
Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 09/3001/09. The contractual start date was in March 2010. The final report began editorial review in January 2012 and was accepted for publication in January 2013. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors' report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors:
none
Permissions
Copyright statement
© Queen's Printer and Controller of HMSO 2013. This work was produced by Crombie et al. under the terms of a commissioning contract issued by the Secretary of State for Health. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
Chapter 1 Structure of the report
Introduction
This study assessed the feasibility of a randomised controlled trial to determine the impact of a novel intervention delivered by text message on drinking behaviour among disadvantaged young to middle-aged men. This was achieved by carrying out all of the stages of a pragmatic randomised controlled trial, with a particular focus on how well each stage was conducted. The aim of this close scrutiny was to identify whether or not a full trial would succeed and what improvements could be made to the conduct and likely effectiveness of the trial. The study was conducted in three phases.
Phase 1 comprised six focus groups to develop the recruitment strategy, to optimise the design of the text messages and images and to determine the most acceptable sequence for their delivery. Five focus groups were conducted with men and one focus group with women. The focus groups explored drinking behaviour and attitudes and beliefs about drinking, its benefits and harms. The findings from this phase were also used to help develop the intervention.
Phase 2 involved the planned recruitment of 60 participants who were randomised to receive either the alcohol intervention or general health promotion messages. This phase was conducted in a series of distinct steps. As the target group was disadvantaged young to middle-aged men, recruitment to the study was given careful attention. The intervention was a series of interactive text messages and images designed using messaging theory, social cognition models, motivational interviewing (MI) and systematic reviews of interventions to tackle alcohol problems. The intervention was delivered to mobile telephones using a programmed computer system. Participants were followed up for 3 months to assess retention, willingness to respond to text messages and to complete the final assessment of drinking behaviour. The aim of this assessment was to determine whether or not the outcomes could be readily measured on the participants. Although the feasibility study was not powered to detect changes in drinking behaviour, it could give an indication of whether or not the intervention might be effective in a full trial.
Phase 3 involved interviews with 20 participants to assess the acceptability of the intervention, the impact it had on their willingness to moderate their drinking and factors that might limit their ability to drink less. The aim was to assess the acceptability of all aspects of the study and to identify opportunities to improve the intervention.
The chapters of the report
This report is laid out as a series of 12 chapters which provide a forensic analysis of the design, conduct and outcome of the feasibility study. Chapter 2 begins with an outline of the research objectives of the feasibility study. Chapter 3 identifies the motivation for the study and then explores the main design challenges which needed to be addressed. This is followed by eight chapters which provide a description of the series of interlinked substudies which were conducted to meet the aims of the feasibility study. Each chapter is self-contained, comprising an introduction, methods and results sections, together with a discussion which summarises the main findings and assesses their significance in the light of previous research. This approach is appropriate because each substudy had a distinct purpose and a specific set of methods. Combining methods or discussion sections into single chapters would lose the close relationship between methods, results and discussion which is essential for a full forensic evaluation. The individual substudies are:
-
Chapter 4 , Understanding drinking motives and behaviours
-
Chapter 5 , Developing the text messages
-
Chapter 6 , Recruitment strategies
-
Chapter 7 , Randomisation and baseline characteristics
-
Chapter 8 , Retention strategy
-
Chapter 9 , Outcome assessment
-
Chapter 10 , Process evaluation
-
Chapter 11 , Post-trial assessment.
Chapter 12, Summary and conclusions, has three linked aims. It presents a concise synthesis of the main findings from the whole feasibility study, together with their implications for future research. It then assesses the extent to which the feasibility study met its aims. Finally, it makes recommendations for modifications to the protocol which will improve the conduct and outcome of the proposed full trial.
Chapter 2 Research objectives
Introduction
The overall objective of this feasibility study was to develop and test the feasibility of an intervention delivered by text messages to reduce the frequency of heavy drinking among young to middle-aged disadvantaged men. This involved conducting all the stages of a randomised controlled trial. The intervention has been developed from brief interventions that have been successful when delivered face to face, but is delivered by a series of text messages and images. This provides a method for reaching large numbers of people at low cost. If the development and feasibility testing are successful, the intervention will be tested in a full-scale randomised controlled trial in a further study for which new funding will be sought.
