

Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 13/90/18. The contractual start date was in September 2015. The final report began editorial review in March 2020 and was accepted for publication in November 2020. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2021. This work was produced by Corder et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2021 Queen’s Printer and Controller of HMSO
Chapter 1 Introduction and background
This report includes text from the authors’ published articles. 1–6 All of these articles are Open Access articles distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/. The text below includes minor additions and formatting changes to the original text.
Adolescent physical activity
Physical inactivity is the fourth largest cause of death worldwide. 7 Globally, physical activity levels are low and are continuing to decline, with less than 1 in 10 adolescents meeting current World Health Organization physical activity recommendations of 60 minutes of moderate-to-vigorous physical activity (MVPA) daily. 8,9 Physical activity declines during adolescence10 and inactive adolescents are at greater risk of long-term ill health. 11 Not only is inactivity associated with poor health and well-being during childhood, but it may have implications for health into adulthood. 12 More physically active adolescents are likely to become active, healthy and successful adults,12 and so tackling the decline in physical activity during adolescence is a major public health priority. 7
Schools should provide an ideal setting for reaching large numbers of young people across a range of differing backgrounds and are therefore an attractive route for adolescent physical activity promotion. Although the reduction in physical activity during adolescence mainly occurs outside school, it is pragmatic to utilise the school setting for recruitment and delivery. 13
The challenge of effectively delivering physical activity interventions in this setting is highlighted by a review13 of school-based trials that were largely ineffective at increasing accelerometer-measured physical activity over the whole day. Of the 17 studies included in this review,13 only one study included participants with a mean age > 13 years at baseline (13.2 years). In another review14 that examined the impact of school-based interventions on objectively measured activity among adolescents, this applied to only 3 of 13 included studies. Lack of intervention fidelity and poor implementation may explain the null findings in many school-based interventions. 15 Taken together, this indicates the need for activity promotion strategies among older adolescents.
Concurrent with physical activity declines, adolescence is also a period of increased risk of mental health problems16 and around half of mental health disorders will have emerged by the age of 14 years. 17 In 2017, it was estimated that 24% of British adolescent girls and 9% of boys experienced depressive symptoms,18 and suicide is one of the major causes of mortality in adolescence and young adulthood. 19 The benefit of physical activity for mental health has been repeatedly observed through meta-analysis of observational studies, as well as in intervention trials, and does not appear to be explained by reverse causality. 20–23 There is increasing consensus on the benefits of physical activity for mental health. These benefits may not be limited to the physiological consequences of physical activity itself, and the wider social and intra/interpersonal aspects of activity should also be considered. 24
Together, this evidence indicated the need for the development and evaluation of an inclusive physical activity promotion initiative that targets adolescents, and this formed the basis for the Get Others Active (GoActive) intervention.
Development of the GoActive intervention
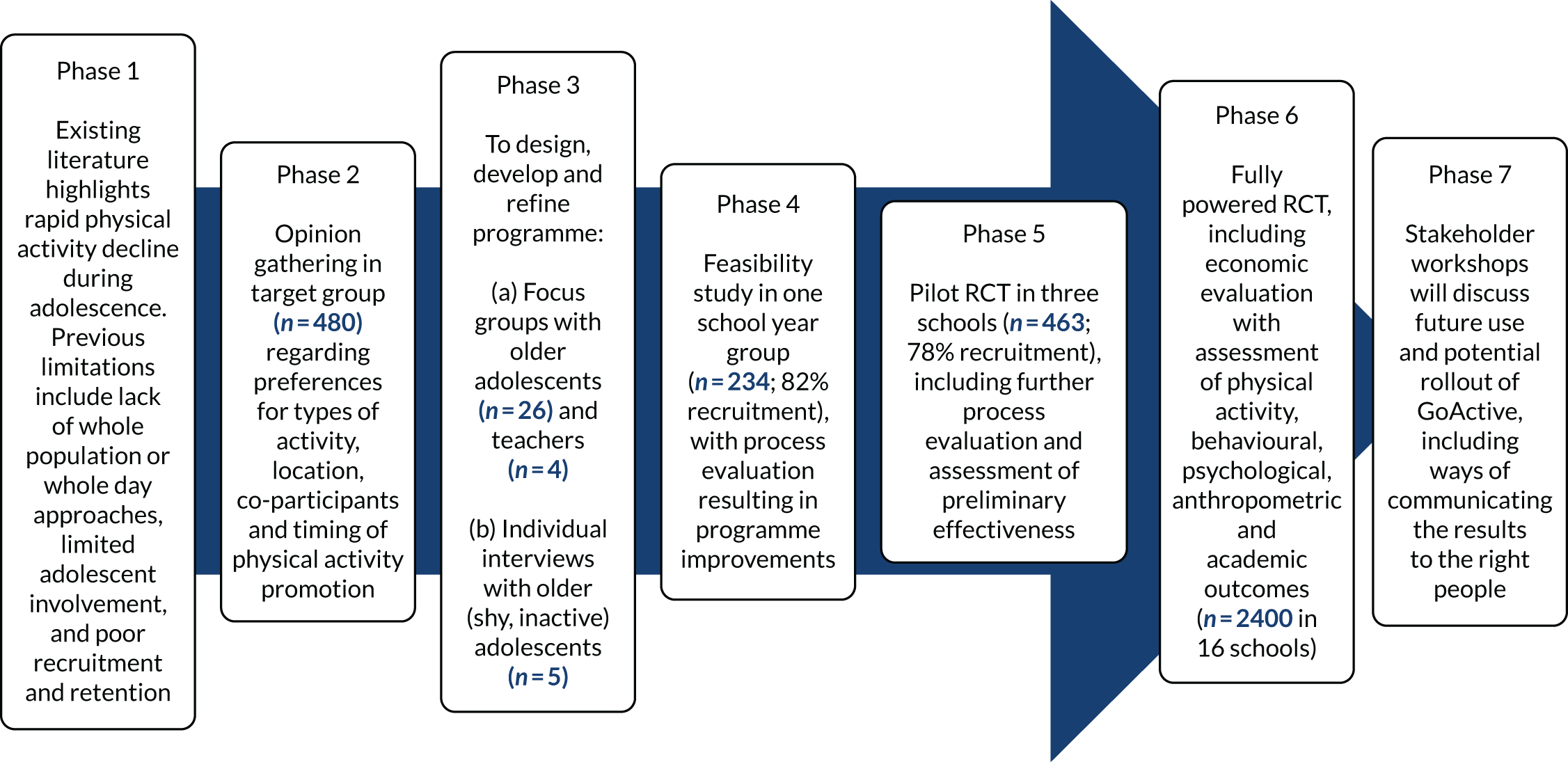
The GoActive physical activity promotion intervention was developed with substantial involvement from adolescents and teachers, and was based on gaps in the existing evidence (Table 1 and Figure 1). Qualitative work with adolescents25 suggested six key themes that may encourage Year 9 students to do more physical activity: (1) choice, (2) novelty, (3) mentorship, (4) competition, (5) rewards and (6) flexibility (Table 2). Although the intervention was broadly aligned with self-determination theory,47 our priority was to co-design the intervention with students and teachers. Therefore, we used theory flexibility to enable the incorporation of components strongly suggested in the development work, irrespective of whether or not they aligned with theory, such as rewards. 6
| Gap in evidence | Key rationale |
|---|---|
| Need for physical activity promotion in older adolescents | Most adolescents are inactive25 and this inactivity tracks into adulthood,26,27 increasing their risk of diabetes, cancer and mortality.28,29 Over 10 minutes/day of physical activity every year is replaced by sedentary time between 9/10 years and 13/14 years25 and a 10-minute increase in MVPA was associated with a smaller waist circumference and lower fasting insulin among young people in a large worldwide meta-analysis.30 Pubertal, brain and social development during adolescence leads to a new capacity for health behaviours,31 increasing the likelihood of long-term change |
| Lack of effective interventions in target group | Reviews highlight limited effectiveness of adolescent physical activity promotion,32–35 with a 4 minutes/day effect size estimated from studies with objective outcomes.35 Only two of these studies included adolescents aged ≥ 13 years,36,37 showing a lack of high-quality research in this important group |
| Lack of whole-population approach | Activity declines among all groups,25 but many interventions target subgroups only.38 A whole-population approach to health promotion overcomes stigmatisation of target groups25 |
| Lack of whole-day approach | The activity decline mainly occurs out of school,39 but many interventions target specific times only (e.g. school time),34,40 PE lessons41 or after-school time |
| Few interventions involve adolescents in intervention development | Adolescent focus groups are mainly used to feedback on existing interventions42 and little research uses adolescent views to develop strategies25 |
| Need for improved adolescent engagement with health promotion interventions | Participation is vital to intervention success, but engaging adolescents to take part in health promotion interventions has challenges,43,44 including transitioning social priorities, biological changes and engagement with minors through schools31,45 |
FIGURE 1.
The GoActive development model.
| Concept | Supporting evidence | Component |
|---|---|---|
| Choice | Adolescents who are given an activity choice have better programme attendance.46 Choice may improve intrinsic motivation, self-efficacy and self-esteem, all of which are important for long-term activity maintenance47,48 | Each tutor group chooses two different activities weekly |
| Novelty | Introducing adolescents to new activities is important. Those given the opportunity to try new activities are more likely to want to do more25 | There are 19 activities available that are designed to utilise little or no equipment. Intervention materials are available on the study website, including Quick Cards (i.e. overviews of chosen activities) |
| Mentorship | Peers are crucial for adolescents to attain the best health behaviours in the transition to adulthood.31 Cross-age mentorship can successfully improve adolescent health behaviours (e.g. substance use,49,50 sexual health51 and nutrition52), but is understudied in physical activity research,53 particularly in young people54 | Older adolescents in the school (i.e. mentors) are paired with each Year 9 class and are responsible for encouraging their class to participate in new activities. Mentors are helped by Year 9 in-class leaders, who change weekly |
| Competition | Competitions improve engagement and retention in health promotion55 | Students gain points every time they do an activity. There is no time limit, students just have to try an activity to get points. Individual points are kept private, with class-level totals announced to encourage interclass competition. Students can enter their points on the GoActive website with individual passwords and login details |
| Rewards | Reward-based interventions appear effective in improving weight management behaviours in children56 | Students gain small individual prizes for reaching certain points levels. Everyone gaining a certain amount of points is entered into a prize draw for a bike |
| Flexibility | A range of co-participants, timing and locations for activity are preferred by Year 9 adolescents, with preferences differing on an individual level25 | One period of tutor time per week was used to do an activity during the feasibility and pilot work. Participants were also encouraged to do activities at other times, especially out of school |
We translated these themes into a physical activity promotion intervention that aimed to increase physical activity among the whole of Year 9.
Feasibility and pilot testing
Feasibility and pilot testing of the GoActive programme was important to demonstrate intervention acceptability, feasibility of recruitment, randomisation and measurement of Year 9 students. 5 Data on preliminary effectiveness was also necessary to inform a realistic estimate of the resources needed for the evaluation of a fully powered randomised controlled trial (RCT). We conducted a feasibility study of the GoActive intervention in one secondary school and a pilot cluster RCT in three schools (two intervention schools and one control school) (ISRCTN31583496). Ethics approval, including for the consent procedures, was obtained for the feasibility and pilot cluster RCT from the Cambridge Psychology Research Ethics Committee, Cambridge, UK (Pre.2013.40).
Feasibility results
The intervention was delivered by one school to the whole of Year 9 for 8 weeks during the summer term of 2013, with limited researcher assistance. Despite initially agreeing to do so, the school was unable to provide mentors, as the older students had examinations. Year 9 form teachers were trained to deliver the intervention prior to the programme commencing. The teachers delivered the intervention with the help of one GoActive team member during tutor time once per week. A total of 234 Year 9 students were exposed to the intervention, as reported by the school, with nine parents (representing 3.8% of eligible students) and 13 students (5.6% of eligible students) opting out of participation in study measures. A total of 183 (78.2%) students assented to participate in measurements, with 29 (12.4%) students not attending a measurement session (because of absence or apathy).
Pilot results
Across the three pilot schools, 596 Year 9 students were invited to participate in the evaluation of GoActive. A total of 458 students provided valid written informed assent and were measured (76.8% response rate; an average of 153 students per school) (Figure 2).
FIGURE 2.
Pilot study recruitment flow chart. All measures include accelerometry, anthropometry and outcomes questionnaire (student-reported physical activity participation, self-efficacy, peer support, friendship quality and mood).
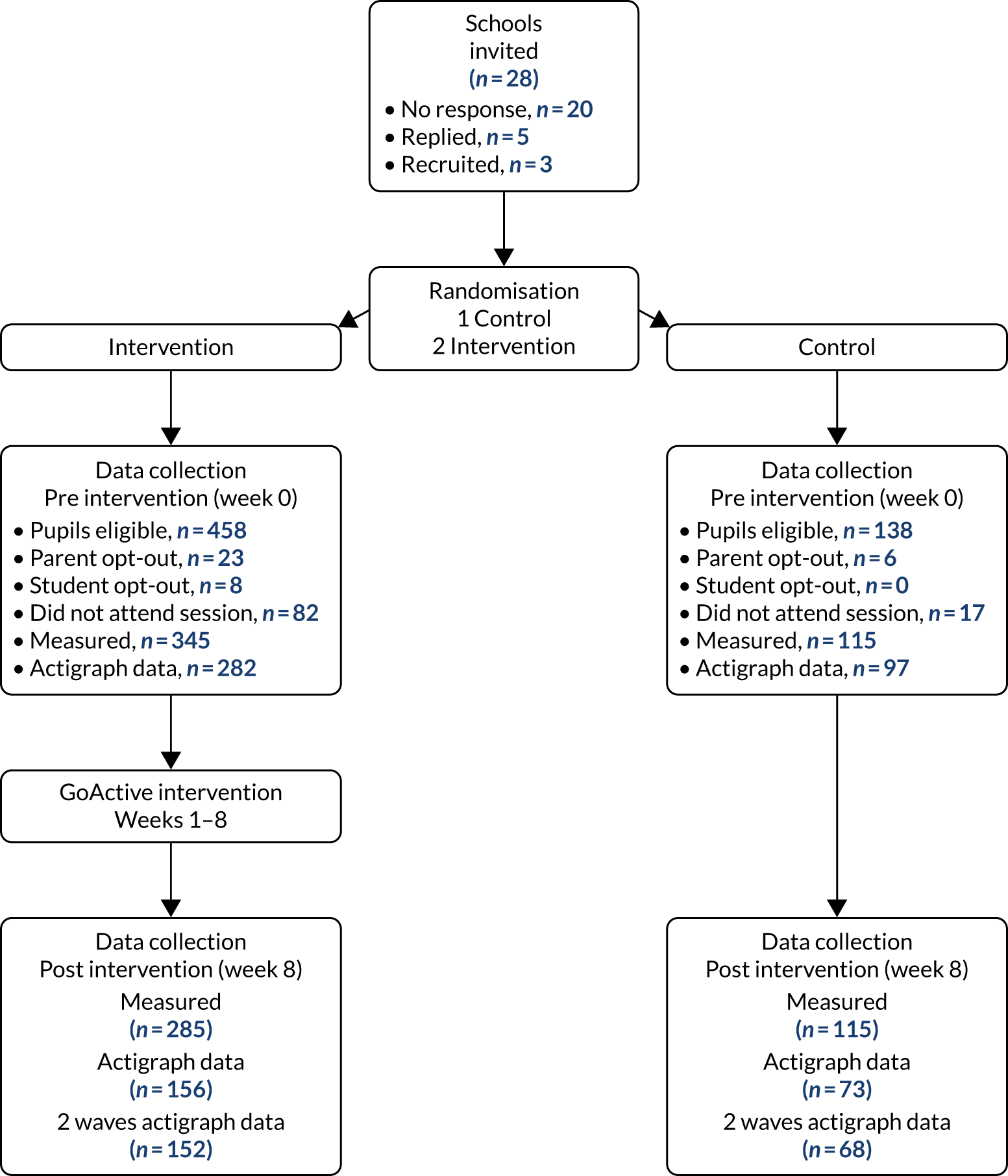
Of the 458 baseline participants, 87.3% attended the follow-up measurement. Of these students, 400 (55%) were available for analysis of the primary outcome [n = 220; ≥ 1 day of ActiGraph data at pre and post intervention (ActiGraph, LLC, Pensacola, FL, USA)] and all 400 completed the questionnaire-based measures that assessed the secondary outcomes. Average days of accelerometer wear were 4.9 (SD 1.8) days pre intervention and 3.8 (SD 1.8) days post intervention.
The results of this pilot cluster RCT provided an indication of the potential effect of GoActive on the main outcome measure (i.e. average daily minutes in MVPA). Change in MVPA was –6.5 (SD 14.0) minutes per day in the control group and –2.5 (SD 15.4) minutes per day in the intervention group, with a change adjusted for baseline of 5.1 [95% confidence interval (CI) 1.1 to 9.2] minutes per day in favour of the intervention group. Furthermore, the results of the questionnaire-based measures indicated tentative positive effects for some secondary outcomes, including well-being and social support.
Year 9 participants
Questionnaire data showed that for boys and girls, respectively, 71% and 74% agreed that taking part in the intervention was ‘fun’ and 56% and 69%, respectively, said that it encouraged them to do more activity. Moreover, 61% of intervention participants indicated that it was fairly likely that they would continue with an activity they had tried during GoActive (boys, 64%; girls, 59%). Of those who had been involved as peer leaders, 81% reported that they thought that it was ‘fun’, 54% said that it had ‘improved their leadership skills’ and 38% said that it took up a lot of time.
Mentors
In focus groups, mentors indicated that although they found it difficult ‘to get their head around’ the GoActive intervention, they quickly picked it up and enjoyed it. Out of the 16 mentors who completed a questionnaire (16 mentors invited), 14 (88%) mentors agreed that GoActive was fun, 15 (94%) mentors said that it improved leadership skills and four (25%) mentors said that it took up a lot of time. Useful suggestions for improvements were made regarding the need for refined points collection, more comprehensive activity explanations, the importance of teacher involvement and more initial training, which were incorporated in the full trial and are summarised in Table 3.
| Issue from feasibility study | Improvements (between feasibility and pilot) | Changes required after pilot | Supporting quotes from student focus groups |
|---|---|---|---|
| Intervention design | |||
| Lack of mentors | |||
| Mentors were not recruited as they had exams |
|
|
. . . so for instance a sixth former came into our form and we was not very motivated, didn’t really want to do it and he’s in there saying, right, we’re all going to go outside, we’re all going to do this, I think probably, I don’t know, I’d probably give it more effort . . .Male participant, post feasibility focus groupMentors would have been helpful especially with large tutor groupsTeacher, post pilot questionnaire |
| Lack of clarity at start | |||
| Researchers did a launch assembly at the beginning of the project, but students suggested the need for clearer initial intervention explanation |
|
|
It was just difficult to get them started but once they were into it, it was fineYear 11 mentor, post pilotNot very sure what was going on, so form [teachers] looked disorganisedTeacher, post pilot |
| Points recording was complicated | |||
| The students found the system for recording points on ‘points cards’ too complicated. This was also a burden for study staff entering the points | Simplified points entry system:
|
|
They [points cards] were like complicated, there was too many like days and numbers and you didn’t know where to like put itFemale participant, post feasibility |
| Activity preferences | |||
| Participant focus groups revealed occasional gender imbalance in activity choices and, with that, differential motivation to participate | Boy and girl leaders each week:
|
|
Yeah, like our sports is for what like the leaders want to do, not the whole class, ‘cos all the boys would pick like boxing and the girls want to do like dancing and Zumba but the boys don’t want to do that so we all go for the boys one, but ‘cos we have a girl and a boy we should like the boys do their thing and the girls do their thing with their leadersFemale Year 9 participant, post feasibility |
| Issue | Proposed change | Changes required after pilot | Supporting information |
| Study design | |||
| Questionnaires | |||
| Some students had difficulty completing questionnaires | Word substitutions and font/colour change:
|
|
Informed by teachers’ suggestions during measurement sessions Rationale for adding additional questions: 44% of pilot participants stated that they asked someone to do physical activity with them during the intervention |
| Measurement session attendance | |||
| A total of 12.4% of eligible students in feasibility study did not attend a measurement session because of absences, illnesses, forgetfulness and apathy |
|
|
In pilot, non-attendance varied (excluding students who opt-out):
|
| Measurement incentives | |||
| Students did not realise that they were receiving vouchers for participating in measurements in feasibility study | No monetary incentives:
|
No further changes | Recruitment and retention was similar in feasibility study and pilot trial |
| Accelerometer data | |||
| Not all participants could be issued with an accelerometer because of resource limitations and 6% of monitors were lost | Strategies for monitor return:
|
|
Pilot study return rate and compliance needs improvement. A total of 36.9% students returned two waves of valid accelerometer data and monitor losses were 8%, 3% and 3% across the three schools |
Teachers
One school had vertical forms, with Year 9 students spread across 66 school forms. The other intervention school had a traditional form structure, with eight Year 9 forms. Eleven teachers completed the questionnaire, five (63%) teachers from the traditional school and six (9%) teachers from the vertical school. Across both schools, 10 (91%) teachers enjoyed the programme, eight (73%) teachers thought that their class did more activity, 11 (100%) teachers thought that their class found it fun, two (18%) teachers thought that it was a lot of work and none (0%) of the teachers thought that their class found it boring. Similar to the feasibility study, most of the free-text comments highlighted the need for improved information provision between the research team and the school. Teacher suggestions are included in Table 3.
Feasibility and pilot summary
The feasibility study and pilot trial of the GoActive intervention showed feasibility of recruitment, measurement, randomisation and the ability to deliver GoActive to a whole-school year group of 13- to 14-year-olds. Both of these stages prompted several key improvements to the intervention and to the study design, including emphasis on monitor return, mentor recruitment, adequate mentor training, clearer and more consistent intervention explanations, and an improved points recording systems. The lessons learnt from each phase of this research were taken forward to the trial reported on here, aiming to evaluate the clinical effectiveness and cost-effectiveness of the GoActive intervention to increase MVPA among 13- to 14-year-olds.
The GoActive study
As outlined, the development of the GoActive intervention followed previous research suggestions. This included basing activity promotion strategies on behaviour change theory, incorporating existing research evidence and including pre-trial qualitative work within the target population in intervention development. 13,16 A further consideration is that whole-group approaches may help overcome some of the stigma associated with targeting particular at-risk groups (particularly shy and inactive adolescents). 17 The overall objective of the GoActive study was to assess the effectiveness of the GoActive intervention in increasing daily MVPA in 13- to 14-year-old (Year 9) adolescents and to establish the cost-effectiveness of the programme. However, responding to calls for more in-depth evaluations of the mechanisms of intervention delivery and effectiveness, the trial was designed to enable the study of mediators of intervention effectiveness and included a comprehensive mixed-methods process evaluation.
Studying mechanisms
We hypothesised that the GoActive intervention components suggested by students and teachers (including mentorship, leadership, teacher support, class-based activity sessions, competition, rewards and online activity tracking) would also influence well-being through social support, self-efficacy, group cohesion, friendship quality and self-esteem. We wanted to investigate if particular engagement with components of GoActive may be associated with mediators and outcomes, for example encouragement provided by older adolescent mentors could be associated with increased self-efficacy and social support, which may be associated with changes in physical activity and mental well-being. 57,58
Mixed-methods process evaluation
The literature on school-based physical activity interventions highlights the need to critically examine the delivery of each component and the processes of any complex intervention. 59 Process evaluation provides detailed evaluative information about the delivery of an intervention from the perspective of participants, mentors, teachers and facilitators, with the aim of contextualising and interpreting its potential effects, providing greater confidence in conclusions about effectiveness. 60
It is also important to understand the primary recipients’ experiences and perspectives of the intervention, as this can not only help to determine the effectiveness of the intervention and its individual components, but can also produce new insights regarding intervention design. There is limited published research of the experiences of those directly involved in receiving these interventions,61–63 particularly using qualitative research methods. Process evaluations of school-based interventions have mainly focused on other stakeholder groups, notably parents and teachers. The process evaluations note the importance of child engagement and autonomy over their own behaviour,64 embedding diet and physical activity across the curriculum and school,64 school resources,64 parental and community engagement,61,64 and the importance of adult role models61,64 in delivering school-based physical activity interventions. However, such stakeholder perspectives cannot replace the sharing of views and experiences of adolescents themselves.
In recent decades, literature and policy have emphasised the importance of capturing views, experiences and actions of those who are the focus of the research. 65 Moore et al. 60 states that the success of an intervention is dependent on the response of the intended audience. This is traditionally considered ‘dose received’,66 and more specifically ‘dose received: satisfaction’. 67 It is argued that ‘dose received’ is a passive term, privileging quantitative measures. 60 Moore et al. 60 advocate for the critical assessment of aspects of dose received, including ‘acceptability’ and ‘satisfaction’, to examine participants’ relationships to the mechanisms through which the intervention works. Additionally, they call for the inclusion of qualitative methods as an effective approach to illuminating participant experiences. Although GoActive was designed as a whole-population approach, aiming to overcome stigmatisation and the potential detrimental mental health consequences of targeting particular subgroups in health promotion strategies,68 we wanted to ensure that the intervention was acceptable to those least likely to engage in physical activity. As such, the intervention was developed to include the opinions of those with characteristics that were deemed as common in those hard to reach for physical activity promotion (including girls, and those with low activity levels and high shyness). 6 Therefore, participants for our process evaluation were purposively sampled to account for perspectives of individuals with those characteristics.
Chapter 2 Methods
GoActive intervention description
Overview
The intervention is titled ‘GoActive’, which stands for ‘Get Others Active’. Each Year 9 class (i.e. tutor group/home room class) are asked to choose 2 of 20 available activities each week. These activities require little or no equipment, and are designed to be appealing to a wide variety of students (e.g. ultimate frisbee, Zumba and hula hoop). Materials available on the GoActive website include activity instructions (Quick Cards), which offer an overview of the chosen activity, a short explanation and suggestions for adaptations, and provide advice, safety tips and ‘factoids’ about each activity (see Appendix 1).
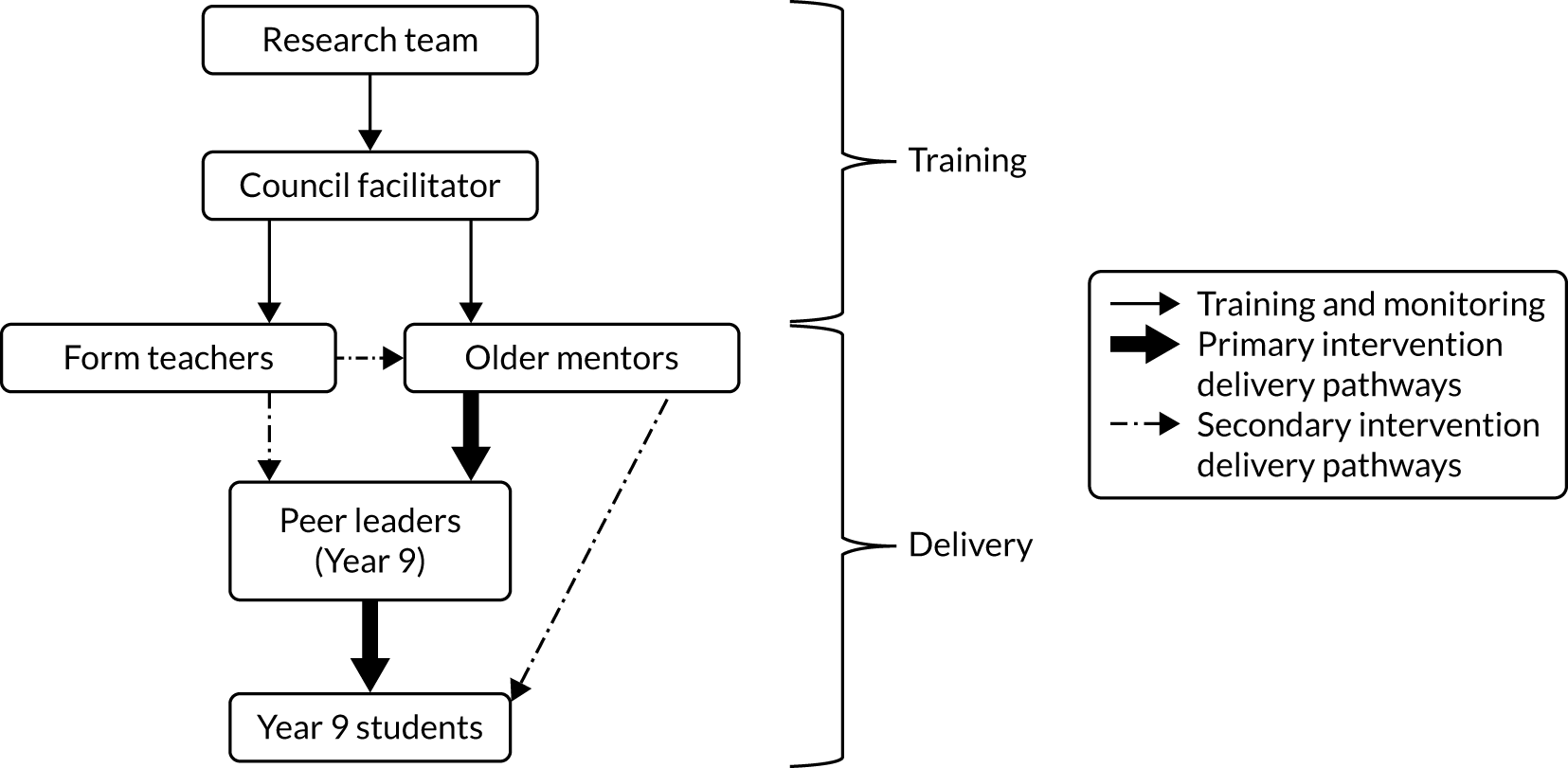
The GoActive intervention is implemented using a tiered leadership system, led by a council-funded facilitator. Schools were requested to select mentors. Mentors (i.e. older adolescents within the school) and peer leaders (i.e. select pupils within each class) encouraged students to try these activities each week (Figure 3). The mentors remain paired with each class for the duration of the intervention, whereas the in-class peer leaders (two per class each week, one male and one female) change every week. Teachers are encouraged to use one period of tutor time (registration/roll call) weekly to do one of the chosen activities as a class; however, students gain points for trying these new activities in or out of school. Points are gained every time a student tries an activity. There is no expectation of time spent in the activity, as points are rewarded for the taking part itself. Individual students keep track of their own points privately on the study website and their points are entered into the between-class competition so that each class competes against each other. Class rankings are circulated each week to encourage teacher support and students receive small rewards (e.g. frisbee, sports bag) for reaching points thresholds (such as 20/50/100 points). As GoActive runs on a weekly cycle, the length of the intervention can vary as appropriate for each individual school.
FIGURE 3.
The GoActive tiered delivery system.
The full intervention ran for 12 weeks, with 6 weeks of weekly facilitator visits and a further 6 weeks with reduced facilitator support. The role of the facilitator was to provide training for mentors and teachers, provide instructions/prompts to teachers, mentors and Year 9 leaders for intervention delivery, support teachers, mentors and leaders to deliver the intervention, provide activity Quick Cards that give overviews and examples of activities, provide basic equipment to facilitate activities if relevant/needed, collect point cards, update points boards in school communal area and class rooms, and to provide prizes. As described in Chapter 1 and clarified in Table 3, several intervention improvements were identified following the pilot intervention and these were incorporated into GoActive. The main differences between the intervention delivered in the pilot evaluation and the GoActive intervention delivered in the trial reported on here were (1) the use of the GoActive website to track points and facilitate communication with the mentor, and (2) delivery was led by a local council-funded facilitator instead of by a member of the research team.
The teachers, mentors and peer leaders delivered the intervention after training from a facilitator (see Facilitator and mentor training). Quick Cards provided information that allows any of these individuals to lead the 20 activities. For example, we suggested using YouTube (YouTube, LLC, San Bruno, CA, USA) for Zumba instruction, as we want the students to be able to try activities without the barrier of needing a specific class. Similarly, we suggested doing these activities at home with a friend or relative to encourage out of school participation.
Table 4 summarises the behaviour change techniques applied in GoActive. Table 5 describes the GoActive intervention’s essential functions (i.e. components of the intervention) that schools were asked to implement. Importantly, these essential functions could be adapted to suit individual settings, offering the schools flexibility to adapt the intervention and its implementation to their context.
| GoActive tenet | Behaviour change technique label | Application in the GoActive intervention |
|---|---|---|
| Novelty, choice, mentorship | 1.1: goal-setting (behaviour) | Form group sets goal to try one new activity per week. Mentors encourage Year 9 students to plan when and with whom they will try the activity |
| Competition | 2.3: self-monitoring of behaviour | Year 9 students record their participation in weekly new activities by entering points online |
| Mentorship | 3.1: social support (unidentified) | Mentors, in-class Year 9 leaders, form teachers and peers provide encouragement and support |
| 4.1: instruction on how to perform behaviour | Quick Cards (i.e. laminated print out resources) and mentors provide activity instructions/tips | |
| 6.1: demonstration of the behaviour | Mentors are encouraged to model the behaviour. Quick Cards show examples of adolescents engaging in the behaviour | |
| Competition | 6.2: social comparison | Points are awarded for trying activities. Anonymised individual points ranking will allow individual-level comparison and class-level competition will be open through the use of school graphs that denote form group leader boards |
| Rewards | 10.1: material incentive (behaviour) | Year 9 students will be informed of the GoActive reward system |
| 10.2: material reward (behaviour) | Year 9 students will be rewarded for obtaining points | |
| 10.4: social reward | Rewards are given out in front of peers. Awards are handed out at full-year assembly at programme end | |
| Mentorship | 10.5: social incentive | Year 9 students are informed that verbal praise will be provided |
| 12.2: restructuring the social environment | A regular short (≈ 20-minute) intervention session is incorporated into the school timetable | |
| 13.1: identification of self as role model | Weekly elected Year 9 peer leaders act as role models. They support and encourage fellow students to try the chosen activities | |
| Rewards | 14.9: reduce reward frequency | Year 9 students receive individual rewards on reaching point milestones [e.g. a sports bag (15 points), t-shirt (50 points) or hoodie (150 points)] |
| Intervention element | Brief description |
|---|---|
| GoActive sessions |
Each tutor group chooses two different activities weekly. Twenty example activities are available, utilising little or no equipment and appealing to a wide variety of students (e.g. ultimate frisbee, Zumba and hula hoop). Materials are available on the GoActive website or in resources provided to schools Teachers are encouraged to use one period of tutor time per week to do one of the chosen GoActive activities as a class |
| Mentors | Older adolescents within the school are paired with each Year 9 tutor group to encourage them to participate in the chosen activities. Mentors remain paired with each class for the duration of the intervention |
| In-class Year 9 leaders | Peer-leaders (two per class each week, one male and one female) assist mentors to encourage students to try activities in GoActive sessions. Peer leaders change every week |
| GoActive website use |
Points: points are gained every time students try a GoActive activity. There is no expectation of time spent in the activity, as points are rewarded for the taking part itself. Individual students keep track of their own points privately on the study website and their points are entered into the between-class competition so that each class competes against each other School graphs: class rankings are circulated each week to encourage teacher support Claiming rewards: students can claim small rewards on reaching individual point thresholds [e.g. a sports bag (15 points), t-shirt (50 points) or hoodie (150 points)] |
Facilitator and mentor training
All facilitators took part in a 1-day training session before the start of the GoActive intervention. Training was provided by members of the GoActive research team and an external consultant specialised in adapting physical activity promotion to different contexts. The contents of the training focused on providing background information on GoActive and its evaluation, a detailed overview of the intervention and the role of the facilitator in intervention delivery, the options for flexibility in intervention implementation, and the resources available to the facilitators and teachers/mentors. All facilitators additionally received a 33-page manual and the research team was available throughout the intervention delivery phase if any questions or concerns arose.
The role of the GoActive intervention facilitator included training teachers and mentors. The audience of this training included Year 9 form tutors and/or house leaders, GoActive mentors and a selected school contact [often physical education (PE) or Year 9 lead]. Training sessions were scheduled for 1 hour. The sessions first provided an overview of the GoActive programme, followed by a question and answer session, during which the audience was encouraged to ask questions or clarify details. Practical training (including role playing, if appropriate) was given for (1) daily intervention delivery, (2) ideas for motivating leaders, (3) overcoming problems and (4) ideas for planning and organising activities. A slide deck and a suggested training schedule were provided to each facilitator to support training and all mentors/teachers received a manual. It was stressed that expectations should be made clear during teacher/mentor training, and the importance of and process for risk assessments was discussed.
Study objective and aims
Overall study
The overall objective was to assess the clinical effectiveness of the GoActive intervention in increasing daily MVPA in 13- to 14-year-old (Year 9) adolescents and to establish the cost-effectiveness of the programme.
The specific aims of the project were as follows:
-
To assess the post-intervention and 10-month effectiveness of the GoActive programme in increasing average daily accelerometer-assessed MVPA among 13- to 14-year-old adolescents.
-
To assess the effect of GoActive on the following secondary outcomes:
-
accelerometer-assessed sedentary time, light physical activity (LPA) and overall physical activity during school time, weekday evenings and weekends
-
student-reported physical activity participation, self-efficacy, peer support, self-esteem, friendship quality and well-being
-
body composition [i.e. body fat percentage and body mass index (BMI) z-score].
-
-
To assess the short-term (within-trial) and potential long-term cost-effectiveness of the programme.
-
To assess programme acceptability, uptake, maintenance and dose.
-
To investigate potential moderation of intervention effects (by gender, socioeconomic status, ethnicity, baseline activity level and weight status) and potential mechanisms of effect by proposed mediators, including peer support, friendship quality, self-efficacy and self-esteem, using a mixed-methods approach.
Mixed-methods process evaluation
Process evaluation is key to being able to assess fidelity and quality of implementation, clarify causal mechanisms and identify contextual factors associated with variation in outcomes. 69 By conducting a thorough process evaluation, combining both quantitative and qualitative data collection methods and insights from different stakeholder groups, it is possible to identify the barriers and facilitators that influence the delivery of the intervention within different contexts, investigating successes and failures of implementation to maximise the learning from the trial delivery of an intervention. 70
The implementation of the programme in each school was assessed through a mixed-methods process evaluation, which included focus groups with and questionnaires completed by students and mentors, as well as individual student, teacher and facilitator interviews and observations of GoActive sessions. The process evaluation protocol has been published previously25 and part of the process evaluation was published prior to analysing intervention efficacy to avoid interpretation bias. 21
The specific objectives of the GoActive process evaluation were as follows:
-
To assess the reach, dose and fidelity of intervention delivery, to document how the intervention was implemented and to ascertain whether or not the intervention’s essential functions (i.e. components of the intervention) were adapted to suit individual settings (see Table 5).
-
To explore the GoActive intervention from the perspective of Year 9 students, mentors, teachers and facilitators, and to describe participants’ views of the intervention (including intervention acceptance).
-
To consider the maintenance and sustainability of the intervention and, if proven effective, the possible dissemination of the GoActive intervention.
The process evaluation was designed to observe the implementation of GoActive and was not used to intervene in how schools implemented the GoActive intervention where deviations from the intervention protocol were detected. The design of the process evaluation was informed by the Medical Research Council (MRC) guidance on the process evaluation of complex interventions. 60,69,71
Study design
We conducted a two-arm cluster RCT with an embedded mixed-methods process evaluation comparing the GoActive intervention with the control condition (i.e. where schools continued to provide their usual physical activity offering). After baseline measurements, participating schools were randomised to the intervention arm or the no-treatment control arm. Allocation used a randomisation list that was prepared in advance by the trial statistician, who was independent from the measurement team, using a random number generator in Stata® version 15.1 (StataCorp LP, College Station, TX, USA). Randomisation was stratified by school-level pupil premium (below or above the county-specific median) and county (Cambridgeshire or Essex). Information on pupil premium is described in Appendix 2.
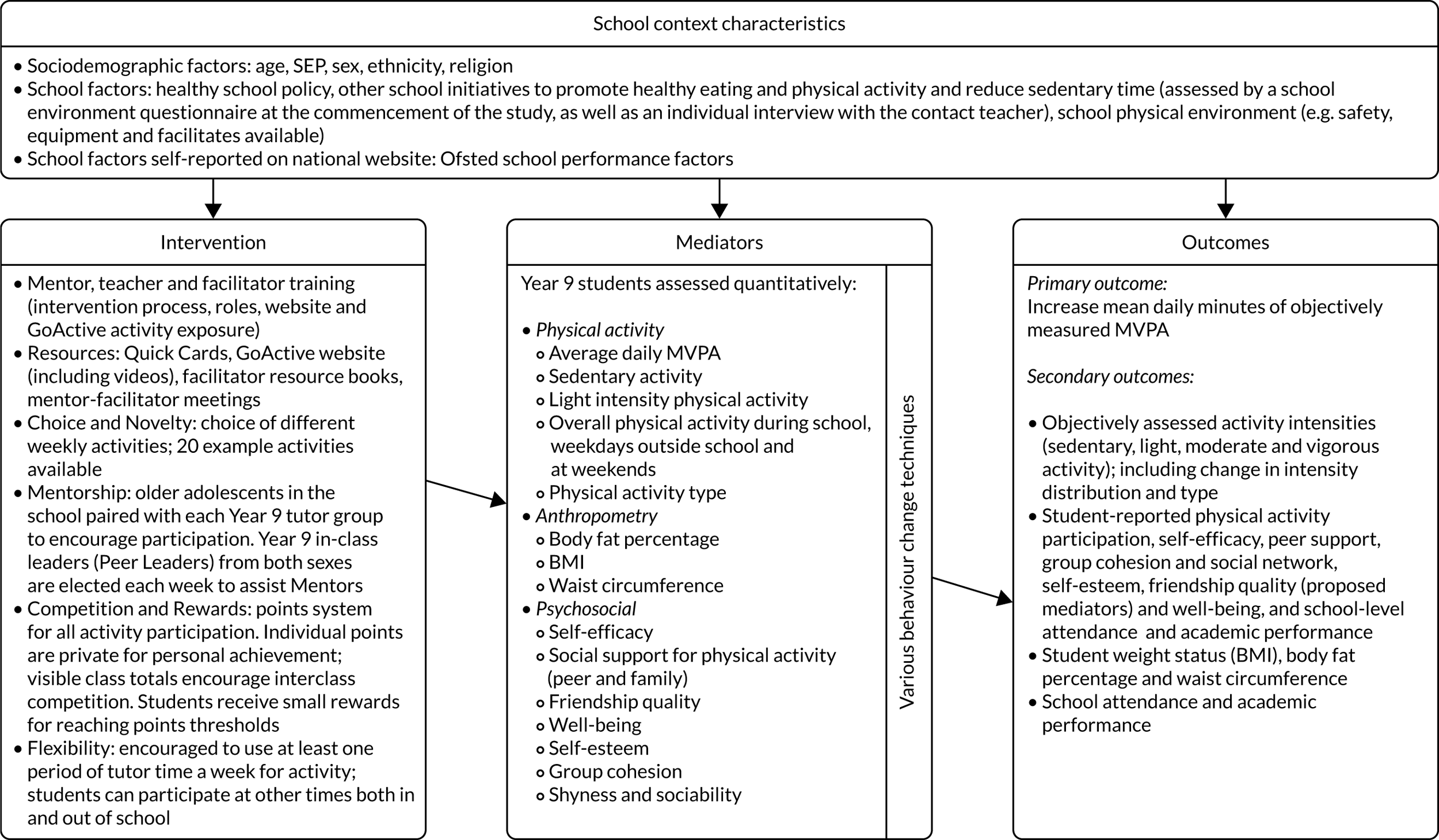
Figure 4 shows the GoActive logic model developed for the overall evaluation.
FIGURE 4.
The GoActive logic model. SEP, socioeconomic position.
Ethics approval was obtained from the University of Cambridge Psychology Research Ethics Committee, Cambridge, UK (PRE.126.2016). The protocol was conducted and reported in accordance with SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) guidance. 27–29 The trial was registered with the ISRCTN registry (trial registration number ISRCTN31583496).
School and participant recruitment
All state-maintained schools that included Year 9 students across Cambridgeshire and Essex (n = 103) were invited to take part in the study between April and July 2016. Although Cambridgeshire and Essex have lower deprivation than the UK median, the areas included wide socioeconomic diversity, including the most deprived place in the UK,20 as well as a mix of urban and rural areas. Schools that expressed interest were provided with further information and senior school staff met with the GoActive study team. Sixteen schools agreed to take part.
All students within Year 9 in the 2016–17 academic year in participating schools were eligible for participation in the study. Students and their parents/guardians/carers were provided with study information. Parents were asked to provide passive consent (meaning that they had to actively opt out their child from study participation). Students provided written informed assent on the data collection day. Parents were provided with information packs that were sent home with students; the packs could also be accessed electronically through the usual school communication channels. Parents were given a 2-week deadline to respond, with the option to respond by telephone or e-mail if they had not returned a form to opt out their child. All those involved in intervention delivery (i.e. mentors, teachers and facilitators) provided informed consent, which was collected by researchers trained in Good Clinical Practice.
Intervention delivery
Irrespective of whether or not students participated in measurements, intervention delivery was at the school tutor group level to all eligible students in intervention schools. Parents were encouraged to speak with the school if they wanted to opt their child out of intervention participation, but no parents chose this option. Control schools received no intervention.
The intervention was delivered over 12 weeks. During the first 6 weeks, a facilitator was provided; however, during the second 6 weeks, external support for the programme was reduced to encourage school-led sustainability. The GoActive intervention targeted peer-led class-based activity, with participation encouraged outside school. Intervention facilitators (i.e. health trainers employed and funded by local councils) provided school staff and older mentors with training, support and resources for intervention delivery. Training sessions consisted of an initial session between facilitators and mentors, lasting at least 1 hour, followed by six 30-minute meetings every week during the first 6 weeks and meetings approximately every 2 weeks thereafter. Mentors were asked to meet with peer leaders weekly.
