
Notes
Article history
The research reported in this issue of the journal was funded by the HS&DR programme or one of its proceeding programmes as project number 10/2001/41. The contractual start date was in October 2011. The final report began editorial review in May 2013 and was accepted for publication in November 2013. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The HS&DR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Two co-authors (names anonymised to protect confidentiality of participants) have received funding from various health service organisations to act as a service user research partner, including some initiatives which were assessed as part of this study. Jane Coad was employed on a partner contract with Coventry University. Rosemary Davies received a University of the West of England bursary for a PhD focused on public involvement in health research.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2014. This work was produced by Evans et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Introduction
Background
This study was concerned with developing the evidence base for public involvement in research in health and social care. From as early as 1993 there was policy commitment to ‘consumer involvement’ (later called ‘public involvement’) in research in the English NHS,1 and there now is significant support for public involvement within the National Institute for Health Research (NIHR), including the work of the INVOLVE Advisory Group and Coordinating Centre. 2 For example, researchers applying for NIHR grants are now strongly encouraged to involve the public in research projects, and lay people are involved in NIHR commissioning groups and as reviewers.
Despite this strong policy commitment, the evidence for the benefits of public involvement within the research and development (R&D) world remains limited. From the early days of the NHS R&D strategy there was some concern to build the evidence base. One of the first acts of the Standing Advisory Group on Consumer Involvement in the NHS R&D programme, established in 1996, was to commission a report on lay involvement in the R&D programme. 3 But such surveys did not overcome the scepticism of many researchers regarding the lack of robust evidence for the impact of involvement. The desire for evidence on the impact of public involvement on research has grown along with wider interest in evidence-based policy making. 4,5
Interest in the evidence base for public involvement in research has grown over the same period, alongside an increasing interest in the evidence regarding public involvement in health care more generally. A number of research projects and evidence reviews on the impact of public involvement in health care have been commissioned by the Department of Health, the NIHR, the NHS and other official and professional bodies over the last decade. 6–10
The first literature reviews commissioned specifically on the impact of public involvement in health research did not appear until 2009–10. 11,12 These reviews identified a number of gaps in the evidence, in particular the lack of primary studies on the impact of involvement and the uneven quality of much of the published literature in this area. Partly in response, the Medical Research Council (MRC) and NIHR commissioned new research on the impact of public involvement in research in 2009 and 2010 respectively, of which this study is one; at the time of writing, however, none of these studies has yet reported.
As with the concept of evidence, the term ‘public involvement’ is often used in R&D policy documents uncritically and generically to encompass a range of very different involvement activities and approaches. People can be involved in research across a wide spectrum of activity including initial priority setting, advising on the design of research, and participating in data collection, analysis and dissemination. A number of authors have sought to conceptualise public involvement in terms of hierarchical levels; for example INVOLVE have previously distinguished between consultation, collaboration and user control. 11 Such models are problematic, however, as public involvement is not well defined in English health policy, either in health services generally10 or in R&D in particular. 12 See Terminology for a further discussion of some of the issues around definition and the terminology we have chosen to use in this report.
The best evidence for the impact of public involvement in research at the start of our study was provided by two recent literature reviews by Staley11 for INVOLVE and Brett et al. 12 for the UK Clinical Research Collaboration. These reviews both independently found that there was huge variation in how the evidence of the impact of involvement had been assessed and reported. Equally, they both found that the impact of involvement was highly context-specific, making it difficult to judge the quality of the evidence or draw general conclusions. Almost all the evidence of impact was based on the retrospective views of researchers and (less commonly) the public. Although there had been no consistent approach to assessing impact, similar benefits and costs were consistently reported. The two reviews concluded that involvement has had a variety of impacts, including on the research, on the public who were involved, on the researchers, on participants, on community organisations and on the wider community. Public involvement has been reported to help identify topics for research, shape research questions and help decide which projects to fund. For research design and delivery, public involvement has helped improve research tools such as questionnaires, and improved recruitment rates by aiding access to potential participants, improving information provided and encouraging people to take part. Many other examples of benefits are given in the two reviews. Most of the identified impacts have been viewed as positive, but some negative impacts of public involvement have been identified, such as additional costs to research projects.
The two reviews reported that there were a number of factors that appeared to influence whether involvement made a difference. 11,12 These included long-term involvement, involvement throughout a project, and training and support for people involved. The reviews concluded with discussions of the difficulties of assessing the impact of public involvement and calls for further research. They noted that public involvement in research was characterised as an area with no economic evaluation and both reviews recommended the development of such approaches. What have been missing in the literature are prospective evaluations of public involvement in research, where the objectives and methods for the evaluation of involvement are identified at the beginning of the studies, and the impact and outcomes are recorded in real time and with robust mechanisms for validating the self-assessments of researchers and the public involved.
There is currently no objective measure of what counts as effective and cost-effective public involvement. In developing an approach to costing public involvement for this study, we found no previous full or partial economic evaluations or economic analyses in which either costs or benefits/impacts have been measured and valued. Such costs include fixed financial costs (e.g. funding for institutional involvement facilitation or training events) and variable costs (e.g. time spent by staff engaging with members of the public or negative impacts such as delay in progressing a project due to conflict between researchers and the public involved).
Aims and objectives
The aim of this project was to assess the impact of public involvement in research through a ‘realist evaluation’13 which emphasises the importance of hypothesising regularities of context, mechanism and outcome (CMO). We examined implementation by asking what context factors (e.g. institutional support for involvement) enable which mechanisms (e.g. training) to lead to what outcomes (e.g. improved research design, cost-effectiveness). We then sought to compare these configurations of ‘CMO regularities’ in a range of research types, for example, qualitative research and clinical trials. We undertook this impact assessment using eight case studies, and special emphasis was given to the involvement of young people and families with children in the research process, as these groups have been relatively neglected in previous literature on public involvement in research.
To date there has been little robust evidence on the effectiveness or cost-effectiveness of public involvement in research. The Staley review recommended strengthening the evidence base by finding more robust ways of assessing the impact of such involvement. 11 The Brett et al. 12 systematic review, which examined the conceptualisation, measurement, impact and outcomes, and cost-effectiveness of public involvement in research, provided a framework to devise a structure for economic evaluation in this area as well as concluding ‘a need to develop economic appraisal of patient and public involvement (PPI) impact’. 12 Our approach to impact assessment and economic evaluation aimed to encompass these recommendations.
Given the finding of these two recent major literature reviews that the impact of public involvement in research is highly context-specific, this proposal adopted a realist evaluation framework in which we sought to map regularities of CMOs. Thus the overarching aim of this research was to identify the contextual factors and mechanisms that are regularly associated with effective and cost-effective public involvement in research. In order to achieve this aim we sought to pursue the following objectives:
-
to identify a sample of eight NIHR and other quality-assured research projects that are diverse in terms of research methodology, participants and extent of public involvement in research
-
to identify the desired outputs and outcomes of public involvement in research in the sample from multiple stakeholder perspectives (e.g. members of the public, researchers, research managers)
-
to track the impact of public involvement in research in this sample from project inception through to completion where possible and, at a minimum, for complete stages of the research process (design, recruitment, data collection, analysis, dissemination)
-
to compare the contextual factors and mechanisms associated with public involvement in research and their impact on desired outcomes of research from stakeholder perspectives, and to make a judgement of the costs of different mechanisms for public involvement in research
-
to undertake a consensus exercise among stakeholders to assess the merit of the realist evaluation approach to ascertain the impact of public involvement in research, and our logic for the measurement and valuation of economic costs of public involvement in research.
Organisation of this report
This report is organised into nine chapters. Following this introduction we describe the project design and research methodology, in particular our realist evaluation approach. In Chapter 3 we describe how our theory of public involvement in research developed over the course of our study. We then present summaries of our eight case studies. The main chapter of the report follows using our case study data to test our emerging theory of public involvement in research. There follows a reflective chapter on our learning from the public involvement in this study. This is followed by a specific chapter on our economic analysis. We then bring all our data and theory development together in our discussion chapter to present our current theory of public involvement in research in terms of our observed regularities of CMO, and our theory’s relationship to the wider literature on public involvement in research. Finally, we present our conclusions and recommendations for future research.
Terminology
We recognise that terminology in public involvement is problematic and sometimes contested, and there is no agreed terminology to describe those members of the public who are actively involved in research. A range of terminology is used (consumer, patient, user, involvement, engagement, participation) with overlapping and sometimes conflicting meanings, and changes over time which sometimes but not always represent policy shifts. 14 We follow the INVOLVE definition of the ‘public’ to include patients, carers, family, service users and those targeted by public health interventions. 2 Thus we use ‘public involvement in research’ as our overarching term rather than the many alternatives such as ‘PPI’ or ‘user involvement’. Where members of the public are actively involved in research we use the term ‘research partner’ to differentiate them from other members of the public, and in particular from research participants or subjects who contribute data but are not involved in design and delivery of research. This terminology is used by some of our case study participants but by no means all, and we recognise that it is not in wide usage, but then neither are any of the alternative terms we might have chosen. From our perspective it is the most all-encompassing term that covers the spectrum of involvement from user researchers who are actively integrated into research teams to members of the public who are infrequently consulted in a project advisory group.
This is not of course just a matter of terminology. There are substantive questions here about the diversity of roles members of the public may play in research, and whether one overarching term is useful to describe all these roles. Some members of the public may be ‘professionalised’, that is, they have developed substantial research expertise as well as the lived experience they bring as a patient or service user. Some researchers are cautious about involving such professionalised research partners, concerned that they may have lost some of the newness to research that enables them to ask seemingly naive but actually profoundly helpful questions. Experienced research partners sometimes have a different concern, that naive members of the public may sometimes be asked to be involved in complex discussions or high-level meetings where their inexperience means they are unable to express a meaningful voice. Whatever terminology we choose, we need to be mindful that such terms as ‘public’ or ‘research partner’ cover a multitude and diversity of roles and experiences.
Finally a note about our usage in describing the research partners in our own project. We originally had four research partner co-applicants, and at a later stage two young people joined us as additional research partners to contribute to case studies concerning young people. Because the original research partners are co-applicants and have been involved from the initial design stages, they have played slightly different roles from the more recently joined young research partners (although those differences have lessened over time). We therefore felt it was sometimes important to distinguish their roles in this report and have struggled to find the right terms to do so. In the end we have settled on the perhaps obvious distinction between our ‘original research partners’ and our ‘young research partners’ and this usage is applied where appropriate, in particular in the reflective Chapter 6.
Chapter 2 Project design and methodology
Introduction
This project was initially designed by a group of academic researchers and research partners drawn from the Service User and Carer Involvement in Research (SUCIR) group at the University of the West of England (UWE). An outline application was submitted in May 2010 to a joint funding call for proposals from the NIHR Health Services and Delivery Research programme (HS&DR) and INVOLVE on public involvement in research (see Research brief). The team were invited to submit a full proposal, which was submitted in October 2010 and approved in February 2011. The HS&DR Board asked the team to consider three points relating to the economic evaluation, the involvement of children and young people and the total number of interviews to be conducted, and changes were made in response in redrafting the project protocol in July 2011 prior to submission for ethical review. A second version of the protocol was drafted once the research fellow was in post in November 2011 and recruitment of case studies had been completed. The overall design and methodology remained similar, but some minor changes were made. In particular, the research fellow appointed was an anthropologist who argued the need for more informal visits at the beginning of the study and observation of case study processes. Because of the time between application, approval and commencing the project other factors became apparent that required additional minor modifications of the planned design. In particular the timescales for public involvement in the agreed case studies were not always optimal for our planned data collection processes and timescales and, as discussed below, research governance processes led to some delays in our starting data collection in some case studies.
Research brief
The NIHR HS&DR Programme and INVOLVE jointly invited proposals in 2010 to address the gap in evidence around the impact of public involvement in research. 15 A background paper summarised the evidence then available, particularly drawing on the reviews by Staley11 and Brett et al. 12 The invitation expressed three key aims for the research: to collect evidence on the impact of public involvement in research, to identify methods of evaluating this involvement, and to identify effective ways of involving the public in research (implementation). The call was open to a range of methodological approaches.
Methodology
Realist evaluation framework
Our research design was based on the application of realist theory of evaluation, particularly drawing on the work of Ray Pawson,13,16,17 which argues that social programmes (in this case public involvement in research) are driven by an underlying vision of change – a ‘programme theory’ of how the programme is supposed to work. The role of the evaluator is to compare the theory and the practice: ‘It is the realist evaluator’s task, and the added value of social science, to identify and explain the precise circumstances under which each theory holds.’17 Moreover, the outcomes of social programmes can be understood by identifying regularities of CMO. Thus the key question for the evaluator is ‘What works for whom in what circumstances . . . and why?’17 The realist approach is increasingly used in the evaluation of complex health programmes, and producing useful analyses. 18,19 After our study began, Staley et al. published a paper calling for the application of realist evaluation to the study of the impact of public involvement in research. 20 The development of our realist theory of public involvement in research over the course of our study is described in more detail in Chapter 3.
Our realist theory of public involvement in research was based on the two recently published literature reviews,11,12 which allowed us to identify a number of contextual factors and mechanisms that we believe were intended by policy-makers and other stakeholders in research policy to enable desired outcomes to be achieved. There has not previously been a robust testing of the underlying ‘programme theory’ of public involvement in research; our study was designed to allow an independent prospective testing of this underlying programme theory for the first time. We included an economic evaluation, designed to complement a realist evaluation design, estimating the resources used for public involvement across eight case studies.
Case study sampling
The setting for this project was within organisations hosting health and social care-related research studies (i.e. universities, NHS trusts and third-sector organisations) in the west of England. Our aim was to recruit a methodologically diverse sample of eight case studies which would have significant elements of public involvement during the period January to December 2012. There was no existing database or other source of routinely available data that enabled such upcoming studies to be identified. To meet our aims the studies needed only to be diverse, not representative, so we took the pragmatic decision to sample through our existing knowledge of studies with public involvement in the west of England and to ‘snowball’ through our existing networks, including the People and Research West of England consortium.
We developed a pro forma to identify from network stakeholders upcoming studies they were involved in or aware of with what they identified as ‘significant’ elements of public involvement. Our key inclusion criterion was evidence of some ongoing public involvement in key stages of the research process (design, recruitment, data collection, analysis, dissemination). A key exclusion criterion was that no study would be included unless both the principal investigator (PI) and at least one research partner agreed to take part. In order to identify generalisable regularities of CMO for public involvement in research, we wanted to identify a maximum variety sample of studies in terms of study type, stages of the research process and public involved. In a relatively small-scale study such as this, however, we knew we would not be able to achieve full diversity in all three dimensions. We therefore prioritised diversity of study type, as different study types can drive very different priorities for public involvement (e.g. emphasis on participant information and recruitment in clinical trials). We also prioritised including some studies involving young people and families with children because they make up a substantial minority of health service users but are underrepresented in the literature on public involvement in research. Our case studies are described in Chapter 4.
In deciding the number of case studies to undertake we recognise that there is always a trade-off between the depth of exploration (which suggests a small number of case studies) and identification of regularities (which benefits from a larger number). There are many ways to categorise research studies (e.g. basic science vs. applied, qualitative vs. quantitative, pilot studies vs. full trials, clinical vs. epidemiological, primary vs. secondary data, action research, translational research) and we could not hope to cover the full diversity in our case studies. From previous experience of case study research,21 we believed that eight case studies would enable us both to examine the CMO regularities in depth and to look for generalisable regularities across the case studies. This number of case studies did not enable us to examine all potential types of research study, but did enable us to include the most common, for example qualitative, mixed methods, feasibility and clinical trials. We received agreement from four PIs with appropriate funded studies taking place in the west of England at the application stage of our study, and the final four between approval and the early months of our study.
Case study data collection
The first stage of data collection involved initial mapping of the eight case studies through informal visits, encompassing observation of research settings and team meetings (where possible) and unstructured interviews.
Intelligence from the informal visits, together with previous findings from the two literature reviews and the CMO configuration, was then used to design an interview guide for semistructured interviews with case study project stakeholders. For each case study we aimed to carry out semistructured interviews with approximately five stakeholders (PIs, other researchers, research managers and two research partners) on three occasions over the course of the year of data collection, January–December 2012 (three interviews × five participants × eight case studies = 120 interviews in total during the year). Potential interviewees were identified in discussion with PIs and invitations forwarded via the PI or an administrative member of the PI’s team.
Interviews were broadly structured around our CMO hypothesis. Data collected include measurable elements (e.g. resources allocated for supporting public involvement and actual spend) and stakeholder perceptions (e.g. respective views of researchers and research partners on whether research partner contributions influenced project decisions). In addition, some of the stakeholders were given a resource log to record over 2 weeks, chosen at random, the amount of time spent contributing to a range of activities linked to public involvement in each case study. These were then costed using prices taken from published or recognised sources (see Chapter 7). Interviews were intended to take place at three broadly evenly spaced times over the 12-month data collection period.
In practice the number and timing of interviews varied widely across the case studies for a variety of reasons including delays in research governance approvals, illness among case study participants and research team members, delays in one research project commencing, and general logistical issues. In two case studies it was possible to carry out only two rounds of interviews rather than three, and the total number of interviews completed was 88 with 42 participants rather than the 120 with 40 participants initially envisaged. Table 1 summarises the total number of interviews (and research partner interviews) undertaken in each round across the case studies.
| Case study | First-round interviews | Second-round interviews | Final interviews | Total interviews |
|---|---|---|---|---|
| 1 | 5 (2) | 2 (0) | 4 (1) | 11 (3) |
| 2 | 6 (2) | 4 (1) | 6 (2) | 16 (5) |
| 3 | 5 (2) | 3 (2) | 4 (2) | 12 (6) |
| 4 | 3 (1) | – | 1 (0) | 4 (1) |
| 5 | 7 (3) | 4 (0) | 4 (2) | 15 (5) |
| 6 | 4 (2) | – | 4 (1) | 8 (3) |
| 7 | 4 (2) | 2 (2) | 2 (0) | 8 (4) |
| 8 | 6 (2) | 3 (1) | 5 (1) | 14 (4) |
| Total | 40 (16) | 18 (6) | 30 (9) | 88 (31) |
Case study 4 was exceptional in that, unexpectedly, no public involvement activity took place during the year. Thus the PI, a research manager and one research partner were interviewed initially and only the research manager at the end of the year. The other case studies where numbers of interviews were relatively low were case study 6, which started much later in the year than expected and where only one research partner chose to participate, and case study 7, where the research team was relatively small, there was relatively little involvement activity, and illness prevented final interviews with the two research partners. The relatively low completion rates on the initially planned 120 interviews were not a problem in themselves, so much as a symptom of lack of involvement activity for long periods in some of the case studies.
Given the small numbers of research partners overall, and the fact that some case studies targeted particular socioeconomic or age groups, we do not believe it would be meaningful to present demographic data on these participants. Our perception was, however, that our experience echoed other reports that those members of the public who choose to get involved in research tend to have attained a higher educational level than the population as a whole.
We recognise that a few interviewees do not fall easily into the categories of researcher, research manager or research partner, but we have kept to a limited number of categories to ensure anonymity.
Each case study was intended to be conducted by pairing an academic researcher and a research partner, under the overall supervision of the PI and co-ordinated by the research fellow. In one case, for logistical reasons, the research fellow undertook the data collection on his own. In the other cases, interviews were conducted by both an academic and research partner, usually separately but on occasion interviewing together.
The first round of interviews focused particularly on understanding the context of the case study and the mechanisms for public involvement planned for the remainder of the year. The second round of interviews was ‘light touch’, intended to capture developments in public involvement since the first round and to identify members of the research team able to nominate at least one research partner per case study who could be approached to complete the resource logs for economic costing. The final round of interviews focused on capturing outcomes and learning from the year, to enable us to assess how the researchers’ initial intentions and aspirations for public involvement turned out in practice. In addition to the semistructured interviews, a flexible approach to capturing data included observation of meetings where possible and/or other group tasks directly related to public involvement, and collection of project documents related to involvement processes. Observations were carried out in case studies 1, 2, 5, 7 and 8 but were not possible in case studies 3, 4 or 6, either because of internal case study project considerations or because no public involvement activity took place during the study period.
Developing a methodology for the economic costing of public involvement
There has been minimal exploration and there is little evidence for the costs and benefits of public involvement in research. El Ansari and Andersson conclude that analysis of the costs and benefits of participatory activities should form part of an overall evaluation of public participation. 22 They state that, for participation to move forward as a field, a broader ‘set of analytical frameworks is required, which captures the richness and unique qualities of participation, [and] that recognises and values the different perspectives that led to its initial development.’22
Our work here is an attempt to develop an analytical framework of how to assess the economic costs of involvement in research. Planning the budget for public involvement in research at the outset is crucial. The budget needs to include all planned research involvement work to be completed by research partners (for example participating in patient advisory groups or undertaking data analysis) as well as time for academics to facilitate research partners. Two key aspects of budgeting for public involvement are the researcher and research partner relationship and contingency planning. For example, research partners may be asked to contribute their expertise to respond to problems arising during a research project, for example poor recruitment of participants to a study (there were several examples of this among our case studies). These contributions generally arose during the research process and were not foreseen.
Payment and reward issues have generally proved controversial. At our second consensus event our case study participants debated the nature of payment and reward for public involvement vigorously, revealing a wide range of strongly held views on this subject. INVOLVE has developed guidelines on payments for involvement research work to respond to these issues. A recent document outlines the issues to bear in mind in paying research partners, gives examples of payments and provides general tips about issues connected with payment and ‘payments in kind’ that need to be carefully considered by project managers. 23 A range of pay rates for different research activities connected with public involvement are mentioned in INVOLVE documents, including a flat rate payment of £19.40 per hour. 23
Our economic analysis aimed to collect data from each case study team, in order to:
-
identify all activities relating to public involvement
-
measure the amounts of activities using a resource log
-
value or put a price on these activities using prices from published or established sources.
Identifying and measuring involvement activity
To gather data from our eight case studies for our economic analysis, we asked selected members of the case study teams (researchers, research managers and research partners) to log all the resources that were used in public involvement work/activities over a snapshot 2-week period. During the 2 weeks each person recorded/logged:
-
all involvement-related activities
-
length of time spent on each activity.
We asked them to include all activities (or inputs) that were undertaken as contributing to or enabling the central objective (or output) of public involvement in research. A sample log sheet for research partners on 1 day is in Appendix 1. Our ethical approval letter stipulated that research staff within each case study were to nominate research partners to provide our data, so we were dependent on these nominations being made successfully from within our case studies, as we were not able to make direct contact with research partners.
We issued user-friendly guidance for completing our resource log, and supported respondents over a 2-week period by e-mail and providing a telephone helpline. Our guidance document for research partners to complete resource logs is in Appendix 2. Our contact and ongoing dialogue with the academics and research partners who used our guidance and completed our resource logs enabled us to become familiar with how involvement activities were working within each case study from the point of view of both academics and their nominated research partners. These exchanges helped us gain a rounded understanding of the nature and diversity of involvement activity and the relationships and issues within each case study.
Economic valuation/costing of involvement activities
We translated the knowledge we had accrued of each case study into some working assumptions about each one. These assumptions are significant but complex, so we have detailed them in Appendices 3–5.
We then used the completed 2-week resource logs to estimate involvement costs for a projected 12-month period. From there we scaled up the 12-month projected costs to the length of each case study. This enabled us to compare the actual budgeted costs from each grant with the projected costs on a like-for-like basis.
We followed a standard economic approach to treat resource use and prices separately to arrive at a cost.
For example:
Ideally the price applied should come from a published source or the next best alternative, a recognised or established source. There are illustrative examples within INVOLVE guidelines of a range of prices for different research activities connected with public involvement. In our own project we had previously paid research partners at a ‘meeting rate’ of £19.77 per hour, but early in this project it became obvious that most work was being done outside meetings, so a lower ‘research associate’ rate of £14.02 per hour was agreed. Research partners kept records of all their work for the project (including e-mails, collecting and analysing data, and writing) and submitted claim forms regularly. Our project did not have a means of costing researcher time for public involvement activities, as working alongside research partners was a continuous process during our project.
A new set of guidelines from INVOLVE to budget for involvement was incomplete at the time of our analysis, but we saw the draft document, which again gave the example of the flat rate payment of £19.40 per hour for public involvement participation, so we used this price when costing research partners’ activities for our case studies. 23
Reflective practice
Data were captured on our reflective learning on the impact of public involvement in our own study. This was done by facilitating and audio-recording short reflective sessions during team meetings on our own experiences as a project team of academic researchers and research partners working together.
Consensus events
Two consensus workshops were organised as part of our plans to develop and test a theory of public involvement in research. Initially we aimed to hold the first event prior to the first round of data collection to inform the interview schedules for this round. As the project developed, however, we realised that this would not be practical in terms of the length of time research governance approval was taking from some NHS trusts and, more importantly, that an event after the first round would be more fruitful in terms of theory development. Thus, the decision was taken to hold the first consensus event between the first and second rounds of data collection.
At the first workshop we presented an overview of our initial findings from our first round of interviews and visits in the eight case studies. The overview was in the form of 12 statements drawn from our initial mapping of the case studies. The statements identify key contextual factors and mechanisms for public involvement in research that we hypothesised were regularly linked to positive impacts on research design and delivery.
The aim of the workshop was to test these statements with case study participants and steering group members, drawing on their experiences and insights regarding public involvement in research, in order to refine or replace the statements, to inform the next phase of data collection and analysis. The workshop was limited to one afternoon in the hope that this relatively short time commitment would make it more feasible for case study participants to attend.
Nineteen participants took part in the first consensus workshop. Six of the eight case studies were represented. The intention had been that all case studies would be represented by both research staff and research partners in their projects, but it was not possible to achieve this because of participants’ other commitments and some last-minute illness.
Participants first voted electronically on the 12 statements with the choices ‘agree’, ‘disagree’ or ‘abstain’. Participants were then divided into three groups, with each group asked to look in depth at four of the statements, discuss and revise them as necessary and identify any omissions, connections or other comments. The groups then fed back to a plenary session and participated in a final discussion.
A second half-day consensus workshop was held at the end of the third round of data collection. On this occasion all eight case studies were represented with a total of 29 participants. Our emerging theory of public involvement was presented in graphic form in a set of four slides covering different aspects of CMO regularities (field of research, leadership and culture, relationships and structures of involvement). Participants were asked to discuss, amend and comment on A1 printed versions of the slides. The output of the workshop was amended slides with marginal commentary, which were further analysed by the project team and used to form the basis of the analysis of findings presented in Chapter 5 and the development of our theory of public involvement as described in Chapter 8, Our revised theory of public involvement in research.
Case study data analysis
All interview data were transcribed and entered into an NVivo 10 database (QSR International, Warrington, Cheshire, UK). A key team discussion was how to most fully involve our research partners in the analysis of these data given that only one of them had experience of using any version of the NVivo software. The decision was made to offer NVivo 10 training to research partners but not to require this, as some did not feel confident of learning and using the programme effectively in the time available. A manual coding alternative was therefore made available. In order to make this practical, we limited the number of codes we identified to a minimum necessary to allow meaningful analysis. Those team members coding in NVivo 10 were supplied with this coding framework. Those coding manually were given a numerical code to use with transcripts and the coding was entered into the NVivo 10 database by the project research associate. For each case study, at least one transcript was coded independently by a researcher and research partner, and any divergence discussed and a joint approach agreed.
Data analysis focused on identifying CMO regularities across our case studies. From the initial CMO configuration identified in the proposal, with amendments from the first consensus workshop, a coding framework was devised with 38 codes (see Appendix 6) organised into six broad themes: relationships, leadership and culture, field of research, structures of involvement, resources and outcomes. We agreed as a team that the codes were the primary unit of analysis and the themes were provisional. Following coding of data, team discussion lead to the codes being reordered in terms of hypothesised CMO regularities presented in Chapter 5. This coding framework was then validated by one academic team member not involved in the case studies, who independently undertook a framework analysis24 of a sample of transcripts and compared her emerging framework with that drawn from the CMO configuration.
Verification of coding
Initial data were analysed by team members identifying codes within interviews. NVivo 10 software was used for data storage, retrieval, coding, analysis, memo writing and theme building across the CMO approach. This was useful in that data coding and development of findings was a collective team activity but an overall verification process was also established. One senior team member, who had not been party to the initial coding discussions, undertook a second verification to ensure consistency and rigor. The coding verification consisted of five transcripts randomly chosen across the case studies and involved two activities: naive reading and structured coding review analysis.
First, transcripts were repeatedly read, blindly from assigned codes, by the independent reviewer, with memo writing with regard to potential codes. Next, data were coded line by line, and each sentence or group of sentences was given a code using the direct meaning of the text. The second reviewer then read the transcripts with the allocated codes assigned by the initial coder. Similarities and differences were recorded. Comparing and contrasting meanings across and within transcripts through the use of memos was used. There was very high agreement found between the coder and second reviewer, which was a very positive result.
Narrative review
There were many issues of agreement in the broader level of understanding. For example, leadership emerged in all five transcripts, as did common terms such as culture (team and organisational), PI beliefs or senior lead issues. Feeling valued, trust and interpersonal relationships and other ‘emotional’-type codes were allocated by coders in all five transcripts. The second reviewer found similar patterns and this showed good overall broad agreement of coders. Power emerged in three transcripts more clearly and repeatedly but was in all five transcripts in some form.
There were minor issues of differences in coding where coders had consistently coded information in a similar way in terms of the value of public involvement. There was only one research partner who coded public involvement not just in terms of value but in terms of impact.
The thematic analysis of each code across the case studies was then used as the basis for the thematic analysis used to test our theory of public involvement in research as presented in Chapter 5.
Research ethics and governance
The study team took the importance of ethical practice extremely seriously and considered whether it raised any substantive ethical issues. As the study was primarily qualitative and did not involve questions around particularly personal health status or behaviours, we came to the view that it was relatively low risk. However, we recognised that, in asking researchers and research partners from the same studies about what was working and not working in terms of public involvement, we could potentially be raising some sensitive interpersonal relationship issues. We therefore sought to address these issues in our study design, participant information sheets and processes for ensuring confidentiality and anonymity. Following the screening questions on the Integrated Research Application System form, our study was identified as eligible for proportionate review. Ethical approval for the study was therefore sought from the County Durham & Tees Valley Research Ethics Committee prior to the commencement of the study and approval was given with minor conditions in August 2011. An application for a substantive amendment was made in December 2011 to include observation of case study meetings, which had not been included in the original application. Approval was given in February 2012.
Research governance approval, which was sought from the three NHS trusts hosting the four NHS-based case studies, proved much more time-consuming and problematic to obtain than expected. This was particularly because of our desire to enable research partners to participate fully in data collection, which required taking them through the NHS research passport system, something that neither the university nor the NHS trust human resources departments appeared familiar with. Final research governance approval for all three NHS trusts was not obtained until late March 2012, thus delaying our planned date for data collection in some case studies by around 3 months.
Throughout the study we sought to adhere to our ethical and research governance approvals by ensuring informed consent for all participants and fully complying with all conditions of our approvals. All case study participants were sent copies of the report in draft form and invited to comment on how their data had been used and any inaccuracies or other comments on their case studies.
Public involvement in our team
Our aim throughout this project has been to model good practice in our own research while studying the impact of public involvement in our case studies. The project was developed by the SUCIR group at UWE, which had strong service user representation. One research partner co-applicant was the cochair of SUCIR. Three other research partner co-applicants had previously worked with the PI and other academic co-applicants on developing the SUCIR scheme and/or on other research projects.
The four research partner co-applicants were involved in all aspects of the project including design, data collection, analysis and dissemination. The case studies were designed to be undertaken by four subteams, each consisting of one academic researcher and one research partner working together on two case studies. The research partners also formed a separate research partner reference group meeting bimonthly.
The initial intention was for two academic co-applicants with extensive experience in working with young people to recruit and support a young persons’ advisory group to work on the two case studies where participants were young people. In the end it did not prove feasible to recruit such a group and a decision was made to develop an alternative model of involving young people in the project. Two young people, one of whom who had worked on a previous study, were recruited to join the project as research partners. Over time they came to play a similar role to the original four research partners, attending team meetings, research partner meetings and other events, and participating in data collection and analysis in their two case studies.
Research partners were involved in our team’s reflective process on what worked well and what did not work well in terms of our own processes around public involvement. A period of approximately 15 minutes was set aside at the beginning of each team meeting and research partner meeting to share reflections and learning about public involvement in our own project. Research partners have co-authored and presented our outputs at the INVOLVE conference and elsewhere, and have contributed to ensuring that this final report is as user-friendly as possible, and that our wider dissemination plans include outputs specifically designed to be accessible to a wide public. The plain English summary of this report was drafted by research partners. Chapter 6 of this report includes the synthesis, led by one research partner, of the shared reflections on public involvement in our project by both the academic researchers and the research partners.
