
Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 10/3004/02. The contractual start date was in June 2011. The final report began editorial review in October 2013 and was accepted for publication in March 2014. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Dr Jean Adams has received funding from NIHR Health Technology Assessment, grants from British Heart Foundation, Cancer Research UK, Economic and Social Research Council, Medical Research Council and the National Institute for Health Research for research activity during the conduct of this study.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2014. This work was produced by Carr et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
This chapter discusses the background to, and an overview of the focus of, this review. Definitions and distinguishing characteristics of Traveller Communities, the demographics of these populations and their commonalities are first discussed. This is followed by an illustration of the health inequalities experienced by these groups and the limited amount of evidence examining the effectiveness of interventions to improve the health of Traveller Communities. Finally, the complex and undertheorised nature of outreach is described, alongside the challenges this poses for evaluation.
Background
Traveller Communities
Definitions and distinguishing characteristics
The term ‘Traveller Communities’ refers to a complex population group that can be characterised by multiple and diverse dimensions. As such, defining Traveller Communities is not straightforward,1 and the use of terms such as ‘Gypsy’ and ‘Traveller’ is contested both within and outside Traveller Communities. 2 The phrase ‘Traveller Communities’ is used as an overarching term to describe multiple cultural and ethnic groups with diverse histories and customs, including Romani Gypsies, Irish Travellers, Welsh Travellers, Scottish Travellers, Roma, New Travellers, Travelling Showpeople, Circus People and Boat Dwellers. 1 While a nomadic lifestyle is one distinguishing dimension of Traveller Communities, frequency of travel may vary within these groups, classified by Niner3 as follows:
-
full-time Travellers
-
seasonal Travellers
-
holiday Travellers
-
special-occasion Travellers
-
settled Travellers.
Although nomadism is often an important component of Traveller Community lives, a definition of Traveller Communities which rests solely on the basis of a travelling lifestyle is inadequate. Ethnic identity is not lost when members of the Communities settle,1 and cultural practices, the importance of extended family, language and preference for self-employment have all been highlighted as important aspects of Traveller Community identity regardless of the frequency of travel. 4 Given this complexity, the definition of Traveller Communities in legal terms has been difficult. 5 The Race Relations Act recognises Roma, Gypsies and Irish Travellers as distinct ethnic groups, but does not afford the same protection to New Travellers and Occupational Travellers. 6 The following definition of Traveller Communities provided by the Housing Act was adopted for this review because of its inclusivity:
Persons with a cultural tradition of nomadism or of living in a caravan; and all other persons of a nomadic habit of life, whatever their race or origin, including: i) such persons who, on grounds only of their own or their family’s or dependent’s educational or health needs or old age, have ceased to travel temporarily or permanently; and ii) members of an organised group of travelling showpeople or circus people (whether or not travelling together as such).
Great Britain 20047
For the purpose of this report, the terms ‘Traveller Communities’, ‘Traveller Community’, ‘Gypsies and Travellers’ will be used to refer to all Traveller Community subgroups, except where referring only to a specific group (e.g. Roma or Showpeople). The term ‘settled community’ will be used to refer to non-Traveller community members.
Population size
Although it is estimated that there are between 10 and 12 million Roma and Travellers in Europe8 and between 120,000 and 300,000 members of Traveller Communities living in the UK,9 no definitive figures exist. The most recent figures from the biannual Gypsy and Traveller caravan count report 18,730 Gypsy and Traveller caravans in England,10 924 caravans in Wales11 and 684 Gypsy and Traveller households living on sites or encampments in Scotland. 12 However, the caravan count has been criticised for its reliability on account of the fact that it counts caravans rather than people and excludes the estimated two-thirds13 of Traveller Community members who live in housing. 14 , 15 Following the longstanding absence of Traveller Communities from national population surveys, Gypsy and Irish Traveller Communities were included as ethnic categories in the national census, the General Household Survey and the Health Survey for England in 2011. 16 The 2011 UK Census reports 57,680 Gypsies and Irish Travellers living in England and Wales. 17 However, this is likely to be a significant underestimate owing to reluctance of Traveller Community members to self-identify due to fear of discrimination, low levels of literacy impacting on ability to complete census forms, failure to engage marginalised groups such as members of Traveller Communities living on unauthorised sites, and the inclusion of only those Traveller Communities recognised as ethnic groups. 18 Drawing together the figures from Local Authority Gypsy and Traveller Accommodation Assessments across England, the Irish Traveller Movement in Britain18 reports that the total population of Traveller Communities in England in 2012 was 122,785.
The lack of reliable data on the demography of Traveller Communities, combined with the mobility of these groups, may lead to their invisibility throughout the planning of health service provision and result in needs being unmet. 19 Dar et al. 16 conducted a geographical mapping of the numbers of Traveller Communities using existing data sources and compared this with knowledge of Traveller Communities, immunisation service provision and estimated immunisation rates among Health Protection Units surveyed in England. Knowledge of Health Protection Units of Traveller Community populations and their uptake of immunisation was found to be low in a number of areas and there was no apparent association between service provision and numbers of Traveller Community members in a local area. Traveller Communities account for a small proportion of the total current UK population of 63.2 million, even when considering upper estimates of numbers. Any intervention targeted at improving Traveller Community health is, therefore, likely to have a very limited impact on overall population health.
Commonalities with other marginalised populations
While Traveller Communities represent a small proportion of the overall population, health policy highlights a number of commonalities with regard to needs and challenges for service provision across a range of socially excluded groups, including Traveller Communities. 20 The synthesis of evidence on outreach interventions for the health improvement of Traveller Communities, therefore, contributes to understanding what works to improve the health of other disengaged or marginalised groups, and therefore to the achievement of ‘resulting economies of scale and purpose by identifying common needs and service specifications across groups’ (p. 6). 20 The life circumstances of marginalised groups and the corresponding lack of responsiveness by services often results in costly patterns of service use by these groups, for example multiple or frequent attendance and reliance on acute services such as accident and emergency (A&E) as opposed to utilisation of primary care. 20 As such, efforts to improve the health of excluded groups and the accessibility and uptake of health services may contribute to reducing costs associated with the treatment of illness. The focus on subsections of the population who experience particularly acute health disparities can also be justified morally. As Marmot21 comments, ‘Reducing health inequalities is a matter of fairness and social justice’ (p. 15). While a focus only on the most disadvantaged sections of the population will not alone alleviate the social gradient of health inequalities, it is acknowledged that the intensity of intervention needs to be tailored to the degree of disadvantage experienced, and that more concentrated efforts will be needed to tackle the multiple and extensive disadvantage experienced by some groups. 21
Health needs of Traveller Communities
This report does not attempt to provide a comprehensive overview of the health status and needs of Traveller Communities, which is reported extensively elsewhere. 6 , 14 , 22–24 Rather, it aims to illustrate the spectrum of health inequalities experienced by Traveller Communities which outreach interventions might be seeking to address.
Traveller Community health status
The lack of data on the Traveller Community population has limited the generation of robust evidence on their comparative health status14 and, as such, findings need to be interpreted with caution. However, the available evidence points to inequalities experienced by Traveller Communities across many domains of health.
General health and well-being
Traveller Communities have been reported to have poorer general health and well-being than other groups. The mortality of Traveller Communities in the Republic of Ireland (ROI) was found to be three and a half times greater than that of the general population, dropping only 13% compared with a decline of 35% in the general population over the last 20 years. 25
The health status of Traveller Communities in the UK is also significantly worse than that of other socioeconomically disadvantaged or ethnic minority groups. 19 , 26 Traveller Communities scored poorer on measures of overall health than age–sex matched comparators [assessed using the European Quality of Life-5 Dimensions (EQ-5D) measure of health, mean difference 0.12; p = 0.001] as well as on all individual dimensions of mobility, self-care, usual activities, pain or discomfort and anxiety and depression. 19 These differences in health status between Traveller and settled communities remain even after controlling for smoking status as well as age and sex. 26 Peters et al. 26 also found Traveller Communities to have significantly poorer health than African Caribbean, Pakistani Muslim and white ethnic groups, as assessed using the EQ-5D (mean scores of 74.9, 83.5, 92.6, and 85.5, respectively; p < 0.001).
Traveller Communities reported higher levels of anxiety (mean scores of 9.0 compared with scores of 6.2 for African Caribbean and Pakistani Muslim participants, and 5.7 for white participants) and depression (mean scores of 6.3 for Traveller Communities, 4.2 for African Caribbean participants, 3.8 for Pakistani Muslim participants and 3.1 for white participants), as assessed using the Hospital Anxiety and Depression Scale (HADS). 26 Qualitative studies which found that Traveller Communities clearly identified with symptoms of mental health and distress27 , 28 provide further evidence in support of concerns around mental health in these groups. Furthermore, high rates of suicide are reported among Traveller Communities, with three times the rates of suicides among Irish Travellers between 2000 and 2006 compared with the general population. 29
Long-term conditions and specific illnesses
Members of Traveller Communities are more likely to have a long-term illness, health problem or disability that limits their everyday activities (42% of Traveller Communities and 31% of age–sex matched comparators; p = 0.009). 19 Traveller Community members more often reported experiencing a number of conditions, including chronic cough (49% vs. 17%), chronic sputum (46% vs. 15%), bronchitis (41% vs. 10%), asthma (65% vs. 40%) and arthritis (22% vs. 10%), than did the comparator group. 19 This study, by Parry et al. ,19 found no difference between Traveller Communities and comparator groups in the prevalence of diabetes, stroke or cancer. However, the authors report that this may be a result of premature death or a reluctance to disclose conditions such as cancer. 19 Since the publication of this study, evidence from Gypsy and Traveller Accommodation Assessments suggests a higher prevalence of diabetes among Traveller Communities (4.6% of those surveyed in Cambridge and 11% in Dorset compared with 3.5% of the general population). 30 A smaller difference was found between Traveller community and African Caribbean and Pakistani groups for health in the past year, asthma and depression after adjustment for age, sex and smoking status. However, significant differences between these groups remained for the cough and sputum items of the respiratory questionnaire. 26 The collation and review of case-management information over a 4-year period revealed a disproportionate incidence of measles among Traveller Communities of more than 100 times that found in the wider population. 31
Maternal and child health
Studies have also raised concerns around the health of Traveller Community mothers and children. A disproportionate number of Traveller Community mothers were represented in the UK maternal mortality statistics for 1997–9 according to the Confidential Enquiry into Maternal Deaths. 32 Members of Traveller Communities more often reported having experienced one or more miscarriages than the comparator group (29% and 16%, respectively; p < 0.001) and the premature death of a child (6.2% of Traveller Community women compared with none of the comparator women; p < 0.001). 19 Results from the All Ireland Traveller Health Study, which suggest that infant mortality is almost four times greater than that of the general population, corroborate these findings. 33
An increased risk of low birthweight (< 2500 g) has been reported among Roma infants in Europe. For example, 14.1% of Roma infants were born with a low birthweight compared with 3.6% of non-Roma infants in the Czech Republic, with a difference of 373 g in birthweight. 34 Similar results have been reported in Hungary, where 26.2% of Gypsy infants were of low birthweight compared with 11.0% in the national sample, and where an overall difference in mean birthweight of 377 g was found. 35 However, the average birthweight of Traveller infants in Ireland was similar to that of the general population, and the growth rate for Traveller children was found to be comparable with the general population at 9 months,33 suggesting that the evidence may be more mixed in this area.
Intragroup differences
A limited amount of evidence exists from which to establish differences between Traveller Community subgroups. Parry et al. 19 found no significant differences between Irish Travellers and English, Welsh or Scottish Gypsies, suggesting that these groups are likely to experience comparable health status. However, there is a lack of evidence on the health of non-ethnic groups, such as Showpeople and Occupational Travellers,16 who share many of the risk factors for health experienced by other Travellers.
Studies suggest a relationship between frequency of travel and health, with those who travel reporting better health status;19 , 36 however, causality is not clear, and this association could reflect a necessity for Traveller Community members with poorer health to settle in order to be close to services. 37
Inequalities of health appear to be particularly great among Traveller Community men. 26 Abdalla et al. 25 report the mortality rate of Traveller Community men in Ireland to be significantly higher than that for women (standard mortality rate of 469 compared with 232 respectively). Traveller Community men have been reported to be over nine times more likely than women to die by suicide, with these gender differences mirroring those found in the general population. 29
Determinants of Traveller Community health
Traveller Communities experience inequalities across the multiple determinants of health represented on Dahlgren and Whitehead’s Social Model of Health. 38 The contributions of these determinants to the poorer health of Traveller Communities are now explored in more detail.
Lifestyle factors
Individual members of Traveller Communities have been found to accept ill health and normalise signs of distress. 37 , 39 Poor health expectations, fear about potential diagnoses and structural constraints resulting from eviction or difficulties in finding appropriate stopping places have all been suggested as factors leading to a lack of prioritisation of preventative health care and services such as screening. 39 , 40 In addition, the literature highlights cultural beliefs of Traveller Communities that govern the body and have a bearing on health practices and which are important for health advisors to be aware of, albeit with the proviso that cultural beliefs and practices may vary across different Traveller Communities and the individuals within them. Okely41 demonstrates the ways in which beliefs about pollution and associated rituals around washing, eating, use of space and placement of objects enacted serve to reinforce a distinction between Travellers and settled communities. For example, the outer body and skin (the interface for engagement with settled community members) is distinguished from and viewed as potentially polluting to the inner body. 41 These beliefs are embodied in practices such as the use of separate washing bowls for items used for cooking and eating from those used for washing the body, and ensuring that anything entering the body through the mouth is ‘ritually clean’. 41 Health practices such as immunisation might, therefore, be viewed as polluting because they transgress the distinction between inner and outer body. While pollution beliefs apply to both men and women, the potential for women to be polluting is greater during menstruation and childbirth as bodily waste from the lower body poses a particular threat of pollution. 41 Women’s sexuality is also potentially polluting and codes of behaviour may be evident to protect against this, for example not revealing certain body parts and women not spending time alone with men other than their husbands. Concerns relating to modesty are likely to impact on the acceptability of behaviours such as breastfeeding and have consequences for health service delivery, including the need to ensure that Traveller Community women are able to access a female health practitioner.
The literature points to a higher number of modifiable risk factors that may contribute to the poorer health of these groups. A greater proportion of Traveller Communities than the general population are current smokers (around 50% compared with around 37%, respectively). 42 Smaller numbers of Traveller Community members report drinking alcohol than the general population, but those who do consume alcohol do so more often (around 65% of male and 40% of female Travellers drink six or more alcoholic drinks on days when they are drinking alcohol compared with around 35% of men and 17% of women in the comparator population). 42
Compared with the general population, fewer Traveller Community members reported eating at least five portions of fruit and vegetables in Ireland (65% and 45%, respectively). 42 A smaller-scale study conducted in Wrexham also reported that Traveller Communities have a poorer diet and lower levels of physical activity than the Welsh and UK population, as well as residents from a deprived local area. 43 Traveller Communities more often reported high blood pressure or cholesterol in the past year (36.5% of Traveller Community members compared with 28.3% of medical card holders in the general population). 42
The literature reports a low uptake of immunisation and well-women services among Traveller Communities. 44 Only around 2.2% of Traveller mothers initiate breastfeeding compared with around 50% of those in the general population. 33
Social and community networks
Extended family provides an important source of social support among Traveller Communities, with family members often expected to provide care for family members who are older or unwell. 37 As such, a positive model of ageing is cited among Traveller Communities, with older Traveller Community members less likely to experience social isolation and loneliness. 45 In addition, elder members of Traveller Communities are often important sources of advice on health, with a higher number of Traveller Community members reporting being supported by parents than the general population (69.6% of Travellers compared with 38.3% of the general population). 42 However, owing to a lack of space on authorised sites, and as Traveller Community members often resort to housed accommodation in order to avoid cycles of frequent eviction, members often find themselves separated from family and community support systems. 46
Living and working conditions
Around one in four Traveller Community members living in caravans do not have a legal place to park their home,5 and are thus forced to live on unauthorised encampments from which they are frequently evicted. Many of the sites provided are of poor quality, are built on contaminated land, are close to motorways, pose significant fire safety risks, are contaminated by vermin, have poor-quality utility rooms, and have chronically decayed sewage and water fittings. 3 , 5 , 6 , 47–49 Traveller Communities experience difficulties in obtaining planning permission for privately owned land due to opposition from local residents. 6 Large numbers of Travellers surveyed in the All Ireland Traveller Health Study who lived on sites or in group housing schemes (designed to enable Travellers to live together in extended family groups) reported a lack of footpaths [40.8% in ROI and 33.0% in Northern Ireland (NI)], public lighting (39.4% in ROI and 20.7% in NI), fire hydrants (73.7% in ROI and 60% in NI) and safe play areas (77.5% in ROI and 79.9% in NI). 42 Places of living were viewed as unhealthy or very unhealthy by around 24.4% of Travellers in the ROI and 24.8% in NI, while 26.4% of Travellers in the ROI and 29% in NI considered thier place of living to be unsafe. 42
Traveller Communities face practical challenges in accessing mainstream services owing to discrimination faced on registering with services, lack of a permanent address and high levels of illiteracy. 6 , 39 Peters et al. 26 report that only 69% of Traveller Communities were permanently registered with a general practitioner (GP) compared with ≥96% of Pakistani Muslim, African Caribbean and white participants. By contrast, findings on Traveller Community access to services in Ireland suggest that Travellers do access preventative screening42 and have similar use of GP services to comparators among the general population (unadjusted rates of 74.2% vs. 75.3%). 50 However, despite these higher rates of access, Traveller Community members rated their experiences of accessing health services less positively. 50 Traveller Communities were less likely than other ethnic groups to have accessed dental services (47% of Gypsies and Travellers compared with 77% of white, 67% of African Caribbean and 63% of Pakistani Muslim participants) or opticians (14% of Gypsies and Travellers compared with 43% of white, 42% of African Caribbean and 49% of Pakistani Muslim participants). 26 As a consequence of difficulties in accessing GP services, Traveller Communities may be more likely to attend acute or reactive services. Beach51 reports that children from Traveller Community sites attend A&E departments twice as often as settled children in the neighbouring areas. Peters et al. 26 found that Gypsies and Travellers had been in contact with A&E departments more often (24% of Traveller Communities) than had African Caribbean (21%), Pakistani Muslim (16%) and white participants (12%) (p = 0.025).
The decline in traditional trades undertaken by Traveller Communities has resulted in many families becoming economically excluded and has necessitated their adaptation or assimilation into mainstream modes of employment. 52 Although there is diversity within the Community with respect to socioeconomic status,52 Travelling Communities overall are cited as experiencing high levels of poverty and low employment. 6 In response to such changes, education is viewed as increasingly important in order to secure the welfare of future generations. 53
Gypsies and Travellers have much poorer educational outcomes, with < 10% of Traveller Community pupils attaining five GCSEs (General Certificates of Secondary Education) or equivalent at A* to C grades, including English and maths, compared with over 50% of the average population. 54 Traveller Community children are noted to have the worst school attendance profile of any ethnic minority group. 55 Absence rates for the years 2007–8 were higher than for other groups for both primary (24.2% for Travellers of Irish heritage, 19.0% for Gypsy/Roma, 5.3% for all pupils) and secondary school (27.3% for Travellers of Irish heritage, 23.5% for Gypsy/Roma, 7.4% for all pupils). 56 Gypsies and Travellers are four times more likely to be excluded from secondary school than any other group. 57 In addition, Traveller Community children are more likely to attend schools with below average results. 56
General socioeconomic, cultural and environmental conditions
There is explicit racism and discrimination directed towards Traveller Communities in society, with this being regarded as the last accepted form of prejudice in England. 58 There is little recognition of the culture or heritage of Traveller Communities and an absence of positive portrayals of Traveller Community lifestyles in mainstream society. 6 A study of media coverage of Traveller Communities in Scotland found a disproportionate amount of coverage relating to these groups (an average of 1.5 articles per day), with nearly half (48%) classified as overly negative portrayals. 59 The under-representation of Traveller Community members in political activities means that they have little voice to challenge such representations. 6 Systems of health service provision contribute to the exclusion of Traveller Communities. For example, it is suggested that GP surgeries might be reluctant to register Traveller Communities due to the extra paperwork required when taking on temporary residents and perceptions that registering Traveller Community members will affect GPs’ ability to meet performance targets around immunisation. 60
Research on the effectiveness of outreach interventions for Traveller Communities
There are efforts to tackle health inequalities faced by Traveller Communities, as evidenced through recent funding sources. 20 , 61–63 Examples of outreach programmes cited as offering potential are diverse, including, for instance, a Community mothers programme,64 trained outreach workers from Traveller Communities,6 , 22 and mobile health clinics or play buses. 6 , 22 A review of health-care interventions for Traveller Communities recommended outreach and the employment of trained health workers from the Community as culturally appropriate and promising components of interventions. 22
However, most initiatives aiming to improve health for Traveller Communities have been initiated in recent years and are as yet unlikely to have yielded significant evidence of impact. Few published reports with robust study designs, such as randomised controlled trials (RCTs) and controlled trials, examine the effectiveness of interventions to improve health in Traveller Communities. A review of the range and quality of evidence on the health of Traveller Communities reveals that studies are rarely well designed and tend to use process rather than outcome measures as indicators of success. 14 While this provides important indicators of culturally sensitive interventions, there is a dearth of reported evidence of improvements in health status. 14 , 65 The heterogeneity of the evidence base, combined with contextual intricacies of a diverse and complex population, raised significant challenges for evidence synthesis.
Outreach
Defining outreach and its purpose
A number of challenges have been identified in meeting the health-care needs of the most socially excluded and vulnerable groups in society. For Traveller Communities and other socially excluded groups who have multiple and complex needs, engagement with and access to preventative care may be afforded a low priority. 66 Mainstream health service provision is often ill adapted to the complicated everyday lives of these groups, for which flexibility and co-ordination across different health- and social-care systems is required. 20 Outreach has, therefore, been utilised as a key strategy to engage those who, through processes of social exclusion or socioeconomic deprivation, occupy a position on the margins of society and are considered ‘hard to reach’. 66 While outreach approaches have, in general, been endorsed in commissioning guidance for improving the health of marginalised groups,67 at present, little detail is given around the specific strategies that are likely to make outreach effective in different contexts.
Owing to the focus of outreach on engagement, and responding to the unique needs of individuals and groups, conceptualisation of approaches to outreach have often been couched in terms of the personal and attitudinal qualities of outreach workers, rather than in terms of methods. 68 For example, the unidirectional nature of the vulnerability between outreach workers and those they attempt to engage, as well as the shared experiences during encounters, are important aspects of the outreach dynamic. 68 However, it is precisely these aspects of outreach that are difficult to articulate and which introduce hidden variability in outreach programmes.
Further diversity in implementation results from the inability to predict the problems that outreach work will need to address. Mackenzie et al. 66 present the following ‘continuum of complexity’ to describe the potential reasons for a lack of engagement that outreach might need to address and the different shapes outreach might take in response:
-
Not receiving engagement invitation letter: outreach works as a ‘health-care postal worker’ to deliver the invitation personally and overcome information gaps in service systems.
-
Literacy or health literacy barriers: outreach worker acts to ‘bridge gaps in understanding’, providing information and responding to questions about services.
-
Lack of priority afforded to preventative health: outreach worker takes a ‘translational role’ to highlight an individual’s candidacy for preventative treatment amid other lifestyle pressures.
-
Psychosocial barriers to engagement: outreach worker utilises strategies such as motivational interviewing and/or signposting to other services to alleviate barriers preventing access.
-
Structural barriers to engagement: outreach workers use signposting, referral and mobilisation of community networks to address broader issues relating to housing, unemployment and debt and co-ordinate the involvement of different agencies.
-
Hidden and multidimensional nature of problem: outreach workers take the role of ‘assessing readiness for action or change’, treating engagement as a process and working incrementally to address multiple issues.
The conditions in which outreach is delivered can be highly unpredictable and beyond the outreach worker’s influence. 68 In addition, the extension of outreach into people’s personal spaces might display aspects of their vulnerability more clearly and evoke feelings of intrusion and potentially unwelcoming responses in those approached. 68 As a result, outreach workers need to be accustomed to the ‘spatial organisation’ of their surroundings and have awareness of social networks and potential change agents, group movements and meeting points. 68 For example, outreach workers in the study reported by Dickson-Gómez et al. 69 had to be sensitive to the social codes and dynamics operating in areas of injection drug use, including the impact that outreach had on the business of drug use through attracting crowds and inviting police attention. In the case of outreach with Traveller Communities, outreach workers may need to demonstrate awareness of the ways Traveller sites and personal spaces are organised to uphold cleanliness and avoid pollution,41 as described above.
Challenges to the evaluation of outreach
The emphasis on the specificity of outreach to particular target groups or contexts has been argued to limit possibilities for the conceptual development of outreach. 68 Indeed, the distinctiveness between outreach implementation models and the boundaries between outreach and other forms of interventions, such as peer support interventions, are not always clear in the literature.
Outreach fits into the category of a complex intervention as defined in the Medical Research Council (MRC) guidance,70 in that it is not standardised and is highly sensitive to local contextual issues. As described above, interventions are often highly individualised,71 implemented in diverse settings and delivered by several different people. 72 In addition, implementation fidelity may be problematic in outreach interventions, as greater flexibility and variability is required in delivery. 71 , 73
The lengthy chain of causality between the delivery of outreach interventions and outcomes also presents a challenge for evaluation. Given the role of outreach in facilitating access to mainstream services, the role of the outreach programme in generating concrete improvements in health behaviour or outcomes may be difficult to disentangle from the impact of other interventions or organisations. 68 Thus, the success of outreach workers in terms of making and sustaining contacts is argued to be a key intermediary outcome in assessing the effectiveness of outreach interventions. 68
Such characteristics pose challenges for articulating71 and documenting the processes of outreach,74 thereby placing it at odds with the emphasis on standardisation in clinical trials. 75 As Mackenzie et al. 66 summarise:
Outreach has been described as eclectic in its purpose, client group and specific mode of practice and, as a direct result of this heterogeneity, little is known about its effectiveness.
Mackenzie et al. 2011,66 p. 352
There is, therefore, a need for greater theoretical development on the particular approaches and underpinning mechanisms of outreach most likely to lead to positive outcomes in particular contexts. 66 , 68 , 76 In doing so, there appears to be a need to achieve a balance between the generalisation and specificity of understandings of outreach across different contexts. 68
Definition of outreach adopted for this review
In order to provide greater focus for this review, and in line with the agenda to tackle health inequalities, the current work will be focused on outreach efforts that aim to engage Traveller Communities in a health-related agenda. For the purpose of this review, the following broad definition of outreach was adopted:
[A] process that involves going out from a specific organisation or centre to work in locations with sets of people who typically do not or cannot avail themselves of the services of that centre.
McGivney 2000,77 p. 11
In addition, following MacKenzie et al. ,66 outreach was considered to involve the alleviation of both ‘physical as well as ideological gaps between services and users’ (p. 2).
Changes in the review process
Initially, it was proposed that a meta-analysis or narrative synthesis (dependent on data quality) and realist synthesis of evidence on outreach interventions for health improvement of Traveller Communities would be undertaken. However, following the processes of searching for and appraising the quality of evidence, it became clear that it was of insufficient quality to lend itself to a narrative synthesis. Of the 407 studies obtained and assessed on full text, only 12 articles described and evaluated outreach interventions and would have been eligible for inclusion in a narrative synthesis. A process of quality assessment categorised two of these 12 items as ‘moderate’ and 10 items as ‘weak’ using the Quality Assessment Tool for Quantitative Studies78 for quantitative studies and the Critical Appraisal Skills Programme checklist for qualitative research. 79 Furthermore, the studies focused on disparate topics, including teenage health, primary health care, support following childbirth, oral health, drug use, prevention of human immunodeficiency virus (HIV) infection, domestic violence, health advocate training, and a health mediator programme. The small number of robust studies examining diverse programmes meant that it would have been impossible to identify patterns of effectiveness of component intervention techniques for the health improvement of Traveller Communities. It was therefore decided to undertake a scoping review in conjunction with the realist synthesis. The study protocol is presented in Appendix 1 .
Characterised by breadth rather than depth of approach,80 the scoping review identifies the extent and range of research activity81 on outreach programmes for the health improvement of Traveller Communities. Scoping reviews are noted to be particularly insightful for areas of emerging evidence not amenable to systematic review,82 as for outreach interventions for Traveller Communities, and have been used successfully to capture the sense of a broad disparate literature base83 such as that described above. The wide-ranging coverage of the literature offered by the scoping review, therefore, provides a comprehensive overview of the available evidence in the area, and scaffolds the realist synthesis by situating the evidence on outreach programmes for Traveller Communities within the wider body of literature on Traveller health.
Objectives and focus of the review
Scoping review
The scoping review aimed to examine the extent, range and nature of research activity and map the range of research rather than describe key findings, in accordance with Arksey and O’Malley’s84 recommendations. It aims to answer the following research question:
What is the extent (quantity) and content of available research evidence concerning the health of Traveller Communities?
Economic evaluation
Following the scoping review, the economic evaluation classifies the different types of outreach interventions, estimates their cost and provides an estimate of whether or not interventions might be considered cost-effective.
Realist synthesis
A realist synthesis acknowledges the complexity of interventions and focuses on the explanation of how, for whom and in what circumstances they work. 85 As such, a realist synthesis necessitates the clarification of the purpose of the review, research questions and key theories that will be addressed, a process that often continues to the later stages of the review. 85 This phase involves ‘a careful dissection of the theoretical underpinnings of the intervention, using the literature in the first instance, not to examine the empirical evidence but to map out in broad terms the conceptual and theoretical territory’ (p. V). 85 In order to facilitate reading and transparency of this continual process, the conceptual and theoretical territory is detailed in Chapter 3.
Four initial theories
An initial exploratory scoping of the literature to clarify the focus of the research concentrated on the origins and nature of Traveller Communities as an ethnic group, their differential health status and outreach as a health intervention. This process was partly formalised through the scoping review and completed by consultation with expert members of the project steering group. This led to the articulation of the following initial programme theories on outreach interventions in Traveller Communities:
-
The cultural distinctiveness and particular needs of Traveller Communities mean that outreach forms a key ‘bridge’ between them and statutory health services (‘by whom’).
-
The cultural background (being a peer) of outreach workers is key to the success of their intervention because that enables them to use the right communication tools to reach out to individual Travellers (‘to whom’).
-
Degree of formality and responsiveness to need are key levers for participation (‘how’).
-
Key aims of outreach are to tackle health inequalities through engagement, advocacy and education (‘what for’).
The focus on Traveller Communities in theory 1 offers an insight into the context of outreach interventions. The reviewers’ expertise in peer and lay intervention guided the formulation of theories 2 and 3 as potential mechanisms of outreach and theory 4 offers an opportunity to delve into the purposes and achievements of outreach in this group (outcomes). Thus, these theories offer an avenue to formulate the kinds of Context–Mechanism–Outcome (CMO) configurations that are the cornerstone of realist thinking. These four initial theories clearly are not designed to be tested against null hypotheses, but rather are explanatory in their formulation. The distinguishing feature of a realist synthesis is the theories it develops, which aim to explain why interventions such as outreach lead to particular outcomes in particular contexts. The overall purpose of the review is to neither confirm nor refute them but rather to improve their explanatory potential. They are designed as a guide to frame the subsequent phases of the research, articulate questions posed of the evidence and refine our understanding of how and in what circumstances outreach interventions in the Communities ‘work’. These initial four theories are also used over and again in the process of extracting and synthesising the evidence, as a way of describing different modes of outreach and as explanations of why some programmes seem to flourish better than others. They therefore form the key objectives and focus of the realist review.
Chapter 2 Methods
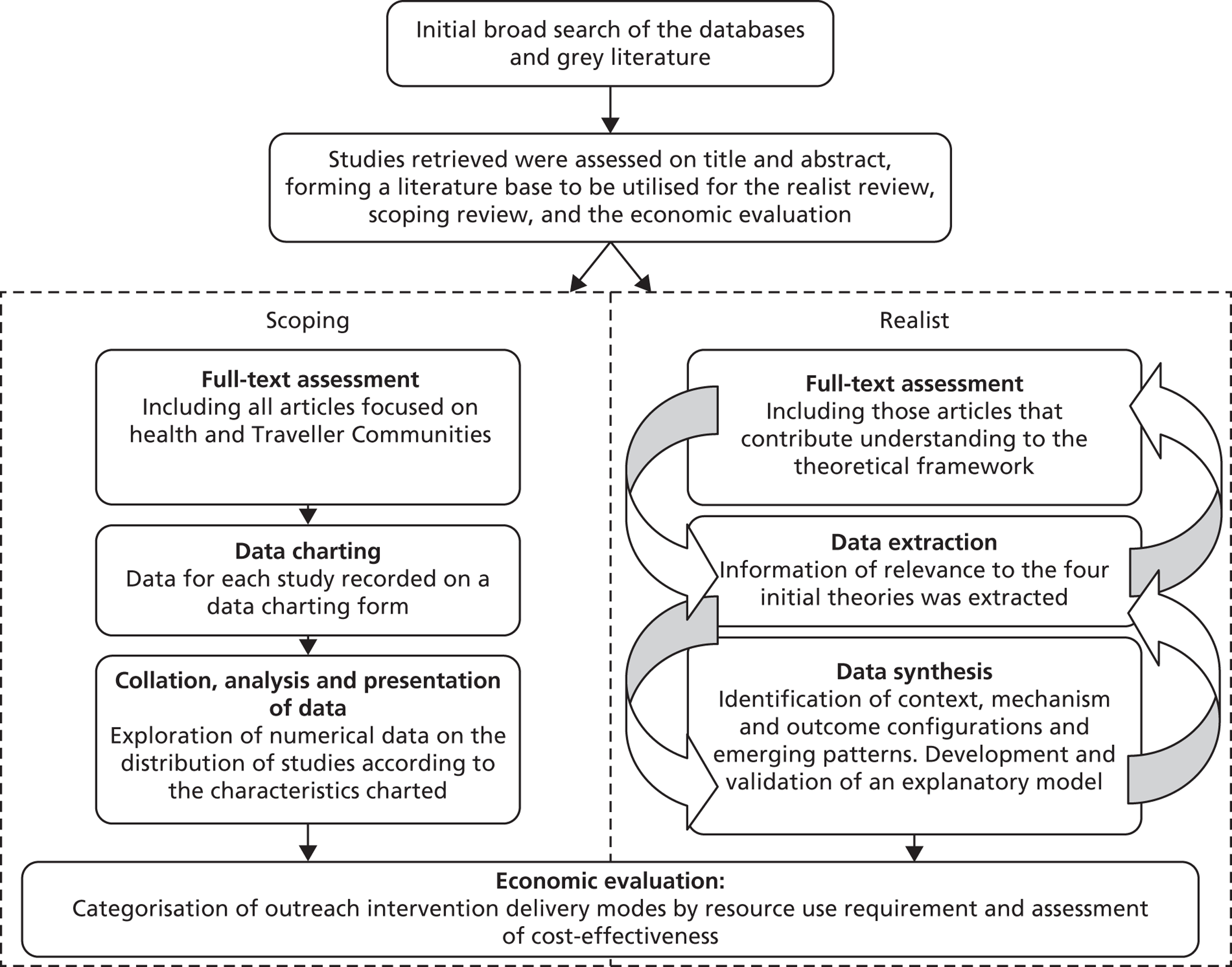
The processes of the primary searching of the evidence base and the screening of studies according to title and abstract are first described, as they informed all review strands. The processes of selection, appraisal on full text and analysis of studies are then discussed independently for the scoping and realist synthesis, respectively, as well as for the economic evaluation. Figure 1 provides a summary of the stages taken for each strand.
FIGURE 1.
Summary of stages for each study strand.
Search strategy development
A short phase of problem definition (2 months) was undertaken in order to refine search strategies and data sources to be utilised, drawing on the expertise of an information specialist as well as the combined knowledge and experience of the project team and steering group members on appropriate terminology for searches.
The search features and structure of the proposed databases were examined to identify and compare keywords, subject headings and thesaurus/index terms. Test searches were undertaken for terms referring to the different Traveller Community groups, such as Romani, Roma, Sinti, ‘Irish Travellers’, ‘Scottish Highland Travellers’, Ceardannan, ‘New Age Travellers’, ‘Bargees’, ‘Pavees’, ‘Showpeople’, ’Circus People’ and Yeniche. The databases examined tended to use used the term ‘Gypsies’ as an overarching term to refer to these different groups. References retrieved by using wider terms, for example ‘transients and migrants’, ‘nomads’, ‘itinerants’ and ‘minority and ethnic groups’, were examined for relevance and found to be beyond the scope of the study. The term ‘outreach’ did not appear as a subject heading term in our sample of databases. The preliminary searches revealed examples of articles describing health interventions for the Traveller Community that featured a number of initiatives, only some of which were termed ‘outreach’.
A ‘citation pearl growing’ exercise was also conducted to identify search terms through examining the terms used to index articles which are relevant to the review (referred to as ‘pearls’). 86 , 87 Pearl articles (see Appendix 2 ) were identified through checking citations in a review of health interventions for Traveller Communities22 and through suggestions for relevant articles from representatives working with Traveller Communities, including those that described a health intervention for Traveller Communities. Pearl articles were indexed under the term ‘Gypsies’ or ‘Travellers’, despite focusing on different subgroups of Traveller Communities such as Roma. While the pearl articles referred to examples of outreach interventions for Travelling Communities, none of the studies were indexed under this term ‘outreach’ in Cumulative Index to Nursing and Allied Health Literature (CINAHL) or MEDLINE. The piloting of searches on the proposed databases and the citation pearl growing exercise, therefore, contributed to the development of a final search strategy which was comprehensive, yet not too unfocused. Together, these exercises suggested that the use of the term ‘outreach’ only in combination with terms for Gypsies and Travellers would be too limiting, leading to the omission of studies describing outreach that were not indexed as such, and that search terms referring to specific groups of Traveller Communities were likely to contribute few unique items.
Searches of electronic databases
Taking the above findings into account, and considering the differing search features provided by the different databases, the following broad and comprehensive approach to searching the literature was taken.
Structured searches were conducted in the following 12 subscription databases available via the University of Northumbria: Web of Knowledge, MEDLINE, The British Library’s Electronic Table of Contents (Zetoc), CINAHL, Applied Social Sciences Index and Abstracts (ASSIA), Social Services Abstracts, British Humanities Index, PsycArticles, Allied and Complementary Medicine Database (AMED), Proquest Nursing and Allied Health Source, International Bibliography of the Social Sciences (IBSS), and Sociological Abstracts.
The searches were conducted between August 2011 and November 2011 by an information specialist working with the research team in order to identify English-language items using the following search strategy: ab,ti(roma or romanies or romany or gipsy or gipsies or gypsy or gypsies or traveler or traveller or travelers or travellers or “travelling community” or “travelling communities” or “traveling community” or “traveling communities”) and (health or outreach).
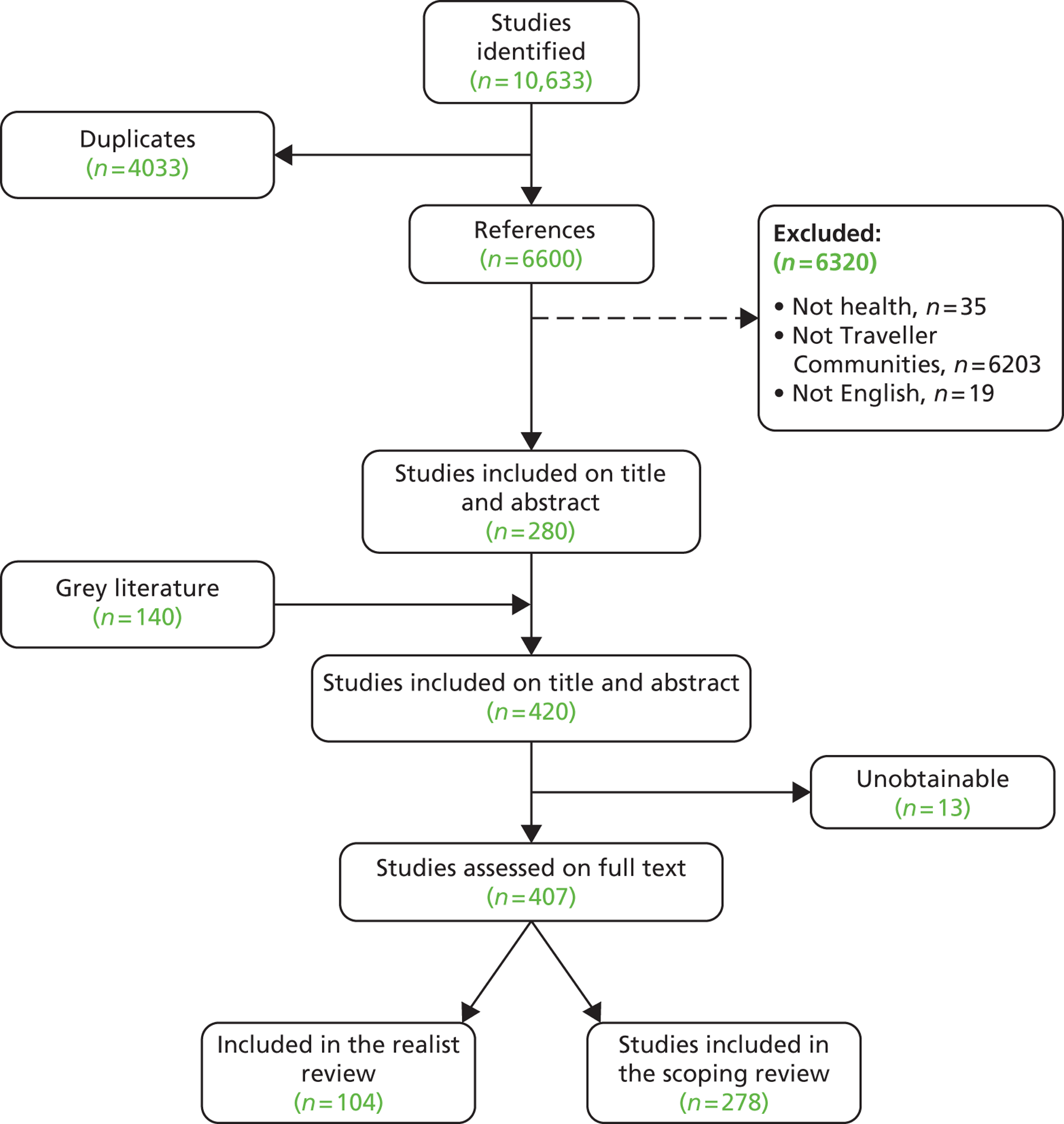
These database searches gathered 10,633 references, of which over 4033 were identified as duplicates (see Figure 3 ). The remaining references were stored in an EndNote library (EndNote, Thomas Reuters, CA, USA). While this strategy resulted in a relatively broad set of references in the first instance, it prevented the exclusion of relevant articles through the adoption of a narrowly focused search strategy.
Searches were also made by two reviewers using The Cochrane Library, The Campbell Collaboration Library of Systematic Reviews, Centre for Reviews and Dissemination (CRD)/Database of Abstracts of Reviews of Effects (DARE) and Evidence for Policy and Practice Information and Co-ordinating Centre (EPPI-Centre) databases.
Searches for grey literature
Initial literature searches prior to the study suggested that the formal literature base (i.e. from peer-reviewed journals) on outreach in Traveller Communities is relatively small. However, there appeared to be a substantial amount of ‘grey’ literature on this subject. A number of search strategies were utilised between July 2011 and November 2011 to retrieve grey literature. Websites of organisations that sponsor and/or conduct relevant research (listed in Box 1 ) were searched to identify publications of interest. Where the function was available, RSS (Really Simple Syndication) feeds or e-mail alerts were set up in order to keep appraised of new literature.
Equality and Human Rights Commission: www.equalityhumanrights.com
Friends Families and Travellers: www.gypsy-traveller.org
Intute: www.intute.ac.uk
Irish Traveller Movement in Britain: www.irishtraveller.org.uk
Local Government Association: www.idea.gov.uk
NHS Evidence: www.evidence.nhs.uk
Pavee Point (human rights organisation for Irish Travellers in Ireland): www.paveepoint.ie
Race for Health: www.raceforhealth.org
Department of Health: www.dh.gov.uk
Home Office: www.homeoffice.gov.uk
Joseph Rowntree Foundation: www.jrf.org.uk
MRC: www.mrc.ac.uk
National Audit Office: www.nao.org.uk
The National Federation of Gypsy Liaison Groups: www.nationalgypsytravellerfederation.org
Department for Communities and Local Government: www.odpm.gov.uk
Society of Behavioural Medicine: www.sbm.org
Urban Institute: www.urban.org
Wellcome Trust: www.wellcome.ac.uk
Searches were also undertaken of the Fade Library, a grey literature library for health (http://fadelibrary.wordpress.com/), as well as of a number of open access resources, including the Directory of Open Access Journals (www.doaj.org/), UK Higher Education Repositories (www.opendoar.org/), BioMed Central Open Access (www.biomedcentral.com/) and UK theses (http://ethos.bl.uk/). The Northumbria University HSWE (Health, Social Work and Education) database, an up-to-date bibliographic database of all journal articles relevant to health, community and education studies, and Government policies, reports and legislation, was also utilised. In addition, contact was made with key representatives working with Traveller Communities to ask for suggestions for relevant literature including unpublished practice accounts or evaluation reports.
In cases where both an internal report and a peer-reviewed paper on the same study were retrieved, both documents were scrutinised.
Screening of studies according to title and abstract
The titles and abstracts of studies identified were scanned by two reviewers to make an initial assessment of relevance. As initially it was envisaged that a meta/narrative synthesis would be undertaken, the Population, Interventions, Comparators, Outcomes and Study design (PICOS) framework88 was used to define inclusion/exclusion criteria at this stage (see Appendix 3 ). However, once it became clear that there was insufficient evidence to undertake a meta/narrative synthesis, eligibility for inclusion was broadened to meet the criteria of the scoping review (i.e. the inclusion criteria was no longer limited to interventions but was broadened to include any article pertaining to the health of Traveller Communities). For the realist synthesis, studies were included if they contributed an understanding to at least one area of the initial theories. If there was any doubt at this stage concerning the relevance for inclusion in the review, the full text of the studies was obtained for assessment. No restrictions on inclusion were imposed according to type of journal, publication date (up to the date of searches) or country of research or practice. Foreign-language publications were excluded. Any disagreements between reviewers with respect to the inclusion or exclusion of studies were resolved by consensus or through consultation with a third reviewer. Thirteen articles included on title and abstract were unobtainable (see Appendix 4 ). The publications included on title and abstract then formed a core set of studies which were assessed on full text according to the specific requirements of each review strand.
The methods of the scoping review and realist synthesis in terms of the selection, appraisal and analysis of studies are now discussed in more detail for each strand. The reporting here follows the methodological framework set out by Arksey and O’Malley84 and Levac et al. 82 for conducting scoping reviews and the Realist And Meta-narrative Evidence Syntheses: Evolving Standards project (RAMESES) publication standards for the reporting of realist syntheses. 89
Scoping review
Study selection
In scoping reviews, as with other systematic review methods, relevant studies are found and considered for inclusion/exclusion in relation to the research question. Poth et al. 90 propose that as scoping reviews are exploratory, all studies on a topic are included in order to identify gaps in research, regardless of study design. As such, the broad search strategy described above generated a comprehensive picture of the available evidence on the health of Traveller Communities, the characteristics of which could then be described and summarised. Thus, the scoping review included all those articles which were screened and included on title and abstract which focused on members of Traveller Communities and which had a health focus. The decision to include not only studies that described outreach interventions but also those that focused more broadly on the health of Traveller Communities was made in order that the evidence on outreach interventions could be placed in the context of the wider literature. As a broad search strategy was used, it is unlikely that any references will have been excluded that would be relevant for the scoping review. Completeness of searching, however, was determined by time and scope constraints.
As in scoping reviews generally, no formal quality assessment of included studies was undertaken. While the challenges in assessing quality among the vast range of published and grey literature that may be included in scoping studies are readily recognised, they have not been resolved, and this lack of quality assessment and the resultant limits on data synthesis and interpretation are known weaknesses. 82 , 91 In this review, key features that characterise the quantity and quality of the literature, such as study design and provenance, are examined in a process that sought to include and classify items rather than exclude them.
Charting the data
The studies included in the scoping review were charted according to the ‘descriptive analytical’ method outlined by Arksey and O’Malley,84 whereby ‘a common analytical framework’ is designed to classify and organise studies according to key issues and themes. The following information was collected from each study and recorded onto a ‘data charting form’84 using NVivo software (QSR International, Warrington, UK):
-
date of publication
-
country of publication
-
type of author (e.g. academic, government/local authority, health service providers, Traveller/third-sector organisations)
-
evidence type (e.g. research study, anecdotal account, literature review, policy/guidelines for practice, theoretical/opinion paper)
-
study design (e.g. qualitative study, controlled clinical trial, pre- and post-intervention study, RCT)
-
whether or not outreach is described
-
outreach worker (e.g. Traveller Community member, health visitor)
-
health focus (e.g. women’s health, child health, dental health).
An early case study of using NVivo for a literature review was presented by di Gregorio92 and while a small amount of published material has since developed this process,93–97 the use of such software does not appear to be commonplace. The use of NVivo software for this review facilitated the management and description of the large number of studies, provided a useful operational tool for the manipulation of data during the analysis process, and helped to ensure transparency in the classification of studies.
Collating, summarising and reporting results
A numerical approach was taken to the collation and presentation of data, which examined the distribution of studies according to the characteristics charted and illustrated these graphically rather than organising the data according to key themes or findings. This approach enabled the presentation of information around how much and what types of evidence is available on the health of Traveller Communities, how much of the overall research evidence on Traveller health reports on the evaluation of outreach interventions, what research designs have been used to do so, who outreach workers are, in which countries are the most/least publications being published, and what kind of authors are publishing on the health of and outreach interventions for Traveller Communities.
Realist synthesis
A realist synthesis is inherently a highly iterative process, each step cumulatively enriching the previous one and informing the following, and each having to be undertaken a number of times over the course of the study. Reporting is, consequently, a recognised challenge. 98 A degree of sanitisation was thus applied in reporting this study, in order to strike a balance between transparency in exposing the methodological audit trail and readability.
Selection and appraisal of documents
The 407 articles selected on title and abstract formed a core set of studies which were then examined for inclusion in the realist review. There was, naturally, significant overlap between the two review strands, but there were exceptions. For example, some outreach interventions could be excluded from the scoping review if they focused on education, but included in the realist review if they gave detailed descriptions of the outreach process. On the other hand, some studies included in the scoping review lacked sufficient detail to inform any of the realist theories and were thus excluded, even if they focused on outreach. A realist synthesis does not seek to come to a verdict about the relevance or quality of whole studies, but ‘requires a series of judgements about the relevance and robustness of particular data for the purposes of answering a specific question’ (p. 8). 89 Study appraisal is, therefore, guided by judgements on the potential for a study to contribute to theoretical developments rather than standard quality assessment tools. The full text of each study was assessed by two reviewers. The Mendeley reference manager programme, which enables the highlighting and annotation of articles as well as the grouping and organisation of articles according to ‘tags’, was used to record decisions about inclusion/exclusion for the different arms of the study, and the particular initial theory to which the studies or section(s) of reported data were thought to contribute. Appendix 5 lists the studies included in the realist review, with comments about the study design, links between articles (when they relate to the same study or organisation) and comments about the particular learning that they could contribute.
Data extraction
Four initial theories (p. 10) guided the data extraction and analysis stages. These formed a framework to extract data as well as offering early explanatory potential. For the purposes of clarity, we report the steps of data extraction, analysis and synthesis as distinct, without all of the iterations that took place in practice. However, in the interest of a decision audit trail, we have sought to thoroughly expose our decision-making process. Pawson et al. 85 state: ‘The process is, within each stage and between stages, iterative. There is a constant to-ing and fro-ing as new evidence both changes the direction and focus of searching and opens up new areas of theory’.
A data extraction sheet was adapted from that reported by McCormack et al. 99 (see Appendix 6 ), developed to mirror the four initial theories. Data extraction was undertaken systematically, by two researchers (periodically reviewing each other’s extraction sheets) until data saturation was reached, that is no new learning was emerging through the studies85 , 98 (38 studies; see Appendix 5 ). The studies were selected for their potential to contribute understanding on each of the four theories. An iterative approach to data extraction was used, with the data providing new insights into the initial theories, and questions to be asked of the data changing in response to the development of our understanding as the analysis progressed. We consulted our Mendeley database regularly in order to ensure that the studies which had not been data extracted could not contribute new insights in the light of emerging findings. An audit trail was kept of all of the decisions that were made during this process, and reviewed regularly by the wider team. This process led to the decision, for example, to focus on perceived and expressed needs in our exploration of ‘to whom’. An extract of our decision trail regarding this is presented in Appendix 7 .
Analysis and synthesis process
This section needs to be preambled by a note on what is expected of a synthesis process in a realist review. There is no pooling of net effects, no ‘aggregation’ or setting of implementation guidelines. Instead, the purpose of the review is a refinement of the initial four theories.
The steps taken to synthesise the data are now described, although in reality the synthesis did not proceed in such a linear sequence, but rather with considerable overlapping or moving back and forth between the different steps. Here, again, the audit trail memos were used to maximise wider team input in the analysis process.
Thematic analysis of the data extracted
The data extracted from each article were separated into the four initial theories (‘to whom’, ‘by whom’, ‘how’ and ‘what for’), and these data were collated and thematically analysed. The list of themes were then classified according to whether they described contexts (C), mechanisms (M) or outcomes (O), and were merged into C, M and O files from which we began to formulate potential CMO configurations. This process enabled immersion in the literature and the search for key terms, abstract ideas and hypotheses that might provide explanatory purchase on how outreach might ‘work’ in Traveller Communities. The net effect of this exercise was, thus, a ‘deconstruction’ of the articles along the lines of our initial theories.
Classifying outcomes
Outcomes were classified following the Dahlgren and Whitehead38 diagram of the social model of health in order to situate intervention impact from the perspective of health inequalities aetiology. Outcomes were thus classified as tackling:
-
General socioeconomic, cultural and environmental conditions. Examples of these include improved communication between members of the Traveller Community and service providers, Community members engaging in a representational role and increased awareness of Traveller culture and needs among service providers.
-
Social and community networks. Examples include building capacity in the Community, participation of Traveller Community members in activities to raise awareness of their culture among the wider community and changing perceptions in the Community about the respective roles of men and women.
-
Individual lifestyle behaviours. Examples of these include improved adherence to prescribed treatment, participants who are engaging and confident to articulate their needs and increased uptake of services.
Working back from outcomes to generate Context–Mechanism–Outcome configurations
Working from this database of classified outcomes, we scrutinised studies for the potential mechanisms that might have led to these outcomes, in context. This was a highly iterative process, whereby theories were developed, populated or countered by a detailed analysis of the studies.
Numerous such CMO configurations were developed from the data extracted, in conjunction with their substantiation and verification through bringing to bear theoretical literature and evidence from interventions in parallel populations. This led to the development of more refined explanatory theories through which outreach interventions may work in Traveller Communities. The net effect of this stage was thus a ‘reconstruction’ of meaning from the previously disaggregated pieces of evidence.
Validation and refining of theories through expert hearings and alternative literature sources
A number of ‘expert hearings’ (EHs) with key stakeholders, including Traveller Community members outreach workers and members of Traveller organisations, were also conducted in order to test and refine the developed theories. Key organisations and individuals were identified and recruited through Internet searches, review of initial documentation and research team networks in the field. The EHs varied in format and consisted of:
-
five consultations with steering group members (Traveller Community members, specialist workers and members of Traveller organisations) (EH1, EH2, EH3, EH4 and EH5)
-
one consultation with a research members’ contact (Gypsy and Traveller liaison officer) (EH6)
-
two focus groups with members of Traveller Communities, facilitated by members of the researchers network (EH7 and EH9)
-
guided discussion around scenarios relating to health needs and services with nine Czech Roma Gypsies (EH8) and five Traveller Community members at Appleby Fair (a traditional horse fair held in Appleby, Cumbria, which is a major annual holiday event and gathering point for members of Traveller Communities) (EH10).
