

Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 13/163/17. The contractual start date was in October 2015. The final report began editorial review in October 2017 and was accepted for publication in May 2018. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
The University of Stirling (Martine Stead and Kathryn Angus), the University of Nottingham (Tessa Langley, Sarah Lewis and Ben Young) and the University of Edinburgh (Linda Bauld) are members of the UK Centre for Tobacco and Alcohol Studies (UKCTAS) (http://ukctas.net). Funding for UKCTAS from the British Heart Foundation, Cancer Research UK, the Economic and Social Research Council, the Medical Research Council and the National Institute for Health Research (NIHR), under the auspices of the UK Clinical Research Collaboration, is gratefully acknowledged. The funders had no role in study design, data collection and analysis, the decision to publish or preparation of the manuscript. Linda Bauld reports that she is a member of the NIHR Public Health Research (PHR) programme Research Funding Board. Srinivasa Vittal Katikireddi reports that he is a NIHR PHR programme Research Funding Board member and received grants from the Medical Research Council and the Scottish Government Chief Scientist Office during the conduct of the study. Sarah Lewis reports that she is a NIHR Health Services and Delivery Research programme Board member.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2019. This work was produced by Stead et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2019 Queen’s Printer and Controller of HMSO
Chapter 1 Introduction
Background and existing research
Behaviour change is crucial to preventing the large burden of non-communicable diseases (NCDs). 1,2 Public health organisations recommend, and spend considerable resources on, mass media campaigns to encourage reductions in risky behaviours or adoption of healthier behaviours. 1,3–5 Mass media campaigns can be run via traditional media channels, such as television, radio, cinema, newspapers, magazines and billboards, or via new digital media, including websites, pop-up and banner advertisements, QR (Quick Response) codes, viral marketing and social media. New media often feature an element of interactivity [e.g. liking, sharing or commenting on content and downloading campaign apps (applications)]. Campaigns aim to increase knowledge, influence attitudes and motivate target groups to change health behaviours. 6 Because they can be delivered at the population level, they can reach large numbers of people at a relatively low cost and are widely agreed to have an important role to play in influencing health behaviour change. 7
Evidence suggests that mass media campaigns can be effective in changing individual health behaviours, for example smoking. 8,9 However, there have been few attempts to synthesise evidence of effectiveness across multiple behaviours. An approach that examines intervention effectiveness across several health topic areas is able to offer a broad overview of evidence, and to bring attention to areas in which no systematic reviews have been conducted. 10 When evidence is scarce or highly heterogeneous (e.g. evidence of effectiveness with population subgroups), a broad overview approach allows evidence to be combined more meaningfully. For commissioners, it can help to guide decision-making regarding in what contexts and for what behaviours mass media campaigns may be most useful.
Aim and objectives
The aim of this research was to provide the NHS, local authorities, government and other organisations with evidence on the effective use of mass media to communicate public health messages.
In order to do so, we aimed to systematically review the evidence of effective uses of mass media campaigns to convey messages that lead to health behaviour change in the target audience – by preventing risky or unhealthy behaviours, by encouraging the cessation of existing risky or unhealthy behaviours, by promoting the uptake of healthy behaviours or by raising awareness of key public health issues.
In addition to the overall aim, the study had the following objectives:
-
Assess the effectiveness of mass media campaigns to communicate public health messages.
-
Examine the components of messages that can be effectively communicated through mass media.
-
Explore how different types and forms of media campaigns can reach and be effective with different target populations (particularly disadvantaged groups).
-
Assess new or emerging evidence about campaigns that employ different forms of media (including new media).
-
Examine the relationship between local, regional and national campaigns and evidence of effectiveness where this exists.
-
Assess the extent to which mass media campaigns can interact with other interventions or services to improve health outcomes.
-
Explore the currency, utility and applicability of findings with key stakeholders.
-
Identify key research gaps in relation to mass media campaigns to communicate public health messages.
Most, but not all, of our objectives were addressed in this study. The first reason for not addressing all of the objectives was that our reviews did not identify evidence to address them. This was the case for objective 4, for which we found very limited evidence on new media, and, to some extent, for objective 5, for which some key findings about campaigns of different scope and scale were available but not enough information applicable to the UK context of local, regional or national was identified. The second reason was that it became apparent that some avenues for exploration were beyond the time and resources available for the study when the volume of literature had been initially assessed. This was the case for objective 6, as it emerged that trying to fully address this objective would have required reviewing a very sizeable body of additional literature in which mass media was just one element of much broader multicomponent interventions. These limitations are discussed in Chapter 7.
Overview of the study
The study comprised a series of evidence reviews informed by a logic model. We have been guided in the write-up of this report by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement,11 although, as this report documents a large review of reviews combined with syntheses of primary studies, we had to develop our own structure to some extent.
Review of reviews
Reviews of reviews are becoming an established component in the repertoire of evidence-informed policy and practice. 12–14 They allow key findings from a range of studies to be easily accessed, while also identifying research gaps. We reviewed and synthesised evidence from English-language systematic reviews published between January 2000 and January 2016 on the effectiveness of mass media campaigns across six health topics that represent the main preventable risk factors for disease morbidity and mortality in developed countries:15 alcohol use, illicit substance use, diet, physical activity, sexual and reproductive health and tobacco use. We registered this review of reviews (review A) with PROSPERO (CRD42013004170)16 (see Chapters 2 and 5).
Reviews of primary studies
No systematic reviews addressing alcohol use or diet met our inclusion criteria for the review of reviews described in the previous section. As a result of this, and as anticipated in our protocol,16 we conducted two reviews of primary studies. The first (review B), a systematic review of English-language primary studies (published by July 2016), was conducted to assess the effectiveness of mass media public health campaigns to reduce alcohol consumption and related harms. Studies examining drink driving mass media interventions and college campus campaigns were excluded. We registered this review with PROSPERO (CRD42017054999)17 (see Chapter 3).
The second (review D) was a systematic review of English-language primary studies of mass media campaigns targeting the same six health topics, conducted in the UK and published between January 2011 and September 2016. The focus of the review was on evidence concerning the characteristics of UK mass media campaigns associated with effectiveness, rather than on the effectiveness of those campaigns per se (see Chapter 5).
Other reviews
We conducted a rapid review of reviews describing the cost-effectiveness of mass media campaigns (review C). We reviewed reviews and systematic reviews, published between January 2000 and January 2017, which assessed economic studies that evaluated both the costs and benefits of mass media campaigns for any of our six health topics of interest (see Chapter 4).
As described previously, no systematic reviews addressing diet met our inclusion criteria for the review of reviews. A scoping search for English-language primary studies (published by August 2016) was conducted for studies of mass media public health campaigns aiming to improve dietary behaviours. The modified search strategy (diet terms and mass media terms) was tested in one database (MEDLINE) and identified > 16,500 hits. A full review and synthesis was too great to conduct within the time and resources of the current project. Project resources were instead directed towards the review of recent UK primary studies (published between January 2011 and September 2016), referred to previously (review D). We focused on UK studies to complement the review of reviews (review A) and enhance the relevance for UK practitioners, policy-makers and commissioners (see Chapter 5).
The logic model
The utility of logic models in systematic reviews
In a broad systematic review such as this, a range of different types of interventions in different contexts are compared and contrasted. Critical to this process is an understanding of how the different interventions are thought (or intended) to work; this provides a conceptual framework to structure the analysis. Based on the idea of programme theory from the evaluation literature, this framework is often described as a ‘logic model’, which is a diagrammatic representation of the key intervention inputs, the activities undertaken in the intervention, and the causal pathway that is triggered by the intervention, resulting in the desired (or not desired) outcome(s). 18 Thinking critically about the causal pathway is important in public health interventions, as there are often long chains of outcomes between the intervention and the ultimate health outcome. For example, in this review, a given mass media campaign might be designed to have a given message to raise awareness about the consequences of a given behaviour. It may adopt a given strategy or intervention theory in order to raise awareness, but merely raising awareness does not necessarily result in improved health. The raised awareness needs to result in a decision to change behaviour; the initial behaviour change, and, ultimately, sustained healthier behaviours, may lead to an improvement in population health.
Many systematic reviews develop a logic model a priori, as this can then drive many of the decisions that need to be made during the systematic review process. First, systematic reviewers need to make consistent decisions about which studies are in the scope of the review and which are not. The logic model can be used to develop inclusion/exclusion criteria in order to delineate the scope of the review. Once the studies for the review have been identified, the logic model can be used to determine what data need to be extracted about studies in a standardised way, in order to structure the comparative analysis. The logic model then helps to structure the analysis, enabling reviewers to identify commonalities and differences in interventions that may help to explain variance between their results. However, although the existence of an a priori logic model can be useful for these reasons, it should be considered provisional and subject to change once the studies have been examined. This is important because once reviewers have seen the range of studies in their review they may find that the logic model does not contain sufficient nuance to capture significant differences in intervention approach, content or in the contextual factors that might influence intervention implementation – or the long causal chain between intervention and health outcome. For this reason, this review contains two logic models: the first, which informed the early stages of the review, helped reviewers to determine what was relevant and irrelevant, and what data should be extracted; the second is based on the first, and also summarised the reviewers’ understanding of the research contained within the review.
Development of the initial logic model for mass media interventions
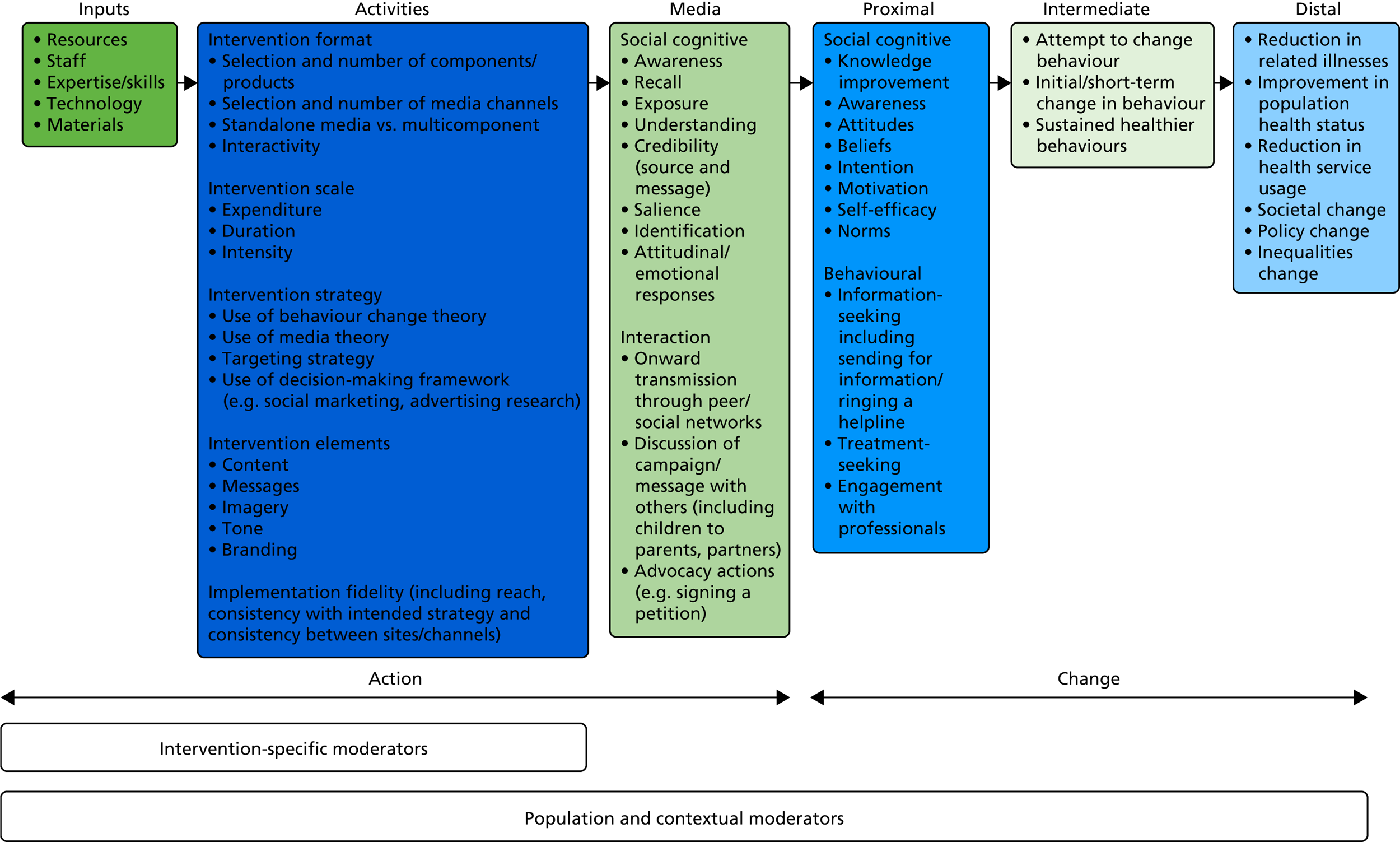
The initial logic model owes much of its overarching structure to the work of Chen. 19 We split the model into two major components: the action model (comprising the intervention inputs, activities and media outcomes) and the change model (made up of proximal, intermediate and distal outcomes). Although this may appear to be rather linear, and not cognisant of relevant theorising about complex interventions (e.g. feedback loops, phase changes and emergent outcomes; see Rogers20), we consider mass media interventions as operating in different ways to other public health interventions, and it is possible to conceptualise the intervention as a coherent entity that is implemented, and then the outcomes that result from it in a linear way (i.e. there may be feedback loops and other manifestations of complexity within the change model, but these can be understood as operating downstream of the mass media intervention, and not interacting with it).
We first developed our initial logic model for mass media interventions separately for each of the public health areas of the review before synthesising these into a common logic model. As well as demonstrating how mass media interventions may work, the resulting logic model was used to guide the evidence synthesis through helping to define inclusion and exclusion criteria, identifying moderators (and potentially subgroup analyses if meta-analyses had been possible at a later stage), and identifying mediating factors and guiding the search for evidence. 21 Our initial model represents a synthesis of logic models developed independently of mass media interventions of smoking cessation and mass media interventions of healthy eating/physical activity. In common with the development of logic models more broadly, both logic models were developed through working backwards across an outcome and action chain starting from the distal outcome.
Beginning with smoking cessation, we first located the small number of systematic reviews of mass media interventions for smoking that included a logic model, and used the model included in the review by Niederdeppe et al. 22 as a starting point. This included detail on the change part of a logic model in particular, but was enhanced with further details that helped to disaggregate some of the intermediate outcomes around behaviour change; this corresponded with other models of ‘stages of change’ in health promotion. The action part of the model was enhanced through examining logic models that were developed in other studies of mass media interventions of public health but that were not necessarily specific to smoking cessation (e.g. Huhman et al. 23), as well as significant components that were identified in reviews of mass media smoking interventions, but that were not conceptualised in a logic model (e.g. Durkin et al. 24). Finally, further stages of change of smoking cessation were identified through examining the logic models that were included in reviews of public health and policy interventions for smoking cessation, but that did not necessarily involve mass media. 25 A similar process was employed to develop the logic model for healthy eating/physical activity. To synthesise the models, common components were identified and the language harmonised; for example, both the physical activity and smoking cessation logic models included common stages of change around the attempts at adopting healthier behaviours and reduction in unhealthy behaviours as precursors to successful behaviour change, although these were originally expressed in language specific to each health topic. Even though the two health topics included here were chosen because they were conceptually relatively different and could affect very different populations (making them suitable candidates to pilot this approach), their synthesis was relatively straightforward as both involved synthesising logic models of mass media interventions to stimulate behavioural change for lifestyle behaviours. However, as we expected that some of the health topics that the review would consider may be more complex, we expected that our process of synthesising logic models and developing an overall logic model might result in topic-specific pathways being depicted within the final model; for example, mass media interventions for some health topics might also attempt to change behaviour through an intermediary party, and this might need to be depicted in the logic model. Thus, our initial logic model is presented here (Figure 1), and it was continually challenged and refined throughout the process of the review.
FIGURE 1.
The National Institute for Health Research mass media review: logic model.
Public and stakeholder engagement
Members of the public and stakeholders from a range of organisations were involved in this study. In particular, public and stakeholder engagement informed the development of the research, our refinement of research plans and the interpretation of findings. Stakeholder engagement was particularly important in shaping the focus and scale of our literature searches, in developing and finalising our logic model, and in supporting the research team to reflect on the implications and key messages from our findings, including for the design of mass media campaigns and future research. Chapter 6 describes our engagement activities in more detail.
Chapter 2 What is the impact of mass media campaigns on behaviour and other outcomes? Findings from the review of reviews (review A)
Overview
This chapter reports evidence from the review of reviews on the impact of mass media campaigns on behavioural and other outcomes, and examines evidence of variations in impact between different target populations. The chapter addresses two of the study objectives:
-
1. assess the effectiveness of mass media campaigns to communicate public health messages
-
3. explore how different types and forms of media campaigns can reach and be effective with different target populations (particularly disadvantaged groups).
Methods
Overviews of reviews are becoming an established component in the repertoire of evidence-informed (or evidence-based) policy and practice. 12–14 In order to fulfil the above objectives, we conducted a review of reviews and carried out a high-level synthesis of the evidence on the effects of mass media campaigns across multiple health behaviours. We registered this review with PROSPERO (reference number CRD42013004170). 16
Identification of reviews
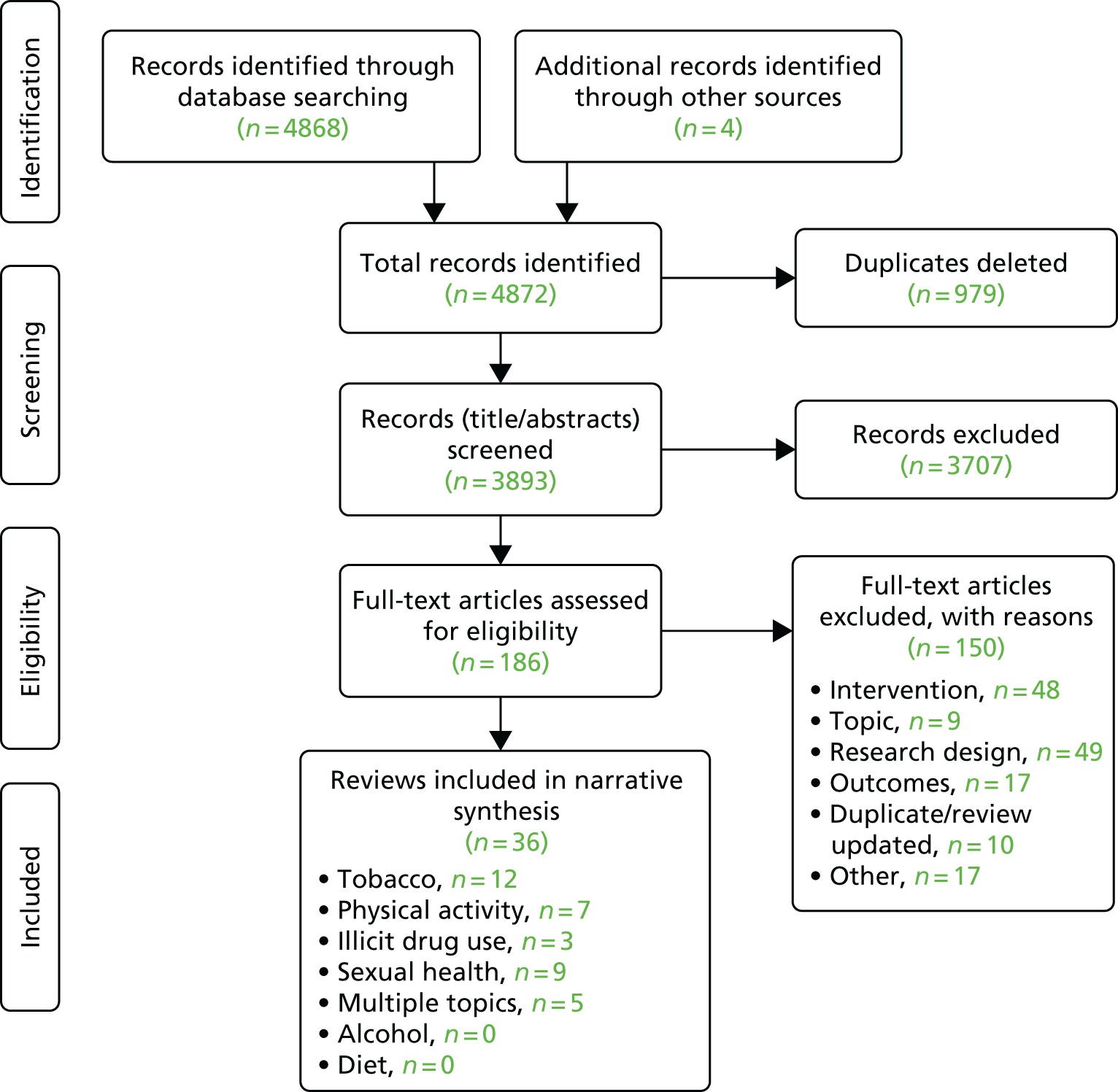
We combined terms concerning mass media campaigns, such as media, ‘mass communication’, ‘social marketing’ and broadcast, with terms denoting systematic reviews and meta-analyses (see Appendix 1). We searched the Database of Promoting Health Effectiveness Reviews, the Cochrane Database of Systematic Reviews, the Database of Abstracts of Reviews of Effects, the Campbell Collaboration Library of Systematic Reviews, the Health Technology Assessment database hosted by the Centre for Reviews and Dissemination, EMBASE, PubMed, the Cumulative Index to Nursing and Allied Health Literature, MEDLINE and Web of Science between 10 December 2015 and 5 January 2016. We did not systematically search the grey literature, which was a departure from our protocol; however, systematic reviews published as reports, rather than in peer-reviewed journals, were still identified by the strategy described above. To check the quality of the searches, we searched the results to find systematic reviews already known to the team. The reference lists of any relevant reviews of reviews were also searched. Results were uploaded to an Evidence for Policy and Practice Information and Co-ordinating Centre (EPPI)-Reviewer 4 database and deduplicated (Figure 2). 26
FIGURE 2.
The PRISMA flow diagram of the identification and selection of reviews (review A).
Review selection
Records were screened against the inclusion criteria listed in Box 1. Reviews were screened on title and abstract by three reviewers. We carried out comparison coding as an inter-rater reliability test, and, when we agreed on the included and excluded reviews at a 90% rate, the reviewers continued individually. Full-text reviews were then retrieved, and individual expert teams assessed the papers in the different health topic categories to reach the final list of reviews. Two researchers from the wider team adjudicated if there was uncertainty about whether or not to include a review. See Appendix 2 for a list of reviews excluded by full-text assessment.
The review:
-
Was published in or after 2000.
-
Was published in English.
-
Concerned human populations.
-
Included interventions that met the definition of a mass media intervention – the intentional use of any media channel(s) of communication by local, regional and national organisations to influence lifestyle behaviour through largely passive or incidental exposure to media campaigns, rather than largely dependent on active help-seeking (adapted from Wakefield et al. 6 and Bala et al. 27). This excludes, for example, health campaign websites that individuals actively searched for or signed up for.
-
Examined one or more of the following health topics – alcohol use, illicit substance use, diet, physical activity (including sedentary behaviour), sexual and reproductive health, and tobacco use. Reviews examining mass media interventions promoting health screening behaviours (e.g. human immunodeficiency virus testing and cervical screening) are excluded because NHS population screenings are not part of the remit of the National Institute for Health Research Public Health Research programme.
-
Was conducted as a systematic review, which was defined as including a specified search strategy from more than one database, an assessment of the quality of studies and some kind of synthesis of the primary studies.
-
Reported sufficient outcome data on behaviour change and/or its individual determinants. In multicomponent interventions, the outcome data had to relate to the mass media component, not to the whole intervention.
Data extraction
Data from reviews identified as meeting the inclusion criteria were extracted into a standardised data extraction form. Data extracted included review characteristics, participant characteristics, types of study design, types of synthesis and outcome data (particularly social cognitive and behavioural outcomes). For each topic, one reviewer extracted the data, and a sample (≥ 25%) was checked by a second reviewer to ensure the consistency of the extraction.
Quality appraisal and relevance assessment
We used the Risk Of Bias In Systematic reviews (ROBIS) tool to assess the risk of bias of included systematic reviews. 28 Included reviews were assessed by one researcher, and a second researcher checked all their assessments against the full-text review and ROBIS guidelines, with any disagreements discussed between the two researchers. We rated the relevance of the included reviews to our aims (high or low relevance), based on two dimensions: its relevance to an Organisation for Economic Co-operation and Development (OECD) context (included studies conducted in OECD countries versus all studies in the review that were conducted in non-OECD countries)29 and whether or not the review’s main focus was on mass media interventions. We also extracted information on the quality of the included studies in each review as assessed by the review authors: good, medium or low quality or not stated.
Data synthesis
Given the highly heterogeneous nature of the interventions and reviews, we did not attempt to conduct meta-analysis, and a narrative synthesis approach was pursued. 30 We initially tabulated all available data according to topic and tried to identify duplicate results. We then created tabular summaries of the full data, with information on potential bias within the included evidence base retained. We investigated patterns in the available results, making comparisons across topics, outcomes and population subgroups [based on the PROGRESS (Place of residence; Race/ethnicity/culture/language; Occupation; Gender/sex; Religion; Education; Socioeconomic status; Social capital) characteristics],31 with due attention paid to contradictory data. Analysis proceeded iteratively, with the whole team regularly meeting to discuss findings. To summarise the results for the outcomes of interest (behaviours, intentions, awareness/knowledge and attitudes), a symbol was applied to indicate how good the evidence was for a positive or negative effect. 32 This incorporated the risk of bias of the relevant reviews and reported effect sizes/directions. Inconsistency statistics were extracted from relevant meta-analyses.
To make conclusions based on the available evidence, we developed a systematic and transparent approach, building on principles of the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach. 33,34 In addition to risk of bias, we also assessed the domains of inconsistency, indirectness and imprecision for each behaviour. Inconsistency assessed whether or not the reported effects for a behaviour differed between assessments of behaviour change and its determinants, as well as whether or not high statistical heterogeneity was observed within meta-analysis. Directness referred to how directly the evidence related to the health topics examined in this review within the UK context. Evidence on behavioural outcomes was considered ‘direct’ whereas evidence regarding awareness/knowledge, attitudes or intentions only was considered ‘indirect’. Similarly, if available evidence was primarily drawn from non-OECD countries then this was considered indirect. Imprecision was assessed on the basis of the precision of the effect estimate [e.g. did the 95% confidence interval (CI) exclude no effect?]. ‘Overall effect’ was assessed by taking into account the direction of effect for behaviour with consideration of the indirect outcomes and the risk of bias in the evidence available. When there was evidence at a low risk of bias that was directly observed for the behaviour of interest, with little imprecision and inconsistency, we considered this to have a high level of certainty. We downgraded to moderate, low or very low certainty if there was a high risk of bias (by two levels), indirect evidence (by two levels), inconsistency (by one level) and imprecision (by one level).
Overview of the included reviews
Thirty-six systematic reviews were included from the initial 3893 records screened (see Figure 2). The reviews examined mass media interventions for tobacco use (12 reviews),27,35–45 sexual health (nine reviews),46–54 physical activity (seven reviews,55–61 of which one focused on reducing sedentary behaviour)55 and illicit drug use (three reviews),62–64 with five reviews addressing ‘mixed topics’65–69 (i.e. more than one of our six health topics) (Table 1). Although no systematic reviews met our inclusion criteria for alcohol use or diet mass media interventions, studies evaluating campaigns targeting alcohol or diet were included in four mixed heath topics reviews. Fourteen reviews were assessed to have a high risk of bias and 22 were considered to have a low risk of bias (see Appendix 3). Approximately half of the reviews focused solely on mass media interventions (n = 17), and the others reviewed broader ranges of behaviour change interventions including mass media campaigns. When geographical data were provided for mass media studies, 15 of the reviews included at least one study from the UK and four reviews included studies from only non-OECD countries (all sexual health topic reviews); the rest were mainly studies of mass media campaigns from OECD countries. On the basis of the focus of the reviews on mass media and geographical data, 18 of the included reviews were judged as highly relevant to the topic. We searched for reviews published between January 2000 and January 2016; the time period covered by the included reviews’ searches ranged from database inception to January 2015, and the most recent included study was published in 2013.
| Review (first author and year); risk of bias (ROBIS) | Health topic | Was mass media the sole focus? | Aim of the review | Relevance to our review of reviews | Type of synthesis | Number of included studies | Number of relevant studies |
|---|---|---|---|---|---|---|---|
| Abioye (2013);55 low risk of bias | Physical activity | Yes | We searched six electronic databases from their inception to August 2012 and selected prospective studies that evaluated the effect of MMCs on physical activity in adults | High | Meta-analysis | 9 | 9 |
| Bala (2013);27 low risk of bias | Tobacco use | Yes | To assess the effectiveness of MMCs in reducing smoking among adults. Four research questions: i) Do MMCs reduce smoking (prevalence, cigarette consumption, quit attempts and quit rates) compared with no intervention in comparison communities? ii) Do MMCs run in conjunction with tobacco control programmes reduce smoking, compared with no intervention or with tobacco control programmes alone? iii) Which study characteristics relate to their efficacy? iv) Do tobacco MMCs cause any adverse effects? | High | Narrative synthesis | 11 | 11 |
| Bertrand (2006);46 low risk of bias | Sexual health | Yes | To review the strength of the evidence for the effects of three types of [broadcast] mass media interventions . . . on HIV/AIDS-related behaviour among young people in developing countries and to assess whether these interventions reach the threshold of evidence needed to recommend widespread implementation | Low | Narrative synthesis | 15 | 15 |
| Brinn (2010);35 low risk of bias | Tobacco use | Yes | To determine the strength of the evidence that mass media interventions to prevent smoking in young people may: 1) reduce smoking uptake among youths (< 25 years), 2) improve smoking attitudes, behaviour and knowledge, 3) improve self-efficacy/self-esteem, 4) improve perceptions about smoking including the choice to follow positive role models | High | Narrative synthesis | 7 | 7 |
| Brown (2012);56 high risk of bias | Physical activity | Yes | The goal of the systematic review described in this summary was to determine the effectiveness of stand-alone MMCs to increase physical activity at the population level | High | Meta-analysis and narrative synthesis | 16 | 16 |
| Brown (2014);37 high risk of bias | Tobacco use | No | To assess the effectiveness of population-level interventions/policies to reduce socioeconomic inequalities in smoking among adults by assessing primary studies of any intervention/policy that reported differential effects on a smoking-related outcome in at least two socioeconomic groups | Low | Narrative synthesis | 117 | 30 |
| Brown (2014);36 high risk of bias | Tobacco use | No | What is the equity impact of interventions/policies to reduce youth smoking? | Low | Narrative synthesis | 38 | 1 |
| Byrne (2005);65 high risk of bias | Multiple – alcohol use, tobacco use, illicit drug use | Yes | Aims to critically review the literature on past and current drug, alcohol, and tobacco use prevention media campaigns, examining the similarities across health communication programme believed to be effective, with the aim of viewing their applicability for the prevention of youth problem gambling | High | Narrative synthesis | 25 | 25 |
| Carter (2015);47 low risk of bias | Sexual health | No | Community education may involve activities that seek to raise awareness and promote behaviour change, using mass media, social media, and other media or interpersonal methods in community settings. This systematic review evaluated the evidence of the effects of community education on select short- and medium-term family planning outcomes | High | Narrative synthesis | 17 | 14 |
| de Kleijn (2015);38 high risk of bias | Tobacco use | No | The primary aim of this review was to determine how effective school-based interventions are in preventing girls smoking, and the secondary objective was to determine which interventions are most successful | Low | Meta-analysis and narrative synthesis | 37 | 4 |
| Derzon (2002);66 high risk of bias | Multiple – alcohol use, tobacco use, illicit drug use | Yes | A synthesis into the capability of media interventions to reduce youth substance-use | High | Meta-analysis | 72 | 72 |
| Ellis (2003);67 low risk of bias | Topics: multiple – diet, tobacco use | No | (1) to provide an overview of the cancer control interventions (adult smoking cessation, adult healthy diet, mammography, cervical cancer screening, control of cancer pain) that are effective in promoting behaviour change and (2) to identify evidence-based strategies that have been evaluated to disseminate these cancer control interventions | Low | Narrative synthesis | 31 | 8 |
| Ferri (2013);62 low risk of bias | Illicit drug use | Yes | To assess the effectiveness of mass media campaigns in preventing or reducing the use of or intention to use illicit drugs among young people | Low | Meta-analysis and narrative synthesis | 23 | 23 |
| Finlay (2005);57 high risk of bias | Physical activity | Yes | The 1998–2002 studies (interventions) were reviewed for their success in impacting message recall and behaviour change. The newer studies plus those identified by Kahn et al. (2002) and Marcus et al. (1998), were assessed for the presence of a more sophisticated understanding of the media processes of inception, transmission and reception | High | Narrative synthesis | 17 | 8 |
| French (2014);48 low risk of bias | Sexual health | Yes | An exploratory review was conducted to assess research examining awareness, acceptability, effects on HIV testing, disclosure and sexual risk, and cost-effectiveness of HIV mass media campaigns targeting MSM | High | Narrative synthesis | 12 | 12 |
| Gould (2013);39 low risk of bias | Tobacco use | Yes | (a) To systematically review and summarise the literature describing attitudes and key responses to culturally targeted anti-tobacco messages [in indigenous and First Nations populations in Australia, New Zealand, USA and Canada] and (b) identify any differences in effect according to whether the messages were addressed to the target population or . . . general population | Low | Narrative synthesis | 20 | 11 |
| Grilli (2000);49 low risk of bias | Sexual health | Yes | To assess the effects of mass media on the utilisation of health services | Low | Narrative synthesis | 21 | 2 |
| Guillaumier (2012);40 low risk of bias | Tobacco use | Yes | 1. Systematically review the published evidence of the effectiveness of MMCs (with the primary purpose of encouraging smokers to quit) with smokers from socially disadvantaged groups. 2. Critique the methodological quality of the evidence for the effectiveness of MMCs with disadvantaged groups | High | Narrative synthesis | 17 | 17 |
| Hemsing (2012);41 high risk of bias | Tobacco use | No | 1. Do interventions that involve partners’ support of their pregnant partners lead to effective smoking cessation among pregnant partners during pregnancy and postpartum? 2. Are there interventions that are effective in encouraging partners who smoke to stop smoking? . . . Do the intensity and modality of the intervention influence effectiveness? | Low | Narrative synthesis | 9 | 1 |
| Hill (2014);42 high risk of bias | Tobacco use | No | To review and synthesise existing evidence on the equity impact of tobacco control interventions by SES | Low | Narrative synthesis | 77 | 12 |
| Jepson (2006);43 low risk of bias | Tobacco use | Yes | To synthesise evidence evaluating the effectiveness of mass media interventions on helping people to quit smoking/tobacco use and/or to prevent relapse. These interventions were considered for both the effectiveness of the channel of communication and also for the effectiveness of message content | High | Narrative synthesis | 44 | 39 |
| Kahn (2002);58 high risk of bias | Physical activity | No | The Guide to Community Preventive Service’s methods for systematic reviews were used to evaluate the effectiveness of various approaches to increasing physical activity: informational, behavioural and social, and environmental and policy approaches. Changes in physical activity behaviour and aerobic capacity were used to assess effectiveness | Low | Narrative synthesis | 94 | 6 |
| Kesterton (2010);50 high risk of bias | Sexual health | No | This review investigates the effectiveness of interventions aimed at generating demand for and use of sexual and reproductive health services by young people, and interventions aimed at generating wider community support for their use | Low | Narrative synthesis | 74 | 3 |
| LaCroix (2014);51 low risk of bias | Sexual health | Yes | This meta-analysis was conducted to synthesize evaluations of mass media–delivered HIV prevention interventions, assess the effectiveness of interventions in improving condom use and HIV-related knowledge, and identify moderators of effectiveness | Low | Meta-analysis | 54 | 54 |
| Leavy (2011);59 high risk of bias | Physical activity | Yes | To assess progress and quality of (i) campaign evaluation design and sampling, (ii) use of theory and formative research in campaign development and (iii) evidence of campaign effects including proximal, intermediate and behavioural outcomes | High | Narrative synthesis | 18 | 18 |
| Matson-Koffman (2005);60 low risk of bias | Physical activity | No | To review selected and recent environmental and policy interventions designed to increase physical activity and improve nutrition as a way to reduce the risk of heart disease and stroke, promote CVH [cardiovascular health], and summarise recommendations | Low | Narrative synthesis | 64 | 7 |
| Mozaffarian (2012);68 low risk of bias | Multiple – diet, physical activity, tobacco use | No | To identify and assess the evidence for the effectiveness of population approaches in changing dietary, physical activity, or tobacco use habits and related health outcomes. Population strategies were . . . media and educational campaigns . . . consumer information . . . economic incentives, school and workplace approaches, local environmental changes and direct restrictions | Low | Narrative synthesis | ≈100 (not stated) | 31 |
| Ogilvie (2007);61 low risk of bias | Physical activity | No | To conduct a systematic review of the best available evidence across all relevant disciplines to determine what characterises interventions effective in promoting walking; who walks more and by how much as a result of effective interventions; and the effects of such interventions on overall physical activity and health | Low | Narrative synthesis | 48 | 2 |
| Richardson (2008);44 low risk of bias | Tobacco use | No | This review examines the effectiveness of: (a) mass media interventions designed to prevent the uptake of smoking in children and young people and (b) interventions that are designed to prevent the illegal sale of tobacco to children and young people | High | Narrative synthesis | 41 | 37 |
| Robinson (2014);69 low risk of bias | Multiple – physical activity, sexual health, tobacco use | Yes | This review aimed to assess the effectiveness of health communication campaigns that include both mass media and health-related product distribution to increase healthy behaviour change. (The criterion requiring campaigns to use a mass media channel was developed to decrease the challenge of distinguishing campaigns from health education interventions) | High | Meta-analysis and narrative synthesis | 25 study arms in 22 included studies | 11 relevant study arms |
| Speizer (2003);52 high risk of bias | Sexual health | No | We review and synthesise this emerging body of evidence with an eye towards advancing our understanding of ‘what works’ in adolescent reproductive health programming in developing countries | Low | Narrative synthesis | 41 | 6 |
| Swanton (2015);53 low risk of bias | Sexual health | No | The aim of the present research was to examine the effect that new-media-based sexual health interventions have on sexual health behaviours in non-clinical populations and to determine the factors that moderate the effect of technology-based sexual health interventions on sexual health behaviours | High | Meta-analysis | 15 | 12 |
| Sweat (2012);54 low risk of bias | Sexual health | No | To examine the relationship between condom social marketing programmes and condom use | Low | Meta-analysis | 11 | 6 |
| Werb (2011);63 high risk of bias | Illicit drug use | Yes | To investigate the state of the research related to the effectiveness of anti-illicit drug public service announcements in modifying behaviour and intention to use illicit drugs among target populations | High | Meta-analysis | 11 | 11 |
| Werb (2013);64 low risk of bias | Illicit drug use | No | To systematically search the existing peer-reviewed scientific literature in order to identify and assess interventions to prevent the initiation of injection drug use | Low | Narrative synthesis | 8 | 1 |
| Wilson (2012);45 low risk of bias | Tobacco use | No | To evaluate the independent effect on smoking prevalence of four tobacco control policies outlined in the WHO MPOWER Package: increasing taxes on tobacco products, banning smoking in public places, banning advertising and sponsorship of tobacco products, and educating people through health warning labels and antitobacco MMCs | High | Narrative synthesis | 84 | 19 |
The reviews focused on a range of target groups, including studies of mass media campaigns targeting by age group, socioeconomic status, ethnicity, sex, sexual orientation, addictive behaviours, morbidity or parental/pregnancy status, in addition to whole-population, untargeted campaigns. Twelve reviews did not report the sample sizes of their included studies, and a further four reviews only reported some samples sizes. Over the other 20 reviews, the sample sizes of included studies ranged from 27 to 130,245 participants.
Most of the reviews included studies of mass media campaigns that had national reach (n = 22), with a third of these including only national campaigns (n = 7); the rest also included regional and local campaigns. Ten reviews included studies of mass media campaigns that had a local reach only or had a local or national reach. Four of the reviews did not report details on the reach of the campaigns.
Twenty-six reviews presented a narrative synthesis of study results, six reviews completed a meta-analysis of the data and four reviews used both methods to synthesise and present findings. The reviews examined a range of direct behavioural outcomes (reducing harmful behaviours, increasing healthy behaviours and help-seeking), indirect behavioural outcomes and sociocognitive outcomes (intentions, awareness and knowledge, attitudes and beliefs, and norms and self-efficacy), and 16 reviews analysed data for subpopulations (see Table 1).
The types of studies included by the reviews in their syntheses were reported in most of the reviews (n = 34). The majority of syntheses included a mixture of study designs, from randomised control trials (RCTs) and trials, cohort studies, pre–post studies and post-test only studies (n = 23). Four reviews synthesised data from RCTs and trials only, six reported data from pre–post-test studies only and one review reported post-test data only (see Appendix 4 for the detailed characteristics of the included systematic reviews).
Evidence of impact on behavioural outcomes
We examined evidence of the effects of mass media campaigns on behavioural outcomes relating to all of our health topics. Rather than present evidence simply by health topic, we synthesised evidence across three broad categories of behavioural outcome: reducing harmful behaviours, increasing healthy behaviours and treatment-seeking. We were interested in examining whether or not the effectiveness of mass media campaigns differs across these three types of behavioural outcome; for example, are mass media campaigns more effective at encouraging or reinforcing positive behaviours than at discouraging negative behaviours? We defined ‘reducing harmful behaviours’ as bringing about a reduction in behaviours that have harmful effects (e.g. preventing young people from taking up smoking or encouraging smoking cessation, reducing other substance use and reducing sedentary behaviour). We defined ‘increasing healthy behaviours’ as encouraging greater engagement in behaviours that are protective of health, such as engaging in physical activity or using a condom. ‘Treatment-seeking’ was defined as engaging in specific actions to secure information, advice, support or treatment relating to the health topics examined in the review, for example using a sexual health service, seeking testing for sexually transmitted diseases or calling a smoking quitline.
Reducing harmful behaviours
Fourteen reviews reported evidence on whether or not mass media campaigns reduced harmful behaviours, as outlined in Table 2. 27,35,38,40,41,43–45,55,62,63,65,66,68 Eleven focused on a specific health topic and three examined mixed health topics. 65,66,68 All 14 reviews included studies based in OECD countries, and seven included studies conducted in the UK. 27,41,43–45,55,68 Ten of the reviews were rated as having a low risk of bias27,35,38,40,43–45,55,62,68 and four were considered to have a high risk of bias. 41,63,65,66 Eleven reviews focused on a specific health topic and three examined mixed health topics. 65,66,68 Three reviews used meta-analysis,55,62,66 with the remainder presenting results in a narrative synthesis.
| Review topic | Outcome | Review (first author and year) | Result | Risk of bias and quality | ||
|---|---|---|---|---|---|---|
| Review risk of biasa | Quality of included studiesb | Mass media focus | ||||
| Physical activity | Reduction in sedentary behaviour | Abioye (2013)55 |
▲ RR 1.15, 95% CI 1.03 to 1.30 (4 studies) ~ I2 = 63% |
✓ | = | All 15 studies on mass media |
| Illicit drugs | Use of illicit drugs | Ferri (2013)62 |
Meta-analysis of RCTs: ● ~ I2 = 70% |
✓ | = | All 23 studies on mass media |
| Illicit drugs | Use of illicit drugs | Ferri (2013)62 |
Other study designs (not RCTs): △ |
✓ | = | All 23 studies on mass media |
| Illicit drugs | Use of illicit drugs | Werb (2011)63 |
▲ ~ I2 = 100% |
✗ | Not stated | All 11 studies on mass media |
| Tobacco | Smoking uptake | Richardson (2008)44 | △ | ✓ | = | 37 of 60 studies on mass media |
| Tobacco | Smoking initiation | Wilson (2012)45 | ◁▷ | ✓ | = | 19 of 84 studies on mass media |
| Tobacco | Smoking uptake | Brinn (2010)35 | ◁▷ | ✓ | ✗ | All 7 studies on mass media |
| Tobacco | Smoking uptake | de Kleijn (2015)38 | △ | ✓ | Not stated | 4 of 37 studies on mass media |
| Tobacco | Smoking prevalence | Bala (2013)27 | ◁▷ | ✓ | ✗ | All 11 studies on mass media |
| Tobacco | Smoking prevalence | Wilson (2012)45 | ◁▷ | ✓ | = | 19 of 84 studies on mass media |
| Tobacco | Smoking consumption | Bala (2013)27 | ◁▷ | ✓ | ✗ | All 11 studies on mass media |
| Tobacco | Quit attempts | Bala (2013)27 | ◁▷ | ✓ | ✗ | All 11 studies on mass media |
| Tobacco | Quit rates | Bala (2013)27 | ◁▷ | ✓ | ✗ | All 11 studies on mass media |
| Tobacco | Quit attempts | Hemsing (2012)41 |
O Based on 1 study |
✗ | = | 1 of 9 studies on mass media |
| Tobacco | Smoking cessation | Wilson (2012)45 | ◁▷ | ✓ | = | 19 of 84 studies on mass media |
| Tobacco | Smoking cessation | Jepson (2006)43 | ◁▷ | ✓ | ✗ | 39 of 44 studies on mass media |
| Tobacco | Smoking cessation | Guillaumier (2012)40 | ◁▷ | ✓ | ✗ | 17 of 17 studies on mass media |
| Tobacco (mixed topics review) | Smoking prevention and cessation | Mozaffarian (2012)68 | △ | ✓ | = | 25 of about 100 studies |
| Mixed topics | Substance use (illicit drugs, alcohol and tobacco) | Derzon (2002)66 | ▲ | ✗ | Not stated | All 72 studies |
| Mixed topics | Substance use (illicit drugs, alcohol and tobacco) | Byrne (2005)65 | △ | ✗ | Not stated | All 25 campaigns in 53 studies |
Effects on sedentary behaviour were examined in one review. A meta-analysis of studies based in OECD countries on the effect of mass media campaigns on physical activity in adults found evidence of mass media campaigns reducing sedentary behaviour [relative risk (RR) 1.15, 95% CI 1.03 to 1.30], with moderate heterogeneity observed (I2 = 63%; p = 0.018). 55
Two reviews reported on whether or not mass media campaigns had an impact on illicit drug use. A meta-analysis of RCT studies of campaigns targeting young people (aged < 26 years) found no effect (standardised mean difference –0.02, 95% CI –0.15 to 0.12), but did find evidence of reductions in the use of illicit drugs in an analysis of non-RCT studies. 62 The other, a review of the effects of anti-illicit drug public service announcements on youth (no definition by age specified) found very small positive reductions in illicit drug use, with considerable inconsistency; however, it should be noted that this review had a high risk of bias. 63
Nine reviews (eight specifically focusing on tobacco27,35,38,40,41,43–45 and one examining a range of health topics68) examined the impact of mass media campaigns on tobacco use. All included OECD-based studies and five included UK studies. 27,41,43–45 Four reviews, all considered to have a low risk of bias, examined the impact on preventing smoking uptake in young people. The review by Richardson et al. ,44 which included one UK study, reported positive results for smoking prevention: the narrative synthesis found evidence to suggest that mass media campaigns can prevent the uptake of smoking in young people (evidence from one review and two studies) and that industry-sponsored studies are less effective (evidence from one study). The other three reviews – Wilson et al. 45 (which included one UK study), de Kleijn et al. 38 and Brinn et al. 35 – all reported mixed results.
Five reviews examined smoking cessation or quit rates. Four reviews with a low risk of bias that included UK or OECD studies reported mixed results. 27,40,43,45 The fifth review reported no effect on quit attempts; the review had a high risk of bias and the evidence was from one study conducted in the UK. 41 Finally, a review that examined a range of health topics reported evidence of mass media campaigns having a positive effect on the combined outcomes of smoking prevention and cessation. 68
The impact of mass media on the use of a combination of substances (alcohol, illicit drugs and alcohol) was examined by two mixed health topic reviews. 65,66 Although both of these reviews reported positive effects, both reviews were rated as having a high risk of bias.
Increasing healthy behaviours
Twelve reviews reported evidence on whether or not mass media campaigns can increase healthy behaviours (Table 3). Ten focused on specific health topics (either physical activity55–61 or sexual health52–54) and two examined a range of topics. 68,69 None of the included reviews focused exclusively on diet/healthy eating, but one of the mixed-topic reviews included evidence on diet-related behaviours. 69 Nine of the reviews included studies conducted in OECD countries,55–61,68,69 four included studies conducted in the UK55,57,58,60 and two did not report the countries. 53,56 Two of the reviews, focusing on sexual health interventions, comprised studies conducted in low- and middle-income countries. 52,54
| Review topic | Outcome | Review (first author and year) | Result | Risk of bias and quality | Mass media focus | |
|---|---|---|---|---|---|---|
| Review risk of biasa | Quality of included studiesb | |||||
| Diet (mixed-topic review) | Consumption of healthy food | Mozaffarian (2012)68 | △ | ✓ | = | 25 of about 100 studies |
| Physical activity | Brisk walking | Abioye (2013)55 |
▲ RR 1.53 (95% CI 1.25 to 1.87) ✓ I2 = 0% |
✓ | = | All 15 studies on mass media |
| Physical activity | Time spent walking | Ogilvie (2007)61 | △ | ✓ | = | 2 of 48 studies on mass media |
| Physical activity | Overall physical activity | Abioye (2013)55 |
● RR 1.02 (95% CI 0.91 to 1.14) ~ I2 = 72% |
✓ | = | All 15 studies on mass media |
| Physical activity (mixed-topic review) | Increases in physical activity | Mozaffarian (2012)68 | △ | ✓ | = | 25 of about 100 studies |
| Physical activity | Self-reported time spent in physical activity | Brown (2012)56 |
▲ Median relative increase of 4.4% |
✗ | = | All 16 studies on mass media |
| Physical activity | Self-reported activity | Brown (2012)56 | △ | ✗ | = | All 16 studies on mass media |
| Physical activity | Changes in physical activity | Finlay (2005)57 | ◁▷ | ✗ | = | All 8 studies on mass media |
| Physical activity | Self-reported activity | Brown (2012)56 | ◁▷ | ✗ | = | All 16 studies on mass media |
| Physical activity | Changes in physical activity | Leavy (2011)59 | ◁▷ | ✗ | ✗ | All 18 studies on mass media |
| Physical activity | Stair use | Matson-Koffman (2005)60 | △ | ✓ | ✓ | 9 of 64 studies on mass media |
| Physical activity (mixed-topic review) | Stair use | Mozaffarian (2012)68 | △ | ✓ | = | 25 of about 100 studies |
| Physical activity | Stair use | Kahn (2002)58 | △ | ✗ | = | 6 of 94 studies on mass media |
| Sexual health | Condom use | Swanton (2015)53 |
▲ OR 1.39 (95% CI 1.06 to 1.83) ~ I2 = 77.2% |
✓ | ✗ | 12 of 15 studies on mass media |
| Sexual health | Condom use – most recent sex encounter | Sweat (2012)54 |
▲ OR 2.01 (95% CI 1.42 to 2.84) ~ (narratively assessed) |
✓ | ✗ | 6 of 11 studies on mass media |
| Sexual health | Condom use – all condom use | Sweat (2012)54 |
▲ OR 2.10 (95% CI 1.51 to 2.91) ~ (narratively assessed) |
✓ | ✗ | 6 of 11 studies on mass media |
| Sexual health | Condom use | Speizer (2003)52 | ◁▷ | ✗ | ✓ | 6 of 41 studies on mass media |
| Sexual health (mixed-topic review) | Condom use | Robinson (2014)69 | △ | ✓ | = | All 22 studies |
Eight of the reviews examined whether or not there was evidence that mass media campaigns could increase physical activity. A range of physical activity outcomes were reported, including walking, overall levels of physical activity, and using the stairs. In reviews that examined impact on stair use, the mass media campaigns typically comprised ‘point-of-decision prompts’, such as posters in locations with high footfall (e.g. public transport hubs and workplaces), encouraging people to use the stairs rather than the lift or escalator.
Two reviews with a low risk of bias reported evidence that mass media campaigns increased walking behaviour. In a meta-analysis of four studies, Abioye et al. 55 found evidence that mass media campaigns could produce an increase in brisk walking (RR 1.53, CI 1.25 to 1.87), whereas Ogilvie et al. 61 found evidence from two studies that mass media campaigns increased the time spent walking. Two reviews with a low risk of bias, one focusing specifically on physical activity60 and one examining a range of topics,68 found that stair use was increased by mass media campaigns comprising point-of-decision prompts (e.g. signs and banners to encourage using stairs). A third review, with a high risk of bias, also reported evidence that mass media campaigns could increase stair use. 58
However, reviews that examined overall levels of physical activity or time spent in physical activity reported generally mixed evidence. A meta-analysis of four studies in one review with a low risk of bias found no clear impact on overall physical activity (RR 1.02, 95% CI 0.91 to 1.14; I2 = 72%). 55 In contrast, a mixed-topic review at low risk of bias found a positive effect on increases in overall physical activity. 68 The evidence from three reviews with a high risk of bias that examined changes in physical activity behaviours was generally mixed. 56,57,59
Four reviews provided evidence on whether or not mass media campaigns could increase healthy sexual health behaviours. Three reviews with a low risk of bias examined the impact of mass media on condom use: two of these reviews conducted meta-analysis and found that media campaigns had a positive effect on condom use, with inconsistency in the effect estimates [odds ratio (OR) 1.39, 95% CI –1.06 to –1.83;53 and OR 2.01, 95% CI 1.42 to 2.84, OR 2.10, 95% CI 1.51 to 2.9154]. The third review, which was of mixed health behaviour topics, also reported positive effects on condom use. 69 The fourth review reported mixed results of the effect of mass media on sexual health behaviours;52 this review was found to have a high risk of bias.
Finally, a mixed-topic review with a low risk of bias reported that mass media campaigns could have a positive effect on the consumption of healthy food. 68
Treatment-seeking
Ten reviews provided information on treatment-seeking: six focused on treatment-seeking in relation to sexual health46–50,52 and four focused on treatment-seeking in relation to tobacco use (Table 4). 27,37,42,43 Seven of the reviews included studies conducted in OECD countries,27,37,42,43,47–49 and all seven included studies conducted in the UK. Six were at a low risk of bias27,43,46–49 and four were at a high risk of bias. 37,42,50,52
| Review topic | Outcome | Review (first author and year) | Result | Risk of bias and quality | Mass media focus | |
|---|---|---|---|---|---|---|
| Review risk of biasa | Quality of included studiesb | |||||
| Sexual health | Use of family planning services | Carter (2015)47 | △ | ✓ | = | 14 of 17 studies on mass media |
| Sexual health | Use of health services | Grilli (2000)49 | ◁▷ | ✓ | ✗ | 2 of 21 studies on mass media |
| Sexual health | Use of health centre | Kesterton (2010)50 |
△ Based on 1 study |
✓ | ✗ | 3 of 74 studies on mass media |
| Sexual health | Use of clinic | Speizer (2003)52 |
△ Based on 1 study |
✗ | ✓ | 6 of 41 studies on mass media |
| Sexual health | HIV testing | French (2014)48 | ◁▷ | ✓ | ✗ | All 12 studies on mass media |
| Sexual health | Use of HIV service/clinic | Bertrand (2006)46 | ◁▷ | ✓ | ✗ | All 15 studies on mass media |
| Tobacco | Calls to quitline | Jepson (2006)43 | △ | ✓ | ✗ | 39 of 44 studies on mass media |
| Tobacco | Calls to quitline | Bala (2013)27 |
△ Based on 1 study |
✓ | ✗ | All 11 studies on mass media |
| Tobacco | Calls to quitline | Hill (2014)42 | ◁▷ | ✗ | ✗ | 12 of 77 studies on mass media |
| Tobacco | Calls to quitline | Brown (2014)37 | ◁▷ | ✗ | ✗ | 30 of 117 studies on mass media |
Of four reviews examining the impact of media campaigns on the use of sexual health services or clinics, one found a positive effect47 and one reported mixed results. 49 Positive results were reported in two further reviews,50,52 but results were from only one study in each review and both reviews were at high risk of bias. The effects of mass media campaigns on the uptake of HIV testing or HIV services was examined in two reviews with a low risk of bias, both reporting mixed evidence. 46,48
There was evidence of mass media campaigns having a positive effect on calls to smoking quitlines from two reviews with a low risk of bias,27,43 although this was based on only one study in one of the reviews. 27 Mixed evidence was reported for the impact of mass media campaigns on smoking quitlines in two reviews with a high risk of bias. 37,42
Evidence of the impact on indirect behavioural outcomes and social cognitive outcomes
We also examined evidence of the effects of mass media campaigns on indirect behavioural outcomes and social cognitive outcomes. Indirect behavioural outcomes were defined as intentions to engage in, reduce or desist from unhealthy behaviours (such as smoking) or to engage in healthy behaviours (such as condom use). Social cognitive outcomes comprised awareness, knowledge, attitudes, beliefs, norms and self-efficacy.