Chapter 3 Developing our realist theory
Introduction
Realist theory needs to be developed and refined by a cumulative process of synthesising the evidence, using the evidence to develop theory and testing theory empirically against new evidence. Our starting point needed to be the best existing synthesis of current evidence, the two recent literature reviews on the impact of public involvement in research. 11,12
Neither review adopted an explicitly realist framework. Staley11 emphasised the importance of context in assessing the impact of public involvement in research but did not seek to provide an explicit conceptual framework linking context with outcomes. Of key relevance was section 4.10, ‘Factors that influence the impact of involvement’, summarised in Box 1. 11
The evidence suggests that public involvement has had the greatest impact when people have been involved throughout an entire research project, rather than just at discrete stages.
Long-term involvementOver a longer term, involvement is reported to have more impact because:
-
members of the public gain more insight into research
-
members of the public and researchers develop more constructive, ongoing dialogue
-
a general ethos of learning from each other is established.
Public involvement is reported to be more likely to have a positive impact if members of the public receive appropriate training and continued support.
Linking involvement to decision-makingSome research projects have established advisory groups. Integrating these groups into the management structure of a project can ensure the public’s views actually influence decisions.
Brett et al. argued the need to develop explicit theory and suggest a model linking context, process and outcome. 12 They did not, however, differentiate between those factors they saw as contextual and those they saw as process. Their table of ‘the architecture of PPI: context and process factors’ contained a single list of undifferentiated context and process factors (Box 2). 12
-
Budget appropriately for the service users’ involvement. This may include contributions to service users for their time, expenses and cost of training.
-
Consider additional time needed for PPI activity in time scales for the study.
-
Involve service users as early as possible in the research, preferably at the beginning of the study and maintain involvement throughout.
-
Define roles of service users and researchers in the PPI activity.
-
Provide service users with adequate training on research skills required for their involvement in the study.
-
Provide service users with the additional knowledge of the disease/condition that is necessary in order for them to contribute.
-
Provide researchers with training on how to involve service users in research and encourage a positive attitude to PPI.
-
Establish good relationships between service users and researchers over time, and avoid recruiting service users in a hurry.
-
Respect the skills, knowledge and experience that service users bring to a research study.
-
Provide personal support and supervision of service users.
-
Encourage good communication to manage conflict and avoid isolation.
-
Involve service users in developing invitation letters, information sheets, consent forms, questionnaires and interview schedules, as service users will assist in developing this information in a patient-relevant way.
-
Involve service users in decisions as to how participants are recruited.
-
If sufficient training is provided, service users can assist in data collection.
-
Service users can identify patient-important themes in the data.
-
Detail in reports/publications how PPI was conducted.
-
Produce a lay summary of the final report so it can be easily understood by the target population.
-
Develop service user advocacies for dissemination and implementation of research to assist in making the results more poignant and more relevant to the target population.
Our initial realist theory of public involvement in research
In developing our realist theory we needed to be clear about what aspects of public involvement in research we were seeking to investigate. Mechanisms to support public involvement have been introduced at many levels within English NHS research systems, for example in strategic leadership, commissioning research, peer review of applications, and supporting research through NIHR research networks. Our focus has been specifically on public involvement within research programmes and projects led by academic and clinical researchers. Thus we were mainly interested in public involvement in the design and conduct of research, for example decision-making around research questions, methods, instrument development, selection of outcomes for measurement, sampling, recruitment, data collection and analysis.
Pawson16 writes that ‘in general, realist analysis admits to the shaping influence of at least four contextual layers’. These layers are:
-
the individual capacities of the key actors
-
the interpersonal relationships supporting the intervention
-
the institutional setting
-
the wider infrastructural system.
These four layers provide a useful framework for structuring the key contextual factors drawn from Staley11 and Brett et al. 12, as summarised in Table 2, first column.
| Context | Mechanism | Outcomes |
|---|---|---|
| Leadership on public involvement by the PI or other senior member of the research team (individual capacities of the key actors) Attitudes of trust and respect towards public involved (interpersonal relationships supporting the intervention) Culture of valuing and support for involvement (institutional setting) Infrastructure that supports involvement, e.g. policy on payment and expenses (wider infrastructural system) |
Involvement throughout a research project Long-term involvement Training and support for the people involved Linking involvement to decision-making Budget for involvement Defined roles |
Impact on research design and delivery – improved quality of:
|
Mechanisms of public involvement can be conceptualised in many different ways. As Brett et al. 12 make clear, there are no agreed definitions or theories of public involvement in research. One of the simplest ways to differentiate the various mechanisms would be in terms of the organisational arrangement by which members of the public are involved in the research process, for example:
-
public (patient/user) advisory groups or panels
-
public membership of a multidisciplinary project steering or advisory group
-
working in partnership with service user-led organisations
-
research partners (working individually alongside researchers but not actually conducting data collection or analysis)
-
coresearchers (conducting data collection and/or analysis).
However, such structures are likely to be specific to different settings, professional disciplines or client groups and so focusing our understanding of mechanisms on them would be unlikely to lead to generalisable learning. Moreover, the reports of the reviews of Staley11 and Brett et al. 12 did not focus on these structures and so do not easily allow us to compare outcomes from these different organisational arrangements for public involvement.
The alternative approach we initially adopted was to define mechanisms in terms of other process factors identified by both Staley11 and Brett et al. 12 such as involvement throughout a research project, training and support offered, and the nature and/or extent of role definition, as indicated in Table 2, second column.
In terms of outcome, both reviews identify very similar areas of impact for public involvement in research, which Staley11 summarised as impact on (1) the research agenda, (2) research design and delivery, (3) research ethics, (4) the public involved, (5) researchers, (6) research participants, (7) the wider community, (8) community organisations and (9) implementation/change. In a relatively small-scale study such as this, it was not possible to assess impact in all of these domains and we chose to focus on impact on (2) research design and delivery and (4) the public involved, as these impacts reflect the policy priorities of improving the quality of research and giving voice to the public involved. For both of these areas there are a number of more specific aspects of impact that can be identified from the two reviews as indicated in Table 2, third column.
Table 2 integrates and synthesises the key context and process factors identified by Staley11 in Box 1 and Brett et al. 12 in Box 2, and summarises key elements of our initial framing of a programme theory for public involvement in research for testing in our case studies. It is recognised that a number of these factors could be broken down into multiple and more specific factors, and that this matrix could be extensively expanded. The temptation to include all relevant specific factors must be balanced, however, with the need to develop a statement of theory that is sufficiently focused to be testable in case studies. The factors identified in Table 2 were not necessarily all explicitly named by both Staley11 and Brett et al. 12 For example, the contextual factor identified here of leadership on public involvement was not explicitly listed by either Staley11 or Brett et al. ,12 but it was implicit in other factors they identify such as linking involvement with decision-making11 and providing researchers with training on how to involve service users. 12
What neither Staley11 nor Brett et al. 12 indicated was whether or not all these factors need to be present (or to what level) to achieve desired outcomes. For example, Brett et al. 12 identified a ‘budget appropriate for the service users’ involvement’ as the first factor in their architecture of public involvement, but did not specify how one might judge appropriateness. 12 This was not a factor explicitly identified by Staley, although it was implicit in her identification of ‘training and support’ as a key factor,11 as these cannot easily be provided without a budget. We thus lacked an evidence base to be able to say that all the identified context and mechanism factors must be present to achieve the desired outcomes. At most we could say that, the more such factors are present, the more likely the desired outcomes were to be achieved. It would require further empirical testing to be able to say more about whether any one or more factors were essential to achieve the desired outcomes or, indeed, if we (and Staley11 and Brett et al. 12) had missed other fundamentally important factors not listed here which need to be incorporated into future revisions of the model.
It is probable that, where one contextual factor is present, others are also likely to be. In particular, if there is leadership supportive of involvement in a department or research team, then it might be expected that culture and the attitudes of other team members are equally likely to be supportive of it. If there is involvement throughout a research project there is also likely to be long-term involvement. Some factor may thus be partly or wholly dependent or contingent on others, and further iterations of our model would therefore need to incorporate such complexities.
This then was the state of play with our theory as we approached the analysis of our case study data in early 2013. The next chapter describes our eight case studies before we go on in Chapter 5 to report the extent to which our case study data supported or challenged our developing theory of public involvement in research.
Chapter 4 Case studies
Introduction
Eight diverse case studies were recruited as described in Chapter 2. Each of the case studies was followed up over the calendar year 2012. Where possible, three rounds of data collection were completed. Because of research governance approvals and logistical factors, data collection did not begin as early as expected, so that in most cases 9 months rather than 12 months separated the first and last rounds of data collection. In two cases (case studies 4 and 6) only two rounds of data collection were possible because of factors internal to the case studies. Key contextual factors, mechanisms and outcomes of involvement are summarised in Table 3 before the CMOs for each case study are described in brief in the rest of this chapter.
| Case study 1 | Case study 2 | Case study 3 | Case study 4 | Case study 5 | Case study 6 | Case study 7 | Case study 8 | |
|---|---|---|---|---|---|---|---|---|
| Context | ||||||||
| Project focus | Evaluation of care provided to first-time mothers | Interventions for preschool children with speech and language impairment | Prevention of recurrent unintentional injury in preschool children | Improving the management of BSIs | Evaluation of personal budgets | Patients’ definition of recovery from chronic pain | Foot problems in people with RA | Longitudinal health research with young people |
| Time period | 5 years 2008–14 |
3 years 2011–13 |
2 years 2011–13 |
6 years 2009–15 |
3 years 2010–13 |
2 years 2012–14 |
5 years 2010–15 |
20 years and ongoing |
| Total funding | £4M | £1.2M | £400,000 | £2M | £430,000 | US$180,000 | £248,000 | Tens of millions of pounds |
| Funding for public involvement | £42,000 | £27,000 stakeholder involvement (£7000 parent involvement) | Not specified separately in bid | Not specified separately in bid | £22,000 | US$15,000 | £2970 | Part of £91,000 for participation |
| Methodology | RCT | Mixed methods | Feasibility RCT | Mixed methods | Mixed methods | Qualitative/Delphi | Mixed methods | Mixed methods/epidemiological |
| Stage of research | Data collection and analysis | Phase 1 parent focus groups | Recruitment, data collection and analysis | Work package 2 – RCT | Phase 2 interview data collection | Phase 1 data collection | Phase 2 survey data collection | Wide range of research in progress |
| Host institution | University | NHS trust | University | NHS trust | Charity | NHS trust | NHS trust | University |
| Collaborating institution | Three universities | Three universities and a third sector organisation | Three universities and one NHS trust | Two universities and five NHS trusts | Two universities and four local authorities | NHS trust and seven international hospitals | NHS trust and two universities | Numerous universities and NHS organisations |
| Mechanism | ||||||||
| Approach to public involvement | Third-sector partners on steering group; involvement of pre-existing groups of young mothers | Parent research panel; rotating parental representation on advisory group | Parent advisory group based in a children’s centre | Patient/carer advisory group | Working with four local service user organisations | Individual research partners at each study site | Two research partners as members of research team | Young people’s advisory group; one young person on ethics committee |
| Frequency of public involvement | Variable | Meeting every 2 months plus ad hoc events | Variable, six in early stages, long gap, final meeting at end of project | Variable, frequent meetings in 2011, none in 2012 | Biannual national meetings; variable local involvement | Once yearly 2-day meeting of research teams; variable in local teams | Variable, two or three times per year | Monthly meetings and regular social media |
| Type of public | Young mothers | Parents of preschool children | Parents of preschool children | Past patients with BSI and their carers | Mental health service users and carers | Patients with complex regional pain syndrome | Patients with RA | Young people involved in cohort |
| Key roles in public involvement | Co-applicant lead on involvement; designated person to support young people | PI, third-sector co-applicant, programme manager, andco-ordinator all with PPI roles | Co-applicant with previous PPI experience leading on PPI | Programme manager lead role | All four researchers had involvement roles | Lead role for junior programme manager | PI lead for PPI, supported by unit director with extensive PPI experience | Executive director, participation team |
| Recruitment of research partners | Approach to existing young mothers’ groups | New group through open advertisement | Via children’s centre staff | Recruited through NHS trust, mainly ITU | Local organisations invited to tender for involvement work | One UK research partner via local user group; others via study hospitals | Recruited through existing involvement process in unit | Invitation to study participants |
| Point involvement began | Early in project life | Third-sector from beginning of bid; parents from early in phase 1 | One parent advised on bid; group recruited early in life of project | Once programme manager came into post (2010) | Individual users involved in bid design; local organisations invited to tender early in project | From early in project life | One research partner involved from beginning; second recruited in phase 1 | Previous ad hoc involvement; group meetings for last 6 years |
| Reward for research partners | Contribution to educational studies | Vouchers and expenses for each meeting | Vouchers given as ‘thank you’ at last meeting | Reimbursed for expenses | Payment to each local organisation and individual payment and expenses for national meetings | Expenses paid for meetings; training in qualitative analysis for three research partners | Honorarium/expenses paid; opportunities for co-authorship | Expenses paid for meetings |
| Outcome | ||||||||
| Research design and delivery | Designed poster for use in recruitment Suggested ideas for retention Contributed to participant website and leaflets Commented on questionnaires |
Advice on parental recruitment strategy taken up by researchers Helped design/redraft recruitment materials Suggested promoting focus groups as play session taken up by researchers Suggested change to telephone interviewing taken up by researchers Commented on bids for future funding Developed and presented a conference poster Helped develop the infrastructure for parental involvement in future projects Helped the researchers work out how best to involve other parents in future |
Suggestions on strategy for trial recruitment taken up by team Supported idea that intervention should be delivered in children’s centres Commented on participant info sheet prior to ethical review Suggestions on draft recruitment poster and proposed injury calendar led to substantial revisions by team |
No outcomes during 2012 as no involvement activity during case study period (In 2011 contributed to ethics application, shaping approach to consent. Commented on bid for future funding) |
Provided local intelligence and insight to the research team Contributed to development of data collection approach and tools Helped recruit and support study participants, including holding two recruitment events Suggested changes to instruments and processes taken up by the team Contributed to data analysis Reviewed and commented on selected excerpts from transcripts Contributed to planning dissemination strategies and designing materials |
Contributed to development of data collection approach and tools Suggestions for design of questionnaire (e.g. splitting questionnaire into two) and changing wording taken up by researchers Insights provided on how questions would be answered, how long it would take to complete |
Contributed to design of questionnaire (changes in layout, order, wording and the inclusion of additional questions) Suggested changes to information sheets and letters taken up by researchers Contributed to planning data collection process |
Contributed to design of individual research projects, suggesting major changes in some projects which were accepted by the programme Contributed to developing policy and practice for the overall programme, e.g. developing generic guidance for consent forms and information sheets Contributed to participant leaflets and data collection tools including on questionnaires Contributed to dissemination through presenting at conferences, making videos and other dissemination materials |
Case studies
Case study 1
Context of public involvement
This research project was a 5-year randomised controlled trial (RCT) involving 1645 young mothers across 18 sites. The PI expressed a strong commitment to public involvement. He had previous experience of working on studies that had a strong element of public involvement and was very committed to public involvement in this project and to having it embedded in the project from the beginning. The PI and his team are based in a clinical trials unit that has had previous experience of public involvement in research and a working group on PPI. A co-applicant based at another university also had significant experience of stakeholder and public involvement in other projects and was identified to lead in this area for the project. Stakeholder organisations have been part of the project from the beginning. A stakeholder management group was therefore an important part of the project.
Another member of the team had interviewed people who belonged to patient organisations and a reason why she was attracted to working for this trial was the fact that public involvement was built into the proposal from the start.
Mechanisms of public involvement
This project had public involvement built into the proposal. Adult stakeholders were part of the stakeholder management group of the project from the beginning and young people were represented at this level through representatives of young people’s organisations. This group met every 2 or 3 months.
The project also worked with a group of young mothers who were already an established and well-supported group who were working together to obtain educational qualifications. Two members of the project team were responsible for engaging directly with this group of young people and supporting their contribution to the project. However, this group closed when funding was cut and so a new group had to be found. There was a goodbye party and presentation of certificates to say thank you for their work and contribution to the project.
A second group was then approached. This was also a well-supported group and the young people were given some information about the project. At the start of our case study period this group had met with the researchers on only one occasion, when the researchers had asked them for some ideas about leaflets. They met a second time during the course of the case study period, but as the RCT was at that point approaching the analysis stage there was less need to seek their input. However, the researchers responsible for the participation of the young people were going to look at ways young people could be involved in dissemination, with the help of a stakeholder group representative from a young people’s organisation.
Outcomes of involvement
The first young people’s group was approached to assist the project in a number of ways – some of which contributed to their educational credits. A poster for the project was designed by the group, supported by a local arts teacher, and this was used during the recruitment phase in all the trial sites. At different points in the trial the group assisted with ideas for retention, a participant website, leaflets and questionnaires. This group worked closely with the project and reportedly had a big impact on how young mothers were recruited and retained in the study. It was too soon to gauge the outcomes of involvement of the second group.
Case study 2
Context of public involvement
Case study 2 took place in a research group with institutional connections to both an NHS trust and a university and with research interests in speech and language therapy (SLT). The PI had a long-term interest in and philosophical commitment to involving parents and children in research, and had previously collaborated with a parent-led third-sector organisation in research, but had relatively little previous experience directly involving parents or children in research. The PI led a small and cohesive team within the group based together in one geographical site. Both the NHS trust and the university had existing initiatives to support public involvement in research, and were collaborating in a subregional initiative to support public involvement. There was no wider experience or culture of public involvement in research in the research group. The PI saw this grant as an opportunity to develop parental involvement not just in the specific programme of SLT research but more widely in the future research work of the group.
As well as the PI and the co-applicant from the parent-led organisation, a research manager was seconded from the NHS trust R&D team to the project team to manage the research programme including taking a strategic lead on parental involvement. Part of her role within the R&D team was to advise other researchers on good practice in public involvement, but she had limited direct experience of it, having previously been in an advisory role, so the SLT role gave her a development opportunity to learn from applying her theoretical knowledge in practice.
The research programme aimed to improve the quality of SLT for preschool children, to develop an evidence-based approach to interventions and to develop a model to support the appropriate targeting of interventions. It was designed to include two phases over 3 years. In the first phase, covered by this case study, the team undertook systematic literature reviews, surveys and case studies involving focus groups with SLT professionals, other health professionals and parents. The second phase will involve the development of an evidence-based typology of interventions. The research programme was funded by a major national funding agency which expected evidence of public involvement in all its funded projects.
Mechanisms of public involvement
The key mechanism for public involvement was the parent research panel, which was set up specifically for this research programme. Parents of preschool children (not necessarily those specifically with speech and language difficulties) were recruited through an advertised open process to establish a panel which met every 2 months. This was a new group of parents who did not previously know each other, and therefore had to form as a new group both with each other and with the research team. It was recognised by the research team that the panel was not diverse and did not include many parents of children with speech and language difficulties or marginalised groups. The research team set the agenda and circulated it prior to the meeting, and facilitated the discussion at each meeting. Activities for the panel included discussing and commenting on recruitment materials and strategies, and on data collection, for the parent focus groups.
The SLT office manager co-ordinated the parent panel and the parental involvement more widely. Halfway through the case study, the post holder left the unit and a new office manager (recruited from within the unit’s administrative team) took on this co-ordination role. Facilitation of the parent panel meetings was shared between the PI and the programme manager, with several research team staff attending each parent panel meeting. The programme manager also produced a written involvement strategy for the research programme.
The parents were not involved in the early design of the research programme, but the intention was that they would help shape later stages of the research programme. Parents were also involved in the study advisory group, with different parents representing the parent panel at different advisory group meetings. Parents were also offered the opportunity to represent the study at conferences and other events, including by presenting a poster on parental involvement. Parents were rewarded with vouchers rather than direct payment as well as in non-monetary ways (e.g. invitation to present at events, thanks).
Outcomes of involvement
The parent research panel were actively involved in shaping parent recruitment strategy and materials. Draft materials were brought to the panel and comprehensively amended and redesigned in discussion at panel meetings. Both researchers and parents agreed the new materials were more accessible and generally more attractive to parents, and the ‘before’ and ‘after’ versions shown to us confirmed this. Alternative recruitment strategies (e.g. recruitment through community rather than NHS venues, marketing the opportunities to participate as fun drama play sessions instead of focus groups) were suggested by the panel and implemented by the research team (although these strategies were not ultimately more effective in enhancing recruitment than the original strategies planned by the research team). The parent panel also commented on bids for future funding.
Case study 3
Context of public involvement
Case study 3 was led by a PI with a public health background leading her first major research project in collaboration with a group of experienced senior researchers. The study participants were parents of young children. Although philosophically in favour of it, the PI did not have previous experience of public involvement in research but several co-applicants did, including one co-applicant who was identified to lead on the parental involvement in the study. The research team were based in different institutions, with the PI and several co-applicants organisationally located in one joint university research centre, but not all physically based in the same geographical location. The PI’s university had an existing scheme to support public involvement in research, and also co-ordinated a collaborative initiative to support involvement across local universities and NHS organisations. Although co-applicants based in the PI’s research centre had previous experience of public involvement, there was no overall approach or system to involve the public within the centre.
The co-applicant who led on parental involvement was partly based in the same research centre as the PI. She had previous experience of public involvement, including the involvement of parents at one children’s centre, which was identified as the potential host for a parent advisory group. She also had a role in a research design service advising other researchers on developing bids, which included advice on public involvement in research.
The study was a feasibility multicentre cluster RCT to develop and test a parenting programme for the prevention of recurrent unintentional injuries in preschool children. The intention was to develop a programme, including first aid and home safety advice, that would be delivered to parents in eight weekly sessions by health visitors. A range of data were collected including pre and post test questionnaires, injury calendars completed by the parents, interviews with parents and health professionals about their experiences of the programme, and numbers agreeing to take part and complete the programme.
Mechanisms of public involvement
The key mechanism for involvement was the parent advisory group. A children’s centre was approached by the co-applicant and agreed to host the group. Centre staff invited a sample of parents to attend who they thought would both be able to contribute to and benefit from participating. The parent advisory group met in the centre at a time when the parents might be using the centre anyway, so that it was easy for the parents to attend, did not require any additional travel or expense and was held in a familiar and safe environment. This was a new group in that the parents had not met together as a specific group before, although they generally knew each other. The sessions were informally facilitated by the co-applicant, with the PI also sometimes attending. The meetings were also informally facilitated by a member of centre staff who was also a local parent. The meetings were held as and when the research team needed input from the parents rather than on a regular schedule. When the team wanted a parent advisory group meeting they contacted the centre and the staff called the parents to invite them to attend the meeting. Refreshments including hot drinks and cakes were provided by the research team to encourage a relaxed and friendly atmosphere. Discussions were informally facilitated without formal agendas, papers or PowerPoint (Microsoft Corporation, Redmond, WA, USA) presentations. Some research materials were brought for discussion, for example the injury calendar and recruitment literature. The group would spend some time discussing issues such as perceived shortcomings and suggest potential improvements to such materials, as well as discussing related issues such as recruitment strategies. The majority of the meetings were held early in the life of the study, with a relatively long gap during the data collection period and a last meeting in the last month of the project to feed back to and thank group participants.
Outcomes of involvement
The parent advisory group commented on a number of aspects of the trial strategy for recruitment and the development of the intervention. The earliest input was on the participant information sheets prior to submission for research ethics committee review. The group made substantial comments on an early draft recruitment poster intended for parents in children’s centres, which was then substantially revised by the research team. ‘Before’ and ‘after’ versions of the poster showed to our team confirmed this. Similarly, the parents initially made a number of critical comments on the first version of the proposed injury calendar, which they suggested might be burdensome to parents to fill in and might not be completed. A revised version addressing the parents’ concern was brought back to the group and much more positively received. Again, the ‘parent-approved’ version seen by our team was dramatically improved. A number of comments were made on the proposed intervention, including the advantages of including children’s centre staff in delivering it, and the need to offer some type of educational incentive to those allocated to the control group as well as the intervention group.
Case study 4
Context of public involvement
Case study 4 was based in an NHS trust department of medical microbiology where the PI was both a consultant in and professor of medical microbiology. The PI did not have significant previous experience of public involvement in research but recognised the need to develop a mechanism for public involvement to meet the funder’s expectations. There was no significant wider experience or culture of public involvement in microbiology research in the research team or in the host microbiology department. The team had not found examples of public involvement in research in the microbiology field more generally. A generic NHS trust patient panel mainly focused on clinical governance was consulted on the original 2008 bid, but no microbiology patients or patient organisations were involved as co-applicants or collaborators. The host NHS trust had an existing initiative within the R&D department to support PPI in research which was referred to in the original funding application, though no specific plans were outlined at that stage. There were some delays to the commencement of the programme of research and thus to the development of the public involvement.
The aim of the research programme was to carry out a series of linked research studies to improve the management of bloodstream infections (BSIs) and so reduce patient mortality. The first work package was an observational study to identify modifiable risk factors for death in patients with BSIs due to four key identified microorganisms. The second work package and the focus of the programme during this case study was a four-centre RCT to assess the impact of laboratory-based rapid diagnostics in patients with BSIs. If the RCT demonstrates that the intervention is effective and further funding is confirmed, the third work package will be the development and evaluation of a blended learning programme for infection practitioners.
Mechanisms of public involvement
The key mechanism for public involvement was the microbiology patient/carer panel at the host NHS trust, which did not exist previously and was set up specifically for this research programme. No public involvement activity took place at the other three research sites. The lead role on public involvement was taken by the programme grant manager, who took up her post in mid-2010. She had previous experience as both a researcher and a research manager, but not of public involvement in research. The grant application had referred to an existing trust patient panel, but this was a generic panel across the trust not specific to microbiology and was more focused on clinical governance rather than research. As part of delivering the grant the research manager and the team recognised the need to establish a patient panel specifically for the microbiology research. The programme grant manager was then supported by the trust R&D team to visit another team in the trust with an existing patient panel and observe how it worked. Recruiting patients in microbiology was a challenge, as patients do not have a long-term relationship with the department. It was thus decided to recruit patients who had previously had BSIs, through the trust’s intensive therapy unit (ITU), and a group of around eight was established. At the first meeting several dropped out but these were balanced by some family members who joined in and added useful carers’ perspectives.
As the first work package involved a study where the patients were not in a position to be able to give informed consent, the patient panel was involved in the ethical review application to the National Information Governance Board, and agreed the questions that were appropriate to ask and the information the researchers would have access to without patient consent.
For the second work package focusing on a RCT, the patient panel again advised on the ethics application, as this was a second non-consenting study. The panel also advised on recruitment processes and information including the patient information sheets. At the same time the panel were consulted by the research team about further research bids the team were considering submitting for funding.
The meetings were held in the early evening from 18.30 to 20.30, as that was the time that was arrived at by consensus that most suited the group. Meals and refreshments were provided and expenses paid, but no payment for time was made. The meetings were facilitated by the programme grant manager and the PI and were managed as an informal discussion. Members of the research team would introduce the topics and themes they would like to discuss and then discussion followed. Brief notes were written up by the programme grant manager and circulated to participants after the meetings.
It was always envisaged there would be a substantial gap in the patient panel meetings due to the lack of substantive issues for them to discuss during the RCT data collection period. In the end the planned autumn 2012 meeting was delayed by illness and other issues, so no meetings were held during 2012.
Outcomes of involvement
Although no meetings of the patient panel were held in 2012, and thus there were no outcomes during the study period, the meetings in late 2011 made significant contributions to the research programme. The panel comments made an important contribution to the application for ethical review, particularly to the non-consenting study, where the ethics review committee made clear that they would not have approved the application without evidence that patients had been consulted and were in agreement with the non-consenting process. The panel also commented on a programme grant application which involved recruitment of patients from the ITU, and as the panel members mainly had been recruited via the ITU they again made helpful comments on recruitment and ethical considerations, although in this case the grant application was not successful.
Case study 5
Context of public involvement
Case study 5 took place in a national mental health charity with a long history of commitment to public involvement across all its activities including board-level representation of service users and carers. Public involvement in research activities was also part of the established culture, with a history of service users working as research partners in a variety of projects and in different ways, including user-researchers being appointed as full members of the research team, to collect and analyse data.
The four members of the research team, based at the charity’s headquarters, all had a strong commitment to meaningful public involvement in research and prior experience of working with research partners. The PI had more than 10 years of experience of conducting research in mental health with strong public involvement. The project manager had 6 years of experience of involving users in research, in this and another organisation. Over the lifetime of the project there were significant research team changes, including a new project manager and two new researchers, who came with a strong involvement focus.
The project on the implementation of personalised budgets involved four study sites, in different geographical locations. Local public involvement activities were affected by differences in the implementation process in the different sites and by the nature of existing relationships between local stakeholders including local authorities, mental health NHS trusts and other service providers. The four local service user- or carer-led organisations also differed in scale, in how they worked with other local stakeholders on personalisation and in their approaches to campaigning in support of personalisation.
The user-led organisation from which we collected data was large and running many different projects, and had its own history of involvement in research. The three research partners we interviewed all had prior experience either as researchers or of working as research partners elsewhere. One had undertaken previous research on personalisation.
Mechanisms of public involvement
A key factor in developing the devolved model whereby the research team worked with the local user-led organisations was the potential to draw on local knowledge of personalisation in the study sites, and to promote personal budgets for recovering mental health service users. The research team spent time considering how to develop meaningful public involvement for this study and the project manager oversaw research partners’ involvement as the study progressed.
The charity and the local user- or carer-led organisation both had a clear commitment to pay for involvement work and to cover out-of-pocket expenses, as specified in a written agreement. The local organisations were responsible for managing and conducting the involvement activities within the study sites, and organising payments to individual partners for local work.
Within the devolved model, involvement work was initially flexible. The PI and research manager were concerned to strike a balance between predefined roles and responding to individual partners’ needs and interests within the study. Later these arrangements were developed into formal agreements between the charity and the local organisations which specified roles, responsibilities and financial rewards. Work was then delivered flexibly by individual partners within the user- or carer-led organisations, which could substitute people to cover during illness. Local organisations could also involve additional members in their activities. Each organisation agreed to submit quarterly reports on local activity and complete other involvement work in the sites, such as recruitment.
The central mechanism used to support local involvement and impact on research design and delivery was the national panel meeting, which had met four times by late 2012. Two representatives from each of the four local organisations attended the national meetings. These meetings provided a forum for feedback about both the study’s progress and the local implementation of personalisation, and for discussion on the design and delivery of the research.
The research team planned the national panel meetings. Research partners liaised with the whole team via e-mail and telephone. Researchers also visited the sites regularly for meetings and to conduct interviews.
Outcomes of involvement
Locally, the role of service user- or carer-led organisations was to provide intelligence to the research team about the implementation of personalisation within the study sites, and to help to recruit and support study participants. Researchers in the team reported positive outcomes from the involvement activities and also valued the experience of being well connected to the lived experience of the study topic within the study sites. They also reported that working with their research partners re-energised them in their work. Research partners were less clear about what difference they had made, but felt valued by the research team. At national panel meetings they contributed to a variety of tasks including developing data collection tools, offering guidance around recruitment and support for participants, data analysis, and developing plans for dissemination. Our team observed national meetings and noted the active involvement of research partners in discussions about developing data collection processes and tools (e.g. advising on types of rewards provided for interviewees, support during and after interviews), analysis and plans for dissemination. The research team intended to involve the research partners in the production of practical toolkits for users, carers and professionals and in the dissemination of study findings to local user or carer groups and professionals.
Case study 6
Context of public involvement
This multicentre international study was hosted in a department within an NHS foundation trust where there was a prior culture of public involvement in research. The project investigated the recovery from a rare chronic pain condition from the patients’ perspectives. The study involved patients in eight countries in order to increase the patient numbers, and to raise the profile of public involvement outside the UK, where public involvement in research is less established.
The PI had previous experience of involving the public in research studies from working on other studies within the host institution. Co-investigators in the other countries involved did not have the same history of experience in public involvement in research. The PI’s experience involves rheumatology research, in which patient opinion is more usually sought. A research partner (described by the PI as an expert patient researcher) has always been allocated to the PI’s research team as a result of this experience. The PI has delegated the co-ordination of the research partners to the junior programme manager in the research team. The programme manager was familiar with the department within the host institution, but had no previous experience of public involvement in research.
The research teams for this study were based across institutions in eight countries, the host institution being in the UK. The aim was to hold one or two international face-to-face meetings per year. The study aimed to explore, via a two-round Delphi technique, what recovery means at different time points across the trajectory of the chronic pain condition (early, intermediate and chronic disease), and to create a list of symptoms in order of priority of importance of resolution by patients who have, or have had, the condition.