Further detail on EH activities, including the rationale for decision-making about the stakeholders involved, the timing of events and key outcomes, are detailed in Appendix 8 . Given the limited number of outcome data available and as the reporting of outreach interventions tended to describe programme strategies and provided a limited amount of insight into underpinning mechanisms, stakeholder involvement was key to eliciting mechanisms leading to particular outcomes. Access to Traveller Communities and facilitation of consultation with them was negotiated by those with established relationships with Community members. This enabled Traveller Communities to have an active role in the validation and refinement of theories. Examples of consultation focus included:
-
trust: what could health-care professionals do to gain the trust of the Community
-
health improvement: what could be done to improve the health of Travellers
-
patterns of nomadism and their impact on access
-
what kinds of services Travellers would access and in relation to what kinds of needs
-
vignettes, used to elucidate what kind of intervention would trigger different levels of engagement.
Appendix 9 provides an illustration of a discussion guide for a focus group with Traveller Communities and how it was informed by the analysis process.
These data were examined in detail and used to substantiate or invalidate our emergent understandings. For example, participants consistently referred to their preference for outreach workers to come from the Community, but some could think of Traveller Community members who would not be accepted because of prior conflicts within the Community. This shaped our understanding of ‘by whom’ in moderating the necessity to belong to the Community in order to offer effective outreach. The emphasis shifted, instead, to the need to have developed trusting relationships with the Community. Trust, in its own right, emerged in the EHs as having crucial importance, as it had in the Traveller Community literature. We searched the broader literature for existent models of trust and how it might be developed, and then subsequently consulted our EH data again, checking if we had evidence of each subdomain of trust.
In realist syntheses, the search process is iterative89 and spans the entire project from the development of research questions through to refining the theories developed through the synthesis. 100 As such, for the realist synthesis the initial search was a preliminary one, which provided the reviewers with a literature base to populate and refine the theories described earlier. Subsequent literature searches were undertaken in order to inform the development of initial theories in the subscription databases detailed on p. 11. At this stage in the process, search strategies are required to be purposive rather than systematic in order to allow the development and substantiation of each initial theory. Three iterative searches focused on:
-
developing an understanding of commonalities in all Traveller Community subgroups, and also what distinguishes them and other disengaged groups (C)
-
understanding of potential underlying mechanisms (M)
-
outcomes (O) measured through ‘stronger’ research designs than those which are predominant in the literature on Traveller Communities ( Figure 2 ).
FIGURE 2.
Flow of citations through the realist review.
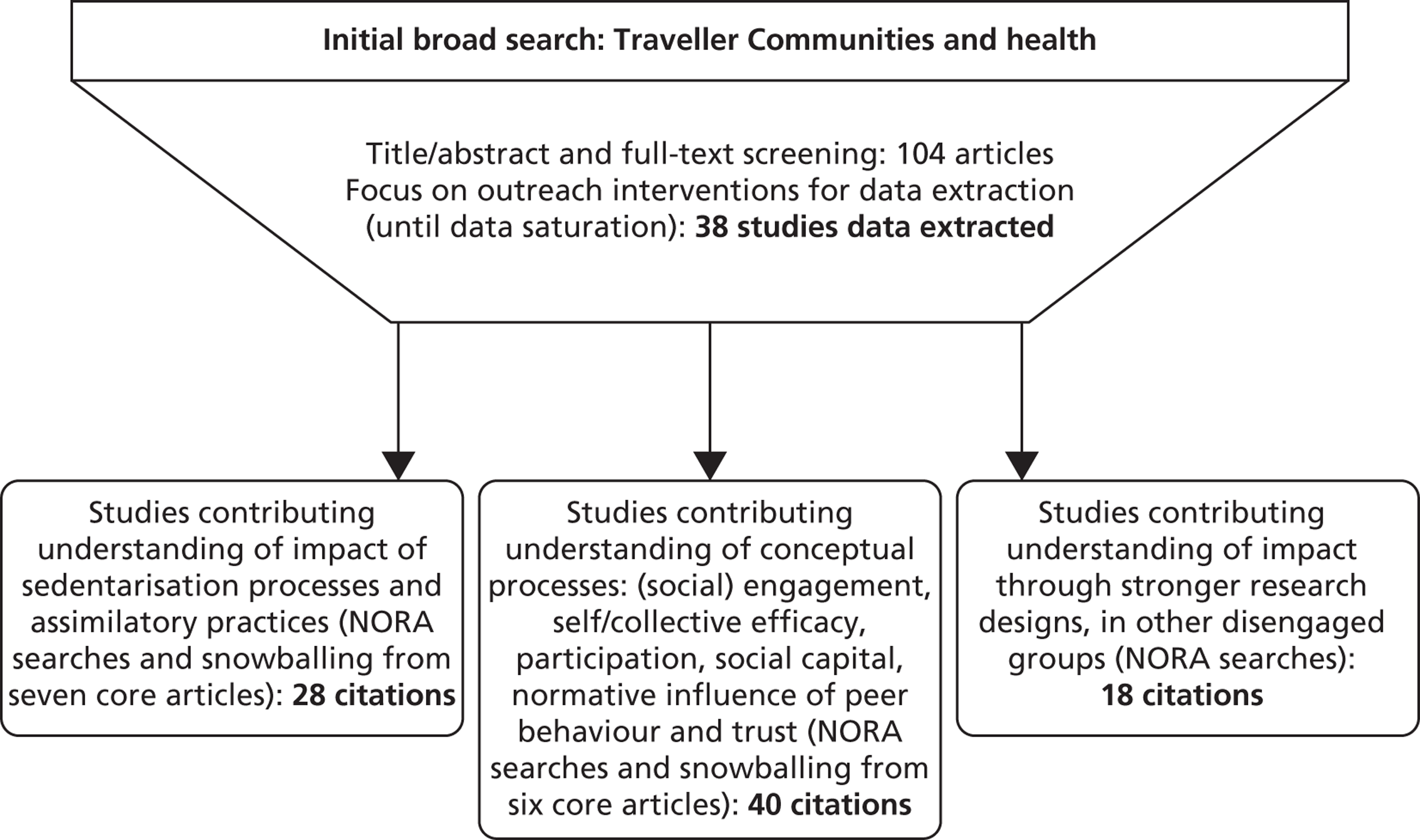
Each subsequent search strategy led to the identification of a number of studies. They all shaped the developing theories, but Figure 2 highlights the citations that provided us with the most explanatory purchase about that particular theory, and that are explicitly cited in this report. However, all of the 28 citations focusing on the particularities of Traveller Communities were used in developing the ‘to whom’ initial theory (see Chapter 3 , ‘To whom’: the context of outreach work), the 40 citations contributing some theoretical understandings contributed to the development of the explanatory framework for outreach detailed in Chapter 3 (see Explanatory framework). The 18 studies featuring stronger research designs (from RCTs to phenomenological studies) included outreach type interventions in aboriginal communities in Australia and Canada,101 homeless people,102 native American,103 , 104 and refugee groups105 as well as disaffected drug users. 106 These studies were used to substantiate the developing theories, for example on p. 57 and p. 64.
Pawson98 notes that in realist syntheses ‘The presentation of the synthesis is difficult because the process of going back and forth from hypothesis to evidence results in the continuous refinement of those hypotheses’ and that the reporting ‘inevitably and like all scientific research, tidies up that process by freezing the running order of hypotheses and evidence’ (p. 13). For example, EHs that have happened chronologically later in the project nevertheless might confirm or illustrate some of the points made earlier in the theory development process. Where this is the case, they are reported in support of the theory in question as if it had been a linear process, for ease of reading. The same applied to additional literature searches as, for example, while the intent of one particular search might have been to elicit measured outcomes of outreach, the results might have shown up the role of trust development in the process.
Economic evaluation
A lack of economic evaluations of outreach interventions was anticipated, hence the original aim of the economic evaluation component was to build on the narrative review of the effectiveness of outreach interventions. This would involve estimation of intervention costs and then evaluation of the potential cost-effectiveness of different modes of intervention and different health behaviours targeted. This approach, which blends evidence review and data synthesis, was used successfully to highlight which health promotional activities undertaken by lay health advisers might be considered cost-effective. 107 However, the lack of quantitative evaluation of the effectiveness of outreach in Traveller Communities rendered this approach infeasible. To maximise learning from the available literature, the initial criteria for inclusion of only articles describing the evaluation of outreach interventions for Traveller Communities was relaxed to include any article that provided a description of the delivery of outreach, the impact of outreach or the resource implications. A table of the studies included in this analysis is presented in Appendix 10 . The available literature was used to define the principal modes of delivery of outreach interventions, to aid estimation of the resulting resource implications and to provide an indication of effectiveness.
The titles and abstracts of all 407 articles unearthed in the literature review were scrutinised to determine the nature and likely content of the article. Articles describing any aspect of outreach were read. Key articles reporting the health of members of Traveller Communities were also read. Information on outreach interventions was extracted, including budgets and indications of resource use; practicalities of delivery; whether or not specific health behaviours were targeted; training and qualifications of staff; the size of the population served; and any measures of outcomes achieved. After extraction, the main modes of delivery were determined and the information previously abstracted was categorised accordingly. Some articles provided information for more than one mode of delivery. Articles within each mode of delivery category were then evaluated. Given the scarcity of data, no formal attempt was made to assess the quality of information. Data on resource use and budgets were assumed to be correct and to represent the cost of delivery of the intervention described. Data on outcomes were scrutinised for potential bias, but the uniformly weak nature of the evidence presented little opportunity to discriminate according to perceived quality of studies.
Chapter 3 Results
A summary of the identification, screening and selection of studies is provided in Figure 3 .
FIGURE 3.
Summary of the systematic identification, screening and selection process.
Scoping review
A total of 278 publications focused on the health of Traveller Communities and formed the evidence base for the scoping review (a list of included studies can be found in Appendix 11 ). As noted earlier, a decision was made to include all articles focused broadly on Traveller health in order to situate the evidence on outreach for Traveller Communities in relation to wider research and practice activity. Of all the articles which focused on the health of Traveller Communities, only around one-quarter (24.8%) described the implementation of outreach. This section describes the characteristics of the overall evidence base on the health of Traveller Communities and on outreach interventions for Traveller Communities according to year of publication, country of research or practice, authors and practitioners, and type of evidence.
Key findings
Year of publication
Interest in improving the health of Traveller Communities appears to have increased in recent years. Half (50.4%) of the articles with available dates were published from 2006 onwards (as shown in Figure 4 ). The publication of a seminal study on the health status of Traveller Communities in England in report form in 200437 , 108 and as peer-reviewed publications in 2007,19 , 39 as well as the initiation of the Decade of Roma Inclusion in 2005,109 are developments that may have contributed to this increasing attention to health of Traveller Communities. Although there appears to be a peak of activity in relation to Traveller health in 2001, this is likely to be an artefact of the separate classification of 13 articles all reported in a journal special issue.
FIGURE 4.
Distribution of publications according to year of publication.
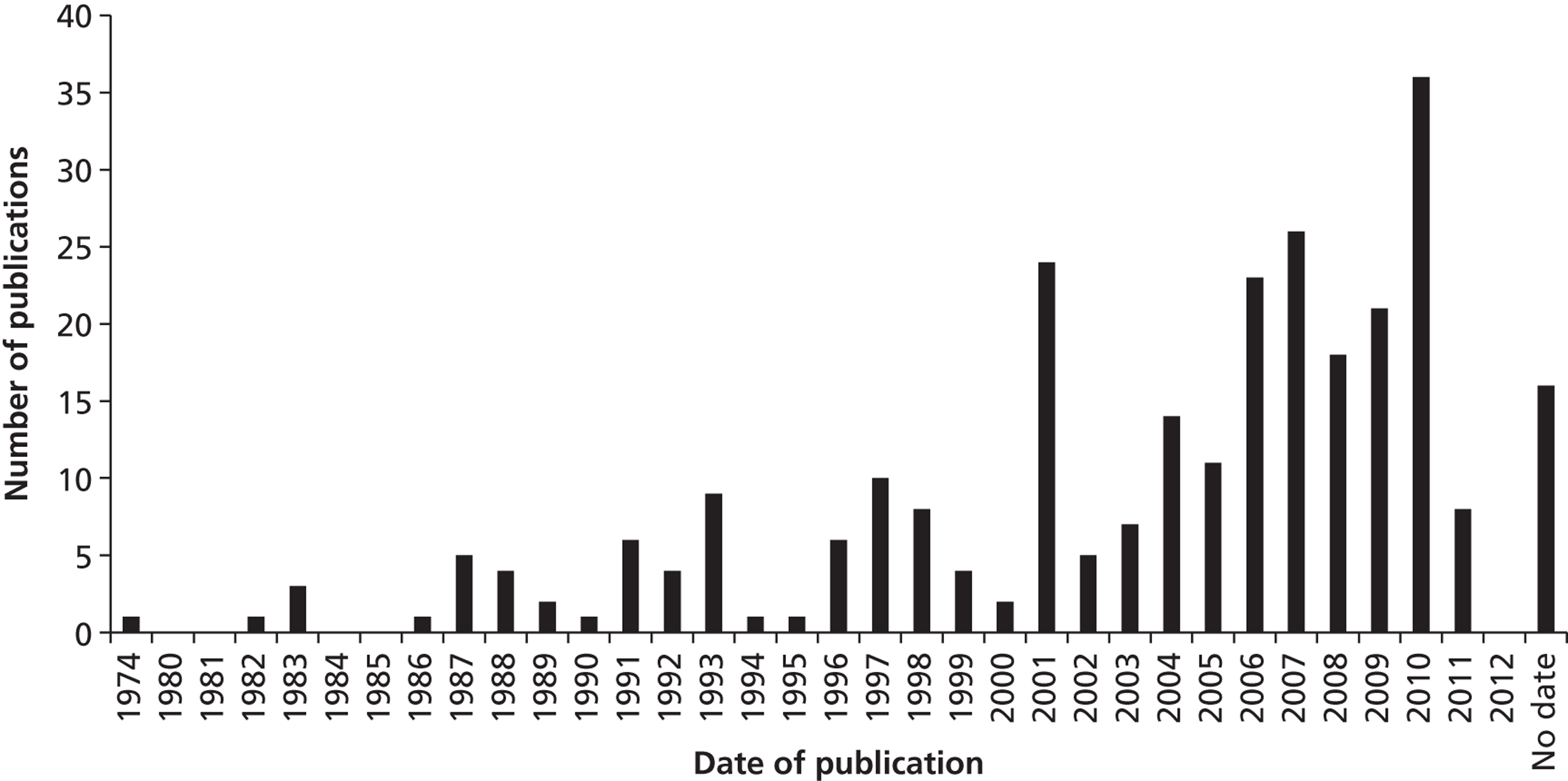
When examining only those articles focused on outreach, a similar distribution is evident, with half (50.7%) published from 2006 onwards.
Country of research or practice
Articles were classified according to the country in which the research or practice was conducted (shown in Figure 5 ). The majority of publications (47.2%) emanated from the UK. Articles from Ireland accounted for the next greatest proportion of articles (18.5%). Taken together, central (10.7%) and eastern Europe (10.7%) contributed just over one-fifth of the overall articles, and only a small proportion of articles originated from the USA (6.6%).
FIGURE 5.
Distribution of publications by country of research or practice.
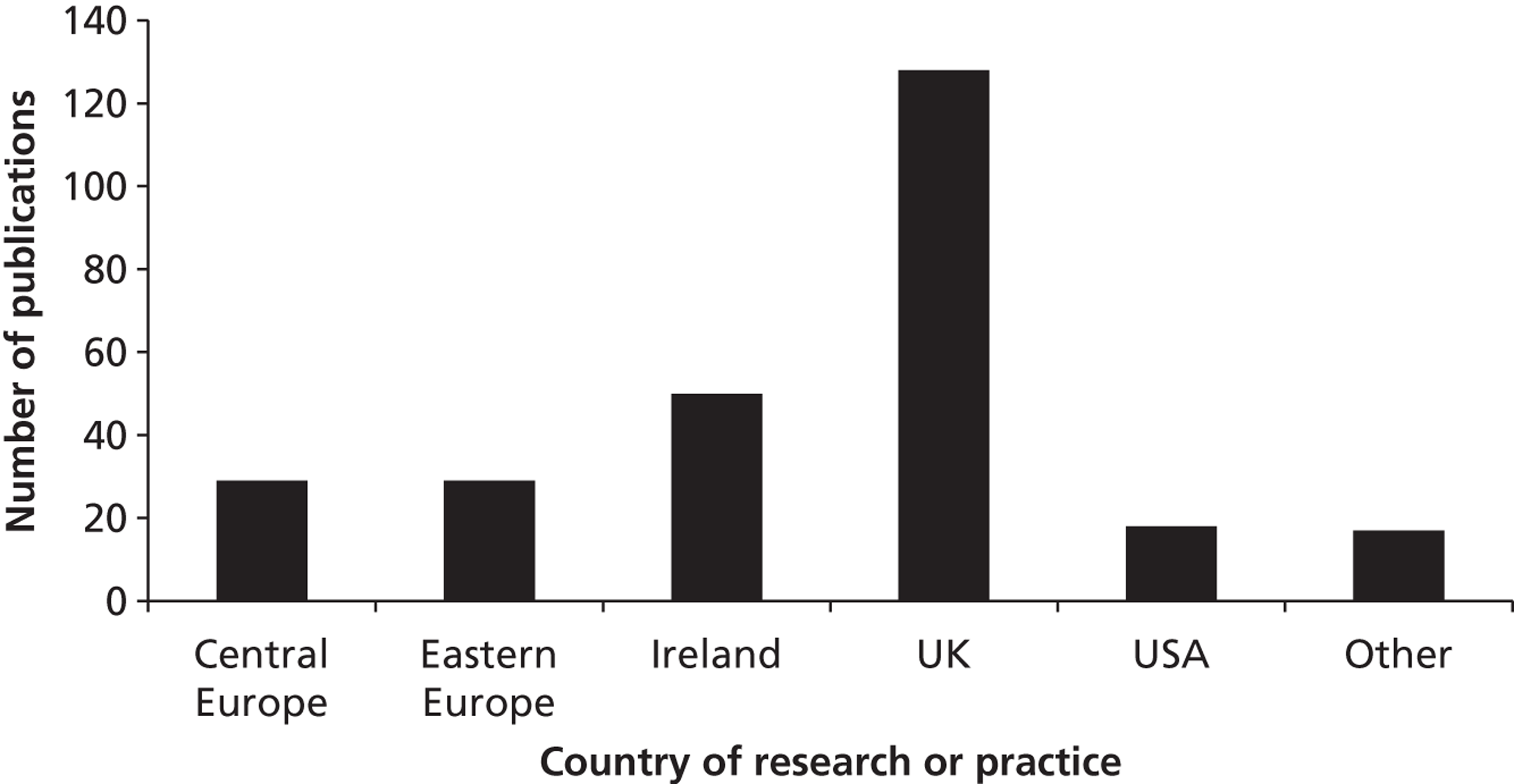
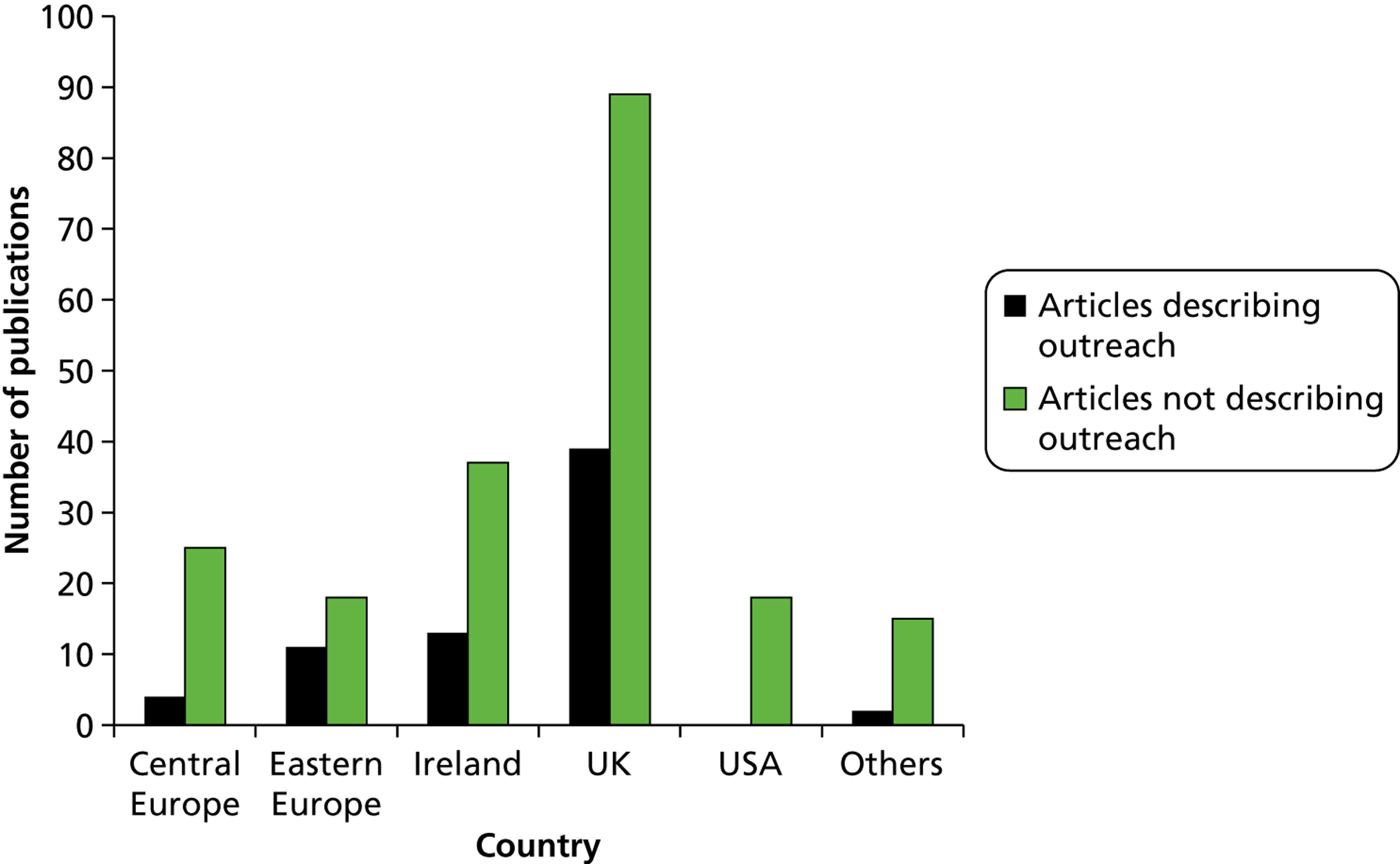
Figure 6 compares the distribution of articles describing outreach with those that do not describe outreach according to country of research or practice. The small amount of evidence describing outreach overall is reflected when studies are broken down by country. However, this difference is particularly pronounced in the USA, in which none of the 18 studies described outreach interventions, and in central Europe, in which only 13.8% of all publications described outreach. Eastern Europe had the highest proportion of articles focused on outreach (37.9%), followed by the UK (30.5%) and Ireland (26%).
FIGURE 6.
Distribution of publications according to country of research and practice and description of outreach.
Authors and practitioners
Almost half of the publications were written by academic authors (48.6%) (described in Figure 7 ). There were also considerable numbers of publications written by Traveller Community specific or third-sector organisations (18.3%) and health service providers (21.2%). Governmental or local authority publications accounted for a much smaller proportion of the overall evidence base (11.9%).
FIGURE 7.
Distribution of publications according to type of author.
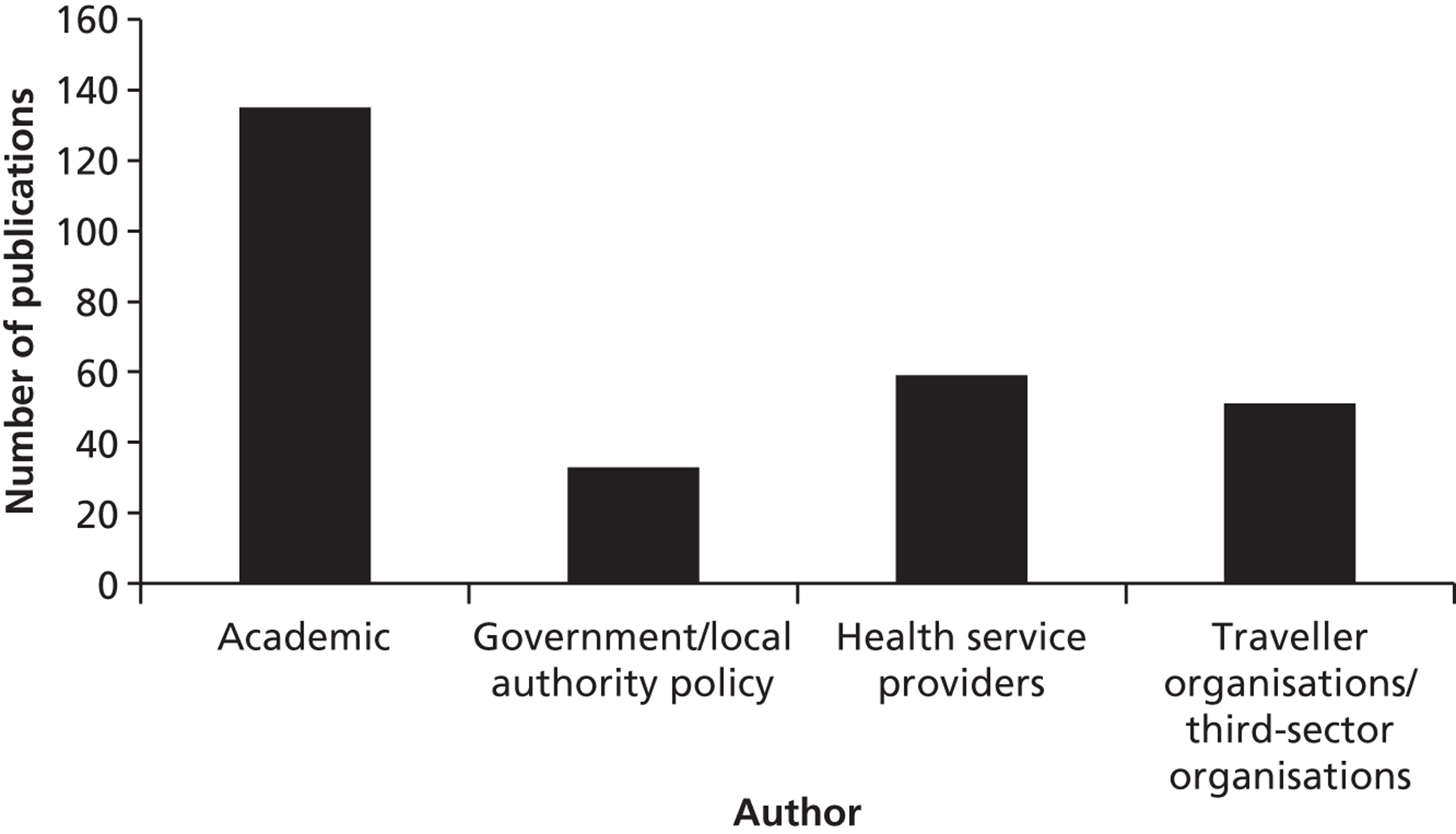
Publications from the UK, Ireland and eastern Europe have the widest range of authors in the sample ( Figure 8 ). On the other hand, authorship in central Europe and the USA is confined to academic, Traveller organisation or third sector, and health service provider authors, and includes no publications written by government or local authority authors. In most countries, articles written by academic authors accounted for the greatest proportion of articles. The dominance of academic authors was particularly pronounced in central Europe (79.3% of overall publications). The regions of eastern Europe and the USA were exceptions, however, with publications by Traveller Community organisations contributing the greatest proportion of all publications (50% of all publications in the USA and 48.3% of all publications in eastern Europe). The USA, the UK and Ireland had the greatest proportion of articles written by health service providers (33.3%, 32.8% and 16%, respectively), with central and eastern Europe each including just one publication (3.4%) written by health service providers. The UK and Ireland contributed the majority (28 out of 33) of publications written by government or local authority authors.
FIGURE 8.
Distribution of publications according to country and type of author.
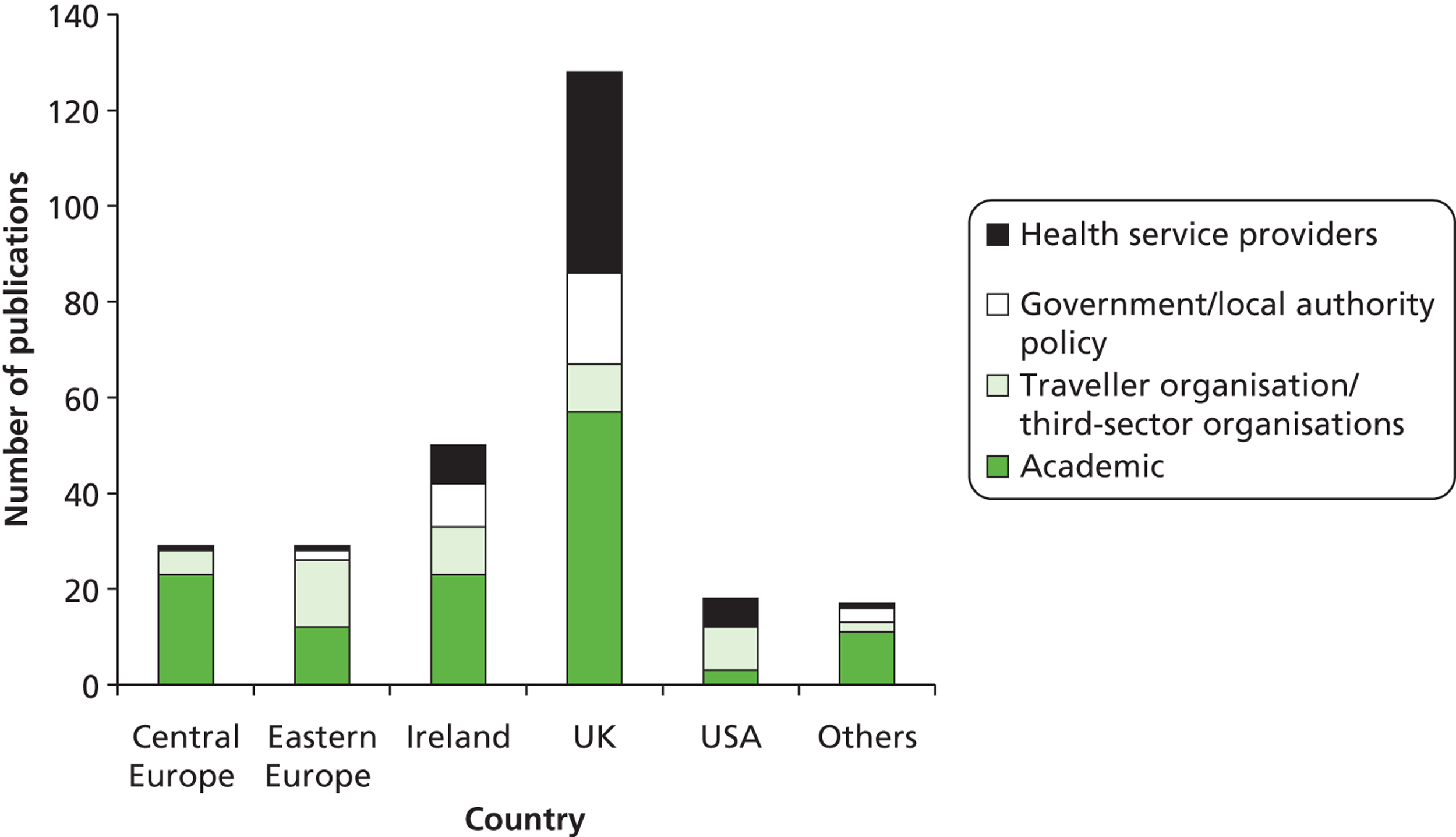
A smaller proportion of those studies describing outreach were written by academic authors (27.5%) than those which did not describe outreach ( Figure 9 ). Studies focused on outreach also contained a higher proportion of publications written by health service providers than those that did not describe outreach (31.9% and 17.7%, respectively), and by Traveller or third-sector organisations (31.9% and 13.9% respectively).
FIGURE 9.
Distribution of publications according to type of author and description of outreach.
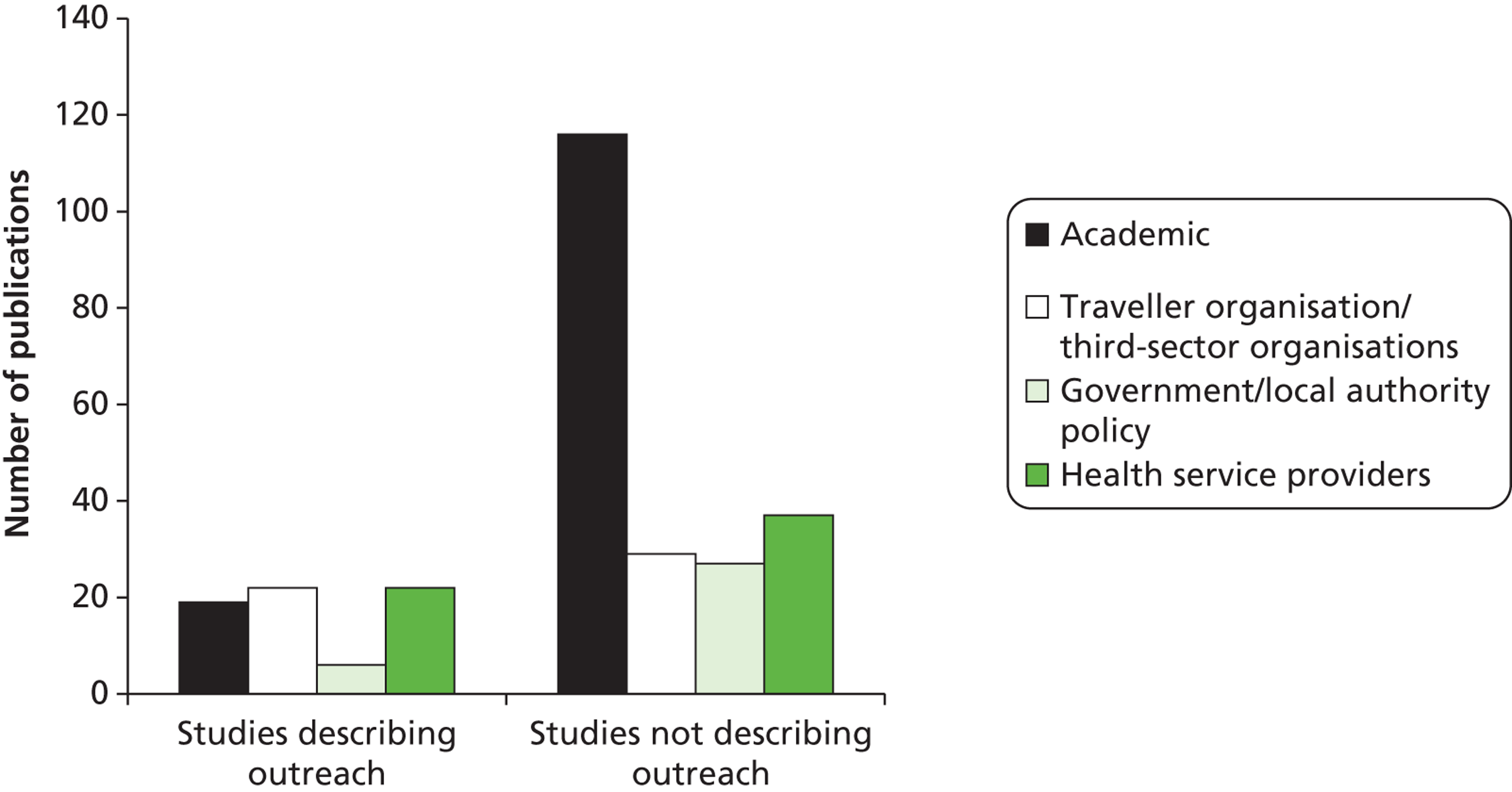
As shown in Figure 10 , those outreach interventions described were delivered either by mainstream service providers (48.3%) (most often health visitors, but also including GPs, nurses, teachers and special education welfare officers), or by members of Traveller Communities (43.3%). The remaining studies described outreach interventions by third-sector or non-governmental organisations which do not focus exclusively on Traveller Communities (3.3%); by both mainstream service providers and Traveller Community members (3.3%); and by lay settled community members with the shared experience of motherhood (1.7%). Nine outreach interventions were not categorised according to the outreach worker due to a lack of sufficient detail.
FIGURE 10.
Distribution of pubications describing outreach according to type of outreach worker. NGO, non-governmental oganisation.
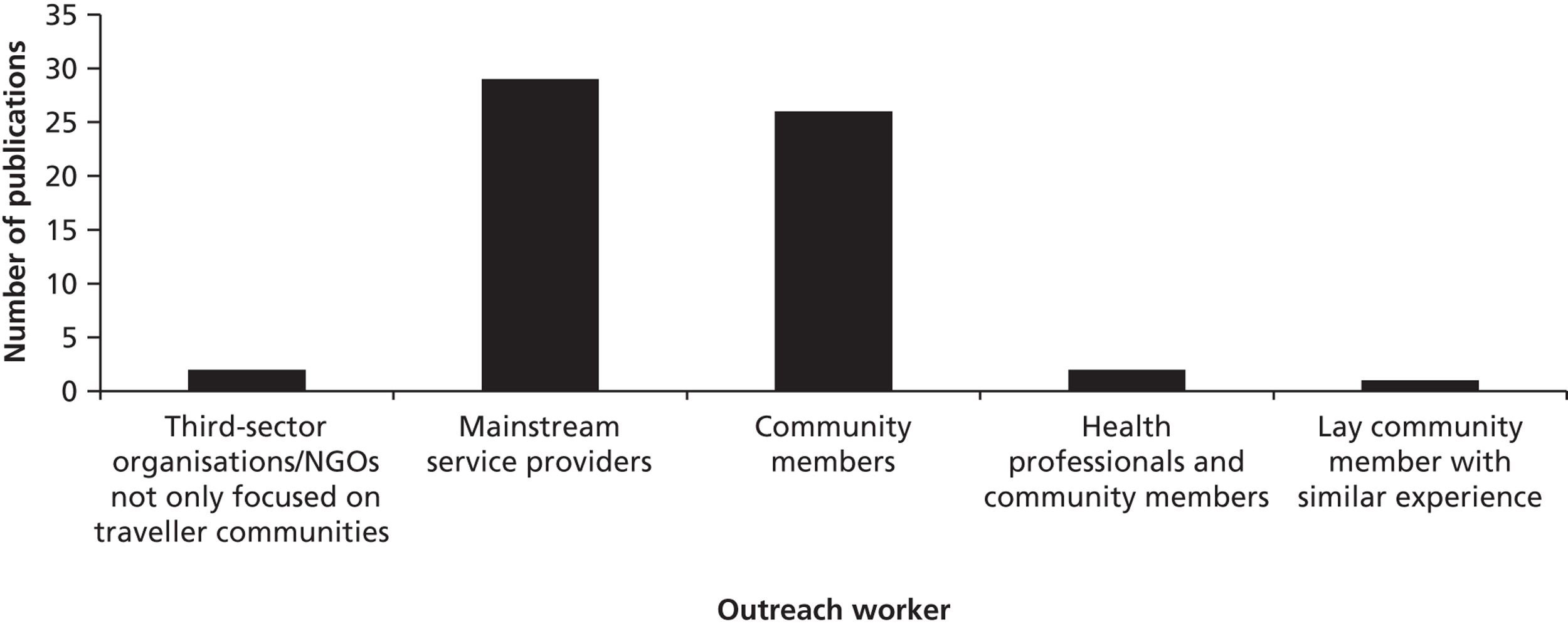
Evidence type
Research studies accounted for the greatest proportion of the overall literature base (42.4%), as shown in Figure 11 . However, in keeping with the developing literature base, anecdotal accounts made the next greatest contribution (27.7%). Theoretical or opinion papers accounted for a small proportion of the available literature (16.2%) and only around one-tenth of articles described policy or guidelines for practice (10.4%).
FIGURE 11.
Distribution of publications according to type of evidence.
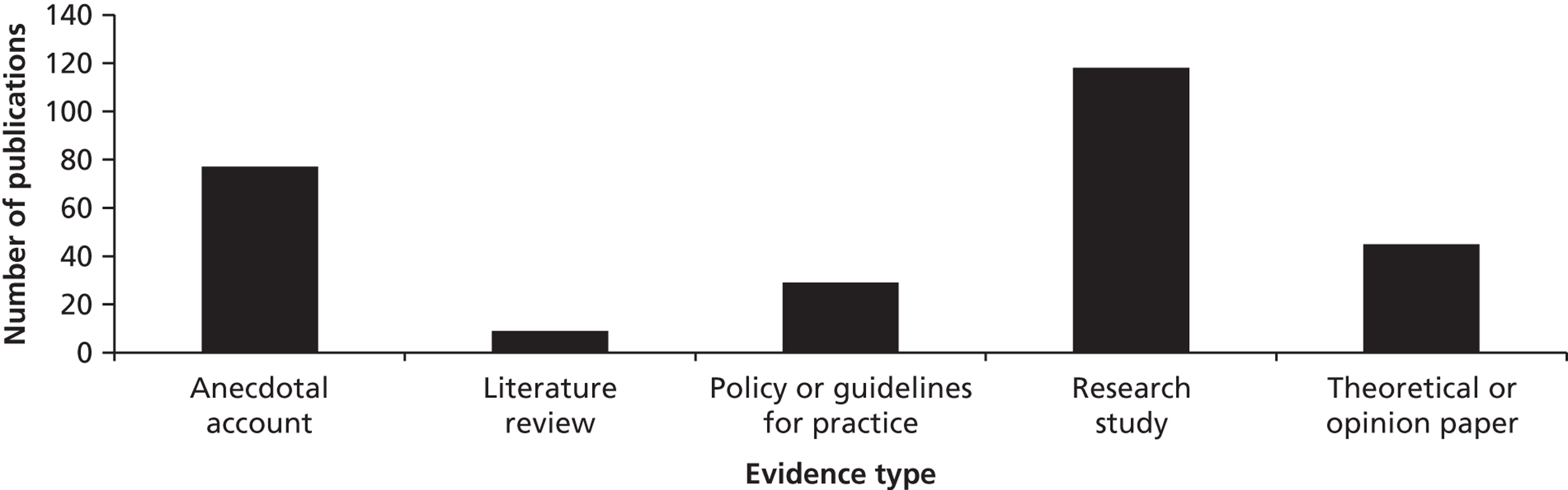
Given that around half of articles were published prior to 2006 and half after, this date was used as the point of comparison for the distribution of articles according to type of evidence and date of publication. As Figure 12 shows, a greater proportion of research articles and a smaller proportion of anecdotal accounts were published in 2006 onwards than in years prior to 2006. This suggests that the literature base on the health of Traveller Communities is starting to shift towards the generation of more robust evidence. In addition, a greater proportion of policy or local authority papers were published in 2006 or afterwards, suggesting that attention to Traveller Community health in health policy may be increasing.
FIGURE 12.
Distribution of publications according to evidence type and date of publication.
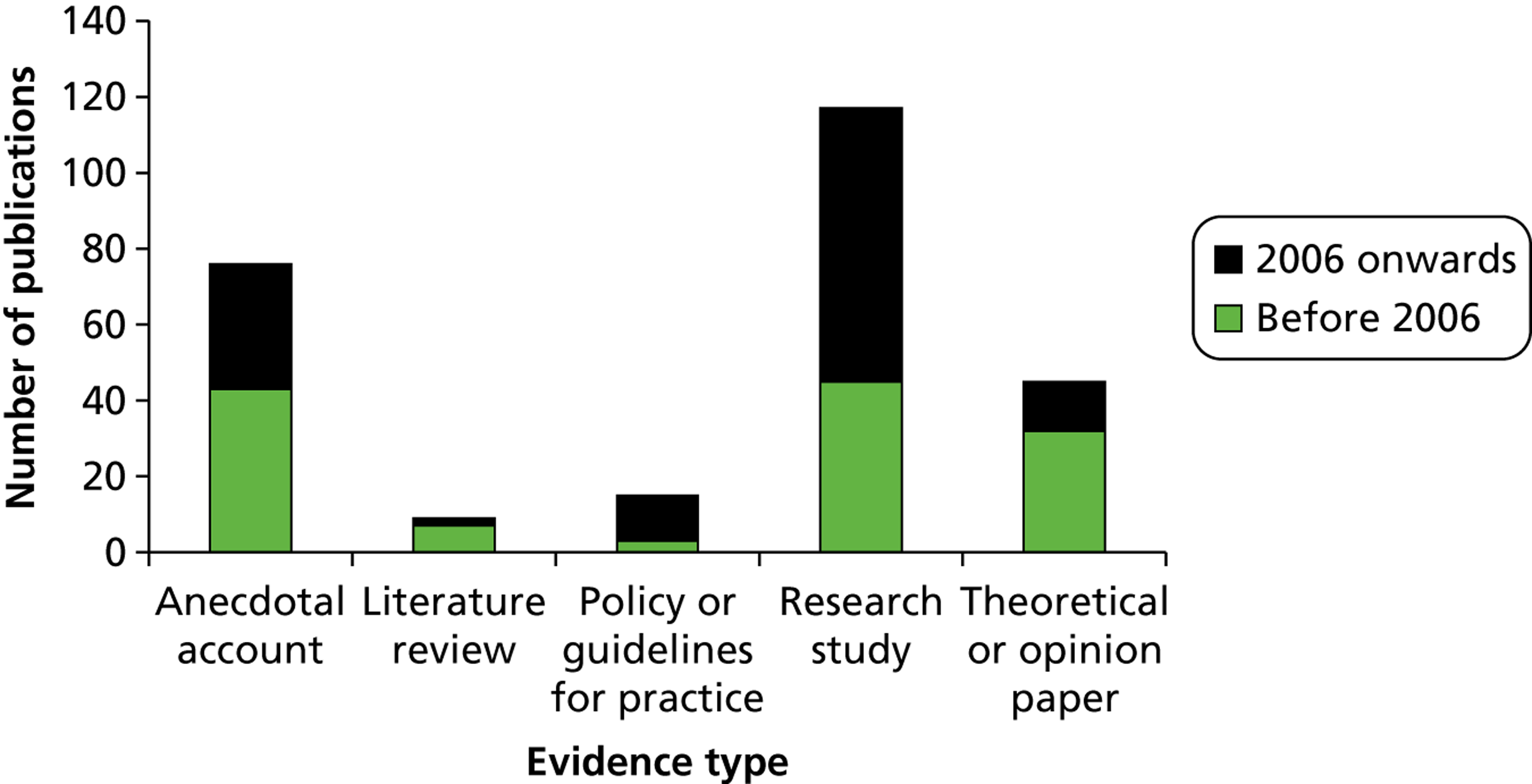
The breakdown of all research studies focused broadly on the health of Traveller Communities according to research design is described in Table 1 . Cross-sectional studies, which examined the health status of Traveller Communities, often with matched control groups, accounted for around one-third of research designs. A further one-third of articles described qualitative approaches, utilising interviews, focus groups, participant observation or a combination of those methods. Studies reporting needs assessments of Traveller Communities accounted for around one-tenth of all research studies. Few research studies reported on the evaluation of interventions to improve the health of Traveller Communities. Only one study reported the results of a RCT and one reported the results of a controlled clinical trial. Two studies reported the results of pre- and post-intervention questionnaires and five reported the results of service evaluations.
| Research approach | Number of articles (%) |
|---|---|
| Cross-sectional study | 41 (34.8) |
| Qualitative | 36 (30.5) |
| Health needs assessment | 11 (9.3) |
| Mixed methods | 11 (9.3) |
| Descriptive questionnaire/survey | 5 (4.2) |
| Service evaluation | 5 (4.2) |
| Action or participatory research | 3 (2.5) |
| Pre- and post-intervention questionnaire | 2 (1.7) |
| Health impact assessment | 2 (1.7) |
| RCT | 1 (0.9) |
| Controlled clinical trial | 1 (0.9) |
Figure 13 describes the distribution of only those publications describing the implementation of outreach according to evidence type. Descriptions of outreach interventions were, for the most part, based on anecdotal or experiential accounts (71%). Only around one-fifth of articles reporting the implementation of outreach were research studies (21.7%).
FIGURE 13.
Distribution of publications describing outreach according to evidence type.
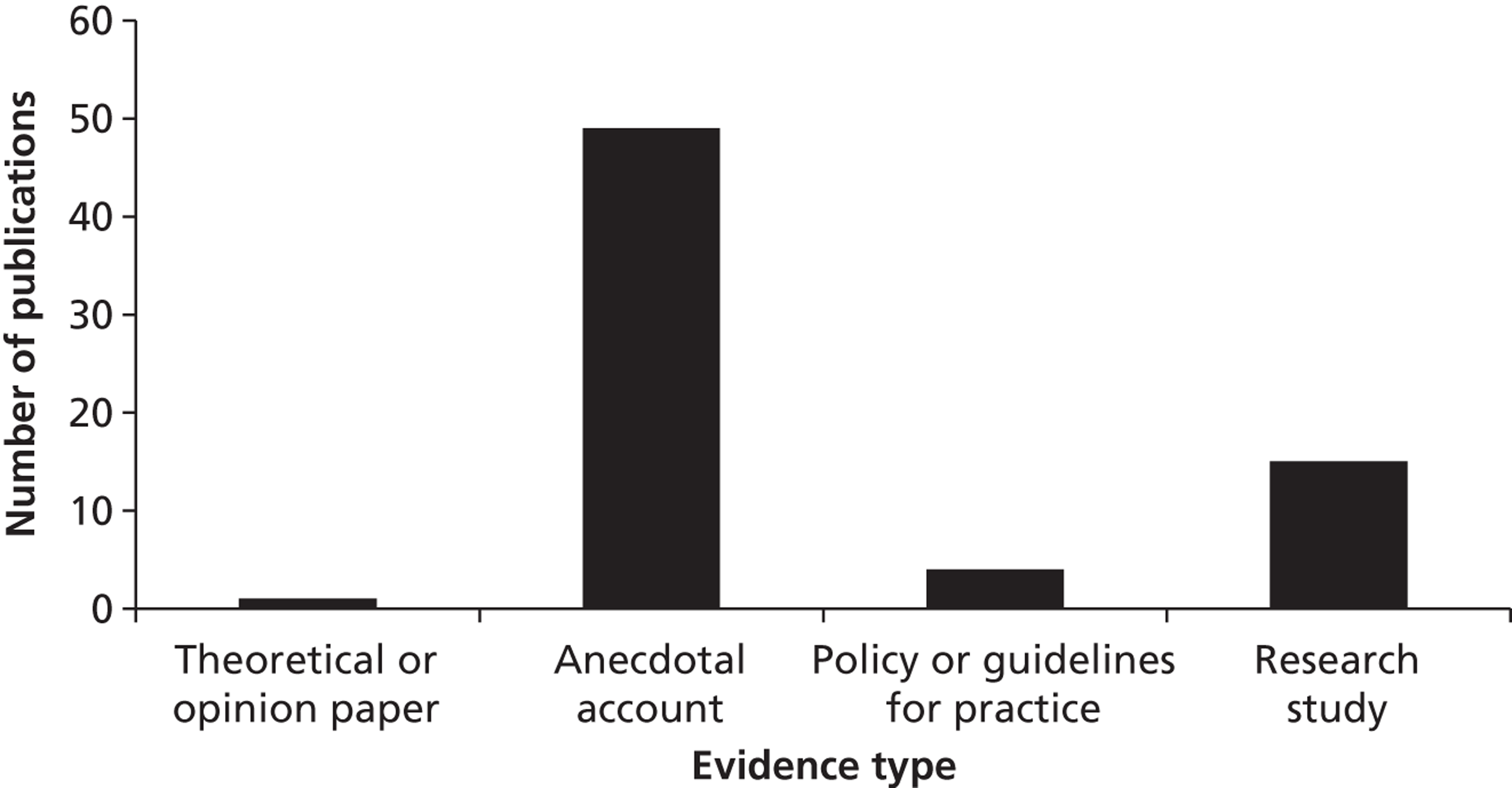
In 5 of the 15 research studies describing outreach, examples were discussed but not related to research findings and as such were, therefore, excluded from analysis of the types of research design. Of the remaining 10 research studies which report the evaluation of outreach interventions, four used qualitative methods, three reported on service evaluations of outreach programmes, one reported on a RCT, one reported on a controlled clinical trial, and one reported on a pre- and post-intervention questionnaire ( Figure 14 ). The articles which reported on research studies of outreach interventions were quality assessed using the Critical Appraisal Skills Programme quality assessment tool79 in the case of qualitative studies and the Effective Public Health Practice Project tool78 for quantitative studies. One study was quality assessed as moderate, with the remainder of studies assessed as weak.
FIGURE 14.
Distribution of research publications describing outreach according to study design.
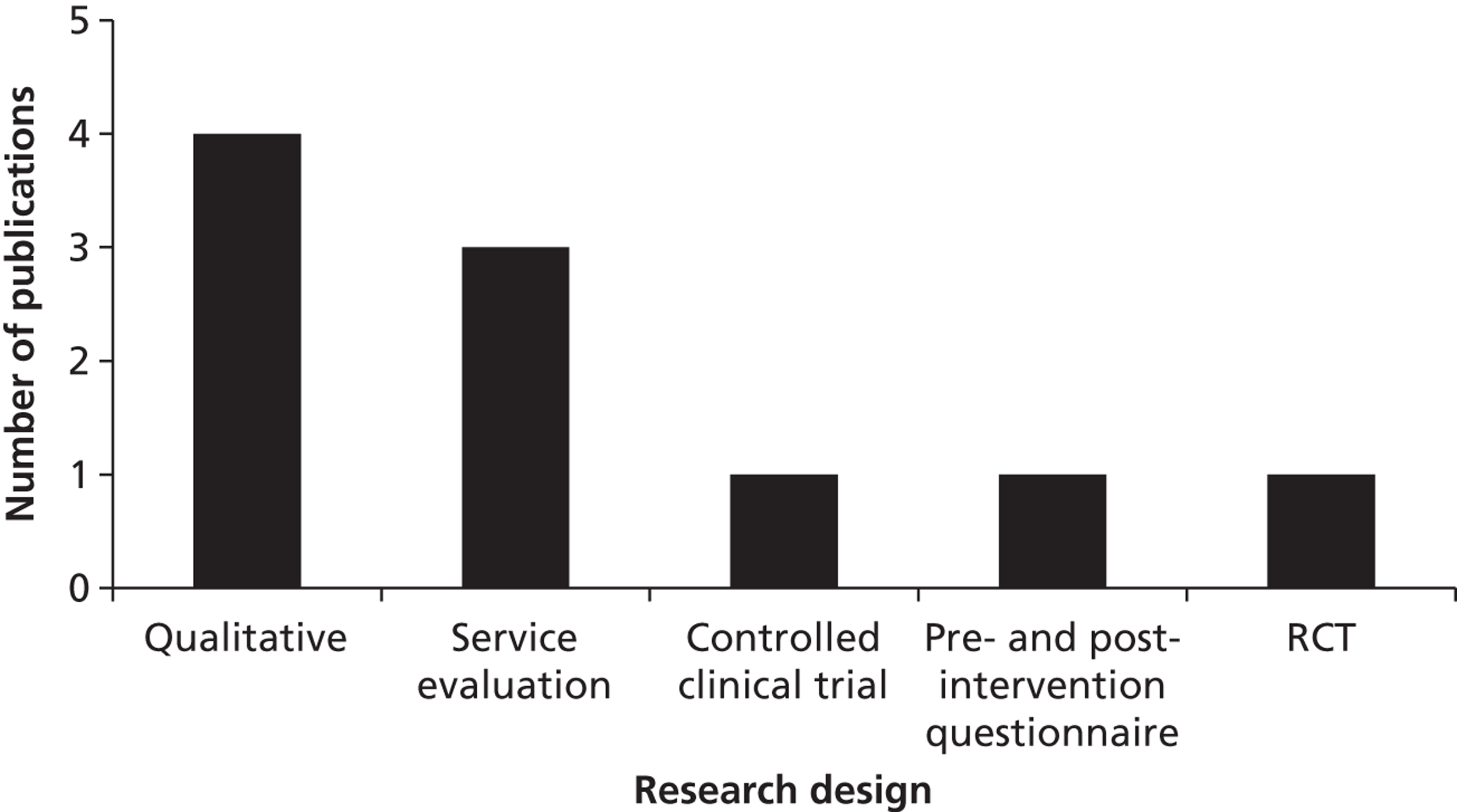
Topic
Publications were grouped into 12 topic areas building on Aspinall’s classification. 22 Some of this classification is, inevitably, arbitrary, as decisions had to be made when articles covered two or more topic areas. Appendix 12 provides examples of studies classified under each topic area in order to enhance transparency over the categorisation process. Given the purpose of the scoping to scaffold the realist synthesis, it is hoped that this will give readers an overview of the amount of evidence on the different health needs of Traveller Communities, as well as the health focus adopted by outreach interventions.
