von Pawel et al. 200158 | Oral topotecan (n = 52) | Intravenous topotecan (n = 54) | |
| TTP (weeks), median (range) | 15 (0.4–69.1) | 13 (0.6–65.1)a |
RR 0.90 95% CI 0.59 to 1.39 |
Quality of life
In the Eckardt and colleagues56 trial, HRQoL was assessed using the Functional Assessment of Cancer Therapy – Lung (FACT-L) scale. This is a 44-item, self-reported instrument, which is reported to be a validated scale and includes four generic dimensions and a subscale that is specific to lung cancer. In addition, the trial outcome index (TOI) was also derived from a subgroup of data. Very few data were presented in the study report, but the authors state that the mean change from baseline indicated no statistical difference between treatment groups for subscale dimension scores or the lung cancer scale (LCS), the TOI or the FACT-L total scores. The mean change from baseline to the last course of treatment also showed no statistical differences between groups (no data were provided). QoL was not assessed in the von Pawel and colleagues58 study.
Symptoms
In those reporting symptoms at baseline, von Pawel and colleagues58 reported the proportion showing an improvement, which was classed as sustained improvement needed until the next treatment cycle. Symptoms were evaluated on a four-point scale (1 = not at all, 2 = a little bit, 3 = quite a bit, 4 = very much) and, although based on the lung cancer symptom score, it was reported that this was not a validated scale. The proportions of participants with improved symptoms were generally between 13% and 42% across all symptoms. The scores were not tested for statistically significant differences between the two groups (see Appendix 6 for full results). In the oral- and i.v. topotecan groups, respectively, the symptoms with the greatest reduction were chest pain (42.1% versus 31.8%), haemoptysis (33.3% versus 40%) and hoarseness (35.7% versus 37.5%). Symptoms scores were not reported by Eckardt and colleagues. 56
Adverse events and toxicity
Eckardt and colleagues56 and von Pawel and colleagues58 report the rates of non-haematological adverse events (Table 18). Rates of grade 3 and grade 4 adverse events generally appeared to be similar across the different routes of administration of treatment in the Eckardt and colleagues56 study, with the exception of grade 3 diarrhoea and anorexia, which were more frequently observed in the oral topotecan group. In the von Pawel and colleagues58 study, rates of non-haematological adverse events were also seen to be similar between the two treatment regimens, with perhaps the exception of vomiting, pneumonia and diarrhoea, which appeared to occur more frequently in the oral topotecan group, and alopecia, which occurred more frequently in the i.v. topotecan group. However, no statistical analyses of these rates were reported. In the Eckardt and colleagues56 study there were six deaths in the oral topotecan group and four in the i.v. topotecan group. The study reports that participants died as a result of haematological toxicity, septic shock related to topotecan treatment or of other causes possibly related to topotecan treatment. In the von Pawel and colleagues58 study, two participants (1.9%) in the oral topotecan group died of sepsis and febrile agranulocytosis.
| Study | Treatment arms | |||||||
|---|---|---|---|---|---|---|---|---|
| Eckardtet al. 200756 | Oral topotecan (n = 153) | Intravenous topotecan (n = 151) | ||||||
| Non-haematological adverse effects, n (%) | Grade 3 | Grade 4 | Grade 3 | Grade 4 | ||||
| Diarrhoea | 11 (7.2) | 1 (0.7) | 3 (2.0) | 1 (0.7) | ||||
| Fatigue | 10 (6.5) | 0 | 10 (6.6) | 2 (1.3) | ||||
| Dyspnoea | 9 (5.9) | 3 (2.0) | 10 (6.6) | 5 (3.3) | ||||
| Anorexia | 8 (5.2) | 0 | 3 (2.0) | 1 (0.7) | ||||
| Nausea | 6 (3.9) | 0 | 3 (2.0) | 1 (0.7) | ||||
| Asthenia | 4 (2.6) | 3 (2.0) | 7 (4.6) | 3 (2.0) | ||||
| Fever | 3 (2.0) | 3 (2.0) | 4 (2.6) | 6 (4.0) | ||||
| von Pawel et al. 200158 | Oral topotecan (n = 52) | Intravenous topotecan (n = 54) | ||||||
| Adverse effects, n (%)a | Grade 3 | Grade 4 | Grade 5 | Grade 3 | Grade 4 | Grade 5 | ||
| Vomiting | 6 (11.5) | 0 | 0 | 2 (3.7) | 0 | 0 | ||
| Dyspnoea | 5 (9.6) | 0 | 0 | 5 (9.3) | 0 | 1 (1.9) | ||
| Fever | 2 (3.8) | 1 (1.9) | 1 (1.9) | 1 (1.9) | 0 | 0 | ||
| Pneumonia | 3 (5.8) | 1 (1.9) | 0 | 0 | 0 | 1 (1.9) | ||
| Diarrhoea | 4 (7.7) | 0 | 0 | 0 | 0 | 0 | ||
| Pulmonary embolism | 1 (1.9) | 0 | 2 (3.8) | 0 | 0 | 1 (1.9) | ||
| Asthenia | 3 (5.8) | 0 | 0 | 5 (9.3) | 0 | 0 | ||
| Fatigue | 3 (5.8) | 0 | 0 | 1 (1.9) | 0 | 0 | ||
| Alopecia | 1 (1.9) | 0 | 0 | 7 (13.0) | 0 | 0 | ||
| Abscess | 0 | 0 | 0 | 2 (3.7) | 1 (1.9) | 0 | ||
Associated toxicities (grades 3 and 4) from the respective treatments were also reported in the studies by Eckardt and colleagues56 and von Pawel and colleagues,58 and can be seen in Table 19. Based on observation of these data, it would appear that rates are similar across the treatment groups in the Eckardt and colleagues56 study. Grade 4 neutropenia and grade 3 anaemia appeared to occur more frequently in the intravenously treated participants than the orally treated participants, while grade 4 thrombocytopenia appeared to occur more frequently in the orally treated participants. In the Eckardt and colleagues56 study the authors also report that fever and/or infection (≥ grade 2) associated with grade 4 neutropenia, together with sepsis, occurred in 5% of courses in both groups. In the von Pawel and colleagues58 study, rates of toxicities were also observed to be similar between the two treatment arms, with the exception of grade 4 neutropenia, which was reported to be statistically significantly more frequently observed in the i.v. topotecan treatment group (p = 0.001). The trial also reports that the median duration of grade 4 neutropenia was similar between groups (oral group 7 days, i.v. group 6 days). Although the trial does not report a statistically significant difference between rates of grade 3 leucopenia, it can be observed that the rates are higher in the i.v. topotecan group than the oral topotecan group.
| Study | Treatment arms | |||
|---|---|---|---|---|
| Eckardt et al. 200756 | Oral topotecan (n = 153) | Intravenous topotecan (n = 151) | ||
| Toxicities, n (%)a | Grade 3 | Grade 4 | Grade 3 | Grade 4 |
| Leucopenia | 64 (42.7) | 34 (22.7) | 74 (49.3) | 39 (26.0) |
| Neutropenia | 39 (26.2) | 70 (47.0) | 35 (23.6) | 95 (64.2) |
| Thrombocytopenia | 30 (20.0) | 43 (28.7) | 38 (25.3) | 27 (18.0) |
| Anaemia | 26 (17.3) | 8 (5.3) | 42 (28.0) | 4 (2.7) |
| von Pawel et al. 200158 | Oral topotecan (n = 52) | Intravenous topotecan (n = 54) | ||
| Toxicities n (%) | Grade 3 | Grade 4 | Grade 3 | Grade 4 |
| Neutropenia | 21.6 | 35.3 | 26.9 | 67.3 |
| Leucopenia | 27.5 | 17.6 | 45.3 | 28.3 |
| Thrombocytopenia | 25.5 | 27.5 | 24.5 | 24.5 |
| Anaemia | 27.5 | 3.9 | 26.4 | 3.8 |
Summary of effectiveness of i.v. versus oral topotecan
There were no statistically significant differences in OS between treatment groups for either of these studies. Similarly, no statistically significant differences were seen in the ORR. Intravenous topotecan appeared to lead to a longer duration before disease progression than oral topotecan in one study,56 but this was not supported by the other. 58 Quality of life was assessed in one of the included studies56 and there appeared to be no statistically significant differences between treatment groups. No statistical analyses of adverse event rates were reported in either study. Associated grade 3 and grade 4 toxicities were similar between i.v. topotecan and oral topotecan in the studies, with the exception of grade 3 or 4 neutropenia, which appeared to occur more frequently in the intravenously treated participants. While these studies suggest that i.v. and oral topotecan are equivalent, it should be noted that neither study was powered to test for equivalence or non-inferiority. In addition, these studies were of unknown methodological quality due to the lack of details reported. Furthermore, it should be considered that there is some uncertainty over whether the Eckardt and colleagues56 study fully meets the inclusion criteria of the current review. For these reasons, it was deemed inappropriate to combine the two trials in a meta-analysis.
Intravenous amrubicin versus i.v. topotecan
Survival
One RCT (Inoue and colleagues63) was included, which compared i.v. topotecan with i.v. amrubicin. In this trial, median OS was not statistically significantly different (p = 0.17) between the amrubicin-treated participants (8.1 months) and the topotecan-treated participants (8.4 months). Progression-free survival between the treatment groups was also not statistically significant (p = 0.16), with a median 3.5 months for the amrubicin group versus 2.2 months for the topotecan group (Table 20). One participant in the amrubicin arm received no treatment due to rapid disease progression, and hence was not included in the analysis. The paper reported a subgroup analysis of OS and PFS according to relapse type. No statistical tests of the difference between treatment groups were presented (see Appendix 6), although for both outcomes the trend was for participants with sensitive disease to do better than those with refractory disease. However, it is unclear if the study was powered for this analysis. Many of the participants received subsequent (third-line or later) chemotherapy after disease progression (48% and 70% in the amrubicin and topotecan groups, respectively) with crossover administration performed in 41% of participants (17% and 63%, respectively). In addition, the dose of topotecan used (1.0 mg/m2) was lower than the UK recommended dose (1.5 mg/m2). It is not clear whether these factors may have had an impact on the OS rates shown.
| Study: Inoue et al. 200863 | Treatment arms | p-value | |
|---|---|---|---|
| Intravenous amrubicin (n = 29) | Intravenous topotecan (n = 30) | ||
| OS, median (months) | 8.1 | 8.4 | p = 0.17 |
| Progression-free survival, median (months) | 3.5 | 2.2 | p = 0.16 |
Response
Response rate was the primary outcome in this study and was assessed according to the RECIST criteria. There was a statistically significant difference in the ORR of 38% (95% CI 21 to 58) for participants who received amrubicin compared with 13% (95% CI 1 to 25) for participants who received topotecan (p = 0.039). Again, it should be noted that a lower dose of topotecan was used. In addition, there were some discrepancies in the reporting of CIs between the full paper, abstract and conference presentation (see Appendix 6). The study reported details of participants with CR or PR, as well as stable or progressive disease in each treatment arm. No participants in either group showed a CR. It can be seen in Table 21 that a greater proportion of participants receiving amrubicin achieved a PR (38% versus 13% topotecan), whereas a greater proportion of participants receiving topotecan were rated as having progressive disease (53% versus 21% amrubicin). Stable disease was reported in 41% and 33% of the amrubicin- and topotecan-treated groups, respectively. However, no statistical analysis for these data were reported.
| Study: Inoue et al. 200863 | Treatment arms | p-value | |
|---|---|---|---|
| Intravenous amrubicin (n = 29) | Intravenous topotecan (n = 30) | ||
| Overall response, n (%), 95% CI | 11 (38), 21 to 58a | 4 (13), 1 to 25b | p = 0.039 |
| Responses, n (%) | |||
| CR | 0 (0) | 0 (0) | |
| PR | 11 (38) | 4 (13) | |
| Stable disease | 12 (41) | 10 (33) | |
| Progressive disease | 6 (21) | 16 (53) | |
Inoue and colleagues63 performed subgroup analyses examining the effects of sensitive and refractory relapse, and PS 0–1 versus 2 on ORRs between treatment groups. No statistically significant differences were shown (all p > 0.05, see Appendix 6), but it should be noted that it is unclear if the study was powered for these analyses. In addition, the trial also reports further analysis of three prognostic factors (age, gender and prior chemotherapy regimen) but no data were presented.
The study also reported disease control rates, but no definition was supplied and these are therefore not reported here.
Time to disease progression
Time to disease progression was not reported by this study.
Quality of life
Quality of life was not reported by this study.
Adverse events and toxicity
Adverse events can be seen in Table 22. Unlike the other included studies, febrile neutropenia was presented as a non-haematological toxicity in this study. Although rates were not tested for statistical significance, it can be observed that participants in the amrubicin treatment arm suffered much higher rates of adverse events of grades 3 and 4, with the exception of diarrhoea, which was more frequently observed in the topotecan group. It is not clear whether the lower dose of topotecan used in this trial affected the rates of adverse events shown.
| Study: Inoue et al. 2008,63 non-haematological toxicity, n | Treatment arms | |||||||
|---|---|---|---|---|---|---|---|---|
| Grade: intravenous amrubicin (n = 29) | Grade: intravenous topotecan (n = 30) | |||||||
| 2 | 3 | 4 | ≥ Grade 3 (%) | 2 | 3 | 4 | ≥ Grade 3 (%) | |
| Fatigue | 4 | 5 | 0 | 17 | 3 | 2 | 0 | 7 |
| Febrile neutropenia | – | 4 | 0 | 14 | – | 1 | 0 | 3 |
| Infection | 0 | 2 | 1 | 10 | 0 | 1 | 0 | 3 |
| Anorexia | 4 | 2 | 0 | 7 | 4 | 0 | 0 | 0 |
| Nausea/vomiting | 1 | 1 | 0 | 3 | 1 | 0 | 0 | 0 |
| Stomatitis | 1 | 1 | 0 | 3 | 0 | 0 | 0 | 0 |
| Diarrhoea | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 3 |
| Fever | 2 | 0 | 0 | 0 | 1 | 0 | 0 | 0 |
| Constipation | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Pneumonitis | 1 | 0 | 0 | 0 | 2 | 0 | 0 | 0 |
Grades of haematological toxicity were also reported in the study by Inoue and colleagues63 and can be seen in Table 23. No statistical analyses of grades or treatment arms were reported. Based on observation, it would appear that participants in the topotecan treatment arm suffered higher rates of associated toxicity of grades 3 or 4 for anaemia and thrombocytopenia, and lower rates of neutropenia, than the amrubicin group. There was a discrepancy between the abstract62 and full publication63 in the reporting of neutropenia, with the abstract62 reporting a higher rate (97%) in the amrubicin arm. One patient in the amrubicin treatment arm is reported to have died of neutropenic sepsis developing from urinary tract infection; no other deaths are reported in the study. 63
| Study: Inoue et al. 2008,63 haematological toxicity, n | Treatment arms | |||||||
|---|---|---|---|---|---|---|---|---|
| Grade: intravenous amrubicin (n = 29) | Grade: intravenous topotecan (n = 30) | |||||||
| 2 | 3 | 4 | ≥ Grade 3 (%) | 2 | 3 | 4 | ≥ Grade 3 (%) | |
| Neutropenia | 0 | 5 | 23 | 93a | 3 | 13 | 13 | 87 |
| Thrombocytopenia | 6 | 7 | 1 | 28 | 5 | 9 | 3 | 40 |
| Anaemia | 15 | 3 | 3 | 21 | 12 | 6 | 3 | 40 |
Summary of effectiveness of i.v. amrubicin versus i.v. topotecan
In this study comparing amrubicin with topotecan, the primary outcome of ORR was shown to be in favour of the amrubicin treatment arm. OS and PFS were not significantly different between the two groups. TTP and QoL were not reported. Based on our observation, rates of adverse events generally appeared to be higher for patients in the amrubicin treatment arm. Rates of toxicity varied; however, neutropenia was higher in the amrubicin group. It should be noted that there is uncertainty over whether this study fully met the inclusion criteria of this review. In addition, the topotecan dose of 1.0 mg/m2/day (the approved dose in Japan) was below the UK recommended dose of 1.5 mg/m2/day and the study is of an unknown quality due to the lack of details reported in the trial.
Ongoing studies
The following studies were identified in searches and are currently ongoing:
-
Wang XS, Hou M, Xue SL, Wu TX. Topotecan for small cell lung cancer. (Protocol) Cochrane Database of Systematic Reviews 2008, Issue 2 (date of most recent substantive amendment – 26 January 2008). This systematic review aims to investigate the role of topotecan in the management of patients with SCLC by considering its clinical effectiveness and safety. (The review will include participants who were previously untreated, will consider topotecan in combination with any other chemotherapy agent, and will also consider topotecan used in first-line treatment.)
-
NCT 00319969. A phase II, randomised trial comparing i.v. amrubicin (40 mg/m2) versus i.v. topotecan (1.5 mg/m2) in adults with extensive-stage SCLC sensitive to first-line (platinum-based) chemotherapy. Study type: open-label, multicentre, phase II, parallel RCT. Sample size: 76. Start date: April 2006. Estimated end date: January 2009 (final data collection date for primary outcome measure). Status: the study is ongoing, but not recruiting participants. Funding: Calgene Corporation. Funding amount: not reported.
-
NCT 00547651. A phase III, randomised trial comparing i.v. amrubicin (40 mg/m2) versus i.v. topotecan (1.5 mg/m2) in adults with extensive-stage or limited-stage SCLC who are sensitive or refractory to first-line (platinum-based) chemotherapy. Study type: open-label, multicentre, phase III, parallel, safety/efficacy RCT. Estimated sample size: 620. Start date: September 2007. Estimated end date: March 2011 (final data collection date for primary outcome measure). Status: the study is currently recruiting participants. Funding: Calgene Corporation. Funding amount: not reported.
Chapter 4 Economic analysis
Methods for economic analysis
The aim of this section is to assess the cost-effectiveness of topotecan compared with existing regimens in second-line chemotherapy for SCLC. The economic analysis comprises the following:
-
systematic review of the literature on the cost-effectiveness of topotecan and a review of the QoL of people suffering with SCLC. An additional search was undertaken to inform different approaches to modelling disease progression
-
review of the MS to NICE
-
presentation of the SHTAC independent economic model and cost-effectiveness evaluation.
Systematic review of the existing cost-effectiveness
A systematic literature search was undertaken to identify economic evaluations of topotecan compared with other regimens as a second-line chemotherapy in SCLC. The details of the search strategy are documented in Appendix 3. The MS was reviewed for any additional studies that were missed by the searches.
Results of the systematic review
A total of 49 potentially relevant publications of economic evaluations relating to topotecan in SCLC were identified in the search. No relevant cost-effectiveness analyses were identified after screening of the titles and abstracts.
Review of research on QoL
The details of the search strategy for QoL are in Appendix 3. A total of 122 publications relating to topotecan in SCLC were identified.
The search identified one potentially relevant study that could be used to populate the model with the relevant outcome measures as specified in the scope. This was the RCT by O’Brien and colleagues,57 which used the EQ-5D to assess HRQoL in trial participants. A further search of recent abstracts was undertaken, which identified one additional QoL abstract based on the O’Brien and colleagues RCT by Chen and colleagues. 64 Both the trial report, by O’Brien and colleagues57 and the abstract by Chen and colleagues64 have been data extracted and critically appraised in the clinical effectiveness section (see Chapter 3, Oral topotecan plus BSC versus BSC alone).
Review of manufacturer’s submission
The MS consisted of a written report and electronic model supporting the cost-effectiveness analyses.
A brief overview of the manufacturer’s cost-effectiveness analysis,51 including the approach taken to model disease progression and the effects of treatment, followed by a critical appraisal of the cost-effectiveness analysis, is presented here.
GlaxoSmithKline submission to NICE – cost-effectiveness analysis
Overview
The stated aim of the analysis was to assess the cost-effectiveness of oral topotecan plus BSC against BSC alone in people with relapsed SCLC in whom treatment with i.v. chemotherapy is not considered appropriate. The cost-effectiveness analysis was based on participant-level data from the O’Brien and colleagues RCT. 57 BSC in the evaluation consisted of analgesics, antibiotics, corticosteroids, appetite stimulants, antidepressants, red blood cell (RBC) transfusions, deep relaxation therapy, and palliative radiotherapy or surgical procedures. Participants with the active treatment were also eligible for BSC alongside treatment with oral topotecan.
The base-case analysis is reported for the whole cohort of participants who received oral topotecan plus BSC compared with BSC alone after relapse of SCLC from the O’Brien and colleagues RCT. 57 Several subgroup analyses were also reported in the MS, including different times to progression, sex, performance status and liver metastases. The maximum survival in the trial was 1480 days, or 71 21-day survival periods.
The perspective of the economic analysis is stated as being that of the NHS and PSS, capturing only those costs and benefits that are directly relevant to the intervention. The submission reports lifetime costs and outcomes (life-years gained and QALYs) for each treatment arm. An incremental analysis of costs and outcomes of topotecan plus BSC compared with BSC alone was undertaken.
Model of cost-effectiveness of topotecan
The MS reports that a systematic review of economic evaluations for oral topotecan in SCLC was undertaken. The search of databases was limited to the NHS EED and PubMed databases. The search identified nine cost-effectiveness studies, with eight being for topotecan in ovarian cancer and a further study in mobilising peripheral blood stem cells – there were no studies identified for topotecan in SCLC. This is consistent with the SHTAC systematic literature search (see Systematic review of the existing cost-effectiveness, above).
The approach taken in the MS model is outlined below. An outline review, based on a checklist suggested for the critical appraisal of cost-effectiveness analysis by Drummond and colleagues,66 the requirements of NICE for the submission on cost-effectiveness (reference case)67 and suggested guideline for good practice in decision modelling by Philips and colleagues,68 is given.
Modelling approach
The model developed by the manufacturer was a trial-based model. The multicentre trial contained 141 participants with participant characteristics being evenly distributed between the two groups. 57 Median survival times were 13.9 weeks (95% CI 11.1 to 18.6) in the BSC alone group and 25.9 weeks (95% CI 18.3 to 31.6) in the oral topotecan plus BSC group. The economic model used the data from the trial up until the final assessment period, when six participants (three in the BSC group and three in the topotecan plus BSC group) were still alive. The model assumed that all surviving participants died the day after this final assessment. The participant level survival data were divided into 21-day periods to reflect the study cycles in the RCT.
Health-state utilities were collected using the EQ-5D during the RCT. This was carried out at the beginning of each cycle, and up to, and including, cycle 12 for all participants in the topotecan plus BSC group and the BSC group. The quality-adjusted survival was calculated by multiplying individual survival in each 21-day period by the corresponding EQ-5D period score for that participant. There were a total of 1548 21-day survival periods across the 141 participants in the RCT. Individual data, however, were available for only 600 periods.
The MS reports that the 948 missing EQ-5D values in the data were mainly due to progression of disease towards death. The MS used the observed mean EQ-5D scores for the first 12 cycles from both arms of the trial to take account of the missing data from each of the corresponding cycles. A last observation carried forward approach (LOCF) was used for the topotecan plus BSC group before participants entered a progressive disease state and after treatment had finished, and, also, in BSC alone group, until five periods from death. For all other missing EQ-5D data, the MS used data from the BSC group’s EQ-5D scores for the five 21-day cycles of disease progression before death, by applying this backwards from the period in which the participant died. This was carried out for both BSC and topotecan groups. If the participant survived more than the five periods in the progressive disease state, the figures for the fourth period before death were applied backwards until the start of progressive disease.
Two categories of adverse events were recorded in the trial and used in the model; haematological adverse events and non-haematological adverse events. The incidence of non-haematological adverse events was reported as a percentage for each grade. Haematological events were reported on the basis of their resource use alone in terms of transfusions and granulocyte colony-stimulating factor (GCSF) and antibiotics. No explicit reduction in QoL was recorded for experiencing an adverse event due to the ongoing recording of EQ-5D valuation throughout the trial.
The costs applied in the MS were split into five main categories:
-
drug cost of oral topotecan
-
oral topotecan drug administration costs
-
drug monitoring costs
-
cost of non-disease progression in the oral topotecan group
-
adverse events associated with oral topotecan.
Not all resource use was collected in the trial and therefore clinical opinion was used to fill in gaps in the resource use.
Oral topotecan used in the trial was administered in 0.25- or 1.00-mg capsules and was dosed at 2.3 mg/m2/day on days 1–5 of 21-day cycles for up to 12 cycles. 57 The drug cost was calculated by multiplying the total drug use of topotecan per participant by the drug acquisition costs. The average cost of oral topotecan in the MS was calculated at £2500. The MS assumed that oral topotecan was delivered on an outpatient basis on days 1–5 and this was verified by clinical opinion. An additional small dispensing fee was also included. The total average cost for drug administration of all topotecan in the trial was £713. Drug monitoring costs for pathology monitoring, haematological toxicity monitoring and biochemical monitoring was taken from a study that included oral topotecan used as a chemotherapy in ovarian cancer, which had an average cost of £39. 69
The cost of progression to death was assumed to be the same for both groups and was not included in the incremental analysis. The cost of non-disease progression for the topotecan plus BSC group was based on clinical feedback and included outpatient visits, GP visits, chest radiographs, and blood tests every 4 weeks. The total costs of non disease progression were £758.
Non-haematological adverse events were reported in terms of a percentage for grades 1 to 4 for diarrhoea, fatigue, nausea and vomiting. Corresponding resource use was then applied to the occurrence of these events. However, haematological adverse events were accounted for in terms of transfusions, GCSF and antibiotics that were used in the trial. The average costs of treating adverse events resulting from oral topotecan in the MS were £1660.
The MS assumed that any PSS costs for additional care given outside a hospital were equally likely to occur in both the BSC alone and topotecan plus BSC groups. Unit costs from different base-years (from 2003 to 2007) were included in the model. The cost-year for the model is 2007/08. All costs reported in other years were inflated to 2007/08 costs using the NHS Hospital and Community Health Service (HCHS) Pay and Prices Index. 70 This includes only data up to the 2006/07 year. An assumption was made, therefore, that the percentage increase in the HCHS pay and prices from 2006/07 to 2007/08 would be the same as that from 2005/06 to 2006/07.
Model/cost-effectiveness results
The MS reports only costs that were likely to be higher in the oral topotecan plus BSC arm of the trial. Outcomes were reported in terms of life-years and QALYs. The oral topotecan plus BSC arm in the base-case analysis resulted in 0.259 years of additional life and 0.211 QALYs over the BSC alone arm of the trial. The incremental cost of the oral topotecan plus BSC arm was £5671 compared with the BSC alone arm. The incremental cost-effectiveness ratio (ICER) per life-year gained is £21,878 and per gained QALY is £26,833.
Drug costs were the largest single component of total costs (44%). The cost of treating adverse events was 29% of the total costs. The cost of non-progressive disease was 13% and monitoring chemotherapy was 13% of total costs. Drug monitoring accounted for 1% of total costs.
The MS concludes that oral topotecan plus BSC versus BSC alone is likely to be a cost-effective therapy in people with relapsed SCLC, who are not considered suitable for standard i.v. chemotherapy.
Outline appraisal of the manufacturer cost-effectiveness analysis
A summary of the MS compared with the NICE reference case requirements is given in Table 24. See Appendix 8 for a tabulation of the critical appraisal of the submission against Drummond and colleagues’ checklist. 66
| NICE reference case requirements | Included in submission |
|---|---|
| Decision problem: as per the scope developed by NICE | ?a |
| Comparator: alternative therapies routinely used in the UK NHS | ?b |
| Perspective on costs: NHS and Personal Social Services | ✓ |
| Perspective on outcomes: all health effects on individuals | ✓c |
| Type of economic evaluation: cost-effectiveness analysis | ✓ |
| Synthesis of evidence on outcomes: based on a systematic review | No evidence synthesis |
| Measure of health benefits: QALYs | ✓ |
| Description of health states for QALY calculations: use of a standardised and validated generic instrument | ✓ |
| Method of preference elicitation for health-state values: choice-based method (e.g. TTO, SG, not rating scale) | ✓ |
| Source of preference data: representative sample of the public | ✓ |
| Discount rate: 3.5% p.a. for costs and health effects | ✓ |
Outline review of the modelling approach
The model used the participant level survival data for the oral topotecan with BSC arm and the BSC alone arm from the O’Brien and colleagues57 trial to estimate survival benefit. The effect of oral topotecan was to increase life expectancy compared to BSC by extending time before the disease progresses. BSC is intended to reduce the impact of disease progression rather than affect disease progression itself.
The time horizon used in the economic evaluation is the length of the trial. No additional modelling was undertaken to extend survival beyond the end of the trial. The MS reported that there were six remaining participants (three in topotecan group and three in the BSC alone group) who were still alive at the end of the trial, and it was assumed that all of these patients died the day after the end of the study. However, from the Kaplan–Meier plot of OS from the O’Brien and colleagues57 trial, this does not appear to be the case. It appears that there are fewer survivors in the BSC arm than the three survivors reported in the MS. The reason for this discrepancy is unclear. Nevertheless, assuming that there are three survivors in each arm, based on the participant level data in the manufacturer’s model, this represents just over 4% of the population in each arm. There is a possibility that this could have underestimated the survival benefit for either arm of the trial.
Adverse events were incorporated into the model through the incidence of grades 1 to 4 non-haematological events as they occurred in the trial. Haematological events were incorporated into the model using resource use of transfusions, the use of GCSF and antibiotics, rather than their incidence. The different methodology used to account for adverse events is thought not to have seriously impacted upon the results of the model. The large amount of missing EQ-5D data in the RCT means it is unclear whether the expected disutility from having an adverse event will have been adequately picked up. Furthermore, it is not clear if the EQ-5D data collected at 3-week intervals captures the impact of the adverse events well.
An assumption was made that there would be a reduction in health utility once the disease progressed in the topotecan group. This was accounted for by using utility data from the BSC participants for the last five periods until death. This seems to be a fair assumption, as there is likely to be a reduction in utility once the disease progresses in the topotecan group that corresponds to the BSC group’s health-state valuations in the five periods preceding death.
Participant level data were taken from the O’Brien study,57 and this provided inputs on the survival length of participants in the trial, resource use and health utilities. Expert opinion was used to give additional information on resource use. The unit cost data were taken from national published sources.
Health utilities were recorded throughout the trial at the beginning of each cycle. However, many of the health-state valuations were missing due to progression of the disease in participants. This causes great uncertainty in the model, as only 39% of the survival periods were available. An average of observed cycle EQ-5D data matched to the corresponding cycle with missing data, and the LOCF technique was used to overcome this missing data. More rigorous modelling methods, for example a regression analysis, could have been used to take account of this missing data.
The average EQ-5D scores used for imputation are highly variable across cycles 1–12. The variability reflects the uncertainties that are involved with using this approach. First, the pooled data on average EQ-5D were used from both arms of the trial. No justification of pooling both groups of participants was given but it is likely to have been adopted due to the small number of observations that occurred as the number of cycles increased. This may have underestimated the health benefit in the topotecan arm in the first five cycles of the trial, as this was when the majority of BSC participants were experiencing disease progression towards death and appear to have reported lower mean EQ-5D scores per cycle at this time. Second, one would expect EQ-5D scores to decline as time goes on and people progress towards death. However, there is an upward trend in the mean EQ-5D scores up to cycle 7. This may reflect sicker participants dying first and leaving a higher proportion of healthier participants who will tend to report higher EQ-5D scores. This is likely to overestimate utility in the topotecan arm of the trial, as these participants lived longer than the BSC participants. Finally, the lack of observations for the last five cycles also causes fluctuations in the average EQ-5D scores, with only one observation from the BSC group accounting for cycles 11 and 12. The impact on the model of using this approach to take account of missing data is unclear, as it is likely to roughly underestimate the utility in the first half of the cycles and roughly overestimate utility in the last half of the cycles.
The MS used a LOCF approach in both groups, prior to disease progression and once the first 12 cycles were completed. This also only affects a very small number of participants in the trial and is unlikely to have a large effect on the model results.
The MS reported that only cost components that were higher in the topotecan arm were included in the model, suggesting that this would probably be most likely to overestimate the incremental costs associated with oral topotecan compared to BSC and was therefore a conservative assumption. 51 This seems reasonable; however, it is likely that palliative care will be experienced at different time periods in both groups and discounting may underestimate incremental costs here in favour of topotecan.
Participant level data for resource use was reported for most of the categories of cost in the model. However, not all resource use was recorded. The manufacturer used expert opinion to estimate resource use that was not recorded in the trial, such as treatment of non-haematological events. We discussed these assumptions with clinical experts who concluded that they appeared to be reasonable.
Uncertainty is addressed using both a deterministic and a bootstrap analysis. The deterministic sensitivity analysis addresses issues of methodological uncertainty (varying discount rates) and parameter uncertainty (different assumptions about utility weights, cost of additional non-progressive disease survival, cost of drug monitoring, cost of treating adverse events, cost of PSS events and assumptions about how the drug is administered). Only the ICER is reported in these analyses and so no comment can be made about the changes in total costs and outcomes. The ICERs were fairly insensitive to the changes made in the deterministic analysis, with a range from £22,512 (for halving the cost of adverse events) to £40,253 (for oral topotecan being administered during a daily outpatient visit for 5 days in each cycle). Other scenarios that raise the ICERs were doubling the cost of treating adverse events (£34,468), the cost of additional non-progressive disease survival being doubled (£30,421), and using the combined mean EQ-5D score at each cycle and LOCF approach to account for missing data (£33,816).
Sample uncertainty was addressed for the base-case analysis using a bootstrap analysis. Non-paramatic bootstrap methods are used to create CIs around a statistic of interest, which are derived from repeatedly drawing samples with replacement from the original treatment arms of the study. 71 In this analysis, the statistic of interest was the ICER for oral topotecan plus BSC and BSC alone. The analysis used 10,000 bootstrap replications and presented the resulting 95% confidence ellipses for the ICERs. Oral topotecan plus BSC in the bootstrap analysis was always associated with increased costs (incremental costs between £4000 and £7500) and usually with improved QALY outcomes (incremental QALYs between 0 and approximately 0.6). The majority of the ICERs (98.31%) for oral topotecan plus BSC (compared with BSC alone) were found in the upper-right quadrant of the cost-effectiveness plane (i.e. oral topotecan plus BSC was more effective and more costly than BSC alone). The remaining 1.69% of replications are in the upper left quadrant, in which oral topotecan plus BSC is less effective and more costly than BSC alone. A cost-effectiveness acceptability curve was presented. Oral topotecan plus BSC had a probability of being cost-effective relative to BSC of 22% at a willingness to pay (WTP) threshold of £20,000 per QALY and 60% at a WTP threshold of £30,000 per QALY.
A subgroup analysis was also presented for TTP that was ≤ 60 days and > 60 days, performance status 0/1, sex and the presence of liver metastases. Oral topotecan plus BSC was more cost-effective per QALY gained in patients for whom the TTP from prior therapy was ≤ 60 days (£17,946), in females (£11,708), and in those patients with no liver metastases (£21,291) and a performance status of 2 (£25,544). The subgroups where ICERs were higher than a WTP threshold of £30,000 per QALY were in males (£74,175) and performance status of zero or 1 (£30,770), liver metastases (£56,534) and TTP of > 60 days (£31,972).
A further analysis was undertaken in the TTP of > 90 days and in the no-liver-metastases subgroups. It is important to note the small sample sizes for these data with only 30 and 51 participants, respectively. No justification was given for more in-depth analysis of these participant subgroups. However, these are the two subgroups that are most likely to benefit from oral topotecan after the ≤ 60 days TTP group. The ICERs for the deterministic analysis, applying the same scenarios as used in the base-case analysis, were in the range of £20,260–38,085 for TTP > 90 days and £17,804–32,043 for no liver metastases. The more conservative assumptions over the measurement of HRQoL, the drug administration costs and cost of treating adverse events, all produced ICERs over a WTP threshold of £30,000 per QALY in the over 90 days to progression subgroup. The only scenario in the no-liver-metastases group that was above the WTP of £30,000 per QALY was the conservative assumption of drug administration cost being provided for 5 days of outpatient visits. A bootstrap analysis with 10,000 bootstrap replications was also undertaken in both subgroups. The bootstrap replications for both groups were predominantly in the upper-right quadrant; 95.85% for the > 90 days to progression and 98.98% in the no-liver-metastases group. At a WTP threshold of £20,000 per QALY, oral topotecan plus BSC would be cost-effective relative to BSC alone in the > 90 days to progression and in the no-liver-metastases subgroups in 33% and 44% of cases, respectively. If the threshold increased to £30,000 then these percentages would increase to 62% and 75%, respectively.
Summary of general concerns
-
It is unclear whether the disutility that would be expected from experiencing an adverse event in the topotecan group has been adequately represented due to the large amount of missing EQ-5D data and 3-week intervals between collections of EQ-5D data. This may be further biased due to healthier participants being more able and willing to fill in EQ-5D questionnaires than those who are experiencing an adverse event. If this is correct then utility, and therefore gain in QoL, compared to BSC is likely to be an overestimation for the topotecan group.
-
No modelling beyond the length of the trial was undertaken. A small, but potentially significant, number of participants were still alive at the end of the trial. However, it is not entirely clear how many participants in the trial were still alive, as the MS and Kaplan–Meier plot from the O’Brien and colleagues RCT57 seem to give conflicting reports. It is assumed here that the MS is correct as the participant-level data are given in the model. Therefore, just over 4% of each arm of the trial were still alive at the end of the study and there is a possibility this could have underestimated the survival benefit for either group.
-
The use of the mean observed EQ-5D scores from both arms of the trial to take account of the missing EQ-5D data raises a number of problems. Utility in both groups of participants in the trial is unlikely to be the same throughout the cycles. The utility for topotecan participants early in the treatment cycles is likely to have been underestimated, as this is when the majority of BSC participants were progressing towards death. In the latter half of the treatment cycles the mean of the observed EQ-5D scores appear to have been overestimated, due to the small number of observations and as the proportion of healthier participants increases. It is not clear what effect this will have had on the model results.
-
The assumptions over the costs in the model appear reasonable. Given that costs for the BSC arm of the trial were not recorded and that this component is common to both arms the conservative assumption may be justified. However, a small percentage of palliative care costs are likely to have occurred in different periods for the topotecan plus BSC and BSC alone groups, and discounting could have been applied here.
-
The description of how utilities were used in the model, and the methods by which EQ-5D values were imputed to allow for missing data, were not entirely clear in the MS.
SHTAC independent economic assessment
Statement of the decision problem and perspective for the cost-effectiveness analysis
We developed a new model to estimate the cost-effectiveness of topotecan as a second-line chemotherapy compared with BSC, in a cohort of adults with relapsed SCLC for whom re-treatment with the first-line regimen was not considered appropriate. The perspective of the cost-effectiveness analysis is that of the NHS and PSS. The type of the economic evaluation was a cost–utility analysis. The health economic outcomes that are evaluated in the model are life-years gained (LYG) and QALYs gained. A discount rate of 3.5% was applied to both costs and benefits over the lifetime of the patients.
Strategies/comparators
The scope for the appraisal states that the interventions to be considered are oral and i.v. topotecan. The comparators for these interventions, including a comparison between the two interventions, are BSC, CAV and any other chemotherapy regimens.
The clinical effectiveness section above highlighted the different study populations that were used in the RCTs involving topotecan and relevant comparators (see Chapter 3, Quantity and quality of research available). It was not felt appropriate to pool the RCTs identified. This resulted in the base-case analysis of our economic model being limited to a comparison of oral topotecan plus BSC and BSC alone, based on the O’Brien and colleagues study. 57 Furthermore, as noted in the MS, CAV is likely to be a more cost-effective option than topotecan as a second-line chemotherapy for SCLC in patients for whom CAV is not contraindicated. Therefore, topotecan would be used only in a small subgroup of patients, for whom CAV was not considered to be an appropriate second-line chemotherapy. The base-case analysis will consist of a comparison between oral topotecan plus BSC compared to BSC alone.
A comparison of i.v. topotecan and BSC, based on an indirect comparison, was also attempted although with reservations (see Estimation of net benefits). This was undertaken to give a complete analysis of the use of topotecan (oral and i.v.) against BSC as a second-line chemotherapy.
Methodology
Model type and rationale for model structure
Figure 2 illustrates the basic survival model which, in its simplest form, contains three states – stable disease (i.e. patients’ state at entry to the trial), progressive disease and death. Movements between these states are usually only permitted in the progressive direction. We have adopted this approach to model the cost-effectiveness of topotecan as a second-line chemotherapy.
FIGURE 2.
Survival model adopted for the cost-effectiveness model. OS, mean overall survival; OS-TTP, mean survival duration with progressive disease; TTP, mean time to progression.
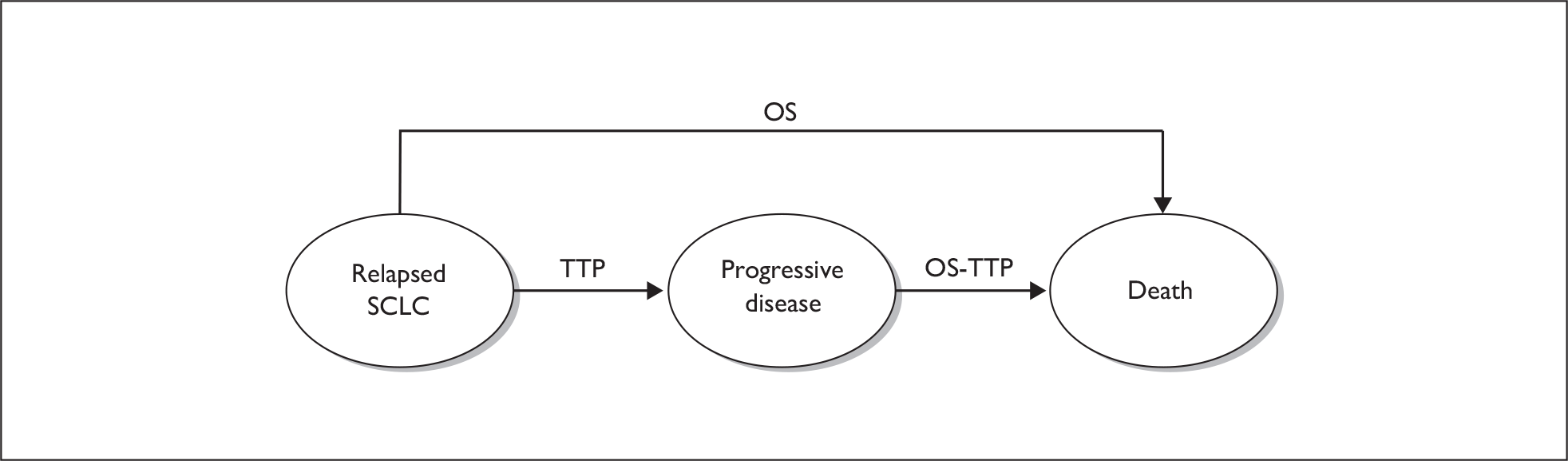
Patients enter the model with relapsed SCLC, are unable or unwilling to undergo i.v. chemotherapy with CAV, and receive either BSC alone or topotecan with BSC. Patients may experience disease progression or may die without experiencing documented disease progression.
The model uses data that are presented in the clinical effectiveness review (see Chapter 3, Results) and the MS to evaluate the most cost-effective strategy for second-line chemotherapy in SCLC. The model is fully probabilistic, to take into account parameter imprecision. In addition, deterministic sensitivity analysis was used to explore different scenarios and assumptions in the model.
The base-case analysis compared the mean OS for oral topotecan plus BSC (meanOST) with the mean OS for BSC (meanOSBSC). The estimate of LYG with the addition of oral topotecan to BSC (LYGT), in the base case, was calculated as: LYGT = meanOST–meanOSBSC.
To estimate the QALY gain associated with the addition of oral topotecan to BSC (QALYGT), treatment-specific utilities (UT and UBSC for oral topotecan plus BSC and for BSC, respectively) reported by O’Brien and colleagues57 and by Chen and colleagues64 were applied to the mean OS estimates. The quality-adjusted life expectancy gain was therefore calculated as: QALYGT = meanOST*UT – meanOSBSC*UBSC. This approach takes no account of the limited duration of follow-up over which the utility data were collected. EQ-5D data were collected for 12 follow-up assessments (up to 36 weeks from randomisation, as stated in the MS), although the abstract by Chen and colleagues64 reports that only data up to 12 weeks were included in the EQ-5D utility analyses. Therefore, the utility data for patients in the oral topotecan plus BSC arm may not reflect patients’ QoL following disease progression. It has been noted elsewhere that there is likely to be a reduction in QoL when patients experience disease progression. As a result, an additional analysis was undertaken to explore the impact of the difference in QoL for patients following the development of progressive disease. The estimate of the QALY gain associated with oral topotecan, taking into account the QoL impact of progressive disease, was calculated as: QALYGT = TTPT*UT + (meanOST – meanTTPT)*UBSC – meanOSBSC*UBSC.
Baseline cohort
The baseline population in the economic model are adults with relapsed SCLC, for whom re-treatment with the first-line regimen is not considered appropriate and who are unsuitable or unwilling to accept i.v. chemotherapy with CAV.
Discounting of future costs and benefits
A discount rate of 3.5% was applied to future costs and benefits, in line with current guidance from NICE. Discount rates of 0% and 6% were applied in the sensitivity analysis.
Presentation of results of the base-case model
We report the results of these comparisons in terms of incremental gain in QALYs and the incremental costs.
Assessment of uncertainty in the SHTAC analysis (sensitivity analysis)
Parameter uncertainty is addressed using probabilistic sensitivity analysis. Probability distributions were assigned to the point estimates used in the base-case analysis.
Deterministic sensitivity analysis is used to address particular areas of uncertainty in the model relating to:
-
model structure
-
methodological assumptions
-
parameters around which there is considerable uncertainty or which may be expected, a priori, to have a disproportionate effect on study results.
The purpose of this analysis is to identify clearly the impact of uncertainty and to test the robustness of the cost-effectiveness results to variation in structural assumptions and parameter inputs.
Estimation of net benefits
Effectiveness data
Oral topotecan plus BSC compared with BSC alone
The model builds upon the Kaplan–Meier curves for OS from the O’Brien and colleagues57 study for topotecan plus BSC and BSC alone. These survival curves were scanned using techdig software and then imported into microsoft excel. In both arms, some of the participants remained alive at the end of the trial. Therefore, the final portions of the survival curves were extrapolated using a regression analysis. A range of parametric survival functions were fit to the observed Kaplan–Meier estimates (full details are included in Appendix 9). The log-logistic survival function provided the best fit to the observed Kaplan–Meier estimates and was used in the economic model.
The extrapolated survival curves are given in Figure 3 and compared to the Kaplan–Meier survival estimates (details of the regression estimates are found in Appendix 9). These show a good fit to the OS curves. The most appropriate measure of OS is the mean rather than the median. Therefore, the associated mean survival times were estimated for the relevant survival curves.
FIGURE 3.
Kaplan–Meier survival estimates from the O’Brien and colleagues trial and log-logistic fits.
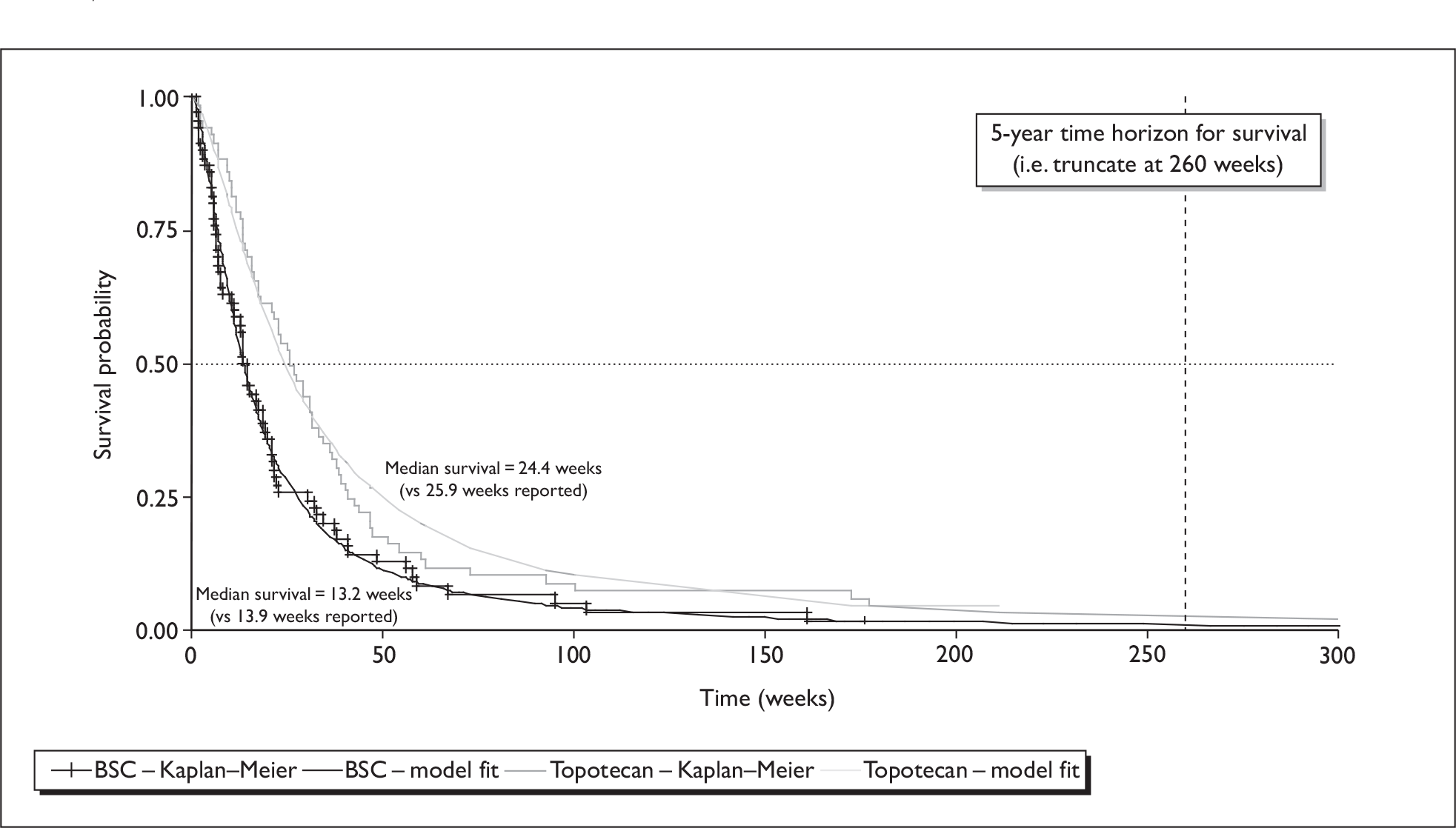
Mean survival (area under the survival curves) estimated directly from the Kaplan–Meier survival function (truncated at the maximum observed survival for each arm in the RCT by O’Brien and colleagues57) and from the log-logistic survival functions (extrapolated to a maximum duration of 5 years) are reported in Table 25.
| Treatment arm | Mean OS (years) | |
|---|---|---|
| Kaplan–Meier estimate | Log-logistic function | |
| Oral topotecan plus BSC | 0.7685 | 0.8271 |
| BSC | 0.4837 | 0.4864 |
The mean OS figures from the Kaplan–Meier estimate and from the log-logistic function are very similar for BSC, at 0.4837 and 0.4864, respectively. For oral topotecan plus BSC, the mean OS from the log-logistic function is greater than the value based on the Kaplan–Meier estimate by 0.06 years, or approximately 3 weeks. If the modelled survival function is truncated at the maximum survival duration observed in the RCT by O’Brien and colleagues,57 the mean reduces to 0.7997 years. The difference between the modelled value and that estimated directly from the Kaplan–Meier curve is reduced to approximately 1.5 weeks.
The RCT by O’Brien and colleagues57 did not report Kaplan–Meier estimates for TTP, but reported only the median TTP for oral topotecan plus BSC. Moreover, no TTP data were reported for the BSC group (see Chapter 3, Oral topotecan plus BSC versus BSC alone). To estimate the mean TTP for oral topotecan plus BSC, the risk of disease progression was derived from the reported median TTP using an exponential approximation:72 λ = –ln(S)/t, where S is the proportion of patients surviving (or in this case without disease progression) at time t. For the median TTP the value of S in the above equation is set, by definition, at 0.5, whereas t = 16.3 weeks (as presented in this report – see Chapter 3, Oral topotecan plus BSC versus BSC alone). The mean TTP was calculated by taking the reciprocal of the risk of disease progression (1/λ), giving a value of 23.52 weeks. This approach has been used in previous Technology Assessment Reports (TARs) looking at second-line chemotherapies for ovarian cancer. 69 The accuracy of this estimate of the mean TTP depends on the adequacy of the exponential approximation, used to convert the median TTP to a risk of disease progression. The appropriateness of this transformation cannot be assessed without reference to the full survival function for TTP, which has not been reported for the RCT by O’Brien and colleagues. 57 This represents a substantial source of uncertainty in the model. See Appendix 9 for additional analysis on TTP, using data from the MS.
Intravenous topotecan versus BSC
An analysis was undertaken to assess the effect of i.v. topotecan on OS, relative to BSC, based on an adjusted indirect comparison using data from three RCTs included in the review. Data from the RCT by O’Brien and colleagues57 were used for the comparison of oral topotecan plus BSC against BSC alone, whereas the trials by Eckardt and colleagues56 and von Pawel and colleagues58 provided data for the comparison of oral topotecan with i.v. topotecan, as discussed in Chapter 3 (see Oral topotecan plus BSC versus BSC alone, and Oral topotecan versus i.v. topotecan).
For the comparison of oral topotecan with i.v. topotecan, data on OS were available in the form of HRs (Eckardt and colleagues56) and RRs (von Pawel and colleagues58). The point estimates and their 95% CIs were entered into Review Manager revman 5.0 software, and combined using the generic inverse variance method. In a fixed-effect meta-analysis there was no statistically significant difference between treatment arms (RR 0.95, 95% CI 0.76 to 1.17, p = 0.62) – see Figure 4. Heterogeneity was not statistically significant (p = 0.56, I2 = 0%).
FIGURE 4.
Fixed-effect meta-analysis of relative risk of overall survival – oral versus intravenous topotecan.
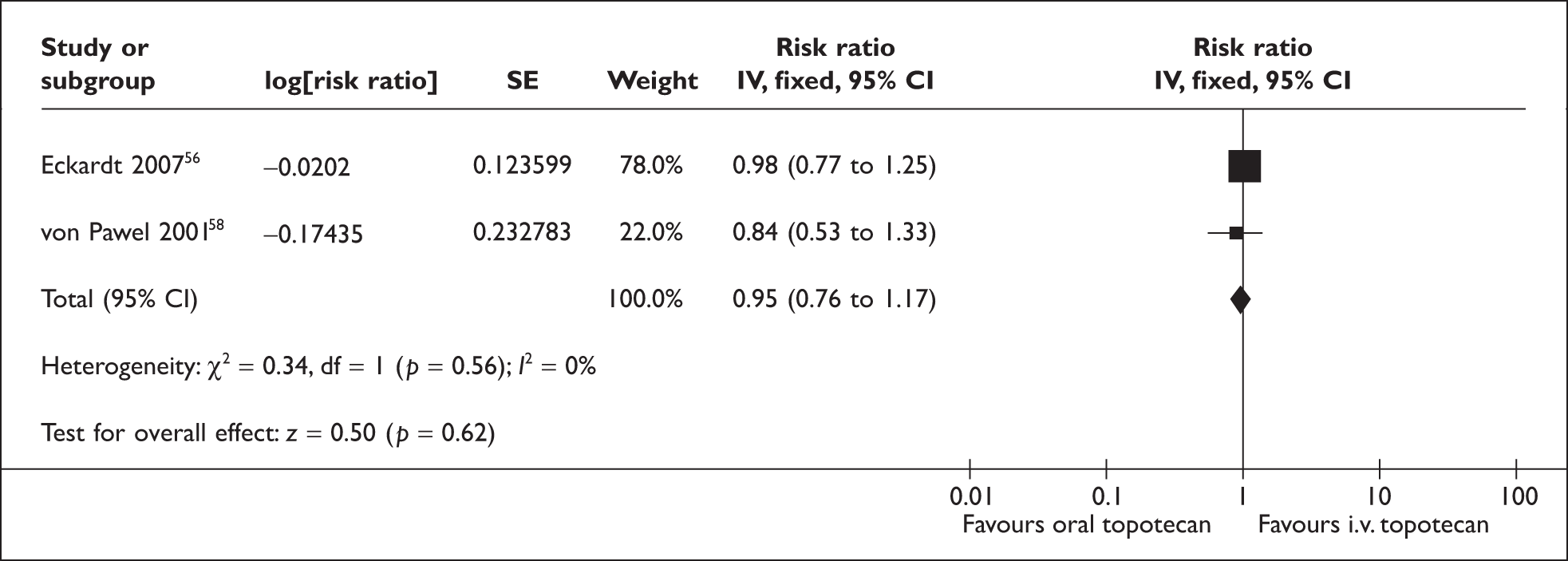
Combining the pooled estimate with the HR for oral topotecan plus BSC compared with BSC alone reported by O’Brien and colleagues,57 and using the method for indirect comparison described by Glenny and colleagues,73 gives a relative risk for OS with i.v. topotecan of 0.68 (95% CI 0.45 to 1.02) compared with BSC (Table 26).
| HR | ln(HR) | se(ln(HR)) | |
|---|---|---|---|
| Oral vs i.v. topotecan | 0.95 | –0.0541 | 0.1092 |
| Oral topotecan vs BSC | 0.64 | –0.4463 | 0.1768 |
| Intravenous topotecan vs BSC | 0.68 | –0.3922 | 0.2078 |
This analysis is highly speculative, given the uncertainty whether these trials fully meet the inclusion criteria for this review (discussed in Chapter 3 under Quantity and quality of research available), particularly regarding the comparability of participant populations in the RCTs and therefore the suitability of pooling their results.
Health-state values/utilities
To calculate QALYs from the mean OS and mean TTP, derived using the methods described above, it was necessary to adjust the survival times for QoL using appropriate utility or health-state valuations. 67 As described in the section ‘Review of research on quality of life’, above, we found only limited data sources on QoL and health-state utility for people with recurrent SCLC.
The utilities used in this analysis are based on those reported for the O’Brien and colleagues’ RCT,57 which used the EQ-5D in both trial arms (see Chapter 3, Oral topotecan plus BSC versus BSC alone). Adopting these utility estimates has the advantage that they were derived:
-
in a relevant population – those with SCLC who responded to first-line treatment, for whom re-treatment with first-line therapy is not considered appropriate and for whom BSC is an appropriate comparator strategy
-
using a measure and methodology (EQ-5D valued using a tariff derived from a representative sample of the general population) that is consistent with the NICE reference case.
In addition, it should be noted that our search for QoL studies and studies reporting utility estimates in this population failed to find any other relevant publications. However, there are shortcomings in the evidence base that need to be borne in mind:
-
The QoL assessment within the trial is reported only very briefly in the main RCT publication. 57 There is very little detail on methods adopted for calculating utilities from the EQ-5D (the value set used is not reported), approaches to handling missing data (baseline data were collected for 96% of participants in the topotecan plus BSC arm and 93% in the BSC arm, whereas the proportions with at least one postbaseline assessment were 89% and 70%, respectively) or methods used to estimate the rate of deterioration in scores over time.
-
It is not clear how far the EQ-5D data, collected at 3-week intervals, capture the impact of treatment-related toxicity for those receiving oral topotecan.
-
There was limited follow-up for the QoL assessments. The main trial publication does not report the duration of the QoL assessment. However, the abstract by Chen and colleagues,64 which reports the same rate of change from baseline to 3 months as the main trial publication,57 states that the data analysed covered a maximum of 12 weeks from baseline (measures were administered at baseline and at four subsequent visits, occurring at 3-week intervals). As a result, these assessments are unlikely to capture the full impact of disease progression in the oral topotecan group.
The RCT reported that the ‘rate of deterioration’ in EQ-5D scores over 3 months was –0.05 for oral topotecan plus BSC and –0.20 for BSC alone. We interpreted this to indicate that for each 3-month period, the mean utility reduces from baseline by 5% for the oral topotecan plus BSC cohort and by 20% for the cohort receiving BSC alone.
Baseline EQ-5D values for all participants, or for each trial arm separately, were not reported in the main publication for the RCT by O’Brien and colleagues. 57 The abstract by Cheng and colleagues64 reported a mean baseline utility (for patients in the RCT by O’Brien and colleagues) of 0.72 for oral topotecan plus BSC arm and 0.68 for BSC alone. These baseline values are for participants included in the pooled analysis (change from baseline to averaged-on-treatment assessments). For the cost-effectiveness model, we assume that the mean baseline utility for all participants is 0.7.
A regression analysis was used to infer the reduction of utility over time from the 0- and 3-month time points, and to model utility beyond the last observation and beyond the trial (see Appendix 11). In the base case, we assumed that any QoL reduction due to toxicity or adverse events would be picked up in the EQ-5D valuations from trial participants.
The base-case analysis assumed that there was an associated loss of utility in people treated with oral topotecan plus BSC once disease had progressed. This was assumed to be the same loss of utility that was associated with participants receiving BSC alone and was applied for survival durations beyond the estimated mean TTP. Quality-adjusted survival curves, showing the effect of assuming a greater reduction in utility following disease progression, are shown in Figure 5.
FIGURE 5.
Impact on quality-adjusted survival of alternative assumptions regarding the utility reduction over time with topotecan.
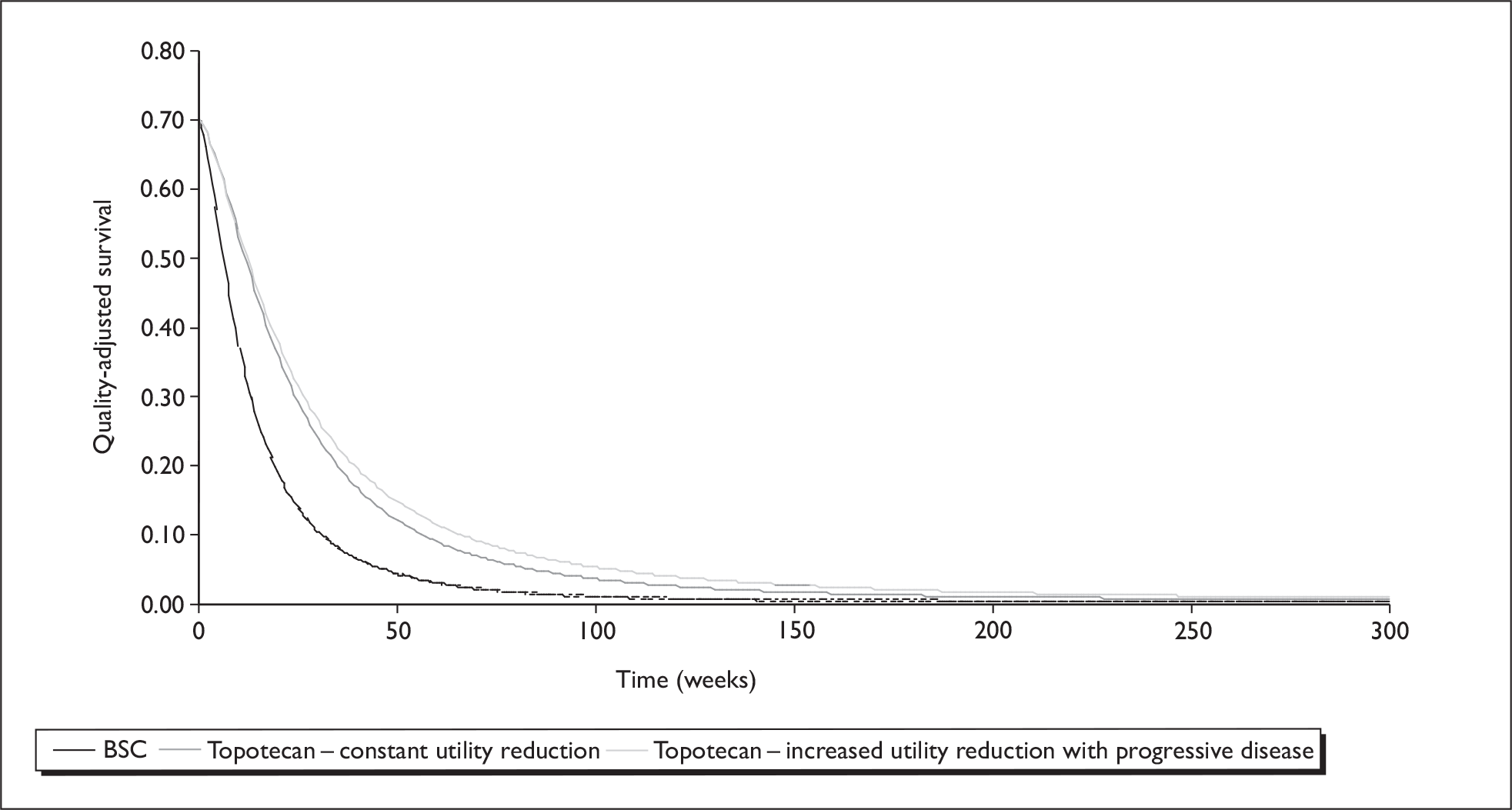
Estimation of net costs
Cost analysis
The cost data were based upon the resource use from the O’Brien and colleagues study. 57 This was supplemented with data from the MS and the other RCTs identified in the clinical effectiveness review. A questionnaire was also sent out to clinical experts to ascertain relevant costing and resource use associated with oral topotecan (see Appendix 13). All cost data and relevant sources are given and discussed, in turn, below.