Research questions of the full-scale trial of the novel intervention
Prior to the feasibility study it was thought that the research questions for the full trial would focus on the effectiveness of the intervention, and on the behavioural antecedents of reduced heavy drinking. Specifically it would investigate whether or not a brief intervention delivered by mobile telephone could:
-
reduce the frequency of heavy drinking by disadvantaged men
-
increase awareness of the harms of excessive drinking
-
increase intentions to avoid becoming drunk
-
increase self-efficacy for refusing drinks.
These questions were to be reassessed in the light of the findings of this feasibility study.
Research questions of the feasibility study
The feasibility study was concerned with the practical issues of recruitment and intervention development and delivery. Successful completion of all these stages is a prerequisite for a full trial of a complex intervention to reduce the frequency of heavy drinking among young to middle-aged disadvantaged men. The specific questions were:
-
What are the best ways to recruit and retain disadvantaged men in a study aimed at reducing the frequency of heavy drinking?
-
What is the type of content and timing of the delivery of a series of text messages and images that is most likely to engage young to middle-aged men?
-
Is the intervention likely to be an acceptable way to influence the frequency of heavy drinking?
Ethical approval
Ethical approval for all aspects of the study was obtained from the East of Scotland Research Ethics Service (reference number 09/S1401/78).
User group representatives
Two men, one a reformed heavy drinker, the other a continuing heavy drinker, were recruited to the Research Group. They attended steering group meetings, where they shared their views on drinking cultures, and the attitudes, beliefs and experiences of drinkers. They were the first to raise two important issues: the prevalence of very heavy binge drinking and the fact that many drinkers in the target age range, 25–44 years, will have suffered, or know someone who has suffered, serious harm from alcohol. They also advised on the construction of the intervention text messages and stressed the importance of phrasing texts in appropriate language. This helped ensure that the interventions were acceptable and the outcomes were relevant and measurable.
Protocol amendments
The intended sample size was exceeded (67 participants instead of 60). This occurred in recruitment of participants through primary care. Invitation letters were sent out in batches and all men who were eligible and willing to take part were included in the study. Recruitment from the final batches of letters led to more men being recruited than intended.
The intervention was modified in the light of findings from the focus groups. MI was added because it provided a convenient technique for presenting components of the intervention. The transtheoretical model (TTM) was added to the intervention design because it offered a logical framework for designing and sequencing of messages. This approach was appropriate because it was anticipated that most participants would be in the pre-contemplation stage.
The number of text messages which was sent was increased from the proposed 28 to 36 for two reasons: (1) texts were inserted which asked participants to respond to specific questions that probed key components of the behaviour change strategy; and (2) some messages were sent in pairs, with the second one sent a few minutes after the first. These devices promoted increased thinking time, a technique used in MI.
The protocol proposed that a post-trial evaluation be conducted to identify ways to improve the study. This was expanded to include an extensive process evaluation of the fidelity of delivery of the intervention. It also assessed the extent of engagement of the study participants with the main behaviour change components of the intervention. The aim of these evaluations was to provide a series of detailed recommendations to improve the acceptability and impact of the intervention.
Chapter 3 Introduction
The morbidity and mortality caused by alcohol are a major public health challenge. The prevalence of alcohol misuse and its cost to society has risen substantially over the last 20 years. 1 It is currently estimated at more than £55B per year in England1 and more than £3.5B per year in Scotland. 2 These costs occur through lost productivity, increased health-care and other public sector costs, and through crime and social disruption. In 2009–10, there were over 1 million hospital admissions in England for alcohol-related conditions. 3 These figures included 177,400 admissions for mental and behavioural disorders and 43,100 for liver disease which were solely due to alcohol. A total of 6584 deaths were due to alcohol, of which two-thirds were due to liver disease. The cost of alcohol to the NHS in England is £2.7B (at 2006–7 prices). The major costs of alcohol to society come from social disruption, crime and costs to the economy. Alcohol was associated with more than 500,000 crimes in England in 2006–7. It was a contributory factor in up to 1 million assaults and 125,000 instances of domestic violence. 4 Some 17 million working days are lost each year because of drinking.
