Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 11/3050/08. The contractual start date was in July 2013. The final report began editorial review in August 2016 and was accepted for publication in March 2017. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
none
Disclaimer
This report contains transcripts of interviews conducted in the course of the research, or similar, and may contain language which offends some readers.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2018. This work was produced by Elsey et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2018 Queen’s Printer and Controller of HMSO
Chapter 1 Background to study
Defining care farming
Care farming (also known as social farming) has been defined as the use of commercial farms and agricultural landscapes as a base for promoting mental and physical health through normal farming activity. 1–3 A care farm (CF) utilises the whole or part of a farm to provide health, social or educational care services for different groups of people, providing a supervised, structured programme of farming-related activities rather than occasional one-off visits (www.carefarming.org.uk; accessed January 2014). 4
Care farming is a truly complex intervention. 5 Farms differ in the type of farming activities (e.g. horticulture and livestock farming), type of other activities (e.g. gardening, conservation and woodwork), the level of support provided (e.g. health promotion, counselling and skills qualifications) and the range of service user groups. A diverse range of activities can be offered to service users at a CF. Activities selected are primarily determined by the particular needs and capabilities of the service user and the type of farm. Likewise, depending on the service user group, they may or may not be involved in agricultural production. The main defining feature of a CF is the involvement in farm activities for a therapeutic purpose. It is not a horticultural- or animal-based therapy per se.
Individuals supported through care farming include those with learning difficulties, those with autism spectrum disorder, those with mental ill health, disaffected youth, people with physical disabilities, older people, people with drugs and alcohol problems, adult probation service users, people with dementia and ex-service personnel. 6 In the UK, the largest service user groups are those with learning difficulties, those with autism spectrum disorder, those with mental ill health and disaffected youth (Table 1).
| Supported group | Percentage of CFs |
|---|---|
| Learning difficulties | 93 |
| Autism spectrum disorder | 84 |
| Mental ill health | 75 |
| Excluded young people | 64 |
| Physical disabilities | 52 |
| Older people | 43 |
| Drug/alcohol history | 36 |
| Adult probation service users | 27 |
| Dementia | 24 |
| Ex-service personnel | 4 |
Green care
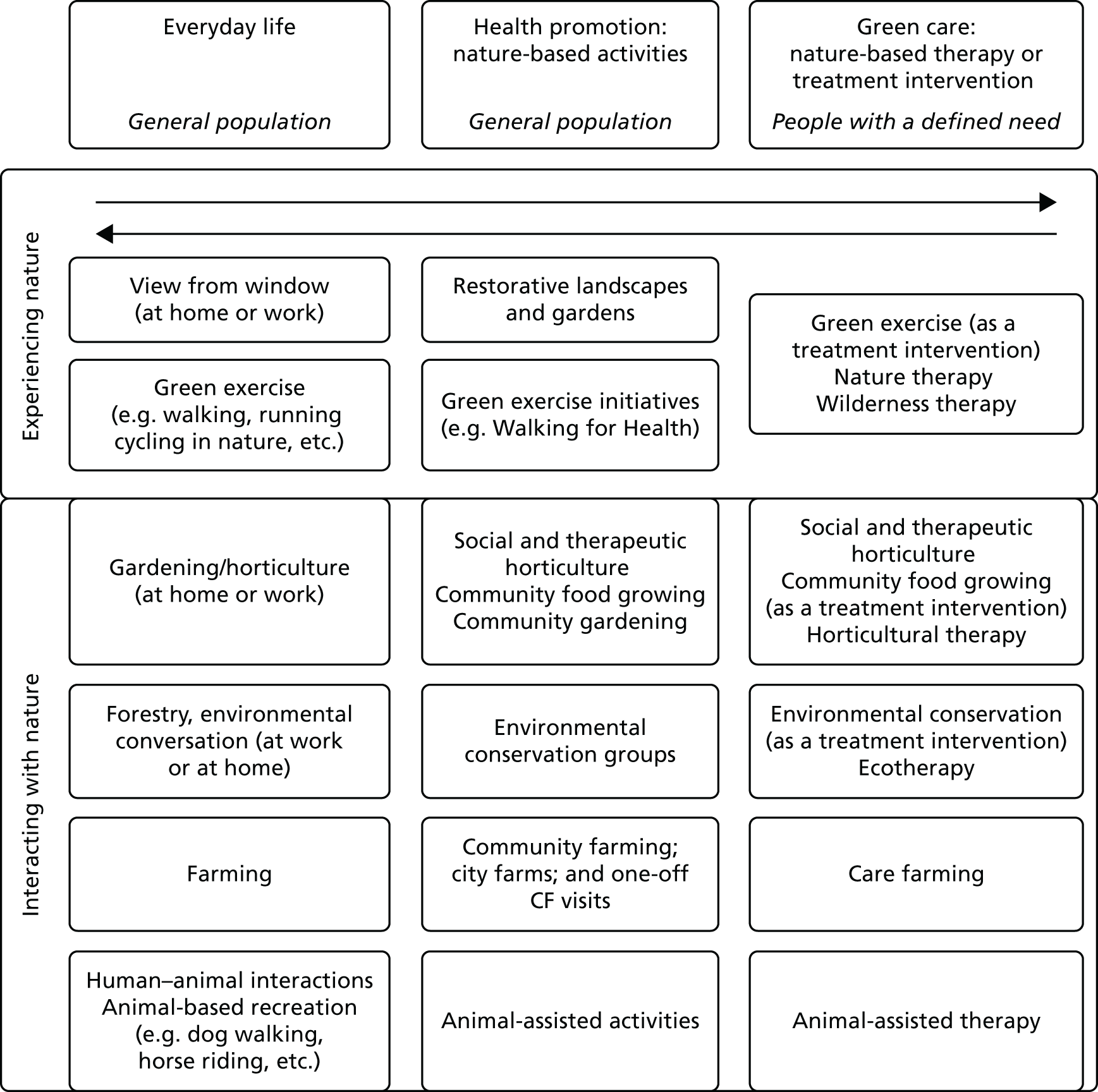
Care farming sits within a broader framework that describes our interactions with nature. These interactions can be viewed as a continuum that ranges from general everyday contact, such as viewing, working or undertaking recreational activities, through to using nature deliberately as a therapeutic or treatment resource (i.e. green care) involving activities, such as wilderness therapy, social and therapeutic horticulture, animal-assisted therapy and care farming (Figure 1).
FIGURE 1.
Continuum of interaction with nature according to human needs. Reproduced from Bragg R, Atkins G. A Review of Nature-Based Interventions for Mental Health Care. Natural England Commissioned Reports, Number 204. York: Natural England; 2016. 7 © Natural England and other parties 2016. Contains public sector information licensed under the Open Government Licence v3.0 (www.nationalarchives.gov.uk/doc/open-government-licence/version/3/). This report is published by Natural England under the Open Government Licence – OGLv3.0 for public sector information. You are encouraged to use, and reuse, information subject to certain conditions. For details of the licence visit http://publications.naturalengland.org.uk/copyright.
Green care has been defined as ‘nature-based therapy or treatment interventions which are specifically designed, structured and facilitated for individuals with a defined need’. 8 Green care utilises plants, animals and landscapes to create interventions to improve health and well-being (i.e. it does not represent a casual encounter with nature). Green care also provides care and support to enable people to reach their true potential; that is, although many of the approaches are termed ‘therapies’ or ‘therapeutic’, they are not necessarily directed at treating or curing conditions and diseases. In the case of people with learning difficulties, for example, green care provides care, support, training and other opportunities to enable those individuals to develop. Such opportunities are often not available elsewhere. 8
How care farming works
As a highly complex intervention comprising multiple activities and involving many service user groups with differing needs, it is likely that multiple mechanisms and interactions will be at work to bring about changes in individuals. At the core of the intervention is the connection with nature, which has value in its own right but also provides the platform for the range of activities. Studies have also shown that connectedness to nature has a positive effect on people’s mental, physical and psychological well-being and spiritual beliefs9,10 and that engaging in nature-based activities, such as farming or gardening, enables people to find solace. 10 As a result, CFs may be beneficial for a wide range of service users.
A number of theories have been mentioned within the care farming literature and some of these speak specifically to the nature element, such as the attention restoration theory11 and biophylia hypothesis. 12 Other theories relate specifically to the service user groups that attend CFs, for example desistence theory for probation service users13 and the recovery model for people with mental ill health. 14 Within these theories are the proposed mechanisms5 that explain how any effective intervention would be expected to bring about change. Within the review we followed the Medical Research Council (MRC)’s definition of a ‘mechanism of impact’, that is, ‘how intervention activities, and participants’ interactions with them, trigger change’ (p. 8). 5 Therefore, identifying these mechanisms within the care farming interventions will provide the links required to understand outcomes. These mechanisms are detailed in the theories we assessed. For example, desistence theory suggests that interventions that lead to a reduction in recidivism involve building human relationships, opportunities for reflection and change,15,16 developing self-efficacy17–19 and social capital by learning and applying new skills to develop a new, more positive identity. 17,20–23 A sense of community and the development of friendships are indeed valued aspects of a CF. 24 Furthermore, farmers are perceived as positive role models with a strong sense of identity, thus offering an essential positive figure that can be emulated through forming a new identity. 25 Both the concepts of building human relationships and creating a new identity are clearly present within care farming interventions.
The need for a study
Green care plays a particularly important role in modern society. Sitting within the third sector, they provide a type of support beyond that which can be provided by statutory health and social care organisations. Utilisation of the third sector by statutory services appears to be increasing, as demonstrated by recent social prescribing initiatives. 26 This has been driven partly by a capacity issue within health services relating to increasing life expectancies over the 20th century27 and an increasing prevalence of long-term conditions. However, it also relates to changing needs and demands of populations within modern societies. Many of the problems presenting to health-care providers (often as the first point of contact) are complex and often are underpinned or exacerbated by social problems (such as poor education, poor housing, unemployment and social isolation) and the skills within health services to address these issues do not exist within this sector. Likewise, among local authorities and probation there appears to be a recognised value in attending for social reasons, such as educational and employment needs and social interactions. Thus, there is the potential for care farming to improve the health and well-being of different population groups. The number of CFs has been growing, particularly in Europe, with an estimated 1000 CFs in the Netherlands,28 over 200 in the UK,4 900 in France, 300 in Belgium, 160 in Germany, 675 in Italy and 100 in Ireland. 29 Despite this growth, however, sustainability is a major challenge. Funding comes from a variety of sources: charitable donations, private sector funding schemes, charity funding schemes, contracts with local authorities, clinical commissioning groups, probation services and through income generated from the sale of farm produce. A key part of the process of securing funding is providing evidence of benefit for health and social outcomes. Although there is a growing body of evidence pointing to the benefits of nature-based interventions for a range of health-based outcomes,30–33 characteristically small sample sizes and a range of methodological limitations allow only tentative conclusions to be drawn. Within care farming research specifically, there have been a number of observational studies published across Europe and a small number of reviews7,34,35 and these studies document the extent and range of care farming initiatives and summarise the evidence for benefits. However, evidence gaps remain and these need to be addressed to ensure that commissioners and policy-makers understand how, and if, care farming is of benefit, and to which service user groups.
Rationale for the study
Health-care commissioners, in general, lack awareness and understanding about care farming. Furthermore, they consider the lack of evidence on the clinical effectiveness and cost-effectiveness to be a barrier to commissioning. 36 Although CFs cater for a wide range of vulnerable population groups and the evidence on all service user groups is of interest, the main focus of this research is one service user group: probation service users undertaking community orders (COs). By removing the wide diversity in need, the activities and support provided on the farm would be considered less complex. Furthermore, a single service user group enables an appropriate comparator group to be selected for the purposes of quantitative evaluation. Given the limited quantitative studies with CF participants and with probation service users, there were many methodological questions that required answers before a larger study could be considered, thus a pilot study was proposed. The key questions posed were:
-
How can recruitment of probation service users undertaking COs on CFs and in comparator settings be maximised?
-
What are the optimum ways to collect baseline and follow-up data (while minimising dropout), cost data from CFs and probation trusts and individual reoffending data from the Police National Computer (PNC)?
-
What are the impacts of CFs on probation service users’ lives and how appropriate are the measures used in the pilot study for identifying changes in quality of life, health and well-being?
-
What is the extent of variation between the activities and approaches used on different CFs and the variation in outcomes for probation service users at different types of CF?
-
What is the influence of seasonality on decisions concerning the allocation of setting to serve a CO, the activities on the CFs and the health and well-being of participants?
-
What factors may lead to selection bias and what are the potential confounders, particularly in terms of factors influencing allocation to CFs and other CO settings, and how can these best be measured?
-
What is the feasibility of measuring key parameters of costs and quality-adjusted life-years (QALYs) to conduct a future cost-effectiveness analysis of CFs in comparison with other CO settings for probation service users?
We formulated these questions into a series of objectives requiring a number of different methodological approaches within one study. In order to address the wider question regarding the evidence across all service user groups, we considered that a systematic literature review would clarify the extent of the evidence and highlight where key gaps remained.
Aims and objectives
The aim of this pilot study was to build knowledge on the mechanisms through which CFs improve the health and well-being of adult probation service users undertaking COs and to explore the feasibility of assessing the cost-effectiveness of CFs in achieving these outcomes in a subsequent study.
Specific objectives were to:
-
Conduct a systematic review of published and grey literature evaluating the impacts and mechanisms within CFs and green care in improving the health and well-being of disadvantaged populations and the impacts of COs and costs of offending to society and health services.
-
Identify factors that drive the decision of CO allocation in order to identify potential selection bias and confounders as well as the most appropriate ways to collect data on these factors.
-
Identify the most appropriate ways to gain informed consent, maximise recruitment and follow-up while minimising dropout and deliver questionnaires effectively among probation service users undertaking COs in CFs and comparator CO settings.
-
Identify the most appropriate ways to collect cost data, including health-care resource use by probation service users, cost of reoffending, costs of crime and gains of employability of probation service users in CFs and comparator CO settings and explore the feasibility of measuring cost–utility.
-
Identify differences in effectiveness in terms of quality of life, mental health, lifestyle behaviours and reoffending rates between the three CFs and between CFs and comparator settings in order to estimate variation and thus determine the intracluster correlation coefficient and sample size required in the follow-on study.
-
To develop a logic model based on probation service users’ experiences of serving their CO on a CF and their perceptions of the impact the CF has on their lives and well-being, taking into consideration seasonal changes, to illustrate the possible mechanisms that lead to changes in health and well-being among probation service users undertaking COs on CFs.
Public involvement
Our aim was to involve a small number of ex-probation service users in the design and interpretation of the study, particularly in relation to the pilot study (see Chapters 3 and 4) and the qualitative interviews (see Chapter 6). At the start of the study we were invited to an established service user board (SUB) group comprising, and facilitated by, ex-probation service users with some staff also present. It was suggested that a researcher should attend the 6-monthly meetings so that a small part of the meeting could be dedicated to the study. During the meetings, there were between 3 and 6 service users in attendance. In total, we were invited to three meetings. Early in the study, the service users contributed to the design of the questionnaire booklet containing the outcome measures, the information sheet and the consent form. They also advised us on what to expect when approaching some probation service users. We were cognisant that the SUB ex-probation service users had previously spent time in prison and that they may not reflect those who had received a CO. As explained in Chapter 3, coincidental with the privatisation of probation services, the SUB facilitator left and meetings stopped. During this time, we located and attended a separate SUB meeting in a different town within the same probation service. The service users’ (three attended the meeting) and facilitators’ expectations of the research were quite different from its actual purpose and because we were not offering a new ‘service’, the group felt that they had other priorities for their meetings and we did not attend further sessions. Service user engagement was therefore interrupted as we tried to identify who was responsible for the SUB group in the original location. On establishing this, we found a new SUB board in place comprising mostly staff and only two service users, which was a change in the dynamics of the group. Interest and knowledge about the study had receded and we were required to outline the purposes of the study again. Ultimately, little progress had been made from the very first visit and our early plans to involve service users in the qualitative work were not realised. On reflection, establishing our own group rather than tapping into an existing group may have, to some extent, militated against the impact that the privatisation of probation services had on the SUB. Our contacts within probation at the start of the study had advised us that volunteers were sparse and that attendance at an additional meeting (to that of the SUB group) may be poor.
About this report
This report comprises four main sections representing the four main workstreams that address the objectives (see Aims and objectives) outlined.
-
Chapter 2 presents the methods and findings from the systematic literature review on the effectiveness of care farming on quality of life for a range of vulnerable groups (objective 1). One of the service user groups within the review is that of probation service users. The review does not include our own pilot study results, as these were not available at the time of conducting the review. We also present a number of developed logic models for particular service user groups but, as a result of the lack of studies, not one for probation service users. Within objective 1, we also included a review of evidence guiding cost-effectiveness analysis. This covered a review of the costs of offending and a review of the impacts of care farming and green care on health-related quality of life (HRQoL). These reviews are included in Chapter 5.
-
Chapter 3 presents the methods for the pilot study, but also includes a summary of probation services and COs and how care farming fits within these. There is a further and important explanation of the major organisational changes that occurred in probation during the period of research and how these impacted on the study. As a consequence of these changes, some of our objectives could not be met in full. Chapter 3 addresses objectives 2, 3 and 4, which are essentially about processes.
-
Chapter 4 presents the quantitative results for the pilot study, specifically addressing objective 5.
-
Chapter 5 presents the methods and findings of the reviews guiding cost-effectiveness analysis (objective 1) and then reports the analysis of the key parameters of costs and utilities collected as part of the feasibility data that would be used for a larger study of cost-effectiveness of CFs in improving the quality of life of probation service users undertaking COs (objective 4).
-
Chapter 6 presents the qualitative study, which involved interviewing probation service user managers regarding allocation decisions (objective 2) and probation service users (objective 6) as well as care farmers. Owing to changes in probation services during the study and other issues that arose in relation to care farming, we were unable to obtain sufficient data to enable us to fully address objective 6. These factors will be explained in Chapter 3. We considered our options and, based on our garnered knowledge regarding probation, we opted to interview a broader range of study participants to explore the role of care farming in probation. We considered that this would be most valuable to probation services going forward.
-
Chapter 7 presents a discussion chapter that brings together the findings from each of the previous chapters and outlines the implications for research and practice.
Chapter 2 The impact of care farms on quality of life among disadvantaged populations: a systematic review
Introduction, aims and objectives
The protocol for this review was registered with the Campbell Collaboration (SW2013–04). The primary objective was to systematically review the available evidence of the effects of CFs on quality of life, health and social well-being on a wide range of service user groups.
We aimed to synthesise the evidence in order to:
-
understand the size of the effect of CFs on the health, well-being or social outcomes of different population groups
-
examine whether or not effects differ depending on the activities and characteristics of the farm or farmer, the duration of time that participants spend at the farm, the number and diversity of the participants on the farm and whether or not the farm is the only intervention
-
understand the mechanisms of change for different population groups attending CFs using a range of study methodologies, including qualitative studies.
The evidence for the effectiveness of care farming is relatively recent (within the last 10 years). The complexities and multifaceted nature of CFs means that randomised controlled trial (RCT) study designs are challenging. In the light of this, our study synthesised the published and unpublished literature using a mixed-methods systematic review design. The review is registered as PROSPERO CRD42014013892 and SW2013–04 (the Campbell Collaboration). The full protocol can be found on the Campbell Collaboration website (www.campbellcollaboration.org/library/impact-of-care-farms-on-quality-of-life-different-population-groups.html; accessed 1 October 2014).
Methods
We conducted a mixed-methods synthesis using a sequential explanatory approach37 that involved the development of an intervention framework based on the theory and qualitative data with subsequent testing using the quantitative evidence. This approach is valuable in identifying possible mechanisms of change to inform the development of a logic model for care farming. We based the design of our logic models on the description and definitions provided by the MRC’s guidance for process evaluation of complex interventions. 5 Here, a logic model is defined as:
A diagrammatic representation of an intervention, describing anticipated delivery mechanisms (e.g. how resources will be applied to ensure implementation), intervention components (what is to be implemented), mechanisms of impact (the mechanisms through which an intervention will work) and intended outcomes.
Given the nature of the evidence base in this area, and the limited studies assessing health outcomes, in our logic models we split outcomes into ‘process outcomes’ and ‘health outcomes’. Examples of process outcomes are those impacts that may well be precursors to health outcomes, for example self-esteem or confidence, and examples of health outcomes include anxiety, depression and quality of life. A narrative approach incorporating a wide range of study designs was planned based on early scoping of the literature that indicated a dearth of RCTs evaluating the effectiveness of CFs.
Selection criteria
Inclusion criteria
We included RCTs, quasi-randomised study designs, cluster quasi-RCTs, interrupted time series and non-randomised observational studies, including cohort studies, case–control studies and controlled before-and-after studies. We also included before-and-after studies that did not have a control group, and qualitative studies. With regard to service user groups, we aimed to include all population groups with participants of any age who would be likely to attend a CF, including those serving COs; those with drug and alcohol problems; those with mental health problems, including anxiety, depression and psychiatric disorders; those with health problems, particularly long-term conditions, including dementia; those with learning difficulties; those receiving palliative care; and young people with challenging behaviour, particularly those excluded/facing exclusion from school or those at risk of offending.
In addition to the included study designs, we retained papers that described any theories offering explanations for how CFs may bring about change in the various population groups under investigation.
Exclusion criteria
Study designs that were excluded from the review were single-subject designs, reviews, overviews, surveys, commentaries and editorials. We also excluded theses in which empirical data had been subsequently published elsewhere. As we were interested in the most disadvantaged service user groups, we excluded studies with participants who were school children visiting for education purposes or adults as conservation volunteers. Studies in which the activity was not part of a working farm (such as community and allotment garden studies or gardening within a hospital or prison) were not included. Single activities such as gardening or horse riding were excluded. Studies evaluating petting farms and one-off farms visits were also excluded. Finally, interventions that were categorised as ‘therapy’ that were not part of a working farm (such as pet therapy and donkey/equine therapy) and those that combined care farming with another intervention (such as music therapy) were not included in the review.
Outcomes
The primary outcomes were quality of life, anxiety and depression as measured using a validated instrument. Secondary outcomes included mental health outcomes such as self-efficacy, self-esteem, stress, coping, mood, mental status, mental functioning, positive affect, rehabilitation and cognitive functioning, empowerment; social outcomes such as social functioning/interaction, group cohesion, recidivism, employment, school exclusion; physical outcomes including functional performance, physical activity and appetite and eating pattern; and behavioural outcomes such as drug use, alcohol intake and smoking.
Identification of studies
We used electronic searching, grey literature searching and hand-searching to identify studies. In November 2014, we searched the following databases: Applied Social Sciences Index and Abstracts (ASSIA) (via ProQuest) from 1987; Cumulative Index to Nursing and Allied Health Literature (CINAHL) (via EBSCOhost) from 1981; The Campbell Library; Criminal Justice Abstracts (via EBSCOhost) from 1830; Conference Proceedings Citation Index – Science [Thomson Reuters’ (New York City, NY, USA) Web of Science] from 1990; Conference Proceedings Citation Index – Social Science & Humanities (Thomson Reuters’ Web of Science) from 1990; EMBASE Classic and EMBASE (via Ovid) from 1947; Education Resources Information Center (ERIC) (via ProQuest) from 1966; Francis (via EBSCOhost) from 1972; Global Health (via Ovid) from 1910; GreenFILE (via EBSCOhost) from 1910; MEDLINE (via Ovid) from 1946; MEDLINE In-Process & Other Non-Indexed Citations (via Ovid) up to 24 November 2014; the National Criminal Justice Reference Service Abstracts Database (via ProQuest) from 1975; PsycINFO (via Ovid) from 1806; Sciences Citation Index (Thomson Reuters’ Web of Science) from 1900; Scopus (Elsevier B.V., Amsterdam, the Netherlands) from 1823; Social Care Online (SCIE) from 1980; Social Sciences Citation Index (SSCI) (Thomson Reuters’ Web of Science) from 1900; Social Services Abstracts (via ProQuest) from 1979; Sociological Abstracts (via ProQuest) from 1925; and Web of Science, Science Citation Index Expanded (SCI-EXPANDED) and SSCI from 1900.
For grey literature we performed the following searches: Health Management Information Consortium from 1983 (via Ovid); ProQuest Dissertations & Theses from 1743 (via ProQuest); Web of Science, Conference Proceedings Citation Index – Science (CPCI-S) from 1990 (Thomson Reuters); Web of Science, Conference Proceedings Citation Index – Social Science & Humanities (CPCI-SSH) from 1990 (Thomson Reuters); and databases of ongoing trials, such as Current Controlled Trials (www.controlled-trials.com; accessed 1 November 2014). We also searched the websites of European Network for Rural Development, UK Ministry of Justice (MoJ), Care Farming UK Social farming in Europe, Farming for Health, European Cooperation in Science and Technology and Green Chimneys (USA and Matmerk, Norway).
In addition, we examined the reference lists of included studies and any relevant systematic reviews identified and tracked citations of key papers using Google Scholar (Google Inc., Mountain View, CA, USA) and Web of Science Citation Indexes. We used social and care farming and relevant academic networks across Europe contact research experts or farmers to request any evaluations they have conducted. Further relevant studies were identified through citation tracking activities. We hand-searched the NJAS – Wageningen Journal of Life Sciences (2000–15) and the abstracts of CF and social farm conferences held in the UK and Europe (2005–15).
A list of search terms is located in Appendix 1.
Study selection, data extraction and management
We performed a two-stage screening process with each stage involving multiple independent reviewers. Stage 1 involved screening titles and abstracts, and stage 2 involved full-text reading. Any disagreements were discussed and resolved by consensus at each stage of the eligibility assessment. Multiple reports from the same study were coded separately before combining information across reports. We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) chart to detail the process of study selection. 38 The PRISMA checklist is also provided in Appendix 2.
To aid the development of theory-informed logic models, during full-paper screening we retained papers that mentioned theories that had been applied or mentioned within care farming studies, regardless of whether or not the study met the inclusion criteria.
We stored all the references identified by the search in EndNote X7 [Clarivate Analytics (formerly Thomson Reuters), Philadelphia, PA, USA]. We recorded in a Microsoft Excel® 2013 (Microsoft Corporation, Redmond, WA, USA) spreadsheet all websites searched and the details of any reports found or further contacts made. EPPI-Reviewer 4 (V.4.5.0.1; Evidence for Policy and Practice Information and Co-ordinating Centre, University of London, London, UK) software was used during full-paper screening to record all eligibility decisions and store extracted data.
Information on study design, sample characteristics, intervention characteristics, including contextual information about the CFs, and outcomes were extracted from studies using an adapted version of the Cochrane Public Health Group Data Extraction and Assessment Template. 39 We used a separate data extraction form for qualitative studies. When data extracting qualitative themes, we extracted negative as well as positive experiences and only included themes that represented the views of the CF service users. In studies involving service users with communication difficulties, we included themes based on the recorded perspectives of significant others (care farmers, carers and parents) on the impact of the CF on the service users. We excluded themes from others that were about their own experiences, for example the care farmers’ views on running a farm.
For papers that reported theories related to care farming, we extracted any summaries explaining how CFs may work and the expected outcomes. If the identified paper failed to provide adequate description of this process, we sought to identify the seminal paper.
Quality assessments
Qualitative studies were assessed using an adapted version of the COnsolidated criteria for REporting Qualitative research (COREQ) tool. 40,41 Three categories of reporting standard were established for each item: clearly met, unsure and not met.
The Effective Practice and Organisation of Care (EPOC) risk-of-bias tool was used to appraise RCTs. 39 The Effective Public Health Practice Project (EPHPP) tool was used to appraise other quantitative studies, such as controlled before-and-after studies or uncontrolled before-and-after (UBA) studies. 42 Studies with the majority of domains categorised as ‘unclear’ in the EPOC risk-of-bias tool were rated as being at a high risk of bias; similarly, studies with two domains categorised as ‘weak’ in the EPHPP tool were rated as being at a high risk of bias.
Each paper was assessed by two independent reviewers and any disagreements were discussed and resolved by consensus. We did not exclude any studies based on these quality assessments.
Measures of treatment effect
We did not find studies with sufficient homogeneity to pool their effect sizes and, therefore, we were unable to conduct our planned meta-analyses. Consequently, odds ratios or mean differences were not calculated.
Assessment of reporting biases
We planned to use funnel plots to assess for reporting bias. A minimum of 10 studies with a common outcome measure is needed to be able to distinguish chance from real asymmetry (i.e. true publication bias) within the funnel plots. 39 As we had fewer than 10 studies, we were unable to assess reporting bias.
Data synthesis
We based our data synthesis on a sequential exploratory approach. 37 This involved four key stages.
Stage 1
The aim of this stage was to develop a preliminary theoretical framework to explain potential mechanisms of change. For this we examined papers that reported theories relating to care farming. We retrieved the seminal articles of theories that lacked adequate description in the paper obtained through the search. Two reviewers (JM and NW) extracted information on the issue being addressed and the mechanism of change that the theory proposed to explain subsequent effectiveness. Each summary was compared with identified areas of overlap to create a condensed set of concepts on which to map the evidence. One reviewer (JM) conducted the extraction and analysis and this was subsequently checked by a second reviewer (NW).
Stage 2
This stage aimed to identify the intervention components, mechanisms of change and process outcomes from the qualitative literature. Extracted themes that were composite, that is, represented multiple discrete findings, were independently deconstructed by three reviewers (NW and JM or HE), checked and then sorted as an intervention component, mechanism or process outcome. Intervention components included the facilities, activities and structure provided as part of the farm. Mechanisms represented subjective experiences, such as feeling and perceptions, that suggested a process by which part of the intervention may result in a particular outcome. 5 Therefore, for example, having physical contact with the animals (the intervention) would provide a sense of warmth and calm (mechanism). Process outcomes were those derived from a particular mechanism within the intervention. Health outcomes, as previously defined in this review, were not categorised as a process outcome.
On agreement between the reviewers, each finding was transcribed onto a sticky note in preparation for a clustering exercise. 43 This exercise involved six additional reviewers (RB, ME, CB, JC, ST and DS) checking the groupings of intervention components, mechanisms and process outcomes on the Post-it® (3M, Maplewood, MN, USA) notes. Then the mechanisms were independently, and without consultation, placed on a blank wall and moved around the wall without consultation according to emerging categories of similar mechanisms. Once completed, the reviewers labelled each category according to composition and meaning. Subsequent detailed additional analysis was performed by three reviewers (JM, NW and HE) to ensure that each of the findings had not been overinterpreted (i.e. assumptions about what the mechanism may lead to), was appropriately allocated and remained true to its original context. For the intervention components, one reviewer (JM) grouped the findings according to congruency and labelled each of the categories. This was subsequently checked by one further reviewer (NW).
As a gauge of the potential relative importance of each of the categories of mechanisms, we assessed the spread of the categories (across all the studies) and the frequency of the findings within each category. We carried this out for all the studies (all population groups) and for each individual population group (whenever possible). We ordered the categories based on this assessment to explore the possibility that CFs may work in different ways for different populations.
Stage 3
This involved mapping of the qualitative mechanisms and process outcomes to the theoretical concepts to create a logic model. This was performed by one reviewer (JM) and checked by a further two reviewers (NW and HE). The aim was to understand the ways in which change occurred and to start testing the theories using empirical data.
Stage 4
The outcomes from the quantitative studies were synthesised narratively, in accordance with the Economic and Social Research Council’s guidance,44 and were then mapped to the logic models.
Findings
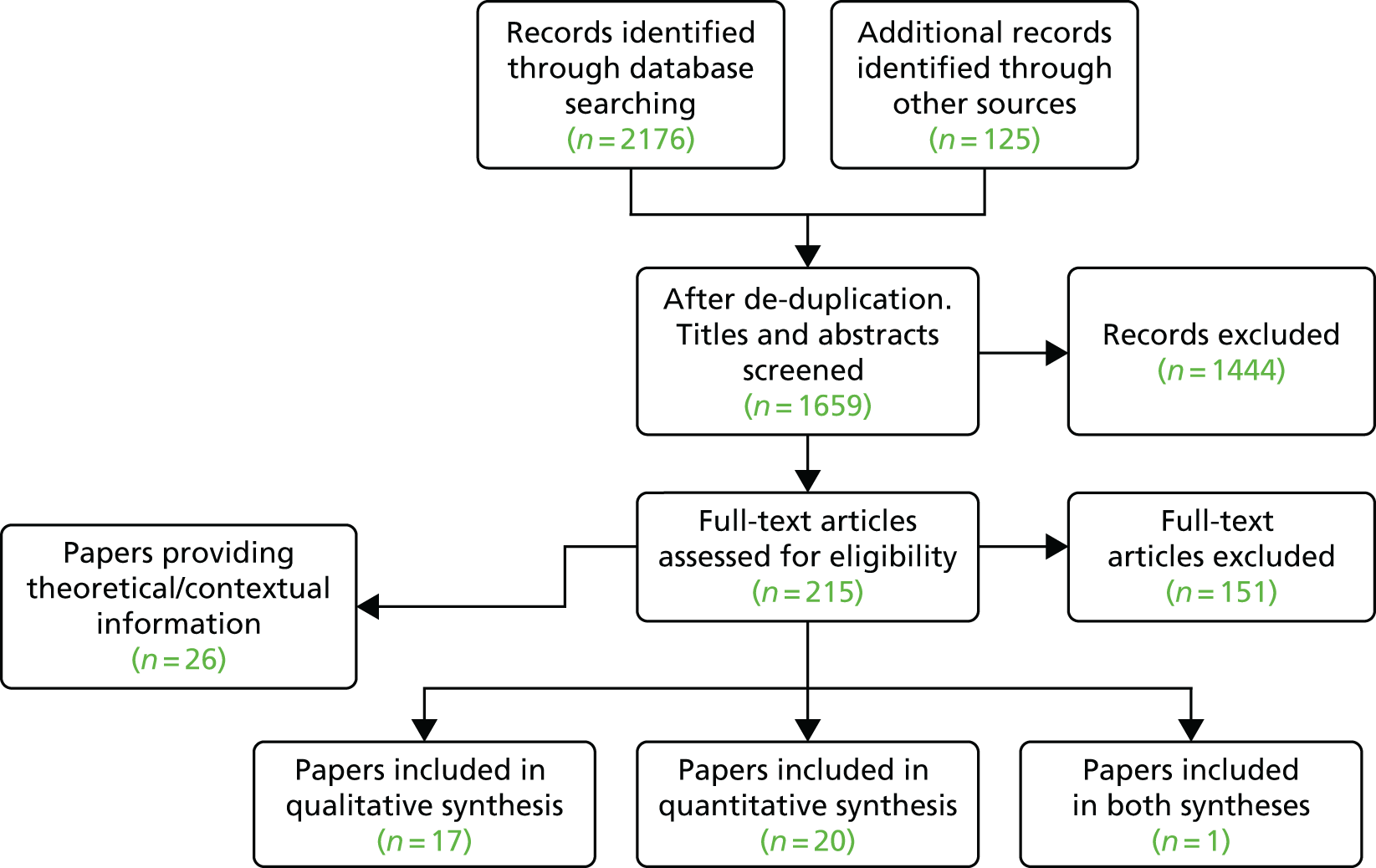
We found 2176 articles through searching of electronic databases and 125 via grey literature retrieval methods (Figure 2). We obtained full copies of 215 articles and, of these, 38 papers (representing 27 studies) met the inclusion criteria. We retained 26 studies that provided theoretical (to support the development of the logic model) and contextual information (to shed light on activities relating to specific service user groups) about the care farming intervention, despite the study’s exclusion from the main review.
FIGURE 2.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Fourteen qualitative studies reported in 17 papers (Table 2), 12 quantitative studies reported in 20 papers (Table 3) and one mixed-methods study28 met the inclusion criteria. From 20 publications, we identified 17 theoretical or philosophical concepts quoted in connection to care farming. From these, we retained 15 that offered a potential explanation for how CFs may work to bring about change in various service user groups.
| References | Country | Client group | Method | Numbers of interviewees | Age (years), mean (range) | Gender (n) | Quality criteria met (%) |
|---|---|---|---|---|---|---|---|
| Baars et al.45 | The Netherlands | Mental ill health | Interviews and photography | 8 | 39 |
Male: 4 Female: 4 |
< 50 |
| Bjørgen and Johansen46 | Norway | Mental ill health | Focus groups | 15 | – | – | < 50 |
| Elings47 | The Netherlands | Learning disabilities | Interviews, participatory observation | 18 | – | – | < 50 |
| Elings and Beerens;48 and, Elings and Hassink49,50 | The Netherlands | Mental ill health: psychiatric; substance misuse | Focus groups | 42 | – | – | < 50 |
| Elings et al.28 | The Netherlands | Mental ill health; substance misuse | Interviews and focus groups | 55 | – | – | < 50 |
| Ferwerda-van Zonneveld et al.51 | The Netherlands | Children with autism spectrum disorder | Interviews | 7 | – |
Male: 1 Female: 6 |
< 50 |
| Granerud and Eriksson52 | Norway | Mental ill health: long-standing severe psychotic disorders, personality disorders; substance misuse | Interviews | 20 | (22–55) |
Male: 8 Female: 12 |
> 50 |
| Hassink;53 and Hassink et al.24 | The Netherlands | Mental ill health; disaffected/excluded youth; older people | Interviews | 41 | – |
Male: 30 Female: 11 |
> 50 |
| Iancu et al.54 | The Netherlands | Mental ill health | Interviews | 26 | – |
Male: 16 Female: 10 |
> 50 |
| Kaley55 | UK | Learning difficulties | Interviews and video recording and photographic method | 7 | – |
Male: 7 Female: 0 |
> 50 |
| Kogstad et al.56 | Norway | Disaffected/excluded youth | Interviews | 9 | 22.5 (17–27) |
Male: 2 Female: 7 |
> 50 |
| Leck et al.57 | UK | Mental ill health; substance misuse; disaffected/excluded youth; learning difficulties | Interviews and focus groups | 33 | – |
Male: 26 Female: 7 |
< 50 |
| Pedersen et al.58 | Norway | Mental ill health: people with depression | Interviews | 8 | 37.6 (27–54) |
Male: 1 Female: 7 |
> 50 |
| Schreuder et al.59 | The Netherlands | Disaffected/excluded youth | Interviews | 11 | (16–23) |
Male: 9 Female: 2 |
> 50 |
| North Essex Research Network and South Essex Service User Research Group60 | UK | Mental ill health | Interviews | 5 | – |
Male: 4 Female: 1 |
< 50 |
| Study design | References | Country | Client group | Control group | Sample size | Age (years), mean ± SD (range) | Gender (n) | Duration | Process outcomes (measures) | Outcomes (measures) | Follow-ups |
|---|---|---|---|---|---|---|---|---|---|---|---|
| RCT | Berget et al.61–63 | Norway | Mental ill health: patients with psychiatric disorders | Treatment as usual | 90 | 34.7 ± 10.7 (18–58) |
Male: 31 (34.4%) Female: 59 (65.6%) |
3 hours, twice a week, for 12 weeks | Coping (Coping Strategies Scale); self-efficacy (Generalized Self-Efficacy Scale); and work abilitiesa,b | Quality of life (the Norwegian version of the Quality of Life Scale); depression (The Beck Depression Inventory); and anxiety (The Spielberger State Anxiety Inventory) | 12 weeks and 6 months |
| RCT | Pedersen et al.64 | Norway | Mental ill health: people with clinical depression | Waiting list control group | 29 |
Intervention: 40.5 ± 10.7 Control: 34.0 ± 6.6 |
Intervention: 5 male, 11 female Control: 1 male, 12 female |
1.5–3 hours, twice a week, for 12 weeks | Self-efficacy (Generalized Self-Efficacy Scale) | Depression (The Beck Depression Inventory); and anxiety (State–Trait Anxiety Inventory-state subscale) | 12 weeks and 3 months after the intervention |
| CBA | de Bruin;65 and de Bruin et al.66 | The Netherlands | Older people > 65 years with dementia | Regular day care facilities | 88 |
Intervention: 77.6 ± 6 Control: 81.9 ± 5.7 |
Intervention: 25 (83%) male, 5 (17%) female Control: 7 (30%) male, 16 (70%) female |
6 hours, 2–3 days a week | Cognitive functioning (Mini Mental State Examination); functional performance (The Barthel Index); medication usage; total number of diseases;a emotional well-being;a number of clinically relevant behavioural symptoms;a and number of medications useda | – | 6 months and 12 months |
| CBA | Elings et al.28 | The Netherlands | Mental ill health; substance misuse | Day activity projects | 113 |
Intervention: (31–50) Control: (31–40) |
Intervention: 80% male, 20% female Control: 62% male, 38% female |
6 hours, approximately 3 days a week | Social functioning (Social Functioning Scale); mental functioning (5-item Mental Health Inventory); and appetite and eating pattern (Simplified Nutritional Appetite Questionnaire) | Quality of life (WHOQOL-BREF) | 6 months and 12 months |
| UBA | Hassink et al.25 | The Netherlands | Disaffected/excluded youth | N/A | 74 |
Male: 16.6, ± 1.0 Female: 15.6 ± 1.2 |
Male: 66 Female: 8 |
24 hours, for half a year at the farm | Problem behaviour (Youth Self-Report); coping (Utrecht Coping List); and self-determination (IPC LOC Scale) | – | 6 months and 12 months |
| UBA | Gonzalez;67 and Gonzalez et al.68–71 | Norway | Mental ill health: people with clinical depression | N/A | 46 | 46.3 (25–65) |
Male: 10 Female: 36 |
3 hours, twice a week, for 12 weeks | Positive affect (Positive and Negative Affect Scale); stress (Perceived Stress Scale); and group cohesion (Therapeutic Factors Inventory – Cohesiveness Scale) | Depression (Beck Depression Inventory); and anxiety (State–Trait Anxiety Inventory–state subscale) | 12 weeks and 3 months after the intervention |
| UBA | Pedersen et al.72 | Norway | Mental ill health: people with clinical depression | N/A | 14 | 37.4 (23–54) |
Male: 3 Female: 11 |
1.5–3 hours, twice a week, for 12 weeks | – | Depression (Beck Depression Inventory); and anxiety (State–Trait Anxiety Inventory-state subscale) | 12 weeks |
| UBA | Javed et al.73 | Pakistan | Mental ill health: diagnosis of schizophrenia | N/A | 25 | 28.18 (20–60) |
Male: 25 Female: 0 |
– | Mental status (Brief Psychiatric Rating Scale); and Rehabilitation (Morningside Rehabilitation Status Scale) | – | 1 year, 2 years and 3 years |
| UBA | Hine et al.74,75 | UK | Mental ill health; substance misuse; older people; and offenders | N/A | 72 | (16–65) |
Male: 55 (76%) Female: 17 (24%) |
5.5 hours (range: 2–8 hours) | Self-esteem (Rosenberg Self–Esteem Scale); and mood (Profile of Mood States questionnaire) | Depression (from the Profile of Mood States questionnaire) | Immediately after the intervention |
| UBA | Hine et al.76 | UK | Mental ill health: asylum seekers and refugees, who are suffering from post-traumatic stress disorder and depression | N/A | 20 | – | – | 10–12 weeks | – | Quality of life (CORE-OM) | End of intervention (10–12 weeks) |
| UBA | Lambert77 | UK | Learning difficulties; mental ill health: anxiety and/or depression; psychosis; personality and/or social issues; and people with brain injury | N/A | 83 | 40.7 ± 12.8 |
Male: 54 (65%) Female: 29 (35%) |
11.5 days | General health and attitudea; and occupational functioninga | Quality of life (EuroQol-5 Dimensions) | End of intervention and morning/afternoon |
| UBA | Marshall and Wakeham78 | UK | Offenders | N/A | 10 | – | – | 5 hours and 15 minutes, over 18 sessions | Reoffending | – | 12 months |
| UBA | Suprise79 | USA | Youth in foster care | N/A | 18 | (9–17) |
Male: 18 Female: 0 |
Up to two times per week with many coming for years | Prosocial behaviour and social competencea defined | – | 6 weeks |
Characteristics of included studies
Across the qualitative studies, five studies45,46,54,58,60 focused solely on people with mental health problems, including people with depression and psychotic and personality disorders. A further three studies included two service user groups for people with mental health problems as well as drug and alcohol misuse. 28,48–50,52 Other studies that involved single service user groups included two for people with learning disabilities,47,55 two for disaffected youth56,59 and one for people with autism. 51 There were 298 service user participants, with study sizes ranging from 5 to 55. Ten studies24,28,46–51,53–55,57,60 did not provide information on the age of the study participants and gender was not reported in four studies. 28,46–50 There were almost twice as many male service users participating in the studies as female service users (ratio of 1.8 : 1).
Among the quantitative studies were two RCTs61–64 and two controlled before-and-after studies,28,65,66 with the remaining nine using an UBA design. 25,67–79 Ten studies evaluated the effects of care farming on a targeted single service user group: six on service users with mental ill health;61–64,67–73,76 one on older people with dementia;65,66 two on disadvantaged youth;25,79 and one on probation service users. 78 Three studies28,74,75,77 used a mixed service user group, with two including four different groups. 74,75,77 Gender was reported in 11 studies,25,28,61–75,77,79 which revealed twice as many male than female participants (male, n = 261; female, n = 117). The mean age of participants in the studies ranged from 9 to 78 years. The intensity and duration of intervention varied, but most commonly involved half-day (1.5–3 hours) or full-day (5–6 hours) sessions two or three times per week over a 12-week period. Most commonly, follow-ups were performed immediately after the intervention with two studies also reporting at 3 months,64,67–71 four studies at 6 months25,28,61–63,65,66 and four studies at 12 months. 25,28,65,66,78 One study reported follow-up at 3 years. 73 Across the studies, 23 different defined outcome measures were applied, only six of which were primary outcomes.
Studies provided limited information about the types of activities available on the farms. The studies fell into four main types: horticultural/land maintenance work,45,65,67,76 conventional farm animal care,28,35,45,52,56,59,61,63,64,74,78 additional animal-based activities73 and other activities. 60 The last type included working in the shop, outdoor recreational activities (camping, campfires, outdoor trips and den building) and indoor activities (baking, meal preparation, crafts, games, general household work and tractor driving). Some studies did not provide enough details about the interventions to be classified.
Quality assessments
Six of the qualitative studies24,52–56,58,59 (40%) met more than 50% of the 37 quality assessment criteria (Table 4). Only one study59 met more than 60% of the criteria. One study met less than 20% of the criteria. 60 Openness about the researcher’s bias and assumptions and evidence of a pre-existing or newly established relationships were each addressed by only one study. Two criteria fundamental to all research practice are evidence of ethics approval and evidence of informed consent. These were not reported in nine (60%) studies. 24,28,45–51,53,59,60 All studies that met more than 50% of the quality criteria used a theoretical framework.
| Section of tool | Items most often addressed (number of studies plus number of studies partially addressing item) | Items least often addressed (number of studies, plus number partially addressing item) |
|---|---|---|
| Background, research team and reflexivity (eight items) |
Is it clear what is being studied? (15 studies)24,45,46,48–60 Is it clear which author(s) conducted the interviews or focus groups? (Seven studies, plus one study)24,46,51–53,55,56,58,59 Is the gender of the researcher clear? (Seven studies, plus one study)24,46,52,53,55–59 |
Were the characteristics of the interviewer reported? (One study)46 Evidence of relationship established between researcher/interviewer and participant before the study commenced? (One study, plus one study)55,57 Did the researcher/interviewer indicate if there was a pre-existing relationship with the participant and, if so, was this described? (One study)58 |
| Study design (16 items) |
Does the study state how many took part in the interviews/focus group/observations? (13 studies, plus one study)24,45,46,48–56,58–60 Does the author say how many interviews/focus group/observations were carried out? (12 studies)24,45,50–60 Were audio or visual methods used to record/collect the data? (12 studies)24,46,48,49,51–56,58–60 |
Does the researcher state if anyone else was present during the interviews? (Three studies, plus one study)46,50,58,60 |
| Data analysis and findings (13 items) |
Do the quotations reflect the findings? (14 studies)24,45–54,56,58–60 Were major themes clearly presented in the findings? (15 studies)24,45,46,48–60 |
Does the study report the number of coders involved? (Three studies)54,56,58 Did the authors report checking back with informants over interpretation? (Two studies)24,46,53 |
All quantitative studies had many limitations and were rated as being at a high risk of bias (Tables 5 and 6). For the two RCTs,61–64 allocation concealment was clearly described in one study. 64 Baseline assessments reported in both studies revealed differences between the intervention and the control groups in one study,25 which were not adjusted for in analysis. Differences in baseline characteristics were also reported in one study61–63 but unclear in the other. 64
| Study | Was the allocation sequence adequately generated? | Was allocation adequately concealed? | Were baseline outcome measurements similar? | Were baseline characteristics similar? | Were incomplete outcome data adequately addressed? | Was knowledge of the allocated intervention adequately prevented during the study? | Was the study adequately protected against contamination? | Are reports of the study free of suggestion of selective outcome reporting? | Global rating for this paper |
|---|---|---|---|---|---|---|---|---|---|
| Pedersen et al.64 | ✓ | ✓ | ✗ | ✗ | ✓ | ✗ | ✓ | ✓ | ✗ |
| Berget et al.61–63 | ✓ | = | ✓ | = | ✗ | ✗ | = | ✓ | ✗ |
| Study | Selection bias | Study design | Confounders | Blinding | Data collection method | Withdrawals and dropouts | Global rating for this paper |
|---|---|---|---|---|---|---|---|
| de Bruin;65 and de Bruin et al.66 | ✗ | = | ✗ | = | = | = | ✗ |
| Elings et al.28 | = | = | ✗ | ✗ | ✓ | = | ✗ |
| Hassink et al.25 | ✓ | = | ✓ | ✗ | = | ✗ | ✗ |
| Gonzalez,67 Gonzalez et al.68–71 | ✗ | = | ✗ | ✗ | ✓ | ✓ | ✗ |
| Pedersen et al.72 | = | = | ✗ | ✗ | ✓ | = | ✗ |
| Javed et al.73 | ✗ | = | = | ✗ | ✗ | = | ✗ |
| Hine et al.74,75 | = | = | = | ✗ | = | ✗ | ✗ |
| Hine et al.76 | ✗ | = | ✗ | ✗ | ✓ | ✗ | ✗ |
| Lambert77 | ✗ | = | = | = | = | ✗ | ✗ |
| Marshall and Wakeham78 | ✗ | = | ✗ | ✗ | ✓ | ✗ | ✗ |
| Suprise79 | ✗ | = | = | ✗ | ✗ | ✗ | ✗ |
The logic models
The MRC’s guidance on the evaluation of complex interventions5 provides the basis for the design of our logic models and the definitions of the terms used within them. For clarity, the MRC’s definition of a logic model is given as:
A diagrammatic representation of an intervention, describing anticipated delivery mechanisms (e.g. how resources will be applied to ensure implementation), intervention components (what is to be implemented), mechanisms of impact (the mechanisms through which an intervention will work) and intended outcomes.
Theoretical concepts
Exploration of the identified theories revealed five theoretical concepts: restorative effects of nature, being socially connected, personal growth, physical well-being and mental well-being. The primary outcomes explicitly suggested by theories were related to depression and anxiety, and quality of life. The process outcomes suggested by theories were related to confidence, stress, coping and self-efficacy, and pro-social behaviours.
Intervention components, mechanisms and process outcomes
Through the process of deconstruction of reported themes, we identified 85 intervention components, 164 mechanisms and 24 process outcomes. Intervention components5 were organised into five categories: being in a group, the farmer, the work, the animals and the setting (Table 7). Overall, care farming intervention components relating to the farmer and the work appeared to be prominent features in the findings. Despite the fact that data were infrequently reported for single service user groups, we did observe some differences in the types of intervention components mentioned that may indicate differences in either the types of activities made available to disparate service user groups or the level of importance of those activities to types of service users.
| Intervention category | Number of findings in each category (%) | |||
|---|---|---|---|---|
| All client groups | Mental ill health and substance misusea | Disaffected youthb | Learning difficultiesc | |
| Being in a group | 13 (15) | 10 (16) | 4 (16) | 4 (19) |
| The farmer | 23 (27) | 17 (27) | 5 (20) | 6 (29) |
| The work | 29 (34) | 20 (31) | 7 (28) | 10 (48) |
| The animals | 11 (13) | 10 (16) | 3 (12) | 0 |
| The setting | 9 (11) | 7 (11) | 6 (24) | 1 (5) |
| All | 85 | 64 | 25 | 21 |
We used the MRC’s definition of mechanisms to guide our identification of mechanisms within CF studies:
The intermediate mechanisms through which intervention activities produce intended (or unintended) effects. The study of mechanisms may include: participant responses – how participants interact with a complex intervention; mediators – intermediate processes which explain subsequent changes in outcomes; unintended pathways and consequences.
Through the iterative clustering exercise, mechanism-based findings were organised into 15 categories of mechanisms (Table 8). Although we identified the frequency that the mechanisms occurred, we do not suggest that any one mechanism is more important than another at an individual level. In terms of frequency and spread of findings, the categories ‘understanding the self’, ‘social relationships’ and ‘belonging and non-judgement’ represented the most common categories across all studies. ‘Creating a new identity’ and the farm as a ‘distraction’ were least often observed across the studies.
| Mechanisms | Description | Frequency of findings in each category (all groups) |
|---|---|---|
| Achievement and satisfaction | Working at the farm gives service users a sense of satisfaction. At the farm, participants learn to perform activities; hence, they spent their days being constructive. There is satisfaction with using their bodies and spending time outdoors | 15 |
| Belonging and non-judgement | The CF is seen by service users as a place of belonging and mutual acceptance. Feelings of solidarity are created through shared experiences. Service users enjoy working with the animals, which are perceived to be non-judgemental | 22 |
| Creating a new identity | Service users view themselves in a new light as a worker, principally as a farmer | 3 |
| Distraction | The farm creates physical work, which offers both a practical and mental distraction from the service users’ own negative thoughts. Conversations centre on work, which offers further distraction | 6 |
| Feeling valued and respected | Service users feel valued, appreciated and needed by the farmer (and the animals) and consider that they are respected ‘for who they are’ | 12 |
| Feeling safe | The atmosphere at the farm creates a feeling of safety and security, providing a mental shield between illnesses and addictions. For some service users this experience is enhanced through physical contact with the animals, but for others there is a need to overcome fear of animals, which can then lead on to a feeling of safety | 12 |
| Learning skills | CFs give service users the opportunity to learn new skills ranging from growing crops to looking after animals, which enables some to gain qualifications, enabling then to (re)enter the work place | 11 |
| Meaningfulness | Service users perceive tasks as meaningful because they are judged to be useful to others and are ‘needed to conduct day-to-day activities at the farm’. Service users also see their role as personally meaningful, contributing to society giving them a sense of purpose, happiness and fulfilment | 11 |
| Nurturing | Through helping each other and caring for the animals/plants, service users become considerate of other people’s needs and recognise that they are doing good for other living creatures | 4 |
| Physical well-being | Through physical activity on the farm, service users improve their physical strength. There is a sense of ‘good’ tiredness from physical work. Service users start to feel more independent and healthier | 10 |
| Reflection | The CF environment is quiet and peaceful, allowing service users to stop and reflect on their problems, their social influences and also the progress they have made. For young people, working at the farm gives space and time away from their family and friends | 3 |
| Social relationships | CFs provide opportunities for participants to interact with the farmer and other service users. For instance, often service users were working together in groups which helped them to develop their communication skills. As the intervention progressed, the service users deepened their relationships with the farmer and considered him or her as a role model. Once service users gained social confidence, their social networks grew. In particular, they found that talking about their farm work was more interesting than talking about their illness in social functions. However, a few service users did not want to interact with others and found it difficult to deal with the diverse range of service users at the farm | 16 |
| Stimulation | Service users find tasks stimulating, giving them more energy and encouraging a mindful approach to work, especially around animals, which are unpredictable. Working with animals offers a sensory experience and the energy derived from the work enables them to work through their own problems better. The experience of being in nature is energising | 7 |
| Structure | The daily farming activities provided a predictable work environment to the service users. This consistency helped the service users to gain a normal rhythm. Moreover, the farmers also allowed service users to work at their own pace as they understood that the service users can have a ‘bad day’ and may not be able to work at full capacity. Similarly, farmers involved participants in deciding tasks for the day | 8 |
| Understanding the self | The CF environment has allowed service users to better understand themselves. Participant’s self-awareness grew while at the CF. For example, learning to master an activity at the farm increased their self-respect and positive self-image. At the farm, participants were free to be themselves, and they also had the opportunity to learn and when they made mistakes they were given time and guidance to learn from their mistakes. This gave them the understanding that tasks at the farm are manageable, which enhanced their self-efficacy and self-confidence. Some found that caring for and cuddling animals helped them to deal with problems | 24 |
In terms of service user groups, findings from the substance misuse and mental ill health service users were reported together and could not be separated. This service user group, as a combined group, was the largest, with 105 findings from 10 studies. No findings relating to ‘reflection’ or ‘creating a new identity’ were found in this combined service user group. For disaffected youth, ‘feeling safe’ was more frequently reported than ‘belonging and non-judgement’. ‘Achievement and satisfaction’ was frequently mentioned in both the combined mental health and substance misuse group and the learning disabilities group, but was reported less often in the disaffected youth group. ‘Reflection’ was also reported more often in the disaffected youth group than in the others. In the learning disability service user group, ‘understanding the self’ was reported less frequently than ‘social relationships’, ‘belonging and non-judgement’, ‘social relationships’ and ‘meaningfulness’.
