

Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as award number NIHR129064. The contractual start date was in March 2020. The draft manuscript began editorial review in July 2023 and was accepted for publication in March 2024. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ manuscript and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this article.
Permissions
Copyright statement
Copyright © 2024 Stenfert Kroese et al. This work was produced by Stenfert Kroese et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaptation in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2024 Stenfert Kroese et al.
Chapter 1 Background to the research
Why is this research important?
A learning disability is characterised by an intelligence quotient below 70 and associated deficits in adaptive functioning, arising before the age of 18 years. It is estimated to affect 1.4–2% of the UK population. 1 Children with a learning disability are four to five times more likely to have a mental health disorder compared with other children and account for 14% of all children with mental health problems. 2 Their parents, especially mothers, are also more likely to report psychological problems. These health inequalities for children with a learning disability and their parents emerge early in the child’s life. 2
Social exclusion and poverty are more likely to be experienced by children and young people with a learning disability, along with other negative life experiences, such as health issues, abuse and bereavement, as well as having fewer friends than other children. These biological, psychological and environmental factors increase their risk of developing mental health difficulties. 2 At least half of children with a learning disability are victimised, rejected or mistreated by peers3 and, compared with their typically developing peers, 75% of children and young people with a learning disability have low social competence4 and low levels of emotional literacy and coping skills, which further increases their risk of developing mental health difficulties. 5 These early negative experiences have long-term consequences, as young people with mental health difficulties are more likely to have further negative life experiences and unequal life chances as they progress into adulthood. 6
Access to specialist mental health support poses challenges and it has been reported that fewer than 30% of children have access to such services. 7 Thus, children with a learning disability and their parents face significant health inequalities and problems gaining access to appropriate and timely services.
For the general population, there is compelling and consistent empirical evidence that social and emotional competencies can be taught and that these competencies lead to positive and significant improvements in mental health and well-being, behaviour and academic achievement. 6 Improved social and emotional literacy may therefore mitigate some of the impact from inequalities experiences by children with a learning disability. Given this evidence, interventions are needed that aim to protect and improve the mental health and resilience of children with a learning disability. Despite higher prevalence rates of mental health problems in children with a learning disability2 and research demonstrating a link between emotional literacy and mental health in adults and adolescents in the general population, there has been limited research that has examined the link between emotional literacy and mental health in children with a learning disability.
A recent systematic review of randomised controlled trials (RCTs)8 indicates that most reported interventions (including school-based interventions) designed to improve psychosocial–behavioural functioning of school-aged (5–18 years) children with a learning disability may be effective. However, the studies included in this review only report on intellectual functioning and adaptive skills (e.g. communication, social skills and educational/vocational functioning) and were not designed to measure impact on emotional literacy.
The findings of our early (uncontrolled) pilot work5 suggest that an adapted school-based intervention, a programme called Zippy’s Friends (ZF) adapted for children with special educational needs and disabilities (SEND), is acceptable to and valued by teachers, with some promise of improvements in mental well-being, social interactions and problem solving in children with a learning disability. It is therefore important to establish in a controlled and systematic manner whether a school-based emotional literacy intervention such as ZF can be effective in protecting and improving the mental health and resilience of children with a learning disability.
Before such research is conducted, a feasibility study is required to investigate whether ZF-SEND can be delivered successfully to small groups of children in special schools by teachers in a classroom setting, and whether it would be feasible to conduct a large-scale RCT of the effectiveness and cost-effectiveness of ZF-SEND.
Conceptualisation of emotional literacy
Emotional literacy has been defined as:
the ability to perceive accurately, appraise and express emotion, the ability to access and/or generate feelings when they facilitate thought, the ability to understand emotion and emotional knowledge; and the ability to regulate emotions to promote emotional and intellectual growth. 9
Bar-On’s10 model of emotional literacy is the most comprehensive and inclusive conceptualisation of this construct, including an array of emotional, personal and social abilities and skills that influence an individual’s ability to cope effectively with environmental demands and pressures. The key factors involved in this model include intrapersonal capacity (understanding, awareness and expression of one’s emotions), interpersonal skills (understanding, awareness and appreciation of others’ feelings), adaptability (altering one’s feeling and thoughts according to different situations and solving interpersonal problems), stress management (coping with stress and strong emotions) and motivational and general mood factors.
Evidence for the positive effects of improving emotional literacy on mental health
Emotional literacy skills have been shown to be associated with resilience to mental health problems. 11 When individuals have a broad repertoire of coping skills they are considered to have ‘coping flexibility’ and research12 has shown that having such flexibility is associated with positive short- as well as long-term outcomes. Studies on coping distinguish between strategies that focus on decreasing the negative feelings a person has after a difficult or stressful situation (‘emotion-focused coping’) and those which attempt to improve or change the situation (‘action-focused coping’). Emotional literacy is associated with (and ZF addresses) both these types of coping strategies.
Research findings suggest that high emotional literacy reduces stress, improves self-esteem and reduces rates of emotional difficulties later in life. A meta-analysis conducted in 2010,13 which includes adult and adolescent participants (from the general population) found evidence that higher emotional literacy is linked to better mental health. A more recent study14 also suggests that emotional literacy predicts mental health in adolescents (without a learning disability) and concludes that teaching emotional literacy is an effective preventative intervention, as emotional literacy was a significant predictor of psychological well-being and adjustment.
Zippy’s Friends, a school-based intervention designed to enhance emotional literacy
Schools have an important role to play in helping to identify mental health difficulties. Early detection and intervention are key so that children get the support they need, when they need it. 6 The UK Government’s Green Paper ‘Transforming Children and Young People’s Mental Health Provision’15 proposes a new joint working approach between schools and the NHS in England to help children and young people live fulfilling and happy lives. National guidance on the social and emotional well-being of children by the National Institute for Health and Care Excellence (NICE) recommends that priority should be given to those children most at risk of mental health problems. 6 However, the recent government ‘SEND and Alternative Provision Improvement Plan’16 fails to mention mental health or emotional literacy promotion as a priority area for children with SEND or a learning disability.
A systematic review17 concludes that schools that promote positive mental health and help children to cope with negative life experiences can create psychological resilience. This review shows school-based psychoeducational interventions to have positive effects on outcomes, including mental health, social, emotional and educational factors for families, children and communities, with the most effective interventions including skills teaching, liaison and education of teachers and parents, involvement in the community, continuity of interventions starting with young children, long-term whole-school approaches, adaptations to the curriculum and a focus on positive mental health. A recent systematic review of classroom-based mental health interventions for children in adverse environments18 also found evidence that such interventions can promote resilience to psychological problems. However, the authors stressed that risk of bias, especially due to confounding variables and deviation from intended intervention delivery, suggests that the findings of most of the 17 included studies should be interpreted with caution.
Zippy’s Friends for mainstream schools has been extensively evaluated in a number of studies in and outside the UK. 19–24 An early (2010) systematic review found support for the effectiveness of ZF for children in mainstream schools, improving coping skills and increasing emotional vocabulary and positive behaviours. 25 The review identified four controlled studies, conducted between 2000 and 2010. Subsequently, research published in 2010 on the effect of ZF on the emotional well-being of 523 primary school children in ‘disadvantaged’ schools in Ireland found a significant positive effect of ZF on emotional literacy, with significant increases in the intervention group’s scores for self-awareness, self-regulation, motivation, empathy and social skills. 20 In 2014, the same authors reported that the significant increase in emotional literacy in the intervention group was maintained at 12-month follow-up. 23 A large RCT with 7- to 8-year-old children (N = 1483) in Norway also found ZF to have a significant positive impact on coping and mental health outcomes. 22
The studies mentioned so far have all been conducted in mainstream schools. Other than the small pilot study carried out by ourselves5 (with no control condition and no recording of feasibility outcomes), to date we have found no studies reporting on trials of whole-class or school-based mental health interventions for children with a learning disability and/or for special schools. Thus, an evidence inequality exists and research on early school-based interventions designed to improve social/emotional functioning and mental health is needed urgently for children with a learning disability.
Rationale for the study
In brief, conducting a feasibility study of ZF-SEND is important because:
-
children with a learning disability experience a range of inequalities, which puts them at greater risk of mental and physical health problems in adulthood;
-
children and young people with a learning disability experience negative life events and adversity more frequently than their non-disabled peers;
-
the construct of emotional literacy has been shown to be a distinct and moderating factor of how life stress affects mental health and well-being;
-
there is evidence that teaching emotional literacy in primary schools is an effective early intervention to promote positive mental health and help children cope with negative life experiences, resulting in better mental health in later life;
-
in mainstream schools, the ZF programme has been shown to be an effective way in which to improve emotional literacy, coping skills and mental health outcomes;
-
emotional literacy is underemphasised in the SEND curriculum and mainstream emotional literacy programmes (except ZF-SEND) do not have SEND adaptations;
-
NICE recommends that help should be given to those most at risk of mental health problems;
-
lack of investment in mental health promotion in primary schools, particularly special schools, has significant costs for society;
-
there is an identified need for SEND-adapted emotional literacy programmes in special schools.
Chapter 2 Study aims, objectives, primary and secondary outcomes
Aims
The primary aim of the study was to evaluate whether it is feasible to conduct a large-scale RCT of the effectiveness and cost-effectiveness of ZF-SEND for children with a learning disability in special schools. We aimed to assess the acceptability and feasibility of: (1) participating in the trial; (2) data collection and (3) the ZF-SEND intervention, through a feasibility RCT which aimed to recruit and randomise 12 special schools to either deliver the ZF-SEND intervention over 1 academic year (6 schools) or continue with practice as usual (PAU; 6 schools) and to collect data from 96 pupils at baseline (pre randomisation) and 12 months post randomisation.
The study explored the following, in relation to each aim:
Participation in the trial:
-
Feasibility of recruiting and retaining eligible schools and participants to the study and to identify the most effective recruitment pathways
-
The acceptability of study processes, including randomisation, to schools, teachers and parents/carers.
Data collection:
-
Feasibility and acceptability of the proposed outcome measures as methods to measure the effectiveness of the intervention and to conduct an embedded health economic evaluation within a large-scale RCT.
The ZF-SEND intervention:
-
The feasibility of recruiting suitable schools and teachers to deliver the intervention
-
Adherence to the intervention and fidelity of implementation
-
Acceptability of the intervention to teachers, pupils and parents/carers.
Objectives
-
To collect quantitative data using a range of standardised measures at baseline and 12 months post randomisation from teachers, pupils and parents/carers.
-
To conduct qualitative interviews with pupils, teachers, senior leadership staff and parents/carers to explore their experiences of participating in the feasibility study (two pupil participants in each ZF-SEND school, one teacher in each school, a senior member of staff in each school and one or two parents/carers in each school).
-
In the ZF-SEND arm, to assess intervention delivery, fidelity and adherence, and factors influencing implementation, mechanisms of impact and context using data from multiple sources, including teacher-completed session records, qualitative interviews and observations of two ZF-SEND lessons in each ZF-SEND school.
-
In the ZF-SEND arm, to explore how children, parents and teachers experience the intervention through qualitative interviews with 10–12 pupil participants, 10–12 parents/carers, 5–6 teachers and 5–6 senior staff.
-
To investigate the validity and reliability of the self-report measure of mental health (‘Me and My School’; MAMS) and its relationship with other (proxy report) measures of mental health and behaviour.
-
To establish what constitutes education as PAU for emotional literacy in special schools for children with a learning disability through a survey of 20 special schools involved in the trial and external to the trial.
-
To undertake a nested ‘study within a trial’ (SWAT) to explore the acceptability of two different study designs: one where PAU does not come with the offer of delayed access to ZF-SEND, and one where it does. The aim of this SWAT will be to explore the extent to which offer of a ‘waitlist’ comparator influences recruitment and retention of schools. The findings from this SWAT will be used to inform the design of a subsequent large-scale effectiveness study, if indicated.
-
To review the feasibility study against the progression criteria and ascertain whether progression to a large-scale RCT is feasible.
Primary outcomes
The primary outcome is to determine the feasibility of conducting a future large-scale trial to establish the impact of ZF-SEND on mental health, behaviour/emotional/social functioning and quality of life and its cost-effectiveness (economic evaluation). To determine these outcomes, the following were assessed:
-
Recruitment of schools, pupils and parents/carers: What are the most effective recruitment pathways to identify special schools? What recruitment rate for parents can be achieved? What are the characteristics of schools and families of children with a learning disability approached and recruited?
-
Recruitment of schools and teachers: Can schools and teachers be recruited to run the ZF-SEND programme over 1 academic year? What factors influence schools’ willingness to take part in the research? Can sufficient teachers be recruited and trained?
-
Acceptability of research design: Are schools and parents willing to be randomised within the context of a RCT? Do they prefer a design with delayed access (after follow-up data collection) to ZF-SEND in the PAU arm or will they accept PAU with no access to ZF-SEND? How does the offer of delayed access to ZF as part of PAU influence recruitment and retention of schools and pupils?
-
Fidelity of implementation: Can teachers deliver ZF-SEND with a high degree of fidelity to the programme manual? What are the key barriers/facilitators for successful implementation of ZF-SEND and how does this vary across different school contexts? Does the implementation of ZF-SEND support the logic model?
-
Adherence: What proportion of children with a learning disability in the intervention arm schools complete the ZF-SEND programme?
-
Retention: What proportion of schools, children and parents/carers are retained in the research study up to the 12-month post-randomisation follow-up?
-
Usual practice: What does PAU consist of for promoting mental health and well-being on a class-wide curriculum basis for children with a learning disability in special schools? How is PAU different from the programme content of ZF-SEND? Does the offer of delayed access to ZF-SEND as part of PAU alter what is offered as part of PAU in the year following randomisation?
-
Estimation of parameters to inform a definitive sample size calculation: What are the estimated standard deviation (SD), intracluster correlation coefficient, average cluster size and coefficient of variation of cluster size for the strengths and difficulties questionnaire (SDQ) at 8–12 months post randomisation?
-
Feasibility of outcome measures: Do children, teachers and parents complete the outcome measures for the study?
-
Design and methods for health economic analysis: What is the feasibility of collecting resource use and health-related quality of life data for parents and the child participants? What sources of unit costs for potential resource consequences are appropriate, and how much primary costing research will be required for a later large-scale trial? What is the most appropriate approach for measuring and valuing child, family and school outcomes for incorporation into a subsequent trial-based economic evaluation?
-
Evidence of harm: Is there evidence on the basis of the outcome measures that the ZF-SEND programme results in harm, in which case progression to a full trial would not be recommended.
Progression criteria
The following progression criteria were determined to inform the feasibility of progression to a large-scale RCT. We used Avery et al. ’s traffic light system26 to prespecify the feasibility outcomes and indicated satisfactory performance that would suggest progression to a large-scale trial is warranted without any amendments (green), progression is only warranted with an amendment to study design and/or processes (amber), or progression is not warranted (red). See Table 1 for each criterion.
| Outcome: metric | Green (%) | Amber (%) | Red (%) |
|---|---|---|---|
| Recruitment of schools: schools randomised/approached | ≥ 50 | 20–40 | ≤ 20 |
| Retention of schools: schools that remain in the study until the end/schools randomised | ≥ 75 | 50–74 | ≤ 49 |
| Recruitment of pupils – consent obtained from parents: parents providing consent for their child to participant/parents approached to provide consent | ≥ 75 | 50–74 | ≤ 49 |
| Fidelity of ZF-SEND delivery: sessions delivered with fidelity to the manual/sessions assessed | ≥ 75 | 50–74 | ≤ 49 |
| Pupil engagement with ZF intervention: pupils actively taking part in at least 50% of sessions/pupils enrolled in the study and in schools allocated to the intervention | ≥ 60 | 40–59 | ≤ 39 |
| Collection of outcome data: pupils with strengths and difficulties questionnaire data available at 8–12 months post randomisation/pupils included in the study | ≥ 75 | 50–74 | ≤ 49 |
Secondary outcomes
The SDQ27 total difficulties score as reported by teachers and parents/carers was anticipated as the primary outcome for a future trial. The SDQ total difficulties score includes 20 behavioural and emotional problems items (5 each for hyperactivity, conduct problems, emotional problems, peer problems). The SDQ is a mental health screening questionnaire used extensively in UK child mental health settings and in research. The SDQ has also been used in research with children with a learning disability in the UK and internationally,28–31 and maintains good psychometric properties with this population including associations with psychopathology scores from the Developmental Behaviour Checklist (a measure that has four times the number of items but was developed specifically for children with a learning disability and validated against clinician-rated psychopathology judgements). Other outcomes (likely to be secondary outcome measures in a large-scale RCT) were selected based on experience in research with children with a learning disability, brevity but with good psychometric properties and match to the key domains of the logic model (see Appendix 1). To inform the design of a future trial, secondary analyses compared the outcomes of each of the secondary measurements from baseline to follow-up between the study arms.
Patient and public involvement
The study had a robust programme of patient and public involvement (PPI) built in. The aim was to gain advice from PPI partners (including teachers and parents of children with a learning disability) in the design and delivery of the study. As the study was carried out during the COVID-19 pandemic, PPI advice was essential to help us understand the pressures on teachers and parents and then plan the study processes accordingly.
Chapter 3 The intervention
Partnership for Children
Zippy's Friends for Special Educational Needs and Disabilities is provided by Partnership for Children, a charitable organisation based in the UK that works in schools and internationally, and trains teachers to promote mental health in children. The ZF and ZF-SEND programmes were developed jointly by Partnership for Children and academics and educational resources specialists. ZF has been implemented around the world since 1998, currently in over 30 countries. To date, the programme has been offered to over 1.6 million children.
The Zippy’s Friends programme
Zippy’s Friends is a manual-based, classroom programme that aims to develop children’s emotional literacy through improving children’s repertoire of coping skills and their ability to adapt those coping skills to various situations. ZF consists of six modules: feelings, communication, making and breaking relationships, conflict resolution, dealing with change and loss and coping.
The ZF programme uses a problem-solving (as opposed to a rule-bound) approach and teaches children to develop different ways of dealing with social and emotional problems and to self-evaluate. The manual comprises session plans and activities. Each session begins with a story about a group of children to introduce a number of situations and concepts relevant to emotional literacy. These situations and concepts are then explained and consolidated by means of a range of exercises. By hearing how the children in the ZF stories cope with interpersonal problems and with their emotions, and by roleplays and other activities, children are taught to choose effective coping strategies and deal with real-life situations. There is evidence that the ZF programme has a number of beneficial outcomes relevant to mental health,19–24 quality of life and relationships, and that mainstream pupils generally like to participate in ZF activities. 20
In mainstream schools, teachers and teaching assistants deliver the programme during routine classroom time over a 24-week period with 45-minute weekly sessions (four sessions per module).
The Zippy’s Friends for Special Educational Needs and Disabilities programme
While the mainstream programme is designed for children aged 5–7 years, our pilot study5 indicated that ZF-SEND, which was adapted from the original ZF programme by the charity Partnership for Children (www.partnershipforchildren.org.uk), caters best for an older age range (9–11 years) with the proviso that teachers take a flexible approach and ensure that the programme is age appropriate, yet at the same time considering levels of cognitive and emotional functioning. The ZF-SEND programme closely aligns with the mainstream programme but has additional resources and supplements developed by Partnership for Children in consultation with teachers of children with SEND to cater for children with a wide range of special needs. It provides a selection of alternative activities (approximately five for each of the mainstream activities to cater for varying levels of learning disability) and the stories have been adapted at four different ability levels and using Widgit® (Widgit Software Ltd, Warwick, UK) symbols. The activities include craft sessions, completion of worksheets, roleplays, discussion and use of metaphors. Completion of ZF-SEND takes longer than the mainstream programme owing to the increased complexity of running the programme with pupils with SEND and to allow for shorter sessions, repetition of sessions and a range of extra activities. Teachers deliver two 45-minute sessions a week to cater for this and to ensure adequate time for completion within 1 academic year. Teachers are asked to send ZF-SEND materials to parents/carers throughout the programme, to be used in the home to reinforce and generalise the principles of ZF-SEND.
In summary, the ZF-SEND programme is an adaptation of the original ZF. The main difference is that the ZF-SEND version has materials and exercises that cater for children with SEND. The content of each of the sessions remains the same as the original but the ZF-SEND programme takes longer to deliver due to shorter sessions, and the need for repetition and more activities to consolidate learning and memory.
Prior to running the ZF-SEND programme, teachers are required to attend a 1-day training course organised by Partnership for Children. Support and supervision via Partnership for Children is available to teachers throughout the six modules.
A logic model was developed (see Appendix 1) to describe the anticipated mechanisms and processes for the ZF-SEND intervention, how this translates into short- and long-term outcomes and the role of other personal, contextual or situational variables.
Programme fidelity and adherence
Programme fidelity
The following statement on fidelity for ZF-SEND was discussed and agreed by the ZF-SEND research team and Hannah Baker from Partnership for Children in October 2022 and subsequently approved by the study management group on 26 January 2023.
The ZF-SEND programme can be implemented flexibly to suit the varying needs of individual pupils and the group as a whole, in fact this is encouraged. For example, teachers can use different ‘levels’ of complexity of the story and choose if and when to the repeat the story. Teachers can also choose how many lessons and how much time is spent on a specific session plan, including the number and range of activities that are used to deliver the session content. The activities themselves can also be adapted to meet the needs of pupils. However, there is a set of minimum requirements for fidelity relevant to the structure and content of delivery that should be met. In the training, teachers are not given a set of rules on fidelity, but rather the programme materials are presented and it is stressed that there is scope for adaptation, as long as it is in line with the lesson objectives.
Essentially, delivery of the ZF-SEND programme should include:
-
Sessions structured to include an introduction followed by activities and feedback.
-
An anchor or introduction to each session is ideal, but there may be occasions, or even a general approach where teachers choose to jump straight into quick activities rather than have lengthy sessions. This would be dependent on the group’s ability to engage for a certain time period.
-
Teachers should work through the manual sequentially; in the order it is presented.
-
The stories are a key component of the intervention and should be presented within each module. Stories may not feature in every session and different levels of story can be used, as presented in ZF-SEND.
-
At least one activity should be used for each part (parts A and B) of each session. This can be selected from all the alternatives within the programme supplement manual or adapted by the teacher to suit the needs of the pupils. However, it should meet at least 50% of the core components of the activity (as identified in the teacher session records). Teachers can edit and modify the activities so long as they meet a majority (at least 50%) of these core components.
Programme adherence
For the present trial, the definition of programme adherence was based on schools’ progress through the programme, and pupils’ attendance in and engagement with the programme, as follows:
-
Completion of/progress through the programme by the school
-
Percentage of children who attend at least one session (i.e. start the intervention)
-
Percentage of children who complete all the sessions delivered by the school
-
Level of engagement of children in the programme.
Chapter 4 Methods
Trial design and setting
The design is a two-arm cluster feasibility trial of the ZF programme adapted for special schools/units (ZF-SEND), with clear progression criteria and incorporating a process evaluation.
Following recruitment, enrolment of pupils, and collection of baseline data, schools were randomised either to receive training in ZF-SEND and implement the programme plus PAU for 1 academic year or to provide PAU. Partnership for Children trained and supervised teachers delivering ZF-SEND. PAU for emotional literacy in special schools/units for children with a learning disability was established through a survey of special schools/units (including the three PAU schools/units) and a sample of teachers and members of senior leadership/teachers with management responsibilities were interviewed for this purpose.
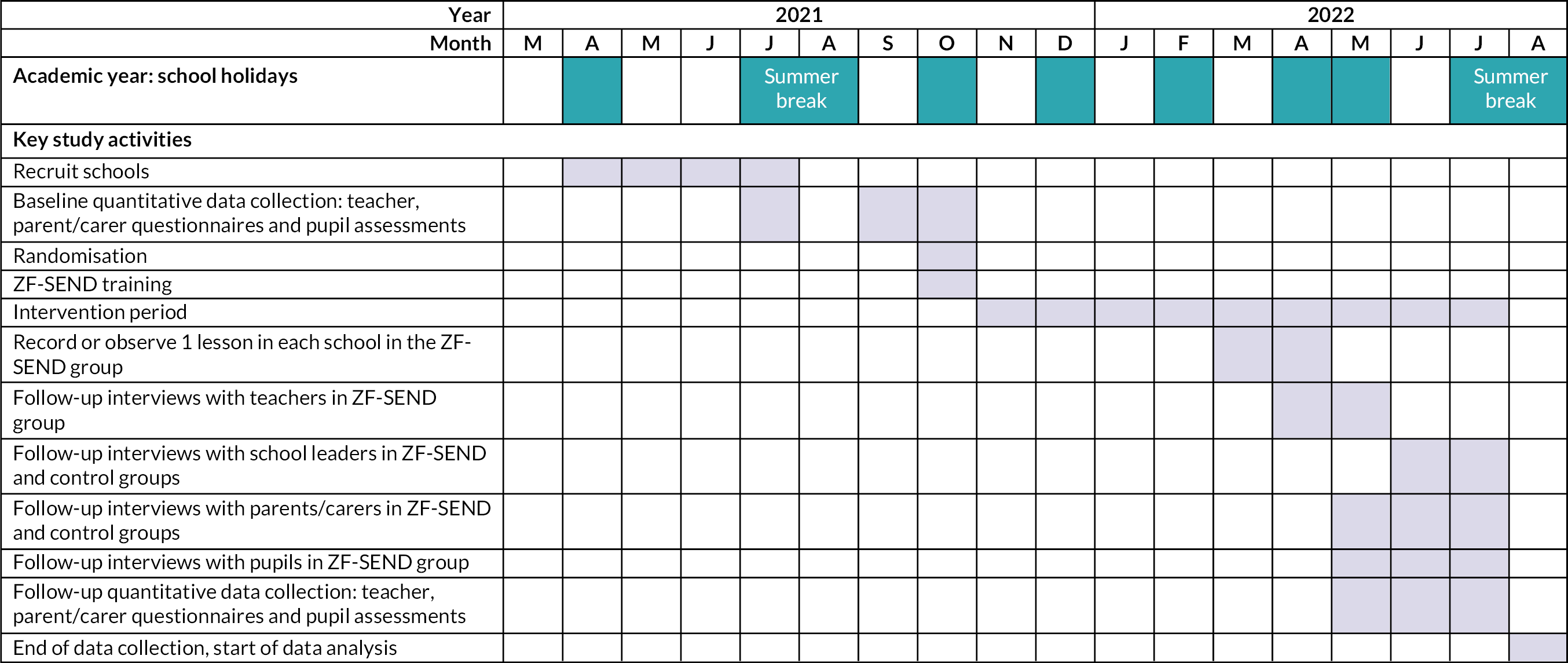
Researchers blind to allocation assessed school-related well-being by interviewing pupil participants. Teacher- and parent-reported data were collected through self-completed questionnaires. Quantitative outcome data were collected at baseline (prior to randomisation) and at 8–12 months follow-up (8–9 months post randomisation). The statisticians remained blind to allocation prior to analysis. Online randomisation used minimisation with a random element, balanced by size of school. Figure 1 provides an overview of the study timeline.
FIGURE 1.
Overview of study timeline.
Training in ZF-SEND was provided to schools in the ZF-SEND arm after randomisation. As Partnership for Children are the only organisation providing the programme there was minimal risk of contamination between arms. Furthermore, the schools were widely spread geographically (Figure 3) and schools were not in contact with each other, further reducing any risk.
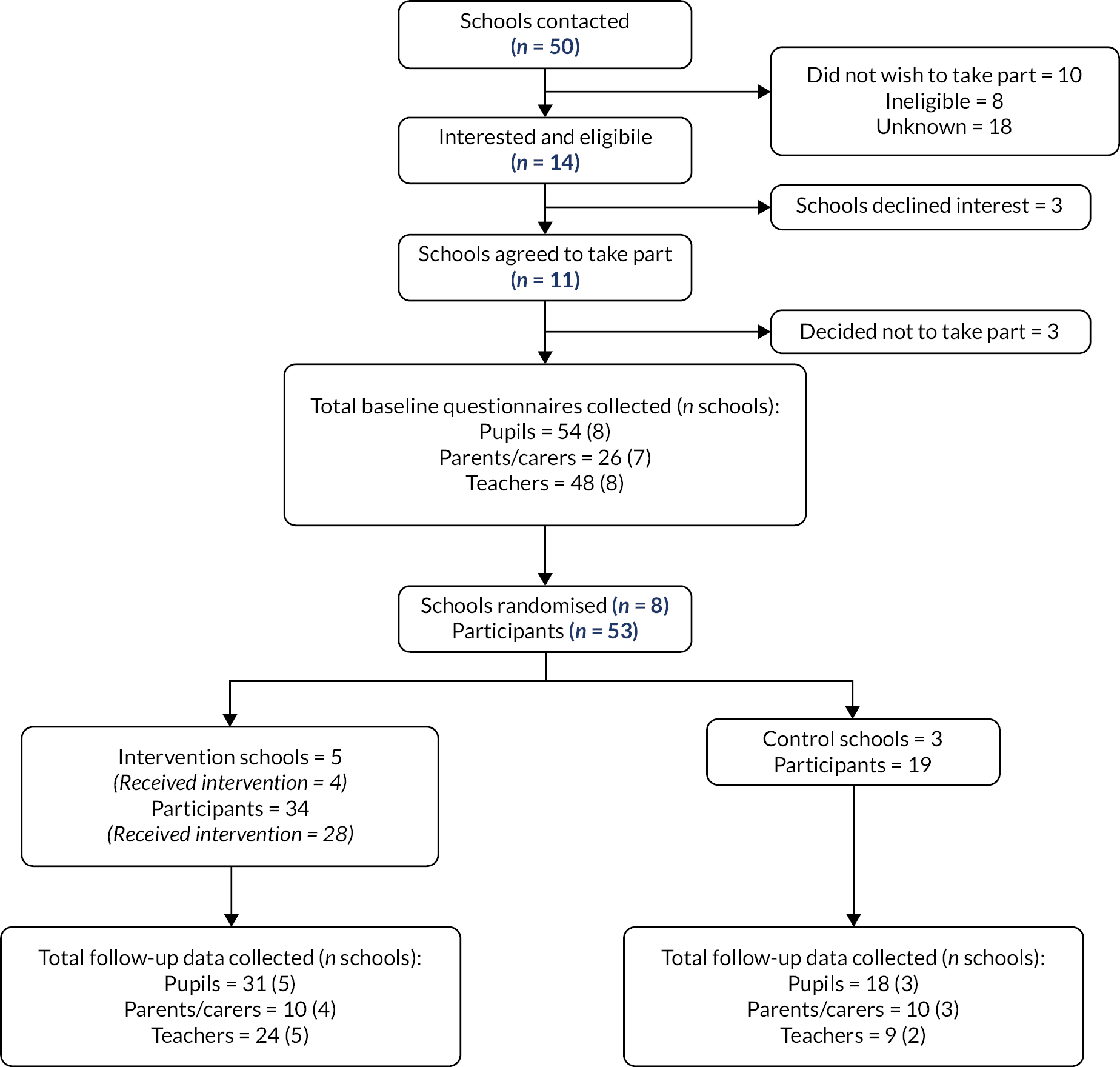
FIGURE 2.
CONSORT diagram of recruitment and data collection process.