Alcohol-related harms are not evenly distributed in the population. People who are socially disadvantaged are at a substantially higher risk of developing alcohol-related diseases. 5,6 Tackling the culture of drinking among this group in order to prevent alcohol-related problems in later life is a priority for research. This introduction reviews the main issues to be addressed for the design and delivery of a brief alcohol intervention to disadvantaged young to middle-aged men.
Alcohol and brief interventions
Extensive evidence shows that brief interventions delivered in health-care settings are effective in reducing alcohol consumption. 7–10 These interventions were developed for middle-aged and older men attending health care. However, the group who binge drink most frequently are young to middle-aged disadvantaged men. 11 Existing brief intervention studies mainly recruit through health-care settings. However, men aged 25–44 years are seldom in contact with health services. They will therefore not be reached by current initiatives to tackle excessive drinking delivered through health-care settings, so alternative approaches are needed. Targeting this group would lead to reductions in heavy drinking before chronic health harms develop. It would also prevent the accidents, violence, social disruption and criminal activities associated with episodes of heavy drinking. This group may be receptive to brief interventions; one recent survey reported that among current drinkers, 32% of men aged 25–44 years felt the need to cut down on their drinking. 11 Thus, there is a need to develop brief interventions which are appropriate for disadvantaged young men.
Brief interventions are commonly based on models from social psychology, such as the theory of planned behaviour (TPB). 12 Many of the interventions use MI,13,14 a person-centred technique which encourages individuals to identify possible inconsistencies between what they do (get drunk) and what they want to achieve (socialise, find a partner). Recent reviews have identified theoretical constructs and specific behaviour change techniques which should form part of behaviour change interventions. 15,16
A further requirement for brief interventions is to reach large numbers of individuals. Traditional face-to-face interventions are limited in the numbers of individuals they can reach. 17 Over 8 million people in England have an alcohol misuse disorder. 18 In England, 26% of men aged 25–44 years exceed the recommended limit of 21 units per week. 3 In Scotland, over 30% of men aged 25–44 years binge drink each week. 11 Given the scale of current problems there is a pressing need for interventions which can be delivered to large numbers of individuals at low cost.
Intervention delivery by mobile telephone
The mobile telephone is an attractive method to deliver interventions to large numbers of people at very low cost. This approach is well suited to young to middle-aged men because their ownership of mobile telephones is high. Text messaging has been used to modify adverse health behaviours19,20 and to increase health-care uptake. 21,22 Recent systematic reviews suggest that brief interventions by mobile telephone are beneficial. 23,24 However, none of the primary studies to date has addressed alcohol and none were directed at disadvantaged men.
Delivering a brief intervention by mobile telephone text messages faces the challenge that the texts are limited to 160 characters (including spaces and punctuation). The challenge for this study was to incorporate the components of behaviour change theory and specific behaviour change techniques in a series of text messages which would be effective with disadvantaged men. Unfortunately, little can be learned from previous text message intervention studies as few of them have been based explicitly on theories of behaviour change. 16
Behaviour change interventions and disadvantaged people
Two recent extensive reviews provide a consistent and deeply worrying assessment of the current situation on social disadvantage. 25,26 Health behaviour varies substantially by socioeconomic status, with disadvantaged individuals being more likely to have adverse health behaviours and to suffer poorer health outcomes. 25 There is a marked social class variation in the uptake of preventive services, with the most disadvantaged being the least likely to take them up. Few intervention studies have addressed the impact of interventions on socially disadvantaged groups. There is some evidence that disadvantaged individuals are harder to recruit and retain in research studies. Available studies on behaviour change are often of poor methodological quality. Most evidence is available from studies of smoking cessation, which show that success rates are lower in individuals from disadvantaged areas. Nonetheless, there is evidence that interventions can be effective in disadvantaged individuals. The recent reviews concluded that there is an urgent need for high-quality studies of interventions targeted at groups of low socioeconomic status.
Recruitment
Participation rates in research studies have been falling over the last 30 years. 27,28 Several studies have found that many trials struggle to recruit their intended sample sizes. 29,30 There is now considerable interest in strategies to increase recruitment rates. 31,32 As people from deprived areas are more difficult to recruit to research studies,33–35 the recruitment strategy for trials targeting this group needs to be designed with particular care. Relying solely on recruitment through health care, the traditional method for trials of brief interventions,8,9,36 may not succeed as the target group is healthy and seldom in contact with health services. Thus, alternative recruitment strategies may be needed.
