

Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 13/117/01. The contractual start date was in November 2014. The final report began editorial review in January 2018 and was accepted for publication in August 2018. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Suzanne Audrey is a member of the National Institute for Health Research (NIHR) Public Health Research (PHR) Research Funding Committee (2017 to present). Chris Metcalfe is co-director of the Bristol Randomised Trials Collaboration. William Hollingworth is a member of the NIHR Health Technology Assessment Clinical Trials Board (2016 to present). Philip Insall is a member of the NIHR PHR Programme Prioritisation Committee (2014 to present).
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2019. This work was produced by Audrey et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2019 Queen’s Printer and Controller of HMSO
Chapter 1 Introduction
Physical activity and health
Physical inactivity increases the risk of many chronic diseases, including coronary heart disease, type 2 diabetes mellitus, obesity and some cancers. 1,2 It is currently recommended that adults should aim to undertake ≥ 150 minutes of moderate-intensity physical activity in bouts of ≥ 10 minutes throughout the week. 3,4 However, because of increasingly sedentary lifestyles, there are concerns that many adults in high-income countries do not achieve this. 1,4–6 For example, in the UK, 41% of adults aged 40–60 years reported no occasions in which they walked continuously for 10 minutes at a brisk pace each month. 5 Increasing physical activity levels, particularly among the most inactive people, is an important aim of the current public health policy in the UK. 1,7
In addition, there is increasing interest in the relationship between time spent sedentary [defined as any waking, sitting or lying behaviour with low energy expenditure (≤ 1.5 metabolic equivalents of task)] and health outcomes. 8 A large amount of time spent sitting has been associated with a greater risk of cardiovascular disease, type 2 diabetes mellitus, and cardiovascular and all-cause mortality. The amount of objectively measured sedentary time has been associated with a poorer metabolic profile in healthy adults and those at risk of and who have developed type 2 diabetes mellitus. 9 It is of note that these associations are independent of the level of moderate to vigorous physical activity (MVPA) and, consequently, UK health guidelines recommend that adults should minimise the amount of time spent sedentary (sitting) in addition to increasing physical activity. 1
Walking as active travel
Evidence from systematic reviews suggests that adult populations that use active modes of transport (walking and cycling) for commuting have overall higher physical activity levels than car commuters, and also have a decreased risk of cardiovascular disease and all-cause mortality. 10,11 Similarly, there is also evidence that people who use public transport, when a portion of the journey is by foot, accumulate more physical activity than car users. 12
Walking is a popular, familiar, convenient and free form of exercise that can be incorporated into everyday life and sustained into older age. 13 It is also a carbon-neutral mode of transport that has declined in recent decades in parallel with the increase in car use. 1 Even walking at a moderate pace of 5 km per hour (3 miles/hour) expends sufficient energy to meet the definition of moderate-intensity physical activity. 14 Hence, there are compelling reasons to encourage people to walk more, not only to improve their health but to address the problems of climate change. 15–18
In the UK, there are substantial opportunities to increase walking by replacing short journeys undertaken by car. For example, the 2016 National Travel Survey showed that 24.5% of all car trips were shorter than 2 miles (3.2 km), and 13% of trips of less than 1 mile (1.6 km) were made by car. 19 An opportunity for working adults to accumulate the recommended moderate activity levels is through the daily commute, and, in addition, replacing using a car with walking for short journeys is likely to reduce sedentary time. Experts in many World Health Organization countries agree that significant public health benefits can be realised through greater use of active transport modes. 20
Systematic reviews have examined the effectiveness of interventions to promote physical activity in general,21–24 but there is less evidence about how best to promote walking to work. A systematic review of interventions to promote change from car to active transport25 examined 19 studies that included workplace-based interventions, architectural and urbanistic adjustments, population-wide interventions and bicycle-renting systems. Sixteen studies reported positive effects on modal shift, but the reviewers concluded that the methodologies used were not of high quality and the interventions were poorly described. 25
Available systematic review evidence has focused on interventions that promote walking, interventions that promote walking and cycling as an alternative to car use and the effectiveness of workplace physical activity interventions. None focuses specifically on employer-led interventions that promote walking to work, although the studies that have been undertaken are included within the available systematic review evidence.
Workplace physical activity interventions
A systematic review of the literature regarding the effectiveness of workplace physical activity interventions, commissioned by the National Institute for Health and Care Excellence (NICE) graded 14 studies as being high quality or good quality. 26 Three public sector studies provided evidence that workplace walking interventions using pedometers can increase daily step counts. One good-quality study reported a positive intervention effect on walking-to-work behaviour (active travel) in economically advantaged female employees. There was strong evidence that workplace counselling influenced physical activity behaviour but the reviewers indicated that there was a dearth of evidence for small- and medium-sized enterprises.
The NICE public health guidance on workplace health promotion concluded that although a range of schemes exist to encourage employees to walk or cycle to work, little is known about their impact. 27 Few studies used robust data-collection methods to measure the impact of workplace interventions on employees’ physical activity levels (most use self-report) and there is a lack of studies examining how workplace physical activity interventions are influenced by the size and type of workplace and the characteristics of employees. 28
Measuring physical activity
The majority of primary studies have depended on self-report measures of both physical activity and mode of travel, which may not provide reliable estimates. 29,30 A systematic review comparing direct measures with self-report measures for assessing physical activity in adults found that self-report measures were higher than objective measures in some cases and lower in others. 30 This calls into question the reliability of self-report measures, and indicates that there is no approach to correcting for self-report measures that will be valid in all cases. However, few studies have objectively measured the contribution of walking, particularly walking to work, to adult physical activity levels. 28,31
In Sweden, two studies examined the association between neighbourhood walkability [measured using a geographic information system (GIS)] and objective physical activity (measured using accelerometers). 32,33 Both studies demonstrated how increased walking rates translated directly to increased MVPA levels. In the USA, a cross-sectional study34 included 2364 participants enrolled in the Coronary Artery Risk Development in Young Adults (CARDIA) study who worked outside the home during year 20 of the study (2005–6) and found active commuting to be positively associated with fitness in men and women, and inversely associated with body mass index (BMI), obesity, triglyceride levels, blood pressure and insulin levels in men. The authors concluded that active commuting should be investigated as a means of maintaining or improving health. In the UK, researchers used accelerometers to examine associations between walking or cycling to work and objective MVPA levels and found that women who reported undertaking ≥ 150 minutes of active commuting per week achieved an estimated 8.50 additional minutes [95% confidence interval (CI) 1.75 to 51.26 minutes; p = 0.01] of daily MVPA compared with those who reported no time in active commuting, but no overall associations were found in men. 35
Costs and benefits of walking as active travel
Experts agree that significant public health benefits can be realised through greater use of active transport modes, and the ratio of benefits to costs is high. 36 However, more evidence is required on the costs and benefits of active travel interventions; a systematic review of interventions to promote walking included 19 randomised controlled trials (RCTs) and 29 non-randomised controlled studies but only six studies included even rudimentary economic evaluation. 37 Despite studies demonstrating the health benefits of active commuting, assessments of the cost-effectiveness of these interventions are relatively scarce. When economic evaluations have been undertaken, cost-effectiveness analyses have been conducted38 and benefit-to-cost ratios have been calculated. 39,40
There are potential benefits to walkers from reduced commuting costs and greater certainty about the timing of the journey to work. Because morbidity and mortality related to physical inactivity disproportionately affect socioeconomically deprived communities, encouraging and enabling walking as physical activity may help to address health inequalities. The potential benefits to employers who promote walking to work may include reduced in sickness costs and absenteeism, improved staff performance and productivity and reduced staff turnover. 41
Using behaviour change techniques to encourage active travel
Behaviour change techniques (BCTs) have been defined as the ‘active ingredients’ within an intervention designed to change behaviour that are observable, replicable and irreducible components, which can be used alone or in combination. 42 A taxonomy of 26 BCTs was identified in 2008,43 with subsequent work undertaken to improve labels and definitions and to reach a wider consensus of agreed distinct BCTs. 44 The 2008 taxonomy has been successfully used to categorise the BCTs used in healthy eating and physical activity interventions with ‘self-monitoring’ combined with at least one other technique identified as the most effective. 45,46
A systematic review of workplace physical activity interventions confirmed that goal-setting, providing instruction and prompting self-monitoring were the main BCTs used. 28 A systematic review and random-effects meta-analysis assessed the effectiveness of 37 worksite interventions and reported that, overall, worksite interventions have small, positive effects on physical activity: those promoting walking as opposed to other forms of physical activity were more effective, and there was some evidence that goal-setting and goal review techniques may enhance fitness gains. 46 Another systematic review of interventions to promote walking37 identified two general characteristics of interventions found to be effective: targeting and tailoring. A systematic review of promoting walking and cycling as alternatives to using cars27 identified 22 studies that met the inclusion criteria and found some evidence that targeted behaviour change programmes can change the behaviour of motivated subgroups.
Of the 46 walking and cycling controlled interventions coded for BCTs by Bird et al. ,47 21 reported a statistically significant effect using a mean number of BCTs of 6.43 [standard deviation (SD) 3.92]. 38 The most commonly used techniques were ‘self-monitoring’ and ‘intention formation’. 47 NICE has issued recommendations advising that interventions should use BCTs based on goals and planning, feedback and monitoring and social support. 48
The Walk to Work feasibility study
Aim and objectives
The current cluster RCT incorporated lessons learned from the Walk to Work feasibility study [National Institute for Health Research (NIHR) Public Health Research (PHR) project number 10/3001/04]. 49 The aim of the feasibility study was to build on existing knowledge and resources to develop an employer-led scheme to increase walking to work and to test the feasibility of implementing and evaluating it in a full-scale cluster RCT. The objectives were to (1) explore with employees and employers the barriers to, and facilitators of, employer-led schemes to promote walking to work, (2) use existing resources and websites to develop a Walk to Work information pack to train work-based Walk to Work promoters, and (3) conduct an exploratory RCT of the intervention to pilot workplace and employee recruitment procedures, examine retention rates, pilot cost and outcome measures and inform a sample size calculation for a full RCT.
Study design
The feasibility study comprised two phases of the Medical Research Council’s framework for evaluating complex interventions. 50 During phase I, a review of resources that promote walking (and in particular the benefits of walking to work) was undertaken. In addition, three focus groups were conducted with employees, and interviews were conducted with three employers, in one small, one medium-sized and one large workplace outside Bristol to finalise the intervention design. Phase II comprised an exploratory randomised trial incorporating process evaluation and an assessment of costs. A cluster trial was required because randomisation of individual employees would risk contamination of the control group: the intervention was to be delivered within workplaces with the potential for employees to share information about the intervention and in which employers would be encouraged to support walking to work.
Recruitment
Workplaces were approached through Bristol Chambers of Commerce for initial expressions of interest. Fifty-five workplaces expressed an interest and were asked to complete a short questionnaire about the size and type of the business. Because the intervention initially aimed to focus on employees within ‘walking distance’ of their workplace, employers were also asked to identify how many of their employees lived within 2 miles of the workplace. This process was aided by the research team supplying the first four digits of postcodes likely to contain employees living within the required range, and an instruction leaflet of how to calculate distance using the website walkit.com (accessed 28 February 2019). Nevertheless, some workplaces found this burdensome and it may have affected recruitment. Of the 55 workplaces initially expressing an interest, 19 were recruited and 17 completed the study. Two workplaces left the study after randomisation to the intervention group: one because of downsizing and one because of heavy workload.
Within participating workplaces, employees living within 2 miles of the workplace were given information about the study and invited to participate. As the study progressed, it was felt that this was too restrictive, and a second round of recuitment was undertaken to include people who lived further away and might be willing to incorporate some walking as part of a mixed-mode commute. A total of 187 participants were recruited to the study: 147 living within 2 miles of the workplace and 40 living further away. In the intervention group, study participants were asked to sign an additional consent form before receiving the intervention. This was also considered to be restrictive and was not thought necessary for a future full-scale trial.
It was felt that naming the study Walk to Work may have restricted interest among some employers and may have encouraged the control group to consider walking to work. Therefore, it was decided to name the full-scale trial the Travel to Work study and to name the intervention the Walk to Work intervention.
Data collection
At baseline, all participating employees were asked to complete a questionnaire giving basic personal data and providing information relating to travel behaviour, costs and health. Participants were also asked to wear accelerometers during waking hours for 7 days to provide an objective measurement of physical activity, and to carry a personal GPS (Global Positioning System) receiver during the commute to confirm the duration of the journey and quantify its contribution to overall physical activity. Post intervention, questionnaires were administered again to explore views and experiences of walking to work, and additional questions about the acceptability of the intervention were included for the intervention group only. The questionnaires, accelerometers and GPS receivers were administered again across the intervention and the control groups (as per the baseline protocol) at a 12-month follow-up data collection point. To examine key issues in more depth, baseline and post-intervention interviews were conducted with employers, Walk to Work promoters and a purposive sample of employees.
The Walk to work intervention
There were several stages of the intervention. Walk to Work promoters, either volunteers or nominated by participating employers, were identified in each workplace in the intervention group of the study. A training session for the Walk to Work promoters was run by experts in the research team and focused on the benefits of walking to work and resources available to promote this, identifying walking routes with participating employees and building confidence to encourage other employees to walk to work. The Walk to Work promoters were provided with the booklets and optional pedometers to assist them in their role. Employees participating in the study were then contacted by the Walk to Work promoter and those who were interested in walking to work were asked to consent to the intervention. The role of the Walk to Work promoter was to distribute booklets and optional pedometers, help identify walking routes, discuss barriers and solutions and encourage goal-setting. The promoters were also asked to provide support through four contacts (face-to-face, e-mail or telephone contacts, as appropriate) with participants over the following 10-week intervention period.
Findings from the process evaluation suggested that the intervention materials were acceptable to participants, with different individuals finding some BCTs more helpful than others. This suggested that a range of BCTs was required to enable participants to choose a ‘package’ to suit their individual needs. Some Walk to Work promoters were more proactive than others. One promoter did not perform the role at all owing to the pressure of work, and others felt that they needed additional support and encouragement during the 10-week intervention period, similar to that provided during the four contacts with study participants. It was also suggested that additional support at an organisational level should be encouraged.
Economic evaluation
All costs (including time, materials, equipment and travel) involved in the intervention were documented. Self-reported general health service use, productivity, absence from work and weekly commuting costs were also measured. The average cost of the intervention for participating workplaces was £441 (with a wide range from £66.33 to £958.38). Costs varied because of different numbers of promoters in each workplace, the number of employees participating in the intervention and the location of promoter training. Mean daily commuting costs were slightly lower in the intervention group than in the control group at follow-up [£2.66 (SD £4.32) vs. £3.64 (SD £12.16)] and mean self-assessed productivity was somewhat better in the intervention group than in the control group [1.51 (SD 1.41) vs. 2.07 (SD 2.24)] (based on a scale of 1 to 10, with 1 being ‘health problems had no effect on my work’ and 10 being ‘health problems completely prevented me from working’), but the study was not powered to provide strong evidence on these outcomes.
Physical activity outcomes
The primary outcome response rate was 80% (149 out of 187 participants) immediately post intervention and 71% (132 out of 187 participants) at the 12-month follow-up. Although not powered to measure effectiveness, the accelerometer data suggested that overall weekday physical activity was lower in the intervention group [434.6 ± 165.0 counts per minute (c.p.m.)] than in the control group (441.9 ± 190.0 c.p.m.) at baseline, but higher in the intervention group (452.0 ± 188.7 c.p.m.) than in the control group (400.6 ± 120.0 c.p.m.) at the 12-month follow-up. MVPA was similar in the intervention (63.4 ± 28.6 minutes per day) and the control (63.3 ± 28.5 minutes per day) groups at baseline, and was higher in the intervention group (61.3 ± 28.4 minutes per day) than in the control group (55.8 ± 22.2 minutes per day) at the 12-month follow-up.
Intracluster correlation coefficient and sample size calculation for a full-scale cluster randomised controlled trial
The intracluster correlation coefficient (ICC) for the fesasibility study was calculated to be 0.12 (95% CI 0.00 to 0.30) and the average cluster size was 8. Based on an ICC of 0.15 to allow for some imprecision in the estimate, it was caluclated that 678 participants across 84 workplaces would be required to give 80% power with a 5% significance level to detect a 15% increase in mean MVPA.
Summary
There are strong public health reasons to promote walking during the commute to and from work, yet there is a paucity of robust evidence relating to the effectiveness of workplace interventions to promote walking to work. A feasibility study showed that a Walk to Work intervention and its evaluation were feasible and acceptable to participants but suggested a need to simplify recruitment procedures and give additional support to the Walk to Work promoters during the 10-week intervention. Qualitative and statistical evidence suggested sufficient evidence of promise to justify a follow-on full-scale cluster RCT. To our knowledge, the Travel to Work cluster RCT is the first study to objectively measure (using accelerometers and GPS receivers) the effectiveness of a workplace intervention to promote walking during the commute to and from work, and to quantify the contribution of walking during the commute to adult physical activity.
Chapter 2 Study design
Trial design
The study was a multicentre, parallel-arm, cluster RCT incorporating process and economic evaluations. The trial protocol was published at the beginning of the study. 51
Aim
The focus of the trial was to evaluate the effectiveness of a workplace-based intervention to increase walking during the commute for adults working in urban and suburban areas.
Primary outcome
Does the intervention lead to an increase in the daily number of minutes of MVPA after 12 months compared with the control group?
Secondary outcomes
As well as the primary outcomes, there were several secondary objectives relating to physical activity and travel mode. These were:
-
Does the intervention lead to an increase in overall physical activity compared with the control group?
-
Does the intervention decrease the daily number of minutes of sedentary time compared with the control group?
-
Does the intervention lead to an increased number of journeys in which walking to work is the major mode of travel compared with the control group?
-
Does the intervention increase MVPA attributable to walking on the commute compared with the control group?
Economic outcomes
There were three key economic outcomes of interest:
-
What are the intervention costs to participating employers and employees?
-
Does the intervention lead to increased or decreased costs in terms of health-care use, commuting costs and productivity losses?
-
Does the intervention lead to improved well-being, as measured by the ICEpop CAPability measure for Adults (ICECAP-A) questionnaire?52
Process outcomes
The purpose of the process evaluation was to examine the context of, delivery of and response to the intervention from the perspectives of employers, Walk to Work promoters and employees. There were two main outcomes of interest:
-
What were the barriers to, and facilitators of, walking during the daily commute?
-
Was there evidence of any social patterning in the uptake of the intervention, particularly in relation to socioeconomic status, age and gender?
Sample size and justification
Using the findings from the feasibility study, the sample size for the full-scale trial was based on an average cluster size of eight, an ICC of 0.15 and participant attrition of 25%. The calculation needed to allow equal numbers of workplaces in the intervention and the control groups. We calculated that we needed 339 participants per study group to detect a 15% difference in MVPA levels (equal to a difference of 0.36 SDs) with 80% power at the 5% significance level. Therefore, 678 employees were required from 84 workplaces.
Setting
The aim was to recruit a variety of workplaces from different urban and suburban settings. Workplace recruitment in the first year of the study was in three areas: South Gloucestershire, Bath and Swansea. This was expanded for the second year of recruitment to include Bristol, Swindon, Neath Port Talbot and Newport. A brief overview of each of these areas is provided in the following sections. The workplace characteristics are described in Chapter 3.
South Gloucestershire
South Gloucestershire, in the south-west of England, comprises multiple towns and population centres to the north and east of the city of Bristol. In 2016, the population of South Gloucestershire was estimated to be 277,600, of whom 174,700 people (62.9%) were aged 16–64 years and 146,700 (52.8%) were economically active. 53 Key employers are local and national government departments, engineering and manufacturing industries and large insurance companies. 54 Many employers are located between the northern edge of Bristol and the M5 motorway. This area includes a large regional shopping centre and surrounding retail and business parks. South Gloucestershire contains a network of roads serving the industries, distribution centres and retail centres in the area. The railway network in South Gloucestershire is connected to major cities and towns across the UK.
Bath
Bath is a city in the south-west of England. In 2016, the population aged 16–64 years in the parliamentary constituency of Bath (which includes the city and surrounding suburbs) was estimated to be 64,900, of whom 49,300 people were economically active. 55 The city has strong software, publishing and service-oriented industries. Other important economic sectors in Bath are education, health, retail, tourism and leisure and business and professional services. 56 Major employers are the NHS, the city’s two universities and Bath and North East Somerset council. In an attempt to reduce car use in the historical centre of Bath, park-and-ride schemes have been introduced through which car drivers are encouraged to use car parks on the edge of the city and travel into the centre by bus. Nevertheless, underground city-centre parking was also provided for a recent large shopping centre development. Bath is served by a main railway station providing connections to major cities, as well as some suburban railway services and a network of bus routes to surrounding towns and cities.
Swansea
Swansea is a coastal city and county in south Wales and has the second highest population of the 22 Welsh local authorities. 57 In 2016, the population of the Swansea local authority area was 244,500, of whom 155,300 people (63.5%) were aged 16–64 years and 113,500 were economically active. 57 The Swansea economy has a proportionately large share of jobs in the public administration, health, hospitality, financial services and retail sectors. Of the people in employment, an estimated 87.5% are employed in the service sectors, with 28.2% working within the public sector. Other main business activities are in the construction and scientific and technical sectors. The M4 motorway and several major trunk roads link Swansea to other cities in Wales and England. Bus services include smaller bus and coach operators, a road-based rapid transport route and two park-and-ride services. 58 There is also a main railway station and three smaller suburban stations.
Bristol
Bristol is a city and county in the south-west of England. In 2016, the population of the city of Bristol was 454,200, of whom 309,900 people (68.2%) were aged 16–64 years and 255,400 were economically active. 59 The main employment opportunities are in wholesale and retail, health and social work, administrative and support services and professional, scientific and technical activities. Bristol is connected to London and other major UK cities by two motorways and connecting major roads, as well as through its main railway station. Sustrans (www.sustrans.org.uk; accessed 19 December 2017), a charity promoting sustainable transport, was founded in Bristol. In 2015, Bristol won the European Union’s European Green Capital award (www.bristol2015.co.uk; accessed 19 December 2017), in which sustainable transport was an important focus.
Swindon
Swindon is a large town in the south-west region of England. In 2016, the Swindon area had a population of 217,900, of whom 139,800 people (64.2%) were aged 16–64 years and 120,600 were economically active. 60 The majority of employment opportunities are in manufacturing (including car production plants), wholesale and retail, administrative and support services, health and social work, and finance. Swindon is on the main railway line linking London with the south west of England and south Wales. The town can be accessed by a strategic road network including two junctions along the M4 motorway. 61 The recent transport plan for Swindon indicates that the development of fast and efficient public transport has ‘lagged behind’ because of the relative ease of car use. 61
Neath Port Talbot
Neath Port Talbot is a County Borough and Unitary Authority in central south Wales. The area stretches from the south coast to the borders of the Brecon Beacons National Park. The majority of the population lives in the principal towns of Neath and Port Talbot. In 2016, the population of Neath Port Talbot was recorded as 141,600, of whom 88,000 people (62.1%) were aged 16–64 years and 67,300 were economically active. 62 Regeneration ‘to make Neath Port Talbot a place that is better connected, better for business and a better place to live’ is an important theme for the county borough council (reproduced with permission from Neath Port Talbot Council63). The main employment opportunities are in manufacturing (including steelworks), wholesale and retail trades, and human health and social work. The towns of Neath and Port Talbot both have railway stations, connecting them to major cities in Wales and England, and are also served by a network of buses. The M4 motorway cuts through Port Talbot, linking it to towns and cities along the M4 corridor. The Port Talbot docks complex is used mostly for the import of iron ore and coal for use by the nearby steelworks.
Newport
Newport is a city and unitary authority area in south-east Wales. In 2016, the population of the city was 149,100, of whom 93,100 people (62.4%) were aged 16–64 years and 73,100 were economically active. 64 Newport was once Wales’ largest coal-exporting port, but the docks declined in importance during the 20th century. The main employment opportunities are now in manufacturing, the wholesale and retail trade, and human health and social work. Newport lies within the M4 corridor and is accessed by a network of major roads. A railway line passes through the centre of the city and a network of buses also serves the city. 65
Research governance
Ethics committee approval
As the study was not a clinical trial, and did not involve patients or users of the NHS, it was not necessary to apply for NHS ethics approval. All protocols and relevant paperwork were submitted to the Faculty of Medicine and Dentistry Research Ethics Committee at the University of Bristol in February 2014 and ethics approval was granted on 20 April 2014.
Adverse events
The Walk to Work intervention was considered low risk, involving generally healthy adults, and no adverse events had been reported during the feasibility study. However, there are potential risks to pedestrians in relation to road traffic safety and personal safety. Furthermore, it was possible that people with low activity and no history of walking might suffer initial muscle stiffness. In most cases, this would be mild and a normal consequence of increased physical activity, but participants were made aware that some symptoms might require medical attention, for example when underlying joint weakness is exposed. Such incidents were monitored throughout the trial.
Participating employers, Walk to Work promoters and employees were provided with guidance about adverse events and how to report them. Because available adverse events forms for health research tended to relate to clinical trials rather than low-risk public health interventions, bespoke forms were designed for the current study and agreed with the University of Bristol Research Governance and Ethics officer (see Appendix 1).
It was agreed that adverse events would be recorded by the key researcher for each site and collated by the study manager and principal investigator. When appropriate, adverse events would be reported to the University of Bristol Research Ethics Committee and the chairperson of the Trial Steering Committee. If adverse events were attributable to the intervention, relevant participants would be informed immediately (e.g. if an incident had happened on a particular route, work colleagues using the same route would be provided with relevant information).
It was also acknowledged that Walk to Work promoters might experience difficulties due to disruption to usual working relationships or employers’ concerns about time taken out of usual work activities. The intervention activities might also present problems for employers and employees, such as disruption to work routines as a result of permitting elements of the intervention during working hours. These issues were considered through the qualitative research undertaken as part of the process evaluation.
Participant recompense
A small amount of recompense, a £10 gift voucher, was given to study participants who returned accelerometers and GPS monitors at the baseline and the 12-month data collections, in recognition of their contribution to the research. Interview participants were also given a £10 gift voucher. This was handled discretely by providing relevant individuals with a plain envelope containing the gift voucher thanking them for their help with the study.
Data storage
All data relating to workplaces and research participants are stored at the University of Bristol in accordance with the Data Protection Act 201866 and University of Bristol research governance requirements. Information collected from the paper questionnaires was transferred onto the study database, which is held on secure file storage at the University of Bristol and protected by a combination of user accounts and file access control lists, limiting access to agreed members of the research team. The data set will be kept, with limited access by agreed members of the research team, for 10 years from the end of the study. Following the transcription of interview recordings, all potentially identifiable personal information was removed to ensure anonymity. Personal information required for routine contact was stored on a separate database that could be linked using the unique participant identification number. The hard copies of the questionnaires and consent forms will be kept at the University of Bristol in a locked filing cabinet for at least 3 years after termination of the study.
Trial management and scrutiny
An overview of the study management structure is provided in Figure 1.
FIGURE 1.
Travel to Work study management structure.
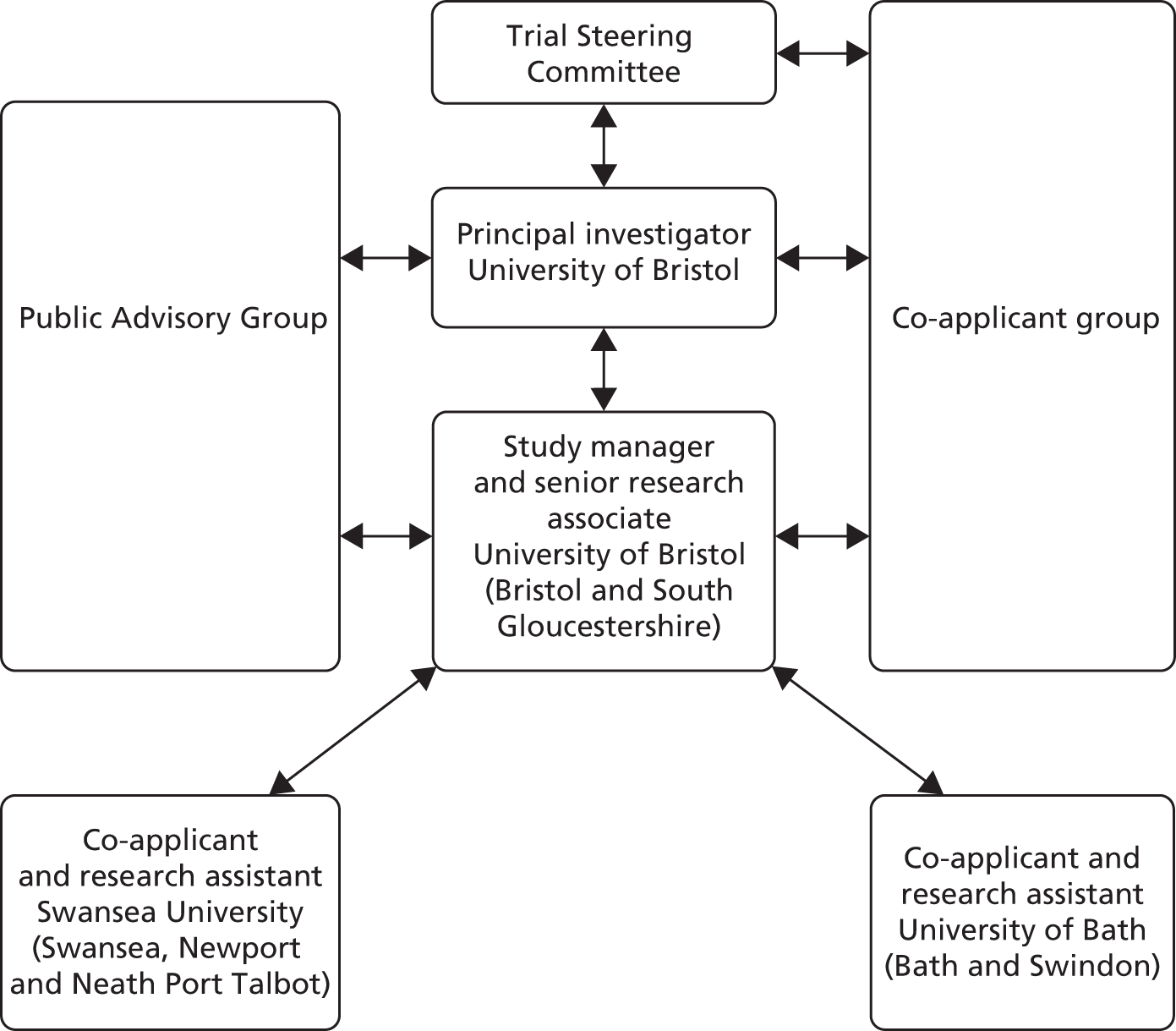
Trial Steering Committee
The Trial Steering Committee met with key members of the research team twice a year throughout the study and comprised an independent chairperson, statistician and health economist plus additional independent experts in travel behaviour, research evaluation, physical activity and health promotion.