Of the 24 process outcomes reported in the qualitative studies (Table 9), 11 related to emotions, such as increased confidence and self-esteem. Improved coping and feelings of well-being were also mentioned in numerous studies, as was independence.
| References | Number of mechanism findings | Categories of mechanisms | Target groups | Outcomes reported by participants | Theoretical basis |
|---|---|---|---|---|---|
| Baars et al.45 | 16 | Achievement and satisfaction; belonging/non-judgement; distraction; feeling valued/respected; learning skills;a nurturing; physical well-being; social relationships; structure; and understanding the selfa | Mental ill health | Less medication | None stated |
| Bjørgen and Johansen46 | 5 | Distraction;a feeling safe; and social relationshipsa | Mental ill health | Increased confidence, physical health and vocational rehabilitation | None stated |
| Elings47 | 20 | Achievement and satisfaction; belonging/non-judgement; creating a new identity; feeling safe; feeling valued/respected;a learning skills; meaningfulness; stimulation; structure; and understanding the self | Mental ill health: service users with intellectual disabilities | Improved self-esteem | None stated |
| Elings and Beerens;48 and Elings and Hassink49,50 | 16 | Achievement and satisfaction; belonging/non-judgement; distraction; learning skills; meaningfulness; physical well-being; stimulation; and understanding the selfa | Mental ill health: psychiatric; substance misuse | Increased confidence | Anthroposophyb |
| Elings et al.28 | 3 | Feeling safe; meaningfulness; and structure | Mental ill health; substance misuse | – | None stated |
| Ferwerda-van Zonneveld et al.51 | 5 | Feeling safe; reflection; stimulation; structure; and understanding the self | Children with autism spectrum disorder | – | None stated |
| cGranerud and Eriksson52 | 13 | Achievement and satisfaction; belonging/non-judgement;a feeling safe; feeling valued/respected; meaningfulness; physical well-being; structure; and understanding the self | Mental ill health: long-standing severe psychotic disorders, personality disorders; and substance misuse | Improved well-being, self-perception; social life and confidence | Recovery model |
| cHassink;53 and Hassink et al.24 | 10 | Belonging/non-judgement;a feeling safe; feeling valued/respected; learning skills; social relationships; structure; and understanding the self | Mental ill health; disaffected/excluded youth; and older people | – | Recovery model |
| cIancu et al.54 | 7 | Belonging/non-judgement; learning skills;a meaningfulness; physical health; social relationships; and understanding the self | Mental ill health | Increased confidence, mood and less tiredness | Recovery model |
| cKaley55 | 22 | Achievement and satisfaction; belonging/non-judgement;a creating a new identity; feeling valued/respected; meaningfulness; nurturing; social relationships; stimulation; and understanding the self | Learning difficulties | Increased independence, well-being and reduced anxiety and healthy lifestyle | Therapeutic landscape concept |
| cKogstad et al.56 | 6 | Feeling safe; meaningfulness; physical well-being; reflection; social relationships; and understanding the self | Disaffected/excluded youth | – | Recovery theory |
| Leck et al.57 | 16 | Achievement and satisfaction; belonging/non-judgement; feeling safe; learning skills; meaningfulness; nurturing; physical well-being; social relationships;a and structure | Mental ill health; substance misuse; disaffected/excluded youth; and learning difficulties | Increased happiness and improved pro-social behaviours | ART, biophilia, PET |
| cPedersen et al.58 | 16 | Achievement and satisfaction;a belonging/non-judgement; distraction; feeling safe; feeling valued/respected; learning skills; meaningfulness; nurturing; physical well-being; stimulation; understanding the self | Mental ill health: people with depression | Increased confidence and independence | Biophilia; self-efficacy theory; |
| cSchreuder et al.59 | 5 | Feeling valued/respected;a reflection; understanding the selfa | Disaffected/excluded youth | – | Salutogenic theory |
| North Essex Research Network, South Essex Service User Research Group60 | 4 | Achievement and satisfaction; social relationships; stimulation; understanding the self | Mental ill health | Increased independence | None stated |
Mapping mechanisms from qualitative studies to the theoretical concepts
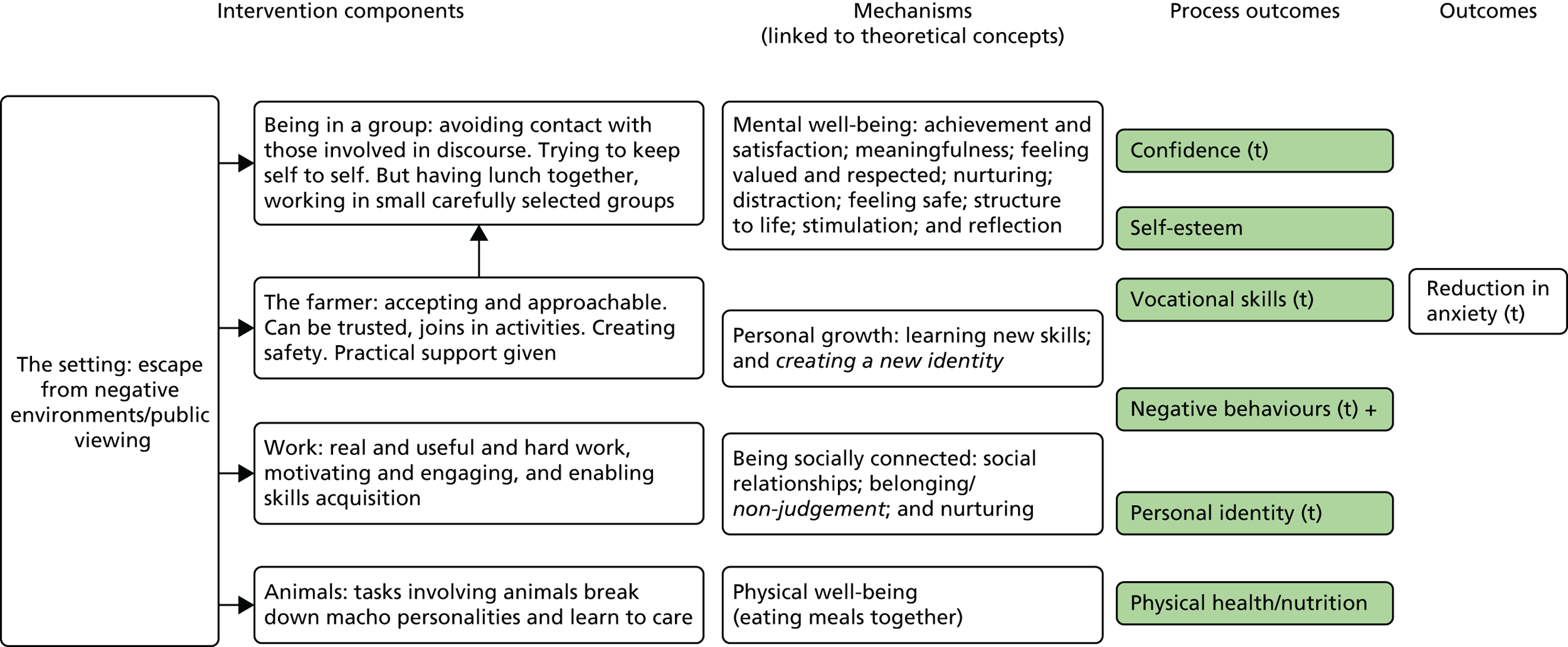
Across the three main service user groups (combined mental health and substance misuse, disaffected youth and learning difficulties), there were some differences in how mechanisms mapped to theoretical concepts. In the combined mental ill health and substance misuse group, the number of mechanism findings that mapped to ‘mental well-being’ was almost double that of any other theoretical concept. In the other service user groups, ‘being socially connected’ and ‘mental well-being’ were similarly represented by the mechanisms. Only four single findings within the mechanism categories of ‘reflection’, ‘stimulation’ and ‘feeling safe’ appeared to map on to the theoretical concept of ‘restorative effects of nature’, but these mapped more appropriately to ‘mental well-being’. The categories of mechanisms were then combined with the intervention components and process outcomes to create a logic model for the following service user groups: all service user groups; combined mental ill health and substance misuse group; disaffected youth group; and learning disabilities group (Figures 3–6). There were insufficient data to develop models for older people and for people with autism spectrum disorder.
FIGURE 3.
Logic model for all service user groups. a, Mechanisms that were most frequently found and with greatest spread across studies. Grey and black symbols show quantitative evidence for which – means no significant difference and + means significant difference; grey represents RCT evidence; two symbols beside each other show different time points within the same study; and shaded process outcomes equate to evidence from qualitative literature. t, theory based.
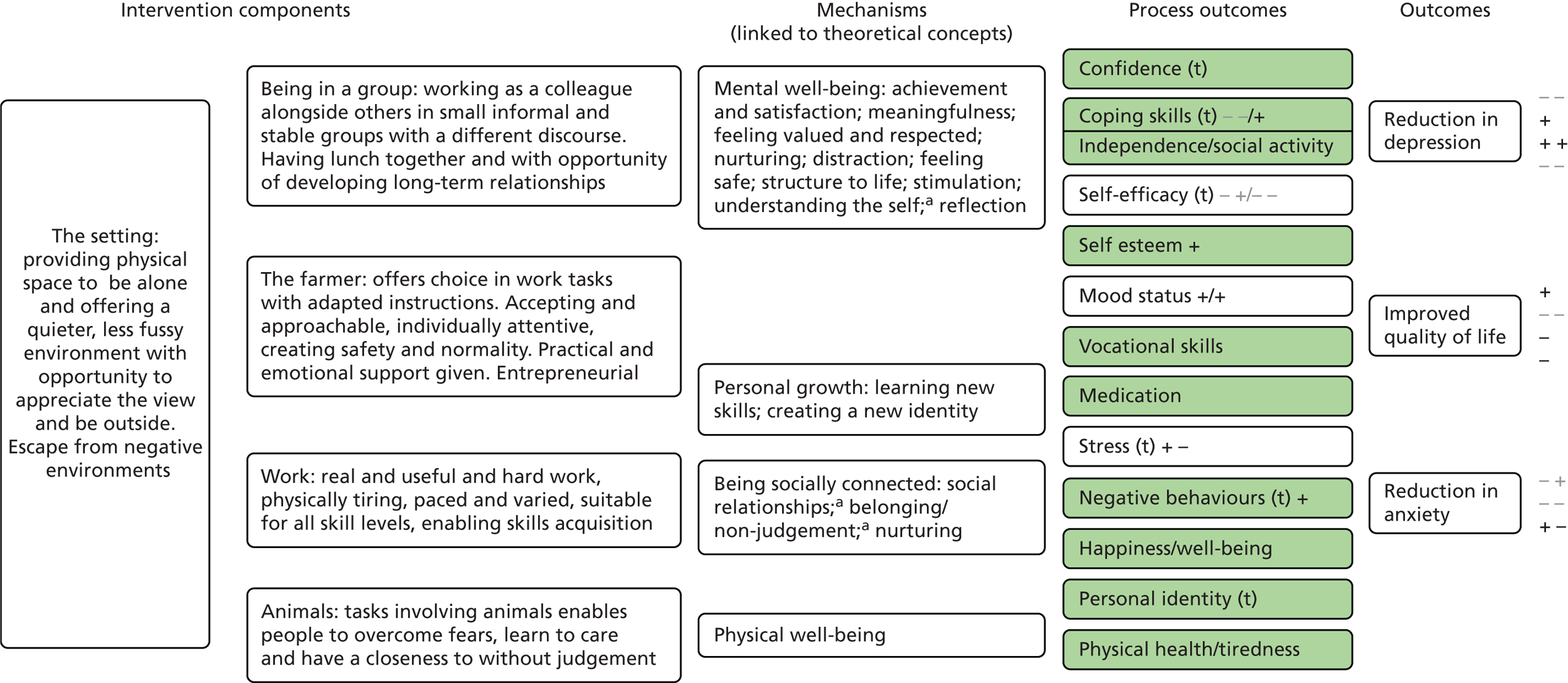
FIGURE 4.
Logic model for combined mental ill health and substance misuse group. a, Mechanisms that were most frequently found and with greatest spread across studies. Grey and black symbols show quantitative evidence for which – means no significant difference and + means significant difference; grey represents RCT evidence; two symbols beside each other show different time points within the same study; and shaded process outcomes equate to evidence from qualitative literature. t, theory based.
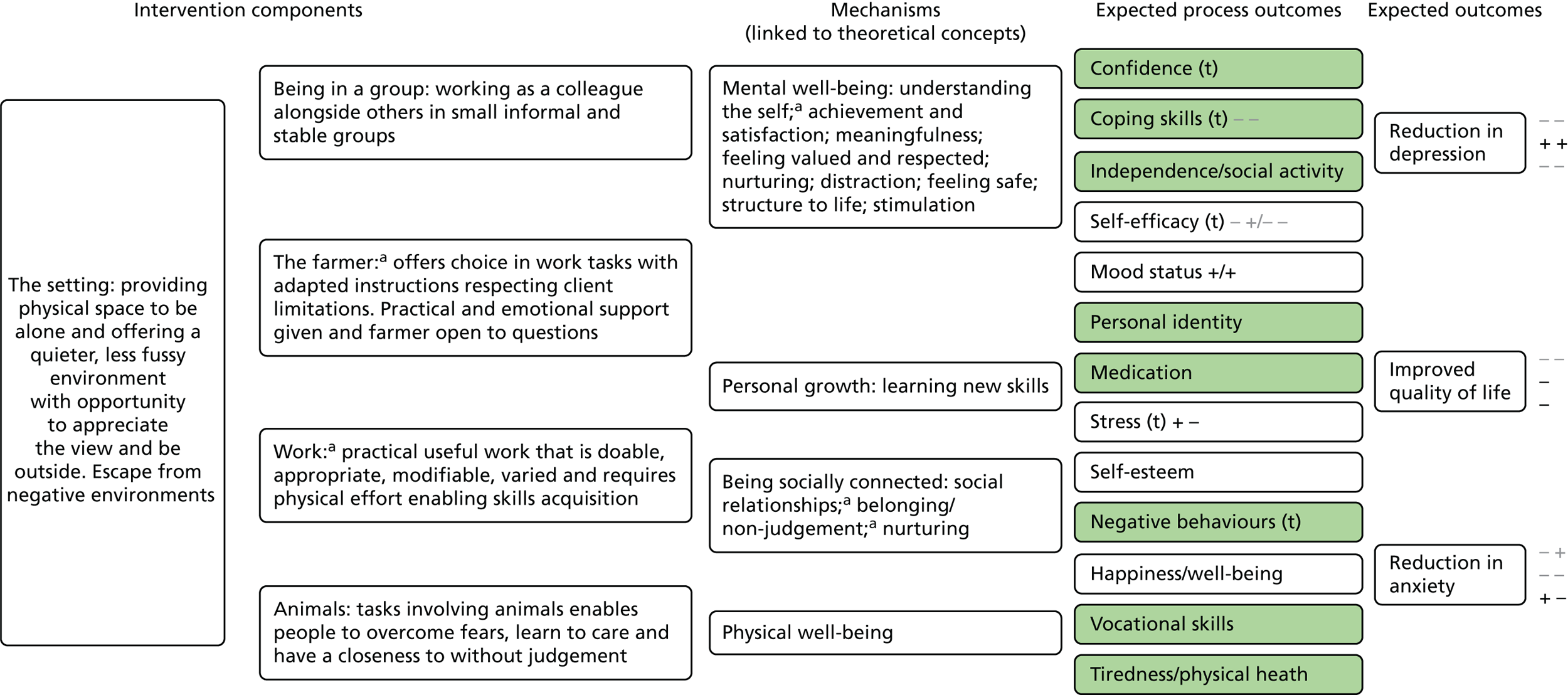
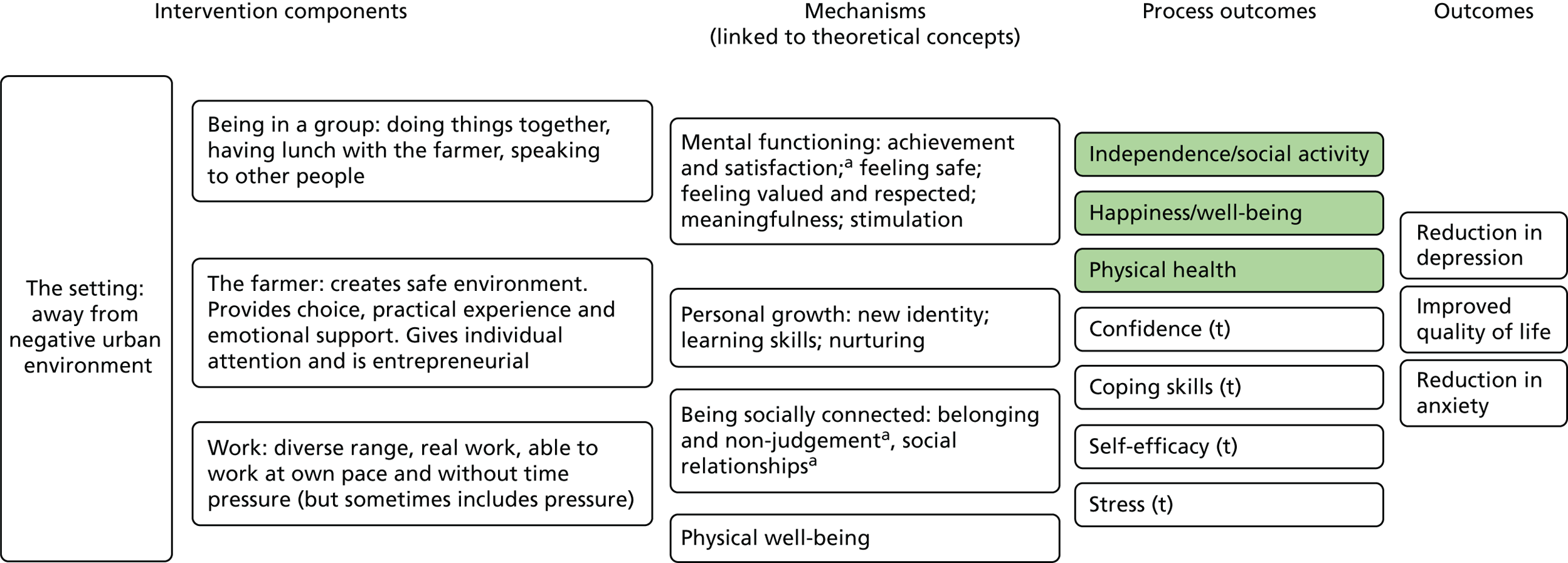
FIGURE 5.
Logic model for disaffected youth group. a, Mechanisms that were most frequently found and with greatest spread across studies. Black symbols show quantitative evidence for which – is no significant difference and + is significant difference; and shaded process outcomes equate to evidence from qualitative literature. t, theory based.
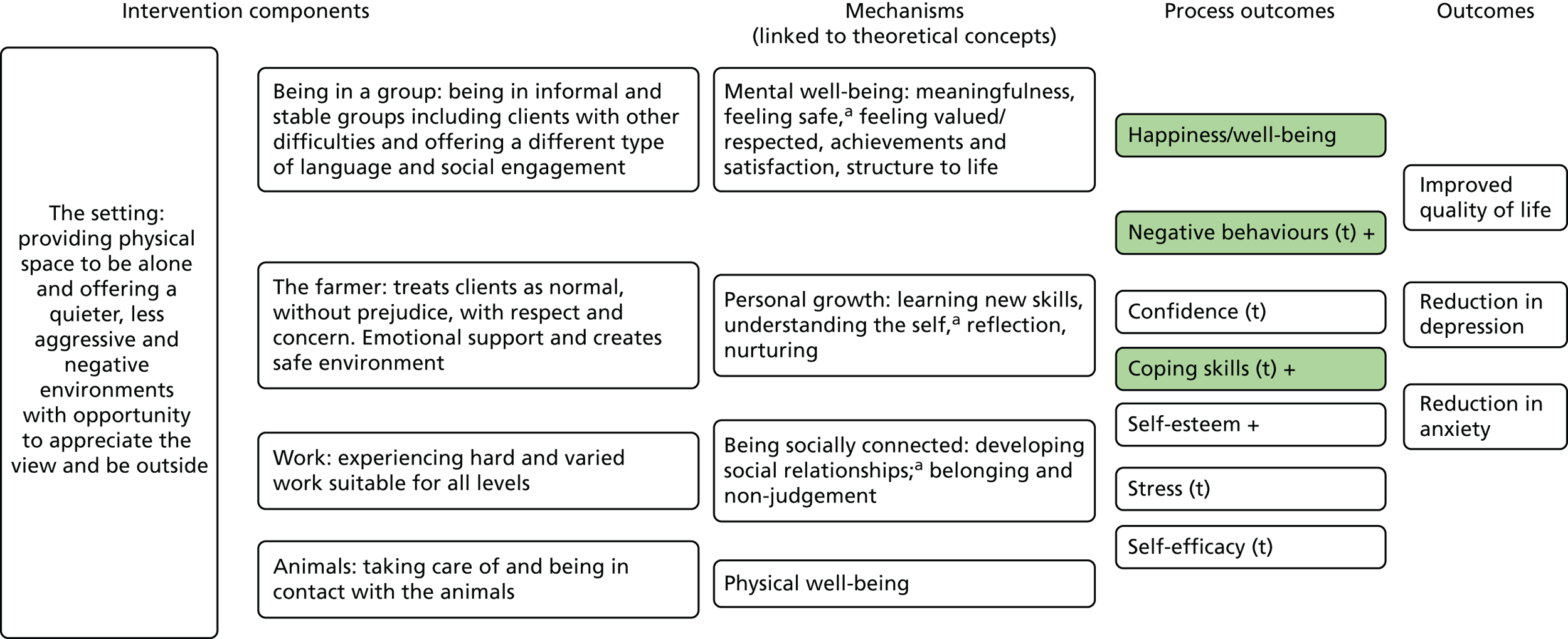
FIGURE 6.
Logic model for learning disabilities group. a, Mechanisms that were most frequently found and with greatest spread across studies. Shaded process outcomes equate to evidence from qualitative literature. t, theory based.
Testing the logic models
Of the expected process and primary outcomes, no quantitative studies were found that evaluated the impact of CFs on confidence, tiredness and physical health. Pro-social behaviours were measured, but only one form (reduction in reoffending) was clearly defined. In addition, vocational skills may have been measured in the form of occupational functioning and work abilities. However, as these outcomes either were not defined or incorporated highly subjective measurements, we cannot be clear.
Despite being able to develop the logic models, an absence of quantitative studies meant that the learning disabilities model could not be tested. The disaffected youth model underwent limited testing of the secondary/process outcome with an absence of any primary outcome data. Based on limited quantitative evidence from only two RCTs, we did not find any significant positive effects of CFs in improving quality of life in the mental ill health or substance misuse groups. We did find some very limited and inconclusive evidence to suggest that care farming can reduce anxiety. For depression, although there appeared to be significant reductions following the intervention, as assessed in UBA studies, when compared with a control group in RCTs no significant difference was found.
For process/secondary outcomes, there were no significant positive effects for either self-efficacy or coping (measured in the RCTs) at the end of the intervention, but there was significant improvement for self-efficacy, but not coping, at follow-up. The possibility that there may be some delayed benefits (as with anxiety) for self-efficacy was not investigated by other studies and, therefore, remains unconfirmed. A number of UBA studies reported significant improvements in self-esteem, stress, affect, mood and group cohesion at the end of the intervention. However, only stress and affect were measured at follow-up (3 months after the intervention ended) and improvements were not sustained. Most of the primary and secondary outcomes were limited to immediately after the intervention with only three (social functioning, eating and appetite and mental status) reported beyond 6 months. With respect to disaffected youth, there was some suggestion that coping may be improved but that there was no impact on self-esteem.
Summary
There is a general trend of evidence to suggest that care farming may be effective for some service user groups; however, this evidence is limited. Small study sizes, evaluations involving mixed service user groups, the use of multiple and sometimes unvalidated outcome measures, short follow-up periods and absence of missing key outcomes that fit with theory have all hampered the development of a more robust evidence base. However, we now have a set of theory-based logic models that offer a framework for research evaluations, and with recommendations in place to address the current research inadequacies there is an opportunity to vastly improve the evidence base for care farming.
Despite the current lack of conclusive evidence from RCTs and robust effectiveness studies, the indications from the available evidence suggest that CFs are a promising alternative or adjunct to mainstream approaches for mental ill health. Lack of choice, gender inequalities and overburdened statutory services indicate the need for a credible alternative treatment option. A concerted effort to increase awareness among commissioners of health care, front-line service providers and potential service users about care farming, and how and for whom it may work, is needed. Models across Europe that offer a more integrated approach between green care and statutory services could provide the learning of this. The evidence for care farming for other service user groups is not as well developed as for mental ill health but that is not to say there is not a need. Disaffected youth, adult probation service users and people with dementia represent significantly large vulnerable population groups for whom current service provisions struggles to meet demand. The need to continue to improve and provide high-quality research in these areas is therefore pressing.
Chapter 3 The pilot study: background and methods
The aim of the study was to pilot the design and methods of a natural experiment and economic evaluation to examine the effectiveness of CFs in improving the quality of life of probation service users undertaking COs. The findings from this study would indicate whether or not a larger, fully powered natural experiment was feasible to assess the cost–utility and/or cost–benefit of CFs in improving probation service user health and well-being and, ultimately, in reducing recidivism.
Objectives
-
Identify factors that drive the decision of CO allocation in order to identify potential selection bias and confounders as well as the most appropriate ways to collect data on these factors.
-
Identify the most appropriate ways to gain informed consent, maximise recruitment and follow-up while minimising dropout and deliver questionnaires effectively among probation service users undertaking COs in CFs and comparator CO settings.
-
Identify the most appropriate ways to collect cost data, including health-care resource use by probation service users, cost of reoffending, costs of crime and gains of employability of probation service users in CFs and comparator CO settings and explore the feasibility of measuring cost–utility.
-
Identify differences in effectiveness in terms of quality of life, mental health, lifestyle behaviours and reoffending rates between the three CFs and between CFs and comparator settings in order to estimate variation and thus determine the intracluster correlation coefficient and sample size required in the follow-on study.
-
To develop a logic model based on probation service users’ experiences of serving their CO on a CF and their perceptions of the impact that the CF has on their lives and well-being, taking into consideration seasonal changes, to illustrate the possible mechanisms that lead to changes in health and well-being among probation service users undertaking COs on CFs.
Care farming and probation service users
Care farming is one possible location where probation service users may be allocated to serve their CO in England. A survey conducted in 2013 estimated that approximately one-quarter of CFs provided support for probation service users. 6 However, more recent work by the study team suggests that at the time of this study, the number of CFs taking service users was much smaller. Our investigations identified only three CFs in England holding contracts with probation services. Our study period coincided with the official disbanding of probation services in May 2014 and subsequent establishment of new organisations as community rehabilitation companies (CRCs) and the National Probation Service (NPS). This organisation change may well have had an impact on the services commissioned by probation.
Community orders and the role of care farming
The most serious crimes and those committed by serial offenders tend to result in a custodial sentence. Offenders whose crime is considered to be less serious in nature can be given a CO, which is completed in the local community under the supervision of probation services. The ultimate purpose of COs is to reduce the risk of reoffending through ‘requirements’ – these are interventions that the probation service user is ‘required’ to comply with to complete the order successfully. There are many types of requirements (Figure 7) and within these there may be multiple programmes, activities and projects. Probation service users can be given one requirement or more depending on the nature of their offence, their offending history and their lifestyle behaviours. COs vary in the degree to which they aim to rehabilitate or punish the probation service user. Probation service users with the greatest needs, for example those with drug or alcohol problems, will be offered a CO with a substantial rehabilitative requirement such as alcohol, drug or mental health treatment. Irrespective of the level of need, all orders, however, must include a punitive element. In predominantly punitive orders, the main requirement might involve a form of community payback (CP) that includes, for example, litter picking or working in a charity shop.
FIGURE 7.
Types of requirements within COs. Adapted from Type of Community Order. 80,81 Crown copyright. Contains public sector information licensed under the Open Government Licence v3.0 (www.nationalarchives.gov.uk/doc/open-government-licence/version/3/).
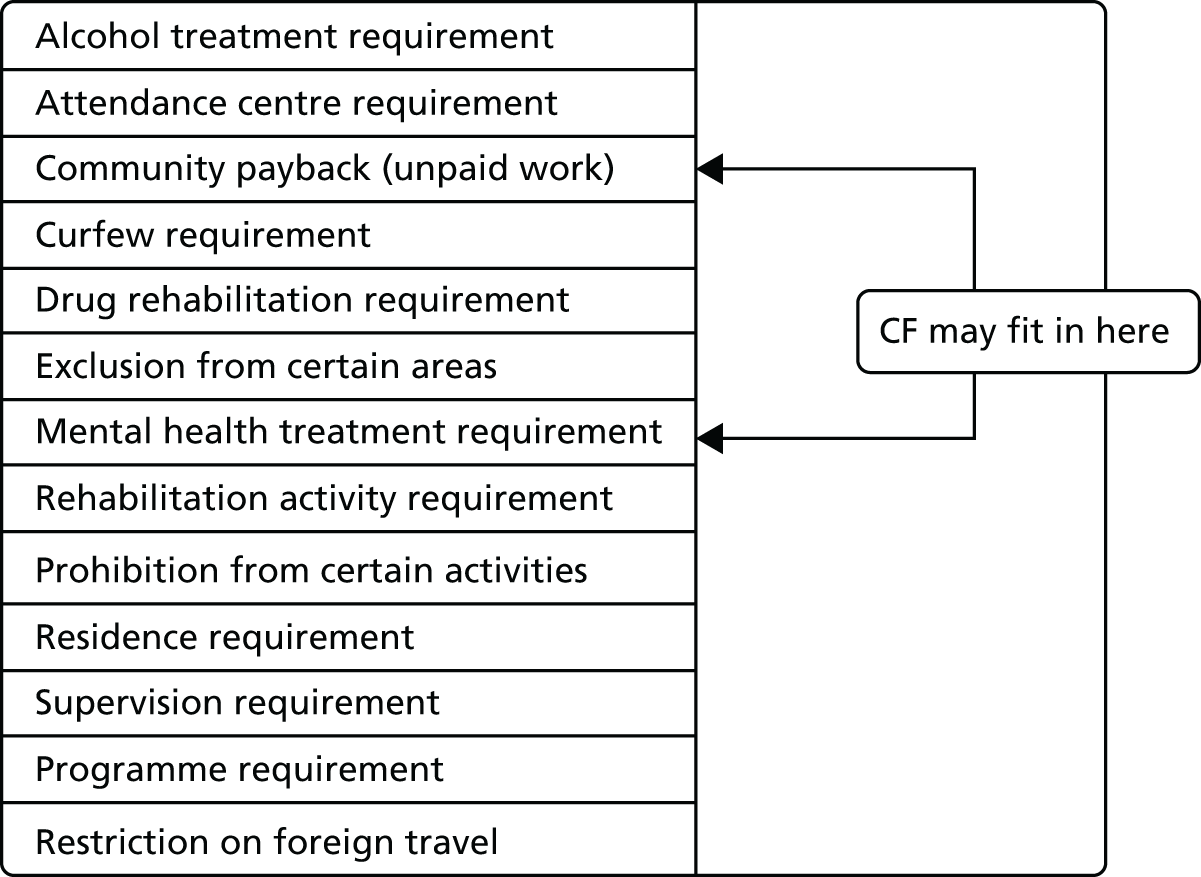
The exact process for allocation of a service user to different CO sites is not clear and differs between probation regions. One of the aims of this study was to understand this process better, particularly to identify any potential confounders, that is, factors that were associated with the allocation decision and with the outcome (i.e. health outcomes and reconvictions)
Care farming as part of a CO can be either rehabilitative or punitive depending on how the probation service views the role of care farming in probation and, in addition, how well the local CF itself has communicated its intentions, services and desired outputs.
Changes to probation services and impact on the research
The privatisation of the NPS was announced as the current research study began. The process lasted for the duration of the study. From the outset, this affected our capacity to carry out our research and the effects of this will be described throughout this report, particularly in relation to the pilot study. Over and above the changes described throughout this chapter, there were three key time points when our study was most affected. The first key time point was June 2014, when the official split in probation services took place, forming a NPS (for the management of higher-risk offenders) and interim CRCs. At this time, the CRCs were not, in fact, new organisations but a temporary reorganisation of existing probation staff. At this time, information technology (IT) services were split, staff were moved and new procedures were put in place. The second major event was the announcement of the preferred bidders in October 2014. Up to this point, various consortia had been preparing their bids, and some of these involved senior staff from existing probation services as well as organisations that were contracted to probation. This included one of the CFs within our pilot study. The third and final key event was in February 2015, when the final contracts were awarded and changes in administrative processes were announced alongside changes in IT services in response to this.
Throughout the study, and particularly at these key time points, staff were leaving or had changing roles, new contracts were being issued and IT staff were under pressure to deliver new IT systems in response to changes in assessments. All of these factors meant that establishing, and maintaining, reliable contacts who could respond to our requests and support our recruitment processes was particularly challenging.
Target population, sample sizes and timelines
This was a pilot study aiming to assess feasibility, recruitment and follow-up rates, clarify selection biases and effects of confounding. As a pilot, the study was not powered to assess effectiveness, so a conventional sample size calculation was not considered appropriate. We estimated that, in order to determine sample size for a follow-on study that took account of between-CF effects and the possible effects of bias (i.e. response rates and dropout), a pilot sample of 300 probation service users would be sufficient.
With an expected loss to follow-up of 40%, this allowed a final sample size of 180 participants (90 CF attendees and 90 comparator location attendees) with both baseline and follow-up data.
We planned to recruit over three centres as follows:
-
Centre 1 – n = 120 (n = 60 from CF; n = 60 from comparator site) over a 12-month period.
-
Centre 2 – n = 90 (n = 45 from CF; n = 45 from comparator site) over a 9-month period.
-
Centre 3 – n = 90 (n = 45 from CF; n = 45 from comparator site) over a 9-month period.
Our monthly targets were therefore set at 10 participants in each centre. Owing to delays in setting up and recruitment, which are explained in the remaining sections of Chapter 3, we made adjustments to these monthly targets. Our initial 12-month recruitment period for centre 1 fell to 10 months, and thus our monthly target became 12 participants. In the other two centres we set a monthly recruitment target of 15 participants, with an expected shortened recruitment period of 6 months.
Outcome measures
The primary outcome of the study was quality of life and well-being, which was derived from the Clinical Outcome in Routine Evaluation–Outcome Measure (CORE-OM). 82 CORE-OM has previously been used to evaluate quality of life of probation service users. In particular, it has been used to assess the risk of self-harm among prisoners83 and among mentally disordered offenders in a high-security hospital. 84 The CORE-OM is also commonly used to measure psychological distress in evaluations of mental health interventions85 and it can be used to derive utilities that can then be transformed into QALYs. 86 The 34 items cover four dimensions: subjective well-being, problems/symptoms, life functioning and risk/harm. 82 The full version of the questionnaire can be found on the CORM-IMS website (www.coreims.co.uk; accessed 1 October 2013).
The secondary outcomes were:
-
individual-level data on reconvictions over a maximum 18-month period obtained from individual-level data from the PNC
-
mental well-being derived from Warwick–Edinburgh Mental Health and Well-Being Scale (WEMWBS)87
-
measures of smoking, alcohol, drug use, diet and physical activity adapted from the General Lifestyle Survey88 and Health Survey of England89
-
exploration of health utility, as derived from the CORE-6D based on the CORE-OM,82 and QALYs permitting a cost–utility analysis86
-
exploration of the health and social care use cost and the cost of a CO as an intervention.
Recruitment and follow-up plan
The logistics of the recruitment and follow-up processes were bespoke to each site; however, the overall plan was to perform recruitment and follow-up face to face by a research assistant (RA). Informed consent was obtained to take part in the study and also, independently, to access personal information from the probation and police services. When follow-up could not be performed face to face because of changes in a probation order, we used postal questionnaires. The overall aim was to complete follow-ups at the end of the CO or if the completion of the order went beyond the 1-year recruitment period participants were followed up for 6 months from the start of their order, regardless of whether or not their order had been completed. For probation service users who were ‘breached’, that is failed to comply with their order, we monitored their return back into the system and followed them up at the end of their subsequent CO or at the end of the follow-up period. For those probation service users not returning back into the system, we offered a financial incentive to complete a postal questionnaire to maximise response rates. If they were given a prison sentence, they were noted as ‘lost to follow-up’ for the quality of life, health and well-being measures; however, their reconviction outcome was still assessed.
Approvals
A critical initial step in gaining access to probation services was gaining both ethics and National Offender Management Service (NOMS) approvals. Ethics approval from the Leeds School of Medicine Research Ethics Committee (SoMREC/13/014) was obtained promptly (December 2013) and approval from the NOMS given in February 2014 (NOMS; 2013–257). The delay in obtaining NOMS approvals impacted on the start date for recruitment in our first site (see Appendix 3, Figure 13, for the impact on recruitment timeline).
Bespoke study documentation
So as to distance ourselves from the probation service and the MoJ, we did not include their logos on any study documentation. Probation staff considered this important because of the possibility that probation service users may not be honest in their questionnaire responses if they thought it would influence their CO. In addition to standard research documentation (information sheet and consent forms), we developed a separate consent form granting permission to access individual data held on probation IT systems and reconvictions data held by the police and MoJ on the PNC. The permission to access personal data form was developed with senior staff in the probation services and was a requirement of the information sharing agreements (ISAs) that were developed later on in the study. In addition, the signed forms were provided (as proof that permission had been granted to us) to the police in one centre in which an ISA was not required under the Freedom of Information Act. 92
We also developed a service user assistance form and a service user details form. The service user assistance form enabled us to assess any difficulty with the outcome measures. The service user details form recorded (in addition to name, address, etc.) information on the type of requirement [i.e. unpaid hours or specified activity (SA)], number of unpaid hours/session, planned attendance days, number of hours completed at baseline and allocated project. This assisted with monitoring progression and changes through the probation order.
Development of the study procedures within the participating centres
Based on information provided by Care Farming UK, we contacted CFs that indicated that they worked with probation service users. Farms that routinely took in probation service users through their local probation service in sufficient numbers to meet our recruitment targets were asked to take part in the pilot study through a telephone call and face-to-face visit. Three CFs, (CF1, CF2 and CF3) agreed to take part. We subsequently sought verbal agreement from the three local probation services (PS1, PS2 and PS3) to conduct the study. Collectively, we refer to these as centres 1, 2 and 3, respectively. Having ethics and NOMS approvals in place was key to progressing the study at each of the three centres.
Although at the time of study set-up probation was a nationalised organisation, there were key organisational differences between each of the probation services that led to the development of bespoke research approaches to probation service user recruitment and data acquisition. At each service, contact points varied from a single individual senior staff member (e.g. head of operations) at one site, to a mix of different levels of staff, both management and front line at the other services (Table 10). These staff were fundamental to establishing key information items that would enable identification, recruitment and follow-up of probation service users from both CF and comparator sites into the study. The key information items included:
-
the type of order given to the probation service users, who were subsequently allocated to CFs
-
the characteristics of probation service users allocated to CFs including, for example, risk of harm, risk of reoffending [Offender Group Reconviction Scale (OGRS)], age range and gender distribution, plus any restrictions (e.g. no one with unstable substance misuse or who was currently in employment)
-
when during the CO the probation service users were allocated to the various requirements and projects
-
who decided on allocation and where this was done
-
when the probation service user commenced their requirement/project during the CO.
| Main study activities | Centre | ||
|---|---|---|---|
| 1a | 2 | 3 | |
| Operations (clarifying characteristics of CF intake and comparators, explaining allocation process, identifying opportunities for embedding research processes; and access to projects) | Operations team manager;b assistant manager for operations; probation office; project officer; case manager; CP supervisor; CP manager; and court managers | Project manager; CP supervisor;b case manager;b director of interventions; and interventions managerb | Director of operations;b and seconded RA |
| IT (development of ISAs and provision of data) | Operations manager; performance and quality officer performing IT searches; and training officer to explain IT system for data requirements | Data provision not started | Information manager (later replacement also information manager) |
| Legal (preparing ISAs) | Staff from legal team | IT manager; and communications manager | Information manager as above |
| HR (staff secondment to study) | Not applicable. Recruitment and follow-up conducted by UoL RA | HR officer; centre manager | Head of operations; and HR staff to assist with interview process for RA |
Having established the type of order and the characteristics of the probation service users who attended CFs, we were then able to establish the characteristics of the comparator group.
In two of the probation services, front-line staff, that is CP supervisors, project officers and some offender managers, were key project contacts. In the third probation service, the head of operations was the key person for liaising and information. Each probation service used a different approach to allocating probation service users to various projects within COs. This meant that the way in which CFs were utilised within COs differed. Therefore, the process of identification and recruitment of service users differed in each centre. The following section describes local service configurations, including the process of probation service user allocation and the approach taken to identification and recruitment at each centre.
Centre 1
Local service configuration and identification of target groups
This probation trust covered five offices: two city-based offices and three more rural locations. One of the city offices acted as a head office.
As with all COs, the time taken between court sentencing and first meeting at probation (during which probation service users are allocated to particular projects) was 2–4 days. Likewise, the time between their initial appointment at probation and starting the CO was often 1–2 days.
In this centre, the CF was close to one of the more rural and smaller probation offices and, in general, only probation service users living in and around the local area could attend the farm. The CF was categorised by probation as a project within a CP requirement. This could be a stand-alone order (i.e. they were just required to work a specified number of hours unpaid) or be part of a multirequirement order in which the probation service user, in addition to completing their unpaid hours, was also required to complete another type of activity (for example, a drink–drive awareness programme). Within this probation service, probation service users who were given a CP order were allocated to a single project to allow completion of the CO in one site. The CF accepted those who:
-
had a low to medium risk of reoffending and harm (as categorised using a suitability model)
-
were judged by probation staff to have a good attitude to work (not formally assessed).
The availability of the probation service users to work on the farm and the capacity of the farm itself were also factors that determined allocation. Discussions with probation staff at the time revealed that the CF catered for 12 stand-alone CP probation service users per day (open 7 days per week). We estimated that we would have sufficient numbers to avoid recruiting people with multirequirement orders who would also be receiving other interventions.
The information outlined above was used to identify a comparator group. We had to select another probation office as the source for the comparator group because the administering office for the CF attendees did not process sufficient numbers of similar probation service users. In order to streamline the recruitment and follow-up process, we sought to identify a single setting for our comparator population. Staff in probation suggested that a clothes-sorting warehouse in the city of the head office would provide a group that was the most comparable and sufficient numbers for our study. The staff at the comparator site were contacted and agreed to support the research study by allowing our team to call them to check each day for new starters and to identify anyone nearing completion of their unpaid hours.
Settings
The care farm
The CF was a small social enterprise set on a reclaimed landfill site on the outskirts of the town. Individuals were required to make their own way to the farm. Open 7 days a week, the farm took in probation service users every day. It did not cater for other vulnerable groups at that time, although it had done in the past. There had recently been a change of management at the farm, which was overseen by a board of trustees. At the time of recruitment, the day-to-day management was the responsibility of a qualified mental health nurse and an ex-community pay back supervisor (both male) from the local probation office. The farm was male dominated and very few, if any, female probation service users attended. A few volunteers also helped, some of whom were ex-probation service users. Activities were a mix of indoor and outdoor work, including woodwork, working with animals (pigs, chickens, rabbits), fish farming, aquaponics and some horticulture and general site maintenance and improvement. Probation service users were encouraged to eat together in the kitchen area, where a mid-day meal was provided using some of the food that had been grown on-site. Probation service users were given tasks to do in small groups or individually depending on their preference and nature. The farm utilised the skills of probation service users to enhance the site, for example using a joiner to fit the kitchen.
The comparator
This was a charity-owned, clothes-sorting warehouse. It was open 7 days a week and managed by three female staff. All activities were indoors and involved steam pressing, labelling and sorting clothes ready for distribution to local charity shops. Most people worked in one main room with the radio on. Lunch was not provided but there was a kitchen where hot drinks were available. Although the warehouse took in probation service users with similar profiles to the CF, they were more stringent about taking in those who could commit to work. Their financial dependence on turnover of clothes meant that they had daily targets to meet. Both male and female probation service users attended the warehouse.
Recruitment set-up
Providing advanced notice of study to participants
Based on the information provided about the process of allocation, we initially planned to recruit probation service users to the study at the head office during their first probation appointment. The ethics committee requested that we attempt to inform potential participants about the study prior to the first appointment. In centre 1, we asked two court team managers attending local magistrates’ courts to give information sheets to all CO probation service users immediately after sentencing. At the subsequent probation appointment, probation service users were then approached by a researcher with a view to recruiting them into the study. We asked probation service users if they had received the information sheet and none remembered receiving it. We therefore opted to provide information about the study during their first appointment and recruit at the same meeting.
Incentivising probation service user participation in the study (centre 1 only)
It was agreed that participation in the study would be enhanced if an incentive was provided. Probation staff felt that probation service users would prioritise reducing their unpaid hours rather than spending time on the study. As we were unable to provide a financial incentive, because the probation service users were in effect working unpaid as their punishment, the most appropriate compromise was for the time taken on the research to count towards their unpaid hours. This was agreed at management level.
Establishing a base for recruitment: strategy 1
During study set-up, the head office was trialling having group inductions twice weekly. Probation service users were invited in batches of approximately 20 to attend a session during which they received health and safety advice and were allocated to their projects. It was suggested that these group inductions would be the best time to recruit and administer baseline measures before COs commenced. To check that we were identifying all potentially eligible participants, we first compared actual attendance rates with planned attendances at the induction appointment. We did this for the first month of recruitment (March 2014). We observed that approximately 61 of the estimated 127 probation service users invited to the induction appointments actually attended. We use approximations here because the paperwork was not always up to date. We also noted that, during this month, 48 of the 61 (79%) service users were ineligible because they had not been allocated to attend either the CF or the comparator site. On checking with the CF and comparator site to identify any new starters whom we had not meet at the induction appointment, we found that some had been missed.
The experience of recruitment at the probation office is also noteworthy. Although the setting provided the opportunity to recruit many individuals within a short space of time, the atmosphere in the area allocated for recruitment was not conducive to informed consent. Time was very limited because immediately after induction and project allocation, many probation service users wanted to leave or were waiting for a minibus to take them back to the other probation office. We were positioned in the waiting room with multiple probation service users and no private space to discuss the study. Thus, we could be in the midst of recruitment with one probation service user but be approached by another. This experience combined with our findings in relation to attendances led us to conclude that the CF and the comparator site would be preferable recruitment locations, as they could provide a more private space.
Establishing a base for recruitment: strategy 2
We approached staff at both sites, obtained permission to contact them on a daily basis to enquire about new starters and recruited on-site as close to the first day of the CO as possible. We found staff to be approachable and accommodating. We monitored recruitment at the CF centre to ensure that we met our target requirements. Our adjusted monthly recruitment target at this centre was 12 participants per month based on a 10-month recruitment period (see Recruitment and follow-up plan). By the end of the third month of recruitment (May 2014), we were meeting our monthly targets; however, we had concerns about sustaining these recruitment rates because of changes in the probation service.
Strategies to increase recruitment
During the first 3 months we recruited those on a stand-alone CO (see Local service configuration and identification of target groups for explanation). The purpose was to measure the impacts of one main intervention rather than multiple interventions (as in the case of a multirequirement order). However, given that the numbers that could be recruited were a potential concern, we opted to expand recruitment to include those on multiple requirement orders. Furthermore, up to this point we performed recruitment on a 5-day standard working week. Both comparator and CF sites operated on a 7-day working week. We considered that by recruiting at the weekends we could both identify more probation service users and also potentially recruit people who attended the project only at weekends because of full-time employment. As being in employment reduces the risk of reoffending,93 it was important to include these people as well. Although our decision to expand the inclusion criteria and recruit at weekends was primarily target driven, it was also underpinned by concerns about the impact that organisational change (through the privatisation of probation services) would have on our capacity to conduct the study at the other centres. By maximising opportunities to recruit at centre 1, it was hoped that we could negate, to some degree, potential under-recruitment at the other centres.
Our monitoring also revealed that, despite telephoning the project sites regularly, some new starters were not being notified to us promptly. Thus, we observed that some new starters had actually been attending the site for a number of days before we were informed. We decided not to recruit people who had completed more than four sessions, as this would be too far into the intervention to obtain a true baseline measure.
Our final inclusion and exclusion criteria for centre 1 were as follows.
Inclusion
-
Adult male or female probation service user serving a CP requirement.
-
Allocated the CF or specified comparator site to complete their unpaid hours.
-
Receiving either a stand-alone or a multirequirement CO.
Exclusion
-
Having completed four or more sessions at the CF or comparator site by the time of recruitment.
Monitoring progress with community orders and conducting follow-up
At recruitment we recorded the number of unpaid hours allocated to the probation service user and also the number of hours already completed. As we were recruiting at the project site [i.e. the CF or the comparator location(s)], we were aware that probation service users were likely to have already completed some hours that may have included their induction at the probation office. In addition, although projects might receive notice of new starters the day before they were due to start, we were advised that they might not turn up. In addition, that time was needed on the first day for on-site inductions and settling in. Therefore, the earliest that probation service users could be recruited to the study was halfway through the morning on their first day. Recording the number of hours completed at baseline enabled us to assess the amount of intervention captured by the research study.
Discussions with probation staff revealed that follow-up would also have to be conducted at the project site, as no official exit interviews at probation offices were conducted. It was also explained that probation service users often did not attend their last day at the project, so attempting follow-up then would inevitably lead to a high loss to follow-up. To complicate matters further, although probation service users would arrange to work their unpaid hours on planned days, the days and frequency of attendance could change, as could the actual project site. Thus, although we could predict when a probation service user might finish their order, it was of little practical value. In order to assist with monitoring users, we made contact with an administration hub and obtained permission to periodically request the number of unpaid hours remaining, the days attending and the actual project site. So as to avoid overburdening the administration hub, we estimated the halfway point for completion of the unpaid hours before contacting them. As a back-up, we continued to ask staff at the project sites if anyone was due to complete their unpaid hours.
Centre-specific changes and their impact on the study
During the pilot study, we observed a number of changes to the organisations at this centre that impacted on our study. The privatisation process that ran throughout the study period coincided with a number of our key contacts either moving within the service or leaving probation all together. Increased workloads on those remaining meant that there was less support for the study in general and a lack of staff continuity resulted in us having to identify new contacts and reiterate the purpose and methods.
A key change in the centre was the closure of the CF. In the seventh month (September 2014) of recruitment, the CF ceased to take in probation service users from the probation service. All probation service users attending the farm were allocated to a range of other projects. Some were reallocated to charity shops and others to supervision (travelling to various sites and supervised by a probation employee). We used our existing contacts in probation to try and trace the reallocated study participants. Probation service users who were allocated to weekend supervision were not followed up because of safety concerns. The office was shut at the weekend and it was an all-male environment, often with probation service users who were considered unsuitable for a project without probation supervision. The CF was not reopened and, therefore, recruitment at this site stopped.
The privatisation of probation meant that IT services were split between the CRC and the NPS. On a practical level, this meant that the administrative hub did not always have access to NPS IT systems; therefore, we experienced difficulty in monitoring the completion of some probation orders.
Barriers to, and enablers of, project administration
This section partly summarises Centre-specific changes and their impact on the study but also describes the system-based challenges that were not a result of the privatisation process. We also summarise the factors that facilitated the operationalisation of the study with probation services, CFs and comparator sites. The barriers were:
-
front-line staff changing – there was a lack of staff continuity
-
staff had very limited research knowledge (both of its practical requirements and strategic importance)
-
staff and probation service users had no knowledge of CFs, which was particularly an issue for the SUB groups
-
sometimes similar levels of staff would hold different views about the characteristics of probation service users attending different projects, and so the most appropriate site for the comparators took time to clarify
-
there was a reliance on project site staff to remember who was new on-site and who was due to complete their CO
-
not having an employee from probation seconded to recruit and follow-up study participants, which might have been an advantage, particularly for recruitment and monitoring with access to IT systems.
The main enablers were:
-
having a probation employee as a co-applicant facilitated access to many staff
-
having multiple contacts, which allowed us to develop relationships with front-line staff, providing direct access to probation service users
-
being able to develop good relationships with project site staff to support recruitment and follow-up.
Centre 2
Local service configuration and identification of target group
This probation service had a throughput of approximately 800 probation service users per year split across four local delivery units: north, west, south and mid. The western local delivery unit was the largest, working with 600 probation service users annually. SA requirements, such as drug and rehabilitation requirements and alcohol treatment requirements, accounted for around one-third of service users, with the remaining two-thirds under a stand-alone CP order. All those attending the CF were serving a CP order. The unemployed or those with an order that included an educational component involving ≥ 20% of their order were not sent to the CF. The numbers attending the CF varied greatly from between 7 per month to 13 per week. The CF was in a rural location and probation service users were transported there from the local office. Only those who could travel to the local office could attend the CF. In addition to the farm, there were 15 other projects that fell under CP orders. These included maintenance of local authority parks, painting railings, litter picking and decorating a children’s centre. Projects would change depending on the completion and cyclical nature of the work, so that some were one-off projects and others were rolling.
Settings
Probation service users on CP orders often attend more than one site throughout the week. The decision on which project probation service users attended depended on the availability and capacity of the project, and this could change on a day-to-day basis. There is some choice available to probation service users, but primarily they are expected to go to wherever they are sent to. Attendance at a number of projects within one CO meant that probation service users were neither pure CF attendees nor comparators. We were advised, however, that the number hours spent at the farm as part of the CO would be recorded and available from the probation service.