Mechanisms of public involvement
The programme manager in the UK host institution was key to informing research partners of updates and activities relating to the study progress by e-mail or telephone at regular intervals. There were two research partners on the research team in the UK and a further six in the other countries involved in the study. The PI and programme manager ensured that, at all times, they sought to express how much they valued the input of the research partners. The research partner within the host institution was a member of the user group in the department. The research partner in the other UK centre was a patient and had worked on another research study within that institution. Public involvement was less established in the other countries involved in the study. In those countries, patients were invited to join the study team by local academic co-applicants who knew them.
Three research partners were being formally trained to analyse qualitative data in the questionnaire responses. This activity had been costed into the project. Research partners were asked whether they would like to be trained and, owing to high levels of interest, names were picked randomly in order to decide who would undertake the training.
Outcomes of involvement
In terms of research design, research partners were involved from the beginning of the project in designing questions for the questionnaire. According to the PI, the research partners made a significant contribution, completely rewriting four questions to make them more patient-focused. The research partners attended a 2-day face-to-face research meeting to plan the project at its inception. A further meeting was held via teleconference 4 months later, but only academics from the research team were invited, as they were discussing practicalities of the project, such as sending out the questionnaires. In hindsight, the PI said that there might have been value in including the research partners at this meeting, and will be inviting them to all future meetings.
As the project was in its early stages, the detailed planning of dissemination and research partner involvement in this had not been undertaken. However, it was the stated intention of the PI to involve research partners at that stage.
Case study 7
Context of public involvement
Case study 7 took place in a rheumatology treatment and research unit where the PI was a doctor of philosophy (PhD) student. The unit has a long-term history and culture of involving patients in both treatment decisions and research projects, which is perceived as normal practice. The PI was a podiatrist with a particular interest in the effect of rheumatoid arthritis (RA) on patients’ feet, which was the topic for her PhD project. The PhD project had two phases. The first was a qualitative phase designed to collect and analyse data to inform the development of a questionnaire. The second phase of the project concerned using the questionnaire to collect and analyse quantitative data from approximately 1000 patients with RA. It was decided to collect data from RA patients attending both the host unit and an RA unit in another local NHS trust.
The director of studies for the PhD project was the clinical director of the host unit, who has played a pivotal role over a number of years in promoting and enabling patient involvement in all the unit activities. Although the PI did not have any previous experience of public involvement in research, she reported having been aware for some time of the need to include patients’ perspectives when thinking about clinical issues. She considered it a natural development to include active patient involvement in her research. She found patient involvement very valuable for her project, and showed evidence of having developed a perception of it as a ‘normal’ component of research. This was no doubt partly the result of her immersion in the culture of the unit. The project team included two other academics overseeing particular topic areas.
There were two patients working as research partners with the PI. One of these individuals had a long-standing relationship with the RA unit, particularly with the director of studies. This patient was a very experienced patient research partner, and had a history of involvement in a variety of activities, including presentation at international conferences concerning ‘Outcome Measures in Rheumatoid Arthritis Clinical Trials’ (OMERACT). The other patient working with the PI attended the RA unit at the second local NHS trust; this was her first experience of being a patient research partner.
Mechanisms of public involvement
A key mechanism for public involvement in research in the unit was a paid part-time post for a patient to co-ordinate and support other patient research partners. Funding for this has been established for some time. This co-ordinator was responsible for facilitating patients’ participation as partners in research projects. When this PhD project was first mooted, the experienced research partner was approached and agreed to be involved from the very early stages of the project; she contributed to the design of interview and focus group schedules, and the analysis of the qualitative data. The second patient partner heard about the project through word of mouth; as she was relatively newly diagnosed and interested in getting more involved in a range of relevant activities, she put herself forward to be a patient research partner, even though she did not attend the RA unit hosting the project.
Both patients attended all the full supervision meetings. Observations of a meeting indicated that they were able to participate fully in the proceedings, which included offering emotional support to the PI. The unit policy was only to pay patient research partners expenses, and not to pay for their time. Both patients reported being satisfied with this arrangement, finding it appropriate for their circumstances.
Outcomes of involvement
The patient research partners reported having been involved in the questionnaire design, and playing a key role in identifying anomalies and repetition in the questionnaire which had not been recognised by any of the clinicians or academics on the team. They also contributed to the decision-making processes concerning where the questionnaire data collection should take place. No specific outcomes of involvement were identified at the meeting we observed, as the focus was on the PI reporting back progress to the supervisory team.
It is expected that research partners will contribute to any papers or presentations arising from the study, and will be offered the opportunity to be co-authors on relevant publications. During the case study period, the main research activity was questionnaire data collection, so the patient research partners’ activities were minimal, consisting only of attending two supervision meetings.
Case study 8
Context of public involvement
This is a longitudinal study that has followed more than 14,000 young people since they were born (between April 1991 and December 1992). Data have been used to establish genetic and environmental determinants of development and health. The founder of the project was keen to ensure that participants were involved in the project. Parents were first involved in the ethics committee towards the end of the 1990s. Participant families have always been kept informed about the project through newsletters and other publications. During the course of the study, the involvement of the participants has developed and public involvement has become embedded within the project. Although initially the focus for involvement was the parents, as the children grew up a young people’s advisory group was established in 2006. This is supported by the project participation team. The current executive director of the study had experience of public involvement prior to leading this project. She is committed to public involvement, to supporting the ongoing development of the group and to seeking funding to enable the young people to become fully involved in the research process.
Mechanisms of public involvement
The primary mechanism for young people’s involvement was an advisory group of about 20 young people who meet regularly, facilitated by a member of the participation team. During the course of our study, the person leading this went on sick leave. However, the commitment of the team to public involvement meant that this role was immediately taken on by another member of the team.
The group was set up when the young people were aged around 15 years and has been meeting for 6 years. Prior to this, participants were involved in some focus group activities. The participation team organised around six advisory group meetings a year, three falling during holiday periods and three falling in between. The team also enabled members to contribute when they were unable to attend meetings in person via electronic resources including social media such as Facebook (Facebook Inc., Menlo Park, CA, USA). Group members and participation workers described how the group has developed as members have grown older and gained a better knowledge and understanding about the project and research processes. Members had the opportunity to comment on various aspects of the project including but not limited to the project website, questionnaires, substudy design and documentation, engagement activities and the dissemination of research findings.
Advisory group members volunteer their time but travel expenses are paid for attendance at meetings and events, and food and refreshments are provided during meetings. The group has developed a role description that lays out the expectations of group members.
Outcomes of involvement
The young people’s advisory group was reported to have significant influence both on individual research proposals within the overall programme of research and on developing policy and practice for the overall programme, for example developing generic guidance for consent forms and information sheets that all collaborators will be asked to use. Examples were also given of comment from the group, when they did not think proposed individual research studies were appropriate, leading to major changes in the design of the research. We observed one group meeting where three researchers presented proposed future studies to the group, and the young people gave helpful feedback which the researchers indicated would be used to revise their proposals. The group were involved in developing and presenting conference posters, videos and other dissemination material about the programme; we observed feedback on a major dissemination event in which the young people had been actively involved. Finally, the young people reported positive outcomes for themselves as individuals in terms of career development.
Chapter 5 Testing our realist theory of public involvement: case study findings
Introduction
Having developed our initial theory of public involvement in research as described in Chapter 3, the key task was to test the theory in our eight case studies. How well then did our case study data support (or not) the configuration of contextual factors and mechanisms we hypothesised would lead to intended outcomes for public involvement in our case studies? We first describe what regularities of outcome we identified across our case studies before going on to discuss what we found about the hypothesised contextual factors and mechanisms.
Outcomes
Influence on research design and delivery
Having hypothesised that influencing research design would be one of the regular intended outcomes of public involvement in our case studies, we found that this was the case in some but not all the case studies; notably, intention to influence design was not as common as an intention to influence the practical aspects of research delivery (e.g. recruitment materials and strategies and data collection tools), which was present in all our case studies. Influencing the design of future studies was a longer-term and somewhat less specific objective in several cases.
There were a number of contextual factors that impacted on the influence members of the public could have on the initial research design. Research funders are often prescriptive in the research they are prepared to fund, outlining specific design requirements and outcome criteria. This had an impact on the degree to which the public could influence an overall design, as reported in case study 1:
Okay. I think they have had more of an impact on the delivery.
Yes.
The initial design had already been written and agreed because it was very influenced by the Department of Health . . . and so it was, it was very controlled . . . so you know it all depends who your funder is.
In addition to the constraints imposed by funders, academic informants often reported managing the public input based on the perceived skill and knowledge of members of the public. This informant suggested that the public required specific knowledge and skills in order to engage in research design:
So with the Big Lottery they are having a bigger input into the design and what we need and what we want to do. So it’s, it’s also the stakeholder involvement and how they matured . . .
Yes.
. . . in their knowledge and skills.
The longer-established and more ongoing the public involvement mechanism, the more this helped support effective public contribution into the development of research design. The advisory group working with case study 8 provided one example of a well-established panel that commented on research projects and activity across this research programme. This group was presented as a powerful mechanism for influencing research project design decisions:
And we often have to spend quite a bit of time explaining to researchers, ‘This is how we do things in [name of programme]. If you want to do the study then it needs to go through the group of participants.’
Yes.
Sometimes they’re going to tell you things that you don’t like. Sometimes they turn round and say, ‘No, that is not okay and that will not be popular.’
Yes.
People will not want to do that. And we always would go with the participant views.
A specific example of the influence this group has had on research design is provided below:
. . . it was quite clear about how that would work and how we would ask those questions and we took it to [the public advisory group] who hated it.
Research manager 1
This advisory group raised new insights for the research team to consider in developing their research design and so had influenced the proposal.
By contrast, newly established and time-limited research partner groups were less involved in influencing research design, but were often able to influence and have impact on the later implementation of the proposed research design. This is evidenced in case study 4, where the input of a patient panel led to changes in the approach to gaining consent from participants:
That was very valuable because that kind of did have an impact on the trial design with that one because it was how we were going to do it. So then with their ideas about that it then dictated our ethics application.
Research manager 2
Influence on recruitment and retention
Recruitment to studies is influenced by many factors; designing good publicity and information sheets is one aspect that public involvement can help with. Participants consistently reported that research partners’ contributions improved recruitment strategies and materials, although these improvements did not necessarily lead to improving participant recruitment to their studies. For example, an advisory group in case study 1 helped develop a poster to support recruitment which was used in all of the trial sites. At a later stage in the trial the group were approached to support the researchers think through ways in which retention might be improved. Their ideas at this stage changed the original strategy:
At some point we had already decided to give out telephone cards to participants for taking part in particular interviews and the [public advisory] group had a look at those cards and they said ‘well it’s not so useful, high street vouchers would be more useful,’ so that kind of input they had.
Researcher 6
An interview recorded at a later stage in the project suggested that recruitment had still been an issue despite the public involvement, though this could be attributed to a number of factors, not merely the recruitment strategies:
It took us longer to recruit; therefore it’ll take longer to follow up for this study.
Researcher 7
Other studies also involved research partners to assist with recruitment. In case study 2 the project was having difficulties in recruitment and sought advice from the advisory group. The group suggested targeting potential participants through the community rather than through NHS services. The parents helped develop fliers to aid recruitment; despite distributing hundreds of these, recruitment remained low:
Clearly the redrafting didn’t do much good, because they didn’t recruit that many parents, so although we put quite a lot of effort into redrafting it, it still wasn’t perfect . . .
Research partner 2
The reasons for low recruitment may not be attributed to the quality of recruitment material alone, and a number of factors related to the project and the target population may have contributed to this outcome.
In case study 5 the local context also impacted on research partners’ efforts to recruit through a programme of local events:
And so we held two events but we didn’t get any people sign up through those events and it was partly due to timing in that we were relying . . . obviously we put word out on our website and through our networks, through our peer specialists, these events are taking place, but we were also relying on the individual teammates and managers and care co-ordinators to tell people about those events and for whatever reason I don’t think the message really got out there.
Research partner 3
Here the research partners’ efforts were thwarted by both a lack of local support from key staff and a lack of people eligible to join the study, due to local authority policy decisions. Recruitment remained problematic despite a number of innovative approaches to recruitment.
In some case studies recruitment and retention strategies developed with public involvement had been more successful. The parents involved in case study 3 made suggestions to aid recruitment to and retention on a training course delivered to parents as part of the feasibility trial. They suggested a number of strategies to help, including making sure a member of the children’s centre, familiar to the parents, was available when the course ran; shortening the length to mirror the school term; and encouraging parents to bring a friend or relative with them to the sessions. They also influenced the scope of recruitment to the study, suggesting that all parents should be invited to the course, not just those with children who had been injured. The research team felt this approach had been successful and intended to use it in the design for a proposed future trial.
Influence on data collection tools and methods
There were a number of examples of research partners influencing the development and use of data collection tools and methods. In case study 6 the research team made a significant change to the order of questions on a questionnaire and the mode of delivery, based on feedback from four patient research partners during a research meeting. One major change was noted:
Yes, so it was going to be one big questionnaire and now we have put in two questionnaires, and that was under the, well it was because of the change, the rephrasing and how they would answer it.
Researcher 8
One research partner in the same study also reported challenging the wording of a question relating to patient recovery, suggesting that patients may see themselves not as ‘recovered’ but as learning to live with the disease, coping with it rather than recovering to their previous level of health. This feedback led to changes in the questions asked, which the research partner felt would have beneficial outcomes for the project:
I think adjusting those questions a little bit is likely to draw out the answers that are really being sought rather than the answers that might have been given otherwise, because they didn’t really understand exactly what was being got at.
Research partner 1
The parent panel in case study 2 influenced the methods of data collection, by commenting during a panel meeting, which resulted in significant design changes:
So they suggested we did this play session instead of direct focus groups and the main headline was, ‘oh, fun drama play session’ . . . We’ve changed to telephone interviews as one of the outcomes of the parent panel recommending that, you know parents who do want to be involved but couldn’t make it to the focus groups.
Researcher 3
This change had been recently implemented and the researchers were unable to comment on the actual impact of the change on the research outcomes. However, it is expected that the change will impact positively on recruitment. Further impact was evidenced in case study 3, where the research team felt members of a parent advisory group added support to their view on where a particular intervention should be delivered:
From a design point of view it’s made a difference in – well it’s reaffirmed our opinion that the setting for delivery of courses should be in children’s centres. The setting for identification of potential participants should be in children’s centres, through children’s centres.
Which was quite different from the plan wasn’t it?
Which is different . . .
Case study 7 also reported changes to a questionnaire design which was influenced by the patient partners’ contributions. These included changes in layout, wording and the inclusion of additional questions. Changes were also made to patient information sheets and letters. Research partner comments at one meeting led to the recognition that a draft questionnaire was being reviewed, rather than the validated version:
Yes because I read through it and basically one question had been duplicated but phrased slightly differently so I told her it should have been this way round and they have now changed it and they are all very impressed with me.
Research partner 4
The advisory panel in case study 8 developed guidelines on the development of information sheets, consent forms and other documentation. These are now provided to all researchers applying to undertake research in the programme, with the intention of helping researchers produce research documents to a specific standard:
I think they have had some real impact in terms of, okay so there are things like the [named] guidelines, so that has gone wider now, so that is not just looking at the information sheets but looking at the consent forms, to look at the invite letters and the reminder letters, and based on the guidance that they gave us, that we then whipped up into a sort of guidance document that fitted with the NIHR guidelines for information sheets and consent forms, we are now taking that and creating templates and a set of guidelines to give to all collaborators when they approach us.
Research manager 4
The experience and insight research partners brought was seen by researchers as valuable, adding an important perspective:
I think I just value their opinion on certain things I guess, especially in terms of how the questionnaire is going to be answered and how long it might take a person to complete . . .
Researcher 8
Case study 5 relied on research partners from a local service-user organisation to gather local intelligence vital to the study:
They are very effective at providing an insight, an on the ground insight, into what’s going on in a way that we wouldn’t have access to especially in the second phase of the study.
Researcher 9
In three of the case studies the researchers suggested it was difficult to separate out the influence of research partners in the development of research design and delivery. The quote below from case study 7 illustrates the difficulties of tracking who is responsible in collaborative teams for the contribution which makes an impact in the research:
Mostly it’s really hard to see what the influence has been because what happens in the research is a synthesis from everybody around the table and you know it’s a bit difficult to say, well, what exactly did [name of research partner] say that made a difference to it . . .
Researcher 5
A number of academics said that they would involve the public again in future research activities and use the learning from their current projects to inform that. Almost universally, research staff stated that involving the public was valuable, was seen as important externally and should be supported in the future:
I think it does add value . . . the ability to involve patients will be a benefit in terms of future research in the sense that we can yes, we have got a patient panel, it’s got this pedigree.
Researcher 10
One academic was sceptical initially of the process of public involvement but was very quickly won over to the benefits:
I think the whole overall process has been helpful, I mean initially I’ve got to be honest and say I thought it was going to be paying lip service to the NIHR and what they were trying to achieve but after the first meeting I think I can quite happily say that was straight out the window.
Research manager 2
Longer-term impact
In several of the case studies participants noted longer-term, strategic or personal impacts of public involvement that might not necessarily contribute directly to the current study, but would contribute to enhancing future research. In case study 2 the team articulated a strategic role for their parent research panel initiative that went beyond contributing to the specific research programme and was intended to help develop an ongoing strategic approach to public involvement for the research group as a whole:
I think we were determined that part of what we would do is work that [role of parents] out really and I think because it is this kind of infrastructure process, part of what we wanted to do was make sure that we had some kind of system that wouldn’t just work for the actual funded project, but it would be something that we could expand and develop into something that works for the whole research unit really . . .
The parent panel is a testing ground for how we involve people in the future and that we start to use them . . . work with them in that kind of broader way so that it’s not just related to that programme of work but others as well. So as I say we’ve taken bids to them that we’re thinking of and got their views about [if] it’s an appropriate one, whether it’s relevant, what parents might think about that, whether the questions would have occurred . . .
Researcher 2
When asked if there were models for this approach elsewhere in the NHS trust, a team member commented:
I think we are quite unique in kind of thinking about it at that strategic level. I think most of the groups we have are very much focused on particular projects whereas we are trying to plan this as a long term, so no, I haven’t seen any other planning or strategy or policy documents, so it’s all kind of feeling my way through it.
Research manager 3
Case study 8 participants commented on the influence of the advisory panel in the development of guidelines that would impact on the processes within the programme. These guidelines had the support of senior programme managers and were being implemented for use by all collaborators:
So like this [named] guidelines is a really good example, I know I keep bringing it up but it is a really good example, because now moving forward we are going to have all our documentation in house in the same format as we would ask collaborators to, all following these templates and these guidelines which I think is the first time we have done that.
Research manager 4
Some case studies reported other intended impacts. Case study 5 planned to involve the research partners in the development of three toolkits to disseminate the study findings, which had the potential for national impact. Research partners from all four local study areas contributed to this through the national public advisory group meetings, organised and facilitated by the research team.
Academics and research partners noted a wide range of potential benefits and impact from public involvement in research on service improvement as well as on research, but were aware of the organisational challenges of achieving this in a meaningful way:
I think there is an organisational issue about how important it is to engage with parents and is it going to be just a tick box exercise? Do you engage parents or is it going to be actually this is really tough? We really want to do this well and we want to design our services with parents informing us of what they want.
Third-sector partner 1
All case study research teams felt they wanted to continue to work with public involvement in future research. Some had long-standing research panels and groups in place that they were continuing to work with, whereas others were considering developing their strategy for public involvement to include the possible use of mechanisms such as formal panels with terms of reference. It was also recognised that investment was needed to support panel development and widen their scope of influence:
I think we want to continue to utilise the panel to . . . you know in terms of validating research questions, I don’t think our panel is developed enough to generate research questions although that may be unfair but I don’t necessarily see that at the moment . . . the more we invest in the panel the more we’ll get out of it because hopefully the people remain relatively constant over a period of time and they possibly understand more about what’s going on and therefore they can make . . . you know a better information base.
Researcher 10
Overall both researchers and research partners felt that research partners brought a crucial perspective to studies which enriched research and research teams:
In the formal governance meetings for the project I’ve certainly found it useful, it’s always useful to have verbal feedback and different points of view being expressed in a constructive environment.
Researcher 7
I think it is making a much richer study, because without their involvement it wouldn’t even be relevant I don’t think.
Researcher 8
For some academics, who were practising clinicians, this impact went beyond the project and into the workplace:
Makes me a better clinician . . .
Researcher 11
In some cases attending external training on public involvement complemented the learning that researchers and research managers gained from their direct involvement activity:
Attending the theory group sessions introduced me to the literature and theoretical discussion on public involvement that in the normal course of events I wouldn’t have been exposed to – and this too may have had an impact on my work with the parent panel.
Research manager 5
Overall, we found consistent evidence that public involvement influences research design and delivery, in particular improving recruitment strategy and materials, and improves data collection tools and methods. Public involvement shaped initial research design only in a minority of our case studies, but there were a number of indications of potentially longer-term influence on future research design, and other intangible impacts such as on researcher learning.
Impact on the public involved
In most of the case studies the primary objective of the public involvement was to improve the quality of the research, particularly around research delivery. Having a positive impact on research partners themselves was not usually an explicit objective of research teams, although it was often recognised that such involvement could be a development opportunity, especially for young people or others who needed to build confidence or develop skills to enhance their career or employment prospects.
Across all the case studies, being involved in research had a range of positive impacts on the research partners, including learning new skills and knowledge, personal development and support, friendship, enjoyment and satisfaction. However, there were a few occasions where research partners were more ambivalent about their involvement.
Developing research skills and knowledge was viewed as a benefit of involvement. One participant commented on the variety of opportunities their involvement brought:
We were invited along to be part of the recruitment interview panel in order to appoint someone to the study, that was not something I would have expected necessarily, but it was quite an interesting opportunity and an interesting way to involve us . . .
Research partner 2
In this example, the public involvement was focused on recruitment rather than data collection. Involvement in some studies enabled research partners to develop dissemination skills, through co-authorship on main papers and contributing to conference presentations.
Involvement in research provided opportunities for development and engagement in stimulating academic work, particularly noted by a respondent in case study 6 who was unable to continue to work:
Having had to give up work because of my condition I do miss the intellectual challenge and so anything like this, which involves me in the academic light again, really is something that I’m very keen to be involved in.
Research partner 1
Taking part in advisory groups led to an increased level of confidence for some research partners. One young group member referred to her experiences gained in the advisory group in her university application, and felt that these skills would be useful at university:
I think definitely when I was younger it helped confidence-wise, just being able to speak in front of people you don’t know and particularly being able to disagree with people politely and not to get frustrated, I think that definitely helped me when I got to uni[versity] as well and I had to talk to irritating people in seminars and so yes, I hope it will help me with my confidence.
Research partner 5
Another research partner noted the personal impact of involvement for some of those participating:
I think the other thing I haven’t said is it has been quite useful in terms of personal contact, if that doesn’t sound selfish.
Research partner 6
Involvement in advisory groups provided research partners with opportunities to learn from others experiences:
One thing that they have said, they really like to come and see what’s going on in other sites, particularly for those sites where they feel like it has been a struggle.
Research manager 6
The struggles (with recruiting study participants) referred to here were also mentioned by a research partner who had felt personally responsible for the lack of progress. The national meeting attended by research partners from the four sites provided a helpful forum for reassurance and support:
Actually we ended up with more participants than [another location, which] has made me feel better.
Researcher 12
One case study reported that research partners had experienced difficulties when other patients made unkind remarks about their involvement in research activity:
About 6 or 7 years ago [name of research partner] brought up a problem, I think it was at one of the training days, that some of the other patients who were sitting in the waiting room who recognise her and a few other people are being sort of involved in the research and things were making nasty remarks about them getting special treatment because they are friends with the doctors.
Researcher 5
While this issue had occurred some time ago, it remained in the thoughts of the researcher and highlights a challenge for some members of the public who become involved in research.
Some of the mechanisms put in place by researchers to support research partners were not used. For example, case study 2 developed a website to facilitate communication between research partners, but they did not use it.
Case study 2 also explored whether payment was an important mechanism to support public involvement, and, for this group, knowing they were making a contribution was a more significant factor:
I’ve been asking parents what they think about payment and whether that was a motivation for becoming involved and actually it’s not really, it’s more about wanting to do something that’s interesting and an interesting subject matter. So I don’t think the payments are particularly . . . well, I think it’s a way of saying you are valued, but the parents don’t seem to see it in that way.
Research manager 3
Providing feedback to research partners which demonstrated that their input had influenced a project was commonly noted as an important motivator:
So again they were quite pleased to see that they had had an input and we had actually listened to them. So you asked about what do we give back to them? But that in itself felt as giving back.
Researcher 6
Only one case study expressed, in an early interview, an explicit objective to promote the development of research partners, who joined the study as delegates from a user-led third-sector organisation:
We are very keen to be not only having users involved but also to be kind of cutting-edge and kind of do something that’s innovative and relevant to the people that we are working with. Because I think it can be relatively easy to involve people who already have skills at a very high level and we wanted to make sure that our approach was inclusive and we allow opportunities for people to learn and develop as part of what we were doing. So we wanted to do something that was innovative and kind of pushing the edges a bit and giving opportunities . . .
Research manager 7
When asked about the impact on the research partners at the end of the data collection period, another researcher in the same project reflected on how difficult it was to assess this:
I don’t know, it depends on what you mean by impact. You know, I think a lot of people are very interested. I am sure they have taken those ideas somewhere else, I am sure they have talked about them with other people, but they were anyway engaged in this kind of work . . . So whether that has impacted beyond what they would have had anyway or maybe it has become part of their other involvement activities I suspect. We haven’t really identified people who have never been involved . . . So it is one of the things that this model does, it brings in people who haven’t had that opportunity before, so in some sense the impact is perhaps less obvious for that reason, it might well be people have gained confidence from it, but I haven’t asked them and it’s very hard to know.
Researcher 6
This was, however, the only case study where research partners reported feeling disappointed or frustrated. The disappointment arose from mismatched expectations about the roles they were to play in the study. The research partners recruited had unusually high levels of experience of working in research, and initially expected to be involved in data collection, which the academics had not planned for or expected. The same research partners also felt frustrated when some distinct local issues hampered recruitment within their study site.
This issue was resolved, and the project continued successfully with the research partners fully engaged. The partners were later encouraged to take on analysis and dissemination work, which they enjoyed. However, this episode illustrates the potentially negative impact of differing expectations or a lack of clarity about roles at the beginning of an involvement partnership.
The example above also exemplifies a more general observation that the case study research teams did not usually have mechanisms to capture the impact of public involvement; this is unsurprising, as many decisions and internal processes in research teams are not recorded or only noted briefly in meeting minutes. Case study 2 was unusual in that it tried out several different mechanisms to try to capture the impact of involvement from the perspective of their parent panel members:
So in terms of actually demonstrating the impact of this involvement from your perspective is . . . to map what the parents are saying in the group discussions and then seeing if we can actually see where that is influencing decisions that are made by the project team?
I think it’s more than that; you’ve got to capture your entry point, where they are now. So hopefully that has been caught and this is why I’m keen that we look at them keeping a ‘diary’ so that we can actually capture how they are feeling, you know what’s changed for them?
Another mechanism later used by case study 2 was cartoon drawing, as observed in one of their parent panel meetings:
Towards the end of the meeting, the PI introduced the idea of ‘cartoon-drawing with speech bubbles’, which the parents took to enthusiastically to ‘capture their journey’. They all said positive things about their participation being more interesting and rewarding than they had expected.
Field notes extract
Outcomes conclusions
Across our case studies the main objective of research teams in involving the public was to improve the practical delivery of research; overall, there was good evidence of some impact by research partners in all of the case studies, except that the impact in case study 4 occurred before the study period. Research partners contributed to a number of aspects of research delivery including improvements to ethical review applications, recruitment materials and strategies, data collection instruments and methods, analysis and dissemination. There was evidence of some longer-term impacts and more strategic impacts, but these were harder to document. A secondary outcome for most of our case studies was the range of positive experiences that research partners reported, with only one negative experience reported early in one case study.
Comparing outcomes with the initial objectives for public involvement was difficult over the relatively short time period of our data collection, particularly for those case studies for which there were substantial further stages of research still to come. Most of the case studies did not themselves have mechanisms to capture the impact of public involvement. The one case study which attempted this found it took some time to develop a mechanism (cartoon drawing) that worked for its parent panel.
The next step in testing our theory must be to turn to the contextual factors and mechanisms we hypothesised were linked to outcomes and assess what these tell us about our theory of public involvement.
Context
Leadership and culture
Our initial theory hypothesised that a number of inter-related contextual factors would influence the extent to which the case studies achieved their intended outcomes. In this section we review the extent to which we observed the anticipated contextual factors of PI belief in public involvement, senior leadership on public involvement, culture and values, and history of public involvement within the wider institution.
Principal investigator belief
A key finding identified in the case studies was the importance of personal commitment to public involvement by PIs (both in research and more generally in service development). In most of our cases the PIs spoke clearly of their personal commitment to public involvement. In case study 2 the personal commitment of the PI was identified by other stakeholders and explicitly expressed by the PI herself:
You know as a clinician when I worked as a speech and language therapist, I always really enjoyed those conversations with parents, you know finding out what they were doing at home with their children and understanding their perspective on how they’d tried to help their children before I started making suggestions. I always really enjoyed those conversation because I just felt . . . it just made me understand how to help them, how to kind of feed my expertise in. You know if you don’t understand that perspective, then you don’t know how to shape your own expertise to help them. So I always really valued it as a clinician . . . So I’ve always enjoyed working with our parents in that way, so it’s nice to kind of feel that coming in to the research more, in that kind of partnership way but we’re still quite a way from that really. I think we’re early days.
Researcher 2
This commitment was recognised by other case study informants including the parent member of the parent research panel:
I was impressed with the way [PI name] makes it feel like we’re really a valued part of the process but it wouldn’t work at all if it was something which had been forced upon her. You can imagine a situation where research has to involve a parent panel and a researcher might resent that and so would be very reluctant or dismissive . . . in the way they communicated with us, but actually she does make us feel like we’re a really valued part of the process so I was really impressed with that.
Research partner 2
In answer to the explicit question of where leadership on public involvement in the project came from, a colleague answered:
It comes from [name 1] the principal investigator, I mean I see there is some things that she has been looking to do for the [research group] and [name 2] mentioned they previously had some patient or parent involvement, but I think [name 1’s] vision [is] to have it you know set up and established for the unit as a whole and obviously having this grant has given us the funding to do that so we are kind of using this as a model and you know when the grant comes to an end we’d hope to kind of expand it to cover, to invite people who would be useful for other projects that we are doing and have that experience. So yeah it’s [name 1] and then, so I am kind of then leading on kind of getting it set up and we can get it from a strategic point of view and [name 2] is doing the kind of admin[istration] around it.
Research manager 3
A consistent message from across the interviews in this case study was that the PI had a long-term commitment to involvement, and had previously involved parents in service improvement projects. She had recently been stimulated to think about involving parents in research, and in particular to take a strategic approach across the unit to develop an ongoing infrastructure for involvement in research in the unit. Several factors had come together to catalyse the PI to take action: her long-term philosophical commitment to involvement, her long-term partnership with key third-sector parent organisations, the increasing requirement for public involvement from NIHR as the prospective funder of the programme grant, and the inspiration of attending a James Lind Alliance meeting:
Around the time I was thinking about working out the programme grant I went to a James Lind Alliance meeting . . . and I found it fascinating. I was just really excited about that meeting and watching how they were supporting that engagement of patients in that context to set up the agenda. So there was quite a lot happening I think around the time.
Researcher 2
In case study 3 the PI was a less experienced researcher, but expressed a similar combination of drives for public involvement, combining recognition that it was a funder’s requirement with personal commitment:
Okay, and when did you start thinking about public involvement in research?
Right at the beginning at the outline stage, partly because it’s a requirement for any [funder’s name] response to one of their calls, they actually have on their application form a section which says how . . . you know what is the user involvement or public involvement, what’s the plan? . . . I knew that I would have to do it from the word go and I knew I would want to do it from the word go, particularly because this is working with parents, our project, and unless we meet the needs of parents they won’t pitch up to our course that we’ve developed. So I mean it was inevitable that we would have to have the parent perspective.
In this case, a co-applicant who was more experienced in research generally, and in public involvement specifically, was identified in the bid to lead on involvement in the project, and has done so. The co-applicant also expressed her personal commitment to public involvement:
When I’m designing projects I do like to make sure that there is a dedicated patient advisory group for each project, just is the way I think is the best way.
Researcher 13
Here the co-applicant had both the experience and the local networks to recruit parents to a new parent advisory group, and continued to take a lead on this activity but with the active support and involvement of the PI, who has also attended the group on occasion. This supports the proposition from the consensus workshop that the PI needs to believe in the value of public involvement and be prepared to support it with resources as necessary, but that another senior member of the research team can effectively take the lead in this area.