Study co-applicant group
The research co-applicant group met on a quarterly basis throughout the study and was chaired by the principal investigator. The group comprised co-applicants from each of the research sites (Bristol, Bath and Swansea), the study manager, a representative of the Bristol Randomised Trials Collaboration (BRTC) and co-applicants with expertise in physical activity measurement, statistical analysis, health economics and sustainable transport.
Research team
A research co-applicant and researcher were based at each research centre (Bristol, Bath and Swansea) and the team met on a quarterly basis. There was frequent and ongoing communication, by e-mail or telephone, between the research sites throughout the trial.
Study registration
The study was listed on the ISRCTN (International Standard Randomised Controlled Trial Number) registry with trial number ISRCTN15009100. 67
Participant and public involvement
The application for a full-scale trial followed on from a feasibility study that included phase I development of the intervention and a phase II exploratory trial. 49 During phase I, focus groups were conducted with employees in three workplaces; their views were sought on the design of the Walk to Work intervention and its evaluation, including the use of accelerometers and GPS monitors. Further interviews were conducted during phase II. A feedback event from the feasibility study was attended by employees, employers and Walk to Work promoters at which the research team presented findings, participants were invited to give feedback on the intervention and its evaluation and we obtained contact details of participants who would consider joining a Public Advisory Group should an application for a full-scale trial be successful.
Data from focus groups, interviews and feedback events helped to shape the intervention and its evaluation for the main trial: the recruitment process was simplified, the arrangements for Walk to Work promoter training were changed to allow group training at an external venue or in-house individual training to suit the workplace and additional booklets were developed that contained information for employers in the intervention group about changes they can make in the workplace to support employees who increase the amount of walking on their commute.
Research co-applicants from non-academic organisations also influenced the feasibility study. A director of Sustrans advised on promoting active travel and a transport consultant with Bristol City Council helped design and implement the training programme. These representatives continued as co-applicants throughout the main trial.
At the beginning of the main trial, 12 people form workplaces involved with the feasibility study were invited to become members of a Public Advisory Group. They were given information about the trial and the role of the group and were informed that reimbursement for time and travel expenses would be provided at a rate of £100 per meeting. Three people accepted membership and fully participated in two meetings towards the beginning of the study. This involved scrutinising the data-collection methods, including questionnaires, travel diary and the instructions for participants using the accelerometers and GPS monitors. They also commented on the intervention materials and suggested that some of the information in the draft booklets for employees, Walk to Work promoters and employers was condescending and repetitive. This was particularly valuable advice and the booklets were shortened and improved as a result.
Project timetable and milestones
The study was originally planned to take 33 months (November 2014 to July 2017) and broadly kept to the proposed timetable for recruitment, delivery of the intervention and data collection. However, a 3-month extension was granted for the core Bristol team to give more time for data analyses and dissemination. The study timetable and key milestones are summarised in Table 1. Because of the potential for seasonality to influence travel behaviour, the study was structured so that the baseline and the 12-month follow-up data collections took place during spring and early summer.
| Milestone | Time point | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2014 | 2015 | 2016 | 2017 | |||||||||
| November to December | January to March | April to June | July to September | October to December | January to March | April to June | July to September | October to December | January to March | April to June | July to October | |
| Staff recruitment (research assistants at three sites) | ✓ | |||||||||||
| Ethics application | ✓ | |||||||||||
| Finalise questionnaires and booklets | ✓ | |||||||||||
| Preparation for baseline data collection | ✓ | |||||||||||
| Prepare Walk to Work packs | ✓ | |||||||||||
| Workplace recruitment | ✓ | ✓ | ||||||||||
| Participant recruitment | ✓ | ✓ | ||||||||||
| Baseline data collection | ✓ | ✓ | ||||||||||
| Randomise workplaces | ✓ | ✓ | ||||||||||
| Recruit and train Walk to Work promoters | ✓ | ✓ | ||||||||||
| Implement Walk to Work intervention | ✓ | ✓ | ✓ | ✓ | ||||||||
| Preparation for post-intervention data collection | ✓ | ✓ | ||||||||||
| Post-intervention data collection | ✓ | ✓ | ||||||||||
| Post-intervention interviews | ✓ | ✓ | ||||||||||
| Data entry and transcription | ✓ | ✓ | ||||||||||
| Preparation for follow-up data collection | ✓ | ✓ | ||||||||||
| Follow-up data collection | ✓ | ✓ | ||||||||||
| Data entry | ✓ | ✓ | ||||||||||
| Data analysis (qualitative and quantitative) | ✓ | ✓ | ||||||||||
| Paper writing and dissemination | ✓ | ✓ | ✓ | |||||||||
Chapter 3 Recruitment
Methods
Lessons from the feasibility study
Following the feasibility study,49 it was felt that the workplace recruitment process should be simplified so that employers were not required to calculate the number of employees who lived within 2 miles of the workplace before being recruited to the study. This requirement had appeared to be onerous for some workplaces that did not sign up for the study after an initial expression of interest. It was also thought that participant eligibility should be expanded to include people living further away from the workplace who might be willing to incoporate walking as part of a mixed-mode commute. Nevertheless, information about the length of the commute was considered valuable to assess how many participants were within a reasonable walking distance (defined as 2 km for the full-scale trial) and might be encouraged to walk the full distance, and how many might be more suited to a mixed-mode commute. The survey questionnaires, following participant consent, were considered to be the most suitable method of collecting postcodes and enabling study researchers to calculate the distances between home and workplace.
Attrition during the feasibility study (29% at the 12-month follow-up) compared well with other workplace-based physical activity interventions. However, no attempt had been made during the feasibility study to contact employees who left the workplace for other employment between baseline and follow-up. To reduce attrition during the main trial, it was agreed that researchers would ask consenting participants to provide contact details if they left the workplace before the 12-month follow-up. This would enable data-collection packs to be sent to them and returned to the researchers by post.
Eligibility criteria
The following exclusion criteria applied at the workplace level: (1) workplaces with a large proportion of staff on short-term or zero-hours contracts, or workplaces with plans to significantly downsize or relocate during the study period, as follow-up data might not be achievable, and (2) workplaces with fewer than five employees, as there was limited potential to recruit a sufficient number of participating employees into a workplace cluster. All employees within participating workplaces were eligible to take part unless they met any of the following exclusion criteria: (1) they already always walked or cycled to work, (2) they were disabled in relation to walking, (3) they were due to retire before the 12-month follow-up data collection or (4) daily driving was a key part of their role.
Workplace recruitment and consent
The aim was to recruit 84 workplaces of different sizes and industrial classifications. Workplace recruitment took place in two phases during May to July 2015 and March to May 2016. The initial intention was to recruit across three urban areas in south-west England and south Wales: South Gloucestershire, Bath and Swansea (Table 2).
| Recruitment phase | Area | |||||
|---|---|---|---|---|---|---|
| Bath | Swansea | South Gloucestershire | ||||
| Number of workplaces | Number of participants | Number of workplaces | Number of participants | Number of workplaces | Number of participants | |
| 2015 | 14 | 113 | 14 | 113 | 14 | 113 |
| 2016 | 14 | 113 | 14 | 113 | 14 | 113 |
| Total | 28 | 226 | 28 | 226 | 28 | 226 |
For the 2015 recruitment round, lists of employers were obtained from relevant Chambers of Commerce and local authorities. The BRTC generated a list of random numbers (blinded to workplace addresses and contact details) for half of the workplaces to be invited to express an interest in the study, with the intention of sending information out to the remaining workplaces in 2016. However, recruitment in 2015 was insufficient to reach the required sample size. Following discussions within the co-applicant group, and subsequently with the Trial Steering Committee and the funders (the NIHR PHR programme), it was agreed that four additional areas would be included in the second recruitment round. In 2016, employers in the other half of the lists for South Gloucestershire, Bath and Swansea were sent information about the study, in addition to all workplaces on available lists of employers for Bristol, Swindon, Neath Port Talbot and Newport.
Workplace recruitment packs
Workplaces were sent a letter of invitation together with an information leaflet and a short form to return to the research team to express interest and provide basic information about the workplace (see Appendix 2).
Following expressions of interest, eligible workplaces were contacted by telephone or e-mail and a meeting was arranged with one member of the research team at which the trial was explained in more detail and written consent was sought for participation in the study.
Participant recruitment and consent
Employers within participating workplaces were provided with an information leaflet (see Appendix 3), describing the study and eligibility criteria, to distribute to all their employees. All eligible employees were invited to participate in the study and given consent forms for their individual participation. This consent was provided before the baseline data collection and subsequent randomisation.
Baseline characteristics
Study participants were asked to complete baseline questionnaires, which included questions about their sociodemographic characteristics, mode of travel to work and occupation.
Results
Workplace recruitment
Approximately 9800 invitation packs were sent out over the two recruitment phases (Table 3). Because of time and resource constraints, it was not possible to check whether or not all the workplaces on the lists were still in existence, or whether or not the packs reached an appropriate person with the authority to decide about workplace participation. For example, of 1892 invitations packs sent out in 2015, 114 (6%) were returned undelivered.
| Research centre and area (recruitment phase) | Number of workplaces |
|---|---|
| Swansea | |
| Swansea (2015 and 2016) | 1265 |
| Neath Port Talbot (2016) | 516 |
| Newport (2016) | 1364 |
| Bath | |
| Bath (2015 and 2016) | 1020 |
| Swindon (2016) | 2027 |
| Bristol | |
| South Gloucestershire (2015 and 2016) | 2263 |
| Bristol (2016) | 1348 |
| Total | 9803 |
Workplaces expressing an interest were checked for eligibility by the research team and those meeting the criteria were contacted and provided with further information about the study. As a result of this process, only 29 workplaces were recruited in the first year (Table 4). The number of areas was increased, and a further 58 workplaces were recruited in the second year, making a total of 87 workplaces. This was in line with the target of recruiting 84 workplaces, but there was not an even spread of workplaces across the different areas and the numbers ranged from 35 in Bristol to three in Neath Port Talbot (see Table 4).
| Area | Recruitment status | |||
|---|---|---|---|---|
| Consented to participate | Withdrew from study | |||
| Number of workplaces | Number of participants | Number of workplaces | Number of participants | |
| 2015 | ||||
| South Gloucestershire | 10 | 110 | 1 | 12 |
| Swansea | 10 | 64 | 0 | 0 |
| Bath | 9 | 49 | 1 | 9 |
| Subtotal | 29 | 223 | 2 | 21 |
| 2016 | ||||
| South Gloucestershire | 2 | 21 | 0 | 0 |
| Bristol | 35 | 266 | 0 | 0 |
| Bath | 2 | 7 | 0 | 0 |
| Swindon | 3 | 19 | 0 | 0 |
| Swansea | 7 | 79 | 0 | 0 |
| Newport | 6 | 35 | 0 | 0 |
| Neath Port Talbot | 3 | 4 | 1 | 1 |
| Subtotal | 58 | 431 | 1 | 1 |
| Total | 87 | 654 | 3 | 22 |
Reasons for workplace withdrawal following expression of interest
Overall, 271 workplaces expressed an interest in the study. These were checked for eligibility and provided with an opportunity to discuss study participation in more detail. At this stage, 162 workplaces did not continue with the study. Reasons for workplaces not consenting to participation after expressing interest are summarised in Table 5: 28% were deemed ineligible by the research team because there were fewer than five employees, 19% reported that their employees already always walk or cycle, 18% felt unable to prioritise the study activities when they were explained in more detail, 12% had consulted their staff and found a lack of interest in participating and 11% indicated that their employees needed to drive as part of their job.
| Reason | Number of workplaces |
|---|---|
| Workplace too small (fewer than five employees) | 46 |
| Employees already walk/cycle | 31 |
| Workplace unable to prioritise the study | 29 |
| Lack of interest from staff | 19 |
| Driving required for job | 18 |
| Researcher unable to make further contact | 11 |
| Workplace unsuitable (shift work/remote sites/staff turnover) | 6 |
| School – lack of time in academic calendar | 1 |
| No reason given | 1 |
| Total | 162 |
Following workplace consent, a further 22 workplaces withdrew before the baseline data collection (Table 6). The main reason for workplaces withdrawing at this stage of the study related to lack of interest among the workforce, despite their employer having an interest in participating.
| Reason | Number of workplaces |
|---|---|
| Lack of interest from staff | 14 |
| Workplace unable to prioritise the study | 4 |
| Not suitable for the workplace at the moment | 1 |
| School – too late to start intervention in academic calendar | 1 |
| No reason given | 2 |
| Total | 22 |
Workplace characteristics
Workplaces were diverse in relation to their function and included public administration, professional and scientific organisations, retail, services and manufacturing (Table 7). 68 The workplaces varied in size: 10 (11.5%) were micro-sized (< 10 employees), 35 (40.2%) were small (10–49 employees), 22 (25.3%) were medium-sized (50–249 employees) and 20 (23.0%) were large (≥ 250 employees). Table 7 shows a good balance of workplace characteristics between the two groups following randomisation.
| Characteristics | Trial group, n (%) | |
|---|---|---|
| Intervention (N = 44) | Control (N = 43) | |
| Location | ||
| Swansea, Newport and Neath Port Talbot | 13 (30) | 13 (30) |
| Bath and Swindon | 8 (18) | 6 (14) |
| South Gloucestershire and Bristol | 23 (52) | 24 (56) |
| Size of business (number of employees) | ||
| Micro (5–9) | 4 (9) | 6 (14) |
| Small (10–49) | 21 (48) | 14 (33) |
| Medium (50–249) | 9 (20) | 13 (30) |
| Large (≥ 250) | 10 (23) | 10 (23) |
| Most often used method of travel to work by employees | ||
| Car or motorised transport | 32 (73) | 31 (72) |
| Public transport | 1 (2) | 1 (2) |
| Walk or cycle | 1 (2) | 0 (0) |
| Unknown | 10 (23) | 11 (26) |
| Proportion of employees who walk or cycle all the way to work | ||
| None or hardly any | 13 (30) | 12 (28) |
| Fewer than half | 23 (52) | 21 (49) |
| Most | 1 (2) | 0 (0) |
| All | 1 (2) | 0 (0) |
| Unknown | 6 (14) | 10 (23) |
| UK-SIC categories 200768 | ||
| C: manufacturing | 4 (9) | 2 (5) |
| D: electricity, gas, steam and air conditioning supply | 0 (0) | 1 (2) |
| F: construction | 1 (2) | 0 (0) |
| G: wholesale and retail trade; repair of motor vehicles and motorcycles | 4 (9) | 2 (5) |
| H: transport and storage | 0 (0) | 1 (2) |
| K: financial and insurance activities | 2 (5) | 2 (5) |
| M: professional, scientific and technical activities | 10 (23) | 11 (26) |
| N: administrative and support service activities | 5 (11) | 3 (7) |
| O: public administration and defence; compulsory social security | 4 (9) | 4 (9) |
| P: education | 5 (11) | 6 (14) |
| Q: human health and social work activities | 6 (14) | 5 (12) |
| R: arts, entertainment and recreation | 1 (2) | 4 (9) |
| S: other service activities | 2 (5) | 2 (5) |
Participant recruitment and characteristics
Across the 87 workplaces, 654 participants were recruited, with a mean cluster size of approximately 8 (as was the case during the feasibility study). 49 The number of participants in each workplace at baseline ranged from 1 to 28. The average age was 40 years and the majority of participants (455, 65.9%) lived in a household with an income of > £30,000 per year (Table 8). There was a slight balance in favour of females (n = 371, 56.7%) and being educated to at least degree level (377, 57.7%). A large majority of participants, 557 of 626 who gave this information (89%), lived > 2 km from their workplace, and two-thirds travelled to work by car at baseline. Table 8 shows a good balance of key participant characteristics in the intervention and the control groups following randomisation.
| Baseline characteristics | Trial group | |
|---|---|---|
| Intervention | Control | |
| Participant demographic characteristics | ||
| Total number of participants | 331 | 323 |
| Gender: male, n (%) | 143 (43) (N = 331) | 140 (43) (N = 323) |
| Age (years), mean (SD) | 41.2 (11.4) (N = 321) | 42.0 (11.3) (N = 314) |
| BMI category, n (%) | N = 331 | N = 323 |
| Underweight and normal | 149 (45) | 144 (45) |
| Overweight | 99 (30) | 92 (28) |
| Obese | 53 (16) | 52 (16) |
| Missing | 30 (9) | 35 (11) |
| Household income, n (%) | N = 313 | N = 305 |
| ≤ £10,000 | 1 (< 1) | 3 (1) |
| £10,001–20,000 | 14 (4) | 25 (8) |
| £20,001–30,000 | 39 (12) | 39 (13) |
| £30,001–40,000 | 51 (16) | 49 (16) |
| £40,001–50,000 | 67 (21) | 53 (17) |
| > £50,000 | 118 (38) | 117 (38) |
| Does not know | 23 (7) | 19 (6) |
| Ethnicity, n (%) | N = 317 | N = 310 |
| White British | 288 (91) | 279 (90) |
| White other | 15 (5) | 14 (5) |
| Mixed ethnic group | 4 (1) | 3 (1) |
| Asian or British Asian | 3 (1) | 6 (2) |
| Black or black British | 7 (2) | 5 (2) |
| Chinese | 0 (0) | 3 (1) |
| Education, n (%) | N = 315 | N = 309 |
| Higher degree, degree or equivalent | 195 (62) | 182 (59) |
| A level or equivalent | 74 (23) | 79 (26) |
| GCSE or equivalent | 41 (13) | 43 (14) |
| No formal qualifications | 5 (2) | 5 (2) |
| Current method of travel to work, n (%) | N = 327 | N = 313 |
| Car | 217 (66) | 205 (65) |
| Public transport | 44 (13) | 32 (10) |
| Walk | 32 (10) | 42 (13) |
| Cycle | 34 (10) | 34 (11) |
| Distance between workplace and home (km), n (%) | N = 319 | N = 307 |
| ≤ 2 km | 35 (11) | 30 (10) |
| > 2 km | 280 (88) | 277 (90) |
| Current occupation, n (%) | N = 315 | N = 299 |
| Sedentary | 239 (76) | 237 (79) |
| Standing | 60 (19) | 42 (14) |
| Manual | 15 (5) | 20 (7) |
| Heavy manual work | 1 (< 1) | 0 (0) |
Summary
Workplace and participant recruitment proved more difficult than anticipated but increasing the number of urban areas in the study enabled the recruitment of a range of workplaces of different sizes, locations and business classifications. The number of participants was close to, but just under, the recruitment target. The sample of participants was broadly balanced by gender, and the participants tended to be well-qualified and have a higher than average annual household income. A large majority did not live within ‘walking distance’ of their workplace.
Chapter 4 Baseline characteristics and physical activity
Parts of this chapter are reproduced from Batista Ferrer et al. ,70 published by Elsevier. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The text below includes minor additions and formatting changes to the original text.
Methods
Data collection
Study participants were asked to complete travel diaries, to wear accelerometers (ActiGraph GT3X+) for 7 days during waking hours and to carry a personal GPS receiver (Qstarz BT-1000X), set to record positional data at 10-second intervals, during their commute. Participants were provided with instructions about how to use the monitors (see Appendix 4) and those who returned the equipment were provided with a £10 gift voucher to acknowledge their contribution to the study.
Objectively measured physical activity and main mode of travel during the commute
Raw accelerometer data were downloaded using ActiLife software (version 6.11.8; ActiGraph, Pensacola, FL, USA) and reintegrated to 10-second epochs for analysis. Reintegrated accelerometer data were processed using KineSoft data reduction software (version 3.3.80; KinesSoft, Loughborough, UK) to generate outcome variables. Continuous periods of ≥ 60 minutes of zero values were considered ‘non-wear’ time and removed. To be included in the analysis of daily physical activity and sedentary behaviours, participants were required to provide ≥ 3 days of valid accelerometer data of ≥ 600 minutes in duration. In relation to mode and physical activity during the commute, participants were required to provide at least 1 valid day of combined accelerometer and GPS (accGPS) data on a working day. Days on which cycling was identified as the main mode of travel to work were excluded owing to the inability of waist-worn accelerometers to accurately record physical activity during cycling. 71
Accelerometer and GPS data were combined for every 10-second epoch (accGPS) based on the timestamp of the ActiGraph data. The participant’s workplace and home were geocoded using the full postcode and imported into a GIS (ArcMap version 10.2.2; Environmental Systems Research Institute, Inc., Redlands, CA, USA). The merged accGPS files were imported into ArcMap and participants’ journeys to and from work were visually identified and segmented from other accGPS data using the ‘identify’ tool. Journeys were identified as a continuous sequence of GPS locations between the participant’s home and workplace, and therefore may include trips to other destinations (e.g. shopping).
Mode of travel (walking, cycling, using public transport or driving) for the outward and return journeys over the measurement week was derived from visual analysis using the following variables: counts per 10 seconds (sustained counts per epoch of < 17 were bus, train, car; sustained counts per epoch of > 325 were walking and cycling);72 changes to the sum of the signal-to-noise ratio (approximate threshold of a drop to < 250 was employed to indicate movement from an indoor to an outdoor environment);73 maximum speed of the journey (walking – not > 10 km/hour; cycling – not > 40 km/hour; bus – 10 to 50 km/hour; train and car speeds of > 50 km/hour);74 and GIS location for each epoch.
For participants who used a mixed mode of travel (e.g. walking and travelling by train), the mode of transport covering the greatest distance was considered the mode for that journey. MVPA accrued from walking during the journey was captured in a separate variable. When an outward/return journey was missing, it was assumed to be the same mode of travel as the outward/return journey on the same day. Any remaining missing data were replaced with the corresponding travel diary mode when available. The most frequent mode of travel during data collection was used to derive an overall mode of travel for each participant.
Time spent being sedentary and in MVPA were defined using validated thresholds [sedentary, < 100 c.p.m.; MVPA, ≥ 1952 c.p.m.]. 72 To examine the proportion of participants who met current physical activity guidelines,1 we calculated the total MVPA accumulated in bouts of ≥ 10 minutes over the data-collection week (by multiplying the mean daily number of bouts of MVPA by 7). In line with another study,75 participants were classified as ‘active’ or ‘inactive’ during the commute if their mean daily MVPA accrued during the commute was ≥ 10 minutes or < 10 minutes, respectively.
Variables
Individual characteristics and interpersonal responsibilities
The following variables were derived from questionnaire data: (1) gender, (2) age group (‘below 35 years old’ or ‘35 years or greater’), (3) annual household income (‘£30,000 or below’ or ‘> £30,000’, representing mean UK household income), (4) level of education (‘degree or above’ or ‘below degree’), (5) occupational activity (‘sedentary’ or ‘non-sedentary’), (6) limited access to a car [absence of a current driving licence and/or household access to car (‘yes’ or ‘no’)] and (7) combines commute with school run or caring responsibilities (‘yes’ or ‘no’). Self-reported height and weight were used to compute BMI and were assigned to either ‘normal or underweight’ (BMI of < 25 kg/m2) or ‘overweight or obese’ (BMI of ≥ 25 kg/m2) categories based on internationally recognised cut-off points. 76
Workplace characteristics
Commute distance was estimated using an online calculator (www.google.co.uk/maps; accessed 28 February 2019) and the participant’s home and work postcodes. Commute distance was categorised as ‘2 km or below’, ‘between 2 km and 4 km’ and ‘4 km and above’. Participants were asked about the following policies and facilities at their workplace: (1) free car parking, (2) entitlement to purchase a car parking permit, (3) secure storage for clothing, (4) employer-subsidised cycling schemes, (5) a safe place for bicycles, (6) showers and changing rooms, (7) employer-subsidised public transport schemes and (8) a travel plan or policy. Variables were categorised as ‘yes’ or ‘no’.
Perception of the commuting environment
To describe the commuting environment, participants reported their level of agreement with nine statements using a five-point Likert scale: (1) ‘there are suitable pavements for walking’, (2) ‘the pavements are well-maintained’, (3) ‘there are not enough safe places to cross roads’, (4) ‘walking is unsafe because of traffic’, (5) ‘it is unsafe because of the level of crime or antisocial behaviour’, (6) ‘the routes for walking are generally well lit at night’, (7) ‘the area is generally free from litter or graffiti’, (8) ‘it is a pleasant environment for walking’ and (9) ‘there is a lot of air pollution’. These statements have been used in other studies,74,77,78 and have acceptable test–retest reliability. 79 Negatively worded items were recoded so that a high score equated to agreement with the statements. A mean substitution approach was used for the seven participants who missed a single item on the scale. As the distribution of scores was positively skewed, a binary variable comprising ‘positive perception’ (less than the mean score) and negative perception (greater than or equal to the mean score) was created.
Reasons for car use
To provide additional understanding of reasons for car use, participants whose main mode of travel was driving were asked to indicate all reasons that applied to them from the following list: (1) quicker than alternatives, (2) reliability, (3) comfort, (4) have to visit more than one place, (5) cheaper than alternatives, (6) lack of alternative, (7) personal safety, (8) dropping off/collecting children, (9) work unsociable hours, (10) car is essential to perform job, (11) dropping off/collecting partner, (12) carry bulky equipment, (13) health reasons, (14) giving someone else a lift and (15) often on call. They were then asked to choose the single most important reason from the list.
Analysis
Initially, descriptive analyses comprising counts, percentages, medians and interquartile ranges, were conducted. Differences in physical activity variables (overall and during the commute) were analysed by main mode of travel (car users, public transport users and walkers) using analysis of variance (ANOVA) and chi-squared statistics. Data related to participants classified as cyclists are not presented because of the inability of waist-worn accelerometers to accurately record physical activity during cycling.
Associations with objectively measured physical activity during the commute
To explore associations with levels of physical activity during the commute, logistic univariable analyses and likelihood ratio tests were conducted. The following explanatory variables for analysis were selected a priori: gender, age group, annual household income, education, weight status, occupational activity and commute distance. A multivariable logistic regression model was developed using ‘inactive during commute’ as the reference group. In the order of the strength of association, variables were selected for inclusion and retained in the model if there was an associated improvement in fit (p < 0.05). The final model adjusted for weight status, occupational activity and commute distance.
Associations with objectively measured mode of travel
The objective of the next stage of the analysis was to identify associations between different modes of travel to work and individual, interpersonal and workplace variables. Analyses were restricted to participants who were classified as ‘walkers’ (n = 74), ‘public transport users’ (n = 76) or ‘car users’ (n = 422). Participants classified as cyclists (n = 68) or whose mode of transport was unknown (n = 14) were excluded. Initially, associations were examined using logistic univariable analyses and likelihood ratio tests. Multicollinearity between variables was tested for through correlations. Using the same methodology as described previously, two separate multivariable logistic regression models were developed for ‘walkers’ and ‘public transport users’, both using ‘car users’ as the reference group. Individual, interpersonal and workplace characteristics and perception-of-commute variables were eligible for inclusion if they were associated with an improvement in fit of model (p < 0.05). The final ‘walkers’ model adjusted for limited access to a car, commute distance and availability of workplace car parking. The final ‘public transport users’ model adjusted for age group, limited access to a car, combines commute with caring responsibilities, availability of workplace car parking and perception of commute environment. Finally, a description of reasons for car use by car users was presented as counts and percentages.
Potential clustering by workplace was adjusted for using a robust standard errors approach allowing for workplace-level random effects in the final model. For each model, results were presented as odds ratios (ORs), adjusted odds ratios (aORs) and corresponding 95% CIs and p-values. Through sensitivity analyses, separate logistic models that were restricted to males only and females only were developed, with no major effect sizes by variables observed. Interactions were not fitted owing to small sample sizes. Analyses were undertaken to explore whether or not associations varied by gender. All analyses were conducted using Stata® version 14 (StataCorp LP, College Station, TX, USA).