Respondent-driven sampling (RDS) was developed to survey hard-to-reach groups, particularly those who engage in stigmatised or illegal behaviours. 37,38 RDS was designed to overcome the limitations of other techniques such as snowball sampling and key informant sampling. The technique assumes that the target population is distributed through a number of socially networked groups, making it suitable for a group behaviour such as drinking. It has been extensively and successfully used with injecting drug users and groups at high risk of human immunodeficiency virus infection. 39
The need for the feasibility study
The intervention used in this project has multiple components and thus is a complex intervention. The Medical Research Council framework for complex interventions recommends that the feasibility of all aspects of the trial be piloted and that the causal mechanism by which the intervention will work be tested in advance of a formal trial. 40 The methods of recruitment to the trial and the retention of participants should also be piloted. This feasibility study was designed to test all components of a full trial from recruitment to outcome measurement. Finally, the potential effectiveness of the intervention would be assessed through an extensive process evaluation.
Chapter 4 Understanding drinking motives and behaviours
Introduction
There is a pressing need for an intervention to tackle harmful drinking in disadvantaged young to middle-aged men which can be rolled out nationally. Although it might be possible to translate existing brief interventions9 for delivery by text message, this would be problematic for two important reasons. The drinking motives, attitudes and beliefs of disadvantaged young to middle-aged men have not been well studied, and may differ from those of men in general. The proposed delivery medium, mobile telephone text message, is markedly different from face-to-face interventions and may not lend itself to the same intervention techniques.
The aim of this phase of the study was to explore these issues to ensure the optimal content for a brief intervention which would exact the greatest behavioural change. Several questions were investigated. To what extent are drinking motives in young to middle-aged disadvantaged men similar to those presumed in brief interventions? Specifically, is drinking influenced by positive alcohol expectancies, social norms and refusal self-efficacy? How are the harms of alcohol perceived and how might these best be used to motivate behaviour change? Could drinking be influenced by other, as yet unknown, factors? How could appropriate interventions be tailored to be delivered by mobile telephone to this target group? What style and content of text message might be effective in reducing the frequency of binge drinking?
Methods
The exploratory nature of the research questions, coupled with a need to identify the breadth of views and experience rather than their frequency, suggested that a qualitative method was most appropriate. 41,42 This phase of the study comprised five focus groups with disadvantaged men and one with female partners of heavy-drinking disadvantaged men. This chapter presents only the findings relevant to the drinking motives, attitudes and beliefs of disadvantaged young to middle-aged men. Two further sets of findings from this phase are presented separately in Chapter 5. These are the results from the women's focus group and the men's views on a draft set of text messages.
Sampling
In accordance with best practice for qualitative research we sought to implement a maximum variation sampling strategy which would achieve diversity in key variables for which views and experience around alcohol would likely differ. 43 Research elsewhere has suggested that the profile of drinking behaviours varies by age; consequently, within our age group (25–44 years) we sought to ensure individuals were represented in both the 25–35 years and 36–44 years age bands. In addition, we sought to include a number of individuals who may be aged between 44 and 60 years in order to obtain their views on past behaviour (with the experience of hindsight).
Recruitment
We purposively sampled from a variety of social venues likely to represent the target group of interest to the study. Venues included Saturday amateur football league clubs, public houses, an employment training centre and a further education college (Table 1). Systematic reviews have shown that the provision of monetary incentives can significantly increase recruitment to research studies. 44,45 Consequently, men agreeing to take part were given a £10 gift voucher and travel expenses. They found the experience rewarding because a prestigious organisation (the university) was interested in their lives and believed what they had to say was valuable. Many said it was therefore something they could share with pride in their social network.
