

Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 12/153/60. The contractual start date was in March 2014. The final report began editorial review in June 2018 and was accepted for publication in November 2018. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Russell M Viner is President of the Royal College of Paediatrics and Child Health. Stephen Scott reports grants from King’s College London during the conduct of the study. Chris Bonell is a member of Public Health Research Research Funding Board. Deborah Christie reports personal fees from Medtronic plc (Dublin, Ireland), personal fees from Pfizer Inc. (New York, NY, USA) and personal fees from ASCEND (Watford, UK), all unrelated to the submitted work.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2019. This work was produced by Bonell et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2019 Queen’s Printer and Controller of HMSO
Chapter 1 Introduction
Parts of this chapter have been reproduced with permission from Bonell et al. 1 This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Scientific background
The study protocol for this trial is available in full in Trials. 1 It is presented again here. Bullying, aggression and violence among children and young people are some of the most consequential public mental health problems apparent today. 2,3 The prevalence and harms of aggressive behaviours among young people makes addressing these a public health priority. 4–7 The World Health Organization (WHO) considers bullying to be a major adolescent health problem, defining this to include the intentional use of physical or psychological force against others. 5,8 This includes verbal and relational aggression that aims to harm the victim or their social relations, such as by spreading rumours or purposely excluding them. 9,10 Some definitions of bullying11 emphasise that bullying refers to abuse that is committed repeatedly over time and that involves a power imbalance between the perpetrator(s) and the victim. The prevalence of bullying among British young people (at around 33%)12 is above the European average,13 with approximately 25% of young people reporting that they have been subjected to serious peer bullying. 14 Cyberbullying, in particular, is rapidly becoming one of the most common forms of bullying. 15 There are marked social gradients: family deprivation and school-level deprivation increase the risk of experiencing bullying. 16 Bullying most commonly occurs in schools17,18 and prevalence varies significantly. 19–22
Being a victim of peer bullying has been associated with an increased risk of physical health problems;23,24 substance use;25–28 long-term emotional, behavioural and mental health problems;29–33 self-harm and suicide;34–36 and poorer educational attainment. 37,38 Students who experience physical, verbal or relational bullying regularly tend to experience the most adverse health outcomes. 39 There has also been evidence that childhood exposure to bullying and aggression may influence lifelong health through biological mechanisms. 23,29,40
The perpetrators of peer bullying are also at risk of a range of adverse emotional and mental health outcomes, including depression and anxiety. 13,19 Therefore, the prevention of bullying, aggression and violence is a major priority for public health and education systems internationally,3,41 with schools a key focus of policy initiatives to improve young people’s mental health and well-being. 42 In England,43 schools have a legal obligation to prevent bullying.
Bullying is often a precursor to more serious violent behaviours. One UK study44 of 14,000 students found that 1 in 10 young people aged 11–12 years reported carrying a weapon, and 8% of this age group admitted that they had attacked another with the intention of hurting them seriously. By the age of 15–16 years, 24% of students reported that they had carried a weapon and 19% had reported attacking someone with the intention of hurting them. 44 Interpersonal violence can cause physical injury and disability, and has been also associated with long-term emotional and mental health problems. Aggression refers to behaviour that is intended to harm, either directly or indirectly, another individual who does not wish to be harmed. 45 There are also links between aggression and antisocial behaviours in young people and violent crime in adulthood. 46,47 This is thought to result from low-level provocation and aggressive behaviours in secondary schools being educationally disruptive and emotionally harmful, and reducing educational attainments and later life chances, and therefore leading to more overt physical aggression over time. 48–50 The economic costs to society as a whole from bullying and violence are extremely high: the total cost of crime attributable to conduct problems in childhood has been estimated to be about £60B per year in England and Wales. 51
Reducing aggression, bullying and violence in British schools has been a consistent priority in public health and education policies. 52–54 The 2009 Steer Review50 concluded that schools’ approaches to discipline, behaviour management and bullying prevention vary widely and are rarely evidence based, and that further resources and research are urgently needed. There is, therefore, a pressing need to determine which interventions are effective in addressing bullying and aggression in schools, and to scale up such interventions to local and national school networks.
Whole-school-based interventions
A number of systematic reviews have assessed school-based interventions to address bullying and aggression. Interventions that promote change across school systems and address different levels of school organisation (i.e. ‘whole-school’ or ‘school environment’ interventions) are particularly effective in reducing victimisation and bullying in comparison with curriculum interventions. 55–57 ‘Whole-school’ or ‘school environment’ interventions are interventions that modify the systemic operations of schools, and they have been shown to have an impact on a range of health outcomes and risk behaviours. 57 A key element of these interventions appears to be increasing student engagement with school, particularly the most socially disadvantaged students, who are at the highest risk of poor health and educational outcomes. 58,59 Two trials have found that such approaches are associated with reductions in risk behaviours, including violence and antisocial behaviour. 60,61
The effectiveness of such interventions may be attributable to the way that they address bullying as a systemic problem meriting an ‘environmental solution’, rather than an individual student issue. 55 Whole-school interventions are also inherently universal in their reach and are likely to provide a cost-effective and non-stigmatising approach to preventing bullying. 56 This is in keeping with other evidence from the UK and internationally, which shows that schools promote health most effectively when they are not treated merely as sites for health education, but also as physical and social environments that can actively support healthy behaviours and outcomes. 62,63
Thus, these school environment interventions take a ‘socio-ecological’64 or ‘structural’65 approach to promoting health, whereby behaviours are understood to be influenced not only by characteristics of individuals, but also by the wider social context. A recent National Institute for Health Research (NIHR)-funded systematic review on the health effects of the school environment found evidence from observational and experimental studies that modifying the way in which schools manage their ‘core business’ (teaching, pastoral care and discipline) can promote student health and potentially reduce health inequalities across a range of outcomes, including reductions in violence and other aggressive behaviours. 63 Other outcomes that are improved by school environment interventions can include mental health and physical activity and reduced substance use, including alcohol, tobacco and drugs. 63
School environment interventions, therefore, are likely to be one of the most efficient ways of addressing multiple health harms in adolescence owing to their potential for modifying population-level risk as well as their reach and sustainability. 63 Multiple risk behaviours in adolescence are subject to socioeconomic stratification, and are strongly associated with poor health outcomes, social exclusion, educational failure, and poor mental health in adult life. 66 A recent King’s Fund report, Clustering of Unhealthy Behaviours Over Time, emphasised the association of multiple risk behaviours with mortality and health across the life-course, and the policy importance of reducing multiple risk behaviours among young people through new interventions that address their common determinants. 67
The INCLUSIVE (initiating change locally in bullying and aggression through the school environment) trial aims to evaluate the Learning Together (LT) intervention. This has been particularly informed by two international evidence-based school environment programmes. The first is the Aban Aya Youth Project (AAYP),61 a multicomponent intervention enabling schools to modify their social environment as well as delivering a social skills curriculum. This approach was designed to increase social inclusion by ‘rebuilding the village’ within schools serving disadvantaged, African American communities. To promote whole-school institutional change at each school, teacher training was provided and an action group (AG) was established (comprising both staff and students) to review policies and prioritise the actions needed to foster a more inclusive school climate. Among boys, the intervention was associated with significant reductions in violence and aggressive behaviour. 61 The intervention also brought benefits in terms of reduced sexual risk behaviours and drug use, as well as provoking behaviour and school delinquency. Second, the Gatehouse Project60,68 in Australia also aimed to reduce health problems by changing the school climate and promoting security, positive regard and communication among students and school staff. As with the AAYP, an AG was convened in each school, facilitated by an external ‘critical friend’ and informed by data from a student survey, alongside a social and emotional skills curriculum. A randomised controlled trial (RCT) found consistent reductions in a composite measure of health risk behaviours, which included violence and antisocial behaviour.
Process evaluation of whole-school health interventions
Most evaluations of interventions taking a whole-school approach to preventing violence and promoting health in schools examine outcomes rather than processes. 63,69 The process evaluation of the Gatehouse Project, which greatly informed LT, found that school staff perceived the various components (needs survey, action team, external facilitator) to function synergistically. Although specific actions varied between schools, these were completed with good fidelity. Implementation was facilitated by supportive school management and the broad participation of staff and students. 70,71 However, this evaluation did not attempt to assess systematically how the completeness of the implementation might have been influenced by schools’ baseline social climate.
The Healthy School Ethos intervention was also informed by the Gatehouse Project and included several elements similar to LT, but without a curriculum or any restorative practice elements. 72,73 Using a structured process modelled closely on the Gatehouse Project, it aimed to enable schools involved in pilots in south-east England to carry out locally determined actions to increase students’ sense of security, positive self-regard, and communication with staff and students. The intervention provided an external facilitator, survey data on student needs and training, and enabled schools to convene action teams to determine priorities and ensure delivery. Students and staff co-revised rules for appropriate conduct and revised policies on bullying and student feedback. Staff were trained to improve classroom management. Process evaluation reported that the intervention was delivered with good fidelity. Locally determined actions (e.g. peer-mediators) were generally more popular than mandatory actions. Implementation was more feasible when it built on aspects of schools’ baseline ethos and when someone on the senior leadership team (SLT) led actions. Student awareness of the intervention was high. Student accounts suggested that benefits might arise as much from participation in intervention processes, such as rewriting rules, as from the effects of subsequent actions. Some components reached a large proportion of students. 72,73
Before the current Phase III trial, the LT intervention had been piloted in four schools. 74 Overall, school staff members were consistently supportive. Although some schools were already deploying some restorative approaches, the intervention was nonetheless attractive because it enabled restorative practices to be delivered more coherently and consistently across the school. The adaptability of the intervention, in contrast to overly prescriptive, ‘one-size-fits-all’ interventions, was also a strong motivating force and a source of acceptability to school managers. Staff valued the ‘external push’ that was provided by the external facilitator. The intervention was highly acceptable to school staff because of its fit with national policies and school metrics focused on attendance and exclusions. Some staff reported that it took time for them to understand how the various intervention components joined up, and this could have been better explained from the outset. Staff were positive about sustainability, with some reporting that activities would continue after the pilot was completed.
Regarding particular components, staff reported that the needs assessment report allowed them to see the ‘big picture’ and identify priorities, but some suggested that the needs assessment could also feel too ‘negative’ at times, especially among established staff, who sometimes viewed this as a reflection on their work at the school. Negative aspects of the needs report could also present problems for schools, because if they were inspected by the Office for Standards in Education, Children’s Services and Skills (Ofsted) they would be expected to share the results with the inspectors. As with the HSE (Healthy School Ethos) evaluation, AGs were viewed positively, and it was suggested that student participation may be an active ingredient in improving relationships and engagement across the school, particularly when these involved students who might be less committed to school and might be involved in antischool peer groups. Again, the presence of a SLT member on the group was seen as critical to driving actions forward. The training, however, was more critically received, with many staff suggesting that this was too didactic and contained too few examples from secondary schools. All schools successfully implemented the curriculum, welcoming its flexibility whereby modules could be implemented using the newly provided or existing materials. The pilot lacked a large enough sample to examine how implementation and processes might vary across a range of different school contexts, and focused only on the first year of implementation, so it could not examine the processes by which the intervention might become normalised within schools’ institutional policies and practices and be sustained once external facilitation is withdrawn.
Restorative justice
The INCLUSIVE trial extends the AAYP and Gatehouse interventions by including a ‘restorative justice’ approach. The Steer Review50 in 2009 called for English schools to consider adopting more restorative approaches to preventing bullying and other aggressive behaviour to help minimise the harms associated with such problems. The central tenet of such approaches is repairing the harms caused to relationships and communities by criminal behaviour, rather than merely assigning blame and enacting punishment. Such approaches have now been adapted for use in schools and can operate at a whole-school level, informing changes to disciplinary policies, behaviour management practices, and the way in which staff communicate with students in order to improve relationships, reduce conflict and repair harm.
Restorative practice aims to prevent and/or resolve conflicts between students or between staff and students to prevent further harms. 75 It enables victims to communicate the impact of the harm to perpetrators, and for perpetrators to acknowledge and take steps to remedy this in order to avoid further harms. Restorative practice can involve methods to prevent incidents (e.g. ‘circle-time’, which brings students together with their teacher during registration periods or other lessons to maintain good relationships) and/or to resolve incidents (e.g. ‘conferencing’, bringing together relevant staff, students, and, where necessary, parents and external agencies such as police or social services). Restorative practice aims to prevent the occurrence or continuation not only of bullying but also of other forms of aggression and classroom disruption. Restorative practice can be delivered instead of, or alongside, more traditional punitive discipline. 76
The theoretical basis for restorative approaches has much in common with the theory of human functioning and school organisation. 59 It is theorised that the process of students coming together, discussing the harm, and working towards a reparative plan develops perpetrators’ competency through accepting responsibility for the actions and contributing to a reparative solution, and develops offenders’ understanding of the realities of others. Victims are also empowered in this process as they become an active participant in the decision-making process, and the acknowledgement of the offenders’ ability to offer some healing to the victim (e.g. via an apology or carrying out a sanction) gives dignity to both parties. This resonates with the ideas of improving relationships as well as promoting practical reasoning and sense of connection to school. By eliciting accountability for the harm caused to the victim and the school community and negotiating a plan for restitution, the young person is encouraged to reclaim an identity as a participant of the school community, not a peripheral outsider. 76 Through this process, the young people involved develop relational competency, and enhance their relationships with staff and other students by improving their ability to empathise and communicate effectively. Restorative approaches might indeed be particularly suitable for ‘alienated’ student offenders as they are given the opportunity to develop the necessary competencies to participate as a responsible member of the school community from which previously they might have felt excluded. 77 It may also be particularly helpful for female young people, as gender theory suggests that female adolescent identity is often based within a framework of relationship and connection. Thus, application of the principles of restorative approaches becomes a natural adjunct to the therapeutic process of self-identity and growth. 77
However, to date, restorative approaches in schools have been evaluated using only non-randomised designs, and systematic reviews have called for more rigorous evaluations of restorative practice in schools. 78 Those studies that have been carried out do suggest that the restorative approach is promising both in the UK79–81 and internationally,82–84 particularly when implemented at the whole-school level. For example, in England and Wales, the Youth Justice Board evaluated the use of restorative approaches at 20 secondary schools and six primary schools, and reported significant improvements in students’ attitudes to bullying and reductions in offending and victimisation in schools that adopted a whole-school approach to restorative practice. Restorative approaches thus appear to have the potential to complement school-environment interventions such as Aban Aya and the Gatehouse Project. They offer a highly promising way forward for reducing aggressive behaviours among British young people. A 2009 Cochrane review85 found no RCTs of interventions employing restorative approaches to reduce bullying in schools and recommended that this be a priority for future research.
Process evaluations report positive results in terms of feasibility and acceptability of restorative practices in schools. In New Zealand,86 case studies of five secondary schools and colleges found that all teachers valued restorative practice and felt that it was a good strategy for managing misbehaviour. In a pilot in London schools,87 students in schools that had implemented restorative practice reported that their school was doing a good job of stopping bullying. Teachers reported that most restorative meetings were effective at addressing bullying, gossiping, and disagreements between students and teachers.
Common challenges reported in process evaluations of restorative practice in schools include consistency in the way restorative practice is implemented. 82,88,89 Evaluations also suggest that restorative practice is implemented most successfully when it is delivered as part of a whole-school approach, when a positive ethos has been established, and when one-to-one problem-solving skills (e.g. listening and responsibility) have been introduced into the curriculum. 90,91
Social and emotional education
Social and emotional education aims to educate students not merely academically but using non-cognitive social skills and emotional self-management skills to enable young people to function at school and in other areas of life and to develop resilience or ‘grit’. There was evidence that classroom curricula that teaches young people the skills needed to manage their emotions and relationships can enhance social relationships, improve mental health and reduce bullying. 92 Many whole-school interventions, including the Aban Aya93 and Gatehouse60 interventions, also include social and emotional education elements, the intention being that these act synergistically with other components, helping students to take part in intervention activities within and beyond the classroom.
Objectives and hypotheses
In 2014, we developed the LT intervention, which aimed to modify the school environment by involving students, building better relationships, using restorative approaches, and developing social and emotional skills to reduce a range of risk behaviours including bullying and aggression. 74 The intervention combined AGs of staff and students to modify the whole-school environment; training for staff to implement restorative approaches; and a social and emotional skills curriculum. These components were intended to address school- and individual-level determinants of bullying and aggression and to be synergistic with one another: the AG ensuring that schools took a whole-school approach to restorative practice and the social and emotional skills curriculum enabling students to participate actively in AGs and restorative practices.
A pilot cluster RCT in eight schools met all of the prespecified feasibility and acceptability criteria. 74 We report here the findings of a full-scale cluster RCT of LT (the INCLUSIVE trial).
We hypothesised that in secondary schools randomly allocated to receive LT there would be lower rates of self-reported bullying and perpetration of aggression among students aged 14–15 years at the 36-month follow-up.
We hypothesised that at the 36-month follow-up student and staff secondary outcomes would be improved in intervention compared with control schools. More specifically, we expected improvements in students’ quality of life (QoL), well-being, psychological function and attainments; reductions in school exclusion and truancy, substance use, sexual risk, NHS use and police contacts among students; and improvements in staff QoL and attendance and reductions in staff burn-out.
We hypothesised that individual-level student socioeconomic status (SES), sex, and school-level stratifying factors (single-sex vs. mixed-sex school, school-level deprivation, and value-added strata) would moderate the effectiveness of the intervention for student outcomes.
We also hypothesised that LT would be cost-effective compared with standard school practice in terms of student quality-adjusted life-years (QALYs) and costs.
Chapter 2 Methods
Parts of this chapter have been reproduced with permission from Bonell et al. 1 This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Trial design
We undertook a two-arm repeat cross-sectional cluster 1 : 1 RCT of the LT trial with an integral economic and process evaluation in 40 secondary schools in south-east England, with schools as the unit of allocation. 1 Our study population consisted of all students in the school at the end of year 7 (aged 11–12 years) at baseline, and at 24-month (end of year 9; aged 13–14 years) and 36-month (end of year 10; aged 14–15 years) follow-up, as well as school teaching and teaching assistant staff at each time point.
Refinements to the trial informed by the pilot
The changes made to the trial informed by the pilot included:
-
identifying the Gatehouse Bullying Scale (GBS) and Edinburgh Study of Youth Transitions and Crime (ESYTC) school misbehaviour subscale as primary outcomes of bullying victimisation and perpetration of aggressive behaviours, respectively
-
including validated measures of drug use, sexual behaviour and educational attendance and attainment as additional secondary outcomes
-
including all ‘state’ schools in the recruitment pool of schools to reflect the overall population profile of schools in south-east England
-
using existing school networks to facilitate timely recruitment
-
using revised timetabling – project initiation in February of the preceding school year, surveys of staff and students to be conducted in the summer term each year, timetabling of intervention and staff training to be undertaken prior to September school-year start
-
enhancing quantitative data on intervention fidelity, including structured independent assessments of intervention delivery
-
undertaking an economic evaluation to use the Child Health Utility 9D (CHU9D) scale and to be supplemented with a cost–consequences analysis.
Refinements to the trial after commencement
During the development of the trial, the following changes to the protocol were made:
-
A meaure of bullying perpetration (the Modified Aggression Scale Bullying subscale) was included after the baseline survey as we elected to add a measure of bullying perpetration as well as one of victimisation.
-
We included administrative documents (e.g. minutes, attendance sheets, training satisfaction feedback) in our assessment of trial arm fidelity to provide us with a wider range of quantifiable data.
The protocol was amended during the trial to refine the methods used. All amendments were approved by the independent study steering committee and the funder of the trial (NIHR). The only change to trial outcomes was the addition of a measure of bullying perpetration (secondary outcome). All refinements were completed before the 36-month surveys were collected and before any trial analyses were conducted.
Participants
The INCLUSIVE trial was a universal intervention aimed at all 11- to 16-year-olds in participating secondary schools in England. Although the intervention was expected to have effects on the whole school, our study population consisted of students at the end of year 7 (aged 11–12 years) at baseline and at the end of year 10 at the 36-month follow-up (aged 14–15 years), as well as all school teaching and teaching assistant staff. This year group should have experienced the intervention for 3 years, including the classroom curriculum for years 8–10. All students in the school in that year and all teaching staff were surveyed at each time point, not only those who participated at baseline.
Eligibility criteria for participants
Participant eligibility was assessed at the school level. Eligible schools were:
-
Secondary schools within the state education system (including community, academy or free schools, and mixed- or single-sex schools) in south-east England. We took the widest definition of a ‘state school’ and excluded only private schools, schools exclusively for those with learning disabilities and pupil referral units. The last two were excluded as the INCLUSIVE study was unlikely to be appropriate for their populations.
-
Schools whose most recent school quality rating by Ofsted was ‘requires improvement’/‘satisfactory’ or better. Schools with an ‘inadequate’/‘poor’ rating were excluded, as these schools would be subject to special measures that were likely to impede LT delivery.
Eligible schools were approached initially by letter and e-mail, with a telephone follow-up, complying with good practice and research governance for undertaking studies within the education system.
As the intervention was delivered at the whole-school level, there were no specific eligibility criteria for students, although parents who did not want their child to participate in the surveys were able to opt out on behalf of their child.
Settings and locations
Schools were recruited between March and June 2014 from secondary schools in Greater London and the surrounding counties (Surrey, Kent, Essex, Hertfordshire, Buckinghamshire and Berkshire) that had a maximum travel time of 1 hour from the study centres in London. To aid recruitment, we partnered with existing school networks, such as the University College London (UCL) Partners Schools Network and the Institute of Education Teaching Schools, and schools that are part of our collaborating schools network, Challenge Partners. We approached approximately 500 eligible schools, initially by letter and e-mail and with a telephone follow-up.
The 40 participating schools did not differ from 450 non-recruited schools in terms of school size, population, deprivation, student attainment or value-added education. However, participating schools were more likely to have an Ofsted rating of good or outstanding (see Appendix 1, Table 26).
Intervention
The INCLUSIVE trial involved 2 years of externally facilitated intervention and a final year without external facilitation. The LT intervention was intended principally to augment, rather than to replace, existing activities (e.g. training and curricula) in intervention schools. However, it was intended to replace existing non-restorative disciplinary school policies and practices when the AG deemed restorative approaches more appropriate. The intervention logic model is shown in Appendix 1 (see Figure 6).
Below we describe the intervention informed by the TIDieR (Template for Intervention Description and Replication) checklist for better intervention reporting. 94 Fidelity assessment is described under process evaluation, the product of which is presented in our results.
Learning Together
Theory of change
Informed by Markham and Aveyard’s59 theory of human functioning and school organisation, the intervention’s theory of change suggests that for young people to choose healthy behaviours over risky behaviours, such as bullying, aggression or substance use, they must possess the autonomy, motivation and reasoning ability to make informed decisions. These capacities and goals are theorised as facilitated by increased engagement with education (the school’s ‘instructional order’) and connection to the school community (the school’s ‘regulatory order’). It is theorised that schools can increase such engagement by improving relationships between students and teachers, between different groups of student and between academic education and broader student development, as well as by reorienting learning and teaching, discipline, social support, and school management and organisation so that these centre on student needs and view conflict as an opportunity for learning. The intervention aims to strengthen relationships between and among staff and students through the use of primary (preventing conflict) and secondary (preventing the escalation of conflict) forms of restorative practice, and by enabling staff and students to work together on an AG co-ordinating intervention delivery in each school (see Appendix 1, Figure 6). AGs also aim to enable student participation in decision-making. Restorative practice aims to increase students’ active participation in discipline systems. A social and emotional skills curriculum delivered in classrooms aims to promote student autonomy and reasoning ability, and to facilitate student participation both in AGs and in restorative practice.
Materials
Schools allocated to receive the intervention were provided with various resources. School staff were offered training in restorative practices, with participants given written summaries of the material covered in training. Schools were provided with a manual to guide the convening and running of an AG. For the first 2 years of the intervention, schools were provided with an external facilitator for the AG. Schools were sent a report on student needs detailing findings from a survey of students aged 11–12 years about their attitudes to and experiences of school, and their experiences of bullying, aggression and other risk behaviours (see Appendix 3). Schools were provided with written lesson plans and slides to guide delivery of a classroom-based social and emotional skills curriculum.
Procedures
Training was given to all staff, and in-depth training was given to selected staff, including training in formal ‘conferencing’ to deal with more serious incidents.
Action groups
Action groups were required to include, at a minimum, six students from the intervention classes (year 7 at the start of the intervention) and six members of staff, including at least one from the senior management team and one member of each of the teaching, pastoral and support staff. Having a member from specialist health staff, such as the school nurse and/or local child and adolescent mental health services staff, was desirable but optional. The AG was required to meet at least six times per school year (approximately once every half-term), and was tasked with developing action plans to co-ordinate the delivery of the intervention outputs:
-
reviewing and revising school rules and policies relating to discipline, behaviour management and staff-student communication to incorporate restorative principles
-
implementing restorative practices throughout the school to prevent and respond to bullying and aggression
-
additional tailored actions to address local priorities
-
delivering the social and emotional skills curriculum for years 8–10.
The facilitator ensured that meetings were scheduled, and attended these to ensure that the meetings were participative and focused on deciding and implementing actions. These actions were informed by findings about their students’ experiences of bullying, aggression and the school environment from our baseline survey (conducted before randomisation) and from a 12-month survey of students at the end of year 8 (aged 12–13 years) in intervention schools only, as well as from the 24-month trial survey. In year 3, facilitation was to be internally led by the AG’s chairperson, usually a SLT member or another experienced staff member. External facilitation in the first 2 years was theorised to be important to enable schools to initiate changes and particularly to empower students to participate in decisions. In year 3, schools were expected to facilitate implementation internally so that the trial could assess whether or not the intervention could be sustained by schools in the absence of an external facilitator.
Social and emotional learning curriculum
Schools delivered classroom-based social and emotional skills education in ‘stand-alone’ lessons, for example ‘personal, social and health education’ (PSHE) lessons, and/or integrated it into tutor time or various subject lessons (e.g. English) to students in the trial cohort as they moved through years 8–10 (aged 12–15 years). They received 5–10 hours of teaching and learning per year on restorative practices, relationships, and social and emotional skills based on the Gatehouse Project curriculum. 60
Schools selected modules for each year from establishing respectful relationships in the classroom and the wider school; managing emotions; understanding and building trusting relationships; exploring others’ needs and avoiding conflict; and maintaining and repairing relationships.
Restorative practice
Primary restorative practices delivered in schools in all three years involved staff using restorative language (the respectful use of language to challenge or support behaviour in a manner that preserves or enhances the relationship) and circle time (classes coming together to discuss their feelings and air any problems so that these may be addressed before they escalate) underpinned by supportive school rules and policies and the social and emotional skills curriculum. Circle time takes place in an informal setting, and is overseen by a member of staff; it provides an opportunity for a class to discuss their relationships in the open. It could be undertaken during registration periods or other lessons and aims to maintain good relationships, or deal with specific problems, as well as making the whole class aware of the issues and responses ongoing.
Secondary restorative practices involve some staff implementing restorative conferences (the parties to a conflict being invited to a facilitated face-to-face meeting to discuss the incident and its impact on the victim and for the perpetrator to take responsibility for their actions and avoid further harms). Conferencing was suggested for use in more serious incidents; this is a more ‘one-on-one’ practice of restorative justice, which brings together relevant staff, students, parents and, where necessary, external agencies to discuss ongoing issues between students.
Training
Staff training was implemented to ensure that teachers understood the necessary skills to engage in restorative practice. Training was provided by trainers accredited by the UK’s Restorative Justice Council. Each school had its own named facilitator, who was a freelance consultant with experience of school leadership or organisational change, co-ordinated by a lead facilitator who trained them in the intervention theory and methods. AGs comprised at least six staff members (including one member of the school’s SLT and one member of the school’s teaching, student support and administrative staff) and at least six students from each school, led by a member of the school’s SLT with support from the external facilitator in the first two years of the intervention but not in the third year. All of these staff attended the all-staff training and some attended the in-depth training. Staff who received basic training in restorative practice implemented this in the form of the use of restorative language and circle time. In addition, 5–10 staff members at each school who received in-depth training in restorative practice implemented this in the form of restorative conferences. The curriculum was delivered by teachers who specialised either in PSHE or in other subjects guided by lesson plans.
Modes of delivery
All intervention components were delivered face to face.
Location
All components were delivered on school premises.
Dose
Training occurred in the first year of intervention, comprising half a day for all staff plus in-depth 3-day training for 5–10 staff members at each school. AGs met six times per year in all 3 years. Restorative practices were delivered as frequently as required in each school. In their curriculum, students received 5–10 hours of teaching per year.
Planned adaptations
The intervention enabled local tailoring, informed by the needs survey and other local data sources. AGs ensured that implementation in their school was appropriate to local needs as identified by members and the survey of student needs. This included ensuring that revisions to policies and rules built on existing work, deciding which curriculum modules to deliver in each year, and implementing locally decided actions aiming to improve relationships and student participation (e.g. cascading restorative practice training to staff who had not attended or to student peer mentors).
Unplanned modifications
There were no unplanned modifications.
Comparator: control schools
Schools randomised to the control group continued with their normal practice and received no additional input. The sample of schools was spread over a wide geographical area and there were no cases in which intervention and control schools were near one another. Head teachers and a small number of staff in control schools were aware that the school was participating in a trial that was described as the INCLUSIVE trial. These individuals were not informed that the name of the intervention was LT and were not informed about the detailed contents of the intervention during recruitment. It is therefore unlikely that schools in the intervention and control arms would have shared information about the intervention.
Assessment and follow-up
Assessment of effectiveness
Student primary and secondary outcomes were assessed at 36 months, at the end of year 10 (when the students were aged 14–15 years), with a baseline survey having been undertaken at the end of year 7 (when the students were aged 11–12 years). Staff secondary outcomes were also assessed at 36 months. Additional student and staff surveys were conducted at 24 months to assess intervention process and intermediate outcomes to be used in the mediation analysis. Student surveys were conducted in exam conditions in schools, maximising privacy. The questionnaires used to collect these data can be found in full in the supplementary material (see Report Supplementary Material 1).
All students in the school in that year and all teachers and teaching assistant staff were surveyed at each time point, not only those who participated at baseline. Paper-based questionnaires were completed confidentially in a 45-minute class session devoted to that purpose. Field workers supervised the class as they completed the questionnaire, with the teacher present (for disciplinary purposes) but unable to see the questionnaires. The field workers assisted students with questions that they did not understand and ensured that the students completed as much of the questionnaire as possible. Students with mild learning difficulties or with limited command of written English were supported by field workers to complete the questionnaires.
We assessed the potential for measurement error and bias by asking the students completing surveys if their responses to questionnaires were completely truthful. We asked students in intervention schools involved in qualitative interviews whether or not their reporting (as opposed to their experience) of bullying and aggression might have been affected by the intervention.
Staff data were often collected on the same days as student data. However, owing to the busy nature of their work, staff questionnaires were often left at the school to be done in private time, and then mailed back to the study team. Staff were allowed to fill in their questionnaires in the staff breakroom, or to take them home to fill in.
Data management
The study centre received class lists for each school in advance of each survey. Participants were allocated a unique identifier (ID) prior to each survey and this ID was recorded on the questionnaire. All questionnaires were anonymous. Questionnaires were completed in classrooms and completed questionnaires were collected in schools on the day of the survey. If a participant was not in school on the day of the survey, a questionnaire was left at the school for them to complete later and was returned to the study centre by post. Completed questionnaires were transported from the school by study personnel to the study centre, where they were stored in a locked room.
Questionnaires were then securely transported for data entry by a third party, where they were double-entered into a database by trained personnel. Each questionnaire was checked at the time of data entry for any handwritten comments. Questionnaires with any additional text, regardless of content, were scanned, and password-protected scans were sent to the study team for safety reporting assessment. Electronic data generated from data entry were transferred via password-protected secure FTP and stored on secure servers at the London School of Hygiene & Tropical Medicine (LSHTM).
Following data entry, questionnaires were securely transported to the LSHTM Clinical Trial Unit (CTU) for archiving. An inventory of all questionnaires was maintained by LSHTM CTU.
Electronic data generated from data entry were transferred via password-protected secure FTP and stored on secure servers at LSHTM. Relevant trial documentation will be kept for a minimum of 15 years after study completion.
Ethics arrangements
The trial was approved by the UCL Ethics Committee (reference 5248/001). Ethics arrangements were informed by recent guidance on ethical issues in cluster RCTs.
Informing participants
Details of the research, including the possible benefits and risks, were provided to schools through written information and personal meetings and were provided to student participants through age-appropriate written information.
Consent
Written, informed consent was obtained at school level (chairperson of governors; head teacher) for random allocation and for the intervention, and at the individual student, staff and intervention facilitator level for data collection. For students, written age-appropriate information sheets were provided in class 2–4 weeks before the baseline survey, together with oral explanation by teachers. Written consent was required from all participating young people, which was collected immediately before conducting the baseline survey. Young people were also asked to take home written information sheets for their parents. Parents who did not want their child to participate were asked to notify this opt-out in writing using a prepared form. This ‘opt-out’ consent is standard practice in trials in secondary schools and was used in our pilot study, proving acceptable to schools, young people and families. Only < 1% of parents exercised an opt-out.
Information sheets and consent forms for student surveys were identical in intervention and control schools and did not refer to the intervention. Parents were informed about the study and could withdraw their children from research activities.
Duty of care and confidentiality
The researchers were experienced with the specific ethical issues involved in undertaking research with young people and other vulnerable participants. All work was carried out in accordance with the requirements of the Data Protection Act 1998. 95 Data storage and IT (information technology) systems were secure. All information remained confidential within the research team, except when child protection issues were raised. We consulted with a child protection social worker to define the issues that would prompt an exemption. The chief investigator, Russell Viner, as a paediatrician with training in child safeguarding, oversaw actions when safeguarding concerns were raised, and sought further advice, when necessary, from appropriate authorities. We followed Economic and Social Research Council ethics guidance and sought research ethics approval from the appropriate bodies. We also sought policy approval from local authorities related to each participating school.
Ethics review
Approval for the study was sought and obtained from the research ethics committees of the two lead universities, LSHTM and UCL. Our trial complied with the Economic and Social Research Council research ethics framework.
Assessment of harms
There were no anticipated risks to participants or to schools. However, as with all interventions, there may have been unanticipated risks. Harms were assessed by examining outcomes at 24 and 36 months. An independent Data Monitoring Committee (DMC) examined any potential harms at 24 months. If any major harms were detected, the DMC was to inform the Trial Steering Committee (TSC), which would decide what action should be taken.
Outcomes
Primary outcomes
Outcomes were collected by a research team (led by RV) independent of the intervention team. The primary outcomes were self-reported experience of bullying victimisation and perpetration of aggression measured at 36 months. The questionnaires used to collect these data can be found in full in Report Supplementary Material 1.
-
Bullying victimisation was assessed with the GBS, a 12-item validated96 self-report measure of being the subject of teasing, name-calling or rumours, being left out of things, and receiving physical threats or actual violence from other students within the previous 3 months. The questions and responses were worded to ensure that these assessed bullying occurring either face to face or online. Students reported the frequency of and upset related to each experience. Items were summed to make a total bullying score (higher scores represented more frequent upsetting bullying, with a maximum score of 3).
-
Perpetration of aggressive behaviour was measured using the ESYTC school misbehaviour subscale, a 13-item scale measuring self-reported aggression towards students and teachers. Each item was coded as occurring hardly ever or never, less than once per week, at least once per week, or most days. Items were summed to provide a total score, with higher scores indicating greater aggressive behaviour (maximum score of 39). 97
Secondary outcomes
The GBS and ESYTC outcomes were measured at 24 months as secondary outcomes. In addition, we measured the following at 24 and 36 months.
Student-level self-report outcomes
These were measured through student survey self-reports.
Quality of life
The Paediatric Quality of Life Inventory (PedsQL) version 4.0 was used to assess overall QoL. The 30-item PedsQL has been shown to be a reliable and valid measure of QoL in normative adolescent populations. 98 It consists of 30 items representing five functional domains – physical, emotional, social, school and well-being – and yields a total QoL score, two summary scores for ‘physical health’ and ‘psychosocial health’, and three subscale scores for ‘emotional’, ‘social’ and ‘school’ functioning.
Health-related quality of life
The CHU9D, a validated, age-appropriate measure of students’ health-related quality of life (HRQoL),99 was used to inform the economic evaluation.
Psychological function and well-being
The Strengths and Difficulties Questionnaire (SDQ)100 is a brief screening instrument for detecting behavioural, emotional and peer problems and prosocial strengths in children and adolescents. It is brief, quick to complete and validated in national UK samples.
The Short Warwick–Edinburgh Mental Well-Being Scale (SWEMWBS)101 is a seven-item scale designed to capture a broad concept of positive emotional well-being, including psychological functioning, cognitive-evaluative dimensions, and affective-emotional aspects, with a total ‘Well-Being Index’ generated.
Risk behaviours
Substance use
Smoking, alcohol use and illicit drug use were assessed. Validated age-appropriate questions were taken from national surveys102 and/or previous trials were used in order to assess smoking (smoking in previous week; ever smoked regularly), alcohol use (use in previous week; number of times really drunk; binge drinking) and illicit-drug use (last month; lifetime use).
Sexual risk behaviours
Age of sexual debut and use of contraception at first sexual encounter were examined with measures used in the RIPPLE trial. 103 We consulted with schools about the acceptability of asking these questions at follow-up (year 10).
The Modified Aggression Scale Bullying subscale (Cronbach’s alpha = 0.83)
This measure came from the Centers for Disease Control and Prevention’s guidance document on bullying measures. 104 It includes a five-item scale assessing the level of bullying perpetration (last 3 months).
Use of NHS services
Self-report use of primary care, accident and emergency, or other service in the previous 12 months.
Contact with police
This was assessed using self-report of whether the young person had been stopped, told off or picked up by the police in the previous 12 months.
Demographic information
Sex and ethnicity
Student self-report.
Socioeconomic status: the Family Affluence Scale
The Family Affluence Scale (FAS) was developed specifically to describe the SES of young people. 105 A composite FAS score was calculated for each student based on his or her responses to four items relating to family car ownership, children having their own bedroom, the number of computers at home, and the number of holidays taken in the past 12 months. For our analyses, scores were collapsed into tertiles of low (score of 0, 1 or 2), medium (score of 3, 4 or 5) and high (score of 6, 7, 8 or 9) family affluence.
Data collected directly from schools
We planned to collect some data directly from schools for each year of the study using data routinely collected by schools:
-
school attendance data, expressed as number of half-days absent over the previous year
-
school rates of temporary and permanent exclusions
-
staff attendance, expressed as number of half-days absent, for which staff members’ informed consent to access was sought.
Individual staff-level outcomes
The following secondary outcomes were measured using survey self-reports from teachers and teaching assistants (the questionnaires used to collect these data can be found in full in Report Supplementary Material 1):
-
staff QoL, measured using the Short Form questionnaire-12 items (SF-12),106 a brief, well-validated measure of adult health-related QoL
-
staff stress and burnout, measured using Maslach Burnout Inventory,107 an established scale that uses a three-dimensional description of exhaustion, cynicism and inefficacy.
School-level outcomes
Value-added education score
School median value-added scores were obtained from UK official statistics108 relating to the progress students make between education Key Stage 2 or 3 (aged 7–14 years) and Key Stage 4 (aged 14–16 years). The value-added score for each student was calculated using the difference between their own output point score (end of Key Stage 4) and the median output point score achieved by others with the same or similar starting point (Key Stage 2 or 3), or input point score. 108 Schools that neither added nor subtracted educational value were given a score of 1000, with positive value added (> 1000) indicating a school where students on average made educational progress and negative value added (< 1000) indicating the reverse.