Results
Associations with undertaking physical activity during the commute
Valid accGPS data from at least 1 day were provided by 597 participants. After adjustment for weight status, occupational activity and commute distance, there was strong evidence that participants were more physically active during their commute if they had sedentary jobs (aOR 1.96, 95% CI 1.26 to 3.04) or had a commute distance of < 2 km (aOR 2.73, 95% CI 1.69 to 4.41) or between 2 km and 4 km (aOR 2.74, 95% CI 1.58 to 4.73). There was weaker evidence that participants in the underweight or normal weight category (aOR 1.48, 95% CI 1.04 to 2.12) were more physically active during the commute (Table 9).
| Variable | Participants, n (%) | OR (95% CI); p-value | aORb (95% CI); p-value | ||
|---|---|---|---|---|---|
| All (N = 654) | Inactivea status (N = 349) | Activea status (N = 248) | |||
| Gender | |||||
| Male | 283 (43.3) | 160 (63.0) | 94 (37.0) | – | NI |
| Female | 371 (56.7) | 189 (55.1) | 154 (44.9) | 1.39 (1.00 to 1.93); 0.05 | |
| Age (years) | |||||
| ≥ 35 | 431 (65.9) | 241 (60.6) | 157 (53.5) | – | NI |
| < 35 | 204 (31.2) | 100 (39.5) | 87 (46.5) | 1.34 (0.94 to 1.90); 0.11 | |
| Annual household income | |||||
| ≤ £30,000 | 121 (18.5) | 65 (59.6) | 44 (40.4) | – | NI |
| > £30,000 | 455 (69.5) | 243 (57.9) | 177 (42.1) | 1.08 (0.70 to 1.65); 0.74 | |
| Education | |||||
| Less than degree level | 247 (37.8) | 138 (59.7) | 93 (40.3) | – | NI |
| Degree level or higher | 377 (57.7) | 195 (56.5) | 150 (43.5) | 1.14 (0.81 to 1.60); 0.44 | |
| Weight status | |||||
| Overweight or obese | 296 (45.3) | 179 (64.2) | 100 (35.8) | – | – |
| Underweight or normal | 293 (44.8) | 143 (54.0) | 122 (46.0) | 1.53 (1.08 to 2.15); 0.02 | 1.48 (1.04 to 2.12); 0.03 |
| Occupational activity | |||||
| Non-sedentary | 130 (19.9) | 87 (69.1) | 39 (31.0) | – | – |
| Sedentary | 450 (68.8) | 229 (55.5) | 184 (44.6) | 1.79 (1.17 to 2.74); < 0.01 | 1.96 (1.26 to 3.04); < 0.01 |
| Commute distance (km) | |||||
| > 4 | 455 (69.6) | 276 (64.9) | 149 (35.1) | – | – |
| Between 2 and 4 | 100 (15.3) | 36 (40.9) | 52 (59.1) | 2.68 (1.67 to 4.28); < 0.001 | 2.73 (1.69 to 4.41); < 0.001 |
| < 2 | 71 (10.9) | 20 (40.6) | 38 (59.4) | 2.71 (1.58 to 4.63); < 0.001 | 2.74 (1.58 to 4.73); < 0.001 |
Of 542 participants (82.4%) who provided 3 days of valid accelerometer data, a minority (n = 60, 11.1%) met current UK public health physical activity guidelines. 1 A substantially higher proportion of walkers (n = 24, 38.7%) and public transport users (n = 10, 16.1%) met public health physical activity guidelines than car users (n = 17, 4.7%) (p < 0.001). There were marked differences in time spent in MVPA by main mode of travel. Overall, both walkers (mean 71.3 minutes, SD 21.3 minutes) and public transport users (mean 59.5 minutes, SD 26.6 minutes) accumulated more MVPA throughout the day than car users did (mean 46.3 minutes, SD 20.6 minutes). Walkers (mean 34.3 minutes, SD 18.6 minutes) and public transport users (mean 25.7 minutes, SD 4.0 minutes) were also, on average, more active during the commute than car users (mean 7.3 minutes, SD 7.6 minutes). There was no strong evidence for differences in time spent in sedentary behaviours (p = 0.12) or accelerometer wear time (p = 0.43) by main mode of travel (Table 10).
| Variable | Main mode of travel | p-valuea | |||
|---|---|---|---|---|---|
| All | Car | Walking | Public transport | ||
| N = 540 | N = 357 | N = 62 | N = 62 | ||
| Meets public health physical activity guidelines,b n (%) | 60 (11.1) | 17 (4.8) | 24 (38.7) | 10 (16.1) | < 0.001a |
| Overall daily physical activity (c.p.m.), mean (SD) | 385.3 (193.1) | 342.7 (120.1) | 507.2 (151.2) | 405.5 (150.7) | < 0.001c |
| Daily time spent in MVPA (minutes), mean (SD) | 52.9 (28.7) | 46.3 (20.6) | 71.3 (21.3) | 59.5 (26.6) | < 0.001c |
| Daily time spent in sedentary behaviours (minutes), mean (SD) | 580.6 (72.6) | 587.6 (69.5) | 568.1 (62.2) | 585.8 (65.2) | 0.12c |
| Daily wear time (minutes), mean (SD) | 798.2 (75.7) | 800.4 (75.0) | 788.6 (70.9) | 792.7 (72.2) | 0.43c |
| N = 597 | N = 404 | N = 71 | N = 73 | ||
| Daily commute time (minutes), mean (SD) | 85.7 (54.2) | 86.6 (51.0) | 53.8 (29.2) | 116.5 (56.2) | < 0.001 |
| Daily time spent in MVPA during commute (minutes), mean (SD) | 13.0 (14.3) | 7.3 (7.6) | 34.3 (18.6) | 25.7 (14.0) | < 0.001 |
Individual characteristics, interpersonal responsibilities and workplace and environmental characteristics associated with mode of travel
After adjustment for having a current driving licence, household access to a car, commute distance to workplace and free work car parking, there was strong evidence that not having a driving licence (aOR 8.74, 95% CI 2.45 to 31.2) and not having access to a car (aOR 23.1, 95% CI 5.0 to 106.5) were positively associated with walking to work. The workplace characteristics ‘commute distance of less than 2 km’ (aOR 51.4, 95% CI 19.7 to 134.3), ‘commute distance between 2 km and 4 km’ (aOR 15.2, 95% CI 5.84 to 39.4) and lack of free parking (aOR 2.97, 95% CI 1.38 to 6.39) were also positively associated with walking (Table 11).
| Variable | Participants, n (%) | OR (95% CI); p-value | aOR (95% CI); p-value | Public transport users (N = 76), n (%) | OR (95% CI); p-value | aOR (95% CI); p-value | ||
|---|---|---|---|---|---|---|---|---|
| All (N = 654) | Car users (N = 422) | Walkers (N = 74) | ||||||
| Individual and interpersonal characteristics | ||||||||
| Gender: female | 371 (56.7) | 241 (57.1) | 44 (59.5) | 1.10 (0.67 to 1.82); 0.71 | NI | 50 (65.8) | 1.44 (0.87 to 2.41); 0.16 | NI |
| Age: < 35 years | 204 (31.2) | 115 (27.3) | 28 (37.8) | 1.69 (1.00 to 2.85); 0.05 | NI | 38 (50.0) | 2.67 (1.62 to 4.41); < 0.001 | 2.05 (1.05 to 4.02); 0.04 |
| Household income: ≤ £30,000 per annum | 121 (18.5) | 80 (19.0) | 17 (23.0) | 1.34 (0.73 to 2.46); 0.34 | NI | 12 (15.8) | 0.84 (0.43 to 1.65); 0.61 | NI |
| Education: lower than degree level | 247 (37.8) | 169 (40.1) | 32 (43.2) | 1.15 (0.69 to 1.90); 0.60 | NI | 29 (38.2) | 0.88 (0.53 to 1.46); 0.62 | NI |
| Weight status: underweight or normal | 293 (44.8) | 178 (42.2) | 44 (59.5) | 2.31 (1.34 to 3.97); < 0.01 | NI | 28 (36.8) | 0.99 (0.58 to 1.70); 0.99 | NI |
| Occupational activity: sedentary | 130 (19.9) | 288 (68.3) | 50 (67.6) | 1.39 (0.71 to 2.72); 0.34 | NI | 61 (80.3) | 2.54 (1.17 to 5.50); 0.02 | NI |
| Limited access to car: no | 62 (9.5) | 9 (2.1) | 21 (28.4) | 20.4 (8.78 to 47.2); < 0.001 | 20.5 (6.01 to 69.8); < 0.001 | 27 (35.5) | 26.8 (11.8 to 60.7); < 0.001 | 29.2 (10.4 to 81.6); < 0.001 |
| Combines commute with caring responsibilities: no | 485 (74.2) | 308 (73.0) | 59 (79.7) | 2.52 (1.05 to 6.05); 0.04 | NI | 64 (84.2) | 5.47 (1.67 to 17.9); < 0.01 | 4.88 (1.17 to 20.3); 0.03 |
| Workplace characteristics | ||||||||
| Commute distance (km) | ||||||||
| > 4a | – | – | – | – | – | – | – | – |
| Between 2 and 4 | 100 (15.3) | 48 (11.4) | 21 (28.4) | 11.3 (5.30 to 24.0); < 0.001 | 15.0 (5.55 to 40.6); < 0.001 | 8 (10.5) | 0.87 (0.39 to 1.93); 0.74 | NI |
| < 2 | 71 (10.9) | 26 (6.2) | 35 (47.3) | 34.7 (16.4 to 73.5); < 0.001 | 63.6 (21.5 to 187.9); < 0.001 | 1 (1.3) | 0.21 (0.03 to 1.60); 0.13 | NI |
| No free work car parking | 253 (38.7) | 147 (34.8) | 38 (51.4) | 3.02 (1.69 to 5.40); < 0.001 | 3.19 (1.38 to 7.39); < 0.01 | 38 (50.0) | 2.88 (1.63 to 5.10); < 0.001 | 3.81 (1.75 to 8.27); < 0.01 |
| No entitlement to purchase a parking permit | 444 (67.9) | 299 (70.9) | 49 (66.2) | 1.62 (0.70 to 3.72); 0.26 | NI | 46 (60.5) | 1.33 (0.60 to 2.94); 0.49 | NI |
| Secure storage for personal belongings | 218 (52.0) | 217 (58.3) | 39 (65.0) | 1.33 (0.75 to 2.34); 0.33 | NI | 37 (59.7) | 1.06 (0.61 to 1.82); 0.84 | NI |
| Employer-subsidised cycling schemes | 214 (32.7) | 142 (33.7) | 25 (33.8) | 1.24 (0.68 to 2.28); 0.47 | NI | 20 (46.5) | 1.04 (0.55 to 1.97); 0.90 | NI |
| Safe place to leave bicycles | 95 (14.5) | 71 (19.6) | 12 (16.2) | 1.03 (0.52 to 2.04); 0.94 | NI | 9 (15.0) | 1.38 (0.65 to 2.93); 0.41 | NI |
| No showers/changing rooms | 195 (29.8) | 131 (31.0) | 25 (33.8) | 1.22 (0.71 to 2.11); 0.48 | NI | 24 (39.3) | 1.20 (0.69 to 2.10); 0.51 | NI |
| No employer-subsidised public transport schemes | 406 (11.2) | 268 (62.1) | 42 (56.8) | 2.15 (0.74 to 6.26); 0.16 | NI | 48 (63.2) | 1.23 (0.55 to 2.75); 0.61 | NI |
| No travel plan or policy | 233 (35.6) | 151 (35.8) | 25 (33.8) | 1.77 (0.79 to 3.94); 0.17 | NI | 35 (46.1) | 1.71 (0.86 to 3.40); 0.13 | NI |
| Environmental characteristics | ||||||||
| Positive perception of environment | 290 (44.3) | 161 (38.2) | 46 (62.2) | 3.44 (1.95 to 6.10); < 0.001 | NI | 19 (25.0) | 2.71 (1.24 to 3.98); 0.01 | 2.71 (1.24 to 5.92); 0.01 |
After adjustment for age group, having a driving licence, household access to a car, combining the commute with caring responsibilities and free work car parking, there was strong evidence that being < 35 years old (aOR 1.98, 95% CI 1.02 to 3.84), not having a driving licence (aOR 20.2, 95% CI 7.25 to 56.2), not having access to a car (aOR 5.00, 95% CI 1.13 to 22.2), not combining the commute with the school run or caring responsibilities (aOR 4.77, 95% CI 1.13 to 20.2) and the workplace characteristic ‘absence of free parking’ (aOR 3.32, 95% CI 1.56 to 7.09) were positively associated with using public transport (see Table 11).
Sensitivity analyses indicated no marked differences by gender across all of the models.
Reasons for car use
The reasons that were frequently provided for car use (Table 12) included that it was quicker than alternative modes of travel (n = 329, 78.0%), reliability (n = 275, 65.2%), comfort (n = 275, 65.2%), having to visit more than one place (n = 179, 42.4%), that it was cheaper than alternative modes of travel (n = 179, 42.2%) and lack of alternatives (n = 174, 41.2%). This order changed slightly when participants were asked to choose their single most important reason (see Table 5). Being quicker than alternatives (n = 100, 28.7%), lack of alternatives (n = 51, 14.7%) and reliability (n = 39, 11.2%) continued as main reasons, but dropping off and collecting children (n = 34, 9.8%) and a car being essential for their job (n = 29, 8.3%) appeared to take priority over comfort, cost or having to visit more than one place.
| Order | |||
|---|---|---|---|
| By all reasons (N = 383) | By most important reason (N = 348) | ||
| Reasons | n (%) | Reasons | n (%) |
| Quicker than alternatives | 329 (78.0) | Quicker than alternatives | 100 (28.7) |
| Reliability | 275 (65.2) | Lack of alternatives | 51 (14.7) |
| Comfort | 275 (65.2) | Reliability | 39 (11.2) |
| Have to visit more than one place | 179 (42.4) | Dropping off/collecting children | 34 (9.8) |
| Cheaper than alternatives | 178 (42.2) | Car is essential to perform job | 29 (8.3) |
| Lack of alternative | 174 (41.2) | Have to visit more than one place | 16 (4.6) |
| Personal safety | 115 (27.3) | Cheaper than alternatives | 15 (4.3) |
| Dropping off/collecting children | 103 (24.4) | Dropping off/collecting partner | 14 (4.0) |
| Works unsociable hours | 99 (23.5) | Comfort | 13 (3.7) |
| Car is essential to perform job | 91 (21.6) | Works unsociable hours | 10 (2.9) |
| Dropping off/collecting partner | 38 (9.0) | Carries bulky equipment and/or cash | 9 (2.6) |
| Carries bulky equipment and/or cash | 80 (19.0) | Health reasons | 6 (1.7) |
| Health reasons | 23 (5.5) | Personal safety | 5 (1.4) |
| Giving someone else a lift | 55 (13.0) | Giving someone else a lift | 4 (1.2) |
| Often on call | 28 (6.6) | Often on call | 3 (0.9) |
Summary
Compared with car users, walkers and public transport users accrued substantially higher levels of daily MVPA during the commute and throughout the day. Participants in non-sedentary occupations were less physically active during their commute. Factors associated with walking to work included shorter commuting distances, limited access to a car and lack of free car parking. Factors associated with public transport use included being aged < 35 years, having limited access to a car, lack of free car parking, not combining the commute with the school run or caring responsibilities and having more-positive perceptions of the commute environment.
Chapter 5 The Walk to Work intervention
Developing the intervention
The intervention aimed to increase the physical activity of participants, and reduce private car use, by focusing on walking as active travel during the commute. Walking and cycling are frequently combined under the term ‘active travel’, but they are discrete behaviours appealing to different population groups and requiring different strategies to increase their use as modes of travel. 80 A number of high-profile active travel initiatives focus on cycling (www.cyclescheme.co.uk; accessed 6 June 2018). However, for shorter journeys, or as part of longer journeys, walking may be perceived as a cheaper and safer option than cycling: it requires no special equipment and is less likely to involve direct competition with motorised traffic for road space.
There were three main stages of the intervention: (1) identification and training of workplace Walk to Work promoters, (2) initial contact between the Walk to Work promoters and participating employees, including the distribution and discussion of intervention materials, and (3) three additional contacts during the following 10 weeks to provide encouragement for participating employees and Walk to Work promoters. Ten weeks is considered a suitable length of time to enable a change of behaviour to become a habit. 81
Lessons from the feasibility study: behaviour change techniques
During the Walk to Work feasibility study, the intervention focused on nine BCTs to guide participants to consider a more active travel mode through to maintaining the new behaviour: intention formation, instruction, barrier identification, goal-setting, general encouragement, self-monitoring, social support, review of goals and relapse prevention. Evidence from the process evaluation suggested that different participants found different BCTs more useful than others. 82 This was supported by other research: for example, ‘intention formation’ was identified by Bird et al. 47 as a key BCT for use in walking and cycling interventions, but not by Malik et al. 28 in their review of workplace physical activity. A qualitative evidence synthesis of workplace smoking interventions concluded that workplace interventions should employ a range of different elements because different employees have different requirements. 83 Overall, the nine BCTs that formed the basis of the Walk to Work intervention during the feasibility study appeared acceptable to participants and were retained for the main trial. However, the term ‘relapse prevention’ had been challenged by some participants as being inappropriate for an intervention that promotes walking. This is supported by Michie et al. ,44 who argue that different BCTs from those used to stop negative behaviour, such as smoking, should be used to support positive behaviours, such as physical activity and healthy eating. Therefore, for the main trial, the techniques used to avoid ‘relapse’ from increased walking back to less active modes of travel were couched in terms of ongoing support and encouragement for walking.
Lessons from the feasibility study: Walk to Work promoter training and support
During the feasibility study, it was originally proposed that the Walk to Work promoters from different workplaces would be invited to an external training event organised by the researchers. However, not all workplaces were able to release an employee for the time and date proposed, and so two smaller external training sessions were organised and some individual workplace-based training was provided. Having received their training and booklets to guide them through their role, the Walk to Work promoters were not provided with any additional support or guidance during the 10-week intervention. However, during post-intervention interviews, the Walk to Work promoters indicated that they would have welcomed additional prompts and encouragement during the intervention period. 82 In the light of these findings, for the main trial an individual training package for Walk to Work promoters was developed for delivery in the workplace and ongoing support for Walk to Work promoters was incorporated into the 10-week intervention.
Lessons from the feasibility study: workplace support for the intervention
Advocates of the socioecological model argue that public health interventions need to consider influences at the policy, community, organisational, interpersonal and intrapersonal levels. 84 During the feasibility study, the importance of support at the workplace (organisational) level was acknowledged. However, the majority of employers who took part in the feasibility study were unclear about how to give practical support for employees who walk to work. 85 Additional materials were, therefore, developed for the main trial to give employers information and ideas about how to support the Walk to Work intervention.
The Walk to Work intervention: methods and resources
The intervention components, linked to BCTs, are summarised in Table 13.
| Contact | BCT | Walk to Work intervention |
|---|---|---|
| Week 1 (getting started) |
|
|
| Week 3 |
|
|
| Week 5 |
|
|
| Week 7 onwards |
|
|
Each stage of the intervention is described in the following sections. A logic model (see Figure 2) summarising the intervention theory, inputs, activities, outputs and anticipated outcomes was developed for the process evaluation.
Walk to Work promoter recruitment
Following randomisation, workplaces in the intervention group were asked to identify a Walk to Work promoter. This could be a volunteer with an interest in the study, someone nominated by their employer as being suitable for the role (e.g. an employee already tasked with developing and implementing a travel plan) or an employer willing to take on the role themselves. Potential Walk to Work promoters were provided with an information leaflet explaining the role (see Appendix 5) and a consent form. Written consent was provided before potential Walk to Work promoters received the training and undertook the role.
Walk to Work promoter training and resources
The research team delivered a training session, lasting for approximately 1 hour, to the Walk to Work promoters at their workplace and at a time and place to suit their needs. The training was summarised in a DVD (digital versatile disc), developed by the research team, which promoters retained after the session. The training included information about the health, social, economic and environmental benefits of walking; using BCTs to promote increased walking, either the whole route or as part of a mixed-mode journey; providing support and encouragement to participating employees; and accessing relevant websites and resources for additional information and resources. Walk to Work promoters were given booklets, also developed by the research team, to assist them in the role. The content of these booklets (see Appendix 6) was discussed in detail as part of the training session.
Walk to Work promoters were given the names of participating employees in their workplace and were asked to provide the employees with Walk to Work booklets and an optional pedometer, highlight the benefits of increased walking, discuss barriers and solutions to walking during the commute, help participants to identify routes and methods of incorporating walking in their journeys and provide ongoing support through four contacts over the following 10 weeks. These contacts could be face to face, via e-mail or via telephone, in groups or on an individual basis, depending on the preferences of the workplace and participants. The Walk to Work promoter’s booklet contained guidance about providing support and encouragement to participating employees over the 10-week intervention period and optional diary pages to record their activities.
Walk to Work promoters were prompted and encouraged in their role through three short newsletters from the research team over the 10-week intervention period (see Appendix 7). These were supplemented by newsletters to pass on to participants (see Appendix 8) focusing on specific BCTs and providing additional information about the benefits of walking. The newsletters were provided by e-mail and/or in paper form to suit the workplace.
Participant booklets
The Walk to Work promoters were given the names of all employees in their workplaces who were participating in the study and were asked to provide each of them with a participant booklet. These booklets provided information and guidance relating to the BCTs that comprised the behavioural intervention (see Appendix 9). To encourage intention formation, the booklets began by considering the benefits of increasing walking during the commute. The focus then moved to identifying personal benefits, barriers and solutions, and goal-setting. Self-monitoring was encouraged through the use of diary pages at the back of the participant’s booklet or the use of optional pedometers, which had been provided free of charge to the study by the charity Living Streets (www.livingstreets.org.uk; accessed 6 June 2018), to record daily steps. Participants were prompted to seek encouragement and social support during their attempts to increase walking during the commute.
Participant newsletters
Three newsletters were sent to the Walk to Work promoters for circulation to participating employees during the following 10 weeks (see Appendix 8). These provided additional information, to stimulate continued interest in the benefits of walking, as well as continuing the focus on key BCTs: highlighting social support at around week 3, reviewing goals at week 5 and following up participants to support the maintenance of behavioural change (relapse prevention) at around week 7.
Information and ideas for employers
An employer pack was provided to all workplaces in the intervention group of the study (see Appendix 10). This comprised a letter outlining the intervention, the booklets being used by the Walk to Work promoters and participants, additional booklets specifically designed for employers and free Walk4Life poster templates for display in the workplace (www.walk4life.info; accessed 6 June 2018). The employer’s booklet contained ideas for promoting walking to work, including providing information about walking distances to train and bus stops, providing lockers or improved cloakroom facilities, giving financial assistance for public transport season tickets or for walking clothes/shoes, offering free incentive items for those who switch to walking (e.g. umbrellas, rucksacks or breakfast vouchers) and supporting competitions and challenges for those who enjoy taking part in such activities. Employers were encouraged to record any support they had provided for the intervention, together with associated costs, in a section at the back of their booklet.
Adverse events
Details of the procedure for reporting adverse events are provided in Chapter 2. No accidents or adverse events relating to the intervention were reported during the study.
Summary
The Walk to Work intervention was based on nine key BCTs and involved three stages: (1) identification and training of workplace Walk to Work promoters, (2) initial contact between the Walk to Work promoters and participating employees, and the distribution and discussion of intervention materials, and (3) additional support and encouragement during the following 10 weeks. Walk to Work promoters, participants and employers were provided with a co-ordinated suite of booklets and resources to support implementation of the 10-week intervention to encourage increased walking during the commute to and from work.
Chapter 6 Process evaluation
Methods
The process evaluation methods were informed by the Medical Research Council guidance on process evaluation of complex public health interventions. 86
Logic model
A logic model was developed, indicating the theoretical underpinning of the Walk to Work intervention, inputs, activities, outputs and outcomes as well as contextual factors likely to have an impact on the implementation of, and response to, the intervention (Figure 2).
FIGURE 2.
Walk to Work intervention logic model.
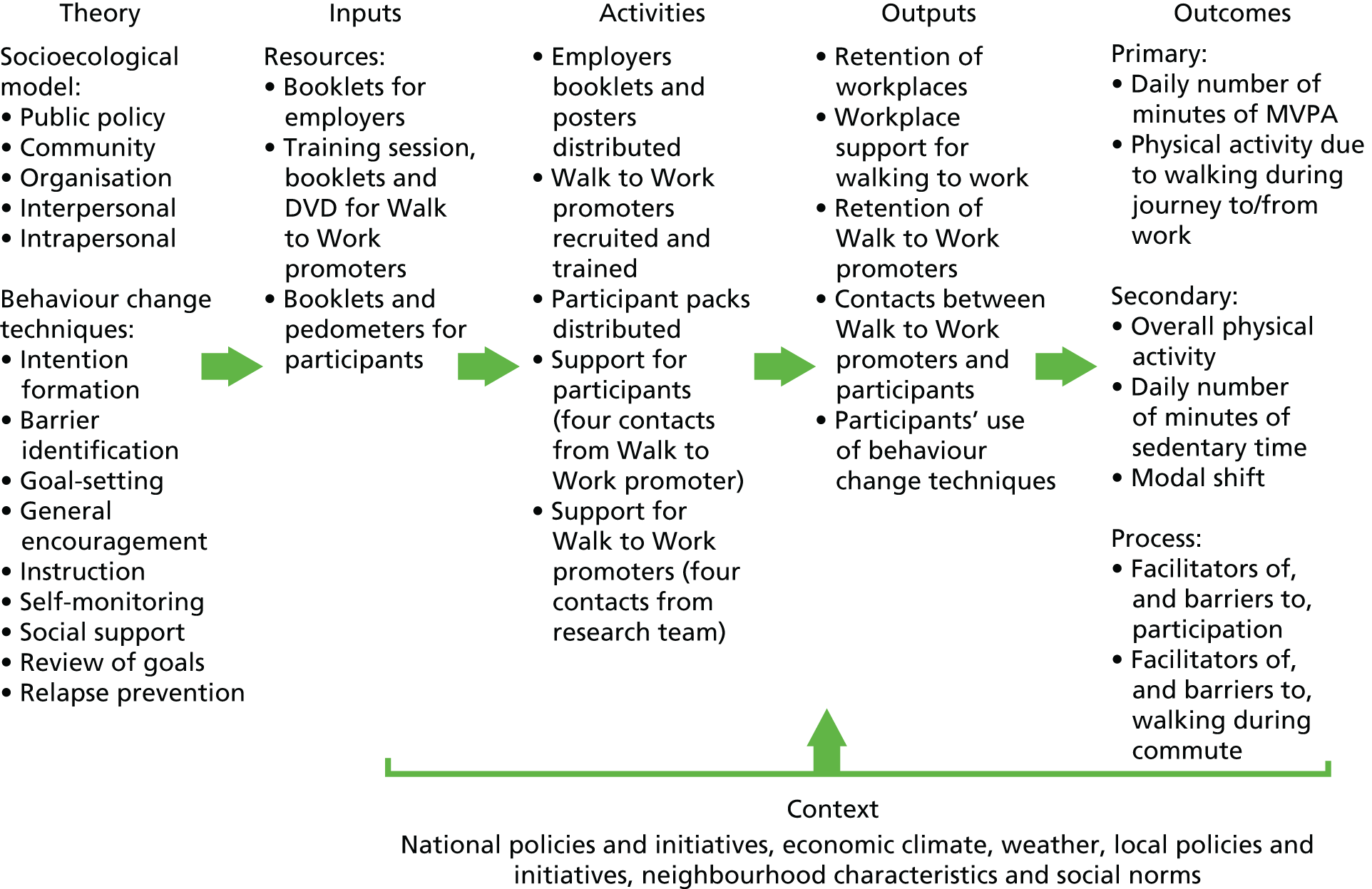
Data collection
The planned process evaluation methods are summarised in Table 14.
| Stage | Method | Issues to be examined |
|---|---|---|
| Recruitment and retention of workplaces |
|
|
| Recruitment and retention of employees |
|
|
| Baseline | Questionnaires administered to all participating employees |
|
| Randomisation | Within ‘matched’ pairs, randomly generated number | Response to randomisation (retention) |
| Training Walk to Work promoters |
|
|
| Contact/support for walkers | Diary completed by Walk to Work promoters | Used as prompt in post-intervention interviews |
| Immediately post intervention |
|
|
|
||
| 12-month follow-up | Questionnaires with all participating employees (intervention and control arms) |
|
Data relating to the context, delivery and response to the intervention were collected from employers, Walk to Work promoters and employees through survey questionnaires at baseline, post intervention and at the 12-month follow-up, and through interviews with a purposive sample of employers, Walk to Work promoters and employees immediately post intervention. Observations and notes were also recorded during contacts with workplaces.