How much evidence of what type is available on the different health needs of Traveller Communities?
As shown in Figure 15 , just under one-quarter (23.7%) of publications on the health of Traveller Communities concerned access to and use of services, constituting the largest proportion of articles. Taken together, the literature on general health needs and health status contributed a sizeable portion of evidence. Lifestyle factors and women’s health each accounted for around one-tenth of the sample of publications (9% and 9.4% respectively). A slightly smaller number of publications focused on the wider determinants of health (7.6%) and very few studies focused on mental health (1.4%), oral health care (1.4%) or cardiovascular disease (2.9%).
FIGURE 15.
Distribution of publications according to topic.
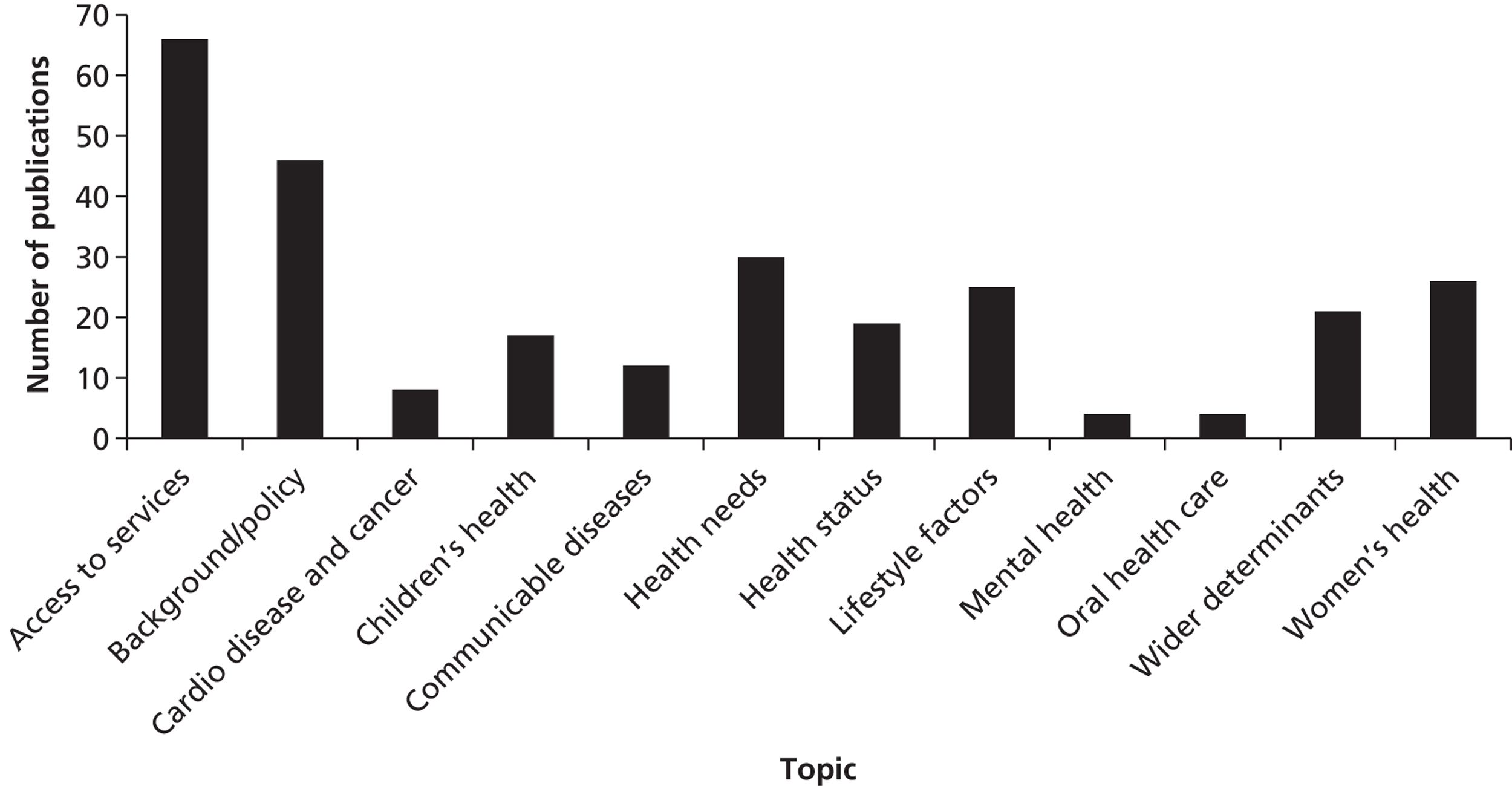
As shown in Table 2 , while research studies made up the majority of publications for most topics within the overall evidence base on Traveller health, over half of publications focused on access to services were anecdotal accounts. Publications on communicable diseases also contained a greater proportion of anecdotal accounts than research studies.
| Topic | Evidence type | |||||
|---|---|---|---|---|---|---|
| Theoretical or opinion paper, n (%) | Anecdotal account, n (%) | Literature review, n (%) | Policy or guidelines for practice, n (%) | Research study, n (%) | Total, N | |
| Access to services | 8 (12.1) | 37 (56.1) | 2 (3) | 0 | 19 (28.8) | 66 |
| Background/policy | 9 (19.6) | 9 (19.6) | 1 (2.2) | 22 (47.8) | 5 (10.9) | 46 |
| Cardio disease and cancer | 1 (12.5) | 0 | 0 | 0 | 7 (87.5) | 8 |
| Children’s health | 4 (23.5) | 1 (5.9) | 0 | 1 (5.9) | 11 (64.7) | 17 |
| Communicable diseases | 0 | 7 (58.3) | 1 (8.3) | 1 (8.3) | 3 (25) | 12 |
| Health needs | 4 (13.3) | 5 (16.7) | 1 (8.3) | 0 | 20 (66.7) | 30 |
| Health status | 4 (21.1) | 0 | 3 (15.8) | 1 (5.3) | 11 (57.9) | 19 |
| Lifestyle factors | 1 (4) | 5 (20) | 0 | 1 (4) | 18 (72) | 25 |
| Mental health | 0 | 2 (50) | 0 | 0 | 2 (50) | 4 |
| Oral health care | 0 | 1 (25) | 0 | 0 | 3 (75) | 4 |
| Wider determinants | 5 (23.8) | 3 (14.3) | 1 (4.8) | 2 (9.5) | 10 (47.6) | 21 |
| Women’s health | 9 (34.6) | 7 (26.9) | 0 | 1 (3.8) | 9 (34.6) | 26 |
How much evidence from which countries is available on the different health needs of Traveller Communities?
As shown in Table 3 , a smaller proportion of research and practice in central Europe focused on access to services than in Ireland, the UK and eastern Europe. As shown above, there appear to be few publications pertaining to cardiovascular disease and cancer in Traveller Communities, with central Europe, eastern Europe and Ireland contributing all of the available evidence in this area. A greater proportion of the overall evidence in central Europe and Ireland focused on child health than did other countries. The UK had a much greater proportion of articles focused on health needs and health status of Traveller Communities, contributing the majority of articles in this area. By contrast, the proportion of evidence in the UK focusing on lifestyle factors was small, with eastern and central Europe containing the greatest proportions of evidence on this topic. All of the four publications pertaining to mental health were published in the UK and articles on oral health were contributed solely by the UK and Ireland. The proportion of publications focusing on the wider determinants of health was highest in eastern Europe and central Europe. While the USA looks to have a vastly greater proportion of background and policy documents than other countries, this is a product of multiple cultural competence guidelines produced by the same organisation on different aspects of Roma culture and health.
| Topic | Country of research/practice | |||||
|---|---|---|---|---|---|---|
| Central Europe, n (%) | Eastern Europe, n (%) | Ireland, n (%) | UK, n (%) | USA, n (%) | Others, n (%) | |
| Access to services | 2 (6.9) | 7 (24.1) | 16 (32) | 35 (27.3) | 3 (16.7) | 3 (17.6) |
| Background/policy | 2 (6.9) | 1 (3.4) | 7 (14) | 22 (17.2) | 13 (72.2) | 0 |
| Cardio disease and cancer | 3 (10.3) | 2 (6.9) | 2 (4) | 0 | 0 | 1 (5.9) |
| Children’s health | 4 (13.8) | 1 (3.4) | 4 (8) | 5 (3.9) | 1 (5.6) | 2 (11.8) |
| Communicable diseases | 0 | 2 (6.9) | 0 | 6 (4.7) | 0 | 3 (17.6) |
| Health needs | 1 (3.4) | 0 | 0 | 25 (19.5) | 0 | 3 (17.6) |
| Health status | 1 (3.4) | 0 | 3 (6) | 10 (7.8) | 1 (5.6) | 0 |
| Lifestyle factors | 6 (20.7) | 8 (27.6) | 8 (16) | 2 (1.6) | 0 | 1 (5.9) |
| Mental health | 0 | 0 | 0 | 4 (3.1) | 0 | 0 |
| Oral health | 0 | 0 | 2 (4) | 2 (1.6) | 0 | 0 |
| Wider determinants | 4 (13.8) | 6 (20.7) | 2 (4) | 7 (5.5) | 0 | 2 (11.8) |
| Women’s health | 6 (20.7) | 2 (6.9) | 6 (12) | 10 (7.8) | 0 | 2 (11.8) |
How much evidence by which authors is available on the different health needs of Traveller Communities?
Academic authors appear to write, for the most part, about health status and health needs, access to and use of services, lifestyle factors, women’s health, children’s health and the wider determinants of health ( Table 4 ). Little work by academic authors focused on communicable diseases, mental health and oral health care. The majority of publications by health service providers and Traveller organisations or third-sector organisations focused on access to services. Only academic authors published on cardiovascular disease and cancer. Children’s health was covered only by academic and health service providers. Health service providers and government or local authority authors were more likely to address communicable diseases. A slightly greater number of academic authors and third-sector organisations addressed the wider determinants of health than did government or health service authors.
| Topic | Type of author | |||
|---|---|---|---|---|
| Academic, n (%) | Traveller organisations/third-sector organisations, n (%) | Government/local authority policy, n (%) | Service providers, n (%) | |
| Access to services | 27 (20) | 15 (29.4) | 3 (9.1) | 21 (35.6) |
| Background/policy | 10 (7.4) | 15 (29.4) | 12 (36.4) | 9 (15.3) |
| Cardiovascular disease and cancer | 8 (5.9) | 0 | 0 | 0 |
| Children’s health | 14 (10.4) | 0 | 0 | 3 (5.1) |
| Communicable diseases | 1 (0.7) | 2 (4) | 4 (12.1) | 5 (8.5) |
| Health needs | 15 (11.1) | 1 (2) | 7 (21.2) | 7 (11.9) |
| Health status | 14 (10.4) | 0 | 2 (6.1) | 3 (5.1) |
| Lifestyle factors | 16 (11.9) | 6 (12) | 1 (3) | 2 (3.4) |
| Mental health | 1 (0.7) | 1 (2) | 0 | 2 (3.4) |
| Oral health care | 0 | 1 (2) | 1 (3) | 2 (3.4) |
| Wider determinants | 14 (10.4) | 5 (10) | 1 (3) | 1 (1.7) |
| Women’s health | 15 (11.1) | 5 (10) | 2 (6.1) | 4 (6.8) |
Which health areas do reported outreach interventions target?
Those studies describing outreach covered 10 of the 12 topics included in the overall sample ( Figure 16 ). The majority of articles describing outreach interventions focused on access to services (44.9%), a much greater proportion than those that did not describe outreach interventions (16.7%). Improving access to services, therefore, seems to be a predominant focus of outreach interventions. Just over one-tenth (11.6%) of articles describing outreach focused on lifestyle factors. Few articles described outreach focused on children’s health, oral health care and mental health care, and no publications described outreach focused on cardiovascular disease or cancer, although this is perhaps unsurprising given the small amount of overall evidence on health focused in these areas.
FIGURE 16.
Distribution of publications according to topic and description of outreach.
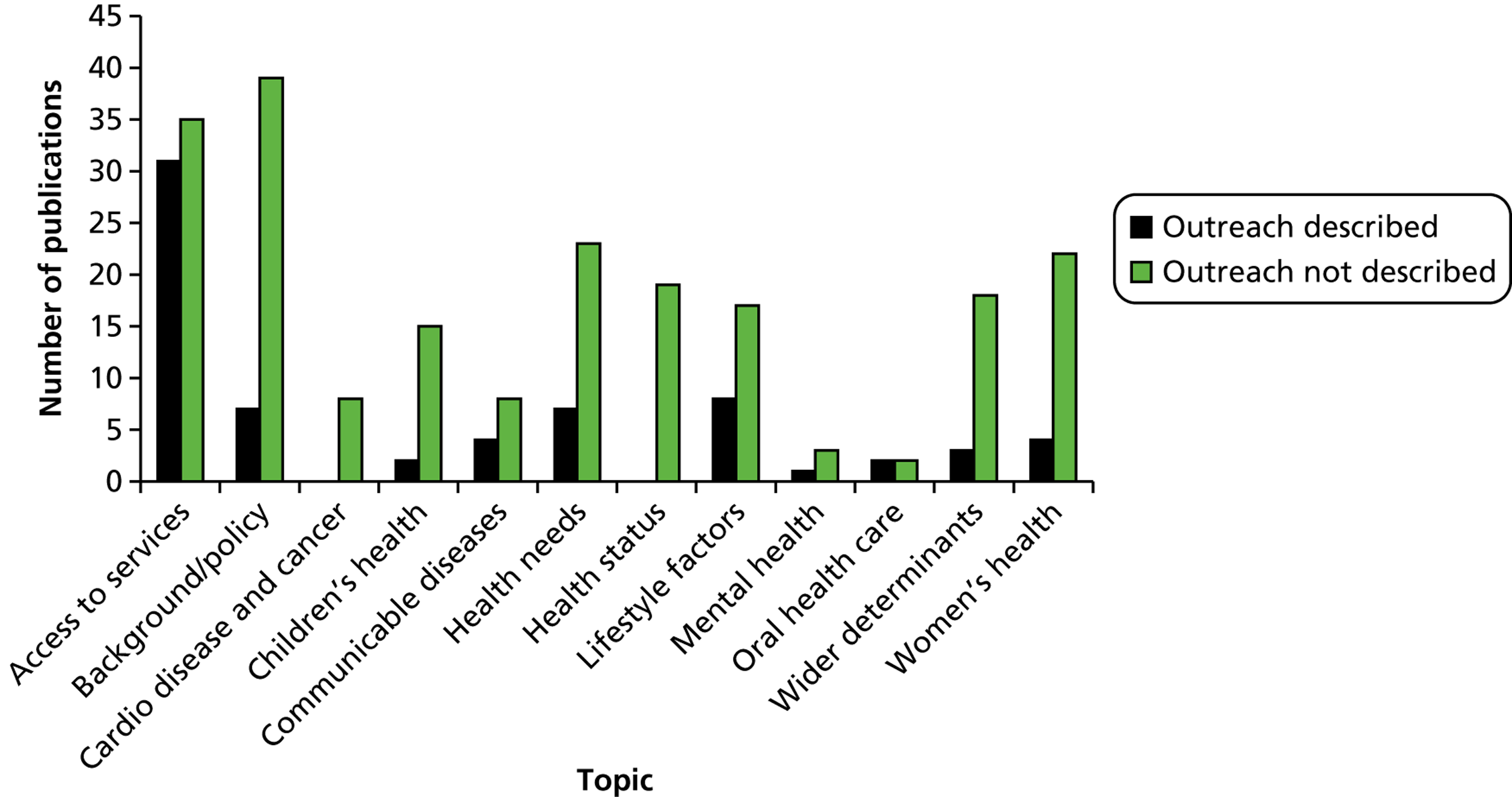
Conclusions
Strengths and weaknesses of the approach
As described in Chapter 1 (see Objectives and focus of the review), this scoping review set out to chart the nature and extent of the broad evidence base on the health of Traveller Communities and on outreach interventions to improve their health. As such, the scoping review did not describe the studies’ findings, but classified the range of included articles in order to generate insights for this review and future research, around the possibilities provided by the existing literature base for the generation and synthesis of evidence.
As this scoping review classifies only those outreach interventions that are reported in the literature, it cannot claim to represent all outreach programmes or activities aiming to improve Traveller health. While this limitation is acknowledged, the scoping review contributes an overview of the published evidence (both peer-reviewed and grey literature) that is available and which is used to inform the decisions of practitioners, policy makers and researchers. Given the broad and systematic search strategy adopted for the review, it is unlikely that studies focused on the health of Traveller Communities will have been missed within the time window examined. However, articles focused on services or interventions that did not lend themselves to outreach, for example genetics, were out of scope for this study and are excluded from this analysis.
Scaffolding the economic and realist review
The review points to a surge of interest in Traveller health, with a predominant focus on describing the particular needs of this group, an underdeveloped literature base on interventions and, at present, a minimal translation of research into specific policy to improve the health of Traveller Communities. These findings corroborate those reported by previous reviews. 14 , 22 The combination of this with a lack of theoretical understanding of outreach as an intervention per se (as described in Chapter 1 , Introduction) makes the field ripe for a realist synthesis of what, in outreach interventions, is likely to lead to favourable outcomes for Traveller Communities and in what circumstances. This emphasises the timeliness of this review and appropriateness of the realist approach.
The scoping study offers a comfortable platform from which to engage in the economic evaluation and in realist thinking. The thoroughness of the search strategies it entailed provided a breadth of literature access, in order to start building some depth. It also provided us with key pointers for theoretical thinking. For example, we now know that the great majority of outreach workers were either mainstream health service providers or members of Traveller Communities, with similar numbers of articles describing each. The fundamental decision of whether to employ trained, mainstream health workers or to train and employ members of Traveller Communities has potential impacts on both costs and outcomes. This also revives a debate about the importance of ‘peerness’ and ‘layness’ that we have had for some time,110 and has helped refine the realist ‘by whom’ initial theory. Just under half of the scoping studies describing outreach focused on improving access to and use of available services, suggesting that this is a key aim of outreach services, and contributing directly to the formulation of the initial theory ‘what for’. This outcome poses challenges for the economic evaluation. Improvements in access to health care may increase costs, at least in the short term. Indeed, success is often judged by measures of increased resource use (such as attendance at antenatal clinics). Assessing the benefit of such interventions requires consideration of the wider literature and is likely to be speculative. Outreach interventions were more commonly described in eastern Europe, suggesting that the context in which the intervention has been more often trialled is the Roma subgroup. Deciphering what could be considered ‘in common’ among all the Traveller subgroups, but also key distinguishing factors between them and other ‘hard-to-reach’ groups, was the focus of the ‘to whom’ initial theory.
This scoping review has thus provided the review team with a solid scaffolding informing both economic and realist elements.
Economic evaluation
Introduction
This section of the report will examine the available evidence on the effectiveness of outreach interventions for Traveller Communities and seek to determine which types of outreach intervention might be considered cost-effective. If outreach interventions are to be cost-effective, then the potential health gains attributable to the intervention must be sufficient to justify the resources required to deliver the intervention. Alongside this efficiency consideration, there are equity issues to consider. Registration with a GP and access to secondary services and dental care is a right of all UK citizens, and indeed citizens of the EU resident in the UK. The extent to which this over-rides efficiency considerations in evaluating interventions that improve access to health services is unclear, but it is clearly a relevant factor. A second consideration is the documented poor health of Traveller Communities. 19 Again, the appropriate trade-off between efficiency and equity considerations in evaluating interventions that target deprived communities is poorly defined. The National Institute for Health and Care Excellence, the body which examines evidence on the effectiveness and cost-effectiveness of treatments and interventions, would typically consider such a factor in deciding on interventions in which the efficiency case was marginal. 111
Much of the evidence considered in this chapter was drawn from grey literature, which was not primarily intended to provide rigorous evidence of effectiveness. Evaluation of outreach interventions was frequently alluded to, but few evaluations were found and those that were available generally consisted of process evaluations or reports on the acceptability of interventions. As a consequence, evidence synthesis in this chapter is, inevitably, speculative.
Classification of outreach interventions
The introduction highlighted the complex nature of outreach interventions (p. 7). The nature of such interventions is typically flexible with protocols and implementation staff varying in response to local circumstances and perceived need. Evaluation of the effectiveness of such interventions is challenging; economic evaluation brings further challenges in assessing both the costs and the long-term consequences of interventions in which implementation protocols and intervention foci adapt to local needs and available infrastructure. 112 , 113 A lack of quantitative evidence on the effectiveness of outreach interventions for Traveller Communities may well reflect the difficulty in conducting such evaluations.
Despite the heterogeneity in intervention protocols, some classification of interventions was evident from the scoping review. The professional status of implementation staff provided a natural architecture with which to classify interventions. Interventions employing members of Traveller Communities as outreach workers were likely to have different costs and operate in a different manner from those employing mainstream health workers. Training costs for members of Traveller Communities might be expected to be high, given the general education and literacy levels of Travellers. However, Travellers might be expected to enjoy greater trust than members of the settled community, allowing outreach workers from the Traveller Community a greater influence on the agenda of interactions. The mode of operation of outreach workers provided another characteristic to classify interventions. The use of mobile clinics to bring services on site to Travellers contrasted with a facilitation role to enable Travellers to access mainstream services. Another mode of delivery could be loosely defined, in which professionals provided advice and help for Travellers to access services while working primarily from offices rather than visiting Travellers. These approaches are not mutually exclusive. Indeed, some degree of assistance to access mainstream services is likely to be a feature of any outreach.
Using the framework outlined above, we considered four types of outreach: mobile clinics, professional outreach, lay (Traveller Community) outreach and office-based outreach. The defining feature of mobile clinics was the use of a modified vehicle to bring medical services to Travellers. Professional outreach was defined as the employment of a trained, settled worker to visit Traveller Community sites to provide advice and assistance in accessing health services. Interventions in this area were primarily delivered by health visitors or community health workers (CHW), although the use of multidisciplinary teams was also described. Lay outreach was defined as the training and employment of members of Traveller Communities in an outreach role. Office-based outreach spanned the employment of trained, settled staff to provide assistance to Travellers in accessing health care without a specific remit to visit Traveller sites. This included the production of promotional materials targeted at Traveller Communities and interventions which aimed to make health-care services more accessible for Travellers.
Few publications provided any detailed information on resource use. Staffing levels and the number of Travellers served by the intervention were sometimes provided. Information on staffing levels allowed an estimate of overall costs in conjunction with yearly cost data for the appropriate grade of staff taken from Unit Costs of Health and Social Care. 114 A few publications reported budgets earmarked for outreach interventions. Where budgets were given, these were assumed to represent the cost of the intervention. Very few quantitative evaluations of outreach interventions were found. Where quantitative evaluation had taken place, measures of process rather than outcomes were evaluated. Some evidence of the impact of outreach on health knowledge and health behaviours was available. Potential effectiveness of interventions was evaluated from implementation descriptions and the broader literature on outreach interventions.
Mobile clinics
The early literature on outreach for Travellers reflects the efforts of dedicated health visitors to improve health care for Travellers. Their work typically focused on child health, although provision of health checks to adults and help in making appointments for health care are commonly described. Moreton115 describes her role in delivering immunisations to Traveller children in Oxfordshire and reports 100 children immunised over the course of 1 year, mainly for polio and diphtheria/tetanus. In addition to this, a number of other duties were undertaken, such as dressing wounds, providing blood pressure checks and giving family planning advice. Streetly116 reports on a similar project in Kent which immunised 42 Traveller children over 1 year. There are other accounts of interventions to increase vaccination rates by health visitors which appear to have been successful, although it is not clear whether or not immunisation was undertaken on site. Lawrie117 reports vaccinating 339 people for polio in 4 days following an outbreak. The success of mobile clinics in increasing immunisation rates has been questioned. 118
More recent initiatives have used mobile services to provide health advice and opportunistic screening for Travellers. The National Assembly for Wales funded a mobile unit with a remit to target coronary heart disease in Travellers as well as provide general health advice and assistance with accessing services. 119 The service ran for 6 years, after which GP registration rates of 95% were reported and 259 Travellers were contacted by the service. 6 A mobile clinic formed part of a package of interventions for Traveller Community members in Dublin and was co-ordinated by the Traveller association Pavee Point. 120 Qualitative data collected as part of a baseline survey of health needs indicated that just under two-thirds of Travellers accessed a mobile clinic which visited a site on which they resided, possibly because the clinic was viewed primarily as a service for children. A number of initiatives have included mobile dental units to try to tackle the extremely poor oral health of many Traveller children. Little evidence on effectiveness is available but a mobile dental unit initiated as part of a larger project in the Scottish Highlands proved too inflexible to ensure continuity of follow-up in addressing oral health needs. 121
Budgets were available for three recent initiatives which used a mobile vehicle to deliver health services on site. The Coronary Heart Disease and Travellers: Redressing the Balance project ran from 2002 to 2008 and was allocated a budget of £531,000. 119 A similar initiative in Essex, Healthy Chance, targeted Travellers and other disadvantaged groups with a service which included cholesterol and blood pressure checks. 122 The budget for this service was £100,000 per year, half of which represented salary costs for a nurse and a project manager. 123 A pilot scheme to provide Traveller Communities with a GP-led mobile clinic in Herefordshire was funded with a £900,000 grant over 3 years, with the aim of registering 1200 Travellers. 22 Alongside a GP, the health team comprised a nurse, two health visitors and a practice administrator. These data would indicate a cost of approximately £100,000 per year to run a mobile clinic staffed by a nurse or health visitor and £300,000 per year to run a mobile clinic staffed by a physician-led team. Based on the outcome of 259 Travellers contacted by Coronary Heart Disease and Travellers: Redressing the Balance, the cost per Traveller assisted was approximately £2000; however, the source does not indicate whether the project was physician or nurse led.
Professional outreach
Much of the early literature documenting professional outreach reflects the response of health visitors to unmet health needs in Traveller Communities. Health promotion, family planning advice and assistance in accessing services are described by Moreton115 and Streetly. 116 Streetly116 reports the delivery of 22 family planning consultations, 26 appointments booked and 60 consultations for general medical problems by two health visitors over 1 year. More recent interventions have employed CHWs, sometimes working alongside a nurse, to provide advice and assistance in accessing health care. CHWs employed by the Highland Gypsy/Traveller Health & Wellbeing Initiative undertook welfare advocacy work as well as facilitating access to health, and secured £150,000 in previously unclaimed benefits for Travellers. 121 The initiative was also successful in raising awareness of Travellers’ culture and needs among health-care staff. However, the evaluation noted that improvements in access to health care were not maintained once the initiative had finished.
Data on caseloads indicate that the number of Travellers served by these initiatives varied from 600 to 2000 Travellers per outreach staff member. There is an almost complete absence of documentation of outcomes following professional outreach. This may reflect the difficulty in collecting this information when compared with process data, and the varied roles that CHWs and specialist health visitors undertake. It might also reflect the need to invest considerable time in building trust with Traveller Communities before any influence on underlying health behaviours can be observed. A number of authors refer to positive achievements in areas such as increased uptake of immunisations, increased uptake of antenatal care, reduction in low-birthweight babies and reductions in perinatal mortality. Aside from immunisations, where some evidence of the effectiveness of professional outreach exists, the extent of effectiveness in meeting unmet needs in Traveller Communities is difficult to estimate.
Very little information on costs was available. The Unit Costs of Health and Social Care reports a total yearly cost of employing a health visitor of £77,000. 114 The closest profession to a CHW for which data were available in this publication was a family support worker, with a yearly cost of £42,000. Assuming a caseload of 1000 Travellers would indicate costs of £42–77 per Traveller. A recent publication described the introduction of a number of changes to a GP practice to facilitate access by Travellers, including training and employment of a practice nurse whose role included visiting Traveller sites to promote health and access to primary health care. 62 The total additional cost of the initiative was reported as £100 per Traveller.
Lay (Traveller Community) outreach
A number of examples of outreach work using trained members of Traveller Communities are documented in the literature. The most prominent examples are the Pavee Point project in Dublin,124 and the Roma Health Mediator programmes in eastern Europe and Finland. 125 Both programmes involved the employment of members of Traveller Communities to provide advice on health issues and to enable access to health care. The majority of the remaining literature on outreach delivered by members of Traveller Communities also describes programmes to train members of Traveller Communities to undertake general health promotion work. Programmes which trained members of the Roma Community in eastern Europe to promote safe sex and injection practices among sex workers and drug users are also described. 126 , 127 Evaluations are more widely available than those for professional outreach, which might reflect the experimental nature of many of these programmes or the need to demonstrate that members of Traveller Communities can be effective in an outreach role. Nevertheless, evidence of improved outcomes resulting from outreach is rarely reported.
The Primary Health Care for Travellers Project in Dublin trained women from Traveller Communities to provide advice on health issues to Travellers and to advise health service providers on improving access by Travellers to health services. 120 , 124 The project evaluation reported increases in child developmental examinations and referrals to specialist services such as speech therapy. Block booking of evening clinics at local dental practices appears to have been particularly successful, with attendance for dental checks increasing from 0% to 80% of the Communities targeted. A very similar project in County Offaly, ROI, targeted oral health. 128 The project evaluation reported an improvement in oral hygiene routines and a reduction of sugary drink consumption. However, an ambitious component of the programme to register all Traveller children in the area and provide them with an oral health needs assessment was judged to have failed.
In Romania, members of Traveller Communities have been trained as mediators to negotiate access to health care for Travellers. There is evidence of increases in vaccination of children and registration with a GP which is attributable to their work. 125 A similar programme in Spain is reported to have increased hepatitis B vaccination rates and increased the proportion of Traveller mothers accessing antenatal care. 129 Further evidence exists of the effectiveness of outreach workers from Traveller Communities in increasing vaccination rates. 130 , 131
Two interventions reported in the literature utilised members of Traveller Communities as peer educators to promote healthier lifestyles within their Communities. Szilagyi132 describes a programme to disseminate knowledge on the risks of tobacco use by schoolchildren predominantly from Traveller Communities. The intervention increased knowledge on tobacco risks and motivated six children (from a class of 50) to attempt to quit smoking. Kelly et al. 133 describes a RCT of the use of influential peers to deliver a safe-sex message to their community. Following the intervention, there was a significantly lower rate of unprotected sex reported by recipients in the intervention arm and a non-significant trend to a lower proportion of sexually transmitted infections.
An example in which an intervention was delivered by lay outreach workers from the settled community to mothers from Traveller Communities is described in the literature. 64 ‘Community mothers’ provided advice on child rearing and development to mothers from the Traveller Communities around Dublin who agreed to participate. Outcomes were compared with results from a RCT undertaken in the settled community in which ‘Community mothers’ were evaluated against usual practice (visits by local public health nurse). Diets of Traveller children and mental stimulation of babies in the Traveller group were on a par with the intervention group and superior to the control group. However, immunisation rates remained stubbornly low and hospitalisation rates were far higher than either settled group.
Very little information on costs was available in the literature. The major cost components are likely to be training costs for Travellers, and employment costs for Travellers and support staff. Training of Roma health mediators appears to have been modest. 125 In contrast, the Travellers employed by the Primary Health Care for Travellers Project in Dublin appear to have received lengthy training consisting of three 30-week courses. 124 No information was available on the cost of this training. However, some of the attendees were preliterate, which would suggest that fairly intensive training was required. After training, eight Travellers worked for 12 hours per week, supported by a CHW and a project nurse. Given the training involved, it seems likely that the employment of Travellers as community health workers in this context would have been at least as expensive as the employment of a trained CHW from the settled community.
Other programmes to train members of Traveller Communities to deliver outreach have been delivered with considerably less training. The One Voice for Travellers project trained 12 women from Traveller Communities to provide health advice and enable access to health care. The women attended a 6-week training course and the project was supported with a £10,000 grant. 134 A project in Leicester trained 30 women to provide awareness sessions of Traveller needs to over 800 health-care staff. The project was supported with a £28,000 grant. 135
Office-based outreach
A number of publications described interventions to improve access to health care for Travellers which did not involve visits to Traveller Communities. The extent to which these interventions might be described as outreach is debatable. However, they support the role of outreach workers in improving access and serve to enable access to health care in the absence of the employment of outreach workers. These interventions consisted of producing Traveller-friendly health-promotion material and information on accessing health care, such as the welcome pack provided to Travellers by Fenland district council in the East of England,136 and the adaptation of health services to facilitate access by Travellers. Service adaptations ranged from texting appointment reminders and providing longer consultations for Travellers to the colocation of health and welfare services.
Unsurprisingly, we found no formal evaluations of this type of outreach work. Work has been undertaken to evaluate the use of patient-held records, which suggests that there are few drawbacks and substantial potential benefits to their use. 137 , 138 However, there is evidence to suggest that Traveller-held records by are underutilised by GPs. 139 We also found no data on the costs of interventions in this category. However, where service reorganisations do not involve the creation of new posts, it seems likely that costs would be modest.
Assessing the cost-effectiveness of outreach
The lowest cost interventions to improve access to health care for Travellers are likely to be those which do not involve site visits. These would include the production of promotional health material which is accessible to Travellers and cultural awareness sessions to educate health professionals. Costs to deliver the latter intervention by trained members of Traveller Communities are in the range of £10,000–30,000. The costs of improving service accessibility (such as texting appointment reminders) or the appointment of champions for Traveller Communities within health-care providers are likely to be modest, provided they do not involve the creation of new posts. The effectiveness of these interventions may also be modest. An equity argument might be made that such interventions are required if the NHS is to fulfil its obligation to provide access to health care to this section of the Community. If this argument is accepted, then these interventions might constitute the minimum acceptable provision of outreach against which other interventions might be evaluated.
The employment of outreach workers from the settled or Traveller Community is likely to be more costly. Literature from the USA suggests a cost of US $420,000 (based on 2011 figures) per annum to run a team of three, CHWs, of which two-thirds was attributed to staff employment costs and one-third to operational costs. 140 This figure is in line with the estimates of cost reported in this chapter. The employment of members of Traveller Communities as outreach workers is likely to involve considerable training costs. This may not be a sensible investment unless trained outreach workers utilise their skills for a considerable period of time. The literature suggests that the potential for lay health workers to save costs over the employment of professional staff is rarely realised. 141 However, lay health workers may enjoy considerable advantages in accessing a community that has traditionally been suspicious of mainstream society. Programmes organised by Traveller organisations, such as Pavee Point, may be best placed to exploit bridges with the Community, provided that longevity of funding can be achieved.
Set against the cost of outreach by lay or professional workers is the potential to reduce costs from inappropriate health-care use. A perception remains that Travellers are prone to use A&E services inappropriately but recent publications have contested this. 122 There is evidence of high rates of attendance at A&E departments among Traveller Communities;26 however, this may be explained, at least in part, by environmental factors such as the proximity of Traveller sites to busy roads. Evidence from the USA indicates the potential for substantial cost savings arising from employment of CHWs to support the management of patients with diabetes. 142 However, the costs of managing the complications which arise from diabetes is high. 143 The scope for potential savings among Traveller Communities is likely to be much lower.
The literature on outreach among Traveller Communities suggests that lay workers can be successful in boosting immunisation rates. A lack of evidence of effectiveness in other areas may reflect a tendency to focus on outcomes that are easily quantified and recorded. Evidence from systematic reviews of the application of CHW programmes suggests that they can be effective in promoting immunisation and breastfeeding. 144 , 145 There is also evidence to show that they are effective in promoting mammography, although effectiveness is modest. 145 , 146 There is less evidence of effectiveness in promoting access to antenatal care and smoking cessation. 144 There is some evidence that CHWs are more effective when they share the ethnicity of the recipients. 146
The benefit from attendance at mammographic screening is small and unlikely to justify a programme to encourage attendance at screening. 107 , 147 The benefits of boosting vaccination rates are less well defined. Around nine deaths and 5500 inpatient days are attributed to pertussis annually in the UK. 148 Hence the scope for health gains among Traveller Communities from increasing pertussis vaccination may be modest. Activities to promote vaccination may be cost-effective if they are sufficiently clinically effective. Our estimates suggest that the costs of employing outreach workers to engage Traveller Communities are likely to be £50–100 per year per Traveller. Whether or not they are able to generate health gains which justify this cost is yet to be demonstrated.
The most expensive modality for conducting outreach is the use of mobile clinics. The provision of mobile clinics to provide health checks and health advice appears to be a very expensive way to reach Travellers. The Coronary Heart Disease and Travellers: Redressing the Balance project cost £2000 per Traveller assisted. The extent to which these Travellers benefited is unclear. The wider literature on the use of mobile clinics is limited. Evidence from developing countries on the cost-effectiveness of mobile clinics is mixed. 149–151 There is evidence to suggest that this form of service is considerably more expensive per patient contact than fixed facilities. 152 However, evidence from the USA suggests that mobile clinics may be cost saving for patients who are high users of A&E services. 153 The meagre evaluation data available do not indicate that mobile clinics are more effective than professional or lay (Traveller Community) outreach, despite the additional costs.
Conclusions
Interventions which use mobile clinics to bring health services to Travellers are associated with the highest costs reported. There has been very little evaluation of these interventions; the brief data on outcomes available give little confidence that they provide value for money. Alongside this is a concern that mobile services specifically targeting Traveller Communities might be stigmatised. While Traveller sites are often located in areas poorly served by public transport, the willingness of Travellers to travel considerable distances to attend preferred health facilities would suggest that physical access to health facilities is not the primary barrier to better access. The use of mobile services appears inappropriate for the majority of Travellers living in houses.
The employment of full-time outreach workers for Traveller Communities appears to be associated with moderate costs. The nature of this type intervention makes evaluation challenging – roles are not clearly defined and a wide variety of health concerns are likely to be targeted. Indeed, the benefits of the intervention may not be primarily improved health. Case work may include considerable advocacy in areas such as benefit claims. Practice nurses are well placed to facilitate access to primary care at the practices in which they work, and they may represent a cost-effective resource to improve access to primary care for Traveller Communities. The wider literature would suggest that outreach workers can be effective in improving vaccination rates and encouraging access to antenatal care. There is evidence that outreach is more effective when delivered by workers who share the ethnicity of the recipients. If this arises from greater levels of trust enjoyed by these workers, we might expect ethnicity to be particularly important in the effectiveness of outreach in Traveller Communities. The training and use of outreach workers from Traveller Communities to promote vaccination and access to antenatal care would merit rigorous evaluation.
The implementation of protocol changes, such as texting appointment reminders, in primary and secondary care is unlikely to be expensive and might be considered the minimum acceptable action to facilitate access to health care by members of Traveller Communities. These changes are likely to require the identification of a champion for Traveller Communities within each care commissioning group. The effectiveness of this role is likely to be enhanced by the involvement of Traveller Communities in selection. Accessibility is unlikely to improve unless health-care staff are aware of the needs and cultural values of Travellers. Examples from the literature suggest that cultural awareness sessions can be delivered successfully by members of Traveller Communities for modest costs. A common theme in the literature documenting GP registration is the perception by GPs that Travellers are ‘expensive’. 154 A recent publication from the Department of Health20 suggested an additional payment to GPs for the registration of Travellers to offset losses in practice income from missed Quality and Outcomes Framework (QOF) points and to incentivise outreach. Such a funding mechanism would require the identification of Travellers. In conjunction with the changes outlined above, an appropriate payment for the registration of Travellers by GPs might be effective in improving access to primary health care for Travellers.
Realist synthesis
The iterative nature of the realist synthesis process and its focus on developing and then testing theories presents an acknowledged challenge for the presentation of results (see p. 18). This section of the report details how initial theories were developed through searches for existing candidate theories which could help explain how, why and in what circumstances certain outcomes were reported. We report the analytical process that led to the development of an explanatory framework for outreach interventions in Traveller Communities, as well as the substantiation of that framework.
Theory refinement process
The following pages develop the initial theories that informed (and were informed by) the data extraction and were articulated around the target of outreach (to whom), the actors (by whom) and process (how) of outreach, as well as its outcomes (what for). Iterative activity between data extraction and early stages of synthesis of the literature, as well as engagement with stakeholders, informed this stage of the process.
‘To whom’: the context of outreach work
While the literature on Traveller Communities is replete with statements of needs, the distinctiveness between these and other groups often remains unclear. Teasing out this distinctiveness has required continual refocusing through consultation with stakeholders as well as engagement with the literature. Instead of directly relating to established or perceived needs, these key contextual factors are most likely to impact on the acceptability and impact of outreach interventions in this group. They are articulated in three strands: a nomadic lifestyle and associated access and environmental health issues; discrimination and historical persecutions; and exposure to assimilatory policies and practices. While none of these strands is particular to Traveller Communities, the fact that they experience the three simultaneously is particular to them. Conversely, not all of the three strands will apply to all people of nomadic lifestyle included under the umbrella term ‘Traveller Communities’, as there is no single common denominator for such a diverse group. However, all are likely to share some or all of the three strands, and, at this stage of the review, this combination offers the most explanatory purchase for the triggering of outreach mechanisms.
A nomadic lifestyle
The reluctance of Traveller Communities to part with a nomadic lifestyle is well documented as being linked to opportunities to escape mundane living, to find employment and as a means to reconnect with people and places that matter. 155 Shubin and Swanson155 stress the misleading oversimplification of complex forms of mobility. Nevertheless, accommodation conditions have significant impacts on the inequalities faced by Traveller Communities. Although conditions vary, many publicly provided sites pose environmental health risks. Faced with the paucity of suitable stopping sites, many Travellers living in caravans are caught in a cycle of evictions and consequent disruption in access to services and schools (EH9). It is estimated that around one-quarter of Travellers living in caravans do not have a legal place on which to park their home, and are thus, in law, homeless. 5 , 156 The stress this generates has been described as inextricably linked to health:
. . . the stress generated by living in a hostile society where discrimination is a constant reality, and this is compounded by frequently enforced change in their way of life. These factors impact adversely on Traveller’s Health and negatively affect their ability to influence access and experience of health services.
McCabe and Keyes 2005,157 p. 6
The threat of eviction poses challenges to the creation of healthy lifestyles through the accompanying stress (EH9) and limiting of resources to, for example, cook and eat healthily (EH2). In order to break a cycle of evictions, improve their living conditions or access services, many families accept the alternative of local authority housing. In a health study focused on Travellers in Ireland, 78.5% of Travellers living in the ROI and 62.6% living in NI had not travelled at all in the past year, and of those who did, this occurred most frequently in the summer period. However, temporary settlement only solves part of the problem, as they are typically housed on the most deprived estates where they often face hostility linked to their ethnic group. 6 , 158
Travellers emphasise the health benefits of a travelling lifestyle, associated with freedom, choice, proximity to extended family, fresh air, and the ability to escape hostility. 158 , 159 They are often reported to describe how a move into housing or permanent accommodation had been detrimental to their mental health:
It used to be different because maybe you’d get two or three weeks in one place and you’d be with all different families and just nice . . . I find it terrible, you miss out, and you miss it. You miss it for the children as well because the children really enjoy it, they like meeting all different people and living in all different places.
Van Cleemput et al. 2007,39 p. 207
At some time during their interviews, all of the women expressed a relationship between how they felt in terms of health and wellbeing and their travelling or non-travelling status. Six of the nine women initially interviewed expressed feelings of stress, panic, anxiety and depression that they associated with not travelling.
Dion 2008,40 p. 33
Other authors report physical impacts of settling:
Away from the road, diets change and families probably take less exercise . . . Smoking is common, exercise less so. A preference for convenience food contributes to many of my clients being overweight, and there is a high incidence of hyper-tension, coronary artery disease and gallstones.
Reid 1993,60 p. 30
More recently, Greenfields and Smith160 have examined how, given the relentless pro-sedentary nature of policy towards Traveller Communities, many have moved into housing, but have nevertheless resisted assimilation and developed strategies to recreate their traditional lifestyle. For example, through a system of exchange, some Travellers living in houses keep a seminomadic lifestyle by moving house frequently. 160 In spite of this, the life expectancy of Travellers living on permanent sites is broadly similar to that of the surrounding settled residents, whereas those resident on unauthorised sites or living in conventional housing have poorer health and a lower life expectancy. 6 A move into housing often impacts negatively on the mental health of Traveller Communities. 39 In addition to housing being an undesirable form of accommodation for many Traveller Community members, settlement in housing has also been highlighted as a costly solution, as a consequence of increased need for social and financial support for families who were previously self-supporting. 161 , 162 A tension is therefore evident between policies of enforced movement or settlement of Traveller Communities that impact on the social support networks of Traveller Communities, and policy drivers to recognise community assets and support resilience. 163
Rather than the more traditional breakdown of Traveller groups per ethnic or occupational origin, in terms of service provision, it appears thus more relevant [as verified through EHs (EH5 and EH9)] to distinguish between:
-
‘Roadsiders’: essentially homeless, these are the people with the most pressing environmental and health needs,3 with (from a provider perspective) time-constrained opportunities to build trust. They are probably most distrustful of authorities due to cycles of eviction and, therefore, disengagement is likely to be entrenched (EH5). However, even frequent travellers will tend to travel seasonally, keep to a circuit of stopping places and be highly visible and easily identifiable (EH5). They might also have created a health service map of ‘trusted’ providers not bound by geographical dimensions, whom they will travel to visit when the need occurs.
-
People who live in caravans but more or less permanently on local authority or privately provided sites. They may have a seasonal pattern of travel, with some authorised sites enabling a nomadic lifestyle by including gaps in occupancy (of varying duration) in people’s tenancy agreement (EH4). This is where most outreach programmes are described in the literature, and there is clear scope for social capital and community engagement activities. However, the Traveller Communities consulted also highlighted that outreach targeted on sites may be difficult to access for male Community members as they are often working away from the site, and taking time off work to access services would entail a loss of income (EH9).
-
People who live in council housing, generally in disadvantaged areas, where they not only have significantly reduced their propensity to travel (though many will still attend Traveller fairs, for example) and to access the critical cultural mass that a site can offer, but are also likely to be exposed to local prejudices and discrimination (EH1 and EH5). From a provider’s perspective, these people are difficult to engage with because of their reluctance to self-identify as Travellers (EH1 and EH9). Living in what they perceive as a hostile environment, they may be even more resistant to engage with non-Traveller institutions. However, because they have an address, at least in theory, access to primary care should be easier. Snowballing strategies have been used successfully in some interventions to recruit Traveller Community members who are living in housing (EH1).
-
A much smaller number of people who may have become homeowners. This subgroup is more likely to have a regular income and better access to health care but, again, self-identification may be an issue.
Belonging to these groups is, of course, fluid; for example, it is estimated that the majority of local authority Traveller Community tenancies end after a year3 and that some people retain a seminomadic lifestyle even when in housing (EH5). There is, however, an overall trend towards settlement, in that an increasing proportion of Travellers have some permanent base, living in caravans or trailers only for occasional trips. Of the four groups above, the first is likely to face the greatest health inequalities, with difficult and interrupted access to health, social care and schooling services. 164 , 165
The need to improve Traveller Community access to health services and other mainstream institutions emerged as a key aim of outreach (and was highlighted in EH1, EH9 and EH10). Particularly for transient Travellers, the design of mainstream services, which often rely on people having a fixed address, is ill adapted. In this case, the role of outreach workers is often to provide a trustworthy link to mainstream services.
The 16 health and sanitary mediators and the 80 community nurses in the county are often the health authorities’ only reliable sources of information about the Roma communities. They are extremely useful because they mediate the relationship between the Roma community and the local health authorities. 166
Vrinceanu 2007,166 p. 7
[W]e go to sites that have got outreach workers and they’ll just tell you ‘It’s great, I’ve been able to register with a GP, I’ve never had access to a GP for 40 years and now I can go to the doctors whenever I want, they’ll give me an appointment’ and the way they speak about [the outreach workers] is just so positive.
EH1
General practitioner surgeries and dentists often refuse to register people without a permanent address, and only 69% of members of Traveller Communities were reported to be permanently registered with a GP in a recent study. 26 Although hand-held records have been piloted in a number of areas, there are not yet widespread systems in place to ensure continuity in care and to ensure swift referrals (EH1 and EH9):
The majority of GP Surgeries throughout Sussex have little or no understanding of the complex needs and experiences of Gypsies and Travellers . . . [those] with no fixed abode have the most difficultly registering with a GP and thus will find it almost impossible to obtain referrals and secondary care.
Atterbury and Bruton 2011,165 p. 3
Peters et al. ’s26 study clearly demonstrates the comparative mismatch between the poor health status of Traveller Communities and low access to primary care, together with a high proportion of reported contacts with social care or accidents and emergency departments (also validated in expert hearings EH9 and EH10). While great anxiety is reported in qualitative studies examining reasons for non-engagement with health services, this is not unavoidable. Van Cleemput et al. 167 also report on examples where Travellers would go to great lengths to maintain continuity with a trusted health-care professional (also corroborated by EH4, EH8 and EH9).
Discrimination and historical persecutions
It is widely acknowledged and documented that Traveller Communities have been subjected to persecutions, harassment and evictions from the fifteenth century onwards,168 , 169 with earlier episodes deemed to have been likely. 170 They were a key target of the Nazi extermination efforts in the Second World War, being referred to as the ‘Gypsy plague’, with Interior Ministry of Württemberg promulgating decrees such as the ‘Gypsy Nuisance decree’, among others. 171 Although the inclusion of Travellers in the Holocaust is disputed (with regards to whether or not Nazi efforts to eradicate them were as systematic as they were for Jewish people), it remains that they suffered considerable losses. 172 Since then, the contrast between compensatory policies and organisation after the war between those accorded to Jewish and Traveller victims has also been highlighted. 173 , 174
Under the communist regime in (the then) Czechoslovakia, Czech Roma were subjected to severe state policies designed to restrict their nomadic lifestyle, seen as a threat to the prevalent social and state order. Harsh measures were introduced to control ‘Gypsies and other work-shy vagabonds’. 175 In 1956, the Act on Permanent Settlement of Nomadic People was passed, forcing Travellers into settlement, and was mirrored in other communist totalitarian European states. Under these policies, Travellers’ horses were killed and caravans were destroyed, thereby much reducing their potential for independent living. 176
Discrimination continues to prevail,6 a phenomenon compounded by negative and widespread media stereotypes. 177 The media, which are often the only way in which settled people learn about Traveller culture, play a particularly important role in perpetuating stereotypes and often overlooking positive interactions between sedentary and nomadic communities. 177
Such historical persecution and discrimination may explain Traveller Communities’ reluctance to invest their trust in settled people. 42 , 178 Although the literature available on outreach interventions tends not to distinguish between different groups of Travellers, consultation with steering group members suggested that European Gypsies are likely to have experienced more extreme levels of racism and discrimination and, therefore, enter interactions with a greater premise of mistrust (EH1). As a result, Travellers often turn to extended family or community for health-care support or advice.
Many Gypsies and Travellers are also afraid that if they disclose having mental health problems social services will get involved and their children will be taken away. There is a reluctance to contact outside agencies for help given negative past experiences with government authorities.
Atterbury and Bruton 2011,165 p. 2
While prejudicial and discriminatory practices are often developed on the basis of the nomadic lifestyles of Traveller Communities, immobility or temporary settlement is also often faced with very public resistance. 155 Greenfields and Smith160 expose how living in hostile environments leads Travellers to rely heavily on close social ties (predominantly within their extended family/kin group) in order to maintain a sense of stability and security. This ‘inward-looking’ tendency may present a stumbling block to developing the kind of bridging social ties on which an outreach programme is likely to rely.
Exposure to assimilatory policies and practices
As exposed above, the historical relationship between European states and Travellers has been fraught, particularly owing to the cultural differences between nomadism and sedentarism. Bancroft176 highlights two practices born out of these tensions: ‘cultural suppression’, which stops Traveller Communities expressing their cultural identity, and ‘forced removal’, which constantly displaces this cultural expression. Some commentators have gone as far as suggesting that policies directed at regulating Traveller movements have amounted to a form of ‘ethnic cleansing’. 179 Across Europe, numerous pieces of legislation are based on a sedentarist logic, in an effort to control what are seen as disorderly lifestyles.
For example, after being forced to settle and accept low-paid, low-skilled forms of employment during the post-war period, Roma from the Czech Republic have been segregated and ghettoised since the 1990s. This spatial exclusion has taken the form of walled areas, featuring Portakabin-type accommodation, and being placed under heavy surveillance. Towards the end of the decade, some Travellers were subsidised to leave the Czech Republic, leading to ‘Roma refugee panics’ in western European countries. 176
Shubin and Swanson155 expose the sedentarist policies and legislations that lead to a near criminalisation of nomadic lifestyles. While they focus on Scotland, their analysis of how policies have pushed many Travellers into either permanent settlement or perpetual motion applies across borders. Despite the fact that it was promulgated nearly 150 years ago and may constitute a violation of human rights, the 1865 Trespass Scotland act is still the legislation most often used to regulate Traveller movements. 155 More recent policies aiming to manage mobility include the 1959 Highways Act in England and the 1984 Roads Scotland Act, which forbid encampments anywhere on or near a road, thus granting authorities the right to displace Travellers parked near any road in the country. The 1986 Public Order Act prevents the gathering of more than 20 individuals, thereby limiting Travellers’ opportunities to maintain extended family networks.
In the UK, in 1968, Parliament passed the Caravan Sites Act that included a statement obliging local authorities to provide caravan sites for Travelling people, although the systematic translation of this act in practice has been questioned. 177 The Cripps report180 and the Government Circular (1977) expressed statements of support for the rights of Traveller Communities to live a nomadic lifestyle, and the right to live on independent sites previously discouraged under the Caravan Sites Act. 41 Nevertheless, the fact that the Caravan Sites Act did not result in Travellers giving up their nomadic lifestyle was cited as an explicit rationale for the legislation that followed in the 1992 Conservative Party Press Release. 181 , 182 In 1994, the UK Parliament passed the Criminal Justice and Public Order Act, which, while acknowledging the enduring shortfall of legal caravan sites, revoked the need to provide legal stopping sites, thereby in effect criminalising nomadic lifestyles. 181 , 182 It also stipulated that convoys of six vehicles or more travelling together could be broken up, thereby making it more difficult for Traveller families to travel together and maintain social networks.
The paragraphs above by no means present an exhaustive review of the kind of assimilatory and sedentarisation efforts that Travellers have been exposed to. It is hoped, however, that they do provide an explanatory hint of Travellers’ resistance, lack of trust in settled institutions and individuals, fear of loss of their cultural identity and over-reliance on close social ties. Traveller Community members consulted expressed an explicit concern about the attempted erosion of their culture and values through enforced settlement into housing (EH9). Understanding the impact of these lifestyle factors and environmental and historical adversities on the formation and maintenance of social networks emerged as key to understanding how outreach workers might interact with the Communities.
Social networks
Mobility is a key distinguishing factor between Traveller Communities and other disadvantaged groups. As exposed above, it is not systematically correlated to living arrangements (trailer/caravan or house). What a nomadic lifestyle does, however, is alter the morphological features of the social networks upon which Travellers rely for health care and information. This generates or curtails opportunities for outreach workers to interact with the Community in a constructive and cumulative manner, particularly when the outreach worker does not belong to the Communities. Therefore, understanding the impact of mobility on forming, maintaining and drawing on relationships within and outwith the Community is key to understanding the potential for outreach workers to develop trusting and effective relationships with a potential to impact on social capital and health. Social network theorists have, however, warned against the systematic expectation of social cohesion among a priori groups, and encourage an assessment of the structural properties of relationships between people not necessarily linked to geography of kinship. 183 This is particularly relevant here, as while mobility may impact on the ability of settled practitioners to form, maintain and develop relationships with Traveller Communities, strong social bonds clearly exist within and between nomadic groups regardless of the duration and frequency of their geographical proximity. At the same time, homogeneity and harmony must not be assumed among Traveller Communities, as conflict between families is said to be a primary motivation for movement (EH4). Thus, using singularly geographically or culturally bounded lenses (e.g. neighbourhood or ethnic group) to understand the nature of Traveller networks would greatly limit the potential for intervention effectiveness.