School size
The total number of students in the school, as identified from the school and college performance tables. 108
School-level deprivation
This was assessed using two variables:
-
Proportions of students eligible for free school meals (FSM) – the percentage of students eligible for FSM at each school at any time during the past 6 years is an accepted summary measure of school deprivation. Data were publicly accessible from the Department for Education. 108
-
The Income Deprivation Affecting Children Index (IDACI) score – a small-area indicator of deprivation specifically affecting children (< 16 years of age), which represents the proportion of children in a postcode who live in low-income households. 109 The value for each school is derived from the school’s postcode and thus represents the deprivation level of the school’s local area, rather than the school itself.
Office for Standards in Education, Children’s Services and Skills rating
Ofsted ratings108 are government inspectorate ratings of the quality of teaching, leadership and management, achievement of students, and behaviour and safety of students of a school. Schools are classified as 1 = ‘outstanding’, 2 = ‘good’, 3 = ‘requires improvement’ or 4 = ‘inadequate’. Owing to eligibility criteria for the INCLUSIVE study, only schools rated from 1 to 3 were included in the sample.
School sex mix
Mixed- or single-sex schools were identified from the school and college performance tables. 108
School type
Our sample comprised five types of school, categorised by the source of school funding. These were (1) converter academy mainstream (n = 18), funded directly from central government; (2) sponsor-led academy (n = 6), which has an independent business or charitable sponsor but is funded directly from central government; (3) foundation (n = 6), where the school owns its premises but is funded by the local authority; (4) community (n = 5), where premises and funding are provided by local authorities; and (5) voluntary-aided (n = 4), where the premises are owned by a charity (e.g. a religious foundation) but funding is at least partly from the local authority. 108
Process evaluation
The process evaluation examined intervention implementation and receipt, and possible causal pathways, in order to facilitate interpretation of the outcome data and enable refinement of the intervention logic model. Informed by existing frameworks,110,111 data were collected to examine the following.
Trial context
We assessed the context of schools in the intervention and control arms, such as discipline systems, staff training, social and emotional skills curricula, and student participation in decision-making. This drew on interviews with intervention facilitators and trainers, members of AGs in intervention schools, staff on school SLTs, and other staff in the intervention and control arms; and focus group discussions with students and staff in schools selected as case studies.
Trial arm fidelity
We assessed the fidelity of intervention delivery by school and facilitator. In addition to the above sources, we drew on follow-up surveys with staff and students; structured researcher observation of AG meetings and staff training; surveys of adults leading curriculum implementation and implementing restorative practice; interviews with adults delivering the curriculum; structured diaries kept by facilitators of AG meetings and by trainers of all-staff training; and administrative documents such as minutes and attendance sheets.
Overall fidelity in the externally facilitated first 2 years was scored out of a possible eight points for each school, as assessed by researchers, based on whether or not (1) at least five staff attended in-depth training (indicated in training registers); (2) each year all six AGs were convened (indicated in minutes); (3) policies and rules were reviewed (indicated in minutes); (4) locally decided actions were implemented (indicated in minutes); (5) AGs were perceived to have had a good or very good range of members (indicated in survey of AG members); (6) AGs were perceived to have been well or very well led (indicated in survey of AG members); (7) schools delivered at least 5 hours and/or at least two modules each year (indicated in survey of lesson deliverers); and (8) at least 85% of staff reported that if there was trouble at the school, staff responded by talking to those involved to help them get on better (indicated in staff survey). Overall intervention fidelity in the internally facilitated third year of the intervention was assessed using a narrower range of data, as the research team’s access to schools was expected to be reduced. Schools were scored out of a possible 4 points, on the basis of interviews with AG members to assess whether or not (1) all six AGs were convened and (2) locally decided actions were implemented; surveys and interviews with curriculum deliverers to assess whether or not (3) schools delivered at least 5 hours and/or at least two modules; and staff survey to assess whether or not (4) at least 85% of staff reported that, if there was trouble at the school, staff responded by talking to those involved to help them get on better.
Participation, reach and dose
We assessed the extent to which students and staff were aware of or involved in intervention delivery. This drew on surveys of AG members as well as follow-up surveys of students and staff and focus group discussions and interviews with students and staff.
Reception and responsiveness
We assessed the experiences of participation in INCLUSIVE, and in school environments shaped by this, to assess acceptability and barriers to facilitators. This drew on satisfaction surveys completed by staff attending in-depth training and of AG members; interviews with AG members, school staff and SLT, and students participating in restorative practice; and focus group discussions with students.
Intermediate outcomes
To assess possible intervention causal pathways, to examine whether or not these might mediate intervention effects, and to assess and refine our logic model, we used the Beyond Blue School Climate Questionnaire 28-item scale to measure students’ perceptions of the school climate, including supportive teacher relationships, sense of belonging, participative school environment, and student commitment to academic values,112 and the Young People’s Development Programme (YPDP) single-item measure of involvement with antischool peer groups. 113
Data collection
The data collection for the process evaluation was prospective and used mixed methods. The process evaluation was designed to explore the same intervention processes using different forms of data, and to compare findings between these. Purposive sampling was used for interviews to involve participants with diversity in terms of characteristics thought important for exploring implementation, and to explore diverse accounts and identify different themes. 114 Samples were large enough to generate diversity, but small enough to keep the analysis manageable. Informed by Medical Research Council (MRC) guidance on process evaluation,115 we sampled participants on the basis of characteristics likely to be associated with diverse perspectives on the intervention and its implementation within schools. We balanced sampling of some participants in all schools to develop an overview of delivery with larger samples in a small number of case study schools to explore processes in more depth. When discrepancies or gaps in the data emerged, these were explored in the next applicable data collection round.
Data collected in all schools
Diaries completed by trainers
Individuals providing the all-staff training in restorative practice were asked to complete a diary for each session delivered, informed by the tool used in the pilot study. They were asked to rate the extent to which they covered topics/materials as intended, and the materials and activities [e.g. Microsoft PowerPoint® (Microsoft Corporation, Redmond, WA, USA) slides, small-group or paired activities] used. Trainers then sent the diaries to the research team.
Observations of training
Researchers aimed to conduct structured non-participant observations of training so that all schools could be observed at least once. Observation guides included what topics were covered and what activities were used, and were informed by the same tools as used in the pilot study.
Satisfaction survey for in-depth training
An anonymous satisfaction survey was given out to the 5–10 staff members from each school who attended the in-depth training on restorative practice. Informed by the same tool as used in the pilot study, questions assessed whether or not participants felt that the training was useful; whether or not they felt confident about putting into practice the skills learnt; whether or not they would recommend the training; and overall how they rated the training provided. Participants placed the questionnaires in an envelope, which the trainers collected and sent to the researchers.
Interviews with trainers
Semistructured interviews with the two trainers were conducted by telephone in year 1 and lasted between 30 and 45 minutes. These aimed to explore the trainers’ views on participant responsiveness, any adaptations and deviations made, and barriers to and facilitators of delivery.
Diaries kept by facilitators of action groups
Facilitators were asked to complete a diary for each AG meeting they attended. Informed by the same tool as used in the pilot study, these explored general meeting information such as duration, date, number of attendees, chairperson and minute-taker names; members’ roles, year group and gender; how and what data were used to inform setting up school actions; priorities set by the school and actions stemming from these; actions concerning the revision of school rules and school policies; identification of which modules of the curriculum were to be implemented and how this was decided; and the participation of AG members. This information was then sent to the research team.
Minutes of action groups
Facilitators were asked to collect minutes from each AG meeting and send these to the researchers. These were used to triangulate the validity of facilitator diary forms.
Observations of action groups
Researchers aimed to conduct structured non-participant observations of AGs in 10 randomly selected schools for each year of intervention. Observation guides focused on the same areas as diaries and were informed by the same tools used in the pilot study.
Survey of action group members
An anonymous survey was handed out to all members of AGs by facilitators at the end of each year of the intervention. Informed by the same tool as used in the pilot study, this explored its acceptability, functioning and composition. It asked questions, for example, on the diversity of staff and students on the AG, how well led they considered the group to be and how empowered members felt to make decisions, using an existing scale. 116 Participants placed the questionnaires in an envelope, which the facilitators collected and sent to the researchers.
Interviews with facilitators of action groups
Semistructured telephone interviews with facilitators (n = 6) were conducted in years 1 and 2 and lasted between 45 and 90 minutes. These aimed to explore views on school culture, responsiveness and priorities; any adaptations and deviations made; and barriers to and facilitators of delivery.
Interviews with members of action groups
We aimed to interview two members of each school’s AG per year. A member of the evaluation team contacted the member of staff tasked with co-ordinating the intervention at each school and asked them to identify two AG members (staff or student) to be interviewed. Identified staff participants were then contacted by e-mail and/or telephone to schedule an interview, which occurred either in person (if possible) in a private room on school premises or over the telephone and lasted between 30 and 60 minutes. Interviews with students were arranged via staff and were always conducted in the school. Interviews were semistructured and explored views on the acceptability of facilitators and the intervention; barriers to and facilitators of AG meetings and how they might be improved; the extent to which actions arising from meetings were implemented in the school; and their perceived impact on the school environment.
Survey of school staff leading implementation of the curriculum
This survey was sent annually to be completed by the teacher in each intervention school who was acting as the LT social and emotional skills co-ordinator. The research team sent the surveys by e-mail termly in the first and second years of the study, and in the final term of the third year. Staff were asked to complete the survey and return it to the research team by e-mail. Informed by the same tool as used in the pilot study, the survey covered what units and lessons were delivered, when, in which subjects, for how many hours, and what intervention materials (e.g. PowerPoint slides, lesson plans), if any, were used to deliver the content.
Interviews with school staff delivering the curriculum
The research team aimed to arrange semistructured interviews in each year of the intervention with the staff member responsible for delivery of the social and emotional curriculum. The curriculum co-ordinator at each school was contacted by e-mail and/or telephone and asked to identify a member of staff delivering the curriculum to participate. Interviews were carried out over the telephone or face to face in a private office on school premises. The interviews gathered views on the fidelity, reach and acceptability of the curriculum; which materials were used; delivery methods; student responsiveness; and contextual barriers to or facilitators of delivery.
Survey of staff implementing restorative practice
This survey aimed to examine the extent to which staff who attended in-depth training in restorative practices were implementing such practices in school. The survey was initially to be completed termly, but for the third year this was changed so that staff were asked to complete it only in the summer term. Staff who had attended the in-depth training were sent an e-mail inviting them to complete the survey. The survey assessed delivery of the use of affective language, circle time, mediation, restorative conferencing, family group conferencing and community conferencing.
Interviews with other school staff
Semistructured interviews were sought across intervention and control schools with one staff member from schools’ SLT (n = 40) and two teaching staff (n = 80) at the beginning of year 1. Each school’s member of staff liaising with the research team was contacted by e-mail and/or telephone and asked to identify three staff members to participate. A member of the research team then contacted these staff by e-mail to schedule a telephone interview. Interviews explored the context of schools, including their policies and practices relating to behaviour management, social and emotional skills education, staff training, and student participation in decisions. In year 3, such interviews were sought with one SLT member in all intervention and control schools. Individuals in control schools were interviewed in the autumn term and in intervention schools in the summer term.
Data collected in case study schools
Six schools in the intervention arm were selected as case studies in order to gather in-depth qualitative data on intervention processes and school context. In these schools, we aimed to conduct focus groups with staff and students, as well as interviews with students participating in restorative practices. To encompass diverse schools, schools were purposively sampled in terms of diversity in relation to the percentage of FSM (above and below national average in 2012 for secondary schools, 16.3%), type of school, the facilitator assigned to the school, and the extent to which the school was responsive (highly responsive, somewhat responsive, poorly responsive) to intervention activities, as rated by the intervention facilitators 3 months into the intervention start date.
Focus groups with staff
In each year of the intervention, we aimed to conduct one focus group with staff in each case study school, each involving four to six members of staff. Staff were purposively selected and invited to participate by the staff member liaising with the research team to include diversity according to degree of participation in the intervention and role within the school (including senior leaders, pastoral staff and classroom teachers). Focus group discussions aimed to explore school culture and ethos, views about the delivery and impacts of the intervention, how restorative practices were applied, and barriers to and facilitators of their use. Focus groups were conducted in private offices on school premises facilitated by one researcher.
Focus groups with students
Each year, we conducted two focus groups with students in each case study school, comprising 4–12 students each: one with students directly involved in intervention activities (e.g. AGs) and one with students not involved in such activities. Students were purposively selected and invited to participate by the staff member in each school liaising with the research team, such that they reflected the diversity of the school in terms of boys and girls, different ethnic groups, and varying degrees of educational engagement. Focus groups were conducted in private offices on school premises facilitated by one researcher.
Interviews with students involved in restorative practices
We aimed to conduct semistructured interviews with two students at each case study school that had been involved in a restorative practice. The staff member at each school liaising with the research team was asked to invite students to participate, recruiting either one boy and one girl or a perpetrator and victim in the same instance of bullying, where possible. Interviews aimed to understand the processes of restorative practice and assess the acceptability of the approach. Restorative interviews were not limited to cases of bullying or aggression but also included classroom misbehaviour or friendship challenges. These interviews were conducted in private offices on school premises facilitated by one researcher.
Interviews and focus groups were audio-recorded and transcribed.
Ethics
All data were collected with research participants’ informed consent. Student and staff participants received written information beforehand and were given the opportunity to ask questions to a member of the research team. They were then invited to give signed consent and reminded that they could skip any questions and/or end the interview at any time. For telephone interviews with staff, an e-mail from participants indicating consent was generally used instead of a written signature. Before the interview began, they were read a statement relating their rights, how the data would be used, and information about anonymity and confidentiality. They were then asked to give verbal consent, which was recorded. All data collected were stored on password-protected drives within separate password-protected folders. However, had any research participants reported that they had been involved in or were at risk of sexual or physical abuse that the school was not already aware of, the research team would have liaised with the safeguarding lead for the school in question, breaking anonymity. Participants were made aware of this policy as part of the consent procedures. No such reports were made.
Economic evaluation
Economic evaluation of the intervention also took place. In accordance with NIHR guidelines, the methodology and results for the economic evaluation are reported separately in Chapter 4.
Changes to trial outcomes
The following deviations from this plan occurred during data collection.
We were unable to collect school-level data on individual student and staff attendance and school rates of temporary and permanent exclusions, despite multiple attempts to contact schools and obtain these data after the intervention was completed. Small numbers of data on school-level exclusions were provided but these were not sufficient for analysis. In response to requests for data, schools either did not respond or notified us that this was a burden they were not prepared to undertake now that the trial had finished. Data were not available similarly across intervention and control schools. A further offer of money towards school staff funds (May 2018; see above) did not motivate schools to provide these data.
In discussion with NIHR, we came up with the following mitigation plan.
-
School attendance data: these data are currently planned to be collected by Manchester University in a planned follow-up to this study in late 2019. These are therefore not reported here.
-
School rates of temporary and permanent exclusions: these data are published at school level by the Department for Education, albeit with a significant delay. We plan to examine these in the future when available, although the data are not reported here.
-
Staff attendance: individual staff attendance levels are not available through other means and these analyses cannot be undertaken.
Amendments to and deviations from the protocol (process evaluation)
All planned amendments were approved by the study steering committee (5 October 2015). We clarified that trainer diaries would be used to examine all-staff training and that a satisfaction survey would instead be used to assess in-depth training. A survey of all-staff training was judged impossible because of the short time available for the training.
We reduced the number of observations of AG meetings from 20 to 10 per year. The rationale was that this was sufficient to explore AGs alongside all the other forms of data on these, and that any greater data collection would be very onerous for schools.
We dropped plans to observe one curriculum session per school per year, replacing this with surveys and interviews examining curriculum implementation, because schools advised us that scheduling observations would be challenging.
We introduced surveys examining implementation of restorative practice to ensure that we examined this important area of implementation. We clarified that we would undertake telephone interviews with one SLT member and two other staff per school in year 1 only and then undertake telephone interviews with one SLT member per school in year 3. The rationale was that this was sufficient to understand the context of trial schools and that any greater data collection would be very time-intensive and onerous for schools.
We reduced the number of case study schools from eight to six, with these being drawn from intervention schools only, rather than from intervention and control schools. The rationale was that six schools was more appropriate for in-depth research and that in-depth case studies in control schools would be informative. We purposively rather than randomly sampled case study schools as this would be more likely to be effective in ensuring the contextual diversity needed for qualitative research.
There were also several deviations from the protocol. We said that we would observe some training in all 20 intervention schools, but a research team error meant that we actually observed a random sample of 10 schools. We said that we would survey staff co-ordinating curriculum delivery annually but in years 1 and 2 we did this termly before reverting to an annual survey in year 3. Our protocol said that we would include as one of our intermediate outcomes a measure of student anti-school actions using the ESYTC self-reported delinquency subscale but this was a drafting error as this measure instead was part of one of our primary outcome measures.
Sample size
We proposed to recruit sufficient participants to detect a difference between groups of 0.25 standard deviation (SD) with 90% power and a 5% level of significance. This is considered to represent a moderate size of effect and is in line with the effect sizes seen in the literature. 117
The average English school has approximately 150 students per year group of students, although this varies across schools. Using a conservative intraclass correlation coefficient (ICC) of 0.04118 and an estimate of 150 students per school, a trial involving 20 schools per arm would have provided 90% power to identify an effect size of 0.25 SD with a 5% significance level. If two schools per arm (i.e. 10%) were to be lost to follow-up over the course of the trial, we would still have 80% power to detect an effect size of 0.23. The total student sample size was estimated to be between 4000 (assuming 100 students per school) and 6000 (assuming 150 students per school). As we were surveying all young people in the relevant school year at each follow-up, this sample was likely to remain similar across the study. The total student sample was therefore planned to be approximately 6000.
No stopping guidelines were put in place for this study; any and all schools and students who agreed to take part were included.
Randomisation
Sequence generation
Schools were randomly allocated in a 1 : 1 ratio to the intervention or control arm immediately after their students and staff had completed the baseline data collection. To promote baseline similarity, randomisation was stratified by key school-level determinants of violence119 data obtained from the Department for Education (www.gov.uk/school-performance-tables, accessed 17 September 2018):
-
single-sex versus mixed-sex school
-
school-level deprivation, as measured by the percentage of students eligible for FSM (low/moderate 0–23% and high > 23%, with 23% being the median for England
-
school ‘best eight value added’ in General Certificate of Secondary Education (GCSE) exams (above and below the median for England of 1000), a school-level measure of students’ attainment in public exams accounting for their attainment on entry to the school.
Data were obtained from the Department for Education (www.gov.uk/school-performance-tables, accessed 17 September 2018).
Schools were allocated randomly within each of these eight strata.
Sequence allocation was generated by the clinical trials unit (CTU) at LSHTM using Stata’s® ‘ralloc’ command (version 15; StataCorp, College Station, TX, USA) and was concealed from schools and the wider evaluation and intervention teams. Allocation was communicated from the CTU to the research team, who communicated this to schools and the intervention team.
Protecting against selection bias
All schools were recruited before the intervention commenced. The randomisation schedule was drawn up once the schools had consented and after the baseline survey, thus guarding against selection biases at entry of clusters to the trial. Retention of control schools was maximised by ensuring regular senior liaison and provision of participation incentives (£500 per school).
We had very high student participation in our pilot study: 96% of students eligible at baseline, and 93% at follow-up. To minimise bias, we used in-school, mail, and telephone contacts to try to include all enrolled students absent at either baseline or follow-up questionnaires. Students absent on the day of questionnaire surveys were provided with the questionnaire to complete and an envelope in which to seal the completed questionnaire, which schools then collated and posted to the research team. We did not attempt to follow up students who had left the school.
Allocation concealment mechanisms
As with most social intervention trial schools, their students, teachers and other staff could not be ‘blinded’ to allocation status. However, field work staff were blinded to allocation, as were data-input staff. Analysis of follow-up quantitative data was undertaken blind to allocation.
Implementation
Randomisation and stratification was undertaken remotely by the CTU at LSHTM.
Blinding
After randomisation, schools, the intervention team and the process evaluators could not be ‘blinded’ to allocation status. However, other field work staff were blinded to allocation, as were the outcome evaluation research team lead (RV) and data input and data analysis staff. Process and economic evaluation researchers could not be blinded.
It was not possible to blind the costing conducted alongside the process evaluation. Researchers remained blinded to the arm and school name while preparing statistical analysis of cost data from questionnaires and the CHU9D until the analysis was completed.
Statistical methods
Primary and secondary outcome analysis
The primary analysis of outcomes was intention to treat, including all randomised schools and participants at each wave. Each measure was analysed using a separate mixed model, with the outcomes from each time point treated as a repeated measures outcome. Fixed effects of treatment (LT vs. control) and time (baseline, 24 months and 36 months) and the interaction between treatment and time were specified, and the estimated baseline measures were constrained to be identical in the two arms of the trial. This is equivalent to adjusting for baseline and permitting the relationship between baseline and follow-up scores to differ at each time point, but offers the additional advantage that the data from all participants contribute to the analysis, even when there were missing data at follow-up. Random effects for school and for participants were specified to allow for correlations within schools, and repeated measures within participants. Statistical significance for these analyses was taken at the 5% level (p < 0.05). As prespecified in the statistical analysis plan, we carried out analyses adjusted only for baseline measures of the outcomes, and the analyses adjusted for baseline measures of outcomes, sex, ethnicity and SES as well as for the school-level stratifying factors (single-sex vs. mixed-sex school; school-level deprivation; value-added strata) as the primary analysis.
For the joint primary outcomes (GBS and ESYTC), mixed linear regression models with random effects at the participant and school levels were used to estimate a mean difference in GBS and ESYTC scores between the two arms of the trial. Formal testing was restricted to a prespecified number of secondary outcomes, and appropriate multilevel models were used to examine the effect of the intervention. For continuous outcomes, we report unadjusted and adjusted mean differences with 95% confidence intervals (CIs) and adjusted effect sizes (standardised mean difference). For binary and ordinal outcomes, we report unadjusted and adjusted odds ratios. Additionally, we report adjusted risk differences for binary outcomes although these cannot be calculated for ordinal outcomes. Evidence for any differential effects of the intervention on the primary and secondary outcomes, by subgroup, was assessed using likelihood ratio tests for the treatment by subgroup interaction terms. The effects in the different subgroups were estimated directly from the regression model with the interaction term included.
The following four subgroups were prespecified: (1) sex; (2) SES, measured using the Health Behaviour in School-aged Children FAS,120 described as low SES for FAS scores of 0–5 and high SES for FAS scores of 6–9; (3) baseline bullying experience (high, defined as frequent – at least weekly – experience of bullying or being upset by it, vs. medium/low, defined as rare – less than weekly – experience of bullying and not being upset by it) based on the GBS; and (4) baseline behaviour problems based on the ESYTC, with high levels of behaviour problems defined as ESYTC scores of > 0 and low levels defined as a score of 0.
When there was evidence of non-normality in the continuous outcome measures, non-parametric bootstrapping, with 1000 samples, was used to estimate the effect of the intervention, and bias-corrected CIs are reported. When this was done, p-values were estimated using permutation tests.
Process evaluation analyses
Quantitative data were entered into CSPro (version 7.2.1; United States Census Bureau, Washington, DC, USA) or Microsoft Excel® (2016; Microsoft Corporation, Redmond, WA, USA) and then transferred and analysed in Stata. Quantitative analysis used descriptive statistics to assess intervention implementation, awareness, reach, satisfaction and empowerment. Quantitative data also examined the association between trial arm and our potential mediators using the same approaches as were used to assess the primary and secondary outcomes. Qualitative data were organised in NVivo (version 11; QSR International, Warrington, UK) and analysed to explore views about intervention processes and contexts. Thematic content analysis of qualitative data was undertaken by Emily Warren and Chris Bonell using the following stages of analysis. 121 First, the researcher created a coding framework based on the research questions and theory guiding the intervention. These starting codes were constructed to reflect the concepts informing our questions and theory, such as the intervention components, the aspects of the school setting included in our inclusion and stratification criteria, and the aspects of implementation such as fidelity, feasibility and acceptability. Other codes were developed inductively to reflect other concepts that featured in interview transcripts, or to subdivide and better describe our starting codes. Transcripts were analysed using in vivo codes to identify key themes that were immediately apparent in participant accounts, as well as axial codes to explore inter-relationships between these in vivo codes (e.g. to explore how implementation varied across different school contexts). Analyses used the method of constant comparisons and examination of deviant cases to refine the emerging analysis.
Data Monitoring Committee
A DMC was established independent of the investigators and of the TSC, but it reported to the TSC and (via the TSC) to the sponsors and the NIHR programme. This consisted of an independent chairperson, a senior statistician and at least one other senior academic independent of the investigators. It met approximately yearly during the study. The DMC monitored data for quality and completeness. The DMC examined the results of an interim analysis at 24 months to consider any potential harms.
Chapter 3 Results
Participant flow
A total of 6667 students in the 40 participating schools provided data at baseline, with the participation rate being 93.6% of the students on the school roll (intervention arm, 92.9%; control arm, 94.3%). Characteristics of the schools and students at baseline and at 24 and 36 months are shown by trial arm in Appendix 1 (see Tables 26 and 27). All schools participated in the follow-up surveys at 24 and 36 months; the numbers of students who completed the questionnaires at baseline, 24 months and 36 months were similar between the arms (Figure 1). Student and school characteristics and outcomes at baseline were well balanced between the arms.
FIGURE 1.
The CONSORT flow diagram. Reproduced from Bonell et al. 122 © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license.
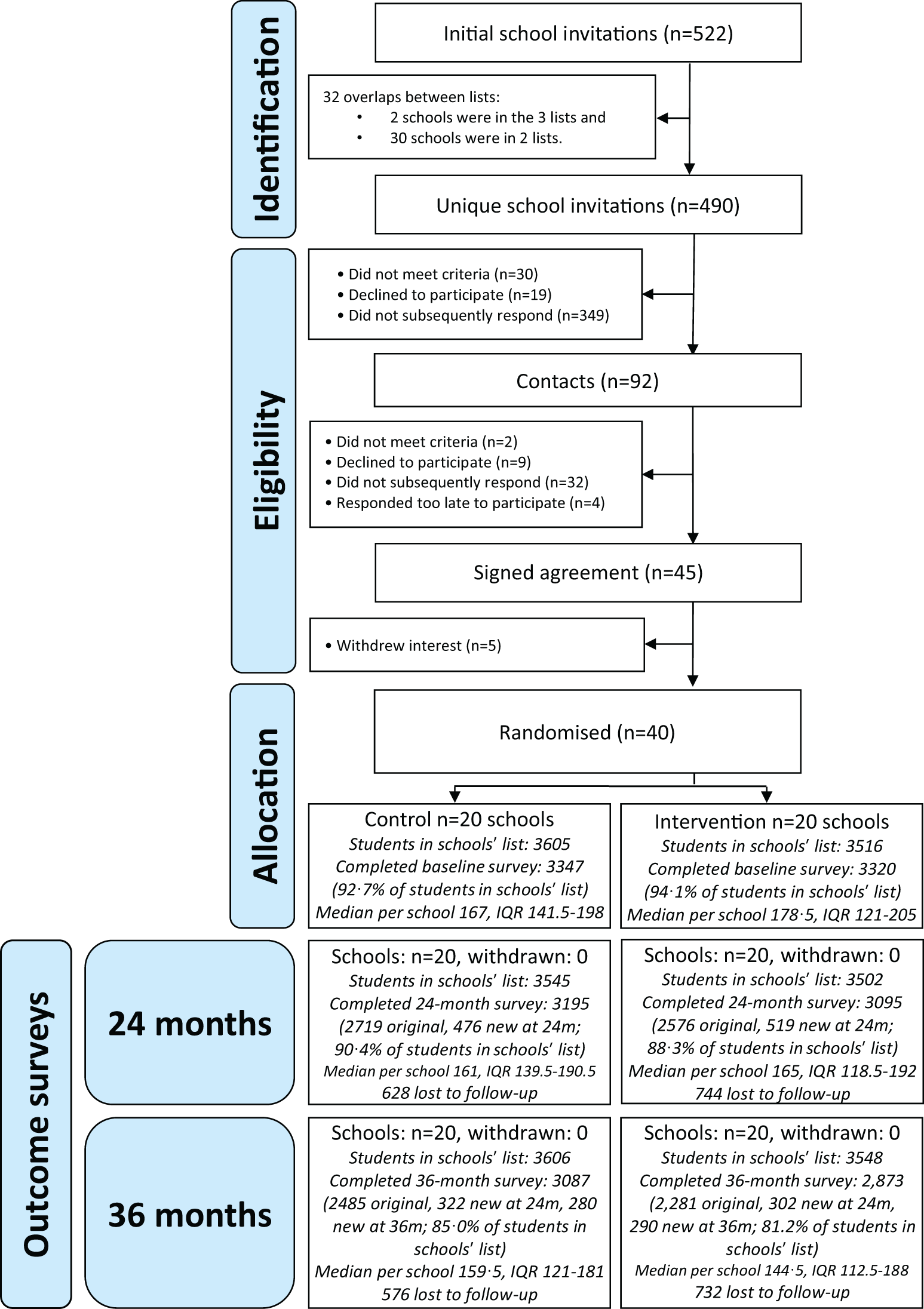
Recruitment
Baseline surveys took place in March–July 2014, with the 24-month follow-up in April–June 2016 and the 36-month follow-up in April–June 2017. The trial ended in summer 2017, as the designated intervention time limit had been reached.
Baseline data
Summaries of demographic characteristics of respondents are presented in Appendix 1 (see Table 27). The arms were well balanced in terms of demographic characteristics and the primary and secondary outcome measures.
The data presented come primarily from mixed-sex schools (80%) with a ‘good’ Ofsted rating (60%). There was a good mix of male and female participants, ethnicities and religions. The majority of student participants came from a two-parent family (72%) in which at least one parent was employed (73%).
In terms of primary and secondary outcomes measures, reports of bullying and aggressive behaviour, emotional difficulties, QoL, risk behaviours, truancy, NHS service use and contact with police were similar between the control and intervention arms at baseline (see Table 1).
| Control (3347 students)† | Intervention (3320 students)† | Overall (6667 students)† | |
|---|---|---|---|
| Primary outcomes | |||
| GBS overall score, mean (SD) | 0.51 (0.63) | 0.48 (0.60) | 0.49 (0.61) |
| Teasing | 0.79 (0.99) | 0.74 (0.95) | 0.76 (0.97) |
| Rumours | 0.52 (0.85) | 0.50 (0.81) | 0.51 (0.83) |
| Deliberate exclusion | 0.40 (0.79) | 0.41 (0.80) | 0.40 (0.79) |
| Threatened or hurt | 0.36 (0.74) | 0.30 (0.68) | 0.33 (0.71) |
| ESYTC overall score, mean (SD) | 2.92 (4.84) | 2.72 (4.77) | 2.82 (4.81) |
| Secondary outcomes | |||
| SDQ total difficulties score, mean (SD) | 11.00 (5.99) | 10.70 (5.76) | 10.85 (5.88) |
| Emotional problems | 3.15 (2.39) | 3.17 (2.35) | 3.16 (2.37) |
| Conduct problems | 2.00 (1.86) | 1.90 (1.83) | 1.95 (1.85) |
| Hyperactivity | 4.00 (2.48) | 3.84 (2.41) | 3.92 (2.45) |
| Peer problems | 1.86 (1.78) | 1.81 (1.75) | 1.83 (1.76) |
| Pro-social strengths | 7.56 (1.91) | 7.65 (1.93) | 7.60 (1.92) |
| SWEMWBS overall score | 24.11 (5.91) | 24.33 (5.91) | 24.21 (5.91) |
| PedsQL overall score | 80.39 (14.31) | 80.98 (14.08) | 80.68 (14.20) |
| Physical | 85.42 (14.88) | 85.75 (14.81) | 85.58 (14.84) |
| Emotional | 75.90 (22.36) | 76.40 (21.80) | 76.15 (22.08) |
| Social | 84.31 (17.88) | 84.88 (17.70) | 84.59 (17.79) |
| School | 72.75 (18.76) | 73.96 (18.55) | 73.34 (18.67) |
| Psychosocial | 77.70 (16.29) | 78.41 (15.84) | 78.04 (16.07) |
| Ever smoked, n (%) | |||
| No | 3083 (94.22) | 3051 (95.28) | 6134 (94.75) |
| Yes | 189 (5.78) | 151 (4.72) | 340 (5.25) |
| If yes, how often in past month, n (%) | |||
| None | 132 (77.65) | 100 (76.34) | 232 (77.08) |
| Once or twice | 30 (17.65) | 20 (15.27) | 50 (16.61) |
| About once a week | 3 (1.76) | 6 (4.58) | 9 (2.99) |
| Daily or almost daily | 5 (2.94) | 5 (3.82) | 10 (3.32) |
| Ever consumed alcohol, n (%) | |||
| No | 2751 (84.96) | 2783 (87.63) | 5534 (86.28) |
| Yes | 487 (15.04) | 393 (12.37) | 880 (13.72) |
| If yes, how often in past month, n (%) | |||
| None | 349 (74.89) | 268 (72.43) | 617 (73.80) |
| Once or twice | 88 (18.88) | 88 (23.78) | 176 (21.05) |
| Once a week or more | 29 (6.22) | 14 (3.78) | 43 (5.14) |
| Ever been offered illicit drugs, n (%) | |||
| No | 2924 (87.36) | 2967 (89.37) | 5891 (88.36) |
| Yes, but did not try them | 258 (7.71) | 175 (5.27) | 433 (6.49) |
| Yes, and tried them | 30 (0.90) | 18 (0.54) | 48 (0.72) |
| Truancy, n (%) | |||
| No | 3019 (94.11) | 2989 (94.26) | 6008 (94.18) |
| Yes | 189 (5.89) | 182 (5.74) | 371 (5.82) |
| Exclusion from school, n (%) | |||
| No | 3154 (95.52) | 3143 (96.92) | 6297 (96.21) |
| Yes | 148 (4.48) | 100 (3.08) | 248 (3.79) |
| Use of NHS services in past year, n (%) | |||
| No | 1836 (55.86) | 1720 (53.33) | 3556 (54.61) |
| Yes | 1451 (44.14) | 1505 (46.67) | 2956 (45.39) |
| Contact with police | |||
| No | 3050 (92.06) | 2982 (91.61) | 6032 (91.84) |
| Yes | 263 (7.94) | 273 (8.39) | 536 (8.16) |
Staff outcomes in relation to stress and burnout and QoL were also similar across control and intervention conditions at baseline (see Appendix 1, Table 28).
Numbers analysed
A total of 3087 participants were included in analysis from the control condition and 2873 were included from the intervention condition. Analysis was undertaken by original assigned group. Details on missing data are shown in Appendix 1 (see Table 43).