| FG | Social network | Venue of FG | No. and age range of participants |
|---|---|---|---|
| FG 1 | Saturday amateur football league clubs | Pub | Five participants aged 27–33 years |
| FG 2 | Unemployed training centre | Training centre | Five participants aged 38–57 years |
| FG 3 | Unemployed training centre | Training centre | Seven participants aged 28–43 years |
| FG 4 | ‘Back to work’ training group | Further education college | Six participants aged 21–55 years |
| FG 5 | Criminal Justice Services | Criminal Justice Office | Five participants aged 37–52 years |
Thus, 28 men aged 21–57 years living in areas of high deprivation were recruited to the study. Deprivation was measured using the Scottish Index of Multiple Deprivation (SIMD),46 which is similar to the English Index of Multiple Deprivation. Individual-level socioeconomic position was also assessed from brief questionnaires on current socioeconomic and demographic characteristics. Summary characteristics of participants are shown in Table 2.
| Variable | Participants (N = 28) |
|---|---|
| Mean age (years) | 37.5 |
| Sex | Male, n = 28 |
| Marital status | Married/living with partner, n = 9 |
| Single, n = 19 | |
| Education (highest level) | Secondary education, n = 19 |
| Diploma (vocational qualification), n = 7 | |
| University degree, n = 2 | |
| Employment status | Employed, n = 4 |
| Unemployed, n = 24 | |
| House type | Owned, n = 3 |
| Rented, n = 25 |
Data collection and analysis
Data were collected using a focus group approach. It was clear that much drinking reflected a social practice influenced in part through group norms and sets of social expectancies. Consequently, enabling men to talk as a group would enable identification of these expectancies, attitudes and values. 47 A topic guide was constructed based on a background search of relevant literature in the area. However, conversations were not limited to these areas. All participants were informed of the confidential nature of the research. All groups were audio-recorded and transcribed. Analysis was conducted by three members of the research team (JC, DWF and BW) using the framework approach. 48 Pseudonyms have been used in direct quotations to protect participant identity.
Results
The majority of the older men in the study believed that their drinking behaviours, motives and desire to change were significantly different from when they were younger. Explanations for current drinking patterns, and the way these change over time, appear rooted in shifts in three interacting conceptual areas: private purpose, social roles and concrete experience. At the heart of this shift is what might be termed the ‘mature drinker’ role. This consists of a set of social expectations stemming from recognition of the person's wider social roles and responsibilities (employee, husband/partner, parent), abilities (self-discipline/control, ability to tolerate alcohol, judge limits and resist social pressure) and life experiences to date.
Private purpose and social roles
Our findings suggest that alcohol consumption behaviours vary in accordance with two parallel drivers: private purpose and public role. Private purpose refers to an individual's personal reasons for and against particular forms of alcohol consumption. While these purposes may sometimes be made public, they are generally tacit. Public role highlights the social role of alcohol in many individuals' lives. As with any role it brings a set of social expectations and duties which must be followed if sanctions are to be avoided. Private purpose may be seen to be a driver of private drinking, while social drinking may be influenced by both private purpose and social role.
Private purpose
All participants clearly identified a range of benefits from alcohol consumption. Predominant among these were reward, relaxation and release. Most men regarded alcohol as having a range of sensory benefits leading to an inherent enjoyment of the experience.
I think just enjoying it. I think as I've got older I just go out to actually have a pint. . . it's actually enjoying it, enjoying a pint of [name of Irish stout], enjoying the ale. You know going into the supermarket and buying the two bottles and thinking right, I might have one of those this week. . . Just enjoying the actual drink for the taste of it and yeah.
Jim, aged 31 years
The positive experiential nature of alcohol meant that it was frequently used as a personal reward. There was a sense that they had earned and therefore deserved the experience. However, although this would suggest that there may be social rules indicating when alcohol was legitimate, i.e. deserved (and thus conversely when it was not), we could not find instances in the data when alcohol was not consumed because it was seen as not deserved. This suggests that drinking as a reward may not so much determine whether or not drinking takes place but rather how one feels about it; the ‘well-deserved drink’ may convey greater satisfaction and pleasure simply because it feels deserved and symbolises an individual's achievements.
Social, but also for me at home it's sometimes a reward. Like if you've had a shit day or you've been working non-stop, it's sometimes good to like have a drink at the end of the night and it's not because you even want one it's because you feel like you deserve something.
Eddie, aged 33 years
A related but slightly different motive for alcohol consumption among this age group was relaxation.
Normally when I drink it's because I feel good about myself. And that way, I could relax at the end of the week, have a drink, knowing that the family is all as it should be. I'd have a drink, not to celebrate, but to relax.