In case study 7 the PI was also less experienced but was developing as a researcher in a unit with a strong ethos and culture of patient involvement:
I was coming from a clinical background and a lot of the literature in rheumatology especially outcome measures were a bit critical of some tools that have been derived [where] the content was derived by expert panel and not patient involvement. So it wasn’t unusual and I wasn’t surprised, you know I just thought it made sense.
Researcher 11
None of our PIs expressed scepticism or doubt about the value of public involvement. One PI, who had previously been unsure of the value of public involvement and undertaken it primarily to meet a funder’s requirement, was then pleasantly surprised at the benefits involvement brought:
We were just entirely naive about the whole thing, or I was, and there had been no previous public involvement in any research that I have done over the previous twenty-odd years and I mean a lot of the research that I’ve done is laboratory based research but I’ve done quite a few clinical trials and things like that as well but not recently. And so it was a relatively new thing so we just had to sort of learn a bit about it and try and understand what it was and how we might deliver it and . . . like I suspect a lot of people you know ‘well, what are we going to put in that box on the application?’
So there was a kind of funding question?
Yes, absolutely, you know what are we going to put in that box? What do they expect us to have in that box? And what do they want us to do? And that’s how we sort of got into it. It wasn’t that we suddenly woke up one morning and thought it was going to be a great thing, it was woke up one morning and suddenly saw box 16 which was patient involvement and I thought what the hell are we going to put in there? . . . Having set up a panel I think we can see advantage in using it now.
Case study 8, with its large size and very different structure, was exceptional in not having a specific PI with a commitment to involvement; but it did have an executive director supportive of involvement and a full-time participation manager acting as an advocate for involvement across a range of studies nested within the overall programme. Thus it had a different structure and leadership on public involvement from the other case studies, which makes it a partial exception to our hypothesis, but essentially it was still consistent, as there was a senior lead within the programme advocating for involvement.
Senior leadership on involvement
In all our case studies a team member was identified to take a lead on public involvement. In most cases this was either a co-applicant researcher or a research manager; in one case of a small postdoctoral study (case study 7) it was the PI herself. Our very large case study 8 had a full-time participation manager. An unusual aspect of case study 2 was the way that leadership on public involvement was shared between four different members of the programme team. Early in the development of the proposal the PI recruited a third-sector senior manager who was a parent of a child with difficulties, and with whom the PI had worked before on other projects, as a co-applicant with a specific oversight role on public involvement. Once the grant had been obtained, two other members of the team, the project manager and an administrator, were asked to take on public involvement leadership roles. The project manager took on the strategic lead for involvement while the administrator co-ordinated the day-to-day involvement. In response to our question about leadership the PI replied:
I think initially from me but I think you know [name] who is our programme manager is also strongly orientated towards that and very keen to see that . . . and I think as we’ve rolled it out each person has kind of really taken to it and is pushing it so they’re kind of promoting their own . . . I maybe kind of kick started it but they’ve each kind of responded to that I think and are driving it hard now themselves. So like [name of administrator] has taken on the kind of organisational role if you like and she’s really promoting that I think now.
Researcher 2
This demonstrates a direct link from the contextual factor of the PI’s personal commitment through the recruitment and structure of the bidding team (including a third-sector/parent co-applicant) to the more concrete mechanisms of allocating staff resource to strategic leadership on involvement (programme manager) and involvement co-ordination (administrator). These staff roles underpinned the ability of the programme team to initiate and develop an ambitious strategic approach to developing a wider infrastructure to support involvement in their research group.
In case study 3, leadership on public involvement was not as widely distributed, but was still shared to some extent. Despite the PI initially delegating public involvement leadership to the co-applicant with expertise in this area, she retained an interest and a role in it. Moreover, at an early stage a second co-applicant, a senior and experienced researcher in another university, had advised the PI on public involvement and facilitated links with third-sector parenting organisations, which were subsequently invited to join the project as collaborators.
In some cases, senior lead roles on public involvement were written into grant applications and explicitly identified; in other cases, team members (in particular research/programme managers) took on this role more informally:
As I understand it you’ve also been the lead person for PPI as well. I mean was that in your job description?
No not at all.
And was there any funding in the original grant application for PPI?
No, no.
So . . .
It’s something I’ve had to absorb in and amongst my other roles.
The crucial factor appears to have been that someone in the project team took on this leadership role, not whether it was formally identified or resourced in the original bid. Leadership can be difficult to define, but in our case studies leadership on public involvement in research included taking responsibility for ensuring research partners were recruited and supported, making sure meetings with them were well organised and facilitated, demonstrating a relaxed and inclusive approach to relationships and good communication – listening to and acting on research partners’ contributions.
Previous experience of involvement
In seven of the eight case studies, the PIs and/or senior researchers all had previous experience of public involvement in research; some of these individuals had extensive and long-term experience. Researches who were clinicians made the point that public involvement in research developed naturally for them because of their clinical experience:
I came from a clinical background . . . I worked for many years in the field of HIV [human immunodeficiency virus] and AIDS [acquired immunodeficiency syndrome]; and I think in many ways that was kind of very much leading the way in terms of our relationships that we had with patients; and so for me coming into research it just felt like a kind of natural progression that that’s what you would do.
Research manager 1
This correspondence between clinical practice and research was also mentioned by other individuals, some of whom had no previous experience of public involvement in research:
I think in a way I still kept it quite separate in my mind . . . It was only when we thought, right, we’ll sit down and think about the PPI side of things, that suddenly I thought, oh, actually the language I use with my research hat on and the language I use with my clinical hat on is quite different; and that challenged me and I suddenly realised, well it’s going to the same parents, why would we necessarily use different terms?
Researcher 3
One participant spoke expressly about the necessity for researchers to acquire the requisite skills to manage public involvement:
Researchers have to learn two new skills that aren’t currently taught in research to enable them to get from the patients the input into their research that makes it better . . . to identify and engage people and support them so that they actually come and take part and make a sensible contribution . . . [and] to listen to what they’re saying in a way which allows them [researchers] to pick out the things which are actually relevant to the research.
Researcher 5
Culture and values
The complex relationship between PI commitment and wider professional or organisational culture towards public involvement became apparent in the data emerging from across the case studies. The relationship between leadership and culture was complex and diverse. In some cases the PI had played a key role in shaping the culture towards public involvement in research. In others, a wider culture of involvement shaped the approach of relatively new PIs. In case study 5 a research manager described the importance of the wider organisational culture:
In research well of course it’s the ethos of the organisation, so the whole ethos of the organisation says we want to be having people’s lived experiences of this, whether it is as directly using services or as carers, to be driving everything we do. So that’s the ethos.
Research manager 7
However, a colleague described how the PI’s approach both reflected this wider organisational culture but also represented his own personal belief and skills:
I think it’s probably [name] because [name] is a very professional person but he also has incredible people skills and he really stresses the importance of working with service users and communicating with people and also the way he approaches everyone is incredible. He is really friendly; he is really open; he remembers about people and he is very approachable and makes me think that maybe it’s partly due to [name’s] personality, but also probably [organisation] approach to running an organisation.
Researcher 12
This organisational ethos of valuing involvement was expressed by all the other researchers in the team as well:
I have a lot of respect for the group who I’m working with who have lived experience and . . . I think it’s important that they’re not just there to tick a box on an ethics form.
Researcher 9
The research partners, recruited from a user-led organisation, were similarly positive about the organisational ethos:
[Name of organisation] wouldn’t want to carry out research that didn’t seek to involve people with lived experience. Which obviously we would feel uncomfortable if they hadn’t come with those values, because that is what we are all about as an organisation.
Research partner 3
The case study 6 PI described the origins of the commitment to public involvement in the project:
I suppose yes, I mean me as the PI on it, I mean I set it that that [public involvement] was absolutely what we were going to do right at the outset; but I guess the influences to that was the cultural environment I work in, research environment that I work in where it is the norm, yes, expected.
Researcher 14
In case study 7 the PI was an early career researcher in a department with a long-term culture and policy of involving patient research partners in all research. A senior professor in the department (and a member of the project team) has a national reputation for involving patients in all research; it was therefore a cultural expectation across the department and an explicit assumption that every new project including this one would involve patient research partners. The department also has a well-developed system of patient research partners working in ones or twos with each project team, so it is assumed that new researchers will also follow this approach.
Culture is of course a complex and contested concept, which can be hard to define or locate. It may vary across a number of dimensions or at different levels (e.g. between clinicians, researchers and patients in different health-care, academic or disciplinary fields such as mental health or rheumatology, between researchers and service user organisations). An insight generated by one case study team was the importance of values underpinning culture in public involvement in research. Case study 5 researchers all expressed a strong commitment to supporting the development of research partners, which was not a value expressed in other case studies. Here one can see a slightly different approach to public involvement in research, with a shared belief that involvement improves the quality of research but also that, by promoting research partners’ personal development, it can lead to longer-term improvements in the quality of the research.
History of public involvement in the institution
All of our case studies had some history of wider institutional support for public involvement in research; however, the individual research teams varied in the extent to which they had linked to the available support. Case study 1 was typical of the nature of the wider institutional arrangements:
We have a working group for public involvement within this trials unit of which I’m the cochair and my cochair is [name] who’s a researcher in nursing and in paediatrics and we have an advisory group who contribute input into how we involve people into studies. And as a unit what we would be trying to do is ensure that all of our studies work to a sort of common standard. Now what we don’t have is a signed off policy on involving people.
Researcher 7
In case study 2 the study-specific research manager, who was relatively new to public involvement, was supported by a central research manager with a remit for NHS trust-wide support for involvement in research:
[Name] has been in post for a couple of years now . . . [Name] and I have been kind of helping each other and trying to work through getting some guidance in place . . . She generally supports all the established or new panels and goes along to their meetings and just kind of provides any thoughts and guidance on that; so that’s really all the support that I know about at [named NHS trust].
Research manager 3
Case study 3 had a different but equally useful history of institutional arrangements including children and young people’s advisory groups:
Parent and child involvement is a key theme of the [research centre name].
Researcher 4
This case study also raised a common issue in that study teams usually work across institutions, in this case four universities and one NHS trust. In most cases each institution will have its own differing arrangements for supporting public involvement, so that different research team members may call upon different individuals and systems for support.
In a few cases, notably case study 4, wider institutional support on public involvement had been available for some time, but had only recently been accessed by the research group. Case study 7 was exceptional in having such a long-term history of patient involvement in research studies in the research grouping, making such involvement the visible norm in the unit.
There are lots of projects going on and . . . lots of patient partners in the other projects . . . there probably isn’t a week that goes by when you don’t see some patient [research partner] or other wandering around the unit.
Researcher 5
Across all our case studies there was consistent evidence of the linked importance of history, leadership and culture in shaping the mechanisms of public involvement that were put in place. A history of institutional support was helpful in several case studies, and this history usually reflected a longer-term culture, but by far the strongest evidence was for the importance of PI leadership on public involvement, or, where this was not apparent, leadership from another senior member of the research team.
Field of research
Following discussion at our two consensus events and analysis of emerging data, we agreed that the term ‘field of research’, although not part of our original theory, reflected an important aspect of the context for public involvement in research which needed to be incorporated into the theory. In part, the concept of ‘field of research’ links to the term ‘research design’ but we felt the need for a broader, more comprehensive term that would capture the complexity of our findings. In particular, studies differ in the extent to which members of the public have an ongoing relationship with researchers and in the degree of diversity among the public. Using the term ‘field of research’ served to highlight that that there is not one way to do research, but actually a number of dimensions to undertaking research. These are defined by complex and often taken-for-granted assumptions, procedures and practices that make one field or discipline distinct from the other.
Academic disciplines and clinical specialties differ markedly in the extent to which they have an ongoing relationship with the public. In our case studies, some groups of researchers did not have such ongoing relationships, for example epidemiologists, microbiologists and social scientists. Other researchers in mainly clinical areas such as rheumatology and SLT did have ongoing relationships with their patients which spanned both their research and clinical or service roles. Even within clinical areas there is diversity, with clinical researchers in rheumatology having longer-term relationships (due to the particularly long-term nature of rheumatology conditions) than clinical researchers in other areas. Relationships between clinicians and patients are also characterised by different levels of continuity and trust; relationships between psychiatrists and their patients may be affected by the legal powers to detain patients that clinicians hold.
The diversity of public involved in our case studies varied from those with very specific health conditions, for example RA in case study 7, to parents of preschool children as a generic group in case studies 2 and 3. But even these two parental involvement processes involved subtly different groups of parents, as case study 3 was particularly seeking to involve parents from disadvantaged communities, who would share more characteristics with the subjects of their research. Case study 4 researchers faced particular difficulties in identifying and recruiting people who had previously had serious BSIs, and chose to focus on a more accessible subset, those who had been patients or carers in an ITU. In case study 5 the collaborating service user groups were required to have specific links to or experience of personal budgets (as well as mental health or carer experience). In case study 8 all the research partners were also study participants, which was not common in other case studies.
Although our informants did not refer directly to the concept of field of research, some did comment about how different disciplines or types of study had particular involvement requirements:
In health care patients become more a part of the team of decision-making but they always have been in rheumatology.
Researcher 5
I think it is implicit in the type of study we were doing, we would have to get help from patients.
Researcher 15
Diversity in types of studies
The field of research where the project was situated influenced the range of options available for public involvement and that this happened as an implicit, taken-for-granted choice, rather than as an explicit conscious decision. For example, in one case study there was a predominance of team members coming from epidemiological backgrounds, rather than more applied clinical backgrounds. When the participation lead suggested more diverse methods for the participants to be involved, the executive group did not support the proposal. The reasons for this may have been completely valid in their own terms, but the issue is that the type of study and methodologies chosen at the outset may not lend themselves to the participants being more involved. In another study, a clinical trial testing a set of interventions, a research partner sits on the Independent Data Monitoring Committee, a requirement of trial-based studies. While this research partner was made very welcome by the chair and committee, they still felt that the nature of the discussions was so technical that their contribution was limited. In several cases the research partners came into a study after inception and funding had been agreed, thus limiting their ability to contribute at the design stage. For each of the studies involving a clinical trial, there were long gaps in involvement activity during the data collection phase; in each case there were good reasons for this, but it does again demonstrate that the field of research does shape the opportunities for involvement.
Context conclusions
We have explored our selection of hypothesised key contextual factors for effective public involvement in research through our eight case studies. As we expected, these factors are interconnected and difficult to interpret separately. The impact of PI leadership on public involvement as a contextual factor to put mechanisms of involvement in place, and on intended outcomes, appears to be a critical factor across our case studies, but has followed a somewhat different pathway in each one. In most cases there were clear expressions of personal commitment from the PI; in some cases this was inextricably linked with a wider institutional culture of public involvement. In two cases with relatively new researchers, their personal commitment appeared to be shaped by this wider culture. In only one case was the initial impetus primarily from a funder’s requirement for involvement; but even here the PI was influenced by their experience of it to value public involvement. Thus PI approaches may be shaped by a culture of public involvement or may help shape it. Most of our case studies were based in organisations with a history of infrastructural support for public involvement, but this did not appear as significant an influence as the PI’s personal approach. It would appear that either a committed PI or a wider institutional culture (or both) is necessary and sufficient to engender effective public involvement. Our case studies have helped us develop a more nuanced view of how contextual factors affect public involvement. Overall, our case study data have broadly validated our theory with respect to the role of context in CMO regularities for public involvement in research with the additional recognition of the importance of the field of research.
Mechanisms
Initially we hypothesised six interconnected mechanisms linked to intended outcomes for public involvement in research: involvement throughout a research project, long-term involvement, training and support for the people involved, linking involvement to decision-making, budget for involvement and defined roles. In the course of our data collection and in particular our two consensus events, we identified that nurturing relationships (including attitudes of trust and respect towards the public), which we had initially conceptualised as a contextual factor, was in fact a key mechanism that underpinned some of the other factors listed above. We thus begin our findings on mechanisms with a discussion of relationships before moving on to consider resource issues (including budgets, training and defined roles) and structures of involvement (including involvement throughout a research project and long-term involvement).
Relationships
Trust
In all the projects, informants identified that developing a relationship of trust between academics and research partners was a critical mechanism that takes time to develop. A trusting relationship depends on a balance of power in relations between everyone involved, on whether there is a mutual respect and on how far research partners feel valued by academics. At its best, trust operates when there is a level of equality between everyone involved; one young research partner described this as being possible when academics are non-judgemental and encourage debate:
I think we actually quite often disagree with the researchers. I mean there’s a really nice atmosphere in the group . . . So everyone’s sort of always encouraged to say whatever they think and, you know, no-one’s judging anyone or anything like that . . . So it’s a really nice sort of atmosphere to be able to say your opinion. I mean the whole sort of study would – not study, the whole group would kind of be pointless if people didn’t feel like they could disagree.
Research partner 5
In the context of the group just described, young people had been working with researchers for 6 years and the mechanism was a group which met regularly six times a year. An academic in the early phase of another study noted that it is challenging to develop a trusting relationship, particularly if staff change and new relationships need to be developed. Some research partners were initially wary, needing time to develop trust and feel confident that they would not be judged:
To begin with possibly because we were a bit slow to start giving comments and you’re sort of thinking . . . is this a test? And you can sort of understand that really, you’re not quite sure what . . . because you’ve just only been in there for sort of an hour you’re not quite sure what the make-up of it all is.
Research partner 2
With time, though, more trusting relationships were established in this case:
. . . and then in the next meeting we did a very similar kind of exercise, you know we were talking about similar kinds of things. You know, ‘this is what we’re thinking of doing’ and ‘what are your comments on that?’ And we all fed in our ideas, so having been to that one as well it became clear that probably yes it was a genuine exercise.
Research partner 2
Even with traditional hierarchical power relations, it appeared to be possible, over time, to minimise differences and to establish trust. In one project where patients and clinicians were working together this required a level of honesty:
I think it is quite frightening for clinicians actually to get patients involved . . . because you have this hierarchy haven’t you and it’s like you know when you see the doctor and say ‘oh I am sorry to bother you Doctor . . .’ So we talked about this and they said we had made it easy for them and we said you’ve made it easy for us because there is that openness and when we are working like that we’re colleagues.
Research partner 7
Across the range of research in the case studies the commonalities were that there needed to be a level of engagement and continuity; once an advisory group or individual research partners had met with academics over a period of time, dialogue became established as a two-way process. Research partners felt:
. . . comfortable in their presence.
Research partner 8
As a result research partners felt trusted enough that even:
. . . stupid questions are answered politely and forthrightly.
Research partner 8
This underlying fear of feeling stupid, however, demonstrated the need for a supportive culture, which in one group with a long history of public involvement meant that they did not:
. . . feel worried about saying anything, you know, we are not going to sound like ignoramuses.
Research partner 7
Getting the right balance between formal and informal contact also seemed to make a difference to the levels of trust. The mechanism in one project was for the researchers to approach a group of parents who already knew each other. However, the researcher needed to get to know the group in a more informal way. A third-sector worker who facilitated the group commented on the group’s relationship with the researcher:
Well although she only met them a few times she obviously knows they chat a little bit in between and even she laughed a few times and they laughed and it’s just good to see how they . . . really talk up now, they don’t even think ‘oh I don’t know whether to say that,’ they actually just openly talk.
Third-sector partner 2
Being able to chat informally enables relationships to develop. One young person explained the importance of this informal time, which in their case also included eating together:
We chat about what we’ve been up to the last few months and that’s nice and then we can sort of get back to it . . . And be serious again . . . But everyone’s feeling sort of happy . . . And well fed.
They’re all friendly and, you know, you feel like you could talk to them . . . which is really, really important I think. Yes. It’s nice to feel that they’re not, you know, members of staff who are expecting results from you, but rather people who are working with you not in charge of you.
Research partner 5
Feedback
Mechanisms for feedback to research partners about the value of their contributions ranged from regular meetings that were minuted and revisited at subsequent meetings, to newsletters and seeing that views had been taken on board through being shown changes that researchers had made to questionnaires, leaflets or posters. In projects where time was taken to offer feedback, research partners felt valued, which in turn motivated future contributions to the project and research partners being prepared to commit to ongoing involvement:
That has been great and very pleasant for us to see that they got really enthusiastic . . . But I guess that’s partly to do with getting the feedback that what they were doing was appreciated and relevant in a very direct, concrete sense.
Research manager 3
Researchers from all the projects recognised that, if research partners are to feel valued, mechanisms were needed to enable researchers to regularly update them, including feeding back information about the overall research process as well as the particular contributions of research partners. One researcher noted that:
Research involves a number of people’s ideas, including the research partners, and which are shared and discussed – so ongoing feedback becomes a kind of iterative process.
Researcher 2
This iterative process was easier where the context of the research enabled a mechanism for involvement such as regular meetings or newsletters. This also meant that research partners could easily see the outcomes of their contributions in those cases where they were sent the minutes of the meeting, and saw that what they had said was recorded. The success of mechanisms such as meetings to enable relationships to develop and be sustained depended on how often meetings were held, how research partners were involved and whether they felt that their contributions were valued. One academic noted that long gaps between meetings could make it more difficult to maintain engagement:
We may not see them again then for several months and we don’t have any contact with them then until the next meeting, so they might have forgotten what we have discussed at the previous meeting. So it’s kind of, it’s much more about thanking them for their contribution at the time.
Researcher 4
There were some concerns expressed about how and what to communicate to research partners. In smaller studies, or during periods when the research was at the data collection stage, whatever mechanism for feedback was used required time, at the right stage of the process, to benefit both academics and research partners. However, a long gap with no feedback did not help to develop or sustain relationships:
Yes it did feel for a long time that nothing was happening and there wasn’t anything for us to do because obviously we needed to wait for some direction, so that was a bit unnerving.
Research partner 3
This year unfortunately from June has been very much data driven and data collection, so what I do try and do is say . . . ‘You know, I’m still here. There’s nothing to report apart from I’ve sent out this number of emails etc.’
Researcher 11
Furthermore, where there were problems with the research for any reason, feedback could be a negative experience for research partners. In one project, feedback to the research partners about how the research was developing could have been dispiriting, but it did not reduce the research partners’ enthusiasm for participating in the research:
I’m sitting there thinking we’re the parent panel and then looking at the response rate, we’ve got about four or eight parents involved and you just think, as a reflection on our contribution it felt like, that’s the sort of thing we should be helping with and we’ve clearly not got very far with what we’ve achieved.
Research partner 2
Overall, however, whatever mechanism for feedback was used, most research partners appeared to feel that, if they were thanked for their contributions and they understood how their involvement in the project made a difference, they were valued and able to develop meaningful relationships with the academics.
Feeling valued
For the most part, partners felt valued through being recognised as experts in their own fields, treated with respect, receiving feedback, understanding how their contribution was assisting the research process and being thanked for their contributions. Academics recognised the importance of ensuring that mechanisms were in place to update partners as:
. . . one way of showing they’re valued
Research manager 3
and making it
. . . explicit that they are equal partners in the process.
Researcher 2
In at least two projects, specific mention was made of a level of equality between partners and academics that clearly demonstrated their sense of feeling valued. In one instance, though, where there appeared to be little relationship between the academics and the young research partners, the fact that their opinions were listened to was sufficient for them to feel valued:
I don’t really see why it would matter but to them it really does seem to because they do come with a load of sheets and then they write on and stuff like that so it must make a difference.
Research partner 9
An interesting observation was made by a young person who attended a meeting for the first time. While there were a large number of documents to read prior to the meeting, she felt she was treated fairly, which made her feel valued:
Luckily people on the committee who paraphrased things for me and said ‘oh obviously you weren’t here but this is what’s been going on, this is what this is about just in case you were wondering,’ so yes it was fine.
Research partner 5
When research partners did not feel valued this was problematic for all involved. This was reported on only a couple of occasions to us; one was the episode referred to earlier in one case study when several research partners felt disappointed that their research skills were not being used:
We felt we were capable of doing the research interviews and we could have done them, we could have done the process here, we could have even have analysed the results, we had the expertise between us.
Research partner 10
Another, who had cancelled a meeting that she had organised to aid recruitment because nobody had signed up, felt upset by a researcher’s response:
So I phoned her and I suppose I thought she’d be really pleased that I was kind of doing this . . . and I felt really put on the spot because you know we really tried our best and I just felt really like . . . it just made me feel a whole lot worse than I did before I started the phone call . . . it made me feel really bad and I went home feeling like a complete failure, but then I got over it.
Research partner 3
In another case study, a young person recalled attending a meeting and felt aggrieved by being treated in a particular way that appeared to be age-related. This young person understood that they might be excluded for part of the meeting because of the confidential nature of what was to be discussed, but felt that if another person attending the group as a guest was not to be asked to leave this was unfair:
They kind of said ‘oh could I leave,’ because . . . they reserve the right to ask guests to leave during discussions and I said, ‘So do me and [other guest] have to leave then?’ . . . but yes, I don’t know whether that’s changed during the years that I have been involved, but, you know, if they want to be fully immersive surely participants should be allowed to stay for the entirety of the meeting?
Research partner 11
Inclusion
When research partners felt trusted and valued as equal partners in the research process and received regular feedback then they enjoyed the experience and felt included as members of a team. In one instance an invitation for research partners to join in a range of activities of the unit (not just the current research) demonstrated such a commitment. Another project recognised that inclusion led to:
. . . growing ownership of our research programme, which I found really quite exciting, you know, that they kind of associate themselves with us, you know, that they’re not just this kind of independent panel that come in and help us out.
Researcher 2
Group meetings as a mechanism for involvement were experienced as positive by most of the research partners, although some research partners did experience some uncertainty for a time about how they were perceived by the academics:
It was running through my mind how they were perceiving us at the meeting . . . I think the fact that they asked us for opinions as to the progress of the research . . . was useful and quite significant.
Research partner 10
Academics chairing meetings which included research partners needed an inclusive approach and chairing skills to enable all to contribute fully and comfortably. A lot of discussion that was difficult to understand led to research partners feeling that their presence could be tokenistic:
I felt really it was talking a lot about data and I personally felt that on some occasions I was out of my depth and I thought well if there is somebody who has got a degree in psychology who is sort of nearly out of their depth so I don’t see how somebody who is not, not meaning to be patronising, but I wasn’t quite sure what they were trying to get out of that apart from ticking a box really.
Research partner 6
People who felt included in meetings described constructive dialogue between everyone involved, an active part in decision-making, bouncing ideas around and a level of informality, described by several respondents in terms of teamwork. Our observation of such informal discussion in a case study 7 team meeting, for example, confirmed the positive accounts of both researcher and research partner participants. One academic also described the need for a good mix between formal and informal relations in order to ensure inclusion – here, as before, the need for an opportunity to chat was mentioned:
What I want it to feel like is it’s a meeting they come to where they have a cup of coffee and a bit of a chat with people who have got something in common with them, that they feel they’re contributing but it isn’t something where they feel intimidated by it and I think the more formal you tend to make these things the more intimidating it is and what I want is for everybody to feel that they’re in the same group, that their opinions are valuable, that they can express their opinions.
Research manager 2
In the context of a national multisite project, there was concern about the practicality of involvement across different sites. Partners found it difficult to feel included when:
. . . it was just ‘go and do it’ sort of thing.
Research partner 8
In a longitudinal project with a large participant cohort, one young person became aware, after attending conferences about the project, that while their contribution was valued within some parts of the programme this was not the case across the whole study:
I mean there are a lot of arguments and people do bring up that we’re tokenistic and we’re not important and they don’t understand what we’re doing.
Research partner 11
Within the mechanism of the young people’s group, the research partners did feel included and valued, thanks to the work of those who co-ordinated the group and had developed good interpersonal relationships with them.
Interpersonal relations
Good interpersonal relationships take time to develop, and continuity was at risk when personnel who were supporting and co-ordinating the involvement of research partners changed. However, in one project the mechanism of involving a group of young people over a period of time meant they had developed the knowledge and skills to survive as a key part of the organisation. This meant that the group was clear about its role and felt valued by the organisation:
They have had several different changes in terms of co-ordination within the organisation, staff members, and they are still going strong and it is still happening, so whilst the management recognise their value . . . and the more we can solidify their role and springboard from what we have done this year, the hope is that they will have more and more involvement and more and more meaningful involvement, so moving to a point where they are asking the research questions and they are more involved in that side of things.
Research manager 4
The issue for some academics was how to develop good working relations when there was a difference in status between academics paid to do a job and research partners who were giving up their time, often without payment, however much they wanted to be involved. For one academic the difficulty was to identify how far she was justified in having her:
. . . put my foot down moments.
Research manager 4
The mix of informal and formal interactions mentioned above was viewed by a number of respondents as important in creating the right atmosphere for developing positive relationships. Academics mentioned how getting to know research partners enabled them to begin to understand the reality of their lives. This in turn had an impact on the research process. For example, one academic described learning about how the research partners faced discrimination, which brought a realisation that the participants in their trial were probably going through something very similar. This in turn influenced how the interview protocol for participants was designed.
Having time to develop good relationships was a key factor, summed up well by one third-sector partner and co-applicant:
You can’t just set up a meeting and go and think you are going to capture some parents, enthuse them by saying you really have to build relationships with them and that takes time. Without creating a dependency culture you really want to genuinely get to know them in what they are thinking. And I think the struggle is how you do it and that face-to-face part is really quite important.
Third-sector partner 1
As researchers and research partners became more confident about working together, positive interpersonal relationships appeared to develop. This seemed to be easier if the research partners either already had a passion about the area of research or were developing a greater interest as a result of their current involvement:
I think it’s really opened his eyes for him because he keeps emailing me with a list of questions about kind of, you know, how does research work or how does, you know, kind of how do you get the funding and kind of quite specific questions about how the programme works as well. So I think he’s finding it really interesting and he’s quite getting into it.
Research manager 3
Developing positive working relationships and involving the public in research was not viewed as an easy option by academics:
But I think working with patient or parent groups or children’s groups as well, you have to . . . it does slow things down, you know it takes . . . it’s a lot of energy and a lot of thinking and a lot of planning so it does . . . you do have to kind of account for that timeline really within a research programme to do that.
Researcher 2
Whatever the context of the research, providing regular and ongoing feedback, so that research partners felt valued and included as members of a team, led to positive outcomes for all involved. For one academic, engaging the public had a wider impact in raising awareness of research and ultimately in ensuring retention of research participants:
I think the more that you can raise the awareness of research within the community as a whole across the whole piece you are going to get a better, you know a better sort of communication with patients and also a greater desire to be participants within research. When they are . . . I think they can then also be reassured that you know, you can still be part of it without it being immensely burdensome.
Research manager 2
Developing good working relations also meant that the research partners were willing to contribute to research in the future. This was seen by one academic as a contribution to the community:
We felt very much that they were happy to contribute as you know giving meaning to their lives as well and it was not just getting together and talking to the other girls but actually doing something for the wider community. But obviously that’s my interpretation. They didn’t say it.
Researcher 6
Power
Power relations had an impact on all the areas of relationships already discussed as well as on the experiences of research partners and academics. The context of some projects meant that there were issues concerning relations between clinicians and national and local patient groups in those projects with a wider geographical spread, and age in projects involving young people. In addition there was, for some research partners, a feeling between academics and research partners of:
. . . us and them . . .
Research manager 1
Even where researchers were able to minimise power relations they still faced the problem that:
You’re trying to make it more equal but actually they are still patients.
Researcher 5
One academic was concerned, when she initially started to work with a group of young people, about how she would be viewed – feeling that they might have issues about authority and concerned about whether, when they met her, they would speak to her. Another expressed concern about ‘using’ research partners, which was not felt to be good, although in another project research partners expressed some frustration about their level of involvement and asked the academics to use them more. In one project it was recognised that:
. . . power dynamics . . .
Research manager 6
appeared to have a significant impact on relationships. In one instance an academic felt that their expertise also needed to be recognised, but this further emphasised the differential power relations:
So I think we just don’t sort of hand it over to them to make all the decisions, we have to, with our expertise, I think we just have to use their advice to make things work.
Researcher 12
Another differential that had an impact on power relations concerned the number of people involved. One research partner found it difficult to speak up in a meeting they attended on their own. In another situation a group of research partners were able to contribute to changing the power relations:
So it felt as though there were fewer of us and I just thought that it made it slightly easier when [PI name] wanted us to talk about things in smaller groups. I think normally we just do exactly what we’re told to do pretty much, but in that meeting we . . . felt we needed to talk about it as the whole group, so we said, ‘let’s talk about it as a group’.
Research partner 2
Across all the case studies the importance of nurturing relationships was emphasised by research staff and research partners alike. Researchers needed the interpersonal skills to make research partners feel valued and included, and to give feedback that convinced them that their contributions were making a difference. Power dynamics and inequalities were recognised but it was generally agreed that these could be overcome through good interpersonal skills and time to develop trusting relationships.
Resources
Resources in the broadest sense was another aspect of the mechanisms of involvement which included budgets for involvement, training and support, defined roles, practical aspects and rewards.