Care farm
The farm at centre 2 was set up as part of a religious movement to support its charitable efforts. It was not originally set up as a CF and the owners had not planned to make the conversion. The move to take probation service users at the care farming came about through a contact at the probation service, who asked if one probation service user could volunteer as part of their CO. The probation service user was supervised by a CP supervisor. Both the farm owners and the probation staff were satisfied with the probation service user’s time at the farm and, subsequently, more probation service users were sent and a more formal arrangement ensued. The farm is situated on the grounds of the religious movement but has its own separate entrance and is distally located to the main buildings so that probation service users do not regularly come in contact with the members of the religious movement. On the farm there is a small outbuilding used by the workers for shelter and break times. Probation service users attend up to 2 days per week and are provided with a mid-day meal cooked onsite. As with the previous CFs, there is a preponderance of male service users. Female probation service users who go to the farm tend to work in the kitchens. The farming activities involve planting and digging vegetables and some on-site maintenance. Activities may also involve sweeping out the cow sheds and driving the tractor to and from the incinerator. Working with the animals directly is rarely permitted. The skill sets of probation service users, such as plumbing and electrics, are used around the main buildings. Although the farm is recognised by Care Farming UK as a CF, it does not have a care farmer. Supervision of probation service users continues to be provided by probation services alongside a volunteer, who acts as a go-between for both the probation services and the religious movement. A farm supervisor from the religious movement is on-site but he is unable to communicate well with the probation service users because he speaks little English. Opportunities to rehabilitate probation service users through learning new skills or by providing counselling are not in place on the farm. However, because probation service users were being sent to the farm as part of a CP supervision (which is seen as a punishment by the probation service) the concept of rehabilitation was possibly not relevant.
Comparator
The intention was to recruit probation service users on CP orders from other local delivery units, assuming that resources would become available to us. We also considered that those service users attending the kitchens at the CF could be comparators as long as they did not undertake any farm work.
Recruitment set-up
The plan was to advertise to a second a member of staff from the local probation service to act as a RA, as in centre 3. This was agreed by senior management and, initially, human resources (HR). However, unlike centre 3 where staff had already been allocated to NPS or CRC some time prior to the official split, this centre waited until May and June to restructure, which was close to the date of the split. Having partly processed the job description, the HR department considered that it would not be able to support the recruitment process further, despite the research co-ordinator and a member of the senior management team offering to process all applications and perform the interviews. The senior manager and the temporary CP project manager asked local offices if they would be willing to ask staff if they wanted extra work or a secondment. No staff were interested and we were informed that many felt insecure about their posts. At the same time, the temporary CP project manager, who had already provided us with some key contacts, also left and was replaced with an agency offender manager. We met with him, the manager at the religious establishment where the CF was located and its local volunteer. The CF was keen to take part and considered the research an important part of progressing its farm, particularly in the light of the changing relationship with probation and the concern that probation service users might not be allocated to the farm in the future. The CF agreed to recruit probation service users and follow them up. Training and documentation were provided and we agreed to pay the farm for each probation service user recruited and followed up. We ensured that there was sufficiently secure storage for the documentation. Both the manager of the religious establishment and its local volunteer received training in recruitment and data management. Unfortunately, despite our best efforts, only four probation service users were recruited, two of whom were based in the kitchens and, therefore, were regarded as comparator respondents.
Centre-specific changes and their impact on the study
Our original contact at the probation service, a CP project manager, informed us in January 2014 that the study had been approved by senior management. We took the learning from centre 3 where input from a senior manager enabled us to progress secondment of an internal RA. Unfortunately, the CP project manager went on sick leave and it was some time before we could identify a replacement. We checked the progress of study approvals with senior management; while the managers were initially unaware of the study, they were supportive, and approval was granted quickly. The probation service managers provided us with the appropriate contacts for the IT, legal, HR and finance departments. As explained above, the HR department declined to support us and this was a significant challenge to the study at this site. Furthermore, the IT department offered to help with the development of the ISA; however, it did not have a working template and, despite sharing an existing one from one of the other centres (with their permission) with it, the ISA did not progress. Our understanding was that their work priorities had changed significantly with new systems being put in place and so our requests were overlooked. We opted to wait until we could assess how recruitment was proceeding and in the end considered that an ISA was inappropriate, as we were able to recruit only four users from this site.
Centre 3
Local service configuration and identification of target groups
Centre 3 included six probation offices across a wide geographical spread. There were approximately 1000 probation service users coming through this probation service, with just over half receiving an unpaid hours or SA requirement.
Within this service the CF was regarded as a SA requirement because of its considered capacity to meet individual needs and, therefore, rehabilitate probation service users. This was part of a minimum 12-month supervision order, that is, probation service users were required to meet with their probation officer on a regular basis. The CF was situated to the north of the probation area and all deemed suitable to attend were transported there from the five closest probation offices by the care farmer. Therefore, unlike CF1, eligibility in general was not geography determined. Instead, suitability was determined by individual need. The farm took in those with an OGRS score of ≥ 75 points, which was indicative of a high risk of reoffending, the unemployed and those in need of drugs rehabilitation (but with a stable habit). A later review of the types of probation service users attending the CF indicated that being unemployed was the main criterion and that OGRS scores varied substantially. Further to this, later discussions with offender managers indicated that those sent to CFs also tended to have social difficulties – one of the more subjective criteria guiding decision allocations. Sex offenders and individuals convicted of domestic violence were not accepted onto the farm.
In comparison with unpaid hours requirements, SA requirements involved the completion of a set number of sessions. In the case of the CF it was 25 sessions, with each probation service user attending two day sessions each week. The first induction session took place at probation. The farm took probation service users in maximum batches of 20–25 service users, allowing all to complete and ‘graduate’ at the same time. For practical reasons, each batch was split into two groups: one group attended on a Tuesday and Wednesday and the other attended on a Thursday and Friday. Not all offices would be included in each batch, which meant that some probation service users could be placed on a waiting list, fulfilling other parts of their order until the next intake to the farm was due to start. There were approximately four intakes per year.
Identification of a comparator group was a challenge. The CF was part of a SA based on a defined need, and all those deemed suitable to attend could go as there was no geographical limit within the probation area. We considered looking at people receiving unpaid hours, but because these individuals have no identified rehabilitative need they were not considered comparable. Having gathered information from probation about the other requirements and discussion with the steering group, we considered that anyone on a requirement or an accredited programme for the same need could be a comparator, even though the types of needs might be different from those attending a CF.
Settings
Care farm
The farm was a cattle farm run by a family. Farming activities were more traditional than in CF1 and included animal work, site maintenance, forestry machinery, woodwork, tractor driving and metalwork. The service users also carried out local community work as and when needed, for example clearing ice from the footpaths. A hot meal was provided each day and a post-lunch group session was also a key part of the day. One-to-one counselling was available. At the end of the 25 sessions, a certificate (of a nationally recognised qualification) was presented to demonstrate the acquisition of skills and to support probation service users’ attempts to secure employment. As transportation to the farm was by minibus and service users were predominantly male, with social problems, it was considered by probation managers to be unsafe and uncomfortable for female probation service users. In the light of this, most service users at the farm were male.
Comparators
Unlike centre 1, the comparators attended different projects. Given the geographical spread of probation offices, we drew service users from one main office at which throughput was considered adequate for the study.
-
The alcohol treatment requirement ran for between 6 and 18 months. Most came with a supervision requirement, which was the same as the CF.
-
The women’s centre ran once a week over 8 weeks and involved furniture restoration and provision of information on employment and finance. Women generally had a low to medium seriousness of offence and, if using drugs, had to be stable users. The requirement came as part of a minimum 6-month order with supervision.
-
The drink-impaired driver’s programme consisted of 14–16 weekly 2-hour group sessions (accredited).
-
The domestic violence group sessions consisted of 27 weekly group sessions plus four individual sessions. It included pre-programme sessions and at least four relapse prevention sessions.
-
General offending.
-
Anger management.
Recruitment set-up
Incentivising probation service user participation in the study
As study participants were those on requirement orders (excluding CP), we could not include time spent on the study as a contribution to completing their order. Therefore, no incentive was possible at this centre.
Establishing recruitment for care farm attendees: strategy 1
In consultation with the farm staff it was agreed that recruitment would begin on-site in April 2014 when the next intake of probation service users commenced. The aim was to recruit probation service users on the third day of their requirement: the first day was off-site induction at the probation office and the second day was on-site health and safety. As there were two groups (see Local service configuration and identification of target groups for fuller explanation) this meant attending the site on two different days within the same week.
We had been working towards advertising to second a member of staff from the local probation service to act as a RA; however, the RA was not yet in place at the time. Therefore, two researchers based at the University of Leeds aimed to travel to the farm to perform recruitment on the two separate days.
At the first session, 8 out of 16 probation service users attended the day. On arrival at the farm, staff had already approached the probation service users and all but four declined. The remaining four were recruited in the presence of a member of staff from the farm. Farm staff considered their presence to be important, as the researcher had not been checked via the Criminal Records Bureau (now the Disclosure and Barring Service) by their organisation, although they were centrally checked. We requested to attend the farm on the Friday of the same week to recruit the second group, but this was declined as a result of farm staff shortages. Our offer to attend the following week to recruit those who had not been approached in the previous week was declined. Furthermore, we were unable to accept its offer to recruit the remaining intakes as, in the absence of any research experience, we could not be sure that the correct ethics procedures for informed consent would be adhered to. On consultation with the steering group, there was consensus that recruitment performed by CF staff would introduce potential bias and invalidate the data. Subsequent discussions with the CF did not resolve the issue.
Establishing recruitment for care farm attendees: strategy 2
We appointed a RA in May (seconded 1 day per week to the project from within the probation service). Through her contacts she arranged for the local unit performance officer to send her a list of who was due to attend the farm so that recruitment could take place before induction at probation. The care farmer had agreed that probation service users could be recruited before coming into contact with CF staff; the purpose being to dissociate the research process from the CF as a SA requirement. The concern was that interference from a researcher might deter individuals from attending the CF if they considered that the paperwork was part of the actual farm experience. The care farmer’s experience was that drop-out rate between the initial probation office induction and the on-site health and safety visit was already quite high.
The next intake was due to start at the farm at the beginning of June. However, the list from the unit performance officer was provided only on the day of induction and, therefore, the small opportunity for recruitment at the probation office was missed. The delay was a result of a large-scale change in administration processes at the probation service as a result of the CRC–NPS split that had occurred at the beginning of the month. We contacted the care farmer who agreed that the RA could attend the farm in the subsequent week to recruit; however, once again, on arrival at the farm the probation service users had already been approached and all had declined.
Establishing recruitment for care farm attendees and comparators: strategy 3
We then opted to identify those on the waiting list for the next intake and start recruitment early. We had previously tried to recruit those who were attending the farm in the initial stages of their order. Using the waiting list presented a separate challenge, as between their recruitment and their attendance at the farm the probation service users would have been receiving supervision, that is another intervention. We decided that this was preferable to losing future attendees through administrative mishaps.
Our RA had access to court results and, therefore, could identify who had been allocated to a waiting list for the CF and the name of their offender manager. The RA made contact with various offender managers to request to attend at the next supervision appointment and perform recruitment at the end. This strategy proved to be successful. As the comparators were also undertaking a range of requirements that involved supervision appointments with their offender managers, this approach also proved to be successful with them.
Meeting our recruitment targets
In centre 1 there was constant throughput of probation service users to both the CF and the comparator sites. In centre 3, however, as the CF took in probation service users in only four annual batches and all probation service users who were eligible to attend were sent there, there was little opportunity to change processes to increase recruitment. Likewise, the comparators attending the other requirements also started at prespecified dates and so opportunities to increase recruitment were limited.
Final inclusion/exclusion criteria for centre 3
Inclusion
-
An adult male or female service user attending a requirement order who was considered rehabilitative in nature.
Exclusion
-
Community pay-back.
-
Requirements that were not seen to be rehabilitative, such as curfews, restrictions on certain areas and residence and restriction on foreign travel requirements.
-
Probation service users convicted of sex offences.
Monitoring progress with requirements and conducting follow-up
Each requirement ran for a predetermined number of weeks or sessions. The RA had access to IT systems that enabled her to determine who was due for a supervision session that aligned with the completion of their requirement. The RA kept in contact with the various offender managers to arrange follow-up immediately after supervision sessions at the probation offices.
Centre-specific changes and their impact on the study
Our initial understanding of eligibility for the CF was that it was primarily available to those with an OGRS score of > 75. However, during our attempts to set up recruitment we reviewed a data set that revealed that most probation service users attending the farm had an OGRS score of < 75 points and that lack of employment was the main criterion. It is unclear if this change in criteria was a response to organisational change in the local probation service. Irrespective of the reason, a lack of clarity about the basis for allocation decisions regarding the CF led to some delays in establishing the make-up of the comparator population.
At the time of the split in probation services into the CRC and the NPS (at the end May 2014) there were large-scale changes in administration. This affected communication between core staff and the RA, which meant that, as a result of the delays, we were unable to recruit a whole cohort (the July intake) for the CF.
Over the course of the privatisation process we observed a fall in the number of probation service users being sent to the CF. Through discussions with staff in the probation offices, our understanding is that probation officers who were now working for the NPS were not promoting the CF in the same way as those working for the CRC. This was confirmed by our RA who, on talking to probation service users, became aware that they had misunderstood the purposes and activities provided on the farm. Senior staff at probation were aware of this and were trying to address it to give all probation service users the same opportunities to attend. However, to our knowledge, this was only addressed towards the end of the recruitment period.
The CRC contract was officially signed at the beginning of February 2015 and with it came a number of new administrative procedures and paperwork. Many staff left the probation service during the privatisation process and so existing staff were spread thinly to cover the workload. This slowed progress and affected both recruitment and follow-up.
Barriers to and enablers of project administration
The following section partly summarises some of the findings from Centre-specific changes and their impact on the study but also describes the system-based challenges that were not a result of the privatisation process. We also summarise the factors that facilitated the operationalisation of the study.
Barriers
-
Having access to one senior member of staff rather than a mix that included front-line staff.
-
Not having someone from inside probation dedicated to the study (initially).
-
Only having a seconded RA for 1 day per week.
-
Being unable to recruit probation service users on the farm or at the induction.
-
Having a reliance on probation officers giving time to the study to enable recruitment and follow-up.
Facilitators
-
Having a seconded RA from within the probation service who had access to systems and was known, or became known, to probation officers during the course of the study.
-
Having a senior member of staff who was able to sanction access to IT systems and the RA appointment.
-
Recruiting the RA prior to the split in probations services.
Data acquisition across all centres
Probation service user demographics and community order data
In order to meet objective 2 (see Chapter 1, Aims and objectives) we required data on the following items from probation services for each probation service user:
-
name
-
criminal record number
-
PNC
-
postcode
-
date of birth
-
ethnicity
-
nationality
-
immigration status
-
disability
-
gender
-
relationship status
-
pregnancy status
-
any other needs to help meet court order
-
employment
-
accommodation
-
index event (i.e. CP)
-
offence
-
sentence
-
requirements and changes
-
tier (pre and post including assessment)
-
OGRS score
-
offender manager
-
-
order outcome
-
requirement outcome
-
previous events (same information as index event)
-
CP hours completed
-
breaches/failures to comply
-
probation service area level (specific to West Yorkshire)
-
registers.
These data were held on an IT case management system called nDelius. In order to access these data, a data sharing agreement (an ISA) was required at each probation service. For full details of the process of obtaining these ISAs (see Appendix 3).
Reconviction data
The second set of data to be obtained from our partner organisations was the reconviction data. These data were a record of the conviction date (court sentencing) and the offence committed. This is held on the PNC and each probation service user has a unique PNC number. For further details of process of obtaining PNC data (see Appendix 3).
Police National Computer numbers provided by NOMS were used to request reconviction data from the MoJ. Ten per cent of probation service users could not be found on the MoJ system, despite all unique PNC identifiers having been checked. The time taken to develop the ISAs for all sites is substantial; therefore, early planning is essential.
The quantitative analysis presented in Chapter 4 is derived from the questionnaire data at baseline and at 6 months, the routine nDelius data and the PNC data to identify reconvictions within 18 months. Statistical methods details the methods used in this analysis.
Statistical methods
All analysis was completed as ‘intention to treat’, that is, it was analysed on the initial allocation of the service user for their CO (i.e. CF: yes or no), ignoring non-compliance, deviations from the CO and anything that happened after CO allocation. Although intention-to-treat analysis can be criticised for being too cautious, and thus being more susceptible to type II error, this approach is recommended in the Consolidated Standards of Reporting Trials (CONSORT) guidelines on the reporting of RCTs,94 and it was felt that, as relatively fewer service users were recruited than originally expected, a comprehensive analysis of non-compliance could not be undertaken.
Differences in the service users’ characteristics at baseline between CO allocation, arrival on site and completion of follow-up questionnaire were summarised and tested using regression models. The service users’ characteristics were placed in four categories: demographics, outcomes from questionnaires, health and lifestyle questions and health and social care use. Depending on the characteristic being tested, the following summary statistics and models were used: median with interquartile range (IQR) and median regression for continuous non-normal characteristics; numbers with percentages and Fisher’s exact test for categorical characteristics; and median IQR and negative binomial regression for counts. The same approach was used to show the differences in follow-up characteristics between CO allocation and nDelius and offending characteristics by CO allocation.
Differences in the changes in outcomes at follow-up between CO allocations were summarised and explored using median (IQR) and median regression for continuous non-normal outcomes and numbers with percentages and multinomial logistic regression for categorical outcomes. The differences were shown as unadjusted and adjusted for baseline.
As the follow-up outcomes were collected in only a fairly small number of service users, no further adjustment for differences in CO allocation was possible. However, the reconviction status at 18 months was available for 120 service users; therefore, further adjustment for this outcome was possible.
The differences in reconviction at 18 months by CO allocation were explored using Cox proportional hazards regression models, for which the time to event was either the first reconviction date since recruitment for those with a reconviction or 18 months if no reconviction occurred within that time. The unadjusted hazard ratio provides an estimate of the risk of 18-month reconviction for those allocated to a CF compared with those with other CO allocations. However, this estimate of the risk is unadjusted for other differences in characteristics between the two CO allocation groups that may also account for any differences in the risk of reconviction. Adjustment for ‘confounding by indication’, as it is known, was carried out by applying the stabilised inverse probability treatment weights (IPTW) to the Cox proportional hazards regression model. The IPTW produces a pseudo-population in which CO allocation is independent of any of the variables considered to be potential confounders, enabling an unbiased estimate of the impact of CFs on 18-month reconviction rates compared with other COs.
To calculate the IPTW, a logistic regression model was used to estimate the probability that the service user was allocated to a CF. Baseline and offending characteristics that showed differences between CO allocation (see Table 30, Appendix 4) were explored further to assess if they were potential confounders and, if so, if they should be included in the model to predict the probability that the service user was allocated to a CF. The associations between the potential confounders and the reconviction rate and CO allocation were tested using Cox proportional hazards regression models and logistic regression models, respectively. Confounders were those characteristics associated with both reconviction rate and CO allocation. Furthermore, those characteristics associated with reconviction rate, but not CO allocation, were also included in the model to predict the probability that the service user was allocated to a CF. However, those characteristics associated with CO allocation, but not reconviction rate, were not included. This method aims to include as many potential predictors as possible, even if their contribution is small, but is balanced in this case with the relatively small sample size (usually recommended to be at least 200 service users). 94 The inverse of the probability (IPTW) was then used to adjust each participant’s risk of reconviction for the confounders, in which the reciprocal of the probability was used if the participant was not allocated to a CF. However, without a numerator this inverse weight is likely to be highly variable and so the inverse probability of treatment weight is stabilised. The numerator was either the proportion of participants allocated to a CF or its reciprocal for those participants allocated to other COs.
The logistic regression models to predict if a participant was allocated to a CF can include only participants with complete data. In total, 600 data items were included in the models used to produce the weights. Of these, 14 (2.3%) were missing. To impute these missing data, we used switching regression, an iterative multivariable regression technique that retains an element of random variation in the estimates. Within Stata® (StataCorp LP, College Station, TX, USA), these methods are incorporated within the mice and mi estimate programs. For each variable, the distributions were compared with and without the imputed data to confirm that the imputed data did not alter the distribution of any of the variables. The imputed data were used only in the prediction of CO allocation and were not included in the reconviction rate models, as the IPTW-adjusted Cox proportional hazards model accounts for these confounders.
A number of different models were employed to explore the differences in the seasonal indicators (season, temperature, rainfall and sunshine) dependent on the outcome. To assess if there any seasonal differences in CO allocation, median regression models were used for temperature, rainfall and sunshine and Fisher’s exact test for season at time of allocation. To explore the association between temperature, rainfall, sunshine and season with CORE-OM and WEMWBS scores at both baseline and follow-up, median regression models were used.
Chapter 4 Results of the pilot study
This chapter outlines the results from the statistical analysis of the pilot data. The methods used in this chapter are outlined in Chapter 3, Statistical methods.
The purpose of the analysis was primarily to identify differences in effectiveness in terms of quality of life, mental health, lifestyle behaviours and reoffending rates between the three CFs and between CFs and comparator settings. This was done by comparing the characteristics at baseline and follow-up and changes in outcomes at follow-up between those allocated to CFs and those not, as well as by comparing the three CF sites. In order to compare the outcomes between the two CO allocation groups, adjustment is required to account for any differences in characteristics within the two groups.
Adjustment for differences in CO allocation was only possible for the reconviction status at 18 months, as a result of smaller numbers at follow-up, and the analysis and results for this outcome are outlined. Consequently, this analysis was also able to identify factors that drive the decision of CO allocation, which was necessary in order to identify potential selection bias and confounders.
Description of sample: characteristics of respondents
Of the 136 respondents initially recruited to the study, two subsequently withdrew from the study and so were removed from all subsequent analysis (Figure 8). For the 134 respondents, 50 (37%) were allocated to a CF for their CO. At baseline, the only factors that were significantly different (at the 5% level) between those allocated or not to care farms were gender, the number of missing CORE-OM questions, whether or not any substances or cannabis were used during the past 4 weeks, smoking status and agreement with the statement ‘Healthy foods are enjoyable’.
FIGURE 8.
The Consolidated Standards of Reporting Trials Diagram (CONSORT) flow diagram: recruitment and follow-up pathways in pilot study. 94 a, For the first 3 months of the study, exclusion criteria included in breach/custody, not allocated to CF or comparator setting, no risk data (not allocated), out of area and CO with other requirement (n = 32). However, after review of the early recruitment period, these criteria were removed. b, The CF closed to probation at the end of September. Prior to this 15 out of 19 (76%) service users completed their CO at their allocated placement, and the closure lead to 11 participants being moved to another placement. c, Lost to follow-up includes being in breach, in custody, not returning the questionnaires, not followed up and dead/terminally ill.
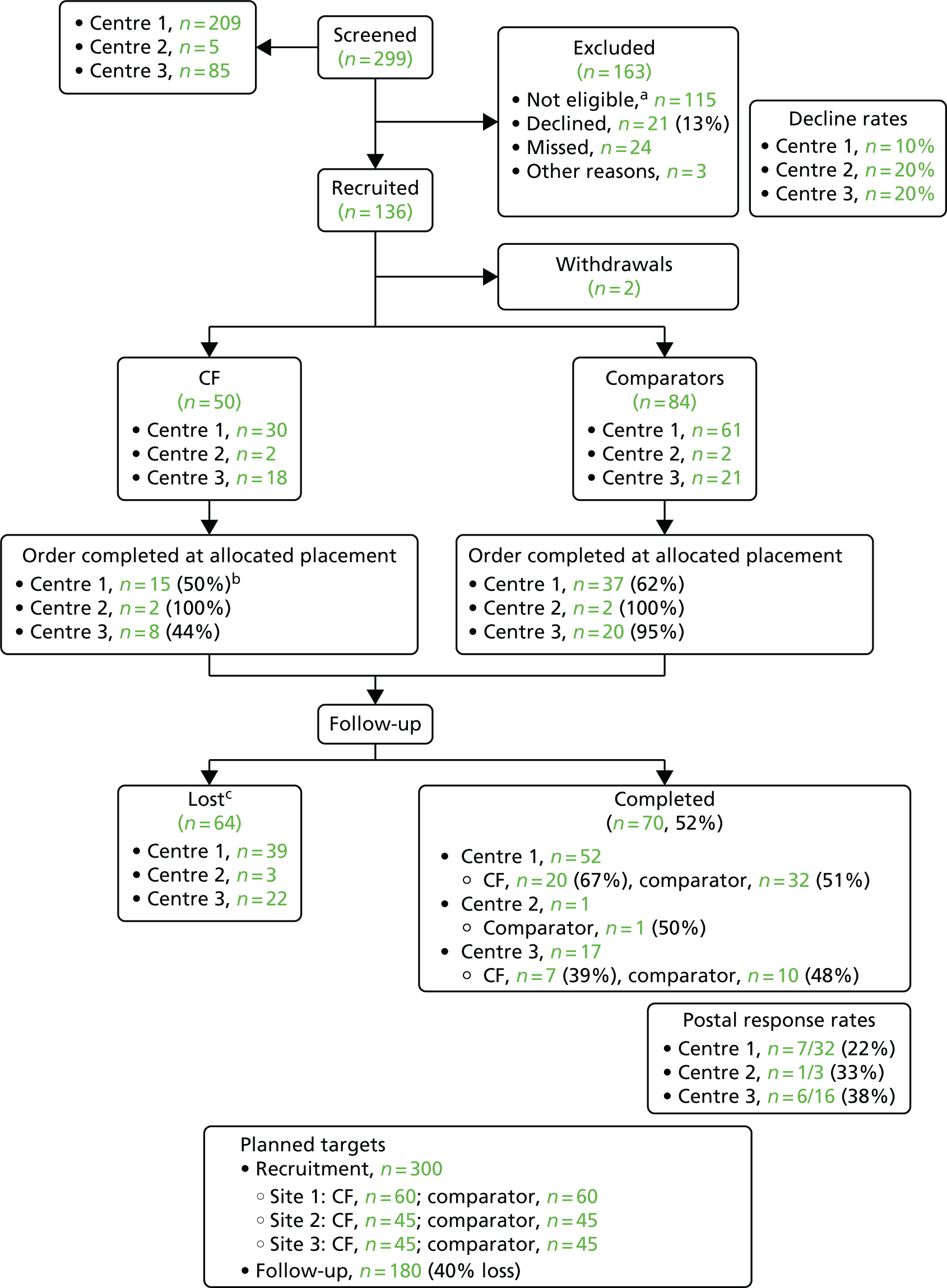
Table 11 shows only those with significant differences. Table 30, Appendix 4, shows all characteristics, whether or not significant. OGRS scores (risk of reoffending) were significantly different (at the 5% level) between those allocated or not to CFs (Table 12).
-
Only 2 out of the 50 (4%) service users allocated to CFs were women, compared with 37 out of the 84 (44%) allocated to other COs (p < 0.001 from Fisher’s exact test).
-
Although the median number of missing CORE-OM questions for those allocated to CFs and to other COs were both zero, there are differences in the variability between the two groups (IQR CF 0–24 and non-CF 0–1). The difference in variability is reflected in the difference in the number of missing CORE-OM questions between the two groups. On average, the CF group had a percentage change of 139% [95% confidence interval (CI) 21% to 370%] more missing questions than those allocated to other COs.
-
Overall, 47% of those allocated to CFs reported that they had used substances in the past 4 weeks compared with 24% of those allocated to other COs (p = 0.01).
-
In total, 34% of those service users allocated to CFs reported that they had used cannabis in the past 4 weeks compared with 16% of those allocated to other COs (p = 0.04).
-
Overall, 78% of those service users allocated to CFs were current smokers compared with 57% of those allocated to other COs (p = 0.02).
-
Proportionally more respondents agreed than disagreed with the statement ‘Healthy foods are enjoyable, of those service users allocated to other COs compared with those allocated to CFs, although more respondents allocated to the CFs neither agreed nor disagreed with the statement (p = 0.003).
-
Mean OGRS scores at the time of disposal of the CO were 26 points higher (95% CI 6.86 to 45.14 points) among CF users than those at comparator sites.
| Characteristic | Valid number | Allocated to CF (all sites, N = 134) | Meanb or percentagec difference between CO allocation | Difference in categories between CO allocation, p-valued | |
|---|---|---|---|---|---|
| No (n = 84) | Yes (n = 50) | ||||
| Demographics | |||||
| Gender: female, n (%) | 134 | 37 (44.1) | 2 (4) | < 0.001 | |
| Outcomes from questionnaires | |||||
| CORE-OM number of missing questions, median (IQR) | 134 | 0 (0–1) | 0 (0–24) | 138.88 (21.3–370.4) | |
| Health and lifestyle questions | |||||
| Used substances during the past 4 weeks: yes, n (%) | 122 | 18 (24) | 22 (46.8) | 0.01 | |
| Number of substances used during the past 4 weeks, mean (95% CI) | 122 | 0 (0 to 0) | 0 (0 to 1)e | 54.43 (–7.47 to 157.74) | |
| Cannabis: yes, n (%) | 117 | 12 (16.4) | 15 (34.1) | 0.04 | |
| Smoker: yes, n (%) | 133 | 47 (56.6) | 39 (78) | 0.02 | |
| ‘Healthy foods are enjoyable’, n (%) | 131 | 0.003 | |||
| Strongly agreee | 43 (52.4) | 13 (26.5) | |||
| Agree | 29 (35.4) | 18 (36.7) | |||
| Neither agree nor disagree | 9 (11) | 14 (28.6) | |||
| Disagree | 0 (0) | 2 (4.1) | |||
| Strongly disagree | 1 (1.2) | 2 (4.1) | |||
| Potential variable | Association with, hazard ratio (95% CI) | Include in IPTW | |
|---|---|---|---|
| Reoffending within 18 months | Allocation to CF | ||
| Age at recruitment: decades | 0.8 (0.60 to 1.07) | 0.87 (0.62 to 1.22) | |
| Gender: female vs. male | 0.58 (0.27 to 1.26) | 0.07 (0.02 to 0.32) | |
| Has disability: yes vs. no | 0.95 (0.42 to 2.18) | 2.84 (1.11 to 7.26) | |
| Probation type: NPS vs. CRC | 0.08 (0.01 to 0.6) | 0.3 (0.08 to 1.09) | ✓ |
| Used substances during the past 4 weeks: yes vs. no | 2.06 (1.08 to 3.93) | 3.53 (1.53 to 8.16) | ✓ |
| Smoker: yes vs. no | 2.44 (1.11 to 5.36) | 2.72 (1.11 to 6.67) | ✓ |
| OGRS score at disposal: point increase | 1.02 (1.01 to 1.03) | 1.02 (1.01 to 1.04) | ✓ |
| IMD: compared with most deprived quintile within cohort | 1.0 | 1.0 | |
| 2 | 2.87 (0.99 to 8.26) | 5 (1.17 to 21.46) | |
| 3 | 1.69 (0.53 to 5.34) | 7 (1.64 to 29.85) | |
| 4 | 1.58 (0.50 to 4.99) | 3.27 (0.72 to 14.73) | |
| 5 – least deprived | 1.34 (0.42 to 4.21) | 2.72 (0.61 to 12.1) | |
| White British according to nDelius: no vs. yes | 0.44 (0.17 to 1.15) | 0.14 (0.03 to 0.61) | |
| Disposal type: suspended sentence order vs. CO | 0.62 (0.30 to 1.28) | 1.56 (0.70 to 3.44) | |
| ‘Healthy foods are enjoyable’: compared with strongly agree/agree | 1.0 | 1.0 | ✓ |
| Neither agree nor disagree | 2.45 (1.17 to 5.14) | 3.51 (1.3 to 9.51) | |
| Disagree/strongly disagree | 2.95 (0.88 to 9.84) | 11.50 (1.22 to 108.02) | |
None of the questionnaire outcome measures was significantly different between the two groups at baseline (Table 30, Appendix 4). For example, the median CORE-OM score was 7.4 in the CF group and 7.1 in those allocated to other COs. Although the mean difference between the medians was 0.3, the 95% CI of this estimate is –3.95 to 4.55, which includes zero; therefore, there is no significant difference in the CORE-OM score between the two groups at the 5% significance level. The 95% CI is dependent on the sample size and, as only 93 out of the 134 respondents completed the CORE-OM to derive scores, missing data will have contributed to a wider estimate of the CI than if all respondents had completed the CORE-OM. Further breakdown of which particular questions were not completed on the CORE-OM, WEMWBS and Connecting with Nature questionnaires can be found in Table 31, Appendix 4.
Using the respondents’ postcode we were able to assign the index of multiple deprivation (IMD) ranking via lower super output area. These rankings were then placed into quintiles: first, for quintiles within the cohort and, second, matched to quintiles for England. The second of these shows that the Evaluating COs (ECO) study cohort was from more deprived quintiles than the English population in both CO allocation groups (see Table 30, Appendix 4). For example, 46% of respondents were from the most deprived quintile in England in both CO allocation groups. Comparing the IMD quintiles of the two CO allocation groups within the cohort shows some differences in the deprivation profile. Proportionally more of those allocated to other COs were in the most deprived quintile than those who had been allocated to a CF (26.5% vs. 10.2%, respectively) and in the least deprived quintile (21.7% vs. 16.3%, respectively). Conversely, proportionally more of those allocated to a CF were in the middle quintile than those allocated to other COs. Although these differences are not significant (p = 0.08), there is some indication that this may be a potential confounder when looking at the difference in the change in outcomes between the two groups.
Table 13 explores whether or not the baseline characteristics of the respondents were different between the three sites. (Table 13 only shows those with significant differences, see Table 32, Appendix 4, for all characteristics.) Although summary statistics for each of the three sites are shown, testing for whether or not there were significant differences in the characteristics between both site and CO allocations could be carried out with only site 1 and 3 because of the small number of service users recruited at site 2. The interaction between site and CO allocations for each characteristic was used to test these differences. Owing to the small numbers in the categorical characteristics within each sites, testing of the interaction was carried out on only a limited number of characteristics.
| Characteristic | Site | p-value for interaction between CO allocation and sitec | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 (N = 91) | 2 (N = 4)b | 3 (N = 39) | ||||||||
| n | Allocated to CF | n | Allocated to CF | n | Allocated to CF | |||||
| No (n = 61) | Yes (n = 30) | No (n = 2) | Yes (n = 2) | No (n = 21) | Yes (n = 18) | |||||
| Demographics | ||||||||||
| Age (years) at recruitment, median (IQR) | 91 | 31 (25–37) | 33.5 (25–43) | 4 | 37.5 (35–40) | 44.5 (38–51) | 39 | 42 (26–53) | 29 (23–37) | 0.02 |
| Outcomes from questionnaires | ||||||||||
| CORE-OM score, mean (95% CI) | 58 | 7.1 (3.8 to 12.6) | 5.6 (3.5 to 9.4) | 3 | 21.2 (21.2 to 21.2) | 2.8 (2.4 to 3.2) | 32 | 7.1 (3.8 to 11.5) | 15.3 (7.4 to 19.7) | 0.04 |
| Health and lifestyle questions | ||||||||||
| Number of days of ≥ 30 minutes’ physical activity in the last week, median (IQR) | 85 | 3 (1–6) | 5 (2–7) | 4 | 4.5 (2–7) | 3.5 (1–6) | 36 | 5 (4–7) | 3 (3–7) | 0.02 |
There are significant differences in the ages of the recruits between sites and between CO allocations within sites (p = 0.02). In site 1, those participants allocated to the CF had a median age of 33.5 years and those allocated to other COs had a median age of 31 years. In site 3, those participants allocated to the CF had a median age of 29 years and those allocated to other COs had a median age of 42 years.
There were significant differences in the CORE-OM scores between sites and between CO allocations within sites but not for the WEMWBS and Connected to Nature scores (CORE-OM, p = 0.04; WEMWBS, p = 0.07; and Connected to Nature, p = 0.16).
There were significant differences in the characteristic of ‘Number of days of ≥ 30 minutes’ physical activity in the last week’ between sites and between CO allocation within sites (p = 0.02). No other baseline characteristics appeared to show differences between sites and between CO allocations within sites, although the comparisons are limited as a result of the relatively small numbers within sites.
Loss to follow-up with reasons
Of the 134 respondents, 70 (52.2%) completed the follow-up (Table 14). Those respondents followed up, through the completion of the questionnaire, were older, more likely to be in the NPS rather than the CRC, did not smoke, used fewer substances in the last week and used fewer health services in the past month than those not followed up. The mean difference in the median age between those followed up and those who were not was 6 years (95% CI 2.59 to 9.41 years). There are no other differences in baseline characteristics between those respondents followed up or not including the proportion allocated to the CFs (p = 1.00) (see Table 33, Appendix 4).
| Characteristic | Valid number | Followed up | Meanb or percentagec (95% CI) difference between follow-up | Difference in categories between follow-up, p-valued | |
|---|---|---|---|---|---|
| No (N = 64) | Yes (N = 70) | ||||
| Demographics | |||||
| Age (years) at recruitment,b median (IQR) | 134 | 29 (23.5–37) | 34.5 (27–45) | 6 (2.59–9.41) | |
| Probation type, n (%) | 134 | ||||
| CRC | 59 (92.2) | 49 (70) | 0.002 | ||
| NPS | 5 (7.8) | 21 (30) | |||
| Health and lifestyle questions | |||||
| Number of substances used during the past 4 weeks,e median (IQR) | 122 | 0 (0–1) | 0 (0–1) | –60.33 (–79.23 to –24.22) | |
| Smoker: yes, n (%) | 133 | 48 (76.2) | 38 (54.3) | 0.01 | |
| Health and social service use | |||||
| Number of health services (out of 10) used during the past month,e median (IQR) | 131 | 1 (0–2) | 0 (0–1) | –36.57 (–55.25 to –10.1) | |
Follow-up and outcomes
For the 70 respondents at follow-up, those that were allocated to a CF (n = 27) were more likely to have changed their CO during the follow-up period, have a higher CORE-OM score, have used substances and used more of them during the past 4 weeks and were less likely to agree with the ‘Healthy foods are enjoyable’ statement (Table 15). In total, 49% of those respondents allocated to a CF had changed their CO, compared with only 28.9% of those allocated to other COs (p = 0.01). There was an indication that those respondents allocated to a CF had, on average, fewer hours to complete of their CO at follow-up than those allocated to other COs (mean difference –7.55 points, 95% CI –16.03 to 0.93 points), although this was not significant (Table 33, Appendix 4).
| Characteristic | Valid number | Allocated to CF (all sites, N = 70) | Meanb or %c (95% CI) difference between CO allocation | Difference in categories between CO allocation, p-valued | |
|---|---|---|---|---|---|
| No (n = 43) | Yes (n = 27) | ||||
| Demographics | |||||
| CO changed during the follow-up period: yes, n (%) | 134 | 23 (27.4) | 26 (52) | 0.01 | |
| Outcomes from questionnaires | |||||
| CORE-OM score,b mean (95% CI) | 58 | 5.3 (2.1 to 11.5) | 9.4 (5 to 14.1) | 4.1 (0.63 to 7.57) | |
| Health and lifestyle questions | |||||
| Used substances during the past 4 weeks: yes, n (%) | 62 | 5 (13.9) | 16 (61.5) | < 0.001 | |
| Number of substances used during the past 4 weeks,c median (IQR)e | 62 | 0 (0–0) | 1 (0–1) | 564.62 (165.79–1561.86) | |
| ‘Healthy foods are enjoyable’, n (%) | 69 | 0.03 | |||
| Strongly agree | 24 (57.1) | 6 (22.2) | |||
| Agree | 11 (26.2) | 11 (40.7) | |||
| Neither agree nor disagree | 6 (14.3) | 7 (25.9) | |||
| Disagree | 1 (2.4) | 2 (7.4) | |||
| Strongly disagree | 0 (0) | 1 (3.7) | |||
Those service users allocated to a CF had a higher CORE-OM score at follow-up, on average 4.1 points higher (95% CI 0.63 to 7.57 points), than those allocated to other COs. The other questionnaire outcomes showed no significant difference between groups. Further breakdown of particular questions on the CORE-OM, WEMWBS and Connecting with Nature questionnaires at follow-up can be found in Table 35, Appendix 4.
For the 134 respondents, it was possible to link 120 with nDelius and reconviction information. Three respondents did not consent to access of their nDelius information and it was not possible to link 11 respondents to their reconviction data. Of the 120 allocated to a CF (n = 40), the respondents had a higher OGRS score at disposal (a term used in the criminal justice system when an order is given by the court once proceedings are complete), were more likely to be white British and more likely to report having a disability than those allocated to other COs (Table 16).
| nDelius and offending characteristic | Valid number | Allocated to CF (all sites, N = 120) | Meana or %b (95% CI) difference between CO allocation | Difference in categories between CO allocation, p-valuec | |
|---|---|---|---|---|---|
| No (n = 80) | Yes (n = 40) | ||||
| Number of days from disposal to recruitment,a median (IQR) | 120 | 28.5 (14 to 80.5) | 41.5 (17.5 to 105) | 13 (–13.77 to 39.77) | |
| OGRS score at disposal,b mean (95% CI) | 120 | 25 (10.5 to 50) | 53.5 (17.5 to 86) | 26 (6.86 to 45.14) | |
| Disposal type, n (%) | 120 | 0.31 | |||
| CJA:95 CO or ORA96 CO | 56 (70) | 24 (60) | |||
| CJA:95 suspended sentence order | 24 (30) | 16 (40) | |||
| Ethnic group, n (%) | 119 | 0.02 | |||
| White British | 57 (72.2) | 38 (95) | |||
| White: other | 3 (3.8) | 1 (2.5) | |||
| Asian or Asian British | 5 (6.3) | 0 (0) | |||
| Black or black British | 11 (13.9) | 0 (0) | |||
| Other or mixed | 3 (3.8) | 1 (2.5) | |||
| Has disability: yes, n (%) | 113 | 11 (14.5) | 12 (32.4) | 0.04 | |
| Mental illness/dyslexia: yes | 6 (7.9) | 5 (13.5) | 0.07 | ||
| Reduced mobility/physical capacity/hearing: yes | 3 (4) | 2 (5.4) | |||
| Other: yes | 2 (2.6) | 5 (13.5) | |||
| Accommodation status at disposal, n (%) | 61 | 0.34 | |||
| Permanent independent housing | 20 (57.1) | 10 (38.5) | |||
| Friends/family | 9 (25.7) | 10 (38.5) | |||
| Transient/short-term accommodation/supported housing/no fixed abode | 6 (17.1) | 6 (23.1) | |||
| Employment status at disposal, n (%) | 100 | 0.35 | |||
| Full-time employed, self-employed, education or training | 33 (49.3) | 12 (36.4) | |||
| Part-time employed or self-employed | 4 (6) | 1 (3) | |||
| Unemployed or unable to work | 27 (40.3) | 16 (48.5) | |||
| Other | 3 (4.5) | 4 (12.1) | |||
| Risk of self-harm at disposal, n (%) | 115 | 0.08 | |||
| Low risk | 60 (76.9) | 22 (59.5) | |||
| Medium risk | 18 (23.1) | 15 (40.5) | |||
| Reconviction within 18 months of recruitment, n (%) | 120 | 17 (21.3) | 21 (52.5) | < 0.001 | |
| Number of days from recruitment to reconviction within 18 months,a median (IQR) | 120 | 442.5 (303 to 535) | 379 (181 to 487.5) | –18.92 (–73.59 to 148.93) | |
| Number of convictions if reconvicted within 18 months of recruitment,b median (IQR) | 120 | 0 (0 to 0) | 1 (0 to 1) | –47.52 (–73.64 to 4.46) | |
The median OGRS score at disposal was, on average, 26 points higher (95% CI 6.86 to 45.14 points) in those service users allocated to a CF than those allocated to other COs. Furthermore, there are significant differences in the OGRS scores between sites and between CO allocations within sites (p = 0.02). In site 1, those service users allocated to the CF had a median OGRS score of 32.5 points (IQR 5–56 points) and those allocated to other COs had a median score of 25 points (IQR 11–49 points). In site 2, those service users allocated to other COs had a median score of 28.5 points (IQR 17–40 points), although only one respondent allocated to a CF had an OGRS score (10 points). In site 3, those service users allocated to the CF had a median OGRS score of 87 points (IQR 70–90 points), although those allocated to other COs had a median OGRS score of 21 points (IQR 7.5–54 points).
The ethnic group stated by the respondents at the time of the disposal shows that 95% of those service users allocated to a CF identified as white British compared with 72% of those allocated to other COs (p = 0.02). At disposal, 32% of those service users allocated to a CF identified as having a disability compared with 15% of those allocated to other COs (p = 0.04).
From the reconviction information, 53% of those service users allocated to a CF had a reconviction within 18 months, compared with 21% of those allocated to other COs (p< 0.001). There were no significant differences in the length of time and the number of convictions for the first reconviction within 18 months between the COs allocation groups. This comparison of the reconvictions rates does not take into account the length of follow-up for each respondent, which is a more appropriate analysis and is outlined in Reconvictions.
The questionnaire outcomes scores at follow-up, outlined in Table 15, are limited in being able to show differences between the CO allocation groups, as it does not account for each respondent’s starting point. The change from baseline to follow-up in the questionnaire outcomes is a better assessment on the impact of CFs compared with other COs (Table 17). In general, there were no differences in the change in the questionnaire outcomes between the CO allocations, even with adjustment for baseline.
| Change in outcome | Valid number | Allocated to CF (all sites, N = 70) | Meana (95% CI) difference between CO allocation | Relative risk ratio (95% CI) of changing category from no change, compared with controlsb | Difference in change in outcome, compared with those not attending CF, adjusted by baseline,a,b mean or relative risk ratio (95% CI) | |
|---|---|---|---|---|---|---|
| No (n = 43) | Yes (n = 27) | |||||
| CORE-OM score,a mean (95% CI) | 42 | –1.5 (–3.05 to 1.15) | –1 (–2 to 0.3) | 0.6 (–0.71 to 1.91) | 1.29 (–3.83 to 6.41) | |
| CORE-OM change category,b n (%) | 42 | |||||
| Clinically significant improvement | 4 (14.3) | 2 (14.3) | 1.28 (0.2 to 8.24) | 1.06 (0.13 to 8.69) | ||
| No clinically significant change | 23 (82.1) | 9 (64.3) | 1.0 | 1.0 | ||
| Clinically significant deterioration | 1 (3.6) | 3 (21.4) | 7.67 (0.7 to 83.73) | 8.58 (0.75 to 97.72) | ||
| WEMWBS score,a median (IQR) | 63 | 4 (–3 to 8) | 3 (–2 to 4) | –1 (–6.19 to 4.19) | –0.32 (–4.63 to 4) | |
| Connected to nature score,a median (IQR) | 64 | –0.16 (–0.34 to 0.34) | 0 (–0.33 to 0.5) | 0.16 (–0.16 to 0.48) | 0.08 (–0.22 to 0.38) | |
| Connecting with nature (nature relatedness scale) change category,b n (%) | 53 | |||||
| More interconnected | 7 (21.2) | 6 (30) | 2.14 (0.55 to 8.38) | 3.13 (0.69 to 14.29) | ||
| No change | 20 (60.6) | 8 (40) | 1.0 | 1.0 | ||
| Less interconnected | 6 (18.2) | 6 (30) | 2.5 (0.62 to 10.11) | 1.46 (0.3 to 7.18) | ||
| Number of substances used during the past 4 weeks,a median (IQR) | 66 | 0 (0 to 0) | 0 (0 to 1) | 0 (–0.45 to 0.45) | 0 (–0.98 to 0.98) | |
| Number of days of ≥ 30 minutes’ physical activity in the last week,a median (IQR) | 58 | 0 (0 to 1) | 0 (–2 to 0.5) | 0 (–0.79 to 0.79) | –0.75 (–2.41 to 0.91) | |
| Number of days out of the last seven drank alcohol,a median (IQR) | 53 | 0 (–1 to 1) | 0 (–1 to 1) | 0 (–1.3 to 1.3) | 0.5 (–0.91 to 1.91) | |
| Number of cigarettes/roll-ups per day,a median (IQR) | 53 | 0 (0 to 2) | 1 (0 to 5) | 1 (–3.78 to 5.78) | 1 (–4.26 to 6.26) | |
| Number of health services (out of 10) used during the past month,a median (IQR) | 33 | 0 (–1 to 1) | 0 (0 to 0) | 0 (0 to 0) | 0 (–0.45 to 0.45) | |
| Number of social services (out of 4) used during the past month,a median (IQR) | 67 | 0 (0 to 0) | 0 (0 to 0) | –c | 0 (0 to 0) | |
| Number of medications prescribed by a doctor or other health-care professional in the past month,a median (IQR) | 62 | 0 (0 to 0) | 0 (0 to 1) | 0 (–0.45 to 0.45) | 0 (–0.46 to 0.46) | |
| bHealthy foods are enjoyable’ agreement change category,b n (%) | 67 | |||||
| More positive view by follow-up | 8 (19.5) | 7 (26.9) | 1.82 (0.54 to 6.1) | 0.8 (0.19 to 3.46) | ||
| No change | 27 (65.9) | 13 (50) | 1.0 | 1.0 | ||
| More negative view by follow-up | 6 (14.6) | 6 (23.1) | 2.08 (0.56 to 7.7) | 2.93 (0.71 to 12.16) | ||
Further details of the results for specific outcomes are outlined in the following sections.
Clinical Outcome in Routine Evaluation–Outcome Measure results
The median change in CORE-OM score in those service users allocated to a CF was –1 point (IQR –2 to 0.3 points) and –1.5 points (IQR –3.05 to 1.15 points) in those allocated to other COs (see Table 17). There was no significant difference in the change in the CORE-OM score between the two groups. On average, there was a 0.6-point difference (95% CI –4.76 to 5.96 points) in the median change in CORE-OM score of those service users allocated to a CF compared with those allocated to other COs. Even with adjustment for baseline CORE-OM score, there is still no significant difference in the change in CORE-OM score between the two groups. On average, there was a 1.29-point difference (95% CI –2.64 to 5.21 points) in the median change in CORE-OM scores between the CO allocation groups. When the change in CORE-OM is classified by clinically significant improvement, deterioration or no change, there still remains no association between CORE-OM change category and CO allocation group; although, with small numbers it is not appropriate to fully interpret these results further.
Warwick–Edinburgh Mental Health and Well-Being Scale
The median change in WEMWBS score in those service users allocated to a CF was 3 points (IQR –2 to 4 points) and in those allocated to other COs was 4 points (IQR –3 to 8 points) (see Table 17). There was no significant difference in the change in WEMWBS score between the two groups. On average, there was a –1-point difference (95% CI –6.19 to 4.19 points) in the median change in WEMWBS score of those service users allocated to a CF compared with those allocated to other COs. Even on adjustment for baseline WEMWBS score there is still no significant difference in the change in WEMWBS score between the two groups. On average, there was a –0.32-point difference (95% CI –4.03 to 4.00 points) in the median change in WEMWBS scores between the CO allocation groups.
Connectedness to nature scale
The median change in connectedness to nature scale score in those service users allocated to a CF was 0 points (IQR –0.33 to 0.5 points) and in those allocated to other COs was –0.16 points (IQR –0.34 to 0.34 points) (see Table 17). There was no significant difference in the change in connectedness to nature scale score between the two groups. On average, there was a 0.16-point difference (95% CI –0.16 to 0.48 points) in the median change in connectedness to nature scale score of those service users allocated to a CF compared with those allocated to other COs. Even with adjustment for the baseline connectedness to nature scale score, there is still no significant difference in the change in connectedness to nature scale score between the two groups. On average, there was a 0.08-point difference (95% CI –0.22 to 0.38 points) in the median change in connectedness to nature scale scores between the CO allocation groups. When the change in Nature Relatedness Scales from baseline to follow-up is classified as more interconnected, less interconnected or no change, there is no association between Nature Relatedness Scales change category and CO allocation group. With adjustment of the baseline Nature Relatedness Scale score, the risk of those service users allocated to the CF being more interconnected rather than no change according to Nature Relatedness Scales was 2.45 points higher (95% CI 0.56 to 10.68 points) than those allocated to other COs.
Health and lifestyle
There was no change in the number of substances used, number of days of physical activity, number of days drank alcohol, number of cigarettes and number of medications prescribed in either CO allocation group (see Table 17). Therefore, there were no differences in the changes in these health and lifestyle indicators, even on adjustment for baseline. For the level of agreement to the statement ‘Healthy foods are enjoyable’ question at baseline and follow-up, which was classified as having a more positive view, more negative view or no change by follow-up; there is no association between ‘Healthy foods are enjoyable’ agreement change category and CO allocation group. With adjustment of the baseline agreement, the risk of those service users allocated to the CF being more positive to the statement rather than no change by follow-up was 20% less likely (95% CI 0.19 to 3.46) and being more negative was almost three times more likely (95% CI 0.71 to 12.06) than that of those allocated to other COs.
Health and social service use
There was no change in the number of health and social services used in either CO allocation group (see Table 17). Therefore, there were no differences in the changes in these the number of health and social services, even with adjustment for baseline.
Reconvictions
The potential confounders for inclusion in the weight to adjust for differences in the CO allocation groups, so as to provide an unbiased estimate of the difference in the risk of reconviction within 18 months, are provided in Table 12. On assessing whether or not these characteristics were associated with reconviction within 18 months or allocation to a CF, five characteristics were identified for inclusion in the IPTW: probation type at baseline; used substances during the past 4 weeks before baseline; smoker at baseline; OGRS score at baseline; and agreement with the ‘Healthy foods are enjoyable’ statement. Apart from probation type, these characteristics were associated with both reconviction within 18 months or allocation to a CF, as indicated by bold text in Table 12. Probation type was found to be associated only with reconviction within 18 months and not allocation to a CF, and so was identified for inclusion in the IPTW.
The unadjusted risk of reconviction within 18 months is over three times higher (95% CI 1.58 to 5.96) in those allocated to CFs than those allocated to other COs (Table 18). With adjustment for differences in the CO allocation groups, so as to provide an unbiased estimate of the difference in the risk of reconviction within 18 months, the risk of reconviction within 18 months is 50% higher in the CF group. However, there is no significant difference in the risk of reconviction between the CO allocation groups (HR 1.50, 95% CI 0.64 to 3.53). This would indicate that any difference in reconviction between the two CO allocation groups results from differences in the characteristics of those service users allocated to a CF and those allocated to other COs.
| Intervention | Association with reconviction within 18 months, HR (95% CI) | |
|---|---|---|
| Unadjusted | Adjusted by IPTW | |
| CF | ||
| No (n = 80) | 1.0 | 1.0 |
| Yes (n = 40) | 3.07 (1.58 to 5.96) | 1.5 (0.64 to 3.53) |
Inverse probability treatment weight diagnostics and sensitivity analysis
To assess the performance of the IPTW to adjust for differences in the CO allocation groups, it is recommended to review the IPTWs between the two groups, including an assessment of the balance of confounders (Table 19). 97 As expected, the unstabilised IPTW is more variable than the stabilised; therefore, the latter is used in the Cox proportional IPTW-adjusted model. The balance of the stabilised IPTWs between the two groups is appropriate (standardised difference < 0.10) in all variables, expect for probation type. This is confirmed when we review the standardised differences for each variable before and after adjustment by IPTWs (Figure 9). The standardised differences are greatly reduced by the IPTW, except for probation type. If we exclude this variable from the IPTW, the adjusted HR would be 1.6 (95% CI 0.71 to 3.64), which is similar to the IPTW-adjusted HR including probation type (HR 1.50, 95% CI 0.64 to 3.53). As exclusion of this variable does not change the overall results of there being no difference in the 18-month reconviction rate between the two CO allocation groups (with adjustment for the difference between groups), it was decided to leave probation type in the IPTW, as it does make some adjustment for the differences between the two groups.