Harry, aged 50 years
However, alcohol-related relaxation was rarely, if ever, associated with alcohol alone; instead, relaxation related to a number of what might be termed ‘alcohol plus’ scripts (i.e. groups of associated behaviours that combine to provide relaxation). Key ingredients in these scripts included alcohol itself, a core activity (watching television, playing pool, darts) and company (existing friends or meeting new people). Location was frequently cited but on closer examination this appeared to be predominantly as a means to access and facilitate these ingredients.
The concept of relaxation suggested a motive that could be engaged in by almost anyone; it represented the pursuit of something positive as much as the removal of anything negative. However, for some men alcohol consumption was sometimes motivated by the latter rather than the former. In these cases alcohol served for some as an emotional release, which would distract or take the edge off perceived problems. It therefore came to be seen by men as an established coping device for stressful times, a means of achieving ‘freedom from’, even if it did not permanently solve, the problem.
You're not worried about money at the end of the night. You're just worried about getting legless and just forgetting about all your problems.
Brian, aged 31 years
I find it a good release. . . I'll just go out and have a laugh and maybe take my head away from things that are going on at the time.
Simon, aged 27 years
Social roles
While some older men used alcohol as a form of release and thus a way of achieving ‘freedom from’ (the stresses and problems of everyday life), for many more it was seen also as a means of achieving ‘freedom to’ – it facilitated the achievement of personal attributes and fulfilling public social roles that they otherwise would not have had the self-confidence to attempt: ‘it can help people, shy people actually come out of their shell, ken.’
However, all quotes relating to this were notable in that they referred to their view of other people's reliance on alcohol to achieve this, or to their own but in earlier years. Using alcohol to improve social confidence and fulfil other social roles and identities was therefore either less important for older men, or was something they were reluctant to admit to personally.
In addition to enhancing one's ability to achieve a valued social identify and fulfil a public role, it became apparent that the social nature of drinking in the pub environment was in fact a social role characterised by a set of expectations, duties and potential sanctions (Box 1). These included expectations to drink alcohol (rather than soft drinks) and to pay one's fair share of rounds. There was evidence of significant disapproval of individuals not conforming, giving rise to a felt pressure to conform and drink.
I know a lot of people that go out, just to have a drink, to look for women, ken what I mean. A lot of the guys that are sober couldn’t chat a woman up unless they’ve had something inside them
Martyn, aged 38 years
I’d say I would probably drink more while I was in the pub, but I probably drink more often at home . . . Whereas when you’re at home, you’re kind of, you’re not as going hell for leather because you’re sitting having a quiet drink rather than having a social piss-up so to speak
Simon, aged 27 years
The drinking role
Expectation to drink alcohol
I’ve been in a pub for a glass of orange. I couldn’t sit all day and do that
Martyn, aged 38 years
Well I’m going to have to say never on that one. That’s how it was. Never. If you go out, pub’s there, that’s it. You have a pint. There’s no way I could ever have walked into a pub and just ordered a coke
Arran, focus group 2
Duty to pay your share of rounds
If we’re in the pub we’re on the rounds, so everybody has pretty much the same amount to drink
Bob, aged 31 years
And if you’re the fastest drinker, you’re buying rounds and you don’t want to see anybody with an empty glass so as soon as someone finishes, the person goes ‘it’s your round’
Simon, aged 27 years
I find that every time I go in the pub it’ll be like ‘what you having mate’ and then that’s me in that round
Simon, aged 27 years
Sanctions and disapproval for transgression
You get the odd people maybe say ‘oh, you lightweight’ or stuff like that
John, aged 27 years
Certain people go out and spend their money and then have to end up borrowing off their pals so they can keep going, you know what I mean. They do it all the time. I get it all the time. ‘You’ve got money with you ‘cos I’ve spent mine.’ It’s always the same people
Fred, aged 34 years
Shifting purpose and role – the importance of age
Participants frequently generated a narrative looking back to earlier times in their lives; in addition, they sometimes compared their own motives, experiences and behaviours to other contemporary younger drinkers. Through these comparisons it became clear that they perceived a very significant shift in both the social role expectations and duties, and the private purpose motives for drinking. Consequently, there was a move towards what might be termed the ‘mature drinker’. Indeed, these were sufficiently consistent as to suggest that there may broader agreement on the existence of younger and mature drinker roles. This shift is shown in Table 3.