Budget for involvement
Whether or not a case study had formally budgeted for public involvement did not appear to be a significant determinant of the extent of their involvement activities or the impact these had in the research project. Across the eight case studies, there was wide variation in the extent of budgeting for public involvement, with no apparent correlation between the budget for and the extent of involvement activity. For example, in case studies 3 and 4 there were no formal budgets for involvement but the research team expended resources drawn from the generic project staffing and expenses budgets in running their respective public advisory group sessions. By contrast, case study 8 explicitly identified in its budget the substantial costs for its full-time participation worker, although this covered promoting participation by study subjects as well as involvement in research. Where public involvement activity was not formally budgeted, it was still recognised as a substantial cost to the research team:
I suppose if you wanted a rough estimate, if you put it down as about a month’s work out of the entirety of a 5-year programme grant of a Band 8A manager that would probably be the cost of our PPI.
Research manager 2
For some studies, PIs felt limited as to how much the funders would offer them for public involvement:
We need more money, but the truth of it was that the funder was unable to give us more money.
Researcher 14
In this case study, extra funding was applied for during the study in order to further support research partner activity in the project:
Since then we’ve gone back to a second funder to apply for additional funding . . . so that they [research partners] can have a night’s rest either side of each meeting.
Researcher 14
Across the case studies, research partners were reimbursed for travel expenses, food, accommodation, and a varying amount of training, but were paid for their time spent on the project in only two cases. Some researchers were ambivalent about the effect that payment could have on the roles and relationships with research partners:
. . . at what point does it stop being public involvement and it becomes like a role that you are paying somebody for and that kind of thing. Yes, it is difficult.
Research manager 4
In the case studies where payment was offered to research partners for their time spent on the project, there were different approaches to how payments were made. In case study 2, vouchers equivalent to £10 per hour were given for attending meetings or doing ad hoc work such as proofreading papers or phone calls. Vouchers were well received by the research partners but were seen as more of a present to say thank you for their hard work. Case study 5 paid partners for attending an advisory panel, working to promote and support the study locally in its four sites, and contributing to analysis and dissemination. However, most of these payments were made via local user- or carer-led organisations, which had contracts with the host organisation, rather than directly to the research partners.
Academics were aware that, if research partners were offered payment for their time, this would have an impact on those people who were receiving benefits. Some research partners said that they did not wish to be offered payment so that they would not experience problems with their benefits. Case study 2 used guidance from the INVOLVE website to help them develop the policy, which made explicit the rewards provided for research partners.
Some academic researchers commented on the time required for dealing with payment and expenses issues for research partners. The case study 2 research team had an administrator to process expense claims. This role assisted in streamlining expense claims and queries from research partners about their payments. Research partners appreciated the consistency that the administrator provided.
For the case studies involving research partners with children, public involvement costs had to include child care costs so that parents could attend meetings. Some academics reflected that they had a heightened awareness of the cost of public involvement in their study as a result of being interviewed for this study, and being asked to supply costing information:
So, certainly we will be doing it differently, costing it differently in the main trial.
. . . I thought that it would be really interesting to know how the INVOLVE study had costed the parent advisory group’s expenses, because I think that gives us better information on forming how we should be covering the costs of a parent advisory group in any future study.
Researcher 4
Training and support
The extent of training provided for research partners varied greatly across the case studies, but did not appear to be a significant factor in the extent of involvement activities or the impact of involvement in the projects. Research partners in all the case studies were grateful for the informal support provided from academics, whether face to face, by e-mail or by telephone. Facebook proved a useful medium for support for the younger research partners.
Even though some case studies had budgeted for training research partners, many academics reported that any training needs tended to emerge during the projects, rather than being obvious at the start. In many projects the individual skills and interests of research partners led to their roles varying accordingly, so training on as ‘as needed’ basis was more appropriate than providing a fixed training programme:
No, I don’t really know much about research, the sort of research process, and I think that’s one of the things I’d like to try and get out of this experience is actually if they’re offering some training would just be to sit down with someone for a bit and sort of talk about what a research process actually constitutes really in this kind of framework.
Research partner 2
Where formal training was offered to research partners, they took it up enthusiastically. Case study 7 offered research partners annual training days and informal mentoring support. Academics in case study 6 offered training for three research partners on qualitative analysis of questionnaires, having included training costs in the project budget. All the research partners involved in the study asked to do the training, so names for the three places were randomly selected. The academic team were pleased with the enthusiasm from the research partners to undertake this training.
How much research partners wanted to be trained during their involvement in the research depended upon their background, the role they were expected to play in the research and their previous experience. While some research partners said that they would like training in the research process, others did not:
. . . I think sometimes the more you are trained in ethics and stuff like that, it can kind of take away from your instinct, you know you don’t say what is immediately on your mind because you’ve been trained to go about something a certain way, sometimes it is better to just go for it.
Research partner 5
Some academics struggled with the concept of why research partners should require training in research skills:
. . . I think it became a bit fuzzy and a bit unclear because we are not asking people to be researchers, so they are not researchers as such, so how helpful is it for them to have research training, this is a bit of a query.
Research manager 7
However, some research partners could clearly see a benefit in having had extra training which increased their ability and confidence to contribute to the study:
I guess with training we kind of did a couple of away days, that’s kind of like team building and I guess I’d call that training . . . it’s building up a relationship and being told that it’s okay to disagree with people . . . having the freedom to speak our mind.
Research partner 11
An academic from case study 4 reflected that there was a learning curve for academics to understand the training required by the research partners.
Academics and research partners recognised the value of the resources offered by INVOLVE and local public involvement collaborations in considering training and support needs of their research partners. However, the suitability of these training courses for research partners was questioned by an academic from case study 4:
. . . when you come to meet our group you will also find that some of the people there will probably find going on some training course like that a bit overwhelming.
Research manager 2
The importance of academics building up a good working relationship with research partners was made evident so that training was experienced as supportive and non-hierarchical.
The staff are young and you can relate to them, they’re friendly. You feel like they are people working with you, rather than academics in charge of you.
Research partner 5
I think I was a little bit worried about scaring them off by making it sound too school-ly. Yes, too much like education.
Researcher 4
Defined roles
In most cases the role of research partners was not tightly defined, which often appeared to suit both the researchers and the research partners. In the study involving teenagers, the academics remarked upon the progress and development of the research partner role as the group matured. A research partner job description was formulated and verified by the group in order to clarify the role. One research partner likened the role to that of a school governor, that is being a critical friend, and coming from a different viewpoint from the academic. Another commented that terms of reference really helped both academics and research partners to focus on clearer roles for individuals in the research team.
In some case studies, research partners liked to have something concrete brought to a meeting by an academic so that they had a clear understanding of what to comment on. Other case studies, however, took less formal and more relaxed approaches to meetings with research partners, which they appreciated.
In most case studies the role of the research partner became clearer as the study developed:
The research partner role was an organic development.
Research manager 7
Academics said how important it was to have some flexibility built into the roles, so that individual research partners could take on different aspects of the research process, for example data analysis.
However, in the one case study referred to earlier, research partners felt frustrated that their existing skills in collecting data were not fully utilised:
Yes, anything to do with research interested me so I say yes, I’ll go ahead but it was after that that [name of researcher] said to me we’re not actually doing the interviews or analysing them, we’re merely recruiting the candidates which put a bit of a downer on it.
Research partner 10
One academic suggested that where organisations had extensive prior history in public involvement, and research partners were more experienced, more formal processes and structures were needed to define the research partner role:
There can be a history of user involvement in mental health research that’s tokenistic and I’m quite proud of the fact that that’s not the case on this project and I think especially in the second phase where we’ve really identified what their role is and how they can work most effectively.
Researcher 9
In most of the case studies there was no formal contract between the host institution and the research partners. In case study 5, which involved four study sites and devolved involvement by working with local user- or carer-led organisations, formal agreements were drawn up for each stage of the project, specifying the work to be done and the payment due. Research partners’ roles were developed flexibly for each research phase. The agreement was a working document, which was revised according to the research partners’ needs, strengths and interests.
Practical aspects
Across the case studies, academics discussed the importance of the nature and effectiveness of meetings with research partners:
Meetings need to be purposeful and not for meetings’ sake.
Researcher 1
An academic from case study 4 highlighted that public involvement relies on a lot of goodwill from the research partners in giving up their own time; therefore, there had to be a fine balance between overburdening the research partner and involving them sufficiently to feel part of the research team. An example of a well-run process was in case study 8, where regular meetings were held with the young research partners. An academic commented that the young people found that a more informal approach to the meeting was valuable, as they were less constrained by agenda items. The meetings were well established, but new people joining the group also felt engaged and welcomed.
In this case, providing the group with clear feedback between meetings on the impact of their contribution allowed for better continuity and understanding of the research process. The academic used Facebook, Twitter (Twitter Inc., San Francisco, CA, USA) and text messaging to keep in touch between meetings, and, even though this was time-consuming, they said it was worth it in order to keep the research partners engaged. Similarly in case study 2, at a research partner’s suggestion, they were given a written report of progress to date with the study before each bimonthly meeting. This helped meetings be meaningful, and research partners felt more integrated with the research team. A research partner from case study 8 commented that academics used Facebook after meetings to conduct polls of what research partners thought, and enabled research partners to vote on topics. This was considered a useful process by the research partners in the case study.
Case study 2 experimented with workshop-style meetings, hoping to make them more productive. The academics commented that they had to allow extra time for public involvement, for example preparing drafts of ideas and documents that needed to be approved by the research partners before moving things forward. The academics were surprised by the enthusiasm of the research partners, who really wanted to be used, so the academics had to be prepared and organised to meet these demands.
A challenge identified by several case study teams was the problem of getting research partners together on a particular date because of outside commitments of work and families, and the time taken to travel to meetings, which were sometimes far from their homes:
We may ideally like a meeting in two to three weeks’ time, but only be able to organise it for four weeks’ time.
Researcher 4
An academic from case study 5 said they encouraged car sharing when travelling to meetings, as this gave a further opportunity to debrief and network. They also found that meetings with smaller numbers of people, fewer than 10, were more effective in allowing the research partner voice to be heard.
Several case study teams highlighted additional resources to be considered. For example, a research partner from case study 2 commented that some research partners had difficulties in accessing a computer at home, so hard copies of papers for meetings were requested. An academic in case study 8 noted the need for administrative support to organise and run meetings, as there was too much to do for the academics to organise this themselves. Several academics across the case studies commented that food provided in meetings was important in making research partners feel welcomed; again, an additional cost to the study:
Setting up a relaxed, friendly atmosphere really helps, for example cakes and a hot drink.
Third-sector partner 2
The practicalities of involving research partners who are parents of young children were highlighted by academics from case study 3. Sometimes meetings were held with the children in the room:
We had the children in the room with us so we were doing the whole thing around toys and noise. Keeping concentration was quite hard for most of them.
Researcher 13
As a result of this, the children were offered a place at the crèche to make the meetings more effective. However, this added further time constraints to the meeting, and added expense to the project. A research partner from case study 3 emphasised that one cannot assume that all panel members have the same requirements; for example, breastfed babies may need to stay with their mother, and some parents may need to pick up older children from school, adding further time limits to meetings.
In some cases, research partners had a long-term condition which affected their ability to participate fully in the research process:
Fatigue is a huge problem for me because of the disease, and that is always a limiter.
Research partner 1
An academic from case study 7, where there was a strong unit culture of public involvement, was mindful of the project length and the impact on the research partner:
Four years is a big time for people to commit to, and especially people who’ve got long-term conditions.
Researcher 11
The academics in case study 7 tried to arrange meetings with research partners when the partner was attending a clinic appointment, so that they did not have to make additional journeys, and in order to maximise effective use of their time.
Reward
Across the case studies, the research partners displayed a strong commitment to the research that they were involved in. This was often because they had experienced the medical condition related to the research themselves, or had a family member or child with the condition being studied:
I think that they are actually interested . . . it’s the thing that motivated them to agree to be part of it in the first place, they are interested to know about research . . . and having been consumers of the local hospital they also feel that they like the idea of influencing what you might be doing because it’s like a two-way feedback.
Research manager 2
The academics were interested and surprised to see how committed the research partners were without the prior offer of reward:
And I think that one of the things that’s impressed me has been the interest in the project and commitment to it considering that they’ve only had cake.
Researcher 4
Research partners were not there to receive rewards; however, they all appreciated the rewards offered by study teams. The simplest form of reward gained by research partners was gratitude, thanks and appreciation from the academic research team for their valuable contributions:
I suppose really we are showing our gratitude by our thanks really and our appreciation of their contribution rather than anything material.
Researcher 4
Academics highlighted the importance of welcoming research partners at each meeting, and reiterating throughout the study that they were integral to the research team. Food or refreshments were provided in some meetings to enhance the welcome. In addition, some studies took research partners out for meals to celebrate success, or to enhance networking, which they appreciated.
Travel expenses were reimbursed to research partners in all eight studies. One research partner from case study 7 used the bus to travel to meetings, and had their own bus pass. They did not claim for their travel expenses as they saw this as their opportunity to give something back to the organisation in which they had previous involvement as a patient.
Case study 2 research partners were invited to a conference to share their involvement in the study. They were not keen to present their work orally, but produced a poster, including quotes describing their involvement, which was well received by delegates. Attending the conference gave them an opportunity for personal development, and increased their feeling of being part of the research team.
Some academics included research partners in the writing of papers, if the research partner showed interest and ability in this. Most academics wanted to acknowledge the contribution of research partners in reports and papers, one saying that, if a research partner made a significant contribution to a paper, they would be a middle author.
As well as financial reward, one research partner stated that the best reward from being involved with the project was making strong friendships within the group, and that they could gain help and advice from this supportive network. Some studies offered a certificate of achievement for their research partners to use as evidence for their contribution. For some of the research partners, particularly young people, being involved in a research study meant that they had something concrete to include on their curriculum vitae (CV) and this would benefit them for future job applications and career development:
Other rewards . . . the main thing I’ve found is the support network you then get. I was writing my applications to university and I had my CV proofread. I have a member of staff on my CV who is my reference.
Research partner 11
One research partner became particularly interested in research during their involvement, and was considering a career shift to develop their new research skills. Case study 1 offered research partners the ability to gain educational credits for working on their research study, which could be added to their educational portfolio and put towards a university programme of studies.
Overall, the allocation of resources was an important set of mechanisms for public involvement in our case studies, but this was not necessarily dependent on formal budgets. Many resources were used without being planned or budgeted for in advance. The commitment of staff time for facilitation, informal support and feedback was critical, and often insufficiently budgeted for. Such resources in kind appeared more important than formal training or payments for research partners, at least in those case studies where they took on a time-limited advisory group role. In two cases where research partners took on more complex roles, either formal training or payment or both were seen as necessary. Further data and discussion on resource allocation are presented in the economic analysis in Chapter 7 of this report.
Structures of involvement
In our initial conceptualisation we identified involvement throughout a research project, long-term involvement and linking involvement to decision-making as potential key mechanisms for public involvement in research. In developing our analysis these interconnected factors all appeared to relate to structures of involvement and we explore them here under that overarching theme. Across the eight case studies, structures varied according to which type of activities research partners were involved in. Case studies differed in how actively members of the public were involved in the projects. In four of the case studies, research staff had initiated and recruited members of the public to a study-specific panel or advisory group. In two other studies researchers had accessed an existing service user or community group. In the final two studies research partners worked more individually, with individual research partners at different study sites in one multisite study, and a pair of research partners working with the other project.
Whatever the structure of involvement, research partners were asked for help and advice with similar aspects of the projects, particularly on recruiting participants and the format or wording of documents, such as information sheets. In the longitudinal study involving young people, the group met frequently and regularly, as well as communicating by e-mail and online. In another case study, meetings were held every 2 months; however, the PI felt that even this frequency did not always guarantee full involvement:
Every two months we’re doing it [holding meetings], but the kind of the meetings or the discussion happen here informally, then by the time their [parent panel] next meeting comes around we‘ve already formulated [issues].
Researcher 2
In the other four studies, the groups/panels met less frequently. Involvement was often characterised by short intervals of focused activity, interspersed by longer periods when the group neither met nor contributed to the study’s progress:
That’s what we found with our patient and public involvement group that we seemed to have periods of quite intense activity and then it seems to fall down.
Research manager 2
A different model of involvement occurred in the two case studies where a few individual patient research partners were included as research team members, attending relevant project meetings. However, despite greater direct engagement, the pattern of involvement resembled that of the other case studies; the research partners contributed to the projects only relatively infrequently, depending on the stage of the research. In these two projects and some others, research partners had input into the study design. However, in a few cases, this input did not involve research partners, who subsequently became members of the panel during the conduct of the study:
So I worked together with those two people to develop the proposal, and we also had a service user and researcher working with us at that time who also was involved in developing the idea.
Research manager 7
I would be really surprised if they hadn’t involved people with experience in the design stage, but I don’t know whether they did.
Research partner 3
The difficulty of involving research partners effectively in the early design stages of a study was described by one researcher:
When you respond to a commissioning brief, you don’t have much time and it is very constrained as to what you can do . . . it would have been nice to have been able to have gone to the group before we put the application in, but that wasn’t possible.
Researcher 13
Four studies involved research partners in developing applications for ethical approval. In at least one case, this input was crucial:
As part of their [ethics committee’s] agreement to allow us to have it as a non-consenting study, we had to demonstrate input from our patient panel that they were happy.
Research manager 2
Some researchers expected that, following their experience in current projects, research partners might get involved in designing future or ongoing studies. There was one incidence reported of the design of a study being fundamentally altered following research partners’ input:
Somebody had got funding to do this particular study on friendships . . . for us it was quite clear about how that would work . . . we took it to [the servicer user panel] who hated it, absolutely hated it and just consistently kept saying this is too private, it’s too complicated . . . it ended up being a very, very, very different study to the study that we had first planned.
Research manager 1
Five of the case studies relied quite heavily on research partners to facilitate access to particular communities and to support recruitment of participants. Researchers reported having found this advice invaluable in some instances, particularly where young people were involved:
On a very practical level with the project . . . I came with our own draft design of some leaflet and the group . . . didn’t even want to look at it, just threw it over the side of the chair and said this is far too much text . . . if we sent such a leaflet out to our participants, it comes through the door and it goes straight in the bin.
Researcher 6
Research partners in seven case studies were asked to comment on and help develop the study instruments, including questionnaires and interview guides. This appeared to be standard practice; all the researchers interviewed were keenly aware of the need to ensure that questions asked were both appropriate and intelligible from the respondents’ perspectives. In the eighth study, research partners were asked to help design materials for an educational programme which was being tested.
There was only one case of research partners being actively engaged in data collection, where some study participants belonged to an underserved ethnic minority community. The researchers found that the most effective way of collecting data from this target population was to work closely with two representatives from the community, who then went on to collect data from a group comprising other community members.
In another study, there had been plans to involve research partners comprehensively in data analysis, but logistical problems had prevented this:
It is difficult to know what to do with the analysis . . . They [research partners] don’t have the time to get involved in kind of analysis systematically across the board; so we are using a framework analysis . . . They are identifying what they think the key things are from [specific transcripts], and those will then be collated by us into an overall framework . . . which can then be systematically applied, but that will be done by the team and not by the lay members.
Research manager 6
In two other studies, findings were brought to the public panel/advisory group for discussion. In one of these studies, the PI explained why he considered this to be important:
Getting a perspective on some of the importance and the meaning of some of the results as well, so we will have a view as researchers and academics about what we think is significant; I don’t mean statistically significant . . . I’m also interested in actually tapping into a lay perspective about what might be important messages for the wider community.
Researcher 7
In the two case studies where research partners were considered team members, they were actively involved in analysing qualitative data. This entailed their receiving appropriate support and training in order to perform this function.
Research partners were involved in dissemination of study findings in half of the case studies, although it should be noted that some others were not yet at a stage to disseminate. In one of the studies where involvement in dissemination had not occurred, this omission was recognised by one of the researchers on the project:
We wrote in our protocol that one of the things we would ask our parent advisory group to do was help on disseminating information . . . and we haven’t fulfilled that bit.
Researcher 4
In another case study, it appeared that plans to involve research partners in dissemination could be inconsistent:
One of the things that was decided in a meeting that I was not at, that we would create a book . . . At no point was I asked ‘Can you engage the cohort and find out what they would like from a book?,’ nothing, it was just decided we would have a book . . . I was like ‘Well let’s maybe get some involvement now’ . . . I got it agreed that we would advertise for a participant to become involved in that working group, who would sit on the interview panel to interview the designers and the editors of the book . . . and I got them to agree that we would have presentations as part of that interview process and they would present to a group of participants and they would feed into who we decide to have.
Research partner 12
I’ve taken a couple of [the young people’s advisory group] members to different conferences with me and they’ve presented about [the group] to those conferences . . . They were involved really heavily with the dissemination and doing the posters . . . like revising the lay posters, and then they created their own film of what [the study] is about and they ran with that project completely.
Research manager 4
However, in most of the studies, there seemed to be a clear intention to ensure future research partner involvement in dissemination of the study findings:
The next thing that they will be involved in is in the dissemination of the results of that study. How we do it, how we tell the doctors, because that’s going to feed in to the educational component. So they will have an input into how we disseminate it on more than one level.
Research manager 2
Planned dissemination activities included co-authoring papers for publication, as well as contributing to the developing and presenting posters and papers at conferences.
Research partners were involved in all project stages, from design through to dissemination, in only one of the case studies. Although engagement was sometimes irregular and infrequent, in most case studies there was input from research partners to most research activities, apart from data collection, at least to some extent. Input into design sometimes involved different research partners from those working with the research teams at later stages.
Some informants raised questions about the changing status of research partners who develop considerable experience in research. Some researchers perceived these individuals no longer functioning purely as patients or service users, and felt this might not be beneficial for projects:
Well the naive patients, if they help and then help again and help again, they become sophisticated patients . . . One of the things that we’ve taught ourselves to do is to always try and get two patients involved, an old one and a new one.
Researcher 5
You could argue that once they have sat through six months of the committee they should be off it, because they are already socialised into the way of a committee, and actually they have already stopped being independent.
Researcher 16
In five of the case studies, involvement appeared to be managed in a systematic fashion, although clear systems had not always been included in the study design. One informant considered this a disadvantage:
Perhaps a slightly more structured approach than we had here . . . work with clearer plans before we go in . . . It might have helped the outputs, I mean, it was great that we got [public involvement], but it could have been even better.
Researcher 6
Two of these case studies involved a two-tier model of involvement. In the third-sector case study, the project design incorporated involving service users at both national and local levels. In the other case study, based in the NHS, some research partners belonged to a formally constituted panel, while others were intended to contribute as and when required:
We’re looking at two levels of participation, the first is a panel. So we have 8 to 10 parents who attend bimonthly meetings to review and discuss some of their project issues . . . On a wider level we realise that some parents can’t commit to being on a panel formally . . . but they’re happy to be involved on an ad hoc basis and to review documents as and when they can.
Research manager 3
In practice, this wider group did not get involved over the course of the year, partly because of time and logistical constraints on the research team, thus illustrating that the absence of relationships with research partners may be a barrier to involvement.
In the two case studies where research partners were regarded as members of the research team, structures for their involvement were relatively informal; this may have been a function of their closer inclusion in the team. In the case study where the PI was involving research partners for the first time, the researchers sought to manage the group responsively to the needs of the moment:
It was a relatively new thing so we just had to sort of learn a bit about it and try and understand what it was and how we might deliver it . . . we sort of sit and think, well that would be an interesting thing to discuss with the patient panel, why don’t we ask them about that? . . . we’re sort of coming at it in a slightly more ad hoc way . . .
Researcher 10
In three cases, practices for managing involvement changed during the course of the project. This appeared to happen for a number of reasons, including trying different approaches and finding that some did not work, as well as pragmatic considerations, including staff changes:
We set up the website for them [the parent panel] to use. I think they were very enthusiastic about that at first but actually I don’t think that’s really adding a lot so I think we’re just going to go back to . . . [doing] most things via email and kind of sending things in the post so . . . I think that something that they wanted introduced actually hasn’t been working so we’re going to get rid of that.
Research manager 3
I think originally the concept was that those groups should to a large extent shape what their involvement would look like themselves . . . But that’s not what actually happened, and it might be to some extent that that has happened less and less as the staff involved in the initial conversations left, and as we had over time to just focus on how do you deliver this project.
Research manager 6
In one case study, the long-standing nature of the research programme necessitated changes in the management of public involvement over the course of time, as environments and wider requirements and standards changed, as did the research partners involved.
In five of the case studies, particular individuals held responsibility for co-ordinating involvement. In some cases the role description was drawn up during the study design process, but in others it developed as it became apparent that involvement co-ordination and management were required. One participant clearly described the requirements of the co-ordinator role:
You do have to be organised and . . . do the administration part of it quite well . . . whether you’re able to establish that relationship or not . . . I can’t think how specifically I’ve done that, I’ve just been there every time that the parents have been in, I’ve been around and met them all and got to know them quite well; but maybe, you know, I’m a parent, so I have something in common [with them].
Research manager 4
In the remaining three case studies, co-ordination of involvement appeared to be shared between different members of the project team. In two of these, research partners were themselves project team members.
Two case studies could access their research partners only through external gatekeepers. One of these studies involved underserved and/or ethnic minority communities, and it was felt to be both practically and ethically necessary to approach service users through individuals with whom they already had established relationships. In the other case study, it was felt that research partners might find it easier to refuse researcher requests if these were channelled through an intermediary:
[Name’s] assumed a sort of gatekeeping role . . . all of the enquiries are filtered through [name] . . . I think one of the fears is that actually if you are approaching the parents and the parent advisory group directly they may feel as though they ought to respond . . . or they ought to co-operate, whereas they may feel able to say no more easily to the gatekeeper, and she can then feed it back through.
Researcher 4
There were very few examples offered by informants of specific practices or mechanisms for managing involvement. Only two participants mentioned arranging meetings at a time which would suit research partners. In only two of the case studies were there specific practices for managing and recording relevant meetings:
The stakeholder work package is represented on the project executive [meeting] . . . we meet monthly . . . because there’s always a long agenda, we cycle through different areas to focus upon . . . Every third month we have a focus on stakeholder involvement.
Researcher 7
Each [advisory group] meeting is minuted, so at the beginning of the minutes it sort of represents the feedback from last time.
Research manager 4
A lack of record keeping, coupled with staff changes, led to different assumptions about payment for involvement in one case study:
Where that has been a real challenge is . . . where people are saying ‘Well, this was agreed’ and we have got no record of that agreement, that conversation; and it makes it very, very hard, because people are working to very different assumptions, and I think probably that has been the biggest implication of the staff changes.
Researcher 12
Overall, there were fewer regularities in the structures of involvement than in other mechanisms of involvement we have explored. The degree of involvement through research projects varied, as did the extent of long-term involvement. The informality of much involvement activity made it more difficult to robustly demonstrate links between involvement and decisions made. There were clear links with operational decisions about recruitment materials and data collection tools, but less clear and less frequent links with more fundamental design decisions.
Mechanisms conclusions
The importance of mechanisms to engender and support good relationships between research teams and research partners was emphasised by informants across all our case studies. While recognising the inevitable power inequalities in the relationship, informants highlighted the actions researchers could take to bring greater equality and trust into these relationships. These included taking time to establish trust in relationships, getting the right balance between formal and informal processes (perhaps emphasising particularly the crucial importance of the informal), and giving feedback to demonstrate how researchers were using and valuing research partners’ contributions. Although we had recognised the importance of attitudes of trust and respect towards the public involved in our initial theory, these findings represent an important development, as we had initially seen them as contextual whereas now we recognise them as key mechanisms that need to be actively nurtured by researchers.
Budgeting and formal training did not appear to be major mechanisms contributing to the impact of public involvement in research in our case studies. However, both researchers and research partners supported and valued ‘payments in kind’ to research partners for the contributions. Only two of the eight case study projects paid research partners for their time. In only one of these cases, our mental health case study, was the payment seen as a significant factor. It is important to recognise the range of reasons why payment may have been regarded differently in this case study. Cultural and political values have influenced expectations about payment for mental health service user involvement in both research and service delivery, and relationships between patients and clinicians are often not as trusting as in other health-care fields.
The policy of not paying some research partners may also reflect the fact that in most case studies involvement took place through advisory groups or panels, which took relatively little time and required fewer skills; payment issues are seen differently where research partners play a more substantial role as coresearchers. Payment was acknowledged more widely as a problematic issue in public involvement in research, for a variety of reasons, including the problems it creates for research partners on welfare benefits. Issues connected with payment and payment in kind are very complex, and are explored in two publications on budgeting from INVOLVE. 23,25
Training was seen as crucial in only one case study, where research partners were offered the opportunity to contribute to the analysis of qualitative data. However, we must caution that training may be less needed in cases, such as the majority of ours, where research partners were mainly taking advisory rather than coresearcher roles. More generally, informal support was seen as much more important in engaging and rewarding research partners. The value felt by both researchers and research partners for ‘payments in kind’, such as access to support networks and information, for the contributions of research partners, was significant.
As with resources, structures of involvement appeared less significant than relationships in shaping the impact of public involvement in research in our case studies. Involvement throughout the research project was not found consistently; in most cases there was little early involvement in bid development and research design. In several of the trials, there were long periods of non-involvement during data collection and processing. Long-term involvement was important in some case studies, but others involved new research partners whose involvement was time-limited to the particular study. Informants made differing comments on the benefits and limitations of involving experienced and new research partners. Similarly, informants reported differing practices on how formally defined or informal and organic the research partner role was, and the benefits and limitations of each approach.
Chapter 6 Reflections on the project’s own public involvement
Introduction
As part of our reflective practice, our team agreed to conduct a brief evaluative review at the end of our project on the public involvement in our own team. This review was led by one research partner, who conducted interviews with most of the other research partners and academics who worked regularly with research partners. The data were anonymised before sharing within the team to encourage honest reflections. While the text follows the themes covered in the case study analysis, there is no attempt to cover all themes equally – the emphasis here is on what people said and what can be learnt from public involvement in our project.
Outcomes
Impact on research design and delivery
Our team included six research partners, who were involved in all research tasks alongside the 12 academics, in an integrated way. Almost all case studies were researched by subteams of an academic and a research partner. It was therefore very difficult to identify and separate out the specific impacts of research partners’ many contributions:
Because the research partners have been involved from the beginning and to some extent have been so integral to the team, it is very difficult to pinpoint the contribution they have made. With hindsight, we should have thought much earlier how we were going to capture the impact of research partners within our own team . . . The overall design and research questions were better because of [research partner] involvement, though it is impossible to track the exact pathways of influence.
Researcher 20
This integrated approach contrasts with, for example, academics in other studies revising a questionnaire after comments from a patient panel, which can then be shown to the panel as evidence of their impact. In this project, the questionnaires emerged from group exercises, including team meetings and consensus workshops, which always included at least some research partners. The same applied to most aspects of the project:
In practice I would say [the research partners] contributed at least as much if not more than some of the academic partners.
Researcher 17
I am most aware of the research partner’s contributions in my own case study team. For me, this partnership has validated our decision to involve research partners in all aspects including data collection. There are a number of times that [the research partner] has contributed important insights that relied on being (a) a service user research partner and (b) involved in data collection and therefore experiencing/observing the issues at first hand.
Researcher 20
Individual research partners observed when their perspectives had an impact:
I’ve noticed various things where I feel, if I hadn’t suggested that, things would have just gone a different way and I feel that’s a very identifiable impact that I’ve had, and it’s carried through to having questions in the interview schedule and it’s carried through to it being a code.
Research partner 16
The academic working with the young research partners found it more difficult to pinpoint their impact:
I’d like to think that I could [unpick how their presence impacted] but I’m not sure I can. I’ve found it very enriching and enjoyed working with them, and they gave me a lot of insights. When we did the coding together, on some occasions we all looked at it from different perspectives, from different angles, but it was still a bit of an academic exercise. I think they have contributed an understanding of what is helpful and what isn’t helpful in terms of involving young people in research, which is important.
Researcher 17
There were also some team perceptions of negative aspects of involving research partners:
I suspect meetings go much slower because of the perceived need to be ‘gentle’ on research partners, and not appear to dismiss our views.
Research partner 16
To enable research partners to contribute to coding, we agreed to allow manual coding, which meant that we artificially restricted ourselves to 38 codes; in retrospect I think we thus failed to include some important codes. The whole process of working with research partners is slower for academics than working on their own; this has contributed to our struggling to finish the project within the allocated time and funding.
Researcher 20
Impact on public involved
Some of our research partners were experienced user researchers, but all expressed similar personal benefits to those identified by Staley:11 acquiring new skills and knowledge (or applying them in the case of experienced research partners); personal development; support and friendship; enjoyment and satisfaction; and being rewarded both by being acknowledged and financially. As with Staley’s analysis, for our research partners both ‘personal development’ and ‘enjoyment and satisfaction’ related to making a useful contribution to worthwhile research.