Study within a trial
A SWAT was included to assess recruitment strategies. For the SWAT, a sampling frame of potentially eligible schools was established and the order in which they were approached was predetermined. The schools were allocated at random to receive information sheets describing a study where PAU either does or does not offer delayed access to ZF-SEND. Following the completion of data collection, all schools in the control arm were offered the programme as delivered by Partnership for Children, whether or not they received an information sheet which described delayed access.
Context for the trial
The study took place during the COVID-19 pandemic. The start of the study was delayed due to the pandemic and subsequently commenced in spring 2021, shortly after schools had reopened after the national lockdown in England at the beginning of 2021. National restrictions were in place throughout the study period and schools and the study team had to respond to changes in these restrictions and fluctuations in COVID-19 infections leading to staff and pupil absence. See Appendix 2 for an overview of the study timeline set against COVID-19 infection rates and national restrictions.
The delayed start and impact of the COVID-19 pandemic affected the anticipated timeline for the study and various study procedures, as discussed throughout this report. For example, recruitment was delayed as schools had just reopened and therefore baseline data collection was not completed before the end of the 2020–1 academic year. Baseline data collection carried over into the 2021–2 academic year and so the follow-up period reduced to 8–12 months rather than 12 months post randomisation. Delays to baseline data collection had a ‘knock on’ effect for randomisation, which was scheduled after data collection was complete, which then impacted on training for those allocated to the ZF-SEND arm of the trial. Training also had to be adapted to be delivered online because of the pandemic and Partnership for Children could only offer one session before the October half-term break. This in turn delayed the start of the ZF-SEND programme and significantly shortened the time ZF-SEND schools had left to deliver the programme, which resulted in some schools not completing the programme before follow-up data collection. Furthermore, adaptation had to be made to data collection procedures to allow remote (online) collection of data from pupils and remote (online) observations of ZF-SEND lessons.
A key aim of this report is therefore to consider the impact of the COVID-19 pandemic on the feasibility study. A summary of the key changes to the protocol are listed on page 28 (Figure 1).
Study setting
Special schools in England. The ZF-SEND intervention was delivered in schools by teaching staff.
Recruitment and follow-up
It was anticipated that 12 schools would be recruited in the summer term starting in April 2021 (8 from England and 4 from Scotland). From each school, a class with 6–10 children eligible to participate and their parents/carers were recruited into the study. Following baseline data collection, those schools allocated to the intervention arm delivered ZF-SEND across the 2021–2 academic year. Follow-up assessments were conducted 8–12 months after baseline data collection in June–July 2022. Data collection concluded in August 2022.
The process evaluation took place throughout the study, from the first approach to schools through to collection of follow-up data and data analysis. Interviews with class teachers and school personnel with management responsibilities were carried out at various time points throughout the follow-up period. Class teachers in the ZF-SEND arm completed session checklists throughout the delivery of the intervention. In addition, observations of ZF-SEND lessons were conducted approximately mid-programme. Data on PAU delivered in the control arm as well as at other special schools were collected at various time points during the 2021–2 academic year.
Research ethics
Prior to opening the study to recruitment, an application was made to University of Birmingham Research Ethics Committee, who reviewed and approved the study (8 March 2023, application number: ERN_20-0191). The study was conducted in accordance with the University of Birmingham’s code of practice for research. In addition, as the study was undertaken during the COVID-19 pandemic, a risk assessment was undertaken in line with the University of Birmingham’s restarting research process.
Risk assessment
A study risk assessment was undertaken prior to commencement to identify the potential hazards associated with the study and to assess the likelihood of those hazards occurring and resulting in harm. This risk assessment included:
-
the known and potential risks and benefits to participants
-
how high the risk is compared with normal standard practice
-
how the risk will be minimised/managed.
The study was categorised as a low risk, where the level of risk is comparable to the risk of usual care or practice. The study risk assessment was used to determine the intensity and focus of monitoring activity. It was therefore agreed that the study steering committee would meet every 6 months throughout the study duration.
Eligibility criteria
The study had three types of participants: pupil participants, parent/carer participants, teacher participants and senior teaching staff participants. In addition, heads of school had to consent to their school taking part in the study. Schools and participants were eligible for the study if they met all of the following inclusion criteria and none of the exclusion criteria applied.
Inclusion criteria for schools
-
Schools must have firm commitment to the research and agree to be randomly allocated to either the intervention or the usual practice arm (either delayed or no access to ZF-SEND) of the study.
-
They should have pupils with a learning disability and be able to identify two teachers who consent to taking part and who are willing to deliver the ZF-SEND intervention over 1 academic year to a group of children with learning disabilities.
-
The teachers must also be willing to complete a 1-day training session, to receive supervision from Partnership for Children and to complete the study records, be video-/audio-recorded and participate in a qualitative interview at follow-up. Where teachers consented to participate in the study but not to having ZF-SEND sessions video-recorded, alternative ways to assess fidelity were explored, for example self-report or through a member of the research team observing sessions with the head teacher’s and teacher’s consent.
-
The schools which host ZF-SEND must have the resources to support the study and must be willing to free up the teachers for training and supervision.
Exclusion criteria for schools
-
Delivering other manual-based classroom interventions designed to address mental health, well-being or emotional literacy.
Inclusion criteria for pupil participants
-
Children with a learning disability in years 5–6 (aged 9–11 years; at the top end of primary school) attending special schools. A learning disability (learning disability/difficulty in UK services terminology) was administratively defined by virtue of attending a special school/unit in England or Scotland.
-
Pupils with the cognitive and communication skills to engage in the intervention, to provide assent and to complete the pupil-completed outcome measures.
Exclusion criteria for pupil participants
-
No parental consent to participate in the research (although this would not exclude the pupil from the intervention).
-
Current child protection concerns relating to the pupil at the point of recruitment or the family are reported by the school to be in a state of current crisis (although this would not exclude the pupil from the intervention).
-
Unable to assent to the pupil-completed outcome measures or to communicate using English (and adaptations to meet their communication needs cannot be put in place in the classroom setting).
-
Specific diagnoses and any comorbid conditions were recorded but not used as a basis for inclusion/exclusion.
Inclusion criteria for parent/carer participants
-
Biological, step-parent, adoptive parent or foster carer, or adult family caregiver of pupil participants.
-
Parents/carers with ability to provide informed consent and a level of English language enabling (verbal) completion of outcome measures. Note that reading skills were not required as measures could be administered via structured telephone interview.
Exclusion criteria for parent/carer participants
-
Insufficient command of the (spoken) English language to complete the outcome measures or lacking capacity to give informed consent to take part in the research.
Recruitment
Recruitment of schools
Special schools in England and Scotland were approached to take part in the study. For schools in England, the National Association for Special Educational Needs (nasen) provided a list of 39 schools that had previously indicated that they were interested in taking part in research. For schools in Scotland, members of the research team worked with colleagues from the University of Glasgow the University of Strathclyde, and the British Institute of Learning Disabilities (BILD) to draw up an initial list of 39 potential schools. This list of Scottish schools was refined to only include schools that were eligible for the study and likely to be open to participating in research, resulting in a list of 11 schools which was passed to the research team.
Each of these 50 schools was contacted by the research team by e-mail and provided with an information sheet describing the study including the process of randomisation to intervention or a control group. For the SWAT, schools were sent, at random, one of two information sheets, which described whether or not, if allocated to the PAU group, they would have access to the intervention at the end of the study. The initial contacts were made after the spring break (i.e. late April 2021). Schools were subsequently followed up by phone call up to a maximum of four times. Initial follow-up phone calls took place between 17 May and 3 June 2021 for schools in England and 5 May and 10 May 2021 for schools in Scotland. As Scottish schools closed earlier for the summer break, they were contacted first. A log of all contacts with schools was kept to allow assessment of the feasibility of recruiting schools and the most effective recruitment pathways.
Recruitment of teachers and selection of classes
Schools interested in the study were provided with the inclusion criteria and asked to select at least one class group of pupils who would be in years 5–6 (aged 9–11 years) at the start of the 2021–2 academic year (September 2021). Teachers of these class groups were given information about the project and asked if they agreed to take part.
Recruitment of pupil participants
A member of the research team discussed the study and inclusion criteria with the selected teachers. They described the communication skills required of the pupils to participate in the study and provided some examples of tasks similar to those used in the ZF-SEND intervention and measures to check that potential pupil participants were likely to have the cognitive and communication skills required to give assent, engage with the intervention and complete the outcome measures. Schools sent out information sheets to parents/carers of all eligible, potential pupil participants, on behalf of the research team.
Teachers in the ZF-SEND group were asked to introduce the intervention to their class as a whole, even if some pupils did not meet the inclusion criteria and were therefore ineligible to participate in the study.
Recruitment of parent/carer participants
To protect potential participants’ (pupils’ and parents’) privacy, schools liaised with parents/carers on behalf of the research team. Materials were distributed using the schools’ usual communication systems including electronic ‘parent mail’ and newsletters. Where parents/carers did not receive information using routine communication systems, schools were asked to use alternative methods of communication. Schools were also asked to display information on school wide forums, for example, school bulletins, to ensure that all parents/carers of children at Key Stage 2 were informed about the trial and were provided with the opportunity to complete a ‘right to object’ form.
Parents/carers for each potential pupil participant were sent information sheets that described how their child would be involved in the study, as well as their involvement in data collection.
Recruitment of participants for interview
All class teachers involved in the study were invited to take part in an interview. A member of senior leadership or a teacher with management responsibilities from each school was also invited to take part in an interview. All parents/carers were invited to take part in an interview through the follow-up questionnaire form. In addition, class teachers were asked, via e-mail, to liaise with parents/carers and pass contact details of those interested in taking part in an interview to the research team. For pupil participants in the ZF-SEND group, class teachers were asked to select two pupils for interview based on their expressive verbal communication.
Agreement and consent
Agreement from schools
Information sheets, outlining the study, were provided to schools that expressed an interest in taking part. For the SWAT, two different information sheets were provided to schools at random: one which described a waitlist control where the school would be offered the intervention after the end of the study, should they be allocated to the control group; and one which did not make such an offer. Informed consent was provided by the head teacher of participating schools and recorded on a memorandum of understanding.
Consent from teachers
After head teachers consented to the participation of their school, class teachers were approached and provided with one of two versions of an information sheet, depending on whether they were in the waitlist control or not. Teachers provided their consent, which was recorded on a consent form. Teachers were asked to consent to receiving appropriate training, running the ZF-SEND programme, providing reports on ZF-SEND sessions and having a session observed, if allocated to the intervention group; and completing assessments and being interviewed by research staff.
Assent from pupil participants
As pupil participants were under 16 years of age, they did not provide informed consent for their participation in the research. Instead, parent/carer consent was provided (see below). Prior to the pupil taking part in the baseline and follow-up assessment, the researcher verbally explained what would be involved, using simple language, and asked if the pupil agreed to take part. This was recorded on an ‘assent form’. In addition, implicit non-assent was tested before each outcome assessment. If pupil participants showed verbal or non-verbal signs of not wanting to take part in the study, the assessment was stopped immediately. Similarly, pupil participants taking part in an interview provided verbal assent prior to interview. Pupil assent was not required to take part in the ZF-SEND programme as this was part of routine school activities.
Consent from parent/carer participants
Parents/carers were provided with information sheets via their child’s school. Information was provided on the aims of the study, the nature of data being collected, how data would be collected, confidentiality, potential benefits of the research and names and contacts for future enquiries. To ensure parents/carers received the information, schools were asked to use multiple methods of communication, such as e-mail, written information, newsletters and displays on notice boards.
Parents were provided with the opportunity to ‘opt out’ of their child taking part in the research study via an ‘opt out’ form attached to the information sheet. Parents/carers were given at least 2 weeks to opt out prior to baseline data collection. The children of parents/carers who opted out were not involved in any of the research processes (namely data collection) but did take part in any emotional literacy programmes, including the ZF-SEND programme, that were delivered in the school. Parent/carer consent for children to take part in the ZF-SEND programme was not required as the programme falls within usual curriculum and other institutional activities.
A subgroup of parents/carers was interviewed about their experiences of the study and the intervention. Prior to interview, these parents/carers were provided with an information sheet about the interview and asked for their consent, which was recorded on a consent form.
Sample size
The target sample size was 12 schools (8 in England and 4 in Scotland) with 6 randomised to each arm of the trial. Based on the pilot study, it was estimated that there would be one class/group per school and an average of eight pupils per class (and therefore eight pupils per school). Recruiting 12 schools would therefore provide a pupil sample size of 96 in total (48 per arm). As this is a feasibility study, a formal, a priori power calculation was not conducted. Instead, this feasibility study aimed to provide estimates of key parameters for a future trial. If two-thirds (66.7%) of schools approached agreed to take part (i.e. 12 of 18 approached), the 95% confidence interval (CI) around the percentage was estimated within ± 21.8% (i.e. 44.9–88.5%). Assuming that 12-month follow-up data were obtained for 75% of children, randomising 96 allowed the 95% CI for retention, to be estimated within ± 8.7%.
Randomisation and masking
For the SWAT, a sampling frame of 50 potentially eligible schools was established. Schools were then allocated at random to information sheets describing a study where PAU either does or does not offer delayed access to ZF-SEND. This randomisation process was carried out by the lead statistician using random permuted blocks with varying block sizes (two and four). Schools were stratified by region (England/Scotland), whether the schools was part of a mainstream school or a standalone special school and school size (< 100 pupils, 100 + pupils).
Following recruitment, enrolment of pupils and baseline data collection, schools were similarly randomised to ZF-SEND or PAU using random permuted blocks. Block sizes were fixed at two, owing to the large number of strata and small overall sample size. Schools were similarly stratified by region, type of school and school size. Randomisation was carried out by a member of staff who was not involved in recruitment or data collection. A member of the research team then informed the schools of their allocation via e-mail.
In the majority of cases, baseline assessments were carried out prior to randomisation, and this was the aim. However, owing to time pressures, randomisation was carried out on some schools before all parent/carer and teacher data were returned. However, the risk of bias was deemed to be low in these circumstances as individual class teachers were not informed of their allocation until after they had completed the baseline assessments and completion of these assessments was not administered by a member of the research team, instead, teachers completed the assessments independently. The same applies for parent/carer assessments.
Pupil assessments were administered by a member of the research team, and these were all completed prior to randomisation. At follow-up, a new member of the research team, who was masked to allocation, administered the pupil assessments and a record was kept of any unmasking.
Withdrawal/changes to participation and loss to follow-up
Withdrawal/changes to participation
Participants (pupil, parent/carer, teacher, senior staff) had the right to withdraw consent for participation in any aspect of the study (except pupil participation in the ZF-SEND programme) at any time, up to the end of follow-up and data collection (August 2021). Participants could withdraw from further data collection with or without permission to use the data already collected. Teacher participants in the ZF-SEND arm could also withdraw from providing the programme and schools could withdraw their involvement in the study. In the case of the latter, contact with parents/carers and pupil participants would also cease as all contacts were made through schools.
While no explicit option for withdrawal from the ZF-SEND intervention was provided to pupils and their parent/carers, teachers were encouraged to follow the same principles as they would for routine lessons. They therefore responded to pupils’ preferences, made accommodations and allowances and, if indicated, allowed pupils to not take part in a lesson or the whole programme.
Attrition
A record of participants lost to follow-up was kept, along with reasons for dropping out of the study.
Experimental intervention: Zippy’s Friends for Special Educational Needs and Disabilities
Those in classes allocated to the intervention arm received the ZF-SEND programme in the 2021–2 academic year. Class teachers were provided with training in ZF-SEND through a 2-hour remote training session, delivered by Partnership for Children in October–November 2021. The session was recorded so that those who were unable to attend could watch the recording. Four teachers from three schools attended the remote session. An additional two teachers from two schools watched the video. These plans were adapted due to the COVID-19 pandemic, as limiting non-essential in-person contact was still preferred by many. The aim was to provide training to at least two teachers from each ZF-SEND class; however, owing to time constraints and capacity of schools to release staff, this was only possible for one class. Follow-up interviews with class teachers in the ZF-SEND arm examined the perceived quality and value of the training. The trainer was also interviewed to explore their experience of delivering the training and the extent to which it was delivered as intended.
Zippy's Friends for Special Educational Needs and Disabilities classes started the intervention between 15 November 2021 and 15 January 2022. It was recommended that schools deliver the ZF-SEND programme at least twice weekly throughout the academic year. However, flexibility was offered in how schools arranged delivery. Schools were encouraged to spend as many lessons as required to work through a session plan as detailed in the manual. However, it was expected that classes would work through the session plans and modules in the specified order, using a variety of activities to explore the topic and provide opportunities for learning. Telephone supervision and support was offered by Partnership for Children on an ad hoc basis and teachers could contact Partnership for Children for advice as required.
Comparator intervention: practice as usual
Classes that were not allocated to receive ZF-SEND received PAU alone. Participants attended their usual classes as well as other services, outside school. No limitations or stipulations were placed on PAU group schools in terms of the emotional literacy initiatives they could implement in the school year. PAU may include any services (mainstream and specialised) provided to families and their children with a learning disability as a part of an education health and care plan in England or equivalent in Scotland. Any schools already delivering a manualised, lesson-based emotional literacy programmes were ineligible to participate. Because Partnership for Children is the only organisation in the UK offering training in the intervention, there was no possibility of contamination within the PAU schools during the study.
Information on PAU in emotional literacy among control schools was collected through three short interviews with one school staff per school: at the end of the winter term (6–15 December 2021) after the spring term (27 April–4 May 2022) and in the follow-up interviews (conducted 27 June–18 July 2022).
Data collection
Data were collected during recruitment, at baseline (pre-randomisation) and throughout the course of the 8- to 12-month follow-up. Baseline quantitative outcome measurement, collecting data from pupils, parents/carers and teachers, was conducted either at the end of the preceding school year (July 2021) or beginning of the new school year (September–October 2021). The same outcome measures were repeated at follow-up towards the end of the 2021–2 academic school year (June–July 2022). The process of follow-up outcome measurement started in June 2022 to allow adequate time for teachers to respond, making allowances for the last few weeks of the school year, which are often off timetable and include special activities and trips.
Measures completed by teachers and parents/carers were self-completed via online or paper questionnaire. Parents/carers were also offered the option to complete via a structured interview over the telephone. Pupil measures were conducted through structured interview by a member of the research team who remained masked to allocation. They were face to face or remote, during school time. Teachers or teaching assistants were available to support the pupil, if required; however, this support was limited to helping the pupil feel comfortable rather than being involved in conducting the assessment. Observational notes were made by the researcher to allow an evaluation of this element of data collection, including the feasibility of conducting remote assessments in this way.
To monitor delivery of the ZF-SEND programme, data were collected throughout the school year through a specially designed session checklist, completed by class teachers. In addition, observations of one ZF-SEND lesson in each ZF-SEND school were made around halfway through the school year.
Qualitative interviews were conducted during the summer term, from April 2022 until the end of the school year. Interviews with teachers from ZF-SEND schools were conducted from the start of the summer term to minimise the competing demands we placed on teachers in these schools as they were also involved in intervention delivery and follow-up outcome assessment. Teachers, members of senior management teams or school staff with managerial roles, parents/carers and pupils from ZF-SEND schools were interviewed about their experience of taking part in the research and, if relevant, the ZF-SEND programme. In addition, a series of interviews with schools involved in the trial as well as other special schools explored PAU in terms of emotional literacy initiatives implemented in schools.
Secondary outcome measures
Questionnaires were completed at baseline and follow-up by the teacher, the parents/carers, and the pupils. Teachers were asked to complete the SDQ, the Emotional Literacy Assessment (ELA), and the Nisonger Child Behaviour Rating form (NCBR); parents/carers were asked to complete SDQ, ELA, the child-friendly EQ-5D version (EQ-5D-Y-3L; Euroqol, Rotterdam, Netherlands), the Child Health Utility instrument (CHU), and the Child and Adolescent Service Use Schedule (CASUS); and pupils were asked to complete EQ-5D-Y, CHU, and the MAMS questionnaire.
Strengths and Difficulties Questionnaire
The SDQ27 is a behavioural screening questionnaire aimed at 2- to 17-year-old children. The SDQ asks about 25 attributes (some positive and some negative) divided into five scales, each with five items: (1) emotional symptoms, (2) conduct problems, (3) hyperactivity/inattention, (4) peer problems and (5) prosocial behaviour. Each question has three levels: (1) not true, (2) somewhat true or (3) certainly true. Individual scores for each scale were generated by summing the items within that scale, and items 1–4 were summed to generate a total difficulties score. Therefore, the individual scores could range from 0 to 10, whereas the total difficulties score could range from 0 to 40, where higher scores indicate more problems for all subscales, except for the prosocial behaviour scale.
Emotional literacy assessment
The ELA32 is a questionnaire used to identify pupils’ level of emotional literacy and covers five scales, each with four items of emotional literacy as addressed in the social and emotional aspects of learning curriculum. These scales include (1) self-awareness, (2) self-regulation, (3) motivation, (4) empathy and (5) social skills. Each question has four levels: (1) not at all true, (2) not really true, (3) somewhat true or (4) very true. Individual scores for each scale were generated by summing the items within that scale, and all items in all scales were summed to generate a total score for emotional literacy. Therefore, the individual scores could range from 4 to 16, whereas the total score could range from 20 to 80, where a higher score indicates better emotional literacy.
Nisonger Child Behaviour Rating form
The NCBR33 is a questionnaire used to assess the behaviour of children with a learning disability and covers two areas of behaviour including (1) positive social behaviour, which contains two subscales including (a) compliant/calm behaviour (five items) and (b) adaptive social behaviour (five items); and (2) problem social behaviour, which contains six subscales including (a) conduct problems (13 items), (b) insecure/anxious (15 items), (c) hyperactive (8 items), (d) self-injurious/stereotypic behaviour (9 items), (e) self-isolated/ritualistic behaviour (11 items) and (f) irritable behaviour (6 items). Each question has four levels: (1) not true, (2) somewhat or sometimes true, (3) very or often true and (4) completely or always true, scored from 0 to 4, respectively. Individual scores for each scale were summed to generate a total score within that scale which could range from 0 up to a maximum score of 60 for the insecure/anxious subscale.
Me and My School
The MAMS34 questionnaire is a self-reported measurement of social, emotional and behavioural challenges in primary school children. The questionnaire consists of two domains, including emotional difficulties and behavioural difficulties. The emotional difficulties domain consists of 10 questions, whereas the behavioural difficulties domain consists of 6 questions, each with 3 possible responses including: (1) never, (2) sometimes or (3) always. The final scores for each domain were summed to produce scores that range from 0 to 20 for the emotional difficulties domain, or 0–12 for the behavioural difficulties domain. A higher score indicates worse emotional or behavioural problems. An adaptive administration, developed for children with a learning disability was used. 35
EQ-5D-Y-3L
The child-friendly version (EQ-5D-Y-3L)36 of the EQ-5D questionnaire was designed as a measurement of quality of life and covers five questions relating to quality of life including: (1) mobility, (2) self-care, (3) usual activity, (4) pain/discomfort and (5) anxiety/depression. Each question had three levels: (1) no problems, (2) some problems or (3) a lot of problems. A total score for EQ-5D-Y-3L was generated using the EQ5D command in Stata 17® (StataCorp LP, College Station, TX, USA), which ranges from –1 to 1, where a higher score indicates better quality of life.
Child Health Utility instrument
The CHU37 is a paediatric generic preference-based measure of health-related quality of life and consists of nine questions with five possible responses to each, scored from 1 to 5. A set of preference weights using values from a sample from the general population to give utility values for each health state described by the descriptive system, which allows the quality-adjusted life-years (QALYs) for use in cost analyses. Coefficients given in previous research38 were used as decrements to calculate utility, which could range from 0.3251 (worst state) to 1 (perfect health).
Child and Adolescent Service Use Schedule
The CASUS39 questionnaire is a parent-reported measurement which reports whether a child has used any health or social services in the past 3 months and, if so, how often they have used them. The questionnaire covers whether the child has had any overnight stays in hospital, hospital appointments that did not require admission, accident and emergency visits, ambulance use, community and school health services not within a hospital setting, use of medication, additional teaching support and living away from home.
Go4Kidds Brief Adaptive Behaviour Scale
The Go4Kidds (Great Outcomes for Kids Impacted by Severe Developmental Disabilities)40 questionnaire includes three questions about a child’s adaptive skills, which includes their support needs, communication, social and self-help skills.
Follow-up interviews
Semistructured interviews were conducted with school staff (class teachers and members of senior leadership/those with managerial responsibilities), parents/carers and pupils. The interviews with school staff and parents/carers were conducted via online video calling. Interviews with pupils were either remote or face to face. All interviews were video- or audio-recorded. Topic guides were developed for each stakeholder group on each arm of the trial to address the feasibility questions. As the study was conducted during the COVID-19 pandemic, interviews also explored the impact of the pandemic on schools and on the conduct of the study (see Appendix 3 for the qualitative results relating to the pandemic). All interviews were transcribed by an external transcription service to allow data analysis.
Interviews were conducted with:
-
eight pupils from four ZF-ZEND schools
-
four parents/carers (two from PAU and two from ZF-SEND schools)
-
seven teachers (three from PAU and four from ZF-SEND schools)
-
four members of senior leadership or teachers with management/oversight roles (two from PAU and two from ZF-SEND schools).
Interviews with school staff
Interviews with school staff on both arms of the trial explored the acceptability of the trial design including recruitment, randomisation and data collection methods. The aim was to interview one class teacher and one member of senior management/teacher with management responsibilities from each school. Follow-up interviews with school staff in the ZF-SEND arm also explored: adherence to the ZF-SEND manual and key influences on implementation; any additions/adaptations made to the manualised content and the reasons for these; attendance and engagement in the intervention by pupils and their parents/carers; the perceived value of ZF-SEND, and its fit with existing school policies/priorities; staff views on intervention aims and the mechanisms through which it operates; and the perceived quality and value of the training.
Interviews with parents/carers
Interviews with parents/carers explored factors affecting recruitment and retention, experiences of being involved in the study and acceptability and feasibility of the outcome measures. In addition, interviews with parents/carers in the ZF-SEND arm also explored the extent to which intervention content was used or discussed at home, and the extent to which schools have involved them in the intervention. The aim was to interview two parents/carers from each of the ZF-SEND schools and one parent/carer from PAU schools. Interviews could be single or joint if two parents/carers wanted to participate together.
Interviews with pupils
Interviews with pupils from ZF-SEND schools explored their experiences of participating in the intervention, acceptability of intervention content and activities, understanding of key intervention messages and the extent to which they used strategies taught. The aim was to interview two pupils from each of the ZF-SEND schools.
Session checklists
To monitor implementation of the ZF-SEND programme and to evaluate adherence and fidelity (see definition in Statistical analysis: primary statistical analysis), class teachers who were responsible for delivery of ZF-SEND were asked to complete session checklists, which were aligned to each of the session plans in the ZF-SEND programme. These checklists were developed with Partnership for Children to evaluate adherence and fidelity to the programme as well as pupil engagement in sessions. Items on the checklists followed the structure of the programme to ascertain the proportion of sessions that were delivered with fidelity to this structure (use of story in module, rules and review of previous sessions, introduction to session, use of activities aligned to each part of the session, and opportunity for review and feedback). Further items explored fidelity of the programme implementation in relation to the key features/processes of the introduction, rules and review, activities and feedback for each session. They also provided information on attendance at each lesson in line with our assessment of adherence. Pupil engagement in each session was assessed by means of four items tailored to the specific session activities (rated as none, some or all pupils engaged). The session checklists were developed to allow analysis that would produce quantitative measures of fidelity, adherence and pupil engagement.
The session checklists were organised into module booklets comprising checklists for each session in the module. These were e-mailed to teachers at appropriate intervals, depending on their progress through the programme. Teachers were asked to complete the checklist as soon as possible after delivery of the session and to return, via e-mail, the completed booklet after each module. As teachers were given flexibility in how many lessons they used to deliver each session plan, the checklists were completed per session rather than per lesson; however, a record was made to capture how many lessons were used for each session. The checklists were designed to be simple and quick to complete, requiring only tick box responses, but with space at the end for teachers to record qualitative observations.
Observations of Zippy’s Friends for Special Educational Needs and Disabilities sessions
Observations were made of one ZF-SEND lesson at each school assigned to the ZF-SEND arm of the trial. Observations took place between 8 March and 29 April 2021. This timing was selected so that schools would be approximately mid programme. Observations were coded initially by two members of the research team (BSK and MS) using a specially prepared checklist and the session checklist corresponding to the session being taught in the lesson. After the first observation, comparisons were made to check interrater agreement. The remaining observations were carried out independently by one researcher (MS).
Observations could be made in one of three formats: direct (live) observation in person, direct (live) observation via remote video call, or through a video recording of the lesson. Increased flexibility was offered in response to the COVID-19 context as some schools were still limiting non-essential, in-person contact/access to school grounds. The observation checklist covered aspects of fidelity including quality of delivery, adaptations made to the materials during delivery, class dynamics, and contextual issues, with space for free-text qualitative observations in relation to lesson delivery, pupil response and environment and context. Rates of agreement to allow observation and the preferred format were recorded to inform the procedures for assessing fidelity within a future large-scale trial. Analysis of the observation notes was undertaken to produce a qualitative understanding of feasibility of implementing ZF-SEND.
Practice as usual interviews
To establish what is currently delivered as PAU for emotional literacy in special schools, a survey of special schools/units (including the control schools) was conducted through short semistructured interviews. A representative from each PAU school was interviewed at the end of each term over the academic year about the emotional literacy initiatives at their school. In addition, special schools known to the research team were also interviewed at one time point about the emotional literacy initiatives in their schools. The follow-up interviews with parents/carers also posed questions about any home-based initiatives to address emotional literacy. The interviewer recorded responses in the form of handwritten notes which were promptly typed up to provide a summary of the interview and a list of all the emotional literacy initiatives mentioned. These interviews provided detailed information about the comparator condition, including any overlap with the experimental intervention, as well as an insight into the emotional literacy initiatives generally in use in special schools.
Statistical analysis
Primary statistical analysis
The primary outcome was to determine the feasibility of conducting a future large-scale RCT to establish the impact of ZF-SEND on mental health, behaviours/emotional/social functioning and quality of life, and its cost-effectiveness (economic evaluation). This included analyses of recruitment rates, retention rates, adherence and fidelity.
Recruitment and retention rates were represented using a Consolidated Standards of Reporting Trials (CONSORT) diagram to demonstrate figures overall and by trial arm, including schools contacted, eligible and recruited.
Adherence (attendance) data was summarised by the percentage of sessions in which at least ‘some’ pupils engaged in at least 50% of the core activities of that session; the percentage of children who attended at least one session (i.e. they started the intervention); percentage of children who completed all of the sessions that were delivered (and rated) by the school; and the average number and range of sessions that were completed by the children, difference between schools, and patterns of completion and engagement over time. Where relevant, proportions are presented alongside two-sided 95% Wilson score CIs. 41
Fidelity of the implementation of the ZF-SEND programme was described using the percentage of ZF-SEND sessions that were delivered with fidelity to the manual, as assessed by teachers (self-rated) on the session checklists. ‘Fidelity’ for these analyses was based on the agreed definition outlined in Chapter 3 and was operationalised as a session meeting the following criteria:
-
session was introduced
-
session included at least two different activities
-
at least some pupils engaged in at least 50% of the core elements of the session.