Outcomes and estimation
Primary and secondary analysis
Overall GBS bullying scores were lower among intervention schools than among control schools at 36 months (adjusted mean difference –0.03, 95% CI –0.06 to 0.00; adjusted effect size –0.08). There was no evidence of a difference in misbehaviour/delinquency ESYTC scores (adjusted mean difference –0.13, 95% CI –0.43 to 0.18; adjusted effect size –0.03) between arms; however, the direction of effect suggests a positive effect of the intervention. These results are shown in Table 2.
| Control group (3087 students)a | Intervention group (2281 students)a | Unadjusted difference (95% CI) | p-value | Adjusted difference (95% CI) | p-value | Adjusted effect size | |
|---|---|---|---|---|---|---|---|
| GBS overall score | 0.34 (0.02) | 0.29 (0.02) | –0.03 (–0.06 to –0.002) | 0.0395 | –0.03 (–0.06 to –0.001) | 0.0441 | –0.08 |
| Teasing | 0.55 (0.03) | 0.47 (0.03) | –0.04 (–0.09 to 0.01) | –0.05 (–0.10 to 0.00) | –0.07 | ||
| Rumours | 037 (0.02) | 0.31 (0.02) | –0.06 (–0.10 to –0.02) | –0.07 (–0.11 to –0.02) | –0.10 | ||
| Deliberate exclusion | 0.24 (0.01) | 0.22 (0.02) | –0.04 (–0.08 to 0.004) | –0.04 (–0.08 to 0.01) | –0.06 | ||
| Threatened or hurt | 0.21 (0.02) | 0.18 (0.02) | 0.01 (–0.02 to 0.05) | 0.01 (–0.03 to 0.05) | 0.02 | ||
| ESYTC overall score | 4.33 (0.20) | 4.04 (0.21) | –0.07 (–0.38 to 0.25) | 0.6820 | –0.13 (–0.43 to 0.18) | 0.4199 | –0.03 |
Secondary outcomes and adjusted and unadjusted intervention effects for the GBS and ESYTC measured at 24 months and other secondary outcomes at 36 months are shown in Table 3. Although the direction of effect was, again, positive, there was no evidence of difference in the GBS overall score or the ESYTC misbehaviour/delinquency scores at 24 months. At 36 months, students in intervention schools had higher QoL (PedsQL adjusted effect 1.44, 95% CI 0.07 to 2.17; adjusted effect size 0.14) and psychological well-being scores (SWEMWBS 0.33, 95% CI 0.00 to 0.66; adjusted effect size 0.07) and lower psychological total difficulties (SDQ total score –0.54, 95% CI –0.83 to –0.25; adjusted effect size –0.14) than students in control schools. There was evidence that those in intervention schools also had lower scores for emotional, conduct, hyperactivity and peer problems (SDQ subscales; see Table 3).
| Outcome | Control (3195 students),a mean (SE) | Intervention (3095 students),a mean (SE) | Unadjusted difference (95% CI); p-value | Adjusted difference (95% CI); p-value | Adjusted effect size (95% CI) |
|---|---|---|---|---|---|
| GBS overall score | 0.42 (0.02) | 0.37 (0.02) | –0.02 (–0.05 to 0.01); 0.2198 | –0.02 (–0.05 to 0.01); 0.1581 | –0.05 (–0.15 to 0.05) |
| Teasing | 0.66 (0.03) | 0.59 (0.03) | –0.02 (–0.07 to 0.03) | –0.03 (–0.08 to 0.01) | –0.05 (–0.14 to 0.04) |
| Rumours | 0.44 (0.02) | 0.41 (0.02) | –0.02 (–0.06 to 0.02) | –0.02 (–0.06 to 0.02) | –0.04 (–0.11 to 0.04) |
| Deliberate exclusion | 0.31 (0.02) | 0.30 (0.02) | –0.03 (–0.07 to 0.01) | –0.03 (–0.07 to 0.01) | –0.05 (–0.13 to 0.03) |
| Threatened or hurt | 0.26 (0.02) | 0.22 (0.02) | 0.01 (–0.02 to 0.05) | 0.01 (–0.03 to 0.04) | 0.01 (–0.07 to 0.09) |
| ESYTC overall score | 4.24 (0.28) | 3.96 (0.28) | –0.04 (–0.34 to 0.27); 0.8113 | –0.06 (–0.35 to 0.24); 0.7206 | –0.01 (–0.12 to 0.09) |
| PedsQL overall score | 79.75 (0.50) | 80.97 (0.51) | 0.77 (0.05 to 1.48) | 0.88 (0.17 to 1.60) | |
| Physical health | 85.39 (0.52) | 86.01 (0.53) | 0.30 (–0.49 to 1.09) | 0.49 (–0.27 to 1.26) | |
| Psychosocial health | 76.71 (0.55) | 78.37 (0.56) | 1.08 (0.28 to 1.89) | 1.15 (0.35 to 1.96) | |
| Emotional functioning | 73.90 (1.07) | 74.65 (1.10) | 0.58 (–0.60 to 1.77) | 0.74 (–0.41 to 1.90) | |
| Social functioning | 85.98 (0.42) | 87.74 (0.43) | 1.15 (0.32 to 1.99) | 1.04 (0.20 to 1.88) | |
| School functioning | 70.19 (0.60) | 72.68 (0.61) | 1.50 (0.50 to 2.50) | 1.66 (0.65 to 2.66) | |
| SDQ total difficulties scoreb | 11.83 (0.16) | 11.23 (0.17) | –0.40 (–0.67 to –0.12) | –0.41 (–0.69 to –0.13) | |
| Emotional problems | 3.46 (0.11) | 3.40 (0.12) | –0.10 (–0.22 to 0.03) | –0.11 (–0.23 to 0.01) | |
| Conduct problems | 2.22 (0.07) | 2.01 (0.07) | –0.12 (–0.21 to –0.03) | –0.13 (–0.22 to –0.04) | |
| Hyperactivity | 4.33 (0.07) | 4.15 (0.07) | –0.05 (–0.17 to 0.07) | –0.05 (–0.17 to 0.07) | |
| Peer problems | 1.84 (0.05) | 1.68 (0.05) | –0.14 (–0.22 to –0.05) | –0.15 (–0.24 to –0.06) | |
| Pro-social strengths | 6.96 (0.10) | 7.18 (0.10) | 0.12 (0.02 to 0.23) | 0.15 (0.04 to 0.25) | |
| SWEMWBS total well-being index | 23.54 (0.20) | 23.79 (0.21) | 0.09 (–0.24 to 0.41) | 0.15 (–0.17 to 0.47) | |
| Age at sexual debut | 12.30 (1.27) | 12.74 (1.29) | 0.06 (–1.53 to 1.66) | –0.22 (–1.60 to 1.16) | |
| Modified aggression scale, bullying subscale | 2.74 (0.23) | 2.61 (0.23) | 0.00 (–0.56 to 0.57) | 0.01 (–0.29 to 0.32) | |
| Ever smoked regularly | |||||
| No | 2568 (83.40) | 2595 (87.97) | 1.00 | 1.00 | |
| Yes | 511 (16.60) | 355 (12.03) | 0.67 (0.48 to 0.92) | 0.63 (0.46 to 0.88) | |
| If yes, how long since last smoked | 1.12 (0.80 to 1.56)c | 1.14 (0.81 to 1.59)c | |||
| < 1 day | 65 (12.87) | 51 (14.66) | |||
| 1–3 days | 29 (5.74) | 20 (5.75) | |||
| 4–7 days | 27 (5.35) | 20 (5.75) | |||
| > 1 week, < 1 a month | 69 (13.66) | 40 (11.49) | |||
| 1–2 months | 64 (12.67) | 41 (11.78) | |||
| 3–6 months | 90 (17.82) | 49 (14.08) | |||
| > 6 months | 161 (31.88) | 127 (36.49) | |||
| Ever drunk alcohol | |||||
| No | 2028 (64.88) | 2127 (70.95) | 1.00 | 1.00 | |
| Yes | 1098 (35.12) | 871 (29.05) | 0.79 (0.62 to 1.02) | 1.26 (0.91 to 1.75) | |
| If yes, had alcohol in the past week | |||||
| No | 885 (83.65) | 675 (81.33) | 1.00 | 1.00 | |
| Yes | 173 (16.35) | 155 (18.67) | 1.16 (0.82 to 1.63) | 1.26 (0.91 to 1.75) | |
| Number of times really drunk | 0.65 (0.37 to 1.14)c | 0.65 (0.41 to 1.02)c | |||
| Never | 911 (66.35) | 771 (70.80) | |||
| Once | 262 (19.08) | 166 (15.24) | |||
| 2–3 times | 120 (8.74) | 97 (8.91) | |||
| 4–10 times | 45 (3.28) | 35 (3.21) | |||
| > 10 times | 35 (2.55) | 20 (1.84) | |||
| Binge drinking (> 5 drinks in a row) in past 30 days | 0.89 (0.60 to 1.33)c | 0.5832 | |||
| 0 | 1204 (81.30) | 978 (81.98) | |||
| 1 to 2 | 181 (12.22) | 143 (11.99) | |||
| 3 to 5 | 20 (3.38) | 46 (3.86) | |||
| 6 to 9 | 17 (1.15) | 6 (0.50) | |||
| ≥ 10 | 29 (1.96) | 20 (1.68) | |||
| Ever been offered illicit drugs | 0.63 (0.41 to 0.96)c | 0.63 (0.44 to 0.92)c | |||
| No | 2346 (75.46) | 2421 (81.19) | |||
| Yes, but did not try them | 618 (19.88) | 469 (15.78) | |||
| Yes, and tried them | 145 (4.66) | 92 (3.09) | |||
| Truancy (skipped school in the past 3 months) | |||||
| No | 2761 (88.95) | 2685 (89.89) | 1.00 | 1.00 | |
| Yes | 343 (11.05) | 302 (10.11) | 0.93 (0.72 to 1.20) | 0.91 (0.70 to 1.18) | |
| Exclusion from school (temporarily or permanently)d | |||||
| No | 2846 (90.18) | 2791 (91.63) | 1.00 | 1.00 | |
| Yes | 310 (9.82) | 255 (8.37) | 0.83 (0.54 to 1.29) | 0.81 (0.55 to 1.21) | |
| Used any contraception at first sex | |||||
| No | 36 (30.51) | 32 (33.68) | 1.00 | 1.00 | |
| Yes | 82 (69.49) | 63 (66.32) | 0.73 (0.28 to 1.88) | 0.71 (0.25 to 1.99) | |
| Use of NHS services in past 12 months | |||||
| No | 1633 (51.91) | 1617 (53.33) | 1.00 | 1.00 | |
| Yes | 1513 (48.09) | 1415 (46.67) | 0.87 (0.75 to 1.00) | 0.87 (0.75 to 1.01) | |
| Contact with police in past 12 months | |||||
| No | 2732 (86.26) | 2673 (87.61) | 1.00 | 1.00 | |
| Yes | 435 (13.74) | 378 (12.36) | 0.83 (0.64 to 1.09) | 0.82 (0.63 to 1.07) | |
Students in intervention schools also had lower odds of having ever smoked regularly (OR 0.58, 95% CI 0.43 to 0.80; adjusted risk difference –0.03, 95% CI –0.05 to –0.01), lower odds of having ever drunk alcohol (OR 0.72, 95% CI 0.56, 0.92; adjusted risk difference –0.03, 95% CI –0.06 to –0.01) and lower odds of having ever been offered or tried illicit drugs (OR 0.51, 95% CI 0.36 to 0.73). There was evidence that among students in the intervention arm who had ever smoked the time since their last cigarette was longer than in the control arm and, similarly, that, among those who had ever drunk alcohol, there were lower odds of having drunk in the past week (OR 0.67, 95% CI 0.50 to 0.91), number of times been really drunk (OR 0.57, 95% CI 0.33 to 0.98) and binge drinking (OR 0.77, 95% CI 0.59 to 1.00). Similarly, students in intervention schools had lower odds of having ever been in contact with the police in the past 12 months than those in control schools (OR 0.74, 95% CI 0.56 to 0.97; adjusted risk difference –0.02, 95% CI –0.04 to –0.00).
We found no evidence of differences in the CHU9D HRQoL score, sexual risk behaviour, use of contraception at most recent sexual contact, bullying perpetration or use of NHS services.
Staff outcome data
No differences were found in relation to staff stress or burnout of QoL between the control and intervention arms of the study at 24 or 36 months (Table 4).
| Measure | 24 months | 36 months | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Arm, mean (SD) | Unadjusted effect | Adjusted effect | Arm, mean (SD) | Unadjusted effect | Adjusted effect | |||||||
| Control | Intervention | Difference (95% CI) | p-value | Difference (95% CI) | p-value | Control | Intervention | Difference (95% CI) | p-value | Difference (95% CI) | p-value | |
| Staff stress and burnout – Maslach Burnout Inventory | ||||||||||||
| Emotional exhaustion score | 23.03 (0.73) | 24.23 (0.75) | 0.81 (–0.24 to 1.86) | 0.1322 | 0.80 (–0.34 to 1.93) | 0.1680 | 23.97 (0.63) | 23.81 (0.63) | –0.46 (–1.52 to 0.61) | 0.3998 | –0.55 (–1.74 to 0.64) | 0.3625 |
| Depersonalisation score | 5.71 (0.32) | 5.91 (0.33) | 0.25 (–0.27 to 0.78) | 0.3434 | 0.26 (–0.30 to 0.81) | 0.3620 | 6.22 (0.36) | 6.07 (0.36) | –0.05 (–0.58 to 0.48) | 0.8414 | 0.03 (–0.55 to 0.60) | 0.9276 |
| Personal achievement score | 34.67 (0.35) | 35.58 (0.37) | 0.80 (0.08 to 1.51) | 0.0291 | 0.88 (0.14 to 1.62) | 0.0195 | 35.12 (0.28) | 35.22 (0.29) | –0.02 (–0.73 to 0.69) | 0.9535 | 0.20 (–0.56 to 0.96) | 0.6127 |
| Staff quality of life – SF-12 v2 Health Survey | ||||||||||||
| Physical health score | 54.97 (0.32) | 55.22 (0.34) | –0.35 (–1.05 to 0.34) | 0.3187 | –0.26 (–0.99 to 0.47) | 0.4825 | 55.62 (0.36) | 55.18 (0.36) | –0.71 (–1.40 to –0.02) | 0.0449 | –0.61 (–1.36 to 0.13) | 0.1058 |
| Mental health score | 44.56 (0.49) | 43.71 (0.52) | –0.66 (–1.64 to 0.32) | 0.1883 | –0.45 (–1.49 to 0.58) | 0.3896 | 43.76 (0.44) | 43.69 (0.45) | 0.15 (–0.83 to 1.13) | 0.7642 | 0.31 (–0.76 to 1.38) | 0.5691 |
Ancillary analyses
Analysis of the primary and secondary outcomes by prespecified subgroup (see Appendix 1, Table 29) suggests that the intervention had a greater effect in boys than in girls for many secondary outcomes [PedsQL overall score; SDQ total difficulties score; SWEMWBS total well-being index; bullying perpetration (modified aggression scale); CHU9D overall score; ever smoked; ever drunk alcohol; contact with police]. The intervention was also more effective in students with higher baseline bullying experience, with greater effects on bullying (GBS score) and psychological secondary outcomes (PedsQL overall score; SDQ total difficulties score; SWEMWBS total well-being index; CHU9D overall score). The intervention was more effective in those with greater baseline aggression, with greater effects on both primary outcomes (GBS score; ESYTC overall score), psychological secondary outcomes (PedsQL overall score; SDQ total difficulties score; SWEMWBS total well-being index; CHU9D overall score) and risk behaviours (ever smoked; ever drunk alcohol). There was no suggestion of any difference in the outcomes by level of SES).
Adverse events
A serious adverse event was defined as (1) any death or event requiring hospitalisation in a young person reported to investigators or (2) a response to study questionnaires that prompted significant concerns about mental health, sexual risk or child safety, which were then communicated to the school. There were 15 reported SAEs to date (Table 5). The total number of reported serious adverse events was similar in each arm.
| SAE | Control | Intervention |
|---|---|---|
| Suicide | 0 | 2 |
| Responses showing potential for self-harm | 0 | 4 |
| Stabbing incidents | 0 | 2 |
| Possible non-consensual sex (including age < 10 years) | 6 | 0 |
| Disability or long-term illness | 1 | 0 |
| Total | 7 | 8 |
Process evaluation
Fidelity was variable, with a reduction in the fidelity of formal intervention activities in year 3. The median fidelity score for years 1 and 2 (maximum possible score 8) was 6 (interquartile range 5–7), whereas for year 3 (maximum score 4) the median was 1 (interquartile range 0–3). In year 3, 15 schools sustained restorative practice. Interviews with AG members and focus groups with staff in case study schools suggested that, in year 3, schools commonly incorporated what they regarded as the most useful AG functions into mainstream school structures and processes. For example, involving students in decision-making and further review of policies to ensure that these supported restorative practice was integrated into existing school committees. Regarding specific components (training, AGs and restorative practices), these were delivered with good fidelity. The fidelity of curriculum delivery was lower. Increased fidelity of delivery in the first 2 years of intervention was associated with lower rates of bullying victimisation at 24 months, but not with rates of aggression. The fidelity score for year 3 was not associated with either primary outcome (see Appendix 1, Table 30).
Slightly over half of staff in intervention schools were aware that the school had been taking steps to reduce bullying and aggression, with this falling slightly between years 2 and 3 (Table 6). About one-third of students reported being aware that the school had been taking steps to reduce bullying (Table 7). About half reported that, if there was trouble at school, staff responded by talking to those involved to help them get on better. About two-thirds of students reported that teachers and students got together to build better relationships or discuss their views and feelings. Other data on the process evaluation are shown in Appendix 1, Tables 31–35.
| Measure | Staff responses | |||||
|---|---|---|---|---|---|---|
| 24 months | 36 months | |||||
| Overall % across intervention group | N schools where school % is > 70% | N schools with no data | Overall % across intervention group | N schools where school % is > 70% | N schools with no data | |
| This school has recently been taking steps to reduce bullying and aggression (% yes) | 58.33 | 6 | 1 | 54.21 | 4 | 3 |
| I support this new work (% yes) | 91.71 | 19 | 2 | 91.40 | 20 | 3 |
| I understand what is meant by ‘restorative practice’ (% yes) | 77.90 | 14 | 1 | 79.52 | 13 | 3 |
| I support using restorative practice in schools (% yes) | 52.85 | 4 | 1 | 55.38 | 3 | 3 |
| If there is trouble at this school, staff response includes talking to those involved to help them get on better (% tick) | 85.99 | 16 | 1 | 89.14 | 17 | 3 |
| Teachers and students at this school get together to build better relationships (% often/sometimes) | 94.55 | 20 | 1 | 94.06 | 20 | 3 |
| Teachers and students at this school get together to discuss their views and feelings (% often/sometimes) | 83.95 | 19 | 1 | 82.39 | 17 | 3 |
| Measure | Staff responses | |||||
|---|---|---|---|---|---|---|
| 24 months | 36 months | |||||
| Overall % across intervention group | N schools where school % is > 70% | N schools with no data | Overall % across intervention group | N schools where school % is > 70% | N schools with no data | |
| This school has recently been taking steps to reduce bullying and aggression (% yes) | 34.29 | 0 | 0 | 33.00 | 0 | 0 |
| If there is trouble at this school, staff response includes talking to those involved to help them get on better (% tick) | 53.69 | 0 | 0 | 50.65 | 0 | 0 |
| Teachers and students at this school get together to build better relationships (% often/sometimes) | 69.68 | 12 | 0 | 67.85 | 9 | 0 |
| Teachers and students at this school get together to discuss their views and feelings (% often/sometimes) | 63.48 | 7 | 0 | 59.84 | 5 | 0 |
Many control schools implemented similar activities to those prescribed in the intervention but with very variable quality. We identified five control schools that delivered restorative practice, social and emotional skills education and consultation with students on policy. A per-protocol analysis excluding these schools showed no discernible differences in the intervention effects compared with the intention-to-treat analyses (Table 8).
| Outcome | Intention-to-treat (adjusted) | Per-protocol (adjusted) | ||
|---|---|---|---|---|
| Difference (95% CI) | p-value | Difference (95% CI) | p-value | |
| GBS overall score | –0.03 (–0.06 to –0.001) | 0.0441 | –0.03 (–0.06 to 0.01) | 0.1211 |
| ESYTC overall score | –0.13 (–0.43 to 0.18) | 0.4199 | –0.12 (–0.46 to 0.22) | 0.4869 |
| PedsQL overall score | 1.44 (0.70 to 2.17) | 0.0001 | 1.02 (0.22 to 1.83) | 0.0122 |
| SDQ total difficulties score | –0.54 (–0.83 to –0.25) | 0.0002 | –0.35 (–0.67 to –0.04) | 0.0289 |
| SWEMWBS total well-being index | 0.33 (0.00 to 0.66) | 0.0487 | 0.31 (–0.05 to 0.66) | 0.0943 |
| CHU9D overall score | 0.01 (–0.00 to 0.01) | 0.0795 | 0.00 (–0.00 to 0.01) | 0.6087 |
| Age of sexual debut | –0.35 (–1.48 to 0.78) | 0.5409 | –0.28 (–1.55 to 0.98) | 0.6589 |
| MAS bullying subscale score | –0.26 (–0.57 to 0.05) | 0.0976 | –0.21 (–0.57 to 0.14) | 0.2342 |
| Outcome | Intention-to-treat (adjusted) | Per-protocol (adjusted) | ||
| Odds ratio (95% CI) | p-value | Odds ratio (95% CI) | p-value | |
| Ever smoked regularly | 0.58 (0.43 to 0.80) | 0.0009 | 0.66 (0.47 to 0.93) | 0.0160 |
| Ever drunk alcohol | 0.72 (0.56 to 0.92) | 0.0094 | 0.79 (0.60 to 1.03) | 0.0764 |
| Ever tried illicit drugs | 0.62* (0.41 to 0.93) | 0.0221 | 0.91* (0.63 to 1.32) | 0.6258 |
| Used any contraception at first sex | 1.08 (0.50 to 2.35) | 0.8410 | 1.29 (0.54 to 3.08) | 0.5741 |
| Use of NHS in past 12 months | 0.96 (0.82 to 1.11) | 0.5652 | 0.93 (0.79 to 1.09) | 0.3685 |
| Contact with police | 0.74 (0.56 to 0.97) | 0.0269 | 0.73 (0.55 to 0.98) | 0.0369 |
Response rates
Some elements of the process evaluation, such as interviews with facilitators, school staff and students, as well as observations of training and AGs, achieved excellent response rates (see Appendix 1, Table 36). However, other elements, such as the surveys of staff delivering the curriculum or restorative practice (RP), achieved poor response rates. This reflected what, in retrospect, was an excessive data collection burden on schools. The low response rates for some elements of the process evaluation in year 3, such as the survey of AG members, also reflected the reality that in this year not all schools delivered all aspects of the intervention, rendering data collection obsolete. However, despite this, our multisource approach meant that we were still able to assess what was happening in most schools, with the exception of a few schools in year 3, where it is reasonable to assume that few, if any, intervention activities were being implemented.
Baseline context of intervention schools
Motivation to participate in the trial
A key theme was the variety in schools’ motivations to participate in the trial. One subtheme focused on a desire to address bullying or an interest in RP, while another subtheme was a desire to provide evidence of performance. For example, in one school, the external facilitator felt that the first year of the trial was focused more on generating evidence for Ofsted than on substantive changes that would benefit students:
Can I just say that the whole of the first year the emphasis was on just getting this Ofsted. I felt anything we did that had as an agenda.
Facilitator 9, school AH, interview, year 2
Another facilitator explained:
There’s also a thing where all schools are like this; they want to make sure . . . there’s an Ofsted agenda which drives all schools. And she wanted to make sure as well that she was . . . they want ‘outstanding’, so she wants to make sure that she’s got all the information possible to make sure that they can get through that.
Facilitator 2, school AD, interview, year 2
Context of control schools
Existing relevant services and practices in control schools during the trial period
Overall, in year 1, five schools delivered some form of RP, social and emotional skills education and student consultation on policy (schools AB, AC, AP, BH and BN), rising to 11 in year 3 (schools AB, AC, AG, AJ, AN, AP, AY, BA, BB, BH and BN).
School discipline systems
A key theme reflected in data from nearly all control schools was that addressing bullying, aggression, and other forms of misbehaviour was generally not schools’ main priority. In almost all schools, staff reported that improving educational attainment was their key priority. Only in one school did participants (school BG) report that addressing bullying was the school’s current main priority, and this was because it had been raised by Ofsted as an area to improve.
Existing use of RP was a common theme. In year 1, 15 schools were reported to use RP to address difficulties between students (schools AA, AB, AC, AG, AI, AJ, AN, AP, AR, BA, BB, BF, BG, BH and BN), with this rising to 17 in year 3 (to also include schools AQ and AY). Staff used the term RP and described processes that brought together each party in cases of conflict, as the following quotation illustrates:
So just going back to bullying and aggression in particular, would you say that your school uses any restorative approaches?
Constantly.
Constantly. OK.
Yeah . . . yesterday morning we had two boys in Year 12 . . . somebody had said something funny that the other boy didn’t find funny . . . He took it quite seriously, it blew out of all proportion; and my parent support advisor and I sat down with the victim . . . no, well . . . the alleged perpetrator, and said, look we need to resolve this. We need to mend this, you’ve got to get back into lessons together. I’m not going to be on anybody’s side . . . will you come and sit and meet? They had a little bit of time. They both said some things, we said things, they shook hands.
SLT member, school AC, interview, year 1
Other quotations, such as the following, offered a more nuanced account of how restorative sessions might focus on recognising and healing social and emotional conflicts:
We have another two students who were saying unkind things to each other in class and it just kept going on . . . And we would just talk through how it made each other feel, you know, what they’d said, what they’d done. And actually get them to come up with how they would resolve . . . how they’re going to resolve it, how they’re going to make each other feel better and what the strategies would be. So it may be, if they’re not going to be friends, how to deal with each other in the community; or if we are able to – quite often we can get them to resolve to the point where . . . they would actually be able to communicate with each other again.
Phase leader for years 7 and 8, school AR, interview, year 1
A recurring idea was that RP was an approach to behaviour management that could be used alongside more traditional, punitive measures, but that could be more effective in addressing the underlying causes of conflict. In the following quotation, a teacher discusses the school’s reasons for using the technique:
It’s about actually sitting down with the victims and the perpetrators and actually having those conversations whereby people are able to express how the situation or the incident or the thing that was said has made them feel you know. And have that opportunity to directly speak to those individuals who have caused the problem. And then for the other ones to be able to respond to that and actually really understand. Because I think sometimes when you sanction and they do their sanction, it’s like . . . OK, has anyone actually stopped to really understand what this has led the other person to feel like or . . . how it’s affected them you know? It’s easy just to give sanctions and then draw a line under it. But really for us it is about actually getting to the root of the problem and understanding and making people aware that this is not acceptable.
Head of year, school AI, interview, year 1
One subtheme was variety in how RP was used. In interviews with staff at some schools, for example in the following quotation, RP was presented as a technique that permeated staff practice in and outside classrooms, and to prevent as well as respond to conflict:
And then also all the teachers are aware of how we should treat each other and how students should treat each other and act as role models. So then if something happens in their lessons they will use restorative justice type conversations with students. And also, if there’s an incident, an argument or an act of unkindness within the lesson, then they’re followed up with a restorative justice meeting that’s usually held by the classroom teacher. So it does permeate across the school.
SLT member, school BH, interview, year 3
However, interviews in some other schools suggested that RP was regarded more as a resource to draw on in particular circumstances:
If it’s a bunch of girls who are generally friends and they can’t seem to get on and there’s constant bickering, we might get one of our behaviour support workers in and they do a restorative thing at lunchtime where they get the girls together and they all have a chance to say their bit about what they’re unhappy about in the relationship or not. And then go on from there. So we sometimes do that although it’s not that often. We probably have about four of those sessions a year with different girls.
SLT member, school BB, interview, year 1
Most of those reporting that their school used RP suggested that it had been used for some time, but a few suggested that it had started after the school had been allocated to the control group in the trial. One SLT member described how, in response to being allocated to the control group, the school had initiated its own programme of RP:
I was really, really upset that we didn’t get picked as one of the schools because we’re actually at a point where we’re going through so much change and what you guys were offering was exactly what we need. But we’re going to do it ourselves, so it’ll be interesting to see . . . how we compare.
SLT member, school BG, interview, year 3
Training was another subtheme. Eight control schools were reported to have trained some staff in using RP in year 1 (schools AB, AC, AG, AI, AW, BB, BH and BL), with this rising to 13 in year 3 (schools AA, AB, AC, AJ, AQ, AR, AY, BA, BB, BG, BH, BL and BN).
The ubiquity of policies and rules was another subtheme. In years 1 and 3, 18 schools were reported to have a policy on bullying or aggression (schools AA, AB, AC, AG, AI, AJ, AN, AP, AQ, AR, AY, BA, BB, BF, BG, BH, BL and BN). In year 1, staff of nine schools reported that their school had revised its policy on bullying or aggression in the last year (schools AA, AI, AN, AP, AR, BA, BB, BF and BN); in year 3 this rose to 11 schools (schools AA, AG, AI, AN, AQ, AR, AY, BB, BF, BH and BL). Policies on bullying and aggression were sometimes part of larger policies, such as on behaviour management or ‘culture for learning’. Schools varied enormously in how staff described the importance of the policies. In most schools, the policies were salient in staff accounts and were said to be reviewed regularly. However, in a few schools, the policies appeared to exist but not to greatly inform practice and to be seldom reviewed, as the quotation below illustrates:
Do you have any formal policies related to bullying and aggression?
Yeah. We have an anti-bullying policy. We also have a behaviour policy. And a cyber-bullying policy.
And how often do you review them and who does this and how long does it take?
Yeah. Well we’re not very good on policies. We’re good at practice, we’re better at practice than we are at policy.
SLT member, school AB, interview, year 1
All schools had rules for student behaviour. Schools varied in whether these were presented primarily in terms of positive expectations or as a list of unacceptable behaviours. However, in all schools, bullying, aggression and other forms of physical or non-physical violence were identified as unacceptable. All schools employed punitive measures. These could work as a complement or an alternative to restorative measures. Many participants reported that punitive measures and RP were used alongside one another.
Personal, social and health education
The provision of PSHE was a recurring theme in staff accounts, with diversity of provision again an important subtheme. About half of schools offered regular timetabled subject lessons and around half delivered PSHE in tutor time or on so-called ‘off-timetable’ or ‘drop-down’ days. In those schools where provision did not occur in specifically timetabled lessons, it was a recurring subtheme, exemplified by the quotation below, that such a format of provision was not ideal:
But obviously we have . . . like the PSHE days. So rather than it being embedded . . . we have 4 PSHE days a year. Like one-off days where the curriculum is changed to focus on exactly like the well-being. But from my point of view I think it would be better run across . . . like weekly during tutor groups, so it’s consistent rather than kind of . . . It seems a bit like an add-on.
Pastoral co-ordinator, school BL, interview, year 1
It was very difficult to assess the extent to which control schools were delivering social and emotional skills curricula to students because staff discussed such provision in very vague terms, generally because they were not directly involved in its delivery. Staff commonly referred in general terms to lessons addressing topics such as ‘well-being’, ‘resilience’, ‘relationships’ or ‘social issues’, but were vague about details. In years 1 and 3, there was some evidence that 13 schools provided their students with some sort of social and emotional skills curriculum (schools AB, AC, AG, AJ, AN, AP, AQ, AR, AY, BA, BB, BH and BN). Staff commonly reported that social and emotional education was integrated into a range of academic subject lessons, but this provision did not appear to be based on a formal curriculum with clear learning objectives. For example, a member of staff described how social and emotional learning occurred in lessons such as drama:
The social and emotional education, is that covered in PSHE?
To some extent, yeah. There’s stuff, there’s definitely lessons and things about healthy relationships and interaction buddying, these kind of things are . . . are covered there.
Are they covered in any other subjects?
I think that, obviously being a drama teacher, we do a lot of stuff to do with well-being and . . . kind of emotional education. But there aren’t any subjects that . . . are kind of . . . responsible for teaching it.
Teacher and deputy head, school AG, interview, year 1
Student participation in decision-making
Student participation in decision-making was a recurring theme. In years 1 and 3, there was evidence that 14 schools had an active student forum (schools AB, AC, AG, AI, AJ, AP, AQ, AR, BA, BB, BF, BG, BH and BN). In years 1 and 3, 15 schools were reported to consult with students on some policy decisions (schools AA, AB, AC, AG, AI, AJ, AN, AP, AQ, AY, BA, BB, BG, BH and BN). In year 1, there was evidence that in seven schools students and staff met together to make decisions (schools AC, AJ, AP, AQ, BA, BN and BG); this rose to 10 schools in year 3 (schools AA, AB, AC, AG, AP, AQ, AY, BB, BG and BN). In year 1, there was some evidence that five schools (schools AB, AJ, AP, AR and BN) surveyed students on health- or well-being-related issues; this rose to six schools (schools AG, AJ, AR, AY, BA and BB) in year 3.
In some schools, staff reported elaborate processes for students’ active participation in decision-making alongside staff. For example, a staff member in one control school reported a parallel student leadership team interacting with the staff SLT:
We have student voice, student council; so we have . . . The same where we have SLT we have JLT [junior leadership team], which is the junior leadership team. These are the students who apply for the job, through an application process. And they have last interviews and then they are selected as member of the JLT. They are attached, each of those is attached to a member of SLT if you like, so they kind of shadow them.
Head of year, school AI, interview, year 1
However, in other schools, staff reported a much more limited and what was sometimes seen as a tokenistic system for participation, as the following quotation from a staff member suggests:
We have the student voice and all those kind of school councils and stuff, which . . . I don’t know; my own personal view is I don’t know, they’re a little bit tokenistic . . . We’ve got our school prefect teams. But I guess ultimately . . . they can propose quite a few things, but it rests with the Head and the senior leadership team whether those things are going to go through or not. So I think students . . . I think certain voices . . . I think they’re heard. But from working, again talking from a pastoral level, and working with the more challenging students; probably they don’t feel like their voice is heard.
Pastoral co-ordinator, school BL, interview, year 1
Existing relevant policies and practices in intervention schools during the trial period
School discipline systems
Another theme was staff interest in RP. At baseline, staff from five schools reported in interviews that they had been interested in moving towards using RP to address student behaviour before taking part in the trial (schools AD, AK, AM, AX and BI). A subtheme was the existing use of the approach. Seven schools (schools AH, AK, AL, AX, BD, BI and BK) were already using some form of RP. Delivery within a school was generally inconsistent:
We also have a guy who works in the internal exclusion room and wherever he has two students who’ve been involved in an incident together, he will sit them down together or talk about the incident just within the room, and approach it from that way. So yeah, the restorative practice does go on. But I think it’s in quite isolated pockets; it’s not across the whole staff.
Year lead, school AH, interview, year 1
Staff in three other schools reported holding conversations to address incidents of bullying or misbehaviour, but did not describe this as RP (schools AD, AS and BE). Some teachers used restorative approaches alongside other approaches. A teacher from school BD explained:
The approach to bullying is more, from my experience and other members of staff, that if there is an issue, having a discussion about it is the first action to take and having the students or who’s involved having a discussion about, you know, this is what’s happened, this is how this person feels, and that, and to express themselves so that the other students can . . . hear you know what they’re doing has an effect. And also they wouldn’t like it. And then usually you might just set a detention, or they sometimes underline the issues where students have been friends before, they’re not friends any more or stuff like that.
Behaviour manager, school BD, interview, year 1
However, another subtheme was the use of more punitive approaches. Intervention facilitators described schools AH, AT and BD as primarily managing student behaviour through quite ‘disciplinarian’ approaches. A teacher from school AT described the school as dealing with misbehaviour ‘quite severely, quite harshly’. When asked if the school had ever used RP before, the teacher replied:
No, not at all. It’s more . . . I feel more accusatory, more . . . ‘you have done this’ and then there’s been the punishment that follows: isolation and then to be expelled for a certain number of days, whatever it is.
Intervention co-ordinator, school AT, interview, year 1
The importance of written policies was another subtheme, with most schools having policies on bullying, and many schools embedding this within their broader behaviour policies. Staff in most schools reported that they were clear about the bullying policy. Occasionally, staff reported not knowing what the bullying policies were (schools AE, AM and AU) or that the policies were not implemented (schools AD and AM).
Training was another subtheme. Several schools had at least a few members of staff who had at some point been trained in RP and who used this technique individually (schools AD, AH, AK, AO, AT, AZ, BE and BM). Staff in only three schools reported having whole-school training (schools AH, AO and BC) and 10 reported receiving no training in dealing with bullying (schools AE, AF, AL, AM, AU, AW, AX, AZ, BE and BK). Some schools offered training on issues indirectly connected with bullying, such as behaviour management (schools AK, AM, AS and BE) or safeguarding (schools AD, AF, AT, BIAD, AF, BI and AT):
We have loads of training on all kinds of different things. We are inundated with training. But directly relating . . . we have child protection training, but that doesn’t really cover bullying, so no, I don’t think there’s anything that specifically deals with bullying.
Subject teacher, school AD, interview, year 1
Personal, social and health education
The variety in provision of PSHE was a prominent theme. Most schools offered distinct PSHE lessons or incorporated such learning into tutor times, generally weekly or twice a week (schools AD, AH, AK, AM, AO, AS, AU, AW, BE and BI). A few supplemented this with teaching PSHE content in assemblies (schools AL, AX and BE) or specific days or part-days when students were taken off their normal timetable of lessons (schools AD, AH, AS, AT and AX). Some schools delivered PSHE through other subjects, including citizenship, religious education and biology (schools AE, AL, AW, AX, BE and BI). The amount of time and scheduling varied greatly, from 20 minutes per fortnight (school AW) to 20 hours per term (school AS). In some schools, teachers reported that the time spent on PSHE had contracted in recent years (schools AW and AU). There was a broad recognition that the time allocated to PSHE was insufficient (schools AD, AL, AO, AT, AW, AX, BD and BE):
I don’t think you can do enough in that short period of time [20 minutes, twice a week]. I think again, it’s almost kind of doing it because . . . we’re obliged to cover the material. I think if it’s a real focus and a genuine focus, I think more time should be devoted to it.
Head of learning, school AX, interview, year 1
Tokenism was a prominent subtheme. Teachers in some schools reported that although PSHE in their schools addressed health and well-being, this was somewhat tokenistic, with the school’s overwhelming focus being on attainment:
I suppose the head teacher superficially would verbalise that, and by signing up to this project has put some resources behind it. But in practice, politically it isn’t easy to get the time or the resources towards that.
Assistant head-teacher, school BD, interview, year 1
I think it comes down, unfortunately comes down to exams, it comes down to . . . It is a very short term . . . you know, if we drop this for an hour we can have an extra maths lesson or an extra English lesson.
Head of department, school AW, interview, year 1
Student participation in decision-making
Student participation in decisions was a recurring theme across schools. Staff reported in interviews that almost all schools had some kind of student council and some had more than one group for discussing student views (schools AF, AK, AL, AS, BC and BE). In some schools, students were invited to share their opinions via surveys or formal discussions with staff (schools AD, AF, AS, AU, AX and BI) or informally (schools AS, BC and BN). Three schools reported no such mechanism (schools AM, BE and BI). Schools aimed either to involve a cross-section of students, including those with a history of misbehaviour (schools AD, AK, AL, AS, AW, AX, BD and BI), or to over-represent students from lower socioeconomic groups (school AS) or those exhibiting challenging behaviour (schools AM, AX and BI).
Intervention implementation
Intervention fidelity
Fidelity per school
Overall fidelity was variable, with a reduction in the fidelity of formal intervention activities in year 3 (see Appendix 1, Tables 37 and 38). The median fidelity score for years 1 and 2 (maximum possible score of 8) was 6 (interquartile range 5–8), whereas for year 3 (maximum score of 4) the median was 1 (interquartile range 0–3). Two schools achieved perfect fidelity in years 1 and 2, six scored 7 out of 8 points, another six scored 6 out of 8 points and the remaining seven scored below this. Two schools achieved perfect fidelity in year 3, whereas another three scored 3 out of 4 points. In year 3, 15 schools sustained RP. Interviews with AG members and focus groups with staff in case study schools suggested that, in year 3, schools commonly incorporated what they regarded as the most useful AG functions into mainstream school structures and processes, for example involving students in decision-making and further reviewing policies to ensure that these supported RP and were integrated into existing school committees. Regarding components, training and AGs were delivered with good fidelity. The fidelity to the curriculum was lower. Schools AF, AM, BE and BI did not engage with the trial in year 3 beyond some teachers’ continued use of RP. A higher fidelity score for years 1 and 2 was associated with lower rates of bullying victimisation at 24 months but not with decreased rates of aggression. The fidelity score for year 3 was not associated with either primary outcome.
Overall fidelity per facilitator
The fidelity of facilitators was judged for those elements of the intervention which they facilitated (in years 1 and 2 only), expressed as the mean score achieved 0–1 across these two years. Most facilitators achieved mean scores in the range 0.55–0.83 (Table 9). Two facilitators scored 1 in their joint work across three schools. One facilitator scored 0.33 working with one school and another scored 0.25 working across four schools. One facilitator was replaced after year 1 and, as a result, this individual’s schools were redistributed to other facilitators.
| Facilitator | Number of schools worked in | Mean fidelity score for their AGs | Mean score overall/1 | ||
|---|---|---|---|---|---|
| Achieving minimum six meetings | Reviewing policies/rules | Implementing locally decided actions | |||
| 1 | 3 | 0.33 | 1 | 1 | 0.77 |
| 2 | 2 | 0.5 | 1 | 1 | 0.83 |
| 3 | 1 | 0 | 1 | 0 | 0.33 |
| 4 | 1 | 1 | 1 | 0 | 0.66 |
| 5 | 4 | 0.25 | 0.5 | 0.75 | 0.25 |
| 6 | 2 | 1 | 0.5 | 1 | 0.83 |
| 7 replaced by 8 | 3 | 1 | 1 | 1 | 1 |
| 9 | 3 | 0.66 | 1 | 0.66 | 0.77 |
| 7 replaced by 2 | 1 | 0 | 1 | 1 | 0.66 |
Fidelity of training in restorative practice
According to the trainers’ diaries, there was very good fidelity of delivery of the all-staff training (Table 10). Data were available for 19 of the 20 schools and, for these, fidelity was as intended, other than less than intended coverage for the three sessions on maintaining relationships after difficult conversations, plus one session in which the intended DVD was not shown.
| Training implementation | Fidelity self-reported in trainer diary, n (%) of schools | |||
|---|---|---|---|---|
| As intended | Less than intended | Not at all | Schools with no data | |
| Covered ‘what is restorative justice/practice’ | 19 (95) | 0 | 0 | 1 (5) |
| Covered ‘the importance of language’ | 19 (95) | 0 | 0 | 1 (5) |
| Covered ‘what we do to challenge bad behaviour/nature of challenge’ | 19 (95) | 0 | 0 | 1 (5) |
| Covered ‘the importance of emotions’ | 19 (95) | 0 | 0 | 1 (5) |
| Covered ‘the importance of listening’ | 19 (95) | 0 | 0 | 1 (5) |
| Covered ‘maintaining the relationship after difficult conversation’ | 16 (80) | 3 (15.79) | 0 | 1 (5) |
| Used PowerPoint slides | 19 (95) | 0 | 0 | 1 (5) |
| Used DVD | 18 (90) | 0 | 1 (5) | 1 (5) |
| Facilitated paired activity | 19 (100) | 0 | 0 | 1 (5) |
| Facilitated small-group activity | 19 (95) | 0 | 0 | 1 (5) |
In total, across all schools, 1878 staff attended all-staff training and 131 staff attended in-depth training. Fifteen schools met the target of having at least five staff members receive in-depth training in using RP, over 3 days (schools AD, AE, AF, AH, AK, AL, AO, AT, AU, AW, AX, AZ, BE, BC and BI). The protocol did not include assessment of the fidelity of in-depth training. A few schools (schools AF, AK, AT, BD, BI and BM) received the training late in the first year of the study, reducing the extent to which RP could be implemented in the first year of intervention. During all six observations of the all-staff training, researchers judged that participants were moderately to very enthusiastic but that the groups were too large. Participatory learning could then be achieved only through small-group or paired activities.
