
Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 09/3005/12. The contractual start date was in March 2011. The final report began editorial review in October 2012 and was accepted for publication in January 2013. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors' report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
none
Permissions
Copyright statement
© Queen's Printer and Controller of HMSO 2013. This work was produced by Shepherd et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Background and rationale for the research
The importance of teachers as health promoters
The role and importance of school health education has been recognised internationally for over 50 years (World Health Organization (WHO) 1951,1 1954,2 cited in Tones and Tilford3). The early focus on health education and hygiene grew over time to recognition of the need to consider the role of the whole school environment in relation to children's health behaviours. The concept of the health-promoting school emerged in the 1990s,4,5 in which all members of the school community (pupils, parents, staff) have the opportunity to contribute to a healthy school environment. During this time there has been a growing recognition of the importance of the school as a setting for health promotion, and the integral role of teachers as promoters of health. In many countries health-promoting schools programmes were established, including the National Healthy Schools Programme (NHSP) in England. 6
Within the school curriculum issues relating to health and well-being can be addressed in a number of ways, including through personal, social, health and economic (PSHE) education (formerly referred to as personal, social and health education – more recently the term economic has been incorporated). PSHE education is a planned, developmental programme of learning designed to help learners develop the knowledge, understanding and skills they need to manage their lives, now and in the future (as defined by the PSHE Association, see www.pshe-association.org.uk). PSHE education includes the concept of personal well-being, which draws together personal, social and health education, including sex education and the social and emotional aspects of learning (SEAL). Although PSHE education is a curriculum-based activity, it may extend to broader school-based activities. Because of its broad nature, health and well-being may also be addressed by the wider curriculum, including subjects such as science, physical education (PE), citizenship and the humanities. The extent to which PSHE education is provided in schools, and more broadly health and well-being is promoted, varies for a number of reasons. Yet teachers are seen to have an increasingly important role in the wider public health workforce. A number of policy strategies have underlined the importance of the school in child health in recent years.
Health and education policies in England
One of the most influential strategies in the area of child health, education and welfare in the last 10 years was Every Child Matters (ECM). 7 ECM stressed the importance of health and safety in all aspects of children's lives, including the school, and underpinned the qualified teacher status (QTS) standards for health.
The NHSP, set up in 1999, was a major initiative to improve health, raise pupil achievement, improve social inclusion and encourage closer working between health and education providers. The NHSP had four themes, including PSHE education, healthy eating, physical activity and emotional health and well-being. A target was set for at least 75% of schools to be accredited with National Healthy Schools status. The Children's Plan: Building Brighter Futures8 emphasised the pivotal role of schools in ensuring that children are healthy and safe. It introduced the concept of ‘extended services’ with its focus on improving access to school activities for disadvantaged children and young people to reduce attainment gaps. It also set a goal for all schools to work with the NHSP. In 2009 the NHSP began rolling out its enhancement model, a universal and targeted approach to pupil well-being offering schools the challenge of meeting specific needs-led healthier behaviour outcomes. Since April 2011, with the new coalition government, the organisation of the NHSP has changed to being a voluntary schools-led initiative rather than one that is centrally driven. The resources to support schools are now in the form of the Healthy Schools toolkit, which is available to schools through the Department for Education (DfE) website. 9
Effective health promotion with children and young people, particularly the early identification and prevention of health inequalities, was also a key aspect of the Choosing Health public health strategy, launched in 2004. 10 The overall aim of the strategy was to develop and build capacity for health improvement at all levels of the system, and to better equip the wider workforce to promote health by ensuring basic skills and knowledge for more people. Furthermore, Healthy Weight, Healthy Lives: a Cross-government Strategy for England11 stated that all schools should be healthy schools, and recognised the need for improvements in staff skills and capabilities.
The Healthy Child Programme from 5 to 19 Years Old, published by the Department of Health and the Department for Children, Schools and Families (DCSF; now the DfE) in 2009,12 set out the early intervention and prevention public health programme for children, young people and their families. It highlighted the need for schools to work together with parents, carers and health professionals and to have an understanding of how to promote health and well-being.
In 2009 the Macdonald review of PSHE education13 recommended that it should be a statutory subject in the curriculum and that all initial teacher training (ITT) courses should include some focus on PSHE throughout the school life. The Macdonald review also recommended that there should be, in time, ‘a cohort of specialist PSHE education teachers’ (p. 8). However, negotiations in April 2010 between the former UK Labour government and opposition parties on the Children, Schools and Families Bill resulted in the removal of the clauses to introduce PSHE education as a statutory subject in the national curriculum at primary and secondary level.
Since the election of the coalition government in 2010, the broad landscape and relationships both within and between education and health has changed. The government published its White Paper, The Importance of Teaching, in November 2010,14 which aims to set out a radical reform programme for the schools system, with schools freed from the constraints of central government direction. It also outlines how the quality of initial training and continuing professional development (CPD) will be transformed. The emphasis will be on more school- or employment-based training. Although the specific focus on health and well-being in this White Paper is less clear, it does acknowledge the fundamental role of school in a pupil's health and well-being:
Good schools play a vital role as promoters of health and wellbeing in the local community and have always had good pastoral systems. They understand well the connections between pupils’ physical and mental health, their safety, and their educational achievement.
2.48, p. 28
In 2011 the DfE published a review of the primary and secondary National Curriculum. 15 The review considered that schools should be given greater freedom over the curriculum, and that the National Curriculum should not absorb the overwhelming majority of teaching time in schools, allowing for a broad and balanced whole school curriculum. The report outlines the requirements for the National Curriculum, to be supported by programmes of study and attainment targets, and the Basic Curriculum, which describes statutory requirements in addition to those for the National Curriculum, which, although compulsory, can be locally shaped by schools. The Basic Curriculum includes sex education. In addition, schools can develop a Local Curriculum, which is non-statutory. The principles underpinning the report's recommendations demonstrate the perceived importance given to PSHE education within the Basic Curriculum. The principles acknowledge the importance of schools contributing to pupils' personal, social and emotional development as well as cognitive development and the crucial role of PSHE education, alongside subject knowledge, in supporting education and learning. Further, the report's overarching aims include:
2.16 The school curriculum should develop pupils' knowledge, understanding, skills and attitudes to satisfy economic, cultural, social, personal and environmental goals.
4. Support personal development and empowerment so that each pupil is able to develop as a healthy, balanced and self-confident individual and fulfil their educational potential.
p. 16
It is suggested that aspects of PSHE education should be included in the Basic Curriculum, and the report welcomed the DfE's internal review of PSHE education. The report also noted that it is important that PSHE education is provided in all stages of education.
The White Paper for public health, Healthy Lives, Healthy People, published in November 2010,16 set out the proposed substantial changes to the public health system in England. It is proposed that joint commissioning of health services will be carried out by local authorities in conjunction with a new body, Public Health England, and the current directors of public health will be employed within local authorities. Health and Wellbeing Boards are being set up in local authorities, comprising local authority directors of public health, social services, children's services, members of local clinical commissioning groups and elected local representatives. The boards will have strategic influence over commissioning decisions across health, public health and social care, with the emphasis on integrated services. These proposed changes will no doubt have a major impact on the way that public health and health-promotion activities are managed, and implications for the support for improvement of health education in schools. The focus will be on local commissioning of services to meet the needs identified in the Joint Strategic Needs Assessment (JSNA) and the Joint Health and Wellbeing Strategy (JWBS). However, although education is mentioned as being represented on the board, there are outstanding questions about how much of the children's agenda the board will cover, and currently little indication of what the relationship will be between schools (maintained or other) and their Health and Wellbeing Board.
Local authorities, through the Health and Wellbeing Board and direct commissioning of public health services, will be held accountable for the delivery of public health outcomes. 17 There are two main public health outcomes: increased healthy life expectancy; and reduced differences in life expectancy and healthy life expectancy between communities. There are four domains (e.g. improving the wider determinants of health, health improvement), each with detailed indicators. Some of these indicators are relevant to children's health and schools (e.g. school readiness, pupil absence, behaviour).
It is unclear how relationships will be sustained across the diversity of types of schools (education authority, academy, free, etc.) and with the Health and Wellbeing Boards and local public health services. The experience of trainee teachers will also vary considerably according to the type of school and locality. As a driver, however, the government's Public Health Outcomes Framework17 – which states the overarching aims of the reformed public health system in England for 2013–16 – may provide some support for the continued emphasis on PSHE education and health-promoting schools. Further, the lack of centralised guidance and direction on healthy schools' implementation policies places more responsibility on teachers and schools to have the skills and knowledge to formulate and deliver their local responses to this agenda.
Organisation of teacher training in England
Initial teacher training
Initial teacher training in England is currently predominantly provided by higher education institutions (HEIs) at undergraduate (e.g. Bachelor of Education, BEd) or postgraduate (e.g. Postgraduate Certificate in Education, PGCE) level. Some postgraduates choose school-centred initial teacher training (SCITT) courses, which provide a greater degree of practice-based learning, while allowing them to retain their student status. An alternative route is through employment-based initial teacher training (EBITT) whereby trainees are employed by schools and train through the Graduate Teacher Programme (GTP) or the Registered Teacher Programme (RTP). Teacher training is funded by the Teaching Agency (part of the DfE and formerly the Training and Development Agency, TDA), but additional health content may be funded from other agencies. Until September 2012, to qualify as a teacher all trainees had to meet QTS standards. 18 The standards specified 33 competencies that teachers need to attain, categorised as professional attributes, professional knowledge and understanding, and professional skills. Standard 21 related specifically to health and well-being, stating that teachers need to know about frameworks and policies around safeguarding and children and young people's health and wellbeing, and how to identify and support pupils' experiencing educational or personal difficulties, including when to refer to other professionals.
New teachers' standards were launched in September 2012, replacing the QTS. 19 Teacher training providers will need to ensure that their programmes are designed and delivered in such a way as to allow all trainees to meet these standards. Newly qualified teachers (NQTs) will also be assessed against the standards at the end of their induction period of employment. Unlike the QTS standards, the new standards do not make explicit reference to health, aside from mentioning the need to create a safe environment and to contribute to the wider life and ethos of the school. Health will be regarded as implicit throughout the standards, as exemplified in phrases such as ‘communicate effectively with parents with regard to pupils' achievements and wellbeing’ (p. 9) and ‘having regard for the need to safeguard pupils' wellbeing’ (p. 10).
A new framework for school inspection came into force in 2012. 20 Again, there is less explicit mention of health but the Office for Standards in Education, Children's Services and Skills (OFSTED) will be considering fundamental aspects such as the behaviour and safety of pupils at the school, including pupils' ability to assess and manage risk appropriately and to keep themselves safe; and the spiritual, moral, social and cultural development of pupils at the school.
The structure of ITT in England is likely to change in the future. In the Importance of Teaching14 the government states that it will reform ITT, to increase the proportion of time that trainees spend in the classroom, focusing on core teaching skills. It will also develop a national network of ‘teaching schools’, based on the model of teaching hospitals, to lead the training and professional development of teachers and head teachers, and increase the number of National and Local Leaders of Education – head teachers of excellent schools who commit to working to support other schools.
It is therefore a changing and challenging time for teacher training in England, and on the surface there appears to be a less explicit role for health and well-being within the framework for training and assessment. This raises questions about the extent to which teacher training providers will feel able to include issues relating to health within their curricula. However, it is also clear that, although less explicit, health and well-being delivered through PSHE education and the wider school ethos is understood to be fundamental to excellent education and improving pupil achievement. The move towards greater self-determination in schools will place more emphasis on teachers and other school staff having the appropriate knowledge and skills, and therefore understanding more about how teachers are currently being trained and how ITT providers are facing up to the future challenges is important. These recent changes to education and health policy are also likely to affect access to training and support around health for qualified teachers in terms of their professional development.
Continuing professional development
Qualified teachers develop their knowledge and skills as part of CPD. Within the context of health, CPD may address the provision of PSHE education or more specifically train teachers to deliver a specific health-promotion intervention (e.g. around a drugs and alcohol initiative, or a sexual health campaign). Training may also encapsulate broader school-wide health-promotion interventions (‘whole-school approaches’) involving others involved in schools with a responsibility for health (e.g. learning assistants, support staff, governors). A variety of people may train teachers around health issues, including Healthy Schools co-ordinators, health professionals (e.g. health-promotion practitioners, health advisers), youth workers, psychologists and educational professionals. Training can be provided in-service (i.e. organised by the school) or externally organised by the organisations responsible for developing specific interventions or teaching methods.
The evidence base for teacher training and health
Early attempts to assess the effectiveness of school health interventions cited a number of effective approaches, but also indicated factors that were not effective and should be discouraged. Amongst other factors, failed programmes were shown to have had little or no investment in teacher training and provision of support resources. 21 These largely related to school-based, mostly intervention-specific training programmes; even less has been written about the initial training of teachers. WHO issued a call for action for schools globally to help them respond more effectively to health, education and development opportunities. Amongst many evidence-based actions, it called for investment in capacity to support professional development programmes to build the capabilities of teachers and health professionals to plan, implement and evaluate school health initiatives. 22
To explore these issues further, ITT and CPD will be considered separately.
Initial teacher training
Since the mid-1980s, research in England and Wales has indicated that teacher education and training in health-related areas is poor and has mostly relied on in-service training, which teachers may or may not receive. 23 Progress on including knowledge and skills regarding health and well-being in the initial training and education of teachers entering the profession has been slow, both in England and elsewhere. 24 There are unanswered questions about the provision and quality of health promotion within ITT courses across England. Our previous survey research has shown that coverage of health and well-being in teacher training curricula is limited and variable in the South East of England region. 25 Using a questionnaire we surveyed 35 organisations offering ITT in 2007 (10 HEIs, 25 employment-based schemes). Fifteen (43%) organisations responded, representing 50% of the total number of trainees in the region (83% from HEIs and 17% from employment-based schemes). The results demonstrated the enormous variability of teacher training provision across the region and the lack of any consistent approach to educating student teachers about their potential roles in promoting children's health. Most organisations were found to be incorporating ECM supported by the NHSP and other external specialists, but to varying extents. Provision of information about the NHSP was also extremely variable, from nothing at all to inclusion in PSHE education or emotional health and well-being. Employment-based training organisations (i.e. EBITT providers) were more likely to have connections with the NHSP. Reasons for lack of inclusion of health issues included insufficient time in a busy curriculum and the extent to which placement schools were actively involved in the NHSP.
The extreme variability found in our survey in the amount of time allocated to health topics demonstrates a lack of consistency in interpretation of the requirements of training, leading to very little provision in many institutions compared with careful attention and innovative good practice in a few others. The survey was limited by the relatively low response rates, its timing (just before a holiday period), the length of the questionnaire (on reflection relatively lengthy) and its confinement to the South East of England. There remains, therefore, a need to assess the adequacy of provision of health initiatives within ITT curricula across England, with a sampling strategy that ensures representation from different types of providers (HEI based, employment based) and types of course (early years, primary, secondary). Such a survey will illuminate variations in practice, identify barriers and facilitators and generate recommendations for effective training and models of effective practice suitable for further evaluation.
More recently there has been further interest in researching ITT, for example considering student teachers' ways of experiencing health education as a school subject26 and guidance for teacher training for health education in France. 27
Continuing professional development and school-based health-promotion training
Personal, social, health and economic education
The 2009 Macdonald review13 suggested that there is wide variability in PSHE education conducted in both primary and secondary schools across England, in terms of content, delivery models and approaches. The DfE commissioned a mapping study of PSHE education in England to determine the prevalent models of delivery and their effectiveness for children and young people. The study, by Formby and colleagues,28 was based on a nationally representative survey of schools in England (with response rates of 22% and 34% for primary and secondary schools respectively) as well as a follow-up case study of 14 schools and sought to address a number of research questions. Three of the questions are particularly pertinent to this report: (1) what are the current skills and qualification levels of PSHE educators? (2) how do staff perceive the professional development that is currently available? and (3) what sources of support are teachers currently using? The survey found that the most effective PSHE education was delivered by well-qualified staff. However, investigation of the skills and qualifications of the PSHE workforce revealed that the vast majority of teaching staff had no PSHE education qualifications, accreditation or CPD training. Only 28% of primary schools had at least one member of staff (including nurses) with the national CPD qualification, largely because it was not easy for primary teachers to be released or funded for PSHE education CPD. The proportion was higher in secondary schools, with 45% of those surveyed reporting that one or more members of staff had the national CPD qualification. Taken as an average across the samples, these figures equate to only 3% and 5% of PSHE education staff in primary and secondary schools, respectively, holding the national qualification.
Although many staff reported good knowledge of available training opportunities, access to training and funding difficulties were rated as perceived barriers to PSHE training, particularly for secondary schools, with over half of schools reporting difficulties in releasing staff and funding them for PSHE education training. Non-accredited CPD PSHE education provided by local authorities was highly valued by primary school staff, particularly in areas where teachers were often lacking in confidence and skills [e.g. sex and relationships education (SRE) and drugs, alcohol and tobacco education]. However, for secondary school teachers, PSHE education was viewed as a low overall priority compared with training for core subjects, even in those schools in which PSHE education had a positive status.
School-based health-promotion training
There is a sizable international evidence base on the effectiveness of school-based health-promotion interventions worldwide. Stewart-Brown29 conducted a synthesis of systematic reviews of school-based health-promotion interventions and health-promoting schools [an update of the previous National Institute for Health Research (NIHR) Health Technology Assessment (HTA) programme-funded systematic review published in 199930]. Fifteen systematic reviews were included, between them comprising approximately 750 primary evaluations of school-based interventions on a variety of health issues (e.g. mental health, healthy eating, physical activity), although not all of these interventions would have been delivered by teachers.
Little has been published, at least in terms of evidence synthesis, on the effectiveness of training teachers to deliver such initiatives (either ITT or CPD), and of the barriers to and facilitators of effective teacher training and their subsequent provision of health promotion. There do not appear to be any published systematic reviews of the evidence for the effectiveness of programmes to train teachers to promote health in schools. However, some relevant primary evaluations have been published in this area evaluating teacher training to deliver specific health-promotion interventions. For example, outcome evaluations compared the effectiveness of different types of teacher training (e.g. video instruction compared with workshop training) on a range of teacher outcomes (e.g. implementation, morale, motivation, self-efficacy). 31,32
In terms of theory, the interventions have been based on a range of well-known theories of education, health and health-related behaviour change such as social learning theory, social cognitive theory, the theory of reasoned action/planned behaviour, diffusion of innovations theory and the social–ecological model. 33 Many of these theories predict the necessary mediators of effective health-related behaviour change. The training that the teachers received was designed to equip them with the knowledge, motivation, confidence and skills to facilitate, in turn, desirable improvements in mediators of pupils' behaviour, such as increasing their knowledge, their self-efficacy and their behavioural skills. For example, Kealey and colleagues,34 who evaluated the Hutchinson Smoking Prevention Project in the USA, conceptualised teacher training as a behaviour change process with a strong emphasis on teacher motivation to facilitate the intended behaviour (i.e. the teacher's effective implementation of the curriculum). Theories such as those mentioned above form part of the conceptual framework for this project.
All studies provided evaluation data on the implementation of the intervention, with varying detail given on the training received by teachers. One of the studies that provided detailed information on training was a Scottish trial of a sexual health education initiative called SHARE (Sexual Health and Relationships – Safe, Happy and Responsible). 35 An extensive process evaluation was carried out, comprising observation, questionnaires and interviews with teachers. The teachers reported that they valued and enjoyed the training very much and felt more confident to teach sex education, but a number of barriers to effective delivery of the curriculum emerged, including a lack of understanding by the teachers of the guiding theory of behaviour change and a lack of confidence to teach behaviour change skills (the key element of the intervention).
These findings, although perhaps not necessarily representative of the wider literature, suggest that additional training and support may be necessary to enable teachers to facilitate health-related behaviour change, an outcome that is considered a key marker of effectiveness by many decision-makers. 3 For example, they may require professional input from health educators to deliver skills-building exercises in the classroom, which may be essential for encouraging healthy behaviours. This will have resource and, therefore, cost implications and it underlines the need for a systematic review of the evidence to identify common overarching barriers to and facilitators of effective and efficient teacher training across a range of health topics. Recommendations would be made for health and education professionals, policy-makers and researchers to ensure that teachers fulfil their potential in promoting health and well-being in schools, ensuring that children adopt and maintain healthy lifestyles into adulthood.
Research objectives
The research questions that this research sought to answer were:
-
In what ways does teacher training prepare teachers to promote health and well-being in schools?
-
How effective are interventions to train and support teachers in health?
-
What are the barriers to, and facilitators of, effective training and delivery?
To answer these questions the project has two research objectives:
-
to conduct a survey, using quantitative and qualitative methods, of a sample of ITT providers in England to assess how health and well-being is covered in teacher training
-
to conduct a systematic review of the effectiveness of and barriers to facilitators of teacher training around health and well-being.
This project adopts a broad concept of health and well-being, based on the definition of health used by the WHO as ‘a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity’. 36 Similarly, a broad perspective on the promotion of health is taken, adopting the definition of Green and Kreuter:37 ‘any combination of educational, organisational, economic and environmental support for conditions of living and behaviour of individuals, groups or communities conducive to health’ (p. 2).
Chapter 2 Methods overview
This chapter provides an overview of the design of the project and the methods used. Further detail on the methods used in each of the components of the project can be found in subsequent chapters of this report.
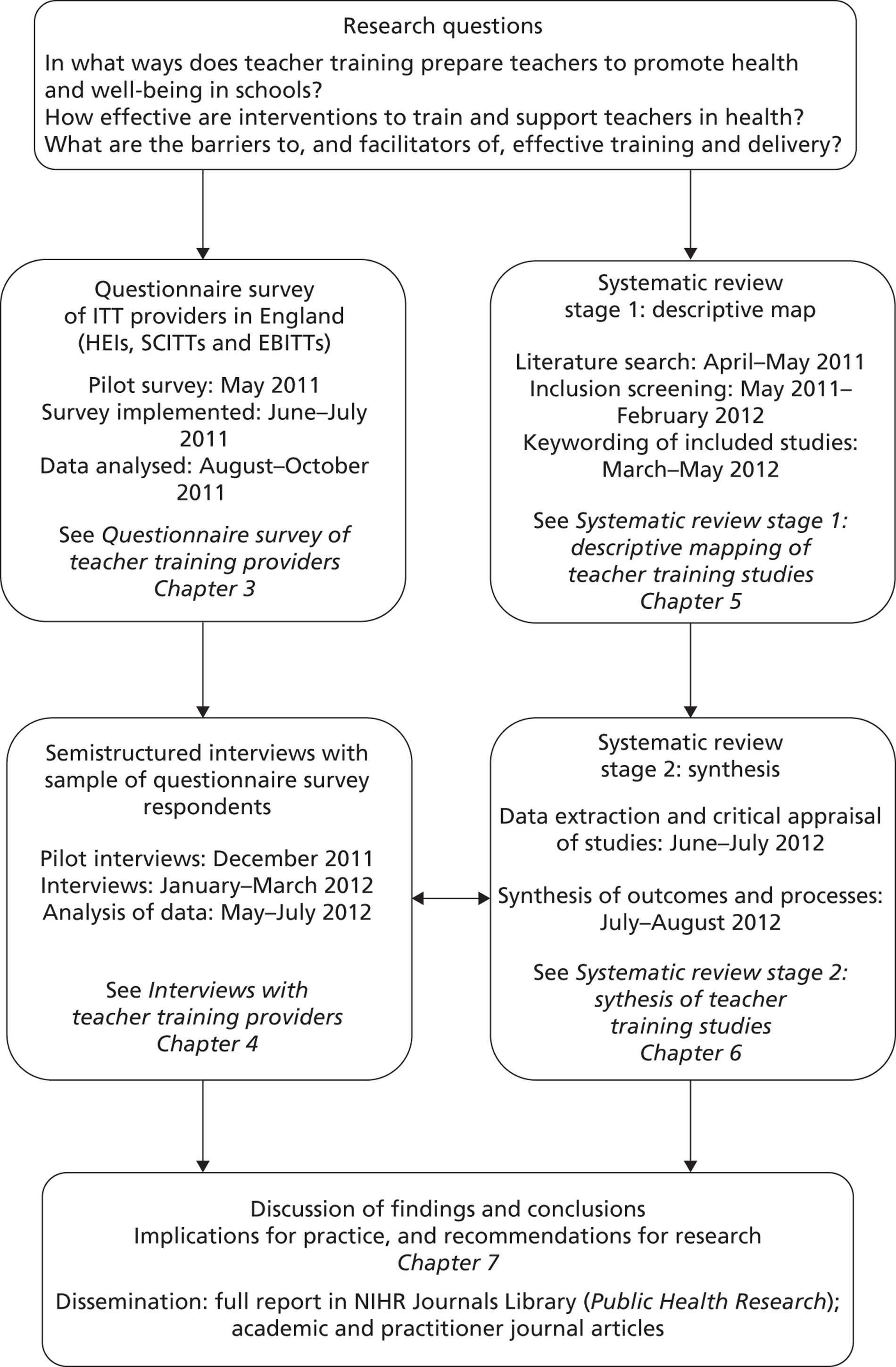
The project comprised two main components: a questionnaire and interview survey of teacher training providers and a two-stage systematic review (descriptive map of study characteristics, followed by an in-depth synthesis of prioritised studies). Figure 1 illustrates the design of the project, showing the stages of the research, including the dates that they were conducted. The two components of the project were designed to complement each other in answering the three research questions. For example, to answer ‘In what ways does teacher training prepare teachers to promote health and well-being in schools?’, the questionnaires and interviews with course managers were able to describe current practice in English ITT institutions. The systematic review was also designed to shed light on this through a descriptive mapping of the characteristics of international research studies evaluating teacher training around health and well-being. The in-depth synthesis of studies included in the systematic review was able to assess ‘How effective are interventions to train and support teachers in health’ through examining the outcomes of the studies (e.g. for teachers and pupils). The questionnaires and the interviews were also able to illuminate effectiveness through course managers' perspectives on the success of their own training in preparing teachers to promote health. Finally, the barriers to and facilitators of effective training and delivery could be assessed from the questionnaires and interviews with the course managers by asking them to discuss the factors that they consider have helped or limited their coverage of health within their training. Barriers and facilitators could also be identified from the studies included in the in-depth synthesis of the systematic review, in terms of process evaluation of training. Chapter 7 of this report discusses the findings of the survey and the systematic review together in relation to each of the three research questions.
Although the two components of the research ran broadly in parallel (see Figure 1), a reciprocal relationship between the two was intended. For example, the findings of the in-depth synthesis of the systematic review were interpreted in terms of the emerging analytical themes from the analysis of the interviews with course managers. The chapters of this report are therefore sequenced to reflect the evolution of the project (i.e. the survey and interview findings followed by the systematic review results).
FIGURE 1.
Overview of the study design.
The protocol for the research was published on the NIHR Public Health Research programme website when the project commenced, and was also registered on the PROSPERO database (international prospective register of systematic reviews; www.crd.york.ac.uk/prospero) (see Appendix 1).
Chapter 3 Questionnaire survey of teacher training providers
Methods for the questionnaire survey of teacher training providers
Questionnaire development
The questionnaire was devised between April and May 2011 and was designed to cover a range of issues in keeping with the aims of the study (e.g. how health and well-being is covered in ITT courses, in terms of who provides training, topics, methods and assessment, and any barriers and facilitators). The questionnaire was based on the one used in our previous survey of ITT providers in the South East of England,25 although it underwent extensive adaptation with the addition of a number of questions (e.g. asking respondents to describe how they think current policy changes in education will affect their courses). A range of question types was used including closed-ended questions, questions with pre-coded response categories, Likert scales and open-ended questions. The draft questionnaire underwent a number of revisions with input from all team members and the project's advisory group, who suggested minor changes. It was intended that the questionnaire would take around 10 minutes to complete and would be administered online via the internet using specialist survey software (SelectSurvey.net, version NETv4.068.002; Classapps, Kansas City, MO, USA).
Once internal revision was complete, the questionnaire was piloted in May 2011 with a sample of one HEI, one EBITT provider and one SCITT provider, randomly selected (using a random number generator in a spreadsheet) from each of the nine English regions (formerly known as the Government Offices for the Regions) (see following section for more detail on sampling). The purpose of piloting was to assess the effectiveness of the questionnaire itself in eliciting relevant information, as well as the process of recruiting, sampling and questionnaire administration. In the first wave of sampling the EBITT and SCITT providers were sent the questionnaire by e-mail, and the head of the education department of each HEI was contacted to introduce the study and to ask for the names and contact details of their course managers. In the second wave the course managers whom the HEI heads of department had named in their institution were sent the questionnaire by e-mail.
The response rate to the pilot was 37% (13/35 course managers surveyed). The data elicited from the questionnaires were variable in terms of the level of detail of the responses to the open-ended questions and the proportion of missing data. Following some minor revisions (e.g. removal of less relevant questions to shorten the questionnaire, some reordering of questions) we considered the questionnaire to be of suitable standard for full implementation. The final version is in Appendix 2.
Sampling
Sampling and recruitment of ITT providers began in May 2011 ready for a planned June survey launch. Our sampling frame was the 208 ITT providers in England listed on the TDA (now the Teaching Agency) website (as of May 2011). This included 74 HEIs, 57 SCITT providers and 77 EBITT providers. It was considered that surveying all providers would not be feasible in terms of time and resources (except for SCITT providers; see later in this section) and so a sampling approach was undertaken.
Initial teacher training courses vary in their duration from a 1-year PGCE to 3- or 4-year undergraduate degrees (BA/BSc with QTS or BEd). There are also variations in the level of education that they specialise in (e.g. primary, secondary, key stage 2/3) (Table 1).
| Type of provider and level of education | Undergraduate | Postgraduate |
|---|---|---|
| HEI (e.g. university) | ||
| Early years | BA/BSc, BEd, RTP | PGCE |
| Primary | BA/BSc, BEd, RTP | PGCE, GTP, OTTP |
| Secondary | BA/BSc, BEd, RTP | PGCE, GTP, OTTP |
| Key stage 2/3 | BA/BSc, BEd, RTP | PGCE |
| Post-compulsory | BA/BSc, BEd, RTP | PGCE |
| SCITT | ||
| Primary | – | PGCE (with QTS)/QTS |
| Secondary | – | PGCE (with QTS)/QTS |
| EBITT | ||
| Primary | RTP | GTP, OTTP |
| Secondary | RTP | GTP, OTTP |
School-centred initial teacher training programmes are designed and delivered by groups of neighbouring schools and colleges. SCITT courses lead to QTS, and some will also lead to a PGCE validated by a HEI. EBITT courses are run by consortia of schools, colleges and local authorities (although note that some universities also offer EBITT courses). On the GTP, graduates can attain QTS while training and working in a paid teaching role. The GTP normally takes between 3 months and 1 school year, working full-time, to complete. The RTP combines work-based teacher training and academic study, allowing non-graduates with some experience of higher education to complete their degree and qualify as a teacher at the same time. This course normally takes 2 years to complete. The Overseas Teacher Training Programme (OTTP) is for qualified teachers from overseas who wish to attain qualified teaching status in England. Courses can last up to 1 year. Key stage 2/3 courses cover children in the age range 8–11 years (key stage 2) and 11–14 years (key stage 3). Early years generally covers the 3–7 years age group.
The ITT providers in England were classified according to the nine English regions. Table 2 shows that the number of providers in each region varied from 14 (North East) to 36 (Eastern). We sampled ITT providers within each of the regions to ensure that all areas of England were represented, given that there may be geographical variations in teacher training practice in relation to health and well-being.
| Region | Type of provider | No. of providers |
|---|---|---|
| Eastern | HEI | 6 |
| SCITT | 15 | |
| EBITT | 15 | |
| Total | 36 | |
| East Midlands | HEI | 7 |
| SCITT | 4 | |
| EBITT | 8 | |
| Total | 19 | |
| London | HEI | 13 |
| SCITT | 7 | |
| EBITT | 12 | |
| Total | 32 | |
| North East | HEI | 4 |
| SCITT | 6 | |
| EBITT | 4 | |
| Total | 14 | |
| North West | HEI | 7 |
| SCITT | 1 | |
| EBITT | 6 | |
| Total | 14 | |
| South East | HEI | 10 |
| SCITT | 5 | |
| EBITT | 14 | |
| Total | 29 | |
| South West | HEI | 8 |
| SCITT | 13 | |
| EBITT | 5 | |
| Total | 26 | |
| West Midlands | HEI | 9 |
| SCITT | 5 | |
| EBITT | 7 | |
| Total | 21 | |
| Yorkshire and the Humber | HEI | 10 |
| SCITT | 1 | |
| EBITT | 6 | |
| Total | 17 |
Our sampling strategy varied according to the type of provider in each region, as follows:
-
Random sample of 50% of each of the HEIs within each region. Our initial course mapping showed that the number and range of courses on offer varied considerably by HEI. For example, in the South East region of England, the University of Portsmouth offered (at that time) just two courses, both at postgraduate level. In contrast, Canterbury Christchurch University offered 10 courses covering undergraduate and postgraduate level. To obtain balance we took a random sample of 50% of HEIs classified as offering a ‘low’ number of courses and 50% of those classified as offering a ‘high’ number of courses (low and high to be determined by the average number of courses per provider in a region). We identified the number of courses offered by a HEI through a systematic mapping of each institution's website, with details logged in a spreadsheet database. A questionnaire was to be sent to each QTS-bearing course offered by the sampled HEIs, resulting in sampling of approximately 50–60% of available courses in each region.
-
A random sample of 50% of EBITT providers in each region. As EBITT providers generally offer fewer courses we did not classify them as high or low. (Note: HEI-run EBITT courses, such as the GTP, were sampled as above in 1.)
-
Survey of all SCITT providers. This was considered feasible as there are relatively fewer of them and they offer only a limited range of courses (e.g. one to two courses per SCITT provider).
Recruitment
Recruitment followed a similar approach to that described in the previous section for the pilot questionnaire. For HEIs we first e-mailed the head of the education department in each institution to introduce the project and to ask them to complete a short structured online proforma providing us with the name and contact details of the tutor of each of their ITT courses. This was primarily to ensure that we had accurate details of all courses, as the institutions' websites did not always appear to be up to date. It was also a courtesy so that the departmental head was aware that staff members were being surveyed, and it was anticipated that their support might potentially increase the response rate. A reminder e-mail was sent 2 weeks after the initial e-mail where a response had not been received. If a response was not received following the reminder we obtained the details that we required from the institution's website, supplemented when necessary with a telephone call to the department administrator to clarify which courses were offered and/or the contact details of the course managers.
When a response had been received from the relevant departmental head we e-mailed the course managers whose details had been provided, asking them to complete the online questionnaire. The e-mail briefly specified the purpose of the study and why they had been chosen, and provided a guarantee that their responses would remain confidential and anonymised in the dissemination of the project. Again, after 2 weeks, if no response had been received an e-mail reminder was sent. If no response was received following the reminder they were logged as a non-responder in our database.
We contacted the course managers directly in each randomly sampled EBITT provider and in each SCITT provider, again by e-mail, and asked them to complete an online questionnaire using the same process as that for the HEI course managers. They were contacted at the same time as the heads of department in the HEIs. In all cases consent to participate in the study was assumed by the response to the questionnaire.
To enhance response rates the course managers were offered a monetary incentive. All responders were entered into a prize draw to win an Amazon gift voucher. The first prize was a £50 voucher and the second a £30 voucher.
Ethical approval for the survey and the subsequent interviews (see Chapter 4) was provided by the University of Southampton Faculty of Medicine Ethics Committee (ethics approval number: SOMSEC080.10). Insurance for the study was provided by the University of Southampton, who acted as research sponsor.
Data analysis
Data were downloaded from the online questionnaire tool (SelectSurvey.net) directly into a spreadsheet. The quantitative questionnaire data were analysed using standard descriptive statistics (e.g. counts and percentages). The data were tabulated and for some questions transformed graphically in bar charts. The qualitative data elicited from the open-ended questions were analysed using a basic content analysis approach, with similar responses grouped together in summary categories.
Results of the questionnaire survey of teacher training providers
Response rates
Table 3 shows the survey response rates stratified according to type of teacher training institution provider sampled and English region. The overall response rate was 34%. As the table shows, the percentage response rate varied by type of provider and by region. The regions with the highest percentage responses were Yorkshire and the Humber (56%), followed jointly by the North East (42%) and the South West (42%). No responses were received from any of the providers sampled in the West Midlands region. The highest rate of response was from the SCITT providers, followed by the HEI course managers and then the EBITT providers.
| Region | HEI (first contact), n/N (%) | HEI (course managers), n/N (%) | SCITT, n/N (%) | EBITT, n/N (%) | Total (not including first contact), n/N (%) |
|---|---|---|---|---|---|
| Eastern | 1/3 (33) | 3/12 (25) | 6/14 (43) | 3/8 (38) | 12/34 (35) |
| East Midlands | 0/3 (0) | 4/12 (33) | 0/3 (0) | 0/4 (0) | 4/19 (21) |
| London | 2/6 (33) | 6/13 (46) | 3/6 (50) | 0/3 (0) | 9/22 (41) |
| North East | 0/3 (0) | 2/12 (17) | 4/5 (80) | 2/2 (100) | 8/19 (42) |
| North West | 0/0 (0) | 1/10 (10) | 1/1 (100) | 2/3 (66) | 4/14 (29) |
| South East | 1/6 (17) | 13/33 (39) | 0/3 (0) | 1/5 (20) | 14/41 (34) |
| South West | 2/4 (50) | 7/17 (41) | 6/12 (50) | 1/4 (25) | 14/33 (42) |
| West Midlands | 1/5 (20) | 0/14 (0) | 0/4 (0) | 0/4 (0) | 0/22 (0) |
| Yorkshire and the Humber | 1/5 (20) | 7/12 (58) | 1/1 (100) | 1/3 (33) | 9/16 (56) |
| Total | 8/35 (23) | 43/135 (32) | 21/49 (43) | 10/36 (28) | 74/220 (34) |
The respondents were asked if they would be willing to be contacted to take part in the follow-up interviews planned for this project (see Chapter 4). Of the 38 HEI respondents who answered this question, 19 (50%) agreed to be contacted; of the 16 SCITT respondents who answered this question, seven (44%) agreed to be contacted; and of the nine EBITT respondents who answered this question, four (44%) agreed to be contacted. The total number of survey respondents who agreed to be contacted was therefore 30.
Details of the respondents
Amongst the HEI respondents, when asked to describe their role, all reported that they managed, led or directed one or more teacher training courses. In some cases this was in addition to other duties such as senior management, assuring the quality of teaching across their institution, developing appropriate CPD and training for staff and conducting research. In some cases more than one person from each HEI sampled responded to the questionnaire. This was a result of the sampling strategy in which providers were sampled at random and all of their course managers were sent questionnaires. Of the SCITT and EBITT respondents, all described themselves as having responsibility for one or more teacher training courses. In addition, some of them also had responsibility for overall management of the organisation itself.
Respondents were asked to tick the ITT course(s) that they managed. Of the 43 HEI course managers who responded, 22 (51%) reported managing one course, 14 (33%) managed two courses, six (14%) managed three courses and one (2%) managed four courses. Between them they managed a total of 72 courses.
Figure 2 displays the number of HEI respondents who managed each type of course.
FIGURE 2.
Types of courses that respondents were responsible for managing: HEIs (n = 43 respondents).
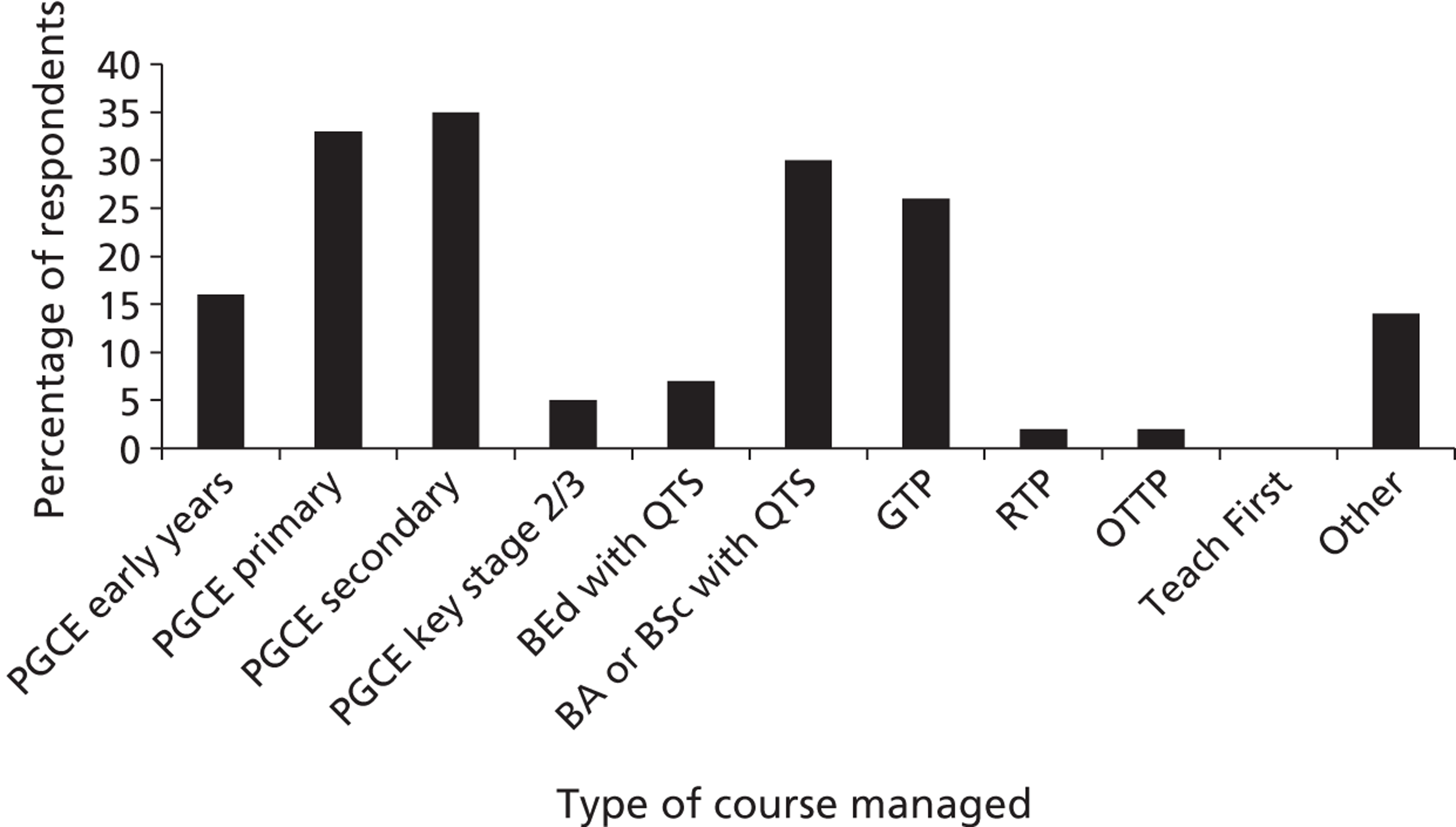
The most commonly managed course was the PGCE (secondary closely followed by primary). At undergraduate level the most commonly managed course was the BA or BSc. Courses classified as ‘other’ included a Training Grant Only Programme and Assessment-Only Route to QTS.
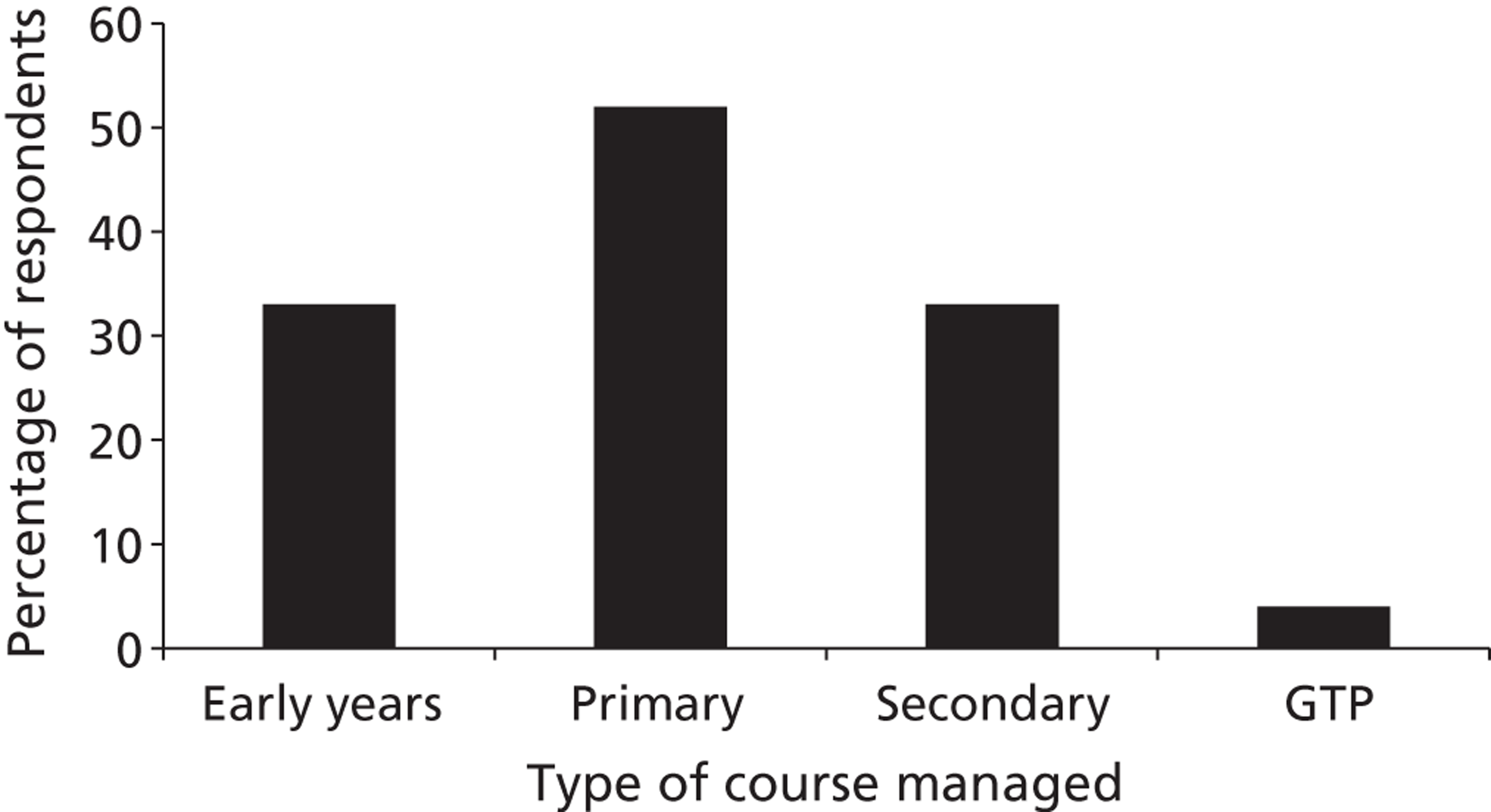
Of the 21 SCITT respondents, 17 (81%) reported managing just one course, three (14%) managed two courses and one (5%) managed three courses. Between them they managed a total of 26 courses. Figure 3 shows the numbers of respondents who managed each type of course. The most common course was the primary course, followed jointly by the early years and secondary courses. One respondent mentioned managing a GTP course under ‘other’. In many cases the respondents mentioned that they managed courses that had PGCE status.
FIGURE 3.
Types of courses that respondents were responsible for managing: SCITTs (n = 21 respondents).
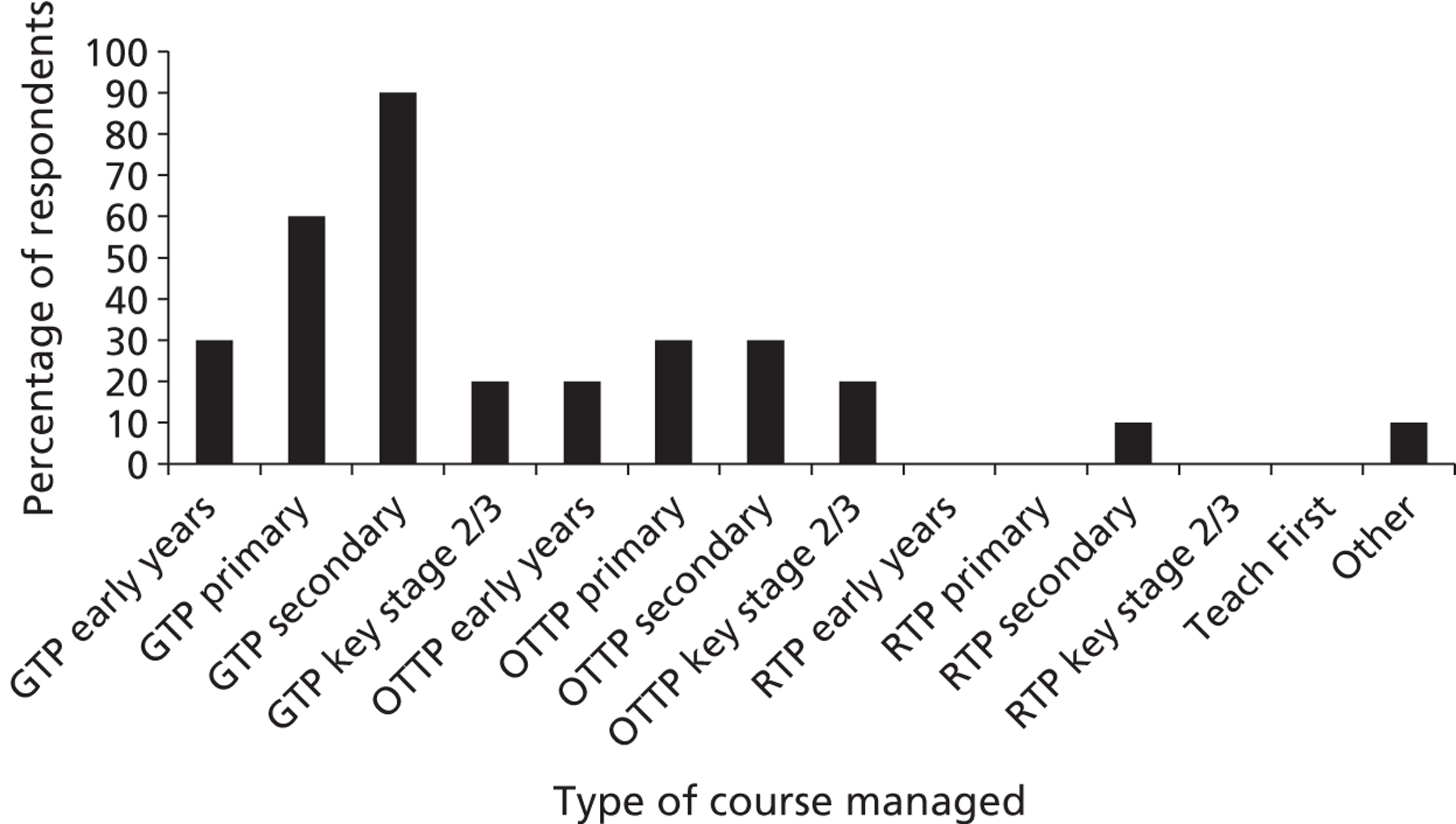
Of the 10 EBITT respondents, two (20%) reported managing one course, five (50%) managed two courses, one (10%) managed four courses and two (20%) managed eight courses. Between them they managed 32 courses. Respondents most commonly managed GTP courses, of which the secondary level was most common, followed by the primary level (Figure 4). They less commonly managed OTTP courses, and only one respondent reported managing a RTP course.
Respondents were asked to specify the numbers of students enrolled on their courses during the 2010–11 year. Table 4 provides the total numbers of students with means and ranges enrolled on courses by respondents in HEIs. In general, more students were enrolled on primary and secondary courses than on early years or key stage 2/3 courses. At postgraduate level, more students were enrolled on primary than on secondary PGCE courses. At undergraduate level, more students were enrolled on BA than on BEd courses, with BSc enrolees in a minority. In terms of employment-based training run by HEIs, students were reported as being enrolled on GTP courses only.
FIGURE 4.
Types of courses that respondents were responsible for managing: EBITTs (n = 10 respondents).
There was considerable variation in the numbers of students enrolled on certain courses. For example, amongst primary BA courses, the lowest number of enrolled students reported was 30, with the highest at 800. For primary and secondary PGCE courses, the lowest number was < 20 and the highest number was > 200.
Table 5 provides the total numbers of students with means and ranges enrolled on courses by respondents in EBITT providers. More students were enrolled on primary and secondary courses than on early years courses and there were none enrolled on key stage 2/3 courses, even though two of the respondents had reported that they had responsibility for courses at this level (see Figure 4). The GTP was the most commonly enrolled EBITT course, followed by the OTTP, although the number of enrolees on the latter was very low. The total number of GTP enrolees was lower at the primary level in the EBITT courses than it was for HEI primary-level GTP courses (see Table 4); however, at the secondary level the opposite was true.
| Course | Early years | Primary | Secondary | Key stage 2/3 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Min. | Max. | Total | Mean | Min. | Max. | Total | Mean | Min. | Max. | Total | Mean | Min. | Max. | Total | |
| PGCE | 49.3 | 12 | 107 | 493 | 115 | 16 | 225 | 1961 | 101 | 10 | 204 | 1614 | 46.5 | 30 | 63 | 93 |
| BEd | 80 | N/A | N/A | 80 | 292 | 214 | 356 | 1170 | 12 | N/A | N/A | 12 | – | – | – | – |
| BA | 112 | 52 | 280 | 560 | 256 | 30 | 800 | 2049 | 255 | 25 | 500 | 1021 | 40 | N/A | N/A | 40 |
| BSc | – | – | – | – | – | – | – | – | 210 | N/A | N/A | 210 | – | – | – | – |
| GTP | 6 | 4 | 8 | 12 | 36 | 8 | 97 | 181 | 21 | 3 | 47 | 147 | – | – | – | – |
| Course | Early years | Primary | Secondary | Key stage 2/3 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Min. | Max. | Total | Mean | Min. | Max. | Total | Mean | Min. | Max. | Total | Mean | Min. | Max. | Total | |
| GTP | 3 | 1 | 4 | 8 | 14 | 7 | 24 | 72 | 31 | 13 | 87 | 248 | – | – | – | – |
| OTTP | – | – | – | – | 2 | 1 | 3 | 4 | 2 | 1 | 3 | 4 | – | – | – | – |
| RTP | – | – | – | – | – | – | – | – | 1 | N/A | N/A | 1 | – | – | – | – |
Table 6 provides the total numbers of students with means and ranges enrolled on courses by respondents in SCITTs. The SCITT course with the largest total number of students was the primary-level course, followed by secondary and then early years courses.
| Course | Mean | Min. | Max. | Total |
|---|---|---|---|---|
| Early years | 22 | 9 | 35 | 153 |
| Primary | 34 | 15 | 78 | 372 |
| Secondary | 34 | 22 | 61 | 236 |
| Key stage 2/3 | – | – | – | – |
| Other | 10 | 10 | 10 | 10 |
Health and well-being topics covered
The respondents were asked to indicate which specific health and well-being topics were covered by their courses. This question was answered by 40 out of the 43 HEI respondents, 19 of 21 SCITT respondents and 9 out of 10 EBITT respondents. Table 7 reports the frequency with which topics were covered by the three types of ITT provider and the overall (ranked) totals. Coverage of topics appeared to be generally similar across the different providers. ECM and child protection were covered by all providers. Comments made in response to open-ended questions illuminated the perceived importance of topics such as ECM, with one respondent stating that it is a:
Strong theme running through all professional . . . modules.
HEI 5
There was also an indication of its changing status:
ECM permeates the programme and was an important assignment (now shifting with ECM no longer core government policy, but principles of ECM remain).
HEI 28
Other commonly covered topics (covered by at least 90% of providers) were SEAL/emotional health, antibullying and working with parents (e.g. seeking parental views on school health policies and initiatives). Some lifestyle-related topics such as healthy eating, SRE, drugs, alcohol and smoking received comparatively less attention. Topics were generally more often reported to have been covered during the college-based component of the course than during the school teaching placement, except for EBITT courses where topics were generally more often covered in the schools that the trainees were working in (data not shown). As discussed later in this report, course managers did not always have full knowledge of how health and well-being was covered in placement schools and so the frequency of topics covered in placement schools may be under-reported.
| Topic | Total (n = 68) | HEIs (n = 40) | SCITTs (n = 19) | EBITTs (n = 9) | ||||
|---|---|---|---|---|---|---|---|---|
| Covered, n (%) | Unsure/not reported as covered, n (%) | Covered, n (%) | Unsure/not reported as covered, n (%) | Covered, n (%) | Unsure/not reported as covered, n (%) | Covered, n (%) | Unsure/not reported as covered, n (%) | |
| ECM | 68 (100) | 0 | 40 (100) | 0 | 19 (100) | 0 | 9 (100) | 0 |
| Child protection | 68 (100) | 0 | 40 (100) | 0 | 19 (100) | 0 | 9 (100) | 0 |
| SEAL/emotional health | 67 (99) | 1 (1) | 39 (98) | 1 (3) | 19 (100) | 0 | 9 (100) | 0 |
| Antibullying | 66 (97) | 2 (3) | 38 (95) | 2 (5) | 19 (100) | 0 | 9 (100) | 0 |
| Working with parents | 65 (96) | 3 (4) | 38 (95) | 2 (5) | 18 (95) | 1 (5) | 9 (100) | 0 |
| Environment education | 55 (81) | 13 (19) | 33 (83) | 7 (18) | 16 (84) | 3 (16) | 6 (67) | 3 (33) |
| Physical activity | 55 (81) | 13 (19) | 33 (83) | 7 (18) | 15 (79) | 4 (21) | 7 (78) | 2 (22) |
| Healthy Schools | 51 (75) | 17 (25) | 29 (73) | 11 (28) | 14 (74) | 5 (26) | 8 (89) | 1 (11) |
| Healthy eating | 43 (63) | 25 (37) | 26 (65) | 14 (35) | 12 (63) | 7 (37) | 5 (56) | 4 (44) |
| SRE | 42 (62) | 26 (38) | 24 (60) | 16 (40) | 13 (68) | 6 (32) | 5 (56) | 4 (44) |
| Trainee teachers' health | 39 (57) | 29 (43) | 20 (50) | 20 (50) | 12 (63) | 7 (37) | 7 (78) | 2 (22) |
| Drugs education | 38 (56) | 30 (44) | 20 (50) | 20 (50) | 11 (58) | 8 (42) | 7 (78) | 2 (22) |
| Careers education | 36 (53) | 32 (47) | 21 (53) | 19 (48) | 10 (53) | 9 (47) | 5 (56) | 4 (44) |
| Alcohol education | 28 (41) | 40 (59) | 14 (35) | 26 (65) | 9 (47) | 10 (53) | 5 (56) | 4 (44) |
| Smoking prevention | 23 (34) | 45 (66) | 10 (25) | 30 (75) | 8 (42) | 11 (58) | 5 (56) | 4 (44) |
| Economic education | 21 (31) | 47 (69) | 8 (20) | 32 (80) | 9 (47) | 10 (53) | 4 (44) | 5 (56) |
| Other | 8 (12) | 60 (88) | 3 (8) | 37 (93) | 3 (16) | 16 (84) | 2 (22) | 7 (78) |
The topics that the respondents specified as ‘other’ were children's and young people's rights; mental and psychological health issues; care for children from vulnerable families; young carers; loss and bereavement; children and cancer; unmet attachment needs and therapeutic approaches; active global citizenship; equality, diversity and discrimination; restorative practice; and trainee health.