Base case: oral topotecan plus BSC versus BSC alone
The groups of health-care costs included in the base-case health economic model are:
-
drug costs
-
chemotherapy administration
-
on-treatment monitoring
-
cost of adverse events
-
post-treatment monitoring
-
palliative care costs.
Drug costs of oral topotecan
Oral topotecan is administered at 2.3 mg/m2/day on five consecutive days of each 21-day course of treatment. 74 Table 27 reports the total dose per day of treatment for oral topotecan used in the cost-effectiveness model. This assumes that patients have a body surface area (BSA) of 1.8 m2 – this assumption is based on the BSA adopted by the SMC for costing i.v. topotecan for treatment of relapsed SCLC,47 with the exact dosage (4.14 mg per day of treatment) rounded up to the nearest 0.25 mg. This allows for the fact that some participants in the RCT by O’Brien and colleagues57 experienced dose reductions (reported as 8% of courses) or dose escalations (reported as 14% of courses). Dose reductions and escalations occurred at increments of 0.4 mg/m2/day to a minimum dose of 1.5 mg/m2/day and to a maximum dose of 3.1 mg/m2/day. We estimated the mean oral topotecan dosages, allowing for dose reductions and escalations, to be between 2.29 and 2.38 mg/m2/day (corresponding to dosages of 4.13–4.28 mg per day of treatment). These were calculated by weighting the standard dosage by the proportion of courses having dose reductions/escalations and assuming that all reductions/escalations were either one or two increments (i.e. either 0.4 mg/m2/day or 0.8 mg/m2/day).
| Total dose per day of treatment | Cost/mg (£) | Cost per day of treatment (£) | Cost per course (£) |
|---|---|---|---|
| 4.25 mga | 30 | 127.50 | 637.50 |
Table 27 reports the unit costs – estimated cost per treatment day and cost per course for oral topotecan – that were used in the cost-effectiveness model. Unit costs for oral topotecan were taken from the current British National Formulary (BNF, no. 57, March 2009). 75 Oral topotecan is available on 10 capsule cards, with a unit cost of £300 per card of 1-mg capsules and £75 per card of 0.25-mg capsules.
The cost per course of oral topotecan has been calculated on the basis of no wastage – we assume that the hospital pharmacy department will supply patients with the exact quantity of capsules to deliver the required dosage over each course of treatment. In the case of the patient with a BSA of 1.8 m2 this would most closely be met by supplying 20 1-mg capsules and five 0.25-mg capsules, which implies that the hospital pharmacy can supply fractions of the 10-capsule card.
The main trial publication57 reports that a total of 278 treatment courses were delivered to the 71 participants randomised to oral topotecan (with a median of 4 per patient, range 1–10). In the cost-effectiveness model we assume that people receive a mean of four courses of oral topotecan, which corresponds to a total drug cost per patient for oral topotecan of £2550. This is similar to the mean cost per patient for oral topotecan of £2500 reported in the MS.
Administration and monitoring costs for oral topotecan
The summary of product characteristics (SmPC) for topotecan states that it should only be prescribed, and therapy should be supervised, by a physician who is experienced in the use of chemotherapeutic agents. We assumed that patients would attend the hospital once, at the beginning of each course, to collect the complete supply of oral topotecan for each course of treatment. At the same time, patients would also receive a supply of an oral antiemetic (domperidone, non-proprietary) and an antidiarrhoeal drug (loperamide) to use as required. Patients attending the hospital to collect oral chemotherapy agents will also have their condition monitored. This will include a consultation with their treating physician (in which their medical history will be assessed for performance status, symptoms and for side effects of treatment) and a series of biochemical, haematological and imaging tests. We have assumed that the medical consultation will be accounted for under standard resource-use assumptions for an outpatient attendance to receive oral chemotherapy. However, we have separately identified a set of tests that is required for patients undergoing chemotherapy with topotecan for relapsed SCLC. All patients will require a FBC prior to administration of the first course of oral topotecan to ensure they have a baseline neutrophil count of ≥ 1.5 × 109/l, a platelet count of ≥ 100 × 109/l and a haemoglobin level of ≥ 9 g/dl (after transfusion if necessary). 74 In addition patients require a repeat of the FBC, liver function tests, renal function tests (urea, creatinine and salts) and a chest radiograph (to assess tumour response) at each attendance. In addition, based on clinical advice, it was assumed that patients receiving active treatment would have a CT scan every two cycles. Clinical advisors confirmed that these were appropriate resource use assumptions for the management of this group of patients.
The unit cost for an outpatient attendance to receive oral chemotherapy has been taken from NHS Reference Costs. 76 This does not include a pharmacy dispensing fee (which is included under ‘procurement costs’ in NHS Reference Costs77). For the base-case analysis we adopt the same pharmacy cost as in the MS, based on contract price per prescription for community pharmacists (£0.90 per prescription at 2007/08 prices). Unit costs for routine tests undertaken to monitor treatment-related toxicity and disease progression were provided by the finance department at Southampton University Hospitals Trust. Table 28 reports the unit costs that were adopted for costing the administration of oral topotecan and for patient monitoring while on treatment. Total cost per course is £274.14, comprising administration costs of £185.87 and monitoring costs of £88.28.
| Item | Unit cost (£)a |
|---|---|
| Outpatient attendance to receive oral chemotherapy | 184.97b |
| Pharmacy cost for dispensing oral chemotherapy | 0.90c |
| FBC | 2.90a |
| LFT | 4.70a |
| U&E | 4.70a |
| Chest radiograph | 28.64b |
| CT scan (every two cycles) | 47.34b |
| Total cost per course of oral topotecan | 274.14 |
Based on the unit cost assumptions in Table 28, the costs of administration of oral topotecan and monitoring for the complete treatment duration of four courses of chemotherapy is £1097 (£743.47 for administration and £353.11 for monitoring).
Adverse events costs
The RCTs included in the clinical effectiveness review reported that treatment with oral topotecan was associated with both haematological and non-haematological adverse events. 56–58 The most common toxicities were haematological, with 61%, 38% and 25% of participants experiencing neutropenia, thrombocytopenia or anaemia, respectively, at grades 3 or 4 in the oral topotecan arm of the RCT by O’Brien and colleagues57 (see Chapter 3, Oral topotecan plus BSC versus BSC alone). Similar proportions were reported for trials including oral topotecan by Eckardt and colleagues56 and by von Pawel and colleagues,58 (see Chapter 3, Oral topotecan versus i.v. topotecan). The proportion of participants with grade 3 and grade 4 non-haematological toxicities associated with treatment for oral topotecan was lower in the three trials – generally below 10% of patients.
O’Brien and colleagues57 followed the usual convention of only reporting toxicity at grades 3 and 4, while the MS included non-haematological toxicity at all grades. Table 29 shows the proportion of participants, treated with oral topotecan, experiencing haematological toxicity, as reported by O’Brien and colleagues57 and also in the MS. Table 29 also shows the proportion of cycles in which participants experienced haematological toxicity when treated with oral topotecan.
| Toxicity | Grade | Proportions of patients reported by O’Brien et al. (%) | Proportions of patients (from CSR) (%) | Proportions of cycles (from CSR) (%) |
|---|---|---|---|---|
| Neutropenia | 3 | 61.2 | 28.4 | 16.4 |
| 4 | 32.8 | 11.5 | ||
| Thrombocytopenia | 3 | 37.7 | 30.4 | 11.4 |
| 4 | 7.2 | 1.8 | ||
| Anaemia | 3 | 24.6 | 14.5 | 5.1 |
| 4 | 10.1 | 9.5 |
Table 30 (and Appendix 12) report the resource use assumptions adopted in our cost-effectiveness model. Resource use assumptions adopted in a previous TAR for topotecan in the treatment of advanced ovarian cancer were updated, based on expert clinical opinion.
| Toxicity | Grade | Resource use | Unit cost (£) | Cost per patient (£) |
|---|---|---|---|---|
| Neutropenia | 3 | Outpatient visit | 207.48a | 103.74 |
| Amoxicillin | 1.37b | 0.69 | ||
| 4 | Inpatient admission (3.5 days) | 249.83a | 874.41 | |
| Piperacillin | 22.99bc | 321.86 | ||
| Thrombocytopenia | 3 | No treatment | ||
| 4 | Day-case admission | 367.29a | 367.29 | |
| Platelet transfusion | 805.67d | 805.67 | ||
| Type and cross | 36.88d | 36.88 | ||
| Anaemia | 3 | Day-case admission | 367.29a | 367.29 |
| Blood transfusion | 90.05d | 90.05 | ||
| Type and cross | 36.88d | 36.88 | ||
| 4 | Day-case admission | 367.29a | 367.29 | |
| Blood transfusion | 535.60d | 535.60 | ||
| Type and cross | 36.88d | 36.88 | ||
| Sepsis | Inpatient admission (10 days): | |||
| 5 days in intensive care unit | 1022.86a | 5114.31 | ||
| 5 days on ward | 249.83a | 1249.15 | ||
| Piperacillin | 22.99bc | 459.80 | ||
| Clarithromycin | 7.47b | 10.70 | ||
| Fluconazole i.v. | 29.28b | 204.96 | ||
The most common grade 3/4 non-haematological adverse events occurring in the oral topotecan plus BSC arm of the RCT by O’Brien and colleagues57 were diarrhoea, vomiting, fatigue and dyspnoea (Table 31). The proportion of participants with grade 3 or 4 fatigue was the same in both arms of the trial and is not included in our model. Table 31 reports the breakdown of non-haematological toxicity between grades 3 and 4, taken from the CSR that was submitted as an appendix to the MS, and used in our cost-effectiveness model. This table includes grade 3 nausea and grade 2 diarrhoea, which was not reported in the publication by O’Brien and colleagues. 57 We have included grade 2 diarrhoea in the model, following advice from clinical experts that this adverse event would require an outpatient attendance and prescription of further antidiarrhoeal medication. We have assumed that grade 1 or 2 nausea and grade 1 diarrhoea occurring in patients treated with oral topotecan will be self-managed using the antiemetic and antidiarrhoeal medication supplied at the outpatient attendance clinic, which initiates each course of chemotherapy.
| Toxicity | Grade | Proportions reported by O’Brien et al. (%) | Proportions reported in CSR (%) |
|---|---|---|---|
| Diarrhoea | 2 | Not reported | 12.9 |
| 3 | 6 | 4.3 | |
| 4 | 1.4 | ||
| Vomiting | 3 | 3 | 2.9 |
| 4 | 0.0 | ||
| Nausea | 3 | Not reported | 1.4 |
| 4 | 0.0 |
Table 32 (and Appendix 12) present details of the cost per patient, as well as unit cost and resource estimates, for managing non-haematological toxicity for patients treated with oral topotecan. Clinical opinion was sought to validate these estimates, which were based on assumptions adopted in a previous TAR, which included topotecan (for advanced ovarian cancer69) and those developed for the MS.
| Toxicity | Grade | Resource use | Unit cost (£) | Cost per patient (£) |
|---|---|---|---|---|
| Diarrhoea | 2 | Outpatient visit | 207.48a | 207.48 |
| Loperamide | 2.15b | 1.40 | ||
| 3 | Inpatient admission (5 days) | 249.83a | 1249.15 | |
| Loperamide | 2.15b | 2.01 | ||
| Buscopan | 2.59b | 2.59 | ||
| Codeine | 0.97b | 0.97 | ||
| 4 | Inpatient admission (5 days) | 249.83a | 1249.15 | |
| Loperamide | 2.15b | 2.01 | ||
| Buscopan | 2.59b | 2.59 | ||
| Codeine | 0.97b | 0.97 | ||
| Ciproflaxin i.v. | 22.00b | 44.00 | ||
| Metronidazole i.v. | 3.41b | 13.64 | ||
| Nausea/vomiting | 3 | Outpatient visit | 207.48a | 207.48 |
| Dexamethasone | 3.27b | 13.08 | ||
| Granisetron | 65.49b | 130.98 | ||
| 4 |
Inpatient admission (5 days) Dexamethasone i.v. |
207.48a 1.00b |
1037.39 5.00 |
|
| Granisetron i.v. | 26.69bc | 80.07 | ||
| Cyclizine | 1.48b | 1.11 |
Cost of non-progressive disease survival
In the base-case model we assumed that patients have a mean duration of treatment of four courses of oral topotecan, which corresponds to 12 weeks. Patients are assumed to continue to attend the outpatients clinic for general medical care and for monitoring of their condition. This continued monitoring is costed in the model until patients develop progressive disease. It is assumed that these patients will also have one chest radiograph and a CT scan to confirm disease progression.
The full package of care for patients during period from ceasing treatment with oral topotecan, until the development of progressive disease, is listed in Table 33 and consists of an outpatient visit, with FBC every 4 weeks, and a GP consultation every 4 weeks. These correspond to a cost of £246.38 for each 4-week period prior to the development of disease progression. We adopted these assumptions based on information in the MS. Clinical experts were asked to comment on the appropriateness of these assumptions and whether there were any additional items of resource use for patients following the cessation of treatment with oral topotecan, and prior to the development of progressive disease, which should be included.
| Resource use item | Frequency of use | Unit cost |
|---|---|---|
| Outpatient attendance | Once every 4 weeks | 207.48a |
| FBC | 2.90b | |
| GP consultation | Once every 4 weeks | 36.00c |
| Chest radiograph | Once, to confirm disease progression | 28.64a |
| CT scan | 94.68a |
Assuming that mean TTP is 23.52 weeks (derived, as described earlier in Methodology, from the median TTP reported by O’Brien and colleagues57) and an average treatment duration of four courses, we estimated that patients with SCLC, treated with oral topotecan, would have an average of 11.52 weeks from treatment cessation until disease progression. This corresponds to an average cost of continued monitoring, from treatment cessation until disease progression, of £709.57 per patient, plus £123.32 for imaging to confirm disease progression.
Cost of palliative care
Best supportive care was available to participants in both arms of the RCT by O’Brien and colleagues,57 and involved the use of analgesics, antibiotics, corticosteroids, appetite stimulants, antidepressants, RBC transfusions, deep-relaxation therapy, and palliative radiotherapy or surgical procedures. The MS, and the main trial publication by O’Brien and colleagues,57 generally provide little detail on the BSC components of care that was provided to participants in the trial (either for participants in the BSC arm or the BSC component for participants receiving topotecan plus BSC). In particular there is no indication of which components of treatment participants were receiving as palliative care. The MS and the trial publication57 note a greater use of medication and radiotherapy in the BSC arm, while there were more blood transfusions for participants in the topotecan plus BSC arm (reflecting the high proportion of participants in this arm experiencing haematological toxicity).
As BSC was common to both arms, and given that recording of resource use in the RCT was not comprehensive, the manufacturer’s economic model did not include palliative care costs (justifying this as a conservative assumption that is most likely to overestimate resource use for topotecan). However, while BSC is a common component in both arms, it is likely that participants will experience palliative care at different times in the two arms, given the survival advantage associated with topotecan. To assess the impact of this assumption, we include a published estimate of the cost of palliative care, derived in a retrospective analysis of case notes for 109 patients with SCLC conducted in the UK49 (Table 34). The study estimated that 28% of the total costs of care occur after recurrence of the disease until death, of which 73% are generated by palliative care. The average cost of palliative care, for the 71 patients (65%) in the study cohort who received such care, was £3495 at 1998 prices.
| Components costed in palliative care (£) | Total | ||||
|---|---|---|---|---|---|
| Hospitalisation | Outpatient visits | Tests and procedures | Surgery/radiotherapy | Other | |
| 3819 (77%) | 251 (5%) | 341 (7%) | 245 (5%) | 322 (6%) | 4977 |
Summary of costs in SHTAC model
Table 35 reports a summary of the costs applied in the SHTAC base-case model, broken down by categories of cost, and identified separately for the oral topotecan plus BSC group and for the BSC alone group.
| Category | BSC (£) | Topotecan and BSC (£) |
|---|---|---|
| Drug cost (per cycle) | 637.50 | |
| Chemotherapy administration cost (per cycle) | 185.87 | |
| Monitoring cost (per cycle) | 88.28 | |
| Managing haematological adverse events (per cycle) | 367.49 | |
| Managing non-haematological adverse events (per patient) | 114.45 | |
| Non-progressive-disease survival (per day) | 8.80a | |
| Palliative care (per patient) | 4977 | 4977 |
Subanalysis of i.v. topotecan versus BSC
Cost analysis
The categories of health care costs included in the model for i.v. topotecan are similar to those included for oral topotecan. The cost data were based upon resource use from the RCTs reported by Eckardt and colleagues56 and von Pawel and colleagues,58 supplemented by responses to the questionnaire that was sent to clinical experts (see Appendix 13).
Drug costs of i.v. topotecan
Intravenous topotecan is administered at 1.5 mg/m2 per day on five consecutive days of each 21-day cycle. The powder for reconstitution and i.v. infusion is available in 1- and 4-mg vials, at unit costs of £97.65 and £390.62, repectively. 50 Table 36 reports the total dose per day of treatment for i.v. topotecan, assuming a BSA of 1.8 m2. The total dosage per day cannot be delivered in exact multiples of 1-mg vials – in the base-case we assumed that all excess was wasted. The impact of this assumption is tested in a sensitivity analysis, as are the potential impact of dose escalation and dose reductions.
| Total dose per day of treatment | Intravenous topotecan cost per day of treatmenta | Cost per cycleb |
|---|---|---|
| 2.70 mg | £298.95 | £1494.75 |
Intravenous topotecan is supplied as a powder, requiring reconstitution with saline (0.9% w/v sodium chloride i.v. infusion or 5% w/v glucose i.v. infusion) to a final concentration of between 25 and 50 µg/ml. The unit cost of sodium chloride i.v. infusion was estimated as £0.06/ml, giving a total cost per day of treatment for i.v. topotecan of £298.95 and a cost per cycle of £1494.75.
The 54 participants in the von Pawel and colleagues RCT58 received a total of 213 courses of treatment. For the base case we assumed that patients would receive four cycles of treatment with i.v. topotecan, giving a total drug treatment cost of £5979 (or £5381.10, assuming reuse of excess).
Administration and monitoring costs for i.v. topotecan
We assumed that i.v. chemotherapy was administered in secondary care, on an outpatient basis, requiring five separate outpatient visits per cycle. The costs of outpatient visits for the administration of chemotherapy were taken from the NHS Reference Costs 2006/07, as detailed in Table 37. Pharmacy costs for chemotherapy by simple i.v. infusion were taken from a previous TAR (£23 at 2004–5 prices were uprated to £25.44 using the HCHS Pay and Prices Index78).
| Item | Unit cost (£) |
|---|---|
| Outpatient attendance to receive i.v. chemotherapy (first attendance of cycle) | 175.53a |
| Outpatient attendance to receive i.v. chemotherapy (subsequent attendances during cycle) | 195.77b |
| Pharmacy cost per cycle | 25.44 |
| FBC | 2.90 |
| LFT | 4.70 |
| U&E | 4.70 |
| Chest radiograph | 28.64 |
| CT scan (every two cycles) | 47.34 |
| Total cost per cycle | 1027.31 |
On the basis of expert clinical opinion, on-treatment monitoring was assumed to be the same as for oral topotecan. The average cost per cycle was therefore £1027.31 for i.v. topotecan administration. Assuming patients receive four cycles of treatment with i.v. topotecan, this gives a total cost of £4289.26 for i.v. chemotherapy administration and on-treatment monitoring, which breaks down as £3936.15 for i.v. chemotherapy administration and £353.11 for on-treatment monitoring.
Adverse events costs for i.v. topotecan
Relative risks for the incidence of adverse events with i.v. topotecan compared with oral topotecan were estimated using data on the proportion of participants experiencing each adverse event from the RCTs by Eckardt and colleagues56 and by von Pawel and colleagues58 (see Tables 18 and 19, Chapter 3, Oral topotecan versus i.v. topotecan for observed proportions, and Appendix 14 for details of the calculation of the pooled estimates).
The proportion of patients receiving i.v. topotecan experiencing haematological toxicity in the model (reported in Table 38, below) was estimated by applying the pooled relative risks to the proportions of participants experiencing each grade of haematological toxicity in the O’Brien and colleagues RCT57 (previously reported in Table 29).
| Toxicity | Grade | Proportion experiencing toxicity (%) |
|---|---|---|
| Neutropenia | 3 | 27.8 |
| 4 | 48.0 | |
| Thrombocytopenia | 3 | 35.6 |
| 4 | 5.1 | |
| Anaemia | 3 | 22.1 |
| 4 | 6.1 | |
| Sepsis | 4.3 |
Combining the above proportions with costs in Table 30 gives estimate of the cost of managing haematological adverse events for patients treated with i.v. topotecan of £1105.
A similar approach was adopted for non-haematological adverse events – deriving relative risks from the RCTs comparing oral and i.v. topotecan and applying these to the proportions observed in the RCT by O’Brien and colleagues. 57 However, given the relatively lower incidence of non-haematological adverse events, there were a number of cases were no adverse events were reported (for example, no cases of grade 2, 3 or 4 diarrhoea for i.v. topotecan and no cases of grade 4 nausea for either arm were reported in the RCT by von Pawel and colleagues58). To take account of this, we increased the numerator and denominator by one – the grey cells in the tables for non-haematological adverse events in Appendix 14 indicate which calculations included zero cells. The estimated proportion of patients receiving i.v. topotecan who experience non-haematological toxicity, in the model, are reported in Table 39.
| Toxicity | Grade | Proportion experiencing toxicity (%) |
|---|---|---|
| Diarrhoea | 2 | 4.1 |
| 3 | 0.8 | |
| 4 | 1.4 | |
| Nausea | 3 | 1.0 |
| 4 | 0.0 | |
| Vomiting | 3 | 1.4 |
| 4 | 0.0 |
Combining the above proportions with the resource use assumptions listed in Table 32 gives an estimate of the cost of £45 for managing haematological adverse events for patients treated with i.v. topotecan.
Cost of non-progressive disease survival for i.v. topotecan
As with oral topotecan, we assume that patients continue to attend outpatients for general medical care and for monitoring of their condition after the completion of their course of treatment with i.v. topotecan. This continued monitoring is costed in the model until disease progression occurs. We assume that the components of this ongoing monitoring are the same as for patients receiving oral topotecan (see Table 33).
Estimates of the relative TTP for i.v. topotecan in comparison with oral topotecan were derived using regression analysis of the Kaplan–Meier estimates reported in von Pawel and colleagues58 and Eckardt and colleagues56 – these are reported in Appendix 15. The estimated mean TTP using data from the RCT by von Pawel and colleagues,58 for which median TTP for i.v. topotecan was shorter than for oral topotecan, was 24.37 weeks. Taking into account the average treatment duration of four cycles of i.v. topotecan, patients are expected to remain in the non-progressive disease state for 12.37 weeks following the end of treatment. This corresponds to an average cost of continued monitoring, from treatment cessation until disease progression, of £885, including for imaging to confirm disease progression. Alternatively, using data from the RCT by Eckardt and colleagues,56 in which the median TTP for i.v. topotecan was longer than that for oral topotecan, the estimated mean TTP was 32.07 weeks. This means that patients are expected to remain in the non-progressive disease state for 20.07 weeks following the end of treatment, giving an average cost of £1360.
Cost of palliative care
Costs of palliative care were assumed to be the same as for BSC and oral topotecan – see Table 34.
Summary of costs in SHTAC model
Table 40 reports a summary of the cost per patient, applied in the SHTAC base-case model. The total costs are broken down by categories of cost and are identified separately for the oral topotecan plus BSC and for the BSC alone groups.
| BSC (£) | Intravenous topotecan plus BSC (£) | |
|---|---|---|
| Drug cost (per cycle) | 1494.75 | |
| Chemotherapy administration cost (per cycle) | 984.04 | |
| Monitoring cost (per cycle) | 88.28 | |
| Managing haematological adverse events (per patient) | 1104.57 | |
| Managing non-haematological adverse events (per patient) | 44.62 | |
| Non-progressive disease survival (per day) | 8.80a | |
| Palliative care (per patient) | 4977 | 4977 |
Summary of the SHTAC cost-effectiveness model
-
The cost-effectiveness model was developed using a survival model methodology.
-
The model includes three states: (1) relapsed SCLC, (2) progressive disease and (3) death. No data on TTP in the BSC alone group were collected. TTP for oral topotecan was included in the model, to allow for poorer QoL with disease progression. QoL weights applied to the BSC group, were applied to oral topotecan patients once they had progressive disease.
-
The survival model was developed using the published Kaplan–Meier estimates for OS and TTP data included in the MS.
-
Utility values reported by O’Brien57 and colleagues and by Chen and colleagues64 were used in the model. Limited published data are available on these QoL values and full details of the methods used to analyse these data are not available in published sources. Limited extra detail was identified in the MS. QoL values were estimated by applying the rate of deterioration, reported by O’Brien and colleagues and by Chen and colleagues,64 to the baseline EQ-5D utility value for participants included in the RCT by O’Brien and colleagues. 57
-
Resource use associated with oral and i.v. topotecan were estimated from included RCTs, the MS and using advice from clinical experts. Where insufficient detail for estimating resource use or costs was available in included studies or the MS (particularly for palliative care) appropriate costs were taken from published sources. Where available, drug costs were taken from the BNF. Other unit costs were taken from NHS reference costs, Southampton University Hospitals Trust or published sources. The cost base for the evaluation was the 2007/08 financial year – where costs were taken from other cost years, these were adjusted using the HCHS Pay and Prices Index.
-
The base-case model has a 5-year time horizon. Alternative scenarios, truncating the survival functions at the maximum follow-up in the RCT (for oral topotecan) or adopting a longer (10 year) horizon, are included in sensitivity analyses to assess whether extrapolation using survival function is likely to introduce bias. Alternative forms of survival function were investigated to determine whether this introduced bias.
-
Discount rates at 3.5% for costs and outcomes are applied.
Estimation of cost-effectiveness
Cost-effectiveness of topotecan – base-case analysis
This section reports cost-effectiveness results for a cohort of patients with relapsed SCLC, for whom re-treatment with the first-line regimen is not considered appropriate and who are unsuitable or unwilling to accept i.v. chemotherapy with CAV, as discussed in Methodology, above. Discounted costs (identifying the contribution of drugs, drug administration and monitoring while receiving oral topotecan, management of adverse events, monitoring prior to disease progression and palliative care) are presented alongside the life expectancy and quality-adjusted life expectancy for patients in the cohort. The results are presented as incremental cost per life-year gained and incremental cost per QALY gained.
Costs and outcomes modelled for cohorts of patients receiving oral topotecan plus BSC or BSC alone are presented in Table 41. Costs and health outcomes in the table have been discounted at 3.5%.
| Treatment | Costs (£) | Life-years | Incremental cost per life-year gained (£) | QALYs | Incremental cost per QALY gained (£) |
|---|---|---|---|---|---|
| BSC | 4854 | 0.4735 | 0.2247 | ||
| Oral topotecan + BSC | 11,048 | 0.7984 | 19,065 | 0.4077 | 33,851 |
The estimated gain in discounted life expectancy, associated with the addition of oral topotecan to BSC is 0.3249 years (16.9 weeks). The equivalent undiscounted values are 0.3407 years (17.7 weeks). The estimated gain in discounted QALYs, associated with the addition of oral topotecan to BSC, is 0.1830. The equivalent undiscounted value is 0.1894 QALYs.
The incremental cost associated with the addition of oral topotecan to BSC is £6194. Table 42 reports a breakdown of treatment costs, by phase of treatment, for each cohort. Palliative care is the only phase of treatment that is identified for patients receiving BSC alone, and this represents 100% of the treatment cost for this cohort. In contrast, for patients receiving treatment with oral topotecan in addition to BSC, while palliative care remains the single most costly phase these have reduced to 43% of total costs for this cohort. Active treatment with oral topotecan (including drug administration and on-treatment monitoring in addition to the costs of the drug itself) represents 33% of total costs for this cohort, with drug costs constituting 70% of active treatment costs. Other significant contributions to total costs for the oral topotecan plus BSC cohort are costs of managing haematological toxicity (13%) and monitoring for disease progression in patients following cessation of treatment (10%).
| Phase of treatment | Oral topotecan (£) | BSC (£) | |
|---|---|---|---|
| Active treatment | Drug | 2550 | |
| Drug administration | 743 | ||
| On-treatment monitoring | 353 | ||
| Adverse event costs | Haematological | 1470 | |
| Non-haematological | 114 | ||
| Non-progressive disease monitoring | 1082 | ||
| Palliative care | 4735 | 4854 | |
| Total | 11,048 | 4854 | |
Oral topotecan as a treatment for patients with relapsed SCLC, for whom re-treatment with the first-line regimen, is not considered appropriate is associated with both improved outcomes (in terms of life expectancy and quality-adjusted life expectancy) and increased costs. QALY outcomes have increased by approximately 80%, while costs have more than doubled, yielding an incremental cost-effectiveness ratio for the addition of oral topotecan to BSC of £33,851 per QALY gained.
Cost-effectiveness of topotecan – deterministic sensitivity analysis
We conducted a sensitivity analysis to consider the effect of uncertainty around the model structure and for variation in certain key parameters that were expected, a priori, to be influential on the cost-effectiveness results. The method adopted in most cases was univariate sensitivity analysis. That is, varying one parameter at a time, leaving all other variables unchanged. This is to highlight the impact, if any, of each selected parameter alone on the cost-effectiveness results. In some situations (such as the analysis of alternative parametric forms for the survival function, or the analysis using the upper confidence limits for all parameters in survival model) a set of related parameters are varied simultaneously. The effects of uncertainty in multiple parameters were addressed using probabilistic sensitivity analysis, which is reported later in the section.
Table 43 reports the results of the sensitivity analysis. Except for the sensitivity analysis with respect to time horizon, all analyses were conducted using a 5-year time horizon. The table is divided to distinguish between analyses undertaken due to uncertainties over structural assumptions in the model, methodological uncertainties (in this case related to the discount rates applied in the model) and uncertainty over parameter values. Where unit costs have been taken from NHS Reference Costs, the upper and lower quartiles have been used in the sensitivity analysis. In all other cases, unit costs have been varied by plus or minus 20%. To test the sensitivity of the cost-effectiveness results to assumptions over the method of estimating adverse event costs, the proportion of patients experiencing adverse events (rather than the proportion of cycles in which adverse events occurred) were used to estimate adverse event costs. In the assessment report by Main and colleagues69 the same transfusion cost was applied for patients experiencing grade 3 and grade 4 anaemia. Clinical advice suggested that patients experiencing grade 4 anaemia would require four units of blood – this was costed in the base case. The final entry in the table shows the cost-effectiveness results using the transfusion cost from Main and colleagues. 69
| Cost (£) | Life-years gained | QALYs gained | ICER (£ per QALY gained) | |
|---|---|---|---|---|
| Base case | 6194 | 0.3249 | 0.1830 | 33,851 |
| Structural assumptions | ||||
| Truncate survival at maximum follow-up for trial | 6160 | 0.3202 | 0.1806 | 34,114 |
| Extrapolate OS up to 10 years | 6302 | 0.3596 | 0.1871 | 33,681 |
| Weibull survival and TTP model | 5940 | 0.3144 | 0.1591 | 37,338 |
| Methodological assumptions | ||||
| Discount rates (0% for both costs and outcomes) | 6283 | 0.3407 | 0.1894 | 33,177 |
| Discount (6% for costs and 1.5% for outcomes) | 6136 | 0.3337 | 0.1866 | 32,889 |
| Parameter uncertainty | ||||
| Lower 95% CI for treatment effect | 6183 | 0.3514 | 0.1909 | 32,381 |
| Upper 95% CI for treatment effect | 6204 | 0.2991 | 0.1751 | 35,432 |
| Lower 95% CI for all parameters in survival model | 6144 | 0.4124 | 0.2009 | 30,579 |
| Upper 95% CI for all parameters in survival model | 6229 | 0.2536 | 0.1660 | 37,515 |
| Lower 95% CI for all parameters in TTP model | 6961 | 0.3249 | 0.2360 | 29,496 |
| Upper 95% CI for all parameters in TTP model | 5676 | 0.3249 | 0.1516 | 37,454 |
| Exclude palliative care costs | 6313 | 0.3249 | 0.1830 | 34,502 |
| Lower limit for utility values | 6194 | 0.3249 | 0.1498 | 41,346 |
| Upper limit for utility values | 6194 | 0.3249 | 0.2492 | 24,859 |
| No adjustment to utility for oral topotecan cohort post progression | 6194 | 0.3249 | 0.2442 | 25,364 |
| Round down oral topotecan dosage | 6044 | 0.3249 | 0.1830 | 33,031 |
| Use proportion of patients with adverse events | 5703 | 0.3249 | 0.1830 | 31,166 |
| Cost of outpatient visit to administer oral chemotherapy: lower quartile | 5714 | 0.3249 | 0.1830 | 31,227 |
| Cost of outpatient visit to administer oral chemotherapy: upper quartile | 6472 | 0.3249 | 0.1830 | 35,373 |
| Cost of palliative care reduced by 20% | 6313 | 0.3249 | 0.1830 | 34,502 |
| Cost of palliative care increased by 20% | 6313 | 0.3249 | 0.1830 | 34,502 |
| Cost of outpatient visit for monitoring: lower quartile | 5858 | 0.3249 | 0.1830 | 32,017 |
| Cost of outpatient visit for monitoring: upper quartile | 6395 | 0.3249 | 0.1830 | 34,949 |
| Cost (per day) of inpatient admission: lower quartile | 6015 | 0.3249 | 0.1830 | 32,871 |
| Cost (per day) of inpatient admission: upper quartile | 6300 | 0.3249 | 0.1830 | 34,432 |
| Cost of day-case admission: lower quartile | 6100 | 0.3249 | 0.1830 | 33,335 |
| Cost of day-case admission: upper quartile | 6294 | 0.3249 | 0.1830 | 34,396 |
| Use transfusion cost from Main and colleagues69 for grade 4 anaemia | 6025 | 0.3249 | 0.1830 | 32,927 |
The cost-effectiveness results appear to be generally robust to variation in the parameters included in the deterministic sensitivity analysis, with ICERs varying between approximately £30,000 and £37,000 per QALY gained. Among the structural sensitivity analyses, the results appear to be most sensitive to assumptions over the functional form for the survival functions. In terms of parameter inputs, the results appear to be most sensitive to variation in utility estimates applied in the model, variation in values of parameters in the survival functions (for OS and TTP) and to the cost of outpatient attendance for the administration of oral chemotherapy.
Time horizon for the model appears to have a very limited impact on the cost-effectiveness estimates. Truncating survival at the maximum duration observed for each arm in the O’Brien and colleagues RCT57 reduces the QALY gain by 0.0024 and costs by £34. The proportionate reduction in outcome (1.3%) is greater than the proportionate reduction in costs (0.5%) hence the ICER increases, but only by a small amount. Increasing the maximum survival duration to 10 years has the opposite effect – a slight increase in QALY gain and a slight increase in costs, with the proportionate change in QALYs being greater than the proportionate increase in costs, leading to a small reduction in the ICER. Adopting an alternative (Weibull) parametric form for the OS and TTP survival functions has a more dramatic effect, resulting in a 13% reduction in QALY gain, a smaller reduction in cost and an increase in the ICER to £37,338.
Varying the discount rates applied has comparatively little effect. Zero discount rates for costs and outcomes result in slight increases in both incremental cost and incremental QALYs compared with baseline values. Applying discount rates of 6% for costs and 1.5% for outcomes leads to a slight reduction in incremental cost and to an increase in incremental QALYs. The resulting ICER is slightly lower than in the base case.
Varying the value of the treatment effect parameter in the OS model, between its upper and lower confidence limits, has a greater effect on outcomes than on cost. In the model, variation in survival (unless it is assumed to be associated with variation in TTP) has an impact on only the duration of postprogression survival, and therefore will only affect the estimate of palliative care costs. A similar situation applies to QALY outcomes where, it is assumed that all gains or losses of life expectancy associated with variation in the treatment effect parameter are weighted by postprogression utility values. This explains why the proportionate variation in QALY gains in less than the variation in life-years gained.
The cost-effectiveness results are more variable if all parameters in the survival models are included (at the 95% confidence limits) in the sensitivity analysis, rather than just the treatment effect estimated in the OS model, with ICERs varying between approximately £30,000 and £37,500 per QALY gained. Variation in the parameters of the TTP survival model has a particularly large impact on incremental cost. This arises from the inclusion of a cost of approximately £9 per day (£246 every 4 weeks) to monitor disease progression in patients following treatment with oral topotecan (see Table 33 and accompanying text for assumptions).
The greatest variation in cost-effectiveness results, associated with parameter inputs, is related to the rate of deterioration in utility values over time. Using the lower 95% confidence limits as an estimate of the higher rate of deterioration (–0.11 for oral topotecan plus BSC, –0.27 for BSC alone – see Table 5) leads to a reduction of 0.03 (18%) in the QALY gain associated with oral topotecan plus BSC. As a result, the ICER increases to £41,346 per QALY gained. In contrast, using the upper 95% confidence limits, giving a lower rate of deterioration (0.02 for oral topotecan plus BSC, –0.12 for BSC alone, – see Table 5) leads to an increase of 0.07 (36%) in the QALY gain associated with oral topotecan plus BSC, with the ICER reducing to £24,859 per QALY gained. To test the sensitivity of the cost-effectiveness results to the assumption that the QoL deterioration for the oral topotecan plus BSC cohort would be significantly greater following disease progression, the utility adjustment for postprogression survival was removed. This meant that the same rate of deterioration (–0.05 reported for oral topotecan plus BSC – see Table 5) was applied for both pre- and postprogression survival. The increase in the incremental QALY gain was almost as great as for the sensitivity analysis using the upper 95% confidence limits, with the ICER reducing to £25,364, compared with the base case.
In terms of cost parameters, the model results appear to be most sensitive to variation in the cost of outpatient attendances for the administration of oral chemotherapy. This is unsurprising as these represent the majority of the administration costs for oral topotecan, and administration cost constitute 7% of total costs for the oral topotecan plus BSC cohort.
Cost-effectiveness of topotecan – probabilistic analysis
In a probabilistic sensitivity analysis, where the parameters of the survival models (both OS and TTP) probabilities of adverse events, proportionate deterioration in health-state utility values, cost of outpatient attendances and patient monitoring, as well as costs of managing adverse events and palliative care were sampled probabilistically, oral topotecan plus BSC is associated with increased QALYs (with a range from 0.13 to 0.31 QALYs), but also increased costs (from £5160 to £8040) in all simulations when compared with BSC alone (Figure 6 – also shows the 95% confidence ellipse).
FIGURE 6.
Cost-effectiveness plane – incremental cost and incremental quality-adjusted life-years for oral topotecan compared with best supportive care.
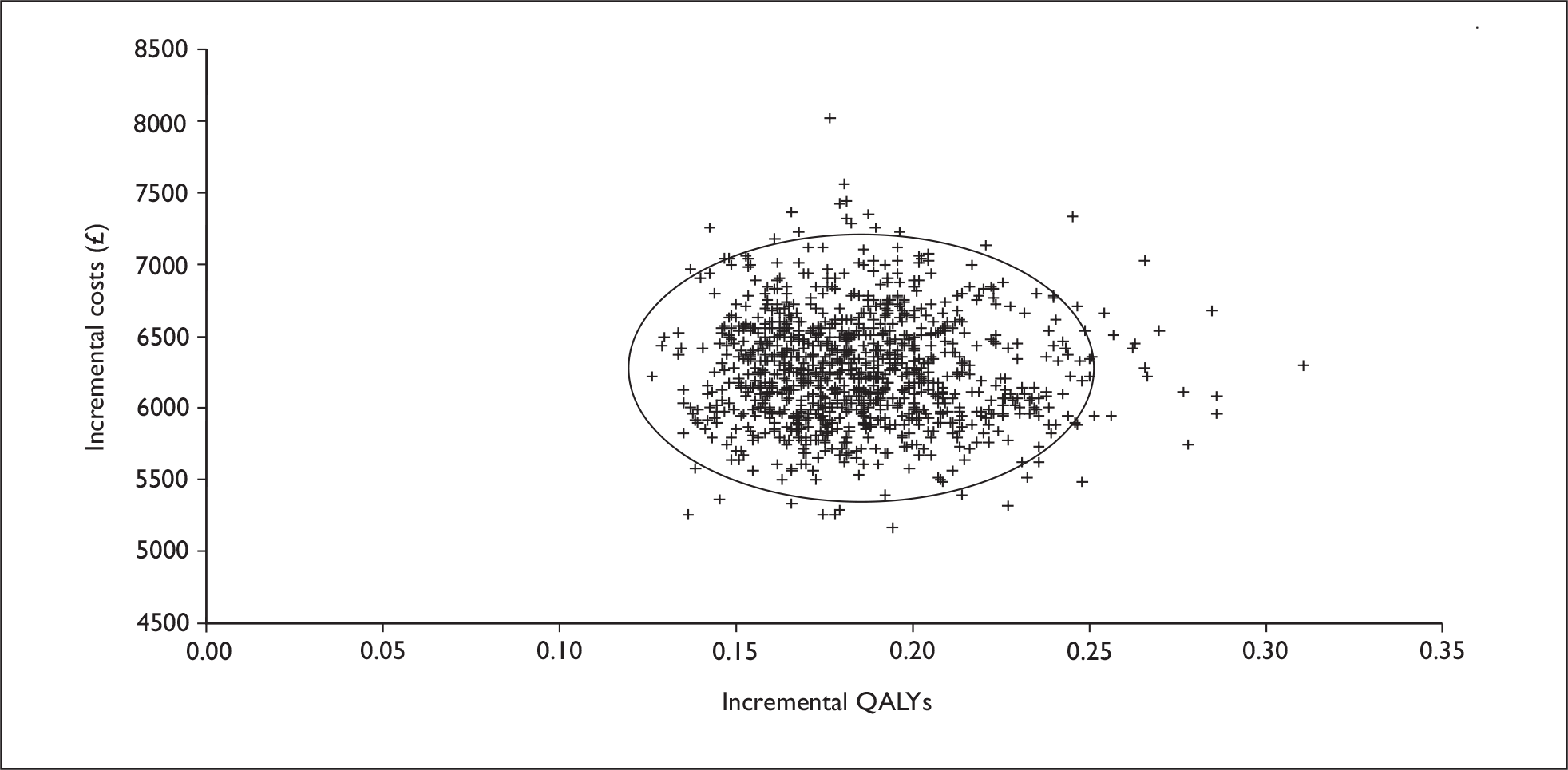
The distributions assigned to each variable included in the probabilistic sensitivity analysis and the parameters of the distribution are reported in Appendix 10. In total, 1000 simulations were run for this analysis. The probabilistic analysis generated cost and QALY estimates for each intervention that were similar to those for the base-case analysis (see Table 41 for the base-case analysis). Table 44 reports the mean costs and outcomes from the probabilistic analysis (including the 2.5th and 97.5th percentiles to give an indication of the range of the simulated values) and the ICER for oral topotecan plus BSC compared with BSC alone, based on the mean values generated in the probabilistic analysis.
| Discounted costs | Discounted QALYs | ICER | |||||
|---|---|---|---|---|---|---|---|
| Mean | 2.5th percentile | 97.5th percentile | Mean | 2.5th percentile | 97.5th percentile | ||
| BSC | 4882 | 2186 | 8584 | 0.2258 | 0.2047 | 0.2522 | |
| Oral topotecan + BSC | 11,153 | 8394 | 14,813 | 0.4116 | 0.3672 | 0.4732 | 33,753 |
The ICER reported in Table 44, calculated using the difference in mean discounted costs and mean discounted QALYs shown in the table, is slightly lower than the mean of the ICERs calculated at each simulation (which was £34,430).
In addition to graphing the incremental cost and incremental QALYs for oral topotecan plus BSC, a cost-effectiveness acceptability curve was derived, representing the proportion of simulations where oral topotecan treatment is cost-effective for a range of WTP thresholds, up to £50,000 (Figure 7). In this analysis oral topotecan plus BSC had a probability of being cost-effective of 0% at a WTP threshold of £20,000 per QALY, 20% at a WTP threshold of £30,000 per QALY and 100% at a WTP threshold of £50,000 per QALY.
FIGURE 7.
Cost-effectiveness acceptability curve for oral topotecan and best supportive care.
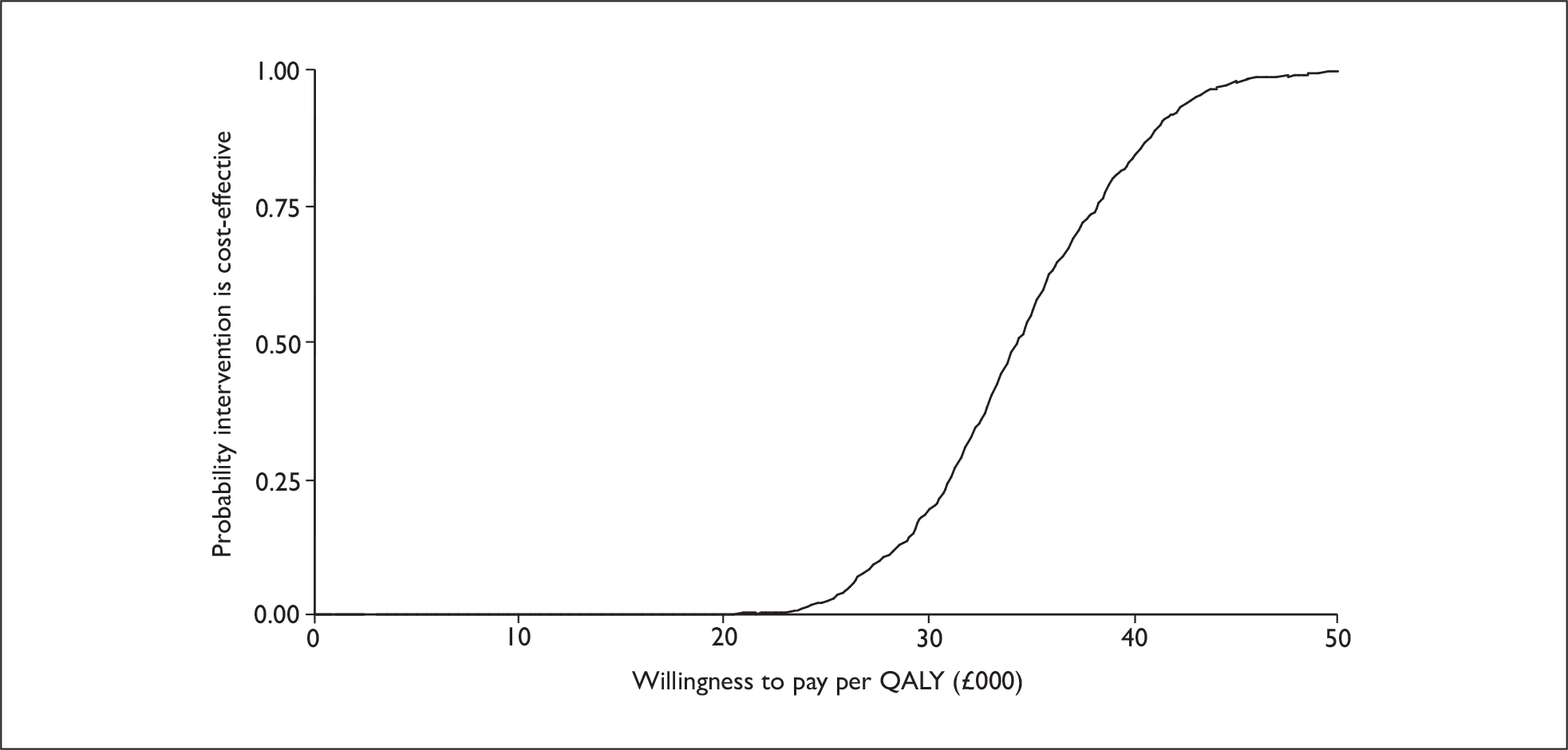
Cost-effectiveness of i.v. topotecan
This section reports cost-effectiveness results for a cohort of patients with relapsed SCLC, for whom re-treatment with the first-line regimen is not considered appropriate and who may be suitable for treatment with i.v. topotecan. As for oral topotecan, discounted costs (identifying the contribution of drugs, drug administration and monitoring, management of adverse events, monitoring prior to disease progression and palliative care) are presented alongside the life expectancy and quality-adjusted life expectancy for patients in the cohort. The results are presented as incremental cost per life-year gained and incremental cost per QALY gained relative to BSC.
Costs and outcomes modelled for cohorts of patients receiving i.v. topotecan plus BSC or BSC alone are presented in Table 45, based on the indirect comparison for OS described in Estimation of net benefits, above, TTP as described in Appendix 15, and relative risks of adverse events (compared with oral topotecan) described in Appendix 14. Costs and health outcomes in the table have been discounted at 3.5%.
| Treatment | Costs (£) | Life-years | Incremental cost per life-year gained (£) | QALYs | Incremental cost per QALY gained (£) |
|---|---|---|---|---|---|
| BSC | 4854 | 0.4735 | 0.2247 | ||
| Intravenous topotecan plus BSC | 16,914a | 0.7784 | 39,552a | 0.3875a | 74,074a |
| 17,369b | 41,043b | 0.4157b | 65,507b |
The estimated gain in discounted life expectancy, associated with the addition of i.v. topotecan to BSC, is 0.3049 years (15.9 weeks) – approximately 1 week shorter than the life expectancy gain in the base-case analysis for oral topotecan, reported above. The equivalent undiscounted values are 0.3196 years (16.6 weeks). As noted in Appendix 15, the two RCTs comparing oral and i.v. topotecan give contradictory results on the relative TTP. This has no effect on the estimated life-year gain with i.v. topotecan. However, given the assumption of a higher rate of deterioration in QoL following disease progression (see Methodology), there is an effect on the QALY gain. The estimated gain in discounted QALYs, associated with the addition of i.v. topotecan to BSC is 0.1628 when TTP is modelled using data from the RCT by von Pawel and colleagues,58 and 0.1910 when TTP is modelled using data from the RCT by Eckardt and colleagues. 56 The equivalent undiscounted values are 0.1683 and 0.1981 QALYs, respectively.
The incremental cost associated with the addition of i.v. topotecan to BSC is substantially higher than for oral topotecan – £12,060, when TTP is modelled using data from the RCT by von Pawel and colleagues,58 and £12,514 when TTP is modelled using data from the RCT by Eckardt and colleagues. 56 Table 46 reports a breakdown of treatment costs, by phase of treatment, for each cohort. For patients receiving treatment with i.v. topotecan, palliative care is no longer the most costly phase (reduced to 27% of total costs) for this cohort, while the costs of active treatment with topotecan constitute 58% of total costs (35% drug costs and 23% for chemotherapy administration).
| Phase of treatment | Intravenous topotecan (£) | BSC (£) | |
|---|---|---|---|
| Active treatment | Drug | 5979 | |
| Drug administration | 3936 | ||
| On-treatment monitoring | 353 | ||
| Adverse event costs | Haematological | 1132 | |
| Non-haematological | 45 | ||
| Non-progressive disease monitoring | 726a | ||
| 1181b | |||
| Palliative care | 4743 | 4854 | |
| Total | 16,914a | 4854 | |
| 17,369b | |||
Intravenous topotecan as a treatment for patients with relapsed SCLC, for whom re-treatment with the first-line regimen is not considered appropriate, is associated with improved outcomes (in terms of life expectancy and quality-adjusted life expectancy) over BSC and similar outcomes to oral topotecan. However, these outcomes are achieved at substantially greater cost – the ICER for i.v. topotecan compared with BSC is £74,074 per QALY gained when TTP is modelled using data from the RCT by von Pawel and colleagues,58 and £65,507 per QALY gained when TTP is modelled using data from the RCT by Eckardt and colleagues. 56 Intravenous topotecan is strictly dominated by oral topotecan (poorer outcomes at higher cost), when TTP is modelled using data from the RCT by von Pawel and colleagues58 and has an ICER of £783,734 per QALY gained compared with oral topotecan, when TTP is modelled using data from the RCT by Eckardt and colleagues. 56
Cost-effectiveness of i.v. topotecan – deterministic sensitivity analysis
Table 47 reports the results of a deterministic sensitivity analysis for i.v. topotecan. Except for the sensitivity analysis with respect to time horizon, all analyses were conducted using a 5-year time horizon. The table is divided to distinguish between analyses undertaken due to uncertainties over structural assumptions in the model, methodological uncertainties (in this case related to the discount rates applied in the model) and uncertainty over parameter values. The upper value in each cell of Table 47 gives the incremental costs, life-years gained, QALYs gained and ICER using TTP based on data from the RCT by Eckardt and colleagues,56 whereas the lower value is based on TTP from the RCT by von Pawel and colleagues. 58
| Cost (£) | Life-years gained | QALYs gained | ICER (£ per QALY gained) | |
|---|---|---|---|---|
| Base case | 12,514 | 0.3049 | 0.1910 | 65,507 |
| 12,060 | 0.1628 | 74,074 | ||
| Structural assumptions | ||||
| Extrapolate OS up to 10 years | 12,638 | 0.3371 | 0.1962 | 64,425 |
| 12,149 | 0.1660 | 73,182 | ||
| Methodological assumptions | ||||
| Discount rates (0% for both costs and outcomes) | 12,611 | 0.3196 | 0.1981 | 63,674 |
| 12,137 | 0.1683 | 72,134 | ||
| Discount (6% for costs and 1.5% for outcomes) | 12,452 | 0.3131 | 0.1950 | 63,868 |
| 12,009 | 0.1659 | 72,408 | ||
| Parameter uncertainty | ||||
| Lower 95% CI for treatment effect | 12,504 | 0.3296 | 0.1985 | 62,984 |
| 12,050 | 0.1703 | 70,755 | ||
| Upper 95% CI for treatment effect | 12,524 | 0.2809 | 0.1836 | 68,200 |
| 12,069 | 0.1554 | 77,664 | ||
| Lower 95% CI for all parameters in survival model | 12,468 | 0.387 | 0.2081 | 59,919 |
| 12,013 | 0.1799 | 66,796 | ||
| Upper 95% CI for all parameters in survival model | 12,547 | 0.2381 | 0.1755 | 71,484 |
| 12,092 | 0.1468 | 82,390 | ||
| Relative treatment effect of i.v. vs oral (lower limit) | 12,542 | 0.2346 | 0.1691 | 74,176 |
| 12,087 | 0.1408 | 85,831 | ||
| Relative treatment effect of i.v. vs oral (upper limit) | 12,476 | 0.3975 | 0.2186 | 57,063 |
| 12,021 | 0.1904 | 63,135 | ||
| Lower 95% CI for all parameters in TTP model | 13,376 | 0.3049 | 0.2815 | 47,514 |
| 12,725 | 0.2066 | 61,581 | ||
| Upper 95% CI for all parameters in TTP model | 11,929 | 0.3049 | 0.1539 | 77,487 |
| 11,614 | 0.1371 | 84,689 | ||
| Exclude palliative care costs | 12,626 | 0.3049 | 0.1910 | 66,089 |
| 12,171 | 0.1628 | 74,756 | ||
| Lower limit for utility values | 12,514 | 0.3049 | 0.1551 | 80,705 |
| 12,060 | 0.1343 | 89,767 | ||
| Upper limit for utility values | 12,514 | 0.3049 | 0.2643 | 47,347 |
| 12,060 | 0.2187 | 55,144 | ||
| No adjustment to utility for oral topotecan cohort post progression | 12,514 | 0.3049 | 0.2335 | 53,585 |
| 12,060 | 0.2335 | 51,638 | ||
| Cost of outpatient visits to administer i.v. chemotherapy: lower quartile | 10,522 | 0.3049 | 0.1910 | 55,076 |
| 10,067 | 0.1628 | 61,833 | ||
| Cost of outpatient visits to administer i.v. chemotherapy: upper quartile | 13,852 | 0.3049 | 0.1910 | 72,510 |
| 13,398 | 0.1628 | 82,291 | ||
| Cost of palliative care (reduced by 20%) | 12,542 | 0.3049 | 0.1910 | 65,653 |
| 12,087 | 0.1628 | 74,244 | ||
| Cost of palliative care (increased by 20%) | 12,487 | 0.3049 | 0.1910 | 65,362 |
| 12,032 | 0.1628 | 73,903 | ||
| Cost of outpatient visit for monitoring: lower quartile | 12,132 | 0.3049 | 0.1910 | 63,507 |
| 11,819 | 0.1628 | 72,594 | ||
| Cost of outpatient visit for monitoring: upper quartile | 12,743 | 0.3049 | 0.1910 | 66,705 |
| 12,204 | 0.1628 | 74,960 | ||
| Use transfusion cost from Main and colleagues69 for grade 4 anaemia | 12,487 | 0.3049 | 0.1910 | 65,366 |
| 12,033 | 0.1628 | 73,908 | ||
The cost-effectiveness results appear to be generally robust to variation in the parameters included in the deterministic sensitivity analysis, with ICERs remaining in most cases above £60,000 per QALY gained. As with oral topotecan, in terms of parameter inputs the results appear to be most sensitive to variation in utility estimates applied in the model, variation in values of parameters in the survival functions (for OS and TTP) and to the cost of outpatient attendance for the administration of chemotherapy. Time horizon for the model appears to have a very limited impact on the cost-effectiveness estimates, as does varying the discount rates applied in the model.
Cost-effectiveness of i.v. topotecan – probabilistic analysis
In a probabilistic sensitivity analysis, where the parameters of the survival models (both OS and TTP) probabilities of adverse events, proportionate deterioration in health-state utility values, cost of outpatient attendances and patient monitoring as well as costs of managing adverse events and palliative care were sampled probabilistically, i.v. topotecan is associated with increased QALYs (with a range from 0.10 to 0.27 QALYs, when TTP is modelled using data from the RCT by von Pawel and colleagues,58 and from 0.11 to 0.33 QALYs, when TTP is modelled using data from the RCT by Eckardt and colleagues56), but also increased costs (from £10,091 to £14,701 and from £9669 to £15,422, when TTP is modelled using data from the RCTs by von Pawel and colleagues,58 and by Eckardt and colleagues,56 respectively) in all simulations, when compared with BSC alone [Figure 8 – also shows 95% confidence ellipses for when TTP is modelled using data from the RCT by von Pawel and colleagues58 (dashed ellipse) and by Eckardt and colleagues56 (solid ellipse)].
FIGURE 8.
Cost-effectiveness plane – incremental cost and incremental quality-adjusted life-years for intravenous topotecan compared with best supportive care, with 95% confidence ellipses.
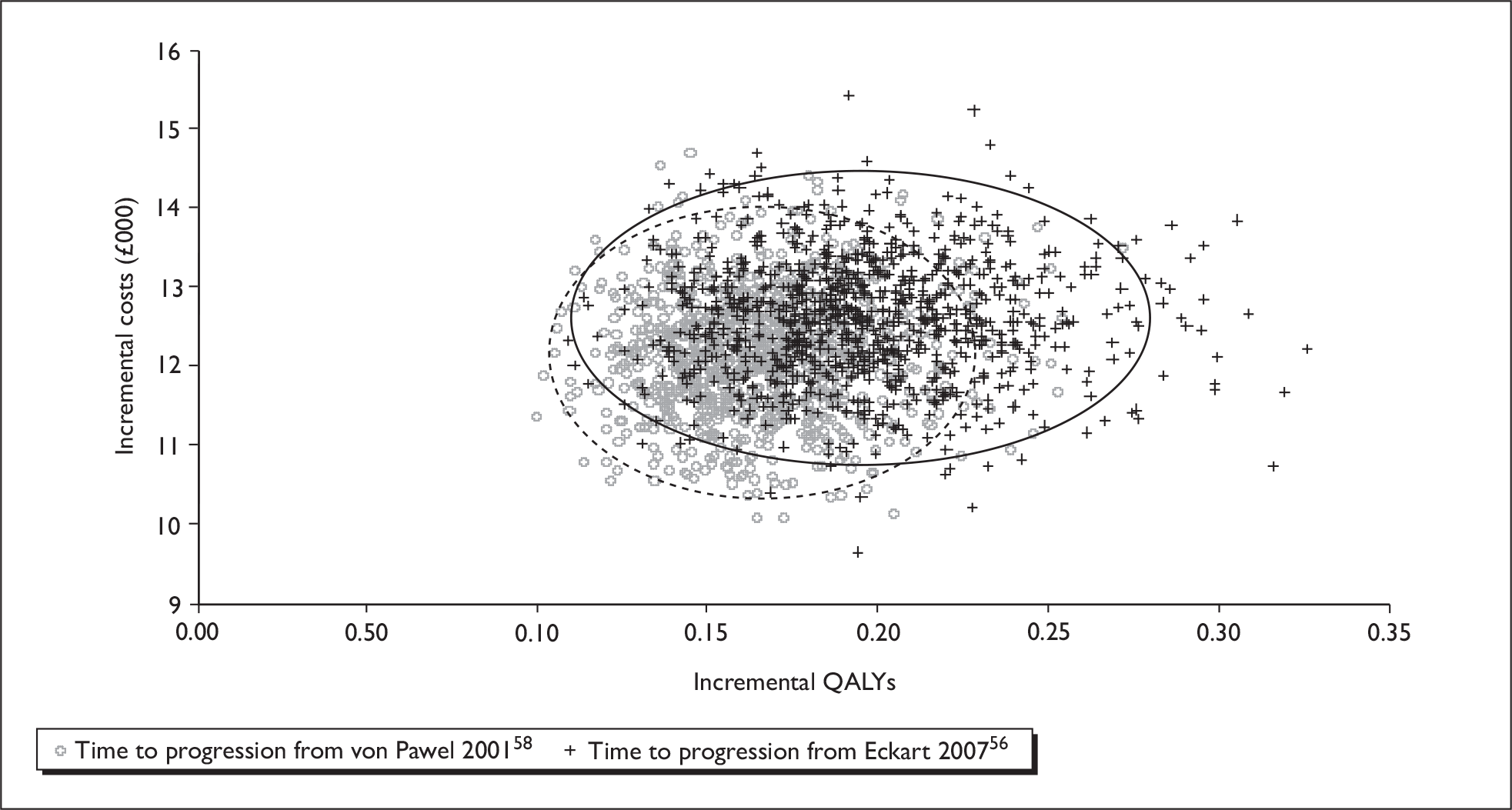
The distributions assigned to each variable included in the probabilistic sensitivity analysis and the parameters of the distribution are reported in Appendix 10. One thousand simulations were run for this analysis. The probabilistic analysis generated cost and QALY estimates for each intervention that were similar to those for the base-case analysis (see Table 45 for the base-case analysis). Table 48 reports the mean costs and outcomes from the probabilistic analysis (including the 2.5th and 97.5th percentiles to give an indication of the range of the simulated values) and the ICER for i.v. topotecan plus BSC compared with BSC alone, based on the mean values generated in the probabilistic analysis.
| Discounted costs | Discounted QALYs | ICER | |||||
|---|---|---|---|---|---|---|---|
| Mean | 2.5th Percentile | 97.5th Percentile | Mean | 2.5th Percentile | 97.5th Percentile | ||
| BSC | 4829 | 2305 | 8652 | 0.2260 | 0.2054 | 0.2527 | 73,579a |
| Intravenous topotecan plus BSC | 17,000a | 14,089a | 20,752a | 0.3915a | 0.3438a | 0.4599a | 64,418b |
| 17,387b | 14,497b | 21,203b | 0.4210b | 0.3615b | 0.4998b | ||
The ICERs reported in Table 48, calculated using the difference in mean discounted costs and mean discounted QALYs shown in the table, are slightly lower than the mean of the ICERs calculated at each simulation (which were £75,325 and £66,444, when TTP is modelled using data from the RCTs by von Pawel and colleagues58 and by Eckardt and colleagues,56 respectively).