Fidelity of needs assessment surveys
Needs assessment surveys were completed in all schools, with generally high response rates (Table 11). In year 1, 11 schools achieved student response rates of ≥ 90%, six achieved response rates in the range 80–89% and three achieved response rates in the range 70–79%. In year 2, these figures were 10, 7 and 3, respectively. In year 3, five schools achieved responses of ≥ 90%, 10 achieved responses in the range 80–89%, three achieved responses in the range 70–79% and four achieved responses < 70%. According to facilitator diaries and meeting minutes, all schools in year 1 and 14 schools in year 2 reported using the needs data to inform priorities and actions. In year 3, four schools (schools AL, AO, AT and BD) reported using the needs data to inform decisions. Three more read the report and used it for discussions (schools AH, AS and AU) and the two schools that most disliked the survey reported that they found the resulting needs assessment report useless (schools AE and AU).
| Needs assessment surveys in intervention schools | Number (%) of schools | ||
|---|---|---|---|
| Year 1 | Year 2 | Year 3 | |
| Conducted | 20 | 20 | 20 |
| Schools with response rate in the range of | |||
| < 70% | 0 (0.0) | 0 (0.0) | 4 (20.0) |
| 70–79% | 3 (15.05) | 3 (15.0) | 1 (5.0) |
| 80–89% | 6 (30.0) | 7 (35.0) | 10 (50.0) |
| ≥ 90% | 11 (55.0) | 10 (50.0) | 5 (25.0) |
Fidelity of action group meetings
In the first year, 19 schools completed all six AG meetings (AGMs) as intended and only one (school AM) convened only four meetings. In the second year, 11 schools completed six AGMs (schools AD, AE, AH, AK, AL, AS, AU, AX, BC, BD and BE), four held five AGMs (AF, AT, AW and BI), three held four AGMs (schools AM, AO and BM), and one held three AGMs (school BK). Thus, 11 schools achieved the target of holding at least six AGMs per year in both years 1 and 2 (schools AD, AE, AH, AK, AL, AS, AU, AX, BC, BD and BE). Of these schools, only AE and AS maintained perfect AG fidelity into the third year of the intervention.
In year 3, several schools (schools AF, AM, BE and BI) did not hold any AGMs, whereas other schools either used AGs for quite different purposes or used other meetings to implement the intervention. Schools AK, AO and AZ began to use AGs to train students or staff in RP or mentoring. Schools AE, AK and AT used student council or student voice committees to fulfil the function of an AG. Seventeen schools succeeded in reviewing school policies and rules during year 1 or 2 (schools AD, AE, AH, AK, AL, AM, AO, AT, AU, AW, AX, AZ, BC, BE, BI, BK and BM). In year 2, four changed school rules (schools AE, AH, AM and AO). In year 3, five schools reviewed their behaviour policies (schools AD, AL, AX, BC and BD).
Most AGs reviewed their rules or policies relating to behaviour (schools AD, AF, AH, AO, AU, AW, AX, AZ, BD and BE) or rewards and sanctions (schools AX, AZ, BC and BM). A recurring theme in interviews with staff members and facilitators was that the school focused considerable energy on revising school policies informed by restorative principles (schools AH, AL, AM, AO, AU, AW, BD and BI):
The behaviour policy has been rewritten now. So restorative practice is part of it. Interactions with parents, interactions with students . . . we’re going to do staff training in terms of how do you talk to parents, how do you talk to students, language used in the classrooms. All [newly qualified teachers]. now have training in restorative practice when they arrive at the school . . .
Senior leader, school AW, interview, year 2
Sixteen schools enacted local decisions in years 1 and 2 (schools AD, AE, AF, AJ, AK, AL, AM, AO, AT, AU, AW, BC, BD, BE, BK and BM). In year 3, 10 schools completed locally decided actions (schools AE, AH, AK, AL, AO, AS, AT, AW, BC and BD). Common locally decided actions included cascading RP training to staff who had not attended the in-depth training, or to students so that those students could work as peer mentors or buddies (schools AH, AK, AS, AU, AW, AX, AZ, BC, BD, BI, BK and BM) or resolve conflicts themselves (schools AS, AU and BM). Others included delivering assemblies on RP (schools AE, AI, AO, AS and BM), instituting specific safe spaces on the school site (schools AF and AW) and various approaches to encouraging girls’ empowerment (school BD). Safety concerns identified by students were addressed in some schools by having staff patrol hallways between classes (schools AF, BD and BI) to discourage aggressive behaviours. Some schools offered more after-school clubs (schools AE, BD, BK), and one offered drop-in services (school AS) to improve school engagement and social and emotional health among students. School BK funded new, external, specialist staff to work with students to improve mental health and well-being, including a counsellor and a boys’ boxing coach. Many of these activities specifically aimed to broaden students’ social circles through engaging with people in other year groups. Other schools made improvements to the physical environment, including decorating the schools with informational or motivational posters (schools AD, AO and BI) and displaying student work (school AS).
According to aggregate data from our survey, all AGs were assessed by their members in years 1 and 2 as having a good or quite good range of staff from across the school, and a good or quite good range of students of different backgrounds and academic ability (see Appendix 1, Table 37). All were assessed by their members in terms of it being definitely or partly true that there was someone from this school on the AG who co-ordinated it and showed leadership.
A rare theme was adaptation of, or deviation from, the intervention manual. One selective school (school AU) did not view itself as having significant problems with bullying or aggression and, therefore, used the AG primarily as a way to revise the homework policy to try to reduce the stress on students arising from receiving multiple homework assignments on the same day. They held double-meetings so that students were removed from lessons less frequently (school AU). Two schools broke the AG into subcommittees (schools AW and BD). This was done in one school so that students were less intimidated to speak in front of a large group and in the other school so that multiple groups could get more done. One school held only one AG meeting in year 2 because its student council already brought students and staff together to make collective decisions and review rules and policies (school AZ).
Schools AS and AD did not formally review their rules as part of the intervention but did incorporate the restorative sentiment into their new interpretation or enforcement of the rules:
So whilst there isn’t an individual rule that has been changed, many policies and practices as a result of the project so far are being flexed and adapted and tweaked accordingly.
Deputy head-teacher, school AS, interview, year 1
Among the AGMs we observed, some were noticeably well led (schools AD, AE, AM, AO, AU and BI), whereas others seemed poorly led (schools AH, AM, BD and BK). Researchers noted that in three schools in particular, students’ comments or concerns did not appear to be taken seriously (schools AH, AM and BD).
Fidelity of restorative practice
Because response rates to the surveys of those trained to deliver RP were very low, we instead assessed the extent of RP by analysing the responses to the 24-month all-staff survey question about RP. In 12 schools (all but schools AF, AH, AK, AM, BD, BE, BI and BM), at least 85% of staff reported that if there was trouble at their school, staff responded by talking to those involved to help them get on better. Qualitative research generally suggested that, in the course of the 3 years of the intervention, there was a continuing increase in the use of restorative approaches. The vast majority of staff reported in surveys that teachers and students got together sometimes or often to build better relationships, or to discuss their views and feelings.
Interviews and focus groups suggested that variability of the form and scope of the RP implemented was a key theme. The majority of schools were reported to be regularly using some form of RP (schools AD, AE, AK, AL, AO, AT, AU, AX, AZ, BD, BI and BM). In some schools, key staff members, particularly the trial champion and pastoral staff, used restorative approaches, but felt frustrated that the school was generally slow to adapt and normalise such work (schools AM, AO, AW, AX, BI and BK), often because the broader culture of the school staff was not supportive or because these schools lacked the management capacity to ensure that restorative approaches were more widely adopted. Schools AU, BD and BM used RP primarily as a strategy to manage classrooms and learning behaviour.
Fidelity of social and emotional education
Response rates to our annual survey of those responsible for delivering the curriculum were poor, so we drew on both this and interviews with curriculum leads to gauge the fidelity of curriculum delivery. This established that in year 1 only 12 schools delivered the curriculum as intended in the protocol (5 hours’ total teaching time or teaching comprising unit 1 as well as one or more additional units) (schools AD, AE, AF, AH, AM, AS, AU, AW, AX, AZ, BC and BE) and in year 2 half as many did so (schools AD, AE, AH, AS, AW and AZ). In year 3, only five schools delivered this threshold of teaching time (schools AD, AL, AS, AT and BC). The curriculum was taught in various forms across the schools, including in 10- to 20-minute sections in tutor time, rarely in specific PSHE lessons, and quite often in off-timetable days focused on PSHE topics.
Many schools did not deliver the curriculum materials as they were packaged. Staff in several schools commented that they needed to adapt the curriculum because it did not address the needs of their students, or because the materials were too simplistic (schools AD, AE, AF, AK, AS and AW). There was some evidence that some schools treated the delivery of the curriculum as a box-ticking exercise. They implemented the minimum required without ensuring that implementation was strong enough to maximise its potential impact. For example, at the end of year 1, a SLT member in school AW admitted that the school had not ensured that the curriculum was delivered by the most appropriate teachers:
Our strongest teachers aren’t our PSHE teachers and our . . . you know . . . RE teachers, they’re not really our . . . our best teachers in the school . . . if we’re really going to place importance in it, how important are we going to think about delivery of it? It’s all very good going through the motions, but unless you do it properly there’s no point doing it.
Assistant head-teacher, school AW, interview, year 1
Participation and reach
We drew on facilitator diaries, AG minutes and training attendance sheets to estimate the numbers of staff and students participating in training and AGs. All-staff training on average reached 103 staff members (range 34–162 staff members) per school in schools for which data were available. In-depth training on average reached 6.35 staff members (range 2–13 staff members) per school in schools for which we have data. Fifteen schools sent at least five staff members on this training (see Appendix 1, Table 39).
On average in year 1, 7.4 staff members (range 3–12 staff members) per school participated in AGs in schools for which data were available, with this falling to 5.4 staff members (range 2–9 members) per school in year 2. On average in year 1, 7.8 students (range 5–14 students) per school participated in AGs in schools for which we have data, with this increasing to 8.8 students (range 4–23 students) per school in year 2. We did not calculate figures on participation in year 3 because schools implemented AGs in such heterogeneous ways.
Schools were encouraged to, and most did, select a diversity of students to serve on the AG, including those with a history of misbehaviour (schools AD, AF, AL, AO, AT, AW, AX, BC, BK, BI and BM), those who struggled academically (schools AD, BC, BI, BK and BM) and those who were at risk of disengagement (AK and BC). Other schools focused recruitment on students who were high achievers (schools AK, AS and AW). These schools sometimes dropped lower-attaining students from AGs. Most schools selected students across school years to participate, but some (schools AF, AL and AW) invited only those in the study cohort.
Just over one-third of staff completing the all-staff survey at the end of year 2 reported that students were involved in developing the behaviour policy or school rules, with this rising slightly by the end of year 3 (Table 12). At the end of years 2 and 3, only about one-third of students reported being aware that the school had been taking steps to reduce bullying. By the end of year 2, around one-third of students reported that they had experienced lessons about relationships or emotions, with this falling to around one-quarter by the end of the third year (Table 13). Only around one-quarter of students reported that students had been involved in developing the behaviour policy or school rules. Across both time points, only about one-sixth of students knew what was meant by the term ‘restorative practices’. About half reported that, if there was trouble at school, staff responded by talking to those involved to help them get on better. About two-thirds of students reported that teachers and students got together to build better relationships or discuss their views and feelings. Focus groups with students not involved in AGs suggested that there was broader awareness of the work of the AG among students in some schools (schools AE, AF, AH, AW and BK) more than others (schools AO, AS, AT, AZ, BC and BD).
| Measure | Staff responses | |||||
|---|---|---|---|---|---|---|
| 24 months | 36 months | |||||
| Overall % across intervention group | Number of schools where school % is > 70% | Number of schools with no data | Overall % across intervention group | Number of schools where school % is > 70% | Number of schools with no data | |
| This school has recently been taking steps to reduce bullying and aggression (% yes) | 58.33 | 6 | 1 | 54.21 | 4 | 3 |
| I support this new work (% yes) | 91.71 | 19 | 2 | 91.40 | 20 | 3 |
| I understand what is meant by ‘restorative practice’ (% yes) | 77.90 | 14 | 1 | 79.52 | 13 | 3 |
| I support using restorative practice in schools (% yes) | 52.85 | 4 | 1 | 55.38 | 3 | 3 |
| If there is trouble at this school, staff response includes talking to those involved to help them get on better (% yes) | 85.99 | 16 | 1 | 89.14 | 17 | 3 |
| Teachers and students at this school get together to build better relationships (% often/sometimes) | 94.55 | 20 | 1 | 94.06 | 20 | 3 |
| Teachers and students at this school get together to discuss their views and feelings (% often/sometimes) | 83.95 | 19 | 1 | 82.39 | 17 | 3 |
| At this school, students were involved in developing the behaviour policy or school rules (% yes) | 38.72 | 1 | 1 | 44.05 | 2 | 3 |
| Measure | Staff responses | |||||
|---|---|---|---|---|---|---|
| 24 months | 36 months | |||||
| Overall % across intervention group | Number of schools where school % is > 70% | Number of schools with no data | Overall % across intervention group | Number of schools where school % is > 70% | Number of schools with no data | |
| This school has recently been taking steps to reduce bullying and aggression (% yes) | 34.29 | 0 | 0 | 33.00 | 0 | 0 |
| This past year in class, we have been learning how to get on well together (% yes) | 37.68 | 0 | 0 | 26.98 | 0 | 0 |
| This past year in class, we have been learning how to manage our emotions (% yes) | 33.28 | 0 | 0 | 24.52 | 0 | 0 |
| This past year in class, we have been learning how to resolve conflict (% yes) | 38.72 | 0 | 0 | 28.49 | 0 | 0 |
| I understand what is meant by ‘Restorative Practice’ (% yes) | 15.42 | 0 | 0 | 13.52 | 0 | 0 |
| If there is trouble at this school, staff response includes talking to those involved to help them get on better (% yes) | 53.69 | 0 | 0 | 50.65 | 0 | 0 |
| Teachers and students at this school get together to build better relationships (% often/sometimes) | 69.68 | 12 | 0 | 67.85 | 9 | 0 |
| Teachers and students at this school get together to discuss their views and feelings (% often/sometimes) | 63.48 | 7 | 0 | 59.84 | 5 | 0 |
| At this school, students were involved in developing the behaviour policy or school rules (% yes) | 28.84 | 0 | 0 | 24.08 | 0 | 0 |
Even if the AG itself was not well known, students on AGs in some schools reported that their peers had noticed changes being made but were unaware of how these had come about (schools AD, AT and BK):
They’re aware of certain changes. But they’re not really aware of why people are doing this. So they see it as, why have they put up a basketball hoop? Oh, that’s probably for people to play on. They don’t see why . . . what caused it to happen. It’s only people on the action group and some teachers are aware of it. Everyone else is oblivious to the situation.
Male, year 9 student, school BK, interview, year 1
Slightly over half of staff in intervention schools were aware that the school had been taking steps to reduce bullying and aggression, with this falling slightly between years 2 and 3 (see Table 12). In interviews with SLT members in year 3, some reported that although the name of the intervention was sometimes not known by all staff members, the push for increased use of RP was more widely known.
Reception and responsiveness
Among the staff who were aware that the intervention was occurring, the vast majority were supportive overall at both time points (see Table 12). With the increasing expectations for educational attainment, some staff resented the work involved in the intervention given its primary focus on health and well-being rather than attainment:
One of the challenges that I foresee is that . . . I’ve worked at a few schools and I don’t think this school is unusual in that teachers feel responsible for academic progress and they don’t . . . feel responsible for student well-being in the same way. And I think that’s a result of accountability measures being focused around those things and so the challenge is to move that perception so that staff take ownership of all of those things. But also then to help them to understand that the two things obviously are linked.
Assistant head-teacher, school BD, interview, year 1
Commitment to the intervention was notably lower in schools where the pre-existing approach to behaviour was disciplinarian or not supportive of student participation in decision-making (schools AH, AT and BD).
Needs assessment surveys
The undertaking of the needs assessment surveys was acceptable to staff and students, evidenced by the high response rates across all schools. The reception given to the reports from these surveys is discussed under AGs.
Training
Those receiving in-depth training reported high satisfaction (Table 14). Participants across all intervention schools reported that they ‘probably’ or ‘definitely’ had learned useful skills, and all indicated that they would recommend the training to colleagues. Over 90% of participants across all schools reported they intended to put into practice the skills learned, felt confident putting into practice the skills learned, and rated the training as good or excellent. Almost 90% rated the training as excellent.
| Measure (response option that indicates satisfaction) | Responses | |
|---|---|---|
| Overall % members responding as indicated | Number of schools where > 70% of members responded as indicated | |
| Do you feel that you learned useful skills at this training? (yes definitely or yes probably) | 100 | 20 |
| Do you feel confident in putting into practice the skills you have learned today? (yes) | 91 | 20 |
| Do you intend to put the skills you learned to use in your everyday practice? (yes) | 95 | 20 |
| Would you recommend this training to a colleague? (yes) | 100 | 20 |
| Overall, how would you rate this training? (good or excellent) | 99 | 20 |
In interviews, staff were very positive about both the all-staff and the in-depth training, with some describing it as ‘brilliant’ (schools AX and AZ), ‘transformational’ (school AW), and helpful with behavioural issues:
I’ve been on two trainings this term and they’re the best two trainings I’ve ever been on in my life. They really, really, really, really helped.
Role unknown, school AH, interview, year 1
Brilliant. Hands down, absolutely amazing. I think every single student, every single teacher should go through that, definitely. It’s been absolutely phenomenal training. And from everybody that I’ve had that’s gone through has found that incredibly useful and are really behind it.
Head of year, school AZ, interview, year 2
Only a few reports about the training were less positive. In three schools (schools AD, AK and AM), some staff were frustrated about the length of the in-depth training, regarding it as condescending to experienced teachers. Conversely, staff in some schools thought that the shorter all-staff training was too short to have a sustainable impact on staff behaviour (schools AD, AO and BK). Some staff sitting on AGs reported that choosing who should attend the in-depth training was a fraught process. A staff member in one school felt that staff were chosen without enough consideration of their roles (school BE). In two schools, an interviewee suggested that too many SLT members attended the training despite having less contact than other staff with students (schools AD and BD). In another school, a staff member suggested that too many teachers and not enough senior leaders were trained, thereby eroding the extent to which training informed school management culture (school BI). In other schools, AG members reported that trainees were selected appropriately (schools AE, AF, AH, AK, AM and BM). Schools AF, AK, AT, BD, BI and BM received the training late in the first year, thus reducing the time available to put RP into action.
Many schools decided to cascade the training so that some of those receiving the in-depth training then trained other staff. Thus, all staff were trained in some schools (schools AE, AK, AO, AZ, BI and BK), whereas others focused this training on key personnel (schools AF, AM, AS and BM) or newly qualified teachers (school AW). Half of the intervention schools trained students to resolve conflict using restorative techniques (schools AE, AK, AM, AO, AS, AW, AZ, BC, BD and BK). In year 3, four schools trained student conflict mediators and anti-bullying mentors (schools AK, AO, AZ and BD). A problem noted across the process evaluation was the tendency for staff who had received the in-depth training to leave the school before the intervention was complete. This meant that schools with high rates of staff turnover had a shortage of staff who had been trained in RP.
Action group meetings
Use of needs data
Over two-thirds of AG members completing the survey reported that they worked hard on the AG because they wanted to, not because they had to (Table 15). Over 80% reported looking forward to meeting and almost 70% reported that meetings were exciting and energising. Our survey of AG members found that most rated the needs assessment report as useful for informing decisions, with the overall percentage of members rating it thus declining slightly from 91% across the 19 schools providing data in year 1 to 88% across the 17 schools providing data in year 2 to 76% among the three schools providing data in year 3. These results appeared broadly consistent across schools, with 17 averaging 70% positive ratings in year 1 and 14 doing so in year 2, and two of the three schools completing the survey in year 3.
| Measure (response option that indicates satisfaction) | Responses | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Year 1 | Year 2 | Year 3 | |||||||
| Overall % of members responding as indicated | Number of schools where > 70% of members responded as indicated | Number of schools with no data | Overall % of members responding as indicated | Number of schools where > 70% of members responded as indicated | Number of schools with no data | Overall % of members responding as indicated | Number of schools where > 70% of members responded as indicated | Number of schools with no data | |
| Was the needs assessment report useful in helping the AG decide what actions to take? (somewhat or very) | 91 | 17 | 1 | 88 | 14 | 3 | 76 | 2 | 17 |
| Was the external facilitator useful in ensuring that all AG members could have their say? (somewhat or very)a | 89 | 18 | 1 | 90 | 15 | 3 | NA | NA | NA |
| Was the external facilitator useful in helping the AG decide what actions to take? (somewhat or very)a | 86 | 16 | 1 | 88 | 17 | 3 | NA | NA | NA |
| Was the external facilitator useful in helping to ensure that actions were actually implemented? (somewhat or very)a | 80 | 13 | 1 | 79 | 13 | 3 | NA | NA | NA |
| Do you think the LT project was a good way to ensure that students contribute to decision-making at this school? (very or quite) | 95 | 19 | 1 | 94 | 16 | 3 | 100 | 3 | 17 |
| Overall do you think the AG made good decisions about what actions to take? (% very or quite) | 94 | 19 | 1 | 93 | 16 | 3 | 98 | 3 | 17 |
| Do you think the AG made sure that these actions were implemented? (% yes) | 70 | 10 | 1 | 72 | 10 | 3 | 69 | 1 | 17 |
In interviews with students and staff on AGs, as well as with facilitators, most reported that they valued the needs reports and used them to identify priorities (schools AD, AE, AF, AH, AK, AL, AM, AO, AS, AT, AU, AW, AX, BC, BE, BI, BK and BM):
And they’ve been drawing on the needs assessment report research to help them think about that as well. It’s feeding into everything they do. So they . . . we focused on it quite a lot in meetings, pored over the data in the first few meetings. And then we still keep coming back to it when we’re thinking about what next, what actions should we be doing? Yeah, so they’ve . . . yeah, they’ve taken it to heart and really want to make a difference.
Facilitator, school BM, interview, year 1
Staff in most schools suggested in interviews that they used the reports as evidence to advocate to school leadership teams that changes were necessary. In school AH, for example, the needs assessment was useful for staff advocating on behalf of students whose concerns, although previously voiced, had not been acted on by school leaders. This was also the case in school AF:
But it certainly gave me some ammunition that I can say, well this is . . . this is proven because the kids have actually said this, so we need to move forward with it.
Assistant head-teacher, school AF, interview, year 2
In some schools (schools AF, AO, BE and BM), staff expressed shock or surprise at the results, particularly about the data on student perceptions of feeling unsafe at school or feeling uncomfortable talking to staff about problems. The reports often highlighted student concerns that staff had previously never considered, particularly relating to feeling safe at school (schools AH, AW and AZ):
I’ve always felt it quite a safe area and a lot of the young people don’t feel it’s particularly safe because of the way they have to come in and out. And obviously that’s being changed now . . . So I think it’s really been useful for us to do that. And quite . . . eye-opening and telling as to the areas that as adults we thought we’d covered and actually, no, the young people don’t think so much.
Head of year, school AZ, interview, year 1
Another school received a report that presented evidence of considerable unmet student needs and this information was accepted as valid by school leaders:
Well the positive thing is, the only way is up. The year group is a challenging year group. And I remember when [facilitator] came to present to SLT and said how terrible our data was . . . it was like a tumbleweed moment; it was so funny. I mean . . . it wasn’t funny in a good way, but . . . but it was a realistic . . . realisation for everyone if you know what I mean . . . Because we all knew it was like that, but we didn’t realise how much the children didn’t actually like us.
Director of Inclusion, school AM, interview, year 1
There were some more negative views expressed. Students or staff in eight schools reported that the reports were difficult to understand (schools AF, AK, AM, AX, AZ, BD, BI and BK). Staff in schools AH, AO and BK misunderstood the reference group to which data on students in their school were being compared, thinking that this was all schools nationally rather than other schools in the intervention arm of the trial. During an observation, it was apparent that the lead staff member in school BK did not understand the concept of statistical significance and needed support to interpret the colour-coding system depicting this.
Staff at two schools felt that the report was not useful or valid (schools AE and BK). In particular, they felt that the questions included vocabulary that was too advanced for students with special educational needs or for those with English as an additional language. They felt that the phrasing, particularly when students were asked to respond to negative statements, was inaccessible and that many of the questions were leading. In school AE, the assistant head teacher reported that, when the school conducted its own surveys, findings from these diverged from the results of this intervention’s needs assessment:
The data from the [your report] is meaningless; completely meaningless . . . It’s the worst . . . it’s a pointless exercise for our students.
Assistant head-teacher, school AE, interview, year 3
Other schools disagreed with some elements of the needs report (schools AD, AL, AT, AU, AW, AX and BC). As with schools BK and AE, school AX reported that the data provided through the study contradicted its internally maintained data. Staff in three schools (schools AF, AS and BD) did not share some or all of the findings with students because the report was seen as either too long and complicated or inappropriate for students to see. When year-on-year trends in such factors did not improve, staff members could sometimes feel dispirited (schools AF and BI). Such disappointments may have contributed to these schools not continuing intervention activities in the final year of the study.
Facilitators
Most AG members rated the facilitator as useful in ensuring that all members could have their say, with the overall percentage of members rating it thus being maintained at 89% across the 19 schools providing data in year 1 and 90% across the 17 schools providing data in year 2 (see Table 15). These results appeared broadly consistent across schools, with 18 schools averaging > 70% positive ratings in year 1 and 15 averaging this in year 2. Most AG members rated the facilitator as useful in helping AGs make decisions, with the overall percentage of members rating it thus being maintained at 86% across the 19 schools providing data in year 1 and at 88% across the 17 schools providing data in year 2. These results appeared broadly consistent across schools, with 16 schools averaging > 70% positive ratings in year 1 and 17 out of 17 averaging this in year 2. Most AG members rated the facilitator as useful in helping to ensure that decisions were implemented, with the overall percentage of members rating it thus being maintained at 80% across the 19 schools providing data in year 1 and at 79% across the 17 schools providing data in year 2. These results were less consistent across schools, with 13 averaging > 70% positive ratings in year 1 and year 2.
However, a theme across interview data was many staff members’ mixed feelings about the facilitation. Some schools reported that the facilitator was relatively passive, listening and taking notes (schools AD, AS and AX), whereas others felt that the facilitator simply did not contribute much or were generally dissatisfied with the facilitator’s work (schools AF and BK):
They don’t really do anything . . . Whether they bring anything to the meeting. I think once or twice they might have asked a couple of questions, but that’s about it. They sit there looking to us.
Role unknown, school AF, interview, year 1
One facilitator was replaced between years 1 and 2, in part because of school dissatisfaction (schools AE, AU, BE and BK). Several of these schools (schools AE, BE and BK) went on to disengage from the intervention or expressed their dissatisfaction with it, although the balance is unclear between the poor facilitation causing the disengagement or the disengagement coming first and informing the criticism. Other schools were not clear about the role of the facilitator and, therefore, had trouble setting reasonable expectations of what the facilitator should or was able to contribute to the group:
I think . . . [facilitator] has been really useful as a . . . So making sure we’re doing what we’re supposed to do in one respect is great. But then it’s sometimes flipped into, well are we doing it right. And having [facilitator]’s presence there has always . . . are we being watched, judged or supported? We’re not quite sure where that . . . what that role is.
SLT member, school AW, Interview, year 2
However, there were also positive feelings. Staff in some schools (schools AE and AT) reported that the facilitator added weight or gravitas to the meetings and reinforced the notion that the school would be held accountable for progress:
So working with a facilitator from outside, that has been quite good at making it . . . just more . . . focused and more effective in that way. Because I think people in schools have really, really good ideas but again, because of the time, you tend to let things slip. Whereas this has kind of imposed a formality to it which means you have to keep to deadlines and move things forward.
Staff member, school AE, interview, year 1
There were mixed reports on what difference the absence of external facilitation made to the third year of the intervention. Most interviewees suggested that external facilitation was not necessary in the final year but a few suggested that this was a significant loss:
The absence of [facilitator] has been incredibly significant because she did, she has, she was able to tie it in all the time to the agenda. And was a touchstone I suppose really for that. And then . . . so that . . . I think that was a loss.
Deputy head-teacher, school AD, interview, year 3
Student participation
Most AG members agreed that the AG was a good way to ensure that students contributed to decision-making, with the overall percentage of members rating it thus being maintained at 95% across the 19 schools providing data in year 1, at 94% across the 17 schools providing data in year 2 and at 100% among the three schools providing data in year 3 (see Table 15). These results appeared broadly consistent across schools, with 19 schools averaging > 70% positive ratings in year 1, 16 in year 2 and 3 out of 3 in year 3.
A recurring theme in student accounts was students joining the AG because they wanted to help change their school (schools AE, AF, AT, AW, BE and BK) or to have more of a voice (schools AD, AM, AT, AW and BC):
Because I felt sometimes frustrated with how the school was sometimes. It felt like a chance where I can say what I want to say now and maybe make a difference so that it wouldn’t be like that anymore, I guess.
Female year-9 student, school AO, interview, year 2
Students valued the opportunity to express their views and highlight where they were unhappy, and AGs provided a calm, structured environment to do this:
I was able to speak from my own point of view not just like statistics and what was on a piece of paper. Because I was able to like . . . relate to it in a sense. And . . . like I started . . . talking about my own experiences, the teachers were acknowledging it and . . . yeah.
Did that feel good . . .?
Yeah. It kind of felt good because it’s like . . . it’s not me having to shout at a teacher or like I want to do this, dadadada. But it was me actually being able to relate to a teacher seeing why if I’m shouting and I’m cussing it’s difficult for a teacher with a class of 30 or more students.
Students often reported that they felt that teachers on the AG listened to students’ views respectfully even when they disagreed with them:
That was good because we didn’t feel intimidated by the teachers. Not that you felt intimidated before, but you didn’t feel like . . . You could say something, all the teachers would listen. If they contradicted, they contradicted, if they agreed, they agreed. But no one disagreed, they’re going to say you’re wrong, but everyone put across their own views with no arguments or anything.
Student of unknown sex and year, school BE, focus group, year 2
Students could grow in confidence in the course of their involvement on the AG. This was most obvious in student accounts from schools AM and BM:
Well at the beginning I was very conscious of not . . . sounding like an idiot, making a mistake, stuttering, something stupid like that. Now . . . it’s completely different. I will . . . sometimes I will interrupt people. Obviously it’s not a good thing but it just shows how I feel I can say what I want in this room.
Student of unknown sex and year, school BM, focus group, year 1
However, a theme across some staff accounts was struggling to manage good interactions between staff and students. Facilitator and interviews suggested that although many students participated meaningfully, others remained disengaged or, at times, combative:
They went down the road of all choosing students who were all, I would say, challenging. And therefore not necessarily always making an appropriate contribution to the group. I mean when I think back on it, out of the six students two of them contributed really well, and the other four were really a challenge.
Facilitator, school BD, interview, year 2
Interviews and focus groups suggested that whereas in many schools student views were described as being taken seriously or very seriously (schools AE, AO, AS, AT, AX, AZ, BI and BM), in other schools staff took note of student views only when these were deemed ‘realistic’ (schools AD, AF, AK, AL, AU, AW and BE). Staff in some schools reported not really valuing student input or that student participation led to conflicts with staff (schools AD, AH and AK). During the interview with a staff member at school AH, these tensions became apparent:
They [students] want some rules to change; so they want to be able to bring their mobiles . . . There were a lot of conversations about, ‘no . . . that’s not [going to happen] . . .’ [. . .]. And I think that they think they had a bigger input than they perhaps did.
Assistant head-teacher, school AH, interview, year 2
The above quotation suggests that students’ participation was, at times, tokenistic. The same staff member continued:
And I guess the limitation is the things that they think . . . having phones will make us feel safer at school, and I know that our . . . part of our health and safety is that no, phones actually make young people more vulnerable. So we say no mobile phones at school. So there are some things which are just . . . not going to happen – so it’s a brick wall. And they don’t like that either. So there is conflict. I always try and say, well I’ll take it to the principal, so that they don’t feel like I’m dismissive.
Assistant head-teacher, school AH, interview, year 2
Taking account of student views could be a challenge to schools’ normal way of working, as one teacher explained:
I think the challenges are twofold, from two different sides. The first from the teachers’ side is that you want to include students but often they’re not equipped to make good decisions for themselves . . . I think from the student side the students often struggle to feel that actually what they say has meaning, because it’s so often just ignored. And therefore I think they can become disillusioned and not really feel it’s worth contributing.
Teacher, school AD, interview, year 1
One staff member reported finding it difficult to take a facilitative approach to managing student inputs:
I’m aware my role is of a facilitator you know, and luckily I’ve done some courses when it comes to teaching about taking a step back; because most teachers want to fix stuff, that’s what we do. And we just think we can fix everything and we’ll tell you what to do and you’ll do it.
Assistant head-teacher, school AF, interview, year 2
However, other schools were enthusiastic about students’ participation in decisions. In school AU, staff on the AG expanded the process of revising school rules so that this involved students beyond the AG alone:
It came about through the Learning Together project. Very nice indeed, because the way it works . . . so the needs analysis said ‘we don’t know what the rules are’. [A teacher] started this exercise and I finished it . . . She got all the forms in form times with their form tutors to come up with rules about living in a community. How should we treat each other at [school AU]? And each form came up with you know lots of suggestions . . . I then took it to the staff and they had their say, and there were a lot of common themes, and we picked out all the favourites. I then took it leadership and we narrowed it down even more.
Assistant head-teacher, school AU, interview, year 2
A recurring theme was the impact of the work on mutual understanding between staff and students, as these four quotations illustrate:
Yeah, because it made me feel like maybe . . . sometimes when teachers do stuff it’s not because they want to do it, it’s because of the rules that maybe they have set. But then when you’re listening to them and they’re agreeing with what you have to say, it’s like they actually do understand and you can see that what I’m saying is being understood.
Female year-9 student, school AO, interview, year 2
It’s also nice to be able to have a conversation with a teacher, because very often they’re just the people at the front of the class . . . And they’re just giving you the work; but when you actually have a conversation and you get to know them, you understand that they’re real people and they’re a lot more relatable.
Female year-10 student, school AU, interview, year 2
Yes [it made me feel differently about teachers], a hundred per cent because it give you a different insight to what they’re really like, especially if you’re with teachers who haven’t taught you before or something like that. Because they’re not as bad as you think.
Male year-11 student, school BM, interview, year 3
I know there is a hierarchy and there are imbalances in power, but with the Learning Together project I’m sat there with a child discussing from my point of view what I think, and from their point of view what they think. We’re almost like putting it in the middle of the table. How can we make that better for both of us?
Role unknown, school AU, focus group, year 1
This could lead to better relationships between staff and students:
I think that’s really good for me to be in something that’s quite positive, because I do deal with quite a lot of negative in my role. So for the students to actually see me in a positive light within things like this I think is good for my role. Because then they’ll stop and talk to me in the corridor: ‘Miss, are you going to the meeting tonight? Yeah, yeah, are you going?’ So it’s nice just to have that. And other people see them talking to me and go ‘Oh OK, she’s not telling everyone off or talking about problems. She’s quite fun actually’. And I think we’ve had a bit of fun in the meetings, had a little bit of a laugh, haven’t we, as well?
Role unknown, school BM, focus group, year 1
Decision-making
Most AG members agreed that the AG made good decisions, with the overall percentage of members rating it thus being maintained at 94% across the 19 schools providing data in year 1, 93% across the 17 schools providing data in year 2 and 98% among the three schools providing data in year 3 (see Table 15). These results appeared broadly consistent across schools, with 19 out of 19 schools providing > 70% positive ratings in year 1, 16 out of 17 in year 2 and three out of three in year 3.
Action group members were less likely to agree that the AG made sure that these decisions were implemented, with the overall percentage of members rating it thus being maintained at 70% across the 19 schools providing data in year 1, 72% across the 17 schools providing data in year 2 and 69% among the three schools providing data in year 3. These results were also less consistent across schools, with 10 out of 19 schools providing > 70% positive ratings in year 1, 10 out of 17 in year 2 and one out of three in year 3.
A common theme in interviews with facilitators and staff was concern about the AG’s capacity to implement actions (schools AF, AL, AM, AT, AW, AX and BK). According to the facilitator, school AF’s AG repeatedly revisited minor issues, such as the school’s policy on make-up, but was largely unable to confront more substantive issues relating to student behaviour, health or well-being. In school AT, the AG proposed numerous actions that were rejected by the head teacher. The amount of work already facing teachers made implementation more difficult. One facilitator said of the individual leading on AG that he had:
. . . been given so much to do I think in his day-to-day role, it’s just another thing for him to do. He does it, he does it with very good grace and he’s obviously very well respected by the students.
Facilitator, school BE, interview, year 2
Schools were better able to implement action when SLTs were represented on action teams or otherwise supported them. In some schools, the staff lead received virtually no support from colleagues (schools AH, AL, AM, AO, AT, AW, AX, BI and BK). In school AH, the staff lead had a committed AG lead but received little tangible support from the head teacher or other teachers:
The head teacher there was completely uninterested when I came to give a talk to the senior leadership team, and it’s the only school where the head has not said anything to me or taken any notice or made any effort to be slightly friendly. It was awful. But I gave a talk to the SLT, they all sat . . . they were terribly . . . first of all, everybody there dresses extremely formally in business suits. And the head never said a thing.
Facilitator, school AH, interview, year 2
However, in school AK, despite there being no senior leaders on the AG, the lead had worked for a long time at the school and was well respected and liked by both students and staff. Thus, it was possible to galvanise action without the formal involvement of senior leaders in some cases.
Throughout the 3-year study, the majority of schools handed over leadership of the project at least once (schools AF, AH, AM, AO, AT, AU, AW, AX, BC, BD, BE, BK and BM). Many went on maternity leave, changed roles or went on sick leave. Through these transitions, schools were sometimes able to transfer the programme to effective leads (schools AT, AW and BD), but some could not.