Secondary analysis
Secondary analyses provided baseline demographics for teachers (who completed the form, how long the teacher has known the pupil, what school year the pupil was in, what the pupil’s primary and secondary needs were and whether the child was eligible to free school meals) and parents/carers (age of the pupil; gender of the pupil; ethnicity of the pupil; the pupil’s current living situation; what the pupil’s primary need was; and whether the pupil had any genetic syndrome, epilepsy or sensory impairments).
Individual measurements and final indices at baseline and follow-up were presented for EQ-5D-Y-3L (as answered by the pupils and parents/carers), SDQ (as answered by the teachers and parents/carers), MAMS (as answered by the pupils), ELA (as answered by the teachers and parents/carers), CHU (as answered by the pupils and parents/carers), NCBR (as answered by the teachers), CASUS (as answered by the parents/carers) and Go4Kidds (as answered by the teachers). Two-level analyses of covariance were performed to compare the outcomes of each of the secondary measurements from baseline to follow-up between the trial arms. It was planned that models were adjusted by balancing factors at randomisation including school size (fewer than 100 pupils compared with 100 or more pupils) and study site. However, all schools recruited were based in England and so the models were only adjusted by school size.
Qualitative analysis
Analysis of the follow-up interview transcripts used framework analysis. Framework analysis is a flexible approach which suits the large and diverse data set generated in the present study. It combines a priori and emergent data-driven themes to guide the framework,42 which fits with the feasibility aims of this study. Data analysis was carried out in NVivo (QSR International, Warrington, UK), with collaboration between team members and leaving a clear record of the process from raw data to the analysis.
Framework analysis has five stages: identifying a framework; indexing; charting; mapping and interpretation. 43 In the initial familiarisation stage, we ‘immersed’ ourselves in the data. The data were then sorted into eight initial categories by a senior member of the research team (GU), providing a preliminary framework. These categories were based on the a priori aims of the study, so that specific topics relevant to the feasibility nature of the RCT, such as the implementation of the programme, were explored in detail. As the interviews were semistructured, we ensured all topics relevant to the aims of the study were explored. The process of familiarisation and developing the framework was a ‘to-and-fro process, in which the familiarisation and development of a framework interact with each other’;42 that is, as we kept readjusting our framework, we became more and more familiar with the data.
To familiarise themselves with the data set and refine the framework, two research assistants (EW and NDC) used the initial framework independently to code a subsample of six transcripts and noted any codes that might have been be missing or did not seem to be relevant to the data, thus refining the framework. The wider qualitative analysis team (including the two research assistants, BSK, GU and JS) then met to discuss the initial experience of using the framework and refine the codes and descriptors. Top-level codes were reorganised to improve consistency in analysis. All changes and updates to the framework were recorded.
The two research assistants both recoded one of the interviews using the updated framework. This allowed the team to check that the codes were being interpreted and used consistently. A further meeting was convened with the qualitative analysis team to make the final adjustments to the framework before moving into the ‘indexing’ phase of the analysis in which the framework was systematically applied to code the entire data set. 42 The data set was split in half randomly and the two research assistants used this final framework to code the data. The data were then merged into the same NVivo file once coding was complete.
The qualitative analysis team then met to discuss the coding of the whole data set. The three senior members of the team (BSK, GU and JS) were allocated a top-level theme each, to audit and check the coding before moving forward. The three densest codes were chosen (‘COVID-19-related issues’, ‘general experience of the research study’ and ‘intervention outcomes’). The team met again to discuss this interpretation of the nodes and the data in each. The two research assistants moved on to formulate code summaries. This formed the ‘charting’ stage of framework analysis,43 where the data collected for each ‘top-level’ code were summarised, including convergence or divergence in perspectives across the different stakeholder groups (teacher, parents/carers and pupils). This process led to concise summaries of the key findings for each code. These were then interpreted alongside the quantitative analysis in an interpretative exercise to inform the feasibility evaluation.
Economic evaluation
The health economic component of the study has two main elements: an estimation of the intervention costs of the programme, and an assessment of the feasibility of collecting data on use of health services and health-related quality of life of children with a learning disability for a future trial. The economic evaluation took a service perspective including costs to education, health and social care services.
To estimate the cost of the ZF-SEND intervention, we collected information on the costs of training, subsistence or travel costs for attending training sessions, the costs of materials such as booklets or access to specialist platforms and the cost of supervision/supervisors’ time.
For health-related quality of life, we assessed completion rates and item ‘missingness’ for both pupil completed and parent/carer report versions of generic paediatric quality of life measures CHU-9D44 and EQ-5D-Y-3L. 45 These measures allow for the calculation of QALYs and would be used as the primary outcome measure for cost-effectiveness analysis in a subsequent large-scale RCT. For the feasibility of collecting data on broader health service use, we modified and tested a version of CASUS, which had been used previously in trials involving school children. 46 Following completion by the parent/carer, we assessed the measure’s comprehensiveness in capturing all relevant services, specifically to identify items that were redundant or important services that had been omitted.
Evaluation of training in Zippy’s Friends for Special Educational Needs and Disabilities
A semistructured interview with the ZF-SEND trainer was conducted shortly after training was provided to teachers in the ZF-SEND group to explore adherence to the training model. Teachers who attended the training were also asked about the perceived quality and value of training in the follow-up interviews. In addition, a researcher (NDC) observed the training session and took notes on the content of the training, teacher response and engagement.
Combining the quantitative and qualitative data
The qualitative and quantitative results are presented for each of the three areas under investigation [feasibility and acceptability of (1) participation in the trial; (2) data collection; (3) the ZF-SEND programme] and then combined and discussed. The quantitative results describe what happened during the study and the qualitative data provide insight into the how and why. The results of the interpretive exercise are presented in discussion sections at the end of Chapter 6, pertaining to each of the three primary aims of the study.
Changes to the protocol
The following changes were made to the protocol during the study:
-
Extension to baseline data collection period to allow baseline data to be collected at the beginning of the school year rather than completed by the end of preceding academic year. This resulted in the follow-up period being 8–12 months post randomisation rather than 12 months.
-
Observation of one ZF-SEND lesson in each ZF-SEND school rather than two.
-
The timing of the PAU interviews with control group schools was adapted to move the first interview to the end of the first term of the school year and include an additional interview around halfway through the academic year so that data were collected retrospectively at the end of each of the three school terms.
-
Adjustment of data collection procedures to include remote observations of ZF-SEND sessions and remote pupil assessments.
Chapter 5 Patient and public involvement and engagement
Aims
There is evidence that PPI can have positive impact on research, enhancing the quality of research and ensuring its appropriateness and relevance46 and that it may have a more positive impact when service users are involved throughout the study and when involved as partners in the research team. We therefore ensured that PPI was integral to: (1) the initial stages of the research (identifying and prioritising relevant topics for the research agenda, providing constructive criticism of the research protocol and commenting on whether research was relevant or appropriate to users); (2) undertaking the research [assessing the appropriateness, wording and timing of research instruments (e.g. questionnaires, interview schedules)] and helping to adapt the language and information for the various participant groups. Moreover, assisting with recruitment to the study and improving response rates, (3) writing up the findings (identifying potential knowledge gaps and grounding the final report in user experiences); (4) dissemination and implementation (ensuring that dissemination and implementation take place in a poignant and user-friendly manner and reach the relevant audiences).
Where PPI is described and reported in this report is indicated by page numbers in the Guidance for Reporting Involvement of Patients and the Public 2, short version checklist (Table 2). 47
| Section and topic | Item | Reported on page no. |
|---|---|---|
| 1: Aim | Report the aim of PPI in the study | 47 |
| 2: Methods | Provide a clear description of the methods used for PPI in the study | 47–49 |
| 3: Study results | Outcomes: report the results of PPI in the study, including both positive and negative outcomes | 49–51 |
| 4: Discussion and conclusions | Outcomes: comment on the extent to which PPI influenced the study overall. Describe positive and negative effects | 92 |
| 5: Reflections/critical perspective | Comment critically on the study, reflecting on the things that went well and those that did not, so others can learn from this experience | 91–94 |
Methods of involvement
The study management group met monthly throughout the project. Members of the group includes all investigators, all employed project staff and two representatives of the PPI advisory group (nasen and BILD representing children and their parents/carers) to discuss study progression and key management issues. Nasen and BILD were co-applicants of the research study.
The NASEN is a charitable membership organisation that exists to support and champion those working with, and for, children and young people with SEND and learning differences. Rooted in research and evidence-informed best practice, their information, training and resources ensure that a wide range of stakeholders are provided with the most up-to-date knowledge and support required to become effective, inclusive practitioners. Nasen is an influential UK-wide organisation that actively contributes to the SEND debate and effects change to improve provision within early years, schools, post-16 and wider settings and, ultimately, outcomes for children and young people with SEND.
The BILD is a national organisation that aims to develop the skills and culture necessary to understand the needs of children and adults with a learning disability and improve their quality of life. They work with universities, government departments, local authorities, NHS trusts, service providers and mainstream organisations to champion rights for people with a learning disability and improve practice. BILD has over 40 years’ experience of supporting people and families with a learning disability and is concerned with workforce development and providing accessible resources and knowledge. Part of BILD’s role is to be a bridge between the academic community and the direct workforce. BILD is internationally known for the quality of their resources and publications and is in an excellent position to facilitate the dissemination of good practice.
Throughout this project, both nasen and BILD have been enthusiastic about the research and keen to continue to work with us, considering ZF as an excellent way to address the health inequalities of children with a learning disability. Their knowledge and expertise informed us on how best to communicate and work with children with a learning disability, their parents, and their teachers and senior staff. Both organisations were uniquely placed to guide the recruitment, research protocol, training of research staff and more recently they have advised on dissemination of research findings as they understand and value the purpose, aims and application of the project, and as third-sector organisations have the well-being of children with a learning disability and their families at the heart of their mission statements.
In addition to PPI representation during the monthly Senior Management Group meetings (held between March 2020 and December 2022), the chief investigator, study manager and research associates met with the PPI partners on a regular basis (at least quarterly) during the course of the study, more frequently at the start to provide input on all materials and procedures. The PPI partners advised and supported the research team in adapting materials, advising on information sheets, consent forms and other study materials, co-producing dissemination outputs (including BILD currently producing an accessible video for the child participants, thanking them and summarising our research findings), acting as ambassadors for the research project, and creating communication pathways with SEND educational organisations and other stakeholder groups for children with a learning disability and their families. The partners offered strategic advice on recruiting and engaging organisations and participants, and to this day contribute to the interpretation of the study’s findings and their dissemination (to be continued over 2024–5).
In addition, nasen coordinated external focus groups to advise the researchers throughout the study. Nasen held 6-monthly meetings with teaching staff in special schools (three focus group meetings held) and (separately) with parents of children with a learning disability (three focus group meetings held) in order to gauge opinions from Experts by Experience, not directly involved in the study, on a number of topics including acceptability of research procedures and how these may impact on the pupil participants, the role of the teachers and the support they may need to deliver ZF-SEND, and the balance between burden imposed on the participants and schools on the one hand and the advantages gained by them on the other. Feedback from these groups was regularly fed into the study management group agenda so members were kept informed, and then to discuss and evaluate the project’s aims and protocol in the light of the views and opinions of Experts by Experience. Teaching staff and parents/carers were paid for their participation in the focus groups.
The research proposal and initial pilot study were prepared in collaboration with the franchise holders of the ZF programmes, Partnership for Children, an organisation that works in schools and trains teachers to promote mental health in children including children with SEND. This brings them in close contact with the setting in which this research was carried out and as providers of evidence-based interventions, they are on the cutting edge of mental health initiatives for children, including children with a learning disability and/or SEND. Their input, in addition to the PPI provided by nasen and BILD, has enabled us to be aware of the needs of these children, and those of their parents and teachers. Partnership for Children will also be involved in future dissemination activities.
All PPI partners received regular feedback about how their advice has been taken forward to ensure they could see how their contributions shaped the project. Where their suggestions were not possible to incorporate, feedback was provided as to the reasons. Both Partnership for Children, BILD and nasen commented on drafts of the original research proposal, which significantly improved and shaped up our recruitment plans and design of the intervention protocol. They also gave significant input into the final report and are currently supporting us to disseminate our findings to the relevant audiences. They have all been enthusiastic and valued contributors throughout this project and they are keen to continue to work with us.
A study steering committee was established and met biannually during the study (between June 2020 and December 2022). It comprised an independent chair with expertise in SEND research and in trials in the SEND field and other independent members: two clinicians who are expert in the learning disability field, a statistician and a parent/carer of a child with a learning disability. The chief investigator and study manager attended the study steering committee as observers and provided information about the progress of the study when requested by the chair. The committee reviewed conduct of the study, provided overall supervision for the study and advice through its independent chair.
COVID-19-related issues: National Association for Special Educational Needs patient and public involvement groups
The PPI groups gave advice on the impact of the COVID-19 pandemic in schools and at home. The parents provided descriptions of how COVID-19 had impacted the children. All parents described that during ‘lockdown’ periods, their children missed the structure of school and the opportunities for social engagement. They also found home schooling to be a huge challenge. Additionally, parents believed that children benefitted from school during the pandemic when they were allowed to go in. This was due to factors such as smaller classes leading to increased attention, shorter days, more child-led work and less of a negative impact on sensory needs. Some parents also described that they were working full time from home, so schoolwork was unfortunately placed as less of a priority.
The teaching professionals reported that the COVID-19 pandemic had meant that there were more disruptions in the timetable and that time had to be spent reintegrating pupils into the school. They described that there had been an exceptional high workload in the schools due to the pandemic. They observed that this had had a negative impact on staff’s mental health and wellbeing due to relocating staff to areas most depleted, exhaustion and serious adverse events such as a pupil dying due to the COVID-19 virus. To cope with staff absences, the curriculum had been reduced to only literacy and numeracy and a focus on meeting pupils’ immediate needs. They also noted that the impact on staff absence due to the pandemic meant that a whole year’s supply budget had already been used up by the end of the autumn term.
Action taken (outcomes of patient and public involvement)
The PPI partners:
-
Provided the researchers with contact details of schools in England that were willing to be approached by the researchers during the recruitment phase.
-
Determined/approved wording, layout, font and illustrations of all communication with participants (children, parents/carers, senior teaching staff and teachers). At a later stage in the research, the nasen parents’ focus group discussions expressed some reservations about some of the wording already used in the pupil questionnaires. These concerns will be addressed in the full trial proposal.
-
Determined/approved the payment (high street vouchers) to adult participants and rewards (stickers) for the child participants. However, later feedback from the nasen focus groups was that £10 vouchers were not really an incentive for teachers and that they were more likely to be motivated by an interest in the research topic and a desire to contribute to worthwhile research that would be of benefit for their pupils. This feedback will influence the full trial proposal; we intend to focus more on public relations during the recruitment phase (e.g. with nasen’s support, we could provide on-line or in-person events for teachers and parents to advertise the research to potential participants).
-
Offered feedback that may inform any potential future trial proposal. Whereas the nasen professionals’ focus group discussions indicated an enthusiasm for taking part in a research trial, such as ZF-SEND, the parents’ focus group appeared to be less convinced. The latter group raised the fear that their children may be used as a ‘guinea pigs’. In future, we propose that the teachers recruited to the project will receive, in addition to their ZF-SEND training, materials for a ‘parents’ information module’, which can be delivered (by teachers and researchers co-presenting) to parents to inform them of the value and the practicalities of being involved in research.
-
Provided the researchers with information about the impact of the COVID-19 pandemic on pupil/teacher absenteeism, the workload/stress levels of special school managers and teachers, and on the well-being being and mental health of the children. Specifically, the professionals’ nasen focus group indicated that: (1) high levels of staff absence had had a negative impact on the delivery of the curriculum as a whole (including the ZF-SEND programme); (2) staff absence had also resulted in staff exhaustion; (3) the pupil deaths due to the COVID-19 virus had an impact on staff morale and causing their anxiety levels to reach levels ‘not seen before’; (4) the number of e-mails teachers received and thus their workload increased dramatically during the COVID-19 pandemic. With bubbles and restricted access to people, all communication became online, with e-mails dominating the communication routes. This meant that staff missed vital e-mails due to overload. This information has been considered when (post hoc) discussing the outcome measures used and the pre/post difference scores and has informed the results, feasibility and acceptability of outcome measurement of this report.
-
Contributed important information to the debate on when to start recruitment in the academic year, when to collect data and the time period during which to deliver the ZF-SEND intervention. The nasen professionals’ focus group discussions indicate that the optimum time for recruitment is well before the Easter holidays and no later than the early part of the summer term as this is when the teaching staff are planning the curriculum and their teaching priorities for the next academic year.
-
When the NIHR call came out in July 2021 to consider expanding existing research projects to include geographical areas that were under-researched, our PPI partners (nasen and BILD) both advised against this due to time constraints – most schools were breaking up that week or the next and it would not be viable to recruit. Nasen would normally be able to stay in touch with senior staff of special schools. However, these networks were not functioning as normal due to the COVID-19 pandemic. It was therefore decided not to apply for this expansion.
-
BILD are currently producing, with input from Experts by Experience, a video for the child participants to thank them and to summarise (in an accessible manner) the main findings of the study.
Chapter 6 Results
School and participant characteristics
Characteristics of schools
Eight schools from England enrolled in the feasibility trial. Five were randomised to run the ZF-SEND intervention and three were allocated to PAU. An additional school was randomised in error, as described in Recruitment of schools. This school was excluded from all analyses. This school would have been allocated to the PAU arm and therefore provided a more balanced study. Exclusion of this school has resulted in more pupil participants in the ZF-SEND arm than in the PAU arm. See Appendix 4, Figure 3 for the geographical locations of the schools. Of the 8 schools, 6 were larger schools (> 100; 2 in the PAU arm and 4 in the ZF-SEND arm).
Participant characteristics
Pupils
A total of 54 pupils were identified by teachers as potential participants at baseline across the 8 schools. One pupil participant was withdrawn from pupil-reported baseline data collection as the class teacher was concerned about their ability and willingness to participate in these assessments. This pupil was also withdrawn by the class teacher from the ZF-SEND programme over concerns about their ability to engage with the programme; 53 pupils therefore participated in the trial. Baseline demographic data on the pupils were collected through parent and teacher report. Teachers provided data on 48 pupil participants (see Appendix 5, Table 8). Parents provided data on 26 pupil participants (see Appendix 5, Table 9).
At baseline (1 September 2021), the mean age of the pupil participants was 9.68 years. The majority of pupils were in year 6. Eight pupils were in year 7 and six were in years 3–4, which fell outside our inclusion criteria of years 5–6. Four pupils were aged 8 years, which was below our target of pupils aged 9–11 years.
Parents provided data on: (1) pupil’s gender: 85% were male across both groups (73% and 93% in the PAU and ZF-SEND arms, respectively); (2) ethnicity: 73% were White British (82% and 67%) and (3) current living situation: 92% lived in the family home with their birth parents (100% and 87%). The most commonly cited primary need by parents was their child’s autism spectrum disorder (ASD; 48% across both arms; 64% and 36% for PAU and ZF-SEND arms, respectively). Similarly, teachers identified ASD as the most common primary need of pupils (63% across both arms; 60% and 64% for the PAU and ZF-SEND arms, respectively). Moderate learning disability was identified as the most common secondary need by teachers (44% across both arms; 40% and 45% for the PAU and ZF-SEND arms, respectively); 29% of pupils were eligible for free school meals (47% and 21% for the PAU and ZF-SEND arms respectively). Pupil demographics were broadly similar across both groups, although slightly more pupils in the ZF-SEND group had free school meals (as per the CONSORT guidelines, no statistical tests for baseline imbalance were conducted).
Teachers
Teacher informants
In 79% of cases, the teacher questionnaire was completed by the pupil’s class teacher. This was more common in the ZF-SEND group (100%) than the PAU group (33%). Teacher informants knew the pupil for almost 20 months in the PAU group and 6 months in the ZF-SEND group (see Appendix 5, Table 10).
Teachers delivering Zippy’s Friends for Special Educational Needs and Disabilities
The teachers who delivered the ZF-SEND programme varied across the five intervention schools. In four schools, it was the class teacher; in one school, it was the head of primary and personal, social, health and economic education (PSHE) coordinator. In two schools, the class teacher also had management responsibilities (key stage 2 and social and emotional well-being lead).
Feasibility and acceptability of participation in the trial
Summary
The feasibility of recruiting eligible schools and participants to the study was assessed through analysis of the recruitment pathways and processes, recruitment rates and retention through the interventions and follow-up period and the acceptability of the study processes, including randomisation, to schools, teachers and parents/carers.
Recruitment of schools
The recruitment process and retention rates are presented in the CONSORT diagram (see Figure 2); 50 schools were formally approached by e-mail invitation and followed up with phone calls/e-mails (39 in England and 11 in Scotland; see Recruitment section for a full description of the recruitment methods). Eight schools responded and informed us that they were not eligible for the study, giving a total of nine reasons: pupils all have severe and profound intellectual disabilities (n = 5); pupils were too young (n = 2); and pupils were too old (n = 2). Ten schools responded to say that they were not interested, citing the following reasons: time restrictions at end of school year (n = 2: both in Scotland); PSHE/emotional literacy already covered in teaching (n = 2); new PSHE curriculum just implemented (n = 1); high levels of COVID-19 cases and self-isolation (n = 1); school moving to a new building (n = 1); new principal starting in at beginning of new academic year (n = 1); misunderstanding regarding timescales (n = 1); and not interested n = 1. Fourteen schools, all in England, were initially interested and eligible to take part (36%); no schools in Scotland agreed to participate. While liaising with schools to set up the study and arrange baseline data collection towards the end of the 2019–20 academic year, three further schools withdrew their interest in participating. Two of these schools ceased contact with the research team and a further cited numerous changes within the school resulting in uncertainty about who and how ZF-SEND could be facilitated as the reason for withdrawing their interest. Therefore, before the summer break, 11 were enrolled in the trial (28% of those approached in England).
In the detailed records of contacts with schools, the following issues were noted:
-
it was difficult to reach head teachers and assistant head teachers on the telephone – often they were unavailable
-
schools in Scotland were contacted in the last few weeks of term when they were busy and preparing to close for the summer break (Scottish schools closed at end June, 3 weeks before English schools).
Contact was re-established with schools at the start of the 2020–1 academic year to arrange baseline data collection. A further two schools withdrew, before baseline data collection commenced, the following reasons were recorded: staffing issues, COVID-19 pandemic-related due to the ‘bubble system’ and contact ceased as the class teacher was off for an extended period and contact could not be re-established. In a further school, baseline data collection with pupils was undertaken but then the school expressed concerns about their capacity to participate in the trial citing staffing issues. The school then ceased contact with the research team. Later, it was decided to randomise the school in case allocation to the control group would allow the school to continue to participate in the trial by alleviating concerns about running the intervention. This school was allocated to the control group, and this was communicated to the school. However, the school had already ceased contact with the research team and therefore the decision to withdraw their agreement to take part was assumed to have been made pre randomisation. This school was therefore excluded from all analyses and was counted as ‘randomised in error’. Eight schools were therefore randomised (20.5% of those approached in England).
Nested study within the trial
The SWAT aimed to estimate differences between waitlist control comparator (WLC) and PAU-only comparator (UCO) arms with regards to recruitment and randomisation, retention following randomisation, usual care and trial outcomes. Of particular importance for the latter two outcomes were the differences between WLC and UCO arms in those subsequently randomised to the comparator. Estimates are presented as absolute and relative percentage differences (i.e. risk differences and relative risks) or mean differences (depending on type of outcome) and provided alongside 95% CIs.
Of the 39 schools in England, 19 were approached following allocation to the WLC comparator arm and 20 were approached following allocation to the UCO comparator arm. From these, 11 schools were initially enrolled into the trial (28.2%, 95% CI 15.0% to 44.9%). By arm, 3/19 schools allocated to the WLC comparator arm were enrolled (15.8%, 95% CI 3.4% to 40.0%) and 8/20 schools allocated to the UCO comparator arm were enrolled (40.0%, 95% CI 19.1% to 63.9%). The absolute risk difference in the percentage of schools enrolled into the trial was 24.0% (i.e. higher in those allocated to the UCO comparator compared with those allocated to the WLC comparator, 95% CI 20.0% to 28.8%) and the relative risk was 2.5 (i.e. 2.5 times higher chance of a school enrolling when allocated to the UCO comparator compared with those allocated to the WLC comparator, 95% CI 0.8 to 8.2).
Eight schools were randomised in total, with only one school initially allocated to the WLC comparator subsequently allocated to the comparator arm. We were therefore unable to conduct any further meaningful comparisons between arms.
Recruitment of participants
It was estimated that eight pupil participants would be recruited from each school. A total of 54 pupils were recruited across the 8 schools with a mean 6.7 (range 5–9) pupils recruited per school. One pupil was subsequently withdrawn resulting in baseline data on 53 pupil participants. No opt-out forms were received from parents/carers.
Retention
No schools withdrew from the trial during the follow-up. Similarly, no parents/carers withdrew consent for the participation of their child. No pupil participants were otherwise withdrawn therefore all 53 pupil participants were followed-up.
Acceptability of study processes to schools, teachers and parents/carers
The qualitative interviews with 11 school staff and 4 parents/carers explored the acceptability of study processes, especially in relation to recruitment and randomisation.
Recruitment/motivation to take part
For senior leads and teachers, motivation to take part centred mostly on perceived value of emotional literacy and well-being. One teacher recognised that that their class struggles to regulate emotions and communicate feelings and therefore felt that the ZF-SEND programme was suitable. Another senior lead spoke about there being limited materials and resources that are appropriate for them and felt that which ZF-SEND filled this gap. Teachers and parents/carers were provided with a £10 gift voucher for completing each questionnaire; however, one senior lead commented that the voucher incentive was not a motivating factor for them, and they felt guilty for receiving payment for something that was going to benefit them:
I’m not going to knock this but I feel quite naughty when you send us the vouchers. I know that sounds random, but I don’t expect payment for something that’s going to benefit us and so I know that’s really lovely and it’s fabulous, but I almost feel I would only sign up to these things if I felt it was a benefit and I really do appreciate that you’ve got to have some incentive for the schools to sign up, but for me I think that I’ m almost a little bit guilty that we’re receiving payment for something that would benefit our school.
Senior lead, school 1
Most parents were motivated to engage with research, especially if it was beneficial to their child and the school. One parent spoke specifically about how their child suffers with anxiety, so they thought the programme might be beneficial.
Parents were asked about how they preferred to be contacted about research opportunities – whether through schools or directly by research teams. One parent preferred to be contacted through the schools as the school knows their child and therefore can articulate the benefits of taking part in the research.
Experience of randomisation
In terms of being randomised, three interviewees in the ZF-SEND arm (one parent, one teacher and one senior lead) all mentioned that they could imagine how disappointing it would have been if their school had been allocated to the control group, due to the ZF programme having so much potential to benefit the children.
However, the senior lead said that if the randomisation process is clear, schools should understand what they are signing up for. Similarly, another teacher and parent agreed that it was an acceptable and necessary process, and it is therefore important to keep an open mind to possibly being allocated to the control group; for example: ‘I think that you’ve got to have both groups to make it worth evaluating at the end’ (teacher, school 11).
Of those allocated to the control group, reported experiences varied. Three interviewees (two teachers and one parent) stated that they did not mind being allocated to the control group and understood that it was a necessary element of a RCT. However, two interviewees (one teacher and a senior lead from a single school) spoke about their disappointment at being allocated to the control group. The senior lead suggested that communication of the risk of being allocated to the PAU group should be made clearer in the initial recruitment of schools, as they believed it was a ‘done deal’ that they would get the ZF-SEND intervention.
If I’m honest I think that we were quite disappointed when we realised we would be in the control group. I have a background in psychology myself and I appreciate that is how research projects work but … I got the impression from conversations that it was a done deal that we would be absolutely part of the research project, so yeah, I think really disappointed. Considering for our pupils, going through that data collection is quite an involved process. I mean it’s great experience … and it’s useful, but it takes up so much resources for that to happen. Yeah, we were left feeling a little bit disappointed.
Senior lead, school 4
General experience of the research study
Almost everyone interviewed expressed that they had a positive experience with the research and that they welcomed research such as the present project. Furthermore, they thought that it was useful and valuable for young people to take part and that not enough research was being done for children and young people with SEND; for example:
I think sometimes that subjects that are kind of about things like this, like PSHE sort of style subjects, people have mixed opinions on how important they are and I think knowing that they’re evidence-based or have been part of research, I think that those people that have an opinion like that, it proves that actually these things are needed and these things are one of the most important things that the children need. So I think that it’s really positive to be honest.
Teacher, school 6
Staff members generally enjoyed being part of a study that could benefit the children they work with and found it an interesting process. Teachers also reported that the pupils enjoyed the research study experience.
One school said that some of their pupils were anxious beforehand and had lots of questions beforehand. Teaching assistants helped these pupils to understand the purpose of the research by explaining, reassuring and answering their questions. Another teacher spoke about it being a useful experience for pupils to talk to an unfamiliar person and learn that they can cope in a new situation.
School staff discussed issues with lack of engagement from parents/carers. One teacher had not realised that there were parent resources to send out: ‘You did say about parent intervention and I literally realised last week, by flicking through the folder, that there are homework sheets and I wasn’t aware of that. So sorry …’ (teacher, school 5).
It was frequently reported that schools had to ‘chase’ parents/carers frequently about completing the questionnaires. One teacher felt that it might be better for the research team to contact parents/carers directly to complete questionnaires. Another teacher recommended that the research team organise a session with parents so that they could learn more about the research and its benefits.
I think for parents perhaps if they were given … more information about what the purpose of the research was and whether that be video links, probably video links are good, you know, short, sharp video links that give people information might be a way to … allow them to see the purpose, so that they might be more encouraged to complete the questionnaire.
Senior lead, school 4
However, the parents we interviewed found the research acceptable and all stated that they were happy with the school contacting them about the research but that they would also not mind being contacted directly by the research team.
Discussion
Eight schools in England were recruited and followed-up over the academic year. The pre-pandemic aim had been to recruit 12 schools across England and Scotland. No schools withdrew between baseline and follow-up. However, there were some issues with initial approaches and interest in the study, especially schools in Scotland, none of which took part. It is likely that the COVID-19 pandemic and timing of the initial approaches were factors here (see Appendix 2 for the study timeline set against COVID-19 rates and pandemic-related restrictions). There was a national lockdown in place early in 2021 and schools were closed to pupils except children of non-essential workers. Schools reopened in late March 2021 but with a range of restrictions. The initial approaches to schools were therefore made from late April to May to allow schools time to settle back. This meant that recruitment was closer to the end of the academic year than originally planned. This was especially the case for Scottish schools, which closed for the summer holidays at the end of June. We know that the end of the academic year is an especially busy time for schools so it is likely that this, combined with the on going restrictions due to the pandemic (e.g. self-isolation for close contacts and formal COVID-19 testing, as part of step 3 restrictions) and an increase in COVID-19 infection in the summer of 2021, meant that schools were under immense pressure during this time. Despite this 36% of schools approached in England were initially interested in participating. The qualitative data show that schools participating in the study did so because they (1) feel that research like this is important and (2) see value in the intervention which indicates that recruitment issues may be due to factors external to the study rather than due to the study design. However, there may be scope to improve communication around the risks and benefits of the randomised design in terms of potential allocation to a control condition.