In addition to providing a graph of the incremental cost and incremental QALYs for i.v. topotecan and BSC, cost-effectiveness acceptability curves were derived for each analysis, representing the proportion of simulations where i.v. topotecan treatment is cost-effective for a range of WTP thresholds, up to £100,000 (Figure 9). In this analysis i.v. topotecan plus BSC had a probability of being cost-effective of 0% at WTP threshold of £20,000 and £30,000 per QALY, and 1% at a WTP threshold of £50,000 per QALY, when TTP is modelled using data from the RCT by von Pawel and colleagues. 58 When TTP is modelled using data from the RCT by Eckardt and colleagues,56 the probability of being cost-effective remained at 0% at the lower WTP thresholds but increased slightly (to 7.6%) at a WTP threshold of £50,000 per QALY.
FIGURE 9.
Cost-effectiveness acceptability curve for intravenous topotecan and best supportive care.
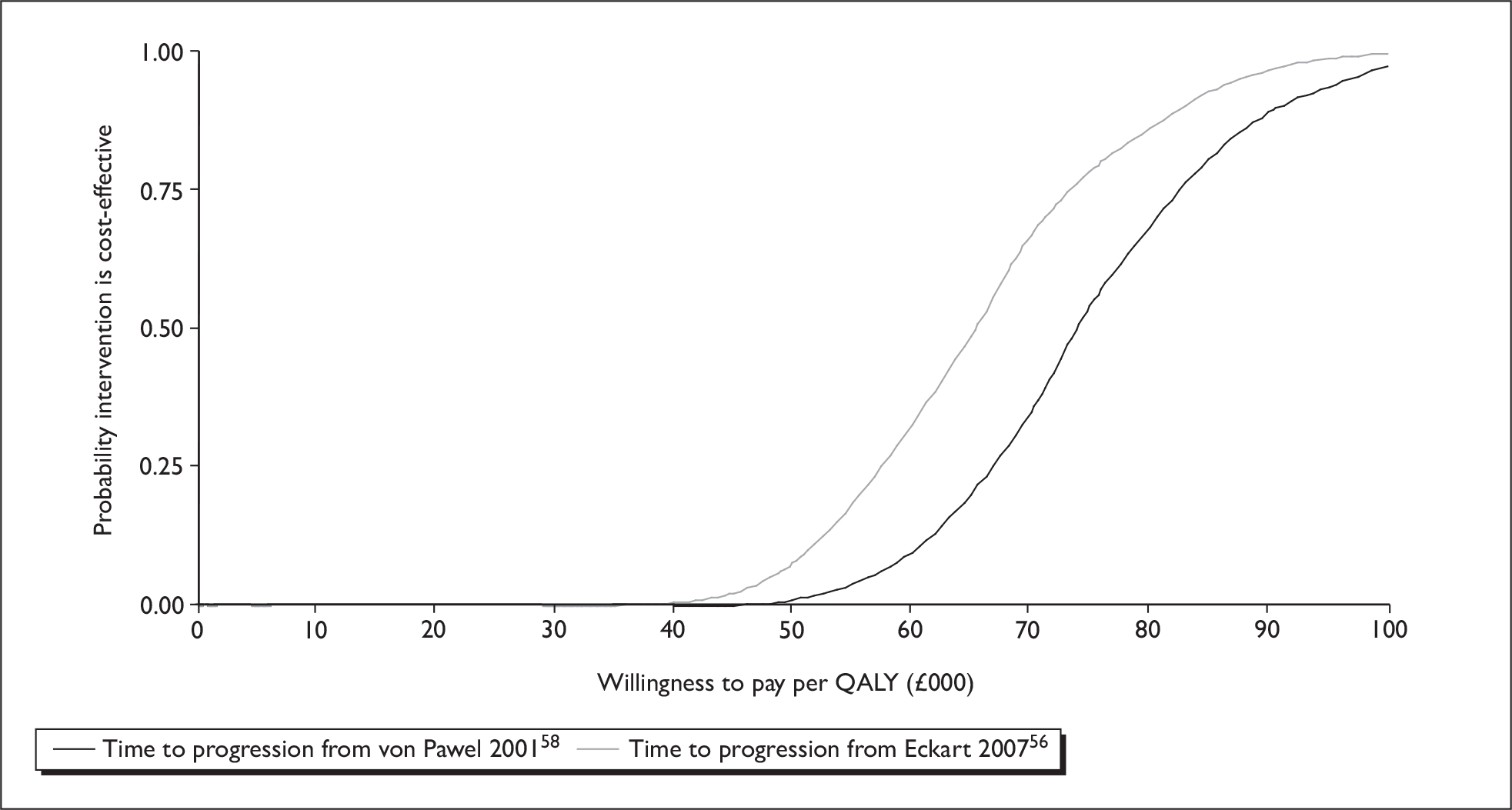
Summary of cost-effectiveness
-
A systematic search of the literature found no fully published economic evaluations of oral or i.v. topotecan as a treatment for patients with relapsed SCLC, for whom re-treatment with the first-line regimen is not considered appropriate.
-
A systematic search for published studies of QoL for patients with relapsed SCLC found no fully published studies other than the main RCT publication by O’Brien and colleagues. 57 There is very little detail on the methods used to analyse the utility data presented in the main trial report. The searches identified an additional publication, available only in abstract form,64 which provided more details (including baseline utility scores for the trial arms). Further methodological detail was extracted from the CSR (submitted as an appendix to the MS to NICE).
-
The manufacturer submitted a dossier in support of oral topotecan, including an economic evaluation based on individual participant data from the RCT reported by O’Brien and colleagues. 57 This compares oral topotecan plus BSC with BSC alone. CAV was excluded from the manufacturer’s analysis on the a priori basis that topotecan (oral or i.v.) would be unlikely to be a cost-effective alternative, given its higher acquisition cost.
-
Mean survival, in the manufacturer’s model, was estimated directly from the survival durations for patients in the O’Brien and colleagues RCT. 57 Censored cases were assumed to have died on the day following censoring – the manufacturer conducted no sensitivity analysis in respect of this assumption.
-
Health-related QoL was recorded using the EQ-5D, for up to 12 cycles (36 weeks), and valued using a general population tariff. 80 Missing values were imputed using data from the trial, using the mean utility score (across both trial arms) for missing values up to cycle 12. Where oral topotecan plus BSC patients survived with non-progressive disease beyond the 36-week data collection, the last observation was carried forward until disease progression occurred. Once these patients developed progressive disease, values for BSC patients were applied.
-
Oral topotecan was costed at the observed total dose for each participant in the topotecan plus BSC arm of the RCT by O’Brien and colleagues57 (with dosage rounded up to the nearest 0.25 mg). Chemotherapy administration was costed for the observed number of cycles for each patient, assuming one attendance per cycle to collect oral chemotherapy and assumed monitoring costs of £10 per cycle (using monitoring costs from a previous TAR,69 which included topotecan, inflated to 2007/08 costs). Haematological adverse events were costed on the basis of the observed prescribing of GCSF and antibiotics, as well as blood products (RBC units and platelet units) delivered to patients in the RCT by O’Brien and colleagues,57 with additional assumptions regarding costs of administration. All blood transfusions were assumed to be provided on a day-case basis. Patients were assumed to be managed as day cases where drugs were administered intravenously, whereas patients receiving oral drugs were assumed to have their adverse events managed in outpatients. Resource use for management of non-haematological adverse events was based on expert opinion and costed according to the proportion of non-haematological adverse events which were deemed to be treatment-related in the RCT by O’Brien and colleagues. 57 Resource use for monitoring patients following the cessation of treatment with topotecan, and prior to disease progression, was also based on expert opinion.
-
In the manufacturer’s base case, the QALY gain for the cohort of patients receiving oral topotecan plus BSC was estimated at 0.211. The cost difference was £5671, giving an ICER of £26,833 per QALY gained.
-
Deterministic sensitivity analysis showed that the results were sensitive to methods of estimating QoL (methods of carrying forward utility scores when patients had missing data), drug administration cost (significantly higher costs if patient attend on 5 days of the cycle to receive chemotherapy) and adverse event costs (halving or doubling adverse event costs).
-
In a bootstrap analysis, treatment with oral topotecan plus BSC was always associated with increased costs (incremental costs between £4000 and £7500) and with improved QALY outcomes (incremental QALYs between 0 and approximately 0.6) in the majority (98%) of replications. Cost effectiveness acceptability curves reported in the MS estimate a probability of oral topotecan plus BSC being cost-effective at 22% at a WTP threshold of £20,000 per QALY and 60% at a WTP threshold of £30,000 per QALY.
-
Subgroup analyses showed that oral topotecan was more likely to be cost-effective in patients whose TTP from prior therapy was less than or equal to 60 days (ICER = £17,946 per QALY gained), in women (ICER = £11,708 per QALY gained) and in those patients without liver metastases (ICER = £21,291 per QALY gained). Treatment with oral topotecan plus BSC also appeared to be more cost-effective for patients with a PS of 2 (ICER = £25,544 per QALY gained) as opposed to those with a PS of 0 or 1 (ICER = £30,770 per QALY gained).
-
We developed an independent model that adopted a survival model methodology, using the published Kaplan–Meier estimates for OS and TTP data included in the MS. The model includes three states – relapsed SCLC, progressive disease and death.
-
Utility values reported for participants in the RCT by O’Brien and colleagues57 were used in the model. QoL data for the trial were reported as a rate of deterioration per 3-month interval for participants in each arm in the trial, controlling for baseline utility. The reported reductions over 3 months were converted to daily utility reductions for use in our model and applied to the baseline utility values for participants in the RCT by O’Brien and colleagues. 57 The rate of deterioration reported for oral topotecan plus BSC was used for participants prior to disease progression. To allow for poorer QoL in participants following disease progression the rate of deterioration reported for BSC alone was applied to oral topotecan patients who had experienced disease progression.
-
Resource use associated with oral and i.v. topotecan were estimated from the included RCTs, the MS and using advice from clinical experts. Where insufficient detail was available (such as for palliative care), appropriate costs were taken from published sources. Drug costs were taken from the BNF. 79 Other unit costs were taken from NHS reference costs, Southampton University Hospitals Trust or published sources. Cost base for evaluation was 2007/08 financial year – where costs were taken from other cost years, these were adjusted using the HCHS Pay and Prices Index.
-
The base-case model has approximate lifetime horizon, with extrapolation of the survival functions up to 5 years in the base case. Alternative scenarios using a longer time horizon or limited to the maximum follow up in the RCT by O’Brien and colleagues57 are reported in the deterministic sensitivity analysis to ascertain whether extrapolation using survival function introduces bias. Alternative forms of survival function were also investigated to assess the sensitivity of the cost-effectiveness to structural assumptions.
-
The gain in discounted life expectancy associated with the addition of oral topotecan to BSC, for patients with relapsed SCLC for whom re-treatment with the first-line regimen is not considered appropriate, is 0.33 years in our model (approximately 16.9 weeks). The discounted QALY gain is 0.1830 QALYs. The incremental cost associated with the addition of oral topotecan to BSC is approximately £6200, resulting in an ICER of £33,851 per QALY gained. Approximately 40% of the incremental cost of the addition of oral topotecan to BSC is associated with drug acquisition costs, while approximately 26% is accounted for by management of adverse events, the majority of which are non-haematological toxicities.
-
The cost-effectiveness results for oral topotecan plus BSC are generally robust to variation in the parameters included in the deterministic sensitivity analysis, with ICERs varying between £30,000 and £37,000 per QALY gained. Among the structural sensitivity analyses, the results are most sensitive to assumptions over the functional form for the survival functions. In terms of parameter inputs, the results are most sensitive to variation in utility estimates applied in the model, variation in values of parameters in the survival functions (for OS and TTP) and the cost of outpatient attendance for the administration of oral chemotherapy.
-
Probabilistic sensitivity analysis shows a 0% probability of oral topotecan plus BSC being cost-effective, compared with BSC alone, at a WTP threshold of £20,000. The equivalent figure for a WTP threshold of £30,000 is 20%.
-
The gain in discounted life expectancy associated with i.v. topotecan, for patients with relapsed SCLC for whom re-treatment with the first-line regimen is not considered appropriate, in our model is 0.30 years (approximately 15.9 weeks) – approximately 1 week shorter than the base-case analysis for oral topotecan. The discounted QALY gain is 0.1628 QALYs when TTP is modelled using data from the RCT by von Pawel and colleagues,58 and 0.1910,when TTP is modelled using data from the RCT by Eckardt and colleagues. 56 The incremental cost associated with i.v. topotecan is approximately £12,000 (£12,060 and £12,514 when TTP is modelled using data from the RCTs by von Pawel and colleagues58 and by Eckardt and colleagues,56 respectively). For patients receiving treatment with i.v. topotecan, palliative care constitutes 27% of total costs for this cohort, while the cost of active treatment with topotecan constitutes 58% of total costs (35% drug costs and 23% for chemotherapy administration). The resulting cost for i.v. topotecan compared with BSC is between £74,074 and £65,507 per QALY gained, depending on assumptions regarding TTP. Compared with oral topotecan, i.v. topotecan is strictly dominated (poorer outcomes at higher cost) when TTP is modelled using data from the RCT by von Pawel and colleagues,58 while the ICER is approximately £783,734 per QALY gained when TTP is modelled using data from the RCT by Eckardt and colleagues. 56
-
In a probabilistic sensitivity analysis, i.v. topotecan had a zero probability of being cost-effective compared with BSC alone at WTP thresholds of £20,000 and £30,000 per QALY. For a WTP threshold of £50,000 the equivalent figure was between 1% and 7.6%, depending on assumptions regarding TTP.
Chapter 5 Implications for other parties
Topotecan (oral or i.v.) appears to provide gains in life expectancy over BSC alone, for people with relapsed SCLC. Recent debates over the assessment of technologies for peoples with short life expectancies have argued that a person’s family and carers may place a high value on relatively small extensions of life expectancy. Such potential benefits need to be weighed against the impact of patients taking up treatment. Attendance at hospital on five consecutive days of each chemotherapy cycle, as would be the case with i.v. topotecan, may be an unacceptable burden for carers. While oral topotecan offers advantages in terms of frequency of attendance for chemotherapy administration, both forms of topotecan are associated with high incidences of grade 3 and grade 4 haematological toxicities, which may have a substantial impact on patients’ carers and families.
Chapter 6 Factors relevant to the NHS
Oral topotecan offers an active treatment option to peoples who were previously deemed only suitable for palliative care, with potential gains in life expectancy over BSC alone. Adoption of oral topotecan as an addition to BSC for people with relapsed SCLC, in whom re-treatment with first-line therapy is not considered appropriate, is likely to require some additional treatment capacity. People undergoing chemotherapy with oral topotecan will be required to attend outpatients once every 3 weeks to collect their medication, to undergo monitoring for treatment-related toxicity and assessment of disease progression as well as for general medical assessment. Additional capacity will be required for management of serious adverse events, when they occur – the RCTs by O’Brien and colleagues57, von Pawel and colleagues58 and Eckardt and colleagues56 suggest that grade 3 or 4 neutropenia will occur in 60–75% of people who are treated with oral topotecan, while 22–32% of people will experience grade 3 or 4 anaemia. Treatment with i.v. topotecan would have similar requirements in terms of managing adverse events, but substantially higher requirements for chemotherapy administration – these are reflected in the treatment cost estimates developed for the independent model. As a consequence, i.v. topotecan appears unlikely to be a treatment of choice in normal NHS practice.
The SmPC for topotecan74 makes clear that the supervision of people receiving treatment requires specialist knowledge and experience of the use of chemotherapeutic agents. On this basis, it seems most likely that the active care component of management will be based in secondary care, under management of clinical oncology, although this may also require co-ordination with primary care. Given the poor prognosis and relatively short life expectancy for those with relapsed SCLC, even those initially responding topotecan, management will also require co-ordination with palliative care services.
Chapter 7 Discussion
Statement of principal findings
Clinical effectiveness
The results from five RCTs were included in this systematic review. One RCT compared oral topotecan plus BSC with BSC alone,57 one compared i.v. topotecan with CAV combination therapy,59 two compared oral topotecan with i.v. topotecan,56,58 and one other compared i.v. topotecan with amrubicin. 63 In one of the included studies of oral versus i.v. topotecan56 and the study comparing topotecan with amrubicin,63 we could not ascertain with any certainty if the population in the trials exactly matched those of the marketing authorisation for topotecan, i.e. participants were inappropriate for re-treatment with their first-line therapy. Therefore, is not clear how generalisable these studies are to the likely eligible participants in a UK setting. In terms of demographic characteristics, these studies, where reported, had similar population groups; the age ranges in each study were similar, with a higher proportion of males and a higher proportion having had extensive SCLC. No studies provided details of the ethnicity of participants, although it may be assumed that a high proportion of the participants in the study by Inoue and colleagues63 were of Asian origin. Assessment of methodological reporting and quality varied between the included studies. There was a risk of selection bias in three studies56,58,63 and a risk of detection bias in all of the studies. Three studies were assessed as having an adequate ITT analysis, however. 57–59
The primary outcome measure in most studies was response rate. For this measure, the evidence showed that there was no difference between i.v. topotecan and i.v. CAV, and no difference between topotecan that was administered orally compared with topotecan administered intravenously. Response rate was seen to be better in those treated with amrubicin, although it is worth noting the lower dose of topotecan in this study. In the trial of oral topotecan compared with BSC, measurement of response rates were appropriate only in the treatment group and hence no comparison on this outcome can be made.
Other outcome measures included duration of response, TTP, OS, symptoms, HRQoL and toxicities/adverse events. The evidence showed that OS was better in those treated with oral topotecan compared to BSC (the primary outcome in this study). There were no differences in OS between i.v. topotecan and CAV therapy, i.v. topotecan and amrubicin, or oral topotecan compared with i.v. topotecan. Health related QoL was seen to favour topotecan in the oral topotecan versus BSC study, although results may need to be viewed critically due to a number of issues (noted above). In one of the studies comparing i.v. topotecan with oral topotecan there were reportedly no differences in QoL between study arms; however no data were reported. Where reported, it would appear that symptoms were favourable to topotecan therapy, although care is required as some scales may not have been validated measures. Toxicities were reported across treatment groups in all studies, except in the O’Brien and colleagues57 study where no treatment was given to those in the BSC group. There were some grades of toxicities that showed higher rates in the topotecan arms of studies, however there were also some grades of toxicities that showed lower rates. This, together with the small sample sizes of the studies and the different comparators evaluated, mean that it is difficult to establish with any degree of certainty if topotecan is more or less toxic in those with SCLC than comparator interventions.
Cost-effectiveness
Systematic searches identified no fully published economic evaluations of oral or i.v. topotecan for the treatment of relapsed SCLC, in patients who were not considered appropriate for re-treatment with their first-line regimen and only limited information on QoL in patients with relapsed SCLC.
The MS included an economic evaluation that compared oral topotecan plus BSC with BSC alone, based on individual participant data from the RCT reported by O’Brien and colleagues. 57 CAV was excluded from the manufacturer’s analysis on the basis that topotecan (oral or i.v.) would be unlikely to be a cost-effective alternative, given its higher acquisition cost. The QALY gain with oral topotecan plus BSC, compared with BSC alone, was estimated at 0.211 in the manufacturer’s base-case analysis. The cost difference was £5671, giving an ICER of £26,833 per QALY gained. Deterministic sensitivity analysis showed that the results were sensitive to methods of estimating QoL, drug administration cost and adverse event costs, although the scenarios examined for costs were extreme. Parametric cost-effectiveness acceptability curves were used in the MS to estimate the probability of oral topotecan plus BSC being cost-effective, compared with BSC alone. The MS reported a probability of being cost-effective of 22% at a WTP threshold of £20,000 per QALY, and 60% at a WTP threshold of £30,000 per QALY.
Subgroup analyses undertaken with the manufacturer’s model showed that oral topotecan was more likely to be cost-effective in patients whose TTP from prior therapy was less than or equal to 60 days (ICER = £17,946 per QALY gained), in women (ICER = £11,708 per QALY gained) and in those patients without liver metastases (ICER = £21,291 per QALY gained). Treatment with oral topotecan plus BSC also appeared to be more cost-effective for patients with a PS of 2 (ICER = £25,544 per QALY gained) as apposed to those with a PS of 0 or 1 (ICER = £30,770 per QALY gained).
The manufacturer’s approach to estimating the cost-effectiveness of oral topotecan appears generally reasonable. However, specific concerns were raised regarding the extent to which the within-trial QoL assessments captured the impact of adverse events for patients in the oral topotecan arm, the adequacy of approaches to imputing values where QoL data were missing and the lack of survival modelling for patients whose data were censored (although the proportion of censored cases is comparatively low).
We developed an independent model to assess the cost-effectiveness of topotecan (oral or i.v.) compared with BSC, using survival analysis. The model consists of three states – relapsed SCLC, progressive disease and death – and includes the utility estimates reported for patients in the RCT by O’Brien and colleagues. 57 In the base case we extrapolate survival up to 5 years.
Resource use associated with oral and i.v. topotecan was estimated from included RCTs, the MS, advice from clinical experts and published sources. Unit costs were taken from the BNF,79 NHS Reference Costs and other published sources. Where published estimates were inadequate we used costs supplied by the Southampton University Hospitals Trust. The cost base for the evaluation was 2007/08 financial year.
The gain in discounted life expectancy associated with the addition of oral topotecan to BSC in our model is 0.33 years (approximately 16.9 weeks). The discounted QALY gain is 0.1830 QALYs. The incremental cost associated with the addition of oral topotecan to BSC is approximately £6200, resulting in an ICER of £33,851 per QALY gained. The cost-effectiveness results for oral topotecan plus BSC are generally robust to variation in the parameters included in the deterministic sensitivity analysis. The results were most sensitive to assumptions over the form of survival functions adopted and variation in values of parameters in the survival functions, variation in utility estimates applied in the model and the cost of outpatient attendance for the administration of oral chemotherapy. In a probabilistic sensitivity analysis we estimated a 0% probability of oral topotecan plus BSC being cost-effective, compared with BSC alone, at a WTP threshold of £20,000 and a 20% probability at a WTP threshold of £30,000 per QALY.
The gain in discounted life expectancy associated with i.v. topotecan, compared with BSC, in our model is 0.30 years (approximately 15.9 weeks) – approximately one week shorter than the base-case analysis for oral topotecan. The discounted QALY gain is between 0.1628 QALYs and 0.1910 QALYs depending on assumptions regarding TTP and the incremental cost is approximately £12,000. The resulting ICER for i.v. topotecan compared with BSC is between £74,074 and £65,507 per QALY gained, depending on assumptions regarding TTP. Compared with oral topotecan, i.v. topotecan is strictly dominated or is associated with a very high ICER. A probabilistic sensitivity analysis for i.v. topotecan showed zero or very low probability of being cost-effective, compared with BSC alone, at WTP thresholds of up to £50,000.
Strengths, limitations and uncertainties
This evidence synthesis has the following strengths:
-
It is independent of any vested interest.
-
It has been undertaken following the principles for conducting a systematic review. The methods were set out in a research protocol (Appendix 2) that defined the research question, inclusion criteria, quality criteria, data extraction process and methods to be used at different stages of the review.
-
An advisory group has informed the review from its initiation. The research protocol was informed by comments received from the advisory group and the advisory group has reviewed and commented on the final report.
-
The review brings together the evidence for the clinical and cost-effectiveness of topotecan for SCLC. This evidence has been critically appraised and presented in a consistent and transparent manner.
-
An economic model has been developed following recognised guidelines and systematic searches have been conducted to identify data for the economic model. The main results have been summarised and presented.
-
Clinical evidence to populate the model has been extracted from reasonable quality RCTs included in the systematic review. The effect of treatment was assessed using appropriate measures (survival and quality-adjusted survival) to model cost and outcome differences over the model time horizons. Additional relevant data on TTP were included to take account of expected differences in QoL following disease progression.
In contrast, this review also has certain limitations and uncertainties, which include:
-
Where possible, the data included in the model are in the public domain. However, additional data inputs, such as TTP and adverse event data, were extracted from the MS where these were not reported in sufficient detail in published sources. The model structure and data inputs are clearly presented in this report. This should facilitate replication and testing of our model assumptions.
-
The resource use assumptions were developed with advice from clinical experts who advised on the development of this review. Our resource-use assumptions and unit cost estimates were compared with those included in the MS to assess their comprehensiveness.
-
There is substantial uncertainty over the QoL data included in the model. However, these are key to assessing the cost-effectiveness of chemotherapeutic interventions for cancer patients. Adverse events associated with highly toxic agents may entirely offset life expectancy or QoL gains for responding patients. To address this uncertainty we have tested the impact of assumptions regarding QoL in the model and attempted to identify which assumptions have greatest impact on the cost-effectiveness results.
-
The validity of applying the survival model approach has been examined by comparing the results from our model with those from the manufacturer’s analysis. The survival model gives a higher estimate of mean survival than the manufacturer’s model using individual participant data. This difference largely results from the assumption, in the manufacturer’s model, that censored patients day on the day following censoring – this appears to have a disproportionately large effect for the oral topotecan plus BSC cohort where one patient is censored after a relatively short period of follow-up, but also involves truncation of the maximum survival duration where up to 5% of patients in the oral topotecan plus BSC arm of the trial were still alive.
Other relevant factors
A number of other issues that need to be taken into account when considering the results of the present review are noted below.
-
Authors of trials were contacted to try to establish with certainty that the participant populations in the included trials met the marketing authorisation. Responses were received from three of these authors (relating to four studies). However, it remains uncertain whether the participant groups in these trials fully meet the licensed indication for topotecan.
-
Only two RCTs reported any assessment of QoL issues; one of these reported no baseline data and reported only minimal information on participants included in the analysis and the other provided no data at all. It is therefore difficult to make any judgement about the impact of topotecan on a person’s QoL.
-
Dose escalations and reductions were permitted in the protocols of each of the included trials. However, full details of these changes are not always presented and it is therefore unknown if these dose changes would have a significant effect on the outcomes.
-
The duration of many of the trials was unclear, but in many was likely to be less than 12 months, in part likely owing to the nature of SCLC, which deteriorates rapidly. However, this does mean that long-term evidence on outcomes and adverse events are limited for those eligible for treatment with topotecan. This may mean that the impact of adverse events are underestimated.
-
All but one of the included trials were multicentre studies and it is unclear whether intercentre variability is an issue within these trials, particularly on measurement of self-report outcomes such as QoL. In addition, all the studies included in this review included participants from countries other than the UK. It is difficult to determine how generalisable the results of the included studies are to the population within the UK.
-
Four of the five included trials were sponsored evaluations by the manufacturer of topotecan.
Chapter 8 Conclusions
Oral topotecan appears to improve survival in people with SCLC when compared with BSC alone. On measures of response there is no evidence that i.v. topotecan is better or worse than treatment with CAV, but i.v. topotecan appears to be less effective than amrubicin. Treatment toxicities and adverse events with i.v. topotecan are comparable to those with CAV or amrubicin, based on the data available. Oral and i.v. topotecan were not seen to be different from one another on survival or measures of response.
In the cost-effectiveness analysis, topotecan (oral or i.v.) for patients with relapsed SCLC was associated with improved health outcomes compared with BSC. However, these improved outcomes were achieved at increased cost. Costs for i.v. topotecan were substantially higher than for oral topotecan, while the health benefits are roughly equivalent (or possibly poorer). ICERs for i.v. topotecan, compared with BSC, were high, and suggest that it is unlikely to be a cost-effective option for this group of patients. The ICER for oral topotecan compared with BSC was lower than for i.v. topotecan, but is at the upper extreme of the range conventionally regarded as cost-effective from an NHS decision-making perspective. Sensitivity analyses suggest that the exact value of the ICER is highly dependent on assumptions regarding QoL for patients with relapsed SCLC who are receiving oral topotecan.
Need for further research
-
While it is desirable for further good-quality RCT evidence on the effectiveness of topotecan, it is neither likely that any further RCTs of topotecan compared to BSC will be ethically acceptable, nor likely for there to be a need to undertake a further comparison with CAV therapy, and there is little to be gained from undertaking further evidence of the effectiveness of i.v. versus oral topotecan. However, given the ongoing RCTs of topotecan versus amrubicin, it would be desirable to update the current review when these report.
-
Further research into the QoL of patients with relapsed SCLC would be beneficial, to identify the impact of disease progression on QoL. In the case of patients receiving active treatment further research is needed on the impact of response (CR or PR) and the impact of treatment-related adverse events on QoL.
-
Further research on the impact of active treatment on resource use for palliative care would improve cost-effectiveness models for topotecan. The data collection on resource use in the RCT by O’Brien and colleagues was not comprehensive. It is difficult to determine whether the lower proportion of patients receiving radiotherapy and palliative medication (in the topotecan plus BSC arm) indicates a genuine reduction in palliative care interventions or a postponement until disease progression occurs.
Acknowledgements
We would like to thank members of our advisory group who provided expert advice and comments on the protocol and/or a draft of this report: Professor Penella Woll, Consultant Medical Oncologist, Clinical Oncology, University of Sheffield; Dr Jason Lester, Consultant Oncologist, Velindre Hospital, Cardiff, Dr Susan Griffin, Research Fellow, Centre for Health Economics, University of York; and Professor John Field, Director of Research, Roy Castle Lung Cancer Research Programme, University of Liverpool Cancer Research Centre. We are also grateful to Jonathan Shepherd, Principal Research Fellow, SHTAC, for reviewing a draft of this report.
Contribution of authors
E Loveman (Senior Research Fellow) developed the research protocol, drafted the background section, assisted in the development of the search strategy, assessed studies for inclusion, extracted data from and quality assessed included studies, synthesised evidence, drafted and edited the final report, and project managed the study.
J Jones (Principal Research Fellow) developed the research protocol, assessed studies for inclusion, extracted data from and quality assessed included studies, synthesised evidence, developed the economic evaluation and drafted the report.
D Hartwell (Research Fellow) developed the research protocol, drafted the background section, assessed studies for inclusion, extracted data from and quality assessed included studies, synthesised evidence and drafted the report.
A Bird (Research Fellow) assessed studies for inclusion, extracted data from and quality assessed included studies, synthesised evidence, developed the economic evaluation and drafted the report.
P Harris (Research Fellow) drafted the background section, assessed studies for inclusion, extracted data from and quality assessed included studies, synthesised evidence and drafted the report.
K Welch (Information Scientist) developed the search strategy, undertook literature searches and edited the final report.
A Clegg (Professor/Director of SHTAC) developed the research protocol, assessed studies for inclusion, extracted data from and quality assessed included studies, synthesised evidence, drafted the report.
Disclaimers
The views expressed in this publication are those of the authors and not necessarily those of the HTA programme or the Department of Health.
References
- Kabir Z, Connolly GN, Clancy L. Sex-differences in lung cancer cell-types? An epidemiologic study in Ireland. Ulster Med J 2008;77:31-5.
- Collins LG, Haines C, Perkel R, Enck RE. Lung cancer: diagnosis and management. Am Fam Physician 2007;75:56-63.
- NICE . The Diagnosis and Treatment of Lung Cancer 2005. www.nice.org.uk/CG024NICEguideline (accessed 3 November 2008).
- Morris DE, Socinski MA, Detterbeck FC, Detterbeck FC, Rivera MP, Socinski MA, et al. Diagnosis and treatment of lung cancer: an evidence-based guide for the practicing clinician. Philadelphia: WB Saunders; 2001.
- Adjei AA, Marks RS, Bonner JA. Current guidelines for the management of small cell lung cancer. Mayo Clin Proc 1999;74:809-16.
- Cheng S, Evans WK, Stys-Norman D, Shepherd FA. Lung Cancer Disease Site Group of Cancer Care Ontario’s Program in Evidence-based Care . Chemotherapy for relapsed small cell lung cancer: a systematic review and practice guideline. J Thorac Oncol 2007;2:348-54.
- Agra Y, Pelayo M, Sacristan M, Sacristán A, Serra C, Bonfill X. Chemotherapy versus best supportive care for extensive small cell lung cancer. Cochrane Database Syst Rev 2003;4.
- Alberg AJ, Samet JM. Epidemiology of lung cancer. Chest 2003;123:S21-49.
- Twigg L, Moon G, Walker S. The smoking epidemic in England. London: Health Development Agency; 2004.
- Rivera MP, Detterbeck FC, Loomis DP, Detterbeck FC, Rivera MP, Socinski MA, et al. Diagnosis and treatment of lung cancer: an evidence-based guide for the practicing clinician. Philadelphia: WB Saunders; 2001.
- Alberg AM, Ford JG, Samet JM. Epidemiology of lung cancer. ACCP evidence-based clinical practice guidelines. Chest 2007;132:S29-55.
- Black C, Bagust A, Boland A, Walker S, McLeod C, De Verteuil R, et al. The clinical effectiveness and cost-effectiveness of computed tomography screening for lung cancer: systematic reviews. Health Technol Assess 2006;10.
- Freedman ND, Leitzmann MF, Hollenbeck AR, Schatzkin A, Abnet CC. Cigarette smoking and subsequent risk of lung cancer in men and women: analysis of a prospective cohort study. Lancet Oncol 2008;9:649-56.
- Bain C, Feskanich D, Speizer FE, Thun M, Hertzmark E, Rosner BA, et al. Lung cancer rates in men and women with comparable histories of smoking. J Natl Cancer Inst 2004;96:826-34.
- Boffetta P, Trichopoulos D, Adami HO, Hunter D, Trichopoulos D. Textbook of cancer epidemiology. Oxford: Oxford University Press; 2002.
- Fabricius P, Lange P. Diet and lung cancer. Monaldi Arch Chest Dis 2003;59:207-11.
- Scottish Intercollegiate Guidelines Network (SIGN) . Management of Patients With Lung Cancer. A National Clinical Guideline 2005.
- Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, et al. Toxicity and response criteria of The Eastern Cooperative Oncology Group. Am J Clin Oncol 1982;5:649-55.
- Karnofsky DA, Abelmann WH, Craver LF, . The use of the nitrogen mustards in the palliative treatment of carcinoma. Cancer 1948;1:634-56.
- Office for National Statistics . Cancer Statistics Registrations: Registrations of Cancer Diagnosed in 2005, England 2008.
- Ferlay J, Autier P, Boniol M, Heanue M, Colombet M, Boyle P. Estimates of the cancer incidence and mortality in Europe in 2006. Ann Oncol 2007;18:581-92.
- Rachet B, Quinn MJ, Cooper N, Coleman MP. Survival from cancer of the lung in England and Wales up to 2001. Br J Cancer 2008;99:S40-2.
- Cancer Research UK . UK Lung Cancer Mortality Statistics 2008.
- Simon GR, Wagner H. Small cell lung cancer. Chest 2003;123:S259-71S.
- Rosti G, Bevilacqua G, Bidoli P, Portalone L, Santo A, Genestreti G. Small cell lung cancer. Ann Oncol 2006;17:ii5-10.
- The Information Centre for Health and Social Care . National Lung Cancer Audit. Key Findings about the Quality of Care for People With Lung Cancer in England and Wales: Report for the Audit Period 2006 2007. www.ic.nhs.uk/our-services/improving-patientcare/more-about-the-audits/audit-reports/lung (accessed 3 November 2008).
- Welsh Cancer Intelligence & Surveillance Unit . Cancer Incidence in Wales 2002–2006 2008. www.wales.nhs.uk/sites3/Documents/242/incpub2006%5F31Jan08.pdf (accessed 6 October 2008).
- Cancer Research UK. UK lung cancer incidence statistics. London: Cancer Research UK; 2008.
- Office for National Statistics . Cancer Survival: England and Wales, 1991–2001 2003.
- Cancer Research UK . UK Lung Cancer Survival Statistics 2008.
- Hyde L, Yee J, Wilson R, Patno ME. Cell type and the natural history of lung cancer. JAMA 1965;193:52-4.
- Simon GR, Turrisi A. Management of small cell lung cancer. ACCP evidence-based clinical practice guidelines. Chest 2007;132:S32-9.
- Lally BE, Urbanic JJ, Blackstock AW, Miller AA, Perry MC. Small cell lung cancer: have we made any progress over the last 25 years?. Oncologist 2007;12:1096-104.
- Johnson BE, Grayson J, Makuch RW, Linnoila RI, Anderson MJ, Cohen MH, et al. Ten-year survival of patients with small-cell lung cancer treated with combination chemotherapy with or without irradiation. J Clin Oncol 1990;8:396-401.
- Rawson NS, Peto J. An overview of prognostic factors in small cell lung cancer. A report from the Subcommittee for the Management of Lung Cancer of the United Kingdom Coordinating Committee on Cancer Research. Br J Cancer 1990;61:597-604.
- Lassen U, Osterlind K, Hansen M, Dombernowsky P, Bergman B, Hansen HH. Long-term survival in small-cell lung cancer: post-treatment characteristics in patients surviving 5 to 18+ years: an analysis of 1,714 consecutive patients. J Clin Oncol 1995;13:1215-20.
- Albain KS, Crowley JJ, Livingston RB. Long-term survival and toxicity in small cell lung cancer. Expanded Southwest Oncology Group experience. Chest 1991;99:1425-32.
- Paesmans M, Sculier JP, Lecomte J, Thiriaux J, Libert P, Sergysels R, et al. Prognostic factors for patients with small cell lung carcinoma: analysis of a series of 763 patients included in 4 consecutive prospective trials with a minimum follow-up of 5 years. Cancer 2000;89:523-33.
- Bremnes RM, Sundstrom S, Aasebo U, Kassa S, Hatlevolh R, Aamdal S. The value of prognostic factors in small cell lung cancer: results from a randomised multicenter study with minimum 5-year follow-up. Lung Cancer 2003;39:303-13.
- Gandhi L, Johnson BE. Paraneoplastic syndromes associated with small cell lung cancer. J Natl Compr Canc Netw 2008;4:631-8.
- Warde P, Payne D. Does thoracic irradiation improve survival and local control in limited-stage small-cell carcinoma of the lung? A meta-analysis. J Clin Oncol 1992;10:890-5.
- Gomersall LN. Imaging in lung cancer. Imaging n.d.;16:2004-9.
- Slotman B, Faivre-Finn C, Kramer G, Rankin E, Snee M, Hattoon M, et al. Prophylactic cranial irradiation in extensive small-cell lung cancer. N Engl J Med 2007;357:664-72.
- Thatcher N, Eckardt J, Green M. Options for first- and second-line therapy in small cell lung cancer: a workshop discussion. Lung Cancer 2003;41:S37-41.
- Cara S, Tannock IF. Retreatment of patients with the same chemotherapy: implications for clinical mechanisms of drug resistance. Ann Oncol 2001;12:23-7.
- von Pawel J. The role of topotecan in treating small cell lung cancer: second-line treatment. Lung Cancer 2003;41:S3-8.
- Scottish Medicines Consortium (SMC) . Topotecan (Hycamtin) for the Treatment of Patients With Relapsed Small Cell Lung Cancer n.d. www.scottishmedicines.org.uk/smc/files/topotecan%20(Hycamtin)%20FINAL%20November%202007%20for%20website.pdf (accessed 7 May 2007).
- All Wales Medicines Strategy Group (AWMSG) . Topotecan (Hycamtin®) for Small Cell Lung Carcinoma 2008. www.pcpoh.bham.ac.uk (accessed 7 October 2008).
- Oliver E, Killen J, Kiebert G, Hutton J, Hall R, Higgins B, et al. Treatment pathways, resource use and costs in the management of small cell lung cancer. Thorax 2001;56:785-90.
- British National Formulary. London: British Medical Association and Royal Pharmaceutical Society of Great Britain; 2007.
- GlaxoSmithKline UK . Multiple Technology Appraisal of Topotecan for the Treatment of Small Cell Lung Cancer 2008.
- National Horizon Scanning Centre . Oral Topotecan (Hycamtin) for Small Cell Lung Cancer 2007. www.pcpoh.bham.ac.uk (accessed 7 October 2008).
- Centre for Reviews and Dissemination . Undertaking Systematic Reviews of Research on Effectiveness: CRD’s Guidance for Those Carrying Out or Commissioning Reviews 2001.
- Miller AB, Hoogstraten B, Staquet M, Winkler A. Reporting results of cancer treatment. Cancer 1980;47:207-14.
- Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, et al. New guidelines to evaluate the response to treatment in solid tumors. J Natl Cancer Inst 2000;92:205-16.
- Eckardt JR, von Pawel J, Pujol JL, Papai Z, Quoix E, Ardizzoni A, et al. Phase III study of oral compared with intravenous topotecan as second-line therapy in small-cell lung cancer. J Clin Oncol 2007;25:2086-92.
- O’Brien ME, Ciuleanu TE, Tsekov H, Shparyk Y, Cucevia B, Juhasz G, et al. Phase III trial comparing supportive care alone with supportive care with oral topotecan in patients with relapsed small-cell lung cancer. J Clin Oncol 2006;24:5441-7.
- von Pawel J, Gatzemeier U, Pujol JL, Moreau L, Bildat S, Ranson M, et al. Phase II comparator study of oral versus intravenous topotecan in patients with chemosensitive small-cell lung cancer. J Clin Oncol 2001;19:1743-9.
- von Pawel J, Schiller JH, Shepherd FA, Fields SZ, Kleisbauer JP, Chrysson NG, et al. Topotecan versus cyclophosphamide, doxorubicin, and vincristine for the treatment of recurrent small-cell lung cancer. J Clin Oncol 1999;17:658-67.
- Eckardt T, von Pawel J, Hainsworth JD, Corso S, Rinaldi D, Preston A, et al. Single agent oral topotecan (PO) versus intravenous topotecan (IV) in patients (pts) with chemosensitive small cell lung cancer (SCLC). An international phase III study [abstract]. Proc Am Soc Clin Oncol 2003;22.
- Schiller J, von Pawel J, Shepherd F, Gralla R, Kleisbauer JP, Clark P, et al. Topotecan (t) versus (vs) cyclophosphamide (c), doxorubicin (a) and vincristine (v) for the treatment (tx) of patients (pts) with recurrent small cell lung cancer (sclc): a phase III study [abstract]. Proc Annu Meet Am Soc Clin Oncol 1998;17.
- Sugawara S, Inoue A, Yamazaki K, Saijo Y, Gomi K, Ishimoto, et al. and North Japan Lung Cancer Study Group . Randomized, phase II trial comparing amrubicin with topotecan in patients (pts) with previously treated small cell lung cancer (SCLC). J Clin Oncol 2008;26.
- Inoue A, Sugawara S, Yamazaki K, Maemondo M, Suzuki T, Gomi K, et al. Randomized Phase II Trial Comparing Amrubicin With Topotecan in Patients With Previously Treated Small-Cell Lung Cancer: North Japan Lung Cancer Study Group Trial 0402. J Clin Oncol 2008;26:5401-6.
- Chen L, Antras L, Duh M, Pickard S, Cella D, Neary M, et al. Is treatment with oral topotecan plus best supportive care associated with better health status compared to best supportive care alone in small cell lung cancer? [abstract]. J Thoracic Oncol 2007;2:S391-2.
- O’Brien ME, Duh MS, Chen L, Antras L, Neary M, Gralla RJ. An analysis of disease control: is major response associated with greater symptomatic benefits than stable disease in small cell lung cancer (SCLC)? Results from the randomized Oral Topotecan (OT) vs. Best Supportive Care (BSC) trial (abstract). J Thoracic Oncol 2007;2.
- Drummond MF, Sculpher MJ, O’Brien BJ, Stoddart GL, Torrance GW. Methods for the economic evaluation of health care programmes. Oxford: Oxford University Press; 2005.
- National Institute for Health and Clinical Excellence . Guide to the Methods of Technology Appraisal n.d. www.nice.org.uk/media/B52/A7/TAMethodsGuideUpdatedJune2008.pdf (accessed 26 January 2009).
- Philips Z, Ginnelly L, Sculpher M, Claxton K, Golder S, Riemsma R, et al. Review of guidelines for good practice in decision-analytic modelling in health technology assessment. Health Technol Assess 2004;8.
- Main C, Bojke L, Griffin S, Norman G, Barbieri M, Mather L, et al. Topotecan, pegylated liposomal doxorubicin hydrochloride and paclitaxel for second-line or subsequent treatment of advanced ovarian cancer: a systematic review and economic evaluation. Health Technol Assess 2006;10.
- Curtis L. Unit costs of health and social care. Canterbury: Personal Social Services Research Unit, University of Kent; 2007.
- Glick HA, Doshi JD, Sonnad SS, Polsky D. Economic evaluation in clinical trials. Oxford: Oxford University Press; 2007.
- Beck JR, Pauker SG, Gottlieb JE, Klein K, Kassirer JP. A convenient approximation of life expectancy (The “DEALE”) II. Use in medical decision making. Am J Med 1982;73:889-97.
- Glenny AM, Altman DG, Song F, Sakarovitch C, Deeks JJ, D’Amico R, et al. Indirect comparisons of competing interventions. Health Technol Assess 2005;9.
- Hycamtin: Summary of Product Characteristics n.d. www.emea.europa.eu/humandocs/PDFs/EPAR/Hycamtin/H-123-PI-en.pdf (accessed 2 February 2009).
- British National Formulary. London: British Medical Association and Royal Pharmaceutical Society of Great Britain; 2009.
- Department of Health . NHS Reference Costs 2006 07 n.d. www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_082571 (accessed 2 February 2009).
- Casemix Service . Guide to Unbundling 2007. www.ic.nhs.uk/webfiles/Services/casemix/Prep%20HRG4/Guide%20to%20Unbundling2.pdf (accessed 2 February 2009).
- Curtis L. Unit costs of health and social care. Canterbury: Personal Social Services Research Unit, University of Kent; 2008.
- British National Formulary. London: British Medical Association and Royal Pharmaceutical Society of Great Britain; 2008.
- Dolan P, Gudex C, Kind P, Williams A. A social tariff for EuroQol: results from a UK general population survey. Centre for Health Economics Discussion Paper no. 138. York: Centre for Health Economics, University of York; 1995.
- NHS Centre for Reviews and Dissemination . NHS Economic Evaluation Database Handbook n.d. www.york.ac.uk/inst/crd/pdf/nhseed-handb07.pdf (accessed 20 August 2008).
- Briggs A, Claxton K, Sculpher M. Decision modelling for health economic evaluation. Oxford: Oxford University Press; 2006.
Addendum
Subsequent to the NICE appraisal committee meeting, SHTAC were requested to provide additional information to their original assessment of topotecan for SCLC. This addendum therefore sets out to answer the following questions:
-
Please could you provide further details of why the comparison of oral topotecan with CAV was not undertaken, highlighting more clearly the various areas of uncertainty?
-
Please could you provide a detailed cost comparison for oral topotecan compared with CAV per cycle and total?
-
Please could you provide a threshold analysis that shows what magnitude of QALY gain would need to be achieved with oral topotecan to make it a cost-effective alternative to CAV?
The rationale for not conducting a formal comparison of oral topotecan with CAV, highlighting the various areas of uncertainty
The rationale for not conducting a formal comparison of oral topotecan with CAV derived from three broad considerations:
-
the lack of any direct comparison of oral topotecan and CAV
-
uncertainties over the comparability of patient populations in included trials (undermining the robustness of formal indirect comparisons)
-
limitations in the available data to support robust economic modelling.
While these considerations are clearly linked – the absence of direct evidence comparing oral topotecan and CAV lead directly to our consideration of the feasibility of conducting a robust indirect comparison using data from the RCTs comparing oral and i.v. topotecan – they are considered here in turn. The inadequacy of the evidence base in relation to each of these points led to our decision not to conduct a formal comparison (for clinical or cost-effectiveness) of oral topotecan with CAV.
Lack of any direct comparison of oral topotecan and CAV
While one RCT of i.v. topotecan versus CAV1 was identified and included in the systematic review, no comparisons of oral topotecan versus CAV were identified. Two trials were identified comparing i.v. topotecan with oral topotecan,2,3 and one comparing oral topotecan plus BSC to BSC alone. 4
Uncertainties over the comparability of patient populations in included trials (undermining the robustness of formal indirect comparisons)
In the absence of direct evidence, comparing oral topotecan and CAV, we considered undertaking an indirect comparison. CAV could be compared with oral topotecan using the RCT of i.v. topotecan versus CAV1 and the two RCTs of i.v. topotecan versus oral topotecan. 2,3 By including the RCT by O’Brien and colleagues4 the set of comparators could be extended to include BSC, thereby covering all standard comparators listed in the scope. This is illustrated in Figure 10.
FIGURE 10.
Potential evidence network for comparing cyclophosphamide, adriamycin (doxorubicin) and vincristine, oral topotecan and best supportive care.

To determine the comparability of the patient populations in these four RCTs we contacted the lead authors to confirm that participants met our inclusion criteria [since, as stated on p. 24 of the assessment report, only one (O’Brien and colleagues4) appeared to fully meet the criteria on inspection of the published article]. We received confirmation that three of the included trials1,2,4 met the criterion that participants were inappropriate for re-treatment with their original first-line chemotherapy, as per the licensed indication for topotecan. No reply was received from the author of the remaining study3 – this is the phase III study comparing oral and i.v. topotecan, with 155 and 154 participants receiving oral and i.v. topotecan, respectively, and represents the best evidence in the hierarchy of clinical trials for this comparison.
In the included trial participants who were ineligible for CAV were excluded from the RCT comparing i.v. topotecan and CAV. 1 It was not clear to the assessment group whether this study represented the patient group who would be appropriate for topotecan in clinical practice, since patients most appropriate for treatment with topotecan may be those for whom CAV therapy is contraindicated.
Inclusion of patients in RCT comparing oral topotecan and CAV1 specified relapse 60 days after completion of first-line therapy. In the O’Brien and colleagues study4 the relapse time was required to be at least 45 days, and in the two trials comparing i.v. topotecan with oral topotecan2,3 the relapse time was specified as 90 days after completion of first-line therapy.
Performance status of the participants across these included trials also varied, for example the proportions with a performance status of 2 were between 27% and 33% in the O’Brien and colleagues study,4 19–23% in the i.v. topotecan versus CAV study,1 and 12–13% in one of the i.v. versus oral topotecan studies3 and 15–30% in the other. 2
Owing to the heterogeneous nature of these trials, at best, this would have been illustrative only.
Limitations in the available data to support robust economic modelling
We constructed an economic model that would be able to include all relevant comparators, where suitable data on disease progression, survival and QoL were available. Key data for the economic model are missing from published articles and from the clinical trial reports included in the submission to NICE. In some cases these data were not collected in the relevant trials and in others they are not reported in sufficient detail. Examples of such missing data would be survival curves for TTP (not reported), and utility data for CAV/IV topotecan (not collected). In our model (as with most economic models of cancer treatment) disease progression is a key event with respect both to costs and QoL. However, only summary data (median TTP) were reported for TTP. Inadequate estimates of the form of the survival curve derived from summary measures such as the median TTP would undermine the robustness of the economic analysis. As stated in the assessment report, no quality-of-life data were collected in the RCT comparing CAV and i.v. topotecan, although some data on symptoms were recorded (using an unvalidated symptom-specific SCLC questionnaire). No QoL or utility data for CAV treatment in this patient population were found in our searches substantially undermining our ability to derive reliable QALY estimates for CAV.
We concluded that, although an adjusted indirect comparison of oral topotecan and CAV was technically feasible, uncertainties over the comparability of patient populations (in particular the exclusion of CAV ineligible patients from the RCT comparing oral topotecan and CAV1) meant that such a comparison would be unreliable. In addition, the absence of key data required to model both costs and outcomes for CAV in our economic model meant that a robust economic evaluation of oral topotecan and CAV could not be conducted.
To summarise, these three considerations were discussed in detail within the assessment group. At this stage no consideration of the possible cost difference between oral topotecan and CAV had been given. The assessment group discussed this with the NICE technical team at a project meeting, and it was agreed that the most appropriate population would be those not eligible for CAV and these (at least in part) will be the population in the O’Brien RCT4 comparing oral topotecan plus BSC with BSC alone (which both SHTAC and the manufacturer modelled).
However, our qualitative assessment of the lack of evidence of significant survival benefits for topotecan (i.v.) over CAV from the von Pawel RCT1 and the lack of evidence of significant survival benefits for oral topotecan over i.v. topotecan, taken together with our assessment of a large cost difference between CAV and oral topotecan, led us to suggest that oral topotecan was unlikely to be a cost-effective option when compared with CAV.
Detailed cost comparison for oral topotecan compared with CAV per cycle and total (drug, administration, pharmacy and monitoring costs, etc.)
Table 49 reports the estimated cost per cycle for CAV, i.v. topotecan and oral topotecan. Oral and i.v. topotecan costs are estimated as in the assessment report (see Appendix 1 for drug costs, chemotherapy administration and patient monitoring costs for oral and i.v. topotecan). CAV has been costed at the dosage used in the RCT by von Pawel and colleagues1 (cyclophosphamide 1000 mg/m2, doxorubicin 45 mg/m2 and vincristine 2 mg), assuming a mean BSA of 1.8 m2 (as for topotecan). It was assumed that patients attend respiratory medicine outpatients (for medical assessment) once per cycle in addition to their chemotherapy administration. NHS Reference Costs5 make a distinction between the cost for a first attendance and follow-up attendances at outpatients. In this case a first attendance is estimated at £182.65 and a follow-up attendance at £111.77 – hence the cost per cycle is higher for the first cycle of CAV. Full details of the resource use and unit cost assumptions underlying these cost estimates for CAV are presented in Appendix 2.
| Costs (£) | |||||
|---|---|---|---|---|---|
| Drugs | Administration | Monitoring | Total | ||
| CAV | First cycle | 208.43 | 443.58 | 88.28 | 740.29 |
| Subsequent cycles | 208.43 | 372.70 | 88.28 | 669.41 | |
| Intravenous topotecan | All cycles | 1494.75 | 984.04 | 88.28 | 2567.06 |
| Oral topotecan | All cycles | 637.50 | 185.87 | 88.28 | 911.64 |
Under these assumptions oral topotecan is estimated to cost between £171 and £242 more per cycle than CAV. This takes no account of possible differences in incidence of adverse events between topotecan and CAV. Table 50 presents estimates of the incidence of haematological adverse events for patients treated with CAV or oral topotecan, along with the estimated costs of managing those adverse events (see Appendix 3 for full details of derivation of adverse events for CAV and oral topotecan, and see Table 30 in the assessment report for details of costs of managing adverse events).
| Toxicity | Grade | Adverse events (%) | Cost per adverse event | Cost of adverse events (£) | ||
|---|---|---|---|---|---|---|
| CAV | Oral topotecan | CAV | Oral topotecan | |||
| Neutropenia | Grade 3 | 15.2 | 18.7 | 104 | 16 | 19 |
| Grade 4 | 71.7 | 48.1 | 1196 | 858 | 575 | |
| Thrombocytopenia | Grade 3 | 9.9 | 24.6 | 0 | 0 | 0 |
| Grade 4 | 5.0 | 41.3 | 1210 | 60 | 500 | |
| Anaemia | Grade 3 | 17.8 | 28.8 | 494 | 88 | 142 |
| Grade 4 | 2.0 | 4.8 | 940 | 19 | 45 | |
| TOTAL | 1040 | 1282 | ||||
This suggests that the costs of managing haematological adverse events may be higher for oral topotecan than for CAV, although there are large differences in the estimated incidences and costs for individual toxicities. Oral topotecan appears to be associated with a lower proportion of grade 4 neutropenia than is the case for CAV, while the situation is reversed for grade 4 thrombocytopenia. These estimates are subject to a large degree of uncertainty, in being derived via an adjusted indirect comparison and due to the questionable comparability of patient populations in the studies included in the indirect comparison.
NHS Reference Costs for 2007/08 have been published since the assessment report was completed (www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_098945). Updated cost estimates for CAV and oral topotecan, using the 2007/08 NHS Reference Costs,6 rather than 2006/07 costs uprated to 2007/08 (as used in the assessment report), are presented in Table 51. These indicate no substantial differences between estimates based on assessment report and those using updated costs.
| Drugs | Administration | Monitoring | Total | ||
|---|---|---|---|---|---|
| CAV | First cycle | 208.43 | 470.41 | 89.44 | 768.28 |
| Subsequent cycles | 208.43 | 402.23 | 89.44 | 700.10 | |
| Oral topotecan | All cycles | 637.50 | 167.53 | 89.44 | 894.47 |
Compared with the costs shown in Table 49 [estimated using 2006/07 NHS Reference Costs (uprated to 2007/08 costs)], cost per cycle for CAV is approximately £30 higher (predominantly due to a higher reference cost for administration of i.v. chemotherapy), while the cost per cycle for oral topotecan is approximately £17 lower (predominantly due to a lower reference cost for administration of oral chemotherapy).
Threshold analysis – what magnitude of QALY gain would be needed with oral topotecan to make it a cost-effective alternative to CAV
Section 2 of this addendum indicates that oral topotecan is likely to be between £171 and £242 more expensive than CAV, per cycle. In the absence of robust data that directly compares oral topotecan with CAV, we have used indirect comparison methods to estimate the relative costs of managing adverse events with oral topotecan and with CAV, which indicate that these may be around £240 higher with oral topotecan than with CAV. This section presents a threshold analysis exploring the magnitude of QALY gain that would be required to make oral topotecan a cost-effective alternative to CAV. The cost-effectiveness thresholds adopted here (£20,000 and £30,000) are those indicated in the current NICE methods guidance. 7
Table 52 reports the estimated costs of chemotherapy for relapsed SCLC based on the costs reported in section 2 of this addendum. The total chemotherapy cost for oral topotecan is based on four treatment cycles, as in the assessment report. Chemotherapy costs for CAV are calculated for three cycles (the median number of cycles in the RCT by von Pawel and colleagues1) and for four cycles (assuming the same treatment duration as for oral topotecan).
| Chemotherapy regimen | Total chemotherapy cost (£) | Cost difference (£) | |
|---|---|---|---|
| Chemotherapy only | Including adverse event costs | ||
| CAV for three cycles | 2079 | 1567 | 1809 |
| CAV for four cycles | 2749 | 898 | 1140 |
| Oral topotecan | 3647 | ||
In the scenario where three cycles of CAV are provided, chemotherapy costs for CAV are 57% those of oral topotecan (with a cost difference of approximately £1600, which rises to £1800 if the costs of managing adverse events are included). If four cycles of CAV are provided, costs are 75% those of oral topotecan (with a cost difference of approximately £900, rising to £1100 if the costs of managing adverse events are included).
Given that the ICER is defined as the change in costs divided by change in outcomes, we can estimate the minimum QALY gain required to meet a cost-effectiveness threshold given a change in costs. For example, in the scenario where three cycles of CAV are provided, the change in costs is £1567, therefore the minimum QALY gain required to meet a cost-effectiveness threshold of £30,000 per QALY gained is 0.05. Table 53 reports the results of this calculation for treatment scenarios where patients receive three or four cycles of CAV, and the impact of including adverse event costs, using cost-effectiveness thresholds of £20,000 and £30,000 per QALY gained.
| Chemotherapy regimen | Chemotherapy costs only (£) | Including adverse event costs (£) | ||
|---|---|---|---|---|
| 20,000 | 30,000 | 20,000 | 30,000 | |
| CAV for three cycles | 0.08 | 0.05 | 0.09 | 0.06 |
| CAV for four cycles | 0.04 | 0.03 | 0.06 | 0.04 |
| Oral topotecan | ||||
The RCT comparing CAV with i.v. topotecan reported no statistically significant differences in survival – median survival was 25.0 weeks (95% CI 20.6 to 29.6) and 24.7 weeks (95% CI 21.7 to 30.3) for patients treated with topotecan and CAV, respectively (RR = 1.039, p = 0.795). Similarly, non-significant survival differences were reported for the RCTs comparing oral and i.v. topotecan [HR of 0.98, 95% CI 0.77 to 1.253 and RR (oral–i.v.) 0.84, 95% CI 0.53 to 1.322]. In the absence of evidence of a survival benefit for topotecan over CAV, it may be argued that the QALY gains indicated in Table 53 would need to arise through quality-of-life improvements associated with treatment with topotecan. These may arise from a preference for oral over i.v. chemotherapy [which will be realised only while patients in both cohorts (oral topotecan and CAV treated) are under treatment] or may arise from differences in symptom relief between the topotecan- and CAV-treated cohorts.
We developed a number of scenarios, based on possible durations of utility gain with oral topotecan, to estimate the utility difference required to achieve the minimum QALY gains reported in Table 53. For example, if patients experience a utility gain by receiving oral, rather than i.v. chemotherapy, we assumed that patients would accrue that utility gain for the expected duration of treatment with i.v. chemotherapy (in the scenario where three cycles of CAV are provided this is 9 weeks, and, when four cycles of CAV are provided, this is 12 weeks). If the minimum QALY gain required to be cost-effective is 0.078 QALYs (at a threshold of £20,000 per QALY gained) and the duration of utility gain is 9 weeks (0.173 years) then we estimate the utility difference would need to be 0.45 (0.078/0.173). Table 54 reports estimated utility differences required to achieve the minimum QALY gains reported in Table 53, by a range of possible durations of utility gain, assuming that three cycles of CAV and four cycles of oral topotecan are provided (Table 55 reports the results of similar calculations assuming four cycles of CAV and four cycles of oral topotecan are provided).
| Duration of utility gain with oral topotecan | Utility difference required to achieve the minimum QALY gain at the given cost-effectiveness thresholds | |||
|---|---|---|---|---|
| Chemotherapy costs only (£) | Including adverse event costs (£) | |||
| 20,000 | 30,000 | 20,000 | 30,000 | |
| Utility gain from receiving oral rather than i.v. chemotherapy | ||||
| 9 weeks (three cycles of CAV) | 0.45 | 0.30 | 0.52 | 0.35 |
| Utility gain from symptom improvements or increased time to worsening of symptoms | ||||
| 20 weeks (mean TTP based on the von Pawel RCT) | 0.20 | 0.14 | 0.23 | 0.16 |
| 28 weeks (mean TTP based on the O’Brien RCT) | 0.15 | 0.10 | 0.17 | 0.11 |
| 9.4 weeks (difference in mean time to worsening of dyspnoea, estimated from data in CSR) | 0.43 | 0.29 | 0.50 | 0.33 |
| Duration of utility gain with oral topotecan | Utility difference required to achieve the minimum QALY gain at the given cost-effectiveness thresholds | |||
|---|---|---|---|---|
| Chemotherapy costs only (£) | Including adverse event costs (£) | |||
| 20,000 | 30,000 | 20,000 | 30,000 | |
| Utility gain from receiving oral rather than i.v. chemotherapy | ||||
| 12 weeks (four cycles of CAV) | 0.20 | 0.13 | 0.24 | 0.16 |
| Utility gain from symptom improvements or increased time to worsening of symptoms | ||||
| 20 weeks (mean TTP based on the von Pawel RCT) | 0.12 | 0.08 | 0.15 | 0.10 |
| 28 weeks (mean TTP based on the O’Brien RCT) | 0.08 | 0.06 | 0.10 | 0.07 |
| 9.4 weeks (difference in mean time to worsening of dyspnoea, estimated from data in CSR) | 0.25 | 0.17 | 0.31 | 0.21 |
The four scenarios considered in Table 54 are that patients receiving oral topotecan rather than CAV experience utility gains by:
-
receiving oral rather than i.v. chemotherapy (duration three cycles)
-
symptom improvements (for example, improvements over baseline assessment for dyspnoea as noted in the RCT by von Pawel and colleagues1); however, as noted in the assessment report, the symptom-specific questionnaire used in this study was not a validated instrument and it is unclear how reliable the results are, and as the duration of symptom improvement was not reported in the RCT by von Pawel and colleagues,1 a range of possible durations for the symptom improvement were considered:
-
– symptom improvement assumed to be maintained until disease progression;
-
– duration based on time to symptom worsening as reported in the clinical study report, submitted to NICE as part of the MS.