My motivation and reward is that . . . I think research is of a better quality, more applicable, more easy to put into practice . . . if the people it’s about are involved in doing the research . . . the fact that I’ve commented, and seen certain things being taken on board, keeps me on board as well.
Research partner 15
I’m not doing it for money. I’m doing it because it’s mentally stimulating. I actually enjoy it.
Research partner 17
There’s no way I would have done it without getting paid. But I greatly value the experience, too. It’s given me the chance to find a way back into the working world, and I feel able to do much more now than when I started.
Research partner 16
The best bits of the project were being able to work with so many different people and feeling valued as part of the team . . . there are so many aspects of it that I can transfer into my own learning.
Research partner 14
Some of these motivations and perceived impacts, such as learning, mental stimulation and money, applied equally to our academics. But there are other academic imperatives, such as publication and reputation, which were never mentioned by our research partners. This was an important reminder that academics and research partners have different motivations.
Context
Leadership and culture
There was an existing culture of involving patients, users and carers in the Health and Life Sciences Faculty at UWE. Our PI played an important role in developing support for public involvement in research, including setting up the SUCIR initiative (now replaced by People and Research West of England), and leading the development of a system for paying research partners early in the bid process:
I feel he has made a tremendous effort in the extent we are involved, consulted, listened to.
Research partner 16
Field of research
Research partners brought different experience and expectations to the project. The young research partners had no experience in research, while one research partner is currently undertaking a PhD at UWE on public involvement in research, having started in research as a service user:
[Our experience] colours the way we’ve seen this project. For me, in some ways it’s not as good as other projects I’ve been involved with. Although it is more, I suppose, solidly academic than some projects where I’ve been a researcher.
Research partner 15
Because we are doing much more, we are a much more integral part of this project than partners usually are [in other projects].
Research partner 13
The young research partners, having joined the project later with little knowledge of research, had their own separate training, including sessions on interviewing and coding for analysis. However, all involved recognised that these arrangements fell short of the ideal:
A lot of you had had previous experience of doing this and were very good at doing the role, that’s probably why we felt more on the outside. People were accommodating us and made us feel welcome, that wasn’t a question, but it was more about understanding . . . I think it would have been really useful to have a really thorough understanding of my role as a research partner.
Research partner 14
[For the young people] we didn’t say at the beginning, well look, this is what we need, this is why we want you to be involved . . . it was a bit organic, which isn’t good in my view.
Researcher 17
Mechanisms
Relationships
Relationships were important for the whole of the research team, but especially for our research partners. Some research partners felt ‘parachuted in’ to an alien environment, so they relied on good relations, with both academics and other research partners, to feel comfortable:
I think if academics are good at being welcoming and friendly and just having goodwill and warmness . . . it makes it easier to say you don’t understand things . . . it also creates the connection – the academics have got there professionally, whereas, for us, we don’t have a right to be there.
Research partner 13
Because research partners had very different motivations from academics in the team, these motivations could be undermined if relations with academics were not good. It was via relationships with academics that research partners received feedback that their contributions were ‘hitting the mark’:
In team meetings, my perception is people really valued what we said.
Research partner 14
I would like somebody to say, that was helpful, that was good. I would like a bit more of that, really.
Research partner 15
Structures of involvement and resources
The idea for the bid grew out of meetings of SUCIR. Most of the original research partners were co-applicants on the bid, and their early involvement was funded through UWE’s policy of paying for public involvement before external funding is granted. The original research partners were involved in all whole-team meetings. One original research partner, in rotation, attended each steering group meeting. Research partners also met separately, with one or more of the academic staff attending only on request:
Meeting as a research partners group is of value. When you’re involving service users [it’s important] to give them time to begin to get to know each other, to feel less isolated.
Research partner 17
Original research partners were able to be involved in virtually all aspects of the project, including interviews, planning and facilitating at consensus workshops, developing the coding framework, analysis, contributing to report writing and planned dissemination.
Public involvement I’ve seen before has involved the public in quite a small role. This project took it to a different level, which is much harder, and I think research partners and academics were sometimes out of their comfort zone.
Researcher 19
Some research partners decided not to undertake some tasks, where they lacked confidence, skills or interest:
It has become very clear during the project that not everyone wants to do everything – what I’ve learned from that is that those possibilities need to be planned for, or at least borne in mind, from early on, so that managing them doesn’t upset the rhythm of what you as a team are trying to do.
Researcher 18
The initial plan was that young people would be involved via an existing young people’s panel. When that did not work out, two individuals were recruited instead. When one original research partner went off long-term sick, the young people were supported to develop into the research partner role. This process left one academic with reservations:
It was all done pretty much on the hoof, and I think it was probably done on the hoof as well as it possibly could have been done. But I’m still left with an uneasy feeling about why did we perhaps not say, well OK because this has happened [the panel not working out], actually now it would be unethical to suddenly bring young people in?
Researcher 17
The delay in starting involvement, a relative lack of prior research experience and less clearly defined roles meant that the young research partners were never as fully integrated into the team. Nonetheless they did come to some whole-team meetings and research partner meetings, and were involved in some interviewing and coding.
Most of the project’s work was organised around four teams, each of which was responsible for two case studies. In response to various factors over the life of the project, these teams morphed into various shapes, though all but one still included a research partner. One case study, though, was undertaken by the research fellow alone, leading to some research partners feeling disappointed:
To me that went totally against what I thought the other seven projects were doing, which was working with a service user. I didn’t understand, and it went against what I thought this project was about.
Research partner 17
An overwhelmingly positive aspect of team members’ reflection focused on how involvement had been integral throughout the project:
From my perspective we definitely have been involved all the way through it from the beginning.
Research partner 13
It’s been very useful having the service user point of view on an ongoing basis – it’s so easy to start a project intending to give that view equal weight to any other, and then for everything to slip because you don’t meet with/work with service users regularly. I think the important thing is face-to-face regular contact.
Researcher 18
Despite research partners being involved throughout the project, involvement processes did not always work seamlessly:
Writing a protocol for the ethics application commits you to quite a lot of detail . . . I don’t think there was as much time as we might have had to talk about some of that. But I think it is that thing about deadlines and the academics having loads of other things they have to do.
Research partner 13
Support for research partners started out being the research fellow’s responsibility, though research partners felt that at times it was squeezed out by the pressure of other work:
You can have all the policies and the right system in place, but when push comes to shove . . . then all the stuff about nurturing public involvement just goes out of the window because the project has got to be delivered.
Research partner 15
Part way through the project a research associate joined the team, and most research partners felt that helped ensure they got the support they needed. One research partner was ill for 6 months, and she felt her return to the project was not smooth:
Given that research partners have illnesses and limitations, [returning to a project] is something that should be managed a bit better . . . For me it is working now because I was offered the support of someone I’ve worked with for a long time . . . and that’s made it all much better.
Research partner 15
It’s clear there’s a need to have some sort of ‘advanced agreement’ with research partners that lays out the process to follow in the case of significant illness or disability during the project.
Researcher 20
Early in the project, the potential need for mentor support for research partners was identified and one of the academics agreed to take on the role, but this did not work as envisaged:
We identified a senior academic that research partners could go to for support, although this did not work in practice, due I think to her not really having a relationship with the research partners. The one research partner who did want external support went to a member of the project steering group and the project was flexible enough to support this financially.
Researcher 20
Conclusion
The project set ambitious goals for its own public involvement, and it is not surprising that research partners had high expectations. Our collective reflection is that, on balance, the benefits of our own public involvement vastly outweighed the costs, and that it would in practice have been impossible to do this research without such integral public involvement. Involvement by research partners was extensive, running throughout from concept to (planned) dissemination. And it was intensive, often involving research partners in detailed, hands-on work such as interviewing and coding transcripts. They have remained involved up to and including contributing to the revisions to the report, and will be involved in further dissemination.
There are lessons to be learnt. For the young research partners, starting involvement later was not ideal. And there were aspects, such as the support of research partners, where the reality did not always match up with their expectations or needs. As with our case studies, the academic researchers collectively underestimated the time required to support research partners and the challenges of balancing meaningful involvement with other academic pressures. There were other support needs that became clear as the project progressed, for example research partners’ access to computer software and training.
What was the impact of public involvement in our project? There were significant positive impacts on research partners, but also some frustrations along the way. We believe there were also significant positive impacts on the research design and delivery, although these were not always easy to pin down. One concrete example was that research partners as well as researchers used their networks to identify and contact potential case studies, and some of our case studies were recruited from this intelligence.
Our experience was that it was important to build flexibility into the research partner role, and this insight also informed our analysis of the case studies. In our team, some research partners took on all research tasks while others took on more limited roles.
Critical learning that we take from our own experience of public involvement is that, the more integrated the involvement, the more difficult it is to demonstrate impact without a significant investment in resources to capture and analyse the impact. Our reflective processes were very beneficial, and helpfully informed our analysis of our case studies; in retrospect, however, it would have been even more valuable if we had sought and obtained the resources to more systematically capture and analyse the impact of public involvement in our own project as well.
Chapter 7 Economic analysis
Introduction
This chapter explains the development process of two new tools, designed to collect data on how public involvement activities used the resources available to them. These tools represent a first attempt to capture the activity of public involvement; like any other tools they will need to be tested, reviewed and refined for future use.
We present estimated costs associated with public involvement we were able to glean by supporting each case study to complete resource logs over a 2-week snapshot period, projected costs over 12 months and for the duration of the case studies, informed by the pattern and intensity of public involvement activities in each case study. We also compare our projections for the costs of public involvement with the budget for public involvement in the original grant proposals for each case study, to examine whether involvement costs were accurately estimated at this point. We discuss the types of public involvement activities, the opportunity costs of resources, our learning about planning resources for public involvement in research grant bidding and the strengths and weaknesses of our approach to costing. Our remit was not to undertake a full economic evaluation, so the benefits or impacts of public involvement are not measured or valued alongside the costs of public involvement in this chapter. Chapter 2, Developing a methodology for the economic costing of public involvement describes the background, methodology and methods of the economic analysis. In the next section, to help the reader, we recap important details of the methods and process of the economic analysis.
Process for costing resource use
Phase 1
Two health economists drew on experiences of the research partners in our research team to develop a resource log checklist which would be simple to use, but also capable of capturing the diversity of resources incurred by various case studies. Detailed feedback was received from the research partners and revised in the light of their comments and specific feedback (see Appendix 1). Our development process within the project team revealed that ‘on the spot’ help was vital to support capture of resource use data and completion of resource logs. As a result, guidance documents were developed to help the case study researchers and research partners to complete resource logs (see Appendix 2). A telephone helpline was set up to resolve any issues and clarify participant understandings of requirements for completion as they arose.
Phase 2
The project research fellow, who had the most complete overview of the eight case studies, worked with the health economists to identify those researchers best placed to complete each case study resource log. In accordance with our ethical approval these identified researchers also nominated a research partner from within their team to complete a resource log. A health economist then had a one-to-one discussion (either in person or by telephone) with each of our case study informants to provide detailed notes and guidance on how to complete the resource logbook. All participants completing the logbook were also given a helpline e-mail or telephone contact, which was monitored during the data collection phase over a 2-week ‘snapshot’ period during 2012. The snapshot period was selected at random; respondents were also asked to assess how typical or indicative each snapshot was of the overall profile of their involvement-related activity. Their assessments within each case study contributed to the process of developing the assumptions for costing (see Appendices 3–5), which we applied to project the overall costs.
Costing price assumptions for researchers
We did not ask participants about pay grades, but assumptions were made based on job title, for example professor or senior research fellow. If titles were not given, assumptions about salary scales were made based on the description (from the resource log) of the specific task that the member of the research team was undertaking, for example preparing paperwork for an advisory group meeting (administrative role) or preparing slides for presentation at an advisory group meeting (more senior role, such as senior research fellow). Where we were unsure we asked case study PIs to clarify grades from information available. Price assumptions are detailed in Appendices 3–5.
Costing involvement activity of research partners
A flat rate payment rate of £19.40 per hour based on an INVOLVE example23 was the price applied to the resource use estimates of research partners.
Findings
Within Tables 4 and 5 there are blocks of estimated, projected and comparative public involvement costs for all case studies. These are:
-
2-week snapshot costs for researchers and research partners from the resource logs (see Table 4)
-
projected costs for advisory meetings where applicable (see Table 5)
-
projected costs at 12 months and for project duration (see Table 5)
-
comparison of our projected costs and actual budgeted costs expressed as a percentage of total project grant (see Table 5).
| Case study number | Research staff | Member of public | Total |
|---|---|---|---|
| 1 | 1668A | Not availableB | 1668 |
| 2 | 1502C | 121D | 1623E |
| 3 | 0 | 0 | 0 |
| 4 | 0 | 0 | 0 |
| 5 | 136F | 0G | 136H |
| 6 | 336I | 16J | 352K |
| 7 | 0 | 0 | 0 |
| 8 | 4494L | Not available | 4494L |
| Case study number | Projected costs PPI | Projected PPI costs vs. budgeted PPI costs in funded grant proposal | |||||
|---|---|---|---|---|---|---|---|
| Advisory meeting | 12 months | Project duration | Total grant | PPI funding in grant | PPI funding as percentage of total grant | Projected PPI costs as percentage of total grant | |
| 1 | Not available | Not available | Not available | £4,034,000 | £42,226 (5 years) | 1.05 | Not able to estimate |
| 2 | £1384M | £9097N | £27,290 (3 years) | £1,196,000 | £7000 (3 years) | 0.60 | 2.28 |
| 3 | £230O | £690P | £1380 (2 years) | £400,000 | No budget (2 years) | 0.00 | 0.35 |
| 4 | Not applicable | £0Q (for 2012) £467Q (to date) | £3616 (5 years) | £1,982,000 | No budget (5 years) | 0.00 | 0.20 |
| 5 | £2232R | £20,464S | £41,391 (3 years) | £432,000 | £22,200 (3 years) | 5.14 | 9.60 |
| 6 | Not applicable | Not available | Not available | $180,000 | $15,345 (2 years) | 8.50 | Not able to estimate |
| 7 | Not applicable | £476.35T £873.30 (to date) | Not known | £248,000 | £2970 (4 years) | 1.20 | Not able to estimate |
| 8 | Not applicable | Not able to estimate | Not able to estimate | Ongoing grant | 91,380U (3 years) | Not able to estimate | Not able to estimate |
Data from the completed resource logs and interviews enabled us to make assumptions from which we created estimates and projections. The assumptions made to arrive at these figures are significant but complicated, so full details are in Appendices 3–5.
In Table 6 we detail the resource log completions for researchers and research partners across all case studies and describe the main costing models associated with public involvement for each case study. Table 4 presents the estimated costs of public involvement in research based on the information in our completed resource logs. Table 5 presents our projected costs for advisory meetings where applicable, projected costs at 12 months and for project duration. We also show a comparison of our projected costs and actual budgeted costs expressed as a percentage of total project grant in Table 5. Based on our projections (where these were possible) we show that, across our case studies, the actual costs of public involvement have sometimes been underestimated in initial application for project funding.
| Case study number | Description of model for costing public involvement | Research staff responses | Research partner responses |
|---|---|---|---|
| 1 | Public involvement activity included representation on various study committees, for example a stakeholder reference group, as well as a stakeholder event due to be delivered towards the end of the project | Two resource diaries | No nominee |
| 2 | The funded grant application did not have separate costing for public involvement. A stakeholder time and travel budget of £27,000 was included to cover all costs of public and stakeholder participation in this research | One resource diary | One resource diary |
| 3 | Public involvement was not a separate costing item in the funded grant proposal and so any costs associated with involvement would have been taken from the general project budget | One resource diary and interview | Summary of costs |
| 4 | Public involvement-related activity was not costed separately in the grant application, so any costs associated with involvement were taken out of the general project budget | Interview | Data from researcher |
| 5 | £22,000, around 5% of the total grant, was budgeted for PPI. A devolved model of public involvement was applied, whereby the lead organisation had a service level agreement with four service user organisations across England | Three resource diaries | One resource diary |
| 6 | The total grant awarded was nearly $180,000 over a 2-year study period. Public involvement-related activity was not separately included, but a travel budget of nearly $33,000 and living expenses of $6900 were included for both project researchers and patient experts to attend international project meetings | One resource diary | One resource diary |
| 7 | The total value of the award is approximately £248,000 with a budget for public involvement of £3000 (around 1.2% of the total grant) for patient partner travel and advisory group meetings including provision for light lunches and study participants‘ travel expenses | One resource diary | One resource diary |
| 8 | This is an ongoing programme grant, which primarily maintains a cohort of individuals and their data. These individuals form a public involvement panel that can be accessed by researchers as required | Three resource diaries | No nominee |
Completed resource logs
Our aim was to have at least one completed resource log for both research staff and for nominated research partners (referred to as members of the public in the resource diary) for each of the eight case studies. All eight case studies responded, and response rates for both resource logs were very good.
Research staff completed 12 resource diaries and one interview, giving 14 responses; no one refused to complete a resource diary. There were four completed resource diaries and a summary of costs (via researcher) for research partners plus data from the researcher (case study 4), giving six responses in total. There were no research partner responses from two case studies (case study 1 and case study 8) for lack of a nominee from researchers within the team.
Discussion
Our analysis has revealed much diversity in the practice of public involvement working, and a mismatch between actual budgeted and projected costs of involvement across the various research designs and grant sizes of our case studies. The range of involvement activity among researchers and research partners is diverse.
This section provides an interpretation of models of public involvement in research costing emerging from the case study evidence. For the benefit of future research teams we identify some of the drivers of variations in costs for public involvement and link these to the models of costing involvement that emerge from our case studies. Strengths and weaknesses of our approach are discussed.
Broadly, there were four types or forms of involvement used with differing associated costs:
-
facilitating a public advisory group or panel that meets at regular intervals throughout the life cycle of the research project – this could include advisory group representation on a project steering group
-
setting up and maintaining a public involvement panel within an ongoing research programme or a variety of research projects to access as required
-
working in partnership with service user-led organisations
-
involving individual members of the public as research partners working with the research team.
Our analysis has revealed a tendency among PIs to underestimate the costs of public involvement in their grant proposals. The range of public involvement activity among researchers and research partners is diverse and requires proper planning.
Where we have been able to make projections for public involvement costing across the time frame of studies, we have found by comparing budgeted involvement costs with projected costs for the duration of projects a fairly significant underestimate ranging from 4.4% of a £432,000 budget (case study 5) to 0.2% of a £1.9M research budget (case study 4). Case studies 3 and 4 had not budgeted public involvement costs as a separate item within the funded grant proposals, so involvement costs would have been taken from elsewhere within the grant. Case study 2 had significantly underestimated the cost by £15,600 or 1.3% of a project grant of £1.2M. Case study 5 had introduced unexpected and additional payments for research partners attending national panel meetings due to changes in project management and lack of continuity in acting on decisions made and recorded in meetings.
In most cases the resources required for public involvement have been taken from elsewhere in the budget, but these findings point to the need to ensure public involvement is planned at the outset as grant proposals are developed.
Describing the range of public involvement activity is necessary because it points us towards clarifying what the potential impacts of this involvement might be, and starting a debate about whether or how these impacts might be captured. Main sources of activity for research staff were preparing for and attending various project team meetings, where a proportion of time was allocated to public involvement issues, often to help manage any problems that emerged during the case studies.
Across those case studies that had public advisory groups, preparation of paperwork, presenting at, and attending public panel meetings, writing up minutes after meetings and administration of the reimbursement costs associated with attending these meetings were significant. Research partners within our case studies also prepared for, attended and presented at regional public involvement conferences. Other activities mentioned included the consideration of research partner involvement in the next phase of a project; contribution to planning analysis of interview data; booking travel arrangements for research partners to attend advisory group meetings; administration of reimbursement of expenses; and responding to e-mail/telephone queries from research partners. The underestimations in the original grant application for one case study meant that the main involvement activity was applying for a further grant to resource research partner travel to four imminent project team meetings in Europe.
In another case study, activities for one researcher included reviewing individual case reports to determine barriers to participation, and involvement in research and planning initiatives to re-engage participants who have not been recently active in research activities. A second informant’s primary responsibility was to maintain the cohort database and related activities. A third informant’s primary role was to meet recruitment targets by linking with study participants to enrol them in new research projects, obtaining consent and encouraging their attendance at clinics.
The main sources of activity and costs for research partners were preparing and attending project advisory group meetings and writing up notes to give updates to subsequent panel meetings. Our study has revealed how an advisory group structure is able to effectively and potentially cost-effectively integrate public involvement within research management processes. Across case studies, project advisory groups with research staff and research partners appear to maximise the value of public involvement within research projects at relatively low cost compared with other ways of working.
There are strengths and important limitations of this economic analysis. We have developed and tested some initial tools to log resource use and guidance to support their use. These tools have been completed by our participants successfully, and can now be further tested, revised and reapplied. We have made an important first step in capturing the nature, level and quantity of resources connected with public involvement work, enabling costs to be estimated and projected. The study findings have revealed a notable underestimation of the budget required for public involvement across the case studies regardless of whether direct monetary payments are made for public involvement.
Limitations of our approach and analysis in this study cannot be ruled out in impacting our findings. Our assumptions in estimating and projecting costs have been made explicit, but it has not been possible to estimate the impact of uncertainty on estimates and projections using sensitivity analyses.
In the light of the strengths and limitations of this analysis it is important to reflect upon the processes for estimating the opportunity costs of public involvement in developing full economic costing within grant applications. Accurate estimation of direct costs, indirect costs, unforeseen costs and overheads is very much dependent on thinking through the hidden intangible costs and benefits of public involvement.
Case study 7 is located in a joint clinical/academic research unit which has a well-established research partner panel supporting a wide range of research projects in the unit. While the two research partners in case study 7 were recruited from this panel, and public involvement is crucial to achieving the study outcomes, there are ‘hidden infrastructure costs’ absorbed by both the local university and the local NHS trust. The unit has two senior clinical academics giving invaluable leadership and support to its research partner panel and providing training. They also employ a patient as a part-time co-ordinator to liaise between the patient panel and the unit. None of the direct costs of these resources has been factored into the resource costs for the study, so they are sizeable ‘hidden’ costs.
Conclusions
These analyses suggest a need for guidance in scoping potential types of public involvement within proposed research projects. We note that a practical guide to budgeting for involving the public in research projects being drafted by Julia Cartwright and others on behalf of the Mental Health Research Network (MHRN) and INVOLVE during our reporting period has been published, and we hope that grant applicants will make use of it. 23
Supporting PIs to scope out and plan public involvement in their projects effectively at the outset and providing tips for this planning are important. Resources for public involvement need to be foreseen and budgeted for with the intention of meeting all payments, payments in kind, rewards, vouchers and expenses of research teams and research partners for public involvement. There should be some element of contingency to support public involvement activities in which research partners might be expected to make further time commitments using their unique perspective; for example, to support researchers who have responsibility for managing recruitment and retention issues arising in projects (nearly all trials experience these issues at some point). More research is needed in how to measure and cost the impacts of public involvement, so that full economic evaluation of public involvement activity can be conducted in the future and enable comprehensive applications for funding to be made.
Chapter 8 Discussion
Introduction
In this chapter we present our theory of public involvement revised in accord with our case study findings, and discuss our developing theory in the light of our reflections on public involvement in our own study. We then consider how our theory relates to the wider literature on the impact of public involvement in research that has appeared since the two seminal literature reviews by Staley11 and Brett et al. 12 that we used as a basis for our initial theory.
Our revised theory of public involvement in research
Having interviewed 42 stakeholders on 88 occasions, and observed public involvement processes in our eight case studies over a year, we are now ready to come to some tentative conclusions about the key contextual factors and mechanisms that lead to intended outcomes in public involvement in research. We should say at the outset that we accept that our conclusions must necessarily be provisional and only incrementally contribute to developing a full theory of public involvement in research. We cannot take what our participants say about outcomes or the contexts and mechanisms that lead to them completely at face value. Researchers and research partners arguably both have interests in claiming impact from public involvement which may be hard to demonstrate conclusively. Nevertheless, we can assess and develop our theory only on the basis of the evidence we have collected and analysed. Our hope and intention is that others will critique and develop our theory to further build our understanding of what works in public involvement in research.
Public involvement achieved at least some of the intended outcomes in all of our case studies. All of the research teams reported that they had valued and acted upon the contributions of research partners, despite the diverse types and scale of research projects and the different structures of public involvement they utilised. In general, research partners’ reports of their experiences of observing changes made following their contributions validated the researchers’ claims. Where we were able to observe, or obtained documentary evidence, this also supported the claims that research teams did listen to and act on the contributions of research partners. This did not necessarily mean that the research partner-inspired changes achieved the project objectives; as we saw in some cases with research partner input into recruitment strategies and materials, research partner input led to improvements in the quality of the materials, but not necessarily to improved recruitment. Clearly there was also some degree of proportionality, as some case studies had little or no public involvement during our data collection period, and so little opportunity to benefit from public input during this period, while other case studies had consistent public input throughout the year. Nonetheless, the overall message from across the case studies was that, when the public were involved as research partners, this helped improved research design and delivery. A secondary but also important message was that, overall, research partners found their involvement rewarding in a number of ways, principally because they consistently felt they were making a useful contribution and felt valued.
If public involvement was having at least some of the intended and desired impact (e.g. the contribution to research design and delivery as detailed in Chapters 4 and 5), what then were the key contextual factors and mechanisms of involvement and how were they related in terms of CMO configurations? Demonstrating the causal pathways is difficult, and again we need to acknowledge the limitations of the evidence we can draw upon and the provisional and incremental nature of our analysis. But some points stand out from our data. Our strongest finding is the importance of the PI’s leadership, belief, commitment and values around public involvement. Where the PI led strongly on public involvement, believed in it, was committed to it and valued it, then the mechanisms and outcomes of public involvement flowed almost inexorably from this.
This is not to say that such PI leadership was absolutely essential. There were several case studies where this was not initially the case. But in these cases there were other factors related to leadership on public involvement that acted as a proxy for PI leadership. In these cases, we would suggest that an essential attribute of the PI is that they need to be open to public involvement, and able and willing either to learn to develop their leadership in this area or, alternatively, to delegate it to another senior member of the team. Thus in one of our case studies a PI undertaking a PhD project, who was new to both the PI role and to public involvement, joined a research unit with an existing strong culture of public involvement. The unit director/director of studies provided a wider leadership role on public involvement and, in this context, the PI naturally developed a commitment to public involvement. Similarly in another case study, a PI new to the role, and to public involvement in research, delegated leadership on involvement to a senior colleague experienced in this area; through the project she also came to value the benefits of involving the public in research. Thus it would appear that, if one has either a committed PI or a culture of public involvement, then one is likely to have an effective approach to public involvement in research, but both are not necessary for effective involvement to take place. What is essential in either case is a PI who is at least open to public involvement and that someone involved (the PI, the senior lead on involvement or another team member) should have or should develop some experience and expertise in public involvement.
A history of public involvement in the institution was another of our hypothesised key contextual factors, but this did not appear as important in our case studies as leadership within the research group or team. All of our case studies had some history of wider institutional support for public involvement, and often this was drawn upon within case studies, but it appeared useful rather than essential. In some cases, such institutional support had been available for some time, but was drawn upon by the PI only for their recent (case study) research. It was also noted in our second consensus workshop that researchers draw upon a range of institutional structures not just within their host institution but also including funding bodies, regional, national, European and international institutions. Essentially, there are a range of resources available to support public involvement in research which PIs and other team members can utilise, and it is not necessarily crucial that they draw on those from their host institutions.
Following discussion at our two consensus events and analysis of the emerging data, it was agreed that a new concept ‘field of research’, although not part of our original theory, reflected an important aspect of the context for public involvement in research which we needed to incorporate into the theory. In particular, as well as research design, studies differ in the extent to which members of the public have an ongoing relationship with researchers and in the degree of diversity among the public. The field of research is defined by complex and often taken-for-granted assumptions, procedures and practices that make one field or discipline distinct from another. One of the clearest ways that the field of research manifested itself in our data was the way the pattern of involvement in clinical trials differed from that in other studies. In all of our trial case studies, there was a lengthy period of data collection when little or no involvement activity took place; in the most extreme example one case study had no involvement activity at all during our entire data collection period of 2012, despite the value the research team ascribed to public involvement earlier in the project. This was very different from other studies, where involvement was more ongoing. Thus the field of research structured the opportunities and boundaries for public involvement and the mechanisms of involvement that were appropriate for those studies.
Bringing the different contextual factors together, we would argue that leadership and culture are the key contextual factors for ensuring that public involvement happens, but the field of research is equally crucial in a more underlying way in determining the opportunities and constraints of what is possible. A history of institutional support for public involvement is helpful but not essential.
Turning to the question of how these contextual factors collectively shape the mechanisms for involvement returns us to the key role of researcher leadership; what was clear from our case studies was the importance of someone senior in the team (whether the PI, a co-applicant or a research manager) being delegated to take a lead on public involvement and, crucially, allocating resources for involvement. This was not necessarily about a formal allocation of budgetary resources. As the economic analysis of the case studies indicates, substantial resources in terms of research team time can be allocated to public involvement without being formally budgeted for. In addition, it was crucial that a member of the team with good interpersonal skills (who might or might not be the same as the senior lead) took on a co-ordination/facilitation role for public involvement. That is, they were the first point of contact, ensured effective communication with research partners, dealt with the practical aspects of meetings and/or sorted expenses. Supporting research partners takes time, and in several of our case studies this time was not formally budgeted for but PIs or the senior lead on involvement ensured that it was made available.
Training has been identified in previous research as an important resource to support the public in getting involved in research but it did not feature very significantly in our data. Some of the research partners played an effective role in case studies without requiring any training. Training appeared most relevant where research partners were taking on more technical research roles such as the analysis of data. More commonly in our case studies research partners were sharing their lived experience and responding as informed patients or service users to draft recruitment or information materials, roles for which they required not training but facilitation and informal support. Thus our theory should be amended to emphasise informal support over formal training, and the need for formal training to be linked to the development of appropriate skills for particular tasks.
The other key resource issue we explored related to how research partners were rewarded for their involvement. Monetary payments were made in only two of our eight case studies, and in one of these it did not appear a significant factor in the research partners’ motivation. Much more important in all our case studies were other types of reward, notably feeling valued, listened to and having feedback that demonstrated that the contribution research partners were making was having an impact. Most of our case studies used advisory groups or panels; arguably these require relatively limited time and skills from research partners. In cases like our own study, where research partners play a coresearcher role requiring a higher level of time commitment and research skills, payment is much more likely to be expected or required. Payment for involvement is perhaps one of the most debated issues in public involvement and we would not wish to make definitive statements on the basis of eight case studies. Members of the public have very different needs and wants around payment, ranging from those for whom it is an absolutely critical statement of the value of their contribution to those who are insulted by the very suggestion that their voluntary gift of time should be demeaned by offers of payment, or those for whom an offer of payment risks their benefit status. The most that we can say at this point in our revised theory is that non-monetary rewards appear more widely valued as a motivating mechanism than payment in cases, such as most of our case studies, where research partners play a relatively time-limited advisory role. We will return to the wider issues of payment later in this discussion.
Another area of debate which emerged through our data was whether or not defined roles were as useful a mechanism as we initially hypothesised. Although in one case study there was an initial tension over the lack of clear agreement on the research partners’ roles, in general most case study participants were content to let the research partner role develop organically without clear definition. Overall it appeared helpful for researchers to make clear their practical expectations of what they would ask research partners to do at each stage of the research project, but this did not necessarily require an overarching or formal role definition.
The crucial factor that did appear to influence outcomes – and one that many discussions with informants came back to – was the importance of building good interpersonal relationships between the research team and research partners. This clearly links back to the need for PI or senior leadership, the role of co-ordination/facilitation and the non-monetary type of rewards that motivate research partners. All of these aspects are mediated through the development of relationships of trust between researchers and research partners, where the latter feel valued and included. The key learning from this research can be summarised in a simple causal pathway as in Figure 1.
FIGURE 1.
Context, mechanism and outcome pathway.