Intentions
Seven reviews examined whether or not there was evidence that mass media campaigns had an impact on intentions to change behaviour (Table 5). 35,39,47,59,62,63,69 All of the reviews included studies from OECD countries but none included studies from the UK. Statistical methods were used in two reviews to assess the impact of mass media campaigns on illicit drug use intentions. 62,63 The remaining five reviews used narrative synthesis. Most of the reviews were of good quality (at a low risk of bias).
| Review topic | Outcome | Review (first author and year) | Result | Risk of bias and quality | Mass media focus | |
|---|---|---|---|---|---|---|
| Review risk of biasa | Quality of included studiesb | |||||
| Illicit drug use | Not to use/to reduce use/to stop use of illicit drugs | Ferri (2013)62 |
◀▶ SMD –0.07 (95% CI –0.19 to 0.04) ~ I2 = 0.0% |
✓ | = | All 23 mass media studies |
| Illicit drug use | To use illicit drugs | Werb (2011)63 |
◀▶ 0.29 (95% CI –0.17 to 0.75) ✓ I2 = 66.1% |
✗ | Not stated | All 11 mass media studies |
| Physical activity | To be more active | Leavy (2011)59 | △ | ✗ | ✗ | All 18 studies on mass media |
| Sexual health | To use contraception | Carter (2015)47 | ◁▷ | ✓ | = | 14 of 17 mass media studies |
| Tobacco use (mixed-topic review) | Intentions to quit, calls to quitlines | Robinson (2014)69 | △ | ✓ | = | All 22 studies |
| Tobacco use | To quit or smoke | Gould (2013)39 | △ | ✓ | ✗ | 11 of 20 studies on mass media |
| Tobacco use | To smoke | Brinn (2010)35 | ◁▷ | ✓ | ✗ | All 7 mass media studies |
Three reviews with a low risk of bias examined tobacco use: two focused solely on tobacco35,39 and one mixed-topic review included tobacco. 69 Positive results for intentions to quit or to smoke were reported in two of the reviews,39,69 whereas one review that focused on reducing smoking prevalence in young people reported largely mixed results for the intention to start smoking. 35 The quality of the included studies was assessed by the reviews themselves as medium to low.
Statistical pooling in two reviews, one at low risk of bias62 and one at high risk of bias,63 found a mixed impact of mass media campaigns on illicit drug use intentions (including not to use, to reduce use or to stop use), with no clear indication of either a positive or negative overall effect.
One sexual health review with a low risk of bias reported largely mixed results for intentions to use contraception,47 whereas a physical activity review reported largely positive results for intentions to be more active,59 but the review had a high risk of bias.
Awareness and knowledge
Fifteen reviews reported on whether or not mass media campaigns had an impact on awareness and knowledge (Table 6). 27,35,39,44,46,47,50–52,57,62,65–68 The reviews had varying levels of relevance to the UK context: three reviews included non-OECD country research only, five reviews included one or two UK studies and the rest were reviews of studies from mainly OECD countries. Two reviews presented statistical results, with the remaining reviews presenting only narrative results. 51,66
| Review topic | Outcome | Review (first author and year) | Result | Risk of bias and quality | Mass media focus | |
|---|---|---|---|---|---|---|
| Review Risk of Biasa | Quality of included studiesb | |||||
| Diet (mixed-topic review) | Healthy diets | Mozaffarian (2012)68 | △ | ✓ | = | 25 of about 100 studies |
| Diet (mixed-topic review) | Dietary counselling helplines | Ellis (2003)67 | △ | ✓ | ✗ | 8 of 31 studies |
| Illicit drug use | Illicit drug effects |
Ferri (2013)62 Effects of illicit drugs use |
◁▷ | ✓ | = | All 23 studies on mass media |
| Physical activity (mixed-topic review) | Physical activity | Mozaffarian (2012)68 | △ | ✓ | = | 25 of about 100 studies |
| Physical activity | Physical activity | Finlay (2005)57 | △ | ✗ | = | All 8 studies on mass media |
| Sexual health | HIV prevention and transmission | LaCroix (2014)51 |
HIV prevention: ▲ d+ = 0.39 (95% CI 0.25 to 0.52), k = 65 HIV transmission: ▲ d+ = 0.30 (95% CI 0.18 to 0.41) |
✓ | Not stated | All 54 studies on mass media |
| Sexual health | Sexual health | Carter (2015)47 | △ | ✓ | = | 14 of 17 studies on mass media |
| Sexual health | Contraception | Carter (2015)47 | △ | ✓ | = | 14 of 17 studies on mass media |
| Sexual health | Health products/service | Bertrand (2006)46 | △ | ✓ | ✗ | All 15 studies on mass media |
| Sexual health | HIV transmission, condom use, HIV risk and prevention methods | Bertrand (2006)46 | ◁▷ | ✓ | ✗ | All 15 studies on mass media |
| Sexual health | How to access services | Kesterton (2010)50 |
△ Based on 1 study |
✓ | ✗ | 3 of 74 studies on mass media |
| Sexual health | Reproductive health |
Speizer (2003)52 Reproductive health |
△ Based on 1 study |
✗ | ✓ | 6 of 41 studies on mass media |
| Tobacco use | Knowledge, attitudes and intentions: towards tobacco use and the tobacco industryc | Richardson (2008)44 | ◁▷ | ✓ | = | 37 of 60 studies on mass media |
| Tobacco use | Knowledge/beliefs: smoking and cardiovascular riskc | Bala (2013)27 | ◁▷ | ✓ | ✗ | All 11 studies on mass media |
| Tobacco use | Smoking | Gould (2013)39 | △ | ✓ | ✗ | 11 of 20 studies on mass media |
| Tobacco use (mixed-topic review) | Smoking cessation helplines | Ellis (2003)67 | △ | ✓ | ✗ | 8 of 31 studies |
| Tobacco use | Smoking | Brinn (2010)35 | ▽ | ✓ | ✗ | All 7 studies on mass media |
| Mixed-topic review | Substance use (illicit drugs, alcohol and tobacco) | Derzon (2002)66 | ▲ | ✗ | Not stated | All 72 studies |
| Mixed topics | Substance use (illicit drugs, alcohol and tobacco) | Byrne (2005)65 | △ | ✗ | Not stated | All 25 campaigns in 53 studies |
There was evidence that mass media campaigns increased knowledge and awareness in relation to sexual health (including knowledge of HIV prevention and transmission, contraception and services). One low-risk-of-bias meta-analysis of 54 studies found consistent positive results for the improvement in knowledge of HIV transmission (d+ = 0.30, 95% CI 0.18 to 0.41, based on 47 reports) and prevention (d+ = 0.39, 95% CI 0.25 to 0.52, based on 65 reports). 51 Positive results regarding sexual health awareness and knowledge outcomes were also reported in four reviews using narrative synthesis,46,47,50,52 but three of these46,50,52 did not include any studies from the UK or other OECD countries, one review had a high risk of bias,52 and both Speizer et al. 52 and Kesterton and Cabral de Mello50 based their results on only one study. The review by Bertrand and Anhang46 also reported some mixed results.
Four reviews with a low risk of bias found mixed evidence that mass media campaigns could improve awareness and knowledge regarding tobacco. Two reviews, which both included studies from the UK,27,44 reported mixed results, whereas the third review reported positive results39 and the fourth review reported negative results. 35 A mixed-topic review with a low risk of bias that examined the effects on knowledge of smoking cessation helplines reported positive results. 67
The effects on knowledge of illicit drugs were examined in one illicit drugs review with a low risk of bias, which reported mixed results. 62 In addition, two mixed-topic reviews65,66 examined the effects on tobacco, alcohol and illicit drugs knowledge. A meta-analysis of the effects on drugs knowledge reported positive results [Δ = 0.05 standard deviation (SD); p < 0.05]66 and a narrative review also reported positive results;65 however, both of these reviews had a high risk of bias.
There was weak evidence that mass media campaigns could have an impact on awareness and knowledge regarding physical activity. Overall positive results, including from UK studies, were reported in one mixed-topic review with a low risk of bias that examined this outcome,68 whereas positive results were also reported by Finlay and Faulkner,57 but the review had a high risk of bias.
Finally, two of the mixed-topic reviews examined evidence of the impact on diet-related awareness and knowledge, both reporting positive results;67,68 the review by Mozaffarian et al. 68 included UK studies.
Attitudes, beliefs, norms and self-efficacy
Ten reviews reported on whether or not mass media campaigns had an impact on attitudes, beliefs, norms and self-efficacy (Table 7). 27,35,44,46,47,52,62,65,66,68 One review conducted a meta-analysis;66 however, only narrative results were presented in the other nine reviews. Most of the reviews were of good quality (low risk of bias), but their relevance to the UK varied.
| Review topic | Outcome | Review (first author and year) | Result | Risk of bias and quality | Mass media focus | |
|---|---|---|---|---|---|---|
| Review risk of biasa | Quality of included studiesb | |||||
| Illicit drug use | Attitudes: illicit drug use |
Ferri (2013)62 Illicit drug use |
◁▷ | ✓ | = | All 23 studies on mass media |
| Illicit drug use | Norms: perceived peer norms | Ferri (2013)62 | ◁▷ | ✓ | = | All 23 studies on mass media |
| Physical activity (mixed-topic review) | Attitudes: physical activity | Mozaffarian (2012)68 | △ | ✓ | = | 25 of about 100 studies |
| Sexual health | Attitudes: use of family planning | Carter (2015)47 |
△ Based on 1 study |
✓ | = | 14 of 17 studies on mass media |
| Sexual health | Attitudes: reproductive health | Speizer (2003)52 |
△ Based on 1 study |
✗ | ✓ | 6 of 41 studies on mass media |
| Sexual health | Beliefs: risk of pregnancy | Carter (2015)47 | △ | ✓ | = | 14 of 17 studies on mass media |
| Sexual health | Beliefs: personal risk of HIV/AIDS | Bertrand (2006)46 | ▽ | ✓ | ✗ | All 15 studies on mass media |
| Sexual health | Self-efficacy: using condoms | Bertrand (2006)46 | ◁▷ | ✓ | ✗ | All 15 studies on mass media |
| Tobacco use (mixed-topic review) | Attitudes: smoking | Mozaffarian (2012)68 | △ | ✓ | = | 25 of about 100 studies |
| Tobacco use | Knowledge, attitudes and intentions: towards tobacco use and the tobacco industryc | Richardson (2008)44 | ◁▷ | ✓ | = | 37 of 60 studies on mass media |
| Tobacco use | Knowledge/beliefs, attitudes, norms and social influences: smoking and cardiovascular riskc | Bala (2013)27 | ◁▷ | ✓ | ✗ | All 11 studies on mass media |
| Tobacco use | Attitudes and norms | Brinn (2010)35 | ◁▷ | ✓ | ✗ | All 7 studies on mass media |
| Tobacco use | Self-efficacy | Brinn (2010)35 | ▽ | ✓ | ✗ | All 7 studies on mass media |
| Mixed topics | Attitudes: substance use (illicit drugs, alcohol and tobacco) | Derzon (2002)66 | ▲ | ✗ | Not stated | All 72 studies |
| Mixed topics | Attitudes: substance use (illicit drugs, alcohol and tobacco) | Byrne (2005)65 | ◁▷ | ✗ | Not stated | All 25 campaigns in 53 studies |
For illicit drugs, the evidence was mixed. A mixed-topic meta-analysis that examined effects on drug use attitudes reported overall positive results (Δ = 0.02 SD; p < 0.05),66 but the review was at high risk of bias, whereas mixed evidence of impact on attitudes to illicit drug use and perceived peer norms was reported in a review with a low risk of bias62 and in a review with a high risk of bias. 65
For sexual health, overall positive results regarding beliefs about risk of pregnancy were reported in one review with a low risk of bias. 47 Positive results regarding other attitude changes were reported in two other sexual health reviews,47,52 but Speizer et al. 52 included only low-income countries and in both cases the reported results were from only one study. Mixed results were reported for the impact on self-efficacy, and negative results were reported for the impact on beliefs by Bertrand and Anhang,46 but this review was limited to low-income country studies and, therefore, it is of less relevance.
The evidence was mixed for tobacco. Three reviews, two including UK studies, reported overall mixed results for the impact on attitudes,27,35,44 and Brinn et al. 35 also reported overall negative results for the impact on self-efficacy. 35 However, a mixed-topic review including UK studies that examined the impact on attitudes to smoking reported overall positive results. 68 The same review also reported overall positive results for attitudes to physical activity.
Evidence of the impact on distal outcomes
In addition to investigating the impact of mass media on proximal outcomes (such as beliefs, attitudes and self-efficacy) and intermediate outcomes (including attempted and sustained behaviour change), evidence on distal outcomes was sought. As noted in the logic model (see Figure 1), this included reduction in illnesses, improved population health, reduced health service usage, societal change, policy change and impact on inequalities. Of all of the systematic reviews included, only one reported on any distal outcomes. 43 The authors noted that:
There is evidence of good quality (1&2 +, C), which shows an effect of mass media interventions on attitudes towards smoking and intentions to smoke among young people under 25 years.
This suggests that mass media programmes may have contributed to the denormalisation of smoking among young people.
Evidence of the impact on different target subpopulations
Summary of the approach to subpopulations in reviews
The majority of the included reviews provide evidence about whether or not the effects of mass media campaigns were comparable across one or more subpopulations. Reviews differ in the extent to which the identification and synthesis of subpopulation differences formed a primary objective. In several reviews, all focusing on tobacco control campaigns, the main aim was to determine the equity or inequity of effects of campaigns across socioeconomic groups. 37,40,42 Some reviews dedicated part of their synthesis to looking at effects in specific subgroups,43–45,54,62 or to looking more generally for factors that moderate sizes of effect51,55 or described results separately for subgroups when this was shown in the original papers. 27,58,61,63 Most reviews provide a narrative synthesis of results for different subpopulations as described by the original studies; very few have conducted a formal statistical subgroup analysis. Some reviews that have included a meta-analysis have examined the factors that cause heterogeneity in study findings,51,55 or analyse in subgroups when available from the original studies. 54,62 A few reviews simply highlighted the subgroups in which statistically significant effects had been found in the original studies; if this was not part of a more formal subgroup analysis, these results have not been included.
When reviews focused on effects of mass media campaigns in a particular target population, those effects have been described earlier according to the relevant outcomes.
The majority of reviews concentrated on behaviour change outcomes, either reducing harmful behaviour or increasing health behaviour, rather than proximal outcomes, when describing and synthesising effects in subpopulations.
Description of the subpopulations that have been considered
The subpopulations considered differ markedly according to health behaviour, with sex27,43,44,51,54,55,58 and age27,44,45,51,55,62 being the only common factors across a number of reviews in different areas. Differences have also been examined according to ethnicity for several health behaviours. 27,39,44,58 Consideration of socioeconomic factors and the equity of effect across socioeconomic groups has been exclusively a feature of reviews of the tobacco control literature, in line with the strong socioeconomic differential in the pattern of smoking and smoking-related morbidity in many developed countries. 27,37,40,42,44 Other subpopulations have been defined according to the pre-campaign level of behaviour, for example by the level of initial physical activity or obesity for campaigns aimed at improving physical activity,58,61 by prior sexual health behaviour for a review of campaigns relating to sexual health,51 and a review of campaigns relating to illicit drugs examined effects according to sensation-seeking behaviour. 63
Effects by subpopulations
Effects by age
Differences by age were reported in terms of youth versus adults, and according to differing age groups of children and adults. For some health behaviours, notably smoking, reviews focused exclusively on youth (smoking uptake) or adults (smoking cessation) and the findings and any contrasting findings of these reviews are described in Reducing harmful behaviours. Six reviews, all at low risk of bias, describe effects by age group: three for tobacco control campaigns,27,44,45 one for illicit drugs,62 one for physical activity55 and one for sexual health. 51 The age groups considered varied markedly between behaviours and between reviews.
Two reviews with a low risk of bias provided evidence that the effects of tobacco control mass media campaigns differ by age, and may be greater for younger children than for older children and greater for youths than for adults. The evidence is relevant to the UK as the reviews concerned included studies only from the UK or OECD countries. The review by Richardson et al. 44 found evidence that tobacco control campaigns appeared to benefit (i.e. decrease intentions to smoke, initiation rates or continuation of smoking) younger children more than older children. Wilson et al. 45 report that findings for youth populations were more consistent than those for adults, with most studies reporting a reduction of 20–40% in the odds of smoking initiation. However, a third low-risk-of-bias review of tobacco mass media campaigns found that the impact of age was contradictory, with three campaigns detecting positive effects among older smokers, and three detecting positive effects among younger smokers (aged up to 34 years). 27
For illicit drugs, Ferri et al. 62 found that campaigns on methamphetamine use affected past-year prevalence only in 12- to 17-year-olds, not in 18- to 24-year-olds.
In relation to other behaviours, the evidence was less consistent. A metaregression of campaigns targeting physical activity found that age was an important determinant of heterogeneity in relation to reducing sedentary behaviour, with stronger effects in older age groups (p = 0.054); each additional 10 years was associated with a 27% greater reduction in sedentary behaviour (p = 0.054). 55 However, age was not a significant determinant of heterogeneity in relation to improving overall physical activity. For sexual health mass media campaigns, LaCroix et al. 51 found that age was not a predictor of effect size for campaigns.
Effects by sex
Seven reviews describe effects by sex: three for tobacco control campaigns,27,43,44 one for physical activity55 and two for sexual health. 51,54
There was evidence in metaregression that sex was not an important determinant of heterogeneity for physical activity mass media campaigns, for either reducing sedentary behaviour or increasing activity. 55
For campaigns on sexual health, there was evidence suggesting slightly greater impact on condom use by females than by males in one review with results stratified by sex; the odds of having used a condom during the most recent sexual encounter were only slightly different, at 1.7% (95% CI 1.1% to 2.7%) higher for males and 2.2% (95% CI 0.5% to 8.7%) higher for females who had been exposed to condom social marketing. 54 However, another review of sexual health mass media campaigns found that no sample characteristics, including sex, were significant predictors of effect size magnitude for any outcome of interest. 51
Two tobacco reviews found that the impact of sex was inconclusive, with some studies showing positive long-term effects for men and some for women. 27,44 One study in the review by Bala et al. 27 found significant differences in intervention quit rates for women but not for men, compared with controls. A third tobacco review reported that few of the included studies evaluated the differential effectiveness in subgroups of the sample but found modest evidence that campaigns were more effective for women than for men only in relation to quit and win and community campaigns. 43
Effects by ethnicity
Four reviews described effects by some marker of ethnicity: three were tobacco control reviews27,39,44 and one focused on physical activity. 58 Guillaumier et al. 40 also refer to ethnicity but use this to identify populations of deprivation, and these results are therefore presented in the section on socioeconomic differences (see Effects by socioeconomic group).
Evidence regarding media campaign effectiveness and ethnicity was generally inconsistent, inconclusive and mixed. Two reviews of tobacco mass media campaigns observed no consistent or conclusive relationship between campaign effectiveness and ethnicity. 27,44 One review examined the effect of generic media on indigenous people compared with the general population,39 and found weak evidence that generic tobacco control messages devised for the whole population can be as effective in terms of recall for indigenous populations as for the general population; however, this may not translate into quit rates.
In a review of physical activity campaigns, Kahn et al. 58 included two studies that reported results separately for black people and found mixed evidence: one study showed a decline in the percentage of black people using the stairs when the sign contained a generic message; however, a message specifically designed for a black population was effective in increasing the percentage of stair users.
Effects by socioeconomic group
Five reviews, all focusing on tobacco mass media campaigns, described differential effects by socioeconomic group. 27,37,40,42,44 For four of these reviews,37,40,42,44 the main aim was to compare the effectiveness of campaigns across socioeconomic groups or to consider effectiveness specifically within deprived populations. Overall, the evidence suggested that tobacco control campaigns have had inconsistent socioeconomic equity effects. However, there is a lack of good-quality studies looking at the differential effects of mass media campaigns, especially those aimed at behaviours other than smoking.
In the review by Brown et al. ,37 12 studies examined the equity impact of mass media campaigns promoting the use of quitlines and/or nicotine replacement therapy (NRT) (i.e. whether or not results differed by socioeconomic status). Five studies were positive (i.e. the campaigns reduced inequality), three were neutral (there was no difference in impact by socioeconomic status) and three were negative (the campaigns were found to increase inequality and one was unclear regarding equity impact). Similarly, of 18 studies examining the equity impact on quitting, three showed a positive equity impact, two were neutral, five were negative (including four Quit & Win competitions), two were mixed and six were unclear. 37
The review by Hill et al. 42 found evidence that mass media campaigns generated greater awareness of quitlines among less educated smokers, with three out of four US studies that evaluated campaigns promoting local quitlines finding higher awareness among less educated smokers.
Other reviews of tobacco mass media campaigns found no consistent relationship between campaign effectiveness and educational status27 or socioeconomic status. 40 Guillaumier et al. 40 reported results from several studies, finding an inconsistent pattern overall. Two studies in the review examined measures of campaign exposure and found that campaigns were either less likely or equally likely to be recalled by disadvantaged groups than by more advantaged smokers. Four studies looked at campaign perceptions: three found no differences in the perceived effectiveness of campaigns regardless of sociodemographic group, and a fourth found that Indigenous Australians perceived a variety of television advertisements as more effective than did non-Indigenous Australians. Motivational responses of smokers (calling quitlines, promoting quit attempts and quit intentions) were assessed in five studies, with mixed results. Four studies assessed the effectiveness of campaigns in promoting cessation: three campaigns were equally effective and one campaign was more effective in reducing smoking rates in disadvantaged smokers than in more advantaged smokers. This review considered the methodological quality of these studies and its main conclusion was that there is poor methodological rigour in research into the effectiveness of mass media campaigns among socially disadvantaged groups. 40
Richardson et al. 44 reported that there was a lack of information regarding the impact of the socioeconomic status of children and young people on the effectiveness of mass media campaigns.
Effects by pre-campaign measures of behaviour
Two reviews, both of physical activity campaigns, defined subpopulations by their pre-campaign level of physical activity or obesity,58,61 and one review of sexual health campaigns defined subpopulations in accordance with pre-campaign sexual activity and use of condoms. 51 One further review focusing on campaigns relating to illicit drug use examined effects according to individuals’ sensation-seeking behaviour. 63
Two physical activity reviews noted evidence of stronger effects in populations who were classified as obese at baseline (Kahn et al. 58) or sedentary at baseline (Ogilvie et al. 61), although the evidence was weak overall, as the review by Kahn et al. 58 was at high risk of bias, and in the Ogilvie et al. 61 review the findings related to only two mass media studies in a review with a wider focus. Kahn et al. 58 found that posters encouraging stair use were effective in both those classified as obese and those not classified as obese, but the median net increase in the percentage of people taking the stairs was higher among the obese group. 58 Ogilvie et al. ,61 examining the two mass media studies in the review, reported that significant net increases in self-reported time spent walking were observed only in the most sedentary subgroup within the study population. 61 Neither prior level of sexual activity nor pre-campaign rate of condom use were significant predictors of effect size magnitude for any outcome of interest in a sexual health review. 51 An illicit drug use review suggested possible stronger effects in a RCT for a subgroup assessed as having a high level of sensation-seeking behaviour, but with no formal synthesis. 63
Overall strength of the evidence
Table 8 presents the findings for our overall summary of findings for the effects of mass media on health behaviours. This overall rating summarises review findings, drawing on the principles of the GRADE approach. 33,34 In particular, we considered the risk of bias of included systematic reviews, potential inconsistency in the results, the extent to which the evidence base reflects behaviour change within a UK context and imprecision in the effect estimates.
| Outcome | Behaviours | Intentions | Awareness/knowledge | Attitudes | Overall effect | Risk of bias | Inconsistency | Directness | Imprecision | Certainty |
|---|---|---|---|---|---|---|---|---|---|---|
| Illicit drugs | ● L | ◀▶ L | ◁▷ L | ◁▷ L | No effect | Low | Inconsistent (I2 = 70%) | Direct | High | Low |
| Sexual health | ▲ L | ◁▷ L | ▲ L | ◁▷ L | Positive | Low | Inconsistent (I2 = 77.22%, no information for other two meta-analyses) | Indirect | Low | Low |
| Physical activity | ● L | △ H | △ L | △ L | No effect | Low |
Inconsistent I2 = 72% I2 = 0% I2 = 63% |
Direct | High (on the basis of overall physical activity) | Low |
| Tobacco | ◁▷ L | △ L | ◁▷ L | ◁▷ L | Mixed | Low | Inconsistent | Direct | High | Low |
| Diet | △ L | – | △ L | – | Positive | Low | Inconsistent | Direct | High | Very low |
| Substance use | ▲ H | – | – | – | Unknown | High | Inconsistent | Direct | High (based on meta-analysis of RCTs) | Very low |
| Alcohol | – | – | – | – | Unknown | – | – | – | – | Very low |
Although our approach is inspired by GRADE,33,34 it has been modified substantially as straightforward implementation is challenging and would have resulted in all assessments being characterised as having very low certainty. This would not have allowed the differing levels of certainty to be communicated. However, it is worth noting that these assessments are not comparable to other GRADE Summary of Findings tables.
With regard to our certainty in mass media campaigns in achieving a positive impact on public health, we conclude that there is:
-
low-certainty evidence for positive effects on improving sexual health behaviour, with existing reviews synthesising evidence that is primarily derived from low-income settings
-
very low-certainty evidence of healthier behaviours in relation to diet and substance use
-
low-certainty evidence for no effect on increased physical activity and reduced use of illicit drugs
-
low-certainty evidence for the effect on tobacco being mixed
-
a large amount of variation in effectiveness across the evidence, suggesting that factors related to the intervention and context are crucial determinants of effectiveness
-
an absence of evidence about the impact on alcohol consumption.
Summary
This review of systematic reviews published between January 2000 and January 2016 brings together the evidence base on the impact of mass media campaigns on health behaviours (including alcohol use, illicit substance use, diet, physical activity, sexual and reproductive health and smoking cessation and prevention) for the first time. Overall, the evidence base for the effectiveness of mass media in promoting behaviour change is mixed. The amount of literature varies. Of the 36 reviews that met our inclusion criteria, the most commonly studied behaviour was tobacco use, followed by sexual health and physical activity. Just three reviews of media campaigns on the use of illicit drugs were identified. A further five systematic reviews looked at campaigns addressing more than one behaviour, of which only four included content on alcohol and/or diet. However, no single review examining the effectiveness of using mass media to address alcohol use or diet was found, identifying an important gap in the literature. The strength of evidence from reviews also varies. Using a modified GRADE approach,33,34 we found moderate evidence for the positive effects of mass media campaigns on reducing sedentary behaviour and sexual health. Low-certainty evidence for positive impacts on diet was found, although the overall volume of evidence on diet was very limited. The impact of mass media campaigns on tobacco use and physical activity was mixed, but with low-certainty evidence in both cases. In contrast, the available and, again, low-certainty evidence on illicit drugs use suggests no impact of mass media. All reviews found considerable variation between individual studies as described in a meta-analysis or narrative synthesis, suggesting that variations in implementation of the campaign and evaluation methods may be important.
For treatment-seeking, there was low-certainty evidence that mass media campaigns can help increase the use of sexual health clinics or services. Whether or not media campaigns can prompt calls to telephone quitlines for smoking cessation has been fairly extensively studied in five reviews. Overall, the direction of effect looks positive, with campaigns serving to prompt calls to quitlines, but variation in results and the quality of studies was identified; therefore, there is only moderate certainty in the strength of this finding.
Mass media campaigns may reach and affect groups in the population differently. Although age differences were not always measured, reviews of tobacco and illicit drug campaigns found that mass media appeared to be more effective for young people and particularly for younger children than for older teenagers. There was modest evidence that mass media outcomes for tobacco, sexual health and physical activity do not differ by sex and no clear consistent evidence was found for ethnicity or socioeconomic status. Looking at baseline measures of health behaviours, physical activity campaigns may be more effective for the less active or for obese people than for others.
Chapter 3 What is the impact of mass media campaigns on alcohol-related behaviour and other outcomes? Findings from the review of primary studies of alcohol campaigns (review B)
This systematic review of primary studies of alcohol campaigns (review B) has been published in full by Young et al. 70 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/. The text in this chapter includes minor additions and formatting changes to the original text. The paper and the supplementary files (including the exclusion criteria and a sample search strategy) are available at https://doi.org/10.1093/alcalc/agx094 (accessed 30 April 2018). In this chapter, we present a scientific summary of the review.
Background
There are approximately 8800 alcohol-related deaths annually in the UK71 and consumption of alcohol is causally linked with > 60 medical conditions including seven types of cancer. 72 In England, 7% of adults regularly consume more than current low-risk guidelines73 and there are an estimated 1.1 million alcohol-related hospital admissions each year. 74 There is a need for effective population-level strategies to reduce consumption and prevent related harm.
Review A highlighted a lack of review-level evidence of the effectiveness of mass media in addressing alcohol use. Two reviews included some evidence on alcohol as part of wider reviews of multiple behaviours;65,66 however, no single comprehensive review was identified that examined the impact of mass media on alcohol consumption and related outcomes.
Other reviews have shown that mass media campaigns can reduce drink driving in some circumstances10,75 although alcohol campaigns may not be effective in school or college campus environments. 76,77 Other than these topics, evaluations of alcohol-related mass media campaigns have not been comprehensively synthesised in a way that can inform current policy.
Objective
The objective was to conduct a systematic review of evidence of the effectiveness of mass media public health campaigns to reduce alcohol consumption and related harms.
Methods
The review protocol17 was registered with PROSPERO (reference number CRD42017054999) and this systematic review (review B) has been published in full. 70 Eligibility criteria are given in Box 2.
-
Purposeful use of mass media channels to influence health behaviours and the individual-level determinants of health behaviours.
-
Mass media channels included television, radio, cinema, online broadcasting, newspapers and magazines, leaflets/booklets, direct mail, outdoor advertising, e-mail and digital media.
-
Aimed at reducing alcohol consumption and its determinants.
-
Multicomponent interventions if they assessed the specific effects of a mass media component.
-
Primary research studies.
-
Any study design.
-
Reported in English.
-
Any country.
-
Reported at least one of the following outcomes – alcohol consumption, alcohol-related social cognitive variables (e.g. knowledge, intentions and social norms), media exposure outcomes (e.g. campaign awareness, exposure and understanding), alcohol-related harm and health service usage.
-
Involved individual person-to-person delivery.
-
Required active engagement before receipt of the message rather than passive message exposure.
-
Used a baseline measure to tailor or target a subsequent mass media message.
-
Targeted drink driving.
-
Promoted alcohol consumption.
-
Based in schools.
-
Targeted college students within university campuses.
-
Social norms campaigns in which it was not evident from the information available that a mass media channel was used.
-
Campaign message testing.
-
Evaluations of alcohol advertisement bans.
-
Evaluations of warning labels on alcohol products.
-
Evaluations of online treatment or self-help programmes.
Eight bibliographic databases were searched from the date of inception to July 2016: MEDLINE, EMBASE, PubMed, The Cochrane Library, Web of Science, Scopus, Applied Social Sciences Index and Abstracts and Education Resources Information Center (ERIC). Each unique search result was screened for relevance by one of a team of four reviewers. Full-text reports of eligible references were assessed for eligibility by one reviewer and random samples were checked by a second reviewer. The references of included studies were examined for any further potentially relevant studies.
Data were extracted from included studies, with outcomes informed by the project logic model, and a sample were double-extracted by a second reviewer. Studies were assessed for quality using the Effective Public Health Practice Project (EPHPP) Quality Assessment Tool for Quantitative Studies,78 with all assessments checked by a second reviewer. Owing to study heterogeneity, a narrative synthesis was conducted, first on behaviour change outcomes and then on behavioural determinants, including social cognitive and campaign exposure outcomes.
Results
There were 10,212 unique search results, 170 of which were assessed for eligibility as a full-text report (Figure 3). Twenty-nine papers were included in the review. They reported 24 different studies that had a range of designs (11 controlled longitudinal and 13 uncontrolled or cross-sectional) and countries (eight in the USA, five in Australia, two in Finland, two in New Zealand, two in the UK, one in Canada, one in Denmark, one in Italy, one in the Netherlands and one in Sri Lanka). Television and/or radio were used in 18 studies. Other media channels that were used were posters, newspapers, pamphlets, e-mails and online video. On EPHPP study quality ratings, two were strong,79,80 four were moderate81–84 and 18 were weak. 85–102 The most common reasons for a weak rating were not reporting reliability and validity of data collection tools, a high risk of selection bias and a weak study design.
FIGURE 3.
The PRISMA flow diagram of the identification and selection of primary studies (review B). This figure has been adapted from Figure 1 in Young et al. 70 This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/.
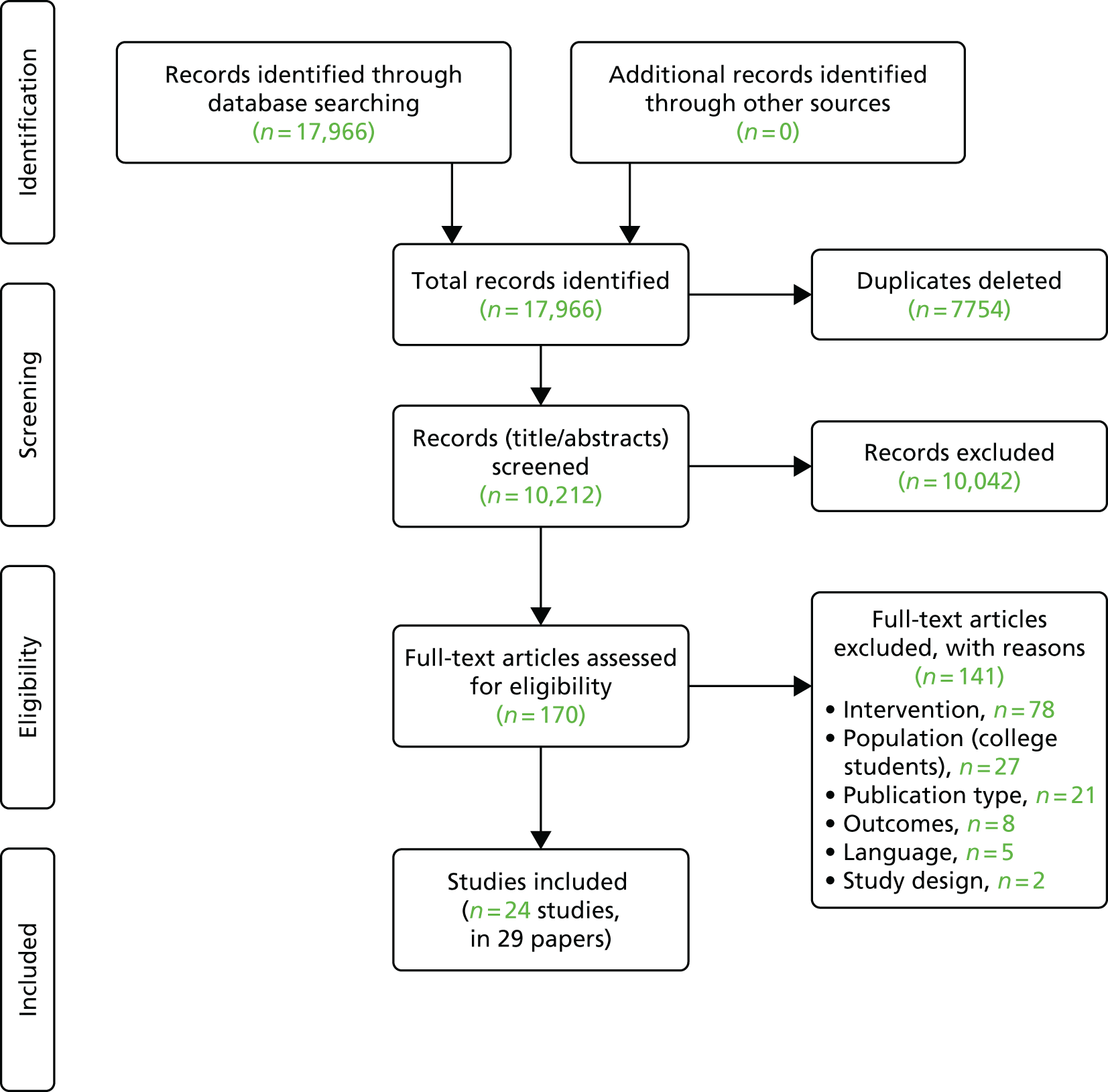
Alcohol consumption
There was little evidence of reductions in alcohol consumption associated with exposure to campaigns based on 13 studies reporting this outcome. 79–82,84,88,91–93,95,97,100,102 Six of these studies compared exposed and non-exposed groups, or exposed groups over time; five reported no statistically significant differences in consumption. 79,81,82,84,95 One study found that participants in a group exposed to a television and mailed letter campaign decreased their consumption on a typical day by 47%, contrasting with increases in the groups receiving either the television or letter components or neither. 88 Other studies examined associations between campaign viewing or awareness and consumption: one reported that increases in awareness in older adolescence, but not younger adolescence, was associated with decreases in binge drinking,80 one reported that campaign viewing significantly predicted drinks consumed102 and two found no significant difference in consumption. 91,97
Treatment- and information-seeking
There was some evidence, from four weak-quality studies, that campaigns generated increases in treatment-seeking or information-seeking. 85,87,92,97 For example, referrals for alcoholism were reported to have increased by 65% following a campaign. 97
Intentions and motivation
Three studies reported intentions to reduce alcohol consumption. In one study, those who reported that they had seen a campaign reported an increase in intentions to decrease alcohol use whereas others decreased their intentions. 102 Another study found an increase in the proportion of people reporting that they were likely to reduce their consumption from pre test to post test. 91 In the other study, the impact of the campaign on intentions was not well described. 84 In a single study reporting motivation to reduce consumption, half of drinkers recognising the campaign reported that it made them feel either very or somewhat motivated to reduce their consumption. 91
Beliefs and attitudes
Five studies reported alcohol-related beliefs or attitudes with mixed findings. 81,84,88,90,97 For example, one study reported an increase in support for some policies aimed at limiting consumption but not for others. 81
Knowledge
There was evidence that alcohol-related knowledge increased, based on eight studies. These included knowledge of unit consumption guidelines,91,92 cancer risk,91 the risks of alcohol use during pregnancy,83,89,93 sources of support for problem drinkers97 and general knowledge about alcohol. 84,96 For example, there was a significant improvement in knowledge of the risks of alcohol use during pregnancy in an exposed group compared with a control group. 83
Other outcomes
Other studies reported self-efficacy,79,96 social norms,102 campaign interaction or discussion,82,83,86,98,99 recall or recognition of campaigns82,83,85,88,89,91,92,94,95,97–100 and attitudinal or emotional responses. 79,92 The evidence was strongest for recall, with the proportions of people remembering campaigns or their messages being generally high.
Discussion
Findings from this review of primary studies published by July 2016 suggest that mass media campaigns have not reduced alcohol consumption, although most did not state that they directly aimed to do so and the evidence is limited by mostly weak study designs and self-reported outcomes. Campaigns can be recalled and increase knowledge, especially in areas where knowledge was initially low (e.g. unit consumption guidelines or cancer risk), suggesting that they can have an impact on important precursors to behaviour change. However, alcohol marketing and pro-alcohol cultural norms create a challenging environment in which alcohol health promotion campaigns must operate.
Conclusion
Mass media public health campaigns about alcohol can often be recalled by individuals, and are associated with changes in knowledge, attitudes and beliefs about alcohol. There is little evidence that campaigns reduced alcohol consumption but most studies did not report consumption as an outcome. Mass media can, however, have an impact on outcomes that could lead to support for other public health actions to reduce alcohol consumption and harm.
Chapter 4 What is the cost-effectiveness of mass media campaigns? Evidence from the cost-effectiveness review (review C)
Background
Mass media campaigns have high upfront costs, and evidence of effectiveness is not sufficient to conclude that they offer value for money. However, the wide reach of mass media campaigns means that they have the potential to offer significant benefits at a low cost per head. The cost-effectiveness of mass media campaigns is an essential consideration for policy-makers.
Methods
We conducted a rapid review of reviews of the cost-effectiveness of mass media campaigns.
Literature searches for reviews of economic evaluations
We combined relevant reviews identified in the original search (see Chapter 2) with additional reviews and systematic reviews identified using a literature search that specifically sought to identify reviews of economic evaluations published between January 2000 and January 2017. We conducted a rapid literature search using Web of Science and Google Scholar. The search strategy is summarised in Appendix 5.
Inclusion and exclusion criteria
We included reviews or systematic reviews describing the cost-effectiveness of paid mass media interventions (including multicomponent interventions in which a major component was mass media) for the relevant health topics. The cost-effectiveness findings had to be described in a results section, even if the findings were that there were no relevant studies. Included reviews were required to assess economic studies that evaluated both costs and benefits of mass media campaigns (i.e. full economic evaluations, not just intervention costs or cost savings). Systematic reviews were defined as those including both a systematic literature search and quality assessment of included papers.
We excluded reviews of reviews and papers that assessed industry-funded mass media campaigns.
Results
Following abstract screening, we screened the full texts of 11 reviews identified in the original searches and a further 29 studies that were identified in the new search. Following full-text screening, we included 20 reviews.
Synthesis of findings
Of the 20 reviews that met the inclusion criteria, 13 were systematic reviews27,35,48,61,103–111 and seven were non-systematic reviews. 24,112–117 The characteristics of the reviews are summarised in Tables 9 and 10.
| Review (first author and year) | Health topic | Review aim | Review type | Is mass media the sole focus of the review? | Is a review of economic evaluations the/a specific aim of the review? | Total number of studies included | Number of relevant studies |
|---|---|---|---|---|---|---|---|
| Brinn (2010)35 | Smoking | To evaluate the effectiveness of mass media interventions to prevent smoking in young people | SR | Yes | No | 7 | 1 |
| Durkin (2011)24 | Smoking | To summarise the impact of mass media campaigns on promoting quitting among adult smokers overall and for subgroups; the influence of campaign intensity and different channels; the effects of different message types | NSR | Yes | No | 26 | 0 |
| Atusingwize (2014)111 | Smoking | To systematically and comprehensively review economic evaluations of tobacco control mass media campaigns | SR | Yes | Yes | 11 | 11 |
| Bala (2013)27 | Smoking | To assess the effectiveness of mass media interventions in reducing smoking among adults | SR | Yes | No | 11 | 0 |
| Flack (2007)104 | Smoking | Assesses the current evidence for the cost-effectiveness of mass media-led smoking cessation interventions | SR | Yes | Yes | 10 | 3 |
| Kahende (2009)113 | Smoking | To review the existing literature on economic evaluations of tobacco control interventions | NSR | No | Yes | 42 | 2 |
| Lantz (2000)114 | Smoking | To provide a comprehensive review of interventions and policies aimed at reducing youth cigarette smoking in the USA | NSR | No | No | Not reported (NSR) | 1 |
| Raikou (2007)110 | Smoking | To undertake a review of the evidence on cost-effectiveness relating to smoking prevention strategies among young people focusing on mass media interventions and point-of-sale measures | SR | No (but key focus) | Yes | 5 | 2 |
| Belaid (2016)103 | Sexual health | To synthesise the evidence on the implementation, costs and cost-effectiveness of demand-generation interventions and their effectiveness in improving uptake of modern contraception methods in LMICs | SR | No | Yes | 20 | 0 |
| French (2014)48 | Sexual health | An exploratory review was conducted to assess research examining awareness, acceptability, effects on HIV testing, disclosure and sexual risk, and cost-effectiveness of HIV mass media campaigns targeting MSM | SR | Yes | Yes | 12 | 0 |
| Lorenc (2011)107 | Sexual health | To systematically review the evidence on the effectiveness and cost-effectiveness of interventions to increase the uptake of HIV screening among MSM | SR | No | Yes | 13 | 0 |
| Vidanapathirana (2005)109 | Sexual health | To assess the effect of mass media interventions and the most effective form of mass media intervention at a general population level or in specific target populations, in relation to changes in HIV testing | SR | Yes | No | 14 | 0 |
| Laine (2014)106 | Physical activity | To synthesise the evidence on the cost-effectiveness of population-level interventions to promote physical activity | SR | No | Yes | 10 (including 1 SR) | 1 |
| Ogilvie (2007)61 | Physical activity | To assess the effects of interventions to promote walking in individuals and populations | SR | No | No | 48 | 0 |
| Hutchinson (2006)112 | Multiple (smoking cessation, sexual health and substance abuse) | To examine the available literature on the cost-effectiveness of health behaviour change communication programme, focusing on communication interventions involving mass media | NSR (some consideration of quality but not formal quality assessment) | No (‘health communication’ includes mass media, counselling and interpersonal communication) | Yes | 45 | 3 |
| Jacob (2014)105 | Multiple | To determine the costs, benefits and overall economic value of communication campaigns that included mass media and distribution of specified health-related products at a reduced price or free of charge | SR (but limited quality assessment) | Yes | Yes | 15 | 0 |
| Mason (2008)108 | Multiple | This paper reports findings from a systematic review of the economic evidence relating to planning, design, delivery or governance of health promotion interventions | SR | No | Yes | 8 | 1 |
| McKinnon (2016)115 | Multiple (obesity – nutrition and physical activity) | To summarise cost–benefit and cost-effectiveness studies of obesity-related policy/environmental interventions for youth and the general population | NSR | No | Yes | 27 | 2 |
| Wang (2011)116 | Diet | To summarise the evidence on the cost-effectiveness of interventions designed to reduce sodium intake | NSR | No | Yes | 11 | 1 |
| Wang (2013)117 | Diet | To summarise recent economic evaluation of interventions to reduce salt intake | NSR | No | Yes | 6 | 1 |
| Review (first author and year) | Country of relevant studies | Target population in relevant studies | Study design of included studies | Perspective of included studies | Relevant findings | Amount of relevant information reported (subjective) – high, medium or low | Authors’ conclusions about cost-effectiveness of MMCs | Cost-effectiveness conclusions (reviewer’s interpretation) |
|---|---|---|---|---|---|---|---|---|
| Brinn (2010)35 | USA: Secker-Walker | Youth | CEA | Not reported | See Table 11 | Low | None | Provides weak evidence that tobacco control MMCs to reduce smoking in young people are cost-effective |
| Durkin (2011)24 | N/A | N/A | N/A | N/A | None | Low | None | None of the included studies assessed cost-effectiveness of MMCs |
| Atusingwize (2014)111 | Australia: Hurley and Matthews. UK: Kotz, Brown, Stevens, Ratcliffe (Scotland), Raikou. USA: Villanti, Fishman, Secker Walker, Holtgrave. Vietnam: Higashi | General population: Hurley and Matthews, Kotz, Brown, Higashi. Adults: Ratcliffe, Villanti. Youth: Secker-Walker, Fishman, Raikou. Specific communities: Stevens (Turkish community in Camden and Islington) | CEA: Hurley, Kotz, Brown, Ratcliffe, Secker-Walker, Fishman, Raikou, Stevens. CUA: Hurley, Villanti, Holtgrave, Raikou, Higashi | Health care: Hurley. Organisational: Kotz, Brown, Ratcliffe, Secker-Walker. Governmental: Higashi. Public health sector: Raikou. Societal: Villanti, Holtgrave. Local authority: Stevens | See Table 11 | High | The evidence on the cost-effectiveness of tobacco control MMCs is limited, but of acceptable quality and consistently suggests that they offer good value for money | Provides moderate evidence that tobacco control MMCs can be cost-effective, but the evidence is likely to be biased as only effective campaigns have been evaluated |
| Bala (2013)27 | N/A | N/A | N/A | N/A | None | Low | None | None of the included studies assessed cost-effectiveness of MMCs |
| Flack (2007)104 | UK: Ratcliffe (Scotland), Stevens. USA: Secker-Walker | Adults: Ratcliffe. Youth: Secker-Walker. Specific communities: Stevens (Turkish community in Camden and Islington) | CEA: Ratcliffe, Stevens, Secker-Walker | Organisational: Ratcliffe, Secker-Walker. Local authority: Stevens | See Table 11 | Medium | Overall there was limited information concerning the cost-effectiveness of mass media-led interventions aimed at smoking cessation | Provides moderate evidence that tobacco control MMCs can be cost-effective |
| Kahende (2009)113 | UK: Ratcliffe (Scotland). USA: Secker-Walker | Adults: Ratcliffe. Youth: Secker-Walker | CEA | Not reported | See Table 11 | Low | No specific conclusions about MMC. General conclusion: although there are obvious gaps in the literature, the existing studies show that in almost every case tobacco control programmes and policies are either cost-saving or highly cost-effective | Provides weak evidence that tobacco control MMCs can be cost-effective |
| Lantz (2000)114 | USA: Secker-Walker | Youth: Secker-Walker | CEA: Secker-Walker | Organisational: Secker-Walker (not reported in review) | See Table 11 | Low | It is believed that mass media interventions can have a significant and cost-effective impact on youth smoking behaviour | Provides weak evidence that MMCs to prevent uptake of smoking in young people are cost-effective |
| Raikou (2007)110 | USA: Secker-Walker, Fishman | Youth: Secker-Walker, Fishman | CEA: Secker-Walker, Fishman | Organisational: Secker-Walker. Societal: Fishman | See Table 11 | Medium | The general conclusion has to be that point-of-sale measures and mass media are cost-effective, often highly so. Although there is a very limited number of studies all studies reviewed find interventions cost-effective | Provides weak evidence that MMCs to prevent uptake of smoking in young people can be cost-effective |
| Belaid (2016)103 | N/A | N/A | N/A | N/A | None | Low | None | None of the included studies assessed the cost-effectiveness of MMCs |
| French (2014)48 | N/A | N/A | N/A | N/A | None | Low | None of the included studies examined the cost-effectiveness of the campaigns | None of the included studies assessed the cost-effectiveness of MMCs |
| Lorenc (2011)107 | N/A | N/A | N/A | N/A | None | Low | None | None of the included studies assessed the cost-effectiveness of MMCs |
| Vidanapathirana (2005)109 | N/A | N/A | N/A | N/A | None | Low | Additional research is needed to identify the effectiveness of different types of mass media interventions, the cost-effectiveness of the interventions and characteristics of messages | None of the included studies assessed the cost-effectiveness of MMCs |
| Laine (2014)106 | Belgium: De Smedt | Not reported | Not reported | Not reported | See Table 11 | Low | None. General conclusions: the number of studies related to the cost-effectiveness of population-level physical activity studies is limited | Provides weak evidence that MMCs that aim to increase physical activity are cost-effective |
| Ogilvie (2007)61 | N/A | N/A | N/A | N/A | None | Low | Only six studies included even a rudimentary economic evaluation. We were therefore unable to synthesise any meaningful data with which to compare these aspects | None of the included studies assessed the cost-effectiveness of MMCs |
| Hutchinson (2006)112 | UK: Ratcliffe (Scotland), Stevens. US: Secker-Walker | Adults: Ratcliffe. Youth: Secker-Walker. Specific communities: Stevens (Turkish community in Camden and Islington) | CEA: Ratcliffe, Stevens, Secker-Walker | Organisational: Ratcliffe, Secker-Walker. Local authority: Stevens | See Table 11 | Medium | There is a clear need for more studies of the cost-effectiveness of health communication interventions. The majority of studies of the cost-effectiveness of health communication that were reviewed here do not pay sufficient attention to methodological rigour | Provides moderate evidence that tobacco control MMCs can be cost-effective. No evidence for other behaviours |
| Jacob (2014)105 | N/A | N/A | N/A | N/A | None | Low | The studies included do not provide evidence to reach a conclusion about the economic merit of health communication campaigns that use mass media combined with product distribution | None of the included studies assessed the cost-effectiveness of MMCs |
| Mason (2008)108 | UK: Ratcliffe (Scotland) | General population: Ratcliffe | CEA: Ratcliffe | Organisation: Ratcliffe | See Table 11 | Low | None | Provides very limited evidence that tobacco control MMCs to reduce smoking in young people are cost-effective |
| McKinnon (2016)115 | Belgium: De Smedt. USA: Peterson | Youth: Peterson. Not reported: De Smedt | CUA: De Smedt. CEA: Peterson | Not reported | See Table 11 | Low | None. General conclusions note the relative paucity of studies located conducting cost–benefit or cost-effectiveness assessments | Provides weak evidence that MMCs that aim to increase physical activity can be cost-effective |
| Wang (2011)116 | Argentina: Rubinstein | General population: Rubinstein | Generalised CEA: Rubinstein | Not stated: Rubinstein | See Table 11 | Low | None | Provides weak evidence that MMCs to reduce salt intake are cost-effective |
| Wang (2013)117 | Vietnam: Ha | General population: Ha | CUA: Ha | Not reported: Ha | See Table 11 | Low | None | Provides weak evidence that MMCs to reduce salt intake are cost-effective |
Eight reviews were on the topic of smoking,24,27,35,104,110,111,113,114 four were on sexual health,48,103,107,109 two were on physical activity61,106 and two were on diet. 116,117 Four reviews covered multiple behaviours. 105,108,112,115
Four of the included reviews had mass media campaigns as the sole focus and reviewing economic evaluations as a specific aim of the review. 48,104,105,111 Four of the reviews had mass media campaigns as the sole focus but did not have reviewing economic evaluations as a specific aim of the review. 24,27,35,109 Ten of the included reviews did not have mass media campaigns as the sole focus but did have reviewing economic evaluations as a specific aim of the review. 103,106–108,110,112,113,115–117 Two of the reviews did not have mass media campaigns as the sole focus or reviewing economic evaluations as a specific aim of the review, but reported on economic evaluations in the results section of the review. 61,114
Eight of the included reviews included no relevant studies. 24,27,48,61,103,105,107,109 Nine reviews included one or two relevant studies. 35,106,108,110,113–117 Three reviews included three or more relevant studies, with a maximum of 11. 104,111,112 Of these, two reviews were on the topic of smoking104,111 and one was a mixed-topic review but all of the relevant included studies were on smoking. 112
A total of 15 individual primary studies were reported in the reviews. The characteristics of the primary studies are summarised in Table 11, based on the information extracted from the reviews. Eleven primary studies were on smoking,118–128 two were on physical activity129,130 and two were on diet. 131,132 The majority of the primary studies were from the UK and the USA.
| Review (first author and year) | Health topic | Country | Target population | Study design | Perspective | Relevant findings |
|---|---|---|---|---|---|---|
| Hurley (2008)118 | Smoking | Australia | General population | CUA | Health care | Prevention of 55,000 deaths, gains of 323,000 life-years and 407,000 QALYs, health-care cost savings of AU$740.6M. Campaign remained cost-saving in sensitivity analysis |
| Kotz (2011)119 | Smoking | UK | General population | CEA | Organisational | ICER of £82.24 per LYG (95% CI £49.70 to £231.60) for 35- to 44-year-olds. £114.29 for those aged < 35 years, £76.19 for those aged 45–54 years and £97.45 for 55- to 64-year-olds. Campaign remained cost-effective in sensitivity analysis |
| Brown (2014)120 | Smoking | UK | General population | CEA | Organisational | ICER for total population of £558 per LYG (95% CI £126 to £989). £414 for 35- to 44-year-olds, £607 for < 35-year-olds, £417 for 45- to 54-year-olds and £566 for 55- to 64-year-olds. Campaign remained cost-effective in sensitivity analysis |
| Stevens (2002)121 | Smoking | UK | Turkish community in London | CEA | Local authority | Study reports mean cost-effectiveness drawn from probability distribution of possible outcomes in sensitivity analysis. ICER of £105 per LYG (95% CI £33 to £391). ICER of £825 per 1-year quitter (95% CI £300 to £3500) |
| Raikou (2008)122 | Smoking | UK | Youth | CEA, CUA | Public health sector | Base case: £49 per QALY gained and £362 per LYG. Campaign remained cost-effective in all sensitivity analyses |
| Ratcliffe (1997)123 | Smoking | UK (Scotland) | Adults | CEA | Organisational | Cost per quitter of £168–363, cost per discounted LYG of £304–656 when parameters are varied. In Kahende: US$341–748 per quitter and US$617–1330 per LYG (results reported in 2005 US$) |
| Villanti (2012)124 | Smoking | USA | Adults | CUA | Societal | Base-case ICER of US$37,355. Sensitivity analysis: 95% uncertainty interval US$10,779–204,976 per QALY |
| Fishman (2005)125 | Smoking | USA | Youth | CEA | Societal | 4-year media campaign combined with US$1 tax increase. If cost = cost of media campaign, cost/LYG = US$528 (low-cost campaign with 3% discount rate) – £19,957 (high-cost campaign with 7% discount rate) (US$615–23,264 in 2006 US$) If cost = campaigns, changes in HC costs and tax revenue, cost saving per LYG = US$583,606–1,449,894 (US$680,310–1,690,141 in 2006 US$) |
| Secker-Walker (1997)126 | Smoking | USA | Youth | CEA | Organisational | Mass media and educational programme compared with educational programme alone. Community level: cost per smoker averted US$754 (95% CI US$531 to US$1296), cost per LYG at 3% DR US$696 (95% CI US$445 to US$1269). National level: cost per smoker averted US$162, cost per LYG at 3% DR US$138 (95% CI US$88 to US$252). Campaign remained cost-effective in sensitivity analysis. In Kahende: cost per smoker averted US$939, cost per LYS US$867 (if campaign run throughout USA) (costs reported in 2005 US$) |
| Holtgrave (2009)127 | Smoking | USA | Youth | CUA | Societal | Base-case: 178,290 QALYs gained, cost-saving. Optimistic case: 1,050,000 QALYs, cost saving. Pessimistic case: US$4302 per QALY |
| Higashi (2011)128 | Smoking | Vietnam | General population | CUA | Governmental | Without health-care cost offset: VND78,300 per DALY averted (95% CI VND43,700 to VND176,300). With cost offset: campaign dominates |
| De Smedt (2012)129 | Physical activity | Belgium | General population | CUA | Not reported | Model based (20 years). In a local-level community campaign to reduce sedentary time and increase walking, the intervention was estimated to improve the average QALY by 0.16 to give 12.23 QALYs for men, and by 0.11 to give 12.77 QALYs for women. Total costs decreased by €576 to €2963 and by €427 to €2454, respectively (€2009). Laine converted physical activity into metabolic equivalent of task: cost per MET-h gained/person $0.014. This is lower than for many of the other interventions assessed |
| Peterson (2008)130 | Physical activity | USA | Youth | CEA | Not reported | State-wide social marketing media campaign to promote physical activity to teens. Average cost of the campaign calculated at US$4.01 per person to see an advertisement, US$7.35 per person to consider being more active and US$8.87 per person increase physical activity. Billboards resulted in the greatest cost-effectiveness (US$2004) |
| Ha (2011)131 | Diet | Vietnam | General population | CUA | Not reported | A mass media education programme to reduce salt intake is cost-effective (US$118/DALY averted). Most cost-effective of 23 strategies to reduce CVD in Vietnam |
| Rubinstein (2009)132 | Diet | Argentina | General population | Generalised CEA | Not reported | The average cost-effectiveness ratio (measured in Argentine pesos) per DALY saved for a mass media campaign to reduce CVD was AR$547 (not strictly a diet campaign) |
Taken together, the reviews and the findings of the primary studies within the reviews provide moderate evidence that tobacco control mass media campaigns can be cost-effective. There is weak evidence in relation to diet (although this is restricted to reductions in salt intake) and physical activity. There is no evidence in relation to the cost-effectiveness of sexual health campaigns, despite efforts to identify such evidence in systematic reviews.