Eight schools that were initially approached informed the research team that they were not eligible for the study, largely due to age restrictions. With hindsight, initial screening of schools should have been more robust to ensure that ineligible schools were not approached. Furthermore, our communications with schools could have been clearer, to avoid any ambiguity about the eligibility criteria. Some participants accepted in the study fell outside of our eligibility criteria, especially in relation to age and therefore these criteria should have been communicated more robustly when schools were selecting classes to participate in the trial. As special schools are not always split into primary and secondary schools, they have a wider age range of pupils. Hence, our age-related eligibility cut off of 9–11 years may have served as a barrier to inclusion for some schools.
We anticipated schools each identifying approximately eight pupils as potential participants; our actual recruitment fell slightly below this. The age-related eligibility criterion may have contributed to this as classes in special schools tend to be based on ability and needs rather than age, as in mainstream schools. Offering greater flexibility in age range may have allowed us to meet our anticipated target. Furthermore, we stipulated that pupils needed to have the cognitive and communication skills to give assent to the pupil assessment. This may have further restricted the number of potential participants from each school. Moreover, for recruitment we only considered children with the capacity and communication skills to engage with the intervention; this was based on a subjective assessment by the teacher. Being more robust in our assessment of the children’s ability to engage in the intervention and/or being more flexible in terms of pupils’ ability levels, may have allowed us to recruit more participants per school.
Schools reported a lack of engagement from parents/carers, especially for parent/carer data collection. The opt out process meant that the research team did not have direct contact with parents. This may have impacted on parent data collection, as discussed in Chapter 7. It may have also contributed to the perceived burden of participating in the study and therefore the school withdrawals at the start of the 2022–3 academic year, as schools were required to send out parent opt out forms and parent questionnaires on behalf of the research team (alongside teacher completing questionnaires and facilitating pupil assessments). If the research team had had direct contact with parents/carers, it could have alleviated some of the pressure on schools. One teacher forgot to send parents ZF-SEND resources to use at home, suggesting that this component of the intervention needs more emphasis during the teacher training sessions.
The nested SWAT indicated that the opportunity to receive the ZF-SEND intervention at the end of the study, if allocate to the PAU group, did not affect schools’ participation in the trial. Future research could therefore omit this offer to strengthen the research design and reduce costs, especially as the ZF-SEND is widely available and accessible to schools.
Feasibility and acceptability of outcome measurement
Summary
Acceptability, reliability and validity of the different outcome measures were assessed. Acceptability and feasibility of all the outcome measures was assessed through analysis of rates of completion of the questionnaires/assessments by teachers, pupils and parents/carers and in the follow-up interviews. Furthermore, the MAMS, used in the pupil assessment, was further evaluated in terms of psychometric properties, as this scale has not been used by children with a learning disability in a RCT before. We also analysed the feasibility of ‘masking’ the researcher administering the pupil assessments and the feasibility of collecting data for a full economic evaluation.
Feasibility of the outcome measurement: questionnaire completion
Baseline data collection commenced as soon as schools were recruited to the study. Pupil assessments were conducted with nine pupils at two schools before the summer break. In addition, four teacher and three parent questionnaires were returned. The rest of the data were collected upon schools reopening in September. Table 3 shows the number of fully completed scales at baseline and follow-up that could be entered into the secondary analyses.
| Outcome | Completed both baseline and follow-up questionnaires/total baseline completed date, N (% baseline completed data) |
|---|---|
| EQ-5D-Y-3L – pupils | 48/53 (91) |
| EQ-5D – parent/carer | 12/24 (50) |
| SDQ – teacher | 30/48 (63) |
| SDQ – parent/carer | 12/22 (55) |
| MAMS – pupils – behaviour | 49/52 (94) |
| MAMS – pupils – emotions | 49/52 (94) |
| ELA – parent/carer | 13/23 (57) |
| ELA – teacher | 31/48 (65) |
| CHU – pupil | 49/53 (92) |
| CHU – parent/carer | 13/25 (52) |
| NCBRF – teacher | 33/48 (69) |
Pupils
Pupil assessments were completed with all 53 pupils at baseline (n = 19 in PAU group; n = 34 in ZF-SEND group). Half of the assessments were conducted face-to-face and half were remote (see Data collection section for a description of data collection methods). At follow-up, 49 pupils were assessed (92% retention; n = 18 in PAU group; n = 31 in ZF-SEND group). Pupils completed the MAMS, CHU-9D and EQ-5D-Y-3L.
Teachers
A total of 48 teacher questionnaires were returned at baseline, comprising the SDQ, ELA and NCBRF (91%; 15 in the PAU group; 33 in the ZF-SEND group). At follow-up, 33 questionnaires were returned (62% retention; n = 9 in PAU group; 24 in ZF-SEND group).
Parents/carers
A total of 26 parent/carer questionnaires, comprising the SDQ, ELA, CHU-9D, EQ-5D-Y and CASUS, were returned at baseline (49%; n = 11 in PAU group; n = 15 in ZF-SEND group). At follow-up, 20 questionnaires were returned (38%; n = 10 in PAU group; n = 10 in ZF-SEND group).
Psychometric properties of the Me and My School
To investigate the validity and reliability of the self-report measure of mental health (MAMS), and its relationship with other (proxy report) measures of mental health and behaviour, we assessed its psychometric properties by calculating Cronbach’s alpha, its factor structure using exploratory factor analysis (using principal factor analysis with orthogonal rotation), described the number of missing items, and described floor and ceiling effects by reporting the percentage of responders who scored the highest or lowest possible scores.
In terms of acceptability, all 53 pupils provided responses to all items, except in 2 instances where 1 item was not answered. There was no evidence of floor/ceiling effects. Based on 52 participants who responded to all 16 items, an exploratory factor analysis indicated that a three-factor solution was the most appropriate, explaining 84% of the total variance. Rotated factor loadings, based on an orthogonal rotation are provided in Appendix 6, Table 11. Factor 1 contains most items related to the original ‘behavioural’ domain of the MAMS. However, the item ‘I am calm’ loads weakly across all three factors and this factor also includes several items related to the original ‘Emotional’ domain of the MAMS. These additional items appear to relate to low mood, and two of these co-load onto other factors (though weaker than their loading on factor 1). Factor 2 contains two items related to sleep, in addition to one item which co-loads to factors 1 and 2 (‘I am unhappy’). Factor 3 contains two items related to shyness and feeling scared and one item which co-loads to factor 1 (‘I cry a lot’). Three items do not load strongly onto any factor (‘I am calm’; ‘I worry a lot’; and ‘I worry when I am in school’).
Despite high levels of acceptability and no floor/ceiling effects, with our limited data set we were unable to replicate a factor structure as implied by the original scale and, hence, we were unable to demonstrate construct validity. We have therefore not undertaken the planned correlations with other scales.
Feasibility of collecting data for an economic evaluation in a full trial (service use and quality of life)
Figure 4 in Appendix 7 shows the completion rates of each health economic measure at baseline and follow-up. Completion rates for the CASUS by parents/carers are detailed in Appendix 7, Table 12. Rates are low at both baseline and follow-up, though consistent for each CASUS item. There are responses for each CASUS item suggesting that the services listed are relevant to this group. Very few items were added as ‘other’ indicating that there were no items not adequately captured by the CASUS.
Completion rates for the CHU-9D by pupils and by parents/carers are detailed in Appendix 7, Tables 13 and 14. All pupils were able to complete the CHU-9D at baseline and 92% at follow-up. Response rates among parents/carers were lower, around half of who completed the CHU-9D at baseline and 44% at follow-up. Completion rates for the EQ-5D follow a similar pattern and are detailed in Appendix 7, Tables 15 and 16. Baseline completion from the pupils was complete, with rates slightly lower at follow-up. In general, there was consistency in completion of each item of the EQ-5D-Y-3L at baseline and follow-up.
Feasibility of masking the assessors to undertake pupil assessments
A researcher who was new to the project and masked to allocation was recruited to undertake the follow-up pupil assessments. Pupil assessments were undertaken both face-to-face and remotely. There was one instance of unblinding out of 49 follow-up assessments (2%). In this case, a member of senior leadership met the researcher onsite and gave the researcher a list of names of the pupils they would be seeing titled ‘control group’. This staff member also discussed their disappointment about being allocated to the control group with the researcher.
Acceptability of outcome measurement
Interviewees in the follow-up interviews provided feedback about outcome measurement. Much of the feedback from school staff concerned the timing of the baseline measures. Staff members were split in their opinion of when the best time for measurements would be: two interviewees felt that July was best and two felt that July was not convenient; they recommended October–November, after settling into the new term.
All school staff who commented on the pupil assessments felt that the data collection process was acceptable to pupils with respondents from three schools commenting that the pupils enjoyed the process. An interviewee from one school commented on pupils being anxious, which was easily ameliorated by providing reassurance. The feedback regarding the pupil questionnaires themselves was positive, with the majority of teachers commenting that the questionnaires were an appropriate length, and that the questions were acceptable. Two teachers commented that the measures would not be appropriate for a cohort with more severe learning disabilities. Feedback regarding the accuracy of pupils’ responses was mixed with one teacher saying that they thought their pupils answered the questions accurately, and another teaching saying their pupils may not have. One of these teachers suggested it might be useful if teachers could access pupil questionnaires before data collection in order to prepare visual supports and other prompts to help their pupils answer the questions accurately.
All the teachers interviewed felt the questionnaires they had to complete were acceptable, both in terms of content and time wise. Three teachers spoke about the questionnaires being helpful in thinking about their pupils’ skills. Three parents commented that the questions and the length of time to fill in the questionnaire were acceptable. One parent commented that the questionnaire was good but some of the questions were not relevant to their son, as he has many complex physical problems and therefore, they felt that the questionnaire was not entirely appropriate for him.
Most teachers commented on the lack of engagement from parents/carers in filling in questionnaires. Three teachers recommended sharing more information about the study with parents/carers regarding the study, either face to face or in online meetings, and that this might improve completion.
Discussion
Despite plans to collect baseline data at the end of the preceding academic year, the majority of data were collected at the beginning of the 2021–2 academic year. As described in the preceding chapter, there were delays to the start of the study and recruitment due to the COVID-19 pandemic. For most schools, baseline data collection took much of the first half of the term, especially the teacher-rated measures, as classes were settling back after the summer break and teachers were busy. This delayed randomisation and, subsequently, the start date for the intervention (discussed in Chapter 5). However, feedback from teachers on the questionnaires provided during their interviews was positive and respondents felt the measures were appropriate and acceptable.
Completion rates for the pupil-rated measures, administered by a researcher, were very high at baseline and follow-up. Teachers were happy to give researchers access to the pupils, either online or face to face, and pupils themselves were willing to take part with some teachers reporting that their pupils enjoyed the process. All forms of assessment (in person or via video calling platform) worked well with pupils engaging with the assessment. This suggests good acceptability and feasibility of the application of these measures. This is an important finding as children with a learning disability are rarely involved directly in data collection; proxy data are most commonly collected. This is a strength of this study and a method of data collection that should be continued in future studies.
Completion rates for the teacher-rated measures were lower, but still well over 60% at follow-up, despite follow-up data collection coinciding with a sharp increase in COVID-19 infection rates (see Appendix 2). Teachers found it hard to find the time to complete the questionnaires; however, around half felt that the assessment process offered them some benefits such as insights into their pupils’ strengths and difficulties. As this is a feasibility study, we collected data on a wide range of measures, some with similar items, which could be streamlined in a future trial based on their statistical properties found for the present cohort. This would reduce the burden on teachers and therefore likely to improve response rates. Extra support for teachers could also be offered such as completion through an interview with a researcher.
Completion rates for the parent-rated measures were below 50%. Teachers identified issues with parent engagement in the interviews and provided recommendations for improving engagement such as in person and online meetings. All contact with parents/carers was through schools and therefore we were reliant on schools sending out information, the questionnaires/online links, and reminders. Schools were asked to send reminders and liaise with parents/carers, but we do not know how many times this was done at baseline and follow-up. In this study, we used opt-out consent procedures. Introducing an element of opt-in consent would allow us to obtain parent/carer contact details and therefore the research team would be able to contact parents/carers directly, alleviating some of the burden on schools as the primary point of contact and also allowing us to monitor and address response rates. Direct contact with parents/carers could also be achieved through online information sharing meetings and webinars. This would improve the knowledge about the study amongst parents/carers and also highlight the importance of completing questionnaires. Alternatively, to make a future trial most cost and time effective, parent measures could be omitted. The completion of parent measures as self-report rather than interview with a researcher also has potential implications for the quality of the data produced.
Psychological research involving children with/out a learning disability routinely relies on proxy-reported measures. These are often behavioural in nature and therefore rely on the assessment of observed behaviour indicative of underlying psychological states. The present study took this approach and, given the nature of the intervention, it was impossible to blind the proxy respondents to treatment allocation. This may have resulted in some inherent bias in responses; however, the measures are designed to be objective and to minimise this bias. Future research could consider using direct observations by blinded members of the research team but these are resource intensive and, depending on the sampling of time periods observed, may not provide a reliable reflection of a child’s functioning over the follow-up period, especially when considering potentially infrequent (yet significant) adaptive or challenging behaviours.
As the MAMS measure has not been used in a large-scale RCT with children with SEND before, analyses were undertaken to investigate the psychometric properties of the measure. Completion rates for the MAMS indicate high levels of face validity with very few missing data points. Similarly, no floor or ceiling effects were detected. However, factor analysis did not support the original factor structure of the scale. Our analyses may have been underpowered. We have access to a data set derived from a similar sample (N = 50) and might therefore be able to repeat the factor analysis on a larger data set which would add power to the analysis.
In terms of health economic measures, for the pupil-rated quality of life measures, completion rates are reasonable and indicate that they would be feasible to collect in a full-scale trial. As previously discussed, response rates were lower for parents/carers, but this could be addressed through improvements in communication and information sharing. The list of health service items included in the CASUS were found to be relevant to this population and few additional items were listed, indicating good coverage of the items. Future research could also use school-held service use data instead of relying solely on parent/carer report. Data from multiple sources could then be triangulated in analyses.
Only one instance of unmasking was reported across 49 follow-up assessments with pupils indicating that masking a researcher to undertake the assessments was feasible. Pupils in the ZF-SEND arm did not routinely disclose information about ZF-SEND, which was anticipated to be the primary source of unmasking. Similarly, the researcher did not see ZF-SEND imagery in the classrooms; conducting assessments online might well have protected against this too. To avoid school staff unmasking the researcher school staff were reminded not to mention allocation so this should be retained and possible strengthened in future research.
Feasibility and acceptability of the Zippy’s Friends for Special Educational Needs and Disabilities intervention
Summary
Feasibility and acceptability of the ZF-SEND intervention across the five schools allocated to the ZF-SEND arm of the trial was assessed in relation t adherence, fidelity of delivery, engagement of pupils (all based on the teacher-rated session checklists and observations of a session), feedback from school staff involved in delivering the intervention, evidence of harm and estimated costs of providing the intervention.
Evaluation of training in Zippy’s Friends for Special Educational Needs and Disabilities
The first phase of the intervention was the training of the teachers who were to deliver the ZF-SEND programme to their pupils. The training (see Experimental intervention: Zippy’s Friends for Special Educational Needs and Disabilities for details) was led by the programme director of Partnership for Children, referred to below as ‘the trainer’.
Interview with the trainer
The trainer was interviewed about her views and experiences of the remote training session. The trainer reported that the online 2-hour training session was shorter than would typically be provided face to face (which would usually be a whole day). However, this compressed version may be more suitable for teachers because they can more easily fit it into their schedules and also reduce the chance of online fatigue. The trainer outlined the support typically provided to schools after training which includes two to four sessions throughout the following year, usually with one occurring a few months after the beginning of delivery of the ZF-SEND programme and one around the middle of the academic year. These sessions usually last for around 30–60 minutes during which teachers can discuss any concerns etc. The follow-up received by each of the intervention schools is described later in this chapter.
In terms of the delivery of the training, the trainer felt that it went as planned with no major issues. The only possible concern she had was that there could have been more time for discussion. However, the trainer commented that the lack of discussion after the video examples (of ZF-SEND being used in the classroom) might have reflected the teachers’ confidence in using the programme in their schools. The trainer also felt that the teachers had prepared themselves for the training by familiarising themselves with the structure and content of the manual.
The trainer reported that the teachers were engaged and focused on the session, that the aims of the training were met and that teachers seemed prepared and enthusiastic to deliver the programme. The teachers particularly enjoyed the well-being section of the training. During the session, the trainer emphasised that the programme’s content could be delivered flexibly and encouraged teachers to be creative and sensitive to each pupil’s specific needs.
The trainer recommended that a ‘train the trainer’ model could be used in future: that is, to train one leader in each intervention school who could then deliver training to other teachers in their school. This would allow more teachers to attend training and thus improve the reach of the programme.
Observation of training
A researcher observed the training and made notes on the teachers’ engagement and response. Throughout the session, the teachers seemed engaged and responded in depth to the questions asked by the trainer. The teachers gave detailed responses to questions. They all gave positive feedback on the programme, could see how it would benefit their pupils, and appeared enthusiastic about it.
Completion of session checklists and schedule of delivery of the Zippy’s Friends for Special Educational Needs and Disabilities programme (adherence)
All teachers in the intervention arm of the study were asked to complete bespoke checklists after each session they taught as well as a schedule of delivery to assess fidelity to the manual. These are described in Chapter 4 of this report.
Four of the five schools allocated to the intervention arm initiated the intervention. One school was unable to start the programme due to the long-term absence of the class teacher. This school therefore withdrew from delivering the programme in April 2022 but did not withdraw from the study and participated in follow-up data collection. It was initially hoped that the teacher would be able to initiate the intervention upon return to the school. However, they soon went on extended leave again and later left the school.
Across the 4 remaining schools, 52 sessions across 16 modules were rated using the session checklists. Table 4 provides an overview of the session checklists returned and the progress through the programme. School 6 only returned the module 1 booklet; however, in this school, a session from module 2 was observed later in the year (see Appendix 7, Table 16) which indicates missing data from the session checklists.
| School | Modules rated (n) | Progress through programme |
|---|---|---|
| 5 | 4 | Up to M4, S3 |
| 6 | 1 | Unknown, M2, S2 observed |
| 9 | 6 | Complete – end of M6 |
| 10 | 0 | Did not start the programme |
| 11 | 5 | End of M5 |
| Overall | 16 | |
Inspection of the session checklists indicates that teachers did not provide complete responses as some questions were left unanswered, for example, the dates of the sessions. The session checklists asked for pupil absence in each session to be recorded. However, we are not at all certain that this was accurately reported by all schools and therefore we have not used these data to calculate pupil attendance across the programme (see Adherence).
Table 5 provides further detail on intervention delivery based on the returned session checklists. All schools started the programme in November 2021, or later. Most schools delivered at least one lesson every week with breaks for school holidays and other events. The number of lessons per module varied widely for module 1 (range 5–19 lessons) and then proceeded with a mean of seven sessions per module (range 4–13 sessions). Each module comprises four session plans, so it took approximately two lessons to deliver each of the session plans. Progress through the programme varied across schools. School 9 was the only school to complete the programme.
| School | Started ZF-SEND | End of M1 (N lessons) | End of M2 (N lessons) | End of M3 (N lessons) | End of M4 (N lessons) | End of M5 (N lessons) | End of M6 (N lessons) |
|---|---|---|---|---|---|---|---|
| 5 | 13 January 2022 | 24 March 2022 (19 lessons) | 25 May 2022 (13 lessons) | 26 Mary 2022 (8 lessons) | 30 June 2022 (6 lessons)a | N/A | N/A |
| 6 | 19 November 2021 | 21 January 2022 (6 lessons) | Unknown, (only M1 session checklists returned) | ||||
| 9 | 17 November 2021 | 14 February 2022 (6 lessons) | 5 April 2022 (4 lessons) | Not recorded (6 lessons) | Not recorded (8 lessons) | Not recorded (6 lessons) | July 2022 (not recorded) |
| 11 | Class a: 15 November 2021 Class b: 13 January 2022 |
6 December 2021 (6 lessons) 3 February 2022 (5 lessons) |
3 February 2022 (7 lessons) | 24 March 2022 (7 lessons) | 26 June 2022 (5 lessons) | 30 June 2022 (4 lessonsa) | |
Fidelity to the intervention
In total, 63 sessions were rated for fidelity, of which 30 (48%) met our threshold for fidelity (i.e. each session was introduced, sessions included at least two different activities, and at least some pupils engaged in at least 50% of the core elements of the session). This varied between schools from 37% (7/19 sessions) to 75% (12/16 sessions) of rated sessions. Where fidelity was not met, this was primarily due to there being no documented evidence that at least 2 different activities were delivered in a session (across 63 sessions, only 31 had evidence of 2 different activities being delivered). This suggests that the session checklists were not fully completed by teachers and therefore the fidelity measure is affected by the incomplete data set.
Attendance (adherence)
Adherence was primarily based on attendance and progress through the programme. All pupils in schools randomised to deliver ZF-SEND and where ZF-SEND was initiated received at least one ZF-SEND session (100%). Pupil absence in sessions varied widely and was high in some schools, with 62% of pupils in school 5 missing at least one of the sessions whereas no absences were reported in school 11.
Owing to the incomplete data set, both across the session checklists and within each checklist, we have not calculated the other attendance-based adherence measures concerning the percentage of children who completed all of the sessions that were delivered (and rated) by the school and the average number of sessions that were completed by the children.
Engagement
In terms of pupil engagement, we were interested in estimating the percentage of sessions in which at least ‘some’ pupils engaged in at least 50% of the core activities of that session. For most sessions, pupil engagement was high (in 59 of the 63 sessions at least some pupils engaged in 50% or more of core session elements). None of the children in two of the schools engaged in one of the activities (‘Reflect on consequences for saying or doing inappropriate things’). All other activities for which there was no engagement from pupils were unique cases.
Observations of Zippy's Friends for Special Educational Needs and Disabilities sessions
Observations were made of one lesson at all four ZF-SEND schools that delivered the programme. All lessons were delivered by the usual ZF-SEND teacher. Table 17 in Appendix 8 provides a summary of the lessons observed.
Lesson delivery
Observational notes were made on the delivery of the lesson in relation to teaching style, changes/omissions to the activities, teacher interactions with the pupils and the role of other staff members present. All four lessons observed started with a recap or rehearsal of previous material. The ZF ‘golden rules’ were used in all lessons. In all lessons, pupils were facilitated to generate and evaluate their own solutions to situations and emotions; group discussion and real-life examples and scenarios were central to this. Roleplay was used in all lessons and in two lessons the teaching assistants demonstrated a roleplay with the teacher before the pupils were asked to act out a scenario. For example, pupils were asked to act out what different emotions look like or they roleplayed excluding someone from a game to experience what this would feel like for the victim. Sheets for pupils to feedback how they found the session were completed for two of the lessons. In one lesson, modifications were made based on the available resources, the teacher modified the activity by using the whiteboard to ‘collect’ solutions to a problem rather than a ‘toolbox’.
All teachers showed good rapport with the pupils and were able to maintain their attention by using a variety of activities, interspersed with discussion. Teachers were able to redirect those who lost focus on the task. Teachers made sure all pupils were involved in discussion, asking specific pupils to respond/input at times and selecting from those with their hand up to contribute at other times. In all four lessons, the environment was judged to be relaxed and inclusive.
Teaching assistants were present in three lessons; it is not known whether they had also attended the ZF-SEND training. Due to staffing shortages, no teaching assistant was present for one of the lessons. The level of involvement from teaching assistants varied: in one lesson, they were not involved in the delivery of ZF SEND; in another, they only contributed to some of the activities and helped to facilitate small group work; and in another, assistants were actively involved in all aspects of the lesson.
Pupil response
The pupils’ responses to the activities were also evaluated, in relation to how pupils interacted with each other, evidence of learning/understanding, variations in pupils’ responses across the lessons, whether pupils asked questions, the number of students who disengaged, and the proportion of time that pupils disengaged. Overall, the pupils were attentive and demonstrated engagement with the lessons. Across all four observed lessons, most of the pupils were attentive most of the time. In all classes, one or two pupils appeared less engaged and wandered around or sat in different areas of the classroom. The atmosphere in the classrooms was generally calm and relaxed and pupils interacted with each other well.
Pupils in all four of the observed lessons demonstrated evidence of learning and understanding of the programme. For example, the pupils in school 5 related emotions in the lesson to the colours used as part of the ‘zones of regulation’ system. Pupils in two schools demonstrated good recall of the ZF story (schools 5 and 6). The lesson in school 6 started with the ZF story and pupils identified how the characters in the story were feeling. In relation to the activities, pupils participated in a range of roleplay and discussion activities. In school 6, the activity centred on how it makes us feel when someone does not listen. Pupils could identify reasons for why someone may ignore you. When they performed their roleplay, some pupils reported feeling angry and annoyed at being interrupted, when they were shouted at or tugged to get attention. In the subsequent roleplay, the aim was to practice how to gain attention appropriately. Pupils were shown how to interrupt politely, such as saying ‘excuse me’ and waiting for other pupils to turn to them and listen.
The lessons in school 9 and 11 addressed feelings of loneliness and rejection. In school 9, pupils discussed loneliness and rejection and shared a situation where these feelings were evoked. Pupils in school 9 identified that loneliness is when a friend is not there or you feel alone, and rejection is when you cannot join in. Some pupils were able to share examples of when they had felt lonely or rejected. Both schools used the ‘circle game’, in which one pupil walked around the circle and the others in the circle could choose to let them in or not. Pupils in both schools identified a range of negative emotions in response to being left out, such as ‘rejected’, ‘sad’, ‘worried’ and ‘anxious’. Conversely, when they were accepted, they were happy. Both lessons then went on to explore responses to feeling rejected and pupils were asked to identify helpful strategies. School 9 did this through a discussion in which pupils shared ‘good’ and ‘bad’ strategies such as finding someone else to play with, playing nicely and asking an adult for help, or (in contrast) swearing, pushing, hurting others and arguing. The teacher posed a scenario of a peer not sharing a toy and asked pupils to give some helpful strategies; pupils responded with ‘walk away’ and ‘ask your turn’. One pupil also mentioned that sometimes you have no choice; you just have to deal with it (acceptance). The teacher then worked with pupils one to one to identify personalised strategies and to write them down in their ZF books. For example, one pupil said when they are rejected and it makes them sad they could meditate. In school 11, two pupils identified that they like to draw when they feel rejected or lonely. Another pupil said that he would ask an adult to help. The teacher discussed another solution with this pupil: to ask someone else to play instead. The pupil then drew a very detailed story and explained how he felt and what he would do. The pupils then reviewed their responses using the ‘golden rules’ to assess whether their solutions ‘worked’.
The observers estimated the proportion of pupils out of the whole class who were engaged in the lesson. Engagement comprised any of the following: paying attention to the teacher; following instructions; contributing to class discussion or seeking to do so (e.g. by raising a hand); and interacting with other pupils as part of the activities. In all lessons, over 75% of pupils evidenced at least one type of engaged behaviour.
Environment and context
The observer made notes on the classroom environment and context, specifically, the general features of classroom (size, noise, etc.), arrangement of desks (e.g. circle, rows), interruptions during the lesson (e.g. visitor, class disruption), and technical challenges (e.g. problems with video). Classrooms were generally quiet and calm. As would be expected, the noise levels increased during roleplay and similar activities. During group discussions, pupils generally sat in chairs facing the teacher, either in a row or semicircle. When in one-to-one activities, pupils sat at a table with a teacher or teaching assistant. During two lessons, other visitors entered the classroom but this did not disrupt the lesson or the observation. During remote observation one pupil appeared curious about the device that was recording the lesson, otherwise the devices did not cause a distraction. During roleplay, it became difficult for the (remote) observer to hear all that was said and in one instance during board-based activities, it was difficult to see what was on the board. However, this did not impact significantly on the researcher’s ability to undertake the observation assessment.
Feedback from school staff on the delivery of Zippy’s Friends for Special Educational Needs and Disabilities
Selection of programme lead or class teachers
We asked staff to comment on how teachers were selected to be involved in delivering the programme. One senior lead stated that this decision was based on the class rather than the teacher’s characteristics. The programme was delivered by a teacher who had a relatively verbal and able class, a class deemed able to engage with ZF-SEND.
Staffing
Five staff members discussed how staffing impacted the delivery of ZF-SEND. One senior lead said that the programme was disrupted when the teacher went on maternity leave and the senior lead struggled to deliver all the sessions on her own. Two other schools described that while teachers or nurses may deliver the programme, they often oversee and support sessions themselves. Four staff members described that the teaching assistants were very involved in supporting roleplaying or other activities in ZF sessions. Teaching assistants had also facilitated smaller groups in ZF sessions when the group was split up for activities.
Programme delivery
Two schools spoke about staff absence being the main barrier to the delivery of the programme. One spoke about the teacher going off on maternity leave part way through the year and another had the class teacher off sick for 3 weeks. Another teacher said that having a dynamic class meant that the programme was not always delivered as described in the manual.
Training and supervision
Most teachers had a positive response to the training, finding it easy to understand and of an appropriate length. Teachers also thought that the training prepared them well to deliver ZF and keen to make a start. However, one teacher believed that while it prepared them to an extent, they did not remember it very well and could have used some more information. They believed that the training could have been more effective if it was in person. Another senior lead thought it may have been beneficial to have more people in their school trained to help with staffing because the untrained teaching assistants could not deliver the programme themselves.
Involvement of parents/carers
Two teachers spoke about a lack of face-to-face contact with the parents, which inhibited them from directly encouraging involvement. One teacher spoke about their group of parents failing to engage with most of the activities they sent home.
Pupil attendance
Pupil attendance was only mentioned by three teachers under this heading because most pupil absences referred to were discussed in the context of the COVID-19 pandemic. Other than COVID-19, one teacher believed that there was nothing else that greatly affected pupil attendance. However, the teacher at school 5 teacher also mentioned that one-off appointments caused absences in participating with the ZF-SEND programme.
Group management
One senior lead and one teacher from two different schools were asked about how they decided which pupils would be involved in the project. Both said the main factor was age appropriateness. The teacher from a different school said some pupils were not chosen due to having profound learning and communication difficulties.
Views on programme content and activities
Four teachers and two pupils discussed their positive views of specific programme contents and activities.
The resources are absolutely brilliant, they are very clear and there is a kind of good range of different activities which suit my class, and it’s kind of – I suppose the core things are about the Zippy’s rules and the golden rules, and they are very understandable and very kind of relatable for the children so it’s kind of I’ve memorized them now, and the actual content is very appropriate … it fits in very nicely with other things that we do in the school like Zones of Regulation and emotion coaching, it just dovetails and it’s just brilliant, and the stories as well, they are very kind of engaging and the characters that the children can relate to and the situations that are happening.
Teacher, school 11
… it all links together as a programme with a story and how everything follows on from the other things, so it’s really – it flows really well, so it’s like a continuation of the things that they’ve learnt and a continuation of the story, which I think helps them to understand better.
Teacher, school 6
The teachers commonly thought that it was useful that the resources were ready to use: ‘I love it, I do love it, I love the worksheets, most of the worksheets and things are really good, the activities are really good’ (teacher, school 5).
They also liked that they were able to use them flexibly and match different activities to different classes and levels of ability. Other programme content that teachers thought were particularly useful included the lesson plans, worksheets, and the story-based activities. The pupils found the roleplays enjoyable and said that they were able to learn from them.