‘By whom’: mechanisms of approaching Traveller Communities
The definition of outreach adopted at the outset of this study was broad, referring to ‘a process that involves going out from a specific organisation or centre to work in locations with sets of people who typically do not or cannot avail themselves of the services of that centre – as a marketing or recruitment strategy; as a delivery mechanism; as a networking process; and a method or approach to working with people’ (p. 11). 77 During initial examination of the literature and consultation with those working with Traveller Communities (EH1, EH10) the success of interventions was frequently attributed to their delivery by members of Traveller Communities. Thus, initially, the focus of the ‘by whom’ theory was on the importance of the characteristics of outreach workers. Workers who are well integrated into the Community readily meet criteria, such as being familiar or similar to the target group, that others might have to work to establish (EH3, EH4). For example, discussion with steering group members suggested that outreach workers who belonged to the Communities were able to talk about family connections to establish initial rapport (EH1). The predominant influence of frequent and close relationships within the group for health knowledge and health-seeking behaviours in Travellers was evident both in expert hearing events (EH9, EH10) and in the literature. 184 Thus, as in many social programmes, interpersonal relationships between the worker and the Community embody the outreach intervention. This takes particular significance in the context of a Community with high level of distrust towards those from outside of the group. 42 , 178 Outreach is thought to work through forming a bridge between health services and Travellers who find it difficult to access services due to their experiences of discrimination and transience.
Trust is an issue that is mentioned throughout the literature on Traveller Communities, and was a key theme throughout expert hearing events (EH1, EH3, EH5, EH8, EH9, EH10). The literature on Traveller Community social networks details the ‘mutual trust and reciprocity upon which social relations operate’ (p. 1198). 184 These trusting relationships help to reinforce the social ties between people and the symbolic boundary between them and settled communities. Smith and Ruston184 highlight the importance accorded to Travellers’ ability to deflect external pressures by maintaining a dense web of social relations within the Community. Through a strong oral tradition, negative experiences with settled communities or professionals circulate through these dense networks and become a distrustful normative consensus from which new relationships are approached. Therefore, careful consideration needs to be given to entry strategies for an outreach programme, in accordance with the likely disposition to trust among the target group [e.g. in cases where previous provision was mostly related to law enforcement, Communities are likely to be more mistrustful of new people (EH3)]. However, oral traditions also work in reverse, in that health professionals with a good reputation are held in high esteem, and Community members will travel considerable distances to consult with them37 (EH4, EH9). So, while there is a reticence to engage with settled communities and professionals and an over-reliance on network relationships for health advice,184 it is not an impossibility for a non-Traveller to develop trusting relationships with the Community.
The literature also suggests that belonging to the Community was a helpful, but not absolutely necessary, condition of success for the outreach worker. Indeed, in some cases, family connections could work to hinder the outreach process in cases where there had been conflict between families (EH1) or the training of outreach workers altered their relationship with the Community:110
I was at Appleby earlier this year and I was talking about community empowerment, not quite in those terms I was doing it in a more informal way and he said well it’s easy for you to say that, you’re not a Gypsy and I said ‘well I am’ and he said well ‘are you?’ and I said ‘well that’s my Dad’ and he said ‘Oh alright then’ and he said ‘well it’s just well you sound really educated’ and I said ‘well I am’, they’re not mutually exclusive but you do have that barrier within the community, so you have barriers from outside the community but you also have them from inside.
EH1
Therefore, a key instrumental step to building trust may be the ability of the outreach worker to ‘place’ themselves in relation to the recipients’ social network map (EH1). Hurley185 and Mayer et al. 186 describe models of trust, which help to unpick how trust might work as a key mechanism of outreach, suggesting that it is built along the six continuums of:
-
similarities (how similar is the outreach worker to the intervention recipients)
-
interests (do outreach workers have Traveller interests at heart)
-
ability (are they in a position to solve problems)
-
benevolence
-
integrity/predictability
-
communication.
We put this model of trust to our experts, in order to see to what extent they thought it applied to Traveller Communities. They suggested that integrity and predictability were the most important domains of trust (EH2, EH4). For example, one stakeholder commented that when beginning to provide outreach services, it is important to visit the Community regularly, even if no one attends, in order to demonstrate commitment (EH4). Traveller Community members consulted highlighted the importance of continuity in health workers and willingness to visit Traveller homes and sites for the development of trust (EH7). Communication was felt to be another important factor (EH2, EH7, EH4), such as friendliness, politeness, listening, being non-judgemental, flexibility, offering clear explanations and being honest and direct (EH7, EH4, EH8), as was cultural awareness and sensitivity (EH7), which is also well reported in the literature. 37 Confidentiality was cited as important to Travellers when making decisions on whether or not an outreach worker was trustworthy. The similarities and ability of workers were also thought to be important in building trust (EH2, EH8).
Thus, we can think of outreach workers as having an initial ‘trust status’ on entering the Community, developing and utilising the following typology:
-
outreach worker is a highly connected member of the Community, already acquainted with the extended family group – high trust
-
outreach worker is a Traveller with no immediate connection to the network – neutral trust
-
outreach worker is a professional or semiprofessional with a long-standing relationship with the Traveller Communities targeted – high trust
-
outreach worker is a professional without a prior relationship with the Traveller Communities targeted – low trust
-
outreach worker is a settled lay person with no prior relationship to the Community – low trust.
‘How’: the mechanisms of successful outreach intervention
Consultations with representatives from Traveller Communities suggested that the main blockage to improving their health is the barriers they experience in accessing health-care services (EH1, EH9, EH10). Outreach interventions, which bring services closer to people (or vice versa), are thought to have the potential to bridge that gap. Engagement with the literature demonstrated the dual role of outreach in both bringing health services to Traveller Communities and enabling Traveller Communities to interact and engage with settled institutions and communities. Discussion with the steering group confirmed the importance of outreach in facilitating access to mainstream services, rather than only providing dedicated services (EH1). Traveller Communities consulted suggested that they lacked information about the range of health services available and how to access them (EH9, EH10). From a provider’s perspective, concerns have been cited regarding the difficulties of ensuring continuity and consistency of care: ‘It’s very difficult; because they might come once in while and maybe come for one appointment and when they need vaccination they don’t show up’ (p. 14). 187 Therefore, ‘How’ complements ‘By whom’ in developing understanding about the nature of the service provider–outreach worker–Traveller Community member relationship and the flow of influences between them.
Outreach work also involved attempts to improve relationships between practitioners and Traveller Communities through raising awareness and challenging discriminatory attitudes (EH1), as well as increasing awareness of rights and knowledge of constraints on service providers among Traveller Communities. 122 , 124 , 165 , 166 , 188 , 189 One study enabled members of Traveller Communities to adopt a representational role in order to inform regional, national and international policy. 157
Given the potential mismatch between health-care service provision and Traveller culture and way of life, and the role of outreach in forming a bridge between them, engagement emerged as a key concept in understanding ‘how’ interventions might work. Following Neufeld et al. ,190 the process of engagement entails cycles of negotiation (when environment and person make adjustments to accommodate each other), participation (active involvement) and evaluation (the degree to which a person has achieved environmental fit). This is further developed on p. 49.
Encouraging Travellers to contribute to setting the agenda for outreach work emerged as a core component of the negotiation stage of the cycle of engagement. For example, the Pavee Point study in Ireland120 , 124 , 157 , 158 and the Friends, Families and Travellers outreach project165 , 191 involved Travellers continually in the planning and implementation of interventions. Both studies allowed phases leading into and throughout the projects to build trust or develop the confidence of Community members to articulate needs and participate in training. The Friends, Families and Travellers project notes how health needs emerged informally, after more general activities such as cooking and eating together had been engaged in191 (EH1). Health-related lifestyle advice may not be considered as a priority by Travellers, who may be experiencing threats to well-being such as lack of appropriate accommodation or access to basic amenities (EH1, EH9, EH10):
Well it’s in the hierarchy of needs, if you haven’t got anywhere to live, that’s the most fundamental thing. You often find that things will be put on the back burner because accommodation is the most dire need.
EH1
In the Pavee Point project,124 Traveller CHWs who had participated in training conducted a needs assessment, before engaging the Community in needs prioritisation and agreeing on strategies to address them. These outreach workers then worked with health service providers to develop and deliver interventions in response to the needs identified. 155 As such, these studies describe interventions which were well sensitised to the needs of Travellers as defined by their experiences and attuned to the contextual factors outlined above. The importance of open dialogue to establish needs was corroborated through expert hearings (EH1, EH2):
[A]lways start by allowing them to define their own needs, and then once you’ve addressed some of those needs or worked with people to develop that trust you can then steer or suggest or give information or give support around the things that we may regard as more pressing.
EH1
The literature highlighted a diverse range of opportunities offered by outreach (programme strategies); opportunities for learning; improved access to services; opportunities to be actively listened to or represent the Community; to reinforce and capitalise on strong community ties; and to receive payment (in kind or otherwise). Van Cleemput et al. 37 describe how a respondent first engaged with the onsite clinic intervention targeting children’s health before feeling able to discuss her own health concerns during the site visits and then making an appointment at the local surgery.
[P]eople will approach us often very tentatively . . . sometimes in a crisis or sometimes they’ll approach you to do with an eviction or something and they’ll have a positive experience with that being managed and being supported through that process. So they will then say ‘actually I found this lump in my breast’. A lot of stuff comes in sideways.
EH5
Thus, processes of trust and engagement were iterative, leading to a more active level of participation, or retreatism, depending on experiences. Processes of gaining trust seem entwined with cycles of engagement, with trust status forming a contextual influence on decisions to engage, which are then re-evaluated following the participation and evaluation, and often shared through word of mouth among other Traveller Community members (EH5).
‘What for’: outcomes
Traveller Community members consulted about what would improve their lives (EH7). This highlighted changes in structural conditions, including the provision of appropriate accommodation and stopping places, employment opportunities and opportunities to pursue traditional trades, specialist support for education and facilitating access to health care. Building on this and the paragraphs above, it seems helpful to map out the potential impacts of outreach on the well-recognised Dahlgren and Whitehead38 diagram, as it includes an explicit acknowledgement of the wider determinants of health ( Box 2 ). This enables the consideration of the potential impacts of outreach from the perspective of health inequalities aetiology.
-
Poor schooling and high rates of illiteracy.
-
Poor living and sanitary conditions on many sites.
-
Policies in favour of sedentarisation.
-
Unemployment.
-
Inappropriate housing.
-
Barriers to access health services.
-
Social exclusion.
-
Marginalised social status.
-
Strong bonding ties within the community.
-
Limited contacts with the settled community.
-
Disengagement entrenched.
-
More sedentary lifestyle with settlement.
-
Poor health literacy.
-
Fatalism/stoicism.
-
Psychological impact of moving into houses.
If one of the key aims of outreach is to provide a bridge between statutory services and Traveller Communities, then an increase in registration with primary care practices and a decrease in use of A&E departments should be key outcomes. However, as exposed in our economic evaluation, the Traveller Community literature is particularly thin on outcome measurement of this kind, making the assessment of effectiveness an impossible task. Consideration of cultural particularities and historical legacy, which have resulted in a strong reliance on close-knit social ties and a distrust of any settled person or institution (e.g. resulting in low rates of self identification3), complicate the situation further. Given the overwhelming accounts of Travellers as a socially excluded group in contemporary society, it seems that considering engagement as an instrumental first step towards health improvement might be key. From the literature, three categories of engagement outcomes could be identified:
-
Participation in a programme. Often, it was difficult from the articles to make a judgement on the underlying reasoning that pushed Traveller Community members to take part in a programme. Clearly, a different level of commitment is required to attend a one-off screening event, than to challenge established behaviour or lifestyle practices. That is not to say that participants at screening events may not change their whole approach to proactive and preventative care, but the studies often provided insufficient detail to make that judgement. A conservative view was therefore taken in classifying outcomes, so that participation at one-off events did not assume more in-depth engagement. This level of participation is unlikely to generate long-term change, but may be sufficient if the focus of the intervention is, for example, immunisation or screening. Although the evidence could not substantiate this with certainty, it could be that participation in a programme produces punctual impacts on impacts on individual lifestyle factors, by, for example, improving health literacy. It is, however, more likely to impact if it is part of a wider programme, i.e. if immunisation or screening interventions are just one of the options on offer, used to ultimately build trust.
-
Engagement in the idea promoted by the programme through explicit questioning of prior knowledge, attitudes, beliefs or behaviours. The aim here is individual development, and it requires a deeper level of engagement than above. This could be manifest through, for example, questioning prior domestic abuse,192 or undertaking further studies. 193 Such engagement could reasonably be expected to impact on individual lifestyle factors (the inner circle of the diagram above).
-
A third level of engagement was evidenced in some of the studies, which entailed taking steps to improve conditions for the wider Community. This is very evident in programmes such as Pavee Point, in which members of the Community initially took part in training sessions and then became outreach workers, and some assumed a representational role with settled local decision-makers. 157 The aim of the engagement endeavour is, thus, much broader than in the two previous cases and could, over time, be expected to impact on social and community networks and general socioeconomic, cultural and environmental conditions. Developing the capacity and confidence of Traveller Community members to improve their living conditions and provide services to their own Community through education and the investment of resources emerged as an important component of some outreach initiatives (EH1). This in itself creates a ‘boost that they themselves get from knowing that they are making a positive impact on their own community’ (EH1) and is consistent with the ‘word-of-mouth culture’ through which health information is passed on within the Community (EH4, EH5).
Enabling professionals and outreach workers to map out their projected impacts, and to distinguish between compliance (e.g. which is sufficient for attendance at a screening event) and true commitment (e.g. necessary to stop smoking), might contribute to bridging the gap between Traveller Communities and statutory services.
Explanatory framework
The scoping review and economic evaluation have highlighted the lack of firm outcome measures and robust research designs. Crucially for the realist synthesis, it also often lacked process detail about what exactly outreach interventions entailed. Therefore, searches of extant literature and expert hearing activities became key in the process of deciphering how and in what circumstances outreach interventions were described to have ‘worked’ (in this case, by engaging Travellers successfully, at any of the three levels described above). These searches initially focused on trust, engagement and mobility, and were subsequently extended to include social capital. Numerous candidate theories were examined for their potential to explain how the interventions described might have reached the outcomes, given the complex contextual fabric of Traveller Community lives. Examples of these, with the reasons for discounting them, are given below.
-
The diffusion of innovation theory194 was discounted because it could only provide an explanation for part of the findings, i.e. when a message was ‘diffused’ through the Community, but this was not always the case or aim of the intervention.
-
Merton’s theory of deviance195 was considered because of the ‘bridging’ function of outreach between settled institutions/services and Traveller Communities, but proved too abstract and difficult to apply to such a disparate group.
-
Self-efficacy and community efficacy theories196–198 were considered to explain when a limited number of outreach workers took on representational roles to improve conditions for the Community as a whole, but this explained only part of the reported outcomes.
-
Hart’s ladder of participation199 was initially used to classify some of the reported outcomes but could not explain why they might have occurred.
The process of considering the explanatory potential of candidate theories impacted on the four initial theories (‘to whom’, ‘by whom’, ‘how’ and ‘what for’); this is detailed in the paragraphs above. ‘To whom’ highlights the importance of mobility, as not only a crude descriptor of a nomadic lifestyle, but also all that an association with the lifestyle implies, and in particular its impact on the formation, development and maintenance of social networks. ‘By whom’ highlights the importance of trust. ‘How’ hinted at the potential of using a model of engagement, such as that developed by Neufeld,190 in order to explain how outreach workers may approach the Community. ‘What for’ highlighted three levels of individual engagement, which can be considered as intermediate outcomes. Thus, engagement emerged as a concept with dual utility in our analysis – it was the process mechanism that could explain most outcomes, but given the lack of trust of Traveller Communities, it was also an important intermediate outcome in its own right. Successions of CMO configurations could thereby be identified in the literature, whereby, for example, a screening intervention would result in participation (O), which then formed the context (C) for another intervention, leading to a deeper level of engagement manifested by behaviour change (O) because trust had been developed (M).
Neufeld’s190 work offers insight into the processes through which outreach workers may approach the Community ( Figure 17 ). This engagement model accounts for a dynamic relationship between a person and their environment, conceptualised as encompassing a set of both physical and social variables. An outreach intervention can be seen as a key component of the social and welfare environment of Traveller Communities. Neufeld et al. 190 define engagement as ‘the quality of a person–environment relationship determined by the extent to which the negotiation, participation and evaluation processes occur during the interaction’ (p. 251). Given that we have hypothesised that outreach workers are key conduits between Traveller Communities and their settled environments, it seems reasonable to think that this model has potential in explaining how and in what circumstances they work best. Neufeld et al. 190 describe negotiation, participation and evaluation as three key elements of a successful person–environment relationship.
FIGURE 17.
The person–environment model of engagement, incorporating a trust development process applied to Traveller Communities.
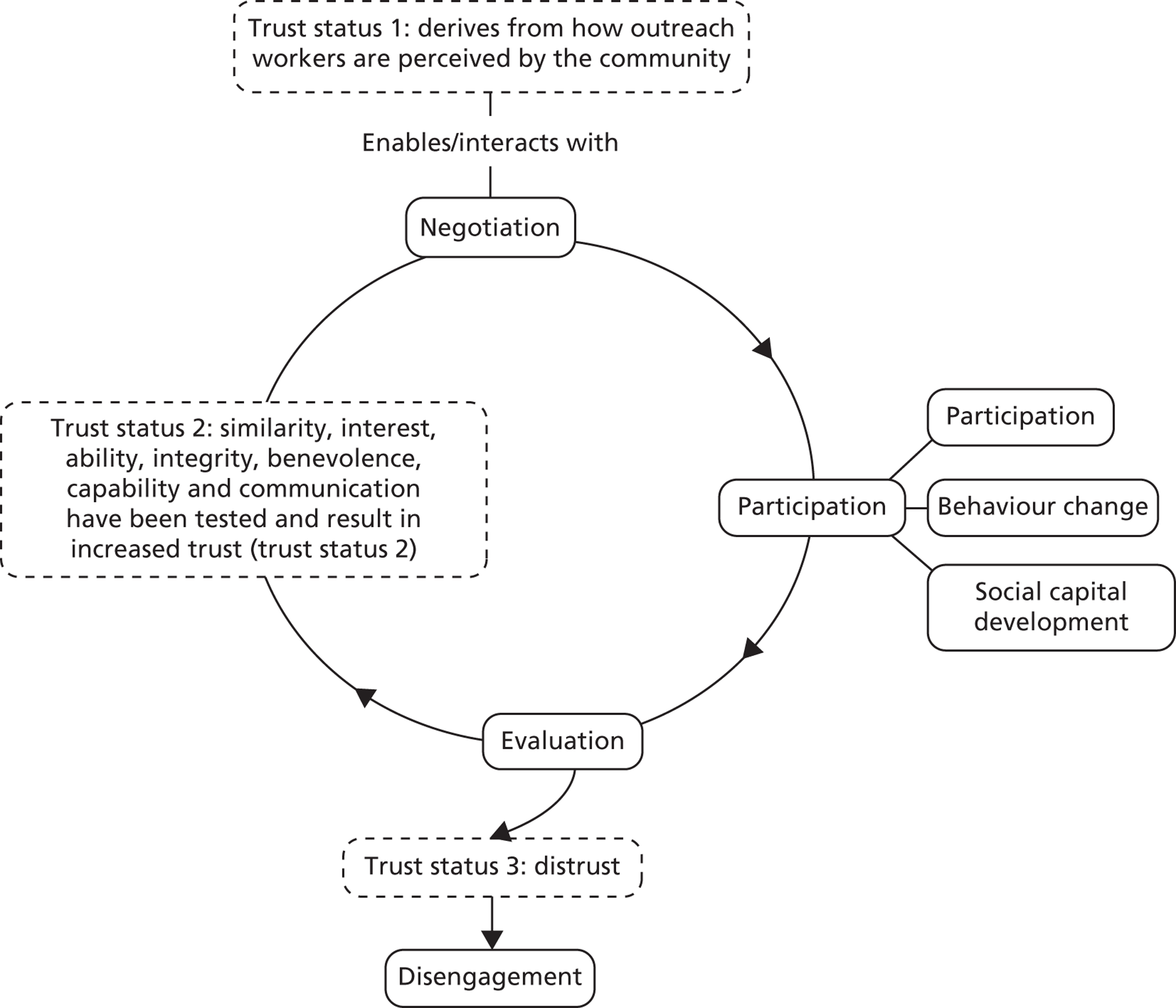
Negotiation refers to a dynamic process in which both an individual and their environment make adjustments to accommodate one another; it presents multiple opportunities for both individual strengths and environmental resources to be capitalised on in an interaction. This negotiation stage could thus refer to the opportunity that outreach workers may afford to negotiate the need tackled by a particular intervention. Expert hearings suggested that opportunities for engagement needed to be matched to people’s readiness for engagement and in accordance with coinciding events in the wider context of people’s everyday lives (EH3, EH5). As such, flexibility and offering a range of potential engagement opportunities is advocated, often starting ‘low key’ or responding to more pressing concerns (as described earlier) and then working opportunistically to address health at appropriate times and given the diversity within the Traveller Community (EH3, EH4, EH5):
People may be smoking quite heavily or whatever but actually if their accommodation is quite perilous and there are other things going on its just not appropriate to remove that crutch at that time . . . its about sowing the seeds so that when people are ready to look at quitting or are at a different point in their lives that they have got the resources, they know where to get the support to do that.
EH3
Indeed, a person’s ability to recognise problems in the environment that may go unnoticed by those outside it (EH3) and to formulate solutions might increase the likelihood of adjustments being made and, thus, of their engagement. In turn, those who engage with services often emerge as peer mentors for others in the Community (EH3). Thus, a successful process of negotiation is likely to feed into a process of incremental trust building, which in turn may impact on how open the recipient may be to messages not previously considered.
Participation refers to the degree of positive psychological, physical and emotional interactions between a person and an environment: ‘the notion of physical participation may involve an individual’s actual behaviour associated with task completion, interpersonal contact, physical exercise, interaction with environmental resources . . . and response to various aspects of the physical surroundings . . .’ (p. 252). 190 We have shown above how the outcomes from the studies included can be mapped on a three-point scale of participation/engagement.
Evaluation is part of a continuous process of engagement. It refers to the appraisal of the participation process, in terms of the degree of ‘fit’ between a person and their environment. A positive evaluation can lead to goal attainment, either from the point of view of individual achievement or in terms of environmental enhancement. Coupled with trust status, negotiation, participation and evaluation can thus describe three stages of the outreach process.
The Pavee Point initiative157 substantiates this model as it reports how positive experiences of attending services led to increased self-efficacy to access services independently. While this study achieved in-depth engagement with a small group of Travellers, the study does not discuss how they dealt with issues of transience. Thus, the study may have engaged those who are more static and less ‘hard to reach’. The Community members who did engage seemed to act as soft and multiple entry points into the wider Community, therefore potentially initiating a new engagement cycle.
In the process of analysis, Neufeld’s model was adapted to include both trust and different levels of participation/engagement (including disengagement), and the CMO configurations formulated from the literature were mapped on to it. This is presented in Appendix 13 . A simplified version is presented in Figure 17 .
Finding, developing and using this model in our analysis proved a key turning point in making sense of the disparate literature we were trying to synthesise. In particular, the cyclical nature of the model helped us to explain how trust and engagement could feed into one another and build into increasingly fruitful relationships over time. We could have used this as our middle range theory and formulated groups of CMOs for each negotiation–participation–evaluation step, and indeed our analysis went so far down that line. However, in many instances, this left some questions unanswered, pertaining to participants’ reasoning (trust and negotiation could explain only some of the underlying reasoning leading to participation). The lack of process detail also made it difficult to systematically highlight, with clarity, the resources that when put in context were likely to trigger that reasoning. We therefore felt the need to access a higher level of abstraction which could explain our observations.
At the individual level, the literature on school engagement200 describes different types of engagement mechanisms, which can conceivably transfer to disengaged groups and complement this outreach process to translate into mechanisms triggered at the micro (individual) level:
-
behavioural engagement relates to participation in social programmes
-
cognitive engagement relates to of personal investment in an idea or project
-
emotional engagement relates to the creation or modification of ties to individuals or programmes. 200
While the person–environment model describes a cycle that Traveller Communities may engage with through outreach workers, Fredricks et al. ’s200 classification offers a menu of potential reasoning mechanisms (M) leading to reported outcomes (O). These also clearly link on the three levels of participation that we identified: behavioural engagement, as a thought mechanism, would logically lead to a kind of participation that does not assume in-depth questioning of one’s prior knowledge, attitudes beliefs or practices. An example of this would be someone who takes part in an event because they think this is expected of them, or they want to be seen to participate – they display a behaviour. Cognitive engagement denotes a deeper level of involvement in a programme and would manifest itself through changes in behaviour or prior established practices. Emotional engagement would manifest itself in the personal investment in improving life for the wider Community.
Drawing on these multiple sources, we constructed an explanatory framework detailing how and in what circumstances outreach interventions may work with Traveller Communities ( Figure 18 ). It was developed from a combination of synthesising the Traveller specific theories exposed thus far: Neufeld’s model of engagement190 with Hurley185 and Mayer et al. 186’s model of trust, and Fredricks et al. ’s200 typology of individual engagement. This framework is literature based, in that these key concepts have been found in extant studies and commentaries. However, the exact formulation of the framework is the result of the insight and judgement of the reviewing team. We have selected those theories which, put together, seem to have the widest explanatory scope, seeking to explain the general rather than every specific instance. The framework is thus the result of a movement from fragmentary evidence sources towards a broader outlook by combining theories to attempt to maximise scope and potential.
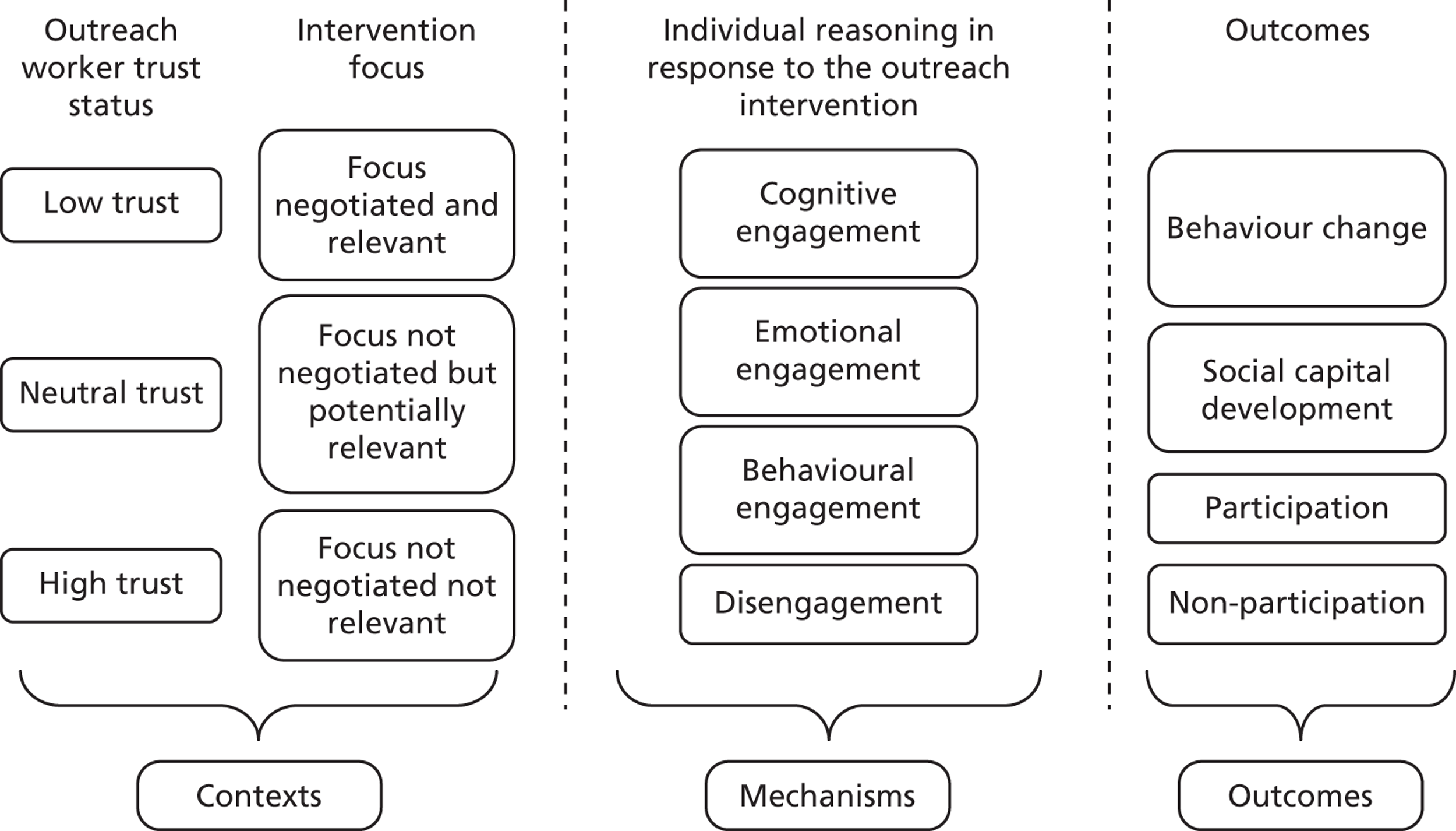
Contexts detail the inverse rule of trust and negotiation. The intervention focus title relates directly to Neufeld’s190 negotiation phase, which, in combination with the outreach worker trust status, is purported to provide a more-or-less fertile ground for intervention strategies (resources) to flourish. Mechanisms detail the engagement reasoning that is likely to have been triggered as a result, based on Fredricks et al. ’s200 typology of engagement. Outcomes are the observable and reported results from this process.
The concepts of engagement and trust provide some explanatory power and, applied in appropriate combinations, can be used to generate hypotheses on what it is about outreach in Traveller Communities that works, for whom, in what circumstances and to what extent. These take the shape of the following seven ‘testable’ theories (‘testable’ theories refer to theories at a close level to the data that were used to break down and test the overarching explanatory framework) about impact on participation, behaviour and social capital that occurred:
-
If they have not got an established place on Traveller Communities’ social network ‘maps’, outreach workers need to create explicit opportunities to build trust. Failure to do this is likely to lead to a lack of participation.
-
There is an inverse rule of trust and negotiation, which means that the higher the initial trust status that the outreach worker has with the Community, the less important the requirement is to negotiate the topic of the intervention so as to respond to a perceived community or individual need and trigger engagement mechanisms.
-
The correlate to theory 2 is that the lower the initial trust status, the more imperative the need is to negotiate the focus of the intervention and to use an opportunistic approach to intervention. Such a responsive and flexible approach is most likely to trigger behavioural engagement and participation.
-
A successful ‘negotiation’ phase will elicit and respond to expressed needs and often use opportunistic strategies for health improvement. This can initiate cycles of engagement, whereby budding trust can become a favourable context for subsequent interventions.
-
A correlate to theory 4 is that a lack of appreciation of the needs and priorities as expressed by the Traveller group targeted is likely to trigger a reasoning of disengagement.
-
Intervention recipients are more likely to change their unhealthy or disengaged behaviour as a result of cognitive engagement, which is likely to be trigged within an established relationship of trust with the outreach worker.
Traveller organisations have developed long-term relationships of trust with outreach workers. This can trigger a transition from cognitive to emotional engagement, manifested through a movement from individual to collective focus. These outreach workers have an established place on Traveller Communities’ social network maps; they tend to have a good understanding of Traveller needs and therefore provide a favourable context for further interventions.
Substantiating the explanatory framework
This section describes the analysis of 16 primary studies, grouped by the degree of participation described as an outcome. The intention is to describe each study briefly, to interrogate the findings in light of the CMO configurations under scrutiny and, in doing so, to add depth and nuance to that theory. In each study described, references are made to other studies, demonstrating some of the complex analytical process that led to these configurations. The analysis below is thus the result of examining the whole of the 104 studies included in the realist review. This led to the development of the model above, and substantiation exemplars are given below.
Participation (theories 1–5)
Participation (with or without further depth of engagement) is by far the most commonly described intervention outcome, and hence this section is the longest of the substantiations. In order to facilitate reading and improve the explanatory potential of the section, studies are grouped by contextual parameters (initial trust status of the outreach worker and the extent of negotiation and relevance of the intervention focus):
-
Barraclough,201 Streetly116 and Reid60 all describe interventions where, on entry in the Community, the outreach worker had a neutral trust status, but the intervention is negotiated and therefore responds to a need expressed by the Community.
-
Darby202 and Chiriac203 describe interventions where, on entry in the Community, the outreach worker had a neutral trust status. The intervention was not negotiated, but potentially relevant.
-
Austerberry204 describes an intervention with a similarly initial neutral trust status, but the intervention is not negotiated, and participation is poor. This is reinforced by Dignan,205 an article focusing on a group of Native American mothers.
-
In Davis,206 the outreach worker has a low trust status on entry, but they negotiate the intervention focus. In Fitzpatrick,64 the initial trust status is low and the intervention is not negotiated, but the reported results are the same as in Davis. 206
Barraclough 2002201
This article describes the work of a specialist health visitor situated within a primary care trust and working with the Nottingham Traveller Team. The multidisciplinary team is led by a teacher and comprises professionals with diverse backgrounds and skills. The programme delivers both health and education services for Traveller Communities and views these as interdependent. Although the article does not describe a detailed negotiation process, the intervention appears to have been responsive to the needs of individuals and families as they emerged. The health visitor offered informational and instrumental support and facilitated access to services through, for example, helping registration with services, making appointments, providing reminders and interpreting letters. This project therefore provides support for theory 4, in that a successful negotiation phase will elicit expressed needs and use opportunistic strategies for health improvement. This leads to participation, in this case in access to health services and school attendance. Examples given include a mother of six children who completed a course of dental treatment while living at seven different addresses in 3 months. Participants cited help with reading, writing and understanding health systems as being particularly beneficial.
[I]f it wasn’t for you we’d be spending 5 hours in casualty every other week.
Grandmother of mobile family group with five children under the age of 1 year – after helping them to obtain a temporary GP, p. 185
Travellers on the team highlighted that trust in health visitors would not be assumed: ‘Travellers is funny about health visitors. We know you and I trust you, but if we go on to another site, we don’t know. We lead a secret life and a free life, we’re careful’ (p. 185). Thus, while the health visitor is unlikely to have entered the Community with low trust status born out of previous negative experiences, they are likely to have a neutral trust status. The CMO configuration for Barraclough201 is represented in Figure 19 .
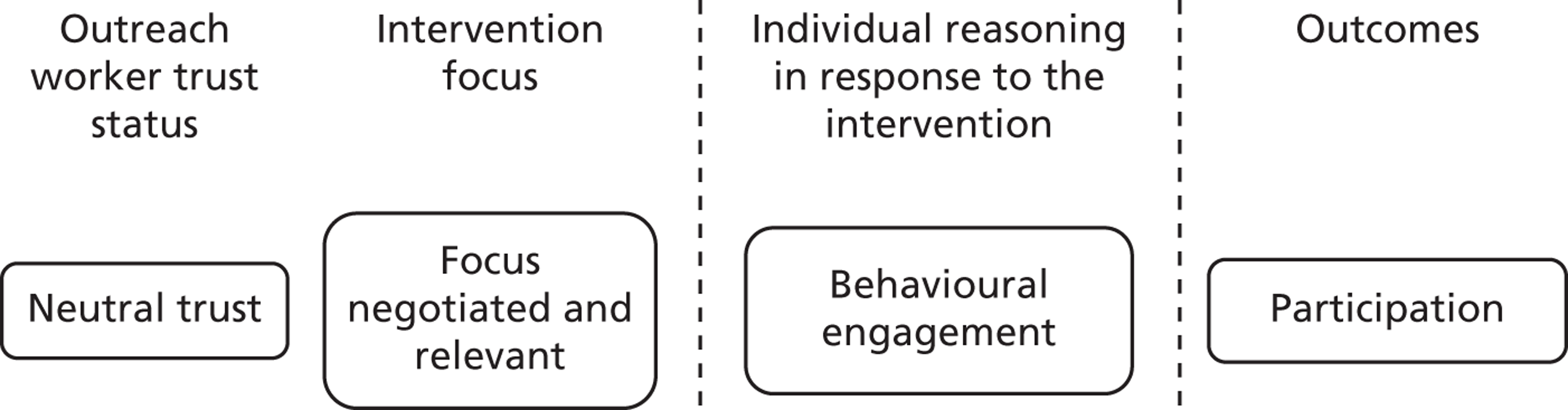
The positive experiences that Travellers describe above led to the development of trust in the health visitor as someone who could be relied upon for help. This led to a conscious decision to participate in activities generated. The article reports that Travellers became ‘increasingly responsive to the team and the work they were doing’ (p. 185). This article lends support to theory 1 and theory 3, of the importance of negotiation when outreach workers do not have an established place on Traveller Community social network maps, and of the establishment of trust, in this case through demonstrating capability, integrity and predictability.
Streetly 1987116
This paper describes a programme of health care for Travellers set up and monitored by a health authority. Two health visitors were given responsibility for a site alongside a clinical medical officer. The service was delivered out of a ‘multipurpose mobile’ which had been bought by the local education project. The health visitors are likely to have started from a position of neutral trust; they worked with teachers working on the site who had built a relationship with Travellers in order to gain acceptance. The service aimed to provide preventative health services on site, as well as facilitate access to existing services. Initially, the help requested from Travellers related to more immediate concerns relating to ‘clothing, welfare, and problems with eviction’; however, once health visitors had helped to address these issues, Travellers raised concerns relating to health care. The intervention, therefore, provides substantiation for theory 4, as health visitors with a neutral trust status worked with Traveller Communities through a process of negotiation, which elicited and responded to needs articulated. In the first instance, the project focused on families with young children and offered immunisation, developmental screening, feeding advice, weighing and family planning services. It later extended its reach to all Travellers in response to concerns around a lack of access to services among men and older people, as well as to those on nearby unauthorised encampments. The outreach workers encouraged attendance at available services, sharing the names of GPs who were willing to register Travellers, booking and accompanying them to appointments with dentists and a chiropodist. Liaison with local services was also undertaken in order to enhance their sensitivity to the needs and situation of this group. Travellers were provided with cards detailing their medical records in an attempt to increase continuity in care. The article reports acceptance of some preventative services, including developmental screening and hearing and vision testing, as well as uptake of family planning facilities, dental, physiotherapy and chiropody appointments, all of which can be classified as ‘participation’. The CMO configuration for Streetly116 is represented in Figure 19 .
The project had less success in encouraging the uptake of immunisation, though this is noted to have improved as the team became more accepted. Uptake of immunisation may necessitate a greater level of engagement (i.e. cognitive engagement in which Traveller Communities invest in the idea of immunisation as opposed to behavioural engagement referring to participation in a programme), particularly given the pollution taboos described earlier relating to the importance of preserving the cleanliness of the inner body,41 and, as such, may have been difficult to achieve in the timescale.
Reid 199360
This paper describes the provision of a weekly clinic for Traveller Community members run by a full-time health visitor. A dentist and chiropodist work in the clinic and a GP practice is situated in the same building. The clinic provides well-women services, including cytology and family planning, as well as child and baby services, with a particular focus on immunisation. It focuses on instrumental support to alleviate barriers to accessing health services and to accommodate the transience of Travellers. As far as possible, the clinic acts as a one-stop service, working opportunistically to conduct immunisations and examinations immediately. In addition, health promotion videos have been produced which take into consideration high levels of illiteracy.
The health visitor conducts outreach on sites and visits those who have just moved into the area to encourage them to attend the clinic and to provide transport where required, as well as providing awareness to other health professionals about the needs of Travellers. The service does not advertise itself as Traveller specific and aims to assist Travellers in accessing mainstream health services. Health promotion advice is also offered opportunistically on site visits:
On a site visit recently we found 15 people, including five children, gathered in one trailer. The father was present so we did not get to talk about family planning, but it was a great opportunity to talk about immunisation.
Reid 1993,60 p. 29
Although the outreach worker is not likely to have started from an initial position of high trust, the responsive approach, which includes offering health advice at appropriate times and places, provides further illustration of a successful process of negotiation (theory 4) and of the relationship between initial trust and the negotiation of the intervention focus (theory 3).
The paper provides examples suggesting high levels of acceptability of the service among Travellers.
Another Traveller mother says: ‘When you can’t read and write it’s difficult to sort things out yourself. I can come here and talk about things, they are explained and I understand. It’s nice to have someone to sort things out for me, someone who understands gypsies.’
Reid 1993,60 p. 28
Communication, through both how things are said and the timing and sensitivity of the advice offered, therefore, seems a key factor in building trust in this intervention.
Barraclough,201 Streetly116 and Reid60 share the CMO configuration drawn in Figure 19 . They provide illustrations of interventions offering social support (instrumental and informational) in a context of neutral trust and negotiation of the topic, leading to behavioural engagement and participation (theory 4). These articles all describe professional or semiprofessional outreach workers who are not from the Community and use explicit strategies to build trust with the Community, through adequate communication and a demonstration of capability, integrity and predictability (theory 1). This leads Traveller Community members to have sufficient levels of trust in the workers to make the conscious decision to participate (behavioural engagement).
Austerberry 2008204
The project was targeted at young people, with an emphasis on specific ‘vulnerable’ target groups, including young people from Traveller Communities. A model of ‘hub and spoke’ was used in one locality, whereby a hub would be in a centrally located setting, serving as a resource and a point of multiagency service delivery. The spokes consisted of a range of outreach provision in different non-health settings around the borough. The evaluation found that the roles of the specialist nurses and the development workers (including a health inclusion worker for Travellers and Gypsies) were particularly key to enhancing participation. Because of the range of these roles, the level of trust that they had as they entered the Community is difficult to assess. The range of issues addressed included healthy eating, exercise, smoking, substance misuse, sexual and reproductive health (including chlamydia screening) and emotional health. The topic was therefore not negotiated, and the relevance or priority of what was on offer is difficult to assess.
A plan to have a mobile bus in an isolated rural area in Northumberland was rejected by young Travellers, who thought that a bus arriving in their site would be too visible and compromise their anonymity. This may have been a key barrier to participation, as there could have been social pressure not to engage in the intervention, particularly if its aims were unclear. Overall, the project achieved high rates of participation, but the proportion of young people from Traveller Communities accessing services remained low over the 2 years, despite early encouraging results from the work of the Traveller specialist worker.
Austerberry204 describes the kind of threat to intervention success described in theory 5, in that the intervention was delivered on an assumption of similarity between Traveller and settled youth, rather than an engagement with the Community. The intervention demonstrated a lack of understanding of the strength of social bonds within the Community, the prevalent mistrust in non-Travellers and the persistence of taboo subjects around, for example, sexual and reproductive health. There were no attempts to build trust with the Community prior to the intervention commencing, with an assumption that, if services were geographically better situated, Travellers would access them. This verifies theory 1, in that without a prior trust-building exercise, this intervention was unlikely to be successful. The combination of low to neutral trust and lack of negotiation over perceived needs verifies theories 2 and 3. The CMO configuration for Austerberry204 is represented in Figure 20 .
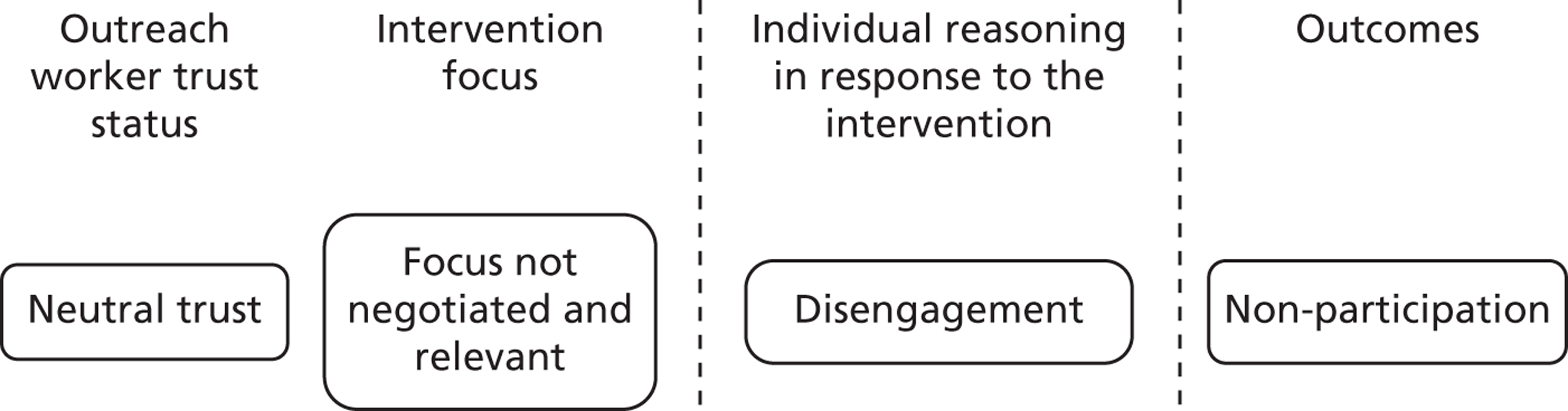
In Austerberry,204 as in the three previous studies, the services offered here are broad and consist of social support strategies. These are, however, implemented in a context where need is assumed rather than understood and the focus of the intervention is not relevant. In this context, social support strategies do not trigger a reasoning of engagement, resulting in poor attendance. Austerberry,204 therefore, substantiates the need for a favourable context (either high trust or responding to an expressed need: theories 2 and 3) in order to enable social support interventions to lead to participation in programmes.
Darby 2007202
This article describes the organisation of breast cancer screening in Hungary by organisations working for the welfare of Romani people. It is very probable that the intervention recipients knew the outreach workers, as one of the workers, at least, who is quoted in the report, was a young Romani woman from Hungary. However, the closeness of their relationship is difficult to assert with any kind of certainty from the text. The screening programme was organised and messages were sent to the Community to encourage women to attend. Given that ‘Romani women are three times more likely to succumb to the disease than non-Romani women’ (p. 1),202 screening is likely to have been seen as relevant, even though the intervention focus was not negotiated. Key elements that triggered participation are described as the fact that mammograms were provided free (a change in national policy), and that screening sites were located nearer to where Romani people live (there was also a mobile scanning unit). The biggest reported barrier to attendance was a fear of discrimination and reluctance to, potentially, being examined by a male doctor, rather than an objection to screening itself. The article describes how a young Traveller with a family history of breast cancer set about convincing other women that they should get screened. As a result, rates of mammograms among Romani women doubled from 26% in 2001–2 to 56% in 2002–3.
Therefore, the resources offered by the outreach programme are mostly in the form of social support (instrumental and appraisal), much like Barraclough,201 Streetly116 and Reid,60 above, although this time the intervention is much more focused and less opportunistic. Although mostly descriptive, the results from this study are not self-reported, suggesting there has been a real impact, at least on screening attendance. The CMO configuration for Darby202 is represented in Figure 21 . The fact that the intervention topic was not negotiated might have been offset by the high prevalence of mortality from breast cancer in the Community (it was relevant), coupled with the fact that at least some of the outreach workers were from the Community. This favourable context enables the programme strategies (free mammograms and convenient location) to trigger decisions to participate, an engagement reasoning that is at least behavioural, if not cognitive (which would involve longer-term lifestyle change and more regular proactive screening – these are described, but only anecdotally).
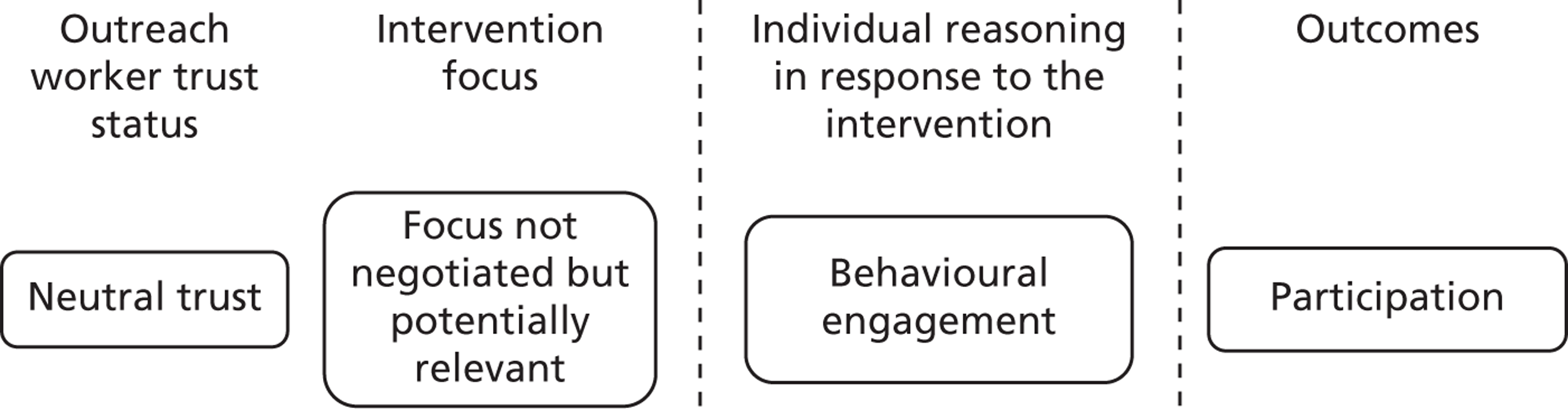
Dignan 2005205
This study was designed to test the relative effectiveness of an intervention delivered face to face or by telephone to urban Native American women. Most prior research on breast cancer among American Indian women has focused on reservation populations, leaving urban populations relatively understudied. The urban Native American population shares with Traveller Communities a consistent exposure to assimilatory practices and policies and mobility, as families may have a base in the city but return regularly to their reserve of origin. In addition, as they travel, many struggle to keep paying their telephone bill and regularly find the line disconnected, rendering even telephone contact difficult. Therefore, this study helps to verify theory 5 on the lack of understanding of needs and priorities as expressed by the target population.
The effectiveness of the intervention was evaluated using a design that included a pre test, a random assignment to a face-to-face or a telephone group, and a post test. Outreach workers were local Native American women (referred to as ‘Native Sisters’) but the exact nature of their relationship to the target group is difficult to assert. The study targeted a total of 929 potential participants living away from their home reserve. It is, therefore, reasonable to assume that while the researchers might have thought the intervention was building on strong community ties, this is unlikely to be the case (as the frequency and intensity of social contacts is likely to be weak). However, it is reasonable to assume that because of their ethnic origin, the Native Sisters entered the Community with a neutral (rather than low) level of trust.
Studies demonstrate that ‘the 5-year breast cancer relative survival rate for American Indian women is 48.8% compared with 75.7% for whites, 73.4% for Hispanics, 62.8% for African Americans, and 69.4% for Native Hawaiians’ (p. 29). In addition, access to mammography screening is described as particularly difficult for Native American women in the area targeted and there are economic and transportation barriers to uptake. However, survey data suggest that cancer may not be seen as a priority by this population. Therefore, the focus of the intervention was not negotiated and it is likely that it was not seen as relevant. This verifies theory 2 on the inverse role of trust and negotiation, according to which, in the absence of high trust, a higher degree of negotiation (and effort to meet perceived needs first) should happen.
The Native Sisters were trained to provide information on the importance of mammography and adherence to guidelines, strategies to overcome barriers to obtaining mammograms and follow-up care, and reinforcement for scheduling and keeping appointments. They, therefore, principally offered informational and instrumental social support. This study, however, introduces a level of negotiation over the delivery mode of the intervention (face to face or by telephone), therefore emphasising opportunities for instrumental social support.
The study compared face-to-face delivery of the intervention with delivery by telephone and a control group. The increase in the proportion of women who reported receiving a mammogram within the past 12 months from pre test to post test was statistically significant (42% for the telephone intervention and 31% for the face-to-face intervention), but there were no significant differences between the intervention and the comparison group. Only 157 out of a potential 929 participants took part in the study and one-third of those participating were lost to follow-up.
This article offers an interesting comparison with the Traveller Community study described by Darby. 202 Both target breast screening, an intervention that requires behavioural engagement only (rather than, necessarily, a longer-term behaviour change) and both sets of outreach workers are likely to have entered the Community with a neutral trust status. The key difference is that in Darby202 the intervention focus is likely to be seen as relevant and instrumental barriers are most likely to explain lack of access. In Darby,202 the intervention also took place near Traveller settlements, so that the influencing potential of strong social ties among women attending could be maximised as a result of the intervention. Dignan,205 on the other hand, reproduces the pattern observed in Austerberry,204 in including a poor understanding of perceived need and a poor appreciation of the importance of strong social ties and the necessity to build, rather than assume, trust in the outreach worker before an intervention can bear fruit. The CMO configuration for Dignan205 is represented in Figure 22 .
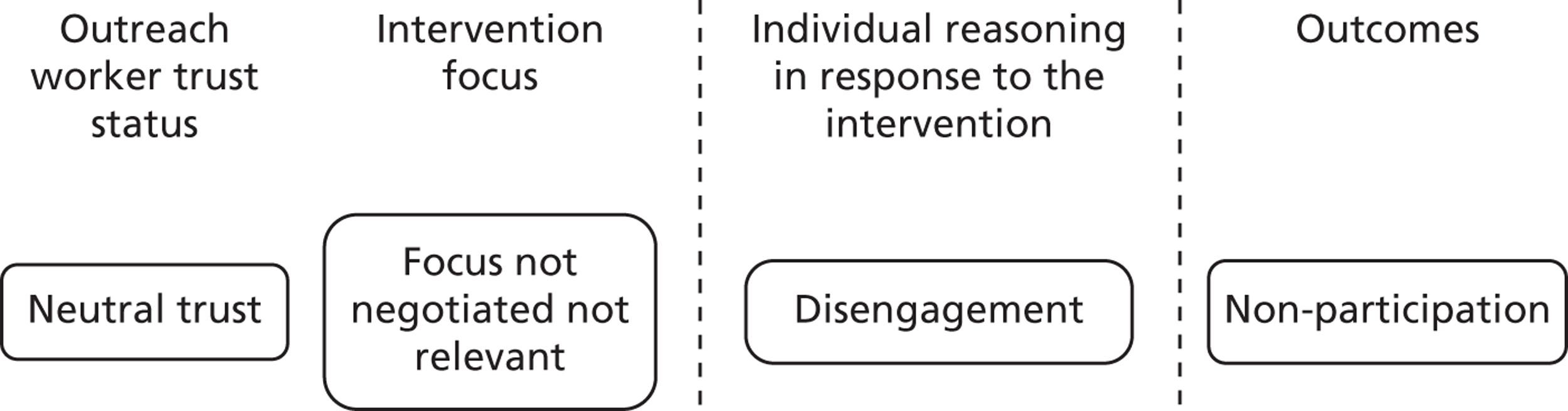
Fitzpatrick 199764
This study was based on a previous one which had been successful in settled mothers, and which had involved lay volunteer community mothers delivering a child development programme to disadvantaged first-time mothers. 207 Given the success of this first trial, this article described the effort to apply the model to Traveller mothers. Outreach workers were experienced settled community mothers who were given additional training to heighten their awareness of and sensitivity to the needs of the Traveller parents. They were not part of the Community and had had no prior contact with it. It is therefore reasonable to assume that they entered the Community with a low trust status.
All travelling mothers giving birth within the area (Dublin) or entering the region within 4 months of delivery were offered the help and support of a settled community mother. However, the intervention did not seem to take into account the fact that Travellers are a very tight-knit community with definite views about childcare, and that mothers are more likely to seek one another’s advice rather than turn to settled mothers who might have different values [as corroborated by expert hearing findings that Traveller Community members expressed concerns about their children mixing with settled children (EH9)]. Therefore, the intervention was not negotiated, and was unlikely to respond to a perceived parenting need (theory 3). However, the authors report behavioural engagement, with better rates of immunisation, maternal well-being and nutrition, and reduced hospitalisations. The programme is also reported to have been well accepted by Traveller mothers.
However, this study establishes the significance of the results against a control group of settled mothers, which makes the significance of the results difficult to establish. Given Traveller mothers’ likely weariness of settled outreach workers, it is likely that they participated in order to be seen to co-operate rather than as a manifestation of belief in the value of advice provided.
The theory refinement process described on p. 38 highlighted a legacy of historical discrimination and persecution, which included the removal of Traveller children from their families. 165 This may lead Travellers to be suspicious of interventions and to fear being perceived as not coping with parenting, as also exposed in Cemlyn. 188 In addition, research highlights that Travellers often prefer not to talk about mental health owing to the fact that it is stigmatised in the Community,39 casting doubts over the validity of self-reported maternal well-being in this study.