Summary
From our rapid review of reviews (published between January 2000 and January 2017) of the cost-effectiveness of mass media campaigns, evidence on cost-effectiveness was extremely limited for all health topics except smoking. The finding that there is moderate evidence that tobacco control mass media campaigns can be cost-effective should be considered in the context of the evidence from the effectiveness review. The cost-effectiveness evidence base is likely to be biased as only effective campaigns have been evaluated. Furthermore, because the majority of the evidence is from the UK and the USA, the cost-effectiveness findings have limited generalisability.
Chapter 5 What characteristics of mass media campaigns are associated with effectiveness?
Overview
In this chapter we review and analyse evidence regarding the characteristics of mass media campaigns that may be associated with effectiveness. First, we first consider the use of adopting theoretical frameworks encompassing communications and/or behavioural theories in the development, implementation and evaluation of campaigns. We then consider the features of campaign design, including type of media channel used, intervention duration and intensity and intervention content (type of messages, targeting strategies and source) associated with effectiveness. Finally, we consider the evidence on the impact of intervention scale (i.e. whether campaigns are implemented at a local, regional or national level).
This chapter seeks to address the following study objectives:
-
2. examine the components of messages that can be effectively communicated through mass media
-
3. explore how different types and forms of media campaigns can reach and be effective with different target populations (particularly disadvantaged groups)
-
4. assess new or emerging evidence about campaigns that employ different forms of media (including new media)
-
5. examine the relationship between local, regional and national campaigns and evidence of effectiveness where this exists.
The first section of this chapter describes a review of reviews of the effectiveness of campaign characteristics based on the reviews identified for Chapter 2 (review A). This review included systematic reviews published between January 2000 and January 2016, but it identified limited evidence on the effectiveness of different campaign characteristics, particularly in relation to the UK context and evidence on new media. However, the research team was aware of recent primary studies that have attempted to shed light on these and that are relevant to UK stakeholders, so we subsequently conducted an additional review to identify primary evidence from UK studies (review D). The second section of this chapter therefore describes a review of primary studies (published between January 2011 and September 2016) that provides recent evidence on campaign characteristics conducted in the UK.
Methods: systematic review of reviews
The methods for the review of reviews have been described in Chapter 2. From the reviews included in Chapter 2, we identified reviews that examined mass media campaign characteristics and synthesised relevant content.
Evidence from the reviews was reviewed and synthesised around the following characteristics of mass media campaigns: theoretical frameworks, intervention duration and intensity, mass media channels used, and intervention content (messages, targeting and source) and intervention scale.
Theoretical frameworks
Given that interventions developed with an explicit theoretical framework are considered more likely to be effective than those lacking any theoretical base,133 we considered that it was important to identify any theories used in the development, implementation and evaluation of campaigns in relation to their effectiveness and whether or not they had used multiple theories to achieve multiple goals. We returned to all the original included review papers to search the full texts for theory in detail. The earlier data extraction did not always include mentions of theories within introductions and discussions of the papers. We defined a theoretical framework in broad terms as a set of interrelated concepts, definitions and propositions that explain or predict events or situations by specifying relations among variables. From our reading of the reviews, we anticipated that theoretical frameworks would encompass two broad areas – communication theories and behaviour change theories – and that these theories would offer different explanatory insights. For instance, communications theories might help us to understand communication processes in the context of campaigns, such as theories underpinning how best to create and target messages, whereas behavioural change theories might help explain how different people might respond to such messages. By being inclusive, we considered that this would provide a comprehensive analysis of the conceptual thinking underpinning any mass media interventions, and identify the important features that might move people through pathways from increased awareness to eventual behaviour change.
Mass media channels used and interactivity
Mass media campaigns can be run via traditional media channels, such as television, radio, cinema, newspapers, magazines and billboards, or via new digital media including websites, pop-up and banner advertisements, QR codes, viral marketing and social media. New media often feature an element of interactivity (e.g. liking, sharing or commenting on content and downloading campaign apps). This ability to actively engage with a campaign may be associated with the increased effectiveness of a public health campaign. We have assessed the evidence relating to the different media channels used in campaigns, including the types of channels used and the use of single versus multiple channels, and on the use of new interactive media.
Intervention duration and intensity/exposure
Duration refers to the overall length of time that a campaign is in operation. Intensity and exposure refer to the overall ‘strength’ or ‘dose’ of a campaign, and can be measured in a number of different ways: the number of different advertisements or media materials produced, the number of times an advertisement is shown, the amount of media spend, the size of the audience reached by the campaign or the percentage of the audience in a given region or area that had a potential opportunity to see the campaign. Duration and intensity/exposure are often closely related, in that the longer a campaign runs, the more likely the audience is to be exposed to it. The two are therefore discussed together in this chapter.
Intervention content: messages, targeting and source
We have examined the evidence on the impact of different types of campaign content. We defined ‘message’ as referring to the types of messages used in campaigns (e.g. ‘positive’ vs. ‘negative’ messages, or messages containing information on the effects of the behaviour or advice on how to change behaviour). ‘Targeting’ referred to whether the campaign as a whole or specific campaign elements were intentionally targeted at specific population groups. Because the strategic decision regarding targeting was often strongly bound up with choice of messages, these two elements are discussed together. ‘Source’ refers to the apparent source of the message, and includes the person delivering the message (e.g. the use of actors or testimonials from real people) and the campaign funder (e.g. government, charities or pharmaceutical companies). As the source is likely to be associated with the type of message used and the intended target group, these elements are discussed together.
Intervention scale: local, regional and national campaigns
Even in the context of evidence that mass media campaigns featuring particular characteristics are likely to be effective, decision-makers need to consider how the scale of a campaign may influence its impact. We review the published evidence that considers the differential impact of local, regional and national campaigns.
Results: systematic review of reviews
Use of theory: findings from the review of reviews
Table 12 summarises the number of included reviews of mass media campaigns that examined various aspects of theory, and the various behaviour change theories mentioned in the reviews.
| Use of theory | Number of reviews |
|---|---|
| Number of reviews with theory as integral to the review process | 8: Brown (2012),56 Byrne (2005),65 Carter (2015),47 Kahn (2002),58 Leavy (2011),59 Matson-Koffman (2005),60 Robinson (2014)69 and Werb (2011)63 |
| Number of reviews listing theories in primary studies | 7: Bala (2013),27 Brinn (2010),35 Ferri (2013),62 Finlay (2005),57 French (2014),48 LaCroix (2014)51 and Leavy (2011)59 |
| Number of reviews analysing the effect of theories | 1: Ferri (2013)62 |
| Number of reviews listing behaviour change theories | 5: Bala (2013),27 Brinn (2010),35 Finlay (2005),57 French (2014)48 and Leavy (2011)59 |
| Behaviour change theories listed | Theory of reasoned action, theory of behaviour, stages of change, health belief model, social learning theory, social cognitive theory, transtheoretical model, social reinforcement for behaviour change and social diffusion theory |
| Number of reviews listing communication theories | 4: Bala (2013),27 Finlay (2005),57 French (2014)48 and Leavy (2011)59 |
| Communication theories listed | Social marketing framework and communication theory |
| Number of reviews with no focus on theory | 23 |
The majority of these reviews did not include a focus on theories or conceptual frameworks or models and, therefore, there was little evidence on the role that theory plays in the effectiveness of the intervention. Eight reviews incorporated theory into the process of their work. Three used logic models to frame their research questions and to identify the outcomes relating to their research. 47,56,58 These models were not adjusted in the light of the results from the review. One review used the presence of a theoretical framework as one of its inclusion criteria, but did not refer to the theories in the primary studies in the results section. 65 Leavy et al. 59 used the hierarchy of effects (HOE) framework to specify levels of impact to typify outcomes. Matson-Koffman et al. 60 and Robinson et al. 69 used theoretical framings to provide the rationale for their reviews. Finally, Werb et al. 63 used theory to explain the findings of their review.
Seven reviews listed the theories they found in their primary studies. Five of these listed behaviour change studies27,35,48,57,59 and four mentioned communication theories, notably social marketing. 27,48,57,59 LaCroix et al. 51 mentioned that 45% of the studies in their review were theory based.
In terms of relating theory to effectiveness, in their analysis of the effects of mass media campaigns on drug use, Ferri et al. 62 discovered that two studies based on social learning theory and the social ecological framework produced better results, whereas the study based on the social influence approach favoured the control group.
Mass media channels used and interactivity: findings from the review of reviews
Table 13 summarises the numbers of included reviews that examined media channels or interactivity as potential mediators of effectiveness.
| Media channels used and media channel interactivity | Number of reviews |
|---|---|
| Number of reviews that focus on channels used and analyse effects | 1: Derzon (2002)66 |
| Number of reviews that focus on channels used | 4: Bertrand (2006),46 Jepson (2006),43 Mozaffarian (2012)68 and Richardson (2008)44 |
| Number of reviews that focus on interactivity and analyse effects | 1: Swanton (2015)53 |
| Number of reviews with no focus on channels used and interactivity | 33 |
Although most of the reviews included information on the media channels used in the individual included studies, most simply listed them when summarising the characteristics of the included studies, and did not examine media channels or degree of interactivity as mediators of campaign outcomes, or discuss the potential relationship between channels and interactivity and effectiveness. The lack of attention paid to interactivity is unsurprising in the older reviews whose included studies would have predated the development of new interactive media. Findings from the five reviews that reported findings specifically relating to channels are summarised below.
Derzon and Lipsey66 conducted a meta-analysis comprising 72 studies of mass media substance use campaigns, with media channels used (radio, television, video or print) as one of the sets of variables in the analysis. Overall, the analysis found that reduced substance use behaviour was associated with exposure to all the different media channels, but that radio was associated with the greatest relative effects (Δ = 0.10) and print with the least (Δ = 0.04). For attitude outcomes, the relative effects were greater for those exposed to video and print rather than other channels. Video was associated with particularly large relative effects on substance use knowledge. In conclusion, the review authors stated that with regard to media channel, messages communicated via video were associated with greater improvements in knowledge, attitudes and behaviour than campaigns that did not use video. It is likely that most of the video-based campaigns would have been implemented in school settings and would have involved discussion and other informational and educational input, in other words in a quite different context from general population mass media campaigns on broadcast media. The age of the Derzon and Lipsey66 review (published in 2002) means that some of the studies are likely to be quite old, which again limits the relevance of the findings to the present UK context.
A review of mass media campaigns on HIV/acquired immunodeficiency syndrome (AIDS)-related behaviour among young people in developing countries specifically examined the strength of the evidence for the effects of three types of mass media interventions (radio only, radio with supporting media or radio and television with supporting media) and assessed whether or not these interventions reach the threshold of evidence needed to recommend widespread implementation. 46 One of the studies included in the review was radio only. Six of the studies evaluated interventions using radio with other supporting media (e.g. written materials, videos, posters, theatre performances and school workshops). The remaining eight interventions involved television and radio with other supporting media.
The review reported that the one radio-only campaign showed mixed results regarding awareness of a helpline but no improvements in social norms, interpersonal communication about HIV/AIDS or various measures of condom use. 46 Of the six studies using radio with other supporting media, all reported some measure of knowledge gain, although results tended not to be significant, and most studies showed some positive effects on skills, knowledge, interpersonal communication and social norms. Findings relating to various sexual behaviours were mixed, although the weight of the evidence across studies reporting condom use was strongly positive.
Eight studies examined the effect of campaigns using television and radio with other supporting media. Evaluations of this type of intervention generally showed improvements in knowledge and skills related to HIV/AIDS, knowledge about health services, interpersonal communication regarding HIV/AIDS and social norms. Data on different measures of condom use showed positive effects in the majority of studies, although evidence regarding other behaviour change (e.g. reduced age of sexual behaviour, number of partners and abstinence) varied but leaned towards having no effect. The review authors concluded that ‘Campaigns that include television require the highest threshold of evidence, yet they also yield the strongest evidence of effects’. 46 The findings have limited relevance for the UK and OECD countries.
In their review of mass media interventions targeting young people smoking, Richardson et al. 44 reported evidence from a single study on mass media channels, one that examined the effects on youths of antismoking cinema advertisements played during a film. Effects included increased disapproval of smoking in films and, among smokers, a desire to quit. In a wide-ranging review of mixed health behaviours, Mozaffarian et al. 68 noted that mass media and education campaigns using ‘multiple modes’ (described as including ‘print, radio, Internet, television, social networking, other promotional materials’) demonstrated effectiveness for increased consumption of specific healthy foods, reduced consumption of less healthful foods and drinks and the promotion of physical activity.
In a review that aimed to synthesise evidence evaluating the effectiveness of mass media interventions on helping people to quit smoking/tobacco use and/or to prevent relapse, Jepson et al. 43 presented data in a format that organised the results by channel of mass media. Interventions that drew on two or more forms of the media (such as newspaper, television and billboard advertising) were referred to as ‘multichannel’ mass media. A particular emphasis was placed on evaluating relevance to the UK setting. Interventions were examined in terms of both the effectiveness of the channel of communication and the effectiveness of message content (see Intervention content: findings from the review of reviews). The review noted that many of the studies used multiple types of media combined with other interventions, which made it difficult to evaluate which particular component was effective or ineffective. It reported some good-quality evidence that the use of technology such as mobile phones could be effective, and offered the potential to deliver culturally specific materials to targeted groups. It also reported evidence that the internet could be an effective way of delivering interventions and may be a particularly appealing channel of communication for young people. Three studies, probably relevant to the UK, found an effect of multichannel mass media on smoking cessation, but there was no evidence about which of the mass media components of the interventions were most effective (or most ineffective), and the review authors cautioned that the results of these studies should be interpreted with caution owing to their poor methodological quality.
One review examined interactivity as a potential moderator of effectiveness. In a meta-analysis of the effects of new-media interventions on sexual health behaviours by Swanton et al. ,53 the interventions examined included websites, SMS (short message service) messages, social media and online video. Components of interventions were coded as interactive (e.g. personalised e-mails) or static (e.g. watching an online video). Moderation analyses found a variation in the effect of new-media interventions on condom use depending on the interactivity of the new-media channel used:53
Interventions using interactive components yielded significant effects (OR 1.79, 95% CI 1.15 to 2.77; p = 0.01); however, this effect was significantly heterogeneous [Q (6) = 28.03; p < 0.01, I2 = 78.59%], suggesting that further factors may influence the size of the effect. Interventions using static content did not yield significant effects, and the effect size was homogeneous.
Swanton et al. 53
In conclusion, the review found that interventions that used interactive components were shown to be more effective than static components in improving condom use.
Intervention duration and intensity/exposure: findings from the review of reviews
Table 14 summarises the number of included reviews of mass media campaigns that examined intervention duration or intensity/exposure.
| Mass media campaign intervention duration and intensity/exposure | Number of reviews |
|---|---|
| Number of reviews with statistical analysis of effect of intervention duration | 2: LaCroix (2014)51 and Swanton (2015)53 |
| Number of reviews with description of an association of effect of intervention duration | 4: Bala (2013),27 Brinn (2010),35 Mozaffarian (2012)68 and Richardson (2008)44 |
| Number of reviews with no focus on intervention duration or intensity/exposure | 30 |
Six of the 36 reviews examined or commented on the relationship between intervention duration or intensity/exposure and effectiveness. Information on duration or intensity/exposure in individual studies was extracted in other reviews, but no attempt was made in the review analysis or synthesis to draw conclusions about the relative effectiveness of different levels of duration or intensity/exposure.
Two of the reviews, both examining sexual health campaigns, conducted statistical analysis to examine whether or not intervention effectiveness was moderated by intervention duration. 51,53 Both found some evidence that effectiveness increases with greater duration and intensity/exposure, although for only some of the outcomes examined. In the meta-analysis of the effects of new-media interventions on sexual health behaviours by Swanton et al. ,53 the interventions examined included websites, SMS messages, social media and online video. They were coded into three duration categories (a single session, ≤ 6 months or > 6 months in duration) and the relationship between duration and effectiveness was examined in moderator analysis. Intervention duration was not related to effectiveness in interventions targeting condom use, but was related to effectiveness when the outcome was participation in testing for sexually transmitted infections (STIs): single-session interventions were less effective than longer interventions (up to 6 months in duration, OR 1.64, 95% CI 1.36 to 1.98; p < 0.01; and > 6 months in duration, OR 2.17, 95% CI 1.36 to 3.47; p < 0.01). A meta-analysis of the impact of sexual health mass media interventions on condom use and HIV-related knowledge51 examined whether or not effectiveness was moderated by various intervention characteristics, including duration and proportion of target population exposed to the campaign. The relationship between campaign characteristics and magnitude of effects was examined using a modified weighted least squares regression analysis. Greater increases in condom use were seen following longer campaigns (k = 51, β = 0.48, p < 0.001).
Three reviews [one National Institute for Health and Care Excellence (NICE) rapid review44 and two Cochrane Database Systematic Reviews27,35] provide some evidence to suggest that intervention duration and intensity/exposure are associated with effectiveness in mass media campaigns targeting tobacco use, but do not examine the relationship statistically. A NICE rapid review of the effectiveness of mass media interventions designed to prevent the uptake of smoking in children and young people examined whether or not the intensity of interventions influenced effectiveness or duration of effect. 44 Evidence statements in the review stated that:
The duration of a mass media intervention influences its effect. Increased exposure to anti-tobacco messages over time decreases intent to smoke and smoking initiation, meanwhile increasing negative attitudes towards the tobacco industry.
Underpinning support for the evidence statement came from a Cochrane Database Systematic Review (Sowden 1998 as cited by Richardson et al. 44), suggesting that intervention duration was an important influence on behaviours, and from three cross-sectional studies, all conducted in the USA, which found that increased exposure to antismoking advertisements over time resulted in a decrease in young people smoking in the past 30 days (compared with those in markets with no exposure to state-sponsored anti-tobacco laws), intent to smoke, initiation of smoking, enhanced perception of risk and negative attitudes about smoking. The same NICE rapid review44 also examined facilitators of and barriers to implementation, and noted that lack of exposure and longevity are barriers to effective mass media interventions, noting that one-off campaigns are not likely to induce behaviour change and that:
Messages must appear frequently enough for audiences to notice them and internalise them.
Bala et al. 27 examined the effectiveness of mass media interventions for smoking cessation in adults in a Cochrane Database Systematic Review. From reviewing 11 campaigns, the review concluded that the intensity and duration of campaigns may influence effectiveness, but length of follow-up and concurrent secular trends and events could make it difficult to quantify the effects. The review cited a UK study (McVey 2000 as cited by Bala et al. 27) that compared the impact of single- and double-weight television campaigns on quit rates and found no significant differences at 6 months, with the single-weight region (Granada) at 6.3% and the double-weight region (Tyne Tees, Yorkshire) at 6.6%, yielding an adjusted OR of 1.02 (p = 0.94). It also discussed studies in other countries that appeared to support the use of longer running or more intense campaigns, but noted that effects may have been confounded by the concurrent presence of other intervention elements such as face-to-face counselling. The authors concluded that ‘The duration and intensity of an intervention may affect its impact on smoking behaviour, but evaluations need to last long enough to detect lasting changes, and to allow for confounders and for secular trends’. 27
Another Cochrane Database Systematic Review examined the effectiveness of mass media interventions for preventing smoking in young people, with seven studies, all using a controlled design, meeting all of the inclusion criteria. 35 The three effective campaigns were all ‘of reasonable intensity over extensive periods of time’; in contrast, the campaigns that did not report positive findings, much more heterogeneous in duration and generally shorter. The three effective campaigns comprised (1) 190 television, 350 cable television and 350 radio spots purchased in each of the 4 years during which the campaign was running (Flynn 1995 as cited by Brinn et al. 35); (2) 167 television and cinema spots in three annual campaigns (Hafstad 1997 as cited by Brinn et al. 35); and (3) television (local, cable and network), radio, websites, magazines, movie theatres and several other media used over 6.5 years (the National Youth Anti-Drug Media Campaign) (Longshore 2006 as cited by Brinn et al. 35).
Finally, a wide-ranging mixed-topic review examining the effectiveness of a range of population approaches reported ‘strong evidence’ that sustained (i.e. longer duration) campaigns are important, particularly for reducing smoking. 68 The review also noted that some of the campaigns found to be effective in improving diet knowledge and behaviours were implemented for many years, suggesting that ‘behavioural changes are sustainable when media and educational campaigns are continued’. However, the effects of mass media campaigns were not distinguished from those of campaigns using multiple approaches including mass media, and the review conducted no statistical analysis of the moderating role of campaign duration. It recommended that media and education campaigns to improve diet, physical activity and smoking should be sustained and should use multiple modes/channels.
Intervention content: findings from the review of reviews
Table 15 summarises the reviews that assess the impact of message type, targeting and source.
| Mass media campaign message type, targeting and source | Number of reviews |
|---|---|
| Number of reviews with message as the primary focus of the review | 0 |
| Number of reviews with targeting of specific groups as the primary focus of the review | 3: de Kleijn (2015, girls),38 Gould (2013, indigenous populations)39 and Guillaumier (2012, disadvantaged groups)40 |
| Number of reviews analysing the effect of the message | 12: Abioye (2013),55 Brinn (2010),35 Brown (2014),36 Byrne (2005),65 Derzon (2002),66 French (2014),48 Hill (2014),42 Jepson (2006),43 LaCroix (2014),51 Mozaffarian (2012),68 Richardson (2008)44 and Wilson (2012)45 |
| Number of reviews analysing the effect of targeting specific groups | 7: Brinn (2010),35 Brown (2014),36 Byrne (2005),65 Derzon (2002),66 Jepson (2006),43 Richardson (2008)44 and Wilson (2012)45 |
| Number of reviews analysing the effect of the ‘source’ of the message | 2: Byrne (2005)65 and Richardson (2008)44 |
| Number of reviews with no specific analysis of message or targeting of specific groups (had intended to look at targeting or messaging but not enough studies) | 20 |
| Types of message | Social norms, guided by theoretical concepts, personal testimony, highly emotive, graphic, negative health consequences, fear campaigns and strategies for refusal |
| Nature of targeting | Low education, low SES, age, youths, girls, cultural indigenous and ethnic groups |
Although the majority of reviews provide some detail on the content of mass media interventions, often including some detail about the message and target population for individual studies and campaigns, only 12 provided some degree of analysis or synthesis of the influence of message type on behavioural or other outcomes. A further 10 provided analysis or synthesis of the effectiveness of the targeting of campaigns. The main focus of three reviews was the effectiveness of targeting campaigns towards specific groups (girls, indigenous populations and disadvantaged groups), whereas none focused solely on the characteristics of effective messages. There is a clear overlap between reviews that provide information on effect of message type and effect of targeting, which is reflected in the summary below.
Message types
A number of reviews provide evidence that intervention content influences effectiveness. An evidence statement in the NICE review on preventing uptake of smoking by children44 states:
The way in which an intervention is delivered does influence effectiveness. However effectiveness is dependent on a number of factors including message content, mode of delivery, target audience, message framing and message elements.
There were some consistent themes among those reviews that compared message types.
Several reviews found that campaign messages that intended to denormalise behaviour, including social norm campaigns, may be more effective across a range of behaviours, including physical activity in adults, smoking in adults and substance use in the young, than some other message types. 44,55,65,66 In their review of health campaigns to increase physical activity, Aboiye et al. 55 noted that campaigns based on ‘social norm’ messages were more likely to lead to a reduction in sedentary behaviour (RR 1.33, 95% CI 1.01 to 1.43) than those using celebrities or based on a ‘risk message’ (RR 1.05, 95% CI 0.92 to 1.21). Richardson et al. 44 provided evidence from one qualitative study that social norms messages were more effective than fear messages at encouraging more committed young smokers to consider their smoking behaviours and reinforcing awareness of the dangers of smoking in less committed smokers. The review by Byrne et al. 65 examining various substance use behaviours in young people found that a denormalisation message was used in 13 campaigns, and most of these (89%) were associated with positive outcomes in the three domains of attitudes, knowledge and behaviour. A meta-analysis on a similar theme by Derzon and Lipsey66 did not report any particularly large effects for their category ‘perceived normative use’ but did note that positive attitudes to non-use, which would arise from denormalisation messaging, were associated with positive outcomes regarding behaviour, attitudes and knowledge.
Several reviews highlighted that messages concerning negative health consequences, mostly anti-tobacco messages, can be effective; however, for the most part negative messages were not directly compared with positive messages. 43–45,65,68 In a broad-ranging review of mixed health behaviours, Mozaffarian et al. 68 noted that factors that increase effectiveness for tobacco campaigns include use of strong negative messages about health. A review by Byrne et al. 65 of campaigns addressing various substance use behaviours in young people found that 14 campaigns, representing 56% of the total number of campaigns evaluated, employed health effects messages using information about the negative health effects of substance use in order to effect change in attitudes, knowledge, behaviour or all of these, and 79% were associated with positive outcomes.
In a review of mass media campaigns promoting antismoking messages, Wilson et al. 45 found that message content and tone contributed to heterogeneity in effects, and suggested that, although it is not clear which types work best, adult audiences are most likely to respond to graphic depictions of health consequences of smoking; this evidence is primarily based on the effectiveness of hard-hitting graphic campaigns from Australia. In the NICE rapid review of campaigns to prevent uptake of smoking by children, Richardson et al. 44 reported evidence from one RCT suggesting that tobacco-related disease messages were effective for increasing anti-tobacco attitudes in the young and another RCT suggesting that message content could change perceptions of health risk severity and intentions not to smoke; both studies were from the USA and the review concludes that it is not clear if these findings are directly applicable to the UK. In a review of mass media campaigns to encourage smokers to quit, Jepson et al. 43 found little direct comparison between message types, but this review resulted in the following evidence statements: (1) there is level 2 evidence, probably relevant to the UK population, which suggests that advertisements depicting suffering as a result of tobacco use may be instrumental in promoting cessation or reinforcing the decision to quit and (2) there is level 3 evidence that shows that graphic mass media messages about negative consequences of smoking among adults also have a positive effect on quit attempts among young people. Finally, there is level 2 evidence providing insufficient evidence that longer positive messages are less effective than short negative messages. However, this review concluded that although a few studies have evaluated different message styles (e.g. fear arousing), there was not enough evidence to determine which messages were more effective than others. They point out that smokers and reasons for smoking are complex and smokers are not simply compelled to quit because of fear/negative messages. 43 One aspect of note here is the addictive impact of nicotine on attempts to quit smoking, although this is rarely mentioned in the context of messaging.
Reviews highlight some messages that appear to be less effective or for which the evidence is less convincing. Both Byrne et al. 65 and Derzon et al. 66 found that those campaigns emphasising resistance or refusal skills for substance use behaviours in the young were less effective. Byrne et al. 65 noted that one campaign promoting such skills was associated with an increase in the intention to take up smoking among young people, although this campaign was funded by a tobacco company and did not contain messages about the harmful effects of smoking. 65 In a similar vein, the review by Derzon et al. 66 showed gain in terms of knowledge with this message but not in terms of behaviour and attitudes.
The effectiveness of tobacco industry deception or truth campaigns for the young was discussed in several reviews with some mixed evidence between studies. 44,45 Richardson et al. 44 reported evidence from several US cross-sectional studies that ‘truth’ messages were effective in decreasing and preventing smoking in youth, although they point out that the American Legacy Foundation’s Truth campaign is a specific US campaign and results may not be directly relevant to other contexts including the UK. 44 They also report a RCT that found that anti-industry advertisements did not decrease young people’s intentions to smoke, and a qualitative study that found that advertisements focused on the marketing and manufacturing practices of the tobacco industry, presenting the industry as greedy and deceitful, were aesthetically appealing but ineffective for preventing the uptake of smoking. Wilson et al. ,45 in their review of interventions for smoking, reported that, among US youths, large-scale campaigns focused on tobacco industry manipulation and deception were shown to be effective at reducing initiation.
Target audience
A dominating theme from a number of reviews is that message effectiveness depends on the target audience and appropriateness of the message to the target audience. 35,43–45,48,51,65,68 The review by Mozaffarian et al. ,68 which examined population approaches across multiple behaviours (diet, physical activity and smoking), noted that ‘broad community-based media and educational programmes that target multiple cardiovascular risk factors and behaviours simultaneously have been less successful, which suggests the importance of focused messages for the target audience’. Byrne et al. ,65 having looked at campaigns across a mixture of behaviours, indicate that mass media messages need to take into account the age, sex, culture, level of engagement in the target activity and personal characteristics, such as sensation-seeking, of the intended audience. Although these reviews considered multiple behaviours, even reviews that have considered only one lifestyle behaviour have suggested that no one message seems to be more or less effective across the board, and reason that we should not expect one style of message to resonate with all. 43,44 The reviews covering smoking alone suggest that smokers are complex and the reasons for smoking are complex, and the outcomes of any message type depends on the context and the values that the audience associates with smoking. 43,44 Broadly, the message needs to have relevance for the target audience and to have the right content, format, tone and level of complexity for the audience; any imagery needs to complement the campaign message. 48
Several reviews examine if and how campaigns should be targeted to reach specific subgroups, for example youths, disadvantaged or less-educated populations, indigenous populations and other ethnic groups. There is evidence of effective campaigns targeting these groups. 35,39,40,43 In the review by Brinn et al. 35 of mass media interventions to prevent smoking in young people, two of the three studies successfully reducing smoking behaviour targeted specific populations: one targeted girls and one targeted higher risk groups, defined by parental education attainment and income levels. Guillaumier et al. 40 reported that antismoking campaigns developed for, marketed to and evaluated with disadvantaged groups only were successful in achieving recall and response. Jepson et al. 43 found a lack of evidence for effectiveness on smoking outcomes of campaigns targeted at pregnant women who smoke and mothers of young children. However, they report that culturally appropriate advertising materials, which target particular ethnicities or communities, have been found to be effective by a number of studies, including materials targeting rural Nebraskan oral tobacco users with cowboy images, using gospel, jazz music and images appropriate to African American communities, or targeting the community with own-language materials, as in the case of Vietnamese Americans. However, they note that ethnicity is also crosscut by different income and educational levels and there is a need to be sensitive to the pitfalls of developing campaigns that may simply reproduce social or cultural stereotypes. It is important that the message does not stereotype or patronise; targeted campaigns need to be culturally appropriate and relevant. 39
Few reviews provide examples of how to target the message for specific populations. A review by Brown et al. 37 considered the equity impact of interventions to reduce smoking in adults; it found mixed evidence in terms of the equity of campaigns overall, but provided evidence from studies showing that highly emotive and personal testimony advertisements were more effective with low-socioeconomic-status groups and that emotive or graphic advertisements were more effective with low-socioeconomic-status smokers. Hill et al. 42 found weak evidence that antismoking television advertisements using personal testimony are more likely to have neutral equity impact for socioeconomic inequalities than traditional information-based advertisements, which tended to have greater impact among high-socioeconomic-status smokers. Gould et al. 39 point out that, for New Zealand Māori, mainstream graphic advertisements showing body parts are inappropriate.
Nevertheless, generic campaigns aimed at the general population can also be effective in reaching specific subgroups such as the young, disadvantaged smokers or indigenous populations. 39,40,44 Adult-focused or general population campaigns are successful in reducing smoking in young people. 44 Looking across different types of substance misuse, Derzon and Lipsey66 suggest that bigger effects are obtained by targeting parents and other youth-influential adults rather than the youths themselves. Although some studies suggested that targeted campaigns are preferred by indigenous populations, even in these subgroups, generic campaigns were as effective in terms of recall as more targeted campaigns, although it was less clear whether or not recall translated into behaviour change. 39 Guillaumier et al. 40 noted that when general population and targeted campaigns, both airing nationally, were compared in disadvantaged-only samples, disadvantaged smokers were more likely to recall and respond to the generic campaigns than to the targeted campaigns, suggesting that general population campaigns have the potential to be effective with disadvantaged population subgroups.
Source
There is some indication that the source of the mass media message can also be important; however, this issue is addressed in only a small number of reviews. Furthermore, the source of the message is often reflected in the message type and, therefore, its effect cannot be easily disentangled. Similarity between the source and the audience may increase persuasive impact, for example teenage actors for campaigns aiming at young people. 65 Several reviews conclude that campaigns produced by the tobacco industry are not effective and may even be harmful, perhaps because the messages used hold less negative emotional appeal to the young than campaigns organised by tobacco control programmes. 44,45 In an evidence statement, Richardson et al. 44 conclude that, when comparing intervention source, prevention campaigns produced by the tobacco industry are less effective than anti-tobacco campaigns produced by tobacco control bodies. Youths perceive industry campaigns to be less effective, less interesting and less engaging.
Intervention scale: findings from the review of reviews
None of the reviews examined scale of campaign as a potential mediator of effectiveness. Although the reviews noted whether their included studies were implemented at local, regional or national levels, most simply listed the information and none of them provided any evidence or commentary regarding the relative effectiveness of campaigns implemented at these different levels or discussed factors that might be associated with effectiveness when campaigns are implemented at the different levels.
Methods: review of recent UK primary studies
In the UK, some primary studies have recently sought to assess the contribution of different media campaign characteristics to campaign effectiveness. In order to address the gaps in the review of reviews and to examine evidence with relevance to the current UK context, we conducted an additional review of UK primary studies published between January 2011 and September 2016 (review D). The focus of this review was on evidence concerning the characteristics of UK mass media campaigns associated with effectiveness, rather than on the effectiveness of those campaigns per se.
Identification of studies
Studies were eligible if the paper was published in or after 2011 and the study was conducted in the UK. Multicountry studies were eligible if findings for the UK were reported separately. The campaigns had to address one of our six health topics: alcohol use, illicit substance use, diet, physical activity, sexual and reproductive health and smoking cessation and prevention. Apart from targeted health topics, the study eligibility criteria for primary research studies evaluating the effectiveness of mass media interventions were the same as those used in the related review of mass media campaigns to reduce alcohol consumption. 17 Box 3 describes the mass media campaign intervention study eligibility criteria. Studies could report data or outcomes of any format for the following outcomes: behavioural or social cognitive outcomes, media outcomes (e.g. recall, understanding and onward transmission of the campaign) and distal (e.g. societal or policy changes) or process (e.g. cost-effectiveness) outcomes. Studies of multicomponent interventions were eligible if they assessed the specific effects of a mass media component, and published conference abstracts were eligible provided there was a description of the campaign and outcome data were reported.
-
Mass media campaigns broadcast using television, radio, cinema, online broadcasting, newspapers and magazines, leaflets/booklets, direct mail, outdoor advertising, text messaging, e-mail and digital media, including websites and banner advertisements.
-
Interventions involving person-to-person contact, requiring active engagement before receipt of the message (e.g. alcohol screening questions) rather than passive message exposure, or online treatment or self-help programmes.
-
Studies in which a baseline measure is used to tailor a subsequent mass media message.
-
Studies testing campaign messages rather than assessing implemented campaigns intended to reach large numbers of people. Exclude studies of messages taken from an implemented campaign but delivered and evaluated outside that campaign (e.g. in laboratory conditions).
-
Studies of multicomponent interventions if they do not assess the specific effects of a mass media component.
-
Studies assessing the impact of advertisement bans.
-
Studies of social norms campaigns unless it is evident from the information available that a mass media channel was used. If an intervention is described only as a social norms or social marketing campaign and there is no information indicating the use of mass media channels then it will be ineligible for inclusion.
-
Studies of obligatory health warnings (e.g. on-pack health warnings and point-of-sale health warnings) and studies evaluating policies rather than campaigns.
The search strategy was a revision of that used for the project’s review of mass media campaigns to reduce alcohol consumption, combining terms for mass media and health communication campaigns and for the target health topics with a UK studies search filter (see Appendix 6 for an example strategy). Sixteen academic databases were searched on 7–9 September 2016 and the results were uploaded to an EPPI-Reviewer 4 database and deduplicated (Figure 4):26
-
Applied Social Sciences Index and Abstracts
-
EMBASE
-
Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Ovid MEDLINE(R) Daily and Ovid MEDLINE(R) – 1946 to present
-
Social Sciences Citation Index – 1900 to present, Arts and Humanities Citation Index – 1975 to present, Conference Proceedings Citation Index – Social Science & Humanities – 1990 to present, Book Citation Index – Social Sciences and Humanities – 2005 to present and Emerging Sources Citation Index – 2015 to present
-
PubMed, via EPPI-Reviewer 4 PubMed direct import
-
EBSCOhost Research Databases Database – Communication Source, Business Source Complete, ERIC
-
The Cochrane Library, Cochrane Central Register of Controlled Trials, issue 8 of 12, August 2016; NHS Economic Evaluation Database; Health Technology Assessment Database, issue 3 of 4, July 2016; Cochrane Methodology Register, issue 3 of 4, July 2012.
FIGURE 4.
The PRISMA flow diagram of the identification and selection of primary studies (review D).
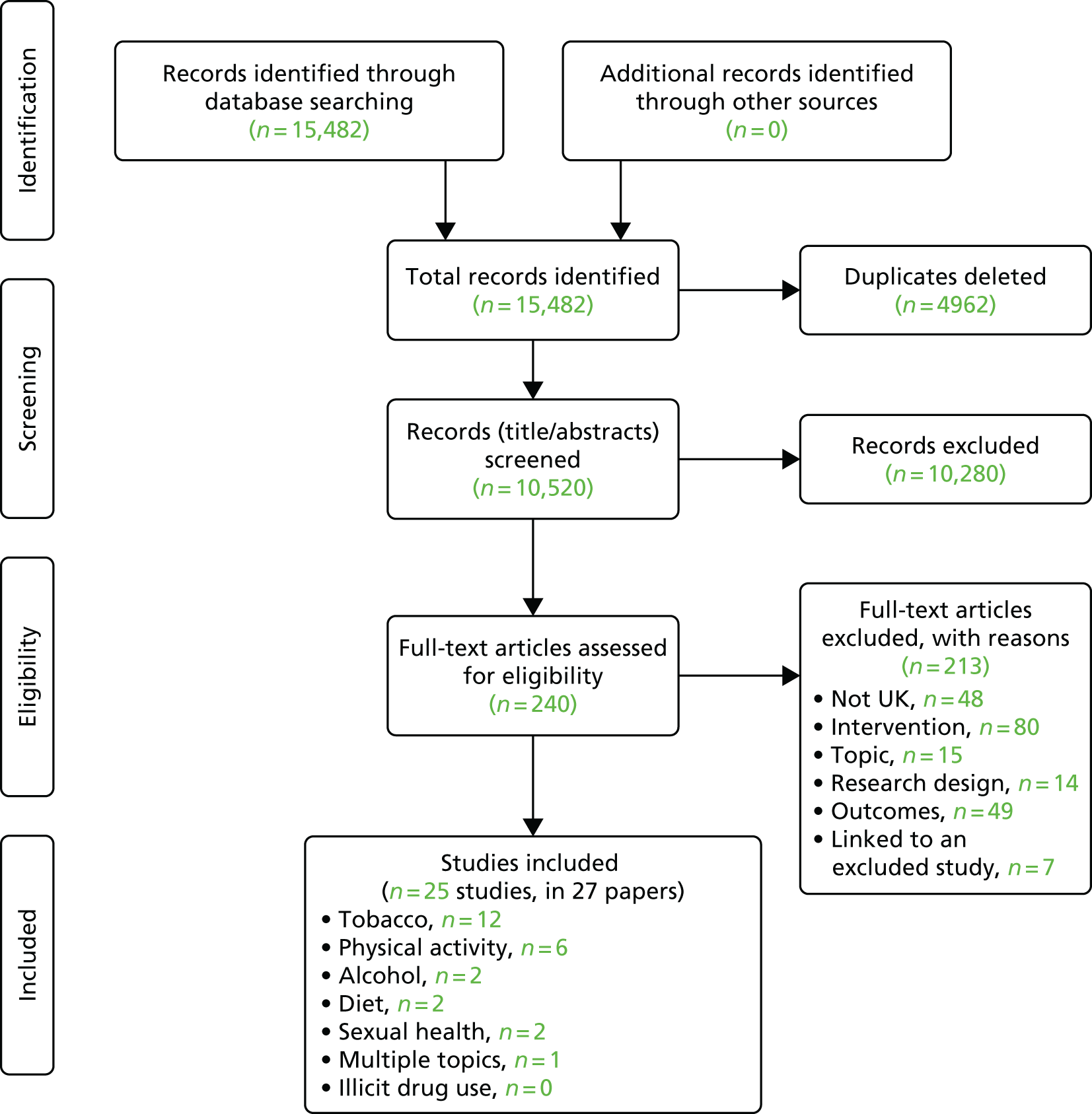
Records (n = 10,520) were screened for initial topic relevance, date and country by two reviewers (KH and KA). One per cent (n = 105) of randomly selected records were double-coded to pilot the screening process and check for inter-rater reliability. Once agreement was > 90% on included and excluded categories, then a proportion of the rest was allocated to each reviewer for single coding. The resulting 240 were retrieved as full texts and all double-coded by the reviewers (KH and KA) for inclusion; any final decision disagreements were resolved by a third reviewer (LB or MS). Twenty-seven papers covering 25 recent evaluations of UK mass media campaigns were included for analysis (see Appendix 7). 119,120,134–158 A list of UK primary studies excluded by full-text assessment is provided in Appendix 8.
The data extraction form was a revision of that used for the project’s review of reviews and designed to capture the study methods and outcome data as well as details of the mass media campaigns (the intervention) towards answering the project’s objectives. Studies were double data extracted independently by three reviewers [KA, KH and Joanne Morrison (JM)], who held telephone meetings in pairs to agree and finalise the data for each study. A pilot data extraction exercise, using two studies independently coded by all three reviewers, familiarised them with the process to ensure consistent interpretation of the headings. No study authors were contacted in order to obtain or confirm data.
In a departure from the review project’s protocol, two additional risk-of-bias appraisal tools were added after study selection to correspond to the included studies’ design. The proposed EPHPP Quality Assessment Tool for Quantitative Studies was used to assess experimental studies,78 with the additional US National Institutes of Health’s assessment tool for observational cohort and cross-sectional studies159 and the Critical Appraisal Skills Programme (CASP) tool for qualitative studies. 160 Studies were appraised for quality and relevance (at a study level) independently in duplicate by three reviewers (KA, KH and JM), who held telephone meetings in pairs to agree and finalise the risk-of-bias assessment for each study. The pilot exercise described above also included an independent appraisal of quality and relevance for the same two studies by all three reviewers.
This review of recent UK primary studies was designed to capture data or outcomes of any format for the following outcomes: (1) behavioural, social cognitive or media outcomes and (2) distal (e.g. societal or policy changes) or process (e.g. cost-effectiveness) outcomes. Thus, from its inclusive nature, we did not expect to be able to carry out a meta-analysis of the data.
Narrative synthesis
Evidence from the UK primary studies was reviewed and synthesised around the following characteristics of mass media campaigns: theoretical frameworks, intervention duration and intensity, mass media channels used and intervention content (messages, targeting and source) and intervention scale. How these characteristics were defined and analysed is described in Methods: systematic review of reviews.
Results: review of recent UK primary studies
Use of theory: findings from the review of UK primary studies
Table 16 summarises the numbers of included UK primary studies that examined various aspects of theory, and the various behaviour change theories mentioned in the studies.
| Use of theory | Number of UK primary studies |
|---|---|
| Number of studies with theory as integral to study or programme design | 6: Brown (2014),120 Brown (2016),136 Eves (2012),139 Eves (2012),140 Richardson (2014)152 and Richardson (2014)153 |
| Number of studies with behaviour change theories | 2: Brown (2016)136 and Eves (2012)139 |
| Behaviour change theories listed | Theory of planned behaviour and prime theory |
| Number of studies with communication theories | 1: Brown (2014)120 |
| Communication theories listed | Social contagion theory |
| Number of studies with no focus on grand theory | 19 |
Out of 23 primary studies, 17 did not include grand theories, conceptual frameworks or models to inform their mass media interventions. Of the six studies that did incorporate theory, three grand theories were identified: ‘social contagion theory’ to amplify a campaign by normalising a behaviour and turning it into a movement;120,136 ‘prime theory’ (plans, responses, impulses/inhibitory forces, motives and evaluations) to alter people’s desires to succeed in changing maintaining patterns of behaviour through increasing motivational inputs;120,136,152,153 and ‘theory of planned behaviour’ to alter behaviour through influencing people’s intentions to perform such behaviours. 139,140 One further study mentioned using theoretical ideas rather than identifying a specific grand theory, by drawing on ideas from social marketing and behaviour change, but in this study it was unclear how these ideas were used. 138 Across the studies, there was no mention of using other theoretical frameworks or logic models to inform their research questions or to identify the outcomes relating to their research.
In terms of how theory was used in the basis of the programme design, in the study by Brown et al. ,120 social contagion theory was used to piggyback onto an annual ‘no smoking day’ that aimed to help smokers stop by providing a nationally supportive environment and drawing attention to available treatments; they also developed a national cessation campaign (Stoptober) to generate a burst of activity around key time points when quit rates had reduced. In a later study, Brown et al. 120 used ‘prime theory’ to refine film content on the basis of focus group testing with a diverse group of smokers. 136 Using ‘theory of planned behaviour’ to alter behaviour through influencing people’s intentions, Eves et al. 139 tested the success of two different messages in encouraging more physical activity in members of the public.
Mass media channels used and interactivity: findings from the review of UK primary studies
Table 17 summarises the different mass media channels examined in the review of UK primary studies.
| Media channels used and media channel interactivity | Number of UK primary studies |
|---|---|
| Number of UK studies that compared effectiveness of different media channels within the same study | 1: Jawad (2015)143 |
| Number of studies with no focus on media channels and interactivity | 24 |
As can be seen, only one of the studies compared different media channels within the same study. 143 This was a tobacco control social media campaign that aimed to raise awareness about the health risks of waterpipe tobacco smoking. The number of Facebook (Facebook, Inc., Menlo Park, CA, USA; www.facebook.com) subscribers, Twitter (Twitter, Inc., San Francisco, CA, USA; www.twitter.com) followers and YouTube (YouTube, LLC, San Bruno, CA, USA; www.youtube.com) views all increased over time (measures taken at 3, 6 and 9 months). In a descriptive comparison of interactions with the social media channels, the authors concluded that Twitter provided the most organisation-based contact (e.g. 8% of tweets were retweeted, and nearly two-thirds were on health effects of waterpipe tobacco and other Twitter users interacted with @shishaware 70 times), whereas Facebook was the most interactive channel (e.g. 69% of status updates had more than one ‘like’, 23% had more than one comment from users). The YouTube channel had also been ‘favourited’, had ‘likes’ and ‘dislikes’ and had a rate of 112.2 comments per 10,000 views.
The remainder of the UK primary studies reported the channel(s) used in the campaigns, but did not provide evidence comparing or commenting on the effectiveness of different channels.
Intervention duration and intensity/exposure: findings from the review of UK primary studies
Table 18 summarises the number of UK primary studies that examined intervention duration or intensity/exposure.
| Mass media campaign intervention duration and intensity/exposure | Number of UK primary studies |
|---|---|
| Number of studies that compared effects of level of intervention duration or intensity/exposure on smoking outcomes. Exposure data used the standard advertising industry measures of a campaign’s reach (gross rating points) and its reach and frequency (television ratings) | 6: Langley (2012),144 Richardson (2014),152 Richardson (2014),153 Sims (2014),155 Lewis (2015)148 and Sims (2016)154 |
| Number of studies that compared effects of level of intensity/exposure, alongside message types/content, on stair use for increasing physical activity | 3: Eves (2012),140 Lewis (2011)145 and Lewis (2012)147 |
| Number of studies that compared effects of sexual health campaign. Exposure calculated by comparing three levels of campaign recall and recognition | 1: Flowers (2013)141 |
| Number of studies that compared effects of level of intervention duration to improve diets | 1: Capacci (2011)137 |
| Number of studies with no focus on intervention duration or intensity/exposure | 14 |
Eleven of the 25 recent UK primary studies commented on or examined the relationship between mass media intervention duration or intensity/exposure and effectiveness.
A series of six related statistical studies evaluated televised tobacco control campaigns broadcast in England (2002–10) by examining existing data sources and indicators of smoking behaviour against detailed population-level campaign exposure data. 144,148,152–155 Exposure data used the standard advertising industry measures of a campaign’s reach [gross ratings points (GRPs)] and its reach and frequency [television ratings (TVRs)]. The standard advertising industry measures of GRPs are equivalent to the summed ratings of individual advertisements across multiple campaigns, giving a per capita measure of advertising exposure. TVRs are defined as the percentage of a particular audience that has seen a commercial break.
An analysis using 4 years of longitudinal panel data from the International Tobacco Control UK Survey found that increased exposure (as measured by GRPs) was associated with higher recall at 6 months, although participants were recalling any advertising or information that talked about the dangers of smoking or encouraged quitting on television – not specifically tobacco control campaigns. 153 The effect was significant only for recent exposure (OR 1.51, 95% CI 1.14 to 2.01); exposure in the 4–6 months before the survey had no impact on recall.
An analysis of monthly Opinions and Lifestyle Survey data found a small association between increased exposure (by 400 GRPs) to television adverts, equivalent to all adults in the population seeing four tobacco control television adverts per month, and a 3% lower odds of smoking (OR 0.97, 95% CI 0.95 to 0.999; p = 0.044) a couple of months later, and a 1.80% (95% CI 0.47 to 3.11; p < 0.01) decline in average daily cigarette consumption 1 month later. 155 Further analyses of exposure by emotive characteristics of the messages in the advertisements are reported in Intervention content: findings from the UK primary studies. 154
In an analysis of time series data of quitline calls and NRT over-the-counter sales and prescribing data against exposure to anti-tobacco mass media advertising and smoking cessation medication advertising,144 there was some evidence that effects on those information- and treatment-seeking behaviours tended to peak in periods of greater campaign exposure (TVRs were higher in January and were highest in January 2005 and 2010). This suggests that exposure is associated with effectiveness. More specifically, a 1% increase in tobacco control TVRs led to a 0.129% increase in quitline calls in the same month (or a 0.085% increase in the seasonally adjusted model, p = 0.007). For NRT, in most years there was a clear peak in prescribing in the first 3 months of the year and a much smaller peak in October and in January to March each year there were generally peaks in over-the-counter NRT sales. A 1% increase in pharmaceutical company TVRs led to a 0.05% increase in sales in the same month; however, this finding was not statistically significant in the adjusted model. A further study evaluated the impact of different types of message in national campaigns on calls to the English NHS Stop Smoking telephone helpline. 152 Exposure to all types of campaign (as measured by GRPs) was associated with increased calls to the helpline (see Intervention content: findings from the UK primary studies for findings for message types).
Looking at the impact of the campaign on smoke-free homes, Lewis et al. 148 found that level of exposure to all tobacco control campaigns (measured by GRPs) was not associated with increased likelihood that a home would be smoke-free, but level of exposure to second-hand smoking campaigns was associated with an increased likelihood that a home would be smoke-free, with increased exposure being associated with increased odds (by 7% for each additional 100 GRPs) at a 1-month lag after the campaigns (OR 1.07, 95% CI 1.01 to 1.13; p = 0.033). There was no significant association during the same month of the campaign (OR 0.99, 95% CI 0.93 to 1.05; p = 0.740) or 2 months after (OR 0.98, 95% CI 0.92 to 1.04; p = 0.490), suggesting that the impact of the second-hand smoking campaign did not happen immediately and that it also fades quickly.
A series of naturalistic studies evaluating local point-of-choice prompts in public places (e.g. multistorey workplaces and railway stations) to encourage stair use for increasing physical activity varied the numbers of posters and signage shown throughout the experimental period. 140,145,147 This variation in intensity of exposure was tested alongside variations in message types, and the findings are reported in Intervention content: findings from the UK primary studies.
One study evaluated a regional 10-month sexual health poster, leaflet and online campaign (2009–10) in the west of Scotland aimed at men who have sex with men. 141 Survey results were analysed by the extent of respondents’ exposure to the campaign (their recall and recognition of the campaign). At the end of the campaign, greater exposure was associated with positive changes for some but not all outcomes. For example, those with no exposure were significantly less likely to report always using appropriate lubricant than those with low exposure (adjusted OR 0.42, 95% CI 0.23 to 0.77; p = 0.005); however, those with high exposure to the campaign did not differ significantly from those with low exposure.
Finally, one study evaluating a 2003–6 national mass media campaign to improve diets reported behavioural outcomes annually throughout the radio, television and online campaign. 137 The campaign to encourage consumption of five portions of fruit and vegetables per day used ‘mini campaign relaunches’ every 6 months; although the overall aim was the same, each relaunch targeted a different subpopulation (by income, age or sex) and used slightly different methods and channels. Significant campaign effects for increased fruit and vegetable intake did not happen until the third year of the campaign and the effect was stronger for those in lower income groups. The fact that significant impacts did not emerge until the third year of the campaign may suggest that campaigns need to last a certain length of time before effects are felt, although the authors suggest that the delay in impact may have been partly attributable to the nature of the activities in different phases of the campaign, with earlier phases involving a lower investment in targeted advertising.
Intervention content: findings from the UK primary studies
Table 19 summarises the UK primary studies that assess the impact of message content.
| Mass media campaign message type, content, targeting and source | Number of UK primary studies |
|---|---|
| Number of studies that compare effects of different types of message or campaign content | 9: Eves (2012),140 Langley (2012),144 Lewis (2011),145 Lewis (2012),147 Lewis (2012),146 Lewis (2015),148 Richardson (2014),152 Richardson (2014)153 and Sims (2016)154 |
| Number of studies that compare effects of different types of message or campaign content on physical activity | 4: Eves (2012),140 Lewis (2011),145 Lewis (2012)147 and Lewis (2012)146 |
| Number of studies that compare effects of different types of message or campaign content on smoking | 5: Langley (2012),144 Lewis (2015),148 Richardson (2014),152 Richardson (2014)153 and Sims (2016)154 |
| Number of studies that compare effects of different types of message or campaign content on other behaviours | 0 |
| Number of studies that compare effects of targeting specific groups | 0 |
| Number of studies that compare effects of the ‘source’ of the message | 1: Langley (2012)144 |
| Type of message/content | Positive vs. negative messages, simple vs. complex, motivational vs. volitional, point of choice, multicomponent, government/charity-funded and second-hand smoke exposure |
The UK evidence on different types of message and campaign content is based on nine studies on two types of behaviour: physical activity (four studies) and smoking (five studies).
The UK has been exposed to very diverse tobacco control campaigns and is therefore a good setting in which to investigate the effect of different types of messages. Several studies on tobacco campaigns investigate the differential impact of ‘positive’ (eliciting happiness, satisfaction or hope) and ‘negative’ (eliciting fear, sadness, guilt, anger or disgust) messages152–154 and find that both are effective. Unlike negative messages, positive messages have not been found to have an effect on recall,153 but both positive and negative messages have been shown to influence information-seeking152 and smoking behaviour,154 with positive campaigns having a bigger effect. This indicates that recall does not necessarily translate into changes in behaviour, which should be taken into account in studies assessing the ‘effectiveness’ of campaigns by measuring recall.
There is evidence from one study that the source of the campaign is important,144 with government- and charity-funded campaigns being more effective at triggering quitting behaviour than pharmaceutical company-funded campaigns. None of the primary studies compared the effects of targeting on specific groups; however, one primary study reports that targeted campaigns about the risks of second-hand smoke exposure increased the odds of a home being smoke-free more than tobacco control campaigns overall. 148
The physical activity studies are based on poster campaigns to increase stair use. They suggest that multicomponent messages (e.g. providing information on calories burned as well as posters directing people to the stairs) delivered at the point of choice (or ‘volitional’ messages) are more effective than those that have a single component and/or are ‘motivational’. 140,145,146 One of the physical activity studies suggests that simple messaging may be more effective in busy settings. 147
Intervention scale: findings from the review of UK primary studies
None of the UK primary studies examined whether or not scale (i.e. whether a campaign was implemented at a local, regional or national level) was a potential mediator of effectiveness.
Summary
We reviewed evidence regarding characteristics of mass media campaigns that may be associated with effectiveness. Evidence was drawn from the review of reviews (reported in the previous sections and see Chapter 2) and from an additional review of recent UK primary studies (published between 2011 and 2016).
Overall, there was limited evidence from the reviews on the contribution of media campaign characteristics to effectiveness, with only a small number of reviews containing statistical analyses to assess the impact of different characteristics. There was little evidence regarding the role that theory may play in campaign effectiveness, with most reviews simply listing which theories, if any, had been referred to in intervention studies. There was limited evidence regarding media channel as a potential moderator of effectiveness in three reviews, with findings varying depending on the types and topics of campaigns, and mostly having limited relevance to the contemporary UK context. Longer intervention duration or greater intensity/exposure were found to be related to effectiveness in several reviews, with most of the evidence relating to tobacco and to a lesser extent to sexual health campaigns; however, there was little clear guidance or consensus on how long or intense campaigns should be to produce effects. Lack of formal statistical analysis in the reviews meant that clear conclusions about the type of messaging content that is most effective could not be drawn. There was evidence from the reviews that social norms campaigns and negative messaging (i.e. hard-hitting messages on health consequences) could change behaviour but little evidence regarding whether or not these were more effective than other approaches. The reviews indicated that targeting can be effective, suggesting that messages need to be appropriate to the target audience taking into account a range of characteristics including age, sex, culture and level of engagement in the activity. There was evidence to suggest that targeting specific subgroups such as the young could be effective, but with caution to avoid patronising or stereotyping. There was no evidence from the reviews on the scale of campaign (i.e. whether it was implemented at a national, regional or local level) acting as a moderator of effectiveness. Regarding source, there was evidence that tobacco industry-sponsored campaigns were not effective.