-
Table 54 suggests that large utility differences (0.30 to 0.52 depending on the cost-effectiveness threshold and whether adverse event costs are included) would need to be associated with receiving oral, rather than i.v. chemotherapy, in order to achieve the minimum QALY gains required for oral topotecan to be cost-effective relative to CAV. With respect to symptom improvement, lower differences (0.10 to 0.23) would be required – if the symptom improvement is assumed to be maintained until disease progression. However, if the duration of symptom improvement is based on the estimated difference in time to symptom worsening for dyspnoea, then the required utility differences are much greater (0.29 to 0.50).
The scenarios considered in Table 55 are identical to those in Table 54, except that the duration of utility gain associated with receiving oral rather than i.v. chemotherapy is increased to four cycles (since the estimates in Table 55 are based on all patients receiving four cycles of chemotherapy).
The pattern of results in Table 55 is similar to that in Table 54. Comparatively large utility differences (0.13–0.20) would need to be associated with receiving oral, rather than i.v. chemotherapy, in order to achieve the minimum QALY gains for oral topotecan to be cost-effective relative to CAV. Lower differences (0.06–0.15) would be required – if symptom improvement is assumed to be maintained until disease progression. However, if the duration of symptom improvement is based on the estimated difference in time to symptom worsening for dyspnoea then the required utility differences are much greater (0.17–0.31).
Summary
Oral topotecan is likely to be between 23% and 36% more expensive than CAV, per cycle, and may be associated with higher costs of managing adverse events. Total costs of chemotherapy for relapsed SCLC are likely to be between £900 and £1800 higher for oral topotecan than CAV (depending on the number of cycles of CAV provided and whether costs of managing adverse events are included). In a threshold analysis, QALY gains of between 0.03 and 0.09 (depending on the number of cycles of CAV provided and whether costs of managing adverse events are included) were required for oral topotecan to be cost-effective relative to CAV. It is unlikely that utility differences associated with receiving oral rather than i.v. chemotherapy, symptom improvements or increased time to worsening of symptoms, such as dyspnoea, would be high enough to realise these QALY gains.
References
- von Pawel J, Schiller JH, Shepherd FA, Fields SZ, Kleisbauer JP, Chrysson NG, et al. Topotecan versus cyclophosphamide, doxorubicin, and vincristine for the treatment of recurrent small-cell lung cancer. J Clin Oncol 1999;17:658-67.
- von Pawel J, Gatzemeier U, Pujol JL, Moreau L, Bildat S, Ranson M, et al. Phase II comparator study of oral versus intravenous topotecan in patients with chemosensitive small-cell lung cancer. J Clin Oncol 2001;19:1743-9.
- Eckardt JR, von Pawel J, Pujol JL, Papai Z, Quoix E, Ardizzoni A, et al. Phase III study of oral compared with intravenous topotecan as second-line therapy in small-cell lung cancer. J Clin Oncol 2007;25:2086-92.
- O’Brien ME, Ciuleanu TE, Tsekov H, Shparyk Y, Cucevia B, Juhasz G, et al. Phase III trial comparing supportive care alone with supportive care with oral topotecan in patients with relapsed small-cell lung cancer. J Clin Oncol 2006;24:5441-7.
- Department of Health . NHS Reference Costs 2006 07 n.d. URL: www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_082571 (accessed 2 February 2009).
- Department of Health . NHS Reference Costs 2007 08 n.d. URL: www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_098945 (accessed 29 July 2009).
- National Institute for Health and Clinical Excellence . Guide to the Methods of Technology Appraisal n.d. URL: www.nice.org.uk/media/B52/A7/TAMethodsGuideUpdatedJune2008.pdf (accessed 26 January 2009).
- British National Formulary. London: British Medical Association and Royal Pharmaceutical Society of Great Britain; 2009.
Appendix I – details of cost calculations for topotecan (oral and i.v.)
| Drug | Dosage: | Cost (£) | |||
|---|---|---|---|---|---|
| mg/m2 | mg/day of treatment | Unit cost per mg | Drug cost per day of treatment | Cost per cycle (5 treatment days) | |
| Oral topotecan | 2.3 | 4.14 | 30.00 | 127.50 | 637.50 |
| Resource item | Resource use per cycle | Reference cost 2006/07 (£) | Uprated to 2007/08 (£) | Reference cost 2007/08 (£) |
|---|---|---|---|---|
| Chemotherapy administrationa | 1 | 178.99 | 184.97 | 166.63 |
| Pharmacy preparation cost | 1 | 0.90 | 0.90 | |
| Total cost per cycle | 185.87 | 167.53 | ||
| Drug | Dosage: | Cost (£) | ||||
|---|---|---|---|---|---|---|
| mg/m2 | mg/day of treatment | Saline (ml) | Unit cost per mg | Drug cost per day of treatment | Total (including saline) per cycle | |
| Intravenous topotecan | 1.5 | 2.7 | 100 | 97.65 | 292.95 | 1494.75 |
| Resource item | Resource use per cycle | Reference cost 2006/07 (£) | Uprated to 2007/08 (£) | Reference cost 2007/08 (£) |
|---|---|---|---|---|
| First chemotherapy administration in cyclea | 1 | 169.85 | 175.53 | 153.40 |
| Subsequent chemotherapy administration in cycleb | 4 | 189.44 | 195.77 | 154.18 |
| Pharmacy preparation cost | 1 | 25.44 | 25.44 | |
| Total cost per cycle | 984.04 | 795.56 | ||
| Resource item | Resource use per cycle | Reference cost 2006/07 (£) | Uprated to 2007/08 (£) | Reference cost 2007/08 (£) |
|---|---|---|---|---|
| FBC | 1 | 2.90 | 2.90 | |
| LFT | 1 | 4.70 | 4.70 | |
| U&E | 1 | 4.70 | 4.70 | |
| Chest radiograph | 1 | 27.71 | 28.64 | ? |
| CT scan (every two cycles) | 0.5 | 91.62 | 94.68 | 97.00 |
| Total cost per cycle | 88.28 | |||
Appendix II – details of cost calculations for CAV
| Drug | Dosage | Cost | |||||
|---|---|---|---|---|---|---|---|
| mg | mg per cycle | Saline (ml) for reconstitution | Unit cost (£) | Cost per mg (£) | Drug cost per cycle | Total cost (including saline) per cycle (£) | |
| Cyclophosphamide | 1000/m2 | 1800 | 100 | 5.04 | 0.01 | 10.08 | 16.08 |
| Doxorubicin | 45/m2 | 81 | 45 | 18.72 | 1.87 | 168.48 | 171.18 |
| Vincristine | 2 | 2 | 21.17 | 10.59 | 21.17 | 21.17 | |
| Total | 199.73 | 208.43 | |||||
| Resource use per cycle | Reference cost 2006/07 (£) | Uprated to 2007/08 (£) | Reference cost 2007/08 (£) | |
|---|---|---|---|---|
| Outpatient first attendancea | 1 | 176.75 | 182.65 | 185.80 |
| Outpatient follow-up attendanceb | 1 | 108.16 | 111.77 | 117.62 |
| Chemotherapy administrationc | 1 | 178.66 | 184.62 | 208.29 |
| Pharmacy preparation cost | 3 | 25.44 | 25.44 | |
| Total cost first cycle | 443.58 | 470.41 | ||
| Total cost subsequent cycle | 372.70 | 402.23 |
On-treatment monitoring per cycle, as for topotecan (see Table 60).
Appendix III – adverse events (haematological toxicity only)
| Toxicity | Grade | CAV | Intravenous top | Per cent events | RR | SE | LCI | UCI | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Event | n | Event | n | CAV | Intravenous top | ||||||
| Neutropenia | Grade 3 | 15 | 99 | 19 | 104 | 15.2 | 18.3 | 0.829 | 0.316 | 0.447 | 1.539 |
| Grade 4 | 71 | 99 | 73 | 104 | 71.7 | 70.2 | 1.022 | 0.090 | 0.857 | 1.218 | |
| Thrombocytopenia | Grade 3 | 10 | 101 | 30 | 104 | 9.9 | 28.8 | 0.343 | 0.337 | 0.177 | 0.665 |
| Grade 4 | 5 | 101 | 30 | 104 | 5.0 | 28.8 | 0.172 | 0.462 | 0.069 | 0.425 | |
| Anaemia | Grade 3 | 18 | 101 | 41 | 104 | 17.8 | 39.4 | 0.452 | 0.246 | 0.279 | 0.732 |
| Grade 4 | 2 | 101 | 3 | 104 | 2.0 | 2.9 | 0.686 | 0.902 | 0.117 | 4.023 | |
| Toxicity | Grade | Study | Oral | Intravenous | Per cent events | RR | SE | w | RRpooled | SE | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Event | n | Event | n | Oral | Intravenous | ||||||||
| Neutropenia | Grade 3 | Eckart | 39 | 149 | 35 | 148 | 26.2 | 23.6 | 1.107 | 0.202 | 24.543 | 1.022 | 0.175 |
| von Pawel | 11 | 51 | 14 | 52 | 21.6 | 26.9 | 0.801 | 0.351 | 8.097 | ||||
| Grade 4 | Eckart | 70 | 149 | 95 | 148 | 47.0 | 64.2 | 0.732 | 0.107 | 88.153 | 0.685 | 0.095 | |
| von Pawel | 18 | 51 | 35 | 52 | 35.3 | 67.3 | 0.524 | 0.213 | 22.081 | ||||
| Thrombocytopenia | Grade 3 | Eckart | 30 | 150 | 38 | 150 | 20.0 | 25.3 | 0.789 | 0.215 | 21.591 | 0.854 | 0.182 |
| von Pawel | 13 | 51 | 13 | 53 | 25.5 | 24.5 | 1.039 | 0.340 | 8.668 | ||||
| Grade 4 | Eckart | 43 | 150 | 27 | 150 | 28.7 | 18.0 | 1.593 | 0.217 | 21.295 | 1.433 | 0.181 | |
| von Pawel | 14 | 51 | 13 | 53 | 27.5 | 24.5 | 1.119 | 0.331 | 9.101 | ||||
| Anaemia | Grade 3 | Eckart | 26 | 150 | 42 | 150 | 17.3 | 28.0 | 0.619 | 0.221 | 20.434 | 0.730 | 0.183 |
| von Pawel | 14 | 51 | 14 | 53 | 27.5 | 26.4 | 1.039 | 0.323 | 9.580 | ||||
| Grade 4 | Eckart | 8 | 150 | 4 | 150 | 5.3 | 2.7 | 2.000 | 0.601 | 2.765 | 1.672 | 0.513 | |
| von Pawel | 2 | 51 | 2 | 53 | 3.9 | 3.8 | 1.039 | 0.981 | 1.040 | ||||
| Toxicity | Grade | CAV vs i.v. topotecan | Oral vs i.v. topotecan | CAV vs oral topotecan | LCI | UCI | |||
|---|---|---|---|---|---|---|---|---|---|
| RR | SE | RR | SE | RR | SE | ||||
| Neutropenia | Grade 3 | 0.829 | 0.316 | 1.022 | 0.175 | 1.232 | 0.361 | 0.607 | 2.498 |
| Grade 4 | 1.022 | 0.090 | 0.685 | 0.095 | 0.670 | 0.131 | 0.518 | 0.866 | |
| Thrombocytopenia | Grade 3 | 0.343 | 0.337 | 0.854 | 0.182 | 2.489 | 0.383 | 1.174 | 5.274 |
| Grade 4 | 0.172 | 0.462 | 1.433 | 0.181 | 8.350 | 0.497 | 3.154 | 22.104 | |
| Anaemia | Grade 3 | 0.452 | 0.246 | 0.730 | 0.183 | 1.616 | 0.306 | 0.887 | 2.944 |
| Grade 4 | 0.686 | 0.902 | 1.672 | 0.513 | 2.436 | 1.038 | 0.319 | 18.617 | |
| Toxicity | Grade | Adverse events (%) | Cost per adverse event | Cost adverse events (£) | ||
|---|---|---|---|---|---|---|
| CAV | Oral topotecan | CAV | Oral topotecan | |||
| Neutropenia | Grade 3 | 15.2 | 18.7 | 104 | 16 | 19 |
| Grade 4 | 71.7 | 48.1 | 1196 | 858 | 575 | |
| Thrombocytopenia | Grade 3 | 9.9 | 24.6 | 0 | 0 | 0 |
| Grade 4 | 5.0 | 41.3 | 1210 | 60 | 500 | |
| Anaemia | Grade 3 | 17.8 | 25.9 | 494 | 88 | 142 |
| Grade 4 | 2.0 | 4.8 | 940 | 19 | 45 | |
| Total | 1040 | 1282 | ||||
Appendix 1 Performance scales and response criteria in SCLC
Performance scales
Eastern Cooperative Oncology Group (ECOG) performance status
| Grade | ECOG |
|---|---|
| 0 | Fully active, able to carry on all pre-disease performance without restriction |
| 1 | Restricted in physically strenuous activity but ambulatory and able to carry out work of a light or sedentary nature, e.g. light housework, office work |
| 2 | Ambulatory and capable of all self-care but unable to carry out any work activities; up and about for more than 50% of waking hours |
| 3 | Capable of only limited self-care; confined to bed or chair for more than 50% of waking hours |
| 4 | Completely disabled; cannot carry on any self-care; totally confined to bed or chair |
| 5 | Dead |
Karnofsky performance index
| Definition | ||
|---|---|---|
| Able to carry on normal activity and to work | 100 | Normal; no complaints; no evidence of disease |
| 90 | Able to carry on normal activity; minor signs or symptoms of disease | |
| 80 | Normal activity with effort; some signs or symptoms of disease | |
| Unable to work; able to live at home, care for most personal needs; a varying amount of assistance is needed | 70 | Cares for self; unable to carry on normal activity or to do active work |
| 60 | Requires occasional assistance but is able to care for most needs | |
| 50 | Requires considerable assistance and frequent medical care | |
| Unable to care for self; requires equivalent of institutional or hospital care; disease may be progressing rapidly | 40 | Disabled; requires special care and assistance |
| 30 | Severely disabled; hospitalisation is indicated, although death is not imminent | |
| 20 | Very sick; hospitalisation necessary; active supportive treatment necessary | |
| 10 | Moribund; fatal processes progressing rapidly | |
| 0 | Dead | |
Treatment response criteria
WHO criteria treatment response (summarised from Miller et al.54)
| Characteristic | Criteria |
|---|---|
| Measurability of lesions at baseline |
|
| Objective response |
|
| Overall response |
|
| Duration of response |
|
RECIST criteria treatment response (summarised from Therasse et al.55)
| Characteristic | Criteria |
|---|---|
| Measurability of lesions at baseline |
|
| Objective response |
|
| Overall response |
|
| Duration of response |
|
Appendix 2 Methods from research protocol
Title of the project
Topotecan for the second-line treatment of small cell lung cancer (SCLC).
Report methods for synthesis of evidence of clinical effectiveness and cost-effectiveness
A review of the evidence for clinical effectiveness and cost-effectiveness will be undertaken systematically following the general principles outlined in CRD Report Number 4 (2nd edn) Undertaking Systematic Reviews of Research on Effectiveness. 53
Search strategy
A search strategy will be developed and tested by an experienced information scientist. The strategy will be designed to identify: (1) clinical effectiveness studies reporting on comparisons between topotecan (oral or i.v., but not combined) and best supportive care (BSC) or other chemotherapy regimens (as described in the economic modelling section) and (2) studies reporting on the cost-effectiveness of topotecan and different second-line treatments, and the relative comparisons. The search strategy will also identify studies reporting resource use and costs, epidemiology and natural history.
The following electronic databases will be searched: The Cochrane library, including the Cochrane Database of Systematic Reviews (CDSR), the Cochrane Central Register of Controlled Trials, CRD (University of York) Database of Abstracts of Reviews of Effectiveness (DARE), the NHS Economic Evaluation Database (NHS EED) and the Health Technology Assessment (HTA) database; MEDLINE (OVID); EMBASE (OVID); PREMEDLINE In-Process and Other Non-Indexed Citations; Web of Knowledge Science Citation Index (SCI); Web of Knowledge ISI Proceedings; PsycInfo; Biosis; UKCRN Study Portfolio and Current Controlled Trials. Key cancer resources (such as the American Society of Clinical Oncology (ASCO), European CanCer Organisation (ECCO), etc.) and relevant cancer symposia will also be searched. The search strategy for MEDLINE will be adapted for other databases.
Bibliographies of related papers will be assessed for relevant studies where possible. The manufacturer’s submission to the National Institute for Health and Clinical Excellence (NICE) will be assessed for any additional studies that meet the inclusion criteria. Experts will be contacted to identify additional published and unpublished evidence.
Searches will be carried out from 1990 and will be limited to the English language. For the cost-effectiveness section, searches for other evidence to inform cost-effectiveness modelling will be conducted as required and may include a wider range of study types (including non-randomised studies). All searches will be updated when the draft report is under review, prior to submission of the final report.
Inclusion and exclusion criteria
Population
-
Adults (≥ 18 years) with relapsed SCLC who responded to first-line treatment and for whom re-treatment with first-line therapy is not considered appropriate (due to contraindications, adverse effects).
-
Patients may have limited-stage disease or extensive-stage disease.
-
Response to initial treatment may be either complete response or partial response.
-
Patients who did not respond to first-line therapy (including patients whose tumours did not respond, or who progressed, during first-line treatment) will not be included.
-
Studies with a mix of untreated and previously treated patients (or responders and non-responders), will not be included unless the groups are reported separately.
Intervention
-
Intravenous topotecan (administered as second-line treatment).
-
Oral topotecan (administered as second-line treatment).
-
Studies with a focus on first-line treatment will not be included.
-
Effectiveness data for oral and i.v. topotecan will not be combined.
Comparators
-
Intravenous and oral topotecan will be compared with each other.
-
BSC (including radiotherapy).
-
CAV (cyclophosphamide, doxorubicin, vincristine).
-
Other chemotherapy regimens.
Outcomes
Studies reporting one or more of the following outcomes will be included:
-
time to disease progression (TTP)
-
progression-free survival (PFS)
-
response rate
-
response duration
-
overall survival (OS)
-
symptom control
-
health-related quality of life (using a validated measure)
-
cost-effectiveness (incremental cost per life-year gained) or cost–utility [incremental cost per quality-adjusted life-year (QALY) gained].
Adverse effects of treatments will be reported if available within trials that meet the other inclusion criteria.
Types of studies
-
Fully published randomised controlled trials (RCTs) will be included. If no RCTs are found, controlled clinical trials and prospective cohort studies (with a concurrent control) will be eligible for inclusion.
-
Studies published as abstracts or conference presentations will only be included if sufficient details are presented to allow an appraisal of the methodology and the assessment of results to be undertaken.
-
For the systematic review of cost-effectiveness, studies will only be included if they report the results of full economic evaluations [cost-effectiveness analyses (reporting cost per life-year gained), cost–utility analyses or cost–benefit analyses].
-
Systematic reviews will be used as a source of references.
-
Case series, case studies, narrative reviews, editorials and opinions will not be included.
-
Non-English language studies will be excluded.
Screening and data extraction process
Reference screening
The titles and abstracts of studies identified by the search strategy will be assessed for potential eligibility using the inclusion/exclusion criteria detailed above. This will be performed by two reviewers. Full papers of studies which appear potentially relevant will be requested for further assessment. These will be screened by two reviewers and a final decision regarding inclusion will be agreed. At each stage, any disagreements will be resolved by discussion, with involvement of a third reviewer where necessary.
Data extraction
Data will be extracted by one reviewer using a standardised data extraction form. Extracted data will be checked by a second reviewer. Discrepancies will be resolved by discussion, with recourse to a third reviewer when necessary.
Quality assessment strategy
The quality of the clinical effectiveness studies will be assessed according to criteria based on Centre for Reviews and Dissemination (CRD) (University of York) criteria. 53 Economic evaluations will be assessed using criteria recommended by Drummond and colleagues,66 and/or the format recommended and applied in the CRD NHS Economic Evaluation Database (using principles outlined in the NHS EED Handbook81). For any studies based on decision models we will also make use of the checklist for assessing good practice in decision-analytic modelling (Philips and colleagues68). Published studies carried out from the UK National Health Service (NHS) and Personal Social Services (PSS) perspective will be examined in more detail.
The quality of the individual studies will be assessed by one reviewer, and independently checked for agreement by a second reviewer. Any disagreements will be resolved by consensus, and, if necessary, a third reviewer will be consulted.
Methods of data analysis/synthesis of clinical effectiveness data
Clinical effectiveness data will be synthesised through a narrative review with tabulation of the results of included studies. Where data are of sufficient quality and homogeneity, a meta-analysis of the clinical-effectiveness studies will be performed to estimate a summary measure of effect on relevant outcomes. If a meta-analysis is appropriate, it will be performed using Review Manager (revman) software.
Methods of data analysis/synthesis of cost-effectiveness data
Published and submitted economic evaluations
Narrative synthesis, supported by the data extraction tables, will be used to summarise the evidence base from published economic evaluations. Any economic evaluation included in sponsor submissions to NICE will be assessed using the same quality criteria as for published economic evaluations, but will be reported separately.
Economic modelling
Where appropriate, an economic model will be constructed by adapting an existing model or developing a new one using best available evidence. The perspective will be that of the NHS and PSS. The incremental cost-effectiveness of the interventions will be estimated in terms of cost per QALY gained, as well as the cost per life-year gained if data permit. Both cost and outcomes will be discounted at 3.5%.
Model structure will be determined on the basis of research evidence and clinical expert opinion of:
-
the biological disease process (i.e. knowledge of the natural history of the disease)
-
the main diagnostic and care pathways for patients in the UK NHS context [both with and without the intervention(s) of interest]
-
the disease states or events which are most important in determining patients’ clinical outcomes, quality of life (QoL) and consumption of NHS or PSS resources.
For patients receiving topotecan, or comparator treatments, for relapsed SCLC following first-line treatment, TTP will be a major factor in defining costs of second-line treatment and is also likely to be a significant determinant of QoL. Any improvements in OS or impacts on QoL that may be associated with changes in PFS will need to be offset by consideration of the toxicity profile of alternative therapies. There is likely to be considerable uncertainty surrounding modes of treatment following disease progression on second-line treatment, which may have an influence on costs and QoL. Clinical guidance will be sought to define appropriate protocols for patient management following disease progression on second-line treatment.
Parameter values will be obtained from relevant research literature, including our own systematic review of clinical effectiveness. Where required parameters are not available from good-quality published studies in the relevant patient group, we may use data from sponsor submissions to NICE or experts’ clinical opinions. Searches for additional information regarding model parameters, patient preferences and other topics will be conducted as required. Sources for parameters will be stated clearly.
Resource use will be specified and valued from the perspective of the NHS and PSS. Cost data will be derived from local sources, extracted from published sources or from sponsor submissions to NICE, as appropriate.
The simulated population will be defined on the basis of both the published evidence about the characteristics of the UK population with SCLC relevant to the licensed indication for topotecan, and the populations for which good-quality clinical effectiveness is available. The base-case results will be presented for the population of UK patients undergoing second-line treatment of SCLC. The time horizon for our analysis will initially be governed by follow-up data available from included clinical trials – we will investigate the feasibility of extrapolating treatment effects beyond the clinical trials.
Methods for estimating QoL
The primary aim of treatment for SCLC is to palliate symptoms, prolong survival and maintain a good QoL with minimal adverse events from treatment. This assessment will aim to identify adverse effects of treatment that are likely to have a substantial impact on patients’ QoL, and to include these in estimates of health-state utility while on treatment. Where presented, QoL information, as well as incidence of adverse events and side effects of treatment, will be extracted from included RCTs. Where QoL data are insufficient to calculate utility estimates, data will be derived from the broader literature or estimated from other sources. Ideally, utility values will be taken from studies that have been based on ‘public’ (as opposed to patient or clinician) preferences elicited using a choice-based method (in accordance with NICE methodological guidance). 67
Analysis of uncertainty
Analysis of uncertainty will focus on cost–utility, assuming that the cost per QALY can be estimated. Uncertainty will be explored through one-way sensitivity analysis and, if the data and modelling approach permit, probabilistic sensitivity analysis (PSA). The outputs of PSA will be presented both using plots on the cost-effectiveness plane and cost-effectiveness acceptability curves.
Handling the company submission(s)
All data submitted by the manufacturers will be considered if received by the Technology Assessment Report (TAR) team no later than 12 December 2008. Data arriving after this date will not be considered. If the data meet the inclusion criteria for the review, they will be extracted and quality assessed in accordance with the procedures outlined in this protocol. Any economic evaluations included in the company submission, provided it complies with NICE’s guidance on presentation,67 will be assessed for clinical validity, reasonableness of assumptions and appropriateness of the data used in the economic model.
Methods adopted, and incremental cost-effectiveness ratios (ICERs) estimated from consultee models will be compared with published economic evaluations of topotecan included in the assessment report and with the results from the Assessment Group’s analysis. Reasons for large discrepancies in estimated ICERs will be explored and, where possible, explained.
Any ‘academic in confidence’ data or ‘commercial in confidence’ data taken from a company submission will be underlined and highlighted in the assessment report.
Appendix 3 Sources of searches and search criteria
The following databases were searched for published studies and recently completed and ongoing research. All searches were limited to English language only. Searches were updated in February 2009.
-
Cochrane Library – Cochrane Database of Systematic Reviews (CDSR)
-
Cochrane Library – Central Register of Controlled Trials (Clinical Trials)
-
MEDLINE (OVID)
-
PREMEDLINE In-Process & Other Non-Indexed citations (OVID)
-
EMBASE (OVID)
-
Web of Knowledge Science Citation Index (SCI)
-
Web of Knowledge ISI Proceedings
-
BIOSIS
-
PsycInfo (EBSCO)
-
CINAHL (EBSCO)
-
DARE (CRD)
-
HTA (CRD)
-
NHS Economic Evaluation Database (CRD)
-
Health Technology Assessment (HTA) database
-
Current Controlled Trials
-
ClinicalTrials.gov
-
Cancer Research UK trials
-
NIHR-Clinical Research Network Portfolio
-
American Society of Clinical Oncology (ASCO)
-
12th World Lung Cancer Conference
Clinical effectiveness searches
The following strategies were used to search MEDLINE (OVID) 1990–2008 and EMBASE (OVID) 1990–2008. These were translated to search the other databases listed above.
MEDLINE
-
Randomized Controlled Trials as Topic/(56584)
-
randomized controlled trial.pt. (263468)
-
controlled clinical trial.pt. (79901)
-
Controlled Clinical Trial/(79901)
-
placebos/(28018)
-
random allocation/(62530)
-
Double-Blind Method/(99912)
-
Single-Blind Method/(12433)
-
(random* adj2 allocat*).tw. (13703)
-
placebo*.tw. (113108)
-
((singl* or doubl* or trebl* or tripl*) adj (blind* or mask*)).tw. (96640)
-
crossover studies/(22777)
-
(crossover* or (cross adj over*)).tw. (42546)
-
Research Design/(54086)
-
((random* or control*) adj5 (trial* or stud*)).tw. (332493)
-
clinical trials.sh. (0)
-
Clinical Trials as Topic/(142719)
-
trial.ti. (76577)
-
randomly.ab. (124831)
-
(randomized or randomised).ab. (205326)
-
Drug Evaluation/(41604)
-
Follow-Up Studies/(377946)
-
prospective studies/(251441)
-
Comparative Study/(1425847)
-
Evaluation Studies as Topic/(120471)
-
or/1–25 (2586344)
-
limit 26 to (english language and humans and yr = “1990 – 2008”) (1257730)
-
Topotecan/(1346)
-
(topotecan or hycamtin).ti,ab. (1661)
-
or/28–29 (1860)
-
27 and 30 (561)
-
SCLC.ti,ab. (3693)
-
Carcinoma, Small Cell/(15715)
-
Lung Neoplasms/(123052)
-
33 and 34 (13271)
-
(small cell* adj3 (cancer* or carcinoma*)).ti,ab. (28814)
-
(lung* adj3 (cancer* or carcinoma* or neoplasm* or tumor* or tumour*)).ti,ab. (82293)
-
32 or 33 or 35 or 36 or 37 (88051)
-
31 and 38 (165)
-
from 39 keep 1–165 (165)
EMBASE (Ovid)
-
Randomized Controlled Trial/(161361)
-
RANDOMIZATION/(26101)
-
PLACEBO/(116829)
-
placebo*.tw. (106937)
-
random*.tw. (377424)
-
Randomization/(26101)
-
Double Blind Procedure/(70149)
-
single blind procedure/(7734)
-
Crossover Procedure/(20539)
-
(crossover* or (cross adj over*)).tw. (38438)
-
Controlled Clinical Trial/(49917)
-
((random* or control* or clinical*) adj5 (trial* or stud*)).tw. (500666)
-
(random adj5 allocat*).tw. (1308)
-
((singl* or doubl* or trebl* or tripl*) adj (blind* or mask*)).tw. (91281)
-
exp clinical trials/(522756)
-
Prospective Study/(76363)
-
Comparative Study/(110563)
-
Evaluation/(52829)
-
or/1–18 (1211004)
-
animal/(18250)
-
human/(6212410)
-
20 not (20 and 21) (14472)
-
19 not 22 (1210216)
-
limit 23 to (english language and yr = “1990 – 2008”) (977835)
-
*topotecan/(1200)
-
hycamtin.ti,ab. (59)
-
topotecan.ti,ab. (1688)
-
or/25–27 (1856)
-
Lung Small Cell Cancer/(9125)
-
SCLC.ti,ab. (3511)
-
(small cell* adj3 (cancer* or carcinoma*)).ti,ab. (27336)
-
(lung* adj3 (cancer* or carcinoma* or neoplasm* or tumor* or tumour*)).ti,ab. (68834)
-
or/29–32 (72839)
-
24 and 28 and 33 (257)
-
from 34 keep 1–257 (257)
Cost-effectiveness searches
The clinical effectiveness strategies above were combined with the following cost-effectiveness filters and run in MEDLINE (OVID) and EMBASE (OVID). The strategies were translated and run in the other databases noted above.
MEDLINE (Ovid)
-
exp economics/(401622)
-
exp economics hospital/(15764)
-
exp economics pharmaceutical/(1958)
-
exp economics nursing/(3849)
-
exp economics dental/(3737)
-
exp economics medical/(12120)
-
exp “Costs and Cost Analysis”/(140560)
-
Cost Benefit Analysis/(44369)
-
value of life/(5057)
-
exp models economic/(6055)
-
exp fees/and charges/(7457)
-
exp budgets/(9937)
-
(economic$or price$or pricing or financ$or fee$or pharmacoeconomic$or pharma economic$).tw. (364284)
-
(cost$or costly or costing$or costed).tw. (215271)
-
(cost$adj2 (benefit$or utilit$or minim$or effective$)).tw. (55616)
-
(expenditure$not energy).tw. (11749)
-
(value adj2 (money or monetary)).tw. (716)
-
budget$.tw. (11787)
-
(economic adj2 burden).tw. (1798)
-
“resource use”.ti,ab. (2425)
-
or/1–20 (831568)
-
(news or letter or editorial or comment).pt. (1037052)
-
21 not 22 (769363)
-
topotecan/(1348)
-
(topotecan or hycamtin).ti,ab. (1664)
-
24 or 25 (1863)
-
SCLC.ti,ab. (3694)
-
Carcinoma, Small Cell/(15724)
-
Lung Neoplasms/(123253)
-
28 and 29 (13275)
-
(small cell* adj3 (cancer* or carcinoma*)).ti,ab. (28891)
-
(lung* adj3 (cancer* or carcinoma* or neoplasm* or tumor* or tumour*)).ti,ab. (82493)
-
26 and (27 or 30 or 31 or 32) (377)
-
23 and 33 (12)
-
26 and 28 (171)
-
23 and 35 (5)
-
34 or 36 (12)
-
from 37 keep 1–12 (12)
EMBASE
-
cost$.ti. (38273)
-
(cost$adj2 (effective$or utilit$or benefit$or minimi$)).ab. (45245)
-
(economic$or pharmacoeconomic$or pharmaco economic$).ti. (14978)
-
(price$or pricing$).ti,ab. (11266)
-
(financial or finance or finances or financed).ti,ab. (23140)
-
(fee or fees).ti,ab. (5171)
-
cost/(20116)
-
cost minimization analysis/(1383)
-
cost of illness/(4659)
-
cost utility analysis/(2350)
-
drug cost/(33975)
-
health care cost/(60374)
-
health economics/(10179)
-
economic evaluation/(4274)
-
economics/(5647)
-
pharmacoeconomics/(91517 budget/(7640)
-
“resource use”.ti,ab. (2184)
-
economic burden.ti,ab. (1743)
-
or/1–19 (207147)
-
(editorial or letter).pt. (638905)
-
20 not 21 (186062)
-
topotecan/(4883)
-
(topotecan or hycamtin).ti,ab. (1695)
-
23 or 24 (4966)
-
Lung Small Cell Cancer/(9151)
-
SCLC.ti,ab. (3517)
-
(small cell* adj3 (cancer* or carcinoma*)).ti,ab. (27408)
-
(lung* adj3 (cancer* or carcinoma* or neoplasm* or tumor* or tumour*)).ti,ab. (69004)
-
or/26–29 (73028)
-
22 and 25 and 30 (33)
-
from 31 keep 1–33 (33)
Quality-of-life searches
The following strategy was used to search MEDLINE (OVID) and EMBASE (OVID) and the strategies were translated and run in the other databases noted above.
MEDLINE
-
“Quality of Life”/(70898)
-
(hql or hqol or “h qol” or hrqol or “hr qol”).ti,ab. (3046)
-
(“hye” or “hyes”).ti,ab. (47)
-
(euroqol or “euro qol” or “eq5d” or “eq 5d”).ti,ab. (1330)
-
Quality-Adjusted Life Year/(3593)
-
“quality adjusted life”.ti,ab. (2709)
-
(qaly$or qald$or qale$or qtime$).ti,ab. (2200)
-
“disability adjusted life”.ti,ab. (475)
-
“quality of wellbeing”.ti,ab. (1)
-
“quality of well being”.ti,ab. (221)
-
daly$.ti,ab. (552)
-
(sf36 or sf 36 or short form 36 or shortform 36 or sf thirtysix or sf thirty six or shortform thirtysix or shortform thirty six or short form thirty six or short form thirtysix or short form thirty six).ti,ab. (7995)
-
health$year$equivalent$.tw. (31)
-
disutil*.ti,ab. (87)
-
“Value of Life”/(5057)
-
rosser.ti,ab. (63)
-
willingness to pay.tw. (1010)
-
standard gamble$.tw. (493)
-
time trade off.tw. (414)
-
time tradeoff.tw. (160)
-
health utilit*.ab. (493)
-
or/1–21 (83056)
-
topotecan/(1348)
-
(topotecan or hycamtin).ti,ab. (58)
-
23 or 24 (1358)
-
SCLC.ti,ab. (3694)
-
“small cell lung cancer”.ti,ab. (19336)
-
Carcinoma, Small Cell/(15724)
-
Lung Neoplasms/(123253)
-
28 and 29 (13275)
-
(small cell* adj3 (cancer* or carcinoma*)).ti,ab. (28891)
-
(lung* adj3 (cancer* or carcinoma* or neoplasm* or tumor* or tumour*)).ti,ab. (82493)
-
25 and (26 or 27 or 30 or 31 or 32) (271)
-
22 and 33 (10)
-
(quality adj5 topotecan).ti,ab. (9)
-
(qol adj5 topotecan).ti,ab. (3)
-
(quality adj5 hycamtin).ti,ab. (1)
-
(qol adj5 hycamtin).ti,ab. (0)
-
or/35–37 (12)
-
22 and 39 (9)
-
34 or 40 (16)
-
from 41 keep 1–16 (16)
-
Survival Analysis/(69669)
-
“symptom palliation”.mp. (141)
-
43 or 44 (69782)
-
33 and 45 (39)
-
46 not 42 (36)
-
from 47 keep 1–36 (36)
-
from 41 keep 1–16 (16)
EMBASE
-
exp quality of life/(94730)
-
quality adjusted life year/(3820)
-
quality adjusted life.ti,ab. (2591)
-
(qaly$or qald$or qale$or qtime$).ti,ab. (2096)
-
disability adjusted life.ti,ab. (428)
-
daly*.ti,ab. (465)
-
(sf36 or sf 36 or short form 36 or shortform 36 or sf thirtysix or sf thirty six or shortform thirtysix or shortform thirty six or short form thirty six or short form thirtysix or short form thirty six).ti,ab. (7682)
-
(sf6 or sf 6 or short form 6 or shortform 6 or sf six or sfsix or shortform six or short form six).ti,ab. (845)
-
(sf12 or sf 12 or short form 12 or shortform 12 or sf twelve or sftwelve or shortform twelve or short form twelve).ti,ab. (953)
-
(sf16 or sf 16 or short form 16 or shortform 16 or sf sixteen or sfsixteen or shortform sixteen or short form sixteen).ti,ab. (11)
-
(sf20 or sf 20 or short form 20 or shortform 20 or sf twenty or sftwenty or shortform twenty or short form twenty).ti,ab. (193)
-
(euroqol or “euro qol” or “eq5d” or “eq 5d”).ti,ab. (1315)
-
(hql or hqol or “h qol” or hrqol or “hr qol”).ti,ab. (2915)
-
(“hye” or “hyes”).ti,ab. (28)
-
health* year* equivalent*.ti,ab. (24)
-
((health or cost) adj5 util*).ti,ab. (10006)
-
(hui or hui1 or hui2 or hui3).ti,ab. (399)
-
disutil*.ti,ab. (88)
-
rosser.ti,ab. (51)
-
quality of well being.ti,ab. (197)
-
quality of wellbeing.ti,ab. (5)
-
qwb.ti,ab. (114)
-
willingness to pay.ti,ab. (972)
-
standard gamble*.ti,ab. (447)
-
time trade off.ti,ab. (392)
-
time tradeoff.ti,ab. (144)
-
tto.ti,ab. (307)
-
(index adj2 well being).mp. (277)
-
(quality adj2 well being).mp. (511)
-
(health adj3 util* adj ind*).mp. (372)
-
((multiattribute* or multi attribute) adj3 (health ind* or theor* or health state* or util* or analys*)).mp. (152)
-
quality adjusted life year*.mp. (4639)
-
(EORTC adj2 “LC-13”).mp. [mp = title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer, drug manufacturer name] (2)
-
FACT-L.mp. (37)
-
LCSS.mp. (35)
-
or/1–35 (108127)
-
topotecan/(4904)
-
topotecan.mp. (4988)
-
hycamtin.mp. (447)
-
or/37–39 (4988)
-
Lung Small Cell Cancer/(9172)
-
SCLC.ti,ab. (3524)
-
(small cell* adj3 (cancer* or carcinoma*)).ti,ab. (27478)
-
(lung* adj3 (cancer* or carcinoma* or neoplasm* or tumor* or tumour*)).ti,ab. (69221)
-
or/41–44 (73251)
-
36 and 40 and 45 (94)
-
(letter or editorial or comment).pt. (641036)
-
46 not 47 (90)
Epidemiology searches
The following strategies were used to search MEDLINE (OVID) and EMBASE (OVID):
-
*carcinoma small cell/ep (161)
-
*lung neoplasms/(94669)
-
1 and 2 (124)
-
*lung small cell cancer/ep (162)
-
((“small cell lung cancer” or SCLC) adj3 (incidence or prevalence or epidemiolog* or mortality or morbidity or aetiology or etiology)).ti,ab. (128)
-
“non small cell lung cancer”.ti. (18884)
-
5 not 6 (80)
-
5 not 7 (48)
-
*carcinoma small cell/et (247)
-
*lung cancer/et (7046)
-
9 and 10 (74)
-
(SCLC and aetiology).ti,ab. (9)
-
(SCLC and etiolog*).ti,ab. (35)
-
(“small cell lung cancer” and etiolog*).ti. (1)
-
(“small cell lung cancer” and aetiolog*).ti. (0)
-
lung cancer trend*.ti,ab. (55)
-
lung cancer pattern*.ti,ab. (24)
-
lung cancer epidemiolog*.ti,ab. (80)
-
3 or 4 or 7 or 11 or 12 or 13 or 14 or 16 or 17 or 18 (624)
-
limit 19 to english language (529)
-
NSCLC.ti. (1555)
-
“non small cell lung cancer”.ti. (18884)
-
21 or 22 (19767)
-
20 not 23 (516)
-
remove duplicates from 24 (395)
-
from 25 keep 1–251 (251) – note this is the medline set downloaded separately for import purposes)
-
from 25 keep 252–395 – note this is the embase record set downloaded separately for import purposes)
Additional searching
Bibliographies: all references of articles for which full papers were retrieved were checked to ensure that no eligible studies had been missed.
Appendix 4 SHTAC peer review of clinical effectiveness in MS of topotecan for SCLC
Other consultee submissions were checked and there was nothing to add.
Comprehensiveness of ascertainment of published studies
Clinical effectiveness
-
Databases and dates of searches were specified in an appendix ‘full systematic review’ (no full check of this was made).
-
Search strategies in annex of appendix (not fully checked).
-
Enough detail provided to be reproducible.
-
Searched for ongoing studies.
-
No direct searching of conference proceedings, although searched using Google.
Cost-effectiveness
-
Search terms specified (although minimal).
-
Only searched NHS EED.
-
However, unlikely that anything was missed.
Searches identified
-
Four clinical trials (oral topotecan versus BSC, i.v. topotecan versus CAV, oral topotecan versus i.v. topotecan × 2).
-
Did not identify our fifth study (i.v. topotecan versus i.v. amrubicin) – possibly as no conferences were directly searched and owing to date of their searches.
-
No cost-effectiveness studies identified.
-
Also searched for indirect comparisons but found no studies of value.
Clinical analysis
-
Evidence reported is similar to ours, with the exception of the amrubicin study, although they do not appear to report the new QOL data from the O’Brien study.
-
Their conclusions are similar to ours.
-
They indirectly compared oral topotecan versus CAV (no real rationale given but see below). They observed the survival data and statistically compared the ORR data only.
-
Adverse event reporting is similar to ours. They undertook a meta-analysis of some data (not checked to see if data are consistent with a meta-analysis).
Interpretation
-
Their interpretation of the clinical data matches their analyses.
Questions
The clinical effectiveness review ran an indirect comparison of oral topotecan versus CAV. Although no justification for this was given directly, it is assumed that this is because CAV is the most likely comparator in this population, and, that although i.v. treatment has been compared to CAV in a trial, a proportion of patients would prefer oral topotecan. In the economic evaluation, however, CAV is not considered as it is reported that this would not be a cost-effective option due to the higher cost of topotecan. So, although on paper the comparator would be CAV, assume the manufacturer’s view is that the comparator should be those who are ineligible for CAV (this population would be a part of those in the O’Brien trial as they were ‘not appropriate’ for further i.v. treatment). In addition, the population in the CAV trial were excluded if they were ineligible for CAV so will not be those ‘eligible’ for topotecan in this sense.
Appendix 5 Quality assessment criteria
Quality criteria for assessment of experimental studies53
| 1. Was the assignment to the treatment groups really random? |
| 2. Was the treatment allocation concealed? |
| 3. Were the groups similar at baseline in terms of prognostic factors? |
| 4. Were the eligibility criteria specified? |
| 5. Were outcome assessors blinded to the treatment allocation? |
| 6. Was the care provider blinded? |
| 7. Was the patient blinded? |
| 8. Were the point estimates and measure of variability presented for the primary outcome measure? |
| 9. Did the analyses include an ITT analysis? |
| 10. Were withdrawals and dropouts completely described? |
Some instructions for using a checklist for RCTs
| Quality item | Coding | Explanation |
|---|---|---|
| Was the assignment to the treatment groups really random? | ||
| Random sequence generation |
Adequate Partial Inadequate Unknown |
Adequate: random numbers table or computer and central office or coded packages Partial: (sealed) envelopes without further description or serially numbered opaque, sealed envelopes Inadequate: alternation, case record number, birth date, or similar procedures Unknown: just the term ‘randomised’ or ‘randomly allocated’, etc. |
| Was the treatment allocation concealed? | ||
| Concealment of randomisation | ||
| The person(s) who decide on eligibility should not be able to know or be able to predict with reasonable accuracy to which treatment group a patient will be allocated. In trials that use good placebos this should normally be the case; however, different modes or timing of drug administration in combination with the use of small block sizes of known size may present opportunities for clinicians who are also involved in the inclusion procedure to make accurate guesses and selectively exclude eligible patients in the light of their most likely treatment allocation; in centres with very low inclusion frequencies combined with very brief follow-up times this may also present a potential problem because the outcome of the previous patient may serve as a predictor of the next likely allocation |
Adequate Inadequate Unknown |
Adequate: when a paper convinces you that allocation cannot be predicted [separate persons, placebo really indistinguishable, clever use of block sizes (large or variable)]; adequate approaches might include centralised or pharmacy-controlled randomisation, serially numbered identical containers, on-site computer-based system with a randomisation sequence that is not readable until allocation, and other approaches with robust methods to prevent foreknowledge of the allocation sequence to clinicians and patients Inadequate: this option is often difficult – you have to visualise the procedure and think how people might be able to circumvent it; inadequate approaches might include use of alternation, case record numbers, birth dates or week days, open random numbers lists, serially numbered envelopes (even sealed opaque envelopes can be subject to manipulation) and any other measures that cannot prevent foreknowledge of group allocation Unknown: no details in text; disagreements or lack of clarity should be discussed in the review team |
| Were the groups similar at baseline regarding the prognostic factors? | ||
| Baseline characteristics | ||
| Main aim is to enable the reviewer to see which patients were actually recruited. It enables one to get a rough idea on prognostic comparability. A real check on comparability requires multivariable stratification (seldom shown) |
Reported Unknown |
Consult the list of prognostic factors or baseline characteristics (not included in this appendix); reviewer decides |
| Were the eligibility criteria specified? | ||
| Prestratification | ||
| Consult the list of prognostic factors or baseline characteristics (not included in this appendix). |
Adequate Partial Inadequate Unknown |
Single-centre study: Adequate: prestratification on at least one factor from the list or no prestratification if the number of patients exceeds a prespecified number Partial: leave judgement to reviewer Inadequate: stratification on a factor(s) not on our list or no stratification, whereas the number of patients is less than the prespecified number Unknown: no details in text and no way to deduce the procedure from the tables Multicentre study: Adequate: must prestratify on centre; within each centre the criteria for single-centre studies also apply Partial: impossible option Inadequate: no prestratification on centre or violating the criteria for single-centre studies (see above) Unknown: no details in text and no way to deduce the procedure from the tables |
| Were outcome assessors blinded to the treatment allocation? | ||
| Blinding of assessors | ||
| The assessor may be the patient (self report), the clinician (clinical scale, blood pressure…) or, ideally, a third person or a panel; very important in judgement of cause of death but unimportant in judgement of death |
Adequate Inadequate Unknown |
Adequate: independent person or panel or (self) assessments in watertight double-blind conditions Inadequate: clinician is assessor in trial on drugs with clear side effects or a different influence on lab results, ECGs, etc. Unknown: no statements on procedures and not deducible |
| Was the care provider blinded? | ||
| Blinding of caregivers | ||
| Look out for good placebos (see, hear, taste, feel, smell), tricky unmasking side effects accounting for the subjectivity of the outcome measurements and the accessibility of cointerventions by the caregivers |
Adequate Partial Inadequate Unknown |
Adequate: placebo described as ‘indistinguishable’ and procedures watertight (use your imagination with the ‘cheat’ in mind, e.g. statement that sensitive/unmasking lab results were kept separate from ward personnel) Partial: just ‘double blind’ in text and no further description of procedures or nature of the placebo Inadequate: wrong placebo (e.g. fructose in trial on ascorbic acid) Unknown: no details in text |
| Cointerventions | ||
| Register when they may have an impact on any of the outcome phenomena; consult the list of cointerventions (not included in this appendix) |
Adequate Partial Inadequate Unknown |
Adequate: percentages of all relevant interventions in all groups Partial: one or more interventions omitted or omission of percentages in each group Inadequate: not deducible Unknown: no statements |
| Was the patient blinded? | ||
| Blinding of patients: this item is hard to define; just the statement ‘double blind’ in the paper is really insufficient if the procedure to accomplish this is not described or reasonably deducible by the reviewer; good placebos (see, hear, taste, feel, smell), tricky unmasking side effects accounting for the subjectivity of the outcome measurements and the accessibility of cointerventions by the patient are required |
Adequate Partial Inadequate Unknown |
Adequate: placebo described as ‘indistinguishable’ and procedures watertight Partial: just ‘double blind’ in text and no further description of procedures or nature of the placebo Inadequate: wrong placebo Unknown: no details in text |
|
Compliance Dosing errors and timing errors |
Adequate Partial Inadequate Unknown |
Adequate: Medication Event Monitoring System (MEMS or eDEM) Partial: blood samples, urine samples (use of indicator substances) Inadequate: pill count or self report Unknown: not mentioned |
| Check on blinding: questionnaire for patients, caregivers, assessors and analysis of the results; the (early) timing is critical because the treatment effect may be the cause of unblinding, in which case it may be used as an outcome measure |
Reported Unknown |
Reviewer decides |
| Were the point estimates and measure of variability presented for the primary outcome measure? | ||
| Results for the primary outcome measure |
Adequate Partial Inadequate Unknown |
Adequate: mean outcome in each group together with mean difference and its standard error (SE) or standard deviation (SD) or any CI around it or the possibility to calculate those from the paper; survival curve with log-rank test and patient numbers at later time points Partial: partially reported Inadequate: no SE or SD, or SD without N (SE = SD/N) Unknown: very unlikely |
| Did the analysis include an intention to treat analysis? | ||
| ITT analysis | ||
| Early dropout can make this very difficult; strictest requirement is sensitivity analysis including early dropouts |
Adequate Inadequate |
Reviewers should not just look for the term ITT but assure themselves that the calculations were according to the ITT principle |
| Dealing with missing values | ||
| The percentage of missing values on potential confounders and outcome measurements (seldom given) is a rough estimate of a trial’s quality; one can carry them forward, perform sensitivity analysis assuming the worst and best-case scenarios, use statistical imputation techniques, etc.; note that the default option (deletion) assumes that the value is randomly missing, which seems seldom justified |
Adequate Partial Inadequate Unknown |
Adequate: percentage of missing values and distribution over the groups and procedure of handling this stated Partial: some statement on numbers or percentages Inadequate: wrong procedure (a matter of great debate) Unknown: no mentioning at all of missing and not deducible from tables |
| Loss to follow-up | ||
| This item examines both numbers and reasons – typically an item that needs checking in the methods section and the marginal totals in the tables; note that it may differ for different outcome phenomena or time points; some reasons may be reasons given by the patient when asked and may not be the true reason; there is no satisfactory solution for this |
Adequate Partial Inadequate Unknown |
Adequate: number randomised must be stated. Number(s) lost to follow-up (dropped out) stated or deducible (from tables) for each group and reasons summarised for each group Partial: numbers, but not the reasons (or vice versa) Inadequate: numbers randomised not stated or not specified for each group Unknown: no details in text |
Appendix 6 Data extraction forms
| Reference and design | Intervention | Participants | Outcome measures |
|---|---|---|---|
|
Author: Eckardt et al. 56 and Eckardt et al. (abstract)60 Year: 2007 Countries: N America, Europe, SE Asia and Australia Study design: Open-label RCT Number of centres: 83 Funding: GlaxoSmithKline |
Group A: Oral topotecan a Dose: 2.3 mg/m2/day Duration: On days 1–5 every 21 days Group B: Intravenous topotecan Dose: 1.5 mg/m2/day, (30-minute infusion) Duration: On days 1–5 every 21 days Patients with CR or PR continued treatment until disease progression or for two courses beyond best response; those with stable disease were recommended to receive at least four courses Dose escalation if no toxicity > grade 2 during course 1. Oral dose increased in increments of 0.4 mg/m2 to a maximum of 3.1 mg/m2/day. i.v. dose increased by 0.25 mg/m2 to a maximum of 2.0 mg/m2/day. Dose reduction if patients had prolonged or severe neutropenia or severe thrombocytopenia. Minimum doses were 1.5 mg/m2/day for oral and 1.0 mg/m2/day for i.v.; study withdrawal if delays of > 2 weeks at these doses Other interventions used: none |
Number of participants: 309 Randomly assigned: oral = 155, i.v. = 154 Received treatment: oral = 153, i.v. = 151 Sample attrition/dropout: Total = 57 (18%), oral = 31/155 (20%), i.v. = 26/154 (17%) Received no treatment: oral = 2, i.v. = 3; protocol violation: oral = 2, i.v. = 0 Withdrew for adverse events: oral = 19 (12%), i.v. = 19 (13%) Withdrew for other reasons: oral = 6, i.v. = 3; lost to follow-up: oral = 1, i.v. = 1 Sample crossovers: n/a Inclusion criteria: Patients with limited- or extensive-stage relapsed SCLC who had CR or PR to first-line therapy with disease recurrence after ≥ 90 days; ≥ 18 years, only one prior chemotherapy regimen, bidimensionally measurable disease (according to WHO criteria), an ECOG performance status of ≤ 2, WBC count ≥ 3500/µl, neutrophils ≥ 1500 µl, platelets ≥ 100,000 µl, Hb ≥ 9.0 g/dl, serum creatinine ≤1.5 mg/dl, bilirubin ≤ 2.0 mg/dl; alkaline phosphatase, AST and ALT ≤ 2 × the ULN or ≤ 5 × ULN with liver metastases; patients with CNS metastases if they were asymptomatic without corticosteroids; prior surgery was allowed if ≥ 4 weeks had passed, as was immunotherapy (≥ 3 months) and radiotherapy (≥ 24 hours) Exclusion criteria: Concurrent chemotherapy, immunotherapy, or radiotherapy; concurrent radiation for palliation of bone or brain lesions unless discussed with the medical monitor Characteristics of participants: Gender (M/F), n (%):Age (years), mean (range):Disease stage, n (%):Performance status, n (%):Maximum lesion diameter (cm), n (%):cPrevious treatment: platinum-based and anthracycline-based combination regimensdDuration of response to first-line chemotherapy, n (%):eLiver metastases, n (%): |
Primary outcomes: Response rate Secondary outcomes:b Time to response, response duration, TTP, OS, toxicities, HRQoL Methods of assessing outcomes: Responses were verified by a central radiologist blinded to study treatment Lesions were assessed at the end of each course (if evaluated by photography or physical examination) or at the end of alternate courses (if evaluated by CT, MRI radiograph or ultrasound); the same method of evaluation was used throughout the study HRQoL was assessed using the Functional Assessment of Cancer Therapy-Lung (FACT-L) 44-item self-reported instrument and validated, and included four generic dimensions and a subscale specific to lung cancer; TOI also derived from a subgroup of data; no details of scoring methods Toxicities were graded according to the National Cancer Institute Common Toxicity Criteria Length of follow-up: Patients received a median of four courses (i.e. 12 weeks); at least 40% of patients in each group received treatment beyond course 4 |
| RESULTS | |||||
|---|---|---|---|---|---|
| Outcomes | Oral topotecan (n = 153) | Intravenous topotecan (n = 151) | Difference | ||
| OS time (weeks), median (range) | n = 153 | n =151 | HRf = 0.98 (95% CI 0.77 to 1.25) | ||
| 33.0 (0.3–185.3) | 35.0 (0.7–205.3) | ||||
| 95% CI | 29.1 to 42.4 | 31.0 to 37.4 | NS | ||
| Survival rate at year 1 (%) | 33 | 29 | |||
| Survival rate at year 2 (%) | 12 | 7 | |||
| f Cox proportional hazards regression. | |||||
| For OS, data were censored for 13.7% and 10.6% of patients in oral and i.v. groups, respectively. | |||||
| Time to progression (weeks), median (range) | n = 153 | n = 151 | |||
| 11.9 (0.3–149.0)g | 14.6 (0.7–177.9)g | ||||
| 95% CI | 9.7 to 14.1 | 13.3 to 18.9 | |||
| g Includes censored events. | |||||
| Progression-free survival | Not reported | Not reported | |||
| ORR, n (%) | 28 (18.3%) | 33 (21.9%) | Difference (oral – i.v.) –3.6% (95% CI –12.6 to 5.5) | ||
| 95% CI | 12.2 to 24.4 | 15.3 to 28.5 | |||
| CR | 2 (1.3%) | 0 | |||
| PR | 26 (17.0%) | 33 (21.9%) | |||
| Of 43 patients with baseline brain or leptomeningeal metastases, one patient (i.v. arm) experienced a PR. | |||||
| Time to response (weeks), median (range) | n = 28 | n = 33 | |||
| 6.1 (4.4–17.7) | 6.1 (2.1–13.9) | ||||
| Response duration (weeks), median (range) | n = 28 | n = 33 | |||
| 18.3 (9.0–65.4) | 25.4 (8.4–132.1)h | ||||
| h Includes censored events. | |||||
| Non-responders, n (%)i | |||||
| Stable disease | 27 (17.6) | 35 (23.2) | |||
| Progressive disease | 78 (51.0) | 65 (43.0) | |||
| Not assessable | 20 (13.1) | 18 (11.9) | |||
| i States that 32 patients were not assessable for response due to death, withdrawal or completion of treatment after one or two courses. These patients received insufficient treatment to assign a response, but n = 38 were classed as not assessable (Table 2). | |||||
| HRQoL | No data reported | ||||
|
The HRQoL questionnaire response was 75% and 78% for oral and i.v. groups, respectively, after two courses of therapy. Rates at which patients failed to complete QoL assessment at one or more courses were similar between groups (no data provided). Least squares estimates for mean change from baseline indicated no statistical difference between treatment groups for subscale dimension scores and lung cancer scale, TOI and FACT-L total scores. Only a small decline in HRQoL was noted for each treatment group compared with declines that may be expected in an untreated lung cancer population (i.e. best supportive care). Mean change from baseline to last course also showed no statistical differences between groups (no data provided). |
|||||
| Oral topotecan | Intravenous topotecan | Difference | |||
| Adverse effects, n (%)j | Grade 3 | Grade 4 | Grade 3 | Grade 4 | Not tested |
| Leucopenia | 64 (42.7) | 34 (22.7) | 74 (49.3) | 39 (26.0) | |
| Neutropenia | 39 (26.2) | 70 (47.0) | 35 (23.6) | 95 (64.2) | |
| Thrombocytopenia | 30 (20.0) | 43 (28.7) | 38 (25.3) | 27 (18.0) | |
| Anaemia | 26 (17.3) | 8 (5.3) | 42 (28.0) | 4 (2.7) | |
| Non-haematological adverse effects, n (%) | Grade 3 | Grade 4 | Grade 3 | Grade 4 | Not tested |
| Diarrhoea | 11 (7.2) | 1 (0.7) | 3 (2.0) | 1 (0.7) | |
| Fatigue | 10 (6.5) | 0 | 10 (6.6) | 2 (1.3) | |
| Dyspnoea | 9 (5.9) | 3 (2.0) | 10 (6.6) | 5 (3.3) | |
| Anorexia | 8 (5.2) | 0 | 3 (2.0) | 1 (0.7) | |
| Nausea | 6 (3.9) | 0 | 3 (2.0) | 1 (0.7) | |
| Asthenia | 4 (2.6) | 3 (2.0) | 7 (4.6) | 3 (2.0) | |
| Fever | 3 (2.0) | 3 (2.0) | 4 (2.6) | 6 (4.0) | |
| Received systemic antibiotic (%) | 41 | 56 | |||
| Received i.v. antibiotic (%) | 14 | 23 | |||
| Death, nk | 6 | 4 | |||
| j Occurring with a frequency of ≥ 10% in either treatment group. | |||||
| k Died as a result of haematological toxicity, septic shock related to topotecan treatment or of other causes possibly related to topotecan treatment. | |||||
| GCSF was administered to 25% (oral) vs 16% (i.v.) of patients, although the proportion of treatment courses was similar in both groups (9% vs 7%, respectively). With the protocolspecified dose adjustments, there was no evidence of cumulative toxicity. | |||||
| At time of analysis, 267 patients had died, and 250 of these deaths were due to disease progression. | |||||
| Fever and/or infection (≥ grade 2) associated with grade 4 neutropenia, together with sepsis, occurred in 5% of courses in both groups. | |||||
| Additional comments | |||||
|
Data collected during poststudy monitoring showed that similar proportions of patients in each group had received third-line chemotherapy – 33% in the oral group and 35% in the i.v. group. Median dose intensity was 3.74 mg/m2 (oral) and 2.31 mg/m2 (i.v.), ratio = 1.61, which reflects the difference in oral and i.v. doses (ratio = 1.53). Dose reductions were made for 31% (oral) and 35% (i.v.) of patients primarily at the end of course 1 due to haematological toxicity. In total, 36% (oral) and 19% (i.v.) had a dose escalation. |
|||||
| Note: If reviewer calculates a summary measure or confidence interval PLEASE INDICATE | |||||
| Methodological comments | |||||
|
Allocation to treatment groups: randomised 1:1. No details on randomisation method. Groups were stratified according to duration of response to first-line therapy (progression ≤ 6 months or > 6 months), gender and presence or absence of liver metastases. Blinding: open-label study. An independent central radiologist who was blinded to study treatment verified all responses, although it is not clear whether this was the case for all outcome measures. Comparability of treatment groups: states that demographics and baseline characteristics were well-matched between groups – not supported statistically, but groups do appear comparable (based on those who received at least one course of treatment). Method of data analysis: ITT population included all patients who received treatment (not all randomised patients). Time to event data were summarised using Kaplan–Meier survival methods. A HR for treatment in the presence of covariates (i.e. duration of prior response, sex and liver metastases) using the Cox proportional hazards model was generated for the survival end point. QoL data were evaluated by calculating the total FACT-L score and the 21-item TOI. Scores recorded before each course of treatment were compared with baseline scores. A repeated measures analysis was performed to compare the rate of change between the two treatment groups for each dimension or subscale. Sample size/power calculation: based on the feasibility of patient accrual and study completion rather than on formal statistical criteria. A study population of 150 patients per treatment arm provided 71% power that the 95% CI would exclude more than 10% difference in favour of i.v. treatment. Attrition/dropout: numbers and reasons reported. However, discrepancy between figure 1 and text regarding number of dropouts for oral therapy (30 vs 31, respectively). |
|||||
| General comments | |||||
|
Generalisability: patients with limited or extensive-stage SCLC who had documented CR or PR to first-line therapy with disease recurrence after ≥ 90 days. Likely to be a mixture of patients groups across a variety of countries but no details on ethnicity or demographics were given. Outcome measures: outcomes are appropriate but uncertain of the reliability of some results that do not have 95% CI or have wide ranges; also no p-values or statistical tests were calculated to compare treatment groups for all but two outcomes. Intercentre variability: not reported. Conflict of interests: supported by GlaxoSmithKline, UK. Many authors are either GSK employees or are consultants to GSK. GSK employees were involved in all aspects of the trial, including study design and data analysis. Many trial authors had potential conflicts of interest noted in the report. |
|||||
Quality criteria for assessment of RCTs
| 1. Was the assignment to the treatment groups really random? | Unknown |
| 2. Was the treatment allocation concealed? | Unknown |
| 3. Were the groups similar at baseline in terms of prognostic factors? | Reported |
| 4. Were the eligibility criteria specified? | Adequate |
| 5. Were outcome assessors blinded to the treatment allocation? | Partial |
| 6. Was the care provider blinded? | Unknown |
| 7. Was the patient blinded? | Unknown |
| 8. Were the point estimates and measure of variability presented for the primary outcome measure? | Adequate |
| 9. Did the analyses include an ITT analysis? | Inadequate |
| 10. Were withdrawals and dropouts completely described? | Adequate |
| Reference and design | Intervention | Participants | Outcome measures |
|---|---|---|---|
|
Author: Inoue et al. 63 and Sugawara et al. (abstract)62 Year: 2008 Country: Japan Study design: RCT (phase II) Number of centres: 12 Funding: states two authors provided financial support |
Group A: Intravenous amrubicin Dose: 40 mg/m2/day Duration: 5-min infusion on days 1–3 every 3 weeks Group B: Intravenous topotecan Dose: 1.0 mg/m2/day Duration: 30-minute infusion on days 1–5 every 3 weeks Patients received at least three cycles (amrubicin: median 3, range 1–7; topotecan: median 2, range 1–4) unless obvious disease progression, patient refusal or intolerable toxicity Other interventions used: GCSF permitted as a therapeutic intervention for neutropenia (but not for use as a prophylactic) Subsequent doses of amrubicin and topotecan were reduced to 35 mg/m2/day or 0.8 mg/m2/day, respectively, if toxicities were observed (grade 4 neutropenia for ≥ 4 days, grade 3 febrile neutropenia, grade 4 thrombocytopenia or grade ≥ 3 non-haematological) Subsequent chemotherapy after disease progression not limited; 14 amrubicin patients and 21 topotecan patients received subsequent chemotherapy |
Number of participants: 60 Amrubicin = 29, topotecan = 30 Sample attrition/dropout: One randomised amrubicin patient was not treated due to rapid disease progression; 1 treatment-related death (amrubicin group) Sample crossovers: crossover for third-line (or later) chemotherapy performed in 41% of patients (amrubicin = 5, topotecan = 19) Inclusion criteria: Patients ≥ 20 years, histologically or cytologically confirmed diagnosis of SCLC, previously treated with platinum-based chemotherapy regimen, ECOG PS of ≥ 2, adequate bone marrow function (absolute neutrophil count ≥ 1500/mm3, platelet count ≥ 100,000 ml, Hb ≥ 9 mg/dl, AST and ALT ≤ 100 IU/l, total bilirubin level ≤ 2.0 mg/dL, serum creatinine ≤ 1.5 mg/dl, arterial oxygen pressure ≥ 60 mmHg, ECG findings within normal range, left ventricular ejection fraction ≥ 60%), resistance to or progressive disease after first-line treatment, measurable disease with RECIST criteria, no chemotherapy or chest radiotherapy within 4 weeks prior to enrolment Exclusion criteria: Patients with symptomatic brain metastases, massive pleural or pericardial effusion requiring drainage, severe comorbidities such as uncontrolled diabetes, heart disease, infectious disease, or pulmonary fibrosis, no prior A or T chemotherapy, symptomatic interstitial pneumonitis or pulmonary fibrosis apparent on chest X-ray, history of drug allergy, lactating or pregnant or possibly pregnant women, or those willing to be pregnant Characteristics of participants: Gender (M/F), n (%):Age (years), median (range):Performance status, n (%):Previous treatment:Response type, n (%): |