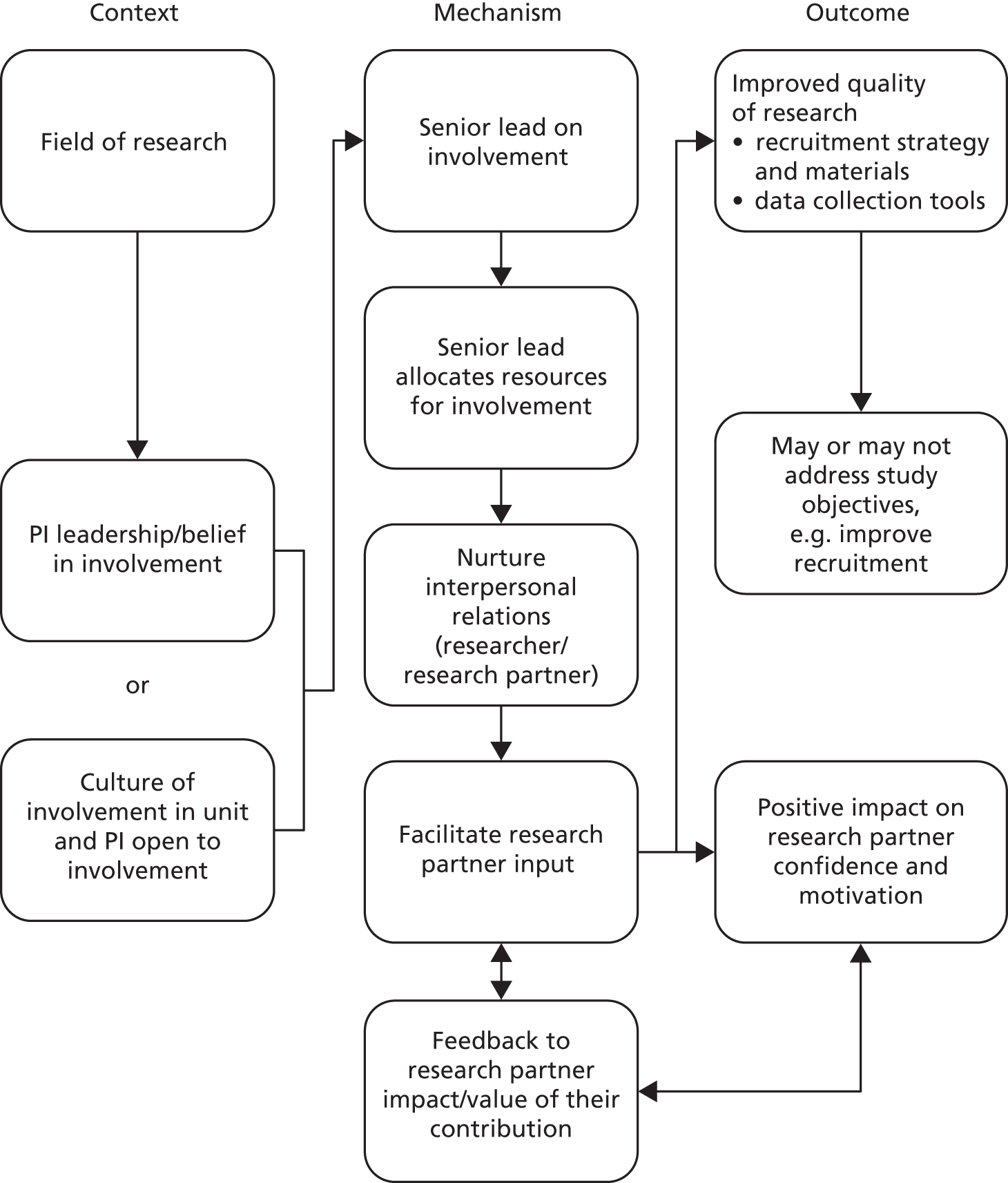
Assessing our developing theory against the experience of public involvement in our own study
As the approach to public involvement in our own study differed significantly from that in all of our case studies in that we adopted much more of a coresearcher model, it is useful to assess the extent to which our own experiences map to the pathway outlined in Figure 1.
There are a number of factors that lead us to argue that our field of research was particularly conducive to public involvement. The funding call we applied to was specifically about public involvement in research, and INVOLVE was a partner in the call. Thus the funders expected strong public involvement in the bid and the research project. As a qualitative study, our project was more accessible to public involvement throughout the life of the study, as research partners would not require highly technical quantitative skills.
Our PI had demonstrated his belief and commitment to public involvement in research through a number of years promoting involvement within his university, in leading a local collaborative project of universities and NHS organisations to support public involvement in research and in national work as a member of the INVOLVE Advisory Group. He took the senior lead role on involvement in this project and in writing the bid allocated significant resources for involvement. In purely monetary terms, £13,000 or 7.2% of the entire budget was allocated to payment for research partners. In non-monetary terms both the PI and the research fellow (and later the research associate) allocated time for supporting research partners including attending research partner meetings to listen to and seek to address any research partner concerns. Conscious attempts were made to create space to nurture interpersonal relations and facilitate research partner input, including allocating time for reflection on what was working or not working in our own public involvement at the beginning of each project team meeting.
An important difference between our research team approach and the majority of our case studies was our policy of including our research partners as coresearchers and paying them on a research staff-related scale (equivalent to the bottom of the research associate grade). Both our academic research staff and research partners were clear that the level of involvement, and the type of work our research partners were engaged in, could not have been expected without payment. This contrasts with most of our case studies, where research partners took on more advisory roles, requiring relatively limited time commitments, and emphasised the intrinsic rewards of satisfaction and gratitude for their contributions rather than monetary rewards. In the two case studies where research partners took on more of a coresearcher role (albeit not to the same extent as our study), the research partners were paid for their time. In summary, non-monetary rewards are always important, and monetary reward becomes increasingly important as the time commitment and level of technical work expected of research partners increases.
A related issue which came up in a number of our informal discussions within the project team and with case study colleagues was the relative value of ‘naive’ versus ‘professionalised’ research partners. Naive research partners are often thought to add value by directly and immediately sharing their lived experience of particular health conditions, while professionalised users often add an understanding of the research process and systems that allows them to voice their experience in professional settings. Some researchers also expressed concerns that professionalised users lose that immediacy of lived experience and may take on the perspective of professionals rather than service users, thus lessening their value to research teams. Our team included research partners with a range of previous experience of research, from our two young research partners, who were relatively inexperienced, to some of the original research partners, who had extensive experience including of user-led research. The nature and implications of professionalised research partners is only just beginning to be explored in the literature. 26 This diversity of extent of professionalisation was also reflected in our case studies, although overall our own research partners were probably nearer the professionalised end of the spectrum than most of the case study research partners. This was not, however, a factor which was captured in our emerging theory and it would be useful for future research to more fully explore the implications of this professionalisation factor in the impact of public involvement in research.
Even more than with our case studies, it was difficult to capture the distinct impact of involving our research partners on our own research design and delivery. Partly this was because of workload and prioritisation issues. We often spoke of our own study as a virtual ‘ninth case study’, and we audio-recorded our reflective sessions at team meetings; but we were fully stretched in collecting and analysing data from our eight formal case studies and did not have the human resources to try to analyse our own involvement processes and outcomes in a systematic way. More fundamentally, it was the very integrated nature of our team, with research partners as co-applicants and coresearchers, that militated against easy impact assessment. Research team meetings had extensive agendas with fast-paced discussions. Determining which team members made what contributions to decisions would have required time-consuming processing of our recordings and analysis, which we did not have the resources for. Thus the best data we have are the post hoc critical reflections captured in Chapter 6, and the most that can be said from these is that the outcomes identified are consistent with the causal pathway outlined in Figure 1.
How our theory relates to the wider literature on the impact of public involvement in research
Other realist evaluations of public involvement in research
At the time we began our study, we were not aware of any studies that had applied the realist evaluation approach to public involvement in research. Subsequently, Staley et al. have produced a paper based on Staley’s earlier literature review11 calling for studies of public involvement in research based on the principles of realist evaluation. 20 They argue that studies based on realist evaluation can test the links between CMO more rigorously than existing observational studies. The key difference in their view is that with a realist evaluation the researcher identifies a specific question, develops a hypothesis about how this type of involvement could make a difference in the context of their study, uses this hypothesis to select appropriate methods for capturing impact, and factors in the contextual and mechanistic factors already known to influence outcome. They identify two recent studies of involving peer interviewers which ‘are more in line with the principles of realist evaluation’. 27,28 Neither of these studies was presented by its authors as a realist evaluation, and the first of the two, by Gillard et al. ,27 is of debatable relevance because the authors neither present a hypothesis nor explore the links between CMO. The second study, by Hamilton et al. ,28 is arguably more relevant, although again there is no explicit discussion of CMO. There were, however, five clear related hypotheses to be tested (e.g. that involving peer interviewers would enable participants to be more open and honest about their experience of stigma and discrimination). Implicit in the study are a number of context factors (e.g. shared experience of stigma and discrimination among mental health service users) and a facilitating mechanism of disclosure (about having used mental health services) by the interviewer leading to the outcome of more complete data collection.
Notably for a study exploring user involvement in research, this paper gives no details of the extent of user involvement in the study itself. One of the paper’s authors is a well-known user researcher, but the significance of this is not discussed in the text. Thus we know nothing about how user members of the research team contributed to the study design, methods or outcomes. It is therefore difficult to see connections with our theory, particularly as none of our case studies involved a peer interviewer model. There is, however, a connection with our team experience of research partner coresearchers. In our study team, academic researchers and research partners shared the interviewing of both case study professionals and research partners. Although we did not do an experimental study as Hamilton et al. 28 did, in terms of our reflections on our interview experiences, we did not notice any consistent differences in response or the openness of either professional or research partner interviewees between our academic and research partner interviewers. To that degree, our experiences have been consistent with the findings of Hamilton et al. 28
The importance of principal investigator leadership
Principal investigator leadership is a critical element in our theory of public involvement in research but was not explicitly identified in the reviews of either Staley11 or Brett et al. 12 although it is implicit in a number of the factors they identify. Subsequently, PI leadership has not been highlighted in more recent reviews, conceptual papers or newer empirical work on public involvement in research. The recent paper by Shippee et al. ,29 which includes both a systematic review and a conceptual framework, does not identify PI leadership as an element of their framework. 29 Other recent literature reviews such as Brett et al.’s 2012 updated article on their systematic review30 or Boote et al. ’s31 bibliometric review similarly do not identify it as a factor. There have been several other recent papers offering conceptual frameworks for making sense of public involvement in research32 but these also have not included any reference to or discussion of PI leadership as a factor. Wider conceptual frameworks for public involvement in service improvement33 equally do not have any comparable component of professional leadership in their conceptual models.
There are two possible explanations for this disjuncture. First, we may have been mistaken in identifying PI leadership as a key contextual factor. But this does not seem likely to us, as this factor was identified so strongly across our data. Second, this may be a crucial factor that has not previously been identified simply because no one else has conceptualised it and examined the hypothesis that it is an important factor in effective public involvement in research. Although leadership as a factor is not explicitly named, there is some evidence in the wider literature to support this. Staley et al. report on service user collaboration in mental health research. 34 Although they do not discuss leadership per se, they discuss the closely related concept of the role researchers play in establishing the boundaries of involvement:
Many researchers have much narrower expectations of involvement, consequently limiting its impact. Some saw enhancing the ‘lay-friendliness’ of research materials and processes as the main purpose, while a smaller number realized the value of incorporating the service-user perspective into research design and delivery. A researcher’s understanding sets constraints on what they ask of the service users involved.
Reproduced from Staley K, Kabir T, Szmukler G. Service users as collaborators in mental health research: less stick, more carrot. Psychol Med 2013; 43:1121–5 http://dx.doi.org/10.1017/S003329171200166334
In most health services research, power lies with the PI and other researchers to determine the extent of any involvement, and we would argue that the opening of opportunities for meaningful public involvement by researchers is usefully understood in terms of leadership.
Our conceptualisation is also consistent with recent research about health researchers’ attitudes towards public involvement. For example, Thompson et al. have conducted a qualitative study of health researchers’ attitudes towards public involvement in health research. 14,35 They found researchers held a range of varying constructions of public involvement in research, with a number of benefits being identified but also some feelings of apprehension expressed. 35 In particular, they identified the issue of ‘epistemological dissonance’ and the ‘know–do gap’. 14 This relates to the tensions between researchers’ perceptions of the potential benefits of public involvement in research and their actual practices, which were often mediated by their perceptions of the limitations of involvement. In terms of our theory, these insights into the impact of researchers’ attitudes and behaviours complement our emphasis on the importance of PI leadership. Those PIs with a smaller know–do gap and less epistemological dissonance are more likely to be open to and allocate resources for involvement, thus enabling it to be more effective.
In most health services research, an academic or clinical researcher will be the PI, assembling the research team, and taking a lead in the distribution of roles and resources within the team. Although the PI will be influenced by external factors (e.g. funders’ requirements) and internal team factors (other team members’ experience, expertise and attitudes towards involvement), the PI’s leadership will be crucial in determining where public involvement in the project lies on the spectrum from tokenism to real partnership. The importance of this PI leadership role has not previously been explicitly identified or discussed in the public involvement in research literature, and represents an importance conceptual insight from our research.
We recognise, however, that more work needs to be done to understand and theorise leadership in public involvement. Leadership is more generally a poorly defined and contested concept. Martin and Learmonth among others have cautioned us on the need to critically analyse the discourse of leadership which has arisen in UK health services over the last 10–15 years. 36 In particular they note the way that leadership has been conferred not only on those in positions of formal power but on frontline clinicians and on patients and the public. In the context of research, this emphasises how we need to critically examine the extent to which researchers, research managers, patients and the public, and other research stakeholders share leadership in public involvement in research.
The question was raised in our second consensus workshop of whether leadership on, and a culture of, public involvement within service user groups was an important factor. This was not an aspect that came up strongly within our data except in the one case where research partners from a local service user-led group and researchers initially had mismatched expectations of the role the research partners would play. This is likely to be a more important issue for some service users with long-term conditions, where greater experience and expertise in involvement in research is likely, and for coresearchers. We are not able to comment from our data on leadership and culture within service user groups but it is arguably an important question for future studies.
To date, public leadership in research has been largely unexplored, except in the concept of user-led or user-controlled research (which represents a tiny proportion of funded research). 37 There is public leadership at a policy level within INVOLVE and more widely in the NIHR in terms of public membership of national advisory groups and commissioning boards. However, at the level of individual research programmes or projects, the PI will be key to the extent to which the public are invited in to take on involvement roles in general and leadership roles in particular. In this sense PIs play a key role in ‘constituting the public’38 in public involvement in research, that is shaping the ways in which the public are seen to have a legitimate voice in research. ‘Patient leadership’ has developed as a strong policy theme in health services more generally;39,40 to date the concept has not yet emerged in the research setting, and it is worthy of further exploration.
Other recent models of public involvement in research
Another important test for our theory is how it compares with other recent theoretical frameworks and models of public involvement in research. Over the last 6 years a number of authors have put forward such models including Oliver et al. ,41 Robinson et al. ,42 Morrow et al. ,32 Brett et al. 12,30 and Shippee et al. 29
Based on a systematic review of the literature, Oliver et al. used framework analysis to propose a ‘multidimensional conceptual framework’ for analysing public involvement in research with three critical dimensions: whether lay people were involved as individuals or as members of organised groups; whether public involvement was at the invitation of the research programme or in response to action by the lay public; and the degree to which the public was involved (consultation, collaboration and lay control). 41 The authors state that the framework combines and extends concepts proposed by Arnstein43 (the often-quoted ladder of participation) and Mullen. 44 Both the second and third dimensions of this model relate to the degree of engagement of the researchers (and implicitly the PI) in facilitating involvement, but do not explicitly consider the role of the PI in particular or the question of leadership. On the other hand, there is nothing in this framework inconsistent with our theory. The authors’ reflections on their framework emphasise the greater value and impact of researchers’ engagement with more collaborative approaches, which is consistent with our emphasis on PI leadership on involvement.
Robinson et al. present a simpler, two-dimensional conceptual model, although the sources of this model are less clear; the authors report having completed a literature review, but give few methodological details. 42 This model identifies two axes: the degree of collaboration (running from less collaborative to more collaborative) and the degree of empowerment (expressed in terms of a top-down or bottom-up approach). Like the Oliver et al. 41 framework, this model does not address PI or researcher leadership on involvement explicitly, but its concern with the potential exclusion of the public from the research process and the balance of power between researchers and the public is wholly consistent with our model’s emphasis on PI leadership and on the importance of nurturing interpersonal relationships between researchers and research partners.
A more complex model of involvement is proposed by Morrow et al. 32 drawing on ‘a range of philosophical and social theories of power and empowerment’ (although these are not detailed). This model focuses on both service user factors (what a person feels able to do, whether or not they feel their potential is being fulfilled and their sense of being valued) and research factors (research relationships, ways of doing research and research structures). The model details personal factors for service users, not researchers, so PI or researcher leadership does not feature explicitly in the model. However, there is a focus on research relationships, with key factors identified including ‘allocating sufficient researcher time for two-way communication in the early stages of the research studies’. 32 Thus, this model mirrors our mechanism of a senior lead allocating resources for involvement and the nurturing of interpersonal relationships. Again, there are no factors identified in this model which are inconsistent with ours.
Stewart and Liabo critique the (now superseded) INVOLVE model of levels of involvement (consultation, collaboration and user control) with its implicit hierarchy devaluing consultation. 45 They join critics such as Tritter33 in arguing that such hierarchies, often based on Arnstein,43 fail to reflect the complexity of public involvement. Instead they argue for a model where patient expertise is integrated with researchers’ and policy-makers’ expertise. In this model, patient expertise comprises knowledge of living with illness and receiving care whereas researcher expertise encompasses knowledge of research design, methods, conduct and analysis. We would argue that this model is unnecessarily restrictive in terms of public contribution to research design and delivery, but it is again consistent with our emphasis on the importance of PI leadership and relationships.
The most recent conceptual framework put forward for public involvement in research is based on a ‘metanarrative systematic review and environmental scan’ conducted by Shippee et al. 29 on what they call patient and service user engagement (PSUE) in research. The authors reviewed 202 sources which met their inclusion criteria and claim to have identified 41 which describe ‘some framework, conceptualisation or planning scheme for the parts of the PSUE process’. Although their methodology for the systematic review was clear and appropriate, the methodology for the synthesis of the 41 frameworks was much less clear, and the 41 sources are not identified. Nonetheless, the synthesis led to a two-part framework: (1) the integral components of PSUE and (2) the phases and stages of PSUE in research. In terms of the integral components, the authors identify four essential components: patient and service user initiation, building reciprocal relationships, colearning, and reassessment and feedback. One of the methodological uncertainties about this framework is how the authors arrive at these four categories from the synthesis of the 41 papers, particularly as the four categories are based on 10, 30, 9 and 2 studies respectively. Without further methodological detail it would appear the ‘building reciprocal relationships’ has greater face validity based on 30 sources than ‘reassessment and feedback’ does with just two sources. The importance of building relationships between researchers and research partners is a recurring theme across the frameworks and models discussed above, as it was in our own research and theory building. Again, explicit discussion of PI or research leadership is conspicuous by its absence.
Allocating resources for involvement
In several of the case studies the lack of a formal budget for public involvement in their projects did not appear to be a significant determinant of the extent of their involvement activities or the impact these had on the research project. But it is possible that lack of a formal budget for public involvement impacted on the type of public involvement adopted within case studies and restricted these activities to less active forms. Case studies without a formal budget for public involvement tended to rely on occasional advisory groups to deliver public involvement in research, which is one of the more inexpensive ways to involve the public in research.
How then does our theorising around the allocation of resources for involvement relate to the wider public involvement literature? There has been little or no previous research on resource allocation for public involvement in research. None of the literature reviews or conceptual models discussed above has given more than cursory attention to resource allocation, budgeting or payment issues for public involvement; for example, Brett et al. 30 include ‘funding’ as one of the contextual factors to check when assessing whether the right conditions for public involvement are in place, but do not explore what this might mean in any further detail. Similarly, we have identified no specific primary papers on costing public involvement in research (although we did find one paper on measuring the costs of public participation in health and social care more generally). 22 Our case studies demonstrated a wide variety of approaches to budgeting for public involvement and in the hidden costs that our economic evaluation identified. What this research demonstrates is that resource allocation is an important but often poorly identified or understood element in the causal pathway leading to impact. The challenges of budgeting and payment for involvement is an area much discussed in the field and has been the focus of recent helpful MHRN/INVOLVE guidance on payment and budgeting, including the provision of a new online budgeting tool. 23
Assessing impact
Our starting point around assessing impact drew on the reviews by Staley11 and Brett et al. 12 Brett et al. 30 have subsequently updated their discussion of their review in their 2012 journal paper but their analysis of the state of the art remains substantially the same, that is, that the evidence base is still relatively weak and requires further substantive development. Our experience echoes this. An honest reflection on our case studies is that we did not capture as much evidence of impact as we had initially hoped. This may partly be a result of the limitations of our methodology, but may also simply reflect the reality of relatively limited impact of public involvement in our particular selection of case studies. On the latter point, our case studies were not, in practice, as diverse as we expected when we recruited them, with more adopting an advisory group model and less coresearch than we initially envisaged. We could report only on impacts which we could document or observe, and these were mainly related to improvements in recruitment materials and processes. In terms of methodology, in hindsight we realise that we probably sought funding for too short a period for data collection and did not sample sufficiently the early period of research design, when research partners are more likely to be able to influence design aspects such as research questions and outcomes to be measured. There were, however, institutional factors that militated against capturing impact on the early design stage, including the long lead time between negotiating case studies for inclusion in our funding application and the eventual commencement of our data collection, with related delays in research governance approvals.
Our study is intended as a contribution to a wider methodological debate on how best to capture the impact of public involvement in research, and indeed the extent to which impact can be measured in any robust and meaningful quantitative way,46 and the relative value of quantitative and qualitative assessment. This debate has been developing for over a decade with an early paper from Telford et al. 47 and recent papers by Barber et al. 48 and Wright et al. 49 Nilsen et al. 50 have also produced a relevant Cochrane review which assesses the effects of ‘consumer’ involvement in research as well as in health-care policy, clinical practice guidelines and patient information materials. The most recent contribution has been the Public Involvement Impact Assessment Framework (PiiAF) developed by Popay et al. through a MRC Methodology Research Programme grant. 51 The PiiAF was disseminated too recently to influence our study but potentially offers the most evidence-based and systematic framework yet available for assessing the impact of public involvement in research. There are also two other larger-scale NIHR HS&DR- or INVOLVE-funded studies (one also based on the principles of realist evaluation) with longer time scales which will report in the near future and contribute to this methodological debate.
More recent empirical studies on the impact of public involvement in research published subsequent to the Staley11 and Brett et al. 12 reviews give some possible avenues for future methodological development. For example, Ennis and Wykes used routine data from the MHRN database to identify positive correlations between levels of patient involvement and recruitment success. 52 Staley et al. also utilised the MHRN database to conduct a qualitative follow-up evaluation of impact in adopted studies. 34 The more that meaningful data on public involvement can be routinely built into such research databases, the easier it will be to conduct larger-scale studies of the impact of public involvement in research. Thus, for example, if data on resource allocation for public involvement were more systematically captured, then these data might be correlated with data on participant recruitment to test our theory on the link between resource allocation and outcome.
Models of public involvement and impact
In revising this report we were specifically asked by the reviewers and editors to say more on the impact of different models and mechanisms of involvement in the studies reviewed on research practice and outcome. This comment stimulated us to think about the different ways in which the term ‘model’ is used and the implications for assessing impact. In most of the literature reviewed earlier in this section, ‘model’ is used to describe a conceptual framework for making sense of the overall complexity of public involvement in research. But the term ‘model’ is also used here by the editors and reviewers to describe the particular form or type of public involvement, for example involvement through an advisory group or by coresearchers. In our eight case studies, there were four such forms of involvement: project-specific public advisory groups (four), individual research partners contributing to research teams (two), working with an existing service user group (one) and a long-term programme advisory panel (one). Each of these broad forms included context-specific aspects; thus one of the individual research partner forms was undertaken in a unit with a long-term history and culture of involvement whereas the other was in a research group with relatively little involvement experience. Similarly, some of the project advisory groups brought together members of the public who were not previously known to each other while others drew from a group of service attendees who knew each other but were not a pre-existing user group. In addition, we also had the opportunity to reflect on our own coresearcher type of involvement. Our analysis did not lead us to judge any one of these forms as more likely to lead to desired outcomes; our focus was on the key context and mechanism factors that we assessed as making a difference (e.g. PI leadership and nurturing relationships) which were relevant to all these forms of involvement and which can be applied to a greater or lesser degree in each and any form. The specific form of involvement adopted by any research team will be determined by a number of contextual factors (e.g. field of research, organisational base, type of study and type of study population).
Discussion conclusion
In this chapter we have drawn on our findings to present our revised theory of public involvement in research in the form of a realist conceptualisation of the links between CMO. We have identified a key contextual factor in terms of PI leadership which has not previously been highlighted in the literature. In terms of mechanism, we have identified the importance of resource allocation, and the significant undercosting of public involvement, in a way that has not been articulated in previous research. Furthermore, we have theorised a causal pathway from PI leadership to senior lead on involvement, allocation of resources and facilitation of research partners, leading to impacts on research design and delivery. This theory offers a more dynamic understanding of the links between CMO than other models of public involvement, which have not addressed the causal pathways between the factors they identify. However, this model is consistent with other models of public involvement in research and other recent empirical work, in particular the importance most other models place on nurturing relationships. Other models have variable evidence bases, and the sources of other models are not always explicit. It is rare for the authors of other models to compare their own with previous models, and the most recent attempt at a synthesis is lacking in methodological detail. 29 Other models, however, also include a number of elements which we have not considered in developing our theory and which are also plausible and consistent with the evidence. There may be other important dimensions omitted from our and other models; one of our steering group members raised the issue of the general lack of attention to equity and diversity issues in our and others’ work. Thus we accept that our theory is by no means comprehensive; rather it is a first attempt to develop a realist model of public involvement in research which we hope other researchers subsequently will build upon.
Chapter 9 Conclusions and recommendations for future research
How well have we achieved our original aim and objectives?
The initially stated overarching aim of this research was to identify the contextual factors and mechanisms that are regularly associated with effective and cost-effective public involvement in research. While recognising the limitations of our analysis, we believe we have largely achieved this in our revised theory of public involvement in research set out in Chapter 8. We have developed and tested this theory of public involvement in research in eight diverse case studies; this has highlighted important contextual factors, in particular PI leadership, which had not previously been prominent in the literature. We have identified how this critical contextual factor shapes key mechanisms of public involvement, including the identification of a senior lead for involvement, resource allocation for involvement and facilitation of research partners. These mechanisms then lead to specific outcomes in improving the quality of research, notably recruitment strategies and materials and data collection tools and methods. We have identified a ‘virtuous circle’ of feedback to research partners on their contribution leading to their improved confidence and motivation, which facilitates their continued contribution. Following feedback from the HS&DR Board on our original application we did not seek to assess the cost-effectiveness of different mechanisms of public involvement but we did cost the different types of public involvement as discussed in Chapter 7. A key finding is that many research projects undercost public involvement.
In our original proposal we emphasised our desire to include case studies involving young people and families with children in the research process. We recruited two studies involving parents of young children aged under 5 years, and two projects involving ‘older’ young people in the 18- to 25-years age group. We recognise that in doing this we missed studies involving children and young people aged under 18 years; in principle we would have liked to have included studies involving such children and young people, but, given the resources at our disposal and the additional resource, ethical and governance issues this would have entailed, we regretfully concluded that this would not be feasible for our study. In terms of the four studies with parental and young persons’ involvement that we did include, we have not done a separate analysis of their data, but the themes emerging from those case studies were consistent with our other case studies and contributed to our overall analysis.
In terms of the initial objectives, we successfully recruited the sample of eight diverse case studies and collected and analysed data from them (objective 1). As intended, we identified the outcomes of involvement from multiple stakeholders‘ perspectives, although we did not get as many research partners‘ perspectives as we would have liked – see limitations below (objective 2). It was more difficult than expected to track the impact of public involvement from project inception through to completion (objective 3), as all of our projects turned out to have longer time scales than our own. Even to track involvement over a stage of a case study research project proved difficult, as the research usually did not fall into neatly staged time periods and one study had no involvement activity over the study period.
Nevertheless, we were able to track seven of the eight case studies prospectively and in real time over time periods of up to 9 months, giving us an unusual window on involvement processes that have previously mainly been observed retrospectively. We were successful in comparing the contextual factors, mechanisms and outcomes associated with public involvement from different stakeholders‘ perspectives and costing the different mechanisms for public involvement (objective 4). We only partly achieved our final objective of undertaking a consensus exercise among stakeholders to assess the merits of the realist evaluation approach and our approach to the measurement and valuation of economic costs of public involvement in research (objective 5). A final consensus event was held, where very useful discussion and amendment of our theory of public involvement took place, and the economic approach was discussed and helpfully critiqued by participants. However, as our earlier discussions developed more fully than expected, we decided to let them continue rather than interrupt them in order to run the final exercise to assess the merits of the realist evaluation approach. We did, however, test our analysis with all our case study participants by sending a draft of this final report for comment. We received a number of helpful comments and corrections but no disagreement with our overall analysis.
What were the limitations of our study?
Realist evaluation is a relatively new approach and we recognise that there were a number of limitations to our study. We sought to follow the approach recommended by Pawson, but we acknowledge that we were not always able to do so. In particular, our theory of public involvement in research evolved over time and initially was not as tightly framed in terms of a testable hypothesis as Pawson recommends. In his latest book Pawson strongly recommends that outcomes should be measured with quantitative data,17 but we did not do so; we were not aware of the existence of quantitative data or tools that would enable us to collect such data to answer our research questions. Even in terms of qualitative data, we did not capture as much information on outcomes as we initially envisaged. There were several reasons for this. The most important was that capturing outcomes in public involvement is easier the more operational the focus of involvement, and more difficult the more strategic the involvement. Thus, it was relatively easy to see the impact of a patient panel on the redesign of a recruitment leaflet but harder to capture the impact of research partners in a multidisciplinary team discussion of research design.
We also found it was sometimes more difficult to engage research partners as participants in our research than researchers or research managers. On reflection this is not surprising. Research partners are generally motivated to take part in research relevant to their lived experience of a health condition or situation, whereas our research was quite detached from their lived experience; in addition people had many constraints on their time, so getting involved in our research as well as their own was likely to be a burden too far for some. Researchers clearly also face significant time pressures but they had a more direct interest in our research, as they are obliged to engage with public involvement to satisfy research funders such as the NIHR. Moreover, researchers were being paid by their employers for their time during interviews with us, while research partners were not paid by us and usually not paid by their research teams. Whatever the reasons, we had less response from research partners than researchers or research managers, particularly for the third round of data collection; thus we have fewer data on outcomes from research partners‘ perspectives and we need to be aware of a possible selection bias towards more engaged research partners. Such a bias could have implications for our findings; for example payment might have been a more important motivating factor for less engaged advisory group members.
There were a number of practical difficulties we encountered. One challenge was when to recruit the case studies. We recruited four of our eight case studies prior to the full application, but this was more than 1 year before our project started and 15 months or more before data collection began. In this intervening period, we found that the time scales of some of the case studies were no longer ideal for our project and we faced the choice of whether to continue with them, although this timing was not ideal, or seek at a late moment to recruit alternative ones. One of our case studies ultimately undertook no involvement activity over the study period, so we obtained fewer data from it, and it contributed relatively little to our analysis. Similarly, one of the four case studies we recruited later experienced some delays itself in beginning and so we had a more limited period for data collection than initially envisaged. Research governance approvals took much longer than expected, particularly as we had to take three of our research partners, who were going to collect data within NHS projects, through the research passport process, which essentially truncated our data collection period from 1 year to 9 months. Even if we had had the full year initially envisaged for data collection, our conclusion with hindsight was that this was insufficiently long. To compare initial plans and intentions for involvement with the reality of what actually happened required a longer time period than a year for most of our case studies.
In the light of the importance we have placed on the commitment of PIs, there is an issue of potential selection bias in the recruitment of our sample. As our sampling strategy explicitly involved a networking approach to PIs of projects where we thought some significant public involvement was taking place, we were likely (as we did) to recruit enthusiasts and, at worst, those non-committed who were at least open to the potential value of public involvement. There were, unsurprisingly, no highly sceptical PIs in our sample. We have no data therefore on how public involvement may work in research where the PI is sceptical but may feel compelled to undertake involvement because of funder requirements or other factors.
What would we do differently next time?
If we were to design this study again, there are a number of changes we would make. Most importantly we would go for a longer time period to be able to capture involvement through the whole research process from initial design through to dissemination. We would seek to recruit far more potential case studies in principle, so that we had greater choice of which to proceed with once our study began in earnest. We would include case studies from the application stage to capture the important early involvement of research partners in the initial design period. It might be preferable to research a smaller number of case studies, allowing a more in-depth ethnographic approach. Although challenging, it would be very informative to seek to sample sceptical PIs. This might require a brief screening exercise of a larger group of PIs on their attitudes to and experience of public involvement.