This study differs from Darby,202 in that the need addressed is assumed by the intervention organisers rather than assessed or negotiated. While the CMO configuration features the same pattern on the face of it, it is likely that the motivational factors that led to participation and report of acceptability were more linked to the historical legacy of Travellers than to the intervention. The decision to participate is thus likely to be informed by a protectionist attitude, rather than an open engagement with the intervention. This provides a verification of theory 5, as reports of well-being and acceptability may be unreliable when interpreted without awareness of the nature and strength of Traveller networks. In the long term, it seems reasonable to expect that this kind of intervention (based on low trust, low negotiation and poor understanding of the nature of Traveller bonds) may lead to further entrenched disengagement. The CMO configuration for Fitzpatrick64 is represented in Figure 23 .
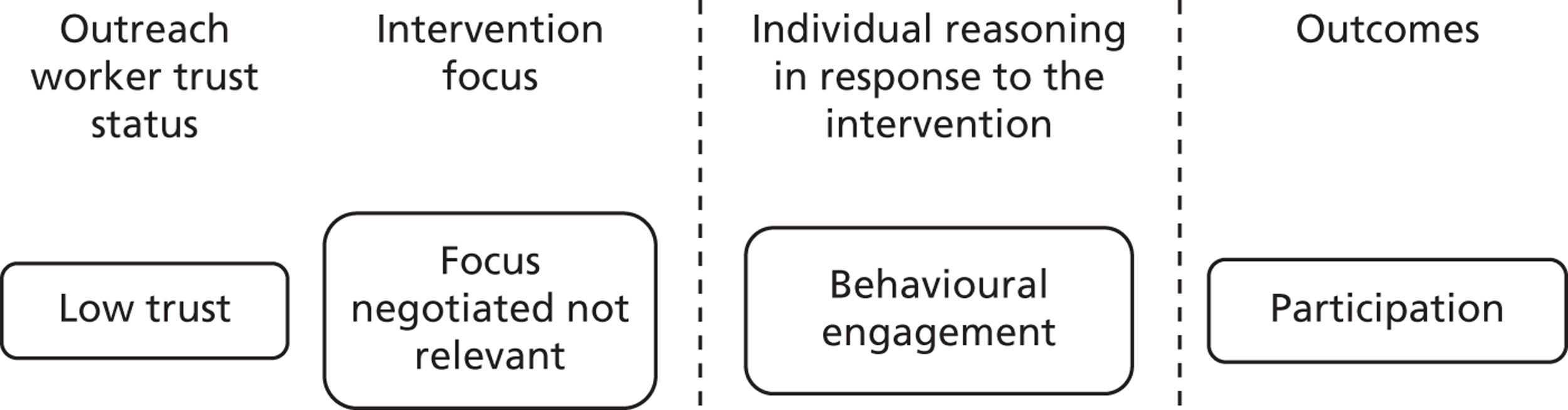
Participation key messages
By far the greatest proportion of the articles we examined in this study reported participation in a way which made it difficult to assess whether it was a sign of a more in-depth engagement or merely, for example, an artefact of social desirability. As stated before, the assumption was therefore made that the latter was more likely and a more in-depth engagement was not assumed. In spite of the paucity of measurable outcomes, these studies do display a pattern which explains why participation may or may not have happened.
The seven articles above provide evidence of the context and mechanism combinations more likely to lead to outcomes of participation in a programme. Each article illustrates how the inverse rule of trust and negotiation (theories 2 and 3) forms a key influencing context, carrying strong explanatory potential. Darby,202 Austerberry,204 Barraclough,201 Streetly116 and Reid60 all describe an initial neutral trust status, offset by a variety of negotiation strategies, concurring to explain either participation or non-participation in a programme. Fitzpatrick64 describes conditions not favourable to participation and yet reports high acceptability, which can be explained by cultural historical legacies of feeling threatened that one’s children may be taken. Some of the studies that we classified as ‘neutral trust’ on the basis of the information provided may have featured high trust, for example in the case of Barraclough,201 who describes long-standing relationships with the Community. If that was the case, it seems reasonable to assume that a team such as this has the potential to implement interventions faster (building on past relationships) and is likely to lead to higher rates of participation. Once trust is established, such interventions therefore have a potential for increased time-effectiveness.
Improved behaviour change (theories 1 and 6)
Leeds GATE 2007192
Leeds GATE was formed in 2003 as a charitable organisation by Gypsy and Irish Travellers to improve the quality of life for their Communities. It is a high-profile organisation within the UK and jointly leads on a National Gypsy and Traveller Health Inclusion project with the Department of Health.
This report describes a project conducted in the UK which aimed to provide opportunities for discussion about domestic violence among Travellers; to increase the self-esteem and confidence of Traveller women to keep themselves safe; and to increase access to available services offering support for those experiencing domestic violence. Much like Pavee Point, the work of Leeds GATE is continuous and the project on domestic violence occurred in the context of many other initiatives focusing on accommodation, health, education and employment, and social inclusion. The project was initiated by a Traveller Community member (who also worked as a youth inclusion worker), following her participation in training on domestic violence and in response to an observed need within the Community. Domestic violence is noted to be a hidden and stigmatised issue within Traveller Communities, and the outreach worker identified a lack of recognition among Community members that domestic violence may involve forms of abuse other than those that are physical: ‘Lots of our women don’t know what domestic violence is, they think it is all based on a good hiding and believe if you don’t get hit then you are not suffering’ (p. 2). 192 The decision around the intervention topic, therefore, responded to a need identified by a Community member; however, it was not negotiated with the wider Community as in the Health Service Executive report128 discussed below. As such, this report provides support for the inverse relationship of trust and negotiation described in theory 2, because the outreach worker’s position as a known and trusted member of the Community enabled the discussion of domestic violence within the Community, despite it being considered a ‘taboo’ topic. The outreach worker herself notes initial concerns about the potential responses of members of her own Community to the project: ‘I didn’t know which way my Community was going to react to it’ (p. 12). This project, therefore, built on the outreach worker’s relationships within the Community in order to initiate discussion and influence social norms around domestic violence (theory 6). The outreach worker spoke informally while spending time with families with whom she was connected, in order to begin ‘sounding out women in her community as to their receptivity to speaking about domestic violence’ (p. 4). The report explicitly states that the outreach worker’s ‘knowledge of the particular sensitivities and context within Gypsy and Irish Traveller families and use of familiar language and concepts are critical to the achievement of shifts of understanding and viewpoint and to the sustainability of change’ (p. 7). The outreach worker describes her own reactions of feeling shocked when learning about what is considered domestic violence and may have been able to draw on this experience to identify with Community members when talking about the issues.
Initially, the outreach worker focused on five women, but she increasingly found that others sought her out to discuss issues relating to domestic violence. Gradually she opened up discussions, when appropriate, and highlighted opportunities to attend further training. In addition, three women known to suffer domestic violence were taken for a meal at a venue where they felt comfortable. They discussed their experiences and highlighted a need to raise awareness of organisations that could help.
As a result of the project, five women attended training on domestic violence and three others attended child protection awareness training. In addition, the project reports an increase in women’s confidence in discussing and addressing domestic violence. Assistance was provided to six women to escape a violent home environment and evidence was found of changing attitudes towards women and a greater consideration of responsibilities for power sharing among men.
A huge outcome for us was a worker witnessing one of the women, two weeks after a full conversation with GATE staff, bringing up the subject of domestic violence in front of her husband . . . informally from the community we have heard that she is more empowered and suffers less violence.
Leeds GATE 2007,192 p. 9
The project reports changed behaviour among Traveller Community members; as a result of learning about the impact of domestic violence on children, one young woman removed her sister’s children during a row. Women shared their understanding and offered support to others:
The worker prompted but it was mainly the two women who had been at the meal telling the other two women that they can go to GATE for help and that they shouldn’t put up with it. This was a long discussion that lasted over 45 minutes and was quite emotional.
Leeds GATE 2007,192 p. 11
The combination of a highly trusted member of the Community who tackles a subject that has resonance in other Traveller women’s lives provided a fertile context within which the discussions (sometimes away from the Community, in a neutral environment) could happen and have an impact on the participants knowledge, attitudes and behaviours surrounding domestic violence (theory 6). It is likely these outcomes happened because the information received triggered a willingness to engage with the subject and gave women the confidence to question the status quo. Cognitive engagement happened because the topic had resonance and the information was delivered in a safe environment, which led to the outcomes observed. The CMO configuration for Leeds GATE is represented in Figure 24 .
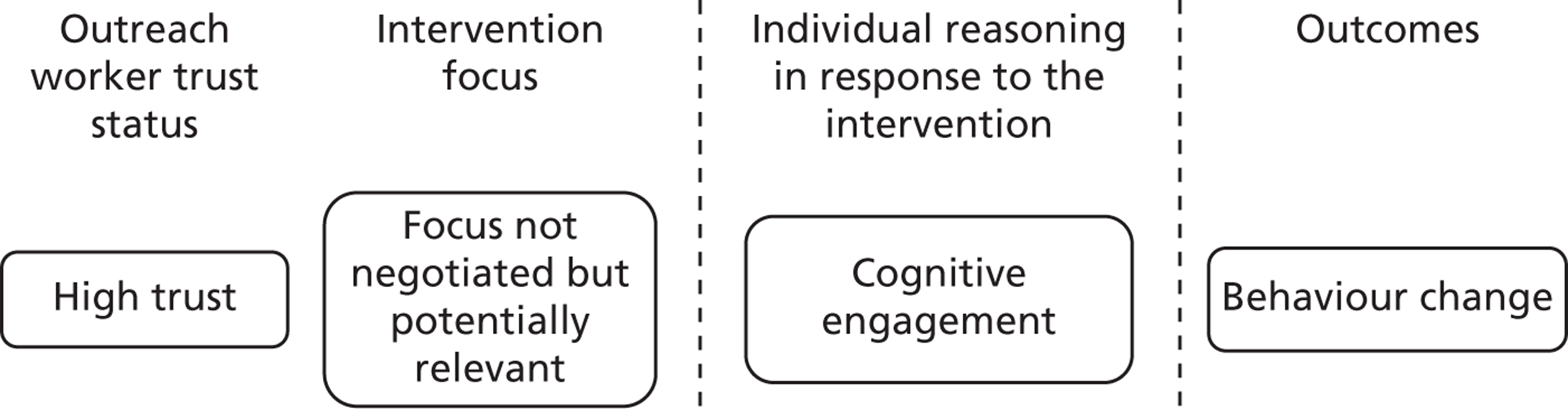
Kelly et al. 2006133
This study took place in one of Bulgaria’s largest Roma communities and was prefaced by an extensive ethnographic phase, which aimed to map out significant networks within the Traveller Community. Workers who were well known from the Community carried out observations in order to identify the presence of ‘social circles’ and the person at their social and affective core. These people were referred to as indexes and became the entry points to access and recruit social networks. Each index provided the research team with a list of network members, who in turn were asked to indicate who on the list they most and least preferred in five domains (including spending time together, trusted for advice, and discussion of important matters). A sociometric analysis was undertaken from this to identify the network lead. Leaders were then provided with training on how to counsel and advise other members of the network on reducing HIV infection risk behaviour. This study, therefore, features an explicit effort to build on close social ties and use them as levers for health promotion, testing the correlate of theory 1 – that interventions are more likely to be successful if they build on existing relationships of trust. The study, however, provided no opportunity for the Community to shape its focus (in terms of ensuring best fit between provision and expressed need). In this, it provides a test of theory 2 on the inverse rule of trust and negotiation. In fact, it provides a significant test, as we know from other studies that sexual behaviour tends to be considered a taboo subject among Traveller Communities, not only in the UK but also in Bulgaria. 167 , 208 So, while Roma groups in eastern Europe are thought to be at increased risk of HIV infection or acquired immunodeficiency syndrome (AIDS), it is unlikely that members of the Community would have highlighted it as an issue to be tackled by an intervention. 209
The programme capitalises on opportunities available to group leaders to exert social influence, leading Community members to alter their behavioural patterns (verifying theory 6). At the core of the intervention was the idea that within Communities with a large degree of distrust of outsiders, ‘advice and recommendations coming from personally known network members . . . carry credibility and influence’ (p. 1101). The study attributes the greater robustness of outcomes reported at 12 months than of those at 3 months to changes in social norms over time. Members of social networks appear to have become cognitively engaged with the intervention as they report a change in behaviour corroborated by a reduction in the incidence of biologically assessed gonorrhoea. The study reports a significantly greater reduction in the prevalence of reported unprotected intercourse (p = 0.01) and significantly increased knowledge of the risk of AIDS, positive attitudes to condoms and strength of intentions to reduce risk behaviours in the intervention group when compared with the control group. The intervention was reportedly most effective for those with casual partners, who were most at risk. This group knew and trusted the leader and it is possible that they viewed the intervention as more relevant given their greater engagement in risky behaviour, or that they experienced greater social pressure to conform, as their behaviour would be furthest from the safer emerging social norm. It therefore seems highly plausible that the underlying mechanism that led to the intervention success was cognitive engagement from the individual risk-takers, and their observed change in behaviour. The CMO configuration for Kelly et al. 133 is represented in Figure 25 .
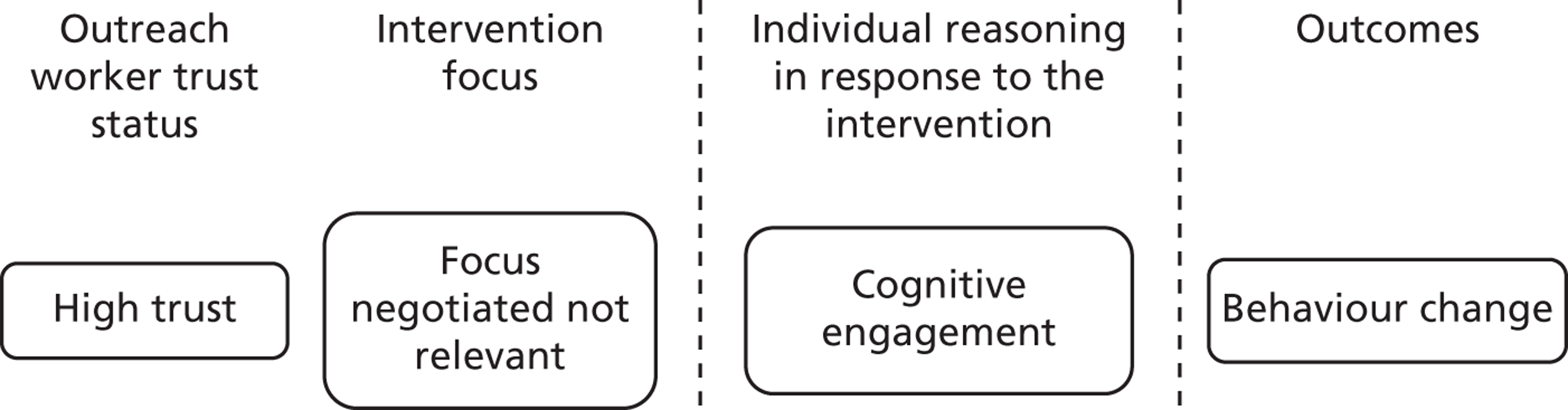
Rather like Leeds GATE,192 this project had a very tight focus and built on strong social ties. 133 The key difference is in the negotiation of the topic, which came from a Community member who then ‘sounded out’ members of her network for their reaction to a sensitive topic in Leeds GATE, but was inexistent in this case. One might wonder why, despite the difference in negotiation, the same strategy of opportunistic conversations triggered cognitive engagement. This may be because while the outreach worker was a trusted member of the Community in Leeds GATE, the authors in Kelly et al. 133 purposefully sought a Community member with pre-existing influence. Thus, the profile of the indexes in Kelly et al. 133 was sufficiently high in the Community to allow for engagement to happen in spite of the fact that the topic was not negotiated and would have been unlikely to be selected. The influential position of index members is likely to have initiated a process whereby talking about risky sexual behaviours, and engaging less in them, became more socially desirable. This leads to participants making the conscious decision to engage with the issue and act upon it. The two studies thus share another common ground, in that they both tackled sensitive subjects within the Community which would have been unlikely to be highlighted as an area of need to members from outside the network.
Chiriac 2007203
This study was conducted in Bucharest, Romania, in a neighbourhood where a majority of the Roma population lives. Living conditions are poor as a result of poverty, lack of education and a lack of initiatives aiming to improve living conditions. The study describes the role of a sanitary mediator working as part of a tuberculosis (TB) prevention and treatment campaign. Mediators were trained members of the local Roma Community, and so while it is plausible that they were known to the group receiving the intervention, the extent to which they were known and trusted is not reported in detail. The article reports barriers to receiving treatment for TB stemming from a lack of knowledge, a lack of awareness that TB treatment is free and the stigmatised nature of TB within the Community as a ‘disease of the poor’, in spite of its prevalence. Thus, the intervention focus was not negotiated but potentially relevant. The programme consisted of an information campaign and home visits to encourage screening and treatment adherence: ‘I finally managed to persuade him to think of himself and the children first and stop being ashamed of his disease . . . At first I would visit him and check if he had taken his medicine. I did that for one year. Finally he understood he had to take care of himself’ (p. 2). 203 Instrumental support was also offered in terms of accompanying people suspected of having TB into medical centres and helping Roma obtain ID (identification) cards or birth certificates so that they could access services. Thus, this programme provides instrumental support in a context of trust which seems to trigger cognitive engagement and behaviour change (acceptance of and adherence to TB treatment – theory 6). The article reports an improvement in the health of this individual and a change in attitude of the Community towards TB, with many people from the local Community attending a caravan in order to be examined by a doctor and approaching the mediator with possible symptoms of TB. Five further cases of TB were identified by the mediator following her work in the Community.
The long-term engagement of the outreach worker is likely to have enabled the development of a trusting relationship, through a demonstration of benevolence, integrity and reliability. Over time, this formed a favourable context for the social support strategies offered by the intervention, leading to a change of attitude towards, and awareness about, TB symptoms and its treatment. Chiriac thus offers a third example of interventions, which, through the use of trusted Community members delivering a range of informational or instrumental support, trigger cognitive engagement with topics that are culturally sensitive. The CMO configuration for Chiriac203 is represented in Figure 26 .
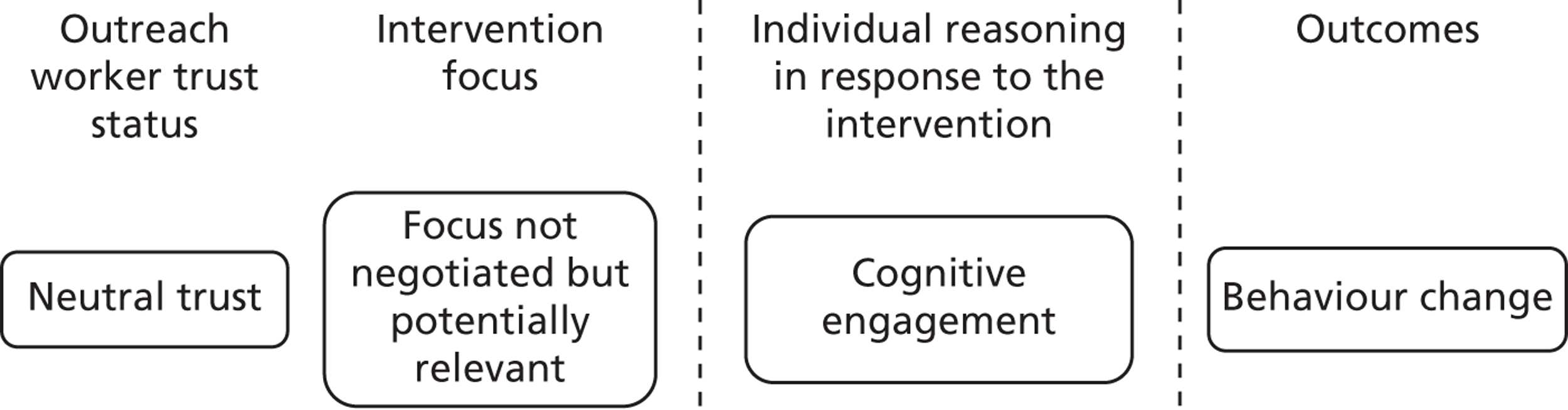
Health Service Executive 2007128
This report describes an intervention associated with Pavee Point, promoting oral health for Travellers in Ireland. A needs assessment and consultation with Traveller Community members was undertaken to elicit their specific dental health needs and the results were used to inform the development of the programme. The intervention focus was, therefore, negotiated and relevant. The outreach workers were Traveller Community members. They had completed a 4-year training programme as part of the Primary Health Care Project and undertook the needs assessment questionnaire. The resulting intervention consisted of two strands. The first trained the outreach workers further in dental health entitlements and available services, oral hygiene, fluoride and its uses, diet and label interpretation, smoking and oral health, trauma to teeth, and fear. This was in the hope that they would then disseminate this knowledge through their Community networks. Five related presentations were also given to the wider Community. Given their previous work as part of the Primary Health Care Project, it is likely that the outreach workers had an established relationship of trust with their target group. This strand of the project was evaluated through pre and post questionnaires.
The second strand was a clinical audit, with all Traveller children under 16 years of age called for a dental assessment and, with consent, added to a register of children entitled to free dental care within the county. These children were then allocated to their nearest dental clinic, which called them in for dental examination and treatment or referral where required. In addition, all dental staff in the area attended a cultural awareness day outlining the need for the programme and providing education on Traveller culture. Procedures were developed in conjunction with the outreach workers in order to ensure that the services were culturally appropriate. This strand was evaluated through questions in the post questionnaire.
Limitations in the evaluation design suggest that findings should be interpreted with care, as results are self-reported. However, the first strand of the programme is reported to have resulted in some improvements in oral hygiene behaviours. The adults questionnaire results showed a 5% increase in respondents reporting brushing their teeth twice a day and a 10% reduction in the use of abrasive toothpastes. Improvements in dietary behaviour are also reported, including a decrease of 15% in the percentage of respondents reporting taking sugar in their tea and a 12% decrease in respondents reporting smoking. A 10% decrease was found in adults reporting feeling nervous when attending the dentist. The mothers’ questionnaire also reported improvements in oral hygiene post intervention, including a 13% increase in use of fluoridated toothpaste among mothers and a 10% increase in the number of mothers who reported their children brushing their teeth twice a day. It also indicated an increase of 17% of respondents reporting that their children were not nervous about attending the dentist. A 31% increase was found in the percentage of mothers reportedly adding fruit to their children’s lunchboxes post intervention, along with a 9% reduction in the use of diluted juice in babies’ bottles. However, the second strand of the programme was less successful, with poor adherence to the service delivery procedures and data collection by dental services.
Although the validity of self-reported outcomes in a context where social desirability is likely to impact on responses has to be interpreted with caution, some learning can nevertheless be drawn from this study. Indeed, informational support alone as a mechanism would have been very unlikely to lead to engagement if the context had been less favourable. The combination of a high trust status and a negotiation phase (meaning that the need targeted by the intervention was also felt and expressed by the Community) may have provided a sufficiently strong basis for people to act on the information provided (theory 6). This is a counter example of theory 2, in that if the only programme strategy is the provision of information, then negotiation may be needed as well as high trust. Cognitive engagement seems to have been activated. The putative CMO configuration for Health Service Executive128 is represented in Figure 27 . Because of the poor design of the study, we can only hypothesise that, were the reported outcome a reality, these mechanisms might have explained them. It has utility here, because it comes to complement Kelly et al. 133 and Leeds GATE192 in explaining how behavioural change may be achieved. The following study (Rowley 2000)210 was sought in order to find somewhat more robust evidence that in a trusting context whereby the focus of the intervention responds to a need identified by the Community, social support resources may be sufficient to trigger behaviour change (through cognitive engagement).
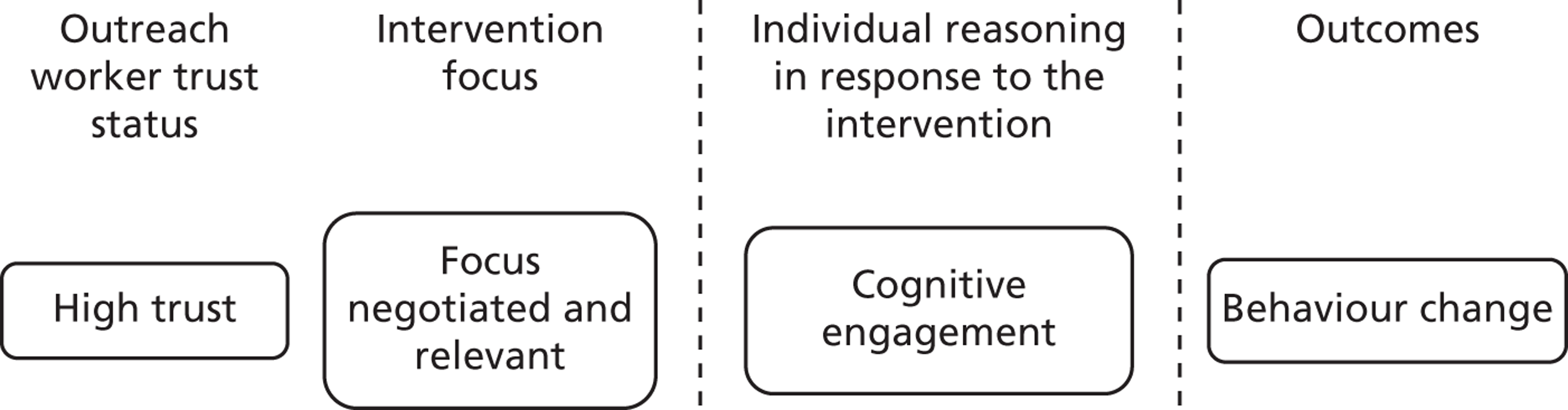
Rowley 2000210
This study took place in the Looma Arboriginal Community in north-west Australia, which was originally built as accommodation for aboriginal stockmen and their families in 1973 (www.loomastore.com.au/community.php). It has an approximate indigenous population of up to 500 people, featuring large, inter-related, extended families who have a cultural bond to that area. Culture and religion are said to link the people, the land and nature through ancestral beings, the pre-existence and reincarnation of spirits, totemism, mythology and ritual. They have a community management team, which in collaboration with the Community council, delivers infrastructure, essential services, employment and training to Community members. They share with Traveller Communities a long history of segregation and assimilation and a strong sense of cultural identity. They are, however, not mobile and are much smaller in number with, it seems, a sense of social capital that can perhaps be best compared with the one described in Pavee Point.
Indeed, the initiative was initiated by the Community itself, who were concerned about high morbidity and mortality from diabetes; the topic is, therefore, highly relevant. Initially, a diabetes nurse educator was employed ‘to assist Looma Community members in the design and implementation of appropriate and potentially sustainable physical activity and dietary modifications’ (p. 137),210 and then Aboriginal health workers were employed and became responsible for running the programme on a day-to-day basis. Therefore, it is reasonable to assume that outreach workers are known (building on close social ties, given the small size of the Community) and trusted members of Looma, although little detail is provided about them.
The intervention was initially implemented in those considered at high risk, for example people who were over-weight or had previously been diagnosed with diabetes, before being implemented with the wider Community. It featured a range of negotiated strategies such as formal and informal education sessions; cooking classes and store tours to help people to identify healthy food choices; physical activity groups such as the organisation of regular hunting trips, two to three basketball or football sport sessions per week and regular walking groups; and weekly body weight and blood glucose checks for those who requested them. When the intervention was implemented in the wider Community, a strong emphasis was placed on the ‘dissemination of messages about diet and physical activity to family members by those persons taking part in the high-risk intervention program’ (p. 137). 210 There is, therefore, an explicit aim to build on trusting strong social ties and activate levers for behaviour change.
This was alongside the invitation of all Community members to the intervention activities implemented initially in order to ‘initiate normative change and enabling conditions’ (p. 137). 210 This included facilitating access to resources needed for changing diet and physical activity (instrumental support). For example, a Community member was appointed to manage the Community store with a mandate to increase sales of fruit and vegetables and reduce the sales of high-fat and high-sugar items.
The Looma Healthy Lifestyle program was associated with sustained, if modest, improvements in biochemical and behavioural risk factors for diabetes and cardiovascular disease, even if it failed to achieve long-term weight loss. There was, however, a marked and sustained increase in the proportion of older Community members reporting regular physical activity and attempts to reduce their intake of fat and sugar. Prior to intervention, few persons reported attempting dietary strategies to reduce their intake of sugar and/or fat. At the 2-year follow-up, there were significantly fewer persons reporting no attempts to lower their intake of fat and/or sugar (χ2 = 42.0, p < 0.001) and this trend was still apparent at 4 years (χ2 = 17.1, p < 0.001). Before intervention, more than 60% of participants reported undertaking no form of regular physical activity. This proportion was significantly lower at 2 years (χ2 = 4.0, p = 0.046) and 4 years (χ2 = 8.1, p = 0.004) compared with baseline. Several family groups also began regular walking independently of the programme, suggesting evidence of cognitive engagement with the idea of healthy eating and physical activity.
The authors attribute the sustainability of impact to the role of Community members in the programme. This study therefore offers the opportunity to verify the correlate of theory 1, in that using strong family ties was an effective way to disseminate a health message. Similar to the Health Service Executive study,128 instrumental support on its own would have been unlikely to produce significant changes, but in conjunction with social influence, it is likely to have contributed to the results. In terms of causal chain, it is likely that social influence opportunities would have been more active within families (as exemplified by family groups undertaking physical activity outside the programme), whereas instrumental support (such as that provided by the Community store) is more likely to have had a lower level of impact (i.e. in itself it would not have been sufficient to change behaviour) but reached a wider group of people. Although results are mostly self-reported in a context where social desirability is likely to influence people, the longitudinality of the study is not matched in the Traveller Community literature, and seems to indicate change. The CMO configuration for Rowley210 is represented in Figure 28 .
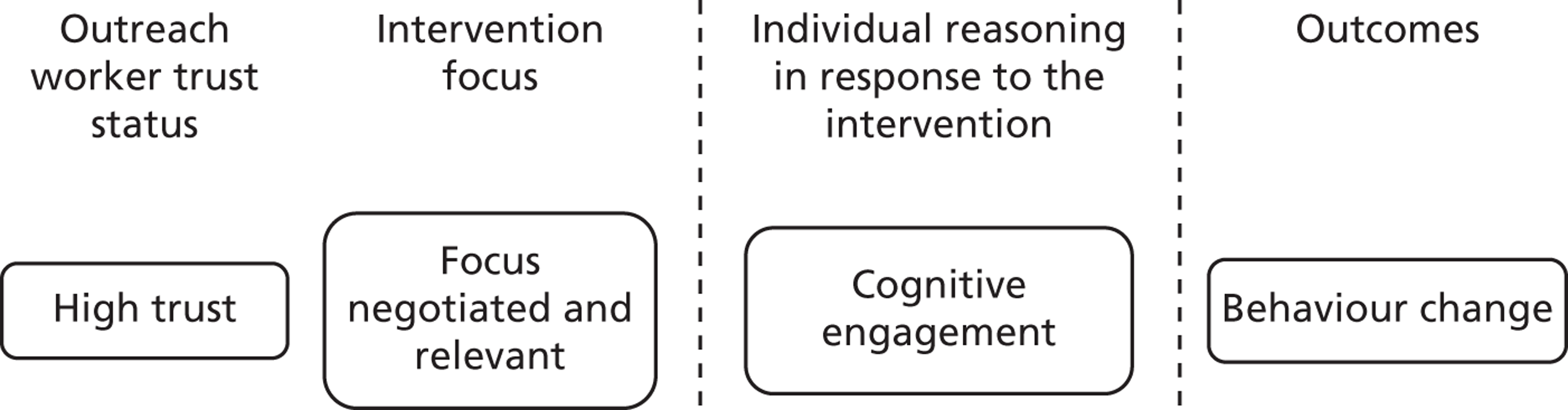
Improved behaviour change key messages
These six articles provide evidence of the context and mechanism combinations more likely to lead to outcomes of behaviour change. In five articles, the outreach worker was part of the Community, and therefore built on pre-existing social bonds. Resources of social influence were offered, alongside instrumental support in the case of Health Service Executive128 and Rowley. 210 This led to reasoning of cognitive engagement, in turn leading to potentially sustainable change. The articles have validated theory 2 (the inverse rule of trust and negotiation), as, like in Kelly et al. ,133 high trust meant that the outreach worker could bypass negotiation. In Leeds GATE,192 this was also bypassed, although the outreach worker did spend some time ‘sounding out’ her peers’ reactions to talking about domestic violence. In the Health Service Executive128 and Rowley,210 the interventions were less focused, more responsive and more opportunistic. These studies featured high levels of trust, which, combined with negotiation, meant that in some cases instrumental support was sufficient to produce an effect. Although the possibility of low trust in the outreach worker, even within close social ties, has been reported and substantiated by expert hearing events (EH1), no articles could be found to illustrate this case scenario. In terms of the strength of the evidence used, Kelly et al. was the strongest study included and, in combination with the others, helps to provide an understanding of how sustainable behaviour change may be achieved.
Social capital development (theory 8)
Pavee Point124 , 157 , 211
Pavee Point is a voluntary organisation dedicated to promoting the rights of Irish Travellers. It comprises members from both Traveller and settled communities and has reported and published aspects of its work since its establishment in the early 1980s. Therefore, the publications discussed below are describing not discrete research projects, but rather a multitude of small-scale interventions that amount to a programme of work. This is quite unique in the Traveller literature and offers insight into the place of voluntary organisations in operationalising the bridging function of outreach. This project features a high level of trust between the outreach workers and the Community. One of the workers reported: ‘When we were starting off, it was a bit overwhelming, we had a big fear of not being accepted. We were very nervous but we needn’t have worried. They accepted us because we were one of their own and we gave them feedback’ (p. 13). Similarly to Kelly et al. ,133 then, this intervention features an explicit effort to build on close social ties, through the use of (in this case self-selected) indexes.
Interventions included facilitating access to dental health services (e.g. two Traveller-specific evening dental clinics were opened and block bookings were organised), thus offering a range of instrumental support and testing theory 4 – the fact that negotiation tends to lead to a demand for instrumental support, which proved successful as the attendance at a dental clinic rose from 0% to 80%.
Traveller families are informed by CHWs of the date of the [specialist audiology] clinic and the benefits of attending with their children. Where necessary, transport is organised. The audiology service continues to be well subscribed . . . many parents book their own appointments and attend the clinic independently.
McCabe and Keyes 2005,157 p. 25
This, thus, denotes a behaviour change vis-à-vis accessing a service, and tests theory 6.
Overall, this aspect of Pavee Point offers evidence of change happening as a result of negotiations to set up health priorities and engineering a range of corresponding participation opportunities. The fact that the outreach workers had close social ties with the Community, but still negotiated the focus of the intervention, fits into the philosophy of Pavee Point of promoting long-term engagement. This does not necessarily, then, contradict theory 2, but capitalises on participation potential (as a result of high trust) to ensure long-term social capital development (theory 7).
A large proportion of the Pavee Point reporting concerns the voluntary organisation’s developing relationship with 16 key Traveller women, who were living in the area targeted in Ireland and employed to work on the project. This further aspect of Pavee Point and its potential to test our theories of outreach is explored below. A key difference from the Kelly et al. 133 study is the longitudinality of the intervention, as it spans 10 years of continuous engagement between the organisation and the outreach workers. This intervention tests theory 7, as longitudinality of engagement leads to the development of trusting relationships, which can foster successive engagement cycles. This has been corroborated by our expert hearings (EH5).
There was a demand for informational support from the outreach workers, and the intervention provided an array of training opportunities in response to their suggestions. The outreach workers ended up acting as Traveller representatives on a range of regional and national committees – demonstrating improved self-efficacy and emotional engagement with the idea of improving the lives of Travellers more broadly. They attended training opportunities and asked for more, also demonstrating engagement in learning. Exposure visits were organised to introduce them to a variety of health services such as the local health centre. Here, Pavee Point operationalised a very clear bridging function of outreach, by enabling the outreach workers to familiarise themselves with statutory health services so that this familiarisation could ‘trickle’ into the Community. ‘One of the best things is that this course happened for Travellers . . . because of Pavee Point we have learned to sit down and talk with the settled people’ (p. 14). 211
The outreach workers were trained to develop, pilot and undertake a survey of Traveller needs in the targeted sites. Survey results were fed back to the Community so that a prioritisation of needs could be drawn up and implemented by the outreach workers, with organisational support, in the form of a formalised collaboration between Pavee Point and the local Health Board. ‘This . . . facilitated the participation of the Community in defining needs, setting priorities and outlining interventions . . . [they] felt this empowered them as they now felt they had control over what was happening to them, as they were involved in an ongoing process which they could feed into’ (p. 18). 157 This level of partnership and negotiation triggered the emotional engagement necessary for the outreach workers to invest themselves in the betterment of their Community as a whole in the long term. The CMO configuration for Pavee Point124 is represented in Figure 29 .
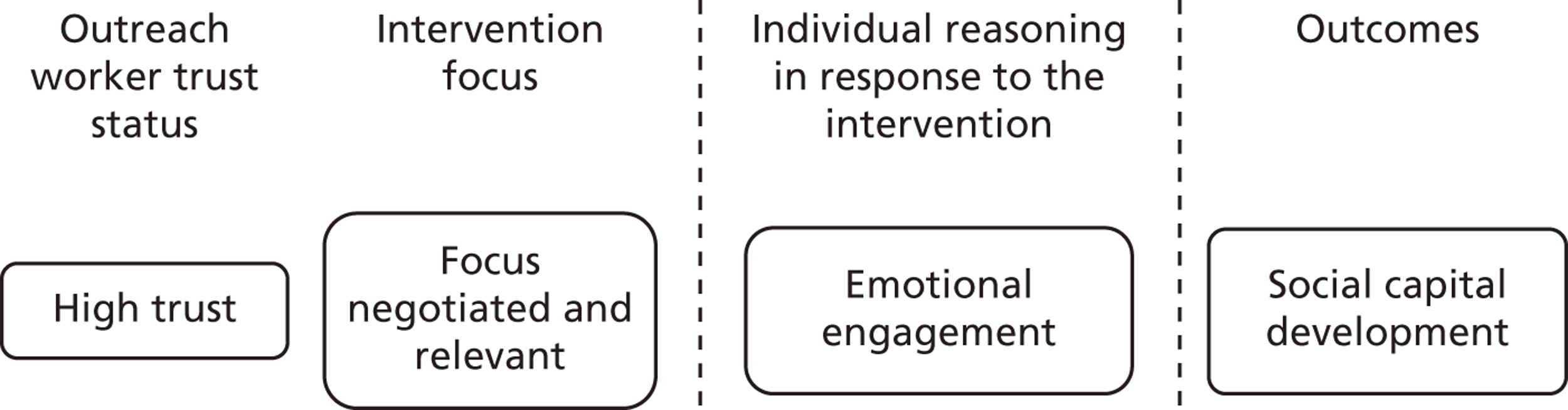
Friends, Families and Travellers165
Friends, Families and Travellers is a charitable organisation promoting equality for Traveller Communities, seeking to end discrimination against them and protect the rights of these groups to live a nomadic lifestyle. This publication describes the Friends, Families and Travellers Sussex Travellers Health Project. Like those models of outreach described by Pavee Point and Leeds GATE, this project refers to a sustained programme of work encompassing many different initiatives to improve Traveller health. It is reported to have taken around 9 years to establish the project and build the trust and confidence of Community members to engage with services. While Traveller Community members did not attend arranged sessions at first, through demonstrating commitment and attending weekly at a set date and time the outreach workers began to see participants attending. Initial attempts to discuss health were rejected by Traveller Community members until trust had been developed through participation in broader activities (theory 1).
We asked about health needs and were told there weren’t any. So we started working with some safer subjects. Women worked on creating individual panels for banners, expressing their own views about what health meant to them.
Atterbury and Bruton 2011,165 p. 4
Following engagement in activities such as collecting traditional recipes to publish a recipe book and cooking and eating together, Traveller women felt comfortable discussing health issues such as domestic and mental health problems and requested further information on drug issues, baby massage and reflexology. Thus, while Traveller Communities clearly regarded outreach workers with suspicion initially, negotiating the focus of outreach and responding to identified issues as they arose led to positive cycles of engagement (validating theory 7). Given the opportunistic approach taken, the outreach project responded to a diverse range of needs and offered a number of forms of social support. A key aim of the outreach project was to facilitate access to existing services, thereby offering instrumental support. The project also provided informational support around available services, and worked with Community members to develop understandable and culturally appropriate ‘food and mood’ booklets, well-being CDs and well-being information flyers, as well as a ‘Know Your Rights and Responsibilities within the NHS’ flyer. This was reported to result in improved knowledge of and access to available health services. The project also involved Traveller Community members in conducting cultural awareness sessions with service providers in order to improve the experiences with services. The opportunity for direct engagement with Community members was felt to have contributed to challenging myths and prejudices about Travellers and to have broken down barriers between service providers and the Community.
In addition to offering informational and instrumental support, the project aimed to empower Community members to develop their own solutions to health issues and provided opportunities for social engagement. The CMO configuration is thus the same as for Pavee Point. Traveller Community women were supported to share positive representations of their culture at the launch of the recipe book, to which significant members of the local Community were invited to attend, and to take a representative role in communicating their needs to commissioners and policy makers. This therefore provides an example of the achievement of emotional engagement leading to the development of social capital in support of theory 7. The CMO configuration for Friends, Families and Travellers is represented in Figure 30 .
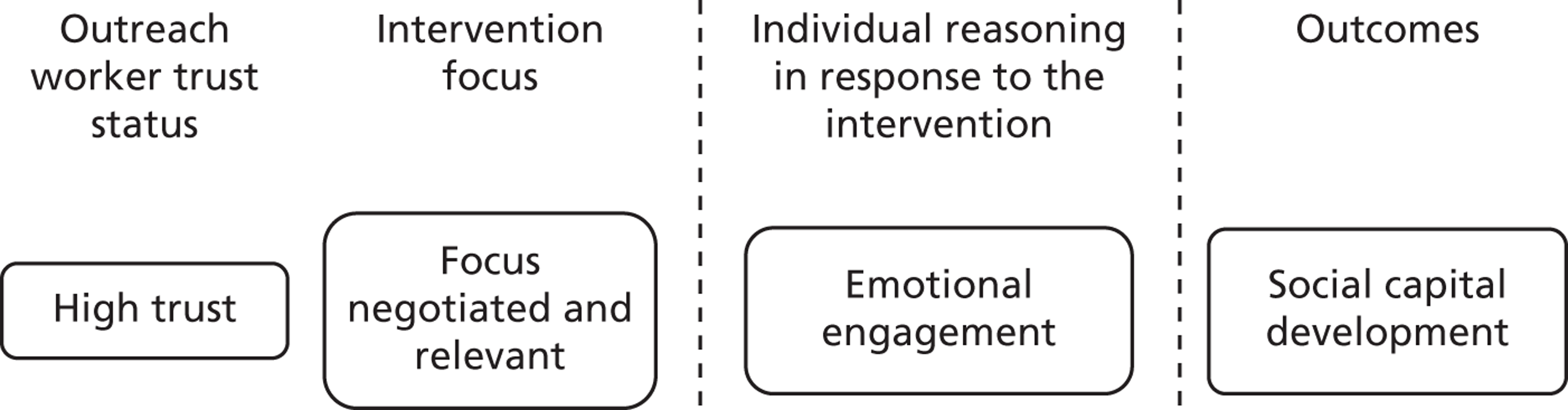
Leeds GATE192
Although the description of the Leeds GATE project192 on domestic violence (described in detail in the earlier section on behaviour change theories) builds predominantly on close social ties, this project can also assist in understanding how social capital may be developed. While the domestic violence project was undertaken by a member of the Traveller Community who initiated discussion through her existing networks, the report also highlights that ‘A great deal of [Community initiated] Community development work has gone into the building up of Leeds GATE as an organisation before we felt able to run a project such as this’ (p. 11). 192 The report describes the need to balance the responsibility to intervene in some circumstances with the maintenance of trust which forms the basis of future interventions in order to increase overall safety and reduce levels of violence within the whole Community. The report suggests that the ‘willingness of women to talk in front of other Leeds GATE staff indicates a growing trust in the organisation to, in the very least do no harm’ (p. 8). 192 As such, this study provides further support for theory 7 in that the established reputation of Leeds GATE as a trusted organisation facilitated engagement with a project focused on a sensitive topic. This trusting context clearly contributed to building capacity in the Community, and to developing social capital. While this study would not traditionally be considered to contribute ‘robust’ research evidence, its conclusions and observations came from the intimate knowledge of the Community and the most likely levers for change. Therefore, over time, they have developed ways to reach their desired outcomes that have stood the test of time – this analysis has merely made these (social engagement opportunities within a context of highly trusted relationships and negotiated or responsive intervention foci) explicit.
Social capital development key messages
The three organisations described above demonstrate the possibility of building trusting and fruitful relationships with Traveller Communities, if sufficient time is invested into engaging with the Community (theory 7). The short-term nature of many funding streams might lead to this time involvement being seen as lacking in measurable outcomes and thus in cost-effectiveness. By the same token, once relationships are established, voluntary and community organisations are in a unique position to implement outreach interventions effectively. Their established links also involve statutory services, funding bodies and educational institutions, and thus they offer opportunities to significantly work towards longer-term goals of capacity building within the Community.
Conclusions
Three sets of CMO configurations were developed, explaining how and in what circumstances outcomes of participation, behaviour change or social capital development may be achieved through outreach interventions. Charting the implications that such understanding has on the implementation of further outreach interventions would lead to the following considerations. From the outset, there needs to be clarity about the purpose of outreach. If it is about promoting attendance to one-off events, such as screening, then the outreach worker may not need to have long-established links with the Community, although, of course, it helps if the target group sees some relevance to the intervention.
Changing behaviour or developing social capital, on the other hand, is a different challenge that needs to build explicitly on long-established and trusting relationships. While true engagement with an issue must not be assumed from participation at an event, this can be used as part of trust-building strategies. Other key impacts of the CMO configurations proposed are the importance of responsiveness to expressed needs (i.e. the outreach worker needs to have some flexibility), clear communication strategies and an acknowledgement of the historical legacy of belonging to Traveller Communities.
Chapter 4 Discussion
In this chapter, we present a summary of the findings, articulate what they add to the wider literature and discuss the strengths and weaknesses of the review. We also draw implications for policy, practice and future research.
Summary of findings
This review aimed to examine the effectiveness of outreach programmes for health improvement of Traveller Communities. Systematic literature searches identified 278 studies, which formed the basis for a scoping review, an evaluation of cost and cost-effectiveness of different models of outreach provision, and a realist review highlighting and testing the mechanisms by which outreach programmes may work, for whom and in what circumstances.
The scoping review classified the range of included articles in order to provide an overview of the available evidence, as a basis from which to produce insights around the possibilities for the generation and synthesis of evidence. The findings are summarised below according to the characteristics used to classify and organise studies.
Date of publication: there appears to be increasing attention to the health of Traveller Communities, with around half of the articles published from 2006 onwards.
Reporting of outreach interventions: only around one-quarter of articles on the health of Traveller Communities described the implementation of outreach interventions.
Evidence type and study design: the overall evidence base on the health of Traveller Communities contained a large proportion (42.4%) of research articles, the majority focused on describing the health needs of Travellers, with very few articles reporting on evaluation designs. Of those articles focused on outreach, the majority were anecdotal accounts (71%) and those research studies that did report on outreach interventions were of poor methodological quality. Few articles reported on policy or legislation to improve the health of Traveller Communities.
Country of publication: the majority of articles included were published in the UK and Ireland, suggesting more established programmes of work in these areas. The small proportion of articles describing outreach appear to be particularly marked in the USA and central Europe, while a greater proportion of articles published within eastern Europe reported on the implementation of outreach.
Type of author and outreach worker: almost half of the overall evidence base on Traveller Communities was contributed by academic authors. However, studies describing outreach were more often written by health service providers and Traveller or third-sector organisations than studies that did not describe outreach. Almost all outreach interventions were delivered either by members of Traveller Communities or by mainstream health service providers such as health visitors, GPs or nurses.
Health focus: just under half of those studies describing outreach focused on improving access to and use of services, suggesting that facilitating access to services is a key aim of outreach interventions. Few articles described outreach focused on children’s health, oral health care and mental health care and none described outreach focused on cardiovascular disease or cancer, reflecting the small amount of overall evidence in these areas.
Overall, the findings suggest that the evidence on outreach interventions for Traveller Communities is emergent. While much research describes the needs of Traveller Communities, as yet there has been little response to this in the form of discussion and evaluation of outreach and other interventions that might improve Traveller Community health. The mapping of the overall evidence base according to the above characteristics provided a scaffold on which the realist synthesis and economic evaluation could build.
With respect to the results of the economic evaluation, interventions which use mobile clinics to bring health services to travellers are associated with the highest costs reported, with little confidence that they provide either value for money or an appealing format for Traveller Communities. The employment of full-time outreach workers for Traveller Communities appears to be associated with moderate costs, with impacts that may not be primarily improved health. Practice nurses are well placed to facilitate access to primary care at the practices in which they work, and they may represent a cost-effective resource to improve access to primary care. There is, however, evidence that outreach is more effective when delivered by workers who share the ethnicity of the recipients. The training and use of outreach workers from Traveller Communities, to promote vaccination and access to antenatal care in particular, would merit rigorous evaluation.
The implementation of protocol changes, such as texting appointment reminders, in primary and secondary care is unlikely to be expensive and might be considered the minimum acceptable action to facilitate access to health care. Examples from the literature also suggest that cultural awareness sessions can be delivered successfully by Traveller Community members for modest costs. A recent publication from the Department of Health20 suggested an additional payment to GPs for the registration of Travellers to offset losses in practice income from missed QOF points and to incentivise outreach. However, such a funding mechanism would require the reliable identification of Travellers, which is an acknowledged issue. In conjunction with the changes outlined above, an appropriate payment for the registration of Traveller Community members by GPs might be effective in improving access to primary health care for Travellers.
The realist review led to the development of an explanatory framework detailing how and for whom outreach interventions may work with Traveller Communities. It was developed from a combination of synthesising the Traveller specific theories, key concepts found in extant studies and commentaries and expert hearings with Traveller Communities, representatives from Traveller Community organisations and outreach workers. The framework is the result of a movement from fragmentary evidence sources towards a broader outlook by combining theories to attempt to maximise explanatory scope and potential. These focused on the entry points into the Community (in terms of trust and negotiation) and the engagement reasoning that intervention strategies are likely to trigger in this context to lead to observable outcomes. It is thus formulated around CMO configurations, which form the cornerstone of realist thinking.
Contexts form the facilitating background in which underlying mechanisms can be triggered by an outreach intervention to lead to favourable outcomes. Engagement in the literature on Traveller Communities highlighted a historical legacy of mistrust ‘by default’ in settled communities and institutions. It thus became clear very quickly that outreach workers enter the Community with a trust status, which is a function of a combination of their ethnic background, their connections to the Traveller Community and their history of working with them. In conjunction with trust, the extent to which the intervention meets the needs expressed by the Community will determine its impact. Negotiation of the focus of the intervention thus became the second key contextual element. Later in this discussion, we detail the nexus formed by trust and negotiation.
Mechanisms are the respondents’ engagement reasoning, which is likely to have been triggered in response to the intervention. Outcomes are the observable and reported results from this process, including participation with or without engagement. This framework offers a structure within which to test seven refined theories, and which are articulated around the outcomes of outreach.
The first set of CMO configurations shows how outreach may lead to participation, without this necessarily entailing a depth of questioning of prior attitudes, beliefs or practices. These interventions were implemented in a context of the outreach worker having an initial neutral trust status, which was then offset by a variety of negotiation strategies and led to reasoning of behavioural engagement. These context–mechanism combinations concurred to explain either participation or non-participation in a programme. Such interventions have a potential to be used as part of a broader trust-building exercise, thus leading to increased time-effectiveness for subsequent interventions. Indeed, the explanatory framework and evidence gathered indicates that when this is the case, interventions can be implemented faster (building on past relationships) and are likely to lead to higher rates of participation.
The second set of CMO configurations demonstrates how outreach interventions may lead to a change in behaviour. This necessitates the participants engaging cognitively with the topic of the intervention, a mechanism that was triggered when the intervention was implemented by a highly trusted, and sometimes influential, individual. In the only case where the initial trusting relationship was difficult to assert,203 the time frame of the intervention was such that it enabled the outreach worker to demonstrate benevolence, integrity and reliability. Over time, this formed a favourable context for social support strategies to lead to a change of attitude towards, and awareness about, TB symptoms and treatment.
The third set of CMO configurations features the impact of organisations that have a long-standing relationship with the Communities, and have demonstrated commitment and reliability. Outreach workers, therefore, come with a ‘trusted brand’ that facilitates early engagement. The time involvement to develop trust is likely to be seen as lacking cost-effectiveness. However, because of their established relationships, voluntary and community organisations are in a unique position to implement outreach interventions effectively. They offer unique opportunities to achieve longer-term goals of capacity building within the Community.
The CMO analysis undertaken in this review has thus enabled us to observe how outreach interventions, if implemented with awareness of (a) the contextual constraints pertaining to this group and (b) the outcomes that the intervention can reasonably be expected to achieve, have the potential to increase the receptiveness of Traveller Communities to health intervention, and their ability to engage with them.
What this study adds to the wider literature
In this section, we discuss the contribution of the review to understanding the distinguishing characteristics of Traveller Communities, facilitating participation in research, the role and function of outreach, theoretical developments and methodological considerations.
Distinguishing characteristics of Travellers
The research team engaged in considerable activity both in searching the literature and in debating with members of the project steering group on the specific characteristics and health needs of Traveller Communities. Our conclusion was that, to a large extent, attempting to distil distinguishing features may be a futile exercise as far as intervention contexts are concerned. While Traveller Communities do present a very complex and multifaceted group, they are nevertheless more often than not conflated under one umbrella. We initially believed that the challenge was to find elements that could both offer a satisfactory explanatory potential (i.e. things in common among all the different subgroups of Travellers) and chart some of the distinctiveness of this group (as opposed to other ‘hard-to-reach’ communities). This was articulated around three aspects: (a) a nomadic lifestyle and associated access and environmental health issues, (b) discrimination and historical persecutions, and (c) exposure to assimilatory policies and practices. Combined, these explain the disengagement tendencies of this group and question the common categorisation of Traveller Communities by cultural or ethnic roots in favour of patterns of movement and their likely impact on services access possibilities. However, the pragmatic impacts of these are on the morphological features of Traveller Community social networks and the closeness of the social bonds which characterise them.
A considerable amount of time was spent identifying and categorising the kind of needs that outreach interventions were responding to (i.e. felt, expressed, measured needs). This exercise in the end led to recognition of the necessity for the outreach worker to negotiate the focus of the intervention, as a key first step in a process of engagement. While the outreach worker, at least ideally, has a commitment to the outreach process, this is not necessarily shared by the recipients of the intervention. Instead, they have a multitude of needs and may use them in order to, for want of a better expression, put the outreach worker to the test. Expressed needs can thus be used as an opportunity for the worker to prove their trustworthiness. While purposive literature searches of outreach in other hard-to-reach groups were undertaken as part of this review, the aim was to explore what works for Traveller Communities, and considerable potential remains to test (and refine) the explanatory potential of our framework in other disengaged groups.
Facilitating participation in research
While not originally thought of as being similar to outreach, encouraging the participation of Traveller Community members in research did share similar features. The analytical hindsight developed through this study helps to explain why some strategies were more successful than others. Embarking on this project, we spent a considerable amount of time and energy attempting to engage members of Traveller Communities in the research process. For example, the use of a research blog reporting on progress generated little response. The undoubtedly low trust status of the research team and the lack of negotiation over the topic of the research highlight the little chance we had of achieving meaningful engagement through informational support only, certainly over the short time scale of the project. We deployed a number of additional strategies to reach out to members of the Communities, which took the form of expert hearing events and proved more conclusive.
A member of the research team’s attendance at Appleby Fair was used as an opportunity both to seek views on emerging findings and to meet a member of the Traveller Community who could facilitate an expert hearing event on our behalf. Participants commented positively on the researcher’s willingness to attend Appleby and learn more about their culture. Thus, while Appleby Fair itself proved to be a difficult place in which to conduct research (due to the busy atmosphere), this was a useful exercise in terms of demonstrating benevolence and integrity, two dimensions of trust according to Hurley’s model185 as discussed earlier in the report.