Primary outcomes: ORR Secondary outcomes: PFS, OS and toxicity profile. Also reports disease control rates but data not extracted here Methods of assessing outcomes: CT scan used to assess ORR according to the Response Evaluation Criteria in Solid Tumours (RECIST) criteria. Toxicity assessed according to National Cancer Institute Common Toxicity Criteria, version 2.0 Length of follow-up: Not stated |
| a One patient received first-line treatment with platinum + etoposide + irinotecan. | |||
| Comments: Refractory relapse defined as no response to first-line chemotherapy or relapse within 90 days after completion of first-line chemotherapy; sensitive relapse defined as relapse at an interval of ≥ 90 days after completion of first-line chemotherapy. | |||
| RESULTS | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Outcomes | Amrubicin (n = 29) | Topotecan (n = 30) | p-value, 95% CI | ||||||
| OS, median (months) | 8.1 | 8.4 | p = 0.17 | ||||||
| OS by relapse type, median (months) | |||||||||
| Sensitive | 9.9 | 11.7 | Not reported | ||||||
| Refractory | 5.3 | 5.4 | Not reported | ||||||
| Comments: The OS of patients who received subsequent chemo (second-line, third-line or later) after the enrolment of this study was presented as survival curves. Additionally, reports that multivariate analysis to examine the effect of age, gender, initial clinical stage, PS, relapse type, and subsequent chemotherapy regimens on OS were presented in an appendix online – data not extracted here. | |||||||||
| Time to progression | Not reported | Not reported | |||||||
| Progression-free survival, median (months) | 3.5 | 2.2 | p = 0.16 | ||||||
| Progression-free survival by relapse type, median (months): | |||||||||
| Sensitive | 3.9 | 3.0 | Not reported | ||||||
| Refractory | 2.6 | 1.5 | Not reported | ||||||
| Overall response, % (n/N), 95% CI | 38 (11/29), 21–58b | 13 (4/30), 1–25c | p = 0.039 | ||||||
| Response, n (%) | |||||||||
| CR | 0 (0) | 0 (0) | Not reported | ||||||
| PR | 11 (38) | 4 (13) | Not reported | ||||||
| Stable disease | 12 (41) | 10 (33) | Not reported | ||||||
| Progressive disease | 6 (21) | 16 (53) | Not reported | ||||||
| Response according to relapse-type,% (n/N) (95% CI): | |||||||||
| Sensitive | 53 (9/17) (28 to 77) | 21 (4/19) (6 to 46) | p = 0.082 | ||||||
| Refractory | 17 (2/12) (2 to 48) | 0 (0/11) (–28) | p = 0.478 | ||||||
| Response according to PS (ECOG), % (n/N) (95% CI): | |||||||||
| 0–1 | 42 (10/24), (22 to 63) | 15 (4/26); (4 to 35) | p = 0.059 | ||||||
| 2 | 20 (1/5); (1 to 72) | 0 (0/4); (–60) | p = 1.000 | ||||||
|
b Different from CIs reported in Sugawara abstract (95% CI 20 to 56). c Different from CIs reported in conference presentation (95% CI 4 to 31). |
|||||||||
| Comment: Reports that better ORRs were observed in amrubicin group regardless of age, gender or prior chemotherapy regimen, but data are not shown. | |||||||||
| Response duration | Not reported | ||||||||
| Others | Not reported | ||||||||
| HRQoL | Not reported | ||||||||
| Haematological toxicity | Amrubicin | Topotecan | |||||||
| Grade (n) | ≥ Grade 3 (%) | Grade (n) | ≥ Grade 3 (%) | ||||||
| 2 | 3 | 4 | 2 | 3 | 4 | ||||
| Neutropenia | 0 | 5 | 23 | 93d | 3 | 13 | 13 | 87 | |
| Thrombocytopenia | 6 | 7 | 1 | 28 | 5 | 9 | 3 | 40 | |
| Anaemia | 15 | 3 | 3 | 21 | 12 | 6 | 3 | 30 | |
| Non-haematological toxicity | |||||||||
| Fatigue | 4 | 5 | 0 | 17 | 3 | 2 | 0 | 7 | |
| Febrile neutropenia | – | 4 | 0 | 14 | – | 1 | 0 | 3 | |
| Infection | 0 | 2 | 1e | 10 | 0 | 1 | 0 | 3 | |
| Anorexia | 4 | 2 | 0 | 7 | 4 | 0 | 0 | 0 | |
| Nausea/vomiting | 1 | 1 | 0 | 3 | 1 | 0 | 0 | 0 | |
| Stomatitis | 1 | 1 | 0 | 3 | 0 | 0 | 0 | 0 | |
| Diarrhoea | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 3 | |
| Fever | 2 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | |
| Constipation | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Pneumonitis | 1 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | |
|
d Total of 97 in Sugawara abstract. e One treatment-related death (grade 5) – patient died of neutropenic sepsis developing from a urinary tract infection. |
|||||||||
| Note: If reviewer calculates a summary measure or confidence interval PLEASE INDICATE | |||||||||
|
Methodological comments Allocation to treatment groups: Randomisation according to stratified factor (PS 0 or 1 vs 2; relapse type, sensitive vs refractory). No other details reported. Blinding: May have been possible due to both treatments being intravenous. Reports that extramural reviewers assessed the eligibility, assessability and response of each patient. No other details reported. Comparability of treatment groups: Groups appear comparable. Paper reports there were no statistically significant differences for demographic characteristics (p-values presented in Sugawara abstract). Patients in topotecan arm were slightly younger than those in amrubicin arm, but not significant (p = 0.195). Method of data analysis: If response rates of subgroups defined in patient characteristics were unusually large or small, additional analyses were performed for these subgroups. The 95% CI was calculated using a binominal distribution. Fisher’s exact test was used to estimate the correlation among different variables between arms. Survival estimation was performed using the Kaplan–Meier method and log-rank test. Stepwise multivariate analysis was used to assess the prognostic significance of several variables. Sample size/power calculation: It is assumed that an ORR of 40% in eligible patients indicates potential usefulness, while an ORR of 15% is the lower limit of interest, with alpha = 0.05 and beta = 0.10, the estimated accrual was 27 patients in each arm. Accrual in both groups was continued if at least three responses were documented in the first 16 assessable patients. Attrition/drop-out: details reported. |
|||||||||
|
General comments Generalisability: Population of previously treated sensitive (relapse ≥ 90 days after completion of first-line therapy) and refractory (no response to first-line chemotherapy or relapse within 90 days after completion of therapy) patients with SCLC. Sensitive relapse, n = 36/59 (61%); refractory relapse, n = 23/59 (39%). Therefore, a proportion were not responders, but this number is unknown. Also, the topotecan dose is lower than that used in the UK (approved dose in Japan is 1.0 mg/m2 compared with 1.5 mg/m2 in UK). Outcome measures: Appropriate. However, median instead of mean reported and no SD provided. Intercentre variability: Not reported. Conflict of interests: Report no conflicts of interest. |
|||||||||
Quality criteria for assessment of RCTs
| 1. Was the assignment to the treatment groups really random? | Unknown |
| 2. Was the treatment allocation concealed? | Unknown |
| 3. Were the groups similar at baseline in terms of prognostic factors? | Reported |
| 4. Were the eligibility criteria specified? | Adequate |
| 5. Were outcome assessors blinded to the treatment allocation? | Unknown |
| 6. Was the care provider blinded? | Unknown |
| 7. Was the patient blinded? | Unknown |
| 8. Were the point estimates and measure of variability presented for the primary outcome measure? | Partial |
| 9. Did the analyses include an ITT analysis? | Inadequate |
| 10. Were withdrawals and dropouts completely described? | Adequate |
| Reference and design | Intervention | Participants | Outcome measures |
|---|---|---|---|
|
Authors: O’Brien et al. 57; Chen et al. (abstract)64, O’Brien et al. (abstract)65 Years: 2006 and 2007 (abstracts) Countries: Europe, Canada, Russia Study design: RCT Number of centres: 40 Funding: sponsored by GlaxoSmithKline (manufacturer) |
Group A: Oral topotecan hydrochloride + BSC Dose: 2.3 mg/m2/day Duration: Days 1–5 every 21 days according to bone marrow recovery. At least four treatment cycles were recommended, depending on tolerability and response. Delays and dose adjustments were prescribed in the protocol if a number of parameters were not met (not reproduced here). Participant withdrawn if delays of more than 2 weeks at minimum dose of 1.5 mg/m2/day Group B: BSC alone Other interventions used: all participants had equal access to supportive care measures (analgesics, antibiotics, corticosteroids, appetite stimulants, antidepressants, RBC transfusions, deep-relaxation therapy, palliative radiotherapy or surgical procedures). All therapies with potential systemic antitumour effect were excluded |
Number of participants: 141: topotecan 71, BSC 70 Sample attrition/dropout: Topotecan 21 (30%), BSC 33 (47%). Reasons for withdrawal were: adverse event [topotecan 13 (18%(; BSC 9 (13%)]; protocol violation [topotecan 0, BSC 7 (10%)]; lost to follow-up [topotecan 2 (3%); BSC 4 (6%)]; other [topotecan 5 (7%, patient choice 4, lack of compliance 1]; BSC 13 (19%, patient choice 6, death 2, progressive disease 2, patient moved 1, patient received terminal care at home 1, patient started second-line therapy 1); ongoing [topotecan 1 (1%); BSC 0] Sample crossovers: None. However, 13 participants in each arm (18.3% BSC, 18.6% topotecan) received poststudy chemotherapy either alone or in combination with other therapy, such as radiotherapy and surgery. In addition, poststudy radiotherapy alone was received by 7 (10%) topotecan participants and 1 (1%) BSC participant Inclusion/exclusion criteria: Only those considered unsuitable for further i.v. chemotherapy were recruited. Unsuitability was based on local policy in patients with resistant (short TFI) SCLC and assessed on an individual basis by the oncologist Initially excluded were those with a TFI of > 90 days for whom treatment with BSC was not acceptable; however, during the trial, some participants with sensitive SCLC who were unsuitable for standard chemotherapy due to comorbidities or who had refused chemotherapy due to the risk of toxicity were eligible Eligibility criteria also included extensive or limited SCLC, one prior chemotherapy regimen, age ≥ 18 years, PS of 0, 1 or 2 (ECOG scale used), haemoglobin ≥ 9.0g/dl, white blood cell count ≥ 3500/mm,3 platelets ≥ 100,000/mm,3 neutrophils ≥ 1500/mm3, calculated creatinine clearance ≥ 60 ml/min, serum bilirubin ≤ 2.0 mg/dl, AST, ALT and alkaline phosphatise ≤ 5 × ULN with liver metastases or ≤ 2 × without, at least 24 hours since last radiotherapy, at least 3 months since last immunotherapy Exclusions – symptomatic CNS metastases, concomitant or previous malignancies within the last 5 years (except SCLC and adequately treated non-melanoma skin cancer, cervical carcinoma in situ, or localised low-grade prostate cancer), infection, severe comorbidities, gastrointestinal conditions or drugs affecting gastrointestinal absorption, prior topotecan therapy, hypersensitivity or other contraindication to the study drugs Characteristics of participants: Gender (M/F), n (%):Age (years), mean (SD) range:Disease stage, n (%):Performance status, n (%):Maximum lesion diameter (cm), n (%):Previous treatment: Any prior treatment, n (%):Response, n (%)Response type, n (%):TFI (TTP since completion of first-line therapy), days, n (%):Median (range): topotecan 84 (34–1996), BSC 90 (14–1409) Liver metastases, n (%) yes/no: topotecan 20/51 (28/72); BSC 14/56 (20/80) |
Primary outcomes: OS (all-cause mortality) Secondary outcomes: Response rate (WHO criteria), TTP, Patient Symptom Assessment (PSA), QOL, safety Methods of assessing outcomes: States independent review of responses was not conducted PSA: Evaluated the degree to which participants experienced nine common and clinically relevant symptoms using a Likert scale for severity [from 1 (not at all) to 4 (very much)] QOL by patient self-report using the EuroQol-5D index and EQ-5D VAS – evaluating five health status dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Rating of 1 (no problem) to 3 (extreme problem). EQ-5D index scored on a scale from 0 (dead) to 1 (perfect health); VAS scored from 0 (worse imaginable) to 100 (best imaginable) health state Patient self-reported lung symptoms assessed using PSALC instrument (but data not extracted here) Length of follow-up: Every 2 months for the full duration of survival. Median time on study 7.8 weeks in the BSC group and 12.3 weeks in the topotecan group |
| RESULTS | |||
|---|---|---|---|
| Outcomes | Topotecan (n = 71) | BSC (n = 70) | p-value, 95% CI |
| OS | |||
| Unadjusted HR for OS was 0.64 (95% CI 0.45 to 0.90) for topotecan relative to BSC. Adjusted HR 0.61 (95% CI 0.43 to 0.87). OS was significantly longer in the topotecan group (log-rank p = 0.01). | |||
| Median survival time, weeks | 25.9 (95% CI 18.3 to 31.6) | 13.9 (95% CI 11.1 to 18.6) | Not tested |
| 6-month survival rate | 49% | 26% | Not tested |
| Subgroup analyses of survival according to stratification factors (HR and 95% CI estimated from figure to one decimal place only as scale on figure is inconsistent, so for illustration only) | |||
|
Gender, male Female |
HR 0.8 (95% CI 0.5 to 1.2) HR 0.4 (95% CI 0.2 to 0.7) |
||
| Performances status: | |||
| PS 0/1 | HR 0.7 (95% CI 0.5 to 1.1) | ||
| PS 2/3/4 | HR 0.5 (95% CI 0.3 to 0.9) | ||
| For those with a PS 2 | Median survival topotecan 20.9 (95% CI 13.4 to 26.9) weeks, BSC 7.7 (95% CI 5.3 to 13.3) weeks | ||
| TTP ≤ 60 days | HR 0.5 (95% CI 0.3 to 0.9), median survival topotecan 23.3 (95% CI 10.7 to 30.9) weeks, BSC 13.2 (95% CI 7.0 to 21.0) weeks | ||
| TTP > 60 days | HR 0.7 (95% CI 0.5, 1.1) | ||
| Presence of liver metastases | HR 0.7 (95% CI 0.3, 1.3) | ||
| No liver metastases | HR 0.6 (95% CI 0.4, 0.9) | ||
| Comment: Paper states that HRs and 95% CIs for all subgroups indicate a survival trend favouring topotecan; however, the 95% CI cross 1.0 for TTP > 60 days, male, PS 0/1 and liver metastases. | |||
| Progression | 59 (83%) | ||
| TTP, median weeks | 16.3 (95% CI 12.9 to 20.0) | ||
| Response rate (all PRs) | 5 (7%) (95% CI 2.33 to 15.67) | Not applicable | |
| Comment: Response not assessed in 11 (16%) participants. | |||
| Achieved stable disease | 31 (44%) | ||
| Progressive disease | 24 (34%) | ||
| Comment: Response according to the stratification factors presented but not extracted as for topotecan group alone. | |||
| EQ-5D, rate of deterioration per 3-month interval | –0.05 (95% CI –0.11 to 0.02) | –0.20 (95% CI –0.27 to –0.12) | Difference + 0.15 (95% CI 0.05 to 0.25) |
| Comments: Baseline EQ-5D questionnaires were completed by 68 (96%) participants in the topotecan group and 65 (93%) participants in the BSC group. At least one postbaseline questionnaire was completed by 63 (89%) participants in the topotecan group and 49 (70%) participants in the BSC group. | |||
| EQ-5D index (pooled analysis a ), mean | n = 239 | n = 167 | Difference 0.09, p = 0.0036 |
| Baseline | 0.72 | 0.68 | |
| Treatment | 0.69 | 0.56 | |
| Change from baseline | –0.03 | –0.12 | |
| EQ-5D index (change b ), mean | n = 61 | n = 51 | Difference 0.2, p = 0.0034 |
| Baseline | 0.70 | 0.65 | |
| Treatment | 0.61 | 0.34 | |
| Change from baseline | –0.10 | –0.30 | |
| EQ-5D VAS (pooled analysis a ), mean | n = 238 | n = 162 | Difference 7.71, p < 0.0001 |
| Baseline | 66.46 | 67.22 | |
| Treatment | 66.76 | 59.80 | |
| Change from baseline | 0.30 | –7.41 | |
| EQ-5D VAS (change b ), mean | n = 60 | n = 48 | Difference 10.48, p = 0.0025 |
| Baseline | 65.75 | 64.29 | |
| Treatment | 61.77 | 49.83 | |
| Change from baseline | –3.98 | –14.46 | |
|
PSALC, Patient Symptom Assessment in Lung Cancer. a Change from baseline to averaged on-treatment assessments. b Change from baseline to last evaluation analysis. O’Brien (2007) abstract presents a subgroup analysis of the association between baseline PSALC total scores and ECOG PS according to PR or stable disease (topotecan arm only), but data not extracted. |
|||
| PSA scores | Odds ratio | 95% CI | p-value |
|
Shortness of breath Cough Chest pain Coughing blood Loss of appetite Interference sleep Hoarseness Fatigue Interference daily activity |
2.18 1.35 2.07 1.95 1.02 2.16 1.35 2.29 1.70 |
1.09 to 4.38 0.68 to 2.66 1.00 to 4.28 0.46 to 8.27 0.57 to 1.84 1.15 to 4.06 0.63 to 2.87 1.25 to 4.19 0.95 to 3.03 |
p < 0.05 NS NS NS NS p < 0.05 NS p < 0.05 NS |
| Comments: Baseline questionnaires were completed by 70 participants in the topotecan group and 67 participants in the BSC group. The numbers of participants with sufficient data to be included in the analyses varied for the symptom scores between 47 and 48 for the BSC group, and between 60 and 61 for the topotecan group. OR > 1 indicates greater likelihood of symptom improvement on topotecan. | |||
| Adverse effects | Topotecan (n = 71) | BSC (n = 70) | p-value, 95% CI |
| Toxicity: grade 3/4 neutropenia | 61% | ||
| Toxicity: grade 3/4 thrombocytopenia | 38% | ||
| Toxicity: grade 3/4 anaemia | 25% | ||
| Febrile neutropenia | 3% | ||
| Non-sepsis infection ≥ grade 2 | 10 (14%) | 8 (12%) | |
| Sepsis | 3 (4%) | 1 (1%) | |
| Diarrhoea | 6% | 0 | |
| Fatigue | 4% | 4% | |
| Vomiting | 3% | 0 | |
| Dyspnoea | 3% | 9% | |
| Cough | 0 | 2% | |
| Toxic deaths | 4 (6%), 3 due to haematological toxicity | ||
| All-cause mortality within 30 days of randomisation | 5 (7%) | 9 (13%) | |
| Comment: Two participants (3%) in the topotecan arm received GSCF or granulocyte–macrophage colony-stimulating factor and two (3%) received erythropoietin. | |||
| Note: If reviewer calculates a summary measure or confidence interval PLEASE INDICATE | |||
|
Methodological comment Allocation to treatment groups: Participants randomly assigned 1 : 1 using a centralised automated registration and randomisation system, stratified by gender, performance status, TFI and presence of liver metastases. Blinding: Blinding of outcome assessors not reported. Blinding of participants or care providers unlikely to be appropriate with these interventions. However, no discussion of why placebo-controlled double-blind study not performed. Comparability of treatment groups: Paper states participant demographics were well matched between arms, particularly with respect to the major prognostic variables of PS and sex. However, p-values not reported. Method of data analysis: States efficacy assessments based on all randomly assigned participants using an ITT population. Safety and QOL were based on all who received at least one postrandom assignment evaluation on the BSC arm or one dose of topotecan (70 participants in topotecan arm, 67 in BSC arm evaluated). OS was analysed using the Kaplan–Meier method and compared using log-rank test. Analysis of secondary outcomes were descriptive with no adjustments made for multiplicity. Response rates were summarised along with a 95% CI and TTP was summarised by Kaplan–Meier. All p-values were two-sided. For PSA a generalised estimating equations model was fitted to longitudinal symptom data to estimate treatment effect on each symptom (response was categorised as favourable or unfavourable). Change from baseline in EQ-5D index and EQ-5D VAS assessed using a pooled analysis (change from baseline to averaged on-treatment assessments) and also considering only change from baseline to last evaluation. The rate of change in EQ-5D index score (rate at which symptoms improved or deteriorated) across treatment groups was evaluated with a longitudinal analysis using a mixed model (to account for repeated measurements over the treatment course) with change from baseline in score as response. Sample size/power calculation: Designed to detect a 66.7% difference in median survival. The expected survival in the BSC arm was 12 weeks, the estimated median survival in the topotecan arm was 20 weeks. Initial sample size calculations determined that 220 participants were required to assess a survival benefit with topotecan with 90% power and a significance level of 0.05. However, recruitment was slower than anticipated, and a formal protocol amendment was implemented to terminate the study once 125 deaths had been reported. This provided an 80% power to assess a survival benefit for topotecan at a 0.05 significance level. This point was reached when 141 participants had been recruited. Attrition/drop-out: Numbers and reasons provided (above). Other comments: Overall, 69 (99%) topotecan participants took ≥ 90% of their prescribed capsules. A median of four courses (range 1–10) of topotecan were administered. Dose reductions occurred in 16 courses (8%) primarily for haematological toxicity (13 courses, 6%). Dose delays occurred in 41 courses (20%), most commonly for haematological toxicity (25 courses, 12%). Dose escalation occurred in 39 courses (14%). The median topotecan dose intensity achieved was 3.77 mg/m2/week, representing 98% of the scheduled dose. BSC participants were observed for the equivalent of a median of three courses (range 1–13). Palliative medications and radiotherapy were used more frequently in the BSC group, while transfusions were used more frequently in the topotecan group (data not extracted as not statistically analysed). General comments Generalisability: Only patients with resistant disease (relapse within 90 days) included initially, but this was widened to include those with sensitive disease (greater than 90 days’ response). Outcome measures: Unclear how valid and reliable Intercentre variability: Not reported whether potential intercentre variability was an issue or how this was handled. Conflict of interests: Supported by GlaxoSmithKline UK, trial designed by GSK, data analysed by GSK. Many trial authors had potential conflicts of interest noted in the report. |
|||
Quality criteria for assessment of RCTs
| 1. Was the assignment to the treatment groups really random? | Adequate |
| 2. Was the treatment allocation concealed? | Adequate |
| 3. Were the groups similar at baseline in terms of prognostic factors? | Reported |
| 4. Were the eligibility criteria specified? | Adequate |
| 5. Were outcome assessors blinded to the treatment allocation? | Inadequate |
| 6. Was the care provider blinded? | Unknown |
| 7. Was the patient blinded? | Unknown |
| 8. Were the point estimates and measure of variability presented for the primary outcome measure? | Adequate |
| 9. Did the analyses include an ITT analysis? | Adequate |
| 10. Were withdrawals and dropouts completely described? | Adequate |
| Reference and design | Intervention | Participants | Outcome measures |
|---|---|---|---|
|
Author: von Pawel et al. 58 Year: 2001 Countries: Europe, South Africa, Australia Study design: RCT (phase II) Number of centres: 31 Funding: SmithKline Beecham |
Group A: oral topotecan Dose: 2.3 mg/m2/day for 5 days every 21 days Duration: depended on response but those with stable disease recommended to have at least four cycles Group B: intravenous topotecan Dose: 1.5 mg/m2/day, 30-minute infusion for 5 days every 21 days Duration: depended on response but those with stable disease recommended to have at least four cycles Other interventions used: Dose escalation permitted if no toxicity greater than grade 2, assessed by National Cancer Institute of Canada Common Toxicity Criteria, was seen in the preceding course. For those in the oral group, daily dose increased by 0.4 mg/m2/day (up to a maximum dose of 3.1 mg/m2/day). For those in the i.v. group, daily dose increased by 0.25 mg/m2/day (up to a maximum dose of 2.0 mg/m2/day). For oral topotecan, dose escalation was made in 17.2% of courses, for i.v. topotecan dose escalation occurred in 6.3% of courses GCSF for therapeutic intervention, not mandatory for prophylaxis against neutropenia for haematological toxicity. Severe or prolonged neutropenia managed through dose reduction during next course. Reduction in oral group by 0.4 mg/m2/day, in i.v. group by 0.25 mg/m2/day. If grade 3/4 toxicity (excluding nausea or vomiting) dose reduced as above, if disease did not respond then patient withdrawn For oral topotecan, dose reduction was made in 6.7% of courses, for i.v. topotecan dose reduction occurred in 16.4% of courses. Haematological toxicity lead to dose delays of ≥ 7 days in only 2.5% of courses with either regimen Treatment also delayed if bone marrow had not recovered and was a clinically significant non-haematological toxicity to study drug |
Number of participants: 106 (oral 52, i.v. 54) Sample attrition/dropout: not reported Sample crossovers: none Inclusion/exclusion criteria: Patients of either sex, aged ≥ 18 years, with limited or extensive SCLC that had recurred ≥ 3 months after the end of first-line therapy, provided only one prior chemotherapy regimen. All had PR or CR. Measurable disease of at least 2 cm in diameter, WHO performance status of no more than 2, life expectancy of at least 2 months, adequate bone marrow function (WBC count ≥ 3.5 × 109/l, neutrophils ≥ 1.5 × 109/l, platelets ≥ 100 × 109/l, haemoglobin ≥ 9 g/dl) and adequate renal and hepatic function (serum creatinine ≤ 1.5 mg/dl; bilirubin ≤ 2.0 mg/dl; alkaline phosphatase, AST and ALT ≤ 2 × the ULN, or ≤ 5 × the ULN if liver metastases were present). At least 4 weeks since previous surgery and at least 24 hours since last radiotherapy. Those with brain or leptomeningeal disease, diagnosed by CT or MRI, could be included provided there were no signs or symptoms on neurological examination that could be attributed to metastases and that the patient was not receiving corticosteroid therapy to control symptoms Excluded: those with previous or current malignancies at other sites, except adequately treated carcinoma of the cervix, or basal or squamous cell carcinoma of the skin. Other severe uncontrolled medical problems Characteristics of participants: Gender (M/F), n (%):Age (years), mean (range):Disease stage, n (%)a:Performance status, n (%):Maximum lesion diameter (cm), n (%):Previous treatment:TTP after end of first-line chemotherapy, n (%) months:Liver metastases, n (%):Previous radiotherapy (%): oral 71.2%, i.v. 72.2% |
Primary outcomes: response, response duration, TTP Secondary outcomes: time to response, survival, symptoms, toxicity Methods of assessing outcomes: Response evaluated according to WHO criteria. CR by disappearance of measurable lesions lasting at least 4 weeks with no appearance of new lesions. PR by a decrease of more than 50% in measurable lesions lasting at least 4 weeks with no appearance of new lesions. Time to response measured from first dose of topotecan to first documented response. Duration of response from time when the response was first documented to disease progression. TTP and survival were measured from first administration of topotecan to progression or death, respectively Symptoms were evaluated on a 4-point symptoms of disease scale (1 = not at all, 2 = a little bit, 3 = quite a bit, 4 = very much). Not a validated scale although based on the LCSS. A symptom improvement needed to be sustained until the next cycle to be reported as a response All radiological responses confirmed by an independent review by a consultant radiologist. The reviewer was blinded as to whether participants received oral or i.v. topotecan Length of follow-up: unclear, although progression was assessed up to 54 weeks and survival up to 64 weeks |
| RESULTS | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Outcomes | Oral topotecan (n = 52) | Intravenous topotecan (n = 54) | p-value, 95% CI | |||||||
| OS, median | 32 weeks | 25 weeks | RR = 0.84 (95% CI 0.53 to 1.32) | |||||||
| 32.3 weeks (0.4 to 69.1)c | 25.1 (0.6 to 65.1)c | |||||||||
| c Report in table which includes censored events. | ||||||||||
|
Comments: States that accounting simultaneously for all prognostic factors the RR of survival was 0.90 (95% CI 0.55 to 1.47). States that two factors (no liver metastases and lower PS) were statistically associated with longer survival (p = 0.001 and p = 0.025, respectively) but no data reported, nor any data for other factors tested. |
||||||||||
| Response rate, n(%) | Difference (ORR) 8.3% (95% CI –6.6% to 23.1%) | |||||||||
| Overall response | 12 (23.1) 95% CI 11.6 to 34.5 | 8 (14.8) 95% CI 5.3 to 24.3 | ||||||||
| CR | 1 (1.9) | 2 (3.7) | ||||||||
| PR | 11 (21.2) | 6 (11.1) | ||||||||
| Non-responders, n (%): | ||||||||||
| Stable disease | 10 (19.2) | 16 (29.6) | Not reported | |||||||
| Progressive disease | 16 (30.8) | 23 (42.6) | Not reported | |||||||
| Not assessable | 14 (26.9) | 7 (13.0) | Not reported | |||||||
| Comments: States true underlying response rate with oral topotecan is at worst 6.6% lower than that of the i.v. topotecan, which is not a clinically meaningful difference. States that two factors (female gender and no previous radiotherapy) were statistically associated with increased probability of response (p = 0.021 and p = 0.015, respectively) but no data reported, nor any data for other factors tested. Accounting simultaneously for all prognostic factors identified in the logistic regression analysis (data not reported), oral topotecan participants 1.6 times more likely to respond than i.v. participants (95% CI for the odds ratio: 0.50 to 5.15). | ||||||||||
| Response duration, median | n = 12 | n = 8 | Not reported | |||||||
| 18 weeks | 14 weeks | |||||||||
| TTP, median (range) | n = 52 | n = 54 | RR = 0.90 (95% CI 0.59 to 1.39) | |||||||
| 15 (0.4–69.1) weeks | 13 (0.6–65.1)d weeks | |||||||||
| d Includes censored events. | ||||||||||
| Comments: Regression modelling of TTP identified female gender (p = 0.041), no liver metastases at baseline (p = 0.020) and lower PS (p = 0.036) as associated with longer TTP. No data were reported for these or any other factors tested in the model. Accounting for all prognostic factors simultaneously the RR of progression was 0.98 (95% CI 0.63 to 1.54). | ||||||||||
| Symptom reduction (in those with symptoms at baseline) | n/N (%) | n/N (%) | Not reported | |||||||
| Chest pain | 8/19 (42.1) | 7/22 (31.8) | ||||||||
| Shortness of breath | 4/29 (13.8) | 9/33 (27.3) | ||||||||
| Cough | 5/31 (16.1) | 8/36 (22.2) | ||||||||
| Haemoptysis | 1/3 (33.3) | 4/10 (40.0) | ||||||||
| Anorexia | 5/27 (18.5) | 9/29 (31.0) | ||||||||
| Insomnia | 8/25 (32.0) | 8/27 (26.6) | ||||||||
| Hoarseness | 5/14 (35.7) | 9/24 (37.5) | ||||||||
| Fatigue | 7/33 (21.2) | 6/36 (16.7) | ||||||||
| Interference daily activity | 8/31 (25.8) | 8/36 (22.2) | ||||||||
| Comments: n = number with improvement, N = number with symptom at baseline. Therefore only a subgroup. Improvement represents improvement for two consecutive assessments after baseline. | ||||||||||
| Adverse effects | % participants oral | % participants i.v. | Difference grade 4 oral – i.v. | |||||||
| Grade 3 | Grade 4e | Grade 3 | Grade 4 | |||||||
| Neutropenia | 21.6 | 35.3 | 26.9 | 67.3 |
Grade 4 neutropenia p = 0.001. no reports of testing others for statistical significance |
|||||
| Leucopenia | 27.5 | 17.6 | 45.3 | 28.3 | ||||||
| Thrombocytopenia | 25.5 | 27.5 | 24.5 | 24.5 | ||||||
| Anaemia | 27.5 | 3.9 | 26.4 | 3.8 | ||||||
| e Two participants (1.9%) in the oral topotecan group died of sepsis and febrile agranulocytosis. | ||||||||||
|
Comments: 52 participants in the oral group received a total of 215 courses of treatment, the 54 i.v. participants received a total of 213 courses of treatment. In both groups a median of four courses per participant were received (range 1–12). The major reason for early discontinuation of treatment was occurrence of adverse experiences. Median duration of grade 4 neutropenia was similar (oral group 7 days, i.v. group 6 days). Data on toxicity by number of courses of the respective therapies not data extracted. GCSF was administered as a treatment of neutropenia for 3 (5.8%) participants in the oral group and 4 (7.4%) participants in the i.v. group. At time of analysis, 85 participants had died, 73 due to progressive disease. |
||||||||||
| Adverse effects occurring in ≥ 5% participants, n(%) | Oral | Intravenous | ||||||||
| Grade 3 | Grade 4 | Grade 5 | Grade 3 | Grade 4 | Grade 5 | |||||
| Vomiting | 6 (11.5) | 0 | 0 | 2 (3.7) | 0 | 0 | Not reported | |||
| Dyspnoea | 5 (9.6) | 0 | 0 | 5 (9.3) | 0 | 1 (1.9) | ||||
| Fever | 2 (3.8) | 1 (1.9) | 1 (1.9) | 1 (1.9) | 0 | 0 | ||||
| Pneumonia | 3 (5.8) | 1 (1.9) | 0 | 0 | 0 | 1 (1.9) | ||||
| Diarrhoea | 4 (7.7) | 0 | 0 | 0 | 0 | 0 | ||||
| Pulmonary embolism | 1 (1.9) | 0 | 2 (3.8) | 0 | 0 | 1 (1.9) | ||||
| Asthenia | 3 (5.8) | 0 | 0 | 5 (9.3) | 0 | 0 | ||||
| Fatigue | 3 (5.8) | 0 | 0 | 1 (1.9) | 0 | 0 | ||||
| Alopecia | 1 (1.9) | 0 | 0 | 7 (13.0) | 0 | 0 | ||||
| Abscess | 0 | 0 | 0 | 2 (3.7) | 1 (1.9) | 0 | ||||
| Note: If reviewer calculates a summary measure or confidence interval PLEASE INDICATE | ||||||||||
|
Methodological comments Allocation to treatment groups: States randomised but no further details. Enrolment was stratified by the extent of disease (limited, extensive), duration of response to chemotherapy after cessation (3–6 months, ≥ 6 months) and liver metastases (presence or not). Blinding: Reports that reviewer blinded to participant group, unclear if this relates just to the radiological outcomes or all outcomes. Comparability of treatment groups: States demographic imbalance between the two groups was generally negligible and was accounted for in the multivariate comparisons of treatment regimens. Baseline characteristics relating to extent of disease appear imbalanced on some factors (PS, lesion diameter). Method of data analysis: Objective radiological response rates were calculated along with 95% CI. Cox proportional hazard regression was used for time to event variables, logistic regression and Cox proportional hazards models for subgroup analyses (duration ≤ 6 months, > 6 months, gender, renal impairment, PS 0 or 1 vs 2 or 3, liver metastases, extent of disease, previous radiotherapy, maximum tumour diameter ≤ 5 cm vs > 5 cm) on response and time to event variables, respectively (data not reported). States all those entering the study were included in the ITT analysis. Sample size/power calculation: Study was designed to give an indication as to the number of participants required in a phase III study of a similar design. To indicate both risk and benefit a study of 100 participants was considered the most appropriate, but no official sample size calculation was provided. Attrition/drop-out: No flow chart provided, no discussion of numbers or reasons for attrition. General comments Generalisability: Population of relapsed SCLC, minimal demographic detail reported. Outcome measures: Appropriate, although symptom score not validated. Intercentre variability: Not reported. Conflict of interests: Sponsored by a grant from SmithKline Beecham pharmaceuticals. Three authors are employees of SKB. |
||||||||||
Quality criteria for assessment of RCTs
| 1. Was the assignment to the treatment groups really random? | Inadequate |
| 2. Was the treatment allocation concealed? | Unknown |
| 3. Were the groups similar at baseline in terms of prognostic factors? | Reported |
| 4. Were the eligibility criteria specified? | Adequate |
| 5. Were outcome assessors blinded to the treatment allocation? | Partial |
| 6. Was the care provider blinded? | Unknown |
| 7. Was the patient blinded? | Unknown |
| 8. Were the point estimates and measure of variability presented for the primary outcome measure? | Adequate |
| 9. Did the analyses include an ITT analysis? | Adequate |
| 10. Were withdrawals and dropouts completely described? | Inadequate |
| Reference and Design | Intervention | Participants | Outcome measures |
|---|---|---|---|
|
Authors: von Pawel et al. 59 and Schiller et al. (abstract)61 Years: 1999 and 1998 (abstract) Countries: Germany, Canada, France, UK, USA Study design: RCT Number of centres: unknown Funding: SmithKline Beecham |
Group A: topotecan Dose: 1.5 mg/m2/day as 30-minute infusion. Duration: five consecutive days every 21 days Group B: cyclophosphamide (C), doxorubicin (D) and vincristine (V) (CAV) Dose: C 1000 mg/m2 (maximum 2000 mg) + D 45 mg/m2 (maximum 100 mg) + V 2-mg infusion Duration: day 1 of each 21-day course Full dose if on treatment day neutrophil count ≥ 1.0 × 109/l, platelet count ≥ 100 x 109/l + Hb count ≥ 9.0 g/dL. Topotecan could be escalated to maximum dose 2.0 mg/m2 in absence of grade ≥ 2 toxicity Patients whose best response was stable disease after four courses could be removed from study or continue at investigator’s discretion; patients whose disease progressed were removed from study Patients in both groups were withdrawn if delay > 2 weeks caused by persistent toxicity at min. doses; patients with CR PR to therapy continued treatment until disease progression or unacceptable toxicity occurred, or for at least six courses past the maximal response Topotecan reduced by 0.25 mg/m2/day and C/D reduced by 25% for: grade 4 neutropenia complicated by fever or infection or lasting ≥ 7 days, grade 3 neutropenia lasting > 21 days of treatment cycle or grade 4 thrombocytopenia. Same dose reduction for grade 3 or 4 non-haematological toxicity (excluding grade 3 nausea) or patient could be withdrawn from study. Minimum dose of topotecan was 1.0 mg/m2/day D discontinued or patient withdrawn from study once lifetime maximum-tolerated dose of D (450 mg/m2) or comparable dose of epirubicin (900 mg/m2) reached or signs of cardiomyopathy evident. D + V dose reductions were required for bilirubin or serum transaminase elevations. V dose reduction of 25% required for grade 2 neurological toxicity: V eliminated for grade 3–4 neurological toxicity until toxicity resolved |
Number of participants: 211 Topotecan: n = 107, CAV n = 104 Sample attrition/dropout: Total number of dropouts not reported and unclear from text (p. 664 reports 20 withdrawal, p. 661 reports 16) In total there were 20 withdrawals due to treatment-related toxicity: 10 topotecan (9.3%) and 10 CAV (9.6%); 16 patients (7 topotecan and 9 CAV) were withdrawn from study, either at patient’s or investigator’s request, because of treatment-related toxicity (haematological toxicity and associated sequelae). Non-haematological reasons: one topotecan patient had tumour lysis syndrome and requested withdrawal and two CAV patients withdrew due to a decline in cardiac status Study also reports that one topotecan and two CAV patients were removed for lack of clinical benefit, but did not have radiological evidence of disease progression Sample crossovers: N/A Inclusion criteria: Documented progressive, limited or extensive SCLC with date of progression at least 60 days after completion of first-line chemotherapy; at least one lesion, bidimensionally measurable by CT, MRI, ultrasound, radiograph, photograph or physical examination; minimum of 4 weeks between prior surgery or immunotherapy and study entry; minimum of 24 hours between radiotherapy and initiation of study drugs; ECOG performance status (PS) ≤ 2, Hb ≥ 9.0 g/dl, WBC count ≥ 3.5 × 109/l, neutrophils ≥ 1.5 × 109/l, platelets ≥ 100 × 109/l, bilirubin ≤ 2.0 mg/dl, transaminase and alkaline phosphatase values ≤ 2 × ULN (or if liver metastases present ≤ 3 ULN), creatine ≤ 1.5 mg/dl or creatine clearance ≥ 60 ml/min |
Primary outcomes: RR and duration of response Secondary outcomes: TTP, time to response, survival and improvement of disease-related symptoms Methods of assessing outcomes: Responses were determined according to WHO criteria. Standard response criteria were used, duration of response measured from time of initial documented response to first sign of disease progression TTP was measured from time of first study drug to documented progressive disease (or initiation of subsequent chemotherapy) Time to response and survival measured from time of first study drug to initial response and death, respectively Symptom scores evaluated for dyspnoea, cough, chest pain, haemoptysis, anorexia, insomnia, hoarseness, fatigue and interference with daily activity; improvement had to be sustained for two consecutive courses. Symptom evaluation included time to symptom worsening as defined by interval from first dose of medication until first evidence of worsening in postbaseline assessment Non-validated, symptom specific ‘symptoms of disease’ SCLC questionnaire used at screening and before each course of treatment, scored on 4-point scale (1 = not at all, 2 = a little bit, 3 = quite a bit, 4 = very much) |
|
Minimum dose C, D + V set by administering physician Other interventions used: GCSF at discretion of investigator |
Exclusion criteria: Symptomatic brain metastases requiring corticosteroids or pre-existing cardiac disease (including clinical congestive heart failure, arrhythmias requiring treatment or a myocardial infraction within preceding 3 months); contraindicated CAV (including history of demyelinating polyneuropathy or poliomyelitis); lifetime cumulative dose of doxorubicin > 270 mg/m2 or cumulative dose of epirubicin > 540 mg/m2; prior topotecan therapy or > 1 previous chemotherapy regimen Characteristics of participants: Age: Not reportedDisease stage, n (%):Performance status, n (%):Maximum lesion diameter (cm), n (%):Missing: topotecan 2 (1.9), CAV 3 (2.9) Previous treatment, n (%): Radiotherapy: topotecan 66 (61.7), CAV 58 (55.8) Immunotherapy: topotecan 0, CAV 2 (1.9) Surgery: topotecan 15 (14), CAV 29 (27.9) Brain irradiation:Platinum (cis or carbo)/etoposide:Both platinum/etoposide + CAV:Cyclo/doxo/etoposide: topotecan 20 (18.7), CAV 16 (15.4) Vincristine/platinum (cis or carbo)/etoposide: topotecan 4 (3.7), CAV 6 (5.8) Other regimes: topotecan 14 (13.1), CAV 18 (17.3) Response, n (%):Response type, n (%):Duration of response to first-line chemotherapy, median (range) weeks:Liver metastases, n (%):Brain metastases, n (%): |
Safety assessment: Minimum weekly complete blood cell counts, blood chemistries on day 15 of each course and urinalysis each cycle. Electrocardiogram and multiple-gated acquisition or echocardiogram performed prior and at end of treatment. Quantitative haematological non-haematological toxicities were assessed prior to each cycle according to National Cancer Institute Common Toxicity Criteria Length of follow-up: minimum of four courses for patients with stable disease, ≥ 6 courses for patients with CR or PR |
| RESULTS | |||||||
|---|---|---|---|---|---|---|---|
| Outcomes | Topotecan (n = 107) | CAV (n = 104) | p-value, 95% CI | ||||
| OS, median weeks, (range) | 25 (0.4–90.7a) | 24.7 (1.3–101.3) | p = 0.795 | ||||
| 6 months’ survival, % | 46.7 | 45.2 | |||||
| 12 months’ survival, % | 14.2 | 14.4 | |||||
| a Censored event. | |||||||
| Comments: At analysis, 11.2% topotecan and 12.5% CAV patients were censored for survival. RR of topotecan/CAV 1.039. Baseline PS and extent of disease statistically significant prognostic factor for survival (p < 0.001). In addition to stratification factors (extent of disease + PS at baseline), gender, baseline liver metastases and baseline brain metastases were statistically significant factors for survival (p < 0.05); after adjustment for covariates, the effect of treatment was not statistically significant (RR 1.17; p = 0.322). | |||||||
| TTP, median weeks (range) | 13.3 (0.4–55.1) | 12.3 (0.1–75.3b) | p = 0.552 | ||||
| b Estimate corresponds to a censored event. | |||||||
| Progression-free survival | Not reported | ||||||
| ORR, n (%) | 26 (24.3) (95% CI 16.2 to 32.4) | 19 (18.3) (95% CI 10.8 to 25.7) | p = 0.285, (difference = 6.0%, 95% CI 6 to 18) | ||||
| CR | 0 | 1 (1) | |||||
| PR | 26 (24.3) | 18 (17.3) | |||||
| Non-responders, overall | 81 (75.7) | 85 (81.7) | |||||
| Stable disease | 21 (19.6) | 12 (11.5) | |||||
| Progressive disease | 49 (45.8) | 55 (52.9) | |||||
| Not assessable | 11 (10.3) | 18 (17.3) | |||||
| Response rate F/M (%) | 30.4 : 19.7 | 30.3 : 12.7 | |||||
| Response rate for relapse patients (60–90 days after first-line treatment) n (%) | 3/22 (13.6) | 1/21 (4.8) | |||||
| Response duration, median weeks (n, range) | 14.4 (n = 26, 9.4–50.1) | 15.3 (n = 19, 8.6–69.9)c | p = 0.300 | ||||
| c Censored event. | |||||||
| Comments: The 95% CI for the difference in the rates of response (6%) was 6 to 18. Three topotecan and five CAV patients were reported as responders, but the responses were not confirmed after independent radiological review. Of the 11 topotecan and 18 CAV patients with an overall response of ‘not assessable’ and classified as non-responders, two topotecan and three CAV patients were ineligible and five patients were not evaluated for response (one topotecan patient relocated to nursing home, two CAV patients were lost to follow-up, one CAV patient died suddenly as a result of an unrelated cause and one CAV patient without lesion assessment after course 2). Response rate for first-line regimen (including cyclophosphamide and an anthracycline) topotecan 26.8% (n = 41) and CAV 20% (n = 45). A logistic regression model (evaluating the effect of baseline characteristics) identified presence of baseline liver metastases and gender as the only significant factors of response (p = 0.043 and p = 0.008, respectively); after adjusting for the covariates, topotecan patients showed a greater propensity to respond than CAV patients, although the result was not statistically significant (OR 1.24, p = 0.557). Paper also reports response rates due to first-line chemotherapy regimen, but data not extracted here. | |||||||
| Time to response, median weeks (n, range) | 6 (n = 26, 2.4–15.7) | 6.1 (n = 19, 5.4–18.1) | p = 0.953 | ||||
| Improvement in disease-related symptoms, n/Nd (%): | Pearson χ2 | ||||||
| Dyspnoea | 19/68 (27.9) | 4/61 (6.6) | 0.002e | ||||
| Cough | 17/69 (24.6) | 9/61 (14.8) | 0.160 | ||||
| Chest pain | 11/44 (25.0) | 7/41 (17.1) | 0.371 | ||||
| Haemoptysis | 4/15 (26.7) | 4/12 (33.3) | 0.706 | ||||
| Anorexia | 18/56 (32.1) | 9/57 (15.8) | 0.042e | ||||
| Insomnia | 19/57 (33.3) | 10/53 (18.9) | 0.085 | ||||
| Hoarseness | 13/40 (32.5) | 5/38 (13.2) | 0.043e | ||||
| Fatigue | 16/70 (22.9) | 6/65 (9.2) | 0.032e | ||||
| Interference with daily activity | 18/67 (26.9) | 7/63 (11.1) | 0.023e | ||||
| Comments: Significant differences in length of time to worsening of dyspnoea (p = 0.046) and anorexia (p = 0.003), with symptoms progressing more slowly in the topotecan group. Verbatim terms used in questionnaire: ‘shortness of breath’ (dyspnoea), ‘coughing up blood’ (haemoptysis) ‘loss of appetite (anorexia), and ‘interference with sleep’ (insomnia). | |||||||
|
d Number of patients with baseline and at least one postbaseline assessment. Improvement defined as two consecutive improvements over the baseline assessment. e p < 0.05. |
|||||||
| Adverse effects, n/Nf (%): haematological toxicities | Topotecan | CAV | |||||
| Patients (n = 107) | Courses (n = 446) | Patients (n = 104) | Courses (n = 359) | ||||
| Leucopenia grade 3 | 57/104 (54.8) | 196/441 (44.4) | 38/101 (37.6) | 160/351 (45.6) | |||
| Leucopenia grade 4 | 33/104 (31.7) | 68/441 (15.4) | 44/101 (43.6) | 77/351 (21.9) | |||
| Neutropenia grade 3 | 19/104 (18.3) | 137/439 (31.2) | 15/99 (15.2) | 71/348 (20.4) | |||
| Neutropenia grade 4 | 73/104 (70.2) | 166/439 (37.8)g | 71/99 (71.7) | 179/348 (51.4)g | |||
| Thrombocytopenia grade 3 | 30/104 (28.8) | 83/441 (18.8) | 10/101 (9.9) | 17/350 (4.9) | |||
| Thrombocytopenia grade 4 | 30/104 (28.8) | 43/441 (9.8) | 5/101 (5.0) | 5/350 (1.4) | |||
| Anaemia grade 3 | 41/104 (39.4) | 73/440 (16.6) | 18/101 (17.8) | 23/351 (6.6) | |||
| Anaemia grade 4 | 3/104 (2.9) | 5/440 (1.1) | 2/101 (2.0) | 2/351 (0.6) | |||
|
f Represents the total number of patients and courses with laboratory data available. g p < 0.001 for courses. |
|||||||
| Comments: Incidences of grade 4 thrombocytopenia (p < 0.001) and grade 3/4 anaemia (p < 0.001) were significantly higher in topotecan patients. Median duration of grade 4 neutropenia in both treatment groups was 7 days. RBC transfusions were administered to 53.2% of topotecan patients in 24.7% of courses vs 26.9% of CAV patients in 24.7% of courses (p < 0.001). No evidence of cumulative toxicity for topotecan patient group. Infections occurred within 2 days of grade 4 neutropenia in 28% (30/107) of T patients and 8.7% (39/446) of courses, and in 26% (27/104) of CAV patients and 12.8% (46/359) of courses. Overall, 4.7% of topotecan patients (1.1% of courses) and 4.8% of CAV patients (1.4% of courses) were associated with sepsis. | |||||||
| Deaths (treatment related haematological toxicity with sepsis) | 4 | 3 | |||||
| Comments: A further two deaths were possibly related or related to therapy. One topotecan death was caused by acute respiratory insufficiency, and one topotecan death was caused by an intracerebral haemorrhage into brain metastases reported as secondary to topotecan-induced thrombocytopenia. One CAV death was caused by progressive disease coincident with reported CAV-related renal failure and pancytopenia. | |||||||
| Related or possibly related non-haematological toxicities occuring in > 10% of patients, n (%) | Topotecan (n = 107) | CAV (n = 104) | |||||
| Common toxicity criteria grade | |||||||
| 1/2 | 3/4 | Total | 1/2 | 3/4 | Total | ||
| Nausea | 38 (35.5) | 4 (3.7) | 42 (39.3) | 36 (34.6) | 6 (5.8) | 42 (40.4) | |
| Alopeciah | 38 (35.5) | 0 (0) | 38 (35.5) | 23 (22.1) | 0 (0) | 23 (22.1) | |
| Fatigue | 23 (21.5) | 5 (4.7) | 28 (26.2) | 26 (25.0) | 9 (8.7) | 35 (33.7) | |
| Vomiting | 24 (22.4) | 2 (1.8) | 26 (24.3) | 22 (21.1) | 3 (2.9) | 25 (24.0) | |
| Anorexia | 19 (17.7) | 1 (0.9) | 20 (18.7) | 20 (19.2) | 3 (2.9) | 23 (22.1) | |
| Stomatitis | 13 (12.2) | 2 (1.8) | 15 (14.0) | 12 (11.5) | 1 (1) | 13 (12.5) | |
| Diarrhoea | 12 (11.2) | 1 (0.9) | 13 (12.1) | 13 (12.5) | 0 (0) | 13 (12.5) | |
| Feveri | 11 (10.3) | 2 (1.9) | 13 (12.1) | Not reported | Not reported | Not reported | |
| Constipation | Not reported | Not reported | Not reported | 16 (15.4) | 0 (0) | 16 (15.4) | |
| Asthenia | Not reported | Not reported | Not reported | 10 (9.6) | 4 (3.8) | 14 (13.5) | |
| Left ventricular ejection fraction | 2/26 (7.7%) | 6/35 (17.1%) | |||||
|
h Reflects the number of patients who developed alopecia on study – approximately 30% in each arm presented to study with alopecia secondary to prior chemotherapy. i Excludes febrile neutropenia. |
|||||||
| Comments: Dose reductions for non-haematological toxicity occurred in one topotecan patient (0.9%) due to grade 3 fatigue and in 11 CAV patients (10.6%), nine due to neurotoxicity (p = 0.003). Incidence of worsening of left ventricular ejection fraction [was based on echocardiogram or multiple-gated acquisition results and can be seen from data in table (100 topotecan and 97 CAV baseline assessments)]. | |||||||
| Note: If reviewer calculates a summary measure or confidence interval PLEASE INDICATE | |||||||
|
Methodological comments Allocation to treatment groups: Patients stratified by extent of disease and PS at baseline and randomised to treatment by a telephone randomisation system. Blinding: All claimed responses were reviewed by an independent radiologist blinded to all claimed responses, but it is unclear whether this was the case for all outcome measures. Blinding of care providers or patients was not reported. No discussion of why a double-blind study was not performed. Comparability of treatment groups: Paper states that stratified randomisation ensured that the distribution of two prognostic variables, baseline PS and extent of disease were comparable between treatment groups. Paper states baseline characteristics were comparable between treatment groups – not supported statistically (no p-values), but groups do appear comparable for most characteristic, except incidence of prior surgery (14% topotecan vs 28% CAV). Gender (topotecan 43% women vs CAV 32%, p = 0.091) and documented brain metastases (topotecan 11.2% vs CAV 24.0%, p = 0.044) were not comparable between groups. Method of data analysis: Paper states that all patients who received a dose of study medication were included in the efficacy evaluations. Two prognostic variables, baseline PS and extent of disease included in multivariate analytical models for time-to-event outcomes. Subgroup analysis included response by gender and TTP relative to first-line chemotherapy; 95% CI for response rates and estimated percentage difference in response rates between treatment groups were calculated. Kaplan–Meier survival estimates used for time-to-event variables, including time to response, response duration, TTP and survival. Time-to-event outcomes were also compared using the Cox regression model. Multivariate statistical methods were applied to survival and response to determine other possible prognostic factors such as gender, PS extent of disease, age, presence of baseline brain and/or liver metastases, response to first-line therapy (CR or PR), response duration and TTP from first-line therapy. As baseline groups were not balanced with respect to the additional covariate, results were adjusted for only the stratification variables. For each of the symptoms of disease, Pearson’s uncorrected chi-squared statistic was used to compare percentage of patients in each treatment group who were experiencing sustained improvement over baseline (patients had to have both baseline and post baseline). For missing baseline measurements and at least one non-missing postbaseline measure of ‘a little bit’ or worse, baseline value was imputed as ‘not at all’ and the patient was included in analysis of that symptom. If symptom assessments not recorded, algorithms were used to impute scores for the course with missing assessments. Kaplan–Meier estimates were obtained and tested using log-rank test for the time to worsening for each symptom. Time to symptom worsening defined as the interval from first dose of study drug until increase in postbaseline assessment score. Patients without worsening of that symptom were censored at their last symptom assessment. Sample size/power calculation: Not reported. Attrition/drop-out: Reported numbers do not add up or is unclear (see column 3, p. 1). Breakdown of numbers and reasons not given. General comments Generalisability: Patients with progressive, limited or extensive SCLC. Paper reports that study was to focus on the sensitive population (relapse > 90 days after first-line chemotherapy, but included patients with date of progression ≥ 60 days after completion of first-line chemotherapy). Outcome measures: Primary and secondary measures are appropriate, but it is unclear how valid and reliable other measures are. No mean or SD reported. Intercentre variability: Number of centres not reported and issues around intercentre variability not discussed. Conflict of interests: Trial supported by SmithKline Beecham and four trial authors were employees of SKB. |
|||||||
Quality criteria for assessment of RCTs
| 1. Was the assignment to the treatment groups really random? | Adequate |
| 2. Was the treatment allocation concealed? | Adequate |
| 3. Were the groups similar at baseline in terms of prognostic factors? | Reported |
| 4. Were the eligibility criteria specified? | Adequate |
| 5. Were outcome assessors blinded to the treatment allocation? | Partial |
| 6. Was the care provider blinded? | Unknown |
| 7. Was the patient blinded? | Unknown |
| 8. Were the point estimates and measure of variability presented for the primary outcome measure? | Adequate |
| 9. Did the analyses include an ITT analysis? | Adequate |
| 10. Were withdrawals and dropouts completely described? | Partial |
Appendix 7 List of excluded studies
| Excluded trials | Reason for exclusion |
|---|---|
| Chen L, Antras L, Neary M, Dharan B, O’Brien ME. Symptom assessment in small cell lung cancer (SCLC) in a randomized trial: a psychometric analysis of Patient Symptom Assessment in Lung Cancer (PSALC). J Clin Oncol 2007;25(Suppl.):18101. | Not an RCT |
| Dy GK, Jett JR, Geoffroy FJ, Krewer KD, Tazelaar H, Maurer M et al. Topotecan and paclitaxel in previously treated patients with relapsed small cell lung cancer: phase II trial of the North Central Cancer Treatment Group. J Thoracic Oncol 2006;1:211–17. | Did not include the right intervention |
| Eckardt JR, Ramlau R, Gervais R, Shepherd F, O’Brien M, Ciuleanu T, et al. Compliance with oral topotecan in patients with non-small cell lung cancer (NSCLC) and small cell lung cancer (SCLC). J Clin Oncol 2006;24(Suppl.):7092. | Not an RCT |
| Gormley N, Edelman MJ, Smith R, Hausner PF, Bedor M, Bisaccia S. Phase II trial of docetaxel and topotecan in recurrent and extensive small cell lung cancer. Lung Cancer 2004;46:S42–3. | Not an RCT |
| Jotte RM, Reynolds CH, Conkling P, Oliver JW, Allen A. A randomized phase 2 trial of amrubicin compared to topotecan as second-line treatments in extensive disease small cell lung cancer (SCLC) sensitive to platinum-based first-line chemotherapy. J Clin Oncol 2007;25(Suppl.):18064. | Abstract – not enough information on methodology |
| Jotte RM, Conkling PR, Reynolds C, Allen AR, Oliver JW. A randomized phase II trial of amrubicin (AMR) vs. topotecan as second-line treatment in extensive-disease small-cell lung cancer (SCLC) sensitive to platinum-based first-line chemotherapy. Journal of Clinical Oncology 2008;26(Suppl.):8040. | Abstract – not enough information on methodology |
| Jotte RM, Reynolds C, Conkling PR, Jungnelius U, Oliver J. Amrubicin (Amr) vs topotecan as second-line treatment of extensive-disease small cell lung cancer (SCLC) sensitive to platinum-based first-line chemotherapy: a randomized phase 2 trial. Ann Oncol 2008;19:116. | Abstract – not enough information on methodology |
| O’Brien ME, Duh M, Chen L, Antras L, Neary M, Dharan B, et al. Is symptom improvement in patients with small cell lung cancer (SCLC) associated with clinical response? An analysis using the Patient Symptom Assessment Lung Cancer (PSALC) scale in a randomized trial comparing oral topotecan (OT) with best supportive care (BSC). J Clin Oncol 2007;25(Suppl.):7725. | Not an RCT |
| Peacock NW, Hainsworth JD, Switzer AB, Burris HA, Barrett C, Nicolau MF, et al. Weekly bolus topotecan as secondary therapy in extensive stage small cell lung cancer: A Minnie Pearl Cancer Research Network phase II trial. J Clin Oncol 2004;22(Suppl.):7278. | Not an RCT |
| Ruotsalainen, Mattson K. Topotecan (T) as second-line therapy following ifosfamide-carboplatin-etoposide (ICE) and maintenance for small cell lung cancer (SCLC). Lung Cancer 2000;29(Suppl.1):217. | Not an RCT |
Appendix 8 Tabulation of the critical appraisal of the MS against Drummond and colleagues’ checklist
| Item | Critical appraisal | Reviewer comment |
|---|---|---|
| Is there a well-defined question? | Yes | Cost effectiveness of oral topotecan plus BSC compared with BSC alone for people with relapsed SCLC, for whom re-treatment with first-line regimen is not considered appropriate, and who are unable or unwilling to receive i.v. chemotherapy |
| Is there a clear description of alternatives? | Yes (see Rationale section at beginning of chapter 4 of MS) |
CAV excluded as ‘topotecan (i.v. and oral) would not provide a cost-effective alternative to CAV in the majority of patients given its relatively higher acquisition cost’ ‘compared with oral topotecan the i.v. formulation has a similar efficacy profile but a higher acquisition and administration costs associated. Thus, it is unlikely to be a cost-effective alternative to oral topotecan’ The economic evaluation therefore focuses only on the use of oral topotecan in relapsed patients with SCLC who are not considered as candidates for standard i.v. therapy with CAV, and for whom BSC represents the main option in the absence of suitable alternative therapies |
| Has the correct patient group/population of interest been clearly stated? | ? | Scope states population as ‘adults with relapsed SCLC, for whom re-treatment with first-line regimen is not considered appropriate’. Does not make reference to those unable or unwilling to receive i.v. chemotherapy – however, this was part of inclusion criteria for O’Brien and colleagues RCT57 |
| Is the correct comparator used? | ? | BSC would be appropriate comparator for patients identified as unsuitable or unwilling to receive standard chemotherapy, having progressed following first-line treatment (and unsuitable for re-treatment with first-line). Appropriate given the inclusion criteria for O’Brien and colleagues RCT,57 but at variance with scope |
| Is the study type reasonable? | Yes | Cost–utility analysis suitable – takes into account life expectancy differences (e.g. median OS of 13.9 and 25.9 weeks for BSC and topotecan, respectively) and QoL differences (deterioration of 0.20 vs 0.05 over 3-month interval for BSC and topotecan respectively) documented in main trial publication |
| Is the perspective of the analysis clearly stated? | Yes |
NHS and PSS for costs (although PSS costs not explicitly included other than in sensitivity analysis) Patient perspective for outcomes – OS weighted for QoL |
| Is the perspective employed appropriate? | Yes |
Costs Only NHS costs included, no PSS costs included. As major difference between groups expected to relate to monitoring and administration costs incurred in NHS setting, then focus on NHS rather than PSS seems appropriate. However, some discussion in sensitivity analysis on inclusion of PSS costs for palliative care Outcomes Patient perspective adopted; OS, QoL weights based on patient responses to EQ-5D (over 12 3-week periods, i.e. maximum follow-up of 36 weeks) with values from population survey (Dolan and colleagues80) |
| Is effectiveness of the intervention established? | Yes | Effectiveness data are taken directly from O’Brien trial. Patient level data, recording:
|
| Has a lifetime horizon been used for analysis (has a shorter horizon been justified)? | Yes | The model has used survival as observed in the study – patients who were still alive at last follow-up were assumed to die the following day. May underestimate life expectancy – may have greater effect on oral topotecan plus BSC group. Unlikely to bias in favour of BSC |
| Are the costs and consequences consistent with the perspective employed? Covered in detail in questions below | Yes |
Costs reported as using NHS and PSS perspective. All included costs are NHS – application of an uplift for PSS costs used in sensitivity analysis Approach to costing is to only include treatment costs for patients receiving topotecan, on the assumption that costs of supportive care/symptom control are the same for both arms. Referred to in text as ‘a conservative approach’ (MS, p. 90). O’Brien and colleagues trial report stated that ‘palliative care and radiotherapy were used more frequently in BSC’ (p. 5444 of journal publication) – see also table 3 of journal publication. Suggests that excluding BSC is unlikely to bias results in favour of BSC Categories of included cost are: |
| Is differential timing considered? | Yes | MS states that 3.5% discount rate has been applied, but with majority of survival below 1 year, this has little effect |
| Is incremental analysis performed? | Yes |
Costs of topotecan acquisition/administration/monitoring and treatment of toxicity, plus costs of non-progressive days (after finishing topotecan treatment) are only costs included. No costs included for BSC Incremental life-years and incremental QALYs are calculated and ICERs presented for both life-years gained and QALYs gained |
| Is sensitivity analysis undertaken and presented clearly? | Yes | Deterministic sensitivity analyses were undertaken on:
|
| Item/study | |
|---|---|
| 1. Patient group | ? subgroup of relapsed patients with SCLC |
| Are the patients in the study similar to those of interest in England and Wales? | MS estimates at approximately 5% of new SCLC cases per year (approximately150 p.a.) |
| 2. Health care system/setting | ✓ |
| Comparability to England and Wales? | |
| Comparability of available alternatives? | |
| Similar levels of resources? | |
| Institutional arrangements comparable? | |
| 3. Treatment | ✓ |
| Comparability with clinical management? | |
| 4. Resource costs | ✓ |
| Comparability between study and setting/population of interest? | Resource use from multicentre trial. Unit costs applied for UK – based on published national sources or expert opinion from UK practitioners |
Appendix 9 Survival modelling methodology
Overall survival
As described in the main body of the text, the survival model adopted for this report was developed using linear regression to estimate the parameters of a linear transformation of the observed Kaplan–Meier estimates for OS from the RCT by O’Brien and colleagues. 57 Two parametric survival functions were estimated, a Weibull survival function and a log-logistic survival function, which were compared for goodness of fit to the observed survival functions for best supportive care and for oral topotecan plus BSC.