Data collection overview
Baseline assessments took place early in the academic year for Year 9 students (September 2016–January 2017), which is the school year in which students will reach 14 years of age.
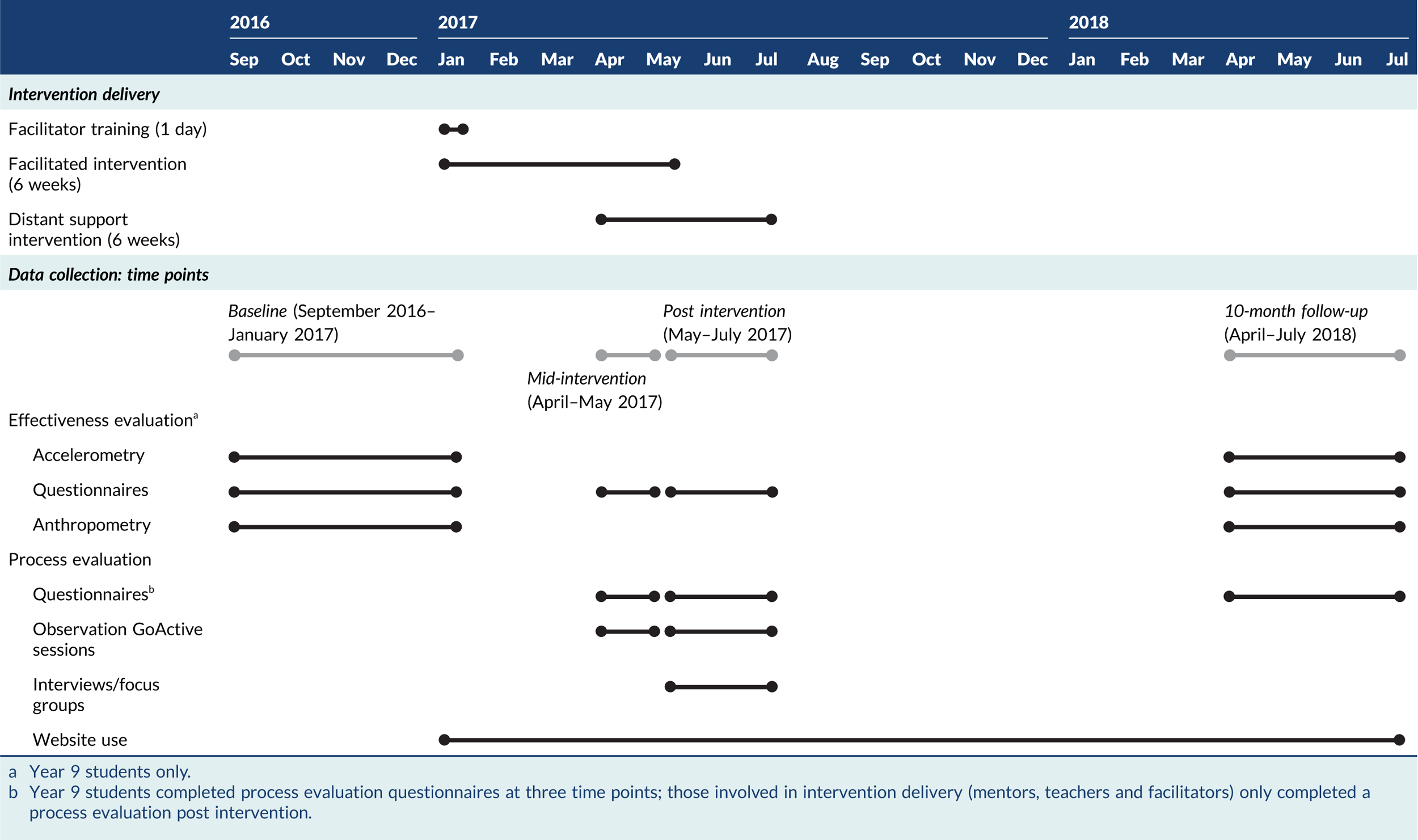
Measurements were taken at four time points:
-
baseline – early in Year 9 (September 2016–January 2017)
-
mid-intervention – 6 weeks after intervention start (April–May 2017)
-
post intervention – 14–16 weeks after intervention start (May–July 2017)
-
10-month follow-up – 10 months after the end of the intervention (April–July 2018).
Outcome assessments using identical procedures were undertaken at baseline and at 10-month follow-up, and these included objective assessment of physical activity for 7 days [i.e. the primary outcome, using a wrist-worn Axivity monitor (Axivity Ltd, Newcastle upon Tyne, UK)], anthropometry (measured), social networks (computer-based assessment), and questionnaires regarding secondary outcomes, including self-reported physical activity, social support, self-efficacy, friendship quality, self-esteem, shyness and sociability. Participant demographic characteristics were additionally included in questionnaires at baseline. Social network data collection, secondary outcomes and objective physical activity assessment were conducted post intervention. Trained measurement staff, blinded to allocation, conducted measurements using standardised protocols and instruments, as detailed in the protocol. 19 Measurement staff were blinded to allocation and our dedicated process evaluation researcher independently verified the success of this blinding by e-mail correspondence shortly after the 10-month follow-up measurements.
Process evaluation measures were collected mid-intervention, post intervention and at 10-month follow-up (Table 6). With regard to quantitative data, all Year 9 participants, regardless of intervention allocation, completed questionnaire-based measures at all time points. In the intervention schools, mentors, facilitators and teachers completed process evaluation questionnaires post intervention. Website analytics were also retrieved from the website, as were facilitator and mentor logs.
| Method of data collection | Data collection participants | Number completed | Response rate | Data collection time frame | Data collected |
|---|---|---|---|---|---|
| Phase 1 | |||||
| Questionnaire | Year 9 students (control and intervention) | 1341 | 86.9% of 1543 baseline participants | Mid-intervention | Experience with the GoActive programme |
| Phase 2 | |||||
| Observation | Form group, mentors and teachers in intervention schools | Eight | Eight out of eight intervention schools had an observation in phase 2 |
During the first 6 weeks of the intervention/during the 12-week intervention Sessions ran from January–July 2017 |
Details on the venue used for the intervention, the number of mentors within the classroom for the intervention and the number of Year 9 students participating in the intervention Delivery and content of GoActive activity Year 9 student engagement and understanding Detailed description of activities Questions, issues or statements from Year 9 students |
| Individual interviews | Year 9 students at intervention schools identified as shy and inactive based on baseline data questionnaire (n = 16) | Two per school | Semistructured interview questions on the following:
|
||
| Contact teacher at each intervention school | Nine (one per school and one school had two contact teachers) | Semistructured interview questions on the following:
|
|||
| Phase 3 | |||||
| Observation | Form group, mentors and teachers in intervention schools | Eight | Eight out of eight schools had an observation |
During the last 6 weeks of the intervention/during the 12-week intervention Sessions ran from April–July 2017 |
Details on the venue used for the intervention and the number of Year 9 students participating in the intervention Delivery and content of GoActive activity Year 9 student engagement and understanding Detailed description of activities Questions, issues or statements from Year 9 students |
| Throughout intervention | |||||
| Website use | Year 9 students (intervention) | 714 | 46.2% of intervention participants | From intervention start to July 2017 |
Proportion of students logging points Number of points logged Number of rewards claimed |
Qualitative process evaluation data were collected from intervention schools only. Qualitative data collection was conducted between April and July 2017 (aligned with post intervention) and included purposively sampled, semistructured individual interviews (participants, teachers and facilitators) and focus group interviews (participants and mentors). Direct observations of two GoActive sessions at each school were conducted.
Table 7 provides an overview of the timing of intervention delivery and data collection in the GoActive study.
TABLE 7.
GoActive study overview
Description of data collection methods
Accelerometer-assessed outcomes (including primary outcome)
The prespecified primary outcome for effectiveness was average daily minutes of MVPA at 10-month follow-up. We measured MVPA at baseline, post intervention and 10-month follow-up using wrist-worn activity monitors (Axivity) that assess acceleration (continuous waveform data). As a change to the published protocol, wrist-worn monitors were used instead of the originally proposed hip-worn ActiGraph monitors (Axivity Ltd, Newcastle upon Tyne, UK) because of the increased likelihood of protocol adherence in the target group compared with what was seen in our pilot work. Participants were asked to wear the monitors continuously for 7 days, 24 hours a day on their non-dominant wrist. Monitor output was processed to provide minutes spent in MVPA and secondary outcomes.
Accelerometery validity and processing
The Axivity monitor has been validated to assess physical activity energy expenditure72 and to have better wear time adherence and acceptability than commonly used hip-worn monitors, among adolescents. 73 Given the 24-hour wear time protocol of the Axivity monitors, a diurnal adjustment was used to reduce any bias caused by imbalances of protocol deviations regarding non-wear. 74 Each day of possible wear was divided into four time quadrants: morning (06.00 to 12.00), afternoon (12.00 to 18.00), evening (20.00 to 24.00) and night (24.00 to 06.00). For participants to be included in analyses, over 6 hours of wear time spread over at least 2 days was required from the possible 42 hours in each daytime quadrant (i.e. ≥ 6 hours from 7 possible mornings, ≥ 6 hours from 7 possible afternoons and ≥ 6 hours from 7 possible evenings). The ‘night’ quadrant (i.e. 24.00 to 06.00) was considered as sleep time and was included in the denominator when calculating daily averages of MVPA, for consistency across all participants. Where individuals did not wear the monitor for ≥ 6 hours at night-time, despite the protocol requesting them to wear it continuously for 7 days, average night-time values were imputed using population averages (n = 91 at baseline and n = 463 at follow-up), created from GoActive participants with 100% protocol compliance regarding monitor wear, to avoid inflation of MVPA estimates. This method was verified by running simulations that exclude night data for a subsample of participants with 100% protocol compliance. For an individual hour to be included for analysis, at least 70% of possible wear time was required, with non-wear time within the hour considered as missing. 74
Monitor output was processed to provide minutes spent in MVPA equivalent to ≥ 2000 ActiGraph counts per minute (c.p.m.). 4 Additional secondary accelerometry-derived outcomes were average daily minutes of sedentary time (equivalent to ≤ 100 ActiGraph c.p.m.), average daily minutes of LPA (equivalent to 101–1999 ActiGraph c.p.m.) and average daily activity (represented by average acceleration). In addition to daily averages, all intensity outcomes (including MVPA) were derived during school time (09.00 to 15.00), during weekday after school time (after 15.00) and at weekends. Participants who met the inclusion criteria for average daily MVPA were included in any analyses for which they had sufficient data (≥ 2 days). 75 As the criteria for deriving average daily MVPA did not require both weekend and weekdays of valid data,76 participant numbers varied by outcome.
Reported demographic data
Participant descriptive characteristics, including prespecified effect modifiers [e.g. gender, individual socioeconomic position (SEP) and ethnicity] were self-reported at baseline. Ethnicity was self-reported by participants who were given 20 response options and additional free-text completion options. For descriptive purposes, the reported values were recoded to five categories in accordance with recommendations:77 (1) ‘white’, (2) ‘mixed ethnicity’ (i.e. identifying with multiple ethnicities), (3) ‘Asian’ (including South Asian and Chinese), (4) ‘African and/or Caribbean’ and (5) ‘other’. Ethnicity was subsequently dichotomised for prespecified moderation analyses (‘white’ vs. remaining categories). Participants completed six items from the Family Affluence Scale (FAS) that relate to family car ownership, holidays, computers, availability of bathrooms, dishwasher ownership and having their own bedroom, which was used as a proxy of individual SEP by summing answers (possible range: 0–13) and dividing into predefined affluence groups (low = 0–6, medium = 7–9 and high = 10–13). 78,79 Shyness and sociability were assessed using five items in the Emotionality, Activity, Shyness and Sociability Scale. 80
Self-reported outcomes
Secondary outcomes were assessed at baseline, post intervention and 10-month follow-up using questionnaires that included measures validated for use in the population (e.g. social support for activity, self-efficacy, group cohesion, friendship quality, self-esteem, shyness, sociability and mental well-being). GoActive questionnaires are available as additional material [see NIHR Journals Library, URL: www.journalslibrary.nihr.ac.uk/programmes/phr/139018 (accessed 12 January 2020)]. Social support for physical activity was a mean derived from nine self-reported items (response range: 1–4) from the European Youth Heart Study. 81 Self-efficacy was a mean of eight self-reported items from Reynolds’ Psychosocial Predictors of Physical Activity: Self-efficacy scale82 (response categories: 1–6). Group cohesion was assessed by an adapted social network modelling tool in which participants were provided with a list of tutor group members on a laptop and were asked to select the names of up to five of their friends from the list provided. These data were used to derive in-degrees (i.e. the number of people identifying the participant as a friend) and out-degrees (i.e. the number of friends that participant lists as a friend). 83 Friendship quality was a mean score of eight self-reported items used in the ‘ROOTS’ study (equally weighted),84 with a response range of 1–5. Self-esteem was a mean score of self-reported items using the 10-item Rosenberg Self-Esteem Scale,85 which had original response options of 1–4. Self-reported physical activity was assessed using the Youth Physical Activity Questionnaire (YPAQ). 86 Activity frequency was calculated as sessions per week of all reported activities (range: 0–160).
The Warwick–Edinburgh Mental Wellbeing Scale was used to assess mental well-being. 87 The 14-item scale asks participants to indicate what best describes their experiences of a collection of statements over the past 2 weeks. Items relate to both hedonic and eudemonic experiences of mental health, including positive affect (e.g. ‘I’ve been feeling optimistic about the future’), relationships (e.g. ‘I’ve been feeling close to other people’) and emotional functioning (e.g. ‘I’ve been dealing with problems well’), each rated on a five-point Likert scale with responses ‘none of the time’, ‘rarely’, ‘some of the time’, ‘often’ and ‘all of the time’ scored 1–5, respectively. The scale has shown good content validity, and correlates well with other mental health and well-being scales, including the Positive and Negative Affect Scale,88,89 Short Depression-Happiness Scale90 and the World Health Organization (Five) Well-Being Index. 91 Cronbach’s alpha has been shown to be 0.89 among a student sample and 0.91 in a population sample. 87 Overall, the scale has shown good internal consistency, good test–retest reliability and good face validity. 92 Participants who responded to all 14 items on the scale were included in the mediation analysis and their score was the average of the item responses (out of a possible 1–5).
Anthropometry
Anthropometry (i.e. height, weight, waist circumference, bioimpedance) was assessed at baseline and at 10-month follow-up by trained staff. BMI z-score was calculated from height, weight, age and gender. 93 BMI z-score was also used to identify participants with overweight or obesity. 94 As a change to the published protocol,4 anthropometry was not assessed at post intervention to reduce the burden on schools and participants, and because no meaningful short-term effect on anthropometry was expected.
Appendix 3 lists further details regarding all outcome variables, including for the primary outcome and all secondary outcome measures.
Process evaluation data collection
As stated earlier, process evaluation measures were collected mid-intervention, post intervention and at 10-month follow-up. Details on the quantitative and qualitative data collected are provided below. An overview of the process evaluation data collected is presented in Table 6.
Quantitative process evaluation data
Quantitative process evaluation data were collected in post-intervention questionnaires adapted from those used in the feasibility study. 5,6 To assess engagement with mentors, students were asked:
Within the GoActive programme, mentors . . . (a) motivated me to be active, (b) were enthusiastic about GoActive, (c) offered lots of different activities to take part in, (d) came in to run GoActive almost every week and (e) explained activities clearly.
Students were also asked to assess engagement with their form tutors (teachers):
Within the GoActive programme, teachers . . . (a) motivated me to be active and (b) were enthusiastic about GoActive.
Response options were from 1, ‘strongly agree’ to 4, ‘strongly disagree’. Items were reverse coded so that higher values were indicative of more positive responses and a mean was calculated. Perception of other intervention components, including class sessions (mean of trying new activities and using tutor time), rewards (individual prizes), competition (mean of class and individual competition) and peer leaders (mean of reported leadership and engagement), were assessed using Likert scales [‘do not like it at all’ (1) to ‘like it a lot’ (5)].
Mentors, teachers and facilitators were also given questionnaires asking them to rate their opinions of the programme and the implementation. All mentors and facilitators involved with the delivery of GoActive were also asked to complete intervention delivery logs on the GoActive website. These logs sought information on, for example, the date each lesson took place, how long it lasted, how many Year 9 students were active in their participation and any comments on the delivery of the session.
Use of the GoActive website was assessed using the points entered on the study website. Participant scores were dichotomised as having entered points compared with not entering points. The website analytics that were included for process evaluation were individual points logged, rewards claimed, activities selected and messages to mentors.
Qualitative process evaluation data
Six process evaluation components were assessed: (1) fidelity, (2) dose delivered, (3) dose received, (4) reach, (5) recruitment and (6) context. 67 Process evaluation quantitative data collection occured in both the control and intervention arms of the trial, whereas qualitative data were collected in the intervention arm only. 3
Qualitative data collection occurred between mid-intervention and 12–14 weeks post baseline (April–July 2017). Data were collected to evaluate the process evaluation measures, to note if findings were consistent with how the intervention was theorised to act in our logic model (see Figure 4) and to note any potential barriers to wider dissemination, should it have proved effective. Qualitative data were collected from all eight intervention schools towards the end of the 12-week intervention. Individual and focus group interviews were conducted by the same experienced qualitative researcher. The interview materials are available as additional material (with color) [see NIHR Journals Library, URL: www.journalslibrary.nihr.ac.uk/programmes/phr/139018 (accessed 12 January 2020)].
Eleven semistructured focus groups with Year 9 students were conducted in a school space familiar to them (total group, n = 48 participants; mean group size, n = 4 participants; range 2–7 participants). Mid-intervention, Year 9 students at intervention schools indicated whether or not they would be willing to be contacted about participating in an interview and those who responded positively were provided with an additional information sheet to clarify the interview procedure (both individual and focus group). Participants for qualitative data collection were purposively sampled to gain information-rich responses, exploring diverse experiences. Focus group participants were grouped by level of participation [determined by tertiles of website points entered: 150 (high), 10–100 (medium), ≤ 10 (low)] and purposively sampled to aim for a mix of gender. An interview guide was developed and iteratively updated as new issues emerged throughout focus groups. 3 Focus groups for six schools were mixed gender. Critical reflection after the first few focus groups led to separating the remaining focus groups by gender, where possible, to maximise the chances of participants feeling comfortable to share experiences openly. Focus groups lasted between 22 and 46 minutes.
Shy/inactive participants were identified using shyness data, and self-reported physical activity participation data (YPAQ) from baseline. Students in the highest tertile for shyness80 and the lowest tertile for self-reported physical activity frequency86 were invited. It was felt that a one-to-one interview may be more comfortable for these individuals. Sixteen individual interviews were conducted (lasting 10–26 minutes). Interviews were semistructured, using a flexible interview guide specifically designed for the interviews.
Interviews focused on the perceptions of the GoActive intervention from diverse student perspectives, including those with high shyness and low physical activity, who may be less likely to engage with physical activity promotion interventions. Both of the interview guides for the focus groups and individual interviews included discussion points on the experience of participating in the GoActive trial, the process of what had been implemented around the GoActive trial within the school and in each class, the depictions of the in-class Year 9 leader, mentor and teacher roles, and perceived barriers to and facilitators of running the GoActive intervention.
Qualitative data were also collected from all of those involved in intervention delivery. Data collection methods included purposively sampled, semistructured individual interviews (teachers and facilitators) and 10 focus group interviews (58 mentors) with individuals involved in intervention delivery. Interview topics included experience of facilitating the GoActive intervention in the school, the process of what had been implemented around the GoActive trial, the depictions of the mentor, teacher and facilitator roles (including self-perceptions), and perceived barriers to and facilitators of running the GoActive intervention. Facilitators implementing across more than one school were asked to discuss school-specific responses.
GoActive sessions observations
Direct observations of two GoActive sessions at each school running the intervention (n = 8) were arranged by contact teachers. Teachers and most mentors that were to be observed were informed of when observations would take place. Data collected during observations comprised detailed written notes that described what took place, where in the school setting, any informal conversation, the role of the mentor, teacher engagement and level of engagement from Year 9 students.
Trial sample size calculation
We estimated that a total of 1310 participants would be required to have 85% power to detect a 5-minute difference in change in MVPA between baseline and 10-month follow-up as significant at the 5% level,4 assuming a standard deviation (SD) of MVPA of 17.8 minutes and a correlation of 0.59 between baseline and follow-up. 19 Assuming a within-school (intraclass) correlation of 0.034 and 30–40% loss to follow-up, we aimed to recruit 16 schools with 150 participants per school. 19
Analytical approach
Analysis of effects on primary and secondary outcomes
The statistical analysis plan was approved by the Trial Steering Committee (TSC) prior to analyses being performed. The full statistical analysis plan is available from the GoActive study website [URL: www.mrc-epid.cam.ac.uk/research/studies/goactive/ (accessed 28 February 2020)]. Statistical quantitative analyses were performed using Stata.
For MVPA at 10-month follow-up (i.e. the primary outcome), the intervention effect, representing the baseline-adjusted difference in change from baseline between the intervention and control groups, was estimated from a linear regression model, including randomisation group, baseline value of the outcome [i.e. analysis of covariance (ANCOVA)] and the randomisation stratifiers (i.e. pupil premium funding and county). Robust standard errors (SEs) were calculated to allow for the non-independence of individuals within schools and the missing indicator method95 was used to ensure the inclusion of participants with a missing baseline value of the outcome variable. All secondary outcome variables were analysed using the same method.
We conducted a complete-case analysis in which participants and schools were included in the group to which they were randomised, although participants with a missing value of an outcome at follow-up were excluded from the analysis of that particular variable. This is a complete-case analysis that is valid under the assumption that the outcome is missing at random, conditional on randomised group and the baseline value of the outcome.
Per-protocol analysis
A further analysis of the primary outcome was performed in a per-protocol population, defined as intervention group participants reporting ‘being active during tutor times at least twice during the last 2 weeks’ [i.e. self-reported intervention engagement mid-intervention (week 6 of the intensely facilitated phase of the intervention)] and logging activity points on the study website at least once during the entire intervention period. This definition was based on a review of quantitative process evaluation data prior to the main analyses and reflects the group with highest intervention engagement, as opposed to delivery of the protocol with fidelity.
Sensitivity analyses
Post hoc sensitivity analyses recommended by the TSC were performed, in which the primary outcome was calculated (1) excluding time between 24.00 and 06.00 and (2) using a stricter inclusion criterion of 12 hours of wear time per quadrant.
Effect modification
For the primary outcome and secondary accelerometer-assessed physical activity outcomes, effect modification was conducted by (1) gender, (2) socioeconomic status (medium or lower vs. high, according to FAS score), (3) ethnicity (white vs. any other ethnic background), (4) baseline physical activity (≥ 60 minutes MVPA/day vs. < 60 minutes) and (5) weight status (with normal weight vs. with overweight or obesity) and was tested with an F-test of the relative multiplicative interaction parameter in the ANCOVA model. Effect modifiers were selected based on previous evidence of potential differential effects. 13,14 Subgroup analyses were performed within all categories defined by these variables.
We used baseline accelerometer-assessed activity data to classify participants’ activity level using 30 and 60 minutes of MVPA, using (average) thresholds. The 60-minute threshold was applied to be consistent with UK physical activity guidelines, whereas the additional 30-minute threshold was applied to achieve greater heterogeneity in the moderator, as activity levels were low at baseline (minutes of MVPA at baseline for whole group: 35.6 ± 18.6 minutes/day). Subgroup analyses were performed for the primary outcome within all categories defined by these variables, but only where interactions showed p < 0.05 for secondary outcomes.
Mediation analyses
We aimed to use mediation analysis as a novel approach to evaluate the potential mediating role of psychosocial factors in the association between engagement in the intervention components suggested by students in our intervention co-design process and changes in physical activity and well-being.
Mediation of effects on the primary outcome (i.e. MVPA) and well-being was assessed using linear regression models stratified by gender (adjusted for age, ethnicity, language, school, BMI z-score and baseline values), assessing associations between (1) exposures and mediators, (2) exposures and outcomes (without mediators) and (3) exposures and mediators with outcomes, using bootstrap resampling.
Economic analysis and cost-effectiveness
A within-trial cost-effectiveness analysis comparing the GoActive intervention with the control was conducted from the perspective of the school funder (assumed to be the local authority). Cost per school and per participant was calculated for intervention group participants based on facilitator and teacher time input, and materials. Quantities of inputs were based on the protocol, supplemented by study records, and unit costs reported in 2019 Great British pounds. As costings considered the additional costs associated with the GoActive intervention only, there were zero costs associated with control.
Outcomes in the economic analysis were the primary outcome (i.e. change in minutes of MVPA) and quality-adjusted life-years (QALYs). QALYs are useful as they measure overall health-related quality and quantity of life. QALYs were assessed using the Child Health Utility-9D, which has been validated for use in adolescents24 and was included in the participant questionnaire at all follow-up time points. Responses were converted to utilities using the recommended published algorithm96 and QALYs were calculated as the area under the curve, with straight-line interpolation between time periods. Total accrued time from baseline to 10-month follow-up, and hence the time horizon for the study, is approximately 2 academic years. Undiscounted and discounted QALYs (at 3.5%) are calculated and an unadjusted and adjusted imputed analysis reported. The latter analysis adjusted for age, socioeconomic status and other demographic variables. Multiple imputation with chained equations was carried out on missing utility data using the predictive mean matching method and five imputed data sets. Analysis was conducted in R (The R Foundation for Statistical Computing, Vienna, Austria). Code is available from the corresponding author on request.
Exploratory economic modelling
The study protocol stated that long-term modelling would be undertaken only if a positive effect on physical activity was observed, on the basis than it is highly unlikely for the intervention to be (cost-) effective in the long term if it is not so in the short term. However, irrespective of the point estimate, incorporating the uncertainty in study results into a previously developed, longer-term model enables analysis of where uncertainties in longer-term cost-effectiveness lie and can be used to guide further research via value-of-information analysis. For example, the treatment effect of the GoActive intervention may be uncertain, which a priori might suggest that further research was warranted. However, the modelling may reveal that greater value would be obtained from a research project investigating, for example, the link between physical activity and blood pressure, or blood pressure and risk of cardiovascular event.
We therefore conducted an exploratory analysis, inserting the results from the GoActive trial into the previously developed PACE (physical activity cost-effectiveness) model,97 adapted to this study question, reporting longer-term costs and QALYs accrued as per the protocol, but also incorporating a value-of-information analysis. Adapting the model to the study question simply comprised converting the study results from minutes of MVPA to metabolic equivalent of task (MET)-hour equivalents. 98
The PACE model has been described previously,97 but, briefly, it generates a cohort of individuals based on English demographic data. The model follows them for a defined number of years under a base case of average physical activity levels, tracking BMI, blood pressure, glucose (glycated haemoglobin) and lipids, the incidence and prevalence of type 2 diabetes and associated complications, cardiovascular events and certain cancers according to a set of risk equations extracted from the literature. Costs and health state utilities are assigned to these events, resulting in a measure of accrued costs and QALYs over the time horizon of the model. A second-order Monte Carlo simulation propagates parameter uncertainty (i.e. uncertainty in coefficients of the risk equations) to decision uncertainty (i.e. uncertainty in costs and QALYs). The model is then repeated under alternative physical activity scenarios, input as mean and SE of difference in MET-hours per day, with assumptions as to the ‘decay’ rate of the intervention effect (base case assumed 55% per annum), yielding a mean and SE cost and QALY gained from each intervention, from which incremental cost-effectiveness ratios can be calculated.
The model simulated a cohort of 10,000 14-year-olds and followed them for a period of 10 years under a ‘do nothing’/control scenario, repeated 10,000 times. This was then repeated, incorporating the distribution of intervention effect described above.
Costs included in the PACE model are health service costs, to which we added the cost to local authorities of the intervention. The cost perspective of the modelled analysis is therefore the public sector.
Results are reported as mean and 95% credibility intervals for costs and QALYs in each arm, as well as increments between the arms, net monetary benefit from each arm and incremental net monetary benefit calculated at £20,000 per QALY gained. Value-of-information analysis estimates the expected value of perfect information (EVPI) and expected value of perfect parameter information (EVPPI), providing a guide as to where future research is likely to be of most value. Population EVPI and EVPPI are calculated based on population projections of the numbers of 14-year-olds in the UK from 2020 to 2029 (i.e. 10-year time horizon), discounted at 3.5%. This yields a beneficial population of 7,169,651.
Analysis of process evaluation data
Quantitative data
Data are presented descriptively as means (SD) or medians (interquartile range) for continuous variables, and as proportions for categorical variables. Between-group differences (boys vs. girls, and shy/inactive vs. others) in data from process evaluation questionnaires, including enjoyment and satisfaction with individual components, were tested, with multilevel linear regression models clustered by school.
Website data collected from Year 9 students entering individual points through the GoActive website (a point per activity completed) included the number of user logins, as well as logs of the pages visited within the GoActive website. Website analytics of the GoActive website were used to generate descriptive statistics to explore the fidelity and dose received of the intervention.
Qualitative data
Qualitative data were audio-recorded, transcribed verbatim and managed using NVivo11 (QSR International, Warrington, UK). Qualitative data were analysed using a realist thematic approach to report the experiences, meanings and reality of participants. 99 Two researchers independently coded a subsample of transcripts. Data were organised into manageable segments of text,100 and patterns and connections between them were identified. 101 All codes were compared, discussed and agreed on prior to coding all other interviews. Interim themes were discussed by members of the research team to reach consensus. Codes were revisited and abridged into broader themes. At first, individual and focus group data were analysed separately; however, because of the identification of common themes, the two data sets were subsequently reviewed together to identify and map overarching themes related to participants experiences of the intervention. A deductive thematic approach was used to provide a focused analysis of the GoActive components.
All data from the website logs, and data from interviews and focus groups from mentors, teachers and facilitators, were analysed using NVivo, using a six-step thematic approach. 99 Codes were generated both from the topics in the interview guides and iteratively from the data. All codes were discussed with another researcher and were categorised as a series of themes. The themes were discussed, refined and agreed by two researchers. Taken with data from participants, the themes exemplify the process evaluation components. These themes combine with an inductive analysis to attain the facilitators and challenges of the intervention. Illustrative anonymised quotes typify the data from interviews. Observation qualitative data were used to provide context, or to support, reaffirm or contradict data from interviews, and were documented as text extracts.
Mixed-methods process evaluation
Qualitative and quantitative data were merged during analysis and interpreted using a mixed-methods convergence matrix, where appropriate. Components were assessed for convergence (i.e. agreement between both sets of results) or dissonance (i.e. disagreement between the sets of results on either the relevance or direction of the determinant/theme under consideration). 102 The process of developing a convergence matrix allowed data sets to be compared, triangulating the data to address completeness, convergence and dissonance of key themes.
Additional mixed-methods analysis included sorting findings based on the process evaluation components (i.e. reach, recruitment, dose and fidelity). Findings were reviewed and compared to assess convergence and dissonance between the data sets, and specific examples of qualitative data were gathered to reflect this convergence or dissonance, or to explain particular process evaluation components. The two researchers involved in the analysis clarified interpretations of the findings, where required. Results were discussed with the research team for review and clarification.
GoActive project management
The overall GoActive project was managed by the GoActive Project Group, which was chaired by the principal investigator and consisted of all applicants, research associates working on the project, the study co-ordinator and research assistants, when relevant. Depending on the project phase, the Project Group met once every 3–6 months. Operational management was led by the GoActive Operational Group, consisting of the principal investigator, study co-ordinator and the main research associates appointed on the grant.
At the start of the project, the GoActive TSC was established. The committee consisted of six independent members and the principal investigator. The independent members represented various scientific disciplines (e.g. young people’s physical activity promotion, public health, health behaviour change, statistics, health economics, physical activity measurement, trial methods) and included stakeholders (physical activity and public health) and members of the public (including school leaders). The GoActive TSC met at least annually for the duration of the trial. Their stated role was to provide oversight for the trial on behalf of the sponsor and funder. The TSC also provided advice, through its independent chairperson, to the Trial Management Group (TMG), sponsor, funder and MRC Epidemiology Unit on all aspects of the trial.
Specific roles of the TSC included:
-
providing expert oversight of the trial
-
making decisions as to the continuation (or otherwise) of the study
-
monitoring recruitment rates and encouraging the TMG to develop strategies to deal with any recruitment problems
-
approving the protocol(s)
-
reviewing regular reports of the trial (sent on behalf of the TMG)
-
assessing the impact and relevance of any accumulating external evidence
-
monitoring completion of adverse events
-
monitoring follow-up rates and review strategies from the TMG to deal with problems
-
approving any amendments to the protocol, where appropriate
-
approving any proposals by the TMG concerning any change to the design of the trial, including additional substudies
-
overseeing the timely reporting of study results
-
commenting and advising on the statistical analysis plan
-
commenting on the publication policy
-
commenting on the main trial manuscript
-
commenting on any abstracts and presentations of any results during the running of the trial
-
liaising with the funder, if required.
The TSC approved all changes to the protocol prior to ethics applications.
Chapter 3 Results
Parts of this chapter are reproduced from Jong et al. 103 © 2020 Published by Elsevier B.V. on behalf of Shanghai University of Sport. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Sample description
The GoActive trial was run between September 2016 and July 2018. Figure 5 shows the trial profile. A total of 103 schools were approached. Sixteen school were initially recruited; however, two dropped out before baseline measurements because of changes in their Senior Leadership Team (SLT) (one school from Essex and one school from Cambridgeshire) and replacements within the same strata were recruited. Of the 3405 Year 9 students eligible for inclusion across all participating schools, 2862 (84.1%) students consented (eight control schools, 1319 participants; eight intervention schools, 1543 participants). A total of 2828 participants (98.8% of those consenting) completed baseline questionnaires and 2638 participants (92.2% of those consenting) had a valid assessment of the primary outcome at baseline. At 10-month follow-up, 2167 (75.7%) participants attended and we obtained a valid measure of primary outcome for 1874 out of 2862 (65.5%) randomised participants. Baseline characteristics were similar between the randomised groups (Table 8). Overall, the mean age was 13.2 (SD 0.2) years, 52.1% of participants were male and 84.7% of participants self-reported as white. More female participants and participants with high socioeconomic backgrounds, from Cambridgeshire, and with underweight or normal weight provided primary outcome data (Table 9). Blinding of measurement staff was largely successful (see Appendix 4); however, a few cases of unblinding occurred due to student and teacher interaction during measurement sessions.
FIGURE 5.
Study flow chart. a, ‘All measures’ includes accelerometry, anthropometry and outcomes questionnaire (student-reported physical activity participation, self-efficacy, peer support, self-esteem, friendship quality and well-being).
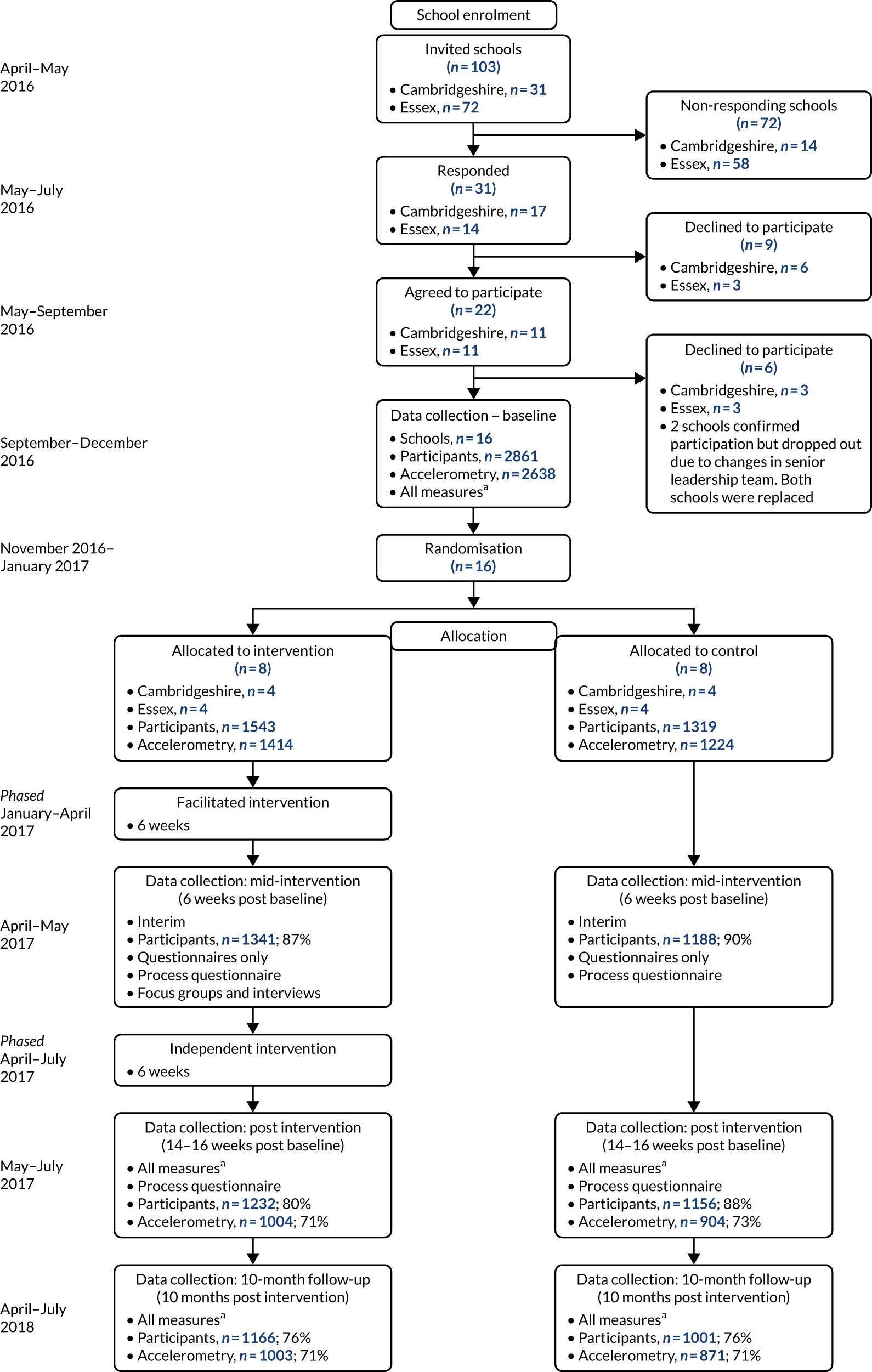
| Characteristic | Control (n = 1319) | Intervention (n = 1543) | ||||
|---|---|---|---|---|---|---|
| % missing | Mean | SD | % missing | Mean | SD | |
| Age (years) | 0.0 | 13.2 | 0.4 | 0.0 | 13.2 | 0.4 |
| BMI SDS | 0.0 | 0.2 | 1.6 | 0.0 | 0.1 | 1.9 |
| Body fat (%) | 3.9 | 20.7 | 10.0 | 5.4 | 20.9 | 9.9 |
| Waist circumference (cm) | 0.5 | 70.0 | 9.6 | 0.6 | 70.4 | 9.7 |
| % | n | % | n | |||
| Gender | 0.0 | 0.0 | ||||
| Male | 53.4 | 704 | 51.1 | 788 | ||
| Female | 46.6 | 615 | 48.9 | 755 | ||
| Ethnicity | 1.1 | 1.3 | ||||
| White | 86.1 | 1135 | 83.5 | 1288 | ||
| Mixed/multiple ethnic background | 6.2 | 82 | 6.3 | 97 | ||
| Asian or Asian British | 3.2 | 42 | 4.3 | 66 | ||
| Black or black British | 2.2 | 29 | 2.7 | 41 | ||
| Other ethnic group | 1.3 | 17 | 2.0 | 31 | ||
| Family socioeconomic status | 0.8 | 1.0 | ||||
| Low | 11.0 | 145 | 16.3 | 252 | ||
| Medium | 40.6 | 536 | 43.4 | 669 | ||
| High | 47.6 | 628 | 39.3 | 606 | ||
| Weight status | 1.4 | 2.7 | ||||
| Underweight | 2.6 | 34 | 2.1 | 33 | ||
| Normal weight | 68.5 | 903 | 66.4 | 1025 | ||
| Overweight | 19.2 | 253 | 18.5 | 285 | ||
| Obese | 8.3 | 110 | 10.2 | 158 | ||
| County | 0.0 | 0.0 | ||||
| Cambridgeshire | 58.8 | 775 | 42.4 | 654 | ||
| Essex | 41.2 | 544 | 57.6 | 889 | ||
| Pupil premium | 0.0 | 0.0 | ||||
| Low | 47.6 | 628 | 49.2 | 759 | ||
| High | 52.4 | 691 | 50.8 | 784 | ||
| Data | Missing (n = 988) | Available (n = 1874) | ||
|---|---|---|---|---|
| Mean | SD | Mean | SD | |
| Age (years) | 13.3 | 0.4 | 13.2 | 0.4 |
| BMI SDS | 0.5 | 1.2 | 0.3 | 1.2 |
| Body fat (%) | 20.8 | 10.0 | 20.8 | 9.9 |
| Waist circumference (cm) | 71.1 | 10.3 | 69.7 | 9.2 |
| % | n | % | n | |
| Gender | ||||
| Male | 55.5 | 548 | 50.4 | 944 |
| Female | 44.5 | 440 | 49.6 | 930 |
| Weight category | ||||
| Underweight/normal weight | 64.6 | 638 | 72.4 | 1357 |
| Overweight/obese | 35.4 | 350 | 27.6 | 517 |
| Ethnicity | ||||
| White | 83.1 | 821 | 85.5 | 1602 |
| Mixed (identifying with multiple ethnicities) | 6.7 | 66 | 6.0 | 113 |
| Asian (including South Asian and Chinese) | 3.2 | 32 | 4.1 | 76 |
| African and/or Caribbean | 3.1 | 31 | 2.1 | 39 |
| Other | 2.0 | 20 | 1.5 | 28 |
| Family socioeconomic status | ||||
| Low | 18.3 | 181 | 11.5 | 216 |
| Medium | 43.2 | 427 | 41.5 | 778 |
| High | 37.2 | 368 | 46.2 | 866 |
| County | ||||
| Cambridgeshire | 38.0 | 375 | 56.2 | 1054 |
| Essex | 62.0 | 613 | 43.8 | 820 |
Primary outcome
Mean accelerometer-assessed MVPA decreased in both randomised groups between baseline and 10-month follow-up. The reduction was slightly larger in the intervention group, although the CI around the intervention effect was wide and inconclusive (Table 10 and Figure 6).
| Control | Intervention | Intervention vs. control: between group difference (95% CI) | |||||
|---|---|---|---|---|---|---|---|
| Baseline | 10 months | Change from baseline | Baseline | 10 months | Change from baseline | ||
| Participants (n) | 1224 | 871 | 1414 | 1003 | |||
| Mean (SD) | 35.6 (18.9) | 27.6 (20.6) | –8.3 (19.3) | 35.6 (18.3) | 25.6 (21.5) | –10.4 (22.7) | –1.91 (–5.53 to 1.70) |
FIGURE 6.
Intervention effect on primary outcome, overall and within subgroups.