Ways in which health and well-being is covered in teacher training
The respondents were asked to ‘Please describe, as fully as possible, examples of how some of the health and well-being/PSHEE (personal, social, health and economic education) topics (as listed in questions 7/8) have been covered in your course’. (Note: the topics listed in questions 7/8 are those discussed in the previous section). In total, 34 of 43 HEI respondents (79%), 16 of 21 SCITT respondents (76%) and 7 of 10 EBITT respondents (70%) answered this question. The responses varied in terms of comprehensiveness, with some people summarising their activities in a few words and others providing more comprehensive accounts. In general, the level of detail provided was considered sufficient for meaningful data analysis.
Following examination of the data the responses were categorised into the following general themes: methods employed, people involved and context. Subthemes (and the frequency with which they were mentioned) were generated for each. The themes are now discussed in turn.
Table 8 provides a classification of the different methods that teacher training providers have used to teach health and well-being. In HEIs, health and well-being was covered generally through a wide range of methods such as lectures, seminars and tutor-led workshops. Some universities commit whole days within their courses to health issues or PSHE education. For example, in one university the students have a joint day-long conference with social work students exploring health (including mental health) and child protection. In several HEIs some health and well-being topics, such as SRE and drugs, are addressed in a lecture to the whole cohort. Topics may then be discussed in cross-curricular group workshops or in subject-specific areas. Some placement schools, which are linked to university courses, have their own professional studies programme, including school-based lectures and seminars.
| Methods | Number (%) of respondents mentioning | ||
|---|---|---|---|
| HEIs (n = 34) | SCITTs (n = 16) | EBITTs (n = 7) | |
| PSHE education and health and well-being are taught in modules/designated sessions | 7 (21) | 4 (25) | 1 (14) |
| Use a combination of some or all of the following: lectures, seminars, presentations, discussion, interactive workshops, e-learning | 22 (65) | 6 (38) | 1 (14) |
| Tutor-led workshops | 1 (3) | – | – |
| Whole cohort/multidisciplinary lectures | 5 (15) | – | – |
| Presentations on PSHE education from trainees, micro-teaching | 3 (9) | 1 (6) | 1 (14) |
| Teach PSHE education in school placement | 1 (3) | – | 1 (14) |
| All students attached to tutor groups in school placement | 1 (3) | – | – |
| Classroom observation/model lessons, directed tasks | – | 3 (19) | – |
| Whole day on PSHE education/citizenship (includes, for example, SRE, drugs and alcohol) | 4 (12) | 1 (6) | 1 (14) |
| Whole day on communicating with parents including SEAL, bullying | – | 1 (6) | – |
| Whole-day workshops organised by trainees | 2 (6) | – | – |
| Whole-group training sessions for lecturers and students | 1 (3) | – | – |
| Whole day on equality and diversity | – | – | 1 (14) |
| Group work | 1 (3) | – | – |
| One-to-one sessions | – | 1 (6) | – |
| Professional studies sessions on PSHE education in university | 4 (12) | – | – |
| Seminars in schools (partnership programme scheme) | 1 (3) | – | – |
| School-based tasks/activities | 8 (24) | – | – |
| School-based professional studies sessions | – | 3 (19) | 2 (29) |
Table 9 provides a classification of the different types of people who were mentioned as participating in teaching around health and well-being.
| People | Number (%) of respondents mentioning | ||
|---|---|---|---|
| HEIs (n = 34) | SCITTs (n = 16) | EBITTs (n = 7) | |
| Use of consultants from the local authority to lead sessions, e.g. ECM, child protection, PSHE education | – | 3 (19) | 1 (14) |
| Working in partnership with other ITT organisations | – | 2 (13) | – |
| Sessions led by university staff | 1 (3) | – | – |
| PSHE education, ECM, SEAL, child protection, teacher health and well-being by leads/experts in own/local schools | 3 (9) | – | 2 (29) |
| Other external organisation/charity | 2 (6) | – | – |
| Guest speakers, not specified | 9 (26) | 1 (6) | – |
| Pupil-led session, e.g. antibullying | – | 1 (6) | – |
| Researcher in SRE-led training (based on research evidence and good practice) | 1 (3) | – | – |
| Peer training | – | – | 1 (14) |
A variety of agents were mentioned, including people from local authorities, schools, charities and within ITT organisations themselves. In some cases the trainee teachers were actively encouraged to carry out the presentations on health topics themselves. For example, at one university the science and PE students organise a health day and there is a focus on the trainees as role models for health:
The aim is to prioritise the corporate responsibility for modelling healthy lifestyles and draw attention to key topics.
HEI 8
‘Micro-teaching’ was another method used in training whereby the student is filmed teaching and later evaluated. At one university (HEI 39) the students are encouraged to work in pairs to produce a lesson for their assessed presentation at the end of the cross-curricular module, which is often on health/PSHE education. On some courses there was an expectation that trainees will teach some PSHE education in their school placements, or through attachment to a tutor group in school, for example:
Teach the full curriculum at 90% contact for the final five weeks of the course, including all PSHCE [personal, social, health and citizenship education] in that part of the year.
SCITT 5
Classroom observation and practice was also mentioned as an important aspect of training.
Employment-based initial teacher training providers tended to use a variety of methods in their training. Several used experts in PSHE education from their own school or from other local schools. One respondent commented:
Our partnership has a core of outstanding and good schools which offer a full range of training to back up central sessions.
EBITT 10
One respondent mentioned that the training involved someone from a research background, taking an evidence-based approach:
A colleague who conducted research on SRE in schools leads session for trainees based on research findings and good practice.
HEI 34
Table 10 reports a classification of issues relating to the context in which health and well-being is addressed, specific to HEIs.
| Context | Number (%) of respondents mentioning |
|---|---|
| Global dimensions | 1 (3) |
| Cross-curricular activities/workshops | 3 (9) |
| Covered through science | 6 (18) |
| Humanities, health and social care, psychology, social work | 2 (6) |
| Child development | 1 (3) |
| Inclusion module | 1 (3) |
| Professional modules/GPS/education studies | 6 (18) |
| Business | 1 (3) |
| PE | 4 (12) |
| PSHE education course | 1 (3) |
In some cases training around health issues was mentioned as being covered in science or PE courses. For example:
Primary science covers healthy eating and environment education.
HEI 7
Sex and drugs are part of a science module in the final year.
HEI 28
However, health was also covered in other areas of the curriculum such as the humanities. One respondent commented:
There are also elements explored in the science sessions e.g. global dimensions’ cross curricula session on science and DT [design technology] related to sustainability and environmental education. Some of these concepts are also explored through the humanities.
HEI 25
Some health topics were covered through broader professional themes in which students from all subject areas are involved. However, the integration of health into broader areas of the ITT curriculum mentioned by some respondents was not universal. One respondent cited evidence to suggest barriers to the infusion of health throughout their programme:
Having completed our own small scale research project on this topic this year, we have identified that beyond PE, geography and science our other training subject areas do not see how this aspect of education is their responsibility. They had little interest in engagement and did not see it as part of the learning package within their area.
HEI 11
Some of the HEI respondents discussed at what stage in their courses health and well-being is addressed. Health topics were covered at various stages of courses, from the first year and beyond. For example, in a BEd course:
In Year 1 an Introduction to PSHE and Citizenship which explores the coverage and what it incorporates and some of the debates around this area of education. We also look at circle time as one way of building relationships with young children. We explore well-being of themselves and children and consider the self-esteem cycles. In Year 2 we have covered a range of things and is usually covered by an outside provider e.g. RSPCA [Royal Society for the Prevention of Cruelty to Animals], SRE, DARE [Drug Abuse Resistance Education].
HEI 25
Assessment
The respondents were asked whether any of the health and well-being aspects of the course were assessed (in general and/or in relation to QTS). In total, 39 out of 43 HEI respondents (91%), 17 out of 21 SCITT respondents (81%) and 9 out of 10 EBITT respondents (90%) answered this question. The majority indicated that assessment was undertaken [overall 44/65 (68%), HEIs 25/39 (64%), SCITT 12/17 (71%) and EBITT 7/9 (78%)]. Those that indicated that assessment took place were then asked to specify which methods were used. Table 11 shows the frequency of use of different methods, overall and for the three types of teacher training providers.
| Assessment method | Total (n = 44), n (%) | HEIs (n = 25), n (%) | SCITTs (n = 12), n (%) | EBITTs (n = 7), n (%) |
|---|---|---|---|---|
| Examination | 3 (7) | 2 (8) | 1 (8) | 0 |
| Portfolio | 21 (48) | 8 (32) | 9 (75) | 4 (57) |
| Assignment | 17 (39) | 10 (40) | 4 (33) | 3 (43) |
| Questionnaire | 0 | 0 | 0 | 0 |
| Teaching observation | 22 (50) | 11 (44) | 9 (75) | 2 (29) |
| Presentation | 15 (34) | 8 (32) | 5 (42) | 2 (29) |
| Other | 13 (30) | 10 (40) | 2 (17) | 1 (14) |
The majority of teacher training providers specified using more than one method of assessment, with the modal class being use of two methods (range 1–5, data not shown). Teaching observation and submission of a portfolio of activities relating to health and well-being were commonly used methods of assessment, particularly so for SCITTs. Less common were methods such as presentations or assignments. Examinations were used by a minority of providers, and no respondents mentioned using questionnaires. In terms of methods listed as ‘other’, the most commonly reported method was the compilation of evidence to support attainment of QTS standards (n = 7, all HEIs). Evidence against the standards could be derived from school placement lesson plans or observational feedback and in some cases students were given the opportunity to select a health and well-being topic for an assignment, essay or their dissertation. Other methods of assessment included ‘professional dialogue’, ‘focused teaching evaluations and reflection’, ‘one-to-one assessments’, ‘tasks during placements assessed as part of their planning files’, ‘online bullying training assessed and certificated’ and ‘implicit through assessment of other aspects of the course’.
External support for teaching health and well-being
The respondents were asked whether they used any external organisations to provide information, resources or teaching to support the delivery of the health and well-being aspects of their courses. In total, 39 out of 43 HEI respondents (91%), 16 out of 21 SCITT respondents (76%) and 9 out of the 10 EBITT respondents (90%) answered this question. For all three types of provider the majority reported use of external organisations [31/39 (79%) HEIs, 10/16 (63%) SCITTs, 6/9 (67%) EBITTs]. Those that indicated that external organisations had been used were then asked to specify which types of organisation were used. Table 12 shows the frequency of use of different external organisations, overall and for the three types of teacher training providers.
| External organisation | Total (n = 47), n (%) | HEIs (n = 31), n (%) | SCITTs (n = 10), n (%) | EBITTs (n = 6), n (%) |
|---|---|---|---|---|
| Health professional | 10 (21) | 4 (13) | 6 (60) | 0 |
| Youth service | 5 (11) | 4 (13) | 0 | 1 (17) |
| Local authority | 35 (74) | 23 (74) | 8 (80) | 4 (67) |
| Voluntary/charitable group | 17 (36) | 13 (42) | 1 (10) | 3 (50) |
| Local university/college | 2 (4) | 3 (1) | 0 | 1 (17) |
| Sports organisation | 10 (21) | 19 (61) | 3 (30) | 1 (17) |
| Local school | 29 (62) | 18 (58) | 7 (70) | 4 (67) |
| Other | 11 (23) | 6 (19) | 4 (40) | 1 (17) |
The majority of respondents specified working with more than one external organisation. For HEIs the median number of external organisations was two (range 1–4, data not shown), for SCITTs the median was three organisations (range 1–4, data not shown) and for EBITTs the median was 2.5 (range 1–5, data not shown).
Local authorities were the most common external organisation that ITT providers worked with to support the health and well-being aspects of their course(s). The delivery of lectures, taught sessions, seminars and workshops by experts were mentioned. These included Healthy Schools co-ordinators, special needs advisors, 14–19 advisors, child protection officers and police liaison officers.
Local schools were also a commonly used external source of support for health and well-being, mentioned by around two-thirds of SCITTs and EBITTs and just over half of the HEIs. The school staff involved included PSHE education experts, PE teachers, senior or head teachers, a teacher specialising in cancer care and teachers with a responsibility for child protection.
Voluntary/charitable groups were used by just over one-third of ITT providers. Specific groups mentioned covered a wide range of health-related issues and included the Teenage Cancer Care Trust, Barnardos, the Red Cross, Rethink Mental Illness (mental health), Nelson's Journey (bereavement), Young Carers, Daisy Chain (autism) and the ABLE project (environmental education). The proportion of ITT providers who worked with health professionals was low overall, and more common for SCITTs. Specific types of health professional mentioned included a clinical psychologist, a speech and language therapist and a cognitive behaviour therapist. The SCITTs who responded did not have any input around health and well-being from a local university or college or youth organisation. The EBITTs made little use of local universities or colleges, sports organisations or youth services (only one used each one).
‘Others’ who support the health aspect of the curriculum in HEIs were the National Society for the Prevention of Cruelty to Children (NSPCC), trade union representatives, police officers responsible for child protection and Association of Teachers and Lecturers (ATL) (education union) consultants. ‘Others’ who were mentioned by SCITTs included child protection specialists (e.g. from the local authority) and ‘the five voices for effective teaching’, a voice development programme for trainees. The only ‘other’ mentioned by an EBITT was a community police officer.
Time spent on health and well-being in the curriculum
The respondents were asked to ‘Please estimate the approximate percentage of time spent, as a whole, covering health and well-being in your course’. In total, 37 of 43 HEI respondents (86%), 16 out of 21 SCITT respondents (76%) and 9 out of 10 EBITT respondents (90%) answered this question. Table 13 presents the percentage of time spent on health by type of provider.
| Time spent on health and well-being (%) | Total (n = 62), n (%) | HEIs (n = 37), n (%) | SCITTs (n = 16), n (%) | EBITTs (n = 9), n (%) |
|---|---|---|---|---|
| < 5 | 14 (23) | 7 (19) | 3 (19) | 4 (44) |
| 5–9 | 26 (42) | 17 (46) | 6 (38) | 3 (33) |
| 10–14 | 16 (26) | 9 (24) | 5 (31) | 2 (22) |
| 15–19 | 4 (6) | 3 (8) | 1 (6) | 0 |
| 20–24 | 2 (3) | 1 (3) | 1 (6) | 0 |
| 25–49 | 0 | 0 | 0 | 0 |
| ≥ 50 | 0 | 0 | 0 | 0 |
The highest percentage of respondents indicated spending 5–9% of time on health and well-being, followed by 10–14% of time. A higher percentage of EBITTs reported spending < 5% of time on health and well-being, and several respondents from EBITTs felt that the health and well-being aspect was mostly the responsibility of the placement schools. The figures presented must be interpreted with some caution as some respondents commented that it was difficult to calculate as aspects of health are embedded throughout the course.
Importance of health and well-being in teacher training
The respondents were asked, ‘How important in your view is it to emphasise the health and well-being of pupils and staff/PSHE in the initial teacher training curriculum?’ In total, 37 out of 43 HEI respondents (86%), 16 of 21 SCITT respondents (76%) and 8 out of 10 EBITT respondents (80%) answered this question. Table 14 illustrates the degree to which respondents considered health and well-being important, by type of provider. For each type of provider, the majority considered health and well-being to be important or very important (although a relatively smaller majority of EBITTs), with only a minority considering it to be of some importance. No respondents indicated that it was not important, although, as acknowledged in Chapter 7 of this report, people who regard health as less important may have chosen not to complete the questionnaire.
| Importance | Total (n = 61), n (%) | HEIs (n = 37), n (%) | SCITTs (n = 16), n (%) | EBITTs (n = 8), n (%) |
|---|---|---|---|---|
| Very important | 23 (38) | 15 (41) | 7 (44) | 1 (13) |
| Important | 31 (51) | 18 (49) | 8 (50) | 5 (63) |
| Of some importance | 7 (11) | 4 (11) | 1 (6) | 2 (25) |
| Not important | 0 | 0 | 0 | 0 |
Several respondents commented that the health and well-being aspects of the course are important. For example:
Health and well-being goes across all curriculum subjects. It is something we as tutors are passionate about.
HEI 19
We do a great deal on the pedagogy of these subject areas, how to deal with controversial issues, how to conduct circle time etc.
HEI 14
However, one respondent was open about the fact that she did not focus enough on health and well-being, but completion of our questionnaire had prompted her to re-evaluate her provision:
In reviewing the list of dimensions provided in this survey I feel that there are areas we have neglected to date and will endeavour to supplement our existing provision accordingly.
HEI 39
It was noted by some respondents that, despite the recognised importance of health, lack of funding and time pressures limited the extent to which it could be covered:
With additional resources (i.e. more time and money) we would focus more on this aspect of the course.
SCITT 8
Future changes to teacher training courses
The respondents were asked, ‘In what ways do you anticipate that the content, delivery or structure of your course is likely to change in the near future? (e.g. in response to changes in educational policy or funding?)’. In total, 30 out of 43 HEI respondents (70%), 13 out of 21 SCITT respondents (62%) and 6 out of 10 EBITT respondents (60%) answered this question. The responses given were examined and a number of key themes to emerge were noted. Subthemes were identified and the frequency with which they were mentioned was noted. Table 15 presents these themes, each of which is discussed in further detail below.
| Theme | HEIs (n = 30), n (%) | SCITTs (n = 13), n (%) | EBITTs (n = 6), n (%) |
|---|---|---|---|
| They will make changes in response to new policies, initiatives and the new QTS standards | 8 (27) | – | – |
| If health is not so high profile/not statutory it may be harder to justify its inclusion and it may be covered less | 5 (17) | 1 (8) | – |
| They will maintain or increase focus on health and well-being despite wider changes, as they see it as important | 7 (23) | 1 (8) | 1 (17) |
| They expect a greater focus on health and well-being as a result of new government priorities | 1 (3) | – | – |
| Changes to the content and delivery of health and well-being/PSHE education in the course (e.g. timing, topics, people delivering health subjects) | 3 (10) | 4 (31) | – |
| No changes to courses in which health and well-being is an essential part of the curriculum – challenge will be other subject routes | 2 (7) | – | – |
| General changes to the course(s) (e.g. reduced course length) | 3 (10) | – | 2 (33) |
| They address issues as necessary/in response to evaluation or feedback | – | 2 (15) | 2 (33) |
| Not sure/not currently known | 3 (10) | 3 (23) | 1 (17) |
| They are concerned about the impact of fewer resources on their courses | 1 (3) | – | 1 (17) |
| No significant changes anticipated | 2 (7) | 3 (23) | – |
| Other expected changes as a result of government changes (e.g. curriculum will become more prescribed or there will be more local flexibility) | 2 (7) | – | – |
| Determining content of a PGCE is a balancing act for institutions as content space is limited – non-statutory subjects cannot be given the same attention as those that are core | 3 (10) | – | – |
The respondents made a range of comments about the ways in which they anticipated that their courses were likely to change in the near future. Five course managers felt that there would be no significant changes to their courses, whereas seven were currently unsure or awaiting the outcomes of the National Curriculum review, information about funding or the new QTS standards. Eight course managers reported that adaptations would be made to their courses in response to these government changes, with six speculating that this might lead to a reduced focus on health and well-being if health was not so high profile in government policy or the QTS standards:
Unfortunately with the central Government’s focus on subject knowledge, we will probably have to spend less time on the health and well-being aspects of the course.
SCITT 8
Conversely, one provider felt that the government's emphasis on special educational needs (SEN), PE and classroom behaviour might raise the profile of health and well-being. Nine of the respondents stated that they would be maintaining or even increasing the health and well-being content of their courses, despite wider educational policy changes. This was often because they felt that it was important:
We will continue to pay attention to this area and give it the importance it deserves.
HEI 33
The respondents also stated other changes that they would be making to their courses, including to the content and methods of delivering PSHE education and health and well-being, and other more general changes:
[We will be] incorporating the elements of health and well-being into the programme much earlier next year in order to prioritise this element in the trainees view of their role as a professional.
HEI 11
One course manager reported that her course would be using external agencies less in the future, with the course staff providing more of the health and well-being sessions. Another said that they would continue to build on delivery from practitioners as evaluation of the course showed that this had the most impact.
Finally, two respondents expressed concerns about the impact of currently operating on ‘lean’ (EBITT 10) resources and anticipated fewer resources in the future:
Despite trends in educational policy and/or funding there is a sense that both expectations and demands to maintain existing high standards of practice will prevail. This will place undue stress on an already overburdened teaching team, who continue to delivery exemplary programmes with increasingly fewer resources.
HEI 39
Summary
A questionnaire survey was conducted on a sample of course managers in ITT providers in England to assess how health and well-being is currently addressed within teacher training.
-
The overall response rate to the survey was 34% (74/220 course managers). In total, 43 out of 135 (32%) of the HEI course managers responded, 21 out of 49 (43%) of the SCITT course managers responded and 10 out of 36 (28%) of the EBITT course managers responded. All of the respondents reported that they managed, led or directed one or more teacher training course. The most commonly managed course in HEIs was PGCE secondary followed by primary, in SCITTs it was primary and in EBITTs it was GTP secondary followed by primary.
-
Nearly all of the respondents reported that their courses covered ECM and child protection. The other most commonly covered topics were SEAL/emotional health and well-being, antibullying, working with parents, environmental education, healthy eating and physical activity.
-
Health and well-being was covered through a wide range of methods including lectures, seminars and tutor-led workshops. A few respondents reported that their institution held whole-day health events or that trainee teachers delivered presentations and sessions themselves.
-
Training around health issues was commonly mentioned as being covered in science or PE courses but could also be addressed through broader professional themes with students from all subject areas being involved.
-
The majority of the respondents reported that the health and well-being aspects of their courses were assessed, with teaching observation and submission of a portfolio being the most commonly used methods.
-
External organisations, especially local authorities and local schools, were used by the majority of the respondents' institutions to support the delivery of health and well-being.
-
The highest percentage of respondents indicated spending 5–9% of time on health and well-being, followed by 10–14% of time. EBITTs tended to spend less time on health than other types of provider.
-
Overall, just under 90% of respondents considered health and well-being in the ITT curriculum to be important or very important. From comments made it was apparent that there was strong support for covering health in training, although there was acknowledgement by some respondents that their coverage of health could be improved.
-
New government policies and the new QTS standards were anticipated by some respondents as likely to result in changes to the health and well-being aspects of their courses in the future, with some speculating that this might lead to a reduced focus on health and well-being. However, other respondents indicated that they would maintain a focus on health and well-being despite wider changes because they felt that it was important.
-
When interpreting the results of this survey it should be acknowledged that those who chose to respond may be considered to be generally more supportive of health and well-being in ITT than those who did not.
Chapter 4 Interviews with teacher training providers
Methods for the interviews with teacher training providers
Development of the interview schedule
The interview schedule was developed between October and November 2011. The interviews were intended to be semistructured in nature with a sequence of mostly open-ended questions with prompts and probes as required. The type of questions used in a research study should be cognisant with the aims and objectives of the study and should be logical, relevant and motivating. 38 As stated earlier, the aim of the interview phase of this project was to investigate in further detail approaches to addressing health and well-being by teacher training providers who had completed the initial questionnaire. It is for this reason that most of the questions used in this study were open-ended, to allow the interviewees to talk at length. The research team decided that the questions would focus on similar issues covered by the questionnaire, but that the questions would be designed to facilitate deeper discussion. In particular, questions would be included to identify and explore barriers to and facilitators of covering health and well-being, as the questionnaire survey did not contain specific questions relating to this. In addition, two questions were included to explore specific findings from the questionnaire survey. One was to assess the extent to which sex education, drugs, alcohol and tobacco were covered by courses and any reasons for lack of coverage relative to other topics (the survey findings suggested that these had received less attention). The second was to assess the extent to which teacher training providers involve health professionals in training teachers about health and well-being, and whether there were any particular barriers to their involvement (the survey findings suggested comparatively less involvement). Other additional questions covered the interviewees' professional background (a warm-up question, designed to explore whether their previous practice or research influenced their current work, specifically in relation to health) and also whether their courses addressed the health and well-being of teachers as well as pupils.
Piloting of the interview schedule took place during December 2011. Three pilot interviews were conducted with teacher training providers in the South East of England. Two of these were HEIs and one was a SCITT. One was a 4-year primary undergraduate course, one a 1-year secondary PGCE course and one a 1-year primary SCITT course. Sampling was partly purposive, to pilot the interview schedule on different types of teacher training providers. Sampling was also undertaken for convenience by selecting contacts of the research team in the local region for ease of access. The variation in terms of teacher training provider and type of course sampled was considered to be sufficiently representative of the intended sample for the main interview study. Furthermore, it was considered by the research team that three pilot interviews were sufficient to test the adequacy of the interview schedule, and as preparation for the interviewers in conducting the interviews.
The pilot interviews lasted for around 45 minutes and were judged by the research team to have been generally successful in terms of testing the comprehensibility of the questions and the suitability of the sequence of questions, and ensuring that the type of information disclosed was sufficient to meet the aims of the project. There was variability in terms of the degree to which health and well-being was covered in the courses of the providers sampled, from dedicated health awareness activities at the start of the course reported by one provider, to relatively minimal focus on health reported by another, and we found that the interview schedule was generally effective in yielding good responses from providers when there was both high and low provision of health training.
The interview schedule underwent a series of generally minor revisions, including suggested revisions from the advisory group, until it was finalised and implemented. Once in use, the interview schedule did not undergo any major changes. However, discussion between the interviewers during the course of the interview period about experiences to date provided the interviewers with a greater awareness of how the questions were being received, and of particular themes and issues that were emerging and in need of probing further in subsequent interviews (see below).
The final interview schedule is provided in Appendix 3.
Sampling and recruitment of interviewees
It was originally estimated that around 20–25 interviews would be a sufficient number for this project. As reported in Chapter 3 (see Response rates), a total of 30 out of 63 survey respondents (48%) who answered the question about whether they were willing to be contacted indicated that they would be. Therefore, the number of questionnaire respondents willing to be approached was sufficient to meet the target number of interviews.
To facilitate selection, key details of each of the 30 consenting survey respondents were tabulated for discussion among the research team (19 HEIs, seven SCITTs and four EBITTs). Details were tabulated for each type of provider including educational course level (i.e. primary/secondary), graduate course status (i.e. undergraduate/postgraduate), course type (e.g. BA, BEd, PGCE, GTP), number of students responsible for, subject specialism (e.g. maths, English) and geographical location (e.g. English region). A qualitative summary was also written based on the key findings of each respondent's questionnaire, including issues such as the degree of importance given to health and well-being (ascertained by responses to Likert-type scales plus qualitative comments describing their views on health in teacher training); the breadth of health topics covered (e.g. many topics covered compared with a relatively small number of topics); innovative examples of approaches to addressing health and well-being (e.g. specific activities such as seminars or workshops, and particular educational techniques or conceptual frameworks); and indications of how health and well-being might be covered as a result of future changes to educational policy and curriculum reorganisation (e.g. retaining or increasing focus on health compared with possibly less emphasis on health).
Once these details were tabulated, the research team discussed the key characteristics of the sample and selected a total of 22 respondents to contact to request an interview (with more to be selected if necessary). We purposively selected interviewees to ensure that the sample reflected the different types and levels of courses, subject specialisms, English regions and approaches to addressing health and well-being. Selection was also weighted according to type of provider consenting to be contacted, the majority being HEIs (and also because a large proportion of ITT provision in England is from HEIs).
We purposively selected course managers from courses using contrasting initiatives to obtain a range of views. We also sampled from the smaller number who appeared to be covering health less overall, or covering health through a narrower range of methods. We also sampled participants to ensure that there was a range of perceptions about the importance of health and well-being, using their responses to the question about its importance in our earlier questionnaire survey to do this (see Chapter 3, Importance of health and well-being in teacher training).
Once selected, a standard e-mail was composed and sent to each respondent from the project's dedicated e-mail account, with an attached participant information sheet providing brief details about the project and the nature and purpose of the interviews. The e-mail thanked them for completing the questionnaire and provided them with their original responses to the questionnaire as a reminder. In cases of non-response a follow-up telephone call was made within 2 weeks of the e-mail request. Only one person did not respond to any contact attempts. A second person declined the invitation to be interviewed, citing work pressure and lack of time. A further two people initially agreed to be interviewed, but subsequently it was not possible to arrange an interview because of their lack of availability.
During the course of the project the research team decided that, if necessary, interviewees could be recruited from other sources, in addition to those who had previously completed the questionnaire. This was a pragmatic decision to enable us to purposively interview teacher training providers who, it appeared, were using approaches to addressing health and well-being that were complementary to those in our existing sample. During the course of sampling and recruitment it was considered that the sample was adequate to reflect a range of approaches and that recruitment of additional teacher training providers would not likely be necessary. However, at the project's advisory group meeting in January 2012, it was noted that there had been no questionnaire responses from the West Midlands region, and therefore this would be the only region not represented in the interview sample. It was recommended that the project attempt to recruit an interviewee from a teacher training institution in this region, for completeness. Our sampling frame from the questionnaire survey showed that in the West Midlands region there were a total of 21 teacher training providers (nine HEIs, five SCITTs, seven EBITTs). We selected one provider (a HEI) from this region, chosen because it provided a range of courses (e.g. undergraduate/postgraduate, level of education) and the ethos and principles of the institution were in contrast to others in our sample (as ascertained from information provided on its website). We contacted three course managers from this institution and one consented to be interviewed.
In summary, a total of 25 people were contacted, of whom 19 were subsequently interviewed in a total of 18 separate interviews (Figure 5) (Note: one of the interviews was conducted jointly with two people from the same institution, at their request).
FIGURE 5.
Flow chart summarising sampling and recruitment of interviewees.
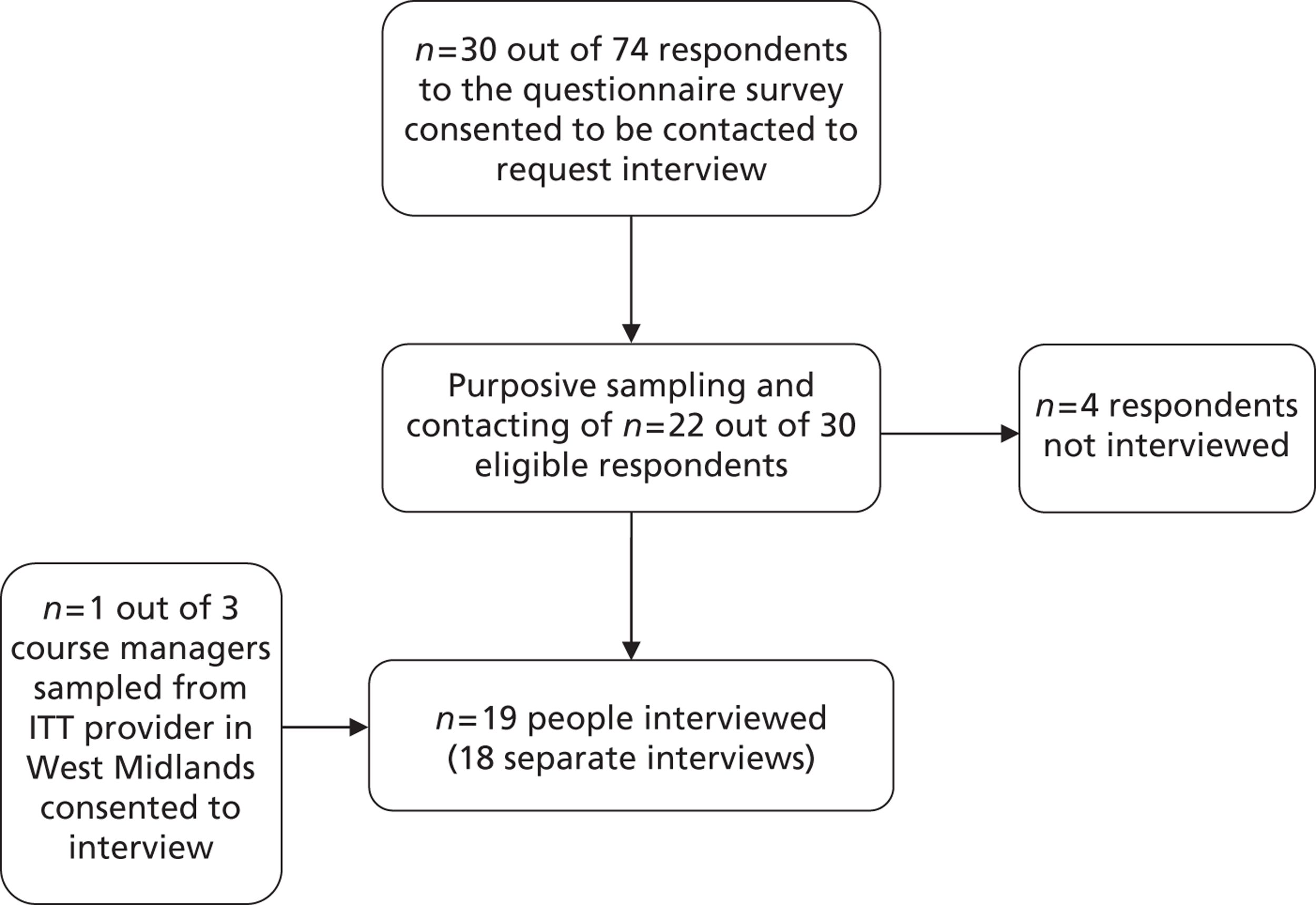
Conducting the interviews
The interviews were conducted by three of the authors (SD, KP and JS) over a 3-month period between January and March 2012. Before each interview the interviewer familiarised himself/herself with the interviewee's questionnaire responses and completed a standard pre-interview proforma containing general details about the interviewee's course(s) (e.g. subject areas) and ways in which health and well-being was covered (as disclosed in the questionnaire). The purpose of the proforma was to help the interviewer to tailor the interview (e.g. through use of specific probes) to the specific circumstances of each interviewee.
All interviews were recorded using a digital voice recorder. The intention was to conduct face-to-face interviews whenever feasible to facilitate rapport and in-depth discussion. Fifteen of the interviews were conducted face-to-face, with the remaining three conducted on the telephone (for reasons of convenience). The telephone interviews were of approximately the same duration as the face-to-face interviews (between 45 minutes and 1 hour) and the quality of discussion was judged to be comparable. All interview recordings were transcribed by a professional academic transcriber.
Data coding
A content analysis approach was used to analyse the data from the interviews. This was chosen as it is a standard and relatively straightforward technique used in the social sciences to categorise and explore qualitative data from interviews. 39,40 At its simplest, content analysis involves reading interview transcripts and recording the frequency with which key terms and issues are mentioned. 41 These can be grouped into response categories and the relevant dialogue coded according to each category. As coding progresses the categories can be amalgamated into broader themes, if appropriate. It was considered to be an appropriate method for the analysis of the type of data to be elicited in this stage of the research, and was in keeping with the inductive nature of the study as a whole.
There are a variety of different computer software programmes available to assist with the analysis of qualitative data. The software has made the process of data management and analysis more efficient, allowing researchers to store and organise data in a format that is easily retrievable, and which automates techniques that researchers used to do by hand. It is important to note, however, that these programmes cannot substitute for the considerable skill necessary to identify themes, explore associations and meanings and draw conclusions from the data. The researcher's analytical and intellectual input therefore remains as important as ever.
NVivo software (version 9; QSR International, Southport, UK) was used to code and analyse the data. This software was chosen as it is a specialist programme suitable for analysis of textual data and was considered adequate for the needs of this project. Once all of the interviews had been conducted, each finalised transcript was imported into NVivo ready for coding. Each interview transcript was coded in turn. Before the start of coding we set up a coding framework in NVivo based on the 12 main questions in the interview schedule (the full interview schedule is available in Appendix 3). A ‘node’ (i.e. a code) for each question was generated when the framework was set up in NVivo, with the aim of the researcher analysing the data to create second-order (or third-order if necessary) subnodes as response categories for each question. The specific nodes set up in NVivo that formed the analytical framework were interviewee background; significant changes to the course; how health and well-being are covered; time spent on and timing of health and well-being in the course; external agencies or external people; sex, relationships, drugs and smoking; funding for health and well-being; assessment of health and well-being; health and well-being of teachers and trainees; challenges and barriers to addressing health and well-being; facilitators to addressing health and well-being; and future changes to course. As part of the framework, a ‘free nodes’ node was also set up where data not directly related to any of the interview questions could be coded, such as any unexpected issues that emerged during the analysis. An example of a code that was created under ‘free nodes’ during the analysis was ‘conceptions of health and well-being’, which captured the interviewees' personal beliefs about the importance of health and well-being, how health and well-being relate to children and young people's education, and what these terms meant – an issue that we did not directly question interviewees about, but which most of the participants spontaneously mentioned during the interviews, and which is a key part of our findings reported below. As the researchers read through the transcript on the computer screen they highlighted passages of text (e.g. a sentence, or a paragraph) and coded them according to which of the interview questions they related to, creating new subnodes if necessary or adding to existing subnodes describing similar issues. For example, the node called ‘challenges and barriers to addressing health and well-being’ was created to categorise responses to the question, ‘What key challenges have you experienced in addressing health and well-being in the teacher training curriculum?’ Responses to this question were assigned to subnodes, with common responses assigned to the same subnode when applicable. Each of these subnodes was therefore classified as a specific barrier. The overall purpose of this exercise was to code each occurrence of a particular issue discussed during the interviews so that those issues could be easily retrieved from the database and the coded text analysed for meaning. The meaning units coded by the researchers were kept sufficiently large so that the context of the interviewees' points was not lost.
Coding of the initial interviews was carried out by the researcher who conducted each interview. Discussion between the interviewers took place after each had coded at least two interviews to ensure shared interpretation of the codes and intercoder reliability. At this point (i.e. at around the sixth coded interview transcript) the number of subnodes had grown to the point at which it was considered necessary to review the subnodes and merge similar or overlapping subnodes to avoid duplication and to keep the coding framework manageable. This was performed by one of the interviewers (KP) and acted as a quality assurance check for accuracy of coding. Following this revision to the coding framework the remaining interview transcripts were generally coded by this interviewer.
Once all 18 interviews had been coded, around 550 separate nodes had been created. A review of the nodes was undertaken by one researcher, to merge similar nodes and merge unnecessary subcodes into the higher-level nodes. Once this review was completed the number of nodes had been reduced to 420. The team then began to analyse the nodes in more detail by examining the passages of interview conversation that had been assigned to them, and noting any patterns in the data (e.g. we noted that, when interviewees had cited a lack of understanding and knowledge about health and well-being as a barrier, they sometimes mentioned this in relation to training provider staff and at other times mentioned it in relation to school placement staff and trainee teachers). From discussion within the team, the barriers to and facilitators of teacher training were considered to fall within the following spheres of influence on how health and well-being was covered in ITT:
-
trainee teachers
-
teacher training providers
-
placement schools and the wider school community (e.g. where trainee teachers spend their placements)
-
external agencies (e.g. local authorities, health services)
-
local culture and geography (e.g. the socioeconomic and cultural profile of the locations where teachers are trained)
-
wider educational culture (e.g. the perceived general culture within education in which providers, schools and trainees work)
-
government policy (e.g. health, education).
It was considered that these spheres encapsulated the main influences on teacher training in relation to health and well-being. To illustrate the relationships between the different spheres we manually (outside of NVivo) constructed a model diagram with arrows showing the direction of influence (e.g. between government policy and teacher training providers, and between teacher training providers and placement schools). This was based on the interview data that we had analysed, but also on our background knowledge of health and education and on broader evidence (e.g. from research, theory and policy). The model was partly informed by the social–ecological model,42,43 which is a theory that explains how individuals' behaviours or social phenomena are influenced by reciprocally related individual and social factors, including intra-individual factors (e.g. attitudes), interpersonal factors (e.g. peers, social networks), the structure of the institutions and organisations in which individuals operate, the wider community (e.g. social norms) and, at the broadest level of the model, social structures, policies and systems (e.g. government policies). During data analysis we considered whether this model could form an explanatory framework for our findings as the barriers and facilitators identified seemed to relate to aspects of the model, but we decided finally that it was not a fully appropriate fit for our data. The social–ecological model therefore helped us to structure our thinking about the analysis and spheres of influence, but we created our own model to explain the findings as this allowed us to create a model that fitted the data better. The model we created became an explanatory framework for our interview findings and also shows the context of teacher training. A draft was discussed with the project's advisory group who made suggestions for minor revisions (the final model can be seen in Figure 7).
The barriers and facilitators that had already been coded were then assigned to each of the spheres of influence as appropriate in NVivo. This process also included some recoding of the barriers and facilitators themselves when necessary. After carrying out this process a total of 515 codes had been generated.
Generating analytical themes
Through the process of coding and analysis described above, a number of overarching themes began to emerge from the data. Two of the research team independently noted down the key themes that they had observed and met to discuss these (JS and KP). These two researchers agreed on the majority of the key themes, resulting in a list of around six. Over time this list of key themes was revised and increased, and then decreased again through discussion with other members of the research team. The reduced list contained six key themes considered to encapsulate the barriers and facilitators identified in the interviews. Once these themes had been defined and agreed by the research team, each of the barriers and facilitators was re-examined and one or more themes were assigned to each. This was done in a series of preliminary tables outside of NVivo, in which the barriers and facilitators were plotted in separate columns and the themes applicable to them were listed in adjacent columns, stratified by the spheres of influence described above (i.e. teacher training providers, placement schools, etc.). The purpose was to describe and discuss the barriers and facilitators operating within each of the six themes. The assignment of themes to the barriers and facilitators was carried out by one researcher and checked by a second for consistency. Minor amendments were made to the categorisation following discussion (mainly to assign additional themes to a barrier or facilitator, rather than reclassify barriers and facilitators altogether). Following this, in NVivo, the barriers and facilitators, labelled by the sphere of influence that they were located within, were then categorised according to the main theme to which they related and, in some cases, subthemes were inferred by comparing differences and similarities between the barriers and facilitators. These data are presented in our findings below and the themes themselves are described in Barriers to and facilitators of effective teacher training.
Results of the interviews with teacher training providers
Characteristics of the study sample
The providers who were interviewed were spread across the country, with representation from every English government administrative region (Table 16). There were slightly more providers interviewed from the South East than from other regions, which may reflect a higher proportion of providers in the South East or perhaps that there may be more trainee teachers in this region. This is difficult to substantiate as the numbers of trainees on individual courses are not always clearly advertised on individual providers' websites, which were consulted before the survey and the interviews.
| Region | Number of interviews | Percentage of total number of interviews |
|---|---|---|
| Eastern | 2 | 11 |
| East Midlands | 1 | 6 |
| London | 2 | 11 |
| North East | 2 | 11 |
| North West | 1 | 6 |
| South East | 4 | 22 |
| South West | 3 | 17 |
| West Midlands | 1 | 6 |
| Yorkshire and the Humber | 2 | 11 |
As stated earlier, the interviewees were sampled according to the type and level of courses that they managed so that they represented a range of courses catering for primary, secondary, early years and key stage 2/3, at undergraduate and postgraduate level, across HEIs, SCITTs and EBITTs. In the HEIs some of the interviewees managed more than one course (e.g. Programme Director for Primary Education) and some managed the whole portfolio of courses provided by their particular institution at undergraduate or postgraduate level (e.g. Head of the Undergraduate Programme) (Figure 6). Others managed one specific course (e.g. Programme Director for PGCE Key Stage 2/3) and had an input, for example as a lecturer, into other courses. SCITT and EBITT managers were responsible for managing postgraduate courses, which for some included courses at more than one level, such as secondary and 14–19 years (e.g. SCITT 15).
The providers of secondary, key stage 2/3 and further education courses generally offered a range of different subjects, some more limited than others, including mathematics, geography, science (physics, biology, chemistry), PE, English, modern foreign languages, religious education, design and technology, information and communications technology and music. Some of the interviewees were subject specialists in their current roles, such as a mathematics lecturer or PE specialist, and they frequently used their subject knowledge and expertise, for example in science or PSHE education, to contribute to the health and well-being content of their training courses.
FIGURE 6.
Role of course managers interviewed. GRTP, Graduate/Registered Teacher Programme.
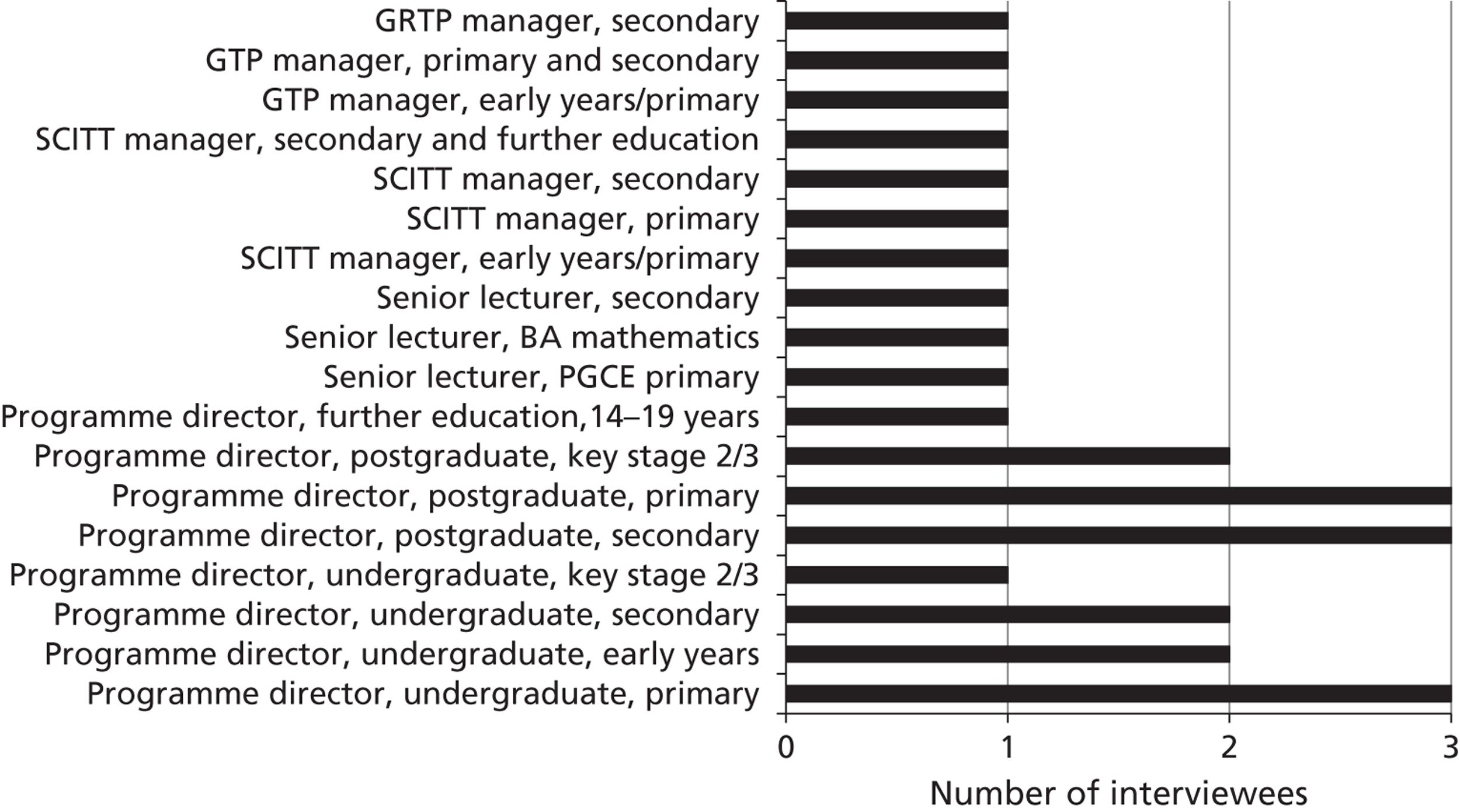
The numbers of students on the courses varied between different institutions and types of organisation. The numbers of students on PGCE courses at SCITTs and EBITTs ranged from three students on an early years GTP course to 79 on a SCITT primary course. In HEIs the numbers of students on the undergraduate courses of those interviewed ranged from around 12 on a BEd in a particular subject to a total of around 800 on a 4-year course. The numbers on 1-year PGCE secondary courses ranged from about 120 to 140 students. On 1-year PGCE primary courses the numbers of students ranged from 60 to 190. On the PGCE 14–19 years course there were 33 students and on the PGCE key stage 2/3 course there were about 60 students. In general, the numbers of student places available in 2012 had been reduced from the time of our questionnaire survey in the previous year because of a reduction in government funding, particularly for training in the teaching of vocational courses in the 14–19 years age group. One course director mentioned that numbers would drop again considerably for vocational courses in the coming academic year.
Background of the study sample
All of the course leaders who were interviewed had teaching qualifications and teaching experience, many at a senior level. Five reported an academic research interest in the area of health and well-being, such as in outdoor play, how children in nursery education make meaning in science and the effect of well-being on children's resilience. A strong personal interest in health was mentioned by seven, as well as a holistic concept of health and well-being, for example through their interests in sport or in nutrition in adolescents, through their previous involvement in schools with the Healthy Schools award, through working with local authorities and children's centres or through their experience of working with parents and community groups. As one person commented:
My whole education background places children at the centre.
HEI 42, primary phase
Some of the course managers were trained in science or in PE and they noted that this has increased their interest in health and well-being. Others had worked with children with SEN or in deprived areas with refugees and asylum seekers, and one worked in the education department within a prison. Overall, seven of the course managers told us about health-related professional experience that they had had (including through their teaching role).
Some course managers had been working in education since their degree and had moved directly from senior roles in schools, which included pastoral responsibilities, to training teachers. Others had had gaps in their careers, to have families or to undertake voluntary work abroad. In some cases their work in schools included a large amount of health education, both with pupils and parents and with the wider school community. Some had worked as local authority advisors and school governors, giving them a broad understanding of how schools function. A few were relatively new to managing a teacher training course and had come to work in a university only within the last 10 years and could therefore draw on their recent experience of working in schools.
In summary, the interviewees came from teaching backgrounds and had progressed to teacher education. They varied in their background experience of health but, in total, 12 interviewees reported that they had either professional or personal experience or interests related to health and well-being.
Course managers' conceptions of health and well-being
In setting the scene for the interviews, the participants were informed that we had a broad definition of health and well-being and therefore anything that they felt was relevant to this theme could be discussed during the interview. Their comments illustrate that health underpinned many aspects of their courses and was often seen as fundamental to effective teaching and learning.
Many course managers mentioned the importance of holistic education, in which health and well-being permeates through the curriculum rather than being addressed in separate modules. They mentioned the importance of the ethos and values that are portrayed by their course which promote health and well-being, such as getting students to understand working across the curriculum, the benefits of different subject staff working together and the sense of health and well-being that this approach brings to staff, trainees and pupils in schools.
On some courses, health was interwoven into the ITT curriculum through a focus on particular themes throughout the course, including SEN, outdoor education and behaviour management – the exact underpinning theme varied from course to course. This did not necessarily mean that health and well-being was comprehensively addressed on these courses, but that there was a particular health-related strand that underpinned them:
We do not explicitly cover a lot of health and well-being in the classroom but it underpins a lot of what we do . . . We do a lot about inclusion and the inclusive classroom, and what an inclusive classroom looks like . . . get them to think about the diverse settings in which they work, which I think again is part of a child's well-being and happiness in school.
HEI 40, primary and secondary phases
As the above course manager explained, health and well-being is not always explicit in teacher training but it is related to issues such as inclusion and special needs. Similarly, in one interview in which two course managers were interviewed jointly, health and well-being was seen as fitting alongside behaviour management, classroom organisation and relationships in school. They highlighted the importance of encouraging their trainee teachers to think about their responsibilities as learners and to one another, and about their own student voice on their course, which would help them to use these approaches with pupils in school:
So it’s important that they have a deeper understanding of how children develop these behaviours, you know the appropriate ones, inappropriate and so on, rather than just being given a strategy if a child is the one child who’s rushing up and down the classroom or whatever, so that they also know about the different sorts of behavioural difficulties and syndromes related to that.
SCITT 19, primary phase
Several course managers acknowledged that subject knowledge is not the only important aspect of teacher training, but that awareness of child development and emotional well-being is also very important. One commented:
How can you run a teacher training programme without thinking about the development of adolescents, about the emotional upheaval, about the hormonal upheaval that’s going on in their lives?
EBITT 6, secondary phase
Conceptions of health and well-being also included awareness about pupils' social and economic backgrounds. One course manager described how a pupil's home environment can affect his or her learning, for example a pupil may be a carer of people within the family:
Class, deprivation, social class, all that sort of stuff, and it’s been my experience that actually a truly effective teacher who can inspire children, needs to take those things into account, and needs to know where their pupils are at, and work with that to improve that.
EBITT 6 secondary phase
The importance of topics such as drugs, alcohol, SRE, smoking, child protection and safety was discussed by several course managers. One commented on the importance of teachers helping pupils to develop health-related skills rather than just providing them with information:
The health and well-being of young people is all to do with more than just you know sex and relationship education, it’s about communication skills, listening skills, developing those skills, and social skills, and you can do that as a classroom teacher and you’ve got a part to play in that.
SCITT 15, secondary phase
Conceptions of health and well-being included teachers' as well as children's health. The fact that an emphasis on exam results can lead to teachers leading unhealthy lives was also mentioned. One organisation provided trainee teachers with the opportunity for self-study and the use of music and books, emphasising the message that part of children's health in your care is your own health:
If schools were more thoughtful and less pressured, given the amount of time that pupils spend in schools . . . we might have happier schools, happier teachers.
HEI 29, primary phase
Model of initial teacher training
From our analysis of the course managers' accounts and our existing knowledge of health and education, we created a model of ITT (shown in Figure 7) which shows the different organisations and people that can influence the delivery of training in health in ITT, and the relationships between them. The purpose of this model is to show the context of ITT and put the findings described in the subsequent sections into context. In particular, we found that the barriers to and facilitators of training in health mentioned by the course managers were each located within one or more of these spheres of influence, and this helps to highlight where changes can be made to promote more effective training in health.
The model shows that government policy (in education and health) partly influences the training provided in ITT and also what placement schools do around health. Our model shows this to be a top-down influence, as this was how course managers portrayed it. They felt that it had a major influence on the content of their courses. We have characterised the relationships between teacher training providers, placement schools and external agencies, as well as trainee teachers, as reciprocal, as the course managers' accounts suggested that these were sometimes two-way relationships. The role of the trainee teachers in our model should not be viewed as a passive one, as simply receivers of training. We found in our analysis that the course managers felt that trainee teachers could also impact on the health training that they received through, for example, the pre-existing knowledge that they brought to courses and their level of interest in and engagement with health issues. The model also shows that health training in ITT was located within the wider contexts of the local culture and geography of the areas in which providers, placement schools and agencies were based, and also the general perceived culture in education, and that these factors could also influence training in health or formed a backdrop to it. The following sections of this report will expand on the relationships between these people, organisations and contexts, and the impact that they have on the provision of health training.
In the following sections we present our findings from our analysis of the interviews with the course managers. We first describe how health and well-being was delivered on courses and then we consider the barriers to and facilitators of effective training in health in ITT in terms of the six analytical themes identified. We present all of the barriers and facilitators identified in the analysis in tables and have shown in the tables how each of the barriers and facilitators mapped onto the spheres of influence shown in the model of ITT in Figure 7.
FIGURE 7.
Model of the spheres of influence on health coverage in ITT and the relationships between them.