For a Weibull distribution the survival function is given by
with scale parameter λ and shape γ. Taking the log of both sides gives
Taking the log of both sides again, gives
which is a linear function and can be fit using least squares methods to provide estimates of λ and γ.
Similarly, the log-logistic survival function, given by
can be transformed to the linear function
This can be fit using least squares methods to provide estimates of λ and β.
The following tables report the parameter estimates and measures of goodness of fit for linear regressions, estimated using stata, for a Weibull survival function and for a log-logistic survival function. In both cases an additional parameter (Treat) was included in the regression – this was a dummy (0,1) variable that indicated whether the observed survival data were for the topotecan plus BSC arm (Treat = 1) or the BSC-only arm (Treat = 0).
Regression output for the Weibull survival function:
Goodness of fit
| Source | SS | df | MS | Number of obs = 240F(2, 237) = 2253.43Prob > F = 0.0000R-squared = 0.9500Adj R-squared = 0.9496Root MSE = .26006 | |||
| ModelResidual | 304.81540816.0291723 | 2237 | 152.407704.067633638 | ||||
| Total | 320.84458 | 239 | 1.3424459 | ||||
| weibull | Coef. | Std. Err. | t | P >|t| | [95% Conf. Interval] | ||
| ln_timetreat_cons | 1.093707–.6442615–5.505614 | .0163295.0344367.0792441 | 66.98–18.71–69.48 | 0.0000.0000.000 | 1.061538–.7121027–5.661727 | 1.125877–.5764203–5.349502 | |
Regression output for the log-logistic survival function:
Goodness of fit
| Source | SS | df | MS | Number of obs = 240F(2, 237) = 5584.19Prob > F = 0.0000R-squared = 0.9792Adj R-squared = 0.9790Root MSE = .23316 | |||
| ModelResidual | 607.17766312.8846967 | 2237 | 303.588831.054365809 | ||||
| Total | 620.06236 | 239 | 2.59440318 | ||||
| logLogistic | Coef. | Std. Err. | t | P >|t| | [95% Conf. Interval] | ||
| ln_timetreat_cons | 1.542566–.9385921–6.984087 | .0146404.0308748.0710474 | 105.36–30.40–98.30 | 0.0000.0000.000 | 1.513724–.9994161–7.124053 | 1.571408–.877768–6.844122 | |
Both models appear to fit the data well, with the log-logistic having a superior fit. This can be more readily identified by graphing the survival functions. For each parametric survival function we first plot the transformed Kaplan–Meier estimates and the fitted linear regressions. In a second figure we show the untransformed Kaplan–Meier estimates and the fitted survival functions for oral topotecan plus BSC and for BSC alone.
FIGURE 11.
Transformed Kaplan–Meier survival curves from O’Brien and colleagues,57 plus linear fit (Weibull).
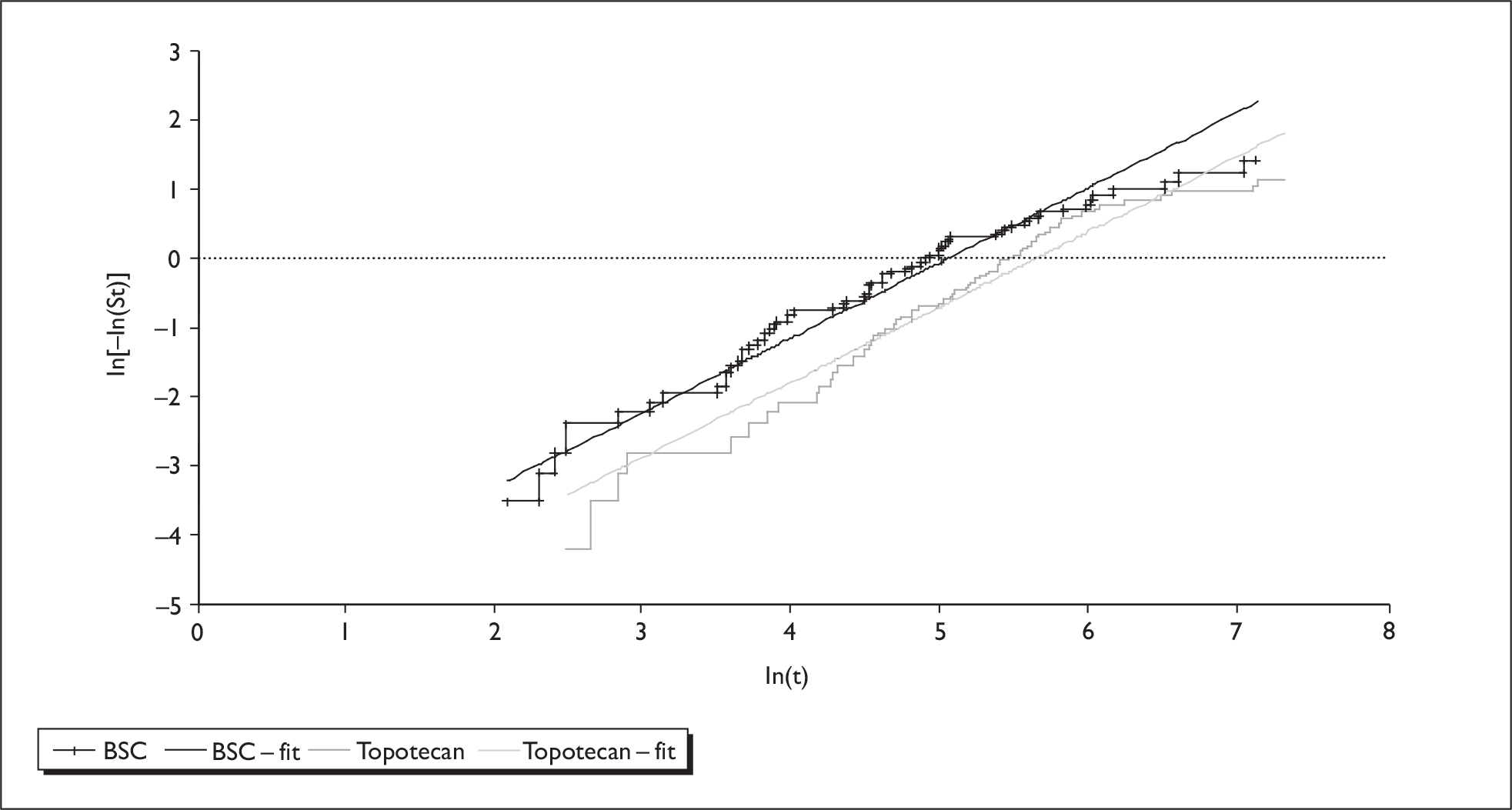
FIGURE 12.
Kaplan–Meier survival curves from O’Brien and colleagues,57 plus Weibull survival curves.

FIGURE 13.
Transformed Kaplan–Meier survival curves from O’Brien and colleagues,57 plus linear fit (log-logistic).
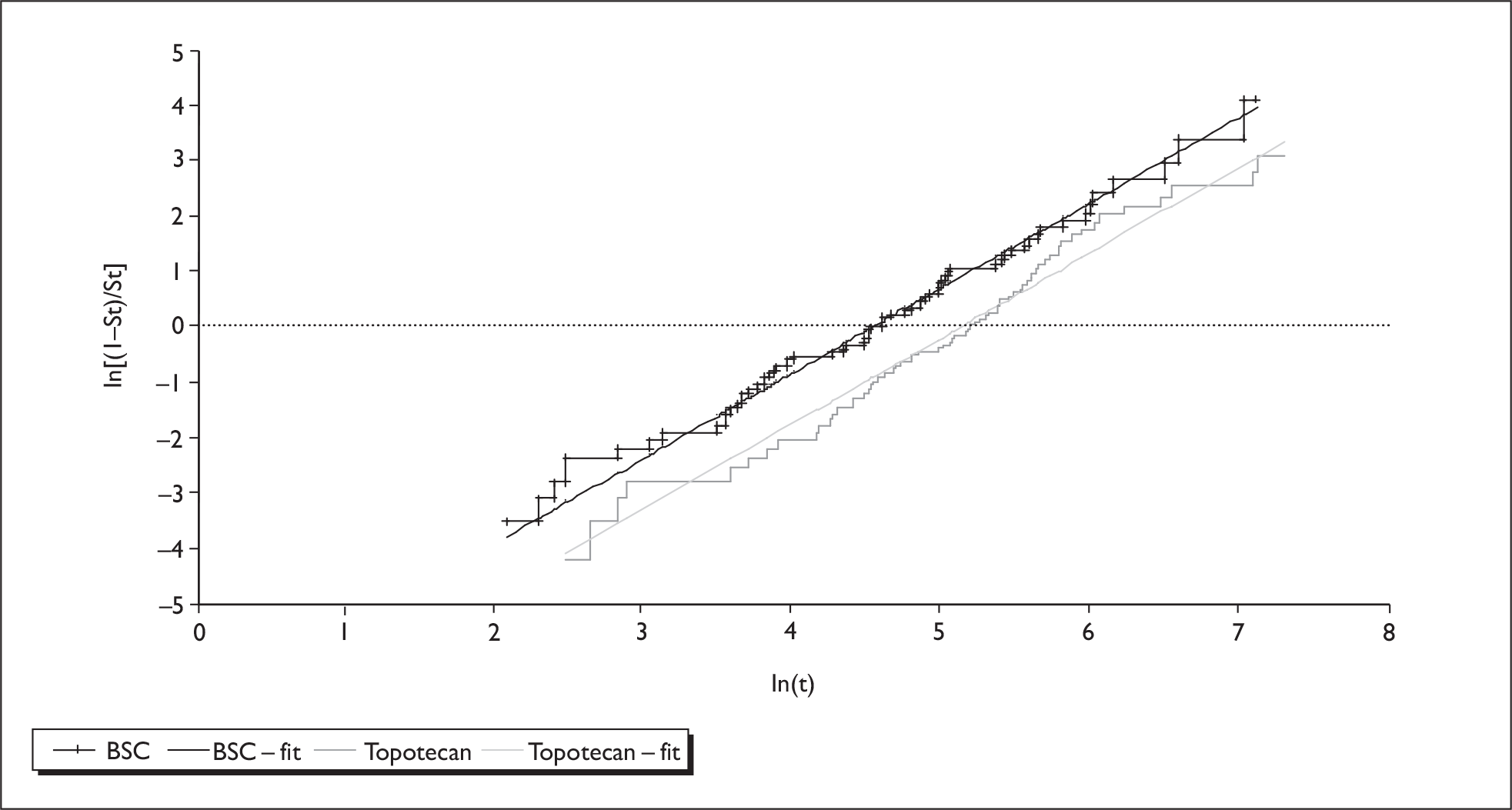
FIGURE 14.
Kaplan–Meier survival curves from O’Brien and colleagues,57 plus log-logistic survival curves.

The transformed log-logistic survival functions appear to be closer to linear functions than the transformed Weibull survival functions. The Weibull survival functions are likely to underestimate survival probabilities at higher survival durations when compared with the Kaplan–Meier estimates. The modelled probability of survival at 100 weeks is very close to zero for the Weibull survival function, whereas the Kaplan–Meier estimate is around 5%. In contrast, for the log-logistic survival function the modelled probability of survival at 100 weeks is around 4%.
The interpretation of the parameter coefficient for the dummy variable Treat is more obscure in the log-logistic model than in the Weibull model, where its absolute value can be interpreted as the HR for oral topotecan plus BSC relative to BSC alone for OS. This value, 0.644, can be compared directly with the unadjusted HR of 0.64 and the adjusted HR of 0.61 reported in the main trial publication by O’Brien and colleagues. 57
Time to progression
A similar procedure was used to estimate an appropriate function to model the mean TTP. In this case, three potential survival functions were modelled, including an exponential function (in addition to the Weibull and log-logistic survival functions).
The risk of disease progression was derived from the reported median TTP using an exponential approximation72
where S is the proportion of patients surviving (or in this case without disease progression) at time t. For the median TTP the value of S in the above equation is set, by definition, at 0.5, while t = 16.3 weeks (as presented in Chapter 3 of this report, under Oral topotecan plus BSC versus BSC alone). The mean TTP can be calculated by taking the reciprocal of the risk of disease progression (1/λ). This approach was used in a previous TAR on second-line chemotherapies for advanced ovarian cancer,69 which included topotecan. The accuracy of the estimate of the mean TTP depends on the adequacy of the exponential approximation, used to convert the median TTP to a risk of disease progression. The appropriateness of this transformation cannot be assessed without reference to the full survival function for TTP, which was not reported in the RCT publication by O’Brien and colleagues. 57 This represents a substantial source of uncertainty in the model.
The economic model submitted with the MS contains participant-level data from the RCT by O’Brien and colleagues, including TTP for patients in the oral topotecan group. The figure below charts the exponential survival function against the Kaplan–Meier estimates for TTP using the patient-level data submitted with manufacturer’s economic model. This suggests that the model fits the observed data well, up to the median survival. However, the fit is much poorer beyond that point and may significantly underestimate PFS when compared with the Kaplan–Meier estimate.
Based on the area under the curve, the estimated mean TTP using the Kaplan–Meier estimates is 30.3 weeks compared with an estimate of 23.52 using the exponential function – thus underestimating PFS by around 48 days. It should be noted that there is considerable uncertainty in the survival functions at longer survival durations, with small numbers of patients included in the analysis above 100 weeks.
To retain compatibility with the methods of estimating the OS functions, the survival function for disease progression was estimated from linear transformations of the Kaplan–Meier estimate of the survival function for TTP.
FIGURE 15.
Kaplan–Meier survival estimate for time to progression with 95% confidence interval, with modelled exponential suvival function.
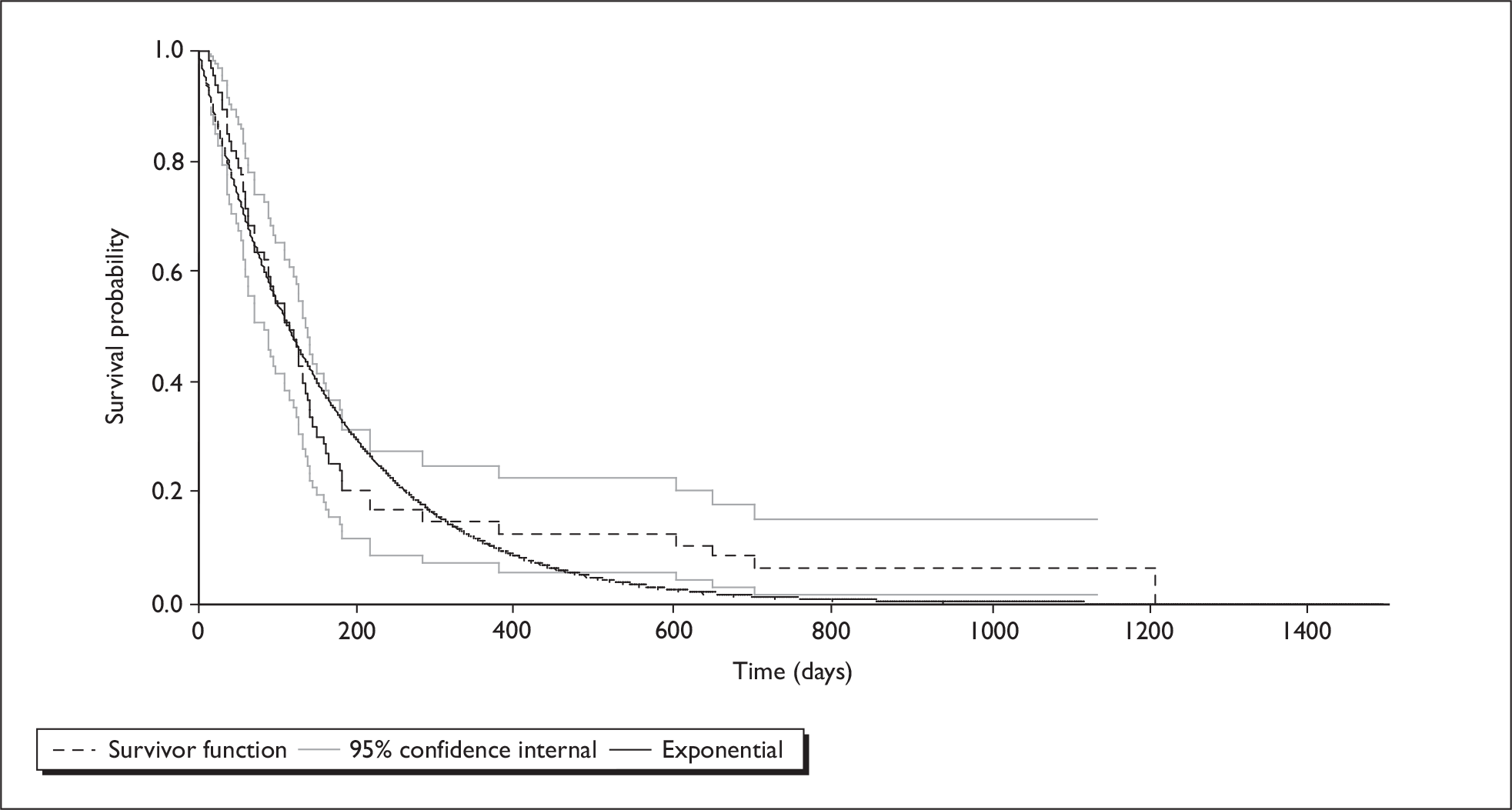
Regression output for the Weibull survival function:
Goodness of fit
| Source | SS | df | MS | Number of obs = 104F(1, 102) = 940.94Prob > F = 0.0000R-squared = 0.9022Adj R-squared = 0.9012Root MSE = .37073 | |||
| ModelResidual | 129.32534214.0191996 | 1102 | 129.325342.137443133 | ||||
| Total | 143.344542 | 103 | 1.39169458 | ||||
| weibull | Coef. | Std. Err. | t | P >|t| | [95% Conf. Interval] | ||
| ln_time_cons | 1.239133–6.361008 | .0403959.1872409 | 30.67–33.97 | 0.0000.000 | 1.159008–6.732399 | 1.319258–5.989616 | |
Regression output for the log-logistic survival function:
Goodness of fit
| Source | SS | df | MS | Number of obs = 104F(1, 102) = 2437.28Prob > F = 0.0000R-squared = 0.9598Adj R-squared = 0.9594Root MSE = .30733 | |||
| ModelResidual | 230.2065189.63412526 | 1102 | 230.206518.094452208 | ||||
| Total | 239.840644 | 103 | 2.32854994 | ||||
| logLogistic | Coef. | Std. Err. | t | P >|t| | [95% Conf. Interval] | ||
| ln_time_cons | 1.653237–7.803979 | .0334875.1552191 | 49.37–50.28 | 0.0000.000 | 1.586814–8.111856 | 1.719659–7.496103 | |
As for OS, the modelled survival functions for TTP were plotted against the Kaplan–Meier estimates.
FIGURE 16.
Kaplan–Meier survival estimate for time to progression with 95% confidence interval, with modelled Weibull suvival function.
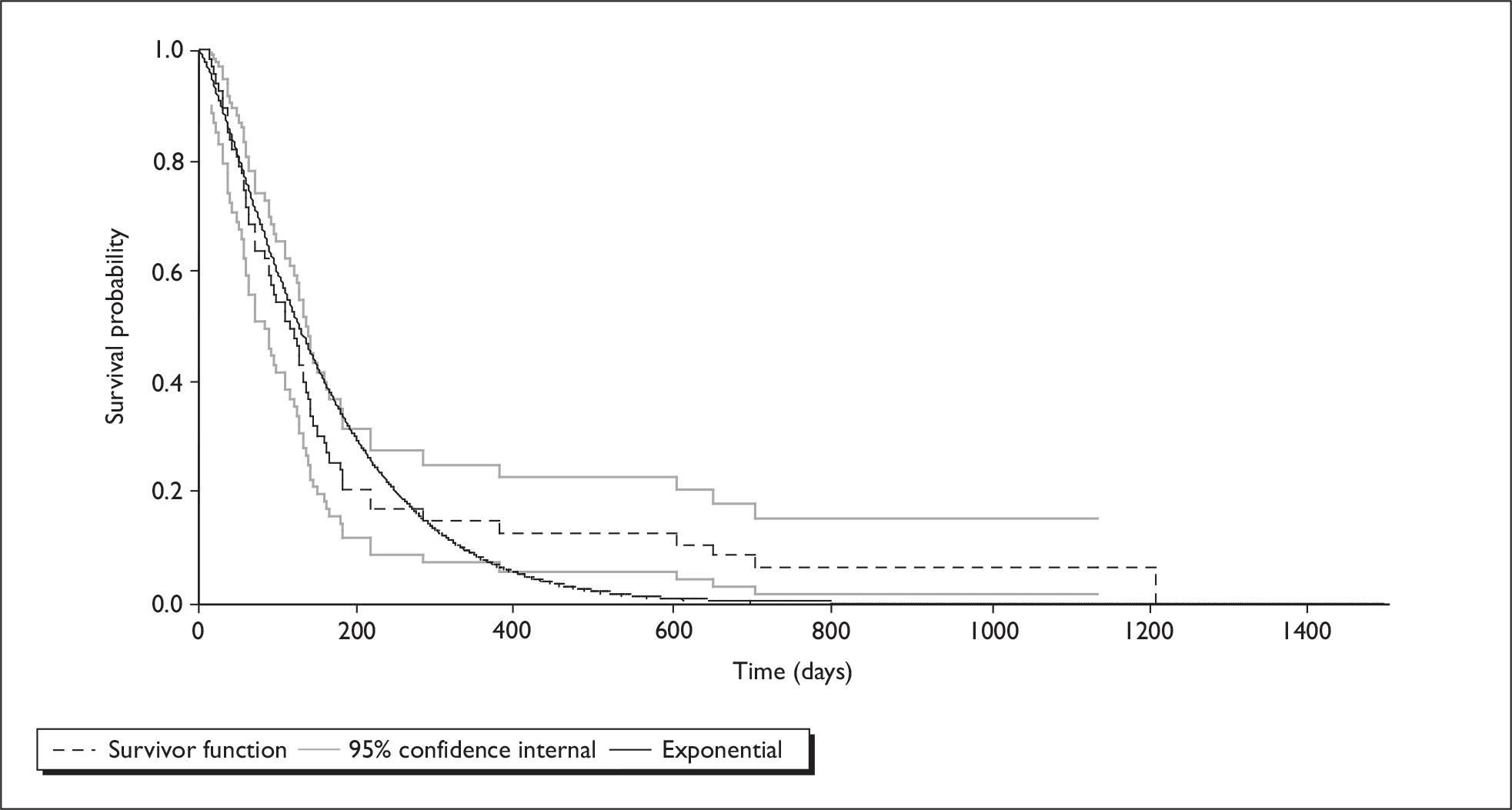
FIGURE 17.
Kaplan–Meier survival estimate for time to progression with 95% confidence interval, with modelled log-logistic suvival function.
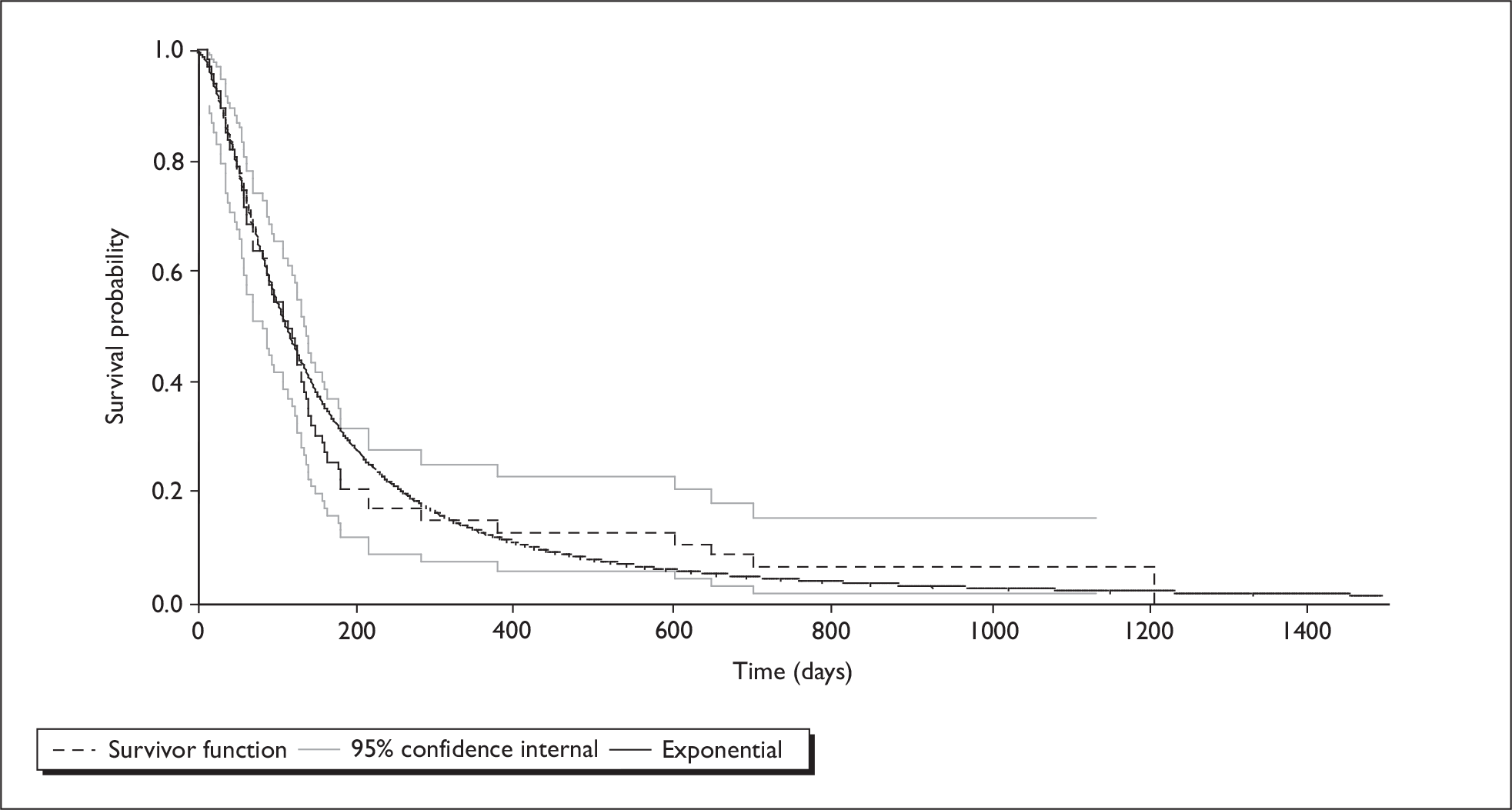
The log-logistic function appears to give a better fit than either the simple exponential approximation or the regression-based Weibull function. Comparing the mean TTP estimated using each of these functions, we get 22.7 weeks with the Weibull function and 28.5 weeks using the log-logistic function. While the log-logistic survival function clearly fits the observed data better than the alternative functions (Weibull and exponential), all three appear to underestimate mean TTP compared with the area under the Kaplan–Meier curve. However, it should be borne in mind, as noted above, that there is considerable uncertainty in the survival functions at longer survival durations, as indicated by the wide 95% CI, with the data contributing to estimated PFS above 110 weeks being contributed by two patients.
Appendix 10 Input parameters for probabilistic sensitivity analysis
Overall survival
Correlation between parameters in the OS regression is handled using the Cholesky decomposition method. 82 The Cholesky decomposition of the variance–covariance matrix for the regression used to fit the log-logistic survival function is shown below:
| ln(t) | Treat | ln(λ) | |
|---|---|---|---|
| ln(t) | 0.014640 | 0.000000 | 0.000000 |
| Treat | –0.006566 | 0.030169 | 0.000000 |
| ln(λ) | –0.067545 | –0.016090 | 0.015051 |
The parameter estimates for the regression are shown below:
| ln(t) | Treat | ln(λ) |
|---|---|---|
| 1.542566 | –0.938592 | –6.984087 |
In each simulation three draws are taken from standard normal distributions (mean = 0, SD = 1), labelled here as z1, z2 and z3. Three new variables (Tz1, Tz2 and Tz3) are defined, by multiplying elements of the Cholesky decomposition matrix (C) by the values drawn from standard normal distributions (z1, z2 and z3). Identifying elements of the Cholesky decomposition matrix as C[i,j] where i is the row number and j the column number, then:
For each simulation the sampled values of the parameter estimates are therefore defined as:
The same approach was used to handle correlation between parameters in the model used to estimate TTP for patients in the oral topotecan cohort.
Probability of adverse events
The probability of adverse events is based on the number of patients experiencing each grade of adverse event, as reported in the CSR for study 487 (included as appendix 5 of the MS). These are sampled using the procedure outlined in Briggs and colleagues82 for sampling from a Dirichlet distribution. Variables x0, x1 … x4 (corresponding to grades 0–4 for a given toxicity) are drawn from independent gamma distributions with shape parameters α0, α1 … α4 (corresponding to the count of patients experiencing the given grades of toxicity) and a common scale parameter of 1.
Thus the simulated count for each grade (j) of a given toxicity is xj ∼ γ(αj,1).
The simulated proportion is calculated by dividing the simulated count for each grade by the sum of the simulated counts for all grades of the relevant toxicity
Health-state utility
The rate of deterioration in QoL per 3-month interval for oral topotecan plus BSC and for BSC is sampled across the 95% CI reported by O’Brien and colleagues. 57 See table below:
| Cohort | Point estimate | LCI | UCI | SE | Distribution |
|---|---|---|---|---|---|
| Topotecan + BSC | –0.05 | –0.11 | 0.02 | 0.03827 | Normal |
| BSC | –0.20 | –0.27 | –0.12 | 0.03316 | Normal |
Chemotherapy courses and BSA
The mean (and SE) for the number of courses of oral topotecan and patients’ BSA were estimated from data included in the manufacturer’s economic model. These were simulated using normal distributions.
| Variable | Mean | SE | Distribution |
|---|---|---|---|
| Number of courses per patient | 3.9296 | 0.2649 | Normal |
| BSA | 1.8404 | 0.0240 | Normal |
Costs
Costs included in the PSA were those related to outpatient provision of chemotherapy, general medical management in outpatients, inpatient and outpatient management of adverse events, and palliative care costs. Drug costs were not sampled during the PSA, but were included at values quoted in the BNF.
Costs derived from NHS Reference Costs were sampled using estimated ‘SEs’. These assumed that a variation of plus or minus 25% was an appropriate CI for the average reference costs. The estimated SEs are shown in column 3 of the table below. Parameters for gamma distributions (shown in columns labelled ‘Alpha’ and ‘Beta’) were derived using the ‘method of moments’,82 based on the means and estimated ‘SEs’. The simulated values were inflated to 2007/08 prices using appropriate inflation indices, as for the base-case and deterministic sensitivity analyses.
The estimated SE for palliative care costs was derived using the minimum and maximum values presented by Oliver and colleagues,49 as these were the only summary data for the distribution of palliative care costs reported.
| Item | Mean | ‘SE’ | Alpha | Beta | Distribution |
|---|---|---|---|---|---|
| Oral topotecan (per mg) | 30.00 | ||||
| Intravenous topotecan (per course) | 1494.75 | ||||
| Outpatient attendance for oral chemotherapy | 178.99 | 15.94 | 126.07 | 1.4198 | Gamma |
| FBC | 2.90 | ||||
| U&E | 4.70 | ||||
| LFT | 4.70 | ||||
| Chest radiograph | 27.71 | 2.47 | 126.07 | 0.2198 | Gamma |
| Day-case admission | 355.43 | 31.66 | 126.07 | 2.8193 | Gamma |
| Inpatient elective excess bed-day | 241.76 | 21.53 | 126.07 | 1.9177 | Gamma |
| Inpatient non-elective excess bed-day | 181.73 | 16.18 | 126.07 | 1.4415 | Gamma |
| Outpatient attendance | 200.78 | 17.88 | 126.07 | 1.5926 | Gamma |
| Intensive care (per day) | 989.82 | 88.15 | 126.07 | 7.8513 | Gamma |
| GP visit | 36.00 | ||||
| Cost of palliative care (per patient) | 3495.00 | 1168.46 | 8.95 | 390.6433 | Gamma |
| Antibody screen | 10.40 | ||||
| Electronic cross-match | 25.00 | ||||
| Serological cross-match | 30.90 | ||||
| Standard red cells (per unit) | 133.90 | ||||
| Platelets (per unit) | 208.46 | ||||
| Blood transfusion (per transfusion) | 78.80 | ||||
| Platelets transfusion (per transfusion) | 705.00 |
Appendix 11 Estimating QALY weights over time (from published values)
O’Brien and colleagues57 and Chen and colleagues64 briefly reported on a pooled analysis of utility data, collected using the EQ-5D and valued using a population tariff, using a mixed model (to account for the inclusion of repeated observations for trial participants). The CSR for Study SK&F-104864/478, submitted to NICE as appendix 5 of the MS, contains slightly more detail on the methods used. The CSR makes clear that the analysis has used EQ-5D utility scores, derived using responses from patients in the RCT by O’Brien and colleagues57 and valued using the tariff reported by Dolan and colleagues. 80 The EQ-5D was administered at baseline and at each clinic visit (every 3 weeks) – missing data for the EQ-5D are not reported or discussed in the main trial publication (O’Brien and colleagues57) or the CSR. The CSR reports that the mixed model was estimated using restricted maximum likelihood and included treatment, baseline EQ-5D utility, time and a treatment-by-time interaction as fixed covariates. The random effects were intercept and time, while course of therapy was included as a repeated effect. An unstructured covariance structure was used for the random effects and a spatial covariance structure for the repeated effect. No further detail of this analysis is provided in the CSR.
Both O’Brien and colleagues57 and Chen and colleagues64 state that the ‘rate of deterioration’ in utility was –0.05 per 3-month period for oral topotecan plus BSC, and –0.20 per 3-month period for BSC. We interpreted this to indicate that for each 3-month period the mean utility reduces from baseline by 5% for the oral topotecan plus BSC cohort and by 20% for the cohort receiving BSC alone.
Assuming a baseline utility for patients in both cohorts of 0.70, based on the reported baseline utility of patients in the RCT by O’Brien and colleagues who contributed data to the pooled analysis (0.72 for oral topotecan plus BSC and 0.68 for BSC), we estimated mean utility over time for each arm over a period of 12 months as:
| Time (months) | Oral topotecan + BSC | BSC |
|---|---|---|
| 0 | 0.7000 | 0.7000 |
| 3 | 0.6650 | 0.5600 |
| 6 | 0.6318 | 0.4480 |
| 9 | 0.6002 | 0.3584 |
| 12 | 0.5702 | 0.2867 |
To estimate a daily rate of deterioration in utility we subtracted the natural log of the baseline utility from the natural log of the value at 3 months, for each arm:
Dividing these values by the mean number of days in 3 months (91.3125) gives –0.000562 for oral topotecan plus BSC and –0.002444 for BSC. To estimate the utility at a given number of days from baseline, simply enter the appropriate values in the following formula:
(where –0.3567 is the natural log of 0.7, the assumed baseline utility value) and exponentiate the result. For example, to calculate the utility value for oral topotecan plus BSC and for BSC at 1 year:
Appendix 12 Detailed calculation of adverse event costs
| Toxicity | Grade | Resource use | Resource-use assumption |
|---|---|---|---|
| Neutropenia | 3 | Outpatient visit | Single attendance by 50% of affected patients |
| Amoxicillin | Oral capsule, non-proprietary; dosage 500 mg every 8 hours, up to 7 days | ||
| 4 | Inpatient admission | All affected patients admitted – average stay of 3.5 days (range 2–5 days) | |
| Piperacillin | Intravenous; 4.5 g every 6 hours for duration of stay (14 for average stay of 3.5 days) | ||
| Saline | 20 ml for dilution of Tazocin + 100 ml for i.v. infusion of piperacillin | ||
| Thrombocytopenia | 3 | No treatment | |
| 4 | Day-case admission | Single attendance for all affected patients | |
| Platelet transfusion | |||
| Type and cross | |||
| Anaemia | 3 | Day-case admission | Single attendance for all affected patients |
| Blood transfusion | |||
| Type and cross | |||
| 4 | Day-case admission | Single attendance for all affected patients | |
| Blood transfusion | |||
| Type and cross | |||
| Sepsis | Inpatient admission | Total stay 10 days: average of 5 (range 3 to 7) ward days and 5 (range 3 to 7) ICU days | |
| Piperacillin | Intravenous, 4.5 g every 6 hours for 5 days (14 for average stay of 3.5 days) | ||
| Clarithromycin | 500 mg, twice daily for 10 days | ||
| Saline | 20 ml for dilution of Tazocin + 100 ml for i.v. infusion of piperacillin | ||
| Fluconazole i.v. | Intravenous, non-proprietary, 100 ml at 2 mg/ml, one per day, for 7 days |
| Toxicity | Grade | Resource use | Resource-use assumption | Unit cost (£) | Unit measure |
|---|---|---|---|---|---|
| Neutropenia | 3 | Outpatient visit | General Medicine (specialty code 300). Consultant Led First Attendance Outpatient Face to Face. Worksheet ‘TCLFASFF’ | 207.48 | Per visit |
| Amoxicillin | 21 × 500-mg capsules (non-proprietary) = £1.37 | 0.065 | Per capsule | ||
| 4 | Inpatient admission | Respiratory Neoplasms with Major CC (DZ17A). Excess bed-day cost. Worksheet ‘TEIXS’ | 249.83 | Per day | |
| Tazocin | 4.5 g of powder for reconstitution | 15.79 | Per infusion | ||
| Saline | Main and colleagues,69 p. 96 | 0.06 | Per ml | ||
| Thrombocytopenia | 3 | No treatment | |||
| 4 | Day-case admission | Respiratory Neoplasms with Major CC (DZ17A). Worksheet ‘TDC’ | 367.29 | Per admission | |
| Platelet transfusion | Main and colleagues69 | 805.67 | Per transfusion | ||
| Type and cross | Southampton University Hospitals Trust | 36.88 | Per transfusion | ||
| Anaemia | 3 | Day-case admission | Respiratory Neoplasms with Major CC (DZ17A). Worksheet ‘TDC’ | 367.29 | Per admission |
| Blood transfusion | Main and colleagues69 | 90.05 | Per transfusion | ||
| Type and cross | Southampton University Hospitals Trust | 36.88 | Per transfusion | ||
| 4 | Day-case admission | Respiratory Neoplasms with Major CC (DZ17A). Worksheet ‘TDC’ | 367.29 | Per admission | |
| Blood transfusion | 4 units red blood cells (expert advice) | 133.90 | Per unit | ||
| Type and cross | Southampton University Hospitals Trust | 36.88 | Per transfusion | ||
| Sepsis | Inpatient admission | ||||
| ICU | Intensive Therapy Unit/Intensive Care Unit: 1 Organ Supported (XC06ZTHE). Worksheet ‘TCCSAL’ | 1022.86 | Per day | ||
| Ward | Respiratory Neoplasms with Major CC (DZ17A). Excess bed-day cost. Worksheet ‘TEIXS’ | 249.83 | Per day | ||
| Tazocin | 4.5 g of powder for reconstitution | 15.79 | Per infusion | ||
| Clarithromycin | Pack of 14 × 500-mg tablets = £7.47 | 0.535 | Per tablet | ||
| Saline | Main and colleagues69 | 0.06 | Per ml | ||
| Fluconazole i.v. | 100-ml bottle at 2 mg/ml = £29.28 | 29.28 | Per infusion | ||
| Toxicity | Grade | Resource use | Resource-use assumption |
|---|---|---|---|
| Diarrhoea | 2 | Outpatient visit | Single attendance by all affected patients |
| Loperamide | Oral tablet, 16 mg per day, for 5 days | ||
| 3 | Inpatient admission | All affected patients admitted – average stay of 5 days | |
| Loperamide | Oral tablet, 16 mg per day, for 7 days. | ||
| Buscopan | Oral tablet, 20 mg, four times per day, for 7 days | ||
| Codeine phosphate | Oral tablet, non-proprietary, 30 mg four times per day, for 7 days | ||
| 4 | Inpatient admission | All affected patients admitted – average stay of 5 days | |
| Loperamide | Oral tablet, 16 mg per day, for 7 days | ||
| Buscopan | Oral tablet. 20 mg, four times per day, for 7 days | ||
| Ciprofloxacin i.v. | 400 mg twice daily, for 2 days – as 2 mg/ml in 200-ml bottle | ||
| Metronidazole i.v. | 500 mg, up to four times per day – as 5 mg/ml in 100-ml container | ||
| Codeine | Oral tablet, non-proprietary, 30 mg four times per day, for 7 days | ||
| Nausea/vomiting | 3 | Outpatient visit | Single attendance for all affected patients |
| Dexamethasone | Oral tablet, 8 mg, twice daily, for 10 days | ||
| Granisetron | Oral tablet, 2 mg daily, for 10 days | ||
| 4 | Inpatient admission | All affected patients admitted – average stay of 5 days | |
| Dexamethasone i.v. | 20-mg single dose | ||
| Granisetron i.v. | 3 mg, three times over 24 hours | ||
| Saline | 15 ml for dilution of Granisetron | ||
| Cyclizine | 50 mg, three times daily, for 5 days |
| Toxicity | Grade | Resource use | Resource-use assumption | Unit cost (£) | Unit measure |
|---|---|---|---|---|---|
| Diarrhoea | 2 | Outpatient visit | General Medicine (specialty code 300). Consultant Led First Attendance Outpatient Face to Face. Worksheet ‘TCLFASFF’ | 207.48 | Per visit |
| Loperamide | Pack of 30 × 2-mg tablets = £2.15 | 0.07 | Per tablet | ||
| 3 | Inpatient admission | Respiratory Neoplasms with Major CC (DZ17A). Excess bed-day cost. Worksheet “TEIXS” | 249.83 | Per day | |
| Loperamide | Pack of 30 × 2- mg tablets = £2.15 | 0.07 | Per tablet | ||
| Buscopan | Pack of 56 × 10- mg tablets = £2.59 | 0.05 | Per tablet | ||
| Codeine phosphate | 28 × 30-mg tablets = £0.97 | 0.035 | Per tablet | ||
| 4 | Inpatient admission | Respiratory Neoplasms with Major CC (DZ17A). Excess bed-day cost. Worksheet ‘TEIXS’ | 249.83 | Per day | |
| Loperamide | Pack of 30 × 2- mg tablets = £2.15 | 0.07 | Per tablet | ||
| Buscopan | Pack of 56 × 10 -mg tablets = £2.59 | 0.05 | Per tablet | ||
| Codeine phosphate | 28 × 30-mg tablets = £0.97 | 0.035 | Per tablet | ||
| Ciprofloxacin i.v. | 200-ml bottle at 2 mg/ml = £22.00 | 22.00 | Per infusion | ||
| Metronidazole i.v. | 100-ml container at 5 mg/ml = £3.41 | 3.41 | Per infusion | ||
| Nausea/vomiting | 3 | Outpatient visit | General Medicine (specialty code 300). Consultant Led First Attendance Outpatient Face to Face. Worksheet ‘TCLFASFF’ | 207.48 | Per visit |
| Dexamethasone | 20 × 2-mg tablets = £3.27 | 0.165 | Per tablet | ||
| Granisetron | 5 × 2-mg tablets = £65.49 | 13.10 | Per tablet | ||
| 4 | Inpatient admission | Respiratory Neoplasms with Major CC (DZ17A). Excess bed-day cost. Worksheet ‘TEIXS’ | 249.83 | Per day | |
| Dexamethasone i.v. | 1-ml ampoule at 4 mg/ml = £1.00 | 5.00 | Per infusion | ||
| Granisetron i.v. | 3-ml ampoule at 1 mg/ml = 25.79 | 25.79 | Per infusion | ||
| Saline | Main and colleagues69 | 0.06 | Per ml | ||
| Cyclizine | 20 × 50-mg tablets = £1.48 | 0.075 | Per tablet |
Appendix 13 Questions to clinical experts – management of patients treated with topotecan (oral or i.v.) and management of treatment-related toxicity
Specific questions regarding the management of patients being treated with topotecan (in oral or i.v. form) are listed below:
What tests would be required prior to starting treatment with topotecan?
Assume that a FBC is required as the SmPC states that ‘prior to administration of the first course of topotecan, patients must have a baseline neutrophil count of ≥ 1.5 × 109/l, a platelet count of ≥ 100 × 109/l and a haemoglobin level of ≥ 9 g/dl (after transfusion if necessary)’.
-
Would any other tests be required prior to starting treatment with topotecan?
What tests would be used to monitor patients receiving chemotherapy with topotecan?
Assume that haematological toxicity is assessed by FBC.
-
Would this be assessed only at start of each treatment cycle or would this happen more frequently?
-
Would assessment/frequency of assessment for haematological toxicity differ between oral versus i.v. topotecan?
-
What tests would be routinely requested for assessing other toxicities? Please specify types of test, the frequency of testing and toxicities being assessed.
-
Would patients receiving oral topotecan have additional monitoring in primary care (e.g. visits by district nurses)? How frequently would patients receiving oral topotecan attend for treatment or monitoring during each treatment cycle?
Would patients attending for topotecan be required to take any premedications or concomitant medication?
-
Would patients require premedication prior to topotecan by i.v. infusion?
-
Would patients require premedication prior to oral topotecan?
-
Would patients require concomitant medication with topotecan by i.v. infusion?
-
Would patients require concomitant medication with oral topotecan?
-
The trial report by O’Brien and colleagues specifically refers to a proportion (3%) of patients receiving GCSF – would this be prescribed as prophylaxis against neutropenia?
-
The trial report by O’Brien and colleagues specifically refers to a proportion of patients (3%) receiving erythropoietin – would this be prescribed as prophylaxis?
Topotecan for i.v. infusion is supplied as powder for reconstitution.
SmPC states ‘saline (0.9% w/v sodium chloride i.v. infusion or 5% w/v glucose i.v. infusion) is required for reconstitution of powder to a final concentration of between 25 and 50 microgram/ml’.
-
Can you indicate the quantity of saline required to achieve this concentration for a patient requiring a dose of 2.7 mg per day (i.e. dosage of 1.5 mg/m2 per day for a patient with a BSA of 1.8 m2)?
Dose escalation/dose reduction
-
If a patient has their chemotherapy dose increased, due to lack of efficacy, in one cycle, does the dose remain at the escalated level for their remaining cycles of treatment on a given agent?
-
If a patient has their chemotherapy dose reduced, due to toxicity, in one cycle, does the dose remain at the reduced level for their remaining cycles of treatment on a given agent?
If the exact dosage of oral topotecan is not available would you recommend rounding the dosage up or down?
For example, the exact dosage for a patient with BSA of 1.8 m2 would be 4.14 mg per day, at a dosing schedule of 2.3 mg/m2 per day. With oral topotecan available in 1- and 0.25-mg capsules would you recommend rounding up to 4.25 mg per day or rounding down to 4.00 mg per day?
Treatment of toxicity/adverse events
A previous review conducted for NICE [Main and colleagues, Health Technol Assess 2006; 10(9)], which included topotecan, reported estimates of the costs of managing treatment-related toxicity. While the review was concerned with the use of topotecan for treatment of advanced ovarian cancer, we are aware that the dosage, frequency of administration and cycle length are the same for advanced ovarian cancer and for SSLC.
Would it be reasonable to adopt similar assumptions for managing (topotecan) treatment-related toxicity in relapsed patients with SCLC as for advanced ovarian cancer patients?
The assumptions and costs adopted in the advanced ovarian cancer review (which were derived from one of the manufacturers’ submissions to the NICE appraisal) are listed below. First, we list the assumptions with regard to how patients are managed, as outpatient, day case or inpatient, and, second, the assumptions regarding drug treatment or specific interventions (such as transfusions) provided.
| Toxicity/adverse event | Grade | Managed as: | Length of stay |
|---|---|---|---|
| Neutropenia | 3 | Outpatient | Single attendance by 50% of affected patients |
| 4 | Inpatient | 3.5 days (range 2–5 days) | |
| Thrombocytopenia | 3 | No treatment | |
| 4 | Day case | All patients attend for platelet transfusion | |
| Anaemia | 3 | Day case | Single attendance for all affected patients |
| 4 | Day case | Single attendance for all affected patients | |
| Sepsis | 3 | Inpatient | Average 4.5 days (range 3–6 days) |
| 4 | Inpatient | Total stay of 10 days on average, with an average of 5 days (range 3–7 days) in ICU and 5 days (range 3–7 days) on the ward |
No assumptions were listed for febrile neutropenia – would it be reasonable to regard these as a subset of Grade 4 neutropenia and apply the same management assumptions?
| Toxicity/adverse event | Grade | Managed as | Length of stay |
|---|---|---|---|
| Diarrhoea | 3 | Inpatient | 5 days |
| 4 | Inpatient | 5 days | |
| Vomiting | 3 | Outpatient | Single attendance for all affected patients |
| 4 | Inpatient | 5 days |
| Toxicity/adverse event | Grade | Drug/intervention | Quantity (total cost) |
|---|---|---|---|
| Neutropenia | 3 | Ciprofloxacin | 6 (£1.50) |
| 4 | Ciprofloxacin | 6 (£1.50) | |
| GCSF | 5 (£77.03) | ||
| Thrombocytopenia | 3 | No treatment | |
| 4 | Platelet transfusion | 1 (£78.80) | |
| Type and cross | 1 (£18.00) | ||
| Anaemia | 3 | Platelet transfusion | 1 (£78.80) |
| Type and cross | 1 (£18.00) | ||
| 4 | Platelet transfusion | 1 (£78.80) | |
| Type and cross | 1 (£18.00) | ||
| Sepsis | 3 | Gentamicin | 1 (£61.25) |
| Tazocin | 1 (£368.48) | ||
| 4 | Gentamicin | 1 (£61.25) | |
| Tazocin | 1 (£368.48) | ||
| Saline | 1 (£42.00) | ||
| Fluconzole i.v. | 1 (£204.96) |
| Toxicity/adverse event | Grade | Drug/intervention | Quantity (total cost) |
|---|---|---|---|
| Diarrhoea | 3 | Buscopan | 1 (£1.39) |
| Ciprofloxacin | 6 (£1.50) | ||
| Codeine | 1 (£0.33) | ||
| Loperamide | 2.5 (£0.08) | ||
| 4 | Buscopan | 1 (£1.39) | |
| Ciprofloxacin | 6 (£1.50) | ||
| Codeine | 1 (£0.33) | ||
| Loperamide | 2.5 (£0.08) | ||
| Vomiting | 3 | Dexamethasone | 6 (£0.51) |
| Granisetron | 1 (£383.95) | ||
| 4 | Saline | 1 (£42.00) | |
| Dexamethasone i.v. | 1 (£6.60) | ||
| Granisetron i.v. | 1 (£360.00) | ||
| Cyclizine | 1 (£8.55) |
Appendix 14 Relative risks of adverse events – i.v. versus oral topotecan
Haematological adverse event
| Neutropenia | RR | SE(lnRR) | 95% CI | |||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Grade 3 | Eckardt | 0.9035 | 0.2019 | 0.6083 | 1.3420 | 75.2 |
| von Pawel | 1.2483 | 0.3514 | 0.6269 | 2.4856 | 24.8 | |
| Pooled | 0.9789 | 0.1750 | 0.6946 | 1.3796 | ||
| Grade 4 | Eckardt | 1.3663 | 0.1065 | 1.1089 | 1.6835 | 80.0 |
| von Pawel | 1.9071 | 0.2128 | 1.2567 | 2.8941 | 20.0 | |
| Pooled | 1.4607 | 0.0952 | 1.2119 | 1.7605 | ||
| Thrombocytopenia | RR | SE(lnRR) | 95% CI | Weight (%) | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Grade 3 | Eckardt | 1.2667 | 0.2152 | 0.8308 | 1.9313 | 71.4 |
| von Pawel | 0.9623 | 0.3397 | 0.4945 | 1.8725 | 28.6 | |
| Pooled | 1.1708 | 0.1818 | 0.8198 | 1.6719 | ||
| Grade 4 | Eckardt | 0.6279 | 0.2167 | 0.4106 | 0.9602 | 70.1 |
| von Pawel | 0.8935 | 0.3315 | 0.4666 | 1.7110 | 29.9 | |
| Pooled | 0.6979 | 0.1814 | 0.4891 | 0.9958 | ||
| Anaemia | RR | SE(lnRR) | 95% CI | Weight (%) | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Grade 3 | Eckardt | 1.6154 | 0.2212 | 1.0471 | 2.4922 | 62.9 |
| von Pawel | 1.3747 | 0.2880 | 0.7817 | 2.4174 | 37.1 | |
| Pooled | 1.5215 | 0.1754 | 1.0788 | 2.1459 | ||
| Grade 4 | Eckardt | 0.5000 | 0.6014 | 0.1538 | 1.6251 | 72.7 |
| von Pawel | 0.9623 | 0.9806 | 0.1408 | 6.5760 | 27.3 | |
| Pooled | 0.5980 | 0.5127 | 0.2189 | 1.6333 | ||
Non-haematological adverse events
| Diarrhoea | RR | SE(lnRR) | 95% CI | Weight (%) | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Grade 2 | Eckardt | 0.3524 | 0.3942 | 0.1627 | 0.7631 | 87.91 |
| von Pawel | 0.1606 | 1.0628 | 0.0200 | 1.2896 | 12.09 | |
| Pooled | 0.3205 | 0.3696 | 0.1553 | 0.6613 | ||
| Grade 3 | Eckardt | 0.1689 | 0.7552 | 0.0384 | 0.7418 | 67.10 |
| von Pawel | 0.1927 | 1.0784 | 0.0233 | 1.5954 | 32.90 | |
| Pooled | 0.1764 | 0.6186 | 0.0525 | 0.5929 | ||
| Grade 4 | Eckardt | 1.0132 | 0.9934 | 0.1446 | 7.1006 | 66.54 |
| von Pawel | 0.9636 | 1.4011 | 0.0618 | 15.0138 | 33.46 | |
| Pooled | 0.9963 | 0.8104 | 0.2035 | 4.8776 | ||
| Nausea | RR | SE(lnRR) | 95% CI | Weight (%) | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Grade 3 | Eckardt | 0.5789 | 0.6163 | 0.1730 | 1.9373 | 62.38 |
| von Pawel | 0.9636 | 0.7935 | 0.2035 | 4.5638 | 37.62 | |
| Pooled | 0.7013 | 0.4867 | 0.2701 | 1.8205 | ||
| Grade 4 | Eckardt | 2.0263 | 1.2194 | 0.1857 | 22.1136 | 56.90 |
| von Pawel | 0.9636 | 1.4011 | 0.0618 | 15.0138 | 43.10 | |
| Pooled | 1.4709 | 0.9198 | 0.2425 | 8.9232 | ||
| Vomiting | RR | SE(lnRR) | 95% CI | Weight (%) | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Grade 3 | Eckardt | 0.6079 | 0.7213 | 0.1479 | 2.4992 | 45.77 |
| von Pawel | 0.4130 | 0.6627 | 0.1127 | 1.5136 | 54.23 | |
| Pooled | 0.4929 | 0.4880 | 0.1894 | 1.2828 | ||
| Grade 4 | Eckardt | 1.0132 | 0.9934 | 0.1446 | 7.1006 | 66.54 |
| von Pawel | 0.9636 | 1.4011 | 0.0618 | 15.0138 | 33.46 | |
| Pooled | 0.9963 | 0.8104 | 0.2035 | 4.8776 | ||
Appendix 15 Estimating relative TTP for i.v. topotecan versus oral topotecan
Plots of the Kaplan–Meier estimates of TTP for patients treated with oral topotecan or i.v. topotecan in the RCTs reported by von Pawel and colleagues58 and Eckardt and colleagues56 were scanned using techdig software and then imported into microsoft excel. These were transformed, as described in Appendix 9, to be fit using least squares methods and the data were analysed using stata 9.
A log-logistic survival function for TTP was estimated, as for oral topotecan (described in Appendix 9), with the addition of a dummy (0,1) variable to indicate whether the data were for the oral topotecan arm (IV_Topo = 0) or the i.v. topotecan arm (IV_Topo = 1).
Regression output for log-logistic survival function for TTP in the RCT reported by von Pawel and colleagues:58
| Source | SS | df | MS | Number of obs = 118F(2, 115) = 1117.30Prob > F = 0.0000R-squared = 0.9511Adj R-squared = 0.9502Root MSE = .39714 | |||
| ModelResidual | 352.43758918.1375774 | 2115 | 176.218795.157718064 | ||||
| Total | 370.575167 | 117 | 3.16730912 | ||||
| logLogistic | Coef. | Std. Err. | t | P >|t| | [95% Conf. Interval] | ||
| ln_timeIV_Topo_cons | 2.00121.2709251–5.217638 | .0423367.07345.125721 | 47.273.69–41.50 | 0.0000.0000.000 | 1.917349.1254348–5.466667 | 2.085071.4164153–4.968609 | |
Regression output for log-logistic survival function for TTP in the RCT reported by Eckardt and colleagues:56
| Source | SS | df | MS | Number of obs = 148F(2, 145) = 1848.82Prob > F = 0.0000R-squared = 0.9623Adj R-squared = 0.9617Root MSE = .34325 | |||
| ModelResidual | 435.65057517.0837308 | 2145 | 217.825288.117818833 | ||||
| Total | 452.734306 | 147 | 3.07982521 | ||||
| logLogistic | Coef. | Std. Err. | t | P >|t| | [95% Conf. Interval] | ||
| ln_timeIV_Topo_cons | 1.812713–.2290531–4.810578 | .0298959.0587501.0955714 | 60.63–3.90–50.33 | 0.0000.0000.000 | 1.753625–.3451704–4.999472 | 1.871801–.1129359–4.621685 | |
The coefficient for the dummy variable, IV_Topo, has opposite signs in the two regressions – as would be expected since the two trials gave inconsistent results in terms of the relative TTP with i.v. and oral formulations of topotecan. In the RCT reported by von Pawel and colleagues58 median TTP was shorter for i.v. topotecan (13 weeks compared with 15 weeks for i.v. and oral topotecan, respectively), whereas in the RCT reported by Eckardt and colleagues56 median TTP was longer for i.v. topotecan (14.6 weeks compared with 11.9 weeks for i.v. and oral topotecan, respectively). Median TTP for oral topotecan in both trials is shorter than that reported in the RCT by O’Brien and colleagues,57 where median TTP for oral topotecan was 16.3 weeks.
IV_Topo was included as an additional covariate in the regression model estimated for TTP (described in Appendix 9), taking values estimated in the regressions above, to estimate the TTP for patients included in the model for oral topotecan, if they were treated with i.v. topotecan. This variable affects only the duration of post-treatment, non-progressive disease survival. Estimated median TTP using the model is reported in Table 77 below.
List of abbreviations
- AC
- adenocarcinoma
- BSA
- body surface area
- BSC
- best supportive care
- CAV
- cyclophosphamide, Adriamycin (doxorubicin) and vincristine
- CI
- confidence interval
- COPD
- chronic obstructive pulmonary disease
- CR
- complete response
- CRD
- Centre for Reviews and Dissemination
- ECOG
- Eastern Cooperative Oncology Group
- EQ-5D
- EuroQol 5 dimension health questionnaire
- ETS
- environmental tobacco smoke
- FACT-L
- Functional Assessment of Cancer Therapy – Lung
- FBC
- full blood count
- GCSF
- granulocyte colony-stimulating factor
- GP
- general practitioner
- HCHS
- Hospital and Community Health Service
- HR
- hazard ratio
- HRQoL
- health-related quality of life
- ICER
- incremental cost-effectiveness ratio
- ITT
- intention-to-treat
- i.v.