All of the expert hearing events with Traveller Communities were arranged with the assistance of organisations and workers with established relationships of trust. This strategy helped to facilitate access to those on the receiving end of outreach, and short-circuit the process of developing trust, much in the way described by our third set of CMO configurations. From the perspective of Traveller Community members, participation in an event, rather than in-depth of engagement in the research process, was required. However, because the discussion topics were bound by the remit of the research, we were not in a position to negotiate them (or solve any expressed need); thus, ready entry routes into the Community proved invaluable.
The process and impacts of outreach
There is an acknowledged need for conceptual development with respect to outreach. 66 Making reference to this publication allows us to expose how this study has contributed to maturing the understanding of the outreach role and function. Mackenzie et al. ’s66 typology of outreach has been articulated around solutions to pragmatic non-engagement ‘problems’, which inhibit participation with a wide spectrum of health-care interventions. Their work represents an attempt to deconstruct outreach into a list of intervention strategies to tackle issues in the target group. Placing this typology beside our explanatory framework highlights how they have focused on a range of social support strategies. Our study allows us to offer additional outreach intervention strategies, as we have demonstrated that workers can use levers of social influence and social engagement when building on trusting and long-standing relationships. In addition, our study also highlights reasoning paths (underlying mechanisms) that result from these strategies and lead to outcomes. This is developed further in this discussion (p. 75).
Bridging the gap between Traveller Communities and statutory services could be achieved by enabling professionals and outreach workers to map out their projected impacts. This should distinguish between compliance (e.g. sufficient for attendance at a screening event) and true commitment (e.g. necessary to stop smoking). Outreach models explicitly building on the workers’ place on the social network maps of their target group have the potential to impact on a wide array of health determinants. This study features examples of social influence levers impacting on individual health behaviour change,133 social engagement levers impacting on health literacy and Community capacity building,124,193 and social support strategies leading to improved access to services. 157,167 This therefore highlights the potential of outreach, in its various forms, to impact on multiple levels of social determinants of health.
Theoretical developments
In debating the explanatory power of trust, we moved away from our initial thinking about the importance of peer and lay qualities to explore the nature of Traveller networks and their impact on outreach. We have substantially refined our understanding of ‘peerness’, its forms and its impacts. Our analysis has led us to use three models found in existing literature in a novel way, which, combined, offer maximal explanatory potential. 185,190,200
Social networks and health
Social networks have the potential to influence individuals’ behaviours and attitudes by shaping the flow of resources which determine access to opportunities and constraints on behaviour. Berkman and Glass183 developed a conceptual model of the causal pathways by which social networks impact on health outcomes. They detail how social-structural conditions (macro ‘upstream factors’, such as culture and socioeconomic factors) condition the shape, extent and nature of social networks (mezzo). They detail how social capital is related to an individual’s ability to mobilise the resources inherent in his or her social network. 183,212 A distinction is made between bridging and bonding social capital. The first term describes the kind of strong connection between people who already know each other and are frequently brought together. It is generally seen as crucial for the social support and mental health of individuals213 and Traveller Communities have been described as featuring a predominance of such bonding ties. 184 Bridging ties typically consist of looser relationships between (rather than within) social groups. They are important, for example, in the development of mobilising movements in society. In Traveller Communities, mobility, homelessness, persecution and discrimination are part of the larger social and cultural context that shape the flow of resources determining trust, access to opportunities and constraints on behaviour. While we have demonstrated that being a member of a Traveller Community is not a prerequisite to successful outreach, trusting relationships are. There is, therefore, a reasonable link between social capital and the distinction between bridging and bonding ties, and the trust status that outreach workers may have when entering the Community. All of the studies included in this review that featured high initial trust status used either members of the Community, therefore building on bonding ties,133,192 or organisations with a long-standing presence in the Community. In this case, not all outreach workers were from the Community, and therefore likely to have bridging ties with the Community, but had high trust as predictability and benevolence had been demonstrated over time. 157 Adding this social network analytical layer onto our analysis enables us to qualify more thoroughly the idea that outreach workers need to be cognisant of, and establish, their ‘place’ on the social network map of Traveller Communities.
Berkman and Glass’183 analysis has additional utility for our analysis, as they conceptualise a causal pathway between social networks and health. They detail how social capital may work through mechanisms of social support, influence and engagement, which in turn impact on, for example, health-related behaviour and self-efficacy. 212
Social influence relates to shared norms around the health behaviour of network members. People obtain normative guidance by comparing their views and behaviours with those of a significant reference group or individual. In this review, this is very evident in Kelly et al. ,133 for example, where the authors have preambled their intervention by an intensive ethnographic phase in order to identify network leaders who could exert influence.
Social engagement relates to the enactment of potential social ties into actual actions. Various groups or training events can present opportunities for social engagement. The programme of work undertaken by Pavee Point157 provides examples of social engagement, whereby outreach workers undertook a number of training opportunities and became advocates for their Community.
Social support includes appraisal support (support in making a decision, e.g. with regards to attending a screening event), emotional support (as provided by confidants or significant others, although it can also be provided by others on emotionally charged topics, e.g. domestic violence), instrumental support (refers to tangible help, e.g. with booking and keeping appointments) and informational support (e.g. in opportunistic health promotion advice). The literature included in this review details numerous social support strategies, which are most likely to lead to participation when they are implemented either in a context of high trust or in response to an expressed need. Social support is transactional in nature, often involving both giving and receiving. According to Berkman and Glass,183 this ‘occurs within a normative framework of exchange in which behaviour is guided by norms of interdependence, solidarity and reciprocity’ (p. 145). This is corroborated by critiques of peer and lay models of lifestyle advice provision110 and by stakeholder consultations, where the necessity for a blurring of professional boundaries was highlighted (EH1, EH7, EH3, EH5).
Social influence, engagement and support can be conceptualised as key strategies that outreach programmes may use. Social capital thus has the potential to form an overarching concept that could help to explain the role of outreach workers in improving the health of Traveller Communities. Indeed, they may ‘work’ in appealing to either the cognitive or structural dimensions of social capital, and improve health through mechanisms of social engagement, support and influence.
Fredricks et al. 200, in reviewing definitions, measures, precursors and outcomes of engagement, provided us with some potential reasoning pathways, which could link Berkman and Glass’183 psychosocial mechanisms with observable outcomes. Fredricks et al. 200 detail processes of behavioural, cognitive and emotional engagement. While they focus their review on learning processes and school engagement, the reasoning can be applied to the recipients of health interventions. As the exemplars in the realist substantiation section detail, the use of outreach strategies in a favourable context of trust/negotiation do seem to trigger reasoning mechanisms of behavioural, cognitive or emotional engagement. Neufeld’s model of engagement190 provided further explanatory purchase, in helping to describe how pragmatically outreach workers could operationalise levers of social support, engagement or influence through initiating a process of negotiation.
Our analysis is thus multilayered and covers the potential operationalisation details of outreach interventions (the engagement cycle and building trust) as well as the underpinning social network levers that may make the intervention ‘work’ and the reasoning triggered by those that lead to observable outcomes.
‘Peerness’ is thus no longer only about belonging to a particular ethnic group or socioeconomic strata, but it is also about the place that one might have in the recipients’ social networks. This can be engineered and developed, rather than being only a fixed characteristic that one is born with. ‘Layness’ on the other hand, provided much less explanatory purchase than originally anticipated, yet the literature suggests that this may be an avenue worth exploring further (we return to this in Chapter 5 ). Professionals have not been reported to have bonding ties with the Traveller Community, but some were held in high esteem (and indeed people would travel from far afield to consult with a specific professional rather than others). Our theories suggest that these professionals have established trust over a period of time through the dimensions of benevolence, communication and predictability, but probably mostly capability. So, although knowledge is held in high regards, knowledge without trust did not trigger engagement mechanisms.
The multiple needs of Traveller Communities occupied a prominent place in the literature and we needed to assert the relationship between those as a potential context and outreach intervention mechanism. One of our early theories was indeed that unless outreach addressed a need that was felt by the Community, the intervention was unlikely to be effective. Bradshaw’s214 classification of need distinguishes:
Normative is identified according to a norm (or set standard); such norms are generally set by experts.
Comparative need concerns problems which emerge by comparison with others who are not in need. One of the most common uses of this approach has been the comparison of social problems in different areas in order to determine which areas are most deprived.
Felt need is need which people feel – that is, need from the perspective of the people who have it.
Expressed need is the need which they say they have. People can feel need which they do not express and they can express needs they do not feel.
Bradshaw 1994,214 p. 46
While the literature reports extensively on normative and comparative needs, the needs considered by our CMO configurations are felt and expressed needs, i.e. how much an outreach intervention is seen to address a need that is of relevance. As this theory became more refined, this work on needs became summarised in the ‘negotiation’ of the intervention topic, which is also the first phase of Neufeld’s190 model of engagement. There was also a clear link between trust and negotiation, in that a worker with a long-standing relationship with Traveller Communities is likely to have a reasonable appreciation of felt and expressed needs, thus reducing the need for negotiation. This was later formulated in one of our key explanatory theories around the inverse rule of trust and negotiation (theory 2). Figure 31 highlights this, and places it in the context of the contrast between bridging and bonding social ties. Bridging ties (looser relationships, typically between social groups) are indeed less likely to feature high trust and therefore the imperative of negotiation is greater. The converse is true, in that bonding ties are more likely to feature high trust and an established understanding of the kinds of needs that the target group would want to see addressed.
FIGURE 31.
The inverse role of trust and negotiation, linked with social capital.
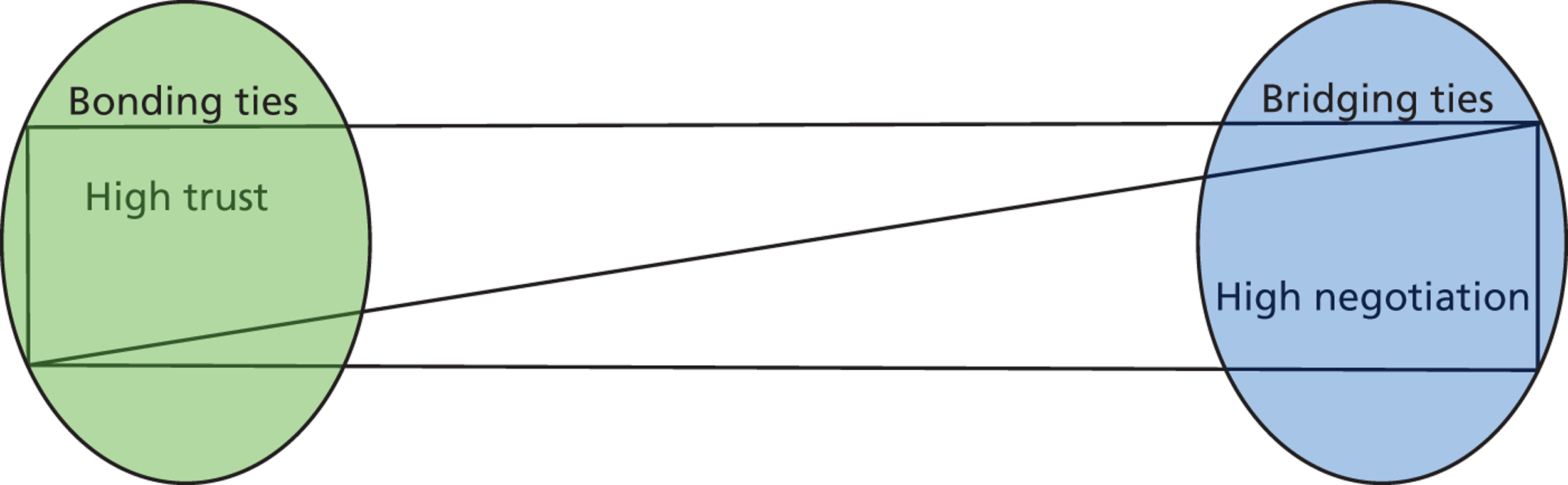
As ever in realist thinking, the theory presented above does not claim universality. It rather provides us with a framework within which to examine the studies included. It has high face validity, credibility and is well substantiated. Through anecdotal accounts and expert hearing consultations, we are aware of examples where there was low trust among bonding ties, which would not be accounted for by this theory. It seems reasonable to assume that if an outreach worker was a member of Traveller Communities but for whatever reason was not trusted by their target group, they would have to develop strategies to build (or rebuild) trusting relationships, and that negotiation might be a reasonable way to do this.
Methodological considerations
This review set out to answer a multilayered question, about the components of outreach programmes for Traveller Communities, and their effectiveness and cost-effectiveness. The outreach programme evidence base is diverse and conceptually immature,66,68 and therefore poses particular challenges to the reviewer. There are a number of additional challenges for methodological rigour in research with ‘hard-to-reach’ populations, including high levels of attrition; the imperative of probability testing which puts challenging demands on recruitment rates; difficulty of achieving ideal sample sizes; the challenge of collecting valid behavioural data in populations with low levels of literacy; and the lack of measurement scales characterised by high reliability and validity to assess particular constructs relevant to disengaged study populations.
Given these limitations, the economic evaluation highlighted the relative cost and potential effectiveness of different models of outreach provision. These pointers have to be put in the context of an argument around fairness and social justice and of the necessity of what Marmot called ‘proportionate universalism’, i.e. that ‘to reduce the steepness of the social gradient in health, actions must be universal, but with a scale and intensity that is proportionate to the level of disadvantage’ (p. 16). If this argument is accepted, then cost-effectiveness must be only one of the yardsticks against which the value of outreach interventions is appraised.
At the next level of evidence production, systematic reviews of complex interventions such as outreach can be problematic, as the methodology on evidence is surfacing and quality assessment and synthesis still require development. As Petticrew states,215 ‘Systematic reviews can be good at answering questions about the effectiveness of specific interventions but often do not yield clear answers to questions about complex interventions that have not themselves been fully evaluated’ (p. 757). The kind of evidence-based characteristic of such complex public health interventions stretch the potential of conventional synthesis approaches to the point that they can often only provide inconclusive results and recommend that stronger evidence should be produced. This highlights a translational chasm that impedes the potential productivity of review outcomes.
In order to guarantee that maximum utility can be made of an anticipated limited evidence base, the research drew on multiple types of synthesis activity. Such pluralism enabled maximum learning to be achieved, regardless of the type and diversity of the evidence accessed. The scoping review offered an effective platform from which to engage in the economic evaluation and in realist reviewing. The thoroughness of the search strategies it entailed provided a breadth of literature access, in order to start building some depth, as well as key pointers for theoretical thinking and cost considerations.
On the realist approach
Reflection on the process
The size of the research team is an issue worthy of comment. In contrast to many reported realist syntheses, this research was undertaken by a very small core research team, supplemented by expert hearings. This impacted on our ability to debate issues around the generative causation of certain mechanisms, or indeed whether or not constructs should be classified as, for example, contexts or mechanisms. These are acknowledged difficulties in realist syntheses,216 which were compounded by our small team size. The correlate to this, however, was our ability to communicate very effectively throughout the project and ensure the timely inclusion of a range of perspectives as the analysis developed. The core team conferred during weekly half-day meetings, ensuring consistency of interpretations and recording the outcomes in a decision trail file on a shared computer drive, which could be consulted and commented on by the wider team, thereby enhancing the validity of our analysis. Pawson85 describes the necessity of engaging with theory at various levels during a realist review. This is so that candidate theories with explanatory potential can be found, applied, discounted or modified as necessary, until a suitable explanation is found for why certain outcomes are reported. With our heterogeneous data set, the tendency was to go higher in theorisation, in order to reach maximum explanatory potential. Retaining the balance between explanatory potential and what could reasonably be inferred from the studies was a challenge, and resulted in multiple draft iterations of the final report. For example, we initially framed the results section around Berkman and Glass’183 causal model between social networks and health. This, however, proved too far removed from the pragmatics described in our studies and was subsequently mentioned only in this discussion.
Study selection process in a conceptually heterogeneous data set
We have described how the Traveller literature is comparatively rich in statements of cultural distinctiveness and needs, which provided us with a vast amount of contextual information. In contrast, the literature on outreach is generally undertheorised and lacks process detail and outcomes measurement. Jagosh et al. 216 describe how, for their realist review on participatory research, the process of refinement of the research question was a key step in defining study inclusion criteria. In order to increase the homogeneity of our data set, we could have undertaken a similar process of refining the parameters of the review. This could have taken the shape, for example, of focusing on outreach intervention strategies leading to behaviour change only. However, our brief was not on outreach, but specifically on outreach in Traveller Communities.
Our initial scope was thus broad and ill-defined and we considered that too early a narrowing of our criteria might have restricted our learning potential quite significantly. We countered this putting particular emphasis on expert hearings and explicitly incorporating them into both our analysis and the report. This enabled the focus on trust and negotiation to emerge over time and in response to our immersion in the whole breadth of the evidence base available. The broad literature base also meant that, as mentioned above, we needed to engage in sufficient theorisation to accommodate the breadth of the evidence base while still retaining explanatory potential. This fits into the kind of methodological customisation recently described in the literature. 216
Selecting theories
Realist reviews are driven by theories, in that theory identification is meant to occur early in the process and to guide the study selection and data extraction protocol so that the adequate evidence can be captured. 85 We did not begin the study with a ‘ready made’ middle-range theory, but rather with our knowledge of the dimensions of peer and lay interventions, from which the initial (‘to whom’, ‘by whom’, ‘how’, ‘what for’) framework emerged. Neufeld’s190 cycle of engagement provided an overarching theoretical framework, which could be considered a middle-range theory; it was not so theoretical that it could not be tested with the evidence at hand, and not so pragmatic that it explained only single occurrences. We therefore tested the three phases of negotiation, participation and evaluation with our studies. The first emerged as key, but only in conjunction with trust, and these became the key contextual ingredients – therefore marking a departure from Traveller-focused literature to maximise translation potential to other groups. Participation was described in a great majority of studies, but did not explain the reasoning which led people to engage to different degrees – this was therefore combined with Fredricks et al. ’s200 model, explaining the kind of engagement decision-making that participants may be going through. Therefore, no single existing theoretical framework could explain the breadth of the literature and we combined three models of engagement and trust in order to obtain maximum explanatory potential.
Linked to this is the existence of ‘layers of mechanisms’ in our analysis. For example, in Fitzpatrick,64 our CMO analysis shows that the underlying mechanism leading to participation was behavioural engagement, because participants made the conscious decision to take part in the intervention and report its high acceptability. However, our understanding of the context leads us to the conclusion that this decision was driven by a protectionist attitude rather than either a trusting relationship with the outreach worker or an intervention that responds to an expressed need. Thus, we could identify different layers, which, combined, could all contribute to explaining reported outcomes. While we initially used Neufeld’s cycle of engagement as an outreach process mechanism, within which cultural and social influencers operated to impact on individual decision-making, engagement was also a key mechanism to making outreach ‘work’. Articulating how these different mechanisms could operate simultaneously, but at various levels (the individual, the group, the intervention, etc.), was a key challenge in formulating our findings.
Strengths and limitations of the review
Realist reviews are at their best when examining complex interventions (e.g. mentoring,98 internet education,217 participatory research218) and test underlying mechanisms of action in a variety of contexts. Here, the context of outreach was stipulated by the funding body.
Another limitation of much research involving Traveller Communities, and thus this review, is their well-acknowledged reluctance to self-identify as such. With an increasing proportion of Travellers turning to ‘bricks and mortar’ accommodation in particular, this poses the issue of the representativeness of research study populations. The expert hearings, encounters, meetings, interviews and focus groups that we conducted with members of the Community, and workers who were well accepted by them, proved a reassuring source of evidence; if study populations may be biased, these people provided an invaluable source of insider knowledge that helped greatly at all stages of the review, and ensured the strong face validity of the explanatory CMO configurations proposed.
One final limitation that readers unfamiliar with realist approaches might highlight is that it does not offer certitude in terms of statistical significance of favourable outcomes. Quite aside from the fact that the literature focusing on Traveller Communities would not allow such numerical aggregation and statistical comparative analyses, this is not the aim of a realist synthesis. As has been stressed throughout the project, the emphasis here is on formulating explanatory statements (theories) that are refined and tested through engagement with a wide range of evidence sources. The resulting explanatory framework can be used as a basis for recommendations for practice and future research. The aim, however, is to provide not an all-encompassing explanatory framework, but rather one that offers the most credible account of what works, for whom and in what circumstances, given the confines of the project remit.
Chapter 5 Conclusions and recommendations for practice and research
Systematic literature searches identified 278 studies, which formed the basis for a scoping review, an evaluation of cost and cost-effectiveness of different models of outreach provision, and a realist review highlighting and testing the mechanisms by which they may work, for whom and in what circumstances. In this section, we draw the implications of the findings for policy, practice and research.
Recommendations for practice
From the outset, there needs to be clarity about the purpose of outreach. If it is about promoting attendance at one-off events, such as screening, then the outreach worker needs cultural awareness but may not need to have long-established links with the Community. Changing behaviour or developing social capital, on the other hand, is a different challenge that is more likely to be met if the intervention builds explicitly on long-established and trusting relationships.
Where outreach workers have such bonding ties to a Community, this may provide greater opportunities for social engagement and influence (as opposed to social support) that are likely to trigger a higher degree of personal investment by Community members. This may facilitate movement from a focus on felt and expressed need to embracement of normative needs that are required not only to improve Traveller health but also to impact on health inequalities.
Peerness, in terms of being a member of the Traveller Communities, may not be the key determinant in achieving successful outreach. Consideration also, and perhaps more importantly, needs to be given to the workers’ place on the specific social network map of the target population.
Practice should guard against interpreting outreach as being unidirectional, i.e. from various degrees of ‘outside’ to impacting ‘inside’ the disengaged Community. Social networks are characterised by the interconnectedness between individuals, thus inherently describing a relational process. Traveller Community individuals should, therefore, be considered not only the passive recipients of a well-designed intervention, but also as key active ‘ingredients’ that, together with outreach workers, make that intervention ‘work’. The emphasis placed in this study on the importance of gaining trust and negotiating the agenda is an example of how such potential can be activated. It cannot be assumed that Traveller Communities have greater degrees of trust with all members of their Community. Rather, relationships between Community members will be built on varying levels of trust as a result of previous experiences, and in the case of health issues to which stigma is attached, Traveller Communities may prefer to seek help from outside the Community. Cultural awareness training delivered by Traveller Community members is a further example of the active participation of Traveller Community members in outreach work.
No evidence could be found for the need to develop Traveller-specific services. Rather, outreach offers the potential to both develop the cultural sensitivity of mainstream services and raise awareness of their existence among Traveller Communities. The limited amount of robust evidence on the effectiveness of interventions to improve the health of Traveller Communities means that recommendations on the cost-effectiveness of different types of outreach are, inevitably, speculative. However, the implementation of protocol changes, such as texting appointment reminders, in primary and secondary care is unlikely to be expensive and might be considered the minimum acceptable action to facilitate access to health care by members of Traveller Communities. The identification of a champion for Traveller Communities within each care commissioning group (selected with the involvement of Traveller Communities) and health and well-being boards would facilitate the implementation of these changes. In addition, examples from the literature suggest that cultural awareness sessions can be delivered successfully by Community members for modest costs. Interventions which use mobile clinics to bring health services to Travellers are associated with the highest costs reported and the brief data on outcomes available give little confidence that they provide value for money. The employment of full-time outreach workers for Traveller Communities appears to be associated with moderate costs with benefits that may not be primarily improved health. Practice nurses are well placed to facilitate access to primary care at the practices in which they work, and they may represent a cost-effective resource to improve access to primary care for Traveller Communities.
Research implications
In a field as specific as Traveller Communities, the scoping review offered a useful scaffold for the other review strands. Interest in the Communities has increased in recent years, and the health inequalities they experience are now well established, but this has yet to translate into robust evaluations of interventions to improve their health. Outreach is mostly reported in eastern European countries, and mostly in the form of descriptive accounts. While this paucity of evidence would be a weakness for most synthesis methods, it makes the realist approach employed in this project particularly timely, as the development of theoretical insights it has allowed can most effectively guide future evaluation efforts.
The economic review highlighted avenues worthy of further exploration, such as the training and use of outreach workers from Traveller Communities to promote vaccination and access to antenatal care. Building trust with Communities through cycles of engagement whereby negotiated needs are addressed involves a considerable time investment. Effectiveness should therefore be evaluated using a continuum of programme impacts, from intermediate outcomes such as engagement through to longer-term outcomes such as improved health status.
Realist synthesis and evaluation offer great potential in developing the kind of cross-cutting theoretical insights that explain how potentially low-cost interventions such as outreach can work, with whom and in what circumstances. Realist researchers internationally are debating the potential of realist syntheses to generate reusable explanatory frameworks, in order to allow syntheses to feed into one another. This is at the very heart of the translational potential offered by realist approaches, as underpinning mechanisms can ‘work’ across whole families of programmes. We anticipate that the inverse role of trust and negotiation identified in this report has, when linked to social network theory, tremendous explanatory potential for why programmes may or may not be successful in engaging other ‘hard to reach’ groups. Capitalising on the inroads into these dense but marginalised social networks offered by Community representative organisations is one of the ways in which research effectiveness might be maximised. Other key additions include the need to consider carefully the entry points in a Community, and the potential and realistic impacts of an intervention. The classification developed here around participation, behaviour change and social capital development presents a useful starting point, which will apply in other families of health improvement interventions.
A lot of the research endeavour surrounding Traveller Communities has been devoted to better understanding their cultural, historical and ethnic differences. While this is an important research field in its own right, its potential to explain why certain interventions work better than others is limited. We suggest that, instead, patterns of mobility and their consequent impact on access to services should be considered, but only with an appreciation of the importance of trust and social bonds. The cost-effectiveness of research and practice efforts in implementing group-specific strategies could be greatly improved by pursuing the kinds theoretical insights developed here.
Acknowledgements
The authors wish to offer their thanks to Jo Crowley, Eva Karchnakova, Irma Karachnakova, Zoe Matthews, Brendan McCormack, Fiona McCredie, Valéry Ridde, Louise Wannop and Gill Westhorp for their support and assistance with the research, and to all the Roma, Gypsies and Travellers who participated in the expert hearings, whose views were hugely important in helping to shape the project results. We also thank the reviewers for their useful comments which helped to improve this report.
Contributions of authors
Professor Susan M Carr was involved in overall project management, research question refinement, search protocol development, data analysis and interpretation, editing of draft reports and final report writing.
Dr Monique Lhussier was involved in research question refinement, search protocol development, realist synthesis lead, editing of draft versions and final report writing.
Natalie Forster was involved in research question refinement, search protocol development, database searching, realist synthesis and scoping review, editing of drafts versions of the report.
Dr Deborah Goodall (until December 2012) was involved in research question refinement, search protocol development, database searching, lead on scoping review.
Lesley Geddes was involved in research question refinement, search protocol development, lead on liaising with Traveller Communities and service providers, commentary on all phases of the reviews, editing of draft versions of report.
Dr Mark Pennington was involved in lead on economic review, research question refinement, commentary on all phases of the reviews, editing of draft versions and final report writing.
Dr Angus Bancroft was involved in research question refinement, commentary on all phases of the reviews, reviewing of draft version of the report.
Dr Jean Adams was involved in research question refinement, commentary on all phases of the reviews, reviewing of draft versions of the report.
Professor Susan Michie was involved in research question refinement, commentary on all phases of the reviews, reviewing of draft versions of the report.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health.
References
- Gypsy, Roma and Traveller Communities – Further Information. London: Department for Children, Schools and Families; 2010.
- Greenfields M, Home R. Assessing Gypsies’ and travellers’ needs: partnership working and ‘The Cambridge Project’. Romani Studies 2006;16:105-31. http://dx.doi.org/10.3828/rs.2006.6.
- Niner P. Local Authority Gypsy/Traveller sites in England. London: Office of the Deputy Prime Minister; 2003.
- Traveller Ethnicity: an Equality Authority Report. Dublin: The Equality Authority; 2006.
- Richardson J. Providing Gypsy and Traveller sites: Contentious Spaces. Coventry: Chartered Institute of Housing, Joseph Rowntree Foundation; 2007.
- Cemlyn S, Greenfields M, Burnett S, Matthews Z, Whitwell C. Inequalities Experienced by Gypsy and Traveller Communities: a Review. London: Equality and Human Rights Commission; 2009.
- Housing Act 2004. London: The Stationery Office; 2004.
- Council of Europe Roma and Travellers. Strasbourg: Council of Europe; n.d.
- Common Ground: Equality, Good Relations and Sites for Gypsies and Irish Travellers. London: Commission for Racial Equality; 2006.
- Count of Gypsy and Traveller Caravans: January 2013. London: Department for Communities and Local Government; 2013.
- Gypsy and Traveller Caravan Count January 2013. Cardiff: Welsh Government; 2013.
- Gypsies/Travellers in Scotland: The Twice Yearly Count – No. 16: July 2009. Edinburgh: Scottish Government; 2010.
- Clark C, Greenfields M. Here to Stay: The Gypsies and Travellers of Britain. Hatfield: University of Hertfordshire Press; 2006.
- Doyal L, Cameron A, Cemlyn S, Nandy S, Shaw M. The Health of Travellers in the South West Region: a Review of Data Sources and a Strategy for Change. Bristol: South West Public Health Observatory; 2002.
- Drakakis-Smith A, Mason K. Out for the count: a critical examination of the DETR (DTLR) bi-annual count of Gypsies/Travellers in England with special reference to Staffordshire. Radic Stats 2001;78:77-90.
- Dar O, Gobin M, Hogarth S, Lane C, Ramsay M. Mapping the Gypsy Traveller Community in England: what we know about their health service provision and childhood immunization uptake. J Public Health 2013;35:404-12. http://dx.doi.org/10.1093/pubmed/fdt052.
- Office for National Statistics . 2011 Census: KS201EW Ethnic Group, Local Authorities in England and Wales 2012. www.ons.gov.uk/ons/search/index.html?pageSize=50&sortBy=none&sortDirection=none&newquery=ks201EW (accessed 9 September 2013).
- Gypsy and Traveller Population in England and the 2011 Census: An Irish Traveller Movement in Britain Report. London: Irish Traveller Movement in Britain; 2013.
- Parry GG, Van Cleemput PP, Peters JJ, Walters SS, Thomas KK, Cooper CC. Health status of Gypsies and Travellers in England. J Epidemiol Community Health 2007;61:198-204. http://dx.doi.org/10.1136/jech.2006.045997.
- Inclusion Health: Improving Primary Care for Socially Excluded People. London: Department of Health; 2010.
- Marmot M. Fair Society, Healthy Lives: The Marmot Review. London: The Marmot Review; 2010.
- Aspinall P. A Review of the Literature on the Health Beliefs, Health Status, and Use of Services in the Gypsy Traveller Population, and of Appropriate Health Care Interventions. Cardiff: Welsh Assembly Government; 2006.
- Hajioff S, McKee M. The health of the Roma people: a review of the published literature. J Epidemiol Community Health 2000;54:864-9. http://dx.doi.org/10.1136/jech.54.11.864.
- Zeman CL, Depken DE, Senchina DS. Roma health issues: a review of the literature and discussion. Ethn Health 2003;8:223-49. http://dx.doi.org/10.1080/1355785032000136434.
- Abdalla S, Quirke B, Daly L, Fitzpatrick P, Kelleher C. All Ireland Traveller Health Study: increasing gap in mortality between Traveller and general populations in the Republic of Ireland over two decades. J Epidemiol Community Health 2010;64. http://dx.doi.org/10.1136/jech.2010.120956.57.
- Peters J, Parry G, Cleemput P, Moore J, Cooper C, Walters S. Health and use of health services: a comparison between Gypsies and Travellers and other ethnic groups. Ethn Health 2009;14:359-77. http://dx.doi.org/10.1080/13557850802699130.
- Hodgins M, Millar M, Barry MM. ‘… It’s all the same no matter how much fruit or vegetables or fresh air we get’: traveller women’s perceptions of illness causation and health inequalities. Soc Sci Med 2006;62:1978-90. http://dx.doi.org/10.1016/j.socscimed.2005.08.052.
- Treise C, Shepherd G. Developing mental health services for Gypsy Travellers: an exploratory study. Clinical Psychology Forum 2006:16-20.
- Walker M. Suicide Among the Irish Traveller Community 2000–2006. Wicklow: Wicklow County Council; 2008.
- Greenfields M. Falling by the wayside. Diabetes Update 2009:24-7.
- Maduma-Butshe A, McCarthy N. The burden and impact of measles among the Gypsy-Traveller communities, Thames Valley, 2006–09. J Pub Health 2012;35:27-31. http://dx.doi.org/10.1093/pubmed/fds052.
- Lewis G, Drife J. Why Mothers Die 1997–1999: the Confidential Enquiries into Maternal Deaths in the United Kingdom. London: Royal College of Obstetricians and Gynaecologists (RCOG) Press; 2001.
- Hamid N, Daly L, Fitzpatrick P. All Ireland Traveller Health Study Technical Repot 2: The Birth Cohort Study Follow Up. Dublin: School of Public Health, Physiotherapy and Population Science, University College Dublin; 2011.
- Bobak M, Dejmek J, Solansky I, Sram RJ. Unfavourable birth outcomes of the Roma women in the Czech Republic and the potential explanations: a population-based study. BMC Pub Health 2005;5. http://dx.doi.org/10.1186/1471-2458-5-106.
- Joubert K. Size at birth and some sociodemographic factors in gypsies in Hungary. J Biosoc Sci 1991;23:39-47. http://dx.doi.org/10.1017/S0021932000019052.
- Van Cleemput P, Parry G. Health status of Gypsy Travellers. J Pub Health Med 2001;23:129-34. http://dx.doi.org/10.1093/pubmed/23.2.129.
- Van Cleemput P, Thomas K, Parry G, Moore J, Cooper CC. The Health Status of Gypsies and Travellers in England: Report of Qualitative Findings. Sheffield: University of Sheffield and Department of Health; 2004.
- Dahlgren G, Whitehead M. Policies and Strategies to Promote Social Equity in Health. Stockholm: Institute of Futures Studies; 1991.
- Van Cleemput P, Parry G, Thomas K, Peters J, Cooper C. Health-related beliefs and experiences of Gypsies and Travellers: a qualitative study. J Epidemiol Community Health 2007;61:205-10. http://dx.doi.org/10.1136/jech.2006.046078.
- Dion X. Gypsies and Travellers: cultural influences on health. Community Pract 2008;81:31-4.
- Okely J. The Traveller-Gypsies. Cambridge: Cambridge University Press; 1983.
- Abdalla S, Cronin F, Drummond A, Fitzpatrick P, Frazier K, Hamid NA, et al. All Ireland Traveller Health Study Technical Report 1: Health Survey Findings. Dublin: University College Dublin; 2010.
- Roberts A, Adkins J, Lewis H, Wilkinson C. Coronary Heart Disease and Mental Health in Gypsies and Travellers in Wrexham: Redressing the Balance. Torquay: Community Practitioners’ and Health Visitors’ Association (CPHVA) Annual Conference; 2007.
- Getting It Right For Every Child: Implementation Plan. Edinburgh: Scottish Executive; 2006.
- Lane P, Spencer S, McCready M. Perspectives on Ageing in Gypsy Families. York: Joseph Rowntree Foundation; 2012.
- Greenfields M, Smith D. A question of identity: the social exclusion of housed Gypsies and Travellers. Res Policy Planning 2011;28:1-14.
- Gypsies and Travellers. A Strategy for the CRE 2004–2007. London: Commission for Racial Equality; 2004.
- Crawley H. Moving Forward: the Provison of Accomodation for Travellers and Gypsies. London: Institiute for Public Policy Research; 2004.
- Review of Service Provision for Gypsies and Travellers. Cardiff: National Assembly for Wales; 2003.
- McGorrian C, Frazer K, Kelleher CC. Do Irish Travellers pose a paradox in terms of healthcare access and engagement? Findings from the All Ireland Traveller Health Study (AITHS). Irish J Med Sci 2011;180.
- Beach H. Comparing the use of an accident and emergency department by children from two local authority Gypsy sites with that of their neighbours. Pub Health 2006;120:882-4. http://dx.doi.org/10.1016/j.puhe.2006.05.017.
- Ryder A, Greenfields M. Roads to Success: Economic and Social Inclusion for Gypsies and Travellers. Buckinghamshire: Irish Traveller Movement in Britain, University of Buckinghamshire; 2012.
- Myers M, McGhee D, Bhopal K. At the crossroads: gypsy and traveller parents’ perceptions of education, protection and social change. Race Ethn Educ 2010;13:533-48. http://dx.doi.org/10.1080/13613324.2010.492138.
- GCSE Attainment by Pupil Characteristics in England (2008/9). London: Department for Children, Schools and Families; 2009.
- Provision of Support for Traveller Pupils. London: Ofsted Publications Centre; 2003.
- Wilkin A, Derrington C, Martin K, Foster B, Kinder K, Rutt S. Improving the Outcomes for Gypsy, Roma and Traveller Pupils: Final Report. London: Department for Education; 2010.
- Moving Forward Together: Raising Gypsy, Roma and Traveller Achievement. Booklet 1: Introduction. London: Department for Children, Schools and Families; 2009.
- Profiles of Prejudice: Detailed Summary of Findings. London: Stonewall; 2003.
- Caught in the Headlines: Scottish Media Coverage of Scottish Gypsy Travellers. Edinburgh: Amnesty international; 2012.
- Reid T. Partners in care. Nurs Times 1993;89:28-30.
- Progress report on Gypsy and Traveller Policy. London: Department for Communities and Local Government; 2009.
- Primary Care Service Framework: Gypsies and Travellers. London: NHS Primary Care Contracting; 2009.
- Van Cleemput P, Bissell P, Harris J. Pacesetters Programme Gypsy, Roma and Traveller Core Strand Evaluation Report for the Department of Health. Sheffield: Public Health Section, ScHARR, The University of Sheffield; 2010.
- Fitzpatrick P, Molloy B, Johnson Z. Community mothers’ programme: extension to the travelling community in Ireland. J Epidemiol Community Health 1997;51:299-303. http://dx.doi.org/10.1136/jech.51.3.299.
- Matthews Z. The Health of Gypsies and Travellers in the UK: Better Health Briefing Paper 12. London: Race Equality Foundation; 2008.
- Mackenzie M, Turner F, Platt S, Reid M, Wang Y, Clark J, et al. What is the ‘problem’ that outreach work seeks to address and how might it be tackled? Seeking theory in a primary health prevention programme. BMC Health Serv Res 2011;11:350-61. http://dx.doi.org/10.1186/1472-6963-11-350.
- Gill P, MacLeod U, Lester H, Hegenbarth A. Improving Access to Health Care for Gypsies and Travellers, Homeless People and Sex Workers. London: Royal College of General Practitioners; 2013.
- Andersson B. Finding ways to the hard to reach – considerations on the content and concept of outreach work. Eur J Social Work 2013;16:171-86. http://dx.doi.org/10.1080/13691457.2011.618118.
- Dickson-Gómez J, Knowlton A, Latkin C. Hoppers and oldheads: qualitative evaluation of a volunteer AIDS outreach intervention. AIDS Behav 2003;7:303-15. http://dx.doi.org/10.1023/A:1025499904469.
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and Evaluating Complex Interventions: New Guidance. London: Medical Research Council; 2008.
- Spillane V, Byrne M, Byrne M, Leathem C, O’Malley M, Cupples M. Monitoring treatment fidelity in a randomised trial of a complex intervention. J Adv Nurs 2007;60:343-52. http://dx.doi.org/10.1111/j.1365-2648.2007.04386.x.
- Hennessey M, Rumrill P. Treatment fidelity in rehabilitation research. Vocational Rehabi 2003;19:123-6.
- Carroll C, Patterson M, Wood S, Booth A, Rick J, Balain S. A conceptual framework for implementation fidelity. Implementation Science 2007;2:40-8. http://dx.doi.org/10.1186/1748-5908-2-40.
- Rots-de Vries C, van de Goor I, Stronks K, Garretsen H. Evaluation of an assertive outreach intervention for problem families: intervention methods and early outcomes. Scand J Caring Sci 2011;25:211-19. http://dx.doi.org/10.1111/j.1471-6712.2010.00811.x.
- Hawe P, Shiell A, Riley T. Complex interventions: how “out of control” can a randomised controlled trial be?. BMJ 2004;328:1561-3. http://dx.doi.org/10.1136/bmj.328.7455.1561.
- Ottoson J, Green L. Communty outreach: from measuring the difference to making a difference with health information. J Med Libr Assoc 2005;93:S49-56.
- McGivney V. Recovering Outreach: Concepts, Issues and Practices. Leicester: National Institute of Adult Continuing Education (UK); 2000.
- Quality Assessment Tool for Quantitative Studies. Ontario: Public Health Research, Education and Development Program (PHRED); 2003.
- Critical Appraisal Skills Programme. 10 Questions to Help You Make Sense of Qualitative Research. England: Public Health Resource Unit; 2006.
- Davis K, Drey N, Gould D. What are scoping studies? A review of the nursing literature. Int J Nurs Stud 2009;46:1386-400. http://dx.doi.org/10.1016/j.ijnurstu.2009.02.010.
- Grant M, Booth A. A typology of reviews: an analysis of 14 review types and associated methodologies. Health Info Libr J 2009;26:91-108. http://dx.doi.org/10.1111/j.1471-1842.2009.00848.x.
- Levac D, Colquhoun H, O’Brien K. Scoping studies: advancing the methodology. Implementation Science 2010;5:1-9. http://dx.doi.org/10.1186/1748-5908-5-69.
- Peat M, Entwistle V, Hall J, Birks Y, Golder S. Scoping review and approach to appraisal of interventions intended to involve patients in patient safety. J Health Serv Res Policy 2010;15:17-25. http://dx.doi.org/10.1258/jhsrp.2009.009040.
- Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodo 2005;8:19-32. http://dx.doi.org/10.1080/1364557032000119616.
- Pawson R, Greenhalgh T, Harvey G, Walshe K. Realist Synthesis: an Introduction. Manchester: ESRC Research Methods Programme; 2004.
- Booth A. Unpacking your literature search toolbox: on search styles and tactics. Health Info Libr J 2008;25:313-7. http://dx.doi.org/10.1111/j.1471-1842.2008.00825.x.
- Papaioannou D, Sutton A, Carroll C, Booth A, Wong R. Literature searching for social science systematic reviews: consideration of a range of search techniques. Health Info Libr J 2010;27:114-22. http://dx.doi.org/10.1111/j.1471-1842.2009.00863.x.
- CRD’s Guidance for Undertaking Reviews in Health Care. York: CRD, University of York; 2009.
- Wong G, Greenhalgh T, Westhorp G, Buckingham J, Pawson R. RAMESES publication standards: realist syntheses. BMC Med 2013;11:1-12.
- Poth C, Ross S. Meta-analysis, systematic review, or scoping review? Comparing methodologies in educational research n.d.
- Armstrong R, Hall B, Doyle J, Waters E. ‘Scoping the scope’ of a Cochrane review. J Pub Health 2011;33:147-50. http://dx.doi.org/10.1093/pubmed/fdr015.
- di Gregorio S. Using NVIVO for your literature review n.d.
- Bandara W. Using Nvivo as a research management tool: a case narrative n.d.
- Bazeley P. Analysing qualitative data: more than identifying themes. Malays J Qual Res 2009;2:6-22.
- Beekhuyzen J, Nielsen S, von Hellens L. The Nvivo Looking Glass: Seeing the Data Through the Analysis n.d.
- Beekhuyzen P. Putting the Pieces of the Puzzle Together: Using NVIVO for a Literature Review n.d.
- Woods MWM. Quality and Impact of Qualitative Research. Brisbane, Australia: Griffith University; 2006.
- Pawson R. Mentoring Relationships: an Explanatory Review. London: ESRC UK Centre for Evidence Based Policy and Practice; 2004.
- McCormack B, Dewar B, Wright J, Garbett R, Harvey G, Ballantine K. Londonderry: University of Ulster; 2006.
- Pawson R. Evidence-based policy: the promise of ‘Realist Synthesis’. Evaluation 2002;8:340-58. http://dx.doi.org/10.1177/135638902401462448.
- Anand S, Atkinson S, Davis D, Blimkie C, Ahmed R, Brouwers M, et al. A family-based intervention to promote healthy lifestyles in an Aboriginal community in Canada. Can J Pub Health 2007;98:447-52.
- Nyamathi A, Liu Y, Marfisee M, Shoptaw S, Gregerson P, Saab S, et al. Effects of a nurse-managed program on hepatitis A and B vaccine completion among homeless adults. Nurs Res 2009;58:13-22. http://dx.doi.org/10.1097/NNR.0b013e3181902b93.
- Lowe J. A cultural approach to conducting HIV/AIDS and hepatitis C virus education among Native American adolescents. J Sch Nurs 2008;24:229-38. http://dx.doi.org/10.1177/1059840508319866.
- Struthers R, Schanche Hodge F, De Cora L, Geishirt-Cantrell B. The experience of native peer facilitators in the campaign against type 2 diabetes. J Rural Health 2003;19:174-80. http://dx.doi.org/10.1111/j.1748-0361.2003.tb00559.x.
- Weine S, Kulauzovic Y, Klebic A, Besic S, Mujagic A, Muzurovic J, et al. Evaluating a multiple family group access intervention for refugees with PTSD. J Marital Fam Ther 2008;34:149-64. http://dx.doi.org/10.1111/j.1752-0606.2008.00061.x.
- Mitchell SG, Peterson JA, Latkin CA. The impact of drug use on perceptions of credibility in indigenous outreach workers. Qual Health Res 2006;16:1108-19. http://dx.doi.org/10.1177/1049732304273934.
- Carr S, Lhussier M, Foster N, Geddes L, Dean K, Pennington M, et al. An evidence synthesis of qualitative and quantitative research on component intervention techniques, effectiveness, cost effectiveness, equity and acceptability of different versions of health-related lifestyle adviser role in improving health. Health Technol Assess 2011;15.
- Parry G, Van Cleemput P, Peters J, Moore J, Walters S, Thomas K, et al. The Health Status of Gypsies and Travellers in England: a Report to the Department of Health. Sheffield: University of Sheffield; 2004.
- Decade of Roma Inclusion Secretariat Foundation . Decade of Roma Inclusion 2005–2015 Hungary. Decade of Roma Inclusion Secretariat Foundation 2012. www.romadecade.org/index (accessed 22 April 2013).
- Lhussier M, Carr SM. Health related lifestyle advice: critical insights. Critical Pub Health 2008;18:299-30. http://dx.doi.org/10.1080/09581590802225738.
- Devlin N, Parkin P. Does NICE have a cost-effectiveness threshold and what other factors influence its decisions? A binary choice analysis. Health Econ 2004;13:437-52. http://dx.doi.org/10.1002/hec.864.
- Shiell A, Hawe P, Gold L. Complex interventions or complex systems? Implications for health economic evaluation. BMJ 2008;336. http://dx.doi.org/10.1136/bmj.39569.510521.AD.
- Pennington M, Dickinson H, Walker I, Gray J, Donaldson C. Economic evaluation of complex social initiatives; feasible, but not practicable at present?. Soc Pub Policy Rev 2014.
- Curtis L. Unit Costs of Health and Social Care 2012. Canterbury: PSSRU, University of Kent; 2012.
- Moreton JJ. Immunization of travellers in Oxfordshire. Nursing 1987;3:723-6.
- Streetly A. Health care for travellers: one year’s experience. Br Med J 1987;294:492-4. http://dx.doi.org/10.1136/bmj.294.6570.492.
- Lawrie B. Travelling families in east London – adapting health visiting methods to a minority group . Gypsies. Health Visitor 1983;56:26-8.
- Taylor JJ. Travellers. Health behaviour and beliefs. Health Visitor 1991;64:223-4.
- Welsh Government . Coronary Heart Disease and Travellers: Redressing the Balance 2012. http://wales.gov.uk/topics/health/improvement/communities/fund/inequalitiesnorth1/balanceproject/?lang=en (accessed 17 August 2013).
- Fay R, Kavanagh D, Quirke B, Malone M. Primary Health Care for Travellers Project: Project Report for Year Ended October 1995. Dublin: Pavee Point; 1996.
- Holden J. The Highland Gypsy/traveller Health & Wellbeing Initiative. NHS England; 2005.
- Thorn H. Gypsy and Travellers’ Health Needs Assessment: Improving the Health of Gypsies and Travellers in the Mid Essex Area. Essex: NHS Mid Essex; 2009.
- theBIGGIVE.org.uk . Disability Essex Healthy Chance Outreach Programme 2013. https://secure.thebiggive.org.uk/projects/view/7540/disability-essex-healthy-chance-outreach-programme (accessed 17 August 2013).
- Murphy P. Primary Health Care for Travellers Project: Implementation Report 1996–1999. Dublin: Pavee Point; 1999.
- Mediating Romani Health: Policy and Program Opportunities. New York, NY: Open Society Institute Network Public Health Program; 2005.
- Hoover J. Persistence Pays: The Challenges and Rewards of One NGO’s Health Promotion Outreach among Roma Drug Users. Sofia: Initiative for Health Foundation; 2007.
- Subata E, Tsukanov J. The work of general practitioners among Lithuanian Roma in Vilnius: incorporating harm reduction into primary medical practice. J Drug Issues 1999;29:805-10.
- An Oral Health Promotion Programme for Traveller Families in County Offaly February 2007. Dublin: Health Service Executive; 2007.
- Health Access for Roma Improves with Award-Winning Programme. Budapest: European Roma Rights Centre; 2006.
- Cámara Medina C, Pérez Garcia A, Quesada Lupiañez P, Sánchez Cantalejo E. Intervention with community health agents in immunization programs in the gypsy population. Aten Primaria 1994;13:415-18.
- Martinez-Campillo Garcia F, Maura da Fonseca A, Santiago Oliva J, Verdú Perez M, Serramia del Prisco A, Ibáñez Molina M, et al. Vaccine coverage study and intervention with health community agents in a marginal gypsy community of Alicante. Aten Primaria 2003;31:234-8. http://dx.doi.org/10.1016/S0212-6567(03)79165-3.
- Szilagyi T. Peer education of tobacco issues in Hungarian communities of Roma and socially disadvantaged children. Cent Eur J Public Health 2002;10:117-20.
- Kelly JA, Amirkhanian YA, Kabakchieva E, Vassileva S, Vassilev B, McAuliffe TL, et al. Prevention of HIV and sexually transmitted diseases in high risk social networks of young Roma (Gypsy) men in Bulgaria: randomised controlled trial. BMJ 2006;333. http://dx.doi.org/10.1136/bmj.38992.478299.55.
- One Voice for Travellers . One Voice for Travellers 2011 n.d. www.idea.org.uk/idk/core/page.do?pageld=30211424 (accessed 18 October 2011).
- Shepherd S. Equality: the open road to greater inclusion. Health Service J 2010;120:16-7.
- Wood S. East Cambridgeshire and Fenland Traveller Health Needs Assessment 2006. www.cambridgeshirejsna.org.uk/book/export/html/1016 (accessed 30 September 2011).
- Gilhooly ML, McGhee SM. Medical records: practicalities and principles of patient possession. J Med Ethics 1991;17:138-43. http://dx.doi.org/10.1136/jme.17.3.138.
- Williams JG, Cheung WY, Chetwynd N, Cohen DR, El-Sharkawi S, Finlay I, et al. Pragmatic randomised trial to evaluate the use of patient held records for the continuing care of patients with cancer. Qual Health Care 2001;10:159-65. http://dx.doi.org/10.1136/qhc.0100159.
- Feder G. Traveller gypsies and primary care. J R Coll Gen Pract 1989;39:425-9.
- Mirambeau AM, Wang G, Ruggles L, Dunet DO. A cost analysis of a community health worker program in rural Vermont. J Community Health 2013;38:1050-7. http://dx.doi.org/10.1007/s10900-013-9713-x.
- Buchan J, DalPoz M. Skill mix in the health care workforce: reviewing the evidence. Bull World Health Organ 2002;80:575-80.
- Fedder DO, Chang RJ, Curry S, Nichols G. The effectiveness of a community health worker outreach program on healthcare utilization of west Baltimore City Medicaid patients with diabetes, with or without hypertension. Ethn Dis 2003;13:22-7.
- American Diabetes Association . Economic costs of diabetes in the US in 2007. Diabetes Care 2008;31:596-615. http://dx.doi.org/10.2337/dc08-9017.
- Swider SM. Outcome effectiveness of community health workers: an integrative literature review. Public Health Nurs 2002;19:11-20. http://dx.doi.org/10.1046/j.1525-1446.2002.19003.x.
- Lewin SA, Dick J, Pond P, Zwarenstein M, Aja G, van Wyk B, et al. Lay health workers in primary and community health care. Cochrane Database Syst Rev 2005;1.
- Wells KJ, Luque JS, Miladinovic B, Vargas N, Asvat Y, Roetzheim RG, et al. Do community health worker interventions improve rates of screening mammography in the United States? A systematic review. Cancer Epidemiol Biomarkers Prev 2011;20:1580-98. http://dx.doi.org/10.1158/1055-9965.EPI-11-0276.
- Pennington M, Visram S, Donaldson C, White M, Lhussier M, Deane K, et al. Cost-effectiveness of health-related lifestyle advice delivered by peer or lay advisors: synthesis of evidence from a systematic review. Cost Eff Resour Alloc 2013;11:1-12. http://dx.doi.org/10.1186/1478-7547-11-30.
- Edmunds W, Brisson M, Melegaro A, Gay N. The potential cost-effectiveness of acellular pertussis booster vaccination in England and Wales. Vaccine 2002;20:1316-30. http://dx.doi.org/10.1016/S0264-410X(01)00473-X.
- Babigumira JB, Sethy AK, Smyth KA, Singer ME. Cost effectiveness of facility-based care, home-based care and mobile clinics for provision of antiretroviral therapy in Uganda. Pharmacoeconomics 2009;27:963-73. http://dx.doi.org/10.2165/11318230-000000000-00000.
- Bailie R. An economic appraisal of a mobile cervical cytology screening service. S Afr Med J 1996;86:1179-84.
- Fox-Rushby JA, Foord F. Costs, effects and cost-effectiveness analysis of a mobile maternal health care service in West Kiang, The Gambia. Health Policy 1996;35:123-43. http://dx.doi.org/10.1016/0168-8510(95)00774-1.
- Walker G, Gish O. Mobile Health Services: a study in cost-effectiveness. Med Care 1977;15:267-76. http://dx.doi.org/10.1097/00005650-197704000-00001.
- Oriol NE, Cote PJ, Vavasis AP, Bennet J, DeLorenzo D, Blanc P, et al. Calculating the return on investment of mobile healthcare. BMC Med 2009;7. http://dx.doi.org/10.1186/1741-7015-7-27.
- Report of the Pilot Health Promotion Project with Travellers in Dorset 1997–1998. Brighton: Friends, Families and Travellers Support Group; 1998.
- Shubin S, Swanson K. “I’m an imaginary figure”: unravelling the mobility and marginalisation of Scottish Gypsy Travellers. Geoforum 2010;41:919-29. http://dx.doi.org/10.1016/j.geoforum.2010.06.006.
- Johnson C, Willers M. Gypsy and Traveller Law. London: Legal Action Group; 2007.
- McCabe C, Keyes F. A Review of Travellers’ Health using Primary Care as a Model of Good Practice: Pavee Point Primary Health Care for Travellers’ Project. Dublin: Pavee Point; 2005.
- Queally M. Health promotion needs of the Travelling Community. J Health Gain Traveller Health 2001;5:9-10.
- Bartlett C. What’s new? Concepts of health – the case of traveller-gypsies. Sociology Review 1998;8:24-5.
- Greenfields M, Smith DM. Housed Gypsy Travellers, social segregation and the reconstruction of communities. Housing Stud 2013;25:397-412. http://dx.doi.org/10.1080/02673031003711022.
- Okely J, Houtman G. The Dale Farm eviction: interview with Judith Okely on Gypsies and Travellers. Anthropo Today 2011;27:24-7. http://dx.doi.org/10.1111/j.1467-8322.2011.00840.x.
- Okely J, Smith DM, Greenfields M. Gypsies and Travellers in Housing: The Decline of Nomadism. Bristol: Policy Press; 2013.
- Campbell F. Improving the Public’s Health: An Overview for Local Authority Leaders. London: The King’s Fund; 2013.