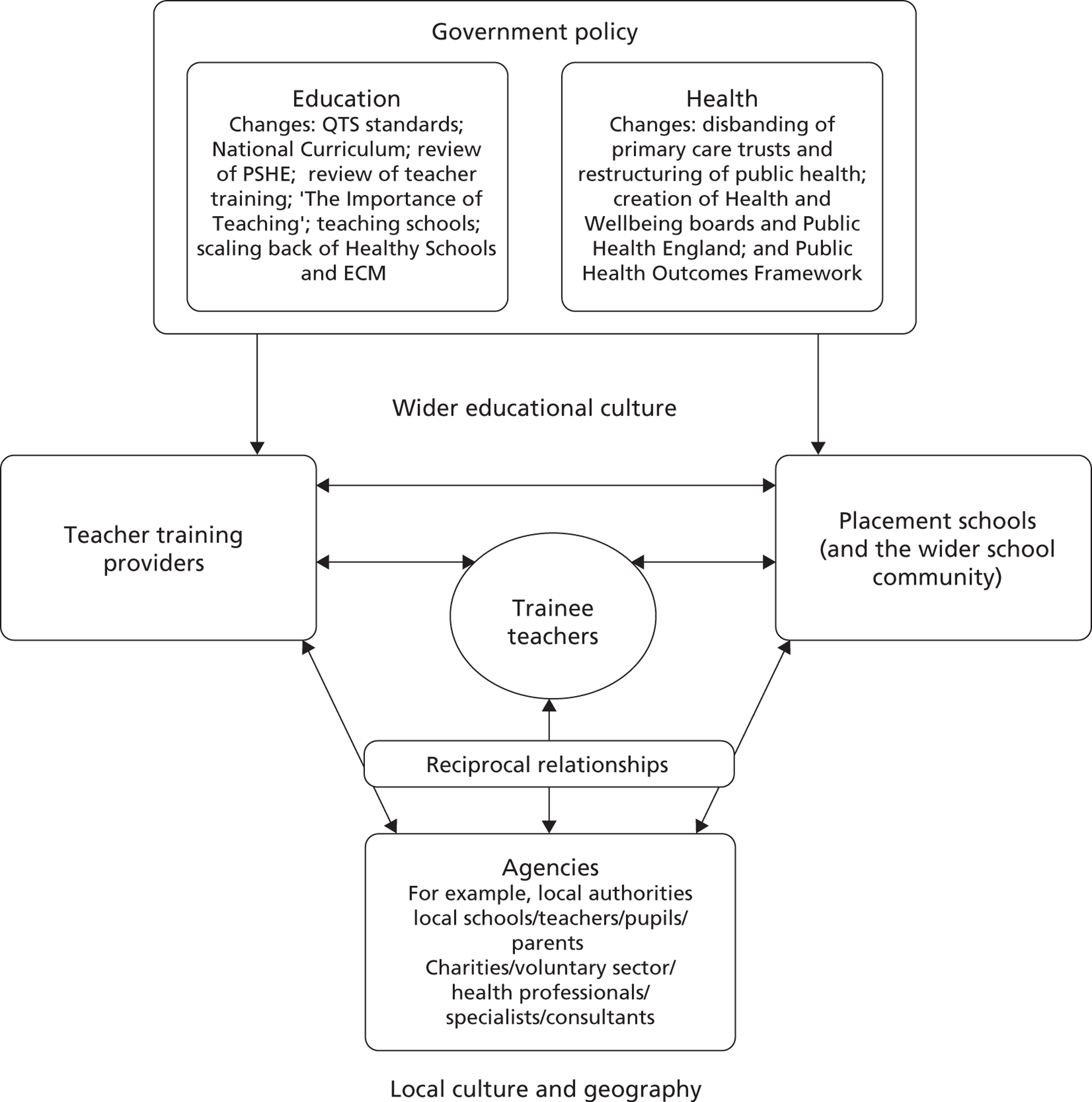
How health and well-being was covered on courses
We found that there was variability in how health and well-being was covered across courses, and also in the amount of time spent covering these topics. Furthermore, course managers were not always clear in the interviews about where health and well-being topics were located within their courses. This was partly because of the perceived wide-ranging nature of what constituted ‘health and well-being’, with a number stating that it came into many aspects of the course indirectly, such as in SEN and behaviour management. However, this was also because of some aspects of health training not being very explicit in some courses. For example, when asked how his course covered SRE, drugs and alcohol education and smoking prevention, one course manager said:
Very incidentally, if I’m very honest . . . I wonder whether we do that at all, but I think it’s more likely to come in the science session than it is in the PSHCE [personal, social, health and citizenship education]. The SEAL materials I think perhaps do wee bit of that, but then it’s more social emotional aspects of learning, and it’s, it’s again it’s only going to be incidentally.
HEI 5, primary phase
From the course managers' accounts we categorised the nature of how health and well-being topics were covered into the following groups – we found that our categories mapped directly onto those created by Arnold and Maio-Taddeo44 to describe teacher education in child protection in Australia, so we used the category names created by these authors:
-
integrated/embedded approach – in which there was an underpinning health-related ethos or structure to the course and health topics were integrated into training across different areas of the course
-
discrete approach – individual sessions or modules that explicitly covered a health topic or PSHE education
-
incidental training – in which a health-related topic was covered incidentally or implicitly as part of another aspect of training, for example SEN, dance or PE, or when trainees chose a health-related topic for an assignment.
These categories are not mutually exclusive. For example, on some courses there were discrete sessions on some topics but other topics were covered more incidentally. The integrated and discrete approaches resulted in health training being much more explicit in the curriculum and contributed to a more coherent approach. There was also variability in terms of whether the trainee teachers across different types of courses (e.g. BEd, PGCE) and subjects within the same institution received similar health input. On some secondary-level courses, course managers said that science and PE trainee teachers were likely to receive more training in health issues because of the nature of their subjects.
Health topics were generally covered within the professional studies modules on courses (Table 17), and discrete sessions on PSHE education were commonly located within this. Specific health issues, such as drugs education and SRE, were sometimes covered as part of the PSHE education sessions, as stand-alone sessions, or were located within subject-specific modules, such as PE or science. All of the secondary phase course managers mentioned that some health topics were covered in professional studies, whereas only four of the seven primary phase course managers said the same. Conversely, more primary phase course managers (four) than secondary phase course managers (one) indicated that health topics were covered in many areas of the curriculum or that they made cross-curricular links.
| Curriculum area | Number of course managers | |||
|---|---|---|---|---|
| All course managers (n = 18) | Primary phase course managers (n = 7) | Secondary phase course managers (n = 8) | Managers of courses spanning both primary and secondary phases (n = 3) | |
| Professional studies | 14 | 4 | 8 | 2 |
| Science | 10 | 5 | 4 | 1 |
| PE | 8 | 5 | 3 | 0 |
| Covered in many areas of the curriculum and/or make cross-curricular links | 7 | 4 | 1 | 2 |
| English or literacy | 4 | 2 | 1 | 1 |
| Humanities | 2 | 2 | 0 | 0 |
| The arts (e.g. music, art, drama) | 2 | 2 | 0 | 0 |
| Other | 4 | 2 | 2 | 0 |
Less attention is given to training teachers to promote healthy lifestyles
On the whole, we found that when the course managers described how health and well-being was covered on their courses they tended to talk about topics such as special or additional educational needs, behaviour management, emotional well-being and SEAL, citizenship, equality and diversity, safeguarding and PSHE education in general (Table 18) – topics that are perhaps seen to be closely related to education and children's learning. They talked less frequently about specific health and lifestyle issues such as healthy eating, alcohol and drugs education, physical activity and smoking prevention. There were no differences between primary and secondary phase course managers in the topics that were mentioned. Six of the course managers told us that they felt that their course provided limited coverage of SRE, alcohol and drugs education and smoking prevention. Furthermore, two course managers made an explicit self-assessment to us that they felt that their courses were not so effective at addressing specific health and lifestyle issues in comparison to other aspects of their courses:
We recognise that there’s room for improvement and I think there are other areas that we tackle better . . . We’re very good on preparing our students while managing behaviour within classrooms . . . I don’t know that we’re so good on preparing our students in understanding the health and well-being of children.
HEI 30, secondary phase
| Topic | Total number of references course managers made to covering topic across the interviews | Number of course managers who mentioned in the interview that they covered topic | |||
|---|---|---|---|---|---|
| All course managers (n = 18) | Primary phase course managers (n = 7) | Secondary phase course managers (n = 8) | Managers of courses spanning both primary and secondary phases (n = 3) | ||
| Special or additional educational needs | 45 | 15 | 5 | 7 | 3 |
| Safeguarding and child protection | 43 | 15 | 4 | 8 | 3 |
| PSHE education | 40 | 14 | 6 | 6 | 2 |
| SRE | 39 | 12 | 5 | 5 | 2 |
| Behaviour management | 30 | 9 | 3 | 3 | 3 |
| Equality and diversity | 24 | 11 | 3 | 5 | 3 |
| Emotional well-being and mental health | 26 | 11 | 5 | 4 | 2 |
| Citizenship | 21 | 7 | 4 | 2 | 1 |
| Drugs and addiction | 12 | 6 | 2 | 2 | 2 |
| Physical activity | 12 | 5 | 2 | 2 | 1 |
| Alcohol | 11 | 5 | 2 | 2 | 1 |
| Healthy eating and nutrition | 10 | 7 | 3 | 3 | 1 |
As we found in our questionnaire survey that SRE, alcohol and drugs education and smoking prevention were covered by fewer courses than other health topics (see Chapter 3), we asked the course managers in the interviews what they felt the challenges were to delivering these topics. We found that the barriers they mentioned were generally the same as those mentioned in relation to the delivery of other aspects of health (e.g. lack of time) (see Barriers to and facilitators of effective teacher training). We did not identify any specific issues associated with these topics, except that the course managers felt that:
-
sometimes trainees were uncomfortable with these topics
-
there was a general lack of comfort with these topics in the wider educational culture
-
the topics could sometimes be seen to be unacceptable to cover in some schools.
The last point demonstrates the impact that the perceived wider educational culture could have on health training. The course manager who raised this point said:
Drugs feature, but I was aiming to sort of try and tackle drugs or addiction through alcohol, because I still think in many schools drugs is just not talked about. It’s still very, very unacceptable . . . So I was wary of going down that route.
HEI 11, secondary phase
Delivery methods
A variety of methods of teaching health-related topics were used across different courses, including lectures, interactive workshops and whole-day events (Table 19). Three of the course managers felt that the whole-day sessions they held had been a particularly successful part of how they addressed health. The themes of the health-related whole-day events held at the institutions included:
-
ECM (n = 1)
-
equality and diversity (n = 2)
-
behaviour management (n = 2)
-
SEN or special educational needs and disability (SEND) (n = 2)
-
Health (n = 3)
-
PSHE education and/or citizenship (n = 5)
-
Interprofessional working (n = 1)
-
Pastoral care (n = 1)
-
Child protection (n = 1).
| Method | Number of course managers who mentioned that this method was used on their course |
|---|---|
| Whole-day events or sessions | 10 |
| Workshops and interactive sessions | 8 |
| Student-led sessions or presentations | 6 |
| Lectures | 5 |
| Materials on the VLE | 5 |
| Tasks or assignments | 5 |
| Self-study | 4 |
| Outside visits | 3 |
| Role play | 3 |
| Reflective diaries | 2 |
| Seminars | 2 |
| Presentations delivered by health professionals | 2 |
| Covered in school and through readings | 1 |
| Distance learning materials | 1 |
| Twilight sessions | 1 |
Six of the course managers said that trainee teachers led workshops and made presentations to each other on health-related topics. Five reported that course tutors sometimes used resources, including Teachers TV and SEAL materials, to support their health delivery, and they commented that these resources were useful.
Four of the course managers said that some of their trainee teachers gained training in health through alternative placements in settings other than schools, including:
-
social services
-
hospital schools
-
prisons
-
homeless shelters
-
sports organisations
-
orphanages abroad.
One course manager commented that these placements had helped to raise their trainee teachers' awareness and understanding of health issues:
We have had some go to a local homeless charity and work with homeless people in [city] essentially, and it was quite powerful what those students said when they returned, about actually how they went with such preconceived ideas, and also they had no knowledge and actually they felt that through their experience they could go, one of them said he could feel that he could go in and teach any PSHE lesson on drugs and alcohol addiction and feel confident that he knew the facts and what the realities are.
HEI 40, primary and secondary phases
Furthermore, at eight of the institutions, the trainees undertook placements in schools for children with additional needs, including SEN, English as an additional language (EAL) and behavioural needs, and, again, the course managers felt that the direct experience of these issues that trainees gained on these placements was beneficial for them. We identified alternative placements in health-related settings as one example of what could be considered innovative practice. Other examples of innovative practice are detailed in Box 1.
-
Raising trainee teachers' awareness of particular initiatives and encouraging them to take them out into schools
-
Science and professional studies tutors team teach health content in professional studies to help trainee teachers understand that health issues are not confined to the remit of particular subjects
-
Students from another course who have a social work background deliver training on interprofessional working
-
Health day located within professional studies, which involves workshops delivered by health professionals and sessions organised and led by science and PE postgraduates
-
Alternative placements in health-related settings (trainee teachers can choose to do their alternative placement in these settings)
-
Peer-organised supervision groups for trainee teachers using a technique applied in medicine for supporting GPs
-
Paired placements
-
Mentoring provided by ex-trainee teachers
Experience on school placement
The course managers said that it was likely that trainee teachers would gain experience of the pastoral side of teaching and PSHE education on school placement, with some also saying that it was a course requirement that their trainee teachers were attached to a tutor group. In some cases the course managers were reliant on trainee teachers gaining experience of some health-related issues in school in the absence of formal training by the provider. However, many of the course managers were not very clear in the interviews about the nature of the training or mentoring around health that the trainee teachers received on placement. Seven told us that they were unsure what was covered and that it was not closely planned or monitored:
PSHE forms part, usually part of their tutorial programmes in schools, so as a tutor they would engage with it. And in my questioning of them, which I was sort of doing on a small group basis, it would seem probably 60% of them have worked on part of the PSHE programme. Whether that’s health, I wouldn't commit. I don’t know.
HEI 11, secondary phase
Furthermore, 15 of the course managers described trainee teachers' experience of health initiatives and teaching PSHE education on placement as variable, with experience being dependent on individual circumstances (e.g. the health-related activities in the school, how high profile health was in the school, and the year group to which trainees were attached), and often incidental:
If there’s something going on and there are things like the collapsed timetable day they [placement schools] often get health professionals in. They often have the school nurses in . . . but then that’s more by good luck than good management on our part. It’s just you know if a trainee happens to, if that happens to happen, then it's usually to do with it being by coincidence, so, which is a good coincidence.
SCITT 15, secondary phase
Some of the course managers also commented that, unlike other aspects of the curriculum, there was no consistency across schools in the way that PSHE education and health topics were delivered or approached. This contributed to the variability of trainee teachers' experience and meant that some were likely to experience a narrow perspective on approaches to it, if they did experience it at all. This was particularly seen to be an issue for students on GTP programmes, who spent much of their time in their employing school and had less contact time at the provider for training than students on other courses.
Cohesion between provider and school placement
On some courses there was some cohesion between the health training at the provider and trainee teachers' experiences on placement. Seven of the course managers told us about tasks that trainee teachers were expected to carry out in school that helped to link their centrally based training with their school experience, including assignments that required trainee teachers to map how health and well-being was delivered in their school, and keeping a reflective log of their tutor group work. Although these tasks provided some link between centrally based training and training on school placement, the interviews showed that practical experience or training relating to health on school placement was generally not systematically planned in courses.
People involved in delivery of health training
On the whole, health-related topics were taught by course tutors, who typically had backgrounds in teaching in schools. The course managers said that they and some of their course tutors had begun to specialise in particular health-related areas during the course of their careers, and that some of the tutors drew on this knowledge to deliver particular health-related sessions on courses. In some cases, PSHE was taught by individuals who had some background in the topic (e.g. through their previous teaching experience), but in many cases it was taught by non-specialist staff who had to prepare themselves to teach it. None of the course managers said that the staff who taught health-related topics had had any specific training in it, but three mentioned that staff might occasionally happen to receive training in it, for example as part of in-service training days. Two course managers mentioned that students or staff from other departments with health-related expertise delivered some of the health content on their courses. More commonly, though, the course managers reported that they brought in external expertise to deliver some health-related elements in their courses.
Working with external agencies or external people
All of the course managers reported that they worked with people from external agencies to deliver some of the health-related content on their courses. In line with our questionnaire findings (see Chapter 3), they most commonly mentioned working with personnel from the local authority or local schools (Table 20). Local authority personnel were especially involved in delivering safeguarding and behaviour management training. The course managers mentioned a wider range of topics being covered by school personnel, including:
-
emotional and behavioural disorders
-
EAL
-
vulnerable children
-
behaviour management
-
SEAL
-
SEN
-
pastoral care and PSHE education
-
the role of the parent in children's learning
-
pupil voice.
On two courses, support staff from schools (a parent support advisor and a teaching assistant) also delivered sessions. Furthermore, one HEI brought pupils from a secondary school in to help facilitate a session on pupil voice. Some course managers also involved theatre groups, charities and the police in delivering health-related content (typically safeguarding, SEN and equality and diversity), among other external people.
Few of the course managers mentioned involving people from external agencies in the delivery of training in health issues such as smoking prevention, healthy eating, physical activity, SRE or mental health issues. On the whole, provision from external agencies usually covered health topics more closely related to education and learning, such as those listed above provided by school personnel, rather than training in health promotion to live healthy lives. This perhaps reflects that this kind of expertise was more immediately available to ITT courses or reflects the sources of expertise that course staff knew about. Indeed, in line with our questionnaire findings, only six of the course managers we interviewed said that they involved health professionals in the course (e.g. nurses, counsellors, midwives, public health-promotion specialists).
| Type of external agency or person | Number of course managers who mentioned that agency or people were involved in delivering health-related content on their courses |
|---|---|
| Local authority | 13 |
| Teachers or other school personnel | 12 |
| Charity or voluntary sector organisation | 8 |
| External specialists (non-specified or unclear) | 8 |
| Health professionals | 6 |
| Consultant | 3 |
| Police | 3 |
| Personnel from other universities | 2 |
| School pupils | 2 |
| Sports organisations or specialists | 2 |
| Theatre groups | 2 |
| Lay people | 1 |
| Local primary care trust personnel | 1 |
| Educational psychologist | 1 |
| Parents | 1 |
| Other | 6 |
As we found in the online questionnaire that few institutions worked with health professionals, we asked the course managers in the interviews what they felt the barriers to this might be. The barriers that course managers mentioned were:
-
it was just not something that they had thought about doing, as they tended to think about education people when engaging external expertise and they felt that it was more appropriate for people with this background to deliver training in ITT
-
difficulties making contacts and not knowing who to approach
-
concern about a lack of understanding of ITT and education among people from external agencies
-
reluctance from the health service to release staff because of the pressures that they were under
-
difficulties finding mutually convenient times to work together.
Ten of the course managers said that working with people from other agencies or departments with health-related expertise had been a particularly successful part of the health training on their courses and they reported that the students liked it. They cited the following benefits of this for the trainee teachers:
-
being exposed to a different perspective
-
being exposed to a facilitator with ‘real-life’, direct experience
-
knowledge for the future of other professionals' roles.
Timing of health in the course
In general, the course managers said that the timing of when health topics were introduced to trainee teachers depended on the trainees' needs and the topic, and that topics were spread throughout the course. Only one course manager said that the timing was incidental (i.e. not based on any specific reason) and another two said that the timing partly depended on timetabling and when contact time at the provider fell. In many cases, topics such as SEN, behaviour management and safeguarding were delivered in the first term, as the course managers felt that the trainees needed to know about these before going on their first school placement. In some institutions, topics such as PSHE education, citizenship and SEAL were also delivered early on in the course. At others, there had been a deliberate choice to introduce some health-related topics either in the middle of the course or later on, as the course managers felt that it was beneficial for the trainees to gain some experience in school before covering some issues:
We look at transfer and transition on their return in the New Year . . . [because they've] had some experience of seeing potential issues and seeing how children slip back and can actually contribute a bit more to those sessions.
HEI 40, primary and secondary phases
Funding of health and well-being
All of the course managers told us that they did not have any specific funding available to them at their institutions for health-related work. Some commented that they could make requests for funds to organise events or activities, with the case having to be made for these. Sometimes funds were available indirectly through other related areas (e.g. funding for SEN training) and sometimes one-off funding was available (e.g. through a funded research project).
In the absence of specific funding, 12 of the course managers said that some of the health-related activities on their courses were partly dependent on free support and the goodwill of others, such as personal contacts, in volunteering their time for minimal cost. Five of the course managers also commented that they had reciprocal relationships with external agencies, whereby the agency offered support on the course and the provider helped them in return, for example by giving them the opportunity to train and to influence their trainee teachers, to broaden the experience of the agency's staff or to advertise their services, or by providing support to the agency:
We’re quite fortunate in that because quite a lot of the close relationships we have with different agencies, a bit of give and take, so you know we support them with something, they support us with something as well.
HEI 25, primary phase
Assessment of health and well-being
Many of the courses did not specifically assess trainee teachers' learning around health and well-being. We characterised the nature of the assessment that took place into the following categories (note that, again, these categories were not mutually exclusive):
-
assessment against the health-related standards in the current QTS standards
-
direct assessment
-
indirect/incidental assessment.
Ten of the course managers said that trainee teachers' learning in health was assessed against the health-related standards in the current QTS standards, and some told us that this was the only method of assessment that they used:
The teaching of PSHEE and elements of citizenship, form tutor roles and all of that kind of area form part of the required standards. Information advice and guidance and things like would come under the current QTS standards, which they’re required to all meet . . . so there’s no sort of necessarily written research-based academic evidence.
HEI 40, primary and secondary phases
Seven reported that their course included direct assessment of some aspects of health and well-being, for example as part of a discrete PSHE education module or on one or two specific health-related topics (e.g. transition and transfer, physical development). Eleven course managers mentioned that trainee teachers' learning in health was indirectly assessed. This was, for example, through assignments required for related subjects such as science or PE or through trainee teachers happening to choose a health-related topic as part of an assignment or research project.
The general lack of direct assessment seemed to be indicative of health and PSHE education sometimes being seen to be lower priority subjects than other aspects of the ITT curriculum. Indeed, the reasons given by some of the course managers for not carrying out direct assessment suggested so:
I suppose it’s because it’s an additional strand, it’s kind of we don’t, we don’t assess them specifically.
SCITT 15, secondary phase
Health and well-being of teachers and trainee teachers
Eight of the course managers acknowledged in the interviews that teacher training is demanding for trainee teachers and they stated that the health and well-being of their trainee teachers was a key concern for them. Five said that it was central to the ethos of their courses. Nearly all of the course managers felt that they addressed trainee teachers' health and well-being well on their course, with only one saying that they felt this could be improved. This was because they felt that they had effective pastoral systems in place, including good liaison with placement schools about trainee teachers' well-being. Six commented that they also got to know their trainee teachers well, and this helped them to ensure trainee teachers' well-being. In addition to the formal pastoral support system, other ways that interviewees stated that they dealt with trainee teachers' well-being on the courses included:
-
encouraging trainees to support each other and share experiences (n = 5)
-
good support services available at their institution which they signposted to trainee teachers (n = 7)
-
encouraging a work–life balance (n = 3)
-
health screening prior to the course (n = 2)
-
raising awareness of union support and employment rights (n = 2)
-
empowering students through the student liaison committee (n = 1)
-
talking to trainee teachers about time management and stress (n = 3)
-
giving trainees opportunities to slow down and take time out during training sessions, to help them understand the importance of this for themselves and pupils (n = 3).
Some of the course managers also mentioned specific initiatives that they had run to support the trainees' pastoral care. These included:
-
paired placements (n = 1)
-
mentoring support from previous trainees (n = 1)
-
school mentor training to raise their awareness of trainee health and well-being (n = 3)
-
supervision groups using a technique used in medicine to support GPs (n = 1).
However, few of the course managers mentioned that they held specific sessions on aspects of teachers' health such as mental health issues or aspects of living a healthy life (e.g. healthy eating and physical activity), although seven of the course managers mentioned that, in some of the training sessions about pupil health, they covered the topic as it related to both pupils' and the trainee teachers' health.
Barriers to and facilitators of effective teacher training
In the interviews, the course managers identified a number of barriers to and facilitators of the delivery of health training in ITT and we also inferred barriers and facilitators from their accounts. We categorised these into the themes shown in Figure 8, which encapsulate the main issues that we identified. The themes are now discussed in turn in terms of the barriers and facilitators relating to each.
FIGURE 8.
The analytical themes that emerged from the course managers' views on the barriers to and facilitators of the delivery of effective teacher training in health and well-being.
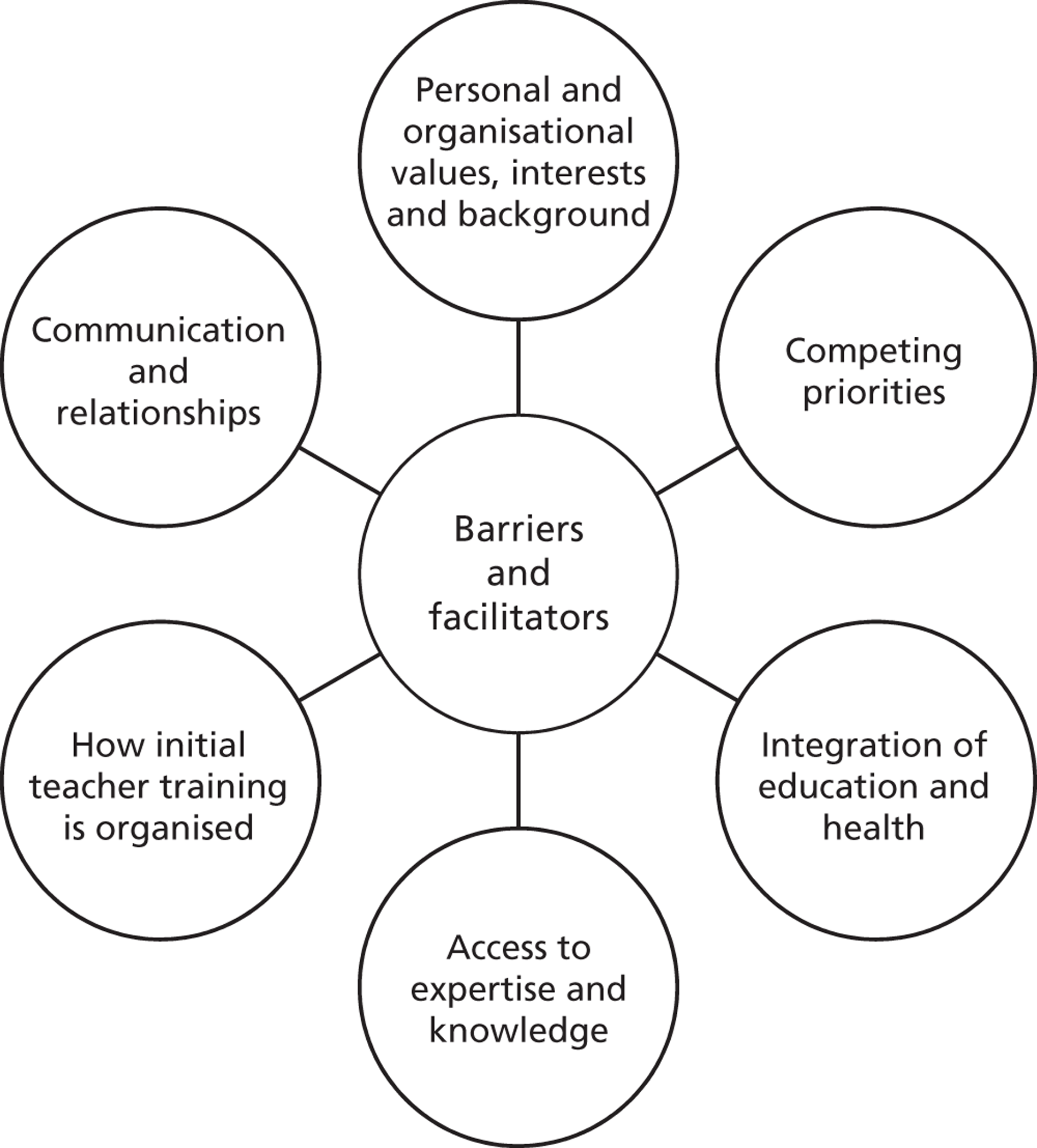
Personal and organisational values, interests and background
The course managers' accounts highlighted how their values, priorities, interests and backgrounds, as well as those of their colleagues, their organisation and placement schools, had influenced the content and delivery of health and well-being on their courses. Table 21 provides a summary of the barriers and facilitators cited by course managers that we categorised under this theme.
Individual and organisational values and commitment
The interviewees' accounts suggested that the delivery of health training in ITT was sometimes dependent on the commitment and personal values of the individuals involved. As discussed above, 13 of the course managers expressed a holistic view of education, and 12 felt that it was important for teachers to develop an understanding of the whole child. Two of the course managers also acknowledged that the role of teachers in school is not limited to teaching an academic subject, but that teachers also often have a pastoral role, and need to be aware of PSHE education and other health initiatives. Three of the interviewees said that they and their colleagues (including colleagues who they worked with from external agencies) shared similar beliefs about this. Their accounts suggested that these personal beliefs about the importance of health and well-being had facilitated the inclusion of some aspects of this in their courses and, in some cases, had helped to shape a course ethos that was centred around health and well-being in some form. Examples of the latter included particular themes that the course managers and/or their colleagues considered to be important being embedded throughout the course, such as SEN, behaviour management, children's well-being and teachers' pastoral care of children; the specific focus varied from course to course. The result was that these particular issues received a high level of attention on these courses:
In terms of preparing the trainees to teach young people, I think we, I think it’s really important. It’s something that I’ve always been quite passionate about, particularly the idea that you’re not just an academic within the school, as teacher you’ve got the role of being a tutor and having a pastoral lead and making sure that you’re aware of the current issues in terms of PSHE, knowing how it links into your subject, so we do quite a lot of how it’s across-curricular. So I think it kind of shapes the course.
SCITT 15, secondary phase
| Individual and organisational values and commitment | |
|---|---|
Facilitators:
|
|
| Personal background and interests | |
Barriers:
|
Facilitators:
|
| Partner school priorities and local culture and geography | |
Barriers:
|
Facilitators:
|
Personal background and interests
The course managers' accounts highlighted that their views and those of their colleagues about the importance of health had often developed from health-related professional or personal experiences they had had or from having worked, during the course of their teaching careers, with disadvantaged children or simply having seen much of children's lives. These experiences had raised their awareness about aspects of health, the link between health and education and the importance of focusing on the whole child, and resulted in these being given more prominence in their courses:
I just think it is that actually the group of us that work together believe in children, and there are a significant amount of us here who have been headteachers and have seen the best of children’s lives and worst of children’s lives. And I think some of the people who are lucky enough to come to study at university haven’t seen either of those things. And you need to be able to prepare them for that, and so there is a real willingness for everybody to encourage everybody to think about it.
HEI 45, primary and secondary phases
Given the broad nature of what health and well-being encompasses, it is difficult for courses to cover everything, and therefore people's backgrounds and interests also tended to influence the focus on particular health topics in the curricula. For example, one course manager's work with people from ethnic minorities had led her to give prominence to this issue in her course, including running a whole-day event on diversity in the previous year.
Four of the interviewees highlighted that the trainee teachers' backgrounds could also be a facilitator or present a challenge to their training in health. They told us that their trainee teachers came from a variety of backgrounds and life experiences, and they felt that these experiences could impact on their awareness and understanding of health issues:
The GTP students do seem to have a rooting in practice and what’s good for children, but I suspect it’s because a lot of them have come up from being teaching assistants, and I think the route develops people who have got this inbuilt sensitivity to children and their needs, and maybe have been quite used to dealing with issues . . . So they seem to be quite switched on and quite responsive, in a way it doesn’t seem to wash over them quite as much as it does BEds and PGCEs.
HEI 22, secondary phase
Competing priorities
The course managers felt that one of the main challenges around incorporating health and well-being into their courses was that there were competing demands on curriculum time, and also in their working lives and those of the trainee teachers and other colleagues. A theme throughout the course managers' accounts was that health was often seen to be or had to be treated as a lower priority area than other aspects of ITT. Table 22 provides a summary of the barriers and facilitators cited by course managers that we categorised under this theme.
| Level of priority placed on health | |
|---|---|
Barriers:
|
Facilitators:
|
| Time | |
Barriers:
|
Facilitators:
|
Level of priority placed on health
Many of the course managers felt that currently there was much uncertainty for ITT, with new educational policy emerging from the coalition government, the National Curriculum review and the introduction of the new teachers' standards. Many felt that that there had been a departure from policy that was supportive of addressing health and well-being in education (e.g. they felt that the new QTS standards emphasised health and well-being less than previously), and that there had been a move towards a greater focus on academic subjects and attainment.
The course managers commented that the main current political priorities for education were subject knowledge, SEN, behaviour management, EAL, black and minority ethnic groups and phonics. They said that these priorities had to take precedence in their courses, as these were the areas that they were assessed against in OFSTED inspections and the NQT survey, and these could also impact on funding and the number of initial teacher education places allocated to institutions each year:
It’s [health and well-being] dropped off the radar of this current government. And one of the things as a provider, and this is what’s quite difficult really, is that providers are required to follow DfE guidance. They’re not required to, in the sense that there’s nothing stopping them doing these things, but . . .there’s a limited amount of time and if you don’t show that your programme is emphasising the government’s priorities, then when OFSTED come along you’re in trouble. So it’s, it’s that that drives it, or that’s what’s driven, drives it out really.
EBITT 6, secondary phase
Fifteen of the course managers said that the lower priority given to health by new government educational policy made it more difficult for them to justify its inclusion in their courses. The personal importance placed on it by some of the course managers and their staff meant that, despite these pressures, time was made for it on their courses to some extent. Even so, these individuals also acknowledged that the realities of the time available meant that, because of the perceived lower profile of health in educational policy, they would probably not be able to cover health to the extent that they would like in the future, and some had already had to reduce the health-related content of their courses.
When the course managers talked about government policy as a facilitator, they tended to talk about previous policy – especially ECM (see Integration of education and health) – or the changes that the government could make in the future to encourage a focus on health, such as adding health-related questions back into the NQT survey. One course manager also commented that the current policy focus on SEN and behaviour management could be a potentially facilitating factor in the inclusion of health in courses, as it might help raise the status of health topics. Another felt that, as the new standards were written in a more general way than the previous ones, this might enable some local flexibility:
They are focusing on pupils making progress, and actually you can’t make progress if you’re not in a good place, whether that’s you know you’re not eating the right things or you’re mentally not well, so actually, and I think that . . . we’ll be able to use those then to change some of the things that we do.
HEI 45, primary and secondary phases
Three interviewees also said that the new areas of priority could be used as ‘ways in’ to delivering health. They described ways that they were adapting their courses to retain a focus on health by addressing the health-related aspects of SEN, disability and behaviour, or by reframing what they already did around the new areas of government priority.
Time
One of the most frequently mentioned challenges by course managers was the lack of adequate time and space to address health and well-being in their courses (mentioned by 16 interviewees). They felt that the range of areas that they had to cover to address government priorities and the need to prepare teachers in terms of their subject knowledge and pedagogical skills left little room to deliver training on some of the wider aspects of teaching life:
Even though I do think it’s important . . .ultimately, the vast majority of the time they spend teaching their subject and the kind of the pressures put onto teachers with the OFSTED framework and learning and progress . . . all of those things now have to take priority. And just getting them to the point where they can use those really efficiently and effectively takes the vast majority of our training time.
SCITT 15, secondary phase
The course managers said that the competing demands on time were particularly a barrier to covering health in depth on 1-year PGCE and GTP programmes. Another perceived challenge for GTP programmes was that trainees spent less time in centrally based training than trainees on other courses.
The course managers felt that having more time available would potentially facilitate the inclusion of health on courses, but the realities of ITT meant that this was not always possible. In this context, six of the course managers had managed to find ways (compromises) to deliver health within these constraints. For example, at two institutions they managed to cover a number of health topics by students self-studying topics and then presenting to each other on them. Finding these compromises facilitated the inclusion of health on some courses.
Integration of education and health
We found from the course managers' accounts that a more integrated approach to education and health was generally perceived to be a facilitator to teacher training in health and well-being. This included the extent to which those involved in ITT and education treat education and health as separate compared with the extent to which a more holistic approach is taken or promoted (e.g. within courses or led by the government). Table 23 provides a summary of some of the barriers and facilitators cited by course managers that we categorised under this theme.
Integration of education and health in government policy
The course managers' accounts highlighted that previous government policy which embedded health in education and promoted interprofessional working and a holistic approach had aided the inclusion of health training in ITT. Six stated that ECM had been particularly successful in doing this. They felt that it had helped to raise the profile of health and make it a higher priority for ITT providers, trainee teachers and schools. Some felt that it had also helped to raise educational personnel's awareness of children's health and had promoted a more holistic and integrated approach in education:
Oh well I think the Every Child Matters agenda . . . with all that exciting talk about partnership working and looking after the whole child, of connecting up services, that meant that there was a push in schools to do something about that, so that meant there was a period of time . . . when school nurses were talking to trainees, police officers were talking to trainees, truancy officers were talking to trainees when they were in school . . . so I would say that was a positive, but it’s turning into a bit of a challenge now, because it feels like it is, it’s not, it’s not disappeared, but it’s I think dissipating.
HEI 27, secondary phase
| Integration of education and health in government policy | |
|---|---|
Barriers:
|
Facilitators:
|
| Interprofessional, inter-agency and interdisciplinary working | |
Barriers:
|
Facilitators:
|
| Acceptability of health promotion in education | |
Barriers:
|
|
The course managers felt that there had been a move towards a disconnection between education and health in current government policy. However, three course managers commented that, despite this, they felt (or hoped) that the legacy of ECM would remain in education and their courses, with some saying that the essence of it would still be covered in their courses even if it did not have the same name. In this sense, ECM continued to be a facilitator in some ways.
Interprofessional, inter-agency and interdisciplinary working
As discussed above, 10 of the course managers felt that working with people from other agencies or departments with health-related expertise had been particularly successful on their courses. Some of the course managers at HEIs acknowledged that there was often a wealth of health-related expertise and input immediately available at their institution in other departments and faculties (e.g. medicine). Although raising the possibility of working with people from other departments in the interviews, only two of the course managers said they had done so. Two course managers felt that they could do more cross-disciplinary working and that this would be a potential facilitator. One course manager had tried to link with the health department at her institution but had found it difficult to arrange because of conflicting university timetables and a lack of staff time.
Acceptability of health promotion in education
Two interviewees commented that a minority of trainee teachers did not feel that health was part of their remit and that this could present a challenge. One course manager said of some workshops on health that the trainee teachers had run:
The feedback was vitriolic I would suggest from two particular subject pathways [English and Religious Education], where they genuinely did not see it as their brief to address health. It was outside their remit, it was outside their knowledge base. They felt that advice they might give might be wrong.
HEI 11, secondary phase
In this instance, the course manager described the trainee teachers' concerns as being centred on a lack of knowledge and worries about dealing with sensitive issues. These trainee teachers did recognise that in their role as a tutor they may need to deal with children's well-being issues, but they saw their role as one of referring identified problems onto someone else. A point for discussion that this raises is also the extent to which addressing health and well-being issues should fall within the remit of teachers and where the boundaries lie between their role and other professionals' roles.
Access to expertise and knowledge
The course managers felt that having access to health-related expertise and knowledge was a facilitator of delivering health on their courses, whereas a lack of access to this kind of expertise and knowledge was perceived to be a barrier. Table 24 provides a summary of some of the barriers and facilitators cited by course managers that we categorised under this theme.
| Comfort and confidence with and understanding of health issues and topics | |
|---|---|
Barriers:
|
Facilitators:
|
| Having and making contacts | |
Barriers:
|
Facilitators:
|
| Knowledge and expertise of trainers from external agencies | |
Barriers:
|
Facilitators:
|
| Resources and information | |
Barriers:
|
Facilitators:
|
Comfort and confidence with and understanding of health issues and topics
Five of the course managers felt that ITT provider staff sometimes lacked confidence and knowledge to be able to deliver health topics effectively, and this was why some valued the specialist knowledge brought by external input. When some course managers and ITT staff had health-related professional or personal backgrounds this was a facilitator, as their experiences had given them the knowledge to be able to teach these topics.
Six of the course managers felt that trainee teachers also often lacked understanding and were not comfortable or confident with health topics (with two commenting that this was also the case among teachers generally in the wider educational culture) and that this presented a challenge. The course managers said that the trainee teachers were especially concerned about teaching SRE and that younger trainee teachers often felt particularly awkward about this. The course managers suggested that this was due to their lack of knowledge. They suggested that the trainees were more comfortable with topics that they were more familiar with, such as alcohol, and comfort with the topics was a facilitator:
The students are . . . well I think are more comfortable, I guess I’m saying more familiar with, that alcohol, they tend to have a lot of questions about alcohol abuse. I think in the media it tends to be a lot about young children in particular. So when we looked at drugs, I think alcohol as one of a drug group is something the students can talk about.
HEI 29, primary phase
Knowledge and expertise of trainers from external agencies
As discussed above, 10 of the course managers said that accessing the expertise and knowledge of people from external agencies had particularly facilitated the delivery of health training on their courses. Four of the course managers emphasised, however, the importance of having access to people with the right experience and skill set to deliver content to trainee teachers. They felt that it was especially important to know that the trainers would be good because, given the time pressures on courses, often a session was the only opportunity to deliver a subject and it needed to be effective. Most of the course managers felt that the people who they had worked with from external agencies on their courses had been very good and engaging trainers. Two, though, expressed concern that people from outside agencies may not necessarily understand the trainees' needs.
And I think I particularly like it when they’re teachers or headteachers from our partnership, because they are likely to understand the students’ needs rather better . . . People who come completely from a separate agency don’t always have a sense of where our students are coming from.
HEI 42, primary phase
Having and making contacts
An important facilitator of working with external agencies was having contacts and making contact with external organisations. Eight of the course managers had made contact with external organisations through their or their colleagues' personal and professional contacts (e.g. from their previous health-related jobs, teaching jobs in local schools or personal role as a school governor). One course manager mentioned that, on her course, the staff had developed a list of external organisations who had hosted successful alternative placements for the trainee teachers and who could be asked to input into the centrally based training. Four of the course managers had simply approached external organisations without any prior contact to see if they would be willing to be involved. The organisational structure of a course could also help course managers make contact with external expertise. Three said that they had brought in external expertise from their placement schools through developing close relationships with these schools during the course of their work. Furthermore, two of the EBITT course managers felt that having a local authority presence on their GTP courses had been useful for identifying and making contact with external expertise:
We’re at a huge advantage in that we’re a local authority provider, so we are embedded within the Local Authority, so we have contacts with the consultants, we have contacts with the local authority safeguarding officer, and those are just there and just established.
EBITT 9, primary and secondary phases
Five course managers commented that a barrier to accessing external expertise was that they did not know who to contact and there was a lack of information about who to approach for this kind of work.
How initial teacher training is organised
The course managers' accounts suggested that aspects of how their courses and ITT in general were structured or organised could be enablers of or barriers to the delivery of health and well-being training. Table 25 provides a summary of some of the barriers and facilitators cited by course managers that we categorised under this theme.
| Course structure and organisation | |
|---|---|
Barriers:
|
Facilitators:
|
| Funding | |
Barriers:
|
Facilitators:
|
| Variability in delivery | |
Barriers:
|
Facilitators:
|
Course structure and organisation
There was a mix of feelings among the course managers about whether or not school-based training was a facilitator of training in health. One HEI course manager felt that the government's move to more school-based training could be a potential facilitator, as the trainee teachers were often focused on their lives in school and training within the school context might make health issues more pertinent to them.
Others also commented that the move to more school-based training might mean that trainee teachers gained more experience of health issues during their training, as they would be spending more time in school. However, others, including current course managers at EBITTs, felt that this was a potential barrier because of the extent to which trainee teachers encountered health on placement being highly variable and context dependent, and they felt that school staff may not necessarily have the skills or capacity to address health.
Funding
A lack of funding was cited as a barrier to the delivery of health and well-being training by nine of the course managers. Some commented that it would be helpful if the government made funding specifically available for health activities, including health training for ITT provider staff (mentioned by four interviewees). They said that hiring external speakers and running special all-day events were particularly costly. In some cases, when they had set up particular health initiatives the funding had run out for these and they had to be stopped.
The current economic climate also presented a challenge to the delivery of health and well-being training on courses as a number of the courses were operating on fewer resources, having undergone a reduction in their trainee teacher numbers for the current year. This meant that some of the health-related initiatives that had previously been in place were not sustainable:
We can’t do special days, which is what we would have done and what we certainly did, and we would have continued that, because it was very successful, but this year it’s been and it’s going to get worse . . . Because they’ve cut the numbers of graduate teacher programme people, so if you have fewer trainees, you’re going to have less money. So I can’t see it getting any better.
EBITT 6, secondary phase
Communication and relationships
We found that communication between and within organisations could be a facilitator of the delivery of health on courses, whereas a lack of communication was a barrier. Table 26 provides a summary of some of the barriers and facilitators cited by course managers that we categorised under this theme.
Seven of the course managers' accounts suggested that there was poor communication between the provider and placement schools about health training. As discussed above, in addition to the course managers saying that trainee experiences of PSHE or health on school placement were variable and dependent on individual circumstances, many were unclear about what trainees covered on placement. They commented that their placement schools were also not always aware of the centrally based training that trainee teachers received. The course managers felt that building a shared understanding and knowledge of the training received at each was easier to achieve if there were only a small number of schools in the partnership and if these were schools who regularly took students.
Barriers:
|
Facilitators:
|
Although some of the course managers suggested that there was poor communication between the provider and placement schools about health training, many felt that they had good relationships and systems in place for communicating about trainee well-being:
We have the close contact with schools so that if schools pick up on anything, we’re in contact with each other quickly and so that we'll deal with it together.
EBITT 9, primary and secondary phases
Furthermore, three of the providers told us that, during their school mentor training, they raised mentors' awareness of issues related to trainee health and well-being. This was because they felt that this was something that it was important for mentors to understand.
Summary of most frequently mentioned barriers and facilitators
Table 27 summarises the most commonly mentioned barriers and facilitators across all of the themes (mentioned in 10 or more of the interviews).
| Barriers | Facilitators |
|---|---|
|
|
Summary
-
We conducted 18 interviews with 19 course managers who responded to the online questionnaire to find out more about how they covered health and well-being on their courses and the barriers to and facilitators of this.
-
Many of the course managers held a holistic view of education and acknowledged the importance of trainee teachers developing an understanding of the health and well-being of pupils.
-
There was variability in how health and well-being was covered across providers and courses. On some courses some health topics were incidentally or implicitly addressed as part of other aspects of the course, whereas in others they were more integrated into the curriculum or discrete sessions were provided (or there was a mix of these approaches). Specific health and lifestyle issues such as healthy eating, alcohol and drugs education, physical activity and smoking prevention appeared to receive less attention on courses than other health topics, and there was wide variability in the methods used to address these topics.
-
A particular issue that we identified was that trainee teachers' experience of teaching PSHE education or exposure to health initiatives on school placement was also inconsistent, with this often being dependent on individual circumstances and the priorities of the school in which they were placed. Many of the course managers were also not clear about the nature of the training that trainee teachers received on placement and their accounts suggested that communication between the provider and the placement schools about this could be improved.
-
We identified some examples of what could be considered innovative practice, including a whole-day health event run in collaboration with health professionals, an interprofessional working day run by students with a social work background from another course and alternative placements in health-related settings.
-
Specific funding for health training was not available to any of the course managers whom we interviewed, and their accounts suggested that health training in ITT was often reliant on free support.
-
Only seven of the course managers reported that they specifically assessed trainee teachers' learning in relation to some health and well-being topics, although 10 reported that they assessed this against the current QTS standards.
-
Most of the course managers felt that they addressed trainee health and well-being well on their courses, and this was usually because they felt that they had effective pastoral support systems in place. Some also had specific initiatives in place to help address trainee teachers' health, including school mentor training. However, few course managers mentioned that they held specific sessions on aspects of teachers' health such as mental health issues or aspects of living a healthy life, suggesting that, again, these topics received less attention in ITT.
-
Working with external agencies or other departments to deliver some aspects of health training was viewed by the course managers to have been particularly successful on their courses. Other commonly mentioned facilitators of the inclusion of health and well-being on courses included the importance placed on it by ITT staff and their commitment to it, having contacts to bring in external expertise and having free or low-cost support.
-
Commonly mentioned barriers to the delivery of health and well-being training included lack of time and space in the ITT curriculum and that health was a lower priority area in current educational policy.
-
The course managers also highlighted that trainee teachers could also impact on the health training that they received through, for example, the pre-existing knowledge that they brought to courses and their level of interest in and engagement with health issues.
-
As with the survey reported in Chapter 3 (from which interviewees were drawn), it should be recognised that the course managers responding may be considered to be generally supportive of health and well-being in ITT. This support may not necessarily be as widespread in practice.
Chapter 5 Systematic review stage 1: descriptive mapping of teacher training studies
To reiterate, the questions that this research sought to answer were:
-
In what ways does teacher training prepare teachers to promote health and well-being in schools?
-
How effective are interventions to train and support teachers in health?
-
What are the barriers to and facilitators of effective training and delivery?
The systematic review (along with the survey) was designed to answer all three of these questions. The first stage of the systematic review was a descriptive map of the research evidence, involving the systematic application of keywords to studies identified from a sensitive literature search.
Preliminary scoping work conducted before this project began suggested that the evidence base in this area was diverse in terms of health topics, country, level of education and types of outcomes and processes investigated. As there had been limited published evidence syntheses of this topic it was therefore considered that a descriptive mapping of the topic would be a useful starting point to provide a greater understanding of the research that has been published, and to determine which issues to focus on in a synthesis. Descriptive mapping has been successfully applied in a number of published systematic reviews of complex health and education interventions as a means of characterising the evidence base to facilitate a focused policy-relevant synthesis. 45–49
Methods
Literature searching
A highly sensitive search strategy was devised and tested on MEDLINE by an experienced information scientist. The strategy comprised a mixture of free-text words and controlled vocabulary terms (Medical Subject Headings). Once finalised, the MEDLINE strategy was then adapted for use on other available bibliographic databases (see Appendix 4 for the MEDLINE search strategy). The following databases were searched, with database platform and search dates in parentheses:
-
MEDLINE (Ovid) (database inception to April 2011)
-
MEDLINE In-Process & Other Non-Indexed Citations (Ovid) (May 2011)
-
EMBASE (Ovid) (database inception to April 2011)
-
The Cochrane Library [Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, Database of Abstracts of Reviews of Effects (DARE), NHS Economic Evaluation Database] (May 2011)
-
The Campbell Library (May 2011)
-
C2-SPECTR (The Campbell Collaboration Social, Psychological, Educational, and Criminological Trials Register)
-
Cumulative Index to Nursing and Allied Health Literature (CINAHL) (EBSCO) (1982–May 2011)
-
PsycINFO (EBSCO) (database inception to May 2011)
-
Social Sciences Citation Index (Web of Knowledge) (1970–May 2011)
-
Conference Proceedings Citation Index – Social Science & Humanities (CPCI-SSH) (Web of Knowledge) (1990–May 2011)
-
Education Resources Information Center (ERIC) (ProQuest Dialog Datastar) (1986–May 2011)
-
EPPI-Centre databases (TRoPHI/Evidence Library) (June 2011)
-
British Education Index (ProQuest Dialog Datastar) (1975–May 2011)
-
Australian Education Index (ProQuest Dialog Datastar) (1979–May 2011)
-
International Bibliography of the Social Sciences (CSA) (May 2011)
-
Sociological Abstracts (CSA) (May 2011).
No language restrictions were applied to the search.
The following websites were searched (in May 2012) for potentially relevant literature:
-
Schools for Health in Europe (www.schoolsforhealth.eu/)
-
Excellence Gateway (www.excellencegateway.org.uk/)
-
Current Education & Children's Services Research (www.ceruk.ac.uk/)
-
British Educational Research Association (www.bera.ac.uk/)
-
National Institute for Health and Care Excellence (www.nice.org.uk/)
-
NHS Evidence (www.evidence.nhs.uk/).
The reference lists of relevant systematic reviews identified by the search were checked for additional potentially relevant studies. All publications of studies included in the synthesis were checked for citations to potentially relevant studies that were not already identified through the sources mentioned above. All references (except those from the EPPI-Centre databases and from websites) were downloaded into a Reference Manager database (version 12; Thomson ResearchSoft, San Francisco, CA, USA) for storage and retrieval.
Inclusion screening
Round 1: screening on titles and abstracts
The inclusion criteria for the first round of screening were intended to be broad, to fully map the varying characteristics of the evidence base in this area. To be included in the first stage of the review (the descriptive mapping) references had to mention all of the following:
-
Health and well-being within schools.
-
This could include any aspect of pupils' or teachers' health and well-being, from specific topics (e.g. drugs, alcohol, sex education, safety, bullying, mental and emotional health) to broader aspects (e.g. life skills training, youth development, financial and economic education, careers education, citizenship education). Mention only of PE without reference to health was not sufficient for inclusion. Studies that reported teacher training without reference to their role as promoters of health were not included. Studies of children and young people with existing illnesses or conditions (e.g. behavioural disorders such as attention deficit hyperactivity disorder or physical conditions such as asthma) were not eligible for inclusion (although studies in which teachers were trained to identify children with previously unrecognised illness and refer to specialist care were eligible). Violence prevention/behaviour management studies were included if conducted within the context of health (e.g. to reduce bullying and improve mental and emotional health). If these studies were only about improving classroom behaviour and educational outcomes they were not included. Other topics excluded if there was no explicit mention of health and well-being included science education, compensatory education (programmes for socioeconomically disadvantaged young people), environmental education and social and interpersonal skills development.
-
References mentioning primary and secondary schools and further education colleges were eligible, but not those mentioning higher education (i.e. university) or preschool. References reporting activities in other settings (e.g. at home, the community, health services) in addition to schools were eligible for inclusion.
-
-
The training of teachers (including head teachers) in relation to the promotion of health and well-being in schools. Studies had to report details of the training received, rather than only stating the occurrence of training (therefore excluding references that just describe the proportion of teachers who have received training, or which survey teachers to assess their knowledge, attitudes, etc. about health and well-being) and/or the implementation of the promotion of health and well-being in schools by teachers (e.g. their general experiences of teaching around health and well-being; any difficulties that they experienced in teaching; the curriculum materials; their professional development; their views on the health and well-being aspect of the curriculum). This criterion was broader than the issue of teacher training (the main focus of this study) and was included in the event that the volume of literature focusing on training was insufficient for evidence synthesis (see Round 2: screening of full papers).
-
Research into the processes and/or outcomes of (2).
-
Research designs could include intervention evaluations [e.g. randomised controlled trials, quasi or non-randomised controlled trials, controlled before-and-after studies, uncontrolled studies and systematic reviews of these studies (systematic reviews to be included for reference checking only)] or non-intervention research (e.g. surveys, questionnaires, interviews, focus groups). Not included were commentaries, editorials, non-systematic review articles, teaching resources, guides, book reviews, curricula descriptions, research protocols/proposals (e.g. research in progress), conference summary reports and bibliographies.
-
Examples of relevant processes could include acceptability to the teachers of the training and of the health-promotion intervention itself (e.g. appeal, enjoyment, relevance to professional goals and personal values); resources and costs used to train the teachers; implementation of the training programme/the health-promotion intervention.
-
Both teacher and pupil outcomes were relevant. Examples of teacher outcomes included knowledge of health in general and of the specific health topic to be addressed; skills (e.g. ability to teach health-related behaviour change skills); and confidence/self-efficacy to provide health-promotion intervention. Examples of pupil outcomes included knowledge, attitudes, behavioural intentions; health-related behaviour change; and biological and physical outcomes (e.g. weight change).
-
Researchers used an inclusion/exclusion worksheet containing the criteria for screening specified above (see Appendix 5). Initially all titles and abstracts were screened alphabetically in batches of 500 by two researchers independently, with disagreements resolved through discussion. The batches were distributed amongst a subset of the research team (JS, KP, JP, DH and SD) in various pairwise combinations. After approximately 4900 (30%) references had been screened it was decided that the remaining references would be screened by one researcher with a random 10% sample independently screened by a second researcher. This decision was taken as inter-rater reliability was adequate (< 10% disagreement rate) and to keep the project manageable. Again, references were screened in a pairwise fashion in batches of 500, with a random 10% of each batch independently screened by the second researcher.
References to studies published before 1990 were not retrieved for further inspection (n = 334). This was decided part way through screening titles and abstracts to keep the workload manageable, and also because more recent studies were considered to be of possible greater relevance.
Round 2: screening of full papers
All papers retrieved for further inspection were screened by one researcher and checked by a second.
The inclusion criteria applied to full papers were similar to those used for titles and abstracts, with two minor revisions (see Appendix 5). First, to be included papers no longer needed to fulfil the following criterion: reporting on the implementation of the promotion of health and well-being in schools by teachers (e.g. their general experiences of teaching around health and well-being; any difficulties that they experienced in teaching; the curriculum materials; their professional development; their views on the health and well-being aspect of the curriculum). This criterion was originally included in case there was an insufficient number of studies reporting specifically on teacher training and health. In such circumstances the project was designed to take a broader perspective by reviewing the evidence base on teachers' more general experience of addressing health in schools (i.e. not within the context of teacher training). However, on completion of screening of titles and abstracts it was apparent that there was likely to be an adequate number of studies specifically about teacher training to ensure a meaningful evidence map and synthesis. Restricting inclusion to studies of teacher training helped keep the review focused and more manageable.
The other change that was made to the inclusion criteria for full papers was a stipulation for an adequate level of detail on the training. This criterion excluded studies that, for example, reported associations between whether or not teachers had previously received training in a particular area of health and well-being and teacher/pupil outcomes, but did not provide any detail about what the training involved. It was considered that this review would not be able to meaningfully assess effectiveness and barriers and facilitators without an adequate description of the training received. Judging the adequacy of reporting can be subjective, but in general reviewers looked for sufficient detail on the training provider, the content and format of the training and the outcomes and processes measured. In cases of doubt over adequacy of reporting, the reviewers discussed and came to a consensus.
The inclusion criteria for full papers were piloted on a total of 75 full papers before being finalised. Only minor revisions were required following piloting.
In summary, the inclusion criteria applied to full papers for inclusion in the map were:
-
health and well-being in schools
-
the training of teachers in relation to the promotion of health and well-being in schools and an adequate description of the training provided
-
research into the processes and/or outcomes of (1) and (2) (e.g. controlled evaluations, surveys).
Development of the keywording tool
The keywording tool was devised specifically for use in this study, although it was based on similar keywording tools used in other systematic reviews in health. 45,47 It was designed to be able to characterise all aspects of the studies considered to be relevant to the aims and objectives of this investigation. A list of descriptive keywords to characterise studies meeting the first two rounds of inclusion screening was therefore generated. The keywords were grouped according to a number of specific aspects of the studies, including basic study details and country, health topic area, study design, level of education, teaching qualification status (e.g. pre-service, in-service), training content and format, training intensity and duration, types of teacher trainer, use of theory and types of processes and outcomes examined. The tool itself was built using Microsoft Excel 2010 software (Microsoft Corporation, Redmond, WA, USA).
A draft of the keywording tool was discussed by the project's advisory group, who suggested some additional keywords, which were subsequently added. The keywording tool was piloted by applying it to a random sample of 10 papers that had met the criteria in the two rounds of inclusion screening described above. The keywords were assigned to each study by one reviewer and checked by a second. The two reviewers discussed and resolved differences in keyword application, as well as the keywording instrument in general. Minor modifications were made to the instrument before it was implemented in full on the studies meeting the inclusion criteria.
Application of the keywording tool
To ensure inter-reviewer reliability, each reviewer carried out a pilot run of keywords on the same 10 studies used to pilot the keywording tool itself (see previous section). Any discrepancies with the keywords applied in the pilot exercise were discussed and resolved before the reviewer began keywording in full on the rest of the studies. Furthermore, to guide the reviewers many of the keywords were defined with explanatory notes to avoid any misinterpretation of meaning.