Questionnaires
For the process evaluation, the post-intervention questionnaires included questions about whether or not participants were aware of efforts within their workplace to increase or support walking during the commute and whether or not the research activities (particularly wearing activity monitors) had influenced their physical activity levels. All questionnaire data were entered into a secure database. Descriptive statistics are displayed as counts and percentages. Some questions allowed participants to add short free-text responses. These were entered in full into the database and grouped in accordance with the issues raised, including identifying similarities and differences in relation to those issues. The quotations included in this chapter were chosen to illustrate the key points that were made.
Interviews
Semistructured interviews were conducted with a purposive sample of employers, Walk to Work promoters and employees in the intervention group. The aim was to include views and experiences from a wide range of workplaces, Walk to Work promoters and employees who self-reported that they had, or had not, increased walking during the commute to work. A gender balance was also sought. Interviews were conducted in the workplace at a time to suit the interviewee. The topic guides were tailored to suit the participant’s role (employer, Walk to Work promoter or employee) and whether they were in the intervention or the control group of the trial (see Appendix 11). Potential interviewees were sent a letter of invitation and written consent was obtained prior to the interview. Interviewees were given a £10 gift voucher to thank them for their contribution to the study.
All interviews were digitally recorded, fully transcribed and anonymised. For this report, preliminary analyses focused on a key outcome for the process evaluation: barriers to, and facilitators of, walking during the commute to and from work. Thematic analysis was undertaken using the Framework method of data management. 87 The Framework method entails examining the transcripts and creating charts of sections of text relevant to key research questions. Streamlined versions of the charts are produced as the process of coding and analysing the data progresses: key terms and phrases are retained, repetition and extraneous text are removed and similarities and differences are examined within emerging themes.
Workplace descriptors
The classification of workplace activities is based on the UK Standard Industrial Classification (SIC) Categories 2007. 68 ‘Micro’ usually refers to workplaces with between one and nine employees,88 but for this study at least five employees were needed to meet the eligibility criteria and so micro refers to workplaces employing between five and nine people. Small workplaces are defined as employing 10–49 people, medium-sized workplaces are defined as employing 50–249 people and large workplaces are defined as employing ≥ 250 people. 88
Participant identification numbers
All participants in the study were given a unique identification number: the first three digits refer to the workplace and the last two digits refer to the participant. IDs (identifiers) preceded by ‘9’ indicate that these participants, either Walk to Work promoters or Walk to Work employers, contributed to the study but did not take part in the outcome data-collection activities.
Results
Workplace and participant recruitment
The process of recruiting workplaces and participants is considered in detail in Chapter 3. Following baseline data collection, 44 workplaces were randomised to receive the intervention. However, two workplaces withdrew from the intervention group: one because of unanticipated relocation to another country and one because the key contact felt that the study activities were too onerous.
Walk to Work promoter recruitment
In the remaining intervention workplaces, the employers were asked to identify a Walk to Work promoter to implement the 10-week intervention. In 19 workplaces, the employer took on this role themselves: of these, six were micro-sized, seven were small, five were medium-sized and one was large (Table 15). One large workplace had two Walk to Work promoters, but in the majority of workplaces one person was identified to undertake the role. Fourteen of the Walk to Work promoters were male and 24 were female.
| Promoter | Workplace | ||||
|---|---|---|---|---|---|
| Gender | Age (years) | Role | ID | Classification | Size |
| Male | 55 | Employer/promoter | 101-01 | Wholesale and retail; vehicle repairs | Small |
| Male | 63 | Employer/promoter | 102-01 | Professional, scientific and technical | Small |
| Female | 52 | Employer/promoter | 127-05 | Other service activities | Micro |
| Female | 52 | Employer/promoter | 127-05 | Other service activities | Micro |
| Male | 43 | Employer/promoter | 165-01 | Financial and insurance | Small |
| Male | 43 | Employer/promoter | 165-01 | Financial and insurance | Small |
| Female | 55 | Employer/promoter | 166-01 | Human health and social work | Micro |
| Female | 55 | Employer/promoter | 166-01 | Human health and social work | Micro |
| Female | 38 | Employer/promoter | 223-01 | Professional, scientific and technical | Medium |
| Female | 52 | Employer/promoter | 228-01 | Human health and social work | Medium |
| Female | 52 | Employer/promoter | 228-01 | Human health and social work | Medium |
| Male | 43 | Employer/promoter | 302-03 | Arts, entertainment and recreation | Small |
| Male | 33 | Employer/promoter | 325-01 | Wholesale and retail; vehicle repairs | Small |
| Male | 33 | Employer/promoter | 325-01 | Wholesale and retail; vehicle repairs | Small |
| Female | 48 | Employer/promoter | 334-01 | Administrative and support services | Micro |
| Female | 48 | Employer/promoter | 334-01 | Administrative and support service | Micro |
| Male | – | Employer/promoter | 9-122-07 | Manufacturing | Large |
| Male | – | Employer/promoter | 9-319-01 | Professional, scientific and technical | Medium |
| Male | – | Employer/promoter | 9-319-01 | Professional, scientific and technical | Medium |
| – | – | No promoter | 207 | Human health and social work | Small |
| – | – | No promoter | 209 | Membership organisation | Small |
| – | – | No promoter | 303 | Wholesale and retail; vehicle repairs | Medium |
| – | – | No promoter | 307 | Administrative and support services | Large |
| – | – | No promoter | 310 | Public administration and defence | Medium |
| Female | 33 | Promoter | 111-02 | Professional, scientific and technical | Large |
| Female | 31 | Promoter | 141-03 | Human health and social work | Medium |
| Female | 31 | Promoter | 141-03 | Human health and social work | Medium |
| Female | 58 | Promoter | 161-02 | Professional, scientific and technical | Small |
| Female | 58 | Promoter | 161-02 | Professional, scientific and technical | Small |
| Female | 58 | Promoter | 305-01 | Manufacturing | Medium |
| Female | 27 | Promoter | 317-03 | Professional, scientific and technical | Small |
| Female | 27 | Promoter | 317-03 | Professional, scientific and technical | Small |
| Male | – | Promoter | 9-122-07 | Manufacturing | Large |
| Female | – | Promoter | 9-226-18 | Public administration and defence | Large |
| Female | – | Promoter | 9-226-18 | Public administration and defence | Large |
| Female | – | Promoter | 9-232-12 | Manufacturing | Small |
| Female | – | Promoter | 9-232-12 | Manufacturing | Small |
| Female | – | Promoter | 9-330-36 | Education | Large |
| Female | – | Promoter | 9-330-36 | Education | Large |
| Male | – | Promoter | 9-335-15 | Administrative and support service | Large |
| Male | – | Promoter | 9-335-15 | Administrative and support service | Large |
| Male | 61 | Promoters (paired) | 106-13 | Public administration and defence | Large |
| Female | – | 9-106-29 | |||
During the first year of recruitment, five workplaces in the intervention group were unable to identify someone to take on the role of Walk to Work promoter. Rather than lose these workplaces from the study altogether, it was decided that the relevant researcher would take on the role of ensuring that the intervention materials were distributed to participating employees. However, it was not felt appropriate for the researcher to go into the workplace to give face-to-face support for employees to encourage them to change their travel behaviour. These workplaces were therefore considered to have received a ‘light-touch’ intervention. In the second year of recruitment, researchers stressed the importance of being able to identify someone in the workplace who might be suitable to be a Walk to Work promoter should the workplace be randomised to the intervention group, and no further workplaces were recorded as not recruiting a Walk to Work promoter.
Walk to Work promoter training and intervention materials
The methods and resources used for the Walk to Work intervention are described in detail in Chapter 5. The training session, DVD and booklets offering guidance about their role were delivered to all designated Walk to Work promoters at the start of the intervention. Three newsletters offering additional information and encouragement were also sent to all Walk to Work promoters during the 10-week intervention. All Walk to Work promoters were provided with booklets and optional pedometers to distribute to participating employees in their workplaces, plus three newsletters to distribute to participants during the 10-week intervention period. The pedometers, which were provided free of charge for participants who wished to use them, were not of high quality. Participants who wanted to self-monitor preferred to use their own wrist-worn monitoring devices or an app (application) on their smartphone, details of which were supplied in newsletter 2 of the intervention.
All employers were provided with the employer pack containing a letter reminding them of the aims of the intervention and the role of Walk to Work promoter, booklets with ideas about how to support the intervention and templates for posters to display as appropriate in their workplaces.
Activities of the Walk to Work promoters
In relation to fidelity (the extent to which the intervention was delivered as planned), we were able to examine the recruitment, training and ongoing support of the Walk to Work promoters but it was not possible to directly observe their activities in their respective workplaces. However, the post-intervention questionnaires included questions to shed light on the Walk to Work promoters’ activities. Questionnaires were administered to all study participants, including those in the control group. Descriptive statistics show that participants in the intervention group were more likely to indicate that someone had tried to encourage them to change their travel behaviour in the last 2–3 months (the intervention period): 19.9% (n = 66) in the intervention group compared with 10.8% (n = 35) in the control group (Table 16).
| Trial group participants | Response, n (%) | No response, n (%) | |
|---|---|---|---|
| Yes | No | ||
| Intervention | 66 (19.9) | 131 (39.6) | 134 (40.5) |
| Control | 35 (10.8) | 228 (70.6) | 60 (18.6) |
The non-response rate for this question was noticeably higher in the intervention group (40.5%) than in the control group (18.6%), and there were noticeably higher non-response rates in the intervention group for other questions relating to intervention activities. It is not clear why this was the case; it may relate to the additional participant burden in the intervention group, as participants had just come to the end of a 10-week intervention, or there may have been some reluctance among participants in the intervention group to confirm that they, or the Walk to Work promoter, had not engaged with the intervention.
In the intervention group, 64 participants from 28 of the 42 intervention workplaces made use of the free-text box to give some additional information about the encouragement they were given. In some cases, the Walk to Work promoter or the Travel to Work study were specifically mentioned; in others, it was less clear if the participant was referring to other active travel initiatives. Half (n = 32) of comments in the intervention group suggested that sustainable transport, active travel and cycling were promoted, rather than specifically focusing on walking. For example:
E-mails about cycling to work, conversations about parking further away from office, e-mails about bike pods.
Employee, ID 106-05
Work colleagues supported my decision to start biking, but also tried suggesting alternatives but unfortunately nothing that would work for me.
Employee, ID 224-08
I have had a workplace induction and the health and safety talk included protecting the environment. They mentioned the benefits (personal and environmental) that can be achieved by alternative travel.
Employee, ID 330-13
The remainder of the comments in the intervention group focused more clearly on encouragement given for walking:
Colleague involved in project gave me a pedometer and suggested I park in the industrial estate and walk the rest of the way to work. Articles on benefits of walking also sent round.
Employee, ID 106-21
Walk to Work champion discussed some strategies to increase number of days I walk.
Employee, ID 141-02
There were posters around the office. Some people who took part in the study live close by so we walked together and encouraged each other to walk. In the past we were sharing car lifts more.
Employee, ID 155-04
Although there was evidence of some interest and enthusiasm, other study participants offered explanations as to why they could not increase walking during the commute:
Talked to [name of Walk to Work promoter] in work, the liaison for Travel to Work. But with weather changes + nights getting darker. I didn’t feel happy to walk more.
Employee, ID 303-02
Tried to get me to park further away, but due to the hours I work, it’s safer for me to park closer to work.
Employee, ID 307-08
I cannot walk to work as I live 6 miles away. I walk most lunchtimes – 1.75 miles but this programme hasn’t adjusted that behaviour.
Employee, ID 335-03
In the control group, there were fewer comments from study participants (n = 35 from 18 of the 43 workplaces). About half (n = 17) who said that they had been encouraged to change their travel behaviour focused on cycling:
Travel to work schemes advertised, car sharing – cycling – new cycle centre opened – discussed with boss whether to cycle to work and he suggested borrowing the electric loan bike to try out for the 10 miles.
Employee, ID 162-14
Posters at work showing examples of employees cycling to work, their routes, how long it takes and the benefits.
Employee, ID 112-12
We have some very good advocates for cycling to work here.
Employee, ID 126-10
Others mentioned more general sustainable transport initiatives:
Conversation with the sustainability leader. Consideration how to try and expand the carshare from my home town.
Employee, ID 104-06
We took part in [name of city] commuter challenge which encourages employees to travel more sustainably/actively for 1 month.
Employee, ID 1151-01
Six respondents indicated that they had been encouraged to walk:
Colleague who lives near me persuaded me to walk home with her one evening rather than get the bus – it was a good experience.
Employee, ID 125-29
Manager encourages us to walk more.
Employee, ID 150-05
The Civil Service walking challenge – an annual campaign to raise money for the Civil Service Benevolent Fund and get us to walk at least 10,000 steps each of 50 days in the summer.
Employee, ID 153-02
Other related activities and campaigns
Descriptive statistics suggest that very few participants were aware of, or taking part in, activities outside the workplace that aimed to change the way they travelled to work (Table 17).
| Trial group participants | Response, n (%) | No response, n (%) | |
|---|---|---|---|
| Yes | No | ||
| Intervention | 11 (3.3) | 188 (56.8) | 132 (39.9) |
| Control | 18 (5.6) | 244 (75.5) | 61 (18.9) |
The free-text box to provide more information about other schemes was completed by 28 participants, of whom five appeared to have misunderstood the question and referred to the Travel to Work study. Ten participants mentioned cycling schemes, for example ‘Cycling UK “cycle-to-work” day’ (Employee, ID 128-09), ‘bike to work campaign’ (Employee, ID 136-05) and ‘cycling schemes to buy bikes’ (Employee, ID 224-07). Only three participants mentioned walking, although not specifically walking to work: ‘I went on a 3-month holiday – trekking’ (Employee, ID 125-07), ‘Living Streets’ (Employee ID 150-04) and ‘I chatted with colleagues about it and walked more after work on a regular basis. I took walks between 6–8 p.m. for around 10–30 mins + took part in an exercise diary’ (Employee, ID 131-01). Other participants referred to more general sustainable transport initiatives: ‘commuter challenge’ (Employee, ID 121-09), ‘Local campaign about car sharing/using the car less’ (Employee, ID 121-10) and ‘Travel Smart in my organisation. Big commuting challenge. Green Impact Award’ (Employee, ID 162-16).
Hawthorne effects
Data from the post-intervention questionnaires provide some evidence of a potential Hawthorne effect in relation to the research activities. Table 18 indicates that around 18–28% of all participants ‘often’ or ‘sometimes’ changed their behaviour (either walking more on journeys to/from work or being more active in general) while wearing the monitors. However, this affect was reported in both the intervention and the control arms and therefore is unlikely to have changed the results of the study.
| While you were wearing the monitors, did you: | Response, n (%) | No response, n (%) | ||
|---|---|---|---|---|
| Often (at least half of the time) | Sometimes (less than half of the time) | Never or hardly ever | ||
| Walk more than usual on journeys to and/or from work? | ||||
| All participants | 44 (6.7) | 83 (12.7) | 306 (46.8) | 221 (33.8) |
| Intervention group participants | 26 (7.9) | 42 (12.7) | 116 (35.1) | 147 (44.4) |
| Control group participants | 18 (5.6) | 41 (12.7) | 190 (58.8) | 74 (22.9) |
| Become more active in general? | ||||
| All participants | 61 (9.3) | 124 (19.0) | 247 (37.8) | 222 (33.9) |
| Intervention group participants | 39 (11.8) | 55 (16.6) | 90 (27.2) | 147 (44.4) |
| Control group participants | 22 (6.8) | 69 (21.4) | 157 (48.6) | 75 (23.2) |
Free-text comments suggest that taking part in the research study, rather than receiving the intervention, appeared to have influenced some participants:
The Travel to Work survey got me to cycle a few days a week in the summer when my wife, a teacher, was on school holiday.
Employee, ID 112-05
This one [Travel to Work questionnaire] made me think. When I was first approached I was tied as I had to pick mum up – although if she could of [sic] walked, she would have – she was known for walking and was on no medication when she died, so I have decided to do more.
Employee, ID 112-21
This study enabled me to think about my activity levels. If I could travel to work by bicycle that would be great, but it is impracticable, and unsafe, too time consuming.
Employee, ID 137-02
Discussed ideas in staff room with other people taking part in Travel to Work survey.
Employee, ID 160-08
To encourage participants to wear the monitors, the research team printed and distributed personal graphs of activity levels and maps showing the routes that were taken. Just over 60% of participants recalled receiving the graphs or maps (Table 19).
| Participants | Response, n (%) | No response, n (%) | |
|---|---|---|---|
| Yes | No | ||
| All | 411 (62.8) | 29 (4.4) | 214 (32.7) |
| Intervention group | 173 (52.3) | 14 (4.2) | 144 (43.5) |
| Control group | 238 (73.7) | 15 (4.6) | 70 (21.7) |
Of those who recalled receiving a graph or map, around 18–28% indicated that they ‘often’ or ‘sometimes’ changed their behaviour (either walking more on journeys to/from work or being more active in general) after seeing the graph or map of their activity (Table 20). This influence appeared to be balanced between the intervention and the control arms in relation to walking to work, but was somewhat higher in the control group in relation to undertaking more activity in general.
| After seeing the graph or map of your activity, did you: | Response, n (%) | No response, n (%) | ||
|---|---|---|---|---|
| Often (at least half of the time) | Sometimes (less than half of the time) | Never or hardly ever | ||
| Walk more than usual on journeys to and/or from work? | ||||
| All participants | 39 (6.0) | 81 (12.4) | 286 (43.7) | 248 (37.9) |
| Intervention group participants | 21 (6.3) | 40 (12.1) | 109 (32.9) | 161 (48.6) |
| Control group participants | 18 (5.6) | 41 (12.7) | 177 (54.8) | 87 (26.9) |
| Become more active in general? | ||||
| All participants | 56 (8.6) | 125 (19.1) | 227 (34.7) | 246 (37.6) |
| Intervention group participants | 28 (8.5) | 54 (16.3) | 88 (26.6) | 161 (48.6) |
| Control group participants | 28 (8.7) | 71 (22.0) | 139 (43.0) | 85 (26.3) |
Workplace support for the Walk to Work intervention
Questions were included in the post-intervention questionnaires to explore the extent to which employees were aware of support for the intervention in the workplace. Again, rates of ‘no response’ were noticeably higher in the intervention group than in the control group. Overall, around 10% of respondents were aware of an increase in their workplace of information about walking. Table 21 suggests that those in the intervention group were more aware than those in the control group of posters (13.6% vs. 7.1%) and information about walking or walking routes (14.0% vs. 4.0%).
| Information and activities | Participants, n (%) | |||||||
|---|---|---|---|---|---|---|---|---|
| Overall | Intervention group | Control group | ||||||
| Response | Response | No response | Response | No response | ||||
| Yes | No | Yes | No | Yes | No | |||
| Posters about walking | 68 (10.4) | 389 (59.5) | 45 (13.6) | 153 (46.2) | 133 (40.2) | 23 (7.1) | 236 (73.1) | 64 (19.8) |
| Information about walking or walking routes | 60 (9.2) | 398 (60.9) | 47 (14.2) | 153 (46.2) | 131 (39.6) | 13 (4.0) | 245 (75.9) | 65 (20.1) |
| Information about public transport | 76 (11.6) | 382 (58.4) | 33 (10.0) | 16.7 (50.5) | 131 (39.6) | 43 (13.1) | 215 (66.6) | 65 (20.1) |
| Walking competitions or events | 72 (11.0) | 386 (59.0) | 36 (10.9) | 165 (49.9) | 130 (39.3) | 36 (11.2) | 221 (68.4) | 66 (20.4) |
| Other information or activities related to walking or transport | 54 (8.3) | 365 (55.8) | 29 (8.8) | 153 (46.2) | 149 (45.0) | 25 (7.7) | 212 (65.6) | 86 (26.6) |
Changes requiring more input from employers (such as improved facilities, changes to parking arrangements, incentives to walk during the commute or subsidised sustainable transport initiatives) were less evident (Tables 22 and 23).
| Changes in workplace facilities | Participants, n (%) | |||||||
|---|---|---|---|---|---|---|---|---|
| Overall | Intervention group | Control group | ||||||
| Response | Response | No response | Response | No response | ||||
| Yes | No | Yes | No | Yes | No | |||
| Improvements to storage, lockers or hanging space | 31 (4.7) | 429 (65.6) | 11 (3.3) | 189 (57.1) | 131 (39.6) | 20 (6.2) | 240 (74.3) | 63 (19.5) |
| Improvements to washing facilities | 24 (3.7) | 438 (67.0) | 11 (3.3) | 190 (57.4) | 130 (39.3) | 13 (4.0) | 247 (76.8) | 62 (19.2) |
| Reduction in the number of workplace parking spaces | 51 (7.8) | 409 (62.5) | 28 (8.5) | 172 (52.0) | 131 (39.6) | 23 (7.1) | 237 (73.4) | 63 (19.5) |
| Increase in the cost of workplace parking | 20 (3.1) | 439 (67.1) | 15 (4.5) | 196 (56.2) | 130 (39.3) | 5 (1.6) | 253 (78.3) | 65 (20.1) |
| Other facilities related to walking or transport | 7 (1.1) | 413 (63.2) | 3 (0.9) | 181 (54.7) | 147 (44.4) | 4 (1.2) | 232 (71.8) | 87 (26.9) |
| Incentives | Participants, n (%) | |||||||
|---|---|---|---|---|---|---|---|---|
| Overall | Intervention group | Control group | ||||||
| Response | Response | No response | Response | No response | ||||
| Yes | No | Yes | No | Yes | No | |||
| Subsidies for public transport use | 32 (4.9) | 429 (65.6) | 18 (5.4) | 182 (55.0) | 131 (39.6) | 14 (4.3) | 247 (76.5) | 62 (19.2) |
| Subsidies for wet-weather clothing or walking shoes | 0 (0.0) | 462 (69.4) | 0 (0.0) | 201 (60.7) | 130 (39.3) | 0 (0.0) | 261 (80.8) | 62 (19.2) |
| Discounts for local outdoor shops | 9 (1.4) | 450 (68.8) | 5 (1.5) | 195 (58.9) | 131 (39.6) | 4 (1.2) | 255 (79.0) | 64 (19.8) |
| Walking mileage allowance | 2 (0.3) | 460 (70.3) | 2 (0.6) | 199 (60.1) | 130 (39.3) | 0 (0.0) | 261 (80.8) | 62 (19.2) |
| Free umbrellas, rucksacks or similar freebies | 10 (1.5) | 450 (68.8) | 8 (2.4) | 192 (58.0) | 131 (39.6) | 2 (0.6) | 258 (79.9) | 63 (19.5) |
Interviews were conducted with 70 participants: 11 employers (Table 24), and a further 12 employers who also took on the role of Walk to Work promoters (Table 25); 11 Walk to Work promoters (Table 26); and 36 employees, of whom 19 self-reported no increase in walking to work (Table 27) and 17 self-reported an increase (Table 28). The age range of interviewees was 24–63 years and there were 33 men and 37 women.
| Employer | Workplace | |||||
|---|---|---|---|---|---|---|
| ID | Gender | Age (years) | Annual household income | Classification | Urban area | Size |
| 9-106-30 | Male | – | – | Public administration and defence | South Gloucestershire | Large |
| 9-128-20 | Male | – | – | Professional, scientific and technical | Bristol | Large |
| 9-226-19 | Female | – | – | Public administration and defence | Swindon | Large |
| 9-232-15 | Female | – | – | Manufacturing | Bath | Small |
| 9-305-10 | Female | – | – | Manufacturing | Swansea | Medium |
| 9-336-01 | Male | – | – | Wholesale and retail trade; repair of motor vehicles | Neath Port Talbot | Small |
| 317-01 | Male | 43 | > £50,000 | Professional, scientific and technical | Swansea | Small |
| 120-08 | Male | 45 | > £50,001 | Professional, scientific and technical | Bristol | Medium |
| 207-03 | Male | 53 | > £50,001 | Other service activities | Bath | Small |
| 303-06 | Female | 53 | > £50,001 | Wholesale and retail | Swansea | Medium |
| 9-335-16 | Male | – | – | Administrative and support services | Swansea | Large |
| Employer/promoter | Workplace | |||||
|---|---|---|---|---|---|---|
| ID | Gender | Age (years) | Annual household income | Classification | Urban area | Size |
| 9-122-07 | Male | – | – | Manufacturing | South Gloucestershire | Large |
| 9-319-01 | Male | – | – | Professional, scientific and technical | Neath Port Talbot | Medium |
| 325-01 | Male | 33 | £30,001–40,000 | Wholesale and retail trade; repair of motor vehicles | Newport | Small |
| 223-01 | Female | 38 | £40,001–50,000 | Professional, scientific and technical | Bath | Medium |
| 165-01 | Male | 43 | > £50,001 | Financial and insurance | Bristol | Small |
| 302-03 | Male | 43 | £40,001–50,000 | Arts, entertainment and recreation | Swansea | Small |
| 334-01 | Female | 48 | > £50,001 | Administrative and support service activities | Newport | Micro |
| 127-05 | Female | 52 | – | Other service activities | Bristol | Micro |
| 228-01 | Female | 52 | > £50,001 | Human health and social work | Swindon | Medium |
| 101-01 | Male | 55 | > £50,001 | Wholesale and retail trade; repair of motor vehicles | South Gloucestershire | Small |
| 166-01 | Female | 55 | £40,001–50,000 | Human health and social work | Bristol | Micro |
| 102-01 | Male | 63 | > £50,001 | Professional, scientific and technical | South Gloucestershire | Small |
| Walk to Work promoter | Workplace | |||||
|---|---|---|---|---|---|---|
| ID | Gender | Age (years) | Annual household income | Classification | Urban area | Size |
| 9-226-18 | Female | – | – | Public administration and defence | Swindon | Large |
| 9-232-12 | Female | – | – | Manufacturing | Bath | Small |
| 9-330-36 | Female | – | – | Education | Swansea | Large |
| 9-335-15 | Male | – | – | Administrative and support service | Swansea | Large |
| 317-03 | Female | 27 | £20,001–30,000 | Professional, scientific and technical | Swansea | Small |
| 141-03 | Female | 31 | £20,001–30,000 | Human health and social work | Bristol | Medium |
| 111-02 | Female | 33 | £40,001–50,000 | Professional, scientific and technical | South Gloucestershire | Large |
| 161-02 | Female | 58 | > £50,001 | Professional, scientific and technical | Bristol | Small |
| 305–01 | Female | 58 | £20,001–30,000 | Manufacturing | Swansea | Medium |
| 106-13 | Male | 61 | £40,001–50,000 | Public administration and defence | South Gloucestershire | Large |
| 9-106-29 | Female | – | – | |||
| Employee | Workplace | |||||
|---|---|---|---|---|---|---|
| ID | Gender | Age (years) | Annual household income | Classification | Urban area | Size |
| 101-05 | Male | 25 | – | Wholesale and retail trade; repair of motor vehicles | South Gloucestershire | Large |
| 106-05 | Female | 32 | £30,001–40,000 | Public administration and defence | South Gloucestershire | Large |
| 122-03 | Male | 52 | > £50,001 | Manufacturing | South Gloucestershire | Large |
| 128-18 | Female | 28 | > £50,001 | Professional, scientific and technical | Bristol | Large |
| 136-05 | Female | 32 | > £50,001 | Administrative and support service | Bristol | Small |
| 158-03 | Female | 45 | > £50,001 | Professional, scientific and technical | Bristol | Small |
| 161-03 | Male | 60 | > £50,001 | Professional, scientific and technical | Bristol | Small |
| 223-02 | Female | 52 | > £50,001 | Professional, scientific and technical | Bath | Medium |
| 223-10 | Male | 41 | – | Professional, scientific and technical | Bath | Medium |
| 226-03 | Male | 48 | £40,001–50,000 | Public administration and defence | Swindon | Large |
| 226-08 | Female | 55 | £30,001–40,000 | Public administration and defence | Swindon | Large |
| 228-03 | Male | 30 | £40,001–50,000 | Human health and social work | Swindon | Large |
| 302-04 | Male | 39 | £10,001–20,000 | Arts, entertainment and recreation | Swansea | Small |
| 305-08 | Female | 49 | £30,001–40,000 | Manufacturing | Swansea | Medium |
| 307-09 | Male | 37 | £40,001–50,000 | Administrative and support service | Swansea | Large |
| 317-02 | Female | 33 | – | Professional, scientific and technical | Swansea | Small |
| 330-29 | Female | 37 | £20,001–30,000 | Education | Swansea | Large |
| 337-02 | Female | 37 | > £50,001 | Human health and social work | Newport | Large |
| 337-05 | Male | 33 | £40,001–50,000 | Human health and social work | Newport | Large |
| Employee | Workplace | |||||
|---|---|---|---|---|---|---|
| ID | Gender | Age (years) | Annual household income | Classification | Urban area | Size |
| 101-06 | Female | 51 | £30,001–40,000 | Wholesale and retail trade; repair of motor vehicles | South Gloucestershire | Small |
| 102-06 | Female | 34 | £10,001–20,000 | Professional, scientific and technical | South Gloucestershire | Small |
| 106-12 | Female | 49 | > £50,001 | Public administration and defence | South Gloucestershire | Large |
| 106-23 | Male | 41 | > £50,001 | Public administration and defence | South Gloucestershire | Large |
| 122-05 | Male | 59 | > £50,001 | Manufacturing | South Gloucestershire | Large |
| 128-08 | Male | 30 | £40,001–50,000 | Professional, scientific and technical | Bristol | Large |
| 155-02 | Female | 63 | £40,001–50,000 | Financial and insurance | Bristol | Small |
| 207-01 | Female | 34 | £40,001–50,000 | Other service activities | Bath | Small |
| 223-08 | Male | 60 | > £50,001 | Professional, scientific and technical | Bath | Medium |
| 226-07 | Female | 52 | > £50,001 | Public administration and defence | Swindon | Large |
| 228-04 | Male | 41 | £40,001–50,000 | Human health and social work | Swindon | Large |
| 232-14 | Female | 24 | £40,001–50,000 | Manufacturing | Bath | Small |
| 305-05 | Male | 47 | £40,001–50,000 | Manufacturing | Swansea | Medium |
| 310-02 | Male | 55 | £40,001–50,000 | Administrative and support service | Swansea | Medium |
| 330-11 | Female | 38 | > £50,001 | Education | Swansea | Large |
| 335-06 | Female | 32 | > £50,001 | Administrative and support service | Swansea | Large |
| 337-07 | Male | 46 | £40,001–50,000 | Human health and social work | Newport | Large |
For the process evaluation, a key outcome of interest was the identification of barriers to, and facilitators of, walking during the daily commute. Preliminary analyses are presented here, examining key issues from the perspectives of employers, Walk to Work promoters and employees. Several key issues were identified: distance, alternatives to car use (public transport and park and walk facilities), caring responsibilities and the stress of the commute.