- intravenous
- LCSS
- lung cancer symptom scale
- LOCF
- last observation carried forward
- LYG
- life-years gained
- MDT
- multidisciplinary team
- MS
- manufacturer’s submission
- NICE
- National Institute for Health and Clinical Excellence
- NSCLC
- non-small cell lung cancer
- OR
- odds ratio
- ORR
- overall response rate
- OS
- overall survival
- PFS
- progression-free survival
- PR
- partial response
- PS
- performance status
- PSA
- patient symptom assessment
- PSS
- Personal Social Services
- QALY
- quality-adjusted life-year
- QoL
- quality of life
- RECIST
- Response Evaluation Criteria in Solid Tumours
- RBC
- red blood cell
- RCT
- randomised controlled trial
- RR
- risk ratio
- SCLC
- small cell lung cancer
- SCC
- squamous cell carcinoma
- SD
- standard deviation
- SMC
- Scottish Medicines Consortium
- SmPC
- summary of product characteristics
- TAR
- Technology Assessment Report
- TFI
- treatment-free interval
- TOI
- trial outcome index
- TTP
- time to disease progression
- ULN
- upper limit of normal
- VAS
- visual analogue scale
- WHO
- World Health Organization
- WTP
- willingness to pay
All abbreviations that have been used in this report are listed here unless the abbreviation is well known (e.g. NHS), or it has been used only once, or it is a non-standard abbreviation used only in figures/tables/appendices, in which case the abbreviation is defined in the figure legend or in the notes at the end of the table.
Notes
Health Technology Assessment reports published to date
-
Home parenteral nutrition: a systematic review.
By Richards DM, Deeks JJ, Sheldon TA, Shaffer JL.
-
Diagnosis, management and screening of early localised prostate cancer.
A review by Selley S, Donovan J, Faulkner A, Coast J, Gillatt D.
-
The diagnosis, management, treatment and costs of prostate cancer in England and Wales.
A review by Chamberlain J, Melia J, Moss S, Brown J.
-
Screening for fragile X syndrome.
A review by Murray J, Cuckle H, Taylor G, Hewison J.
-
A review of near patient testing in primary care.
By Hobbs FDR, Delaney BC, Fitzmaurice DA, Wilson S, Hyde CJ, Thorpe GH, et al.
-
Systematic review of outpatient services for chronic pain control.
By McQuay HJ, Moore RA, Eccleston C, Morley S, de C Williams AC.
-
Neonatal screening for inborn errors of metabolism: cost, yield and outcome.
A review by Pollitt RJ, Green A, McCabe CJ, Booth A, Cooper NJ, Leonard JV, et al.
-
Preschool vision screening.
A review by Snowdon SK, Stewart-Brown SL.
-
Implications of socio-cultural contexts for the ethics of clinical trials.
A review by Ashcroft RE, Chadwick DW, Clark SRL, Edwards RHT, Frith L, Hutton JL.
-
A critical review of the role of neonatal hearing screening in the detection of congenital hearing impairment.
By Davis A, Bamford J, Wilson I, Ramkalawan T, Forshaw M, Wright S.
-
Newborn screening for inborn errors of metabolism: a systematic review.
By Seymour CA, Thomason MJ, Chalmers RA, Addison GM, Bain MD, Cockburn F, et al.
-
Routine preoperative testing: a systematic review of the evidence.
By Munro J, Booth A, Nicholl J.
-
Systematic review of the effectiveness of laxatives in the elderly.
By Petticrew M, Watt I, Sheldon T.
-
When and how to assess fast-changing technologies: a comparative study of medical applications of four generic technologies.
A review by Mowatt G, Bower DJ, Brebner JA, Cairns JA, Grant AM, McKee L.
-
Antenatal screening for Down’s syndrome.
A review by Wald NJ, Kennard A, Hackshaw A, McGuire A.
-
Screening for ovarian cancer: a systematic review.
By Bell R, Petticrew M, Luengo S, Sheldon TA.
-
Consensus development methods, and their use in clinical guideline development.
A review by Murphy MK, Black NA, Lamping DL, McKee CM, Sanderson CFB, Askham J, et al.
-
A cost–utility analysis of interferon beta for multiple sclerosis.
By Parkin D, McNamee P, Jacoby A, Miller P, Thomas S, Bates D.
-
Effectiveness and efficiency of methods of dialysis therapy for end-stage renal disease: systematic reviews.
By MacLeod A, Grant A, Donaldson C, Khan I, Campbell M, Daly C, et al.
-
Effectiveness of hip prostheses in primary total hip replacement: a critical review of evidence and an economic model.
By Faulkner A, Kennedy LG, Baxter K, Donovan J, Wilkinson M, Bevan G.
-
Antimicrobial prophylaxis in colorectal surgery: a systematic review of randomised controlled trials.
By Song F, Glenny AM.
-
Bone marrow and peripheral blood stem cell transplantation for malignancy.
A review by Johnson PWM, Simnett SJ, Sweetenham JW, Morgan GJ, Stewart LA.
-
Screening for speech and language delay: a systematic review of the literature.
By Law J, Boyle J, Harris F, Harkness A, Nye C.
-
Resource allocation for chronic stable angina: a systematic review of effectiveness, costs and cost-effectiveness of alternative interventions.
By Sculpher MJ, Petticrew M, Kelland JL, Elliott RA, Holdright DR, Buxton MJ.
-
Detection, adherence and control of hypertension for the prevention of stroke: a systematic review.
By Ebrahim S.
-
Postoperative analgesia and vomiting, with special reference to day-case surgery: a systematic review.
By McQuay HJ, Moore RA.
-
Choosing between randomised and nonrandomised studies: a systematic review.
By Britton A, McKee M, Black N, McPherson K, Sanderson C, Bain C.
-
Evaluating patient-based outcome measures for use in clinical trials.
A review by Fitzpatrick R, Davey C, Buxton MJ, Jones DR.
-
Ethical issues in the design and conduct of randomised controlled trials.
A review by Edwards SJL, Lilford RJ, Braunholtz DA, Jackson JC, Hewison J, Thornton J.
-
Qualitative research methods in health technology assessment: a review of the literature.
By Murphy E, Dingwall R, Greatbatch D, Parker S, Watson P.
-
The costs and benefits of paramedic skills in pre-hospital trauma care.
By Nicholl J, Hughes S, Dixon S, Turner J, Yates D.
-
Systematic review of endoscopic ultrasound in gastro-oesophageal cancer.
By Harris KM, Kelly S, Berry E, Hutton J, Roderick P, Cullingworth J, et al.
-
Systematic reviews of trials and other studies.
By Sutton AJ, Abrams KR, Jones DR, Sheldon TA, Song F.
-
Primary total hip replacement surgery: a systematic review of outcomes and modelling of cost-effectiveness associated with different prostheses.
A review by Fitzpatrick R, Shortall E, Sculpher M, Murray D, Morris R, Lodge M, et al.
-
Informed decision making: an annotated bibliography and systematic review.
By Bekker H, Thornton JG, Airey CM, Connelly JB, Hewison J, Robinson MB, et al.
-
Handling uncertainty when performing economic evaluation of healthcare interventions.
A review by Briggs AH, Gray AM.
-
The role of expectancies in the placebo effect and their use in the delivery of health care: a systematic review.
By Crow R, Gage H, Hampson S, Hart J, Kimber A, Thomas H.
-
A randomised controlled trial of different approaches to universal antenatal HIV testing: uptake and acceptability. Annex: Antenatal HIV testing – assessment of a routine voluntary approach.
By Simpson WM, Johnstone FD, Boyd FM, Goldberg DJ, Hart GJ, Gormley SM, et al.
-
Methods for evaluating area-wide and organisation-based interventions in health and health care: a systematic review.
By Ukoumunne OC, Gulliford MC, Chinn S, Sterne JAC, Burney PGJ.
-
Assessing the costs of healthcare technologies in clinical trials.
A review by Johnston K, Buxton MJ, Jones DR, Fitzpatrick R.
-
Cooperatives and their primary care emergency centres: organisation and impact.
By Hallam L, Henthorne K.
-
Screening for cystic fibrosis.
A review by Murray J, Cuckle H, Taylor G, Littlewood J, Hewison J.
-
A review of the use of health status measures in economic evaluation.
By Brazier J, Deverill M, Green C, Harper R, Booth A.
-
Methods for the analysis of quality-of-life and survival data in health technology assessment.
A review by Billingham LJ, Abrams KR, Jones DR.
-
Antenatal and neonatal haemoglobinopathy screening in the UK: review and economic analysis.
By Zeuner D, Ades AE, Karnon J, Brown J, Dezateux C, Anionwu EN.
-
Assessing the quality of reports of randomised trials: implications for the conduct of meta-analyses.
A review by Moher D, Cook DJ, Jadad AR, Tugwell P, Moher M, Jones A, et al.
-
‘Early warning systems’ for identifying new healthcare technologies.
By Robert G, Stevens A, Gabbay J.
-
A systematic review of the role of human papillomavirus testing within a cervical screening programme.
By Cuzick J, Sasieni P, Davies P, Adams J, Normand C, Frater A, et al.
-
Near patient testing in diabetes clinics: appraising the costs and outcomes.
By Grieve R, Beech R, Vincent J, Mazurkiewicz J.
-
Positron emission tomography: establishing priorities for health technology assessment.
A review by Robert G, Milne R.
-
The debridement of chronic wounds: a systematic review.
By Bradley M, Cullum N, Sheldon T.
-
Systematic reviews of wound care management: (2) Dressings and topical agents used in the healing of chronic wounds.
By Bradley M, Cullum N, Nelson EA, Petticrew M, Sheldon T, Torgerson D.
-
A systematic literature review of spiral and electron beam computed tomography: with particular reference to clinical applications in hepatic lesions, pulmonary embolus and coronary artery disease.
By Berry E, Kelly S, Hutton J, Harris KM, Roderick P, Boyce JC, et al.
-
What role for statins? A review and economic model.
By Ebrahim S, Davey Smith G, McCabe C, Payne N, Pickin M, Sheldon TA, et al.
-
Factors that limit the quality, number and progress of randomised controlled trials.
A review by Prescott RJ, Counsell CE, Gillespie WJ, Grant AM, Russell IT, Kiauka S, et al.
-
Antimicrobial prophylaxis in total hip replacement: a systematic review.
By Glenny AM, Song F.
-
Health promoting schools and health promotion in schools: two systematic reviews.
By Lister-Sharp D, Chapman S, Stewart-Brown S, Sowden A.
-
Economic evaluation of a primary care-based education programme for patients with osteoarthritis of the knee.
A review by Lord J, Victor C, Littlejohns P, Ross FM, Axford JS.
-
The estimation of marginal time preference in a UK-wide sample (TEMPUS) project.
A review by Cairns JA, van der Pol MM.
-
Geriatric rehabilitation following fractures in older people: a systematic review.
By Cameron I, Crotty M, Currie C, Finnegan T, Gillespie L, Gillespie W, et al.
-
Screening for sickle cell disease and thalassaemia: a systematic review with supplementary research.
By Davies SC, Cronin E, Gill M, Greengross P, Hickman M, Normand C.
-
Community provision of hearing aids and related audiology services.
A review by Reeves DJ, Alborz A, Hickson FS, Bamford JM.
-
False-negative results in screening programmes: systematic review of impact and implications.
By Petticrew MP, Sowden AJ, Lister-Sharp D, Wright K.
-
Costs and benefits of community postnatal support workers: a randomised controlled trial.
By Morrell CJ, Spiby H, Stewart P, Walters S, Morgan A.
-
Implantable contraceptives (subdermal implants and hormonally impregnated intrauterine systems) versus other forms of reversible contraceptives: two systematic reviews to assess relative effectiveness, acceptability, tolerability and cost-effectiveness.
By French RS, Cowan FM, Mansour DJA, Morris S, Procter T, Hughes D, et al.
-
An introduction to statistical methods for health technology assessment.
A review by White SJ, Ashby D, Brown PJ.
-
Disease-modifying drugs for multiple sclerosis: a rapid and systematic review.
By Clegg A, Bryant J, Milne R.
-
Publication and related biases.
A review by Song F, Eastwood AJ, Gilbody S, Duley L, Sutton AJ.
-
Cost and outcome implications of the organisation of vascular services.
By Michaels J, Brazier J, Palfreyman S, Shackley P, Slack R.
-
Monitoring blood glucose control in diabetes mellitus: a systematic review.
By Coster S, Gulliford MC, Seed PT, Powrie JK, Swaminathan R.
-
The effectiveness of domiciliary health visiting: a systematic review of international studies and a selective review of the British literature.
By Elkan R, Kendrick D, Hewitt M, Robinson JJA, Tolley K, Blair M, et al.
-
The determinants of screening uptake and interventions for increasing uptake: a systematic review.
By Jepson R, Clegg A, Forbes C, Lewis R, Sowden A, Kleijnen J.
-
The effectiveness and cost-effectiveness of prophylactic removal of wisdom teeth.
A rapid review by Song F, O’Meara S, Wilson P, Golder S, Kleijnen J.
-
Ultrasound screening in pregnancy: a systematic review of the clinical effectiveness, cost-effectiveness and women’s views.
By Bricker L, Garcia J, Henderson J, Mugford M, Neilson J, Roberts T, et al.
-
A rapid and systematic review of the effectiveness and cost-effectiveness of the taxanes used in the treatment of advanced breast and ovarian cancer.
By Lister-Sharp D, McDonagh MS, Khan KS, Kleijnen J.
-
Liquid-based cytology in cervical screening: a rapid and systematic review.
By Payne N, Chilcott J, McGoogan E.
-
Randomised controlled trial of non-directive counselling, cognitive–behaviour therapy and usual general practitioner care in the management of depression as well as mixed anxiety and depression in primary care.
By King M, Sibbald B, Ward E, Bower P, Lloyd M, Gabbay M, et al.
-
Routine referral for radiography of patients presenting with low back pain: is patients’ outcome influenced by GPs’ referral for plain radiography?
By Kerry S, Hilton S, Patel S, Dundas D, Rink E, Lord J.
-
Systematic reviews of wound care management: (3) antimicrobial agents for chronic wounds; (4) diabetic foot ulceration.
By O’Meara S, Cullum N, Majid M, Sheldon T.
-
Using routine data to complement and enhance the results of randomised controlled trials.
By Lewsey JD, Leyland AH, Murray GD, Boddy FA.
-
Coronary artery stents in the treatment of ischaemic heart disease: a rapid and systematic review.
By Meads C, Cummins C, Jolly K, Stevens A, Burls A, Hyde C.
-
Outcome measures for adult critical care: a systematic review.
By Hayes JA, Black NA, Jenkinson C, Young JD, Rowan KM, Daly K, et al.
-
A systematic review to evaluate the effectiveness of interventions to promote the initiation of breastfeeding.
By Fairbank L, O’Meara S, Renfrew MJ, Woolridge M, Sowden AJ, Lister-Sharp D.
-
Implantable cardioverter defibrillators: arrhythmias. A rapid and systematic review.
By Parkes J, Bryant J, Milne R.
-
Treatments for fatigue in multiple sclerosis: a rapid and systematic review.
By Brañas P, Jordan R, Fry-Smith A, Burls A, Hyde C.
-
Early asthma prophylaxis, natural history, skeletal development and economy (EASE): a pilot randomised controlled trial.
By Baxter-Jones ADG, Helms PJ, Russell G, Grant A, Ross S, Cairns JA, et al.
-
Screening for hypercholesterolaemia versus case finding for familial hypercholesterolaemia: a systematic review and cost-effectiveness analysis.
By Marks D, Wonderling D, Thorogood M, Lambert H, Humphries SE, Neil HAW.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of glycoprotein IIb/IIIa antagonists in the medical management of unstable angina.
By McDonagh MS, Bachmann LM, Golder S, Kleijnen J, ter Riet G.
-
A randomised controlled trial of prehospital intravenous fluid replacement therapy in serious trauma.
By Turner J, Nicholl J, Webber L, Cox H, Dixon S, Yates D.
-
Intrathecal pumps for giving opioids in chronic pain: a systematic review.
By Williams JE, Louw G, Towlerton G.
-
Combination therapy (interferon alfa and ribavirin) in the treatment of chronic hepatitis C: a rapid and systematic review.
By Shepherd J, Waugh N, Hewitson P.
-
A systematic review of comparisons of effect sizes derived from randomised and non-randomised studies.
By MacLehose RR, Reeves BC, Harvey IM, Sheldon TA, Russell IT, Black AMS.
-
Intravascular ultrasound-guided interventions in coronary artery disease: a systematic literature review, with decision-analytic modelling, of outcomes and cost-effectiveness.
By Berry E, Kelly S, Hutton J, Lindsay HSJ, Blaxill JM, Evans JA, et al.
-
A randomised controlled trial to evaluate the effectiveness and cost-effectiveness of counselling patients with chronic depression.
By Simpson S, Corney R, Fitzgerald P, Beecham J.
-
Systematic review of treatments for atopic eczema.
By Hoare C, Li Wan Po A, Williams H.
-
Bayesian methods in health technology assessment: a review.
By Spiegelhalter DJ, Myles JP, Jones DR, Abrams KR.
-
The management of dyspepsia: a systematic review.
By Delaney B, Moayyedi P, Deeks J, Innes M, Soo S, Barton P, et al.
-
A systematic review of treatments for severe psoriasis.
By Griffiths CEM, Clark CM, Chalmers RJG, Li Wan Po A, Williams HC.
-
Clinical and cost-effectiveness of donepezil, rivastigmine and galantamine for Alzheimer’s disease: a rapid and systematic review.
By Clegg A, Bryant J, Nicholson T, McIntyre L, De Broe S, Gerard K, et al.
-
The clinical effectiveness and cost-effectiveness of riluzole for motor neurone disease: a rapid and systematic review.
By Stewart A, Sandercock J, Bryan S, Hyde C, Barton PM, Fry-Smith A, et al.
-
Equity and the economic evaluation of healthcare.
By Sassi F, Archard L, Le Grand J.
-
Quality-of-life measures in chronic diseases of childhood.
By Eiser C, Morse R.
-
Eliciting public preferences for healthcare: a systematic review of techniques.
By Ryan M, Scott DA, Reeves C, Bate A, van Teijlingen ER, Russell EM, et al.
-
General health status measures for people with cognitive impairment: learning disability and acquired brain injury.
By Riemsma RP, Forbes CA, Glanville JM, Eastwood AJ, Kleijnen J.
-
An assessment of screening strategies for fragile X syndrome in the UK.
By Pembrey ME, Barnicoat AJ, Carmichael B, Bobrow M, Turner G.
-
Issues in methodological research: perspectives from researchers and commissioners.
By Lilford RJ, Richardson A, Stevens A, Fitzpatrick R, Edwards S, Rock F, et al.
-
Systematic reviews of wound care management: (5) beds; (6) compression; (7) laser therapy, therapeutic ultrasound, electrotherapy and electromagnetic therapy.
By Cullum N, Nelson EA, Flemming K, Sheldon T.
-
Effects of educational and psychosocial interventions for adolescents with diabetes mellitus: a systematic review.
By Hampson SE, Skinner TC, Hart J, Storey L, Gage H, Foxcroft D, et al.
-
Effectiveness of autologous chondrocyte transplantation for hyaline cartilage defects in knees: a rapid and systematic review.
By Jobanputra P, Parry D, Fry-Smith A, Burls A.
-
Statistical assessment of the learning curves of health technologies.
By Ramsay CR, Grant AM, Wallace SA, Garthwaite PH, Monk AF, Russell IT.
-
The effectiveness and cost-effectiveness of temozolomide for the treatment of recurrent malignant glioma: a rapid and systematic review.
By Dinnes J, Cave C, Huang S, Major K, Milne R.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of debriding agents in treating surgical wounds healing by secondary intention.
By Lewis R, Whiting P, ter Riet G, O’Meara S, Glanville J.
-
Home treatment for mental health problems: a systematic review.
By Burns T, Knapp M, Catty J, Healey A, Henderson J, Watt H, et al.
-
How to develop cost-conscious guidelines.
By Eccles M, Mason J.
-
The role of specialist nurses in multiple sclerosis: a rapid and systematic review.
By De Broe S, Christopher F, Waugh N.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of orlistat in the management of obesity.
By O’Meara S, Riemsma R, Shirran L, Mather L, ter Riet G.
-
The clinical effectiveness and cost-effectiveness of pioglitazone for type 2 diabetes mellitus: a rapid and systematic review.
By Chilcott J, Wight J, Lloyd Jones M, Tappenden P.
-
Extended scope of nursing practice: a multicentre randomised controlled trial of appropriately trained nurses and preregistration house officers in preoperative assessment in elective general surgery.
By Kinley H, Czoski-Murray C, George S, McCabe C, Primrose J, Reilly C, et al.
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) Acute day hospital versus admission; (2) Vocational rehabilitation; (3) Day hospital versus outpatient care.
By Marshall M, Crowther R, Almaraz- Serrano A, Creed F, Sledge W, Kluiter H, et al.
-
The measurement and monitoring of surgical adverse events.
By Bruce J, Russell EM, Mollison J, Krukowski ZH.
-
Action research: a systematic review and guidance for assessment.
By Waterman H, Tillen D, Dickson R, de Koning K.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of gemcitabine for the treatment of pancreatic cancer.
By Ward S, Morris E, Bansback N, Calvert N, Crellin A, Forman D, et al.
-
A rapid and systematic review of the evidence for the clinical effectiveness and cost-effectiveness of irinotecan, oxaliplatin and raltitrexed for the treatment of advanced colorectal cancer.
By Lloyd Jones M, Hummel S, Bansback N, Orr B, Seymour M.
-
Comparison of the effectiveness of inhaler devices in asthma and chronic obstructive airways disease: a systematic review of the literature.
By Brocklebank D, Ram F, Wright J, Barry P, Cates C, Davies L, et al.
-
The cost-effectiveness of magnetic resonance imaging for investigation of the knee joint.
By Bryan S, Weatherburn G, Bungay H, Hatrick C, Salas C, Parry D, et al.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.
By Forbes C, Shirran L, Bagnall A-M, Duffy S, ter Riet G.
-
Superseded by a report published in a later volume.
-
The role of radiography in primary care patients with low back pain of at least 6 weeks duration: a randomised (unblinded) controlled trial.
By Kendrick D, Fielding K, Bentley E, Miller P, Kerslake R, Pringle M.
-
Design and use of questionnaires: a review of best practice applicable to surveys of health service staff and patients.
By McColl E, Jacoby A, Thomas L, Soutter J, Bamford C, Steen N, et al.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.
By Clegg A, Scott DA, Sidhu M, Hewitson P, Waugh N.
-
Subgroup analyses in randomised controlled trials: quantifying the risks of false-positives and false-negatives.
By Brookes ST, Whitley E, Peters TJ, Mulheran PA, Egger M, Davey Smith G.
-
Depot antipsychotic medication in the treatment of patients with schizophrenia: (1) Meta-review; (2) Patient and nurse attitudes.
By David AS, Adams C.
-
A systematic review of controlled trials of the effectiveness and cost-effectiveness of brief psychological treatments for depression.
By Churchill R, Hunot V, Corney R, Knapp M, McGuire H, Tylee A, et al.
-
Cost analysis of child health surveillance.
By Sanderson D, Wright D, Acton C, Duree D.
-
A study of the methods used to select review criteria for clinical audit.
By Hearnshaw H, Harker R, Cheater F, Baker R, Grimshaw G.
-
Fludarabine as second-line therapy for B cell chronic lymphocytic leukaemia: a technology assessment.
By Hyde C, Wake B, Bryan S, Barton P, Fry-Smith A, Davenport C, et al.
-
Rituximab as third-line treatment for refractory or recurrent Stage III or IV follicular non-Hodgkin’s lymphoma: a systematic review and economic evaluation.
By Wake B, Hyde C, Bryan S, Barton P, Song F, Fry-Smith A, et al.
-
A systematic review of discharge arrangements for older people.
By Parker SG, Peet SM, McPherson A, Cannaby AM, Baker R, Wilson A, et al.
-
The clinical effectiveness and cost-effectiveness of inhaler devices used in the routine management of chronic asthma in older children: a systematic review and economic evaluation.
By Peters J, Stevenson M, Beverley C, Lim J, Smith S.
-
The clinical effectiveness and cost-effectiveness of sibutramine in the management of obesity: a technology assessment.
By O’Meara S, Riemsma R, Shirran L, Mather L, ter Riet G.
-
The cost-effectiveness of magnetic resonance angiography for carotid artery stenosis and peripheral vascular disease: a systematic review.
By Berry E, Kelly S, Westwood ME, Davies LM, Gough MJ, Bamford JM, et al.
-
Promoting physical activity in South Asian Muslim women through ‘exercise on prescription’.
By Carroll B, Ali N, Azam N.
-
Zanamivir for the treatment of influenza in adults: a systematic review and economic evaluation.
By Burls A, Clark W, Stewart T, Preston C, Bryan S, Jefferson T, et al.
-
A review of the natural history and epidemiology of multiple sclerosis: implications for resource allocation and health economic models.
By Richards RG, Sampson FC, Beard SM, Tappenden P.
-
Screening for gestational diabetes: a systematic review and economic evaluation.
By Scott DA, Loveman E, McIntyre L, Waugh N.
-
The clinical effectiveness and cost-effectiveness of surgery for people with morbid obesity: a systematic review and economic evaluation.
By Clegg AJ, Colquitt J, Sidhu MK, Royle P, Loveman E, Walker A.
-
The clinical effectiveness of trastuzumab for breast cancer: a systematic review.
By Lewis R, Bagnall A-M, Forbes C, Shirran E, Duffy S, Kleijnen J, et al.
-
The clinical effectiveness and cost-effectiveness of vinorelbine for breast cancer: a systematic review and economic evaluation.
By Lewis R, Bagnall A-M, King S, Woolacott N, Forbes C, Shirran L, et al.
-
A systematic review of the effectiveness and cost-effectiveness of metal-on-metal hip resurfacing arthroplasty for treatment of hip disease.
By Vale L, Wyness L, McCormack K, McKenzie L, Brazzelli M, Stearns SC.
-
The clinical effectiveness and cost-effectiveness of bupropion and nicotine replacement therapy for smoking cessation: a systematic review and economic evaluation.
By Woolacott NF, Jones L, Forbes CA, Mather LC, Sowden AJ, Song FJ, et al.
-
A systematic review of effectiveness and economic evaluation of new drug treatments for juvenile idiopathic arthritis: etanercept.
By Cummins C, Connock M, Fry-Smith A, Burls A.
-
Clinical effectiveness and cost-effectiveness of growth hormone in children: a systematic review and economic evaluation.
By Bryant J, Cave C, Mihaylova B, Chase D, McIntyre L, Gerard K, et al.
-
Clinical effectiveness and cost-effectiveness of growth hormone in adults in relation to impact on quality of life: a systematic review and economic evaluation.
By Bryant J, Loveman E, Chase D, Mihaylova B, Cave C, Gerard K, et al.
-
Clinical medication review by a pharmacist of patients on repeat prescriptions in general practice: a randomised controlled trial.
By Zermansky AG, Petty DR, Raynor DK, Lowe CJ, Freementle N, Vail A.
-
The effectiveness of infliximab and etanercept for the treatment of rheumatoid arthritis: a systematic review and economic evaluation.
By Jobanputra P, Barton P, Bryan S, Burls A.
-
A systematic review and economic evaluation of computerised cognitive behaviour therapy for depression and anxiety.
By Kaltenthaler E, Shackley P, Stevens K, Beverley C, Parry G, Chilcott J.
-
A systematic review and economic evaluation of pegylated liposomal doxorubicin hydrochloride for ovarian cancer.
By Forbes C, Wilby J, Richardson G, Sculpher M, Mather L, Riemsma R.
-
A systematic review of the effectiveness of interventions based on a stages-of-change approach to promote individual behaviour change.
By Riemsma RP, Pattenden J, Bridle C, Sowden AJ, Mather L, Watt IS, et al.
-
A systematic review update of the clinical effectiveness and cost-effectiveness of glycoprotein IIb/IIIa antagonists.
By Robinson M, Ginnelly L, Sculpher M, Jones L, Riemsma R, Palmer S, et al.
-
A systematic review of the effectiveness, cost-effectiveness and barriers to implementation of thrombolytic and neuroprotective therapy for acute ischaemic stroke in the NHS.
By Sandercock P, Berge E, Dennis M, Forbes J, Hand P, Kwan J, et al.
-
A randomised controlled crossover trial of nurse practitioner versus doctor-led outpatient care in a bronchiectasis clinic.
By Caine N, Sharples LD, Hollingworth W, French J, Keogan M, Exley A, et al.
-
Clinical effectiveness and cost – consequences of selective serotonin reuptake inhibitors in the treatment of sex offenders.
By Adi Y, Ashcroft D, Browne K, Beech A, Fry-Smith A, Hyde C.
-
Treatment of established osteoporosis: a systematic review and cost–utility analysis.
By Kanis JA, Brazier JE, Stevenson M, Calvert NW, Lloyd Jones M.
-
Which anaesthetic agents are cost-effective in day surgery? Literature review, national survey of practice and randomised controlled trial.
By Elliott RA Payne K, Moore JK, Davies LM, Harper NJN, St Leger AS, et al.
-
Screening for hepatitis C among injecting drug users and in genitourinary medicine clinics: systematic reviews of effectiveness, modelling study and national survey of current practice.
By Stein K, Dalziel K, Walker A, McIntyre L, Jenkins B, Horne J, et al.
-
The measurement of satisfaction with healthcare: implications for practice from a systematic review of the literature.
By Crow R, Gage H, Hampson S, Hart J, Kimber A, Storey L, et al.
-
The effectiveness and cost-effectiveness of imatinib in chronic myeloid leukaemia: a systematic review.
By Garside R, Round A, Dalziel K, Stein K, Royle R.
-
A comparative study of hypertonic saline, daily and alternate-day rhDNase in children with cystic fibrosis.
By Suri R, Wallis C, Bush A, Thompson S, Normand C, Flather M, et al.
-
A systematic review of the costs and effectiveness of different models of paediatric home care.
By Parker G, Bhakta P, Lovett CA, Paisley S, Olsen R, Turner D, et al.
-
How important are comprehensive literature searches and the assessment of trial quality in systematic reviews? Empirical study.
By Egger M, Jüni P, Bartlett C, Holenstein F, Sterne J.
-
Systematic review of the effectiveness and cost-effectiveness, and economic evaluation, of home versus hospital or satellite unit haemodialysis for people with end-stage renal failure.
By Mowatt G, Vale L, Perez J, Wyness L, Fraser C, MacLeod A, et al.
-
Systematic review and economic evaluation of the effectiveness of infliximab for the treatment of Crohn’s disease.
By Clark W, Raftery J, Barton P, Song F, Fry-Smith A, Burls A.
-
A review of the clinical effectiveness and cost-effectiveness of routine anti-D prophylaxis for pregnant women who are rhesus negative.
By Chilcott J, Lloyd Jones M, Wight J, Forman K, Wray J, Beverley C, et al.
-
Systematic review and evaluation of the use of tumour markers in paediatric oncology: Ewing’s sarcoma and neuroblastoma.
By Riley RD, Burchill SA, Abrams KR, Heney D, Lambert PC, Jones DR, et al.
-
The cost-effectiveness of screening for Helicobacter pylori to reduce mortality and morbidity from gastric cancer and peptic ulcer disease: a discrete-event simulation model.
By Roderick P, Davies R, Raftery J, Crabbe D, Pearce R, Bhandari P, et al.
-
The clinical effectiveness and cost-effectiveness of routine dental checks: a systematic review and economic evaluation.
By Davenport C, Elley K, Salas C, Taylor-Weetman CL, Fry-Smith A, Bryan S, et al.
-
A multicentre randomised controlled trial assessing the costs and benefits of using structured information and analysis of women’s preferences in the management of menorrhagia.
By Kennedy ADM, Sculpher MJ, Coulter A, Dwyer N, Rees M, Horsley S, et al.
-
Clinical effectiveness and cost–utility of photodynamic therapy for wet age-related macular degeneration: a systematic review and economic evaluation.
By Meads C, Salas C, Roberts T, Moore D, Fry-Smith A, Hyde C.
-
Evaluation of molecular tests for prenatal diagnosis of chromosome abnormalities.
By Grimshaw GM, Szczepura A, Hultén M, MacDonald F, Nevin NC, Sutton F, et al.
-
First and second trimester antenatal screening for Down’s syndrome: the results of the Serum, Urine and Ultrasound Screening Study (SURUSS).
By Wald NJ, Rodeck C, Hackshaw AK, Walters J, Chitty L, Mackinson AM.
-
The effectiveness and cost-effectiveness of ultrasound locating devices for central venous access: a systematic review and economic evaluation.
By Calvert N, Hind D, McWilliams RG, Thomas SM, Beverley C, Davidson A.
-
A systematic review of atypical antipsychotics in schizophrenia.
By Bagnall A-M, Jones L, Lewis R, Ginnelly L, Glanville J, Torgerson D, et al.
-
Prostate Testing for Cancer and Treatment (ProtecT) feasibility study.
By Donovan J, Hamdy F, Neal D, Peters T, Oliver S, Brindle L, et al.
-
Early thrombolysis for the treatment of acute myocardial infarction: a systematic review and economic evaluation.
By Boland A, Dundar Y, Bagust A, Haycox A, Hill R, Mujica Mota R, et al.
-
Screening for fragile X syndrome: a literature review and modelling.
By Song FJ, Barton P, Sleightholme V, Yao GL, Fry-Smith A.
-
Systematic review of endoscopic sinus surgery for nasal polyps.
By Dalziel K, Stein K, Round A, Garside R, Royle P.
-
Towards efficient guidelines: how to monitor guideline use in primary care.
By Hutchinson A, McIntosh A, Cox S, Gilbert C.
-
Effectiveness and cost-effectiveness of acute hospital-based spinal cord injuries services: systematic review.
By Bagnall A-M, Jones L, Richardson G, Duffy S, Riemsma R.
-
Prioritisation of health technology assessment. The PATHS model: methods and case studies.
By Townsend J, Buxton M, Harper G.
-
Systematic review of the clinical effectiveness and cost-effectiveness of tension-free vaginal tape for treatment of urinary stress incontinence.
By Cody J, Wyness L, Wallace S, Glazener C, Kilonzo M, Stearns S, et al.
-
The clinical and cost-effectiveness of patient education models for diabetes: a systematic review and economic evaluation.
By Loveman E, Cave C, Green C, Royle P, Dunn N, Waugh N.
-
The role of modelling in prioritising and planning clinical trials.
By Chilcott J, Brennan A, Booth A, Karnon J, Tappenden P.
-
Cost–benefit evaluation of routine influenza immunisation in people 65–74 years of age.
By Allsup S, Gosney M, Haycox A, Regan M.
-
The clinical and cost-effectiveness of pulsatile machine perfusion versus cold storage of kidneys for transplantation retrieved from heart-beating and non-heart-beating donors.
By Wight J, Chilcott J, Holmes M, Brewer N.
-
Can randomised trials rely on existing electronic data? A feasibility study to explore the value of routine data in health technology assessment.
By Williams JG, Cheung WY, Cohen DR, Hutchings HA, Longo MF, Russell IT.
-
Evaluating non-randomised intervention studies.
By Deeks JJ, Dinnes J, D’Amico R, Sowden AJ, Sakarovitch C, Song F, et al.
-
A randomised controlled trial to assess the impact of a package comprising a patient-orientated, evidence-based self- help guidebook and patient-centred consultations on disease management and satisfaction in inflammatory bowel disease.
By Kennedy A, Nelson E, Reeves D, Richardson G, Roberts C, Robinson A, et al.
-
The effectiveness of diagnostic tests for the assessment of shoulder pain due to soft tissue disorders: a systematic review.
By Dinnes J, Loveman E, McIntyre L, Waugh N.
-
The value of digital imaging in diabetic retinopathy.
By Sharp PF, Olson J, Strachan F, Hipwell J, Ludbrook A, O’Donnell M, et al.
-
Lowering blood pressure to prevent myocardial infarction and stroke: a new preventive strategy.
By Law M, Wald N, Morris J.
-
Clinical and cost-effectiveness of capecitabine and tegafur with uracil for the treatment of metastatic colorectal cancer: systematic review and economic evaluation.
By Ward S, Kaltenthaler E, Cowan J, Brewer N.
-
Clinical and cost-effectiveness of new and emerging technologies for early localised prostate cancer: a systematic review.
By Hummel S, Paisley S, Morgan A, Currie E, Brewer N.
-
Literature searching for clinical and cost-effectiveness studies used in health technology assessment reports carried out for the National Institute for Clinical Excellence appraisal system.
By Royle P, Waugh N.
-
Systematic review and economic decision modelling for the prevention and treatment of influenza A and B.
By Turner D, Wailoo A, Nicholson K, Cooper N, Sutton A, Abrams K.
-
A randomised controlled trial to evaluate the clinical and cost-effectiveness of Hickman line insertions in adult cancer patients by nurses.
By Boland A, Haycox A, Bagust A, Fitzsimmons L.
-
Redesigning postnatal care: a randomised controlled trial of protocol-based midwifery-led care focused on individual women’s physical and psychological health needs.
By MacArthur C, Winter HR, Bick DE, Lilford RJ, Lancashire RJ, Knowles H, et al.
-
Estimating implied rates of discount in healthcare decision-making.
By West RR, McNabb R, Thompson AGH, Sheldon TA, Grimley Evans J.
-
Systematic review of isolation policies in the hospital management of methicillin-resistant Staphylococcus aureus: a review of the literature with epidemiological and economic modelling.
By Cooper BS, Stone SP, Kibbler CC, Cookson BD, Roberts JA, Medley GF, et al.
-
Treatments for spasticity and pain in multiple sclerosis: a systematic review.
By Beard S, Hunn A, Wight J.
-
The inclusion of reports of randomised trials published in languages other than English in systematic reviews.
By Moher D, Pham B, Lawson ML, Klassen TP.
-
The impact of screening on future health-promoting behaviours and health beliefs: a systematic review.
By Bankhead CR, Brett J, Bukach C, Webster P, Stewart-Brown S, Munafo M, et al.
-
What is the best imaging strategy for acute stroke?
By Wardlaw JM, Keir SL, Seymour J, Lewis S, Sandercock PAG, Dennis MS, et al.
-
Systematic review and modelling of the investigation of acute and chronic chest pain presenting in primary care.
By Mant J, McManus RJ, Oakes RAL, Delaney BC, Barton PM, Deeks JJ, et al.
-
The effectiveness and cost-effectiveness of microwave and thermal balloon endometrial ablation for heavy menstrual bleeding: a systematic review and economic modelling.
By Garside R, Stein K, Wyatt K, Round A, Price A.
-
A systematic review of the role of bisphosphonates in metastatic disease.
By Ross JR, Saunders Y, Edmonds PM, Patel S, Wonderling D, Normand C, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of capecitabine (Xeloda®) for locally advanced and/or metastatic breast cancer.
By Jones L, Hawkins N, Westwood M, Wright K, Richardson G, Riemsma R.
-
Effectiveness and efficiency of guideline dissemination and implementation strategies.
By Grimshaw JM, Thomas RE, MacLennan G, Fraser C, Ramsay CR, Vale L, et al.
-
Clinical effectiveness and costs of the Sugarbaker procedure for the treatment of pseudomyxoma peritonei.
By Bryant J, Clegg AJ, Sidhu MK, Brodin H, Royle P, Davidson P.
-
Psychological treatment for insomnia in the regulation of long-term hypnotic drug use.
By Morgan K, Dixon S, Mathers N, Thompson J, Tomeny M.
-
Improving the evaluation of therapeutic interventions in multiple sclerosis: development of a patient-based measure of outcome.
By Hobart JC, Riazi A, Lamping DL, Fitzpatrick R, Thompson AJ.
-
A systematic review and economic evaluation of magnetic resonance cholangiopancreatography compared with diagnostic endoscopic retrograde cholangiopancreatography.
By Kaltenthaler E, Bravo Vergel Y, Chilcott J, Thomas S, Blakeborough T, Walters SJ, et al.
-
The use of modelling to evaluate new drugs for patients with a chronic condition: the case of antibodies against tumour necrosis factor in rheumatoid arthritis.
By Barton P, Jobanputra P, Wilson J, Bryan S, Burls A.
-
Clinical effectiveness and cost-effectiveness of neonatal screening for inborn errors of metabolism using tandem mass spectrometry: a systematic review.
By Pandor A, Eastham J, Beverley C, Chilcott J, Paisley S.
-
Clinical effectiveness and cost-effectiveness of pioglitazone and rosiglitazone in the treatment of type 2 diabetes: a systematic review and economic evaluation.
By Czoski-Murray C, Warren E, Chilcott J, Beverley C, Psyllaki MA, Cowan J.
-
Routine examination of the newborn: the EMREN study. Evaluation of an extension of the midwife role including a randomised controlled trial of appropriately trained midwives and paediatric senior house officers.
By Townsend J, Wolke D, Hayes J, Davé S, Rogers C, Bloomfield L, et al.
-
Involving consumers in research and development agenda setting for the NHS: developing an evidence-based approach.
By Oliver S, Clarke-Jones L, Rees R, Milne R, Buchanan P, Gabbay J, et al.
-
A multi-centre randomised controlled trial of minimally invasive direct coronary bypass grafting versus percutaneous transluminal coronary angioplasty with stenting for proximal stenosis of the left anterior descending coronary artery.
By Reeves BC, Angelini GD, Bryan AJ, Taylor FC, Cripps T, Spyt TJ, et al.
-
Does early magnetic resonance imaging influence management or improve outcome in patients referred to secondary care with low back pain? A pragmatic randomised controlled trial.
By Gilbert FJ, Grant AM, Gillan MGC, Vale L, Scott NW, Campbell MK, et al.
-
The clinical and cost-effectiveness of anakinra for the treatment of rheumatoid arthritis in adults: a systematic review and economic analysis.
By Clark W, Jobanputra P, Barton P, Burls A.
-
A rapid and systematic review and economic evaluation of the clinical and cost-effectiveness of newer drugs for treatment of mania associated with bipolar affective disorder.
By Bridle C, Palmer S, Bagnall A-M, Darba J, Duffy S, Sculpher M, et al.
-
Liquid-based cytology in cervical screening: an updated rapid and systematic review and economic analysis.
By Karnon J, Peters J, Platt J, Chilcott J, McGoogan E, Brewer N.
-
Systematic review of the long-term effects and economic consequences of treatments for obesity and implications for health improvement.
By Avenell A, Broom J, Brown TJ, Poobalan A, Aucott L, Stearns SC, et al.
-
Autoantibody testing in children with newly diagnosed type 1 diabetes mellitus.
By Dretzke J, Cummins C, Sandercock J, Fry-Smith A, Barrett T, Burls A.
-
Clinical effectiveness and cost-effectiveness of prehospital intravenous fluids in trauma patients.
By Dretzke J, Sandercock J, Bayliss S, Burls A.
-
Newer hypnotic drugs for the short-term management of insomnia: a systematic review and economic evaluation.
By Dündar Y, Boland A, Strobl J, Dodd S, Haycox A, Bagust A, et al.
-
Development and validation of methods for assessing the quality of diagnostic accuracy studies.
By Whiting P, Rutjes AWS, Dinnes J, Reitsma JB, Bossuyt PMM, Kleijnen J.
-
EVALUATE hysterectomy trial: a multicentre randomised trial comparing abdominal, vaginal and laparoscopic methods of hysterectomy.
By Garry R, Fountain J, Brown J, Manca A, Mason S, Sculpher M, et al.
-
Methods for expected value of information analysis in complex health economic models: developments on the health economics of interferon-β and glatiramer acetate for multiple sclerosis.
By Tappenden P, Chilcott JB, Eggington S, Oakley J, McCabe C.
-
Effectiveness and cost-effectiveness of imatinib for first-line treatment of chronic myeloid leukaemia in chronic phase: a systematic review and economic analysis.
By Dalziel K, Round A, Stein K, Garside R, Price A.
-
VenUS I: a randomised controlled trial of two types of bandage for treating venous leg ulcers.
By Iglesias C, Nelson EA, Cullum NA, Torgerson DJ, on behalf of the VenUS Team.
-
Systematic review of the effectiveness and cost-effectiveness, and economic evaluation, of myocardial perfusion scintigraphy for the diagnosis and management of angina and myocardial infarction.
By Mowatt G, Vale L, Brazzelli M, Hernandez R, Murray A, Scott N, et al.
-
A pilot study on the use of decision theory and value of information analysis as part of the NHS Health Technology Assessment programme.
By Claxton K, Ginnelly L, Sculpher M, Philips Z, Palmer S.
-
The Social Support and Family Health Study: a randomised controlled trial and economic evaluation of two alternative forms of postnatal support for mothers living in disadvantaged inner-city areas.
By Wiggins M, Oakley A, Roberts I, Turner H, Rajan L, Austerberry H, et al.
-
Psychosocial aspects of genetic screening of pregnant women and newborns: a systematic review.
By Green JM, Hewison J, Bekker HL, Bryant, Cuckle HS.
-
Evaluation of abnormal uterine bleeding: comparison of three outpatient procedures within cohorts defined by age and menopausal status.
By Critchley HOD, Warner P, Lee AJ, Brechin S, Guise J, Graham B.
-
Coronary artery stents: a rapid systematic review and economic evaluation.
By Hill R, Bagust A, Bakhai A, Dickson R, Dündar Y, Haycox A, et al.
-
Review of guidelines for good practice in decision-analytic modelling in health technology assessment.
By Philips Z, Ginnelly L, Sculpher M, Claxton K, Golder S, Riemsma R, et al.
-
Rituximab (MabThera®) for aggressive non-Hodgkin’s lymphoma: systematic review and economic evaluation.
By Knight C, Hind D, Brewer N, Abbott V.
-
Clinical effectiveness and cost-effectiveness of clopidogrel and modified-release dipyridamole in the secondary prevention of occlusive vascular events: a systematic review and economic evaluation.
By Jones L, Griffin S, Palmer S, Main C, Orton V, Sculpher M, et al.
-
Pegylated interferon α-2a and -2b in combination with ribavirin in the treatment of chronic hepatitis C: a systematic review and economic evaluation.
By Shepherd J, Brodin H, Cave C, Waugh N, Price A, Gabbay J.
-
Clopidogrel used in combination with aspirin compared with aspirin alone in the treatment of non-ST-segment- elevation acute coronary syndromes: a systematic review and economic evaluation.
By Main C, Palmer S, Griffin S, Jones L, Orton V, Sculpher M, et al.
-
Provision, uptake and cost of cardiac rehabilitation programmes: improving services to under-represented groups.
By Beswick AD, Rees K, Griebsch I, Taylor FC, Burke M, West RR, et al.
-
Involving South Asian patients in clinical trials.
By Hussain-Gambles M, Leese B, Atkin K, Brown J, Mason S, Tovey P.
-
Clinical and cost-effectiveness of continuous subcutaneous insulin infusion for diabetes.
By Colquitt JL, Green C, Sidhu MK, Hartwell D, Waugh N.
-
Identification and assessment of ongoing trials in health technology assessment reviews.
By Song FJ, Fry-Smith A, Davenport C, Bayliss S, Adi Y, Wilson JS, et al.
-
Systematic review and economic evaluation of a long-acting insulin analogue, insulin glargine
By Warren E, Weatherley-Jones E, Chilcott J, Beverley C.
-
Supplementation of a home-based exercise programme with a class-based programme for people with osteoarthritis of the knees: a randomised controlled trial and health economic analysis.
By McCarthy CJ, Mills PM, Pullen R, Richardson G, Hawkins N, Roberts CR, et al.
-
Clinical and cost-effectiveness of once-daily versus more frequent use of same potency topical corticosteroids for atopic eczema: a systematic review and economic evaluation.
By Green C, Colquitt JL, Kirby J, Davidson P, Payne E.
-
Acupuncture of chronic headache disorders in primary care: randomised controlled trial and economic analysis.
By Vickers AJ, Rees RW, Zollman CE, McCarney R, Smith CM, Ellis N, et al.
-
Generalisability in economic evaluation studies in healthcare: a review and case studies.
By Sculpher MJ, Pang FS, Manca A, Drummond MF, Golder S, Urdahl H, et al.
-
Virtual outreach: a randomised controlled trial and economic evaluation of joint teleconferenced medical consultations.
By Wallace P, Barber J, Clayton W, Currell R, Fleming K, Garner P, et al.
-
Randomised controlled multiple treatment comparison to provide a cost-effectiveness rationale for the selection of antimicrobial therapy in acne.
By Ozolins M, Eady EA, Avery A, Cunliffe WJ, O’Neill C, Simpson NB, et al.
-
Do the findings of case series studies vary significantly according to methodological characteristics?
By Dalziel K, Round A, Stein K, Garside R, Castelnuovo E, Payne L.
-
Improving the referral process for familial breast cancer genetic counselling: findings of three randomised controlled trials of two interventions.
By Wilson BJ, Torrance N, Mollison J, Wordsworth S, Gray JR, Haites NE, et al.
-
Randomised evaluation of alternative electrosurgical modalities to treat bladder outflow obstruction in men with benign prostatic hyperplasia.
By Fowler C, McAllister W, Plail R, Karim O, Yang Q.
-
A pragmatic randomised controlled trial of the cost-effectiveness of palliative therapies for patients with inoperable oesophageal cancer.
By Shenfine J, McNamee P, Steen N, Bond J, Griffin SM.
-
Impact of computer-aided detection prompts on the sensitivity and specificity of screening mammography.
By Taylor P, Champness J, Given- Wilson R, Johnston K, Potts H.
-
Issues in data monitoring and interim analysis of trials.
By Grant AM, Altman DG, Babiker AB, Campbell MK, Clemens FJ, Darbyshire JH, et al.
-
Lay public’s understanding of equipoise and randomisation in randomised controlled trials.
By Robinson EJ, Kerr CEP, Stevens AJ, Lilford RJ, Braunholtz DA, Edwards SJ, et al.
-
Clinical and cost-effectiveness of electroconvulsive therapy for depressive illness, schizophrenia, catatonia and mania: systematic reviews and economic modelling studies.
By Greenhalgh J, Knight C, Hind D, Beverley C, Walters S.
-
Measurement of health-related quality of life for people with dementia: development of a new instrument (DEMQOL) and an evaluation of current methodology.
By Smith SC, Lamping DL, Banerjee S, Harwood R, Foley B, Smith P, et al.
-
Clinical effectiveness and cost-effectiveness of drotrecogin alfa (activated) (Xigris®) for the treatment of severe sepsis in adults: a systematic review and economic evaluation.
By Green C, Dinnes J, Takeda A, Shepherd J, Hartwell D, Cave C, et al.
-
A methodological review of how heterogeneity has been examined in systematic reviews of diagnostic test accuracy.
By Dinnes J, Deeks J, Kirby J, Roderick P.
-
Cervical screening programmes: can automation help? Evidence from systematic reviews, an economic analysis and a simulation modelling exercise applied to the UK.
By Willis BH, Barton P, Pearmain P, Bryan S, Hyde C.
-
Laparoscopic surgery for inguinal hernia repair: systematic review of effectiveness and economic evaluation.
By McCormack K, Wake B, Perez J, Fraser C, Cook J, McIntosh E, et al.
-
Clinical effectiveness, tolerability and cost-effectiveness of newer drugs for epilepsy in adults: a systematic review and economic evaluation.
By Wilby J, Kainth A, Hawkins N, Epstein D, McIntosh H, McDaid C, et al.
-
A randomised controlled trial to compare the cost-effectiveness of tricyclic antidepressants, selective serotonin reuptake inhibitors and lofepramine.
By Peveler R, Kendrick T, Buxton M, Longworth L, Baldwin D, Moore M, et al.
-
Clinical effectiveness and cost-effectiveness of immediate angioplasty for acute myocardial infarction: systematic review and economic evaluation.
By Hartwell D, Colquitt J, Loveman E, Clegg AJ, Brodin H, Waugh N, et al.
-
A randomised controlled comparison of alternative strategies in stroke care.
By Kalra L, Evans A, Perez I, Knapp M, Swift C, Donaldson N.
-
The investigation and analysis of critical incidents and adverse events in healthcare.
By Woloshynowych M, Rogers S, Taylor-Adams S, Vincent C.
-
Potential use of routine databases in health technology assessment.
By Raftery J, Roderick P, Stevens A.
-
Clinical and cost-effectiveness of newer immunosuppressive regimens in renal transplantation: a systematic review and modelling study.
By Woodroffe R, Yao GL, Meads C, Bayliss S, Ready A, Raftery J, et al.
-
A systematic review and economic evaluation of alendronate, etidronate, risedronate, raloxifene and teriparatide for the prevention and treatment of postmenopausal osteoporosis.
By Stevenson M, Lloyd Jones M, De Nigris E, Brewer N, Davis S, Oakley J.
-
A systematic review to examine the impact of psycho-educational interventions on health outcomes and costs in adults and children with difficult asthma.
By Smith JR, Mugford M, Holland R, Candy B, Noble MJ, Harrison BDW, et al.
-
An evaluation of the costs, effectiveness and quality of renal replacement therapy provision in renal satellite units in England and Wales.
By Roderick P, Nicholson T, Armitage A, Mehta R, Mullee M, Gerard K, et al.
-
Imatinib for the treatment of patients with unresectable and/or metastatic gastrointestinal stromal tumours: systematic review and economic evaluation.
By Wilson J, Connock M, Song F, Yao G, Fry-Smith A, Raftery J, et al.
-
Indirect comparisons of competing interventions.
By Glenny AM, Altman DG, Song F, Sakarovitch C, Deeks JJ, D’Amico R, et al.
-
Cost-effectiveness of alternative strategies for the initial medical management of non-ST elevation acute coronary syndrome: systematic review and decision-analytical modelling.
By Robinson M, Palmer S, Sculpher M, Philips Z, Ginnelly L, Bowens A, et al.
-
Outcomes of electrically stimulated gracilis neosphincter surgery.
By Tillin T, Chambers M, Feldman R.
-
The effectiveness and cost-effectiveness of pimecrolimus and tacrolimus for atopic eczema: a systematic review and economic evaluation.
By Garside R, Stein K, Castelnuovo E, Pitt M, Ashcroft D, Dimmock P, et al.
-
Systematic review on urine albumin testing for early detection of diabetic complications.
By Newman DJ, Mattock MB, Dawnay ABS, Kerry S, McGuire A, Yaqoob M, et al.
-
Randomised controlled trial of the cost-effectiveness of water-based therapy for lower limb osteoarthritis.
By Cochrane T, Davey RC, Matthes Edwards SM.
-
Longer term clinical and economic benefits of offering acupuncture care to patients with chronic low back pain.
By Thomas KJ, MacPherson H, Ratcliffe J, Thorpe L, Brazier J, Campbell M, et al.
-
Cost-effectiveness and safety of epidural steroids in the management of sciatica.
By Price C, Arden N, Coglan L, Rogers P.
-
The British Rheumatoid Outcome Study Group (BROSG) randomised controlled trial to compare the effectiveness and cost-effectiveness of aggressive versus symptomatic therapy in established rheumatoid arthritis.
By Symmons D, Tricker K, Roberts C, Davies L, Dawes P, Scott DL.
-
Conceptual framework and systematic review of the effects of participants’ and professionals’ preferences in randomised controlled trials.
By King M, Nazareth I, Lampe F, Bower P, Chandler M, Morou M, et al.
-
The clinical and cost-effectiveness of implantable cardioverter defibrillators: a systematic review.
By Bryant J, Brodin H, Loveman E, Payne E, Clegg A.
-
A trial of problem-solving by community mental health nurses for anxiety, depression and life difficulties among general practice patients. The CPN-GP study.
By Kendrick T, Simons L, Mynors-Wallis L, Gray A, Lathlean J, Pickering R, et al.
-
The causes and effects of socio-demographic exclusions from clinical trials.
By Bartlett C, Doyal L, Ebrahim S, Davey P, Bachmann M, Egger M, et al.
-
Is hydrotherapy cost-effective? A randomised controlled trial of combined hydrotherapy programmes compared with physiotherapy land techniques in children with juvenile idiopathic arthritis.
By Epps H, Ginnelly L, Utley M, Southwood T, Gallivan S, Sculpher M, et al.
-
A randomised controlled trial and cost-effectiveness study of systematic screening (targeted and total population screening) versus routine practice for the detection of atrial fibrillation in people aged 65 and over. The SAFE study.
By Hobbs FDR, Fitzmaurice DA, Mant J, Murray E, Jowett S, Bryan S, et al.
-
Displaced intracapsular hip fractures in fit, older people: a randomised comparison of reduction and fixation, bipolar hemiarthroplasty and total hip arthroplasty.
By Keating JF, Grant A, Masson M, Scott NW, Forbes JF.
-
Long-term outcome of cognitive behaviour therapy clinical trials in central Scotland.
By Durham RC, Chambers JA, Power KG, Sharp DM, Macdonald RR, Major KA, et al.
-
The effectiveness and cost-effectiveness of dual-chamber pacemakers compared with single-chamber pacemakers for bradycardia due to atrioventricular block or sick sinus syndrome: systematic review and economic evaluation.
By Castelnuovo E, Stein K, Pitt M, Garside R, Payne E.
-
Newborn screening for congenital heart defects: a systematic review and cost-effectiveness analysis.
By Knowles R, Griebsch I, Dezateux C, Brown J, Bull C, Wren C.
-
The clinical and cost-effectiveness of left ventricular assist devices for end-stage heart failure: a systematic review and economic evaluation.
By Clegg AJ, Scott DA, Loveman E, Colquitt J, Hutchinson J, Royle P, et al.
-
The effectiveness of the Heidelberg Retina Tomograph and laser diagnostic glaucoma scanning system (GDx) in detecting and monitoring glaucoma.
By Kwartz AJ, Henson DB, Harper RA, Spencer AF, McLeod D.
-
Clinical and cost-effectiveness of autologous chondrocyte implantation for cartilage defects in knee joints: systematic review and economic evaluation.
By Clar C, Cummins E, McIntyre L, Thomas S, Lamb J, Bain L, et al.
-
Systematic review of effectiveness of different treatments for childhood retinoblastoma.
By McDaid C, Hartley S, Bagnall A-M, Ritchie G, Light K, Riemsma R.
-
Towards evidence-based guidelines for the prevention of venous thromboembolism: systematic reviews of mechanical methods, oral anticoagulation, dextran and regional anaesthesia as thromboprophylaxis.
By Roderick P, Ferris G, Wilson K, Halls H, Jackson D, Collins R, et al.
-
The effectiveness and cost-effectiveness of parent training/education programmes for the treatment of conduct disorder, including oppositional defiant disorder, in children.
By Dretzke J, Frew E, Davenport C, Barlow J, Stewart-Brown S, Sandercock J, et al.
-
The clinical and cost-effectiveness of donepezil, rivastigmine, galantamine and memantine for Alzheimer’s disease.
By Loveman E, Green C, Kirby J, Takeda A, Picot J, Payne E, et al.
-
FOOD: a multicentre randomised trial evaluating feeding policies in patients admitted to hospital with a recent stroke.
By Dennis M, Lewis S, Cranswick G, Forbes J.
-
The clinical effectiveness and cost-effectiveness of computed tomography screening for lung cancer: systematic reviews.
By Black C, Bagust A, Boland A, Walker S, McLeod C, De Verteuil R, et al.
-
A systematic review of the effectiveness and cost-effectiveness of neuroimaging assessments used to visualise the seizure focus in people with refractory epilepsy being considered for surgery.
By Whiting P, Gupta R, Burch J, Mujica Mota RE, Wright K, Marson A, et al.
-
Comparison of conference abstracts and presentations with full-text articles in the health technology assessments of rapidly evolving technologies.
By Dundar Y, Dodd S, Dickson R, Walley T, Haycox A, Williamson PR.
-
Systematic review and evaluation of methods of assessing urinary incontinence.
By Martin JL, Williams KS, Abrams KR, Turner DA, Sutton AJ, Chapple C, et al.
-
The clinical effectiveness and cost-effectiveness of newer drugs for children with epilepsy. A systematic review.
By Connock M, Frew E, Evans B-W, Bryan S, Cummins C, Fry-Smith A, et al.
-
Surveillance of Barrett’s oesophagus: exploring the uncertainty through systematic review, expert workshop and economic modelling.
By Garside R, Pitt M, Somerville M, Stein K, Price A, Gilbert N.
-
Topotecan, pegylated liposomal doxorubicin hydrochloride and paclitaxel for second-line or subsequent treatment of advanced ovarian cancer: a systematic review and economic evaluation.
By Main C, Bojke L, Griffin S, Norman G, Barbieri M, Mather L, et al.
-
Evaluation of molecular techniques in prediction and diagnosis of cytomegalovirus disease in immunocompromised patients.
By Szczepura A, Westmoreland D, Vinogradova Y, Fox J, Clark M.
-
Screening for thrombophilia in high-risk situations: systematic review and cost-effectiveness analysis. The Thrombosis: Risk and Economic Assessment of Thrombophilia Screening (TREATS) study.
By Wu O, Robertson L, Twaddle S, Lowe GDO, Clark P, Greaves M, et al.
-
A series of systematic reviews to inform a decision analysis for sampling and treating infected diabetic foot ulcers.
By Nelson EA, O’Meara S, Craig D, Iglesias C, Golder S, Dalton J, et al.
-
Randomised clinical trial, observational study and assessment of cost-effectiveness of the treatment of varicose veins (REACTIV trial).
By Michaels JA, Campbell WB, Brazier JE, MacIntyre JB, Palfreyman SJ, Ratcliffe J, et al.
-
The cost-effectiveness of screening for oral cancer in primary care.
By Speight PM, Palmer S, Moles DR, Downer MC, Smith DH, Henriksson M, et al.
-
Measurement of the clinical and cost-effectiveness of non-invasive diagnostic testing strategies for deep vein thrombosis.
By Goodacre S, Sampson F, Stevenson M, Wailoo A, Sutton A, Thomas S, et al.
-
Systematic review of the effectiveness and cost-effectiveness of HealOzone® for the treatment of occlusal pit/fissure caries and root caries.
By Brazzelli M, McKenzie L, Fielding S, Fraser C, Clarkson J, Kilonzo M, et al.
-
Randomised controlled trials of conventional antipsychotic versus new atypical drugs, and new atypical drugs versus clozapine, in people with schizophrenia responding poorly to, or intolerant of, current drug treatment.
By Lewis SW, Davies L, Jones PB, Barnes TRE, Murray RM, Kerwin R, et al.
-
Diagnostic tests and algorithms used in the investigation of haematuria: systematic reviews and economic evaluation.
By Rodgers M, Nixon J, Hempel S, Aho T, Kelly J, Neal D, et al.
-
Cognitive behavioural therapy in addition to antispasmodic therapy for irritable bowel syndrome in primary care: randomised controlled trial.
By Kennedy TM, Chalder T, McCrone P, Darnley S, Knapp M, Jones RH, et al.
-
A systematic review of the clinical effectiveness and cost-effectiveness of enzyme replacement therapies for Fabry’s disease and mucopolysaccharidosis type 1.
By Connock M, Juarez-Garcia A, Frew E, Mans A, Dretzke J, Fry-Smith A, et al.
-
Health benefits of antiviral therapy for mild chronic hepatitis C: randomised controlled trial and economic evaluation.
By Wright M, Grieve R, Roberts J, Main J, Thomas HC, on behalf of the UK Mild Hepatitis C Trial Investigators.
-
Pressure relieving support surfaces: a randomised evaluation.
By Nixon J, Nelson EA, Cranny G, Iglesias CP, Hawkins K, Cullum NA, et al.
-
A systematic review and economic model of the effectiveness and cost-effectiveness of methylphenidate, dexamfetamine and atomoxetine for the treatment of attention deficit hyperactivity disorder in children and adolescents.
By King S, Griffin S, Hodges Z, Weatherly H, Asseburg C, Richardson G, et al.
-
The clinical effectiveness and cost-effectiveness of enzyme replacement therapy for Gaucher’s disease: a systematic review.
By Connock M, Burls A, Frew E, Fry-Smith A, Juarez-Garcia A, McCabe C, et al.
-
Effectiveness and cost-effectiveness of salicylic acid and cryotherapy for cutaneous warts. An economic decision model.
By Thomas KS, Keogh-Brown MR, Chalmers JR, Fordham RJ, Holland RC, Armstrong SJ, et al.