We used an adapted version of the Learner Empowerment Scale to assess the extent to which staff and student AG members felt empowered to make decisions. The mean percentage of positive responses across all items among AG members in intervention schools for which data were available was 75% in year 1, rising to 79% in year 2 and 80% in year 3 (Table 16). In year 1, 13 out of 19 schools that provided data had a rate of positive reports > 70% across all members and items. In years 2 and 3, these figures were 12 out of 17 and two out of three, respectively.
| Learner Empowerment Scale item (response option that indicates empowerment) | Responses | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Year 1 | Year 2 | Year 3 | |||||||
| Overall % of members responding as indicated | Number of schools where > 70% of members responded as indicated | Number of schools with no data | Overall % of members responding as indicated | Number of schools where > 70% of members responded as indicated | Number of schools with no data | Overall % of members responding as indicated | Number of schools where > 70% of members responded as indicated | Number of schools with no data | |
| During AGMs, I felt confident that I could do what was expected (yes) | 90 | 18 | 1 | 91 | 14 | 3 | 98 | 3 | 17 |
| I had the power to make a difference to how things were done at AGMs (yes) | 78 | 14 | 1 | 82 | 10 | 3 | 89 | 3 | 17 |
| The AGs work fits with what I believe in (yes) | 88 | 17 | 1 | 92 | 17 | 3 | 89 | 3 | 17 |
| My participation was important to the success of the AG (yes) | 83 | 16 | 1 | 81 | 14 | 3 | 86 | 3 | 17 |
| Other people on the AG made me feel like I was not good enough (no) | 92 | 19 | 1 | 79 | 15 | 3 | 89 | 2 | 17 |
| I actively took part in the tasks undertaken on the AG (yes) | 90 | 19 | 1 | 89 | 16 | 3 | 91 | 3 | 17 |
| I usually did more work than I had to do on the AG (yes) | 23 | 0 | 1 | 34 | 0 | 3 | 33 | 0 | 17 |
| I was overwhelmed by all of the work required of the AG (no) | 75 | 14 | 1 | 74 | 15 | 3 | 86 | 3 | 17 |
| I worked hard on the AG because I wanted to, not because I had to (yes) | 83 | 17 | 1 | 83 | 14 | 3 | 84 | 2 | 17 |
| I had a choice in the way I went about doing work on the AG (yes) | 86 | 17 | 1 | 90 | 17 | 3 | 86 | 3 | 17 |
| The things I had to do on the AG meant a lot to me personally (yes) | 61 | 5 | 1 | 74 | 10 | 3 | 69 | 1 | 17 |
| I liked to talk about what I was doing on the AG with friends or family (yes) | 55 | 2 | 1 | 61 | 11 | 3 | 66 | 1 | 17 |
| I felt nervous about what was expected of me on the AG (no) | 76 | 15 | 1 | 73 | 12 | 3 | 80 | 2 | 17 |
| I was able to affect the way things were done on the AG (yes) | 76 | 12 | 1 | 84 | 14 | 3 | 75 | 1 | 17 |
| I looked forward to the AGMs (yes) | 73 | 11 | 1 | 84 | 13 | 3 | 91 | 3 | 17 |
| Those leading the AG believed that they must control how I contributed to the AG (no) | 63 | 9 | 1 | 61 | 4 | 3 | 79 | 2 | 17 |
| I got positive responses when I expressed my own attitudes and ideas on the AG (yes) | 85 | 15 | 1 | 92 | 17 | 3 | 84 | 2 | 17 |
| I agree with the things that were done on the AG (yes) | 90 | 17 | 1 | 94 | 16 | 3 | 93 | 3 | 17 |
| I had the skills needed to contribute to the AG (yes) | 89 | 18 | 1 | 91 | 17 | 3 | 80 | 2 | 17 |
| My ability to contribute to the AG was under my control (yes) | 85 | 17 | 1 | 88 | 13 | 3 | 82 | 2 | 17 |
| Those leading the AG felt that they were always right (no) | 71 | 11 | 1 | 69 | 9 | 3 | 72 | 2 | 17 |
| I found the AG to be exciting and energising (yes) | 62 | 17 | 1 | 71 | 8 | 3 | 84 | 2 | 17 |
| I found the AG to be interesting (yes) | 87 | 17 | 1 | 90 | 15 | 3 | 86 | 1 | 17 |
| The things I did on the AG were valuable to me (yes) | 75 | 14 | 1 | 80 | 13 | 3 | 78 | 2 | 17 |
| The things I learned and did on the AG will be helpful for my future (yes) | 77 | 13 | 1 | 86 | 15 | 3 | 78 | 1 | 17 |
| This AG was one of the first times I felt like I was able to contribute to something important (yes) | 43 | 0 | 1 | 45 | 3 | 3 | 27 | 0 | 17 |
| This AG taught me how to work well together with others (yes) | 56 | 3 | 1 | 64 | 3 | 3 | 75 | 1 | 17 |
| This AG helped me better understand some of the problems in my school (yes) | 84 | 14 | 1 | 88 | 15 | 3 | 91 | 3 | 17 |
| This AG gave me the chance to do something about the problems in my school (yes) | 82 | 15 | 1 | 92 | 16 | 3 | 88 | 2 | 17 |
| Mean across all items | 75 | 13 | 1 | 79 | 12 | 3 | 80 | 2 | 17 |
Restorative practice
Restorative practice was widely regarded as extremely useful for dealing with behavioural problems and conflicts. It appeared acceptable to most staff and students in most schools. Over three-quarters of staff responding to the all-staff survey understood the term ‘restorative practice’. Around half supported the use of RP (see Table 12).
The presence of a staff member who championed the use of RP was critical to its broader use, and hence to its reach. Schools AO and AS had such a champion. In school AS, the staff member had a strong academic background in RP. He began working with students who misbehaved in class, expanding to use it with students who had particular pastoral needs, and then to the sixth form, and eventually to the entire range of year groups for which he was responsible. He set up voluntary training for all staff and unofficially trained students in restorative techniques. Having an important middle management role in the school and being an established and well-liked teacher placed this teacher in a strong position to champion RP.
In some schools, RP was used by most of those staff who had attended the in-depth training but some of these staff felt frustrated that the school was not adopting RP quickly enough (schools AM, AO, AW, AX, BI and BK). Some schools where this was the case had cultural norms that acted as barriers to implementation, such as an authoritarian ethos, or did not have adequate commitment from the SLT to ensure more widespread adoption. Schools that faced challenges, particularly in terms of poor results or Ofsted ratings, often struggled to adopt RP fully because it was not seen as a priority for the SLT to lead.
Where it was used, staff generally felt that RP allowed them to resolve problems more easily, because it allowed them to focus on restoring relationships rather than being bogged down in culpability:
And before I found we were spending a lot of time in ‘Billy said (a), Johnny said (b)’. And we’re arguing about (a) and (b) forever and ever and you probably never get to the end of it. And now Billy gets to give his view, Johnny gets to give his view, and then we move on to how we’re going to move on and what this is going to look like in the future.
Role unknown, school AO, focus group, year 1
In other schools (schools AU, BD and BM), RP was used primarily as a strategy to manage classroom and learning behaviour. This often took the form of requiring a restorative conversation before a student who had breached expected norms of behaviour could be readmitted to the classroom.
The RP sessions benefited from their being facilitated by trained staff. Many students acknowledged this:
Well I got excluded for overheated arguments and when I came back from exclusion [the teacher] sat with me and the boy and we kind of . . . because before, if we tried to resolve it ourselves it would just end up, like the same thing that happened, we start overheating each other and then someone would get hit. But when you’re in restorative justice it’s more calm. Because the teacher’s there, the presence of the teacher or whoever’s there, it helps calm down the situation and you actually listen to them. So I reckon that helped a lot.
Student of unknown sex and year, school AO, focus group, year 2
School AO often brought in parents or family members to restorative conferences and their presence could further calm the interactions that ensued. Students reportedly felt more pressure to be more honest and mature in such meetings, not wanting to embarrass their parents:
You have to act a lot more mature. You can’t just be bickering and you know . . . let it get heated in front of your parents. You have to really think about what it is you’re saying and what you mean.
Female year 10 student, school AO, RP interview, year 2
Students in general reported positive experiences of RP. Several students in schools AM and BE felt that restorative conferences could improve relationships where these had been conflicting. Students did not necessarily leave conferences as friends but were better able to manage their relationships:
I thought it [restorative conference] was useful because if we wouldn’t have had it there would have been many, many, many more problems would have happened. It’s not like it’s completely gone. It’s not because there’s still a bit of tension between all of us . . . It’s not as big as it used to be.
Student of unknown sex and year, school BE, interview, year 1
Sessions could force perpetrators to appreciate the hurt they had caused. A student with a history of bullying perpetration learned through a difficult restorative discussion the extent to which his bullying had hurt another boy in his class:
I just felt so sorry . . . the boy was just crying. When he was speaking he could barely speak and it just reminded me why did I do that? You shouldn’t have done that. It just . . . made me realise . . . And when we came in, it’s just like . . . at first I was laughing . . . But then when I just saw him there sitting down at this table and his eyes were all red from the tears . . . I just don’t . . . it just came to me and just shocked me. That could have that had happened to me really.
Male student of unknown year, school AM, interview, year 1
After a restorative conversation, a student in school BD not only forgave the student who had been mean, but also saw that that he was capable of change and personal growth:
I could tell he kind of regretted it, what he did. But at the same time, I saw that he could actually change. Bad people are not always that bad at the same time they can always change.
Male student of unknown year, school BD, interview, year 1
Social and emotional education
A recurring theme in staff interviews was the very mixed responses to the curriculum. There were some subthemes concerning positive evaluations. Some teachers appreciated the clear structure of sessions (schools AK, AL, AS and AZ). Many students also found the lessons acceptable because they provided a good opportunity for discussions (schools AE and AL) or felt that the topics covered were highly relevant to their life (schools AK, AS and AW). Some staff commented that the curriculum as with the RP sessions could provide students with the skills needed to resolve disputes themselves:
And training for students is important. Because if we can teach the students how to monitor and measure themselves, and use this process, that’s where you’re going to have the biggest breakthrough. Because if students are taught the skill of sitting down and talking through problems and have a structure to do it, that’s where you’re going to have a win.
Role unknown, school AO, focus group, year 1
Other staff commented that although some of the skills focused on in the curriculum were basic, they were nonetheless important:
So I was given . . . the learning objective around how we can get our students to work together more cohesively in teams. And it was really, really interesting because a lot of the lesson . . . initially when I looked at the lesson plan I thought, this is quite basic stuff, because as an adult you do just think it’s second nature. [. . .]. What’s always really interesting to see is that some of these things are not obvious to students. Like stopping to listen to someone when they’re speaking, or taking roles in groups or . . . different things like that which seem really obvious to us, which was really lovely. And also they’re very easily achievable learning outcomes from the lessons. Also the students are left with a real sense of being equipped, and they left with a sense of achievement in terms of having very easily achieved a learning outcome.
Trainee teacher, school BD, interview, year 2
However, another theme was how lessons could be improved. One concern was that the materials had been sent too late in the year to be incorporated into lesson plans (schools AE, AF and AU), which was repeated in all three years of the study. Teachers also said they felt they had to adapt the lessons because they were too simplistic (schools AD, AE, AF, AK, AS and AW) or so that they could be used as evidence for Ofsted inspections (school AK):
Increasingly, the further along with the units we went the more we used our own resources [. . .] we have a lot of PowerPoints and teacher notes, but not very much to evidence the students’ learning. And that’s a big focus for our school you know; we have to evidence their progression.
PSHE teacher, school AK, interview, year 1
Some teachers said that they adapted materials to make the curriculum more engaging for their pupils. This was often felt necessary because the lessons were viewed as unfocused, simplistic or boring (schools AF, AK, AS and AX):
Sometimes to make it . . . I had to make it sometimes a little bit more visual or include videos or try to . . . sometimes approach it from a different . . . in a slightly different way.
Teacher, school AX, interview, year 1
They [students] felt it was a little bit repetitive and they thought that some of it at least was a bit boring for them because it was relatively straightforward. It was things that they do anyway, things they think about anyway.
Teacher, school AF, interview, year 1
Teachers found it time-consuming to adapt lessons to the needs of their classes (schools AD, AE, AS and AW):
Teachers don’t have time to rewrite things and . . . it does take a lot of time. You know planning an hour lesson can take up to 3 hours. And if you’re then messing around with what someone else has done as well . . . it gets very complicated.
Teacher, school AW, interview, year 2
We did have to tweak them quite a lot just to make sure that all children would be able to do it. So I would say they probably spent quite a bit of time just tweaking them.
Teacher, school AE, interview, year 2
Intermediate outcomes and mediation
Quantitative analyses examined effects of the intervention on school climate and involvement with anti-school peer groups as pre-hypothesised intermediate outcomes and potential mediators of intervention effects on our primary and secondary student outcomes. The measures of potential mediators had good response rates and reliability, with > 90% of all participants completing all items and with multi-item scales and subscales having alphas of > 70% in all cases (Table 17).
| Measure | Response rates, n (%) | Internal consistency | ||||||
|---|---|---|---|---|---|---|---|---|
| Baseline | 24 months | Baseline | 24 months | |||||
| Completed all items | Completed half or more of items | Completed all items | Completed half or more of items | Alpha (standardised) | Ordinal alpha | Alpha (standardised) | Ordinal alpha | |
| BBSCQ | ||||||||
| Overall BBSCQ | 5733 (85.99) | 6635 (99.52) | 5549 (8.22) | 6265 (99.60) | 0.9137 | 0.9373 | 0.9170 | 0.9371 |
| Student sense of belonging subscale | 6293 (94.39) | 6613 (99.19) | 5965 (94.83) | 6240 (99.21) | 0.7952 | 0.8345 | 0.8225 | 0.8576 |
| Student commitment to academic values subscale | 6519 (97.78) | 6581 (98.71) | 6190 (98.41) | 6231 (99.06) | 0.7394 | 0.8407 | 0.7732 | 0.8619 |
| Student perception of supportive teacher relationships subscale | 6221 (93.31) | 6631 (99.46) | 5935 (94.36) | 6247 (99.32) | 0.8804 | 0.9115 | 0.8938 | 0.9207 |
| Student perception of participative school environment subscale | 6396 (95.94) | 6600 (99.00) | 6071 (96.52) | 6231 (99.06) | 0.8005 | 0.8540 | 0.8313 | 0.8712 |
| YPDP measure of student involvement with anti-school peer groups (single item) | 6494 (97.41) | NA | 6167 (98.04) | NA | NA | NA | NA | NA |
The intervention had statistically significant effects on our overall measure of a positive school climate as well as its constituent subscales (supportive relationships with teachers; sense of belonging; perception of a participative school environment; and commitment to academic values) at 36-month but not 24-month follow-up. The intervention had a statistically significant effect on our measure of involvement with anti-school peer groups at 24 months but one slightly short of statistical significance at 36 months (Table 18). We undertook a per-protocol analysis to examine the effect of additionally adjusting for our potential mediators measured at 24 months on the associations previously found between the intervention and our primary and secondary outcomes measured at 36 months. This analysis found no evidence that this additional adjustment made any difference except marginally in the case of the intervention effect on well-being, where adjustment for both school climate and for involvement with anti-school peers at 24 months removed the previously statistically marginal intervention effect at 36 months (see Appendix 1, Table 40).
| Measure | 24 months | 36 months | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Arm, mean (SE) | Unadjusted effect | Adjusted effect | Arm, mean (SE) | Unadjusted effect | Adjusted effect | |||||||
| Control | Intervention | Difference (95% CI) | p-value | Difference (95% CI) | p-value | Control | Intervention | Difference (95% CI) | p-value | Difference (95% CI) | p-value | |
| Beyond Blue School Questionnaire | ||||||||||||
| BBSQ overall score | 2.92 (0.03) | 2.90 (0.03) | –0.00 (–0.02 to 0.02) | 0.915 | –0.00 (–0.02 to 0.02) | 0.993 | 2.82 (0.03) | 2.85 (0.03) | 0.05 (0.03 to 0.07) | < 0.001 | 0.05 (0.03 to 0.08) | < 0.001 |
| Student perception of supportive teacher relationships subscale | 2.76 (0.04) | 2.70 (0.04) | –0.03 (–0.06 to 0.00) | –0.02 (–0.05 to 0.01) | 2.64 (0.03) | 2.66 (0.03) | 0.05 (0.02 to 0.08) | 0.06 (0.03 to 0.09) | ||||
| Student sense of belonging | 2.84 (0.03) | 2.88 (0.03) | 0.04 (0.01 to 0.07) | 0.04 (0.01 to 0.07) | 2.78 (0.02) | 2.84 (0.02) | 0.06 (0.03 to 0.09) | 0.06 (0.03 to 0.09) | ||||
| Student perception of participative school environment subscale | 2.96 (0.03) | 2.91 (0.03) | –0.02 (–0.05 to 0.01) | –0.03 (–0.06 to 0.01) | 2.81 (0.04) | 2.82 (0.04) | 0.05 (0.02 to 0.08) | 0.05 (0.01 to 0.08) | ||||
| Student commitment to academic values subscale | 3.51 (0.01) | 3.53 (0.01) | 0.00 (–0.02 to 0.03) | 0.00 (–0.02 to 0.03) | 3.42 (0.01) | 3.46 (0.01) | 0.03 (0.01 to 0.06) | 0.03 (0.01 to 0.06) | ||||
| Measure | 24 months | 36 months | ||||||||||
| Arm, n (%) | Unadjusted effect | Adjusted effect | Arm, n (%) | Unadjusted effect | Adjusted effect | |||||||
| Control | Intervention | Odds ratio (95% CI) | p-value | Odds ratio (95% CI) | p-value | Control | Intervention | Odds ratio (95% CI) | p-value | Odds ratio (95% CI) | p-value | |
| YPDP measure of student involvement with anti-school peer groups, single item | ||||||||||||
| Friends cautioned/stopped/picked up by police | ||||||||||||
| No | 2203 (70.05) | 2271 (75.15) | 0.80 (0.66 to 0.97) | 0.024 | 0.80 (0.66 to 0.96) | 0.020 | 2073 (68.64) | 2044 (73.21) | 0.84 (0.69 to 1.02) | 0.074 | 0.83 (0.69 to 1.01) | 0.066 |
| Yes | 942 (29.95) | 751 (24.85) | 947 (31.36) | 748 (26.79) | ||||||||
Chapter 4 Economic evaluation
Methodology
Study question, selection of alternatives and form of evaluation
A cost-effectiveness analysis (CEA) was undertaken to assess the relative cost-effectiveness of the LT intervention compared with standard school-based practices for managing aggression. The economic evaluation was undertaken in conjunction with the analysis of the effectiveness of the LT intervention at 24 and 36 months since randomisation. The primary economic evaluation was a cost–consequences analysis with all main outcomes. In addition, a cost–utility analysis was conducted, with health outcomes expressed in terms of QALYs.
Resource use and outcome data collected as part of the cluster RCT were used to report cost-effectiveness at 24 and 36 months since randomisation. The CEA involved estimation of resource use, costs, HRQoL and QALYs at 24 and 36 months. In the cost–consequences analysis, we report incremental costs and incremental effects of all main outcomes. The cost–utility analysis used information on QoL collected at 24 and 36 months’ follow-up to report QALYs at each time point. We compared randomised groups by reporting incremental costs, incremental QALYs and an incremental cost-effectiveness ratio (ICER). The main assumptions of the CEA were subjected to sensitivity analyses. The results are illustrated on the cost-effectiveness planes (Figures 2 and 3).
FIGURE 2.
Uncertainty in the mean costs (£) and QALY differences and their distribution for intervention versus control at 24 months.
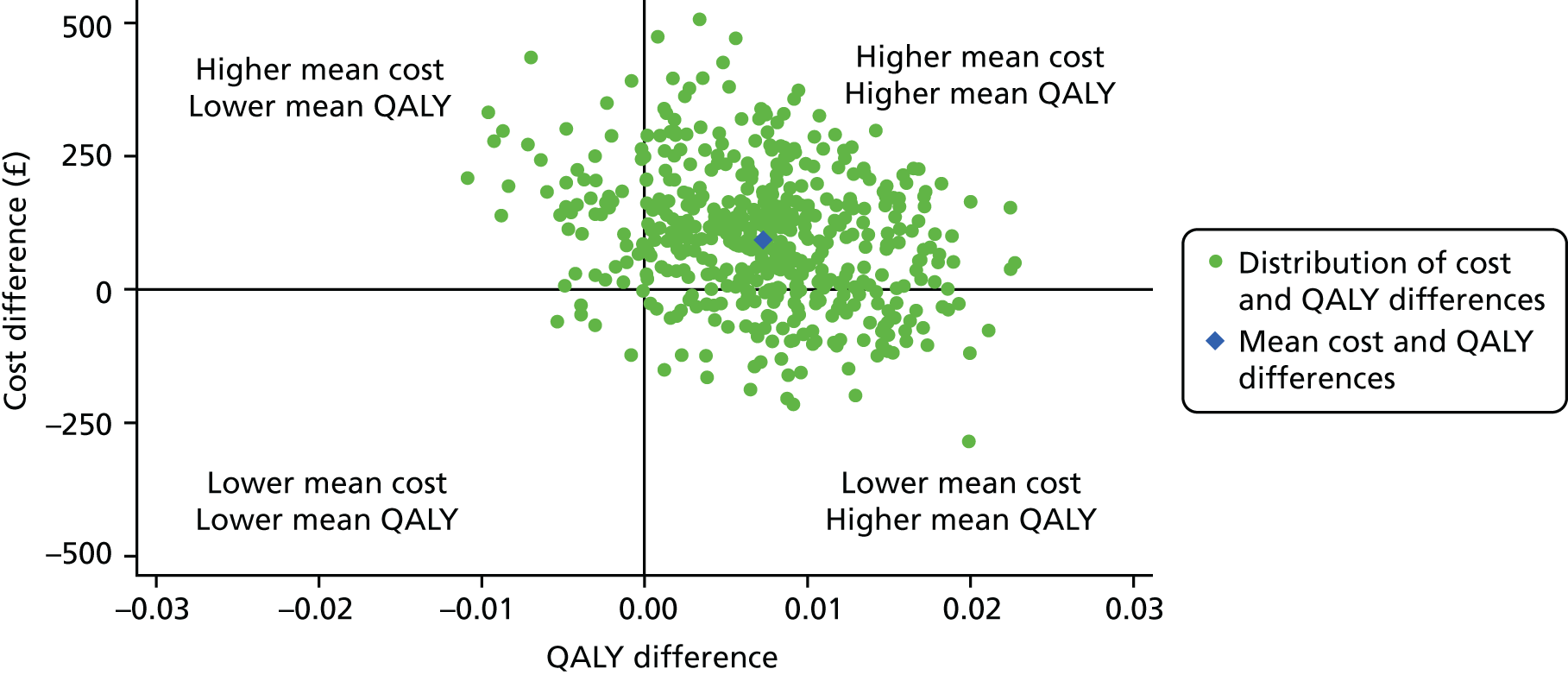
FIGURE 3.
Uncertainty in the mean costs (£) and QALY differences and their distribution for intervention versus control at 36 months.
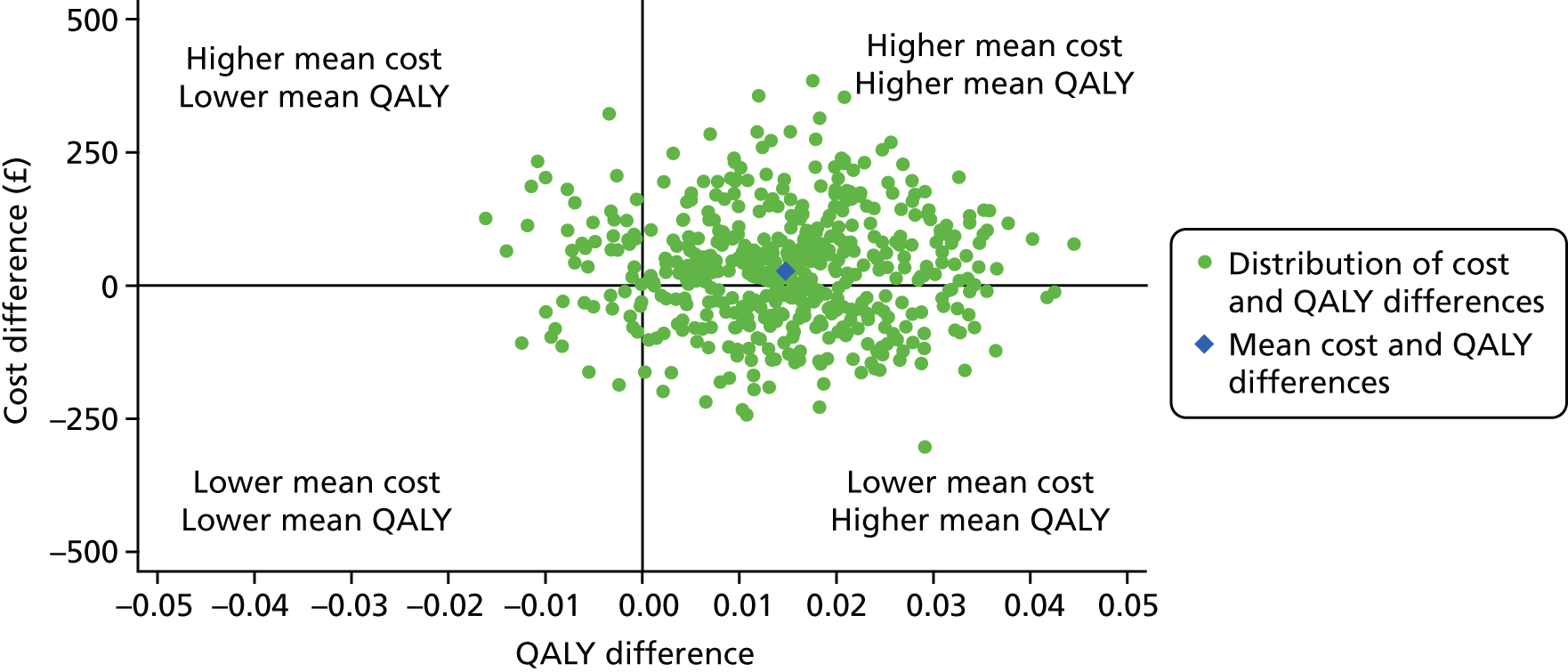
Effectiveness data and benefit measurement and evaluation
The CHU9D measure99 was used to assess HRQoL as part of the economic evaluation. Utility values were collected using the CHU9D questionnaire at baseline and 24 and 36 months. We calculated QALYs for each participant using the ‘area under the curve’ approach, that is, the weighted average of time spent in the study and HRQoL. 127
However, the analysis of the pilot study data suggested that there was only a weak correlation between the CHU9D and the proposed primary outcome measures. Therefore, there was a concern that QALYs were unlikely to capture all of the intervention effects. We therefore planned to also perform a cost–consequences analysis as the ‘primary analysis’, as recommended by the National Institute for Health and Care Excellence (NICE)’s public health methods guidance. 128
Resource use measurement and costing
The cost analyses took a public sector perspective following NICE’s method guidelines. 129 NICE’s guidelines for interventions with health and non-health outcomes in public sector settings129 recommend that the base-case cost-effectiveness estimate is presented from a public sector perspective. We used a public sector perspective to cover education, NHS and police costs. The main resource use items and sources of these data are detailed in Appendix 1, Table 41.
The costs of the intervention (trainer, facilitator and staff costs) and costs of the NHS and police resources used by the students were considered. In calculating the total cost per school, the attribution of costs such as facilitator and staff time recognised that only a percentage of time is going to the year group under study relative to the total number of students in each school. For the main trial analysis outcomes for the 11- to 12-year-old cohort, the costs have to be a proportion of the total number of students in the school to be consistent. The only exception is that the curriculum was delivered only in that year group so will be costed at 100%.
We collected costs on the delivery of the intervention as incurred during the trial. The costs of the trainers’ and facilitators’ time were available from the trainers’ and facilitators’ invoices, which capture preparation and organisation time.
Staff time included staff time spent dealing with bullying or aggression that was identified in the teacher survey. The amount of time spent with AGs was taken from the facilitator diary and, in addition, there were questions in the AG survey about the related time involved in preparation and follow-up. The staff time involved in curriculum change was taken from the curriculum logs. The amount of time spent training was taken from the trainer diaries and the number of teachers attending was recorded on attendance sheets. In the interviews with staff, we enquired whether our training was additional or instead of other training and, if the latter, what it replaced.
Teacher salaries for each intervention and control school were obtained from the Department for Education website. 130 To estimate an hourly rate, we divided salaries by the Department for Education statutory guidance on school teachers’ pay and conditions document detailing the annual hours of work. The student costs included the implications for NHS resource use in terms of visits and hospital stays, and policing costs associated with stopping children and arrests. These items were identified with specific questions in the student survey. The unit cost of inpatient stay in hospital was £298. 131 The unit cost of an NHS visit was calculated as the weighted average unit costs of general practitioner (GP) consultation and outpatient visit. 131,132 The percentages of GP visits and outpatient visits reported in another published study133 were applied. The unit costs for police attendance were £267 for those who were not arrested and £457 for those who were arrested. These unit costs were obtained from previously published work. 134 Total costs up to 24 and 36 months were calculated by combining the resource use with unit costs. Where there were missing costs at the school level we used mean imputation unless there was evidence from the process evaluation that these costs had not been incurred.
Modelling and adjustments for timing of costs and benefits
We considered the potential for longer-term modelling as part of the pilot phase and concluded that, although there are longer-term implications for bullying, given the inherent limitations of the existing evidence base such an exercise would be likely to produce cost-effectiveness estimates that are so uncertain that they would be of little practical use.
The time horizon captured costs and outcomes within the trial. We conducted the analysis at 2 years to capture the time when there was a facilitator, and at 3 years where there was no facilitator for the final year. A discount rate of 3.5% was applied to both costs and outcomes.
Statistical analysis and uncertainty
The CEA followed the intention-to-treat principle, and used multilevel linear regression models that allowed for clustering of pupils at school level135 to report mean (95% CI) incremental costs and main outcomes of LT interventions compared with standard practice at 24 and 36 months. The cost–utility analysis also allowed for correlation between costs and QALYs136 to report mean (95% CI) incremental costs and QALYs of LT interventions compared with standard practice at 24 and 36 months.
Both cost–consequences and cost–utility analyses reported unadjusted and adjusted differences in mean (95% CI) costs and outcomes (mentioned above) between the randomised groups. In the adjusted analysis, the following baseline variables were adjusted: baseline measures of outcomes, sex, ethnicity and SES, and school-level stratifying factors (single-sex vs. mixed-sex school; school-level deprivation; value-added strata). The differences in average costs and QALYs between the randomised groups were used to calculate the ICER of the LT intervention versus standard school-based practices. The CIs around the ICER were constructed by applying Taylor series expansion137 on the incremental estimates of cost and QALY of LT interventions. We also reported cost-effectiveness acceptability curves by calculating the probability that, compared with standard school-based practices, the LT intervention was cost-effective, given the data, at alternative levels of willingness to pay for a QALY gain.
We also performed a number of sensitivity analyses. The sensitivity analysis explored the inclusion of police and NHS costs and the exclusion of costs of school staff time training. The implications of fidelity measures and compliance on cost-effectiveness was explored as per statistical analysis of primary outcomes.
Results
Resource use and costs
Table 19 reports the school staff time associated with delivering the intervention and dealing with bullying and aggression per student. The main time component for school staff was attending the training and curriculum development. The interviews with staff in year 1 revealed that the training was attended not as an additional training but as part of an existing inset training period, suggesting that these staff costs might not need to be included; the implications of this are further explored in the sensitivity analysis. Interestingly, in the intervention arm, school staff spent slightly more time dealing with bullying than in the control arm. The effect of this was more marked in years 1 and 2 than in year 3.
| Control, mean (SD) | Intervention, mean (SD) | |
|---|---|---|
| A: Years 1 and 2 i.e. facilitated intervention years | ||
| School staff time (minutes) | ||
| School staff time training (year 1) | . | 20.04 (6.82) |
| Curriculum development (year 1) | . | 16.98 (9.32) |
| School staff time at action groups (year 1) | . | 2.62 (1.44) |
| School staff time preparing/after action groups (year 1) | . | 3.72 (2.04) |
| Curriculum development (year 2) | . | 9.73 (9.86) |
| School staff time at action groups (year 2) | . | 2.18 (1.58) |
| School staff time preparing/after action groups (year 2) | . | 2.26 (1.49) |
| School staff time dealing with bullying and aggression (year 1 and 2) | 219.30 (85.44) | 224.33 (113.49) |
| Total school staff time years 1 and 2 | 219.30 (85.44) | 281.85 (120.71) |
| B: Year 3 i.e. unfacilitated intervention year | ||
| School staff time (minutes) | ||
| Curriculum development | . | 6.40 (9.43) |
| School staff time at action groups | . | 1.87 (3.45) |
| School staff time preparing/after action groups | . | 2.47 (4.56) |
| School staff time dealing with bullying and aggression | 115.29 (56.04) | 117.44 (56.34) |
| Total school staff time year 3 | 115.29 (56.04) | 128.21 (57.70) |
| Total school staff time years 1 to 3 | 334.58 (119.99) | 410.07 (163.10) |
Table 20 shows the costs of trainers, facilitators and staff associated with the delivery of the intervention and dealing with bullying and aggression per student. The average cost for trainers was £3.44 and for facilitators and staff was £5.00 and £3.36, respectively. The largest component of cost for school staff relate to curriculum delivery and staff training. Overall, in the first 3 years, the mean (SD) total cost of trainers, facilitators and school staff time was £116 (£47) in the control arm compared with £163 (£69) in the intervention arm. As expected, in the third year the difference in cost was much smaller as no training or facilitators were required and, in addition, school staff spent less time dealing with bullying. In the third year, the mean (SD) total cost of trainers, facilitators and staff was £63 (£33) in the control group and £74 (£37) in the intervention group.
| Costs (£) | Control, mean (SD) | Intervention, mean (SD) |
|---|---|---|
| A: Years 1 and 2 i.e. facilitated intervention years | ||
| Trainer and facilitator | ||
| Trainer (year 1) | . | 3.44 (1.43) |
| Facilitator action groups (year 1) | . | 5.00 (2.28) |
| Facilitator action groups (year 2) | . | 3.36 (1.35) |
| School staff time costs | ||
| Staff time training (year 1) | . | 10.74 (3.55) |
| Curriculum development (year 1) | . | 9.79 (5.34) |
| School staff time at action groups (year 1) | . | 1.43 (0.87) |
| School staff time preparing/after action groups (year 1) | . | 2.23 (1.46) |
| Curriculum development (year 2) | . | 5.39 (5.37) |
| School staff time at action groups (year 2) | . | 1.16 (0.90) |
| School staff time preparing/after action groups (year 2) | . | 1.21 (0.88) |
| Staff time dealing with bullying and aggression (year 1 and 2) | 115.64 (46.62) | 119.27 (62.75) |
| Total cost years 1 and 2 | 115.64 (46.62) | 163.02 (68.78) |
| B: Year 3 i.e. unfacilitated intervention year | ||
| School staff time costs | ||
| Curriculum development | . | 3.25 (4.80) |
| School staff time at action groups | . | 0.91 (1.59) |
| School staff time preparing/after action groups | . | 1.21 (2.09) |
| School staff time dealing with bullying and aggression | 63.21 (33.49) | 68.70 (36.94) |
| Total costs year 3 | 63.21 (33.49) | 74.08 (36.60) |
| Total costs years 1 to 3 | 178.85 (67.42) | 237.10 (97.61) |
Table 21 presents the student health service and police resource use and shows the related costs. Overall, the health service and police resource use is similar in both trial arms. However, slightly more students were stopped or told off by police in the control arm. Unexpectedly, more nights in hospital related to accident or injury occurred in the intervention arm, but it was not determined whether or not these were directly related to bullying. As these additional costs of nights in hospital in the intervention arm may not be directly related to bullying, this is further explored in the sensitivity analysis by excluding police and NHS costs.
| Resource use | Control, mean (SD) | Intervention, mean (SD) |
|---|---|---|
| Resource use up to 24 months | ||
| Health service and police | ||
| Visits to health service for accident or injury | 1.56 (3.60) | 1.51 (2.58) |
| Nights in hospital for accident or injury | 0.59 (4.76) | 1.03 (20.61) |
| Stopped or told off by police | 0.34 (1.06) | 0.31 (1.04) |
| Formally cautioned or arrested by police | 0.11 (0.60) | 0.11 (0.65) |
| Resource use 24 to 36 months | ||
| Health service and police | ||
| Visits to health service for accident or injury | 0.60 (1.53) | 0.92 (9.45) |
| Nights in hospital for accident or injury | 0.30 (2.71) | 0.57 (9.64) |
| Stopped or told off by police | 0.18 (0.58) | 0.11 (0.45) |
| Formally cautioned or arrested by police | 0.06 (0.33) | 0.04 (0.26) |
| Student health service and police costs (£) | ||
| Costs up to 24 months | ||
| Visits to health service for accident or injury | 63.29 (145.70) | 61.12 (104.32) |
| Nights in hospital for accident or injury | 172.38 (1395.69) | 303.60 (6037.89) |
| Stopped or told off by police | 88.22 (278.93) | 82.42 (273.50) |
| Formally cautioned or arrested by police | 48.71 (271.14) | 48.29 (292.78) |
| Total costs up to 24 months | 372.60 (1686.06) | 495.44 (6203.27) |
| Costs 24 to 26 months | ||
| Visits to health service for accident or injury | 23.21 (58.76) | 35.31 (363.19) |
| Nights in hospital for accident or injury | 83.09 (754.93) | 158.34 (2682.37) |
| Stopped or told off by police | 44.69 (143.45) | 27.87 (111.88) |
| Formally cautioned or arrested by police | 24.96 (139.66) | 15.52 (110.07) |
| Total costs 24 to 36 months | 175.95 (871.10) | 237.04 (3107.29) |
| Total costs up to 36 months | 483.33 (1827.44) | 507.81 (3482.45) |
Health outcomes
The HRQoL utility scores indicate that utility scores were slightly higher at baseline in the control arm and there is no clear pattern of a difference in utility scores between arms (see Appendix 1, Table 42a–c).
Cost-effectiveness
There was no significant difference between groups in staff QoL as measured with the overall CHU9D or the SF12 (Table 22). However, as noted earlier in the report, there was a significant effect on the primary outcomes of the GBS and ESYTC scores. The mean total costs per pupil at 24 and 36 months for the control school were £493 and £667, respectively. The mean total costs per pupil were higher for the intervention school at both 24 months (£650) and 36 months (£719). The unadjusted incremental costs were £157 (95% CI –£83 to £397) at 24 months and £62 (95% CI –£165 to £288) at 36 months. The adjusted incremental costs were £57 (95% CI –£183 to £297) at 24 months and £71 (95% CI –£73 to £214) at 36 months. Overall, the intervention is associated with higher costs, but the incremental costs are surrounded by statistical uncertainty.
| Measure | Trial arm, mean (SD) | Unadjusted effect estimate, difference (95% CI); p-value | Adjusted effect estimate, difference (95% CI); p-value | |
|---|---|---|---|---|
| Control | Intervention | |||
| At 24 months | ||||
| Total costs (£) | 493 (1687) | 650 (6203) | 157 (–83 to 397); 0.199 | 57 (–183 to 297); 0.642 |
| Bullying victimisation – GBS overall score | 0.42 (0.02) | 0.37 (0.02) | –0.02 (–0.05 to 0.01); 0.2198 | –0.02 (–0.05 to 0.01); 0.1581 |
| Misbehaviour/delinquency – ESYTC | 4.24 (0.28) | 3.96 (0.28) | –0.04 (–0.34 to 0.27); 0.8113 | –0.06 (–0.35 to 0.24); 0.7206 |
| CHU9D – student HRQoL | 0.86 (0.01) | 0.87 (0.01) | 0.00 (–0.00 to 0.01); 0.4883 | 0.00 (–0.00 to 0.01); 0.2640 |
| SF-12 – staff HRQoLa physical health score | 54.97 (0.32) | 55.22 (0.34) | –0.35 (–1.05 to 0.34); 0.3187 | –0.26 (–0.99 to 0.47); 0.4825 |
| SF-12 – staff HRQoLa mental health score | 44.56 (0.49) | 43.71 (0.52) | –0.66 (–1.64 to 0.32); 0.1883 | –0.45 (–1.49 to 0.58); 0.3896 |
| At 36 months | ||||
| Total costs (£) | 667 (1829) | 719 (3486) | 62 (–165 to 288); 0.593 | 71 (–73 to 214); 0.334 |
| Bullying victimisation – GBS overall score | 0.34 (0.02) | 0.29 (0.02) | –0.03 (–0.06 to –0.00); 0.0395 | –0.03 (–0.06 to –0.00); 0.0441 |
| Misbehaviour/delinquency – ESYTC | 4.33 (0.20) | 4.04 (0.21) | –0.07 (–0.38 to 0.25); 0.6820 | –0.13 (–0.43 to 0.18); 0.4199 |
| CHU9D – student HRQoL | 0.85 (0.00) | 0.86 (0.01) | 0.01 (–0.00 to 0.01); 0.2423 | 0.01 (–0.00 to 0.01); 0.0795 |
| SF-12 – staff HRQoLa physical health score | 55.62 (0.36) | 55.18 (0.36) | –0.71 (–1.4 to 0.02); 0.0449 | –0.61 (–1.36 to 0.13); 0.1058 |
| SF-12 – staff HRQoLa mental health score | 43.76 (0.44) | 43.69 (0.45) | 0.15 (–0.83 to 1.13); 0.7642 | 0.31 (–0.76 to 1.38); 0.5691 |
Overall, the intervention is associated with higher costs (Table 23) but the mean gain in CHU9D score is slightly higher in the intervention arm even though it has not reached a significant level (see Table 22), leading to small QALY gains. The adjusted ICERs are £13,284 (95% CI –£32,175 to £58,743) and £1875 (95% CI –£12,945 to £16,695) per QALY at 2 and 3 years, respectively. These baseline ICERs are well below the threshold at which NICE considers interventions to be cost-effective, which is £20,000 to £30,000 per QALY gained. However, assessment of the CIs around ICERs indicates that there is uncertainty in the results about whether or not the intervention is cost-effective at 2 years, whereas at 3 years it is within the threshold.
| Measure | Trial arm, mean (SD) | Incremental effect (unadjusted), mean (95% CI) | Incremental effecta (adjusted), mean (95% CI) | |
|---|---|---|---|---|
| Control | Intervention | |||
| At 24 months | ||||
| Total costs (£) | 493 (1687) | 650 (6203) | 108 (–119 to 335) | 96 (–151 to 343) |
| QALY | 1.6833 (0.1710) | 1.6834 (0.1710) | 0.0106 (–0.0113 to 0.0325) | 0.0072 (–0.0043 to 0.0188) |
| ICER | 10,214 (–20,190 to 40,616) | 13,284 (–32,175 to 58,743) | ||
| At 36 months | ||||
| Total costs | 667 (1829) | 719 (3485) | 46 (–154 to 246) | 28 (–187 to 242) |
| QALY | 2.4858 (0.2496) | 2.4937 (0.2473) | 0.0240 (–0.0097 to 0.0578) | 0.0148 (–0.0057 to 0.0353) |
| ICER | 1905 (–5938 to 9748) | 1875 (–12,945 to 16,695) | ||
Graphically we present the uncertainty in cost-effectiveness acceptability curves in Figures 4 and 5. At 2 years, there is a 65% probability that the intervention is cost–effective at a willingness-to-pay threshold of £20,000 per QALY. At 3 years, there is a 90% probability that the intervention is cost-effective at the £20,000 per QALY threshold. Overall, there is some uncertainty at 2 years that the intervention is cost-effective, but at 3 years there is a high degree of certainty that it is.