Each study report was read by a reviewer who then applied keywords from the keyword instrument based on the information given by the study authors. The first 30 papers were checked by a second researcher for accuracy, with all differences in judgement resolved through discussion. Once the level of agreement was considered satisfactory through discussion between the reviewers, the remaining studies were keyworded by one researcher and a random sample of 20% was checked by a second researcher. The level of agreement between researchers in the random sample (98%) was considered acceptable.
Analysis of the keywords
The Microsoft Excel spreadsheet housing the keywording instrument was designed to enable frequencies to be calculated for each keyword. Frequencies for each group of keywords were used as the basis for the data tables presented in the following section. The spreadsheet was also designed to allow subsets of studies with particular keyworded characteristics to be easily identified (e.g. studies keyworded as being about drugs and alcohol, which were classified as outcome evaluations, in which the teachers were taught skills for promoting health behaviour change). The purpose was to be able to generate various contrasting subsets of studies that could be examined in more detail for potential in-depth synthesis (e.g. ‘scenarios’ that were proposed in Inclusion criteria, Chapter 6).
Results of the literature search
The original literature search of electronic databases generated a total of 20,281 references. Following deduplication (to eliminate duplicate references identified from more than one source) the total number of references to be screened was 16,620 (Figure 9).
After screening titles and (when available) abstracts, a total of 1050 (6%) references appeared relevant and full papers were sought for further screening [of which 973 (93%) were able to be retrieved]. Electronic versions of papers were sought online via academic journals, or via interlibrary loan when necessary. A total of 170 (16%) references25,26,31,32,34,35,44,50–211,213 met the inclusion criteria for the descriptive mapping exercise. A total of 757 (72%) full papers did not meet the inclusion criteria and were excluded. The most common reason for exclusion (around 70% of these papers) was that the papers did not report research findings on relevant processes or outcomes of teacher training around health and well-being. These tended to be reports discussing health in schools that mentioned teacher training to promote health but did not report the results of relevant evaluation of the training.
The remaining 30% of papers that did not meet the inclusion criteria were excluded primarily because, although they mentioned health initiatives in schools, there was no or minimal focus on the teacher training aspect of the initiative.
FIGURE 9.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)212 flow chart.
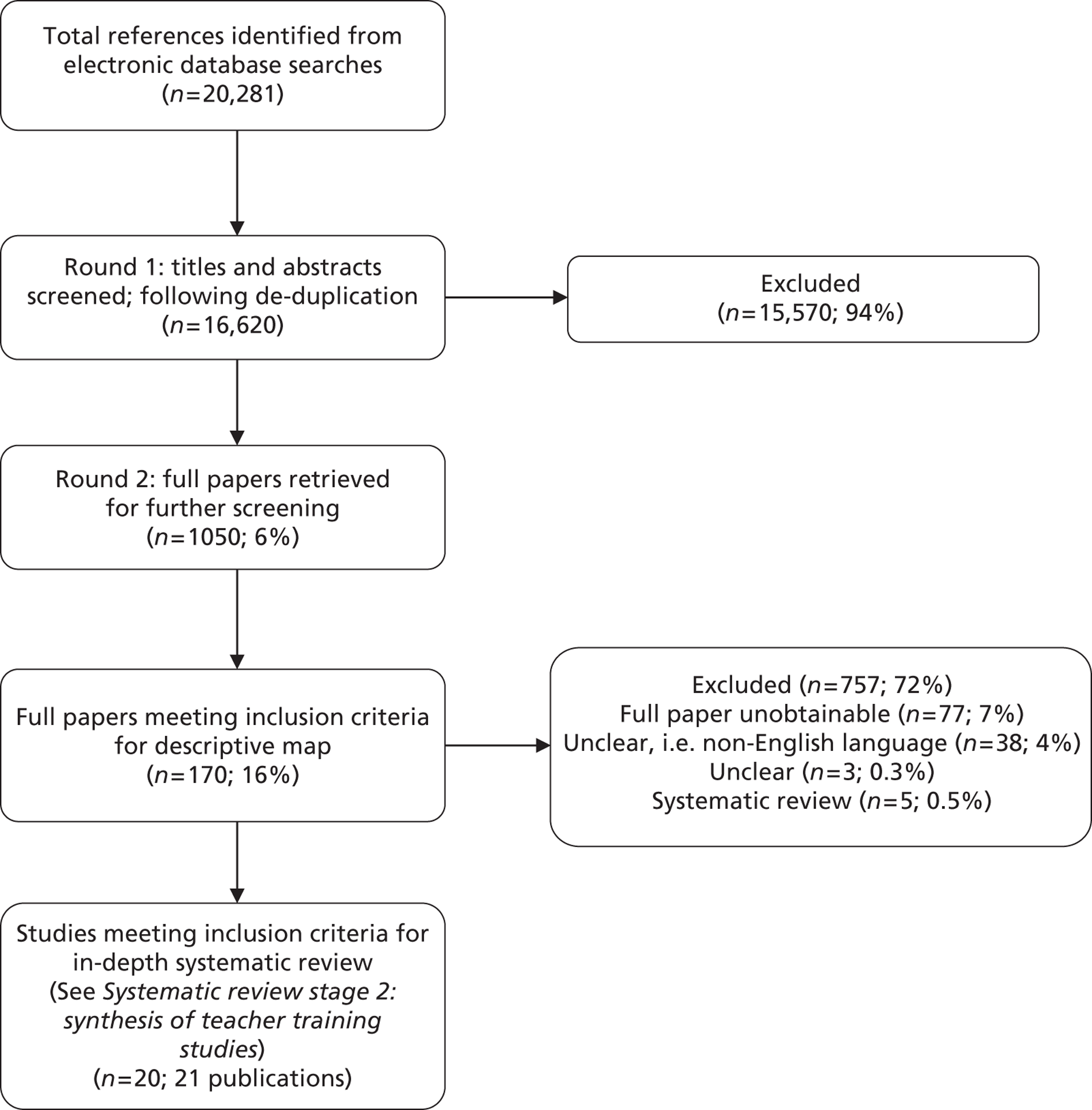
A total of 38 (4%) full papers were judged unclear as they were non-English language (predominantly Spanish, Portuguese, French or German). It was not feasible in the project timescale to seek translation of these papers. We were unable to obtain full copies of 77 (7%) of the references. These were mainly dissertations and reports from overseas (and therefore unlikely to be available from the British Library) and it was not feasible to try alternative methods to obtain them. Systematic reviews were not included, but their reference lists were scanned to identify any potentially relevant references.
The following sections describe the characteristics of the 170 publications included in the descriptive mapping exercise. Some publications report more than one study, and some studies may have been reported by more than one included publication (it was not possible for us to discern how many at the mapping stage). Therefore, we report the number of publications rather than the number of actual studies.
(Note: an update of the literature search was conducted in April 2012, which identified 1690 additional references, of which 14 references214–227 met the inclusion criteria for the descriptive map. Because of time constraints these references were not included in the map but will be included in any future updates of this systematic review. Further details can be found in Appendix 6.)
Results of the descriptive mapping exercise
Origin of study
Table 28 gives a breakdown of the origin of each publication, by country or region. The country with the largest proportion of publications was the USA (42%). A similar proportion of publications reported studies conducted in Africa, Australia and the UK (11–13%).
| Country/region | n (%) |
|---|---|
| USA | 72 (42) |
| Africa | 22 (13) |
| Australia | 19 (11) |
| UK | 18 (11) |
| Europe (non-UK) | 12 (7) |
| Asia | 10 (6) |
| Canada | 5 (3) |
| South America | 4 (2) |
| Middle East | 3 (2) |
| Not stated | 5 (3) |
The African countries represented included South Africa, Nigeria, Tanzania, Kenya and Zimbabwe; the non-UK European countries represented included Italy, the Netherlands, Norway and Finland; and the Asian countries represented included China, India and Thailand. In two of the five publications in which a country was not explicitly stated it was inferred that the study was probably carried out in the USA.
Health topic areas covered
Publications were keyworded according to the main health topics addressed by the study. As Table 29 shows, the most commonly covered health topic areas were sexual and reproductive health (22%), drugs/alcohol (18%) and mental and emotional health (16%).
| Topics | n (%) |
|---|---|
| Sexual and reproductive health | 38 (22) |
| Drugs/alcohol | 31 (18) |
| Mental and emotional health | 27 (16) |
| Health education/promotion in general | 22 (13) |
| Tobacco | 17 (10) |
| Physical activity | 15 (9) |
| Bullying/aggression/violence | 14 (8) |
| Child protection/safeguarding | 14 (8) |
| Youth development/life skills training | 13 (8) |
| Healthy eating | 10 (6) |
| Social development | 6 (4) |
| Diversity | 4 (2) |
| Hygiene/infection prevention | 4 (2) |
| Dental and oral health | 3 (2) |
| Obesity/cardiovascular health | 3 (2) |
| PSHE education | 3 (2) |
| Environmental education | 3 (2) |
| Citizenship | 2 (1) |
| Delinquency | 2 (1) |
| Eating disorders | 1 (1) |
| Eyes and vision | 1 (1) |
| Safety | 0 |
| Economic education | 0 |
| Cancer prevention | 0 |
| Other | 7 (4) |
| Topic area not stated | 0 |
Other noteworthy topics were tobacco use prevention; studies addressing bullying, aggression and/or violence; child protection or safeguarding; physical activity; and youth development/life skills training. In total, 13% of the publications were classified as health education/promotion in general. These were papers that tended not to focus on a particular topic area but which addressed a range of health issues. Publications classed as PSHE education were only classified as such if there was explicit mention of that term, and publications classed as social development were those in which PSHE education was not mentioned but which could include elements similar to the social development aspect of PSHE education. Publications classified as ‘other’ included topics such as diabetes prevention and support to children experiencing cancer in their lives.
Study design
The papers were classified according to a study design typology, broadly defined as outcome evaluations, process evaluations and surveys. A total of 124 (73%) publications were classified as outcome evaluations, reporting the impact of teacher training on teachers, pupils or both (e.g. in terms of changes in health-related knowledge, attitudes). These tended to be evaluations of school-based health-promotion interventions delivered by teachers in which the training of the teachers was a particular focus of the study. Table 30 shows a typology of outcome evaluation study designs used. Just over half of the outcome evaluations were classed as controlled trials, of which 39 (31%) reported using random allocation of teachers and/or pupils to study groups.
| Type of outcome evaluation | n (%) |
|---|---|
| Randomised controlled trial | 39 (31) |
| Controlled trial (non-random allocation) | 30 (24) |
| Controlled cohort before-and-after study (prospective) | 7 (6) |
| Single cohort before-and-after study | 36 (29) |
| Single cohort study (after only) | 6 (5) |
| Single cohort (other) | 2 (2) |
| Interrupted time series | 0 |
| Design unclear/not reported | 4 (3) |
A total of 36 (29%) publications were classified as single cohort before-and-after studies, in which outcomes were assessed in a group of teachers and/or pupils before and after teacher training had taken place, without any comparison to a group receiving an alternative form of training or not receiving any teacher training.
A total of 79 (46%) publications were classified as reporting a process evaluation. Some publications defined themselves as reporting a process evaluation whereas others did not provide an explicit definition of the study design, but we classified them as evaluating processes if it appeared that they empirically measured one or more process indicators (e.g. in terms of assessing how training was implemented and received by participants, see Table 44 for more information). Table 31 reports the data collection methods that the process evaluations used. Questionnaires were the most commonly used method, followed by interviews and observation. Methods classed as ‘other’ included teachers' written training responses and reflections (e.g. written in journals, in essays and on online discussion boards) and training attendance records.
| Process evaluation methods | n (%) |
|---|---|
| Focus groups | 15 (19) |
| Interviews | 28 (35) |
| Questionnaire | 49 (62) |
| Observation | 17 (22) |
| Other (specify) | 21 (27) |
| Unclear/not reported | 2 (3) |
A total of 49 (29%) publications were classified as reporting both an outcome evaluation and a process evaluation. These publications evaluated a range of outcomes and processes (see Outcomes and processes measured) and were representative of the sample of publications as a whole in terms of study characteristics.
Nineteen (11%) of the publications were classified as reporting a survey. A publication was classed as a survey rather than a process evaluation if it reported an evaluation of teacher training in general (e.g. a survey of a sample of training courses in an area) rather than in relation to a specific training programme (although surveys could report process indicators). Table 32 reports the survey data collection methods used.
| Survey method | n (%) |
|---|---|
| Focus groups | 1 (5) |
| Interviews | 10 (53) |
| Questionnaire | 12 (63) |
Level of education
The publications were classified according to whether the teacher training was at the UK primary or the UK secondary educational level (or equivalent in other countries). Table 33 shows that slightly more publications reported training at the secondary than the primary level. Just over 20% of the studies featured both primary- and secondary-level training, and in 20% of publications it was not possible to classify level of education as it was unclear or not reported.
| Level | n (%) |
|---|---|
| Primary only | 45 (26) |
| Secondary only | 56 (33) |
| Primary and secondary | 35 (21) |
| Unclear/not stated | 33 (19) |
Study population
The publications were classified in terms of whether the recipients of the training were teachers only or a mixed population of teachers and others who work with children and young people. Table 34 shows that in the majority of publications (72%) only teachers received training. The remaining 28% of publications provided health training for teachers and people such as counsellors, school administrators and health-care professionals.
| Study population | n (%) |
|---|---|
| Teachers only | 122 (72) |
| Mixed population (teachers and others) | 48 (28) |
Characteristics of the training
Table 35 shows that the vast majority of publications (84%) reported training teachers classified as in-service (i.e. qualified). Only 18% of publications referred to ITT, although 2% of the studies included both in-service and pre-service teachers.
| Status | n (%) |
|---|---|
| Pre-service | 31 (18) |
| In-service | 143 (84) |
| Training content | n (%) |
|---|---|
| Information provision | 131 (77) |
| Skills development (general) | 66 (39) |
| Skills development (behaviour change techniques) | 11 (6) |
| Skills development (to identify health problems and/or how to refer) | 27 (16) |
| Skills development (pedagogy of health) | 45 (26) |
| Awareness and attitudes | 37 (22) |
| Planning and implementation methods | 54 (32) |
| Training content not stated/unclear | 16 (9) |
The publications were also classified in terms of the content of the health training. Table 36 shows the frequency with which publications reported different types of content. Provision of factual information was a key aspect of training, featured in 77% of publications. Skills development for promoting health was also included in a number of publications, classified most commonly as general skills development (39%), skills to identify health problems and/or how to refer children with health problems to specialist help (16%), pedagogical skills (e.g. strategies for teaching about health and how to develop pupils' understanding of health and well-being issues, 26%) and skills development for teaching behaviour change techniques (e.g. communication skills in relationships; assertiveness skills to resist peer pressure to smoke, drink, take drugs, etc., 6%). Just under one-third of publications (32%) were concerned with how teachers can manage and plan how to promote health and well-being. It was common for training to cover a range of aspects, for example providing factual information about a health issue and also developing health-related skills that teachers could apply in their practice.
A classification of the format of the teacher training is provided in Table 37. It was common for training to be multiformat using a combination of lectures, workshops, group work (e.g. discussions, or planning a lesson on health) and activities to practice skills (e.g. role play and modelling). A total of 32% of the studies provided support to teachers after initial training, including during the course of teacher delivery of a health intervention, and refresher training after a period of time. In total, 10% of studies included a period of school teaching practice as part of the training, in addition to other training formats such as discussion and group work. The publications classified as ‘other’ (38%) included a range of activities, most common of which was the provision of training manuals, materials and teaching resources. The ‘other’ category also included self-directed learning, tele- and videoconferencing, essays and assignments, feedback and coaching. In only one study classified as ‘other’ was this the only format used – all of the other studies classified as ‘other’ used multiple formats.
| Training format | n (%) |
|---|---|
| Lecture/seminar/presentation | 59 (35) |
| Workshop | 64 (38) |
| Discussion groups/group work | 60 (35) |
| Computer/digital media | 16 (9) |
| Teaching practice | 17 (10) |
| Skills demonstration/practice | 64 (38) |
| Support post initial training | 54 (32) |
| Video | 27 (16) |
| Other | 65 (38) |
| Training format not stated/unclear | 28 (16) |
The publications were also classified according to how long the training lasted for, in terms of intensity and total duration. The intensity of the training was categorised in terms of total ‘contact time’ in days (Table 38). One-quarter of publications reported training lasting for 1 day or less. Some of these involved training that was spread out over a period of time but which, in terms of hours, added up to a day.
Just over one-third of the publications (35%) reported training lasting between 2 and 5 days. Training lasting longer than a total of 5 days was in the minority (9%). The classification of training intensity was limited by lack of reporting in 34% of the publications.
| Training intensity (days) | n (%) |
|---|---|
| ≤ 1 | 43 (25) |
| 2–5 | 60 (35) |
| 6–10 | 11 (6) |
| > 10 | 5 (3) |
| Training length not stated/unclear | 58 (34) |
The total period of the training, in terms of the period of time that it was spread out over, is reported in Table 39. In one-third of the publications the training period was 7 days or less. The percentage of publications reporting longer training periods varied from 4% (training occurring for between 1 week and 4 weeks) to 10% (training occurring over a 7- to 12-month period). Again, the classification of training period was limited by lack of reporting in 40% of the publications.
| Training duration | n (%) |
|---|---|
| ≤ 1 day | 29 (17) |
| 2–7 days | 27 (16) |
| > 1 week–4 weeks | 7 (4) |
| > 1 month–3 months | 12 (7) |
| 4–6 months | 8 (5) |
| 7–12 months | 17 (10) |
| > 12 months | 10 (6) |
| Training duration not stated/unclear | 68 (40) |
Table 40 shows the range of providers of the teacher training in the publications mapped. Specialist trainers were reported by the highest percentage of studies (29%); these were classified as specialists in the health topics being addressed, for example specialist trainers in substance abuse prevention, or experts in child protection. In total, 16% of publications reported training delivered by education practitioners, including schoolteachers, college tutors and other people working in education. Health professionals (e.g. doctors, nurses, health advisors) were reported in only 10% of publications. Some training was delivered by more than one provider, for example practitioners in health, education or psychology working in partnership, or practitioners delivering training alongside computer and video training.
| Teacher trainer | n (%) |
|---|---|
| Researcher | 18 (11) |
| Health professional | 17 (10) |
| Specialist trainer | 49 (29) |
| Education practitioner | 27 (16) |
| Psychologist/counsellor | 10 (6) |
| Computer | 9 (5) |
| Video | 7 (4) |
| Lay person/volunteer | 3 (2) |
| Other | 15 (9) |
| Trainer unclear/not stated | 77 (45) |
Table 41 shows that the majority of the publications did not report that the training was based on a theory or model (e.g. theory of education or health-related behaviour change). Only 18% of studies did make reference to theory, although given the complex and overlapping nature of theoretical models in this area we did not attempt to classify them.
| Theory based | n (%) |
|---|---|
| Theory reported | 31 (18%) |
| Theory not reported | 139 (82%) |
Outcomes and processes measured
The publications were classified in terms of which outcome and process measures were reported.
A total of 133 (78%) studies reported the impact of training on the teachers themselves. [Note: this is in excess of the 124 (73%) publications classified as outcome evaluations in Study design – this is because nine studies classified as process evaluations reported impacts on teachers within the context of the process evaluation, for example how teachers considered their knowledge, skills, etc. had changed, without these necessarily being defined by the study as outcomes.]
A range of teacher outcomes was measured (Table 42), commonly including the rate of delivery of health promotion in schools by teachers (41%), changes in teachers' knowledge of health (37%), teachers' confidence or self-efficacy to address health in schools (32%), teachers' skills in addressing health (e.g. to promote healthy behaviours or to identify and assist pupils at risk of health problems) (25%) and attitudes towards promoting children's health (25%). Publications assessing teachers' values (22%) were classed as such if they reported teachers' views and beliefs around health and their role as teachers of health. Publications classed as ‘other’ (18%) included teachers' dissemination of health information to other teachers, teachers' perceptions of risk, teachers' own health-related behaviours and teachers' perceptions of their own health and well-being.
| Teacher outcomes | n (%) |
|---|---|
| Knowledge of health in general and specific health topic to be addressed | 63 (37) |
| Skills (e.g. ability to teach health-related behaviour change skills) | 43 (25) |
| Confidence/self-efficacy to provide health-promotion intervention | 54 (32) |
| Attitudes towards health-promotion intervention | 43 (25) |
| Motivation and intentions to provide health-promotion intervention | 10 (6) |
| Awareness and understanding of whole-school approaches to health promotion, and wider determinants of health | 11 (6) |
| Health literacy | 0 |
| Rates of delivery of the intervention/implementation (e.g. fidelity) | 70 (41) |
| Unintended/unanticipated outcomes (e.g. increasing health inequalities) | 0 |
| Teachers' values | 37 (22) |
| Biological and physical outcomes (e.g. weight change) | 1 (1) |
| Mental health outcomes | 5 (3) |
| Other (specify) | 30 (18) |
| Teacher outcomes not stated | 37 (22) |
The impact of teacher training on pupils was less commonly evaluated [reported in 59 (35%) publications]. These tended to be controlled evaluations (many of which were randomised) of school-based health initiatives delivered by in-service (qualified) teachers, covering topics such as sexual and reproductive health and drugs/alcohol and tobacco use prevention. The training that teachers received in these studies included a range of activities to develop their knowledge and skills to deliver these health interventions. Table 43 shows the range of pupil outcomes measured, the most common being health-related behaviour (22%), knowledge of health issues (19%) and attitudes towards health (12%).
| Pupil outcomes | n (%) |
|---|---|
| Knowledge of relevant health topic (e.g. risk factors, prevention, well-being) | 32 (19) |
| Attitudes towards health-related behaviour/intervention | 21 (12) |
| Intentions to adopt health-related behaviour | 9 (5) |
| Self-efficacy to adopt health-related behaviour | 8 (5) |
| Biological and physical outcomes (e.g. weight change) | 8 (5) |
| Health-related behaviour (e.g. smoking) | 37 (22) |
| Health literacy | 0 |
| Educational attainment | 1 (1) |
| Mental health outcomes | 11 (6) |
| Unintended/unanticipated outcomes (e.g. differential health gain) | 0 |
| Other (specify) | 18 (11) |
| Pupil outcomes not stated | 111 (65) |
Table 44 reports a classification of the processes evaluated in the publications. The most commonly reported measure was the acceptability and adequacy of the training (41%). This measure included assessment of the views of the training recipients (and other study participants) on the content and format of the training (e.g. perceived usefulness of activities such as role play or didactic learning), whether it met their needs or expectations (e.g. in changing their knowledge, attitudes or abilities to address health issues in school) and whether the health topics covered conflicted with their personal beliefs and values (e.g. sensitive issues such as sexual and reproductive health).
| Processes | n (%) |
|---|---|
| Acceptability and adequacy to the teachers of the training | 69 (41) |
| Resources and costs used to train the teachers | 9 (5) |
| Teachers' general reflexivity of their health-promoting role and practice | 57 (34) |
| Implementation of the training programme/health-promotion intervention | 65 (38) |
| General organisation/administration of the training | 6 (4) |
| Other (specify) | 8 (5) |
| Processes unclear/not stated | 63 (37) |
Another common process measure was the implementation of the teacher training (38%). Publications were classified according to this measure if they reported an assessment of any aspect of the design or delivery of the training, such as its content or format (e.g. timing or location), exposure to training (e.g. number of people trained, how much of the available training participants received, which topics teachers received training on) and any reported barriers to or facilitators of teacher training (e.g. sufficiency of training length, ability to attend training). In total, 34% of the publications were classed as assessing teachers' general reflexivity of their health-promoting role and practice. This was defined as whether teachers reflected on what impact the training had, or was expected to have, on their teaching practice in relation to health and well-being. It could also include broader perspectives of teachers on their role in addressing health.
Summary of mapping results
A total of 170 publications were systematically keyworded to characterise the evidence base for the evaluation of teacher training in health. There is an international literature with studies conducted in Europe, the USA, Africa, Asia, Australia, South America and the Middle East, with a predominance of studies from the USA. The training covered a wide range of health topics, notably sexual and reproductive health, drugs/alcohol and mental and emotional health. Just under three-quarters of the publications were outcome evaluations (just over half of which used controlled study designs, including some randomised controlled trials) and just under half reported a process evaluation of training (using methods such as questionnaires, focus groups and interviews).
The majority of publications reported training for teachers only, although in just under 30% of publications training was given to teachers and other people working with children and young people, such as school counsellors. Training was given at both primary and secondary education level, and the vast majority (84%) of publications reported training for qualified teachers as opposed to pre-service teachers undergoing ITT.
In terms of content, factual information provision about health was a feature of many training programmes, sometimes accompanied by the development of skills for promoting health (e.g. health-related behaviour change) and how to plan and implement health promotion in schools. Training was often multiformat in nature, involving lectures and presentations, group work, discussion, skills practice and, in a minority of cases, teaching practice. The length of the training, in terms of total ‘contact time’, varied from < 1 day to > 10 days, but was most commonly up to 5 days in total. Training periods varied from < 1 day to > 12 months but in general training was delivered over a period of up to 3 months. Training was rarely reported to be based on a theoretical model.
A greater number of publications reported training outcomes for teachers (78%) than outcomes for pupils (35%). Commonly reported teacher outcomes included their delivery of health promotion in schools; their knowledge of health topics; their confidence, self-efficacy and skills to address health in schools; and their attitudes towards promoting health. Commonly reported pupil outcomes included health-related behaviour, knowledge of health issues and attitudes to health.
A range of processes was evaluated, including how acceptable and adequate the training was considered to be by its recipients, how the training was implemented in terms of content and format, and teachers' reflexivity on their role and their health teaching practice following training.
For some study characteristics the results of the descriptive map are limited by unclear or missing details in the publications. How the results of the descriptive mapping were used to set the inclusion criteria for the in-depth synthesis is discussed in the next chapter.
Chapter 6 Systematic review stage 2: synthesis of teacher training studies
Methods for the synthesis
Inclusion criteria
As mentioned earlier in this report, the inclusion criteria for the synthesis were based on the results of the descriptive map. The results of the map were presented to the project's advisory group along with a number of different sets of studies with selected characteristics that the synthesis could potentially focus on. The sets of studies were presented as contrasting ‘scenarios’, including:
-
A set of studies focusing on a particular health area or combination of areas (e.g. some of the most prevalent topics from the mapping, such as sexual and reproductive health, mental health, drugs and alcohol) examining outcomes and processes (i.e. categorised as an outcome evaluation and a process evaluation). The rationale for this scenario was to investigate teacher training within the context of specific health areas, facilitating a detailed analysis of relevant issues. Also, restricting the analysis to studies that measure both outcomes and processes (as opposed to one or the other) could, in theory, provide a more informative investigation into factors associated with effectiveness (or lack of).
-
A set of studies focusing on a particular topic or combination of health areas and examining processes (i.e. including process evaluations but not outcome evaluations). The rationale was that process evaluations may provide more data on barriers to and facilitators of teacher training. The review could examine some of the processes categorised in the mapping exercise such as teachers' general reflexivity of their health-promoting role and practice in general, or the implementation of the teacher training programme and/or implementation by teachers of health promotion.
-
A set of studies focusing on teacher training that included an aspect of health-related skill development, examining outcomes and processes. One or more ‘types’ of skill could be examined (e.g. skills development to encourage health-related behaviour change; pedagogy of health; identifying children with health problems). Equipping teachers with health-related skills arguably is a key aspect of improving health and well-being, more so than just providing information or influencing norms and attitudes.
-
A set of studies examining pre-service teacher training. The studies would be diverse in terms of country, health issues, types of training provided and processes and outcomes, but they would all be conducted within the context of ITT. The advantage of this scenario was that it would mean the focus of the project as a whole would be on issues relating to ITT. Some of the themes arising from the interviews could be taken into account when analysing the literature, to identify commonalities and differences.
-
A set of studies conducted in the UK. As with scenario (4), the studies would be diverse in characteristics. The advantage of this scenario is that it would overcome the challenges of drawing generalisations from international studies in which values, culture and educational policy and systems vary considerably. Also in common with scenario (4), there could be greater linkage between themes identified from our interviews and the UK literature, such as issues relating to PSHE education. The project could therefore make specific recommendations relating to UK practice.
The advisory group discussed the merits and possible limitations of these scenarios with the project team. All of the scenarios were considered relevant. However, it was considered that a focus on studies of pre-service teachers was the highest priority as it provided continuity with the survey component of the project (i.e. it could inform/be informed by the survey), and was particularly relevant during a time of great change in policy and practice in ITT and education more broadly. There were 31 such study reports included in the descriptive mapping exercise. 25,26,44,57,61,63,67,70,81,83,85,88,92,94,116,117,142,148,156,174,179,189,191,192,195,199–202,206,213
It was noted by the research team that there was marked variability in the stated aims and research questions of these 31 publications, and that some appeared to be more focused on pre-service teachers than others. For example, some investigated a particular health topic or type of teacher training in pre-service teachers but with little or no rationale for studying this group as opposed to qualified teachers. These reports were therefore examined in more detail to ascertain the degree to which issues relating to pre-service teachers were investigated by the studies. The aim was to potentially exclude studies in which there was no explicit rationale for studying pre-service teachers or no exploration of issues pertinent to this group, so that the synthesis would be more focused. To be included a report had to meet at least one of the following three criteria:
-
Does the study provide a rationale for specifically studying pre-service teachers?
-
Does the aim/objective/purpose of the study make reference to studying pre-service teachers?
-
Do the results of the study specifically mention issues that affect/involve pre-service teachers (e.g. their attitudes towards their role as teachers in relation to health; their teaching practice)?
If the report met one or more of the above criteria the following criteria were also applied:
-
Is the training reported in sufficient detail?
-
Are the results reported in sufficient detail?
These criteria were applied to the reports by one reviewer and checked by a second. In summary, inclusion criteria for the synthesis were:
-
publications (published from 1990 onwards) in the English language
-
reporting (in adequate detail) evaluation research (of any design) into the processes and/or outcomes of teacher training in relation to the promotion of health and well-being
-
training of pre-service (not yet qualified) teachers.
Data extraction
A standardised data extraction template was designed and piloted for use on studies included in this systematic review (see Appendix 7). It was designed to capture all of the data reported in study publications relevant to the aims of this investigation, and was partially based on the keywording instrument used in the descriptive map reported earlier (see Chapter 5, Development of the keywording tool). The template was split into subsections for basic study details (e.g. date, country, aims and objectives), health topics studied, details of study participants (e.g. sociodemographic characteristics, level of education taught), details of the teacher training (e.g. content, format, duration/intensity), processes and outcomes evaluated (when applicable), study methodological characteristics (e.g. study design, data collection instruments, data analysis methods), study results and reviewer's general comments on the study. Data were extracted by one reviewer and checked by a second.
Quality assessment
Methodological quality and risk of bias were assessed with published critical appraisal criteria (see Appendix 8). 37,47 Studies reporting outcomes were appraised using risk of bias criteria adapted from the Cochrane Collaboration's Effective Practice and Organisation of Care (EPOC) Group. 228 The EPOC Group has adapted the standard Cochrane risk of bias criteria for randomised controlled trials37 for use in evaluation studies that are non-experimental in design (i.e. without a control or comparison group). The methodological quality of process evaluation data was appraised with criteria devised and used in our previous systematic review of process evaluations of school-based behavioural interventions to prevent sexually transmitted infections in young people,229 based, in turn, on previous research assessing the methodological quality of process evaluations and qualitative research. 230–232 The criteria assess whether steps were taken to minimise bias and error in sampling, data collection procedures and data analysis. They also assess whether the findings are grounded in the data, and overall whether the findings presented are reliable and useful (to put this into context see Critical appraisal of process evaluation for the results of the quality assessment of process evaluations). Quality assessment criteria were applied by one reviewer and checked by a second, with any disagreements resolved through discussion and involvement of a third reviewer when necessary. Studies were not excluded from the synthesis on the basis of quality; however, methodological limitations (e.g. because of evaluation design) of particular studies are mentioned in the synthesis when relevant.
Synthesis methods
The results of the studies were analysed in a narrative synthesis, based on the data that had been systematically extracted from each study publication. Quantitative synthesis using meta-analysis was not possible because of the lack of studies using a controlled evaluation design. Because of the heterogeneous characteristics of the studies, particularly the methods used to report outcomes, summary tabulation of results was difficult. It is for this reason that the study outcomes (see Assessment of the effectiveness of training on teacher outcomes) are presented only textually.
A thematic analysis of the process evaluation data was conducted, similar to methodology described by Thomas and Harden. 233 One researcher (JS) read all of the results that had been extracted from the studies reporting processes and identified a list of five emerging themes which summarised the results. These themes were then discussed and agreed with other members of the project team. A second researcher (KP) also read the extracted results and then systematically coded the extracted data in a NVivo database. As part of this process she revised the five themes and identified a further three. A narrative account was then written summarising the results of the process evaluations for each theme, including barriers and facilitators that had been reported by, or inferred from, the studies. The first researcher then reviewed and agreed the final list of themes and cross-checked a sample of the coded study results against the narrative account for reliability of interpretation.
Results of the synthesis
After applying the inclusion criteria described in the previous section to the 31 pre-service publications, 20 studies reported in a total of 21 publications25,26,44,61,63,70,81,83,92,94,117,142,148,156,174,189,191,195,200,201,213 were included in the synthesis (one study was reported in two separate publications,26,156 and data from both of these were extracted for this report), with 10 references57,67,85,88,116,179,192,199,202,206 being excluded.
Characteristics of the included studies
Table 45 provides an overview of the key characteristics of the included studies. The level of reporting detail in the study publications varied, and in some cases the study characteristics were unclear. (Note: we requested and received further information from the authors of two of the studies25,142.) As the table shows, the studies varied in a number of respects, including the study population, the health topics addressed by the training, the content and length of the training and the study measures and designs.
In terms of country, the highest percentage of studies were conducted in the UK (n = 9,25,63,70,83,92,117,142,174,191 45%), followed by Australia (n = 7,44,94,189,195,200,201,213 35%). There was one study each from Finland,26,156 Zimbabwe81 and the USA,61 with one study not explicit about the country but it most likely being the USA. 148
Health topics covered
The studies tended to focus on one or two health areas, although a few studies had a broader focus on health in general, with some covering a number of specific areas (see Table 45). The area of health covered by the highest proportion of studies was mental and emotional health (n = 7,70,148,189,195,200,201,213 35%). These studies covered issues such as depression, self-esteem, suicide prevention, resilience, stress and body image, with one study covering training to support children affected by cancer in their lives. Child protection was another common topic area (n = 5,44,63,94,117,174 25%), with studies covering a wide variety of issues relating to protection from abuse. PSHE education and sexual and reproductive health were each covered in three studies (15%),92,142,191 drugs/alcohol were covered in two studies (10%)148,213 and tobacco was featured in one study. 148 Other health topics included citizenship,142 diversity61 and healthy eating148 (all in one study each).
Study participants
The participants in the majority of studies were pre-service teachers enrolled in teaching qualification courses at HEIs. Generally these institutions were universities, although in some studies the type of institution was not specified. One of the UK studies was based on a SCITT. 117 When stated the courses were predominantly postgraduate, although there was a minority of undergraduate Bachelor degree courses. In terms of the level of education, eight studies26,70,92,156,189,191,195,200,201 provided training for teachers at the secondary level, two94,142 provided training at the primary level and six25,44,81,117,148,213 provided training at both primary and secondary level, with four studies61,63,83,174 not stating the level of training. The subject areas of the teaching degrees were rarely specified; however, in two studies26,156,213 the teachers were studying PE and health, one study191 included PGCE science and geography teachers and in another70 the teachers were enrolled on psychology, business and creative and media secondary PGCE courses.
| Study | Country | Study population | Topics covered | Training content | Level of education | Study measures | Study design classification |
|---|---|---|---|---|---|---|---|
| Outcome evaluations | |||||||
| Bostock 201070 | UK | 73 PGCE students at university in north-west England; 35 experienced teachers from partner secondary schools; five NQTs who had received the training 18 months ago | Mental health | Information provision | Secondary | Outcomes (teacher) | Single cohort before-and-after study |
| Myers-Clack 2001148 | USA | 119 students enrolled in a teaching major at Montana State University | Drugs/alcohol, health education/promotion in general, healthy eating, mental and emotional health, physical activity, sexual and reproductive health, tobacco | Drug and Health Issues for Educators. Information provision, skills development, awareness and attitudes, planning and implementation | Primary and secondary | Outcomes (teacher) | Single cohort before-and-after study |
| Thomas 2005191 | UK | 57 PGCE science and geography trainees | PSHE education | Information provision, skills development, planning and implementation | Secondary | Outcomes (teacher) | Survey |
| Weatherby-Fell 2004200 | Australia | 96 secondary education teachers in their final year at Southern Cross University | Mental and emotional health | Response Ability, MindMatters. Information provision, skills development, awareness and attitudes | Secondary | Outcomes (teacher) | Design unclear |
| Process evaluations | |||||||
| Arnold 200744 | Australia | Teacher training providers and representatives of the teacher registration body | Child protection | Not reported in detail (survey of a number of courses) | Primary and secondary | Processes | Survey |
| Fenton 200894 | Australia | 19 pre-service teachers studying ‘Early Childhood Education’, a semester-long subject | Child protection | Strengths Approach Child Protection module. Information provision, skills development, awareness and attitudes; 13-week module | Primary | Processes | Survey |
| Hodgkinson 2000117 | UK | Pre-service teachers (number not reported); 14 course managers from SCITTs | Child protection | Information provision | Primary and secondary | Processes | Survey |
| Mead 2004142 | UK | 102 students (BEd/PGCE) on final school-based placements | PSHE education, citizenship, SRE, diversity | Skills development, awareness and attitudes, planning and implementation | Primary | Processes | Survey |
| Paakkari 201026,156 | Finland | 20 PE students specialising in health education at the University of Jyvaskyla | Health education/promotion in general | Information provision, skills development | Secondary | Processes | Survey |
| Rossato 2009174 | UK | Four recent graduate sports/PE teachers; 126 course leaders at 55 HEIs providing PE ITT and sport-related degrees | Child protection, physical activity | Information provision, skills development, planning and implementation | Not explicit (probably secondary) | Processes | Survey |
| Taylor 2008189 | Australia | 10 students studying for a Graduate Diploma of Education | Health education/promotion in general, mental and emotional health | Information provision, skills development, planning and implementation, health and well-being ‘infused’ throughout the 1-year course | Secondary | Processes | Survey |
| Yager 2009213 | Australia | 182 first-year BEd and Bachelor of Health and Physical Education students | Health education/promotion in general, mental and emotional health, sexual health, drugs/alcohol, physical activity, healthy eating, environmental education | Concepts of Wellbeing. Information provision, skills development, awareness and attitudes; course lasted for 13 weeks, spanning a semester | Primary and secondary | Processes | Process evaluation |
| Outcomes and process evaluations | |||||||
| Athanases 200361 | USA | 98 students enrolled in graduate and postgraduate education degrees at a large California public state university | Diversity – respecting, understanding and supporting lesbian and gay youth | Cultural Diversity and Education. Information provision, skills development, planning and implementation; once weekly for 2 hours over a 10-week academic quarter | Not explicit but likely to be primary and secondary | Outcomes (teacher); processes | Process evaluation |
| Baginsky 200563 | UK | 1247 students from 13 HEIs | Child protection/safeguarding | Child Protection in Initial Teacher Training Tutor Pack. Information provision, skills development | Not stated | Outcomes (teacher); processes | Single cohort study (after only) |
| Chifunyise 200281 | Zimbabwe | 1562 students from 20 institutions of higher learning | Sexual and reproductive health – HIV infection/AIDS prevention | AIDS and Life Skills Education programme. Information provision, skills development, planning and implementation; course appears to take place over 2–3 years, with HIV/AIDS education throughout that period | Primary and secondary | Outcomes (teacher); processes | Single cohort before-and-after study |
| Cleave 199783 | UK | 11 PGCE students at Sheffield University; 19 practising teachers; 13 volunteers with the Cancer Aid and Listening Line (CALL) | Mental and emotional health – children who have experienced cancer in their lives | Information provision, skills development, awareness and attitudes; 2-day course | Not stated | Outcomes (teacher); processes | Single cohort before-and-after study |
| Evans 200792 | UK | 21 NQTs who had studied PGCE English at Edge Hill College of Higher Education between 2002 and 2004 | PSHE education | Skills development; planning and implementation | Secondary | Outcomes (teacher); processes | Survey |
| Speller 201025 | UK | 384 pre-service PGCE teachers at the University of Southampton, and the University of Brighton; survey of 35 ITT course providers in south-east England | Health education/promotion in general | Not stated | Primary and secondary | Outcomes (teacher); processes | Single cohort before-and-after study; survey |
| Vincent 2005195 | Australia | Approximately 250 pre-service teachers based at teaching training providers in regional New South Wales, Sydney and regional Victoria | Mental and emotional health | Information provision | Secondary | Outcomes (teacher); processes | Single cohort before-and-after study |
| Weatherby-Fell 2005201 | Australia | 13 early career secondary teacher graduates (eight from Southern Cross University) | Mental and emotional health | Response Ability, MindMatters | Secondary | Outcomes (teacher); processes | Single cohort study (after only) |
In some studies the teachers had qualified and entered service and were being assessed in relation to the health training that they had received prior to service (and also since, in some cases). The study by Evans and Evans,92 published in 2007, included NQTs who had studied PGCE English between 2002 and 2004, with the aim of assessing their confidence in teaching PSHE education since entering practice. Weatherby-Fell and Vincent201 included ‘early career secondary teacher graduates’ approximately 12 months after they had completed their university training. A further study included pre-service teachers, NQTs and experienced teachers. 70 In this study a brief training course was given to PGCE teacher trainees to raise their awareness of their role in the early detection of mental illness in children. A comparison was made with NQTs who had received the training 18 months before to assess the longer-term impact of the training. A further comparison was made with the attitudes of practising teachers towards their role in the early detection of mental illness and whether or not these were different from the attitudes of PGCE trainee teachers. In the study by Cleave and Charlton83 both pre-service teachers and practising teachers (separately) received training on supporting children who have experienced cancer in their lives.
A handful of studies included representatives from teacher training providers, to survey the provision of health content within courses. 25,117,174 In all but one case the survey of providers was reported in addition to assessment of health training for trainee teachers themselves. The exception was the study by Arnold and Maio-Taddeo,44 which assessed the coverage of child protection by university teacher training providers, surveying course managers and representatives of the teacher registration body of each Australian state or territory.
Rationale for studying initial teacher training
All of the studies provided a rationale for assessing training specifically in pre-service teachers (as this was a requirement of our inclusion criteria for the synthesis – see Inclusion criteria). The explicitness of the rationale varied across the studies. For example, the focus of the study by Athanases and Larrabee61 was the social challenges facing young lesbian and gay people and ways that educators can be mindful of these issues in schools. Although the rationale for studying pre-service teachers was implicit, the findings explore the trainee teachers' views of their roles as ‘future educators’ in relation to issues affecting these young people. In contrast, Yager213 provided a more explicit rationale. She acknowledged the important role of the school in health promotion but notes that there has not been an increase in health education training for primary school teachers. The focus of the health training in the study was to influence trainee teachers' own health-related behaviour, but ‘also so they could reflect on the process and use this in their teaching’ (p. 62).
Some of the UK studies included in the systematic review made explicit reference to changes to educational policy or regulations in the rationale and design of the study. A chronology can be observed in terms of the development of policy and the research response over recent years. For example, Hodgkinson and Baginsky,117 in their study assessing training for teachers in child protection, refer to the new requirements for all teacher training courses as outlined in the Children Act 1989 and subsequent government circulars. Later, Baginsky and Macpherson63 evaluated a child protection training pack for trainee teachers to encourage consistency in training provision by ITT providers. This was in the context of child protection legislation in the Children Act 2004 and government guidance on safeguarding children in education,234 which they suggest ‘recognises that teachers should receive training as part of their initial training but does not elaborate upon what this should entail’ (p. 318). Rossato and Brackenridge,174 in their study of child protection in sport-related degrees, cite ECM and new TDA professional standards for teachers as providing a framework to promote child protection. The study investigated teacher educators' perceived impact of ECM and new ITT guidelines for child protection training within higher education sport/PE courses.
In terms of PSHE education, Mead's study, published in 2004,142 was conducted within the context of the 2002 professional standards for QTS,235 which state that trainee teachers should be able to understand the values, aims and purposes of the National Curriculum and be familiar with the programmes of study for PSHE and citizenship. The QTS guidance makes a link between teachers' values relating to the curriculum (inclusion) and explicit expression of those values through PSHE and citizenship. The link has implications for values education for trainee teachers, hence the rationale for examining the implications of this for the school-based element of teacher education. Evans and Evans92 cited concerns about the adequacy of provision of support for PSHE education and ITT and CPD raised by Mead's study142 and an OFSTED review of PSHE education in 2005,236 particularly in relation to the integration of PSHE education within main curriculum subject training. This underpinned their study of secondary English PGCE trainee teachers and the training in PSHE education that they received in their PGCE course.
Training content
In common with the general trend observed from the descriptive map presented earlier in this report, the studies included in the synthesis reported training that was diverse in terms of content (e.g. providing information and practical skills development) and which was delivered through a variety of formats (e.g. lectures, practical activities) (see Table 45).
A key aspect of the training courses was the provision of factual information about health, in 15 (75%) of the studies. 26,61,63,70,81,83,94,117,148,174,189,191,195,200,213 The comprehensiveness of the information, as reported by the study authors, varied. For example, Chifunyise and colleagues,81 who provided training to teachers to support the acquired immunodeficiency syndrome (AIDS) and Life Skills Education programme in primary and secondary schools in Zimbabwe, specified that teachers were taught ‘basic facts’ about transmission, symptoms and prevention of sexually transmitted diseases and human immunodeficiency virus (HIV) infection/AIDS, but no further detail was given (p. 378). Other studies provided teachers with more extensive information, such as that by Bostock and colleagues,70 which covered the incidence, classification and diagnosis of mental health problems in teenagers, and the early signs of mental health problems. Similarly, Fenton94 provided trainee teachers with child abuse statistics, types of abuse, indicators and signs of abuse and mandatory reporting and policy requirements. Information was also provided on how teachers could deal with a health issue once they had identified it.
Fourteen (70%) of the studies26,61,63,81,83,92,94,142,148,156,174,189,191,200,213 were classified as teaching skills that would enable teachers to promote health. We subclassified studies according to different types of skill. The most common of these was health pedagogical skills, defined as strategies for teaching about health and how to develop pupils' understanding of health and well-being issues (eight studies,26,61,81,92,94,142,189,191 40%). For example, Thomas and Jones191 aimed to help trainee teachers acquire key skills so that they can develop high levels of critical health literacy in their students. Their training provided trainee teachers with the opportunity to develop communication skills to deliver PSHE issues effectively, sensitively and confidently using a variety of teaching strategies such as role play and discussion groups. There were four (20%) studies63,148,174,200 that we classified as helping teachers learn how to identify that a child has, or is at risk of, a health problem, and how to refer them to appropriate services. For example, the training provided by Baginsky and Macpherson63 on child protection was built around a series of headings: ‘recognizing, responding, reporting, roles and responsibilities, and reflecting’ (p. 319).
Training for teachers to plan and implement activities to promote health was addressed by six (30%) of the studies. 81,92,142,148,161,191 For Thomas and Jones,191 enabling trainee teachers to gain experience of curriculum planning was a key aspect of training to teach PSHE education. Each of the 15 groups of trainee teachers had to provide an overview of their intended PSHE lesson, stating the teaching and learning strategies to be employed and the learning outcomes to be achieved by the pupils. Also in relation to PSHE, Mead142 examined the extent to which BEd and PGCE trainee teachers were given the opportunity to plan and teach PSHE while on school placement. In the study by Chifunyise and colleagues,81 the trainee teachers worked in groups after a weekly mass lecture to prepare lessons that they were to present to each other on the prevention of HIV infection and AIDS.
In five of the studies (25%)94,142,148,200,213 one of the aspects of the training was to increase trainee teachers' awareness of health issues and to promote favourable attitudes towards health in education. Two of the hypotheses proposed by Myers-Clack and Christopher148 were that their training course, Drug and Health Issues for Educators, would increase teachers' belief in the importance of health to a child's learning and would increase the value that they place on school health education. Limited detail is given on how, explicitly, the training attempted to do this, although the teachers did write essays on controversial health issues and participated in group presentations on a controversial health issue. This may have helped them to explore their attitudes towards health and the importance of enabling children to be healthy. In another example, Mead142 investigated opportunities for trainee teachers to understand and experience within their school placements the relationship between values, personal and social development and learning. He suggested that there has been little attention to the process of change that professionals undergo during and after PGCE training which enables them to articulate values that underpin their delivery of PSHE education.
Training format
Table 46 illustrates the format of the training provided in the studies. As evident from the table, the training was generally multiformat, comprising lectures/seminars with group work involving discussion or specific tasks, in some cases accompanied by activities to enable trainee teachers to practice skills. Training with the use of computer programmes or videos also featured in some studies. The training format classified as ‘other’ in Table 46 included use of distance learning materials,174 assigned readings from health textbooks and writing essays on controversial health issues,148 development by trainee teachers of resource files81 and critical reflection on lesson delivery. 191
There were six (30%) studies26,63,81,142,156,189,191 in which teachers had the opportunity to teach health in the classroom as part of their training. In Mead's study142 teaching practice was the main aspect of the training evaluated. BEd and PGCE trainee teachers taught PSHE and citizenship while on their final school placements, with the former collecting data for a PSHE education/citizenship dissertation. The Child Protection in Initial Teacher Training Tutor Pack evaluated by Baginsky and Macpherson63 included directed time tasks that could be undertaken while trainee teachers were on their school placements. In the study by Thomas and Jones191 the PGCE science and geography trainees worked in small groups to plan and deliver a 1-hour lesson on peer pressure to year 7/8 pupils. Taylor189 analysed teachers' developing views on health in education in the contexts of university coursework combined with two major practical sessions in schools, followed by a period of independent ‘real-world’ teaching employment (although evaluation of the latter aspect was ongoing at the time of the study publication, so the results of the study mainly focus on the coursework and practical sessions).
| Study | Lecture/seminar/presentation | Workshop | Discussion groups/group work | Computer/digital media | Teaching practice | Skills demonstration/practice | Support post initial training | Video | Other | Training format not stated/unclear |
|---|---|---|---|---|---|---|---|---|---|---|
| Arnold 200744 | ✓ | |||||||||
| Athanases 200361 | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| Baginsky 200563 | ✓ | ✓ | ✓ | ✓ | ||||||
| Bostock 201070 | ✓ | ✓ | ✓ | ✓ | ||||||
| Chifunyise 200281 | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| Cleave 199783 | ✓ | ✓ | ||||||||
| Evans 200792 | ✓ | |||||||||
| Fenton 200894 | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| Hodgkinson 2000117 | ✓ | |||||||||
| Mead 2004142 | ✓ | ✓ | ||||||||
| Myers-Clack 2001148 | ✓ | ✓ | ✓ | |||||||
| Paakkari 201026,156 | ✓ | |||||||||
| Rossato 2009174 | ✓ | ✓ | ✓ | ✓ | ||||||
| Speller 201025 | ✓ | |||||||||
| Taylor 2008189 | ✓ | ✓ | ✓ | |||||||
| Thomas 2005191 | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| Vincent 2005195 | ✓ | ✓ | ✓ | ✓ | ||||||
| Weatherby-Fell 2004200 | ✓ | ✓ | ✓ | ✓ | ||||||
| Weatherby-Fell 2005201 | ✓ | |||||||||
| Yager 2009213 | ✓ | ✓ | ✓ | ✓ | ✓ |
The study by Chifunyise and colleagues81 in Zimbabwe provided the most extensive period of teaching practice. During the first year of the degree course teachers attended weekly lectures and participated in group activities. This was followed by teaching practice for 22 months during which they were required to teach AIDS education. After this they returned for a final two terms to complete their training.
An example of training that was delivered through a number of formats was that reported by Fenton,94 who evaluated the Strengths Approach Child Protection module within an Early Childhood Education, semester-long module in Australia. The training involved whole-group formal lecture presentations, workshop sessions, small-group tutorials, the use of online discussion boards and practical skill development. In terms of the last, the trainee teachers listened to a range of stories written for use with children explaining the topic of child abuse and discussed their use in the classroom. Dolls, puppets and picture prompt cards were used in demonstrations to model practice in identifying expressions, role-play situations and examining personal strengths with children. The teachers kept a portfolio of subject materials, which included a personal journal entry each week as part of the formal subject requirements. A subject website was available and the teachers also used an online discussion board or placed a journal entry in their subject portfolio regarding their own information, stories and perspectives on the issue of child protection to add to the formal subject materials.
In terms of the training provider, in the majority of studies in which the provider was specified, training was classified as being given by someone with an education background (Table 47). These could include schoolteachers or other school personnel, as well as lecturers and tutors from HEIs in which the teaching degree courses were based. For example, Bostock and colleagues,70 in their study of training around mental health promotion with PGCE trainee teachers, mentioned involvement of lecturers and graduate teaching assistants, both of whom had educational backgrounds in health. Trained undergraduate teaching assistants were also involved, who were from either an education or a health background.
| Teacher trainer | n (%) |
|---|---|
| Researcher/academic | 5 (25) |
| Health professional | 1 (5) |
| Specialist trainer | 4 (20) |
| Education practitioner | 9 (45) |
| Psychologist/counsellor | 1 (5) |
| Computer | 2 (10) |
| Video | 2 (10) |
| Lay person/volunteer | 0 |
| Other | 3 (15) |
| Trainer unclear/not stated | 6 (30) |
Four studies reported that specialist trainers were used, including trainers from the NSPCC63 and child protection specialists and local National Union of Teachers (NUT) representatives. 117 In two of these studies, the specialist trainers were not clearly defined and were referred to as ‘facilitators’,83 and ‘specialists’. 174 Only one study was classified as including a health professional. Thomas and Jones191 involved a Local Unitary Authority Health Promotion Officer to deliver a ‘review of strategies, such as role play used to get pupils to communicate about health issues’ (p. 168). However, Mead142 mentions that the trainee teachers in his study had the opportunity to observe SRE being taught in placement schools by outside specialists, including nurses. It is also possible that the specialist trainers in the studies mentioned above may have also included people with a health professional background.
The studies did not always explicitly report the amount of training received and the total duration of the training period. However, it was possible to discern between studies providing relatively brief training and those providing training over longer periods of time. The shortest training period was reported by Hodgkinson and Baginsky,117 who provided child protection training lasting up to 3 hours to PGCE trainee teachers. Other short-term training included that in the studies by Bostock and colleagues70 (1 day) and Cleave and Charlton83 (2 full days). There were two studies that reported a total training period lasting around a month: Weatherby-Fell and Kean200 gave a 1-hour lecture every week for 4 weeks, and Thomas and Jones191 reported a series of activities covering around 12 hours in total over 6 weeks. In some studies training spanned an academic term or semester, such as that by Athanases and Larrabee,61 who provided sessions once weekly for 2 hours over a 10-week academic quarter (total of 20 hours contact time), or that by Fenton,94 who evaluated a 13-week module on child protection integrated within an existing Early Childhood Education subject over a semester. Myers-Clack and Christopher148 referred to the ‘semester they took the course’ (p. 465) but provided no other information. In two studies26,156,189 the training appeared to be delivered over the period of an academic year. In one of these studies189 training around health and well-being was said to be ‘infused’ throughout the Graduate Diploma in Education course (p. 26), and teachers spent 1 day per week on teaching practice in secondary schools for the first 6 weeks of the course. As stated above, the HIV infection/AIDS training given by Chifunyise and colleagues81 provided the most extensive period of training, comprising college-based training for two terms (6 months) and a period of teaching practice involving teaching AIDS education spanning 22 months.
Theoretical basis of training
Only two94,213 of the 20 studies explicitly reported that the training was theory-based. Yager213 designed training for first-year BEd and Bachelor of Health and Physical Education trainee teachers based on three theories of behaviour change: the transtheoretical model, cognitive dissonance theory and the theory of planned behaviour. These theories reflect the focus of the study on influencing trainee teachers' own health-related behaviour so that they can use this learning in their own teaching of health to pupils. Fenton94 described training based on the Strengths Approach to child protection education, a theoretical framework that evolved out of recent practice in social work which she applied to teaching and addressing moral and ethical issues such as child abuse.
Although not explicitly described as a theoretical model, Mead142 appears to propose a model of teacher education that places experience of PSHE education and citizenship (in terms of discussion about, observation of and teaching of) at the heart of a process of learning which helps trainee teachers to make their values explicit. Myers-Clack and Christopher148 did not explicitly report that their training was based on a theory; however, it is stated that the questionnaire used to assess outcomes was developed based on Fullan's theory of educational change and the course objectives and goals. Cleave and Charlton83 did not report a theory but did report that the course was designed in line with ‘humanistic principles of education’ (p. 401).
Outcome and process measures
Twelve (60%) studies25,61,63,70,81,83,92,148,191,195,200,201 measured outcomes associated with health teacher training (see Table 45). Teacher outcomes were measured in all of these studies; no studies reported pupil outcomes. The teacher outcomes reported were knowledge of health issues (n = 7; 35%), health-related teaching skills (n = 4; 20%), confidence/self-efficacy to teach health (n = 7; 35%), attitudes towards promoting health (n = 4; 20%), motivation/intentions to teach health (n = 2; 10%), teaching of health in school (n = 3; 15%), teachers' values (views and beliefs around health and their role as a teacher of health) (n = 8; 40%), teachers' mental health (n = 1; 5%) and ‘other’ outcomes (n = 3; 15%).
Sixteen (80%) studies25,26,44,61,63,81,83,92,94,117,142,156,174,189,195,201,213 evaluated the processes of health teacher training. The studies were classified in terms of the same types of processes used in the descriptive map earlier in this report (see Chapter 5, Outcomes and processes measured). These were acceptability and adequacy to the teachers of the training (n = 12; 60%), resources and costs used to train the teachers (n = 3; 15%), teachers' general reflexivity of their health-promoting role and practice (n = 13; 22%), implementation of the training programme (n = 8; 40%) and ‘other’ processes (n = 2; 10%).