There was limited evidence from the review of UK primary studies (which were mostly concerned with tobacco, plus a small number of physical activity interventions) regarding the use of theory as a potential moderator of campaign effectiveness. Only one study compared different media channels within the same study (a comparison of audience engagement through different social media channels). Evidence from the primary studies regarding intervention duration or intensity/exposure as moderators of effectiveness was consistent with that from the reviews, generally finding that more sustained and greater intensity campaigns were more effective. A benefit of reviewing the UK primary studies’ evidence was that a greater mix of message types have been evaluated, and this evidence suggests that positive messages may also be important, with both positive and negative messages affecting smoking behaviour. Regarding messages for physical activity, there was mixed evidence regarding effective messages for poster campaigns promoting stair use. There was limited evidence that government and charity campaigns may be more effective than those from pharmaceutical companies. As with the reviews, there was no evidence regarding scale as a moderator of effectiveness.
Chapter 6 Stakeholder engagement
Stakeholders have been engaged throughout the study but particularly in the development and initiation of the research and the interpretation of findings. This includes public engagement. In this chapter, we describe stakeholder and public engagement in:
-
developing the study
-
refining research plans
-
interpreting findings.
Development of the study
The research questions for the study were shaped by the commissioning brief from NIHR, but we involved stakeholders and particularly the public in preparing the application. The principal investigator (PI) of the study is the public engagement lead for the UK Centre for Tobacco and Alcohol Studies (UKCTAS). UKCTAS convenes public engagement groups on smoking and alcohol use: two of the main public health issues covered by our research. The PI set up a smokers’ panel (of smokers and recent ex-smokers) in Bath, when she was based at the University of Bath prior to this study, and the panel started meeting in 2008. The panel was reconstituted at the University of Nottingham, another UKCTAS university also involved in this study, from 2011, when the PI moved to Stirling. The Nottingham panel helped shape the study scope, particularly commenting on key aspects of the proposal including the plain English summary. After the study was initially considered for funding by NIHR, the PI had established an alcohol public engagement panel at the University of Stirling and the research proposal was discussed with the university at the time when the proposal was resubmitted before funding was secured.
Two initial lay members for the study were identified from the smokers’ panel when it was held in Bath and another previous study from the team on smoking in pregnancy. However, 2 years passed between the initial development of the outline for the study and funding being secured and contact was lost with the Bath-based panel member while the smoking in pregnancy lay adviser moved on to support another study conducted by the PI’s research team. When the study began, we were pleased to secure the involvement of Mr George Vekic, who served as public and patient involvement (PPI) representative on the study advisory group. Mr Vekic is a member of the UKCTAS alcohol discussion group and also works as a digital media officer, so had an interest in the study topic.
Stakeholders from a range of organisations were also involved in developing the study. The research team consulted colleagues at Health Scotland, the Scottish Government and the Department of Health and Social Care while developing the study proposal. We also engaged academic and practice colleagues who subsequently agreed to join our advisory group. This included representatives from two Collaborations for Leadership in Applied Health Research and Care (CLAHRCs): one in north London (links facilitated by research team members at University College London) and the other in the East Midlands (links facilitated by research team members at the University of Nottingham).
Refining research plans
As the study developed, we continued to engage with professionals and the public. In particular, we sought input on the development of the logic model for the study. The initial model was discussed with the project advisory group, the UKCTAS smokers’ panel, the UKCTAS alcohol public engagement group (including our PPI representative Mr Vekic) and representatives of two CLAHRCs: East Midlands and North Thames. Their response to the model helped refine its content and make more explicit the assumptions underpinning the relationship between the resources and activities in the model and the range of possible outcomes that we expected might arise from public health mass media campaigns.
Initial findings from the review of reviews element of the study were circulated to members of both the UKCTAS public engagement panels and members reflected on their own experiences of viewing public health mass media campaigns. Panel members were not convinced that campaigns alone can change health behaviours but did agree that memorable campaigns help build knowledge and awareness around the benefits of taking up health behaviours (i.e. physical exercise) or modifying harmful behaviours (i.e. smoking cessation). They also agreed that campaigns, if well resourced, designed and sustained, can help change social norms around some behaviours (such as condom use to promote sexual health or promote compliance with smoke-free legislation).
One challenge we encountered was in discussing emerging findings with groups other than our public engagement panels. The research team were focused on trying to complete the literature reviews in the face of a large volume of material and had limited time to prepare interim finding briefs, particularly when it became clear how complex the findings of the literature were and that clear directions of effect or impact on key outcomes were difficult to distil into simple summaries. We did approach both CLAHRCs to see if we could discuss review progress at CLAHRC public engagement or planning meetings but we were not able to secure appropriate slots at these meetings and CLAHRC colleagues felt that final outputs from the study might be more appropriate for dissemination. In addition, owing to limited research team time we were not able to engage one youth organisation, Young Scot, in discussing interim findings and as a result of this public engagement activity not taking place we had an underspend (now returned to NIHR) in our public engagement budget. Instead, we were able to involve young people in discussing findings from our final report through a separate organisation (City of Edinburgh Council), as set out in the following section, and this proved very valuable.
Therefore, a primary focus for our stakeholder engagement was end-of-study dissemination and discussion and this is described in the following sections.
Interpreting findings
Once findings from the study were available, the research team invested considerable time and effort in organising a national event to discuss and help interpret results as well as a youth engagement meeting. Each of these events is described here.
End-of-study event
On 28 September 2017, an end-of-study event was hosted in the conference centre at the Iris Murdoch Building, University of Stirling. A series of presentations on the project’s background, methodology and results was given by the research team, which represented all the academic teams involved (University College London and the Universities of Nottingham, Glasgow and Stirling). In addition to sharing the findings of the review, the purpose of the event was to discuss the findings with interested stakeholders and experts to identify strengths and limitations of the evidence, to identify implications for commissioning/using mass media campaigns and to identify recommendations for future research. The event was also intended to inform the final report for the study.
An open invitation (see flyer in Appendix 9) was issued to relevant policy and practice networks in the UK. Personal invitations were also sent to the study advisory group and key organisations that design and deliver mass media campaigns for public health, such as Public Health England and the Scottish Government. Forty-nine delegates attended the event. These included representatives from local and national charities and advertising agencies, NHS staff, civil servants, clinical academics, public health and marketing researchers, research students and the PPI representative for the study. Delegates had a range of experience, from a deputy director of a Scottish Government department to master’s students. There was also representation from across the UK: attendees had travelled from Northern Ireland, Orkney, Shetland, the north-east and north-west of England and London, in addition to those from other UK regions.
The event included a series of presentations from the research team on all the elements of the study. The PI opened the day and began by showing a series of videos of past mass media public health campaigns (Box 4). Presentations of study findings were then followed by question-and-answer sessions and small-group discussions with feedback to the room (see the event agenda in Appendix 10). Both the event’s presenters and attendees were encouraged to share slides and views via social media.
-
HEBS (1995): Gavin Hastings ‘Did you know that walking a mile . . .’.
-
HEBS (1997): The Lifesaver ‘You can save a life. Your own’.
-
Central Office of Information and the Department of Transport (1996): Christmas anti drink-drive: accident-scarred woman at mirror.
-
HEBS (c. 1998): ‘Night out’, Think About It ‘You spend ages thinking about what you put on your body, how long do you spend thinking about what you put in it?’.
-
NHS Smokefree (2007): Hooked (fish-hook).
-
NHS (2005): Family and friends watching TV ‘Secondhand smoke is a killer’.
-
This Girl Can and the National Lottery (2017): ‘Phenomenal Woman’.
HEBS, Health Education Board for Scotland (now NHS Health Scotland).
Key points raised among those attending related to a range of themes. Some of these focused on the limitations of the evidence our study identified. Overall, delegates had expected the evidence on the effectiveness of mass media campaigns to be more conclusive. There was a general perception, particularly among those involved in planning or delivering services or promoting public health interventions, that tobacco control mass media in general was highly effective and cost-effective and that this might be the case for mass media on other public health topics. Our review did find that tobacco control campaigns can be effective but this varied based on the type, duration and content of the campaign. Evidence for campaigns on other behaviours was also mixed and in some cases very limited. This challenged the views of some delegates and meant that some of the questions and discussion at the event were not straightforward.
Delegates had a range of questions and useful feedback on the limitations of our reviews and the evidence in general; for example, they discussed the parameters of our review of systematic reviews, the changing media landscape and how this might affect the available evidence, the time lag between campaigns and evaluations being published and the fact that the results of many campaigns, particularly at a regional level, are not captured in the peer-reviewed literature. Attendees also reflected on their own experience (in both research and practice) compared with the review evidence. This included issues to do with fitting mass media campaigns into wider political messages, the fact that diet and nutrition campaigns can come from commercial or industry sources (in contrast to the tobacco industry, which is not permitted to conduct marketing in the UK) and also that commercial advertising involves large budgets, which it is difficult for public health campaigns to counteract (alcohol advertising was highlighted as a particular example). There are also limited available resources for public health campaign evaluations and, when decisions have to be made, resources will focus on designing and delivering the campaign rather than research around it. Limited resources also result in difficult choices being made around the medium of communication, with a more recent focus just on social marketing or online campaigns. The literature identified by the study had limited evidence on campaigns run via digital media only, and evaluating these should be a priority for the future.
Discussions also focused on why the evidence differs between health topics; for example, for some health behaviours, it can be more difficult to define what the ‘message’ should be. Those planning campaigns may favour positive rather than fear-based messaging, but questions remain about which is more effective. With limited budgets, how should campaigns be targeted? The evidence is unclear for campaigns aiming to reach particular population groups. Some of the evidence in our review suggests that a whole-population approach may be desirable, but again this has cost implications. Finally, delegates discussed how indicative evidence identified in our reviews suggests that campaigns focused on increasing healthy behaviours may be more appealing or effective than those focused on reducing unhealthy behaviours. This may be influenced by some of the unhealthy behaviours involving dependence-forming products including tobacco, alcohol and illegal drugs and using mass media to change behaviour around these may be particularly challenging. The insights and suggestions raised by delegates have helped inform how we have approached key sections of this final report and have directly informed how we describe the context and implications of our findings.
Engagement with young people
Two members of the research team (Professor Linda Bauld and Dr Srinivasa Vittal Katikireddi) met with 15 young people on 29 September 2017 to discuss the findings of the study and the logic model that had been developed to inform the research. The meeting took place in a City of Edinburgh Council leisure facility: the Royal Commonwealth Pool, Edinburgh. The young people were attending a youth club that provides access to gym and pool facilities at the venue along with snacks, board games and art materials; it is held every Friday evening during term. The club is known as ‘Open All Hours’ and is funded by City of Edinburgh Council in partnership with Edinburgh Leisure. Research team attendance at the club was made possible by Laurene Edgar, a youth work organiser, whom Dr Katikireddi contacted after obtaining her contact details from a member of the study advisory group.
The researchers met with two separate groups of young people between the ages of 11 and 15 years. In the first group there were six boys and two girls, and in the second group there were seven girls. The researchers showed some examples of public health mass media campaigns on a television screen connected to a laptop. These ranged from television campaigns on physical activity, alcohol and chronic disease prevention from the early 1990s to slightly more recent NHS campaigns on smoking cessation and second-hand smoke from around 2005–7 and concluded with a current online video of the ‘This Girl Can’ physical activity campaign funded by the National Lottery. Young people had mixed views about the advertisements, perhaps preferring more contemporary examples, and just one or two of them recognised the ‘This Girl Can’ film.
The researchers then asked the young people to note down on paper what they thought constituted a ‘good’ or ‘appealing’ advertisement. Some of the main suggestions are included in Box 5.
-
Music.
-
Strong colours.
-
Something unusual or strange that makes you notice.
-
Cartoons.
-
Featuring normal/real people.
-
Outdoor/green areas.
-
Before-and-after images of the same person.
-
Attractive people.
-
People doing silly things.
-
Showing what needs to be changed (i.e. smoking, drinking).
-
Logos that people recognise.
-
Bright, positive images.
-
Featuring a celebrity.
-
Humour.
-
Making scientific information simple.
-
Not too long – a short advertisement.
-
Words on the screen as well as spoken.
With the first group (which spent slightly longer discussing the campaigns than did the second group) the researchers also distributed copies of the study logic model with the details of the model removed and just the headings showing. The researchers explained the purpose of the model and the young people then wrote down some of the elements they thought might connect a public health advertisement with short-term, medium-term and longer term outcomes.
They were able to describe in some detail the key ‘inputs’ needed for a mass media campaign, including funding, staffing, equipment, ideas and production. They were also adept at identifying key activities after inputs were secured, including where advertisements or other forms of marketing should be placed (television, social media, YouTube, etc.) and how the public and others should be informed about the release of a campaign. They were less sure about the pathway after that between people viewing an advertisement or other campaign output and longer term outcomes. They articulated very clearly what the ideal behavioural outcomes would be in terms of reducing harmful behaviours (stopping smoking and being less sedentary) or increasing healthy behaviours (eating a more balanced diet and being more physically active). They also understood that these behavioural outcomes would be linked to longer life or reducing the risk of chronic diseases such as cancer. However, unsurprisingly, the mechanisms for change between viewing a mass media campaign and possible behaviour change were much more difficult for them to describe.
Despite this, the concept of the logic model and how inputs and activities could be linked to longer term outcomes was something that appeared to resonate with them and supports the concept of the logic model approach. Their notes also illustrate how an unappealing or perhaps not well-sustained campaign could be ignored and might make little difference. They also talked about how young people could view a campaign (e.g. on second-hand smoke) and discuss behaviour change with parents or carers. One girl in the second group gave examples of a friend who had seen campaigns about the harms of second-hand smoke exposure and talked to both her parents about their smoking and smoking cessation.
The discussions with these young people were informative at the stage when the team was drafting the final report for the study and their views have been useful in assisting us to write the discussion section of the report, the further description of the logic model and our summary of findings.
Chapter 7 Discussion and conclusions
The aim of this study was to provide the NHS, local authorities, government and other organisations with evidence on the effective use of mass media to communicate public health messages. We conducted four reviews underpinned by a logic model of how mass media campaigns influence behaviour. These were:
-
A review of existing systematic reviews (review A). This comprised a review of 36 English-language systematic reviews published between January 2000 and January 2016 on the effectiveness of mass media campaigns across six health topics. We identified 12 reviews of mass media addressing tobacco use, nine addressing sexual health, seven addressing physical activity and three addressing illicit drug use, with five reviews addressing ‘mixed topics’ (i.e. more than one of our six health topics). Despite none of the reviews meeting our inclusion criteria for alcohol use or diet mass media interventions, studies evaluating campaigns targeting alcohol or diet were included in four mixed-heath-topic reviews. Findings from this review are presented in Chapters 2 and 5.
-
A review of primary studies examining alcohol mass media campaigns (review B). This was conducted because review A found no reviews specifically addressing alcohol and limited evidence relating to alcohol in the reviews covering mixed topics. The parameters for the review were English-language primary studies (published up to July 2016) that assessed the effectiveness of mass media public health campaigns to reduce alcohol consumption and related harms. Studies examining drink driving mass media interventions and college campus campaigns were excluded. Findings from this review, which included 24 studies, are presented in Chapter 3.
-
A rapid review of cost-effectiveness evidence (review C). This involved a rapid review of 13 systematic and seven non-systematic reviews, published between January 2000 and January 2017, which assessed economic studies that evaluated both the costs and benefits of mass media campaigns for any of our six health topics. Findings from this review are presented in Chapter 4.
-
A review of primary studies of mass media campaigns conducted in the UK and published between January 2011 and September 2016 (review D). The main aim of this review was to provide additional, UK-relevant evidence and evidence on new media to complement evidence from review A regarding campaign characteristics that might be associated with effectiveness. Studies were eligible for inclusion in this review if the paper was published in or after 2011 and the study was conducted in the UK; multicountry studies were eligible if findings for the UK were reported separately. The campaigns had to address one of our six health topics. Findings from this review, which included 25 studies, are presented in Chapter 5.
In addition, we conducted stakeholder engagement work, which is described in Chapter 6.
In the remainder of this chapter, we aim to synthesise our findings across the different chapters, to reflect on implications for our logic model and gaps in the evidence and to identify pointers for future research.
How effective are mass media campaigns?
We addressed this question with three reviews: a review of 36 systematic reviews (review A), a review of 24 primary studies on alcohol mass media campaigns (review B) and a cost-effectiveness review of 20 reviews and systematic reviews (review C).
Review A, which included 36 systematic reviews, brought together evidence on the impact of mass media campaigns on health behaviours (including alcohol use, illicit substance use, diet, physical activity, sexual and reproductive health and smoking cessation and prevention) for the first time. Overall, the evidence base for the effectiveness of mass media for behaviour change is mixed. First, the amount of evidence varies across health topics, with most evidence relating to campaigns addressing tobacco use, followed by sexual health and physical activity. The strength of evidence from reviews also varies. Using a modified GRADE approach,33,34 we found moderate evidence for the positive effects of mass media campaigns on reducing sedentary behaviour and sexual health-related behaviours such as condom use. Low-certainty evidence for positive impacts on diet was found, although the overall volume of evidence on diet was very limited. The impact of the mass media on tobacco use and physical activity, such as stair use and brisk walking, was mixed, but with low-certainty evidence in both cases. In contrast, the available and again low-certainty evidence on illicit drugs suggests no impact of mass media. All reviews found considerable variation between individual studies as described in a meta-analysis or narrative synthesis, suggesting that variations in implementation of the campaign and evaluation methods may be important.
For treatment-seeking behaviours, there was low-certainty evidence that mass media campaigns can help increase the use of sexual health clinics or services. Whether or not media campaigns can prompt calls to telephone quitlines for smoking cessation has been fairly extensively studied in five reviews. Overall, the direction of effect looks positive, with campaigns serving to prompt calls to quitlines, but variation in results and the quality of studies was identified – therefore, there is only moderate certainty in the strength of this finding. A recent study examining the impact of Scottish tobacco control mass media campaigns (2003–12) found a cumulative increase in calls to a quitline, sustained for 6 months. 161 This is further evidence of a positive direction of effect; however, the study found no impact on NRT prescription volumes.
Evidence on distal outcomes (reduction in illnesses, improved population health, reduced health service usage, societal change, policy change and impact on inequalities) was also examined, and little evidence was found. However, distal outcomes can be defined in different ways to those adopted in our logic model, and can, for example, include denormalisation and longer term shifts in public attitudes regarding the acceptability of a behaviour. One systematic review noted that:
There is evidence of good quality (1&2+, C), which shows an effect of mass media interventions on attitudes towards smoking and intentions to smoke among young people under 25 years.
This suggests that mass media programmes may have contributed to the denormalisation of smoking among young people.
Changes in health behaviour are the ideal outcome of mass media health campaigns. However, theories of health behaviour change are generally based on an assumption that behaviour change happens incrementally or via changes in mediating variables such as changes in knowledge, attitudes, self-efficacy and intentions. 7,162,163 A more realistic assessment of the value and effectiveness of mass media campaigns takes into account the impact of such campaigns not only on behaviour but also on these mediating variables. Our review of reviews examined evidence regarding indirect behavioural outcomes (intentions to engage in, reduce or desist from unhealthy behaviours or to engage in healthy behaviours) and social cognitive outcomes (awareness, knowledge, attitudes, beliefs, norms and self-efficacy).
In the 15 reviews examining the impact of mass media campaigns on knowledge and awareness, there was evidence of positive impacts on increased knowledge and awareness in relation to sexual health, such as knowledge of HIV prevention, contraception and sexual health services. Positive results were also reported for increased knowledge and awareness of tobacco risks and services to help quit, increased knowledge and awareness for diet and for physical activity. There was mixed evidence regarding the impact on knowledge and awareness of illicit drug use. In the seven reviews examining the impact of mass media campaigns on intentions, there was generally positive evidence of impacts on intention to increase physical activity (although from a review with a high risk of bias), and there was some evidence of positive impacts on intention to quit smoking. There was mixed evidence regarding intention to stop the use of illicit drugs and to use contraception. In 10 reviews reporting on attitudes, beliefs and self-efficacy, there was evidence of positive impacts on beliefs about risk of pregnancy and the use of condoms, from reviews of studies in low-income countries. There was mixed evidence of the impact on attitudes towards illicit drug use and tobacco. A mixed-topic review that included studies from the UK reported positive results on attitudes towards reducing tobacco use and increasing physical activity.
Some previous reviews and meta-analyses have reported stronger evidence that media health campaigns can produce positive effects on behaviour change, but have also suggested that this differs with the type of behaviour. Anker et al. ,164 in a meta-analysis, found a significant effect for the use of mass mediated health campaigns on behaviour across 51 primary studies, but the size and significance of campaign effects varied across target behaviours, with campaigns working best for increased transport safety and also better than controls for cardiovascular disease, physical activity and nutrition. Wakefield et al. 6 reviewed the outcomes of mass media campaigns in the context of a wide range of health-risk behaviours (e.g. use of tobacco, alcohol, other drugs, heart disease risk factors, sex-related behaviours, road safety, cancer screening and prevention, child survival and organ or blood donation), and concluded that mass media campaigns can produce positive changes or prevent negative changes in health-related behaviours. They concluded that the success of mass media campaigns was greater when the target behaviour was one-off or episodic (e.g. screening, vaccination and children’s aspirin use) rather than habitual or ongoing (e.g. food choices, sun exposure and physical activity). Many of these one-off behaviours were not included in our review, and our focus on lifestyle behaviours may have contributed to the overall weaker evidence of success in actual behaviour change as opposed to its mediating factors. Of the behaviours that were included in our review, the strongest evidence of success in behaviour change was seen for reducing sedentary behaviour and improving sexual health behaviour (e.g. wearing a condom). The Anker et al. 164 meta-analysis identified a weighted mean effect size of 0.05 for effects of campaigns on behaviour change, and proposed that this 5% benchmark could provide a standard against which future media intervention studies could assess success. In the reviews that we identified, when there were sizes of effect for campaigns to reduce sedentary behaviour or increase physical activity, these generally met or exceeded this benchmark for success, and those for condom use tended to produce somewhat greater effects. One interpretation of these findings is that media campaigns are most successful when the behavioural goal is simple, a conclusion also drawn in an NHS Health Development Agency report from 2004. 165 It might be anticipated that the more complex the behaviour change (e.g. if it involves a component of addiction as with tobacco or illicit drugs), the more back-up is required to supplement the mass media campaign. Although our review was limited in its evaluation of contextual moderators, some of the included reviews (e.g. the Cochrane Database Systematic Review of tobacco control campaigns27) conclude that these can be important in the context of wider or multiple interventions, such as a comprehensive tobacco control programme. This should include the appropriate support services. Looking across health behaviours, Wakefield et al. 6 highlight that concurrent availability of and access to key services and products are crucial to persuade individuals motivated by media messages to act on them.
A further aspect of context is the prevalence of the behaviour in the population. Naugle and Hornik,166 in reviewing the literature on child survival in low- and middle-income countries, highlight that, for mass media campaign effects to be detected, there ‘must be room to move the population on the target behaviour’. It is possible that this contributes to the positive outcomes of some mass media sexual health campaigns in non-OECD countries where baseline rates of condom use were low.
We found additional evidence regarding the effectiveness of mass media campaigns in review B. Our systematic review of primary studies of mass media campaigns targeting alcohol was the first comprehensive synthesis of evidence from such campaigns. The overall quality of the evidence base was low, predominantly owing to the use of weak study designs, risk of participant selection bias and self-reported outcome data.
Overall, we found very limited evidence that campaigns were associated with reductions in alcohol consumption, although the majority of reports did not state that reducing consumption had been an aim of the campaign. Most campaigns had aims such as improving knowledge of, awareness of and communication about alcohol. Despite this, it is likely that reducing consumption was an implicit long-term aim of all campaigns, as they all targeted outcomes that can be considered precursors to consumption within our logic model. Longer term evaluations following repeated exposure to campaign messages may be needed to detect changes in consumption, of which we found few. There are important social, cultural and environmental barriers to alcohol behaviour change, such as widespread alcohol advertising and pro-alcohol cultural norms. This provides a challenging context that contrasts with tobacco, for example, for which advertising is highly restricted and norms are antismoking. Other reviews have concluded that social norms interventions were ineffective at reducing alcohol consumption by university and college students and that reductions in drink driving could not be attributed to mass media campaigns alone. 77,167 Our findings add to this evidence and are consistent with the conclusion of Snyder et al. 168 that mass media campaigns should have modest expectations of effect on health behaviour. Alcohol campaigns in particular face a number of competing forces that may limit their effectiveness at reducing consumption.
There was some evidence in review B, from mainly weak-quality studies, that alcohol mass media campaigns were associated with increases in information-seeking and treatment-seeking behaviour. There were mixed findings regarding other proximal outcomes, such as attitudes, beliefs, intention and self-efficacy. Mass media campaigns face a number of challenges in terms of these sorts of outcomes: they may be perceived to be aimed only at very heavy drinkers (meaning that many in the population disregard them as not relevant) and can lack a clear call to action, typically advising limiting units consumed rather than abstinence. There was mixed evidence of interaction with campaigns and discussion or onward transmission of campaign messages, from mostly weak-quality studies. More encouragingly, studies reported high levels of campaign recall, and evidence that campaigns were associated with increases in knowledge about alcohol, especially where it had initially been low. This is a key finding and perhaps indicates where mass media messages about alcohol are currently best targeted to achieve change. This is particularly important given that knowledge about alcohol unit consumption guidelines and the health risks associated with alcohol consumption is reported to be very low. 169
Our searches for published English-language evaluations with no time limit applied produced only 24 campaigns (in July 2016). In comparison, a content analysis study by Dunstone et al. 170 identified 72 English-language campaigns conducted between 2006 and 2014. This suggests that a large proportion of alcohol campaigns have not been evaluated and published. A greater investment in alcohol campaign evaluation is needed in order to better understand its effectiveness. We found only two reports of campaigns that used online or social media as a primary channel. 86,102 An important challenge for future research is therefore to evaluate the effectiveness of newer digital media channels to communicate alcohol health messages.
Regarding the cost-effectiveness of mass media campaigns, review C examined evidence from 20 systematic and non-systematic reviews (published between January 2000 and January 2017), reporting on 15 individual primary studies. Included reviews were required to assess economic studies that evaluated both costs and benefits of mass media campaigns (i.e. full economic evaluations, not just intervention costs or cost savings). Taken together, the reviews and the findings of the primary studies within the reviews provided moderate evidence that tobacco control mass media campaigns can be cost-effective. There was weak evidence in relation to diet campaigns (restricted to a campaign seeking to reduce salt intake) and physical activity, and no evidence in relation to the cost-effectiveness of sexual health campaigns, despite efforts to identify such evidence in systematic reviews.
Recent work by Marsh et al. 171 on how to prioritise investments in public health ranked 14 intervention types in order of cost-effectiveness (cost per quality-adjusted life-year gained). Increasing alcohol and tobacco tax by 5% topped the list, national mass media campaigns for smoking were third in the list and national mass media campaigns for obesity were fifth in the list. However, overall, evidence on the cost-effectiveness of mass media campaigns was extremely limited for all health behaviours except smoking. Regarding smoking, the studies in the included reviews generally found tobacco mass media campaigns to be cost-effective. However, the fact that only effective interventions tend to be taken forward to an economic evaluation, and hence the potential for bias in reviews on this topic, should be taken into account.
How effective are mass media campaigns with different target populations?
The majority of the 36 reviews included in review A provided evidence on whether the effects of mass media campaigns were similar or different across subpopulations. Our analysis of this evidence found that mass media campaigns may reach and affect groups in the population differently. Although age differences were not always measured, reviews of tobacco and illicit drug campaigns found that mass media appeared to be more effective for young people, and particularly for younger children rather than for older teenagers. There was modest evidence that mass media outcomes for tobacco, sexual health and physical activity do not differ by sex and no clear consistent evidence was found for ethnicity or socioeconomic status. Looking at baseline measures of health behaviours, physical activity campaigns may be more effective for less active or obese people than for others.
This paucity of good-quality evidence on the differential effects of campaigns on behaviour across different population groups is a concern. It has been suggested that health promotion interventions might increase rather than decrease inequalities, and particularly socioeconomic inequalities, in health, because messages and interventions may have a differential take-up and success across different social class groups. 37,40,43 The reviews included in review A, all based on tobacco control campaigns in contexts in which there are marked inequalities in smoking prevalence and morbidity, provide mixed evidence regarding whether or not effects on behavioural outcomes vary across socioeconomic groups. Nevertheless, the evidence is more consistent that interventions will be more effective if appropriately developed and targeted to reach the intended audience, and this will be important to ensure that campaigns work to reduce inequality. We are aware of an ongoing systematic review on targeted mass media interventions promoting healthy behaviours to reduce risk of NCDs in adults from ethnic minority groups. 172
Evidence for the greater effectiveness of campaigns among the young, mostly based on tobacco control campaigns, is consistent with much of the communications literature. Advertising is well known to work effectively in children and young people,173,174 and advertisers seek to use this to establish behaviour and brand preference at an early age. The evidence from this review suggests that anti-tobacco mass media messages can also be effective in the young, and that the impact may be greater on uptake of smoking than on cessation in adults, possibly because it is simpler to change behaviour before the onset of addiction.
What characteristics of mass media campaigns are associated with effectiveness?
We sought to identify characteristics of mass media campaigns that may be associated with effectiveness, drawing on evidence from the review of reviews (review A) and from the additional review of UK primary studies (review D). Overall, there was limited evidence on the contribution of media campaign characteristics to effectiveness, with only a small number of reviews and studies containing statistical analyses to assess the impact of different characteristics.
Across all the reviews included in review A, there was little evidence regarding the role that theory may play in campaign effectiveness, with most reviews simply listing which theories, if any, had been referred to in intervention studies. There was limited evidence regarding media channel as a potential moderator of effectiveness in three reviews, with findings varying depending on the types and topics of campaigns, and mostly having limited relevance to the contemporary UK context. Longer intervention duration or greater intensity/exposure were found to be related to effectiveness in several reviews, with most of the evidence relating to tobacco and to a lesser extent sexual health campaigns; however, there was little clear guidance or consensus on how long or intense campaigns should be to produce effects. One of the reviews noted a recommendation from the US Centers for Disease Control and Prevention that advertisements should be aired for a minimum of 6 months to affect awareness and up to 24 months to have an impact on behaviours, and should be aired as frequently as possible. 44
Lack of formal statistical analysis in the reviews included in review A meant that clear conclusions about the type of messaging content that is most effective could not be drawn. There was evidence from the reviews that social norms campaigns and negative (i.e. hard-hitting messages on health consequences) messaging could change behaviour, but little evidence regarding whether or not these were more effective than other approaches. The reviews included in review A indicated that targeting can be effective, suggesting that messages needed to be appropriate to the target audience, taking into account a range of characteristics including age, sex, culture and level of engagement in the activity. There was evidence to suggest that targeting specific subgroups such as the young could be effective, but with caution to avoid patronising or stereotyping. There was no evidence from the reviews on the scale of campaign (i.e. whether it was implemented at a national, regional or local level) acting as a moderator of effectiveness. Regarding source, there was evidence that tobacco industry-sponsored campaigns were not effective.
The UK primary studies that we examined in review D for evidence regarding campaign characteristics were mostly concerned with tobacco, plus a small number of physical activity interventions. This limited the value of the evidence for other health behaviour topics, but an advantage of examining this evidence was that all the studies were relevant to the UK context, and when examining the role of message the primary studies examined a wider range of message types than did the reviews. The evidence from the UK primary studies in review D suggested that positive messages may also be important, with both positive and negative messages affecting smoking behaviour. Regarding messages for physical activity, there was mixed evidence regarding effective messages for poster campaigns promoting stair use. Evidence from the primary studies included in review D regarding intervention duration or intensity/exposure as moderators of effectiveness was consistent with that from the reviews, generally finding that more sustained and greater intensity campaigns were more effective. There was limited evidence that government and charity campaigns may be more effective than those from pharmaceutical companies (e.g. NRT manufacturers). Only one study compared different media channels within the same study (a comparison of audience engagement through different social media channels). As with review A, there was little evidence regarding the use of theory as a potential moderator of campaign effectiveness, and no evidence regarding scale as a moderator of effectiveness; the latter was not surprising, as any statistical comparison of the effect of scale (e.g. national vs. local-level campaigns) is more likely to happen at a review level than in a primary study, although none of our included reviews examined this.
Evidence from other literature regarding the characteristics of mass media campaigns associated with effectiveness is limited. A recent review by the US Centers for Disease Control and Prevention175 of physical activity mass media campaign design suggested that campaign success was more likely if a number of campaign principles (formative research, audience segmentation, message design, channel placement, process evaluation and theory-based) were used as part of campaign design and planning. Some of these principles were tested in a recent meta-analysis, published while our study was ongoing. 164 Five campaign design principles thought to be associated with effectiveness were examined in the meta-analysis: (1) the use of formative research to help develop messages and campaign content, (2) the use of theory, (3) message, (4) channel and (5) ‘environmental supplements’, in this case defined as efforts to educate health-care providers and supplementary materials/services (such as free condoms or reduced-cost screening). The study differed from ours in that it reviewed primary studies rather than reviews, and included a wider range of health topics. In total, data from 63 articles were included in the meta-analysis, which, overall, found little evidence that principles of effective campaign design explained a significant amount of heterogeneity in effect sizes. Some results were described by the authors as ‘puzzling’, such as findings that the use of formative research significantly reduced effects on behaviour change or that there was no improvement in outcomes when campaigns were theory driven, or that the use of more channels to disseminate messages was associated with lower effects on knowledge. The authors suggested that some inconsistent or unexpected findings may have been explained by small numbers of studies in some of the moderator analyses, by confounding by multiple moderators, or simply by studies failing to report certain moderators. 164
A recent review of mass media tobacco campaigns that focused on the relative effectiveness of different campaign characteristics found that young people were more likely to recall and think about advertising that includes personal testimonials, a surprising narrative, and intense images, sound and editing; however, it found mixed evidence regarding use of health consequences messages, a second-hand smoke theme or a social norms theme. 176 Since commencing our own review of systematic reviews, the Cochrane Database Systematic Review on mass media interventions for preventing smoking in young people has been updated,35,177 adding one more RCT to the evidence base but not changing the overall findings. Regarding mass media channels used in this updated review, the authors note that the ‘inclusion of only two studies from the last 10 years is concerning, particularly considering the rising use of social media among youth. More high-quality studies are needed’. 177
What are the implications for our logic model?
Our four reviews indicate that there is a lack of theory employed in the development of mass media campaigns and their evaluation. In this respect, our logic model provides a useful starting point for researchers, practitioners and commissioners planning future campaigns. The lack of theory underpinning current campaigns suggests a greater need to recognise the importance of utilising existing theories, concepts and logic models and to apply this knowledge in a systematic manner to the processes of campaign planning, development, implementation and evaluation. In particular, there is a need for future campaigns to be based on a deeper understanding of the fundamental principles of communication, persuasion and changing social norms, as well as an appreciation of the interplay between communication theories, behaviour change theories and the wider sociopolitical context in which mass media campaigns often operate. Indeed, mass media campaigns rarely operate in a vacuum, and our logic model would be further strengthened by empirical research that better explores the interplay between the political and mass media campaigns’ agenda-setting functions. Such insights would aim to explore the opportunities and challenges encountered in attempting to explore causal pathways and disentangling the effects of campaign activities from external influences – including political influences. Such research would develop better understanding of the complexity of mass media campaigns in the process of health improvement. McCoy and Hargie178 echo this when referring to the prerequisite of effective evaluation as the deep understanding of its ‘nature, purposes and concepts’. Mass media campaigns can, if developed in a strategic way and informed by principles and theories of effective communication, be successful in conveying health messages to large sections of the population at a relatively low cost and, for this reason, are a useful tool to promote health. However, it is imperative to invest in research that develops a strong evidence base for understanding what works and in what context in order to maximise the effectiveness of mass media interventions.
The original logic model we developed (see Figure 1) did not adequately reflect the body of literature we found from the review of systematic reviews. The outcomes we identified at the outset were not discussed as proximal, intermediate or distal in the papers, which tended to refer to them as outcomes without distinguishing between them. In some ways this is understandable because behaviour change is rarely a linear affair, as many behaviour change theories suggest a more iterative process. Therefore, we conclude that, although the terms ‘proximal’, ‘intermediate’ and ‘distal’ were not useful labels in the data extraction tool, they may be useful in thinking through how to better identify the evaluation outcomes of an intervention.
Strengths and limitations of the study
Strengths
This review adds value to the current literature on mass media interventions by bringing together a large amount of evidence for a variety of health topics and enabled a comparison between them. It combined the breadth that is offered when looking across review-level evidence with the depth obtainable from examining individual primary studies. In response to frequent calls for in-depth analysis of how campaigns work (e.g. Cassidy et al. 179), it examined intervention characteristics that are associated with effectiveness. The review has particular relevance to the UK context, and we sought feedback from stakeholders to assess its usefulness.
Methodological limitations
We were unable to conduct statistical synthesis owing to the considerable heterogeneity across the studies. This makes it difficult to draw firm explanatory conclusions about the causes of the variability in results, noted by Ferri et al. 62 among others. In the review of reviews, some of the primary studies were published in the 1980s and 1990s and, thus, were discussing technologies that are no longer relevant. The searches for review A, the review of reviews, were conducted in January 2016. Searches for the subsequent reviews were conducted later (up to January 2017 for review C), reflecting the sequential nature of the project. Although offering a breadth that would have been unachievable if only primary studies had been examined, the focus on reviews meant that, at times, we lacked contextual and intervention details, and there may have been some overlap in studies between reviews. It was difficult to assess bias within the existing reviews because this would have entailed redoing their analyses. Inevitably, our results are limited by the quality of the primary studies, and reflect a publication bias in which weaker campaigns are rarely evaluated, and interventions with poor results are less likely to be written up and published. 166
As noted above, there are a number of issues involved in assessing the cost-effectiveness of mass media campaigns. Data are generally limited, with few studies; this is the case even regarding tobacco use, the health topic that tends to be most frequently examined in mass media studies and reviews. Part of the reason for the lack of studies is likely to be the challenges associated with extrapolating short-term effects (e.g. increase in quit attempts) to long-term costs and outcomes, which requires expertise in mathematical modelling. The evidence is also likely to be biased, with ineffective evaluations being unlikely to undergo economic evaluation, thereby running the risk that the intervention under examination is likely to look more cost-effective than it is on average. Finally, approaches to the synthesis of economic evidence are still being developed. Cost-effectiveness analyses, in particular, are very context specific, and it is challenging to conduct systematic reviews of such studies while maintaining global relevance.
Limitations in scope/definitions of our study
Although the study was wide-ranging, necessary parameters in terms of scope and how mass media campaigns were defined meant that there were inevitable gaps in the evidence we could review. We focused on six topics relating to preventable risk factors for disease: alcohol use, diet, illicit substance use, physical activity, sexual and reproductive health and smoking. The focus on disease prevention meant that campaigns addressing related behaviours but with a different focus were excluded: we did not include alcohol campaigns whose main focus was drink driving. Mass media campaigns seeking to raise awareness, counter stigma and encourage help-seeking behaviour in relation to mental health issues were excluded, as were road safety campaigns (e.g. targeting speeding or seat belt use) and campaigns encouraging skin cancer protection behaviours. Mass media campaigns whose primary aim was to encourage participation in screening programmes were excluded, although campaigns that sought to encourage screening in addition to more lasting behaviour change (such as campaigns that encouraged condom use and HIV/AIDS testing) were included because of the behaviour component. Because of our focus on population behaviour change, we excluded evidence relating to the use of the media in a media advocacy context, in which news media coverage and other forms of media messages are used to foster public and policy-maker support for policies or legislation to promote health, such as changes in taxation, drink driving laws or restrictions on marketing activity. 180–182 Previous research has suggested that media coverage achieved as part of a multifaceted advocacy campaign can be one of the factors leading to successful policy change, although the challenges of demonstrating the particular contribution of media to the outcomes are considerable. 183
We defined mass media campaigns as the intentional use of any media channel(s) of communication by local, regional and national organisations to influence lifestyle behaviour through largely passive or incidental exposure to media campaigns, rather than largely dependent on active help-seeking (adapted from Wakefield et al. 6 and Bala et al. 27). We adopted this definition of mass media as it is potentially the most useful for campaign planners seeking an estimate of the effectiveness of campaigns implemented in naturalistic settings that do not require active audience engagement with a given channel to achieve message exposure. 164 However, this meant that certain types of communications-based intervention were excluded. Interventions that require individuals actively to seek out the information (such as websites) or to opt in or sign up (such as SMS/text messaging for smokers trying to quit) would have been excluded because they require active engagement by target populations. Not including these interventions has limited what the review can say about new/digital/interactive media interventions. However, that missing evidence may be limited in itself. A fairly recent scoping review of how digital media (including visual, electronic and online media) are used in the area of public health184 found that current public health usage is predominantly the ‘outmoded approach of “telling and selling” and cast[s] the recipient in an individual and passive role’, based on 221 systematic reviews published between 2000 and 2013.
Large multifaceted community interventions that included a media element were included only if it was possible to relate effects to the media component of the campaign. For example, a review of interventions that involved a mass media campaign combined with health-related product distribution was included because the outcomes that related specifically to the mass media were reported and synthesised by the authors. 69 However, this meant that evidence from reviews such as the Cochrane Database Systematic Reviews of universal multicomponent prevention programmes for alcohol misuse and community interventions for preventing smoking76,185 and the ‘Change4Life Smart Swaps’ intervention study (Wrieden and Levy186) was not included in our reviews. We are therefore limited in what we can conclude about the extent to which mass media campaigns can interact with other interventions or services to improve health outcomes, which was one of our original objectives. However, our review of reviews found promising evidence regarding the ability of mass media campaigns to stimulate engagement with other services. We found that, overall, media campaigns can prompt calls to telephone quitlines for smoking cessation (although there is only moderate certainty in the strength of this finding). For helping to foster engagement with sexual health clinics or services, there was low-certainty evidence that campaigns can increase use of such services.
In examining characteristics of mass media campaigns that may be associated with effectiveness, we focused on campaign components that featured in the ‘Activities’ box of our logic model. We did not examine mass media campaign ‘Inputs’, which in our logic model included resources, staff, expertise/skills, technology and materials, although the full economic evaluation reviews in our rapid review of cost-effectiveness (review C) would have taken into account the upfront costs (resources) of mass media campaigns, when information was reported.
Gaps in the evidence and implications for future research
As noted above, the amount of evidence relating to mass media campaigns varies considerably across different health behaviours. The most commonly studied behaviour, as reflected in the number of existing reviews we found that met our criteria, was tobacco use, followed by sexual health and physical activity. Although there were a relatively large number of reviews of sexual health mass media campaigns, many of the studies in these reviews were conducted in non-OECD countries and so had limited relevance to the UK context. Just three reviews of media campaigns on illicit drugs were identified, and no single review examining the effectiveness of mass media for addressing alcohol use or diet was found, although these behaviours were addressed in reviews examining multiple health behaviours. We partially addressed this latter gap by conducting the first (to our knowledge) review of mass media campaigns on alcohol use, but were unable, within the time and resources available, to conduct a similar review for mass media campaigns addressing diet. This remains a gap.
In part, the variations in the amount of evidence reflect the amount and nature of activity in each topic area (e.g. several major campaigns on smoking cessation and second-hand smoke in the 1990s/2000s and a decline in mass media campaigns on sexual health in the UK after the 1980s/early 1990s). Another contributory factor to the apparent lack of evidence we found in some health behaviour topic areas is that our definition of mass media campaigns would have excluded media activity implemented and evaluated as part of multicomponent community interventions such as the Department of Health and Social Care’s Change4Life public health programme. In other words, the gaps in evidence we found in some areas do not necessarily mean that there has been no mass media activity or that this activity has not been evaluated, but rather that sometimes this mass media activity has taken place in the context of wider multifaceted interventions in which the specific contribution of mass media cannot be examined separately. The challenge of disentangling the contribution of mass media elements from the contribution of other intervention elements, in multifaceted interventions, is recognised elsewhere. 6,58
Naugle and Hornik166 recommend that:
In the future, evaluators should address threats to inference of mass media effects by using unbiased samples, multiple comparison groups across time, levels of exposure, and treatment and control sites, statistical controls and advanced statistical methods, and data triangulation. The written report should reflect the measures taken to mitigate threats to inference. Published evaluations of mass media campaigns should provide detailed information about the campaign, exposure, and the evaluation to permit meta-analyses as the literature base grows.
After starting our reviews of the evidence, we became aware that the evaluation methods for social media and public health mass communication interventions are being appraised as an ongoing registered systematic review. 187
One of our objectives was to assess new or emerging evidence about campaigns employing different types of media, including new media. Overall, we found limited evidence regarding such campaigns. The nature of reviews of reviews is such that newer evidence tends not to be included; in our review of reviews published from 2000 to early 2016 (review A), the years covered by the identified reviews ranged from database inception to January 2015, with the most recent reviews including studies up to 2013. The review of UK primary studies published between 2011 and 2016 (review D) included some more recent evidence relating to interventions using newer media, but this was limited. In part, the limited evidence we found regarding campaigns using newer media reflected our definition of mass media campaigns as those involving incidental exposure, which as noted above would have excluded interventions that required individuals to engage in active information-seeking or to opt in to campaign participation (e.g. joining the Smokefree Facebook community or downloading the Public Health England One You Drinks tracker app). Reviews in this area have suggested that new digital media have the potential to be ‘user controlled and shareable’,188 crucial elements for reaching a large population while at the same time providing interpersonal support to heighten the effects of public health campaigns;189 and the scoping review of reviews by Clar et al. 184 showed that all six of our health topics are targets of digital media for public health. A review of 10 studies that evaluated the impact of new digital media interventions on adolescents’ sexual health found changes in sociocognitive outcomes (although not always in a positive direction), and two interventions showed a reduced risk of sexual initiation among young teenagers. 188
The ‘user controlled and shareable’ aspects of new/digital media interventions mean that they are not standardised products, and this poses challenges for evaluation. McGloin and Eslami190 note that ‘although web-based, social-media-based and mobile-based studies tend to show positive results for dietary behaviour change, methodologies have yet to be developed that go beyond basic evaluation criteria and move towards true measures of behaviour change’. Guse et al. 188 suggest that evaluations using RCTs ‘can be laborious, with timelines that are inconsistent with the paces of technology and youth culture’. More research that tests new/social media interventions using rigorous methods, and that compares them with interventions using more traditional media (e.g. Jane et al. 191), is needed and we note that research into reviewing the evaluation methods for social media interventions is ongoing. 187
Another original objective of our study was to examine the relationship between local, regional and national campaigns and evidence of effectiveness where this exists. Although the reviews included in the review of reviews sometimes noted at what scale included interventions had been implemented (i.e. local, regional or national scale), none of the reviews compared or reflected on scale as a potential moderator of campaign effectiveness. There was similarly no evidence on scale of a campaign as a moderator of effectiveness in the review of UK primary studies; however, it is interesting to note that the review of UK primary studies included studies at both ends of the spectrum, ranging from national whole-population television campaigns on smoking to highly localised poster campaigns promoting stair use in a specific area or building. Future research could explore the potential relationship between scale of campaign and type of health behaviour change in more detail. For example, is physical activity more effectively promoted with a highly localised campaign focusing on physical activity in a particular location, or with a national campaign focusing on physical activity in general, and could highly localised campaigns be used to promote other types of health behaviour than physical activity? For commissioners of campaigns interested in how local/regional and national campaigns can be designed to work synergistically, it may be useful to examine process and other evaluations of campaigns that are designed to be implemented at both national and local/regional levels, such as National No Smoking Day or Dry January.
Chapter 8 Conclusion
This study provides a new synthesis of existing research on the use of mass media to communicate public health messages. Informed by a logic model, the study involved a review of evidence on the effectiveness of mass media campaigns across six health topics that represent the main preventable risk factors for disease morbidity and mortality in developed countries:15 alcohol use, diet, illicit substance use, physical activity, sexual and reproductive health and tobacco use.
First, we conducted a review of systematic reviews (review A). This was informative and provided a high-level overview of what is known on this topic, including identification of gaps in the evidence. We found no systematic reviews of mass media campaigns specifically addressing alcohol use that met our inclusion criteria, and thus we conducted our own original review on this topic (review B). The overall study also aimed to examine the cost-effectiveness of mass media campaigns for the six health topics of interest, and this was addressed in a third review (review C). The final element of our study involved a systematic review of English-language primary studies of mass media campaigns targeting the same six health topics, conducted recently in the UK (review D). This was conducted to provide additional evidence on campaign characteristics that might be associated with effectiveness that was directly relevant to the current or recent UK context.
Our review of reviews also found no systematic reviews of the effectiveness of mass media campaigns to improve or modify diet. We conducted a scoping search for this, which resulted in > 16,500 references being identified in MEDLINE. Within this study, we did not have the available time or resources to conduct a full, new systematic review on this topic.
Our study had a number of limitations, as described in Chapter 7. However, key messages and priorities for future research emerged.
Key findings
First, logic models provide a useful basis for planning and conducting systematic reviews on complex topics such as mass media for public health messages. Our model proved essential in helping us to develop the scope and focus of our reviews, in partnership with stakeholders, and was refined as the study progressed. We hope that our logic model will prove useful to others studying this topic or indeed those designing campaigns and considering what issues to assess or measure in any evaluation.
In addition, a number of systematic reviews of mass media campaigns have been conducted but there is significantly more literature on tobacco control mass media campaigns than on campaigns focusing on other topics, although campaigns on sexual health and physical activity have been evaluated in a number of studies and these findings have been brought together in reviews.
Looking across reviews, the strength of the evidence varies. The impact of the mass media on tobacco use and physical activity is mixed, based on the available literature. There is moderate evidence for the positive effects of mass media campaigns on reducing sedentary behaviour and sexual health. Review-level evidence was of low certainty for the impact of campaigns on illicit drugs.
Mass media campaigns can prompt people to contact or access services (treatment-seeking). There is evidence that tobacco control mass media campaigns can prompt people to call smoking quitlines and some, but more limited, evidence that mass media campaigns can help to increase the use of sexual health clinics or services.
Mass media campaigns on alcohol have been evaluated to a modest degree in the literature. Campaigns can be memorable and can influence knowledge, attitudes and beliefs about drinking, but there is limited evidence that these campaigns can help reduce alcohol consumption.
There is moderate evidence that tobacco control mass media campaigns can be cost-effective. We found almost no data on the cost-effectiveness of mass media campaigns for other health behaviours, and this requires further research.
How effective a mass media campaign is may depend on its characteristics, and we examined this in both review A and review D. Campaigns that run for longer and are more intensive (with people exposed to them more often, for example) are likely to be more effective, based on evidence from tobacco and sexual health campaigns in particular.
Targeting a campaign at different audiences (such as young people) can be effective. Targeted campaigns need to be designed and tested to be appropriate to the target audience taking into account age, sex, culture and level of engagement in the behaviour of interest.
The messages featured in a campaign may also make a difference. We found some evidence in review A that those focusing on ‘hard-hitting’ (negative) messages, for example, or on shifting social norms, may change behaviour, whereas the UK studies in review D found evidence that campaigns with both positive and negative messages may affect smoking behaviour. However, few direct comparisons of different messages were identified and we also found gaps relating to the use of theory, the type of media channel used and the scale of a campaign (national, regional or local).
Future research
Our study identifies clear priorities for future research. These include the need for a systematic review of mass media campaigns on diet. Evaluations of mass media campaigns need to be rigorous and to include detailed information on the campaign itself, and on target population exposure. In addition, more information is required on the cost-effectiveness of mass media campaigns for public health messages, particularly on topics other than tobacco. Researchers should aim to include cost data and ideally assess cost-effectiveness in future studies. We identified some findings on new media (see Chapter 5), but the data were mixed and it was difficult to offer firm conclusions in this area, at least partially because of the time lag between campaigns being run and evaluations being conducted and published.
More studies and reviews on the effectiveness of new-media (including digital and social media) campaigns are needed. In addition, and although very difficult to achieve, a separate study could be commissioned to examine the specific contribution of mass media campaigns when delivered as part of multicomponent community interventions. In reality, mass media campaigns do not exist in isolation but are often designed to complement other public health programmes or interventions, but unpicking their ‘independent’ effect in this context may be very difficult in practice. Finally, a better understanding of how local, regional or national campaigns can work together is needed to inform commissioning decisions, particularly in a UK context.
Acknowledgements
The authors wish to acknowledge the contribution of a number of colleagues during the study. Kathleen Massie, Carol Anne Greenan, Aileen Paton and Graeme Docherty provided administrative and organisational support to the project and we are very grateful for their input. Two University of Stirling postgraduate students assisted with the study and provided very valuable contributions to the research. Naomie Crispin assisted with defining inclusion criteria, review screening, data extraction and quality assessments (for review A) and Joanne Morrison assisted with screening, data extraction, quality assessments and results synthesis (for reviews C and D). We would also like to acknowledge the contribution of members of the study advisory group, in particular George Vekic who provided PPI input throughout.
Advisory group membership
-
Professor Annie S Anderson, Professor of Public Health Nutrition, School of Medicine, University of Dundee.
-
Professor Kamlesh Khunti, Professor of Primary Care Diabetes and Vascular Medicine, University of Leicester.
-
Ms Tara MacLeod, Deputy Director: Strategy, Engagement and Innovation, Public Health England.
-
Ms Dona Milne, Deputy Director of Public Health, NHS Lothian.
-
Dr Catherine Pritchard, UKCTAS, University of Nottingham.
-
Professor Harry Rutter, Director, Halsa Consulting Ltd, Oxford Centre for Healthcare Transformation.
-
Mr Paul Thorne, Press Officer, Cancer Research UK.
-
Mr George Vekic, Lay Member.
Contributions of authors
Ms Martine Stead (Deputy Director, Institute for Social Marketing, University of Stirling) contributed to the original grant application, was responsible for day-to-day co-ordination of project elements, conducted data appraisal, conducted review and synthesis for Chapters 2 and 5 and prepared results for publication, drafted Chapter 7, devised the overall report structure and contributed to report editing.
Ms Kathryn Angus (Information Specialist, Institute for Social Marketing, University of Stirling) conducted searches, data extraction and appraisal and made a substantial contribution to synthesis and write-up. She contributed to structuring and co-ordinating the final report and managing the referencing for the final report.
Dr Tessa Langley (Associate Professor in Health Economics, Division of Epidemiology and Public Health, University of Nottingham) contributed to the original grant application, supported the management of research staff, conducted data extraction and appraisal, made a substantial contribution to synthesis and write-up, commented on drafts and facilitated stakeholder engagement events.
Dr Srinivasa Vittal Katikireddi (Senior Clinical Research Fellow, Medical Research Council/Chief Scientist Office Social and Public Health Sciences Unit, University of Glasgow) contributed to the original grant application, supported the management of research staff, conducted data extraction and appraisal, made a substantial contribution to synthesis and write-up, commented on drafts and helped facilitate public engagement activities.
Ms Kate Hinds (Systematic Reviewer, Institute of Education, University College London) conducted searches, screened records, developed data extraction tools, data extracted and quality appraised the papers and contributed to the methods and the characteristics chapters in the report.
Dr Shona Hilton (Deputy Director, Medical Research Council/Chief Scientist Office Social and Public Health Sciences Unit, University of Glasgow) contributed to the original grant application, conducted data extraction and appraisal and provided a substantial contribution to synthesis and write-up of the report, in particular in Chapter 7 on characteristics.
Professor Sarah Lewis (Professor of Medical Statistics, Division of Epidemiology and Public Health, University of Nottingham) contributed to study design, data extraction and analysis of subgroup effects on main outcomes, impact of message type and co-supervised the alcohol mass media review.
Professor James Thomas (Professor of Social Research and Policy, Institute of Education, University College London) contributed to the original grant application, co-ordination and team management, the development of tools and methods and writing the final report.
Ms Mhairi Campbell (Systematic Reviewer, Medical Research Council/Chief Scientist Office Social and Public Health Sciences Unit, University of Glasgow) contributed to the literature search of diet studies, conducted quality appraisal, data extraction and synthesis of behavioural outcomes for the review of reviews and prepared the results for publication.
Mr Ben Young (Research Assistant, Division of Epidemiology and Public Health, University of Nottingham) carried out data extraction and quality assessment and conducted the systematic review of alcohol primary studies.
Professor Linda Bauld (Bruce and John Usher Chair in Public Health, Usher Institute, College of Medicine and Veterinary Medicine, University of Edinburgh) was the PI with overall responsibility for the design, co-ordination and delivery of the study and liaising with NIHR. With co-investigators, she conceived, designed and led the original grant application. She made substantial contribution to synthesis and write-up of chapters in the report, commented on drafts and outputs of the study and facilitated stakeholder and public engagement activities.
All authors contributed to the interpretation of findings, writing and editing of the final report and outputs from the study.
Publications
Young B, Lewis S, Katikireddi SV, Bauld L, Stead M, Angus K, et al. Effectiveness of mass media campaigns to reduce alcohol consumption and harm: a systematic review. Lancet 2017;390(Suppl. 3):98.
Young B, Lewis S, Katikireddi SV, Bauld L, Stead M, Angus K, et al. Effectiveness of mass media campaigns to reduce alcohol consumption and harm: a systematic review. Alcohol Alcohol 2018;53:302–16.
Data-sharing statement
All data requests should be submitted to the corresponding author for consideration. Access to available anonymised data may be granted following review.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care.
References
- Gateway to Health Communication & Social Marketing Practice. Atlanta, GA: Centers for Disease Control and Prevention; 2017.
- Noncommunicable Diseases. Factsheet. Geneva: World Health Organization; 2017.
- Marketing Strategy 2014–2017. London: Public Health England; 2014.
- Davis RM, Gilpin EA, Loken B, Viswanath K, Wakefield MA. Monograph 19: The Role of the Media in Promoting and Reducing Tobacco Use. Bethesda, MD: U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute; 2008.