Distance
The distance between home and work was frequently highlighted as an important factor in whether or not walking was a feasible mode of travel to work:
I suppose the most important is distance the person lives away from their workplace and that’s how, and I think is the main consideration of how they decide how they’re going to get to work.
Employer promoter, ID 302-03
Distance was expressed in terms of both mileage and time:
1 to 2 miles, I think, you know, most people would walk, which they do, um, there are a lot of people who just live within probably yeah, probably three or four live in a mile, or mile and a half, radius so they walk to work.
Employee, ID 161-03
For staff that live more than a mile or so away it’s not a convenient route to be able to walk into work.
Employer promoter, ID 228-01
I live literally 15 minutes approximately from here. I always have tried to walk to work with most of my jobs, um, it’s only once I had to commute ‘cos I worked at a hospital which was a bit too far away. So I always try to walk as much as possible, um, anywhere really, but yeah I think living close to my workplace is what gives me the motivation to do it really.
Promoter, ID 141-03
I walk to work, but only because of the distance, like it’s only a 20-minute walk.
Employer, ID 9-232-15
Interviewees also linked distance with location:
I would walk to work if I worked in town, like in the centre, I would walk to work definitely but it’s just too far here.
Employee, ID 102-06
Distance is a big one I mean where we live, um, we’re in [name of city] but I know a lot of people here especially at work live quite rurally, live a long way away from [name of city], um so distance is a big factor.
Employee, ID 335-06
If you are in a business park, it’s, it’s too long a hike for most people.
Employer, ID 9-128-20
Some workplaces suggested that the majority of employees taking part in the study lived too far away from the workplace to walk the entire commute:
There was something about this project that attracted people from a long way away. I’m not quite sure what there was in our pre-marketing recruitment and I don’t know whether that’s been the same with other workplaces, but we’ve had people from [English city] and [English town] and [English city] and all over that um commute hours each way . . . I think yeah they would have had that barrier from the beginning.
Promoter, ID 9-226-18
Everybody was like ‘Look, we just live too far, too far away to get here’ so whether that was because of the group make-up, um, if it was a larger group maybe we would have had people that were closer.
Promoter, ID 9-335-15
The location of workplaces was also linked to perceptions of available walking routes:
We don’t park on site, we park a little further away and then it takes about sort of ten minutes to walk from the car park to the door and it’s, it sounds really daft it’s probably not that much quicker than walking from my house but it’s safer. Where I live I have to walk along to the dual carriageway, down a lane which is incredibly creepy, um and sort of through another car park in order to get here um and especially with the light, with the nights being darker. In summer months it wouldn’t be so much of an issue but where it’s later, it’s darker, it’s really creepy so where, where we park now is lovely and light, lovely bright um and just generally feels a little less like somethings going to jump out in the bushes . . . there’s probably nothing to be concerned about um I don’t think this area’s got a particularly high crime rate but it’s um, it’s more of a comfort thing.
Promoter, ID 111-02
It’s some distance for me but the routes, I wouldn’t even know the safest route, and the route that I drive in, half of that has no pavements that you could walk anyway. So I wouldn’t even know which route to take um to get to work, safely and on my own, I mean especially in the nights or in the um in the mornings when it’s dark.
Employee, ID 317-02
At one workplace, concerns about the safety of a walking route had led to calls for improvements:
Since they’ve build the new houses up by um junction – up by the [Welsh village] roundabout . . . They’ve actually now put in the new footpath for those houses on that side of the road, so they can get, so that the children can go from that site straight into the primary school. Um and one of the girls who works in [workplace], she lives there and she’s saying it takes her 20 minutes to get by car from there to here, so she’s been looking at walking but of course the other pavement that we need to come in, which is the opposite side of the road, is the one where there’s no lighting and you have to cross the dual carriageway, so it’s the safety aspect of that and it’s the same with me if I parked um on [Welsh village] and walked back that way, it’s crossing that dual carriageway is the problem. Now further up they’ve put, now put the um traffic lights with the pelican crossing facilities on it, and we were just wondering whether they would have considered doing it further down so that we can use, so people can actually walk across there.
Promoter, ID 305-01
At the time of the interview, as a result of this concern, the local authority had set up monitoring devices to check vehicle speeds at the site of a requested new crossing.
Analyses of baseline characteristics (see Table 8) confirmed that a large majority of participants lived > 2 km from their workplace. This meant that increased walking was more likely to be part of a mixed-mode journey involving the use of public transport or combining a car journey with walking.
Public transport
There were some positive comments about the availability of public transport:
We’re very lucky we’ve got a train station you know not even a 3-minute walk up the road so um you know location to public transport helps um I’m not familiar with the bus but I’ve used the train a few times so I know that, I know the train station’s very close.
Employee, ID 106-23
Access to this workplace is good because we’re in the centre of [name of city] so you’ve got buses, the trains, a bit of a walk, it’s a 15-minute walk, some people are OK with that, some people are not OK with that.
Employer promoter, ID 165-01
There is good public transport links so I don’t think that will be a major problem for people to change from using a car to public transport really.
Employer promoter, ID 302-03
However, the majority of interviewees expressed dissatisfaction with public transport as a means of travelling to and from work. Although the study had focused on workplaces in urban areas, this did not mean that their employees lived in urban areas served by regular bus or train services:
It is either ‘Do I get in the car?’ or ‘Do I get the bus?’. You know it is that simple for me. That may not be the case for somebody who lives a little bit closer who could walk all the way, but the four of us that participated, none of us are in that category. In fact, the other three, I don’t know how they’d get to work with public transport. They would be hours if they had to do that. Because one lives down at [English village] I think it is, and the other at [English village] so they are miles outside of [English city] so I think they’re limited to what changes they could make really.
Promoter, ID 161-02
Because we’re quite rural the public transport isn’t great, um you couldn’t get a train from where I live to here, you couldn’t get one bus from, from, where I live to here, you’d have to catch several.
Employee, ID 335-06
There were also concerns about whether or not public transport would enable employees to get to work on time:
A bus from my house [laughs] would actually get me to [name of town] town centre about 15 minutes after I was supposed to start work so, you know, that, the timing of the bus probably, you know, is probably the biggest influence.
Employee, ID 226-08
I have to be in work for 7 o’clock in the morning, there’s no buses, there’s no trains, I am forced to use a car. If there were public transport I would use it, so that’s a big factor.
Employee, ID 310-02
Because of concerns about getting to work on time, the idea of getting off the bus a few stops early to include additional walking in the journey could be problematic:
It’s whether you are running late or not, and that can be down to the public transport being late. You know, you might, you might intend to get off the bus earlier and then the bus might not turn up till 10 minutes later so that cuts your getting to work time . . . you might go out thinking ‘Right, I am going to get off the bus two stops earlier’ but then the bus might be 10 minutes late and you think ‘Actually I can’t because I am not going to get into work on time’.
Promoter, ID 161-02
In some areas, using public transport might result in quite complex journeys compared with a single-mode car journey:
I live in the [name of place] which is about 30 miles away from here where I work, um, it’s quite a remote village, um, there’s very little public transport, unless it’s a Tuesday or a Thursday [laugh] so travel by public transport would mean a cab to a rail station and then three changes of train, or a cab to a local town (name of place) and then two buses at least, so the only practical way to travel to work is really by car.
Employee, ID 122-05
More-complex journeys may also be perceived as extending the working day:
The bus station is only a very short walk from the office so anyone travelling in by bus wouldn’t have a problem, the same as the train station that’s not far away. Whether or not there would be a direct bus or a direct train, I suspect a direct train is more likely, um but if they were to come in by train they may have to get a bus to the train station and vice versa. I think for a lot of people one of the deterrents there would be the fact that it makes the working day that much longer.
Employer promoter, ID 9-319-01
In some areas, public transport was also perceived as being expensive:
Financially it would be far more expensive. I can’t, I can’t remember how much it is something like £4.50 one way to get on the bus to come to work, and I think I can probably drive that for a lot less.
Employee, ID 226-08
I think public transport is relatively expensive in this area, on a few occasions I’ve used it um I‘ve been surprised how expensive it is, I’m sure if someone was using it on a regular basis and they’re buying season tickets that type of thing it’s probably cheaper, but I think um sort of on an ad hoc basis given that the price of public transport would probably put people off as well.
Employer promoter, ID 9-319-01
Park and walk
Where public transport was not perceived to be a viable alternative to car use, increased walking might be achieved by parking further away from the workplace and walking the remainder of the journey:
What I do now is I park 10 minutes away from the office, so I drive, it’s probably, yeah it’s probably just 2 and a bit miles and so I park 10 minutes away and then I have that 10-minute walk into the office, and I do that most of the time . . . I’ve done it in the rain and I’ve done it when I’ve not been feeling great, and I’ve done it when I’ve had a lot to carry, so all those things that previously I would have said ‘I can’t do it today’ because I’ve, because I think that was one of your questions in one of your booklets wasn’t it . . . I guess that made me think about it and I thought well it’s, you know, it’s not really a valid excuse because you, I can carry that or I might feel better – feeling a bit grotty I might feel a bit better after a walk and sure enough you were right [laugh] and I did.
Employee, ID 106-12
Other interviewees encountered difficulties in finding a suitable place to park their car:
I haven’t found a way of making the walk part of the commute and making the journey times the same for me. The, the, my main route to work there isn’t actually anywhere I can leave the car to walk that last bit, so for me to, to park further away I am actually increasing the journey in terms of the driving part of it as well as the walking part.
Promoter, ID 106-13
One of the options was to park in a local park and then walk um and then they changed the parking restrictions so you can only park there for 2 hours before you move on, rather than all day . . . I guess having somewhere to park for free which then allows me a short walk to work would be useful but the, yeah, with the parking restrictions going crazy all over the place that’s becoming less and less feasible.
Employee, ID 207-01
There isn’t anywhere around here where you could actually park your car to be able to walk in, sort of thing. I think it’s more down to the council and the government then, who are actually stopping anybody from doing it because there aren’t facilities around here to do be able to leave your car off the premises where you can walk that distance then into work.
Employee, ID 305-08
One participant decided to pay for the park-and-ride facility but then walk to work rather than take the bus. This led to some confusion when an attendant at the park-and-ride said it was not permitted and attempted to issue a fine:
There’s been quite a few changes at the park and ride, one of which was introducing civilian um security guards who seem to be of the opinion they could issue fines for people that left their car and walked, um that was misdirection it now appears, um but it did cause 2 weeks where um we couldn’t walk at all because of the threat of being fined . . . through various emails and correspondence we managed to clarify the position and find out that it wasn’t the case you couldn’t walk – it was a misunderstanding and they were happy for you to walk.
Employee, ID 310-02
Where workplaces provided free or relatively stress-free parking, this could undermine attempts to encourage study participants to park and walk:
The only thing that could seriously affect it [current park-and-walk journey] is if I reached the holy grail and get a parking space in the basement car park . . . it’s not only financial but obviously the ease. I can come straight in to work and literally jump in the lift and I’m at work so it’s a big time saving as well. I mean with the best will in the world I spend at least half an hour getting to and from work where if I could park in work I could drive straight in and drive straight out again.
Employee, ID 310-02
If there’s somewhere I know I can park, and I can walk in, like a 25- to 30-minute walk, and I used to do that quite a lot, but then we had more parking at work so, I actually feel bad [laugh], so they can buy you more parking and so it’s so much easier now to come and drive in and park whereas before it wasn’t and so I had to use this park and walk thing um but now we’ve got more parking.
Employee, ID 223-02
They often live a fair distance out, there’s convenient parking at the place of work, so if somebody was to try and drive part-way and park somewhere it would actually make life a lot more difficult for them. Um most of the streets around the office are either residents’ parking or you’ve got to pay to park and people aren’t going to do that if they can just drive straight to the office and make life easier for themselves.
Employer promoter, ID 9-319-01
One possible solution would be for workplaces to provide parking facilities away from the workplace itself to encourage employees to park and walk:
I suppose one thing that might help if there was spaces that the company, I just don’t think it’s really viable so I wouldn’t even, I don’t [laugh], but if there were spaces that were a 10-minute walk way. If the company kind of had, were going to buy more parking spaces, it almost would be a good thing in a way but to be a 10-minute walk.
Employer promoter, ID 223-01
They’re putting a charge on it [parking] so it’s £20 a month if you park in one of the car parks close by but if you then park on site it’s £40 a month . . . for £20 a month you can’t really beat that so um it’s about £1 a day so um yeah the car park’s probably about half a mile away so then I’d walk about half a mile . . . if I park in the car parks which are a little bit, little bit further away then just walking that half mile in is now probable.
Employee, ID 226-03
Car drivers appeared to discount the cost of purchasing and maintaining their vehicle, and focused on the immediate costs of running and parking their vehicles. This resulted in perceptions that car driving was cheaper and more convenient than other modes of transport, especially where workplaces provided free or subsidised parking:
One person said she used to get the bus and walk the rest of the way but um, it didn’t save any money and the weather’s always rubbish so she couldn’t really be bothered with that. Um, most of the employees feel it’s too far to walk and as the building has free parking, and we’re in the city centre there’s nowhere really to park further away um, without paying or getting parking tickets.
Promoter, ID 317-03
We get free parking at work but if you park further away there’s a lot of residential parking zones so there aren’t many areas where you can actually park [laugh] and leave your car all day without paying . . . I think this project has prompted people higher up than myself such as [name] to um thinking about actually our policy on car parking isn’t an incentive at all to make people walk or cycle to work so, and we knew that anyway, and we did have a try a few years ago to bring in car park charging, but it got thrown out. But now perhaps is the time in the days of austerity to try again [laugh] . . . there’s lack of incentives really, in terms of just providing people free and ample parking, to try and change behaviour.
Promoter, ID 9-226-18
If people had to pay for parking and we didn’t have um, parking here, then I think it would change how people would travel to work. It would definitely be more of an encouragement for them to, to look at alternatives, possibly to walk.
Employer, ID 317-01
Caring responsibilities
Interviewees with caring responsibilities, especially for young children, appeared to feel that they had no alternative but to combine the journey to work with transporting their children to school or child-care facilities:
My children go to school near here and I bring them here to work and then they walk to school from here. Um, they could all, we could all walk but actually, you know, they have, during their spring and summer terms they have cricket bags. They are at different ages so the days that they bring their stuff to school is different and, you know, yes they could walk with their cricket bags and their school bags and their sports bags but actually it’s a lot!
Employee, ID 158-03
My personal family life is definitely one of the barriers. I have a young son who is at a childminder and my wife works part-time hours so it’s a combination of making sure we were picking him up at the childminder and my wife also works evenings and making sure I was back in time for that.
Employee, ID 228-04
My journeys include dropping the kids off to childminders/school and then coming in to work and finishing early to get back for the school run and so on, so I’m restricted with times.
Employee, ID 317-02
Concerns about timing the journey were particularly evident in relation to public transport:
I have to drive for my daughter because there’s no other option um well there is a bus, but it doesn’t, the timing isn’t really, doesn’t work for everyone taking their daughters to school so that’s, so that’s not an option.
Employer promoter, ID 223-01
I’ve for example got two children and I often have to drop them off and pick them up at the same time to, as I go to and from work, so um that makes public transport impossible for me.
Employee, ID 337-02
One participant who was keen to change his travel arrangements was able to negotiate a solution with his employer:
Getting the children, well picking them up for me from school um was something to consider so, how much walking or public transport could I do, you know, with that in mind um and actually some things I would change, I have changed my hours since I filled in the questionnaire and I should mention that, so it makes it easier for me to catch the train um three times a week to [Welsh city] and then I get home in time to pick my daughter up then from the childminder . . . I always find the train times don’t quite correlate, so I tend to have about a half an hour wait in the station. Um so I think obviously more regular transport would help but I have found work have been a bit more flexible I think, with thinking about how people do get to and from work now and they have been flexible by giving me 15 minutes at the end of 4 days a week to catch the train.
Employee, ID 337-05
The stress of the commute
For some participants, it was clear that the journey to and from work was a stressful part of the day. Some interviewees felt that changing their mode of travel would be complicated, less convenient and would increase the level of stress:
For maybe half of the team they possibly could get a bus, but then they would have to walk from the bus stop, but a lot of that, they would probably choose not to do it because of the reliability of the bus. Um, that being the biggest factor, it would be the reliability. They would probably end up having to leave a lot earlier to get to work, but yeah, I would say that probably, definitely, half of them are on a bus route that comes this direction. I wouldn’t say it’s necessarily round the corner but it’s this direction. They’d have to then maybe do a walk. ‘Cos even myself, I could get a bus to the top of [name of road] and I could walk down and have done that, but then it would take me, I would have to get, make sure that that bus is 100 per cent guaranteed to leave at that time, so, cos I’d be panicking.
Employer promoter, ID 127-05
If I had the time, I’d have quite a good walk in to work and back. I would definitely prefer to do it. Um but yeah just, just the last few months has been mental . . . I just have to get kids to school, get to work, not you know as quickly as I possibly can. Um I don’t have time to walk, um I don’t have time for lunch breaks. I work on reduced, I’d be working, I have a break because I have to have a break but I have the shortest break that I, you know, because I just have, I have to leave the office early to get my daughter so to work my hours I don’t have, I can’t have, an hour lunch break um and so really I supposed I felt like why, why set myself targets that I can’t, you know, I haven’t, I just thought, I haven’t got the space in my life right now to set myself goals . . . it would just go down the source of stress.
Employer promoter, ID 223-01
I thought I would try to increase my levels of activity across the board um by walking a little bit on my way in to work, etc., and then the things such as the park closing and then having to take a detour or um having to get on to the main road from my parking space and it adding another 15 minutes to my day, these – what would consider to be relatively minor incidents in the grand scheme of things, just to have such a negative knock-on effect on my, onto my, the most stressful part of my day which is getting to work and getting, with the kids, and getting home from work with the kids, um that it left me very little wiggle room and I just found it stressful and unhelpful so I stopped doing it.
Employee, ID 337-02
Others felt able to adjust their journey and found some enjoyment in doing so:
When we started doing it, it became quite enjoyable and we got the maps back and we saw [laugh] where we had walked. We’re all there then going ‘How much did you do?’. It’s all about like gamification you almost want to be ‘Oh I’ve done the most steps’ or ‘I’ve walked the furthest’ that’s, creates a bit of team building really’.
Employer promoter, ID 165-01
I have walked more, um, my commute’s about 4 miles but over the summer I was trying to do it once a week and I’ll, I’m a little bit embarrassed to admit that it was Pokémon GO that started me doing that. So I found that the commute was a great time to catch Pokémon on the way to work.
Promoter, ID 9-226-18
I’ve found a really pretty route. I’ve also started listening to serialised podcasts on my walk to and from the bus, so like it’s time that I can spend on my own listening to something . . . I go from working with loads of people to being with my partner all the time so having like half an hour or so on my own listening to something and chilling out is really nice.
Employee, ID 335-06
When you first contacted me I was working 20 miles, or 18 miles away, um, and I looked into the train, couldn’t use the train, um, because of times to get to work and certainly when I’m on call at the weekends, nights and so on it just doesn’t happen so I didn’t have any option other than to drive . . . now it’s completely different because it’s 12 minutes’ walk for me so I’m not going to drive . . . now I live and work in the same town, I do not drive, and even though I know the parking is going to be OK I elect not to drive.
Employee, ID 337-07
Summary
Descriptive statistics from the process evaluation suggest that a majority of participants in the intervention group of the study were aware of the Walk to Work promoters in their workplaces, and attempts were made to encourage increased walking during the commute. Workplace support for the intervention tended to focus on the provision of information rather than improvements to facilities or incentives with cost implications. Key factors influencing whether or not participants increased walking during the commute were identified through the behavioural questionnaires and qualitative interviews, and included commuting distance and workplace location, availability and cost of alternatives to private car use, caring responsibilities and stress during the commute.
Chapter 7 Outcome evaluation
Parts of this chapter are reproduced from Audrey et al. ,69 published by BMC Public Health journal. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The text below includes minor additions and formatting changes to the original text.
Methods
Data collection
The physical activity outcomes, data-collection methods and timings are summarised in Table 29.
| Outcome | Method | Timing |
|---|---|---|
| Primary outcome | ||
| 1. Daily number of minutes of MVPA | Accelerometers | Baseline and 12-month follow-up |
| Secondary outcomes | ||
| 2. Overall level of physical activity (c.p.m.) | Accelerometers | Baseline and 12-month follow-up |
| 3. Daily number of minutes of sedentary time | Accelerometers | Baseline and 12-month follow-up |
| 4. Daily number of minutes of moderate to vigorous activity during the commute (mean MVPA over the number of valid working follow-up days completed) | Accelerometers, GPS and travel diaries | Baseline and 12-month follow-up |
| 5. Modal shift (number of journeys, when walking was the main mode of travel to/from work) | Accelerometers, GPS and travel diaries | Baseline and 12-month follow-up |
Outcome measures
Physical activity was objectively measured using accelerometers (ActiGraph GT3X+). Validated accelerometer thresholds were used to compute daily time spent in MVPA (all 10-second epochs with ≥ 1952 c.p.m.) and being sedentary (all 10-second epochs with < 100 c.p.m.);72 these are listed in Table 30. The primary outcome was the daily number of minutes of MVPA. To be included in the analyses, participants were required to provide at least 3 valid days of accelerometer data: any 3 days were permissible, as our primary aim was to see if increasing walking during the commute led to an increase in overall physical activity, rather than on work days only. The secondary outcomes were overall levels of physical activity (c.p.m.), daily number of minutes of sedentary time, daily number of minutes of MVPA during the commute and modal shift (number of journeys, over the previous 5 working days, when walking was the major commuting mode). Primary and secondary outcomes were measured at baseline and at the 12-month follow-up.
| Procedure | Settings |
|---|---|
| Initialising | Accelerometers were initialised to start recording on the day after distribution and to store data for 7 days including a weekend |
| Protocol | Single ActiGraph GT3X+ monitor, worn around the waist over the same hip during waking hours (except when swimming/bathing/showering) |
| Wear time | Waking hours (usually 06.00 to midnight but this was modified, e.g. for shift workers) |
| Valid length of day | ≥ 10 hours (600 minutes) |
| Days required | Any 3 days89 |
| Epoch length | 10 seconds |
| Zero counts | Bouts of 60 minutes of continuous/consecutive zero counts excluded |
| Spurious data | > 15,000 c.p.m. |
| Missing data | No alternative source of information |
| Activity cut-off points | Sedentary, < 100 c.p.m.; MVPA, ≥ 1952 c.p.m.72 |
To identify physical activity during the commute, participants wore a GPS receiver (QStarz BT-1000X) during their journeys, set to record positional data every 10 seconds; GPS settings are listed in Table 31. As described in Chapter 4, participants’ workplaces and homes were geocoded using the full postcode and imported into a GIS (ArcMap v10.2.2). The merged accGPS files were imported into ArcMap and participants’ journeys to and from work were visually identified and segmented from other accGPS data using the ‘identify’ tool to provide a measure of duration of the journey and associated MVPA.
| Procedure | Settings |
|---|---|
| Initialising | GPS records when switched on |
| Protocol | Switch on to ‘log’ before leaving for work. Switch to ‘off’ when finishing the commute |
| Wear time | Commute and working hours |
| Days required | 1 valid working day |
| Valid data | One journey on given day required |
| Spurious data |
Aberrant speed: all GPS points recorded as travelling at > 100 km/hour Outliers for each participant: removal of GPS points that are > 500 m from any other GPS points |
| Missing data | Use mode of travel from self-reported travel diary |
Randomisation procedures
Randomisation took place at the workplace level after consent to participate was secured and baseline data were collected, thus ensuring allocation concealment. Employers in participating workplaces completed a short questionnaire to optimise matching pairs (or triples) of workplaces with similar characteristics, including size (micro-sized, 5–9 employees; small, 10–49 employees; medium-sized, 50–249 employees; large, ≥ 250 employees), location (south Wales, Bath, Swindon, Bristol and South Gloucestershire) and type of business [using UK Standard Industrial Classification (SIC) Categories]. 68 The assignment of workplaces was carried out at the BRTC by a statistician not involved in workplace recruitment. Allocation was based on random numbers generated by Stata version 14, such that one workplace from a matched set was randomised to the control group and one (or two in a triple) to the intervention group. Given the nature of the intervention, it was not possible to blind participants following randomisation.
Statistical methods
The primary statistical analysis was prespecified in a statistical and health economics analysis plan, which was made publicly available prior to release of outcome data to the statistical team. 90 Individuals providing a measurement of the primary outcome were included in the primary analysis, which compared workplaces allocated to the intervention and workplaces allocated to usual practice. The treatment effect was estimated as the mean difference between the intervention and the control groups using multivariable linear regression (adjusted for baseline MVPA), accelerometer wear time at follow-up, workplace size, location and type of business as covariates. A normally distributed random effect accommodated any variation between workplaces in the mean outcome of their employees. This model was adapted for the continuous secondary outcome measures (overall levels of physical activity, daily number of minutes of sedentary time and daily number of minutes of MVPA during the commute). A zero-inflated negative binomial regression model, with robust standard errors, estimated the treatment effect on the modal shift measure (number of journeys when walking was the major mode of travel). This model was adjusted for baseline modal shift, workplace size and location, with variation across participants in the total number of journeys recorded being accommodated (as an offset). In this model, variation between workplaces in the average outcome of their employees was accommodated by the robust standard errors. 91
Sensitivity analyses on the primary outcome only were pre-planned to assess the impact on the primary analysis of any imbalance in baseline covariates, any non-normality in the distribution of the primary outcome missing data (through the use of multiple imputation) and different quality-assurance thresholds for accelerometer data. This last analysis included a greater number of participants in the primary analysis and so explored the influence of missing values. Prespecified subgroup analyses of the primary outcome measure explored whether or not age at baseline (above/below the median), gender (male/female) or household income (above/below £30,000) modified the intervention effect; these analyses proceeded by adding interaction terms to the regression models used in the primary analysis. The statistician was blinded while the code for analysis was developed and unblinded to run the final analysis.
Results
Recruitment and retention
Recruitment is discussed in detail in Chapter 3. Recruitment took place in two phases: May to July 2015 and March to May 2016. The initial intention was to recruit across three urban areas in south-west England and south Wales. However, because fewer workplaces were recruited during the first year, we included four additional urban areas in the same regions during the second year. We received 271 expressions of interest and, after screening for eligibility and giving further information about the study, we recruited 87 workplaces (Figure 3): 10 micro-sized, 35 small, 22 medium-sized and 20 large.
FIGURE 3.
Flow of workplaces and participants through the study. This figure is reproduced from Audrey et al. ,69 published by BMC Public Health journal. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The figure includes minor additions and formatting changes to the original.