Eight (40%) studies25,61,63,81,83,92,195,201 measured both outcomes and processes. Further detail on the outcomes and processes measured are given in Assessment of the effectiveness of training on teacher outcomes and Assessment of processes, which report the results of the studies.
Critical appraisal of the included studies
As stated earlier, the methodological quality of all of the included studies was appraised using standard criteria (see Appendix 8). The level of detail of study methods and findings reported in the publications varied considerably. In a number of cases detail was minimal, prohibiting a full appraisal of quality, although it is acknowledged that many academic journals impose word limits limiting the extent to which authors can describe methods.
The sample sizes of the studies varied considerably, from < 10 to around 1500 participants, with the majority including up to 100 participants (see Table 45). Some of these studies could be considered to be relatively small; however, to put the research into perspective, some authors pointed out that the status of their study was a ‘preliminary investigation’,201 a ‘pilot evaluation’,63 a ‘small-scale study’142 and ‘a case study methodological approach’. 70
Only two studies26,83,156 reported who had funded the research and it was therefore unclear in the majority of studies whether funding status represented a possible conflict of interests (e.g. whether the funder had a financial interest in the outcome of the research). In the majority of studies there was no explicit statement of whether informed consent was sought from the study participants.
Data collection methods
A range of data collection methods was used by the studies to assess outcomes and processes, with some studies using multiple methods (Table 48). The most common method was questionnaires. Many of these were structured, with pre-coded response categories and rating scales, although some also included open-ended questions allowing respondents to elaborate in more detail on particular issues. Interviews were another commonly used method, mainly conducted on a one-to-one basis using open-ended questions. In one of the two studies that used observation as a method, the study author observed the guest presenter who addressed the trainee teachers, as well as the trainee teachers' verbal and non-verbal responses to the guest presentation. 61 The other study that used observation did not provide any further detail on this method. 63
| Study | Focus group | Interview | Questionnaire | Observation | Other |
|---|---|---|---|---|---|
| Arnold 200744 | ✓ | ✓ | |||
| Athanases 200361 | ✓ | ✓ | |||
| Baginsky 200563 | ✓ | ✓ | ✓ | ✓ | |
| Bostock 201070 | ✓ | ✓ | ✓ | ||
| Chifunyise 200281 | ✓ | ✓ | |||
| Cleave 199783 | ✓ | ✓ | |||
| Evans 200792 | ✓ | ✓ | |||
| Fenton 200894 | ✓ | ✓ | ✓ | ||
| Hodgkinson 2000117 | ✓ | ✓ | |||
| Mead 2004142 | ✓ | ✓ | |||
| Myers-Clack 2001148 | ✓ | ||||
| Paakkari 201026,156 | ✓ | ✓ | |||
| Rossato 2009174 | ✓ | ✓ | |||
| Speller 201025 | ✓ | ✓ | |||
| Taylor 2008189 | ✓ | ||||
| Thomas 2005191 | ✓ | ||||
| Vincent 2005195 | ✓ | ||||
| Weatherby-Fell 2004200 | ✓ | ||||
| Weatherby-Fell 2005201 | ✓ | ||||
| Yager 2009213 | ✓ | ✓ |
The eight studies classified as ‘other’ used a variety of methods, the most common of which were trainee teachers' reflections on the training elicited using essays,26,156 ‘written responses’ and ‘anonymous students' evaluations’,61 ‘critical incident reflections’,70 ‘written narratives’,92 ‘electronic discussion board that allows anonymous postings’94 and ‘e-mails and posts on an online discussion board’. 213 Also classified as ‘other’ were curriculum mapping of the content of a PGCE course against qualified teacher standards and the Public Health Skills and Career Framework (PHSCF)25 and analysis of trainee teachers' mentor reports. 142 One study mentioned receiving feedback from experts in the fields of education and child protection, but provided no further information. 63 In general, the studies did not report whether data collection instruments had been validated, although some did mention that they had been piloted before use.
Critical appraisal of outcome evaluation
The studies varied in terms of their evaluation design (see Table 45) and, because of the way that some of them were conducted and reported, they did not always fit easily into standard categories of study design. In only a few studies did the authors themselves provide a definition of the design.
In terms of the 12 studies that reported outcomes,25,61,63,70,81,83,92,148,191,195,200,201 the most commonly classified design was a single cohort of teachers, with outcomes assessed before and after their training (single cohort before-and-after study). 25,70,81,83,148,191,195 (Note that the term ‘single cohort’ does not prohibit more than one group of teachers in the study but means that all teachers received the same training with no control or comparison group.) Two studies evaluated training in single cohorts of teachers with outcomes assessed only after the training. 63,201 Another study appeared to be primarily a process evaluation of training in a single cohort of teachers, but some outcomes were also reported during the course of the training, and also at the end. 61 In a further study that reported outcomes the design was classified as unclear. 200 This appeared to be a single cohort of teachers receiving training, but there were conflicting details in the publication about the possible inclusion of a before-training assessment. The seven single cohort before-and-after training studies were critically appraised using the Cochrane EPOC Group risk of bias criteria228 (Table 49).
All studies were judged unclear in terms of whether the intervention, in this case the teacher training, was independent of other changes. Only three studies81,148,191 commented on the limitations of the study design in this respect. For example, Myers-Clack and Christopher148 commented that, because of the lack of a control group, it was inconclusive whether or not the observed changes were due to the training: ‘discussions with other students or teachers, other courses, or experiences in the classroom, actual teaching experience, paraprofessional experiences, volunteering – might have influenced the outcome variables’ (p. 465).
| Question | Low, n | High, n | Unclear, n |
|---|---|---|---|
| 1. Was the intervention independent of other changes? | 0 | 0 | 7 |
| 2. Was the intervention unlikely to affect data collection? | 7 | 0 | 0 |
| 3. Were incomplete outcome data adequately addressed? | 4 | 0 | 3 |
| 4. Was the study free from selective outcome reporting? | 5 | 0 | 2 |
| 5. Was the study free from other risks of bias? | 4 | 2 | 1 |
All studies were judged at low risk of bias in terms of the data collection being affected by the training (e.g. sources and methods of data collection were the same before and after the intervention for consistency in measurement). Incomplete data were adequately addressed in four of the studies25,70,148,191 (e.g. the proportion of missing data at the post-training assessment was considered low and unlikely to bias the outcome measurement) and this was unclear in three81,83,195 (e.g. not reported whether or not there were any missing data at the post-training assessment, or unmatched samples of teachers assessed before and after training). Most of the studies were judged at low risk of bias from selective outcome reporting (e.g. all outcomes that were stated to have been measured were reported on in terms of results). In one study195 it was unclear because no detail was provided on which items and measures were included in the surveys, and in another study25 the authors state that selected outcomes are reported but it is not possible to tell which outcomes were omitted.
Critical appraisal of process evaluation
Table 50 reports the critical appraisal judgements for the 16 studies that evaluated the processes of teacher training (see Appendix 8 for more detail on the criteria used). As stated earlier, the studies that we have classified as examining processes of teacher training did not always define themselves explicitly as process evaluations.
Twelve of the studies25,26,44,63,81,83,92,94,117,156,189,201,213 were judged to have taken at least a few steps to minimise bias in the sampling of research participants (e.g. using a sampling strategy appropriate to the study aims; including all stakeholders in the research; reporting the characteristics of the study sample). One study61 was judged to have made a fairly thorough attempt. In this study the evaluation involved all people involved in the training, including the trainee teachers, the training instructors and the guest presenter.
| Unclear, n | A few steps taken, n | Several steps taken, n | Fairly thorough attempt, n | |
|---|---|---|---|---|
| 1. Were steps taken to minimise bias/increase rigour in sampling? | 3 | 8 | 4 | 1 |
| 2. Were steps taken to increase rigour/minimise bias and error in the process data collected? | 6 | 4 | 5 | 1 |
| 3. Were steps taken to increase rigour/minimise bias and error in the analysis of the process data? | 12 | 1 | 1 | 2 |
| Limited grounding/support, n | Fairly well grounded/supported, n | Reasonably well grounded/supported, n | ||
| 4. Were the findings of the process evaluation grounded in/supported by the data? | 6 | 9 | 1 | |
| Limited breadth and depth, n | Good/fair breadth, limited depth, n | Good/fair depth, limited breadth, n | Good breadth and depth, n | |
| 5. Breadth and depth of findings | 8 | 2 | 1 | 5 |
Similarly, nine of the studies25,26,44,92,94,117,156,174,189,213 were judged to have taken at least a few steps to minimise any error in the process of data collection (e.g. validation and piloting of data collection instruments; ensuring that all participants were able and willing to contribute; assurances of confidentiality). The one study judged to have taken a fairly thorough attempt was again that by Athanases and Larrabe. 61 In this study the authors discuss the efforts made to encourage the trainee teachers to provide candid responses in their evaluation of the training, and a combination of data collection methods was used (e.g. written responses; anonymous trainee teacher feedback, observation, interviews) providing a comprehensive set of evaluation methods. It was not stated, however, whether data collection instruments were validated.
Fewer studies were judged to have taken steps to minimise bias and error in the analysis of the process data. Twelve25,44,63,81,83,92,117,142,174,195,201,213 of the 16 studies were judged unclear on this criterion, mainly because of lack of detail given about which methods had been used to analyse the data (e.g. type of approach to analysing qualitative data from interviews and focus groups), who participated in the data analysis and whether they accounted for their role in the training and the research, and whether data were independently analysed by more than one person. One of the two studies that was classified as providing a fairly thorough attempt was that by Paakkari and colleagues,26,156 who provided a detailed account of their approach, which they describe as phenomenographic research. A process was followed to minimise the influence on the research of the authors' own perspectives, and the authors also describe a holistic approach to the data analysis with full integration of data from trainee teachers' essays and interview transcripts.
The findings of the majority of the studies25,26,61,92,94,117,142,156,201,213 were classed as fairly well grounded in/supported by the data. In some studies quantitative results were provided in tabular form (e.g. counts and frequencies illustrating the predominance of certain issues or themes) with further elaboration in the text and with supporting illustrative quotes from the research participants illustrating the range of perspectives. The ‘qualitative case study’ by Taylor and colleagues189 was the only study judged to be reasonably well grounded in its findings, with several illustrative participant quotations to support the analytical observations made. (Note: the distinction between ‘fairly well’ and ‘reasonably well’ grounded can be seen as ‘average/satisfactory’ and ‘good’ respectively.) Although the quotations are not numbered or otherwise identified, the author does demonstrate that quotes come from a range of research participants. In six studies,44,63,81,83,174,195 however, only limited process data were given, which made it difficult to interpret the authors' overall conclusions (e.g. key results only summarised in terse bullet points, or findings reported in general terms making it difficult to discern between data and the authors' interpretations and general opinions).
The studies were judged in terms of the breadth and depth of findings, with ‘breadth’ being the extent of description of the findings and ‘depth’ being the extent to which data have been transformed into themes or concepts. The findings of half of the studies25,63,81,83,174,195,201,213 were judged to be of limited breadth and depth. Generally, these studies were reported in brief detail with limited analytical exploration of the findings and their implications. Only five of the studies26,61,92,94,156,189 were judged as providing good breadth and depth of findings [e.g. the perspectives of participants are fully explored in terms of breadth (contrast of two or more perspectives) and depth (insight into a single perspective)]. An example is the study by Evans and Evans,92 which explored the confidence of trainee teachers and NQTs of English in teaching PSHE education. There was reasonable breadth to the findings with a number of illustrative quotes and discussion of the implications for teacher training. In terms of depth there was some translation of the data into key areas for discussion and reflection, although there was no explicit attempt at theoretical development.
A final step in the critical appraisal process was for studies to be judged in terms of their ‘weight of evidence’. A weight (low/medium/high) was assigned to the reliability or trustworthiness of the findings (e.g. the extent to which the methods used were rigorous/could minimise bias and error in the findings – items 1–4 in Table 50). A second weight was assigned according to the usefulness of the findings in terms of how well the teacher training was described and whether or not the process data could illuminate the relationship between the process of delivering the training and outcomes, and barriers to and facilitators of successful implementation (taking into account items 4 and 5 in Table 50). The majority of the studies (n = 10) were judged to be medium or high in reliability and usefulness of findings (Table 51). The three studies that were judged high on reliability and/or usefulness were those by Athanases and Larrabee,61 Taylor and colleagues189 and Paakkari and colleagues. 26,156
Assessment of the effectiveness of training on teacher outcomes
Knowledge of health
Seven studies reported the impact of training on teachers' knowledge of health. Five25,70,81,191,195 were classified as single cohort before-and-after study designs and two61,200 included single cohorts of trainee teachers with outcomes measured at various time points during the study. Knowledge was assessed in a variety of ways.
Athanases and Larrabee61 reported that a ‘dominant theme’ in their study was the trainee teachers' positive value placed on new learning about issues faced by lesbian and gay people (p. 247). Seventy-four of the 97 trainee teachers (76%) were classified as placing a value on developing knowledge of issues about lesbian and gay people, including issues in relation to school.
Chifunyise and colleagues81 report changes in Zimbabwean trainee teachers' knowledge of HIV infection/AIDS prevention, symptomology and epidemiology from baseline to follow-up 4 years after the start of training. There was an increase in knowledge of symptoms, diagnosis and treatment. No statistical tests were reported for the changes presented. The authors' overall summary of knowledge acquisition was that the increase was ‘small’ (p. 383).
Speller and colleagues25 reported changes in PGCE trainee teachers' knowledge of physical activity and healthy eating over the course of a year. There were mixed findings, with a low proportion of trainee teachers correctly identifying recommended physical activity guidelines for children, but a higher proportion aware of the five-a-day recommendation for fruit and vegetables. No statistical tests were reported for the changes presented.
| Study | Reliability of findings | Usefulness of findings | ||||
|---|---|---|---|---|---|---|
| Low | Medium | High | Low | Medium | High | |
| Arnold 200744 | ✓ | ✓ | ||||
| Athanases 200361 | ✓ | ✓ | ||||
| Baginsky 200563 | ✓ | ✓ | ||||
| Chifunyise 200281 | ✓ | ✓ | ||||
| Cleave 199783 | ✓ | ✓ | ||||
| Evans 200792 | ✓ | ✓ | ||||
| Fenton 200894 | ✓ | ✓ | ||||
| Hodgkinson 2000117 | ✓ | ✓ | ||||
| Mead 2004142 | ✓ | ✓ | ||||
| Paakkari 201026,156 | ✓ | ✓ | ||||
| Rossato 2009174 | ✓ | ✓ | ||||
| Speller 201025 | ✓ | ✓ | ||||
| Taylor 2008189 | ✓ | ✓ | ||||
| Vincent 2005195 | ✓ | ✓ | ||||
| Weatherby-Fell 2005201 | ✓ | ✓ | ||||
| Yager 2009213 | ✓ | ✓ | ||||
| Total | 5 | 9 | 2 | 5 | 9 | 2 |
Vincent and colleagues195 reported changes in two questionnaire knowledge items following implementation of the Response Ability programme to prepare teachers for dealing with mental health issues affecting children. Pre- and post-training changes in knowledge are reported for five geographically separate cohorts in Australia who received the programme. There was a statistically significant increase in understanding of how schools can respond to youth suicide in all five cohorts, and in understanding of a range of mental health problems in adolescence (depression, eating disorders, anxiety and schizophrenia) in three of the cohorts. Weatherby-Fell and Kean200 also report an evaluation of Response Ability, using the same knowledge measures as Vincent and colleagues. 195 They do not appear to have measured knowledge before the training but they do make a comparison with a (non-concurrent) control group who did not receive the training. There were no statistically significant differences in ‘understanding of mental health problems in adolescence’ between the training and control groups (mean ratings were high in both groups); however, the training group showed a statistically significant higher understanding than the control group of how schools can address suicide prevention and respond to youth suicide.
Bostock and colleagues70 reported that the PGCE trainee teachers who received training on mental health issues affecting children became more aware of the incidence and early signs of mental illness in children and adolescents. These results were reported narratively with no supporting quantitative data.
Finally, Thomas and Jones191 reported a highly statistically significant increase in trainee teachers' self-rating of knowledge in relation to the health aspects of PSHE education following training (p < 0.0001).
Confidence/self-efficacy to teach health
Seven studies63,70,83,191,195,200,201 reported the impact of training in terms of changes to teachers' confidence/self-efficacy to address health in schools. All but two of these63,200 were before-and-after single cohort study designs. Confidence was generally measured by trainee teachers' self-ratings against statements about perceived ability to identify with and respond to children with health issues.
Baginsky and Macpherson63 report changes in confidence following implementation of the Child Protection in Initial Teacher Training Tutor Pack in 13 HEIs in the UK. At the first questionnaire, completed at the end of the first training input, 59% of trainee teachers said that they were confident in their role and responsibilities in relation to child protection. This figure increased to 73% once they had completed their teaching practice. Despite the high levels of confidence identified by the questionnaire, there were a ‘significant number of respondents expressing some anxiety and confusion’ (p. 320).
Bostock and colleagues70 stated narratively that PGCE trainee teachers showed a big increase in confidence in their ability to detect early warning signs of mental health problems after a 1-day training course. The confidence ratings of the PGCE trainee teachers for knowing what to do if they did detect a mental health problem were much higher after the training. No quantitative data are provided to support this assertion and details of the rating scale used are not given. A small sample of five NQTs who received the training 18 months previously were reported to remain confident that they would know what to do if they detected a problem with a pupil, without having had any further training.
Cleave and Charlton83 evaluated a 2-day training course for teachers to enable them to support children experiencing cancer-related life crises. The authors report that after training the majority felt more confident in being able to identify children under stress (73%) and negotiate some form of action with the child (82%). In total, 45% of the participants felt more confident immediately after the course in being able to accurately reflect what a child was saying or feeling, whereas 55% felt about the same as they had before the course. No participants rated themselves as feeling less confident in any of the skills at either of the two post-training assessments. Caution is advised in the interpretation of these findings because of the small number of trainee teachers in the study (n = 11).
Improving confidence to teach PSHE education was the focus of the study by Thomas and Jones. 191 Mean post-test scores for total confidence on a PSHE Key Skills Confidence Scale were reported to have increased substantially compared with pre-test scores. Following training there was a highly statistically significant increase in 25 skill items relating to working with others, and in 20 items relating to confidence in communication following training (p < 0.0001).
There were statistically significant increases in the mean agreement with the two confidence statements assessed by Vincent and colleagues. 195 The statement relating to feeling confident about responding to a young person considering suicide was statistically significant for all five geographical cohorts in the study. The statement about responding to and working with a young person with a mental health problem was statistically significant for four of the five cohorts (p-values not reported).
Weatherby-Fell and Vincent201 reported a moderate to high level of agreement with the statement about feeling more confident about identifying young people in need of support in a small sample of early career teachers (n = 13) approximately 12 months after they had completed their university training. (Note: Weatherby-Fell and Kean200 report a separate evaluation of the same training; however, because of the unclear nature of the study design and ambiguities in reporting of data for confidence we have not reported results for this outcome.)
Teachers' values
Eight studies25,61,70,81,148,195,200,201 reported outcomes classified as teachers' values (teachers' views and beliefs around health and their role as a teacher of health). All but two of these61,200 were single cohort before-and-after study designs. As with the outcomes presented above, methods for assessing values varied.
One of the themes of the qualitative evaluation of diversity training by Athanases and Larrabee61 was ‘developing strategies for advocating for lesbian and gay youth’. The authors report that following the training the teachers re-examined their roles as future educators and many considered that it was part of their duty to treat all of their future pupils with respect, including those who are lesbian or gay.
Bostock and colleagues70 compared PGCE trainee teachers' pre- and post-training responses and experienced teachers' responses to six Likert scale attitude statements relating to the perceived importance of the teacher's role in identifying and addressing mental illness in pupils. There were statistically significant differences between these groups in relation to five of the six statements. The Likert scale mean scores were ranked for each question, with PGCE trainee teachers after the training showing the most positive attitudes and the experienced teachers showing the least positive. The authors also report that a larger number of PGCE trainee teachers after the training than before it expressed a neutral opinion towards the idea that they have an important role to play in detecting early signs of mental illness in their pupils (no numerical data provided).
Trainee teachers who participated in focus groups in the study by Chifunyise and colleagues81 discussed what qualities a teacher should have to be able to teach AIDS education. It is reported that they all agreed that such a teacher should be a strong role model for pupils. They recognised that AIDS education is a difficult and sensitive subject and that they did not always feel competent to teach it. To overcome this they recognised that they should be able to identify up-to-date information.
Myers-Clack and Christopher,148 who evaluated the training course Drug and Health Issues for Educators, hypothesised that the training would increase the teachers' value of school health education and belief in the importance of health to a student's learning. There was a statistically significant increase in the former (p = 0.000) but not the latter (p = 0.320) over the course of the semester.
Speller and colleagues25 reported the percentage of trainee teachers agreeing with five statements relating to the role and ability of teachers/schools to influence children's health (e.g. ‘Teachers can be role models for health’ and ‘As a teacher I will be able to positively influence young people's health behaviours’). A high proportion of trainee teachers agreed with the statements at baseline (ranging from 74% to 96%). At the end of the academic year there was a slight decrease in agreement with four of the five statements, only one of which was statistically significant (‘The school environment affects students' food choices’; p < 0.01). There was a slight increase in agreement with one statement (‘The nutritional health of students should be a school priority’) but this was not statistically significant.
There was a statistically significant increase in mean agreement with the statement ‘It is important for student teachers to learn about mental health promotion and suicide prevention at university or college’ between baseline and follow-up in three of the five cohorts in the study by Vincent and colleagues. 195 There was a statistically significant increase in mean agreement with the statement ‘Schools and teachers can have a positive effect on the mental health of young people and help to prevent suicide’ between baseline and follow-up in four of the five cohorts. No p-values were provided for these results. The authors also report selected quotes from two of the trainee teachers about how they considered the course would help them to address the mental health of their pupils. Weatherby-Fell and Kean200 also report an evaluation of this training (Response Ability) using these same two statements. They do not appear to have measured these statements before the training but they do make a comparison with a control group (non-concurrent). They report that mean scores for the statements were very high for both groups, and no statistically significant difference was found between the training group and the control group.
Approximately 12 months after they completed their university training, Weatherby-Fell and Vincent201 asked their small sample of 13 early career teachers to rate the statement that teachers have an important role in creating supportive school environments and building resilience. The teachers agreed strongly with this (mean scores ranging from 8 to 10 on a scale of 1–10). The teachers were also asked to indicate their level of agreement with the statement that young people's social and emotional well-being, or resilience, can impact on school performance, behaviour or learning outcomes. There was strong agreement with this statement (mean scores between 9 and 10).
Teaching of health and well-being in school
Three studies70,92,191 reported the impact of training in terms of various aspects of the teaching about health and well-being issues in school.
The study that investigated this in most depth was that of Evans and Evans,92 which assessed the confidence of a small group of 21 NQTs to teach PSHE education in relation to their initial training received (secondary PGCE English) and subsequent training through early CPD. It is reported that one-third of the study respondents had never taught PSHE education as a separate subject during their PGCE teaching placement, with only half having done so in more than one lesson. Once in post the NQTs reported significant responsibility for PSHE education delivery. Based on the questionnaire responses and written narratives the authors suggest that there is a significant disparity between experience gained as trainees and expectations of teachers during the NQT year regarding the delivery of PSHE education.
Respondents were also asked to rate the usefulness (‘most useful’) of 10 particular teaching methods for both PSHE education as a separate subject and PSHE education through English. Common rated methods included ‘question and answer’ (five respondents), ‘small group or paired discussion’ (five respondents), ‘whole class discussion’ (six respondents) and ‘guided, practical activity’ (four respondents). Drama techniques was the most popular choice for teaching PSHE education through English (10 respondents), but was rated ‘most useful’ by only three respondents when teaching PSHE education as a separate subject. Responses to open-ended questions agreed with these ratings, highlighting the usefulness of interactive and practical tasks for PSHE education. The authors suggest that these teachers do recognise the usefulness of, and do use, interactive methods in teaching PSHE education. When asked, ‘How often do you deliberately target PSHE education learning objectives when planning English/media lessons?’, one-third of the participants responded ‘often/quite often’, one-third responded ‘not very often/not often enough’ and one-third responded ‘spontaneously only’, ‘never’ or ‘when instructed’. The authors suggest that there is a lack of overt awareness of how much PSHE education teaching could be planned for in English lessons.
The training evaluated by Thomas and Jones191 provided PGCE science and geography trainees with the opportunity to plan and deliver a 1-hour lesson on peer pressure to year 7/8 pupils. As stated earlier (see Confidence/self-efficacy to teach health), the impact of the training was assessed through self-ratings of confidence to teach PSHE education through the PSHE Key Skills Confidence Scale. Some of the items on this scale related to the teaching of PSHE education, including items such as ‘During PSHE lessons I listen and respond sensitively, developing ideas and encouraging other pupils to contribute; encourage pupils to recognise and express their ideas, feelings, attitudes, beliefs, values and personal experiences’. There was a highly statistically significant increase in scores for all items following training, indicating good practice around the teaching of PSHE education.
Finally, Bostock and colleagues,70 in their study of mental health training for PGCE trainee teachers, reported that trainees took a very positive and proactive approach once they identified mental health problems in their pupils during their training school placements. They reported taking responsibility and referred the problem to appropriate colleagues and took advice. These findings were based on critical incident reflections written by the trainee teachers for their assignments.
Summary of teacher outcomes
Twelve studies25,61,63,70,81,83,92,148,191,195,200,201 reported teacher outcomes, based on evaluation of teacher training that varied in a range of characteristics. The majority of the studies measured outcomes before and after training in a single group of trainee teachers, with few comparisons with teachers who did not receive training. Outcomes were measured in a variety of ways, predominantly through self-ratings on structured scales, although some studies reported trainee teachers' written reflections and qualitative methods from focus groups. The changes in outcomes were not always confirmed by statistical tests and caution is advised in the interpretation of the findings in the absence of control or comparison groups.
The studies demonstrated some increases in trainee teachers' factual knowledge of health issues following training, in areas as varied as HIV/AIDS, healthy eating and physical activity, mental health, health aspects of PSHE education and diversity. There was a general increase in teachers' confidence in relation to teaching PSHE education, and in identifying and helping children with mental health problems or child protection issues. Likewise, there was a general increase in positive beliefs about the role of teachers and schools in promoting children's health, including tentative evidence for beliefs about the relationship between good health and effective learning. There was some limited evidence on teachers' experiences of teaching health in schools, specifically PSHE education lessons. Teachers' self-ratings showed increases in scores for their ability to facilitate effective discussion of health issues. Teaching methods such as interactive and practical tasks for PSHE education were popular.
Assessment of processes
During data extraction we classified the process evaluation findings according to the categories shown on the left-hand side of Figure 10. We then analysed these to identify overall themes within the findings. This resulted in a list of eight themes that encapsulated the findings of the process evaluations. Figure 10 shows the themes identified and which of the original data extraction categories most of the findings relating to each theme came from. We next discuss the process evaluation findings relating to each theme and the barriers to and facilitators of health training in ITT that can be inferred from these findings.
Acceptability of teacher training in relation to health
Eight studies61,81,83,92,94,195,201,213 reported findings on trainee teachers' and training providers' perceptions of the acceptability of the training in health that they had received or delivered. These studies reported on the perceived acceptability of the training overall61,81,83,92,201,213 (which included training in health education and promotion in general,213 sexual diversity,61 HIV infection/AIDS prevention,81 working with children who have experienced cancer in their lives,83 PSHE education92 and mental and emotional health201) and the resources used to support delivery. 94,195,213 The studies reported that, in the main, the training was seen to be acceptable and was well received by trainee teachers. 61,81,83,92,201,213 The authors of only one study, that by Athanases and Larrabee,61 reported that a minority of trainee teachers were resistant to the training. This study was conducted at a university in the USA and was published in 2003. It examined trainee teachers' responses to training about respecting sexual diversity and understanding and supporting lesbian and gay youth in schools, with the training delivered in part by a gay-identified guest speaker. The resistant trainee teachers had difficulty reconciling the topic with their religious beliefs, with one trainee teacher refusing to attend a class meeting with the guest speaker.
FIGURE 10.
How the process evaluation findings themes related to the original data extraction categories.
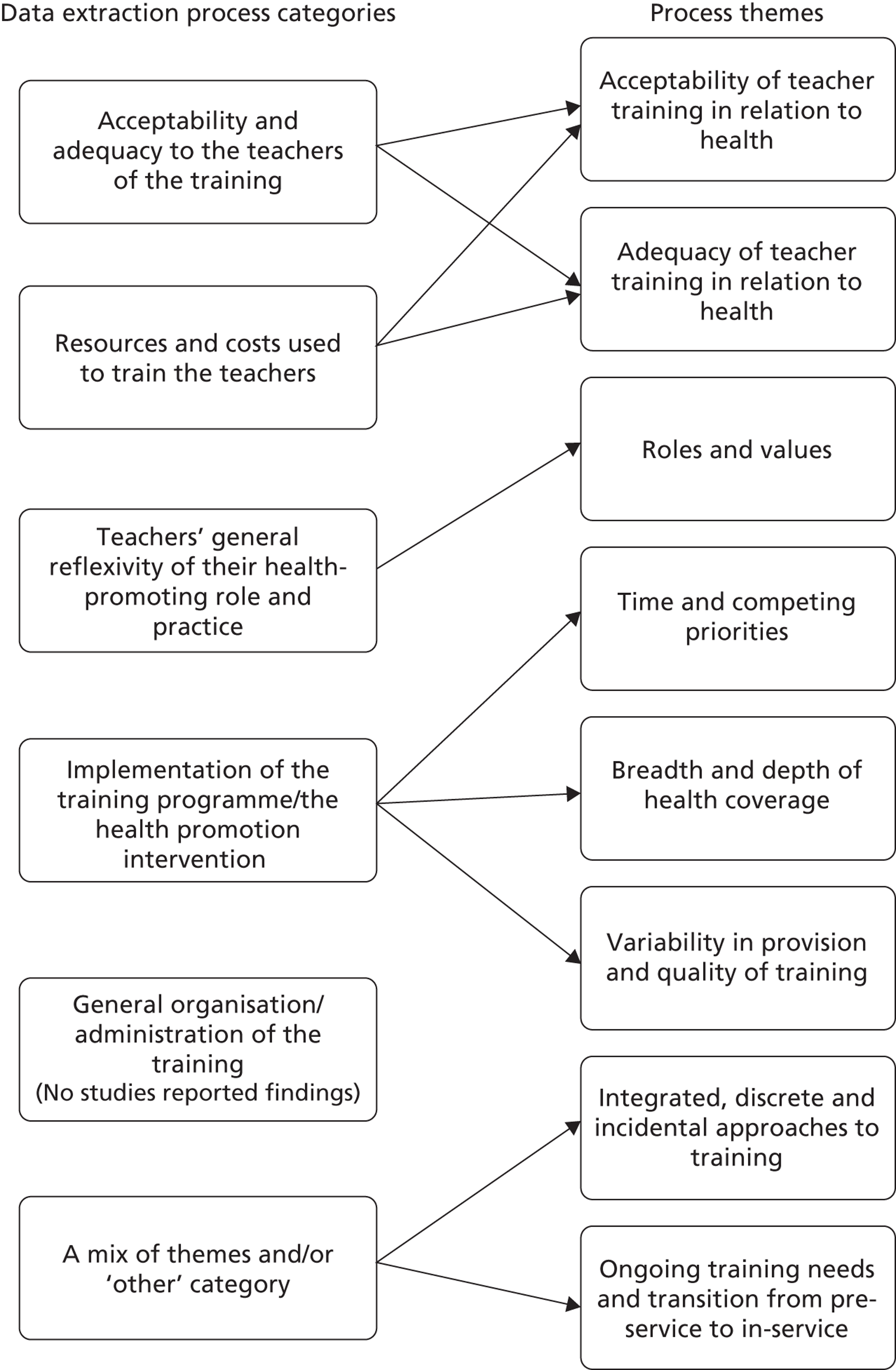
The findings of this study, along with those of Chifunyise and colleagues,81 who evaluated a HIV infection/AIDS prevention training programme in Zimbabwe, also highlighted that the creation of a non-threatening atmosphere was helpful for trainee teachers to discuss these sensitive diversity61 and sexual health81 topics.
Two94,195 of the three studies that reported on trainee teachers' and training providers' responses to resources and materials used as part of the training also suggested that these resources and materials were generally well received. Fenton94 stated that trainee teachers responded well to case studies that were included as part of child protection training, as these helped trainee teachers to explore different perspectives on child protection issues. Vincent and colleagues195 reported that 96% of the teacher educators in their study found it easy to use a multimedia resource package called Response Ability, which was distributed to pre-service education providers in Australia to support mental health training. Furthermore, 96% said that their trainee teachers were receptive to the material.
The other study that reported on trainee teachers' responses to resources and materials used as part of the training213 suggested that training delivered using online materials may not be effective in engaging the interest of all trainee teachers. Over the semester-long course about health issues relevant to trainee teachers, the majority of the trainee teachers (67%) engaged with these materials for fewer hours than they were guided to. Yager213 noted anecdotal evidence of ‘online overload’ and suggests that trainee teachers might be more likely to complete activities if they are provided in a hard-copy format.
Adequacy of teacher training in relation to health
Trainee teachers' views of the adequacy of the training that they had received varied. Two studies83,92 suggested that PGCE trainee teachers (along with NQTs in one of the studies92) were generally positive that the training that they had received in communication skills for working with children experiencing cancer in their lives (conducted at one university in England)83 and in incorporating PSHE education into their English teaching (conducted at another university in England)92 had met their needs. The trainee teachers and NQTs in the latter study felt that the training that they had received had had a beneficial impact on their practice in school, as did trainee teachers who had participated in HIV infection/AIDS prevention training in Zimbabwe in another study. 81 After training in how to incorporate PSHE education into their English teaching,92 some of the trainee teachers felt, however, that they still lacked knowledge and that further knowledge-based input would have been useful. One study of mental health training (using the Response Ability resources) in Australia201 showed that four of the seven trainee teachers surveyed felt that the training had helped them to become ‘a better teacher’, whereas three were neutral about this. A study of teacher training in issues related to their health213 found that only around half of the trainee teachers involved felt that it had enhanced their personal well-being or had helped them to reflect on this. Other authors reported that, after receiving training in PSHE education,92 child protection,63,94,117,174 sexual diversity61 and mental and emotional health,189 some trainee teachers still had ongoing concerns about teaching PSHE education92 and dealing with sensitive issues in practice. 61,63,94,117,174,189 This was especially the case in the studies about child protection training,63,94,117,174 which reported that trainee teachers often did not feel fully prepared to deal with this issue if it arose in school and that they expressed concerns about the complex issues facing teachers.
For health training to meet trainee teachers' needs, the findings of the process evaluations suggested that it may be important for it to:
-
include practical experience92 or training in practical skills63,94,174,189,201
-
be made personally relevant to trainee teachers61,94,213 and take into account individual needs63,83
Practical experience or skills
Six studies reported that trainee teachers felt that more practical experience of teaching PSHE education92 or training in practical strategies for dealing with issues such as pupil well-being189,201 (e.g. working with parents) and child protection63,94,174 (e.g. reporting strategies, dealing with disclosure) would have been useful in the training that they received or in their future training. Two studies found, however, that some trainee teachers believed that, although training was helpful, they would learn better from their own experience once they were working within schools how to teach PSHE education (with observation and feedback)92 or deal with student well-being. 189 Teacher educators in another study,44 which surveyed teacher training providers across Australia about the child protection content of their courses and ran a focus group with teacher educators about this, also acknowledged that practical experience of child protection issues on school placement teaching might be useful for trainee teachers to help contextualise and broaden their understanding of this issue. They also felt, however, that this would have organisational implications for ITT providers in terms of a need to closely monitor the training that took place.
Personal relevance and individual needs
Findings from the studies by Fenton94 and Athanases and Larrabee61 suggest that it may be important for the delivery methods used in training to engage trainee teachers on a personal level. Fenton94 states that, during child protection training that used the Strengths Approach in a 13-week module with 19 pre-service teachers studying Early Childhood Education in Australia, the trainee teachers appreciated more informal statistics about child abuse presented in case studies rather than national statistics, because the case studies translated the statistics into a more tangible format, and enabled the trainee teachers to make connections between the statistics and their experiences. Fenton94 also states that trainee teachers sharing their personal and professional experiences of child protection issues during training enabled them to more fully explore these issues and ‘made it harder for pre-service teachers to ignore the likelihood of encountering children in situations of abuse in their careers or to have thoughts of ignoring the issue as irrelevant for their practice’ (p. 229). In their study of training about understanding and supporting gay and lesbian youth in schools, Athanases and Larrabee61 found that trainee teachers felt that the delivery of some of the training by a gay-identified guest speaker helped to bring the statistics that they were presented with alive and they appreciated the opportunity to gain insight into an insider's perspective.
The findings of three of the process evaluations63,83,213 also suggested that in some cases training did not fully meet teachers' needs as they felt that the delivery methods needed to be tailored more to individual circumstances, including different levels of teaching experience (found in a study83 evaluating teacher training about working with children experiencing cancer in their lives, which was delivered to both PGCE students and practicing teachers) and previous training (found in a study63 that evaluated a child protection training pack, which had been developed by the NSPCC, among 1247 students at 13 HEIs in the UK). In the study of training in health issues relevant to the trainee teachers' own health by Yager,213 only 50% of the trainees reported that they felt that the training was personally relevant to them. For example, the author provided a quote from a mature trainee teacher who commented that the training was more relevant to younger trainee teachers.
Relevance to teachers’ practice in schools
Three studies61,63,94 suggested that it may be important to make information presented to trainee teachers during training relevant to their practice as teachers. Fenton94 and Athanases and Larrabee61 found that trainee teachers responded well to training in child protection and supporting gay and lesbian youth in schools, respectively, when the materials and methods used were specifically related to education. Baginsky and Macpherson63 conducted a study to examine how to improve a child protection training pack, developed by the NSPCC, to be used in ITT. Among other improvements, trainee teachers suggested that the materials could be made more relevant to what happens in schools and that they could highlight the responsibilities of the agencies who would be involved in a case.
Roles and values
Some of the studies that included process evaluations explored trainee teachers' perspectives on their health-promoting role and how these changed after training; there is some overlap between the findings of the process evaluations reported here and the findings of the outcome evaluations reported earlier. In the process evaluations, there were mixed findings in these studies about the extent to which trainee teachers had assimilated responsibility for health promotion into their role as a teacher and their understanding about their role. Three of these studies explored trainee teachers' attitudes about this after their ITT in England25,117 and the UK174 – these studies did not include a specific health training intervention or enhanced training. Speller and colleagues25 found that only a minority of the trainee teachers whom they surveyed in the 2008–9 academic year did not feel that health promotion was part of a teacher's responsibility and that teachers could influence children and young people's health. They did, however, find a small, statistically significant increase in the proportion of trainee teachers who endorsed this view over time, from 3% at the start of their PGCE year to 7% at the end of the year. In 1997, Hodgkinson and Baginsky117 examined how child protection training was covered in ITT in SCITTs in England following new requirements from the government that teachers receive training in child protection. They found that some trainee teachers were resistant to the idea that child protection was their responsibility as a teacher and some felt that little could be done to help children experiencing abuse. The trainee teachers expressed a lack of clarity about what their role in child protection entailed and had little understanding of interprofessional responsibilities for dealing with these issues. In a similar study, Rossato and Brackenridge174 examined how child protection was covered in sports degrees and PE ITT degrees in the UK following the introduction of ECM. They found that trainee teachers generally did not feel prepared for their role in child protection following their ITT, and that they saw their role as one of identifying situations and referring the issue to others who were more knowledgeable.
Four of the studies94,189,201,213 that evaluated a specific health training intervention reported that these were associated with a positive impact on some trainee teachers' attitudes towards and their understanding of their health-promotion role. Fenton94 states that early on in a 13-week child protection module using the Strengths Approach, some of the trainee teachers expressed a disengagement with child protection issues. Over the course of the module, however, they all came to acknowledge the importance of their role in this as teachers and expressed more personal engagement with the issue. Taylor and colleagues189 found that, after receiving training in pupil well-being, which was ‘infused’ into their ITT course (including two practicum experiences), trainee teachers generally felt that they had developed a greater awareness of the importance of their and schools' roles in health promotion. They had also developed an increased understanding of the complexities of student well-being and developed a more holistic and broader understanding of the factors that affect it and how it can affect pupils' education. Weatherby-Fell and Vincent201 provided three quotes from their small sample of early career secondary school teachers in Australia who had received mental health training during their pre-service training, delivered by the Professional Experience Coordinator using the Response Ability and MindMatters resources, which suggested that the training had made them more aware of the importance of teachers being sensitive to these issues and how to deal with them. Yager213 found that 49% of the trainee teachers who had received training in issues related to their health, the aim of which was also to prepare them for their health education role, agreed that the training had helped them to develop a broader perspective of well-being as it related to their teaching role. In the discussion of this study, the author suggests that they should have made the links between health and teaching clearer in the training so that the trainee teachers could recognise the role of health in their teaching.
Although some of the studies indicated that training had a positive impact on trainee teachers' beliefs about their role in health promotion as teachers, the studies also indicated that trainee teachers felt that there were limitations to their role. One study83 reported that trainee teachers had experienced benefits from training in working with children experiencing cancer in their lives, but that they felt that there was a limit to what they could do in their role as teachers to support pupils' health and well-being, particularly given the academic requirements expected of them. Baginsky and Macpherson63 found that, after child protection training in 2000–1, which had been delivered to 1247 trainee teachers in the UK using a package developed by the NSPCC, trainee teachers recognised their responsibilities as teachers, but they had a number of ongoing concerns about this. They were concerned that it would be difficult to deal with child protection issues in reality and that they might not respond appropriately to a disclosure.
The authors of two studies in this review advocated that it is important for trainee teachers to become aware of their values142 and personal approaches156 to health in their development as teachers. In a study of pre-service teachers' conceptions of approaches to teaching health education conducted in Finland, Paakkari and colleagues156 provide a hierarchy of approaches, from a deliverer of knowledge and skills to being a reflective fellow-learner. The authors argue that it is important in health education that trainee teachers become aware of the personal approaches and beliefs that they hold about it, as these might affect the level of understanding that pupils develop. Paakkari and colleagues,156 however, did not explicitly link the conceptions held by trainee teachers to the training that they had received. In a study of 102 BEd and PGCE students in the UK who were on their final school placement, Mead142 found that trainee teachers' opportunities to discuss their values in relation to teaching PSHE education and citizenship on their school placement were variable.
Time and competing priorities
Six studies25,44,63,81,142,189 indicated that a perceived lack of time in an already crowded curriculum in pre-service training could be a challenge for implementing health training. One study81 also indicated that training in health (specifically training in HIV/AIDS prevention delivered to 1562 trainee teachers from 20 institutes of higher learning in Zimbabwe), although well received, was treated as a lower priority by lecturers and trainee teachers as it was not an assessed subject. The authors of this study recommend assessment to help address this.
Breadth and depth of health coverage
Five studies44,63,83,117,189 suggested that balancing breadth and depth of coverage could also be a challenge in teacher training in health. Two studies that examined child protection coverage in ITT courses, one carried out in Australia in 2005 and 200644 and one in SCITTs in England in 1997,117 found that training sometimes provided narrow perspectives on this issue, with little contextualisation of abuse in terms of its prevalence, defining features117 and how it is linked to wider family or mental health issues. 44 Teacher educators in the study conducted in Australia44 felt that, if trainee teachers were exposed to broader perspectives on child protection, this might better prepare them to identify children experiencing these issues. Some felt, however, that within the time available on their courses they were able to provide only an overview of the issue.
Three studies63,83,189 reported concerns about breadth and depth of coverage from the trainee teachers' perspective. Two reported that trainee teachers recognised that, because of time constraints, they had received limited depth of coverage. 63,189 In one of these studies,63 in which child protection training was delivered to UK trainee teachers using a package developed by the NSPCC, the trainee teachers felt that as a result of the limited depth of coverage they did not feel prepared to deal with these issues. In the other study,189 about training in pupil well-being that was ‘infused’ into a pre-service training course in Australia, trainee teachers expressed concern that the limited time spent in school practicums meant that they were not able to fully engage with the wide range of approaches taken within schools to address this. The authors report, however, that after two school practicums, trainee teachers showed a deeper knowledge of this issue. In the other study,83 trainees expressed concern about limited breadth in the training that they had received in working with children who had experienced cancer in their lives. They felt that it was too specific to cancer and could have been broader to enable them to help children with other problems.
Variability in provision and quality of training
Four studies25,44,117,174 surveyed teacher training providers about how health topics were covered in their courses (three of these studies were conducted in the UK25,117,174 and one in Australia44) and one142 surveyed trainee teachers about their experiences of teaching or observing PSHE education and citizenship on school placement in the UK. These studies generally found variation in the provision and quality of training across different providers25,44,117 and course types25,44 and on school placement. 25,142 In a survey of ITT providers in the South East of England in 2007, Speller and colleagues25 found that coverage of health topics was variable. They state that few institutions explicitly covered healthy eating, and the amount of time spent covering physical activity and PE varied, with trainee teachers on secondary PGCE courses specialising in PE receiving the most training time on the latter.
In terms of training in child protection, in a survey of the child protection content of SCITT-based courses in England in 1997, Hodgkinson and Baginsky117 found that 9 of the 14 responding course managers reported that their courses did not contain any specific child protection training. They report that only a minority of courses provided comprehensive coverage of this issue. Furthermore, most of the trainee teachers were not briefed about child protection on school placement. This study was conducted immediately after the introduction of new requirements for covering child protection in teacher training and therefore reflects provision at that time. A similar survey of HEI course leaders174 following the introduction of ECM found that child protection was covered on all of the PGCE courses related to sport. In a survey of child protection training in Australia in 2005 and 2006, Arnold and Maio-Taddeo44 examined the extent to which training was delivered in an explicit integrated or discrete way on courses. They found that 47% of respondents reported integrated content and 23% reported discrete training. There was also variability in the extent to which it was a compulsory part of the course, with around three-quarters of the providers who said that they provided each of these types of training stating that it was a core rather than an elective part of their courses. They also found variation across states and course types in the extent to which integrated or discrete approaches were used, with integrated training more commonly reported in undergraduate than in graduate, postgraduate and other course types. Undergraduate trainee teachers also on average received more incidental training in child protection (in which related issues were taught but not explicitly linked to child protection) as part of other aspects of their courses than did graduate or postgraduate trainee teachers. In this study, teacher educators stated that they felt that it was important to achieve consistency in delivery across courses in the future to improve provision in Australia.
In a study of 31 BEd and 71 PGCE primary phase trainee teachers conducted in the UK between 2000 and 2003, Mead142 found that opportunities to teach and discuss elements of PSHE and citizenship on school placement, and the quality of these opportunities, varied, especially for SRE. He found that up to 90% of trainee teachers reported that they had taught PSHE education or citizenship, but only up to 42% and 23% of the trainee teachers had had the opportunity to discuss how PSHE education and citizenship contribute to multicultural awareness in pupils or to teach SRE respectively. Of those who taught PSHE education, 81% reported working from a scheme of work, whereas a minority did not, with some of these individuals saying that they had to draw on their own ideas and experience to teach this. Although many of the trainee teachers had the opportunity to teach PSHE education in general, Mead142 states that few had been able to discuss the scheme of work with a co-ordinator or had been able to observe an experienced teacher delivering PSHE education. Opportunities for trainee teachers to discuss their personal values also varied. Around three-quarters of the trainee teachers (73%) in the 2002–3 cohort reported that they had discussed how PSHE education and citizenship can contribute to social and cultural development, whereas the remaining trainee teachers (27%) said that the discussions they had had tended to focus on planning methods and outcomes. Mead142 found that opportunities to teach and discuss PSHE education and citizenship issues were dependent on the nature of the school in which trainee teachers were placed (e.g. the mentoring available, whether the school had discrete PSHE education time and the importance placed on multiculturalism in PSHE). Speller and colleagues25 also found that opportunities for training in healthy eating in ITT in England partly depended on the extent to which placement schools were involved in the Healthy Schools programme. Furthermore, Speller and colleagues noted that some providers were reliant on trainee teachers receiving training in physical activity and healthy eating on their school placement in the absence of formal training at the provider, but that this did not necessarily happen.
Integrated, discrete and incidental approaches to training
In the literature, studies have not evaluated the impact of different approaches to structuring health content within ITT courses, such as integrated, discrete and incidental approaches on trainee teacher outcomes. However, the authors of two studies in this review25,63 state that integrated training may be a desirable approach. Speller and colleagues25 mapped the content of one English HEI's primary and secondary PGCE courses and found that the health and well-being elements of the course were individually planned and not integrated across the curriculum. The authors speculate that this discrete approach may result in trainee teachers developing a fragmented knowledge of health and well-being rather than a holistic understanding, and advocate that an integrated approach may be better. In a study by Baginsky and Macpherson,63 trainee teachers in the UK suggested that they would appreciate child protection training being integrated into the curriculum rather than provided as discrete training. Baginsky and Macpherson63 highlight, though, that in reality this may be difficult for providers to do as it would require a restructure of courses.
Ongoing training needs and the transition from pre-service to in-service
Findings from the process evaluations indicated that training in health may need to be addressed beyond one-off sessions or limited-duration courses, and be addressed beyond ITT and into in-service training. Fenton94 argued that a 13-week-long child protection module for trainee teachers was more effective in engaging trainee teachers with this subject than a one-off session would have been (although the effectiveness of these different approaches was not assessed in this study). Hodgkinson and Baginsky117 stated that trainee teachers reported that it was difficult to take on board information about child protection on their course and felt that information to take away would have been helpful. Baginsky and Macpherson63 found that trainee teachers felt that child protection training in ITT was a first step and that there was a need for ongoing professional training. Similarly, trainee teachers in another study201 felt that follow-up training on mental health once they had some in-service experience as a teacher would be useful. Speller and colleagues25 reported that, when trainee teachers were asked at the end of their PGCE training what would help teachers most to promote health in schools, 75% felt that training would be useful. It is not clear from the studies in this review to what extent teachers might receive in-service training in the period following entering practice, as only two studies92,174 reported this. In one of these studies174 the findings were not clear and so we have not reported them here. The other study92 reported that 5 of 21 trainee teachers had taken part in further PSHE education training in their NQT or second year of practice in the UK.
Summary of processes
We classified 16 studies as containing process evaluations. 25,26,44,61,63,81,83,92,94,117,142,156,174,189,195,201,213 The majority of these studies (n = 10) were judged to be medium or high in reliability and usefulness of findings. These studies showed that pre-service teacher training interventions in health were generally seen to be acceptable and were well received by trainee teachers and training providers. Trainee teachers' views on the adequacy of the training that they had received were more variable, with the child protection studies in particular reporting that trainee teachers did not always feel well prepared to deal with this issue after training. The evidence suggested that, for training to meet trainee teachers' needs, it may be important that it includes practical experience and training in practical skills (especially strategies for dealing with sensitive issues); is made personally relevant and takes into account individual needs; and is clearly relevant to teachers' practice in schools. There were mixed findings about the extent to which trainee teachers had assimilated responsibility for health promotion into their roles as teachers and their understanding about their role after training. The findings suggest, however, that generally trainee teachers recognised their role in health promotion and that training helped them to develop broader perspectives about health issues. A lack of time in an already overcrowded pre-service curriculum was perceived to be a challenge in implementing health training, with one study suggesting that it may be perceived to be a lower priority than other aspects of the ITT curriculum. Balancing breadth and depth was also challenging. The studies also found variation in the provision and quality of training across different providers, course types and school placements. Furthermore, studies indicated that training in health may need to be continued beyond one-off sessions or courses, and that trainee teachers feel that follow-up or ongoing professional training once they have transitioned to in-service teaching posts might be useful.
Chapter 7 Discussion
In this chapter we draw together the findings of the survey and systematic review in relation to each of the research questions proposed earlier in this report (see Chapter 1, Research objectives)
In what ways does teacher training prepare teachers to promote health and well-being in schools?
Coverage of health and well-being
There was strong support for the inclusion of health and well-being in the ITT curriculum, with around 90% of the course managers surveyed in our study agreeing that it is important or very important (notwithstanding a potential sample bias in favour of health – see Strengths and limitations of this research). When interviewed some of the managers commented that they were passionate about health in education, and take it very seriously. Many showed a commitment to health despite policy shifts in favour of a focus on core education issues. There was also evidence of a holistic conception of health and well-being, with good health seen as important for effective learning. Although this is encouraging, the question arises whether the content of ITT courses reflects this enthusiasm. To some extent it does, with ECM and child protection included in courses by all of the managers in our survey, and topics such as social and emotional health, bullying and working with parents reported to be covered by at least 90% of the course managers. Furthermore, when asked how much time is spent covering health and well-being on their courses, 42% of the managers reported this to be between 5% and 9% of the time, and a further 26% estimated 10–14%. This could be considered generous given the numerous time constraints on the curriculum that some of the course managers who were interviewed mentioned exist (see Chapter 3).
An important overall finding of this research, however, is that coverage of health and well-being in ITT courses is variable, in terms of content, format and methods.
Variation in content
Although, as mentioned above, some health-related topics were covered universally, others – mainly lifestyle-related issues – were given comparatively less attention. Our survey found that smoking, alcohol, drugs and SRE were reported to be covered by only up to two-thirds of course managers. This seems surprising given the high profile of these topics in public health. Our descriptive map of the literature showed that sexual and reproductive health, drugs and alcohol were some of the most commonly addressed topics in evaluations of teacher training. During interviews we asked the course managers to comment further on coverage of these topics in their courses. In some cases there was detailed coverage through dedicated workshops and other events, whereas in other cases it was incidental. Some course managers acknowledged limited coverage and the need for improvement. The barriers to covering these topics did not appear to be different from barriers to covering health in general (e.g. lack of time in the curriculum – see What are the barriers to, and facilitators of, effective training and delivery?), although for SRE there was the suggestion of a lack of comfort in dealing with sensitive personal issues such as sex. Given that sexual health, drugs, alcohol and tobacco are public health priorities,16,237–240 it is important that these topics are covered adequately within any health training that trainee teachers receive.
Another prominent finding from both the survey and the systematic review is that trainee teachers' experiences of health issues while on school teaching placement are variable. Opportunities to discuss, observe or teach health-related issues, including PSHE education, varied according to how much of a priority the school itself gave to health or to practicalities such as timetabling of PSHE education in the school in relation to when the placement took place. Some course managers commented that they assumed that trainee teachers learned about particular health topics, such as SRE, while on placement and therefore these topics were given less exposure at college. There was also a perception that some trainee teachers' experiences of health on placement were better than others, depending on a school's commitment to health promotion. The likely increase in time that trainee teachers will spend training in schools as a result of ITT reforms14 (e.g. the introduction of teaching schools), and increased diversity in types of schools (e.g. free schools run by local groups and independent of local authorities), may compound the inconsistency in trainee teachers' experiences of health and well-being in ITT. With the decentralisation of the NHSP, which provided a national framework for health promotion in schools, it is uncertain how this will be addressed.
Variation in format and methods
Our survey also found variation in terms of where in the ITT curriculum health and well-being was covered. Health was not confined to traditional areas such as science or PE, but was also covered in broader areas such as professional studies, English and the humanities. Some ITT providers covered health issues across the curriculum and made cross-curricular links. Integrating health throughout the curriculum could be considered beneficial so that trainee teachers do not associate health as being confined within particular subject areas. One of the studies included in our systematic review critiqued the scientific emphasis on health in schools and aimed to encourage PGCE trainee teachers to recognise that their wider skills, developed through their main subject of English, could be applied in the teaching of PSHE education to enable pupils to grow emotionally and socially. 92 The authors reported that the trainees had a lack of overt awareness of how much PSHE education teaching could be planned for in English lessons, and suggested that they have a limited definition of PSHE education as being a scientific subject knowledge-based curriculum. To ensure adequate capacity for the teaching of health in schools it would appear to be useful to help trainee teachers to recognise how the skills that they develop in their subject specialisms can be applied in the teaching of PSHE education (and health more broadly). To be effective, training would need to encourage trainee teachers to recognise that health and well-being is part of their role as a teacher (see below). However, integration of health within the ITT curriculum might be more appropriate to broader issues that underpin many aspects of health, rather than specific health topics such as those discussed earlier (e.g. drugs, alcohol, SRE), which may need to be covered in discrete topic-focused sessions.
Our survey found a great deal of variation in the methods used to address health and well-being in the ITT courses. Some courses devoted whole-day sessions focusing on topics such as PSHE education, citizenship, equality and diversity, behaviour management and health in general. Workshops and interactive sessions were also common, as well as student-led presentations. It was common for multiple methods to be used, including various combinations of lectures, seminars, presentations, discussion groups, interactive workshops and electronic resources (e.g. virtual learning environment). Although health training was often provided by course managers and tutors themselves, external agencies were also very commonly used (e.g. representatives from local authorities and local schools), particularly to address specific health-related topics (e.g. emotional health, SEN, behaviour management). Engaging external expertise, including interprofessional working, was viewed by many of the course managers to have been a successful part of their delivery of health training. It was also reported by some course managers that trainees gained health experience through placements in non-educational settings such as social services, hospital schools, prisons and sports organisations. One course manager commented that this had been effective in raising trainee teachers' awareness of health issues. An implication of this is that inter-agency and interprofessional working could be encouraged where possible and the effectiveness of this could be subjected to further evaluation, including the effectiveness of alternative placements in health-related settings, which could be considered to be innovative practice.
Furthermore, few of the course managers we interviewed reported that they had worked with other departments at their institutions to deliver health training, although some raised this as a possibility in the interviews. It may be beneficial in the future to raise ITT providers' awareness of the possibilities for multidisciplinary working within their institutions – particularly HEIs, which may have more immediate access to a range of potential health inputs in their institutions than EBITTs or SCITTs – and encourage sharing of expertise within institutions (e.g. through existing networks or groups). The course managers whom we interviewed did not always know how to make contact with health professionals, and it could be argued that accessing this input from health-related departments at their institutions may be easier than making contact with external expertise. In common with the ITT courses surveyed, many of the studies included in the systematic review evaluated training that was multiformat and multimethod and delivered by a range of providers, reflecting the broad nature of health promotion in education.
How effective are interventions to train and support teachers in health?