-
A systematic literature review of the effectiveness of non-pharmacological interventions to prevent wandering in dementia and evaluation of the ethical implications and acceptability of their use.
By Robinson L, Hutchings D, Corner L, Beyer F, Dickinson H, Vanoli A, et al.
-
A review of the evidence on the effects and costs of implantable cardioverter defibrillator therapy in different patient groups, and modelling of cost-effectiveness and cost–utility for these groups in a UK context.
By Buxton M, Caine N, Chase D, Connelly D, Grace A, Jackson C, et al.
-
Adefovir dipivoxil and pegylated interferon alfa-2a for the treatment of chronic hepatitis B: a systematic review and economic evaluation.
By Shepherd J, Jones J, Takeda A, Davidson P, Price A.
-
An evaluation of the clinical and cost-effectiveness of pulmonary artery catheters in patient management in intensive care: a systematic review and a randomised controlled trial.
By Harvey S, Stevens K, Harrison D, Young D, Brampton W, McCabe C, et al.
-
Accurate, practical and cost-effective assessment of carotid stenosis in the UK.
By Wardlaw JM, Chappell FM, Stevenson M, De Nigris E, Thomas S, Gillard J, et al.
-
Etanercept and infliximab for the treatment of psoriatic arthritis: a systematic review and economic evaluation.
By Woolacott N, Bravo Vergel Y, Hawkins N, Kainth A, Khadjesari Z, Misso K, et al.
-
The cost-effectiveness of testing for hepatitis C in former injecting drug users.
By Castelnuovo E, Thompson-Coon J, Pitt M, Cramp M, Siebert U, Price A, et al.
-
Computerised cognitive behaviour therapy for depression and anxiety update: a systematic review and economic evaluation.
By Kaltenthaler E, Brazier J, De Nigris E, Tumur I, Ferriter M, Beverley C, et al.
-
Cost-effectiveness of using prognostic information to select women with breast cancer for adjuvant systemic therapy.
By Williams C, Brunskill S, Altman D, Briggs A, Campbell H, Clarke M, et al.
-
Psychological therapies including dialectical behaviour therapy for borderline personality disorder: a systematic review and preliminary economic evaluation.
By Brazier J, Tumur I, Holmes M, Ferriter M, Parry G, Dent-Brown K, et al.
-
Clinical effectiveness and cost-effectiveness of tests for the diagnosis and investigation of urinary tract infection in children: a systematic review and economic model.
By Whiting P, Westwood M, Bojke L, Palmer S, Richardson G, Cooper J, et al.
-
Cognitive behavioural therapy in chronic fatigue syndrome: a randomised controlled trial of an outpatient group programme.
By O’Dowd H, Gladwell P, Rogers CA, Hollinghurst S, Gregory A.
-
A comparison of the cost-effectiveness of five strategies for the prevention of nonsteroidal anti-inflammatory drug-induced gastrointestinal toxicity: a systematic review with economic modelling.
By Brown TJ, Hooper L, Elliott RA, Payne K, Webb R, Roberts C, et al.
-
The effectiveness and cost-effectiveness of computed tomography screening for coronary artery disease: systematic review.
By Waugh N, Black C, Walker S, McIntyre L, Cummins E, Hillis G.
-
What are the clinical outcome and cost-effectiveness of endoscopy undertaken by nurses when compared with doctors? A Multi-Institution Nurse Endoscopy Trial (MINuET).
By Williams J, Russell I, Durai D, Cheung W-Y, Farrin A, Bloor K, et al.
-
The clinical and cost-effectiveness of oxaliplatin and capecitabine for the adjuvant treatment of colon cancer: systematic review and economic evaluation.
By Pandor A, Eggington S, Paisley S, Tappenden P, Sutcliffe P.
-
A systematic review of the effectiveness of adalimumab, etanercept and infliximab for the treatment of rheumatoid arthritis in adults and an economic evaluation of their cost-effectiveness.
By Chen Y-F, Jobanputra P, Barton P, Jowett S, Bryan S, Clark W, et al.
-
Telemedicine in dermatology: a randomised controlled trial.
By Bowns IR, Collins K, Walters SJ, McDonagh AJG.
-
Cost-effectiveness of cell salvage and alternative methods of minimising perioperative allogeneic blood transfusion: a systematic review and economic model.
By Davies L, Brown TJ, Haynes S, Payne K, Elliott RA, McCollum C.
-
Clinical effectiveness and cost-effectiveness of laparoscopic surgery for colorectal cancer: systematic reviews and economic evaluation.
By Murray A, Lourenco T, de Verteuil R, Hernandez R, Fraser C, McKinley A, et al.
-
Etanercept and efalizumab for the treatment of psoriasis: a systematic review.
By Woolacott N, Hawkins N, Mason A, Kainth A, Khadjesari Z, Bravo Vergel Y, et al.
-
Systematic reviews of clinical decision tools for acute abdominal pain.
By Liu JLY, Wyatt JC, Deeks JJ, Clamp S, Keen J, Verde P, et al.
-
Evaluation of the ventricular assist device programme in the UK.
By Sharples L, Buxton M, Caine N, Cafferty F, Demiris N, Dyer M, et al.
-
A systematic review and economic model of the clinical and cost-effectiveness of immunosuppressive therapy for renal transplantation in children.
By Yao G, Albon E, Adi Y, Milford D, Bayliss S, Ready A, et al.
-
Amniocentesis results: investigation of anxiety. The ARIA trial.
By Hewison J, Nixon J, Fountain J, Cocks K, Jones C, Mason G, et al.
-
Pemetrexed disodium for the treatment of malignant pleural mesothelioma: a systematic review and economic evaluation.
By Dundar Y, Bagust A, Dickson R, Dodd S, Green J, Haycox A, et al.
-
A systematic review and economic model of the clinical effectiveness and cost-effectiveness of docetaxel in combination with prednisone or prednisolone for the treatment of hormone-refractory metastatic prostate cancer.
By Collins R, Fenwick E, Trowman R, Perard R, Norman G, Light K, et al.
-
A systematic review of rapid diagnostic tests for the detection of tuberculosis infection.
By Dinnes J, Deeks J, Kunst H, Gibson A, Cummins E, Waugh N, et al.
-
The clinical effectiveness and cost-effectiveness of strontium ranelate for the prevention of osteoporotic fragility fractures in postmenopausal women.
By Stevenson M, Davis S, Lloyd-Jones M, Beverley C.
-
A systematic review of quantitative and qualitative research on the role and effectiveness of written information available to patients about individual medicines.
By Raynor DK, Blenkinsopp A, Knapp P, Grime J, Nicolson DJ, Pollock K, et al.
-
Oral naltrexone as a treatment for relapse prevention in formerly opioid-dependent drug users: a systematic review and economic evaluation.
By Adi Y, Juarez-Garcia A, Wang D, Jowett S, Frew E, Day E, et al.
-
Glucocorticoid-induced osteoporosis: a systematic review and cost–utility analysis.
By Kanis JA, Stevenson M, McCloskey EV, Davis S, Lloyd-Jones M.
-
Epidemiological, social, diagnostic and economic evaluation of population screening for genital chlamydial infection.
By Low N, McCarthy A, Macleod J, Salisbury C, Campbell R, Roberts TE, et al.
-
Methadone and buprenorphine for the management of opioid dependence: a systematic review and economic evaluation.
By Connock M, Juarez-Garcia A, Jowett S, Frew E, Liu Z, Taylor RJ, et al.
-
Exercise Evaluation Randomised Trial (EXERT): a randomised trial comparing GP referral for leisure centre-based exercise, community-based walking and advice only.
By Isaacs AJ, Critchley JA, See Tai S, Buckingham K, Westley D, Harridge SDR, et al.
-
Interferon alfa (pegylated and non-pegylated) and ribavirin for the treatment of mild chronic hepatitis C: a systematic review and economic evaluation.
By Shepherd J, Jones J, Hartwell D, Davidson P, Price A, Waugh N.
-
Systematic review and economic evaluation of bevacizumab and cetuximab for the treatment of metastatic colorectal cancer.
By Tappenden P, Jones R, Paisley S, Carroll C.
-
A systematic review and economic evaluation of epoetin alfa, epoetin beta and darbepoetin alfa in anaemia associated with cancer, especially that attributable to cancer treatment.
By Wilson J, Yao GL, Raftery J, Bohlius J, Brunskill S, Sandercock J, et al.
-
A systematic review and economic evaluation of statins for the prevention of coronary events.
By Ward S, Lloyd Jones M, Pandor A, Holmes M, Ara R, Ryan A, et al.
-
A systematic review of the effectiveness and cost-effectiveness of different models of community-based respite care for frail older people and their carers.
By Mason A, Weatherly H, Spilsbury K, Arksey H, Golder S, Adamson J, et al.
-
Additional therapy for young children with spastic cerebral palsy: a randomised controlled trial.
By Weindling AM, Cunningham CC, Glenn SM, Edwards RT, Reeves DJ.
-
Screening for type 2 diabetes: literature review and economic modelling.
By Waugh N, Scotland G, McNamee P, Gillett M, Brennan A, Goyder E, et al.
-
The effectiveness and cost-effectiveness of cinacalcet for secondary hyperparathyroidism in end-stage renal disease patients on dialysis: a systematic review and economic evaluation.
By Garside R, Pitt M, Anderson R, Mealing S, Roome C, Snaith A, et al.
-
The clinical effectiveness and cost-effectiveness of gemcitabine for metastatic breast cancer: a systematic review and economic evaluation.
By Takeda AL, Jones J, Loveman E, Tan SC, Clegg AJ.
-
A systematic review of duplex ultrasound, magnetic resonance angiography and computed tomography angiography for the diagnosis and assessment of symptomatic, lower limb peripheral arterial disease.
By Collins R, Cranny G, Burch J, Aguiar-Ibáñez R, Craig D, Wright K, et al.
-
The clinical effectiveness and cost-effectiveness of treatments for children with idiopathic steroid-resistant nephrotic syndrome: a systematic review.
By Colquitt JL, Kirby J, Green C, Cooper K, Trompeter RS.
-
A systematic review of the routine monitoring of growth in children of primary school age to identify growth-related conditions.
By Fayter D, Nixon J, Hartley S, Rithalia A, Butler G, Rudolf M, et al.
-
Systematic review of the effectiveness of preventing and treating Staphylococcus aureus carriage in reducing peritoneal catheter-related infections.
By McCormack K, Rabindranath K, Kilonzo M, Vale L, Fraser C, McIntyre L, et al.
-
The clinical effectiveness and cost of repetitive transcranial magnetic stimulation versus electroconvulsive therapy in severe depression: a multicentre pragmatic randomised controlled trial and economic analysis.
By McLoughlin DM, Mogg A, Eranti S, Pluck G, Purvis R, Edwards D, et al.
-
A randomised controlled trial and economic evaluation of direct versus indirect and individual versus group modes of speech and language therapy for children with primary language impairment.
By Boyle J, McCartney E, Forbes J, O’Hare A.
-
Hormonal therapies for early breast cancer: systematic review and economic evaluation.
By Hind D, Ward S, De Nigris E, Simpson E, Carroll C, Wyld L.
-
Cardioprotection against the toxic effects of anthracyclines given to children with cancer: a systematic review.
By Bryant J, Picot J, Levitt G, Sullivan I, Baxter L, Clegg A.
-
Adalimumab, etanercept and infliximab for the treatment of ankylosing spondylitis: a systematic review and economic evaluation.
By McLeod C, Bagust A, Boland A, Dagenais P, Dickson R, Dundar Y, et al.
-
Prenatal screening and treatment strategies to prevent group B streptococcal and other bacterial infections in early infancy: cost-effectiveness and expected value of information analyses.
By Colbourn T, Asseburg C, Bojke L, Philips Z, Claxton K, Ades AE, et al.
-
Clinical effectiveness and cost-effectiveness of bone morphogenetic proteins in the non-healing of fractures and spinal fusion: a systematic review.
By Garrison KR, Donell S, Ryder J, Shemilt I, Mugford M, Harvey I, et al.
-
A randomised controlled trial of postoperative radiotherapy following breast-conserving surgery in a minimum-risk older population. The PRIME trial.
By Prescott RJ, Kunkler IH, Williams LJ, King CC, Jack W, van der Pol M, et al.
-
Current practice, accuracy, effectiveness and cost-effectiveness of the school entry hearing screen.
By Bamford J, Fortnum H, Bristow K, Smith J, Vamvakas G, Davies L, et al.
-
The clinical effectiveness and cost-effectiveness of inhaled insulin in diabetes mellitus: a systematic review and economic evaluation.
By Black C, Cummins E, Royle P, Philip S, Waugh N.
-
Surveillance of cirrhosis for hepatocellular carcinoma: systematic review and economic analysis.
By Thompson Coon J, Rogers G, Hewson P, Wright D, Anderson R, Cramp M, et al.
-
The Birmingham Rehabilitation Uptake Maximisation Study (BRUM). Homebased compared with hospital-based cardiac rehabilitation in a multi-ethnic population: cost-effectiveness and patient adherence.
By Jolly K, Taylor R, Lip GYH, Greenfield S, Raftery J, Mant J, et al.
-
A systematic review of the clinical, public health and cost-effectiveness of rapid diagnostic tests for the detection and identification of bacterial intestinal pathogens in faeces and food.
By Abubakar I, Irvine L, Aldus CF, Wyatt GM, Fordham R, Schelenz S, et al.
-
A randomised controlled trial examining the longer-term outcomes of standard versus new antiepileptic drugs. The SANAD trial.
By Marson AG, Appleton R, Baker GA, Chadwick DW, Doughty J, Eaton B, et al.
-
Clinical effectiveness and cost-effectiveness of different models of managing long-term oral anti-coagulation therapy: a systematic review and economic modelling.
By Connock M, Stevens C, Fry-Smith A, Jowett S, Fitzmaurice D, Moore D, et al.
-
A systematic review and economic model of the clinical effectiveness and cost-effectiveness of interventions for preventing relapse in people with bipolar disorder.
By Soares-Weiser K, Bravo Vergel Y, Beynon S, Dunn G, Barbieri M, Duffy S, et al.
-
Taxanes for the adjuvant treatment of early breast cancer: systematic review and economic evaluation.
By Ward S, Simpson E, Davis S, Hind D, Rees A, Wilkinson A.
-
The clinical effectiveness and cost-effectiveness of screening for open angle glaucoma: a systematic review and economic evaluation.
By Burr JM, Mowatt G, Hernández R, Siddiqui MAR, Cook J, Lourenco T, et al.
-
Acceptability, benefit and costs of early screening for hearing disability: a study of potential screening tests and models.
By Davis A, Smith P, Ferguson M, Stephens D, Gianopoulos I.
-
Contamination in trials of educational interventions.
By Keogh-Brown MR, Bachmann MO, Shepstone L, Hewitt C, Howe A, Ramsay CR, et al.
-
Overview of the clinical effectiveness of positron emission tomography imaging in selected cancers.
By Facey K, Bradbury I, Laking G, Payne E.
-
The effectiveness and cost-effectiveness of carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma: a systematic review and economic evaluation.
By Garside R, Pitt M, Anderson R, Rogers G, Dyer M, Mealing S, et al.
-
Drug-eluting stents: a systematic review and economic evaluation.
By Hill RA, Boland A, Dickson R, Dündar Y, Haycox A, McLeod C, et al.
-
The clinical effectiveness and cost-effectiveness of cardiac resynchronisation (biventricular pacing) for heart failure: systematic review and economic model.
By Fox M, Mealing S, Anderson R, Dean J, Stein K, Price A, et al.
-
Recruitment to randomised trials: strategies for trial enrolment and participation study. The STEPS study.
By Campbell MK, Snowdon C, Francis D, Elbourne D, McDonald AM, Knight R, et al.
-
Cost-effectiveness of functional cardiac testing in the diagnosis and management of coronary artery disease: a randomised controlled trial. The CECaT trial.
By Sharples L, Hughes V, Crean A, Dyer M, Buxton M, Goldsmith K, et al.
-
Evaluation of diagnostic tests when there is no gold standard. A review of methods.
By Rutjes AWS, Reitsma JB, Coomarasamy A, Khan KS, Bossuyt PMM.
-
Systematic reviews of the clinical effectiveness and cost-effectiveness of proton pump inhibitors in acute upper gastrointestinal bleeding.
By Leontiadis GI, Sreedharan A, Dorward S, Barton P, Delaney B, Howden CW, et al.
-
A review and critique of modelling in prioritising and designing screening programmes.
By Karnon J, Goyder E, Tappenden P, McPhie S, Towers I, Brazier J, et al.
-
An assessment of the impact of the NHS Health Technology Assessment Programme.
By Hanney S, Buxton M, Green C, Coulson D, Raftery J.
-
A systematic review and economic model of switching from nonglycopeptide to glycopeptide antibiotic prophylaxis for surgery.
By Cranny G, Elliott R, Weatherly H, Chambers D, Hawkins N, Myers L, et al.
-
‘Cut down to quit’ with nicotine replacement therapies in smoking cessation: a systematic review of effectiveness and economic analysis.
By Wang D, Connock M, Barton P, Fry-Smith A, Aveyard P, Moore D.
-
A systematic review of the effectiveness of strategies for reducing fracture risk in children with juvenile idiopathic arthritis with additional data on long-term risk of fracture and cost of disease management.
By Thornton J, Ashcroft D, O’Neill T, Elliott R, Adams J, Roberts C, et al.
-
Does befriending by trained lay workers improve psychological well-being and quality of life for carers of people with dementia, and at what cost? A randomised controlled trial.
By Charlesworth G, Shepstone L, Wilson E, Thalanany M, Mugford M, Poland F.
-
A multi-centre retrospective cohort study comparing the efficacy, safety and cost-effectiveness of hysterectomy and uterine artery embolisation for the treatment of symptomatic uterine fibroids. The HOPEFUL study.
By Hirst A, Dutton S, Wu O, Briggs A, Edwards C, Waldenmaier L, et al.
-
Methods of prediction and prevention of pre-eclampsia: systematic reviews of accuracy and effectiveness literature with economic modelling.
By Meads CA, Cnossen JS, Meher S, Juarez-Garcia A, ter Riet G, Duley L, et al.
-
The use of economic evaluations in NHS decision-making: a review and empirical investigation.
By Williams I, McIver S, Moore D, Bryan S.
-
Stapled haemorrhoidectomy (haemorrhoidopexy) for the treatment of haemorrhoids: a systematic review and economic evaluation.
By Burch J, Epstein D, Baba-Akbari A, Weatherly H, Fox D, Golder S, et al.
-
The clinical effectiveness of diabetes education models for Type 2 diabetes: a systematic review.
By Loveman E, Frampton GK, Clegg AJ.
-
Payment to healthcare professionals for patient recruitment to trials: systematic review and qualitative study.
By Raftery J, Bryant J, Powell J, Kerr C, Hawker S.
-
Cyclooxygenase-2 selective non-steroidal anti-inflammatory drugs (etodolac, meloxicam, celecoxib, rofecoxib, etoricoxib, valdecoxib and lumiracoxib) for osteoarthritis and rheumatoid arthritis: a systematic review and economic evaluation.
By Chen Y-F, Jobanputra P, Barton P, Bryan S, Fry-Smith A, Harris G, et al.
-
The clinical effectiveness and cost-effectiveness of central venous catheters treated with anti-infective agents in preventing bloodstream infections: a systematic review and economic evaluation.
By Hockenhull JC, Dwan K, Boland A, Smith G, Bagust A, Dundar Y, et al.
-
Stepped treatment of older adults on laxatives. The STOOL trial.
By Mihaylov S, Stark C, McColl E, Steen N, Vanoli A, Rubin G, et al.
-
A randomised controlled trial of cognitive behaviour therapy in adolescents with major depression treated by selective serotonin reuptake inhibitors. The ADAPT trial.
By Goodyer IM, Dubicka B, Wilkinson P, Kelvin R, Roberts C, Byford S, et al.
-
The use of irinotecan, oxaliplatin and raltitrexed for the treatment of advanced colorectal cancer: systematic review and economic evaluation.
By Hind D, Tappenden P, Tumur I, Eggington E, Sutcliffe P, Ryan A.
-
Ranibizumab and pegaptanib for the treatment of age-related macular degeneration: a systematic review and economic evaluation.
By Colquitt JL, Jones J, Tan SC, Takeda A, Clegg AJ, Price A.
-
Systematic review of the clinical effectiveness and cost-effectiveness of 64-slice or higher computed tomography angiography as an alternative to invasive coronary angiography in the investigation of coronary artery disease.
By Mowatt G, Cummins E, Waugh N, Walker S, Cook J, Jia X, et al.
-
Structural neuroimaging in psychosis: a systematic review and economic evaluation.
By Albon E, Tsourapas A, Frew E, Davenport C, Oyebode F, Bayliss S, et al.
-
Systematic review and economic analysis of the comparative effectiveness of different inhaled corticosteroids and their usage with long-acting beta2 agonists for the treatment of chronic asthma in adults and children aged 12 years and over.
By Shepherd J, Rogers G, Anderson R, Main C, Thompson-Coon J, Hartwell D, et al.
-
Systematic review and economic analysis of the comparative effectiveness of different inhaled corticosteroids and their usage with long-acting beta2 agonists for the treatment of chronic asthma in children under the age of 12 years.
By Main C, Shepherd J, Anderson R, Rogers G, Thompson-Coon J, Liu Z, et al.
-
Ezetimibe for the treatment of hypercholesterolaemia: a systematic review and economic evaluation.
By Ara R, Tumur I, Pandor A, Duenas A, Williams R, Wilkinson A, et al.
-
Topical or oral ibuprofen for chronic knee pain in older people. The TOIB study.
By Underwood M, Ashby D, Carnes D, Castelnuovo E, Cross P, Harding G, et al.
-
A prospective randomised comparison of minor surgery in primary and secondary care. The MiSTIC trial.
By George S, Pockney P, Primrose J, Smith H, Little P, Kinley H, et al.
-
A review and critical appraisal of measures of therapist–patient interactions in mental health settings.
By Cahill J, Barkham M, Hardy G, Gilbody S, Richards D, Bower P, et al.
-
The clinical effectiveness and cost-effectiveness of screening programmes for amblyopia and strabismus in children up to the age of 4–5 years: a systematic review and economic evaluation.
By Carlton J, Karnon J, Czoski-Murray C, Smith KJ, Marr J.
-
A systematic review of the clinical effectiveness and cost-effectiveness and economic modelling of minimal incision total hip replacement approaches in the management of arthritic disease of the hip.
By de Verteuil R, Imamura M, Zhu S, Glazener C, Fraser C, Munro N, et al.
-
A preliminary model-based assessment of the cost–utility of a screening programme for early age-related macular degeneration.
By Karnon J, Czoski-Murray C, Smith K, Brand C, Chakravarthy U, Davis S, et al.
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.
By Shepherd J, Jones J, Frampton GK, Tanajewski L, Turner D, Price A.
-
Absorbent products for urinary/faecal incontinence: a comparative evaluation of key product categories.
By Fader M, Cottenden A, Getliffe K, Gage H, Clarke-O’Neill S, Jamieson K, et al.
-
A systematic review of repetitive functional task practice with modelling of resource use, costs and effectiveness.
By French B, Leathley M, Sutton C, McAdam J, Thomas L, Forster A, et al.
-
The effectiveness and cost-effectivness of minimal access surgery amongst people with gastro-oesophageal reflux disease – a UK collaborative study. The reflux trial.
By Grant A, Wileman S, Ramsay C, Bojke L, Epstein D, Sculpher M, et al.
-
Time to full publication of studies of anti-cancer medicines for breast cancer and the potential for publication bias: a short systematic review.
By Takeda A, Loveman E, Harris P, Hartwell D, Welch K.
-
Performance of screening tests for child physical abuse in accident and emergency departments.
By Woodman J, Pitt M, Wentz R, Taylor B, Hodes D, Gilbert RE.
-
Curative catheter ablation in atrial fibrillation and typical atrial flutter: systematic review and economic evaluation.
By Rodgers M, McKenna C, Palmer S, Chambers D, Van Hout S, Golder S, et al.
-
Systematic review and economic modelling of effectiveness and cost utility of surgical treatments for men with benign prostatic enlargement.
By Lourenco T, Armstrong N, N’Dow J, Nabi G, Deverill M, Pickard R, et al.
-
Immunoprophylaxis against respiratory syncytial virus (RSV) with palivizumab in children: a systematic review and economic evaluation.
By Wang D, Cummins C, Bayliss S, Sandercock J, Burls A.
-
Deferasirox for the treatment of iron overload associated with regular blood transfusions (transfusional haemosiderosis) in patients suffering with chronic anaemia: a systematic review and economic evaluation.
By McLeod C, Fleeman N, Kirkham J, Bagust A, Boland A, Chu P, et al.
-
Thrombophilia testing in people with venous thromboembolism: systematic review and cost-effectiveness analysis.
By Simpson EL, Stevenson MD, Rawdin A, Papaioannou D.
-
Surgical procedures and non-surgical devices for the management of non-apnoeic snoring: a systematic review of clinical effects and associated treatment costs.
By Main C, Liu Z, Welch K, Weiner G, Quentin Jones S, Stein K.
-
Continuous positive airway pressure devices for the treatment of obstructive sleep apnoea–hypopnoea syndrome: a systematic review and economic analysis.
By McDaid C, Griffin S, Weatherly H, Durée K, van der Burgt M, van Hout S, Akers J, et al.
-
Use of classical and novel biomarkers as prognostic risk factors for localised prostate cancer: a systematic review.
By Sutcliffe P, Hummel S, Simpson E, Young T, Rees A, Wilkinson A, et al.
-
The harmful health effects of recreational ecstasy: a systematic review of observational evidence.
By Rogers G, Elston J, Garside R, Roome C, Taylor R, Younger P, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of oesophageal Doppler monitoring in critically ill and high-risk surgical patients.
By Mowatt G, Houston G, Hernández R, de Verteuil R, Fraser C, Cuthbertson B, et al.
-
The use of surrogate outcomes in model-based cost-effectiveness analyses: a survey of UK Health Technology Assessment reports.
By Taylor RS, Elston J.
-
Controlling Hypertension and Hypotension Immediately Post Stroke (CHHIPS) – a randomised controlled trial.
By Potter J, Mistri A, Brodie F, Chernova J, Wilson E, Jagger C, et al.
-
Routine antenatal anti-D prophylaxis for RhD-negative women: a systematic review and economic evaluation.
By Pilgrim H, Lloyd-Jones M, Rees A.
-
Amantadine, oseltamivir and zanamivir for the prophylaxis of influenza (including a review of existing guidance no. 67): a systematic review and economic evaluation.
By Tappenden P, Jackson R, Cooper K, Rees A, Simpson E, Read R, et al.
-
Improving the evaluation of therapeutic interventions in multiple sclerosis: the role of new psychometric methods.
By Hobart J, Cano S.
-
Treatment of severe ankle sprain: a pragmatic randomised controlled trial comparing the clinical effectiveness and cost-effectiveness of three types of mechanical ankle support with tubular bandage. The CAST trial.
By Cooke MW, Marsh JL, Clark M, Nakash R, Jarvis RM, Hutton JL, et al. , on behalf of the CAST trial group.
-
Non-occupational postexposure prophylaxis for HIV: a systematic review.
By Bryant J, Baxter L, Hird S.
-
Blood glucose self-monitoring in type 2 diabetes: a randomised controlled trial.
By Farmer AJ, Wade AN, French DP, Simon J, Yudkin P, Gray A, et al.
-
How far does screening women for domestic (partner) violence in different health-care settings meet criteria for a screening programme? Systematic reviews of nine UK National Screening Committee criteria.
By Feder G, Ramsay J, Dunne D, Rose M, Arsene C, Norman R, et al.
-
Spinal cord stimulation for chronic pain of neuropathic or ischaemic origin: systematic review and economic evaluation.
By Simpson, EL, Duenas A, Holmes MW, Papaioannou D, Chilcott J.
-
The role of magnetic resonance imaging in the identification of suspected acoustic neuroma: a systematic review of clinical and cost-effectiveness and natural history.
By Fortnum H, O’Neill C, Taylor R, Lenthall R, Nikolopoulos T, Lightfoot G, et al.
-
Dipsticks and diagnostic algorithms in urinary tract infection: development and validation, randomised trial, economic analysis, observational cohort and qualitative study.
By Little P, Turner S, Rumsby K, Warner G, Moore M, Lowes JA, et al.
-
Systematic review of respite care in the frail elderly.
By Shaw C, McNamara R, Abrams K, Cannings-John R, Hood K, Longo M, et al.
-
Neuroleptics in the treatment of aggressive challenging behaviour for people with intellectual disabilities: a randomised controlled trial (NACHBID).
By Tyrer P, Oliver-Africano P, Romeo R, Knapp M, Dickens S, Bouras N, et al.
-
Randomised controlled trial to determine the clinical effectiveness and cost-effectiveness of selective serotonin reuptake inhibitors plus supportive care, versus supportive care alone, for mild to moderate depression with somatic symptoms in primary care: the THREAD (THREshold for AntiDepressant response) study.
By Kendrick T, Chatwin J, Dowrick C, Tylee A, Morriss R, Peveler R, et al.
-
Diagnostic strategies using DNA testing for hereditary haemochromatosis in at-risk populations: a systematic review and economic evaluation.
By Bryant J, Cooper K, Picot J, Clegg A, Roderick P, Rosenberg W, et al.
-
Enhanced external counterpulsation for the treatment of stable angina and heart failure: a systematic review and economic analysis.
By McKenna C, McDaid C, Suekarran S, Hawkins N, Claxton K, Light K, et al.
-
Development of a decision support tool for primary care management of patients with abnormal liver function tests without clinically apparent liver disease: a record-linkage population cohort study and decision analysis (ALFIE).
By Donnan PT, McLernon D, Dillon JF, Ryder S, Roderick P, Sullivan F, et al.
-
A systematic review of presumed consent systems for deceased organ donation.
By Rithalia A, McDaid C, Suekarran S, Norman G, Myers L, Sowden A.
-
Paracetamol and ibuprofen for the treatment of fever in children: the PITCH randomised controlled trial.
By Hay AD, Redmond NM, Costelloe C, Montgomery AA, Fletcher M, Hollinghurst S, et al.
-
A randomised controlled trial to compare minimally invasive glucose monitoring devices with conventional monitoring in the management of insulin-treated diabetes mellitus (MITRE).
By Newman SP, Cooke D, Casbard A, Walker S, Meredith S, Nunn A, et al.
-
Sensitivity analysis in economic evaluation: an audit of NICE current practice and a review of its use and value in decision-making.
By Andronis L, Barton P, Bryan S.
-
Trastuzumab for the treatment of primary breast cancer in HER2-positive women: a single technology appraisal.
By Ward S, Pilgrim H, Hind D.
-
Docetaxel for the adjuvant treatment of early node-positive breast cancer: a single technology appraisal.
By Chilcott J, Lloyd Jones M, Wilkinson A.
-
The use of paclitaxel in the management of early stage breast cancer.
By Griffin S, Dunn G, Palmer S, Macfarlane K, Brent S, Dyker A, et al.
-
Rituximab for the first-line treatment of stage III/IV follicular non-Hodgkin’s lymphoma.
By Dundar Y, Bagust A, Hounsome J, McLeod C, Boland A, Davis H, et al.
-
Bortezomib for the treatment of multiple myeloma patients.
By Green C, Bryant J, Takeda A, Cooper K, Clegg A, Smith A, et al.
-
Fludarabine phosphate for the firstline treatment of chronic lymphocytic leukaemia.
By Walker S, Palmer S, Erhorn S, Brent S, Dyker A, Ferrie L, et al.
-
Erlotinib for the treatment of relapsed non-small cell lung cancer.
By McLeod C, Bagust A, Boland A, Hockenhull J, Dundar Y, Proudlove C, et al.
-
Cetuximab plus radiotherapy for the treatment of locally advanced squamous cell carcinoma of the head and neck.
By Griffin S, Walker S, Sculpher M, White S, Erhorn S, Brent S, et al.
-
Infliximab for the treatment of adults with psoriasis.
By Loveman E, Turner D, Hartwell D, Cooper K, Clegg A
-
Psychological interventions for postnatal depression: cluster randomised trial and economic evaluation. The PoNDER trial.
By Morrell CJ, Warner R, Slade P, Dixon S, Walters S, Paley G, et al.
-
The effect of different treatment durations of clopidogrel in patients with non-ST-segment elevation acute coronary syndromes: a systematic review and value of information analysis.
By Rogowski R, Burch J, Palmer S, Craigs C, Golder S, Woolacott N.
-
Systematic review and individual patient data meta-analysis of diagnosis of heart failure, with modelling of implications of different diagnostic strategies in primary care.
By Mant J, Doust J, Roalfe A, Barton P, Cowie MR, Glasziou P, et al.
-
A multicentre randomised controlled trial of the use of continuous positive airway pressure and non-invasive positive pressure ventilation in the early treatment of patients presenting to the emergency department with severe acute cardiogenic pulmonary oedema: the 3CPO trial.
By Gray AJ, Goodacre S, Newby DE, Masson MA, Sampson F, Dixon S, et al. , on behalf of the 3CPO study investigators.
-
Early high-dose lipid-lowering therapy to avoid cardiac events: a systematic review and economic evaluation.
By Ara R, Pandor A, Stevens J, Rees A, Rafia R.
-
Adefovir dipivoxil and pegylated interferon alpha for the treatment of chronic hepatitis B: an updated systematic review and economic evaluation.
By Jones J, Shepherd J, Baxter L, Gospodarevskaya E, Hartwell D, Harris P, et al.
-
Methods to identify postnatal depression in primary care: an integrated evidence synthesis and value of information analysis.
By Hewitt CE, Gilbody SM, Brealey S, Paulden M, Palmer S, Mann R, et al.
-
A double-blind randomised placebo-controlled trial of topical intranasal corticosteroids in 4- to 11-year-old children with persistent bilateral otitis media with effusion in primary care.
By Williamson I, Benge S, Barton S, Petrou S, Letley L, Fasey N, et al.
-
The effectiveness and cost-effectiveness of methods of storing donated kidneys from deceased donors: a systematic review and economic model.
By Bond M, Pitt M, Akoh J, Moxham T, Hoyle M, Anderson R.
-
Rehabilitation of older patients: day hospital compared with rehabilitation at home. A randomised controlled trial.
By Parker SG, Oliver P, Pennington M, Bond J, Jagger C, Enderby PM, et al.
-
Breastfeeding promotion for infants in neonatal units: a systematic review and economic analysis.
By Renfrew MJ, Craig D, Dyson L, McCormick F, Rice S, King SE, et al.
-
The clinical effectiveness and cost-effectiveness of bariatric (weight loss) surgery for obesity: a systematic review and economic evaluation.
By Picot J, Jones J, Colquitt JL, Gospodarevskaya E, Loveman E, Baxter L, et al.
-
Rapid testing for group B streptococcus during labour: a test accuracy study with evaluation of acceptability and cost-effectiveness.
By Daniels J, Gray J, Pattison H, Roberts T, Edwards E, Milner P, et al.
-
Screening to prevent spontaneous preterm birth: systematic reviews of accuracy and effectiveness literature with economic modelling.
By Honest H, Forbes CA, Durée KH, Norman G, Duffy SB, Tsourapas A, et al.
-
The effectiveness and cost-effectiveness of cochlear implants for severe to profound deafness in children and adults: a systematic review and economic model.
By Bond M, Mealing S, Anderson R, Elston J, Weiner G, Taylor RS, et al.
-
Gemcitabine for the treatment of metastatic breast cancer.
By Jones J, Takeda A, Tan SC, Cooper K, Loveman E, Clegg A.
-
Varenicline in the management of smoking cessation: a single technology appraisal.
By Hind D, Tappenden P, Peters J, Kenjegalieva K.
-
Alteplase for the treatment of acute ischaemic stroke: a single technology appraisal.
By Lloyd Jones M, Holmes M.
-
Rituximab for the treatment of rheumatoid arthritis.
By Bagust A, Boland A, Hockenhull J, Fleeman N, Greenhalgh J, Dundar Y, et al.
-
Omalizumab for the treatment of severe persistent allergic asthma.
By Jones J, Shepherd J, Hartwell D, Harris P, Cooper K, Takeda A, et al.
-
Rituximab for the treatment of relapsed or refractory stage III or IV follicular non-Hodgkin’s lymphoma.
By Boland A, Bagust A, Hockenhull J, Davis H, Chu P, Dickson R.
-
Adalimumab for the treatment of psoriasis.
By Turner D, Picot J, Cooper K, Loveman E.
-
Dabigatran etexilate for the prevention of venous thromboembolism in patients undergoing elective hip and knee surgery: a single technology appraisal.
By Holmes M, C Carroll C, Papaioannou D.
-
Romiplostim for the treatment of chronic immune or idiopathic thrombocytopenic purpura: a single technology appraisal.
By Mowatt G, Boachie C, Crowther M, Fraser C, Hernández R, Jia X, et al.
-
Sunitinib for the treatment of gastrointestinal stromal tumours: a critique of the submission from Pfizer.
By Bond M, Hoyle M, Moxham T, Napier M, Anderson R.
-
Vitamin K to prevent fractures in older women: systematic review and economic evaluation.
By Stevenson M, Lloyd-Jones M, Papaioannou D.
-
The effects of biofeedback for the treatment of essential hypertension: a systematic review.
By Greenhalgh J, Dickson R, Dundar Y.
-
A randomised controlled trial of the use of aciclovir and/or prednisolone for the early treatment of Bell’s palsy: the BELLS study.
By Sullivan FM, Swan IRC, Donnan PT, Morrison JM, Smith BH, McKinstry B, et al.
-
Lapatinib for the treatment of HER2-overexpressing breast cancer.
By Jones J, Takeda A, Picot J, von Keyserlingk C, Clegg A.
-
Infliximab for the treatment of ulcerative colitis.
By Hyde C, Bryan S, Juarez-Garcia A, Andronis L, Fry-Smith A.
-
Rimonabant for the treatment of overweight and obese people.
By Burch J, McKenna C, Palmer S, Norman G, Glanville J, Sculpher M, et al.
-
Telbivudine for the treatment of chronic hepatitis B infection.
By Hartwell D, Jones J, Harris P, Cooper K.
-
Entecavir for the treatment of chronic hepatitis B infection.
By Shepherd J, Gospodarevskaya E, Frampton G, Cooper, K.
-
Febuxostat for the treatment of hyperuricaemia in people with gout: a single technology appraisal.
By Stevenson M, Pandor A.
-
Rivaroxaban for the prevention of venous thromboembolism: a single technology appraisal.
By Stevenson M, Scope A, Holmes M, Rees A, Kaltenthaler E.
-
Cetuximab for the treatment of recurrent and/or metastatic squamous cell carcinoma of the head and neck.
By Greenhalgh J, Bagust A, Boland A, Fleeman N, McLeod C, Dundar Y, et al.
-
Mifamurtide for the treatment of osteosarcoma: a single technology appraisal.
By Pandor A, Fitzgerald P, Stevenson M, Papaioannou D.
-
Ustekinumab for the treatment of moderate to severe psoriasis.
By Gospodarevskaya E, Picot J, Cooper K, Loveman E, Takeda A.
-
Endovascular stents for abdominal aortic aneurysms: a systematic review and economic model.
By Chambers D, Epstein D, Walker S, Fayter D, Paton F, Wright K, et al.
-
Clinical and cost-effectiveness of epoprostenol, iloprost, bosentan, sitaxentan and sildenafil for pulmonary arterial hypertension within their licensed indications: a systematic review and economic evaluation.
By Chen Y-F, Jowett S, Barton P, Malottki K, Hyde C, Gibbs JSR, et al.
-
Cessation of attention deficit hyperactivity disorder drugs in the young (CADDY) – a pharmacoepidemiological and qualitative study.
By Wong ICK, Asherson P, Bilbow A, Clifford S, Coghill D, R DeSoysa R, et al.
-
ARTISTIC: a randomised trial of human papillomavirus (HPV) testing in primary cervical screening.
By Kitchener HC, Almonte M, Gilham C, Dowie R, Stoykova B, Sargent A, et al.
-
The clinical effectiveness of glucosamine and chondroitin supplements in slowing or arresting progression of osteoarthritis of the knee: a systematic review and economic evaluation.
By Black C, Clar C, Henderson R, MacEachern C, McNamee P, Quayyum Z, et al.
-
Randomised preference trial of medical versus surgical termination of pregnancy less than 14 weeks’ gestation (TOPS).
By Robson SC, Kelly T, Howel D, Deverill M, Hewison J, Lie MLS, et al.
-
Randomised controlled trial of the use of three dressing preparations in the management of chronic ulceration of the foot in diabetes.
By Jeffcoate WJ, Price PE, Phillips CJ, Game FL, Mudge E, Davies S, et al.
-
VenUS II: a randomised controlled trial of larval therapy in the management of leg ulcers.
By Dumville JC, Worthy G, Soares MO, Bland JM, Cullum N, Dowson C, et al.
-
A prospective randomised controlled trial and economic modelling of antimicrobial silver dressings versus non-adherent control dressings for venous leg ulcers: the VULCAN trial
By Michaels JA, Campbell WB, King BM, MacIntyre J, Palfreyman SJ, Shackley P, et al.
-
Communication of carrier status information following universal newborn screening for sickle cell disorders and cystic fibrosis: qualitative study of experience and practice.
By Kai J, Ulph F, Cullinan T, Qureshi N.
-
Antiviral drugs for the treatment of influenza: a systematic review and economic evaluation.
By Burch J, Paulden M, Conti S, Stock C, Corbett M, Welton NJ, et al.
-
Development of a toolkit and glossary to aid in the adaptation of health technology assessment (HTA) reports for use in different contexts.
By Chase D, Rosten C, Turner S, Hicks N, Milne R.
-
Colour vision testing for diabetic retinopathy: a systematic review of diagnostic accuracy and economic evaluation.
By Rodgers M, Hodges R, Hawkins J, Hollingworth W, Duffy S, McKibbin M, et al.
-
Systematic review of the effectiveness and cost-effectiveness of weight management schemes for the under fives: a short report.
By Bond M, Wyatt K, Lloyd J, Welch K, Taylor R.
-
Are adverse effects incorporated in economic models? An initial review of current practice.
By Craig D, McDaid C, Fonseca T, Stock C, Duffy S, Woolacott N.
-
Multicentre randomised controlled trial examining the cost-effectiveness of contrast-enhanced high field magnetic resonance imaging in women with primary breast cancer scheduled for wide local excision (COMICE).
By Turnbull LW, Brown SR, Olivier C, Harvey I, Brown J, Drew P, et al.
-
Bevacizumab, sorafenib tosylate, sunitinib and temsirolimus for renal cell carcinoma: a systematic review and economic evaluation.
By Thompson Coon J, Hoyle M, Green C, Liu Z, Welch K, Moxham T, et al.
-
The clinical effectiveness and cost-effectiveness of testing for cytochrome P450 polymorphisms in patients with schizophrenia treated with antipsychotics: a systematic review and economic evaluation.
By Fleeman N, McLeod C, Bagust A, Beale S, Boland A, Dundar Y, et al.
-
Systematic review of the clinical effectiveness and cost-effectiveness of photodynamic diagnosis and urine biomarkers (FISH, ImmunoCyt, NMP22) and cytology for the detection and follow-up of bladder cancer.
By Mowatt G, Zhu S, Kilonzo M, Boachie C, Fraser C, Griffiths TRL, et al.
-
Effectiveness and cost-effectiveness of arthroscopic lavage in the treatment of osteoarthritis of the knee: a mixed methods study of the feasibility of conducting a surgical placebo-controlled trial (the KORAL study).
By Campbell MK, Skea ZC, Sutherland AG, Cuthbertson BH, Entwistle VA, McDonald AM, et al.
-
A randomised 2 × 2 trial of community versus hospital pulmonary rehabilitation for chronic obstructive pulmonary disease followed by telephone or conventional follow-up.
By Waterhouse JC, Walters SJ, Oluboyede Y, Lawson RA.
-
The effectiveness and cost-effectiveness of behavioural interventions for the prevention of sexually transmitted infections in young people aged 13–19: a systematic review and economic evaluation.
By Shepherd J, Kavanagh J, Picot J, Cooper K, Harden A, Barnett-Page E, et al.
-
Dissemination and publication of research findings: an updated review of related biases.
By Song F, Parekh S, Hooper L, Loke YK, Ryder J, Sutton AJ, et al.
-
The effectiveness and cost-effectiveness of biomarkers for the prioritisation of patients awaiting coronary revascularisation: a systematic review and decision model.
By Hemingway H, Henriksson M, Chen R, Damant J, Fitzpatrick N, Abrams K, et al.
-
Comparison of case note review methods for evaluating quality and safety in health care.
By Hutchinson A, Coster JE, Cooper KL, McIntosh A, Walters SJ, Bath PA, et al.
-
Clinical effectiveness and cost-effectiveness of continuous subcutaneous insulin infusion for diabetes: systematic review and economic evaluation.
By Cummins E, Royle P, Snaith A, Greene A, Robertson L, McIntyre L, et al.
-
Self-monitoring of blood glucose in type 2 diabetes: systematic review.
By Clar C, Barnard K, Cummins E, Royle P, Waugh N.
-
North of England and Scotland Study of Tonsillectomy and Adeno-tonsillectomy in Children (NESSTAC): a pragmatic randomised controlled trial with a parallel non-randomised preference study.
By Lock C, Wilson J, Steen N, Eccles M, Mason H, Carrie S, et al.
-
Multicentre randomised controlled trial of the clinical and cost-effectiveness of a bypass-surgery-first versus a balloon-angioplasty-first revascularisation strategy for severe limb ischaemia due to infrainguinal disease. The Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) trial.
By Bradbury AW, Adam DJ, Bell J, Forbes JF, Fowkes FGR, Gillespie I, et al.
-
A randomised controlled multicentre trial of treatments for adolescent anorexia nervosa including assessment of cost-effectiveness and patient acceptability – the TOuCAN trial.
By Gowers SG, Clark AF, Roberts C, Byford S, Barrett B, Griffiths A, et al.
-
Randomised controlled trials for policy interventions: a review of reviews and meta-regression.
By Oliver S, Bagnall AM, Thomas J, Shepherd J, Sowden A, White I, et al.
-
Paracetamol and selective and non-selective non-steroidal anti-inflammatory drugs (NSAIDs) for the reduction of morphine-related side effects after major surgery: a systematic review.
By McDaid C, Maund E, Rice S, Wright K, Jenkins B, Woolacott N.
-
A systematic review of outcome measures used in forensic mental health research with consensus panel opinion.
By Fitzpatrick R, Chambers J, Burns T, Doll H, Fazel S, Jenkinson C, et al.
Health Technology Assessment programme
-
Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Medical Care Research Unit, University of Sheffield
Prioritisation Strategy Group
-
Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Medical Care Research Unit, University of Sheffield
-
Dr Bob Coates, Consultant Advisor, NETSCC, HTA
-
Dr Andrew Cook, Consultant Advisor, NETSCC, HTA
-
Dr Peter Davidson, Director of Science Support, NETSCC, HTA
-
Professor Robin E Ferner, Consultant Physician and Director, West Midlands Centre for Adverse Drug Reactions, City Hospital NHS Trust, Birmingham
-
Professor Paul Glasziou, Professor of Evidence-Based Medicine, University of Oxford
-
Dr Nick Hicks, Director of NHS Support, NETSCC, HTA
-
Dr Edmund Jessop, Medical Adviser, National Specialist, National Commissioning Group (NCG), Department of Health, London
-
Ms Lynn Kerridge, Chief Executive Officer, NETSCC and NETSCC, HTA
-
Dr Ruairidh Milne, Director of Strategy and Development, NETSCC
-
Ms Kay Pattison, Section Head, NHS R&D Programme, Department of Health
-
Ms Pamela Young, Specialist Programme Manager, NETSCC, HTA
HTA Commissioning Board
-
Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Director, Medical Care Research Unit, University of Sheffield
-
Senior Lecturer in General Practice, Department of Primary Health Care, University of Oxford
-
Professor Ann Ashburn, Professor of Rehabilitation and Head of Research, Southampton General Hospital
-
Professor Deborah Ashby, Professor of Medical Statistics, Queen Mary, University of London
-
Professor John Cairns, Professor of Health Economics, London School of Hygiene and Tropical Medicine
-
Professor Peter Croft, Director of Primary Care Sciences Research Centre, Keele University
-
Professor Nicky Cullum, Director of Centre for Evidence-Based Nursing, University of York
-
Professor Jenny Donovan, Professor of Social Medicine, University of Bristol
-
Professor Steve Halligan, Professor of Gastrointestinal Radiology, University College Hospital, London
-
Professor Freddie Hamdy, Professor of Urology, University of Sheffield
-
Professor Allan House, Professor of Liaison Psychiatry, University of Leeds
-
Dr Martin J Landray, Reader in Epidemiology, Honorary Consultant Physician, Clinical Trial Service Unit, University of Oxford?
-
Professor Stuart Logan, Director of Health & Social Care Research, The Peninsula Medical School, Universities of Exeter and Plymouth
-
Dr Rafael Perera, Lecturer in Medical Statisitics, Department of Primary Health Care, Univeristy of Oxford
-
Professor Ian Roberts, Professor of Epidemiology & Public Health, London School of Hygiene and Tropical Medicine
-
Professor Mark Sculpher, Professor of Health Economics, University of York
-
Professor Helen Smith, Professor of Primary Care, University of Brighton
-
Professor Kate Thomas, Professor of Complementary & Alternative Medicine Research, University of Leeds
-
Professor David John Torgerson, Director of York Trials Unit, University of York
-
Professor Hywel Williams, Professor of Dermato-Epidemiology, University of Nottingham
-
Ms Kay Pattison, Section Head, NHS R&D Programme, Department of Health
-
Dr Morven Roberts, Clinical Trials Manager, Medical Research Council
Diagnostic Technologies & Screening Panel
-
Professor of Evidence-Based Medicine, University of Oxford
-
Consultant Paediatrician and Honorary Senior Lecturer, Great Ormond Street Hospital, London
-
Professor Judith E Adams, Consultant Radiologist, Manchester Royal Infirmary, Central Manchester & Manchester Children’s University Hospitals NHS Trust, and Professor of Diagnostic Radiology, Imaging Science and Biomedical Engineering, Cancer & Imaging Sciences, University of Manchester
-
Ms Jane Bates, Consultant Ultrasound Practitioner, Ultrasound Department, Leeds Teaching Hospital NHS Trust
-
Dr Stephanie Dancer, Consultant Microbiologist, Hairmyres Hospital, East Kilbride
-
Professor Glyn Elwyn, Primary Medical Care Research Group, Swansea Clinical School, University of Wales
-
Dr Ron Gray, Consultant Clinical Epidemiologist, Department of Public Health, University of Oxford
-
Professor Paul D Griffiths, Professor of Radiology, University of Sheffield
-
Dr Jennifer J Kurinczuk, Consultant Clinical Epidemiologist, National Perinatal Epidemiology Unit, Oxford
-
Dr Susanne M Ludgate, Medical Director, Medicines & Healthcare Products Regulatory Agency, London
-
Dr Anne Mackie, Director of Programmes, UK National Screening Committee
-
Dr Michael Millar, Consultant Senior Lecturer in Microbiology, Barts and The London NHS Trust, Royal London Hospital
-
Mr Stephen Pilling, Director, Centre for Outcomes, Research & Effectiveness, Joint Director, National Collaborating Centre for Mental Health, University College London
-
Mrs Una Rennard, Service User Representative
-
Dr Phil Shackley, Senior Lecturer in Health Economics, School of Population and Health Sciences, University of Newcastle upon Tyne
-
Dr W Stuart A Smellie, Consultant in Chemical Pathology, Bishop Auckland General Hospital
-
Dr Nicholas Summerton, Consultant Clinical and Public Health Advisor, NICE
-
Ms Dawn Talbot, Service User Representative
-
Dr Graham Taylor, Scientific Advisor, Regional DNA Laboratory, St James’s University Hospital, Leeds
-
Professor Lindsay Wilson Turnbull, Scientific Director of the Centre for Magnetic Resonance Investigations and YCR Professor of Radiology, Hull Royal Infirmary
-
Dr Tim Elliott, Team Leader, Cancer Screening, Department of Health
-
Dr Catherine Moody, Programme Manager, Neuroscience and Mental Health Board
-
Dr Ursula Wells, Principal Research Officer, Department of Health
Pharmaceuticals Panel
-
Consultant Physician and Director, West Midlands Centre for Adverse Drug Reactions, City Hospital NHS Trust, Birmingham
-
Professor in Child Health, University of Nottingham
-
Mrs Nicola Carey, Senior Research Fellow, School of Health and Social Care, The University of Reading
-
Mr John Chapman, Service User Representative
-
Dr Peter Elton, Director of Public Health, Bury Primary Care Trust
-
Dr Ben Goldacre, Research Fellow, Division of Psychological Medicine and Psychiatry, King’s College London
-
Mrs Barbara Greggains, Service User Representative
-
Dr Bill Gutteridge, Medical Adviser, London Strategic Health Authority
-
Dr Dyfrig Hughes, Reader in Pharmacoeconomics and Deputy Director, Centre for Economics and Policy in Health, IMSCaR, Bangor University
-
Professor Jonathan Ledermann, Professor of Medical Oncology and Director of the Cancer Research UK and University College London Cancer Trials Centre
-
Dr Yoon K Loke, Senior Lecturer in Clinical Pharmacology, University of East Anglia
-
Professor Femi Oyebode, Consultant Psychiatrist and Head of Department, University of Birmingham
-
Dr Andrew Prentice, Senior Lecturer and Consultant Obstetrician and Gynaecologist, The Rosie Hospital, University of Cambridge
-
Dr Martin Shelly, General Practitioner, Leeds, and Associate Director, NHS Clinical Governance Support Team, Leicester
-
Dr Gillian Shepherd, Director, Health and Clinical Excellence, Merck Serono Ltd
-
Mrs Katrina Simister, Assistant Director New Medicines, National Prescribing Centre, Liverpool
-
Mr David Symes, Service User Representative
-
Dr Lesley Wise, Unit Manager, Pharmacoepidemiology Research Unit, VRMM, Medicines & Healthcare Products Regulatory Agency
-
Ms Kay Pattison, Section Head, NHS R&D Programme, Department of Health
-
Mr Simon Reeve, Head of Clinical and Cost-Effectiveness, Medicines, Pharmacy and Industry Group, Department of Health
-
Dr Heike Weber, Programme Manager, Medical Research Council
-
Dr Ursula Wells, Principal Research Officer, Department of Health
Therapeutic Procedures Panel
-
Consultant Physician, North Bristol NHS Trust
-
Professor of Psychiatry, Division of Health in the Community, University of Warwick, Coventry
-
Professor Jane Barlow, Professor of Public Health in the Early Years, Health Sciences Research Institute, Warwick Medical School, Coventry
-
Ms Maree Barnett, Acting Branch Head of Vascular Programme, Department of Health
-
Mrs Val Carlill, Service User Representative
-
Mrs Anthea De Barton-Watson, Service User Representative
-
Mr Mark Emberton, Senior Lecturer in Oncological Urology, Institute of Urology, University College Hospital, London
-
Professor Steve Goodacre, Professor of Emergency Medicine, University of Sheffield
-
Professor Christopher Griffiths, Professor of Primary Care, Barts and The London School of Medicine and Dentistry
-
Mr Paul Hilton, Consultant Gynaecologist and Urogynaecologist, Royal Victoria Infirmary, Newcastle upon Tyne
-
Professor Nicholas James, Professor of Clinical Oncology, University of Birmingham, and Consultant in Clinical Oncology, Queen Elizabeth Hospital
-
Dr Peter Martin, Consultant Neurologist, Addenbrooke’s Hospital, Cambridge
-
Dr Kate Radford, Senior Lecturer (Research), Clinical Practice Research Unit, University of Central Lancashire, Preston
-
Mr Jim Reece Service User Representative
-
Dr Karen Roberts, Nurse Consultant, Dunston Hill Hospital Cottages
-
Dr Phillip Leech, Principal Medical Officer for Primary Care, Department of Health
-
Ms Kay Pattison, Section Head, NHS R&D Programme, Department of Health
-
Dr Morven Roberts, Clinical Trials Manager, Medical Research Council
-
Professor Tom Walley, Director, NIHR HTA programme, Professor of Clinical Pharmacology, University of Liverpool
-
Dr Ursula Wells, Principal Research Officer, Department of Health
Disease Prevention Panel
-
Medical Adviser, National Specialist, National Commissioning Group (NCG), London
-
Director, NHS Sustainable Development Unit, Cambridge
-
Dr Elizabeth Fellow-Smith, Medical Director, West London Mental Health Trust, Middlesex
-
Dr John Jackson, General Practitioner, Parkway Medical Centre, Newcastle upon Tyne
-
Professor Mike Kelly, Director, Centre for Public Health Excellence, NICE, London
-
Dr Chris McCall, General Practitioner, The Hadleigh Practice, Corfe Mullen, Dorset
-
Ms Jeanett Martin, Director of Nursing, BarnDoc Limited, Lewisham Primary Care Trust
-
Dr Julie Mytton, Locum Consultant in Public Health Medicine, Bristol Primary Care Trust
-
Miss Nicky Mullany, Service User Representative
-
Professor Ian Roberts, Professor of Epidemiology and Public Health, London School of Hygiene & Tropical Medicine
-
Professor Ken Stein, Senior Clinical Lecturer in Public Health, University of Exeter
-
Dr Kieran Sweeney, Honorary Clinical Senior Lecturer, Peninsula College of Medicine and Dentistry, Universities of Exeter and Plymouth
-
Professor Carol Tannahill, Glasgow Centre for Population Health
-
Professor Margaret Thorogood, Professor of Epidemiology, University of Warwick Medical School, Coventry
-
Ms Christine McGuire, Research & Development, Department of Health
-
Dr Caroline Stone, Programme Manager, Medical Research Council
Expert Advisory Network
-
Professor Douglas Altman, Professor of Statistics in Medicine, Centre for Statistics in Medicine, University of Oxford
-
Professor John Bond, Professor of Social Gerontology & Health Services Research, University of Newcastle upon Tyne
-
Professor Andrew Bradbury, Professor of Vascular Surgery, Solihull Hospital, Birmingham
-
Mr Shaun Brogan, Chief Executive, Ridgeway Primary Care Group, Aylesbury
-
Mrs Stella Burnside OBE, Chief Executive, Regulation and Improvement Authority, Belfast
-
Ms Tracy Bury, Project Manager, World Confederation for Physical Therapy, London
-
Professor Iain T Cameron, Professor of Obstetrics and Gynaecology and Head of the School of Medicine, University of Southampton
-
Dr Christine Clark, Medical Writer and Consultant Pharmacist, Rossendale
-
Professor Collette Clifford, Professor of Nursing and Head of Research, The Medical School, University of Birmingham
-
Professor Barry Cookson, Director, Laboratory of Hospital Infection, Public Health Laboratory Service, London
-
Dr Carl Counsell, Clinical Senior Lecturer in Neurology, University of Aberdeen
-
Professor Howard Cuckle, Professor of Reproductive Epidemiology, Department of Paediatrics, Obstetrics & Gynaecology, University of Leeds
-
Dr Katherine Darton, Information Unit, MIND – The Mental Health Charity, London
-
Professor Carol Dezateux, Professor of Paediatric Epidemiology, Institute of Child Health, London
-
Mr John Dunning, Consultant Cardiothoracic Surgeon, Papworth Hospital NHS Trust, Cambridge
-
Mr Jonothan Earnshaw, Consultant Vascular Surgeon, Gloucestershire Royal Hospital, Gloucester
-
Professor Martin Eccles, Professor of Clinical Effectiveness, Centre for Health Services Research, University of Newcastle upon Tyne
-
Professor Pam Enderby, Dean of Faculty of Medicine, Institute of General Practice and Primary Care, University of Sheffield
-
Professor Gene Feder, Professor of Primary Care Research & Development, Centre for Health Sciences, Barts and The London School of Medicine and Dentistry
-
Mr Leonard R Fenwick, Chief Executive, Freeman Hospital, Newcastle upon Tyne
-
Mrs Gillian Fletcher, Antenatal Teacher and Tutor and President, National Childbirth Trust, Henfield
-
Professor Jayne Franklyn, Professor of Medicine, University of Birmingham
-
Mr Tam Fry, Honorary Chairman, Child Growth Foundation, London
-
Professor Fiona Gilbert, Consultant Radiologist and NCRN Member, University of Aberdeen
-
Professor Paul Gregg, Professor of Orthopaedic Surgical Science, South Tees Hospital NHS Trust
-
Bec Hanley, Co-director, TwoCan Associates, West Sussex
-
Dr Maryann L Hardy, Senior Lecturer, University of Bradford
-
Mrs Sharon Hart, Healthcare Management Consultant, Reading
-
Professor Robert E Hawkins, CRC Professor and Director of Medical Oncology, Christie CRC Research Centre, Christie Hospital NHS Trust, Manchester
-
Professor Richard Hobbs, Head of Department of Primary Care & General Practice, University of Birmingham
-
Professor Alan Horwich, Dean and Section Chairman, The Institute of Cancer Research, London
-
Professor Allen Hutchinson, Director of Public Health and Deputy Dean of ScHARR, University of Sheffield
-
Professor Peter Jones, Professor of Psychiatry, University of Cambridge, Cambridge
-
Professor Stan Kaye, Cancer Research UK Professor of Medical Oncology, Royal Marsden Hospital and Institute of Cancer Research, Surrey
-
Dr Duncan Keeley, General Practitioner (Dr Burch & Ptnrs), The Health Centre, Thame
-
Dr Donna Lamping, Research Degrees Programme Director and Reader in Psychology, Health Services Research Unit, London School of Hygiene and Tropical Medicine, London
-
Mr George Levvy, Chief Executive, Motor Neurone Disease Association, Northampton
-
Professor James Lindesay, Professor of Psychiatry for the Elderly, University of Leicester
-
Professor Julian Little, Professor of Human Genome Epidemiology, University of Ottawa
-
Professor Alistaire McGuire, Professor of Health Economics, London School of Economics
-
Professor Rajan Madhok, Medical Director and Director of Public Health, Directorate of Clinical Strategy & Public Health, North & East Yorkshire & Northern Lincolnshire Health Authority, York
-
Professor Alexander Markham, Director, Molecular Medicine Unit, St James’s University Hospital, Leeds
-
Dr Peter Moore, Freelance Science Writer, Ashtead
-
Dr Andrew Mortimore, Public Health Director, Southampton City Primary Care Trust
-
Dr Sue Moss, Associate Director, Cancer Screening Evaluation Unit, Institute of Cancer Research, Sutton
-
Professor Miranda Mugford, Professor of Health Economics and Group Co-ordinator, University of East Anglia
-
Professor Jim Neilson, Head of School of Reproductive & Developmental Medicine and Professor of Obstetrics and Gynaecology, University of Liverpool
-
Mrs Julietta Patnick, National Co-ordinator, NHS Cancer Screening Programmes, Sheffield
-
Professor Robert Peveler, Professor of Liaison Psychiatry, Royal South Hants Hospital, Southampton
-
Professor Chris Price, Director of Clinical Research, Bayer Diagnostics Europe, Stoke Poges
-
Professor William Rosenberg, Professor of Hepatology and Consultant Physician, University of Southampton
-
Professor Peter Sandercock, Professor of Medical Neurology, Department of Clinical Neurosciences, University of Edinburgh
-
Dr Susan Schonfield, Consultant in Public Health, Hillingdon Primary Care Trust, Middlesex
-
Dr Eamonn Sheridan, Consultant in Clinical Genetics, St James’s University Hospital, Leeds
-
Dr Margaret Somerville, Director of Public Health Learning, Peninsula Medical School, University of Plymouth
-
Professor Sarah Stewart-Brown, Professor of Public Health, Division of Health in the Community, University of Warwick, Coventry
-
Professor Ala Szczepura, Professor of Health Service Research, Centre for Health Services Studies, University of Warwick, Coventry
-
Mrs Joan Webster, Consumer Member, Southern Derbyshire Community Health Council
-
Professor Martin Whittle, Clinical Co-director, National Co-ordinating Centre for Women’s and Children’s Health, Lymington