FIGURE 9.
Standardised difference in IPTW of variables included.
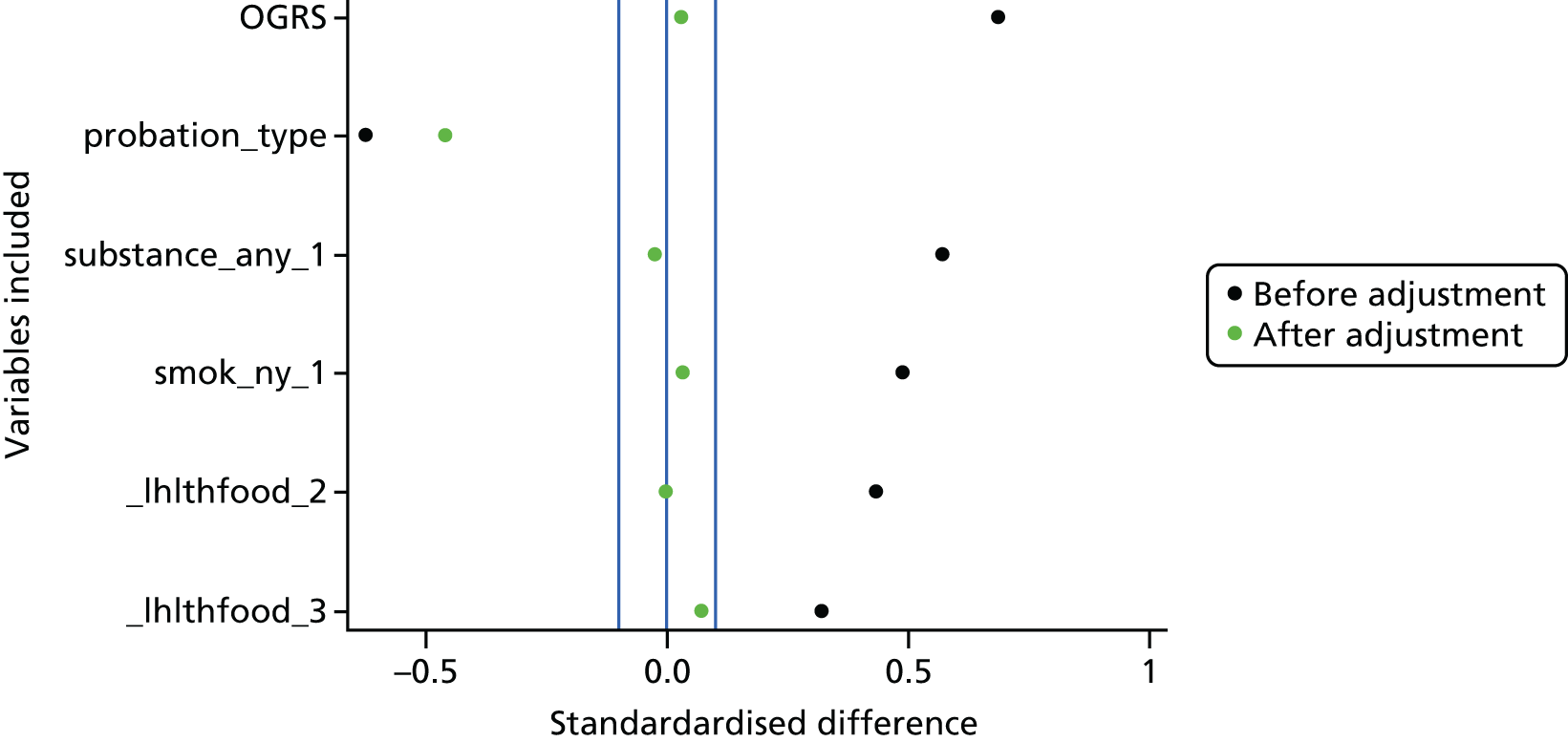
| Variable included in IPTW | CF (all sites, N = 120) | Standardised difference | |
|---|---|---|---|
| No (n = 80) | Yes (n = 40) | ||
| Overall unstabilised IPTW | |||
| Mean (95% CI) | 1.45 (1.34 to 1.57) | 3.17 (2.29 to 4.05) | |
| Median (IQR) | 1.3 (1.21–1.43) | 2.24 (1.5–3.87) | |
| Minimum, maximum | 1.05, 4.11 | 1.05, 16.53 | |
| Overall stabilised IPTW | |||
| Mean (95% CI) | 0.97 (0.89 to 1.04) | 1.06 (0.76 to 1.35) | |
| Median (IQR) | 0.87 (0.81–0.95) | 0.75 (0.5–1.29) | |
| Minimum, maximum | 0.7, 2.74 | 0.35, 5.51 | |
| Mean stabilised IPTW | Standardised difference | ||
| Probation type: NPS vs. CRC | 0.19 | 0.04 | –0.459 |
| Used substances during the past 4 weeks: yes vs. no | 0.34 | 0.33 | –0.025 |
| Smoker: yes vs. no | 0.64 | 0.66 | 0.032 |
| OGRS score at disposal: point increase | 38.07 | 38.94 | 0.029 |
| Healthy foods are enjoyable’: compared with strongly agree/agree | |||
| Neither agree nor disagree | 0.2 | 0.19 | –0.005 |
| Disagree/strongly disagree | 0.02 | 0.03 | 0.071 |
Seasonality
There are no differences in the seasonal indicators between the CO allocation groups, at the time of disposal (Table 20), indicating that there were no seasonal differences in allocation. There was no difference in the median temperatures, mean percentage difference from average centimetres of rain and mean percentage difference from average hours of sunshine between those allocated to a CF and other COs. There were no significant differences in CO allocation by season (p = 0.85).
| Season characteristic at time of disposal | Valid number | CF (all sites, N = 134) | Meana (95% CI) difference between CO allocation | Difference in categories between CO allocation, p-valueb | |
|---|---|---|---|---|---|
| No (n = 84) | Yes (n = 50) | ||||
| Temperature (°C), median (IQR) | 129 | 11.2 (6.7 to 13.9) | 11.2 (6.7 to 13.9) | 0 (–3.1 to 3.1) | |
| Rain percentage difference from average, median (IQR) | 128 | –10 (–18 to 57) | –17 (–23 to 60.5) | –7 (–51.7 to 37.7) | |
| Sunshine percentage difference from average, median (IQR) | 128 | –3.5 (–9 to 27) | 6 (–8 to 31) | 10 (–4.7 to 24.7) | |
| Season, n (%) | 129 | 0.85 | |||
| Spring | 30 (37) | 21 (43.8) | |||
| Summer | 20 (24.7) | 12 (25) | |||
| Autumn | 16 (19.8) | 7 (14.6) | |||
| Winter | 15 (18.5) | 8 (16.7) | |||
At baseline, the only seasonal indicator that showed a significant association was between the WEMWBS score and rainfall (Table 21). With each point increase in WEMWBS score, the percentage difference from average rainfall is increased by almost 5% (median 4.93%, 95% CI 0.45% to 9.41%). There were no significant differences in the CORE-OM and WEMWBS scores at baseline based on which season the baseline questionnaire was completed. No associations were found between CORE-OM score at baseline and temperature, rainfall or sunshine and between WEMWBS score with temperature or sunshine. At follow-up, there are no seasonal indicators associated with the CORE-OM or WEMWBS scores. Furthermore, our findings show that collection and linkage of seasonality data would be feasible in a larger study.
| Baseline and follow-up characteristic | Valid number | Season | ||||
|---|---|---|---|---|---|---|
| All | Spring | Summer | Autumn | Winter | ||
| At baseline questionnaire or recruitment | ||||||
| CORE-OM score, median (IQR) | 93 | 7.65 (3.2–15) | 7.1 (3.5–12.9) | 7.1 (4.7–11.5) | 9.1 (3.8–12.9) | |
| Mean (95% CI) difference from springa | – | –1.4 (–8.24 to 5.44) | –1.4 (–7.9 to 5.1) | 0.6 (–7.71 to 8.91) | ||
| WEMWBS score, median (IQR) | 124 | 47 (43–55) | 52 (41–59) | 51 (45–54) | 56 (47.5–65.5) | |
| Mean (95% CI) difference from springa | – | 5 (–2.31 to 12.31) | 4 (–2.4 to 10.4) | 9 (–1.32 to 19.32) | ||
| Temperature: average for month | ||||||
| Correlation (95% CI), at baselinea | ||||||
| With CORE-OM | 93 | –0.1 (–0.53 to 0.34) | ||||
| With WEMWBS | 124 | –0.14 (–0.73 to 0.46) | ||||
| CF, median (IQR) temperature | ||||||
| No | 84 | 11.1 (6.7–13.9) | ||||
| Yes | 50 | 11.15 (6.7–13.9) | ||||
| Rain: percentage difference from average | ||||||
| Correlation (95% CI), at baselinea | ||||||
| With CORE-OM | 93 | –0.77 (–5.69 to 4.14) | ||||
| With WEMWBS | 124 | 4.93 (0.45 to 9.41) | ||||
| CF, median (IQR) percentage difference from average | ||||||
| No | 84 | –10 (–23 to 21) | ||||
| Yes | 50 | –23 (–25 to 15) | ||||
| Sunshine: percentage difference from average | ||||||
| Correlation (95% CI), at baselinea | ||||||
| With CORE-OM | 134 | 6.06 (–7.33 to 19.45) | ||||
| With WEMWBS | 2.5 (–14.86 to 19.86) | |||||
| CF, median (IQR) percentage difference from average | ||||||
| No | 84 | 5 (–9 to 27) | ||||
| Yes | 50 | 5 (–6 to 20) | ||||
| At follow-up questionnaire | ||||||
| CORE-OM score, median (IQR) | 58 | 5 (2.4–10.6) | 6.5 (5–13.2) | 6.9 (2.4–12.9) | 10.25 (1.3–18.8) | |
| Mean (95% CI) difference from springa | – | 1.5 (–3.1 to 6.1) | 3.2 (–2.14 to 8.54) | –2.4 (–20.13 to 15.33) | ||
| WEMWBS score, median (IQR) | 66 | 54 (47–62) | 51 (49–55) | 53 (48–56) | 57 (37–67) | |
| Mean (95% CI) difference from springa | – | 1.5 (–4.31 to 7.31) | 3.2 (–3.76 to 10.16) | –2.4 (–19.13 to 14.33) | ||
| Temperature: average for month | ||||||
| Correlation (95% CI), at follow-upa | ||||||
| With CORE-OM | 58 | 0.5 (–0.24 to 1.24) | ||||
| With WEMWBS | 66 | –0.42 (–1.27 to 0.43) | ||||
| Rain: percentage difference from average | ||||||
| Correlation (95% CI), at follow-upa | ||||||
| With CORE-OM | 58 | –1.72 (–7.59 to 4.14) | ||||
| With WEMWBS | 66 | 2.63 (–6.7 to 11.96) | ||||
| Sunshine: percentage difference from average | ||||||
| Correlation (95% CI), at follow-upa | ||||||
| With CORE-OM | 58 | –2 (–14.68 to 10.68) | ||||
| With WEMWBS | 66 | 0 (–16.51 to 16.51) | ||||
Discussion of statistical methods
The relatively small number of service users, particularly those at follow-up, should be considered when we review the conclusions of the results from the pilot study. In that context, we should also consider the number of statistical tests and models included in the analysis, that is, the potential problem of multiple testing. To negate multiple testing we have focused the analysis on the estimates of differences and changes (and corresponding 95% CI) rather than relying solely on p-values. This does not fully invalidate the problem, as the 95% CI indicates whether or not there are significant differences or changes at the 5% level and so correspond to the p-values. However, by estimating the differences and changes, we can better understand the impact of any change or difference between the CO allocation groups.
To assist the consideration of the sample sizes involved and their impact on what differences or changes can be estimated, Table 22 shows a post hoc analysis of numbers involved in the four main outcomes. For the three questionnaire outcome measures (CORE-OM, WEMWBS and connectedness to nature scale) we used the mean change score at follow-up [and standard deviation (SD)] by CO allocation group with the number of respondents to calculate the corresponding effect size that this difference in change represents. From this, we can then calculate the power (given α = 0.05) for that effect size and number of respondents, that is, the probability that the test correctly rejects the null hypothesis (no difference) when the alternative hypothesis (difference in groups) is true.
| Outcome measure | Mean change in score (SD) | Effect size | Power | |
|---|---|---|---|---|
| Non-CF | CF | |||
| CORE-OM score | –1.05 (4) | 0.53 (5) | 0.186 | 0.22 |
| WEMWBS score | 2.6 (8.6) | 1.24 (7.4) | 0.083 | 0.10 |
| Connected to nature score | 0.026 (0.9) | 0.058 (0.6) | 0.017 | 0.05 |
| Reconviction with 18 months | ||||
| Unadjusted | Hazard ratio 3.0 | ≈1.00 | ||
| Adjusted by IPTW | Hazard ratio 1.5 | 0.61 | ||
As can be seen, there is insufficient power to estimate a significant difference (at the 5% level) between the CO allocation groups in the change in scores at follow-up for the three questionnaire outcomes.
For the reconviction within 18 months outcome, we used the hazard ratio (both unadjusted and adjusted by IPTW) for the risk of reconviction in the CF group compared with the other CO allocation along with the number of respondents to each to, again, estimate the power. Here we see that we have sufficient respondents (n = 120) to estimate the unadjusted differences in reconviction risk between the two groups (i.e. power > 0.90), but not the adjusted differences in reconviction risk.
Although these calculations indicate that we do not have the number of respondents required to estimate significant differences, they do not take into account that there may not be differences in these outcomes between the CO allocation groups in the first place.
The other major statistical consideration is the adjustment for the decision to allocate to a CF rather than other COs and other differences between these two groups. A variety of methods have been suggested for this adjustment, including propensity scores. 98 Four methods have been outlined in the statistical literature for how to use propensity scores: covariate adjustment, stratification or subclassification, propensity score-matching and the IPTW. We have used IPTW as it has been found that, even in small study samples, propensity score-matching and the IPTW can yield correct estimations of treatment effect (in this study the effect of CFs). 99 However, this recommendation applies if only true confounders are included and those variables related only to the outcome and not the exposure are not included in the propensity score model, which we followed when developing the logistic model to predict the propensity scores.
Consideration is also required in regard to the number of variables included in the models used to produce the propensity weights. The recommended sample size is between 200 and 400 service users or 10–20 cases for each variable included. 100 Therefore, we had adequate power to use propensity score models in this context, that is, 120 service users with five variables.
There is a continuing debate as to which variables should be included in the models to estimate the propensity weights. Results from simulation experiments101 suggest that variables related to outcome but not to treatment should always be included because they decrease the variance of estimates without increasing bias, that is, overfitting is a positive aspect of these models. As part of this process, the diagnostics of the IPTW are important to determine whether or not conditioning on the estimated propensity score has removed observed systematic differences between CF and other CO allocation groups, which we followed as recommended for IPTWs. 97 However, the possibility of residual confounding remains because of unmeasured variables that are associated either with CO allocation decisions or with reconviction rates. Although we included variables that cover the spectrum of characteristics, unmeasured confounders may include service user preferences and compliance with COs.
Summary
Taking into consideration the statistical methods employed, this analysis was able to illustrate the feasibility of comparing outcomes between CO allocation groups with robust and valid adjustment for factors that drive the decision of CO allocation. The use of propensity scores provides a viable method for comparison despite differences in participant characteristics at CFs and comparator sites. These methods are becoming more common, particularly in the evaluation of complex interventions in which it is not, as in probation, possible to randomise.
As discussed in Chapter 3 and highlighted from these results, retention for follow-up was problematic. However, using reconviction data linked from police data without the need to directly follow-up subjects was shown to be a robust outcome with the appropriate adjustment. The weights used in the adjustment were calculated based on relatively few variables (the largest being OGRS score), highlighting that the data required to adjust appropriately for differences between CO allocation and sites are not extensive. Furthermore, the methods for adjustment for CO decision can also be employed to adjust for those lost to follow-up and so could be employed in future studies with a primary outcome of reconviction based on linked records.
Chapter 5 Economic evaluation
Despite the widespread use of CFs in Europe, studies that evaluate the economic impact of CFs are scarce. Nevertheless, evaluating the economic impact as well as the value for money of this kind of public health intervention is key to policy-makers and robust economic analyses would provide them with elements to make decisions regarding resource allocation in the future. 102
The health economics component in this project was twofold: to review the evidence to guide any type of economic evaluation (cost–benefit, cost-effectiveness and cost–utility), and to collect and use data from the pilot study to understand the feasibility of conducting an economic evaluation in a future study. This chapter therefore compiles the evidence from the literature on (1) the economic evaluation of CFs as an intervention for vulnerable people, especially probation service users, (2) the use of HRQoL measures to evaluate their effectiveness and, finally, (3) the evaluation of the cost of crime. In this report, we have summarised the evidence of the three reviews for space restrictions; however, full reviews are available on request to the health economics lead. Second, it calculates the cost related to the social and health care use data and the calculation of utility at baseline and follow-up as collected as part of the pilot study.
Economic evaluation of care farms: a review of the evidence
Introduction and aims
The aim of this review was to examine the methods used in the economic evaluation of CF or related community interventions for prisoners.
Methods
Search strategy
A systematic search strategy was conducted in December 2013 in the following databases: EMBASE, Health Management and Information Consortium, MEDLINE, MEDLINE In-Process & Other Non-Indexed Citations, PsycINFO (all via Ovid); ASSIA, National Criminal Justice Reference Service Abstracts, Sociological Abstracts, Social Services Abstracts (all via ProQuest); CINAHL, Criminal Justice Abstracts (all via EBSCOhost); The Campbell Library; the NHS Economic Evaluation Database (The Cochrane Library via Wiley Online Library); RePeC Ideas; and Conference Proceedings Citation Indexes – Science, Social Science and Humanities (via the Web of Science, Thomson Reuters).
Inclusion criteria
Studies were selected based on whether or not they contained quantitative economic data, such as a cost-effectiveness analysis, cost–benefit analysis, cost–utility analysis and cost-savings analysis of CFs or related community interventions for prisoners. Studies were excluded if the intervention setting was not in the community or if the study was not in a developed country, lacked quantitative data or focused primarily on juvenile offenders or was a review or guideline.
Data collection and analysis
Search results were screened by a researcher, and a second reviewer was consulted if the decision to include or exclude a study was not obvious. Full-text copies were retrieved and data extracted using a standardised form. The quality of the economic evaluations was assessed using the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist. 103 The findings were discussed narratively.
Results
The literature search identified 8520 articles and, after duplicates were removed, 6277 titles and abstracts were screened. Full-text copies of 66 potentially relevant studies were assessed for eligibility, of which 10 papers were included in this review. Three papers specifically evaluated CFs as an intervention for probation service users1,104,105 and seven other papers evaluated other types of interventions for probation service users in the community setting. 106
Summary of the evidence
The literature review showed that current available evidence on the economic evaluation of CFs is scarce; most cost analyses are rudimentary and based only on estimated cost savings. There is no study using a cost-effectiveness analysis.
Most studies did not consider all relevant costs in the analysis. For instance, some authors considered only the costs to the criminal justice system and did not include any costs to society. On the other hand, others conducted sensitivity analyses by first using costs to the criminal justice system and then adding direct and indirect societal costs to address uncertainty surrounding their analysis. Moreover, as a result of data unavailability and restrictions in measuring some offence types, often the estimated cost of reoffending was underestimated. Furthermore, on several occasions, the authors omitted the cost year, discounting of the costs or adjustments for inflation. This is problematic, as it is uncertain whether or not all of the costs included in the analysis were from the same year. Only one paper presented a cost analysis of CFs104 and it found that there were possible savings after probation service users participated in the CF programme; however, only two participants were included. Apart from this cost analysis, two other scoping studies of CFs from the UK6 and the Netherlands25 collected data on the average cost of a CF, per service user, per day. Regarding other similar interventions, we found one cost–benefit analysis that evaluated a ‘circle of support’ intervention for probation service users.
Owing to the heterogeneity in the collected data, it was difficult to directly compare the results of these interventions. We were particularly interested in collecting information on the specific cost types the authors considered when costing the intervention. The following costs were frequently included in the different analyses: cost of treatment, staff training costs, transportation costs, staff salaries, cost of monitoring probation service users, staff and probation service user recruitment costs, telephone costs, premises costs and cost of equipment. Furthermore, several studies also calculated the cost of reoffending, cost of offences to the criminal justice system, money paid by probation service users as fees for enrolling in a particular programme and cost of court appearances.
The impact of care farms on health-related quality of life: a systematic review
Introduction and aims
This scoping review was conducted prior to the Campbell Review (see Chapter 2) and identified any existing literature on the impact of CFs and similar interventions using HRQoL measures in adult populations. The main objective was to focus on HRQoL measures that could be used for a cost-effectiveness or cost–utility analysis. HRQoL is increasingly used as an outcome to measure effectiveness in both medical and social interventions. 107
Methods
Search strategy
The search strategy was based on the search concepts ‘green care’ and ‘quality of life’ (see Appendix 5).
Inclusion criteria
Studies that met the following criteria were included: RCTs, cluster RCTs, non-randomised studies (provided that baseline characteristics were comparable), adult participants, and CFs or green care. Any comparison group was considered, that is, no intervention, care as usual or alternative intervention. Studies that measured HRQoL using any validated measures were considered.
Data collection and analysis
Titles and abstracts were screened by a researcher, and a second reviewer was consulted if the decision to include or exclude a study was not obvious. Full-text copies were retrieved and data were extracted using a standardised form. The detailed process of study selection was presented in a PRISMA flow diagram. 108 To assess reliability and validity of RCTs, we used the Cochrane six-item risk-of-bias checklist. 39 Studies were rated as being at a high risk, low risk or unclear risk of bias. For all other non-RCTs, the suggested risk-of-bias criteria for EPOC reviews was used. The findings were discussed narratively.
Results
The literature search identified 1132 potentially relevant studies. After the removal of duplicates, 948 titles and abstracts were screened, of which 937 studies were excluded. Eleven possibly relevant studies were retrieved for full-text assessment. 106 After full-text review, five studies were included in the analysis. 106 A flow diagram can be found in Figure 10.
FIGURE 10.
Flow diagram of excluded and included studies in HRQoL review.
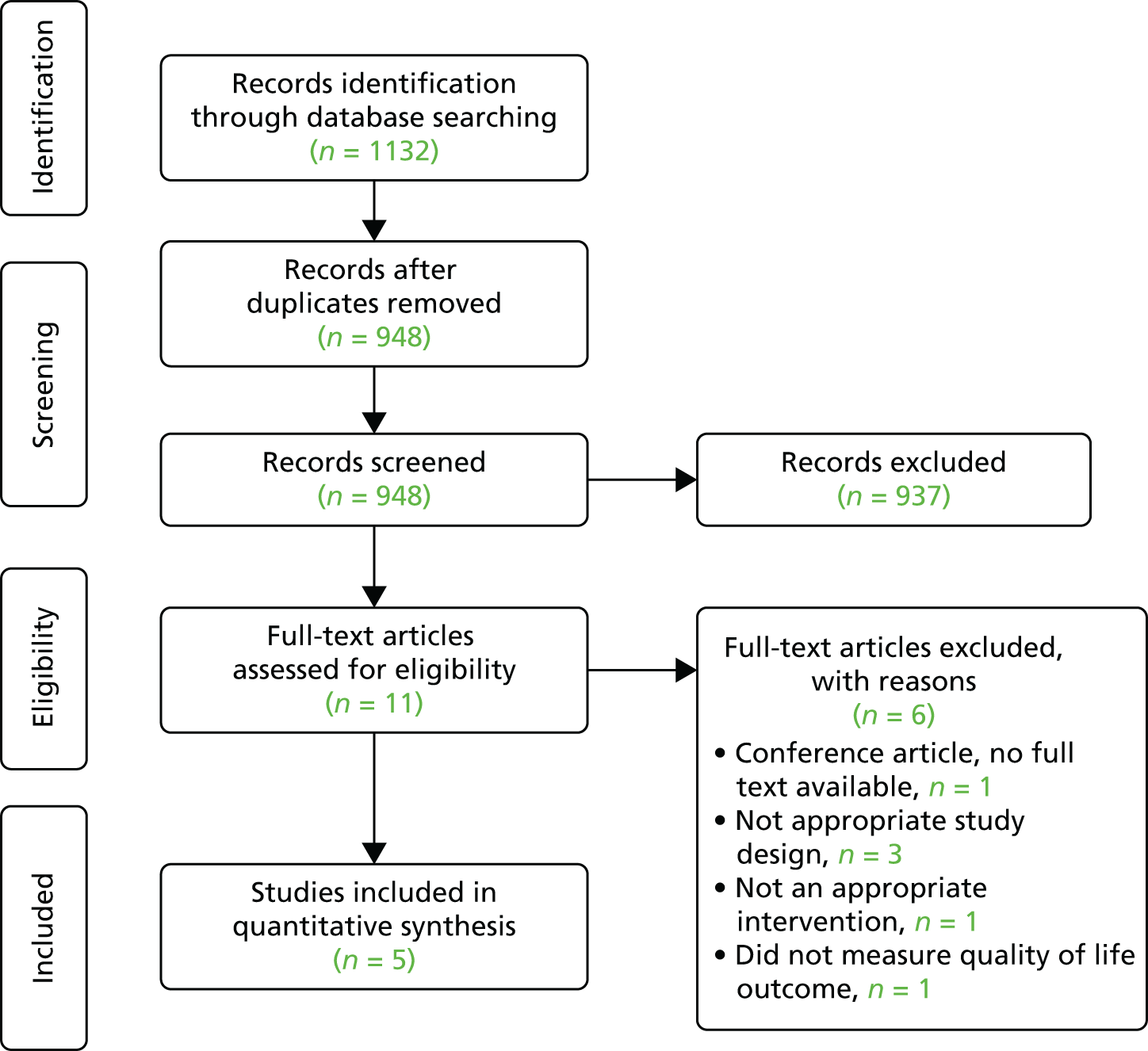
Summary of the evidence
Four hundred and eighty-four participants were included in this review. All included studies delivered different types of green-care interventions, such as CFs, animal-assisted therapy or horticultural therapy, or a combination of these. Only two studies were conducted in a farm setting. 106 Most studies had small sample sizes and, therefore, may have been insufficiently powered to detect an effect.
One of the most important findings from this review was the paucity of research that evaluated the impact of CFs using HRQoL. We found no studies that included any direct measure of utility. Instead, two studies used the Short Form questionnaire-36 items instrument,106 which could be used to generate utility via Short Form questionnaire-6 Dimensions. 86
Cost of crime: a systematic review
This review was published during the duration of the project; please refer to Wright et al. 106 for details.
Aims and objective
This review aimed to systematically search the literature to identify all published studies that estimated the cost of crime imposed by adult offenders. We defined cost of crime as ‘all costs that would not exist in the absence of illegal behaviour’. 109
Methods
Search strategy
In December 2013 we searched the following databases: EMBASE, Health Management and Information Consortium, MEDLINE, MEDLINE In-Process & Other Non-Indexed Citations, PsycINFO (all via Ovid); ASSIA, National Criminal Justice Reference Service Abstracts, Sociological Abstracts, Social Services Abstracts (all ProQuest); CINAHL, Criminal Justice Abstracts (all EBSCOhost); The Campbell Library; NHS Economic Evaluation Database (The Cochrane Library, Wiley Online Library); RePeC Ideas; and Conference Proceedings Citation Indexes – Science, Social Science and Humanities (Web of Science, Thomson Reuters). Searches were designed to identify studies of the health and societal costs of offending by combining the search concept ‘offending’ with the concepts ‘health costs’ or ‘societal costs’. In addition, grey literature was sought by scanning the UK government website (www.gov.uk, accessed December 2013) and by screening bibliographies of included studies or literature reviews (see Appendix 5).
Inclusion criteria
We considered studies that quantified the cost of crime and excluded studies that reported qualitative data, literature reviews, policy papers, studies that only discussed methodology of costing crime, economic evaluations of crime prevention interventions and studies that reported only costs for juvenile offenders, as the focus of our review was to assess costs imposed by adult offenders.
Data collection and analysis
Titles and abstracts were screened by a researcher, and a second reviewer was consulted if the decision to include or exclude a study was not obvious. As studies varied considerably when estimating the cost of crime, results were synthesised descriptively and presented according to crime category.
Results
The literature search yielded 8520 potentially relevant studies. After removal of duplicates, 6265 were identified for screening. In addition, twelve studies were identified through hand-searching of references and in total 6277 titles and abstracts were screened. During full-text review, 21 studies were included in the analysis. 109–129 A PRISMA chart describing the inclusion and exclusion processes can be found in Figure 11.
FIGURE 11.
Flow diagram of excluded and included studies cost of crime review.
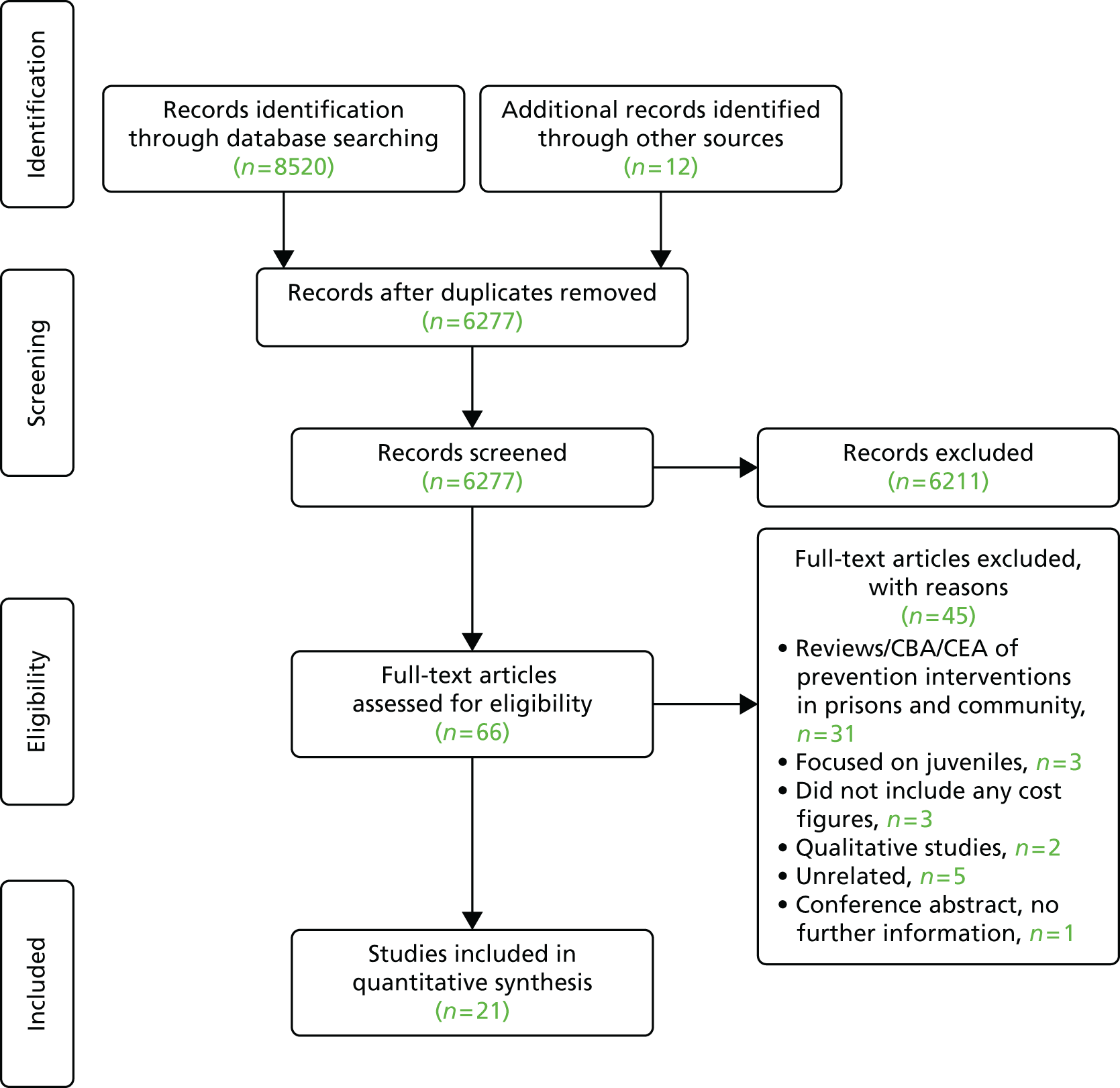
Summary of the evidence
Overall, 21 studies reported estimates of the costs of crime, of which 14 estimated the cost of crime to society and victims, six focused only on the cost of crime to victims and one study measured the costs to society of career offenders. The findings show that the total costs of crime varied considerably between studies. Furthermore, each offence category also provided substantially different cost estimates. This was reflected in the large standard deviations estimated for each category with the exception of serious traffic offence, criminal damage and fraud. In addition, homicide ranked as the offence that was most costly, followed by drug offence, fraud, sexual assault, assault and serious traffic offence, all of which account for more than 9% of the total cost of crime. Crime categories that involved violence to a person, such as homicide, assault and sexual assault, were all associated with higher intangible costs.
There are several possible reasons that could explain the variations in the cost estimates. The dispersion may be due to the differences in the year when the study was conducted, inflation, changes in unit costs, under-reporting of crime or changes in crime trends. In addition, officially recorded crime statistics may underestimate the actual incidence of crime because victims have under-reported incidents of crime or police have not recorded a reported crime. 130 As a result, studies that calculated costs based only on recorded crimes provided a conservative estimate of the total cost of crime. To address this problem, authors used multipliers to calculate the actual crime rate. Multipliers were calculated by computing the ratio of the actual estimated number of crimes to the number of crimes recorded. However, owing to lack of data availability, some authors also used proxy multipliers from different studies.
The lack of a standardised approach to measure cost of crime was also problematic. When calculating the total cost of crime it was clear that the types of offences that were considered by authors were not the same, and the exclusion of some crime categories in the overall cost calculations could therefore underestimate the overall cost of crime.
Inconsistency in the definitions of crime categories was also observed; some authors aggregated two similar crime categories, such as criminal damage and arson, whereas others disaggregated crime categories and presented cost estimates, for example for sexual assault and rape, separately. The inconsistency in the definitions is problematic, as it can increase the variability in the cost estimates when comparing studies in the review and interpreting the findings.
Although direct costs were relatively straightforward to calculate, intangible costs such as fear, pain and suffering required a more intricate approach. Diverse methods were used for this purpose, such as the jury awards approach, the willingness-to-pay approach and the QALY approach. These different methods introduced considerable heterogeneity to the estimated results.
To the best of our knowledge this was the first systematic review conducted to estimate the cost of crime; consequently, we were able to assess similarities and differences of the methodologies used to estimate the cost of crime.
Analysis of key parameters for a future cost-effectiveness analysis
Introduction
The health economics analysis was designed to identify the feasibility of conducting an economic evaluation of CFs in comparison with other CO settings by (1) improving the health and well-being of offenders over 6 months and in (2) reducing reconviction rates over 18 months. As identified in Chapter 4, this pilot study was not designed to detect a significant difference in quality of life or reconvictions, particularly with adjustment for important confounders. In the light of this, we do not present the results of the cost-effectiveness analysis here, but instead discuss the feasibility of conducting this analysis in a larger follow-up study.
Methods
Perspective
We designed our analysis of the cost-effectiveness of CFs as a CO from the perspective of the health and social care. This includes costs incurred in the provision of the intervention, as well as health-care resource and social service utilisation, as reported by users as part of the pilot study follow-up. All costs were adjusted to 2014 prices using the Campbell and Cochrane Economics Methods Group, Evidence for Policy and Practice Information Centre (EPPI-Centre) Cost Converter (version 1.4) (https://eppi.ioe.ac.uk/costconversion, accessed June 2015). The analysis would be within the study period (6 months) and, therefore, discounting for future cost and health outcome would not be necessary. The currency was UK pounds sterling.
Quality of life
In line with the National Institute for Health and Care Excellence reference case,131 the primary outcome for a cost-effectiveness analysis would be QALYs. In the pilot study, users’ HRQoL was assessed using the CORE-OM,82 and was assessed at baseline and at the 6-month follow-up. The CORE-OM is a self-reported questionnaire that is commonly used to measure psychological distress in evaluations of mental health interventions. 132 A preference-based measure, CORE-6D, was developed from the CORE-OM combining a number of answers to the CORE-OM into a utility using an algorithm developed by Mavranezouli et al. 133 These utilities represent users’ overall quality of life and are multiplied by the time spent in each state to generate QALYs. The average numbers of QALYs between adjacent time points are calculated to generate smoothed estimates between those time points. QALYs represent a quality-weighted survival value in which 1 QALY is the equivalent of 1 year of full health.
Resource use and valuation
The total cost of each arm of the study was calculated combining the reported resource usage at follow-up and unit cost data along with the intervention cost.
The health and social care resource usage data were collected as part of a questionnaire that was conducted with all participants in centres 1, 2 and 3 at the same time points: baseline and 6 months. The recall period was the past month for both questionnaires. The questionnaires included number of health services visits [e.g. general practitioner (GP), practice nurse, physiotherapist, occupational therapist, psychiatrist, mental health counsellor, drug and alcohol worker, family planning service, health trainer] and number of social services visits (e.g. social worker, helpline, family support of self-help groups). Service users also reported any use of hospital services including outpatient and inpatient and medication use. As our study duration was 6 months’ follow-up, we generated an average health-care resource use using both collection points and multiplied this average by six to estimate the average level of health-care use per offender over 6 months.
Resource usage figures were then converted into costs using unit cost figures from the Personal Social Services Research Unit (PSSRU)’s Unit Costs of Health and Social Care 2014. 134 Unit costs for medications were obtained from the British National Formulary. 135 Probation service users reported details for medications that were taken. The total medication costs were then calculated using the average cost per dose for each product. Tables 23 and 24 present a summary of health-care use and medication data collected, along with associated unit costs.
| Resource | Unit cost (£, 2013–14) | Source |
|---|---|---|
| GP | 46 | PSSRU’s Unit Costs of Health and Social Care 2014,134 p. 195 |
| Practice or district nurse | 37 | NHS Reference Costs 2013 to 2014 136 |
| Physiotherapist | 51 | PSSRU’s Unit Costs of Health and Social Care 2014,134 p. 179 |
| Occupational therapist | 36 | PSSRU’s Unit Costs of Health and Social Care 2014,134 p. 180 |
| Psychiatrist | 103 | PSSRU’s Unit Costs of Health and Social Care 2014,134 p. 259 |
| Mental health counsellor | 50 | PSSRU’s Unit Costs of Health and Social Care 2014,134 p. 51 |
| Drug and alcohol worker | 48 | PSSRU’s Unit Costs of Health and Social Care 2014,134 p. 67 |
| Family planning service | 50 | PSSRU’s Unit Costs of Health and Social Care 2014,134 p. 212 |
| Health trainer | 53 | NHS Reference Costs 2013 to 2014 136 |
| Social worker | 79 | PSSRU’s Unit Costs of Health and Social Care 2014,134 p. 206 |
| Helpline | 29 | NHS direct cost in 2007, £25, adjusted for inflationa |
| Family or patient support or self-help groups | 52 | PSSRU’s Unit Costs of Health and Social Care 2014,134 p. 154 |
| Any other social services | 50 | PSSRU’s Unit Costs of Health and Social Care 2014,134 p. 212 |
| Dentist | 125 | NHS Reference Costs 2013 to 2014 136 |
| Support worker | 52 | PSSRU’s Unit Costs of Health and Social Care 2014,134 p. 154 |
| Hospital inpatient stay | 275 | NHS Reference Costs 2013 to 2014 136 |
| Hospital outpatient clinic | 109 | PSSRU’s Unit Costs of Health and Social Care 2014,134 p. 189 |
| Hospital accident and emergency department | 124 | NHS Reference Costs 2013 to 2014 136 |
| Radiography | 40 | PET-NECK study137 |
| Drug name | Package size | Package cost (£) | Description | Source |
|---|---|---|---|---|
| Amiloride | 28 | 11.02 | 5-mg tablets | BNF138 |
| Amitriptyline | 28 | 1.11 | 10-mg, 25-mg or 50-mg tablets | BNF138 |
| Amoxicillin | 21 | 0.36 | 250-mg or 500-mg capsules | eMIT139 |
| Aspirin | 28 | 0.94 | 75-mg tablets | BNF138 |
| Atorvastatin | 28 | 0.74 | 10-mg tablets | eMIT139 |
| Bisoprolol | 28 | 1.02 | 10-mg tablets | BNF138 |
| Buspirone | 30 | 7.67 | 10-mg tablets | BNF138 |
| Candesartan | 28 | 1.02 | 4-mg, 8-mg, 16-mg or 32-mg tablets | eMIT139 |
| Celecoxib (CELEBREX®, Pfizer Ltd, Tadworth, UK) | 30 | 21.55 | 100-mg capsules | BNF138 |
| Citalopram | 28 | 1.14 | 10-mg, 20-mg, 40-mg or 80-mg tablets | BNF138 |
| Co-codamol | 100 | 1.27 | 30-mg to 500-mg tablets or 8-mg to 500-mg tablets | eMIT139 |
| Codeine | 28 | 0.79 | 30-mg tablets | eMIT139 |
| Cyanocobalamin | 50 | 6.24 | 50-µg tablets | BNF138 |
| Diazepam | 28 | 0.19 | 2-mg, 5-mg or 10-mg tablets | eMIT139 |
| Diclofenac sodium | 84 | 1.17 | 25-mg or 50-mg tablets | BNF138 |
| Ferrous sulfate (Ferrograd®, Teofarma, Pavia, Italy) | 30 | 2.58 | 325-mg tablet | BNF138 |
| Finasteride (Propecia®, Merck Sharp & Dohme Ltd, Hoddesdon, UK) | 28 | 26.99 | 1-mg tablet | BNF138 |
| Fluoxetine | 30 | 14.11 | 20-mg or 60-mg capsules | eMIT139 |
| Fluoxetine (PROZAC®, Eli Lilly and Company Ltd, Basingstoke, UK) | 30 | 1.50 | 20-mg capsules | BNF138 |
| Fluticasone propionate (Seretide, GlaxoSmithKline UK Ltd, London, UK) | 60 | 40.92 | 500-µg inhaler | BNF138 |
| Folic acid | 90 | 2.71 | 500-µg tablets | eMIT139 |
| Furosemide | 28 | 10.29 | 10-mg, 40-mg or 500-mg tablets | BNF138 |
| Hydroxyzine hydrochloride (Atarax®, Alliance Pharmaceuticals Ltd, Chippenham, UK) | 28 | 1.22 | 25-mg tablets | BNF138 |
| Hyoscine butylbromide (Buscopan®, Boehringer Ingelheim Ltd, Bracknell, UK) | 56 | 3.00 | 10-mg tablets | BNF138 |
| Hypromellose [Artelac®, Bausch & Lomb (UK) Ltd, Kingston upon Thames, UK] | 1 | 4.99 | 10-ml bottle | BNF138 |
| Insulin detemir | 1 | 42.00 | 100-ml injection | BNF138 |
| Lansoprazole | 28 | 1.52 | 30-mg capsules | BNF138 |
| Mesalazine (PENTASA®, Ferring Pharmaceuticals Ltd, West Drayton, UK) | 100 | 30.74 | 500-mg tablets | BNF138 |
| Metformin | 56 | 5.32 | 500-mg tablets | BNF138 |
| Methadone | 50 | 3.39 | 5-mg tablets | BNF138 |
| Mirtazapine | 28 | 1.60 | 30-mg tablets | BNF138 |
| Morphine sulphate | 1 | 2.60 | 10-mg/ml, 15-mg/ml, 20-mg/ml or 30-mg/ml injection | eMIT139 |
| Naproxen | 56 | 9.78 | 500-mg tablets | BNF138 |
| Olanzapine | 28 | 1.59 | 10-mg tablets | BNF138 |
| Omeprazole | 28 | 1.23 | 20-mg capsules | BNF138 |
| Paracetamol | 100 | 0.41 | 500-mg tablets | eMIT139 |
| Paroxetine | 30 | 2.12 | 20-mg or 30-mg tablets | BNF138 |
| Propranolol | 28 | 3.05 | 10-mg, 40-mg or 160-mg tablets | eMIT139 |
| Quetiapine | 60 | 2.36 | 100-mg tablets | BNF138 |
| Quetiapine (SEROQUEL, AstraZeneca UK Ltd, Luton, UK) | 60 | 113.10 | 100-mg tablets | BNF138 |
| Ramipril | 28 | 1.33 | 10-mg capsules | BNF138 |
| Salbutamol (Salamol®, Teva UK Ltd, Castleford) | 1 | 6.30 | 100-µg inhaler | BNF138 |
| Salbutamol (Ventolin, GlaxoSmithKline UK Ltd, London, UK) | 1 | 3.00 | 200-µg | BNF138 |
| Sertraline | 28 | 1.56 | 50-mg or 100-mg tablets | BNF138 |
| Sitagliptin (JANUVIA®, Merck Sharp & Dohme Ltd, Hoddesdon, UK) | 28 | 33.26 | 25-mg, 50-mg or 100-mg tablets | BNF138 |
| Temazepam | 28 | 13.70 | 20-mg tablets | BNF138 |
| Thiamine | 100 | 7.87 | 50-mg or 100-mg tablets | BNF138 |
| Tramadol | 30 | 1.20 | 50-mg capsules | BNF138 |
| Zopiclone | 28 | 1.68 | 3.75-mg tablets | BNF138 |
The intervention cost was based on interviews with the business manager who had responsibility for interventions (including CP). Neither of the sites (CFs or comparator) were contacted to get full details of the activities and the costs of running these. Data on the intervention and comparator site cost were collected from only one centre (centre 1) in the study. Accessing cost data from the probation service at a time when it was tendering for new CRC contracts was particularly challenging. Collecting comparator and CF costs at only one site was a pragmatic response. We estimated the costs incurred in the provision of the COs and collected from sites the number of hours in each setting in which probation service users were supervised.
The number of supervised hours over the study year is reported in Table 25. The number of hours was then multiplied by the estimated hourly rate. In CFs, the hourly rate was reported by the probation services to be £3.10; however, it was reported as £3.17 in the comparator settings.
| Service users (month) | Supervised hours | |
|---|---|---|
| CF | Comparator CO location | |
| April | 1957 | 1530 |
| May | 3740 | 1050 |
| June | 1795 | 1055 |
| July | 1314 | 884 |
| August | 1298 | 1363 |
| September | 1313 | 1327 |
| October | 1583 | 1418 |
| November | 1501 | 1231 |
| December | 548 | 1454 |
| January | 1408 | 1577 |
| February | 1534 | 1621 |
| March | 1771 | 1291 |
| Total (hours) | 19,762 | 15,801 |
We also collected travel expenses, although offenders had to meet the first £2.20 of their travel costs. The business manager informed us that the probation trusts reimburse the difference to the service user upon production of a bus ticket via petty cash, and this was estimated to equal an average of £1 per reporting occasion. The CF site reported 2820 occasions, although the comparator site reported 2260 occasions. The total annual cost per site was £65,466 in the comparator site and £51,234 in the CF site; the comparator CO was, therefore, £14,232 more expensive than the CF.
Missing data
The mean total costs per patient from a health and social perspective was calculated adding the cost of inpatient stay, outpatient visit, consultations, medication and intervention costs for all service users for whom response data were available. Respondents who failed to complete individual items of the CORE-OM at baseline could not be allocated a utility index score and, therefore, would be excluded from the analysis. This was the case for 38.32% of the sample, and the complete-case data set consisted of 18 probation service users in the CF arm and 35 probation service users in the control arm.
Results
Quality of life
Table 26 details the CORE-6D scores at baseline and 6 months. The index score is between 0 and 1, for which 0 represents a health status of death and 1 represents full health. In line with the results on the CORE-OM score in the statistical analysis, the CORE-6D index scores showed improvements in quality of life from baseline to the 6-month follow-up point in both groups. It appeared that the increase between the two time points was larger for users in the comparator arm than in the CF arm. Although CF users had marginally higher utility at baseline, the reverse was observed at the 6-month follow-up; in both cases, there were no significant differences between the CORE-6D scores at baseline or follow-up for the two study arms.
| Parameter | Study arm | Difference p-value of t-test | |
|---|---|---|---|
| CO (n = 35) | CF (n = 18) | ||
| Baseline | |||
| Mean (SD) | 0.825 (0.175) | 0.830 (0.132) | |
| Median (minimum, maximum) | 0.87 (0.16, 0.95) | 0.87 (0.5, 0.95) | 0.906 |
| 6 months – complete case | |||
| Mean (SD) | 0.849 (0.122) | 0.835 (0.118) | |
| Median (minimum, maximum) | 0.92 (0.5, 0.95) | 0.87 (0.61, 0.95) | 0.679 |
Health-care resource usage
Resource use was broadly comparable between the two arms (Table 27). Probation service users were frequent users of drug and alcohol workers and mental health counsellors in the past month. Although no probation service users in the CF arm reported any visit to a nurse, four probation service users reported a visit in the control arm. The number of visits to the GP was slightly higher in the control arm.
| Health or social service resource | Use of the service | Number of visits | ||
|---|---|---|---|---|
| CO, n (%) | CF, n (%) | CO, n (SD) | CF, n (SD) | |
| GP | 12 (34.29) | 3 (16.67) | 1.7 (0.37) | 1 (0) |
| p-value of t-test | 0.214 | 0.089 | ||
| Practice or district nurse | 4 (11.43) | 0 (0) | 1.33 (1.15) | N/A |
| p-value of t-test | 0.043 | N/A | ||
| Physiotherapist | 1 (2.86) | 1 (5.56) | 2 (0) | 2 (–) |
| p-value of t-test | 0.659 | N/A | ||
| Psychiatrist | 1 (2.86) | 1 (5.56) | – | – |
| p-value of t-test | 0.659 | – | ||
| Mental health counsellor | 2 (5.71) | 1 (5.56) | 0.5 (0.71) | 1 (–) |
| p-value of t-test | 0.977 | N/A | ||
| Drug and alcohol worker | 3 (8.57) | 3 (16.67) | 1.66 (0.58) | 5 (–) |
| p-value of t-test | 0.473 | N/A | ||
| Health trainer | 2 (5.71) | 0 (0) | 4 (–) | – |
| p-value of t-test | 0.534 | N/A | ||
| Social worker | 1 (2.86) | 1 (5.56) | 2 (–) | – |
| p-value of t-test | 0.695 | N/A | ||
| Support or self-help groups | 1 (2.86) | 0 (0) | 8 (–) | N/A |
| p-value of t-test | N/A | N/A | ||
| Other social services | 0 (0) | 2 (11.12) | – | 1 (1.41) |
| p-value of t-test | 0.163 | N/A | ||
Costs
The total health and social service resource use costs in the past month, averaged over the two collection points, were, respectively, £93 for users in the comparator group and £33.50 for CF users, which was significantly different at the 5% level (Table 28). Total medication costs were marginally higher in the CF sample (£5.50 vs. £3.00); however, the difference was not significant. When including the cost of the intervention in the mean total cost of health-care resource use, the total costs over the last month were marginally higher in the control arm (£95.70 vs. £67.20).
| Parameter | Study arm | Difference p-value of t-test | |
|---|---|---|---|
| CO (n = 35) | CF (n = 18) | ||
| Health and social services usage costs (£) | |||
| Mean (SD) | 92.96 (145.04) | 33.47 (65.48) | |
| Median (minimum, maximum) | 23.00 (0, 650) | 0.00 (0, 263.5) | 0.045* |
| Total medication costs (£) | |||
| Mean (SD) | 2.92 (6.80) | 5.46 (14.59) | |
| Median (minimum, maximum) | 0.00 (0, 31.62) | 0.00 (0, 58.59) | 0.492 |
| Total costsa (£) | |||
| Mean (SD) | 95.74 (135.16) | 67.23 (119.43) | |
| Median (minimum, maximum) | 22.21 (22.21, 644.21) | 21.71 (21.71, 315.98) | 0.343 |
Summary
The health economics component of this project aimed to (1) conduct a review of published and grey literature evaluating the impacts of COs and costs of offending to society and health services and (2) identify the most appropriate ways to collect cost data, including health-care resource use by probation service users, cost of reoffending, costs of crime and gains of employability of probation service users in CFs and comparator CO settings and explore the feasibility of measuring cost–utility.
The first review objective was completed with three useful reviews. The review of the economic evaluation of CFs concluded that most cost analyses were rudimentary and, based on only estimated cost savings, there was no study using a cost-effectiveness analysis. The second review on the impact of CFs or green care on HRQoL measures showed the paucity of research that used utility and preference-based instruments to measure benefits, despite the fact that HRQoL is increasingly used as an outcome to measure effectiveness in both medical and social interventions. 107 Finally, the third review of the cost of crime was substantial and gathered evidence on cost of crime that could be easily integrated in a future decision-analysis model evaluating interventions in crime area.
Regarding the second objective, we were able to collect health-care resource used by probation service users in self-reported questionnaires completed at baseline and at the 6-month follow-up; we also surveyed and summarised costs of crime via the third literature review.
We found that the CORE-OM is a suitable outcome measure to generate utilities for probation service users undertaking COs. We found that only 13.9% of the participants requested help or clarification from the RA. The results indicate a large number of missing data at baseline; however, this was mainly attributable to human error as the questionnaire package was missing two pages of the CORE-OM. At follow-up, the number of true missing data were small. Although it is possible that the participants found the questionnaire suitable, several items stood out as being particularly challenging for some participants. The participants requested help from the RA to seek clarification of words, such as overwhelming, warmth and affection, and optimistic. This suggests that if the CORE-OM is administered, it is better to employ a RA so that the participant can ask for any clarifications, which will reduce the rate of missing values. Using the CORE-6D we were able to generate utilities from which QALYs could be generated to undertake a cost–utility analysis.
The total annual cost per site was estimated to be £51,234 in the CF and £65,466 in the comparator site. A limit to the costing of the intervention we faced in the study is that, although we were able to appropriately cost CFs as an intervention from the perspective of the probation trust, the cost of the comparator intervention was based on only one type of CO within centre 1 and we had to assume that all other COs would cost the same amount to implement. It is likely that this assumption may be inappropriate and some COs may be cheaper or more expensive.
Considering the small complete-case data set (n = 53), it is likely that the exploratory cost–utility analysis would lead to incremental cost-effectiveness ratios with a high level of uncertainty and it would therefore be difficult to generalise the results of this study.
An interesting complementary analysis would be a cost-effectiveness analysis using reconviction rates as the outcome of benefit; the sample for this secondary analysis would be larger than the study sample using QALYs as reconviction rates are available for 120 participants (vs. only 53 participants for QALYs). However, we collected health and social services usage costs over only the baseline and 6-month time points and we would have to assume that probation service users pursue the same use of health and social care over 18 consecutive months.
Furthermore, if the type of reoffence had been collected we could have used the results of the systematic cost review to extrapolate the incremental costs of reconviction in the analysis and construct a full decision-analysis model.