The systematic review found some evidence for the effectiveness of training in terms of improving teachers' knowledge and confidence to address health and well-being, and influencing their beliefs about the ability of teachers and schools to address the health needs of pupils. However, studies tended to measure the impact of training in the short term, with many studies assessing outcomes at the completion of training, or at most 1–2 years afterwards. The longer-term impact of training teachers is therefore unclear. In fact, some studies reported that after training teachers still had ongoing concerns about their ability to teach PSHE education, and they found certain health-related situations that they encountered, or anticipated encountering, in schools challenging (e.g. topics such as mental health or child protection). The transition phase between ITT and entering practice appears to be a demanding one for teachers in many respects as they adjust to the realities of teaching. One of the studies included in our systematic review92 reported that teachers received little support for teaching PSHE education in the first couple of years of qualified teaching. This finding was echoed by a recent survey of schools in England showing barriers to accessing PSHE education training, particularly in secondary schools. 28
Furthermore, Evans and Evans92 report in their evaluation of PSHE education training that some of the teachers commented that, although initial training is useful, most of their learning came from experience of teaching in school. Covering health and well-being in ITT may therefore be viewed as a necessary and important first step, to be reinforced by experiential learning in practice. An implication of this is that it would be useful for ITT providers to provide trainee teachers with the opportunity to plan and teach PSHE education while on school placement (experience of this was variable in our survey) and for adequate ‘scaffolded’ follow-up training and support around health (e.g. from a school-based mentor, a PSHE education co-ordinator or an external specialist) in the NQT year and the early teaching career period to be provided. Evaluations of the effectiveness of health-related training spanning ITT and the early career years are therefore required.
It should also be acknowledged that many of the studies evaluating health training in ITT in our systematic review lacked control or comparison groups, making it difficult to discern whether the favourable outcomes observed were due to the training or to other competing influences. When possible, future evaluations should employ controlled designs, preferably with random allocation of ITT providers to different forms of health-related training. Such designs may be appropriate for evaluating particular curriculum approaches, which could be standardised across providers. Given the variation in schools' approaches to health and well-being identified in this study, other, more flexible study designs might be more appropriate for evaluating health training that is predominantly school based (given the variation in schools' coverage of health as discussed earlier). Assessing the impact of ITT health-related training on pupils themselves (e.g. in terms of their knowledge, attitudes, health-related behaviour) is also desirable given the lack of available evidence identified by the systematic review. However, this may be challenging given that trainee teachers and NQTs will be distributed across a number of schools, with one or two trainees per school, making it difficult to attribute changes in pupil outcomes to the training that the teachers received rather than other influences (e.g. a school's health-promotion policies and ethos and other local factors).
As described earlier in this report (see Chapter 6, Inclusion criteria), we prioritised studies evaluating health training in pre-service teachers for inclusion in the synthesis. The purpose was to provide cohesion with the findings of our survey of ITT providers in answering our research questions. However, the majority of the studies included in our descriptive map evaluated training for in-service (qualified) teachers. These studies evaluated a variety of training approaches (e.g. information provision, skill development for addressing health issues), using a number of formats (e.g. lectures, discussion groups, workshops, skills demonstration), addressing a diverse range of health topics and conducted in a number of countries (e.g. the USA, Europe, Africa). Further evidence synthesis is needed to assess the effectiveness of health training for in-service teachers, as there has been a lack of published systematic reviews of this evidence. Given the large volume of evidence on in-service training that we identified in the descriptive map (just under 150 studies), a prioritisation exercise would be useful to focus on health topics or training approaches that are considered most relevant to policy and practice. For example, some of the scenarios (sets of studies) discussed earlier in this report (see Chapter 6, Inclusion criteria) could be reviewed, such as a synthesis focused on training to address key public health priorities (e.g. sexual and reproductive health, mental health, drugs and alcohol).
What are the barriers to, and facilitators of, effective training and delivery?
The interviews with course managers and the findings of the process evaluations included in the systematic review enabled us to identify some of the barriers to and facilitators of effective teacher training around health and well-being. The barriers and facilitators were seen to be operating in relation to six themes, discussed in turn below.
Personal and organisational values, interests and background
A number of facilitators, as well as some barriers, were associated with the personal and organisational values, interests and background of those involved in ITT. As discussed above, there was much commitment and enthusiasm for health in ITT from the course managers, with a prevalent holistic conception of health in education. Accordingly, their personal and professional experience influenced the prominence of health in the content and format of courses, albeit within the constraints placed on ITT providers by recent educational policy shifts (see following section). For example, some had taught in schools in areas of social and economic deprivation and considered it important that trainees were aware of the needs of children from such areas. When teaching placements were in schools in deprived areas it was considered that this was beneficial to trainee teachers' development as they were more likely to encounter children with health issues than in schools in more affluent areas (where more emphasis might be placed on educational attainment rather than pastoral issues; this was seen as a potential barrier). Given the continuing commitment to tackling health inequalities it is important that all trainee teachers are aware of the health and educational needs of children from low socioeconomic status backgrounds. 16
The trainee teachers' own interests could be both a barrier and a facilitator. In some institutions in our survey trainee teachers were given the choice to pursue health-related topics through assignments or alternative placements (e.g. in sports organisations). However, it was noted that a minority of trainee teachers do not necessarily see health as being within their role as a teacher. The studies included in our systematic review that assessed teachers' roles and values generally found that trainee teachers became more aware and accepting of their health-promoting role over the course of their training. It would be useful for trainee teachers to be given the opportunity to explore their personal values and beliefs in relation to health, and to engage in critical reflection with tutors, mentors and each other. Opportunities could be provided to trainees motivated enough to want to pursue health issues further, for example through designing and organising events such as workshops or seminars, or taking placements with relevant organisations.
Competing priorities
A common theme in the data collected was that teacher training courses are constrained by competing priorities which act as a barrier to addressing health and well-being. However, pragmatic ways of overcoming these barriers were described.
One of the key issues discussed by the course managers was the changing policy landscape in education. There was a perception that recent developments such as the review of the National Curriculum, the revised teachers' standards and the withdrawal of ECM as a government policy signalled less overt support for health and well-being in education. The standards in particular no longer contain an explicit standard for promoting children's health, and there is more of an emphasis on developing teachers' subject knowledge, SEN and behaviour management. This conflicted with the commitment of many course managers to covering health within the ITT curriculum, and they felt that they were expected to give more attention to these priorities. However, some course managers commented that they intended to use these priority areas as ‘ways in’ to maintain a focus on health, such as considering health issues related to disability. The general way in which some policies have been written, such as the revised teacher standards, was considered by some to offer flexibility, giving them the opportunity to cover health issues. Although these pragmatic strategies are encouraging for addressing certain aspects of health, they may not offer scope for covering specific lifestyle-related issues discussed earlier, which, despite being health priorities, seem to receive comparatively less attention in ITT. As the survey and interviews were conducted during a period of policy change, and course managers were starting to revise their courses accordingly, it would be useful to conduct further research with ITT providers in the next few years to assess how successful they have been in terms of addressing health in a new policy era.
The difficulties of addressing health issues within a busy ITT curriculum was also a commonly mentioned issue, both by the course managers interviewed and in some of the studies in the systematic review. This was a particular issue in PGCE and GTP courses, which are run over relatively shorter time periods. Preparing trainee teachers to acquire subject and pedagogical skills necessarily took a priority over wider issues such as health. However, some providers found solutions to this such as encouraging trainees to self-study health topics.
Integration of health and education
We have already discussed the emerging policy shifts in which health and well-being appears to have a more implicit role in education, juxtaposed with the prevailing holistic conception of health in education from the course managers interviewed. The course managers in this study considered that integration of health and education was important as, for example, it fostered interprofessional and interdisciplinary working and was appreciated by trainee teachers. In particular, ECM was generally highly regarded by the course managers as a way of making essential links between education and health. The dissipation of ECM was lamented by some course managers, who expressed an intention to retain it as a theme underpinning their courses. However, as the new educational policy agenda takes hold, ITT providers may find it increasingly challenging to retain the principles and ethos of ECM and it would be useful to investigate how their courses adapt to the new agenda.
As touched on above, although trainee teachers generally came to accept and embrace their health-promoting role over the course of their training, a minority did not consider health to be part of their remit as a teacher. A move away from an explicit framework for the integration of health and education may exacerbate this view. Two of the process evaluations in our systematic review found that making training more personally relevant (e.g. encouraging trainees to discuss their personal experiences in relation to a health issue) was appreciated by the trainee teachers, and was more likely to encourage them to see health as more relevant to their practice. 61,94 This might be one practical method that ITT providers can incorporate into training to stimulate trainee teachers' interest in this area.
Another issue is that trainee teachers may not fully appreciate their potential health role because of a perceived lack of knowledge or confidence, particularly to address complex or sensitive areas. This raises the wider question of how extensive should the teacher's role be with regard to health, and at what point should he or she refer to more specialist professional input? Our systematic review found that training can improve trainee teachers' confidence in being able to identify children at risk of, or experiencing, health-related problems. However, trainee teachers recognised that there were limits to what they could realistically do to address problems and they felt reassured by the availability of specialist help to liaise with.
Our descriptive map identified a number of studies which evaluated the development of other skills that teachers can use to promote health, including health-related behaviour and lifestyle change skills. These studies have generally been conducted in schools in which teachers have been trained to implement a specific health-promotion intervention. Our previous systematic review of behavioural interventions to prevent sexually transmitted infections in young people in schools explored process evaluation findings about teachers' experiences of delivering skills-based sex education. 47 In a large UK randomised controlled trial (SHARE35) included in the review it was found that teachers did not engage with the theoretical basis of the programme that was fundamental to achieving health-related behaviour change. For example, they did not always facilitate role-play activities to model and practice skills required by the intervention. It was suggested that many teachers viewed such activities as too far removed from their teaching role, and some experienced discomfort in discussing personal and sensitive issues with pupils. Furthermore, in another study included in that review [the RIPPLE (Randomized Intervention of PuPil-Led sex Education) study241], peer-delivered sex education was more acceptable to pupils than teacher-delivered sex education. These findings suggest a potential limit to the teacher's role in relation to lifestyle areas such as sexual health. However, they may also signal the need for greater training and support for teachers to recognise the conceptual basis of health promotion, and to acquire the skills, confidence and values to enable pupils to develop healthy lifestyle skills. Further evidence synthesis, drawing on the studies included in the descriptive map, would be valuable to assess how applicable the findings from our previous systematic review are across other health lifestyle areas, and also to assess the effectiveness of teacher training programmes in relation to teachers' skills, confidence and values.
Access to expertise and knowledge
Course managers valued having knowledge of health issues, and some expressed that training for ITT provider staff on health issues would be beneficial. However, few mentioned receiving training and in a number of cases course managers drew on knowledge gained through their own personal and professional background, utilising their experience of teaching children from vulnerable backgrounds, for example, or using their contacts and networks to arrange external workers to provide training (sometimes for free or reduced rate). However, access to external agencies may become harder given recent budget cuts and pressure on services, as discussed below.
The interviews with course managers also revealed that trainee teachers could be uncomfortable about addressing certain health topics with pupils, particularly SRE. One of the process evaluations in the systematic review found that a minority of trainee teachers expressed resistance to discussing issues relating to homosexuality, although for personal or religious beliefs as opposed to embarrassment about the topic. Creating a non-threatening atmosphere was reported to facilitate discussion about sensitive issues such as diversity61 and sexual health. 81 This would be a prerequisite to increased coverage of such topics in ITT, which, as discussed earlier, is necessary.
How initial teacher training is organised
Barriers and facilitators were identified in relation to the way in which ITT courses were organised. As discussed earlier, trainee teachers' experience of addressing health on school teaching placements was variable, with some having more opportunities to engage with health issues than others. The course managers did not always have awareness of, or input into, what health issues were covered on placement. Again, this underlines the need for consistency in how health is addressed in ITT given the likely increase in school-based training in the future. 14 The course managers had mixed views on the appropriateness of a move to greater school-based training. Some thought that trainee teachers' experience of health would be fragmented because of the variability noted above in experience on placements. However, others felt that it would provide greater context as the teachers would have the opportunity to learn about pupils' health and well-being directly through practice, rather than indirectly through study. Both approaches have merits as well as drawbacks and it seems logical that a degree of balance between ‘theory’ and ‘practice’ should be aimed for. Research would be useful with trainee teachers themselves and school staff (e.g. mentors) to establish how health and well-being is covered within school-based training, and any barriers or facilitators experienced. The research could also include teaching schools and free schools, investigating trainee teachers' general experiences of these new initiatives and assessing any variations in health-related training across different types of school.
One of the key findings from our survey and interviews was that little or no specific funding was available for specific activities to cover health and well-being in ITT (notwithstanding, however, the fact that health was an integral theme underpinning routine aspects of some courses). Many of the initiatives described by course managers were supported by either existing course resources or, as we have mentioned above, through goodwill and reciprocal favours between ITT providers and external agencies. However, some ITT providers had experienced cuts to their core funding and were enrolling fewer trainees, which put pressure on budgets, resulting in some previously run health initiatives ceasing. Likewise, cuts to the budgets of some external agencies meant that they were in less of a position to work with ITT providers, at least without adequate remuneration, which, as said, was difficult.
Communication and relationships
Communication and relationships between ITT providers and others involved in teacher training were associated with a number of barriers and facilitators. ITT providers had good, often long-standing relationships with external organisations with a role in health and well-being. This was considered to facilitate effective training as providers were reassured of the quality of the training. There were mutual benefits, with providers sometimes offered the training for free, allowing the external organisations to gain experience of providing training to a trainee teacher audience.
Although communication between course managers and placement schools about coverage of health topics at respective institutions was lacking, communication between them about trainee teachers' own health and well-being was said to be more effective. Trainee teachers' health was considered to be important by a number of course managers, and was something they monitored through pastoral support and regular contact with trainees, although it was noted by one course manager that trainee teachers themselves did not always disclose issues that they were experiencing. Although trainee teachers' health is important in its own right, it could be argued that encouraging trainee teachers to be aware of their own health and well-being might increase their awareness of the importance of health more generally in schools, and in particular the needs of their pupils. This was the aim of one of the studies in our systematic review,213 which evaluated the use of behaviour change theory to improve trainee teachers' personal health behaviours and eventually prepare them for teaching about such health issues in schools. Only around half of the teachers agreed that the training had enhanced their own personal well-being, and found the issues covered to be personally relevant. The authors suggested that, with hindsight, the training should have made more specific links between the training topics and the teaching of health issues with pupils, as the trainee teachers did not yet understand the variety of demands of the teacher's role in the classroom and in the school community. This was echoed by other studies in the systematic review61,63,94 which suggested that training should be more relevant to trainee teachers' practice as teachers. ITT providers could therefore usefully explore more integrated forms of training in which teacher and pupil health are on an equal footing and viewed as mutually reinforcing.
Strengths and limitations of this research
Standard procedures for conducting questionnaire and interview surveys were followed. The response rate to the survey and the quantity and quality of the data generated were considered adequate to meet the study's objectives. Although it was encouraging that in general there was support for health and well-being in the courses that we surveyed, it should be acknowledged that our sample might be biased towards course managers who are more supportive of health in teacher training. Health, therefore, may not necessarily be a consistent feature of all ITT courses. Course managers with less awareness of, or interest in, health may have been less likely to respond to the survey. It was not possible to discern any consistent differences in characteristics between responders and non-responders in terms of variables such as type of ITT provider or type of course offered. There was a little variation in the response rate between different geographical regions, with most regions having a response rate within the range of 21–56% (see Table 3). The outlier was the West Midlands region with a response rate of 0%. It is not clear whether there was a specific reason for this or whether it was due to chance. We endeavoured to maximise the response by approaching heads of departments first to ascertain correct details of course managers and to encourage general support for the survey among their staff. Monetary incentives were used to encourage questionnaire completion (e.g. voucher draw) and e-mail reminders were sent to non-responders (it was not practical to use telephone reminders, which may have been more successful). We also conducted the survey at a time in the academic year (June/July) when it was anticipated that course managers would be planning the curriculum for the following year and therefore would be receptive to participating in an investigation of course content. However, on reflection, a higher response may have been achieved if the survey had taken place slightly earlier in the year to avoid exam periods and end-of-term preparations.
The systematic review was conducted according to rigorous, standard methods for evidence synthesis (e.g. sensitive literature searches of a range of sources, systematic screening of studies for relevance, critical appraisal of evidence). Data extraction and critical appraisal were performed by one reviewer and checked by a second, which is regarded as an accepted minimum standard,242 although independent extraction and appraisal by two reviewers is preferable where resources allow. The two-stage systematic review was particularly useful as it allowed us to become acquainted with a diverse evidence base that had not been systematically characterised before. The descriptive map is therefore a useful resource for anyone wanting to gain an overview of the key characteristics of this evidence base. The knowledge gained was helpful in prioritising the focus for an in-depth assessment of the evidence. The heterogeneous nature of the studies included in the synthesis made it challenging to summarise across the studies; however, we have endeavoured to assess and present the evidence as succinctly as possible. Although much of the evidence included in the systematic review synthesis is from the UK, some of the other studies conducted in Australia, the USA and Africa may not be wholly generalisable to the UK. The findings of the systematic review, particularly the impact of training on teachers, should be interpreted with caution given the limitations of the study designs used (e.g. single cohort before-and-after study with no control or comparison group). The systematic review was restricted to studies in the English language and so there may be a potential publication bias.
Finally, although this project adopted a broad perspective on health and well-being, it was challenging to be consistent about what could be classed as health, and therefore be relevant to the project. At the start of each interview with course managers we informed them that we had a broad conception of health and that they should discuss any aspects of their courses that they considered relevant. As our findings have shown, they tended to see health holistically, as fundamental to effective learning and vice versa. At the data analysis stage it became apparent that, although they expressed this view, few were talking about key health topics and children living healthy lives – their focus was on the meaning of health (usually in terms of SEAL/emotional well-being, diversity, behaviour management and SEN) for children's education and learning. That is when the research team realised that important public health topics were more neglected, and that these did not tend to be the focus for many interviewees. Our recommendation for further research on these topics within ITT could be seen as adopting a narrower, perhaps fragmented perspective on health, but this should be seen as complementary to a holistic approach.
Further, a discord between the survey and the systematic review component of the project emerged in terms of perspectives on health. The inclusion criteria for the systematic review (see Chapter 5, Inclusion screening) aimed to be as inclusive as possible, but for consistency (and to keep the workload manageable) we had to draw boundaries around what literature could be considered relevant to health and well-being. For example, studies of behaviour management were not included unless the study acknowledged a link with health. Although we recognise that classroom behaviour management and health are intertwined concepts (and indeed some of the interviewees described behaviour management as fundamental to child health), unless studies explicitly aimed to investigate this link (e.g. in terms of their stated aim, hypothesis or outcome measures) we felt that it would be too tenuous for us to make that link on their behalf. If we had included such studies in our systematic review they may have provided evidence for the effectiveness of behaviour management in terms of academic outcomes, but with only a theoretical impact on health. The process of inclusion screening was therefore challenging, requiring much discussion and reflection by the research team, with acknowledgement that the scope of the systematic review, although broad, is not necessarily in accord with that of the survey.
Conclusions
This research has been conducted at a time of significant change in ITT, and more generally in education and health. It has investigated how a sample of ITT providers in England prepare trainee teachers to promote health and well-being, using a questionnaire survey and then in more detail through interviews with course managers. It has also systematically assembled and charted the voluminous and disparate international evidence base on teacher training and health, and conducted a detailed assessment of the effectiveness of training specifically in ITT.
From those surveyed there appears to be much support and enthusiasm for health and well-being in ITT, although there was variation in the breadth and depth of coverage and in the methods and approaches used. Health was often considered fundamental to effective teaching and learning in schools, and was something that a number of course managers felt strongly about. They benefited from knowledge and experience gained through their personal and professional background, and from access to expertise from external agencies. However, they were constrained by a number of factors, including a perceived policy shift away from health and well-being towards areas such as subject knowledge and behaviour management; lack of time in a busy curriculum; and limited knowledge of, or control over, trainee teachers' experience of health issues in school placements.
The literature has shown that training can be effective in improving teachers' knowledge and confidence to address health, and can influence their beliefs about the value of promoting health in school (albeit with methodological limitations in the studies). Teachers generally appreciated the training around health and well-being that they received and became more aware and accepting of their potential to influence pupils' health over time. However, some noted ongoing concerns about their ability to deal with particular complex issues, and expressed the need for ongoing support. A similar variation in the breadth and depth of coverage and the methods that was found in our survey was also evident in the literature.
Implications for practice
Below is a summary of the main implications for teacher educators arising from this research.
A broad holistic conception of health enabled course managers to integrate health-related issues throughout the ITT curriculum, rather than necessarily addressing health in isolation. Although this approach was seen to have advantages, it is important that education for specific health priority topics, such as sexual health, smoking, alcohol and drugs, is not overlooked in favour of a general approach to health.
To be successful health promoters, teachers need to see health promotion as part of their role. Evidence from this research suggests that trainee teachers gradually accept this role over time, and that training which emphasises how health is relevant to them personally (i.e. their own health) and professionally (e.g. addressing local health needs) is a facilitator. Further, trainee teachers recognise limits to their health-promoting role when referral of pupils to specialist support is appropriate. Teacher training should therefore encourage a realistic role for teachers, throughout the training period, to help establish their confidence, emphasising the benefits of good health for themselves as well as their pupils, and familiarising them with other practitioners (e.g. health professionals) who they can liaise with to provide specialist help when required.
Experiential learning, such as that gained during school teaching placements, was considered an important way for trainee teachers to develop knowledge, values and the confidence to address health. The planned increase in emphasis on school-based training in England will provide greater opportunities for trainees to address child health, which may be advantageous as it will be within context. However, a good level of support and feedback from tutors, mentors and, when relevant, external practitioners will be necessary to ensure effective teacher learning and development.
Our research found that creation of a non-threating atmosphere was important when addressing complex and sensitive health issues such as child protection, sexual and reproductive health and sexuality and diversity. Training should therefore aim to minimise any discomfort that may impede effective discussion of such issues (e.g. through establishing confidentiality, trust, respect for others' views).
Research recommendations
-
There is limited published research on the longer-term impact of ITT around health and well-being, particularly in the period when NQTs enter service. Evidence from our systematic review suggested that, although initial training was associated with improved knowledge and confidence, some teachers had continued concerns about their ability to address children's health needs. They valued the opportunity for experiential learning through practice with ongoing support from mentors and specialists, particularly when addressing complex or sensitive health-related issues. Further evaluation of the effectiveness of health-related training spanning ITT and the early career years is therefore required, using controlled designs when possible. Teacher and, when possible, pupil outcomes should be assessed, including health literacy, which has received little attention in the literature reviewed. All outcome assessment should ideally be accompanied by process evaluation to assess implementation, acceptability and adequacy, and other factors that may influence effectiveness.
-
Evaluation of ITT as recommended in (1) could also assess aspects of training that were found to be beneficial, such as inter-agency and interprofessional working to deliver health training; increasing the personal relevance of health issues to trainees themselves (to their own health, and pupils' health too); and creating a supportive and non-threatening atmosphere for discussion of sensitive topics and issues.
-
Given the likely increase in school-based ITT it would be useful to conduct research with mentors and tutors located in placement schools, and trainee teachers themselves, to ascertain barriers to and facilitators of covering health and well-being. It would be particularly important to explore potential variations in coverage between schools (particularly given provision in the new National Curriculum for schools to shape aspects of the curriculum according to local needs), and between different types of schools (e.g. free schools, academies, teaching schools). A relevant question would be how can schools maintain a balance between being sensitive to the needs of the local community (e.g. social, economic and cultural concerns) and keeping in mind national public health policy priorities. Research would be valuable to assess the feasibility and effectiveness of inter-agency and interdisciplinary collaboration, particularly given the reorganisation of education and health services (e.g. integration of public health within local authorities, establishment of Health and Wellbeing Boards).
-
Further evidence synthesis is needed to assess the effectiveness of health training for in-service teachers. Our descriptive map identified around 150 studies of in-service training, which have not been subjected to detailed synthesis. One or more of the scenarios proposed in Chapter 6 of this report (see Inclusion criteria) could be reviewed, including:
-
a topic-focused review, selecting studies of training around a health topic area or combination of areas (e.g. sexual and reproductive health, mental health, drugs and alcohol), focusing on outcomes of training, training processes or both
-
a pedagogical-focused review, selecting studies that evaluate how teachers can acquire the varied skills and competencies that a health promoter needs, such as teaching health-related behaviour and lifestyle change skills, or the ability to identify children experiencing, or at risk of experiencing, health problems
-
a geographical-focused review, selecting studies conducted in a particular country or region, with the aim of drawing out implications for practice and policy of specific interest to an area.
-
-
Follow-up research should be conducted with ITT providers over the next few years to assess the longer-term impact of government policy changes in education and health on the coverage of health and well-being in their courses. Many were in the process of revising their curricula in response to changes in teachers' standards, and exploring ways to retain a health ethos. It would be useful to further investigate how they have adapted their courses according to the new policy agenda and the barriers and facilitators experienced.
Acknowledgements
Thanks to the advisory group for their input throughout the course of the project and for commenting on a draft of this report.
Members of the advisory group: Hannah Chanter, Product Manager, Careers Resources & Consultancy, Babcock International Group, UK; Rachel Bailey, Independent Education Consultant (Health and Well-being); Didier Jourdan, Professor and Dean, Faculty of Education, Université Blaise Pascal Clermont-Ferrand II, France; Nick Mead, Senior Lecturer in RE and Citizenship, Oxford Brookes University, UK; Glynis Wright, County Inspector/Adviser Personal Development Learning, Hampshire County Council, UK.
Thanks also to Karen Welch [(Information Scientist, Southampton Health Technology Assessment Centre (SHTAC)] for literature searching; Jackie Bryant (Principal Research Fellow, SHTAC) for reviewing a draft of this report; Jo Picot (Research Fellow, SHTAC) for screening studies for inclusion/exclusion in the systematic review; and Petra Harris (Research Fellow, SHTAC) for retrieving full reports for the systematic review.
This report presents independent research commissioned by the NIHR. The views and opinions expressed by the authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the NIHR Evaluation, Trials and Studies Coordinating Centre (NETSCC), the Public Health Research programme or the Department of Health. The views and opinions expressed by the interviewees in this publication are those of the interviewees and do not necessarily reflect those of the authors, the NHS, the NIHR, the NETSCC, the Public Health Research programme or the Department of Health.
Contributions of authors
Dr Jonathan Shepherd (Principal Research Fellow) was principal investigator and managed all aspects of the project. He conducted the questionnaire survey (sampling, questionnaire design and administration, data analysis), the interview survey (interview schedule design, conducting and analysing interviews) and the systematic review (screening studies for inclusion/exclusion, keywording of included studies, data extraction and quality assessment, and data synthesis) and wrote the final report.
Ms Sue Dewhirst (Research Fellow) was co-investigator and conducted the questionnaire survey (sampling, questionnaire design and administration, data analysis), the interview survey (interview schedule design, conducting and analysing interviews) and the systematic review (screening studies for inclusion/exclusion, data extraction and quality assessment) and wrote the final report.
Dr Karen Pickett (Research Fellow) conducted the questionnaire survey (data analysis), the interview survey (interview schedule design, conducting and analysing interviews) and the systematic review (screening studies for inclusion/exclusion, keywording of included studies, data extraction and quality assessment, and data synthesis) and wrote the final report.
Dr Jenny Byrne (Lecturer) was co-investigator and provided strategic guidance on all aspects of the research. She conducted the questionnaire survey (questionnaire design and data analysis) and the interview survey (interview schedule design and analysis) and wrote the final report.
Dr Viv Speller (Independent Consultant) was co-investigator and provided strategic guidance on all aspects of the research. She conducted the questionnaire survey (questionnaire design and data analysis) and the interview survey (interview schedule design) and wrote the final report.
Dr Marcus Grace (Senior Lecturer) was co-investigator and provided strategic guidance on all aspects of the research. He conducted the questionnaire survey (questionnaire design and data analysis), the interview survey (interview schedule design and data analysis) and the systematic review (data extraction and quality assessment) and wrote the final report.
Dr Palo Almond (Lecturer) was co-investigator and provided strategic guidance on all aspects of the research. She conducted the questionnaire survey (questionnaire design and data analysis) and the interview survey (interview schedule design and data analysis) and wrote the final report.
Dr Debbie Hartwell (Research Fellow) conducted the questionnaire survey (sampling, questionnaire design and administration) and the systematic review (screening studies for inclusion/exclusion, keywording of included studies) and wrote the final report.
Professor Paul Roderick (Professor of Public Health) was co-investigator and provided strategic guidance on all aspects of the research. He conducted the questionnaire survey (questionnaire design and analysis) and the interview survey (interview schedule design and data analysis) and wrote the final report.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health.
References
- Technical Report Series 30, Expert Committee on School Health Services. Geneva: WHO; 1951.
- Technical Report Series 89, Expert Committee on Health Education of the Public. Geneva: WHO; 1954.
- Tones K, Tilford S. Health promotion: effectiveness, efficiency and equity. Cheltenham: Nelson Thornes; 2001.
- The health-promoting school – an investment in education, health and democracy: conference report 1997.
- Barnekow Rasmussen V, Rivett D, Burgher M. The European network of health-promoting schools: the alliance of education and health. Copenhagen: WHO Regional Office for Europe; 1999.
- Warwick I, Aggleton P, Chase E, Schagen S, Blenkinsop S, Schagen I, et al. Evaluating healthy schools: perceptions of impact among school-based respondents. Health Educ Res 2005;20:697-708. http://dx.doi.org/10.1093/her/cyh024.
- Every child matters: change for children. London: HMSO; 2004.
- The children’s plan: building brighter futures. London: HMSO; 2007.
- Department for Education . Healthy Schools Toolkit n.d. www.education.gov.uk/childrenandyoungpeople/healthandwellbeing/a0075278/healthy-schools-toolkit (accessed 5 July 2011).
- Choosing health: making healthy choices easier. London: HMSO; 2004.
- Healthy weight, healthy lives: a cross government strategy for England. London: HMSO; 2008.
- Healthy child programme from 5 to 19 years old. London: Department of Health; 2009.
- Macdonald A. Independent review of the proposal to make personal, social, health and economic education (PSHE) statutory. London: HMSO; 2009.
- The importance of teaching: schools White Paper. London: The Stationary Office; 2010.
- Department for Education . The Framework for the National Curriculum – a Report by the Expert Panel for the National Curriculum Review n.d. www.education.gov.uk/publications/standard/publicationDetail/Page1/DFE-00135–2011 (accessed 16 August 2012).
- Healthy lives, healthy people: our strategy for public health in England. London: The Stationary Office; 2010.
- Improving outcomes and supporting transparency. Part 1: a public health outcomes framework for England, 2013–2016. London: Department of Health; 2012.
- Professional standards for qualified teacher status and requirements for initial teacher training (revised 2008). London: Training and Development Agency for Schools; 2008.
- Department for Education . Teachers’ Standards. n.d. www.education.gov.uk/publications/eOrderingDownload/teachers%20standards.pdf (accessed 16 August 2012).
- Department for Education . The Framework for School Inspection from January 2012. n.d. www.ofsted.gov.uk/resources/framework-for-school-inspection-january-2012 (accessed 10 August 2012).
- St Leger L, Nutbeam D. The evidence of health promotion effectiveness. Shaping public health in a New Europe. Brussels: ESCS-EC-EAEC; 1999.
- Tang KC, Nutbeam D, Aldinger C, St Leger L, Bundy D, Hoffmann AM, et al. Schools for health, education and development: a call for action. Health Promot Int 2009;24:68-77. http://dx.doi.org/10.1093/heapro/dan037.
- Denman S, Moon A, Parsons C, Stears D. The health promoting school: policy, research and practice. London: Routledge Falmer; 2002.
- Jourdan D, Samdal O, Diagne F, Carvalho GS. The future of health promotion in schools goes through the strengthening of teacher training at a global level. Promot Educ 2008;15:36-8. http://dx.doi.org/10.1177/1025382308095657.
- Speller V, Byrne J, Dewhirst S, Almond P, Mohebati L, Norman M, et al. Developing trainee school teachers’ expertise as health promoters. Health Educ 2010;110:490-507. http://dx.doi.org/10.1108/09654281011087288.
- Paakkari L, Tynjala P, Kannas L. Student teachers’ ways of experiencing the objective of health education as a school subject: a phenomenographic study. Teach Teach Educ 2010;26:941-8. http://dx.doi.org/10.1016/j.tate.2009.10.035.
- Jourdan D. Health education in schools. The challenge of teacher training. Saint-Denis: Inpes, coll. Santé en action; 2011.
- Formby E, Coldwell M, Stiell B, Demack S, Stevens A, Shipton L, et al. Personal, social, health and economic (PSHE) education: a mapping study of the prevalent models of delivery and their effectiveness. Sheffield: Sheffield Hallam University; 2011.
- Stewart-Brown S. What Is the Evidence on School Health Promotion in Improving Health or Preventing Disease And, Specifically, What Is the Effectiveness of the Health Promoting Schools Approach? 2006.
- Lister-Sharp D, Chapman S, Stewart-Brown S, Sowden A. Health promoting schools and health promotion in schools: two systematic reviews. Health Technol Assess 1999;3.
- Basen-Engquist K, O’Hara-Tompkins N, Lovato CY, Lewis MJ, Parcel GS, Gingiss P. The effect of two types of teacher training on implementation of Smart Choices: a tobacco prevention curriculum. J Sch Health 1994;64:334-9. http://dx.doi.org/10.1111/j.1746-1561.1994.tb03323.x.
- Rohrbach LA, Graham JW, Hansen WB. Diffusion of a school-based substance abuse prevention program: predictors of program implementation. Prev Med 1993;22:237-60. http://dx.doi.org/10.1006/pmed.1993.1020.
- Shek DT, Wai CL. Training workers implementing adolescent prevention and positive youth development programs: what have we learned from the literature?. Adolescence 2008;43:823-45.
- Kealey KA, Peterson AV, Gaul MA, Dinh KT. Teacher training as a behavior change process: principles and results from a longitudinal study. Health Educ Behav 2000;27:64-81. http://dx.doi.org/10.1177/109019810002700107.
- Wight D, Buston K. Meeting needs but not changing goals: evaluation of in-service teacher training for sex education. Oxf Rev Educ 2003;29:521-43. http://dx.doi.org/10.1080/0305498032000153061.
- Preamble to the Constitution of the World Health Organization n.d.
- Green L, Kreuter M. Health promotion planning: an educational and ecological approach. Boston: McGraw-Hill; 1999.
- Gorden R. Basic interviewing skills. Ithaca, NY: Peacock; 1992.
- Bowling A, Ebrahim S. Handbook of health research methods: investigation, measurement and analysis. Maidenhead: Open University Press; 2005.
- Weber P. Basic content analysis. Thousand Oaks, CA: Sage; 1990.
- Low J, Saks M, Allsop J. Researching health: qualitative, quantitative and mixed methods. London: Sage; 2007.
- Gregson J, Foerster SB, Orr R, Jones L, Benedict J, Clarke B, et al. System, environmental, and policy changes: using the social–ecological model as a framework for evaluating nutrition education and social marketing programs with low-income audiences. J Nutr Educ 2003;33:S4-13. http://dx.doi.org/10.1016/S1499-4046(06)60065-1.
- McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecological perspective on health promotion programs. Health Educ Q 1988;15:351-77. http://dx.doi.org/10.1177/109019818801500401.
- Arnold L, Maio-Taddeo T. Professionals protecting children: child protection and teacher education in Australia. Magill: University of South Australia, Australian Centre for Child Protection; 2007.
- Rees R, Kavanagh J, Harden A, Shepherd J, Brunton G, Oliver S, et al. Young people and physical activity: a systematic review matching their views to effective interventions. Health Educ Res 2006;21:806-25. http://dx.doi.org/10.1093/her/cyl120.
- Shepherd J, Harden A, Rees R, Brunton G, Garcia J, Oliver S, et al. Young people and healthy eating: a systematic review of research on barriers and facilitators. Health Educ Res 2006;21:239-57. http://dx.doi.org/10.1093/her/cyh060.
- Shepherd J, Kavanagh J, Picot J, Cooper K, Harden A, Barnett-Page E, et al. The effectiveness and cost-effectiveness of behavioural interventions for the prevention of sexually transmitted infections in young people aged 13 to 19: a systematic review and economic evaluation. Health Technol Assess 2010;14.
- Oliver S, Harden A, Rees R, Shepherd J, Brunton G, Oakley A. Young people and mental health: novel methods for systematic review of research on barriers and facilitators. Health Educ Res 2008;23:770-90. http://dx.doi.org/10.1093/her/cym038.
- Oliver S, Sutcliffe K, Gough D, Oliver S, Thomas J. An introduction to systematic reviews. London: Sage; 2012.
- United States, General Accounting Office . AIDS Education. Public School Programs Require More Student Information and Teacher Training 1990.
- Prenatal exposure to substances of abuse: an evaluation of the Drug Free Schools and Communities Act Emergency Grants Program. New York, NY: Office of Research, Evaluation, and Assessment; 1993.
- Title IV safe and drug-free schools and communities evaluation report, 1998–99. Principles of effectiveness as the building blocks of Title IV school-based programming. Austin, TX: Austin Independent School District, TX, Office of Program Evaluation; 1999.
- Adegbenro C, Adeniyi JD, Oladepo O. Effect of training programme on secondary schools teachers’ knowledge and attitude towards reproductive health education in rural schools Ile-Ife, Nigeria. Afr J Reprod Health 2006;10:98-105. http://dx.doi.org/10.2307/30032476.
- Ahmed N, Flisher AJ, Mathews C, Jansen S, Mukoma W, Schaalma H. Process evaluation of the teacher training for an AIDS prevention programme. Health Educ Res 2006;21:621-32. http://dx.doi.org/10.1093/her/cyl031.
- Ajuwon AJ, Oladepo OO, Sati B, Otoide P. Improving primary school teachers’ ability to promote visual health in Ibadan, Nigeria. Int Q Community Health Educ 1996;16:219-27. http://dx.doi.org/10.2190/26K0-Q59J-D6R2-2PMD.
- Allison KR, Silverman G, Dignam C. Effects on students of teacher training in use of a drug education curriculum. J Drug Educ 1990;20:31-46. http://dx.doi.org/10.2190/HDRV-3RYR-56FY-YM1X.
- Apostolidou M, Fontana D. Teacher attitudes towards health education in Greek-speaking Cyprus schools. Health Educ 2003;103:75-82. http://dx.doi.org/10.1108/09654280310467690.
- Aquilani R, Parisi U, Bigoni N, Maggi L, Ghioni G, Zucchella M, et al. School teachers can effectively manage primary prevention of adult cardiovascular disease. The Stradella Project. Prev Med 2007;45:290-4. http://dx.doi.org/10.1016/j.ypmed.2007.06.018.
- Araji SK, Fenton R, Straugh T. Child sexual abuse: description and evaluation of a K–6 prevention curriculum. J Prim Prev 1995;16:149-64. http://dx.doi.org/10.1007/BF02407337.
- Arcand J-L, Wouabe ED. Teacher training and HIV/AIDS prevention in West Africa: regression discontinuity design evidence from the Cameroon. Health Econ 2010;19:36-54. http://dx.doi.org/10.1002/hec.1643.
- Athanases SZ, Larrabee TG. Toward a consistent stance in teaching for equity: learning to advocate for lesbian- and gay-identified youth. Teach Teach Educ 2003;19:237-61. http://dx.doi.org/10.1016/S0742-051X(02)00098-7.
- Aune T, Stiles TC. Universal-based prevention of syndromal and subsyndromal social anxiety: a randomized controlled study. J Consult Clin Psychol 2009;77:867-79. http://dx.doi.org/10.1037/a0015813.
- Baginsky M, Macpherson P. Training teachers to safeguard children: developing a consistent approach. Child Abuse Rev 2005;14:317-30. http://dx.doi.org/10.1002/car.905.
- Beffa N, Cohen N, Laus M, McLandsborough L. Development and evaluation of an online, inquiry-based food safety education program for secondary teachers and their students. J Food Sci Educ 2007;6:66-71.
- Belansky ES, Romaniello C, Morin C, Uyeki T, Sawyer RL, Scarbro S, et al. Adapting and implementing a long-term nutrition and physical activity curriculum to a rural, low-income, biethnic community. J Nutr Educ Behav 2006;38:106-13. http://dx.doi.org/10.1016/j.jneb.2005.11.011.
- Bell CD, Raczynski KA, Horne AM. Bully Busters abbreviated: evaluation of a group-based bully intervention and prevention program. Group Dynam 2010;14:257-67. http://dx.doi.org/10.1037/a0020596.
- Black DR, Frauenknecht M. Developing entry-level competencies in school health educators: evaluation of a problem-solving curriculum for stress management. Educ Treat Child 1997;20:404-24.
- Blenkinsop S, Taylor G, Wade P, Schagen S. Alcohol and Tobacco Teacher Training Package: Longitudinal Study of Teaching 2004.
- Borgia P, Spadea T, Perucci CA, De Pascali V, Fano V, Schifano P, et al. The contribution of interagency collaboration to the promotion of young people’s sexual health. Eur J Public Health 1997;7:411-17.
- Bostock J, Kitt R, Kitt C. Why wait until qualified: the benefits and experiences of undergoing mental health awareness training for PGCE students. Pastor Care Educ 2010;29:103-15. http://dx.doi.org/10.1080/02643944.2011.573494.
- Botvin GJ, Baker E, Dusenbury L, Botvin EM, Diaz T. Long-term follow-up results of a randomized drug abuse prevention trial in a white middle-class population. JAMA 1995;273:1106-12. http://dx.doi.org/10.1001/jama.273.14.1106.
- Botvin GJ, Tortu S, Baker E, Dusenbury L. Preventing adolescent cigarette smoking: resistance skills training and development of life skills. Spec Serv Schools 1990;6:37-61. http://dx.doi.org/10.1300/J008v06n01_03.
- Brink SG, Basen-Engquist KM, O’Hara-Tompkins NM, Parcel GS, Gottlieb NH, Lovato CY. Diffusion of an effective tobacco prevention program. Part I: evaluation of the dissemination phase. Health Educ Res 1995;10:283-95. http://dx.doi.org/10.1093/her/10.3.283.
- Brown JL, Jones SM, LaRusso MD, Aber JL. Improving classroom quality: teacher influences and experimental impacts of the 4Rs program. J Educ Psychol 2010;102:153-67. http://dx.doi.org/10.1037/a0018160.
- Cain G, Carnellor Y. ‘Roots of empathy’: a research study on its impact on teachers in Western Australia. J Student Wellbeing 2008;2:52-73.
- Cameron R, Brown KS, Best JA, Pelkman CL, Madill CL, Manske SR, et al. Effectiveness of a social influences smoking prevention program as a function of provider type, training method, and school risk. Am J Public Health 1999;89:1827-31. http://dx.doi.org/10.2105/AJPH.89.12.1827.
- Campbell H, Macdonald S. Child protection in schools: an evaluation of a training course for Fife schools’ co-ordinators of child protection. Public Health 1996;110:37-40.
- Carter DSG. A whole-school approach to adolescent peer-leader development for affective learning in health-related curricula. Res Papers Educ Policy Pract 1999;14:295-319. http://dx.doi.org/10.1080/0267152990140305.
- Chao L-W, Gow J, Akintola G, Pauly M. HIV/AIDS stigma attitudes among educators in KwaZulu-Natal, South Africa. J Sch Health 2010;80:561-9. http://dx.doi.org/10.1111/j.1746-1561.2010.00542.x.
- Chao L-W, Gow J, Akintola O, Pauly M. Perceptions of community HIV prevalence, own HIV infection, and condom use among teachers in KwaZulu-Natal, South Africa. AIDS Behav 2007;11:453-62. http://dx.doi.org/10.1007/s10461-006-9154-y.
- Chifunyise T, Benoy H, Mukiibi B. An impact evaluation of student teacher training in HIV/AIDS education in Zimbabwe. Eval Prog Plann 2002;25:377-85. http://dx.doi.org/10.1016/s0149-7189(02)00049-6.
- Chubb H. Developing and implementing a comprehensive AIDS education program in a public school district. Fort Lauderdale, FL: Nova Southeastern University; 1994.
- Cleave H, Charlton A. Evaluation of a cancer-based coping and caring course used in three different settings. Child Care Health Dev 1997;23:399-413. http://dx.doi.org/10.1111/j.1365-2214.1997.tb00907.x.
- Cothran D, McCaughtry N, Kulinna P, Martin J. Top-down public health curricular change: the experience of physical education teachers in the United States. J Serv Educ 2006;32:533-47. http://dx.doi.org/10.1080/13674580601024556.
- Davidson MW, Range LM. Are teachers of children and young adolescents responsive to suicide prevention training modules? Yes. Death Stud 1999;23:61-7. http://dx.doi.org/10.1080/074811899201190.
- Deutschlander S. An analysis of training effects on school personnel’s knowledge, attitudes, comfort, and confidence levels toward educating students about HIV/AIDS in Pennsylvania. Int J Ment Health Addiction 2010;8:444-52. http://dx.doi.org/10.1007/s11469-009-9221-5.
- Dewit DJ, Timney CB, Silverman G, StevensLavigne A. A process evaluation of a comprehensive drug education training package. J Alcohol Drug Educ 1996;41:102-22.
- Dusenbury LA, Hansen WB, Giles SM. Teacher training in norm setting approaches to drug education: a pilot study comparing standard and video-enhanced methods. J Drug Educ 2003;33:325-36. http://dx.doi.org/10.2190/LH8K-G404-CJAW-PER0.
- Dusenbury L, Hansen WB, Jackson-Newsom J, Pittman DS, Wilson CV, Nelson-Simley K, et al. Coaching to enhance quality of implementation in prevention. Health Educ 2010;110:43-60. http://dx.doi.org/10.1108/09654281011008744.
- el Katsha S, Watts SJ. School-based summer clubs: venues for health education using a partnership model in Egypt. Promot Educ 1994;1:24-8. http://dx.doi.org/10.1177/102538239400100211.
- Impact evaluation study on the professional development course for teachers in sexual health education and the use of the ‘Growing and Developing Healthy Relationships Curriculum Support Materials’ and preferred models of teacher professional development in sexual health education. Perth, WA: Department of Health; 2009.
- Evans C, Evans B. More than just worksheets?: a study of the confidence of newly qualified teachers of English in teaching personal, social and health education in secondary schools. Pastor Care Educ 2007;25:42-50. http://dx.doi.org/10.1111/j.1468-0122.2007.00424.x.
- Favaro A, Zanetti T, Huon G, Santonastaso P. Engaging teachers in an eating disorder preventive intervention. Int J Eat Disord 2005;38:73-7. http://dx.doi.org/10.1002/eat.20148.
- Fenton A, Bottrell D, Meagher G. Communities and change: selected papers. Sydney: Sydney University Press; 2008.
- Frencken JE, Borsum-Andersson K, Makoni F, Moyana F, Mwashaenyi S, Mulder J. Effectiveness of an oral health education programme in primary schools in Zimbabwe after 3.5 years. Community Dent Oral Epidemiol 2001;29:253-9. http://dx.doi.org/10.1034/j.1600-0528.2001.290403.x.
- Gaglianone C, Taddei J, Colugnati F, Magalhaes C, Davanco G, Macedo L, et al. Nutrition education in public elementary schools of São Paulo, Brazil: the Reducing Risks of Illness and Death in Adulthood project. Rev Nutr 2006;19:309-20. http://dx.doi.org/10.1590/S1415-52732006000300002.
- Geiger BF, Petri CJ, Myers O, Lan J, Binkley D, Aldige CR, et al. Using technology to teach health: a collaborative pilot project in Alabama. Journal School Health 2002;72:401-7. http://dx.doi.org/10.1111/j.1746-1561.2002.tb03548.x.
- Gibson CA, Smith BK, DuBose KD, Greene JL, Bailey BW, Williams SL, et al. Physical activity across the curriculum: year one process evaluation results. Int J Behav Nutr Phys Activ 2008;5. http://dx.doi.org/10.1186/1479-5868-5-36.
- Givaudan M, Leenen I, Van de Vijver FJ, Poortinga YH, Pick S. Longitudinal study of a school based HIV/AIDS early prevention program for Mexican adolescents. Psychol Health Med 2008;13:98-110. http://dx.doi.org/10.1080/13548500701295256.
- Goenka S, Tewari A, Arora M, Stigler MH, Perry CL, Arnold JP, et al. Process evaluation of a tobacco prevention program in Indian schools – methods, results and lessons learnt. Health Educ Res 2010;25:917-35.
- Goldman J. Australian undergraduate primary school student-teachers’ responses to child sexual abuse and its mandatory reporting. Pastor Care Educ 2010;28:283-94. http://dx.doi.org/10.1080/02643944.2010.530679.
- Gonzalez GM, Moreno VK. Drug-education in Bolivian schools – a feasibility study for cross-cultural application of a preventive curricular unit. Int Rev Educ 1995;41:439-58. http://dx.doi.org/10.1007/BF01263140.
- Graham A, Moore L, Sharp D, Diamond I. Improving teenagers’ knowledge of emergency contraception: cluster randomised controlled trial of a teacher led intervention. BMJ 2002;324:1179-83. http://dx.doi.org/10.1136/bmj.324.7347.1179.
- Greytak E, Kosciw J. Year one evaluation of the New York City Department of Education ‘Respect for All’ training program. New York, NY: Gay, Lesbian and Straight Education Network (GLSEN); 2010.
- Gueldner B, Merrell K. Evaluation of a social-emotional learning program in conjunction with the exploratory application of performance feedback incorporating motivational interviewing techniques. J Educ Psychol Consult 2011;21:1-27. http://dx.doi.org/10.1080/10474412.2010.522876.
- Gyarmathy VA, Mcnutt LA, Molnar A, Morse DL, DeHovitz J, Ujhelyi E, et al. Evaluation of a comprehensive AIDS education curriculum in Hungary – the role of good educators. J Adolesc 2002;25:495-508.
- Hahn EJ, Noland MP, Rayens MK, Christie DM. Efficacy of training and fidelity of implementation of the life skills training program. J Sch Health 2002;72:282-7. http://dx.doi.org/10.1111/j.1746-1561.2002.tb01333.x.
- Hamm JV. Enhancing the effects of teacher attunement to student peer group affiliations on the school social-affective context: promotive effects of the SEALS intervention. Evanston, IL: Society for Research on Educational Effectiveness (SREE); 2011.
- Hanson RF, Ralston E, Self-Brown S, Ruggiero KJ, Saunders BE, Love AG, et al. Description and preliminary evaluation of the child abuse school liaison program: a secondary prevention program for school personnel. J Psychol Trauma 2008;7:91-103. http://dx.doi.org/10.1080/19322880802231783.
- Harel R. Teacher’s knowledge and attitudes towards health education and its teaching in schools. Kinesiology 1996;28:57-61.
- Harthun ML, Dustman PA, Reeves LJ, Hecht ML, Marsiglia FF. Culture in the classroom: developing teacher proficiency in delivering a culturally-grounded prevention curriculum. J Prim Prev 2008;29:435-54. http://dx.doi.org/10.1007/s10935-008-0150-z.
- Harvey-Berino J, Ewing JF, Flynn B, Wick JR. Statewide dissemination of a nutrition program: Show the Way to 5-a-Day. J Nutr Educ 1998;30:29-36. http://dx.doi.org/10.1016/S0022-3182(98)70272-9.
- Hausman AJ, Ruzek SB. Implementation of comprehensive school health education in elementary schools: focus on teacher concerns. J Sch Health 1995;65:81-6. http://dx.doi.org/10.1111/j.1746-1561.1995.tb03352.x.
- Hawkins R, McCallum C. Mandatory notification training for suspected child abuse and neglect in South Australian schools. Child Abuse Neglect 2001;25:1603-25. http://dx.doi.org/10.1016/S0145-2134(01)00296-4.
- Hendrix K, Gilbert G, Kozlowski L, Bradley E, Austin L, Valois R. The impact of teacher training on utilization of problem-based learning in classroom health education. Am J Health Educ 2002;33:258-64. http://dx.doi.org/10.1080/19325037.2002.10604741.
- Hillman SJ, Siracusa AJ. The effectiveness of training teachers to identify and intervene with children of alcoholics, abuse, and neglect. J Alcohol Drug Educ 1995;41:49-61.
- Hodgkinson K, Baginsky M. Child protection training in school-based initial teacher training: a survey of school-centred initial teacher training courses and their trainees. Educ Stud 2000;26:269-79. http://dx.doi.org/10.1080/03055690050137105.
- Holcomb JD, Kingery PM, Sherman LD, Smith QW, Smith DW, Cullen KW, et al. Evaluation of a diabetes education program for fifth-grade students. J Health Educ 1999;30:73-84.
- Howard NM, Horne AM, Jolliff D. Self-efficacy in a new training model for the prevention of bullying in schools. J Emot Abuse 2001;2:181-91. http://dx.doi.org/10.1300/J135v02n02_11.
- Huber MJ, Workman J, Ford JA, Moore D, Mayer T. Evaluating the Prevention through Alternative Learning Styles program. J Drug Educ 2009;39:239-59. http://dx.doi.org/10.2190/DE.39.3.b.
- Irish HS, Goldberg JP, Wilde P, Bers M, Ioannone L, Economos CD. Comparison of online and face-to-face dissemination of a theory-based after school nutrition and physical activity training and curriculum. J Health Comm 2010;15:859-79.
- Jackson GJ. Professional development in HIV prevention education for teachers using flexible learning and tutor support. Bentley, Western Australia: Curtin University of Technology; 2004.
- Jameson CP, Glover PH. AIDS education in schools – awareness, attitudes and opinions among educators, theology students and health professionals. S Afr Med J 1993;83:675-9.
- Jorm AF, Kitchener BA, Sawyer MG, Scales H, Cvetkovski S. Mental health first aid training for high school teachers: a cluster randomized trial. BMC Psychiatry 2010;10. http://dx.doi.org/10.1186/1471-244X-10-51.
- Kafle KK, Karkee SB, Shrestha N, Prasad RR, Bhuju GB, Das PL, et al. Community intervention to improve knowledge and practices on commonly used drugs. Kathmandu Univ Med J 2010;8:29-34. http://dx.doi.org/10.3126/kumj.v8i1.3218.
- Kaivola T, Cabral S. Implementing education for active citizenship and sustainability. Geography 2004;89:278-81.
- Kantor G, And O. Project impact: teaching the teachers to intervene in student substance abuse problems. J Alcohol Drug Educ 1992;38:11-29.
- Khatib IM, Hijazi SS. Adaptation of the school health index to assess the healthy school environment in Jordan. East Med Health J 2011;17:62-8.
- Kulinna PH, McCaughtry N, Martin JJ, Cothran D, Faust R. The influence of professional development on teachers’ psychosocial perceptions of teaching a health-related physical education curriculum. J Teach Phys Educ 2008;27:292-307.
- Lillehoj C, Spoth R, Trudeau L. Rural teacher training. Rural Educat 2002;24:3-12.
- Lokanc-Diluzio W, Cobb H, Harrison R, Nelson A. Building capacity to talk, teach, and tackle sexual health. Can J Hum Sex 2007;16:135-43.
- Martin J, McCaughtry N, Kulinna P, Cothran D. The impact of a social cognitive theory-based intervention on physical education teacher self-efficacy. Prof Dev Educ 2009;35:511-29. http://dx.doi.org/10.1080/19415250902781814.
- Martin J, McCaughtry N, Hodges K, Cothran D. The influences of professional development on teachers’ self-efficacy toward educational change. Phys Educ Sport Pedagog 2008;13:171-90. http://dx.doi.org/10.1080/17408980701345683.
- Maticka-Tyndale E, Wildish J, Gichuru M. Thirty-month quasi-experimental evaluation follow-up of a national primary school HIV intervention in Kenya. Sex Educ 2010;10:113-30. http://dx.doi.org/10.1080/14681811003666481.
- McBride N, Farringdon F, Midford R. Implementing a school drug education programme: reflections on fidelity. Int J Health Promot Educ 2002;40:40-5.
- McBride N. The Western Australian School Health Project: comparing the effects of intervention intensity on organizational support for school health promotion. Health Educ Res 2000;15:59-72. http://dx.doi.org/10.1093/her/15.1.59.
- McBride NT, Farringdon FH, Kennedy CA. Research to practice – formal dissemination of the School Health and Alcohol Harm Reduction Project (SHAHRP) in Australia. Drug Alcohol Rev 2007;26:665-72. http://dx.doi.org/10.1080/09595230701613510.
- McKenzie TL, Sallis JF, Faucette N, Roby JJ, Kolody B. Effects of a curriculum and inservice program on the quantity and quality of elementary physical education classes. Res Q Exerc Sport 1993;64:178-87. http://dx.doi.org/10.1080/02701367.1993.10608795.
- McKenzie TL, Sallis JF, Kolody B, Faucette FN. Long-term effects of a physical education curriculum and staff development program: SPARK. Res Q Exerc Sport 1997;68:280-91. http://dx.doi.org/10.1080/02701367.1997.10608009.
- McLaughlin RJ, Holcomb JD, Jibaja-Rusth ML, Webb J. Teacher ratings of student risk for substance use as a function of specialized training. J Drug Educ 1993;23:83-95. http://dx.doi.org/10.2190/EUGT-G9HA-RM65-GLM6.
- McVey G, Gusella J, Tweed S, Ferrari M. A controlled evaluation of web-based training for teachers and public health practitioners on the prevention of eating disorders. Eat Disord 2009;17:1-26. http://dx.doi.org/10.1080/10640260802570064.
- Mead N. The provision for personal, social, health education (PSHE) and citizenship in school-based elements of primary initial teacher education. Pastor Care Educ 2004;22:19-26.
- Meers BW, Werch CE, Hedrick B, Lepper J. Prevention training for teachers: a contemporary challenge. J Alcohol Drug Educ 1995;40:47-51.
- Miller D, Eckert T, DuPaul G, White G. Adolescent suicide prevention: acceptability of school-based programs among secondary school principals. Suicide Life Threat Behav 1999;29:72-85.
- Moor S, Sharrock G, Scott J, McQueen H, Wrate R, Cowan J, et al. Evaluation of a teaching package designed to improve teachers’ recognition of depressed pupils – a pilot study. J Adolesc 2000;23:331-42. http://dx.doi.org/10.1006/jado.2000.0318.
- Moor S, Maguire A, McQueen H, Wells EJ, Elton R, Wrate R, et al. Improving the recognition of depression in adolescence: can we teach the teachers?. J Adolesc 2007;30:81-95. http://dx.doi.org/10.1016/j.adolescence.2005.12.001.