- Thomason C. Here to Stay: An Exploratory Study into the Needs and Preferences of Gypsy/Traveller Communities in Cheshire, Halton and Warrington. Cheshire Halton & Warrington Racial Equality Council; 2006.
- Atterbury J, Bruton L. DRE West Sussex Black and Ethnic Minorities CDW Service May 2008–April 2011: Final Report. Brighton: Friends, Families and Travellers; 2011.
- Vrinceanu S. Playing Russian Roulette With Roma Health 2007. www.soros.org/initiatives/health/focus/roma/articles_publications/articles/roulette_20070910 (accessed 13 September 2011).
- Van Cleemput P, Parry G, Thomas K, Peters J. Gypsies and Travellers in England – what are their perceived barriers to accessing health care?. Eur J Public Health 2004;14:12-3.
- Fraser A. The Gypsies. Oxford: Blackwell; 1992.
- Liegeois J, Gheorghe N. Roma/Gypsies: A European Minority. London: Minority Rights Group; 1995.
- Clark C, Campbell E. ‘Gypsy Invasion’: a critical analysis of newspaper reaction to Czech and Slovak Romani asylum-seekers in Britain, 1997. Romani Stud 2000;10:23-47. http://dx.doi.org/10.3828/rs.2000.2.
- Lewy G. Nazi Persecution of the Gypsies. Oxford: Oxford University Press; 2000.
- Davis Lutz B. Gypsies as victims of the Holocaust. Holocaust Genocide Stud 1995;9:346-59. http://dx.doi.org/10.1093/hgs/9.3.346.
- New York Times . Gypsies and the Holocaust. New York Times 2000.
- Catterall T. Gypsies Genocide was Hidden Holocaust. Chicago Tribune 1985.
- Crowe D. A History of the Gypsies of Eastern Europe and Russia. London: IB Taurius; 1995.
- Bancroft A. Closed spaces, restricted places: marginalisation of Roma in Europe. Space Polity 2001;5:145-57. http://dx.doi.org/10.1080/13562570120104454.
- Kabachnik P. Place invaders: constructing the nomadic threat in England. Geogr Rev 2010;100:90-108. http://dx.doi.org/10.1111/j.1931-0846.2010.00008.x.
- Hawes D, Perez B. The Gypsy and the State: The Ethnic Cleansing of British Society. Oxford: Alden Press; 1995.
- Hawes D, Perez B. The Gypsy and the State: the Ethnic Cleansing of British Society. Bristol: Policy Press; 1996.
- Cripps J. Accommodation for Gypsies: A Report on the Working of the Caravan Sites Act 1968. Cardiff: Department of Environment Welsh Office; 1977.
- Bancroft A. The Right to Roam: Scotland’s Travelling People. Edinburgh: Save the Children; 1996.
- Bancroft A. ‘No interest in land’: legal and spatial enclosure of gypsy-travellers in Britain. Space Polity 2000;4:41-56. http://dx.doi.org/10.1080/713697750.
- Berkman LF, Glass T, Berkman LF, Kawachi I. Social Epidemiology. Oxford: Oxford University Press; 2000.
- Smith D, Ruston A. ‘If you feel that nobody wants you you’ll withdraw into your own’: Gypsies/Travellers, networks and healthcare utilisation. Sociol Health Illn 2013;35:1196-210. http://dx.doi.org/10.1111/1467-9566.12029.
- Hurley RF. The Decision to Trust. Harvard Bus Rev 2006. http://altfeldinc.com/pdfs/Trust.pdf (accessed 14 June 2013).
- Mayer RC, Davis JH, Schoorman FD. An integrative model of organisational trust. Acad Manage Rev 1995;20:709-34.
- Walsh CA, Krieg B. Roma refugees: a profile of health and social service needs. J Immigrant Refugee Stud 2007;5:5-28. http://dx.doi.org/10.1300/J500v05n01_02.
- Cemlyn S. From neglect to partnership? Challenges for social services in promoting the welfare of Traveller children. Child Abuse Rev 2000;9:349-63. http://dx.doi.org/10.1002/1099-0852(200009/10)9:5<349::AID-CAR647>3.0.CO;2-1.
- Ambulance Not On The Way: The Disgrace of Health Care for Roma in Europe. Hungary: European Roma Rights Centre; 2006.
- Neufeld J, Rasmussen H, Lopez S, Ryder J, Magyar-Moe J. The engagement model of person–environment interaction. Counsel Psychol 2006;34:245-59. http://dx.doi.org/10.1177/0011000005281319.
- Local Government Improvement and Development . Health Needs of Gypsies and Travellers 2010. www.idea.gov.uk/idk/core/page.do?pageId=17917440 (accessed 8 October 2011).
- Leeds GATE. One Punch Kills: Leeds Gypsy and Traveller Exchange Domestic Violence Project Report. Leeds: Leeds GATE Gypsy and Traveller Exchange; 2007.
- Local Government Improvement and Development . Unabridged Version: One Voice for Travellers 2010.
- Winett RA, Anderson ES, Desiderato L, Solomon LJ, Perry M, Kelly JA, et al. Enhancing social diffusion theory as a basis for prevention intervention: a conceptual and strategic framework. Appl Prev Psychol 1995;4:233-45. http://dx.doi.org/10.1016/S0962-1849(05)80025-3.
- Merton R. Social Theory and Social Structure. New York, NY: Free Press; 1968.
- Sampson R, Morenoff J, Earls F. Beyond social capital: spatial dynamics of collective efficacy for children. Am Sociol Rev 1999;64:633-60. http://dx.doi.org/10.2307/2657367.
- Earls F. Toward a science of citizenship. Am J Orthopsychiat 2011;81:447-52. http://dx.doi.org/10.1111/j.1939-0025.2011.01120.x.
- Carlson M, Brennan R, Earls F. Enhancing adolescent self-efficacy and collective efficacy through public engagement around HIV/AIDS competence: a multilevel, cluster randomised-controlled trial. Soc Sci Med 2012;75:1078-87. http://dx.doi.org/10.1016/j.socscimed.2012.04.035.
- Hart R. Children’s Participation from Tokenism to Citizenship. Florence: UNICEF Innocenti Research Centre; 1992.
- Fredricks J, Blumenfeld P, Paris A. School engagement: potential of the concept, state of the evidence. Rev Educ Res 2004;74:59-109. http://dx.doi.org/10.3102/00346543074001059.
- Barraclough C. Nottingham Traveller Team. Community Pract 2002;75.
- Darby S. Malignant Neglect 2007. www.soros.org/initiatives/health/focus/roma/articles_publications/artic (accessed 12 September 2011).
- Chiriac M, Ganga D. Ferentari: Life in the Fast Lane 2007. www.soros.org/initiatives/health/focus/roma/articles_publications/articles/ferentari_20070926 (accessed 13 September 2011).
- Austerberry H, Sawtell M, Ingold A, Wiggins M, Arai L, Strange V. Evaluation of the Teenage Health Demonstration Site Programme: 1st Annual Report 2007. London: Social Science Research Unit, Institute of Education, University of London; 2008.
- Dignan M, Burhansstipanov L, Hariton J, Harjo L, Rattler T, Lee R, et al. A comparison of two Native American navigator formats: face-to-face and telephone. Cancer Control 2005;12:28-33.
- Davis R. Specialist team earns trust of travellers. Community Care 2010:20-1.
- Johnson Z, Howell F, Molloy B. Community mothers’ programme: randomised controlled trial of non-professional intervention in parenting. BMJ 1993;306:1449-52. http://dx.doi.org/10.1136/bmj.306.6890.1449.
- Dimitrijevic T. Improving Access to Health Care of Roma Community in Valjevo. Valjevo: Roma Centre for Democracy; 2009.
- Social Assessment of Roma and HIV/AIDS in Central East Europe. Bucharest: UNDP–Romania; 2004.
- Rowley K, Daniel M, Skinner K, Skinner M, White G, O’Dea K. Effectiveness of a community-directed ‘healthy lifestyle’ program in a remote Australian Aboriginal community. Aust NZ J Public Health 2000;24:136-44. http://dx.doi.org/10.1111/j.1467-842X.2000.tb00133.x.
- Fay R, Kavanagh D, Quirke B, Malone M. Primary Health Care for Travellers Project: Project Report for Year Ended October 1995. Dublin: Eastern Health Board; 1996.
- Kawachi I, Berkman LF, Berkman LF, Kawachi I. Social Epidemiology. Oxford: Oxford University Press; 2000.
- Dahl E, Malmberg-Heimonen I. Social inequality and health: the role of social capital. Sociol Health Illn 2010;32:1102-19. http://dx.doi.org/10.1111/j.1467-9566.2010.01270.x.
- Bradshaw J, Popay J, Williams G. Researching the People’s Health. London: Routledge; 1994.
- Petticrew M. Why certain systematic reviews reach uncertain conclusions. BMJ 2003;326:756-8. http://dx.doi.org/10.1136/bmj.326.7392.756.
- Jagosh J, Pluye P, Wong G, Cargo M, Salsberg J, Bush PL, et al. Critical reflections on realist review: insights from customizing the methodology to the needs of participatory research assessment. Res Synth Methods 2013;5:131-41. http://dx.doi.org/10.1002/jrsm.1099.
- Wong G, Greenhalgh T, Pawson R. Internet-based medical education: a realist review of what works, for whom and in what circumstances. BMC Med Educ 2010;10:1-10. http://dx.doi.org/10.1186/1472-6920-10-12.
- Macaulay A, Jagosh J, Seller R, Henderson J, Cargo M, Greenhalgh T, et al. Assessing the benefits of participatory research: a rationale for a realist review. Global Health Promo 2011;18:45-8. http://dx.doi.org/10.1177/1757975910383936.
- Kósa Z, Széles G, Kardos L, Kósa K, Németh R, Országh S, et al. A comparative health study of the inhabitants of Roma settlements in Hungary. Am J Public Health 2007;97:853-9. http://dx.doi.org/10.2105/AJPH.2005.072173.
- Gill G. The health needs of the Slovak Roma community in Sheffield. Community Pract 2009;82:34-7.
- Jenkins L. Preparation Study of Gypsy/Traveller Health Needs. Kent: Centre for Health Services Studies, University of Kent; 2010.
- Ambulance Not on the Way: The Disgrace of Health Care for Roma in Europe. Budapest: European Roma Rights Centre; 2006.
- Hall V, Sadouni M, Fuller A. Gypsies’ and Travellers’ Experience of Using Urgent Care Services within NHS Brighton and Hove Boundaries. Sussex: Friends, Families and Travellers; 2009.
- Kearney P, Kearney P. The prevalence of asthma in schoolboys of Travellers’ families. Ir Med J 1998;91:203-6.
- Dostal M, Topinka J, Sram RJ. Comparison of the health of Roma and non-Roma children living in the district of Teplice. Int J Public Health 2010;55:435-41. http://dx.doi.org/10.1007/s00038-010-0133-8.
- Schaaf M. Confronting a Hidden Disease: TB in Roma Communities. New York, NY: Open Society Institute; 2007.
- Slattery D, Brennan M, Canny C, Sweeney K, Ward M, O’Shea P, et al. Cardiovascular health in the Irish Traveller community. Br J Diabetes Vasc Dis 2010;10:305-7. http://dx.doi.org/10.1177/1474651410390150.
- Vozarova de Courten B . Higher prevalence of type 2 diabetes, metabolic syndrome and cardiovascular diseases in gypsies than in non-gypsies in Slovakia. Diabetes Res Clin Pract 2003;62:95-103. http://dx.doi.org/10.1016/S0168-8227(03)00162-1.
- Gerevich J, Bácskai E, Czobor P, Szabó J. Substance use in Roma and non-Roma adolescents. J Nerv Ment Dis 2010;198:432-6. http://dx.doi.org/10.1097/NMD.0b013e3181e07d51.
- Petek D, Rotar Pavlic D, Svab I, Lolić D. Attitudes of Roma toward smoking: qualitative study in Slovenia. Croat Med J 2006;47:344-7.
- Van Hout MC. Alcohol use and the Traveller community in the west of Ireland. Drug Alcohol Rev 2010;29:59-63. http://dx.doi.org/10.1111/j.1465-3362.2009.00085.x.
- Goward P, Repper J, Appleton L, Hagan T. Crossing boundaries. Identifying and meeting the mental health needs of Gypsies and Travellers. J Ment Health 2006;15:315-27. http://dx.doi.org/10.1080/09638230600700888.
- Treise C, Shepherd G. Developing mental health services for Gypsy Travellers: an exploratory study. Clinical Psychology Forum 2006;163:16-20.
- Edwards DM, Watt RG. Oral healthcare in the lives of Gypsy Travellers in east Hertfordshire. Br Dent J 1997;183:252-7. http://dx.doi.org/10.1038/sj.bdj.4809479.
- Kolarcik P, Geckova AM, Orosova O, van Dijk JP, Reijneveld SA. To what extent does socioeconomic status explain differences in health between Roma and non-Roma adolescents in Slovakia?. Soc Sci Med 2009;68:1279-84. http://dx.doi.org/10.1016/j.socscimed.2008.12.044.
- Molnár A, Adány R, Adám B, Gulis G, Kósa K. Health impact assessment and evaluation of a Roma housing project in Hungary. Health Place 2010;16:1240-7. http://dx.doi.org/10.1016/j.healthplace.2010.08.011.
- Reid B, Taylor J. A feminist exploration of Traveller women’s experiences of maternity care in the Republic of Ireland. Midwifery 2007;23:248-59. http://dx.doi.org/10.1016/j.midw.2006.03.011.
- Francis G. Developing the Cultural Competence of Health Professionals Working with Gypsy Travellers. London: Department of Health; 2010.
Appendix 1 Study protocol
Appendix 2 Articles used for pearl growing
Camara Medina C, Pérez García A, Quesada Lupiañez P, Sanchez CE. [Intervention with community health agents in immunisation programs in the gypsy population.] Aten Primaria 1994;13:415–18.
Davis R. Specialist team earns trust of Travellers. Community Care 2010;20–1.
Fitzpatrick P, Molloy B, Johnson Z. Community mothers’ programme: extension to the Travelling Community in Ireland. J Epidemiol Community Health 1997;51:299–303.
Martinez-Campillo Garcia F, Maura de Fonseca A, Santiago Oliva J, Verdú Pérez M, Serramia del Prisco A, Ibañez Molina M, et al. [Vaccine coverage study and intervention with health community agents in a marginal gypsy community of Alicante.] Aten Primaria 2003;31:234–8.
Greenfields M. Reaching Gypsies and Travellers. Prim Health Care 2009;19:26–7.
Lawrence H. On the road to better health. Emerg Nurs 2007;15:12–17.
Lynch E. Travellers’ tales. Nurs Stand 2006;20:20–1.
Moreton J. HIB Educating parents and professionals. Health Visit 1992;65:266–7.
Pickersgill F. Moving in the right direction. Nurs Stand 2010;24:72.
Szilagyi T. Peer education of tobacco issues in Hungarian communities of Roma and socially disadvantaged children. Cent Eur J Public Health 2002;10:117–20.
Appendix 3 Population, Interventions, Comparators, Outcomes and Study design framework
| Include | Exclude |
|---|---|
| Populations | |
| Gypsies Roma Gypsies Roma Scottish Travellers Welsh Travellers Irish Travellers New Travellers Bargees or Boat Travellers Showpeople Circus People No restrictions on inclusion according to country of research or practice |
Non-Gypsy and Traveller communities |
| Interventions | |
| Outreach (interventions which take place beyond usual limits of
the delivering organisation) aimed at Traveller
Communities Outreach intervention (e.g. housing related) that have an explicit health improvement aim One-to-one or group interventions, as long as it involves at least one person going to places where Traveller Communities live at least once |
Interventions without an explicit health improvement
focus Interventions that are not outreach Intervention that do not focus on Traveller Communities Publicity or health promotion campaigns, if delivered through posters or advertisement only |
| Comparators | |
| Comparable travelling community, without outreach programme and/or with standard care | Any other community |
| Outcomes | |
| Physiological measures of general health Other measures of general health Health behaviour Health-care beliefs and knowledge Health-care use/uptake of statutory services Effect on socialisation Effects on relatives/carers Adverse outcome, e.g. complaints Quality of life Networking/connecting with community Social capital development |
|
| Study designs | |
| RCT Non-RCTs Cohort studies Case control Interrupted time series Ethnographic Phenomenological In-depth qualitative evaluations Combined designs Intervention descriptions Evaluations Combined designs |
Other evidence/literature reviews |
Appendix 4 Unobtainable articles
Acton T, Mundy G. Romani Culture and Gypsy Identity. Hatfield: University of Hertfordshire Press; 1997.
Appleton L, Hagan T, Goward P, Repper J, Wilson R. Smail’s contribution to understanding the needs of the socially excluded: the case of Gypsy and Traveller women. Clin Psychol 2003;24:40–6.
Boyd C. Poverty and Health Care in the Context of Romanian Postcommunism. PhD thesis. Washington, DC: American University; 2008.
Bradley CM, Khan FA. The oral health of Irish travellers – a qualitative study. J Dent Res 1999;78:1050.
Bunce C. Travellers: Travellers’ nomadic lifestyle, coupled with the prejudice they face, makes access to health care difficult. Nurs Times 1996;92:34–7.
Graham F, Whelton H, et al. Study of the oral health of schoolchildren of the Irish Traveller community. J Dent Res 1998;77:707.
Hawes D. Gypsies, Travellers and the Health Service: a Study in Inequality. Bristol: Policy Press; 1997.
Manrique N. Corpo-real Identities: Perspectives from a Gypsy Community. In Edwards J, Salazar C, editors. European Kinship in the Age of Biotechnology. New York, NY: Berghahn Books; 2009.
Milanov K, Georgiev P, Todorova M. Eradication of poliomyelitis in Bulgaria--problem encountered. Cent Eur J Public Health 1994;2:23–6.
Ormandy D. No fixed abode: should local authorities have to provide sites for travellers? Environ Health J 1999;107:102–3.
Rodin U, Uhernik AI. Reducing health inequality of Roma minority in Croatia. Eur J Public Health 2005;15:65–6.
Rustom A. Family planning for travellers. Community Outlook 1990;15–8.
Wilson G. On the road ... travellers to use mainstream health services. Nurs Times 1988;84:26–7.
Appendix 5 Realist table of included studies
| Reference | Notes | Data extracted |
|---|---|---|
| Anonymous. Traveller women train to become health and wellbeing advocates. Prim Health Care 2010;20:5 | Brief statement of intent of training | Yes |
| Atterbury J, Bruton L. DRE West Sussex Black and Ethnic Minorities CDW Service May 2008–April 2011 Final Report. 2011. pp. 1–10 | Describes outreach efforts in minorities including Travellers | Yes |
| Austerberry H, Sawtell M, Ingold A, Wiggins M, Arai L, Strange V. Evaluation of the Teenage Health Demonstration Site Programme: 1st Annual Report 2007. London: Social Science Research Unit, Institute of Education, University of London; 2008 | Outreach to enhance young people’s health, included Travellers and some qualitative outcomes | Yes |
| Barraclough C. Nottingham Traveller team. Community Pract 2002;75:185 | Descriptive account from a Traveller specialist health visitor | Yes |
| Bunce C. A hard road to travel. Nurs Times 1996;92:34–6 | Descriptive account of Traveller life, access to services and outreach intervention | |
| Cemlyn S. Health and social work: working with Gypsies and Travellers. Practice 1993;6:246–61 | Experiential account of an outreach worker | |
| Cemlyn S. Human rights and Gypsies and Travellers: an exploration of the application of a human rights perspective to social work with a minority community in Britain. Br J Soc Work 2008;38:153–73 | Opinion piece on the need to understand the needs of Travellers through a human rights framework | Yes |
| Cemlyn S. From neglect to partnership? Challenges for social services in promoting the welfare of Traveller children. Child Abuse Rev 2000;9:349–63 | Exploratory two-stage study including descriptive quantitative data on social services for Travellers | Yes |
| Charikar L. Setting the pace on health equality: the Pacesetters Programme in Leicester. J Family Health Care 2008;18:212–15 | Descriptive account of Travellers becoming ‘health ambassadors’ for their community | |
| Chiriac M, Ganga D. Ferentari: Life in the Fast Lane. 2007. URL: www.soros.org/initiatives/health/focus/roma/articles_publications/articles/ferentari_20070926 (retrieved 13 September 2011) | Descriptive account of the health status of Roma communities in Romania and the tensions surrounding health-care provision | Yes |
| Crout E. Trailer bound. Community Outlook 1987;12–14 | Descriptive account of a specialist health visitor | |
| Darby S. Malignant Neglect. 2007. URL: www.soros.org/initiatives/health/focus/roma/articles_publications/articles/malignant_20071010 (retrieved 12 September 2011) | Description of a screening programme for Traveller women in Hungary | Yes |
| Davies M. Eradicating Child Poverty: the Role of Key Policy Areas. The Effects of Discrimination on Families in the Fight to End Child Poverty. York: Joseph Rowntree Foundation; 2008 | About vulnerable groups more generally but includes a breakdown of components which are likely to make outreach successful | Yes |
| Davis R. Specialist team earns trust of travellers. Community Care 2010;1822:20–1 | Details the process of developing trust (descriptive account) | Yes |
| Department of Health. Healthcare for Single Homeless People. London: Department of Health; 2010 | Not specifically about Travellers, but is part of the wider Department of Health Inclusion Health programme which also targets Traveller Communities. Details proposed models of service provision | Yes |
| Department of Health. Inclusion Health: Improving Primary Care for Socially Excluded People. London: Department of Health; 2010 | Details the potential role of outreach in relation to other services for disengaged groups | Yes |
| Department of Health Social Services and Public Safety. Oral Health Strategy: General Dental Services, Equality Impact Assessments – Preliminary Consultation Report. Department of Health Social Services and Public Safety; 2001 | Description of needs and needs assessments in dental health, including focus groups with Travellers | Yes |
| Dimitrijevic T. Improving access to health care of Roma Community in Valjevo. Chart 2009;1–62 | Includes descriptive findings about perceived and assessed needs in Roma communities | Yes |
| Dion X. Gypsies and Travellers: cultural influences on health. Community Pract 2008;81:31–4 | Interviews with Traveller women, focusing on needs and cultural attitudes/understanding of health | Yes |
| Doyal L, Cameron A, Cemlyn S, Nandy S, Shaw M. The Health of Travellers in the South West Region: a Review of Data Sources and a Strategy for Change. Bristol: Public Health Intelligence Team, South West Public Health Observatory; 2002 | Review of the extent and quality of the evidence on Traveller health | |
| European Roma Rights Centre. Ambulance Not On The Way: The Disgrace of Health Care for Romain Europe. Budapest: European Roma Rights Centre; 2006 | Statement of needs, detailing historical persecution and discrimination in access. Describes health mediators programmes and when they work best | Yes |
| Fay R, Kavanagh D, Quirke B, Malone M. Primary Health Care for Travellers Project: Project Report for Year Ended October 1995. Dublin: Eastern Health Board; 1996 | Part of the Pavee Point project. Describes outreach workers’ training, needs assessment and descriptive process evaluation | Yes |
| Feder G. Traveller gypsies and primary care. Br J Gen Pract 1989;39:425–9 | Statements of needs and access (linked to the thesis below) | |
| Feder GS. Traveller Gypsies and Primary Health Care in East London. PhD thesis. London: University of London; 1994 | Three-part study of Traveller primary health-care needs and provision of preventative services | |
| Fitzpatrick P, Molloy B, Johnson Z. Community mothers’ programme: extension to the travelling community in Ireland. J Epidemiol Community Health 1997;51:299–303 | Detailing a settled community mothers intervention applied to Traveller mothers. Includes outcomes measurement | Yes |
| Fountain J. An Overview of the Nature and Extent of Illicit Drug Use Amongst the Traveller Community: an Exploratory Study. Dublin: National Advisory Committee on Drugs; 2006 | Literature review and thematic analysis of interviews with 137 Travellers and 37 agency workers | |
| Francis G. Developing the Cultural Competence of Health Professionals Working with Gypsy Travellers. London: Department of Health; 2010 | Project focused on health professionals and their understanding of Travellers’ needs and culture | |
| Francis G. Traveller Voices. Chief Executive; 2010 | Booklet developed following the project above | |
| Fred M. Training cultural brokers: practicing theory in anthropology. Ethnos 1986;51:246–58 | Focuses on cross-cultural training workshops. Interesting in terms of discussion about role development | |
| Gammon J. Health services for travelling gypsies: a day in the life of Judith Moreton. Auditorium 1997;6:12–15 | Descriptive account of a specialist health visitor | |
| Ghose D. Rights for Young Travellers. Young People Now. London: The National Youth Agency; 2004 | Descriptive account of a Traveller outreach worker | |
| Greenfields M. Reaching Gypsies and Travellers. Prim Health Care 2009;19:26–7 | Description of an outreach project | Yes |
| Greenfields M, Home R. Assessing Gypsies and Travellers needs: partnership working and ‘the Cambridge Project’. Romani Stud 2006;16:105–31 | Needs assessment of the Traveller Community. Describes the partnership approach adopted | |
| Health Service Executive. An Oral Health Promotion Programme for Traveller Families in County Offaly. HSE Dublin Mid-Leinster, Co. Offaly; 2007 | Evaluates an intervention to improve dental health which included the use of Community health workers to educate people on oral health | Yes |
| Henriques J. Hard travelling. Community Pract 2001;74:330–2 | Focused on New Age Travellers. Descriptive account of a specialist worker | |
| Hodgins M, Millar M, Barry MM. ‘... It’s all the same no matter how much fruit or vegetables or fresh air we get’: Traveller women’s perceptions of illness causation and health inequalities. Soc Sci Med 2006;62:1978–90 | Focus groups with 41 Traveller women exploring cultural attitudes and beliefs in relation to health | |
| Hoover J. The Challenges and Rewards of One NGO’s Health Promotion Outreach among Roma Drug Users. Sofia; 2007 | Descriptive report of an outreach programme implementation | Yes |
| Horan T. Travellers doing it for themselves. Nurs Community 2006;7:8–10 | Descriptive account of a similar approach to Pavee Point | |
| Jackson C. On the road. Health Visitor 1990;63:204–6 | Experiential account from a specialist health visitor | |
| Jarosová D, Dusová B, Vrublová Y. The education of Romany health and social assistants in the Czech Republic. Int Nurs Rev 2009;56:264–8 | Questionnaire-based evaluation of the impact of Romani health assistants | |
| Jenkins L. Preparation Study of Gypsy/Traveller Health Needs. Kent: Centre for Health Services Studies, University of Kent; 2010 | Literature review and statement of needs | |
| Jones K. Midwives and Travellers. In Richens Y, editor. Challenges for Midwives, Volume 2. London: Quay Books; 2005. pp. 163–9 | Account of the challenges of providing midwifery services for Travellers | |
| Kellleher K, McGinley A, Healy C. Traveller Health Services: Regional Strategy Statement and Action Plan 2003–2005. Limerick: Mid-Western Health Board; 2005 | Details of a national strategy in Ireland. Includes some discussion of resources required for programmes | |
| Kelly H. Health Needs of Travellers and Gypsy Community in Northumberland. Northumberland; 2009 | Descriptive account. Includes interviews with specialist workers and Travellers | |
| Kelly JA, Amirkhanian YA, Kabakchieva E, Vassileva S, Vassilev B, McAuliffe TL, DiFranceisco WJ, et al. Prevention of HIV and sexually transmitted diseases in high risk social networks of young Roma (Gypsy) men in Bulgaria: randomised controlled trial. BMJ 2006;333:1098 | Two-arm randomised controlled trial of a behavioural intervention to prevent sexually transmitted diseases. Purposefully builds on network theories and includes an ethnographic phase to identify network leaders | Yes |
| Kennedy P. Travellers in Ireland, training and health issues: lessons for social policy. Reg Dev Dialogue 2001;22:79–89 | Linked to the Pavee Point articles on primary health care. Details the training and role of community health workers | Yes |
| Krumova T, Ilieva M. The Health Status of Romani Women in Bulgaria. Veliko Tarnovo: Center for Interethnic Dialogue and Tolerance ‘AMALIPE’; 2008. pp. 1–56 | Detailing of Roma women’s health status and needs in Bulgaria | |
| Lane P, Tribe R. Towards an understanding of the cultural health needs of older gypsies. Working Older People 2010;14:23–30 | Clear expose of how policies impact on people and their health. Highlights how/why people may be transient and the consequences of that for health and access to health-care services | |
| Lawrie B. Travelling families in east London – adapting health visiting methods to a minority group. Health Visitor 1983;56:26–8 | Experiential account of a specialist health visitor | |
| Leeds GATE Gypsy and Traveller Exchange. One Punch Kills: Leeds Gypsy and Traveller Exchange Domestic Violence Project Report. Leeds GATE Gypsy and Traveller Exchange; 2007 | Project led by Traveller women – needs identification and outreach approaches detailed | Yes |
| Local Government Improvement and Development. Unabridged Version: One Voice for Travellers. 2010. URL: www.idea.gov.uk/idk/core/page.do?pageId=30211424 (retrieved 18 October 2011) | Short descriptive report of 12 Traveller women selected to become health advocates | Yes |
| Local Government Improvement and Development. Health Needs of Gypsies and Travellers. 2010. URL: www.idea.gov.uk/idk/core/page.do?pageId=17917440 (retrieved 18 October 2011) | Experiential account of setting up an outreach programme, gaining trust and engaging Travellers | Yes |
| Local Government Improvement and Development. Two Communities Come Together to ImproveGypsy and Traveller Health. 2011. URL: www.idea.gov.uk/idk/core/page.do?pageId=25454507 (retrieved 18 October 2011) | Short descriptive account | |
| Magyari-Vincze E. Roma Women’s Reproductive Health as a Human Rights Issue in Romania Roma. Budapest: Central European University Center for Policy Studies; 2006 | Includes a rationale for selecting women as Roma mediators | |
| Malan M, Schreedhar J. Time Bomb for Roma. 2007. URL: www.tol.cz/look/TOL/article.tpl?IdLanguage=1&IdPublication=4&NrIssue=220&NrSection=3&Nr Article=18752 (retrieved 13 September 2011) | Descriptive account of preventative health needs | |
| Mason P, Plumridge G, Barnes M, Beirens H, Broughton K. Preventative Services for Gypsy/Traveller Children. Education. Birmingham; 2006 | Describes engagement strategies and ‘entry points’ into the Community | |
| Mason P, Broughton K. Gypsy/Traveller children and families: the potential of working with networks. Soc Policy Society 2007;6:243–53 | Includes a focus on working with Traveller networks in order to work with the Community | |
| Matthews Z, Velleman R. “New age” Travellers, urban slum dwellers, Aborigines and drug users: experiences of collecting sensitive data from marginalised communities. Bull Méthodologie Sociologique 1997;57:65–85 | Highlights engagement strategies with ‘hard-to-reach’ communities | |
| Matthews Z. The Health of Gypsies and Travellers in the UK: A Race Equality Foundation Briefing Paper. London: Race Equality Foundation; 2008. pp. 1–11 | Statements of needs and examples of outreach practice | |
| Matthews Z, Edwards T, Sillman S, Benwel S. A Collaborative Programme to Improve the Oral Health of the Gypsy and Travelling Communities in Sussex. Sussex: Friends, Families and Travellers; 2010 | Descriptive and experiential accounts of health needs and health-care provision | |
| McCabe C, Keyes F. A Review of Travellers’ Health using Primary Care as a Model of Good Practice: Pavee Point Primary Health Care for Travellers’ Project. Dublin: Pavee Point; 2005 | Part of the Pavee Point project in Ireland | Yes |
| McCann V. Health education for a Traveller Community. Health Visitor 1987;60:293–5 | Example of breakdown in trust | |
| McCarthy D. Drugs and Diversity: Exploring Drug Issues amongst New Communities and the Traveller Community: Seminar report. Ethnicity. Dublin; 2006 | Gives information about what works in outreach or why take an outreach approach with Traveller Communities to promote drugs awareness | |
| Moore R, Turner J, Nic Charthaigh R, Quirke B, Hamid NA, Drummond A, Kilroe J, et al. All Ireland Traveller Health Study Technical Report 3. Dublin: University College Dublin; 2010 | Qualitative approaches (case studies, focus groups and interviews). Highlights perceptions of health and need | |
| Moreton J. Immunization of travellers in Oxfordshire. Nursing 1987;3:723–6 | Describes problems in implementing an immunisation programme among Traveller families and describes outreach approach | |
| Moreton J. HIB 2 Educating parents and professionals. Health Visitor 1992;65:266–7 | Describes on-site provision of education and immunisation | |
| Murphy P. Primary Health Care for Travellers Project: Implementation Report 1996–1999. Dublin: Pavee Point; 1999 | Part of the Pavee Point study. Gives details about the implementation of the primary care for Travellers project which involved some outreach and some of the lessons learned | Yes |
| NHS Primary Care Contracting. Primary Care Service Framework: Gypsy & Traveller Communities. London: NHS Primary Care Contracting; 2009 | Focus on recommendations to facilitate access to services and puts outreach strategies forward as a solution | |
| Open Society Institute. Mediating Romani Health: Policy and Program Opportunities. New York, NY: Open Society Institute; 2005 | Describes outreach strategies through Roma Health mediators | |
| Open Society Institute. How the Global Fund Can Improve Roma Health: An Assessment of HIV and TB Programs in Bulgaria, Macedonia, Romania, and Serbia. New York, NY: Open Society Institute; 2007 | Emphasis on the necessity for the outreach workers to be from the Community | |
| O’Neill R. Health inequalities: travelling communities. Health Service Journal, 6 October 2008 | Account from a Traveller providing advice on working with the Community | |
| Pahl J, Vaile M. Health and health care among travellers. J Soc Policy 1988;17:195–213 | Descriptive health status and statement of needs | |
| Papadopoulos I. The health promotion needs and preferences of Gypsy Travellers in Wales. Diversity Health Soc Care 2007;4:167–77 | Focus groups with Travellers to find out attitudes towards, and health promotion needs | |
| Parry G, Cleemput PV, Peters J, Moore J, Walters S, Thomas K, Cooper C. The Health Status of Gypsies & Travellers in England. Sheffield: University of Sheffield; 2004 | Interview and survey of Travellers to establish health status and needs | |
| Patterson J. On the road: reflections on Travellers and their children. Nurs Times 1982;78:1617–20 | Descriptive account of mobile education and health services | |
| Peck B. Gypsies – a Sheffield experience. Health Visitor 1983;56:365 | Anecdotal account from a specialist health visitor | |
| Queally M. Health promotion needs of the Travelling Community. J Health Gain 2001;5:1–32 | Talks about the involvement of Travellers in defining health needs and gives examples of health initiatives | Yes |
| Quirke B. Primary health care for Travellers project. J Health Gain 2001;5:12–14 | Part of a special issue on Traveller health. The primary health care for Travellers was organised by the Pavee Point organisation | Yes |
| Raper M. Travelling families in Northumberland. Health Visitor 1986;59:345–7 | Anecdotal account of health visiting | |
| Reid B. Cross-border Traveller health initiative. World Irish Nurs Midwifery 2006;14:45–6 | Description of a cross-border network of health visitors and public health nurses in NI and the ROI | |
| Reid B. Networking for traveller health. Community Pract? 2005;78:312–13 | Same initiative as above | |
| Reid B, Taylor J. A feminist exploration of Traveller women’s experiences of maternity care in the Republic of Ireland. Midwifery 2007;23:248–59 | Interviews with 13 Traveller women to explore their experiences of maternity care | |
| Reid T. Partners in care. Nurs Times 1993;89:28–30 | Descriptive account of a health visitor’s work, coupled with a clinic | Yes |
| Rose V. On the road: Val Rose, a health visitor in a rural area, describes how she meets travellers’ health needs by providing a tailor-made mobile service. Nurs Times 1993;89:31 | Anecdotal account from a health visitor using a mobile clinic | |
| Ryder A, Greenfields M. Roads to Success: Economic and Social Inclusion for Gypsies and Travellers. London: Irish Traveller Movement in Britain; 2008 | Participatory research including interviews focusing on inequalities and employment issues. Includes experiences of Travellers working as community development workers | |
| Streetly A. Health care for travellers: one year’s experience. BMJ 1987;294:492–4 | Description of health visitor programme set up and monitored by a health authority. Describes early stages of developing trust | Yes |
| Tavares M. ‘Gypsies and Travellers in Leeds – Making a Difference’: An Exploratory Study on the Health Needs of Gypsies and Travellers. Leeds: Travellers Health Partnership; 2001 | Summary on the ingredients for successful specialist health visitor services and also a suggestion that on-site primary health care is most likely to be effective. Identifies health needs and gaps in provision | Yes |
| The Highland Council, NHS Highland. The Highland Gypsy/Traveller Health & Wellbeing Initiative. Int J Toxicol 2005;30(3 Suppl.):1–72 | Description of a heath provision initiative responsive to expressed needs | |
| Thomason C. Here to Stay: An Exploratory Study into the Needs and Preferences of Gypsy/Traveller Communities in Cheshire, Halton and Warrington – July 2006. Cheshire, Halton & Warrington Racial Equality Council; 2006 | Participatory research approach to assess needs | Yes |
| Thorn H for NHS Mid-Essex. Gypsy & Travellers’ Health Needs Assessment: Improving the Health of Gypsies and Travellers in the Mid Essex Area. NHS Mid-Essex; 2009 | Health needs assessment – includes lay health workers as an example of good practice, mapping of provision and access issues | Yes |
| Traveller health initiatives – health board regions. J Health Gain 2001;5:17–22 | ||
| Treise C, Shepherd G. Developing mental health services for Gypsy Travellers: an exploratory study. Clin Psychol Forum 2006;163:16–19 | Small scale qualitative study on mental health issues | |
| Valente T. Opinion leader interventions in social networks can change HIV risk behaviour in high risk communities. BMJ 2006;333:1082–3 | Linked to Kelly study | Yes |
| Van Cleemput P. Health care needs of travellers. Arch Dis Child 2000;82:32–7 | Review of health-care needs | Yes |
| Van Cleemput P, Thomas K, Parry G, Moore J, Cooper C. The Health Status of Gypsies and Travellers in England: Report of Qualitative Findings. Sheffield: University of Sheffield; 2004 | Thorough review of Traveller Community cultural and health beliefs and attitudes, access issues, environmental issues | Yes |
| Van Hout MC. Traveller health and primary care in Ireland: a consultative forum. Community Pract 2010;83:27–30 | Focus group leading to statement of needs and recommendations for health-care provision | Yes |
| Van Hout MC, Connor S. The normalisation of substance abuse among young Travellers in Ireland: implications for practice. J Ethn Subst Abuse 2008;7:5–22 | Qualitative comparison of Traveller vs. settled youth attitudes and knowledge of drug-related issues and services | |
| Vivian C, Dundes L. The crossroads of culture and health among the Roma (Gypsies). J Nurs Scholarship 2004;36:86–91 | Cultural understanding of beliefs and behaviours related to health and health-care provision | |
| Voicu M, Tufis CD. Roma life stories. Cult Med Psychiat 2008;19 | Highlights the way relationships within Roma may change with education | |
| Vrinceanu S. Playing Russian Roulette with Roma Health. 2007. URL: www.soros.org/initiatives/health/focus/roma/articles_publications/articles/roulette_20070910 (retrieved 13 September 2011) | Journalistic report on health needs, health-care provision and discrimination in Romania | Yes |
| Walsh CA, Krieg B. Roma refugees: a profile of health and social service needs. J Immigr Refugee Stud 2007;5:5–27 | Concerns Roma refugees in Canada – health needs and health-care provision | Yes |
| Weber L. Cambridgeshire Travellers Review Research Report Number 4: Location Studies. Cambridgeshire: Cambridgeshire County Council; 1998 | Reflects on the process of consultation about needs to inform outreach service provision | Yes |
| Windess B. One year working with the Travellers. Health Visitor 1987;60:289–91 | Anecdotal account of a health visitor work. Describes process of gaining trust | |
| Wood S. East Cambridgeshire and Fenland Traveller Health Needs Assessment. Cambridgeshire; 2006. pp. 1–11 | Health needs assessment – expressed needs | Yes |
Appendix 6 Final data extraction sheet
Adapted from McCormack et al. 99
Appendix 7 Extract from realist decision trail file
Appendix 8 Mapping of stakeholder activity
| Project phase | Issue/need for consultation | Consultation activity | Rationale for which stakeholders were involved | Key outcomes |
|---|---|---|---|---|
| Problem definition | Raising awareness of the project and its aims and generating interest among Traveller Community members and workers in becoming involved in the project | Initial blog post introducing the project and regular updates throughout the project, inviting participation in defining search terms, finding relevant information and involvement expert hearing events to be held later in the project | A blog post was the chosen method of communication as it is able to reach a wide target audience | A range of contacts were made ranging from Cumbria through to
Brighton and include representation from Traveller Community
members, voluntary and public sector working at a local,
regional and national level A number of unpublished reports were shared of needs assessments and implementation of health work with Traveller Communities |
| Initial orientation regarding how outreach works in practice, in the context of wider influences on the health and well-being in the everyday lives of Gypsies and Travellers | Opening meeting with a Gypsy and Traveller liaison officer to discuss general socioeconomic cultural and environmental conditions and approach and communicate with the Community | Gypsy and Traveller liaison officers work in an outreach role often as a first point of contact with Traveller Communities who move into an area and will make an initial assessment of needs before referring Travellers to available services (education, health) | Enhanced insight around the strategies for communication with Gypsies and Travellers (being open and honest; consultation with Traveller Community to identify needs); differential positioning of practitioners in terms of legitimate knowledge about and attitudes towards Traveller Communities and negotiating access; structural influences on health arising from different forms of accommodation | |
| Development of theories | Further development of initial programme theories about how outreach is expected to work for Traveller Communities which can then be tested through the evidence synthesis | Discussion with steering group members around the four initial theories (‘to whom’, ‘by whom’, ‘how’, ‘what for’) and blog post asking for suggestions about those factors that are important for successful outreach in each of these domains | Drawing on expertise and experience of steering group | ‘By whom’: importance of investing in Traveller
Communities to deliver outreach to their own communities;
personal connection to the family is more important than
belonging to the same Traveller Community subgroup in gaining
trust; some issues are best disclosed to those outside the
Community ‘To whom’: outreach needs to address wider needs than those strictly related to health; importance of Traveller Communities identifying their own needs; different needs are experienced by those living in different forms of accommodation ‘How’: need for time to build trust and establish familiarity with Traveller Community members; need for reliability in meeting expectations; need to build capacity within the Community; need for interventions to be delivered in a culturally sensitive way (e.g. use of appropriate language) ‘What for: need to consider outcomes at the general socioeconomic, cultural environmental level; key outcome of outreach is to provide links and facilitate access to mainstream services |
| Refinement of theories | Engagement and trust emerged as key to successful outreach interventions. However, the literature tended to report only on the pragmatics of outreach (i.e. what they did) and little material was available from which to infer the mechanisms underpinning decisions about whether or not to trust in or engage with outreach interventions | Steering group exercise and discussion to elicit and prioritise the mechanisms associated with programme strategies that were likely to have fired in a given context | The experiences of two key stakeholders working with Traveller Communities were drawn upon for examples of Traveller Community responses to the implementation of similar programme strategies to those reported in the reviewed studies | Validation of the importance of co-setting the agenda in order
to ensure that Travellers feel that their voices are
included Domains of trust that were perceived as most important for Traveller Communities were similarities; communication; ability; and integrity and predictability |
| Obtaining the perspectives of Traveller Community members on decision making processes surrounding engagement with interventions and trust in outreach workers | Focus group with five Romani Gypsy women to discuss factors that would improve the lives of Traveller Communities; what leads to Traveller Community members having trust in health professionals; and visualise the best possible health services for Traveller Communities | Seeking the voices of Gypsies and Travellers enabled us to better understand the reasoning of Traveller Communities themselves as they make initial decisions about whether or not to engage with outreach programmes | Travellers highlighted the importance of permanent living and working conditions, suggesting the need for the general socioeconomic, cultural and environmental conditions to be addressed. Key attributes of the outreach worker which are likely to engender trust were good communication skills, cultural awareness, confidentiality and continuity. An ideal health service for Travellers would be culturally sensitive and use appropriate means of communication (leaflets, recall system before appointments). An ideal service would reach out to Traveller sites, but would not necessarily need to be Traveller specific | |
| Substantiation of theories | Further detailing of the resources outreach programmes have at their disposal in order to create engagement opportunities (e.g. provision of training, facilitating access to health services) which were often only discussed minimally in the literature | In-depth interview with member of Traveller Community organisation to discuss examples of the implementation of engagement strategies and why they were thought to be successful/unsuccessful | This stakeholder was consulted due to her experience of community development work with Traveller Communities within a community and voluntary sector organisation. This organisation has often facilitated a wide range of activities beyond those associated with health therefore bringing to bear experience with a range of different engagement opportunities | There is no ‘one size fits all’ model of engagement. Engagement options will depend on people’s initial propensity to trust (built through previous experiences) and need to be matched with people’s readiness for engagement and with coinciding events in people’s everyday lives. There is a need for flexibility and negotiation in the engagement opportunities provided and for an opportunistic approach to raising issues and offering engagement activities |
| Verification and testing of the model describing how the opportunities offered by outreach interventions might interact with the initial trust status of outreach workers and the reasoning of participants to produce particular pathways through outreach interventions | Interview with mainstream health service provider to discuss how the different pathways developed map onto experiences of implementing outreach interventions and the weighting of different contextual factors (e.g. trust status of outreach worker and negotiation of topic) in influencing the outcomes of outreach | This stakeholder was consulted for her experience of working at a strategic level within a department of public health in order to generate examples pathways through outreach interventions with Traveller Communities | Examples of pathways included: A community member who conducted a needs assessment (outreach worker known and trusted) where immunisation was highlighted as a concern (topic negotiated and relevant) and, as a result, a pathway was implemented to immunise Travellers on site without requiring registration with a GP (facilitating access) An outbreak of measles on a campsite created concern among Traveller Community members who were nevertheless still worried about the potential side effects of the vaccine (topic negotiated but potentially relevant). A Traveller family support worker provided an entry point into the community, however the immunisation co-ordinator was not known to the community outreach worker neutral trust). The outreach worker adopted a straightforward communication style which treated Travellers respectfully, provided time for families to discuss the decision and delivered the intervention in a culturally appropriate way |
|
| Understanding which forms of service provision would best address the needs of Travellers with respect to different health issues; how transience facilitates or hinders access to services; and what needs Traveller Communities may have that are distinct from those of other marginalised groups | Guided discussion around scenarios relating to health needs and services with fiveTraveller Community members (four female and one male) at Appleby Fair (a traditional horse fair held in Appleby, Cumbria, which is a major annual holiday event and gathering point for members of Traveller Communities) | Accepting that only brief interviews may be achieved, this offered an alternative recruitment strategy to the identification of Travellers through services and enabled access to the views of Traveller Community members who travel for calendar events | Traveller Communities described a lack of knowledge of the available services and how to access them. A reactive rather than preventative approach to health-care seeking was described and A&E was used for both urgent and non-urgent health issues. Family was cited as an important source of advice about health. Examples were cited of discrimination experienced and the importance of trust in health professionals was stressed | |
| Guided discussion around scenarios relating to health needs and services with nineCzech Roma women in Newcastle. The majority of the women who participated did not speak English | Roma are a distinct group of Traveller Communities who are likely to experience particular barriers to accessing services such as those relating to language | The Roma women appeared to have relatively good access to GP services; however, access to dental services was generally reported to be low and sometimes only in relation to problems experienced. Roma women considered that it was important for immunisation to be conducted by a doctor. The importance of trust in GPs and the ‘friendliness’ of staff was important to their acceptance | ||
| Discussion and verification of the different engagement pathways depending on the context and programme resources with Traveller Community members | Focus group with 12Traveller Community members (11 women and one man of mixed ages and accommodation arrangements) in Cumbria to discuss short vignettes exemplifying different models of outreach provision | Understanding the reasoning of Traveller Communities throughout the process of engagement with outreach programmes | Traveller Community members agreed that the categorisation of Travellers developed were appropriate. Achieving continuity of care was felt to be particularly difficult for Roadsiders. Outreach targeted at sites may not reach male Traveller Community members who are often off site working. Those who live in housing were felt to be difficult for outreach initiatives to locate and access as a result of reluctance to self-identify | |
| Understanding how transience relates to service provision, possible ways of developing groupings according to circumstances of transience and accommodation in order to understand the different forms outreach may need to take with the different groupings | Interview with member of Traveller Community organisation | Following the views of Travellers collected at Appleby on which services they access for particular health issues while maintaining a transient lifestyle. This stakeholder’s experience of providing outreach for Traveller Communities, as well as involvement in the National Inclusion Health programme for vulnerable groups more generally was drawn upon in order to disentangle in what ways outreach for Travellers may need to differ than that provided to other marginalised groups | The transience of Traveller Communities is a key distinguishing characteristic that may facilitate or hinder the development of trust with outreach workers and the maintenance of Traveller Community culture and social networks in the face of assimilation. Word of mouth is a key mechanism mediating the development of trust with individuals and with the wider community. However, the approach to outreach with Traveller Communities in terms of building trust, and working informally and opportunistically in order to remain responsive to the different needs of community members are likely to be similarly appropriate to other disadvantaged and marginalised groups |
Appendix 9 Discussion guide for feedback with Traveller Community members (EH7)
-
If you could dream up the best possible health service for Travellers – what would it be like?
-
Notes to facilitator: The commissioning brief specified for us to look at outreach, but we are finding that some of the mechanisms that make outreach ‘work’ could well apply to other kinds of services. Examples of these are finding ‘indexes’ in the community that people know and trust; negotiating the purpose and format of a service; improving Travellers’ confidence in their own ability to do things, etc. The first question is therefore trying to ascertain what Travellers would mostly look for in an ‘ideal’, Traveller friendly, health service.
-
-
What are the key things that a health professional needs to say or do to gain Travellers’ trust?
-
Notes to facilitator: This question follows on from our previous communication about trust – our review so far highlights how trust in the person delivering the service is important in leading to successful outcomes. We think this might build on social diffusion theory – when key people in the community change their behaviour and talk about it, change begins to happen in the community. We are thus seeking to understand better what kinds of things/characteristics/behaviour/language lead to this key trusting relationship.
-
-
Name three things that would improve the lives of Travellers and what could be done to make them happen.
Notes to facilitator
In reviewing the literature, we are becoming aware that interventions targeting the wider determinants of health may be at least as relevant as interventions targeting individual health behaviour change. The kind of key (broad but relevant to health) outcomes we have found are engagement (i.e. community members become receptive to an intervention, for example a training course – this then leads them to be more likely to engage in other interventions); social diffusion (as before); capacity building (we have articles describing Travellers going to training courses and then taking on a leading role for health and quality of life improvement in their community). This question therefore aims to generate discussion about the things that impact on Travellers’ life more broadly, and how these things could be improved (we could then see if engagement, social diffusion and capacity building could help tackling these).
Appendix 10 Table of studies included in the economic evaluation
| Reference | Classification | Source |
|---|---|---|
| American Diabetes Association. Economic costs of diabetes in the US in 2007. Diabetes Care 2008;31:596–615 | Costing study | Peer-reviewed journal |
| Aspinall P. A Review of the Literature on the Health Beliefs, Health Status, and Use of Services in the Gypsy Traveller Population, and of Appropriate Health Care Interventions. Cardiff: Welsh Assembly Government; 2006 | Narrative review | Commissioned study |
| Babigumira JB, Sethy AK, Smyth KA, Singer ME. Cost effectiveness of facility-based care, home-based care and mobile clinics for provision of antiretroviral therapy in Uganda. Pharmacoeconomics 2009;27:963–73 | Cost-effectiveness analysis | Peer-reviewed journal |
| Bailie R. An economic appraisal of a mobile cervical cytology screening service. S Afr Med J 1996;86:1179–84 | Cost-minimisation analysis | Peer reviewed journal |
| Buchan J, Dalpoz M. Skill mix in the health care workforce: reviewing the evidence. Bull World Health Organ 2002;80:575–80 | Narrative review | Peer-reviewed journal |
| Cámara Medina C., Pérez García A, Quesada Lupiañez P, Sánchez Cantalejo E. [Intervention with community health agents in immunization programs in the gypsy population.] Aten Primaria 1994;13:415 | Observational study | Peer-reviewed journal |
| Carr S, Lhussier M, Foster N, Geddes L, Dean K, Pennington M, et al. An evidence synthesis of qualitative and quantitative research on component intervention techniques, effectiveness, cost effectiveness, equity and acceptability of different versions of health-related lifestyle adviser role in improving health. Health Technol Assess 2011;15(9) | Systematic review | Peer-reviewed journal |
| Cemlyn S, Greenfields M, Burnett S, Matthews Z, Whitwell C. Inequalities Experienced by Gypsyand Traveller Communities: A Review. Equality and Human Rights Commission; 2009 | Narrative review | Commissioned study |
| Department of Health. Inclusion Health: Improving Primary Care for Socially Excluded People. London: Department of Health; 2010 | Commissioning guidance | Report |
| Edmunds W, Brisson M, Melegaro A, Gay N. The potential cost-effectiveness of acellular pertussis booster vaccination in England and Wales. Vaccine 2002;20:1316–30 | Cost-effectiveness analysis | Peer-reviewed journal |
| El Pais. Health Access for Roma Improves with Award-Winning Programme. Budapest: European Roma Rights Centre; 2006. URL: www.errc.org/cikk.php?cikk=2505 (accessed 7 October 2011) | Project evaluation | Newspaper article |
| Fedder DO, Chang RJ, Curry S, Nichols G. The effectiveness of a community health worker outreach program on healthcare utilization of west Baltimore City Medicaid patients with diabetes with or without hypertension. Ethn Disease 2003;13:22–7 | Uncontrolled before-and-after study | Peer-reviewed journal |
| Feder GG. Traveller gypsies and primary care. J R Coll Gen Pract 1989;39:425–9 | Questionnaire survey | Peer-reviewed journal |
| Fay R, Kavanagh D, Quirke B, Malone M. Primary Health Care for Travellers Project: Project Report for YearEnded October 1995. Dublin: Pavee Point; 1996 | Project evaluation | Report |
| Fitzpatrick P, Molloy B, Johnson Z. Community mothers’ programme: extension to the travelling community in Ireland. J Epidemiol Community Health 1997;51:299–303 | Observational study | Peer-reviewed journal |
| Fox-Rushby JA, Foord F. Costs, effects and cost-effectiveness analysis of a mobile maternal health care service in West Kiang, The Gambia. Health Policy 1996;35:123–43 | Cost-effectiveness analysis | Peer-reviewed journal |
| Friends, Families and Travellers support group. Report of the Pilot Health Promotion Project with Travellersin Dorset 1997–1998. Brighton; 1998 | Project evaluation | Report |
| Garcia FMC, Da Fonseca AM, Oliva JS, Perez MV, Del Prisco AS, Molina MI, et al. Vaccine coverage study and intervention with health community agents in a marginal gypsy community of Alicante. Aten Primaria 2003;31:234–8 | Observational study | Peer-reviewed journal |
| Gilhooly ML, McGhee SM. Medical records: practicalities and principles of patient possession. J Med Ethics 1991;17:138–43 | Narrative review | Peer-reviewed journal |
| Health Service Executive. An Oral Health Promotion Programme for Traveller Families in County Offaly February 2007. Dublin: Health Service Executive; 2007 | Project evaluation | Report |
| Holden J. The Highland Gypsy/traveller Health & Wellbeing Initiative. Final Report. NHS England; 2005 | Project evaluation | Report |
| Hoover J. Persistence Pays: The Challenges and Rewards of One NGO’s Health Promotion Outreach amongRoma Drug Users. Sofia: Initiative for Health Foundation; 2007 | Project evaluation | Report |
| Kelly JA, Amirkhanian YA, Kabakchieva EE, Vassileva SS, Vassilev BB, McAuliffe TL, et al. Prevention of HIV and sexually transmitted diseases in high risk social networks of young Roma (Gypsy) men in Bulgaria: randomised controlled trial. BMJ 2006;333:1098 | RCT | Peer-reviewed journal |
| Lawrie B. Travelling families in east London – adapting health visiting methods to a minority group ... Gypsies. Health Visitor 1983;56:26–8 | Personal account of health visitor | Peer-reviewed journal |
| Lewin S, Judy D, Pond P, Zwarenstein M, Aja G, Van Wyk BE, et al. Lay health workers in primary and community health care. Cochrane Database Syst Rev 2005;1:CD004015 | Systematic review | Peer-reviewed journal |
| Mirambeau AM, Wang G, Ruggles L, Dunet DO. A cost analysis of a community health worker program in rural Vermont. J Community Health 2013;38:1050–7 | Costing study | Peer-reviewed journal |
| Moreton JJ. Immunization of travellers in Oxfordshire. Nursing 1987;3:723–6 | Personal account of health visitor | Peer-reviewed journal |
| Murphy P. Primary Health Care for Travellers Project: Implementation Report 1996–1999. Dublin: Pavee Point; 1999 | Project evaluation | Report |
| NHS Primary Care Contracting. Primary Care Service Framework: Gypsies and Travellers. London: NHS Primary Care Contracting; 2009 | Service framework | Report |
| One Voice for Travellers. One Voice for Travellers. 2011. URL: www.idea.org.uk/idk/core/page.do?pageld=30211424 (accessed 18 October 2011) | Project evaluation | Report |
| Open Society Institute. Mediating Romani Health: Policy and Program Opportunities. New York, NY: Open Society Institute Network Public Health Program; 2005 | Project evaluation | Report |
| Oriol NE, Cote PJ, Vavasis AP, Bennet J, Delorenzo D, Blanc P, et al. Calculating the return on investment of mobile healthcare. BMC Med 2009;7:27 | Cost–benefit analysis | Peer-reviewed journal |
| Peters J, Parry G, Cleemput P, Moore J, Cooper C, Walters S. Health and use of health services: a comparison between Gypsies and Travellers and other ethnic groups. Ethn Health 2009;14:359–77 | Questionnaire survey | Peer-reviewed journal |
| Shepherd S. Gypsies’ and Travellers’ health: the road to greater inclusion. Health Service Journal, 17 August 2010 | Brief project description | Professional journal |
| Streetly A. Health care for travellers: one year’s experience. Br Med J 1987;294:492–4 | Personal account of health visitor | Peer-reviewed journal |
| Subata E, Tsukanov J. The work of general practitioners among Lithuanian Roma in Vilnius: incorporating harm reduction into primary medical practice. J Drug Issues 1999;29:805–10 | Case study | Peer-reviewed journal |
| Swider SM. Outcome effectiveness of community health workers: an integrative literature review. Public Health Nurs 2002;19:11–20 | Systematic review | Peer-reviewed journal |
| Szilagyi T. Peer education of tobacco issues in Hungarian communities of Roma and socially disadvantaged children. Cent Eur J Public Health 2002;10:117–20 | Observational study | Peer-reviewed journal |
| Taylor JJ. Travellers. Health behaviour and beliefs. Health Visitor 1991;64:223–4 | Brief review | Peer-reviewed journal |
| TheBigGive.org.uk. Disability Essex Healthy Chance Outreach Programme. 2013. URL: https://secure.thebiggive.org.uk/projects/view/7540/disability-essex-healthy-chance-outreach-programme (accessed 17 August 2013) | Brief project description | Website |
| Thorn H. A Gypsy and Travellers’ Health Needs Assessment: Improving the Health of Gypsies and Travellers in the Mid Essex Area. Essex: NHS Mid Essex; 2009 | Health needs assessment | Report |
| Walker G, Gish O. Mobile health services: a study in cost-effectiveness. Med Care 1977;15:267–76 | Cost-effectiveness analysis | Peer-reviewed journal |
| Wells KJ, Luque JS, Miladinovic B, Vargas N, Asvat Y, Roetzheim RG, et al. Do community health worker interventions improve rates of screening mammography in the United States? A systematic review. Cancer Epidem Biomar 2011;20:1580–98 | Systematic review | Peer-reviewed journal |
| Welsh Government. Coronary Heart Disease and Travellers: Redressing the Balance. 2012. URL: http://wales.gov.uk/topics/health/improvement/communities/fund/inequalitiesnorth1/balanceproject/?lang=en (accessed 17 August 2013) | Brief project description | Website |
| Williams JG, Cheung WY, Chetwynd N, Cohen DR, El-Sharkawi S, Finlay I, et al. Pragmatic randomised trial to evaluate the use of patient held records for the continuing care of patients with cancer. Qual Health Care 2001;10:159–65 | RCT | Peer-reviewed journal |
| Wood S. East Cambridgeshire and Fenland Traveller Health Needs Assessment. Cambridge; 2006 | Health needs assessment | Report |
Appendix 11 Studies included in the scoping review
Abdalla S, Cronin F, Drummond A, Fitzpatrick P, Frazier K, Hamid NA, et al. All Ireland Traveller Health Study Technical Report 1: Health Survey Findings – Physiotherapy. Dublin; 2010.