- Road Safety Mass Media Campaigns: a Toolkit. 10 Steps for Developing Road Safety Mass Media Campaigns in Low- and Middle-Income Countries. Geneva: World Health Organization; 2016.
- Wakefield MA, Loken B, Hornik RC. Use of mass media campaigns to change health behaviour. Lancet 2010;376:1261-71. https://doi.org/10.1016/S0140-6736(10)60809-4.
- Atkin CK, Rice RE, Sharrer E. The International Encyclopedia of Media Studies. London: Wiley Blackwell; 2013.
- McVey D, Stapleton J. Can anti-smoking television advertising affect smoking behaviour? Controlled trial of the Health Education Authority for England’s anti-smoking TV campaign. Tob Control 2000;9:273-82. https://doi.org/10.1136/tc.9.3.273.
- Hornik RC. Public Health Communication: Evidence for Behavior Change. Abingdon: Lawrence Erlbaum Associates; 2002.
- Jepson RG, Harris FM, Platt S, Tannahill C. The effectiveness of interventions to change six health behaviours: a review of reviews. BMC Public Health 2010;10. https://doi.org/10.1186/1471-2458-10-538.
- Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group . Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLOS Med 2009;6. https://doi.org/10.1371/journal.pmed.1000097.
- Caird J, Sutcliffe K, Kwan I, Dickson K, Thomas J. Mediating policy-relevant evidence at speed: are systematic reviews of systematic reviews a useful approach?. Evid Policy 2015;11:81-97. https://doi.org/10.1332/174426514X13988609036850.
- Smith V, Devane D, Begley CM, Clarke M. Methodology in conducting a systematic review of systematic reviews of healthcare interventions. BMC Med Res Methodol 2011;11. https://doi.org/10.1186/1471-2288-11-15.
- Thomson D, Russell K, Becker L, Klassen T, Hartling L. The evolution of a new publication type: Steps and challenges of producing overviews of reviews. Res Synth Methods 2010;1:198-211. https://doi.org/10.1002/jrsm.30.
- Forouzanfar MH, Afshin A, Alexander LT, Anderson HR, Bhutta ZA, Biryukov S, et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016;388:1659-724. https://doi.org/10.1016/S0140-6736(16)31679-8.
- Langley T, Bauld L, Stead M, Lewis S, Thomas J, Hilton S, et al. A Systematic Review of the Effectiveness of Mass Media Public Health Interventions n.d. www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42015029205 (accessed 6 March 2017).
- Young B, Lewis S, Langley T, Bauld L, Stead M, Thomas J, et al. Mass Media Campaigns to Reduce Alcohol Consumption n.d. www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42017054999 (accessed 12 July 2017).
- Kneale D, Thomas J, Harris K. Developing and optimising the use of logic models in systematic reviews: exploring practice and good practice in the use of programme theory in reviews. PLOS ONE 2015;10. https://doi.org/10.1371/journal.pone.0142187.
- Chen H. Practical Program Evaluation: Assessing and Improving Planning, Implementation, and Effectiveness. Thousand Oaks, CA: Sage Publications Inc.; 2005.
- Rogers PJ. Using programme theory to evaluate complicated and complex aspects of interventions. Evaluation 2008;14:29-48. https://doi.org/10.1177/1356389007084674.
- Anderson LM, Petticrew M, Rehfuess E, Armstrong R, Ueffing E, Baker P, et al. Using logic models to capture complexity in systematic reviews. Res Synth Methods 2011;2:33-42. https://doi.org/10.1002/jrsm.32.
- Niederdeppe J, Kuang X, Crock B, Skelton A. Media campaigns to promote smoking cessation among socioeconomically disadvantaged populations: what do we know, what do we need to learn, and what should we do now?. Soc Sci Med 2008;67:1343-55. https://doi.org/10.1016/j.socscimed.2008.06.037.
- Huhman ME, Potter LD, Duke JC, Judkins DR, Heitzler CD, Wong FL. Evaluation of a national physical activity intervention for children: VERB campaign, 2002–2004. Am J Prev Med 2007;32:38-43. https://doi.org/10.1016/j.amepre.2006.08.030.
- Durkin S, Brennan E, Wakefield M. Mass media campaigns to promote smoking cessation among adults: an integrative review. Tob Control 2012;21:127-38. https://doi.org/10.1136/tobaccocontrol-2011-050345.
- Amos A, Brown T, Platt S. A Systematic Review of the Effectiveness of Policies and Interventions to Reduce Socio-economic Inequalities in Smoking Among Adults. Final Report. Edinburgh: Centre for Population Health Sciences, University of Edinburgh; 2013.
- Thomas J, Brunton J, Graziosi S. EPPI-Reviewer 4: Software for Research Synthesis. EPPI-Centre Software. London: Social Science Research Unit, University College London Institute of Education; 2010.
- Bala MM, Strzeszynski L, Topor-Madry R, Cahill K. Mass media interventions for smoking cessation in adults. Cochrane Database Syst Rev 2013;6. https://doi.org/10.1002/14651858.CD004704.pub3.
- Whiting P, Savović J, Higgins JP, Caldwell DM, Reeves BC, Shea B, et al. ROBIS: a new tool to assess risk of bias in systematic reviews was developed. J Clin Epidemiol 2016;69:225-34. https://doi.org/10.1016/j.jclinepi.2015.06.005.
- Members and Partners. Paris: OECD; n.d.
- Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, et al. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews. A Product from the ESRC Methods Programme. Lancaster: Institute for Health Research, Lancaster University; 2006.
- Tugwell P, Petticrew M, Kristjansson E, Welch V, Ueffing E, Waters E, et al. Assessing equity in systematic reviews: realising the recommendations of the Commission on Social Determinants of Health. BMJ 2010;341. https://doi.org/10.1136/bmj.c4739.
- Thomson HJ, Thomas S. The effect direction plot: visual display of non-standardised effects across multiple outcome domains. Res Synth Methods 2013;4:95-101. https://doi.org/10.1002/jrsm.1060.
- Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE Working Group . GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008;336:924-6. https://doi.org/10.1136/bmj.39489.470347.AD.
- Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol 2011;64:383-94. https://doi.org/10.1016/j.jclinepi.2010.04.026.
- Brinn MP, Carson KV, Esterman AJ, Chang AB, Smith BJ. Mass media interventions for preventing smoking in young people. Cochrane Database Syst Rev 2010;11. https://doi.org/10.1002/14651858.CD001006.pub2.
- Brown T, Platt S, Amos A. Equity impact of interventions and policies to reduce smoking in youth: systematic review. Tob Control 2014;23:e98-105. https://doi.org/10.1136/tobaccocontrol-2013-051451.
- Brown T, Platt S, Amos A. Equity impact of population-level interventions and policies to reduce smoking in adults: a systematic review. Drug Alcohol Depend 2014;138:7-16. https://doi.org/10.1016/j.drugalcdep.2014.03.001.
- de Kleijn MJ, Farmer MM, Booth M, Motala A, Smith A, Sherman S, et al. Systematic review of school-based interventions to prevent smoking for girls. Syst Rev 2015;4. https://doi.org/10.1186/s13643-015-0082-7.
- Gould GS, McEwen A, Watters T, Clough AR, van der Zwan R. Should anti-tobacco media messages be culturally targeted for Indigenous populations? A systematic review and narrative synthesis. Tob Control 2013;22. https://doi.org/10.1136/tobaccocontrol-2012-050436.
- Guillaumier A, Bonevski B, Paul C. Anti-tobacco mass media and socially disadvantaged groups: a systematic and methodological review. Drug Alcohol Rev 2012;31:698-70. https://doi.org/10.1111/j.1465-3362.2012.00466.x.
- Hemsing N, Greaves L, O’Leary R, Chan K, Okoli C. Partner support for smoking cessation during pregnancy: a systematic review. Nicotine Tob Res 2012;14:767-76. https://doi.org/10.1093/ntr/ntr278.
- Hill S, Amos A, Clifford D, Platt S. Impact of tobacco control interventions on socioeconomic inequalities in smoking: review of the evidence. Tob Control 2014;23:e89-97. https://doi.org/10.1136/tobaccocontrol-2013-051110.
- Jepson R, Harris F, Rowa-Dewar N, MacGillivray S, Hastings G, Kearney N, et al. A Review of the Effectiveness of Mass Media Interventions Which Both Encourage Quit Attempts and Reinforce Current and Recent Attempts to Quit Smoking. London: NICE; 2008.
- Richardson L, Allen P, McCullough L, Bauld L, Assanand S, Greaves L, et al. Interventions to Prevent the Uptake of Smoking in Children and Young People. London: NICE; 2008.
- Wilson LM, Avila Tang E, Chander G, Hutton HE, Odelola OA, Elf JL, et al. Impact of tobacco control interventions on smoking initiation, cessation, and prevalence: a systematic review. J Environ Public Health 2012;2012. https://doi.org/10.1155/2012/961724.
- Bertrand JT, Anhang R. The effectiveness of mass media in changing HIV/AIDS-related behaviour among young people in developing countries. World Health Organ Tech Rep Ser 2006;938:205-41.
- Carter MW, Tregear ML, Moskosky SB. Community education for family planning in the U.S.: a systematic review. Am J Prev Med 2015;49:107-15. https://doi.org/10.1016/j.amepre.2015.03.030.
- French RS, Bonell C, Wellings K, Weatherburn P. An exploratory review of HIV prevention mass media campaigns targeting men who have sex with men. BMC Public Health 2014;14. https://doi.org/10.1186/1471-2458-14-616.
- Grilli R, Freemantle N, Minozzi S, Domenighetti G, Finer D. Mass media interventions: effects on health services utilisation. Cochrane Database Syst Rev 2000;2.
- Kesterton AJ, Cabral de Mello M. Generating demand and community support for sexual and reproductive health services for young people: a review of the Literature and Programs. Reprod Health 2010;7. https://doi.org/10.1186/1742-4755-7-25.
- LaCroix JM, Snyder LB, Huedo-Medina TB, Johnson BT. Effectiveness of mass media interventions for HIV prevention, 1986–2013: a meta-analysis. J Acquir Immune Defic Syndr 2014;66:329-40. https://doi.org/10.1097/QAI.0000000000000230.
- Speizer IS, Magnani RJ, Colvin CE. The effectiveness of adolescent reproductive health interventions in developing countries: a review of the evidence. J Adolesc Health 2003;33:324-48. https://doi.org/10.1016/S1054-139X(02)00535-9.
- Swanton R, Allom V, Mullan B. A meta-analysis of the effect of new-media interventions on sexual-health behaviours. Sex Transm Infect 2015;91:14-20. https://doi.org/10.1136/sextrans-2014-051743.
- Sweat MD, Denison J, Kennedy C, Tedrow V, O’Reilly K. Effects of condom social marketing on condom use in developing countries: a systematic review and meta-analysis, 1990-2010. Bull World Health Organ 2012;90:613-622A. https://doi.org/10.2471/BLT.11.094268.
- Abioye AI, Hajifathalian K, Danaei G. Do mass media campaigns improve physical activity? A systematic review and meta-analysis. Arch Public Health 2013;71. https://doi.org/10.1186/0778-7367-71-20.
- Brown DR, Soares J, Epping JM, Lankford TJ, Wallace JS, Hopkins D, et al. Stand-alone mass media campaigns to increase physical activity: a community guide updated review. Am J Prev Med 2012;43:551-61. https://doi.org/10.1016/j.amepre.2012.07.035.
- Finlay SJ, Faulkner G. Physical activity promotion through the mass media: inception, production, transmission and consumption. Prev Med 2005;40:121-30. https://doi.org/10.1016/j.ypmed.2004.04.018.
- Kahn EB, Ramsey LT, Brownson RC, Heath GW, Howze EH, Powell KE, et al. The effectiveness of interventions to increase physical activity. A systematic review. Am J Prev Med 2002;22:73-107. https://doi.org/10.1016/S0749-3797(02)00434-8.
- Leavy JE, Bull FC, Rosenberg M, Bauman A. Physical activity mass media campaigns and their evaluation: a systematic review of the literature 2003–2010. Health Educ Res 2011;26:1060-85. https://doi.org/10.1093/her/cyr069.
- Matson-Koffman DM, Brownstein JN, Neiner JA, Greaney ML. A site-specific literature review of policy and environmental interventions that promote physical activity and nutrition for cardiovascular health: what works?. Am J Health Promot 2005;19:167-93. https://doi.org/10.4278/0890-1171-19.3.167.
- Ogilvie D, Foster CE, Rothnie H, Cavill N, Hamilton V, Fitzsimons CF, et al. Scottish Physical Activity Research Collaboration. Interventions to promote walking: systematic review. BMJ 2007;334. https://doi.org/10.1136/bmj.39198.722720.BE.
- Ferri M, Allara E, Bo A, Gasparrini A, Faggiano F. Media campaigns for the prevention of illicit drug use in young people. Cochrane Database Syst Rev 2013;6. https://doi.org/10.1002/14651858.CD009287.pub2.
- Werb D, Mills EJ, Debeck K, Kerr T, Montaner JS, Wood E. The effectiveness of anti-illicit-drug public-service announcements: a systematic review and meta-analysis. J Epidemiol Community Health 2011;65:834-40. https://doi.org/10.1136/jech.2010.125195.
- Werb D, Buxton J, Shoveller J, Richardson C, Rowell G, Wood E. Interventions to prevent the initiation of injection drug use: a systematic review. Drug Alcohol Depend 2013;133:669-76. https://doi.org/10.1016/j.drugalcdep.2013.08.017.
- Byrne AM, Dickson L, Derevensky JL, Gupta R, Lussier I. The application of youth substance use media campaigns to problem gambling: a critical evaluation. J Health Commun 2005;10:681-700. https://doi.org/10.1080/10810730500326658.
- Derzon JH, Lipsey MW, Crano WD, Burgoon M, Oskamp S. Mass Media and Drug Prevention: Classic and Contemporary Theories and Research. Mahwah, NJ: Lawrence Erlbaum Associates; 2002.
- Ellis P, Robinson P, Ciliska D, Armour T, Raina P, Brouwers M, et al. Diffusion and dissemination of evidence-based cancer control interventions. Evid Rep Technol Assess 2003;79:1-5.
- Mozaffarian D, Afshin A, Benowitz NL, Bittner V, Daniels SR, Franch HA, et al. Population approaches to improve diet, physical activity, and smoking habits: a scientific statement from the American Heart Association. Circulation 2012;126:1514-63. https://doi.org/10.1161/CIR.0b013e318260a20b.
- Robinson MN, Tansil KA, Elder RW, Soler RE, Labre MP, Mercer SL, et al. Mass media health communication campaigns combined with health-related product distribution: a community guide systematic review. Am J Prev Med 2014;47:360-71. https://doi.org/10.1016/j.amepre.2014.05.034.
- Young B, Lewis S, Katikireddi SV, Bauld L, Stead M, Angus K, et al. Effectiveness of mass media campaigns to reduce alcohol consumption and harm: a systematic review. Alcohol Alcohol 2018;53:302-16. https://doi.org/10.1093/alcalc/agx094.
- Alcohol-Related Deaths in the UK: Registered In 2015. ONS; 2017.
- The Public Health Burden of Alcohol and the Effectiveness and Cost-Effectiveness of Alcohol Control Policies: An Evidence Review. London: Public Health England; 2016.
- Adult Drinking Habits in Great Britain: 2005 to 2016. Newport: ONS; 2017.
- Public Health England . Local Alcohol Profiles for England: February 2018 Update 2018. www.gov.uk/government/statistics/local-alcohol-profiles-for-england-february-2018-update (accessed 30 April 2018).
- Elder RW, Shults RA, Sleet DA, Nichols JL, Thompson RS, Rajab W. Task Force on Community Preventive Services . Effectiveness of mass media campaigns for reducing drinking and driving and alcohol-involved crashes: a systematic review. Am J Prev Med 2004;27:57-65. https://doi.org/10.1016/j.amepre.2004.03.002.
- Foxcroft DR, Tsertsvadze A. Universal school-based prevention programs for alcohol misuse in young people. Cochrane Database Syst Rev 2011;5. https://doi.org/10.1002/14651858.CD009113.
- Foxcroft DR, Moreira MT, Almeida Santimano NM, Smith LA. Social norms information for alcohol misuse in university and college students. Cochrane Database Syst Rev 2015;1. https://doi.org/10.1002/14651858.CD006748.pub3.
- Quality Assessment Tool for Quantitative Studies. Hamilton, ON: EPHPP; 2010.
- Flynn BS, Worden JK, Bunn JY, Dorwaldt AL, Dana GS, Callas PW. Mass media and community interventions to reduce alcohol use by early adolescents. J Stud Alcohol 2006;67:66-74. https://doi.org/10.15288/jsa.2006.67.66.
- Scheier LM, Grenard JL. Influence of a nationwide social marketing campaign on adolescent drug use. J Health Commun 2010;15:240-71. https://doi.org/10.1080/10810731003686580.
- Barber JJ, Grichting WL. Australia’s media campaign against drug abuse. Int J Addict 1990;25:693-708. https://doi.org/10.3109/10826089009061328.
- Kypri K, Dean J, Kirby S, Harris J, Kake T. ‘Think before you buy under-18s drink’: evaluation of a community alcohol intervention. Drug Alcohol Rev 2005;24:13-20. https://doi.org/10.1080/09595230500102731.
- Lowe JB, Baxter L, Hirokawa R, Pearce E, Peterson JJ. Description of a media campaign about alcohol use during pregnancy. J Stud Alcohol Drugs 2010;71:739-41. https://doi.org/10.15288/jsad.2010.71.739.
- Wallack L, Barrows DC. Evaluating primary prevention: the California ‘winners’ alcohol program. Int Q Community Health Educ 1982;3:307-36. https://doi.org/10.2190/YJDA-24KY-TTUC-9TRA.
- Allamani A, Forni E, Ammannati P, Sani IB, Centurioni A. Alcohol carousel and children’s school drawings as part of a community educational strategy. Subst Use Misuse 2000;35:125-39. https://doi.org/10.3109/10826080009147690.
- Atkinson AM, Sumnall H, Measham F. Depictions of alcohol use in a UK Government partnered online social marketing campaign: Hollyoaks ‘The Morning after the night before’. Drugs 2011;18:454-67.
- Awopetu O, Brimacombe M, Cohen D. Fetal alcohol syndrome disorder pilot media intervention in New Jersey. Can J Clin Pharmacol 2008;15:e124-31.
- Barber JG, Bradshaw R, Walsh C. Reducing alcohol consumption through television advertising. J Consult Clin Psychol 1989;57:613-18. https://doi.org/10.1037/0022-006X.57.5.613.
- Casiro OG, Stanwick RS, Pelech A, Taylor V. Public awareness of the risks of drinking alcohol during pregnancy: the effects of a television campaign. Child Health Committee, Manitoba Medical Association. Can J Public Health 1994;85:23-7.
- Casswell S, Ransom R, Gilmore L. Evaluation of a mass-media campaign for the primary prevention of alcohol-related problems. Health Promot Int 1990;5:9-17. https://doi.org/10.1093/heapro/5.1.9.
- Dixon HG, Pratt IS, Scully ML, Miller JR, Patterson C, Hood R, et al. Using a mass media campaign to raise women’s awareness of the link between alcohol and cancer: cross-sectional pre-intervention and post-intervention evaluation surveys. BMJ Open 2015;5. https://doi.org/10.1136/bmjopen-2014-006511.
- Grønbaek M, Strøger U, Strunge H, Møller L, Graff V, Iversen L. Impact of a 10-year nation-wide alcohol campaign on knowledge of sensible drinking limits in Denmark. Eur J Epidemiol 2001;17:423-7. https://doi.org/10.1023/A:1013765827585.
- Hanson JD, Winberg A, Elliott A. Development of a media campaign on fetal alcohol spectrum disorders for Northern Plains American Indian communities. Health Promot Pract 2012;13:842-7. https://doi.org/10.1177/1524839911404232.
- Kääriäinen J, Aalto M, Kääriäinen M, Seppä K. Audit questionnaire as part of community action against heavy drinking. Alcohol Alcohol 2008;43:442-5. https://doi.org/10.1093/alcalc/agn028.
- Karlsson T, Raitasalo K, Holmila M, Koski-Jännes A, Ollikainen H, Simpura J. The impact of a self-help pamphlet on reducing risk drinking among 30- to 49-year-old men in Helsinki, Finland. Subst Use Misuse 2005;40:1831-47. https://doi.org/10.1080/10826080500318533.
- Kelley K, Stanley L, Edwards R. The impact of a localized anti-alcohol and tobacco media campaign on adolescent females. Soc Market Q 2000;6:39-43. https://doi.org/10.1080/15245004.2000.9961116.
- Plant MA, Pirie F, Kreitman N. Evaluation of the Scottish Health Education Unit’s 1976 campaign on alcoholism. Soc Psychiatry 1979;14:11-24. https://doi.org/10.1007/BF00583569.
- Siriwardhana P, Dawson AH, Abeyasinge R. Acceptability and effect of a community-based alcohol education program in rural Sri Lanka. Alcohol Alcohol 2013;48:250-6. https://doi.org/10.1093/alcalc/ags116.
- Surkan PJ, Dejong W, Herr-Zaya KM, Rodriguez-Howard M, Fay K. A paid radio advertising campaign to promote parent-child communication about alcohol. J Health Commun 2003;8:489-95. https://doi.org/10.1080/713852114.
- Trees K. Mobile media: communicating with and by Indigenous youth about alcohol. Aust Aboriginal Studies 2015;1:97-106.
- van Gemert C, Dietze P, Gold J, Sacks-Davis R, Stoové M, Vally H, et al. The Australian national binge drinking campaign: campaign recognition among young people at a music festival who report risky drinking. BMC Public Health 2011;11. https://doi.org/10.1186/1471-2458-11-482.
- van Leeuwen L, Renes RJ, Leeuwis C. Televised entertainment-education to prevent adolescent alcohol use: perceived realism, enjoyment, and impact. Health Educ Behav 2013;40:193-205. https://doi.org/10.1177/1090198112445906.
- Belaid L, Dumont A, Chaillet N, Zertal A, De Brouwere V, Hounton S, et al. Effectiveness of demand generation interventions on use of modern contraceptives in low- and middle-income countries. Trop Med Int Health 2016;21:1240-54. https://doi.org/10.1111/tmi.12758.
- Flack S, Taylor M, Trueman P. Cost-ffectiveness of Interventions for Smoking Cessation: Mass Media Interventions. Supplementary Report. London: NICE; 2007.
- Jacob V, Chattopadhyay SK, Elder RW, Robinson MN, Tansil KA, Soler RE, et al. Economics of mass media health campaigns with health-related product distribution: a community guide systematic review. Am J Prev Med 2014;47:348-59. https://doi.org/10.1016/j.amepre.2014.05.031.
- Laine J, Kuvaja-Köllner V, Pietilä E, Koivuneva M, Valtonen H, Kankaanpää E. Cost-effectiveness of population-level physical activity interventions: a systematic review. Am J Health Promot 2014;29:71-80. https://doi.org/10.4278/ajhp.131210-LIT-622.
- Lorenc T, Marrero-Guillamón I, Aggleton P, Cooper C, Llewellyn A, Lehmann A, et al. Promoting the uptake of HIV testing among men who have sex with men: systematic review of effectiveness and cost-effectiveness. Sex Transm Infect 2011;87:272-8. https://doi.org/10.1136/sti.2010.048280.
- Mason AR, Carr Hill R, Myers LA, Street AD. Establishing the economics of engaging communities in health promotion: what is desirable, what is feasible?. Crit Pub Health 2008;18:285-97. https://doi.org/10.1080/09581590802277366.
- Vidanapathirana J, Abramson MJ, Forbes A, Fairley C. Mass media interventions for promoting HIV testing. Cochrane Database Syst Rev 2005;3. https://doi.org/10.1002/14651858.CD004775.pub2.
- Raikou M, McGuire A. A Review of the Cost-Effectiveness of Interventions (Specifically Point of Sales Measures and Mass Media) to Prevent the Uptake of Smoking in Young People Under 18 Years Old. London: NICE; n.d.
- Atusingwize E, Lewis S, Langley T. Economic evaluations of tobacco control mass media campaigns: a systematic review. Tob Control 2015;24:320-7. https://doi.org/10.1136/tobaccocontrol-2014-051579.
- Hutchinson P, Wheeler J. The cost-effectiveness of health communication programs: what do we know?. J Health Commun 2006;11:7-45. https://doi.org/10.1080/10810730600973862.
- Kahende JW, Loomis BR, Adhikari B, Marshall L. A review of economic evaluations of tobacco control programs. Int J Environ Res Public Health 2009;6:51-68. https://doi.org/10.3390/ijerph6010051.
- Lantz PM, Jacobson PD, Warner KE, Wasserman J, Pollack HA, Berson J, et al. Investing in youth tobacco control: a review of smoking prevention and control strategies. Tob Control 2000;9:47-63. https://doi.org/10.1136/tc.9.1.47.
- McKinnon RA, Siddiqi SM, Chaloupka FJ, Mancino L, Prasad K. Obesity-related policy/environmental interventions: a systematic review of economic analyses. Am J Prev Med 2016;50:543-9. https://doi.org/10.1016/j.amepre.2015.10.021.
- Wang G, Labarthe D. The cost-effectiveness of interventions designed to reduce sodium intake. J Hypertens 2011;29:1693-9. https://doi.org/10.1097/HJH.0b013e328349ba18.
- Wang G, Bowman BA. Recent economic evaluations of interventions to prevent cardiovascular disease by reducing sodium intake. Curr Atheroscler Rep 2013;15. https://doi.org/10.1007/s11883-013-0349-1.
- Hurley SF, Matthews JP. Cost-effectiveness of the Australian national tobacco campaign. Tob Control 2008;17:379-84. https://doi.org/10.1136/tc.2008.025213.
- Kotz D, Stapleton JA, Owen L, West R. How cost-effective is ‘No Smoking Day’?. Tob Control 2011;20:302-4. https://doi.org/10.1136/tc.2009.034397.
- Brown J, Kotz D, Michie S, Stapleton J, Walmsley M, West R. How effective and cost-effective was the national mass media smoking cessation campaign ‘Stoptober’?. Drug Alcohol Depend 2014;135:52-8. https://doi.org/10.1016/j.drugalcdep.2013.11.003.
- Stevens W, Thorogood M, Kayikki S. Cost-effectiveness of a community anti-smoking campaign targeted at a high risk group in London. Health Promot Int 2002;17:43-50. https://doi.org/10.1093/heapro/17.1.43.
- Raikou M, McGuire A. Cost-Effectiveness of a Mass Media Campaign and a Point of Sale Intervention to Prevent the Uptake of Smoking in Children and Young People: Economic Modelling Report. London: NICE; 2008.
- Ratcliffe J, Cairns J, Platt S. Cost effectiveness of a mass media-led anti-smoking campaign in Scotland. Tob Control 1997;6:104-10. https://doi.org/10.1136/tc.6.2.104.
- Villanti AC, Curry LE, Richardson A, Vallone DM, Holtgrave DR. Analysis of media campaign promoting smoking cessation suggests it was cost-effective in prompting quit attempts. Health Aff 2012;31:2708-16. https://doi.org/10.1377/hlthaff.2012.0277.
- Fishman PA, Ebel BE, Garrison MM, Christakis DA, Wiehe SE, Rivara FP. Cigarette tax increase and media campaign cost of reducing smoking-related deaths. Am J Prev Med 2005;29:19-26. https://doi.org/10.1016/j.amepre.2005.03.004.
- Secker-Walker RH, Worden JK, Holland RR, Flynn BS, Detsky AS. A mass media programme to prevent smoking among adolescents: costs and cost effectiveness. Tob Control 1997;6:207-12. https://doi.org/10.1136/tc.6.3.207.
- Holtgrave DR, Wunderink KA, Vallone DM, Healton CG. Cost-utility analysis of the National truth campaign to prevent youth smoking. Am J Prev Med 2009;36:385-8. https://doi.org/10.1016/j.amepre.2009.01.020.
- Higashi H, Truong KD, Barendregt JJ, Nguyen PK, Vuong ML, Nguyen TT, et al. Cost effectiveness of tobacco control policies in Vietnam: the case of population-level interventions. Appl Health Econ Health Policy 2011;9:183-96. https://doi.org/10.2165/11539640-000000000-00000.
- De Smedt D, De Cocker K, Annemans L, De Bourdeaudhuij I, Cardon G. A cost-effectiveness study of the community-based intervention ‘10 000 Steps Ghent’. Public Health Nutr 2012;15:442-51. https://doi.org/10.1017/S1368980011001716.
- Peterson M, Chandlee M, Abraham A. Cost-effectiveness analysis of a statewide media campaign to promote adolescent physical activity. Health Promot Pract 2008;9:426-33. https://doi.org/10.1177/1524839907313722.
- Ha DA, Chisholm D. Cost-effectiveness analysis of interventions to prevent cardiovascular disease in Vietnam. Health Policy Plan 2011;26:210-22. https://doi.org/10.1093/heapol/czq045.
- Rubinstein A, García Martí S, Souto A, Ferrante D, Augustovski F. Generalized cost-effectiveness analysis of a package of interventions to reduce cardiovascular disease in Buenos Aires, Argentina. Cost Eff Resour Alloc 2009;7. https://doi.org/10.1186/1478-7547-7-10.
- Glanz K, Bishop DB. The role of behavioral science theory in development and implementation of public health interventions. Annu Rev Public Health 2010;31:399-418. https://doi.org/10.1146/annurev.publhealth.012809.103604.
- Ayers B, Myers LB. Do media messages change people’s risk perceptions for binge drinking?. Alcohol Alcohol 2012;47:52-6. https://doi.org/10.1093/alcalc/agr052.
- Shankar B, Brambila-Macias J, Traill B, Mazzocchi M, Capacci S. An evaluation of the UK Food Standards Agency’s salt campaign. Health Econ 2013;22:243-50. https://doi.org/10.1002/hec.2772.
- Brown J, Michie S, Walmsley M, West R. An online documentary film to motivate quit attempts among smokers in the general population (4Weeks2Freedom): a randomized controlled trial. Nicotine Tob Res 2016;18:1093-100. https://doi.org/10.1093/ntr/ntv161.
- Capacci S, Mazzocchi M. Five-a-day, a price to pay: an evaluation of the UK program impact accounting for market forces. J Health Econ 2011;30:87-98. https://doi.org/10.1016/j.jhealeco.2010.10.006.
- Croker H, Lucas R, Wardle J. Cluster-randomised trial to evaluate the ‘Change for Life’ mass media/ social marketing campaign in the UK. BMC Public Health 2012;12. https://doi.org/10.1186/1471-2458-12-404.
- Eves FF, Webb OJ, Griffin C, Chambers J. A multi-component stair climbing promotional campaign targeting calorific expenditure for worksites; a quasi-experimental study testing effects on behaviour, attitude and intention. BMC Public Health 2012;12. https://doi.org/10.1186/1471-2458-12-423.
- Eves FF, Olander EK, Webb OJ, Griffin C, Chambers J. Likening stairs in buildings to climbing a mountain: self-reports of expected effects on stair climbing and objective measures of effectiveness. Psychol Sport Exerc 2012;13:170-6. https://doi.org/10.1016/j.psychsport.2011.11.002.
- Flowers P, McDaid LM, Knussen C. Exposure and impact of a mass media campaign targeting sexual health amongst Scottish men who have sex with men: an outcome evaluation. BMC Public Health 2013;13. https://doi.org/10.1186/1471-2458-13-737.
- Goodwin DM, Peerbhoy D, Murphy R, Stratton G. From design to interpretation: lessons from a public health campaign promoting physical activity. Health Educ J 2014;73:554-65. https://doi.org/10.1177/0017896913508275.
- Jawad M, Abass J, Hariri A, Akl EA. Social media use for public health campaigning in a low resource setting: the case of waterpipe tobacco smoking. Biomed Res Int 2015;2015. https://doi.org/10.1155/2015/562586.
- Langley TE, McNeill A, Lewis S, Szatkowski L, Quinn C. The impact of media campaigns on smoking cessation activity: a structural vector autoregression analysis. Addiction 2012;107:2043-50. https://doi.org/10.1111/j.1360-0443.2012.03958.x.
- Lewis AL, Eves FF. Specific effects of a calorie-based intervention on stair climbing in overweight commuters. Ann Behav Med 2011;42:257-61. https://doi.org/10.1007/s12160-011-9283-z.
- Lewis A, Eves F. Prompt before the choice is made: effects of a stair-climbing intervention in university buildings. Br J Health Psychol 2012;17:631-43. https://doi.org/10.1111/j.2044-8287.2011.02060.x.
- Lewis AL, Eves FF. Prompts to increase stair climbing in stations: the effect of message complexity. J Phys Act Health 2012;9:954-61. https://doi.org/10.1123/jpah.9.7.954.
- Lewis S, Sims M, Richardson S, Langley T, Szatkowski L, McNeill A, et al. The effectiveness of tobacco control television advertisements in increasing the prevalence of smoke-free homes. BMC Public Health 2015;15. https://doi.org/10.1186/s12889-015-2207-2.
- Lyons J, Smith D, Armitage C. LARC: how is the message getting through?. Eur J Contracept Reprod Health Care 2013;18.
- McNeill A, Iringe-Koko B, Bains M, Bauld L, Siggens G, Russell A. Countering the demand for, and supply of, illicit tobacco: an assessment of the ‘North of England Tackling Illicit Tobacco for Better Health’ Programme. Tob Control 2014;23:e44-50. https://doi.org/10.1136/tobaccocontrol-2013-050957.
- Naughton F, Cooper S, Bowker K, Campbell K, Sutton S, Leonardi-Bee J, et al. Adaptation and uptake evaluation of an SMS text message smoking cessation programme (MiQuit) for use in antenatal care. BMJ Open 2015;5. https://doi.org/10.1136/bmjopen-2015-008871.
- Richardson S, Langley T, Szatkowski L, Sims M, Gilmore A, McNeill A, et al. How does the emotive content of televised anti-smoking mass media campaigns influence monthly calls to the NHS Stop Smoking helpline in England?. Prev Med 2014;69:43-8. https://doi.org/10.1016/j.ypmed.2014.08.030.
- Richardson S, McNeill A, Langley TE, Sims M, Gilmore A, Szatkowski L, et al. The impact of televised tobacco control advertising content on campaign recall: evidence from the International Tobacco Control (ITC) United Kingdom survey. BMC Public Health 2014;14. https://doi.org/10.1186/1471-2458-14-432.
- Sims M, Langley T, Lewis S, Richardson S, Szatkowski L, McNeill A, et al. Effectiveness of tobacco control television advertisements with different types of emotional content on tobacco use in England, 2004-2010. Tob Control 2016;25:21-6. https://doi.org/10.1136/tobaccocontrol-2013-051454.
- Sims M, Salway R, Langley T, Lewis S, McNeill A, Szatkowski L, et al. Effectiveness of tobacco control television advertising in changing tobacco use in England: a population-based cross-sectional study. Addiction 2014;109:986-94. https://doi.org/10.1111/add.12501.
- Stautz K, Marteau TM. Viewing alcohol warning advertising reduces urges to drink in young adults: an online experiment. BMC Public Health 2016;16. https://doi.org/10.1186/s12889-016-3192-9.
- Sutherland J, Edwards P, Shankar B, Dangour AD. Fewer adults add salt at the table after initiation of a national salt campaign in the UK: a repeated cross-sectional analysis. Br J Nutr 2013;110:552-8. https://doi.org/10.1017/S0007114512005430.
- Wyness LA, Butriss JL, Stanner SA. Reducing the population’s sodium intake: the UK Food Standards Agency’s salt reduction programme. Public Health Nutr 2012;15:254-61. https://doi.org/10.1017/S1368980011000966.
- Quality Assessment for Observational Cohort Studies. Bethesda, MA: National Heart, Lung and Blood Institute; 2014.
- 10 Questions to Help You Make Sense of Qualitative Research. CASP; 2013.
- Haghpanahan H, Mackay DF, Pell JP, Bell D, Langley T, Haw S. The impact of TV mass media campaigns on calls to a National Quitline and the use of prescribed nicotine replacement therapy: a structural vector autoregression analysis. Addiction 2017;112:1229-37. https://doi.org/10.1111/add.13793.
- Finnegan JR, Viswanath K, Glanz K, Rimer BK, Viswanath K. Health Behavior and Health Education: Theory, Research, and Practice. San Francisco, CA: Jossey-Bass; 2008.
- Griffiths W, Knutson AL. The role of mass media in public health. Am J Public Health Nations Health 1960;50:515-23. https://doi.org/10.2105/AJPH.50.4.515.
- Anker AE, Feeley TH, McCracken B, Lagoe CA. Measuring the effectiveness of mass-mediated health campaigns through meta-analysis. J Health Commun 2016;21:439-56. https://doi.org/10.1080/10810730.2015.1095820.
- The Effectiveness of Public Health Campaigns. HDA Briefing No. 7. London: HDA; 2004.
- Naugle DA, Hornik RC. Systematic review of the effectiveness of mass media interventions for child survival in low- and middle-income countries. J Health Commun 2014;19:190-215. https://doi.org/10.1080/10810730.2014.918217.
- Yadav RP, Kobayashi M. A systematic review: effectiveness of mass media campaigns for reducing alcohol-impaired driving and alcohol-related crashes. BMC Public Health 2015;15. https://doi.org/10.1186/s12889-015-2088-4.
- Snyder LB, Hamilton MA, Mitchell EW, Kiwanuka-Tondo J, Fleming-Milici F, Proctor D. A meta-analysis of the effect of mediated health communication campaigns on behavior change in the United States. J Health Commun 2004;9:71-96. https://doi.org/10.1080/10810730490271548.
- Buykx P, Li J, Gavens L, Hooper L, Lovatt M, Gomes de Matos E, et al. Public awareness of the link between alcohol and cancer in England in 2015: a population-based survey. BMC Public Health 2016;16. https://doi.org/10.1186/s12889-016-3855-6.
- Dunstone K, Brennan E, Slater MD, Dixon HG, Durkin SJ, Pettigrew S, et al. Alcohol harm reduction advertisements: a content analysis of topic, objective, emotional tone, execution and target audience. BMC Public Health 2017;17. https://doi.org/10.1186/s12889-017-4218-7.
- Marsh K, Dolan P, Kempster J, Lugon M. Prioritizing investments in public health: a multi-criteria decision analysis. J Public Health 2013;35:460-6. https://doi.org/10.1093/pubmed/fds099.
- Mosdøl A, Lidal IB, Straumann GH, Vist GE. Targeted Mass Media Interventions Promoting Healthy Behaviours to Reduce Risk of Non-Communicable Diseases in Adult, Ethnic Minorities n.d. www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42015026560 (accessed 27 September 2017).
- Strasburger VC. Committee on Communications, American Academy of Pediatrics. Children, adolescents, and advertising. Pediatrics 2006;118:2563-9. https://doi.org/10.1542/peds.2006-2698.
- Norman J, Kelly B, Boyland E, McMahon A. The impact of marketing and advertising on food behaviours: evaluating the evidence for a causal relationship. Current Nutrition Reports 2016;5:139-49. https://doi.org/10.1007/s13668-016-0166-6.
- Lankford T, Wallace J, Brown D, Soares J, Epping JN, Fridinger F. Analysis of physical activity mass media campaign design. J Phys Act Health 2014;11:1065-9. https://doi.org/10.1123/jpah.2012-0303.
- Allen JA, Duke JC, Davis KC, Kim AE, Nonnemaker JM, Farrelly MC. Using mass media campaigns to reduce youth tobacco use: a review. Am J Health Promot 2015;30:e71-82. https://doi.org/10.4278/ajhp.130510-LIT-237.
- Carson KV, Ameer F, Sayehmiri K, Hnin K, van Agteren JE, Sayehmiri F, et al. Mass media interventions for preventing smoking in young people. Cochrane Database Syst Rev 2017;6. https://doi.org/10.1002/14651858.CD001006.pub3.
- McCoy M, Hargie OD. Evaluating evaluation: implications for assessing quality. Int J Health Care Qual Assur Inc Leadersh Health Serv 2001;14:317-27. https://doi.org/10.1108/09526860110409081.
- Cassidy T, Bowman B, McGrath C, Matzopoulos R. Brief report on a systematic review of youth violence prevention through media campaigns: Does the limited yield of strong evidence imply methodological challenges or absence of effect?. J Adolesc 2016;52:22-6. https://doi.org/10.1016/j.adolescence.2016.07.002.
- Chapman S, Lupton D. The Fight for Public Health: Principles and Practice of Media Advocacy. London: BMJ Publishing; 1994.
- Treno AJ, Breed L, Holder HD, Roeper P, Thomas BA, Gruenewald PJ. Evaluation of media advocacy efforts within a community trial to reduce alcohol-involved injury. Preliminary newspaper results. Eval Rev 1996;20:404-23. https://doi.org/10.1177/0193841X9602000403.
- Wallack L, Dorfman L, Jernigan D, Themba M. Media Advocacy and Public Health: Power for Prevention. Thousand Oaks, CA: Sage; 1993.
- Stead M, Hastings G, Eadie D. The challenge of evaluating complex interventions: a framework for evaluating media advocacy. Health Educ Res 2002;17:351-64. https://doi.org/10.1093/her/17.3.351.
- Clar C, Dyakova M, Curtis K, Dawson C, Donnelly P, Knifton L, et al. Just telling and selling: current limitations in the use of digital media in public health: a scoping review. Public Health 2014;128:1066-75. https://doi.org/10.1016/j.puhe.2014.09.009.
- Carson KV, Brinn MP, Labiszewski NA, Esterman AJ, Chang AB, Smith BJ. Community interventions for preventing smoking in young people. Cochrane Database Syst Rev 2011;7. https://doi.org/10.1002/14651858.CD001291.pub2.
- Wrieden WL, Levy LB. ‘Change4Life Smart Swaps’: quasi-experimental evaluation of a natural experiment. Public Health Nutr 2016;19:2388-92. https://doi.org/10.1017/S1368980016000513.
- O’Kane N, Gough A, Hunter R, McKinley M. Social Media and Public Health Mass Communication Interventions: A Systematic Review of Evaluation Methods 2016. www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42016049280 (accessed 27 September 2017).
- Guse K, Levine D, Martins S, Lira A, Gaarde J, Westmorland W, et al. Interventions using new digital media to improve adolescent sexual health: a systematic review. J Adolesc Health 2012;51:535-43. https://doi.org/10.1016/j.jadohealth.2012.03.014.
- Cugelman B, Thelwall M, Dawes P. Online interventions for social marketing health behavior change campaigns: a meta-analysis of psychological architectures and adherence factors. J Med Internet Res 2011;13. https://doi.org/10.2196/jmir.1367.
- McGloin AF, Eslami S. Digital and social media opportunities for dietary behaviour change. Proc Nutr Soc 2015;74:139-48. https://doi.org/10.1017/S0029665114001505.
- Jane M, Foster J, Hagger M, Pal S. Using new technologies to promote weight management: a randomised controlled trial study protocol. BMC Public Health 2015;15. https://doi.org/10.1186/s12889-015-1849-4.
Appendix 1 Review of reviews example search strategy (review A)
Cumulative Index to Nursing and Allied Health Literature (via EBSCOhost)
Date searched: 5 January 2016.
Date range searched: January 2000 to present.