- Moore L, Graham A, Diamond I. On the feasibility of conducting randomised trials in education: case study of a sex education intervention. Br Educ Res J 2003;29:673-89. http://dx.doi.org/10.1080/0141192032000133712.
- Myers-Clack SA, Christopher SE. Effectiveness of a health course at influencing preservice teachers’ attitudes toward teaching health. J Sch Health 2001;71:462-6. http://dx.doi.org/10.1111/j.1746-1561.2001.tb07327.x.
- Newman-Carlson D, Horne AM. Bully Busters: a psychoeducational intervention for reducing bullying behavior in middle school students. J Counsel Dev 2004;82:259-67.
- Nyandindi U, Milen A, Palin-Palokas T, Mwakasagule S, Mbiru F. Training teachers to implement a school oral health education programme in Tanzania. Health Promot Int 1995;10:93-100. http://dx.doi.org/10.1093/heapro/10.2.93.
- O’Donnell J, Hawkins JD, Catalano RF, Abbott RD, Day LE. Preventing school failure, drug use, and delinquency among low-income children: long-term intervention in elementary schools. Am J Orthopsychiatry 1995;65:87-100. http://dx.doi.org/10.1037/h0079598.
- O’Moore AM, Minton SJ. Evaluation of the effectiveness of an anti-bullying programme in primary schools. Aggress Behav 2005;31:609-22. http://dx.doi.org/10.1002/ab.20098.
- Okabayashi H, Thongthien P, Singhasvanon P, Waikagul J, Looareesuwan S, Jimba M, et al. Keys to success for a school-based malaria control program in primary schools in Thailand. Parasitol Int 2006;55:121-6. http://dx.doi.org/10.1016/j.parint.2005.11.056.
- Ollis D. ‘I haven’t changed bigots but . . . . ’: reflections on the impact of teacher professional learning in sexuality education. Sex Educ 2010;10:217-30. http://dx.doi.org/10.1080/14681811003666523.
- Orpinas P, Horne AM, Staniszewski D. School bullying: changing the problem by changing the school. School Psychol Rev 2003;32:431-44.
- Paakkari L, Tynjala P, Kannas L. Student teachers’ ways of experiencing the teaching of health education. Stud High Educ 2010;35:905-20. http://dx.doi.org/10.1080/03075070903383229.
- Perez F, Dabis F. HIV prevention in Latin America: reaching youth in Colombia. AIDS Care 2003;15:77-8. http://dx.doi.org/10.1080/0954012021000039789.
- Petersen PE, Peng B, Tai B, Bian Z, Fan M. Effect of a school-based oral health education programme in Wuhan City, Peoples Republic of China. Int Dent J 2004;54:33-41. http://dx.doi.org/10.1111/j.1875-595X.2004.tb00250.x.
- Phuphaibul R, Thanooruk R, Leucha Y, Sirapo-ngam Y, Kanobdee C. The impacts of the ‘Immune of Life’ for teens module application on the coping behaviors and mental health of early adolescents. J Pediatr Nurs 2005;20:461-8. http://dx.doi.org/10.1016/j.pedn.2005.08.003.
- Plummer ML, Wight D, Obasi AI, Wamoyi J, Mshana G, Todd J, et al. A process evaluation of a school-based adolescent sexual health intervention in rural Tanzania: the MEMA kwa Vijana programme. Health Educ Res 2007;22:500-12. http://dx.doi.org/10.1093/her/cyl103.
- Pruitt BE, And O. Researchers and teachers: partners in comprehensive school health education. Health Values 1993;17:17-25.
- Pruski LA, Plaetke R, Blalock CL, Marshall CE, Lichtenstein MJ. The Stealth Gerontology (TM) program: training teachers to infuse aging and age-related content into public school classrooms. Educ Gerontol 2004;30:691-710.
- Randolph MK, Gold CA. Child sexual abuse prevention – evaluation of a teacher training program. School Psychol Rev 1994;23:485-95.
- Reis C, Cornell D. An evaluation of suicide gatekeeper training for school counselors and teachers. Prof Sch Counsel 2008;11:386-94. http://dx.doi.org/10.5330/PSC.n.2010-11.386.
- Remafedi G. The impact of training on school professionals’ knowledge, beliefs, and behaviors regarding HIV/AIDS and adolescent homosexuality. J Sch Health 1993;63:153-7. http://dx.doi.org/10.1111/j.1746-1561.1993.tb06105.x.
- Renju J, Nyalali K, Andrew B, Kishamawe C, Kimaryo M, Remes P, et al. Scaling up a school-based sexual and reproductive health intervention in rural Tanzania: a process evaluation describing the implementation realities for the teachers. Health Educ Res 2010;25:903-16. http://dx.doi.org/10.1093/her/cyq041.
- Resnicow K, Davis M, Smith M, Baranowski T, Lin LS, Baranowski J, et al. Results of the TeachWell worksite wellness program. Am J Public Health 1998;88:250-7. http://dx.doi.org/10.2105/AJPH.88.2.250.
- Ringwalt CL, Pankratz MM, Hansen WB, Dusenbury L, Jackson-Newsom J, Giles SM, et al. The potential of coaching as a strategy to improve the effectiveness of school-based substance use prevention curricula. Health Educ Behav 2009;36:696-710. http://dx.doi.org/10.1177/1090198107303311.
- Rohrbach LA, Sun P, Sussman S. One-year follow-up evaluation of the Project Towards No Drug Abuse (TND) dissemination trial. Prev Med 2010;51:313-19. http://dx.doi.org/10.1016/j.ypmed.2010.07.016.
- Rohrbach LA, Gunning M, Sun P, Sussman S. The Project Towards No Drug Abuse (TND) dissemination trial: implementation fidelity and immediate outcomes. Prev Sci 2010;11:77-88. http://dx.doi.org/10.1007/s11121-009-0151-z.
- Romano JL. School personnel prevention training: a measure of self-efficacy. J Educ Res 1996;90:57-63. http://dx.doi.org/10.1080/00220671.1996.9944444.
- Romano JL. School personnel training for the prevention of tobacco, alcohol, and other drug use: issues and outcomes. J Drug Educ 1997;27:245-58. http://dx.doi.org/10.2190/HYEW-1EEJ-74PD-P1E3.
- Ross JG, Luepker RV, Nelson GD, Saavedra P, Hubbard BM. Teenage health teaching modules: impact of teacher training on implementation and student outcomes. J Sch Health 1991;61:31-4. http://dx.doi.org/10.1111/j.1746-1561.1991.tb07856.x.
- Rossato C, Brackenridge C. Child protection training in sport-related degrees and initial teacher training for physical education: an audit. Child Abuse Rev 2009;18:81-93. http://dx.doi.org/10.1002/car.1052.
- Sallis JF, McKenzie TL, Kolody B, Lewis M, Marshall S, Rosengard P. Effects of health-related physical education on academic achievement: project SPARK. Res Q Exerc Sport 1999;70:127-34. http://dx.doi.org/10.1080/02701367.1999.10608030.
- Salmivalli C, Kaukiainen A, Voeten M. Anti-bullying intervention: implementation and outcome. Br J Educ Psychol 2005;75:465-87. http://dx.doi.org/10.1348/000709905X26011.
- Sarkar A, Dutta S, Biswas R. Development of a training programme for school teachers on school health service. Indian J Publ Health 2003;47:29-34.
- Scott DM, Merkel PA, Barlow TW. Process evaluation of Nebraska’s Team Training Project. J Drug Educ 1994;24:269-79. http://dx.doi.org/10.2190/5BV9-92EW-TXWC-AAXC.
- Seabert DM, Pigg RM, Weiler RM, Behar-Horenstein LS, Miller MD, Varnes JW. The influence of preservice instruction in health education methods on the health content taught by elementary teachers in Indiana. J Sch Health 2002;72:422-8. http://dx.doi.org/10.1111/j.1746-1561.2002.tb03553.x.
- Shah P, Misra A, Gupta N, Hazra DK, Gupta R, Seth P, et al. Improvement in nutrition-related knowledge and behaviour of urban Asian Indian school children: findings from the ‘Medical education for children/Adolescents for Realistic prevention of obesity and diabetes and for healthy aGeing’ (MARG) intervention study. Br J Nutr 2010;104:427-36. http://dx.doi.org/10.1017/S0007114510000681.
- Shechtman Z, Levy M, Leichtentritt J. Impact of life skills training on teachers’ perceived environment and self-efficacy. J Educ Res 2005;98:144-54. http://dx.doi.org/10.3200/JOER.98.3.144-155.
- Shek DT, Wong KK. Subjective outcome evaluation of the training program of the Project P.A.T.H.S. based on qualitative findings. Int J Adolesc Med Health 2010;22:437-47. http://dx.doi.org/10.1515/IJAMH.2010.22.3.437.
- Shek DTL, Wong KKL. Qualitative evaluation of the training program of the project P.A.T.H.S. in Hong Kong. Int J Adolesc Med Health 2010;22:413-23. http://dx.doi.org/10.1515/IJAMH.2011.034.
- Sherman J, Muehlhoff E. Developing a nutrition and health education program for primary schools in Zambia. J Nutr Educ Behav 2007;39:335-42. http://dx.doi.org/10.1016/j.jneb.2007.07.011.
- Sherman JB, Bassett MT. Adolescents and AIDS prevention: a school-based approach in Zimbabwe. Appl Psychol 1999;48:109-24. http://dx.doi.org/10.1080/026999499377556.
- Shollar B. Project AAPT: Alcohol Abuse Prevention Training Evaluation Report 1993.
- Sulak PJ, Herbelin S, Kuehl AL, Kuehl TJ. Analysis of knowledge and attitudes of adult groups before and after attending an educational presentation regarding adolescent sexual activity. Am J Obstet Gynecol 2005;193:1945-54. http://dx.doi.org/10.1016/j.ajog.2005.05.059.
- Syed EU, Hussein SA. Increase in teachers’ knowledge about ADHD after a week-long training program: a pilot study. J Attention Disord 2010;13:420-3.
- Taylor L, Prain V, Rosengren R. Pre-service teachers’ engagement with student wellbeing. Curriculum Perspect 2008;28:21-34.
- Telljohann SK, Everett SA, Durgin J, Price JH. Effects of an inservice workshop on the health teaching self-efficacy of elementary school teachers. J Sch Health 1996;66:261-5. http://dx.doi.org/10.1111/j.1746-1561.1996.tb06282.x.
- Thomas M, Jones S. The impact of group teaching on the acquisition of key skills to teach personal, social and health education. Health Educ 2005;105:164-85. http://dx.doi.org/10.1108/09654280510595245.
- Thompson S, Anderson A. National survey of health education for elementary teacher candidates: are elementary teachers ready to teach health education?. AVANTE 2005;11:1-15.
- Turner SA. Children’s understanding of food and health in primary classrooms. Int J Sci Educ 1997;19:491-508. http://dx.doi.org/10.1080/0950069970190501.
- Van der Westhuizen D, Kruger C. Observing a decline in general school functioning associated with depressive disorders in children – a potential role for teachers?. S Afr J Psychiatr 2005;11:96-8.
- Vincent K, Hazell T, Allen J, Griffiths T, Cooper M. Teacher education: local and global. Surfers Paradise: Griffith University; 2005.
- Visser MJ. Life skills training as HIV/AIDS preventive strategy in secondary schools: evaluation of a large-scale implementation process. SAHARA J 2005;2:203-16.
- Walker SL, Smith DJ. ‘Children at risk’: development, implementation, and effectiveness of a school-based violence intervention and prevention program. J Prev Intervention Community 2009;37:316-25. http://dx.doi.org/10.1080/10852350903196316.
- Warwick I, Aggleton P, Rivers K. Accrediting success: evaluation of a pilot professional development scheme for teachers of sex and relationship education. Sex Educ 2005;5:235-52. http://dx.doi.org/10.1080/14681810500171425.
- Watts V, Laskey L. Preparing teachers for effective child protection: a pre-service curriculum approach. S Pac J Teach Educ 1994;22:117-27. http://dx.doi.org/10.1080/0311213940220202.
- Weatherby-Fell N, Kean B. Mental health and teacher education – implications of the rural perspective for beginning teachers. Int PEPE 2004;8:6-18.
- Weatherby-Fell N, Vincent K, Cooper M. Teacher education: local and global. Surfers Paradise: Griffith University; 2005.
- Webb P, Gripper A. Developing teacher self-efficacy via a formal HIV/AIDS intervention. SAHARA J 2010;7:28-34. http://dx.doi.org/10.1080/17290376.2010.9724966.
- Webster-Stratton C, Jamila RM, Stoolmiller M. Preventing conduct problems and improving school readiness: evaluation of the Incredible Years Teacher and Child Training Programs in high-risk schools. J Child Psychol Psychiatry 2008;49:471-88. http://dx.doi.org/10.1111/j.1469-7610.2007.01861.x.
- Weich L, Philip R. Evaluation of the expanded and enhanced model system-wide 7–9 drug/alcohol abuse prevention training program, 1991–1992. New York, NY: New York City Board of Education, Division of Strategic Planning/Research and Development; 1993.
- Wiefferink CH, Poelman J, Linthorst M, Vanwesenbeeck I, van Wijngaarden JC, Paulussen TG. Outcomes of a systematically designed strategy for the implementation of sex education in Dutch secondary schools. Health Educ Res 2005;20:323-33. http://dx.doi.org/10.1093/her/cyg120.
- Wilson D, Mparadzi A, Lavelle S. An experimental comparison of two AIDS prevention interventions among young Zimbabweans. J Soc Psychol 1992;132:415-17. http://dx.doi.org/10.1080/00224545.1992.9924719.
- Wolfe DA, Crooks C, Jaffe P, Chiodo D, Hughes R, Ellis W, et al. A school-based program to prevent adolescent dating violence: a cluster randomized trial. Arch Pediatr Adolesc Med 2009;163:692-99. http://dx.doi.org/10.1001/archpediatrics.2009.69.
- Wood LA. ‘Not only a teacher, but an ambassador’: facilitating HIV/AIDS educators to take action. Afr J AIDS Res 2009;8:83-92. http://dx.doi.org/10.2989/AJAR.2009.8.1.9.722.
- Wood L, Olivier T. Addressing the needs of teachers in disadvantaged environments through strategies to enhance self-efficacy. Teach Dev 2008;12:151-64. http://dx.doi.org/10.1080/13664530802038154.
- Wright J, Konza D, Hearne D, Okely T. The gold medal fitness program: a model for teacher change. Phys Educ Sport Pedagog 2008;13:49-64. http://dx.doi.org/10.1080/17408980701345592.
- Wyman PA, Brown CH, Inman J, Cross W, Schmeelk-Cone K, Guo J, et al. Randomized trial of a gatekeeper program for suicide prevention: 1-year impact on secondary school staff. J Consult Clin Psychol 2008;76:104-15. http://dx.doi.org/10.1037/0022-006X.76.1.104.
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009;6. http://dx.doi.org/10.1371/journal.pmed.1000097.
- Yager Z. Developing wellbeing in first year pre-service teachers: a trial of a personal approach to professional education. J Student Wellbeing 2009;3:52-7.
- Armour KM, Makopoulou K. Great expectations: teacher learning in a national professional development programme. Teach Teach Educ 2012;28:336-46. http://dx.doi.org/10.1016/j.tate.2011.10.006.
- Bernard ME, Walton K. The effect of You Can Do It! Education in six schools on student perceptions of wellbeing, teaching learning and relationships. J Student Wellbeing 2011;5:22-37.
- Breslin G, Murphy M, Mckee D, Delaney B, Dempster M. The effect of teachers trained in a fundamental movement skills programme on children’s self-perceptions and motor competence. Eur Phys Educ Rev 2012;18:114-26. http://dx.doi.org/10.1177/1356336X11430657.
- Burns ER. Healthy Lungs: cancer education for middle school teachers using a ‘train and equip’ method. J Cancer Educ 2012;27:179-85. http://dx.doi.org/10.1007/s13187-011-0274-3.
- Darvin J. Situated performances in a graduate teacher education course: an inquiry into the impact of Cultural and Political Vignettes (CPVs). Teachers Teach 2011;17:345-64. http://dx.doi.org/10.1080/13540602.2011.554710.
- Fahlman M, McCaughtry N, Martin J, Shen B. Efficacy, intent to teach, and implementation of nutrition education increases after training for health educators. Am J Health Educ 2011;42:181-90. http://dx.doi.org/10.1080/19325037.2011.10599185.
- Kulinna PH, McCaughtry N, Martin J, Cothran D. Effects of continuing professional development on urban elementary students’ knowledge. Res Q Exerc Sport 2011;82:580-4. http://dx.doi.org/10.1080/02701367.2011.10599792.
- Panunzio MF, Caporizzi R, Antoniciello A, Cela EP, D’Ambrosio P, Ferguson LR, et al. Training the teachers for improving primary schoolchildren’s fruit and vegetables intake: a randomized controlled trial. Ann Ig 2011;23:249-60.
- Riggs AD, Rosenthal AR, Smith-Bonahue T. The impact of a combined cognitive-affective intervention on pre-service teachers’ attitudes, knowledge, and anticipated professional behaviors regarding homosexuality and gay and lesbian issues. Teach Teach Educ 2011;27:201-9. http://dx.doi.org/10.1016/j.tate.2010.08.002.
- Robinson DB, Meyer M. Health education and interactive drama: findings from a service learning project. Health Educ J 2012;71:219-28. http://dx.doi.org/10.1177/0017896911398811.
- Shek DT, Chak YL. Training evaluation of the Secondary 3 Training Program of the Project P.A.T.H.S. in Hong Kong. Int J Adolesc Med Health 2011;23:333-9. http://dx.doi.org/10.1515/IJAMH.2011.030.
- Suarez-Mutis MC, Coura JR, Massara CL, Schall VT. Effect of a participatory educational program on primary school teachers’ knowledge of malaria. Rev Saude Publica 2011;45:931-7.
- Till J, Ferkins L, Handcock P. Physical activity based professional development for teachers: the importance of whole school involvement. Health Educ J 2011;70:225-35. http://dx.doi.org/10.1177/0017896910396218.
- Wood L, Goba L. Care and support of orphaned and vulnerable children at school: helping teachers to respond. S Afr J Educ 2011;31:275-90.
- Cochrane Effective Practice and Organisation of Care (EPOC) Group . Suggested Risk of Bias Criteria for EPOC Reviews. n.d. http://epoc.cochrane.org/sites/epoc.cochrane. org/files/uploads/Suggested%20risk%20of%20bias%20criteria%20for%20EPOC%20reviews.pdf (accessed 23 April 2013).
- Shepherd J, Kavanagh J, Picot J, Cooper K, Harden A, Barnett-Page E, et al. The effectiveness and cost-effectiveness of behavioural interventions for the prevention of sexually transmitted infections in young people aged 13–19: a systematic review and economic evaluation. Health Technol Assess 2010;14.
- Popay J, Arai L, Roberts H, Roen K. Preventing accidents in children – how can we improve our understanding of what really works?. London: Health Development Agency; 2003.
- Harden A, Oakley A, Oliver S. Peer-delivered health promotion for young people: a systematic review of different study designs. Health Educ J 2001;60:339-53. http://dx.doi.org/10.1177/001789690106000406.
- Harden A, Gough D, Gough D, Oliver S, Thomas J. An introduction to systematic reviews. London: Sage; 2012.
- Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med 2008;8. http://dx.doi.org/10.1186/1471-2288-8-45.
- Safeguarding children in education. London: Department for Education and Skills; 2004.
- Qualifying to teach handbook of guidance. London: Teacher Training Agency; 2002.
- Personal, social and health education in schools. Manchester: OFSTED; 2005.
- One to one interventions to reduce the transmission of sexually transmitted infections (STIs) including HIV, and to reduce the rate of under 18 conceptions, especially among vulnerable and at risk groups. London: NICE; 2007.
- Interventions in schools to prevent and reduce alcohol use among children and young people. London: NICE; 2007.
- School-based interventions to prevent the uptake of smoking among children and young people. London: NICE; 2010.
- Community-based interventions to reduce substance misuse among vulnerable and disadvantaged children and young people. London: NICE; 2007.
- Stephenson JM, Strange V, Forrest S, Oakley A, Copas A, Allen E, et al. Pupil-led sex education in England (RIPPLE study): cluster-randomised intervention trial. Lancet 2004;364:338-46. http://dx.doi.org/10.1016/S0140-6736(04)16722-6.
- Systematic reviews: CRD’s guidance for undertaking reviews in health care. York: University of York, Centre for Reviews and Dissemination; 2009.
Appendix 1 Protocol
1 September 2011 (minor revision 19/4/12)
1. Aims/Objectives
The main research questions are:
In what ways does teacher training prepare teachers to promote health and well-being in schools? How effective are interventions to train and support teachers? What are the barriers to, and facilitators of, effective training and delivery?
To answer this question the project has 2 research objectives:
-
To conduct a survey, using quantitative and qualitative methods, of a sample of initial teacher training providers in England to assess how health and well-being is covered in teacher training.
-
To conduct a systematic review of effectiveness, and barriers/facilitators, of teacher training around health and well-being.
2. Background and rationale for the research
2.1.1 The importance of teachers as health promoters
The importance of teachers as promoters of health in schools has been acknowledged for some time. 1 However, pressure on busy curricula has meant that health and well-being has not always been covered in as much detail as desirable. Yet, teachers are playing an increasingly important role in the wider public health workforce. A number of Government policy strategies have underlined the importance of the school in children's health in recent years. For example, ‘Every Child Matters’ (2004)2 was a key policy for children's health, education and welfare, which stressed the importance of health and safety, and still underpins the current Qualified Teacher Status (QTS) standards for health. ‘The Children's Plan: Building Brighter Futures’ (2007)3 emphasised the pivotal role of schools in ensuring children are healthy and safe. It introduced the concept of Extended Services with its focus on improving access to school activities for disadvantaged children and young people to reduce attainment gaps. It also set a goal for all schools to work with the National Healthy Schools Programme (NHSP) by 2009.
Also in 2009 the NHSP began rolling out its Enhancement Model, a universal and a targeted approach to pupil well-being offering schools the challenge of meeting specific needs-led healthier behaviour outcomes. Since April 2011 the organisation of the NHSP has changed to being a schools-led initiative rather than one that is Government-led. The resources to support schools are now in the form of the ‘Healthy Schools Toolkit’ which is available to schools via the Department for Education website. 4
Effective health promotion with children and young people, particularly the early identification and prevention of health inequalities, was also a key aspect of the ‘Choosing Health’ strategy, launched in 2004. 5 The overall strategy was to develop and build capacity for health improvement at all levels of the system, and to better equip the wider workforce to promote health by ensuring basic skills and knowledge for more people. Furthermore, ‘Healthy Weight, Healthy Lives: a cross-government strategy for England’ (2008)6 stated that all schools should be healthy schools, and recognised the need for improvements in staff skills and capabilities.
The ‘Healthy Child Programme 5–19 years’, published by the Department for Health and the Department for Children, Schools and Families in 2009,7 set out the early intervention and prevention public health programme for children, young people and their families. It highlighted the need for schools to work together with parents, carers and health professionals and to have an understanding of how to promote health and well-being.
Importantly, the 2009 Macdonald Review of Personal, Social and Health Education (PSHE) recommended that it should be a statutory subject in the curriculum and that all ITT courses should include some focus on PSHE throughout the school life. 8 The Macdonald review also recommended that there should be in time, ‘a cohort of specialist PSHE education teachers’ (page 8). Since the recent change in government the Department for Education is currently conducting a review of the primary and secondary National Curriculum, which also includes an internal Government review of the non-statutory status of PSHE.
Since the election of the Coalition government in May 2010, the broad landscape and relationships both within and between health and education is changing. The Government published its White Paper ‘The Importance of Teaching’ in November 20109 which states:
We will recognise that schools have always had good pastoral systems and understand well the connections between pupils’ physical and mental health, their safety, and their educational achievement and that they are well placed to make sure additional support is offered to those who need it.
Page 9
The White Paper for public health, ‘Healthy Lives, Healthy People’, published in November 2010, set out the proposed substantial changes to the public health system in England over the next two years. 10 It is planned that joint commissioning of health services will be carried out by local authorities in conjunction with a new body, ‘Public Health England’, and the current Directors of Public Health will be employed within these organisations. The Commons Select Health Committee has held an inquiry into the proposed changes (though the results of the enquiry have not yet been reported). These proposed changes will no doubt have a major impact on the way that public health and health promotion activities are managed, and implications for the support for improvement of health education in schools.
2.1.2 Teacher training in the UK
Initial Teacher training in the UK is currently predominantly provided by Higher Education Institutions (HEIs) at under-graduate (e.g. Bachelor of Education) or post-graduate level (e.g. Post-Graduate Certificate in Education, PGCE). Some post-graduates choose school-centred ITT courses (SCITTs) which provide a greater degree of practice based learning, while retaining their student status. An alternative route is through employment-based ITT (EBITT) whereby trainees are employed by schools and train via the Graduate Teacher Programme (GTP) or the Registered Teacher Programme (RTP). Teacher training is funded by the Training and Development Agency for schools (TDA) (to become a new body called ‘The Teaching Agency’ from April 2012), but additional health content may be funded from other agencies.
This nature of teacher training is likely to change in the future. In the ‘Importance of Teaching’9 the Government states that it will:
-
Reform initial teacher training, to increase the proportion of time trainees spend in the classroom, focusing on core teaching skills.
-
Develop a national network of Teaching Schools on the model of teaching hospitals to lead the training and professional development of teachers and head teachers, and increase the number of National and Local Leaders of Education – head teachers of excellent schools who commit to working to support other schools.
Training is also provided to qualified teachers as part of continuing professional development (CPD). Within the context of health CPD may address the provision of PSHE, or more specifically train teachers to deliver a specific health promotion intervention (e.g. around a drugs and alcohol initiative, or a sexual health campaign). Training may also encapsulate broader school-wide health promotion interventions (‘whole-school approaches’). A variety of people may train teachers around health issues, including Healthy Schools Co-ordinators, health professionals (e.g. health promotion practitioners, health advisers), youth workers, psychologists, educational professionals, and educational professionals. Training is provided in-service (i.e. organised by the school), or externally organised by the organisations responsible for developing specific interventions or teaching methods.
It is unclear how current policy changes will ensure continued support for schools in actively promoting health and well-being. A key question is to what extent do teacher training courses adequately prepare teachers for this pivotal role?
2.2.1 Initial teacher training
Since the mid 1980s research in England and Wales has indicated that teacher education and training in health-related areas is poor, and has mostly relied on in-service training which teachers may or may not receive. 1 Progress on including knowledge and skills regarding health and well-being in the initial training and education of teachers entering the profession has been slow, both in England and elsewhere. 11 There are unanswered questions about the provision and quality of health promotion within ITT courses across England. Our previous survey research has shown that coverage of health and well-being in teacher training curricula is limited and variable in the South East of England region. 12 We surveyed, via questionnaire, 35 organisations offering ITT in 2007 (10 HEIs, 25 employment-based schemes). Fifteen (43%) organisations responded, representing 50% of the total number of trainees in the region (83% from HEIs, and 17% from employment-based schemes). The results demonstrated the enormous variability of teacher training provision across the region and the lack of any consistent approach to educating student teachers about their potential roles in promoting children's health. Most organisations were found to be incorporating Every Child Matters (ECM) supported by Healthy Schools and other external specialists, but to varying extents. Provision of information about the NHSP was also extremely variable, from nothing at all to inclusion in PSHE or emotional health and well-being. Employment-based schemes were more likely to have connections with the NHSP. Reasons for lack of inclusion of health issues included insufficient time in a busy curriculum, and the extent to which placement schools were actively involved in the NHSP.
The extreme variability in the amount of time allocated to health topics in our survey demonstrates a lack of consistency in interpretation of the requirements of training leading to very little provision in many institutions, versus careful attention and innovative good practice in a few others. The survey was limited by the relatively low response rates, its timing (just before holiday period), the length of the questionnaire (on reflection relatively lengthy) and its confinement to the SE of England. There remains, therefore, a need to assess the adequacy of provision of health initiatives within ITT curricula across England, with a sampling strategy that ensures representation from different types of providers (HEI based, employment-based) types of course (primary, secondary teaching). Such a survey will illuminate variations in practice, identify barriers and facilitators, and will generate recommendations for effective training, and models of effective practice suitable for further evaluation.
2.2.2 Continuing professional development, and intervention-specific training
There is a sizable evidence base on the effectiveness of school-based health promotion interventions worldwide. Stewart-Brown (2006)13 conducted a synthesis of systematic reviews of school-based health promotion interventions and health promoting schools (an update of the previous NIHR HTA funded systematic review published in 199914). Fifteen systematic reviews were included, between them comprising approximately 750 primary evaluations of school-based interventions on a variety of health issues (e.g. mental health, healthy eating, physical activity). There was little overlap between the reviews in terms of their constituent studies, suggesting that this figure has probably not been over-estimated by double counting and is therefore an accurate estimate of the size of the evidence.
2.2.3 The evidence base
Despite the volume of evidence for school-based health promotion interventions, little has been published, at least in terms of secondary research, on the effectiveness of training teachers to deliver such initiatives (either ITT or CPD), and of the barriers and facilitators to effective teacher training and their subsequent provision of health promotion. Scoping searching of electronic databases conducted for this protocol (e.g. Educational Resources Information Center (ERIC), Medline) and key websites (EPPI-Centre, National Foundation for Educational Research) did not identify any published systematic reviews of the evidence for the effectiveness of programmes to train teachers to promote health in schools. However, we did identify 18 potentially relevant primary studies (some of which were included in a broader published literature review of 26 studies investigating training of workers to implement adolescent prevention and positive youth development15).
The majority of these studies evaluated teacher training to deliver specific health promotion interventions. They covered a range of topic areas including sexual health,16–20 tobacco,21–24 drugs and alcohol,25–27 physical activity,28–30 injury prevention,31 and youth development/life skills training. 15;32 In terms of publication dates the studies spanned the last two decades with the most recent published in 200931, indicating that this remains a fertile area for research. The studies were conducted in a number of countries (e.g. Australia, Hong Kong, South Africa) though many were from the USA, with one notable example from the UK (see below). 17 A mixture of study designs were used, including process evaluations of teacher training as part of a randomised controlled trial (RCT) or other type of outcome evaluation of a school-based health promotion intervention, or process only evaluations of school-based interventions. At least three outcome evaluations compared the effectiveness of different types of teacher training (e.g. video instruction versus workshop training) on a range of teacher outcomes (e.g. implementation, morale, motivation, self-efficacy)21;25;26 and one of these also assessed changes in pupil outcomes (e.g. use of drugs, tobacco and alcohol). 25
In terms of theory, the interventions were based upon a range of well known theories of education, health and health-related behaviour change such as Social Learning Theory, Social Cognitive theory, and the Theory of Reasoned Action/Planned Behaviour, Diffusion of Innovations theory and the Social–Ecological Model. 15 Many of these theories predict the necessary mediators of effective health-related behaviour change. The training the teachers received was designed to equip them with the knowledge, motivation, confidence and skills, to facilitate, in turn, desirable improvements in mediators of pupils' behaviour, such as increasing their knowledge, their self-efficacy and their behavioural skills. For example Kealey et al. (2000),22 who evaluated the Hutchinson Smoking Prevention Project in the USA, conceptualized teacher training as a behaviour change process with a strong emphasis on teacher motivation to facilitate the intended behaviour (i.e. the teacher's effective implementation of the curriculum). Theories such as those mentioned above form part of the conceptual framework for this project (see Section 4.2.2.5).
All studies provided evaluation data on the implementation of the intervention, with varying detail given to the training received by teachers. One of the studies that provided detailed information on training was a Scottish trial of a sexual health education initiative called SHARE (Sexual Health Relationships Education). 17 An extensive process evaluation was carried out, comprising observation, questionnaires and interviews with teachers. The teachers reported that they valued and enjoyed the training very much and felt more confident to teach sex education, but a number of barriers to effective delivery of the curriculum emerged, including a lack of understanding by the teachers of the guiding theory of behaviour change and a lack of confidence to teach behaviour change skills (the key element of the intervention). This was echoed by other studies identified by our scoping searches such as Ward et al. (2006)29 who, in a process evaluation of a physical activity promotion programme for high school girls, reported that the teachers found it difficult to understand and implement behavioural skills concepts to encourage physical activity.
These findings, though perhaps not necessarily representative of the wider literature, suggest that additional training and support may be necessary to enable teachers to facilitate health-related behaviour change, an outcome that is considered as a key marker of effectiveness by many decision makers. 33 For example, they may require professional input from health educators to deliver skills-building exercises in the classroom which may be essential for encouraging healthy behaviours. This will have resource, and therefore, cost implications and it underlines the need for a full systematic review of the evidence to identify common over-arching barriers and facilitators to effective and efficient teacher training across a range of health topics. Recommendations would be made for health and education professionals, policy makers, and researchers to ensure teachers fulfil their potential in promoting health and well-being in schools, ensuring children adopt and maintain healthy lifestyles into adulthood.
3. Methods
The project comprises two main components: a survey of teacher training providers; and a systematic review. They will run in parallel with each other, with a reciprocal relationship between the two. For example, emerging findings from the systematic review may influence the issues explored in the semi-structured interviews with teacher training providers.
3.1 Survey of teacher training providers
3.1.1 Setting
We will undertake a survey of a sample of ITT providers in England to map the ways in which they incorporate health and PSHE in their curricula to enable trainee teachers to develop knowledge and skills to promote health and well-being. The survey will focus on how ITT providers address the health issues embraced within policies such as, ‘Healthy Lives, Brighter Futures: the strategy for children and young people's health’,34 and ‘Your child, your schools, our future: building a 21st century schools system’,35 that are underpinned by the five outcomes of the ‘Every Child Matters’ strategy. 2 We will build on our previous survey experience of this topic in SE England (see Section 2.2.1) to ensure optimal response rates and high quality data are collected. 12
3.1.2 Data collection
3.1.2.1 Sampling
We will use the 208 ITT providers in England listed in the TDA website as our sampling frame. This includes 74 Higher Education Institutions (HEIs), 57 school-centred Initial Teacher Training providers (SCITTs) and 77 Employment-Based Initial Teacher Training providers (EBITTS).
Courses vary in their duration from a 1-year PGCE to 3–4-year undergraduate degrees (BA/BSc with QTS or BEd), as well as variations in the phase of education that they specialise in (i.e. primary, secondary, key stage 2/3) (Table 1). SCITT programmes are designed and delivered by groups of neighbouring schools and colleges. SCITT courses lead to qualified teacher status (QTS), and some will also lead to a PGCE validated by a HEI. EBITTs are run by consortia of schools, colleges and local authorities (though note that some Universities also offer EBITTs courses). On the Graduate Teacher Programme (GTP), graduates can attain QTS while training and working in a paid teaching role. The GTP normally takes between three months and one school year, working full-time, to complete. The Registered Teacher Programme (RTP) combines work-based teacher training and academic study, allowing non-graduates with some experience of higher education to complete their degree and qualify as a teacher at the same time. This course normally takes two years to complete. The Overseas Teacher Training Programme (OTTP) is for qualified teachers from overseas who wish to attain qualified teaching status in England. Courses can last up to one year. Key stage 2/3 courses covers children in the age range 8–11 (key stage 2) and 11 to 14 (key stage 3). Early years generally covers the 3 to 7 age group.
| Type of provider | Undergraduate | Post-graduate |
|---|---|---|
| Higher Education Institution (HEI) (e.g. University) | ||
|
BA/BSc; BEd | PGCE |
|
BA/BSc; BEd | PGCE, GTP, OTTP |
|
BA/BSc; BEd | PGCE, GTP, OTTP |
|
BA/BSc; BEd | PGCE |
|
BA/BSc; BEd | PGCE |
| RTP | ||
| School Centred Initial Teacher Training (SCITT) | ||
|
PGCE (with QTS)/QTS | |
|
PGCE (with QTS)/QTS | |
| Employment Based Initial Teacher Training (EBITT) | ||
|
RTP | GTP, OTTP |
|
RTP | GTP, OTTP |
The ITT providers in England have been classified according to the 9 Government administrative regions. Table 2 shows that the number of providers in each region varies from 14 (North East) to 36 (Eastern).
We aim to sample the ITT providers within each of the regions to ensure all areas of England are represented, given that there may be geographical variations in teacher training practice in relation to health and well-being. Our sampling strategy will vary according to the type of provider in each region, as follows:
-
We will randomly sample 50% of each of the HEIs within each of the 9 English regions. Our initial mapping work has shown that the number and range of courses on offer varies considerably by HEI. For example in the South East region of England, the University of Portsmouth currently offers just 2 courses, both at post-graduate level. In contrast, Canterbury Christchurch University offers 10 courses covering undergraduate and postgraduate level. To obtain balance we will take a random sample of 50% of HEIs classified as offering a low number of courses, and 50% of those classified as offering a high number of courses (low and high to be determined by the average number of courses per provider in a region). A questionnaire will be sent to each course offered by the sampled HEIs, and should result in sampling approximately 50% to 60% of available courses in each region.
-
We will also randomly sample 50% of EBITTs in each region. However, as EBITTs generally offer fewer numbers of courses we will not be classifying them as high or low. (NB. HEI-run EBITT courses, such as GTP, will be sampled as above in 1.)
-
We will survey all SCITTs rather than take a sample as there are relatively fewer of them, and because they offer only a limited range of courses (e.g. one to two courses per SCITT).
| Eastern | London | East Midlands | |||
|---|---|---|---|---|---|
| HEI | 6 | HEI | 13 | HEI | 7 |
| SCITT | 15 | SCITT | 7 | SCITT | 4 |
| EBITT | 15 | EBITT | 12 | EBITT | 8 |
| Total | 36 | Total | 32 | Total | 19 |
| North East | South East | South West | |||
| HEI | 4 | HEI | 10 | HEI | 8 |
| SCITT | 6 | SCITT | 5 | SCITT | 13 |
| EBITT | 4 | EBITT | 14 | EBITT | 5 |
| Total | 14 | Total | 29 | Total | 26 |
| Yorks and the Humber | West Midlands | North West | |||
| HEI | 10 | HEI | 9 | HEI | 7 |
| SCITT | 1 | SCITT | 5 | SCITT | 1 |
| EBITT | 6 | EBITT | 7 | EBITT | 6 |
| Total | 17 | Total | 21 | Total | 14 |
3.1.2.2 Recruitment
It is planned to recruit and survey ITT providers in the 2011 spring/summer term (see Table 5, Section 4). This is a time when many courses begin to review the current curriculum and think about planning for the subsequent academic year. We believe this would be an optimal time to gather data from ITT providers.
We will approach, by e-mail, the head of the education department in each HEI in our sample to introduce the project and to ask them to provide us with the name and contact details of the tutor of each of their ITT courses. We will then contact, via e-mail, the tutors of those courses that are in the sample directly and ask them to complete an online questionnaire (see below). The e-mail will specify the purpose of the study, why they have been chosen, and a guarantee that their responses will be confidential and anonymised in the dissemination of the project. We will contact directly the course leader/manager in each randomly-sampled EBITT, and in each SCITT, again via e-mail, and ask them to complete an online questionnaire.
3.1.2.3 Survey Instruments
An online questionnaire will be developed for ITT providers to complete, using SelectSurvey.NET software (www.som.soton.ac.uk/quest). The questionnaire will be piloted on a small random sub-sample of ITT providers in each region prior to full implementation.
We will request information about what ITT providers do to address health and well being, how much time they devote within their course to health issues, and how trainees gather evidence about health related matters. In particular we will ask about:
-
The type of course.
-
Approximate amount of time spent on health issues – in institution based training and in school-based training.
-
Specific health issues addressed (education on sex and relationships, alcohol, smoking and drugs; healthy eating; physical activity and emotional well-being).
-
Who teaches the health aspects of the curriculum (e.g. use of external agencies).
-
Whether and how health and well-being training is assessed (e.g. portfolio; questionnaire).
-
Who funds the health and well-being activities undertaken (e.g. primary care trusts; TDA).
-
Examples of successful initiatives around health and well-being.
Non-responders will be followed up with a reminder e-mail.
Following an initial analysis of the questionnaires a purposive sub-sample of around 20 to 25 providers will be selected for follow-up qualitative semi-structured qualitative interviews to gain detailed insights into how health and well-being is addressed in their curricula. We will interview those providers that are currently covering health and well-being in some depth to identify contrasting models of what potentially might be considered good practice. We will also select providers who, from the questionnaire, do not appear to cover health and well-being to a great extent to identify and explore any particular barriers. Where appropriate we may also purposively select other ITT providers for interview (i.e. who were not included in the questionnaire survey), if it is considered that their health and well-being initiatives would be useful to investigate.
Specific issues that the interviews will focus on include:
-
Coverage of specific aspects in the course and curriculum relevant to the Public Health Skills and Careers Framework including:
-
Awareness raising of health-related policies/practice (e.g. whole school health policies, PSHE, healthy eating, physical activity, anti-bullying, etc.).
-
Awareness raising of the determinants of health and current health policies (e.g. reducing health inequalities).
-
Encouragement and awareness raising about the processes of monitoring and evaluating relevant health-related data.
-
-
Who teaches/facilitates the health aspects of the course, and whether there are links with external agencies available to support schools (e.g. sports partnerships, teenage pregnancy & family planning agencies, NHS public health agencies, youth workers, drug and alcohol teams, Healthy Schools Programme, school food trust/nutritionists, etc.).
-
Description of specific initiatives or events that providers mount or engage in to raise awareness of health and well-being (e.g. in collaboration with external agencies, as above).
-
Elucidation and exploration of barriers to addressing health and well-being in teacher training.
3.1.3 Data analysis
For analysis of the questionnaire data and some of the interview questions we will use standard descriptive statistics (e.g. proportions, median, or mean with standard deviation for continuous measures). We may undertake a limited number of comparisons using standard statistics (e.g. Chi-square tests for proportions, Mann–Whitney for non-normal continuous data) with results analysed in a suitable statistical package such as the Statistical Package for the Social Sciences (SPSS). Qualitative data yielded by the interviews will be analysed in a standard content analysis, with data coded and categorised into themes, using an appropriate programme such as NVivo (Version 9.0, QSR international).
4.2 Systematic review of teacher training interventions
Our proposed systematic review will use rigorous methods to identify, appraise and synthesise relevant evidence, drawing on established processes and procedures in evidence synthesis,36–38 with particular consideration given to wider determinants of health and health inequalities. 39 Figure 1 provides an overview of the key stages of the review.
FIGURE 1.
Key stages of the systematic review.
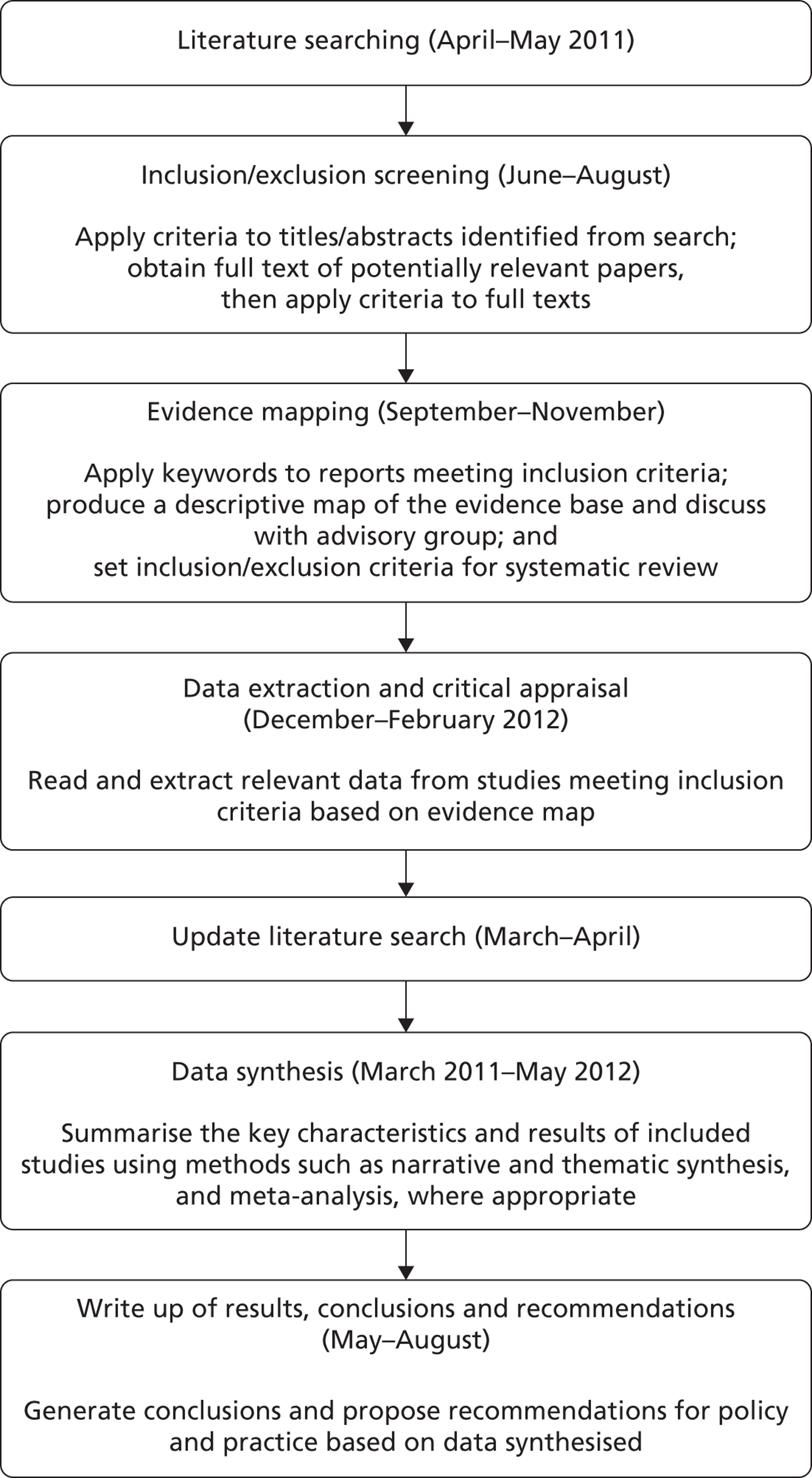
4.2.1 Literature Searching
An extensive search will be conducted to identify relevant literature. A highly sensitive search strategy will be devised and tested by an experienced information scientist. The strategy will comprise a mixture of free-text words and controlled vocabulary terms (see Appendix 1).
The strategy will be applied to the following electronic bibliographic databases (database platform in parentheses)
-
Medline (Ovid)
-
Medline In-Process (Ovid)
-
Embase (Ovid)
-
The Cochrane Library (Cochrane Database of Systematic Reviews; Cochrane Central Register of Controlled Trials)
-
Database of Abstracts of Reviews of Effectiveness (DARE)
-
The Campbell Library
-
C2 Spectr (The Campbell Collaboration's Social, Psychological, Educational, and Criminological Trials Register).
-
CINAHL (Ebsco)
-
Psychinfo (Ebsco)
-
Social Science Citation Index (Web of Science)
-
Conference Proceedings Citation Index- Social Science & Humanities (CPCI-SSH) (Web of Science)
-
ERIC (Dialog Datastar)
-
EPPI-Centre databases (TRoPHI/Evidence Library)
-
British Educational Index (Datastar/Dialog Web)
-
Australian Educational Index (Dialog Datastar)
-
International Bibliography of the Social Sciences (CSA)
-
Sociological Abstracts (CSA)
Although databases will be searched from inception to the current date, only studies published from 1990 onwards will be eligible for inclusion (this was a decision taken during the course of the project. The rationale was that older studies were considered to be less relevant to current practice, are generally poorly reported, and also because it would make the workload more manageable).
Key websites will be searched, including the National Foundation for Educational Research, the International Union for Health Promotion and Education and others. We will be particularly interested in locating relevant studies from the grey (unpublished) literature and will make contact with experts in the field, including our advisory group, to identify relevant studies. Bibliographies of relevant studies will be screened to identify further potentially relevant studies.
Studies published in the English language will be prioritised for inclusion in the review. Any non-English language studies will be included if translation is possible.
Relevant systematic reviews identified by the search will only be used as a source of additional relevant studies.
The search will be updated in March/April 2012 (approximately a year after the original search – see Table 5) to identify any new literature published since the initial search. Depending on the volume of literature identified it may be possible to integrate any new relevant studies into the systematic review. Where this is not feasible the newly identified studies will be listed in an appendix with brief details of their key characteristics.
4.2.2 Inclusion criteria
4.2.2.1 Population
-
Teachers
-
Pupils in primary, secondary and further education
Studies of children and young people with existing illness or conditions (e.g. physical illnesses such as asthma, or behavioural disorders such as attention-deficit hyperactivity disorder) are not eligible for inclusion.
4.2.2.2 Intervention
-
Health and well-being training component of the ITT curriculum
-
Teacher training either as part of CPD (e.g. for PSHE), or to facilitate a specific school-based health promotion intervention.
Interventions may delivered in the context of any area of health including general well-being and personal and social development (e.g. life skills training, youth development), as well as on specific topics such as substance abuse, healthy eating and physical activity, sexual health, bullying and mental and emotional health, etc. (NB. Differences in findings according to topic areas will be explored as part of the synthesis, see Section 4.2.6).
4.2.2.3 Comparator
For comparative outcome evaluations studies any type of comparison will be eligible. For example, a study may compare a new method of teacher training (e.g. interactive programme using computers and video) with standard methods of teacher training (e.g. facilitator-led workshop).
4.2.2.4 Study type
For both types of intervention the following study types are relevant:
-
Outcome evaluations (e.g. preferably randomised controlled trials (RCTs), but non-random or uncontrolled studies will be considered where there is a lack of RCTs). These studies aim to measure effects of teacher training interventions either on the teachers themselves, the pupils, or both. This excludes studies of school-based health promotion interventions where the aim is only to assess the effectiveness of the school-based intervention itself, rather than the training the teachers received.
-
Process evaluations (e.g. integrated within an outcome evaluation, or a process only evaluation). These studies assess how the intervention was implemented (e.g. the resources used, acceptability of the intervention, unanticipated barriers and facilitators), and can provide insights into the outcomes achieved. They can use qualitative or quantitative methods or use both (e.g. surveys; questionnaires; interviews; focus groups). In this review we will include process evaluations that report on: the acceptability and adequacy to the teachers of the training, and of the health promotion intervention itself (e.g. appeal, enjoyment, relevance to professional goals and personal values); Teachers' general reflexivity of their health promoting role and practice; implementation of the teacher training programme/the health promotion intervention.
4.2.2.5 Outcomes and processes
Table 3 summarises possible relevant outcome measures for both teachers and pupils, while Table 4 specifies some of the relevant processes which can inform our understanding of barriers and facilitators.
For studies which only evaluate processes (i.e. they do not necessarily aim to measure impact on pupils or teachers) some of the outcomes in Table 1 may be discussed within the context of delivery of the intervention. For example, a process evaluation may not formally measure changes in teachers' motivation to deliver a health promotion intervention, but nonetheless report that lack of motivation was an impediment to effective delivery.
These outcomes and processes reflect the conceptual framework of this study, which is effective teacher training for health as essentially, though not limited to, a behaviour change process (see Section 2.2.2). Our starting point is that equipping teachers with basic competencies in their initial training means they will be more motivated to address health and well-being and be better able to contribute to health promoting schools when teaching. The framework also recognises wider structural influences on health, including political, social and economic factors that constrain or enable individuals and groups to make informed decisions about their health (to be taken into account in the thematic analysis of barriers and facilitators – see Section 4.2.6).
| Outcomes | |
|---|---|
| Teachers | Pupils |
| Knowledge of health in general and the specific health topic to be addressed | Knowledge of relevant health topic (e.g. risk factors, prevention, well-being) |
| Skills (e.g. ability to teach health-related behaviour change skills) | Attitudes towards health-related behaviour |
| Confidence/self-efficacy to provide health promotion intervention | Intentions to adopt health-related behaviour |
| Attitudes towards health promotion intervention | Self-efficacy to adopt health-related behaviour |
| Motivation and intentions to provide health promotion intervention | Biological and physical outcomes (e.g. weight change) |
| Awareness and understanding of whole-school approaches to health promotion, and wider determinants of health | Health-related behaviour (e.g. smoking) |
| Health literacy | Health literacy |
| Rates of delivery of the intervention | Educational attainment |
| Unintended/unanticipated outcomes (e.g. increasing health inequalities) | Unintended/unanticipated outcomes (e.g. differential health gain) |
| Processes |
|---|
| Acceptability to the teachers of the training, and of the health promotion intervention itself (e.g. appeal, enjoyment, relevance to professional goals and personal values) |
| Resources and costs used to train the teachers |
| Teachers' general reflexivity of their health promoting role and practice |
| Implementation of the teacher training programme/the teacher-led health promotion intervention |
Inclusion criteria will initially be applied to each title and abstract (where available) independently by two reviewers. Reviewer agreement will be monitored during the first few batches of references screened and once an acceptable level of agreement has been reached (e.g. 90% or greater) all remaining references will be screened by a single person. A random sample of 10% of each batch of remaining references will be independently screened by a second person. This will enable the team to monitor on-going levels of agreement. In cases where agreement cannot be reached a third reviewer will be consulted.
4.2.3 Descriptive mapping stage
As the evidence base is likely to be diverse (e.g. in terms of health issues, country, type of school, outcomes/processes etc.), and uneven in terms of volume (e.g. there may potentially be more outcome evaluations from the United States), an intermediate descriptive mapping stage is proposed. Descriptive mapping has been successfully applied in a number of published systematic reviews of complex health and education interventions as a means of characterising the evidence base to facilitate a focused policy-relevant synthesis. 40–43 It is particularly useful in systematic reviews such as this, where sensitive literature searches are necessary. All studies meeting the inclusion criteria described above in Section 4.2.2 will be classified through the systematic application of pre-specified keywords. Each study will be keyworded by one reviewer and a random sample checked by a second for fairness in accuracy in interpretation. The keywords will cover a number of study characteristics including the:
-
country the study was conducted in,
-
level of education (e.g. primary/secondary),
-
type of school (including whether mainstream or schools for children with special educational requirements),
-
topic area (e.g. substance abuse, sexual health etc.),
-
outcomes measured (where applicable),
-
processes evaluated (where applicable).
The keywording will not, however, characterise the results of studies.
The descriptive map will be presented to the project's advisory group for discussion (likely to be during meeting 2, see Table 5). Based on their guidance a policy-relevant focussed set of inclusion criteria will be set for the systematic review. For example, based on the evidence available it might be decided to focus on studies of teacher training in schools for minority children or those with special educational requirements who may be at particular risk of poor health outcomes. The mapping stage may also be used to ensure that the volume of evidence to be reviewed is manageable, ensuring the project is conducted within its resources and to its timetable. As well as helping to set the focus for the proposed systematic review the map will be a useful resource of its own as it will provide an outline of the key attributes literature over a fairly extensive area. It will be published as part of the final report to the NIHR PHR, and potentially also published separately in journal or in practice publications.
4.2.4 Data extraction of included studies
Following the mapping exercise each study meeting the inclusion criteria for the systematic review will be read by one researcher and will then have relevant data extracted from it into a standardised template. A second researcher will check the data for accuracy and interpretation, and any disagreements resolved through discussion.
Data to be extracted include:
-
Markers of health and health inequalities and SES (e.g. pupil educational attainment, parental income, residential status, ethnicity, locality)
-
Type of teacher training (e.g. didactic education, skills training)
-
Format of the training (e.g. length, duration, intensity, maintenance)
-
Setting for the teacher training (e.g. school, or other venue)
-
Details of any specific intervention for the teachers to provide (e.g. PSHE in general, or focus on particular health topic)
-
Materials and media used (e.g. use of video, computers, course materials)
-
Theory underpinning the teacher's training, and the health promotion intervention
-
Training provider (e.g. type of provider, their own training/qualification)
-
Costs and resources (e.g. training provider costs, cost of materials used)
-
Results of the outcome and process evaluation (as specified in Section 4.2.2).
4.2.5 Critical appraisal
Each study will be data extracted and critically appraised by one researcher, and checked by a second with any disagreements resolved through discussion and recourse to a third researcher if necessary. The criteria will assess risk of bias and aspects of methodological quality of outcome evaluations using standard methodological criteria (e.g. selection bias, attrition bias, selective reporting) based on that used by the Cochrane Collaboration37 and the Centre for Reviews and Dissemination36. Process evaluation studies will be appraised by criteria specifically applied in our recently published systematic review of school-based sexual health promotion,40 in turn based on criteria proposed by experts in the field. 44–46 These criteria assess the rigour of methods for sampling, data extraction, data analysis, and whether adequate breadth and depth was achieved in the interpretation of the findings.
4.2.6 Synthesis
The results of the outcome evaluations will be tabulated and summarized textually in a narrative synthesis. Quantitative meta-analysis will be performed if the studies are not considered too heterogeneous (in terms of intervention characteristics, participants and methods) and where sufficient data are available to allow statistical pooling. 37 Cochrane Review Manager software will be used to perform any meta-analysis. Results will be analysed according to markers of health and health inequalities where reported in the primary studies.
The results from the process evaluations (in terms of the process markers described in Table 2) will also be tabulated and summarised. In addition they will undergo a more detailed thematic analysis using methods applied in our previous systematic review of sexual health promotion in schools,40 in turn devised by colleagues at the EPPI-Centre, London. 47;48 Two researchers will independently identify any reported or inferred barriers and facilitators to effective teacher training and delivery from each study, and compile them into higher order themes (e.g. teacher skills, school organization, school ethos, health inequalities). The two researchers will compare their themes and propose a draft agreed set. A brief description of each of the themes will be written up and the draft set will be discussed and finalized by the research team (and, if possible, the advisory group at meeting 3 – see Table 5). The analysis will explore differences in findings between health topic area (e.g. sexual health, physical activity) and look for common themes across all topic areas. Specialist NVivo software (Version 9.0, QSR international) for analysing qualitative data such as will be used to facilitate this synthesis. The thematic analysis will adhere to the principles of qualitative research in evidence synthesis. 47
The analysis of both outcome and process evaluations will take into consideration the generalisability of the evidence from international studies to the UK, in terms of cultural and socio-economic relevance, and replicability of education and health services. Potential temporal changes will also be examined, given that the findings of older studies may not be wholly relevant to current practice.