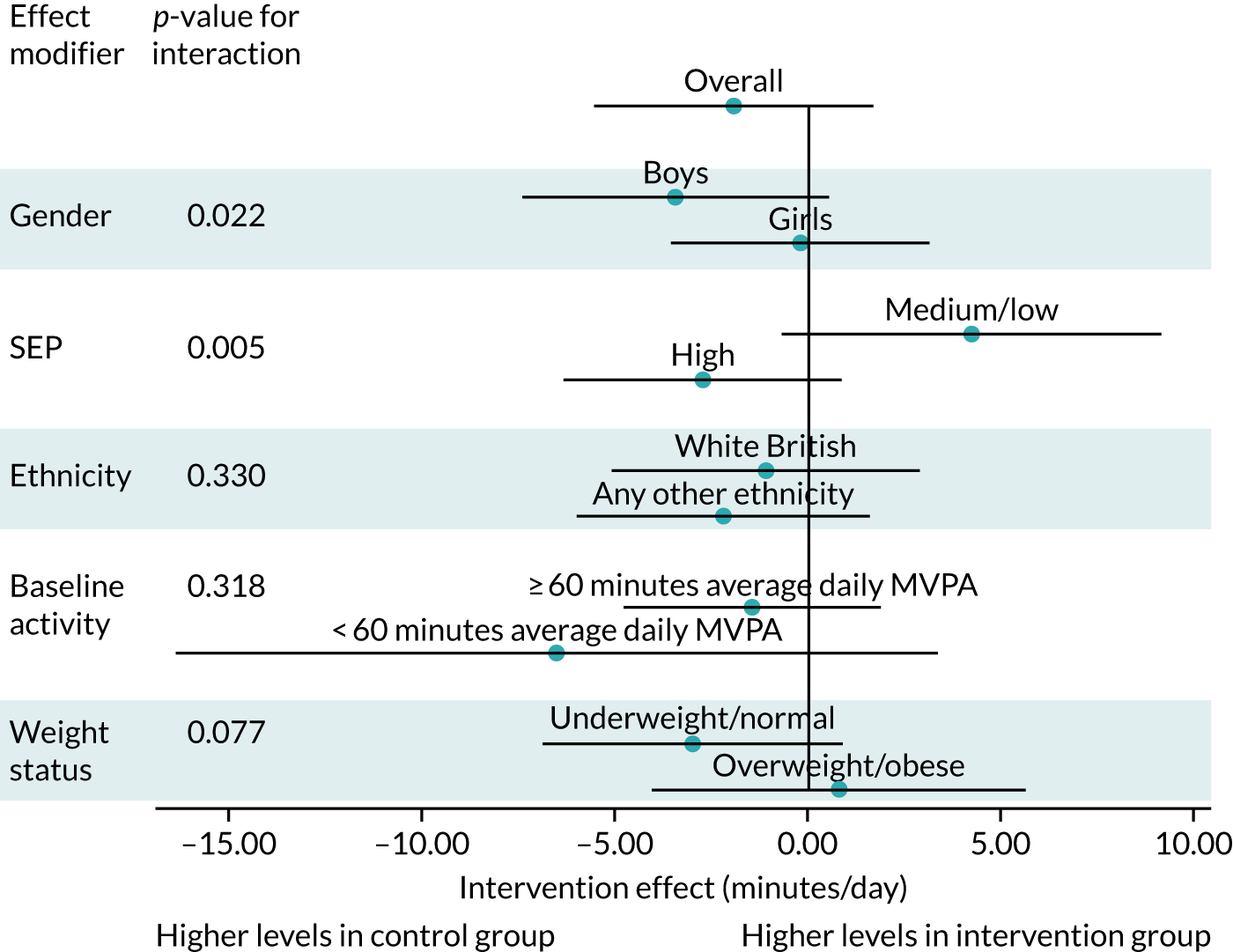
Secondary outcomes
In the whole population, over the duration of the study, overall time spent sedentary increased and LPA decreased (Table 11). There was no evidence of an intervention effect on average daily accelerometer-based outcome measures post intervention or at 10-month follow-up (Tables 12 and 13, respectively). Time-specific accelerometry-based outcomes showed that on schooldays (weekdays) changes over time were more favourable in the control group (both during school and after school), while at weekends more favourable changes were observed in the intervention group, particularly at 10-month follow-up (Figures 7 and 8; see also Tables 12 and 13 for full details).
| Intention-to-treat population | Control | Intervention | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Post intervention | 10-month follow-up | Baseline | Post intervention | 10-month follow-up | |||||||||||||
| n | Mean | SD | n | Mean | SD | n | Mean | SD | n | Mean | SD | n | Mean | SD | n | Mean | SD | |
| Average daily minutes of MVPA | ||||||||||||||||||
| Overall | 1224 | 35.6 | 18.9 | 904 | 35.5 | 21.4 | 871 | 27.6 | 20.6 | 1414 | 35.6 | 18.3 | 1004 | 33.6 | 22.1 | 1003 | 25.6 | 21.5 |
| School time | 1176 | 13.2 | 7.1 | 770 | 13.5 | 7.3 | 657 | 11.3 | 6.9 | 1367 | 13.3 | 7.0 | 852 | 13.1 | 8.2 | 703 | 10.2 | 7.4 |
| Weekdays after school | 1176 | 18.7 | 12.5 | 770 | 21.3 | 14.2 | 655 | 17.9 | 14.0 | 1367 | 18.6 | 12.4 | 851 | 20.0 | 15.5 | 700 | 15.4 | 13.6 |
| Weekends | 1121 | 28.2 | 24.0 | 711 | 33.2 | 30.5 | 562 | 22.3 | 24.2 | 1222 | 28.4 | 24.5 | 770 | 31.2 | 28.9 | 599 | 24.0 | 29.3 |
| Average daily minutes spent sedentary | ||||||||||||||||||
| Overall | 1224 | 1103.8 | 61.8 | 904 | 1106.7 | 73.5 | 871 | 1147.0 | 75.5 | 1414 | 1100.6 | 60.8 | 1004 | 1115.4 | 78.8 | 1003 | 1151.7 | 85.9 |
| School time | 1176 | 243.5 | 22.1 | 770 | 243.0 | 24.0 | 657 | 254.8 | 24.9 | 1367 | 242.1 | 22.7 | 852 | 244.6 | 26.0 | 703 | 259.1 | 28.1 |
| Weekdays after school | 1176 | 331.6 | 38.8 | 770 | 321.0 | 44.1 | 655 | 335.2 | 45.6 | 1367 | 330.2 | 39.5 | 851 | 326.8 | 46.2 | 700 | 345.1 | 46.4 |
| Weekends | 1121 | 805.0 | 101.3 | 711 | 785.8 | 121.9 | 562 | 832.4 | 116.0 | 1222 | 799.7 | 100.8 | 770 | 792.6 | 121.7 | 599 | 824.7 | 138.7 |
| Average daily minutes spent in light-intensity activity | ||||||||||||||||||
| Overall | 1224 | 284.2 | 59.7 | 904 | 269.4 | 78.6 | 871 | 224.7 | 83.6 | 1414 | 286.6 | 57.1 | 1004 | 261.1 | 83.8 | 1003 | 214.8 | 94.1 |
| School time | 1176 | 102.5 | 18.0 | 770 | 102.2 | 20.2 | 657 | 92.2 | 21.5 | 1367 | 103.6 | 18.3 | 852 | 100.6 | 21.9 | 703 | 88.6 | 25.0 |
| Weekdays after school | 1176 | 128.1 | 31.7 | 770 | 135.0 | 37.0 | 655 | 122.4 | 38.7 | 1367 | 129.2 | 32.6 | 851 | 129.6 | 38.5 | 700 | 114.1 | 40.7 |
| Weekends | 1121 | 240.2 | 93.6 | 711 | 250.6 | 113.3 | 562 | 207.4 | 114.6 | 1222 | 244.7 | 92.3 | 770 | 245.5 | 112.1 | 599 | 212.6 | 134.8 |
| Overall activity (average acceleration in milli-g) | ||||||||||||||||||
| Overall | 1176 | 42.7 | 13.2 | 770 | 43.6 | 14.1 | 657 | 37.6 | 12.7 | 1367 | 43.0 | 12.7 | 852 | 42.2 | 13.9 | 703 | 35.9 | 14.1 |
| School time | 1176 | 45.2 | 13.9 | 770 | 45.0 | 13.9 | 657 | 39.5 | 13.2 | 1367 | 45.3 | 13.5 | 852 | 43.7 | 14.8 | 703 | 36.9 | 14.0 |
| Weekdays after school | 1176 | 45.3 | 18.9 | 770 | 48.8 | 21.1 | 655 | 42.6 | 19.7 | 1367 | 44.7 | 17.7 | 851 | 45.9 | 20.8 | 700 | 38.4 | 19.2 |
| Weekends | 1121 | 34.4 | 17.8 | 711 | 37.5 | 22.1 | 562 | 28.6 | 18.5 | 1222 | 34.8 | 18.3 | 770 | 35.6 | 20.4 | 599 | 29.8 | 22.4 |
| Self-reported physical activity | 1311 | 16.8 | 15.0 | 1160 | 13.2 | 10.6 | 1020 | 11.6 | 10.6 | 1529 | 17.4 | 15.6 | 1267 | 14.2 | 11.3 | 1202 | 11.6 | 10.3 |
| Psychosocial | ||||||||||||||||||
| Physical activity self-efficacy score | 1302 | 2.7 | 1.1 | 1160 | 2.7 | 1.1 | 1012 | 2.9 | 1.2 | 1523 | 2.7 | 1.1 | 1267 | 2.8 | 1.2 | 1201 | 2.9 | 1.2 |
| Social support for physical activity score | 1304 | 2.1 | 0.6 | 1158 | 2.0 | 0.6 | 1009 | 1.8 | 0.6 | 1522 | 2.1 | 0.7 | 1264 | 2.0 | 0.7 | 1195 | 1.9 | 0.6 |
| Friendship quality score | 1305 | 2.0 | 0.6 | 1158 | 2.0 | 0.7 | 1009 | 2.1 | 0.7 | 1520 | 1.9 | 0.6 | 1265 | 2.0 | 0.6 | 1196 | 2.0 | 0.6 |
| Well-being score | 1303 | 3.5 | 0.7 | 1159 | 3.4 | 0.8 | 1010 | 3.3 | 0.8 | 1520 | 3.5 | 0.7 | 1265 | 3.4 | 0.8 | 1192 | 3.3 | 0.8 |
| Self esteem score | 1304 | 2.0 | 0.5 | 1158 | 2.1 | 0.6 | 1010 | 2.2 | 0.6 | 1522 | 2.0 | 0.5 | 1265 | 2.1 | 0.6 | 1192 | 2.1 | 0.6 |
| Anthropometry | ||||||||||||||||||
| BMI SDS | 1319 | 0.2 | 1.6 | NR | NR | NR | 990 | 0.2 | 1.7 | 1543 | 0.1 | 1.9 | NR | NR | NR | 1147 | 0.1 | 1.9 |
| Body fat (%) | 1267 | 20.7 | 10.0 | NR | NR | NR | 903 | 20.7 | 10.4 | 1460 | 20.9 | 9.9 | NR | NR | NR | 1022 | 20.6 | 10.3 |
| Waist circumference (cm) | 1313 | 70.0 | 9.6 | NR | NR | NR | 974 | 72.2 | 9.3 | 1534 | 70.4 | 9.7 | NR | NR | NR | 1119 | 72.5 | 8.9 |
| Accelerometer-assessed physical activity | Post intervention | ||||||
|---|---|---|---|---|---|---|---|
| Control | Intervention | Intervention vs. control | |||||
| Mean | SD | Mean | SD | Difference | 95% CI | Model n | |
| Average daily minutes of MVPA | |||||||
| Overall | –0.81 | 18.89 | –1.70 | 19.88 | –0.81 | –5.28 to 3.66 | 1908 |
| During school time | 0.22 | 6.16 | 0.16 | 7.22 | –0.11 | –1.94 to 1.73 | 1622 |
| During weekdays after school | 2.31 | 13.19 | 1.87 | 14.91 | –0.72 | –3.33 to 1.89 | 1621 |
| At weekends | 4.17 | 30.88 | 3.31 | 29.28 | –0.79 | –5.81 to 4.24 | 1481 |
| Average daily minutes of sedentary time | |||||||
| Overall | 6.34 | 70.27 | 16.17 | 74.01 | 8.34 | –6.44 to 23.13 | 1908 |
| During school time | –0.45 | 22.68 | 2.58 | 24.98 | 2.00 | –3.49 to 7.48 | 1622 |
| During weekdays after school | –8.76 | 42.04 | –2.74 | 44.02 | 5.46 | –4.81 to 15.72 | 1621 |
| At weekends | –14.51 | 134.20 | –3.43 | 128.46 | 3.98 | –10.17 to 18.13 | 1481 |
| Average daily minutes of light-intensity physical activity | |||||||
| Overall | –19.84 | 71.82 | –30.05 | 76.11 | –8.54 | –21.70 to 4.63 | 1908 |
| During school time | –0.41 | 19.12 | –3.63 | 21.17 | –2.12 | –6.17 to 1.93 | 1622 |
| During weekdays after school | 4.97 | 34.38 | –1.21 | 36.32 | –5.30 | –13.28 to 2.69 | 1621 |
| At weekends | 3.40 | 123.82 | –7.49 | 118.43 | –2.87 | –15.66 to 9.91 | 1481 |
| Average daily minutes of overall physical activity | |||||||
| Overall | 0.81 | 12.08 | –0.35 | 12.45 | –1.06 | –3.83 to 1.70 | 1622 |
| During school time | –0.36 | 12.52 | –1.08 | 13.82 | –0.82 | –4.13 to 2.49 | 1622 |
| During weekdays after school | 2.79 | 19.96 | 1.55 | 20.36 | –1.87 | –5.95 to 2.20 | 1621 |
| At weekends | 2.19 | 23.26 | 0.52 | 21.50 | –1.18 | –4.66 to 2.29 | 1481 |
| Accelerometer-assessed physical activity | 10-month follow-up | ||||||
|---|---|---|---|---|---|---|---|
| Control | Intervention | Intervention vs. control | |||||
| Mean | SD | Mean | SD | Difference | 95% CI | Model n | |
| Average daily minutes of MVPA | |||||||
| Overall | –8.26 | 19.33 | –10.44 | 22.75 | –1.91 | –5.53 to 1.70 | 1874 |
| During school time | –1.59 | 6.30 | –2.74 | 8.02 | –1.17 | –2.74 to 0.41 | 1360 |
| During weekdays after school | –0.37 | 14.04 | –2.71 | 16.10 | –2.43 | –4.96 to 0.11 | 1355 |
| At weekends | –5.25 | 26.44 | –2.73 | 32.19 | 2.96 | –1.05 to 6.96 | 1161 |
| Average daily minutes of sedentary time | |||||||
| Overall | 44.31 | 78.11 | 52.78 | 88.19 | 5.34 | –7.59 to 18.27 | 1874 |
| During school time | 10.30 | 23.60 | 16.14 | 29.55 | 5.14 | 0.82 to 9.46 | 1360 |
| During weekdays after school | 3.60 | 46.62 | 12.90 | 51.13 | 9.52 | 0.52 to 18.51 | 1355 |
| At weekends | 30.97 | 126.85 | 23.57 | 148.55 | –13.43 | –31.81 to 4.95 | 1161 |
| Average daily minutes of light-intensity physical activity | |||||||
| Overall | –62.87 | 82.82 | –73.35 | 93.02 | –9.46 | –23.35 to 4.44 | 1874 |
| During school time | –9.81 | 20.48 | –14.52 | 25.45 | –4.15 | –7.17 to –1.13 | 1360 |
| During weekdays after school | –6.76 | 39.22 | –13.94 | 42.03 | –7.62 | –13.72 to –1.52 | 1355 |
| At weekends | –40.12 | 121.98 | –34.71 | 139.19 | 11.86 | –3.39 to 27.11 | 1161 |
| Average daily minutes of overall physical activity | |||||||
| Overall | –4.29 | 11.92 | –6.37 | 15.33 | –1.94 | –4.94 to 1.06 | 1360 |
| During school time | –4.94 | 12.59 | –7.47 | 15.41 | –2.60 | –5.47 to 0.26 | 1360 |
| During weekdays after school | –1.93 | 20.18 | –5.55 | 22.73 | –3.99 | –7.83 to –0.15 | 1355 |
| At weekends | –5.73 | 20.52 | –4.14 | 24.63 | 2.29 | –0.66 to 5.24 | 1161 |
FIGURE 7.
10-month intervention effect on continuous secondary physical activity outcomes in minutes per day (acceleration in milli-g). a, For interpretation of sedentary time, please note that, in contrast to physical activity, higher levels are undesirable.
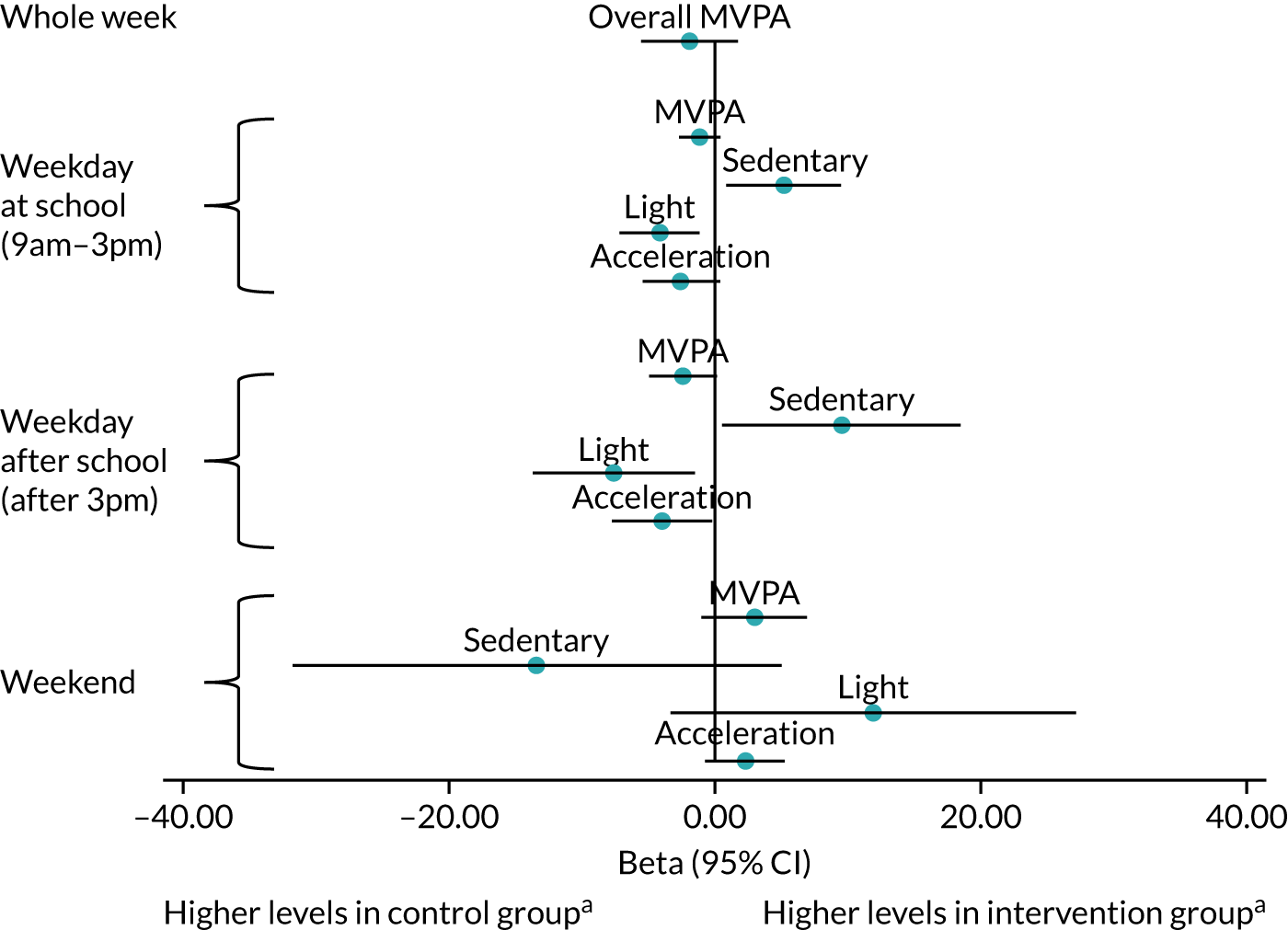
FIGURE 8.
Post-intervention effect on continuous secondary physical activity outcomes in minutes per day (acceleration in milli-g). a, For interpretation of sedentary time, please note that, in contrast to physical activity, higher levels are undesirable.
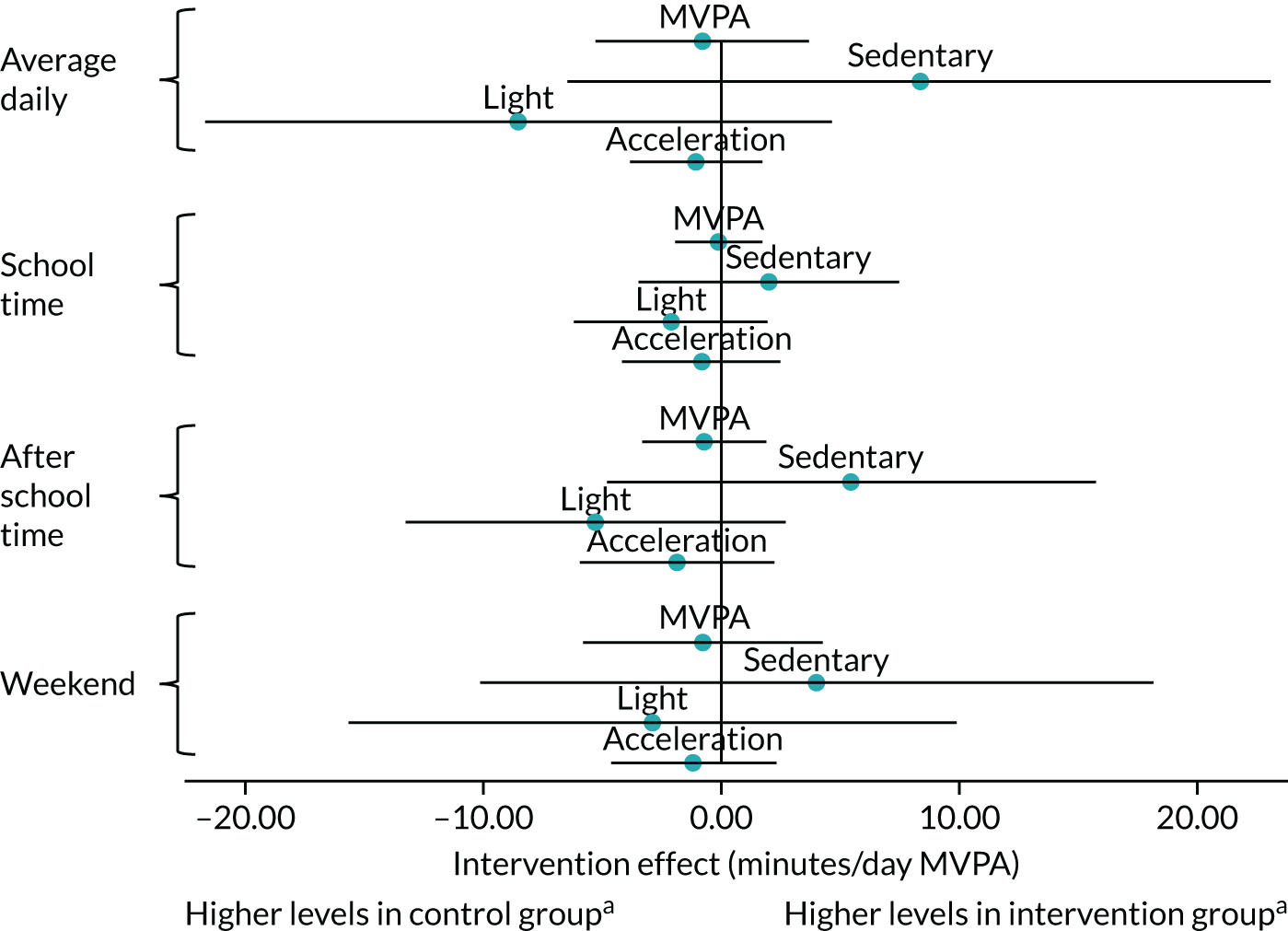
Self-reported physical activity declined over the duration of the study, whereas little change over time was observed for self-efficacy, social support, friendship quality, well-being and self-esteem (see Table 11). Overall, the intervention did not affect self-reported outcomes (including the assessment of harm assessed using well-being) or anthropometry, with the exception of higher self-efficacy among intervention participants post intervention (Table 14).
| Outcome | Control | Intervention | Intervention vs. control | ||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Difference | 95% CI | Model n | |
| Post intervention | |||||||
| Self-reported physical activity | –3.46 | 13.88 | –3.43 | 13.47 | 0.62 | –0.15 to 1.38 | 2427 |
| Psychosocial | |||||||
| Physical activity self-efficacy | 0.04 | 0.95 | 0.16 | 0.97 | 0.12 | 0.02 to 0.23 | 2427 |
| Social support for physical activity | –0.12 | 0.55 | –0.13 | 0.56 | 0.00 | –0.06 to 0.06 | 2422 |
| Friendship quality | 0.07 | 0.62 | 0.09 | 0.57 | 0.00 | –0.05 to 0.05 | 2423 |
| Well-being | –0.02 | 0.72 | –0.09 | 0.74 | –0.04 | –0.11 to 0.02 | 2424 |
| Self-esteem | 0.01 | 0.46 | 0.03 | 0.48 | 0.02 | –0.02 to 0.06 | 2423 |
| 10-month follow-up | |||||||
| Self-reported physical activity | –5.10 | 15.60 | –5.42 | 15.37 | 0.06 | –1.03 to 1.15 | 2222 |
| Psychosocial | |||||||
| Physical activity self-efficacy | 0.17 | 1.12 | 0.24 | 1.06 | 0.05 | –0.03 to 0.14 | 2213 |
| Social support for physical activity | –0.22 | 0.59 | –0.22 | 0.60 | 0.02 | –0.04 to 0.09 | 2204 |
| Friendship quality | 0.11 | 0.71 | 0.09 | 0.61 | –0.04 | –0.14 to 0.06 | 2205 |
| Well-being | –0.20 | 0.83 | –0.19 | 0.78 | 0.03 | –0.07 to 0.13 | 2202 |
| Self-esteem | 0.11 | 0.55 | 0.08 | 0.51 | –0.03 | –0.10 to 0.05 | 2202 |
| Anthropometry | |||||||
| BMI SDS | 0.05 | 0.49 | 0.05 | 0.51 | 0.01 | –0.05 to 0.07 | 2089 |
| Body fat (%) | 0.01 | 4.56 | 0.30 | 4.48 | 0.26 | –0.94 to 1.46 | 1925 |
| Waist circumference (cm) | 2.41 | 4.91 | 2.86 | 4.57 | 0.48 | –0.19 to 1.15 | 2093 |
Intervention effect is the difference in mean change (baseline to post intervention, or baseline to 10-month follow-up) in outcome (adjusted for baseline) between the intervention and control groups. Difference is estimated from a linear regression model, including parameters for randomised group (i.e. control, intervention), baseline value of the outcome (i.e. ANCOVA), pupil premium (i.e. low, high) and county (i.e. Cambridgeshire, Essex). Robust SEs were calculated to allow for the non-independence of individuals within schools. Missing indicator method is used to enable participants with a missing baseline value of the outcome to be included in the analysis. Participants with a missing value of the outcome at the relevant follow-up visit (either post intervention or at 10-month follow-up) are excluded from this analysis. Anthropometry was not assessed post intervention.
Per-protocol and sensitivity analyses
Only 382 intervention group participants (24.8% of those recruited at baseline and randomised to the intervention) met the criteria for inclusion in the per-protocol analysis. The results of the per-protocol analysis did not differ from those of the complete-case analysis (Table 15). Post hoc sensitivity analyses indicated that results were unaffected by participants with missing data (see Appendix 5) or different approaches to data processing decisions (Table 16).
| Control | Intervention | Intervention vs. control: difference (95% CI) | |||||
|---|---|---|---|---|---|---|---|
| Baseline | 10-month follow-up | Change from baseline | Baseline | 10-month follow-up | Change from baseline | ||
| Participants included in analyses (n) | 1224 | 871 | 365 | 285 | |||
| Mean (SD) | 35.6 (18.9) | 27.6 (20.6) | –8.3 (19.3) | 36.9 (19.1) | 25.9 (20.7) | –11.1 (23.3) | –1.87 (–6.80 to 3.06) |
| Control | Intervention | Intervention vs. control: difference (95% CI) | |||||
|---|---|---|---|---|---|---|---|
| Baseline | 10-month follow-up | Change from baseline | Baseline | 10-month follow-up | Change from baseline | ||
| Night-time excluded from pre processing | |||||||
| Participants included in analyses (n) | 1176 | 657 | 1367 | 703 | 1360 | ||
| Mean (SD) | 37.1 (19.9) | 31.9 (19.3) | –4.1 (17.3) | 37.3 (19.5) | 29.7 (22.0) | –6.7 (23.4) | –2.52 (–7.33 to 2.29) |
| Using 12 hours of wear per quadrant | |||||||
| Participants included in analyses (n) | 1097 | 537 | 1262 | 535 | 1072 | ||
| Mean (SD) | 36.8 (19.2) | 31.8 (18.2) | –3.4 (15.4) | 36.9 (18.9) | 31.5 (22.2) | –3.4 (21.4) | –0.15 (–5.25 to 4.95) |
Adverse events
One participant (in the intervention group) reported an unrelated hospital admission during the baseline measurement period.
Effect modification
Main outcome
Tests for effect modification indicated differences in the effect of the intervention between subgroups, in particular between boys and girls, and between high and medium/low socioeconomic status (Table 17 and Figure 6). The results of the subgroup analyses suggested a negative intervention effect among boys and a positive intervention effect for those with low and medium socioeconomic status. However, the subgroup results are inconclusive, as the CIs included zero (Table 18).
| Interaction between randomised group and . . . | Estimate | 95% CI | p-value |
|---|---|---|---|
| Gender (boys vs. girls) | –2.97 | –5.24 to –0.70 | 0.022 |
| Socioeconomic status (medium/low vs. high) | –6.89 | –11.04 to –2.74 | 0.005 |
| Ethnicity (white vs. any other ethnicity) | –1.81 | –5.33 to 1.71 | 0.330 |
| Baseline physical activity (≥ 60 minutes average daily MVPA vs. < 60 minutes) | –6.04 | –17.52 to 5.43 | 0.318 |
| Weight status (with underweight/normal weight vs. with overweight/obesity) | 4.64 | –0.15 to 9.43 | 0.077 |
| Effect modifier | Control | Intervention | Intervention vs. control | ||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Difference | 95% CI | ||
| Gender | |||||||
| Boys | –10.15 | 22.30 | –13.77 | 24.94 | –3.44 | –7.42 | 0.54 |
| Girls | –6.43 | 15.75 | –7.20 | 19.88 | –0.20 | –3.56 | 3.16 |
| Socioeconomic status | |||||||
| Medium/low | –10.07 | 18.46 | –2.71 | 21.67 | 4.25 | –0.66 | 9.16 |
| High | –8.04 | 19.47 | –11.54 | 22.79 | –2.72 | –6.33 | 0.89 |
| Ethnicity | |||||||
| White | –4.62 | 19.04 | –8.07 | 24.83 | –1.08 | –5.06 | 2.89 |
| Any other ethnicity | –8.66 | 19.39 | –10.91 | 22.46 | –2.18 | –5.97 | 1.62 |
| Baseline physical activity | |||||||
| ≥ 60 minutes average daily MVPA | –5.92 | 16.25 | –7.83 | 20.11 | –1.45 | –4.77 | 1.87 |
| < 60 minutes average daily MVPA | –29.10 | 29.59 | –36.08 | 30.19 | –6.51 | –16.40 | 3.37 |
| Weight status | |||||||
| Underweight/normal weight | –8.58 | 20.30 | –11.58 | 22.30 | –3.14 | –7.02 | 0.74 |
| Overweight/obese | –7.39 | 16.43 | –7.42 | 23.66 | 0.99 | –3.80 | 5.79 |
Secondary accelerometry outcomes
In addition to indications of differential effectiveness by demographic characteristics, analyses of the secondary accelerometer-assessed outcomes also showed some suggestion of temporal patterning of effectiveness, with changes on weekdays (both during and after school) generally favouring the control participants, with the reverse on weekend days (see Figures 7 and 8). To examine these distributions of effect across time and subgroups in more detail, we explored potential differential effects of the GoActive intervention on accelerometer-assessed outcomes across the week by subgroups for SEP, weight status, ethnicity, baseline activity level and gender.
Moderate-to-vigorous physical activity
No differences in effect on MVPA were observed by ethnicity or baseline activity level (Table 19). The long-term effects on MVPA were generally more negative for boys than for girls. Although a statistically significant difference in effect between boys and girls was observed for school-based MVPA at 10-month follow-up, the stratified results revealed small and non-significant effects in both genders.
| Moderatora | Whole week | School | After school | Weekend | ||||
|---|---|---|---|---|---|---|---|---|
| Post intervention | 10-month follow-up | Post intervention | 10-month follow-up | Post intervention | 10-month follow-up | Post intervention | 10-month follow-up | |
| Gender | –0.60 (–4.38 to 3.18) | –2.97 (–5.24 to –0.70) | –0.45 (–1.98 to 1.09) | –1.28 (–2.52 to –0.05) | 0.21 (–3.16 to 3.58) | –1.65 (–4.14 to 0.84) | 3.33 (–6.52 to 13.18) | –6.87 (–15.7 to 1.96) |
| SEP | –4.81 (–10.1 to 0.45) | –6.89 (–11.04 to –2.74) | –1.06 (–2.51 to 0.39) | –2.68 (–4.45 to –0.91) | –2.46 (–5.32 to 0.40) | –4.31 (–6.97 to –1.66) | –4.11 (–11.35 to 3.13) | –5.49 (–13.72 to 2.74) |
| Ethnicity | 2.87 (–4.05 to 9.79) | –1.81 (–5.33 to 1.71) | 1.75 (–1.50 to 5.00) | –0.07 (–2.55 to 2.42) | 3.98 (–2.09 to 10.05) | –0.99 (–6.50 to 4.52) | 0.10 (–9.10 to 9.31) | 0.35 (–8.03 to 8.73) |
| Baseline MVPA ≥ 30 minutes | 0.60 (–4.20 to 5.40) | –2.41 (–7.08 to 2.27) | 0.21 (–1.00 to 1.41) | –1.34 (–3.24 to 0.56) | 0.01 (–3.39 to 3.40) | –2.23 (–6.45 to 1.99) | –1.42 (–8.19: 5.35) | –0.85 (–6.45 to 4.75) |
| Baseline MVPA ≥ 60 minutes | 2.14 (–7.54 to 11.82) | –6.04 (–17.52 to 5.43) | 1.32 (–1.59 to 4.24) | –2.17 (–7.27 to 2.93) | 2.34 (–3.9 to 8.68) | –6.00 (–14.32 to 2.31) | –7.57 (–28.98 to 13.85) | –4.61 (–17.05 to 7.83) |
| Weight status | 4.81 (0.53 to 9.09) | 4.64 (–0.15 to 9.43) | 1.75 (0.33 to 3.17) | 2.50 (0.47 to 4.53) | 4.52 (1.50 to 7.54) | 3.94 (–0.25 to 8.12) | 6.74 (0.41 to 13.08) | 0.64 (–7.35 to 8.63) |
Across all MVPA outcomes, those from high SEP backgrounds appeared to have benefited least. This difference in effect was statistically significant at 10-month follow-up both in and out of school. Stratified analyses for both settings showed statistically significant negative intervention effects for participants from high SEP backgrounds and no evidence of intervention effect in participants from low/medium SEP backgrounds.
Finally, participants with overweight or obesity at baseline appeared to have consistently benefited more from the intervention than those with underweight or normal weight. Stratified results revealed that this difference in effect was largely because of small negative effects in participants with underweight or normal weight, and moderate positive effects in those with overweight or obesity, particularly after school and at weekends at post intervention.
Light physical activity
The results revealed limited evidence for differential intervention effect on LPA across time points and time of the week (Table 20). Notably, participants from other ethnic backgrounds had a 22.91-minute larger negative effect on overall LPA at 10-month follow-up than those of white ethnic background. Stratified results showed a strong negative intervention effect for those of other ethnic backgrounds (–31.81 minutes, 95% CI –52.72 to –10.90 minutes), with a smaller negative effect in white participants (–7.13 minutes, 95% CI –22.77 to 8.51 minutes).
| Moderatora | Whole week | School | After school | Weekend | ||||
|---|---|---|---|---|---|---|---|---|
| Post intervention | 10-month follow-up | Post intervention | 10-month follow-up | Post intervention | 10-month follow-up | Post intervention | 10-month follow-up | |
| Gender | 8.06 (–9.50 to 25.62) | 5.55 (–11.68 to 22.77) | 1.28 (–3.92 to 6.47) | 0.01 (–3.63 to 7.59) | 4.18 (–3.29 to 11.65) | 5.28 (–2.50 to 13.05) | 16.25 (–14.19 to 46.69) | –5.70 (–53.16 to 41.75) |
| SEP | –17.76 (–36.41 to 0.89) | –6.15 (–28.23 to 15.94) | –1.16 (–4.91 to 2.59) | –4.67 (–10.24 to 0.92) | –4.45 (–10.86 to 1.97) | –7.19 (–17.68 to 3.30) | –20.14 (–45.20 to 4.92) | 3.91 (–24.08 to 31.9) |
| Ethnicity | –8.16 (–35.78 to 19.47) | –22.91 (–44.37 to –1.45) | 1.53 (–6.34 to 9.40) | –4.04 (–12.69 to 4.60) | 6.33 (–10.43 to 23.1) | –2.91 (–19.95 to 14.13) | –8.10 (–28.76 to 12.57) | –31.34 (–85.28 to 22.59) |
| Baseline MVPA ≥ 30 minutes | 12.71 (–2.84 to 28.26) | 8.21 (–13.22 to 29.64) | 2.69 (–1.16 to 6.53) | –0.81 (–5.57 to 3.95) | 1.98 (–3.21 to 7.17) | –0.10 (–10.89 to 10.69) | 15.81 (–8.34 to 39.96) | 12.60 (–22.65 to 47.85) |
| Baseline MVPA ≥ 60 minutes | 1.98 (–25.11 to 29.08) | –12.54 (–40.42 to 15.34) | 1.55 (–7.29 to 10.38) | 0.26 (–10.37 to 10.89) | 1.70 (–13.66 to 17.06) | 3.29 (–7.66 to 14.24) | 14.00 (–28.75 to 56.76) | –2.40 (–65.27 to 60.46) |
| Weight status | 12.30 (–4.05 to 28.64) | 4.57 (–19.51 to 28.64) | 2.29 (–2.65 to 7.23) | 3.95 (–2.62 to 10.53) | 3.84 (–4.51 to 12.20) | 6.77 (–5.14 to 18.68) | 4.21 (–32.71 to 41.13) | 0.86 (–38.02 to 39.73) |
Sedentary time
No differential intervention effects on time spent sedentary were identified for gender, ethnicity, weight status and baseline activity level (Table 21). However, participants from high SEP backgrounds had a fall in sedentary time on weekdays and those from low/medium SEP backgrounds did not. Stratified analyses of the statistically significant interaction for school-based time spent sedentary at post intervention revealed a strong positive intervention effect for those from high SEP (8.66, 95% CI 3.64 to 13.68), but no effect in participants from low/medium SEP backgrounds (1.60, 95% CI –3.85 to 7.06). Similarly, a strong positive intervention effect was observed for those from high SEP for time spent sedentary outside school at 10-month follow-up (15.6, 95% CI 3.4 to 27.8), but not for those from low/medium SEP (4.0, 95% CI –5.1 to 13.09).
| Moderatora | Whole week | School | After school | Weekend | ||||
|---|---|---|---|---|---|---|---|---|
| Post intervention | 10-month follow-up | Post intervention | 10-month follow-up | Post intervention | 10-month follow-up | Post intervention | 10-month follow-up | |
| Gender | –3.70 (–20.63 to 13.23) | 1.40 (–12.93 to 15.74) | 0.02 (–6.17 to 6.20) | –0.27 (–6.46 to 5.91) | –4.10 (–14.03 to 5.83) | –0.29 (–10.22 to 9.63) | –16.70 (–57.51 to 24.11) | 16.22 (–24.56 to 67.00) |
| SEP | 14.66 (–3.12 to 32.43) | 12.49 (–5.18 to 30.15) | 7.32 (0.87 to 13.77) | 2.05 (–2.89 to 7.00) | 6.28 (–2.39 to 14.95) | 11.94 (2.57 to 21.31) | 19.49 (–8.68 to 47.66) | –1.36 (–29.70 to 26.97) |
| Ethnicity | –4.40 (–26.22 to 25.33) | 1.84 (19.85 to 23.54) | 3.90 (–6.22 to 14.01) | –3.56 (–13.94 to 6.82) | –10.66 (–32.84 to 11.52) | 3.35 (–15.75 to 22.45) | 6.72 (–19.91 to 33.35) | 21.89 (–23.52 to 67.3) |
| Baseline MVPA ≥ 30 minutes | –12.34 (–28.35 to 3.68) | –3.34 (–22.03 to 15.36) | 2.12 (–3.37 to 7.61) | –2.79 (–7.20 to 1.63) | –1.88 (–9.11 to 5.35) | 3.29 (–10.05 to 16.64) | –11.74 (–42.03 to 18.55) | –15.38 (–50.63 to 19.88) |
| Baseline MVPA ≥ 60 minutes | –1.86 (–31.32 to 27.59) | 14.88 (–16.75 to 46.51) | 1.48 (–12.22 to 15.17) | –2.83 (–13.24 to 7.58) | –3.28 (–23.22 to 16.66) | 2.01 (–14.92 to 18.94) | –15.64 (–74.40 to 43.12) | –0.23 (–70.91 to 70.45) |
| Weight status | –13.81 (–28.28 to 0.66) | –10.64 (–27.01 to 5.73) | –4.08 (–9.73 to 1.56) | –6.46 (–14.08 to 1.16) | –8.03 (–18.03 to 1.96) | –11.28 (–24.83 to 2.27) | –9.92 (–45.88 to 26.04) | –3.73 (–40.45 to 32.99) |
Effects on mental well-being
The GoActive intervention provides an opportunity to investigate the impact of a school-based physical activity intervention on the mental health status of adolescents. The likelihood of GoActive reaching mental health domains, we propose, is likely to be greater than that of previous physical activity interventions that do not incorporate multidisciplinary techniques and focus primarily on physiological aspects of physical activity. The intervention used co-design methods, involving young people and other school key informants, which are potential enablers of improved mental health and well-being outcomes. Additionally, we propose that the unique design of the GoActive intervention, with the focus on psychosocial support, may have an impact on subgroups and this warrants specific exploration. Based on the above evidence, we sought to examine whether or not the GoActive intervention had an impact on mental well-being outcomes and whether or not specific outcomes differed by gender, SEP and weight status.
The final included sample in this subanalysis included those with complete baseline and 10-month follow-up mental well-being, baseline demographic (i.e. gender, age, ethnicity, school SEP) and study design (i.e. school randomisation identifier, study condition) data (n = 2068) (see Table 19). Excluded participants (n = 977), compared with included participants, were more likely to be from low SEP schools (56% vs. 46%, respectively; p = 0.000), identify as non-white compared with white ethnicity (17% vs. 14%, respectively; p = 0.047) and have higher standardised BMI scores at baseline (0.44 vs. 0.33, respectively; p = 0.037). Tables 22 and 23 show the participant characteristics. Briefly, half (49%) of the participating sample were female and three-quarters (77%) were aged 13 years at baseline. The proportion of participants from low and high SEP schools was similar (46% vs. 54%, respectively). Overweight/obesity was observed in one-quarter (28%) of the included sample.
| Demographic | Control | Intervention | Total |
|---|---|---|---|
| Participants, n (%) | 945 (45.7) | 1123 (54.3) | 2068 |
| Gender, n (%) | |||
| Male | 485 (51.3) | 581 (51.7) | 1066 (51.6) |
| Female | 460 (48.7) | 542 (48.3) | 1002 (48.5) |
| Age at baseline (years), n (%) | |||
| 13 | 722 (76.4) | 872 (77.5) | 1593 (77.0) |
| 14 | 223 (23.6) | 252 (22.5) | 475 (23.0) |
| School socioeconomic status, n (%) | |||
| Low | 452 (47.8) | 491 (43.7) | 943 (45.6) |
| High | 493 (52.2) | 632 (56.3) | 1125 (54.4) |
| Weight, n (%) | |||
| Underweight/normal weight | 676 (72.1) | 798 (72.4 | 1474 (72.3) |
| Overweight/obese | 262 (27.9) | 304 (27.6) | 566 (27.8) |
| Warwick–Edinburgh Mental Wellbeing Scale, mean (SD) | |||
| Baseline | 48.7 (9.2) | 49.4 (9.4) | 49.1 (9.3) |
| Follow-up | 45.7 (11.8) | 46.6 (11.1) | 46.2 (11.4) |
| Subgroup | Time point | Total score, mean (SD) | ||
|---|---|---|---|---|
| Control | Intervention | Total | ||
| Gender | ||||
| Male | Baseline | 50.3 (8.9) | 51.3 (9.1) | 50.9 (9.1) |
| Follow-up | 47.5 (12.2) | 48.6 (11.8) | 48.1 (12.0) | |
| Female | Baseline | 47.0 (9.3) | 47.3 (9.3) | 47.1 (9.3) |
| Follow-up | 43.9 (11.1) | 44.5 (9.9) | 44.2 (10.4) | |
| School SEP | ||||
| Low | Baseline | 48.3 (10.0) | 49.0 (9.7) | 48.7 (9.9) |
| Follow-up | 44.4 (12.4) | 46.9 (11.3) | 45.7 (11.9) | |
| High | Baseline | 49.0 (8.5) | 49.6 (9.2) | 49.3 (8.9) |
| Follow-up | 46.9 (11.2) | 46.4 (10.9) | 46.6 (11.0) | |
| Weight status | ||||
| Healthy weight | Baseline | 49.1 (9.5) | 49.5 (9.3) | 49.3 (9.4) |
| Follow-up | 46.2 (11.7) | 46.7 (10.8) | 46.5 (11.2) | |
| Overweight/obesity | Baseline | 47.7 (8.6) | 49.3 (9.9) | 48.5 (9.3) |
| Follow-up | 44.5 (12.1) | 46.6 (11.9) | 45.6 (12.0) | |
Table 24 reports the intervention effects for well-being. As described for the full sample, the intervention did not have an impact on mental well-being, and the non-significant interaction terms with gender and weight status indicated that this was similar for boys and girls, and for participants with different weight status at baseline. The interaction term for SEP showed that the intervention had a positive effect on students’ mental well-being in lower SEP schools (β = 3.01, 95% CI 0.22 to 5.81; p = 0.036) compared with students’ mental well-being in higher SEP schools (Figure 9).
| Exposure variables | β | 95% CI | p-value |
|---|---|---|---|
| Overall | |||
| Study conditiona | 0.54 | –1.18 to 2.27 | 0.510 |
| Subgroup | |||
| Genderb | |||
| Study condition × gender | –0.18 | –2.08 to 1.71 | 0.839 |
| School SEPc | |||
| Study condition × school SEP | 3.01 | 0.22 to 5.81 | 0.036 |
| Weight statusd | |||
| Study condition × weight status | 0.96 | –1.09 to 3.01 | 0.334 |
FIGURE 9.
Mental well-being change by condition, school and SEP.