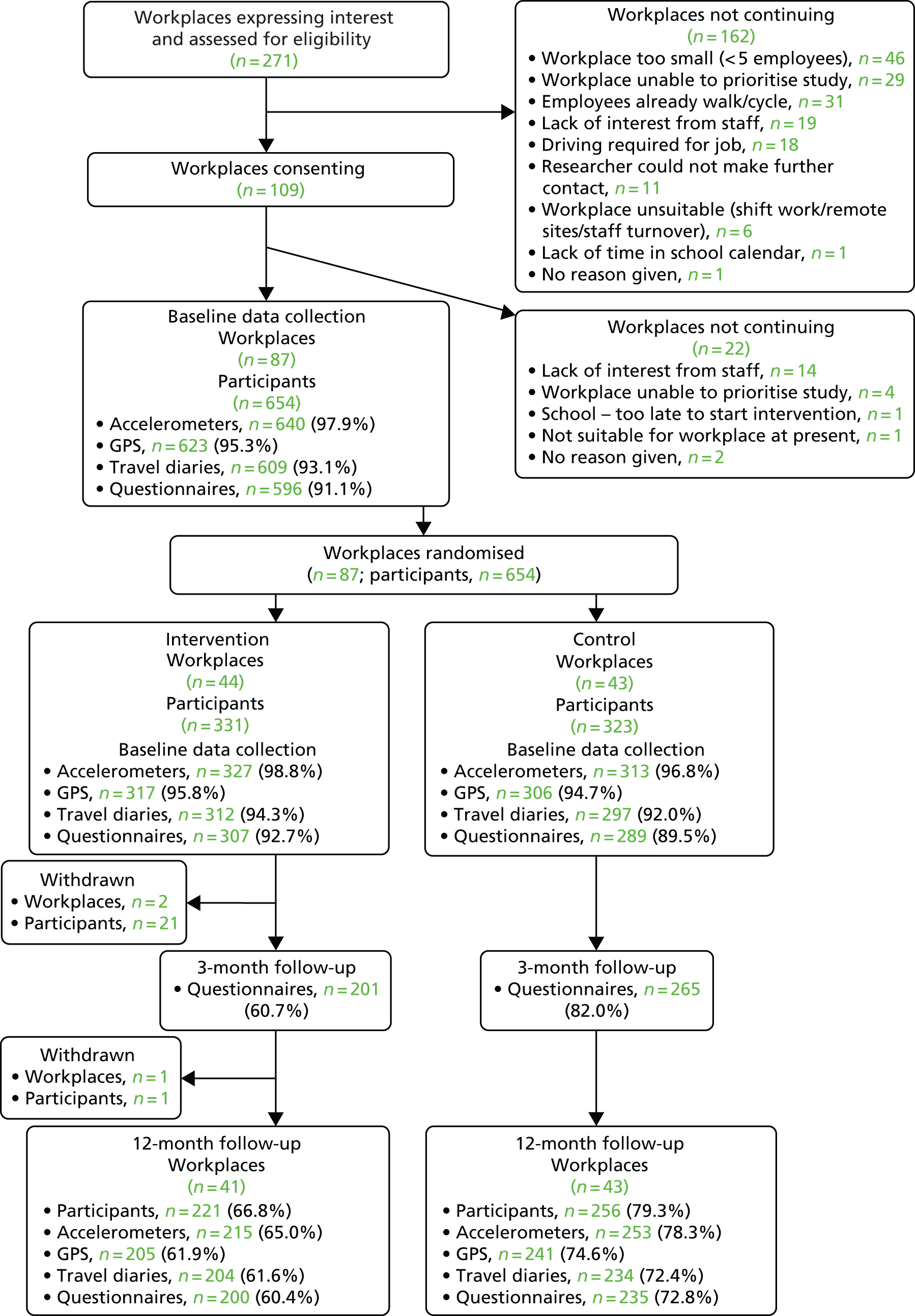
Following baseline data collection, 44 workplaces (331 participants) were randomised to receive the intervention and 43 workplaces (323 participants) were randomised to the control group (see Figure 3). Two workplaces (21 participants) withdrew during the 10-week intervention period: one relocated overseas, and in the other workplace the main contact indicated that they were too busy to continue with the study. A further intervention workplace (with only one participant) withdrew at the follow-up data-collection point because of a lack of interest among staff. At the 12-month follow-up, 84 workplaces (41 intervention and 43 control) and 477 employees (73% of those originally recruited to the study) took part in data-collection activities. Response rates in the control group were higher than those in the intervention group (Tables 32 and 33; see Figure 3).
| Characteristics | Trial group, outcome data | |||
|---|---|---|---|---|
| Intervention (N = 331) | Control (N = 323) | |||
| Complete (N = 160) | Incomplete (N = 171) | Complete (N = 192) | Incomplete (N = 131) | |
| Participant demographics | ||||
| Gender: male, n (%) | 64 (40) (N = 160) | 79 (46) (N = 171) | 75 (39) (N = 192) | 65 (50) (N = 131) |
| Age (years), mean (SD) | 42.7 (10.1) (N = 160) | 39.8 (12.3) (N = 161) | 43.3 (10.9) (N = 191) | 40.0 (11.7) (N = 123) |
| BMI category, n (%) | ||||
| Underweight and normal | 71 (44) (N = 160) | 78 (46) (N = 171) | 99 (52) (N = 192) | 45 (34) (N = 131) |
| Overweight | 56 (35) (N = 160) | 43 (25) (N = 171) | 52 (27) (N = 192) | 40 (31) (N = 131) |
| Obese | 26 (16) (N = 160) | 27 (16) (N = 171) | 33 (17) (N = 192) | 19 (15) (N = 131) |
| Missing | 7 (4) (N = 160) | 23 (13) (N = 171) | 8 (4) (N = 192) | 27 (21) (N = 131) |
| Household income, n (%) | ||||
| ≤ £10,000 | 0 (0) (N = 159) | 1 (1) (N = 154) | 3 (2) (N = 188) | 0 (0) (N = 117) |
| £10,001–20,000 | 8 (5) (N = 159) | 6 (4) (N = 154) | 10 (5) (N = 188) | 15 (13) (N = 117) |
| £20,001–30,000 | 17 (11) (N = 159) | 22 (14) (N = 154) | 21 (11) (N = 188) | 18 (15) (N = 117) |
| £30,001–40,000 | 26 (16) (N = 159) | 25 (16) (N = 154) | 30 (16) (N = 188) | 19 (16) (N = 117) |
| £40,001–50,000 | 39 (25) (N = 159) | 28 (18) (N = 154) | 33 (18) (N = 188) | 20 (17) (N = 117) |
| > £50,000 | 58 (36) (N = 159) | 60 (39) (N = 154) | 79 (42) (N = 188) | 38 (32) (N = 117) |
| Not known | 11 (7) (N = 159) | 12 (8) (N = 154) | 12 (6) (N = 188) | 7 (6) (N = 117) |
| Ethnicity, n (%) | ||||
| White British | 146 (92) (N = 159) | 142 (90) (N = 158) | 171 (90) (N = 190) | 108 (90) (N = 120) |
| White other | 8 (5) (N = 159) | 7 (4) (N = 158) | 9 (5) (N = 190) | 5 (4) (N = 120) |
| Mixed ethnic group | 1 (1) (N = 159) | 3 (2) (N = 158) | 0 (0) (N = 190) | 3 (3) (N = 120) |
| Asian or British Asian | 0 (0) (N = 159) | 3 (2) (N = 158) | 5 (3) (N = 190) | 1 (1) (N = 120) |
| Black or black British | 4 (3) (N = 159) | 3 (2) (N = 158) | 2 (1) (N = 190) | 3 (3) (N = 120) |
| Chinese | 0 (0) (N = 159) | 0 (0) (N = 158) | 3 (2) (N = 190) | 0 (0) (N = 120) |
| Education, n (%) | ||||
| Higher degree, degree or equivalent | 103 (65) (N = 158) | 92 (59) (N = 157) | 117 (62) (N = 190) | 65 (55) (N = 119) |
| A level or equivalent | 38 (24) (N = 158) | 36 (23) (N = 157) | 45 (24) (N = 190) | 34 (29) (N = 119) |
| GCSE or equivalent | 16 (10) (N = 158) | 25 (16) (N = 157) | 24 (13) (N = 190) | 19 (16) (N = 119) |
| No formal qualifications | 1 (1) (N = 158) | 4 (3) (N = 157) | 4 (2) (N = 190) | 1 (1) (N = 119) |
| Current method of travel to work (by journeys), n (%) | ||||
| Car | 106 (66) (N = 160) | 111 (66) (N = 167) | 124 (65) (N = 190) | 81 (66) (N = 123) |
| Public transport | 17 (11) (N = 160) | 27 (16) (N = 167) | 16 (8) (N = 190) | 16 (13) (N = 123) |
| Walking | 18 (11) (N = 160) | 14 (8) (N = 167) | 26 (14) (N = 190) | 16 (13) (N = 123) |
| Cycling | 19 (12) (N = 160) | 15 (9) (N = 167) | 24 (13) (N = 190) | 10 (8) (N = 123) |
| Distance between workplace and home (km), n (%) | ||||
| ≤ 2 | 22 (14) (N = 159) | 17 (11) (N = 160) | 14 (7) (N = 187) | 18 (15) (N = 120) |
| > 2 | 137 (86) (N = 159) | 143 (89) (N = 160) | 173 (93) (N = 187) | 102 (85) (N = 120) |
| Current occupation, n (%) | ||||
| Sedentary | 122 (76) (N = 160) | 117 (75) (N = 155) | 150 (80) (N = 187) | 87 (78) (N = 112) |
| Standing | 31 (19) (N = 160) | 29 (19) (N = 155) | 26 (14) (N = 187) | 16 (14) (N = 112) |
| Manual | 7 (4) (N = 160) | 8 (5) (N = 155) | 11 (6) (N = 187) | 9 (8) (N = 112) |
| Heavy manual work | 0 (0) (N = 160) | 1 (1) (N = 155) | 0 (0) (N = 187) | 0 (0) (N = 112) |
| Characteristics | Trial group, outcome data | |||
|---|---|---|---|---|
| Intervention (N = 331) | Control (N = 323) | |||
| Complete | Incomplete | Complete | Incomplete | |
| Primary outcome: daily number of minutes of MVPA, mean (SD) | 55.0 (24.9) (N = 142) | 48.2 (22.3) (N = 136) | 57.7 (37.0) (N = 180) | 46.1 (20.5) (N = 82) |
| Secondary outcomes, mean (SD) | ||||
| Overall physical activity (c.p.m.) | 390.5 (144.2) (N = 142) | 361.0 (140.9) (N = 136) | 417.1 (267.4) (N = 180) | 346.7 (126.5) (N = 82) |
| Sedentary time (minutes per day) | 585.8 (63.2) (N = 142) | 581.6 (72.0) (N = 135) | 581.8 (79.9) (N = 179) | 567.2 (71.8) (N = 82) |
| Daily number of minutes of MVPA during the commute | 13.3 (14.6) (N = 142) | 13.1 (13.6) (N = 156) | 13.7 (15.1) (N = 174) | 11.5 (13.9) (N = 120) |
| Number of journeys when walking was the major mode of travel to and from work, n (%) | ||||
| 0 | 130 (81) (N = 160) | 136 (81) (N = 167) | 152 (80) (N = 190) | 99 (80) (N = 123) |
| 1 | 8 (5) (N = 160) | 7 (4) (N = 167) | 5 (3) (N = 190) | 4 (3) (N = 123) |
| 2 | 2 (1) (N = 160) | 8 (5) (N = 167) | 4 (2) (N = 190) | 4 (3) (N = 123) |
| 3 | 3 (2) (N = 160) | 0 (0) (N = 167) | 3 (2) (N = 190) | 2 (2) (N = 123) |
| 4 | 0 (0) (N = 160) | 3 (2) (N = 167) | 3 (2) (N = 190) | 1 (1) (N = 123) |
| 5 | 2 (1) (N = 160) | 2 (1) (N = 167) | 2 (1) (N = 190) | 2 (2) (N = 123) |
| 6 | 5 (3) (N = 160) | 2 (1) (N = 167) | 3 (2) (N = 190) | 1 (1) (N = 123) |
| 7 | 0 (0) (N = 160) | 1 (1) (N = 167) | 1 (1) (N = 190) | 0 (0) (N = 123) |
| 8 | 3 (2) (N = 160) | 5 (3) (N = 167) | 6 (3) (N = 190) | 6 (5) (N = 123) |
| 9 | 0 (0) (N = 160) | 1 (1) (N = 167) | 2 (1) (N = 190) | 1 (1) (N = 123) |
| 10 | 5 (3) (N = 160) | 2 (1) (N = 167) | 9 (5) (N = 190) | 1 (1) (N = 123) |
| 11 | 2 (1) (N = 160) | 0 (0) (N = 167) | 0 (0) (N = 190) | 0 (0) (N = 123) |
| 12 | 0 (0) (N = 160) | 0 (0) (N = 167) | 0 (0) (N = 190) | 2 (2) (N = 123) |
Outcomes and estimation
At baseline, study participants were achieving, on average, > 50 minutes of MVPA per day (Table 34). At the 12-month assessment point, no increase in MVPA was observed in either the intervention group or the control group, and hence there was no evidence of an effect of the Walk to Work intervention on the primary outcome measure (p = 0.92) (see Table 34). The ICC for the primary outcome was estimated at 0.020 (95% CI 0.001 to 0.292).
| Outcome | Trial group, mean (SD) | Adjusted difference in meansa (95% CI) | p-valuea | |||
|---|---|---|---|---|---|---|
| Intervention | Control | |||||
| Baseline | Follow-up | Baseline | Follow-up | |||
| Primary | ||||||
| 1. Daily number of minutes of MVPA | 55.0 (24.9) (n = 142) | 53.3 (23.7) (n = 142) | 57.7 (37.0) (n = 180) | 53.9 (27.6) (n = 180) | 0.3 (–5.3 to 5.9) | 0.917 |
| Secondary | ||||||
| 2. Overall physical activity (c.p.m.) | 390.5 (144.2) (n = 142) | 387.6 (148.5) (n = 142) | 417.1 (267.4) (n = 180) | 392.7 (168.8) (n = 180) | 3.5 (–30.3 to 37.4) | 0.838 |
| 3. Sedentary time (minutes per day) | 585.5 (63.3) (n = 141) | 580.0 (97.0) (n = 141) | 581.9 (80.1) (n = 178) | 585.4 (108.6) (n = 178) | 1.0 (–11.7 to 13.6) | 0.882 |
| 4. Daily number of minutes of MVPA during commute | 13.9 (14.1) (n = 183) | 13.8 (14.0) (n = 183) | 13.3 (15.1) (n = 213) | 16.2 (19.0) (n = 213) | –3.1 (–6.0 to –0.2) | 0.036 |
Including participants with at least 1 day of valid accelerometer data, at least 2 weekdays and 1 weekend day, using data from either working days or non-working days only, or log-transforming the primary outcome data (at baseline and follow-up, to model the non-normality), in sensitivity analyses supported the same conclusion (Table 35). We did not carry out the multiple imputation of the primary outcome as specified in the statistical and health economics analysis plan88 as it was clear that using at least 1 day of valid data did not change our conclusions and, therefore, it was agreed with the Trial Steering Committee that this was acceptable. We also did not further adjust our primary outcome analysis by any baseline characteristics, as there was no imbalance in these between the intervention and the control groups at baseline.
| Outcome | Trial group, mean (SD) | Adjusted difference in meansa (95% CI) | p-valuea | |||
|---|---|---|---|---|---|---|
| Intervention | Control | |||||
| Baseline | Follow-up | Baseline | Follow-up | |||
| At least 1 day of valid data | 52.6 (25.0) (n = 189) | 51.1 (23.7) (n = 189) | 55.5 (35.1) (n = 217) | 52.6 (28.1) (n = 217) | –0.4 (–5.3 to 4.5) | 0.876 |
| At least 2 weekdays and 1 weekend day | 53.9 (20.3) (n = 86) | 54.3 (22.3) (n = 86) | 59.8 (40.3) (n = 121) | 56.6 (29.0) (n = 121) | 1.6 (–6.5 to 9.7) | 0.691 |
| Data from working days only | 55.7 (26.2) (n = 131) | 51.2 (23.0) (n = 131) | 54.7 (27.8) (n = 163) | 51.9 (26.1) (n = 163) | –2.4 (–7.2 to 2.5) | 0.339 |
| Data from non-working days only | 52.1 (28.2) (n = 87) | 53.9 (29.2) (n = 87) | 60.8 (46.3) (n = 121) | 56.7 (40.2) (n = 121) | 4.9 (–5.7 to 15.5) | 0.364 |
| Log-mean (SD) | Adjusted ratio of geometric meansa (95% CI) | p-valuea | ||||
| Log-transformed daily number of minutes of MVPA | 3.9 (0.5) (n = 142) | 3.9 (0.5) (n = 142) | 3.9 (0.5) (n = 179) | 3.9 (0.6) (n = 179) | 1.0 (0.9 to 1.1) | 0.898 |
The unadjusted means of the primary outcome of daily number of minutes of MVPA and the secondary outcome of overall physical activity decreased in both the intervention group and the control group over the 12-month follow-up (see Table 35). There was no evidence of an effect of the intervention on these measures for any of the adjusted analyses. The unadjusted means of sedentary time increased over the 12-month follow-up in the control group but reduced in the intervention group, again with no evidence of an intervention effect. However, daily number of minutes of MVPA during the commute increased in the control group but reduced in the intervention group, with evidence of a differential effect after adjustment for covariates (p = 0.036). For both the intervention group and the control group, at all assessment points, the median number of journeys walked to work was 0 (interquartile range 0–0), with no evidence of an effect of the intervention on this measure (p = 0.395).
There was no evidence that the effect of the intervention differed between different age groups, men and women or participants with different household incomes (Table 36).
| Outcome | Trial group, mean (SD) | Adjusted difference in means between control and intervention within the subgroupa (95% CI) | Interaction test p-valuea | |||
|---|---|---|---|---|---|---|
| Intervention | Control | |||||
| Baseline | Follow-up | Baseline | Follow-up | |||
| Age | ||||||
| Less than the median | 55.2 (23.2) (n = 61) | 56.3 (24.7) (n = 61) | 63.2 (46.7) (n = 77) | 60.6 (26.8) (n = 77) | –1.9 (–9.8 to 6.0) | 0.496 |
| More than or equal to the median | 54.9 (26.3) (n = 81) | 51.0 (22.8) (n = 81) | 53.6 (27.2) (n = 103) | 48.9 (27.2) (n = 103) | 1.6 (–5.5 to 8.6) | |
| Gender | ||||||
| Male | 58.1 (24.8) (n = 57) | 56.4 (23.7) (n = 57) | 61.8 (50.1) (n = 71) | 56.0 (31.3) (n = 71) | 1.5 (–6.8 to 9.9) | 0.664 |
| Female | 53.0 (24.9) (n = 85) | 51.1 (23.6) (n = 85) | 55.0 (24.9) (n = 109) | 52.6 (25.0) (n = 109) | –0.8 (–7.7 to 6.2) | |
| Household income | ||||||
| ≤ £30,000 or missing | 52.4 (24.2) (n = 32) | 54.4 (23.2) (n = 32) | 54.6 (25.5) (n = 41) | 53.8 (24.6) (n = 41) | 2.6 (–8.3 to 13.5) | 0.628 |
| > £30,000 | 55.8 (25.2) (n = 110) | 52.9 (24.0) (n = 110) | 58.6 (39.8) (n = 139) | 54.0 (28.5) (n = 139) | –0.4 (–6.6 to 5.8) | |
| Distance from work | ||||||
| ≤ 2 km | 58.7 (26.3) (n = 20) | 57.2 (25.4) (n = 20) | 59.9 (22.7) (n = 12) | 64.5 (34.0) (n = 12) | –6.8 (–23.2 to 9.7) | 0.419 |
| > 2 km | 54.7 (24.7) (n = 121) | 52.9 (23.4) (n = 121) | 57.3 (38.0) (n = 164) | 53.1 (27.1) (n = 164) | 0.4 (–5.5 to 6.3) | |
Summary
We conducted a robust outcome evaluation of the Walk to Work intervention in line with a prespecified statistical analysis plan. The results presented here show that the intervention was not effective in increasing participants’ MVPA or in changing travel mode.
Chapter 8 Economic evaluation
Parts of this chapter are reproduced from Audrey et al. ,69 published by BMC Public Health journal. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The text below includes minor additions and formatting changes to the original text.
Methods
The economic evaluation is presented as a cost–consequences analysis whereby costs and consequences have been estimated but no attempt has been made to combine the results (e.g. in an incremental cost-effectiveness ratio). A broad perspective was taken, including employer, employee and health-care costs and individual well-being over the 1-year follow-up period. Given the follow-up period, discounting was not carried out.
Assessment of costs
Promoter training was conducted in the workplace. Trainer and promoter time and trainer travel costs were recorded on time sheets during the 10-week intervention period. Trainer time was costed using University of Bristol pay scales and included basic salary, National Insurance and superannuation (Table 37). Trainer travel costs were self-reported. If trainers travelled by car, they reported the number of miles travelled and the cost was estimated using a cost per mile of 59.9 pence. 92 The numbers of promoters and employers and the numbers of individuals participating in the intervention at each workplace were recorded. The unit cost of promoter time was calculated by dividing the upper quartile weekly earnings by the median number of hours worked per week, as reported in the annual survey of hours and earnings. 93 The upper quartile was applied as some promoters were also the employer and it was believed that promoters were likely to be on a higher wage than the average worker.
| Staff role | Unit cost per hour (£) |
|---|---|
| Research associate | 28.16 |
| Senior research associate | 31.77 |
| Senior research fellow | 44.59 |
| Senior lecturer | 44.59 |
| Promoter | 18.39 |
The intervention resources required at each workplace included employee, employer and promoter booklets and folders, employer letters, newsletters, incident forms, poster sets, postage, optional pedometers and DVDs. Materials were printed by the University of Bristol print services, with 60% of the costs covered by Living Streets (www.livingstreets.org.uk; accessed 6 June 2018), a UK charity that promotes everyday walking. Pedometers were donated by Living Streets but were costed at £3.00 per unit in the analysis to reflect the true cost if the intervention was to be rolled out.
Health service use in the previous 4 weeks was self-reported by study participants at baseline and at the 12-month follow-up. Unit costs that were used to value health service use are presented in Table 38.
| Health-care resource | Unit cost per resource (£) |
|---|---|
| Face-to-face appointment with a doctor at the GP surgery | 36.00 |
| Face-to-face appointment with a nurse at the GP surgery | 14.47 |
| Telephone consultation with a doctor at the GP surgery | 27.72 |
| Telephone consultation with a nurse at the GP surgery | 11.14 |
| Hospital accident and emergency department | 137.74 |
| Hospital outpatient appointment | 116.92 |
| Hospital admission | 1243.86 |
| Telephone call to NHS Direct/NHS 111 | 12.89 |
| Out-of-hours visit | 69.83 |
| Chiropractor appointment | 55.00 |
| Osteopath appointment | 42.50 |
| Other non-hospital-based appointments | Varies by item94,95 |
| Other hospital-based appointments | Varies by item96 |
| Prescribed medication | Varies by item97 |
Primary care, including general practitioner (GP) visits, nurse visits, GP calls and nurse calls, was costed using national unit cost estimates. 94,95 Hospital-based care was costed using NHS Reference Costs 2015–16. 96 Osteopathic and chiropractic care were costed using the NHS Choices website. 98,99 Out-of-hours care and NHS 111/NHS Direct use were costed using published estimates. 100,101 Admitted care and all other care reported by participants, including use of NHS 111/NHS Direct, out-of-hours care, osteopathic care and chiropractic care were grouped together under ‘other care’ for the analysis. All health service use was valued for the year 2016; when 2016 unit costs were not available, costs were inflated to 2016 prices using the Hospital and Community Health Services Index. 94 For five appointments in which participants were asked to provide details of other care they received, some participants reported only the type of care and not the number of appointments; for these, we assumed that the participant had one appointment. Routine dental and optician appointments and pharmacist contacts were excluded from the analysis and a few health-care items were excluded because of a lack of information on what service the participant had received. Medications were costed using the Prescription Cost Analysis – England. 97 When medications could not be costed because of missing information on the number of days taken, it was assumed that medications for chronic conditions and contraception were taken daily. For medications with missing information on the number of doses per day, an assumption of one dose was made. Any medications that could not be costed owing to a lack of sufficient information were excluded.
Self-assessed productivity was measured on a 10-point scale based on the extent to which health problems had affected productivity in the previous 7 days at baseline and in the previous 3 months at the post-intervention and the 12-month follow-ups: 1 indicated that health problems had no effect on an individual’s work and 10 indicated that health problems had completely prevented work. 102 Self-assessed lost productivity was valued using median weekly earnings,93 assuming that a 1-point decrement on the scale equated to a 10% loss in productivity. Absence from work was also self-reported, whereby participants were asked to report the number of hours of work they had missed because of health problems in the previous 7 days at baseline and the number of days they had missed because of health problems in the previous 3 months at the post-intervention and the 12-month follow-ups. Lost productivity due to hours and days of missed work was also valued using median weekly earnings. 93
Workplaces were contacted after the 12-month follow-up and asked to report the total number of sickness absence days and the number of full-time-equivalent employees between baseline and the 12-month follow-up. The overall workplace absentee rates were estimated assuming that full-time employees have 28 days of paid annual leave per year.
Information regarding the commute was recorded for 1 week at baseline and the 12-month follow-up in a travel diary. Time spent commuting by mode of transport, daily expenses (such as bus fares) associated with the commute and occasional commuting expenses (including bus and train passes and parking permits) were all recorded. When reported commute modes and times were found to be inaccurate when compared with GPS data, diary data were replaced with GPS data. For some participants, it was observed that their commute time included time spent doing other activities (such as shopping); for these journeys, when possible, the commute time was replaced with the participant’s average commute time for the given mode of transport. A cost per mile of 59.9 pence92 and an average speed of 23.43 miles per hour19 were used to calculate a cost per minute of driving; this was multiplied by the number of minutes of driving in order to estimate the cost of commuting by car. Costs and durations of parking permits, bus passes and train passes were used to estimate daily parking permit, bus and train costs. Car sharing was incorporated into the costs of car travel by deducting the contribution from passengers from the cost of commuting by car.
Quality of life
Scores on the ICECAP-A, a measure of well-being, were collected at baseline, post intervention and at the 12-month follow-up to capture participant well-being. 52 ICECAP-A is a five-attribute questionnaire, with each attribute containing four levels, which range from no capability to full capability. The ICECAP-A tariff was applied to questionnaire scores to estimate participant quality of life. 103 ICECAP-A scores are anchored on 0 indicating no capability and 1 indicating full capability.
Results
Costs of intervention materials
The costs of intervention materials to deliver the intervention are provided in Table 39.
| Item | Number of units | Cost (£) | |
|---|---|---|---|
| Unit | Total | ||
| Employer booklet | 73 | 0.35 | 25.55 |
| Employer folder | 26 | 5.00 | 130.00 |
| Employer letter | 43 | 0.05 | 2.15 |
| Promoter/employer folder | 15 | 5.00 | 75.00 |
| Promoter booklet | 73 | 0.40 | 29.20 |
| Promoter folder | 32 | 5.00 | 160.00 |
| Employee booklet | 357 | 0.45 | 160.65 |
| Newsletters 1, 2 and 3 | 993 | 0.05 | 49.65 |
| Promoter newsletters 1, 2 and 3 | 144 | 0.05 | 7.20 |
| Incident form 1 | 150 | 0.05 | 7.50 |
| Incident form 2 | 181 | 0.06 | 10.86 |
| Poster sets | 73 | 2.40 | 175.20 |
| Postage | 482 | 0.54 | 260.28 |
| Pedometers | 331 | 3.00 | 993.00 |
| DVDs | 48 | 1.50 | 72.00 |
| Average cost per workplace | 50.19 | ||
| Average cost per participating employee | 6.52 | ||
Cost per employer and participating employee
The costs of the intervention per workplace and employee, by workplace size, are presented in Table 40. Costs varied because of different numbers of promoters in each workplace and depending on the number of employees participating in the intervention at each workplace. The number of trainers delivering the promoter training and travel distance and cost also affected the overall cost. The costs per workplace and per participating employee by workplace size demonstrate that there is no clear association between employer size and cost per participating employee; this may be in part because the number of participants recruited was not consistently larger in larger workplaces.
| Workplace sizea | Costs (£) | ||||
|---|---|---|---|---|---|
| Intervention materialsb | Promoter training | Total per workplace | Per participating employee | ||
| Training deliveryc | Promoterd | ||||
| Micro | 31.58 | 130.50 | 20.69 | 182.77 | 43.01 |
| Small | 42.78 | 97.86 | 19.05 | 159.68 | 25.60 |
| Medium | 44.55 | 134.19 | 29.12 | 207.86 | 34.01 |
| Large | 81.40 | 118.98 | 27.59 | 227.96 | 16.03 |
| All | 50.19 | 112.92 | 23.09 | 186.20 | 24.19 |
Health service use
Table 41 provides the mean number of units and the mean cost of each service per participant, by group and by time point. There was a total of 331 participants in the intervention group and 323 participants in the control group. At baseline, the response rate varied between 88% and 91% in the intervention group and between 81% and 88% in the control group, depending on the question asked. At the 12-month follow-up, response rates, including only participants who also recorded their baseline health-care use, varied between 52% and 56% in the intervention group and between 63% and 67% in the control group. On average, the response rate was 36% lower than baseline in the intervention group and 21% lower than baseline in the control group at follow-up.
| Health service use | Trial group | Incremental difference (£) (95% CI) | |||||
|---|---|---|---|---|---|---|---|
| Intervention | Control | ||||||
| n | Mean number of units | Cost (£), mean (SD) | n | Mean number of units | Cost (£), mean (SD) | ||
| Baseline | |||||||
| GP appointment | 300 | 0.18 | 6.48 (17.20) | 284 | 0.18 | 6.46 (15.11) | 0.02 (–2.62 to 2.65) |
| Nurse appointment | 299 | 0.08 | 1.21 (4.18) | 282 | 0.07 | 1.03 (3.72) | 0.18 (–0.46 to 0.83) |
| GP telephone call | 300 | 0.04 | 1.20 (6.09) | 284 | 0.10 | 2.73 (11.56) | –1.53 (–3.02 to –0.04) |
| Nurse telephone call | 298 | 0.01 | 0.07 (0.91) | 283 | 0.01 | 0.16 (1.62) | –0.08 (–0.30 to 0.13) |
| A&E visit | 300 | 0.02 | 2.30 (20.95) | 284 | 0.02 | 2.91 (25.73) | –0.61 (–4.42 to 3.19) |
| Hospital outpatient visit | 299 | 0.11 | 12.90 (50.39) | 285 | 0.09 | 10.67 (43.67) | 2.24 (–5.44 to 9.92) |
| Other care | 298 | 0.16 | 20.18 (126.75) | 279 | 0.12 | 10.04 (81.76) | 10.15 (–7.42 to 27.72) |
| Medication | 291 | 7.86 (57.38) | 263 | 27.48 (198.73) | –19.62 (–43.54 to 4.29) | ||
| Total | 284 | 50.43 (174.64) | 254 | 60.61 (236.81) | –10.18 (–45.19 to 24.82) | ||
| 12-month follow-up | |||||||
| GP appointment | 183a | 0.46 | 16.52 (31.28) | 216a | 0.62 | 22.17 (36.84) | –5.45 (–12.17 to 1.27)b |
| Nurse appointment | 181a | 0.33 | 4.80 (10.68) | 215a | 0.27 | 3.84 (8.84) | 0.79 (–1.10 to 2.68)b |
| GP telephone call | 183a | 0.11 | 3.18 (11.37) | 216a | 0.24 | 6.55 (17.43) | –3.06 (–5.94 to –0.18)b |
| Nurse telephone call | 181a | 0.03 | 0.37 (2.00) | 216a | 0.04 | 0.41 (2.37) | –0.04 (–0.48 to 0.39)b |
| A&E visit | 184a | 0.06 | 8.23 (35.77) | 215a | 0.07 | 8.97 (41.14) | 0.16 (–7.35 to 7.67)b |
| Hospital outpatient visit | 180a | 0.36 | 41.57 (136.85) | 215a | 0.46 | 53.84 (191.71) | –11.67 (–45.13 to 21.80)b |
| Other care | 178a | 0.43 | 68.47 (264.84) | 212a | 0.35 | 34.64 (151.26) | 33.93 (–8.25 to 76.10)b |
| Medication | 173a | 13.20 (99.08) | 202a | 18.83 (123.55) | 2.20 (–17.64 to 22.04)b | ||
| Totalc | 158a | 139.75 (372.56) | 191a | 140.51 (339.55) | 23.19 (–56.09 to 102.47)b | ||
At baseline, the mean total cost of health services, including medications, in the intervention group was lower than that in the control group, at £50.43 (SD £174.64) compared with £60.61 (SD £236.81). At the 12-month follow-up, the mean cost of health service use was similar in both arms, at £139.75 (SD £372.56) in the intervention group and £140.51 (SD £339.55) in the control group. The adjusted incremental difference of £23.19 (95% CI –£56.09 to £102.47) at the 12-month follow-up was not statistically significantly different from zero.