5. Project Management
This project is a collaboration between a multi-disciplinary team of people with both academic and practice experience in this topic, drawn from the University of Southampton (Medicine, Education) and Anglia Ruskin University. Collectively the team has extensive expertise in evidence synthesis, surveys, and qualitative interviews. The project will be based within Southampton Health Technology Assessments Centre (SHTAC), part of the Faculty of Medicine, under the supervision of the Principal Investigator, Dr Jonathan Shepherd.
The co-investigators of the project are:
-
Dr Marcus Grace (Senior Lecturer/Deputy Head of School of Education, University of Southampton)
-
Dr Jenny Byrne (Learning and Teaching Co-ordinator, School of Education, University of Southampton)
-
Professor Paul Roderick (Director of Public Health Sciences and Medical Statistics, School of Medicine, University of Southampton),
-
Dr Viv Speller (Independent consultant in public health development)
-
Ms Sue Dewhirst (Research Fellow, Public Health Sciences and Medical Statistics, School of Medicine, University of Southampton).
-
Dr Palo Almond (Head of Primary and Public Health, Faculty of Health and Social Care, Anglia Ruskin University).
The co-investigators will have strategic input all aspects of the project, and participate directly in some project tasks.
The research team also comprises:
-
Dr Debbie Hartwell, Research Fellow, Southampton Health Technology Assessments Centre (SHTAC).
-
Dr Karen White, Research Fellow, Southampton Health Technology Assessments Centre (SHTAC).
-
Karen Welch, Information Scientist, Southampton Health Technology Assessments Centre (SHTAC).
-
Other research fellows from within SHTAC will work on the project as required.
The research team will carry out the key project tasks, including survey related activities (e.g. questionnaire design, sampling, data analysis, interviews) and systematic review activities (e.g. inclusion/exclusion screening; data extraction; data synthesis).
Table 5 outlines the timelines for the project. Although the specific stages of the survey and systematic review are sequential there is likely to be overlap between them (e.g. studies meeting the inclusion criteria for the systematic review can be keyworded for the descriptive map while other studies are still being screened for inclusion).
| Month | Component of the study | |
|---|---|---|
| Survey | Systematic review | |
| 1. March 2010 | Devise + pilot survey questionnaire | Write protocol, devise and test search strategy |
| 2. April 2011 | Run literature searches | |
| 3. May (AG 1) | Sample + recruit ITT providers, survey ITT providers | |
| 4. June | Apply inclusion criteria | |
| 5. July | ||
| 6. August | Analysis of survey results | |
| 7. September | Evidence mapping | |
| 8. October (AG 2) | ||
| 9. November | Devise + pilot interview schedule | |
| 10. December | Data extraction + critical appraisal, update literature searches | |
| 11. January 2012 | Conduct follow-up interview with sub-sample of 20–25 providers | |
| 12. February | ||
| 13. March | Analyse interview results | Synthesis of outcome and process evaluations |
| 14. April 2012 (AG 3) | ||
| 15. May | Write-up of results (final report + journal articles) | |
| 16. June | External review of draft final report by Advisory Group, and other selected experts | |
| 17. July | Finalise report and submit to funder, finalise journal articles and submit to relevant journals | |
| 18. August | ||
6. Service users/public involvement
The project will be supported by a multi-disciplinary advisory group comprising: academics in the area of health and education; health and educational professionals (e.g. from the National Healthy Schools Programme); and methodologists (e.g. with experience of qualitative evidence synthesis). We will also endeavour to seek public participation by inviting teachers (e.g. with a responsibility for PSHE) and lay people with an interest in education and child health to join the group.
The aims of the group include: to provide advice and guidance to the research team on the scope and the conduct of the study; to notify the research team of any relevant research literature for the systematic review; to advise on dissemination of the findings.
As mentioned earlier, the advisory group will meet (at the University of Southampton) up to three times during the course of the project at strategic milestones. Advisory group members will be consulted where necessary between meetings (e.g. via e-mail or telephone) regarding specific issues.
References
- Denman S, Moon A, Parsons C, Stears D. The health promoting school: policy, research and practice. London: Routledge Falmer; 2002.
- Every child matters: change for children. London: HMSO; 2004.
- The children’s plan: building brighter futures. London: HMSO; 2007.
- Department for Education . Healthy Schools Toolkit n.d. URL: www.education.gov.uk/childrenandyoungpeople/healthandwellbeing/a0075278/healthy-schools-toolkit (accessed 5 July 2011).
- Choosing health: making healthy choices easier. London: HMSO; 2004.
- Healthy weight, healthy lives: a cross government strategy for England. London: HMSO; 2008.
- Healthy child programme from 5 to 19 years old. London: Department of Health; 2009.
- Macdonald A. Independent review of the proposal to make personal, social health and economic education (PSHE) statutory. London: HMSO; 2009.
- The importance of teaching: schools White Paper. London: The Stationary Office; 2010.
- Healthy lives, healthy people: our strategy for public health in England. London: The Stationary Office; 2010.
- Jourdan D, Samdal O, Diagne F, Carvalho GS. The future of health promotion in schools goes through the strengthening of teacher training at a global level. Promot Educ 2008;15:36-8.
- Speller V, Byrne J, Dewhirst S, Almond P, Mohebati L, Norman M, et al. Developing trainee school teachers’ expertise as health promoters. Health Educ 2010;110:490-507.
- Stewart-Brown S. What is the evidence on school health promotion in improving health or preventing disease and, specifically, what is the effectiveness of the health promoting schools approach?. Health Evidence Network report. Copenhagen: WHO Regional Office for Europe; 2006.
- Lister-Sharp D, Chapman S, Stewart-Brown S, Sowden A. Health promoting schools and health promotion in schools: two systematic reviews. Health Technol Assess 1999;3.
- Shek DT, Wai CL. Training workers implementing adolescent prevention and positive youth development programs: what have we learned from the literature?. Adolescence 2008;43:823-45.
- Ahmed N, Flisher AJ, Mathews C, Jansen S, Mukoma W, Schaalma H. Process evaluation of the teacher training for an AIDS prevention programme. Health Educ Res 2006;21:621-32.
- Wight D, Buston K. Meeting needs but not changing goals: evaluation of in-service teacher training for sex education. Oxf Rev Educ 2003;29:521-43.
- Gyarmathy VA, McNutt LA, Molnar A, Morse DL, DeHovitz J, Ujhelyi E, et al. Evaluation of a comprehensive AIDS education curriculum in Hungary – the role of good educators. J Adolesc 2002;25:495-508.
- Kinsman J, Harrison S, Kengeya-Kayondo J, Kanyesigye E, Musoke S, Whitworth J. Implementation of a comprehensive AIDS education programme for schools in Masaka District, Uganda. AIDS Care 1999;11:591-60.
- Deutschlander S. An analysis of training effects on school personnel’s knowledge, attitudes, comfort, and confidence levels toward educating students about HIV/AIDS in Pennsylvania. Int J Ment Health Addiction 2010;8:444-52.
- Basen-Engquist K, O’Hara-Tompkins N, Lovato CY, Lewis MJ, Parcel GS, Gingiss P. The effect of two types of teacher training on implementation of Smart Choices: a tobacco prevention curriculum. J Sch Health 1994;64:334-9.
- Kealey KA, Peterson AV, Gaul MA, Dinh KT. Teacher training as a behavior change process: principles and results from a longitudinal study. Health Educ Behav 2000;27:64-81.
- Perry CL, Murray DM, Griffin G. Evaluating the statewide dissemination of smoking prevention curricula: factors in teacher compliance. J Sch Health 1990;60:501-4.
- Ross JG, Luepker RV, Nelson GD, Saavedra P, Hubbard BM. Teenage health teaching modules: impact of teacher training on implementation and student outcomes. J Sch Health 1991;61:31-4.
- Botvin GJ, Baker E, Dusenbury L, Tortu S, Botvin EM. Preventing adolescent drug abuse through a multimodal cognitive-behavioral approach: results of a 3-year study. J Consult Clin Psychol 1990;58:437-46.
- Rohrbach LA, Graham JW, Hansen WB. Diffusion of a school-based substance abuse prevention program: predictors of program implementation. Prev Med 1993;22:237-60.
- Dewit DJ, And O. A process evaluation of a comprehensive drug education training package. J Alcohol Drug Educ 1996;41:102-22.
- Taggart VS, Bush PJ, Zuckerman AE, Theiss PK. A process evaluation of the District of Columbia ‘Know Your Body’ project. J Sch Health 1990;60:60-6.
- Ward DS, Saunders R, Felton GM, Williams E, Epping JN, Pate RR. Implementation of a school environment intervention to increase physical activity in high school girls. Health Educ Res 2006;21:896-910.
- Young DR, Steckler A, Cohen S, Pratt C, Felton G, Moe SG, et al. Process evaluation results from a school- and community-linked intervention: the Trial of Activity for Adolescent Girls (TAAG). Health Educ Res 2008;23:976-86.
- Buckley L, Sheehan M. A process evaluation of an injury prevention school-based programme for adolescents. Health Educ Res 2009;24:507-19.
- Hahn EJ, Noland MP, Rayens MK, Christie DM. Efficacy of training and fidelity of implementation of the life skills training program. J Sch Health 2002;72:282-7.
- Tones K, Tilford S. Health promotion: effectiveness, efficiency and equity. Cheltenham: Nelson Thornes; 2001.
- Healthy lives, brighter futures: the strategy for children and young people’s health. London: The Stationery Office; 2009.
- Your child, your schools, our future: building a 21st century schools system. London: The Stationery Office; 2009.
- Systematic reviews: CRD’s guidance for undertaking reviews in health care. York: University of York, Centre for Reviews and Dissemination; 2009.
- Higgins JP, Green S. Cochrane handbook for systematic reviews of interventions. The Cochrane Collaboration; 2009.
- Petticrew M, Roberts H. Systematic reviews in the social sciences: a practical guide. Oxford: Blackwell; 2006.
- Oliver S, Thomas J, Harden A, Shepherd J, Oakley A, Killoran A, et al. Public health evidence: tackling health inequalities. Oxford: Oxford University Press; 2006.
- Shepherd J, Kavanagh J, Picot J, Cooper K, Harden A, Barnett-Page E, et al. The effectiveness and cost-effectiveness of behavioural interventions for the prevention of sexually transmitted infections in young people aged 13 to 19: a systematic review and economic evaluation. Health Technol Assess 2010;14.
- Rees R, Kavanagh J, Burchett H, Shepherd J, Brunton G, Harden A, et al. HIV health promotion and men who have sex with men (MSM): a systematic review of research relevant to the development and implementation of effective and appropriate interventions. London: EPPI-Centre, Institute of Education, University of London; 2004.
- Harden A, Garcia J, Oliver S, Rees R, Shepherd J, Brunton G, et al. Applying systematic review methods to studies of people’s views: an example from public health research. J Epidemiol Community Health 2004;58:794-800.
- Thomas J, Kavanagh J, Tucker H, Burchett H, Tripney J, Oakley A. Accidental injury, risk-taking behaviour and the social circumstances in which young people (aged 12–24) live: a systematic review. London: EPPI-Centre, Social Science Research Unit, Institute of Education, University of London; 2007.
- Harden A. The quality of qualitative evidence: a review of assessment tools n.d.
- Harden A. Does Study Quality Matter in Systematic Reviews That Include Qualitative Research? n.d.
- Popay J, Arai L, Roberts H, Roen K. Preventing accidents in children – how can we improve our understanding of what really works?. London: Health Development Agency; 2003.
- Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med 2008;8.
- Oliver S, Oliver S, Peersman G. Using research for effective health promotion. Buckingham: Open University Press; 2001.
Protocol appendix 1: Search strategy for systematic review (Medline, via Ovid)
-
(train* adj2 (teacher* or schoolteacher* or educator*)).tw.
-
(teacher* adj2 (learn* or course* or development* or self?development* or program* or materials or seminar* or workshop* or conference* or inset or package* or video* or leaflet* or self?study or study)).tw.
-
1 or 2
-
teaching/
-
(teacher* or schoolteacher or educator* or pedagogy).tw.
-
4 or 5
-
education continuing/
-
inservice training/
-
continu* professional development.tw.
-
(curricul* adj5 (train* or development)).tw.
-
(inservice adj2 (train* or educat* or development)).tw.
-
(pre?service adj2 (train or educat* or development*)).tw.
-
(PGCE or ITT or SCITT or EBITT or “certificate in education”).tw.
-
“train* the trainer*”.tw.
-
“provider training”.tw.
-
“practice based learning”.tw.
-
“professional development”.tw.
-
(skill* adj2 (develop* or updat* or train* or gain*)).tw.
-
(implement* adj5 (intervention* or strateg* or program* or initiative* or pilot* or scheme*)).tw.
-
(program* adj2 (deliver* or implement*)).tw.
-
6 and (7 or 8 or 9 or 10 or 11 or 12 or 14 or 15 or 18 or 19 or 20)
-
(“teach the teacher*” or teaching the teacher*).tw.
-
3 or 21 or 22
-
Schools/ or (Curriculum/ and school*.tw.)
-
(school* or classroom* or “class room*” or pupil* or student* or adolescen* or teen* or child* or yout* or “young person” or “young people”).tw.
-
(“primary education” or “secondary education” or “elementary education” or “educational system*” or “educational setting*”).tw.
-
(“key stage 1” or “key stage 2” or “key stage 3” or “key stage 4”).tw.
-
(school* and (curriculum* or curricula*)).tw.
-
24 or 25 or 26 or 27 or 28
-
23 and 29
-
exp health promotion/ or exp health education/ or exp health behavior/
-
exp risk reduction behavior/
-
exp public health/
-
exp primary prevention/
-
exp preventive health services/
-
exp preventive medicine/
-
attitude to health/ or health knowledge, attitudes, practice/
-
(health adj2 (educat* or information or awareness or issue* or pilot* or program* or promot* or improv* or intervention* or initiative* or empower* or strateg* or prevent* or project* or campaign* or skill*)).tw.
-
(“good health” or “better health” or “healthy life” or “healthy lives” or “healthy lifestyle” or “healthy life style” or “healthy living” or “balanced life*”).tw.
-
((health adj2 child*) or adolesc*).tw.
-
(“healthy child*” or healthy adolesc*).tw.
-
(wellbeing or “well being” or safe*).tw.
-
exp sex education/ or exp sexual behavior/ or exp sexology/ or exp safe sex/ or exp unsafe sex/ or exp sexual abstinence/ or exp sexually transmitted diseases/ or exp sexually transmitted diseases, bacterial/
-
((prevent* or reduc* or educat* or promot* or increas* or decreas* or facilitat* or barrier* or encourag* or discourag*) adj2 (sex* or HIV or STI or STIs or STD* or chlamydia)).tw.
-
(sexual* transmit* adj3 (infect* or disease*)).tw.
-
(sexual adj2 (health or knowledge or behavio?r*)).tw.
-
“safe* sex”.tw.
-
(pregnancy adj2 prevent*).tw.
-
Contraception, Barrier/ or Contraception, Postcoital/ or Contraception/ or Contraception, Immunologic/ or Contraception Behavior/ or Pregnancy in Adolescence/
-
(contraception or contraceptive*).tw.
-
(STI or STIs or STD or STDs).tw.
-
herpes genitalis/ or exp acquired immunodeficiency syndrome/ or exp HIV infection/ or exp gonorrhea/ or exp syphilis/ or chlamydia/
-
condom*.tw.
-
Condoms, Female/ or Condoms/
-
Sexual Abstinence/
-
Coitus/
-
“sexual intercourse”.tw.
-
reproductive medicine/
-
puberty.mp.
-
Marijuana Abuse/ or Marijuana Smoking/
-
Substance-Related Disorders/
-
((prevent* or reduc* or educat* or promot*) adj2 (drug* or smoke or smoking or cigarette* or tobacco or substance* or glue or anti?smoking or alcohol or marijuana)).tw.
-
Smoking/ or Behavior, Addictive/ or Alcoholism/
-
((drug* or substance* or alcohol or cigarette* or marijuana) adj2 (“use” or misuse or abuse or abusing)).tw.
-
exp Exercise/
-
“Physical Education and Training”/
-
(“physical activit*” or “physical education” or exercise).tw.
-
((walk* or cycle or cycling or “active commut*”) adj3 school).tw.
-
“walking bus”.tw.
-
(games adj3 school*).tw.
-
“healthy lifestyle*”.tw.
-
(health* adj2 (diet* or food or eat*)).tw.
-
nutriti*.tw.
-
food habits/
-
(obes* or anti?obes*).tw.
-
exp Obesity/
-
exp Eating Disorders/
-
bulimia/ or bulimia nervosa/
-
(bulimia or bulimic).tw.
-
(unhealthy adj2 (diet* or food or eat*)).tw.
-
exp Mental Health/
-
exp Depression/
-
(depression or depressed or sucide or suicidal).tw.
-
Emotions/
-
(“emotional health” or “emotional wellbeing” or “emotional well-being” or “emotional inhibition*”).tw.
-
(bereav* or death or grief or grieving or sorrow).tw.
-
(“health and safety” or “road safety”).tw.
-
Accident Prevention/
-
(prevent* adj2 (injury or injuries)).tw.
-
exp First Aid/
-
Cardiopulmonary Resuscitation/
-
(“first aid” or CPR).tw.
-
Bullying/
-
(bullying or anti?bullying or cyberbullying or violence).tw.
-
exp Hygiene/ or Oral Hygiene/
-
Handwashing/
-
(“oral health” or “oral hygiene” or dentist*).tw.
-
Adaptation, Psychological/ or Social Adjustment/
-
(skill* adj2 (life or lives or living)).tw.
-
environment/ or social environment/
-
cancer*.tw.
-
unhealthy.tw.
-
(safe* adj2 sun).tw.
-
Skin Neoplasms/
-
(“keeping safe” or citizenship or “youth development”).tw.
-
exp cardiovascular diseases/
-
exp heart diseases/
-
child abuse/ or child abuse sexual/
-
((abuse or abusing) adj2 (physical* or mental*)).tw.
-
child advocacy/ or child welfare/
-
(“self image” or “self respect” or “self confidence” or “self esteem”).tw.
-
or/31–111
-
30 and 112
-
School Health Services/
-
School Nursing/
-
“national child measurement program*”.tw.
-
(school* adj2 health*).tw.
-
(PSHE or PSHEE).mp.
-
“whole school”.tw.
-
“personal social health”.tw.
-
“health promoti* school*”.tw.
-
(school* adj2 prevention).tw.
-
or/114–122
-
23 and 123
-
113 or 124
-
(editorial or comment or letter).pt.
-
125 not 126
-
(“medical student*” or “student doctor*” or “student nurs*” or “nurs* student*”).tw.
-
127 not 128
Appendix 2 Survey questionnaire (higher education institution course managers)
-
Please give your full name and title.
-
What is your job title?
-
Please state the name of your department and institution.
-
Please briefly describe your role.
-
Please tick the initial teacher training (ITT) course(s) that you manage. Tick as many as apply.
-
PGCE Early Years
-
PGCE Primary
-
PGCE Secondary
-
PGCE Key Stage 2/3
-
BEd with Qualified Teaching Status
-
BA or BSc with Qualified Teaching Status
-
Graduate Teacher Programme (GTP)
-
Registered Teacher Programme (RTP)
-
Overseas Teacher Training Programme (OTTP)
-
Teach First
-
-
Please enter the total numbers of students enrolled in 2010–11 for each level (i.e., primary/secondary, key stage 2/3) and for each programme that you manage.
-
Which of the following health and well-being/personal, social, health and economic education (PSHEE) topics are covered in your course? Tick as appropriate (e.g. in the university or on school placement or both).
-
If you ticked ‘Other’ in response to Question 7 please specify.
-
Please describe, as fully as possible, examples of how some of the health and well-being/PSHEE topics (as listed in Question 7/8) have been covered in your course. For example, through seminars, presentations, interactive workshops, e-learning, use of specialised resources, use of additional expertise, etc.
-
Are any of the health and well-being aspects of the course assessed? (in general and/or in relation to Qualified Teacher Status)?
-
Yes (go to Question 11)
-
No (go to Question 12)
-
-
(If your answer to Question 10 was ‘Yes’) Which method(s) of assessment for the health and well-being aspects of your course do you use? (Tick as many as apply)
-
Exam
-
Portfolio
-
Assignment
-
Questionnaire
-
Teaching observation
-
Presentation
-
Other (please specify)
-
-
Do you use any external organisations to provide information, resources or teaching to support the delivery of the health and well-being aspects of your course?
-
Yes (go to Question 13)
-
No (go to Question 15)
-
-
(If you ticked ‘Yes’ to question 12) Please tick which type of external organisation you use to support the delivery of the health and well-being aspects of your course. (Tick as many as apply)
-
Health Professional (e.g. Nurse, Dietitian, Health promotion specialist)
-
Youth Services
-
Local Authorities (e.g. Children's services, Healthy schools, Schools Advisory Service, Child Protection Officer)
-
Voluntary Organisation/Charity
-
Local University or College
-
Sports Organisation (e.g. sports coaches, sports partnerships)
-
Local School
-
Other (please specify)
-
-
For each of the external organisations you have ticked in Question 13 please provide brief details of the support you have received.
-
Please estimate the approximate percentage of time spent, as a whole, covering health and well-being in your course
-
Less than 5%
-
5 to 9%
-
10 to 14%
-
15 to 19%
-
20 to 24%
-
25 to 49%
-
50% and higher
-
-
Do you have further comments you would like to make about the health and well-being aspects of your course? (If none then please go to Question 17)
-
How important in your view is it to emphasise the health and well-being of pupils and staff/PSHEE in the initial teacher training curriculum? (Please choose one option)
-
Very important
-
Important
-
Of some importance
-
Not important
-
-
In what ways do you anticipate that the content, delivery or structure of your course is likely to change in the near future? (e.g. in response to changes in educational policy or funding)
-
We may contact you again in a few months to request a research interview to find out more about some of the things you've told us about in this questionnaire. Would you be willing to be contacted?
-
Yes (go to Question 20)
-
No (go to Question 21)
-
-
If your answer to question 19 was ‘Yes’, please provide us with details so we can contact you.
-
It would be very helpful to receive copies of any of the course materials for the health and well-being aspects of your course that you would be prepared to share with us. You could send these by e-mail or by post to: Dr Jonathan Shepherd, Southampton Health Technology Assessments Centre (SHTAC), University of Southampton, 1st Floor Epsilon House, Enterprise Road, Southampton Science Park, Southampton, SO16 7NS (e-mail: jps@soton.ac.uk). Please list the materials available in the box below.
Appendix 3 Interview schedule
Question 1
Before we start discussing the detail of your course I wondered if you could you tell me a bit about your professional background?
Probe a): What professional experience or training have you had, if any, around health and well-being [issues]?
If they mention training or experience specific to health and well-being, then
Probe b): How do you think your professional background/previous experience has influenced your approach to health and well-being in the course(s) that you manage, if at all?
Probe c): Have you been involved with setting up any health and well-being aspects to the course?
Question 2
Refer to the individual organisation proforma to recap on the information supplied in the questionnaire, course information on the organisation website and any other background information such as any relevant research areas on the website.
Prompt: I'd like to start by recapping on the information you supplied on the questionnaire and other information on your organisation website.
Can you tell me whether there have been any significant changes to your course(s) since the start of the new academic year?
Then recap on the numbers of trainees, course overview, course(s) content.
Question 3
Ask as appropriate, according to questionnaire responses.
On the questionnaire you mentioned . . . (named initiative, etc.) the health and well-being/PSHE aspects of your course. Can you tell me more about that?
Probe a): What influenced the inclusion of this on your course?
Probe b): What has helped you to implement particular changes?
Probe c): What has hindered the implementation?
Probe d): How successful, or otherwise, are they?
Probe e): If not successful, what are the barriers?
If not mentioned on the questionnaire:
Please can you tell me whether health and well-being/PSHE is covered in your course(s). Yes/no? If so, how is it covered?
Probe f): Do you have any particular initiatives in place to promote health and well-being?
If so, can you describe these initiatives?
Probe g): How successful, or otherwise are they?
Probe h): What difference have they made in your opinion (to the students/course/staff, etc.)?
Probe i): Do they take place in school and/or university settings?
Probe j): On school placements who in the school is responsible for ensuring that there is an opportunity for students to teach PSHEE? Who provides the mentoring for this activity? (e.g. the form tutor/professional tutor/subject mentor)
Probe k): How long? (a session, lecture, whole day, module, etc.)
Probe l): Compulsory or optional?
Probe m): Subject based or whole cohort?
Question 4
For any health and well-being aspects that do take place, when in the course and at what time during the academic year are they addressed?
Prompt: Beginning of the course/before school placements, middle/between placements, towards the end? If undergraduate course, which year?
Probe a): Why do they take place at that time? What are the advantages/disadvantages?
Probe b): Do you feel there is enough time given to health and well-being in general on the course?
Probe c): If no, do you think it's important to include more? If so how would you do this?
Question 5
You mentioned on the questionnaire that [external agency(ies)/staff member(s)] have an input into the health and well-being aspects of your course. Can you describe how/why this input came about?
Probe a): For external agencies (if not already explained): Who? Where are they from? Which organisation? How were they contacted? Do they require payment? How long have they worked with you? What are the advantages/disadvantages of working with them?
Probe b): For internal staff/course tutors are leading on health issues ask: How are the tutors/directors trained to facilitate the health and well-being aspects of the course? What is their expertise in this field?
Probe c): From the initial survey results it appears that health professionals are not widely used to train teachers. Is this the same in your institution? (refer to their questionnaire responses)
Probe d): If so why? What do you think are the challenges of involving health professionals in teacher training?
Prompt: Health professionals could include: teenage pregnancy & family planning agencies, NHS public health agencies, Healthy Schools co-ordinators, health promotion specialists, dieticians, drug and alcohol agencies, voluntary agencies.
Question 6
We have observed in our analysis of the questionnaire that sex and relationships, drugs, alcohol and smoking education receive less attention compared to other topics in teacher training courses.
-
(a) In your view how important is it that these topics are covered?
Probe a): (If not already covered) How do you address these topics on your course, if at all?
Probe b): Do students have to teach SRE while on their placement, do they have to observe an SRE lesson, or neither?
Probe c): Who mentors students in the teaching of SRE in the school?
-
(b) In your view (or, if appropriate, in your experience) what are the particular challenges to including these on a teacher training course?
Question 7
Is there funding available to include particular aspects of health and well-being on your course(s) or for the initiatives mentioned on questionnaire? (Yes/no)
(Ask the next few questions/probes sensitively)
If so, can you indicate how much funding there is approximately?
Who provides the funding for this work/where does it come from?
Prompts: For example, your institution, your department, local education authority/Children's Services, the TDA, health services, voluntary sector.
(If not already covered)
Probe a): What type of work around health and well-being on the course(s) requires funding?
Probe b): Has the cost/funding of health and well-being ever been an issue?
Probe c): If there is no ‘extra’ funding, how do you address the provision of training in health and well-being?
Probe d): What do you think will be the state of funding for health and well-being on your course in the future?
Probe e): What kind of funding do you think should be available in the future for H&W in teacher training courses, if any?
Question 8
You mentioned in the questionnaire that your students are/are not assessed in the area of health and well-being. Please can you tell me more about this? Which elements of health and well-being are assessed?
Probes: Why do you assess in this way? How do you carry out the assessment? In which setting? (University or in school) By whom?
Prompt: For example, are they measured against criteria, such as QTS Standard 21, which refers to health and safety?
Probe: If they are not assessed, is there a reason why? Is there likely to be an element of assessment in the future?
Question 9
Does your course(s) address the issue of the health and well-being of teachers in schools? If so how?
Probe a): How effective do you think it is in addressing staff health?
Probe b): If not, is this something that you might address in future?
Probe c): If so why do you feel it's important to address staff health?
Probe d): How do you address the health and well-being of the trainees themselves?
Or, if mentioned on the questionnaire . . .
You indicated that staff health and well-being was covered/an important aspect of your course. How is this addressed?
The following 2 questions may have already been covered*. If so, you can reiterate the key challenges and facilitators at this point.
Question 10*
What key challenges have you experienced/would you experience in addressing health and well-being in the teacher training curriculum?
OR
You mentioned this/these challenges in the questionnaire, please can you expand on this . . .
OR
You didn't mention any challenges, is there a reason for this?
Prompts: For example: Lack of time? Lack of resources? Lack of expertise? Organisational/departmental/administrative considerations? Health considered a relatively low priority? Lack of student engagement?
Probe: How do you think you might address these challenges?
Question 11*
(May be no need for this question if already covered)
What has helped/would help you or your organisation in addressing health and well-being in the teacher training curriculum?
Prompts: For example: Your own background/interest/and those around you? Good professional networks/contacts? Protected time/resources within the curriculum? Supportive school placement staff? Ethos of your own organisation/school(s)?
Question 12
Please can you tell me about any changes that might be happening to your course(s) in the future that we have not already covered.
Prompt: Check if any changes were mentioned in questionnaire responses.
Probe a): If yes, ask What? When? How? Why? If no, why not?
Prompt: For example, better timing, more time/resources, more institutional support, making it more relevant/meaningful to the students, the inclusion of further topics?
Probe b): How will this affect the health and well-being components of the course(s)?
Probe c): How, if at all, do you think training around health and well-being could be improved/organised differently in your course(s)?
Probe d): Does this apply to all the courses you are responsible for or do they vary?
Probe e): For example, how do you think any changes in education policy may affect the course or it's health and well-being content?
Probe: Do you have a support mechanism or network to help you face any changes that may occur? (e.g. TDA, other training organisations)
Question 13
Is there anything else you would like to say in relation to what you've said already?
Notes to interviewer:
-
Tell them that this concludes the interview and switch off the tape recorder.
-
Before finishing ask the interviewee if they would like to see a copy of the interview transcript and whether they would like to be kept informed of the findings.
-
Thank them for their time.
Appendix 4 MEDLINE (Ovid) literature search strategy
-
(train* adj2 (teacher* or schoolteacher* or educator*)).tw.
-
(teacher* adj2 (learn* or course* or development* or self?development* or program* or materials or seminar* or workshop* or conference* or inset or package* or video* or leaflet* or self?study or study)).tw.
-
1 or 2
-
teaching/
-
(teacher* or schoolteacher or educator* or pedagogy).tw.
-
4 or 5
-
education continuing/
-
inservice training/
-
continu* professional development.tw.
-
(curricul* adj5 (train* or development)).tw.
-
(inservice adj2 (train* or educat* or development)).tw.
-
(pre?service adj2 (train or educat* or development*)).tw.
-
(PGCE or ITT or SCITT or EBITT or “certificate in education”).tw.
-
“train* the trainer*”.tw.
-
“provider training”.tw.
-
“practice based learning”.tw.
-
“professional development”.tw.
-
(skill* adj2 (develop* or updat* or train* or gain*)).tw.
-
(implement* adj5 (intervention* or strateg* or program* or initiative* or pilot* or scheme*)).tw.
-
(program* adj2 (deliver* or implement*)).tw.
-
6 and (7 or 8 or 9 or 10 or 11 or 12 or 14 or 15 or 18 or 19 or 20)
-
(“teach the teacher*” or teaching the teacher*).tw.
-
3 or 21 or 22
-
Schools/ or (Curriculum/ and school*.tw.)
-
(school* or classroom* or “class room*” or pupil* or student* or adolescen* or teen* or child* or yout* or “young person” or “young people”).tw.
-
(“primary education” or “secondary education” or “elementary education” or “educational system*” or “educational setting*”).tw.
-
(“key stage 1” or “key stage 2” or “key stage 3” or “key stage 4”).tw.
-
(school* and (curriculum* or curricula*)).tw.
-
24 or 25 or 26 or 27 or 28
-
23 and 29
-
exp health promotion/ or exp health education/ or exp health behavior/
-
exp risk reduction behavior/
-
exp public health/
-
exp primary prevention/
-
exp preventive health services/
-
exp preventive medicine/
-
attitude to health/ or health knowledge, attitudes, practice/
-
(health adj2 (educat* or information or awareness or issue* or pilot* or program* or promot* or improv* or intervention* or initiative* or empower* or strateg* or prevent* or project* or campaign* or skill*)).tw.
-
(“good health” or “better health” or “healthy life” or “healthy lives” or “healthy lifestyle” or “healthy life style” or “healthy living” or “balanced life*”).tw.
-
((health adj2 child*) or adolesc*).tw.
-
(“healthy child*” or healthy adolesc*).tw.
-
(wellbeing or “well being” or safe*).tw.
-
exp sex education/ or exp sexual behavior/ or exp sexology/ or exp safe sex/ or exp unsafe sex/ or exp sexual abstinence/ or exp sexually transmitted diseases/ or exp sexually transmitted diseases, bacterial/
-
((prevent* or reduc* or educat* or promot* or increas* or decreas* or facilitat* or barrier* or encourag* or discourag*) adj2 (sex* or HIV or STI or STIs or STD* or chlamydia)).tw.
-
(sexual* transmit* adj3 (infect* or disease*)).tw.
-
(sexual adj2 (health or knowledge or behavio?r*)).tw.
-
“safe* sex”.tw.
-
(pregnancy adj2 prevent*).tw.
-
Contraception, Barrier/ or Contraception, Postcoital/ or Contraception/ or Contraception, Immunologic/ or Contraception Behavior/ or Pregnancy in Adolescence/
-
(contraception or contraceptive*).tw.
-
(STI or STIs or STD or STDs).tw.
-
herpes genitalis/ or exp acquired immunodeficiency syndrome/ or exp HIV infection/ or exp gonorrhea/ or exp syphilis/ or chlamydia/
-
condom*.tw.
-
Condoms, Female/ or Condoms/
-
Sexual Abstinence/
-
Coitus/
-
“sexual intercourse”.tw.
-
reproductive medicine/
-
puberty.mp.
-
Marijuana Abuse/ or Marijuana Smoking/
-
Substance-Related Disorders/
-
((prevent* or reduc* or educat* or promot*) adj2 (drug* or smoke or smoking or cigarette* or tobacco or substance* or glue or anti?smoking or alcohol or marijuana)).tw.
-
Smoking/ or Behavior, Addictive/ or Alcoholism/
-
((drug* or substance* or alcohol or cigarette* or marijuana) adj2 (“use” or misuse or abuse or abusing)).tw.
-
exp Exercise/
-
“Physical Education and Training”/
-
(“physical activit*” or “physical education” or exercise).tw.
-
((walk* or cycle or cycling or “active commut*”) adj3 school).tw.
-
“walking bus”.tw.
-
(games adj3 school*).tw.
-
“healthy lifestyle*”.tw.
-
(health* adj2 (diet* or food or eat*)).tw.
-
nutriti*.tw.
-
food habits/
-
(obes* or anti?obes*).tw.
-
exp Obesity/
-
exp Eating Disorders/
-
bulimia/ or bulimia nervosa/
-
(bulimia or bulimic).tw.
-
(unhealthy adj2 (diet* or food or eat*)).tw.
-
exp Mental Health/
-
exp Depression/
-
(depression or depressed or sucide or suicidal).tw.
-
Emotions/
-
(“emotional health” or “emotional wellbeing” or “emotional well-being” or “emotional inhibition*”).tw.
-
(bereav* or death or grief or grieving or sorrow).tw.
-
(“health and safety” or “road safety”).tw.
-
Accident Prevention/
-
(prevent* adj2 (injury or injuries)).tw.
-
exp First Aid/
-
Cardiopulmonary Resuscitation/
-
(“first aid” or CPR).tw.
-
Bullying/
-
(bullying or anti?bullying or cyberbullying or violence).tw.
-
exp Hygiene/ or Oral Hygiene/
-
Handwashing/
-
(“oral health” or “oral hygiene” or dentist*).tw.
-
Adaptation, Psychological/ or Social Adjustment/
-
(skill* adj2 (life or lives or living)).tw.
-
environment/ or social environment/
-
cancer*.tw.
-
unhealthy.tw.
-
(safe* adj2 sun).tw.
-
Skin Neoplasms/
-
(“keeping safe” or citizenship or “youth development”).tw.
-
exp cardiovascular diseases/
-
exp heart diseases/
-
child abuse/ or child abuse sexual/
-
((abuse or abusing) adj2 (physical* or mental*)).tw.
-
child advocacy/ or child welfare/
-
(“self image” or “self respect” or “self confidence” or “self esteem”).tw.
-
or/31-111
-
30 and 112
-
School Health Services/
-
School Nursing/
-
“national child measurement program*”.tw.
-
(school* adj2 health*).tw.
-
(PSHE or PSHEE).mp.
-
“whole school”.tw.
-
“personal social health”.tw.
-
“health promoti* school*”.tw.
-
(school* adj2 prevention).tw.
-
or/114-122
-
23 and 123
-
113 or 124
-
(editorial or comment or letter).pt.
-
125 not 126
-
(“medical student*” or “student doctor*” or “student nurs*” or “nurs* student*”).tw.
-
127 not 128
Appendix 5 Inclusion/exclusion criteria
Inclusion/exclusion worksheet for round 1 screening (titles and abstracts)
| Study name or number: | |||
| Does the reference mention health and well-beinga within schools?b (e.g. health promotion, health education) | Yes | Unclear | No |
| ↓ | ↓ | → | |
| next question | next question | EXCLUDE | |
| Does the reference mention: | Yes | Unclear | No |
| the training of teachers in relation to the promotion of health and well-being in schools? | ↓ | ↓ | → |
| and/or | next question | next question | EXCLUDE |
| the implementation of the promotion of health and well-being in schools by teachers?c | (However, if reference reports an evaluation of a school-based health and well-being intervention, but there is no mention of teachers then mark as ‘RETRIEVE 1’) | ||
| (either trainee or qualified teachers) | |||
| Does the reference report researchd into: | Yes | Unclear | No |
| the processes of teacher training in relation to the promotion of health and well-being in schools? (see Box A)/the implementation of the promotion of health and well-being in schools by teachers?c | ↓ | ↓ | → |
| and/or | next question | next question | EXCLUDE |
| the outcomes of teacher training in relation to the promotion of health and well-being in schools? (see Box B) | |||
| Final decision | RETRIEVE | UNCLEAR (discuss) | EXCLUDE |
-
Acceptability to the teachers of the training and of the health-promotion intervention itself (e.g. appeal, enjoyment, relevance to professional goals and personal values)
-
Resources and costs used to train the teachers
-
Teachers' general reflexivity of their health-promoting role and practice
-
Implementation of the training programme/the health-promotion intervention
-
Skills and training of the teachers
-
Accessibility/programme reach
-
Collaboration and partnerships
-
Quality of intervention materials
| Outcomes | |
|---|---|
| Teachers | Pupils |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Inclusion/exclusion worksheet for round 2 screening (full papers)
Text in bold represents amendments made to the criteria during their piloting for full papers in November 2011.
| Study name or number: | |||
| Does the reference mention health and well-beinga within schools?b (e.g. health promotion, health education) | Yes | Unclear | No |
| ↓ | ↓ | → | |
| next question | next question | EXCLUDE1 | |
| Does the reference mention the training of teachers in relation to the promotion of health and well-being in schools? (either trainee or qualified teachers, including head teachers) | Yes | Unclear | No |
| ↓ | ↓ | → | |
| next question | next question | EXCLUDE2 | |
| Does the reference report research findingsc into: | Yes | Unclear | No |
| the processes of teacher training in relation to the promotion of health and well-being in schools? (see Box A) | ↓ | ↓ | → |
| and/or | next question | next question | EXCLUDE3 |
| the outcomes of teacher training in relation to the promotion of health and well-being in schools? (see Box B) | |||
| The training provided and results of the research should be reported in adequate detail. When there is minimal reporting the reviewer should exclude the study. If in doubt about the adequacy of the detail the reviewer should include it and if necessary discuss with the second reviewer | |||
| Final decision | INCLUDE | UNCLEAR (discuss) | EXCLUDE |
-
Acceptability and adequacy to the teachers of the training and of the health-promotion intervention itself (e.g. appeal, enjoyment, relevance to professional goals and personal values)
-
Resources and costs used to train the teachers
-
Teachers' general reflexivity of their health-promoting role and practice
-
Implementation of the training programme/the health-promotion intervention
| Outcomes | |
|---|---|
| Teachers | Pupils |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Appendix 6 Results of the updated literature search
The literature search of electronic bibliographic databases described in Chapter 5 (see Literature searching) was updated in April 2012 to identify any relevant research published since the initial search in April 2011.
A total of 1897 references were identified:
-
following deduplication a total of 1690 references were screened on title and abstract (round 1)
-
1643 references were excluded
-
47 references were to be retrieved for further inspection (round 2)
-
40 full papers were retrieved and screened:
-
14 papers met inclusion criteria for the descriptive map
-
25 papers were excluded
-
one paper was judged unclear (non-English language)
-
-
seven references were unobtainable (e.g. dissertations, unpublished reports).
Only two of the 14 papers meeting the inclusion criteria evaluated the training of pre-service teachers (Riggs et al. 222 and Robinson et al. 223) and would therefore be relevant for the in-depth synthesis (meeting the inclusion criteria reported in Chapter 6 of this report), increasing the total number of studies to 22. It is unlikely that inclusion of these two studies would significantly alter the findings of the review.
References for the 14 studies
- Armour KM, Makopoulou K. Great expectations: teacher learning in a national professional development programme. Teach Teach Educ 2012;28:336-46.
- Bernard ME, Walton K. The effect of You Can Do It! Education in six schools on student perceptions of wellbeing, teaching learning and relationships. J Student Wellbeing 2011;5:22-37.
- Breslin G, Murphy M, Mckee D, Delaney B, Dempster M. The effect of teachers trained in a fundamental movement skills programme on children’s self-perceptions and motor competence. Eur Phys Educ Rev 2012;18:114-26.
- Burns ER. Healthy Lungs: cancer education for middle school teachers using a ‘train and equip’ method. J Cancer Educ 2012;27:179-85.
- Darvin J. Situated performances in a graduate teacher education course: an inquiry into the impact of Cultural and Political Vignettes (CPVs). Teachers Teach 2011;17:345-64.
- Fahlman M, McCaughtry N, Martin J, Shen B. Efficacy, intent to teach, and implementation of nutrition education increases after training for health educators. Am J Health Educ 2011;42:181-90.
- Kulinna PH, McCaughtry N, Martin J, Cothran D. Effects of continuing professional development on urban elementary students’ knowledge. Res Q Exerc Sport 2011;82:580-4.
- Panunzio MF, Caporizzi R, Antoniciello A, Cela EP, D’Ambrosio P, Ferguson LR, et al. Training the teachers for improving primary schoolchildren’s fruit and vegetables intake: a randomized controlled trial. Ann Ig 2011;23:249-60.
- Riggs AD, Rosenthal AR, Smith-Bonahue T. The impact of a combined cognitive-affective intervention on pre-service teachers’ attitudes, knowledge, and anticipated professional behaviors regarding homosexuality and gay and lesbian issues. Teach Teach Educ 2011;27:201-9.
- Robinson DB, Meyer M. Health education and interactive drama: findings from a service learning project. Health Educ J 2012;71:219-28.
- Shek DT, Chak YL. Training evaluation of the Secondary 3 Training Program of the Project P.A.T.H.S. in Hong Kong. Int J Adolesc Med Health 2011;23:333-9.
- Suarez-Mutis MC, Coura JR, Massara CL, Schall VT. Effect of a participatory educational program on primary school teachers’ knowledge of malaria. Rev Saude Publica 2011;45:931-7.
- Till J, Ferkins L, Handcock P. Physical activity based professional development for teachers: the importance of whole school involvement. Health Educ J 2011;70:225-35.
- Wood L, Goba L. Care and support of orphaned and vulnerable children at school: helping teachers to respond. S Afr J Educ 2011;31:275-90.
Appendix 7 Systematic review synthesis data extraction form
1. Basic study details
Data extracted by:
Checked by:
| Study lead author & ID | Publication year | Year study conducted |
| Country | Location (e.g. town/city/region) | Funder |
| Study aims/objective/purpose (summarise the rationale for the study, including the rationale for studying pre-service teachers) | ||
| Research question(s) |
2. Topic areas
| Topic(s)* | Description (where applicable) |
|---|---|
3. Details of study population
| Type of population | Description (where applicable) |
|---|---|
| Pre-service [e.g. type of course enrolled in, including subject area; demographic details (e.g. age/gender/ethnicity)] | |
| Number of pre-service teachers | |
| In-service (e.g. type of school located in, subject areas taught, teaching experience) | |
| Number of in-service teachers | |
| Level of education |
4. Details of training/intervention
| Name of the intervention/training programme (e.g. any specific name given) | |
| Training content | Description (where applicable) |
|---|---|
| Information provision | |
| Skills development (general) | |
| Skills development – behaviour change techniques | |
| Skills development – to identify health problems and/or how to refer | |
| Skills development – pedagogy of health | |
| Awareness and attitudes | |
| Planning and implementation methods | |
| Other (specify) | |
| Training content not stated/unclear | |
| Training format | Description (where applicable) |
| Lecture/seminar/presentation | |
| Workshop | |
| Discussion groups/group work | |
| Computer/digital media | |
| Teaching practice | |
| Skills demonstration/practice | |
| Support post-initial training | |
| Video | |
| Other (specify) | |
| Training format not stated/unclear | |
| Training intensity | Description (where applicable) |
| ≤ 1 day | |
| 2–5 days | |
| 6–10 days | |
| > 10 days | |
| Training length not stated/unclear | |
| Training duration | Description (where applicable) |
| ≤ 1 day | |
| 2–7 days | |
| > 1–4 weeks | |
| > 1–3 months | |
| 4–6 months | |
| 7–12 months | |
| > 12 months | |
| Training duration not stated/unclear | |
| Teacher trainer | Description (where applicable) |
| Researcher/academic | |
| Health professional | |
| Specialist trainer | |
| Education practitioner | |
| Psychologist/counsellor | |
| Computer | |
| Video | |
| Lay person/volunteer | |
| Other (specify) | |
| Trainer unclear/not stated | |
| Theory based | Describe (where applicable) |
| Theory reported | |
| Theory not reported |
5. Study measures
| Processes/issues examined | Description (where applicable) |
|---|---|
| Acceptability and adequacy to the teachers of the training, and of the health-promotion intervention | |
| Resources and costs used to train the teachers | |
| Teachers' general reflexivity of their health-promoting role and practice | |
| Implementation of the training programme/the health-promotion intervention | |
| General organisation/administration of the training | |
| Other (specify) | |
| Processes unclear/not stated |
| Outcomes of teacher training | Description (where applicable) |
|---|---|
| Teacher outcomes | |
| Knowledge of health in general and specific health topic to be addressed | |
| Skills (e.g. ability to teach health-related behaviour change skills) | |
| Confidence/self-efficacy to provide health-promotion intervention | |
| Attitudes towards health promotion | |
| Motivation and intentions to provide health-promotion intervention | |
| Awareness and understanding of whole-school approaches to health promotion, and wider determinants of health | |
| Health literacy | |
| Delivery of the intervention/teaching practice around health | |
| Unintended/unanticipated outcomes (e.g. increasing health inequalities) | |
| Teachers' values | |
| Biological and physical outcomes (e.g. weight change) | |
| Mental health outcomes | |
| Other (specify) | |
| Teacher outcomes not stated | |
| Pupil outcomes | |
| Knowledge of relevant health topic (e.g. risk factors, prevention, well-being) | |
| Attitudes towards health-related behaviour/intervention | |
| Intentions to adopt health-related behaviour | |
| Self-efficacy to adopt health-related behaviour | |
| Biological and physical outcomes (e.g. weight change) | |
| Health-related behaviour (e.g. smoking) | |
| Health literacy | |
| Educational attainment | |
| Mental health outcomes | |
| Unintended/unanticipated outcomes (e.g. differential health gain) | |
| Other (specify) | |
| Pupil outcomes not stated | |
6. Methodological characteristics and critical appraisal
| Description (where applicable) | |
|---|---|
| Study design classification* | |
| Author's description of study design | |
| Data collection instrument(s) used (e.g. questionnaire/interview/clinical test/observation) | |
| Were data collection instruments reported to be validated? (note if they have been used in previous studies) | |
| Timing of data collection (e.g. in relation to the training/intervention, pre–post measurements) | |
| Data analysis method (for controlled designs – e.g. intention to treat/treatment received) | |
| Unit of data analysis (for controlled designs – were the results reported according to the unit of allocation?) | |
| Statistical procedures used (summarise any statistical procedures/tests used) | |
| Qualitative data analysis procedures used (summarise the methods used to analyse any qualitative data collected) | |
| Were participants asked for their informed consent? | |
| Reviewer's comments on study methodological characteristics and quality (add in any comments that may be relevant) |
7. Study results
[Summarise the results of the study in the subsections below. It is difficult to specify how much detail to go into, as this will vary from study to study. You may need to report some results verbatim for clarity using quotation marks and specifying the page number (e.g. where description by the authors might be ambiguous and open to misinterpretation). As a general guide do not reproduce results wholesale, especially where data are extensive. However, it is ok to describe what results are given and how they are presented, and if necessary say ‘data not extracted’. Note that sometimes results may be reported within the discussion section of a publication.]
Teacher outcomes
(Add rows to the table for all the outcomes reported. Where data have been reported but are not extracted summarise and state ‘data not extracted’)
Pupil outcomes
(Add rows to the table for all the outcomes reported)
Process
(Add rows to the table for all the processes reported)
Barriers and facilitators
Summarise any data reported which the authors state to be barriers and/or facilitators to teacher training around health. If none are explicitly reported as barriers/facilitators but can be inferred by the reviewers state them here (noting that they have been inferred).
8. Reviewer's general comments on the study
(Write in any comments on the study in general, e.g. your interpretation of the findings, methodological quality, etc.)
9. Mapping discrepancies
List any discrepancies for this study that have you have noticed with the keywording database
10. Bibliography check
Check to see whether any studies are cited in the publication that may meet our inclusion criteria, and if so list them below. If none, state so.
Appendix 8 Systematic review synthesis critical appraisal criteria
Risk of bias criteria for single cohort before-and-after studies (adapted from the Cochrane Effective Practice and Organisation of Care Group criteria228 for interrupted time series designs)
-
Was the intervention independent of other changes?
Score ‘low risk’ if there are compelling arguments that the intervention occurred independently of other changes over time and the outcome was not influenced by other confounding variables/historic events during the study period. If events/variables identified, note what they are. Score ‘high risk’ if reported that intervention was not independent of other changes in time.
-
Was the intervention unlikely to affect data collection?
Score ‘low risk’ if reported that intervention itself was unlikely to affect data collection (e.g., sources and methods of data collection were the same before and after the intervention). Score ‘high risk’ if the intervention itself was likely to affect data collection (e.g. any change in source or method of data collection reported).
-
Were incomplete outcome data adequately addressed?*
Score ‘low risk’ if missing outcome measures were unlikely to bias the results (e.g. the proportion of missing data was similar in the pre- and post-intervention periods or the proportion of missing data was less than the effect size, i.e. unlikely to overturn the study result). Score ‘high risk’ if missing outcome data were likely to bias the results. Score ‘unclear risk’ if not specified in the paper (do not assume 100% follow-up unless stated explicitly).
-
Was the study free from selective outcome reporting?
Score ‘low risk’ if there is no evidence that outcomes were selectively reported (e.g. all relevant outcomes in the methods section are reported in the results section). Score ‘high risk’ if some important outcomes are subsequently omitted from the results. Score ‘unclear risk’ if not specified in the paper.
-
Was the study free from other risks of bias?
Score ‘low risk’ if there is no evidence of other risk of biases, e.g. should consider if seasonality is an issue (i.e. if January to June comprises the pre-intervention period and July to December the post, could the ‘seasons’ have caused a spurious effect).
*If some primary outcomes were assessed blindly or affected by missing data and others were not, each primary outcome can be scored separately.
| Question | Judgement (high risk, low risk, unclear) | Reviewer's comment |
|---|---|---|
| 1. Was the intervention independent of other changes? | ||
| 2. Was the intervention unlikely to affect data collection? | ||
| 3. Were incomplete outcome data adequately addressed? | ||
| 4. Was the study free from selective outcome reporting? | ||
| 5. Was the study free from other risks of bias? |
Quality assessment criteria for process evaluations (adapted from Shepherd and colleagues47)
| Question | Judgement (underline as appropriate) | Reviewer's comments (add in comments to support your judgement) |
|---|---|---|
| 1. Were steps taken to increase rigour/minimise bias and error in the sampling for the process evaluation? Consider whether the sampling strategy was appropriate to the questions posed in the process evaluation (e.g. was the strategy well reasoned and justified?); attempts were made to include all relevant stakeholders and/or obtain a diverse sample (think about who might have been excluded who may have had a different perspective to offer); characteristics of the sample critical to the understanding of the study context and findings were presented (i.e. do we know who the participants are in terms of, for example, role in the intervention/evaluation, basic sociodemographics, etc.) | 1.1 Yes, a fairly thorough attempt was made (please specify) | |
| 1.2 Yes, several steps were taken (please specify) | ||
| 1.3 Yes, a few steps were taken (please specify) | ||
| 1.4 Unclear (please specify) | ||
| 1.5 No, not at all (please specify) | ||
| 2. Were steps taken to increase rigour/minimise bias and error in the data collected for the process evaluation? Consider whether data collection tools were piloted/(if quantitative) validated data collection was comprehensive, flexible and/or sensitive enough to provide a complete and/or vivid and rich description/evaluation of the processes involved in the intervention [e.g. Did the researchers spend sufficient time at the site/with participants? Did they keep ‘following up’? Were steps taken to ensure that all participants were able and willing to contribute (e.g. confidentiality, language barriers, power relations between adults and young people)? Was more than one method of data collection used? Was there a balance between closed and open-ended data collection methods?] | 2.1 Yes, a fairly thorough attempt was made (please specify) | |
| 2.2 Yes, several steps were taken (please specify) | ||
| 2.3 Yes, a few steps were taken (please specify) | ||
| 2.4 Unclear (please specify) | ||
| 2.5 No, not at all (please specify) | ||
| 3. Were steps taken to increase rigour/minimise bias and error in the analysis of the process data? Consider whether data analysis methods were systematic (e.g. was a method described/can a method be discerned?); diversity in perspective was explored; the analysis was balanced in the extent to which it was guided by preconceptions or by the data (i.e. participants' views, researcher observations, etc.); the analysis sought to rule out alternative explanations for findings (in qualitative research this could be done by, for example, searching for negative cases/exceptions, feeding back preliminary results to participants, asking a colleague to review the data, or reflexivity; in quantitative research this may be done by, for example, significance testing) | 3.1 Yes, a fairly thorough attempt was made (please specify) | |
| 3.2 Yes, several steps were taken (please specify) | ||
| 3.3 Yes, a few steps were taken (please specify) | ||
| 3.4 Unclear (please specify) | ||
| 3.5 No, not at all (please specify) | ||
| 4. Were the findings of the process evaluation grounded in/supported by the data? Consider whether enough data are presented to show how the authors arrived at their findings; the data presented fit the interpretation/support claims about patterns in data; the data presented illuminate/illustrate the findings; (for qualitative studies) quotes are numbered or otherwise identified so that the reader can see that they do not just come from one or two people | 4.1 Reasonably well grounded/supported (please specify) | |
| 4.2 Fairly well grounded/supported (please specify) | ||
| 4.3 Limited grounding/support (please specify) | ||
| 5. Please rate the findings of the process evaluation in terms of its breadth and depth. Consider whether (NB: it may be helpful to consider ‘breadth’ as the extent of description and ‘depth’ as the extent to which data has been transformed/analysed) a range of processes/issues were covered in the evaluation; the perspectives of participants are fully explored in terms of breadth (contrast of two or more perspectives) and depth (insight into a single perspective); both the strengths and weaknesses of the intervention are described/explored; the context of the intervention has been fully described/explored; richness and complexity has been portrayed (e.g. variation explained, meanings illuminated); there has been theoretical/conceptual development | 5.1 Limited breadth or depth | |
| 5.2 Good/fair breadth but very little depth | ||
| 5.3 Good/fair depth but very little breadth | ||
| 5.4 Good/fair breadth and depth | ||
| 6. Overall, what weight would you assign to this process evaluation in terms of the reliability of its findings? Guidance: think (mainly) about the answers you have given to questions 1–4 above | 6.1 Low | |
| 6.2 Medium | ||
| 6.3 High | ||
| 7. What weight would you assign to this process evaluation in terms of the usefulness of its findings? Guidance: think (mainly) about the answers you have given to questions 4 and 5 above and consider (a) how well intervention processes are described (e.g. does it provide useful information on barriers and facilitators to implementation – factors that others implementing the intervention would need to consider?) (b) whether the findings can help us to explain the relationship between intervention process and outcome (e.g. why the intervention worked or did not work; factors influencing effectiveness; how the intervention achieved its effects) | 7.1 Low | |
| 7.2 Medium | ||
| 7.3 High |
List of abbreviations
- AIDS
- acquired immunodeficiency syndrome
- BEd
- Bachelor of Education
- CPD
- continuing professional development
- DfE
- Department for Education
- EAL
- English as an additional language
- EBITT
- employment-based initial teacher training
- ECM
- Every Child Matters
- EPOC
- Effective Practice and Organisation of Care
- GTP
- Graduate Teacher Programme
- HEI
- higher education institution
- HIV
- human immunodeficiency virus
- ITT
- initial teacher training
- NHSP
- National Healthy Schools Programme
- NIHR
- National Institute for Health Research
- NQT
- newly qualified teacher
- NSPCC
- National Society for the Prevention of Cruelty to Children
- OFSTED
- Office for Standards in Education, Children's Services and Skills
- OTTP
- Overseas Teacher Training Programme
- PE
- physical education
- PGCE
- Postgraduate Certificate in Education
- PSHE
- personal, social, health and economic
- PSHEE
- personal, social, health and economic education
- QTS
- qualified teacher status
- RTP
- Registered Teacher Programme
- SCITT
- school-centred initial teacher training
- SEAL
- social and emotional aspects of learning
- SEN
- special educational needs
- SHARE
- Sexual Health and Relationships – Safe, Happy and Responsible Education (Scotland)
- SHTAC
- Southampton Health Technology Assessments Centre
- SRE
- sex and relationships education
- TDA
- Training and Development Agency (now the Teaching Agency)
- WHO
- World Health Organization
All abbreviations that have been used in this report are listed here unless the abbreviation is well known (e.g. NHS), or it has been used only once, or it is a non-standard abbreviation used only in figures/tables/appendices, in which case the abbreviation is defined in the figure legend or in the notes at the end of the table.