Intervention outcomes
Impact on pupils
One pupil said that he recalled the ZF-SEND lessons if a difficult situation arose in the playground. When people were being ‘mean’ in the playground and it made him feel annoyed and upset, he could tell the teacher and ask for their help. Another pupil spoke about learning about loss and agreed that this lesson had helped him cope with his own experiences of loss. Two teachers both commented that ZF-SEND had helped their pupils label their emotions in real life situations, for example recognising when they felt jealous of other classmates. One teacher spoke about one of their pupils reporting they felt jealous, which was a ‘bit like a wow moment’ (teacher, school 5).
One parent reported that their child had learned to discuss their emotions:
… instead of having complete meltdowns about an unexplained feeling that he has about any situation … [he] seemed to be more open to discussion about it … so where we used to get lots of tears when he came home from school, because he would at school keep it all to himself and then come home and say, ‘this happened’ or ‘I told them this and no one listened’ or ‘I felt like this and I don’t understand’, do you know what I mean? But I feel like he must be discussing it more within school and feels more comfortable at discussing himself.
Parent, school 5
Two teachers commented on their pupils’ empathy, listening skills and conflict-resolution skills improving slowly.
Pupil engagement in the programme
The response regarding pupil engagement in the programme was very positive, with all four teachers interviewed reporting that the pupils engaged well and enjoyed the programme: ‘As well as me loving it my class do as well, so when I tell them it’s Zippy today they get really excited and they engaged very well with every session’ (teacher, school 11). Teachers commented on the stories being engaging and the pupils liking and remembering the characters from them although not all pupils were actively engaged all the time:
In my class there are eight children and I would say that six of them consistently join in and want to be part of it and the other two are a bit hit and miss but will also join in, so it’s great that they don’t access everything but they do still want to be part of a lot of it.
Teacher, school 11
What the pupils learnt
Three teachers spoke about their pupils transferring the skills and messages learnt outside of the lessons, for example recognising that they were jealous:
Because we’ve done it at a whole class level, they are all benefitting from it and in other moments now you will hear children say ‘Oh, I felt a bit jealous/a bit embarrassed’ so they are actually transferring the learning outside of the sessions.
Teacher, school 11
One teacher felt as though their pupils understood most key messages but struggled to understand what jealousy was. The teacher felt that it was too big of a jump from everyday emotions in the programme to something quite abstract, with no particular facial expressions or body language to teach:
And do the pupils understand the key messages? [Interviewer] Ermm, jealousy they didn’t. They weren’t getting jealousy. I think that is just such a kind of a high level. I get that they need to understand jealously, but it just seemed a big jump from their everyday emotions into something really, really abstract.
Teacher, school 5
One parent (school 5) spoke about her child experienced jealousy when his friends wouldn’t play with him at school and when she told him this emotion was jealousy, he referred to learning this ‘with Zippy’s’. His parent felt as though he hadn’t been able to understand this emotion during the session as he hadn’t experienced it yet, and this real-life experience helped him understand it better.
Two pupils mentioned the change and loss module, with one recognising that if a pet died (like Zippy does in the story), he would be sad (school 11). Five pupils spoke about the conflict resolution module. Two pupils spoke about telling a teacher if someone was unkind to them (schools 5 and 6), and two of these pupils (schools 11 and 5) identified that someone being unkind would make them feel sad. One pupil (school 9) spoke about how the best thing about ZF-SEND is that you can use the things you learn if you have a similar problem. Another pupil (school 6) spoke about how they remembered learning that jealousy can make you annoyed at someone and sad, demonstrating a reasonable understanding of the concept of jealousy, its causes and its emotional impact.
Do you remember any other lessons? So any other sort of topics that you’ve looked at, except for bullying? [Interviewer] We looked at jealousy and how that can make you annoyed at someone. We’ve looked at how if your best friend is going with someone else … and you’re feeling bad and then that other person says ‘They’re my friend now’ that would make me sad, it’s quite bad, and yeah.
Pupil, school 6
Acceptability of the intervention
Views on programme content and activities
Four teachers and two pupils discussed their views of specific programme contents and activities. The teachers commonly thought that it was useful that the resources were ready to use. They also liked that they were able to use them flexibly and suit different activities to different classes and levels of ability. As already reported above, specific aspects of the programme that teachers thought were useful included the lesson plans, worksheets and the story-based aspect. The pupils described the roleplays as enjoyable and that they were able to learn from them. One parent pointed out how the programme allows the children to talk about their emotions and its long-term positive impact on well-being:
I tell you what I like about the Zippy programme, is that you can put all these children into counselling and talks, but that is so direct about feelings, and it also provokes feelings that probably aren’t really there … but with the Zippy programme it’s done in a way that is fun and it’s about someone else, you know what I mean, and so it is almost like in a sense – it provokes them to talk and for them to be okay about these – not to be locked in their own heads, do you know what I mean? To be open and honest … it’s so important for these children because I’m very big on what happens now has a massive effect on you when you’re a grown up.
Parent, school 5
Acceptability to pupils
All the pupils interviewed said they liked ZF-SEND and there was nothing they did not like. One teacher (school 6) noted that the only negative feedback they had was when the topic discussed was death.
Programme strengths
Four staff members and one parent discussed a range of general strengths about the programme. A common strength that was mentioned was that the programme worked well in tandem with PSHE and other resources, such as ‘zones of regulation’. Furthermore, two staff members mentioned that the ‘ready-made’ resources were much welcomed in their time pressured work environment. Senior leads also discussed that it was good that the programme covered issues that were important and relevant for the pupils and that they could relate to in their current life.
Views on programme aims
The majority of teachers and parents had a positive view of the aims of ZF-SEND, describing it correctly as aiming to develop the emotional literacy and well-being of the children. Three specific elements identified as particularly useful included the programme aiming to: (1) make children aware of their emotions; (2) cope with certain feelings and situations; and (3) improve social skills and communication.
Future use of Zippy's Friends for Special Educational Needs and Disabilities
Every teacher interviewed said they saw a future for ZF-SEND at their school. Four schools said they would continue to use the programme as a whole and the fifth school said they would ‘dip in and out’ of the resources.
Supervision provided to schools
Partnership for Children provided supervision to schools, in line with what they typically offer. Supervision was voluntary and attendance/uptake varied. Below is a summary of the supervision received by each school. In addition, all class teachers were on mailing lists and received half termly newsletter with blogs, new research, advice and so on, and invitations to termly support drop-in sessions. We have no evidence that any of the teachers in the intervention arm attended these drop-in sessions.
School 5: A 30- to 45-minute phone call 2 months after the training; programme support discussion was around implementation due to staff shortages and COVID. Follow-up e-mail in January 2022 to check in, no further support requested.
School 6: Follow up e-mail/check in in January 2022; response all positive, no support needed.
School 9: No support needed after training and no response to support e-mail in January 2022.
School 10: Phone call in February 2022 to offer support with implementation due to staff sickness/shortages. E-mail communication in May 2022 due to more staff shortage to offer advice on how to implement with limited resources.
School 11: E-mail support in January 2022; no follow-up support needed.
Rates of adverse events/evidence of harm
No serious adverse events were reported during the study period. There was no evidence of harm from the intervention in any of the data collected.
Economic costs associated with the programme
Training in ZF-SEND is now delivered online, with the training costs estimated at £50 per person. Schools in the trial received physical sets of resources costing £325 + £30 postage per class of 15, which also includes access to online resources. However, schools can choose to just buy online resources for £150 per year. Partnership for Children is developing an online platform to improve online access to resources and envisage phasing out providing printed materials in the future.
Review of the logic model
A logic model for ZF-SEND was produced, together with the application for funding for the study (see Appendix 1). The results in this chapter support the validity of the model, especially the processes involved, such as ‘engaging and enjoyable lessons for teachers and children’, individualisation that responds to the varied needs of children’. Feedback on the ZF-SEND programme suggests that the lesson were engaging and enjoyable for teachers and children. Teachers delivered the programme through incremental sessions, individualised delivery to meet the needs of pupils (e.g. number of lessons for each module and choice of activities) and adhered to the aims and goals of the sessions. However, as highlighted in the logic model, external factors affected the delivery of the delivery of the programme and 80% of ZF-SEND schools could not complete the programme over the academic year. Similarly, pupil and staff absence further impacted on the delivery with one school being unable to start the programme and attendance in lessons varying widely.
The logic model emphasises parent/carer engagement through home activities to achieve consistency in school/home approach. There was little evidence of use of the home activities and parents generally had little knowledge of the programme. Furthermore, teachers generally did not take up support offered by Partnership for Children. The logic model refers to three follow-up support meeting and class observations to ensure competent and accurate delivery and sharing of good practice. This aspect of programme delivery could therefore be improved and may enhance the engagement of parents/carers by reminding teachers of the home activities and the importance this aspect of the programme.
The qualitative data provide anecdotal evidence of the short-term outcomes outlined in the logic model. Most interviewees identified examples of pupils showing improved emotional literacy skills (e.g. understanding emotions) communication and coping skills. However, as most schools did not complete the programme, it may be premature for even short-term outcomes to become apparent. There was also some evidence of medium-term outcomes in the transfer of learning from school to the home context.
Discussion
Four of five schools randomised to the ZF-SEND arm started the intervention. One school was unable to initiate the programme because of the long-term absence of the teacher who was trained to deliver the intervention. Owing to delays in randomisation due to COVID-19 restrictions resulting in the majority of baseline data collection occurring at the beginning of the academic year, we were only able to offer one online training session which limited teachers’ ability to attend and meant that we were unable to train at least two teachers per school, as originally intended. The training session was recorded to allow those unable to attend to watch it, but this option was not taken up by every school. Delivering online training is cost-effective and allows us to be more flexible and future research should allow time to provide multiple sessions to ensure that multiple teachers at each school are trained and can therefore act as cover for teachers who are absent. Similarly, having a strategy to cover teacher absence at each school at the outset would mitigate these issues.
Schools started the ZF-SEND intervention from November 2022 onwards. This was later than anticipated and resulted in only one school completing the programme by the end of the academic year. Once the programme was initiated, progress was steady and schools delivered around two lessons per week, taking around seven lessons to complete a module. Starting the programme in September would require schools to complete two modules each term (12–14 weeks; 4 sessions per 6–7 weeks) which, based on the progress of the schools in this study, would be feasible.
According to the session checklists, adherence varied across schools and engagement of pupils was acceptable. However, overall fidelity was lower with only 48% of rated sessions being recorded as delivery with fidelity. Inspection of the data set shows that it is incomplete, despite numerous requests to schools to supply the data, and some sessions, which were delivered, were not rated. For example, module 2, session 2 was observed in school 6 but this school only rated module 1 sessions. In addition, some of the checklists were incomplete with missing, and sometimes conflicting data. Our measure of fidelity stipulated that sessions needed to include two different activities, covering part A and part B of each session. While it is highly likely that schools did this, it was often not recorded in the session checklist and therefore the session had to be coded as not being delivered with fidelity. The observational and interview data may have provided a more reliable indicator of fidelity.
Furthermore, we asked about pupil absence rather than attendance and therefore teachers may not have accurately reported absences leading to an inflated measure of adherence. We therefore have not reported detailed analysis of attendance-based adherence. This makes it hard to draw firm conclusions from these data and indicates that improvements need to be made to more accurately capture engagement data. For example, the checklists could be broken down into individual session trackers rather than a module booklet. They could also be embedded more into the intervention, rather than supplied separately by the research team. Discussions with Partnership for Children have indicated a move to accessing the ZF-SEND materials online and they have agreed for the checklists to be displayed along with the content for each module with prompts for teachers to complete them before moving on in the programme. Online completion would also allow us to monitor return rates throughout the follow up period and prompt where necessary.
One session in each of the intervention schools was observed, which provides a detailed ‘snapshot’ of how the programme was being delivered and the response of pupils. The sessions observed were delivered with good fidelity to the programme. Pupils were engaged and teachers managed the classroom dynamics well. Furthermore, the methods for observation, face to face, live remote, as well as video recording, all worked well and these modes of observation appear to be feasible and acceptable.
There was little use of supervision among the teachers, which was optional. This may have been due to the pressures caused by the COVID-19 pandemic and resultant staff absences etc. The qualitative data also indicate that, despite positive feedback from teachers about the training, it perhaps did not fully equip teachers to deliver the programme. For example, there was little evidence of homework and parent information being sent. Amending the delivery of training to provide two sessions, one as an introduction to the programme and to equip teachers with the knowledge to get started, and then a follow-up training session once teachers had delivered a few lessons to review progress and act as supervision, may enhance fidelity of implementation and allow key messages, such as those relevant to home tasks, to be reiterated. This would increase training from the 2 hours delivered in the present study while maintaining the advantages of shorter training sessions.
The qualitative data collected during interviews with teachers, parents and pupils suggest that both the research participation as well as the ZF-SEND intervention had been experienced in a positive way. The general consensus across the three groups of participants was that ZF-SEND is an acceptable, feasible, useful, enjoyable and time-efficient programme that can have an observable positive impact on individual children’s coping skills and wellbeing. The estimated cost of online training (£50) and of online access to the programme (£150 per year) also suggests that this is an affordable option for schools.
Practice as usual
Summary
The aim was to understand: (1) the breadth of emotional literacy initiatives currently in use in England and Scotland; (2) who provided them; (3) how they were delivered; and (4) any other observations/impressions reported by school staff. A broad definition of ‘emotional literacy initiative’ was used to include anything used in the school to improve emotional recognition, coping with emotions and coping with personal/emotional problems.
Interviews were conducted with the teachers from all three schools in the PAU arm of the trial at three time points to collect data on the emotional literacy interventions in their school. The interviews were conducted towards the end of each academic term to collect information about the preceding term (term 1: 6–15 December 2021; term 2: 27 April–4 May 2022; term 3: 8–18 July 2022). In addition, a scoping exercise was undertaken to understand PAU in terms of emotional literacy across special schools not involved in the trial. Eight short (approximately 20 minutes) interviews were carried out between December 2021 and March 2022 with representatives from special schools who were already known to the research team in England and Scotland.
Methods
A semistructured interview schedule was developed to scope the emotional literacy initiatives in use at each school. Initially, 11 participants were provided with a definition of emotional literacy and then asked a general question about any initiatives and then specifically asked about school-wide, classroom-based, individual-level (one to one) and manual-based initiatives. For each initiative mentioned, the interviewer probed on the aims of the initiative, mode of delivery, people involved in delivery, whether it was specifically designed for children with SEND, and the interviewees’ views and impressions of the initiative. The interviewer recorded responses in the form of handwritten notes, which were promptly typed up to provide a summary of the interview and a list of all the emotional literacy initiatives mentioned.
This resulted in a wide range of responses, many of which did not fit within our definition of ‘emotional literacy initiative’. It became evident that different school representatives had different views of what ‘emotional literacy’ initiatives were. A classification system was therefore developed, based on the initial scoping exercise (interviews with three schools in the PAU arm and eight schools external to the study) to better understand the breadth of emotional literacy interventions in use across the schools and to provide a more detailed framework for the following rounds of interviews with the schools in the PAU arm of the study. The interview schedule was refined to reflect the classification system and then used in the following two rounds of interviews with schools in the control group.
Results: a classification system for emotional literacy initiatives used in special schools
The following types of emotional literacy initiative were identified, with examples:
-
Integrated into the curriculum/curriculum-based (e.g. as part of PSHE in England, Curriculum of Excellence in Scotland, mental health or emotion-focused curriculum).
-
Involving parents/carers (e.g. coaching sessions for carers, family support worker providing support for families experiencing difficulties at home, school nurses offering support, home diaries to improve communication with families which includes information on feelings and well-being, phone applications and messaging to allow schools and families to communicate).
-
Teacher-level/training, including training to deliver an intervention as well as training to up-skill [e.g. training teachers in psychological understanding of emotional literacy and how to deliver individualised support plans for pupils via the Emotional Literacy Support Assistant (ELSA) Network; www.elsanetwork.org; training for teachers from an educational psychologist in coaching; training to provide small group interventions, nurture groups www.nurtureuk.org; training in the Attachment, Regulation and Competency Framework (https://arcframework.org/)].
-
Individual-level/personal plans [e.g. one-to-one or small group interventions led by ELSA for pupils identified as in need; nurture groups for those who are younger or have more complex needs (may include discussion, art therapy or music therapy); one-to-one sessions with an educational psychologist; one-to-one sessions with a pupil support worker; educational health and care plan in which ‘emotional literacy’ is named as a target outcome of development; positive behaviour support plans].
-
(Informal) emotional literacy tools [e.g. activities to identify feelings and worries; visual cards/cues to show emotions; ‘jar’ of well-being, daily feelings charts; worry monsters; worry boxes; breathing exercises; yoga, mindfulness; Zones of Regulation (www.zonesofregulation.com); playfulness, acceptance, curiosity and empathy approach]; TACPAC® (TACPAC, Oxford, UK) communication through touch and music (www.tacpac.co.uk); Emotion Works (www.emotionworks.org.uk) cogs; ROCK (Reach Out Centre for Kids: www.rockonline.ca); songs, poems and chants, etc.
-
(Formal) lesson-based/lesson-format (e.g. learning skills for life, including communication and how to interact with people; sensory play activities and stories; well-being days with a focus on well-being).
-
Externally provided programmes, which may provide lessons plans or a manual [e.g. Emotion Works programme; SCERTS® model for children with autism spectrum disorder (www.scerts.com); skills groups delivered by teaching assistant, ‘Making Me’ Primary School Emotional Well-being Programme (www.makingme.org.uk)].
-
Creating an emotionally literate environment, including passive approaches (e.g. working with body language, encouraging positive language and demonstrations that teachers understand how a pupil is feeling, modelling positive/adaptive behaviour, providing safe spaces and relaxing environments, understanding that ‘behaviour is communication’, making lessons practical and meaningful to pupils; staff labelling emotions regularly with/for pupils, Makaton symbols to communicate emotions.
-
Assessments of emotional literacy [e.g. Pupil Attitudes to Self and School measure (PASS; www.gl-assessment.co.uk); Boxall Profile® (Nurture UK, Stansted Mountfitchet, UK; www.boxallprofile.org), Thrive assessments (Fronting the Challenge Projects Ltd, Newton Abbott, UK;www.thriveapproach.com)].
-
Emotional literacy leads/people responsible for co-ordinating (e.g. mental health lead; ELSA Networks; educational psychologists; occupational therapists; high-level teaching assistants; PSHE lead; family support workers; individual class teachers).
-
School policies (e.g. policies on the language that can be used to describe a pupil’s behaviour, behaviour policy, guidebook on how the school supports emotional health and well-being).
Results: practice as usual in the control arm of the study
The three schools in the PAU arm of the trial employed a range of the approaches described above, most commonly daily feelings charts, use of the Zones of Regulation, ad hoc sessions on emotions and individualised plans for those identified as in need. Only one approach was similar to ZF-SEND in that it was a manual-based programme that provides a structure to and resources for teaching emotional literacy. The ‘Making Me’ primary school emotional well-being programme was used in one of the control group schools. However, this programme had been implemented 2–3 years before the study and the school representative reported that it had lost momentum. A small number of teachers were still using a small element of the programme to start the day with how ‘Kispy the caterpillar’ is feeling; they reported that it seems to work well. However, the school representative reported that the whole programme does not work well with their students.
The ‘Making Me’ programme is a whole-school approach and includes a staff induction, a programme for children along with information for parents/carers and a pack of resources. It is designed for primary schools but is not specifically for children with a learning disability or SEND. It aims to enable children to learn how to look after their own mental and emotional health. We are not aware of any formal evaluation of the effectiveness of this programme.
Additionally, another PAU school reported using the Thrive approach, which is a whole-school approach to well-being. Thrive provides an online tool for the profiling, action planning and progress monitoring of pupils, as well as staff training, which focuses on the needs of different age groups. The primary aim of Thrive is to reduce exclusions and improve attendance but it has no specific remit to improve emotional literacy. It was not specifically designed for special schools but has been implemented in special schools. We are not aware of any formal evaluations of the Thrive approach. While resources are provided as part of the approach, it does not provide class-based lesson plans to deliver teaching on emotional literacy.
The same PAU school also reported using ‘Boxall Profile’ and ‘PASS’ to assess pupils’ social and emotional well-being. These tools are designed to support teachers in planning to address any concerns relating to individual pupils. They are not specifically designed for children with a learning disability or SEND and do not provide a manualised, lesson-based programme for the whole class, rather they are focused on identification of pupils who may require additional support.
Analysis of secondary outcome data
See Appendix 9 for a summary of the scores for the secondary outcomes at baseline and follow-up.
Regression/ANCOVA analyses were carried out on all the outcome measures, including subscale scores, to estimate effect sizes across outcomes and ascertain if there were any signals of differences between the ZF-SEND and PAU groups at follow-up. Table 6 shows the results of these analyses, together with an interpretation of the results. The results indicate that the participants allocated to the ZF-SEND group tended to have better outcomes in terms of behavioural problems and prosocial behaviour and also for the teacher-rated NCBR, apart from adaptive social behaviour. For those allocated to the intervention group, there was a difference in NCBR self-isolated/ritualistic behaviour and irritable behaviour compared with the control group.
| Outcome | Sample size (n) | Adjusted mean differencea (95% CI) | ICC 95% (CI) | Interpretation |
|---|---|---|---|---|
| EQ-5D-Y-3L – pupils | 48 | –0.04 (–0.19 to 0.11) | 0.14 (0.01 to 0.73) | Higher scores indicate improved quality of life. No difference between groups |
| EQ-5D – parent/carer | 12 | 0.36 (–0.24 to 0.97) | Not estimable | Higher scores indicate improved quality of life. No difference between groups |
| SDQ – teacher (emotional problems score) | 30 | –1.49 (–3.32 to 0.34) | Not estimable | Lower scores indicate reduced emotional problems. No difference between groups |
| SDQ – teacher (conduct problems score) | 30 | –0.56 (–2.61 to 1.48) | 0.41 (0.07 to 0.86) | Lower scores indicate reduced conduct problems. No difference between groups |
| SDQ – teacher (hyperactivity score) | 30 | –0.84 (–2.49 to 0.81) | Not estimable | Lower scores indicate reduced hyperactivity. No difference between groups |
| SDQ – teacher (peer problems score) | 30 | –0.49 (–2.00 to 1.02) | Not estimable | Lower scores indicate reduced peer problems. No difference between groups |
| SDQ – teacher (prosocial behaviour score) | 30 | 0.71 (–1.40 to 2.82) | Not estimable | Higher scores indicate improved prosocial behaviour. No difference between groups |
| SDQ – teacher (total difficulties score) | 30 | –2.64 (–7.00 to 1.73) | Not estimable | Lower scores indicate reduced behavioural difficulties. No difference between groups |
| SDQ – parent/carer (emotional problems score) | 12 | 1.67 (–3.18 to 6.51) | Not estimable | Lower scores indicate reduced emotional problems. No difference between groups |
| SDQ – parent/carer (conduct problems score) | 12 | 0.47 (–2.10 to 3.03) | 0.31 (0.00 to 0.99) | Lower scores indicate reduced conduct problems. No difference between groups |
| SDQ – parent/carer (hyperactivity score) | 12 | –2.00 (–4.91 to 0.92) | Not estimable | Lower scores indicate reduced hyperactivity. No difference between groups |
| SDQ – parent/carer (peer problems score) | 12 | –1.24 (–3.81 to 1.34) | Not estimable | Lower scores indicate reduced peer problems. No difference between groups |
| SDQ – parent/carer (prosocial behaviour score) | 12 | 0.01 (–2.78 to 2.80) | Not estimable | Higher scores indicate improved prosocial behaviour. No difference between groups |
| SDQ – parent/carer (total difficulties score) | 12 | –6.58 (–17.37 to 4.21) | 0.30 (0.00 to 0.99) | Lower scores indicate reduced behavioural difficulties. No difference between groups |
| MAMS – pupils (emotional difficulties) | 49 | –0.46 (–0.03 to 0.55) | Not estimable | Lower scores indicate reduced emotional difficulties. No difference between groups |
| MAMS – pupils (behavioural difficulties) | 49 | 0.06 (–1.64 to 1.76) | 0.13 (0.01 to 0.71) | Lower scores indicate reduced behavioural difficulties. No difference between groups |
| ELA – teacher (self-awareness) | 31 | –1.25 (–6.01 to 3.51) | 0.52 (0.11 to 0.91) | Higher scores indicate improved self-awareness. No difference between groups |
| ELA – teacher (self-regulation) | 31 | –0.34 (–3.12 to 2.45) | Not estimable | Higher scores indicate improved self-regulation. No difference between groups |
| ELA – teacher (motivation) | 31 | 0.74 (–1.50 to 2.97) | Not estimable | Higher scores indicate improved motivation. No difference between groups |
| ELA – teacher (empathy) |
31 | 1.03 (–1.63 to 3.69) | Not estimable | Higher scores indicate improved empathy. No difference between groups |
| ELA – teacher (social skills) | 31 | 0.95 (–3.63 to 5.52) | 0.43 (0.06 to 0.90) | Higher scores indicate improved social skills. No difference between groups |
| ELA – teacher (final score) | 31 | 1.66 (–11.52 to 14.84) | 0.12 (0.00 to 0.97) | Higher scores indicate improved emotional literacy. No difference between groups |
| ELA – parent/carer (self-awareness) | 13 | –5.12 (–12.47 to 2.22) | 0.84 (0.33 to 0.98) | Higher scores indicate improved self-awareness. No difference between groups |
| ELA – parent/carer (self- regulation) | 13 | –3.73 (–9.83 to 2.38) | 0.28 (0.00 to 0.99) | Higher scores indicate improved self-regulation. No difference between groups |
| ELA – parent/carer (motivation) | 13 | –0.75 (–11.69 to 10.20) | 0.76 (0.17 to 0.98) | Higher scores indicate improved motivation. No difference between groups |
| ELA – parent/carer (empathy) | 13 | –4.70 (–12.39 to 3.00) | 0.85 (0.39 to 0.98) | Higher scores indicate improved empathy. No difference between groups |
| ELA – parent/carer (social skills) | 13 | –4.44 (–13.82 to 4.93) | 0.96 (0.75 to 0.99) | Higher scores indicate improved social skills. No difference between groups |
| ELA – parent/carer (final score) | 13 | –22.08 (–62.42 to 18.25) | 0.88 (–0.44 to 0.98) | Higher scores indicate improved emotional literacy. No difference between groups |
| CHU – pupil | 49 | –0.01 (–0.07 to 0.06) | Not estimable | Higher scores indicate improved health. No difference between groups |
| CHU – parent/carer | 12 | 0.03 (–0.19 to 0.25) | Not estimable | Higher scores indicate improved health. No difference between groups |
| NCBR – teacher (positive social – compliant/calm) | 31 | 1.14 (–1.40 to 3.68) | Not estimable | Higher scores indicate improved compliant/calm behaviour. No difference between groups |
| NCBR – teacher (positive social – adaptive social) | 31 | –0.20 (–2.51 to 2.11) | 0.04 (0.00 to 1.00) | Higher scores indicate improved adaptive social behaviour. No difference between groups |
| NCBR – teacher (conduct problems score) | 31 | –3.14 (–7.80 to 1.51) | Not estimable | Lower scores indicate reduced conduct problems. No difference between groups |
| NCBR – teacher (insecure/anxious) | 31 | –5.90 (–11.89 to 0.08) | Not estimable | Lower scores indicate reduced insecurity/anxiety. No difference between groups |
| NCBR – teacher (hyperactive) | 31 | –2.86 (–8.07 to 2.34) | 0.02 (0.00 to 1.00) | Lower scores indicate reduced hyperactivity. No difference between groups |
| NCBR – teacher (self-injurious/stereotypic) | 31 | –1.24 (–3.88 to 1.29) | 0.13 (0.00 to 0.97) | Lower scores indicate reduced self-injurious/stereotypic behaviour No difference between groups. |
| NCBR – teacher (self-isolated/ritualistic) | 31 | –5.14 (–8.85 to –1.42) | 0.12 (0.00 to 1.00) | Lower scores indicate reduced self-isolated/ritualistic behaviour. For those allocated to the intervention group, there was a reduction in NCBR Self-Isolated/Ritualistic score compared to the control group between baseline and follow-up. A lower score indicates better outcomes |
| NCBR – teacher (irritable) | 31 | –3.71 (–7.04 to –0.37) | Not estimable | Lower scores indicate reduced irritable behaviour. For those allocated to the intervention group, there was a reduction in NCBR Irritable score compared to the control group between baseline and follow-up. A lower score indicates better outcomes |
Parent-rated scores were limited by low sample sizes and wide CIs.
Discussion
Our findings provide useful estimates for effect sizes achievable in a large-scale effectiveness study. Encouragingly, we also demonstrate that effects tended to be in the direction of a benefit from the intervention arm, though we were not powered to detect intervention effects in this study, so caution is urged in overinterpreting these findings.
The analysis of parent-reported outcomes was limited by the relatively small number of parents completing measures and a future study will need to consider parent involvement more if these outcome data are to form a core part of the trial outcome package.
Review of progression criteria
Avery et al.’s traffic light system26 was used to prespecify progression criteria against which feasibility outcomes were evaluated. Achieving ‘green’ criteria would suggest progression to a large-scale trial is warranted without any amendments, achieving ‘amber’ would suggest progression is only warranted with an amendment to the study design and/or processes, while only achieving ‘red’ would indicate that progression is not warranted. See Table 7 for each criterion and performance against it. A narrative summary of the results is presented following the table and then the results are further discussed in the discussion section in Chapter 7.
| Outcome: metric | Green (%) | Amber (%) | Red (%) | Result (%) |
|---|---|---|---|---|
| Recruitment of schools: schools randomised/approached | ≥ 50 | 20–40 | ≤ 20 | 8/39 = 20.5 |
| Retention of schools: schools that remain in the study until the end/schools randomised | ≥ 75 | 50–74 | ≤ 49 | 8/8 = 100 |
| Recruitment of pupils – consent obtained from parents: parents providing consent for their child to participant/parents approached to provide consent | ≥ 75 | 50–74 | ≤ 49 | 54/54 = 100 |
| Fidelity of ZF-SEND delivery: sessions delivered with fidelity to the manual/sessions assessed | ≥ 75 | 50–74 | ≤ 49 | 48 |
| Pupil engagement with ZF intervention: pupils actively taking part in at least 50% of sessions/pupils enrolled onto the trial and in schools allocated to the intervention | ≥ 60 | 40–59 | ≤ 39 | 59/63 rated sessions = 93.7 |
| Collection of outcome data: pupils with SDQ data available at 8–12 months post randomisation/pupils included in the trial | ≥ 75 | 50–74 | ≤ 49 | 33/53 teacher-rated SDQ = 62.3 |
Owing to the difficulties recruiting in Scotland (because recruitment started near the end of the school year in Scotland as outlined in the Feasibility and acceptability of participation in the trial), we calculated the ‘recruitment of schools’ metric based on schools in England only. This achieved an amber result. The COVID-19 pandemic is likely to have contributed to the recruitment rate, as well as the study timeline, and the research team have identified a range of modifications to the study that could improve this. All eight schools randomised remained in the study and participated in follow-up data collection achieving a green result. Similarly, the parents/carers of all 54 pupils who were invited to take part provided their consent. Only one pupil was subsequently withdrawn by a teacher.