Commute
A summary of the commute data is presented in Table 42. At baseline, 90% of the intervention participants and 90% of the control participants provided information on their weekly commute to and from work. This information was provided at both baseline and the 12-month follow-up for 56% of the intervention participants and 65% of the control participants.
| Mode of Transport | Trial group, mean (SD) daily number of minutes | Incremental difference (95% CI) | |
|---|---|---|---|
| Intervention (N = 299) | Control (N = 290) | ||
| Baseline | n = 187a | n = 211a | |
| Walking | 11.69 (16.90) | 10.46 (17.28) | 1.23 (–1.54 to 4.00) |
| Cycling | 6.75 (20.84) | 6.39 (15.22) | 0.35 (–2.61 to 3.31) |
| Bus | 5.32 (15.06) | 5.74 (16.25) | –0.42 (–2.96 to 2.11) |
| Train | 6.24 (21.61) | 4.97 (17.46) | 1.27 (–1.91 to 4.46) |
| Car | 39.55 (36.84) | 41.31 (35.08) | –1.75 (–7.58 to 4.07) |
| Other | 1.27 (6.87) | 1.05 (5.12) | 0.21 (–0.77 to 1.20) |
| Inactive travelb | 52.38 (45.35) | 53.07 (39.66) | –0.69 (–7.59 to 6.21) |
| Total | 70.82 (50.50) | 69.93 (42.69) | 0.89 (–6.69 to 8.47) |
| Follow-up | n = 187a | n = 211a | |
| Walking | 11.49 (19.63) | 12.92 (21.62) | –2.15 (–5.46 to 1.15)c |
| Cycling | 6.37 (18.03) | 7.37 (17.53) | –0.69 (–3.67 to 2.29)c |
| Bus | 3.13 (10.04) | 4.87 (13.77) | –1.45 (–3.48 to 0.58)c |
| Train | 4.72 (18.98) | 7.14 (23.83) | –1.44 (–4.95 to 2.07)c |
| Car | 34.56 (31.06) | 39.70 (35.84) | –2.09 (–6.63 to 2.45)c |
| Other | 0.62 (3.12) | 1.56 (7.48) | –0.94 (–2.10 to 0.22)c |
| Inactive travelb | 43.03 (35.46) | 53.27 (47.75) | –6.03 (–12.98 to 0.93)c |
| Total | 60.90 (41.48) | 73.56 (57.40) | –9.17 (–18.05 to –0.28)c |
At baseline, the average daily time of commuting to work was similar between groups, at approximately 71 and 70 minutes for the intervention and the control groups, respectively. At the 12-month follow-up, there was a trend for a lower total daily mean commute time in the intervention group [60.90 minutes (SD 41.48 minutes)] than in the control group [73.56 minutes (SD 57.40 minutes)], with an adjusted incremental difference of –9.17 minutes (95% CI –18.05 to –0.28 minutes).
The percentage of participants with complete information available for costing was 78% of the intervention group and 72% of the control group at baseline. This number dropped at the 12-month follow-up, with 42% of the intervention participants and 41% of the control participants with complete information available for costing. As shown in Table 43, at baseline the mean daily commuting cost was £11.03 (SD £9.74) in the intervention group and £11.37 (SD £10.21) in the control group. At the 12-month follow-up, the mean daily commuting cost was £9.32 (SD £7.67) in the intervention group and £10.99 (SD £12.19) in the control group. The adjusted incremental difference at follow-up was £1.15 (95% CI –£3.10 to £0.79).
| Costs | Trial group, mean (SD) daily cost | Incremental difference (95% CI) | |||
|---|---|---|---|---|---|
| Intervention | Control | ||||
| Baseline | n = 259 | n = 233 | |||
| Daily commuting cost | £11.03 | (£9.74) | £11.37 | (£10.21) | –£0.34 (–£2.11 to £1.43) |
| 12-month follow-up | n = 140a | n = 131a | |||
| Daily commuting cost | £9.32 | (£7.67) | £10.99 | (£12.19) | –£1.15 (–£3.10 to £0.79)b |
Productivity
Response rates to the questions on self-rated productivity and absenteeism declined over the study period (Table 44). At baseline, approximately 89% of participants in the intervention group and 88% of participants in the control group answered these questions. At the 12-month follow-up, response rates had fallen to approximately 59% in the intervention group and 72% in the control group.
| Productivity | Trial group | Incremental difference in wages lost (£) (95% CI) | |||||
|---|---|---|---|---|---|---|---|
| Intervention (N = 331) | Control (N = 323) | ||||||
| n | Mean number of units | Value of wages lost (£), mean (SD)a | n | Mean number of units | Value of wages lost (£), mean (SD)a | ||
| Self-assessed productivity | |||||||
| Post intervention | 200 | 2.23 | 701.32 (1067.41) | 263 | 2.56 | 891.04 (1238.79) | –189.72 (–405.04 to 25.60) |
| Follow-up | 195 | 2.26 | 719.30 (1041.80) | 231 | 2.85 | 1056.44 (1397.15) | –337.13 (–575.53 to –98.73) |
| Average of post-intervention and follow-up differencesb | –231.35 (–424.77 to –37.92) | ||||||
| Self-reported number of days of work missed | |||||||
| Post intervention | 199 | 1.01 | 88.16 (245.15) | 262 | 1.44 | 126.39 (449.57) | –38.23 (–107.58 to 31.12) |
| Follow-up | 194 | 2.01 | 176.57 (536.05) | 232 | 1.71 | 149.92 (401.70) | 26.65 (–62.78 to 116.08) |
| Average of post-intervention and follow-up differencesb | –12.50 (–84.34 to 59.33) | ||||||
At baseline, the mean productivity score in both the intervention group and the control group was low [1.77 (SD 1.47) and 2.02 (SD 1.83), respectively], suggesting a low self-perceived impact of health on productivity. Productivity scores were slightly lower (better) in the intervention group than in the control group at the 12-month follow-up [2.26 (SD 1.83) and 2.85 (SD 2.45), respectively]. When converted to lost wages, on average, the control participants lost more wages than the intervention participants did [£1056.44 (SD £1397.15) and £719.30 (SD £1041.80), respectively], with a difference in wages of –£231 (95% CI –£424.77 to –£37.92) based on a repeated-measures analysis.
The average number of hours missed from work because of health problems was slightly higher in the control group at baseline, at 0.60 hours (SD 3.48 hours) compared with 0.45 hours (SD 2.36 hours) in the intervention group. Immediately post intervention, the mean number of days missed was higher in the control group, at 1.44 days (SD 5.13 days) than 1.01 days (SD 2.79 days) in the intervention group. At the 12-month follow-up, the mean number of days was higher in the intervention group [2.01 days (SD 6.11 days)] than in the control group [1.71 days (SD 4.58 days)]. Conversion into wages suggested that the intervention participants lost, on average, more wages than the control participants [£176.57 (SD £536.05) and £149.92 (SD £401.70), respectively]; however, this result was not statistically significant (mean –£12.50, 95% CI –£84.34 to £59.33).
Data required to estimate overall workplace absentee rates were reported by 15 intervention and 13 control workplaces. The average overall workplace absentee rate between baseline and the 12-month follow-up was 1.68% in intervention workplaces and 2.91% in control workplaces.
Quality of life
At baseline, 90% of the intervention participants and 88% of the control participants completed the ICECAP-A questions. For both trial arms, the percentage reduced over the follow-up period; however, the reduction was larger in the intervention group, with 59% of the intervention participants and 82% of the control participants answering the ICECAP-A questions at the 12-month follow-up.
The ICECAP-A scores, presented in Table 45, were similar between trial arms at baseline, with the mean intervention score being 0.839 (SD 0.133) and the mean control score being 0.831 (SD 0.136). A repeated-measures analysis suggests that the mean ICECAP-A score in the intervention group was higher than that in the control group over the follow-up period (mean 0.018, 95% CI 0.000 to 0.036; scores anchored at 0 indicated ‘no capability’ and scores anchored at 1 indicated ‘full capability’).
| Time point | Trial group | Incremental difference (95% CI) | |||
|---|---|---|---|---|---|
| Intervention (N = 331) | Control (N = 323) | ||||
| n | Score, mean (SD) | n | Score, mean (SD) | ||
| Baseline | 298 | 0.839 (0.133) | 284 | 0.831 (0.136) | 0.008 (–0.014 to 0.030) |
| Post intervention | 197 | 0.852 (0.136) | 264 | 0.825 (0.143) | 0.027 (0.001 to 0.053) |
| Follow-up | 196 | 0.840 (0.134) | 228 | 0.823 (0.152) | 0.017 (–0.010 to 0.045) |
| Average of post-intervention and follow-up differencesa | 0.018 (0.000 to 0.036) | ||||
Summary
On average, the Walk to Work intervention cost £186.20 per workplace and £24.19 per participating employee, representing a relatively inexpensive and ‘light-touch’ intervention for employers to adopt. Participants in the intervention group had better self-rated productivity and well-being scores over the 12-month follow-up period; however, the small differences and higher loss to follow-up in the intervention group caution against overinterpreting these findings.
Chapter 9 Discussion
Main findings
Recruitment and retention
Recruitment took place in two phases, during May to July 2015 and March to May 2016, across seven urban areas in south-west England and south Wales. Information sheets with invitations for expressions of interest were sent to approximately 9800 workplace addresses. We received 271 expressions of interest and 87 workplaces were recruited (10 micro-sized, 35 small, 22 medium-sized and 20 large workplaces) involving 654 participants. Following baseline data collection, 44 workplaces were randomised to receive the intervention and 43 workplaces were randomised to the control group. At the 12-month follow-up, 84 workplaces (41 intervention and 43 control) and 477 employees (73% of those originally recruited to the study) took part in data-collection activities. Response rates in the control group were higher than those in the intervention group at the 12-month follow-up.
Baseline characteristics and physical activity
In line with other studies reporting objective measures of physical activity,104–106 a low proportion of participants in our study (≈11%) met current physical activity recommendations of ≥ 150 minutes of MVPA per week in bouts of ≥ 10 minutes. 1 Compared with car users, walkers and public transport users accrued substantially higher levels of daily MVPA during the commute. The absence of free workplace car parking was independently related to walking to work and using public transport. Shorter commuting distances were also related to walking to work, and public transport users were less likely to combine their commute with caring responsibilities.
Intervention delivery
Of the 44 workplaces that were randomised to receive the intervention, two workplaces withdrew during the intervention. A total of 37 workplaces identified a Walk to Work promoter who received training and materials to undertake the role; however, five workplaces were unable to identify a Walk to Work promoter and the local researcher took on the role of distributing intervention materials to participating employees. All employers in the intervention group were provided with booklets and posters encouraging them to support the intervention.
Process evaluation
Descriptive statistics from the process evaluation suggested that a majority of participants in the intervention group were aware of the Walk to Work promoters in their workplace. Employers’ support for the intervention tended to focus on the provision of information rather than initiatives with a higher cost or requiring organisational change, such as improved washing and changing facilities, changes to parking arrangements, incentives to walk during the commute or subsidised sustainable transport initiatives. Key factors influencing whether or not participants increased walking during the commute were identified through the behavioural questionnaires and qualitative interviews, and included commuting distance and workplace location; the availability, reliability and cost of alternatives to private car use; and caring responsibilities, especially child care.
Outcome evaluation
At the 12-month follow-up, we found no effect on the participants’ MVPA levels, overall physical activity or travel mode. There was no evidence that the effect of the intervention differed between different age groups, males and females or participants with different household incomes.
Economic evaluation
On average, the Walk to Work intervention cost £186.20 per workplace and £24.19 per participating employee, representing a relatively inexpensive intervention for employers to adopt. There was weak evidence that self-rated productivity and well-being scores were better in the intervention group than in the control group over the 12-month follow-up period. However, the small differences, the lack of improvement in MVPA and active commuting and the higher loss to follow-up in the intervention group caution against overinterpreting these findings.
Limitations and strengths
Recruitment
Although the target for workplace recruitment was achieved, this was after a large mailout to workplaces across seven urban areas. It was not possible to check if all workplaces on the lists were extant, if addresses and contact details were accurate and if the information reached someone with the authority to make a decision on study participation. However, with only 271 responses from > 9000 letters, we can conclude that the study, which was clearly related to workplace travel behaviour with an emphasis on changing travel mode to increase walking, was not of interest to the majority of employers. Furthermore, there was a relatively low cluster size, even within larger workplaces.
Baseline characteristics and physical activity
There are some notable strengths of this study. To our knowledge, this is the largest study that has combined robust, objectively measured data derived from accelerometer and GPS devices to identify characteristics associated with physical activity and walking as the main mode of travel to work. Data were collected over a relatively short period of time (May to July 2015 and March to May 2016) to minimise the effect of seasonality on physical activity and travel behaviours. In this study, 65% and 11% of the study participants were categorised as car users and walkers, respectively. Similarly, findings from the National Travel Survey: England 2016 showed that 64% and 11% of commute journeys were made by car and walking, respectively. 19 This suggests that the findings we report are similar to national patterns of commuting behaviour and could be more widely generalisable. However, as analyses were undertaken on cross-sectional data, we are unable to establish causal relationships between the variables of interest. We used perceptions of the commute environment, rather than objectively quantified characteristics of the environment through a GIS. Participants of the study were relatively young, predominantly well-educated and employed in sedentary occupations. Therefore, the findings may not be applicable to a population with different characteristics.
Process evaluation
The promoters all received the Walk to Work training session and DVD, booklets and resources relevant to their role and four newsletters during the intervention period. However, they were encouraged to deliver the intervention to colleagues in a way that suited their workplace routines. This model was relatively cheap to deliver, as shown by the economic evaluation, but leaves room for variation and uncertainty about fidelity and reach. On the other hand, the results may be more relevant to a ‘real-world’ situation than an intervention that is highly monitored throughout and is therefore more likely to accrue Hawthorne effects.
The post-intervention questionnaires sent to all study participants, which included questions about interventions relating to travel to work, had noticeably higher non-response rates in the intervention group than in the control group. It is not clear why this is the case; it may relate to the additional participant burden in the intervention group, as these participants had just come to the end of a 10-week intervention, or it may be that there was a reluctance among participants in the intervention group to confirm that they, or the Walk to Work promoter, had not engaged with the intervention in their workplace. A strength of the process evaluation is the number of interviews (n = 70) with employers, Walk to Work promoters and employees. This has provided a substantial data set that has provided additional understanding of some of the statistical findings and will be subject to detailed future analyses.
Outcome evaluation
The use of objective measures, and a 12-month follow-up period, contribute valuable evidence for those who have called for greater rigour in assessing the effectiveness of physical activity interventions,26,28 and interventions aiming to change the travel mode of commuters. 25 It would have been interesting to collect these objective measures immediately post intervention to assess whether or not there was an immediate impact of the intervention on physical activity and commuting behaviour, and the response rate may have been higher. However, this would have increased the burden on research participants and would not have addressed the important concern that long-term follow-up has been identified as a weakness in other studies.
The study included workplaces in geographically distinct areas and of different sizes and industrial classifications, which might add to its generalisability. However, it should be noted that participants were predominantly educated to degree level and with a household income above the national average. It might be thought that study participants were fairly active with a baseline mean daily number of minutes of MVPA of > 50 minutes; however, this was largely not achieved in the recommended bouts of ≥ 10 minutes. Furthermore, there are concerns that feedback from activity monitors is not easily reconciled with current physical activity recommendations because the guidelines refer to the amount of activity required on top of normal activities. 107
Missing data
Three workplaces, all randomised to the intervention group, did not continue with the study. The loss of these workplaces contributed to a higher response rate in the control group at the 12-month follow-up than in the intervention group, but does not completely explain the difference observed. In the intervention group, 142 out of 331 participants (43%) provided a measure of the primary outcome; in the control group, 180 out of 323 participants (56%) provided that measure. The number of missing data is disappointing, and the reasons are unclear. It may be that the interest in the research, and especially the novelty of wearing the monitors, decreased over the 12-month period. At the follow-up data collection point, 477 participants (73%) were still involved with the study and returned some data (questionnaire, travel diary, accelerometer or GPS data). However, it may be that those who had not changed their travel behaviour were less inclined to have this confirmed by wearing the monitors. Moreover, the waist-worn accelerometer involves a research burden for the participants: it is usually worn on an elastic belt (as was the case with our study) and requires a degree of commitment to remember to put it on at the beginning of the day and to wear it for ≥ 10 hours, especially if a change of clothes is required when arriving home.
Although this low response rate is clearly a limitation to the strength of conclusions that can be drawn, we do not believe that the missing measurements cause the study results to be misleading. If the lower completion rate in the intervention group was due to some individuals who did not benefit from the intervention not wanting to have their physical activity assessed, had these participants provided outcome data it would have been in line with the same conclusion of no intervention effect. Furthermore, measuring the primary outcome for all participants who provided 1 day or more of accelerometer data (rather than 3 days or more) provided an outcome measure for 189 out of 331 participants (57%) in the intervention group and 217 out of 323 participants (67%) in the control group; repeating the analysis with these data led to the same conclusion of no effect of the intervention.
Measuring physical activity
The primary outcome of the Travel to Work study was compromised by missing data at the 12-month follow-up and this may have related to the burden of wearing waist-worn accelerometers in free-living conditions. Wrist-worn monitors are easier to wear and may increase compliance. 108 At the outset of this study, wrist-worn accelerometry was evolving and we wished to use an established technology so that we could relate the findings to other studies. Research suggests that the results from wrist-worn accelerometers differ from waist-worn accelerometers, with the wrist attachment producing a higher average step count than the waist attachment in free-living conditions. 109 A study comparing the wrist-worn Fitbit Flex (Fitbit, San Francisco, CA, USA) and waist-worn ActiGraph wGT3X-BT (ActiGraph, Pensacola, FL, USA) in free-living adults found that the Fitbit Flex and ActiGraph respectively classified 51.5% and 37.5% of the days as active. 110 Clearly, caution is needed in the choice of instrument used to measure physical activity in free-living conditions. The potential of wrist-worn devices to collect more data over a longer period of time and in larger samples is obviously attractive to researchers and health professionals. However, more work needs to be done to examine the accuracy of wrist-worn devices in measuring walking-related physical activity.
Economic evaluation
There was a high percentage of missing health economic data, in particular for commuting costs: at the 12-month follow-up, costs could only be estimated for 42% of the intervention participants and 41% of the control participants. To estimate daily commuting costs, participants were required to record complete times and costs for each work day at baseline and follow-up. It was evident that some participants reported details of bus and train costs in multiple places in the travel diary; when possible, this information was included only once. When possible, fuel and parking permit costs were excluded from daily costs as these costs were also recorded elsewhere in the diaries. Some participants reported that they were reimbursed for travel costs by their employer, but these costs were still included in the analyses. Some missing information was observed in the medication section of the questionnaire; as a result, some medications could not be costed and were not included. Consequently, the medication cost for these participants is an underestimate. Although we could have used multiple imputation to impute missing data and obtain estimates for all participants, given that no evidence of an intervention effect was observed, imputation was not conducted as it would not have altered the conclusion.
Conclusions
Recruitment
Overall, it can be concluded that a large proportion of workplaces that were sent information about the study were unwilling or unable to participate. This would suggest that active travel interventions may need to be carefully targeted at workplaces. Issues such as the location of the workplace, the type of business activities, working hours and the availability and reliability of public transport are important factors to be taken into consideration.
Two decisions taken by the research team may have restricted workplace recruitment and employee participation in the intervention. The first relates to the size of workplaces. The research team decided that workplaces with fewer than five employees would be ineligible. This was because of the increased cost of delivering the intervention to only one or two people. However, in the UK in 2014, micro-sized businesses (0–9 employees) accounted for 96% of all businesses and 33% of all employees,87 and so a large pool of workplaces were ineligible for the intervention.
The second issue relates to the distance between where the study participants lived and their workplaces. The original feasibility study,49 which was not powered to provide evidence of effectiveness, had nevertheless shown some promise that the intervention might have an effect. However, the feasibility study had initially focused on recruiting employees who lived within 2 miles of their workplace. After discussion within the team, it was felt that this might have been an unnecessary restriction, making recruitment difficult and failing to reach people who might be willing to increase walking as part of a mixed-mode journey. For the current study, the baseline statistical analyses and qualitative analyses of interview transcripts suggest that commuting distance is a critical factor in whether or not people walk during the commute. Focusing on those who live within walking distance of their workplace but who do not currently walk to work may narrow the field of participants but may increase the likelihood of success in changing travel mode.
Changing travel mode
Our findings suggest that workplace-based interventions focusing on travel mode are more likely to be of interest to ‘motivated subgroups’, as Ogilvie et al. 24 also suggest, rather than a broad spectrum of workplaces and employees. It is worth noting that 89% of participants in our study lived > 2 km from their place of work and, to increase walking during the commute, mixed-mode travel would be more feasible than walking the whole route. Our findings indicate that such a change is likely to be influenced by the availability, cost, convenience and reliability of public transport. The analyses of the baseline data in Chapter 4 indicate that other contextual factors, such as the location of the workplace and the availability of car parking, influence travel mode. 76,111 In addition, interventions may be more effective when they coincide with naturally occurring disruption in travel habits,112 such as moving house, changing employment or reductions in workplace parking, suggesting that tailoring the timing or target group of travel mode interventions in accordance with the wider context could also be an important factor in their impact.
Implications for policy and practice
We have shown that walking to work, either the whole route or combined with public transport, is an important contributor to objectively measured physical activity levels in a large sample of adult employees recruited from diverse workplaces and settings in the UK. We believe that the picture is sufficiently clear to assert that supporting walking during the daily commute (either as the main mode or as part of a mixed-mode journey) should be a priority for both transport and public health disciplines. However, interventions to increase walking to work should take into account the wider determinants of commuting behaviour. Our research suggests that, at organisational and policy levels, consideration needs to focus on commuting distances, availability of car parking and the availability of convenient and reliable public transport. Our findings support the argument that attention should be directed towards a systems approach that focuses on interactions between the correlates of physical inactivity, rather than BCTs focusing on individuals. 113
Previous qualitative research has suggested that child-care commitments may restrict choice of travel mode for the commute. 114,115 Within our sample of employees, we found that child-care commitments were perceived as an important reason why participants were unable to change travel mode from private car use. This was particularly evident in relation to the reliability, frequency and timing of public transport, suggesting that employees with caring responsibilities may require greater flexibility in their working hours if they are to be encouraged to use public transport.
We found that walking and public transport use were both positively associated with a lack of free car parking at work. The removal of this ‘perk’ is unlikely to be popular with employees who value driving to work. Previous qualitative research has suggested that, where removing parking might be perceived as punitive, employers would prefer this to be imposed from outside the workplace. 49 This might, for example, be a directive from a more distant ‘head office’ or because of policies imposed by the local or national government.
In other UK-based studies, a short distance to the workplace75,76,116 and a lack of on-site car parking84,112,117 have been shown to act as facilitators of walking travel modes. In the current study, the majority of participants had a commute distance of > 2 km (n = 555, 84.8%). Therefore, switching to walking as the main mode of travel to work may not have been feasible for many of our study population. However, a mixed-mode commute, combining walking with public transport, may be possible. A case study of 20 UK workplaces showed that limiting parking, by either introducing parking charges or reducing the number of spaces available, and providing payments for public transport users were critical factors contributing to decreased car use. 118 The implementation of workplace policies to limit or charge for workplace car parking, while offering subsidies for public transport, may make modes of travel other than a car more appealing. Providing, or subsidising, car parking away from city-centre workplaces, to enable and encourage employees to park and walk, may be a more palatable option for employees than the removal of parking ‘perks’ altogether, and may be attractive to employers if it proves to be cheaper than the provision of city-centre parking.
In our study, although univariable analyses suggested that walkers and public transport users had more positive perceptions of their commute environment that car users, there was no evidence of a difference after adjustment for other variables. As we did not objectively quantify characteristics of the environment through GIS-based measures, we cannot eliminate physical differences in participants’ commute environments. Our qualitative data suggest that concerns about the walking environment may be a deterrent to walking. However, Guell et al. 119 suggest that some participants will walk despite adverse environmental conditions, having overcome the issue through experience or weighing up the perceived benefits and costs. In the UK, nationwide construction of walking and cycling routes has been shown to be associated with increased physical activity levels and walking and cycling as modes of travel. 120,121 However, distance to the infrastructure was identified as a mediating factor, suggesting that fragmented improvements to infrastructure may not be sufficient to bring about behaviour changes. 122
Recommendations for future research
We believe that there is sufficient reliable evidence to show that walking to work, or incorporating walking into a mixed-mode commute, can enable working adults to build physical activity into their daily routine and meet the physical activity recommendations. We would also argue that there is sufficient evidence to suggest that focusing on individual behaviour change has limited capacity to change travel mode at the population level.
We would recommend that future research considers targeted interventions for particular subgroups (e.g. employees with good public transport links between their workplace and home and employees wanting to increase physical activity for health reasons), interventions that address specific barriers that have been identified in this and other research (e.g. employees with caring responsibilities) and interventions that operate at organisational, environmental and policy levels (e.g. reductions in car parking and improvements to pedestrian routes). Some of the environmental and policy research may be more suited to evaluation as high-quality natural experiments rather than in RCTs.
Some areas for future research to encourage active travel include the acceptability, impact and cost-effectiveness of interventions relating to the reduction or relocation of workplace parking, examining the links between the school run and the commute to work, the effectiveness and cost-effectiveness of targeting travel-to-work interventions at micro-sized workplaces and the impact of infrastructure changes to the walking environment on travel mode.
Future work
The current study has a comprehensive dissemination plan, including publications and presentations to academics, practitioners and policy-makers. This focuses on analysing both the statistical and the qualitative data to (1) further interpret and explain the results relating to physical activity and travel mode, (2) examine contextual issues and (3) explore the wider determinants of workplace travel behaviour.
Acknowledgements
We would like to thank all of the workplaces and participants who contributed to this study. We are grateful to the following members of the Public Advisory Group: Julie Hughes, Martha Webb and Paul Coombs. Our thanks are also given to the Trial Steering Committee for its guidance and support throughout the study. Dr David Ogilvie (Programme Leader, Medical Research Council Epidemiology Unit, University of Cambridge) chaired the Trial Steering Committee. Dr Obi Ukoumunne (Associate Professor in Medical Statistics, University of Exeter) was the independent statistician and Dr Emma Frew (Reader in Health Economics, Institute of Applied Health Research, University of Birmingham) was the independent health economist. The other members of the Trial Steering Committee were Dr Kiron Chatterjee (Associate Professor in Travel Behaviour, University of the West of England), Dr Emma Adams (Research and Evaluation Manager, British Heart Foundation National Centre for Physical Activity and Health) and Natalie Grohmann (Environmental Science and Technology, Welsh Assembly Government). We would also like to acknowledge the contribution of Professor Martyn Standage, Claire Shovelton and Rhiannon Edwards (all University of Bath) and Professor Rona Campbell (University of Bristol).