Chapter 6 The qualitative study
Introduction
As outlined in Chapter 1, objective 6, we aimed to develop a logic model based on the experiences of probation service users of serving their CO at a CF. In Chapter 2, we reported the findings from our systematic literature review, in which we developed a theoretically based logic model to explain the mechanisms for how care farming might work for different groups of vulnerable people. Briefly, the development of the logic model involved identifying theoretical concepts as a basis for the model and exploring the qualitative literature to unearth the potential intervention components, mechanisms and process outcomes that were of importance to the various groups.
The plan for this part of the pilot study was to conduct 24 in-depth interviews with probation service users and six with CF staff to further contribute to the development the logic model. However, we took the decision to refocus our qualitative work to explore the relationship between probation services and CFs in depth. One of our early observations during the study was the different approaches taken by the three probation services in their approach to the use of CFs for service users on COs. Two services had positioned CFs within CP requirements (centres 1 and 2) and the third placed the CF as a SA rehabilitation requirement (centre 3). CP is regarded as primarily punitive and is offered to those with limited or no identified rehabilitative needs. Punitive CP orders can include activities such as litter picking, park maintenance and warehouse work. In contrast, SA requirements aim to rehabilitate service users with an identified need to reduce the risk of reoffending. Given the therapeutic aims of care farming to use agricultural and farming practices to support vulnerable groups,4 its approach is more closely aligned to the rehabilitation rather than the punishment of probation service users. We wanted to understand, therefore, if, and how, care farming could support probation service user rehabilitation if it was viewed by probation as part of a punitive order. We considered that exploring this in more depth would be of value to probation services and also to care farming. We therefore aimed to conduct a qualitative study to understand the role of care farming in COs.
Methods
In the light of the changed focus of this qualitative study, we addressed the following specific objectives:
-
to understand the extent to which probation services in other regions in England utilise CFs
-
to understand the perspective of probation service users on serving their CO on a CF
-
to explore, from the perspective of the probation services, the use of CFs within COs, including the allocation process
-
to explore, from the perspective of care farmers, the relationship of the care farmer with probation services and their experiences of supporting probation service users on their farms.
Identification and recruitment
Care farms working with probation
To meet our first objective, which was to understand the extent to which probation services in England utilise CFs, we approached Care Farming UK, which provided us with a list of CFs that had indicated in a previous survey6 that they worked with probation services. Twenty-nine farms were subsequently contacted. Only one of the 29 farms reported providing support for probation service users. In addition, we located another farm that was not listed with Care Farming UK that had been part of a study involving probation service users and had been included in the literature review (see Chapter 2). 78
Service users
Neither of the two farms identified outside our study sites were able to offer us access to recruit probation service users. One farm only received a few ad hoc service users and had none at the time of our study. The other farm took service users in batches and had only one ex-probation service user at the time of our study. They were unsure if they would receive any more probation service users in the future, as a result of the privatisation and restructuring of probation services.
Therefore, we only recruited service users in our existing three CF sites. We planned to purposefully sample service users to explore differences by gender, age range, employment status and responses to the quantitative questionnaires (see Chapter 2, Outcomes for a list of outcomes). However, the closure of one farm (just as we were organising the interviews), the limited access to service users at the second farm, along with low recruitment rates and a reliance on probation supervisors to select service users, forced us to use a convenience sample. The sample therefore included any service user attending one of our three CFs as part of a CO.
We identified and recruited service users using a number of approaches. As centre 1 was in the process of closing and having all service users removed, only one ex-probation service user could be approached. He had served his CO at the farm and then continued to work on the farm as a volunteer. We attempted to follow-up, by mobile phone, all of those who had been reallocated to other CO projects. We rang and then followed up with one text message that included a link to a short YouTube video (YouTube, LLC, San Bruno, CA, USA) describing our study. Of the five service users that were approached, three declined to participate or failed to respond to a telephone call. One service user who initially agreed to take part failed to attend for the interview. Only one other service user responded. Unfortunately, he had spent a limited amount of time at the farm before being moved so his contribution to the discussions about the CF were somewhat limited.
At centre 2 a group of service users was approached at the farm in the presence of a CP supervisor. The meeting had been planned in advance and approved by all relevant parties. After providing an initial overview of the study and inviting anyone within the group to attend, the CP supervisor took the group away to have a discussion in private and returned to the researcher stating that all the probation service users had declined. We decided to review our approach and 6 months later a different CP supervisor arranged interviews with six service users who were attending for supervision appointments. These interviews were conducted over 1 day for the convenience of the service users and the researcher. Unfortunately, two of the interviewees had been placed in the kitchens at the CF. As they had not undertaken any farm work they were ineligible for the study. In centre 3, the seconded RA, based within the probation service, liaised with probation service user managers to arrange an interview that coincided with a supervision appointment.
All service users were given a £20 high-street voucher as a thank you for taking part. This was agreed with the probation service.
Care farmers and probation staff
The research team had been in regular face-to-face contact with the care farmer at centre 1; therefore, he was approached directly. At centre 2, as there was no designated farmer, we interviewed the manager of the overall setting (a religious movement) and the farm volunteer who acted as liaison point between probation and the religious movement. The care farmer at centre 3 did not respond to our requests to be interviewed. Two further farmers and one of the farmers’ wives who had been identified while searching for other CFs also consented to be interviewed. One of these farmers worked with the same probation service as the farmer who had declined, provided care farming within the same type of requirement (a SA) and worked with a similar profile of service users. This farmer and his wife are regarded as part of centre 3.
Probation staff were selected on the basis that they worked directly with service users and were responsible for allocating service users to particular projects and thus had knowledge about what each project offered.
Topic guide
We developed an interview guide based on theories of desistence15,17,20,22,140–142 and green care. 11,143–149 The green theories (relating to any nature-based approach) presented seven key elements to suggest how care farming might work (for any group). These included looking at nature, being active in nature, shaping and nurturing nature, interacting with living creatures, social interaction, worthwhile purpose and skills building. At the time of the qualitative interviews, the literature review reported in Chapter 2 had not been completed; therefore, the logic model was not available to inform the topic guides. This was instead used to guide the analysis.
We tailored this to each group of participants: care farmers, service users and probation staff. The interview guides (see Appendix 6) included questions on what the CF aimed to achieve, the experience of being on a farm, the rehabilitation of service users, the allocation process and how care farming fitted with the aims of probation.
Interviewing and analysis
All interviews were conducted face to face except three that were conducted over the telephone. All participants were given an information sheet and asked to sign a consent form. Interviews were conducted by three researchers (JM, ZR and RL) at CFs and at probation service offices. All current service users were interviewed at a probation office. Although a more neutral location would have been preferred, this needed to be balanced with offering a convenient time and location to service users.
Only the ex-service user was interviewed at the CF. Prior to the interview, we had established working relationships with four of the probation staff and three care farming staff. Other than for recruitment into the quantitative study, we had no prior relationship with any of the service users.
Out of necessity, the service user interviews were conducted in close succession. This meant that we were not always able to read transcripts between interviews to inform any necessary modifications to the guide. We did, however, make notes during each interview to identify topics to be explored with subsequent service users. All interviews were digitally recorded and transcribed verbatim. Data were stored and managed in NVivo version 10 (QSR International, Warrington, UK).
We applied a mainly theoretical approach to a thematic analysis,150 but were open to new potential themes that were not represented by the theories. Our analytic framework was based on theories of desistence and our own theoretically based logic model from the systematic review of care farming. The combination of these two theoretical stances clearly showed areas of overlap. For example, social reintegration in desistance theory was clearly represented in our logic model through the mechanisms of developing social relationships, belonging/non-judgement, and feeling valued and respected.
For our analysis we (JM, HE and ZR) individually read a selection of transcripts and then discussed potential codes and key observations. Each transcript was coded, allowing for back coding as new codes emerged. Codes that were repeated across transcripts or appeared to be linked were grouped into initial themes and subthemes (see Appendix 6). To understand potential relationships between themes, we constructed visual maps. The themes were then reviewed against the original coded data and then against the data set as a whole to ensure that each theme represented a coherent story that fit within the aims of our study. We looked for deviant cases, comparing across centres and across types of interviewees. Once the themes had developed, these were compared with the concepts identified in the logic model derived from our systematic review (see Chapter 2). The themes were then compared and contrasted with the descriptions for each of the intervention components and mechanisms within the ‘all-service user’ logic model. This first involved gathering the descriptions for the components and mechanisms from the all-service user logic model and transferring them to a grid. From this, we extracted any descriptions sourced from existing theories and studies78,151 pertaining to probation services users to create a new probation-specific logic model. By aligning the two models side by side, we were able to retain complete descriptions for intervention component and mechanism while it also enabled us to identify contrasting descriptions and gaps within the probation framework. We then began the process of translating the contents of the themes from the qualitative study into the existing all-service user logic model. This was an iterative process moving back and forth between the content of the themes and the logic model grid to ensure that findings representing possible intervention components and mechanism within the theme were extracted out into the developing logic model. Given that the logic model aimed to explain how care farming may work at achieving health outcomes, we were looking for data that suggested an enabling process, thus findings pertaining to other outcomes, for example lack of choice, were not included in the model as they did not help to explain a mechanism to explain how CFs might work. Understanding the barriers to an effective intervention are also clearly important, so these themes have been described in this chapter. Once translation of the qualitative findings into the probation service user logic model was complete, we were then able to compare the emerging contents of intervention components and mechanisms with those of the all-service user logic model. As the model is only based on this limited empirical work, it has clear limitations and will require further detailing as more evidence becomes available.
Ethics
Ethics approval from the Leeds School of Medicine Research Ethics Committee (reference number SoMREC/13/14) and permissions from NOMS (reference number 2013-247) granted for the pilot study also covered the qualitative work.
Findings
Characteristics of sample
We interviewed seven current service users, one ex-probation service user, six CF staff and five probation staff (Table 29). All the service users were male; this was expected as only two of the service users who were recruited to the quantitative pilot study and who had attended a CF were female.
| Interviewees | Gender | Details |
|---|---|---|
| Service users | ||
| Centre 1 | ||
| SU60 | Male | Aged 31 years, ex-probation service user and previously served 150 hours of CP at a farm |
| SU42 | Male | Aged 47 years, was given 140 hours of CP and part was spent at a farm and then reallocated to other project after farm closure (telephone interview) |
| Centre 2 | ||
| SU1 | Male | Aged 52 years and was given 200 hours of CPa |
| SU4 | Male | Aged 20 years and was given 80 hours of CPa |
| SU5 | Male | Aged 25 years and was given 200 hours of CPa |
| SU6 | Male | Aged 31 years and was given 150 hours of CPa (telephone interview) |
| Centre 3 | ||
| SU305 | Male | Aged 30 years and was given a SA requirement involving 25 sessions at a farm plus supervision appointments at probation offices |
| SU311 | Male | Aged 22 years and was given a SA requirement involving 25 sessions at farm plus supervision appointments at probation offices (telephone interview) |
| Care farmers | ||
| Centre 1 | ||
| CF1 | Male | Previously a mental health nurse, acted as care farmer for 1.5 years and the farm was offered as a CP requirement |
| Centre 2 | ||
| CF5 | Male | Manager for overall setting that included a farm, he had limited involvement in farm itself but responsible for who worked on the farm and the farm was offered as part of CP requirement |
| CF6 | Male | Volunteer and retired accountant |
| Centre 3b | ||
| CF3 | Male | Beef cattle farmer, he had been involved in care farming for 7 years and the CF was provided as a SA requirement (rehabilitation) |
| CF4 | Female | Farmer’s wife (of CF3), she was a qualified teacher and was involved in care farming for 7 years |
| Centre 5 | ||
| CF2 | Male | Background in engineering and property management with later qualifications in child care, most of intake is for disadvantaged children, with no formal contract in place between farm and probation service and service users attending occasionally |
| Probation staff | ||
| Centre 1 | ||
| PO1 | Male | Project officer for 4 years and his role was to allocate service users to various CP projects |
| PO2 | Female | Probation service officer for 1 year and her role was to allocate service users to various CP projects |
| Centre 2 | ||
| PO3 | Male | CP supervisor for 4 years and his role was to allocate service users to various CP projects |
| Centre 3 | ||
| PO4 | Female | Probation service officer for 11 years and her role was to serve service users needs, suggest CO requirements and projects and make recommendations to court prior to sentencing |
| PO5 | Male | Probation officer for 9 years and his role was to serve service users’ needs, suggest CO requirements and projects and make recommendations to court prior to sentencing |
General findings
Eight themes emerged from the data. These were easy environment, the farmer or supervisor, developing relationships, the animals, the work, personal growth, belief in the farm and looking back. The extent to which the findings within these themes reflects the process of probation service user rehabilitation according to both desistence and the CF theoretical logic model is described in Themes. In terms of where the CFs were positioned within the COs (as punitive or rehabilitative), the evidence suggested that there were three, rather than two, working approaches. These were that the CF was:
-
part of a punitive CP order (centre 2 and centre 5)
-
part of a rehabilitative environment (centre 3 and centre 4)
-
a mixture of both punitive and rehabilitation (centre 1).
Interviews with probation staff regarding allocation decisions offered some explanation for how the characteristics and needs of service users were matched to the various types of COs, including CFs. Some of these characteristics and needs were regarded as ‘hard’ data, being recorded on nDelius systems within probation services. Factors that were specifically mentioned also contributed to the OGRS score, such as age, gender and offence committed as well as employment status, place of residence, risk of harm (to themselves and to others) and caring responsibilities. Other data were more nuanced and subjective and seemed to be involved in making final decisions that could, at times, conflict with what the hard data suggested would be appropriate for a placement, for example the service user’s demeanour, their attitude to obtaining qualifications and the likelihood that the service user would complete their placement. Probation staff in centre 1 also talked about the ‘neediness’ of service users doing CP placements (as opposed to specified needs to be meet through a SA). This seemed to refer mostly to whether or not the project supervision staff at the placement would be able to cope with the service users. Within centre 3, probation staff talked about employment needs and participants who were leading a very antisocial life as key factors in allocating service users to the CF. The probation staff suggested that those service users who perhaps were not as entrenched in their behaviours would benefit from a different venue than the CF:
[T]hey will develop them [social skills] anyway with the number of people that they have to work on [CF] anyhow, but there is also kind of in the reverse of that looking at how vulnerable an individual may be, how mixing with some of the very entrenched offenders will have, the effect will have on that individual.
P04, centre 3
I wouldn’t recommend [CF] for someone who just had an education training and employment need.
P05, centre 3
The care farmer who also worked with the same probation service concurred that service users attending his farm had very entrenched behaviours, often with substance misuse and mental health problems.
At centre 1, probation staff tended to talk about the capacity of various placement staff to cope with the needs and characteristics of service users. So charity shops would typically, but not exclusively, receive female service users with a low risk of reoffending whose criminal offence had not included theft. Specifically, they mentioned the comparator site (that was part of the pilot study), referring to its capacity to cope with more challenging individuals.
All the interviewees who contributed to the discussions about the CFs as a rehabilitation requirement (within centre 3) concurred. The two CFs here provided a good fit with the theories on desistence. Within centre 2, the experiences of service users were often neutral or negative and this was at odds with the perceptions of the care farmer or supervisor. Opportunities for activities that could contribute to the process of rehabilitation were essentially provided through probation as an entirely separate activity. Perhaps the least clear approach was that offered at centre 1, where the CF was offered as a CP punitive order, but the experiences of the care farmer and service users suggested activities and mechanisms of change that were clearly compatible with the process of desistence. At the time of the study, the farm in centre 1 did not provide qualifications to improve employment prospects and this was regarded by all probation staff as key in the rehabilitation of service users. Although plans had been made to introduce formal qualifications at the farm, there was no suggestion that the farm would move from a CP to a SA requirement once in place. The offer of a CP placement (not related to care farming) that also offered elements of rehabilitation was also evident at centre 3, where the concept of providing ‘that helping hand . . . that little nudge’ (PO4) for younger offenders was considered important. The view here was that putting younger people (< 24 years) into unpaid work groups could ‘often lead them further astray’ (PSO4).
Themes
Easy environment
The majority of service users expressed an appreciation for the outdoors. The service users explained that the fresh air and open space created a sense of freedom and peace, allowing them to relax, escape the hectic pressures of life and reflect on their stressful weeks:
It just gives me the open spaces you know, I keep repeating that but it’s just the open fields and that, you know, you’re not confined anywhere, just free, you really feel free.
SU1, centre 2
It is peaceful up there as well, it’s quite relaxing, it’s just nice to get away from manic life really, it’s just hectic, all the time, hectic, hectic, hectic, and then you go up there and it’s just a little bit of peace, to get away from everything, cause it is in the middle of nowhere.
SU4, centre 2
In addition, service users at one farm (centre 2) enjoyed being away from the public, not having to wear high-visibility jackets and working in an environment in which everyone was treated equally. However, one service user from a different farm (centre 1) felt that the high-visibility jackets should be worn as a punishment and others suggested that they were a badge of honour.
Care farmers mirrored many of the positive expressions of the services users and, in addition, considered that the CF offered a peaceful, judgement-free environment. Furthermore, this environment enabled service users to shed the personas that they had had to develop to fit with their turbulent social circumstances. In particular, farmers felt that the sense of freedom from the open space allowed service users to be more open about their problems. Although service users did not discuss the presence of a persona as such, in one of the three farms (centre 2) they did describe how the farmer, rather than the environment, was helping them to learn to trust again:
[W]e try to look at it as though you can take a break from society, take a break from it for these few hours that you’re down here, and spend that time on yourself, look at yourself, if you want to speak to us about owt, if there’s owt worrying let us know, we’ll help you.
CF1, centre 1
[I]f I walked into [name of town] with one of my offenders now, their attitude would change, because they are putting up a wall, they are putting up a defence, they do not want to be seen as a softie . . . out here they are different people altogether, I’ve seen that, I’ve seen that time and time again, they come here their shell comes off, they go back to town they put their shell back on . . .
CF3, centre 3
I think that’s more likely to be the case, I think it’s the atmosphere, the ambience, the, it’s a chill-out zone, in fact that’s almost the wording that they use, this isn’t a place to lose your temper, you know, we’re relaxed, we’re happy here, why spoil it? And of course for many of this group they’ve never experienced that in their life to date, they come from obviously disturbed backgrounds or whatever, people they hang out with tend to be very aggressive in their nature, and this is so outwith their normal experience.
CF6, centre 2
Care farmers further felt that the open space of the outdoors and the lack of walls created the perception of a lack of barriers. This provides a sense of freedom that makes it easier for service users to open up and talk. This highlights how an easy environment could encourage the development of relationships between people at the CF. The open space also gave service users room to be themselves and focus on their issues and developing themselves. One care farmer described the outdoors as a large classroom that created a learning environment that was suitable for individuals who struggled to learn in an enclosed classroom setting:
[T]hat’s important part because there’s no barriers or nothing, we’re out here, and it’s just, people can’t get it in to their heads, it just, there’s no barrier, that’s it, there’s no barriers, cause there’s no walls, we’re not going to take you in to a little room and talk to you and do all these things, that’s all I, people become nervous or they clam up or we have various reactions to all that, I compare it really to going to a job interview, for a really important job and if you don’t get this job, you know, amount of nerves and things what everybody goes through, but majority only is because we’re going in to that room and they’re going to be sat behind a desk and they’re going to be judging me and they’re going to be this that and the other, It’s not about, it’s just, it’s far easier to counsel people through problems by doing sommat to start with and go outside and do it, not in a confined space.
CF1, centre 1
Probation staff, who were all responsible for discussing the various orders and project options with the service users, made little mention of the environment, with only one (PO5) promoting the nature side of the farm with selected service users at the time of allocation. Desistence theory emphasises that an environment conducive to reflection is an important early stage in the process of desistence. However, this possibility within CFs was not alluded to by probation staff. Further reflection is a recognised mechanism within the care farming theoretical logic model:
[S]ome of them yeah will come back and say oh I really liked working with the sheep or we did this with the sheep or whatever, but personally that wouldn’t be something I would pursue with them.
PO4, centre 2
The farmer or supervisor
This was core to the themes of developing relationships, the ease of the environment and experiencing personal growth as part of the formation of a new identity. The majority of service users spoke highly of the CFs and probation supervisors. The service users commented that, although the probation supervisors were authority figures, they were still welcoming, easy to talk to, guiding and wanting to help. This was particularly the case at centres 1 and 3, but at centre 2, where the authority figures were staff from probation services, there were conflicting experiences:
Just nice people, just, you know, they want to help, they want to help, that’s it, they want to help people, they don’t want people reoffending they’re there to, you know, obviously they’re on a salary or an hourly rate, but that’s regardless to me, I don’t care if they earn 50 grand a year or five grand a year, obviously I’d prefer it if they earn 50 grand a year cause they all do a good job.
SU305, centre 2
Supervisor, it’s not [name of supervisor] so I don’t know what associations they have, I’ve never really asked them, yeah, they just tell us what to do and we do it, they supervise it or manage it or whatever you want to call it, they don’t really get involved in doing a lot of the work themselves, they just make sure the work is being done to a good standard.
SU5, centre 2
Care farmers themselves had insight into the skills required for, and utilised in, their role, balancing supervision with support and teaching to earn respect and trust. They described how the nature/personality of care farmers and probation officers played an important role in care farming. They mentioned that the ideal care farmer is someone who genuinely wanted to help service users and was willing to spend the time and effort developing relationships:
[S]o it’s all about the delivery, about the person and are you passionate about nature, are you passionate about farming, and if you are, you’ve got to be able, the second thing you’ve got to be is passionate about people, if you’re passionate about them both it’s easy, well not easy but it’s easier, but if you’re not passionate about this it’s probably like you doing this project, it’s like you either have passion to do it or you don’t. The passion will take you that extra mile, so yes I will say nature does work, and yes the farm does work, but you’ve got to have the right person delivering it to young, mental health, to every different part of society there is, with passion.
CF3, centre 3
Skilled supervision is a key component of desistance theory; however, staff in probation did not discuss this in the context of care farmers. Within the context of CP requirements across the CF and comparator sites, probation staff recognised the importance of matching service users to the skills and requirements of the project supervisor (often a charity shop manager or warehouse supervisor) to ensure that orders were completed with minimal disruption. A number of probation staff were keen to ensure that they ‘did not set people up to fail’, but for some this seemed less to do with rehabilitation and more about ensuring a smooth CO:
[Y]ou’ve got to look at the individual themselves, they might be really needy, and they’d be ideal for a placement, but you just couldn’t put that weight on a shop manager, so then you’d pair them up with a supervisor, I mean all supervisors have got strengths and weaknesses, so if you’ve got somebody really needy, got two sisters on at the moment who are really needy, we tried them in [warehouse] and [name] the manager couldn’t cope with them just because they were so needy, so we’ve now put them with a supervisor who is, that’s what he’s good at, he’ll give them time and what have you.
PO1, centre 1
The work
A wide variety of activities were undertaken at two of the farms (centres 1 and 3). These activities required the users to acquire new skills and use existing skills to contribute to the everyday working of the farm. The service users at the other farm (centre 2) provided conflicting descriptions of activities, with most users indicating that they were predominantly involved in site maintenance and not in horticulture activities or contact with animals:
I’ve done welding, I’ve done fabricating, I’ve done woodwork, cooking, looking after livestock, planting, generally everything that happens on a farm really, driving some of the machinery, done some mechanics.
SU305, centre 2
Gardening, cleaning the site up, I’ve done painting and decorating, planting all the plants, I did that car park over there.
SU6, centre 2
Get there in a morning have a cup of tea, then we go and do the rubbish, it’s a compactor, take it down to the compactor which is a machine that compacts all the rubbish, then we go up, we do a couple of journeys with that till all the rubbish cleared. Then we go and do the cardboard, put that in the cardboard skip, have another cup of tea, and then we go up and do a bit of maintenance on the tractor, and probably go and feed the cows, not groom the cows, clear the cows out, sweep the yards and that’s it really.
SU1, centre 2
Most services users discussed enjoying the work they did on the farm. One service user, at centre 1, explained that he felt motivated by the work, suggesting a link to personal growth, as identified in both desistance theory and our own logic model. Service users at centre 3 described how they enjoyed being able to do a variety of activities:
I’m more motivated here and look forward to coming down here cause there’s always something to do and I can get on with sommat, it felt like, people like, if you started sommat there’s always sommat else to do after.
SU6, centre 2
I liked the woodwork, quite a lot, cause we were always building something new but, I liked the mechanical side more, because we was always, you know using the tools, driving around, and just having a bit of fun really, playing, well not playing up but having some fun like.
SU311, centre 3
You’re always doing sommat different, and obviously on a farm, for me as a welder it’s great cause there’s always sommat broke which I can fix, so that’s cool, but just doing different stuff.
SU305, centre 3
The extent of enjoyment at the other farm (centre 2) was very mixed. Two younger service users explained that they just wanted to complete their order and move on with their lives; these individuals did not have much connection with nature during their stay at the farm but still preferred the farm to other project types. The fact that the work was ‘unpaid’ was alluded to, re-enforcing their awareness of the order as a punishment:
I was looking forward to getting it out of the way, getting it finished. I don’t mind it, but nobody likes working for nothing anyway do they?
SU4, centre 2
Care farmers provided a more detailed insight into how the activities were planned and adapted to take account of the skills, capabilities (whether or not they were under the influence of drugs or alcohol) and expected behaviours of the service users, as well as the daily work requirements of the farm. This was partly to ensure the safety of the service users but also to provide work that was deemed worthwhile (by the service users) to maximise engagement. Again, farmers used their personal skills to decide when, and how, to introduce different activities that might seem either daunting (e.g. sheep handling) or mundane but necessary, such as litter picking on-site:
You can’t plan it too much, it is almost spur of the moment, but the good thing about the farm is it’s so diverse, farming skills are so wide ranged where if you just say, let’s say we were just going to do one specific activity say like fork-lift, well not fork-lift driving but driving, tractor driving, straight away if you had a course . . . these guys have got to go on a course and drive a tractor I guarantee you that out of eight of them four of them, five of them, maybe six of them wouldn’t be able to do it, because they’re not in the right frame of mind.
CF3, centre 3
Yeah it’s real, so if they should, it’s because fencing actually needs doing on the farm, and you know if it’s sheep handling then they get in a flock of sheep and they dip them because that’s what’s needed, so, and it’s seasonal, so they appreciate that there’s some activities available at certain time of the year, and that we feel has a big impact on the success, because when the service users come and they do the activities they know that [supervisor’s name] hasn’t just made them up that morning to keep them occupied, that they feel that they are on a working farm and the activities they’re asked to do are part of that working day, I mean obviously you have to adapt it a little bit, cause you’ve got to keep them occupied and entertained and there are some activities that you have to save for the end of the working day and we do ourselves because they’re dangerous, but on the whole all the activities are real, and that’s a really important ethic.
CF4, centre 3
Litter picking is outdoors yeah, a lot of people find litter picking degrading, it is, it is, it’s a bit like, ‘oh god do we have to pick al the rubbish up?’ I cannot stand doing it at home; putting the bins out. So when you have 34 acres to pick all the rubbish up, but we just expect it, if we do not do this it’ll just pile up and pile up and pile up and we’ll get rats and we get this that and other. It’s just simply explaining that that has to go because it has to because it’s not clean.
CF1, centre 1
Probation staff based in centre 3 considered the farm to be a ‘massively productive way to spend the day’ (PO5). This referred to the work and also the therapeutic support, the thinking skills and the support with job searching. They talked about people achieving and gaining confidence and self-esteem, concepts that are closely aligned with desistence theory and the mechanisms of change within the CF logic model:
[I]t provides skills, so there are practical skills in terms of whatever work they need to do there, but also kind of a bit of life skills as well in terms of how you interact with other people, you know, how you behave when you’re asked to do something and when you’re told to do something and whatever else, and I think there is a general, also the kind of confidence building things that are there, there are people that take great kind of joy really in somebody achieving something in somebody improving and certainly in somebody completing the work, there’s the kind of confidence and self-esteem stuff.
PO5, centre 3
The animals
The theme consisted of discussions about the nature of interaction with service users and the animals. Service users differed in their willingness to engage with animals but also in the extent to which they had access to them. In contrast to other service users at centre 3, one individual found the experience of working with the cows therapeutic and gave a sense of worth. He also described how this created an avenue for him to interact with the non-farming staff on-site who facilitated a desire to change. One other service user suggested that they were not ‘hands-on’ with the cows indicating that interaction was limited and seemed somewhat disappointed at this. A service user at another farm also described feeding and caring for livestock, explaining how this had contributed to his new qualifications. Here the link between the presence of animals and personal growth through the acquisition of new skills is clear:
Well it’s what I said, feeding the cows and that, gives me a sense of worth and things like that, you know.
SU1, centre 2
[I]t’s nice to be able to, rather than seeing rats and pigeons you get to see deers and ducks, you know what I mean?
SU305, centre 3
We don’t get hands-on with the cows either, it’s like one of my friends outside, he’s on a project at a farm, and there one of the mums stood on the leg of the baby and he’s been wrapping the leg up and fixing the leg and next week he’s got to help the lambs give birth, so he’s proper hands-on with it all.
SU4, centre 2
From the perspective of care farmers, animals were considered to exert positive influences in three ways: through the acquisition of skills; by developing a sense of responsibility through the meaningful activity of caring for the animals; and by exposing fear in service users, which meant that their macho personas were shed and contributed to the creation of an easy environment on the farm. The novelty of working with animals created a stimulating environment that supported engagement and the acquisition of new skills. Animals were considered a calming influence that encouraged service users to look beyond their own needs and desires and perceive their work to be meaningful:
[W]e’ve got things from like Chinese painted quails, a baby quail is about the size of a bumble bee, and you know when I look at the faces of these people that have never seen them it’s like ‘wow, what’s that?’, I say ‘it’s a quail’, ‘blimey’, and these little things are running all over the place, you know, or then the Aylesbury duck, all fluff aren’t they, I put a chick in their hand and they’re ‘wow’.
CF2, centre 5
I think that, if you look at the care element side of things you are, that animal’s your responsibility in some way, when you come down, ‘oh so, right the chickens need to be cleaned out and all this’. You might get a couple of lads who’ll say ‘I’m not cleaning chickens out they stink’ and this, that and other, but at the end of the day them chickens need to be cleaned out, it’s about a responsibility to sommat else, and not just to yourself, it’s not that take, take, take; it’s about giving, you have to care for that animal, it has be looked after, it has to be protected it has to be fed, watered, all them things, and I think it’s a great way of doing it, it’s just, we can’t bring kids in and say here look after that kid, you need to look after this, so using animals that way, and the response is different again, it’s, when people are around certain animals it’s very calming, because it’s either respect for the animal that they can’t be shouting or they frighten it, but people just adhere to it.
CF1, centre 1
[T]he animals are good because you’ve got these lads coming out, or young men, and even ladies, who are talking machoness, some of them from violent backgrounds, been out fighting, stuff like that, and then you put like a chicken in front of them and they’re scared of a chicken.
CF3, centre 3
Animals clearly provide a tangible opportunity for change, by giving something back to society and the developing new skills. These factors are identified within desistance theory as leading to positive change. Probation staff in centre 3 concurred that people enjoyed the contact with animals. This was despite interaction with animals and nature appearing to be a very limited part of their discussions with users during allocations:
. . . anecdotally, lots of people like working with the animals, you know, I know it might sound like a bit of a trivial thing but particularly if someone is going there around lambing time, it’s just a kind of little bit of a feel good factor thing, so that will be by far the tiniest rehabilitative thing of all the examples I’ve just given you.
P05, centre 3
Developing relationships
This theme revealed contrasting experiences, particularly between the younger (aged < 30 years old) and the older (aged ≥ 30 years) service users. Although only a few interviews (three) were conducted with service users in the < 30-year age group, the reflections from care farmers during their interviews have also helped to deepen this theme. Positive relationships, although not necessarily friendships, developed between care farmers and the older services users. However, among the younger service users there was unwillingness to make meaningful relationships with other service users and they did not discuss any relationships with care farmers. One in particular described how he felt it would be beneficial to avoid making friends with other service users because they had committed a criminal offence:
Well cause he’s the team leader isn’t he, he’s in charge of us, what he says goes isn’t it really? But he’s not like that, he’s like one of us you know.
SU1, centre 2
Yeah the staff were welcoming, they’re like easy to get on with, and they listen to you, if you’ve got a problem they’ll talk to you about it, like I was, I had a bit of anxiety, not due down to this place, it was sommat to do with outside, and I spoke to [care farmer] about it and he come and he says ‘what’s up?’ and I actually felt a lot better after I’d spoke to him cause, it’s like he helped me with it, he said all you have to do is talk to somebody, I got talking to him and I felt a lot better after.
SU6, centre 2
I don’t really want to make friends, I get on with everyone, I don’t really want to make friends on the course, because they’re all on the course for the wrong reason, and it’s just trouble isn’t it, it’s trouble you don’t know . . . You just keep to yourself, I stick with my brother a little bit, but just keep myself to myself cause I don’t want to get involved with the wrong crowd again, and that’s just an easy way, they’re at community service, they might not have changed around, they might still be doing naughty stuff, and you get back in with them then you start getting arrested again.
SU4, centre 2
OK, development of friendships in there?
No, not really, I mean I say hi to everyone I’m not rude to anyone or anything, they’re not rude to anyone else, everyone just is on the same playing field when you’re there, so yeah.
Centre 2
Care farmers on the other hand were much more positive about social interactions on the farms. They considered that the work on the farm created the opportunity for people develop relationships and that the non-judgemental atmosphere and nature of the care farmers encouraged the development of relationships between service users and care farmers. Care farmers explained that actively working alongside other people in the CF/working in teams encouraged the development of relationships between people on the CF. This illustrates the relationship between work and the development of relationships. They explained that this helped alleviate the social isolation that some service users may experience, especially those who were unemployed. They discussed the importance of creating a sense of community that extended beyond the time on the CF:
It stops them being isolated for one thing, because there’s nowhere for them to go, I mean that’s really sad, I mean people used to go to the pub, didn’t they, none of that any more really, not round here, very few pubs, plus if you’re unemployed which quite a few of them are.
CF2, centre 5
I think they like coming here, they like the camaraderie, they like the enjoyment, they like the biscuits and the tea, that’s for sure, I mean I made that point, but it’s the way they’re treated.
CF6, centre 2
The probation staff interviewed were less familiar with the way in which service users interacted with each other and the care farming staff, as they did not have any observational experience upon which to recall. One probation officer did, however, seem to offer some explanation for how groups managed on the farm:
Once you get people there who are all there all committed they tend to drag each other along, and they know everybody is there to do, you know, they know everyone is there because they have to be there but they know the people are at least trying to change, and then it gets better I think as time goes on really.
PO5, centre 3
Belief in the care farm
All but one of the service users who attended the farms at centres 1 and 3 mentioned that they were initially cynical and reluctant about attending a CF but soon realised the benefits. They emphasised that they had gained from and enjoyed their time on the CF and wished more resources were available to the farm so it could expand and continue to help other service users in the way it had benefited them. It is of little surprise that service users in centre 2 did not voice a belief in the CF to the same extent as those at other farms:
I think it’s a really good idea, it helped me out, helped a lot of other people out, and I think they should keep it up, try and expand their farm a little bit more or something.
SU311, centre 3
It’s everything, just the niceness of the staff, and everything, just the whole thing, and you could speak to [supervisor’s name] and even the drive on the first day I was like no I don’t like this, I ain’t doing it, I ain’t going to no farm, I ain’t planting no potatoes, and then for me to go through it from what I’ve gone through for the farm, you know, and for me to say I will come in here out of my own time and tell people hang on a minute bruv, A I probably know you off the street and B I’m telling you now it’s alright, [CF] is alright man.
SU305, centre 3
Oh yeah, I just wish somebody would give it a chance down here just to see the better things, the positive things down here instead of all the negatives, cause there’s no negatives down here, cause somebody give it that one chance, just to show, just for us to show them that it would work and everything could be a lot better.
SU6, centre 2
Probation staff in centre 3 appeared to hold positive beliefs about the benefits of the CP projects. They often identified projects that had the potential to rehabilitate probation service users and each seemed have a particular favourite:
[P]ersonally I tend to recommend the senior attendance centre requirement for those between 18 and 24, rather than putting them on an unpaid work party, because I don’t believe that that will actually help them to do anything and also the senior attendance centre is a punishment, it’s deemed a punitive element but there’s a lot of rehabilitation within the sessions that they attend.
PO4, centre 3
The farm is the only project that we have that’s anything like that in terms of the length of time it runs for and in terms of the fact that it takes up a whole day, we don’t have anything else here that, if we’re to say to someone OK look you need to change your lifestyle, there isn’t that much else that we could say to someone OK well I’m going to put you in touch with somebody that’s going to take a day or two out of your week, but isn’t just punitive, because we’ve got unpaid work, but you know actually has that more rehabilitative slant.
PO5, centre 3
In contrast, the probation staff who worked with service users undertaking unpaid hours did not seem to hold any special regard for the CF over and above any of the other projects, possibly reflecting the fact that those with specific needs were already perceived to have been supported within other orders.
Looking back
This theme consists of descriptions of instances in which service users reflected on their past lives, specifically their criminogenic attitudes and behaviours. Some service users on all three CFs recounted the drug use, homelessness, stress, chaos and unhappiness that characterised their lives prior to their convictions and presence on the CFs. They explained that at the time, they were carried away in these activities and neither could see the pointlessness and selfishness of their behaviours, nor were they aware of their own unhappiness:
Yeah I stopped going raving, I used to, cause I’d done all the squatting and we used to do squat raving and I used to take loads of drugs every week, and I stopped taking all the drugs.
So who has helped you with that then, the drugs side of things, or did you just do it yourself?
I just did, I just didn’t want to do it any more, I was taking all the raving drugs every weekend, all the party drugs to keep you awake all night, and I just, it’s a never-ending circle just goes round and round.
So I suppose you get to a point where you can’t see a reason to not do that?
Yeah, and you can’t see a way out either, it’s just a vicious circle, you don’t know what you’re doing, all your friends are doing it, you don’t see the bad in it, until afterwards, and now I think, what was I doing?
Centre 2
I didn’t have no moods and emotions, I didn’t give a monkey’s, I was taking amphetamines but getting psychosis, and was just, I didn’t realise how unhappy you are, you don’t realise how unhappy you are until sommat changes in your life.
SU6, centre 2
One of the service users in centre 2 mentioned that the easy environment of the CF allowed them to think, reflect on their behaviour and plan their future activities. The other service user who discussed reflecting on the past stated that they had done this prior to attending the CF. The two younger service users in centre 2 mentioned that they often thought about their criminogenic behaviours on the way to and from the CF but explained that this resulted from having to complete a CO and was not specific to attending the CF:
OK, and reflecting on things a little bit more?
Yeah a little bit to be fair yeah.
Is that the thing about being outdoors a little bit, being away from it all?
No, just not saying this is where you’ll end up, or prison, if you reoffend again, so yeah.
Cause I do think about things I do think about it, while I’m on my way there and on my way home.
But you could do that to any [CO] couldn’t you?
Yeah I could do that to anything, I would be doing that to anything, and I don’t want to be there, I don’t want to be at any community project, but nobody does, but it’s one of the better tasks that you can do for community service.
Centre 2
Personal growth and new identities
This theme consisted of a number of subthemes relating to (1) gaining skills and knowledge, (2) having a sense of worth and achievement, (3) feeling the change and (4) breaking up and making up. It should be noted that this theme was not as well supported in the interviews as the other identified themes. This may be due to the challenge that service users felt in talking about their experiences in depth; however, the data there are provide valuable insight into the personal growth of service users. For example, most service users mentioned that they had acquired useful skills from working on the farms:
The atmosphere is different, you can learn more things, you can get a trade if you thought about it, there’s a lot of various things to do, you just need a push in the right direction.
SU6, centre 2
Yeah I’ve got qualifications, in rustic furniture making and horticultural seed sowing, things like that, a mechanical one, which was quite good.
SU311, centre 3
However, younger service users at the farm in centre 2 who were both employed did not derive the same benefits:
Right, OK. So have you learned any skills while you’ve been on the farm? You can be honest.
Not really . . . No, not really. It’s just, normal stuff, anyone can do it, it’s just straightforward.
Yeah learned how to garden and be a rubbish man and, I don’t know, work in a stables, whatever, yeah, . . . I’m not really that sort of person I’m more of a business person, sales person, so whatever, so even though it’s good I’ll never need it.
Centre 2
Service users described feeling a sense of worth and achievement in two ways. The first way given was in relation to the completion of a task or the attainment of a reward. The second was the knowledge that they were contributing positively to the environment around them. This could be by feeding the cows, caring for the animals around or by keeping the environment tidy and creating a nice atmosphere for others on the CF:
[W]hen I achieved sommat, it looked good, did all the greenhouses, I just took pictures of all the cabbage patches I did and that . . . I’ve got it all on my [social media page] and that, all the pictures and stuff that I did.
SU6, centre 2
You get a hot dinner, which is alright, nice food, not monetary rewards or anything, but I just, I think it would be more personal rewards in your own head really.
SU305, centre 3
All care farmers discussed seeing changes among service users who had attended their CFs. The care farmer at centre 1 recounted instances in which former service users used the skills they had acquired while on the CF and set-up businesses that allowed them to earn a living without resorting to crime. Other care farmers reported how they observed a positive change in behaviours while on the farm:
I’ve got lads now that have set up businesses and all they’re doing is building benches, they’re building planters, they’re earning a living and they’re spending their time building, making, selling, than thieving, getting caught, you know, and they come back.
CF1, centre 1
[I]t’s more about the nature of the work that they’re given, it’s work that can be seen, when we can find work that immediately shows a result . . . in fact there was a situation literally with the strimming, where two guys, and they wouldn’t go home when they were told to go home they said, ‘no we want to finish it’. Now I’m not, you know, I just had to let them get on with that, you don’t interfere with that, because to me that showed real value added in terms of the change in their behaviour as individuals. And that’s come from within, it’s not come from without.
CF6, centre 2
Development of a logic model on care farming for probation service users
By combining the findings from the current qualitative study with the existing theory on care farming and desistance151 and the logic model developed from the literature review (see Chapter 2) we were able to construct a logic model that was specific for probation service users (Figure 12). This involved fitting the themes from the qualitative findings to the mechanisms identified in all service user logic model (see Figure 3). The new logic model for probation service users differs from those that were constructed as part of the literature review, as it included the views of care farmers rather than just service users. As explained in Chapter 7, we consider this to strengthen the logic model. Only the process and final outcomes measured in the published studies included in the systematic review are shown in Figure 12. Other process and final outcomes displayed in the other logic models are likely to be relevant here, but as yet these have not been measured for probation service users.
FIGURE 12.
Logic model on care farming for probation service users. t, theory based; coloured process outcomes equates to evidence from qualitative literature; black + symbols = qualitative evidence where – is no significant difference and + is significant difference.
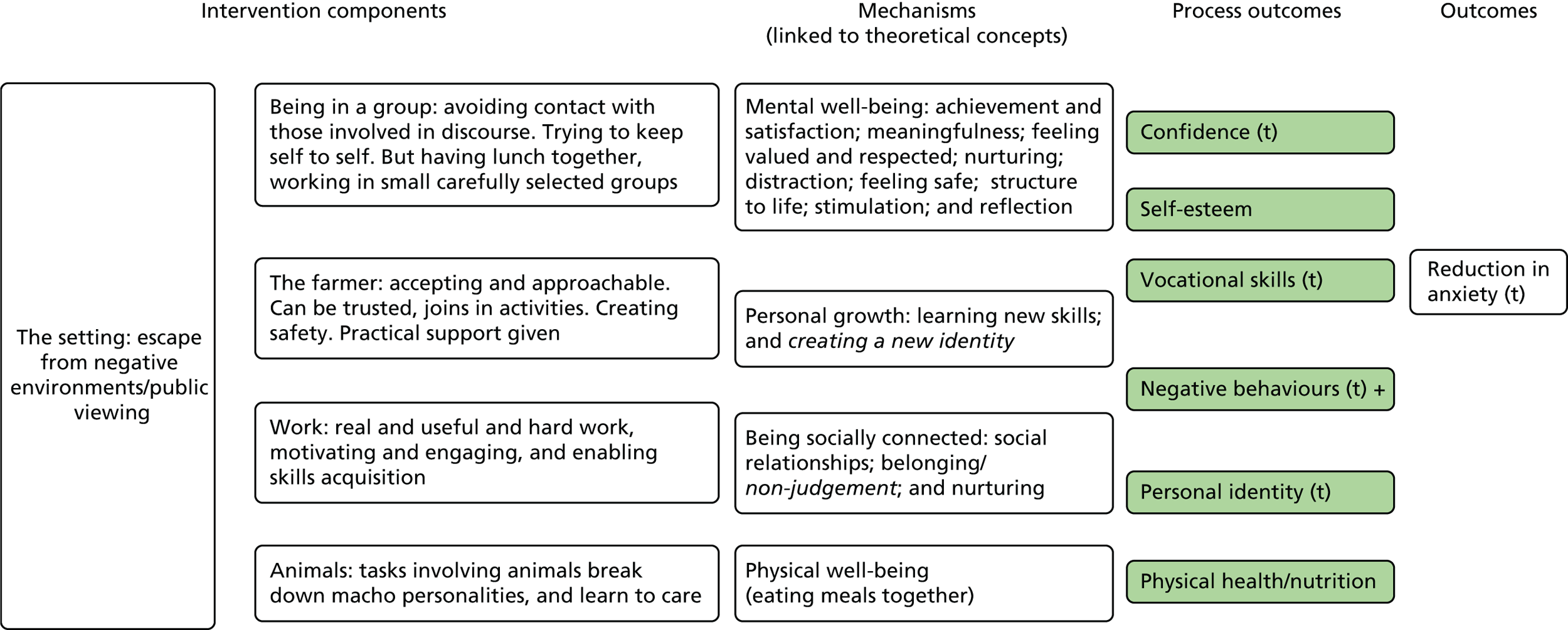
Summary
This qualitative study provides contextual insights into probation services and the use of CFs that can support the interpretation of key findings in the pilot study. It also suggests which mechanisms appear to be operating to further aid the development of the logic model for this particular service user group.
Probation officers confirmed a range of factors that influence allocation decisions for service users that are not always recorded in the probation system. These added a layer of complexity in establishing the influence of various confounders on health outcomes. In centre 3, probation staff confirmed that those attending the CF had the most entrenched behaviours and were the most challenging to support. In centre 1, the probation staff worked only with those on unpaid hours with no specific identified needs; however, within this there was recognition that some service users were more challenging to support than others. Probation staff tended to talk about whether or not staff at the various unpaid work placements (particularly charity shops and the comparator site warehouse) could cope with certain service users but they did not mention staff at the CF in this context. This supports informal discussions that were held at the probation services at the time of the pilot study set-up. Both the manager at the comparator site (warehouse) and staff at probation services talked about the types of individuals who would be appropriate. Specifically, as a business, the comparator site had targets to meet for their employer. It, therefore, expressed a preference for individuals who were willing to work with minimal disruption. The CF, on the other hand, did not rely on production to support itself and, therefore, it was not subject to the daily pressures of the warehouse. This meant that the CF could take service users who had more challenging behaviours. These early discussions also indicated that the CF even took in some high-risk (of harm and reoffending) probation service users, even though officially it was allocated as a placement for medium- to low-risk probation service users.
Our qualitative study included care farmers, service users and probation staff. Many of the studies included in our literature review (see Chapter 2) only included service users and, indeed, in studies that included others we used data only from service users to construct our logic model. The benefit of including care farmers here is twofold. We were able to interview only a small number of service users, and many of them were distrustful of authority figures. Although we attempted to interview people in neutral locations, there was little motivation for people to take part outside their unpaid hours or supervision sessions. Thus, the institutional setting of the probation offices became the setting for interviews. This created a natural divide between the interviewers and the service users, who did appear reluctant at times to reveal personal feelings. By also including care farmers as interview participants, we were able to gain insights from one individual about many of the service users. We were aware that care farmers could have referred to only positive changes within service users, but they did mention that some service users were ultimately not suited to the farm and were asked to leave. This was supported by probation staff, who also talked about service users dropping out and not completing their time at the farm. The additional benefit of including care farmers in the interviews was that they discussed changes in individuals that the individuals might not recognise in themselves. The care farmers suggested that service users were not always aware that care farmers were working on their personal development through specific interactions, such as presenting a sheep to them with the implicit aim of breaking down the bravado or even sitting down to eat a hot meal together with the unspoken aim of creating a social environment. This insight and different perspective have enriched the data collected in this study.
The themes that emerged provide an interesting fit with existing theories on desistance and other theories that have been connected with care farming that contributed to the logic models. The five intervention components represented within the logic model were all represented thematically within the interview data. In particular, the farmer and the animals seemed to be core to many of themes and mechanisms suggested within the logic model. For example, the farmer was undoubtedly responsible for creating and maintaining the easy environment that promoted a sense of non-judgement, value and respect. By creating tasks that were novel and interesting, service users felt motivated and satisfied and they gained more skills. These concepts are clearly present within desistance theory. The role of animals on the farms offered a unique insight into how care farming might work in a different way for probation service users compared with other vulnerable groups. No other studies have talked about the role of farm animals in breaking down macho personas. Here it appeared that working with animals enabled the more vulnerable side of service users to be exposed, thus paving the way for more open and honest interactions. Although these almost seemed like pivotal moments to care farmers they were not mentioned by service users. A number of possible explanations exist: the setting and the lack of established relationships limited the extent to which service users were able to open-up during interviews; those who experienced this chose not to be interviewed, perhaps as part of their continued macho persona; or the service users did not recognise this as a key moment or factor in their changing attitudes.
One theme, in particular, stands out as conflicting with the existing logic model for other service user groups. The importance of developing social relationships as a mechanism within the logic model featured strongly across many of the studies within the literature review. Among the probation service users, however, there was a clear message that social contact was to be avoided. There was a desire to just complete the order with minimal interaction, either to avoid negative influences (as appeared to be the case for centre 3) or to just compartmentalise the experience and banish it from memory (as suggested at centre 2). Interaction between care farmers and service users did appear to be more open and service users seemed to value the contact. Care farmers were more positive about developing relationships between service users and, again, this difference in experiences might partly reflect the interview sample.
In contrast to a number of other qualitative studies about care farming, we have identified service users with negative experiences. Most of these experiences relate to CF 2, where the work was considerably less varied, there was a lack of a therapeutic element and it was without a clear care farmer role. However, this further helps to clarify what it is that a CF needs to provide to benefit probation service users.
It was clear from the interviews at centre 3 that the experiences of service users, the care farmer and the probation staff concurred. There was a collective sense that care farming offered structured rehabilitation, meeting the needs of service users in a unique way. The positioning of care farming as a SA was clearly well-thought through, with probation staff and care farmers closely aligned in their understanding of what care farming could offer and who would be suitable to attend. The views of the care farmer in centre 1 appeared to be misaligned with that of the probation services. Whereas it was offered as unpaid work to service users and, therefore, was viewed as more of a punishment, the care farmer talked about non-judgement, social reintegration, safety and nurturing, which are concepts that feature in desistance theories. It is unclear if service users attending the CF here, or even probation staff, considered a need for rehabilitation. Furthermore, as a punishment it is unclear if service users felt less able to draw on the potential benefits of the CF because of the overriding message that it was there to punish rather than to support. Discussions between the care farmer and the probation staff about the positioning of care farming and its role in supporting targeted rehabilitation could be of value to service users and probation staff. In centre 2, although the CF was officially recognised by Care Farming UK, it was clear that the over-riding intention was to support the CF’s charitable efforts to help the homeless, and the farm was a means to do that with free labour from probation service users. Service users in general found this to be a less therapeutic environment with routine site maintenance being the main activity. Probation staff also did not seem to favour the CF over and above any other unpaid work placement. In this respect, apart from the farm being labelled as a ‘CF’, both the service users and probation were aligned in their views about this particular placement.
Care farms aim to offer therapeutic benefits through farming activities. CFs that can clearly demonstrate this should therefore be used as a rehabilitative requirement. Care farmers need a clear understanding about how they can contribute to the process of rehabilitation so that they can communicate to probation services and appropriately position themselves within the right type of CO.
Chapter 7 Discussion and conclusions
This final chapter brings together the four different elements of this study: the mixed-methods systematic review of the impact of care farming; the quantitative findings of the pilot study; the health economics findings; and the qualitative exploration of the relationship between probation and care farming and the CF experiences of service users. The discussion points below are structured to align with the objectives of the study, highlighting the key findings and setting them within the context of the existing literature when appropriate.
Systematic review evaluating the impacts of care farms
The studies included approximately 980 participants from a range of service user groups. The largest single service user group (albeit spanning a range of conditions within) was those with mental health problems (11 out of 27 studies).
Based on data from 15 qualitative studies (including the mixed-methods study) and information from 15 theories we were able to develop logic models to explain the mechanisms for change for four service user groups: mental ill health, substance misuse, disaffected youth and learning disabilities. As studies reported combined data for mental ill health and substance misuse, there is one logic model for both groups. Although there were some data on older people and individuals with autistic spectrum disorder, they were insufficient to develop a service user-specific logic model. The developed overall model (for all service user groups) highlights the importance of being in a non-judgemental, structured, stimulating and safe environment that allows for reflection, helping individuals to understand themselves, to feel that they belong, are valued and respected, to support them to develop social relationships, to have a sense of achievement, satisfaction and meaningfulness and to learn new skills, to allow for the development, and nurturing, of a new identity if wanted and to help them become physically healthy. These mechanisms are a good fit with a number of theories that have been, up until now, mentioned only in connection with care farming.
Although we ordered mechanisms based on frequency and spread, we do not suggest that any one mechanism is any more important than another at an individual level. However, as a gauge, and based on available data, we observed potential differences in the way CFs work for particular service user groups. For example, a sense of achievement and satisfaction may be more important to the combined substance misuse and mental ill health group and the learning disabilities service user group than the disaffected youth, for whom feeling safe may be a priority. In this last service user group, having the opportunity to reflect seemed to be valued. Although we do not have sufficient data to be able to robustly link the intervention components to the mechanisms, we do tentatively suggest that in the disaffected youth group the emphasis on reflection appears to fit with the greater focus on the ‘setting’ aspect of the intervention. As with the causal pathway between intervention components and mechanisms, the relationship between many of the mechanisms and process outcomes is unclear. For example, ‘understanding the self’ (a mechanism category), which included findings such as increasing self-respect and understanding of tasks that are manageable, was clearly linked to process outcomes relating to self-efficacy and improved confidence. However, the connection of other, seemingly important, mechanisms such as ‘belonging and non-judgement’ to outcomes is less clear. It is likely that many of these mechanisms interact in a way that is not yet understood to influence outcomes. These hidden features of complex interventions are commonly observed within logic models. 5
A key finding within this aspect of the review was that the theoretical concept ‘restorative effects of nature’ was represented by the intervention components (but to a notably lesser extent than ‘the work’ and ‘the farmer’ components) but was not represented at all in the categories of mechanisms. This was somewhat surprising, given that, informally at least, one of the most lauded attributes of care farming is its nature-based approach. Only four findings of the 164 that mapped to the theoretical concept about mental well-being could potentially relate to nature. We suggest that the absence, or near absence, of ‘the restorative effects of nature’ is not a true absence. Rather, nature is the essential component of the intervention that triggers other, more overt, mechanisms to be acted out. Thus, as individuals recall their experiences on the farm, it is primarily the mechanisms promoted through the work and the interactions with the farmer that are at the forefront in thought. It is not clear exactly what individuals were asked about in the qualitative studies, but given that the aims were primarily about exploring the experience and benefits of care farming, more specific questioning about nature would not have been part of the topic guides.