Acton T, Caffrey S, Dunn S, Vinson P. Gendered health policies and a women’s movement: the Gypsy case. Health Place 1998;4:45–54.
Anderson E. Health concerns and needs of traveller families. Health Visitor 1997;70:148–50.
Anonymous. Focus on Gypsies and Travellers’ health. Community Pract 2001;74:2–3.
Anonymous. Roma/Gypsy: Diet and Nutrition. CultureVision; 2008.
Anonymous. Roma/Gypsy: Beliefs, Religion and Spirituality. CultureVision; 2008.
Anonymous. Roma/Gypsy: Concept of Health. CultureVision; 2008.
Anonymous. Roma/Gypsy: Health Promotion/Disease Prevention. CultureVision; 2008.
Anonymous. Roma/Gypsy: An Overview. CultureVision; 2008.
Anonymous. Roma/Gypsy: Language & Communication. CultureVision.
Anonymous. Roma/Gypsy: Treatment Issues. CultureVision.
Anonymous. Roma/Gypsy: Labor, Birth and Aftercare. CultureVision.
Anonymous. Roma/Gypsy: Illness-related Issues. CultureVision.
Aspinall P. A Review of the Literature on the Health Beliefs, Health Status, and Use of Services in the Gypsy Traveller Population, and of Appropriate Health Care Interventions. Cardiff: Welsh Assembly Government; 2005.
Atterbury J. Fair Access for All? Gypsies and Travellers in Sussex, GP Surgeries and Barriers to Primary Healthcare. Friends, Families and Travellers; 2010.
Atterbury J, Bruton L. DRE West Sussex Black and Ethnic Minorities CDW Service May 2008–April 2011: Final Report. Friends, Families and Travellers; 2011.
Austerberry H, Sawtell M, Ingold A, Wiggins M, Arai L, Strange V. Evaluation of the teenage health demonstration site programme: 1st Annual Report 2007. London: Social Science Research Unit; 2008.
Aylward RB, Porta D, Fiore L, Ridolfi B, Chierchini P, Forastiere F. Unimmunized Gypsy populations and implications for the eradication of poliomyelitis in Europe. J Infect Dis 1997;175 (Suppl):S86–8.
Ballinger P. Travel news. Community Pract 1998;71:345.
Barraclough C. Nottingham Traveller Team. Community Pract 2002;75:185.
Bartlett C. Concepts of health: the case of traveller-gypsies. Sociology Rev 1998;8:24–5.
Batstone J. Meeting the health needs of gypsies. Nurs Stand 1993;7:30–2.
Bell EJE, Riding MH, Collier PW, Wilson NC, Reid D. Susceptibility of itinerants in Scotland to poliomyelitis. Bull World Health Organ 1983;61:839–43.
Birchard K. Asthma linked to settled and affluent lifestyle. Lancet 1999;353:564.
Bobak M, Dejmek J, Solansky I, Sram RJ. Unfavourable birth outcomes of the Roma women in the Czech Republic and the potential explanations: a population-based study. BMC Public Health 2005;5:106.
Bodner A. Leininger M. Transcultural nursing care values, beliefs, and practices of American (USA) Gypsies. J Transcult Nurs 1992;4:17–28.
Bowers J. Health inequalities: Travellers’ tales. Health Service J 2004;114:26–8.
Brighton & Hove LINk, Friends, Families and Travellers. Gypsy & Traveller Health: What Might be Helpful – Tipsfor Practitioners. Friends, Families and Travellers.
Bunce CC. Travellers are the unhealthiest people in Britain. BMJ 1996;313:963.
Bunce C. A hard road to travel. Nurs Times 1996;92:34–6.
Carnicer-Pont D, Bagaria J, Paranthaman K, Smith A, Barber S, Benrhaut J. Hepatitis A cases in a travelling community in South East England. Euro Surveill 2006;11:3067.
Cemlyn S. Health and social work: working with Gypsies and Travellers. Practice 1993;6:246–61.
Cemlyn S, Greenfields M, Burnett S, Matthews Z, Whitwell C. Inequalities Experienced by Gypsy and Traveller Communities: A Review. Manchester: Equality and Human Rights Commission; 2009.
Charikar L. Setting the pace on health equality: the Pacesetters Programme in Leicester. J Fam Health Care 2008;18:212–15.
Chiriac M, Ganga D. Ferentari: Life in the Fast Lane. 2007. URL: www.soros.org/initiatives/health/focus/roma/articles_publications/articles/ferentari_20070926 (retrieved 13 September 2011).
Clements L, Morris R. Traveller children: educational and health deprivation. Childright 2001;179:7–9.
Cohuet S. Outbreak of measles among Irish Travellers in England. Euro Surveill 2007;12:3216.
Collins M. A Day in the Life of a Traveller Woman. In Quigley T, Brennan M-A, McCloskey M, McFarlane G, O’Connor A, O’Donovan D, et al. , editors. Report of the Conference on “Creating Connections”: Health Inequalities on the Island of Ireland – an Agenda for Change! Maynooth: Public Health Alliance Ireland; 2004.
Crickley A. Community development, discrimination and Traveller health. J Health Gain 2001;5:2–3.
Crout E. Trailer bound. Community Outlook 1987;12–14.
Crowley N. The Equal Status Act 2000 and the implications for health service provision. J Health Gain 2001;5:11.
Daniel K. Travellers’ friend. Nurs Times 1999;95:32–3.
Danis S. The Gypsy culture in South Florida. Fla Nurse 1996;44:17.
Darby S. Malignant Neglect. 2007. URL: www.soros.org/initiatives/health/focus/roma/articles_publications/articles/malignant_20071010 (retrieved 12 September 2011).
Davies W, Ohri A. Investing in Equality/Improving Services. Communities. Dublin: Equality Authority, Ireland; 2010.
Davis R. Specialist team earns trust of travellers. Community Care 2010;20–1.
Department for Health and Children. Traveller Health: A National Strategy of Health 2002–2005. Department for Health and Children; 2002.
Department of Health. Inclusion Health: Improving Primary Care for Socially Excluded People. London: Department of Health; 2010.
Department of Health, Social Services and Public Safety. Oral Health Strategy General Dental Services Equality Impact Assessments Preliminary Consultation Report. October. Belfast: Department of Health Social Services and Public Safety; 2001.
Dimitrijevic T. Improving Access to Health Care of Roma Community in Valjevo. Valijevo: Roma Centre for Democracy; 2009.
Dion X. Gypsies and Travellers: cultural influences on health. Community Pract 2008;81:31–4.
Doherty L. Nurses’ network shines light on the health issues of Traveller and Gypsy children. Paediatr Nurs 2010;22:6–7.
Dorkova Z, Sopkova Z, Tkacova R. Risk factors and severity of obstructive sleep apnoea in central European Roma and non-Roma patients referred for a diagnostic polysomnography [corrected]. Int J Public Health 2010;55:429–34.
Dostal M, Topinka J, Sram RJ. Comparison of the health of Roma and non-Roma children living in the district of Teplice. Int J Public Health 2010;55:435–41.
Doyal L, Cameron A, Cemlyn S, Nandy S, Shaw M. The Health of Travellers in the South West Region: A Review of Data Sources and a Strategy for Change. Bristol: Public Health; 2002.
Duggan-Jackson A. The voice of Traveller women through research. J Health Gain 2001;5:16.
Durst J. Fertility and childbearing practices among poor Gypsy women in Hungary: the intersections of class, race and gender. Communist Post Communcist 2002;35:457–74.
Edwards DM, Watt RG. Oral healthcare in the lives of Gypsy Travellers in east Hertfordshire. Brit Dent J 1997;183:252–7.
Edwards DM, Watt RG. Diet and hygiene in the lives of Gypsy Travellers in Herfortshire. Community Dent Health 1997;14:41–6.
Ekuklu G. Utilisation of primary health care services by Turkish gypsies and members of the general population at Muradiye Health Unit District in Edirne, Turkey. Yonsei Med J 2003;44:414–23.
European Roma Rights Centre. Ambulance Not On The Way: The Disgrace of Health Care for Roma in Europe. Budapest: European Roma Rights Centre; 2006.
European Roma Rights Centre. Health Access for Roma Improves with Award-Winning Programme. European Roma Rights Centre; 2006. URL: www.errc.org/cikk.php?cikk=2505 (retrieved 7 October 2011).
European Roma Rights Centre. Differences in Access to Primary Healthcare: Structures, Equal Opportunity and Prejudice – The Results of an Empirical Study. European Roma Rights Centre; 2004. URL: www.errc.org/cikk.php?cikk=2017 (accessed 7 October 2011).
European Union Agency for Fundamental Rights. Roma in the EU – A Question of Fundamental Rights Implementation. Vienna: European Union Agency for Fundamental Rights; 2010. pp. 11–26.
Evans D. Traveller friendly services: the Western health board experience. J Health Gain 2001;5:23–4.
Fay R, Crowley N. Ethnicity, culture and health. J Health Gain 2001;5:6–7.
Fay R, Kavanagh D, Quirke B, Malone M. Primary Health Care for Travellers Project: Project Report for Year Ended October 1995. Dublin: Eastern Health Board; 1996.
Fay R, Quirke B. Mainstreaming equality: Travellers access to the health services. J Health Gain 2001;5:30–2.
Feder G. Traveller gypsies and primary care. J R Coll Gen Pract 1989;39:425–9.
Feder GS, Vaclavik T, Streetly A. Traveller Gypsies and childhood immunization: a study in east London. Br J Gen Pract 1993;43:281–4.
Feder G, Salkind M, Sweeney O. Current Comment (xxii) Traveller-Gypsies and general practitioners in East London: the role of the Traveller health visitor. Health Trends 1989;21:93–4.
Fitzpatrick P, Molloy B, Johnson Z. Community mothers’ programme: extension to the travelling community in Ireland. J Epidemiol Community Health 1997;51:299–303.
Fonai M. Poverty, health and ethnicity: the empirical experiences of researchers in North East Hungary. Rev Sociology 2008;14:63–91.
Forrest E. Working with travellers: “the worst part is the hassle and discrimination”. Health Serv J 2004;114:28.
Fountain J. An Overview of the Nature and Extent of Illicit Drug Use Amongst the Traveller Community: An Exploratory Study. Dublin: National Advisory Committee on Drugs; 2006.
Francis G. Developing the Cultural Competence of Health Professionals Working with Gypsy Travellers. London: Department of Health; 2010.
Francis G. Traveller Voices. London: Department of Health; 2010.
Francis G, Anionwu E. Gillian fights prejudice against Gypsies. Nurs Stand 2011;25:10–11.
Franklin A. Travellers on the road to nowhere. Poverty 1993;84:11–13.
Friends, Families and Travellers. Good Practice Examples in Healthcare Provision for Gypsies and Travellers. Friends, Families and Travellers; 2011.
Gallagher A, Cvorović J, Strkalj G. Body mass index in Serbian Roma. Homo 2009;60:567–78.
Gammon J. Health services for travelling gypsies: a day in the life of Judith Moreton. Auditorium 1997;6:12–15.
Garcia J. Here everything is poison. Va Quart Rev 2010;86:122–37.
Gerevich J, Bácskai E, Czobor P, Szabó J. Substance use in Roma and non-Roma adolescents. J Nerv Ment Dis 2010;198:432–6.
Ghose D. Rights for Young Travellers. Young People Now. London: The National Youth Agency; 2004
Gill G. The health needs of the Slovak Roma community in Sheffield. Community Pract 2009;82:34–7.
Gordon M, Gorman D, Hashem S, Stewart D. The health of Travellers’ children in Northern Ireland. Public Health 1991;105:387–91.
Goward P, Repper J, Appleton L, Hagan T. Crossing boundaries. Identifying and meeting the mental health needs of Gypsies and Travellers. J Ment Health 2006;15:315–27.
Greenfields M. “A Good Job for a Traveller?” Exploring Gypsy and Travellers’ Perceptions of Health and Social Care Careers: Barriers and Solutions to Recruitment, Training and Retention of Social Care Students. Buckinghamshire; 2008.
Greenfields M. Reaching Gypsies and Travellers. Prim Health Care 2009;19:26–7.
Greenfields M, Home R. Assessing Gypsies’ and Travellers’ needs: partnership working and “the Cambridge Project”. Romani Stud 2006;16:105–31.
Grellier J, Soltesova K. Healthcare Policy and Provision for Roma in Slovakia and the Czech Republic. European Roma Rights Centre; 2004. URL: www.errc.org/cikk.php?cikk=2065 (accessed 7 October 2011).
Gualdi-Russo E, Zironi A, Dallari GV, Toselli S. Migration and health in Italy: a multiethnic adult sample. J Travel Med 2008;16:88–95.
Gulland A. The road less travelled. Nurs Times 1997;93.
Gyukits G, Csoboth C, Ürmös A, Purebl G, Kopp MS. Health and health behaviour of young Roma women in Hungary. Cogn Brain Behav 2006;69–84.
Hajioff S, McKee M. The health of the Roma people: a review of the published literature. J Epidemiol Community Health 2000;54:864–9.
Hall V, Sadouni M, Fuller A. Gypsies’ and Travellers’ Experience of Using Urgent Care Services Within NHS Brighton and Hove Boundaries, April 2008–August 2009. Friends, Families and Travellers; 2009.
Harrison S. Drive to improve mental health care for travellers. Nurs Stand 2003;18:8.
Hayman M, Matthews Z. Social exclusion: Gypsies, Travellers and health. Community Health UK Action 2003;60:14.
Health Service Executive. An Oral Health Promotion Programme for Traveller Families in County Offaly February 2007. Dublin: Health Service Executive; 2007.
Health Service Executive. HSE South: Implementing the National Service Plan – Management. Health Service Executive; 2010.
Hemmingway E. Travellers – a subculture from a transcultural nursing perspective. J Community Nurs 1999;13:12–17.
Henriques J. On the road. Nurs Stand 2001;15:16–17.
Henriques J. Hard travelling. Community Pract 2001;74:330–2.
Ho T, Cordovilla L. Our dilemma: the self-marginal people. EDTNA ERCA J 2004;30:230–3.
Hodgins M, Millar M, Barry MM. ‘... It’s all the same no matter how much fruit or vegetables or fresh air we get’: Traveller women’s perceptions of illness causation and health inequalities. Soc Sci Med 2006;62:1978–90.
Holt E. Roma women reveal that forced sterilisation remains. Lancet 2005;365:927–8.
Home R, Greenfields M. Cambridge Sub-Region Traveller Needs Assessment. Cambridgeshire: Cambridgeshire County Council; 2006.
Honer D, Hoppie P. The enigma of the Gypsy patient. RN 2004;67:33–6.
Hoover J. The Challenges and Rewards of One NGO’s Health Promotion Outreach among Roma Drug Users. Sofia; 2007.
Horan T. Travellers doing it for themselves. Nurs Community 2006;7:8–10.
House of Commons, Health Committee. Inequalities in Access to Maternity Services: Eighth Report of Session 2002–03 (HC 696). London: The Stationery Office; 2003.
Howley T. Poor accommodation and its impact on Travellers’ health. J Health Gain 2001;5:24–5.
Hudson LW. Hearing the human rights voices of Gypsy and traveller mothers in the UK. J Soc Welfare Fam Law 2009;31:121–32.
Hujová Z, Desatnikova J, Gabor D. Some cardiovascular risk factors in Gypsy children and adolescents from Central Slovakia. Bratisl Lek Listy 2009;110:233–9.
Hujová Z, Alberty R, Ahlers I, Ahlersová E, Paulíková E, Desatniková J, et al. Cardiovascular risk predictors in central Slovakian Roma children and adolescents: regional differences. Cent Eur J Public Health 2010;18:139–44.
Hussey RM. Travellers and preventive health care: what are health authorities doing? Br Med J (Clin Res Ed) 1988;296:1098.
Jackson C. On the road. Health Visitor 1990;63:204–6.
Janevic T, Petrovic O, Bjelic I, Kubera A. Risk factors for childhood malnutrition in Roma settlements in Serbia. BMC Public Health 2010;10:509.
Jarosová D, Dusová B, Vrublová Y. The education of Romany health and social assistants in the Czech Republic. Int Nurs Rev 2009;56:264–8.
Jenkins L. Preparation Study of Gypsy/Traveller Health Needs. Kent: Centre for Health Services Studies; 2010.
Jesper E, Griffiths F, Smith L. A qualitative study of the health experience of Gypsy Travellers in the UK with a focus on terminal illness. Prim Health Care Res Devel 2008;9:157–65.
Jones A. Working with Older Gypsies and Travellers. Age UK.
Jones K. Midwives and travellers. In Richens Y, editor. Challenges for Midwives, Volume 2. London: Quay Books; 2005. pp. 163–9.
Joubert K. Size at birth and some sociodemographic factors in gypsies in Hungary. J Biosoc Sci 1991;23:39–47.
Kabakchieva E, Amirkhanian Y, Kelly J, McAuliffe TL, Vassileva S. High levels of sexual HIV/STD risk behaviour among Roma (Gypsy) men in Bulgaria: patterns and predictors of risk in a representative community sample. Int J STD AIDS 2002;13:184–91.
Kabakchieva E, Vassileva S, Kelly J, Amirkhanian Y, DiFranceisco WJ, McAuliffe TL, et al. HIV risk behavior patterns, predictors, and sexually transmitted disease prevalence in the social networks of young Roma (Gypsy) men in Sofia, Bulgaria. Sex Transm Dis 2006;33:485–90.
Kaditis AG, Gourgoulianis K, Tsoutsou P, Papaioannou AI, Fotiadou A, Messini C, et al. Spirometric values in Gypsy (Roma) children. Respir Med 2008;102:1321–8.
Kanapeckiene V, Valinteliene R, Berzanskyte A, Kevalas R, Supranowicz P. Health of Roma children in Vilnius and Ventspils. Medicina (Kaunas) 2009;45:153–61.
Kearney P, Kearney P. The prevalence of asthma in schoolboys of Travellers’ families. Ir Med J 1998;91:203–6.
Kellleher K, McGinley A, Healy C. Traveller Health Services: Regional Strategy Statement and Action Plan 2003–2005. Strategy. Limerick: Mid-Western Health Board; 2005.
Kelly C, Gavin A, Molcho M, Gabhainn SN. Food consumption and dietary behaviour of children from the Traveller community: data from the 2006 Health Behaviour in School-aged Children (HBSC) survey. Proc Nutr Soc 2009;67(OCE7).
Kelly H. Health Needs of Travellers and Gypsy Community in Northumberland. Northumberland; 2009.
Kelly J, Amirkhanian Y, Kabakchieva E, Csepe P, Seal DW, Antonova R, et al. Gender roles and HIV sexual risk vulnerability of Roma (Gypsies) men and women in Bulgaria and Hungary: an ethnographic study. AIDS Care 2004;16:231–45.
Kelly J, Amirkhanian Y, Kabakchieva E, Vassileva S, Vassilev B, McAuliffe TL, et al. Prevention of HIV and sexually transmitted diseases in high risk social networks of young Roma (Gypsy) men in Bulgaria: randomised controlled trial. BMJ (Clin Res Ed) 2006;333:1098.
Kennedy P. Travellers in Ireland, training and health issues: lessons for social policy. Reg Dev Dialogue 2001;22:79–89.
Kolarcik P, GeckovaM, Orosova O, van Dijk JP, Reijneveld S. Predictors of health-endangering behaviour among Roma and non-Roma adolescents in Slovakia by gender. J Epidemiol Community Health 2010;64:1043–8.
Kolarcik P, Geckova AM, Orosova O, van Dijk JP, Reijneveld S. To what extent does socioeconomic status explain differences in health between Roma and non-Roma adolescents in Slovakia? Soc Sci Med 2009;68:1279–84.
Kosa K. Rapid health impact appraisal of eviction versus a housing project in a colony-dwelling Roma (Gypsy) community. J Epidemiol Community Health 2007;61:217.
Koupilová I, Epstein H, Holcík J, Hajioff S, McKee M. Health needs of the Roma population in the Czech and Slovak Republics. Soc Sci Med 2001;53:1191–204.
Krajčovičová-Kudláčková M, Blazícek P, Ginter E, Valachicová M. Homocysteine and its nutritional determinants in two ethnic groups of Slovakia. Cent Eur J Public Health 2004;12:217–19.
Krumova T, Ilieva M. The Health Status of Romani Women in Bulgaria. Centre for Interethnic Dialogue and Tolerance; 2008.
Kósa Z, Széles G, Kardos L, Kósa K, Németh R, Országh S, et al. A comparative health survey of the inhabitants of Roma settlements in Hungary. Am J Public Health 2007;97:853–9.
Lane P, Tribe R. Towards an understanding of the cultural health needs of older gypsies. Working Older People 2010;14:23–30.
Lauer C. Legacy of Shame. Open Society Foundations; 2007. URL: www.soros.org/initiatives/health/focus/roma/articles_publications/articles/legacy_20070703 (retrieved 13 September 2011).
Lawrence H. On the road to better health. Emerg Nurse 2007;15:12–17.
Lawrie B. Travelling families in east London – adapting health visiting methods to a minority group. Health Visitor 1983;56:26–8.
Leeds Gate Gypsy and Traveller Exchange. One Punch Kills: Leeds Gypsy and Traveller Exchange Domestic Violence Project Report. Leeds: Leeds GATE Gypsy and Traveller Exchange.
Lehti A, Mattson B. Health, attitude to care and pattern of attendance among gypsy women-a general practice perspective. Fam Pract 2001;18:445–8.
Local Government Improvement and Development. Dorset – Toby’s Youth Café. 2009. URL: www.idea.gov.uk/idk/core/page.do?pageId=14278226 (retrieved 18 October 2011).
Local Government Improvement and Development. Health Needs of Gypsies and Travellers. 2010. URL: www.idea.gov.uk/idk/core/page.do?pageId=17917440 (retrieved 18 October 2011).
Local Government Improvement and Development. Two Communities Come Together to Improve Gypsy and Traveller Health. 2011. URL: www.idea.gov.uk/idk/core/page.do?pageId=25454507 (retrieved 18 October 2011).
Loewenberg S. Plight of Roma worsens in Italy. Lancet 2010;375:17–18.
London Network for Nurses and Midwives. Moving On: Does Every London Traveller and Gypsy Child Matter? Observatory. 2009.
Løvoll Ø. An outbreak of measles among a travelling community from England in Norway. Euro Surveill 2007;12:3198.
Løvoll Ø. Outbreak of measles among Irish travellers in Norway: an update. Euro Surveill 2007;12:3217.
Lowenberg S. The health of Europe’s most marginalised populations. Lancet 2006;368:2115.
Lynch E. Travellers’ tales. Nurs Stand 2006;20:20–1.
MacAuley D. Uptake of cervical smear testing among travellers. BMJ 1991;303:191.
MacGabhann C. Voices unheard: a study of Irish Travellers in prison. Sex Reprod Healthcare 2010;1:143–8.
Magyari-Vincze E. Roma Women’s Reproductive Health as a Human Rights Issue in Romania Roma. Budapest: Central European University Center for Policy Studies; 2006.
Malan M, Schreedhar J. Time Bomb for Roma. 2007. URL: www.tol.cz/look/TOL/article.tpl?IdLanguage=1&IdPublication=4&NrIssue=220&NrSection=3&Nr Article=18752 (retrieved 13 September 2011).
Mandell F. Gypsies: culture and child care. Pediatrics 1974;54:603–7.
Mason P. The Travellers’ friend. Nurs Times 1991;87:20–1.
Masseria C, Mladovsky P, Hernández-Quevedo C. The socio-economic determinants of the health status of Roma in comparison with non-Roma in Bulgaria, Hungary and Romania. Eur J Public Health 2010;20:549–54.
Matthews Z, Velleman R. “New Age” Travellers, urban slum dwellers, Aborigines and drug users: experiences of collecting sensitive data from marginalised communities. Bull Méthodologie Sociologique 1997;57:65–85.
Matthews Z. The Health of Gypsies and Travellers in the UK: A Race Equality Foundation Briefing Paper. London: Race Equality Foundation; 2008.
Matthews Z, Edwards T, Sillman S, Benwel S. A Collaborative Programme to Improve the Oral Health of the Gypsy and Travelling Communities in Sussex. Sussex: Friends, Families and Travellers; 2010.
McCabe C, Keyes F. A Review of Travellers’ Health using Primary Care as a Model of Good Practice: Pavee Point Primary Health Care for Travellers’ Project. Dublin: Pavee Point; 2005.
McCann V. Health education for a Traveller community. Health Visitor 1987;60:293–5.
McCarthy D. Drugs and Diversity: Exploring Drug Issues Amongst New Communities and the Traveller Community: Seminar Report. Ethnicity. Dublin; 2006.
McKee M. The health of gypsies: lack of understanding exemplifies wider disregard of the health of minorities in Europe. BMJ (Clin Res Ed) 1997;315:1172–3.
McLeish J. Gypsy and Traveller women: the road to better care. Pract Midwife 2008;11:12–14.
Merino L. When the Gypsies come. An insider’s view into a mysterious culture. An interview by Jeanne M. Burger. J Chris Nurs 1996;13:4–9.
Minority Rights Centre. Decade of Roma: Yearly Report of the League for the Decade 2007. 2008. URL: www.soros.org/reports/decade-roma-inclusion-2007-serbia-report (accessed 6 October 2011).
Molnár A, Adány R, Adám B, Gulis G, Kósa K. Health impact assessment and evaluation of a Roma housing project in Hungary. Health Place 2010;16:1240–7.
Monasta L, Andersson N, Ledogar RJ, Cockcroft A. Minority health and small numbers epidemiology: a case study of living conditions and the health of children in 5 foreign Romá camps in Italy. Am J Public Health 2008;98:2035–41.
Moore R, Turner J, Nic Charthaigh R, Quirke B, Hamid NA, Drummond A, et al. All Ireland Traveller Health Study Technical Report 3. Dublin: University College Dublin; 2010.
Moreton J. Immunization of travellers in Oxfordshire. Nursing 1987;3:723–6.
Moreton J. Control of fertility amongst Travellers. Midwife Health Visit Community Nurse 1988;24:314–17.
Moreton J. HIB 2 Educating parents and professionals. Health Visitor 1992;65:266–7.
Morris M. Traveller health care: stopped in their tracks. Community Outlook 1987;16–19.
Morris R, Clements L. Disability, Social Care, Health and Travelling People. Cardiff: Cardiff Law School, Traveller Law Research Unit; 2001.
Murphy P. Primary Health Care for Travellers Project: Implementation Report 1996–1999. Dublin; 1999.
NHS Primary Care Contracting. Primary Care Service Framework: Gypsy & Traveller Communities. London: NHS Primary Care Contracting; 2009.
NHS Race for Health. NHS Suffolk Peer Review: Developing Staff Competencies to Build and Sustain Effective Relationships with Minority Ethnic Communities. Race for Health; 2008.
Neff-Smith M, Erickson GP, Campbell J. Gypsies: health problems and nursing needs. J Multicultural Nurs Health 1996;2:36–42.
Neile E. Sick-birth caravans. Nurs Stand 1993;7:49.
Office for Democratic Institutions and Human Rights. Implementation of the Action Plan on Improving the Situation of Roma and Sinti Within the OSCE Area. Poland: Organization for Security and Co-operation in Europe; 2008. pp. 1–69.
Open Society Institute. Mediating Romani Health: Policy and Program Opportunities. New York, NY: Open Society Institute; 2005.
Open Society Institute. How the Global Fund Can Improve Roma Health: An Assessment of HIV and TB Programs in Bulgaria, Macedonia, Romania, and Serbia. New York, NY: Open Society Institute; 2007.
Open Society Institute Public Health Program. Understanding Risk: Roma and HIV Prevention. New York, NY: Open Society Institute; 2007.
Ormiston Children and Families Trust, Cambridgeshire Community Services. An Insight into the Health of Gypsies and Travellers: A Booklet for Health Professionals in Cambridgeshire. Ipswich and St Ives: Ormiston Children and Families Trust, Cambridgeshire Community Services; 2008.
O’Neill R. Health inequalities: travelling communities. Health Service Journal, 6 October 2008.
Pahl J, Vaile M. Health and health care among travellers. J Soc Policy 1988;17:195–213.
Papadopoulos I. The health promotion needs and preferences of Gypsy Travellers in Wales. Divers Health Soc Care 2007;4:167–77.
Parry G, Cleemput PV, Peters J, Moore J, Walters S, Thomas K, et al. The Health Status of Gypsies & Travellers in England. Sheffield: University of Sheffield; 2004.
Parry G, Van Cleemput P, Peters J, Walters S, Thomas K, Cooper C. Health status of Gypsies and Travellers in England. J Epidemiol Community Health 2007;61:198–204.
Patterson J. On the road: reflections on Travellers and their children. Nurs Times 1982;78:1617–20.
Pavee Point. Irish Travellers. J Health Gain 2001;5:3–5.
Peck B. Gypsies – a Sheffield experience. Health Visitor 1983;56:365.
Petek D, Rotar Pavlic D, Svab I, Lolić D. Attitudes of Roma toward smoking: qualitative study in Slovenia. Croat Med J 2006;47:344–7.
Peters J, Parry GD, Cleemput PV, Moore J, Cooper CL, Walters SJ. Health and use of health services: a comparison between Gypsies and Travellers and other ethnic groups. Ethn Health 2009;14:359–77.
Pickersgill F. Moving in the right direction. Nurs Stand 2010;24:72.
Popova S. Reaching the hard to reach. World Health 1995;48:29.
Power C. Room to Roam: England’s Irish Travellers. Community Fund; 2004
Queally M. Health promotion needs of the Travelling Community. J Health Gain 2001;5:1–32.
Quirke B. Primary Health Care for Travellers Project. J Health Gain 2001;5:12–14.
Quirke B, Bennet P. Newly established Traveller health structures. J Health Gain 2001;5:8.
Rambousková J, Dlouhý P, Krízová E, Procházka B, Hrncírová D, Andel M. Health behaviors, nutritional status, and anthropometric parameters of Roma and non-Roma mothers and their infants in the Czech Republic. J Nutr Educ Behav 2009;41:58–64.
Raper M. Travelling families in Northumberland. Health Visitor 1986;59:345–7.
Rechel B, Blackburn CM, Spencer NJ, Rechel B. Access to health care for Roma children in Central and Eastern Europe: findings from a qualitative study in Bulgaria. Int J Equity Health 2009;8:24.
Reid B. Networking for traveller health. Community Pract 2005;78:312–13.
Reid B. Re-visioning the provision of maternity care for traveller women. Evid Based Midwifery 2005;3:21–5.
Reid B, Taylor J. A feminist exploration of Traveller women’s experiences of maternity care in the Republic of Ireland. Midwifery 2007;23:248–59.
Reid T. Partners in care. Nurs Times 1993;89:28–30.
Rhodes S. Gypsies’ and travellers’ health. Community Pract 2005;78:303.
Rose V. On the road: Val Rose, a health visitor in a rural area, describes how she meets travellers’ health needs by providing a tailor-made mobile service. Nurs Times 1993;89:31.
Sandiford R. Caring without prejudice. Nurs Times 2005;101:26–7.
Schaaf M. Confronting a Hidden Disease: TB in Roma Communities. New York, NY: Open Society Institute; 2007.
Sepkowitz KA. Health of the world’s Roma population. Lancet 2006;367:1707–8.
Shepherd S. Gypsies’ and Travellers’ health: the road to greater inclusion. Health Service J, 17 August 2010.
Simko V, Ginter E. Short life expectancy and metabolic syndrome in Romanies (gypsies) in Slovakia. Cent Eur J Public Health 2010;18:16–8.
Skarić-Jurić T, Klarić IM, Narancić NS, Drmić S, Salihović MP, Lauc LB, et al. Trapped between tradition and transition--anthropological and epidemiological cross-sectional study of Bayash Roma in Croatia. Croat Med J 2007;48:708–19.
Slattery D, Brennan M, Canny C, Sweeney K, Ward M, O’Shea P, et al. Cardiovascular health in the Irish Traveller community. Br J Diabetes Vasc Dis 2010;10:305–7.
Smart H, Titterton M, Clark C. A literature review of the health of Gypsy/Traveller families in Scotland: the challenges for health promotion. Health Educ 2003;103:156–65.
Smith T. Romani “Gypsy” women and mainstream health services. Eur J Womens Stud 1997;4:183–96.
Streetly A. Traveller mothers and babies. BMJ 1990;301:342.
Subata E, Tsukanov J. The work of general practitioners among Lithuanian Roma in Vilnius: incorporating harm reduction. J Drug Issues 1999;29:805–10.
Sutherland A. Health and illness among the Roma of California. J Gypsy Lore Society 1992;2:19–59.
Sutherland A. Gypsies and health care. West J Med 1992;157:276–80.
Szilagyi T. Peer education of tobacco issues in Hungarian communities of Roma and socially disadvantaged children. Cent Eur J Public Health 2002;10:117–20.
Tan S, Avalos G, Dineen B, Burke A, Gavin J, Brennan M, et al. Traveller health: prevalence of diabetes, pre diabetes and the metabolic syndrome. Ir Med J 2009;102:176–8.
Tavares M. ‘Gypsies and Travellers in Leeds – Making a Difference’: An Exploratory Study on the Health Needs of Gypsies and Travellers. Leeds: Travellers Health Partnership; 2001.
Taylor J. Health behaviour and beliefs. Health Visitor 1991;64:223–4.
The Highland Council, NHS Highland. The Highland Gypsy/Traveller health & wellbeing initiative. Int J Toxicol 2005;30(3 Suppl.):1–72.
Theophanous H. “On The Move”: A Mobile Midwifery Programme for the Women of the Gypsy and Traveller Community. PhD thesis. 2011.
Thomas JD. Health Care of American Gypsies: Social and Medical Aspects. In DeSilva C, Grumet J, Nemeth DJ, editors. Papers from the Eighth and Ninth Annual Meetings Gypsy Lore Society, North American Chapter. New York, NY: Gypsy Lore Society; 1988. pp. 128–38.
Thomas JD. Tales of a Gypsy doc: perspectives on social and medical aspects of care of the American Gypsy population. Clev Clin J Med 1993;60:427–9.
Thomason C. Here to Stay: An Exploratory Study into the Needs and Preferences of Gypsy/Traveller communities in Cheshire, Halton and Warrington. Chester: Cheshire Halton & Warrington Racial Equality Council; 2006.
Thorn H. Gypsy & Travellers’ Health Needs Assessment: Improving the Health of Gypsies and Travellers in the Mid Essex Area. Essex: NHS Mid Essex; 2009. pp. 1–63.
Traveller health initiatives – health board regions. J Health Gain 2001;5:17–22.
Treise C, Shepherd G. Developing mental health services for Gypsy Travellers: an exploratory study. Clin Psychol Forum 2006;163:16–19.
Tyler C. Travellers’ tale. Nurs Times 1993;89:26–7.
Valente T. Opinion leader interventions in social networks: can change HIV risk behaviour in high risk communities. BMJ 2006;333:1082–3.
Van Cleemput P. Health care needs of travellers. Arch Dis Child 2000;82:32–7.
Van Cleemput P. Abstract of thesis: Gypsies and Travellers accessing primary health care: interactions with health staff and requirements for “culturally safe” services. J Res Nurs 2009;14:365–9.
Van Cleemput P. Social exclusion of Gypsies and Travellers: health impact. J Res Nurs 2010;15:315–27.
Van Cleemput P, Parry G. Health status of Gypsy Travellers. J Public Health Med 2001;23:129–34.
Van Cleemput P. Health impact of Gypsy sites policy in the UK. Soc Policy Society 2007;7:103–17.
Van Cleemput P, Parry G, Thomas K, Peters J, Cooper C. Health-related beliefs and experiences of Gypsies and Travellers: a qualitative study. J Epidemiol Community Health 2007;61:205–10.
Van Cleemput P, Thomas K, Parry G, Moore J, Cooper C. The Health Status of Gypsies and Travellers in England: Report of Qualitative Findings. Sheffield: University of Sheffield; 2004.
Van Doorslaer O, Quirke B. Current research initiatives on Traveller health in Ireland 2000. J Health Gain 2001;5:26–9.
Van Hout M. Travellers and substance use – implications for service provision. Int J Health Promotion Educ 2006;48:36–41.
Van Hout MC. The Irish Traveller Community: social capital and drug use. J Ethn Subst Abuse 2010;9:186–205.
Van Hout MC. Traveller health and primary care in Ireland: a consultative forum. Community Pract 2010;83:27–30.
Van Hout MC. Alcohol use and the Traveller community in the west of Ireland. Drug Alcohol Rev 2010;29:59–63.
Van Hout MC, Connor S. The normalisation of substance abuse among young Travellers in Ireland: implications for practice. J Ethn Subst Abuse 2008;7:5–22.
Van Hout MC. Traveller drug use and the school setting: friend or foe? J Alcohol Drug Educ 2010;54:7–16.
Vernon D. The health of traveller-Gypsies. Br J Nurs 1994;3:969–72.
Vivian C, Dundes L. The crossroads of culture and health among the Roma (Gypsies). J Nurs Scholarship 2004;36:86–91.
Vozarova de Courten B. Higher prevalence of type 2 diabetes, metabolic syndrome and cardiovascular diseases in gypsies than in non-gypsies in Slovakia. Diabetes Res Clin Pr 2003;62:95–103.
Vrinceanu S. Timboiesti: Welfare Revisions Leave Roma Without Medical Insurance. Ziarul de Vrancea. 2007. URL: www.soros.org/initiatives/health/focus/roma/articles_publications/articles/timboiesti_20070913 (retrieved 13 September 2011).
Vrinceanu S. Luncile – the Roma Village That is Losing Ground. 2007. URL: www.soros.org/initiatives/health/focus/roma/articles_publications/articles/luncile_20070917 (retrieved 13 September 2011).
Vrinceanu S. Playing Russian Roulette with Roma Health. 2007. URL: www.soros.org/initiatives/health/focus/roma/articles_publications/articles/roulette_20070910 (retrieved 13 September 2011).
Walsh CA, Este D, Krieg B, Giurgiu B. Needs of refugee children in Canada: what can Roma refugee families tell us? J Comp Fam Stud 2011;42:599–613.
Walsh CA, Este D, Krieg B. The enculturation experience of Roma refugees: a Canadian perspective. Br J Soc Work 2006;38:900–17.
Walsh CA Krieg B. Roma refugees: a profile of health and social service needs. J Immigr Refugee Stud 2007;5:5–27.
Weber L. Cambridgeshire Travellers Review Research Report Number 3: Travellers in Cambridgeshire. Cambridgeshire: Cambridgeshire Country Council; 1998.
Weber L. Cambridgeshire Travellers Review Research Report Number 1: Identification of Key Issues. Cambridgeshire: Cambridgeshire Country Council; 1998.
Weber L. Cambridgeshire Travellers Review Research Report Number 4: Location studies. Cambridgeshire: Cambridgeshire Country Council; 1998.
Weber L. Cambridgeshire Travellers Review Research Report Number 5: Suggestions for Good Practice. Cambridgeshire: Cambridgeshire Country Council; 1998.
West Sussex Local Involvement Network. Health & Social Care needs of Gypsy and Traveller Families and communities in West Sussex. Sussex: West Sussex Local Involvement Network; 2010.
Windess B. One year working with the Travellers. Health Visitor 1987;60:289–91.
Wood S. East Cambridgeshire and Fenland Traveller Health Needs Assessment. Cambridgeshire; 2006. pp. 1–11.
Zeman CL, Depken DE, Senchina DS. Roma health issues: a review of the literature and discussion. Ethn Health 2003;8:223–49.
van Hout M-C. Assimilation, habitus and drug use among Irish Travellers. Crit Public Health 2011;21:203–20.
Živković TB, Marjanović M, Prgomelja S, Soldatović I, Koprivica B, Acković D, et al. Screening for diabetes among Roma people living in Serbia. Croat Med J 2010;51:144–50.
Appendix 12 Examples of the categorisation of scoping studies using Aspinall’s framework
| Health status: publications assessing the health status of Traveller Communities | |
|---|---|
| Abdalla et al. (2010)42 | A health survey of Traveller Communities living in Ireland |
| Kosa et al. (2007)219 | A comparative health survey of the inhabitants of Roma settlements with the general population in Hungary |
| Parry et al. (2007)19 | An epidemiological survey on the health of Gypsies and Travellers in England compared with an age- and sex-matched non-Traveller sample from different socioeconomic groups |
| Peters et al. (2009)26 | A cross-sectional survey comparing the health of Gypsies and Travellers with other ethnic groups in England |
| Health needs: publications reporting on health needs assessments or on the range of health needs experienced by Traveller Communities | |
| Gill (2009)220 | Described the health needs of Slovak Roma community in Sheffield, including those related to poverty, housing and access to services |
| Jenkins (2010)221 | A preparation study on the health needs of Traveller Communities in Kent, uptake of services and of interventions to improve their health |
| Walsh and Krieg (2007)187 | Identifies the health and social service needs of Roma Communities in Canada through interviews and focus groups with members of the Roma Community and service providers |
| Access to and use of services: publications examining barriers and inequalities in accessing health services and experiences of health care (including primary care, acute services and health promotion services) | |
| European Roma Rights Centre (2006)222 | Describes the inequalities in access to health care by Roma communities and recommendations for health-care reform |
| Feder (1989)139 | Discusses the difficulties accessing primary care services by Traveller Communities and the role of general practitioners in improving health care for these groups |
| Hall et al. (2009)223 | Investigated Traveller Communities use of urgent care services and how services offered can be improved |
| Children’s health: including asthma, diet and malnutrition, morbidity, birth size and teenage health | |
| Kearney and Kearney (1998)224 | Compares the prevalence of asthma in Traveller schoolboys compared with a control group of children in the settled community |
| Dostal et al. (2010)225 | Compares the morbidity of Roma and non-Roma children in the first 6 years of life |
| Joubert (1991)35 | Compares the birthweight, birth length and gestational age of Gypsies in Hungary with a national reference sample |
| Communicable diseases: including immunisation, polio, TB, measles | |
| Moreton (1987)115 | Describes an immunisation programme for Traveller Communities in Oxfordshire |
| Schaaf (2007)226 | Examines data on and current initiatives to address TB in Roma Communities |
| Cardiovascular disease and cancer: studies examining cardiovascular health and associated risk factors | |
| Slattery et al. (2010)227 | Assesses the point prevalence of diabetes, pre-diabetes and the metabolic syndrome in a sample population of Irish Travellers |
| Vozarova de Courten (2003)228 | Investigates the prevalence of type 2 diabetes mellitus, metabolic syndrome and cardiovascular diseases in Gypsies and non-Gypsies living in the same region of southern Slovakia |
| Lifestyle factors: includes smoking, substance use, diet and nutrition and HIV infection prevention | |
| Gerevich et al. (2010)229 | Assesses substance use of Roma as compared with non-Roma adolescents |
| Petek et al. (2006)230 | Examines attitudes of Roma towards smoking in Slovenia |
| Van Hout (2010)231 | An exploratory account of Travellers and alcohol use according to perspectives of Travellers and key service providers in the west of Ireland |
| Mental health | |
| Goward et al. (2006)232 | Explores the mental health needs and service provision for Gypsies and Travellers in Sheffield |
| Treise and Shepherd (2006)233 | Qualitative study exploring Gypsies’ and Travellers’ perceptions of mental health problems |
| Oral health | |
| Edwards and Watt (1997)234 | Explores Gypsies’ and Travellers’ perceptions of dental health and service use |
| Health Service Executive (2007)128 | Describes an oral health promotion programme for Traveller Communities in Ireland |
| Wider determinants of health: publications discussing environmental factors such as housing and socioeconomic factors such as employment, income and poverty | |
| Kolarcik et al. (2009)235 | Explores the relationship between socioeconomic status and differences in health between Roma and non-Roma adolescents |
| Molnar et al. (2010)236 | Health impact assessment of a Roma housing project in Hungary |
| Van Cleemput (2007)39 | Explores the health impact of Gypsy sites policy in the UK |
| Women’s health including maternal health and use of maternity services, cervical and other screening, family planning and contraception, domestic violence | |
| Darby (2007)202 | Describes a programme to increase mammography uptake in Romani women in Hungary |
| Leeds GATE192 | Describes a project initiated by a Traveller Community member to raise awareness of domestic violence |
| Reid and Taylor (2007)237 | Explores Traveller women’s experiences of maternity care in the ROI |
| Background and policy: includes policy documents and cultural and health information for professionals | |
| NHS Primary Care Contracting62 | Primary Care Service Framework for Gypsies and Travellers |
| Francis (2010)238 | Booklet informing health-care professionals about the cultural identity and health needs of Gypsies and Travellers |
Appendix 13 Neufeld’s model of engagement populated with Context–Mechanism–Outcome configurations
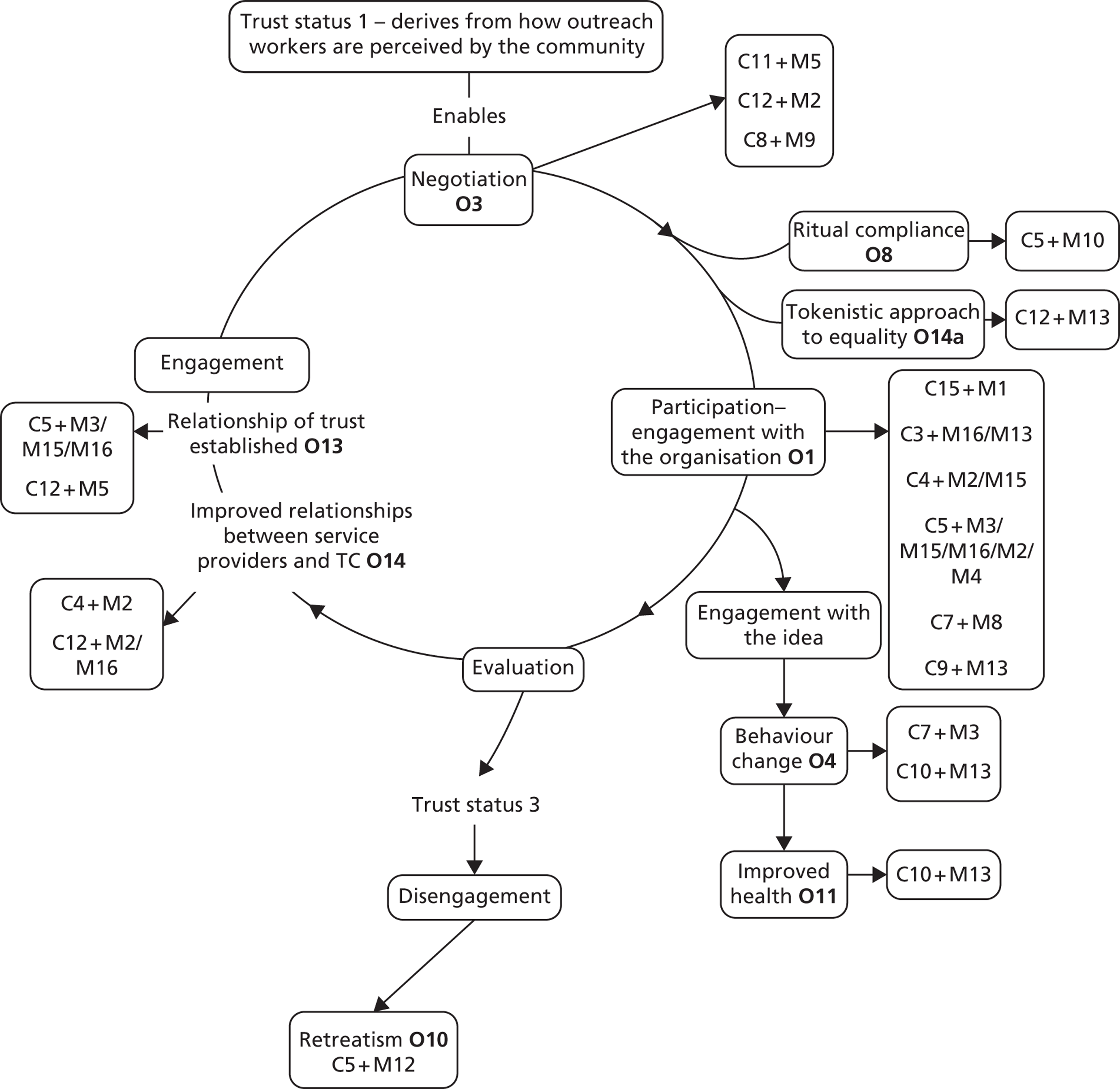
| CMO configuration | Meaning |
|---|---|
| C = context | |
| C3 | Cultural beliefs pertaining to health |
| C4 | Transience, lack of permanent address |
| C5 | Mistrust due to history of assimilation/acculturation, institutions ill adapted to Traveller Community lifestyles |
| C7 | Tight-knit community |
| C8 | Increased understanding of health issues |
| C9 | Traveller Communities are engaging and confident to articulate their needs |
| C10 | Destigmatisation of a health issue |
| C11 | Previous lack of consultation with Traveller Community about needs |
| C12 | Practitioners’/settled communities’ lack of knowledge of Traveller Communities and discrimination towards them |
| C15 | Low expectations with respect to employment opportunities |
| M = mechanism | |
| M1 | Self-efficacy |
| M2 | Rights awareness |
| M3 | Trust – communication |
| M4 | Demystification of environments and processes |
| M5 | Feeling valued and accepted |
| M8 | Compliance with social norms |
| M9 | Questioning existing practices |
| M10 | Fear of acculturation/being perceived as not coping |
| M12 | Lack of negotiation with Traveller Communities |
| M13 | Strategic compliance (based on desire not to disappoint the worker) |
| M15 | Trust in the integrity/benevolence of the professional |
| M16 | Trust – aligned interests |
| O = outcome | |
| O1 | Participation |
| O3 | Cognitive engagement (Traveller Communities are engaging and confident to articulate their needs) |
| O4 | Behaviour change |
| O8 | Ritual compliance |
| O10 | Retreatism |
| O11 | Improved health |
| O13 | Relationship of trust established |
| O14 | Improved relationships between service providers and Traveller Communities/increased awareness of Traveller Community culture and lifestyles |
| O14a | Tokenistic approach to equality |
Glossary
- Anecdotal account
- An account of Traveller Community needs or the delivery of an intervention that is based on the experiences of outreach workers or Traveller Communities and not on research evidence.
- Candidate theories
- Candidate theories refer here to existing theories from the literature that were accessed, confronted to the data and rejected, retained or amended to provide maximum explanatory potential.
- Context–Mechanism–Outcome configurations
- Following Jagosh et al. (Jagosh J, Pluye P, Wong G, Cargo M, Salsberg J, Bush PL, et al. Critical reflections on realist review: insights from customizing the methodology to the needs of participatory research assessment. Res Synth Methods 2013;5:131–41. http://dx.doi.org/10.1002/jrsm.1099), Context–Mechanism–Outcome configurations refer to ‘a heuristic used to generate causative explanations pertaining to outcomes in the observed data . . . One CMO may be embedded in another or configured in a series (in which the outcome of one CMO becomes the context for the next in the chain of implementation steps)’.
- Initial programme theories
- Initial theories were used for their early explanatory potential and as a framework for study selection and data extraction.
- Middle range theories
- Following Jagosh et al. middle range theory ‘is an implicit or explicit explanatory theory that can be used to explain specific parts of programmes and interventions. “Middle-range” means that it can be tested with the observable data and is not abstract to the point of addressing larger social or cultural forces (i.e. grand theories)’.
List of abbreviations
- A&E
- accident and emergency
- AIDS
- acquired immunodeficiency syndrome
- CHW
- community health worker
- CINAHL
- Cumulative Index to Nursing and Allied Health Literature
- CMO
- Context–Mechanism–Outcome
- EH
- expert hearing
- EQ-5D
- European Quality of Life-5 Dimensions
- GP
- general practitioner
- HIV
- human immunodeficiency virus
- MRC
- Medical Research Council
- NI
- Northern Ireland
- QOF
- Quality and Outcomes Framework
- RCT
- randomised controlled trial
- ROI
- Republic of Ireland
- TB
- tuberculosis