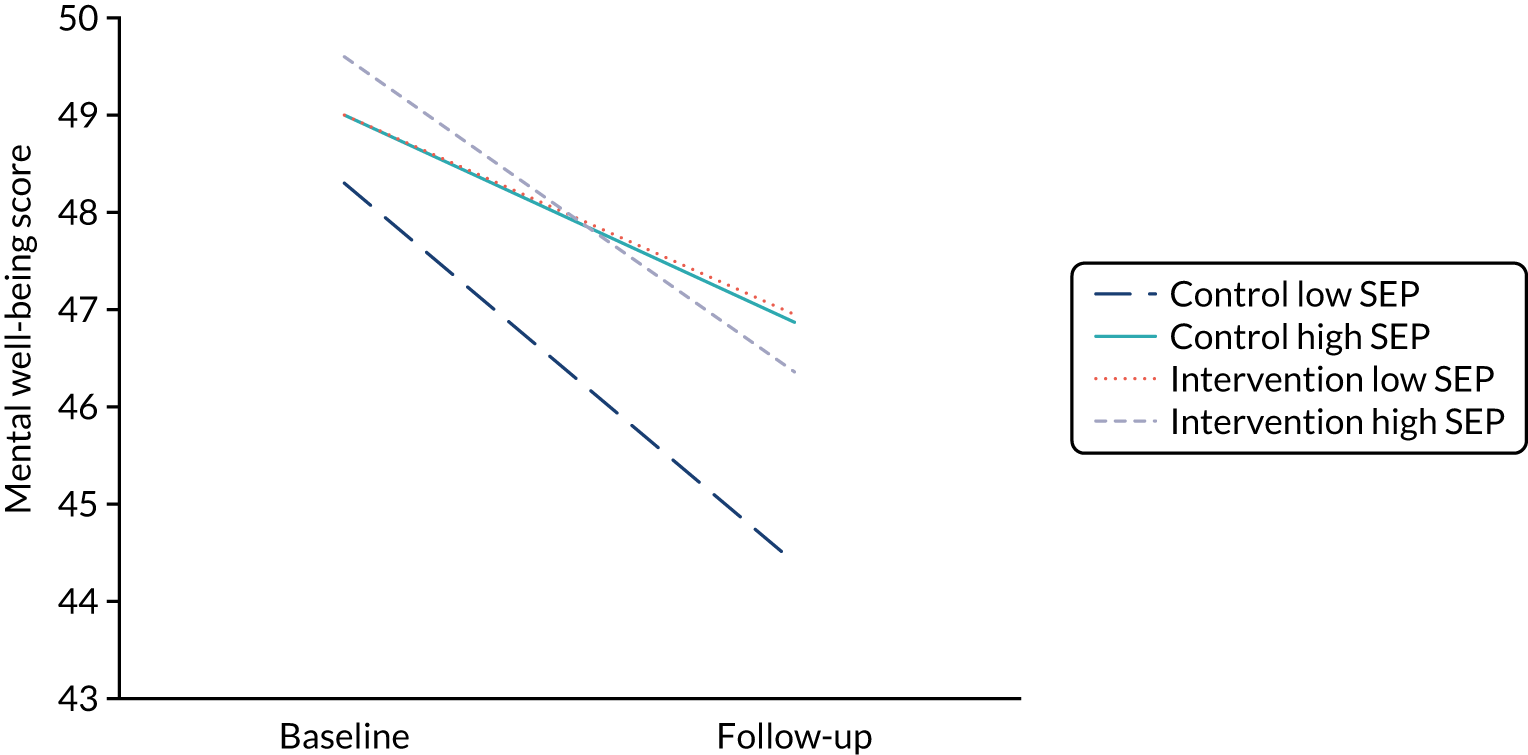
Mediation analysis
Table 25 shows the descriptive characteristics of participants included in the mediation analysis. Table 26 shows the associations between each exposure (i.e. intervention component) and potential mediator individually and with both outcomes (i.e. average daily MVPA and mental well-being). Associations between intervention components and potential mediators are shown in Table 27. Although perceived teacher support and perception of rewards were directly positively associated with MVPA among boys, no potential mediators were associated with MVPA. Among girls, no exposures or potential mediators were associated with MVPA. Various intervention components and proposed mediators were associated with increased well-being. The variables that were identified differed for boys and girls.
| Descriptive characteristic | Boys (n = 360) | Girls (n = 311) | p-value for gender difference |
|---|---|---|---|
| Baseline age (years), mean (SD) | 13.23 (0.42) | 13.24 (0.43) | 0.966 |
| BMI z-score, mean (SD) | 0.19 (1.25) | 0.38 (1.15) | 0.077 |
| Language (English only), % | 91.64 | 93.06 | 0.490 |
| Ethnicity (white), % | 84.89 | 87.50 | 0.327 |
| Outcome, mean (SD) | |||
| MVPA change (minutes/day) | –1.98 (23.40) | –1.55 (17.04) | 0.901 |
| Well-being change (score) | –0.03 (0.79) | –0.11 (0.72) | 0.146 |
| Exposure | |||
| Perceived teacher support (score), mean (SD) | 2.47 (0.93) | 2.58 (0.91) | 0.113 |
| Perceived mentor support (score), mean (SD) | 2.61 (0.83) | 2.80 (0.77) | 0.002 |
| Web-based points entered (% entering scores) | 52.73 | 48.89 | 0.321 |
| Perceived peer leaders support (score), mean (SD) | 0.47 (0.50) | 0.36 (0.48) | 0.006 |
| Rewards, mean (SD) | 3.53 (1.17) | 3.76 (1.35) | 0.024 |
| Competition, mean (SD) | 3.40 (1.07) | 3.42 (1.25) | 0.745 |
| Class sessions, mean (SD) | 3.42 (1.16) | 3.42 (1.24) | 0.462 |
| Potential mediator, mean (SD) | |||
| Self-efficacy change (score) | –0.09 (0.91) | –0.10 (0.87) | 0.955 |
| Self-esteem change (score) | –0.02 (0.50) | –0.06 (0.45) | 0.108 |
| Social support change (score) | –0.11 (0.55) | –0.12 (0.46) | 0.629 |
| Group cohesion in-degree | –0.16 (1.37) | –0.28 (1.30) | 0.159 |
| Group cohesion out-degree | –0.05 (1.44) | –0.03 (1.24) | 0.883 |
| Friendship quality change (score) | –0.23 (0.55) | –0.21 (0.55) | 0.990 |
| Perception of intervention component | Boys | Girls | ||
|---|---|---|---|---|
| Physical activity | Well-being | Physical activity | Well-being | |
| Teacher support | 2.93 (0.31 to 5.54) | 0.08 (0.01 to 0.16) | –0.50 (–2.41 to 1.43) | 0.06 (–0.02 to 0.14) |
| Mentor support | 1.47 (–1.51 to 4.45) | 0.14 (0.03 to 0.23) | 0.31 (–1.87 to 2.50) | 0.11 (0.02 to 0.20) |
| Class sessions | 1.83 (–0.31 to 3.96) | 0.10 (0.03 to 0.18) | 0.20 (–1.18 to 1.57) | 0.04 (–0.02 to 0.05) |
| Peer leadership | –4.42 (–9.25 to 0.41) | 0.11 (–0.04 to 0.25) | –0.91 (–4.56 to 2.74) | –0.09 (–0.23 to 0.06) |
| Rewards | 2.53 (0.35 to 4.71) | 0.07 (0.01 to 0.14) | 0.35 (–0.97 to 1.67) | 0.10 (0.05 to 0.15) |
| Competition | 1.26 (–1.16 to 3.67) | 0.06 (–0.02 to 0.14) | 0.53 (–0.87 to 1.92) | 0.13 (0.07 to 0.18) |
| Online intervention component | ||||
| Web-based points | –0.04 (–4.79 to 4.71) | 0.06 (–0.09 to 0.20) | –1.74 (–5.15 to 1.67) | 0.06 (–0.07 to 0.19) |
| Potential mediator | ||||
| Self-efficacy | –1.10 (–3.94 to 1.75) | 0.08 (–0.01 to 0.16) | 1.75 (–0.32 to 3.82) | 0.20 (0.12 to 0.28) |
| Self-esteem | 4.19 (–1.25 to 9.63) | 0.66 (0.51 to 0.80 | 1.22 (–2.71 to 5.15) | 0.95 (0.83 to 1.08) |
| Social support | –2.90 (–7.51 to 1.71) | 0.43 (0.29 to 0.56) | 1.25 (–2.47 to 4.98) | 0.28 (0.14 to 0.42) |
| Friendship quality | 4.86 (–0.05 to 9.76) | 0.42 (0.28 to 0.57) | 2.29 (–1.19 to 5.78) | 0.66 (0.53 to 0.78) |
| Group cohesion in-degree | 0.65 (–1.42 to 2.71) | –0.01 (–0.08 to 0.07) | 0.08 (–1.44 to 1.60) | –0.01 (–0.07 to 0.06) |
| Group cohesion out-degree | –0.87 (–3.00 to 1.26) | 0.04 (–0.03 to 0.12) | –0.38 (–2.08 to 1.33) | 0.04 (–0.03 to 0.11) |
| Intervention component | Self-efficacy | Self-esteem | Social support | Friendship quality | Group cohesion in-degree | Group cohesion out-degree |
|---|---|---|---|---|---|---|
| Boys | ||||||
| Teacher support | 0.12 (0.01 to 0.22) | 0.02 (–0.04 to 0.07) | 0.09 (0.03 to 0.15) | 0.00 (–0.05 to 0.06) | –0.14 (–0.29 to 0.01) | 0.01 (–0.14 to 0.15) |
| Mentor support | 0.15 (0.04 to 0.27) | 0.07 (0.01 to 0.13) | 0.14 (0.07 to 0.21) | 0.06 (–0.01 to 0.13) | –0.09 (–0.26 to 0.09) | 0.12 (–0.05 to 0.28) |
| Class sessions | 0.02 (–0.07 to 0.11) | 0.05 (0.01 to 0.10) | 0.05 (0.01 to 0.10) | 0.09 (0.04 to 0.13) | 0.01 (–0.12 to 0.13) | 0.20 (0.08 to 0.31) |
| Peer leadership | 0.15 (–0.05 to 0.34) | –0.08 (–0.18 to 0.02) | 0.06 (–0.05 to 0.17) | –0.04 (–0.15 to 0.08) | –0.22 (–0.50 to 0.53) | 0.14 (–0.14 to 0.41) |
| Rewards | 0.06 (–0.03 to 0.14) | 0.01 (–0.04 to 0.06) | 0.04 (–0.01 to 0.09) | 0.04 (–0.02 to 0.09) | –0.07 (–0.21 to 0.08) | 0.01 (–0.15 to 0.16) |
| Competition | 0.02 (–0.07 to 0.12) | –0.02 (–0.07 to 0.03) | 0.04 (–0.02 to 0.10) | 0.04 (–0.01 to 0.08) | –0.14 (–0.29 to 0.02) | –0.02 (–0.19 to 0.14) |
| Web-based points | 0.11 (–0.09 to 0.31) | –0.03 (–0.13 to 0.07) | 0.06 (–0.05 to 0.17) | –0.04 (–0.15 to 0.07) | 0.25 (–0.02 to 0.52) | 0.32 (0.06 to 0.58) |
| Girls | ||||||
| Teacher support | 0.06 (–0.03 to 0.16) | 0.04 (–0.01 to 0.09) | 0.03 (–0.01 to 0.08) | 0.05 (–0.01 to 0.11) | –0.16 (–0.02 to –0.29) | –0.05 (–0.17 to 0.06) |
| Mentor support | 0.10 (–0.01 to 0.20) | 0.11 (0.05 to 0.17) | 0.06 (0.01 to 0.12) | –0.01 (–0.08 to 0.06) | –0.21 (–0.04 to –0.37) | –0.01 (–0.16 to 0.14) |
| Class sessions | 0.05 (–0.02 to 0.12) | 0.07 (0.03 to 0.10) | 0.06 (0.02 to 0.10) | 0.05 (0.01 to 0.09) | 0.03 (–0.07 to 0.13) | 0.04 (–0.05 to 0.13) |
| Peer leadership | 0.04 (–0.14 to 0.22) | –0.01 (–0.10 to 0.09) | 0.00 (–0.10 to 0.10) | –0.02 (–0.13 to 0.09) | –0.16 (–0.43 to 0.11) | –0.07 (–0.31 to 0.17) |
| Rewards | 0.10 (0.03 to 0.16) | 0.08 (0.04 to 0.11) | 0.04 (0.01 to 0.07) | 0.04 (0.01 to 0.08) | –0.07 (–0.17 to 0.04) | 0.06 (–0.04 to 0.16) |
| Competition | 0.10 (0.03 to 0.17) | 0.10 (0.06 to 0.13) | 0.04 (0.01 to 0.08) | 0.03 (–0.02 to 0.09) | –0.04 (–0.15 to 0.08) | 0.12 (0.01 to 0.23) |
| Web-based points | 0.12 (–0.04 to 0.28) | 0.00 (–0.09 to 0.09) | 0.01 (–0.11 to 0.08) | 0.02 (–0.08 to 0.12) | –0.06 (–0.30 to 0.19) | 0.01 (–0.21 to 0.23) |
Results of mediation models are displayed in Figures 10–13. Among boys, higher perceived teacher support was associated with increased well-being via increased social support (see Figure 10). In addition, higher perceived mentor support was associated with increased well-being via increases in social support, self-esteem and self-efficacy (see Figure 10). For boys, a higher perception of class-based activity sessions was associated with increased well-being via self-esteem, social support and friendship quality (see Figure 11). Among girls, higher perception of mentor support was positively associated with increased well-being via increased self-esteem and increased social support (see Figure 12). Perception of both competition and rewards was associated with increased well-being via self-efficacy, self-esteem and social support, but only among girls (see Figure 13).
FIGURE 10.
Mediation models of potential psychological mediators in the association between perceived support and well-being among boys: (a) model A; (b) model B; and (c) model C. Adjusted for age, ethnicity, language, school, BMI z-score and baseline values of change variables. E-value estimates (in relative risk): model A, 1.26; model B, 1.33; and model C, 1.39.
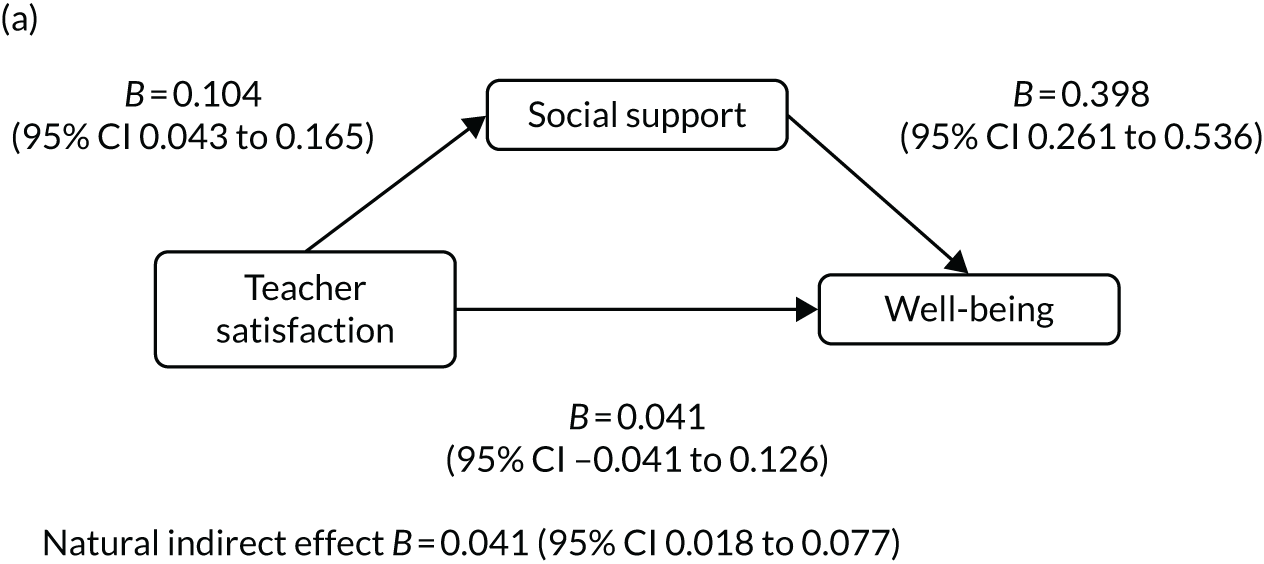
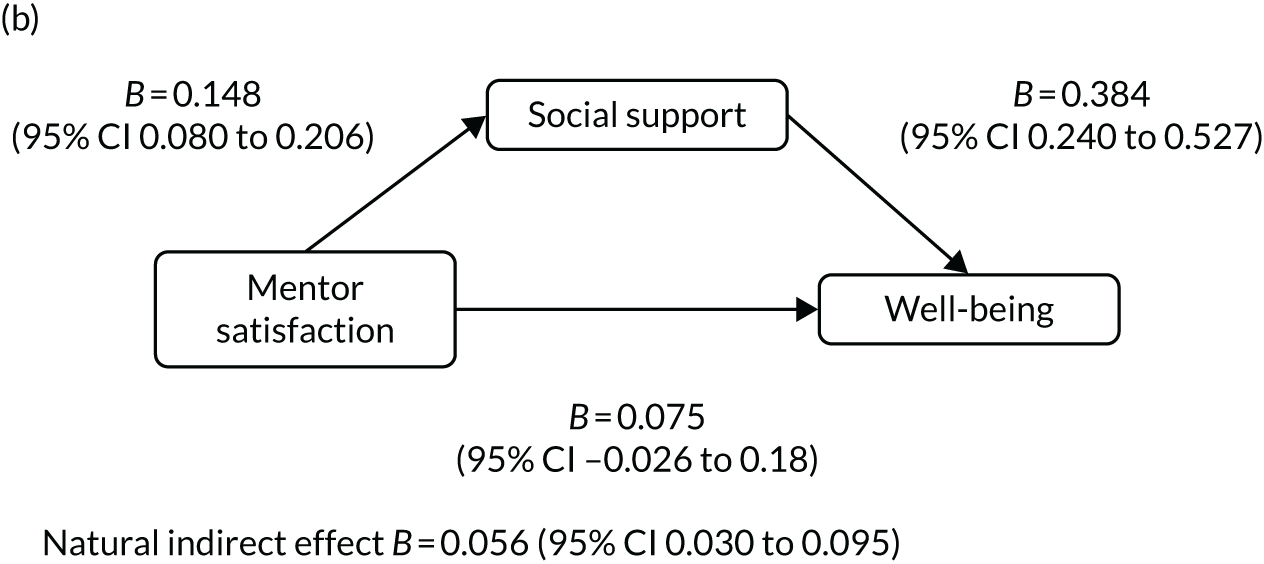
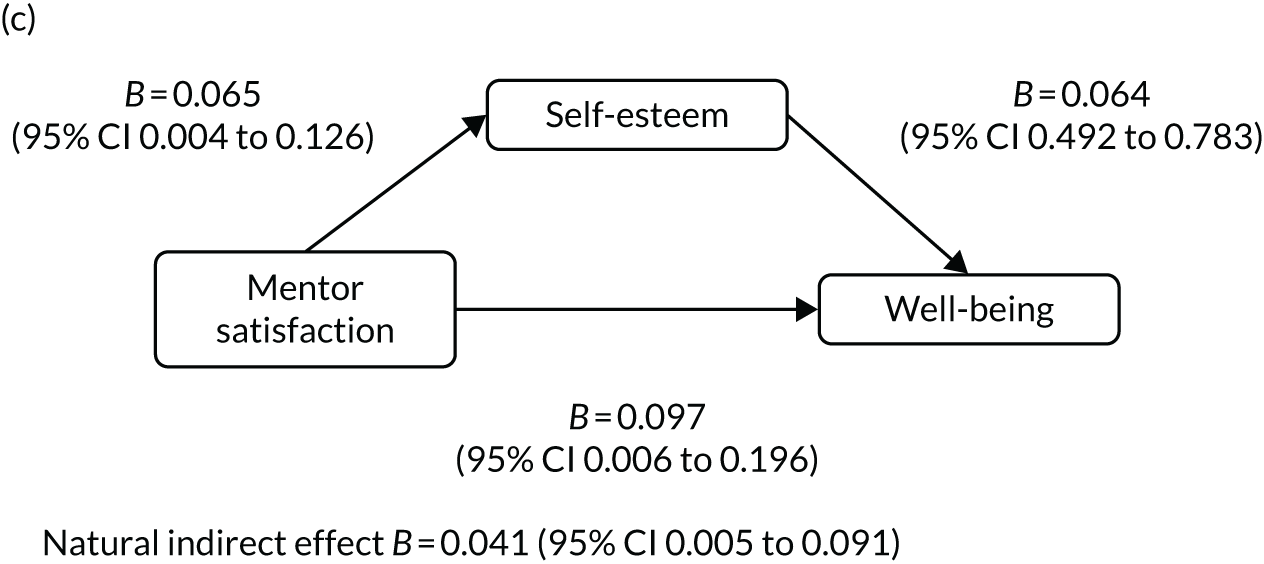
FIGURE 11.
Mediation models of potential psychological mediators in the association between perception of class and well-being among boys: (a) model A; (b) model B; and (c) model C. Adjusted for age, ethnicity, language, school, BMI z-score and baseline values of change variables. E-value estimates (in relative risk): model A, 1.34; model B, 1.29; and model C, 1.25.
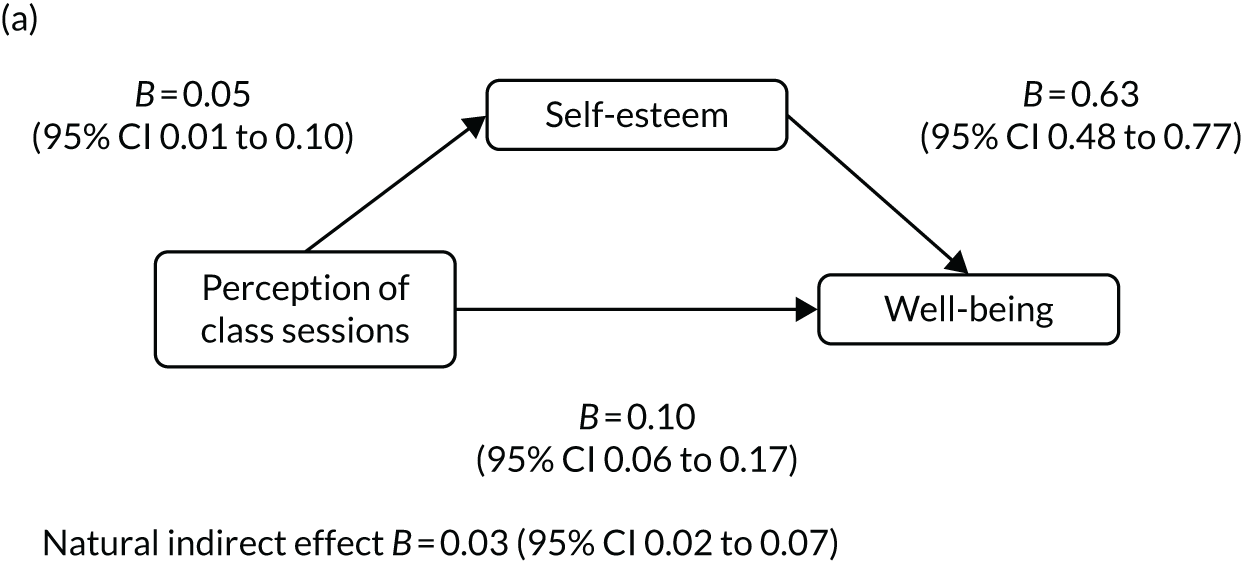
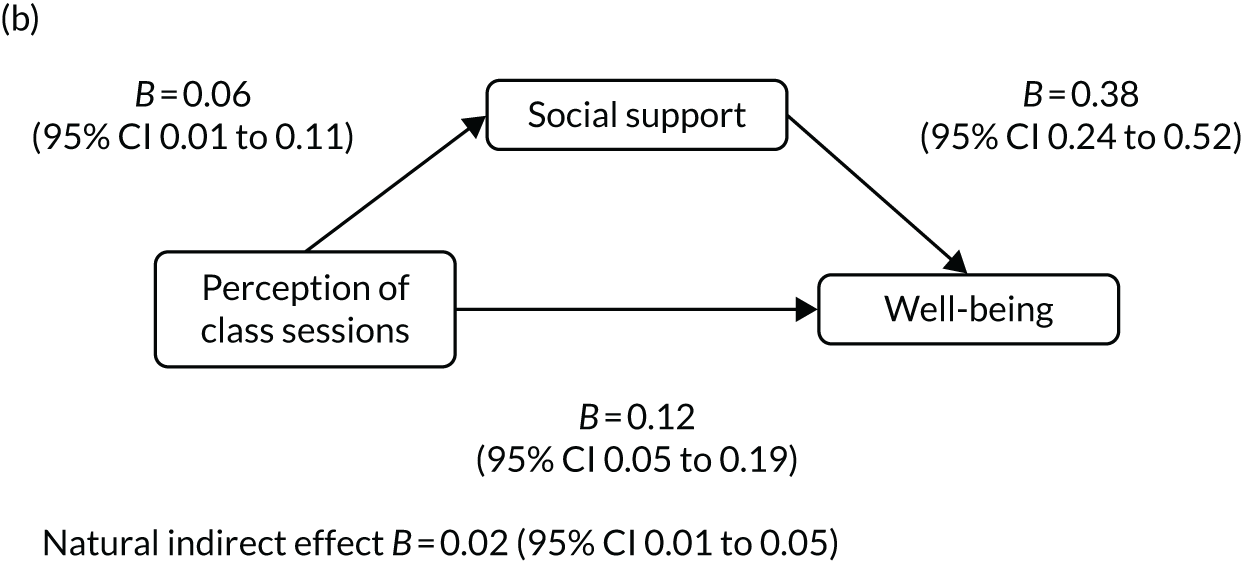
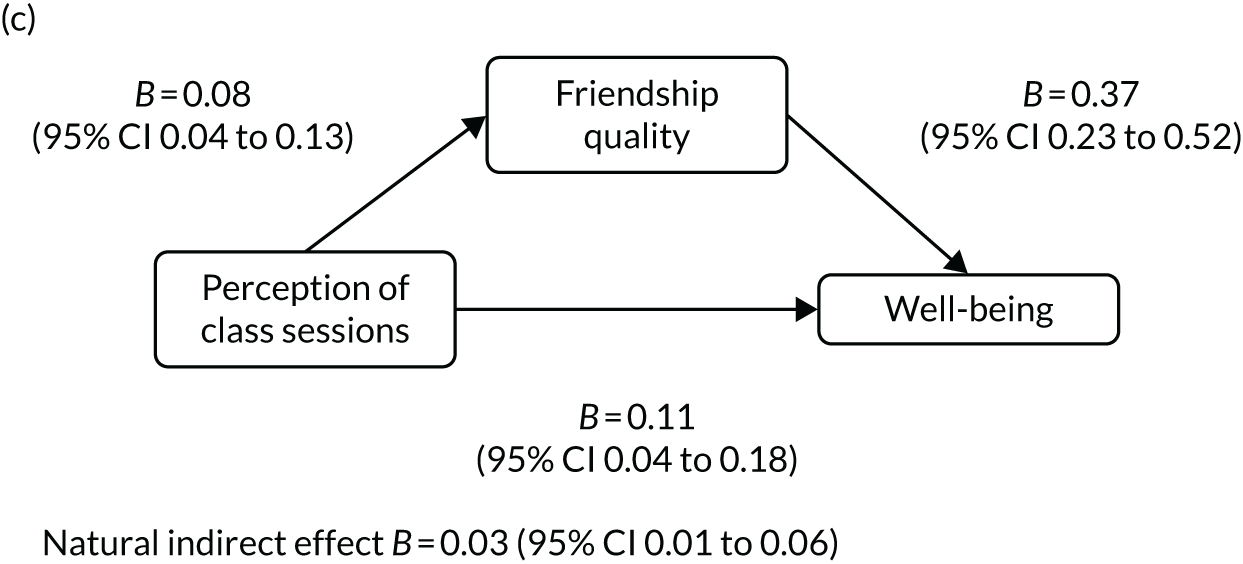
FIGURE 12.
Mediation models of potential psychological mediators in the association between intervention components and well-being among girls: (a) model A; and (b) model B. Adjusted for age, ethnicity, language, school, BMI z-score and baseline values of change variables. E-value estimates (in relative risk): model A, 1.51; and model B, 1.16.
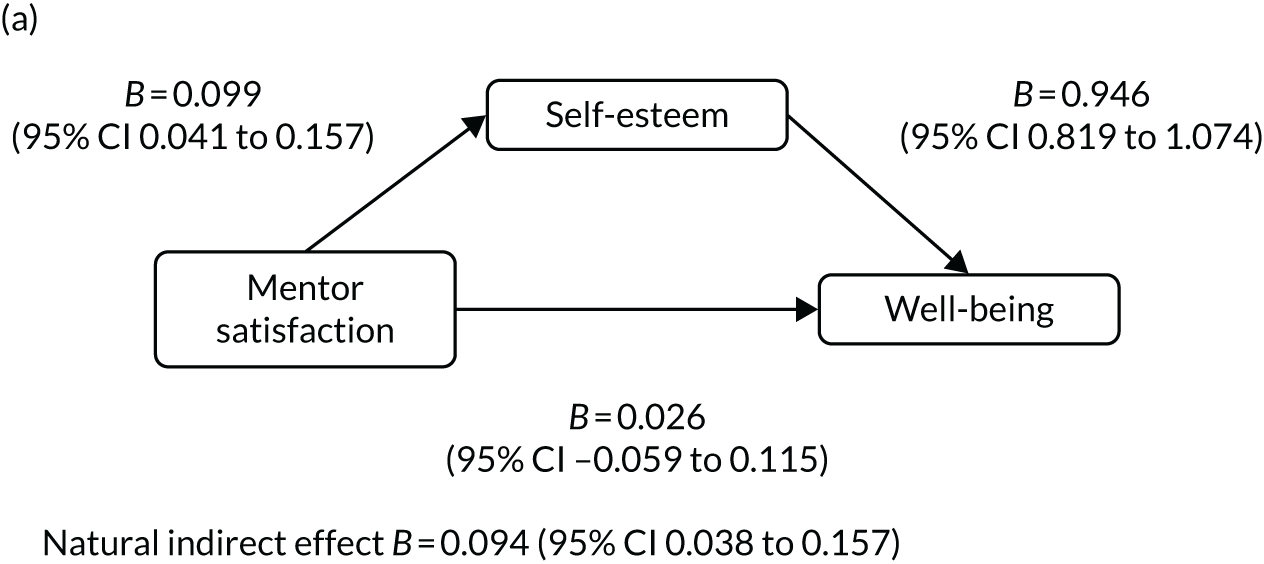
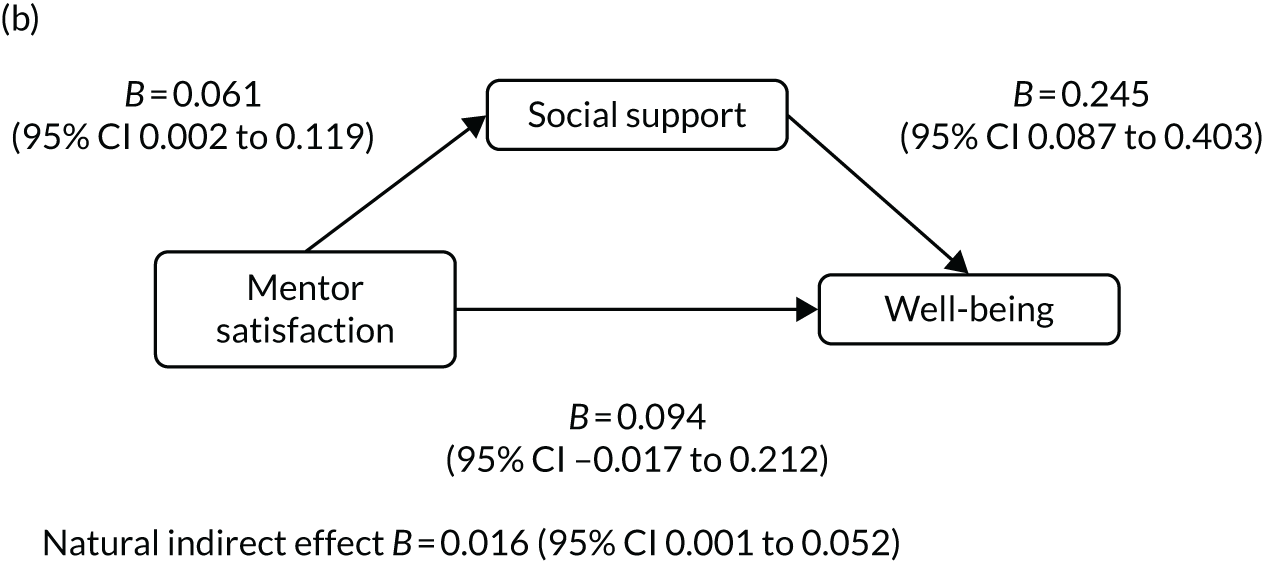
FIGURE 13.
Mediation models of potential psychological mediators in the association between intervention components and well-being among girls: (a) model A; (b) model B; (c) model C; (d) model D; (e) model E; and (f) model F. Adjusted for age, ethnicity, language, school, BMI z-score and baseline values of change variables. E-value estimates (in relative risk): model A, 1.32; model B, 1.19; model C, 1.33; model D, 1.39; model E, 1.18; and model F, 1.38.
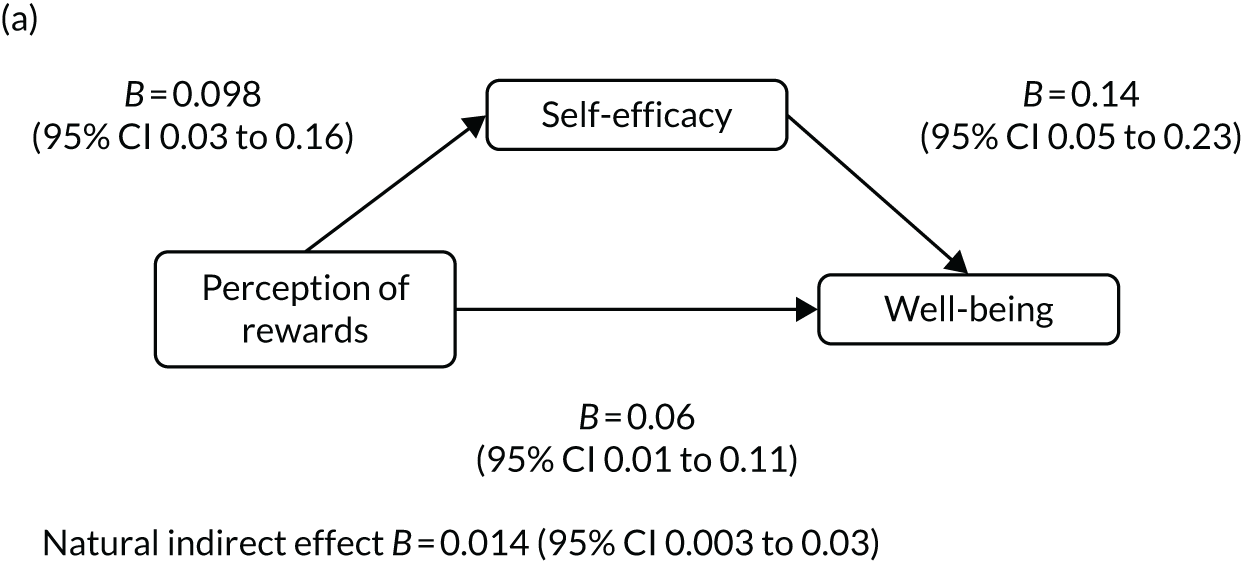
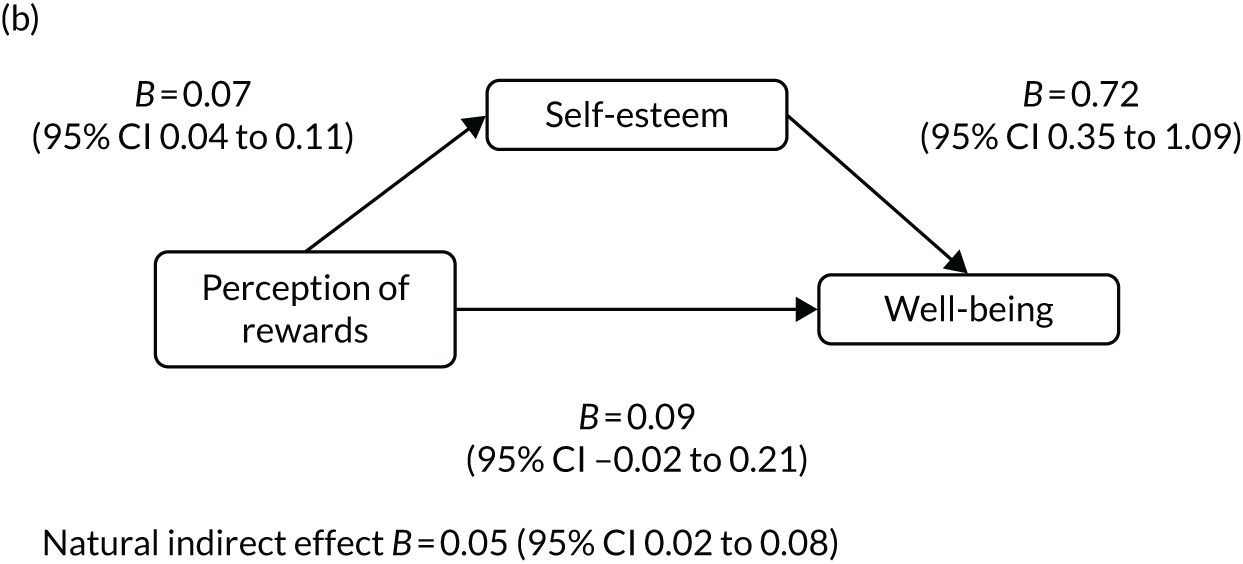
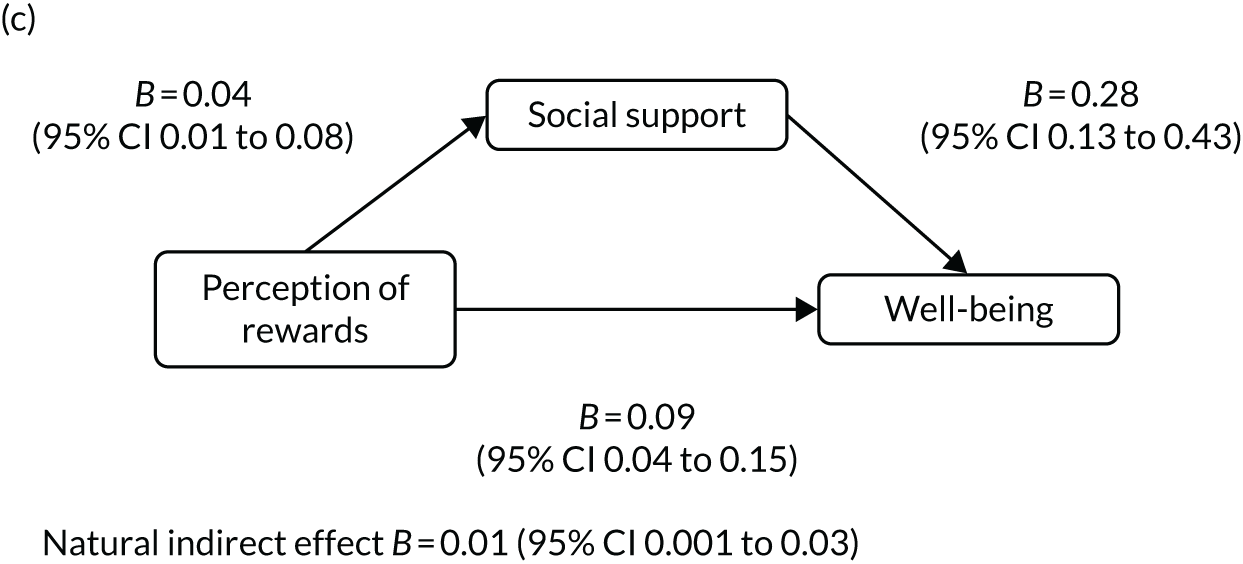
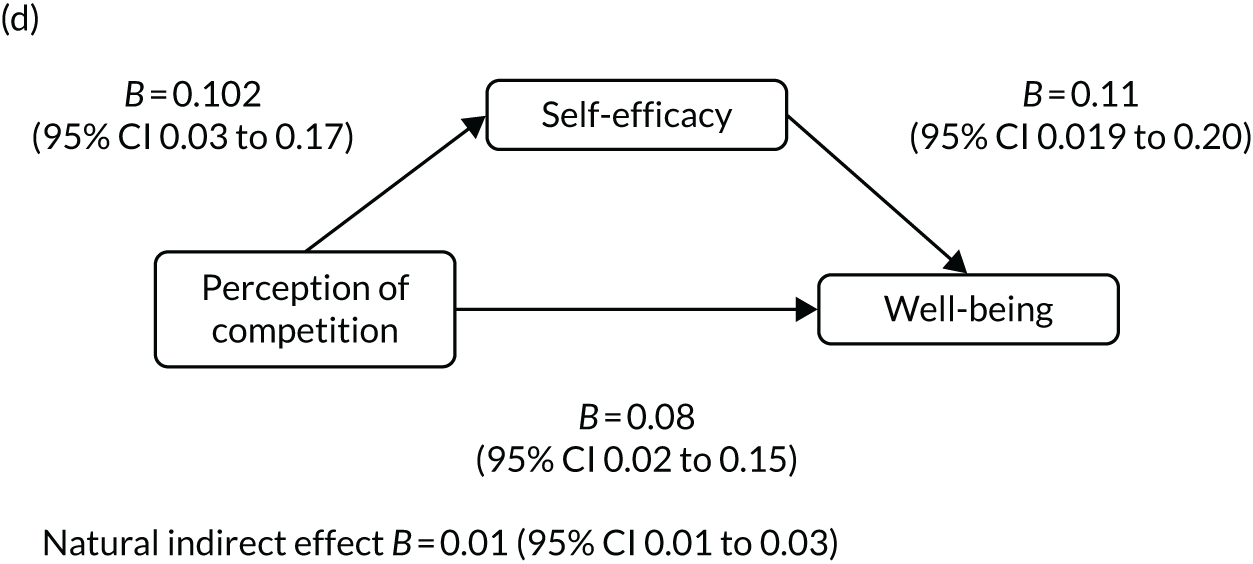
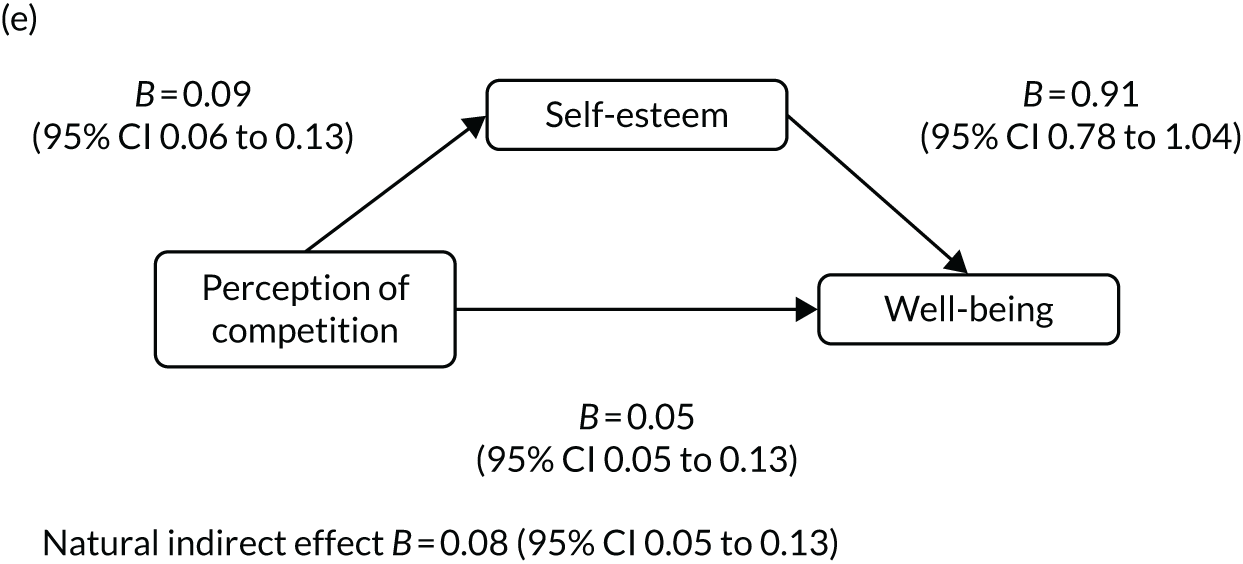
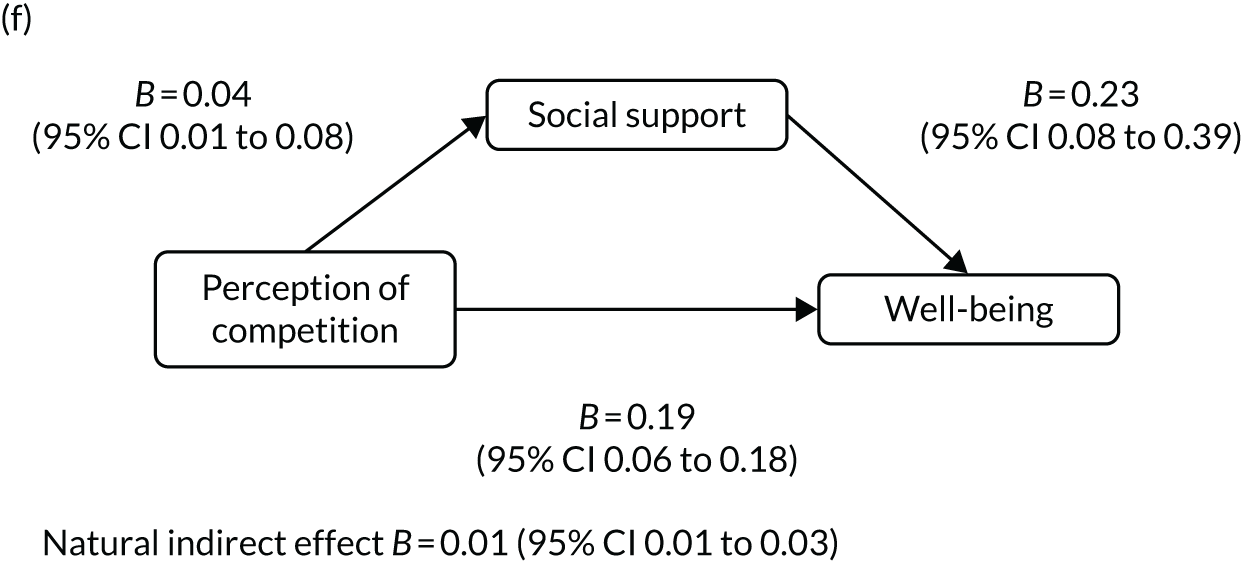
Economic analysis
Within-trial cost-effectiveness analysis
The cost of delivering the intervention was estimated to be £2520 per school, compared with control schools. The average cost per student was £13.06 (Tables 28 and 29). The mean QALYs accrued was 1.242 (SE 0.005) in the intervention group compared with 1.244 (SE 0.005) in the control group (difference adjusted for baseline data –0.006, 95% CI –0.017 to 0.005) (Table 30). Therefore, the ‘most plausible’ interpretation is that the GoActive intervention is dominated by control, that is it increases costs and leads to lower QALY gains (albeit noting that we did not detect a statistically significant difference in QALYs).
| Cost | Unit cost (£) | Units | Quantity | Total (£) | Unit cost source/notes |
|---|---|---|---|---|---|
| Facilitator time | |||||
| Facilitator training day | 15.26 | Hour | 8 | 122.05 | Hourly rate, assuming 46 working weeks of 37.5 hours104 |
| 2 hours per week per school × 12 weeks | 15.26 | Hour | 24 | 366.15 | |
| Facilitator training school staff | 15.26 | Hour | 8 | 122.05 | |
| Materials | |||||
| Activity cards | 5.00 | 1 | 5.00 | Representative cost | |
| Facilitator training manual | 5.00 | 1 | 5.00 | Representative cost | |
| Teacher time | |||||
| Training day (led by facilitator) | 17.26 | Hour | 32 | 552.44 | Assuming four teachers being trained 8 hours per day105 |
| 30 minutes per week | 17.26 | Hour | 78 | 1346.57 | Assuming 46 working weeks of 37.5 hours, 39 weeks in school year = 19.5 hours of teacher time × four teachers105 |
| Total | 2519.26 | ||||
| Factor | Cost (£)/n |
|---|---|
| Cost per school (£) | 2519.26 |
| Number of schools | 8 |
| Number of students | 1543 |
| Cost per student (£) | 13.06 |
| Intervention | Control | Increment, mean (SE) | Increment (adjusted),a mean (SE) | |||
|---|---|---|---|---|---|---|
| n | Mean (SE) | n | Mean (SE) | |||
| Baseline | 1515 | 0.854 (0.003) | 1298 | 0.848 (0.003) | ||
| Mid-intervention | 1377 | 0.839 (0.003) | 1205 | 0.839 (0.003) | ||
| Post intervention | 1257 | 0.842 (0.003) | 1153 | 0.844 (0.004) | ||
| 10-month follow-up | 1187 | 0.826 (0.004) | 1002 | 0.829 (0.004) | ||
| QALYs | 919 | 1.256 (0.005) | 885 | 1.258 (0.005) | –0.004 (0.006) | –0.006 (0.006) |
| QALYsb | 1.242 (0.005) | 1.244 (0.005) | –0.004 (0.006) | –0.006 (0.006) | ||
Economic evaluation explanatory modelling results
At 10-month follow-up, the intervention group engaged in 1.91 fewer minutes of MVPA per day (95% CI –5.53 to 1.70 minutes) than the control group (see Table 10). The PACE model requires physical activity expressed as MET-hours. MVPA is assumed as an intensity of six METs. 98 This equates to a difference of –1.91 × 6/60 = –0.191 MET-hours per day, with a SE of 0.92 minutes of MVPA, equating to 0.092 MET-hours per day. The cost of the intervention is assumed to be £13.10 per student, incurred in the first year of the model only. These values were inserted into the model to predict longer-term costs and outcomes, and to conduct the value-of-information analysis.