The economic evaluation was challenging in a number of ways, particularly in seeking to obtain completed resource logs from case study research partners. Having a 2-week data collection period was also problematic in a field such as public involvement, where activity may be very episodic and infrequent. Thus, collecting economic data alongside other case study data in a more integrated way, and particularly with interviews and more ethnographic observation of case study activities, might be advantageous. The new budgeting tool developed by INVOLVE and the MHRN may provide a useful resource for future economic evaluations. 23
We have learned much from the involvement of research partners in our research team and, although many aspects of our approach worked well, there are some things we would do differently in future. Even though we included substantial resources for research partner involvement in all aspects of our study, we underestimated how time-consuming such full involvement would be. We were perhaps overambitious in trying to ensure such full involvement with the number of research partners and the number and complexity of the case studies. We were also perhaps naive in expecting all the research partners to play the same role in the team; different research partners came with different experiences and skills, and, like most of our case studies, we might have been better to be less prescriptive and allow the roles to develop more organically within the project.
Implications for research practice and funding
If one of the objectives of R&D policy is to increase the extent and effectiveness of public involvement in research, then a key implication of this research is the importance of influencing PIs to value public involvement in research or to delegate to other senior colleagues in leading on involvement in their research. Training is unlikely to be the key mechanism here; senior researchers are much more likely to be influenced by peers or by their personal experience of the benefits of public involvement. Early career researchers may be shaped by training but again peer learning and culture may be more influential. For those researchers sceptical or agnostic about public involvement, the requirement of funders is a key factor that is likely to make them engage with the involvement agenda. Therefore, funders need to scrutinise the track record of research teams on public involvement to ascertain whether there is any evidence of commitment or leadership on involvement.
One of the findings of the economic analysis was that PIs have consistently underestimated the costs of public involvement in their grant applications. Clearly the field will benefit from the guidance and budgeting tool recently disseminated by MHRN and INVOLVE. It was also notable that there was a degree of variation in the real costs of public involvement and that effective involvement is not necessarily costly. Different models of involvement incur different costs and researchers need to be made aware of the costs and benefits of these different options.
One methodological lesson we learned was the impact that conducting this research had on some participants’ reflection on the impact of public involvement. Particularly for research staff, the questions we asked sometimes made them reflect upon what they were doing and change aspects of their approach to involvement. Thus, the more the NIHR and other funders can build reporting, audit and other forms of evaluation on the impact of public involvement directly into their processes with PIs, the more likely such questioning might stimulate similar reflection.
Recommendations for further research
There are a number of gaps in our knowledge around public involvement in research that follow from our findings, and would benefit from further research, including realist evaluation to extend and further test the theory we have developed here:
-
In-depth exploration of how PIs become committed to public involvement and how to influence agnostic or sceptical PIs would be very helpful. Further research might compare, for example, training with peer-influencing strategies in engendering PI commitment. Research could explore the leadership role of other research team members, including research partners, and how collective leadership might support effective public involvement.
-
More methodological work is needed on how to robustly capture the impact and outcomes of public involvement in research (building as well on the PiiAF work of Popay et al. 51), including further economic analysis and exploration of impact when research partners are integral to research teams.
-
Research to develop approaches and carry out a full cost–benefit analysis of public involvement in research would be beneficial. Although methodologically challenging, it would be very useful to conduct some longer-term studies which sought to quantify the impact of public involvement on such key indicators as participant recruitment and retention in clinical trials.
-
It would also be helpful to capture qualitatively the experiences and perspectives of research partners who have had mixed or negative experiences, since they may be less likely than enthusiasts to volunteer to participate in studies of involvement in research such as ours. Similarly, further research might explore the (relatively rare) experiences of marginalised and seldom-heard groups involved in research.
-
Payment for public involvement in research remains a contested issue with strongly held positions for and against; it would be helpful to further explore the value research partners and researchers place on payment and its effectiveness for enhancing involvement in and impact on research.
-
A final relatively narrow but important question that we identified after data collection had finished is: what is the impact of the long periods of relative non-involvement following initial periods of more intense involvement for research partners in some types of research, particularly clinical trials?
Acknowledgements
We would like to express our deepest thanks and gratitude to everyone who has contributed to this research including in particular all the participants in the case studies for this research, attendees at our consensus workshops and our steering group members (Alan Emond, Selena Gray, Tara Mistry, Kate Oliver, Sophie Staniszewska, Pat Taylor and Nicda Williams). Special thanks to Sarah Hewlett. We are grateful to Jo Brett and the UKCRC for permission to reproduce the material in Chapter 3, Box 2. We would also like to thank colleagues in NHS trust research governance departments and the County Durham and Tees Valley Research Ethics Committee who scrutinised and approved our research. Without their help this research could not have been completed. We are also very grateful for the comments from the editors and anonymous referees on our first draft. Needless to say they are not responsible for any errors or misinterpretations remaining in this report.
Contributions of authors
Professor David Evans (Professor in Health Services Research – Public Involvement) conducted study design and delivery including interviews and coding of interview transcripts, the analysis of the ‘leadership and culture’ section and production of the final report.
Professor Jane Coad (Professor in Children and Family Nursing) conducted study design and delivery including verification of coding of interview transcripts across the case studies and the analysis of the ‘field of research’ section.
Kiera Cottrell (research partner) conducted study design and delivery including interviews and coding of interview transcripts.
Dr Jane Dalrymple (lecturer) conducted study design and delivery including interviews and coding of interview transcripts, and the analysis of the ‘relationships’ section.
Rosemary Davies (research partner) conducted study design and delivery including interviews and coding of interview transcripts, the analysis of the ‘field of research’ section and the plain English summary.
Christine Donald (research partner) conducted study design and delivery including interviews.
Dr Vito Laterza (research fellow) co-ordinated and conducted study design and delivery including interviews and coding of interview transcripts.
Amy Long (research partner) conducted study design and delivery including interviews and coding of interview transcripts.
Dr Amanda Longley (Deputy Head of Research, Business and Innovation) conducted study design, delivery and analysis of the economic analysis section of the project.
Professor Pam Moule (Professor of Health Services Research – Service Evaluation) conducted study design and delivery including interviews and coding of interview transcripts, and analysis of the ‘outcomes’ section.
Dr Katherine Pollard (senior research fellow) conducted study design and delivery including interviews and coding of interview transcripts, and the analysis of the ‘structures of involvement’ section.
Professor Jane Powell (Professor of Public Health Economics) conducted study design, delivery and analysis of the economic analysis section of the project.
Anna Puddicombe (research associate) conducted study design and delivery including coding of interview transcripts, analysis of the ‘resources’ section and production of the final report.
Cathy Rice (research partner) conducted study design and delivery including interviews and coding of interview transcripts, analysis of the ‘reflections on our public involved’ section and proofreading of the final report.
Ruth Sayers (research partner) conducted study design and delivery including interviews and coding of interview transcripts, and contributed to the writing of the economic analysis and proofreading of the final report.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the HS&DR programme or the Department of Health.
References
- Research for Health. London: Her Majesty’s Stationery Office; 1993.
- INVOLVE . About INVOLVE 2012. www.invo.og.uk (accessed 30 September 2012).
- Oliver S, Buchanan P. Examples of Lay Involvement in Research and Development. London: EPI-Centre, Institute of Education; 1997.
- Cameron A, Salisbury C, Lart R, Stewart K, Peckham S, Calnan M, et al. Policy makers’ perceptions of the use of evidence from evaluations. Evid Policy 2011;7:429-47. http://dx.doi.org/10.1332/174426411X603443.
- Nutley S, Walter I, Davies H. Using Evidence: How Research Can Inform Public Service. Bristol: Policy Press; 2007.
- Crawford M, Rutter D, Manley C, Weaver, T, Kamaldeep B, Fulop N, et al. Systematic review of involving patients in the planning and development of health care. BMJ 2002;325. http://dx.doi.org/10.1136/bmj.325.7375.1263.
- Crawford M, Rutter D, Thelwell S. User Involvement in Change Management: A Review of the Literature. London: NCCSDO; 2003.
- Simpson E, House A. Involving users in the delivery and evaluation of mental health services: systematic review. BMJ 2002;325. http://dx.doi.org/10.1136/bmj.325.7375.1265.
- Daykin N, Evans D, Petsoulas C, Sayers A. The impact of patient and public involvement initiatives on UK health services: a literature review. Evid Policy 2007;3:47-65. http://dx.doi.org/10.1332/174426407779702201.
- Mockford C, Staniszewska S, Griffiths F, Herron-Marx S. The impact of patient and public involvement on UK NHS health care: a systematic review. Int J Qual Health Care 2011;24:28-3. http://dx.doi.org/10.1093/intqhc/mzr066.
- Staley K. Exploring Impact: Public Involvement in NHS, Public Health and Social Care Research. Eastleigh: INVOLVE; 2009.
- Brett J, Staniszewska S, Mockford C, Seers K, Herron-Marx S, Bayliss H. The PIRICOM Study: A Systematic Review of the Conceptualisation, Measurement, Impact and Outcomes of Patients and Public Involvement in Health and Social Care Research. London: UKCRC; 2010.
- Pawson R, Tilley N. Realistic Evaluation. London: Sage; 1997.
- Ward P, Thompson J, Barber R, Armitage C, Boote J, Cooper C, et al. Critical perspectives on ‘consumer involvement’ in health research: Epistemological dissonance and the know–do gap. J Sociol 2009;46:63-82. http://dx.doi.org/10.1177/1440783309351771.
- Background Notes for Applicants: HS&DR/INVOLVE Joint Funding Call: Public Involvement in Research. Southampton: University of Southampton; 2010.
- Pawson R. Evidence-Based Policy: A Realist Perspective. London: Sage; 2006.
- Pawson R. The Science of Evaluation. London: Sage; 2013.
- Greenhalgh T, Humphrey C, Hughes J, MacFarlane F, Butler C, Pawson R. How do you modernise a health service? A realist evaluation of whole-system transformation in London. Milbank Q 2009;87:391-416. http://dx.doi.org/10.1111/j.1468-0009.2009.00562.x.
- Marchal B, Dedzo M, Kegels G. A realist evaluation of a well-performing regional hospital in Ghana. BMC Health Serv Res 2010;10. http://dx.doi.org/10.1186/1472-6963-10-24.
- Staley K, Buckland S, Hayes H, Tarpey M. ‘The missing links’: understanding how context and mechanism influence the impact of public involvement in research. Health Expect 2012. http://dx.doi.org/10.1111/hex.12017.
- Evans D, Booker S, Daykin N, Powell J, Taylor P, Weil S. National Evaluation of Patient Advice and Liaison Services (PALS): Final Report. Bristol: UWE; 2008.
- El Ansari W, Andersson E. Beyond value? Measuring the costs and benefits of public participation. Journal of Integrated Care 2011;19:45-57. http://dx.doi.org/10.1108/14769011111191467.
- Budgetting for Involvement: Practical Advice on Budgeting for Activity Involving the Public in Research Studies. London and Eastleigh: Mental Health Research Network and INVOLVE; 2013.
- Ritchie J, Spencer L, Bryman A, Burgess R. Analyzing Qualitative Data. London: Routledge; 1994.
- Payment for Involvement: A Guide for Making Payments to Members of the Public Actively Involved in NHS, Public Health and Social Care Research. Eastleigh: INVOLVE; 2010.
- Thompson J, Bissell P, Cooper C, Armitage C, Barber R. Credibility and the ‘professionalized’ lay expert: Reflections on the dilemmas and opportunities of public involvement in health research. Health 2012;16:602-18. http://dx.doi.org/10.1177/1363459312441008.
- Gillard S, Borschmann R, Turner K, Goodrich-Purnell N, Lovell K, Chambers M. ‘What difference does it make?’ Finding evidence of the impact of mental health service user researchers on research into the experiences of detained psychiatric patients. Health Expect 2010;13:185-94. http://dx.doi.org/10.1111/j.1369-7625.2010.00596.x.
- Hamilton S, Pinfold V, Rose D, Henderson C, Lewis-Holmes E, Flach C, et al. The effect of disclosure of mental illness by interviewers on reports of discrimination experienced by service users: a randomised study. Int Rev Psychiatry 2011;23:47-54. http://dx.doi.org/10.3109/09540261.2010.545367.
- Shippee N, Domecq Garces JP, Prutsky Lopez G, Wang Z, Elraiyah T, Nabhan M, et al. Patient and service user engagement in research: a systematic review and synthesized framework. Health Expect 2013. http://dx.doi.org/10.1111/hex.12090.
- Brett J, Staniszewska S, Mockford C, Herron-Marx S, Hughes J, Tysall C, et al. Mapping the impact of patient and public involvement on health and social care research: a systematic review. Health Expect 2012. http://dx.doi.org/10.1111/j.1369-7625.2012.00795.x.
- Boote J, Wong R, Booth A. ‘Talking the talk or walking the walk?’ A bibliometric review of the literature on public involvement in health research published between 1995 and 2009. Health Expect 2012. http://dx.doi.org/10.1111/hex.12007.
- Morrow E, Ross F, Grocott P, Bennett J. A model and measure for quality service user involvement in health research. Int J Consum Stud 2010;34:532-9. http://dx.doi.org/10.1111/j.1470-6431.2010.00901.x.
- Tritter J. Revolution or evolution: the challenges of conceptualising patient and public involvement in a consumerist world. Health Expect 2009;12:275-87. http://dx.doi.org/10.1111/j.1369-7625.2009.00564.x.
- Staley K, Kabir T, Szmukler G. Service users as collaborators in mental health research: less stick, more carrot. Psychol Med 2013;43:1121-5. http://dx.doi.org/10.1017/S0033291712001663.
- Thompson J, Barber R, Ward P, Boote J, Cooper C, Armitage C, et al. Health researchers’ attitudes towards public involvement in health research. Health Expect 2009;12:209-20. http://dx.doi.org/10.1111/j.1369-7625.2009.00532.x.
- Martin G, Learmonth M. A critical account of the rise and spread of ‘leadership’: the case of UK healthcare. Soc Sci Med 2012;74:281-8. http://dx.doi.org/10.1016/j.socscimed.2010.12.002.
- Faulkner A. Changing Our Worlds: Examples of User-Controlled Research in Action. Eastleigh: INVOLVE; 2010.
- Barnes M, Newman J, Knops A, Sullivan H. Constituting ‘the public’ in public participation. Public Administration 2003;81:379-99. http://dx.doi.org/10.1111/1467-9299.00352.
- Woodard F, Bovill L, Freedman D, Greenhalgh T, Humphrey C, Woodard F. User Involvement in Health Care. Chichester: Wiley-Blackwell; 2011.
- Gilbert D, Doughty M. Patient leaders: taking the revolution one hurdle at a time. Health Serv J 2013;123:29-31.
- Oliver S, Rees R, Clarke-Jones L, Milne R, Oakley A, Gabbay J, et al. A multidimensional conceptual framework for analysing public involvement in health services research. Health Expect 2008;11:72-84. http://dx.doi.org/10.1111/j.1369-7625.2007.00476.x.
- Robinson L, Newton J, Dawson P. Professionals and the public: power or partnership in health research?. J Eval Clin Pract 2010;18:276-82. http://dx.doi.org/10.1111/j.1365-2753.2010.01572.x.
- Arnstein S. A ladder of citizen participation. J Am Inst Plann 1969;35:216-24. http://dx.doi.org/10.1080/01944366908977225.
- Mullen P. Public involvement in health care priority setting: an overview of methods for eliciting values. Health Expect 1999;2:222-34. http://dx.doi.org/10.1046/j.1369-6513.1999.00062.x.
- Stewart R, Liabo K. Involvement in research without compromising research quality. J Health Serv Res Policy 2012;17:248-51. http://dx.doi.org/10.1258/jhsrp.2012.011086.
- Staniszewska S, Adebajo A, Barber R, Beresford P, Brady L-M, Brett J, et al. Developing the evidence base of patient and public involvement in health and social care research: the case for measuring impact. Int J Consum Stud 2011;35:628-32. http://dx.doi.org/10.1111/j.1470-6431.2011.01020.x.
- Telford R, Boote J, Cooper C. What does it mean to involve consumers successfully in NHS research? A consensus study. Health Expect 2004;7:209-20. http://dx.doi.org/10.1111/j.1369-7625.2004.00278.x.
- Barber R, Boote J, Parry G, Cooper C, Yeeles P, Cook S. Can the impact of public involvement in research be evaluated? A mixed methods study. Health Expect 2012;15:229-41. http://dx.doi.org/10.1111/j.1369-7625.2010.00660.x.
- Wright D, Foster C, Amir Z, Elliot J, Wilson R. Critical appraisal guidelines for assessing the quality and impact of user involvement in research. Health Expect 2010;13:359-68. http://dx.doi.org/10.1111/j.1369-7625.2010.00607.x.
- Nilsen E, Myrhaug H, Johansen M, Oliver S, Oxman A. Methods of consumer involvement in developing healthcare policy and research, clinical practice guidelines and patient information material. Cochrane Database Syst Rev 2006;3. http://dx.doi.org/10.1002/14651858.CD004563.pub2.
- Popay J, Collins M. PiiAF: The Public Involvement Impact Assessment Framework Guiance. Lancaster: University of Lancaster; 2014.
- Ennis L, Wykes T. Impact of patient involvement in mental health research: longitudinal study. Br J Psychiatry 2013;203:381-6. http://dx.doi.org/10.1192/bjp.bp.112.119818.
- Salary Costings August 2011 payround. Bristol: University of the West of England; 2012.
- NHS . NHS Payscales 2012 n.d. http://www.nhscareers.nhs.uk/working-in-the-nhs/pay-and-benefits/agenda-for-change-pay-rates/ (accessed 8 January 2013).
Appendix 1 Sample daily log sheet for research partners
Appendix 2 Guidance for research partners to complete resource logs
Appendix 3 Cost-pricing assumptions for researchers’ time
-
Salary costing for research staff is based on the ‘Salary costing August 2011 payround’ amended and National Insurance updated on 1 May 2012. 53 The exception is case study 4, where NHS Band 8a Manager was used. 54
-
Academic salary grades: table for period commencing 1 August 2012. Mid-point of scale used wherever possible, hourly rate based on 1650 hours per annum. 21
-
Research salary grades: table for period commencing 1 August 2012. Mid-point of scale used wherever possible, hourly rate based on 1650 hours per annum. 21
-
Administrative, professional, technical and clerical salary grades: table for period commencing 1 August 2012. Mid-point of scale used wherever possible, hourly rate based on 1650 hours per annum. 21
-
UWE PhD bursary stipend = £13,590 for 2012/13. Full-time = 1650 hours per annum. Hourly rate = £8.24.
Appendix 4 Assumptions made for case study projections from information gained during data collection
Case study 1
Public involvement activity included representation on various study committees, for example a stakeholder reference group, as well as a stakeholder event due to be delivered towards the end of the project.
Case study 2
The funded grant application did not include a separate costing for public involvement, but a stakeholder time and travel budget of £27,000 was included to cover all costs for both public and stakeholder participation in this research. Of this, £7000 was allocated for public involvement activity over a 3-year study period: £2000 per year, plus £1000 contingency.
Case study 3
Public involvement was not a separate costing item in the funded grant proposal, so any costs associated with involvement would have been taken from the general project budget.
Case study 4
Public involvement-related activity was not costed separately in the grant application, so any costs associated with involvement were taken out of the general project budget. During the interview, the researcher estimated that there would be approximately 1 month of her time devoted to public involvement activity over the 5-year research programme. We were able to put a value on this person’s time using an hourly wage rate in order to calculate the amount of input used. The total research project costs associated with facilitating public involvement in research were £3616; this did not include reimbursement of travel costs/refreshment costs and so forth.
Case study 5
£22,200, around 5% of the total grant, was budgeted for PPI. A devolved model of public involvement was applied, whereby the lead organisation had a service level agreement with four service user organisations across England. We have collected resource data from one of the service user organisations, £3000, and have made the assumption that the other three organisations will have similar resource inputs: £12,000 in total. A further service level agreement has been written between the lead organisation and the service user organisation up until the end of the project. Two further national advisory meetings are planned = £4464. In addition, there have been two previous national advisory meetings prior to November 2011 at a cost of £4464. Total project costs = £41,391.
Case study 6
The total grant awarded was nearly $180,000 over a 2-year study period. Public involvement-related activity was not separately included, but a travel budget of nearly $33,000 and living expenses of $6900 were included for both project researchers and patient experts to attend international project meetings. We can estimate that of this amount approximately $11,900 was for travel and $3500 for living expenses of four or five patient experts to attend project meetings in Europe and North America. Given this reasoning and assumptions the public involvement budget is approximately $15,345 (around 8.5% of the total grant).
Case study 7
The total value of the award is approximately £248,000, with a budget for public involvement of £2970 (around 1.2% of the total grant) for patient partner travel and advisory group meetings including provision for light lunches and study participants‘ travel expenses.
Case study 8
This is an ongoing programme grant, which primarily maintains a cohort of individuals and their data. These individuals form a public involvement panel that can be accessed by researchers as required.
Appendix 5 Detailed assumptions corresponding with letters in Tables 5 and 6
A. The research project estimated that costs associated with facilitating public involvement in research over a 2-week snapshot period were £1668.
B. The research team were unable to identify a research partner that could be given a resource diary – costs for participating in research activity over a 2-week snapshot period are unknown.
C. We were able to put a value on time for six researchers using an hourly wage rate in order to calculate the amount of input used. In addition, refreshment costs, travel costs and reimbursement for research partners were recorded in the resource log. The research project estimated that costs associated with facilitating public involvement in research over a 2-week snapshot period were £1502.
D. A flat rate of £19.40 per hour was applied (INVOLVE, 2010). 25 The research partner estimated that costs for participating in research activity over a 2-week period were £121. The main costs associated with PPI activity by the research partner were the person’s own time and travel costs to/from meetings. The respondent noted that ‘relatively speaking this has been an active 2 weeks. In a typical 2-week period between the parent panel meetings I’d do very little/no work on this.’
E. C + D = £1623.
F. We were able to put a value on time for three researchers using an hourly wage rate in order to calculate the amount of input used. In addition, refreshment costs, travel costs and reimbursement for research partners were recorded in the resource log. The research project estimated that costs associated with facilitating public involvement in research over a 2-week snapshot period were £136.13.
G. One resource diary was completed by a representative from the service user organisation who noted that there was no PPI activity during the 2-week snapshot period.
H. F + G = £136.13.
I. The research project estimated that costs associated with facilitating public involvement in research over a 2-week snapshot period were £336.48.
J. The research partner noted that there was very little activity over the 2-week snapshot period. A flat rate of £19.40 per hour was applied (INVOLVE, 2010). 25 The research partner estimated that costs for participating in research activity over a 2-week snapshot period were £16.
K. The total estimated costs associated with facilitating public involvement in research over a 2-week snapshot period were £352.48.
L. We were able to put a value on time for seven research team members using an hourly wage rate in order to calculate the amount of input used. In addition, refreshment costs and paper costs were recorded in the resource log. The research project estimated that costs associated with facilitating public involvement in research over a 2-week snapshot period were £4494.
M. Advisory meetings: research project projected costs = £899.92; research partners projected costs (n = 4) = £484; total projected costs = £1383.92.
N. Projected 12-month costs: research project projected costs = £6077.05; research partner projected costs = £3019.95; total projected costs = £9097.
O. During the 2-week snapshot for PPI, there had been no parent advisory group meeting – the main form of PPI in this case study. Therefore there were zero costs for both the research project and the research partners. However, we were able to obtain data on research project costs associated with facilitating public involvement in research through the group meeting for the research project (£139.83) and the direct costs for hosting/facilitating an advisory group meeting (£90) for the organisation representing the research partners. Total estimated costs for associated with facilitating one parent advisory group meeting were £229.83.
P. Assumption that there were three group meetings in a 12-month period: £229.83 × 3 = £689.49.
Q. The researcher noted that there had been no PPI activity in the project during 2012, so zero costs were recorded for both the research project and the research partners during the 2-week snapshot period. However, we were able to value the amount of PPI activity undertaken so far in the project based on 21 hours of the researcher’s time plus refreshments for meeting = £467.26. Similarly, the researcher thought that there would be around 1 month of her time devoted to public involvement activity during the 5-year research programme. Once again, we were able to put a value on this person’s time using an hourly wage rate in order to calculate the amount of input used. The total projected research project costs associated with public involvement activity = £3615.67.
R. The National Advisory Meetings were held in London. Two representatives from each of the four service user organisations attended these meetings. Travel arrangements were made in advance by the research team in agreement with local service user representatives.
We have made an assumption that service users based outside London will travel by economy train to London King’s Cross, leaving around 08.00 from the station of origin to London and returning after 18.00 from London to the station of origin. Train fares are based on the cheapest available direct route (March 2013 prices).
In addition, local representatives get a flat rate of £100 for attending the national meetings, and subsistence allowance for breakfast, morning coffee, lunch, tea and evening meal.
We have been able to put a value on each of these resource inputs and can therefore estimate the total cost of bringing service user representatives (n = 8) to one national advisory group meeting in London at around £2231.80.
S. Devolved model – we have made the assumption that each of the four service user organisations have been allocated the same amount of resources to undertake public involvement activity over a 12-month period, so we were able to calculate the total projected costs for a 12-month period, which included two national advisory group meetings. Total = £20,464.
Projected total costs for the duration of the project were also estimated. Again we have made the assumption that each of the four service user organisations has been allocated the same amount of resources to undertake public involvement activity over the study period, and that there were six national advisory group meetings. Total = £41,391.
T. Although there was no PPI activity during the 2-week snapshot period, the PhD student had kept a record of all the face-to-face contact with the two research partners associated with her research project. Therefore, we were able to estimate public involvement in research costs over a 12-month period = £476.35; and for the research project to date (22 months) = £873.30.
U. This project team primarily maintains a cohort of individuals and their data, which can then be accessed by other researchers working on specific research projects. The proposed budget for the next 3 years is £91,380. This is primarily allocated to the ‘participation team’ in the project for recruitment and retention of the cohort of individuals and not just for PPI.
Appendix 6 Coding framework
| Number | Coding framework | |
|---|---|---|
| Code | Description | |
| Theme A: relationships | ||
| 1 | Trust | There is evidence of trust between academics and research partners involved in the project and/or extracts where interviewees explicitly talk about trust (positively or negatively) |
| 2 | Feedback to research partners | Extracts where interviewees discuss anything to do with academics giving feedback to research partners about the impact of their involvement, how well it works (if at all), problems, challenges, and successful cases |
| 3 | Feeling valued | The extent to which research partners feel valued and/or appreciated by the academics in their team. This includes negative feelings, i.e. not feeling valued |
| 4 | Inclusion | The extent to which research partners feel included and/or integrated into the research team (this includes negative feelings, i.e. not feeling included) and/or discussions and references to team building |
| 5 | Interpersonal relationships | Extracts where interviewees discuss the nature, extent, history and/or quality of interpersonal relationships between academics and research partners and/or extracts about how these relationships evolve and change through time and/or extracts indicating specific dynamics between the formal structures of the project and the informal interpersonal relationships between academics and research partners |
| 6 | Power | Extracts where interviewees discuss issues relating to power, equality, inequality, and hierarchy, especially in the relationships between research partners and academics |
| 7 | Relationships (other) | Anything researchers coding the interviews find absolutely crucial about this theme and that does not fit in any of the previous codes |
| Theme B: leadership and culture | ||
| 8 | Principal investigator belief | The PI demonstrates their personal belief in and commitment to PPI by the actions they take including ensuring adequate resources and/or strong leadership in PPI by the PI by example and/or seniority does not matter and PI is open and approachable in relationships with research partners |
| 9 | Senior lead on PPI | Where a senior member of the research team (but not the PI) has designated responsibility to lead on PPI within the project |
| 10 | Culture and history of PPI in institution | There is evidence of a history/culture of PPI in the unit or wider institution that predates the specific research project |
| 11 | Values | Specific values and principles driving PPI and/or awareness of values and principles driving PPI in the team |
| 12 | Organisational vs. team culture | The extent to which there is a tension (or a match) between the team culture and the wider organisational culture |
| 13 | Leadership and culture (other) | Anything researchers coding the interviews find absolutely crucial about this theme and that doesn’t fit in any of the previous codes |
| Theme C: field of research and understanding of research by research partners | ||
| 14 | Field of research | Indication of field of research of academics and/or institutions and/or funders involved in the case study and/or funding call under which the case study has been funded |
| 15 | Understanding of research by research partners | The extent to which research partners understand the research they are involved in. Areas they feel comfortable with. Areas they struggle with |
| 16 | Mechanisms to increase understanding of research | Formal and informal activities carried out in the case study to equip research partners with an adequate/better understanding of the research |
| 17 | Fit between type of involvement and field of research | Cases where there is close fit between the type of involvement and the field of research of the case study |
| 18 | Limits | Limits and constraints posed by the field of research of the case study on the type and quality of involvement activities |
| 19 | Understanding of research (other) | Anything researchers coding the interviews find absolutely crucial about this theme and that does not fit in any of the previous codes |
| Theme D: structures of involvement | ||
| 20 | Type of involvement | Type of involvement activities (team meetings, research partners’ panels, data collection activities, etc.) |
| 21 | Host institution structures | Structures of involvement of the host institution of the case study (i.e. independent from the case study structures of involvement) |
| 22 | PPI facilitation | A team member is identified who effectively facilitates public involvement in the research and/or presence and importance (if any) of individuals external to the team acting as gatekeepers mediating the relationship between academics and research partners |
| 23 | Practices, systems and structures of PPI | The extent to which there are practices, systems and structures of PPI within the research team/unit and whether these are being used |
| 24 | Involvement throughout | There is evidence of the public being involved from the very beginning of the project (or even before the beginning) through to the current stage/final dissemination stage of the project and/or lack of involvement throughout or limited involvement |
| 25 | Previous experience of involvement | Previous experience of involvement of principal investigators, academics, clinical researchers, participation or programme managers, and members of the public. Specific references to these experiences |
| 26 | Structures of involvement (other) | Anything researchers coding the interviews find absolutely crucial about this theme and that does not fit in any of the previous codes |
| Theme E: resources | ||
| 27 | Budget for involvement | Whether there is a specific and explicit budget for involvement including facilitation costs, payment, expenses, training, conference attendance, etc. |
| 28 | Training and support | Where members of the public involved have been offered and/or provided with training, mentoring, facilitation and/or other forms of support |
| 29 | Defined roles | A clear shared understanding between researchers and the members of public involved of the role and contribution of the members of the public in the research and/or lack of clearly defined roles |
| 30 | Practical aspects | Factors such as pleasant rooms for meetings, timing and frequency of meetings, refreshments, written information in advance, access to equipment, etc. |
| 31 | Reward | All the different ways in which the public involved may be rewarded including payment, expenses, acknowledgement, thanks, co-authorship, feedback, etc. and/or the extent to which academics on the team show altruism and a sharing attitude towards research partners |
| 32 | Resources (other) | Anything researchers coding the interviews find absolutely crucial about this theme and that does not fit in any of the previous codes |
| Theme F: actual and intended outcomes | ||
| 33 | Research design | Where the involvement of members of the public has impacted on research design including the overall choice of research methods, questions to be asked, outcomes to be measured, etc. (including intended and/or negative outcomes) |
| 34 | Research delivery | Where the involvement of members of the public has impacted on the delivery or implementation of the research including the recruitment of participants, the wording of information sheets, questionnaires and other documents, etc. (including intended and/or negative outcomes) |
| 35 | Impact on public involved | Where the involvement of members of the public has impacted on themselves including new skills and knowledge, personal development, support and friendship, enjoyment and satisfaction, etc. (including intended and/or negative outcomes) |
| 36 | Impact on academic researchers | Where the involvement of members of the public has impacted on academic researchers including new skills and knowledge, personal development, different ways of carrying out research, support and friendship, enjoyment and satisfaction, etc. (including intended and/or negative outcomes) |
| 37 | Strategic impact | Where the involvement of members of the public has impacted beyond the specific research project or programme on the wider approach to involvement in the unit or institution (including intended and/or negative outcomes) |
| 38 | Outcomes (other) | Anything researchers coding the interviews find absolutely crucial about this theme and that does not fit in any of the previous codes |
Glossary
- Delphi technique
- A method of building consensus among a pre-selected group of participants through a series of questionnaires with multiple iterations of statements and group responses.
- INVOLVE
- National Institute for Health Research advisory group on public involvement in research.
List of abbreviations
- BSI
- bloodstream infection
- CMO
- context, mechanism and outcome
- CV
- curriculum vitae
- HS&DR
- Health Services and Delivery Research programme
- ITU
- intensive therapy unit
- MHRN
- Mental Health Research Network
- MRC
- Medical Research Council
- NIHR
- National Institute for Health Research
- PhD
- doctor of philosophy
- PI
- principal investigator
- PiiAF
- Public Involvement Impact Assessment Framework
- PPI
- patient and public involvement
- PSUE
- patient and service user engagement
- R&D
- research and development
- RA
- rheumatoid arthritis
- RCT
- randomised controlled trial
- SLT
- speech and language therapy
- SUCIR
- Service User and Carer Involvement in Research group at UWE
- UWE
- University of the West of England