FIGURE 4.
Cost-effectiveness acceptability curve, reporting the probability that the intervention is cost-effective (at 24 months) at alternative willingness to pay for a QALY gain.
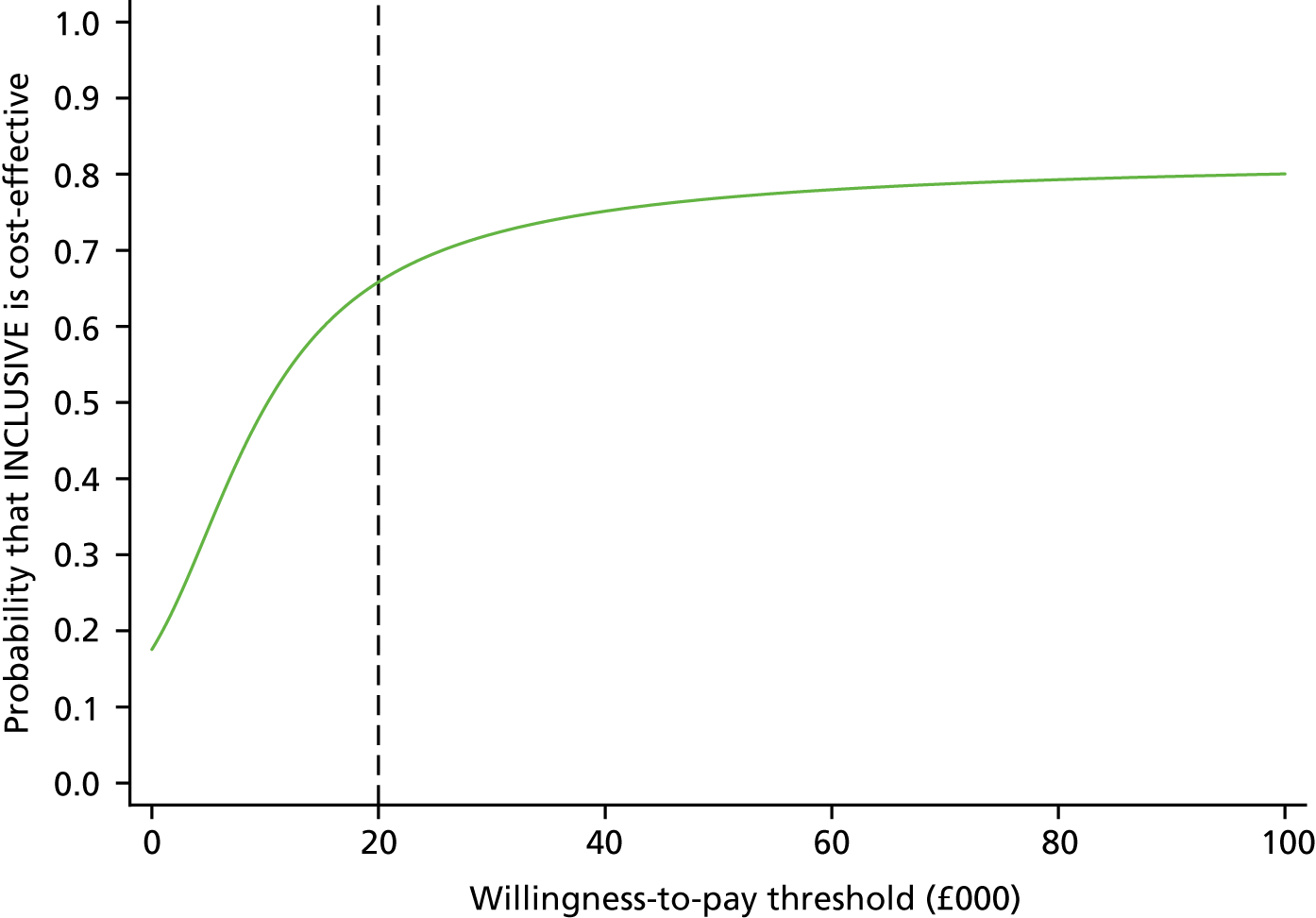
FIGURE 5.
Cost-effectiveness acceptability curve, reporting the probability that the intervention is cost-effective (at 36 months) at alternative willingness to pay for a QALY gain.
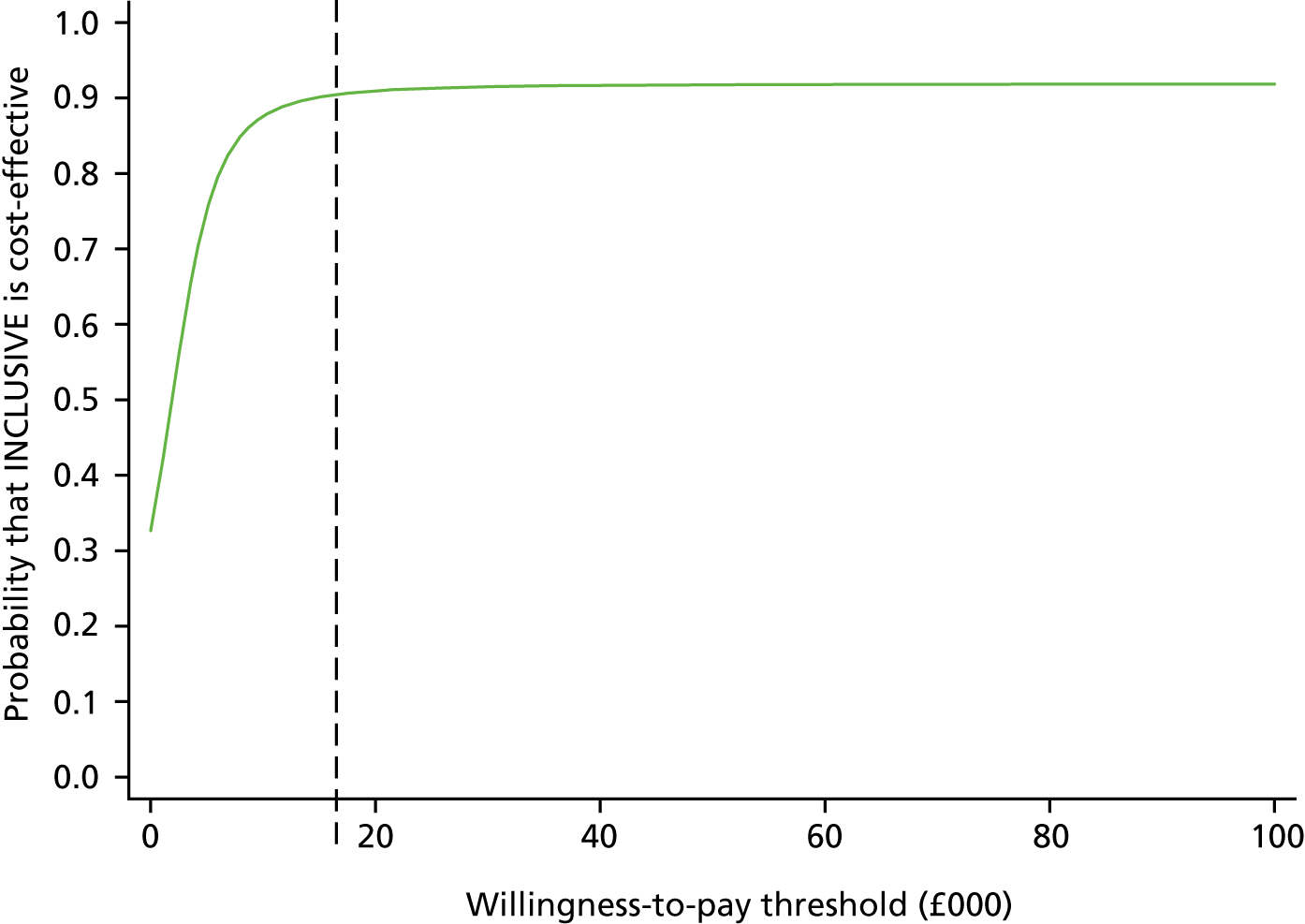
In the sensitivity analysis we explored the impact of not including teacher training time, as this was provided as part of routine inset days (Table 24). This had little impact on results and conclusions. Again, there was some uncertainty about whether or not the increased hospital days in the intervention arm were related to the trial, but exclusion of NHS and police costs did not have a significant impact on results. The fidelity analysis shows (Table 25) that a higher fidelity score was associated with lower costs and QALYs in the unadjusted analysis. When other baseline variables are adjusted, higher fidelity score was associated with lower costs but higher QALYs, although the results were surrounded by statistical uncertainty.
| Measure | Trial arm, mean (SD) | Incremental effect (unadjusted), mean (95% CI) | Incremental effect (adjusted), mean (95% CI) | |
|---|---|---|---|---|
| Control | Intervention | |||
| Excluding staff time training costs | ||||
| Total costs (£) | 667 (1829) | 709 (3486) | 35 (–164 to 235) | 28 (–187 to 242) |
| QALY | 2.4858 (0.2496) | 2.4937 (0.2473) | 0.0241 (–0.0097 to 0.0577) | 0.0148 (–0.0057 to 0.0353) |
| ICER | 1476 (–6393 to 9345) | 1175 (–13,470 to 15,820) | ||
| Excluding NHS and police costs | ||||
| Total costs (£) | 184 (66) | 215 (84) | 17 (12 to 22) | 32 (28 to 36) |
| QALY | 2.4858 (0.2496) | 2.4937 (0.2473) | 0.0129 (–0.0035 to 0.0294) | 0.0106 (–0.0009 to 0.0221) |
| ICER | 1314 (–371 to 2999) | 3008 (–275 to 6291) | ||
| Alternative discount rate | ||||
| Total costs (£) | 681 (1862) | 735 (3605) | 47 (–158 to 252) | 29 (–191 to 249) |
| QALY | 2.5509 (0.2562) | 2.5591 (0.2538) | 0.0247 (–0.0099 to 0.0593) | 0.0152 (–0.0059 to 0.0362) |
| ICER | 1918 (–5907 to 9743) | 1917 (–12,900 to 16,734) | ||
| Measure | Analysis, mean (95% CI) | |
|---|---|---|
| Unadjusted | Adjusted | |
| Total costs (£) | –16 (–92 to 61) | –13 (–73 to 46) |
| QALY | –0.0007 (–0.0112 to 0.0098) | 0.0043 (–0.0017 to 0.0102) |
Chapter 5 Discussion
We present here the first randomised trial of restorative approaches to reducing bullying and aggression and to promote student health in schools, within a multicomponent whole-school intervention engaging students in school decision-making, and providing restorative practice and social and emotional skills education. LT resulted in a very broad range of benefits for behaviour and health outcomes when delivered as a universal intervention over 3 years.
Primary and secondary results
Learning Together reduced student reports of bullying victimisation, both overall and in terms of teasing and rumour-spreading, compared with schools continuing their standard practice. We did not identify a reduction in student reports of aggression across the whole sample. Additionally, LT appeared to have larger beneficial impacts on a wide range of important secondary outcomes among students, ranging from improved psychological function, well-being and QoL to reductions in police contact, smoking and alcohol and drug use. The effects seen for bullying and other continuous outcomes by the third year approximate 0.1 SD, which are potentially highly important at the population level. The impact of LT on risk behaviours at 36 months was also substantial. We found intervention effects both in the whole sample and in those with higher levels of bullying or aggression at baseline, implying that the intervention worked to curtail existing bullying and aggression (secondary prevention) as well as prevent new bullying (primary prevention).
We found a small effect of the intervention on bullying at 36 months (as hypothesised for our primary outcome) but not at 24 months, and we found a similar strengthening of effects over time for most secondary outcomes, suggesting that this was a broad intervention effect. We had anticipated that this would be the case, reflecting the time needed for changes made in the first 2 years to be translated into organisational change within schools. Although many schools did not deliver formal intervention components so well in year 3 as earlier, our process evaluation suggested that by year 3 schools had integrated some of the AG functions into mainstream school structures and processes, enhancing their ability to implement whole-school change. This strengthening of intervention effects with time is consistent with evidence from the Gatehouse Project, in which effects increased among student cohorts subsequently moving through intervention schools after the initial 2-year intervention was completed. 68
We found that although LT was delivered as a universal intervention, exploratory analyses suggest that it was most powerful for students with higher baseline levels of bullying or aggressive behaviours, regardless of the prevalence of bullying or aggression in their school. This is reassuring in that LT appears to benefit those who most need it regardless of the level of problems in a school, and reflects similar findings in other school aggression programmes,93 but is also likely to reflect greater room for improvement among those with higher baseline problems. We also found LT to have greater effects for boys than for girls for secondary psychological and behavioural outcomes, although not for primary outcomes.
There are few other studies to which we can appropriately compare our findings. Our study is unique for the breadth of positive outcomes across bullying, well-being, QoL, psychological problems and substance use. We did not find an effect of our intervention on perpetration of aggressive behaviours, which is contrary to the Ayan Aba study,61 although consistent with the Gatehouse study68 and findings from reviews that school-based studies consistently have stronger effects for victimisation than perpetration. 57 Among comparable trials, the Gatehouse Project identified no impact on bullying or psychological problems, in contrast to our findings,60 although it identified similar impacts on risky behaviours, including substance use. 68 As predicted by the theory of human functioning and school organisation,59 which underpinned our intervention theory of change, intervention effects were concentrated on risk behaviours that may function as overt manifestations of anti-school rebelliousness, such as bullying, smoking and drunkenness, rather than on outcomes that are less manifest, such as sexual health outcomes.
We hypothesised that the intervention would increase the age at sexual debut and increase use of contraception because there is evidence that engagement with school is protective against early sexual debut and lack of contraception use. 138 However, we found no effects on these outcomes, perhaps because our intervention did not explicitly address sexual health, or because, unlike bullying and substance use, sexual behaviours occur off the school site and in private. We did not assess sexual debut or contraception use at baseline at the request of the ethics committee because of the age of the baseline cohort. It is possible that, despite good balance generally in the trial between the intervention and control arms, there were chance imbalances in these outcomes that might have obscured intervention effects on these outcomes.
Intervention cost and cost-effectiveness
The intervention was low cost, falling into the ‘very low cost’ category for school interventions according to the Educational Endowment Foundation guidance. 139 The costs of trainers, facilitators and school staff were an additional £58 per pupil in the intervention compared with control schools over the 3 years, and approximately £47 if LT training costs were regarded as replacing other teacher training rather than being additional. In terms of cost per QALY, at 2 years there was uncertainty about the cost-effectiveness (ICER £13,284, 95% CI –£32,175 to £58,743), but over 3 years the intervention was cost-effective (ICER £1875, 95% CI –£12,945 to £16,695).
Trial context
Schools recruited to the trial were commonly already taking actions to implement RP, student participation in decisions, and/or social and emotional skills education, but these were not being implemented as part of a coherent, guided intervention. Despite reporting the value of RP, most schools used discipline systems focused on traditional punitive responses and only a few schools had staff trained in RP. Schools allocated to the control group did, in some cases, act to implement elements of what they perceived the intervention to involve, in particular RP. However, only a handful of control schools implemented RP, student participation in decisions and social and emotional skills education, and none did so as part of a coherent intervention.
Fidelity and acceptability
The intervention was implemented with variable fidelity and acceptability between components. The training, needs reports and AGs were well delivered and generally acceptable. AGs generally succeeded in reviewing policies and rules, and this was perceived as useful. There were mixed views about the facilitators. On balance, they appeared useful to keep schools focused on scheduling meetings and delivering action, but they may not have needed to attend every meeting. Meetings became less frequent after facilitators were withdrawn, but this may have reflected the mainstreaming of their function (see below). The curriculum was delivered patchily and there were more negative views than positive from teachers. Although data on implementation were poor, interviews and surveys suggest that RP, particularly in the form of conferences, was widely delivered and acceptable. However, time constraints and perceived threats to authority were listed as barriers. The intervention was developed with lower formal fidelity in year 3 but there was some evidence that schools prioritised the components that they most valued and adapted and mainstreamed these components into normal school policies and systems.
Determinants of implementation
The intervention was delivered more completely when led by a member of staff with sufficient authority and support to make decisions and drive delivery. In many, but not all, cases, this required that the staff member was on the school’s SLT. Fidelity, in terms of both success in delivering specific components and ensuring that activity was focused on improving relationships and supporting students’ overall well-being, also appeared stronger when the intervention could build on a pre-existing school culture that was at least starting to address such issues.
Reach and awareness
There was low awareness of the intervention among both staff and students not directly involved in implementation. Staff and students who were involved in delivery did not view this as a barrier to the intervention achieving impacts, as what counted was piecemeal actions to improve the school environment whether or not these were branded as part of the intervention.
Intermediate outcomes
There was some evidence that the intervention did improve students’ sense of a positive school climate, but as this did not manifest until year 3 it was not possible to conclude that this mediated intervention effects on primary and secondary outcomes that also did not manifest until year 3. There was some evidence that the intervention reduced student contact with anti-school peer groups in year 2 but not year 3 and with no evidence that this mediated intervention effects on primary or secondary outcomes. Qualitative data showed how intervention components and processes improved empathy between students and students and staff.
Strengths and limitations
We undertook a well-conducted, large, cluster RCT of an intervention of proven feasibility (LT) in a group of schools that are larger, are more ethnically and culturally diverse, and have notably greater levels of student deprivation than the English average. Participating schools were representative of the approximately 500 schools initially approached and all schools were retained in the trial. Our follow-up was sufficiently lengthy to allow time both for intervention effects to develop and for investigation of persistence of intervention effects after the end of the facilitated intervention. Student participation was high. Our outcome research team and intervention team remained independent throughout the trial and blinding of lead researchers was maintained. Outcomes were assessed using age-appropriate validated instruments. Although self-report outcomes can be open to recall bias, baseline data were collected before randomisation, instruments were used with standardised recall periods and actions at the school level are very unlikely to have biased reporting between intervention and control arms. Analysis used an intention-to-treat approach and appropriate mixed-effects models.
Our data are subject to a number of limitations. In terms of generalisability, our trial was carried out in a representative sample of urban and periurban settings in and around London. Although our study did not include schools in rural England, our process evaluation identified no factors that might suggest that implementation or effects would be different in such schools. The absence of students at some waves may have introduced bias. However, given that non-responders are more likely to have experienced bullying or behaviour problems, this is likely to have underestimated the intervention effect. The large number of secondary outcomes investigated necessitated multiple statistical testing. However, to mitigate this, we restricted ourselves to testing only prespecified secondary and subgroup analyses. A sensitivity analysis allowing for a very stringent Bonferroni correction to the p-values led to little change in our conclusions; the evidence of an effect of the intervention remained for QoL, psychological total difficulties, ever smoked regularly, been offered or tried illicit drugs and number of times really drunk. Subgroup analyses were underpowered. We have not yet assessed the impact of the intervention on staff outcomes or on educational outcomes (attainments, attendance and exclusions), as these rely on routine administrative data which will be available 1–2 years after the end of the trial. We used the GBS, a well-established tool, to measure the occurrence of bullying victimisation in schools. The measure aligns with the WHO definition of bullying described in Chapter 1. 8 It focuses on different forms of abuse committed face to face or online, as well as the frequency of victimisation and the hurt caused. The tool aligns less well with some other definitions of bullying, such as that of Olweus,11 which focuses on repeat victimisation from the same perpetrator(s) as well as power imbalances between perpetrator(s) and victim. We used the ESYTC school misbehaviour subscale to assess broader forms of violence and aggression at school. 72 It should be noted that, as well as assessing forms of behaviour that clearly involve interpersonal aggression, the measure includes items on some behaviours that might best be regarded as anti-social, such as arriving late for classes, refusing to do work, wandering around school in class time and cheating when doing homework or tests.
Self-report of student outcomes, although providing the most useful data for the majority of outcomes, has limitations. There is evidence that peer reports identify a higher prevalence of bullying perpetration than self-reports,140 but we are unaware of any evidence that peer reports identify a higher prevalence of bullying victimisation than self-reports. The use of multiple respondents may have improved the accuracy of mental health data. Parental report or the use of linked routine administrative data is likely to have improved the accuracy of policy contacts and health service use. Our process evaluation was both broad in collecting data from all schools and deep in exploring some processes in depth in case study schools. It also enabled a longitudinal evaluation of implementation across 3 years. Although response rates for process data collection were generally high, some aspects, such as the surveys of teachers delivering the curriculum, had lower response rates. Despite this, our multisource approach meant that we were still able to assess what was happening in most schools, with the exception of a few schools in year 3, when it is reasonable to assume that few, if any, intervention activities were being implemented.
Fidelity of implementation of LT was variable. Some schools in the control arm implemented activities that resembled some elements of LT. However, only five control schools implemented what might be regarded as three of the key elements of our intervention (RP, social and emotional skills education and student participation in decision-making) and implemented these with less support than was the case in intervention schools. A per-protocol analysis excluding these control schools found similar intervention effects. A sensitivity analysis excluding the six case study schools selected for more intensive process evaluation data collection and showed no discernible differences in intervention effects from the intention-to-treat analyses, although CIs were wider as these analyses were underpowered.
The economic evaluation also had some limitations. We have not incorporated the staff outcomes (HRQoL) into the QALY estimates, although we do report physical and mental health scores of staff in the cost–consequences analysis. This was because it is difficult to know how staff and student QoL should be combined. It is possible that we have not captured all of the costs incurred in the control arm, as these were difficult to capture without changing the control arm status. Finally, we have only conducted a within-trial analysis and have not modelled the longer-term impact of bullying on health outcomes, costs and QoL.
Chapter 6 Conclusions
Learning Together offers the potential for broad improvements in behaviour and health to be promoted in secondary schools and provides strong support for further development of restorative approaches in such settings. Positive effects were found, despite the intervention being delivered with variable fidelity. It may be that, for this sort of organisational change intervention, traditional fidelity of ‘form’ (what intervention components were delivered) was less important than overall ‘fidelity of function’ (whether or not overall the intervention achieved benefits in the ways theorised, albeit locally appropriate). 141 Our findings are particularly encouraging given that many of the control schools were delivering broadly similar activities, including RP and student involvement in decision-making. This suggests that the intervention packaged and promoted these activities more effectively than most schools could do on their own.
We have demonstrated the effectiveness and cost consequences of the LT intervention for a broad range of key public health targets for young people. At a time when young people’s mental health is a major public health concern internationally,42,142 countries such as the UK42 and Australia142 have identified schools as a key policy platform for improving mental health. Universal school environment interventions such as LT are likely to be one of the most efficient ways of promoting mental health and well-being and simultaneously addressing other health harms in adolescence, owing to their potential for modifying population-level risk as well as their wide reach across health outcomes and likely sustainability. 143
Implications for research and practice
Our study adds to the evidence that whole-school approaches to preventing bullying and aggression and promoting student health are feasible to implement and have positive effects on a range of outcomes in a broad range of high-, middle- and low-income settings. 57,60,61,144 LT offers the potential for broad improvements in behaviour and health in secondary schools and, as the first RCT of school-based RP, provides strong support for further development of restorative approaches in secondary schools. The results are important for public health policy in that a single, very low-cost intervention had an impact on a clustered set of outcomes of public health importance including bullying, mental health, well-being and QoL, as well as on the use of tobacco, alcohol and drugs. The findings are also of broader scientific interest in that they provide the first experimental evidence that it is possible to promote multiple health outcomes by transforming the school environment and increasing educational engagement rather than via health services or traditional health education, as we theorised.
The wider value of LT must be examined in further trials in diverse settings, such as nations within the UK that have different education systems (e.g. Scotland). We recommend that some future studies examine the effectiveness of interventions that do not include a curriculum component in order to assess whether or not whole-school elements alone are sufficient to achieve health outcomes. We also recommend that other studies examine the effectiveness of an intervention that incorporates a strengthened curriculum element, where more thought is given to ensuring that lessons are culturally appropriate and can be delivered within busy school timetables. Curriculum components may prove more feasible to deliver in schools or school systems that have dedicated time in school timetables for personal, social and/or health education. We further recommend that future studies explore whether external facilitation is essential to initiate implementation or training for schools on implementing whole-school change would be an alternative. We recommend that, in future studies, training be repeated annually to compensate for staff turnover.
We are currently undertaking further analyses to investigate which elements of the intervention may have been the most beneficial. The poor fidelity for the curriculum element suggests this was less likely to have contributed significantly to the benefits detected, although it is possible that schools were already implementing social and emotional learning in other ways.
Future work will examine staff and educational outcomes, explore the sustainability of the intervention within LT intervention schools once the trial was complete, and examine hypothesised mechanisms by which the intervention had an impact on outcomes and whether or not these varied between schools. Work is also needed to establish the generalisability of our findings. However, given that participating schools were representative of those invited to participate and included a good range in terms of attainment, deprivation and inspectorate ratings, this suggests that LT may achieve similar effects in other schools in England and beyond. Given the extent to which control schools were implementing quite similar activities to those included in the intervention, effects of LT might be greater in settings and countries where schools are less involved in such activities. Future work is needed to examine broader implementation of LT and evaluate any modification of the intervention.
Chapter 7 Other information
Patient and public involvement
This trial has strongly benefited from service user and public involvement. Our trial involved young people from the National Children’s Bureau young researchers’ group (YRG) in advising on intervention and research methods.
We consulted with the YRG on refinements to the intervention and trial methods during the set-up phase. This ensured that the intervention remained acceptable and appropriate to young people, as they were in the pilot. Three meetings took place with the YRG on these issues. Note that training and support to the YRG was routinely provided by the National Children’s Bureau. At the trial summation, the YRG was again consulted about the meaning of the results to students and schools, and the most effective ways to disseminate the findings to schools and charities. One group’s feedback on this is provided in Appendix 2.
School AGs during the intervention ensured that implementation in their school was appropriate to local needs that were identified by members and the survey of student needs. This included ensuring that revisions to policies and rules built on existing work, deciding which curriculum modules to deliver in each year, and implementing locally decided actions aiming to improve relationships and student participation (e.g. cascading restorative practice training to staff who had not attended or to student peer mentors).
The study student advisory group comprised students and staff drawn from intervention schools in the pilot who had signalled their willingness to undertake this. This was used to consolidate learning from the pilot, particularly regarding implementation issues.
We convened an advisory group of research and service users. This included representatives who were key policy-makers and clinicians. This group met twice during the study and provided an opportunity for the research team to consult about the research design and methods for data collection, choice of outcomes and methods for data analyses. The advisory group also aided in interpreting the initial findings and developing the dissemination strategies.
Research governance
Trial documentation
Relevant trial documentation will kept for a minimum of 15 years.
Trial registration and conduct
The pilot study was registered with controlled-trials.com (ISRCTN88527078) and the full trial was similarly registered. Note that as the trial was not carried out clinical settings and did not use clinical samples or a medicinal product, there was no requirement to comply with the The Medicines for Human Use (Clinical Trials) Regulations 2004. 145 We followed the MRC’s Guidelines on Good Clinical Practice in Clinical Trials. 146 Note that the CI and the majority of the other investigators have been trained in Good Clinical Practice for clinical trials. The protocol for this trial can be found online. 1
Sponsor
This paper presents independent research funded by NIHR in England under its Public Health Research Board (12/153/60) and the Education Endowment Foundation.
Trial Steering Committees
The trial was overseen by a TSC, including an independent chairperson, at least two other independent members, and a patient and public involvement representative, and an investigator representative of each institution involved in the research. The TSC formed for the pilot trial agreed to continue for the full trial (chairperson: Professor Rona Campbell, Bristol University; other members listed in the uploaded pilot trial report). Observers from the Health Technology Assessment (HTA) programme were invited to all TSC meetings. The TSC met 6-monthly throughout the pilot. A monitoring schedule covering the roles and responsibilities of the researcher, project team, management committee and TSC for monitoring recruitment, data quality, compliance, safety and ethics was developed and agreed.
Data Monitoring and Ethics Committee
A DMC was established independent of the investigators and of the TSC, but reporting to the TSC and (via the TSC) to the sponsors and the HTA programme. This committee comprised an independent chairperson, a senior statistician and at least one other senior academic independent of the investigators. They met approximately yearly during the study. The DMC monitored data for quality and completeness. Data quality, follow-up and trial monitoring were facilitated through the development of a trial-specific database, including validation, verification, monitoring and compliance reports and follow-up report functionalities. The DMC examined the results of an interim analysis at 24 months to consider any potential harms.
Study management
Russell Viner directed the study together with Chris Bonell as co-director. The intervention and research teams were functionally independent. The research team was managed by Russell Viner with Chris Bonell and an experienced full-time trial manager based at the UCL Institute of Child Health. Chris Bonell will direct the process evaluation. An executive of Russell Viner, Chris Bonell, Adam Fletcher, Meg Wiggins and Elizabeth Allen met monthly with the trial manager. The trial manager had day-to-day responsibility for the conduct of the trial and the operations of the research team, and reported to the study executive and ultimately to Russell Viner. The investigator group formed the Scientific Steering Committee for the study and met four-monthly throughout the trial. Responsibility for data integrity and analysis were held by the CTU at the LSHTM.
The intervention team was managed by Meg Wiggins at the Institute of Education, together with an intervention manager who directed day-to-day operation of the intervention and co-ordinated the educational facilitators. Note that Meg Wiggins formed part of the Scientific Steering Committee.
Acknowledgements
Miranda Perry played a key role in developing the intervention and co-ordinated its implementation in the pilot and Phase III trials.
We are grateful to the staff and students of participating schools for their dedication to the intervention and completion of the outcome surveys and process evaluation surveys and interviews. We are very grateful for the advice and support of our TSC and DMC.
We acknowledge the work of, and mourn the loss of, Dr Farah Jamal during the trial, whose death at the age of 30 years was a tragic loss for public health research.
Contributions of authors
Chris Bonell (Professor, Public Health Sociology) co-led development of the LT intervention, conceptualised the study, led design of the trial, led the research and writing of the manuscript. He directed the study, together with Russell M Viner. Chris Bonell conducted the trial’s progress review, including staff and resources. He ensured that the trial was administered in a financially responsible manner. The research team was managed by Russell M Viner with Chris Bonell. Chris Bonell led the process evaluation and intervention teams. Chris Bonell planned and led the process evaluation.
Elizabeth Allen (Professor, Medical Statistics) contributed to the trial design, and was responsible for randomisation of schools, for entry and cleaning of all quantitative data, and for all quantitative analyses.
Emily Warren (Research Fellow, Behaviour and Intervention Use) was responsible for process evaluation.
Jennifer McGowan (Research Associate, Health Psychology) conducted the review of the progress of the trial, looking at staff and resources issues. She reported to the NIHR on study’s progress and achievements. She had day-to-day responsibility for the conduct of the trial and the operations of the research team, and writing of the final report.
Leonardo Bevilacqua (Research Assistant, Developmental Psychopathology) conducted schools recruitment, dissemination of surveys in schools, overall management of the trial, and led the process evaluation activities.
Farah Jamal (Social Researcher, School Environment) conducted schools recruitment, surveys in schools, overall management of the trial, and led the process evaluation activities.
Zia Sadique (Lecturer, Economic Evaluation) conducted the economic evaluation with Rosa Legood.
Rosa Legood (Associate Professor, Health economics) conducted overviews of progress, advice, implementation, publications and dissemination strategy. She was responsible for the economic evaluation.
Meg Wiggins (Research Officer, Education) managed the intervention team at the Institute of Education. She was part of the Scientific Steering Committee.
Charles Opondo (Honorary Assistant Professor, Medical Statistics) conducted the qualitative statistical analysis with Elizabeth Allen.
Anne Mathiot (Trial Manager) conducted the review of the progress of the trial, looking at staff and resources issues. She reported to the NIHR on study’s progress and achievements, before passing the role to Jennifer McGowan.
Joanna Sturgess (Research Fellow, Clinical Trials) was responsible for randomisation of schools, for entry and cleaning of all quantitative data, and for the quantitative analyses. She managed the trial data and contributed to the analysis.
Sara Paparini (Honorary Research Fellow, Social and Environmental Health) contributed to the fieldwork and analysis within the process evaluation.
Adam Fletcher (Senior Lecturer, Public Health Improvement) conducted overviews of the intervention progress, advice, implementation, publications and dissemination strategy.
Miranda Perry (Education Consultant) was responsible for the information required for delivering the intervention in the schools.
Grace West (Research Assistant, Developmental Psychology) conducted schools recruitment, dissemination of surveys in schools, overall management of the trial, and led the process evaluation activities.
Tara Tancred (Assistant Professor, Public Health) contributed to the fieldwork and analysis within the process evaluation.
Stephen Scott (Professor, Child Health and Behaviour) conducted overview of the intervention progress, implementation, publications and dissemination strategy.
Diana Elbourne (Professor, Health-Care Evaluation) contributed to the trial design, was responsible for randomisation of schools, for entry and cleaning of all quantitative data and for quantitative analyses. She also conducted overviews of the intervention progress, advice, implementation, publications and dissemination strategy.
Deborah Christie (Professor, Paediatric and Adolescent Psychology) conducted overviews of the intervention progress, advice, implementation, publications and dissemination strategy.
Lyndal Bond (Professor, Population Health and Evaluation) conducted overviews of the intervention progress, advice, implementation, publications and dissemination strategy.
Russell M Viner (Professor, Adolescent Health) co-led development of the LT intervention, conceptualised the study, led design of the trial, led the research and led the writing of the manuscript. He directed the study, together with Chris Bonell as co-director. Russell M Viner conducted the trial’s progress review, including staff and resources. He ensured that the trial was administered in a financially responsible manner. The research team was managed by Russell M Viner with Chris Bonell. Russell M Viner led the outcome evaluation team.
All authors contributed to writing the manuscript, with the exception of Farah Jamal.
Publications
Bonell C, Allen E, Christie D, Elbourne D, Fletcher A, Grieve R, et al. Initiating change locally in bullying and aggression through the school environment (INCLUSIVE): study protocol for a cluster randomised controlled trial. Trials 2014;15:381.
Hargreaves D, Bevilacqua L, Shackleton N. Association between ethnic minority status at school and bullying and mental health outcomes in early adolescence: cross-sectional analysis of data from the INCLUSIVE study. Lancet 2015;386:S42.
Jamal F, Fletcher A, Shackleton N, Elbourne D, Viner R, Bonell C. The three stages of building and testing mid-level theories in a realist RCT: a theoretical and methodological case-example. Trials 2015;16:466.
Bonell C, Shackleton N, Fletcher A, Jamal F, Allen E, Mathiot A, et al. Student- and school-level belonging and commitment and student smoking, drinking and misbehaviour. Health Educ J 2016;76:206–20.
Bonell C, Warren E, Fletcher A, Viner R. Realist trials and the testing of context-mechanism-outcome configurations: a response to Van Belle et al. Trials 2016;17:478.
Shackleton N, Hale D, Bonell C, Viner RM. Intraclass correlation values for adolescent health outcomes in secondary schools in 21 European countries. SSM Popul Health 2016;2:217–25.
Bonell C, Mathiot A, Allen E, Bevilacqua L, Christie D, Elbourne D, et al. Initiating change locally in bullying and aggression through the school environment (INCLUSIVE) trial: update to cluster randomised controlled trial protocol. Trials 2017;18:238.
Shackleton N, Fletcher A, Jamal F, Markham W, Aveyard P, Mathiot A, et al. A new measure of unhealthy school environments and its implications for critical assessments of health promotion in schools. J Crit Pub Health 2017;27:248–62.
Bonell C, Allen E, Warren E, McGowan J, Bevilacqua L, LeGood R, et al. A multi-component school environment intervention reduces bullying and risky behaviour and improves mental health and quality of life: findings from the INCLUSIVE cluster randomised controlled trial. J Adolesc Health 2018;62:S9.
Bonell C, Moore G, Warren E, Moore L. Are randomised controlled trials positivist? Reviewing the social science and philosophy literature to assess positivist tendencies of trials of social interventions in public health and health services. Trials 2018;19:238.
Fantaguzzi C, Allen E, Miners A, Christie D, Opondo C, Sadique Z, et al. Health-related quality of life associated with bullying and aggression: a cross sectional study in English secondary schools. Eur J Health Econ 2018;19:641–51.
McGowan J, Bonell C, Allen E, Warren E, Aswathikutty A, Bevilacqua L, et al. The relationship between school-level factors and adolescent student well-being: cross-sectional findings from the INCLUSIVE trial. J Adolesc Health 2018;62:S14–15.
Bonell C, Allen E, Warren E, McGowan J, Bevilacqua L, Jamal F, et al. Effects of the Learning Together intervention on bullying and aggression in English secondary schools (INCLUSIVE): a cluster randomised controlled trial. Lancet 2018;392:2452–64.
Bonell C, Allen E, Opondo C, Warren E, Elbourne D, Sturgess J, et al. Examining intervention mechanisms of action using mediation analysis within a randomised trial of a whole-school health intervention. J Epidemiol Community Health 2019;73:455–64.
Bonell C, Beaumont E, Dodd M, Elbourne D, Bevilacqua L, Mathiot A, et al. The effects of school environments on student risk behaviours: evidence from longitudinal study of secondary schools in England. J Epidemiol Community Health 2019;73:502–8.
Bonell C, Allen E, Opondo C, Warren E, Elbourne DR, Sturgess J, et al. Examining intervention mechanisms of action using mediation analysis within a randomised trial of a whole-school health intervention. J Epidemiol Community Health 2019;73:455–64.
Warren E, Bevilacqua L, Opondo C, Allen E, Mathiot A, West G, et al. Action groups as a participative strategy for leading whole-school health promotion: results on implementation from the INCLUSIVE trial in English secondary schools. Br Educ Res J 2019;45:979–1000.