As expected, the point estimate incremental net benefit is negative (given a willingness to pay of £20,000 per QALY), but with substantial decision uncertainty (95% credibility interval –£252 to £229). Therefore, the GoActive intervention is not cost-effective at a £20,000 per QALY willingness-to-pay threshold. It is certain that the intervention will impose a cost on schools/local authorities, but there is virtually no difference in QALYs accrued over the subsequent 10 years. Overall, uncertainty in cost and QALYs (and hence incremental net benefit) is due to uncertainty in longer-term incidences of cardiovascular events and the associated cost of treatment, rather than uncertainty in the ‘treatment effect’ of the GoActive intervention. This is borne out by the value-of-information analysis, which finds zero value in a further study of the GoActive intervention. The greatest gains from reducing uncertainty are in unit costs of subsequent events (accounting for 19% of the EVPI), the risks of cardiovascular and stroke events (14.3% and 7.9%, respectively) and the future pathways of blood pressure, cholesterol and glucose levels (6.5%). Given the young age of the cohort, the absolute numbers of such events will be extremely small, but they have large impacts on costs and quality of life, therefore driving the majority of the uncertainty in the results. As stated previously, this analysis should be considered highly exploratory in nature, with the emphasis placed on the value-of-information analysis, illustrating where the key uncertainties lie, rather than a robust estimate of the long-term cost-effectiveness of the GoActive intervention (Tables 31 and 32).
| Cost (£), mean (95% CrI) | QALYs, mean (95% CrI) | Net monetary benefit (£), mean (95% CrI) | |
|---|---|---|---|
| Status quo | 406.31 (253.99 to 599.64) | 8.05 (6.953 to 8.579) | 160,587.18 (138,534.06 to 171,299.58) |
| GoActive | 432.94 (279.56 to 629.31) | 8.05 (6.954 to 8.579) | 160,576.48 (138,516.77 to 171,284.25) |
| Increment | 26.63 (–105.25 to 160.05) | 0 (–0.008 to 0.009) | –10.70 (–252.47 to 228.55) |
| Parameter | Per person EVPPI (SE) (£) | Percentage of overall EVPI | Population EVPPI (£) |
|---|---|---|---|
| GoActive intervention effect | 0.00 (0.00) | 0.0 | 0 |
| Risks of cardiac events (AF, IHD, MI, CHF) | 5.51 (0.88) | 14.3 | 39,507,794 |
| Risks of stroke | 3.07 (0.77) | 7.9 | 22,014,997 |
| Risk of complications from diabetes | 0.00 (0.01) | 0.0 | 0 |
| Blood markers (SBP, cholesterol and glucose) | 2.50 (0.70) | 6.5 | 17,945,181 |
| Smoking behaviour | 1.35 (0.35) | 3.5 | 9,692,455 |
| Health state utilities | 2.07 (0.59) | 5.4 | 14,866,375 |
| Unit costs | 7.35 (1.00) | 19.0 | 52,663,376 |
| All parameters (EVPI) | 38.66 (n/a) | 100 | 277,192,896 |
Process evaluation findings 1: adolescent perspectives
Process evaluation data from Year 9 students was analysed to determine satisfaction with intervention components and interpret adolescents’ experience of the intervention process. The key highlights from the deductive analysis of adolescent experiences and perspectives of the GoActive intervention using mixed-methods process evaluation included the following:
-
Gender disparity was consistent throughout components.
-
Competition was disliked by girls and shy/inactive students.
-
Adolescents liked the idea of older mentors, but mentors did not meet their expectations.
-
Boys enjoyed trying new activities more than girls did.
-
Participants wanted to try new activities, but identified barriers to choosing them.
Table 33 shows the Year 9 participants included in qualitative process evaluation and Table 34 provides an overview of the characteristics of participants included for quantitative process evaluation analysis. Quantitative results (Table 35) indicate that for most components, overall responses were around the mid-point of the scale, but towards the positive end. However, for mentorship and leadership, responses dipped below the central scale point, indicating low acceptability of these components. A small number of differences in intervention acceptability and satisfaction were seen between genders and shy/inactive subgroups, with boys consistently preferring most intervention components compared with girls. Although the magnitude of these differences were relatively small and may not represent meaningful differences between groups, the qualitative findings provided context to these observed differences. Participants were purposively sampled for invitation to focus groups based on tertiles of website usage (as a proxy for intervention engagement). However, the quantitative results are not stratified by participation, instead this is used to ensure a balanced mixture of participation levels in qualitative work to represent views across differing participation levels in the study.
| School label | Website usage classification | Number/gender (focus group) | Number/gender (individual interview: shy and inactive participants) | |
|---|---|---|---|---|
| Focus group 1 | Focus group 2 | |||
| A | Medium | 1 boy, 3 girls | 2 boys | |
| B | Low | 3 boys, 2 girls | 2 girls | |
| C | Medium | 2 girls | 1 girl, 2 boys | 1 boy, 1 girl |
| D | High | 4 boys | 2 girls | 1 boy, 1 girl |
| E | High | 1 boy, 4 girls | 1 boy, 1 girl | |
| F | Low | 4 girls | 2 girls | |
| G | Low | 5 girls | 2 boys | |
| H | Medium | 7 girls | 7 boys | 1 boy, 1 girl |
| Total | 48 | 16 | ||
| Characteristic | Boys | Girls | Shy and inactive | Others |
|---|---|---|---|---|
| Participants, n (%) | 790 (51.2) | 752 (48.8) | 221 (14.3) | 1322 (85.7) |
| Age (years), mean (SD) | 13.2 (0.4) | 13.2 (0.4) | 13.2 (0.4) | 13.2 (0.4) |
| Ethnicity, n (%) | ||||
| White | 646 (42.7) | 635 (42.0) | 184 (12.0) | 1104 (72.6) |
| Mixed/multiple background | 52 (3.4) | 44 (2.9) | 10 (0.7) | 87 (5.7) |
| Asian or Asian British | 38 (2.5) | 27 (1.8) | 20 (1.4) | 46 (3.0) |
| Black or black British | 23 (1.5) | 18 (1.2) | 2 (0.1) | 39 (2.6) |
| Other ethnic group | 12 (0.8) | 17 (1.1) | 3 (0.2) | 28 (1.8) |
| SEP, n (%) | ||||
| Low (i.e. FAS score 0–6) | 132 (7.9) | 135 (8.4) | 39 (2.5) | 228 (13.9) |
| Medium (i.e. FAS score 7–9) | 324 (21.3) | 345 (22.7) | 119 (7.6) | 551 (36.1) |
| High (i.e. FAS score 10–13) | 334 (21.7) | 272 (18.0) | 63 (4.2) | 543 (35.5) |
| Participants visiting website, n (%) | 366 (46.3) | 348 (46.3) | 93 (42.1) | 621 (47.0) |
| Component (scale 1–5) | Boys, mean (SD) | Girls, mean (SD) | Difference, beta (95% CI) | Shy/inactive, mean (SD) | Others, mean (SD) | Difference, beta (95% CI) | Convergence and qualitative interpretation |
|---|---|---|---|---|---|---|---|
| Class sessions (tutor time) | 3.4 (1.3) | 3.2 (1.2) | 0.2 (0.1 to 0.3) | 3.0 (1.2) | 3.3 (1.3) | –0.4 (–0.9 to 0.1) | Congruence: participants liked using form time, but acknowledged the limited time. Some suggested using lessons or having the mentors come in more often |
| Suggesting new activities | 3.2 (1.1) | 3.1 (1.0) | 0.1 (0.1 to 0.3) | 3.0 (0.9) | 3.1 (1.1) | –0.2 (–0.5 to 0.1) | Dissonance: qualitative findings suggest that Year 9 students did not wish to suggest new activities (potentially linked with self-consciousness/embarrassment) |
| Activity choice | 3.3 (1.1) | 3.1 (1.0) | 0.2 (0.1 to 0.3) | 3.0 (0.9) | 3.2 (1.1) | –0.2 (–0.5 to 0.2) | Dissonance: interviews revealed that choices did not appeal and were self-limited. Qualitative data show boys preferring choice, but girls indicated a wish to try new activities more than boys in qualitative interviews |
| Novel activities | 3.3 (1.1) | 3.2 (1.0) | 0.1 (0.1 to 0.2) | 3.1 (1.0) | 3.3 (1.1) | –0.2 (–0.6 to 0.1) | Congruence: quantitative results are neutral, which may indicate hesitation. Qualitative findings provide justification of these hesitations |
| Class competition | 3.2 (1.2) | 3.0 (1.1) | 0.2 (0.2 to 0.3) | 2.8 (1.1) | 3.1 (1.1) | –0.3 (–0.5 to –0.1) | Congruence: boys referred to the fun of competition much more than girls. Girls indicated that competition exasperated by boys was at times a barrier to their participation in the intervention |
| Mentors | 2.9 (1.1) | 2.7 (1.0) | 0.2 (–0.1 to 0.4) | 2.8 (0.9) | 2.8 (1.1) | –0.1 (–0.3 to 0.2) | Dissonance: participants liked the idea of working with older mentors; however, their expectations were not met |
| In-class leaders | 2.9 (1.1) | 2.8 (1.0) | 0.2 (0.1 to 0.3) | 2.8 (0.9) | 2.9 (1.0) | –0.1 (–0.4 to 0.2) | Dissonance: qualitative findings indicate that Year 9 students did not want to be leaders among their peers. Where this element was not implemented, some suggested it and suggested that those selected should be ‘popular’ (influencers) |
| Rewards (points) | 3.1 (1.2) | 3.0 (1.1) | 0.2 (0.1 to 0.3) | 2.9 (1.0) | 3.1 (1.1) | –0.2 (–0.4 to 0.1) | Dissonance: participants liked the idea, but may have conflated thoughts on gaining individual points and adding points to their account, which may indicate why they did not like individual points |
| Rewards (prizes) | 3.2 (1.2) | 3.2 (1.1) | –0.1 (–0.3 to 0.2) | 3.0 (1.0) | 3.3 (1.2) | –0.3 (–0.6 to –0.1) | Congruence: participants liked the idea of rewards, but discussed barriers as to why they did not like rewards more than presented |
| Acceptability of intervention (scales 1–4) | |||||||
| Was it fun? | 2.4 (0.9) | 2.5 (0.8) | –0.1 (–0.3 to 0.1) | 2.6 (0.9) | 2.4 (0.9) | 0.2 (0.1 to 0.4) | Dissonance: qualitative results were resoundingly positive compared with the average feeling from the quantitative data |
| Was it boring? | 2.6 (0.9) | 2.5 (0.9) | 0.1 (0.1 to 0.3) | 2.4 (0.9) | 2.6 (0.9) | –0.2 (–0.3 to –0.1) | Congruence: qualitative findings revealed rationale behind ‘boring’ statements related to lack of activity variability |
Quantitative and qualitative results on the GoActive components are discussed below and summarised in the mixed-methods convergence matrix (see Table 35).
Reflections on the GoActive sessions
Participants reflected on a number of key GoActive components, including their enjoyment of the intervention (e.g. fun), competition, choice and novelty. Analysis of participant responses indicated that many of these overlapped and ultimately had an impact on enjoyment and participation.
Enjoyment
Shy/inactive participants reported finding the GoActive intervention less fun than the remaining participants. This was supported by the qualitative data, where participants identified sociability and fun as the main features of GoActive sessions. Some participants saw the sessions as an opportunity to socialise with their form group (i.e. tutor group, roll-call/registration class) and with students outside their usual friendship circle:
So 2 months ago would you have spoken to these people in your form group?
No, not really, I normally keep my head down and read my book or something in form. But it’s kind of quite fun, it’s something different, and I think, because we’re all on the same team as such, we all kind of get along and want to play.
When asked about the appeal of participating, the participant responded:
I don’t know, I think it’s just the fact I can go up there with my friends and you can have a mess around, have a laugh and try and hit people with the dodgeball [laughs].
School A, individual interview, I1
Some students recognised that the fun and enjoyment of the activities were a mechanism affecting behaviour change:
When our form like misbehave loads and then we have to do silent reading, but as soon as GoActive came into place, like they started misbehaving less and less the more GoActive happened. So I think, because they’re enjoying it they stopped messing about so they could go out and do more fun things in form.
School E, focus group, S1
Qualitative data helped to understand differentiated experiences between subgroups. Fun was connected to sociability, but not always, and only for the ‘right’ kind of interactions. Socialising with people was a positive intervention element for some, but others would have preferred to socialise with a particular group of people, potentially those outside the intervention. Some girls suggested that at times they preferred to be sociable without participating in the activity or would rather study, prioritising this over one morning of physical activity per week.
Using form time
The GoActive sessions were designed to allow for diversity in a range of co-participants, and for variability in timing and locations for activity. Flexibility was also present as a choice as to when to run a session in a school day. All schools, except one, used morning form time to run the GoActive intervention. Qualitative data indicated that students preferred engaging in a session, having something to do rather than traditional form time activities (e.g. sitting and talking, reading or personal reflection activities):
I like trying new things and I find it [the intervention] really fun and it’s just fun, and it’s better than just sitting there and doing nothing, because that’s what we always do in form.
School A, focus group 1, S3
Competition
Boys preferred the class competition compared with girls and the main sample enjoyed class competition more than shy/inactive students (see Table 4). Similarly, the consensus from the focus groups was that the competitive element of the activities was a source of fun for boys. Boys stated that ‘boys are more competitive than the girls’. Competition was always linked to the social nature of activities for boys, including teams within forms and competing against other form groups within the school. One boy commented:
In our form we’ve done competitions against other forms, so the boys from one form and the boys from another form, we went into the sports hall and played dodgeball, that was fun.
School E, focus group, S1
Girls often discussed the competition shown from the boys when participating in the sessions:
You could see it, like they wanted to win, you could tell they did.
School A, focus group, F1S1
However, quantitative results showed that girls and shy/inactive participants did not enjoy competition. Interview discussions revealed that this was, instead, a deterrent to participation.
Choice and novelty
Questionnaire data suggests that boys liked choosing new activities more than girls. Qualitative data revealed that choices were limited by the Year 9 students themselves: students were too shy, displayed apathy towards suggesting an activity, or were discontented with the selected activities. Engagement varied depending on the activity offered:
I think it’s because like dodgeball, it’s competitive, it’s fun and we all know how to do it, and it’s a pretty easy game to learn, and it’s pretty easy to get people to do it with you as well.
School B, individual interview, I2
Other participants reiterated that their form group would prefer to do activities that were familiar and that they had participated in previously:
In our class not so much, they just wanted to do football or dodgeball or, you know, that sort of, things that they like and do normally.
School E, focus group, S5
Boys and shy/inactive participants stated that some of the activities on the GoActive website ‘didn’t appeal’ and specified that they would rather engage in ‘a sport that makes you do like more running’ (school H, individual interview, I2).
For boys, the desire for higher intensity activities was matched with a desire for competition:
I think yoga’s too calm . . .
School B, focus group, S2
There’s no competitive side to it.
School B, focus group, S3
Conversely, girls seemed interested to try different activities (e.g. yoga, Zumba and Pilates). A class vote to decide on an activity usually resulted in one person or a small group, usually boys, determining the activity for the entire class. More often than not, football was selected. However, on the rare occasion girls were able to choose and run an activity, not many students participated. In one focus group, a group of girls described their experiences:
We tried yoga, but there was only a few people that actually wanted to do it, and everyone else kind of just took the mick and just sat on the floor.
School E, focus group, S3
Yeah, we tried Zumba, but nobody, there were about three people that were really going for it, but then nobody else was.
School E, focus group, S5
Although no significant between-group differences were seen in preference for choosing new activities between shy/inactive participants and others, when discussing variety in choosing an activity, one shy/inactive participant stated:
I don’t mind, it’s just whatever’s chosen I’ll just play.
School C, individual interview, I1
However, self-imposed choice restriction or repetition also resulted in boredom and disengagement:
Some people just got sort of like bored because it was just like we’re doing the same thing every single week, so we’d just sort of like talk because there’s just not really anything to do.
School C, individual interview, I1
One group of participants suggested that those who do a lot of sport may be less keen to do an organised sporting activity within school time. To ameliorate some of these concerns, participants suggested embedding activity sessions into their routine or curriculum, calling for a more structured approach. The ad hoc nature of the GoActive intervention was perceived not to fit within the traditional prescribed and timetabled structure of the school day:
No, or if they gave us any information as to how to get there, you know, you know, there wasn’t a timetable or anything so it wasn’t very helpful.
School F, individual interview, I1
Participants suggested set weeks to do particular activities, timetabled to fit into the school day. Participants expressed a desire for consistency and momentum in running the intervention:
We could do like more activities more frequently, because I feel like doing it like once every now and again wasn’t as good.
School H, individual interview, I1
Reflections on mentorship
Mentors
Questionnaire data showed that mentorship (from older students) and in-class leaders were the least acceptable components and qualitative discussions identified mentors as a barrier to participating. Qualitative data showed that girls were more critical of their mentors than boys, despite no gender difference in questionnaire responses. Girls expressed issues with disorganisation and a lack of consistency in attendance, resulting in the form group not doing any GoActive intervention activities:
A couple of times they’ve shown us the cards with the different selection of activities and we’ll talk about which ones we want to do and generally there’s only football that we want to do and that everyone’s happy with. But then they don’t book a place to do it or they don’t have a football next time so we don’t end up doing it.
School D, focus group, F2S2
Participants additionally reported that teachers/tutors and mentors seemed confused with their roles within the intervention. One student explained:
I think our form tutors were relying on the mentors to come and get us but because our mentors didn’t, our form tutors just forgot that we had to do it.
School H, focus group, F2S3
Qualitative data revealed disparity in student thoughts about mentor enthusiasm. Many students felt that their mentors were unenthusiastic and showed a lack of care and seriousness. Conversely, some boys expressed positive affirmations, such as mentors providing verbal encouragement:
They said, ‘Come on, it’ll be fun. You’ll get points on the website and stuff and you could win prizes from that’. Saying like, ‘Even if you don’t do as well as others, you’ve still participated so that’s the best part of it’, stuff like that.
School D, individual interview, I1
Positive descriptions placed value on mentor participation, keen observation, helpfulness, ability to provide advice and teaching of the rules:
Because they taught us the rules, yeah.
And they participated.
And they got involved on the teams.
And do you think that helps?
Makes the game more interesting.
It was evident that students valued consistency and organisation:
They turned up, our mentors, they turned up every week, which was really good, and they had a new sport plan every week.
School E, focus group, S5
In an effort to increase participation time in activity, participants suggested that mentors should have a plan in place to select the activity and organise equipment so that Year 9 student time was spent participating in the activity rather than getting and setting up equipment. Participants suggested additional training to establish clarity in the week-to-week organisational routine:
Some sort of like, not really training for form tutors and Year 10 leaders but a sort of discussion where you introduce it more formally and set out sort of expectations where you want them to try and get everyone to participate and help to lead the activities.
School D, focus group, F2S1
Participants also suggested the inclusion of additional lead-in time, as one participant commented:
I’d like to like introduce it more into our tutor, like not just bam go straight into it, like introduce it slowly so maybe start talking about it more because we have discussion lessons on Thursdays, normally it’s about the assemblies but like sometimes it’s not much to talk about, about assembly because we’ve already had the assembly but I think we should like start discussing it bit-by-bit and start to like try and get involved and like discuss ideas so everyone gets a bit of understanding, so then they’re more likely to like like it, yeah.
School G, focus group, S1
In-class Year 9 leaders
Quantitative results indicate that boys preferred having in-class leaders more than girls, but qualitative discussions revealed that implementation of in-class leaders was low. Participants stated there was a reluctance to be a leader:
Ours was a bit confusing because no one really wanted to be the leader, I don’t know why but, yeah, no one wanted to do it.
School E, focus group, S5
One shy/inactive participant suggested that self-consciousness may provide rationale as to why there was a lack of people interested in being an in-class leader, a sentiment shared by a few other students:
I think it just makes people self-conscious because people want to hide in the group.
School F, individual interview, I1
Participants from one form group reported that their teacher resorted to selecting a new boy and girl each week to be in-class leaders. A participant from another form felt that adoption of this approach would be beneficial:
Our form teacher normally forces them to put their hand up so. It’s like, ‘So you haven’t actually put your hand up for anything yet so you’re it!’ [Laughs.]
School E, individual interview, I2
Those within the form group who were considered ‘good’ at particular activities by the teacher were the first to be selected as leaders for that activity. Some participants expressed that this meant that they were less likely to volunteer themselves as a leader, as they did not feel as if they had sufficient skills:
I don’t know, like I don’t normally get like too involved with those things, and there’s like, I feel like there’s more people, the people that might have done better in doing it.
School H, individual interview, I1
Disparity in implementation, both between and within schools, led to discussions about the value of having in-class leaders, but views were primarily negative. Participants stated that there would be no difference and that in-class leaders would not have helped the intervention. Some participants suggested behaviour of the cohort as rationale for this:
I don’t think it’d help, some people are just a bit defiant and they’ll only listen to like the people who are certain, they wouldn’t take us probably serious enough.
School A, focus group, S1
Responses to monitoring and rewards
Website use
Participants reported three main issues with using the GoActive intervention website: (1) they did not receive enough information about how to use the site, (2) they found the website hard to access or (3) they lost their username and/or password:
We never really got to use it though because we weren’t sure . . . because we never got explained how to do it properly really or anything.
School H, focus group, S2
Yeah, in form we never like knew how to get on it or how to use it so none of us used it because we didn’t know what to do.
School H, focus group, S3
Points
Boys preferred the points element of the intervention compared with girls. Qualitative data suggested that all participants enjoyed keeping track of their physical activity and acknowledged the potential for it to act as a motivator for behaviour change:
Yeah, I think it did, sometimes if I thought, like, ‘Should I go and do something or should I not?’ well, actually, if I go and do it then I can go and log a point on.
School E, focus group, S5
One shy/inactive participant reinforced this:
I can like keep track of, I can see myself like how active I’ve been and it’d probably encourage me to do more activity.
School D, individual interview, I1
Participants admitted to forgetting to log their points and expressed irritation with needing to add multiple activities concurrently to ensure they were up to date:
Yeah, because I’m going to have to add on like sixty things because I’ve forgotten them for so long, and then like I get reminded and then I’ve forgotten the password or whatever, and then you have to e-mail them and it’s a bit . . .
School E, focus group, S4
After the initial attraction of the intraform group competition tapered off, participants acknowledged that website use was not continued. There was limited discussion on other form groups’ point tally accumulated through the GoActive website and intraform group competition using the school graphs. One participant described the effect of the school graphs on their form:
I’d logged my points like after every week. [ . . . ] And then my class, everyone, like most people in my class logged them because we were like trying to like win the competition to have the most points in a form. I think everyone, like, most people did that. It was like a good way of recording it.
School D, focus group 2, S1
Rewards
Boys liked the rewards more than girls, but most participants described the rewards positively, intimating that they were a means of motivation to do physical activity:
I know a couple of people did like once they knew that there was like a reward system, thought OK, I’ll try harder now to get rewards.
School D, focus group 1, S2
Confusion mounted over who was in charge of reward distribution. Although the intervention protocol indicated that mentors would do this, this was not implemented at every school, with form teachers or GoActive contact teachers tasked with reward distribution. Although rewards were distributed to the GoActive schools at the start of the intervention, participants discussed disappointment with the time it took to receive the reward after logging points and claiming the prize:
I’m disappointed with that to be honest . . . I logged all my points to get my stuff ages ago and they haven’t come yet.
School D, focus group 1, S2
Lack of action on the reward distribution meant that students lacked the desire and care to log points and use the GoActive intervention website:
At the end no one [Year 9 students] really cared because like, you know how you could win things like jumpers? At the very beginning I won a jumper and I asked for it, and they were like, ‘Yeah, I’ll get it for you’.
Who?
Our mentors . . .
We were never given ours . . .
Conversation arose from one school about the timing of the intervention and rewards. For those who felt as if they started the intervention ‘late’, they deemed the rewards ‘unachievable’. This was reflected in limited or no use of the website.
Smartphone applications (apps) were suggested as a way of overcoming some of the barriers to logging points and removing the need to rely on remembering the password and username. A points-logging reminder could be an added feature to ensure a more accurate accumulation of points over the course of the intervention and potentially beyond. A conversation from one focus group divulged:
It would be a really good idea, an app.
Yeah, like saying, a reminder saying like, ‘Add points now’, or a certain day where you get, I don’t know reminded to add the points, I think, like people spend ages like every day on their phone like looking at it for 5 minutes, you could easily add points then, and then it would stop people from forgetting and stuff.
Yeah, because it would keep you logged on, so then people wouldn’t forget their passwords and keep having to go back and . . . You’d literally just have to go in, do your balance, and then you’re done.
Process evaluation results 2: reach, dose and fidelity
Descriptive findings of quantitative assessments of reach, recruitment, dose delivered (completeness) and implementation fidelity are presented in Table 36. Qualitative data provide a more nuanced picture to contextualise questionnaire data and are presented below alongside key quantitative results. Individual school case studies that include more detailed information regarding school variability are described in Appendix 6. The final section of the results will focus on the perceived challenges to intervention implementation.
| GoActive intervention: essential component | Implementation per school | |||||||
|---|---|---|---|---|---|---|---|---|
| A (n = 140) | B (n = 169) | C (n = 207) | D (n = 229) | E (n = 232) | F (n = 116) | G (n = 219) | H (n = 231) | |
| School-level socioeconomic status | Low | Low | High | High | High | High | Low | Low |
| Baseline MVPAa (minutes/day), mean (SD) | 34.3 (14.2) | 33.9 (16.9) | 39.1 (20.3) | 38.2 (19.8) | 32.3 (16.1) | 37.4 (17.8) | 37.4 (19.4) | 33.3 (18.5) |
| Reported GoActive sessions at post intervention (average): percentage of Year 9 student reporting at least one GoActive session in last 2 weeks | 21.3 | 11.2 | 49.5 | 63.2 | 47.9 | 20.4 | 554 | 13.5 |
| Mentors | ||||||||
| Number of mentors per school | 23 | 7 | 6 | 17 | 20 | 9 | 0 | 20 |
| Number of meetings recorded in the website log | 5 | 0 | 0 | 10 | 4 | 1 | 0 | 13 |
| In-class Year 9 leaders: percentage of Year 9 students reporting having leaders in the class | 8.6 | 10.0 | 17.8 | 54.6 | 72.9 | 30.2 | 33.1 | 27.1 |
| GoActive website use | ||||||||
| Percentage of Year 9 students who recorded points | 77.1 | 8.9 | 35.7 | 60.7 | 75.0 | 19.8 | 38.8 | 41.6 |
| Median (IQR) points recorded | 8 (2–25) | 44 (17–58) | 12.5 (6–53) | 38 (5–43) | 58.5 (15–153) | 13 (4–39) | 24 (10–70) | 4 (2–4) |
Reach
The reach, or proportion of participants who attended GoActive sessions, calculated from a self-reported Year 9 student questionnaire, was 39.4%. The reported dose of at least one GoActive class session in the last 2 weeks during the distant support phase ranged from 11.2% to 63.2% between schools, as reported from Year 9 students (see Table 36). This was in contrast to 93.7% of the mentors and 84.2% of the teachers who reported that the sessions had been delivered at least once over the last 2 weeks. GoActive sessions were delivered over a median time frame of 12 weeks.
Interview data indicated that dose had changed in response to competing priorities, which had an impact on resourcing (e.g. school space availability, a lack of time or engagement issues). One contact teacher explained:
When it’s exam season it’s exam season for [Year] 9, 10 and 11, so we had to stop for a certain point . . . we had to stop because of the sports hall and gym were being used and we couldn’t get the kids out during registration because their exams started at 9 o’clock.
Contact teacher, school H
Recruitment
Procedures to attract and maintain participant involvement in the intervention included rewards. On a five-point Likert scale that ranged from ‘do not like it at all’ (1) to ‘like it a lot’ (5), 38.3% of Year 9 students reported liking rewards [mean 3.8 (SD 1.4)]. Additional ‘thank you’ gifts were provided after each measurement session. These included pens, earphones, mints and stationery, which may have facilitated sustained involvement. In turn, 87% of Year 9 students were retained at mid-intervention, 80% were retained post intervention and 76% were retained at 10 months post intervention.
The top three reasons for mentors joining the programme reported from the questionnaire data were (1) for the incentives/prizes (i.e. £20 vouchers and a hoodie), (2) to be more active themselves and (3) because a teacher encouraged them. In the focus group discussions, mentors suggested that their continued involvement was linked to ‘fun’ and enjoyment, or the social aspect of spending time with their peers. Others stated that they believed in the aims of the GoActive intervention for Year 9 students and that their involvement was linked to the perceptions that the GoActive intervention was ‘good for their [Year 9 students’] health’.
Dose delivered (completeness)
The dose delivered (completeness), or the number of GoActive intervention components implemented, differed between and within schools. The complete GoActive programme was not implemented by any school. Table 36 depicts the implementation of the four GoActive essential components3 per school, as reported by Year 9 students, website analytics, and logged by mentors and facilitators.
Intervention fidelity
From the data presented in Table 36, the fidelity, or the extent to which the GoActive intervention was implemented as planned, varied between schools. It should be noted that despite reporting that no similar programmes were running at the school pre intervention, interviews with Year 9 students, mentors and the contact teacher revealed that school D had been running a weekly ‘healthy active form time’ activity session with all year groups in the school.
The GoActive intervention used specific behaviour change techniques to increase adolescents’ daily MVPA (e.g. novelty, choice, flexibility, competition, mentorship and rewards). 3 A description of the application of the tenet in the GoActive programme will be shown to demonstrate GoActive protocol, as opposed to actual implementation.
GoActive sessions
Qualitative data from individual and focus group interviews indicated that most schools attempted to implement the GoActive sessions as planned. Most descriptions of the GoActive sessions included the class going to a location within the school [e.g. AstroTurf (Equistone Partners Europe, Dalton, GA, USA), hall, field, etc.] and mentors facilitating an activity session. One Year 9 participant described:
We normally like go into form and we get told where to go and then we meet the mentors where we were supposed to be.
Year 9 focus group, school C
A Year 9 participant from school E describes a similar process:
We usually just go on the field and do like rounders, football, any sport on the GoActive website, and just go on the field and do it as a form.
Year 9 focus group, school E
Time for the GoActive intervention varied between schools because of contextual school differences in timetabling. Most schools used their form time (i.e. registration/tutor time) at the beginning of the day, which varied from 15 to 25 minutes. One school used their afternoon form time and another school implemented after school sessions in line with their after-school clubs.
Quantitative and qualitative data on GoActive sessions present dissonance between data sets. For example, 57.3% of Year 9 students from school G reported receiving at least one GoActive session in the last 2 weeks (see Table 36). However, data from individual interviews with Year 9 students, and the two observations, raised questions as to whether or not the GoActive intervention had been implemented at the school at all, aside from one observation. At one observation, anecdotal comments from Year 9 students revealed that the GoActive session was a ‘one-off’ session run for the purpose of the observation. Other indications from the day of observation, including teacher’s comments, led to further questions around implementation. The following is an excerpt from a narrative on the day of the second observation:
As we packed up the equipment and walked over to the gate I met one of the form tutors. In the absence of older mentors, I asked, ‘Do you have any older mentors helping to run GoActive?’ She replied ‘no’. She paused and then stated, ‘I don’t know if I was support to say that’.
Table 37 reports on the relevant GoActive intervention tenets within the implementation of the GoActive sessions.
| GoActive essential element | GoActive tenet | School implementation |
|---|---|---|
| GoActive sessions | Novelty, choice and flexibility |
Reports from Year 9 students and older mentors revealed that there was limited time to discuss the choice of activity for the session. Choice and novelty were hindered because of a number of reasons: continuous choice of the same activity (often football) or the same ‘favourites’ were ‘picked for captains’ and they decided on the choice of activity Very few Year 9 students stated that they participated in a ‘novel’ activity. Year 9 students did not engage with the choices provided or had no desire to choose a novel activity. This resulted in mentors making the novel activity choice on behalf of the students |
| Mentors | Mentorship |
Evidence of mentorship was mixed from observations and views from Year 9 focus groups:Year 9 focus group, school DYear 9 focus group, school CData from the observations indicated that some mentors modelled the behaviour, whereas others did not engage with the activity at all, aside from explaining rules and adjudicating Year 9 students heavily relied on the mentor role, and attributed most of the interventions successes and failures to this role. Mentors did not meet the expectations of the Year 9 students Year 9 students reported that Quick Cards resource were seldom used |
| In-class Year 9 peer leaders | Mentorship | The qualitative evidence suggested that very few tutor groups were able to implement in-class Year 9 peer leaders, if at all. The quantitative data suggested that in-class Year 9 peer leaders were implemented at every school and in at least two GoActive sessions |
| GoActive website use: points logged | Competition |
46.5% (n = 717) of students in intervention schools assessed at baseline entered points on the GoActive website Year 9 students discussed technical challenges to accessing the website, along with an inability to remember their password and sign-in for the website to log points, as key barriers |
| Class-level competition, displayed using school graphs, was rarely referred to in individual and focus group interviews with all subgroups. One Year 9 focus group discussed being shown the graphs by their tutor. One mentor focus group revealed that they had shown their tutor groups the graph. In an interview with a contact teacher, the teacher described receiving the school graph from the GoActive facilitator, with whom they discussed the intention of showing the graph at an assembly. One facilitator mentioned the graphs when describing tutor group participation in an individual interview | ||
| GoActive website site: rewards claimed | Rewards |
Year 9 students were informed of the GoActive reward system in a pre-intervention assembly held with every school. A total of 1014 rewards were claimed by at least 195 Year 9 students Reports of delayed reward distribution and confusion with where and from whom to claim and collect rewards occurred. Rewards seemed to be collected by mentors and/or the GoActive contact teacher, who presented these to students independently, rather than presenting them in class |
On observation, many schools implemented the GoActive sessions as intended in the design of the intervention; however, some modifications were present. From the interviews and observations, modifications of the GoActive sessions included the following:
-
The role of the mentor. Some mentors were given greater responsibility to organise, run and facilitate the delivery of the session than others. Some teachers employed greater control over the organisation and delivery of the session than others.
-
An omission of the mentor role.
-
Combined class GoActive sessions.
-
Gender-segregated GoActive sessions.
-
Non-GoActive activities selected for GoActive sessions.
-
Separate activities for those who did not want to participate in the main session (e.g. some Year 9 students were asked to walk around the playing fields if they did not want to participate in the main activity).
School B amended the GoActive sessions to account for vertical forms (i.e. where the form/tutor group is made up of students from all year groups, as opposed to a single year group). Instead of conducting an activity with the whole form, the mentors recruited Year 9 students using a sign-up sheet to different GoActive activities run throughout the week. Year 9 students were required to remember about the session, turn up at the time and place of where it was held and participate. In turn, this led to some Year 9 students reporting that ‘I wasn’t really asked’ to participate in the session and, as such, they did not participate. Quantitative results offer a complimentary perspective, as Year 9 participants at school B reported the fewest class sessions (11.9%). Despite having traditional form groups, school F employed a similar mechanism of recruitment to GoActive sessions, trialling after school sessions. Few participants in School F reported GoActive class sessions (20.8%).
Noteworthy, some Year 9 students described that they did not receive any GoActive sessions. One participant stated that ‘We didn’t do anything’ (Year 9 focus group discussion, school H). This is reflected in the quantitative data, with only 13.7% of Year 9 students reporting participation in a GoActive session in the last 2 weeks, when schools were still meant to be running the GoActive intervention.
Mentors
Data from the observations and Year 9 student and mentor focus group interviews revealed that each tutor group had between two and seven mentors. Mentor age ranged from 14–15 years old (Year 10 students) through to 17–18 years old (Year 13 students) within one school. Some mentors demonstrated their engagement with the GoActive programme by discussing their pre-GoActive session plans, working with the Year 9 students in multiple tutor time sessions, demonstrating how to play, joining in and working with Year 9 students to encourage their participation in GoActive sessions. In an observation at school A, one mentor demonstrated their engagement:
The mentor walked over to the boy who stood in the corner and gave him a ball. He looked to encourage the boy to participate, and urged the boy to throw the ball at an opposing player. The mentor moved away and the boy moved forward to throw it.
Observational data revealed diverse actions of the mentors between schools. The following is an excerpt from an observation at school D:
We walked over to the sport shed. The contact teacher had given her keys to a Year 10 mentor in order for them to gather the equipment they needed. The two mentors were throwing a frisbee between themselves. They did not appear to speak to any Year 9 students, nor give any eye contact to anyone. They purely played between themselves.
Interview data from Year 9 students further depicted the disparity of the implementation of the mentor role. Some Year 9 students reported that they had not seen their mentors ‘for a couple of weeks’ and that they only ‘sometimes turned up’. At some schools, as a result of mentor non-attendance, the GoActive sessions would not run:
A couple of times they’ve [mentors] shown us the cards [Quick Cards GoActive resources] with the different selection of activities and we’ll talk about which ones we want to do . . . but then they don’t book a place to do it or they don’t have a football next time so we don’t end up doing it.
In-class Year 9 peer leaders
Contact teachers, mentors and facilitators reported that all schools found it difficult to implement the in-class Year 9 peer leader GoActive component. Observation suggested that no schools had implemented in-class Year 9 peer leaders. Reports from Year 9 individual and focus groups, as well as individual interviews with contact teachers, supported this. A contact teacher from school D explained their rationale for taking the focus off of in-class Year 9 peer leaders:
I think we haven’t had any Year 9 peer leaders, I think that’s a difficult thing to try and do because it’s difficult to lead your own peer group, and some, it’s something that I would maybe explore further next time. If I’m honest I haven’t invested much time into that aspect of it, I invested more time in the coordination of it and the Year 10 leaders [mentors] going out. I can see how some peer leaders do encourage and motivate some others, you know, the enthusiastic ones, that might help, but I think it’s, that’s, it’s another thing for teachers or leaders to have to do, who’s going to be the leader next time and rotate it round, it’s just another extra thing which I’m not sure is necessarily needed.
However, qualitative and quantitative results are dissimilar. Quantitative data from Year 9 student questionnaires suggest some implementation of in-class peer leaders at every school, with the lowest implementation at two sessions (see Table 36).
GoActive website use: points logged
Engagement with the recording of points varied per school, for both the percentage of Year 9 students who recorded points and the average points that were claimed (see Table 36). Overall, only 714 Year 9 students (46.2%) logged points on the GoActive website. Year 9 students reported that they were aware of their requirement to log their individual points on the GoActive website in individual and focus group interviews. Year 9 students discussed challenges with forgetting their individual profile password to the GoActive website, forgetting to log their points and subsequently adding numerous points at one time, and having to recall activity participation from memory, as well as issues with school resourcing of laptops/computers to facilitate logging points. There was substantial reliability on using form time to log points from Year 9 students, as very few Year 9 students reported logging points outside school hours:
. . . because some people did log at home, like I think I logged on at home once, one week and then between like 4 weeks I didn’t log my points, I had to log on the fifth week my points from the 4 weeks.
Year 9 focus group, school D, male
Table 37 reports the relevant GoActive tenets within the implementation of the GoActive mentors.
GoActive website use: claimed rewards
All schools had Year 9 participants who claimed rewards. However, there was great variation in the claimed rewards from participants by school (see Table 37). For example, only three prizes were claimed by one participant at school H, whereas 230 prizes were claimed by 106 participants at school E.
In most of the individual and focus group discussions, Year 9 students acknowledged the GoActive intervention rewards on the website. There was confusion regarding who to contact about claimed rewards from the website and who would distribute the rewards. Year 9 students also reported disappointment with the time it took to receive the reward after logging points and claiming the reward online. One student reported:
Ours tried, they [mentors] wrote down like who’d received the jumpers and stuff, but then they didn’t give us them one week, the next week they didn’t again, and then the next week they were off on exams so we haven’t actually seen them since then.
Year 9 focus group, school E
There was additional confusion about how the rewards worked generally. For example, some Year 9 students did not understand the process of claiming the rewards. A few students stated that they were saving their points to claim a GoActive hoodie, instead of claiming the other GoActive rewards along the way. In another focus group, one Year 9 asked if they were required to buy the rewards. The other Year 9 students in the focus group were able to inform them of the process of acquiring rewards.
Table 37 reports on the GoActive tenet of rewards within the implementation of the GoActive intervention.
Dose received (satisfaction): multisubgroup response to the intervention
Questionnaire data revealed that 55.7% of Year 9 students thought that GoActive was fun. Qualitative data were resoundingly positive, revealing that Year 9 students found the programme fun and preferred it to how they traditionally used their form time. Of the mentors, 87.3% thought that participating in the programme was enjoyable. A large proportion of the teachers (50%, 10/20) reported that they enjoyed facilitating the GoActive intervention and 70% (14/20) indicated that they would recommend it to a colleague. The vast majority (85.7%, 6/7) of facilitators would recommend the GoActive programme to a colleague.