Search strategy
AB “systematic review” OR TI meta-analysis OR AB meta-analysis OR TX meta-analy* OR TI “systematic literature review” OR AB “systematic literature review” OR TI “meta-synthesis” OR AB “meta-synthesis” OR AB “integrative review” OR AB “integrative research review” OR AB “rapid review” OR TI “evidence based” OR AB “evidence based” OR TX “exclusion criteri*” OR research synthesis OR “narrative synthesis OR narrative review” OR “critical interpretive synthesis” OR “rapid review” OR “scoping review” OR “evidence synthesis” OR “research synthesis” OR “evidence review”
TI media OR AB media OR TI “mass communication” OR AB “mass communication” OR TI “social marketing” OR AB “social marketing” OR TI broadcast* OR AB broadcast* OR (MH “Communications Media”) OR (MH “Social Media”) OR “media” OR health campaigns
Appendix 2 List of reviews excluded from the systematic review of reviews (review A) at the full-text assessment stage
| Reference | Reason for exclusion |
|---|---|
| Adeigbe RT, Baldwin S, Gallion K, Grier S, Ramirez AG. Food and beverage marketing to Latinos: a systematic literature review. Health Educ Behav 2015;42:569–82 | Did not include interventions that met the definition of a mass media interventiona |
| Afshin A, Abioye AI, Ajala ON, Nguyen AB, See KC, Mozaffarian D. Abstract P087: Effectiveness of mass media campaigns for improving dietary behaviors: a systematic review and meta-analysis. Circulation 2013;127(Suppl. 12):AP087 | A dual publication or the review has since been updated |
| Agostinelli G, Grube JW. Alcohol counter-advertising and the media. A review of recent research. Alcohol Res Health 2002;26:15–21 | Did not meet the definition of a systematic reviewb |
| Akers AY, Holland CL, Bost J. Interventions to improve parental communication about sex: a systematic review. Pediatrics 2011;127:494–510. https://doi.org/10.1542/peds.2010-2194 | Did not examine one or more of the relevant health behaviours |
| Allara E, Ferri M, Bo A, Gasparrini A, Faggiano F. Are mass-media campaigns effective in preventing drug use? A Cochrane systematic review and meta-analysis. BMJ Open 2015;5:e007449. https://doi.org/10.1136/bmjopen-2014-007449 | A dual publication or the review has since been updated |
| Allen JA, Duke JC, Davis KC, Kim AE, Nonnemaker JM, Farrelly MC. Using mass media campaigns to reduce youth tobacco use: a review. Am J Health Promot 2015;30:e71–82. https://doi.org/10.4278/ajhp.130510-LIT-237 | Did not meet the definition of a systematic reviewb |
| Anonymous. Population-based smoking cessation strategies: a summary of a select group of evidence-based reviews. Ont Health Technol Assess Ser 2010;10 | Did not meet the definition of a systematic reviewb |
| Arora M, Mathur MR, Singh N. A framework to prevent and control tobacco among adolescents and children: introducing the IMPACT model. Indian J Pediatr 2013;80(Suppl. 1):55–62. https://doi.org/10.1007/s12098-012-0768-y | Did not meet the definition of a systematic reviewb |
| Azagba S, Burhoo P, Chaloupka FJ, Fong GT. Effect of cigarette tax increase in combination with mass media campaign on smoking behaviour in Mauritius: findings from the ITC Mauritius Survey. Tob Control 2015;24(Suppl. 3):iii715. https://doi.org/10.1136/tobaccocontrol-2014-052096 | Did not meet the definition of a systematic reviewb |
| Beauchamp A, Backholer K, Magliano D, Peeters A. The effect of obesity prevention interventions according to socioeconomic position: a systematic review. Obes Rev 2014;15:541–54. https://doi.org/10.1111/obr.12161 | Did not include interventions that met the definition of a mass media interventiona |
| Backinger CL, Fagan P, Matthews E, Grana R. Adolescent and young adult tobacco prevention and cessation: current status and future directions. Tob Control 2003;12(Suppl. 4):IV46–53 | Did not meet the definition of a systematic reviewb |
| Baker PR, Francis DP, Soares J, Weightman AL, Foster C. Community wide interventions for increasing physical activity. Cochrane Database Syst Rev 2015;1:CD008366. https://doi.org/10.1002/14651858.CD008366.pub3 | Did not include interventions that met the definition of a mass media interventiona |
| Balatsoukas P, Kennedy CM, Buchan I, Powell J, Ainsworth J. The role of social network technologies in online health promotion: a narrative review of theoretical and empirical factors influencing intervention effectiveness. J Med Internet Res 2015;17:e141. https://doi.org/10.2196/jmir.3662 | Did not include interventions that met the definition of a mass media interventiona |
| Kiran B, Bhusan G. Scenario of adolescent sexual and reproductive health with opportunities for information communication and technology use in selected South Asian countries. Health Sci J 2015;9:1–7 | Excluded on outcomes data |
| Bardus M, Smith JR, Samaha L, Abraham C. Mobile phone and web 2.0 technologies for weight management: a systematic scoping review. J Med Internet Res 2015;17:e259. https://doi.org/10.2196/jmir.5129 | Excluded on outcomes data |
| Bauman A, Chau J. The role of media in promoting physical activity. J Phys Act Health 2009;6(Suppl. 2):196–210 | Did not meet the definition of a systematic reviewb |
| Beauchamp A, Backholer K, Magliano D, Peeters A. The effect of obesity prevention interventions according to socioeconomic position: a systematic review. Obes Res Clin Pract 2013;7:e48 | Excluded on outcomes data |
| Bélanger-Gravel A, Godin G, Amireault S. A meta-analytic review of the effect of implementation intentions on physical activity. Health Psychol Rev 2013;7:23–54 | Excluded on outcomes data |
| Berg RC, Denison E. Interventions to reduce the prevalence of female genital mutilation/cutting in African countries. Campbell Syst Rev 2012;8:9 | Excluded on outcomes data |
| Bertrand JT, O’Reilly K, Denison J, Anhang R, Sweat M. Systematic review of the effectiveness of mass communication programs to change HIV/AIDS-related behaviors in developing countries. Health Educ Res 2006;21:567–97 | A dual publication or the review has since been updated |
| Bessell TL, McDonald S, Silagy CA, Anderson JN, Hiller JE, Sansom LN. Do Internet interventions for consumers cause more harm than good? A systematic review. Health Expect 2002;5:28–37 | Did not include interventions that met the definition of a mass media interventiona |
| Biddle SJ, Petrolini I, Pearson N. Interventions designed to reduce sedentary behaviours in young people: a review of reviews. Br J Sports Med 2014;48:182–6. https://doi.org/10.1136/bjsports-2013-093078 | Did not meet the definition of a systematic reviewb |
| Blanchette L, Brug J. Determinants of fruit and vegetable consumption among 6-12-year-old children and effective interventions to increase consumption. J Hum Nutr Diet 2005;18:431–43 | Did not include interventions that met the definition of a mass media interventiona |
| Brusse C, Gardner K, McAullay D, Dowden M. Social media and mobile apps for health promotion in Australian Indigenous populations: scoping review. J Med Internet Res 2014;16:e280. https://doi.org/10.2196/jmir.3614 | Did not meet the definition of a systematic reviewb |
| Carins JE, Rundle-Thiele SR. Eating for the better: a social marketing review (2000–2012). Public Health Nutr 2014;17:1628–39. https://doi.org/10.1017/S1368980013001365 | Excluded on outcomes data |
| Carson KV, Brinn MP, Labiszewski NA, Esterman AJ, Chang AB, Smith BJ. Community interventions for preventing smoking in young people. Cochrane Database Syst Rev 2011;7:CD001291. https://doi.org/10.1002/14651858.CD001291.pub2 | Did not include interventions that met the definition of a mass media interventiona |
| Carson KV, Brinn MP, Labiszewski NA, Peters M, Chang AB, Veale A, et al. Interventions for tobacco use prevention in Indigenous youth. Cochrane Database Syst Rev 2012;8:CD009325. https://doi.org/10.1002/14651858.CD009325.pub2 | Did not include interventions that met the definition of a mass media interventiona |
| Cavill JL, Jancey JM, Howat P. Review and recommendations for online physical activity and nutrition programmes targeted at over 40s. Glob Health Promot 2012;19:44–53. https://doi.org/10.1177/1757975912441227 | Did not include interventions that met the definition of a mass media interventiona |
| Cavill N, Bauman A. Changing the way people think about health-enhancing physical activity: do mass media campaigns have a role? J Sports Sci 2004;22:771–90. https://doi.org/10.1080/02640410410001712467 | Did not meet the definition of a systematic reviewb |
| Centers for Disease Control and Prevention. Increasing physical activity. A report on recommendations of the Task Force on Community Preventive Services. MMWR Recomm Rep 2001;50:1–14 | A dual publication or the review has since been updated |
| Chambers SA, Freeman R, Anderson AS, MacGillivray S. Reducing the volume, exposure and negative impacts of advertising for foods high in fat, sugar and salt to children: a systematic review of the evidence from statutory and self-regulatory actions and educational measures. Prev Med 2015;75:32–43. https://doi.org/10.1016/j.ypmed.2015.02.011 | Did not include interventions that met the definition of a mass media interventiona |
| Chang T, Chopra V, Zhang C, Woolford SJ. The role of social media in online weight management: systematic review. J Med Internet Res 2013;15:e262. https://doi.org/10.2196/jmir.2852 | Did not include interventions that met the definition of a mass media interventiona |
| Chavez NR, Shearer LS, Rosenthal SL. Use of digital media technology for primary prevention of STIs/HIV in adolescents and young adults: a systematic review of the literature. J Adolesc Health 2013;52:S84–5 | Did not meet the definition of a systematic reviewb |
| Chou WY, Prestin A, Lyons C, Wen KY. Web 2.0 for health promotion: reviewing the current evidence. Am J Public Health 2013;103:e9–18. https://doi.org/10.2105/AJPH.2012.301071 | Did not include interventions that met the definition of a mass media interventiona |
| Clar C, Dyakova M, Curtis K, Dawson C, Donnelly P, Knifton L, Clarke A. Just telling and selling: current limitations in the use of digital media in public health: a scoping review. Public Health 2014;128:1066–75. https://doi.org/10.1016/j.puhe.2014.09.009 | Did not meet the definition of a systematic reviewb |
| Clayforth C, Pettigrew S, Mooney K, Lansdorp-Vogelaar I, Rosenberg M, Slevin T. A cost-effectiveness analysis of online, radio and print tobacco control advertisements targeting 25-39 year-old males. Aust N Z J Public Health 2014;38:270–4. https://doi.org/10.1111/1753-6405.12175 | Did not meet the definition of a systematic reviewb |
| Cugelman B, Thelwall M, Dawes P. Online interventions for social marketing health behavior change campaigns: a meta-analysis of psychological architectures and adherence factors. J Med Internet Res 2011;13:e17. https://doi.org/10.2196/jmir.1367 | Excluded by another of the criteria |
| Dalziel K, Segal L. Time to give nutrition interventions a higher profile: cost-effectiveness of 10 nutrition interventions. Health Promot Int 2007;22:271–83 | Did not meet the definition of a systematic reviewb |
| De Bruijn A, Angus K, Gordon R, Hastings G, Anderson P. Impact of alcohol advertising and media exposure on adolescent alcohol use: a systematic review of longitudinal studies. Alcohol Alcohol 2009;44:229–43 | Did not include interventions that met the definition of a mass media interventiona |
| De Leon E, Fuentes LW, Cohen JE. Characterizing periodic messaging interventions across health behaviors and media: systematic review. J Med Internet Res 2014;16:e93. https://doi.org/10.2196/jmir.2837 | Excluded on outcomes data |
| DeJong W. The role of mass media campaigns in reducing high-risk drinking among college students. J Stud Alcohol Suppl 2002;14:182–92 | Did not meet the definition of a systematic reviewb |
| Ditter SM, Elder RW, Shults RA, Sleet DA, Compton R, Nichols JL, Task Force on Community Preventive Services. Effectiveness of designated driver programs for reducing alcohol-impaired driving: a systematic review. Am J Prev Med 2005;28(Suppl. 5):280–7 | Did not examine one or more of the relevant health behaviours |
| Durkin S, Brennan E, Wakefield M. Mass media campaigns to promote smoking cessation among adults: an integrative review. Tob Control 2012;21:127–38. https://doi.org/10.1136/tobaccocontrol-2011-050345 | Did not meet the definition of a systematic reviewb |
| Ekpu VU, Brown AK. The economic impact of smoking and of reducing smoking prevalence: review of evidence. Tob Use Insights 2015;8:1–35. https://doi.org/10.4137/TUI.S15628 | Did not meet the definition of a systematic reviewb |
| Elder JP. Preventing smoking in multiethnic communities. Am J Health Behav 2001;25:200–5 | Did not meet the definition of a systematic reviewb |
| Elder RW, Shults RA, Sleet DA, Nichols JL, Thompson RS, Rajab W. Task Force on Community Preventive Services. Effectiveness of mass media campaigns for reducing drinking and driving and alcohol-involved crashes: a systematic review. Am J Prev Med 2004;27:57–65. https://doi.org/10.1016/j.amepre.2004.03.002 | Did not examine one or more of the relevant health behaviours |
| Escobar-Chaves SL, Tortolero SR, Markham CM, Low BJ, Eitel P, Thickstun P. Impact of the media on adolescent sexual attitudes and behaviors. Pediatrics 2005;116:303–26 | Did not include interventions that met the definition of a mass media interventiona |
| Evans WD, Horn KA, Gray T. Systematic review to inform dual tobacco use prevention. Pediatr Clin North Am 2015;62:1159–72. https://doi.org/10.1016/j.pcl.2015.05.003 | Excluded on outcomes data |
| Fjeldsoe BS, Marshall AL, Miller YD. Behavior change interventions delivered by mobile telephone short-message service. Am J Prev Med 2009;36:165–73. https://doi.org/10.1016/j.amepre.2008.09.040 | Did not include interventions that met the definition of a mass media interventiona |
| Flay BR. Approaches to substance use prevention utilizing school curriculum plus social environment change. Addict Behav 2000;25:861–85 | Did not meet the definition of a systematic reviewb |
| Flynn BS, Worden JK, Bunn JY, Solomon LJ, Ashikaga T, Connolly SW, Ramirez AG. Mass media interventions to reduce youth smoking prevalence. Am J Prev Med 2010;39:53–62. https://doi.org/10.1016/j.amepre.2010.03.008 | Did not meet the definition of a systematic reviewb |
| Foxcroft DR, Tsertsvadze A. Universal multi-component prevention programs for alcohol misuse in young people. Cochrane Database Syst Rev 2011;9:CD009307. https://doi.org/10.1002/14651858.CD009307 | Did not include interventions that met the definition of a mass media interventiona |
| Free C, Phillips G, Galli L, Watson L, Felix L, Edwards P, et al. The effectiveness of mobile-health technology-based health behaviour change or disease management interventions for health care consumers: a systematic review. PLOS Med 2013;10:e1001362. https://doi.org/10.1371/journal.pmed.1001362 | Did not include interventions that met the definition of a mass media interventiona |
| Friend K, Levy DT. Reductions in smoking prevalence and cigarette consumption associated with mass-media campaigns. Health Educ Res 2002;17:85–98 | Did not meet the definition of a systematic reviewb |
| Gavin LE, Williams JR, Rivera MI, Lachance CR. Programs to strengthen parent-adolescent communication about reproductive health: a systematic review. Am J Prev Med 2015;49(Suppl. 2):65–72. https://doi.org/10.1016/j.amepre.2015.03.022 | Did not include interventions that met the definition of a mass media interventiona |
| Gibbons MC. Personal health and consumer informatics. The impact of health oriented social media applications on health outcomes. Yearb Med Inform 2013;8:159–61 | Did not include interventions that met the definition of a mass media interventiona |
| Gittelsohn J, Lee-Kwan SH, Batorsky B. Community-based interventions in prepared-food sources: a systematic review. Prev Chronic Dis 2013;10:E180. https://doi.org/10.5888/pcd10.130073 | Did not include interventions that met the definition of a mass media interventiona |
| Graham AL, Milner P, Saul JE, Pfaff L. Online advertising as a public health and recruitment tool: comparison of different media campaigns to increase demand for smoking cessation interventions. J Med Internet Res 2008;10:e50. https://doi.org/10.2196/jmir.1001 | Did not meet the definition of a systematic reviewb |
| Guse K, Levine D, Martins S, Lira A, Gaarde J, Westmorland W, Gilliam M. Interventions using new digital media to improve adolescent sexual health: a systematic review. J Adolesc Health 2012;51:535–43. https://doi.org/10.1016/j.jadohealth.2012.03.014 | Excluded on outcomes data |
| Hackman CL, Knowlden AP. Theory of reasoned action and theory of planned behavior-based dietary interventions in adolescents and young adults: a systematic review. Adolesc Health Med Ther 2014;5:101–14. https://doi.org/10.2147/AHMT.S56207 | Did not include interventions that met the definition of a mass media interventiona |
| Hamel LM, Robbins LB. Computer- and web-based interventions to promote healthy eating among children and adolescents: a systematic review. J Adv Nurs 2013;69:16–30. https://doi.org/10.1111/j.1365-2648.2012.06086.x | Did not include interventions that met the definition of a mass media interventiona |
| Hamm MP, Shulhan J, Williams G, Milne A, Scott SD, Hartling L. A systematic review of the use and effectiveness of social media in child health. BMC Pediatr 2014;14:138. https://doi.org/10.1186/1471-2431-14-138 | Did not include interventions that met the definition of a mass media interventiona |
| Hammond D, Wakefield M, Durkin S, Brennan E. Tobacco packaging and mass media campaigns: research needs for Articles 11 and 12 of the WHO Framework Convention on Tobacco Control. Nicotine Tob Res 2013;15:817–31. https://doi.org/10.1093/ntr/nts202 | Did not meet the definition of a systematic reviewb |
| Heath GW, Parra DC, Sarmiento OL, Andersen LB, Owen N, Goenka S, et al. Evidence-based intervention in physical activity: lessons from around the world. Lancet 2012;380:272–81. https://doi.org/10.1016/S0140-6736(12)60816-2 | Did not meet the definition of a systematic reviewb |
| Hieftje K, Edelman EJ, Camenga DR, Fiellin LE. Electronic media-based health interventions promoting behavior change in youth: a systematic review. JAMA Pediatr 2013;167:574–80. https://doi.org/10.1001/jamapediatrics.2013.1095 | Excluded by another of the criteria |
| Hoffman SJ, Tan C. Overview of systematic reviews on the health-related effects of government tobacco control policies. BMC Public Health 2015;15:744. https://doi.org/10.1186/s12889-015-2041-6 | Did not meet the definition of a systematic reviewb |
| Hopkins DP, Briss PA, Ricard CJ, Husten CG, Carande-Rulis VG, Fielding JE, et al. Reviews of evidence regarding interventions to reduce tobacco use and exposure to environmental tobacco smoke. Am J Prev Med 2001;20:16–66 | Did not meet the definition of a systematic reviewb |
| Hopson L, Wodarski J, Tang N. The effectiveness of electronic approaches to substance abuse prevention for adolescents. J Evid Inf Soc Work 2015;12:310–22 | Did not include interventions that met the definition of a mass media interventiona |
| Hou SI, Charlery SA, Roberson K. Systematic literature review of Internet interventions across health behaviors. Health Psychol Behav Med 2014;2:455–81. https://doi.org/10.1080/21642850.2014.895368 | Did not include interventions that met the definition of a mass media interventiona |
| Jackson NW, Howes FS, Gupta S, Doyle JL, Waters E. Interventions implemented through sporting organisations for increasing participation in sport. Cochrane Database Syst Rev 2005;2:CD004812. https://doi.org/10.1002/14651858.CD004812.pub2 | A dual publication or the review has since been updated |
| Jacob V, Chattopadhyay SK, Elder RW, Robinson MN, Tansil KA, Soler RE, et al. Economics of mass media health campaigns with health-related product distribution: a community guide systematic review. Am J Prev Med 2014;47:348–59. https://doi.org/10.1016/j.amepre.2014.05.031 | A dual publication or the review has since been updated |
| Jacobs MA, Cobb CO, Abroms L, Graham AL. Facebook apps for smoking cessation: a review of content and adherence to evidence-based guidelines. J Med Internet Res 2014;16:e205. https://doi.org/10.2196/jmir.3491 | Did not meet the definition of a systematic reviewb |
| Janssen MM, Mathijssen JJ, van Bon-Martens MJ, van Oers HA, Garretsen HF. Effectiveness of alcohol prevention interventions based on the principles of social marketing: a systematic review. Subst Abuse Treat Prev Policy 2013;8:18. https://doi.org/10.1186/1747-597X-8-18 | Did not meet the definition of a systematic reviewb |
| Jenkins A, Christensen H, Walker JG, Dear K. The effectiveness of distance interventions for increasing physical activity: a review. Am J Health Promot 2009;24:102–17. https://doi.org/10.4278/ajhp.0801158 | Did not include interventions that met the definition of a mass media interventiona |
| Jepson RG, Harris FM, Platt S, Tannahill C. The effectiveness of interventions to change six health behaviours: a review of reviews. BMC Public Health 2010;10:538. https://doi.org/10.1186/1471-2458-10-538 | Excluded by another of the criteria |
| Jones K, Eathington P, Baldwin K, Sipsma H. The impact of health education transmitted via social media or text messaging on adolescent and young adult risky sexual behavior: a systematic review of the literature. Sex Transm Dis 2014;41:413–19. https://doi.org/10.1097/OLQ.0000000000000146 | Did not examine one or more of the relevant health behaviours |
| Jones L, Bates G, Downing J, Sumnall H, Bellis MA. A Review of the Effectiveness and Cost Effectiveness of Alcohol and Sex and Relationship Education for all Children and Young People Aged 5–19 Years in Community Settings. Liverpool: Centre for Public Health, Liverpool John Moores University; 2010 | Excluded by another of the criteria |
| Kabir Z, Alpert HR, Goodman PG, Haw S, Behm I, Connolly GN, et al. Effect of smoke-free home and workplace policies on second-hand smoke exposure levels in children: an evidence summary. Pediatric Health 2010;4:391–403 | Did not include interventions that met the definition of a mass media interventiona |
| Bastien S, Kajula LJ, Muhwezi WW. A review of studies of parent-child communication about sexuality and HIV/AIDS in sub-Saharan Africa. Reprod Health 2011;8:25. https://doi.org/10.1186/1742-4755-8-25 | Did not include interventions that met the definition of a mass media interventiona |
| Kang M, Skinner R, Usherwood T. Interventions for young people in Australia to reduce HIV and sexually transmissible infections: a systematic review. Sex Health 2010;7:107–28. https://doi.org/10.1071/SH09079 | Did not meet the definition of a systematic reviewb |
| Kelley MJ, McCrory DC. Prevention of lung cancer: summary of published evidence. Chest 2003;123(Suppl. 1):50–9 | Did not meet the definition of a systematic reviewb |
| Kelly SA, Melnyk BM. Systematic review of multicomponent interventions with overweight middle adolescents: implications for clinical practice and research. Worldviews Evid Based Nurs 2008;5:113–35. https://doi.org/10.1111/j.1741-6787.2008.00131.x | Did not include interventions that met the definition of a mass media interventiona |
| Cole-Lewis H, Kershaw T. Text messaging as a tool for behavior change in disease prevention and management. Epidemiol Rev 2010;32:56–69. https://doi.org/10.1093/epirev/mxq004 | Excluded by another of the criteria |
| Kesten JM, Griffiths PL, Cameron N. A systematic review to determine the effectiveness of interventions designed to prevent overweight and obesity in pre-adolescent girls. Obes Rev 2011;12:997–1021. https://doi.org/10.1111/j.1467-789X.2011.00919.x | Excluded by another of the criteria |
| Knai C, Pomerleau J, Lock K, McKee M. Getting children to eat more fruit and vegetables: a systematic review. Prev Med 2006;42:85–95 | Did not include interventions that met the definition of a mass media interventiona |
| Kraak VI, Story M, Wartella EA. Government and school progress to promote a healthful diet to American children and adolescents: a comprehensive review of the available evidence. Am J Prev Med 2012;42:250–62. https://doi.org/10.1016/j.amepre.2011.10.025 | Excluded on outcomes data |
| Laine J, Kuvaja-Köllner V, Pietilä E, Koivuneva M, Valtonen H, Kankaanpää E. Cost-effectiveness of population-level physical activity interventions: a systematic review. Am J Health Promot 2014;29:71–80. https://doi.org/10.4278/ajhp.131210-LIT-622 | Excluded on outcomes data |
| Laranjo L, Arguel A, Neves AL, Gallagher AM, Kaplan R, Mortimer N, et al. The influence of social networking sites on health behavior change: a systematic review and meta-analysis. J Am Med Inform Assoc 2015;22:243–56. https://doi.org/10.1136/amiajnl-2014-002841 | Did not include interventions that met the definition of a mass media interventiona |
| Lopez LM, Steiner M, Grimes DA, Hilgenberg D, Schulz KF. Strategies for communicating contraceptive effectiveness. Cochrane Database Syst Rev 2013;4:CD006964. https://doi.org/10.1002/14651858.CD006964.pub3 | Did not include interventions that met the definition of a mass media interventiona |
| Lorenc T, Marrero-Guillamón I, Aggleton P, Cooper C, Llewellyn A, Lehmann A, Lindsay C. Promoting the uptake of HIV testing among men who have sex with men: systematic review of effectiveness and cost-effectiveness. Sex Transm Infect 2011;87:272–8. https://doi.org/10.1136/sti.2010.048280 | Did not include interventions that met the definition of a mass media interventiona |
| Macdonald HM. Interventions to promote walking: a review. Clin J Sport Med 2007;17:516–17. https://doi.org/10.1097/01.jsm.0000299225.75020.b7 | A dual publication or the review has since been updated |
| Macfarlane A. What are the Main Factors that Influence the Implementation of Disease Prevention and Health Promotion Programmes in Children and Adolescents? Copenhagen: WHO Regional Office for Europe’s Health Evidence Network; 2005 | Did not meet the definition of a systematic reviewb |
| Magnée T, Burdorf A, Brug J, Kremers SP, Oenema A, van Assema P, et al. Equity-specific effects of 26 Dutch obesity-related lifestyle interventions. Am J Prev Med 2013;44:e57–66. https://doi.org/10.1016/j.amepre.2012.11.041 | Excluded by another of the criteria |
| Maher CA, Lewis LK, Ferrar K, Marshall S, De Bourdeaudhuij I, Vandelanotte C. Are health behavior change interventions that use online social networks effective? A systematic review. J Med Internet Res 2014;16:e40. https://doi.org/10.2196/jmir.2952 | Did not include interventions that met the definition of a mass media interventiona |
| Manhas M, Kuo MH. Information technologies to improve public health: a systematic review. Stud Health Technol Inform 2015;208:258–63 | Did not examine one or more of the relevant health behaviours |
| Marlatt GA, Witkiewitz K. Harm reduction approaches to alcohol use: health promotion, prevention, and treatment. Addict Behav 2002;27:867–86 | Did not meet the definition of a systematic reviewb |
| Marshall AL, Owen N, Bauman AE. Mediated approaches for influencing physical activity: update of the evidence on mass media, print, telephone and website delivery of interventions. J Sci Med Sport 2004;7(Suppl. 1):74–80 | Did not meet the definition of a systematic reviewb |
| Martineau F, Tyner E, Lorenc T, Petticrew M, Lock K. Population-level interventions to reduce alcohol-related harm: an overview of systematic reviews. Prev Med 2013;57:278–96. https://doi.org/10.1016/j.ypmed.2013.06.019 | Did not meet the definition of a systematic reviewb |
| Lee JG, Matthews AK, McCullen CA, Melvin CL. Promotion of tobacco use cessation for lesbian, gay, bisexual, and transgender people: a systematic review. Am J Prev Med 2014;47:823–31. https://doi.org/10.1016/j.amepre.2014.07.051 | Did not meet the definition of a systematic reviewb |
| McAfee TA. Quitlines a tool for research and dissemination of evidence-based cessation practices. Am J Prev Med 2007;33(Suppl. 6):357–67 | Did not include interventions that met the definition of a mass media interventiona |
| Momin B, Neri A, McCausland K, Duke J, Hansen H, Kahende J, et al. Traditional and innovative promotional strategies of tobacco cessation services: a review of the literature. J Community Health 2014;39:800–9. https://doi.org/10.1007/s10900-014-9825-y | Did not meet the definition of a systematic reviewb |
| Montague E, Perchonok J. Health and wellness technology use by historically underserved health consumers: systematic review. J Med Internet Res 2012;14:e78. https://doi.org/10.2196/jmir.2095 | Excluded by another of the criteria |
| Montano D, Hoven H, Siegrist J. Effects of organisational-level interventions at work on employees’ health: a systematic review. BMC Public Health 2014;14:135. https://doi.org/10.1186/1471-2458-14-135 | Did not examine one or more of the relevant health behaviours |
| Montoya ID, Atkinson J, McFaden WC. Best characteristics of adolescent gateway drug prevention programmes. J Addict Nurs 2003;14:75–83 | Excluded by another of the criteria |
| Müller AM, Khoo S. Non-face-to-face physical activity interventions in older adults: a systematic review. Int J Behav Nutr Phys Act 2014;11:35 | Excluded on outcomes data |
| Naugle DA, Hornik RC. Systematic review of the effectiveness of mass media interventions for child survival in low- and middle-income countries. J Health Commun 2014;19(Suppl. 1):190–215. https://doi.org/10.1080/10810730.2014.918217 | Did not examine one or more of the relevant health behaviours |
| Neville S, Adams J, Holdershaw J. Social marketing campaigns that promote condom use among MSM: a literature review. Nurs Prax N Z 2014;30:5–16 | Did not meet the definition of a systematic reviewb |
| Nguyen B, Kornman KP, Baur LA. A review of electronic interventions for prevention and treatment of overweight and obesity in young people. Obes Rev 2011;12:e298–314 | Did not include interventions that met the definition of a mass media interventiona |
| Niederdeppe J, Kuang X, Crock B, Skelton A. Media campaigns to promote smoking cessation among socioeconomically disadvantaged populations: what do we know, what do we need to learn, and what should we do now? Soc Sci Med 2008;67:1343–55. https://doi.org/10.1016/j.socscimed.2008.06.037 | Did not meet the definition of a systematic reviewb |
| Nocon M, Müller-Riemenschneider F, Nitzschke K, Willich SN. Review article: increasing physical activity with point-of-choice prompts – a systematic review. Scand J Public Health 2010;38:633–8. https://doi.org/10.1177/1403494810375865 | Did not meet the definition of a systematic reviewb |
| Nour MM, Chen J, Allman-Farinelli M. Efficacy and external validity of electronic and mobile phone-based interventions promoting vegetable intake in young adults: a systematic review protocol. JMIR Res Protoc 2015;4:e92. https://doi.org/10.2196/resprot.4665 | Did not meet the definition of a systematic reviewb |
| O’Dea J. School-based health education strategies for the improvement of body image and prevention of eating problems: an overview of safe and successful interventions. Health Education 2005;105:11–33 | Did not include interventions that met the definition of a mass media interventiona |
| Bertrand JT, O’Reilly K, Denison J, Anhang R, Sweat M. Systematic review of the effectiveness of mass communication programs to change HIV/AIDS-related behaviors in developing countries. Health Educ Res 2006;21:567–97 | Excluded by another of the criteria |
| Poorman E, Gazmararian J, Parker RM, Yang B, Elon L. Use of text messaging for maternal and infant health: a systematic review of the literature. Matern Child Health J 2015;19:969–89. https://doi.org/10.1007/s10995-014-1595-8 | Did not meet the definition of a systematic reviewb |
| Priest N, Armstrong R, Doyle J, Waters E. Interventions implemented through sporting organisations for increasing participation in sport. Cochrane Database Syst Rev 2008;3:CD004812. https://doi.org/10.1002/14651858.CD004812.pub3 | Excluded on outcomes data |
| Primack BA, Carroll MV, McNamara M, Klem ML, King B, Rich M, et al. Role of video games in improving health-related outcomes: a systematic review. Am J Prev Med 2012;42:630–8. https://doi.org/10.1016/j.amepre.2012.02.023 | Excluded by another of the criteria |
| Purcell KR, O’Rourke K, Rivis M. Tobacco control approaches and inequity – how far have we come and where are we going? Health Promot Int 2015;30(Suppl. 2):ii89–101. https://doi.org/10.1093/heapro/dav075 | Did not meet the definition of a systematic reviewb |
| Scher L, Maynard RA, Stagner M. Interventions intended to reduce pregnancy-related outcomes among adolescents: a systematic review. Campbell Syst Rev 2006;2:2 | Did not include interventions that met the definition of a mass media interventiona |
| Shamblen SR, Derzon JH. A preliminary study of the population-adjusted effectiveness of substance abuse prevention programming: towards making IOM program types comparable. J Prim Prev 2009;30:89–107. https://doi.org/10.1007/s10935-009-0168-x | Excluded by another of the criteria |
| Shepherd J, Harden A, Rees R, Brunton G, Garcia J, Oliver S, Oakley A. Young people and healthy eating: a systematic review of research on barriers and facilitators. Health Educ Res 2002;165 | Did not include interventions that met the definition of a mass media interventiona |
| Short CE, James EL, Plotnikoff RC, Girgis A. Efficacy of tailored-print interventions to promote physical activity: a systematic review of randomised trials. Int J Behav Nutr Phys Act 2011;8:113. https://doi.org/10.1186/1479-5868-8-113 | Did not include interventions that met the definition of a mass media interventiona |
| Shults RA, Elder RW, Nichols JL, Sleet DA, Compton R, Chattopadhyay SK, Task Force on Community Preventive Services. Effectiveness of multicomponent programs with community mobilization for reducing alcohol-impaired driving. Am J Prev Med 2009;37:360–71. https://doi.org/10.1016/j.amepre.2009.07.005 | Did not examine one or more of the relevant health behaviours |
| Silver MZ. Efficacy of anti-tobacco mass media campaigns on adolescent tobacco use. Pediatr Nurs 2001;27:293–6 | Did not meet the definition of a systematic reviewb |
| LaCroix JM, Snyder LB, Huedo-Medina TB, Johnson BT. Effectiveness of mass media interventions for HIV prevention, 1986-2013: a meta-analysis. J Acquir Immune Defic Syndr 2014;66(Suppl. 3):329–40. https://doi.org/10.1097/QAI.0000000000000230 | Excluded by another of the criteria |
| Snyder LB, Hamilton MA. A Meta-Analysis of U.S. Health Campaign Effects on Behavior: Emphasize Enforcement, Exposure, and New Information, and Beware the Secular Trend. In Hornik RC (editor). Public Health Communication: Evidence for Behavior Change. Mahwah, NJ: Lawrence Erlbaum Associates, Inc.; 2002. pp. 357–83 | Excluded by another of the criteria |
| Snyder LB, Hamilton MA, Mitchell EW, Kiwanuka-Tondo J, Fleming-Milici F, Proctor D. A meta-analysis of the effect of mediated health communication campaigns on behavior change in the United States. J Health Commun 2004;9(Suppl. 1):71–96 | Did not meet the definition of a systematic reviewb |
| Sowden A, Arblaster L. Community interventions for preventing smoking in young people. Cochrane Database Syst Rev 2000;2:CD001291 | A dual publication or the review has since been updated |
| Sowden AJ, Arblaster L. Mass media interventions for preventing smoking in young people. Cochrane Database Syst Rev 2000;2:CD001006 | A dual publication or the review has since been updated |
| Sreevatsava M, Narayan KM, Cunningham SA. Evidence for interventions to prevent and control obesity among children and adolescents: its applicability to India. Indian J Pediatr 2013;80(Suppl. 1):115–22. https://doi.org/10.1007/s12098-012-0881-y | Did not meet the definition of a systematic reviewb |
| Stead M, Gordon R, Angus K, McDermott L. A systematic review of social marketing effectiveness. Health Education 2007;107:126–91 | Excluded on outcomes data |
| Thomas J, Sutcliffe K, Harden A, Oakley A, Oliver S, Rees R, et al. Children and Healthy Eating: a Systematic Review of Barriers and Facilitators. London: EPPI; 2003 | Did not include interventions that met the definition of a mass media interventiona |
| Thomas R, Perera R. School-based programmes for preventing smoking. Cochrane Database Syst Rev 2006;3:CD001293 | Did not include interventions that met the definition of a mass media interventiona |
| Thomson G, Wilson N, Howden-Chapman P. Population level policy options for increasing the prevalence of smokefree homes. J Epidemiol Community Health 2006;60:298–304 | Did not meet the definition of a systematic reviewb |
| Carter MW, Tregear ML, Moskosky SB. Community education for family planning in the U.S.: a systematic review. Am J Prev Med 2015;49:S107–15 | Excluded by another of the criteria |
| Vélez LF, Sanitato M, Barry D, Alilio M, Apfel F, Coe G, et al. The role of health systems and policy in producing behavior and social change to enhance child survival and development in low- and middle-income countries: an examination of the evidence. J Health Commun 2014;19(Suppl. 1):89–121. https://doi.org/10.1080/10810730.2014.939313 | Did not include interventions that met the definition of a mass media interventiona |
| Vidanapathirana J, Abramson MJ, Forbes A, Fairley C. Mass media interventions for promoting HIV testing. Cochrane Database Syst Rev 2005;3:CD004775. https://doi.org/10.1002/14651858.CD004775.pub2 | Did not include interventions that met the definition of a mass media interventiona |
| Villanti AC, McKay HS, Abrams DB, Holtgrave DR, Bowie JV. Smoking-cessation interventions for U.S. young adults: a systematic review. Am J Prev Med 2010;39:564–74. https://doi.org/10.1016/j.amepre.2010.08.009 | Did not include interventions that met the definition of a mass media interventiona |
| Vuori I. Promoting cycling: a review of interventions. Clin J Sport Med 2011;21:542–4 | A dual publication or the review has since been updated |
| Wakefield M, Chaloupka F. Effectiveness of comprehensive tobacco control programmes in reducing teenage smoking in the USA. Tob Control 2000;9:177–86 | Did not meet the definition of a systematic reviewb |
| Wakhisi AS, Allotey P, Dhillon N, Reidpath DD. The effectiveness of social marketing in reduction of teenage pregnancies: a review of studies in developed countries. Soc Mar Q 2011;17:56–90 | Did not include interventions that met the definition of a mass media interventiona |
| Webb OJ, Eves FF, Kerr J. A statistical summary of mall-based stair-climbing interventions. J Phys Act Health 2011;8:558–65 | Did not meet the definition of a systematic reviewb |
| Webb TL, Joseph J, Yardley L, Michie S. Using the internet to promote health behavior change: a systematic review and meta-analysis of the impact of theoretical basis, use of behavior change techniques, and mode of delivery on efficacy. J Med Internet Res 2010;12:e4. https://doi.org/10.2196/jmir.1376 | Did not include interventions that met the definition of a mass media interventiona |
| Wei C, Herrick A, Raymond HF, Anglemyer A, Gerbase A, Noar SM. Social marketing interventions to increase HIV/STI testing uptake among men who have sex with men and male-to-female transgender women. Cochrane Database Syst Rev 2011;9:CD009337. https://doi.org/10.1002/14651858.CD009337 | Did not include interventions that met the definition of a mass media interventiona |
| Williams DM, Matthews CE, Rutt C, Napolitano MA, Marcus BH. Interventions to increase walking behavior. Med Sci Sports Exerc 2008;40(Suppl. 7):567–73. https://doi.org/10.1249/MSS.0b013e31817c7006 | Did not meet the definition of a systematic reviewb |
| Williams G, Hamm MP, Shulhan J, Vandermeer B, Hartling L. Social media interventions for diet and exercise behaviours: a systematic review and meta-analysis of randomised controlled trials. BMJ Open 2014;4:e003926. https://doi.org/10.1136/bmjopen-2013-003926 | Excluded by another of the criteria |
| Xiao Z, Noar SM, Zeng L. Systematic review of HIV prevention interventions in China: a health communication perspective. Int J Public Health 2014;59:123–42. https://doi.org/10.1007/s00038-013-0467-0 | Excluded on outcomes data |
| Yadav RP, Kobayashi M. A systematic review: effectiveness of mass media campaigns for reducing alcohol-impaired driving and alcohol-related crashes. BMC Public Health 2015;15:857. https://doi.org/10.1186/s12889-015-2088-4 | Did not examine one or more of the relevant health behaviours |
| Yamada J. Review: health education interventions offering information plus sexual negotiation skill development promote increased condom use in women [commentary on Shepherd J, Weston R, Peersman G, et al. Interventions for encouraging sexual lifestyles and]. Evid Based Nurs 2000;16-16 1p | Excluded by another of the criteria |
| Yancey AK, Kumanyika SK, Ponce NA, McCarthy WJ, Fielding JE, Leslie JP, Akbar J. Population-based interventions engaging communities of color in healthy eating and active living: a review. Prev Chronic Dis 2004;1:A09 | Did not meet the definition of a systematic reviewb |
| Yang L, Sahlqvist S, McMinn A, Griffin SJ, Ogilvie D. Interventions to promote cycling: systematic review. BMJ 2010;341:c5293. https://doi.org/10.1136/bmj.c5293 | Excluded on outcomes data |
| Yonker LM, Zan S, Scirica CV, Jethwani K, Kinane TB. ‘Friending’ teens: systematic review of social media in adolescent and young adult health care. J Med Internet Res 2015;17:e4. https://doi.org//jmir.3692 | Excluded on outcomes data |
Appendix 3 Summary of the results of the Risk Of Bias In Systematic reviews assessment (low or high risk of bias) for all inclusions in the review of reviews (review A)
| Review (first author and year) | ROBIS28 results | ||||
|---|---|---|---|---|---|
| Phase 2 | Phase 3 | ||||
| Study eligibility criteria | Identification and selection of studies | Data collection and study appraisal | Synthesis and findings | Risk of bias in the review | |
| Abioye (2013)55 | Low | Low | High | Low | Low |
| Bala (2013)27 | Low | Low | Low | Low | Low |
| Bertrand (2006)46 | Low | Low | Low | High | Low |
| Brinn (2010)35 | Low | Low | Low | Low | Low |
| Brown (2012)56 | High | High | Low | High | High |
| Brown (2014)37 | High | High | Low | High | High |
| Brown (2014)36 | High | High | Low | Unclear | High |
| Byrne (2005)65 | Low | Low | High | High | High |
| Carter (2015)47 | Low | Low | Low | Low | Low |
| de Kleijn (2015)38 | Low | High | Low | High | High |
| Derzon (2002)66 | Low | Low | High | High | High |
| Ellis (2003)67 | Low | Low | Low | Low | Low |
| Ferri (2013)62 | Low | Low | Low | Low | Low |
| Finlay (2005)57 | High | High | High | High | High |
| French (2014)48 | Low | Low | Low | Low | Low |
| Gould (2013)39 | Low | Low | Low | Low | Low |
| Grilli (2000)49 | Low | Low | Low | Low | Low |
| Guillaumier (2012)40 | Low | Low | Unclear | Low | Low |
| Hemsing (2012)41 | High | Low | Unclear | Low | High |
| Hill (2014)42 | Low | High | High | Low | High |
| Jepson (2006)43 | Low | Low | Low | Low | Low |
| Kahn (2002)58 | Low | High | Low | Unclear | High |
| Kesterton (2010)50 | Low | Low | High | High | High |
| LaCroix (2014)51 | Low | Low | Low | Low | Low |
| Leavy (2011)59 | Low | High | High | High | High |
| Matson-Koffman (2005)60 | Low | Low | High | Low | Low |
| Mozaffarian (2012)68 | Low | Low | Low | Low | Low |
| Ogilvie (2007)61 | Low | Low | Low | Unclear | Low |
| Richardson (2008)44 | Low | Low | Unclear | Low | Low |
| Robinson (2014)69 | Low | Unclear | Low | High | Low |
| Speizer (2003)52 | Low | High | High | High | High |
| Swanton (2015)53 | Low | Low | High | Low | Low |
| Sweat (2012)54 | Low | Low | Low | Low | Low |
| Werb (2011)63 | Low | High | High | High | High |
| Werb (2013)64 | Low | High | Low | Low | Low |
| Wilson (2012)45 | Low | Low | Unclear | Low | Low |
Appendix 4 Characteristics of included systematic reviews (review A)
This table is grouped by the reviews’ relevance to our review of reviews: high-relevance reviews are at the top and lower relevance reviews are below them.
| Review (first author and year); risk of bias (ROBIS); relevance to our review of reviews | Review’s health topic, aims, coverage and theoretical framework (if used) | Date range of included studies (date range of searches/inclusion criterion) | Number of relevant studies (number of included studies) | Country: UK studies, OECD countries or non-OECD countries | Types of intervention | Types of population/target groups; range of study sample sizes | Synthesis: study design type/subgroup analysis | Types of outcomes:a media outcomes, proximal outcomes, intermediate outcomes and distal outcomes |
|---|---|---|---|---|---|---|---|---|
|
Abioye (2013)55 Low risk of bias High relevance |
Topic: Physical activity Was mass media sole focus? Yes Aim of review: |
Date range of included studies: 2001–8 (campaign years 1996–2005) (Date range of searches: Database inception to August 2012) |
Number of studies: Nine relevant studies (of nine included studies) |
UK studies: 1 OECD countries: USA (3), Australia (1), Canada (1), UK (1), New Zealand (1), the Netherlands (1), Norway (1) |
Definition of mass media: Studies reporting mass media campaigns that were implemented simultaneously with other interventions were also excluded Characteristics of the mass media interventions collected by the reviewers: Theoretical framework Basis of programme design: Prior research, or consultation with experts Components Duration of the programme:Coverage/reach of included campaigns Scope Reach of included campaigns: Local Regional National |
Target population: Age: adults ≥ 19 years Range of study sample sizes: The nine studies enrolled a total of 27,601 participants |
Type of synthesis: Meta-analysis Type(s) of studies synthesised: RCTs/trials before-and-after designs with comparison groups. Cohort/Longitudinal study prospective cohort design Pre/Post test Subgroup analysis: None reported |
Media: None reported Proximal: None reported Intermediate: Behaviour: decreased sedentary behaviour Behaviour: increased brisk walking Behaviour: increased overall physical activity Distal: None reported |
|
Bala (2013)27 Low risk of bias High relevance |
Topic: Tobacco use Was mass media sole focus? Yes Aim of review: |
Date range of included studies: 1977–2010 (Date range of searches: Search range not reported, searches done in February 2013) |
Number of studies: 11 relevant studies (of 11 included studies) |
UK studies: 1 OECD countries: 7 USA, 1 UK, 2 Australia, 1 South Africa |
Definition of mass media: Characteristics of the mass media interventions collected by the reviewers: Theoretical framework Basis of programme design Start date Duration of the programme Dose intensity Coverage/reach of included campaigns: In analysis 1.2 Scope Target populations Intervention Aim Setting Other: Whether part of a wider tobacco control programme Reach of included campaigns: Local Community programmes Regional: US states (e.g. California and Massachusetts) |
Target population: Age: ≥ 25 years. Studies which cover all adults as defined in studies were included Morbidity: target behaviour – regular smokers. Interventions for pregnant women were ineligible Range of study sample sizes: 311–5468 from two studies (sample size not reported in nine studies) |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: RCTs/trials Described as quasi-experimental or quasi-randomised Repeated cross-sectional Interrupted time series Subgroup analysis: Age Gender Education Race/ethnicity Duration of intervention |
Media: Awareness Proximal: Awareness/knowledge: beliefs or knowledge of smoking and cardiovascular risk Attitudes: attitudes, norms, social influences on smoking and cardiovascular risk Behaviour: calls to quitline Intermediate: Behaviour: smoking prevalence Behaviour: smoking consumption Behaviour: quit attempts Behaviour: quit rates Distal: None reported Process outcomes: Intervention costs |
|
Brinn (2010)35 Low risk of bias High relevance |
Topic: Tobacco use Was mass media sole focus? Yes Aim of review: |
Date range of included studies: 1983–2010 (Date range of searches: 1997–July 2010, date of last search) |
Number of studies: Seven relevant studies (of seven included studies) | OECD countries: USA (6), Norway (1) |
Definition of mass media: Channels of communication such as television, radio, newspapers, bill boards, posters, leaflets or booklets intended to reach large numbers of people and which are not dependent on person to person contact Characteristics of the mass media interventions collected by the reviewers: Theoretical framework Basis of programme design Components Start date Duration of the programme Target populations Reach of included campaigns: Local Regional |
Target population: Age: < 25 years Range of study sample sizes: 2534–2742; not reported for most |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: RCTs/trials Subgroup analysis: None reported |
Media: Awareness Proximal: Intention to smoke Awareness/knowledge: smoking Attitudes: smoking norms Attitudes: smoking efficacy Intermediate: Behaviour: smoking uptake Distal: None reported |
|
Brown (2012)56 High risk of bias High relevance |
Topic: Physical activity Was mass media sole focus? Yes Aim of review: Theoretical Framework |
Date range of included studies: 1980–2010 (Date range of searches: 1980–2011) |
Number of studies: 16 relevant studies (of 16 included studies) | Countries: Not reported |
Definition of mass media: Stand-alone mass media campaigns:Characteristics of the mass media interventions collected by the reviewers: Components Duration of the programme Dose intensity Coverage/reach of included campaigns Target populations: For updated review Only four studies,32–34,36 two conducted among children and two among adults, met inclusion criteria Cost Reach of included campaigns: National: 1 national campaign, the rest not reported |
Target population: No target defined Range of study sample sizes: n = 9755 to n = 74 |
Type of synthesis: Meta-analysis narrative synthesis Type(s) of studies synthesised: RCTs/trials three controlled trials Cohort/longitudinal study: five cohort studies Observational/correlational: 5 Pre/Post test: three single-group studies using before–after designs19,21,30 Subgroup analysis: None reported |
Media: None reported Proximal: None reported Intermediate: Behaviour: increased self-report time spent in physical activity Behaviour: increased self-reported activity Distal: None reported Process: Intervention costs |
|
Byrne (2005)65 High risk of bias High relevance |
Topics: Multiple – alcohol use, tobacco use, illicit drug use Was mass media sole focus? Yes Aim of review: |
Date range of included studies: 1990–2003 (Date range of searches: 1990–2003) |
Number of studies: 25 relevant studies (of 25 included studies, reported in 53 articles) | OECD countries: Restricted to North American interventions only. Majority developed and disseminated in the USA, but includes at least one Canadian campaign |
Definition of mass media: Characteristics of the mass media interventions collected by the reviewers: Components Target populations Reach of included campaigns: Local: From the campaign titles in table 1 (e.g. The Rowan University Social Norms Project) Regional: From the campaign titles in table 1 (e.g. Massachusetts Tobacco Control Program, Oregon’s Tobacco Prevention and Education Program) National: From the campaign titles in table 1 [e.g. Office of the National Drug Control Policy (ONDCP) National Youth Anti-Drug Media Campaign] |
Target population: Age: ≤ 21 years Range of study sample sizes: Not reported |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: Pre/Post test Post test Subgroup analysis: Age Gender Race/ethnicity Personality traits Message |
Media: Awareness Credibility Proximal: Awareness/knowledge: substance use (illicit drugs, alcohol and tobacco) Attitudes: substance use (illicit drugs, alcohol and tobacco) Intermediate: Behaviour: substance use (illicit drugs, alcohol and tobacco) Distal: None reported |
|
Carter (2015)47 Low risk of bias High relevance |
Topic: Sexual health Was mass media sole focus? No Aim of review:Theoretical Framework See figure 1 |
Date range of included studies: 1989–2011 (Date range of searches: January 1985 to February 2011) |
Number of studies: 14 relevant studies (of 17 included studies) |
UK studies: 2 OECD countries: USA (11), UK (2), Australia (2), Sweden (2) |
Definition of mass media: Studies that focused on condom use or sexual health promotion, when it was done not solely for HIV or STD prevention but also included pregnancy prevention messaging as a component Characteristics of the mass media interventions collected by the reviewers: Components Intervention Aim: Studies were diverse in terms of aims, the evaluated interventions, and the evaluation approach Reach of included campaigns: Local Regional National |
Target population: Not reported Range of study sample sizes: 57 (Hall 1996) to 6122 (Bull 2008) |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: RCTs/trials: 4 studies Cohort/Longitudinal study: 2 were retrospective cohort studies, 1 was a longitudinal cohort study Pre/Post test: 2 used pre–post designs Repeated cross-sectional: 8 used time series cross-sectional study designs, 3 with comparison or control groups, and 5 without Subgroup analysis: None reported |
Media: None reported Proximal: Intention: to use contraception Awareness/knowledge: sexual health Awareness/knowledge: contraception Attitudes: use of family planning Beliefs: risk of pregnancy Behaviour: use of family planning services Intermediate: None reported Distal: None reported |
|
Derzon (2002)66 High risk of bias High relevance |
Topics: Multiple – alcohol use, tobacco use, illicit drug use Was mass media sole focus? Yes Aim of review: |
Date range of included studies: Not reported (Date range of searches: Not reported) |
Number of studies: 72 relevant studies (of 72 included studies) | OECD countries: Developed Western countries |
Definition of mass media: Eligible media interventions included messages designed for dissemination to a specific audience or the general public and delivered via print, audio, video or electronic media or some combination thereof Characteristics of the mass media interventions collected by the reviewers: Components Reach of included campaigns: Not reported |
Target population: Age: youth ≤ 21 years Other: Parents:Range of study sample sizes: 90 distinct subject samples |
Type of synthesis: Meta-analysis Type(s) of studies synthesised: RCTs/trials quasi experimental designs Subgroup analysis: Age Gender Risk status |
Media: Channel Approach Duration of intervention Message Target Proximal: Awareness/knowledge: substance use (illicit drugs, alcohol and tobacco) Attitudes: substance use (illicit drugs, alcohol and tobacco) Intermediate: Behaviour: substance use (illicit drugs, alcohol and tobacco) Distal: None reported |
|
Ferri (2013)62 Low risk of bias High relevance |
Topic: Illicit drug use Was mass media sole focus? Yes Aim of review: Theoretical Framework Health belief model, theory of reasoned action/theory of planned behaviour, social norms theory, super peer theory, social learned theory |
Date range of included studies: 1992–2011 (Date range of searches: 1974–2013) |
Number of studies: 23 relevant studies (of 23 included studies) | OECD countries: 21 in USA, 1 in USA and Canada, 1 Australia |
Definition of mass media: Characteristics of the mass media interventions collected by the reviewers: Theoretical framework: Table on page 10 records ‘explicit underpinning theory’ Components Target populations: characteristics of studies tables for each study includes any targeting of the intervention. No studies had subjects younger than age 10 years. 21 studies were between the age of 10 and 20. 2 studies had subjects older than 20, younger than 26. Setting 11 studies conducted in 1 setting, (8 studies in school/college setting, 2 in community setting, 1 a national state-wide setting). 12 conducted in multiple settings (3 in schools/community, 8 in community and national settings) Reach of included campaigns: Local: school/college/community settings Regional: state National: nationwide campaign |
Target population: Age: Young people Range of study sample sizes: 79 (Kelly 1992) to 130,245 (Carpenter 2011) |
Type of synthesis: Meta-analysis Narrative synthesis Type(s) of studies synthesised: RCTs/Trials Cohort/Longitudinal study Pre/Post test Other: interrupted time series Subgroup analysis: Age |
Media: None reported Proximal: Intentions: use of illicit drugs Awareness/knowledge: use of illicit drugs Attitude: use of illicit drugs Intermediate: Behaviour: use of illicit drugs Distal: None reported |
|
Finlay (2005)57 High risk of bias High relevance |
Topic: Physical activity Was mass media sole focus? Yes Aim of review: |
Date range of included studies: 1998–2002 (part 1), 1980–2002 (part 2) (Date range of searches: 1997 (since inclusion in the Marcus et al. 1998 review) to December 2002) |
Number of studies: Eight relevant studies (of eight included in initial effectiveness analysis plus an additional nine in the critical media analysis, n = 17) |
UK studies: Three (reported for 1998- studies only) OECD countries: USA (3), UK (3), Australia (1), Canada (1) (reported for 1998 studies only) |
Definition of mass media: An intervention using a component of community-wide mass media (interpersonal communication, workplace or school-based campaigns and small group settings were excluded). Inclusion criterion for ‘media’ in the title or abstract of the study Characteristics of the mass media interventions collected by the reviewers: Theoretical framework Components Coverage/reach of included campaigns Target populations: see table 1 Reach of included campaigns: Local: e.g. Towns Regional: States in USA e.g. Virginia National: e.g. England |
Target population: Not reported Range of study sample sizes: Not reported |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: Pre/Post test Third, the study consisted of a pre–post design assessing a physical activity intervention using a component of community-wide mass media. Studies had to meet this inclusion criteria – no further info given Subgroup analysis: Education Ethnicity |
Media: Recall Proximal: Awareness/knowledge: physical activity Intermediate: Behaviour: increased changes in physical activity Distal: None reported |
|
French (2014)48 Low risk of bias High relevance |
Topic: Sexual health Was mass media sole focus? Yes Aim of review: An exploratory review was conducted to assess research examining awareness, acceptability, effects on HIV testing, disclosure and sexual risk, and cost-effectiveness of HIV mass media campaigns targeting MSM |
Date range of included studies: 1995–2011 (Date range of searches: between 1990 and May 2011) |
Number of studies: 12 relevant studies (of 12 included studies) |
UK studies: 7 OECD countries: 7 UK, 4 USA, 1 Canada |
Definition of mass media: Mass media campaigns relating to HIV health promotion that targeted MSM were included. Unpaid for media coverage and interactive media health promotion interventions (such as use of internet chat rooms) were excluded. Interventions that only included small media were excluded, but those where mass media were complemented with small media were included Characteristics of the mass media interventions collected by the reviewers: Theoretical framework:Basis of programme design:The authors note that this:Components Target populations: Seven targeted all MSM. The remainder targeted specific subgroups of MSM by age or ethnic subgroups, recent unprotected sexual intercourse with men of unknown or discordant HIV status and perceived HIV-negative serostatus. None reported aiming to target MSM according to sexual identity Cost: Campaign costs were reported in four studies. Costs ranged from CA$250,000 for the national campaign in Canada to £9500 for media placement, artists’ fees and staff time for the ‘Stella Seattle’ newspaper comic strip Intervention Aim: Most aimed to provide information on HIV prevention strategies and encourage HIV testing. Despite most moving away from basic ‘use a condom’ messages, few aimed to provide men with information on negotiating safer sex or disclosing their HIV status to a sexual partner Reach of included campaigns: Local: Six city-wide Regional: One US state National: Four country-wide |
Target population: Other: sexual orientation – men having sex with men Range of study sample sizes: 55,270–242 |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: RCTs/trials Pre/Post test Post test Subgroup analysis: Message (campaign) |
Media: Awareness Identification Proximal: Behaviour: HIV testing Intermediate: None reported Distal: None reported Process outcomes: Intervention costs |
|
Guillaumier (2012)40 Low risk of bias High relevance |
Topic: Tobacco use Was mass media sole focus? Yes Aim of review: |
Date range of included studies 1992–2011 (Date range of searches: Published before March 2012, start of date range not reported) |
Number of studies: 17 studies (of 17 included studies) | OECD countries: USA (10), Australia (5), New Zealand (2) |
Definition of mass media: Channels of communication such as television, radio, newspapers, billboards, posters, leaflets or booklets intended to reach large numbers of people, and which are not dependent on person-to-person contact Characteristics of the mass media interventions collected by the reviewers: Start date Duration of the programme Dose intensity Scope Target populations: Ethnic groups (as a marker of disadvantage) Intervention Aim Reach of included campaigns: Local: At least four studies conducted at a community/city level National: At least one study conducted at a national level |
Target population: Age: > 18 years Socioeconomic status:Ethnicity: See SES Range of study sample sizes: 198–2714 from five studies (‘n’ not reported for 12 studies) |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: RCTs/trials Cohort/longitudinal study Observational/correlational Pre/Post test Repeated cross-sectional Subgroup analysis: Socioeconomic status |
Media: Awareness Credibility Attitudinal/emotional responses Proximal: Intention Motivation Behaviour: information-seeking Intermediate: Behaviour: smoking cessation Distal: None reported |
|
Jepson (2006)43 Low risk of bias High relevance |
Topic: Tobacco use Was mass media sole focus? Yes Aim of review: |
Date range of included studies: 1990–2006 (Date range of searches: 1990–2006) |
Number of studies: 39 relevant studies (of 44 included studies – 5 systematic reviews) |
UK studies: 4 OECD countries: USA, New Zealand, Canada, Switzerland, Australia, Wales, Norway, Finland, the Netherlands, UK |
Definition of mass media: Channels of communication which are not dependent on person-to-person contact such as:Characteristics of the mass media interventions collected by the reviewers: Scope Target populations Intervention Aim Setting Reach of included campaigns: Local Regional National |
Target population: Other: People who use tobacco products Range of study sample sizes: Not reported |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: RCTs/trials Cohort/longitudinal study Pre/Post test Post test Repeated cross-sectional Other: Process evaluation; ‘observation/ethnography’ Subgroup analysis: Gender Education Channel Approach Message style Race/Ethnicity |
Media: Awareness Proximal: Behaviour: calls to quitline Intermediate: Behaviour: smoking cessation Distal: Societal change (stigma) Process outcomes: Intervention costs |
|
Leavy (2011)59 High risk of bias High relevance |
Topic: Physical activity Was mass media sole focus? Yes Aim of review: Theoretical Framework Campaign impact was classified as: |
Date range of included studies: 2003–10 (Date range of searches: 2003–10) |
Number of studies: 18 relevant studies (of 18 included studies) |
OECD countries: USA (n = 8), Australia (n = 3), Canada (n = 3), Belgium (n = 1) and New Zealand (n = 1) Non-OECD countries: two were conducted in middle-income countries in South America (Colombia and Brazil) |
Definition of mass media: a clear mass media and/or social marketing component that relates specifically to physical activity OR fitness OR exercise; paid or unpaid media or a combination of both Characteristics of the mass media interventions collected by the reviewers: Theoretical framework Over the 18 campaigns, ‘included: theory of reasoned action and planned belief, theory of planned behaviour, McGuire’s HOE, stages of change, health belief model, social ecological model and a social marketing framework.’ Seven reported a combination. Only half reported formative research Basis of programme design formative evaluations Components Start date Duration of the programme: Campaign duration ranged from: as short as 8–13 weeks (n = 6); around 6 months (n = 3), 12 months (n = 2); several phases over 12–24 months (n = 2) and greater than 2 years (n = 5) Dose intensity Coverage/reach of included campaigns Target populations Cost Reach of included campaigns: Regional National |
Target population: Age: Adult Range of study sample sizes: 297 – 7217 (Wray and Craig) |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: RCTs/Trials: quasi-experimental Observational/correlational: ‘Post–only’ cross-sectional designs Pre/Post test: Pre– post–campaign cross-sectional design, repeated cross-sectional Other: Non-experimental, mixed methods design Subgroup analysis: None reported |
Media: Awareness Exposure Proximal: Intention: to be more active Intermediate: Behaviour: increased change in physical activity Distal: None reported Process: Intervention costs |
|
Richardson (2008)44 Low risk of bias High relevance |
Topic: Tobacco use Was mass media sole focus? No Aim of review: |
Date range of included studies: 1994–2007 (Date range of searches: 1990 – July 2007) |
Number of studies: 37 relevant studies (of 41 included studies – 4 systematic reviews) |
UK studies: 1 OECD countries: USA (32), Australia (2), UK (1), Sweden (1) Non-OECD countries: South Korea (1) |
Definition of mass media: Programmes or campaigns aimed at reaching large numbers of people via television, internet, radio, newspapers, bill boards, posters leaflets, booklets and new media. New media includes media such as podcasts, text messaging, Bebo, Facebook, and social networking websites Characteristics of the mass media interventions collected by the reviewers: Basis of programme design Duration of the programme Target populations Reach of included campaigns: Local Regional |