Data-sharing statement
All data requests should be submitted to the corresponding author for consideration. Access to anonymised data may be granted following review.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care.
References
- Bonell C, Allen E, Christie D, Elbourne D, Fletcher A, Grieve R, et al. Initiating change locally in bullying and aggression through the school environment (INCLUSIVE): study protocol for a cluster randomised controlled trial. Trials 2014;15. https://doi.org/10.1186/1745-6215-15-381.
- World Health Organization . Global Status Report on Violence Prevention 2014 2014.
- Department of Health and Social Care . Public Mental Health Priorities: Investing in the Evidence. Annual Report of the Chief Medical Officer 2013 2014.
- Scott S, Knapp M, Henderson J, Maughan B. Financial cost of social exclusion: follow up study of antisocial children into adulthood. BMJ 2001;323. https://doi.org/10.1136/bmj.323.7306.191.
- Krug EG, Mercy JA, Dahlberg LL, Zwi AB. The world report on violence and health. Lancet 2002;360:1083-8. https://doi.org/10.1016/S0140-6736(02)11133-0.
- McKee M, Raine R. Riots on the streets. BMJ 2011;343. https://doi.org/10.1136/bmj.d5248.
- Fletcher A, Gardner F, McKee M, Bonell C. The British government’s Troubled Families Programme. BMJ 2012;344. https://doi.org/10.1136/bmj.e3403.
- World Health Organization . World Report on Violence and Health 2002. www.who.int/violence_injury_prevention/violence/world_report/en/full_en.pdf (accessed 29 September 2017).
- Craig WM, Henderson K, Murphy JG. Prospective teachers’ attitudes toward bullying and victimization. School Psychol Int 2000;21:5-21. https://doi.org/10.1177/0143034300211001.
- Newman RS, Murray B, Lussier C. Confrontation with aggressive peers at school: students’ reluctance to seek help from the teacher. J Educ Psychol 2001;93:398-410. https://doi.org/10.1037/0022-0663.93.2.398.
- Olweus D. Bullying at school: basic facts and effects of a school based intervention program. J Child Psychol Psychiatry 1994;35:1171-90. https://doi.org/10.1111/j.1469-7610.1994.tb01229.x.
- Brooks F, Magnusson J, EKlemera E, Chester K, Spencer N, Smeeton N. HBSC England National Report 2014 2015.
- Nansel TR, Craig W, Overpeck MD, Saluja G, Ruan WJ. Health Behaviour in School-Aged Children Bullying Analyses Working Group . Cross-national consistency in the relationship between bullying behaviors and psychosocial adjustment. Arch Pediatr Adolesc Med 2004;158:730-6. https://doi.org/10.1001/archpedi.158.8.730.
- Radford L, Corral S, Bradley C, Fisher H, Bassett C, Howat N, et al. Child Abuse and Neglect in the UK Today. London: National Society for the Prevention of Cruelty to Children; 2011.
- Bevilacqua L, Shackleton N, Hale D, Allen E, Bond L, Christie D, et al. The role of family and school-level factors in bullying and cyberbullying: a cross-sectional study. BMC Pediatr 2017;17. https://doi.org/10.1186/s12887-017-0907-8.
- Jansen DE, Veenstra R, Ormel J, Verhulst FC, Reijneveld SA. Early risk factors for being a bully, victim, or bully/victim in late elementary and early secondary education. The longitudinal TRAILS study. BMC Public Health 2011;11. https://doi.org/10.1186/1471-2458-11-440.
- Chamberlain T, George N, Golden S, Walker F, Benton T. Tellus4 National Report 2010.
- Offending, Crime and Justice Survey, 2006. 2006.
- Wolke D, Woods S, Stanford K, Schulz H. Bullying and victimization of primary school children in England and Germany: prevalence and school factors. Br J Psychol 2001;92:673-96. https://doi.org/10.1348/000712601162419.
- Stansfeld S, Haines M, Booy R, Taylor S, Viner RM, Head JJ, et al. Health of Young People in East London: The RELACHS Study 2001. London: Institute of Community Health Sciences, Barts and The London Queen Mary’s School of Medicine & Dentistry; 2003.
- Battistich V, Hom A. The relationship between students’ sense of their school as a community and their involvement in problem behaviors. Am J Public Health 1997;87:1997-2001. https://doi.org/10.2105/AJPH.87.12.1997.
- National Center for Educational Statistics . Indicators of School Crime and Safety: 2007 2007.
- Arseneault L. Annual research review: the persistent and pervasive impact of being bullied in childhood and adolescence: implications for policy and practice. J Child Psychol Psychiatry 2018;59:405-21. https://doi.org/10.1111/jcpp.12841.
- Arseneault L, Walsh E, Trzesniewski K, Newcombe R, Caspi A, Moffitt TE. Bullying victimization uniquely contributes to adjustment problems in young children: a nationally representative cohort study. Pediatrics 2006;118:130-8. https://doi.org/10.1542/peds.2005-2388.
- Hair EC, Park MJ, Ling TJ, Moore KA. Risky behaviors in late adolescence: co-occurrence, predictors, and consequences. J Adolesc Health 2009;45:253-61. https://doi.org/10.1016/j.jadohealth.2009.02.009.
- Forero R, McLellan L, Rissel C, Bauman A. Bullying behaviour and psychosocial health among school students in New South Wales, Australia: cross sectional survey. BMJ 1999;319:344-8. https://doi.org/10.1136/bmj.319.7206.344.
- Kaltiala-Heino R, Rimpelä M, Rantanen P, Rimpelä A. Bullying at school – an indicator of adolescents at risk for mental disorders. J Adolesc 2000;23:661-74. https://doi.org/10.1006/jado.2000.0351.
- Juvonen J, Graham S, Schuster MA. Bullying among young adolescents: the strong, the weak, and the troubled. Pediatrics 2003;112:1231-7. https://doi.org/10.1542/peds.112.6.1231.
- Copeland WE, Wolke D, Angold A, Costello EJ. Adult psychiatric outcomes of bullying and being bullied by peers in childhood and adolescence. JAMA Psychiatry 2013;70:419-26. https://doi.org/10.1001/jamapsychiatry.2013.504.
- Lereya ST, Copeland WE, Costello EJ, Wolke D. Adult mental health consequences of peer bullying and maltreatment in childhood: two cohorts in two countries. Lancet Psychiatry 2015;2:524-31. https://doi.org/10.1016/S2215-0366(15)00165-0.
- Hawker DS, Boulton MJ. Twenty years’ research on peer victimization and psychosocial maladjustment: a meta-analytic review of cross-sectional studies. J Child Psychol Psychiatry 2000;41:441-55. https://doi.org/10.1111/1469-7610.00629.
- Bond L, Carlin JB, Thomas L, Rubin K, Patton G. Does bullying cause emotional problems? A prospective study of young teenagers. BMJ 2001;323:480-4. https://doi.org/10.1136/bmj.323.7311.480.
- Arseneault L, Bowes L, Shakoor S. Bullying victimization in youths and mental health problems: ‘much ado about nothing’?. Psychol Med 2010;40:717-29. https://doi.org/10.1017/S0033291709991383.
- Fisher HL, Moffitt TE, Houts RM, Belsky DW, Arseneault L, Caspi A. Bullying victimisation and risk of self harm in early adolescence: longitudinal cohort study. BMJ 2012;344. https://doi.org/10.1136/bmj.e2683.
- Winsper C, Lereya T, Zanarini M, Wolke D. Involvement in bullying and suicide-related behavior at 11 years: a prospective birth cohort study. J Am Acad Child Adolesc Psychiatry 2012;51:271-82.e3. https://doi.org/10.1016/j.jaac.2012.01.001.
- van der Wal MF, de Wit CA, Hirasing RA. Psychosocial health among young victims and offenders of direct and indirect bullying. Pediatrics 2003;111:1312-7. https://doi.org/10.1542/peds.111.6.1312.
- Glew GM, Fan MY, Katon W, Rivara FP, Kernic MA. Bullying, psychosocial adjustment, and academic performance in elementary school. Arch Pediatr Adolesc Med 2005;159:1026-31. https://doi.org/10.1001/archpedi.159.11.1026.
- Woods S, Wolke D. Direct and relational bullying among primary school children and academic achievement. J School Psychol 2004;42:135-55. https://doi.org/10.1016/j.jsp.2003.12.002.
- Crick NR, Ostrov JM, Werner NE. A longitudinal study of relational aggression, physical aggression, and children’s social-psychological adjustment. J Abnorm Child Psychol 2006;34:131-42. https://doi.org/10.1007/s10802-005-9009-4.
- Price LH, Kao HT, Burgers DE, Carpenter LL, Tyrka AR. Telomeres and early-life stress: an overview. Biol Psychiatry 2013;73:15-23. https://doi.org/10.1016/j.biopsych.2012.06.025.
- Steer A. Learning Behaviour: Lessons Learned. A Review of Behaviour Standards and Practices in Our Schools. London: Department for Children, Families and Schools; 2009.
- Department of Health and Social Care and Department for Education . Transforming Children and Young People’s Mental Health Provision: A Green Paper 2017.
- Department for Education . Preventing and Tackling Bullying: Advice for Headteachers, Staff and Governing Bodies 2017.
- Beinart S, Anderson B, Lee S, Utting D. Youth at risk? A National Survey of Risk Factors, Protective Factors and Problem Behaviour Among Young People in England, Scotland and Wales. York: Joseph Rowntree Foundation; 2002.
- Baron RA, Richardson DR. Perspectives in Social Psychology. Human Aggression. New York, NY: Plenum Press; 1994.
- Olweus D. Bullying at School: What We Know and What We Can Do. Hoboken, NJ: Wiley–Blackwell; 1993.
- Bender D, Lösel F. Bullying at school as a predictor of delinquency, violence and other anti-social behaviour in adulthood. Crim Behav Ment Health 2011;21:99-106. https://doi.org/10.1002/cbm.799.
- Brame B, Nagin DS, Tremblay RE. Developmental trajectories of physical aggression from school entry to late adolescence. J Child Psychol Psychiatry 2001;42:503-12. https://doi.org/10.1111/1469-7610.00744.
- Boxer P, Edwards-Leeper L, Goldstein SE, Musher-Eizenman D, Dubow EF. Exposure to ‘low-level’ aggression in school: associations with aggressive behavior, future expectations, and perceived safety. Violence Vict 2003;18:691-705. https://doi.org/10.1891/vivi.2003.18.6.691.
- Steer A. Learning Behaviour: Lessons learned – A Review of Behaviour Standards and Practices in our Schools. London: DCSF; 2009.
- Parsonage M. Diversion: A Better Way for Criminal Justice and Mental Health. London: Sainsbury Centre for Mental Health; 2009.
- Department for Education and Skills (DfES) . White Paper: The Future of Higher Education 2003.
- Department for Children, Families and Schools (DfCFS) . Your Child, Your Schools, Our Future: Building a 21st Century Schools System 2009.
- Department of Health and Social Care . Healthy Lives, Brighter Futures 2009.
- Vreeman RC, Carroll AE. A systematic review of school-based interventions to prevent bullying. Arch Pediatr Adolesc Med 2007;161:78-8. https://doi.org/10.1001/archpedi.161.1.78.
- Smith JD, Schneider B, Smith PK, Ananiadou K. The effectiveness of whole-school antibullying programs: a synthesis of evaluation research. Sch Psychol Rev 2004;33:547-60.
- Langford R, Bonell CP, Jones HE, Pouliou T, Murphy SM, Waters E, et al. The WHO health promoting school framework for improving the health and well-being of students and their academic achievement. Cochrane Database Syst Rev 2014;4. https://doi.org/10.1002/14651858.CD008958.pub2.
- Bonell C, Fletcher A, McCambridge J. Improving school ethos may reduce substance misuse and teenage pregnancy. BMJ 2007;334:614-16. https://doi.org/10.1136/bmj.39139.414005.AD.
- Markham WA, Aveyard P. A new theory of health promoting schools based on human functioning, school organisation and pedagogic practice. Soc Sci Med 2003;56:1209-20. https://doi.org/10.1016/S0277-9536(02)00120-X.
- Bond L, Patton G, Glover S, Carlin JB, Butler H, Thomas L, et al. The Gatehouse Project: can a multilevel school intervention affect emotional wellbeing and health risk behaviours?. J Epidemiol Community Health 2004;58:997-1003. https://doi.org/10.1136/jech.2003.009449.
- Flay BR, Graumlich S, Segawa E, Burns JL, Holliday MY. Aban Aya Investigators . Effects of 2 prevention programs on high-risk behaviors among African American youth: a randomized trial. Arch Pediatr Adolesc Med 2004;158:377-84. https://doi.org/10.1001/archpedi.158.4.377.
- Viner RM, Ozer EM, Denny S, Marmot M, Resnick M, Fatusi A, et al. Adolescence and the social determinants of health. Lancet 2012;379:1641-52. https://doi.org/10.1016/S0140-6736(12)60149-4.
- Bonell C, Jamal F, Harden A, Wells H, Parry W, Fletcher A, et al. Systematic review of the effects of schools and school environment interventions on health: evidence mapping and synthesis. Public Health Res 2013;1.
- Dahlgren G, Whitehead M. Policies and Strategies to Promote Social Equity in Health. Stockholm: Institute for Future Studies; 1991.
- Marmot MG. Creating healthier societies. Bull World Health Organ 2004;82.
- Viner R. Co-occurrence of adolescent health risk behaviors and outcomes in adult life: findings from a national birth cohort. J Adolescent Health 2005;36:98-9. https://doi.org/10.1016/j.jadohealth.2004.11.012.
- Buck D, Frosini F. Clustering of Unhealthy Behaviours Over Time. London: The King’s Fund; 2012.
- Patton GC, Bond L, Carlin JB, Thomas L, Butler H, Glover S, et al. Promoting social inclusion in schools: a group-randomized trial of effects on student health risk behavior and well-being. Am J Public Health 2006;96:1582-7. https://doi.org/10.2105/AJPH.2004.047399.
- Langford R, Bonell C, Komro K, Murphy S, Magnus D, Waters E, et al. The Health Promoting Schools Framework: known unknowns and an agenda for future research. Health Educ Behav 2017;44:463-75. https://doi.org/10.1177/1090198116673800.
- Bond L, Glover S, Godfrey C, Butler H, Patton GC. Building capacity for system-level change in schools: lessons from the Gatehouse Project. Health Educ Behav 2001;28:368-83. https://doi.org/10.1177/109019810102800310.
- Glover S, Butler H, Moodie R, Hulme A. Hands-on Health Promotion. Melbourne, VIC: IP Communications; 2004.
- Bonell C, Sorhaindo A, Allen E, Strange V, Wiggins M, Fletcher A, et al. Pilot multi-method trial of a school-ethos intervention to reduce substance use: building hypotheses about upstream pathways to prevention. J Adolesc Health 2010;47:555-63. https://doi.org/10.1016/j.jadohealth.2010.04.011.
- Bonell C, Sorhaindo A, Strange V, Wiggins M, Allen E, Fletcher A, et al. A pilot whole-school intervention to improve school ethos and reduce substance use. Health Educ 2009;110:252-72. https://doi.org/10.1108/09654281011052628.
- Bonell C, Fletcher A, Fitzgerald-Yau N, Hale D, Allen E, Elbourne D, et al. Initiating change locally in bullying and aggression through the school environment (INCLUSIVE): a pilot randomised controlled trial. Health Technol Assess 2015;19. https://doi.org/10.3310/hta19530.
- Morrison B, Elliot E, Gordon RM. New Directions in Restorative Justice: Issues, Practices, Evaluation. Cullompton: Willan Publishing; 2005.
- Bazemore G. Young people, trouble, and crime restorative justice as a normative theory of informal social control and social support. Youth Soc 2001;33:199-226. https://doi.org/10.1177/0044118X01033002004.
- Pepi C. Children without childhoods: a feminist intervention strategy utilizing systems theory and restorative justice in treating female adolescent offenders. Women Ther 1998;20:85-101. https://doi.org/10.1300/J015v20n04_07.
- Farrington DP, Ttofi MM. School-based programs to reduce bullying and victimization. Campbell Syst Rev 2009;6. https://doi.org/10.1037/e528362010-001.
- National Evaluation of the Restorative Justice in Schools Programme 2004.
- Lloyd G, Kane J, McCluskey G, Stead J, Riddell S. Restorative Approaches in Scottish Schools: Transformations and Challenges. Edinburgh: Scottish Executive Education Department; 2006.
- Skinns L, Du Rose N, Hough M. An Evaluation of Bristol RAiS. London: ICPR, King’s College London; 2009.
- Minnesota Department of Children, Families & Learning . In-School Behavior Intervention Grants: A Three-Year Evaluation of Alternative Approaches to Suspensions and Expulsions. Report to the Legislature 2001.
- Shaw G. Restorative practices in Australian schools: changing relationships, changing culture. Conflict Resolution Q 2007;25:127-35. https://doi.org/10.1002/crq.198.
- Wong DS, Cheng CH, Ngan RM, Ma SK. Program effectiveness of a restorative whole-school approach for tackling school bullying in Hong Kong. Int J Offender Ther Comp Criminol 2011;55:846-62. https://doi.org/10.1177/0306624X10374638.
- Farrington DP, Ttofi MM. School-Based Programs to Reduce Bullying and Victimization, Systematic Review for the Campbell Collaboration Crime and Justice Group. Oslo: Campbell Collaboration Crime and Justice Group; 2009.
- Buckley S, Maxwell GM. Respectful Schools: Restorative Practices in Education: A Summary Report 2007.
- Youth Justice Board . National Evaluation of the Restorative Justice in Schools Programme 2004.
- Sumner MD, Silverman CJ, Frampton ML. School-Based Restorative Justice as an Alternative to Zero-Tolerance Policies: Lessons From West Oakland. Berkeley, CA: Thelton E Henderson Center for Social Justice; 2010.
- Kokotsaki D, White C, Hopkins B. Capturing change: a review of the implementation of Restorative Approaches and its outcomes within a local authority in North East England. Online Educ Res J 2014;5.
- Bitel M. The Evaluation of Year 3 of Leicestershire Mediation Services Conflict Resolution in Schools Programme. London: Charities Evaluation Services; 2001.
- Youth Justice Board for England and Wales . National Evaluation of the Restorative Justice in Schools Programme 2004.
- Durlak JA, Weissberg RP, Dymnicki AB, Taylor RD, Schellinger KB. The impact of enhancing students’ social and emotional learning: a meta-analysis of school-based universal interventions. Child Dev 2011;82:405-32. https://doi.org/10.1111/j.1467-8624.2010.01564.x.
- Segawa E, Ngwe JE, Li Y, Flay BR. Evaluation of the effects of the Aban Aya Youth Project in reducing violence among African American adolescent males using latent class growth mixture modeling techniques. Eval Rev 2005;29:128-48. https://doi.org/10.1177/0193841X04271095.
- Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014;348. https://doi.org/10.1136/bmj.g1687.
- Great Britain . Data Protection Act 1998 1998.
- Bond L, Wolfe S, Tollit M, Butler H, Patton G. A comparison of the Gatehouse Bullying Scale and the peer relations questionnaire for students in secondary school. J Sch Health 2007;77:75-9. https://doi.org/10.1111/j.1746-1561.2007.00170.x.
- Smith DJ. School Experience and Delinquency at Ages 13 to 16. Edinburgh: University of Edinburgh, Centre for Law and Society; 2006.
- Varni JW, Burwinkle TM, Seid M. The PedsQL 4.0 as a school population health measure: feasibility, reliability, and validity. Qual Life Res 2006;15:203-15. https://doi.org/10.1007/s11136-005-1388-z.
- Stevens K. Assessing the performance of a new generic measure of health-related quality of life for children and refining it for use in health state valuation. Appl Health Econ Health Policy 2011;9:157-69. https://doi.org/10.2165/11587350-000000000-00000.
- Goodman R, Ford T, Simmons H, Gatward R, Meltzer H. Using the Strengths and Difficulties Questionnaire (SDQ) to screen for child psychiatric disorders in a community sample. Br J Psychiatry 2000;177:534-9. https://doi.org/10.1192/bjp.177.6.534.
- Clarke A, Friede T, Putz R, Ashdown J, Martin S, Blake A, et al. Warwick-Edinburgh Mental Well-being Scale (WEMWBS): validated for teenage school students in England and Scotland. A mixed methods assessment. BMC Public Health 2011;11. https://doi.org/10.1186/1471-2458-11-487.
- Bridges S, Gill V, Omole T, Sutton R, Wright V. Smoking, drinking and drug use among young people in England in 2010. London: NHS Information Centre; 2011.
- Stephenson JM, Strange V, Forrest S, Oakley A, Copas A, Allen E, et al. Pupil-led sex education in England (RIPPLE study): cluster-randomised intervention trial. Lancet 2004;364:338-46. https://doi.org/10.1016/S0140-6736(04)16722-6.
- Hamburger ME, Basile KC, Vivolo AM. Measuring Bullying Victimization, Perpetration, and Bystander Experiences: A Compendium of Assessment Tools. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control; 2011.
- Boyce W, Torsheim T, Currie C, Zambon A. The family affluence scale as a measure of National Wealth: validation of an adolescent self-report measure. Soc Indic Res 2006;78:473-87. https://doi.org/10.1007/s11205-005-1607-6.
- Farivar SS, Cunningham WE, Hays RD. Correlated physical and mental health summary scores for the SF-36 and SF-12 Health Survey, V.I. Health Qual Life Outcomes 2007;5. https://doi.org/10.1186/1477-7525-5-54.
- Maslach C, Jackson SE. The measurement of experienced burnout. J Occupational Behav 1981;2. https://doi.org/10.1002/job.4030020205.
- Department for Education . School and College Performance Tables: Statements of Intent 2017.
- McLennan D, Noble M, Davies J, Garatt E, Dibben C. The English Indices of Deprivation 2010: Technical Report 2011.
- May C. Towards a general theory of implementation. Implement Sci 2013;8. https://doi.org/10.1186/1748-5908-8-18.
- Moore G, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process Evaluation of Complex Interventions: UK Medical Research Council (MRC) Guidance. London: MRC Population Health Science Research Network; 2014.
- Sawyer MG, Pfeiffer S, Spence SH, Bond L, Graetz B, Kay D, et al. School-based prevention of depression: a randomised controlled study of the beyond blue schools research initiative. J Child Psychol Psychiatry 2010;51:199-20. https://doi.org/10.1111/j.1469-7610.2009.02136.x.
- Wiggins M, Bonell C, Sawtell M, Austerberry H, Burchett H, Allen E, et al. Health outcomes of youth development programme in England: prospective matched comparison study. BMJ 2009;339. https://doi.org/10.1136/bmj.b2534.
- Green J, Thorogood N. Qualitative Methods for Health Research. London: Sage; 2009.
- Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015;350. https://doi.org/10.1136/bmj.h1258.
- Frymier AB, Shulman GM, Houser M. The development of a learner empowerment measure. Communication Education 1996;45:181-99. https://doi.org/10.1080/03634529609379048.
- Mytton J, DiGuiseppi C, Gough D, Taylor R, Logan S. School-based secondary prevention programmes for preventing violence. Cochrane Database Syst Rev 2006;3. https://doi.org/10.1002/14651858.CD004606.pub2.
- Hale DR, Patalay P, Fitzgerald-Yau N, Hargreaves DS, Bond L, Görzig A, et al. School-level variation in health outcomes in adolescence: analysis of three longitudinal studies in England. Prev Sci 2014;15:600-10. https://doi.org/10.1007/s11121-013-0414-6.
- Tobler AL, Komro KA, Dabroski A, Aveyard P, Markham WA. Preventing the link between SES and high-risk behaviors: ‘value-added’ education, drug use and delinquency in high-risk, urban schools. Prev Sci 2011;12:211-21. https://doi.org/10.1007/s11121-011-0206-9.
- Currie C, Molcho M, Boyce W, Holstein B, Torsheim T, Richter M. Researching health inequalities in adolescents: the development of the Health Behaviour in School-Aged Children (HBSC) family affluence scale. Soc Sci Med 2008;66:1429-36. https://doi.org/10.1016/j.socscimed.2007.11.024.
- Green J, Thorogood N. Qualitative Methods for Health Research. London: Sage; 2004.
- Bonell C, Allen E, Warren E, McGowan J, Bevilacqua L, Jamal F, et al. Effects of the Learning Together intervention on bullying and aggression in English secondary schools (INCLUSIVE): a cluster randomised controlled trial. Lancet 2018;392:2452-64. https://doi.org/10.1016/S0140-6736(18)31782-3.
- Ofsted . Low-Level Disruption in Classrooms: Below the Radar 2014.
- Angus M. Pipeline Project: Trajectories of Classroom Behaviour and Academic Progress : A Study of Student Engagement with Learning. Mount Lawley, WA: Edith Cowan University; 2010.
- Lasher S, Baker C. Bullying: Evidence from the Longitudinal Study of Young People in England 2, Wave 2. London: Department of Education; 2015.
- Warren E, Bevilacqua L, Opondo C, Allen E, Mathiot A, West G, et al. Action groups as a participative strategy for leading whole-school health promotion: results on implementation from the INCLUSIVE trial in English secondary schools. Br Educ Res J 2019;45:979-1000. https://doi.org/10.1002/berj.3547.
- Manca A, Hawkins N, Sculpher MJ. Estimating mean QALYs in trial-based cost-effectiveness analysis: the importance of controlling for baseline utility. Health Econ 2005;14:487-96. https://doi.org/10.1002/hec.944.
- National Institute for Health and Care Excellence . Methods for the Development of NICE Public Health Guidance (3rd Edition) 2012.
- National Institute for Health and Care Excellence . Developing NICE Guidelines: The Manual 2014.
- Department for Education n.d. www.gov.uk/government/organisations/department-for-education (accessed 29 September 2017).
- Department of Health and Social Care . NHS Reference Costs 2015–2016 2016.
- Curtis L, Burns A. Unit Costs of Health and Social Care. Canterbury: Personal Social Services Research Unit, University of Kent; 2016.
- The King’s Fund . Improving the Quality of Care in General Practice 2011.
- Heslin M, Callaghan L, Barrett B, Lea S, Eick S, Morgan J, et al. Costs of the police service and mental healthcare pathways experienced by individuals with enduring mental health needs. Br J Psychiatry 2017;210:157-64. https://doi.org/10.1192/bjp.bp.114.159129.
- Grieve R, Nixon R, Thompson SG, Normand C. Using multilevel models for assessing the variability of multinational resource use and cost data. Health Econ 2005;14:185-96. https://doi.org/10.1002/hec.916.
- Willan AR, Briggs AH, Hoch JS. Regression methods for covariate adjustment and subgroup analysis for non-censored cost-effectiveness data. Health Econ 2004;13:461-75. https://doi.org/10.1002/hec.843.
- Willan AR, Briggs AH. Statistical Analysis of Cost-effectiveness Data. Chichester: Wiley; 2006.
- Bonell C, Allen E, Strange V, Copas A, Oakley A, Stephenson J, et al. The effect of dislike of school on risk of teenage pregnancy: testing of hypotheses using longitudinal data from a randomised trial of sex education. J Epidemiol Community Health 2005;59:223-30. https://doi.org/10.1136/jech.2004.023374.
- Higgins S, Matsipataki M, Kokotsaki D, Coe R, Major LE, Coleman RE. The Sutton Trust-Education Endowment Foundation Teaching and Learning Toolkit: Technical Appendices. London: Educational Endowment Foundation; 2013.
- Branson CE, Cornell DG. A comparison of self and peer reports in the assessment of middle school bullying. J App School Psychol 2009;25:5-27. https://doi.org/10.1080/15377900802484133.
- Hawe P, Shiell A, Riley T. Complex interventions: how ‘out of control’ can a randomised controlled trial be?. BMJ 2004;328:1561-3. https://doi.org/10.1136/bmj.328.7455.1561.
- Scott S, Kearney J. $100m Funding Boost for School Mental Health Programs and Headspace centres. ABC News Online 2018. www.abc.net.au/news/2018-01-08/more-dollars-for-kids-mental-health/9310172 (accessed 27 September 2017).
- Bonell C, Wells H, Harden A, Jamal F, Fletcher A, Thomas J, et al. The effects on student health of interventions modifying the school environment: systematic review. J Epidemiol Community Health 2013;67:677-81. https://doi.org/10.1136/jech-2012-202247.
- Shinde S, Weiss HA, Varghese B, Khandeparkar P, Pereira B, Sharma A, et al. Promoting school climate and health outcomes with the SEHER multi-component secondary school intervention in Bihar, India: a cluster-randomised controlled trial. Lancet 2018;392:2465-77.
- Great Britain . The Medicines for Human Use (Clinical Trials) Regulations 2004) 2004. www.legislation.gov.uk/uksi/2004/1031/contents/made (accessed 27 September 2017).
- Medical Research Council . MRC Guidelines on Good Clinical Practice in Clinical Trials 1998.
Appendix 1 Tables and figures
| England average | Inclusive trial schools | Non-recruited schools | Comparison of recruited and non-recruited schools | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Mean (SD) | Median | Range | N | Mean (SD) | Median | Range | p-value | ||
| School IDACI (mean) | Not available | 40 | 0.262 (0.198) | 0.239 | 0.028–0.698 | 427 | 0.251 (0.186) | 0.199 | 0.007–0.765 | 0.5* |
| School population size (mean) | 939 | 40 | 1081 (324) | 1075 | 446–1786 | 427 | 1073 (379) | 1058 | 60–2405 | 0.9 |
| Special educational need (SEN) (%) | 2.8 | 40 | 5.2 (4.4) | 5.9 | 0.03–14.4 | 422 | 5.6 (5.9) | 5.1 | 0.1–42.7 | 0.5* |
| English as a foreign language (%) | 13.60 | 40 | 34.7 (25.9) | 29.5 | 3.3–90.3 | 424 | 30.5 (25.0) | 23.3 | 0–92.8 | 0.2* |
| Eligible for free school meals (%) | 16.30 | 40 | 36.8 (19.4) | 38.1 | 3.9–75.8 | 427 | 34.7 (20.8) | 31.2 | 1.6–94.0 | 0.3* |
| Number with ≥ 5 GCSEs at A to C grade (%) | 59.30 | 40 | 60.6 (14.5) | 56.5 | 35–99 | 399 | 63.4 (16.0) | 63.0 | 14–100 | 0.3 |
| Value added (best 8) (median score) | 1000 | 40 | 1013 (24) | 1014 | 925–1064 | 399 | 1015 (22) | 1016 | 949–1081 | 0.3 |
| Student absence (annual) (%) | 5.8 | 40 | 5.2 (1.2) | 5.1 | 2.7–9.1 | 419 | 5.0 (1.0) | 4.9 | 2.1–10.5 | 0.3 |
| OFSTED rating Outstanding | 12% | 13 | 32.5% | 144 | 33.8% | |||||
| Good | 60% | 23 | 57.5% | 194 | 45.5% | |||||
| Requires improvement | 15% | 3 | 7.5% | 68 | 16.0% | |||||
| Inadequate | 13% | 0 | 0% | 3 | 0.7% | |||||
| Not available | – | 1 | 2.5% | 17 | 4.0% | |||||
| Combined either outstanding or good | 72% | 40 | 90% | 426 | 79.3% | 0.04 | ||||
| School sex makeup | 40 | % | 427 | % | ||||||
| Boys only | 2 | 5 | 28 | 6.6 | 0.9 | |||||
| Mixed sex | 32 | 80 | 356 | 83.4 | ||||||
| Girls only | 6 | 15 | 43 | 10.1 | ||||||
Ofsted ratings were not available for one INCLUSIVE school and a number of non-recruited schools for a variety of reasons, including being new schools that had not yet been rated.
Data sources for England averages
Because recruitment was undertaken in 2014, we used the most recently available data for 2013/14. Data for England averages were taken from Department for Education statistics (www.gov.uk/government/organisations/department-for-education/about/statistics, accessed 24 April 2017) and www.compare-school-performance.service.gov.uk/ (accessed 25 July 2017).
| Outcome | Baseline | 24 months | 36 months | |||
|---|---|---|---|---|---|---|
| Control n = 3347 | Intervention n = 3320 | Control n = 3195 | Intervention n = 3095 | Control n = 3087 | Intervention n = 2873 | |
| Age, mean (SD) | 11.75 (0.44) | 11.76 (0.43) | 13.72 (0.59) | 13.76 (0.45) | 14.75 (1.20) | 14.70 (0.82) |
| Sex, n (%) | ||||||
| Male | 1639 (49.85) | 1464 (44.88) | 1580 (49.45) | 1357 (43.84) | 1462 (47.36) | 1232 (42.88) |
| Female | 1649 (50.15) | 1804 (55.20) | 1543 (48.29) | 1675 (54.12) | 1521 (49.27) | 1563 (54.40) |
| Ethnicity, n (%) | ||||||
| White British | 1391 (41.47) | 1221 (37.32) | 1265 (39.59) | 1028 (33.21) | 1127 (36.51) | 966 (33.62) |
| White other | 291 (8.78) | 273 (8.34) | 308 (9.64) | 285 (9.21) | 322 (10.43) | 273 (9.50) |
| Asian/Asian British | 859 (25.92) | 786 (24.02) | 837 (26.20) | 762 (24.62) | 816 (26.43) | 687 (23.91) |
| Black/Black British | 384 (11.59) | 535 (16.35) | 365 (11.42) | 489 (15.80) | 377 (12.21) | 473 (16.46) |
| Chinese/Chinese British | 11 (0.33) | 35 (1.07) | 14 (0.44) | 29 (0.94) | 15 (0.49) | 26 (0.90) |
| Mixed ethnicity | 238 (7.18) | 224 (6.85) | 231 (7.23) | 229 (7.40) | 217 (7.03) | 191 (6.65) |
| Other | 140 (4.22) | 198 (6.05) | 145 (4.54) | 232 (7.50) | 170 (5.51) | 219 (7.62) |
| Religion, n (%) | ||||||
| None | 983 (29.59) | 787 (23.99) | 1037 (32.46) | 808 (26.11) | 1043 (33.79) | 802 (27.92) |
| Christian | 1073 (32.30) | 1173 (35.76) | 923 (28.89) | 1019 (32.92) | 871 (28.22) | 900 (31.33) |
| Jewish | 9 (0.27) | 13 (0.40) | 11 (0.34) | 17 (0.55) | 15 (0.49) | 18 (0.63) |
| Muslim/Islam | 878 (26.46) | 817 (24.91) | 843 (26.38) | 774 (25.01) | 810 (26.24) | 726 (25.27) |
| Hindu | 90 (2.71) | 176 (5.37) | 79 (2.47) | 149 (4.81) | 83 (2.69) | 144 (5.01) |
| Sikh | 71 (2.14) | 88 (2.68) | 69 (2.16) | 87 (2.81) | 70 (2.27) | 81 (2.82) |
| Do not know | 145 (4.36) | 126 (3.84) | 148 (4.63) | 114 (3.68) | 91 (2.95) | 91 (3.17) |
| Other | 73 (2.20) | 100 (3.05) | 57 (1.78) | 85 (2.75) | 69 (2.24) | 67 (2.33) |
| Family structure, n (%) | ||||||
| Two parents | 2393 (71.91) | 2369 (72.05) | 2200 (68.86) | 2137 (69.05) | 2073 (67.15) | 1958 (68.15) |
| Single mothers | 604 (18.15) | 626 (19.04) | 627 (19.62) | 649 (20.97) | 624 (20.21) | 584 (20.33) |
| Single fathers | 37 (1.11) | 56 (1.70) | 52 (1.63) | 60 (1.94) | 51 (1.65) | 62 (2.16) |
| Reconstituted | 246 (7.39) | 204 (6.20) | 237 (7.42) | 182 (5.88) | 240 (7.77) | 177 (6.16) |
| Other | 48 (1.44) | 33 (1.00) | 63 (1.97) | 37 (1.20) | 65 (2.11) | 56 (1.95) |
| At least one parent in work, n (%) | ||||||
| No | 298 (8.73) | 233 (7.18) | 187 (5.85) | 200 (6.46) | 179 (5.80) | 155 (5.40) |
| Yes | 2437 (74.03) | 2381 (73.35) | 2648 (82.88) | 2529 (81.71) | 2612 (84.61) | 2423 (84.34) |
| Do not know | 566 (11.19) | 632 (19.47) | 317 (9.92) | 313 (10.11) | 242 (7.84) | 246 (8.56) |
| Housing tenure, n (%) | ||||||
| One rented from the council or housing association | 474 (14.41) | 559 (17.26) | 523 (16.37) | 612 (19.77) | 575 (18.63) | 629 (21.89) |
| One rented from a landlord | 391 (11.88) | 396 (12.23) | 382 (11.96) | 428 (13.83) | 438 (14.19) | 423 (14.72) |
| One owned by my family | 1451 (44.10) | 1273 (39.31) | 1569 (49.11) | 1354 (43.75) | 1511 (48.95) | 1312 (45.67) |
| Other | 62 (1.88) | 59 (1.82) | 55 (1.72) | 45 (1.45) | 41 (1.33) | 30 (1.04) |
| Do not know | 912 (27.72) | 951 (29.37) | 616 (19.28) | 600 (19.39) | 467 (15.13) | 422 (14.69) |
| Family affluence scale, mean (SD) | 6.03 (1.84) | 6.10 (1.81) | 6.13 (1.77) | 6.16 (1.76) | 6.03 (1.81) | 6.17 (1.75) |
| Control, mean (SD) | Intervention, mean (SD) | Overall, mean (SD) | |
|---|---|---|---|
| Staff Stress and Burnout – Maslach Burnout Inventory | |||
| Emotional exhaustion score | 22.49 (11.28) | 22.17 (11.36) | 22.34 (11.32) |
| Depersonalisation score | 5.52 (5.07) | 5.48 (5.48) | 5.51 (5.08) |
| Personal achievement score | 35.30 (7.14) | 35.69 (6.99) | 35.48 (7.07) |
| Staff QoL – SF-12 v2 Health Survey | |||
| Physical health score | 55.22 (7.31) | 56.01 (6.32) | 55.59 (6.88) |
| Mental health score | 44.64 (9.63) | 44.91 (9.62) | 44.77 (9.62) |
| Measure | Main adjusted effect | By sex | By baseline bullying | By baseline aggression | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Effect size* | p-value | Boys (95% CI) | Girls (95% CI) | p interaction | Low (95% CI) | High (95% CI) | p interaction | Low (95% CI) | High (95% CI) | p interaction | |
| Continuous outcomes | |||||||||||
| GBS overall score | –0.03 (–0.06 to –0.001) | 0.0441 | –0.04 (–0.08 to 0.001) | –0.03 (–0.06 to 0.01) | 0.6113 | 0.15 (0.12 to 0.18) | –0.41 (–0.45 to –0.36) | < 0.0001 | 0.01 (–0.03 to 0.05) | –0.06 (–0.10 to –0.02) | 0.0024 |
| ESYTC overall score | –0.13 (–0.43 to 0.18) | 0.4199 | –0.33 (–0.73 to 0.06) | 0.04 (–0.32 to 0.39) | 0.0890 | 0.02 (–0.34 to 0.37) | –0.17 (–0.63 to 0.29) | 0.4422 | 0.71 (0.33 to 1.10) | –0.65 (–1.03 to –0.27) | < 0.0001 |
| PedsQL overall score | 1.44 (0.70 to 2.17) | 0.0001 | 3.85 (2.89 to 4.80) | –0.41 (–1.28 to 0.46) | < 0.0001 | 0.34 (–0.52 to 1.19) | 3.93 (2.81 to 5.04) | < 0.0001 | –0.14 (–1.13 to 0.85) | 2.70 (1.74 to 3.65) | < 0.0001 |
| SDQ total difficulties score | –0.54 (–0.83 to –0.25) | 0.0002 | –1.29 (–1.67 to –0.92) | 0.04 (–0.30 to 0.39) | < 0.0001 | –0.08 (–0.42 to 0.26) | –1.61 (–2.05 to –1.17) | < 0.0001 | 0.34 (–0.05 to 0.72) | –1.31 (–1.69 to –0.94) | < 0.0001 |
| SWEMWBS total well-being index | 0.33 (0.00 to 0.66) | 0.0487 | 1.32 (0.89 to 1.74) | –0.42 (–0.81 to –0.04) | < 0.0001 | 0.14 (–0.24 to 0.53) | 0.93 (0.43 to 1.43) | 0.0034 | –0.18 (–0.62 to 0.26) | 0.78 (0.36 to 1.21) | 0.0001 |
| Age at sexual debut (years) | –0.35 (–1.48 to 0.78) | 0.5409 | –0.63 (–1.99 to 0.74) | 0.01 (–1.51 to 1.53) | 0.4879 | –0.14 (–1.34 to 1.05) | –0.46 (–1.89 to 0.98) | 0.7085 | –0.63 (–2.40 to 1.15) | –0.42 (–1.58 to 0.73) | 0.8308 |
| Modified aggression scale | –0.26 (–0.57 to 0.05) | 0.0978 | –0.53 (–0.89 to –0.18) | –0.03 (–0.37 to 0.31) | 0.0029 | –0.18 (–0.52 to 0.17) | –0.22 (–0.62 to 0.18) | 0.8100 | 0.03 (–0.33 to 0.39) | –0.25 (–0.60 to 0.10) | 0.0933 |
| Categorical outcomes | |||||||||||
| Ever smoked | 0.58 (0.43 to 0.80) | 0.0009 | 0.33 (0.22 to 0.50) | 0.87 (0.60 to 1.25) | < 0.0001 | 0.66 (0.46 to 0.96) | 0.52 (0.33 to 0.80) | 0.2887 | 0.93 (0.58 to 1.49) | 0.46 (0.32 to 0.68) | 0.0053 |
| Ever drunk alcohol | 0.72 (0.56 to 0.92) | 0.0094 | 0.52 (0.38 to 0.70) | 0.95 (0.71 to 1.26) | 0.0002 | 0.81 (0.61 to 1.07) | 0.57 (0.41 to 0.81) | 0.0541 | 1.08 (0.78 to 1.49) | 0.56 (0.41 to 0.75) | 0.0009 |
| Been offered illicit drugs | 0.51† (0.36 to 0.73) | 0.0003 | 0.44† (0.29 to 0.68) | 0.57 (0.38 to 0.86) | 0.2350 | 0.46† (0.31 to 0.68) | 0.58† (0.37 to 0.93) | 0.2895 | 0.62† (0.40 to 0.96) | 0.50† (0.34 to 0.74) | 0.3137 |
| Used any contraception at first sex | 1.08 (0.50 to 2.35) | 0.8410 | 1.02 (0.39 to 2.69) | 1.19 (0.36 to 3.90) | 0.8409 | 0.55 (0.20 to 1.57) | 2.63 (0.61 to 11.35) | 0.0905 | 0.18 (0.02 to 1.45) | 1.35 (0.45 to 4.13) | 0.1003 |
| Use of NHS in past 12 months | 0.96 (0.82 to 1.11) | 0.5652 | 0.96 (0.79 to 1.17) | 0.95 (0.80 to 1.14) | 0.9590 | 0.96 (0.81 to 1.16) | 1.02 (0.80 to 1.29) | 0.6717 | 1.12 (0.90 to 1.38) | 0.93 (0.76 to 1.14) | 0.1556 |
| Contact with police in past 12 months | 0.74 (0.56 to 0.97) | 0.0269 | 0.62 (0.45 to 0.85) | 0.93 (0.66 to 1.31) | 0.0371 | 0.66 (0.48 to 0.92) | 0.79 (0.53 to 1.17) | 0.4280 | 0.93 (0.58 to 1.47) | 0.67 (0.49 to 0.93) | 0.1917 |
Bullying
Low and high bullying subgroups were defined on the basis of baseline bullying experience based on the GBS. High was defined as frequent – at least weekly – experience of bullying or being upset by it; low or medium was defined as rare – less than weekly – experience of bullying and not being upset by it.