Challenges to implementing the GoActive intervention
Based on observations of the GoActive sessions, and individual and focus group interview data from all subgroups, primary factors that may have contributed to the lack of implementation include uncertainty of the roles subgroups played within the GoActive intervention, a lack of Year 9 engagement, a lack of institutional support for contact teachers and school-level constraints (e.g. uniform requirements, limited facility space, resources and time). Additional school-level constraints that had a negative impact on implementation included teacher absence and the timing of the intervention within the school year. These will be discussed in greater detail below.
Roles and responsibility and institutional support
One of the key factors contributing to the lack of implementation appeared to be the uncertainty of the roles that each subgroup played. Most of the contact teachers stated that they were tasked with their role in implementing the GoActive intervention by their SLT, or one of the heads of year levels. A few contact teachers stated that some members of the SLT were extremely supportive and proactive, taking a keen interest in physical activity:
Because our school are very proactive, the head teacher likes the idea of physical activity and our heads of year are engaged with it, they are happy for a form time to be used in that manner.
Contact teacher, school D
Other contact teachers indicated that their SLT did not fully comprehend the intervention. Most of the time, responsibility remained solely with this member of staff:
Initially I didn’t realise how much was involved and, to be honest, I don’t think my head [head teacher] knew how much was involved, I think he thought it would be, I don’t think he’d maybe read the information through and he didn’t realise, I think he thought it might be a month or two thing, done, he didn’t realise it was going to go on.
Contact teacher, school A
This was reinforced by the contact teacher at school G:
I’ve found that that has been the biggest pressure of it, that I may . . . Because I am the head of year by myself, I haven’t got an assistant, I haven’t got anyone else helping me and I’ve found that this has been, not something that, but I just haven’t been able to impart as much of my time on this as maybe I want to but I’m just unable to do that, so again, maybe someone else within the school could have taken it on but they’re so busy, staff are so busy so I would say that’s because of my tutor team and I’m relying on them to be more proactive with it and they’re not.
Contact teacher, school G
At school D, the contact teacher held a SLT role within the school, aligning with health and well-being. The contact teacher at school D felt that their position within the school helped to facilitate intervention implementation and whole year-level adoption of the GoActive intervention. For example, they were able to use their presence in the team to facilitate staff engagement and schedule GoActive sessions into their timetable, creating a sense of routine, which was highly valued by Year 9 students.
Year 9 students held mentors and tutors responsible for the successful implementation of the GoActive programme. The following comment exemplifies this:
I think our form tutors were relying on the mentors to come and get us but because our mentors didn’t, our form tutors just forgot that we had to do it.
Year 9 focus group, school H
Actions of tutors described by mentors and Year 9 students also indicated that more responsibility was placed on the mentors. Year 9 students relied on the mentors to be competent at the GoActive activities, prepare the equipment, explain the rules, interact with those who were not engaging, and continuously encourage those who did not participate. Furthermore, mentors felt that they had to manage the classroom and Year 9 student behaviour. For some tutor groups, if mentors or tutors did not organise an activity, the GoActive sessions did not take place:
We tried to [organise] but we’re a bit wimpy and our form tutor doesn’t really want to and then our year 10 leaders [mentors] aren’t very good so we don’t really get to actually do it.
Year 9 focus group, school D
A Year 9 focus group from school F reiterated this confusion with roles and responsibilities:
I think more on like our side of the school as opposed to the actual project because we just haven’t really done it like done much.
And I don’t think there’s like that many people like in our form for example like willing to take responsibility for setting it up.
Yeah.
Because everyone’s like, oh if I don’t do it we won’t have to do the sport.
Yeah, I think we’re just like relying on our mentors but then if they don’t . . .
Year 9 student behaviour, attitude and engagement
Year 9 student behaviour, attitudes and engagement were discussed as a challenge to implementation by mentors and Year 9 students themselves. The age gap between the year groups, mostly for those mentors who were in Year 10, was constantly cited by mentors as an issue for managing attitudes and behaviour within the Year 9 cohort. Mentors expressed concerns with what they described as a lack of ‘respect’ shown by Year 9 students:
They wouldn’t listen to us because we’re just students as well. So you’d tell them what to do and then they’d do it for like 5 minutes and then it’d just turn into like a free-for-all.
Mentor focus group, school E
One contact teacher (school F) stated that mentors ‘complained of apathy and, “Oh, they [Year 9 students] don’t want to know, they’re not bothered”’. Another contact teacher commented that mentors reported finding it difficult to ‘motivate’ the Year 9 students. Despite some mentors working through disengaging behaviours and attitudes, there were still reported difficulties:
Once we kind of got them involved, we kind of had like a few, like maybe three or four boys that weren’t involved and they were kind of like swaying the whole class.
Mentor focus group, school D
Facilitators and contact teachers encouraged mentors to promote participation from Year 9 students. Concerns were continually expressed about the lack of Year 9 students engaging with activities. One contact teacher explained how they tried to reassure the mentors:
A little bit of worry about what the expectation is as well, so you know, I was sort of saying to them ‘if you decide to do this Zumba session that you did inside and only five people do it, it’s fine, just go with it, you know, you’re not there to make people do it, you’re there to facilitate’, and I think there’s a little bit of a maybe worry with that, like ‘I can’t get everybody to do it’ or an embarrassment maybe as well about being that sort of enthusiastic and then not responding to that maybe, I don’t know.
At some schools, there was a trade agreed, that is if Year 9 students did not want to participate in the chosen activity then they were permitted to walk around the activity space to attain GoActive points (walking was an activity that could be logged to attain GoActive points). The following is an abstract from an observation from one school:
A girl approaches one form tutor with a small group of girls and asks ‘Ma’am, do we have to do it?’ with a sad, whining tone. This was followed by a ‘Yeah’ in agreement from her peers. The tutor informs them that they will have to ‘Ask Sir’, who is running the session. They walk over to the male teacher who is surrounded by the group of Year 9 students. He informs them that they can participate in the session, or if they choose not to then they need to walk around the field instead. Some girls leave the group [those who asked the female tutor if they could not participate]. A different girl watches the girls leave the group, raises her hand to point towards them, and begins to ask ‘why is everyone . . . ?’ She does not finish her question, but she continues to stare at those walking. Twelve girls in total decide to walk. Two boys also decide to walk around in the opposite direction.
School-level factors
Uniform
The school uniform was a challenge to Year 9 participation that was mentioned by Year 9 students, mentors and contact teachers. Many schools required the Year 9 students to change into their PE sporting uniform to participate. At observed sessions, this change took approximately 5–10 minutes of a 15- to 25-minute form time. At some schools, Year 9 students were excluded from participating because of not bringing sport shoes. Some schools allowed Year 9 students to wear their traditional school uniform during GoActive sessions. However, this brought other challenges that had an impact on Year 9 participation, including sweating and smelling in their uniform after participating in a GoActive session or wearing skirts, which was a key barrier to girls’ participation noted by multiple subgroups:
Just the fact that girls wear skirts and that can be a bit difficult when you’re like really trying to go for basketball or something, I mean we were just standing around and a ball bounced up a girl’s skirt [laughs], yeah. So I guess it can be embarrassing in that kind of way.
Mentor focus group, school D
An observation at school E further cemented this as an issue for participation for girls:
Whilst walking back to the boys game the teacher says ‘its like getting blood out of a stone for some of the girls . . . even the sporty ones’. After a brief interaction he indicated that ‘its cos of their skirts’. He said that even if they did want to run they were in their school skirts which made the girls feel uncomfortable.
Resources and facilities
Another challenge mentioned by a number of schools was the resourcing of facilities. Mentors discussed that they ‘didn’t have the equipment’ they wanted for running the activities. Space was limited by exam provision, but also by other form groups using the space or the school not having the space to run activities:
One of the main frustrations was getting the facilities, because we ended up, what was it, we had like two or three forms all doing dodgeball.
Mentor focus group, school E
Mentors and contact teachers also discussed difficulties with booking computer rooms. Mentors noted that they did not possess the ability to access booking computer rooms. Schools either lacked the resources for Year 9 students to access computer rooms to log points or the computer rooms were used by other form groups during registration time. A contact teacher from school F added that the quality of facilities was also a challenge:
Our IT [information technology] facilities aren’t very good at the moment, and if you want the students to log their points, they may not remember at home because maybe they won’t regard it as extra homework or something, I don’t know, or they might just forget to do it . . . So, if you want to try and encourage them to log their points, it’s best to book like an IT facility during registration time, which we’ve tried, but because our facility’s quite slow and you’ve only got 20 minutes to do it in, by the time you’ve logged on it’s time to log off again and then.
Contact teacher, school F
Timing in the school year: examinations
There were several school-level factors that had an impact on the full implementation of the GoActive programme. Interviews with contact teachers, Year 9 students and mentors revealed that exam timings and other school priorities had an impact on implementation. This had implications for the practical running of GoActive sessions. Exam timings created inconsistencies in mentor availability and where the programme could be run within the school. For some forms where the programme had been run, these challenges contributed to the programme losing momentum. Some contact teachers recognised that this challenge was due to the later start of the programme than originally intended:
We didn’t get involved quickly and early enough, partly just through being busy and then, by the time we’d done the first measurements and so on, everything sort of got knocked on. So by the time we started looking at doing some intervention it was into exam period time, which meant we didn’t have an indoor space we could use when we needed to, and then there are barriers to using the outdoor space, which is really that the students need a lot of supervision.
Contact teacher, school F
Staffing
For a few schools, teacher staffing was an issue. Merging of schools through trusts created sharing of staff across campuses. One contact teacher explained:
The Year 9 tutors, that’s another, I guess, a barrier, in a way, is our Year 9 tutors. There’s only one form who has a consistent tutor throughout the week, all the other teachers have got at least two, perhaps three in some cases, of people coming in taking their register. So, you know, that’s an issue in school itself – that group of teachers, some of them might be teaching at [school 1], which is our other school up the road, in a morning, so they won’t be in [school 2], necessarily. So those people, who obviously have a bit more vested interest for these form groups, haven’t been around so much . . .
Contact teacher, school F
As such, the training provided to teaching staff may have reached only a minority of those who were involved. Additionally, turnover of staff or staff absence left supply (relief or substitute) teachers to facilitate running a programme that they were unfamiliar with:
We had supply teachers, so like, it would be like, they didn’t know what was going on, so it was sort of like, ‘You can go with them’, but like it would be like, ‘Shall we let them out before the mentors arrive?’, or something like that.
Year 9 focus group, school E
It was revealed from an interview with a contact teacher that one school had Ofsted (Office for Standards in Education, Children's Services and Skills) inspections that led to the deprioritisation of the GoActive programme within the school.
Chapter 4 Lessons learnt from dissemination
Following completion of the GoActive project, the study team organised a dissemination event that attracted delegates from a variety of fields, including researchers, policy-makers and practitioners. The aim of this event was to provide insights into best practice for future school-based research and health promotion more broadly. The notes are included in this report to provide more insight into the lessons learnt from the team’s engagement with key stakeholders.
On the day, delegates attended an introduction session outlining the GoActive journey so far and an overview of the topic area more generally, before attending each of four discussion topics that were selected from discussions between the project team and TSC:
-
Student voices: what have we learnt? Unpicking inequalities.
-
How can the school environment be used to influence adolescent physical activity?
-
What is the future of school-based activity promotion?
-
Can physical activity improve adolescent well-being?
These sessions generated some excellent discussion and collaboration between delegates.
Theme 1: student voices – what have we learnt? Unpicking inequalities
The importance of considering gender differences when implementing programmes such as the GoActive programme was highlighted. Similarly, it was acknowledged that different groups of students had different preferences and interests. Delegates suggested that student personality should be matched to the type of sport promoted and that topics that may motivate students, such as Instagram (URL: www.instagram.com, Facebook, Inc., Menlo Park, CA, USA) and Love Island (ITV plc, London, UK), should be investigated. Efforts should be made to work out how these can be used as promotors of physical activity.
The importance of establishing role models within the school was discussed, including the importance of making sure that these individuals are on board with programmes to encourage a whole-school approach. Discussions continued around the need for a teacher/leader within the school to provide opportunities for all students to be physically active, such as an active schools co-ordinator. The group suggested that all teachers should also have well-being training and be made aware of different opportunities for and the importance of physical activity.
Delegates discussed whether or not programmes such as GoActive are actually inclusive and whether or not they actually provide absolute beginners with the opportunity to be physically active, as they may be attracting the competitive and sporty students only.
There may be no one-size-fits-all schools approach and there appears to be a need to work with schools on an individual basis to plan how to make physical activity a priority within that school. Schools are already aware that physical activity is important, but there is a need to make it a school-level priority and easy for teachers to implement.
Theme 2: how can the school environment be used to influence adolescent physical activity?
There was general agreement that the school social, policy and physical environment areas are important areas to research and that these can influence adolescent physical activity. The most popular discussion topic revolved around pinpointing the most influential members of classrooms and schools (both teachers and pupils) and using these individuals as leaders to influence physical activity. Delegates showed a clear passion to help adolescents become more active and agreed that it was likely that almost every school had a teacher/pupil who enjoyed sport/physical activity, and it should not necessarily be up to the PE teachers to encourage/champion physical activity.
It was agreed that teachers can have a significant impact on adolescents’ behaviour and that adolescents may model their teacher’s behaviours. Providing examples of how teachers spend their free time (e.g. if they have a physically active hobby) could help adolescents feel more connected to the teachers.
Changing into kit to be physically active (e.g. for PE) was reported as a major barrier to participation in activity for many pupils. Rules that require or prohibit changing of clothes, or scheduling sufficient time to prepare for PE and the next lesson can influence physical activity. Scheduling PE at the start or end of the day may maximise participation when coupled with the provision of showers and allowing pupils to use other amenities (e.g. hair dryers, hair straighteners). Delegates were aware that girls and boys may have different needs when it comes to scheduling PE.
It was acknowledged that financial pressures of schools influence physical activity (e.g. ‘it would be a great idea to offer physical activity after school or at lunch times but teachers are unlikely to want to give up their time unless they are paid’). Offering a free lunch for someone to run a physical activity session at lunch time was not considered suitable reimbursement.
The need to consider the influence of the neighbourhood environment (e.g. the way that adolescents get to school each day) on adolescent physical activity was acknowledged. An example was given where one side of a school was countryside and the other well-connected streets. Delegates suggested that those living on either side of the school should be supported with specific strategies to encourage physical activity (e.g. there would be more barriers to cycling in the countryside where the infrastructure is not designed to support cyclists and ‘so it would be inappropriate to push cycling for these kids’).
There was general agreement that strategies must be simple and free to achieve whole-school engagement. It was suggested that the GoActive intervention was quite complicated and may have hampered implementation and effectiveness.
Parents’ behaviours were also mentioned as important:
A home environment may negate the positive effects of the school environment.
Theme 3: what is the future of school-based activity promotion?
The need to identify differing motivations for participating in activity was suggested, including differences between reasons for participating in team/individual sports and differences between genders.
It was acknowledged that all schools are incredibly different and therefore success may need to be assessed in different ways. It is therefore incredibly hard to design an intervention that fits all schools.
It was thought that teaching team sports regularly may be more practical for schools because of limited resources, staff and experience. Although some schools will bring in external coaches to teach different or new activities in place of the PE teacher, it was suggested that the PE teachers should stay around for these external coach-led sessions so that they could replicate sessions in future.
A lot of discussions focused around the change in guidelines for schools regarding physical activity not becoming mandatory if the school had a more ‘education-based’ approach. They suggested that this could be ruining students’ perceptions of physical activity; if the school did not think physical activity was important, then why would they? A group member did point out that Ofsted were implementing a new framework that included school’s having to demonstrate that they were making steps towards implementing 30 minutes of healthy behaviours a week, although the group were concerned about how this could be interpreted.
The idea of having a ‘physical activity champion’ in schools was discussed. Not necessarily a PE teacher, this could be someone employed specifically for the role. If added to school development plans and potentially given a role on the SLT, then it would make the physical activity champion more accountable and development would have to be monitored.
Delegates said that for any increase in physical activity to happen, there needs to be a whole change in the way schools teach PE or any lessons. Perhaps schools can be educated more on the benefits of active learning in all subjects, with less responsibility solely attributed to the PE department to get students active. It was suggested that perhaps the answer is not school-based interventions at all. The idea was discussed that more emphasis should be made to changing habits at home and that potentially a more ‘home/life/family’-based approach should be taken for interventions.
It was suggested that RCTs of school-based interventions that attempt to promote physical activity should be stopped and that researchers should make use of the very large data sets already available. This led on from the discussion around how different each school can be and how hard it was to design an intervention that can fit into the way that a school works. This also led to the idea that instead of a structured intervention being implemented, a council-funded member of staff could work with a school (or across a few schools) to identify how more physical activity could fit into their school day and support them through implementing this.
It was suggested that a good way to encourage physical activity is to disguise it. Being subtle about encouraging physical activity, with some students not identifying that is the sole aim of an activity, can be a great way to engage students who would not necessarily sign up to or engage in a ‘physical activity-promoting activity’.
For PE teaching to be more successful in schools, it was suggested that perhaps the way it is taught could be changed. Some suggestions for this included the following:
-
Using technology to PE teaching’s advantage (e.g. step count challenges).
-
Asking students to complete a questionnaire at the start of the year/term, with answers dictating which PE group they would be placed into (i.e. team/individual sports could be separated).
-
Multisport lessons rather than one main focus.
-
Treating students more like adults by giving them more freedom and choice.
Some students may not want to make a choice that has an impact on the whole class and so maybe structured choice could work in a practical sense. For example, each lesson allows students to have a choice between two or three activities.
Theme 4: can physical activity improve adolescent well-being?
The overwhelming majority of participants agreed that aligning physical activity and mental well-being objectives was a worthy endeavour, and that there was an understanding among educators that physical and mental health were closely linked. Despite such agreement, there were concerns in terms of the best methods for aligning objectives. For example, the heterogeneity of schools and the unique needs in terms of physical activity and mental health posed difficulties in developing solutions that could be widely implemented.
School leadership was identified as a major enabler to developing school focus on mental well-being. In addition to a commitment to the culture and ethos of the school adopting a mentally healthy approach, it was frequently commented that, like physical activity and health promotion broadly, mental well-being promotion should be implemented as a whole-school approach, as opposed to standalone individual efforts.
There are a number of existing initiatives in the UK to support emotional development and mental health of children, and it was noted that such efforts are ever evolving and greatly welcomed in schools, but only when adequate support and training for educators is provided so that they are equipped with the skills and competencies to respond appropriately to student mental health concerns.
Furthermore, it was suggested that physical health and mental health should fall under ‘whole-child development’ and that refocusing the goals and objectives of such efforts to contributing to whole-child development could hold great promise for schools.
There were suggestions that the overwhelming focus on academic achievements in place of student health may be a barrier to successful implementation of mental well-being and physical activity support. A stronger understanding and clearer translation of the evidence base for positive mental well-being and academic outcomes would be welcomed.
There were preconceptions that PE comprised sport and exercise, and that schools could make shifts to incorporate broader health topics and curricula, including mental health and well-being. This would allow mental health prevention to become integrated into the curricula.
There have been shifts in the public understanding of mental health and this has worked in positive ways, including reducing stigma. Educators and school leadership were acknowledged to be major influencers of working towards reducing stigma. Sensitivities should be allowed whereby young people do not feel further stigmatised by activities, but are supported to seek help for problems when they occur.
Physical activity was identified as a widely understood mechanism through which student behaviour and well-being could be supported. In particular, there was a strong recommendation that activities available to young people foster benefits beyond physical exertion, including relationship building, resilience, goal-setting and other protective benefits.
Cost and other resources is an area of concern. In particular, on whom do the responsibilities of mental well-being fall and what support is available for implementation?
Overall, mental well-being was noted as a major concern nationally and schools were accepted as an ideal environment for implementation of mental well-being objectives. Despite the recognised changes above, there was a consensus that mental and physical health should be pursued as dual objectives and that doing so was likely to lead to the best outcomes for young people.
Chapter 5 Discussion
Summary of main findings
The results of the GoActive trial show that all adolescents became less physically active over time, with no difference between those exposed to the GoActive intervention and those who attended normal school activities. There were inconclusive indications of a more negative effect among boys and a more favourable effect for adolescents with low and medium SEP. Secondary physical activity outcomes showed differential impact across weekdays and weekends, with small between-group differences favouring the control group on weekdays for LPA and sedentary time. The findings also indicate that the GoActive intervention is not cost-effective and that intervention implementation was variable. There was no evidence that the intervention had an impact on well-being, although there was a suggestion of more favourable effects in low SEP schools.
Subgroup effects tended towards a narrowing in inequalities, with lower SEP students and those who with overweight or obesity experiencing more positive effects of the programme. Furthermore, there were indications of attenuated declines in well-being among students in schools with lower SEP when receiving the GoActive intervention. Certain intervention components, particularly mentorship, could potentially warrant consideration for future use in lower SEP settings in interventions targeting well-being and physical activity. This is supported by the results from the mediation analyses, which showed that intervention components traditionally used to increase physical activity could have the potential to be used in school-based interventions aiming to improve well-being, despite no evidence to support their use in increasing physical activity. Higher perception of mentorship was associated with greater increases in well-being among both boys and girls. Class-based sessions and perceived teacher support may be particularly beneficial among boys, whereas rewards and competition require further investigation for use in improving well-being among girls.
The embedded mixed-methods process evaluation helps shed light on some of the reasons for these findings. Two apparent overarching issues were identified regarding adolescent views of the intervention. First, although components may have been liked in principle, varying degrees of implementation undesirably had an impact on participant satisfaction (e.g. self-limited activity choice led to feelings of boredom). Second, some components were differentially liked by subgroups (e.g. competition was disliked by girls and shy/inactive participants). Mentorship seemed the easiest component to implement across all school sites; however, the mentor–facilitator meetings were poorly attended. Mentorship was liked by Year 9 students in principle, but, undesirably, implementation issues had an impact on satisfaction. Mentors did not meet expectations. Year 9 student engagement and attitudes had a negative impact on mentors’ ability to deliver the programme. Triangulation of process evaluation data revealed that the GoActive programme was not consistently implemented, which may additionally help explain the lack of effectiveness. The GoActive intervention was implemented, to some extent, in all of the schools, but reach was low (only 39.4% of participants in intervention schools received the GoActive sessions). At some schools, the mentor and/or in-class Year 9 peer leader roles were omitted. Multiple challenges and varying contextual considerations hindered the implementation of the GoActive programme in multiple school sites, such as an uncertainty of the roles of teachers and mentors, and school-level constraints (e.g. lack of teacher time and other conflicting priorities, including exams).
Low intervention fidelity has implications for the conclusions drawn. As the intervention was not delivered, and therefore not engaged with by students, as intended, then no matter how robust the trial design, methods and analysis are, they can only give certainty to findings pertaining to a low fidelity intervention. In concluding that the intervention was not effective, there is a caveat that it was not effectively delivered.
Relationship with previous evidence
Overall effects
Our findings are in line with emerging review-level evidence, which has identified the limited effectiveness of research-driven physical activity promotion interventions on whole-day MVPA. 14,15 Of note is that high-quality evaluations of school-based interventions targeting adolescent physical activity are still rare, and this evaluation therefore significantly adds to a limited evidence base. The absence of an intervention effect on time spent in MVPA could be partly because of inadequate implementation. The per-protocol population was small and our process evaluation findings indicate that some intervention components, such as mentorship, were not adequately implemented. However, the per-protocol analysis produced similar results to the main analyses, indicating that if the intervention had been implemented with higher fidelity then it may still not have been effective at a whole-population level. The per-protocol definition focused on website use and reported activity sessions. Use of the website was low and contrasts with the high engagement observed in the pilot trial,5 which indicated preliminary effectiveness. This pattern is common in behavioural interventions, with 75% lower effectiveness seen for behavioural interventions across various health behaviours at the full trial stage compared with feasibility and pilot testing. 26 This is thought to be at least partly due to adaptations needed to implement programmes at scale, which highlights the challenge of scaling-up health promotion interventions. 26 Since its inception, the GoActive intervention has been designed to be scalable by including a website and flexibility for use in multiple school structures. However, implementation difficulties may have arisen from the provision of implementation flexibility for schools – an issue also identified in the National Institute for Health Research-funded Girls Active study75 – as well as a lack of clarity in the conceptualisation of the mentor and teacher roles. Additionally, the delivery agent of the intervention changed between the pilot (research staff) and full trial (local authority-funded health trainer, supported by the research team), which may have contributed to the reduced effectiveness. This points to the challenge for researchers to design interventions that are scalable at the outset, which would minimise the need for major adaptions.
Secondary outcomes suggested a negative impact of the intervention on LPA and sedentary time on weekdays (both in school and out of school), with the opposite effect seen on weekends. Adolescent-focused process evaluation results indicate that, at times, the intervention may have fostered a climate that was not conducive to physical activity within school (e.g. the sessions appeared to have a lack of social cohesion and connection, and activity choice was often dominated by boys). 103 However, this may not have extended to weekends. One of the main aims of the GoActive programme was to use school time to encourage participation in activities with friends and family outside school. On a population level, most of the decline in physical activity during adolescence happens on weekends. 106,107 Therefore, it would be worthwhile teasing out what intervention components may be associated with weekend activity. The negative findings for LPA and sedentary time on weekdays were reversed for weekends. These opposing associations largely cancelled each other out, leading to no effect for daily averages, with the intervention not appearing to increase activity of higher intensity (i.e. MVPA).
The evidence base for school-based physical activity interventions for mental well-being among young people is inconsistent108,109 and often overlooked in place of physical health outcomes. 13,110–112 Although a secondary analysis, the examination of the effect of the GoActive programme on mental well-being is an important contribution to a relatively underexplored area of research. We found no overall intervention effect on mental well-being among participating adolescents. This finding was unexpected, given the utilisation of psychological techniques in the GoActive intervention to engage young people to promote physical activity. Such techniques were hypothesised to protect mental well-being through building peer support, self-efficacy, self-esteem and strengthened friendships, all of which are known enablers for positive mental well-being. 113 It is possible that in focusing on such psychological techniques, in place of physical activity levels itself, as done in this current study, we may have overlooked the physiological role of activity in promoting positive mental well-being. Indeed, this is concordant with the GoActive pilot study findings, which found both improved mental well-being and an overall positive impact of the intervention on physical activity levels of young people. 5
Effects in subpopulations
To the best of our knowledge, this is one of the first adolescent physical activity promotion trials to comprehensively investigate which population subgroups may benefit more or less from the exposure to the intervention, and whether or not this differs across activity intensity and time of week. Although the GoActive intervention was not effective in changing the main outcome measure, average daily MVPA at long-term follow-up, there was evidence that the intervention had an impact on population subgroups differentially. The differences in effects between subgroups were small, but potentially meaningful at a population level. 30 The intervention appeared to have a more negative effect among boys, as well as those reporting high SEP. These findings contrast with results from a recent review, which showed no difference between subgroups for intervention effectiveness when assessing whole-day MVPA. However, this was mainly in primary school-based studies. 20 Across subgroups, our results provide a tentative suggestion of a narrowing of inequalities in physical activity levels, as boys are often reported to have higher activity levels than girls,5 although differences in activity levels by SEP are less clear. 57,58 The unfavourable impact among boys for average daily MVPA contrasts with our insights from the mixed-methods process evaluation paper exploring satisfaction with the dose received. This evaluation reported higher intervention acceptability among boys and found that activity choice appeared to be largely driven by boys. 33 These results indicate that gender differences in intervention delivery may not have manifested as expected regarding intervention effect. These contrasting results reinforce the importance of a thorough process evaluation, including observations of delivery, and highlight the complexity of psychosocial issues surrounding activity promotion.
The GoActive intervention appeared to be more effective among individuals with low SEP, which is in contrast to a recent meta-analysis showing no differential effectiveness by SEP. 20 Exploratory moderator analyses demonstrated that participants from a high SEP background appeared to have been negatively impacted, both during and after school, and the reasons for this are unclear. Despite the fact that evidence regarding socioeconomic differences in activity levels is equivocal,58 individuals with lower SEP may do less-vigorous activity59 and may have less opportunity for a variety of structured activities. 60 This lack of equity contributes to health inequalities throughout the life course,61 and reducing health inequalities in behaviours and health is therefore a public health priority. 62 It is possible that individuals of low SEP may have particularly benefited from the chance to try a variety of activities in the GoActive intervention, as the opportunities may not have been available to them otherwise. There appears to be some utility of comprehensive school physical activity interventions for increasing adolescents’ physical activity behaviour, particularly in disadvantaged neighbourhoods, and such interventions could be particularly relevant among certain population groups. 63
The intervention effect on mental well-being for students in lower socioeconomic schools is an important finding because there are known specific mental health vulnerabilities of young people in disadvantaged settings, such as low family income, multiple insecurities (e.g. employment, safety, food provision) and increased risk of chronic physical conditions. 114,115 It is possible that students within more disadvantaged settings may have been particularly sensitive to benefits from the enhanced social support and mentoring provided in the GoActive intervention, in the context of wider home and environmental circumstances that may pose unique mental health risks.
Moreover, participants with overweight or obesity at baseline particularly benefited from the intervention in increasing their out-of-school activity in the short term. Living with overweight or obesity may be associated with increased barriers to participating in group physical activities. 116 The GoActive intervention may have increased self-efficacy among these potentially marginalised individuals, as adolescents who have tried an activity are more likely to want to do it again. 25 This could at least partly explain why the group with overweight or obesity appeared to increase their activity out of school, as they may have particularly benefited from the provision of opportunities to try new activities.
Contextualising the findings
The GoActive trial presented in this report was strengthened by the inclusion of an in-depth mixed-methods process evaluation, involving all relevant actors in the intervention process. This enabled the team to understand both the potential mechanisms of effect and the contextual factors that may help or hinder effectiveness, irrespective of the overall effect observed. Below we provide a reflection on the results from this process evaluation and how they help identify ways to not only improve the GoActive intervention, but also to move the field of secondary school-based physical activity promotion forward.
Implementation
The GoActive intervention was implemented, to some extent, in all of the schools. As the programme was often placed in the hands of one teacher within the school, usually by senior school management, there were issues with workload, lowering the GoActive intervention on the priority list. Additionally, this meant that the programme was not embedded across the whole-school year group as intended and this increased the time pressure on the contact teacher who was leading the GoActive intervention. Teachers highlighted and appreciated the support from the GoActive team; however, most teachers suggested that it would have been useful to have a member of the GoActive staff come in to run the sessions. This directly contradicted suggestions from students and teachers in the development work, which strongly advocated for in-school older mentors to take control of the programme and the request for distance from the researchers. Contact teachers and mentors voiced support for the GoActive programme and what it was trying to achieve; however, implementation of programme components was slow and often occurred late in the evaluation time frame, meaning that the potential for impact on outcomes of interest, including MVPA, was limited.
Enablers of the implementation of the GoActive intervention included school support, embedding a routine, and mentor and tutor support. Challenges that had a negative impact on implementation included school-level constraints, such as having limited space for physical activity, lack of time, uncertainty of the roles subgroups played within the GoActive intervention and sustaining Year 9 student engagement. This is supported by mediation analyses that suggest that, even though no evidence was found to support the use of GoActive intervention components in increasing physical activity, higher perceived mentor and teacher support was associated with improved well-being among boys and girls via various mediators, including self-efficacy, self-esteem and social support. 2
The context of an intervention cannot be overlooked or undervalued. Although the intervention itself was complex in nature, its interaction with its context was also highly complex. For example, once exams were scheduled, one school did not have the space for the physical activity required for the intervention. Another school already had the infrastructure and support from the SLT to embed the GoActive intervention in school practice. The disparity of resources, staffing, equipment and space between schools imposed clear barriers to the implementation of the intervention.
In a change from the feasibility and pilot studies,5,6 in the trial reported here, council-funded facilitators were the official entry point of the intervention within the school and there were several challenges surrounding this role, including facilitator staff changes between training and programme start and also during the programme. In addition, school and facilitator availability did not always align, exacerbating limited school access for some facilitators. Facilitator website logs were not fully completed and, as such, they provided only a partial picture of what happened during the facilitator visits to schools and within the facilitator–mentor meetings. There is potential for bias if only those who felt particularly strongly about the intervention returned their questionnaires or completed their website logs. A number of steps were taken to minimise these issues, including building rapport with the programme staff at meetings and over e-mail. Although facilitators stated that they understood the programme during the training, this was not consistent throughout their post-intervention process evaluation. Perhaps this could be at least partly due to the complexity of implementing the programme in varied school settings and dealing with school preferences for programme implementation. Although appropriate for potential future programme dissemination, having facilitators outside the study team added another level of substantial complexity to implementation. This role was only a small part of a busy health trainer role for the facilitators and therefore it is unlikely that they were as dedicated to the programme as the research team. Incorporating more strategies to increase buy-in from the facilitators of the programme could have been helpful.
GoActive intervention components
The proposed logic model was tested in examining the association between perception of intervention components and physical activity and well-being via a range of proposed psychosocial mediators. 5 The logic model was partly supported, with mentorship being the most consistent component leading to change in well-being, although not physical activity, via a range of psychosocial mediators for both boys and girls. We also identified different patterns of mediation for boys and girls, with teacher support and class sessions identified for boys and competition and rewards identified for girls. Many interventions use components such as mentorship, leadership, class-based activity sessions and online activity tracking to increase physical activity. The potential for these physical activity interventions to additionally target well-being are becoming increasingly salient. 21,24,117 Despite this widespread use, relatively little is known about the mechanisms by which these intervention components may target outcomes via proposed mediators. We provide a reflection of the implementation and effectiveness of the GoActive intervention components below.
Mentorship
Mentorship was strongly suggested in the co-design phase and was associated with increased well-being, but not physical activity, among both girls and boys. Mentorship is commonly incorporated into adolescent physical activity promotion strategies. 5,118,119 Although mentorship was liked in principle, implementation difficulties negatively influenced acceptability, as student expectations of mentors were not met. However, when mentorship was carried out well, the sessions flourished and the feedback was positive.
Combining the mentorship role with challenges, including staff resourcing, limited space, time constraints and examinations, meant that implementation was hindered and at times took longer than anticipated. A more structured approach where facilitators demonstrate GoActive activities to mentors using the Quick Cards may help this inexperienced group maximise the time available and develop confidence. Findings also indicate a potential need for continued training regarding how to promote engagement and targeted attention for participants showing decreasing participation early on, either by non-participation in the GoActive sessions or by not logging points on the GoActive websites. Additionally, because of the reliance on time, it may have been better to build GoActive mentorship into pre-existing sport mentorship roles within the school.
Owing to the primary aim of the programme to increase physical activity, mentors were often chosen by schools as students who were ‘sporty’, whereas focusing on a mentor’s interpersonal skills, social standing and approachability may have been more important.
The importance of recruiting appropriate mentors and of ensuring high-quality and consistent ongoing training is crucial. 120 Mentors may require more substantive training and their contribution clearly supported and, potentially, enforced by the school. Providing specific mentorship training that addresses the importance of developing a sense of connection and creating a positive and inclusive social context would appear important for future behavioural interventions that incorporate these elements. It has been previously suggested that mentors who represent, advance, create and embed a shared sense of social identity can aid participation in physical activity. 121 Even though this was not supported here, regarding MVPA, our results suggest that this may extend to well-being. When successfully implemented, mentorship can facilitate positive feelings of relatedness, which in turn has an impact on an individual’s motivation to make a positive health behaviour change. 122 If implemented well, mentorship from older adolescents could have the potential to increase social support, self-esteem and well-being among adolescents.
Peer leadership
We encouraged the use of weekly in-class peer leaders (which was intended to promote autonomy); however, this was met with reluctance by participants. This may be linked to embarrassment, self-consciousness or fear of judgement from peers. 123,124 In addition, it is possible that being led by someone who is perceived as good at an activity may have put off those who perceived themselves to be less competent.
Peer leadership was not associated with changes in MVPA or well-being and this is in contrast to previous evidence. 75,125 It should be noted that this intervention component may have potential for behaviour change, irrespective of our results. This is at least partly because there were implementation issues within and across participating schools that could have had an impact on the effectiveness of different components. The difficulty of establishing what really went on during implementation is exacerbated by differences between process evaluation data obtained from focus groups, interviews, questionnaires and observations. Despite the questionnaire data reporting on quality of peer leadership, observations suggest that this component was rarely embraced by schools. 103
For peer mentors to be effective, consideration should be given to the mentor selection process. For example, previous studies have used a peer nomination questionnaire to identify ‘influential’ peers to undertake mentor training, provide support and encourage participation in the trial. 126,127 In addition, because of the reliance on mentor time, it may be best to build mentorship into pre-existing leadership roles within the school. Note that the leadership role should be about wider participation, rather than a leadership role exclusively designed with a sports remit, to avoid exacerbation of existing inequalities in schools.
Teacher support
The GoActive programme proposed a tiered leadership approach, with mentors taking on substantial responsibility for organisation and planning, including helping to lead GoActive intervention activities, as well as working with facilitators. In addition, in-class peer leaders worked with mentors to facilitate the choice of activities, team selection, and set up and pack up. Although teachers did not feature in this delivery structure, they often ended up with more responsibility than planned, as mentors struggled to motivate the class. This had an impact on the time required of teaching staff who have multiple competing priorities. Teachers and mentors found their roles in the programme difficult to conceptualise. At times, teachers took on more responsibility than intended; however, this was because the teachers chose to do so, and therefore mentors were not allowed to fulfil their role at the school. On the other hand, mentors often struggled to motivate the class, but it was often reported that teachers did not help with this at all. Both facilitators and mentors reported that teachers did not help or support them with their role in the programme. Issues with teacher buy-in to the programme may link to insufficient training, lack of consistent teacher attendance at training and consistency in training provision across schools, as well as how often facilitators were allowed to come into the school. On reflection, acknowledging the barriers continually faced in general school-based work, there is potential for simple, brief interventions to be the interventions of choice for schools. 128
Competition and rewards
Competition and rewards were identified to increase well-being via self-efficacy, self-esteem and social support among girls. This is contrary to what is expected from the literature and our own process evaluation of adolescent perceptions, in that girls are often stated not to like competition. 42 The discrepancy between the process evaluation and mediation results could be explained by the mediation analysis examining perceptions of competition: girls who perceived competition more highly experienced increased well-being, whereas the focus group participants may not have positively experienced competition. It is unlikely that any one component will be acceptable for all individuals in any population subgroup, although this aligns with our co-design work refining our intervention, where we conducted individual interviews with five students (three girls) who did support including competition. 6 One additional possible explanation for the differential results is that proximal rewards are preferred by some groups more than others. For example, individuals from lower socioeconomic backgrounds129 and individuals with overweight or obesity may be more sensitive to rewards because of increased salience of the rewarding qualities of the stimulus. 130 This is consistent with our observation of differential effectiveness in favour of these subgroups. As girls may be seen as a marginalised community within a school, especially with regard to physical activity,131 it is possible that this could be an explanation of why these components may have been particularly salient to girls. As suggested in our development work with adolescents, a sensitive approach to competition may be worth further consideration. Further work with girls on exactly what elements of competition are acceptable could be useful for future intervention design.
Online activity tracking website
The GoActive intervention had been designed to be scalable by including a website and flexibility for use in multiple school structures. In hindsight, we perhaps afforded schools too much flexibility, potentially leading to inferior implementation because of increased uncertainty about what was ‘supposed’ to be carried out. However, we also identified issues with the implementation of the reward system that was operationalised through the website. Despite their assumed digital literacy,132 many participants reported wanting prescriptive details about how to use the website. Although results indicate that a rewards system is worthwhile, it is currently unclear how it can be operationalised most effectively. Our experience suggests that complex functionality and infrastructure is necessary for rewards tracking. The students had a preference for an app and highlighted the importance of immediacy and attainability of rewards.
Although there was a range of reach reported across schools, there was a relatively low proportion of Year 9 students who reported attending a GoActive session. Many factors contributed to this, including the choice of activity for the session, the competitive nature of the sessions and the organisational factors (based on the perceived mentor role). Other factors, such as the embeddedness of the intervention in and across school institutions, may also have had an impact on reach of the intervention. Overall, the elements that were implemented were potentially those considered the easiest to implement for schools. For example, mentorship was something most schools implemented, drawing on those who had previously been identified as mentors or leaders in the school. The low implementation of in-class peer leaders across all schools may have linked to the input required from mentors and teachers, and the lack of conceptualisation of their roles, as well as the resistance from Year 9 students. Additionally, programme elements that were under greater control of the participants, such as adding points to the GoActive website and claiming rewards from the website, were inconsistent across schools and between participants. Future research should explore different strategies to engage adolescents with physical activity interventions (e.g. with wearable technology, progressive digital technology/mobile apps), as well as investigating ways of maximising the embeddedness of interventions, to promote reach and engagement with future interventions.
Gender differences in physical activity interventions
The whole-school approach of GoActive aimed to avoid the stigmatisation of targeting particular groups;68 however, the results indicate that separate activities for boys and girls may warrant further investigation. The detrimental impact among boys for average daily MVPA contrasts with our insights from the process evaluation, indicating higher intervention acceptability among boys and that activity choice appeared largely driven by boys. 21 These results indicate that gender differences in intervention delivery experience may not have manifested as expected regarding intervention effect.
Aside from mentor support, the results of the mediation analyses differed for boys and girls, with teacher support and class-based activity sessions identified as important for boys, whereas rewards and competition were identified for girls. These gender differences could be at least partly explained by differences in attitudes to physical activity among boys and girls, the complex nature of girls’ relationship with physical activity, and the gendered societal pressures and expectations that can enable or inhibit physical activity. 133,134 We conducted our co-design work with 26 students (18 boys and 8 girls) and it is possible that these students had particular views that did not represent the majority of those in the full trial. 6 Gender differences in our results may perhaps have been exacerbated by the larger amount of boys included in the co-design phase. 6
The results showed that teacher encouragement of physical activity and co-educational class-based sessions could be more appropriate for boys. It is possible that girls may not have felt comfortable co-participating in activities, as PE in the UK is usually segregated by gender and girls may be particularly self-conscious of doing physical activity. 135 Body image is a strong predictor of MVPA in both boys and girls,136 and is also linked to well-being. 137 Concerns around masculine and feminine ideologies of health-related behaviour and body image are very relevant to physical activity promotion in a school setting, but are rarely central to physical activity provision in schools. It follows that considering social identity in physical activity promotion may have particular value in schools, as it has been proposed to have the potential to facilitate the promotion of exercise behaviour and to impact physical activity norms positively, and this has also been identified as facilitating successful mentorship. 121 We proposed that boys’ opinions may hold more weight in the class environment. 103 If this is the case, class-based activity sessions may not have fostered increased social support among girls and could be a potential explanation for why the class-based activity sessions and perceived teacher support were identified as mediators among boys only.
Reflections from theory
The process evaluation results indicate that there was high variability in intervention fidelity for some components, for example the regularity of GoActive sessions (choice and novelty), mentors and in-class peer leaders. These GoActive essential elements were linked to two facets of motivation informed by self-determination theory: (1) extrinsic motivation and (2) intrinsic motivation. 47,138 Despite intervention components aligning with the basic needs for competence, autonomy and relatedness, linked to self-determination theory, modifications or implementation issues potentially remove key underpinning principles of motivation and subsequent behaviour change. Additionally, the considerable variance in the length of GoActive activities may suggest inconsistency.
Despite intervention components aligning with the basic needs for competence, autonomy and relatedness, results suggest that implementation issues and gender differences may have limited, or even reversed, the intended effect. Gender differences were identified, potentially leading to the perpetuation of disparities in perceived competence and autonomy regarding physical activity among girls, which we had aimed to avoid with a whole-population approach. Both autonomy and competence are experiences that are readily affected by conditions in the social environment (i.e. facing non-optimal, overwhelming challenges can lead to feelings of incompetence and disengagement). 122 It appears that elements of the intervention (such as competition and choice) may have undermined girls’ autonomy and perceived competence and led to disengagement. Largely, among boys, choice may have facilitated autonomous motivation and, when carried out well, mentorship and class-based activity appeared to have a positive impact on relatedness. Rewards were generally liked as a strategy but, along with competition, these elements did not adequately support perceived competence and autonomy and risked further marginalising girls and shy/inactive individuals. The results highlight the importance and difficulty of creating activity and needs-supporting environments, and demonstrate how easy it is to inadvertently perpetuate activity-thwarting environments because of issues with intervention implementation.
Mentorship was intended to increase relatedness and social cohesion with older students who were tasked with fostering a sense of connection and positive social climate to facilitate participant interest in physical activity. 54 Both increased self-esteem and social support appeared to mediate the association between higher perceived mentor support and increased well-being, but not physical activity. The ‘quality’ of mentorship may be particularly important when considering the potential impact on psychosocial factors, as mentorship may work successfully only if the recipients are satisfied with the mentorship on offer. 103 Participants seldom reported feelings of connectedness from mentor interaction, and some of the mentors may have perpetuated social environments that were less conducive to physical activity. It is likely that these activity- ‘conducive or thwarting’ environments could influence well-being through the same mediators proposed for physical activity and our results suggest that the associations appear stronger with well-being than physical activity.
Rewards were considered a positive aspect of the intervention and this is consistent with previous findings in behavioural research. 139,140 Using rewards to influence behaviour is a controversial method in health promotion and is contrary to some elements of self-determination theory,47 as it has been suggested that all types of reward may undermine intrinsic motivation. 141 Rewards may be successfully used in behaviour change, but they need to be for behaviour that is desirable, enjoyable and perceived as important. 140 It appears that these criteria were not met in this case, as the intervention did not do enough to encourage students to perceive activity as important. For some students, the GoActive intervention seems to have constituted desirable behaviour and been enjoyable, but implementation may have been a barrier to facilitating this.