For the ZF-SEND programme, 48% of sessions that were rated were delivered with fidelity, according to the definition described in Chapter 4. These data were derived from the session checklists that were an incomplete data set so the results should be interpreted with caution. The observations of ZF-SEND lessons suggest that ZF-SEND sessions were delivered with adequate fidelity. Therefore the ‘red’ result on this criterion is more suggestive of the need to improve data collection on delivery of the ZF-SEND programme rather than fidelity.
Pupil engagement in ZF-SEND sessions was rated on the session checklists across pupils, rather than at the individual level so we were unable to calculate the ‘pupil engagement’ metric as intended. Instead, we calculated the proportion of sessions that were rated in which ‘at least some’ of the pupils engaged in at least 50% of the core activities of that session. We have rated this metric as amber and the observational data support this. However, there are issues in assessing pupil engagement in the programme using teacher report. This requires pupils to display behavioural indicators of engagement; however, the ZF-SEND programme does not require pupils to play an active role in the programme – much can be learnt from passive observation. Interpretation of this metric therefore requires caution and is confounded by the aforementioned issues in collecting the session checklist data.
At follow-up, 62% of teacher-rated SDQ measures were returned, achieving an amber result. We have already identified ways to improve response rate, discussed in Chapter 6. We have based this metric on a teacher-rated measure, as this is likely to be the primary outcome for a large-scale trial. The parent/carer response rate was lower, with 38% of parents/carers completing the questionnaire at follow-up. Engagement with parents/carers has been identified as an area for improvement for a large-scale trial and this is discussed in more detail in Chapter 7.
Chapter 7 Discussion, conclusions and recommendations for future research
Discussion
This feasibility, cluster RCT aimed to evaluate whether it was possible to conduct a large-scale RCT of the ZF-SEND programme for children with a learning disability in special schools. A total of 8 schools and 53 pupil participants were recruited to the study and followed up over the 2021–2 academic year. Emotional literacy, behaviour, health and service use were measured at baseline (before the start of the intervention) and at follow-up (8–12 months post randomisation), collecting data from pupils, parents/carers and teachers.
The eight schools were randomised to provide PAU or the ZF-SEND programme. Three schools were randomised to the PAU group and five to the ZF-SEND group. Teachers in the ZF-SEND group were trained in ZF-SEND through a 2-hour online training session (either joining remotely or watching the recorded session) and provided with supervision throughout the study period from Partnership for Children. Interview and observational data were collected to evaluate the training provided.
Towards the end of the academic year (from May 2022), follow-up interviews were conducted with eight pupils from four of the ZF-SEND schools, four parents/carers (two from PAU and two from ZF-SEND schools), seven class teachers or those responsible for delivering the ZF-SEND programme (three from PAU and four from ZF-SEND schools) and four members of senior leadership or teachers with management/oversight roles (two from PAU and two from ZF-SEND schools). To assess ZF-SEND delivery, teachers in the ZF-SEND group completed session checklists and had one ZF-SEND lesson observed by the researchers. To gather information on PAU in the control group, members of staff from the control groups were interviewed three times, towards the end of each academic term about the emotional literacy initiatives in their school. Additionally, staff from other special schools (not involved in the study) were also interviewed to gain insight into PAU with respect to emotionally literacy in special schools.
The quantitative and qualitative data were brought together to assess the feasibility and acceptability of: (1) participation in the trial; (2) data collection; and (3) the ZF-SEND intervention. The predetermined progression criteria were reviewed to further inform whether progression to a large-scale trial was warranted.
The study started in April 2021; 50 schools were invited to take part in the trial, 39 in England and 11 in Scotland. Eight schools were recruited, all from England. This is likely due to the start of the study being delayed due to the COVID-19 pandemic combined with schools in Scotland closing for the summer break earlier than ones in England. The recruitment rate of schools in England was therefore 20.5%, which is an amber result according to our predefined progression criteria (see Chapter 6). The UK was just emerging form a national lockdown when the study started and schools were under immense pressure to resettle pupils and implement a host of COVID-19-related procedures. We are therefore confident that the recruitment rate for schools could be improved through modifications to the study design. A future study should open for recruitment earlier in the preceding academic year, for example in January, to allow adequate time for initial discussions, selection of classes and baseline data collection before the end of the academic year. This would facilitate other aspects of the study, as described later. Furthermore, schools in England were identified through nasen and this proved to be a useful route for recruitment that could be extended to Scotland, Wales and Northern Ireland, as they are a UK-wide charity.
All randomised schools remained in the study showing high levels of retention and achieving a green result according to our predefined progression criteria. Moreover, the qualitative interview data and 100% (of those invited to take part) rate of pupil recruitment, indicate that the trial was acceptable to pupils, parents/carers and teachers. Any issues with recruitment of schools may therefore be due to factors external to the study rather than reflecting schools’ willingness to participate. Some teachers had concerns about the lack of clarity on randomisation and therefore the risk of being allocated to the control group. Communication with schools and teachers could therefore be strengthened to make this clearer. However, the SWAT indicated that the offer of the ZF-SEND programme at the end of the study, if allocated to the control group, did not result in increased recruitment rates so the RCT design itself may not deter schools from participating and access to the ZF-SEND intervention was not the only motivating factor for schools. Indeed, the qualitative data suggest that schools are supportive of this kind of research, acknowledge the importance of emotional literacy and are invested in improving access to evidence-based interventions for their pupils.
We anticipated recruiting eight pupils per school; however, a mean of 6.7 pupils were recruited per school. We also aimed to recruit 96 pupils across 12 schools: 54 pupils were recruited. Pupil eligibility criteria stipulated an age range of 9–11 years, or those in years 5–6. A minority of pupils who were recruited fell outside of this range and there was nothing to indicate that they were less suitable for the research. Future research could therefore broaden the age-related eligibility criteria to include 8- to 12-year-olds. This would facilitate delivery in special schools in which classes are not exclusively age-based, instead, classes may be based on abilities and may cross over from primary to secondary. This may allow more pupils to be recruited per school and therefore improve the feasibility of meeting sample size targets.
A key aspect of the study design was to collect data directly from pupils rather than rely solely on proxy report. This is an important step for research involving children with a learning disability, which rarely gives voice to those participants. High response rates were achieved to the researcher-administered pupil assessment and pupils generally enjoyed the process, suggesting that pupil assessment, both in-person and remotely were both acceptable and feasible. To achieve this, one of the eligibility criteria stipulated that pupils needed the cognitive and communication skills to agree to the pupil assessment. This may have excluded some pupils from the trial who may have otherwise been eligible. To improve access to the trial and recruitment rates of pupils per school, future research could seek to collect data from pupils where possible, but not use this as a criterion for eligibility. For example, a simple screening instrument with appropriate cut-off scores could determine which pupils to involve in pupil-rated measures. This would provide a more robust and systematic measure for suitability for pupil assessment.
The sample of pupil participants in this trial had a range of conditions, primarily ASD, followed by moderate learning disabilities. The study was designed to evaluate ZF-SEND for children with a learning disability; however, there was no formal assessment of this, so it is possible that some participants did not have a learning disability. Future research could use a measure of a learning disability or adaptive behaviour with thresholds to reflect presence/absence/severity of a learning disability. A further threshold could then be used to ascertain whether the pupil could participate in the aforementioned pupil assessments. Future research could then include both those with and without a learning disability (given that the ZF-SEND programme is usually provided to whole classes in special schools) and then undertake subgroup analyses on those with/out a learning disability. Similarly, only pupils with the capacity and communication skills to engage in the intervention were recruited, based on a subjective assessment by the teacher. A more formal evaluation would ensure that sampling was consistent across schools and would also allow analysis according to severity of a learning disability, which would ascertain which pupils might benefit more from the ZF-SEND programme.
Acceptable return rates were achieved for the teacher-rated measures with SDQ data available at follow-up on 62% of pupils included in the trial. This achieved an amber result against our progression criteria. The qualitative data indicate that teachers, parents and pupils found the process of completing outcome measures acceptable. However, it is important to note that the COVID-19 pandemic and subsequent national restrictions and changing circumstances for children and their parents/carers may have impacted in unanticipated ways on return rates. A number of studies48 and a recent scoping review49 suggest that pre-existing inequalities for children with SEND and their families became greater during the pandemic and affected parents/carers’ stress levels and mental health. These negative consequences for parents/carers as a result of the COVID-19 pandemic are likely to have had an adverse impact on their motivation and capacity to complete and return research questionnaires. Nevertheless, future research should seek to maximise response rates, especially of parents/carers.
As this was a feasibility study, with little previous research to inform the selection of outcome measures, a wide range of measures were included in the teacher and parent/carer questionnaires resulting in a rather long and, at times, repetitive process of data collection. Based on the results of this study, future research could reduce the number of measures and therefore shorten the length taken to collect data, which may improve the return rates at both baseline and follow-up.
Schools reported a lack of engagement from parents/carers. This was also a likely factor in the response rate of parents/carers to the questionnaires (38% of questionnaires containing all the parent-rated measures were returned at follow-up). We used opt out parental consent for pupil participants. Therefore, all communication with parents/carers was through schools and the research team did not have access to parent/carer contact details (except for those agreeing to be contacted for interview). Future research could use a combination of both opt-out (to pupil’s participation in the trial) and opt-in consent (to parents/carers completing the measures), which would allow the research team access to parent/carer contact details by requesting contact details on consent forms. Further engagement activities could include webinars and events to inform parents/carers about the study, its aims and how they will be involved. Starting the study earlier in the preceding academic year would provide adequate time for this.
In the schools allocated to deliver ZF-SEND, feasibility and acceptability of the intervention were assessed in a number of ways: through the session checklists, observation of ZF-SEND lessons, in the follow-up interviews and through evaluation of the training provided. We measured engagement, adherence and fidelity to the intervention through data collected on the teacher-completed session checklists so that quantitative measures of each could be provided and then assessed against the predetermined progression criteria. Pupil engagement for each session was assessed against three core elements of the session plan. We determined that at least some of the pupils present for the session should be engaged in at least 50% of the core elements of that session. High levels of engagement were recorded (94% of sessions rated). However, we acknowledge the challenges of rating pupil engagement in a programme like ZF-SEND, especially children with a learning disability who may not always show stereotypical markers of participation and engagement. For example, a pupil may choose to passively observe a session rather than participate in a roleplay but may still acquire the key learning from the roleplay. This is further complicated by the incomplete session checklists and reliance on teacher report. However, the observational and interview data provide evidence that pupils are actively engaged in ZF-SEND and found the lessons enjoyable and interesting.
We calculated adherence based on attendance of pupils and schools’ progress through the programme. Measurement of attendance was hampered by the incomplete session checklists; however, all pupils enrolled in the study in the four schools that started the programme, attended at least one ZF-SEND session. Rates of attendance varied and the COVID-19 pandemic was a factor in this. Progress through the programme also varied and only one school completed the programme within the academic year. However, schools started the programme later than anticipated as baseline data collection and therefore randomisation was pushed into the first half term of the year. Therefore, schools could not start the programme until after the autumn half term. This coincided with an increase in COVID-19 rates and high levels of pupil and teacher absence, so some schools did not state the programme until the beginning of 2022. Bringing forward recruitment, baseline data collection randomisation and a first instalment of training in ZF-SEND to before the end of the preceding academic year would allow schools allocated to ZF-SEND to start the programme immediately after settling into the new academic year. Based on schools’ progress through the programme in this study, once they got started, this would give adequate time to complete the programme in 1 academic year. Having more time for training would also allow us to provide more training sessions and train more teachers and teaching assistants in each school who could, in the event of class teacher absence, provide cover and therefore continue the programme. A further benefit of this is that we would achieve a full 12-month follow-up and baseline and follow-up measures would be taken at the same point in the school year. Furthermore, randomising schools early in the summer term would allow those in the ZF-SEND arm time to build the programme into their lesson planning from September.
As mentioned, the session checklists were partially completed. We know that some schools did not return checklists for all the sessions they provided. Similarly, analysis of the data indicates that teachers did not fully record the information requested making interpretation of the data difficult. This is especially relevant to the measure of fidelity: only 48% of sessions were rated with fidelity to the programme. The main issue was lack of recording of two different activities for each session. However, observational and interview data suggest that the programme was delivered with good fidelity, so this score is likely to reflect an issue with reporting rather than delivery. Future research should therefore improve data collection through the session checklists. We have liaised with Partnership for Children who oversee the ZF-SEND intervention and they have agreed to embed the checklists into the programme resources, as access to the programme is moved online. Each checklist will need to be completed before teachers access the next module. The checklists will therefore become part of the intervention, but will also serve research purposes, rather than as an additional task for teachers. Online completion and submission of the checklists will also allow us to monitor completion and chase up on missing data.
Furthermore, Partnership for Children has agreed to modify the programme of training. As mentioned earlier, we will provide a first, introductory training session before the end of the preceding academic year. This would equip teachers with the knowledge of the programme and materials to begin delivery after the summer break. This will incorporate the 2-hour online session provided as part of this study. A second training session will be scheduled for early in the academic year, after giving time for teachers to start the programme and deliver a few sessions. In this second training session, implementation issues will be discussed, and teachers will be asked and reminded about completion of the session checklists. The home activities and involvement of parents will also be discussed to ensure teachers are providing parents with the home activities, which was reported to be lacking in the present study.
Data from pupils, parents/carers and teachers suggest that the ZF-SEND programme is acceptable and feasible and addresses issues that are important for children with a learning disability. It is a relatively low-cost intervention, especially with the move to online resources and training. However, the costs of teachers’ time to deliver the programme should also be included in future costing models. The intervention can be adapted and delivered flexibly to meet the needs of pupils and teachers especially appreciated the comprehensive resources that, unlike other programmes, do not require any further adaptation for children with a learning disability. We are therefore confident that, with the modifications to the study design as previously discussed, the study, data collection and ZF-SEND programme are acceptable and feasible to stakeholders.
Practice as usual in the control group and in a wider sample of special schools was assessed. A wide range of emotional literacy initiatives were used in special schools, ranging from ‘feelings check ins’ during the day, visual displays relating to emotions, and the Zones of Regulation and behavioural support plans. However, no schools were using a manualised, modular classroom-based programme specifically designed for children in special schools.
Patient and public involvement
Public involvement was a key aspect of the study throughout. We sought advice from teachers and parents during study set up, data collection and analysis. Their advice helped shape the study procedures and our understanding of contextual issues, especially in identifying issues relating to the COVID-19 pandemic and their impact on the study. A representative from nasen, who sat on the study management group, was the key contact for the PPI groups, taking matter to the groups and then feeding back at study management group meetings. This process worked well and should be retained in future research.
Equality, diversity and inclusion
Participant representation
Child participants
This ZF-SEND study has as its central focus a group of children that, despite their many complex needs, have until recently been neglected by researchers as well as clinicians, namely children with a learning disability. We designed the study specifically to give these children, who traditionally have rarely been consulted, a voice, allowing them to report on their own mental health and well-being and to learn more about expressing and dealing with their emotions. Our recruitment strategy was to contact special schools in order to reach this population and we are confident that our sample is representative of children of primary school age.
Judging from the demographics tables presented in Appendix 5 of this report, we are confident that the child participant population that engaged in this research is inclusive. Gender and ethnicity percentages are representative of the general child population. By definition of our inclusion criteria, all the child participants had SEND, and many had developmental and physical disabilities. The percentages recorded for these additional special needs are largely representative of the general child learning disability population.
Parent/carer participants
The study design also incorporated participation from parents/carers. They were asked to complete questionnaires about their children’s special needs, their emotional intelligence, behaviour and well-being. We asked schools to communicate with parents/carers, as we knew that they already had ‘tried and tested’ communication systems set up for this. We provided the teachers with accessible information leaflets, questionnaires etc. to pass on to parents/carers and the teachers also ensured that the parents/carers who participated in the research received their high street vouchers, as a token of appreciation for their participation. We tasked the schools with ‘selling’ the research to parents/carers on our behalf and also with reminding parents to complete the questionnaires and to return them. We anticipated that the teachers would be more successful in these tasks than the researchers who were unknown to the parents/carers and therefore less likely to hold sway with them. With hindsight, we think that this may have possibly resulted in the exclusion of certain groups and are, therefore, less certain about inclusivity with regard to the parent participants.
It is possible that we failed to recruit a significant proportion of parents/carers from disadvantaged backgrounds. These parents/carers may have been less inclined to complete our questionnaires due to a variety of reasons including lower levels of literacy (including information technology literacy, as they were given the choice of completing the questionnaires online or on paper and most respondents opted for the former). Moreover, compared with the general population, it is more likely that parents of a child with a learning disability have a learning disability themselves, thus requiring more support and guidance to complete and return the questionnaires. To address these issues, parents/carers were given the option of requesting a phone call to complete the measures with a researcher; however, this was not taken up by any parent/carer.
To improve inclusivity in a future study, we propose that as researchers we take a more active part in the recruitment of parents/carers. We aim to improve and expand our efforts to publicise the research, and make contact with potential parent/carer participants instead of depending on (already very busy) teaching and school administrative staff.
Teacher participants
Our teacher participants make up a relatively homogeneous group (all female professionals of working age) and we consider them to be representative of teachers in special school in England. However, we did not note age, ethnic background or disability details for these participants and aim to address this gap in the data collection in a future trial.
Inclusivity and accessibility of materials
The materials that we chose or designed were carefully adapted to the participant groups. The children’s questionnaires used age-appropriate language, simplified Likert scales and were short enough to maintain the children’s attention. The researchers were trained and experienced in working with children with a learning disability and made sure that each child was relaxed and engaged throughout the assessment sessions. This ensured an almost complete data set for the child participants.
The qualitative interview conducted with teachers and with a subset of the child participants confirmed that completing the questionnaires with the support of the researcher was feasible within the context of their intellectual capacity and had been a positive and interesting experience for the children.
We plan, however, to shorten the questionnaire packs for the teachers and the parents as there are a number of items that are repeated, especially in the emotional literacy measures. The qualitative interviews with both these participant groups indicate that some participants at least found completing the questionnaires arduous
Reflections on the research team and wider involvement
We were fortunate to be able to form a team of researchers and advisors with a wide range of ages (from early 20s to 60 +), ethnic backgrounds (including North African, South Asian, Central and North European) and from a number of different UK countries (England, Wales, Scotland), and, as the project was conducted in England, a number of English regions (London, West Midlands, North-East).
A wide range of experience, expertise and skills were present across the research team that included academics as well as experienced clinicians and scientist practitioners with backgrounds rooted in psychology, sociology, social policy, health economics and statistics. The two researchers employed both had MSc Research in Psychology qualifications. During the duration of the study, they were provided with ample opportunities to expand their quantitative and qualitative research skills and were centrally involved in designing the session tracker forms, observation checklist and the framework analysis. Their contributions to the project are acknowledged and where appropriate, they will be involved in report writing and listed as co-authors on the publications and presentations that will constitute the dissemination of the study findings.
Patient and public involvement
The study steering committee included a parent of a child with a learning disability and autism. The focus groups (Chapter 5) conducted by nasen were attended by parents/carers of children with a learning disability and SEND and, as a separate group, by experienced teaching staff in special schools. We also had representation on the study management group from nasen and from BILD. The varied and useful PPI contributions (described in Chapter 5 of this report) have been highly influential in the preparation, execution and dissemination phases of this feasibility study. Although we introduced pupils’ self-reported well-being as an outcome measure, a first as far as we know in controlled studies of children with SEND, we did not include them into our PPI consultations. This will be addressed in the proposal for a full trial.
Impact and learning
This feasibility study has highlighted a number of modifications that could be made to enhance the design of a large-scale RCT such as starting recruitment earlier in the preceding academic year, broadening the inclusion criteria for pupils, improving engagement and communication with parents/carers, improving the way that ZF-SEND session are rated, and reducing the number of behavioural outcome measures for parents/carers and teachers. A large-scale trial would provide much-needed evidence on effective emotional literacy interventions for children with a learning disability. This study has also generated impact for the participants in the study. The teacher reported a range of positive impacts on the children who took part in the ZF-SEND programme. Schools allocated to the PAU group were also provided with the programme at the end of the study so 12 schools have been given access to the programme as part of the study. In the interviews, teachers commented that they would continue to use the programme in their schools, potentially giving access to well over the 53 pupils involved in this study.
Another aspect of key learning from this study is the collection of data from pupils using both in-person and remote techniques. Both modes were acceptable and feasible and the MAMS has good face validity. Further work is required to validate this measure for children with a learning disability, as the study did not replicate the factor structure of the MAMS; however, we are keen to highlight the importance of self-rating in research for children with a learning disability.
Implications for decision makers
This feasibility study does not warrant us to identify implications for practice or local service delivery. Once a full trial has been conducted, we will be in a position to set out implications for decision makers in the context of the evidence. The current study was not designed to produce such evidence. We are therefore keen to prepare a proposal for a large-scale RCT which can do this, as research that can produce evidence to support clear and achievable action points is more likely to encourage uptake.
Recommendations for future research
As this is a feasibility RCT, the primary recommendation for future research, based on the outcome of this study is to conduct a large-scale effectiveness trial of ZF-SEND for children with a learning disability in special schools. Currently, there are no evidence-based, emotional literacy interventions for children with a learning disability, despite emotional literacy being a proven moderator of a range of negative health and social conditions and children with a learning disability being at higher risk of such negative health and social conditions. Providing evidence of effectiveness of an intervention would enable special schools to make a case to purchase and provide the programme within their school and give their pupils the opportunity to develop their emotional literacy. In addition, research on how to improve parent/carer engagement in both school-based interventions and research is warranted.
Conclusions
This study sought to evaluate whether a large-scale trial of an emotional literacy programme (ZF-SEND) for children with a learning disability is warranted. The feasibility of: (1) study processes, (2) data collection and (3) the ZF-SEND programme were evaluated through a feasibility RCT which aimed to recruit 96 pupils across 12 schools and collect teacher-, parent/carer- and pupil-rated data at baseline (pre-randomisation) and then at 12 months post randomisation. A series of predetermined progression criteria were defined, against which feasibility outcomes were evaluated.
The study was planned before the COVID-19 pandemic. Recruitment, data collection and follow-up all took place during the pandemic and while various national restrictions were in place and therefore the results of this study are impacted by the pandemic. It is likely that the pandemic resulted in reduced capacity and interest of schools to participate in research, higher staff and pupil absence in schools, increased pressure on schools and teachers, increased pressure on parents/carers and difficult family dynamics and poorer response rates of teachers and parents/carers. Despite this, 53 pupils across 8 schools were recruited and followed-up with high rates of recruitment of pupils invited to take part and retention. Acceptable response rates at baseline and follow-up from teachers on the outcome measures were achieved. Moreover, data collection from pupils was feasible and acceptable with high response rates.
Owing to the difficulties in recruiting schools, baseline data collection was later than originally planned, resulting in delayed randomisation and ZF-SEND schools starting the programme, and a shorter follow-up period of 8–12 months post randomisation. Only one school therefore completed the programme. Observational and interview data suggest that stakeholders found ZF-SEND feasible and acceptable and teachers were especially positive and enthusiastic about it. However, there were issues in collecting data about programme delivery on the session checklists, which means that quantitative measure of fidelity, adherence and engagement need to be interpreted with caution.
This study indicates that a large-scale RCT of ZF-SEND is feasible and would provide important evidence about emotional literacy interventions for children with a learning disability. The study design can be enhanced by approaching schools in January in the preceding academic year, randomising schools early in the summer term, providing training to teachers in the ZF-SEND arm both before the summer break and shortly after starting the programme early in the school year, refining and reducing the outcome measures, embedding data collection on ZF-SEND delivery into the programme and engaging more with parents/carers.
Additional information
CRediT contribution statement
Biza Stenfert Kroese (https://orcid.org/0000-0002-3027-7954): Conceptualisation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – editing and reviewing.
Gemma Unwin (https://orcid.org/0000-0002-5205-3150): Conceptualisation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualisation, Writing – original draft, Writing – editing and reviewing.
Richard Hastings (https://orcid.org/0000-0002-0495-8270): Conceptualisation, Funding acquisition, Methodology, Resources, Writing – editing and reviewing.
Andrew Jahoda (https://orcid.org/0000-0002-3985-6098): Conceptualisation, Funding acquisition, Methodology.
Rachel McNamara (https://orcid.org/0000-0002-7280-1611): Conceptualisation, Data curation, Funding acquisition, Methodology, Supervision, Writing – editing and reviewing.
David Gillespie (https://orcid.org/0000-0002-6934-2928): Conceptualisation, Data curation, Formal analysis, Funding acquisition, Methodology, Resources, Software, Supervision, Validation, Visualisation, Writing – editing and reviewing.
Jeremy Segrott (https://orcid.org/0000-0001-6215-0870): Conceptualisation, Formal analysis, Methodology, Resources, Supervision, Validation, Writing – editing and reviewing.
Kate Ingarfield (https://orcid.org/0000-0002-6910-0267): Data curation, Formal analysis, Writing – editing and reviewing.
Myrsini Gianatsi (https://orcid.org/0000-0003-3664-4302): Data curation, Formal analysis, Writing – editing and reviewing.
Elizabeth Randell (https://orcid.org/0000-0002-1606-3175): Conceptualisation, Data curation, Funding acquisition, Methodology, Writing – editing and reviewing.
Zoe Mather (https://orcid.org/0009-0009-8213-7855): Methodology, Writing – editing and reviewing.
Barbara Barrett (https://orcid.org/0000-0002-0270-6256): Conceptualisation, Formal analysis, Funding acquisition, Methodology, Resources, Supervision.
Poushali Ganguli (https://doi.org/0000-0002-1764-5273): Conceptualisation, Formal analysis, Methodology, Resources.
John Rose (https://orcid.org/0000-0003-2672-9767): Conceptualisation, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision.
Mariam Sahle (https://orcid.org/0009-0006-2533-2222): Investigation, Project administration, Resources, Visualisation.
Emily Warren (https://orcid.org/0009-0007-3242-0535): Formal analysis, Investigation, Project administration.
Nathan Da Cruz (https://orcid.org/0009-0006-6106-6240): Formal analysis, Investigation.
Claire Wilson: Conceptualisation, Methodology. Sarah Leitch: Conceptualisation, Funding acquisition.
Acknowledgements
This study would not have been possible without the hard work and dedication of the teachers who took part. The team expresses their sincere gratitude to these teachers who showed impressive commitment, despite challenges during the study. Our thanks also go to members of senior leadership in the schools for agreeing to take part in research at a time of such uncertainty. Similarly, to the parents and carers who completed questionnaires and took part in interviews – we thank you for your time and energy in making this study a success. Finally, to the pupils who took part, thank you for speaking with us, we are proud to have included your voice in this study.
Data-sharing statement
All data requests should be submitted to the corresponding author for consideration. Access to anonymised data may be granted following review.
Ethics statement
Ethical approval was granted by the University of Birmingham (UK) Ethics Committee on 8 March 2021 (ERN_20-0191).
Information governance statement
University of Birmingham is committed to handling all personal information in line with the UK Data Protection Act (2018) and the General Data Protection Regulation (EU GDPR) 2016/679. Under the Data Protection legislation, University of Birmingham is the Data Controller, and you can find out more about how we handle personal data, including how to exercise your individual rights and the contact details for our Data Protection Officer here (https://www.birmingham.ac.uk/university/leadership/governance/policies-regs/data-protection.aspx). The Data Processor was the Centre for Trials Research at Cardiff University.
Disclosure of interests
Full disclosure of interests: Completed ICMJE forms for all authors, including all related interests, are available in the toolkit on the NIHR Journals Library report publication page at https://doi.org/10.3310/JTJY8001.
Primary conflicts of interest: The following authors held the following NIHR Committee memberships: David Gillespie: HTA Associate Board 2020; HTA Commissioning Committee 2021–5, John Rose: HTA MPOH Panel 2015–18; HTA Prioritisation Committee 2015–19.
Disclaimers
This article presents independent research funded by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the PHR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, the PHR programme or the Department of Health and Social Care.
References
- Hatton C, Glover G, Emerson E, Brown I. People With Learning Disabilities in England 2015: Main Report 2015.
- Emerson E, Hatton C. The mental health of children and adolescents with learning disabilities in Britain. Adv Ment Health Learn Disab 2007;1:62-3. https://doi.org/10.1108/17530180200700033.
- Baumeister AL, Storch EA, Geffken GR. Peer victimization in children with learning disabilities. Child Adolesc Social Work J 2008;25:11-23. https://doi.org/10.1007/s10560-007-0109-6.
- Forness SR, Kavale KA. Treating social skill deficits in children with learning disabilities: a meta-analysis of the research. Learn Disabil Q 1996;19:2-13. https://doi.org/10.2307/1511048.
- Unwin GL, Stenfert Kroese B, Blumson J. An evaluation of a mental health promotion programme to improve emotional, social and coping skills in children and young people attending special schools. Front Educ 2018;3. https://doi.org/10.3389/feduc.2018.00093.
- National Institute for Health and Care Excellence . Social and Emotional Wellbeing in Primary Education 2008.
- Jacobs M, Downie H, Kidd G, Fitzsimmons L, Gibbs S, Melville C. Mental health services for children and adolescents with learning disabilities: a review of research on experiences of service users and providers. Br J Learn Disabil 2015;44:225-32. https://doi.org/10.1111/bld.12141.
- Windsor C, Zhang T, Wilson NJ, Blyth K, Ballentine N, Speyer R. Psychosocial-behavioural interventions for school-aged children with intellectual disabilities: a systematic review of randomised control trials. J Appl Res Intellect Disabil 2023;36:458-85. https://doi.org/10.1111/jar.13086.
- Mayer JD, Salovey P. Emotional Development and Emotional Intelligence: Educational Implications. New York: Harper Collins; 1997.
- Bar-On R. The Emotional Quotient Inventory (EQ-I): A Test of Emotional Intelligence. Toronto, ON, Canada: Multi-Health Systems; 1997.
- Fenwick-Smith A, Dahlberg EE, Thompson SC. Systematic review of resilience-enhancing, universal, primary school-based mental health promotion programs. BMC Psychol 2018;6. https://doi.org/10.1186/s40359-018-0242-3.
- Cheng C, Lau HPB, Chan MPS. Coping flexibility and psychological adjustment to stressful life changes: a meta-analytic review. Psychol Bull 2014;140:1582-607. https://doi.org/10.1037/a0037913.
- Martins A, Ramalho N, Morin E. A comprehensive meta-analysis of the relationship between Emotional Intelligence and Health. Pers Individ Dif 2010;49:554-64. https://doi.org/10.1016/j.paid.2010.05.029.
- Salguero JM, Palomera R, Fernández-Berrocal P. Perceived emotional intelligence as predictor of psychological adjustment in adolescents: a 1-year prospective study. Eur J Psychol Educ 2001;27:21-34. https://doi.org/10.1007/s10212-011-0063-8.
- Department of Health and Department for Education . Cm 9523. Transforming Children and Young People’s Mental Health Provision: A Green Paper 2017.
- Gov.UK . CP 800. Special Educational Needs and Disabilities (SEND) and Alternative Provision (AP) Improvement Plan Right Support, Right Place, Right Time 2023.
- Weare K, Nind M. Mental health promotion and problem prevention in schools: what does the evidence say?. Health Promot Int 2011;26:i29-69. https://doi.org/10.1093/heapro/dar075.