Aggression
Low and high aggression subgroups were defined on the basis of baseline behaviour problems based on the ESYTC, with high levels of behaviour problems defined as ESYTC scores greater than zero and low levels defined as scores of zero.
| Measure | 24 months | 36 months | ||||||
|---|---|---|---|---|---|---|---|---|
| Unadjusted (95% CI) | p-value | Adjusted (95% CI) | p-value | Unadjusted (95% CI) | p-value | Adjusted (95% CI) | p-value | |
| GBS overall score | –0.02 (–0.04 to –0.003) | 0.0206 | –0.02 (–0.04 to –0.003) | 0.0220 | –0.001 (–0.01 to 0.01) | 0.7433 | –0.001 (–0.01 to 0.01) | 0.8019 |
| ESYTC overall score | –0.14 (–0.34 to 0.07) | 0.1949 | –0.12 (–0.32 to 0.08) | 0.2297 | 0.02 (–0.08 to 0.11) | 0.7600 | 0.02 (–0.07 to 0.12) | 0.5985 |
| Year 1 | Year 2 | Year 3 | Total | |||
|---|---|---|---|---|---|---|
| All schools | Interviews | Facilitators | 8/8 | 8/8 | NA | 16/16 |
| AGM members | 28/40 | 41/40 | 28/40 | 97/120 | ||
| Senior leadership team | 36/40 | NA | 35/40 | 71/80 | ||
| Other staff | 66/80 | NA | NA | 66/80 | ||
| Curriculum deliverers | 6/20 | 10/20 | 8/20 | 24/60 | ||
| Observations | AGMs | 10/10 | 9/10 | 7/10 | 26/30 | |
| All-staff training | 9/10 | NA | NA | 9/10 | ||
| Surveys | Curriculum | 20/60 | 21/60 | 2/20 | 43/140 | |
| In-depth training satisfaction | 129/100a | NA | NA | 129/100 | ||
| AGM members | 228/240b | 184/240b | 32/240b | 444/720 | ||
| Staff delivering RP | 189/300c | 82/300c | 34/100d | 305/700 | ||
| Diaries | Facilitators | 115/120e | 101/120e | NA | 118/240 | |
| Trainers | 18/20f | NA | NA | 18/20 | ||
| Minutes | AGMs | 115/120 | 101/120 | NA | 216/240 | |
| Case study schools | FGDs | Students | 12/12 | 10/12 | 8/12 | 30/36 |
| Staff | 6/6 | 5/6 | 4/6 | 15/18 | ||
| Interviews | Students involved in RP | 12/12 | 6/12 | 6/12 | 24/36 | |
| Intervention element | N schools implementing this element | ||
|---|---|---|---|
| Year 1/2 | Year 3 | ||
| Action groups | Minutes or diaries indicate min. 6 meetings in years 1 and 2 | 11 | 3 |
| Minutes or diaries indicate review of policies/rules in year 1 or 2 | 17 | NA | |
| Minutes or diaries indicate implementation of locally decided actions in years 1 and 2 | 16 | 8 | |
| Survey of members indicated good range of students and staff members (mean score for two measures at or below 2) | 20 | NA | |
| Survey of members indicated well led (mean score at or below 2) | 20 | NA | |
| Curriculum | Surveys or interviews indicates five hours/> 1 unit delivered in years 1 and 2 | 9 | 5 |
| RP | Attendance logs indicated at least five staff received in-depth training | 15 | NA |
| Staff survey indicates at least 85% staff report that if there is trouble at this school, staff respond by talking to those involved to help them get on better | 12 | 15 | |
| Median fidelity score | 6/8 | 1/4 | |
| Training implementation |
Fidelity self-reported in trainer diary N (%) of schools |
|||
|---|---|---|---|---|
| As intended | Less than intended | Not at all | Schools with no data | |
| Covered ‘what is restorative justice/practice’ | 19 (95) | 0 | 0 | 1 (5) |
| Covered ‘the importance of language’ | 19 (95) | 0 | 0 | 1 (5) |
| Covered ‘what we do to challenge bad behaviour/nature of challenge’ | 19 (95) | 0 | 0 | 1 (5) |
| Covered ‘the importance of emotions’ | 19 (95) | 0 | 0 | 1 (5) |
| Covered ‘the importance of listening’ | 19 (95) | 0 | 0 | 1 (5) |
| Covered ‘maintaining the relationship after difficult conversation’ | 16 (80) | 3 (15) | 0 | 1 (5) |
| Used Power point slides | 19 (95) | 0 | 0 | 1 (5) |
| Used DVD | 18 (90) | 0 | 1 (5) | 1 (5) |
| Facilitated paired activity | 19 (95) | 0 | 0 | 1 (5) |
| Facilitated small group activity | 19 (95) | 0 | 0 | 1 (5) |
| Measure (response option which indicates satisfaction) | Responses | |
|---|---|---|
| Overall % members responding as indicated | N schools where > 70% of members responded as indicated | |
| Do you feel you learnt useful skills at this training? (yes definitely or yes probably) | 100% | 20 |
| Do you feel confident in putting into practice the skills you have learnt today? (yes) | 91% | 20 |
| Do you intend to put the skills you learnt to use in your everyday practice? (yes) | 95% | 20 |
| Would you recommend this training to a colleague? (yes) | 100% | 20 |
| Overall, how would you rate this training? (good or excellent) | 99% | 20 |
| Measure (response option which indicates satisfaction) | Responses | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Year 1 | Year 2 | Year 3 | |||||||
| Overall % members responding as indicated | N schools where > 70% of members responded as indicated | N schools with no data | Overall % members responding as indicated | N schools where > 70% of members responded as indicated | N schools with no data | Overall % members responding as indicated | N schools where > 70% of members responded as indicated | N schools with no data | |
| Was the needs-assessment report useful in helping the action group decide what actions to take? (somewhat or very) | 91% | 17 | 1 | 88% | 14 | 3 | 76% | 2 | 17 |
| Was the external facilitator useful in ensuring that all action group members could have their say? (somewhat or very) | 89% | 18 | 1 | 90% | 15 | 3 | NA | NA | NA |
| Was the external facilitator useful in helping the action group decide what actions to take? (somewhat or very) | 86% | 16 | 1 | 88% | 17 | 3 | NA | NA | NA |
| Was the external facilitator useful in helping to ensure that actions were actually implemented? (somewhat or very) | 80% | 13 | 1 | 79% | 13 | 3 | NA | NA | NA |
| Do you think the LT Project was a good way to ensure students contribute to decision-making at this school? (very or quite) | 95% | 19 | 1 | 94% | 16 | 3 | 100% | 3 | 17 |
| Overall do you think the action group made good decisions about what actions to take? (% very or quite) | 94% | 19 | 1 | 93% | 16 | 3 | 98% | 3 | 17 |
| Do you think the action group made sure that these actions were implemented? (% yes) | 70% | 10 | 1 | 72% | 10 | 3 | 69% | 1 | 17 |
| Year 1 | Year 2 | Year 3 | Total | |||
|---|---|---|---|---|---|---|
| All schools | Interviews | Facilitators | 8/8 | 8/8 | NA | 16/16 |
| AGM members | 28/40 | 41/40 | 28/40 | 97/120 | ||
| Senior leadership team | 36/40 | NA | 35/40 | 71/80 | ||
| Other staff | 66/80 | NA | NA | 66/80 | ||
| Curriculum deliverers | 6/20 | 10/20 | 8/20 | 24/60 | ||
| Observations | AGMs | 10/10 | 9/10 | 7/10 | 26/30 | |
| All-staff training | 9/10 | NA | NA | 9/10 | ||
| Surveys | Curriculum | 20/60 | 21/60 | 2/20 | 43/140 | |
| In-depth training satisfaction | 129/100a | NA | NA | 129/100 | ||
| AGM members | 228/240b | 184/240b | 32/240b | 444/720 | ||
| Staff delivering RP | 189/300c | 82/300c | 34/100d | 305/700 | ||
| Diaries | Facilitators | 115/120e | 3/120e | NA | 118/240 | |
| Trainers | 18/20f | NA | NA | 18/20 | ||
| Minutes | AGMs | 115/120 | 101/120 | NA | 216/240 | |
| Case study schools | FGDs | Students | 12/12 | 10/12 | 8/12 | 30/36 |
| Staff | 6/6 | 5/6 | 4/6 | 15/18 | ||
| Interviews | Students involved in RP | 12/12 | 6/12 | 6/12 | 24/36 | |
| School | AGs | Curriculum | RP | Overall score/8 | |||||
|---|---|---|---|---|---|---|---|---|---|
| Minutes or diaries indicated minimum of six meetings in years 1 and 2 | Minutes or diaries indicated review of policies/rules in year 1 or 2 | Minutes or diaries indicated implementation of locally decided actions in years 1 and 2 | Survey of members indicated good range of students and staff members (mean score for two measures at or below 2) | Survey of members indicated well led (mean score at or below 2) | Surveys or interviews indicated five hours/> 1 unit delivered in years 1 and 2 | Attendance logs indicated at least five staff received in-depth training | Staff survey indicated at least 85% of staff report that if there is trouble at this school, staff respond by talking to those involved to help them get on better | ||
| BE | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 6 |
| AW | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| AO | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 6 |
| AZ | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 6 |
| AX | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 7 |
| AS | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 5 |
| AD | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| AK | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 6 |
| BD | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 4 |
| AU | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 7 |
| AF | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 5 |
| AH | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 6 |
| AM | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 5 |
| BK | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 5 |
| AE | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| BI | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 5 |
| BM | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 4 |
| AT | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 6 |
| BC | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 7 |
| AL | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 7 |
| School | AGs | Curriculum | RP | Overall score | |
|---|---|---|---|---|---|
| Interviews indicate minimum of six meetings in year 3 | Interviews indicate implementation of locally decided actions in year 3 | Surveys or interviews indicates five hours/> 1 unit delivered in year 3 | Staff survey indicates at least 85% of staff report that if there is trouble at this school, staff respond by talking to those involved to help them get on better | ||
| BE | 0 | 0 | 0 | 1 | 1 |
| AW | 1 | 1 | 0 | 1 | 3 |
| AO | 0 | 1 | 0 | 1 | 2 |
| AZ | 0 | 0 | 0 | 1 | 1 |
| AX | 0 | 0 | 0 | 1 | 1 |
| AS | 1 | 1 | 1 | 1 | 4 |
| AD | 0 | 0 | 1 | 1 | 2 |
| AK | 0 | 1 | 0 | 1 | 2 |
| BD | 0 | 1 | 0 | 1 | 2 |
| AU | 0 | 0 | 0 | 1 | 1 |
| AF | 0 | 0 | 0 | 1 | 1 |
| AH | 0 | 1 | 0 | 1 | 2 |
| AM | 0 | 0 | 0 | 0 | 0 |
| BK | 0 | 0 | 0 | 0 | 0 |
| AE | 0 | 0 | 0 | 0 | 0 |
| BI | 0 | 0 | 0 | 0 | 0 |
| BM | 0 | 0 | 0 | 0 | 0 |
| AT | 0 | 1 | 1 | 1 | 3 |
| BC | 1 | 1 | 1 | 1 | 4 |
| AL | 0 | 1 | 1 | 1 | 3 |
| School | N staff participating in all-staff training | N staff participating in in-depth training | N staff in total participating in AGM (year 1) | N staff in total participating in AGM (year 2) | N students in total participating in AGM (year 1) | N students in total participating in AGM (year 2) |
|---|---|---|---|---|---|---|
| BE | 84 | 7 | 11 | 7 | 13 | 12 |
| AW | 58 | 5 | 5 | 3 | 6 | 6 |
| AO | 90 | 7 | 7 | 8 | 8 | 8 |
| AZ | Unknown | 6 | 12 | Unknown | 12 | 7 |
| AX | Unknown | 6 | 7 | 5 | 8 | 7 |
| AS | 93 | 5 | 7 | 7 | 10 | 10 |
| AD | 131 | 8 | 6 | 6 | 6 | 7 |
| AK | 153 | 8 | 6 | 7 | 5 | 5 |
| BD | 162 | 5 | 6 | Unknown | 7 | 7 |
| AU | 93 | 2 | 8 | 3 | 8 | 8 |
| AF | 150 | 7 | 3 | 8 | 14 | 14 |
| AH | 145 | 9 | 9 | 2 | 6 | 8 |
| AM | 80 | 4 | 9 | 2 | 9 | 9 |
| BK | 60 | 3 | Unknown | 4 | Unknown | 10 |
| AE | 34 | 13 | 6 | 6 | 9 | 23 |
| BI | Unknown | 5 | 6 | 3 | 7 | 10 |
| BM | 88 | 4 | 11 | 5 | 5 | 9 |
| AT | 124 | 5 | 8 | 5 | 9 | 4 |
| BC | Unknown | 8 | 7 | 7 | 6 | 7 |
| AL | 103 | 8 | 7 | 9 | 6 | 5 |
| Overall mean | 103 | 6.25 | 7.4 | 5.4 | 8.1 | 8.8 |
| Measure | Arm | Unadjusted effect | Adjusted effect (baseline covariates) | Adjusted effect (baseline covariates plus BBSQ) | Adjusted effect (baseline covariates plus YPDP) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Control, mean (SE) | Intervention, mean (SE) | Difference (95% CI) | p-value | Difference (95% CI) | p-value | Difference (95% CI) | p-value | Difference (95% CI) | p-value | |
| Continuous student outcomes | ||||||||||
| GBS overall score | 0.34 (0.02) | 0.29 (0.02) | –0.03 (–0.06 to –0.00) | 0.039 | –0.03 (–0.06 to –0.00) | 0.044 | –0.04 (–0.08 to –0.01) | 0.007 | –0.04 (–0.07 to –0.01) | 0.016 |
| ESYTC overall score | 4.33 (0.20) | 4.04 (0.21) | –0.07 (–0.38 to 0.25) | 0.684 | –0.13 (–0.43 to 0.18) | 0.421 | –0.20 (–0.52 to 0.13) | 0.229 | –0.12 (–0.44 to 0.20) | 0.469 |
| PedsQL overall score | 78.82 (0.54) | 80.65 (0.55) | 1.16 (0.41 to 1.90) | 0.002 | 1.44 (0.70 to 2.17) | < 0.001 | 1.42 (0.64 to 2.21) | < 0.001 | 1.26 (0.49 to 2.03) | 0.001 |
| SDQ total difficulties score | 12.20 (0.18) | 11.51 (0.19) | –0.51 (–0.80 to –0.22) | < 0.001 | –0.54 (–0.83 to –0.25) | < 0.001 | –0.62 (–0.92 to –0.31) | < 0.001 | –0.54 (–0.85 to –0.24) | < 0.001 |
| SWEMWBS total well-being index | 22.88 (0.19) | 23.32 (0.19) | 0.27 (–0.06 to 0.60) | 0.115 | 0.33 (0.00 to 0.66) | 0.048 | 0.27 (–0.08 to 0.62) | 0.141 | 0.23 (–0.13 to 0.58) | 0.210 |
| CHU9D overall score | 0.85 (0.00) | 0.86 (0.01) | 0.01 (–0.00 to 0.01) | 0.244 | 0.01 (–0.00 to 0.01) | 0.080 | 0.00 (–0.00 to 0.01) | 0.153 | 0.00 (–0.00 to 0.01) | 0.217 |
| Age of sexual debut | 13.11 (0.43) | 12.54 (0.49) | –0.58 (–1.97 to 0.81) | 0.416 | –0.35 (–1.48 to 0.78) | 0.541 | –0.24 (–1.48 to 1.00) | 0.703 | –0.40 (–1.65 to 0.84) | 0.525 |
| MAS bullying subscale score | 2.75 (0.21) | 2.33 (0.21) | –0.28 (–0.84 to 0.29) | 0.334 | –0.26 (–0.57 to 0.05) | 0.097 | –0.29 (–0.57 to –0.00) | 0.047 | –0.16 (–0.45 to 0.13) | 0.279 |
| Measure | Arm | Unadjusted effect | Adjusted effect (baseline covariates) | Adjusted effect (baseline covariates plus BBSQ) | Adjusted effect (baseline covariates plus YPDP) | |||||
| Control, n (%) | Intervention, n (%) | Odds ratio (95% CI) | p-value | Odds ratio (95% CI) | p-value | Odds ratio (95% CI) | p-value | Odds ratio (95% CI) | p-value | |
| Categorical student outcomes | ||||||||||
| Ever smoked | ||||||||||
| No | 2293 (77.70) | 2318 (84.17) | 0.59 (0.43 to 0.81) | 0.001 | 0.58 (0.43 to 0.80) | 0.001 | 0.55 (0.39 to 0.78) | 0.001 | 0.57 (0.40 to 0.81) | 0.002 |
| Yes | 658 (22.30) | 436 (15.83) | ||||||||
| Ever drunk alcohol | ||||||||||
| No | 1677 (56.43) | 1735 (62.43) | 0.75 (0.58 to 0.79) | 0.029 | 0.72 (0.56 to 0.92) | 0.009 | 0.72 (0.55 to 0.95) | 0.019 | 0.74 (0.56 to 0.97) | 0.028 |
| Yes | 1295 (43.57) | 1044 (37.57) | ||||||||
| Ever been really drunk | ||||||||||
| No | 788 (53.14) | 721 (61.21) | 0.50 (0.29 to 0.87) | 0.014 | 0.47 (0.31 to 0.71) | < 0.001 | 0.42 (0.27 to 0.65) | < 0.001 | 0.47 (0.31 to 0.71) | < 0.001 |
| Yes | 695 (46.86) | 457 (38.79) | ||||||||
| Been offered illicit drugs | ||||||||||
| No | 1913 (64.41) | 1997 (72.54) | 0.52 (0.34 to 0.79) | 0.002 | 0.51 (0.36 to 0.73) | < 0.001 | 0.44 (0.30 to 0.64) | < 0.001 | 0.51 (0.36 to 0.73) | < 0.001 |
| Yes, but did not try them | 744 (25.05) | 567 (20.60) | ||||||||
| Yes, and tried them | 313 (10.54) | 189 (6.87) | ||||||||
| Used contraception at last sex | ||||||||||
| No | 64 (23.10) | 36 (21.95) | 1.18 (0.56 to 2.48) | 0.658 | 1.08 (0.50 to 2.35) | 0.841 | 1.60 (0.65 to 3.91) | 0.305 | 1.34 (0.56 to 3.22) | 0.511 |
| Yes | 213 (76.90) | 128 (78.05) | ||||||||
| Use of the NHS in past 12 months | ||||||||||
| No | 1605 (53.22) | 1472 (52.59) | 0.96 (0.83 to 1.12) | 0.639 | 0.96 (0.82 to 1.11) | 0.565 | 0.96 (0.81 to 1.13) | 0.600 | 0.99 (0.84 to 1.17) | 0.916 |
| Yes | 1411 (46.78) | 1327 (47.41) | ||||||||
| Contact with police | ||||||||||
| No | 2626 (86.52) | 2485 (88.43) | 0.75 (0.57 to 0.99) | 0.041 | 0.74 (0.56 to 0.97) | 0.027 | 0.66 (0.49 to 0.88) | 0.004 | 0.72 (0.54 to 0.95) | 0.022 |
| Yes | 409 (13.48) | 325 (11.57) | ||||||||
| Measure sub-components | Tool | Questions |
|---|---|---|
| Trainer time | Costed based on trainer invoices | |
| Facilitator cost | Costed based on facilitator invoices | |
| School staff time | ||
|
Training AGM Preparation of AGM Staff time dealing with bullying Curriculum delivery Delivery of bullying strategy in control schools |
Trainer attendance sheet Facilitator diary forms AG questionnaire Staff survey Curriculum log Staff interviews |
Questions 20 and 21 |
| Staff costs | Salaries from routinely collected data | |
| Other resource use | ||
| NHS resource use | Questions in the student survey | Questions 34 and 35 |
| Police resource use | Questions in the student survey | Questions 31 and 32 |
| Other resource costs | PSSRU, police data | |
| Health-related quality of life (HRQoL) | ||
| Student HRQoL | CHU-9D in student survey | Question 50 |
| Staff HRQoL | SF12 in teacher survey | Questions 23 to 29 |
| Measure sub-components | 1, N (%) | 2, N (%) | 3, N (%) | 4, N (%) | 5, N (%) |
|---|---|---|---|---|---|
| Control | |||||
| Worried | 2249 (70.28) | 567 (17.72) | 212 (6.63) | 100 (3.13) | 72 (2.25) |
| Sad | 2508 (78.35) | 406 (12.68) | 152 (4.75) | 75 (2.34) | 60 (1.87) |
| Pain | 2163 (67.59) | 640 (20.00) | 236 (7.38) | 99 (3.09) | 62 (1.94) |
| Tired | 983 (30.67) | 1127 (35.16) | 500 (15.60) | 332 (10.36) | 263 (8.21) |
| Annoyed | 2356 (73.53) | 493 (15.39) | 162 (5.06) | 103 (3.21) | 90 (2.81) |
| Sleep | 1890 (59.06) | 729 (22.78) | 321 (10.03) | 146 (4.56) | 114 (3.56) |
| School work | 2176 (68.11) | 679 (21.25) | 239 (7.48) | 64 (2.00) | 37 (1.16) |
| Daily routine | 2646 (83.05) | 390 (12.24) | 104 (3.26) | 25 (0.78) | 21 (0.66) |
| Activities | 2197 (69.11) | 512 (16.11) | 187 (5.88) | 142 (4.47) | 141 (4.44) |
| Intervention | |||||
| Worried | 2093 (68.09) | 605 (19.68) | 203 (6.60) | 109 (3.55) | 64 (2.08) |
| Sad | 2322 (75.64) | 429 (13.97) | 151 (4.92) | 100 (3.26) | 68 (2.21) |
| Pain | 2114 (68.88) | 591 (19.26) | 226 (7.36) | 90 (2.93) | 48 (1.56) |
| Tired | 938 (30.44) | 1092 (35.44) | 469 (15.22) | 319 (10.35) | 263 (8.54) |
| Annoyed | 2159 (70.14) | 514 (16.70) | 194 (6.30) | 102 (3.31) | 109 (3.54) |
| Sleep | 1868 (60.71) | 692 (22.49) | 276 (8.97) | 133 (4.32) | 108 (3.51) |
| School work | 2103 (68.57) | 661 (21.55) | 204 (6.65) | 64 (2.09) | 35 (1.14) |
| Daily routine | 2587 (84.54) | 343 (11.21) | 86 (2.81) | 21 (0.69) | 23 (0.75) |
| Activities | 2150 (70.58) | 456 (14.97) | 195 (6.40) | 132 (4.33) | 113 (3.71) |
| Measure sub-components | 1, N (%) | 2, N (%) | 3, N (%) | 4, N (%) | 5, N (%) |
|---|---|---|---|---|---|
| Control | |||||
| Worried | 2074 (66.18) | 579 (18.47) | 237 (7.56) | 164 (5.23) | 80 (2.55) |
| Sad | 2366 (75.54) | 407 (12.99) | 162 (5.17) | 120 (3.83) | 77 (2.46) |
| Pain | 2177 (69.51) | 560 (17.88) | 237 (7.57) | 93 (2.97) | 65 (2.08) |
| Tired | 815 (26.01) | 949 (30.28) | 556 (17.74) | 463 (14.77) | 351 (11.20) |
| Annoyed | 2072 (66.09) | 563 (17.96) | 225 (7.18) | 130 (4.15) | 145 (4.63) |
| Sleep | 1765 (56.43) | 754 (24.10) | 318 (10.17) | 165 (5.27) | 126 (4.03) |
| School work | 2099 (67.28) | 666 (21.35) | 236 (7.56) | 77 (2.47) | 42 (1.35) |
| Daily routine | 2542 (81.61) | 385 (12.36) | 114 (3.66) | 44 (1.41) | 30 (0.96) |
| Activities | 2117 (67.98) | 455 (14.61) | 193 (6.20) | 163 (5.23) | 186 (5.97) |
| Intervention | |||||
| Worried | 1929 (64.62) | 539 (18.06) | 269 (9.01) | 168 (5.63) | 80 (2.68) |
| Sad | 2162 (72.57) | 402 (13.49) | 200 (6.71) | 129 (4.33) | 86 (2.89) |
| Pain | 2073 (69.56) | 514 (17.25) | 260 (8.72) | 82 (2.75) | 51 (1.71) |
| Tired | 800 (26.87) | 870 (29.22) | 535 (17.97) | 424 (14.24) | 348 (11.69) |
| Annoyed | 1960 (65.77) | 522 (17.52) | 229 (7.68) | 141 (4.73) | 128 (4.30) |
| Sleep | 1660 (55.84) | 721 (24.25) | 324 (10.90) | 183 (6.16) | 85 (2.86) |
| School work | 2029 (68.22) | 645 (21.69) | 211 (7.09) | 67 (2.25) | 22 (0.74) |
| Daily routine | 2440 (82.13) | 361 (12.15) | 115 (3.87) | 34 (1.14) | 21 (0.71) |
| Activities | 2062 (69.47) | 428 (14.42) | 186 (6.27) | 140 (4.72) | 152 (5.12) |
| Measure sub-components | 1, N (%) | 2, N (%) | 3, N (%) | 4, N (%) | 5, N (%) |
|---|---|---|---|---|---|
| Control | |||||
| Worried | 1847 (62.40) | 553 (18.68) | 290 (9.80) | 180 (6.08) | 90 (3.04) |
| Sad | 2101 (71.05) | 401 (13.56) | 213 (7.20) | 143 (4.84) | 99 (3.35) |
| Pain | 2057 (69.59) | 521 (17.63) | 208 (7.04) | 94 (3.18) | 76 (2.57) |
| Tired | 705 (23.87) | 808 (27.36) | 567 (19.20) | 429 (14.53) | 444 (15.04) |
| Annoyed | 1956 (66.15) | 505 (17.08) | 225 (7.61) | 135 (4.57) | 136 (4.60) |
| Sleep | 1553 (52.55) | 735 (24.87) | 355 (12.01) | 171 (5.79) | 141 (4.77) |
| School work | 1846 (62.83) | 657 (22.36) | 280 (9.53) | 85 (2.89) | 70 (2.38) |
| Daily routine | 2387 (81.19) | 346 (11.77) | 132 (4.49) | 45 (1.53) | 30 (1.02) |
| Activities | 1881 (67.66) | 390 (13.32) | 182 (6.22) | 150 (5.12) | 225 (7.68) |
| Intervention | |||||
| Worried | 1591 (58.15) | 537 (19.63) | 266 (9.72) | 205 (7.49) | 137 (5.01) |
| Sad | 1929 (70.50) | 368 (13.45) | 203 (7.42) | 129 (4.71) | 107 (3.91) |
| Pain | 1916 (70.11) | 444 (16.25) | 211 (7.72) | 91 (3.33) | 71 (2.60) |
| Tired | 671 (24.52) | 784 (28.64) | 472 (17.25) | 403 (14.72) | 407 (14.87) |
| Annoyed | 1796 (65.64) | 487 (17.80) | 189 (6.91) | 123 (4.50) | 141 (5.15) |
| Sleep | 1518 (55.44) | 653 (23.85) | 323 (11.80) | 146 (5.33) | 98 (3.58) |
| School work | 1756 (64.89) | 603 (22.28) | 244 (9.02) | 68 (2.51) | 35 (1.29) |
| Daily routine | 2222 (82.27) | 326 (12.07) | 89 (3.30) | 37 (1.37) | 27 (1.00) |
| Activities | 1919 (71.23) | 345 (12.81) | 159 (5.90) | 127 (4.71) | 144 (5.35) |
| Outcome | Baseline | 24 months | 36 months | |||
|---|---|---|---|---|---|---|
| Control n = 3347 | Intervention n = 3320 | Control n = 3195 | Intervention n = 3095 | Control n = 3087 | Intervention n = 2873 | |
| GBS overall score | 9.3% | 9.4% | 7.8% | 8.0% | 9.0% | 8.5% |
| ESYTC overall score | 5.6% | 6.4% | 5.4% | 5.0% | 5.1% | 5.2% |
| PedsQL overall score | 2.6% | 5.1% | 1.3% | 2.6% | 3.1% | 4.1% |
| SDQ total difficulties score | 2.7% | 4.2% | 2.0% | 2.6% | 2.7% | 3.0% |
| SWEMWBS total well-being index | 3.9% | 6.8% | 2.1% | 3.3% | 4.0% | 4.9% |
| CHU9D overall score | 7.1% | 9.8% | 4.2% | 5.7% | 7.1% | 7.8% |
| Age of sexual debut | NA | NA | 12.6% | 10.5% | 12.5% | 13.7% |
| Ever smoked | 2.2% | 3.6% | 3.6% | 4.7% | 4.4% | 4.1% |
| Ever drunk alcohol | 3.3% | 4.3% | 2.2% | 3.1% | 3.7% | 3.3% |
| Been offered illicit drugs | 4.0% | 4.8% | 2.7% | 3.7% | 3.8% | 4.2% |
| Truancy | 4.2% | 4.5% | 2.8% | 3.5% | 3.0% | 3.0% |
| Exclusion from school | 1.3% | 2.3% | 1.2% | 1.6% | 1.9% | 2.4% |
| Used contraception at last sex | NA | NA | 18.8% | 14.3% | 9.2% | 9.7% |
| Use of NHS in past 12 months | 1.8% | 2.9% | 1.5% | 2.0% | 2.3% | 2.6% |
| Contact with police | 1.0% | 1.1% | 0.9% | 1.4% | 1.7% | 2.2% |
FIGURE 6.
The INCLUSIVE logic model. Reproduced from Bonell et al. 122 © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license.
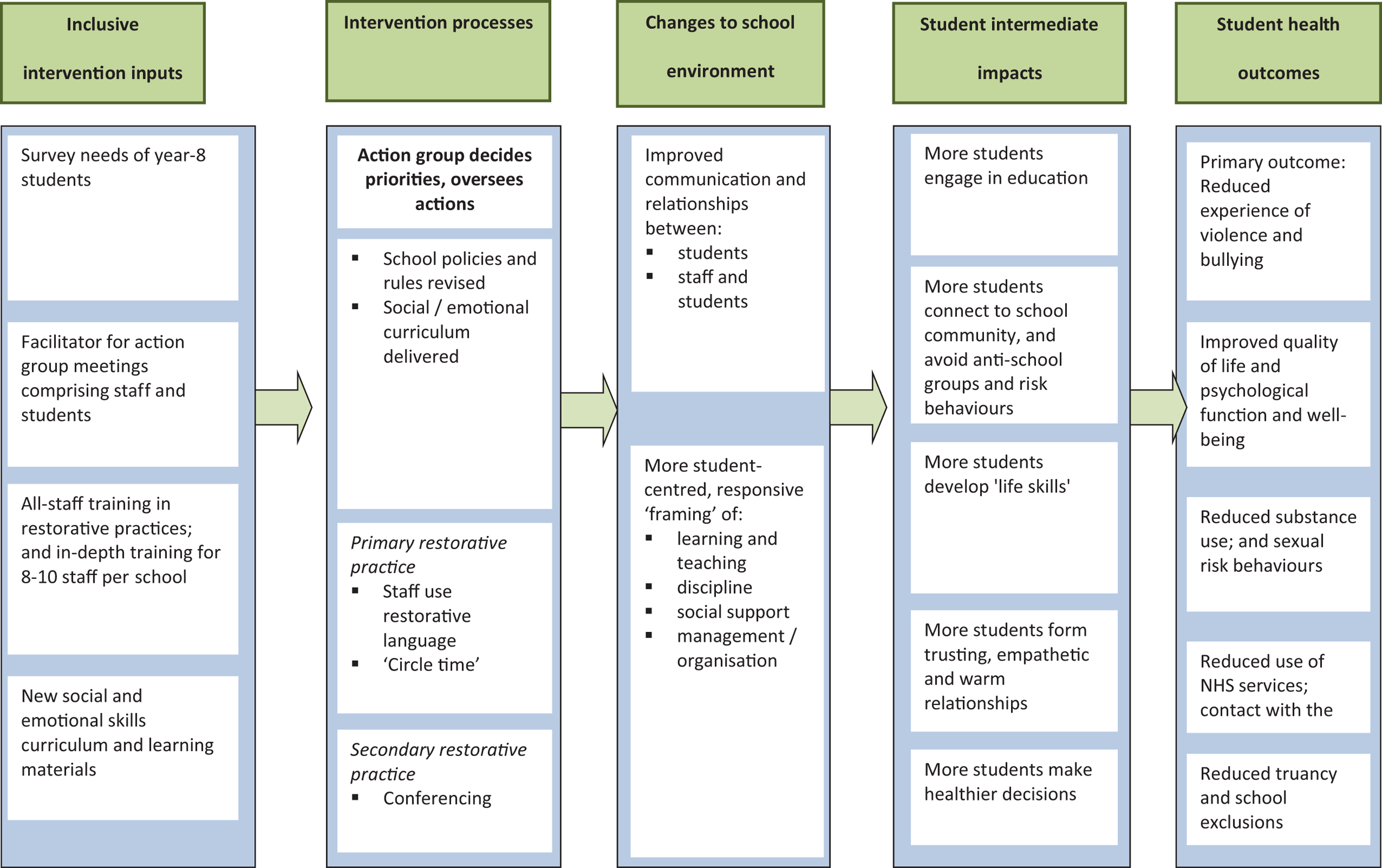
Appendix 2 The young researchers group feedback example
Appendix 3 Example school report, year 3 (anonymised)
List of abbreviations
- AAYP
- Aban Aya Youth Project
- AG
- Action Group
- AGM
- action group meeting
- CEA
- cost-effectiveness analysis
- CHU9D
- Child Health Utility 9D
- CI
- confidence interval
- CTU
- Clinical Trial Unit
- DMC
- Data Monitoring Committee
- ESYTC
- Edinburgh Study of Youth Transitions and Crime
- FAS
- Family Affluence Scale
- FSM
- free school meals
- GBS
- Gatehouse Bullying Scale
- GCSE
- General Certificate of Secondary Education
- GP
- general practitioner
- HRQoL
- health-related quality of life
- HTA
- Health Technology Assessment
- ICER
- incremental cost-effectiveness ratio
- ID
- identifier
- IDACI
- Income Deprivation Affecting Children Index
- INCLUSIVE
- initiating change locally in bullying and aggression through the school environment
- LSHTM
- London School of Hygiene & Tropical Medicine
- LT
- Learning Together
- MRC
- Medical Research Council
- NICE
- National Institute for Health and Care Excellence
- NIHR
- National Institute for Health Research
- Ofsted
- Office for Standards in Education, Children’s Services and Skills
- PedsQL
- Paediatric Quality of Life Inventory
- PSHE
- personal, social and health education
- QALY
- quality-adjusted life-year
- QoL
- quality of life
- RCT
- randomised controlled trial
- RP
- restorative practice
- SD
- standard deviation
- SDQ
- Strengths and Difficulties Questionnaire
- SES
- socioeconomic status
- SF-12
- Short Form questionnaire-12 items
- SLT
- senior leadership team
- SWEMWBS
- Short Warwick–Edinburgh Mental Well-being Scale
- TSC
- Trial Steering Committee
- UCL
- University College London
- WHO
- World Health Organization
- YPDP
- Young People’s Development Programme
- YRG
- young researchers group
Notes
-
Staff and student questionnaires, consent forms and information sheets
Supplementary material can be found on the NIHR Journals Library report project page (www.journalslibrary.nihr.ac.uk/programmes/phr/1215360/#/documentation).
Supplementary material has been provided by the authors to support the report and any files provided at submission will have been seen by peer reviewers, but not extensively reviewed. Any supplementary material provided at a later stage in the process may not have been peer reviewed.