Activity choice in our intervention design was intended to target autonomous motivation, but the process evaluation findings indicated that boys dominated class discussion in choosing activities for the class. Although some girls made suggestions for activity selection, the social context of the form group and the dominant voices of the boys seemingly deterred girls from persevering with their choice. This may be due to a number of factors, including social context, comfortability and empowerment of autonomy; however, it is noteworthy that these Year 9 students did not actually express the desire to exert autonomy over the choices provided. Additionally, girls’ novel activity choices led to a lack of participation, which may have deterred others from making suggestions in case it proved an unpopular choice. In turn, rather than supporting feelings of autonomy, the process of choices becoming limited may link to feelings of incompetence and disengagement. Focusing more on empowering Year 9 students to assert autonomy and make a choice may have been beneficial. Additionally, the provision of activity choice from set options on the GoActive website may have further limited autonomy by not encouraging participant input. 142
Although we hypothesised that incorporating novel activities would improve perceived competence, participants often selected familiar activities, which may have been strategic in avoiding the demonstration of a lack of perceived competence. Overall, participants did consider the sessions fun if there was a social element; however, some girls intimated that participating in GoActive sessions kept them from being sociable elsewhere. Although social aspects of the intervention appeared important, qualitative data indicated that peer support, particularly relating to in-class leaders or mentors, was not always well received. This missed opportunity to develop a sense of belonging and connection has important implications on a participant’s intrinsic motivation.
Finally, it has been suggested that for a school-based intervention to work, it needs to include a mechanism from at least one category outlined in the Theory of Expanded, Extended, and Enhanced Opportunities,143 and the GoActive intervention targeted two of these. The ‘expansion’ mechanism suggests providing new occasions to be active by replacing sedentary time with physical activity, such as adding activity to previously sedentary tutor times. Another suggested mechanism implemented in the GoActive intervention is ‘extension’, which suggests lengthening the time currently allocated to activity, such as by encouraging students to be active out of school and in tutor times. 143 Process evaluation data revealed that the GoActive programme was not consistently implemented and therefore may not have led to sufficient expansion or extension of student activity provision.
Reflections on context
Insight gained from the current process evaluation has prompted greater reflection regarding the implementation of complex interventions and the consideration of using the school environment as a context for physical activity interventions. Our findings have a number of implications for the development and evaluation of public health improvement interventions for use in educational settings. Given the limited success of school-based physical activity promotion to date,13 we call for a step change in our approach to intervention design and implementation.
The results presented here raise the question of the appropriateness and value of standardised intervention protocols across a multisite approach. The context of an intervention cannot be overlooked or undervalued. Although the GoActive intervention itself was complex in nature, its interaction with its context was also highly complex. Our analysis highlights the importance of gaining both breadth and depth in understanding of the context of individual schools. The disparity of resources, staffing, equipment and space between schools posed clear challenges for the implementation of the intervention. Each school is different, with competing priorities, as well as resource and time constraints. Future research should consider how best to utilise schools as an intervention setting. Although schools might provide significant reach to adolescents, there are multiple other factors that create challenges, for example teacher/student rapport or school culture around physical activity. A well-resourced intervention can create time and opportunities in the current school system, while minimising the burden of delivery for schools.
Co-production is seen as an inclusive method of intervention development, which may be thought to take into consideration contextual concerns. 144 The GoActive study demonstrates that, if we are to continue to embrace schools as an intervention setting, we need to do more than co-produce interventions, that is we need to understand each school’s culture, particularly as contexts change (e.g. moving to multiacademy trust or an academy chain). We should endeavour to understand how a school’s culture can be a part of intervention design or a complex intervention, for example attitudes towards physical activity. An approach with greater emphasis on school empowerment through the selection of an appropriate and relevant programme to implement in their context, or implementing a protocol followed by input from schools to tailor the intervention, could work best. 145 However, this more practice-based intervention may require new modes of evaluation other than RCTs.
Reflections on the participatory co-design approach
Our results highlight several impasses between suggestions made by students in the co-design phase and the perception of components when implemented. In our process evaluation, students stated that they would have preferred the intervention integrated into the school timetable;103 however, this contrasts directly with the suggestion in the co-design phase to have older students run the programme with distance from teachers and researchers. 6 Although participants indicated a desire to try non-standard activities in the development phase, when implemented, students were reluctant to choose and participate in unfamiliar activities, contrasting the requests for novelty that were central to the participatory input in the earlier phase. 103
Some components developed in the co-design phase were well liked, such as mentorship. Mentorship was strongly suggested in the co-design phase and when mentorship was carried out well it was highly acceptable. Although, in theory, intervention components such as mentorship and leadership align with student and teacher requests, in reality the implementation of these components may not be easily incorporated in the school context. The logistical challenges of mentor recruitment and scheduling training became apparent during the full trial, but this was not perceived to be a challenge by students or teachers during participatory design work.
The diverse range of opinions and preferences across individuals makes it challenging to incorporate multiple student ideas into programmes that can be implemented widely at scale. A different group of students, from different schools, participated in the co-design work to those that were participants in the RCT, and this could offer one explanation for why some components in the co-design process did not lead to change in physical activity and/or well-being. Conducting a participant-led design with the same students who receive the intervention may overcome some of this incongruence, but that appears problematic when aiming to implement a consistent programme at scale and evaluate it in a RCT. Whole-systems approaches with varied, detailed and documented stakeholder input are increasingly being promoted,146 but pragmatic applications of RCTs may be required to assess such approaches.
Future studies may consider a detailed co-design phase that focuses on the practicalities of implementation, including the organisation of training and facilitator retention. It is also important to conduct honest and rigorous process evaluations (including observations) to better establish the underlying barriers to and facilitators of the use of individual intervention components in a school setting.
Overall study strengths and limitations
We recruited a population representative of the east of England and our results are relevant to many schools across the UK and to many other high-income settings. Limitations include the adolescent-reported measure of socioeconomic status and the relative lack of participants of low socioeconomic status and non-white participants. However, the percentage of pupils eligible for Pupil Premium funding in the participating schools was similar to the east of England average (20.9% vs. 22.7%). 31 Moreover, the ethnic diversity of the participants was similar to that of England and Wales (86.1% vs. 87.4% white). 32 Device-measured MVPA as the primary outcome aligns with public health research recommendations for objective and comprehensive evaluation of health promotion programmes. 147 Our recruitment to measurement sessions was high, with 84% of eligible pupils measured at baseline. Although retention on the primary outcome at 10-month follow-up could be perceived as a limitation, we achieved our intended sample size and the proportion of participants with valid data at follow-up is comparable to that of similar trials. 148 Although female participants and participants from higher SEP backgrounds, from Cambridgeshire, and participants with underweight or normal weight were more likely to provide primary outcome data, post hoc sensitivity analyses indicated that the main results were unaffected by participants with missing data. The long-term economic modelling was exploratory and demonstrates its potential utility in adolescent physical activity promotion research. To our knowledge, this effectiveness trial was the largest trial with device-measured physical activity. In addition, the trial addressed many weaknesses of previous trials by including iterative development with the target group and school stakeholders, well-measured prespecified outcomes, long-term follow-up, detailed process evaluation and economic evaluation, and by having sufficient statistical power to assess effectiveness. However, it is likely that an insufficient dose of the intervention was delivered to achieve the desired effect, and it therefore remains unclear whether or not the GoActive intervention, if delivered as intended, is effective in changing adolescents’ overall MVPA.
It should be noted that all of the effect sizes presented in mediation models are relatively small and it was not possible to derive standardised coefficients for these, making it challenging to easily compare the strength of the different associations. The coefficients for change in well-being roughly align with group-level change in well-being, with an average score of –0.03 (SD 0.79) and –0.11 (SD 0.72) for boys and girls, respectively. This average score can be translated to decreases of 0.5 and 1.5 for boys and girls, respectively, on the total Warwick–Edinburgh Mental Wellbeing Scale score, which ranges from 14 to 70, with a cut-off point for probable depression of ≤ 40. 149 Despite small effect sizes, we used E-values to conduct sensitivity analyses for potential unmeasured confounding. E-values on a risk ratio scale represent the minimal strength that confounders would need to have with both the exposure and outcome variable to explain away the indirect effect and to fully explain away the associations we found. It would be necessary for unmeasured confounders to have a relative risk between 1.18 and 1.5. Therefore, despite these modest coefficients, the mediation findings support further exploration of using specific intervention components when targeting well-being in school-based interventions, as this change appears relevant on a population level. However, these suggestions should be taken in the context of the null results for the primary outcome of MVPA and well-being being a secondary outcome in this trial.
Strengths of the process evaluation include the mixed-methods design, and the purposeful sampling to specifically include shy/inactive participants and participants with diversity in levels of intervention participation. Observations were also conducted in addition to interviews with those involved in intervention delivery (i.e. facilitators, teachers and mentors). All effect sizes were small for process evaluation related quantitative results and when interpreted in the context of the four- or five-point scale used, and therefore these are unlikely to represent substantial between-group differences. Approaching shy/inactive students for interview, and designing and evaluating based on their opinions,67 is a novel contribution to the field. It is possible that the intervention was differentially experienced by other subgroups, such as participants with low SEP, but focus groups were not set up to explore these differences. The critical process evaluation presented here provides transferable insights for future intervention design. Including observations from and interviews with individuals from all intervention schools and all levels of intervention delivery enabled exploration of the importance of variability in school context. The researcher had some prior knowledge of participating schools as a result of earlier process evaluation visits, which may have affected participant responses. With its qualitative component the findings from this study are not generalisable, but, nonetheless, provide transferable insights for similar intervention studies. The large sample size of the quantitative data and the in-depth insight gained into students’ perspectives provides insights into the mechanisms of complex interventions in a complex environment.
Evaluation of the training for intervention delivery provided to facilitators, teachers and mentors was not conducted. Observation or survey data collection on these dates would have provided insight into the consistency of what was delivered, the attendance at the sessions for each school and the preparedness perspectives of those who were facilitating the programme. Only a small number of teacher questionnaires were returned, and facilitator and mentor website logs were not completed consistently. This may lead to a biased evaluation, as those with strong views might have been more likely to provide their views. The team attempted to minimise this by creating a contact point within the school to act as a project champion, and by building rapport with teachers and facilitators at meetings and by e-mail. The views of teachers in school-based interventions is vital, particularly in terms of implementation. Barriers to this data collection need to be overcome in future research. Moreover, the lack of website logs means that we were unable to assess how many GoActive intervention sessions were conducted. Although development of the questions used to evaluate the GoActive intervention’s essential components provides specificity, a limitation of this approach is the lack of evidence for reliability or validity of the scores that such scales generate, and this is an issue that has broader applicability for other studies.
The value of in-depth process evaluations should not be underestimated in the initial design of a study,59 as these highlight the need to critically examine the delivery of each component and the processes or underlying mechanisms of any complex intervention. In the GoActive intervention, an extensive process evaluation, following the guidance for process evaluation of complex interventions,150 was conducted, collecting data from a variety of sources and using a variety of methods. We employed questionnaires, focus groups, interviews, website analytics, website logs and observer notes to gain breadth and depth in our understanding of how the GoActive intervention was implemented. Although time-consuming and researcher intensive, the diversity in data from all schools, including the perspectives of multiple subgroups, allowed the triangulation of sources, which is an important factor to consider for interpreting our findings. The mixed-methods nature of the process evaluation allowed us to gain different insights to build a full picture of what the programme actually looked like in schools. It is considered ‘best practice’ to publish process evaluation protocols and this recognises the importance of doing so to improve the standards of trials. 151 It is pivotal when using a mixed-methods approach that the process of data collection and analysis is planned from the beginning. Understanding how and when the data will come together, or ‘interact’,152 enhances the knowledge that mixed-methods process evaluation generates. Without this integration, the knowledge gained may have been limited.
Implications for practice and research
Physical activity across both groups decreased by 10 minutes per day over 2 school years, reflecting the population-level decline seen in physical activity over adolescence. 19,64 Even at baseline, the average activity level of participants was half of the recommended 60 minutes per day, potentially increasing the risk of poor health in the future. It is important to continue to try to increase, or at least prevent the decline of, physical activity among adolescents on a population level and schools remain a convenient way to reach large numbers of adolescents in one place. However, there may be insurmountable barriers to this approach, given limitations on resources and time in school. UK schools now have very tight budgets and, given statutory requirements, the additional curriculum time they can allocate to each subject or activity is constrained. Evidence suggests that the majority of the physical activity decline in adolescence occurs out of school and it has been suggested that the structured nature of the school day may already be somewhat protective of maintaining activity levels. 65 Given the limited success of most school-based interventions in increasing objectively measured whole-day physical activity,20,21 higher-level structural changes based on a more in-depth understanding of how physical activity is best integrated in the school appears increasingly worthwhile. Complementary to this, further exploration of how best to promote physical activity in the out-of-school setting is required. Family-based physical activity promotion appears effective, but the evidence based on family-based interventions is dominated by studies targeted at younger children, and is limited by low-quality evaluations and issues with recruitment and reach. 153 Moreover, adolescent-based research on community-based or social media-driven approaches is limited and requires further investment.
Taken together with recent reviews that highlight the lack of effectiveness of research driven by school-based physical activity promotion strategies,14,15 the current evidence suggests that school-based approaches on the whole do not work to increase adolescent physical activity. However, schools have massive potential to have a positive impact on the health of young people. An overhaul of our approach to secondary school-based physical activity promotion is needed to encourage school-driven approaches with support from the wider school system through the use of frameworks such the Comprehensive School Physical Activity Program,154, the World Health Organization’s Health Promoting Schools155 or the Creating Active Schools Framework. 156 A common feature of these frameworks is the importance of senior leadership buy-in. It should be noted, however, that the utility and effectiveness of these frameworks has yet to be established comprehensively. The GoActive intervention was not initiated by senior leaders and in most cases their involvement was for consent sign-off only. This may indicate limited buy-in, which may have affected the GoActive intervention’s potential for effect.
The challenge of designing a replicable intervention offering the flexibility needed across settings is clearly highlighted in this and other trials where small-scale feasibility and pilot studies appeared successful, but experienced implementation issues when scaled up. 157–159 There are likely to be multiple reasons for this phenomenon, including greater distance from the research team to the target population and less time for individual focus on each school. Although some school-based adolescent physical activity interventions have demonstrated effectiveness on a large scale,160 more emphasis on implementation and scale-up from the initial design phase is often necessary. The importance of strong leadership, active participation of multiple actors in the setting and tailoring to the individual local context have been identified as important for scaling up public health programmes. 161 Scaling up and sustaining whole-school interventions of any description is of course challenging, particularly given the resource and time constraints of leaders and staff, and other competing school priorities.
Time and competing school priorities are a constant challenge for school-based physical activity interventions. Compounding pressures on schools and educational systems requires physical activity researchers to do more to link health and educational outcomes. We affirm the importance of this recommendation from previous research. 145 Linking interventions to the priorities and needs of the schools, for example the National Curriculum Framework or Education Inspection Framework, may establish greater importance of the interventions and justify the prioritisation of time to invest in health improvement interventions for their students. Curriculum-based approaches report high reach and dose of lessons taught. 162 Understanding the broader applicability of these lessons to out-of-school hours is the next challenge.
In addition, a stronger focus on implementation science in the initial design phase of school-based adolescent physical activity interventions is necessary. Working with schools to facilitate an approach nformed by implementation science will provide a greater understanding of implementation factors that affect the successful implementation of evidence-based interventions. Furthermore, a focus on school context in implementation science may empower schools with choice in developing their own programme of implementation that suits their particular context. Evidence of physical activities with embedded implementation adoption strategies is developing. 163 Following the PRACTIS (PRACTical planning Implementation and Scale-up) guide steps, this comes under characterising the parameters of the implementation setting, step 1. 164 A stronger emphasis on the concepts of readiness and resourcing,164 recognising the 10 domains that cover the core principles and methods of implementation science, will be important. 165
Each school is a unique system with its own culture, and during this research the team experienced barriers to intervention implementation that varied on a school level because of, what we often perceived as, differences in school culture, ethos or attitudes. 21 This led us to consider that a RCT that expects the same intervention to be replicable, let alone effective, across multiple schools may be an unrealistic expectation and that perhaps aiming for success at a school-by-school level may be more realistic. Although schools are unique microenvironments, standardisation in approaches to every aspect of the curriculum is increasingly becoming normal practice and appears welcome in schools. There is a need to pursue real and interdisciplinary understanding and collaboration that is likely to deviate from the path of subject-specific research agendas. This should lead to a deeper understanding of the educational system and culture, and may require a shift in the field’s ideological principles on physical activity interventions and their delivery in the educational system. Interdisciplinary techniques and disciplines, such as ethnography, education, anthropology, sociology and social networks, could progress further understanding of the cultural context of physical activity behaviour in the educational setting.
Physical activity promotion initiatives are proliferating throughout schools worldwide without evidence adequately assessing their effect or potential harms. 166,167 However, the simplicity of such initiatives has achieved what many designers of complex school-based physical activity interventions aspire to in terms of scale-up, reach and adoption, and there is also a lot to be learnt from them. Our results from this rigorous and honest evaluation may be uncomfortable. However, they highlight the importance of the thorough testing of outcomes and unexpected negative consequences, and could serve as a warning to those wishing to implement interventions without a candid evaluation. Current research-led approaches to school physical activity promotion do not appear to be effective in their current forms and are unlikely to lead to population-level changes in adolescents’ behaviour. 14 The GoActive intervention was rigorously designed with students and teachers and iteratively tested and refined, but despite this rigorous and costly process, when implemented at scale it was no better than the normal school curriculum at preventing declines in adolescent physical activity. We recommend that authorities are cautious about commissioning and rolling-out school-based health promotion strategies, that potential unintended negative consequences are considered and that they are realistic about the scale of behaviour change that can be achieved at a population level and the challenges of implementing a programme as intended.
Research recommendations
-
It is important to continue to try to increase, or at least prevent the decline of, physical activity among adolescents on a population level and schools remain a convenient way to reach large numbers of adolescents in one place. Given the limited effectiveness of school-based physical activity research efforts to date, we recommend that higher-level structural changes, based on a more in-depth understanding of how physical activity is best integrated in schools and the educational system more broadly, appear increasingly worthwhile.
-
There is a need to pursue real and interdisciplinary understanding and collaboration that is likely to deviate from the path of subject-specific research agendas. This should lead to a deeper understanding of the educational system and culture, and may require a shift in the field’s ideological principles on physical activity interventions and their delivery in the educational system. Interdisciplinary techniques and disciplines, such as ethnography, education, anthropology, sociology and social networks, could progress a further understanding of the cultural context of physical activity behaviour in the educational setting.
-
More work needs to consider a link between health and educational outcomes. Time and competing school priorities are a constant challenge for school-based physical activity interventions. Linking interventions to the priorities and needs of the schools may establish the greater importance of the interventions and justify the prioritisation of time to invest in health improvement interventions for their students.
-
Future behaviour change interventions should give more emphasis to implementation and scale-up from the initial design phase. The importance of strong leadership, active participation of multiple actors in the setting and tailoring to the individual local context have been identified as important for scaling up public health programmes. Working with schools to facilitate an approach informed by implementation science may empower schools with choice in developing their own programme of implementation that suits their particular context.
-
The value of in-depth process evaluations should not be underestimated in the initial design of an evaluation of a complex behavioural intervention. They enable the critical examination of the delivery of each component and the processes, or underlying mechanisms, of any complex intervention.
-
Cost-effectiveness evaluations remain rare in youth physical activity promotion and this study demonstrates its feasibility and utility. Future trial should include cost-effectiveness evaluations to enhance the value of the overall research and provide decision-makers within public health and education with the much-needed information to inform how to best spend scarce resources.
-
Exploratory economic modelling showed that the greatest gains of reducing the uncertainty in the results lie in the unit costs of subsequent events, the risks of cardiovascular and stroke events, and the future pathways of blood pressure, cholesterol and glucose levels. Future research should aim to reduce these uncertainties.
-
Co-design is considered a critical component of effective intervention design. Future research is required to understand how best to implement co-design in the development of interventions for large-scale implementation. Conducting a participant-led design with those directly exposed to the intervention may be problematic when aiming to implement a consistent programme at scale and evaluate it in a RCT. Future studies may consider a detailed co-design phase that focuses on the practicalities of implementation, including organisation of training and facilitator retention. Moreover, more flexible research designs should be applied and tested to enable robust evaluation of actual real-world implementation of interventions.
-
Although important from the perspective of scalability and sustainability, having facilitators outside the study team added substantial complexity to implementation and may have affected effective implementation of the GoActive intervention. In this instance, it was important for the research team to recognise that the role is a small part of a busy health trainer role for the facilitators and that they are unlikely to be as dedicated to the programme as the research team. Future interventions should incorporate (behaviour change) strategies to increase buy-in from the facilitators of the programme, recognising that such training is an intervention in itself. Additionally, further involvement of intended external facilitators in the design phase of the intervention allows researchers to draw on local experiences with schools and can lead to increased engagement with the intervention implementation.
-
This study shows the potential of using mentorship and peer mentors, particularly in promoting well-being. However, future behavioural interventions should consider providing specific mentorship training that addresses the importance of developing a sense of connection and creating a positive and inclusive social context. Moreover, consideration should be given to the mentor selection process, for example through use of a peer nomination questionnaire to identify ‘influential’ peers to undertake mentor training.
-
Ways to advance adolescent activity tracking warrants further investigation. The experience here suggests that complex functionality and infrastructure is necessary for rewards tracking. The students had a preference for an app and highlighted the importance of immediacy and attainability of rewards.
-
Although GoActive’s whole-school approach aimed to avoid stigmatisation of targeting particular groups, its results indicate that separate activities for boys and girls may warrant further investigation. Further work with girls could include identification of exactly what elements of competition are acceptable, which could be useful for future intervention design.
Chapter 6 Conclusion
The GoActive school-based intervention was not effective in countering the age-related decline in adolescent physical activity. Together with other recent evidence, this suggests that current research-driven approaches to school-based adolescent physical activity promotion are not effective, with implementation challenges in a complex and stretched educational system likely playing an important role in the lack of effect. Interdisciplinary research should seek to further understand the cultural context of physical activity behaviour in the educational setting. Funders, researchers and local authorities should be realistic about expectations of the effect of school-based adolescent physical activity promotion strategies implemented at scale.
Acknowledgements
We thank Active Essex (Essex, UK) and Everyone Health (Hinckley, UK) for providing facilitators for intervention delivery and we are grateful to the facilitators who delivered the programme. We are grateful to participating schools and students for their involvement in the study and we acknowledge GoActive and MRC Epidemiology Unit staff past and present for their involvement in the project. We also thank the TSC and patient and public involvement groups that have provided valuable advice throughout the project. We are grateful to Dr Charlotte Curtis for acting as scientific editor in leading, co-ordinating and preparing this report for submission. This work was additionally supported by the MRC (unit programme number MC_UU_12015/7) and undertaken under the auspices of the Centre for Diet and Activity Research (Cambridge, UK), a UK Clinical Research Collaboration Public Health Research Centre of Excellence. Funding from the British Heart Foundation (London, UK), Cancer Research UK (London, UK), Economic and Social Research Council (Swindon, UK), MRC, the National Institute for Health Research (Southampton, UK) and the Wellcome Trust (London, UK), under the auspices of the UK Clinical Research Collaboration, is gratefully acknowledged (087636/Z/08/Z; ES/G007462/1; MR/K023187/1).
Contributions of authors
Kirsten L Corder (https://orcid.org/0000-0002-2744-3501) (Senior Investigator Scientist, Behavioural Epidemiology) gained funding, conceptualised the study, acted as chief investigator of the trial, prepared the results for publication, conducted secondary statistical analyses, interpreted results and drafted this report.
Helen E Brown (https://orcid.org/0000-0001-7632-1714) (Research Associate, Behavioural Epidemiology) operationalised the intervention and led the quantitative data collection.
Caroline HD Croxson (https://orcid.org/0000-0003-1225-4713) (Senior Researcher, Primary Care) gained funding, initially conceptualised the process evaluation, and advised on the conduct and analyses of process evaluation.
Stephanie T Jong (https://orcid.org/0000-0002-5012-7187) (Lecturer, Health Sciences) conceptualised the process evaluation, led the qualitative data collection, conducted the mixed-methods process evaluation and prepared the process evaluation results for publication.
Stephen J Sharp (https://orcid.org/0000-0003-2375-1440) (Senior Statistician, Epidemiology) prepared the randomisation schedule, implemented all of the predefined statistical analyses and provided input into the publication.
Anna Vignoles (https://orcid.org/0000-0002-9268-212X) (Professor, Education) gained funding, conceptualised the study and provided an educational perspective on the interpretation of results.
Paul O Wilkinson (https://orcid.org/0000-0003-3302-9662) (University Senior Lecturer and Honorary Consultant, Developmental Psychiatry) gained funding, conceptualised the study and provided a psychiatric perspective on the interpretation of results.
Edward CF Wilson (https://orcid.org/0000-0002-8369-1577) (Senior Lecturer, Health Economics) gained funding, conceptualised the study, conducted the cost-effectiveness analysis and presented it for publication.
Esther MF van Sluijs (https://orcid.org/0000-0001-9141-9082) (Group Leader, Behavioural Epidemiology) gained funding, conceptualised the study, acted as chief investigator of the trial and provided a public health perspective on the interpretation of results.
Publications
Publications arising from this grant
Brown HE, Whittle F, Jong ST, Croxson C, Sharp SJ, Wilkinson P, et al. A cluster randomised controlled trial to evaluate the effectiveness and cost-effectiveness of the GoActive intervention to increase physical activity among adolescents aged 13–14 years. BMJ Open 2017;7:e014419.
Jong ST, Brown HE, Croxson CHD, Wilkinson P, Corder KL, van Sluijs EMF. GoActive: a protocol for the mixed methods process evaluation of a school-based physical activity promotion programme for 13–14 year old adolescents. Trials 2018;19:282.
Corder K, Sharp S, Foubister F, Brown HE, Jong ST, Wells EK, et al. Effectiveness of the GoActive intervention to increase physical activity in adolescents aged 13–14 years: a cluster randomised controlled trial. Lancet 2019;394.
Corder K, Sharp SJ, Jong ST, Foubister C, Brown HE, Wells EK, Armitage SM, et al. Effectiveness and cost-effectiveness of the GoActive intervention to increase physical activity among UK adolescents: a cluster randomised controlled trial. PLOS Med 2020;17:e1003210.
Corder K, Werneck AO, Jong ST, Hoare E, Brown HE, Foubister C, et al. Pathways to increasing adolescent physical activity and wellbeing: a mediation analysis of intervention components designed using a participatory approach. Int J Environ Res Public Health 2020;17:E390.
Jong ST, Croxson CHD, Guell C, Lawlor ER, Foubister C, Brown HE, et al. Adolescents’ perspectives on a school-based physical activity intervention: a mixed method study. J Sport Health Sci 2020;9:28–40.
Related publications
Corder K, Schiff A, Kesten JM, van Sluijs EM. Development of a universal approach to increase physical activity among adolescents: the GoActive intervention. BMJ Open 2015;5:e008610.
Corder K, Brown HE, Schiff A, van Sluijs EM. Feasibility study and pilot cluster-randomised controlled trial of the GoActive intervention aiming to promote physical activity among adolescents: outcomes and lessons learnt. BMJ Open 2016;6:e012335.
Data-sharing statement
All data requests should be submitted to the corresponding author for consideration. Access to anonymised data may be granted following favourable review of a research proposal.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care.
References
- Corder K, Sharp SJ, Jong ST, Foubister C, Brown HE, Wells EK, et al. Effectiveness and cost-effectiveness of the GoActive intervention to increase physical activity among UK adolescents: a cluster randomised controlled trial. PLOS Med 2020;17. https://doi.org/10.1371/journal.pmed.1003210.
- Corder K, Werneck AO, Jong ST, Hoare E, Brown HE, Foubister C, et al. Pathways to increasing adolescent physical activity and wellbeing: a mediation analysis of intervention components designed using a participatory approach. Int J Environ Res Public Health 2020;17. https://doi.org/10.3390/ijerph17020390.
- Jong ST, Brown HE, Croxson CHD, Wilkinson P, Corder KL, van Sluijs EMF. GoActive: a protocol for the mixed methods process evaluation of a school-based physical activity promotion programme for 13–14 year old adolescents. Trials 2018;19. https://doi.org/10.1186/s13063-018-2661-0.
- Brown HE, Whittle F, Jong ST, Croxson C, Sharp SJ, Wilkinson P, et al. A cluster randomised controlled trial to evaluate the effectiveness and cost-effectiveness of the GoActive intervention to increase physical activity among adolescents aged 13–14 years. BMJ Open 2017;7. https://doi.org/10.1136/bmjopen-2016-014419.
- Corder K, Brown HE, Schiff A, van Sluijs EM. Feasibility study and pilot cluster-randomised controlled trial of the GoActive intervention aiming to promote physical activity among adolescents: outcomes and lessons learnt. BMJ Open 2016;6. https://doi.org/10.1136/bmjopen-2016-012335.
- Corder K, Schiff A, Kesten JM, van Sluijs EM. Development of a universal approach to increase physical activity among adolescents: the GoActive intervention. BMJ Open 2015;5. https://doi.org/10.1136/bmjopen-2015-008610.
- World Health Organization (WHO) . Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks 2009.
- Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U. Lancet Physical Activity Series Working Group . Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet 2012;380:247-57. https://doi.org/10.1016/S0140-6736(12)60646-1.
- Cooper AR, Goodman A, Page AS, Sherar LB, Esliger DW, van Sluijs EM, et al. Objectively measured physical activity and sedentary time in youth: the International children’s accelerometry database (ICAD). Int J Behav Nutr Phys Act 2015;12. https://doi.org/10.1186/s12966-015-0274-5.
- Corder K, Winpenny E, Love R, Brown HE, White M, Sluijs EV. Change in physical activity from adolescence to early adulthood: a systematic review and meta-analysis of longitudinal cohort studies. Br J Sports Med 2019;53:496-503. https://doi.org/10.1136/bjsports-2016-097330.
- Shrestha R, Copenhaver M. Long-term effects of childhood risk factors on cardiovascular health during adulthood. Clin Med Rev Vasc Health 2015;7:1-5. https://doi.org/10.4137/CMRVH.S29964.
- Aberg MA, Pedersen NL, Toren K, Svartengren M, Backstrand B, Johnsson T, et al. Cardiovascular fitness is associated with cognition in young adulthood. Proc Natl Acad Sci U S A 2009;106:20906-11. https://doi.org/10.1073/pnas.0905307106.
- Love R, Adams J, van Sluijs EMF. Are school-based physical activity interventions effective and equitable? A meta-analysis of cluster randomized controlled trials with accelerometer-assessed activity. Obes Rev 2019;20:859-70. https://doi.org/10.1111/obr.12823.
- Borde R, Smith JJ, Sutherland R, Nathan N, Lubans DR. Methodological considerations and impact of school-based interventions on objectively measured physical activity in adolescents: a systematic review and meta-analysis. Obes Rev 2017;18:476-90. https://doi.org/10.1111/obr.12517.
- Koopman JS, Chick SE, Riolo CS, Adams AL, Wilson ML, Becker MP. Modeling contact networks and infection transmission in geographic and social space using GERMS. Sex Transm Dis 2000;27:617-26. https://doi.org/10.1097/00007435-200011000-00010.
- Gunnell D, Kidger J, Elvidge H. Adolescent mental health in crisis. BMJ 2018;361. https://doi.org/10.1136/bmj.k2608.
- Kessler RC, Angermeyer M, Anthony JC, DE Graaf R, Demyttenaere K, Gasquet I, et al. Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization’s World Mental Health Survey Initiative. World Psychiatry 2007;6:168-76.
- Patalay P, Gage SH. Changes in millennial adolescent mental health and health-related behaviours over 10 years: a population cohort comparison study. Int J Epidemiol 2019;48:1650-64. https://doi.org/10.1093/ije/dyz006.
- World Health Organization (WHO) . Adolescents: Health Risks and Solutions 2017.
- Cairns KE, Yap MB, Pilkington PD, Jorm AF. Risk and protective factors for depression that adolescents can modify: a systematic review and meta-analysis of longitudinal studies. J Affect Disord 2014;169:61-75. https://doi.org/10.1016/j.jad.2014.08.006.
- Biddle SJH, Ciaccioni S, Thomas G, Vergeer I. Physical activity and mental health in children and adolescents: an updated review of reviews and an analysis of causality. Psychol Sport Exerc 2019;42:146-55. https://doi.org/10.1016/j.psychsport.2018.08.011 (accessed 29 September 2020).
- Mammen G, Faulkner G. Physical activity and the prevention of depression: a systematic review of prospective studies. Am J Prev Med 2013;45:649-57. https://doi.org/10.1016/j.amepre.2013.08.001.
- Schuch FB, Vancampfort D, Firth J, Rosenbaum S, Ward PB, Silva ES, et al. Physical activity and incident depression: a meta-analysis of prospective cohort studies. Am J Psychiatry 2018;175:631-48. https://doi.org/10.1176/appi.ajp.2018.17111194.
- Lubans D, Richards J, Hillman C, Faulkner G, Beauchamp M, Nilsson M, et al. Physical activity for cognitive and mental health in youth: a systematic review of mechanisms. Pediatrics 2016;138. https://doi.org/10.1542/peds.2016-1642.
- Corder K, Atkin AJ, Ekelund U, van Sluijs EM. What do adolescents want in order to become more active?. BMC Public Health 2013;13. https://doi.org/10.1186/1471-2458-13-718 (accessed 29 September 2020).
- Raustorp A, Ekroth Y. Tracking of pedometer determined physical activity: a 10 years follow-up study from adolescence to adulthood in Sweden. J Phys Act Health 2013;10:1186-92. https://doi.org/10.1123/jpah.10.8.1186.
- Telama R, Yang X, Viikari J, Välimäki I, Wanne O, Raitakari O. Physical activity from childhood to adulthood: a 21-year tracking study. Am J Prev Med 2005;28:267-73. https://doi.org/10.1016/j.amepre.2004.12.003.
- Khaw KT, Wareham N, Bingham S, Welch A, Luben R, Day N. Combined impact of health behaviours and mortality in men and women: the EPIC-Norfolk prospective population study. PLOS Med 2008;5. https://doi.org/10.1371/journal.pmed.0050012.
- Gill JM, Cooper AR. Physical activity and prevention of type 2 diabetes mellitus. Sports Med 2008;38:807-24. https://doi.org/10.2165/00007256-200838100-00002.
- Ekelund U, Luan J, Sherar LB, Esliger DW, Griew P, Cooper A. International Children’s Accelerometry Database (ICAD) Collaborators . Moderate to vigorous physical activity and sedentary time and cardiometabolic risk factors in children and adolescents. JAMA 2012;307:704-12. https://doi.org/10.1001/jama.2012.156.
- Viner RM, Ozer EM, Denny S, Marmot M, Resnick M, Fatusi A, et al. Adolescence and the social determinants of health. Lancet 2012;379:1641-52. https://doi.org/10.1016/S0140-6736(12)60149-4.
- Salmon J, Booth ML, Phongsavan P, Murphy N, Timperio A. Promoting physical activity participation among children and adolescents. Epidemiol Rev 2007;29:144-59. https://doi.org/10.1093/epirev/mxm010.
- van Sluijs E, McMinn A, Griffin S. Effectiveness of interventions to promote physical activity in children and adolescents: systematic review of controlled trials. BMJ 2007;6. https://doi.org/10.1136/bmj.39320.843947.BE.
- Dobbins M, De Corby K, Robeson P, Husson H, Tirilis D. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6–18. Cochrane Database Syst Rev 2009;1. https://doi.org/10.1002/14651858.CD007651.
- Metcalf B, Henley W, Wilkin T. Effectiveness of intervention on physical activity of children: systematic review and meta-analysis of controlled trials with objectively measured outcomes (EarlyBird 54). BMJ 2012;345. https://doi.org/10.1136/bmj.e5888.
- Jago R, Baranowski T, Baranowski JC, Thompson D, Cullen KW, Watson K, et al. Fit for Life Boy Scout badge: outcome evaluation of a troop and Internet intervention. Prev Med 2006;42:181-7. https://doi.org/10.1016/j.ypmed.2005.12.010.
- Haerens L, Deforche B, Maes L, Cardon G, Stevens V, De Bourdeaudhuij I. Evaluation of a 2-year physical activity and healthy eating intervention in middle school children. Health Educ Res 2006;21:911-21. https://doi.org/10.1093/her/cyl115.
- Jago R, Sebire SJ, Cooper AR, Haase AM, Powell J, Davis L, et al. Bristol girls dance project feasibility trial: outcome and process evaluation results. Int J Behav Nutr Phys Act 2012;9. https://doi.org/10.1186/1479-5868-9-83.
- Brooke HL, Corder K, Griffin SJ, Ekelund U, van Sluijs EM. More of the same or a change of scenery: an observational study of variety and frequency of physical activity in British children. BMC Public Health 2013;13. https://doi.org/10.1186/1471-2458-13-761.
- Kriemler S, Meyer U, Martin E, van Sluijs EM, Andersen LB, Martin BW. Effect of school-based interventions on physical activity and fitness in children and adolescents: a review of reviews and systematic update. Br J Sports Med 2011;45:923-30. https://doi.org/10.1136/bjsports-2011-090186.
- Lonsdale C, Rosenkranz RR, Peralta LR, Bennie A, Fahey P, Lubans DR. A systematic review and meta-analysis of interventions designed to increase moderate-to-vigorous physical activity in school physical education lessons. Prev Med 2013;56:152-61. https://doi.org/10.1016/j.ypmed.2012.12.004.
- Jago R, Davis L, McNeill J, Sebire SJ, Haase A, Powell J, et al. Adolescent girls’ and parents’ views on recruiting and retaining girls into an after-school dance intervention: implications for extra-curricular physical activity provision. Int J Behav Nutr Phys Act 2011;8. https://doi.org/10.1186/1479-5868-8-91.
- Elder JP, Shuler L, Moe SG, Grieser M, Pratt C, Cameron S, et al. Recruiting a diverse group of middle school girls into the trial of activity for adolescent girls. J Sch Health 2008;78:523-31. https://doi.org/10.1111/j.1746-1561.2008.00339.x.
- Strunin L, Douyon M, Chavez M, Bunte D, Horsburgh CR. The GirlStars program: challenges to recruitment and retention in a physical activity and health education program for adolescent girls living in public housing. Prev Chronic Dis 2010;7.
- Cardy A, Holden S, Watson D, Nelson D, Turner S. Recruiting children onto research studies by the Scottish Primary Care Research Network: a real team effort. Qual Prim Care 2012;20:199-206.
- Thompson C, Wankel L. The effect of perceived activity choice upon frequency of exercise behavior. J Appl Soc Psychol 1980;10:436-43. https://doi.org/10.1111/j.1559-1816.1980.tb00722.x.
- Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol 2000;55:68-7. https://doi.org/10.1037/0003-066x.55.1.68.
- Wilson DK, Kitzman-Ulrich H, Williams JE, Saunders R, Griffin S, Pate R, et al. An overview of ‘The Active by Choice Today’ (ACT) trial for increasing physical activity. Contemp Clin Trials 2008;29:21-3. https://doi.org/10.1016/j.cct.2007.07.001.
- Beier SR, Rosenfeld WD, Spitalny KC, Zansky SM, Bontempo AN. The potential role of an adult mentor in influencing high-risk behaviors in adolescents. Arch Pediatr Adolesc Med 2000;154:327-31. https://doi.org/10.1001/archpedi.154.4.327.
- Yancey AK, Siegel JM, McDaniel KL. Role models, ethnic identity, and health-risk behaviors in urban adolescents. Arch Pediatr Adolesc Med 2002;156:55-61. https://doi.org/10.1001/archpedi.156.1.55.
- Davey-Rothwell MA, Tobin K, Yang C, Sun CJ, Latkin CA. Results of a randomized controlled trial of a peer mentor HIV/STI prevention intervention for women over an 18 month follow-up. AIDS Behav 2011;15:1654-63. https://doi.org/10.1007/s10461-011-9943-9.
- Black MM, Hager ER, Le K, Anliker J, Arteaga SS, Diclemente C, et al. Challenge! Health promotion/obesity prevention mentorship model among urban, black adolescents. Pediatrics 2010;126:280-8. https://doi.org/10.1542/peds.2009-1832.
- Smith LH. Cross-age peer mentoring approach to impact the health outcomes of children and families. J Spec Pediatr Nurs 2011;16:220-5. https://doi.org/10.1111/j.1744-6155.2011.00286.x.
- Ginis KA, Nigg CR, Smith AL. Peer-delivered physical activity interventions: an overlooked opportunity for physical activity promotion. Transl Behav Med 2013;3:434-43. https://doi.org/10.1007/s13142-013-0215-2.
- Tate D, Larose J, Espeland M, Wing R. Study of Novel Approaches to Prevention (SNAP) of Weight Gain in Young Adults: Rationale, Design and Development of Interventions n.d.
- Hendy HM, Williams KE, Camise TS. Kid’s Choice Program improves weight management behaviors and weight status in school children. Appetite 2011;56:484-94. https://doi.org/10.1016/j.appet.2011.01.024.
- Chen H, Sun H, Dai J. Peer support and adolescents’ physical activity: the mediating roles of self-efficacy and enjoyment. J Pediatr Psychol 2017;42:569-77. https://doi.org/10.1093/jpepsy/jsw103.
- Mendonça G, Júnior JC. Physical activity and social support in adolescents: analysis of different types and sources of social support. J Sports Sci 2015;33:1942-51. https://doi.org/10.1080/02640414.2015.1020842.
- Grant A, Treweek S, Dreischulte T, Foy R, Guthrie B. Process evaluations for cluster-randomised trials of complex interventions: a proposed framework for design and reporting. Trials 2013;14. https://doi.org/10.1186/1745-6215-14-15.
- Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015;350. https://doi.org/10.1136/bmj.h1258.
- Clarke JL, Griffin TL, Lancashire ER, Adab P, Parry JM, Pallan MJ. WAVES study trial investigators . Parent and child perceptions of school-based obesity prevention in England: a qualitative study. BMC Public Health 2015;15. https://doi.org/10.1186/s12889-015-2567-7.
- Sebire SJ, Banfield K, Campbell R, Edward MJ, Kipping R, Kadir B, et al. Development and feasibility cluster randomised controlled trial of a Peer-Led physical Activity iNtervention for Adolescent girls (PLAN-A). Public Health Res 2017;7. https://doi.org/10.3310/phr07160.
- van Nassau F, Singh AS, Hoekstra T, van Mechelen W, Brug J, Chinapaw MJ. Implemented or not implemented? Process evaluation of the school-based obesity prevention program DOiT and associations with program effectiveness. Health Educ Res 2016;31:220-33. https://doi.org/10.1093/her/cyw007.
- Jago R, Rawlins E, Kipping RR, Wells S, Chittleborough C, Peters TJ, et al. Lessons learned from the AFLY5 RCT process evaluation: implications for the design of physical activity and nutrition interventions in schools. BMC Public Health 2015;15. https://doi.org/10.1186/s12889-015-2293-1.
- Larsson I, Staland-Nyman C, Svedberg P, Nygren JM, Carlsson IM. Children and young people’s participation in developing interventions in health and well-being: a scoping review. BMC Health Serv Res 2018;18. https://doi.org/10.1186/s12913-018-3219-2.
- Steckler AB, Linnan L. Process Evaluation for Public Health Interventions and Research. San Francisco, CA: Jossey-Bass; 2002.
- Saunders RP, Evans MH, Joshi P. Developing a process-evaluation plan for assessing health promotion program implementation: a how-to guide. Health Promot Pract 2005;6:134-47. https://doi.org/10.1177/1524839904273387.
- Shochet IM, Dadds MR, Holland D, Whitefield K, Harnett PH, Osgarby SM. The efficacy of a universal school-based program to prevent adolescent depression. J Clin Child Psychol 2001;30:303-15. https://doi.org/10.1207/S15374424JCCP3003_3.
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ 2008;337. https://doi.org/10.1136/bmj.a1655.
- van de Glind I, Bunn C, Gray CM, Hunt K, Andersen E, Jelsma J, et al. The intervention process in the European Fans in Training (EuroFIT) trial: a mixed method protocol for evaluation. Trials 2017;18. https://doi.org/10.1186/s13063-017-2095-0.
- Medical Research Council (MRC) . Process Evaluation of Complex Interventions: UK Medical Research Council (MRC) Guidance 2014.
- White T, Westgate K, Wareham NJ, Brage S. Estimation of physical activity energy expenditure during free-living from wrist accelerometry in UK Adults. PLOS One 2016;11. https://doi.org/10.1371/journal.pone.0167472.
- Scott JJ, Rowlands AV, Cliff DP, Morgan PJ, Plotnikoff RC, Lubans DR. Comparability and feasibility of wrist- and hip-worn accelerometers in free-living adolescents. J Sci Med Sport 2017;20:1101-6. https://doi.org/10.1016/j.jsams.2017.04.017.
- Collings PJ, Wijndaele K, Corder K, Westgate K, Ridgway CL, Dunn V, et al. Levels and patterns of objectively-measured physical activity volume and intensity distribution in UK adolescents: the ROOTS study. Int J Behav Nutr Phys Act 2014;11. https://doi.org/10.1186/1479-5868-11-23.
- Harrington DM, Davies MJ, Bodicoat DH, Charles JM, Chudasama YV, Gorely T, et al. Effectiveness of the ‘Girls Active’ school-based physical activity programme: a cluster randomised controlled trial. Int J Behav Nutr Phys Act 2018;15. https://doi.org/10.1186/s12966-018-0664-6.
- Ricardo LIC, Wendt A, Galliano LM, de Andrade Muller W, Niño Cruz GI, Wehrmeister F, et al. Number of days required to estimate physical activity constructs objectively measured in different age groups: findings from three Brazilian (Pelotas) population-based birth cohorts. PLOS One 2020;15. https://doi.org/10.1371/journal.pone.0216017.