Target population: Age: < 18 years Range of study sample sizes: 27–103,172 from 36 studies (1 study ‘n’ not reported – Table 5) |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: RCTs/trials Cohort/longitudinal study Post test Other: Qualitative Subgroup analysis: Age Gender Socioeconomic status Race/ethnicity |
Media: Awareness Understanding Credibility Attitudinal/emotional responses Proximal: Awareness/knowledge: Knowledge, attitudes, intentions towards tobacco use and the tobacco industry Attitudes: knowledge, attitudes, intentions towards tobacco use and the tobacco industry Intermediate: Behaviour: smoking uptake Distal: None reported |
|
Robinson (2014)69 Low risk of bias High relevance |
Topics: Multiple – physical activity, sexual health, tobacco use Theoretical Framework Conceptual model on p. 363 Was mass media sole focus? Yes Aim of review: |
Date range of included studies: 1999–2010 (Date range of searches: Not reported) |
Number of studies: 11 relevant study arms (of 25 study arms in 22 included studies) | OECD countries: nine study arms in the US (six condoms use and three smoking cessation), one study arm in Australia (phys act), and one study arm in Belgium (physical activity) |
Definition of mass media: Two criteria: (i) to use messages designed to increase awareness of, demand for, and appropriate use of a product. (ii) to distribute a product to enable the adoption or maintenance of health-promoting behaviours, or to sustain cessation of harmful behaviours, or to protect against behaviour-related disease or injury Characteristics of the mass media interventions collected by the reviewers: Theoretical framework Components Duration of the programme Cost: Whether the related product was distributed for free or at reduced price Reach of included campaigns: Not reported |
Target population: No target defined Range of study sample sizes: Not reported |
Type of synthesis: Meta-analysis Narrative synthesis Type(s) of studies synthesised: Unclear Subgroup analysis: Approach: Product distribution Race/ethnicity Sexual orientation/gender identity |
Media: None reported Proximal: Intention: to call smoking quitlines Intermediate: Behaviour: condom use Distal: None reported Process outcomes: Intervention costs |
|
Swanton (2015)53 Low risk of bias High relevance |
Topic: Sexual health Was mass media sole focus? No Aim of review: |
Date range of included studies: 2007–13 (Date range of searches: Searched in September 2013 and updated in September 2014) |
Number of studies: 12 relevant studies (of 15 included studies) | Countries: Not reported |
Definition of mass media: Delivered exclusively through new media Characteristics of the mass media interventions collected by the reviewers: Components Reach of included campaigns: Not reported |
Target population: No target defined Range of study sample sizes: Not reported |
Type of synthesis: Meta-analysis Type(s) of studies synthesised: RCTs/trials Subgroup analysis: Age Gender Approach: Interactive/static Duration of intervention Sexual orientation/gender identity Research design |
Media: None reported Proximal: None reported Intermediate: Behaviour: increased condom use Distal: None reported |
|
Werb (2011)63 High risk of bias High relevance |
Topic: Illicit drug use Was mass media sole focus? Yes Aim of review: |
Date range of included studies: 1991–2008 (Date range of searches: Searched for studies published between 1989 and 2008) |
Number of studies: 11 relevant studies (of 11 included studies) | OECD countries: USA (10), Australia (1) |
Definition of mass media: national anti-drug youth media campaign, public service announcement, ‘PSA’. PSAs were defined as ‘produced for a variety of media channels including tv, radio, print and the internet’ Characteristics of the mass media interventions collected by the reviewers: Duration of the programme: Table 1 notes duration of programme – the length of the included studies ranged from immediate post-test up to 5 years post test. The table also reports if available on the number of weeks the intervention ran for Dose intensity: Table 1 records the number of the public service announcements, and the time of exposure Target populations: Table 1 notes where any of the studies targeted specific populations (e.g. public school students, college students) Setting: Table 1 notes the setting = country (USA or Australia) Reach of included campaigns: Unclear; at least one national campaign |
Target population: Age: Youth (review did not give any exact age range) Range of study sample sizes: From 93 to 9598 |
Type of synthesis: Meta-analysis Type(s) of studies synthesised: RCTs/trials: seven RCTs included Observational/correlational: four observational studies included Subgroup analysis: Research design Personality traits |
Media: None reported Proximal: Intentions: Use of illicit drugs Intermediate: Behaviour: Use of illicit drugs Distal: None reported |
|
Wilson (2012)45 Low risk of bias High relevance |
Topic: Tobacco use Was mass media sole focus? No Aim of review: Theoretical Framework WHO MPOWER Package |
Date range of included studies: 1991–2011 (Date range of searches: MEDLINE 1990–January 2012; other databases 1990–February 2009) |
Number of studies: 19 relevant studies (of 84 included studies) |
UK studies: 1 OECD countries: USA, Norway, the Netherlands, UK, Australia, South Africa |
Definition of mass media: Any campaign intended to reduce tobacco use using channels of communication such as television, radio, newspapers, billboards, posters, leaflets, or booklets intended to reach large numbers of people, which are not dependent on person-to-person contact Characteristics of the mass media interventions collected by the reviewers: Start date Duration of the programme Target populations Reach of included campaigns: Not reported |
Target population: No target defined Range of study sample sizes: 310–343,835 where reported, n not reported for six studies |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: RCTs/trials Cohort/longitudinal study Pre/Post test Controlled before and after; uncontrolled before and after Repeated cross-sectional Time series Subgroup analysis: Age |
Media: None reported Proximal: None reported Intermediate: Behaviour: smoking initiation Behaviour: smoking prevalence Behaviour: smoking cessation Distal: None reported |
|
Bertrand (2006)46 Low risk of bias Low relevance |
Topic: Sexual health Was mass media sole focus? Yes Aim of review: |
Date range of included studies: 1995–2006 (Date range of searches: 1990 to 2004) |
Number of studies: 15 relevant studies (of 15 included studies) | Non-OECD countries: 11 examined interventions in Africa, 2 in Latin America, 1 in Asia, and 1 examined a programme that took place in 44 developing countries |
Definition of mass media:Authors categorised the most common types of mass media interventions to prevent HIV transmission used in developing countries: radio only, radio with other supporting media, and radio and television with other supporting media Characteristics of the mass media interventions collected by the reviewers: Components Reach of included campaigns: Local Regional National |
Target population: Age: Young people Range of study sample sizes: 297–11,904 |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: Other: No randomised trials Subgroup analysis Channel (campaign) Dose response relationship (campaign) |
Media: None reported Proximal: Awareness/knowledge: health products/service Awareness/knowledge: HIV transmission; condom use; HIV risk; prevention methods Beliefs: personal risk of HIV/AIDS Self-efficacy: using condoms Behaviour: use of HIV service/clinic Intermediate: None reported Distal: None reported |
|
Brown (2014)37 High risk of bias Low relevance |
Topic: Tobacco use Was mass media sole focus? No Aim of review: |
Date range of included studies: 2000–13 (Date range of searches: 1995–2012/13, dates varied between databases) |
Number of studies: 30 relevant studies (of 117 included studies) |
UK studies: 1 OECD countries: USA (16), the Netherlands (5), Australia (3), Canada (2), UK (1), New Zealand (1) Non-OECD countries: Croatia (1), Russia (1) |
Definition of mass media: Not reported Characteristics of the mass media interventions collected by the reviewers: Components Duration of the programme Reach of included campaigns: National: One national, the rest unclear |
Target population: Age: ≥ 18 years plus studies measuring children’s reports of parental smoking Socioeconomic status: Studies had to report differential smoking-related outcomes for at least two socioeconomic groups Range of study sample sizes: Not reported |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: RCTs/trials Cohort/longitudinal study Observational/correlational Cross-sectional, comparison between different types of intervention Pre/Post test Repeated cross-sectional Subgroup analysis: Socioeconomic status |
Media: Awareness Proximal: Behaviour: calls to quitline Intermediate: None reported Distal: None reported |
|
Brown (2014)36 High risk of bias Low relevance |
Topic: Tobacco use Was mass media sole focus? No Aim of review: |
Date range of included studies: 1997–2013 (relevant study 2009) (Date range of searches: Published since 1995 to October 2013) |
Number of studies: 1 relevant study (of 38 included studies) | OECD countries: USA (1) |
Definition of mass media: Not reported Characteristics of the mass media interventions collected by the reviewers: Components Target populations Reach of included campaigns: National |
Target population: Age: 0–25 years Socioeconomic status: Studies had to report outcomes for two or more SES groups Range of study sample sizes: 30,512 (one study) |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: Post test Subgroup analysis: Socioeconomic status |
Media: Awareness Salience Proximal: None reported Intermediate: None reported Distal: None reported |
|
de Kleijn (2015)38 High risk of bias Low relevance |
Topic: Tobacco use Was mass media sole focus? No Aim of review: |
Date range of included studies: 1997–2014 (relevant studies 1996–2006) (Date range of searches: 1992–January 2015) (date of searches) |
Number of studies: 4 relevant studies (of 37 included studies) | OECD countries: USA (3), Norway (1) |
Definition of mass media: Antismoking advertisements Characteristics of the mass media interventions collected by the reviewers: Duration of the programme Dose intensity Target populations Reach of included campaigns: Local Regional |
Target population: Age: < 18 years Gender: Female (non-targeting interventions were included, but only studies that present results for girls were included) Range of study sample sizes: Described as final sample: 325–101,70 (from three studies – one other study ‘n’ not reported) |
Type of synthesis: Meta-analysis None of the four relevant studies included in the pooled analysis Narrative synthesis Type(s) of studies synthesised: RCTs/trials: one RCT; three ‘other controlled trial’ Subgroup analysis: None reported |
Media: None reported Proximal: None reported Intermediate: Behaviour: smoking uptake Distal: None reported |
|
Ellis (2003)67 Low risk of bias Low relevance |
Topics: Multiple – diet, tobacco use Was mass media sole focus? No Aim of review: |
Date range of included studies: 1986–1998 (Date range of searches: 1980–2001/02, varied between databases) |
Number of studies: 8 relevant studies (of 31 included studies) | OECD countries: 7 USA, 1 Australia |
Definition of mass media: Not reported Characteristics of the mass media interventions collected by the reviewers: Target populations Reach of included campaigns: Local Regional National |
Target population: Age: Reports focusing exclusively on children or adolescents were excluded Other: Excluded: studies exclusively focused on prenatal smoking cessation, tobacco sale to minors, prenatal/antenatal diets Range of study sample sizes: 353–279,681 from four studies, four not reported |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: RCTs/trials Pre/Post test: pre/post with control group Post test: post-test with control group and post-test with 1 group Repeated cross-sectional interrupted time series Unclear: ‘descriptive study’ Subgroup analysis: None reported |
Media: Awareness Understanding Proximal: Awareness/knowledge: dietary counselling helplines Awareness/knowledge: smoking cessation helplines Intermediate: None reported Distal: None reported |
|
Gould (2013)39 Low risk of bias Low relevance |
Topic: Tobacco use Was mass media sole focus? Yes Although sometimes referred to as ‘media’. Some interventions may not meet our definition of mass media Aim of review: |
Date range of included studies: 1998–2011 (Date range of searches: Earliest to October 2011) |
Number of studies: 11 relevant studies (of 20 included studies) | OECD countries: Australia, New Zealand, USA |
Definition of mass media: Search terms were communication media, or mass media or social marketing, or advertising or health promotion or health education or internet or mobile phone or arts or arts therapy Characteristics of the mass media interventions collected by the reviewers: Components: eight TV/radio, three mobile phone, four print media, two internet, one CD-ROM, one video, one ‘edutainment’ Target populations: Seven studies described impact of interventions among youth, two addressed women, one aimed at pregnant women, two studies included health staff or health professionals Setting: All studies were in community settings covering a range of urban, rural and remote locations Reach of included campaigns: Local: 4 National: 6 |
Target population: Ethnicity: Indigenous populations with Australia, New Zealand, USA and Canada including Australian Aboriginal or Torres Strait Islanders, NZ Maori, American Indians, Alaska Natives, Pacific Islanders, First Nations or Inuit Range of study sample sizes: Not reported |
Type of synthesis: Narrative synthesis using Popay’s guidelines for narrative synthesis Type(s) of studies synthesised: RCTs/trials Pre/Post test Post test Other: Database analysis, mixed methods or qualitative Subgroup analysis: None reported |
Media: Recall Credibility Proximal: Intention: to quit or smoke Awareness/knowledge: smoking Behaviour: information-seeking Behaviour: treatment-seeking Intermediate: Behaviour: smoking uptake/quitting Distal: None reported |
|
Grilli (2000)49 Low risk of bias Low relevance |
Topic: Sexual health Was mass media sole focus? Yes Aim of review: |
Date range of included studies: 1979–99 (Date range of searches: no restrictions up to 1996) |
Number of studies: 2 relevant studies (of 21 included studies) | UK studies: 2 |
Definition of mass media: Based on the use of mass media, including radio, television, newspapers, magazines, leaflets, posters and pamphlets (alone or in conjunction with other interventions) Characteristics of the mass media interventions collected by the reviewers: Components Reach of included campaigns: National: 2 UK-wide campaigns |
Target population: Other: Health-care providers, patients, and the general public Range of study sample sizes: Not reported |
Type of synthesis: Narrative synthesis Results from individual studies addressing the same aspect of care were not pooled, due to the substantial heterogeneity in both the setting and subjects between studies Type(s) of studies synthesised: Observational/Correlational Pre/Post test Subgroup analysis: None reported |
Media: None reported Proximal: Behaviour: Use of health services Intermediate: None reported Distal: None reported |
|
Hemsing (2012)41 High risk of bias Low relevance |
Topic: Tobacco use Was mass media sole focus? No Aim of review: |
Date range of included studies: 1994–2008 (relevant study 1994) (Date range of searches: 1990–May 2009) |
Number of studies: One relevant study (of nine included studies) |
UK studies: 1 OECD countries: UK (1) |
Definition of mass media: Not reported Characteristics of the mass media interventions collected by the reviewers: Components Coverage/reach of included campaigns Target populations Intervention Aim Setting Other: Source of funding Reach of included campaigns: National: Described as including adverts in six tabloid newspapers therefore assumed to be a national campaign |
Target population: Other: Pregnant women and their partners Range of study sample sizes: Not reported |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: Pre/Post test Before-and-after study Subgroup analysis: None reported |
Media: None reported Proximal: None reported Intermediate: Behaviour: quit attempts Distal: None reported |
|
Hill (2014)42 High risk of bias Low relevance |
Topic: Tobacco use Was mass media sole focus? No Six tobacco control interventions: price increases, smoke-free policies, advertising bans, mass media campaigns, warning labels, smoking cessation support and community-based programmes combining several interventions Aim of review: Theoretical Framework World Bank tobacco control strategies |
Date range of included studies: 2006–11 (Date range of searches: January 2006–September 2010) |
Number of studies: 12 relevant studies (of 77 included studies) |
UK studies: 1 OECD countries: USA (9), Holland (1), UK (1), Canada (1) |
Definition of mass media: Not reported Characteristics of the mass media interventions collected by the reviewers: Components Channels Intervention Aim Reach of included campaigns: local |
Target population: Age: ≥ 18 years Range of study sample sizes: Not reported |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: Not reported Subgroup analysis: Socioeconomic status |
Media: Awareness Proximal: Behaviour: calls to quitline Intermediate: None reported Distal: None reported |
|
Kahn (2002)58 High risk of bias Low relevance |
Topic: Physical activity Was mass media sole focus? No Aim of review: Theoretical framework Conceptual model in figure 1The authors categorise the modifiable determinants of behaviour: (1) information-based determinants (e.g. knowledge and attitudes about physical activity and behaviours that precede physical activity; motivations to be active; and intentions to engage); (2) social and behavioural skills that facilitate the adoption and maintenance of physical activity behavioural change; and (3) environmental characteristics (e.g. safe and accessible parks and recreation facilities) that increase the possibility and likelihood of physical activity occurring |
Date range of included studies: 1980 and 2000 (Date range of searches: 1980–2000) |
Number of studies: 6 relevant studies (of 94 included studies) |
UK studies: Point of decision prompts: one in England and one in Scotland OECD countries: Point of decision prompts: four in US, two in UK |
Definition of mass media: Informational approaches to change knowledge and attitudes about the benefits of and opportunities for physical activity within a community Characteristics of the mass media interventions collected by the reviewers: Components Point of decision prompts: All interventions evaluated in this category were single-component interventions, in which placement of the sign was the only intervention activity Reach of included campaigns: Local Point of decision prompts |
Target population: Not reported Range of study sample sizes: Not reported |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: RCTs/Trials: mass media – one non-randomised trial Pre/Post test: Mass media one pre post design Repeated cross-sectional: Point of decision prompts All studies were of moderate suitability, using time-series designs. Mass Media Time series design Subgroup analysis: Race/ethnicity Weight status |
Media: None reported Proximal: None reported Intermediate: Behaviour: increased physical activity Distal: None reported |
|
Kesterton (2010)50 High risk of bias Low relevance |
Topic: Sexual health Was mass media sole focus? No Aim of review: |
Date range of included studies: 2001 (Date range of searches: Not before 1990) |
Number of studies: 3 relevant studies (of 74 included studies) | Non-OECD countries: Zimbabwe 2, Burkina Faso 1 |
Definition of mass media: Not reported Characteristics of the mass media interventions collected by the reviewers: Components Reach of included campaigns: Local: Community based Regional: Cities and centres of small towns in rural areas |
Target population: Age: Programmes targeting young people Other: Programmes targeting communities to improve their support for young people’s services Range of study sample sizes: 1400 (reported for one study) |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: RCTs/trials: quasi-experimental – two Pre/Post test Subgroup analysis: None reported |
Media: Interaction: discussion of campaign or message with others Proximal: Awareness/knowledge: how to access services Behaviour: use of health centre Intermediate: None reported Distal: None reported |
|
LaCroix (2014)51 Low risk of bias Low relevance |
Topic: Sexual health Was mass media sole focus? Yes Aim of review: |
Date range of included studies: 1986–2010 (Date range of searches: in 2013) |
Number of studies: 54 relevant studies (of 54 included studies) | Continents: Africa 27, Asia 9, Europe 6, USA 6, South/Central America 5, Australia 1 |
Definition of mass media: Characteristics of the mass media interventions collected by the reviewers: Theoretical framework Components Duration of the programme: Range 1–1456 Intervention Aim Other: condom demonstration/condom distribution Reach of included campaigns: Local: community based Regional: state or province wide National |
Target population: Age: Youth Other: General population Range of study sample sizes: Range of sample pre intervention – 53–6000 range of sample post intervention – 47–6000 |
Type of synthesis: Meta-analysis Type(s) of studies synthesised: Pre/Post test Subgroup analysis: Age Gender Pre-campaign behaviour |
Media: None reported Proximal: Awareness/knowledge: HIV prevention and transmission Intermediate: None reported Distal: None reported |
|
Matson-Koffman (2005)60 Low risk of bias Low relevance |
Topic: Physical activity Was mass media sole focus? No Aim of review: Theoretical framework Social ecological model |
Date range of included studies: 1995–2001 (Date range of searches: 1970 – October 2003) |
Number of studies: 7 relevant studies (of 64 included studies) |
UK studies: 1 England + 1 Scotland OECD countries: USA, UK |
Definition of mass media: Not reported; however, review excluded media-only campaigns Characteristics of the mass media interventions collected by the reviewers: Components Duration of the programme Scope Setting Reach of included campaigns: Local: Cities/communities Regional: States/counties |
Target population: No target defined Range of study sample sizes: 5050–115,113 |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: Other: Categorised as ‘quasi-experimental’ and ‘non-experimental’ Subgroup analysis: None reported |
Media: None reported Proximal: None reported Intermediate: Behaviour: increased stair use Distal: None reported |
|
Mozaffarian (2012)68 Low risk of bias Low relevance |
Topics: Multiple – diet, physical activity, tobacco use Was mass media sole focus? No Aim of review: Theoretical framework CDC Evaluation Framework |
Date range of included studies: 1987–2010 (Date range of searches: not reported) |
Number of studies: 31 relevant studies [22 media and educational campaign intervention studies + 3 Multicomponent Interventions (Including Major Components Beyond Media and Education); 6 point-of-decision stairs prompt studies (in Labelling and Consumer Information Category)] [of ≈100 (not stated) included studies] |
UK studies: 2 OECD countries: US, Finland, Australia, Great Britain Non-OECD countries: Singapore, Mauritius, China, Pakistan, US-Mexico border |
Definition of mass media: Media and Education Campaigns; category From the results:Characteristics of the mass media interventions collected by the reviewers: Components Duration of the programme Target populations Setting Reach of included campaigns: Local: Population = communities or neighbourhoods Regional: Targets whole US state National: Target whole country |
Target population: No target defined Range of study sample sizes: n = 374 to the US population |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: RCTs/trials: cluster-randomised trials (diet) Unclear for the PA and tobacco studies Other: Ecological studies, quasi-experimental studies (diet) Subgroup analysis: Duration of intervention: Sustained vs. shorter term |
Media: None reported Proximal: Awareness/knowledge: healthy diets Awareness/knowledge: physical activity Attitudes: physical activity Attitudes: smoking Intermediate: Behaviour: smoking prevention and cessation Behaviour: consumption of healthy food Behaviour: increases in physical activity Behaviour: stair use Distal: None reported |
|
Ogilvie (2007)61 Low risk of bias Low relevance |
Topic: Physical activity Was mass media sole focus? No Aim of review: |
Date range of included studies: 2002–5 (Date range of searches: 1990–2007) |
Number of studies: 2 relevant studies (of 48 included studies) | OECD countries: 2 USA |
Definition of mass media: Not reported Characteristics of the mass media interventions collected by the reviewers: Components:Duration of the programme Target populations Reach of included campaigns: Local |
Target population: No target defined Range of study sample sizes: study population range: 173 [Reger-Nash (Wheeling) study) to 730 (Reger-Nash (Welch) study] |
Type of synthesis: Narrative synthesis includes forest plots showing each study, (visually represents each study in relation to the others) but no overall analysis Type(s) of studies synthesised: Unclear: non-randomised studies Subgroup analysis: None reported |
Media: None reported Proximal: None reported Intermediate: Behaviour: increased time spent walking Distal: None reported Process outcomes: Intervention costs |
|
Speizer (2003)52 High risk of bias Low relevance |
Topic: Sexual health Was mass media sole focus? No Aim of review: |
Date range of included studies: All but a few of these studies were undertaken after 1990, with the bulk being undertaken during the 1995–2001 period (Date range of searches: Not reported) |
Number of studies: 6 relevant studies (of 41 included studies) | Non-OECD countries: 1 in Paraguay, 5 in Sub-Saharan Africa |
Definition of mass media: Not reported Characteristics of the mass media interventions collected by the reviewers: Components Duration of the programme Target populations Other: Social marketing of condoms, education sessions, peer counselling Reach of included campaigns: Local: One in Soweto National: Three national campaigns in Botswana, Cameroon, Guinea |
Target population: Age: Adolescents (aged 10–19 years) or young adults (aged 20–24 years) Range of study sample sizes: 226 to 2396 |
Type of synthesis: Narrative synthesis Type(s) of studies synthesised: RCTs/trials: quasi-experimental trials – repeat cross sectional studies with control groups – one without control group Subgroup analysis: None reported |
Media: Awareness Exposure Interaction: discussion of campaign or message with others Proximal: Awareness/knowledge: reproductive health Attitudes: reproductive health Behaviour: use of clinic Intermediate: Behaviour: increased condom use Distal: None reported |
|
Sweat (2012)54 Low risk of bias Low relevance |
Topic: Sexual health Was mass media sole focus? No Aim of review: |
Date range of included studies: The six mass media studies conducted between 1995 and 2008 (Date range of searches: Studies published between January 1990 and March 2010) |
Number of studies: 6 relevant studies (of 11 included studies) | Non-OECD countries: India – 1, Sub-Saharan Africa – 5 |
Definition of mass media: Characteristics of the mass media interventions collected by the reviewers: Components Duration of the programme: In the four serial cross-sectional studies, follow-up ranged from 12 to 36 months Target populations Reach of included campaigns: National: Two studies were described as national in scope |
Target population: No target defined Range of study sample sizes: Serial cross-sectional studies: baseline range: 928–2401, follow-up range: 200–3370 Cross-sectional studies: range 9803 to 541,212 |
Type of synthesis: Meta-analysis Type(s) of studies synthesised: Observational/correlational: Cross-sectional design Pre/Post test: Serial cross-sectional design Subgroup analysis: Gender |
Media: None reported Proximal: None reported Intermediate: Behaviour: condom use – most recent sex encounter Behaviour: condom use – all condom use Distal: None reported |
|
Werb (2013)64 Low risk of bias Low relevance |
Topic: Illicit drug use Was mass media sole focus? No Aim of review: |
Date range of included studies: 1992–2011, relevant study published 2007 (Date range of searches: Inception to 1 June 2012) |
Number of studies: One relevant study (of eight included studies) |
OECD countries: 7 (1 relevant study is from Canada) Non-OECD countries: 1 from Uzbekistan and Kyrgyzstan |
Definition of mass media: Not reported Characteristics of the mass media interventions collected by the reviewers: Theoretical framework: Relevant study – social marketing intervention to prevent injecting initiation Duration of the programme: 2.5 months Coverage/reach of included campaigns: ‘Data from in-depth qualitative interviewing suggested that campaign penetration was high’ Target populations: ‘Montreal street youth’ Setting: ‘61 participating establishments catering to street youth in Montreal’ Reach of included campaigns: Local: One relevant study used targeted dissemination of addiction-themed posters to Montreal street youth over the period of two and a half months. Combined with public postering around 61 participating establishments catering to street youth in Montreal |
Target population: Other:Range of study sample sizes: Not reported |
Type of synthesis: Narrative synthesis Descriptive summary of included studies and some learning across the studies in the discussion Type(s) of studies synthesised: RCTs/trials: 2 irrelevant studies Cohort/longitudinal study: 3 irrelevant studies Repeated cross-sectional: 2 lagged cross-sectional Other Relevant study:Subgroup analysis: None reported |
Media: Awareness Attitudinal response Proximal: None reported Intermediate: None reported Distal: None reported |
Appendix 5 Rapid review of reviews of the cost-effectiveness example search strategy (review C)
A literature search was conducted to identify reviews not identified in the original review of reviews search.
Web of Science
Date searched: 17 January 2017.
Date ranged searched: January 2000 to present.
Search strategy
Combined with OR:
-
TOPIC: (mass media) AND TOPIC: (economic evaluation) AND TOPIC: (review)
-
TOPIC: (mass media) AND TOPIC: (cost-effectiveness) AND TOPIC: (review)
-
TOPIC: (mass media) AND TOPIC: (cost-effectiveness) AND TOPIC: (review) AND TOPIC: (tobacco)
-
TOPIC: (mass media) AND TOPIC: (cost-effectiveness) AND TOPIC: (review) AND TOPIC: (alcohol)
-
TOPIC: (mass media) AND TOPIC: (cost-effectiveness) AND TOPIC: (review) AND TOPIC: (diet)
-
TOPIC: (mass media) AND TOPIC: (cost-effectiveness) AND TOPIC: (review) AND TOPIC: (drugs)
-
TOPIC: (mass media) AND TOPIC: (cost-effectiveness) AND TOPIC: (review) AND TOPIC: (physical activity)
-
TOPIC: (mass media) AND TOPIC: (cost-effectiveness) AND TOPIC: (review) AND TOPIC: (sexual health).
Google Scholar
Date searched: 17 January 2017.
Date ranged searched: January 2000 to present.
Search strategy
-
mass media cost-effectiveness review
-
mass media economic evaluation review.
Appendix 6 Review of recent UK primary studies example search strategy (review D)
MEDLINE [Epub ahead of print, In-Process and Other Non-Indexed Citations, Ovid MEDLINE(R) daily and Ovid MEDLINE(R)] (via Ovid)
Date searched: 9 September 2016.
Date range searched: 1946 to present.
Search strategy
-
1 exp Mass Media/
-
2 exp Communications Media/
-
3 exp Social Media/
-
4 exp Health Promotion/
-
5 Pamphlets/
-
6 exp Serial Publications/
-
7 Electronic Mail/
-
8 media.ab,ti.
-
9 mass communication?.ab,ti.
-
10 social marketing.ab,ti.
-
11 “broadcast*”.ab,ti.
-
12 advert*.mp.
-
13 campaign*.mp.
-
14 health campaign*.mp.
-
15 mass media.mp.
-
16 communications media.mp.
-
17 social media.mp.
-
18 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17
-
19 Diet/
-
20 diet.mp.
-
21 nutrition.mp.
-
22 eating.mp.
-
23 calorie*.ab,ti.
-
24 fruit.ab,ti.
-
25 vegetable?.ab,ti.
-
26 over-eating.ab,ti.
-
27 fast food.ab,ti.
-
28 food preferences.ab,ti.
-
29 healthy eating.ab,ti.
-
30 unhealthy eating.ab,ti.
-
31 (fat adj9 food).ab,ti.
-
32 Street Drugs/
-
33 Designer Drugs/
-
34 (illicit adj1 drug$).mp.
-
35 (illicit adj1 substance$).mp.
-
36 (substance$ adj1 us*).mp.
-
37 (substance$ adj1 misus*).mp.
-
38 (drug$ adj1 us*).mp.
-
39 (drug$ adj1 misus*).mp.
-
40 Exercise/
-
41 Motor Activity/
-
42 (physical* adj1 activ*).mp.
-
43 (physical* adj1 fitness).mp.
-
44 (physical* adj1 exertion).mp.
-
45 (activ* adj1 travel*).mp.
-
46 exercise.ti,ab.
-
47 sport*.ti,ab.
-
48 exp Sexual Behavior/
-
49 Sexually Transmitted Disease/
-
50 Sexual Health/
-
51 Sex.mp.
-
52 Tobacco/
-
53 Smoking/
-
54 tobacco.mp.
-
55 smoking.mp.
-
56 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 or 48 or 49 or 50 or 51 or 52 or 53 or 54 or 55
-
57 exp Great Britain/
-
58 (“united king*” or uk or “U.K.” or “UK.” or “U.K” or britain).ab,in,ti.
-
59 (british or english or scottish or welsh or irish).ab,in,ti.
-
60 (scotland or ireland).ab,in,ti.
-
61 (england not “new england”).ab,in,ti.
-
62 (wales not “new south wales”).ab,in,ti.
-
63 (london or manchester or birmingham or leeds or sheffield or liverpool or newcastle or edinburgh or glasgow or cardiff or oxford or bristol).ab,in,ti.
-
64 ((london adj2 ontario) or (london adj on) or new london).ab,in,ti.
-
65 (manchester adj3 (USA or massach*)).ab,in,ti.
-
66 (newcastle adj4 (australia* or “new south wales” or nsw)).ab,in,ti.
-
67 (liverpool adj4 (australia* or “new south wales” or nsw)).ab,in,ti.
-
68 64 or 65 or 66 or 67
-
69 63 not 68
-
70 (nhs or “national health service”).ab,in,ti.
-
71 57 or 58 or 59 or 60 or 61 or 62 or 69 or 70
-
72 18 and 56 and 71
-
73 limit 72 to ed=20110901-20160831
-
74 limit 73 to yr=“2011-2016”
Source of lines 57–71: Wright J (2010). UK studies search filters. Academic Unit of Health Economics, University of Leeds; unpublished. URL: https://medhealth.leeds.ac.uk/download/363/uk-based_studies (accessed 6 September 2016).
Appendix 7 Characteristics of included recent UK primary studies (review D)
| Study (first author and year) quality rating | Study topic and aim | Mass media intervention | Sample and study design | Subgroup analyses | Types of outcomes: media outcomes, proximal outcomes, intermediate outcomes, distal outcomes, process outcomes |
|---|---|---|---|---|---|
|
Ayers (2012)134 EPHPP: 2 Moderate |
Health topic: Alcohol use Aim of study: Was mass media sole focus? Yes |
Campaign setting: UK (no further breakdown) Characteristics: Campaign aim: anti-binge drinking – targeted having an accident when under the influence of alcohol Duration of the programme: < 1 minute advertisement [broadcast 2006–2007] Dose intensity The advertisement had aired on UK national television, although at the time of the experiment was not currently being aired. It was played once for two of three experimental conditions Scope: national Target populations: binge/heavy episodic drinkers Components: Channels TV Messages: Source: funded by the UK Department of Health and Social Care and the Home Office Branding Know Your Limits |
Study country: England (Uxbridge, Middlesex) Sample size: n = 124 students from Brunel University who drank alcohol 1–7 times per week (mean = 4.76, SD = 2.66) and drank 1–20 units of alcohol per episode (mean = 5.65, SD = 3.8). 48 males, 75 females, aged 18–30 years (mean = 21.94, SD = 3.57) Date of data collection: Not reported Study design: RCTs/trials A between-participants experimental design. Sample randomly assigned to 1 of 3 conditions (1. questionnaire only, 2. watch alcohol ad, 3. watch alcohol ad and told ‘to imagine that it is personal and involves you’) before completing a post-exposure survey Data collection method Survey: Participants gave informed consent. The study was completed in a ‘quiet testing room’. Participants watched the video clip of the ad . . . on a PC then turned over the questionnaire to complete . . . Ratings, and subsequent scoring, were on a 5-point scale), demographic info and whether they held a driving licence |
Subgroup analyses: Age Gender Other: alcohol drinking behaviour |
Media outcomes: None reported Proximal outcomes Social cognitive: beliefs Intermediate outcomes: None reported Distal outcomes: None reported Process outcomes: None reported |
|
Brown (2014)120 OCCS: good |
Health topic: Tobacco use Aim of studyWas mass media sole focus? Yes |
Campaign setting: England Other: Likely UK shared-media channelsCharacteristics: Campaign aimTheoretical framework: 3 psychological principles: Basis of programme designDuration of the programme: month of October Scope: National campaign in England Target populations: All smokers CostComponents: ChannelsChannel InteractivityMessagesTargeting strategies includedBranding: Not described as a brand, but:Other support materials |
Study country: England |
Subgroup analyses: Age Gender Socioeconomic status Time |
Media outcomes: None reported |
|
Sample size: n = 31,566 adult (≥ 16 years) past-year smokers Date of data collection: 2007–12 Study design: Repeated Cross SectionalData collection method Survey: |
Proximal outcomes: None reported Intermediate outcomes: Behavioural: attempt to change behaviour Distal outcomes: Improvement in population health status Process outcomes: Cost-effectiveness data |
||||
|
Brown (2016)136 EPHPP: 1 Strong |
Health topic: Tobacco use Aim of study:Was mass media sole focus? Yes |
Campaign setting: UK (no further breakdown) Characteristics: Campaign aim: Thus the current study addressed the question of whether a novel online motivational film designed to boost motivation and self-efficacy and provide role-models to promote ex-smoker identities was effective in promoting quit attempts in the general population of smokers Theoretical framework: PRIME Theory has many components but in this case the one that was considered most relevant was the idea that one could create a momentary desire and therefore intention to stop smoking by creating a vivid positive image . . . in a way that smokers could identify with Basis of programme design: Early versions of the film were refined on the basis of focus-group testing with a diverse group of smokers Duration of the programme: The final film consisting of both the diaries and the analysis was 90 minutes. Showing how people can quit over 4 weeks Scope: national Target populations: Adults (> = 18 years) who smoked cigarettes (including hand-rolled) daily or occasionally Cost: ‘low cost’ Components: Channels online film Messages: The aim of this advice was to encourage those who made a quit attempt to use support that would give the highest probability of success Branding: 4weeks2freedom Other support materials: other support materials were promoted but not provided |
Study country: UK (no further breakdown) Sample size: Individual assignment to a no intervention control (n = 1016), an informational film (n = 1004), or 4Weeks2Freedom (n = 999). Participants were adults (aged ≥ 18 years) from the UK Date of data collection: between February and March 2014 Study design: RCTs/trials Data collection method Survey: Measures recorded for outcome assessment at the 4-week endpoint were: self-report of a serious attempt to quit smoking permanently in the previous 4 weeks and . . . whether nonsmoking was continued since the start of the attempt to the time of the survey, and which (if any) smoking cessation aids were used |
Media outcomes: Social cognition: exposure Proximal outcomes: Behavioural: treatment-seeking Intermediate outcomes: Behavioural: attempt to change behaviour Distal outcomes: None reported Process outcomes: None reported |
|
|
Capacci (2011)137 OCCS: Good |
Health topic: Diet Aim of study: We provide an ex-post assessment of the UK 5-a-day information campaign, where the positive effects of information are disentangled from potentially conflicting price dynamics Was mass media sole focus? Yes: sole focus of this study although the campaign had other elements – not described |
Campaign setting: UK (no further breakdown) Characteristics: Campaign aim: The ultimate objective of the program is to reach 5 portions of fruit and vegetables per day for the whole UK population by the year 2015, with intermediate objectives of 4 (by 2005) and 4.5 (by 2010) Duration of the programme: April 2003 – 2015 (study period 2003–2006) March 2003 to December 2006 (mini campaign relaunches every 6 months: in Jan–Jun 2004, Jul–Dec 2004, Jan–Jun 2005, Jul–Dec 2005 and Jan–Dec 2006) Scope: national Target populations: Consumers: General UK population Commercial: Market agents and commercial partners (grocery retail brands, fast-food outlets, caterers and food manufacturers). Separate mini-relaunches targeted at mothers in younger and older lower socioeconomic families; teenage girls and boys living at home; older (7–11 years), lower socioeconomic group children; independent young women and men; younger, lower socioeconomic group children Cost: Planned budget for 2003–2006 was around £1.5m/year, although average actual spending was less than £1/m/year (budget spent 2003: £1,026,000; 2004: £904,000; 2005: £923,000) Components: Channels: radio, TV online Channel Interactivity: on-line and interactive marketing for the campaign mini-relaunches targeted at teenage boys and girls living at home and targeted at older children (7–11) in lower socioeconomic groups Messages: An over-arching theme for the campaign was based on the proposition ‘Helping you to enjoy the benefits of eating more fruit and vegetables’, which was then tailored in different forms depending on target groups Targeting strategies: The information campaign does not target consumers only, but also all market agents . . . The national campaign has started the development of a logo and portion indicator, whose license can only be granted by the Department of Health to products, which meet a set of nutritional criteria Branding: Official logo launched on 25 March 2003Other support materials: |
Study country: UK (no further breakdown) Sample size: 27,501 roughly 7000 samples over 4 years from 2002 to 2006 Date of data collection: 2002/3 to 2005/6 Study design Other: modelling using secondary analysis Data collection method Survey: EFS data are collected from a sample of households in the UK using self-reported diaries of all purchases, including food, over a 2-weeks period Other: secondary data – food diaries |
Subgroup analyses: Socioeconomic status |
Media outcomes: None reported Proximal outcomes: None reported Intermediate outcomes: Behavioural: behaviour change Distal outcomes: None reported Process outcomes: None reported |
|
Croker (2012)138 EPHPP: 2 Moderate |
Health topic: Diet, physical activity Aim of study:Was mass media sole focus? No |
Campaign setting: England Characteristics: Campaign aim:Theoretical framework:Duration of the programme: Launched January 2009 and families completed HTK questionnaires as part of the national C4L campaign between February 2009 and August 2011 Scope: national Target: populations parents of primary school aged children targeted at lower SES parents Phase 4 supported ‘at risk’ families (primarily lower SES) with regular booster materials by mail or online Components: Channels: TV, print and poster advertising Messages:Branding: Change4Life Other: support materials A helpline, a website, accompanying material resources (e.g. families in intervention schools were mailed the C4L print materials and the ‘How are the Kids’ questionnaire; those returning the questionnaire were sent personalised feedback and others received generic materials) |
Study country: England:Sample size: **Survey BASELINE: 16,029 children were given invitation letters at their schools; 3774 families with 4419 children returned the baseline questionnaire (28% response rate) Date of data collection: summer 2009 to summer 2010 Study design: RCTs/trials: cluster-randomised trial (clustered by school) Qualitative Data collection method Survey: self-completion, before and after (postal questionnaires) Interviews: home-based |
Subgroup analyses: Age Socioeconomic status Education |
Media outcomes: Social cognition: awareness Social cognition: attitudinal/emotional responses Proximal outcomes: Social cognitive: attitudes Social cognitive: intention Intermediate outcomes: Behavioural: behaviour change Distal outcomes: None reported Process outcomes: None reported |
|
Eves (2012)139 EPHPP: 1 Strong |
Health topic: Physical activity Aim of study:Was mass media sole focus? Yes |
Campaign setting: England (West Midlands) (two worksites) Characteristics: Campaign aim: aimed at attitudinal change on stair climbing Theoretical framework: Theory of Planned Behaviour (‘behaviour is determined by intentions to perform it’) Basis of programme design: Message pre-testing: Duration of the programme: 4 weeks (baseline week after intervention installed, 3 follow-up weeks) Dose intensity: posters in the foyer and halfway up each flight of stairs; arrow at the lift button with the message ‘Stairs this way’, above this arrow, another poster ‘Poster and stairwell messages’ worksite (5 floors): six different messages were positioned on the wall beside the stair risers between each floor Scope: Local (‘Posters alone; City Council building, 1200 employees, five floors: Posters + Stairwell messages; Water Supply company, 500 employees, four floors’) Components: Channels: Posters: Messages: Source: |
Study country: England (West Midlands) Sample size: two worksites (1200 employees – posters only site, 500 employees – posters+ stairwell site); the follow-up questionnaire was returned by 165 (13.8%) and 123 (24.6%) employees Date of data collection: Not reported Study design: Repeated cross sectional quasi-experimental/interrupted time series Data collection method Survey: a follow-up questionnaire distributed through the worksite internal mail Other: Automated observations of stair and lift ascent and descent at baseline and for 3 weeks during intervention |
Subgroup analyses: Gender Message |
Media outcomes: Social cognition: Credibility Social cognition: salience Proximal outcomes: Social cognitive: intention Intermediate outcomes: Behavioural: behaviour change Distal outcomes: None reported Process outcomes: None reported |
|
Eves (2012)140 OCCS: Fair |
Health topic: Physical activity Was mass media sole focus? Yes |
Campaign setting: England West Midlands (one office building/worksite) Characteristics: Campaign aim: to encourage stair use in buildings Theoretical framework: Tested whether individual’s self-categorisation of their level of physical activity might affect preferred campaign message. Categories were based on Stage of Change for physical activity (Laforge, Velicer, Richmond, and Owen, 1999) Basis of programme design: Message pre-testingDuration of the programme: 18 working week days (13 days baseline phase and 18 days after intervention installed) (2 days lost at each phase from technical issues) Dose intensity: Posters at point of choice, outside 2 lifts, insides 2 lifts and on each of 12 floors in the stairwell Scope: Local (1 city worksite) Components: Channels: Posters/prompts: green A2 poster at the point-of-choice; an arrow at the 2 lifts buttons pointed to the stairs with the message ‘Stairs this way’, above this arrow, a yellow A4 prompt; yellow A4 prompt inside the lifts Messages: A health goal:Source: Both the A2 and A4 posters ‘prominently displayed logos for the University of Birmingham, Healthy Living and Heart of Birmingham Teaching, Primary Care Trust NHS’ |
Study country: England West Midlands Sample size: one worksite [office building n = 803 employees (50.9% male)] Date of data collection: Not reported Study design: Repeated cross sectional quasi-experimental/interrupted time series Data collection method Other: Automated observations of stair and lift ascent and descent at baseline and for 3 weeks during intervention |
Media outcomes: None reported Proximal outcomes: None reported Intermediate outcomes: Behavioural: behaviour change Distal outcomes: None reported Process outcomes: None reported |
|
|
Flowers (2013)141 OCCS: Fair |
Health topic: Sexual health Aim of study:Was mass media sole focus? Yes |
Campaign setting: Scotland across the West of Scotland Characteristics: Campaign aim:Theoretical framework: As far as we are aware, there was no explicit attempt to use any theoretical behaviour change techniques within the campaign development Basis of programme design: The development of the campaign involved consultation with voluntary sector agencies and representatives of the target group (through focus groups), prior to commissioning a creative agency to develop the materials. The consultations and focus groups centred on obtaining views on setting, medium, imagery and tone Duration of the programme: It ran from October 2009 to July 2010 Audience Exposure Scope: west of Scotland Target populations: gay men Components: ChannelsMessages: It had two key aims: to promote the use of condoms and water-based lubricant with each episode of anal intercourse; and to promote regular sexual health check ups and HIV testing every 6 months, or more often if the individual had put himself at risk Targeting strategies:Branding ‘make your position clear’ logo |
Study country: Scotland west Sample size: The maximum sample included in the analysis was 784. The total sample was 822 men Date of data collection: July 2010 Study design: Post test: The current study involved one cross-sectional survey of men recruited from seven bars frequented by gay men and other MSM in Glasgow in July 2010, ten months after the campaign had been launched (i.e. post-test only) Data collection method Survey: |
Subgroup analyses: Age Education Other Employment status Geographical area Use of gay scene |
Media outcomes Social cognition: awareness Social cognition: exposure Proximal outcomes Social cognitive: intention Behavioural: treatment-seeking Intermediate outcomes Behavioural: behaviour change Distal outcomes: None reported Process outcomes: None reported |
|
Goodwin (2014)142 CASP: fair |
Health topic: Physical activity Aim of study:Was mass media sole focus? Yes |
Campaign setting: England Liverpool Characteristics: Campaign aim:Basis of programme design: a point of choice strategy used for the mass media Channels, but ‘there was no public consultation by way of a pilot assessment prior to the launch of the campaign’ Duration of the programme: 1 month, January 2007 (to coincide with the UK sales period) Scope: Local (city-wide) Target populations: None (‘The design was not aimed directly at obese people: we wanted to increase awareness on levels of obesity within Liverpool . . . we were looking to get people to understand what is a local issue’ and the selected image was non-gender specific) Components: Channels: Messages:Branding: Liverpool Active City brand was included in the image |
Study country: England Liverpool (and the Public Survey was specifically, ‘various locations around Liverpool city centre’) Sample size: n = 1 campaign lead designer interview; n = 100 public survey with current residents of Liverpool [62 women, 38 men; mean age 37 years (SD 11, range 16–82)]; n = 5 formative evaluation feedback [group discussion n = 4 and e-mail n = 1] Date of data collection: 2007 Study design: Post test cross-sectional survey Qualitative campaign lead designer interview (and emailed feedback); formative evaluation feedback (group discussion) Data collection method Survey: On-street public survey:[NB the reported outcomes data all come from this element of the data collection] Focus groups: Formative evaluation feedback: a group session with key stakeholders, asked for their views on the raw comments from survey respondents. (Plus e-mail correspondence with the lead designer) Interviews: In-depth open-ended 50-minute interview with the campaign lead designer, plus post-test e-mail correspondence to ask for views on the raw comments from survey respondents |
Media outcomes Social cognition: awareness Social cognition: understanding Social cognition: identification Social cognition: attitudinal/emotional responses Proximal outcomes: Social cognitive: intention Intermediate outcomes: None reported Distal outcomes: None reported Process outcomes: None reported |
|
|
Jawad (2015)143 OCCS: Poor |
Health topic: Tobacco use Aim of study:Was mass media sole focus? Yes |
Campaign setting: Other Online Characteristics: Campaign aim: To raise awareness about the health risks of waterpipe tobacco smoking via a YouTube video and posting of ‘shisha facts’ and global news articles in social media Basis of programme design: A ‘grassroots initiative’ and the video was designed by young people Duration of the programme: 9 months Audience exposure: Facebook: 130 status updates over 9 months Twitter: tweeted 373 times over 9 months, longitudinal ‘tweeting rate’ declined over time, from 2.2 ‘tweets’/day from months 0–3 to 1.1 ‘tweets’/day from months 3–6 and then to 0.8 ‘tweets’/day from months 6–9. 73.2% current affairs tweets YouTube: posted 1 video Scope: global Target populations:Cost: An unfunded initiative: used free website-building program and free to access media platforms; campaign team used volunteers Components: Channels: A website and 3 social media channels: Facebook, Twitter and YouTube Channel Interactivity All 3 social media channels involved user interactivity with the campaign Messages: The video ‘maintained an “It’s your choice” message throughout’ Targeting strategies: ‘ShishAware was advertised by posting content on other, related social media accounts’, although the authors did not specify how they were related Source: The campaign video contained excerpts from interviews with (i) young people who had just attended a workshop on waterpipe smoking, (ii) an ex-waterpipe smoker, who detailed reasons for cessation, (iii) one of the ShishAware members, who explained the aims of this campaign, and (iv) general public Branding: ShishAware |
Study country: England London Borough of Brent Other global online community Sample size: Not reported Date of data collection: Not reported Study design: Repeated cross sectional Data collection method Other: Social media usage data (page traffic, page views, unique trends, and views) at 3, 6, and 9 months; likes/comments; and user interaction data (Facebook only) |
Subgroup analyses: Age Gender Reach |
Media outcomes: Social cognition: exposure Interaction: other (with Twitter, Facebook) Proximal outcomes: None reported Intermediate outcomes: None reported Distal outcomes: None reported Process outcomes: Other |
|
Kotz (2011)119 OCCS: Good |
Health topic: Tobacco use Aim of study:Was mass media sole focus? Yes |
Campaign setting: UK (no further breakdown) Characteristics: Campaign aim: ‘helps smokers who want to stop smoking by creating a supportive environment and highlighting the help available for smokers who want to stop’ Duration of the programme: 1 day annually but not reported when the campaign begins around this Scope: National (UK-wide) Target populations: Smokers who want to quit Cost: Total annual direct cost of campaign delivery is approx. £750,000 Components: Channels: ‘It involves a national social marketing campaign and provides materials such as posters and leaflets to local organisations to use in events and promotional activities’ Targeting strategies: ‘works closely with local National Health Service Stop Smoking Services and others . . . provides materials to local organisations’ Branding: No Smoking Day (2nd Wednesday in March) Other support materials: works closely with local NHS Stop Smoking Services and others to provide ongoing support |
Study country: England Sample size: n = 1309 respondents in April 2007–2009 and n = 2672 respondents in the adjacent March and May 2007–9 reported that they had smoked cigarettes or any other tobacco product daily or occasionally at the time of the survey or during the preceding 12 months Date of data collection: March, April and May 2007–9 Study design: Repeated Cross Sectional The ‘Smoking Toolkit Study’ – monthly household survey Data collection method Survey: ‘Smoking Toolkit Study’: computer-assisted face-to-face household surveys (monthly) |
Subgroup analyses: Age Gender Time Other |
Media outcomes: None reported Proximal outcomes: None reported Intermediate outcomes: Behavioural: behaviour change Distal outcomes: None reported Process outcomes: Cost-effectiveness data |
|
Langley (2012)144 OCCS: Good |
Health topic: Tobacco use Was mass media sole focus? Yes |
Campaign setting: England Wales Characteristics: Campaign aim: Campaigns for smoking cessation Tobacco control mass media campaigns (overall, not single campaign): to decrease smoking prevalence and/or increase smoking cessation. Pharmaceutical-company funded campaigns for NRT (overall, not single campaign): to increase the use and sales of NRT Duration of the programme: Tobacco control campaigns: January 2002 – May 2010 Pharmaceutical campaigns: January 2005 – December 2009 Audience Exposure:Scope: national Target populations: smokers Components: Channels: TV Source: Tobacco control campaigns: the government, Cancer Research UK, the British Heart Foundation. Pharmaceutical campaigns: pharmaceutical companies |
Study country: England all outcomes (helpline calls data, NRT prescribing and over-the-counter sales Wales NRT prescribing and over-the-counter sales only (not helpline calls data) Sample size: records from 500 general practices Not reported Not applicable – no sampling beyond the time period selected. All calls to helpline and sales included Date of data collection: TVRs purchased monthly for tobacco control campaigns from January 2002 to May 2010 and by pharmaceutical companies to advertise NRT from January 2005 to December 2009. Number of calls to the NHS helpline per month from November 2004 to June 2010. Unit sales each month from November 2003 to September 2008. Numbers of prescriptions per month from January 2002 to June 2009 Study design Other: Multiple time series analysis:Data collection method Other: data from routine processes not created for the research Outcomes: 1) number of calls to NHS Stop Smoking Services helpline per month . . . 2) NRT over-the-counter sales data from Electronic Point of Sales scanner data . . . 3) divided the numbers of prescriptions by the total person/months . . . derive the rate of prescribing |
Subgroup analyses: Time |
Media outcomes: None reported Proximal outcomes: Behavioural: information-seeking Behavioural: treatment-seeking Intermediate outcomes: None reported Distal outcomes: None reported Process outcomes: None reported |
|
Lewis (2011)145 OCCS: Good |
Health topic: Physical activity Aim of study:Was mass media sole focus? Yes |
Campaign setting: England West Midlands, a Midland Metro station ‘with a 43-step staircase (height = 6.45 m) positioned 16.5 m beyond the escalator’ Characteristics: Campaign aim:Basis of programme design: Based on previous research by these authors:Duration of the programme; 8 weeks (2 weeks point-of-choice prompt at base of stairs only, then 6 weeks with additional posters at the top summarising the calorific consequences) Dose intensity: 1 poster at the base, 2 posters at the top. ‘Pedestrian traffic volume . . . was entered as a continuous variable (mean = 78 pedestrians per tram, range 21–156)’ Scope Local – 1 metro station Components: Channels: Posters: Messages: |
Study country: England (West Midlands) Sample size: n = 23,121 pedestrians leaving trams were coded at 1 metro station (57.9% female, 22.4% overweight). Baseline stage 1, n = 3829; Intervention stage 2, n = 4737; Intervention stage 3, n = 6766; Intervention stage 4, n = 7789 Date of data collection: 2008 Study design: Repeated cross sectional a quasi-experimental, interrupted time-series design Data collection method Other: Observation: 4 inconspicuous observers recorded stair/escalator choices of ascending travellers, between 08:00 and 09:59, on Tuesday and Thursday each week |
Subgroup analyses: Gender Weight status Time |
Media outcomes: None reported Proximal outcomes: None reported Intermediate outcomes: Behavioural: behaviour change Distal outcomes: None reported Process outcomes: None reported |
|
Lewis (2012)146 OCCS: Good |
Health topic: Physical activity Aim of study:Was mass media sole focus? Yes |
Campaign setting: England four buildings at the University of Birmingham: Characteristics: Campaign aim: To increase stair-climbing Basis of programme design: Based on previous research by these authors:Duration of the programme: 13 working week days (5 days motivational intervention only; 8 days volitional intervention plus motivational intervention) Dose intensity: Stage 2 posters inside lifts only (8 lifts in 4 buildings); Stage 3 as Stage 2, plus posters at point of choice and outside 2 liftsScope: Local (one city worksite/four buildings) Components: Channels: Posters: all buildings, stage 2 – yellow A2 motivational poster inside each lift; all buildings, stage 3 – as stage 2 plus same yellow A2 poster between lift and stairs at point of choice plus green A4 poster plus yellow arrow pointing to stairs at the external lift control panel Messages:Source: |
Study country: England Birmingham Sample size: four buildings in one worksite. n = 14,138 observations were recorded (stage 1, n = 4623; stage 2 n = 3853; stage 3, n = 5662), of which 46% were women Date of data collection: December 2009 Study design: Repeated cross sectional quasi-experimental, interrupted-time-series design Data collection method Other: Observation: 4 discrete observers (1 per building) recorded stair/lift choices of ascending pedestrians, between 08:00–10:00 and 14:15–16:15 each weekday (excluding Wednesday afternoons, and excluding 08:45–08:59, 09:45–09:59, 14:45–14:59, and 15:45–15:59) |
Subgroup analyses: Gender Message Time |
Media outcomes: None reported Proximal outcomes: None reported Intermediate outcomes: Behavioural: behaviour change Distal outcomes: None reported Process outcomes: None reported |
|
Lewis (2012)147 Quality not assessed |
Health topic: Physical activity Aim of study:Was mass media sole focus? Yes |
Campaign setting: England West Midlands, a West Midlands Travel rail station ‘with 2 independent platforms exited by identical 39-step staircases and adjacent escalators (height = 6.64 m)’ Characteristics: Campaign aim: to increase stair climbing in the station Theoretical framework:Basis of programme design:Duration of the programme: 3 weeks (2 weeks baseline, 3 weeks poster intervention) Dose intensity: 1 poster at the point of choice (base) on each platform. The simple message platform had higher average pedestrian traffic levels (161.6 ± 87.3 pedestrians.train-1) than the complex message platform (130.7 ± 85.6 pedestrians.train-1) Scope: Local (1 rail station) Components: Channels Posters:Messages: |
Study country: England West Midlands Sample size: n = 48,697 pedestrians were coded (54.7% female overall) for ascending by stair/escalator as they left the train; simple message platform, n = 23,626 (56.7% female); complex message platform n = 25,071 (52.9% female) Date of data collection: February and March 2008 Study design: Repeated cross sectional A quasi-experimental, interrupted time series designData collection method Other: Observation: 4 discretely positioned observers recorded stair/escalator choices of ascending travellers, between 08.00 and 10.00, on Tuesday and Thursday each week 2 weeks baseline observations; point of choice poster phase for 3 weeks, simple message on one side’s platform and complex message on the other side’s platform |
Subgroup analyses: Gender Message Time |
Media outcomes: None reported Proximal outcomes: None reported Intermediate outcomes: Behavioural: behaviour change Distal outcomes: None reported Process outcomes: None reported |
|
Lewis (2015)148 OCCS: Good |
Health topic: Tobacco use Aim of study: Was mass media sole focus? Yes |
Campaign setting: UK (no further breakdown) Characteristics: Campaign aim: Duration of the programme: 75-month study period (Jan 2004 to Apr 2010): second-hand smoking theme broadcast in only 12 of those months Audience Exposure:Scope: National campaigns Target populations: Smokers Components: Channels Television Messages: Smoking cessation theme and second-hand smoking theme campaignsSource: |
Study country: England Data from the Health Survey for England . . . designed to be representative of adults and children living in private households in England Sample size: n = 9872 households with at least one adult smoker (≥ 18 years, responded ‘Yes’ to ‘Do you smoke cigarettes at all nowadays?’) Date of data collection: January 2004 – April 2010 (inclusive) Study design: Repeated cross sectional Analysed annual cross-sectional household survey with Gross Rating Points (GRPs) measure of advertising exposure to national televised tobacco control campaigns Data collection method Survey: Health Survey for EnglandOther: |
Subgroup analyses: Age Gender Socioeconomic status Time Other Households with children |
Media outcomes: None reported Proximal outcomes: None reported Intermediate outcomes: Behavioural: other (smoke-free homes) Distal outcomes: None reported Process outcomes: None reported |
|
Lyons (2013)149 OCCS: Poor |
Health topic: Sexual health Aim of study:Was mass media sole focus? No |
Campaign setting: England UK Department of Health (England, most of the health items devolved) Characteristics: Campaign aim: A campaign ‘Worth Talking About’ with two main strands; one focusing on contraception and in particular increasing awareness of LARCs (long-acting reversible contraception) and the other focusing on chlamydia Duration of the programme: Launched November 2009 Components: Channels: not reported, described as a ‘media campaign’ Branding: ‘Worth Talking About’ |