Despite being able to develop the logic models, we could not test the learning disabilities model because of an absence of quantitative data. Although we could test the combined substance misuse and mental ill health group and the disaffected youth logic models, only very limited testing of secondary outcomes was possible with the disaffected youth group. Based on limited quantitative evidence from only two RCTs we did not find any significant positive effects of CFs in improving quality of life. We did find some limited and inconclusive evidence to suggest that care farming can reduce anxiety. For depression, although there appeared to be significant reductions following the intervention, as assessed in UBA studies in the context of a RCT, no significant differences were found between the intervention and the control groups.
For process and secondary outcomes, there were no significant positive effects for self-efficacy and coping (measured in the RCTs) at the end of the intervention. However, a significant improvement in self-efficacy (but not coping) was reported at follow-up. The possibility that there may be some delayed benefits (as with anxiety) for self-efficacy requires confirmation by future studies. A number of UBA studies reported significant improvements in self-esteem, stress, affect, mood and group cohesion at the end of the intervention. However, only stress and affect were measured at follow-up (3 months after the intervention ended) and improvements were not sustained. Most of the primary and secondary outcomes were limited to immediately post intervention with only three (social functioning, eating and appetite, and mental status) reported beyond 6 months. With respect to disaffected youth, there was some suggestion that coping might be improved, but that it had no impact on self-esteem.
By far the most studied service user group in care farming research is people with mental ill health. Although in the UK currently there are more CFs providing support for people with learning difficulties (93% of farms) and autism spectrum disorder (84% of farms) than there are for those with mental ill health (75%),6 only 3 of the 15 qualitative studies explored the experience of care farming for learning disabilities and autistic spectrum disorder. Similarly, disaffected youth, who as a group are supported by around 64% of UK CFs,6 were again the focus of only four studies,25,56,59,79 with two being quantitative. 25,79
Yet even with this, green-care services are used relatively infrequently when compared with traditional approaches. 7 Given that, in the UK at least, CFs are underutilised,6 lack of capacity across the broader green-care service is not the issue. Lack of access may contribute, specifically within more urban areas, which have fewer green spaces, higher deprivation and lack of transport. Lack of understanding and awareness is, however, likely to be a major factor. In some countries, such as Norway, Sweden and the Netherlands, where care farming is well established and research is most active, there is greater integration with statutory services. In Northern Ireland and Republic of Ireland there has been an active push to market care farming directly to commissioners, combined with the establishment of a network of farms supported by European Union funding,152 and this could be an option in areas where engagement has been low.
Maximising recruitment, data collection and follow-up
Throughout the pilot study we tried several different approaches to recruitment, data collection and follow-up. It must be noted, however, that the dissolving of probation trusts in 2014, subsequent privatisation during our study implementation period and the closure of one of our CF sites had significant impacts on the feasibility of identifying, recruiting and following up participants. These adverse circumstances meant that of the 300 participants that we planned to recruit across the CFs and comparators in all sites, we were able to recruit only 134, 50 of whom were allocated to CFs and 84 to comparator locations. Once approached, however, users were willing to consent to participate in the study, with only 21 not wanting to consent. As described in Chapter 3, the main challenges to recruitment were, above all, found in our interactions with the probation system, and many of these were as a result of the impact of probation changes on staff turn over, redundancies and IT and other systems. A stable probation service could facilitate more successful recruitment and, once identified, the high level of service user willingness to complete the questionnaires indicates that recruitment could be feasible, particularly drawing on the lessons learned from this study to maximise recruitment.
In summary, the lessons learned on maximising recruitment and data collection included having a RA seconded from probation services within the centre (centre 3), having a co-investigator working at a senior level within a probation service (centre 1), incentivising users by allowing time spent with the researchers to count towards their unpaid hours (centre 1), including probation service users with multiple requirement orders and recruiting at weekends as well as during the week. The differences in operations in each probation service required bespoke recruitment strategies; however, our lessons on enablers of recruitment may well be of use to other research teams working with probation services.
Our attempts at follow-up were less successful, with only 52% of our participants successfully followed up to complete questionnaires. We tried several approaches. Linking with scheduled probation meetings proved particularly effective, and contacting users by short messaging service (SMS), telephone and letter were of limited effectiveness, even with high-street vouchers offered as incentives. We found systematic differences between those followed up and those lost to follow-up, with those followed up less likely to smoke, and more likely to have a better quality of life (as measured by the CORE-OM but not by the WEMWBS), to find healthy foods enjoyable and to be employed. This is clearly an area of concern of bias in any future study.
In terms of the feasibility of data collection and the differences between the CORE-OM and WEMWBS questionnaires, our experience and data on the questions answered point to greater challenges with the CORE-OM than with the WEMWBS questionnaire. The positive framing of the WEMWBS has been identified as helping questionnaire completion by other studies. 153 Given the benefit of deriving QALYs through use of the transformation of the CORE-OM into the CORE-6D, which is not currently a possibility with the WEMWBS, the CORE-OM is still considered a valuable measure that can feasibly be used among this population. This is reinforced by the fact that only 14% of the participants requested help or clarification from the RA in completing the CORE-OM.
The challenges of following up probation service users to fill in any of the questionnaire measures still present a limitation to feasibility. However, our use of pre-existing routine data, namely reconviction rates from the PNC, did prove to be a feasible approach to gaining sufficient outcome data for this group. Participants consented to, and we were able to access and link, probation service and reconviction data for 90% of respondents. Given the challenges and potential bias in following up probation service users to fill in questionnaires, the feasibility of using existing PNC data to assess reconvictions among our participants at 6 months (or more) after completing their CO is a valuable finding to inform future studies. It should be noted that reducing reoffending is the main performance indicator for the new CRCs. 154 Using the reconviction data would, therefore, be of clear policy relevance to the new probation services, as they consider the services to commission.
We have shown that users are prepared to consent to providing questionnaire data and the vast majority were willing to consent to access to their probation records (nDelius) and PNC data on reconvictions. Furthermore, that with sufficient time and energy built into the study plan to secure the required data sharing agreements, these routine data can be retrieved from the MoJ and from probation services and then linked to an individual’s questionnaire data. Although most of the data could be linked to PNC and nDelius records, a small proportion (11 out of 134) could not. Failure to access certain records may relate to changes that occurred to information systems as part of the privatisation of probation services during the study or also because special permissions (over and above usual informed consent) to access individual records are needed. This would be the case for those who were publicly known or for whom the release of their data would put them at risk of harm. Although we are only speculating on the former, we know that the latter situation does exist. The possibility that individuals provided incorrect personal details at the time of recruitment into the study has been ruled out because we were able to track the progress of COs with the administrative hub, which needed the name and date of birth of the offender in order to check the records. Ultimately, our study suggests that data linkage is possible.
Any future study must take into consideration the time required to build the necessary relationships and agreements with the MoJ and the required number of probation services, and the time required to recruit sufficient participants into any study and establish the necessary agreements to access the routine probation data and reconviction data from the PNC.
Collecting cost data and feasibility of measuring cost–utility
The collecting of cost data from probation services and CFs proved challenging, particularly as our request came during the process of tendering for the new CRCs. In the light of this, we collected cost data from probation services at only one of the sites. However, we were able to access sufficient data on the costs of sessions and this, in combination with the data found during the systematic reviews of the cost of crime and the results of the health service use questionnaires, provided us with sufficient data to run an exploratory cost-effectiveness analysis.
Feasibility of measuring differences in effectiveness between care farms and comparators
Although our systematic review highlights the need for further sufficiently powered studies to assess the effectiveness of CFs in improving quality of life, mental well-being and other outcomes, the experience of this pilot study highlights the challenges of doing so. We identified significant differences between the CFs and between probation services. Service users had different relationships with CFs and different levels of engagement and interaction with nature. Our qualitative findings show this diversity, as the farms that we studied ranged from having very well-developed rehabilitative elements, able to support clients with challenging behaviour and substance abuse issues, to very little support available and limited opportunities for clients to interact with nature. Similarly, probation services showed considerable difference in how CFs were used, with some using CFs as a punitive intervention and others as rehabilitative or a mixture of the two, and in the type of service user allocated to the CFs in each setting, with one farm being allocated users who had a high risk of reoffending, higher levels of substance misuse and low unemployment, although other CFs took lower-risk users. These differences in the users allocated to CFs have not happened as a result of chance but because of a recognition (even if not formally) within probation services, particularly when the focus is on rehabilitation, that the CF may offer a more suitable and beneficial environment for users with greater needs.
Identifying comparators with ‘comparable’ users was challenging, with the comparator in centre 3 taking users with very different special requirements (e.g. to counteract drink driving) compared with those at the CF. Given the continued, and even increased, diversity of approaches within the new CRCs,154 these differences are unlikely to lessen. Although these issues of comparability clearly undermine a standard controlled study design, our statistical methods, particularly the use of propensity scores, detailed in Chapter 4, present a robust way to deal with these differences, allowing comparison between sites with participants with different characteristics.
In particular, it should be noted that the OGRS score, which is a predictor of reoffending combining age, gender and criminal history,155 proved to be a valuable composite measure for adjusting for the differences between those allocated to CFs and comparators. We were able to collect OGRS scores from 90% of the sample through linkage with the nDelius data held by probation. With a suitable sample size and the use of the propensity score method, we believe that a robust and reliable study of the effectiveness of CFs in reducing recidivism and improving offender health could be conducted.
As a pilot study, the study was not designed to detect a difference in quality of life between users at the CFs and comparator sites. It should be emphasised that the small sample size of this pilot study limits any interpretation of the primary and secondary outcomes and cost-effectiveness results. The differences initially seen in the unadjusted reconviction rates between CF and comparator users disappeared once the differences between the two groups had been adjusted for in the analysis. The analysis of confounders highlighted the value of the OGRS score as a composite measure of the factors associated with reoffending. Utilising this score in any future study is vital in order to adjust for the differences between groups, particularly as, in some probation services, those with high OGRS scores are actively sent to CFs.
As all necessary variables were available from the study for both the exploratory statistical and health economic analysis, a larger study could be conducted. Our study has also demonstrated that it is feasible to include an analysis of the impact of seasonality and, although this was not found to drive allocation decisions, this is another element that may potentially moderate effectiveness so needs to be included in any future study.
However, a major challenge to the conduct of such a definitive study in future is the limited number of CFs that are currently contracted by probation services to receive probation service users on COs. This reduction in the number of CFs working with probation may reflect the instability of this period of transition to CRCs and NPS. Once the new system is firmly established, it may be that more CFs are commissioned to work with probation. This would facilitate the recruitment of sufficient participants for a fully powered study in improvements in quality of life and fewer reconvictions in CFs compared with other CO placements. It is encouraging that recent parliamentary assessment of the Transforming Rehabilitation programme emphasises the need for MoJ to overcome the ‘significant barriers to encouraging the promised innovative practice in rehabilitating offenders’ and to realise the ‘full potential of the third sector’ (p6–7154). These recommendations bode well for CFs, which are clearly third-sector organisations that are able to provide innovative solutions with the potential to reduce recidivism.
Understanding community order allocation
Conducting the study in three different probation service regions, and the in-depth qualitative study, helped to shed light on very different approaches within probation services, in particular how CFs are viewed (as a punitive or rehabilitative intervention) and the different approaches taken to allocation of users to the CFs or other setting. These differences are exemplified by the fact that centre 3 used the CF as a SA, allocating users who were unemployed and who had a high risk of reoffending. This was very different in the other two centres, where probation service users had a lower risk of offending and many were employed. In centre 1, the qualitative findings highlighted that the comparator CO sites were often unwilling to take challenging users with complex needs and who had a high risk of reoffending; this was not the same in the CFs, where all users were accepted. The impacts of this are seen in the quantitative data, in which the CF users had significantly higher OGRS scores on allocation to the CF. CFs are clearly a resource for probation in being able manage and support offenders who had a higher-risk profile.
Our analysis of the characteristics of users allocated to the CFs as opposed to the comparator sites highlights significant gender difference in the allocation (4% of those service users sent to CFs were women compared with 44% sent to the comparator sites). This gender bias is reflected across many of the care farming studies found in our review. 25,28,75,77 This may well reflect the preconceived ideas of probation staff about which locations are appropriate for men and women to serve their CO. Probation staff who were interviewed considered CFs to be male dominated and, therefore, not an appropriate environment for women; how the farms became predominantly male in the first instance is not clear. The availability of independent placements (that require minimal supervision from non-probation staff) for lower-risk probation service users may be more appealing to women. In addition, given that CFs seem to take higher-risk probation service users, these placements have an over-representation of men over and above the preponderance of male probation service users. However, this does not mean that women cannot potentially benefit from nature-based interventions as part of their CO and probation services may want to consider this option. We know that, at the time of the study, one CF was looking into the possibility of supporting women through a residential scheme as part of a suspended sentence order and this will be worth further investigation.
Our qualitative findings highlight how probation officers, responsible for allocation particularly in centres 1 and 2 (West Yorkshire and Hertfordshire), rarely considered the potential of CFs as a rehabilitative location in which the beneficial elements of the CF, so closely linked to desistance theory, could reduce recidivism. Instead, the concern was for the order to be completed as smoothly and efficiently as possible. Such an approach may appear to support short-term benefits for the service; however, it may reduce life improvements for individual users and, ultimately, long-term benefits in reducing recidivism. When the CF was seen as aiding rehabilitation, particularly for those seen as having a higher risk of recidivism and more challenging needs, probation officers were more aware of the potential benefits of the farm environment.
Logic model of mechanisms for change among probation service users
A significant contribution of this study is the development of a logic model that elucidates the mechanisms of change leading to potential improvements in health outcomes. The logic model derived from the mixed-methods review guided the analysis of the qualitative data collected from users, care farmers and probationers as part of this study.
The qualitative themes that emerged were well aligned with the all-service user logic model presented in the review. For example, the easy environment identified by the users in our study fits well with the description of the ‘setting’ provided by other CF service user groups, the themes from our participants highlight the important and supportive role of the farmer or supervisor and the interaction with animals and the work fits well with the logic model from the review. The mechanism of ‘personal growth’ was also clearly identified by our participants and those from the synthesised evidence. One area in which there are differences, however, is in developing relationships; the building of friendships and opportunity to spend time in a group was seen as a positive benefit of the CF for all service user groups in the review; however, for the probation service users in our study, many were keen to keep to themselves, serve their order and not build any new friendships with other probation service users that might get them into trouble again at a later date. It may be that for a probation service user attending CFs, building relationships with the farm staff and probation supervisors may be more acceptable and valuable to aid service users build a new non-offending identity. The idea of ‘looking back’ emerged as a distinctive theme among the probation service users, whereas this concept was seen as integral to the setting among the other service users studied in the review. In fact, probation service users rarely identified the farm as a setting for ‘looking back’, and this was more likely to happen on the journey to and from the farm. It may be that the distractive elements of the farm – which is a very important element for mental health CF users – were sufficient to keep probation service users from looking back on their past. According to attention restoration theory,11 this opportunity for space or time-out from anxiety-inducing thoughts is part of mental health recovery, and it may also be that probation service users are able to benefit from this time-out to gain a new perspective on their offending behaviour and its impact on their lives.
Strengths and limitations of the research
The limitations of each component of the study are presented in each corresponding chapter. Here, the overall limitation of conducting this pilot study during a period of major transformation of probation services should be noted. In particular, the changes in staffing within probation, managing relationships with CFs when they faced contractual uncertainty with probations services, the challenges of co-ordinating researchers’ site visits with the availability of service users and the need to establish multiple data sharing agreements with both the old and new organisations significantly affected our ability to recruit, both to the qualitative and quantitative study, the follow-up of participants and the timely implementation of the study. A strength of this study is that, with all these challenges, we have been able to try a number of different mechanisms for recruiting and following up participants, and the learning gained from these is presented throughout the report, particularly in Chapter 3. However, with changing systems it may be that the process would need further adaptions in future.
A further limitation of the study is the limited engagement of service users. Although at the design phase we had hoped for significant engagement in the design, implementation and analysis of the study, we were successful in gaining inputs only into the early stage of designing information sheets and recruitment processes. In part, this was attributable to our strategy of linking into existing service user structures established by probation services. With hindsight, a more productive and rewarding engagement could have been nurtured if we had established our own service user group with a core group of participants who were interested in our study. We could have supported participants in building their understanding of the concept of the study, and care farming, strengthening their capacity for understanding research. Although this would have engaged only a small, and perhaps unrepresentative group, it would have brought valuable user perspectives to bear on our work.
Recommendations for future research
Our study has highlighted that, although challenging, it is feasible to collect the data required to conduct a cost-effectiveness analysis of CFs compared with other COs. We recommend that future studies consider a primary outcome of reconvictions. Data on this outcome can be acquired, with the correct permissions and arrangements, from the MoJ, and our study shows that participant consent to, and linkage of, individual data is feasible. Furthermore, this outcome is of utmost importance to policy-makers and commissioners within probation services.
Our study has also shown that health and social outcomes for probation service users can be collected. The constraints to following up this participant group to complete outcome questionnaires should not be underestimated. In the light of this, we recommend that health and social outcomes are considered as secondary outcomes in future research.
The lack of CFs currently contracted by probation services would make a larger study unfeasible at the present time; however, it may be that this changes as the restructured probation services re-establish contracts with a wider range of providers, particularly those in the third sector, with a view to encouraging innovation and ultimately reducing recidivism.
Our study highlights the challenges of finding ‘comparable’ comparator sites and participants. We recommend that the propensity score analysis methods used in this study be considered and used more extensively in natural experiments to respond to this inevitable lack of comparability found when assessing cost-effectiveness in complex social and public health interventions.
Methodologically, conducting such a study with probation service users as participants has many advantages, not least because while serving their CO they are continually monitored by probation services, enabling some degree of follow-up and, most encouragingly, reconviction data can be used as provide outcome data for 90% of participants. Furthermore, data on confounders can be gathered from probation services, particularly the OGRS score, which can be used within the study analysis.
However, it should also be noted that with increasing emphasis on third-sector provision of health and social services for mental health (including long-term conditions and dementia) that commissioners across the health, social and criminal justice economy are seeking evidence of the effectiveness of CFs. Further studies to determine effectiveness in improving mental and physical health for these client groups would clearly be of value.
Our review found much similarity across the qualitative studies on the mechanism and process outcomes for a range of service user groups attending CFs. We would therefore recommend that conducting further similar qualitative studies would need a clear justification and explorations in new directions. One group that we identified as consistently absent, both in the qualitative and quantitative studies in the review, was those service users who decided to leave the CF. Although these participants may be more challenging to identify and interview, such work would be valuable in providing greater depth of understanding of who may benefit from CFs and may not. For probation service users, this issue is somewhat different, as they must serve their order where they are allocated or they are in breach of their CO and return to court. However, among service user groups that can leave the farm out of choice, a great exploration of the reasons for this would be valuable. This may be of particular relevance to female service users; as CFs are male dominated it may be that some women are de-incentivised to stay. A further area to be explored, which may lend itself to both quantitative – the connectedness-to-nature scales used in this study are valuable here – and qualitative research, is the link between interaction with nature and health. Our review identified how the relationships were rarely explored explicitly within studies, and yet this could provide more detailed information on this characteristic of CFs that is rarely found in other similar interventions.
Recommendations for practice
Although further research is needed to determine the cost-effectiveness of CFs in reducing recidivism, our review and qualitative study highlight the potential of CFs to provide innovative rehabilitation interventions to benefit the well-being of probation users and, ultimately, to reduce recidivism. In the light of this, we recommend that probation services, both CRCs and NPS, build an understanding of the CFs within their catchment areas, identifying their potential to support the rehabilitation of probation service users. Our study highlights that not all CFs are the same, and an understanding of the ethos and aims of the farm is therefore important before considering allocating service users. CFs that can clearly demonstrate that they offer therapeutic benefits through farming activities should be used as a rehabilitative requirement.
Aligning probation service goals and practice to focus on rehabilitation, rather than a purely punitive focus, is clearly a first step in this process. Considering specific rehabilitation needs of individuals and aligning these with the intervention components of local CFs will help ensure that those most likely to benefit gain access to CFs. Our logic model indicates that probation service users who might benefit from learning new skills and participating in meaningful, structured work with a strong role model figure of the farmer, would be particularly suited to a placement on a CF.
In order to ensure that probation services understand the potential benefits of CF, care farmers need a clear understanding of how they can contribute to the process of rehabilitation and an ability and means to communicate this to probation services. This will allow CFs to appropriately position themselves within the right type of CO.
Despite the turbulence within probation services during the time frame of this study, we have benefited from the willingness of probation services and the MoJ to establish data sharing agreements that have enabled us to use existing probation and PNC data. We strongly recommend that requests to access and link individual data continue to be supported within the new probation structures. This will allow further robust research, which can take into consideration important confounders, to understand the effect of different probation interventions on recidivism.
Acknowledgements
Joyce Croker (Research Fellow, Public Health) led the qualitative data analysis and contributed to the preparation of a manuscript for publication.
Judy Wright (Senior Information Specialist) designed and conducted the searches for the systematic reviews.
Thomas Fleming (Data Management Manager) designed the outcomes database, provided guidance during the development of data sharing agreements with partner organisations and performed the data linkage and anonymisation.
Rachel Lunt (NPS Administrator) performed recruitment in one centre and qualitative interviews.
Jen Ball (Finance Officer) managed the budgets and liaised with partner organisations to arrange invoicing.
David Brennan (Research Support Secretary in Public Health) organised the steering group meetings and the minutes from them, led in organising the Way Forward Workshop and transcribed the qualitative interviews.
Adrian Slater (Legal Adviser) and Kevin Darley (Head of IT security) reviewed and advised on data protection and the development of the ISAs.
We also wish to thank the following people: the many probation staff who assisted us in various ways during the study at a particularly difficult time. The care farmers and staff at New Gokul who were also generous with their time. The comparator site staff who accommodated us, enabling us to perform recruitment and follow-up efficiently. The staff at the MoJ and the police services who made the development of ISAs and a memorandum of understanding possible and performed data extraction diligently and efficiently. Marina Garcia Llorente who contributed to the Campbell literature review.
Contributions of authors
Helen Elsey (Lecturer in Public Health) led the design, overall implementation and synthesis of the project, ensuring that milestones were met and the overall objectives of the project were addressed.
Rachel Bragg (Director of Care Farming UK) provided support and guidance throughout the duration of the study.
Marjolein Elings (Scientist and Researcher in Agriculture and Health) provided support and guidance throughout the duration of the study.
Cathy Brennan (Lecturer in Public Health) was an active member of the steering committee, providing guidance throughout.
Tracey Farragher (Statistician and Public Health Epidemiologist) carried out the statistical analysis for the main pilot study.
Sandy Tubeuf (Associate Professor in Health Economics) designed the health economics analysis, led the health economics systematic reviews and performed the cost-effectiveness analysis.
Rochelle Gold (previously Manager of the Research Department at West Yorkshire Probation Trust) provided access to a number of contacts within probation and provided guidance on a number of procedures within probation.
Darren Shickle (Professor in Public Health) was an active member of the steering committee, providing guidance throughout.
Nyantara Wickramasekera (Research Fellow, Public Health) took a lead role in the systematic review on quality of life and conducted the systematic review on cost of reoffending.
Zoe Richardson (Research Fellow, Public Health) undertook recruitment and follow-up during the pilot study and contributed to screening during the literature review on quality of life.
Janet Cade (Epidemiologist, leading the Nutritional Epidemiology Group) was an active member of the steering committee providing guidance throughout.
Jenni Murray (Senior Research Fellow, Public Health) co-ordinated the project and took lead roles in the systematic review on quality of life, quantitative pilot study and the qualitative study.
Publications and presentations
Publications
Elsey H, Bragg R, Elings M, Cade JE, Brennan C, Farragher T, et al. Understanding the impacts of care farms on health and well-being of disadvantaged populations: a protocol of the Evaluating Community Orders (ECO) pilot study. BMJ Open 2014;4:e006536.
Elsey H, Bragg R, Brennan C, Murray J, Elings M, Richardson Z, et al. The Impact of Care Farms on Quality of Life Among Different Populations Groups: Protocol for a Systematic Review. Oslo: the Campbell Collaboration; 2014. URL: www.campbellcollaboration.org/lib/project/321 (accessed 1 June 2016).
Wickramasekera N, Wright J, Elsey H, Murray J, Tubeuf S. Cost of crime: a systematic review. J Crim Justice 2015;43:218–28.
Elsey H, Murray J, Bragg R. Green fingers and clear minds: prescribing ‘care farming’ for mental illness. Br J Gen Pract 2016;66:99–100.
Murray J, Elsey H, Gold R. Care Farming and Probation in the UK. In Barton J, Bragg R, Wood C, Pretty J, editors. Green Exercise: Linking Nature, Health and Wellbeing. London: Routledge; 2016.
Presentations
Murray J. The Impact of Care Farms on Quality of Life among Different Population Groups: Systematic Review. Agriculture in an Urbanizing Society, Rome, Italy, 14–17 September. URL: www.agricultureinanurbanizingsociety.com/?cat=13 Rome (accessed September 2015).
Tubeuf S. Happiness is in the Field: Economic Evaluation of Care Farms for Probation Service users Undertaking Community Orders. French Health Economists Days, Dijon, France, 3–4 December 2015.
Elsey H. The Impact of Care Farms on Quality of Life Among Different Population Groups: Systematic Review. Faculty of Public Health Conference, Brighton, UK, 14–15 June 2016.
Nyantara W. The Impact of Care Farms on Quality of Life Among Different Population Groups: Systematic Review. HSRUK Symposium, Nottingham Conference Centre, Nottingham, UK, 13 July 2016.
Data sharing statement
All available data can be obtained by contacting the corresponding author.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care.
References
- Hassink J, Zwartbol C, Aricola HJ, Elings M, Thissen JTNM. Current status and potential of care farms in the Netherlands. NJAS-Wagening J Life Sci 2007;55:21-36. https://doi.org/10.1016/S1573-5214(07)80002-9.
- Hassink J. Combining Agricultural Production and Care for Persons with Disabilities: A New Role of Agriculture and Farm Animals. Florence: Wageningen University/Fifth IFSA European Symposium; 2003.
- Hine R. Care farming: bringing together agriculture and health. ECOS 2008;29:42-51.
- Care-Farming UK n.d. www.carefarming.org.uk (accessed January 2016).
- Moore G, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process Evaluation of Complex Interventions UK Medical Research Council (MRC) Guidance. London: MRC; 2011.
- Bragg R, Egginton-Metters I, Elsey, Wood C. Care Farming: Defining the ‘Offer’ in England. York: Natural England; 2014.
- Bragg R, Atkins G. A Review of Nature-Based Interventions for Mental Health Care. York: Natural England; 2016.
- Sempik J, Bragg R, Gallis C. Green Care: For Human Therapy, Social Innovation, Rural Economy and Education. New York, NY: Nova Science Publishers; 2013.
- Bragg R. Care Farming in the UK – Key Facts and Figures. Colchester: University of Essex; 2013.
- Sempik J, Hine R, Wilcox D. Green Care: a Conceptual Framework. Loughborough: Loughborough University; 2010.
- Kaplan R, Kaplan S. The Experience of Nature: A Psychological Perspective. Cambridge: Cambridge University Press; 1989.
- Wilson EO. Biophilia. Cambridge, MA: Harvard University Press; 1984.
- McNeill F, Weaver B. Changing Lives? Desistance Research and Offender Management. Glasgow: Scottish Centre for Crime and Justice Research and Glasgow School of Social Work; 2010.
- Anthony W. Recovery from mental illness: the guiding vision of the mental health service system in the 1990s. Psychosoc Rehabil J 1993;16. https://doi.org/10.1037/h0095655.
- Farrall S, Bowling B. Structuration, human development and desistance from crime. Br J Criminol 1999;17:252-67. https://doi.org/10.1093/bjc/39.2.253.
- Weaver B, McNeill F. Giving Up Crime: Directions for Policy. Glasgow: The Scottish Centre for Crime and Justice Research; 2007.
- Maruna S. Making Good: How Ex-Convicts Reform and Rebuild their Lives. Washington, DC: American Psychological Association; 2001.
- McCulloch T. Probation, social context and desistance: retracing the relationship. Probat J 2005;52:8-22. https://doi.org/10.1177/0264550505050623.
- McNeill F. A desistance paradigm for offender management. Criminol Crim Just 2006;6:39-62. https://doi.org/10.1177/1748895806060666.
- Farrell S, Maruna SaIR. After Crime and Punishment: Pathways to Offender Reintegration. Cullomptom: Willan Publishing; 2004.
- Giordano PC, Cernkovich SA, Rudolph JL. Gender, crime and desistance: toward a theory of cognitive transformation. AJS 2002;107:990-1064. https://doi.org/10.1086/343191.
- Laub JH, Samson RJ. Turning points in the life course: why change matters to the study of crime. Criminology 1993;31:301-25. https://doi.org/10.1111/j.1745-9125.1993.tb01132.x.
- McNeill F, Maruna S, McIvor G, Raynor P. Developments in Social Work with Offenders. London: Jessica Kingsley; 2007.
- Hassink J, Elings M, Zweekhorst M, van den Nieuwenhuizen N, Smit A. Care farms in the Netherlands: attractive empowerment-oriented and strengths-based practices in the community. Health Place 2010;16:423-30. https://doi.org/10.1016/j.healthplace.2009.10.016.
- Hassink J, De Meyer R, van der Sman P, Veerman JW. Effectiviteit van ervarend leren op de boerderij. Tijdschr Orthoped 2011;50:51-63.
- Evidence to Inform the Commissioning of Social Prescribing. York: Centre for Reviews and Dissemination, University of York; 2015.
- Christensen K, Doblhammer G, Rau R, Vaupel JW. Ageing populations: the challenges ahead. Lancet 2009;374:1196-208. https://doi.org/10.1016/S0140-6736(09)61460-4.
- Elings M, Haubenhofer D, Hassink J, Rietberg P, Michon H. Effecten van Zorgboerderijen en Andere Dagbestedingsprojecten Voor Mensen Met een Psychiatrische en Verslavingsachtergrond. Wageningen: Plant Research International, Wageningen; 2011.
- Di Lacovo F, O’Connor D. Supporting Policies for Social Farming in Europe Progressing Multifunctionality in Responsive Rural Areas 2009.
- Kamioka H, Tsutani K, Yamada M, Park H, Okuizumi H, Honda T, et al. Effectiveness of horticultural therapy: a systematic review of randomized controlled trials. Complement Ther Med 2014;22:930-43. https://doi.org/10.1016/j.ctim.2014.08.009.
- Lovell R, Husk K, Cooper C, Stahl-Timmins W, Garside R. Understanding how environmental enhancement and conservation activities may benefit health and wellbeing: a systematic review. BMC Public Health 2015;15. https://doi.org/10.1186/s12889-015-2214-3.
- Barton J, Griffin M, Pretty J. Exercise, nature and socially interactive based initiatives improve mood and self-esteem in the clinical population. Perspect Public Health 2011;132:89-96. https://doi.org/10.1177/1757913910393862.
- Thompson Coon J, Boddy K, Stein K, Whear R, Barton J, Depledge MH. Does participating in physical activity in outdoor natural environments have a greater effect on physical and mental wellbeing than physical activity indoors?. Environ Sci Technol 2011;45:1761-72. https://doi.org/10.1021/es102947t.
- Elings M. Effects of Care Farms: Scientific Research on the Benefits of Care Farms for Clients. Wageningen UR: Trimbos Institute and Practikon/Radbound University; 2012.
- Iancu S, Hoogendoorn A, Zweekhorst M, Veltman D, Bunders J, van Balkom A. Farm-based interventions for people with mental disorders: a systematic review of literature. Disabil Rehabil 2013;37:379-88. https://doi.org/10.3109/09638288.2014.932441.
- Bragg R, Egginton-Metters I, Leck C, Wood C. Expanding Delivery of Care Farming Services to Health and Social Care Commissioners. York: Natural England; 2015.
- Pluye P, Hong QN. Combining the power of stories and the power of numbers: mixed methods research and mixed studies reviews. Annu Rev Public Health 2014;35:29-45. https://doi.org/10.1146/annurev-publhealth-032013-182440.
- Moher D, Liberati A, Tetzalaff J, Altman DG. PRISMA Group . Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. PLOS Med 2009;6. https://doi.org/10.1371/journal.pmed.1000097.
- Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. (updated March 2011). London: The Cochrane Collaboration; 2011.
- Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ) a 32-item checklist for interviews and focus groups. Int J Qual Health Care 2007;19:349-57. https://doi.org/10.1093/intqhc/mzm042.
- Long AF, Godfrey M. An evaluation tool to assess the quality of qualitative research studies. Int J Social Research Methodology 2004;7:181-96. https://doi.org/10.1080/1364557032000045302.
- Armijo-Olivo S, Stiles CR, Hagen NA, Biondo PD, Cummings GG. Assessment of study quality for systematic reviews: a comparison of the Cochrane Collaboration Risk of Bias Tool and Effective Public Health Practice Project Quality Assessment tool: methodological research. J Eval Clin Pract 2012;18:12-8. https://doi.org/10.1111/j.1365-2753.2010.01516.x.
- Backoff RW, Nutt PC, Bryson J, Einsweiler R. Strategic Planning: Threats and Opportunities for Planners. Chicago, IL: Planners Press; 1988.
- Popay J. Narrative Synthesis Guidance. Lancaster: Narrative Synthesis in Systematic Reviews; 2006.
- Baars E, Elings M, Hassink J. De Hoge Born Verbindt: Kwaliteiten en Effecten van Zorgboerderij De Hoge Born. Wageningen: Plant Research International, Wageningen; 2009.
- Bjørgen D, Johansen KJ. Bruker Spør Bruker: Evaluering Av Inn På Tunet. Trondheim: Mental helse i Sør-Trøndelag; 2007.
- Elings M. Boer, Zorg Dat je Boer Blijft: Een Onderzoek Naar de Specifieke Waarden van een Bedrijfsmatige Zorgboerderij. Wageningen: Wetenschapswinkel; 2004.
- Elings M, Beerens A. The added value and effects of care farms on clients with psychiatric or addiction problems. Acta Hortic 2012;954:57-66. https://doi.org/10.17660/ActaHortic.2012.954.6.
- Elings M, Hassink J. Green care farms, a safe community between illness or addiction and the wider society. Ther Communities 2008;29:310-22.
- Elings M, Hassink JC. The Added Value of Care Farms and Effects on Clients n.d.
- Ferwerda-van Zonneveld R, Oosting SJ, Kijlstra A. Care farms as a short-break service for children with autism spectrum disorder. NJAS Wagening J Life Sci 2012;59:35-40. https://doi.org/10.1016/j.njas.2012.01.001.
- Granerud A, Eriksson BG. Mental health problems, recovery, and the impact of green care services: a qualitative, participant-focused approach. Occup Ther Ment Health 2014;30:317-36. https://doi.org/10.1080/0164212X.2014.938558.
- Hassink J. Zorgboerderijen Dragen bij aan Empowerment en Eigen Kracht van Deelnemers. Wageningen: Plant Research International, Wageningen; 2009.
- Iancu SC, Zweekhorst MBM, Veltman DJ, van Balkom A, Bunders JFG. Mental health recovery on care farms and day centres: a qualitative comparative study of users’ perspectives. Disabil Rehabil 2014;36:573-83. https://doi.org/10.3109/09638288.2013.804595.
- Kaley A. Green Care in Agriculture: Interim Report. Lancaster: Lancaster University; 2015.
- Kogstad RE, Agdal R, Hopfenbeck MS. Narratives of natural recovery: youth experience of social inclusion through green care. Int J Environ Res Public Health 2014;11:6052-68. https://doi.org/10.3390/ijerph110606052.
- Leck C, Upton D, Evans N. Growing well-beings: The positive experience of care farms. Br J Health Psychol 2015;20:745-62. https://doi.org/10.1111/bjhp.12138.
- Pedersen I, Ihlebaek C, Kirkevold MC. Important elements in farm animal-assisted interventions for persons with clinical depression: a qualitative interview study. Disabil Rehabil 2012;34:1526-34. https://doi.org/10.3109/09638288.2011.650309.
- Schreuder E, Rijnders M, Vaandrager L, Hassink J, Enders-Slegers M-J, Kennedy L. Exploring salutogenic mechanisms of an outdoor experiential learning programme on youth care farms in the Netherlands: untapped potential?. Int J Adolesc Youth 2014;19:139-52. https://doi.org/10.1080/02673843.2014.896267.
- Evaluation of the Care Farm Pilot for Mental Health Service Users. Cambridge: Anglia Ruskin University; 2013.
- Berget B, Ekeberg Ø, Braastad BO. Animal-assisted therapy with farm animals for persons with psychiatric disorders: effects on self-efficacy, coping ability and quality of life, a randomized controlled trial. Clin Pract Epidemiol Ment Health 2008.
- Berget B, Ekeberg O, Pedersen I, Braastad B. Animal-assisted therapy with farm animals for persons with psychiatric disorders: effects on anxiety and depression, a randomized controlled trial. Occup Ther Ment Health 2011;27:50-64. https://doi.org/10.1080/0164212X.2011.543641.
- Berget B, Skarsaune I, Ekeberg O, Braastad B. Humans with mental disorders working with farm animals: a behavioral study. Occup Ther Ment 2007;23:101-17. https://doi.org/10.1300/J004v23n02_05.
- Pedersen I, Martinsen EW, Berget B, Braastad BOC. Farm animal-assisted intervention for people with clinical depression: a randomized controlled study. Anthrozoos 2012;25:149-60. https://doi.org/10.2752/175303712X13316289505260.
- de Bruin SR. Sowing in the Autumn Season: Exploring Benefits of Green Care Farms for Dementia Patients. Wageningen: Wageningen University; 2009.
- de Bruin SR, Oosting SJ, Tobi H, Enders-Slegers MJ, van der Zijpp A, Schols J. Comparing day care at green care farms and at regular day care facilities with regard to their effects on functional performance of community-dwelling older people with dementia. Dementia 2012;11:503-19. https://doi.org/10.1177/1471301211421074.
- Gonzalez MT, Gallis C. Green Care: For Human Therapy, Social innovation, Rural Economy, and Education. New York, NY: Nova Science Publishers; 2013.
- Gonzalez MT, Hartig T, Patil GG, Martinsen EW, Kirkevold M. Therapeutic horticulture in clinical depression: a prospective study. Res Theory Nurs Pract 2009;23:312-28. https://doi.org/10.1891/1541-6577.23.4.312.
- Gonzalez MT, Hartig T, Patil GG, Martinsen EW, Kirkevold M. Therapeutic horticulture in clinical depression: a prospective study of active components. J Adv Nurs 2010;66:2002-13. https://doi.org/10.1111/j.1365-2648.2010.05383.x.
- Gonzalez MT, Hartig T, Patil GG, Martinsen EW, Kirkevold M. A prospective study of group cohesiveness in therapeutic horticulture for clinical depression. Int J Ment Health Nurs 2011;20:119-29. https://doi.org/10.1111/j.1447-0349.2010.00689.x.
- Gonzalez MT, Hartig T, Patil GG, Martinsen EW, Kirkevold M. A prospective study of existential issues in therapeutic horticulture for clinical depression. Issues Ment Health Nurs 2011;32:73-81. https://doi.org/10.3109/01612840.2010.528168.
- Pedersen I, Nordaunet T, Martinsen EW, Berget B. Braastad BOCTJZI . Farm animal-assisted intervention: relationship between work and contact with farm animals and change in depression, anxiety, and self-efficacy among persons with clinical depression. Issues Ment Health Nurs 2011;32:493-500. https://doi.org/10.3109/01612840.2011.566982.
- Javed MA, Chaudhry UR, Suleman T, Chaudhry MR. Agrotherapy – new concept of rehabilitation for chronic schizophrenics in Pakistan. J Pak Med Assoc 1993;43:251-3.
- Hine R, Peacock J, Pretty J. Care farming in the UK: contexts, benefits and links with therapeutic communities. Ther Communities 2008;29:245-60.
- Hine R, Peacock J, Pretty JN. Care Farming in the UK: Evidence and Opportunities. Colchester: University of Essex; 2008.
- Hine R, Barton J, Pretty J. Evaluation of the Traumatic Stress Service at Vauxhall City Farm: A City Farm-based Psycho-Education Group for Asylum Seekers and Refugees. Colchester: University of Essex; 2009.
- Lambert R. Service Evaluation for Clinks Care Farm, Beccles. Beccles and Norwich: Clinks Care Farm and University of East Anglia; 2014.
- Marshall D, Wakeham C. SHIFT Care Farm: Evaluation Report for One Cohort of Offenders under the SHIFT Pathways Approach for the Use of a Care Farm for the Management of Offenders. Hereford: Bulmer Foundation; 2015.
- Suprise KL. The Efficacy of Therapeutic Horticulture and Animal-Assisted Therapy to Promote Prosocial Behavior in Foster Youth. Long Beach, CA: California State University; 2013.
- CRC WM. Type of Community Order 2017. www.westmerciaprobation.org.uk/page.php?Plv=2&P1=12&P2=25 (accessed August 2015).
- MoJ . Types of Community Order n.d. http://open.justice.gov.uk/how-it-works/sentencing-and-rehabilitation/ (accessed August 2015).
- Gray P, Mellor-Clark J. CORE: A Decade of Development. Rugby: CORE IMS; 2007.
- Horton M, Wright N, Dyer W, Wright-Hughes A, Farrin A, Mohammed Z, et al. Assessing the risk of self-harm in an adult offender population: an incidence cohort study. Health Technol Assess 2014;18. https://doi.org/10.3310/hta18640.
- Tapp J, Fellowes E, Wallis N, Blud L, Moore E. An evaluation of the Enhanced Thinking Skills (ETS) programme with mentally disordered offenders in a high security hospital. Legal Criminol Psychol 2009;14:201-12. https://doi.org/10.1348/135532508X336178.
- Barkham M, Gilbert N, Connell J, Marshall C, Twigg E. Suitability and utility of the CORE-OM and CORE-A for assessing severity of presenting problems in psychological therapy services based in primary and secondary care settings. Br J Psychiatry 2005;186:239-46. https://doi.org/10.1192/bjp.186.3.239.
- Brazier J. Measuring and valuing mental health for use in economic evaluation. J Health Serv Res Policy 2008;13:70-5. https://doi.org/10.1258/jhsrp.2008.008015.
- Tennant R, Hiller L, Fishwick R, Platt S, Joseph S, Weich S, et al. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): development and UK validation. Health Qual Life Outcomes 2007;5. https://doi.org/10.1186/1477-7525-5-63.
- General Lifestyle Survey. Newport: Office for National Statistics; 2010.
- Health Survey for England. Leeds: NHS Digital; 2012.
- Nisbet EK, Zelenski JM, Murphy SA. The nature relatedness scale: linking individuals’ connection with nature to environmental concern and behavior. Environ Behav 2009;41:715-40. https://doi.org/10.1177/0013916508318748.
- Schultz W, Schmuck P, Schultz W. Psychology of Sustainable Development. Dordrecht: Kluwer Academic Publishers; 2002.
- Freedom of Information Act 2000. London: The Stationery Office; 2000.
- Transforming Rehabilitation: A Summary of the Evidence on Reducing Re-offending. London: MoJ; 2013.
- Moher D, Schulz K, Altman D. The CONSORT statement: revised recommendations for improving the quality of reports of parallel-group randomized trials. Ann Intern Med 2001;134:657-62. https://doi.org/10.7326/0003-4819-134-8-200104170-00011.
- Criminal Justice Act 2003. London: The Stationery Office; 2003.
- Offender Rehabilitation Act 2014. London: The Stationery Office; 2014.
- Austin P, Stuart E. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat Med 2015;34:3661-79. https://doi.org/10.1002/sim.6607.
- Rosenbaum P, Rubin D. The central role of the propensity score in observational studies for causal effects. Biometrika 1983;70. https://doi.org/10.1093/biomet/70.1.41.
- Pirracchio R, Resche-Rigon M, Chevret S. Evaluation of the propensity score methods for estimating marginal odds ratios in case of small sample size. BMC Med Res Methodol 2012;12. https://doi.org/10.1186/1471-2288-12-70.
- Stevens J. Applied Multivariate Statistics for the Social Sciences. Hillsdale, NJ: Lawrence Erlbaum Associates, Inc.; 1996.
- Brookhart MA, Schneeweiss S, Rothman KJ, Glynn RJ, Avorn J, Stürmer T. Variable selection for propensity score models. Am J Epidemiol 2006;163:1149-56. https://doi.org/10.1093/aje/kwj149.
- Cohen MA. Measuring the costs and benefits of crime and justice. Crim Justice 2000;4:263-315.
- Husereau D, Drummond M, Petrou S, Carswell C, Moher D, Greenberg D, et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) – explanation and elaboration: a report of the ISPOR health economic evaluation publication guidelines good reporting practices task force. Value Health 2013;16:231-50. https://doi.org/10.1016/j.jval.2013.02.002.
- Care Farming: Harvesting the Benefits – A Review of Herefordshire PPO Scheme Use of SHIFTBODS Care Farm. Worcester: West Mercia Constabulary; 2008.
- Bragg R, Wood C, Barton J. Ecominds Effects on Mental Wellbeing. London: Mind; 2013.
- Wickramasekera N, Wright J, Elsey H, Murray J, Tubeuf S. Cost of crime: a systematic review. J Crim Justice 2015;43:218-28. https://doi.org/10.1016/j.jcrimjus.2015.04.009.
- Wilson IB, Cleary PD. Linking clinical variables with health-related quality of life. A conceptual model of patient outcomes. JAMA 1995;273:59-65. https://doi.org/10.1001/jama.1995.03520250075037.
- Liberati A, Altman D, Tetzlaff J, Mulrow C, Gøtzsche P, Ioannidis J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLOS Med 2009;6. https://doi.org/10.1371/journal.pmed.1000100.
- Anderson D. The Cost of Crime. Found Trends Microeconomics 2012;7:209-65. https://doi.org/10.1561/0700000047.
- Ambrey C, Fleming C, Manning M. The Life Satisfaction Approach to Estimating the Cost of Crime: An Individual's Willingness-to-pay for Crime Reduction. Southport, QLD, Australia: Griffith Business School; 2013.
- Atkinson G, Healey A, Mourato S. Valuing the costs of violent crime: a stated preference approach. OEP 2005;57:559-85. https://doi.org/10.1093/oep/gpi036.
- Brand S, Price R. The Economic and Social Costs of Crime. London: The Home Office; 2000.
- Cohen M, Miller T. The cost of mental health care for victims of crime. J Interpers Violence 1998;13:93-110. https://doi.org/10.1177/088626098013001006.
- Czabanski J. The feasibility of cost of crime estimations in Eastern Europe – the case of Poland. Eur J Crim Pol Res 2009;15:327-42. https://doi.org/10.1007/s10610-009-9106-y.
- DeLisi M, Gatling J. Who pays for a life of crime? An empirical assessment of the assorted victimization costs posed by career criminals. Crim Justice Stud Crit J Crime Law Soc 2003;16:283-93. https://doi.org/10.1080/0888431032000183489.
- DeLisi M, Kosloski A, Sween M, Hachmeister E, Moore M, Drury A. Murder by numbers: monetary costs imposed by a sample of homicide offenders. J Forens Psychiatry Psychol n.d.:501-13. https://doi.org/10.1080/14789940903564388.
- Dolan P, Loomes G, Peasgood T, Tsuchiya A. Estimating the intangible victim costs of violent crime. Br J Criminol 2005;45:958-76. https://doi.org/10.1093/bjc/azi029.
- Dolan P, Peasgood T. Estimating the economic and social costs of the fear of crime. Br J Criminol 2007;47:121-32. https://doi.org/10.1093/bjc/azl015.
- Dubourg R, Hamed J, Thorns J. The Economic and Social Costs of Crime Against Individuals and Households 2003/04. London: The Home Office; 2005.
- Leung A. Cost of Pain and Suffering from Crime in Canada. Ottawa, ON: Department of Justice Canada; 2004.
- Mayhew P. Counting the Costs of Crime in Australia. Canberra, NSW: Australian Institute of Criminology; 2003.
- McCollister KE, French MT, Fang H. The cost of crime to society: new crime-specific estimates for policy and program evaluation. Drug Alcohol Depend 2010;108:98-109. https://doi.org/10.1016/j.drugalcdep.2009.12.002.
- Miller T, Cohen M, Wiersema B. Victim Costs and Consequences: A New Look. Washington, DC: US Department of Justice; 1996.
- Piquero AR, Jennings WG, Farrington D. The monetary costs of crime to middle adulthood: findings from the Cambridge study in delinquent development. JRCD 2013;50:53-74. https://doi.org/10.1177/0022427811424505.
- Rollings K. Counting the Costs of Crime in Australia: A 2005 Update. Canberra, NSW: Australian Institute of Criminology; 2008.
- Roman JK. What is the price of crime? New estimates of the cost of criminal victimization. Diss Abstr Int A 2010;71.
- Roper T, Thompson A. Estimating the Costs of Crime in New Zealand in 2003/04. Wellington: New Zealand Treasury; 2006.
- Russell S. Costs of Crime in Victoria. Melbourne, VIC: Monash University; 2011.
- Walker J. Estimates of the Costs of Crime in Australia in 1996. Canberra, NSW: Australian Institute of Criminology; 1997.
- MacDonald Z. Revisiting the dark figure: a microeconometric analysis of the under-reporting of property crime and implications. Br J Criminol 2001;41:127-49. https://doi.org/10.1093/bjc/41.1.127.
- Guide to the Methods of Technology Appraisal. London: NICE; 2008.
- Barkham M, Leach C, Lucock M, Evans C, Margison F, Mellor-Clark J, et al. Service profiling and outcomes benchmarking using the CORE-OM: toward practice-based evidence in the psychological therapies. Clinical Outcomes in Routine Evaluation-Outcome Measures. J Consult Clin Psychol 2001;69:184-96. https://doi.org/10.1037/0022-006X.69.2.184.
- Mavranezouli I, Brazier JE, Young TA, Barkham M. Using Rasch analysis to form plausible health states amenable to valuation: the development of CORE-6D from a measure of common mental health problems (CORE-OM). Qual Life Res 2011;20:321-33. https://doi.org/10.1007/s11136-010-9768-4.
- Curtis L. Unit Costs of Health and Social Care 2014. Canterbury PSSRU: University of Kent; 2014.
- British National Formulary (online). London: BMJ Group and Pharmaceutical Press; n.d.
- NHS Reference Costs 2013 to 2014. London: DH; 2014.
- Mehanna H, Wong WL, McConkey CC, Rahman JK, Robinson M, Hartley AG, et al. PET-CT Surveillance versus Neck Dissection in Advanced Head and Neck Cancer. N Engl J Med 2016;374:1444-54. https://doi.org/10.1056/NEJMoa1514493.
- British National Formulary. London: BMJ Group and Pharmaceutical Press; 2015.
- Department of Health . Drugs and Pharmaceutical Electronic Market Information 2014. www.gov.uk/government/publications/drugs-and-pharmaceutical-electronic-market-information-emit (accessed June 2015).
- Farrall S, Calverley A. Understanding Desistance from Crime: Theoretical Directions in Resettlement and Rehabilitation. Oxford: McGraw-Hill Education, Oxford University Press; 2006.
- Cusson M, Pinsonneault P, Cornish DB, Clarke RV. The Reasoning Criminal. New York, NY: Springer-Verlag; 1986.
- Maruna S, LeBel TP. Welcome home? Examining the ‘Reentry Court’ concept from a strengths-based perspective. West Crim Rev 2003;4:91-107.
- Ulrich R, Altman I, Wohlwill JF. Behavior and the Natural Environment. New York City, NY: Springer; 1983.
- Peacock J, Hine R, Pretty J. Got the Blues? Then Find some Greenspace: The Mental Health Benefits of Green Exercise Activities and Green Care. Colchester: University of Essex; 2007.
- Lebel J. Health: An Ecosystem Approach. Ottawa, ON: International Development Research Centre; 2003.
- Berget B. Animal-Assisted Therapy: Effects on Persons with Psychiatric Disorders Working with Farm Animals. As: Norwegian University of Life Sciences; 2006.
- Sempik J, Spurgeon J. Lesson Learnt – Evidence from Practice: The Use of Plants and Horticulture in Promoting Health and Well-Being n.d.
- Boardman J. Work employment and psychiatric disability. Advan Psychiatr Treat 2003;9:327-34. https://doi.org/10.1192/apt.9.5.327.
- Kolb DA, Boyatzis RE, Mainemelis C, Sternberg RJ, Zhang LF. Perspectives on Thinking, Learning, and Cognitive Styles. Abingdon: Routledge; 2001.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol 2006;3:77-101. https://doi.org/10.1191/1478088706qp063oa.
- Evans S, Evans A. Theory of Change for SHIFT Hereford n.d. www.clinks.org/sites/default/files/SHIFT%20Hereforshire%20ToC.pdf (accessed 1 December 2014).
- Institutional Arrangements for Promoting and Enabling Social Farming in Ireland and Northern Ireland. Drumshanbo: Social Farming Across Borders; 2014.
- Stewart-Brown SL, Platt S, Tennant A, Maheswaran H, Parkinson J, Weich S, et al. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): a valid and reliable tool for measuring mental well-being in diverse populations and projects. J Epidemiol Community Health 2011;65:A38-A9. https://doi.org/10.1136/jech.2011.143586.86.
- Transforming Rehabilitation: Seventeenth Report of Session 2016–17. London: House of Commons; 2016.
- Howard P, Francis B, Soothill K, Humphreys L. OGRS 3: the Revised Offender Group Reconviction Scale. London: MoJ; 2009.
Appendix 1 Search strategy for the quality-of-life systematic review
The following databases were searched in November 2014:
-
ASSIA (via ProQuest): 1987 to current
-
CINAHL (via EBSCOhost): 1981 to current
-
The Campbell Library
-
Criminal Justice Abstracts (via EBSCOhost): 1830 to current
-
Conference Proceedings Citation Index – Science (Thomson Reuters’ Web of Science): 1990 to current
-
Conference Proceedings Citation Index – Social Science & Humanities (Thomson Reuters’ Web of Science): 1990 to current
-
EMBASE Classic and EMBASE (via Ovid): 1947 to 24 November 2014
-
ERIC (via ProQuest): 1966 to current
-
Francis (via EBSCOhost): 1972 to current
-
Global Health (Ovid): 1910 to week 46 2014
-
GreenFILE (via EBSCOhost): 1910 to current
-
MEDLINE (via Ovid): 1946 to week 2 November 2014
-
MEDLINE In-Process & Other Non-Indexed Citations (via Ovid): 24 November 2014
-
National Criminal Justice Reference Service Abstracts (via ProQuest): 1975 to current
-
PsycINFO (via Ovid): 1806 to week 3 November 2014
-
Sciences Citation Index (Thomson Reuters’ Web of Science): 1900 to current
-
Scopus (Elsevier B.V.): 1823 to current
-
SCIE: 1980 to current
-
SSCI (Thomson Reuters’ Web of Science): 1900 to current
-
Social Services Abstracts (via ProQuest): 1979 to current
-
Sociological Abstracts (via ProQuest): 1952 to current
-
Web of Science, SCI-EXPANDED, SSCI: 1900 to current.
Search strategies included the search concepts care farming and agricultural-based rehabilitation therapies. Subject headings and free-text words were identified for use in the search concepts by the information specialist and project team members. Further terms were identified and tested from known relevant papers. Experimental animal studies were removed from the search. There were no language or publication date restrictions.