- Johnson MRD, Bhopal RS, Ingleby JD, Gruer L, Petrova-Benedict RS. A glossary for the first World Congress on Migration, Ethnicity, Race and Health. Public Health 2019;172:85-8. https://doi.org/10.1016/j.puhe.2019.05.001.
- Currie C, Molcho M, Boyce W, Holstein B, Torsheim T, Richter M. Researching health inequalities in adolescents: the development of the Health Behaviour in School-Aged Children (HBSC) family affluence scale. Soc Sci Med 2008;66:1429-36. https://doi.org/10.1016/j.socscimed.2007.11.024.
- Voráčová J, Sigmund E, Sigmundová D, Kalman M. Family affluence and the eating habits of 11- to 15-year-old Czech adolescents: HBSC 2002 and 2014. Int J Environ Res Public Health 2016;13. https://doi.org/10.3390/ijerph13101034.
- Buss P. Temperament. Early Developing Personality Traits. Hillsdale, NJ: Lawrence Erlbaum Associates; 1984.
- Ommundsen Y, Page A, Ku PW, Cooper AR. Cross-cultural, age and gender validation of a computerised questionnaire measuring personal, social and environmental associations with children’s physical activity: the European Youth Heart Study. Int J Behav Nutr Phys Act 2008;5. https://doi.org/10.1186/1479-5868-5-29.
- Saunders RP, Pate RR, Felton G, Dowda M, Weinrich MC, Ward DS, et al. Development of questionnaires to measure psychosocial influences on children’s physical activity. Prev Med 1997;26:241-7. https://doi.org/10.1006/pmed.1996.0134.
- Valente TW. Social Networks and Health: Models, Methods, and Applications. Oxford: Oxford University Press; 2010.
- Goodyer IM, Herbert J, Tamplin A, Secher SM, Pearson J. Short-term outcome of major depression: II. Life events, family dysfunction, and friendship difficulties as predictors of persistent disorder. J Am Acad Child Adolesc Psychiatry 1997;36:474-80. https://doi.org/10.1097/00004583-199704000-00009.
- Rosenberg M. Conceiving the Self. New York, NY: Basic Books; 1979.
- Corder K, van Sluijs EM, Wright A, Whincup P, Wareham NJ, Ekelund U. Is it possible to assess free-living physical activity and energy expenditure in young people by self-report?. Am J Clin Nutr 2009;89:862-70. https://doi.org/10.3945/ajcn.2008.26739 (accessed 29 September 2020).
- Tennant R, Hiller L, Fishwick R, Platt S, Joseph S, Weich S, et al. The Warwick–Edinburgh Mental Well-being Scale (WEMWBS): development and UK validation. Health Qual Life Outcomes 2007;5. https://doi.org/10.1186/1477-7525-5-63.
- Watson D, Clark LA. The PANAS-X: Manual for the Positive and Negative Affect Schedule-Expanded Form. Iowa, IA: University of Iowa; 1999.
- Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol 1988;54:1063-70. https://doi.org/10.1037//0022-3514.54.6.1063.
- Joseph S, Linley PA, Harwood J, Lewis CA, McCollam P. Rapid assessment of well-being: The Short Depression-Happiness Scale (SDHS). Psychol Psychother 2004;77:463-78. https://doi.org/10.1348/1476083042555406.
- Bech P, Olsen LR, Kjoller M, Rasmussen NK. Measuring well-being rather than the absence of distress symptoms: a comparison of the SF-36 Mental Health subscale and the WHO-Five Well-Being Scale. Int J Methods Psychiatr Res 2003;12:85-91. https://doi.org/10.1002/mpr.145.
- Taggart F, Stewart-Brown S, Parkinson J. Warwick–Edinburgh Mental Well-being Scale (WEMWBS) User Guide. Edinburgh: NHS Health Scotland; 2015.
- Cole TJ, Lobstein T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr Obes 2012;7:284-94. https://doi.org/10.1111/j.2047-6310.2012.00064.x.
- Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ 2000;320:1240-3. https://doi.org/10.1136/bmj.320.7244.1240.
- White IR, Thompson SG. Adjusting for partially missing baseline measurements in randomized trials. Stat Med 2005;24:993-1007. https://doi.org/10.1002/sim.1981.
- Stevens K. Valuation of the Child Health Utility 9D Index. PharmacoEconomics 2012;30:729-47. https://doi.org/10.2165/11599120-000000000-00000.
- Gc VS, Suhrcke M, Hardeman W, Sutton S, Wilson ECF. Very Brief Interventions Programme Team . Cost-effectiveness and value of information analysis of brief interventions to promote physical activity in primary care. Value Health 2018;21:18-26. https://doi.org/10.1016/j.jval.2017.07.005.
- US Department of Health and Human Services . 2008 Physical Activity Guidelines for Americans 2008. https://health.gov/paguidelines/2008/appendix1.aspx (accessed 14 January 2020).
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol 2006;3:77-101. https://doi.org/10.1191/1478088706qp063oa.
- Bryman A. Social Research Methods. Oxford: Oxford University Press; 2012.
- Richards L. Handling Qualitative Data: A Practical Guide. London: SAGE Publications Ltd; 2005.
- Farmer T, Robinson K, Elliott SJ, Eyles J. Developing and implementing a triangulation protocol for qualitative health research. Qual Health Res 2006;16:377-94. https://doi.org/10.1177/1049732305285708.
- Jong TS, Croxson CHD, Guell C, Lawlor ER, Foubister C, Brown HE, et al. Adolescents’ perspectives on a school-based physical activity intervention: a mixed method study. J Sport Health Sci 2020;9:28-40. https://doi.org/10.1016/j.jshs.2019.06.007.
- National Education Union . Support Staff Pay and Conditions n.d. https://neu.org.uk/advice/support-staff-pay-and-conditions (accessed 9 March 2020).
- National Association of Schoolmasters Union of Women Teachers . England Pay Scales n.d. www.nasuwt.org.uk/advice/pay-pensions/pay-scales/england-pay-scales.html (accessed 9 March 2020).
- Brooke HL, Atkin AJ, Corder K, Ekelund U, van Sluijs EM. Changes in time-segment specific physical activity between ages 10 and 14 years: a longitudinal observational study. J Sci Med Sport 2016;19:29-34. https://doi.org/10.1016/j.jsams.2014.10.003.
- Corder K, Sharp SJ, Atkin AJ, Griffin SJ, Jones AP, Ekelund U, et al. Change in objectively measured physical activity during the transition to adolescence. Br J Sports Med 2015;49:730-6. https://doi.org/10.1136/bjsports-2013-093190.
- Costigan SA, Eather N, Plotnikoff RC, Taaffe DR, Lubans DR. High-intensity interval training for improving health-related fitness in adolescents: a systematic review and meta-analysis. Br J Sports Med 2015;49:1253-61. https://doi.org/10.1136/bjsports-2014-094490.
- Ha AS, Burnett A, Sum R, Medic N, Ng JY. Outcomes of the rope skipping ‘STAR’ programme for schoolchildren. J Hum Kinet 2015;45:233-40. https://doi.org/10.1515/hukin-2015-0024.
- Watson A, Timperio A, Brown H, Best K, Hesketh KD. Effect of classroom-based physical activity interventions on academic and physical activity outcomes: a systematic review and meta-analysis. Int J Behav Nutr Phys Act 2017;14. https://doi.org/10.1186/s12966-017-0569-9.
- Hynynen ST, van Stralen MM, Sniehotta FF, Araújo-Soares V, Hardeman W, Chinapaw MJ, et al. A systematic review of school-based interventions targeting physical activity and sedentary behaviour among older adolescents. Int Rev Sport Exerc Psychol 2016;9:22-44. https://doi.org/10.1080/1750984X.2015.1081706.
- Russ LB, Webster CA, Beets MW, Phillips DS. Systematic review and meta-analysis of multi-component interventions through schools to increase physical activity. J Phys Act Health 2015;12:1436-46. https://doi.org/10.1123/jpah.2014-0244.
- Lippman LH, Ben-Arieh A, Casas F, Frones I, Korbin J. Handbook of Child Well-being: Theories, Methods and Policies in Global Perspective. New York, NY: Springer; 2014.
- Schneiders J, Drukker M, van der Ende J, Verhulst FC, van Os J, Nicolson NA. Neighbourhood socioeconomic disadvantage and behavioural problems from late childhood into early adolescence. J Epidemiol Community Health 2003;57:699-703. https://doi.org/10.1136/jech.57.9.699.
- Leventhal T, Brooks-Gunn J. The neighborhoods they live in: the effects of neighborhood residence on child and adolescent outcomes. Psychol Bull 2000;126:309-37. https://doi.org/10.1037/0033-2909.126.2.309.
- World Health Organization (WHO) . Report of the Commission on Ending Childhood Obesity 2016.
- O’Neil A, Jacka FN, Quirk SE, Cocker F, Taylor CB, Oldenburg B, et al. A shared framework for the common mental disorders and non-communicable disease: key considerations for disease prevention and control. BMC Psychiatry 2015;15. https://doi.org/10.1186/s12888-015-0394-0.
- Owen MB, Kerner C, Taylor SL, Noonan RJ, Newson L, Kosteli MC, et al. The feasibility of a novel school peer-led mentoring model to improve the physical activity levels and sedentary time of adolescent girls: the Girls Peer Activity (G-PACT) Project. Children 2018;5. https://doi.org/10.3390/children5060067.
- Sebire SJ, Edwards MJ, Campbell R, Jago R, Kipping R, Banfield K, et al. Protocol for a feasibility cluster randomised controlled trial of a peer-led school-based intervention to increase the physical activity of adolescent girls (PLAN-A). Pilot Feasibility Stud 2016;2. https://doi.org/10.1186/s40814-015-0045-8.
- Gorely T, Harrington DM, Bodicoat DH, Davies MJ, Khunti K, Sherar LB, et al. Process evaluation of the school-based girls active programme. BMC Public Health 2019;19. https://doi.org/10.1186/s12889-019-7493-7.
- Stevens M, Rees T, Coffee P, Steffens NK, Haslam SA, Polman R. A Social identity approach to understanding and promoting physical activity. Sports Med 2017;47:1911-18. https://doi.org/10.1007/s40279-017-0720-4.
- Ryan R, Williams G, Patrick H, Deci E. Self-determination theory and physical activity: the dynamics of motivation in development and wellness. Hellenic J Psychol 2009;6:107-24.
- Coleman L, Cox L, Roker D. Girls and young women’s participation in physical activity: psychological and social influences. Health Educ Res 2008;23:633-47. https://doi.org/10.1093/her/cym040.
- Martins J, Marques A, Sarmento H, Carreiro da Costa F. Adolescents’ perspectives on the barriers and facilitators of physical activity: a systematic review of qualitative studies. Health Educ Res 2015;30:742-55. https://doi.org/10.1093/her/cyv042.
- Sebire SJ, Edwards MJ, Campbell R, Jago R, Kipping R, Banfield K, et al. Update to a protocol for a feasibility cluster randomised controlled trial of a peer-led school-based intervention to increase the physical activity of adolescent girls (PLAN-A). Pilot Feasibility Stud 2016;2. https://doi.org/10.1186/s40814-016-0110-y.
- James ML, Christian D, Scott SC, Todd CE, Stratton G, Demmler J, et al. Active children through individual vouchers evaluation: a mixed-method RCT. Am J Prev Med 2020;58:232-43. https://doi.org/10.1016/j.amepre.2019.10.005.
- Starkey F, Audrey S, Holliday J, Moore L, Campbell R. Identifying influential young people to undertake effective peer-led health promotion: the example of A Stop Smoking In Schools Trial (ASSIST). Health Educ Res 2009;24:977-88. https://doi.org/10.1093/her/cyp045.
- Tercedor P, Villa-González E, Ávila-García M, Díaz-Piedra C, Martínez-Baena A, Soriano-Maldonado A, et al. A school-based physical activity promotion intervention in children: rationale and study protocol for the PREVIENE Project. BMC Public Health 2017;17. https://doi.org/10.1186/s12889-017-4788-4.
- Pepper GV, Nettle D. The behavioural constellation of deprivation: causes and consequences. Behav Brain Sci 2017;40. https://doi.org/10.1017/S0140525X1600234X.
- Small DM. Individual differences in the neurophysiology of reward and the obesity epidemic. Int J Obes 2009;33:44-8. https://doi.org/10.1038/ijo.2009.71.
- Cockburn C, Clarke G. ‘Everybody’s looking at you!’: girls negotiating the ‘femininity deficit’ they incur in physical education. Womens Stud Int Forum 2002;25:651-65. https://doi.org/10.1016/S0277-5395(02)00351-5.
- Lenhart A. Teens, Social Media & Technology Overview 2015. Washington, DC: Pew Research Centre; 2015.
- Spencer RA, Rehman L, Kirk SF. Understanding gender norms, nutrition, and physical activity in adolescent girls: a scoping review. Int J Behav Nutr Phys Act 2015;12. https://doi.org/10.1186/s12966-015-0166-8.
- Hill J. Girls’ active identities: navigating othering discourses of femininity, bodies and physical education. Gend Educ 2015;27:666-84. https://doi.org/10.1080/09540253.2015.1078875.
- Robbins L, Pender N, Kazanis M. Barriers to physical activity perceived by adolescent girls. J Midwifery Womens Health 2003;48:206-12. https://doi.org/10.1016/S1526-9523(03)00054-0.
- Kantanista A, Osiński W, Borowiec J, Tomczak M, Król-Zielińska M. Body image, BMI, and physical activity in girls and boys aged 14–16 years. Body Image 2015;15:40-3. https://doi.org/10.1016/j.bodyim.2015.05.001.
- Dyremyhr AE, Diaz E, Meland E. How adolescent subjective health and satisfaction with weight and body shape are related to participation in sports. J Environ Public Health 2014;2014. https://doi.org/10.1155/2014/851932.
- Ryan RM, Deci EL, Deci EL, Ryan RM. Handbook of Self-Determination Research. Rochester, NY: University of Rochester Press; 2002.
- Lowe CF, Horne PJ, Tapper K, Bowdery M, Egerton C. Effects of a peer modelling and rewards-based intervention to increase fruit and vegetable consumption in children. Eur J Clin Nutr 2004;58:510-22. https://doi.org/10.1038/sj.ejcn.1601838.
- Horne PJ, Tapper K, Lowe CF, Hardman CA, Jackson MC, Woolner J. Increasing children’s fruit and vegetable consumption: a peer-modelling and rewards-based intervention. Eur J Clin Nutr 2004;58:1649-60. https://doi.org/10.1038/sj.ejcn.1602024.
- Deci EL, Koestner R, Ryan RM. A meta-analytic review of experiments examining the effects of extrinsic rewards on intrinsic motivation. Psychol Bull 1999;125:627-68. https://doi.org/10.1037/0033-2909.125.6.627.
- How Y, Whipp P, Dimmock J, Jackson B. The effects of choice on autonomous motivation, perceived autonomy support, and physical activity levels in high school physical education. J Teach Phys Educ 2013;32:131-48. https://doi.org/10.1123/jtpe.32.2.131.
- Beets MW, Okely A, Weaver RG, Webster C, Lubans D, Brusseau T, et al. The theory of expanded, extended, and enhanced opportunities for youth physical activity promotion. Int J Behav Nutr Phys Act 2016;13. https://doi.org/10.1186/s12966-016-0442-2.
- Hawkins J, Madden K, Fletcher A, Midgley L, Grant A, Cox G, et al. Development of a framework for the co-production and prototyping of public health interventions. BMC Public Health 2017;17. https://doi.org/10.1186/s12889-017-4695-8.
- Campbell R, Rawlins E, Wells S, Kipping RR, Chittleborough CR, Peters TJ, et al. Intervention fidelity in a school-based diet and physical activity intervention in the UK: Active for Life Year 5. Int J Behav Nutr Phys Act 2015;12. https://doi.org/10.1186/s12966-015-0300-7.
- Daly-Smith A, Quarmby T, Archbold VSJ, Routen AC, Morris JL, Gammon C, et al. Implementing physically active learning: future directions for research, policy, and practice. J Sport Health Sci 2020;9:41-9. https://doi.org/10.1016/j.jshs.2019.05.007.
- All-Party Commission on Physical Activity . Tackling Physical Inactivity – A Coordinated Approach 2014. https://parliamentarycommissiononphysicalactivity.files.wordpress.com/2014/04/apcopa-final.pdf (accessed 4 January 2021).
- Howie EK, Straker LM. Rates of attrition, non-compliance and missingness in randomized controlled trials of child physical activity interventions using accelerometers: a brief methodological review. J Sci Med Sport 2016;19:830-6. https://doi.org/10.1016/j.jsams.2015.12.520.
- Bianca D. Performance of the Warwick–Edinburgh Mental Well-Being Scale (WEMWBS) As a Screening Tool for Depression in UK and Italy n.d. https://warwick.ac.uk/fac/sci/med/research/platform/wemwbs/using/howto/donatella_bianco-thesis.pdf (accessed 20 December 2016).
- Medical Research Council (MRC) . A Framework for the Development and Evaluation of RCTs for Complex Interventions to Improve Health 2000.
- Grant A, Dreischulte T, Treweek S, Guthrie B. Study protocol of a mixed-methods evaluation of a cluster randomized trial to improve the safety of NSAID and antiplatelet prescribing: data-driven quality improvement in primary care. Trials 2012;13. https://doi.org/10.1186/1745-6215-13-154.
- O’Cathain A, Murphy E, Nicholl J. Three techniques for integrating data in mixed methods studies. BMJ 2010;341. https://doi.org/10.1136/bmj.c4587.
- Brown HE, Atkin AJ, Panter J, Wong G, Chinapaw MJ, van Sluijs EM. Family-based interventions to increase physical activity in children: a systematic review, meta-analysis and realist synthesis. Obes Rev 2016;17:345-60. https://doi.org/10.1111/obr.12362.
- National Center for Chronic Disease Prevention and Health Promotion . Increasing Physical Education and Physical Activity: A Framework for Schools n.d. www.cdc.gov/healthyschools/physicalactivity/pdf/17_278143-A_PE-PA-Framework_508.pdf (accessed 4 January 2021).
- World Health Organization (WHO) . Health Promoting School: An Effective Approach for Early Action on NCD Risk Factors 2017.
- Daly-Smith A, Quarmby T, Archbold VSJ, Corrigan N, Wilson D, Resaland GK, et al. Using a multi-stakeholder experience-based design process to co-develop the Creating Active Schools Framework. Int J Behav Nutr Phys Act 2020;17. https://doi.org/10.1186/s12966-020-0917-z.
- Adab P, Pallan MJ, Lancashire ER, Hemming K, Frew E, Barrett T, et al. Effectiveness of a childhood obesity prevention programme delivered through schools, targeting 6 and 7 year olds: cluster randomised controlled trial (WAVES study). BMJ 2018;360. https://doi.org/10.1136/bmj.k211.
- Kipping RR, Howe LD, Jago R, Campbell R, Wells S, Chittleborough CR, et al. Effect of intervention aimed at increasing physical activity, reducing sedentary behaviour, and increasing fruit and vegetable consumption in children: active for Life Year 5 (AFLY5) school based cluster randomised controlled trial. BMJ 2014;348. https://doi.org/10.1136/bmj.g3256.
- Jago R, Edwards MJ, Sebire SJ, Tomkinson K, Bird EL, Banfield K, et al. Effect and cost of an after-school dance programme on the physical activity of 11–12 year old girls: the Bristol Girls Dance Project, a school-based cluster randomised controlled trial. Int J Behav Nutr Phys Act 2015;12. https://doi.org/10.1186/s12966-015-0289-y.
- Sutherland RL, Campbell EM, Lubans DR, Morgan PJ, Nathan NK, Wolfenden L, et al. The Physical Activity 4 Everyone Cluster Randomized Trial: 2-year outcomes of a school physical activity intervention among adolescents. Am J Prev Med 2016;51:195-20. https://doi.org/10.1016/j.amepre.2016.02.020.
- Milat AJ, Bauman A, Redman S. Narrative review of models and success factors for scaling up public health interventions. Implement Sci 2015;10. https://doi.org/10.1186/s13012-015-0301-6.
- Hall WJ, Zeveloff A, Steckler A, Schneider M, Thompson D, Pham T, et al. Process evaluation results from the HEALTHY physical education intervention. Health Educ Res 2012;27:307-18. https://doi.org/10.1093/her/cyr107.
- Sutherland R, Campbell E, Lubans DR, Morgan PJ, Okely AD, Nathan N, et al. ‘Physical Activity 4 Everyone’ school-based intervention to prevent decline in adolescent physical activity levels: 12 month (mid-intervention) report on a cluster randomised trial. Br J Sports Med 2016;50:488-95. https://doi.org/10.1136/bjsports-2014-094523.
- Koorts H, Eakin E, Estabrooks P, Timperio A, Salmon J, Bauman A. Implementation and scale up of population physical activity interventions for clinical and community settings: the PRACTIS guide. Int J Behav Nutr Phys Act 2018;15. https://doi.org/10.1186/s12966-018-0678-0.
- King’s College London . Implementation Science Research Development (ImpRes) Tool 2018. https://impsci.tracs.unc.edu/wp-content/uploads/ImpRes-Guide.pdf (accessed 29 September 2020).
- Breheny K, Adab P, Passmore S, Martin J, Lancashire E, Hemming K, et al. A cluster randomised controlled trial evaluating the effectiveness and cost-effectiveness of the daily mile on childhood obesity and wellbeing; the Birmingham daily mile protocol. BMC Public Health 2018;18. https://doi.org/10.1186/s12889-017-5019-8.
- Chesham RA, Booth JN, Sweeney EL, Ryde GC, Gorely T, Brooks NE, et al. The Daily Mile makes primary school children more active, less sedentary and improves their fitness and body composition: a quasi-experimental pilot study. BMC Med 2018;16. https://doi.org/10.1186/s12916-018-1049-z.
- Clarke A, Friede T, Putz R, Ashdown J, Martin S, Blake A, et al. Warwick–Edinburgh Mental Well-being Scale (WEMWBS): validated for teenage school students in England and Scotland. A mixed methods assessment. BMC Public Health 2011;11. https://doi.org/10.1186/1471-2458-11-487.
- White IR, Carpenter J, Horton NJ. Including all individuals is not enough: lessons for intention-to-treat analysis. Clin Trials 2012;9:396-407. https://doi.org/10.1177/1740774512450098.
Appendix 1 Quick Card example
Appendix 2 Pupil premium
Pupil premium is used as a proxy for school-level deprivation; it is school funding that aims to reduce the effects of deprivation. Prior to April 2018, schools received money for every child whose families received income support and had an annual gross income of ≤ £16,190.
Department for Education. Pupil Premium: Funding and Accountability for Schools. URL: www.gov.uk/guidance/pupil-premium-information-for-schools-and-alternative-provision-settings (accessed 5 September 2019).
Appendix 3 GoActive study outcomes
| Outcome | Description | Time point |
|---|---|---|
| Primary outcome | ||
| Accelerometry-derived physical activity outcomes: continuous waveform data from wrist-worn Axivity monitor (minutes/day) | ||
| MVPA | Average daily minutes | 10 months |
| Secondary outcomes | ||
| MVPA | Average daily minutes | Post intervention |
|
School time (09.00–15.00) Weekdays after school (15.00 onwards) Weekends |
Post intervention and 10 months | |
| Sedentary time |
Average daily minutes School time (09.00–15.00) Weekdays after school (15.00 onwards) Weekends |
Post intervention and 10 months |
| Light-intensity activity |
Average daily minutes School time (09.00–15.00) Weekdays after school (15.00 onwards) Weekends |
Post intervention and 10 months |
| Average acceleration |
Average daily acceleration in milli-g School time (09.00–15.00) Weekdays after school (15.00 onwards) Weekends |
Post intervention and 10 months |
| Questionnaire-derived physical activity outcome at post intervention and 10 months | ||
| Self-reported physical activity |
Continuous Self-reported participation frequency based on 28 activities from the YPAQ. 86 For each activity, participation was reported as never, once, two or three times, or four or more times. Participation was recoded to 0, 1, 2.5, and 4.5, respectively, and summed to obtain outcome measure |
|
| Questionnaire-derived psychosocial outcomes at post intervention and 10 months | ||
| Physical activity self-efficacy |
Continuous (range 1–6) Mean score of eight self-reported items from Reynolds’ Psychosocial Predictors of Physical Activity: Self-efficacy scale82 |
|
| Social support for physical activity |
Continuous (range 1–4) Mean score of nine self-reported items from European Youth Heart Study81 |
|
| Friendship quality |
Continuous (range 1–5) Mean score of eight self-reported items used in the ROOTS project (equally weighted)84 |
|
| Well-being |
Continuous (range 1–5) Mean score of self-reported items using the 14-item Warwick–Edinburgh Mental Well-being Scale168 |
|
| Self-esteem |
Continuous (range 1–4) Mean score of self-reported items using the 10-item Rosenberg Self-Esteem Scale85 |
|
| Anthropometry at 10 months | ||
| BMI SDS |
Continuous; z-score BMI SDS calculated from height and weight data [i.e. weight/height2 (kg/m2)] collected onsite by trained research staff. Later categorised according to age- and gender-standardised IOTF thresholds94 |
|
| Body fat percentage |
Continuous; percentage Data collected onsite using bioelectrical impedance scales |
|
| Waist circumference |
Continuous; whole number (cm) Data collected onsite by trained research staff |
|
Appendix 4 GoActive intervention blinding summary
Staff involved in measurements at follow-up (n = 15) were asked the following questions:
-
What schools are control?
-
What schools are intervention?
If they listed any, then they were asked to state how they knew this. Please note that school names are pseudonyms.
| Staff | Role | Confirmed school | How they found out | Staff member response to question |
|---|---|---|---|---|
| 1 | Dedicated GoActive research assistant | If assisting with questionnaire checking (this was rare, i.e. checking less than five questionnaires at each school) I would often be asked by pupils to help explain what was meant by the question ‘Was my school intervention or control?’. After hearing another member of staff respond to this question by saying that ‘intervention schools would have had access to a website’, I adopted this habit. Participants would often reply to this by saying they did or did not remember using a website, but I never retained this information | ||
| 2 | Dedicated GoActive research assistant | A (control) | I cannot remember how I found out, I think through pupils discussing | I think I kept pretty much blinded throughout the measurement sessions. There may have been a couple of occasions when a pupil said that the school didn’t engage with any of the activities or carry on GoActive but I can’t remember which schools those pupils was from as I just tried to block anything like that out |
| J (intervention) | The school teacher passed us lots of unused equipment (hoodies, t-shirts and the activity cards) | |||
| 3 | Dedicated GoActive research assistant | B (control) | I think the teacher or a few pupils mentioned something about not having the intervention | There are a few schools that I think are control and intervention but only thought this after the measurement sessions had taken place |
| J (intervention) | The teacher handed back intervention materials to us at the final session | |||
| K (intervention) | There were boxes around the office labelled with pupil rewards given out at previous intervention stages | |||
| L (intervention) | Pupils and the teacher were discussing the control/intervention question and spoke about the activities they had done in form time | |||
| 4 | Unit staff employed to work on other projects (occasional support) | I cannot recall anything from my time in the schools that would indicate which arm of the study they were in | ||
| 5 | Unit staff employed to work on other projects (occasional support) | I cannot tell you which Go Active schools were control or intervention schools | ||
| 6 | Unit staff employed to work on other projects (occasional support) | I have no idea on either control or intervention schools. At the time of session when checking questionnaires you can see what the majority of students put for the question asking them which group they thought they were in so you can kind of assume from that. I can’t remember now what they were | ||
| 7 | University bank staff (occasional support) | There were some schools I knew that were control because of the students lack of knowledge about the whole process at which they were undergoing/the type of questions they would ask. Intervention schools were not always as clear cut and most of the time I couldn’t be entirely sure however I would base it off their knowledge of the process and the questions they would askOn the other hand there were schools where I had no clue, which was due to the mixed responses of the students | ||
| 8 | Unit staff employed to work on other projects (occasional support) | You must have done a good job because I had no idea if the schools I attended were control or intervention | ||
| 9 | Unit staff employed to work on other projects (occasional support) | I legit couldn’t even tell you the name of the schools I attended for data collection. I never asked about a school’s allocation and wasn’t told by any of the others | ||
| 10 | Unit staff employed to work on other projects (occasional support) | I think I may have only come to one school during [follow-up]. I cannot even remember what school I went to, let alone if anything was mentioned about if they were control or not. I think this helped because we are at a measuring station we didn’t really get much interaction with the students to be asked any questions. So to answer you e-mail below, I went to one school and have no idea as to whether or not this is a control or intervention school | ||
| 11 | Unit staff employed to work on other projects (occasional support) | I haven’t a clue which arm any of the schools were recruited into | ||
| 12 | University bank staff (occasional support) | As far as I remember was I not aware about what schools were interventions and controls | ||
| 13 | University bank staff (occasional support) | I don’t know which schools were controls and which intervention | ||
| 14 | University bank staff (occasional support) | J (intervention) | The teachers gave back a lot of items (such as sweatshirts and bags) that I assume were provided to incentivise participation in the study | |
| 15 | University bank staff (occasional support) | I am unsure as to which schools were intervention or control within the study |
Appendix 5 Impact of deviations from the missing at random assumption on the results for the primary outcome
The primary analysis assumes that missing data in MVPA at 10-month follow-up are missing at random. Figure 14 shows the impact of deviations from this assumption on the estimated intervention effect, based on a pattern mixture analysis169 and using the ‘rctmiss’ command in Stata. The results show that even when those with missing data could be assumed to do at least 10 minutes more or 10 minutes less MVPA than those with available data, the intervention effects and 95% CIs are very similar to those in the primary analysis.
FIGURE 14.
Impact of deviations on the estimated intervention effect.
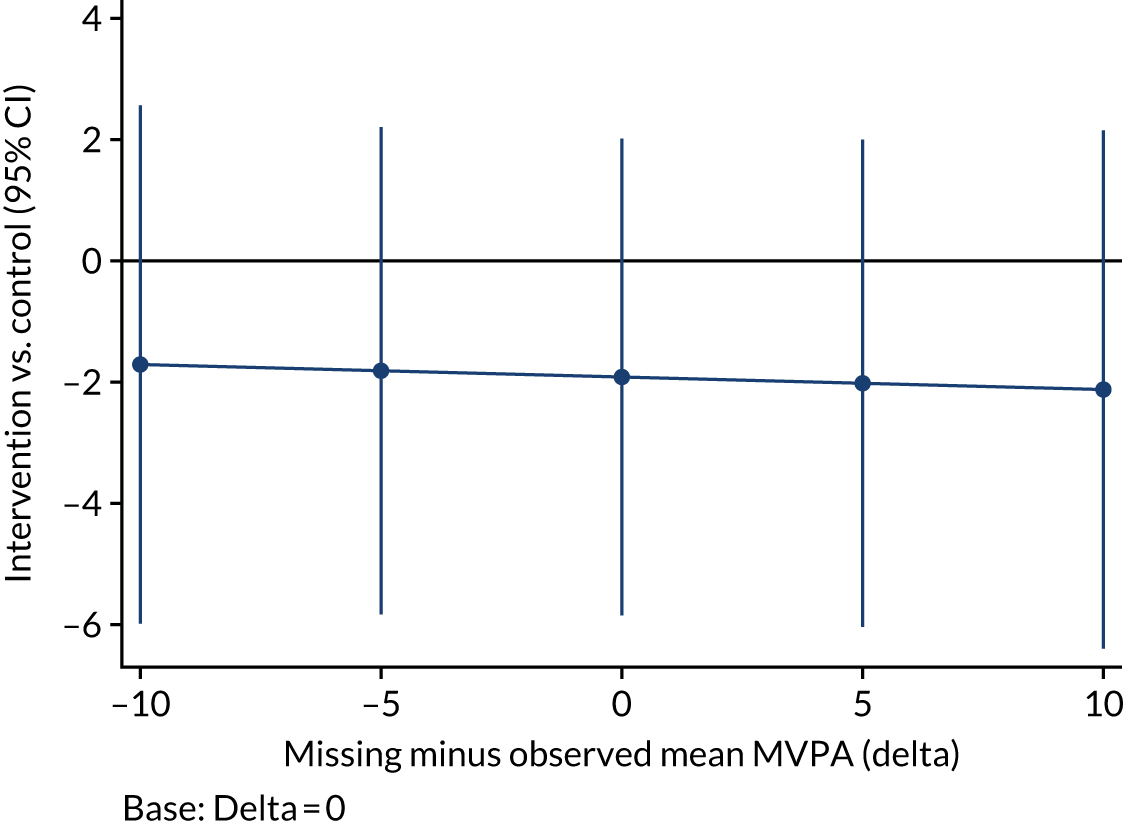
Appendix 6 School case studies
Short case studies that outline the participation of each intervention school with the intervention components are presented in Boxes 1–8. It is evident from these case studies that engagement, participation and implementation varied between schools. Generally, all schools deviated from the per protocol timeline for implementation.
School A quantitative data collection dates: (mid-intervention) 1 March 2017; (post intervention) 26 April 2017 and 3 May 2017.
School A process evaluation observation and interview (individual and focus group) collection dates: (1) 11 May 2017 and (2) 26 May 2017.
Contact teacher: library/resource centre manager, female.
Teacher/mentor training conducted: 9 January 2017.
Launch assembly scheduled: 8 September 2016.
Intervention launch assembly/per protocol start date: 18 January 2017.
Intervention components GoActive sessionsApproximated number of GoActive sessions: a Year 9 student in one focus group indicated that at the time of interview on the 26 April 2017 that they had not conducted the GoActive intervention for 3 weeks. In an individual interview, one Year 9 student indicated that they had been participating in GoActive for approximately 2.5 months. In another individual interview, it was revealed that one student perceived they had participated in the GoActive intervention for 1 month.
MentorsNumber of mentors: 23.
Mentor selection: contact teacher e-mailed out a call for volunteers to a number of teachers, including the head of PE. Mentors indicated that they were selected by their PE teachers based on their perceived leadership skills and their work experience visits conducted by PE teachers. There was no limit placed on numbers.
Mentor reimbursement: the contact teacher decided to distribute Year 10 mentors vouchers to those she considered actively involved only, and gave the remaining mentors a chance to ‘earn’ the vouchers over the following term by sustaining GoActive. She will hang on to ‘spare’ vouchers in meantime.
Age of mentors: Year 10 students aged 14–15 years.
Year 9 class leaders: n = 0; did not implement.
Year 9 class leader selection: not applicable.
Contextual factors-
In March 2018, the allocated facilitator had resigned from their post. A GoActive staff member went in to visit mentors in the first instance (9 March 2018).
School B process evaluation quantitative data collection dates: (mid-intervention) 27 February 2017; (post intervention) 24 April 2017 and 28 April 2017.
School B process evaluation observation and interview (individual and focus group) collection dates: (1) 22 May 2017 and (2) 8 June 2017.
Contact teacher: head of year 9, male.
Teacher/mentor training conducted: 12 January 2017.
Launch assembly scheduled: 17 October 2016.
Intervention launch assembly/per protocol start date: 1 February 2017.
Intervention componentsContact teacher indicated that students were in their third week of participating in the GoActive intervention as of the 24 April 2017. In an individual interview, one student noted that they had been to two or three GoActive sessions.
MentorsNumber of mentors: seven.
Mentor selection: mentors were asked to volunteer for the positions. Generally, mentors volunteered because they all enjoyed sports.
Age of mentors: Year 11, aged 16/17 years; sixth formers (Year 13); aged 16–18 years.
Year 9 class leaders: n = 0; did not implement.
Year 9 class leader selection: not applicable.
Challenges to implementation specific to the school-
School form group structure had a great impact on implementation. Instead of running with form groups, students were offered the option to participate in the GoActive intervention outside their form groups.
-
Had a sign-up sheet for those who wanted to participate because of vertical forms.
-
One overarching mentor from Year 13 was tasked to run the GoActive programme with Year 10 mentors.
-
In March 2018, the allocated facilitator had resigned from their post. A GoActive staff member went in to visit mentors in the first instance (9 March 2018).
-
Vertical forms.
-
Owing to vertical forms, there was no form teacher input to the intervention.
-
No prize-giving assembly, as a date was unable to be arranged.
School C process evaluation quantitative data collection dates: (mid-intervention) 8 March 2017 and 15 March 2017; (post intervention) 10 May 2017 and 28 April 2017.
School C process evaluation observation and interview (individual and focus group) collection dates: (1) 18 May 2017 and (2) 25 May 2017.
Contact teacher: head of PE (newly appointed), female.
Teacher/mentor training conducted: 11 January 2017.
Launch assembly scheduled: 12 September 2016.
Intervention launch assembly/per protocol start date: 16 January 2017.
Intervention componentsOne student reported participating in the GoActive intervention for around 3 months. A Year 9 student in another focus group indicated that it stopped before Easter break (2017).
MentorsNumber of mentors: six.
Mentor selection: mentors indicated that they were selected because they held the role as ‘sports captains’ for their respective houses. One mentor indicated that they did not fulfil this role and, instead, they volunteered to be a mentor. An other mentor stated that they were not a sports captain, but that they were heavily involved in school sport and were asked by their teachers to take on the mentor role.
Year 9 class leaders: n = 0; did not implement.
Year 9 class leader selection: not applicable.
Facilitators of implementation-
Contact teacher was the head of PE for girls, which facilitated the implementation of the GoActive intervention, with the whole of PE ‘buy-in’.
School D process evaluation quantitative data collection dates: (mid-intervention) 16 March 2017; (post intervention) 15 May 2017.
School D process evaluation observation and interview (individual and focus group) collection dates: (1) 16 June 2017 and (2) 30 June 2017.
Contact teacher: head of PE and assistant principal, female.
Teacher/mentor training conducted: 24 January 2017.
Launch assembly scheduled: 23 February 2016.
Intervention launch assembly/per protocol start date: Year 9 students shown introduction video in lieu of launch assembly. Scheduled for a later date because of school timetable (22 February 2017).
Intervention components MentorsNumber of mentors: 17.
Mentor selection: selected Year 10 and Year 11 students were unable to be taken out of lessons, and contact teacher worked closely with Year 10 students, rather than sixth form students. This school also engages with an external Leadership Academy for their Year 10 students. Mentors were selected from this academy. In particular, those who were in the ‘leadership group for PE’.
Age of mentors: Year 10, aged 14–15 years.
Year 9 class leaders: experienced difficulty in implementing. The intervention did not carry on for more than 1 week. One focus group with mentors revealed that one class ‘tried’ to implement in the first week, but ‘they [Year 9 students] just didn’t want to do it’. This was supported by a focus group with Year 9 students who indicated ‘they [Year 9 leaders] didn’t do anything and we never did it again’. Another focus group with mentors indicated that they tried to implement Year 9 leaders, but the form tutor ‘brushed off’ the idea. One mentor focus group described their Year 9 class leaders as ‘strong at the start’, but then behavioural issues dampened their efforts (e.g. lack of listening from peers).
Year 9 class leader selection: not applicable.
Facilitator-
Facilitator reported to have completed six sessions with the mentors (2 May 2019).
-
Prior implementation of active form time.
-
Support from SLT as the programme was initially facilitated by an assistant principal as the contact teacher.
-
Issues with website logins. Resolved mid-intervention.
-
Active form time already implemented in the school, every 2 weeks. This meant that their usual active form times were rebranded as the GoActive intervention.
School E process evaluation quantitative data collection dates: (mid-intervention) 29 March 2017; (post intervention) 12 July 2017.
School E process evaluation observation and interview (individual and focus group) collection dates: (1) 24 May 2017 and (2) 7 June 2017.
Contact teachers (× 2): pastoral manager years 9–11, female; head of year 9, male.
Teacher/mentor training conducted: 31 January 2017.
Launch assembly scheduled: 1 November 2016.
Intervention launch assembly/per protocol start date: 21 February 2017.
Intervention components MentorsNumber of mentors: 20.
Mentor selection: Year 11 and Year 12 students were selected because of their ‘sense of authority’ and because of their relationship with the contact teacher, as the previous head of Year 11. Mentors were recruited through an assembly. It was thought to have been a good opportunity to put on the students’ UCAS applications. Initially, 30 students volunteered, but this number ‘whittled down over the weeks’ and one of the contact teachers decided who would be allocated to which class.
Age of mentors: sixth formers, aged 16–18 years.
Year 9 class leaders: n unknown.
Year 9 class leader selection: for some classes, a girl and boy each week were selected by mentors and for others this was implemented once only.
Facilitators-
Minimal facilitator visits (approximately four) because of difficulty finding time in the school and contact teachers’ schedule.
-
Issues with logins to the website reported on the 23 February 2017 by contact teacher.
-
Issues with logins to the website reported to staff on 31 March 2017.
-
Facilitator raised concerns that ‘fake’ points had been added (5 March 2017). Contact teachers enforced removal of points from students.
-
A 20-minute training session was conducted for the mentors by their facilitator on the 27 February 2017.
UCAS, Universities and Colleges Admissions Service.
School F process evaluation quantitative data collection dates: (mid-intervention) 23 May 2017; (post intervention) 12 July 2017.
School F process evaluation observation and interview (individual and focus group) collection dates: 19 June 2017.
Contact teacher: head of PE, male.
Teacher/mentor training conducted: 10 March 2017 (after three rescheduled sessions).
Launch assembly scheduled: 7 November 2016.
Intervention launch assembly/per protocol start date: 20 March 2017.
Intervention componentsCommenced the week after Easter break (2017).
MentorsNumber of mentors: nine.
Mentor selection: Year 10 was selected as the best age group, as the contact teacher worked closely with Year 10 students. Year 13 was considered ‘too late’ and Year 12 students were offered the role through a general announcement, but they ‘weren’t forthcoming’. It was perceived that a different and more personalised approach to Year 12 student recruitment would have facilitated excellent Year 12 mentors. Year 10 students were approached by their PE teachers who asked for volunteers and then selected the mentors.
Age of mentors: Year 10, aged 14–15 years.
Year 9 class leaders: n = 0; did not implement.
Year 9 class leader selection: not applicable.
Facilitators-
Minimal facilitator visits.
-
Difficulties expressed in finding time for students to get involved (tried to implement out of school hours, e.g. in lunch or after school).
-
Lack of resources (space).
-
Lack of resources and availability of school grounds was an issue because of space confinement.
School G process evaluation quantitative data collection dates: (mid-intervention) 24 March 2017 and 21 April 2017; (post intervention) 13 July 2017.
School G process evaluation observation and interview (individual and focus group) collection dates: (1) 12 May 2017 and (2) 22 June 2017.
Contact teacher: PE teacher, male.
Teacher/mentor training conducted: 2 February 2017.
Launch assembly scheduled: 21 September 2016.
Intervention launch assembly/per protocol start date: 22 February 2017.
Intervention components GoActive sessionsApproximated number of GoActive sessions: in an individual interview, one Year 9 student indicated that they had not conducted a GoActive session (21 April 2017).
MentorsNumber of mentors: zero.
Mentor selection: not applicable.
Year 9 class leaders: n = 0; did not implement.
Year 9 class leader selection: not applicable.
Challenges to implementation-
Disclosed that the 15 minutes for tutor group was not enough time to conduct a GoActive session.
-
Unsure of responsibility to the programme. For example, in an interview with the contact teacher, it was suggested that aspects of the intervention had not been ‘pushed forward enough’ and it was admitted that this was not pushed by them as the contact teacher.
-
No prize-giving intervention assembly.
-
Several form groups together.
-
School’s choice not to implement facilitator.
School H process evaluation quantitative data collection dates: (mid-intervention) 17 March 2017; (post intervention) 30 June 2017.
School H process evaluation observation dates: (1) 10 July 2017.
Contact teacher: head of performing arts, female
Teacher/mentor training conducted: 26 January 2017.
Launch assembly scheduled: 2 November 2016.
Intervention launch assembly/per protocol start date: 1 February 2017.
Intervention components GoActive sessionsApproximated number of GoActive sessions: one students from a Year 9 focus group reported only two sessions. Another Year 9 student reported three sessions.
MentorsNumber of mentors: 20.
Mentor selection: some mentors volunteered based on a recruitment call at an assembly. Other mentors were selected because they had previously led in a different capacity within the school. For example, some mentors alluded to the fact that they were ‘peer mentors’, a role within the school.
Age of mentors: Year 10, aged 14–15 years.
Year 9 class leaders: n = 0; did not implement.
Year 9 class leader selection: not applicable.
Challenges to implementation specific to the school-
Mentors had exams from the 1 June and indicated that they needed to stop conducting the GoActive intervention at the end of May.
-
Owing to it being exam time, the hall was in use and often had tables set up.
-
Mentors indicated that their GCSE timetables were ‘quite hectic’ during the time of running the GoActive intervention.
-
The school had 10 Year 9 classes and so needed to roster four classes a week to conduct the GoActive intervention.
GCSE, General Certificate of Secondary Education.
List of abbreviations
- ANCOVA
- analysis of covariance
- app
- application
- BMI
- body mass index
- CI
- confidence interval
- c.p.m.
- counts per minute
- EVPI
- expected value of perfect information
- EVPPI
- expected value of perfect parameter information
- FAS
- Family Affluence Scale
- GoActive
- Get Others Active
- LPA
- light physical activity
- MET
- metabolic equivalent of task
- MRC
- Medical Research Council
- MVPA
- moderate-to-vigorous physical activity
- PACE
- physical activity cost-effectiveness
- PE
- physical education
- QALY
- quality-adjusted life-year
- RCT
- randomised controlled trial
- SD
- standard deviation
- SE
- standard error
- SEP
- socioeconomic position
- SLT
- Senior Leadership Team
- TMG
- Trial Management Group
- TSC
- Trial Steering Committee
- YPAQ
- Youth Physical Activity Questionnaire