Study country: England Leeds Sample size: 400 women who had an etonogestrel contraceptive implant (Nexplanon®) Merck Sharp & Dohme Corp., Merck & Co., Inc., Whitehouse Station, NJ, USA fitted Date of data collection: October 2010 Study design: Post test (described as prospective study; however the results reported here are cross-sectional, post-campaign) Data collection method: Survey asked at the their fitting appointment |
Subgroup analyses: Gender |
Media outcomes: Social cognition: awareness Proximal outcomes: None reported Intermediate outcomes: None reported Distal outcomes: None reported Process outcomes: None reported |
|
McNeill (2014)150 OCCS: Fair |
Health topic: Tobacco use Aim of study:Was mass media sole focus? No; mostly about the set up of the programme some information from views |
Campaign setting: Other: two North of England Department of Health Regions: Northwest and Northeast Characteristics: Campaign aim:Components: Channels: a range of media, including websites Channel Interactivity: hotlines for reporting illegal tobacco Messages: Its two main messages were that IT made it easier for children to start smoking, and that IT brought crime into the community. The campaign . . . proposed that people should ‘get some answers’ to key questions about illicit tobacco . . . Branding Logos: ‘illegal tobacco’ and ‘keep it out’ |
Study country: Other: Northern England – North East, North West and Yorkshire and Humber Sample size: A representative sample of around 2300 people was attained and this was then supplemented with a boosted sample of around 1800 smokers . . . Stakeholder Interviews I: 16 interviews Stakeholder Interviews I: 9 follow-up interview + 5 others Date of data collection: Two independent cross-sectional surveys were carried out, in July 2009 and March/April 2011 Study design: Pre/post test surveys about two years apart Repeated cross-sectional qualitative ethnography Data collection method Survey: Hotline data (calls to Crimestoppers and Customs Hotline concerning illicit tobacco); Consumer Research (commissioned a market research company, used telephone number sampling and street interviews) Interviews: Stakeholder Interviews with the Programme’s Governance Board (comprising representatives from local and national enforcement agencies, regional health agencies, and marketing and communication professionals); 45 minutes, face to face or telephone |
Media outcomes: None reported Proximal outcomes: Social cognitive: awareness Behavioural: engagement with professionals Intermediate outcomes Behavioural: behaviour change Behavioural: other Distal outcomes: None reported Process outcomes Other |
|
|
Naughton (2015)151 OCCS: Fair |
Health topic: Tobacco use Aim of study:Was mass media sole focus? No |
Campaign setting: England King’s Mill Hospital (KMH), Sherwood Forest Hospitals NHS Foundation Trust, Sutton-In-Ashfield, Nottinghamshire Characteristics: Campaign aim: To promote uptake of the MiQuit text service by pregnant smokers. Duration of the programmeScope: local (single site, antenatal care in one hospital) Target populations: pregnant smokers Cost: Described as ‘low-cost’. . . . the low cost of delivering MiQuit (approximately £3.20 per user based on trial data plus maintenance costs) and low dissemination costs to promote it would likely make it highly cost-effective’ Components: Channels: Leaflets, posters, promotions pens and information cards. A single-sheet A5 leaflet describing MiQuit was inserted into maternity notes folders (given to all pregnant women at midwife ‘booking’ appointment) alongside two other health advice leaflets unrelated to smoking. A3 posters in the ultrasound clinic area and antenatal ward. ‘Banner’ pens and credit card-sized information cards in the ultrasound clinic area Messages: Informational [‘In addition to providing information about the support provided and potential costs associated with activating MiQuit, the leaflet explained how to activate MiQuit support . . . and how to discontinue text support’] Targeting strategies: Distribution of promotional materials in booking notes, and in ultrasound clinic area and antenatal ward Branding: MiQuit |
Study country: England King’s Mill Hospital (KMH), Sherwood Forest Hospitals NHS Foundation Trust, Sutton-In-Ashfield, Nottinghamshire Sample size: n = 1775 (6-month, strict), including n = 499 smokers (25.3%); n = 2356 (9-month, extended), including n = 585 smokers (24.8%) Date of data collection: January to August 2013 (6-month period Jan-Jun 2013 (Strict); 9-month period Jan-Sep 2013 (Extended – due to lag in packs handed out by midwives)) Study design: Post test ‘A single-site service evaluation . . . where initiation and subsequent discontinuation rates for a smoking cessation text message support system (MiQuit) were recorded among a cohort of pregnant women’. It was promoted without ‘active health professional endorsement’ Data collection method Other: Community midwife booking appointment attendance data (routine data for smoker information) were analysed with MiQuit activation requests |
Subgroup analyses: Other Pregnancy status |
Media outcomes: None reported Proximal outcomes: Behavioural: treatment-seeking Intermediate outcomes: None reported Distal outcomes: None reported Process outcomes: Other: (equivalent local Stop Smoking Service access rates) |
|
Richardson (2014)152 OCCS: Good |
Health topic: Tobacco use Aim of study:Was mass media sole focus? Yes |
Campaign setting: UK (no further breakdown) Characteristics: Campaign aim:Theoretical framework:Audience exposure:Components: Channels: TV Messages: positive and negative emotive content Source: government funded Other: some had helplines |
Study country: England calls to English quitline Sample size: 1,227,189 calls Date of data collection: between April 2005 and April 2010 Study design: Repeated cross sectional Data collection method Other: secondary data analysis The outcome variable was generated using UK Department of Health data on calls to the English NHS Stop Smoking helpline between April 2005 and April 2010, expressed as monthly count data |
Subgroup analyses: Message |
Media outcomes: Social cognition: exposure Proximal outcomes: Behavioural: information-seeking Intermediate outcomes: None reported Distal outcomes: None reported Process outcomes: None reported |
|
Richardson (2014)153 OCCS: Good |
Health topic: Tobacco use Aim of study:Was mass media sole focus? Yes |
Campaign setting: UK (no further breakdown) Characteristics: Campaign aim: ITC survey measure: ‘advertising or information that talks about the dangers of smoking, or encourages quitting on television’ (not a single campaign, but ‘government-funded televised tobacco control mass media campaigns’) Theoretical framework: Not as reported by campaign designers, but the researchers categorised campaigns ‘using a coding framework based on PRIME Theory [(plans, responses, impulses/inhibitory forces, motives and evaluations); West R: The multiple facets of cigarette addiction and what they mean for encouraging and helping smokers to stop. COPD 2009, 6:277–283]’ Duration of the programme: April 2005 to March 2009 Dose intensity:Scope: national (UK) Target populations: Smokers (not specified in paper) Components: Channels TV Messages: ‘Campaigns were categorised as having either ‘positive’ (eliciting happiness, satisfaction or hope) or ‘negative’ (eliciting fear, sadness, guilt, anger or disgust) emotional content.’ 42.4% of campaign GRPs from campaigns featuring positive emotive content, 52.6% of campaign GRPs from campaigns featuring negative emotive content (5.0% classified as ‘neutral’ and removed) Source: |
Study country: England Sample size: n = 1968 adult smokers residing in England through four waves of the International Tobacco Control (ITC) United Kingdom Survey. Provided 3932 observations over four waves of follow-up, implying a mean of 2.0 observations per participant Date of data collection: April 2005 to March 2009 [UK ITC Waves 4–7: 4 (2005–2006), 5 (2006–2007), 6 (2007–2008), 7 (2008–2009)] Study design: Cohort/longitudinal study ITC United Kingdom Survey, a prospective longitudinal cohort study Other: Secondary data analysis (of ITC UK Survey and campaign reach data) Data collection method Survey: Telephone survey: |
Subgroup analyses: Time to follow-up Dose response: relationship for each Message |
Media outcomes: Social cognition: awareness Proximal outcomes: None reported Intermediate outcomes: None reported Distal outcomes: None reported Process outcomes: None reported |
|
Sims (2014)155 Quality not assessed |
Health topic: Tobacco use Aim of study:Was mass media sole focus? Yes |
Campaign setting: UK (no further breakdown) Characteristics: Campaign aim: ‘The United Kingdom has not shown anti-industry messages, focusing instead on both the negative health impacts of smoking and campaigns with positive messages about how to quit’. Not a single campaign, but public sector tobacco control advertising (funded by government and charities) Duration of the programme: January 2002 to April 2010 Dose intensity: Time–series plot of gross rating points (GRPs) shows ‘during the period covered by the study . . . [GRPs] are characterized by peaks and troughs with no clear secular trend’ Scope: National Cost: ‘Government expenditure on television advertising campaigns from January 2002 to December 2009 was £78 million’ Components: Channels: television Messages:Source: |
Study country: England Sample size: n = 81,256 adults (≥ 18 years) living in England in the smoking prevalence analyses; n = 19,488 adults (≥ 18 years) living in England in the cigarette consumption analyses Date of data collection: February 2002 to April 2010 (inclusive, no Office for National Statistics survey in January 2002) Study design: Repeated cross-sectional Opinions and Lifestyle Survey (OS), a monthly cross-sectional survey Other: Secondary data analysis of monthly cross-sectional surveys and campaign reach data ‘using generalised additive models’ Data collection method Survey:Other: |
Media outcomes: None reported Proximal outcomes: None reported Intermediate outcomes Behavioural: behaviour change Distal outcomes: Improvement in population health status Process outcomes: Cost-effectiveness data |
|
|
Sims (2016)154 OCCS: Good |
Health topic: Tobacco use Aim of study:Was mass media sole focus? Yes |
Campaign setting: England, smokers in England Characteristics: Campaign aim: To change adult tobacco use, specifically to decrease smoking prevalence and cigarette consumption Duration of the programme: January 2004 to April 2010 inclusive; ads screened in 60 of the 76 months (negative emotive campaigns 19 months, positive emotive campaigns 17 months, both 24 months) Dose intensity: The intensity of each campaign type changed . . . with more negative emotive campaigns in the earlier years and positive emotive campaigns in later years. Of the 26,222 GRPs during the study, 53% were for negative emotive campaigns, 42% for positive emotive campaigns and the remaining 5% were emotionally neutral Scope: National Target populations: Adult Components: Channels: Television (basic information, either a telephone number, website or text number that would lead to further information on quitting would appear on the screen) Messages:Source: ‘Negative emotive adverts . . . were mostly testimonial or acted adverts with a very few showing graphic imagery . . . Positive campaigns . . . all were acted.’ Campaigns were government-funded plus campaigns by Cancer Research UK and the British Heart Foundation funded by the Department of Health |
Study country: England Sample size: ≈60,000 adults (≥ 18 years) (≈14,000 self-reported current smokers for cigarette consumption outcomes) Date of data collection: January 2004 to April 2010 inclusive Study design: Repeated cross sectional More specifically, an ‘analysis of monthly cross-sectional surveys using generalised additive models’ Data collection method Survey: |
Subgroup analyses: Message |
Media outcomes: None reported Proximal outcomes: None reported Intermediate outcomes: Behavioural: behaviour change Distal outcomes: None reported Process outcomes: Cost-effectiveness data |
|
Stautz (2016)156 EPHPP: 1 Strong |
Health topic: Alcohol useAim of study:The primary aim of this [online] pilot study is to assess whether exposure to alcohol warning advertising is effective in reducing the urge to drink alcohol, and whether affective responses to advertising help to explain any such effectWas mass media sole focus? Yes |
Campaign setting: UK (no further breakdown) (seven advertisements) Other Australia (four advertisements), New Zealand (1), the Republic of Ireland (1), Sweden (1), and Iceland (1) Characteristics: Campaign aim: Not a specific mass media campaign. Described as ‘advertisements [that] were professionally produced, appeared to be relevant to young adults, and highlighted short-or long-term negative consequences of alcohol consumption’ Basis of programme design: ‘Categories [of message content and presentation style] were adapted from a study of obesity prevention advertisements [19 Dixon et al. BMC Public Health. 2015;15:804.], and were coded by the first author’ Duration of the programme: Selected ads were produced between 2006 and 2015, ads ranged from 30 to 69 seconds long Scope: National Target populations: Ads selected for study on appearing ‘to be relevant to young adults’. Two UK ads gender targeted [Know your limits (Male); Know your limits (Female)] Components Channels: video advertising (via television or internet – sample were asked about their typical use of both channels) Messages:‘Categories of presentation style were: graphic; depiction; testimonial; and animated text’ |
Study country: UK (no further breakdown) Sample size: n = 152 18- to 25-year-old drinkers (≥ 1 alcoholic beverage per typical week); 50% female, 49.3% male, n = 1 not reported); mean age 21.47 SD± 1.31; 65.1% ‘White British’, 17.8% ‘Any other white background’. Recruited from a UK online panel Date of data collection: Not reported. The advertisements (stimuli) were selected in 2015 and the paper submitted in 2015 Study design: RCTs/trials A between-participants experimental design. Sample randomly assigned to one of three conditions (1. alcohol warning advertisements, 2. alcohol promoting advertisements, 3. non-alcohol advertisements) before completing a post-exposure survey Data collection method: Survey: The study was completed entirely online. Participants gave informed consent and then completed . . . questionnaires. . . . participants were presented with a random selection of six advertisements . . . participants reported their current pleasure and arousal, and the degree to which they perceived the advertisement to be effective. . . . participants reported their urges to drink alcohol |
Subgroup analyses: Other: heaviness of drinking |
Media outcomes: Social cognition: credibility Social cognition: attitudinal/emotional responses Proximal outcomes: Social cognitive: motivation Intermediate outcomes: None reported Distal outcomes: None reported Process outcomes: None reported |
|
OCCS: Good |
Health topic: Diet Aim of study:Was mass media sole focus? No: two pronged campaign – also looked to reduce salt in ready meals |
Campaign setting: UK (no further breakdown) Characteristics: Campaign aim: First, by a gradual reduction in the salt content of foods through engagement with the food industry on reformulation of industrially processed foods and, second, by increasing consumer awareness of the impact of salt on health via a public awareness campaign using a variety of media outlets Duration of the programme: 4 years – 2004–2008 Target populations: The public awareness campaign’s main target group comprised women aged 25–65 years in social demo- graphic groups C1, C2 and D, as women in the household are considered to be the main gatekeepers when it comes to food and health Components: Channels: The campaign involved television, radio, press and poster advertisements; leaflets, interactive activities at supermarkets, digital advertising, Food Standards Agency website Channel interactivity: experiential activity at supermarkets (interactive activity involving quizzes, provision of information and product tasting) Messages: Phase 1 . . . featured ‘Sid the Slug’ . . . Phase 2, . . . encouraged consumers to ‘check the label’ . . . Phase 3, . . . focused on informing consumers . . . Phase 4 reinforced messages from the previous phases and highlighted . . . ‘hidden’ salt and offered practical solutions Targeting strategies: During the second and third phases of the campaign, some food companies and some NGO carried out work to help disseminate the campaign messages to hard-to-reach groups The target groups for the initiatives included black and minority ethnic groups, inner-city communities, young parents, Hindu and Sikh populations and housing association staff and residents Branding: Sid the Slug; Talking Food; Full of it |
Study country: England Sample size: 67 980 individuals answered the Health Survey for England salt behaviour question between 1997 and 2007 Date of data collection: In the years 1997, 1998, 2003, 2005, 2006 and 2007 Study design: Repeated cross-sectional Data collection method Survey: Health Survey of England Data were obtained from repeated cross-sections of the Health Survey for England (HSE), an annual survey of a nationally representative sample of the general population living in households in England. Specifically, participants were asked to categorise their salt use at the table . . . |
Subgroup analyses: Age Gender Socioeconomic status Race/Ethnicity Other region of England |
Media outcomes: None reported Proximal outcomes: None reported Intermediate outcomes: Behavioural: behaviour change, Behavioural: sustained healthier behaviours Distal outcomes: None reported Process outcomes: None reported |
Appendix 8 List of UK primary studies excluded from the rapid review at the full-text assessment stage (review D)
| Reference | Reason for exclusion |
|---|---|
| Adams E. Walking Works! Evaluation of a workplace walking project in England. J Sci Med Sport 2012;15:S236 | Intervention did not meet the mass media definitiona |
| Ainsworth H, Shah S, Ahmed F, Amos A, Cameron I, Fairhurst C, et al. Muslim communities learning about second-hand smoke (MCLASS): study protocol for a pilot cluster randomised controlled trial. Trials 2013;14:295. https://doi.org/10.1186/1745-6215-14-295 | Excluded on outcomes data |
| Ajay VS, Praveen PA, Millett C, Kinra S, Prabhakaran D. Role of mobile phone technology in tobacco cessation interventions. Glob Heart 2012;7:167–74. https://doi.org/10.1016/j.gheart.2012.03.004 | Intervention did not meet the mass media definitiona |
| Al-Alawy K, Roche T, Alwali W. Implementing public health in secondary care: a Rotherham perspective on strategy development and implementation. Perspect Public Health 2011;131:137–43. https://doi.org/10.1177/1757913911400141 | Intervention did not meet the mass media definitiona |
| Allmark P, Tod AM, McDonnell A, Al-Alawy K, Mann K, Hollis E, et al. Evaluation of the impact of a smoke-free home initiative in Rotherham, a deprived district in Northern England. Eur J Public Health 2012;22:248–51. https://doi.org/10.1093/eurpub/ckr072 | Intervention did not meet the mass media definitiona |
| Anderson AS, Macleod M, Mutrie N, Sugden J, Dobson H, Treweek S, et al. Breast cancer risk reduction – is it feasible to initiate a randomised controlled trial of a lifestyle intervention programme (ActWell) within a national breast screening programme? Int J Behav Nutr Phys Act 2014;11:156. https://doi.org/10.1186/s12966-014-0156-2 | Intervention did not meet the mass media definitiona |
| Anokye NK, Lord J, Fox-Rushby J. Is brief advice in primary care a cost-effective way to promote physical activity? Br J Sports Med 2014;48:202–6. https://doi.org/10.1136/bjsports-2013-092897 | Intervention did not meet the mass media definitiona |
| Armitage A, Crosse C, Bridger A. Sex undressed: developing a website for young people around sex and body image. BMJ 2015;91:84 | Excluded on outcomes data |
| McCarthy OL, French RS, Baraitser P, Roberts I, Rathod SD, Devries K, et al. Safetxt: a pilot randomised controlled trail of an intervention delivered by mobile phone to increase safer sex behaviours in young people. BMJ Open 2016;6:e013045 | Excluded on outcomes data |
| Aventin Á, Lohan M, O’Halloran P, Henderson M. Design and development of a film-based intervention about teenage men and unintended pregnancy: applying the Medical Research Council framework in practice. Eval Program Plann 2015;49:19–30. https://doi.org/10.1016/j.evalprogplan.2014.11.003 | Excluded on outcomes data |
| Baguley S. Texting or talking: which is the more effective intervention for hazardous drinking? Int J STD AIDS 2013;24:1–60 | Intervention did not meet the mass media definitiona |
| Bailey J, McCarthy O, Carswell K, Murray E, Rait G, Hart G, et al. The Sexunzipped Website for Sexual Wellbeing for Young People: Early Results of a Pilot Online RCT. Paper presented at 20th World Congress of Sexual Health, Glasgow, UK, 12–16 June 2011 | Excluded on outcomes data |
| Bailey JV, Pavlou M, Copas A, McCarthy O, Carswell K, Rait G, et al. The Sexunzipped Trial: optimizing the design of online randomized controlled trials. J Med Internet Res 2013;15:278 | Excluded on outcomes data |
| Bailey JV, Webster R, Hunter R, Freemantle N, Rait G, Michie S, et al. The Men’s Safer Sex (MenSS) trial: protocol for a pilot randomised controlled trial of an interactive digital intervention to increase condom use in men. BMJ Open 2015;5:e007552. https://doi.org/10.1136/bmjopen-2014-007552 | Excluded on outcomes data |
| Bath R, O’Connell R, Lascar M, Ferrand R, Matin N, Basnett I, et al. #Testmeeast@Eurohivtestingweek: a Celebrity-Endorsed, Newsworthy NHS Campaign Across Six Hospitals to Test 2500 Patients (500/Day) Based in Outpatients (OPD) and Emergency Departments (ED): the Results. 3rd Joint Conference of the British HIV Association, BHIVA with the British Association for Sexual Health and HIV, and BASHH, Liverpool, UK, 1–4 April 2014 | Intervention did not meet the mass media definitiona |
| Bath R, O’Connell R, Lascar M, Ferrand R, Strachan S, Matin N, et al. TestMeEast: a campaign to increase HIV testing in hospitals and to reduce late diagnosis. AIDS Care 2016;28:608–11. https://doi.org/10.1080/09540121.2015.1120855 | Intervention did not meet the mass media definitiona |
| Beeken RJ, Wardle J. Public beliefs about the causes of obesity and attitudes towards policy initiatives in Great Britain. Public Health Nutr 2013;16:2132–7. https://doi.org/10.1017/S1368980013001821 | Excluded on outcomes data |
| Best C, Haseen F, van der Sluijs W, Ozakinci G, Currie D, Eadie D, et al. Relationship between e-cigarette point of sale recall and e-cigarette use in secondary school children: a cross-sectional study. BMC Public Health 2016;16:310. https://doi.org/10.1186/s12889-016-2968-2 | Did not examine one or more of the relevant health behaviours |
| Bhogal MS, Langford R. Gender differences in weight loss; evidence from a NHS weight management service. Public Health 2014;128:811–13 | Intervention did not meet the mass media definitiona |
| Bird W. Activating a whole community. Beat the Street. J Sci Med Sport 2014;18:145–6 | Intervention did not meet the mass media definitiona |
| Blyth A, Maskrey V, Notley C, Barton GR, Brown TJ, Aveyard P, et al. Effectiveness and economic evaluation of self-help educational materials for the prevention of smoking relapse: randomised controlled trial. Health Technol Assess 2015;19(59). https://doi.org/10.3310/hta19590 | Intervention did not meet the mass media definitiona |
| Boddington EL, McDermott MR. Predicting resistance to health education messages for cannabis use: the role of rebelliousness, autic mastery, health value and ethnicity. J Health Psychol 2013;18:157–66. https://doi.org/10.1177/1359105312438111 | Intervention did not meet the mass media definitiona |
| Bradshaw D, Hughes A, Day S. A novel service promotion campaign using the social media site Facebook. Sex Transm Infect 2013;89:104. https://doi.org/10.1136/sextrans-2012-050877 | Excluded on outcomes data |
| Brady M, Nardone A, Buenaventura E, Qureshi F, Edwardes D, Kelly P, et al. Home HIV sampling linked to national HIV testing campaigns: a novel approach to improve HIV diagnosis. HIV Medicine 2014;15(Suppl. 3):7–8 | Intervention did not meet the mass media definitiona |
| Brennan LK, Brownson RC, Kelly C, Ivey MK, Leviton LC. Concept mapping: priority community strategies to create changes to support active living. Am J Prev Med 2012;43(Suppl. 5):337–50. https://doi.org/10.1016/j.amepre.2012.07.015 | Excluded on outcomes data |
| Bromley H, Lloyd Williams F, Orton L, Mcgill R, Anwar E, Taylor Robinson D, et al. Using a Novel Framework to Categorise Public Health Nutrition Actions in 30 European Countries. Paper presented at EuroPRevent Amsterdam, the Netherlands, 8–10 May 2014 | Excluded on outcomes data |
| Buckton CH, Lean ME, Combet E. ‘Language is the source of misunderstandings’ – impact of terminology on public perceptions of health promotion messages. BMC Public Health 2015;15:579. https://doi.org/10.1186/s12889-015-1884-1 | Excluded on outcomes data |
| Burton J, Brook G, McSorley J, Murphy S. The utility of short message service (SMS) texts to remind patients at higher risk of STIs and HIV to reattend for testing: a controlled before and after study. Sex Transm Infect 2014;90:11–13. https://doi.org/10.1136/sextrans-2013-051228 | Intervention did not meet the mass media definitiona |
| Buyuktuncer Z, Kearney M, Ryan CL, Thurston M, Ellahi B. Fruit and vegetables on prescription: a brief intervention in primary care. J Hum Nutr Diet 2014;27(Suppl. 2):186–93. https://doi.org/10.1111/jhn.12109 | Intervention did not meet the mass media definitiona |
| Cameron D, Epton T, Norman P, Sheeran P, Harris PR, Webb TL, et al. A theory-based online health behaviour intervention for new university students (U@Uni:LifeGuide): results from a repeat randomized controlled trial. Trials 2015;16:555. https://doi.org/10.1186/s13063-015-1092-4 | Intervention did not meet the mass media definitiona |
| Cameron LD, Williams B. Which images and features in graphic cigarette warnings predict their perceived effectiveness? Findings from an online survey of residents in the UK. Ann Behav Med 2015;49:639–49 | Intervention did not meet the mass media definitiona |
| Carswell K, McCarthy O, Murray E, Bailey JV. Integrating psychological theory into the design of an online intervention for sexual health: the sexunzipped website. JMIR Res Protoc 2012;1:e16. https://doi.org/10.2196/resprot.2114 | Excluded on outcomes data |
| Cavill N, Muller L, Mulhall C, Rutter H. Cycling Demonstration Towns: a Cost-Effective Investment to Promote Physical Activity. Paper presented at 18th European Congress on Obesity, ECO, Istanbul, Turkey, 25–28 May 2011 | Excluded on outcomes data |
| Clarke J, Gill H. I Was Planning on Coming but the Programme Pushed Me to Do It: Staff Response and Clinic Attendee Reactions to Participation of a UK Sexual Health Service in a Reality TV Series. Paper presented at 2014 STD Prevention Conference Atlanta, USA, 9–12 June 2014 | Excluded on outcomes data |
| Clarke J, Gill H. Not Enough HIV Stories!: Staff Reactions to a UK Sexual Health Reality TV Series. Paper presented at 3rd Joint Conference of the British HIV Association, BHIVA with the British Association for Sexual Health and HIV, BASHH, Liverpool, UK, 1–4 April 2014 | Linked to a previously excluded study |
| Cobb NK, Jacobs MA, Saul J, Wiley to EP, Graham AL. Diffusion of an evidence-based smoking cessation intervention through Facebook: a randomised controlled trial study protocol. BMJ Open 2014;4:e004089. https://doi.org/10.1136/bmjopen-2013-004089 | Excluded on outcomes data |
| Collins M, Mason H, O’Flaherty M, Guzman-Castillo M, Critchley J, Capewell S. An economic evaluation of salt reduction policies to reduce coronary heart disease in England: a policy modelling study. Value Health 2014;17:517–24 | Intervention did not meet the mass media definitiona |
| Cooper AJ, Dearnley K, Williams KM, Sharp SJ, van Sluijs EM, Brage S, et al. Protocol for Get Moving: a randomised controlled trial to assess the effectiveness of three minimal contact interventions to promote fitness and physical activity in working adults. BMC Public Health 2015;15:296. https://doi.org/10.1186/s12889-015-1654-0 | Excluded on outcomes data |
| Corcoran N, Ahmad F. The readability and suitability of sexual health promotion leaflets. Patient Educ Couns 2016;99:284–6. https://doi.org/10.1016/j.pec.2015.09.003 | Excluded on outcomes data |
| Dahl S, Eagle L, Ebrahimjee M. Golden moves: developing a transtheoretical model-based social marketing intervention in an elderly population. Social Marketing Quarterly 2013;19:230–41 | Excluded on outcomes data |
| Dawson J, Huikuri S, Armada F. Liverpool Active City 2005-2010: Increasing Population Physical Activity Levels Through Intersectoral Action. J Phys Act Health 2015;12:749–55. https://doi.org/10.1123/jpah.2013-0397 | Intervention did not meet the mass media definitiona |
| Day S, Hughes A. A highly cost-effective and targeted service promotion campaign using the social media site Facebook. BMJ 2012;88:44 | Excluded on outcomes data |
| de Visser RO, Wheeler Z, Abraham C, Smith JA. Drinking is our modern way of bonding: young people’s beliefs about interventions to encourage moderate drinking. Psychology & Health 2001;28:1460–80 | Excluded on outcomes data |
| de Vocht F, Higgerson J, Oliver K, Verma A. Incorporating uncertainty in aggregate burden of disease measures: an example of DALYs-averted by a smoking cessation campaign in the UK. J Epidemiol Community Health 2011;65:751–6. https://doi.org/10.1136/jech.2010.119842 | Excluded on outcomes data |
| Derges J, Clow A, Lynch R, Jain S, Phillips G, Petticrew M, et al. ‘Well London’ and the benefits of participation: results of a qualitative study nested in a cluster randomised trial. BMJ Open 2014;4:e003596. https://doi.org/10.1136/bmjopen-2013-003596 | Intervention did not meet the mass media definitiona |
| Dewhurst H, Neild P. Attitudes, Experience and Expectations of Health Service Users Regarding Nutritional Advice and Its Source. Paper presented at Malnutrition Matters, Joint BAPEN and Nutrition Society Meeting, Harrogate, UK, 29–30 November 2011 | Intervention did not meet the mass media definitiona |
| Dixon H, Scully M, Cotter T, Maloney S, Wakefield M. Healthy weight and lifestyle advertisements: an assessment of their persuasive potential. Health Educ Res 2015;30:569–79. https://doi.org/10.1093/her/cyv031 | Excluded on outcomes data |
| Dobbie F, Hiscock R, Leonardi-Bee J, Murray S, Shahab L, Aveyard P, et al. Evaluating Long-term Outcomes of NHS Stop Smoking Services (ELONS): a prospective cohort study. Health Technol Assess 2015;19(95). https://doi.org/10.3310/hta19950 | Intervention did not meet the mass media definitiona |
| Dovey TM, Taylor L, Stow R, Boyland EJ, Halford JC. Responsiveness to healthy television (TV) food advertisements/commercials is only evident in children under the age of seven with low food neophobia. Appetite 2011;56:440–6. https://doi.org/10.1016/j.appet.2011.01.017 | Intervention did not meet the mass media definitiona |
| Eaton JW, Hallett TB, Epstein H. 2012. What might be the impact of sexual partnership ‘concurrency’ behavior change communication campaigns? Sex Transm Dis 2012;39:899 | Intervention did not meet the mass media definitiona |
| Eddy F, Thomas B, Gill E. Use of the Internet for Sexual Health Information, Can We Engage Young People Online? 11th Spring Meeting of the British Association for Sexual Health and HIV, and BASHH, Bristol, UK, 15–17 May 2013 | Excluded on outcomes data |
| Edmunds S, Stephenson D, Clow A. The effects of a physical activity intervention on employees in small and medium enterprises: a mixed methods study. Work 2013;46:39–49. https://doi.org/10.3233/WOR-121523 | Intervention did not meet the mass media definitiona |
| Edwardson CL, Harrington DM, Yates T, Bodicoat DH, Khunti K, Gorely T, et al. A cluster randomised controlled trial to investigate the effectiveness and cost effectiveness of the ‘Girls Active’ intervention: a study protocol. BMC Public Health 2015;15:526. https://doi.org/10.1186/s12889-015-1886-z | Excluded on outcomes data |
| Elliott L, Henderson M, Nixon C, Wight D. Has untargeted sexual health promotion for young people reached its limit? A quasi-experimental study. J Epidemiol Community Health 2013;67:398–404. https://doi.org/10.1136/jech-2012-201034 | Intervention did not meet the mass media definitiona |
| Epton T, Norman P, Sheeran P, Harris PR, Webb TL, Ciravegna F, et al. A theory-based online health behavior intervention for new university students: study protocol. BMC Public Health 2013;13:107. https://doi.org/10.1186/1471-2458-13-107 | Excluded on outcomes data |
| Epton T, Norman P, Dadzie AS, Harris PR, Webb TL, Sheeran P, et al. A theory-based online health behaviour intervention for new university students (U@Uni): results from a randomised controlled trial. BMC Public Health 2014;14:563. https://doi.org/10.1186/1471-2458-14-563 | Intervention did not meet the mass media definitiona |
| Evans RE, Fawole HO, Sheriff SA, Dall PM, Grant PM, Ryan CG. Point-of-choice prompts to reduce sitting time at work: a randomized trial. Am J Prev Med 2012;43:293–7. https://doi.org/10.1016/j.amepre.2012.05.010 | Intervention did not meet the mass media definitiona |
| Fairclough SJ, Hackett AF, Davies IG, Gobbi R, Mackintosh KA, Warburton GL, et al. Promoting healthy weight in primary school children through physical activity and nutrition education: a pragmatic evaluation of the CHANGE! randomised intervention study. BMC Public Health 2013;13:626. https://doi.org/10.1186/1471-2458-13-626 | Intervention did not meet the mass media definitiona |
| Fernando KA, Matthews S, Jaleel H, Salimee S. Multidisciplinary Approach to Managing a Syphilis Outbreak in Southend-On-Sea, Essex UK. STI and AIDS World Congress 2013 Vienna, Austria, 14–17 July 2013 | Intervention did not meet the mass media definitiona |
| Flanagan S. Call the Radio Doctor! Experiences of a Sexual Health Doctor on BBC Radio 1’s Surgery. Paper presented at 3rd Joint Conference of the British HIV Association, BHIVA with the British Association for Sexual Health and HIV, BASHH, Liverpool, UK, 1–4 April 2014 | Intervention did not meet the mass media definitiona |
| Forwood SE, Ahern A, Hollands GJ, Marteau TM. Impact on Food Preferences of Priming a Healthy Eating Goal. Paper presented at 20th European Congress on Obesity, ECO, Liverpool, UK, 12–15 May 2013 | Linked to a previously excluded study |
| Forwood SE, Ahern AL, Hollands GJ, Ng YL, Marteau TM. Priming healthy eating. You can’t prime all the people all of the time. Appetite 2015;89:93–102. https://doi.org/10.1016/j.appet.2015.01.018 | Intervention did not meet the mass media definitiona |
| Frew EJ, Bhatti M, Win K, Sitch A, Lyon A, Pallan M, Adab P. Cost-effectiveness of a community-based physical activity programme for adults (Be Active) in the UK: an economic analysis within a natural experiment. Br J Sports Med 2014;48:207–12. https://doi.org/10.1136/bjsports-2012-091202 | Intervention did not meet the mass media definitiona |
| Gamble T, Walker I, Laketa A. Bicycling campaigns promoting health versus campaigns promoting safety: a randomised controlled online study of ‘dangerization. Journal of Transport & Health 2015;2:369–78 | Intervention did not meet the mass media definitiona |
| Gholami M, Wiedemann A, Knoll N, Schwarzer R. Mothers improve their daughters’ vegetable intake: a randomized controlled trial. Psychol Health Med 2015;20:1–7. https://doi.org/10.1080/13548506.2014.902485 | Intervention did not meet the mass media definitiona |
| Gillespie DO, Allen K, Guzman-Castillo M, Bandosz P, Moreira P, McGill R, et al. The Health Equity and Effectiveness of Policy Options to Reduce Dietary Salt Intake in England: Policy Forecast. PLOS ONE 2015;10:e0127927. https://doi.org/10.1371/journal.pone.0127927 | Excluded on outcomes data |
| Gobin M, Verlander N, Maurici C, Bone A, Nardone A. Do sexual health campaigns work? An outcome evaluation of a media campaign to increase chlamydia testing among young people aged 15-24 in England. BMC Public Health 2013;13:484. https://doi.org/10.1186/1471-2458-13-484 | Did not examine one or more of the relevant health behaviours |
| Gorely T, Morris JG, Musson H, Brown S, Nevill A, Nevill ME. Physical activity and body composition outcomes of the GreatFun2Run intervention at 20 month follow-up. Int J Behav Nutr Phys Act 2011;8:74. https://doi.org/10.1186/1479-5868-8-74 | Intervention did not meet the mass media definitiona |
| Goyder E, Hind D, Breckon J, Dimairo M, Minton J, Everson-Hock E, et al. A randomised controlled trial and cost-effectiveness evaluation of booster interventions to sustain increases in physical activity in middle-aged adults in deprived urban neighbourhoods. Health Technol Assess 2014;18(13) | Intervention did not meet the mass media definitiona |
| Grewe ME, Tucker JD. Syphilis cure posters. Sex Transm Infect 2015;91:71. https://doi.org/10.1136/sextrans-2014-051782 | Intervention did not meet the mass media definitiona |
| Guerriero C, Cairns J, Roberts I, Rodgers A, Whittaker R, Free C. The cost-effectiveness of smoking cessation support delivered by mobile phone text messaging: Txt2stop. Eur J Health Econ 2013;14:789–97. https://doi.org/10.1007/s10198-012-0424-5 | Intervention did not meet the mass media definitiona |
| Hamilton-Shield J, Goodred J, Powell L, Thorn J, Banks J, Hollinghurst S, et al. Changing eating behaviours to treat childhood obesity in the community using Mandolean: the Community Mandolean randomised controlled trial (ComMando) – a pilot study. Health Technol Assess 2014;18(47) | Intervention did not meet the mass media definitiona |
| Harris HE, Tweedie F, Skaparis Y, White M, Scott N, Samson K. Success of a Smoking and Rheumatoid Arthritis Awareness Campaign in Fife, Scotland. British Society for Rheumatology and British Health Professionals in Rheumatology Annual Meeting 2013, and Rheumatology 2013, Birmingham, UK, 23–25 April 2013 | Linked to a previously excluded study |
| Harris H, Tweedie F, Skaparis Y, White M, Scott N, Samson K. Impact of a Smoking Cessation Awareness Campaign on Smokers with Rheumatoid Arthritis in Scotland. Annual European Congress of Rheumatology of the European League Against Rheumatism, and EULAR 2012, Berlin, Germany, 6–9 June 2012 | Intervention did not meet the mass media definitiona |
| Harris H. How Can We Persuade Patients with Rheumatoid Arthritis to Stop Smoking? Annual European Congress of Rheumatology of the European League Against Rheumatism, and EULAR 2013, Madrid, Spain, 12–15 June 2013 | Intervention did not meet the mass media definitiona |
| Harris PR, Brearley I, Sheeran P, Barker M, Klein WMP, Creswell JD, et al. Combining self-affirmation with implementation intentions to promote fruit and vegetable consumption. Health Psychol 2014;33:729–36 | Intervention did not meet the mass media definitiona |
| Hartland D, Duffton R, Home J, D’Aguilar C, Berktay L, Tomkinson A, et al. Health Promotion (HP) and Health Outcomes: Impacts of Old and New Media Campaigns on Referral Patterns For HIV Testing: Implications for The National HIV Saving Lives Campaign. Paper presented at 17th Annual Conference of the British HIV Association, BHIVA 2011, Bournemouth, UK, 6–8 April 2011 | Did not examine one or more of the relevant health behaviours |
| Hawkes N. Campaign seeks to make Britons active every day. BMJ 2014;349:g6441. https://doi.org/10.1136/bmj.g6441 | Intervention did not meet the mass media definitiona |
| He FJ, Brinsden HC, MacGregor GA. Salt reduction in the United Kingdom: a successful experiment in public health. J Hum Hypertens 2014;28:345–52. https://doi.org/10.1038/jhh.2013.105 | Intervention did not meet the mass media definitiona |
| Hickson F, Tomlin K, Hargreaves J, Bonell C, Reid D, Weatherburn P. Internet-based cohort study of HIV testing over 1 year among men who have sex with men living in England and exposed to a social marketing intervention promoting testing. Sex Transm Infect 2015;91:24–30. https://doi.org/10.1136/sextrans-2014-051598 | Did not examine one or more of the relevant health behaviours |
| Hitchman SC, Mons U, Nagelhout GE, Guignard R, Mcneill A, Willemsen MC, et al. Effectiveness of the European Union text-only cigarette health warnings: findings from four countries. Eur J Public Health 2012;22:693–9 | Intervention did not meet the mass media definitiona |
| Hodgkins CE, Raats MM, Fife-Schaw C, Peacock M, Gröppel-Klein A, Koenigstorfer J, et al. Guiding healthier food choice: systematic comparison of four front-of-pack labelling systems and their effect on judgements of product healthiness. Br J Nutr 2015;113:1652–63. https://doi.org/10.1017/S0007114515000264 | Intervention did not meet the mass media definitiona |
| Hrobonova E, Lewis E, Dunsford EA, Vamos EP. Community-Based Pilot to Tackle Childhood Obesity in a London Borough: a Whole-System Approach. 22nd Congress of the European Congress on Obesity, and ECO 2015, Prague, Czech Republic, 6–9 May 2015 | Excluded on outcomes data |
| Hughes A, Day S. A highly cost-effective and targeted service promotion campaign using Facebook. HIV Medicine 2012;13:13 | Did not examine one or more of the relevant health behaviours |
| Hum O, Lee RL. Marketing sexual health in a brand conscious world: can we make services more accessible to young people? Sex Transm Infect 2012;88:56–7 | Excluded on outcomes data |
| Jago R, Sebire SJ, Bentley GF, Turner KM, Goodred JK, Fox KR, et al. Process evaluation of the Teamplay parenting intervention pilot: implications for recruitment, retention and course refinement. BMC Public Health 2013;13:1102. https://doi.org/10.1186/1471-2458-13-1102 | Intervention did not meet the mass media definitiona |
| Johnson F, Wardle J. The association between weight loss and engagement with a web-based food and exercise diary in a commercial weight loss programme: a retrospective analysis. Int J Behav Nutr Phys Act 2011;8:83. https://doi.org/10.1186/1479-5868-8-83 | Intervention did not meet the mass media definitiona |
| Johnstone AM, Giles K, O’Connor D, Cooper C, Fyfe C, Horgan G. Workplace Stress and Eating Behaviour: Influence of Health Promotion? Basel, Switzerland: S. Karger AG; 2013 | Intervention did not meet the mass media definitiona |
| Jones M, Aderogba K, Drunis L. Providing Rapid HIV Testing in Their Homes for Men Who Have Sex with Men, Recruited via Social Media. Paper presented at 21st Annual Conference of the British HIV Association, BHIVA 2015, Brighton, UK, 21–24 April 2015 | Did not examine one or more of the relevant health behaviours |
| Kearney M, Holton K, Moger A, Clarke J, Winter R, Hill S. Shifting the focus to prevention and early identification-a national toolkit to support behaviour change interventions in chronic obstructive pulmonary disease. Am J Respir Crit Car Med 2012;185:2873 | Excluded on outcomes data |
| Kesten JM, Cohn S, Ogilvie D. The contribution of media analysis to the evaluation of environmental interventions: the commuting and health in Cambridge study. BMC Public Health 2014;14:482. https://doi.org/10.1186/1471-2458-14-482 | Excluded on outcomes data |
| Keyworth C, Nelson PA, Cordingley L, Griffiths CEM, Bundy C. Health Promotion for Patients with Psoriasis: Examining Current Signposting in U.K. Health Centres. 7th International Congress of Psoriasis: From Gene to Clinic, London, UK, 11–13 December 2011 | Excluded on outcomes data |
| Kinsella K, Cross R, South J. An evaluation of the condom distribution scheme (C-Card) with young people in Northeast England. Perspect Public Health 2014;134:25–30. https://doi.org/10.1177/1757913913483245 | Intervention did not meet the mass media definitiona |
| Knox EC, Esliger DW, Biddle SJ, Sherar LB. Lack of knowledge of physical activity guidelines: can physical activity promotion campaigns do better? BMJ Open 2013;3:e003633. https://doi.org/10.1136/bmjopen-2013-003633 | Intervention did not meet the mass media definitiona |
| Knox EC, Taylor IM, Biddle SJ, Sherar LB. Awareness of moderate-to-vigorous physical activity: can information on guidelines prevent overestimation? BMC Public Health 2015;15:392. https://doi.org/10.1186/s12889-015-1705-6 | Intervention did not meet the mass media definitiona |
| Knox EC, Webb OJ, Esliger DW, Biddle SJ, Sherar LB. Using threshold messages to promote physical activity: implications for public perceptions of health effects. Eur J Public Health 2014;24:195–9. https://doi.org/10.1093/eurpub/ckt060 | Linked to a previously excluded study |
| Knox EC, Biddle SJ, Taylor IM, Latimer-Cheung AE, Webb OJ, Sherar LB. Messages to promote physical activity: Are descriptors of required duration and intensity related to intentions to be more active? J Educ Health Promot 2015;4:77. https://doi.org/10.4103/2277-9531.171790 | Intervention did not meet the mass media definitiona |
| Knox EC, Taylor IM, Biddle SJ, Sherar LB. Awareness of moderate-to-vigorous physical activity: can information on guidelines prevent overestimation? BMC Public Health 2015;15:392. https://doi.org/10.1186/s12889-015-1705-6 | Intervention did not meet the mass media definitiona |
| Kuipers MA, Beard E, Hitchman SC, Brown J, Stronks K, Kunst AE, et al. Impact on smoking of England’s 2012 partial tobacco point of sale display ban: a repeated cross-sectional national study. Tob Control 2017;26:141–8 | Intervention did not meet the mass media definitiona |
| Kyle RG, Nicoll A, Forbat L, Hubbard G. Adolescents’ awareness of cancer risk factors and associations with health-related behaviours. Health Educ Res 2013;28:816–27. https://doi.org/10.1093/her/cyt055 | Intervention did not meet the mass media definitiona |
| Langley T, Lewis S, McNeill A, Gilmore A, Szatkowski L, West R, Sims M. Characterizing tobacco control mass media campaigns in England. Addiction 2013;108:2001–8 | Excluded on outcomes data |
| Langley T, Szatkowski L, Lewis S, McNeill A, Gilmore AB, Salway R, Sims M. The freeze on mass media campaigns in England: a natural experiment of the impact of tobacco control campaigns on quitting behaviour. Addiction 2014;109:995–1002 | Intervention did not meet the mass media definitiona |
| Levy DT, Huang AT, Currie LM, Clancy L. The benefits from complying with the framework convention on tobacco control: a SimSmoke analysis of 15 European nations. Health Policy Plan 2014;29:1031–42. https://doi.org/10.1093/heapol/czt085 | Intervention did not meet the mass media definitiona |
| Li L, Borland R, Yong HH, Hitchman SC, Wakefield MA, Kasza KA, Fong GT. The association between exposure to point-of-sale anti-smoking warnings and smokers’ interest in quitting and quit attempts: findings from the International Tobacco Control Four Country Survey. Addiction 2012;107:425–33 | Intervention did not meet the mass media definitiona |
| Lloyd-Williams F, Bromley H, Orton L, Hawkes C, Taylor-Robinson D, O’Flaherty M, et al. Smorgasbord or symphony? Assessing public health nutrition policies across 30 European countries using a novel framework. BMC Public Health 2014;14:1195 | Intervention did not meet the mass media definitiona |
| Malcolm E, Evans-Lacko S, Henderson C, Thornicroft G. 2011. Community Based Physical Activity Programmes to Increase Levelso Fitness, Empowerment and Reduce Stigma. Paper presented at 9th International Conference of the European Network for Mental Health Service Evaluation, ENMESH 2011, Ulm, Germany, 23–25 June 2011 | Intervention did not meet the mass media definitiona |
| Manyiwa S, Brennan R. Fear appeals in anti-smoking advertising: how important is self-efficacy? Journal of Marketing Management 2012;28:1419–37 | Excluded on outcomes data |
| Marsland N, Twenefour D, Kelly T. Impact of ‘Enjoy Food’: Diabetes UK’s Programme to Promote Healthy Eating. Paper presented at Diabetes UK Professional Conference 2016, Glasgow, UK, 2–4 March 2016 | Intervention did not meet the mass media definitiona |
| Mason D, Gilbert H, Sutton S. Effectiveness of web-based tailored smoking cessation advice reports (iQuit): a randomised trial. Addiction 2012;107:2183–90 | Intervention did not meet the mass media definitiona |
| McCarthy O, Carswell K, Murray E, Free C, Stevenson F, Bailey JV. What young people want from a sexual health website: design and development of Sexunzipped. J Med Internet Res 2012;14:e127. https://doi.org/10.2196/jmir.2116 | Excluded on outcomes data |
| McClinchy J, Dickinson A, Barron D, Thomas H. Practitioner and lay perspectives of the service provision of nutrition information leaflets in primary care. J Hum Nutr Diet 2011;24:552–9. https://doi.org/10.1111/j.1365-277X.2011.01200.x | Excluded on outcomes data |
| Mehta G, Macdonald S, Maurice JB, Al-Khatib SH, Piao S, Rosselli M, et al. Short term abstinence from alcohol improves insulin resistance and fatty liver phenotype in moderate drinkers. Heptology 2015;62:267 | Excluded on outcomes data |
| Menon-Johansson A. Post (zip) code power: a new web/SMS tool to market providers and sign post clients. Sex Transm Infect 2012;88:45 | Excluded on outcomes data |
| Michie S, Brown J, Geraghty AW, Miller S, Yardley L, Gardner B, et al. Development of StopAdvisor: A theory-based interactive internet-based smoking cessation intervention. Transl Behav Med 2012;2:263–75. https://doi.org/10.1007/s13142-012-0135-6 | Excluded on outcomes data |
| Milton K, Grix J. Public health policy and walking in England-analysis of the 2008 ‘policy window’. BMC Public Health 2015;15:614. https://doi.org/10.1186/s12889-015-1915-y | Intervention did not meet the mass media definitiona |
| Morgan G. Health promotion for older people in Wales: preliminary evaluation of the national service framework for older people. Int J Health Promot Educ 2012;50:45–9 | Intervention did not meet the mass media definitiona |
| Mulka L, Lock E, Salim M, Cameron D, Mann S. Alcohol and Sexual Health: a Pilot Study of Screening and Brief Intervention. 3rd Joint Conference of the British HIV Association, BHIVA with the British Association for Sexual Health and HIV, and BASHH, Liverpool, UK, 1–4 April 2014 | Intervention did not meet the mass media definitiona |
| Munafo MR, Roberts N, Bauld L, Leonards U. Plain packaging increases visual attention to health warnings on cigarette packs in non-smokers and weekly smokers but not daily smokers. Addiction 2011;106:1505–10 | Intervention did not meet the mass media definitiona |
| Myers LB. Changing smokers’ risk perceptions – for better or worse? J Health Psychol 2014;19:325–32. https://doi.org/10.1177/1359105312470154 | Intervention did not meet the mass media definitiona |
| Naughton F, Prevost AT, Gilbert H, Sutton S. Randomized controlled trial evaluation of a tailored leaflet and SMS text message self-help intervention for pregnant smokers (MiQuit). Nicotine Tob Res 2012;14:569–77. https://doi.org/10.1093/ntr/ntr254 | Intervention did not meet the mass media definitiona |
| Nikolaou CK, Hankey CR, Lean ME. Elearning approaches to prevent weight gain in young adults: A randomized controlled study. Obesity 2015;23:2377–84. https://doi.org/10.1002/oby.21237 | Intervention did not meet the mass media definitiona |
| Norwood P, Eberth B, Farrar S, Anable J, Ludbrook A. Active travel intervention and physical activity behaviour: an evaluation. Soc Sci Med 2014;113:50–8. https://doi.org/10.1016/j.socscimed.2014.05.003 | Intervention did not meet the mass media definitiona |
| Nothwehr F, Andsager J, Haines H. The rural restaurant healthy options program: response of rural, local newspapers to a program press release. Health Promot Pract 2014;15:217–22. https://doi.org/10.1177/1524839912466870 | Excluded on outcomes data |
| Phillips G, Bottomley C, Schmidt E, Tobi P, Lais S, Yu G, et al. Well London Phase-1: results among adults of a cluster-randomised trial of a community engagement approach to improving health behaviours and mental well-being in deprived inner-city neighbourhoods. J Epidemiol Community Health 2014;68:606–14. https://doi.org/10.1136/jech-2013-202505 | Intervention did not meet the mass media definitiona |
| Portman M, Aung S, Brigstock-Barron O, Hunt T, Doyle T, Smith A, et al. T’hiv’k Goes North: Outcomes and Experience of UK HIV Testing Week in a Northern UK City. 19th Annual Conference of the British HIV Association, and BHIVA 2013, Manchester, UK, 16–19 April 2013 | Did not examine one or more of the relevant health behaviours |
| Portman M, Doyle T, Hill E, Hirst J, Smith A, Aung S, et al. National HIV testing week – a celebration! 3rd Joint Conference of the British HIV Association, BHIVA with the British Association for Sexual Health and HIV, and BASHH, Liverpool, UK, 1–4 April 2014 | Did not examine one or more of the relevant health behaviours |
| Power L, McClelland B. National HIV Testing Week: An intervention for Raising Awareness and Encouraging HIV testing. Paper presented at 19th Annual Conference of the British HIV Association, BHIVA 2013, Manchester, UK, 16–19 April 2013 | Did not examine one or more of the relevant health behaviours |
| Reeves I, Hodson M, Figueroa J, Horne P. A Great Way of Doing It from the Comfort of My Home: Expanding Opportunities For HIV Testing through Home Sampling. Paper presented at 3rd Joint Conference of the British HIV Association, BHIVA with the British Association for Sexual Health and HIV, BASHH, Liverpool, UK, 1–4 April 2014 | Did not examine one or more of the relevant health behaviours |
| Robinson N, Lorenc A. ‘No one wants to be the face of Herpes London’: a qualitative study of the challenges of engaging patients and the public in sexual and reproductive health and HIV/AIDS services. Health Expect 2015;18:221–32. https://doi.org/10.1111/hex.12024 | Excluded on outcomes data |
| Rowsell A, Muller I, Murray E, Little P, Byrne CD, Ganahl K, et al. Views of People With High and Low Levels of Health Literacy About a Digital Intervention to Promote Physical Activity for Diabetes: A Qualitative Study in Five Countries. J Med Internet Res 2015;17:e230. https://doi.org/10.2196/jmir.4999 | Excluded on outcomes data |
| Rutten GM, Savelberg HH, Biddle SJH, Kremers SPJ. Interrupting long periods of sitting: good STUFF. International Journal of Behavioral Nutrition and Physical Activity 2013;10:1 | Intervention did not meet the mass media definitiona |
| Ryder J, Davies L, Bibby J. Smoking Cessation Educational Poster Campaign. Paper presented at British Thoracic Society Winter Meeting 2011, London, United Kingdom, 7–9 December 2011 | Intervention did not meet the mass media definitiona |
| Sahlqvist S, Goodman A, Cooper AR, Ogilvie D, iConnect Consortium. Change in active travel and changes in recreational and total physical activity in adults: longitudinal findings from the iConnect study. Int J Behav Nutr Phys Act 2013;10:28 | Intervention did not meet the mass media definitiona |
| Shan LC, Panagiotopoulos P, Regan A, De Brun A, Barnett J, Wall P, McConnon A. Interactive communication with the public: qualitative exploration of the use of social media by food and health organizations. J Nurt Educ Behav 2015;47:104–8 | Excluded on outcomes data |
| Short CE, James EL, Girgis A, D’Souza MI, Plotnikoff RC. Main outcomes of the Move More for Life Trial: a randomised controlled trial examining the effects of tailored-print and targeted-print materials for promoting physical activity among post-treatment breast cancer survivors. Psycho-oncology 2015;24:771–8 | Intervention did not meet the mass media definitiona |
| Skår S, Sniehotta FF, Molloy GJ, Prestwich A, Araújo-Soares V. Do brief online planning interventions increase physical activity amongst university students? A randomised controlled trial. Psychol Health 2011;26:399–417. https://doi.org/10.1080/08870440903456877 | Intervention did not meet the mass media definitiona |
| Slack S, Wilson L. The pleasure principle in sexual health promotion. Eur J Contracept Reprod Health Care 2012;17(Suppl. 1):8 | Intervention did not meet the mass media definitiona |
| Smith SA, O’Malley C, Summerbell C, Araujo Soares V, Hillier Brown F, Lake AA. Exploring the Feasibility and Implementation of Workplace Dietary Interventions: Views of the Intervention Deliverers. European Obesity Summit (EOS): 1st Joint Congress of EASO and IFSO-EC, Gothenburg, Sweden, 1–4 June 2016 | Excluded on outcomes data |
| Song F, Holland R, Barton GR, Bachmann M, Blyth A, Maskrey V, et al. Self-help materials for the prevention of smoking relapse: study protocol for a randomized controlled trial. Trials 2012;13:69. https://doi.org/10.1186/1745-6215-13-69 | Excluded on outcomes data |
| Spice W, Clamp R, Palmer C. What kind of information do patients want to see in sexual health clinic waiting rooms? Sex Transm Infect 2015;91:65–6 | Intervention did not meet the mass media definitiona |
| Springvloet L, Willemsen MC, Mons U, van den Putte B, Kunst AE, Guignard R, et al. Educational differences in associations of noticing anti-tobacco information with smoking-related attitudes and quit intentions: findings from the International Tobacco Control Europe Surveys. Health Educ Res 2015;30:719–30. https://doi.org/10.1093/her/cyv037 | Intervention did not meet the mass media definitiona |
| Srinivasan CS. Can adherence to dietary guidelines address excess caloric intake? An empirical assessment for the UK. Econ Hum Biol 2013;11:574–91. https://doi.org/10.1016/j.ehb.2013.04.003 | Intervention did not meet the mass media definitiona |
| Stamp M, Cattan M. Men’s Behaviour Change Following a Positive and Negative Diagnosis for Chlamydia Trachomatis. 11th Spring Meeting of the British Association for Sexual Health and HIV, and BASHH 2013, Bristol, UK, 15–17 May 2013 | Intervention did not meet the mass media definitiona |
| Stepney M. The rise and fall of ‘girlsdrinkdiaries.com’: dilemmas and opportunities when creating online forums to investigate health behaviour. Health Place 2014;27:51–8. https://doi.org/10.1016/j.healthplace.2014.01.001 | Excluded on outcomes data |
| Syred J, Naidoo C, Woodhall SC, Baraitser P. Would you tell everyone this? Facebook conversations as health promotion interventions. J Med Internet Res 2014;16:e108. https://doi.org/10.2196/jmir.3231 | Excluded on outcomes data |
| Taylor C, Darby H, Upton P, Upton D. Can a school-based intervention increase children’s fruit and vegetable consumption in the home setting? Perspect Public Health 2013;133:330–6. https://doi.org/10.1177/1757913913506575 | Intervention did not meet the mass media definitiona |
| Taylor J, Taylor A, Lewis S, McNeill A, Britton J, Jones LL, et al. A qualitative evaluation of a novel intervention using insight into tobacco industry tactics to prevent the uptake of smoking in school-aged children. BMC Public Health 2016;16:539. https://doi.org/10.1186/s12889-016-3205-8 | Excluded on outcomes data |
| Thomas EL, Ribera AP, Senye-Mir A, Greenfield S, Eves F. Testing messages to promote stair climbing at work. Int J Workplace Health Manag 2015;8:189–205 | Intervention did not meet the mass media definitiona |
| Turner K, Clarke B, Priestley C, Scofield S, Chapman C. Uptake and Acceptance of Combined HIV POCT and STI Screening for MSM in Community Settings during National HIV Testing Week. BASHH Spring Conference 2015, Glasgow, UK, 1–3 June 2015 | Did not examine one or more of the relevant health behaviours |
| Ubhi HK, Michie S, Kotz D, Wong WC, West R. A mobile app to aid smoking cessation: preliminary evaluation of SmokeFree28. J Med Internet Res 2015;17:e17. https://doi.org/10.2196/jmir.3479 | Intervention did not meet the mass media definitiona |
| Upton D, Upton P, Taylor C. Increasing children’s lunchtime consumption of fruit and vegetables: an evaluation of the Food Dudes programme. Public Health Nutr 2013;16:1066–72. https://doi.org/10.1017/S1368980012004612 | Linked to a previously excluded study |
| Warriner J, Harbottle J, James C. National HIV testing week: normalising HIV testing for at-risk communities through a yearly community/clinical campaign. HIV Medicine 2014;15:97 | Did not examine one or more of the relevant health behaviours |
| Warriner J, Harbottle J, Tooke B, Mowlabocus S. Reaching out online: researching the benefits and challenges of an internet-based, sexual health community outreach model. HIV Medicine 2014;15:23 | Intervention did not meet the mass media definitiona |
| West R, Daniels D. Sexual Networking: Does Targeting Online Sexually Transmitted Infection Booking Appointments to Men Who Have Sex With Men on Grindr Improve Access to Sexually Transmitted Infection Testing Services? 29th European Conference on Sexually Transmitted Infections, Brisbane, Australia, 13–16 September 2015 | Did not examine one or more of the relevant health behaviours |
| West R, Okecha E, Forbes K. Keeping ‘app’ to date: using geolocation apps to signpost to local sexual health services. Sex Transm Infect 2015;91:32–3 | Did not examine one or more of the relevant health behaviours |
| Wilsher SH. The Impact of Emotional Health on Fruit and Vegetable Consumption in Young Men: a Qualitative Study. Nutrition Society Summer Meeting 2013, Newcastle-upon-Tyne, UK, 15–18 July 2013 | Intervention did not meet the mass media definitiona |
| Withal J, Jago R, Fox KR. Who attends physical activity programmes in deprived neighbourhoods? Health Education Journal 2011;70:206–16 | Linked to a previously excluded study |
| Withall J, Jago R, Fox KR. The effect a of community-based social marketing campaign on recruitment and retention of low-income groups into physical activity programmes – a controlled before-and-after study. BMC Public Health 2012;12:836. https://doi.org/10.1186/1471-2458-12-836 | Intervention did not meet the mass media definitiona |
| Witzel TC, Guise A, Nutland W, Bourne A. It Starts With Me: Privacy concerns and stigma in the evaluation of a Facebook health promotion intervention. Sex Health 2016;13:228–33. https://doi.org/10.1071/SH15231 | Excluded on outcomes data |
| Wressell A, Twaites H, Taylor S, Hartland D, Gove-Humphries T. Saving Lives through visual health communication: a multidisciplinary team approach. J Vis Commun Med 2014;37:81–90. https://doi.org/10.3109/17453054.2014.981800 | Did not examine one or more of the relevant health behaviours |
| Wrieden WL, Levy LB. ‘Change4Life Smart Swaps’: quasi-experimental evaluation of a natural experiment. Public Health Nutr 2016;19:2388–92. https://doi.org/10.1017/S1368980016000513 | Intervention did not meet the mass media definitiona |
| Xiao D, Chen Z, Wang C. Effects of a short-term mass-media campaign against smoking. Lancet 2013;382:1964–6 | Intervention did not meet the mass media definitiona |
| Yong HH, Borland R, Cummings KM, Hammond D, O’Connor RJ, Hastings G, King B. Impact of the removal of misleading terms on cigarette pack on smokers’ beliefs about ‘light/mild’ cigarettes: cross-country comparisons. Addiction 2011;106:2204–13. https://doi.org/10.1111/j.1360-0443.2011.03533.x | Intervention did not meet the mass media definitiona |
| Yong HH, Borland R, Thrasher JF, Thompson ME, Nagelhout GE, Fong GT, et al. Mediational pathways of the impact of cigarette warning labels on quit attempts. Health Psychol 2014;33:1410–20. https://doi.org/10.1037/hea0000056 | Intervention did not meet the mass media definitiona |
Appendix 9 Event flyer for ‘Using the mass media for public health: what’s the evidence?’ stakeholder event, September 2017
Examples of mass media posters and images were removed from the flyer to be reproduced for this report.
Appendix 10 Agenda for ‘Using the mass media for public health: what’s the evidence?’ stakeholder event, September 2017
Date: 28 September 2017.
Venue: Iris Murdoch Building, University of Stirling.
Time: 12–4 p.m.
AgendaChairperson: Professor Linda Bauld, Institute for Social Marketing, University of Stirling.
12.00–12.30 Sandwich lunch on arrival.
12.30–12.45 Background to the study and examples of campaigns – Professor Linda Bauld, University of Stirling.
12.45–13.00 Developing and using logic models – Professor James Thomas, EPPI Centre, University College London.
13.00–13.20 Outcomes and costs: mass media campaigns – Dr Vittal Katikireddi, University of Glasgow, and Dr Tessa Langley, University of Nottingham.
13.20–13.40 Public health mass media campaigns on alcohol – Professor Sarah Lewis and Ben Young, University of Nottingham.
13.40–14.15 Discussion in small groups: what does the evidence tell us about the effective use of mass media?
14.15–14.35 Coffee.
14.35–15.00 What makes a successful mass media campaign? Focus on characteristics – Dr Shona Hilton, University of Glasgow.
15.00–15.15 Gaps and opportunities: what our reviews tell us about future research on mass media campaigns for public health – Martine Stead, University of Stirling.
15.15–15.45 Discussion in small groups: priorities for future monitoring, evaluation and research.
15.45–16.00 Summing up – Professor Linda Bauld, University of Stirling.
The study is funded by the National Institute for Health Research, PHR project 13/163/17.
List of abbreviations
- AIDS
- acquired immunodeficiency syndrome
- CASP
- Critical Appraisal Skills Programme
- CI
- confidence interval
- CLAHRC
- Collaboration for Leadership in Applied Health Research and Care
- EPHPP
- Effective Public Health Practice Project
- EPPI
- Evidence for Policy and Practice Information and Co-ordinating Centre
- ERIC
- Education Resources Information Center
- GRADE
- Grading of Recommendations, Assessment, Development and Evaluation
- GRP
- gross ratings point
- HIV
- human immunodeficiency virus
- HOE
- hierarchy of effects
- NCD
- non-communicable disease
- NICE
- National Institute for Health and Care Excellence
- NIHR
- National Institute for Health Research
- NRT
- nicotine replacement therapy
- OECD
- Organisation for Economic Co-operation and Development
- OR
- odds ratio
- PI
- principal investigator
- PPI
- public and patient involvement
- PRISMA
- Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- QR
- Quick Response
- RCT
- randomised controlled trial
- ROBIS
- Risk Of Bias In Systematic reviews
- RR
- relative risk
- SD
- standard deviation
- SMS
- short message service
- STI
- sexually transmitted infection
- TVR
- television rating
- UKCTAS
- UK Centre for Tobacco and Alcohol Studies