Appendix 2 Preferred Reporting Items for Systematic Reviews and Meta-Analyses Checklist for the care farm mixed-method systematic review
| Section/topic | # | Checklist item | Reported on page number |
|---|---|---|---|
| Title | |||
| Title | 1 |
Identify the report as a systematic review, meta-analysis or both: The impact of care farms on quality of life among disadvantages populations: a systematic review |
p. 7 |
| Abstract | |||
| Structured summary | 2 | Provide a structured summary including, as applicable: background; objectives; data sources; study eligibility criteria, participants and interventions; study appraisal and synthesis methods; results; limitations; conclusions and implications of key findings; systematic review registration number | p. xix |
| Introduction | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known | p. 7 |
| Objectives | 4 | Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons, outcomes and study design (PICOS) | p. 7 |
| Methods | |||
| Protocol and registration | 5 | Indicate if a review protocol exists, if and where it can be accessed (e.g. web address), and, if available, provide registration information including registration number | p. 7 |
| Eligibility criteria | 6 | Specify study characteristics (e.g. PICOS, length of follow-up) and report characteristics (e.g. years considered, language, publication status) used as criteria for eligibility, giving rationale | p. 8 |
| Information sources | 7 | Describe all information sources (e.g. databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched | pp. 8–9, and Appendix 1 |
| Search | 8 | Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated | Appendix 1 |
| Study selection | 9 | State the process for selecting studies (i.e. screening, eligibility, included in systematic review, and, if applicable, included in the meta-analysis) | p. 8, Chapter 2, Inclusion and Exclusion |
| Data collection process | 10 | Describe method of data extraction from reports (e.g. piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators | p. 9, Chapter 2, Study selection, data extraction and management |
| Data items | 11 | List and define all variables for which data were sought (e.g. PICOS, funding sources) and any assumptions and simplifications made | pp. 9–10, Chapter 2, Study selection, data extraction and management |
| Risk of bias in individual studies | 12 | Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis | p. 10, Chapter 2, Quality assessments and Assessment of reporting biases |
| Summary measures | 13 | State the principal summary measures (e.g. risk ratio, difference in means) | pp. 10–11 |
| Synthesis of results | 14 | Describe the methods of handling data and combining results of studies, if done, including measures of consistency (e.g. I2) for each meta-analysis | pp. 10–11, Chapter 2, Data synthesis |
Appendix 3 Data sharing agreements
Information sharing agreements with probation services
Initially, creating ISAs with probation services meant developing three ISAs; however, the split in probation into the NPS and the individual CRCs meant that the process became more complex. The ISAs that had been developed with probation services prior to the split remained with the CRCs. For probation service users who were moved to the NPS, a one-off memorandum of understanding was developed with NOMS. In centre 1, access to NPS offender data was no longer possible; therefore, these data were obtained from NOMS. In centre 2, a lack of progress with recruitment and high staff turnover in probation meant that the ISA was not developed. Instead we sought nDelius data directly from NOMS. In centre 3, the IT service at the CRC was able to access NPS offender data and provided nDelius data for all study participants apart from those they were unable to trace (through name and date of birth). See Figure 13 for the data acquisition timeline.
FIGURE 13.
Timeline for data acquisition. The light blue line denotes the point that probation split into CRCs and NPS. Planned targets were n = 300 recruitment (centre 1: CF, n = 60; comparator, n = 60), (centre 3: CF, n = 45; comparator, n = 45; centre 2: CF, n = 45; comparator, n = 45). n = 180 were followed up (40% loss).
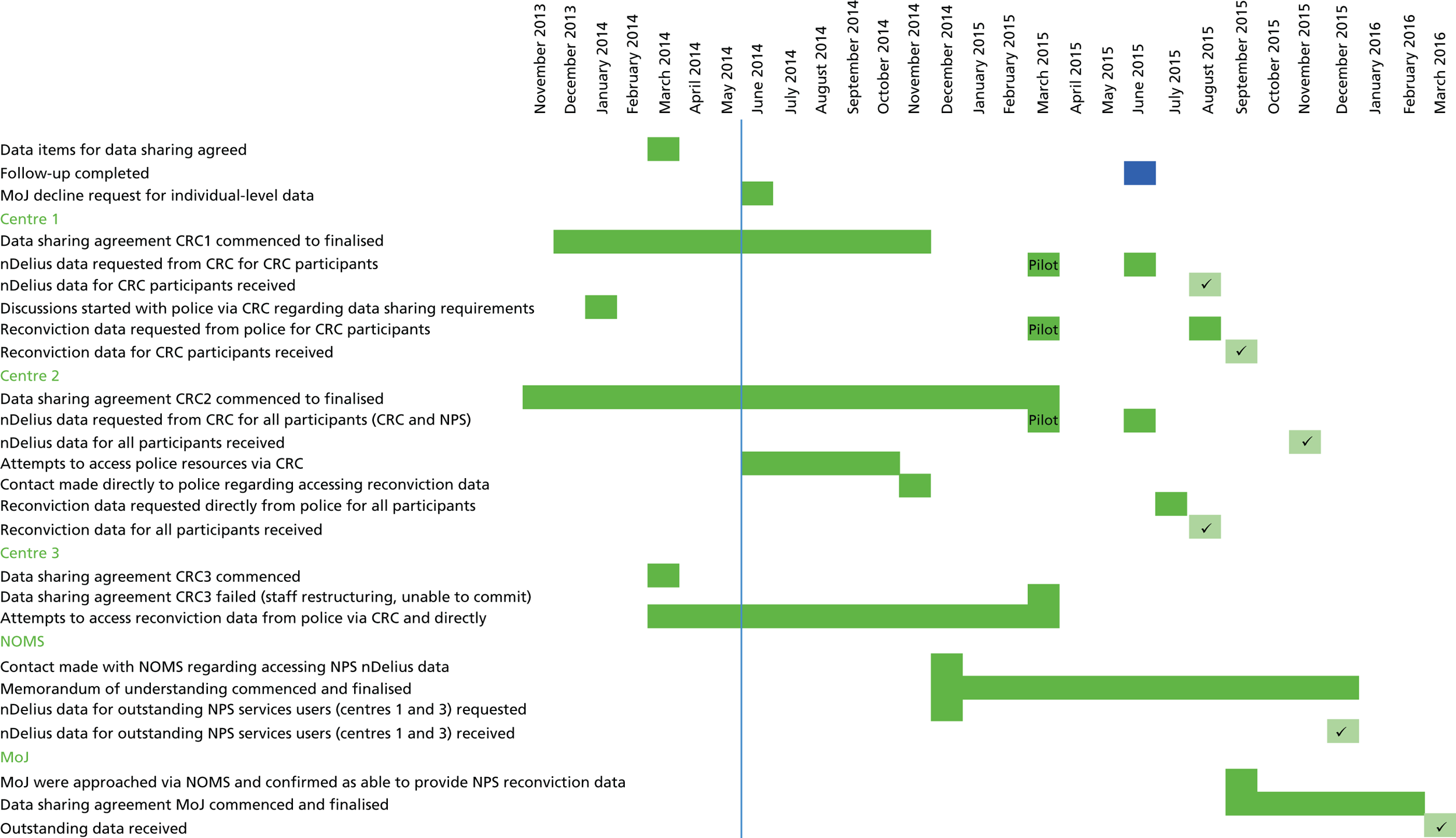
Obtaining data from the Police National Computer
Based on the premise that it was a national system, we approached the MoJ to identify if reconviction data could be obtained from one source. This was requested prior to any recruitment. At the time, the MoJ were piloting the ‘DataLab’, which held aggregated offending history data, and it was suggested that this could be used as a source of outcome data for the comparator group. As the DataLab did not hold WEMWBS outcome data and it did not allow access to individual-level data for the identification of potential confounders, we could not use this source. The MoJ were subsequently willing to provide anonymised individual-level data, but were unable to commit the time required to develop a data sharing agreement and so our request was declined. As a consequence, we approached the police services linked with each of the three probation services.
In centre 1, the local probation service held an existing ISA with the local police force. The request for reconviction data therefore went through the local probation service (with which we held an ISA). At the time of request, the probation service had already become the CRC and it did not have access to NPS offender data. Its request to the police (from us) contained only the PNC numbers for CRC probation service users. Therefore, PNC data from this source did not include NPS reconviction data.
At centre 2, a local police disclosure manager contacted us regarding what he understood to be the development of a nationwide ISA between the Department of Health and the police. After clarification about the nature of our study, the development of an ISA was provisionally agreed. Over a number of months, however, no progress was made despite attempts, and as there was lack of progress in recruiting probation service users at this site the decision was taken not to pursue the ISA further.
At centre 3, we tried a number of routes to access reconviction data. The approach used in centre 1 did not work in centre 3. Our contact in probation identified the business development manager as being the appropriate person to liaise with the PNC manager within the local police force. Unfortunately, our request for access to data was declined. We subsequently approached a contact in the police and crime commissioners office; however, this attempt proved fruitless as well. We finally identified an information request service on the police website and our request was approved. As we were able to provide written proof of consent to access criminal record data, the information service considered that an ISA would not be required. The service was also satisfied that data could be transferred safely, as we had acquired an account with the criminal justice secure e-mail system. Data provided at this centre included both NPS and CRC reconviction data.
Having developed a memorandum of understanding with NOMS for the nDelius data, we enquired about the possibility of obtaining reconviction data on NPS probation service users. This time the MoJ agreed to develop an ISA. Data on all service users that could not be found through other sources were subsequently requested from the MoJ. PNC numbers provided by NOMS were used to request reconviction data from the MoJ. Ten per cent of probation service users could not be found on the MoJ system, despite all unique PNC identifiers being checked. We have, however, clarified that future reconviction data could be obtained from MoJ with the development of a single ISA. The time taken to develop the ISAs for all sites is substantial, so early planning is essential.
Appendix 4 Full tables from statistical analysis of pilot (see Chapter 4)
| Characteristic | Valid number | Allocated to CF (all sites, N = 134) | Meana or %b (95% CI) difference between CO allocation | Difference in categories between CO allocation, p-valuec | |
|---|---|---|---|---|---|
| No (n = 84) | Yes (n = 50) | ||||
| Demographics | |||||
| Age (years) at recruitmenta | 134 | 32 (25.5 to 41) | 33 (25 to 41) | 1 (–3.57 to 5.57) | |
| Gender: female | 134 | 37 (44.1) | 2 (4) | < 0.001 | |
| IMD | |||||
| Quintiles within cohort | 132 | 0.08 | |||
| 1 – most deprived | 22 (26.2) | 5 (10.4) | |||
| 2 | 16 (19.1) | 10 (20.8) | |||
| 3 | 12 (14.3) | 15 (31.3) | |||
| 4 | 16 (19.1) | 10 (20.8) | |||
| 5 – least deprived | 18 (21.4) | 8 (16.7) | |||
| English quintiles | 132 | 0.83 | |||
| 1 – most deprived | 39 (46.4) | 22 (45.8) | |||
| 2 | 18 (21.4) | 11 (22.9) | |||
| 3 | 11 (13.1) | 9 (18.8) | |||
| 4 | 9 (10.7) | 4 (8.3) | |||
| 5 – least deprived | 7 (8.3) | 2 (4.2) | |||
| Employment status | 130 | 0.5 | |||
| Full-time employed, self-employed, in education or training | 20 (25) | 13 (26) | |||
| Part-time employed or self-employed | 13 (16.3) | 4 (8) | |||
| Unemployed or unable to work | 32 (40) | 25 (50) | |||
| Other | 15 (18.8) | 8 (16) | |||
| Ethnic group | 134 | 0.07 | |||
| White British | 57 (67.9) | 44 (88) | |||
| White: other | 3 (3.6) | 2 (4) | |||
| Asian or Asian British | 5 (6) | 1 (2) | |||
| Black or black British | 11 (13.1) | 1 (2) | |||
| Other or mixed | 8 (9.5) | 2 (4) | |||
| Probation type | 134 | 0.5 | |||
| CRC | 66 (78.6) | 42 (84) | |||
| NPS | 18 (21.4) | 8 (16) | |||
| Outcomes from questionnaires | |||||
| CORE-OM scorea | 93 | 7.1 (3.8 to 12.1) | 7.4 (3.5 to 15.15) | 0.3 (–4.1 to 4.7) | |
| CORE-OM category | 93 | ||||
| Healthy | 56 (91.8) | 28 (87.5) | 0.49 | ||
| Low level | 5 (8.2) | 4 (12.5) | |||
| CORE-OM number of missing questionsb | 134 | 0 (0 to 1) | 0 (0 to 24) | 138.88 (21.3 to 370.4) | |
| WEMWBS scorea | 124 | 52 (44 to 57) | 51 (43 to 55) | –1 (–6.9 to 4.9) | |
| Connected to nature scorea | 130 | 3.67 (2.67 to 4.17) | 3.42 (2.83 to 4.17) | –0.34 (–0.76 to 0.08) | |
| Connecting with nature (nature relatedness scale) | 111 | 0.97 | |||
| 1 – least interconnected | 6 (8.5) | 4 (10) | |||
| 2 | 13 (18.3) | 7 (17.5) | |||
| 3 | 18 (25.4) | 12 (30) | |||
| 4 | 19 (26.8) | 9 (22.5) | |||
| 5 – most interconnected | 15 (21.1) | 8 (20) | |||
| Health and lifestyle questions | |||||
| Number of days of ≥ 30 minutes’ physical activity in the last weekb | 125 | 4 (1 to 7) | 4 (3 to 7) | 9.81 (–9.04 to 32.58) | |
| Used substances during the past 4 weeks: yes | 122 | 18 (24) | 22 (46.8) | 0.01 | |
| Number of substances used during the past 4 weeksb | 122 | 0 (0 to 0) | 0 (0 to 1) | 54.43 (–7.47 to 157.74) | |
| Cannabis: yes | 117 | 12 (16.4) | 15 (34.1) | 0.04 | |
| Amphetamines: yes | 104 | 2 (2.9) | 0 (0) | 0.55 | |
| Tranquillisers, sedatives and antidepressants: yes | 108 | 6 (8.6) | 6 (15.8) | 0.34 | |
| Heroin: yes | 106 | 1 (1.4) | 2 (5.6) | 0.27 | |
| Methadone: yes | 108 | 2 (2.9) | 5 (13.2) | 0.09 | |
| Crack: yes | 106 | 2 (2.9) | 1 (2.7) | 1 | |
| Cocaine: yes | 107 | 5 (7.1) | 1 (2.7) | 0.66 | |
| Anabolic steroids: yes | 105 | 1 (1.5) | 0 (0) | 1 | |
| Number of days out of last 7 drank alcoholb | 103 | 2 (0 to 3) | 2 (0 to 4) | 18.43 (–24.04 to 84.66) | |
| Smoker: yes | 133 | 47 (56.6) | 39 (78) | 0.02 | |
| Number of cigarettes/roll-ups per dayb | 85 | 10 (8 to 20) | 15 (10 to 20) | 5.22 (–16.67 to 32.86) | |
| ‘Healthy foods are enjoyable’: strongly agree | 131 | 43 (52.4) | 13 (26.5) | 0.003 | |
| Agree | 29 (35.4) | 18 (36.7) | |||
| Neither agree nor disagree | 9 (11) | 14 (28.6) | |||
| Disagree | 0 (0) | 2 (4.1) | |||
| Strongly disagree | 1 (1.2) | 2 (4.1) | |||
| Health and social service use | |||||
| Number of health services (out of 10) used during the past monthb | 131 | 1 (0 to 1) | 0.5 (0 to 2) | 2.68 (–37.48 to 68.62) | |
| Used GP during the past month: yes | 129 | 38 (48.1) | 23 (46) | –d | |
| Number of times used GP in the past month | 50 | 1 (1 to 2) | 1 (1 to 2) | –d | |
| Used practice or district nurse during the past month: yes | 110 | 7 (10.5) | 3 (7) | –d | |
| Number of times used practice or district nurse in the past month | 6 | 1 (1 to 1) | 1.5 (1 to 2) | –d | |
| Used physiotherapist during the past month: yes | 108 | 5 (7.6) | 2 (4.8) | –d | |
| Number of times used physiotherapist in the past month | 5 | 1 (1 to 2.5) | 4 (4 to 4) | –d | |
| Used occupational therapist during the past month: yes | 105 | 1 (1.5) | 0 (0) | –d | |
| Number of times used occupational therapist in the past month | 1 | 1 (1 to 1) | – | –d | |
| Used psychiatrist during the past month: yes | 110 | 4 (6) | 5 (11.6) | –d | |
| Number of times used psychiatrist in the past month | 8 | 4 (1 to 4) | 1 (1 to 1) | –d | |
| Used mental health counsellor during the past month: yes | 111 | 3 (4.5) | 3 (6.8) | –d | |
| Number of times used mental health counsellor in the past month | 6 | 4 (1 to 31) | 2 (2 to 4) | –d | |
| Used drug and alcohol worker during the past month: yes | 123 | 7 (9.2) | 6 (12.8) | –d | |
| Number of times used drug and alcohol worker in the past month | 9 | 2.5 (1 to 4) | 2 (1 to 4) | –d | |
| Used family planning service during the past month: yes | 118 | 2 (2.7) | 1 (2.2) | –d | |
| Number of times used family planning service in the past month | 2 | 2 (2 to 2) | 2 (2 to 2) | –d | |
| Used health trainer during the past month: yes | 116 | 2 (2.8) | 2 (4.4) | –d | |
| Number of times used health trainer in the past month | 1 | 1 (1 to 1) | – | –d | |
| Used other health services during the past month: yes | 94 | 2 (3.6) | 0 (0) | –d | |
| Number of times used other health services in the past month | 1 | 1 (1 to 1) | – | –d | |
| Number of social services (out of four) used during the past monthb | 120 | 0 (0 to 0) | 0 (0 to 0) | 43.37 (–46.98 to 287.7) | |
| Used social worker during the past month: yes | 119 | 8 (11.1) | 8 (17) | –d | |
| Number of times used social worker in the past month | 13 | 2 (1 to 2) | 3 (2 to 4) | –d | |
| Used helpline during the past month: yes | 113 | 0 (0) | 0 (0) | –d | |
| Number of times used helpline in the past month | 0 | – | – | –d | |
| Used family or patient support or self-help groups during the past month: yes | 115 | 3 (4.2) | 2 (4.6) | –d | |
| Number of times used family or patient support or self-help groups in the past month | 4 | 19 (2 to 36) | 2 (1 to 3) | –d | |
| Used any other social services during the past month: yes | 114 | 2 (2.8) | 2 (4.7) | –d | |
| Number of times used any other social services in the past month | 4 | 4 (2 to 6) | 5.5 (1 to 10) | –d | |
| Number of medications prescribed by a doctor or other health-care professional in the past monthb | 134 | 0 (0 to 1) | 0 (0 to 0) | –32.09 (–69.11 to 49.34) | |
| Inpatient stay during the last month: yes | 127 | 1 (1.2) | 2 (4.4) | 0.3 | |
| Number of inpatient night’s stay during the last month | 3 | 3 (3 to 3) | 1.5 (1 to 2) | –d | |
| Visited outpatients during the last month: yes | 126 | 7 (8.8) | 3 (6.5) | 0.75 | |
| Number of outpatient visits during the last month | 9 | 2.5 (1 to 4) | 2 (1 to 6) | –d | |
| Visited A&E during the last month: yes | 126 | 5 (6.2) | 3 (6.7) | 1 | |
| Number of A&E visits during the last month | 8 | 1 (1 to 1) | 1 (1 to 2) | –d | |
| Question number and CF allocation | Valid number | Response, n (%) | ||||
|---|---|---|---|---|---|---|
| Not at all | Only occasionally | Sometimes | Often | Most of the time | ||
| CORE-OM | ||||||
| 1 | ||||||
| No | 133 | 54 (65.1) | 6 (7.2) | 15 (18.1) | 4 (4.8) | 4 (4.8) |
| Yes | 22 (44.0) | 8 (16.0) | 11 (22.0) | 7 (14.0) | 2 (4.0) | |
| 2 | ||||||
| No | 130 | 20 (25.0) | 26 (32.5) | 22 (27.5) | 8 (10.0) | 4 (5.0) |
| Yes | 15 (30.0) | 7 (14.0) | 16 (32.0) | 3 (6.0) | 9 (18.0) | |
| 3 | ||||||
| No | 131 | 22 (27.2) | 17 (21.0) | 13 (16.0) | 10 (12.3) | 19 (23.5) |
| Yes | 20 (40.0) | 9 (18.0) | 10 (20.0) | 6 (12.0) | 5 (10.0) | |
| 4 | ||||||
| No | 132 | 32 (38.6) | 15 (18.1) | 15 (18.1) | 11 (13.3) | 10 (12.0) |
| Yes | 14 (28.6) | 12 (24.5) | 9 (18.4) | 8 (16.3) | 6 (12.2) | |
| 5 | ||||||
| No | 131 | 31 (38.3) | 14 (17.3) | 18 (22.2) | 11 (13.6) | 7 (8.6) |
| Yes | 21 (42.0) | 11 (22.0) | 13 (26.0) | 4 (8.0) | 1 (2.0) | |
| 6 | ||||||
| No | 132 | 72 (87.8) | 5 (6.1) | 2 (2.4) | 3 (3.7) | 0 (0.0) |
| Yes | 46 (92.0) | 2 (4.0) | 1 (2.0) | 1 (2.0) | 0 (0.0) | |
| 7 | ||||||
| No | 131 | 30 (37.0) | 20 (24.7) | 15 (18.5) | 4 (4.9) | 12 (14.8) |
| Yes | 12 (24.0) | 13 (26.0) | 11 (22.0) | 8 (16.0) | 6 (12.0) | |
| 8 | ||||||
| No | 131 | 36 (44.4) | 8 (9.9) | 17 (21.0) | 10 (12.3) | 10 (12.3) |
| Yes | 18 (36.0) | 6 (12.0) | 16 (32.0) | 5 (10.0) | 5 (10.0) | |
| 9 | ||||||
| No | 133 | 68 (81.9) | 7 (8.4) | 3 (3.6) | 3 (3.6) | 2 (2.4) |
| Yes | 31 (62.0) | 5 (10.0) | 9 (18.0) | 4 (8.0) | 1 (2.0) | |
| 10 | ||||||
| No | 132 | 50 (61.0) | 6 (7.3) | 19 (23.2) | 4 (4.9) | 3 (3.7) |
| Yes | 23 (46.0) | 9 (18.0) | 11 (22.0) | 3 (6.0) | 4 (8.0) | |
| 11 | ||||||
| No | 108 | 47 (64.4) | 5 (6.8) | 12 (16.4) | 7 (9.6) | 2 (2.7) |
| Yes | 18 (51.4) | 4 (11.4) | 6 (17.1) | 0 (0.0) | 7 (20.0) | |
| 12 | ||||||
| No | 108 | 25 (34.2) | 13 (17.8) | 23 (31.5) | 7 (9.6) | 5 (6.8) |
| Yes | 17 (48.6) | 5 (14.3) | 6 (17.1) | 5 (14.3) | 2 (5.7) | |
| 13 | ||||||
| No | 109 | 45 (60.8) | 10 (13.5) | 9 (12.2) | 6 (8.1) | 4 (5.4) |
| Yes | 22 (62.9) | 3 (8.6) | 6 (17.1) | 4 (11.4) | 0 (0.0) | |
| 14 | ||||||
| No | 110 | 38 (50.7) | 16 (21.3) | 12 (16.0) | 7 (9.3) | 2 (2.7) |
| Yes | 19 (54.3) | 2 (5.7) | 11 (31.4) | 3 (8.6) | 0 (0.0) | |
| 15 | ||||||
| No | 110 | 55 (73.3) | 6 (8.0) | 8 (10.7) | 5 (6.7) | 1 (1.3) |
| Yes | 26 (74.3) | 1 (2.9) | 4 (11.4) | 3 (8.6) | 1 (2.9) | |
| 16 | ||||||
| No | 110 | 71 (94.7) | 1 (1.3) | 2 (2.7) | 1 (1.3) | 0 (0.0) |
| Yes | 30 (85.7) | 1 (2.9) | 3 (8.6) | 0 (0.0) | 1 (2.9) | |
| 17 | ||||||
| No | 109 | 39 (52.0) | 16 (21.3) | 13 (17.3) | 4 (5.3) | 3 (4.0) |
| Yes | 19 (55.9) | 4 (11.8) | 4 (11.8) | 6 (17.6) | 1 (2.9) | |
| 18 | ||||||
| No | 110 | 26 (34.7) | 14 (18.7) | 18 (24.0) | 5 (6.7) | 12 (16.0) |
| Yes | 16 (45.7) | 4 (11.4) | 3 (8.6) | 8 (22.9) | 4 (11.4) | |
| 19 | ||||||
| No | 109 | 29 (39.2) | 18 (24.3) | 9 (12.2) | 6 (8.1) | 12 (16.2) |
| Yes | 13 (37.1) | 12 (34.3) | 4 (11.4) | 0 (0.0) | 6 (17.1) | |
| 20 | ||||||
| No | 109 | 34 (45.9) | 8 (10.8) | 23 (31.1) | 5 (6.8) | 4 (5.4) |
| Yes | 17 (48.6) | 3 (8.6) | 8 (22.9) | 4 (11.4) | 3 (8.6) | |
| 21 | ||||||
| No | 109 | 35 (47.3) | 18 (24.3) | 16 (21.6) | 2 (2.7) | 3 (4.1) |
| Yes | 13 (37.1) | 11 (31.4) | 9 (25.7) | 1 (2.9) | 1 (2.9) | |
| 22 | ||||||
| No | 109 | 66 (89.2) | 3 (4.1) | 4 (5.4) | 1 (1.4) | 0 (0.0) |
| Yes | 30 (85.7) | 0 (0.0) | 3 (8.6) | 2 (5.7) | 0 (0.0) | |
| 23 | ||||||
| No | 110 | 50 (66.7) | 10 (13.3) | 7 (9.3) | 7 (9.3) | 1 (1.3) |
| Yes | 23 (65.7) | 1 (2.9) | 6 (17.1) | 2 (5.7) | 3 (8.6) | |
| 24 | ||||||
| No | 109 | 62 (83.8) | 6 (8.1) | 3 (4.1) | 2 (2.7) | 1 (1.4) |
| Yes | 26 (74.3) | 2 (5.7) | 4 (11.4) | 1 (2.9) | 2 (5.7) | |
| 25 | ||||||
| No | 110 | 44 (58.7) | 13 (17.3) | 12 (16.0) | 3 (4.0) | 3 (4.0) |
| Yes | 15 (42.9) | 7 (20.0) | 7 (20.0) | 3 (8.6) | 3 (8.6) | |
| 26 | ||||||
| No | 109 | 60 (80.0) | 1 (1.3) | 7 (9.3) | 4 (5.3) | 3 (4.0) |
| Yes | 22 (64.7) | 3 (8.8) | 6 (17.6) | 0 (0.0) | 3 (8.8) | |
| 27 | ||||||
| No | 109 | 35 (46.7) | 14 (18.7) | 16 (21.3) | 7 (9.3) | 3 (4.0) |
| Yes | 14 (41.2) | 3 (8.8) | 11 (32.4) | 2 (5.9) | 4 (11.8) | |
| 28 | ||||||
| No | 109 | 44 (59.5) | 7 (9.5) | 8 (10.8) | 10 (13.5) | 5 (6.8) |
| Yes | 24 (68.6) | 1 (2.9) | 4 (11.4) | 4 (11.4) | 2 (5.7) | |
| 29 | ||||||
| No | 111 | 43 (56.6) | 13 (17.1) | 13 (17.1) | 6 (7.9) | 1 (1.3) |
| Yes | 16 (45.7) | 8 (22.9) | 7 (20.0) | 2 (5.7) | 2 (5.7) | |
| 30 | ||||||
| No | 104 | 18 (26.1) | 10 (14.5) | 21 (30.4) | 13 (18.8) | 7 (10.1) |
| Yes | 15 (42.9) | 6 (17.1) | 5 (14.3) | 3 (8.6) | 6 (17.1) | |
| 31 | ||||||
| No | 108 | 22 (30.1) | 21 (28.8) | 15 (20.5) | 5 (6.8) | 10 (13.7) |
| Yes | 9 (25.7) | 12 (34.3) | 6 (17.1) | 4 (11.4) | 4 (11.4) | |
| 32 | ||||||
| No | 109 | 21 (28.4) | 15 (20.3) | 17 (23.0) | 9 (12.2) | 12 (16.2) |
| Yes | 9 (25.7) | 6 (17.1) | 13 (37.1) | 5 (14.3) | 2 (5.7) | |
| 33 | ||||||
| No | 111 | 49 (64.5) | 11 (14.5) | 11 (14.5) | 4 (5.3) | 1 (1.3) |
| Yes | 26 (74.3) | 3 (8.6) | 3 (8.6) | 2 (5.7) | 1 (2.9) | |
| 34 | ||||||
| No | 111 | 71 (93.4) | 2 (2.6) | 0 (0.0) | 3 (3.9) | 0 (0.0) |
| Yes | 29 (82.9) | 2 (5.7) | 3 (8.6) | 1 (2.9) | 0 (0.0) | |
| WEMWBS | ||||||
| 1 | ||||||
| No | 133 | 3 (3.6) | 6 (7.1) | 21 (25.0) | 35 (41.7) | 19 (22.6) |
| Yes | 1 (2.0) | 4 (8.2) | 17 (34.7) | 20 (40.8) | 7 (14.3) | |
| 2 | ||||||
| No | 132 | 3 (3.7) | 11 (13.4) | 18 (22.0) | 31 (37.8) | 19 (23.2) |
| Yes | 1 (2.0) | 6 (12.0) | 17 (34.0) | 20 (40.0) | 6 (12.0) | |
| 3 | ||||||
| No | 132 | 2 (2.4) | 15 (18.1) | 37 (44.6) | 17 (20.5) | 12 (14.5) |
| Yes | 2 (4.1) | 9 (18.4) | 16 (32.7) | 17 (34.7) | 5 (10.2) | |
| 4 | ||||||
| No | 133 | 0 (0.0) | 11 (13.3) | 22 (26.5) | 33 (39.8) | 17 (20.5) |
| Yes | 2 (4.0) | 11 (22.0) | 13 (26.0) | 16 (32.0) | 8 (16.0) | |
| 5 | ||||||
| No | 132 | 6 (7.2) | 19 (22.9) | 34 (41.0) | 12 (14.5) | 12 (14.5) |
| Yes | 2 (4.1) | 12 (24.5) | 18 (36.7) | 10 (20.4) | 7 (14.3) | |
| 6 | ||||||
| No | 134 | 5 (6.0) | 10 (11.9) | 25 (29.8) | 26 (31.0) | 18 (21.4) |
| Yes | 2 (4.0) | 5 (10.0) | 19 (38.0) | 17 (34.0) | 7 (14.0) | |
| 7 | ||||||
| No | 133 | 1 (1.2) | 10 (12.0) | 25 (30.1) | 24 (28.9) | 23 (27.7) |
| Yes | 1 (2.0) | 5 (10.0) | 18 (36.0) | 15 (30.0) | 11 (22.0) | |
| 8 | ||||||
| No | 132 | 4 (4.8) | 8 (9.6) | 30 (36.1) | 26 (31.3) | 15 (18.1) |
| Yes | 3 (6.1) | 6 (12.2) | 17 (34.7) | 19 (38.8) | 4 (8.2) | |
| 9 | ||||||
| No | 132 | 0 (0.0) | 13 (15.5) | 28 (33.3) | 28 (33.3) | 15 (17.9) |
| Yes | 1 (2.1) | 4 (8.3) | 16 (33.3) | 21 (43.8) | 6 (12.5) | |
| 10 | ||||||
| No | 134 | 3 (3.6) | 12 (14.3) | 22 (26.2) | 29 (34.5) | 18 (21.4) |
| Yes | 0 (0.0) | 6 (12.0) | 21 (42.0) | 16 (32.0) | 7 (14.0) | |
| 11 | ||||||
| No | 134 | 0 (0.0) | 5 (6.0) | 15 (17.9) | 27 (32.1) | 37 (44.0) |
| Yes | 2 (4.0) | 2 (4.0) | 12 (24.0) | 15 (30.0) | 19 (38.0) | |
| 12 | ||||||
| No | 133 | 2 (2.4) | 8 (9.6) | 20 (24.1) | 25 (30.1) | 28 (33.7) |
| Yes | 1 (2.0) | 3 (6.0) | 15 (30.0) | 19 (38.0) | 12 (24.0) | |
| 13 | ||||||
| No | 134 | 2 (2.4) | 12 (14.3) | 18 (21.4) | 23 (27.4) | 29 (34.5) |
| Yes | 1 (2.0) | 5 (10.0) | 10 (20.0) | 19 (38.0) | 15 (30.0) | |
| 14 | ||||||
| No | 134 | 3 (3.6) | 9 (10.7) | 28 (33.3) | 23 (27.4) | 21 (25.0) |
| Yes | 2 (4.0) | 3 (6.0) | 17 (34.0) | 19 (38.0) | 9 (18.0) | |
| Connecting with nature | ||||||
| 1 | ||||||
| No | 133 | 20 (24.1) | 13 (15.7) | 22 (26.5) | 17 (20.5) | 11 (13.3) |
| Yes | 5 (10.0) | 9 (18.0) | 15 (30.0) | 8 (16.0) | 13 (26.0) | |
| 2 | ||||||
| No | 134 | 4 (4.8) | 14 (16.7) | 12 (14.3) | 30 (35.7) | 24 (28.6) |
| Yes | 2 (4.0) | 7 (14.0) | 11 (22.0) | 22 (44.0) | 8 (16.0) | |
| 3 | ||||||
| No | 134 | 15 (17.9) | 11 (13.1) | 18 (21.4) | 25 (29.8) | 15 (17.9) |
| Yes | 11 (22.0) | 11 (22.0) | 14 (28.0) | 8 (16.0) | 6 (12.0) | |
| 4 | ||||||
| No | 134 | 5 (6.0) | 8 (9.5) | 14 (16.7) | 22 (26.2) | 35 (41.7) |
| Yes | 3 (6.0) | 3 (6.0) | 8 (16.0) | 13 (26.0) | 23 (46.0) | |
| 5 | ||||||
| No | 131 | 8 (9.6) | 13 (15.7) | 13 (15.7) | 27 (32.5) | 22 (26.5) |
| Yes | 5 (10.4) | 7 (14.6) | 17 (35.4) | 6 (12.5) | 13 (27.1) | |
| 6 | ||||||
| No | 134 | 8 (9.5) | 9 (10.7) | 13 (15.5) | 24 (28.6) | 30 (35.7) |
| Yes | 3 (6.0) | 7 (14.0) | 17 (34.0) | 14 (28.0) | 9 (18.0) | |
| Characteristic | Site | p-value for interaction between CO allocation and sitea,b | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 (N = 91) | 2 (N = 4) | 3 (N = 39) | ||||||||
| n | CF | n | CF | n | CF | |||||
| No (n = 61) | Yes (n = 30) | No (n = 2) | Yes (n = 2) | No (n = 21) | Yes (n = 18) | |||||
| Demographics | ||||||||||
| Age (years) at recruitmenta | 91 | 31 (25 to 37) | 33.5 (25 to 43) | 4 | 37.5 (35 to 40) | 44.5 (38 to 51) | 39 | 42 (26 to 53) | 29 (23 to 37) | 0.02 |
| Gender: female | 91 | 26 (42.6) | 0 (0) | 4 | 2 (100) | 0 (0) | 39 | 9 (42.9) | 2 (11.1) | –c |
| IMD: quintiles within cohort | 91 | –c | ||||||||
| 1 – most deprived | 22 (36.1) | 3 (10) | 4 | – | – | 37 | 0 (0) | 2 (12.5) | ||
| 2 | 15 (24.6) | 8 (26.7) | – | – | 1 (4.8) | 2 (12.5) | ||||
| 3 | 8 (13.1) | 12 (40) | – | – | 4 (19) | 3 (18.8) | ||||
| 4 | 6 (9.8) | 5 (16.7) | 2 (100) | 1 (50) | 8 (38.1) | 4 (25) | ||||
| 5 – least deprived | 10 (16.4) | 2 (6.7) | - | 1 (50) | 8 (38.1) | 5 (31.3) | ||||
| IMD: English quintiles | 91 | –c | ||||||||
| 1 – most deprived | 38 (62.3) | 18 (60) | 4 | – | – | 37 | 1 (4.8) | 4 (25) | ||
| 2 | 9 (14.8) | 7 (23.3) | 1 (50) | – | 8 (38.1) | 4 (25) | ||||
| 3 | 5 (8.2) | 4 (13.3) | 1 (50) | 1 (50) | 5 (23.8) | 4 (25) | ||||
| 4 | 5 (8.2) | 1 (3.3) | – | – | 4 (19) | 3 (18.8) | ||||
| 5 – least deprived | 4 (6.6) | 0 (0) | – | 1 (50) | 3 (14.3) | 1 (6.3) | ||||
| Employment status | 89 | –c | ||||||||
| Full-time employed, self-employed, education or training | 15 (25.4) | 12 (40) | 4 | 1 (50) | 1 (50) | 37 | 4 (21.1) | 0 (0) | ||
| Part-time employed or self-employed | 10 (16.9) | 2 (6.7) | 1 (50) | – | 2 (10.5) | 2 (11.1) | ||||
| Unemployed or unable to work | 24 (40.7) | 10 (33.3) | – | 1 (50) | 8 (42.1) | 14 (77.8) | ||||
| Other | 10 (16.9) | 6 (20) | – | – | 5 (26.3) | 2 (11.1) | ||||
| Ethnic group | 91 | –c | ||||||||
| White British | 37 (60.7) | 25 (83.3) | 4 | 1 (50) | 2 (100) | 39 | 19 (90.5) | 17 (94.4) | ||
| White: other | 2 (3.3) | 2 (6.7) | – | – | 1 (4.8) | 0 (0) | ||||
| Asian or Asian British | 5 (8.2) | 1 (3.3) | – | – | – | – | ||||
| Black or black British | 11 (18) | 1 (3.3) | – | – | – | – | ||||
| Other or mixed | 6 (9.8) | 1 (3.3) | 1 (50) | – | 1 (4.8) | 1 (5.6) | ||||
| Probation type | 91 | –c | ||||||||
| CRC | 43 (70.5) | 22 (73.3) | 4 | 2 (100) | 2 (100) | 39 | 21 (100) | 18 (100) | ||
| NPS | 18 (29.5) | 8 (26.7) | – | – | – | – | ||||
| Outcomes from questionnaires | ||||||||||
| CORE-OM scorea | 58 | 7.1 (3.8 to 12.6) | 5.6 (3.5 to 9.4) | 3 | 21.2 (21.2 to 21.2) | 2.8 (2.4 to 3.2) | 32 | 7.1 (3.8 to 11.5) | 15.3 (7.4 to 19.7) | 0.04 |
| CORE-OM category | 58 | –c | ||||||||
| Healthy | 38 (92.7) | 16 (94.1) | 3 | – | 2 (100) | 32 | 18 (94.7) | 10 (76.9) | ||
| Low level | 3 (7.3) | 1 (5.9) | 1 (100) | – | 1 (5.3) | 3 (23.1) | ||||
| CORE-OM number of missing questions | 91 | 0 (0 to 1) | 0 (0 to 24) | 4 | 14 (0 to 28) | 0 (0 to 0) | 39 | 0 (0 to 0) | 0 (0 to 1) | –c |
| WEMWBS scorea | 83 | 51.5 (44.5 to 56) | 54 (47 to 59) | 4 | 54.5 (42 to 67) | 63 (56 to 70) | 37 | 52 (40 to 58) | 45 (38.5 to 47) | 0.07 |
| Connected to nature scorea | 87 | 3.5 (2.5 to 4.17) | 3.6 (2.9 to 4.17) | 4 | 4.17 (4.0 to 4.33) | 4.25 (3.67 to 4.83) | 39 | 3.83 (3.33 to 4) | 3 (2.67 to 3.67) | 0.16 |
| Connecting with nature (nature relatedness scale) | 77 | –c | ||||||||
| 1 – least interconnected | 6 (11.8) | 3 (11.5) | 4 | – | – | – | 0 (0) | 1 (8.3) | ||
| 2 | 11 (21.6) | 5 (19.2) | – | – | – | 2 (11.1) | 2 (16.7) | |||
| 3 | 12 (23.5) | 7 (26.9) | 1 (50) | – | 5 (27.8) | 5 (41.7) | ||||
| 4 | 12 (23.5) | 6 (23.1) | 1 (50) | 1 (50) | 6 (33.3) | 2 (16.7) | ||||
| 5 – most interconnected | 10 (19.6) | 5 (19.2) | – | 1 (50) | 5 (27.8) | 2 (16.7) | ||||
| Health and lifestyle questions | ||||||||||
| Number of days of ≥ 30 minutes’ physical activity in the last weekb | 85 | 3 (1 to 6) | 5 (2 to 7) | 4 | 4.5 (2 to 7) | 3.5 (1 to 6) | 36 | 5 (4 to 7) | 3 (3 to 7) | 0.02 |
| Used substances during the past 4 weeks: yes | 82 | 16 (29.6) | 10 (35.7) | 4 | 2 (100) | 2 (100) | 36 | 2 (10.5) | 12 (70.6) | –c |
| Number of substances used during the past 4 weeks | 82 | 0 (0 to 1) | 0 (0 to 1) | 4 | 0 (0 to 0) | 0 (0 to 0) | 36 | 0 (0 to 0) | 1 (0 to 2) | –c |
| Cannabis: yes | 81 | 11 (20.8) | 9 (32.1) | 4 | 0 (–) | 0 (–) | 32 | 1 (5.6) | 6 (42.9) | –c |
| Amphetamines: yes | 73 | 2 (4.1) | 0 (0) | 4 | 0 (–) | 0 (–) | 27 | 0 (–) | 0 (–) | –c |
| Tranquillisers, sedatives and antidepressants: yes | 74 | 5 (10) | 1 (4.2) | 4 | 0 (–) | 0 (–) | 30 | 1 (5.6) | 5 (41.7) | –c |
| Heroin: yes | – | – | – | 4 | 0 (–) | 0 (–) | 29 | 1 (5.3) | 2 (20) | –c |
| Methadone: yes | 73 | 1 (2) | 0 (0) | 4 | 0 (–) | 0 (–) | 31 | 1 (5.3) | 5 (41.7) | –c |
| Crack: yes | 73 | 2 (4.1) | 0 (0) | 4 | 0 (–) | 0 (–) | 29 | 0 (0) | 1 (9.1) | –c |
| Cocaine: yes | 75 | 5 (10) | 1 (4) | 4 | 0 (–) | 0 (–) | 28 | – | – | –c |
| Anabolic steroids: yes | – | – | – | 4 | 0 (–) | 0 (–) | 28 | 1 (5.6) | 0 (0) | –c |
| Number of days out of last 7 drank alcoholb | 65 | 2 (0 to 3) | 1 (0 to 3) | 4 | 5.5 (4 to 7) | 1.5 (1 to 2) | 34 | 1 (0 to 2) | 3 (1 to 5) | 0.2 |
| Smoker: yes | 90 | 31 (51.7) | 20 (66.7) | 4 | 2 (100) | 2 (100) | 39 | 14 (66.7) | 17 (94.4) | –c |
| Number of cigarettes/roll-ups per dayb | 51 | 10 (8 to 15) | 15 (10 to 20) | 4 | 12.5 (10 to 15) | 10 (10 to 10) | 30 | 15 (10 to 20) | 15 (10 to 20) | 0.15 |
| ‘Healthy foods are enjoyable’ | 89 | –c | ||||||||
| Strongly agree | 32 (53.3) | 9 (31) | 4 | – | 2 (100) | 38 | 11 (55) | 2 (11.1) | ||
| Agree | 21 (35) | 13 (44.8) | 2 (100) | – | 6 (30) | 5 (27.8) | ||||
| Neither agree nor disagree | 6 (10) | 5 (17.2) | – | – | 3 (15) | 9 (50) | ||||
| Disagree | – | – | – | – | 0 (0) | 2 (11.1) | ||||
| Strongly disagree | 1 (1.7) | 2 (6.9) | – | – | – | – | ||||
| Health and social service use | ||||||||||
| Number of health services (out of 10) used during the past monthb | 90 | 0.5 (0 to 1) | 0 (0 to 1) | 4 | 1 (1 to 1) | 0.5 (0 to 1) | 37 | 1 (0 to 2) | 1.5 (1 to 2) | 0.08 |
| Number of social services (out of four) used during the past month | 84 | 0 (0 to 0) | 0 (0 to 0) | 4 | 0 (0 to 0) | 0 (0 to 0) | 32 | 0 (0 to 0) | 0 (0 to 1) | –c |
| Number of medications prescribed by a doctor or other health-care professional in the past month | 91 | 0 (0 to 0) | 0 (0 to 0) | 4 | 0 (0 to 0) | 0 (0 to 0) | 39 | 0 (0 to 1) | 0 (0 to 1) | –c |
| Inpatient stay during the last month: yes | 88 | 0 (0) | 1 (3.4) | 4 | 0 (–) | 0 (–) | 35 | 1 (5) | 1 (6.7) | –c |
| Number of inpatient night’s stay during the last month | 1 | – | 1 (1 to 1) | 0 | – | – | 2 | 3 (3 to 3) | 2 (2 to 2) | –c |
| Visited outpatients during the last month: yes | 88 | 5 (8.5) | 1 (3.4) | 4 | 0 (–) | 0 (–) | 34 | 2 (10.5) | 2 (13.3) | –c |
| Number of outpatient visits during the last month | 6 | 3 (2 to 4) | 2 (2 to 2) | 0 | – | – | 3 | 1 (1 to 1) | 3.5 (1 to 6) | –c |
| Visited A&E during the last month: yes | 89 | 4 (6.7) | 2 (6.9) | 4 | 0 (–) | 0 (–) | 33 | 1 (5.3) | 1 (7.1) | –c |
| Number of A&E visits during the last month | 6 | 1 (1 to 2.5) | 1 (1 to 1) | 0 | – | – | 2 | 1 (1 to 1) | 2 (2 to 2) | –c |
| Characteristic | Valid number | Followed up | Meana or percentageb (95% CI) difference between follow-up | Difference in categories between follow-up, p-valuec | |
|---|---|---|---|---|---|
| No (n = 64) | Yes (n = 70) | ||||
| Demographics | |||||
| CF: yes | 134 | 24 (37.5) | 27 (38.6) | 1 | |
| Age (years) at recruitmenta | 134 | 29 (23.5 to 37) | 34.5 (27 to 45) | 6 (2.59 to 9.41) | |
| Gender: female | 134 | 15 (23.4) | 24 (34.3) | 0.19 | |
| IMD: quintiles within cohort | |||||
| 1 – most deprived | 132 | 12 (19.1) | 15 (21.7) | 0.73 | |
| 2 | 14 (22.2) | 12 (17.4) | |||
| 3 | 15 (23.8) | 12 (17.4) | |||
| 4 | 12 (19.1) | 14 (20.3) | |||
| 5 – least deprived | 10 (15.9) | 16 (23.2) | |||
| IMD: English quintiles | |||||
| 1 – most deprived | 132 | 30 (47.6) | 31 (44.9) | 0.42 | |
| 2 | 14 (22.2) | 15 (21.7) | |||
| 3 | 12 (19.1) | 8 (11.6) | |||
| 4 | 5 (7.9) | 8 (11.6) | |||
| 5 – least deprived | 2 (3.2) | 7 (10.1) | |||
| Employment status | 130 | 0.51 | |||
| Full-time employed, self-employed, in education or training | 14 (22.6) | 19 (27.9) | |||
| Part-time employed or self-employed | 6 (9.7) | 11 (16.2) | |||
| Unemployed or unable to work | 31 (50) | 26 (38.2) | |||
| Other | 11 (17.7) | 12 (17.7) | |||
| Ethnic group | 134 | 0.19 | |||
| White British | 53 (82.8) | 48 (68.6) | |||
| White: other | 2 (3.1) | 3 (4.3) | |||
| Asian or Asian British | 3 (4.7) | 3 (4.3) | |||
| Black or black British | 2 (3.1) | 10 (14.3) | |||
| Other or mixed | 4 (6.3) | 6 (8.6) | |||
| Probation type | 134 | 0.002 | |||
| CRC | 59 (92.2) | 49 (70) | |||
| NPS | 5 (7.8) | 21 (30) | |||
| Outcomes from questionnaires | |||||
| CORE-OM scorea | 93 | 9.25 (3.8 to 15.3) | 6.8 (3.5 to 12.6) | –2.6 (–6.16 to 0.96) | |
| CORE-OM category | 93 | 0.32 | |||
| Healthy | 40 (87) | 44 (93.6) | |||
| Low level | 6 (13) | 3 (6.4) | |||
| CORE-OM number of missing questionsb | 134 | 0 (0 to 1.5) | 0 (0 to 1) | 11.02 (–48.34 to 138.58) | |
| WEMWBS scorea | 124 | 51 (42 to 56) | 51 (45 to 58) | 0 (–7.71 to 7.71) | |
| Connected to nature scorea | 130 | 3.5 (2.67 to 4) | 3.67 (2.83 to 4.17) | 0.17 (–0.26 to 0.6) | |
| Connecting with nature (nature relatedness scale) | 111 | 3 (5.8) | 7 (11.9) | 0.31 | |
| 1 – least interconnected | |||||
| 2 | 12 (23.1) | 8 (13.6) | |||
| 3 | 17 (32.7) | 13 (22) | |||
| 4 | 11 (21.2) | 17 (28.8) | |||
| 5 – most interconnected | 9 (17.3) | 14 (23.7) | |||
| Health and lifestyle questions | |||||
| Number of days of ≥ 30 minutes’ physical activity in the last weekb | 125 | 4 (2 to 6) | 4 (2 to 7) | 5.85 (–11.02 to 25.91) | |
| Used substances during the past 4 weeks: yes | 122 | 23 (40.4) | 17 (26.2) | 0.12 | |
| Number of substances used during the past 4 weeksb | 122 | 0 (0 to 1) | 0 (0 to 1) | –60.33 (–79.23 to –24.22) | |
| Cannabis: yes | 117 | 16 (30.2) | 11 (17.2) | 0.12 | |
| Amphetamines: yes | 104 | 1 (2.1) | 1 (1.8) | 1 | |
| Tranquillisers, sedatives and antidepressants: yes | 108 | 9 (18) | 3 (5.2) | 0.06 | |
| Heroin: yes | 106 | 2 (4.1) | 1 (1.8) | 0.59 | |
| Methadone: yes | 108 | 5 (10) | 2 (3.5) | 0.25 | |
| Crack: yes | 106 | 3 (6.1) | 0 (0) | 0.1 | |
| Cocaine: yes | 107 | 5 (10) | 1 (1.8) | 0.1 | |
| Anabolic steroids: yes | 105 | 1 (2.1) | 0 (0) | 0.46 | |
| Number of days out of last 7 drank alcoholb | 103 | 1.5 (0 to 4) | 2 (1 to 3) | 3.5 (–30.94 to 55.11) | |
| Smoker: yes | 133 | 48 (76.2) | 38 (54.3) | 0.01 | |
| Number of cigarettes/roll-ups per dayb | 85 | 11 (10 to 20) | 10 (8 to 20) | –7.53 (–25.17 to 14.27) | |
| ‘Healthy foods are enjoyable’ | 131 | 29 (46) | 27 (39.7) | 0.53 | |
| Strongly agree | |||||
| Agree | 21 (33.3) | 26 (38.2) | |||
| Neither agree nor disagree | 12 (19.1) | 11 (16.2) | |||
| Disagree | 1 (1.6) | 1 (1.5) | |||
| Strongly disagree | 0 (0) | 3 (4.4) | |||
| Health and social service use | |||||
| Number of health services (out of 10) used during the past monthb | 131 | 1 (0 to 2) | 0 (0 to 1) | –36.57 (–55.25 to –10.1) | |
| Used GP during the past month: yes | 129 | 35 (58.3) | 26 (37.7) | –d | |
| Number of times used GP in the past month | 50 | 1 (1 to 2) | 1 (1 to 2) | –d | |
| Used practice or district nurse during the past month: yes | 110 | 5 (11.1) | 5 (7.7) | –d | |
| Number of times used practice or district nurse in the past month | 6 | 1 (1 to 1.5) | 1 (1 to 1) | –d | |
| Used physiotherapist during the past month: yes | 108 | 5 (11.1) | 2 (3.2) | –d | |
| Number of times used physiotherapist in the past month | 5 | 2.5 (1 to 4) | 1 (1 to 1) | –d | |
| Used occupational therapist during the past month: yes | 105 | 0 (0) | 1 (1.6) | –d | |
| Number of times used occupational therapist in the past month | 1 | – | 1 (1 to 1) | –d | |
| Used psychiatrist during the past month: yes | 110 | 6 (12.5) | 3 (4.8) | –d | |
| Number of times used psychiatrist in the past month | 8 | 2 (1 to 4) | 1 (1 to 1) | –d | |
| Used mental health counsellor during the past month: yes | 111 | 4 (8.5) | 2 (3.1) | –d | |
| Number of times used mental health counsellor in the past month | 6 | 3 (1.5 to 17.5) | 3 (2 to 4) | –d | |
| Used drug and alcohol worker during the past month: yes | 123 | 8 (14.6) | 5 (7.4) | –d | |
| Number of times used drug and alcohol worker in the past month | 9 | 2 (1 to 4) | 3 (3 to 3) | –d | |
| Used family planning service during the past month: yes | 118 | 2 (3.9) | 1 (1.5) | –d | |
| Number of times used family planning service in the past month | 2 | 2 (2 to 2) | 2 (2 to 2) | –d | |
| Used health trainer during the past month: yes | 116 | 2 (3.9) | 2 (3.1) | –d | |
| Number of times used health trainer in the past month | 1 | – | 1 (1 to 1) | –d | |
| Used other health services during the past month: yes | 94 | 1 (2.4) | 1 (1.9) | –d | |
| Number of times used other health services in the past month | 1 | 1 (1 to 1) | – | –d | |
| Number of social services (out of four) used during the past monthb | 120 | 0 (0 to 0) | 0 (0 to 0) | –47.26 (–79.89 to 38.32) | |
| Used social worker during the past month: yes | 119 | 10 (18.9) | 6 (9.1) | –d | |
| Number of times used social worker in the past month | 13 | 2 (1 to 3) | 2.5 (1.5 to 6.5) | –d | |
| Used helpline during the past month: yes | 113 | 0 (0) | 0 (0) | –d | |
| Number of times used helpline in the past month | 0 | – | – | –d | |
| Used family or patient support or self-help groups during the past month: Yes | 115 | 3 (5.9) | 2 (3.1) | –d | |
| Number of times used family or patient support or self-help groups in the past month | 4 | 3 (1 to 36) | 2 (2 to 2) | –d | |
| Used any other social services during the past month: yes | 114 | 2 (4) | 2 (3.1) | –d | |
| Number of times used any other social services in the past month | 4 | 1.5 (1 to 2) | 8 (6 to 10) | –d | |
| Number of medications prescribed by a doctor or other health-care professional in the past monthb | 134 | 0 (0 to 1) | 0 (0 to 0) | 3.23 (–51.24 to 118.54) | |
| Inpatient stay during the last month: yes | 127 | 2 (3.4) | 1 (1.5) | 0.6 | |
| Number of inpatient night’s stay during the last month | 3 | 1.5 (1 to 2) | 3 (3 to 3) | –d | |
| Visited outpatients during the last month: yes | 126 | 5 (8.5) | 5 (7.5) | 1 | |
| Number of outpatient visits during the last month | 9 | 3.5 (2.5 to 5) | 1 (1 to 2) | –d | |
| Visited A&E during the last month: yes | 126 | 4 (6.7) | 4 (6.1) | 1 | |
| Number of A&E visits during the last month | 8 | 1 (1 to 1.5) | 1 (1 to 2.5) | –d | |
| Characteristic | Valid number | CF (all sites, N = 70) | Meana or %b (95% CI) difference between CO allocation | Difference in categories between CO allocation, p-valuec | |
|---|---|---|---|---|---|
| No (n = 43) | Yes (n = 27) | ||||
| Demographics | |||||
| Days to follow-up since baselinea | 70 | 105 (56 to 194) | 121 (68 to 233) | 16 (–64.09 to 96.09) | |
| Hours left on CO at follow-upa | 55 | 11 (4 to 18) | 3.45 (0 to 12) | –7.55 (–16.03 to 0.93) | |
| Proportion of CO left at follow-upa | 54 | 0.84 (0.76 to 0.93) | 0.91 (0.79 to 0.98) | 0.07 (–0.06 to 0.2) | |
| CO changed during follow-up: yes | 134 | 23 (27.4) | 26 (52) | 0.01 | |
| Employment status | 65 | 0.19 | |||
| Full-time employed, self-employed, in education or training | 7 (18) | 5 (19.2) | |||
| Part-time employed or self-employed | 10 (25.6) | 3 (11.5) | |||
| Unemployed or unable to work | 10 (25.6) | 13 (50) | |||
| Other | 12 (30.8) | 5 (19.2) | |||
| Outcomes from questionnaires | |||||
| CORE-OM scorea | 58 | 5.3 (2.1 to 11.5) | 9.4 (5 to 14.1) | 4.1 (0.63 to 7.57) | |
| CORE-OM category | 58 | 0.51 | |||
| Healthy | 33 (94.3) | 23 (100) | |||
| Low level | 2 (5.7) | 0 (0) | |||
| CORE-OM number of missing questionsb | 134 | 12 (0 to 34) | 1 (0 to 34) | –7.4 (–33.82 to 29.56) | |
| WEMWBS scorea | 66 | 53.5 (48 to 61) | 53 (48 to 56) | –1 (–4.49 to 2.49) | |
| Connected to nature scorea | 66 | 3.5 (3.17 to 4.17) | 3.67 (2.83 to 4.17) | 0.17 (–0.56 to 0.90) | |
| Connecting with nature (nature relatedness scale) | 57 | 0.24 | |||
| 1 – least interconnected | 2 (6.1) | 2 (8.3) | |||
| 2 | 3 (9.1) | 6 (25) | |||
| 3 | 9 (27.3) | 9 (37.5) | |||
| 4 | 11 (33.3) | 3 (12.5) | |||
| 5 – most interconnected | 8 (24.2) | 4 (16.7) | |||
| Health and lifestyle questions | |||||
| Number of days of ≥ 30 minutes’ physical activity in the last weekb | 69 | 5 (3 to 7) | 4 (1 to 5) | –18.91 (–42.53 to 14.42) | |
| Used substances during the past 4 weeks: yes | 62 | 5 (13.9) | 16 (61.5) | < 0.001 | |
| Number of substances used during the past 4 weeksb | 62 | 0 (0 to 0) | 1 (0 to 1) | 564.62 (165.79 to 1561.86) | |
| Cannabis: yes | 62 | 1 (2.8) | 13 (50) | –d | |
| Amphetamines: yes | 56 | 0 (0) | 1 (5) | –d | |
| Tranquillisers sedatives and antidepressants: yes | 56 | 1 (2.8) | 3 (15) | –d | |
| Heroin: yes | 56 | 0 (0) | 1 (5) | –d | |
| Methadone: yes | 56 | 0 (0) | 3 (15) | –d | |