This study was designed and conducted in collaboration with the BRTC, a UK Clinical Research Collaboration (UKCRC)-registered clinical trials unit in receipt of NIHR clinical trials unit support funding. Study data were collected and managed using REDCap (Research Electronic Data Capture),123 hosted at the University of Bristol.
The work was undertaken with the support the Centre for the Development and Evaluation of Complex Interventions for Public Health Improvement (DECIPHer), a UKCRC Public Health Research Centre of Excellence. Joint funding (reference MR/KO232331/1) from the British Heart Foundation, Cancer Research UK, Economic and Social Research Council, Medical Research Council, the Welsh Government and the Wellcome Trust, under the auspices of the UKCRC, is gratefully acknowledged.
Contributions of authors
Dr Suzanne Audrey (Senior Research Fellow in Public Health) was principal investigator and lead qualitative researcher, and drafted Chapters 1, 3–5 and 9.
Dr Harriet Fisher (Senior Research Associate in Mixed Methods) was the lead researcher on physical activity measurement, drafted Chapter 4 and contributed analyses for Chapter 6.
Professor Ashley Cooper (Physical Activity and Public Health) led the physical activity measurement and contributed to the analyses for Chapters 4 and 7.
Ms Daisy Gaunt (Senior Research Associate in Medical Statistics) conducted the statistical analyses of the outcome data, contributed to Chapter 2 and drafted Chapter 7.
Professor Chris Metcalfe (Medical Statistics) led the outcome evaluation and contributed to Chapters 2 and 7.
Ms Kirsty Garfield (Research Associate in Health Economics) analysed the health economic data and drafted Chapter 8.
Professor William Hollingworth (Health Economics) led the economic evaluation and contributed to Chapters 2 and 8.
Dr Sunita Procter (Trial Manager) co-ordinated the study activities and contributed to Chapters 1 and 5.
Dr Marie Gabe-Walters (Research Fellow) was the lead researcher in Swansea.
Dr Sarah Rodgers (Associate Professor) led the study at the Swansea University.
Dr Fiona Gillison (Senior Lecturer in Exercise and Health Psychology) led the study at the University of Bath.
Dr Adrian Davis (Visiting Professor and Independent Consultant in Health and Transport) contributed expertise in transport and health.
Mr Philip Insall (Lead Consultant at Insall & Coe) contributed lay expertise in active and sustainable transport.
All authors contributed to the design and conduct of the study.
Publications
Travel to Work: randomised controlled trial
Audrey S, Cooper A, Hollingworth W, Metcalfe C, Procter S, Davis A, et al. Study protocol: the effectiveness and cost effectiveness of an employer-led intervention to increase walking during the daily commute: the Travel to Work randomised controlled trial. BMC Public Health 2015;15:154.
Batista Ferrer H, Cooper A, Audrey S. Associations of mode of travel to work with physical activity, and individual, interpersonal, organisational, and environmental characteristics. J Transp Health 2018;9:45–55.
Audrey S, Fisher H, Cooper A, Gaunt D, Garfield K, Metcalfe C, et al. Evaluation of an intervention to promote walking during the commute to work: a cluster randomised controlled trial. BMC Public Health 2019;19:427.
Walk to Work: feasibility study
Audrey S, Procter S, Cooper AR. The contribution of walking to work to adult physical activity levels: a cross sectional study. Int J Behav Nutr Phys Act 2014;11:37.
Procter S, Mutrie N, Davis A, Audrey S. Participants’ views of using behaviour change techniques to encourage walking to work: a qualitative study. BMC Public Health 2014;14:868.
Audrey S, Procter S, Cooper A, Mutrie N, Hollingworth W, Davis A, et al. Employer schemes to encourage walking to work: feasibility study incorporating an exploratory randomised controlled trial. Public Health Res 2015;3(4).
Audrey S, Procter S. Employers’ views of promoting walking to work: a qualitative study. Int J Behav Nutr Phys Act 2015;12:12.
Data-sharing statement
All data requests should be submitted to the corresponding author for consideration. Access to available anonymised data may be granted following review.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care.
References
- Start Active, Stay Active. A Report on Physical Activity for Health From the Four Home Countries. London: Chief Medical Officer; 2011.
- Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Lancet Physical Activity Series Working Group . Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet 2012;380:219-29. https://doi.org/10.1016/S0140-6736(12)61031-9.
- UK Physical Activity Guidelines. London: Chief Medical Office; 2011.
- Global Recommendations on Physical Activity for Health. Geneva: WHO; 2010.
- Public Health England . 6 Million Adults Do Not Do a Monthly Brisk 10 Minute Walk 2017. www.gov.uk/government/news/6-million-adults-do-not-do-a-monthly-brisk-10-minute-walk (accessed 6 June 2018).
- Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U. Lancet Physical Activity Series Working Group . Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet 2012;380:247-57. https://doi.org/10.1016/S0140-6736(12)60646-1.
- Be Active, Be Healthy: A Plan for Getting the Nation Moving. London: DHSC; 2009.
- Wilmot EG, Edwardson CL, Achana FA, Davies MJ, Gorely T, Gray LJ, et al. Sedentary time in adults and the association with diabetes, cardiovascular disease and death: systematic review and meta-analysis. Diabetologia 2012;55:2895-905. https://doi.org/10.1007/s00125-012-2677-z.
- Jeon CY, Lokken RP, Hu FB, van Dam RM. Physical activity of moderate intensity and risk of type 2 diabetes: a systematic review. Diabetes Care 2007;30:744-52. https://doi.org/10.2337/dc06-1842.
- Kelly P, Kahlmeier S, Götschi T, Orsini N, Richards J, Roberts N, et al. Systematic review and meta-analysis of reduction in all-cause mortality from walking and cycling and shape of dose response relationship. Int J Behav Nutr Phys Act 2014;11. https://doi.org/10.1186/s12966-014-0132-x.
- Saunders LE, Green JM, Petticrew MP, Steinbach R, Roberts H. What are the health benefits of active travel? A systematic review of trials and cohort studies. PLOS ONE 2013;8. https://doi.org/10.1371/journal.pone.0069912.
- Rissel C, Curac N, Greenaway M, Bauman A. Physical activity associated with public transport use – a review and modelling of potential benefits. Int J Environ Res Public Health 2012;9:2454-78. https://doi.org/10.3390/ijerph9072454.
- Morris JN, Hardman AE. Walking to health. Sports Med 1997;23:306-32.
- Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, et al. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc 2000;32:498-504. https://doi.org/10.1097/00005768-200009001-00009.
- A Walking Strategy for Scotland: Consultation Document. Edinburgh: Scottish Executive Development Department; 2003.
- Walking and Cycling: An Action Plan. London: Department for Transport; 2004.
- A Walking and Cycling Action Plan for Wales. Cardiff: Welsh Assembly Government; 2008.
- Coote A. What health services could do about climate change. BMJ 2006;332:1343-4. https://doi.org/10.1136/bmj.332.7554.1343.
- National Travel Survey: England 2016. London: Department for Transport; 2017.
- Economic Assessment of Transport Infrastructure and Policies: Methodological Guidance on the Economic Appraisal of Health Effects Related to Walking and Cycling. Copenhagen: WHO; 2007.
- Hillsdon M, Foster C, Cavill N, Crombie H, Naidoo B. The Effectiveness of Public Health Interventions for Increasing Physical Activity Among Adults: A Review of Reviews. London: Health Development Agency; 2005.
- Kahn EB, Ramsey LT, Brownson RC, Heath GW, Howze EH, Powell KE, et al. The effectiveness of interventions to increase physical activity. A systematic review. Am J Prev Med 2002;22:73-107. https://doi.org/10.1016/S0749-3797(02)00434-8.
- Hillsdon M, Foster C, Thorogood M. Interventions for promoting physical activity. Cochrane Database Syst Rev 2005;1. https://doi.org/10.1002/14651858.CD003180.pub2.
- Ogilvie D, Egan M, Hamilton V, Petticrew M. Promoting walking and cycling as an alternative to using cars: systematic review. BMJ 2004;329. https://doi.org/10.1136/bmj.38216.714560.55.
- Scheepers CE, Wendel-Vos GCW, den Broeder JM, van Kempen EEMM, van Wesemael PJV, Schuit AJ. Shifting from car to active transport: a systematic review of the effectiveness of interventions. Transp Res Part A Policy Pract 2014;70:264-80. https://doi.org/10.1016/j.tra.2014.10.015.
- Dugdill L, Brettle A, Hulme C, McCluskey S, Long AF. Workplace physical activity interventions: a systematic review. Int J Workplace Health Manag 2008;1:20-4. https://doi.org/10.1108/17538350810865578.
- NICE Public Health Guidance 13. Promoting Physical Activity in the Workplace. Manchester: NICE; 2008.
- Malik SH, Blake H, Suggs LS. A systematic review of workplace health promotion interventions for increasing physical activity. Br J Health Psychol 2014;19:149-80. https://doi.org/10.1111/bjhp.12052.
- Tully MA, Panter J, Ogilvie D. Individual characteristics associated with mismatches between self-reported and accelerometer-measured physical activity. PLOS ONE 2014;9. https://doi.org/10.1371/journal.pone.0099636.
- Prince SA, Adamo KB, Hamel ME, Hardt J, Connor Gorber S, Tremblay M. A comparison of direct versus self-report measures for assessing physical activity in adults: a systematic review. Int J Behav Nutr Phys Act 2008;5. https://doi.org/10.1186/1479-5868-5-56.
- Vuillemin A, Rostami C, Maes L, Van Cauwenberghe E, Van Lenthe FJ, Brug J, et al. Worksite physical activity interventions and obesity: a review of European studies (the HOPE project). Obes Facts 2011;4:479-88. https://doi.org/10.1159/000335255.
- Arvidsson D, Kawakami N, Ohlsson H, Sundquist K. Physical activity and concordance between objective and perceived walkability. Med Sci Sports Exerc 2012;44:280-7. https://doi.org/10.1249/MSS.0b013e31822a9289.
- Sundquist K, Eriksson U, Kawakami N, Skog L, Ohlsson H, Arvidsson D. Neighborhood walkability, physical activity, and walking behavior: the Swedish Neighborhood and Physical Activity (SNAP) study. Soc Sci Med 2011;72:1266-73. https://doi.org/10.1016/j.socscimed.2011.03.004.
- Gordon-Larsen P, Boone-Heinonen J, Sidney S, Sternfeld B, Jacobs DR, Lewis CE. Active commuting and cardiovascular disease risk: the CARDIA study. Arch Intern Med 2009;169:1216-23. https://doi.org/10.1001/archinternmed.2009.163.
- Yang L, Panter J, Griffin SJ, Ogilvie D. Associations between active commuting and physical activity in working adults: cross-sectional results from the Commuting and Health in Cambridge study. Prev Med 2012;55:453-7. https://doi.org/10.1016/j.ypmed.2012.08.019.
- Davis A. Value for Money: An Economic Assessment of Investment in Walking and Cycling. Bristol: Department of Health and Social Care and Government Office of the South West; 2010.
- Ogilvie D, Foster CE, Rothnie H, Cavill N, Hamilton V, Fitzsimons CF, et al. Scottish Physical Activity Research Collaboration . Interventions to promote walking: systematic review. BMJ 2007;334. https://doi.org/10.1136/bmj.39198.722720.BE.
- Shaw R, Fenwick E, Baker G, McAdam C, Fitzsimons C, Mutrie N. ‘Pedometers cost buttons’: the feasibility of implementing a pedometer based walking programme within the community. BMC Public Health 2011;11. https://doi.org/10.1186/1471-2458-11-200.
- Sinnett D, Powell J. Fitter for Walking Economic Evaluation Report in Economic Evaluation of Living Streets’ Fitter for Walking Project. Loughborough: University of Loughborough; 2012.
- Health Inequalities. Third Report of Session 2008–09. London: House of Commons Health Committee; 2009.
- Paths for All . Our Support for Workplaces n.d. www.pathsforall.org.uk/pfa/walk-at-work/the-benefits-of-workplace-walking.html (accessed 6 June 2018).
- Michie S, Richardson M, Johnston M, Abraham C, Francis J, Hardeman W, et al. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: building an international consensus for the reporting of behavior change interventions. Ann Behav Med 2013;46:81-95. https://doi.org/10.1007/s12160-013-9486-6.
- Abraham C, Michie S. A taxonomy of behavior change techniques used in interventions. Health Psychol 2008;27:379-87. https://doi.org/10.1037/0278-6133.27.3.379.
- Michie S, Ashford S, Sniehotta FF, Dombrowski SU, Bishop A, French DP. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: the CALO-RE taxonomy. Psychol Health 2011;26:1479-98. https://doi.org/10.1080/08870446.2010.540664.
- Michie S, Abraham C, Whittington C, McAteer J, Gupta S. Effective techniques in healthy eating and physical activity interventions: a meta-regression. Health Psychol 2009;28:690-701. https://doi.org/10.1037/a0016136.
- Abraham C, Graham-Rowe E. Are worksite interventions effective in increasing physical activity? A systematic review and meta-analysis. Health Psychol Rev 2009;3:108-44. https://doi.org/10.1080/17437190903151096.
- Bird EL, Baker G, Mutrie N, Ogilvie D, Sahlqvist S, Powell J. Behavior change techniques used to promote walking and cycling: a systematic review. Health Psychol 2013;32:829-38. https://doi.org/10.1037/a0032078.
- Behaviour Change: Individual Approaches. NICE Public Health Guidance 49. Manchester: NICE; 2014.
- Audrey S, Procter S, Cooper A, Mutrie N, Hollingworth W, Davis A, et al. Employer schemes to encourage walking to work: feasibility study incorporating an exploratory randomised controlled trial. Public Health Res 2015;3.
- Developing and Evaluating Complex Interventions: New Guidance. London: Medical Research Council; 2008.
- Audrey S, Cooper AR, Hollingworth W, Metcalfe C, Procter S, Davis A, et al. Study protocol: the effectiveness and cost effectiveness of an employer-led intervention to increase walking during the daily commute: the Travel to Work randomised controlled trial. BMC Public Health 2015;15. https://doi.org/10.1186/s12889-015-1464-4.
- University of Birmingham . ICECAP-A 2015. www.birmingham.ac.uk/research/activity/mds/projects/HaPS/HE/ICECAP/ICECAP-A/index.aspx (accessed 19 December 2017).
- Labour Market Profile – South Gloucestershire. Newport: Office for National Statistics; n.d.
- South Gloucestershire Council . South Gloucestershire Economic Review, March 2017 n.d. www.southglos.gov.uk/Documents/COS70146.pdf (accessed 17 April 2019).
- Labour Market Profile – Bath Parliamentary Constituency. Newport: Office for National Statistics; n.d.
- Bath in Focus . Business Matters. Archived from the Original on 1 March 2012 n.d. www.web.archive.org/web/20120301081407/http://www.business-matters.biz/site.aspx?i=pg64 (accessed 17 April 2019).
- Labour Market Profile – Swansea. Newport: Office for National Statistics; n.d.
- Swansea Council . About Swansea 2019. www.swansea.gov.uk/keyfacts (accessed 19 December 2017).
- Labour Market Profile – Bristol, City of. Newport: Office for National Statistics; n.d.
- Labour Market Profile – Swindon. Newport: Office for National Statistics; n.d.
- Swindon Borough Council . Swindon Local Transport Plan 3: 2011–2026 Main Strategy 2011. www.swindon.gov.uk/download/downloads/id/3584/local_transport_plan.pdf (accessed 17 May 2019).
- Nomis Official Labour Market Statistics. Newport: Office for National Statistics; n.d.
- Neath Port Talbot County Borough Council . Regeneration n.d. www.npt.gov.uk/1308 (accessed 19 December 2017).
- Labour Market Profile – Newport. Newport: Office for National Statistics; n.d.
- Newport City Council . Newport City Council Local Transport Plan, January 2015 n.d. www.newport.gov.uk/documents/Transport-and-Streets/Local-Transport-Plan-January-2015.pdf (accessed 19 December 2017).
- Data Protection Act 2018. London: The Stationery Office; 2018.
- ISCRTN Registry . Travel to Work Study n.d. www.isrctn.com/ISRCTN15009100 (accessed 6 June 2018).
- Companies House . UK Standard Industrial Classification (SIC) Categories 2007 2008. www.gov.uk/government/publications/standard-industrial-classification-of-economic-activities-sic (accessed 6 June 2018).
- Audrey S, Fisher H, Cooper A, Gaunt D, Garfield K, Metcalfe C, et al. Evaluation of an intervention to promote walking during the commute to work: a cluster randomised controlled trial. BMC Public Health 2019;19. https://doi.org/10.1186/s12889-019-6791-4.
- Batista Ferrer H, Cooper A, Audrey S. Associations of mode of travel to work with physical activity, and individual, interpersonal, organisational, and environmental characteristics. J Transp Health 2018;9:45-5. https://doi.org/10.1016/j.jth.2018.01.009.
- Wetten AA, Batterham M, Tan SY, Tapsell L. Relative validity of 3 accelerometer models for estimating energy expenditure during light activity. J Phys Act Health 2014;11:638-47. https://doi.org/10.1123/jpah.2011-0167.
- Freedson PS, Melanson E, Sirard J. Calibration of the Computer Science and Applications, Inc. accelerometer. Med Sci Sports Exerc 1998;30:777-81. https://doi.org/10.1097/00005768-199805000-00021.
- Kerr J, Norman G, Godbole S, Raab F, Demchak B, Patrick K. Validating GPS data with the PALMS system to detect different active transportation modes. Med Sci Sports Exerc 2012;44:S25-9.
- Stopher P, FitzGerald C, Zhang J. Search for a global positioning system device to measure person travel. Transp Res Part C: Emerg Technol 2008;16:350-69. https://doi.org/10.1016/j.trc.2007.10.002.
- Panter J, Desousa C, Ogilvie D. Incorporating walking or cycling into car journeys to and from work: the role of individual, workplace and environmental characteristics. Prev Med 2013;56:211-17. https://doi.org/10.1016/j.ypmed.2013.01.014.
- Obesity: Preventing and Managing the Global Epidemic. Report of a WHO Consultation. Geneva: WHO; 2000.
- Panter J, Griffin S, Jones A, Mackett R, Ogilvie D. Correlates of time spent walking and cycling to and from work: baseline results from the commuting and health in Cambridge study. Int J Behav Nutr Phys Act 2011;8. https://doi.org/10.1186/1479-5868-8-124.
- Adams E, Bull F, Foster C. Are perceptions of the environment in the workplace ‘neighbourhood’ associated with commuter walking?. J Transp Health 2016;3:479-84. https://doi.org/10.1016/j.jth.2016.01.001.
- Ogilvie D, Mitchell R, Mutrie N, Petticrew M, Platt S. Perceived characteristics of the environment associated with active travel: development and testing of a new scale. Int J Behav Nutr Phys Act 2008;5. https://doi.org/10.1186/1479-5868-5-32.
- National Institute for Health and Care Excellence . Physical Activity: Walking and Cycling 2012. www.nice.org.uk/guidance/ph41/resources/physical-activity-walking-and-cycling-pdf-1996352901061 (accessed 6 June 2018).
- Gardner B, Lally P, Wardle J. Making health habitual: the psychology of ‘habit-formation’ and general practice. Br J Gen Pract 2012;62:664-6. https://doi.org/10.3399/bjgp12X659466.
- Procter S, Mutrie N, Davis A, Audrey S. Participants’ views of using behaviour change techniques to encourage walking to work: a qualitative study. BMC Public Health 2014;14. https://doi.org/10.1186/1471-2458-14-868.
- Carroll C, Rick J, Leaviss J, Fishwick D, Booth A. A qualitative evidence synthesis of employees’ views of workplace smoking reduction or cessation interventions. BMC Public Health 2013;13. https://doi.org/10.1186/1471-2458-13-1095.
- McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecological perspective on health promotion programmes. Health Educ Q 1988;15:351-77. https://doi.org/10.1177/109019818801500401.
- Audrey S, Procter S. Employers’ views of promoting walking to work: a qualitative study. Int J Behav Nutr Phys Act 2015;12. https://doi.org/10.1186/s12966-015-0174-8.
- Moore G, Audrey S, Barker M, Bond L, Bonell C, Hardeman Wl, et al. Process Evaluation of Complex Interventions. London: Medical Research Council Population Health Science Research Network; 2014.
- Ritchie J, Lewis J. Qualitative Research Practice: A Guide for Social Science Students and Researchers. London: Sage; 2003.
- Ward M, Rhodes C. Small Businesses and the UK Economy. Economic Policy and Statistics. London: House of Commons; 2014.
- Hart TL, Swartz AM, Cashin SE, Strath SJ. How many days of monitoring predict physical activity and sedentary behaviour in older adults?. Int J Behav Nutr Phys Act 2011;8. https://doi.org/10.1186/1479-5868-8-62.
- Travel to Work Statistical and Health Economics Analysis Plan Version 1.1 (21 April 2017). Bristol: University of Bristol; 2017.
- Kirkwood BR, Sterne JAC. Essential Medical Statistics. Oxford: Blackwell Science; 2003.
- The Automobile Association . The AA Schedule of Motoring Costs n.d. www.theaa.com/motoring_advice/running_costs/ (accessed 24 September 2017).
- Annual Survey of Hours and Earnings. 2016 Provisional Results. Newport: Office for National Statistics; 2016.
- Curtis L. Unit Costs of Health and Social Care 2016. Canterbury: Personal Social Services Research Unit, University of Kent; 2016.
- Curtis L. Unit Costs of Health and Social Care 2012. Canterbury: Personal Social Services Research Unit, University of Kent; 2012.
- NHS Reference Costs 2015–16. London: DHSC; 2016.
- Prescription Cost Analysis – England, 2016. Leeds: NHS Digital; 2017.
- NHS . Osteopathy 2017. www.nhs.uk/conditions/Osteopathy/Pages/Introduction.aspx (accessed 23 September 2017).
- NHS . Chiropractic 2017. www.nhs.uk/Conditions/chiropractic/Pages/Introduction.aspx (accessed 23 September 2017).
- Out-of-hours GP Services in England. London: National Audit Office; 2014.
- Turner J, O’Cathain A, Knowles E, Nicholl J, Tosh J, Sampson F, et al. Evaluation of NHS 111 pilot sites. Final Report to the Department of Health. Sheffield: Medical Care Research Unit, University of Sheffield; 2012.
- Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. PharmacoEconomics 1993;4:353-65. https://doi.org/10.2165/00019053-199304050-00006.
- Flynn TN, Huynh E, Peters TJ, Al-Janabi H, Clemens S, Moody A, et al. Scoring the Icecap-a capability instrument. Estimation of a UK general population tariff. Health Econ 2015;24:258-69. https://doi.org/10.1002/hec.3014.
- Craig R, Mindell J, Hirani V. Health Survey for England 2008: Physical Activity and Fitness. Leeds: National Information Centre; 2009.
- Mutikainen S, Helander E, Pietilä J, Korhonen I, Kujala UM. Objectively measured physical activity in Finnish employees: a cross-sectional study. BMJ Open 2014;4. https://doi.org/10.1136/bmjopen-2014-005927.
- Hagströmer M, Oja P, Sjöström M. Physical activity and inactivity in an adult population assessed by accelerometry. Med Sci Sports Exerc 2007;39:1502-8. https://doi.org/10.1249/mss.0b013e3180a76de5.
- Thompson D, Batterham AM, Peacock OJ, Western MJ, Booso R. Feedback from physical activity monitors is not compatible with current recommendations: a recalibration study. Prev Med 2016;91:389-94. https://doi.org/10.1016/j.ypmed.2016.06.017.
- McLellan G, Arthur R, Buchan DS. Wear compliance, sedentary behaviour and activity in free-living children from hip-and wrist-mounted ActiGraph GT3X+ accelerometers. J Sports Sci 2018;36:2424-30. https://doi.org/10.1080/02640414.2018.1461322.
- Tudor-Locke C, Barreira TV, Schuna JM. Comparison of step outputs for waist and wrist accelerometer attachment sites. Med Sci Sports Exerc 2015;47:839-42. https://doi.org/10.1249/MSS.0000000000000476.
- Chu AH, Ng SHX, Paknezhad M, Gauterin M, Koh D, Brown MS, et al. Comparison of wrist-worn Fitbit Flex and waist-worn ActiGraph for measuring steps in free-living adults. PLOS ONE 2017;12. https://doi.org/10.1371/journal.pone.0172535.
- Brockman R, Fox KR. Physical activity by stealth? The potential health benefits of a workplace transport plan. Public Health 2011;125:210-16. https://doi.org/10.1016/j.puhe.2011.01.005.
- Verplanken B, Walker I, Davis A, Jurasek M. Context change and travel mode choice: combining the habit discontinuity and self-activation hypotheses. J Environ Psychol 2008;28:121-7. https://doi.org/10.1016/j.jenvp.2007.10.005.
- Kohl HW, Craig CL, Lambert EV, Inoue S, Alkandari JR, Leetongin G, et al. Lancet Physical Activity Series Working Group . The pandemic of physical inactivity: global action for public health. Lancet 2012;380:294-305. https://doi.org/10.1016/S0140-6736(12)60898-8.
- Faulkner GE, Richichi V, Buliung RN, Fusco C, Moola F. What’s’ quickest and easiest?’: parental decision making about school trip mode. Int J Behav Nutr Phys Act 2010;7. https://doi.org/10.1186/1479-5868-7-62.
- Jain J, Line T, Lyons G. A troublesome transport challenge? Working round the school run. J Transp Geogr 2011;19:1608-615. https://doi.org/10.1016/j.jtrangeo.2011.04.007.
- Dalton AM, Jones AP, Panter JR, Ogilvie D. Neighbourhood, route and workplace-related environmental characteristics predict adults’ mode of travel to work. PLOS ONE 2013;8. https://doi.org/10.1371/journal.pone.0067575.
- Panter JR, Jones AP, van Sluijs EM, Griffin SJ, Wareham NJ. Environmental and psychological correlates of older adult’s active commuting. Med Sci Sports Exerc 2011;43:1235-43. https://doi.org/10.1249/MSS.0b013e3182078532.
- Cairns S, Newson C, Davis A. Understanding successful workplace travel initiatives in the UK. Transp Res Part A Policy Pract 2010;44:473-94. https://doi.org/10.1016/j.tra.2010.03.010.
- Guell C, Panter J, Ogilvie D. Walking and cycling to work despite reporting an unsupportive environment: insights from a mixed-method exploration of counterintuitive findings. BMC Public Health 2013;13. https://doi.org/10.1186/1471-2458-13-497.
- Goodman A, Sahlqvist S, Ogilvie D. iConnect Consortium . New walking and cycling routes and increased physical activity: one- and 2-year findings from the UK iConnect Study. Am J Public Health 2014;104:e38-46. https://doi.org/10.2105/AJPH.2014.302059.
- Panter J, Ogilvie D. iConnect consortium . Can environmental improvement change the population distribution of walking?. J Epidemiol Community Health 2017;71:528-35. https://doi.org/10.1136/jech-2016-208417.
- Song Y, Preston J, Ogilvie D. iConnect consortium . New walking and cycling infrastructure and modal shift in the UK: a quasi-experimental panel study. Transp Res Part A Policy Pract 2017;95:320-33. https://doi.org/10.1016/j.tra.2016.11.017.
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009;42:377-81. https://doi.org/10.1016/j.jbi.2008.08.010.
Appendix 1 Adverse event forms
Appendix 2 Employer recruitment leaflet and expression-of-interest form
Appendix 3 Information leaflet for employees
Appendix 4 Instructions for participants
Appendix 5 Walk to Work promoters’ information leaflet
Appendix 6 Walk to Work promoter’s booklet and diary
Appendix 7 Walk to Work promoters’ newsletters
Appendix 8 Participant newsletters
Appendix 9 Participant booklet
Appendix 10 Walk to Work employers’ pack
Appendix 11 Example of interview topic guide
List of abbreviations
- accGPS
- combined accelerometer and Global Positioning System
- ANOVA
- analysis of variance
- aOR
- adjusted odds ratio
- BCT
- behaviour change technique
- BMI
- body mass index
- BRTC
- Bristol Randomised Trials Collaboration
- CI
- confidence interval
- c.p.m.
- counts per minute
- DVD
- digital versatile disc
- GIS
- geographic information system
- GP
- general practitioner
- GPS
- Global Positioning System
- ICC
- intracluster correlation coefficient
- ICECAP-A
- ICEpop CAPability measure for Adults
- ID
- identifier
- MVPA
- moderate to vigorous physical activity
- NICE
- National Institute for Health and Care Excellence
- NIHR
- National Institute for Health Research
- OR
- odds ratio
- PHR
- Public Health Research
- RCT
- randomised controlled trial
- SD
- standard deviation
- UKCRC
- UK Clinical Research Collaboration