- Higgin S, Mueller J, Mösko MR. Universal mental health interventions for young students in adverse environments: a systematic review of evaluated interventions. Child Adolesc Ment Health 2022;27:281-93. https://doi.org/10.1111/camh.12493.
- Monkeviciené O, Mishara BL, Dufour S. Effects of the Zippy’s Friends programme on children’s coping abilities during the transition from Kindergarten to Elementary School. Early Child Educ J 2006;34:53-60. https://doi.org/10.1007/s10643-006-0104-0.
- Clarke AM, Barry MM. An Evaluation of the Zippy’s Friends Emotional Wellbeing Programme for Primary Schools in Ireland. Galway, Ireland: National University of Galway; 2010.
- Dufour S, Denoncourt J, Mishara BL. Improving children’s adaptation: new evidence regarding the effectiveness of Zippy’s Friends, a school mental health promotion program. Adv Sch Ment Health Promot 2011;4:18-2. https://doi.org/10.1080/1754730x.2011.9715633.
- Holen S, Waaktaar T, Lervåg A, Ystgaard M. The effectiveness of a universal school-based programme on coping and mental health: a randomised, controlled study of Zippy’s friends. Educ Psychol 2012;32:657-77. https://doi.org/10.1080/01443410.2012.686152.
- Clarke AM, Bunting B, Barry MM. Evaluating the implementation of a school-based emotional well-being programme: a cluster randomized controlled trial of Zippy’s Friends for children in disadvantaged primary schools. Health Educ Res 2014;29:786-98. https://doi.org/10.1093/her/cyu047.
- Kim M, Ko H, Kim S, Kim B. The effect of Zippy’s Friends program based on stress-coping model on early-child in convergence era. J Korea Converg Soc 2019;10:359-67. https://doi.org/10.15207/JKCS.2019.10.5.359.
- Wills J. A Systematic Review of the Zippy’s Friends Programme 2010.
- Avery KN, Williamson PR, Gamble C, O’Connell Francischetto E, Metcalfe C, Davidson P, et al. Members of the Internal Pilot Trials Workshop Supported by the Hubs for Trials Methodology Research . Informing efficient randomised controlled trials: exploration of challenges in developing progression criteria for Internal Pilot Studies. BMJ Open 2017;7. https://doi.org/10.1136/bmjopen-2016-013537.
- Goodman R. The Strengths and Difficulties Questionnaire: a research note. J Child Psychol Psychiatry 1997;38:581-6. https://doi.org/10.1111/j.1469-7610.1997.tb01545.x.
- Bailey T, Totsika V, Hastings RP, Hatton C, Emerson E. Developmental trajectories of behaviour problems and prosocial behaviours of children with intellectual disabilities in a population‐based cohort. J Child Psychol Psychiatry 2019;60:1210-8. https://doi.org/10.1111/jcpp.13080.
- Kaiser S, Halvorsen MB. The Strengths and Difficulties Questionnaire self-report-, parent-, and teacher version in children with intellectual and developmental disabilities. Res Dev Disabil 2022;123. https://doi.org/10.1016/j.ridd.2022.104194.
- Kleefman M, Jansen DE, Stewart RE, Reijneveld SA. The effectiveness of Stepping Stones Triple P parenting support in parents of children with borderline to mild intellectual disability and psychosocial problems: a randomized controlled trial. BMC Med 2014;12. https://doi.org/10.1186/s12916-014-0191-5.
- Murray C, Hastings R, Totsika V. Clinical utility of the parent-reported Strengths and Difficulties Questionnaire as a screen for emotional and behavioural difficulties in children and adolescents with intellectual disability. Br J Psychiatry 2021;218:323-5. https://doi.org/10.1192/bjp.2020.224.
- Southampton Psychology Service . Emotional Literacy: Assessment and Intervention 2003.
- Aman MG, Tassé MJ, Rojahn J, Hammer D. The Nisonger CBRF: a child behavior rating form for children with developmental disabilities. Res Dev Disabil 1996;17:41-57. https://doi.org/10.1016/0891-4222(95)00039-9.
- Deighton J, Tymms P, Vostanis P, Belsky J, Fonagy P, Brown A, et al. The development of a school-based measure of Child Mental Health. J Psychoeduc Assess 2012;31:247-57. https://doi.org/10.1177/0734282912465570.
- Jackson-Terblanche E. Mental Health and Emotional Literacy in Children and Young People with Special Educational Needs and Disabilities: Self Report and Performance Measures Versus Teachers Ratings. Birmingham: University of Birmingham; 2020.
- Wille N, Badia X, Bonsel G, Burström K, Cavrini G, Devlin N, et al. Development of the EQ-5D-Y: a child-friendly version of the EQ-5D. Qual Life Res 2010;19:875-86. https://doi.org/10.1007/s11136-010-9648-y.
- Stevens K, Ratcliffe J. Measuring and valuing health benefits for economic evaluation in adolescence: an assessment of the practicality and validity of the Child Health Utility 9D in the Australian adolescent population. Value Health 2012;15:1092-9. https://doi.org/10.1016/j.jval.2012.07.011.
- Stevens K. Valuation of the child health utility 9D index. PharmacoEconomics 2012;30:729-47. https://doi.org/10.2165/11599120-000000000-00000.
- Goodyer I, Dubicka B, Wilkinson P, Kelvin R, Roberts C, Byford S, et al. A randomised controlled trial of cognitive behaviour therapy in adolescents with major depression treated by selective serotonin reuptake inhibitors: the ADAPT trial. Health Technol Assess 2008;12:iii–iv-ix–60. https://doi.org/10.3310/hta12140.
- Perry A, Taheri A, Ting V, Weiss J. The GO4KIDDS brief adaptive scale. J Appl Res Intellect Disabil 2015;28:594-7. https://doi.org/10.1111/jar.12143.
- Newcombe RG. Improved confidence intervals for the difference between binomial proportions based on paired data. Stat Med 1998;17:2635-50. https://doi.org/10.1002/(sici)1097-0258(19981130)17:22<2635::aid-sim954>3.0.co;2-c.
- Parkinson S, Eatough V, Holmes J, Stapley E, Midgley N. Framework analysis: a worked example of a study exploring young people’s experiences of depression. Qual Res Psychol 2016;13:109-29. https://doi.org/10.1080/14780887.2015.1119228.
- Ritchie J, Spencer L. Analyzing Qualitative Data. London: Routledge; 1994.
- Stevens K. Developing a descriptive system for a new preference-based measure of health-related quality of life for children. Qual Life Res 2009;18:1105-13. https://doi.org/10.1007/s11136-009-9524-9.
- Ravens-Sieberer U, Wille N, Badia X, Bonsel G, Burström K, Cavrini G, et al. Feasibility, reliability, and validity of the EQ-5D-Y: results from a multinational study. Qual Life Res 2010;19:887-97. https://doi.org/10.1007/s11136-010-9649-x.
- Brett J, Staniszewska S, Mockford C, Herron-Marx S, Hughes J, Tysall C, et al. Mapping the impact of patient and public involvement on health and social care: a systematic review. Health Expect 2012;17:637-50. https://doi.org/10.1111/j.1369-7625.2012.00795.x.
- Staniszewska S, Brett J, Simera I, Seers K, Mockford C, Goodlad S, et al. GRIPP2 reporting checklists: tools to improve reporting of patient and public involvement in research. BMJ 2017;358. https://doi.org/10.1136/bmj.j3453.
- Willner P, Rose J, Stenfert Kroese B, Murphy GH, Langdon PE, Clifford C, et al. Effect of the COVID-19 pandemic on the mental health of carers of people with intellectual disabilities. J Appl Res Intellect Disab 2020;33:1523-33. https://doi.org/10.1111/jar.12811.
- Paterson J, McCarthy M, Triantafyllopulou P. The impact of the coronavirus pandemic on the lives of children and young people who have special educational needs and/or disabilities in the UK: a scoping review. J Res Spec Educ Needs 2023;24:12-24. https://doi.org/10.1111/1471-3802.12608.
Appendix 1 Logic model for Zippy’s Friends for Special Educational Needs and Disabilities intervention
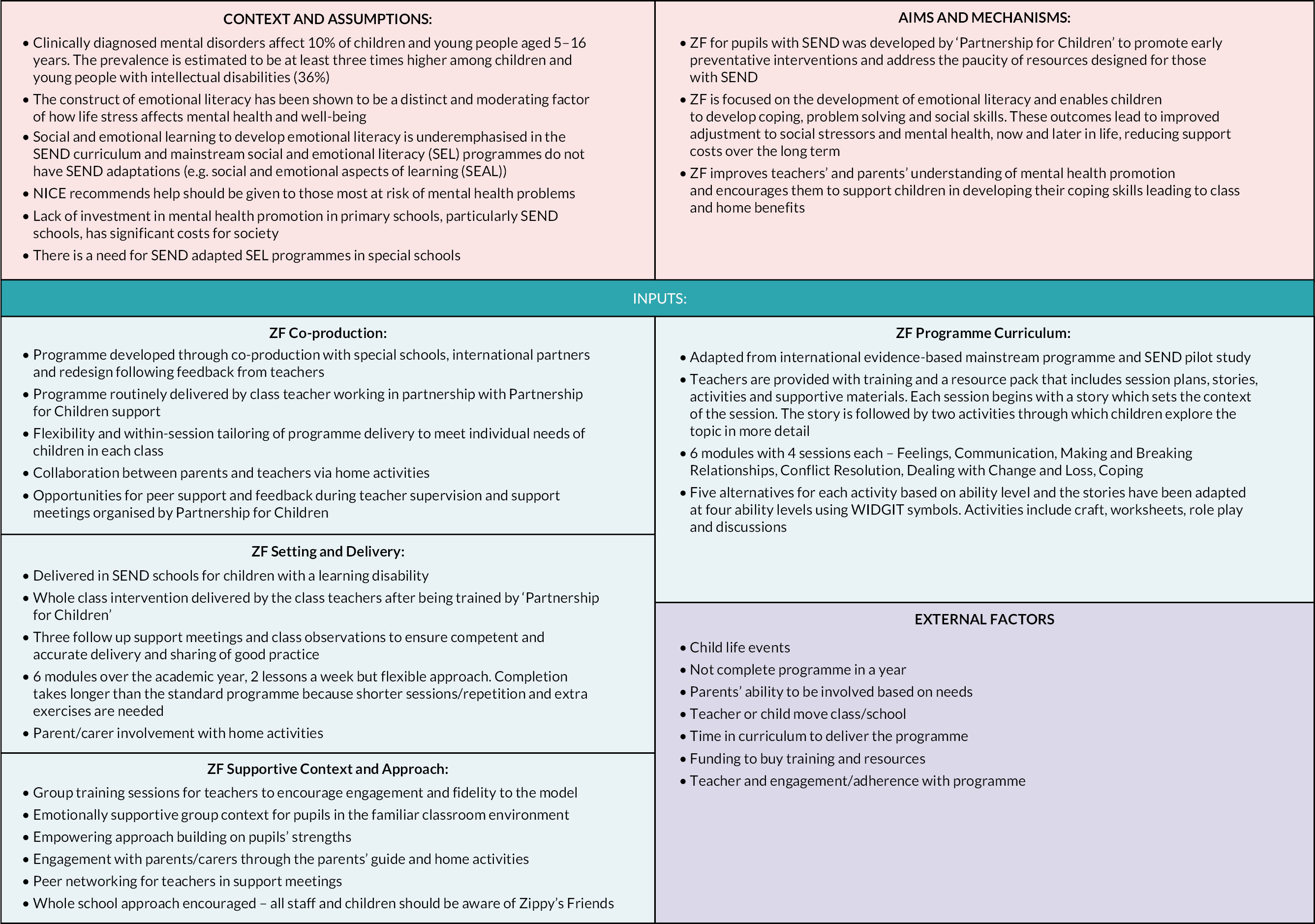
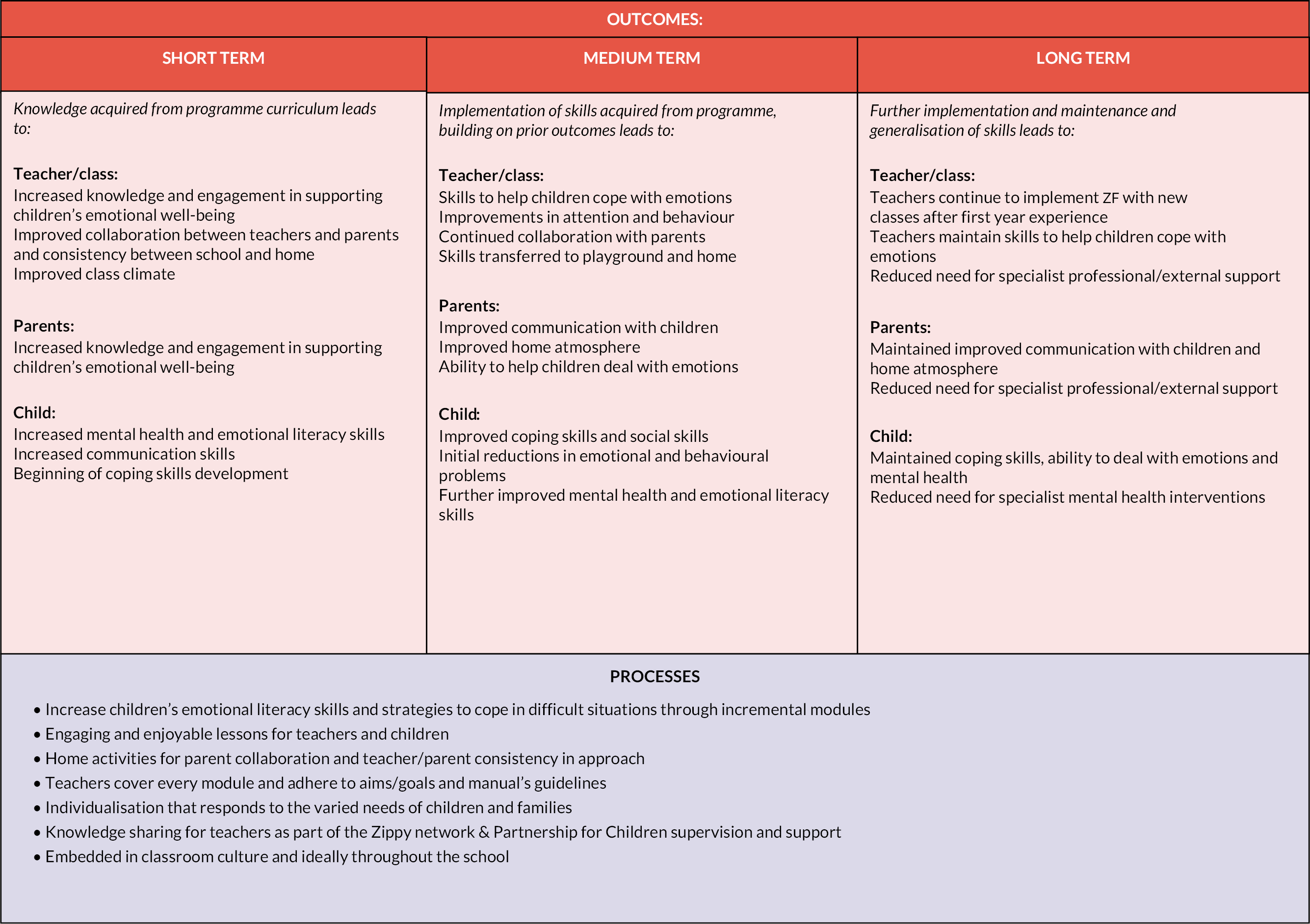
Appendix 2 Zippy’s Friends for Special Educational Needs and Disabilities: study timeline in relation to pandemic and academic year COVID-19 infection rates
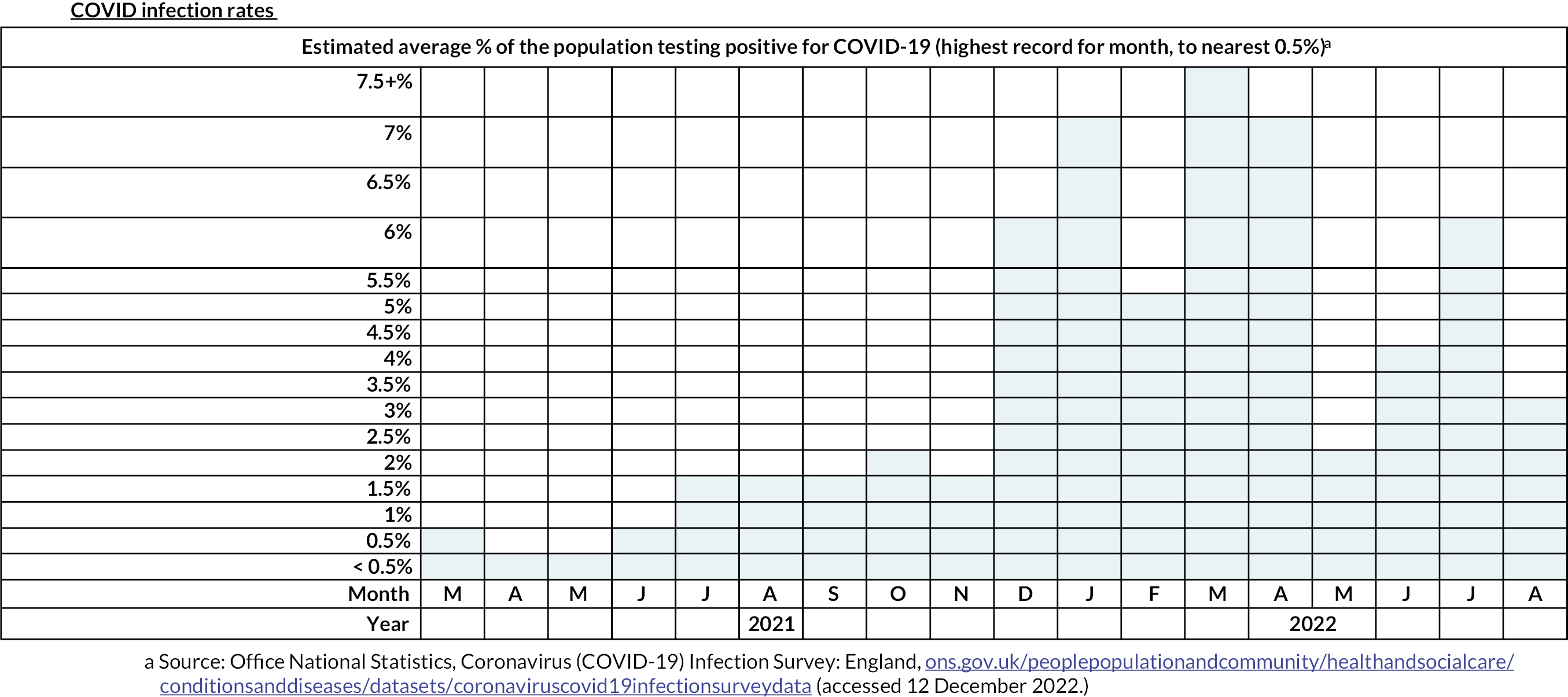
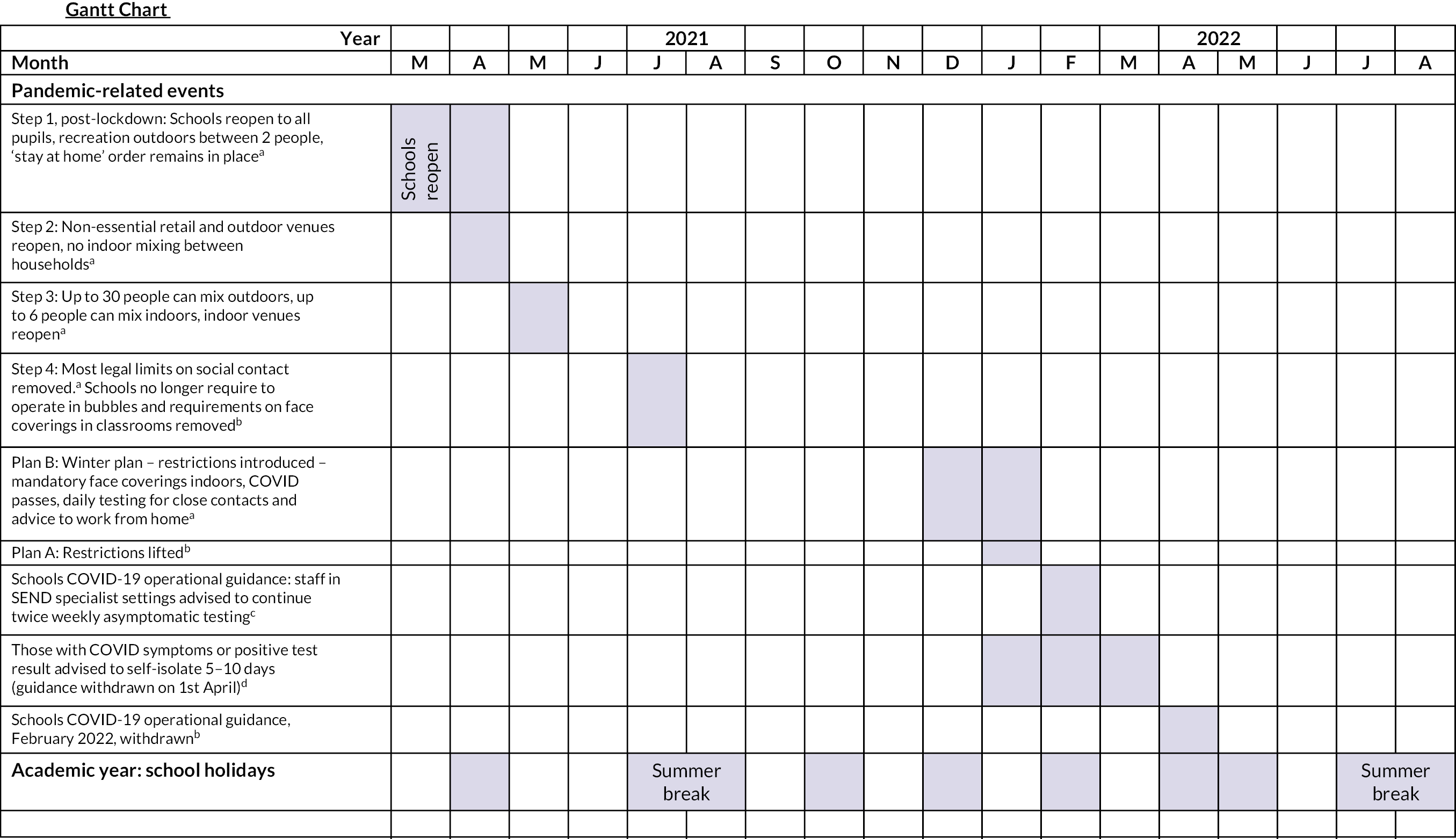
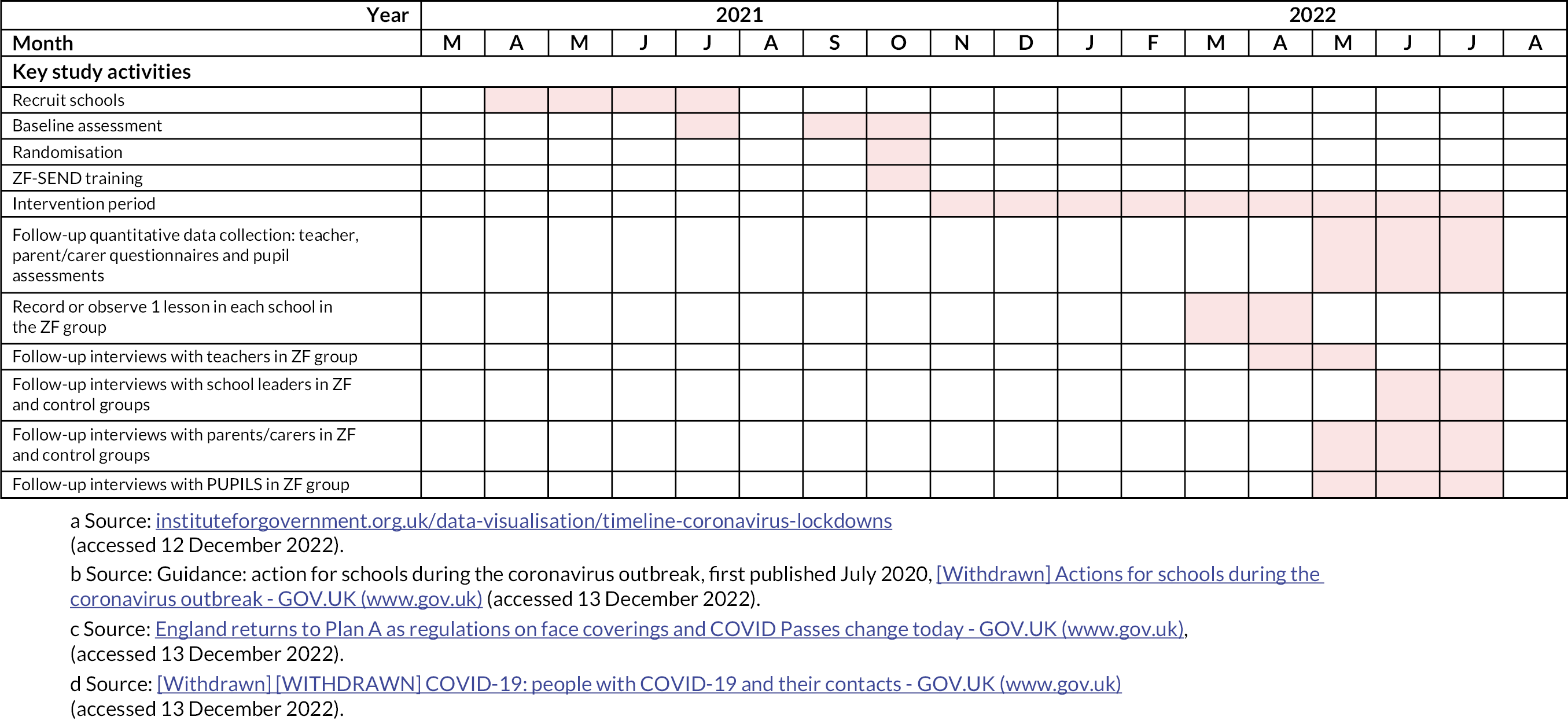
Appendix 3 COVID-19-related issues
Factors affecting delivery of Zippy’s Friends for Special Educational Needs and Disabilities programme
Seven teachers or senior leads mentioned how COVID-19 has impacted the delivery of ZF-SEND. The staff split in their opinion, with two teachers (schools 1 and 11) describing that the pandemic has had minimal impact due to online communication methods and staffing issues only causing disruption for no more than a week. However, the other schools (schools 5, 10 and 9) did stress that COVID-19 had had a profound impact on how ZF-SEND could be delivered. These schools described how staff absences caused large disruptions, preventing the programme being delivered on a regular basis. The teacher from school 9 also mentioned that children often missed sessions of ZF-SEND because of being absent due to COVID-19.
Factors affecting delivery of other newly introduced programmes
Four teachers or senior leads talked about COVID-19 potentially impacting the delivery of new programmes or initiatives. All of them stated that COVID-19 has not had a serious impact on any new initiatives that year. However, three of these interviewees (schools 2, 1 and 4) explained that one of the reasons for this was because no new initiatives were being put in place, due to the schools using this year to adapt to changes necessary due to the pandemic. One teacher also mentioned that their school had to cope with the post-pandemic impacts on some of the children including the worsening of emotional dysregulation.
Impact of COVID-19 on schools
Nine teachers or senior leads discussed the impact that COVID-19 has had on schools in the past year. Staffing issues were commonly mentioned as the largest issue, but many teachers and senior leads believed that they were able to cope because there were adaptations in place to deal with difficulties that could arise due to COVID-19. Most staff however also agreed that COVID-19 had caused a significant change in schools compared to pre-COVID-19 years, with measures such as social restrictions (in assemblies or meals) and bubbles still in practice. Three teachers (teachers 5 and 9, school 4) also suggested that the impact of COVID-19 was as significant, if not more significant, in that academic year compared with previous years since the onset of the pandemic. For example, the teacher from school 4 believed that children and families coped well during the pandemic but the biggest issues are being seen now due to children struggling to adapt to returning to the school and community.
Some of the teachers mentioned that COVID-19 had a worse impact on special schools because of the extra social, health, emotional and psychological needs which children with SEND experience. Furthermore, it was described that children with SEND are less able to deal with change or loss (senior lead, school 10) and that they are less able to learn from bubble or remote learning (teacher, school 5). Staff from schools 1 and 10 also reported that the disruption caused by COVID-19 has meant that there has been less focus on non-core subjects such as art or history. Schools instead have prioritised what they perceive to be essential teaching of mathematics and English.
Impact of COVID-19 on the research experience
Most teachers who talked about COVID-19’s impact on the research reported this to be minor, especially in the schools in the PAU group. The school 1 senior lead and school 6 teacher mentioned the use of technology such as video calls and the remote observation as useful tools in enabling the school to participate in the research. However, COVID-19 was mentioned to have a negative impact on the ability to participate in the research by the school 9 teacher; she mentioned that because of staff and pupil absences caused by COVID-19, the data collection had been delayed.
Pupil absence
Nine staff members described how COVID-19 has impacted pupil attendance. All reported that COVID-19 had significantly reduced pupil attendance that year compared to the years before the pandemic. The school 1 senior lead mentioned that it was the lowest attendance they had ever recorded. The school 10 senior lead on the other hand believed that while large student absences had caused partial closures of the school, the absences had not caused as many disruptions as in the previous (pandemic) year. Teachers from schools 2 and 6 noted that when pupil absences occurred, programmes such as ZF-SEND would continue as normal and that students who were absent would miss sessions.
Staff absence
All staff members stated that COVID-19 had caused high rates of staff absence and that there had been significantly more absences compared to previous years. The school 4 senior lead and school 2 teacher reported that while staff absences due to COVID-19 had caused issues, their schools had been able to cope relatively well because staff absences had not been long term, and they were able to still cover the curriculum. However, the rest of the schools found it difficult to cope with staffing issues because of the unpredictability of their occurrence and staff contracting the virus multiple times. Three schools (schools 10, 11 and 6) also described that staff absences due to COVID-19 disrupted the delivery of programmes such as ZF-SEND because other teachers could not fill in because they had not been trained in the programme. This resulted in the programmes stopping and starting on multiple occasions.
Appendix 4 Location of schools in the study
FIGURE 3.
Map of locations of schools in the study. Source: Reproduced from Mapsland. Detailed administrative map of England. Published under the Creative Commons Attribution-ShareAlike 3.0 Licence. URL: https://www.mapsland.com/europe/united-kingdom/england/detailed-administrative-map-of-england (accessed 16 November 2023).