| Crack: yes | 57 | 0 (0) | 0 (0) | –d | |
| Cocaine: yes | 56 | 0 (0) | 1 (4.8) | –d | |
| Anabolic steroids: yes | 57 | 0 (0) | 1 (4.6) | –d | |
| Number of days out of last 7 drank alcoholb | 55 | 2 (0 to 3) | 1.5 (1 to 4) | 41.67 (–15.16 to 136.56) | |
| Smoker: yes | 70 | 19 (44.2) | 16 (59.3) | 0.33 | |
| Number of cigarettes/roll-ups per dayb | 63 | 10 (7 to 20) | 20 (10 to 20) | 39.44 (–6.62 to 108.23) | |
| ‘Healthy foods are enjoyable’ | 69 | 0.03 | |||
| Strongly agree | 24 (57.1) | 6 (22.2) | |||
| Agree | 11 (26.2) | 11 (40.7) | |||
| Neither agree nor disagree | 6 (14.3) | 7 (25.9) | |||
| Disagree | 1 (2.4) | 2 (7.4) | |||
| Strongly disagree | 0 (0) | 1 (3.7) | |||
| Health and social service use | |||||
| Number of health services (out of 10) used during the past month | 68 | 0 (0 to 1) | 0 (0 to 1) | –d | |
| Used GP during the past month: yes | 67 | 17 (40.5) | 8 (32) | –d | |
| Number of times used GP in the past month | 21 | 1 (1 to 2) | 1 (1 to 2) | –d | |
| Used practice or district nurse during the past month: yes | 55 | 4 (11.8) | 0 (0) | –d | |
| Number of times used practice or district nurse in the past month | 3 | 2 (0 to 2) | – | –d | |
| Used physiotherapist during the past month: yes | 54 | 3 (9.1) | 1 (4.8) | –d | |
| Number of times used physiotherapist in the past month | 3 | 2 (2 to 2) | 2 (2 to 2) | –d | |
| Used occupational therapist during the past month: yes | 53 | 0 (0) | 0 (0) | –d | |
| Number of times used occupational therapist in the past month | 0 | – | – | –d | |
| Used psychiatrist during the past month: yes | 54 | 1 (3) | 1 (4.8) | –d | |
| Number of times used psychiatrist in the past month | 1 | 0 (0 to 0) | – | –d | |
| Used mental health counsellor during the past month: yes | 54 | 3 (9.1) | 1 (4.8) | –d | |
| Number of times used mental health counsellor in the past month | 4 | 1 (0 to 3) | 1 (1 to 1) | –d | |
| Used drug and alcohol worker during the past month: yes | 60 | 3 (8.6) | 5 (20) | –d | |
| Number of times used drug and alcohol worker in the past month | 4 | 2 (1 to 2) | 5 (5 to 5) | –d | |
| Used family planning service during the past month: yes | 60 | 0 (0) | 0 (0) | –d | |
| Number of times used family planning service in the past month | 0 | – | – | –d | |
| Used health trainer during the past month: yes | 58 | 3 (8.6) | 1 (4.4) | –d | |
| Number of times used health trainer in the past month | 2 | 2.5 (1 to 4) | – | –d | |
| Used other health services during the past month: yes | 50 | 2 (6.7) | 0 (0) | –d | |
| Number of times used other health services in the past month | 0 | – | – | –d | |
| Number of social services (out of four) used during the past month | 64 | 0 (0 to 0) | 0 (0 to 0) | –d | |
| Used social worker during the past month: yes | 61 | 1 (2.9) | 2 (7.7) | –d | |
| Number of times used social worker in the past month | 2 | 2 (2 to 2) | 3 (3 to 3) | –d | |
| Used helpline during the past month: yes | 61 | 0 (0) | 0 (0) | –d | |
| Number of times used helpline in the past month | 0 | – | – | –d | |
| Used family or patient support or self-help groups during the past month: yes | 62 | 1 (2.8) | 0 (0) | –d | |
| Number of times used family or patient support or self-help groups in the past month | 1 | 8 (8 to 8) | – | –d | |
| Used any other social services during the past month: yes | 63 | 1 (2.8) | 3 (11.1) | –d | |
| Number of times used any other social services in the past month | 4 | 3 (3 to 3) | 2 (0 to 4) | –d | |
| Number of medications prescribed by a doctor or other health-care professional in the past month | 58 | 0 (0 to 1) | 0 (0 to 1) | –d | |
| Inpatient stay during the last month: yes | 66 | 0 (0) | 0 (0) | –d | |
| Number of inpatient night’s stay during the last month | 0 | – | – | –d | |
| Visited outpatients during the last month: yes | 66 | 2 (5.1) | 3 (11.1) | –d | |
| Number of outpatient visits during the last month | 3 | 1 (1 to 1) | 1 (1 to 1) | –d | |
| Visited A&E during the last month: yes | 66 | 1 (2.6) | 1 (3.7) | –d | |
| Number of A&E visits during the last month | 1 | 1 (1 to 1) | – | –d | |
| Question number and CF allocation | Valid number | Response, n (%) | ||||
|---|---|---|---|---|---|---|
| Not at all | Only occasionally | Sometimes | Often | Most of the time | ||
| CORE-OM | ||||||
| 1 | ||||||
| No | 70 | 26 (60.5) | 6 (14.0) | 8 (18.6) | 1 (2.3) | 2 (4.7) |
| Yes | 19 (70.4) | 2 (7.4) | 5 (18.5) | 1 (3.7) | 0 (0.0) | |
| 2 | ||||||
| No | 69 | 22 (52.4) | 8 (19.0) | 7 (16.7) | 3 (7.1) | 2 (4.8) |
| Yes | 13 (48.1) | 5 (18.5) | 6 (22.2) | 2 (7.4) | 1 (3.7) | |
| 3 | ||||||
| No | 69 | 21 (50.0) | 5 (11.9) | 12 (28.6) | 2 (4.8) | 2 (4.8) |
| Yes | 7 (25.9) | 8 (29.6) | 7 (25.9) | 3 (11.1) | 2 (7.4) | |
| 4 | ||||||
| No | 69 | 20 (47.6) | 6 (14.3) | 14 (33.3) | 1 (2.4) | 1 (2.4) |
| Yes | 7 (25.9) | 11 (40.7) | 8 (29.6) | 1 (3.7) | 0 (0.0) | |
| 5 | ||||||
| No | 68 | 21 (51.2) | 9 (22.0) | 7 (17.1) | 4 (9.8) | 0 (0.0) |
| Yes | 8 (29.6) | 9 (33.3) | 5 (18.5) | 3 (11.1) | 2 (7.4) | |
| 6 | ||||||
| No | 69 | 40 (95.2) | 2 (4.8) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Yes | 23 (85.2) | 2 (7.4) | 1 (3.7) | 0 (0.0) | 1 (3.7) | |
| 7 | ||||||
| No | 70 | 25 (58.1) | 7 (16.3) | 7 (16.3) | 2 (4.7) | 2 (4.7) |
| Yes | 7 (25.9) | 10 (37.0) | 8 (29.6) | 2 (7.4) | 0 (0.0) | |
| 8 | ||||||
| No | 68 | 13 (31.0) | 7 (16.7) | 10 (23.8) | 8 (19.0) | 4 (9.5) |
| Yes | 9 (34.6) | 4 (15.4) | 7 (26.9) | 5 (19.2) | 1 (3.8) | |
| 9 | ||||||
| No | 70 | 37 (86.0) | 4 (9.3) | 1 (2.3) | 0 (0.0) | 1 (2.3) |
| Yes | 24 (88.9) | 1 (3.7) | 2 (7.4) | 0 (0.0) | 0 (0.0) | |
| 10 | ||||||
| No | 69 | 27 (64.3) | 6 (14.3) | 4 (9.5) | 2 (4.8) | 3 (7.1) |
| Yes | 18 (66.7) | 5 (18.5) | 4 (14.8) | 0 (0.0) | 0 (0.0) | |
| 11 | ||||||
| No | 68 | 29 (70.7) | 5 (12.2) | 7 (17.1) | 0 (0.0) | 0 (0.0) |
| Yes | 15 (55.6) | 4 (14.8) | 5 (18.5) | 0 (0.0) | 3 (11.1) | |
| 12 | ||||||
| No | 69 | 19 (45.2) | 13 (31.0) | 6 (14.3) | 1 (2.4) | 3 (7.1) |
| Yes | 9 (33.3) | 9 (33.3) | 7 (25.9) | 0 (0.0) | 2 (7.4) | |
| 13 | ||||||
| No | 68 | 29 (70.7) | 1 (2.4) | 7 (17.1) | 3 (7.3) | 1 (2.4) |
| Yes | 18 (66.7) | 3 (11.1) | 3 (11.1) | 3 (11.1) | 0 (0.0) | |
| 14 | ||||||
| No | 70 | 25 (58.1) | 5 (11.6) | 8 (18.6) | 4 (9.3) | 1 (2.3) |
| Yes | 14 (51.9) | 5 (18.5) | 7 (25.9) | 1 (3.7) | 0 (0.0) | |
| 15 | ||||||
| No | 69 | 33 (78.6) | 5 (11.9) | 3 (7.1) | 1 (2.4) | 0 (0.0) |
| Yes | 22 (81.5) | 1 (3.7) | 3 (11.1) | 1 (3.7) | 0 (0.0) | |
| 16 | ||||||
| No | 70 | 39 (90.7) | 2 (4.7) | 0 (0.0) | 1 (2.3) | 1 (2.3) |
| Yes | 25 (92.6) | 0 (0.0) | 1 (3.7) | 1 (3.7) | 0 (0.0) | |
| 17 | ||||||
| No | 68 | 26 (63.4) | 5 (12.2) | 6 (14.6) | 4 (9.8) | 0 (0.0) |
| Yes | 14 (51.9) | 4 (14.8) | 6 (22.2) | 2 (7.4) | 1 (3.7) | |
| 18 | ||||||
| No | 70 | 19 (44.2) | 7 (16.3) | 8 (18.6) | 5 (11.6) | 4 (9.3) |
| Yes | 7 (25.9) | 3 (11.1) | 8 (29.6) | 4 (14.8) | 5 (18.5) | |
| 19 | ||||||
| No | 68 | 17 (40.5) | 5 (11.9) | 9 (21.4) | 4 (9.5) | 7 (16.7) |
| Yes | 10 (38.5) | 6 (23.1) | 5 (19.2) | 2 (7.7) | 3 (11.5) | |
| 20 | ||||||
| No | 68 | 24 (58.5) | 6 (14.6) | 5 (12.2) | 4 (9.8) | 2 (4.9) |
| Yes | 10 (37.0) | 6 (22.2) | 6 (22.2) | 3 (11.1) | 2 (7.4) | |
| 21 | ||||||
| No | 68 | 24 (58.5) | 5 (12.2) | 10 (24.4) | 1 (2.4) | 1 (2.4) |
| Yes | 8 (29.6) | 9 (33.3) | 9 (33.3) | 0 (0.0) | 1 (3.7) | |
| 22 | ||||||
| No | 69 | 40 (95.2) | 1 (2.4) | 1 (2.4) | 0 (0.0) | 0 (0.0) |
| Yes | 21 (77.8) | 3 (11.1) | 2 (7.4) | 1 (3.7) | 0 (0.0) | |
| 23 | ||||||
| No | 70 | 31 (72.1) | 6 (14.0) | 4 (9.3) | 2 (4.7) | 0 (0.0) |
| Yes | 20 (74.1) | 2 (7.4) | 3 (11.1) | 2 (7.4) | 0 (0.0) | |
| 24 | ||||||
| No | 70 | 36 (83.7) | 4 (9.3) | 1 (2.3) | 2 (4.7) | 0 (0.0) |
| Yes | 24 (88.9) | 0 (0.0) | 3 (11.1) | 0 (0.0) | 0 (0.0) | |
| 25 | ||||||
| No | 68 | 29 (70.7) | 5 (12.2) | 4 (9.8) | 2 (4.9) | 1 (2.4) |
| Yes | 14 (51.9) | 6 (22.2) | 2 (7.4) | 4 (14.8) | 1 (3.7) | |
| 26 | ||||||
| No | 70 | 36 (83.7) | 1 (2.3) | 2 (4.7) | 3 (7.0) | 1 (2.3) |
| Yes | 19 (70.4) | 3 (11.1) | 4 (14.8) | 1 (3.7) | 0 (0.0) | |
| 27 | ||||||
| No | 70 | 21 (48.8) | 7 (16.3) | 10 (23.3) | 3 (7.0) | 2 (4.7) |
| Yes | 13 (48.1) | 5 (18.5) | 6 (22.2) | 2 (7.4) | 1 (3.7) | |
| 28 | ||||||
| No | 68 | 25 (61.0) | 3 (7.3) | 7 (17.1) | 5 (12.2) | 1 (2.4) |
| Yes | 16 (59.3) | 5 (18.5) | 3 (11.1) | 2 (7.4) | 1 (3.7) | |
| 29 | ||||||
| No | 68 | 27 (65.9) | 10 (24.4) | 2 (4.9) | 2 (4.9) | 0 (0.0) |
| Yes | 17 (63.0) | 6 (22.2) | 3 (11.1) | 1 (3.7) | 0 (0.0) | |
| 30 | ||||||
| No | 67 | 18 (43.9) | 5 (12.2) | 12 (29.3) | 3 (7.3) | 3 (7.3) |
| Yes | 8 (30.8) | 7 (26.9) | 5 (19.2) | 3 (11.5) | 3 (11.5) | |
| 31 | ||||||
| No | 68 | 18 (42.9) | 8 (19.0) | 9 (21.4) | 2 (4.8) | 5 (11.9) |
| Yes | 5 (19.2) | 8 (30.8) | 7 (26.9) | 2 (7.7) | 4 (15.4) | |
| 32 | ||||||
| No | 69 | 19 (45.2) | 6 (14.3) | 11 (26.2) | 3 (7.1) | 3 (7.1) |
| Yes | 4 (14.8) | 8 (29.6) | 9 (33.3) | 3 (11.1) | 3 (11.1) | |
| 33 | ||||||
| No | 70 | 34 (79.1) | 3 (7.0) | 3 (7.0) | 2 (4.7) | 1 (2.3) |
| Yes | 20 (74.1) | 3 (11.1) | 4 (14.8) | 0 (0.0) | 0 (0.0) | |
| 34 | ||||||
| No | 70 | 39 (90.7) | 1 (2.3) | 1 (2.3) | 1 (2.3) | 1 (2.3) |
| Yes | 19 (70.4) | 7 (25.9) | 1 (3.7) | 0 (0.0) | 0 (0.0) | |
| Response | ||||||
| None of the time | Rarely | Some of the time | Often | All of the time | ||
| WEMWBS | ||||||
| 1 | ||||||
| No | 69 | 2 (4.8) | 5 (11.9) | 11 (26.2) | 13 (31.0) | 11 (26.2) |
| Yes | 1 (3.7) | 2 (7.4) | 12 (44.4) | 9 (33.3) | 3 (11.1) | |
| 2 | ||||||
| No | 69 | 3 (7.1) | 1 (2.4) | 10 (23.8) | 17 (40.5) | 11 (26.2) |
| Yes | 1 (3.7) | 2 (7.4) | 7 (25.9) | 12 (44.4) | 5 (18.5) | |
| 3 | ||||||
| No | 70 | 1 (2.3) | 6 (14.0) | 15 (34.9) | 12 (27.9) | 9 (20.9) |
| Yes | 1 (3.7) | 3 (11.1) | 11 (40.7) | 9 (33.3) | 3 (11.1) | |
| 4 | ||||||
| No | 70 | 2 (4.7) | 2 (4.7) | 14 (32.6) | 13 (30.2) | 12 (27.9) |
| Yes | 0 (0.0) | 3 (11.1) | 14 (51.9) | 8 (29.6) | 2 (7.4) | |
| 5 | ||||||
| No | 69 | 2 (4.7) | 8 (18.6) | 10 (23.3) | 15 (34.9) | 8 (18.6) |
| Yes | 2 (7.7) | 5 (19.2) | 4 (15.4) | 12 (46.2) | 3 (11.5) | |
| 6 | ||||||
| No | 70 | 0 (0.0) | 3 (7.0) | 8 (18.6) | 20 (46.5) | 12 (27.9) |
| Yes | 1 (3.7) | 0 (0.0) | 12 (44.4) | 12 (44.4) | 2 (7.4) | |
| 7 | ||||||
| No | 70 | 2 (4.7) | 1 (2.3) | 8 (18.6) | 18 (41.9) | 14 (32.6) |
| Yes | 1 (3.7) | 1 (3.7) | 4 (14.8) | 18 (66.7) | 3 (11.1) | |
| 8 | ||||||
| No | 70 | 2 (4.7) | 3 (7.0) | 11 (25.6) | 14 (32.6) | 13 (30.2) |
| Yes | 0 (0.0) | 2 (7.4) | 7 (25.9) | 10 (37.0) | 8 (29.6) | |
| 9 | ||||||
| No | 70 | 1 (2.3) | 2 (4.7) | 13 (30.2) | 14 (32.6) | 13 (30.2) |
| Yes | 0 (0.0) | 2 (7.4) | 9 (33.3) | 14 (51.9) | 2 (7.4) | |
| 10 | ||||||
| No | 70 | 2 (4.7) | 1 (2.3) | 10 (23.3) | 14 (32.6) | 16 (37.2) |
| Yes | 0 (0.0) | 4 (14.8) | 4 (14.8) | 15 (55.6) | 4 (14.8) | |
| 11 | ||||||
| No | 69 | 2 (4.8) | 4 (9.5) | 10 (23.8) | 0 (0.0) | 26 (61.9) |
| Yes | 0 (0.0) | 2 (7.4) | 14 (51.9) | 0 (0.0) | 11 (40.7) | |
| 12 | ||||||
| No | 69 | 2 (4.8) | 4 (9.5) | 9 (21.4) | 11 (26.2) | 16 (38.1) |
| Yes | 0 (0.0) | 2 (7.4) | 7 (25.9) | 7 (25.9) | 11 (40.7) | |
| 13 | ||||||
| No | 69 | 2 (4.8) | 2 (4.8) | 10 (23.8) | 15 (35.7) | 13 (31.0) |
| Yes | 1 (3.7) | 1 (3.7) | 2 (7.4) | 14 (51.9) | 9 (33.3) | |
| 14 | ||||||
| No | 70 | 3 (7.0) | 3 (7.0) | 10 (23.3) | 14 (32.6) | 13 (30.2) |
| Yes | 0 (0.0) | 3 (11.1) | 5 (18.5) | 13 (48.1) | 6 (22.2) | |
| Valid number | Response, n (%) | |||||
| Disagree strongly | Disagree a little | Neither agree or disagree | Agree a little | Agree strongly | ||
| Connecting with nature | ||||||
| 1 | ||||||
| No | 69 | 6 (14.3) | 7 (16.7) | 11 (26.2) | 12 (28.6) | 6 (14.3) |
| Yes | 4 (14.8) | 5 (18.5) | 5 (18.5) | 7 (25.9) | 6 (22.2) | |
| 2 | ||||||
| No | 69 | 1 (2.4) | 2 (4.8) | 11 (26.2) | 16 (38.1) | 12 (28.6) |
| Yes | 0 (0.0) | 2 (7.4) | 6 (22.2) | 13 (48.1) | 6 (22.2) | |
| 3 | ||||||
| No | 67 | 4 (10.0) | 6 (15.0) | 11 (27.5) | 11 (27.5) | 8 (20.0) |
| Yes | 3 (11.1) | 4 (14.8) | 9 (33.3) | 8 (29.6) | 3 (11.1) | |
| 4 | ||||||
| No | 69 | 2 (4.8) | 4 (9.5) | 6 (14.3) | 11 (26.2) | 19 (45.2) |
| Yes | 3 (11.1) | 0 (0.0) | 5 (18.5) | 9 (33.3) | 10 (37.0) | |
| 5 | ||||||
| No | 69 | 6 (14.3) | 2 (4.8) | 9 (21.4) | 14 (33.3) | 11 (26.2) |
| Yes | 2 (7.4) | 2 (7.4) | 12 (44.4) | 8 (29.6) | 3 (11.1) | |
| 6 | ||||||
| No | 69 | 2 (4.8) | 5 (11.9) | 8 (19.0) | 12 (28.6) | 15 (35.7) |
| Yes | 2 (7.4) | 2 (7.4) | 10 (37.0) | 9 (33.3) | 4 (14.8) | |
Appendix 5 Search strategy for cost-effectiveness systematic review
Applied Social Sciences Index and Abstracts (via ProQuest)
Date range searched: 1987 to current.
Search strategy
(((SU.EXACT(‘Young adult offenders’) OR SU.EXACT(‘Fine defaulters’) OR SU.EXACT(‘Remand offenders’) OR SU.EXACT(‘Recidivists’) OR SU.EXACT(‘Violent offenders’) OR SU.EXACT(‘Ex-offenders’) OR SU.EXACT(‘Offenders’) OR SU.EXACT(‘Murderers’) OR SU.EXACT(‘Prisoners’) OR SU.EXACT(‘Drunken offenders’) OR SU.EXACT(‘Probationers’) OR SU.EXACT(‘Sex offenders’) OR SU.EXACT(‘Dangerous offenders’) OR SU.EXACT(‘Suspected offenders’)) OR (convict OR convicts OR convicted OR offender* OR reoffender* OR criminal* OR prisoner* OR inmate* OR detainee* OR cellmate* OR incarcerated* OR felon* OR probation OR probationer* OR ‘ex offender*’ OR parole OR correctional))
AND
((SU.EXACT(‘Cost containment’) OR SU.EXACT(‘Social costs’) OR SU.EXACT(‘Functional cost analysis’) OR SU.EXACT(‘Cost analysis’) OR SU.EXACT(‘Cost effectiveness’) OR SU.EXACT(‘Health costs’) OR SU.EXACT(‘Cost benefit analysis’) OR SU.EXACT(‘Unemployment benefit’) OR SU.EXACT(‘Cost effective analysis’) OR SU.EXACT.EXPLODE(‘Family fund’ OR ‘Food stamps’ OR ‘Income support’ OR ‘Nonincome tested transfers’ OR ‘Supplementary benefits’ OR ‘Welfare benefits’)) OR (((polic* or crime OR criminal* OR violence OR correctional*) n/5 (cost or costs or economic*)) OR ((‘vocational training’) n/5 (cost or costs or economic*) OR (social or housing or health or societ* or communit*) n/2 (cost or costs or economic*))) OR ((housing OR welfare OR state OR income OR family OR child OR entitle*) NEAR/3 (support OR benefit* OR allowance)) OR ti(cost OR costs OR economic*)))
NOT (SU.EXACT(‘Violent juvenile offenders’) OR SU.EXACT(‘Suspected juvenile offenders’) OR SU.EXACT(‘Juvenile offenders’) OR SU.EXACT(‘Children’) OR SU.EXACT(‘Violent adolescents’) OR SU.EXACT(‘Adolescents’))
Cumulative Index to Nursing and Allied Health Literature: via EBSCOhost databases
Date range searched: 1 January 1960 to current.
Search strategy
S22 S18 not S21
S21 S19 NOT S20
S20 ( (MH ‘Child+’) OR (MH ‘Adolescence+’) OR (MH ‘Infant+’) OR (MH ‘Minors (Legal)’) ) AND (MH ‘Adult+’)
S19 (MH ‘Child+’) OR (MH ‘Adolescence+’) OR (MH ‘Infant+’) OR (MH ‘Minors (Legal)’)
S18 S5 AND S17
S17 S6 OR S7 OR S8 OR S9 OR S12 OR S13 OR S14 OR S15 OR S16
S16 (MH ‘Job Re-Entry’)
S15 (MH ‘Employment, Supported’) OR (MH ‘Rehabilitation, Vocational’)
S14 (MH ‘Public Assistance+’) OR (MM ‘Insurance, Health’)
S13 (MM ‘Costs and Cost Analysis+’)
S12 S10 AND S11
S11 (MM ‘Economics+’)
S10 (MH ‘Social Welfare’) OR (MH ‘Socioeconomic Factors’)
S9 TX health n3 (cost or costs)
S8 TX (housing or welfare or state or ‘low income’ or ‘job seeker*’ or family or child or entitle*) w2 (support or benefit* or allowance*)
S7 TX ( (societ* or ‘social care’ or communit*) n5 (cost or costs) ) OR TX ( (‘criminal activit*’ or crime or violence or polic* or correctional) n5 (cost or costs) ) OR TX ( (unemploy* or ‘vocational training’ or employment or ‘job seeker*’) n5 (cost or costs) )
S6 TI cost or costs or economic*
S5 S1 OR S2 OR S3 OR S4
S4 (MH ‘Mentally Ill Offenders’) OR (MH ‘Public Offenders’) OR (MH ‘Repeat Offenders’) OR (MH ‘Sex Offenders’)
S3 (MH ‘Correctional Facilities’)
S2 (MH ‘Prisoners’)
S1 TX convict or convicts or convicted or offender* or reoffend* or criminal* or prisoner* or inmate* or detainee* or cellmate* or incarcerated* or felon* or probation or probationer* or ‘ex offender*’ or parole or recidiv*
The Campbell Library
Date range searched: 1 January 2004 to current.
Search strategy
-
cost* or economic* in Title or Keywords limited to Crime and Justice Coordinating group = 1 hit
-
prison* or crime or criminal* or offender* or reoffend* or convict* or inmate* or detainee* or cellmate* or incarcerated or felon* or probation* or parole or recidiv* or correctional in Title or Keywords limited to Social Welfare Coordinating group = 2 hits
Criminal Justice Abstracts: via EBSCOhost databases
Date range searched: 1 January 1830 to current.
Search strategy
S10 S6 OR S9 (1490)
S9 S7 AND S8 (25)
S8 (ZU ‘prisoners’) or (ZU ‘criminals’) or (ZU ‘prisons’) (21,226)
S7 (ZU ‘cost analysis’) or (ZU ‘cost control’) or (ZU ‘cost effectiveness’) (842)
S6 S1 AND S5 (1473)
S5 S2 OR S3 OR S4 (6692)
S4 TI (housing OR welfare OR state OR income OR family OR child OR entitle*) w2 (support OR benefit* OR allowance) (352)
S3 TI (economic n3 (analysis OR impact OR burden OR evaluation OR model OR factors OR perspective*)) (560)
S2 TI (cost or costs or economics) (6349)
S1 TX (convicts or convicted or offender* or reoffend* or criminals or criminal or prisoner* or inmate* or detainee* or cellmate* or incarcerated* or felon* or probation or probationer* or ‘ex offender*’ or parole or recidiv*) (141,548)
EMBASE Classic and EMBASE
Date range searched: 1947 to 13 December 2013.
Search strategy
-
(cost or costs or economic*).ti. (130,794)
-
((societ* or ‘social care’ or communit*) adj5 (cost or costs)).tw. (8256)
-
((‘criminal activit*’ or crime or violence or polic* or correctional) adj5 (cost or costs)).tw. (3154)
-
((unemploy* or ‘vocational training’ or employment or ‘job seeker*’) adj5 (cost or costs)).tw. (479)
-
((housing or welfare or state or ‘low income’ or ‘job seeker*’ or family or child or entitle*) adj2 (support or benefit* or allowance*)).tw. (9577)
-
(health adj3 (cost or costs)).tw. (25,767)
-
or/1-6 [Societal and Health Costs Textwords] (159,806)
-
exp *social problem/ or social care/ or *caregiver support/ or *social insurance/ or *social security/ or *social support/ (413,841)
-
exp *economic aspect/ (351,607)
-
(cost or costs).tw. (413,146)
-
8 and (9 or 10) (21,553)
-
return to work/ (506)
-
*vocational rehabilitation/ (5452)
-
exp *‘health care cost’/ (47,918)
-
exp *economic evaluation/ (33,879)
-
or/11-15 [Societal and Health Costs MeSH] (104,512)
-
7 or 16 [Societal and Health Costs] (218,512)
-
exp *prisoners/ or exp offender/ or exp *prison/ (21,289)
-
(convict or convicts or convicted or offender* or reoffend* or criminal or criminals or prisoner* or inmate* or detainee* or cellmate* or incarcerated* or felon* or probation or probationer* or ‘ex offender*’ or parole or recidiv*).tw. (46,370)
-
correctional.tw. (2745)
-
or/18-20 [Offenders] (55,220)
-
17 and 21 (1125)
-
(exp adolescent/ or exp child/ or exp newborn/) not ((exp adolescent/ or exp child/ or exp newborn/) and (adult/ or exp aged/ or middle aged/)) (1,951,636)
-
22 not 23 (1042)
Health Management Information Consortium
Date range searched: 1983 to current.
Search strategy
-
(convict or convicts or convicted or offender* or reoffend* or criminal* or prison* or inmate* or detainee* or cellmate* or incarcerated* or felon* or probation or probationer* or ‘ex offender*’ or parole or recidiv*).tw. (4075)
-
correctional.tw. (52)
-
1 or 2 [Offenders] (4080)
-
(cost or costs or economic*).ti. (9065)
-
((societ* or ‘social care’ or communit*) adj5 (cost or costs)).tw. (718)
-
((‘criminal activit*’ or crime or violence or polic* or correctional) adj5 (cost or costs)).tw. (408)
-
((unemploy* or ‘vocational training’ or employment or ‘job seeker*’) adj5 (cost or costs)).tw. (65)
-
((housing or welfare or state or ‘low income’ or ‘job seeker*’ or family or child or entitle*) adj2 (support or benefit* or allowance*)).tw. (1621)
-
(health adj3 (cost or costs)).tw. (1908)
-
or/4-9
MEDLINE (via Ovid)
Date range searched: 1946 to week 3 November 2013.
Search strategy
-
(convict or convicts or convicted or offender* or reoffend* or criminal* or prisoner* or inmate* or detainee* or cellmate* or incarcerated* or felon* or probation or probationer* or ‘ex offender*’ or parole or recidiv*).tw. (32,721)
-
correctional.tw. (2123)
-
prisoners/ or criminals/ (13,458)
-
exp prisons/ (7791)
-
or/1-4 [Offenders] (41,967)
-
exp *economics/ (261,559)
-
exp *socioeconomic factors/ (121,894)
-
6 and 7 (20,744)
-
exp public assistance/ (59,349)
-
employment, supported/ or return to work/ (1110)
-
Vocational Education/ (1774)
-
exp Health Care Costs/ (47,394)
-
exp *‘Costs and Cost Analysis’/ (46,412)
-
or/8-13 [Societal and Health Costs MeSH] (143,762)
-
(cost or costs or economic*).ti. (96,282)
-
((societ* or ‘social care’ or communit*) adj5 (cost or costs)).tw. (5651)
-
((‘criminal activit*’ or crime or violence or polic* or correctional) adj5 (cost or costs)).tw. (2441)
-
((unemploy* or ‘vocational training’ or employment or ‘job seeker*’) adj5 (cost or costs)).tw. (353)
-
((housing or welfare or state or ‘low income’ or ‘job seeker*’ or family or child or entitle*) adj2 (support or benefit* or allowance*)).tw. (7643)
-
(health adj3 (cost or costs)).tw. (18,802)
-
or/15-20 [Societal and Health Costs Textwords] (117,824)
-
14 or 21 (223,617)
-
(adolescent/ or exp child/ or exp infant/) not (exp adult/ and (adolescent/ or exp adult/ or exp child/ or exp infant/)) (1,525,970)
-
(5 and 22) not 23 [Health and society offenders costs, children excluded] (773)
MEDLINE In-Process & Other Non-Indexed Citations (via Ovid)
Date range searched: 12 December 2013.
Search strategy
-
(convict or convicts or convicted or offender* or reoffend* or criminal* or prison* or inmate* or detainee* or cellmate* or incarcerated* or felon* or probation or probationer* or ‘ex offender*’ or parole or recidiv*).tw. (2349)
-
correctional.tw. (137)
-
1 or 2 [Offenders] (2399)
-
(cost or costs or economic*).ti. (7332)
-
((societ* or ‘social care’ or communit*) adj5 (cost or costs)).tw. (515)
-
((‘criminal activit*’ or crime or violence or polic* or correctional) adj5 (cost or costs)).tw. (163)
-
((unemploy* or ‘vocational training’ or employment or ‘job seeker*’) adj5 (cost or costs)).tw. (31)
-
((housing or welfare or state or ‘low income’ or ‘job seeker*’ or family or child or entitle*) adj2 (support or benefit* or allowance*)).tw. (580)
-
(health adj3 (cost or costs)).tw. (1394)
-
or/4-9 [Societal and Health Costs Textwords] (9106)
-
3 and 10 (52)
National Criminal Justice Reference Service Abstracts Database (via ProQuest)
Date range searched: 1 January 1975 to current.
Search strategy
((((ti(cost OR costs OR economics) OR ti((economic NEAR/3 (analysis OR impact OR burden OR evaluation OR model OR factors OR perspective*)))) OR ti((housing OR welfare OR state OR income OR family OR child OR entitle*) NEAR/2 (support OR benefit* OR allowance))) AND (convicts OR convicted OR offender* OR reoffender* OR criminal OR criminals OR prisoner* OR inmate* OR detainee* OR cellmate* OR incarcerated* OR felon* OR probationer* OR ‘ex offender*’ OR correctional))
OR
((su.Exact(‘cost analysis (04660)’ OR ‘operating costs (03979)’ OR ‘law enforcement costs (05431)’ OR ‘crime costs (04384)’ OR ‘evaluation costs (04483)’ OR ‘court costs (05161)’ OR ‘murder trial costs (10297)’ OR ‘corrections costs (08994)’ OR ‘prison costs (08651)’ OR ‘probation costs (10128)’ OR ‘cost effectiveness analysis (04491)’ OR ‘business crime costs (01880)’ OR ‘medical costs (00638)’ OR ‘costs (04379)’ OR ‘cost benefit analysis (03601)’) OR su.Exact(‘economic analysis of crime (09862)’ OR ‘economic impact of prisons (10112)’ OR ‘economic analysis (05024)’ OR ‘socioeconomic impact of terrorism (08270)’)) AND su.Exact(‘offender profiles (08370)’ OR ‘first offenders (03670)’ OR ‘offender supervision (08984)’ OR ‘federal prisoners (09830)’ OR ‘female offenders (00411)’ OR ‘drug offenders (04683)’ OR ‘offender mental health services (08565)’ OR ‘elderly offenders (08542)’ OR ‘ex-offender employment (03884)’ OR ‘convicted offender incapacitation (05012)’ OR ‘ex-offenders (04211)’ OR ‘barriers to ex-offender employment (09630)’ OR ‘offender financial assistance (04900)’ OR ‘foreign offenders (11184)’ OR ‘electronic monitoring of offenders (10113)’ OR ‘drunk offenders (08347)’ OR ‘female sex offenders (10437)’ OR ‘offender tracking systems (11286)’ OR ‘offenders college-credit-programs (05223)’ OR ‘offender participatn in rehab goals (09655)’ OR ‘habitual offenders (00936)’ OR ‘elderly sex offenders (09867)’ OR ‘offenders (00715)’ OR ‘homeless offenders (09939)’ OR ‘adult offenders (00010)’ OR ‘prisoner reentry (92000)’ OR ‘offender reclassification (08731)’ OR ‘offender participation programs (09209)’)))
NOT su(juvenile*)
NHS Economic Evaluation Database (The Cochrane Library via Wiley Online Library)
Date range searched: Issue 4 of 4, October 2013.
Search strategy
#1. MeSH descriptor: [Prisoners] this term only
#2. MeSH descriptor: [Criminals] explode all trees
#3. MeSH descriptor: [Crime] explode all trees
#4. convict or convicts or convicted or offender* or reoffend* or criminal* or prisoner* or inmate* or detainee* or cellmate* or incarcerated* or felon* or probation or probationer* or ‘ex offender*’ or parole or recidiv* or correctional
#5. MeSH descriptor: [Prisons] explode all trees
#6. #1 or #2 or #3 or #4 or #5
PsycINFO
Date range searched: 1806 to week 2 December 2013.
Search strategy
-
(convict or convicts or convicted or offender* or reoffend* or criminal* or prisoner* or inmate* or detainee* or cellmate* or incarcerated* or felon* or probation or probationer* or ‘ex offender*’ or parole).tw. (64,800)
-
correctional.tw. (5475)
-
prisoners/ or criminals/ or exp Prisons/ or exp Mentally Ill Offenders/ (22,963)
-
or/1-3 [Offenders] (68,659)
-
(cost or costs or economic*).ti. (18,832)
-
(recidiv* and (cost or costs or economic*)).tw. (364)
-
((societ* or ‘social care’ or communit*) adj5 (cost or costs)).tw. (1920)
-
((‘criminal activit*’ or crime or violence or polic* or correctional) adj5 (cost or costs)).tw. (1124)
-
((unemploy* or ‘vocational training’ or employment or ‘job seeker*’) adj5 (cost or costs)).tw. (272)
-
((housing or welfare or state or ‘low income’ or ‘job seeker*’ or family or child or entitle*) adj2 (support or benefit* or allowance*)).tw. (10,138)
-
(health adj3 (cost or costs)).tw. (4680)
-
or/5-10 [Societal and Health Costs Textwords] (31,166)
-
social issues/ or exp homeless/ or exp social discrimination/ or exp social equality/ or exp social integration/ or exp unemployment/ or exp social programs/ (34,710)
-
‘welfare services (government)’/ or community welfare services/ (3516)
-
government programs/ or social security/ or shelters/ or exp social services/ (35,962)
-
vocational rehabilitation/ or supported employment/ or rehabilitation counseling/ (6625)
-
housing/ or assisted living/ or group homes/ or shelters/ (5718)
-
13 or 14 or 15 or 16 or 17 (79,798)
-
exp *economics/ (11,077)
-
18 and 19 [Societal cost MeSH] (760)
-
health care costs/ or exp ‘costs and cost analysis’/ (17,919)
-
12 or 20 or 21 [Societal Health Costs] (42,298)
-
juvenile delinquency/ or juvenile gangs/ or juvenile justice/ or predelinquent youth/ or adolescent psychiatry/ or adolescent psychology/ or adolescent psychopathology/ or adolescent psychotherapy/ (25,204)
-
4 and 22 (1204)
-
24 not 23 (1059)
Research Papers in Economics Ideas
Date range searched: 1997 to current.
Search strategy
(prison | convict | criminal | offender | reoffend | probationer | incarcerated | correctional | crime) + (cost | economic) in Title
Sociological Abstracts (via ProQuest)
Date range searched: 1 January 1952.
Search strategy
(((convict OR convicts OR convicted OR offender* OR reoffender* OR criminal* OR prisoner* OR inmate* OR detainee* OR cellmate* OR incarcerated* OR felon* OR probation OR probationer* OR ‘ex offender*’ OR parole OR correctional)
AND
((((polic* or crime OR criminal* OR violence OR correctional*) n/3 (cost or costs)) OR ((‘vocational training’) n/3 (cost or costs ) OR (social or housing or health or societ* or communit*) n/2 (cost or costs)) OR ((housing OR welfare OR state OR income OR family OR child OR entitle*) n/2 (support OR benefit* OR allowance))) OR ti(cost OR costs or economics))) OR ti(economic NEAR/3 (analysis OR impact OR burden OR evaluation OR model OR factors OR perspective*)))) OR SU.EXACT(‘Prisoners’) AND (SU.EXACT(‘Cost-Benefit Analysis’) OR SU.EXACT(‘Cost Containment’) OR SU.EXACT(‘Housing Costs’) OR SU.EXACT(‘Costs’) OR SU.EXACT(‘Benefits’) OR SU.EXACT(‘Social Security’) OR SU.EXACT(‘Health Care Costs’))))
NOT (SU.EXACT(‘Juvenile Correctional Institutions’) OR SU.EXACT(‘Juvenile/Juveniles’) OR SU.EXACT(‘Juvenile Offenders’) OR SU.EXACT(‘Juvenile Delinquency’) OR SU.EXACT(‘Juvenile Courts’) OR SU.EXACT(‘Children’) OR SU.EXACT(‘Adolescents’) OR SU.EXACT(‘Juvenile Justice’))
Social Services Abstracts (ProQuest CSA)
Date range searched: 1979 to current.
Same search strategy as Sociological Abstracts (via ProQuest).
Web of Science Conference Proceedings Citation Index-Science, Web of Science Conference Proceedings Citation Index – Social Science & Humanities and Web of Science (Thomson Reuters)
Date ranges searched: 1990 to current.
Date searched: 20 December 2013.
Search strategy
#1. Topic=(convict or convicts or convicted or offender* or reoffend* or criminal* or prisoner* or inmate* or detainee* or cellmate* or incarcerated* or felon* or probation or probationer* or ‘ ex offender*’ or parole or recidiv* or correctional) (6111)
#2. Topic=((polic* or crime OR criminal* OR violence OR correctional*) near/3 (cost or costs)) OR Topic=((‘ vocational training‘ ) near/3 (cost or costs )) OR Topic= ((social or housing or health or societ* or communit*) near/2 (cost or costs)) (4230)
#3. Topic=((housing OR welfare OR state OR income OR family OR child OR entitle*) near/2 (support OR benefit* OR allowance)) OR Title=((cost OR costs or economics)) OR Title=((economic NEAR/3 (analysis OR impact OR burden OR evaluation OR model OR factors OR perspective*))) (47,217)
#4. #3 OR #2 (50,017)
#5. #4 AND #1 (124)
Appendix 6 Topic guides and coding frame from the qualitative study
Service users topic guide
-
How are you finding things here/how did you find it on the farm?
-
Looking back to before you were convicted, how were things for you then?
-
(Tease out; personal/quality of life; social life/work, housing, emotions, attitudes, lifestyles.)
-
What were your initial impressions of the care farm?
-
(Expectations, could include why they thought they were sent here/past experience of working with nature.)
-
Tell me about the things (activities) you have done here?
-
(Tease out activities, working with nature, friendships, mentoring, skills, respect, responsibilities, choices, rewards, general behaviours of people on farm, purposefulness, outdoors work vs. indoors.)
-
How did you get on with the staff at the farm?
-
(About relationship.)
-
What do you think about those (activities) (if doesn’t expand on question 3)?
-
What’s been good or not so good? OR question below . . .
-
What do you think about the general idea of people coming to a care farm as part of a community order
-
(teasing out things to do with time out, being away from the public, comparing with other orders – experience or perception, choice, nature element)
-
If you look back what changed for you since coming to the farm?
Care farmers topic guide
-
What do you think the care farm is all about (what problem is it trying to address), what is it hoping to achieve? Discuss how the care farm contributes to rehabilitation
-
(Thinking about seven pathways to reoffending: (1) education; (2) training and employment; (3) health; (4) drugs; (5) alcohol; (6) finance, benefits and debt; and (7) attitude, thinking and behaviour) – where do care farms fit in?
-
-
In what way do the activities provided on-site support that aim?
-
With the activities provided on-site how do you decide who does what?
-
(Looking at extent to which tasks are allocated as determined by farm requirements or whether or not there is a choice, use of existing skills vs. developing new skills, seasonally dependent.)
-
-
What changes, if any, do you see in the people serving community orders that come here? What do you put that down to?
-
(Link with increased environmental awareness.)
-
-
What factors might influence the care farms ability to create change in service users?
-
Tell me about your relationship with the offenders on the farm?
-
What do you think this farm offers as part of a community order that other placements perhaps don’t? (Nature element, variety, skills enhancement.)
Probation staff topic guide
-
Explain the process by which you allocate a service user to a type of project (free agency placement/larger project/CP supervision) to serve their community order?
-
How do you balance the various factors that influence decisions?
-
What does the term ‘rehabilitation’ mean to you in this environment?
-
(Dig deeper to get beyond stopping reoffending, think about desistance theory; link this back to the care farm; see if they mention any of the green theory elements – could prompt here.)
-
-
How do the various projects offer opportunities for rehabilitation (exclude alcohol, addiction treatment and education, training and employments)? How does this fit with service user potential for rehabilitation? Who needs rehabilitation? (With particular reference to the care farm.) Have any of your views about this changed with the privatisation?
-
What sort of projects fit with the punishment element of a community order? What are your views on the role of punishments?
-
How do care farms or nature-based activities fit with community orders either as a rehabilitation/punishment? Why was the care farm placed where it was within the order?
Coding frame used in the qualitative analysis
Table 36 shows a copy of the coding framework used in the qualitative analysis of the care farmers and service users interviews.
| Theme or code | Number of interviews containing this theme or code | Number of times coded |
|---|---|---|
| A new identity | 16 | 117 |
| Enjoying the work | 14 | 45 |
| Feeling the change | 14 | 61 |
| Renewed relationships and social networks | 6 | 11 |
| Allocation to CO | 4 | 64 |
| Employment status | 4 | 8 |
| Gender | 4 | 7 |
| Geographic location and transportation | 4 | 7 |
| Information acquisition or process | 4 | 19 |
| Mental or physical health | 4 | 12 |
| Offence | 4 | 11 |
| Animals | 11 | 33 |
| Believing in it | 5 | 15 |
| CF vs. other COs | 7 | 10 |
| Developing relationships | 15 | 67 |
| Belonging | 15 | 54 |
| Refusal to belong | 6 | 9 |
| Easy environment – the setting | 16 | 93 |
| Judgement-free atmosphere | 9 | 38 |
| The outdoors and getting away | 14 | 55 |
| Lack of choice | 13 | 69 |
| Feeling powerless | 6 | 11 |
| Presence or absence of choice about activities on the farm | 8 | 34 |
| Presence or absence of choice about COs | 11 | 24 |
| Looking back | 7 | 16 |
| Negative aspects of being on the CF | 7 | 16 |
| People | 16 | 147 |
| Authority figures | 15 | 85 |
| Other service users – group membership | 14 | 42 |
| Others on the CF | 6 | 18 |
| Personal growth | 15 | 104 |
| Sense of worth and achievement | 11 | 35 |
| Skills, knowledge and employment | 15 | 69 |
| Rehabilitation vs. punishment | 4 | 13 |
| Structure of the CF | 9 | 189 |
| Capacity of CF | 3 | 7 |
| Components or activities of the CF | 5 | 45 |
| Funding | 4 | 14 |
| Issues faced by CFs | 8 | 63 |
| Selection of service users | 4 | 10 |
| Vision of CF or motivation for setting up CF | 6 | 50 |
| The work | 15 | 84 |
Appendix 7 Example electronic search: MEDLINE (via Ovid)
Date range searched: 1946 to week 2 November 2014.
Search strategy
-
(care adj3 (farm or farms or farming or ranch or ranches)).tw. (61)
-
(rehab* adj3 (farm or farms or farming or ranch or ranches)).tw. (6)
-
(‘social farm*’ or ‘therapeutic farm*’).tw. (2)
-
or/1-3 [care/rehab farms or ranches] (69)
-
(farm* or farms* or ranch or ranches or land).tw. (69,177)
-
(agricultur* adj2 (setting* or environment* or facility or facilities)).tw. (990)
-
(aquacultur* or hydroponic* or ‘market garden*’ or ‘horticult* unit*’ or ‘horticult* garden*’ or (small adj3 holding*) or (nurser* adj1 garden*)).tw. (6152)
-
Agriculture/ and *‘Delivery of Health Care’/ (45)
-
‘green space*’.tw. (266)
-
or/5-9 [farms] (75,335)
-
exp nature/ (615)
-
(nature* adj1 (therap* or intervention* or rehabilitation)).tw. (94)
-
(green adj2 (care or exercise)).tw. (48)
-
((Heal or healing or sensory) adj3 garden*).tw. (19)
-
exp Horticultural Therapy/ (14)
-
exp animal assisted therapy/ or exp equine-assisted therapy/ (218)
-
‘animal* assisted’.tw. (172)
-
((riding or equine) adj1 (therap* or intervention* or rehabilitation)).tw. (71)
-
(horticultur* adj1 (treatment* or ‘vocation* program*’ or therap* or intervention* or rehabilitation)).tw. (31)
-
(forest adj (therap* or intervention*)).tw. (10)
-
onotherap*.tw. (1)
-
hippotherap*.tw. (72)
-
ecotherap*.tw. (3)
-
social horticultur*.tw. (0)
-
or/11-22 [specific agric/gardening therapies] (1218)
-
exp agriculture/ (61,996)
-
exp *Gardening/ (336)
-
(garden* or horticultur*).tw. (7720)
-
((cart or carts) adj2 (drive or driving)).tw. (0)
-
craft*.tw. (3143)
-
woodwork*.tw. (319)
-
(woodland* adj3 (restor* or manage*)).tw. (29)
-
exp ‘Conservation of Natural Resources’/ (32,365)
-
conservation*.tw. (51,521)
-
(paddock* adj2 maintenance).tw. (0)
-
farm mechanics.tw. (0)
-
((bird* or nature) adj3 watch*).tw. (44)
-
(apiar* or beekeep* or ‘bee keep*’ or ‘bee yard*’ or beehive*).tw. (674)
-
or/26-38 [Agriculture, Gardening, Countryside activities] (144,409)
-
rehabilitation/ or ‘activities of daily living’/ or animal assisted therapy/ or equine-assisted therapy/ or art therapy/ or bibliotherapy/ or dance therapy/ or early ambulation/ or exercise therapy/ or motion therapy, continuous passive/ or muscle stretching exercises/ or plyometric exercise/ or resistance training/ or occupational therapy/ or recreation therapy/ or rehabilitation, vocational/ (119,772)
-
rehabilitation centers/ (7047)
-
rh.fs. (173,336)
-
correctional.tw. (2183)
-
(therapy or therapies).tw. (1,313,901)
-
th.fs. (1,496,682)
-
or/40-45 [Rehabilitation or Therapy] (2,692,671)
-
39 and 46 [Agric/Garden/Countryside Rehab or Therapy] (5028)
-
25 or 47 [All Agric related therapies or rehab] (6198)
-
10 and 48 [Farms and Agric related therapies or rehab] (386)
-
4 or 49 [Care Farms or Agric therapy/rehab at farm setting] (444)
-
exp Horticultural Therapy/ or ‘re-entry garden*’.tw. [feedback from campbell, with less emphasis on farm or Agri setting] (14)
-
4 or 49 or 51 [Care Farms or Agric therapy/rehab at farm setting] (458)
-
exp Veterinary Medicine/ or exp Animal Experimentation/ (28,317)
-
exp animals/ not (exp animals/ and exp humans/) (4,094,644)
-
53 or 54 [Items to remove] (4,110,647)
-
52 not 55 (290)
Appendix 8 Questionnaires: Clinical Outcome in Routine Evaluation–Outcome Measure, Warwick–Edinburgh Mental Health and Well-Being Scale, service use and connectedness to nature scale
List of abbreviations
- ASSIA
- Applied Social Sciences Index and Abstracts
- CF
- care farm
- CI
- confidence interval
- CINAHL
- Cumulative Index to Nursing and Allied Health Literature
- CO
- community order
- CORE-OM
- Clinical Outcome in Routine Evaluation–Outcome Measure
- CP
- community payback
- CRC
- community rehabilitation company
- EPHPP
- Effective Public Health Practice Project
- EPOC
- Effective Practice and Organisation of Care
- ERIC
- Education Resources Information Center
- GP
- general practitioner
- HR
- human resources
- HRQoL
- health-related quality of life
- IMD
- Index of Multiple Deprivation
- IPTW
- inverse probability treatment weight
- IQR
- interquartile range
- ISA
- information sharing agreement
- IT
- information technology
- MoJ
- Ministry of Justice
- MRC
- Medical Research Council
- NOMS
- National Offender Management Service
- NPS
- National Probation Service
- OGRS
- Offender Group Reconviction Scale
- PNC
- Police National Computer
- PRISMA
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- PSSRU
- Personal Social Services Research Unit
- QALY
- quality-adjusted life-year
- RA
- research assistant
- RCT
- randomised controlled trial
- SA
- specified activity
- SCIE
- Social Care Online
- SCI-EXPANDED
- Science Citation Index Expanded
- SD
- standard deviation
- SSCI
- Social Sciences Citation Index
- SUB
- service user board
- UBA
- uncontrolled before-and-after
- WEMWBS
- Warwick–Edinburgh Mental Health and Well-Being Scale