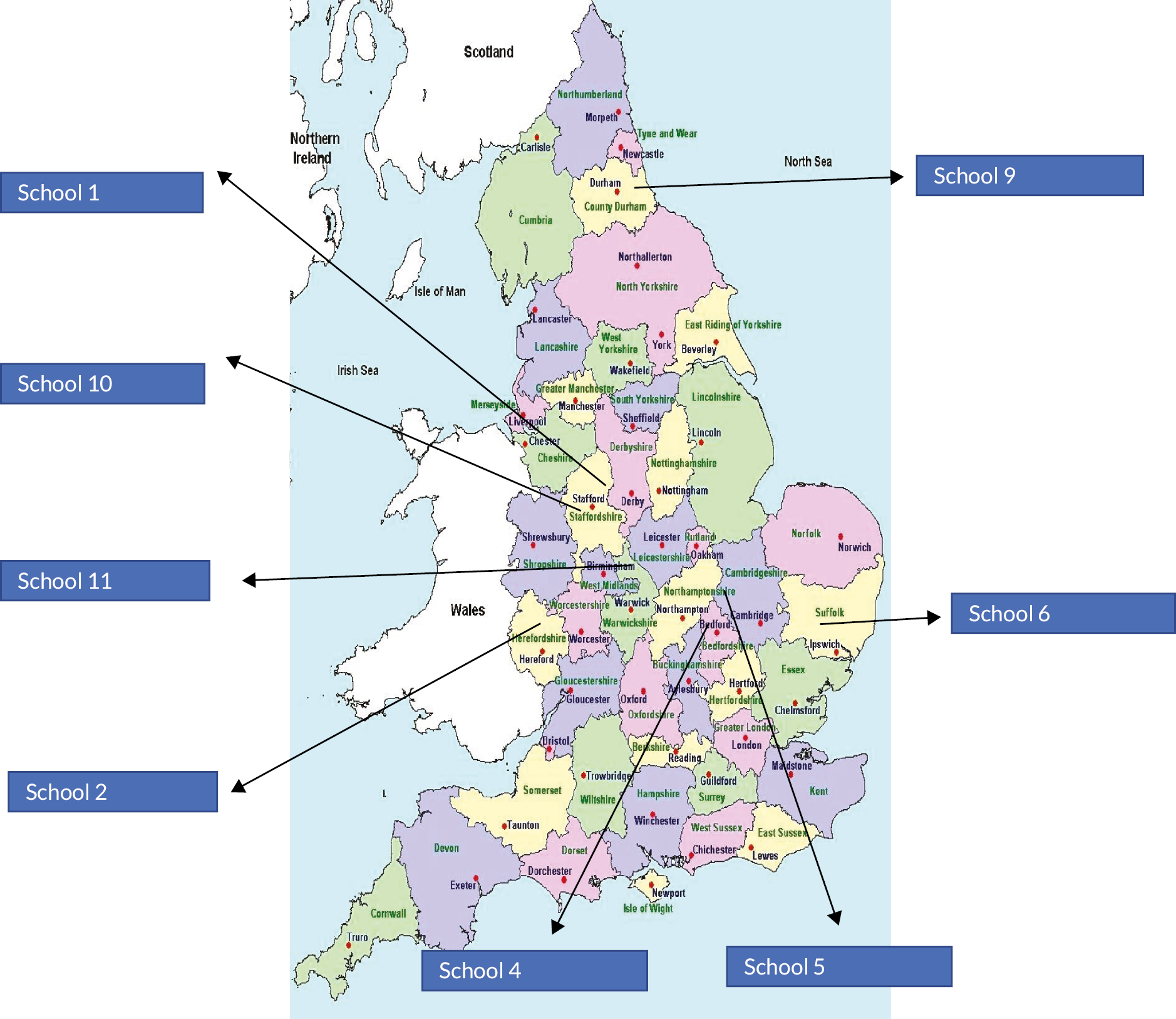
Appendix 5 Tables of demographic profile of the sample
| Variable | Control (N = 15), n (%) | Intervention (N = 33), n (%) | Total (N = 48), n (%) |
|---|---|---|---|
| School year | |||
| 3 | 0 (0) | 1 (3) | 1 (2) |
| 4 | 1 (7) | 4 (12 | 5 (10) |
| 5 | 7 (47) | 7 (21) | 14 (29) |
| 6 | 7 (47) | 13 (39) | 20 (42) |
| 7 | 0 (0) | 8 (24) | 8 (17) |
| What is the child’s primary need? | |||
| Autism spectrum disorder | 9 (60) | 21 (64) | 30 (63) |
| Moderate learning difficulties | 4 (27) | 4 (12) | 8 (17) |
| Severe learning difficulties | 0 (0) | 5 (15) | 5 (10) |
| Profound and multiple learning difficulties | 0 (0) | 1 (3) | 1 (2) |
| Behaviour | 2 (13) | 0 (0) | 2 (4) |
| Complex medical needs | 0 (0) | 1 (3) | 1 (2) |
| Visual and hearing impairment | 0 (0) | 1 (3) | 1 (2) |
| What is the child’s secondary need? | |||
| Autism spectrum disorder | 1 (7) | 4 (12) | 5 (10) |
| Moderate learning difficulties | 6 (40) | 15 (45) | 21 (44) |
| Severe learning difficulties | 0 (0) | 1 (3) | 1 (2) |
| Profound and multiple learning difficulties | 0 (0) | 1 (3) | 1 (2) |
| Medical needs | 0 (0) | 1 (3) | 1 (2) |
| Physical and medical | 0 (0) | 1 (3) | 1 (2) |
| Developmental delay | 0 (0) | 1 (3) | 1 (2) |
| No secondary need recorded | 8 (53) | 9 (27) | 17 (35) |
| Is the child eligible for free school meals? | |||
| Yes | 7 (47) | 7 (21) | 14 (29) |
| No | 8 (53) | 16 (48) | 24 (50) |
| Not known | 0 (0) | 10 (30) | 10 (21) |
| Variable | Control (N = 11), n (%) | Intervention (N = 15), n (%) | Total (N = 26), n (%) |
|---|---|---|---|
| Age of child | |||
| 8 years | 1 (9) | 1 (7) | 2 (8) |
| 9 years | 5 (45) | 9 (60) | 14 (54) |
| 10 years | 5 (45) | 2 (13) | 7 (27) |
| 11 years | 0 (0) | 3 (20) | 3 (12) |
| Mean (SD), years | 9.9 (0.6) | 10.0 (1.0) | 10.0 (0.8) |
| Median (IQR), years | 9.9 (9.5–10.3) | 9.6 (9.4–10.7) | 9.8 (9.5–10.5) |
| Gender of child | |||
| Male | 8 (73) | 14 (93) | 22 (85) |
| Female | 3 (27) | 1 (7) | 4 (15) |
| Ethnicity of child | |||
| White British | 9 (82) | 10 (67) | 19 (73) |
| White other | 1 (9) | 1 (7) | 2 (8) |
| Asian/Asian British: Bangladeshi | 0 (0) | 1 (7) | 1 (4) |
| Black/Black British: African | 1 (9) | 0 (0) | 1 (4) |
| British/Asian | 0 (0) | 1 (7) | 1 (4) |
| British/Turkish | 0 (0) | 1 (7) | 1 (4) |
| White/Black Caribbean | 0 (0) | 1 (7) | 1 (4) |
| Current living situation | |||
| Family home (with birth parents) | 11 (100) | 13 (87) | 24 (92) |
| Family home (with one parent) | 0 (0) | 1 (7) | 1 (4) |
| Lives with grandparents with special guardianship order | 0 (0) | 1 (7) | 1 (4) |
| What is your child’s primary need? | |||
| Autism spectrum disorder | 7 (64) | 5 (36) | 12 (48) |
| Moderate learning difficulties | 3 (27) | 2 (14) | 5 (20) |
| Severe learning difficulties | 0 (0) | 3 (21) | 3 (12) |
| Attention deficit hyperactivity disorder | 0 (0) | 1 (7) | 1 (4) |
| Special educational plan | 0 (0) | 1 (7) | 1 (4) |
| Behaviour | 1 (9) | 0 (0) | 1 (4) |
| Cerebral palsy and global development delay | 0 (0) | 1 (7) | 1 (4) |
| Unknown | 0 (0) | 1 (7) | 1 (4) |
| Missing | 0 (0) | 1 (7) | 1 (4) |
| Genetic syndrome | |||
| Down syndrome | 0 (0) | 1 (9) | 1 (6) |
| 10Q26 deletion | 0 (0) | 1 (9) | 1 (6) |
| Fetal valproate syndrome | 0 (0) | 1 (9) | 1 (6) |
| Neurofibromatosis type 1 | 0 (0) | 1 (9) | 1 (6) |
| Retinitis pigmentosa and primary ciliary dyskinesia | 0 (0) | 1 (9) | 1 (6) |
| SAMS syndrome | 0 (0) | 1 (9) | 1 (6) |
| Unknown | 7 (100) | 5 (45) | 12 (67) |
| Missing | 4 (36) | 4 (27) | 8 (31) |
| Epilepsy | |||
| Yes | 0 (0) | 4 (29) | 4 (17) |
| No | 10 (100) | 10 (71) | 20 (83) |
| Missing | 1 (9) | 1 (9) | 2 (8) |
| Sensory impairments (vision, hearing) | |||
| Yes | 1 (9) | 9 (60) | 10 (38) |
| No | 10 (91) | 6 (40) | 16 (62) |
| Variable | Control (N = 15), n (%) | Intervention (N = 33), n (%) | Total (N = 48), n (%) |
|---|---|---|---|
| Baseline questionnaire completed by | |||
| Class teacher | 5 (33) | 33 (100) | 38 (79) |
| Deputy head | 5 (33) | 0 (0) | 5 (10) |
| Pathway leader | 5 (33) | 0 (0) | 5 (10) |
| How long have you known the child? (Months) | |||
| 12 months or less | 6 (40) | 18 (55) | 24 (50) |
| More than 12 months | 9 (60) | 15 (45%) | 24 (50) |
| Mean (SD) | 22.7 (13.4) | 16.3 (20.2) | 18.3 (18.5) |
| Median (IQR) | 20.0 (12.0–29.0) | 6.0 (3.0–24.0) | 12.5 (6.0–25.5) |
Appendix 6 Results of factor analysis on the Me and My School
| Original MAMS domain | Item | Factor 1 | Factor 2 | Factor 3 |
|---|---|---|---|---|
| Behavioural | I get very angry | 0.73 | 0.13 | 0.18 |
| I lose my temper | 0.71 | 0.08 | 0.05 | |
| I hit out when I am angry | 0.66 | 0.26 | 0.14 | |
| I do things to hurt people | 0.55 | 0.08 | –0.14 | |
| I am calm (reverse-scored) | 0.17 | –0.12 | 0.34 | |
| I break things on purpose | 0.61 | 0.18 | –0.11 | |
| Emotional | I feel lonely | 0.45 | 0.01 | 0.28 |
| I cry a lot | 0.48 | 0.20 | 0.41 | |
| I am unhappy | 0.55 | 0.44 | 0.27 | |
| Nobody likes me | 0.49 | –0.15 | 0.05 | |
| I worry a lot | 0.32 | 0.34 | 0.31 | |
| I have problems sleeping | 0.17 | 0.76 | 0.01 | |
| I wake up in the night | 0.07 | 0.82 | 0.04 | |
| I am shy | –0.04 | 0.04 | 0.67 | |
| I feel scared | 0.24 | 0.07 | 0.56 | |
| I worry when I am in school | 0.38 | 0.30 | –0.05 |
Appendix 7 Tables of completion rates for the health economic measures
FIGURE 4.
Summary of completion rates.
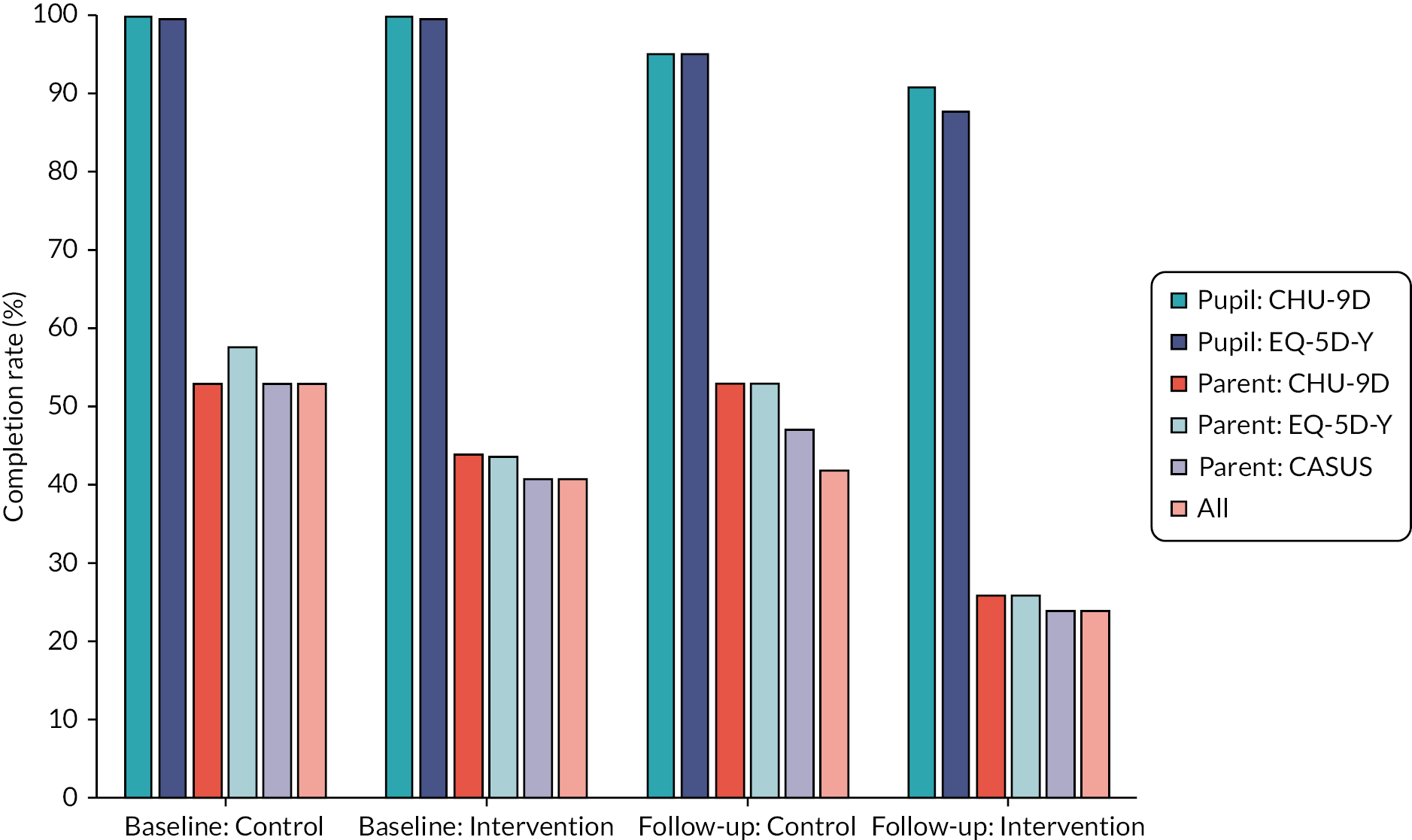
| CASUS items | At baseline | At follow-up | ||||||
|---|---|---|---|---|---|---|---|---|
| Control, complete responses (N = 19) | Intervention, complete responses (N = 34) | Control, complete responses (N = 19) | Intervention, complete responses (N = 34) | |||||
| (n) | (%) | (n) | (%) | (n) | % of all | (n) | (%) | |
| General practitioner/other doctor | 10 | 53 | 14 | 41 | 9 | 47 | 8 | 24 |
| Nurse or midwife | 10 | 53 | 14 | 41 | 9 | 47 | 8 | 24 |
| CAMHS | 10 | 53 | 14 | 41 | 9 | 47 | 8 | 24 |
| Social worker | 10 | 53 | 14 | 41 | 9 | 47 | 8 | 24 |
| Pharmacist | 10 | 53 | 14 | 41 | 9 | 47 | 8 | 24 |
| School nurse | 10 | 53 | 14 | 41 | 9 | 47 | 8 | 24 |
| School counsellor or educational psychologist | 10 | 53 | 14 | 41 | 9 | 47 | 8 | 24 |
| Speech and language therapist | 10 | 53 | 14 | 41 | 9 | 47 | 8 | 24 |
| Counselling (talking therapy) | 10 | 53 | 14 | 41 | 9 | 47 | 8 | 24 |
| Other therapy (e.g. music, drama) | 10 | 53 | 14 | 41 | 9 | 47 | 8 | 24 |
| Medication for depression, anxiety, eating disorders | 10 | 53 | 14 | 41 | 9 | 47 | 8 | 24 |
| Medication for attention deficit hyperactivity disorder | 10 | 53 | 14 | 41 | 9 | 47 | 8 | 24 |
| Medication for sleep disorders | 10 | 53 | 14 | 41 | 9 | 47 | 8 | 24 |
| Medication for tics/Tourette’s | 10 | 53 | 14 | 41 | 9 | 47 | 8 | 24 |
| Respite care | 10 | 53 | 14 | 41 | 9 | 47 | 8 | 24 |
| Complete cases | 10 | 53 | 14 | 41 | 9 | 47 | 8 | 24 |
| CHU-9D items | Responses at baseline | Responses at follow-up | ||||||
|---|---|---|---|---|---|---|---|---|
| Control (N = 19) | Intervention (N = 34) | Control (N = 19) | Intervention (N = 34) | |||||
| (n) | (%) | (n) | (%) | (n) | (%) | (n) | (%) | |
| Worry | 19 | 100 | 34 | 100 | 18 | 95 | 31 | 91 |
| Sad | 19 | 100 | 34 | 100 | 18 | 95 | 31 | 91 |
| Pain | 19 | 100 | 34 | 100 | 18 | 95 | 31 | 91 |
| Tired | 19 | 100 | 34 | 100 | 18 | 95 | 31 | 91 |
| Annoyed | 19 | 100 | 34 | 100 | 18 | 95 | 31 | 91 |
| Sleep | 19 | 100 | 34 | 100 | 18 | 95 | 31 | 91 |
| School work | 19 | 100 | 34 | 100 | 18 | 95 | 31 | 91 |
| Daily routine | 19 | 100 | 34 | 100 | 18 | 95 | 31 | 91 |
| Activities | 19 | 100 | 34 | 100 | 18 | 95 | 31 | 91 |
| Complete cases | 19 | 100 | 34 | 100 | 18 | 95 | 31 | 91 |
| CHU-9D items | Responses at baseline | Responses at follow-up | ||||||
|---|---|---|---|---|---|---|---|---|
| Control (N = 19) | Intervention (N = 34) | Control (N = 19) | Intervention (N = 34) | |||||
| (n) | (%) | (n) | (%) | (n) | (%) | (n) | (%) | |
| Worry | 10 | 53 | 15 | 44 | 10 | 53 | 9 | 26 |
| Sad | 10 | 53 | 15 | 44 | 10 | 53 | 9 | 26 |
| Pain | 10 | 53 | 15 | 44 | 10 | 53 | 9 | 26 |
| Tired | 10 | 53 | 15 | 44 | 10 | 53 | 9 | 26 |
| Annoyed | 10 | 53 | 15 | 44 | 10 | 53 | 9 | 26 |
| Sleep | 10 | 53 | 15 | 44 | 10 | 53 | 9 | 26 |
| School work | 10 | 53 | 15 | 44 | 10 | 53 | 9 | 26 |
| Daily routine | 10 | 53 | 15 | 44 | 10 | 53 | 9 | 26 |
| Activities | 10 | 53 | 15 | 44 | 10 | 53 | 9 | 26 |
| Complete cases | 10 | 53 | 15 | 44 | 10 | 53 | 9 | 26 |
| EQ-5D items | Responses at baseline | Responses at follow-up | ||||||
|---|---|---|---|---|---|---|---|---|
| Control (N = 19) | Intervention (N = 34) | Control (N = 19) | Intervention (N = 34) | |||||
| (n) | (%) | (n) | (%) | (n) | (%) | (n) | (%) | |
| Mobility | 19 | 100 | 34 | 100 | 18 | 95 | 31 | 91 |
| Self-care | 19 | 100 | 34 | 100 | 18 | 95 | 31 | 91 |
| Usual activities | 19 | 100 | 34 | 100 | 18 | 95 | 31 | 91 |
| Pain | 19 | 100 | 34 | 100 | 18 | 95 | 31 | 91 |
| Anxiety/depression | 19 | 100 | 34 | 100 | 18 | 95 | 30 | 88 |
| Complete cases | 19 | 100 | 34 | 100 | 18 | 95 | 30 | 88 |
| EQ-5D items | Responses at baseline | Responses at follow-up | ||||||
|---|---|---|---|---|---|---|---|---|
| Control (N = 19) | Intervention (N = 34) | Control (N = 19) | Intervention (N = 34) | |||||
| (n) | (%) | (n) | (%) | (n) | (%) | (n) | (%) | |
| Mobility | 11 | 58 | 15 | 44 | 10 | 53 | 9 | 26 |
| Self-care | 11 | 58 | 15 | 44 | 10 | 53 | 9 | 26 |
| Usual activities | 11 | 58 | 15 | 44 | 10 | 53 | 9 | 26 |
| Pain | 11 | 58 | 15 | 44 | 10 | 53 | 9 | 26 |
| Anxiety/depression | 11 | 58 | 15 | 44 | 10 | 53 | 9 | 26 |
| Complete cases | 11 | 58 | 15 | 44 | 10 | 53 | 9 | 26 |
Appendix 8 Zippy’s Friends for Special Educational Needs and Disabilities lessons observed
| School | Date of observation | Session observed | Mode of observation | Typical sessions/week (n) | Teaching assistants present (n) | Pupils present, n (N participants enrolled in the study; % present of those enrolled) | Length of lesson (minutes) | Researcher estimate of pupils engaged (%) |
|---|---|---|---|---|---|---|---|---|
| 5 | 7 April 2022 | Module 1 session 4 | Video recording | 2 most weeks | 2 | 8 (5; 63) | 22 | 76–100 |
| 6 | 8 March 2022 | Module 2 session 2 | Direct – remote video call | 1–2, depending on pupil needs | 2–3 | 13 (6; 100) | 40 | 76–100 |
| 9 | 29 April 2022 | Module 3 session 2 | Direct – remote video call | 2–3 | 0 due to short staffing | 8 (2; 22) | 45 | 76–100 |
| 11 | 10 March 2022 | Module 3 session 2 | Direct – in person | 2 | 2 | 8 (2; 40) | 45 | 76–100 |
Appendix 9 Summary on the secondary outcome measures
| Outcome | Baseline | Follow-up | ||||
|---|---|---|---|---|---|---|
| Control | Intervention | Total | Control | Intervention | Total | |
| EQ-5D-Y – pupils, median (IQR) | 0.8 (0.6–1) | 0.8 (0.7–0.8) | 0.8 (0.7–0.8) | 1 (0.8–1) | 1 (0.8–1) | 1 (0.8–1) |
| EQ-5D – parents/carers, median (IQR) | 0.7 (0.7–0.8) | 0.5 (0.1–0.7) | 0.7 (0.2–0.8) | 0.6 (0.3–0.8) | 0.5 (0.1–0.6) | 0.5 (0.2–0.8) |
| SDQ – teacher – emotional problems score – mean (SD) | 3.9 (2.1) | 2.9 (2.4) | 3.3 (2.3) | 4.9 (2.3) | 2.9 (2.3) | 3.4 (2.4) |
| SDQ – teacher – conduct problems score – mean (SD) | 2.8 (2.4) | 2.1 (1.7) | 2.3 (1.9) | 2.3 (3) | 2.5 (2.2) | 2.4 (2.4) |
| SDQ – teacher – hyperactivity score – mean (SD) | 5.9 (1.6) | 5.8 (2.6) | 5.9 (2.4) | 5.7 (2.6) | 6.3 (2.8) | 6.2 (2.7) |
| SDQ – teacher – peer relationship score – mean (SD) | 2.8 (2) | 3.5 (2) | 3.3 (2) | 3.3 (2.7) | 3.5 (1.9) | 3.4 (2.1) |
| SDQ – teacher – prosocial score – mean (SD) | 4.9 (1.7) | 4.8 (2.9) | 4.9 (2.6) | 5.2 (3.5) | 5.7 (2.4) | 5.6 (2.7) |
| SDQ – teacher – total difficulties score – mean (SD) | 15.4 (4.5) | 14.3 (5.6) | 14.6 (5.2) | 16.6 (10.1) | 15.2 (5.9) | 15.5 (6.9) |
| SDQ – parent/carer – emotional problems score – mean (SD) | 3.4 (1.7) | 3.9 (2.2) | 3.7 (2) | 4.1 (2.5) | 5.5 (2.5) | 4.8 (2.5) |
| SDQ – parent/carer – conduct problems score – mean (SD) | 2.4 (2.1) | 3.1 (1.6) | 2.8 (1.8) | 3.6 (2.8) | 3 (2.5) | 3.3 (2.6) |
| SDQ – parent/carer – hyperactivity score – mean (SD) | 6.6 (2.2) | 7.3 (2.1) | 7 (2.1) | 7.1 (2.6) | 6.9 (1.7) | 7 (2.2) |
| SDQ – parent/carer – peer relationship score – mean (SD) | 3.1 (1.6) | 4.4 (1.8) | 3.8 (1.8) | 3.4 (2.3) | 4.4 (2.5) | 3.9 (2.4) |
| SDQ – parent/carer – prosocial score – mean (SD) | 6.5 (2.3) | 6.8 (2.8) | 6.7 (2.5) | 6.7 (2.1) | 7.1 (2.5) | 6.9 (2.2) |
| SDQ – parent/carer – total difficulties score – mean (SD) | 15.5 (4.6) | 18.7 (4.4) | 17.4 (4.7) | 18.2 (8) | 19.8 (7.3) | 18.9 (7.5) |
| MAMS – pupils – emotional difficulties, mean (SD) | 6.1 (3.6) | 6.9 (3.1) | 6.6 (3.3) | 5.9 (2.8) | 5.9 (3.9) | 5.9 (3.5) |
| MAMS – pupils – behavioural difficulties, mean (SD) | 2.8 (2.5) | 3.2 (2.2) | 3.1 (2.3) | 3.3 (2.3) | 3.4 (2.3) | 3.4 (2.3) |
| ELA teacher, self-awareness, mean (SD) | 10.1 (1.5) | 9.6 (1.7) | 9.8 (1.6) | 9.3 (1.6) | 9.7 (3) | 9.6 (2.6) |
| ELA teacher, self- regulation, mean (SD) | 8.2 (2.8) | 9 (3) | 8.7 (2.9) | 10.1 (3.4) | 10.3 (3.7) | 10.2 (3.6) |
| ELA teacher, motivation, mean (SD) | 9.8 (1.6) | 9.6 (2.7) | 9.7 (2.4) | 10.9 (1.9) | 10.3 (2.9) | 10.5 (2.7) |
| ELA teacher, empathy, mean (SD) | 10.1 (2.3) | 10.9 (2.7) | 10.6 (2.6) | 9.9 (3.2) | 8.6 (3.1) | 8.9 (3.1) |
| ELA teacher, social skills, mean (SD) | 13 (1.4) | 12.9 (1.8) | 12.9 (1.6) | 7.9 (1.8) | 6.5 (2) | 6.9 (2.1) |
| ELA teacher, final score, mean (SD) | 51.2 (5.1) | 52 (9.1) | 51.7 (8) | 48.1 (9.8) | 45.3 (12.9) | 46.1 (12.1) |
| ELA parent/carer, self-awareness, mean (SD) | 11.4 (4.8) | 12.3 (4.5) | 11.9 (4.6) | 11.8 (4.8) | 11.2 (6.2) | 11.5 (5.4) |
| ELA parent/carer, self-regulation, mean (SD) | 11.5 (4.9) | 13.3 (4.7) | 12.5 (4.8) | 12.5 (5.8) | 10.8 (6.7) | 11.6 (6.2) |
| ELA parent/carer, motivation, mean (SD) | 12.7 (4.8) | 13.1 (4.2) | 12.9 (4.4) | 13 (5.3) | 12 (7) | 12.5 (6.1) |
| ELA parent/carer, empathy, mean (SD) | 9.2 (4) | 9.9 (3.2) | 9.6 (3.5) | 10 (4.6) | 8.8 (5.4) | 9.4 (4.9) |
| ELA parent/carer, social skills, mean (SD) | 8.2 (4.1) | 9.5 (3.7) | 9 (3.9) | 8.6 (4.3) | 8.9 (5.1) | 8.8 (4.6) |
| ELA parent/carer, final score, mean (SD) | 52.9 (19.6) | 58.2 (16.8) | 56.0 (17.8) | 55.9 (23.3) | 51.7 (28.4) | 53.8 (25.4) |
| CHU – Pupil, mean (SD) | 0.8 (0.1) | 0.8 (0.1) | 0.8 (0.1) | 0.9 (0.1) | 0.9 (0.1) | 0.9 (0.1) |
| CHU – Parent/carer, mean (SD) | 0.9 (0.1) | 0.8 (0.1) | 0.8 (0.1) | 0.8 (0.1) | 0.7 (0.1) | 0.8 (0.1) |
| NCBR teacher, positive social, mean (SD) | 16 (6.1) | 15.1 (6.3) | 15.4 (6.2) | 17 (7.9) | 14.8 (5.8) | 15.4 (6.4) |
| NCBR teacher, conduct problems score, mean (SD) | 7.3 (8.6) | 5.5 (5.8) | 6.1 (6.7) | 8.8 (13.2) | 5.1 (6.6) | 6.1 (8.8) |
| NCBR teacher, insecure/anxious score, Mean (SD) | 13.3 (8.6) | 8.3 (6.5) | 9.9 (7.5) | 14.9 (10.3) | 8.5 (6.8) | 10.2 (8.2) |
| NCBR teacher, hyperactive score, mean (SD) | 6.7 (4.6) | 7.1 (6.3) | 7 (5.7) | 8 (6.6) | 8.6 (6.6) | 8.5 (6.5) |
| NCBR teacher, self-injurious/stereotypic score, mean (SD) | 1.9 (2.6) | 0.8 (1.2) | 1.1 (1.8) | 2.3 (3.2) | 1.2 (2) | 1.5 (2.4) |
| NCBR teacher, self-isolated/ritualistic score, mean (SD) | 4.9 (3.7) | 4.1 (3.2) | 4.3 (3.3) | 7.7 (5.2) | 3.5 (2.6) | 4.6 (3.9) |
| NCBR teacher, irritable score, mean (SD) | 5.1 (4.4) | 5.2 (4.9) | 5.1 (4.7) | 7.2 (6.3) | 5.1 (4.9) | 5.7 (5.3) |
List of abbreviations
- ASD
- autism spectrum disorder
- BILD
- British Institute of Learning Disabilities
- CASUS
- Child and Adolescent Service Use Schedule
- CHU
- Child Health Utility
- CONSORT
- Consolidated Standards of Reporting Trials
- ELA
- Emotional Literacy Assessment
- ELSA
- Emotional Literacy Support Assistant
- MAMS
- Me and My School
- nasen
- National Association for Special Educational Needs
- NCBR
- Nisonger Child Behaviour Rating
- PAU
- practice as usual
- PPI
- patient and public involvement
- PSHE
- personal, social, health and economic education
- QALY
- quality-adjusted life-year
- RCT
- randomised controlled trial
- SDQ
- strengths and difficulties questionnaire
- SEND
- special educational needs and disabilities
- SWAT
- study within a trial
- UCO
- practice as usual-only comparator
- WLC
- waitlist control comparator
- ZF
- Zippy’s Friends
- ZF-SEND
- Zippy’s Friends for Special Educational Needs and Disabilities