| Drinking motive | Age → | |
|---|---|---|
| The young drinker | The ‘mature’ drinker | |
| Private purpose | Freedom to:
|
Freedom from:
|
| Social role | Expectation:
|
Similar expectation:
|
Increased expectation regarding:
|
||
There was a general view that older drinkers were less likely to be drinking in order to get drunk and more likely to drink for general relaxation, social company, reward and as a means of escaping from daily pressures. In addition, older drinkers saw themselves as more able to know their limits and more likely to be able to ‘hold’ their drink. Some felt that they had more money to drink now that they were older while others found that finance was a major obstacle. Consequently, these drivers meant that more mature drinkers might well consume greater volumes of alcohol but be drunk less frequently.
Although these issues suggested that greater quantities of alcohol might frequently be consumed, there were multiple examples of explanations of changes in drinking behaviour rooted in the adoption of multiple new social roles which competed and were sometimes incompatible with their past drinking behaviours. These provided a new and perhaps wider ‘perspective’ on the role and impact of alcohol in their lives:
Yeah because maybe if you're seeing a lassie, you’ll maybe get a bottle of wine and a DVD or have a glass of wine with my tea most nights or a couple of beers maybe watching the Champions League. You've got a different perspective on drink because you’re older.
Simon, aged 27 years
A commonly reported shift was with regard to their obligations within family roles and relationships. This included both partners and children:
But you do, even like when kids come on the scene, if you’ve got your partner, you split up, you get your bairn one week, you get the bairn weekends. That changes yourself as well. That’s like me, I get [inaudible] every weekend, so I don’t go out. I go out every Wednesday, that’s when I got out.
Fred, aged 34 years
More frequently expressed were their current identities and obligations as employees. When they were younger such responsibilities were not of concern, but now they constrained what the men could do:
With my job and responsibilities, I can’t just go out, I’m not working in a warehouse like I was when I was 18 where you can just do what you want the next day, it doesn’t matter. But now, during the week, it just can’t happen, with my job the next day, I just couldn’t function properly.
Jim, aged 31 years
There was recognition that the adoption of these wider life roles and responsibilities were appropriate and to be expected as part of the process of becoming more mature. They were not expressed in pejorative forms and there was little sense of nostalgia about what they were losing in terms of past drinking behaviour. Consequently, even among those older men who were still drinking significantly there was a willingness to publicly express their intention to change as these new roles emerged for them:
Well I don’t want to be, my ideal at some point would be to settle down and have some sort of family unit that my focus was on them, and go for the occasional night out with the boys and the odd couple of pints. But certainly not drink socially the way we drink now and I wouldn’t want to be drinking to that extent when I get older. I’m not saying I might, what I want and what will happen might be two different things but certainly, for the picture of where I want my life to go I don’t want to be still having the nights out the way I have them just now in say 5–10 years’ time. I would rather want my focus to be somewhere more important.
Simon, aged 27 years
Awareness of consequences and the importance of concrete personal experience over abstract risk
High levels of alcohol consumption among the older men do not appear to be rooted in a lack of awareness of the consequences of drink. There was ample evidence, and graphic examples, of the consequences including hangovers, significant financial cost, changed character, poor health and violence with its associated implications.
Underpinning many of the consequences was recognition that during the drinking process their usual selves, with their typical motives, intentions, values and self-discipline diminish, culminating with a complete disappearance and a lack of awareness or memory of anything that occurred:
Your judgement could be all wrong.
Martyn, aged 38 years
You forget a lot, you don’t ken what you’ve done. You lose your identity as well because you don’t know what you’ve done.
Derek, aged 28 years
Yeah me, I have. Quite a few years ago. I was out with a mate, a friend of mine and ended up having quite a few drinks and the next thing I knew I woke up in hospital.
Jeff, aged 40 years
I woke up in Orkney Street in Govan and I thought ‘How did I get here?’
Brian, aged 31 years
Consequently, while alcohol had been described as facilitating the achievement of social roles and valued personal identity in their earlier years through improved social confidence (‘freedom to’), alcohol now frequently proved to be an obstacle to achieving such an identity (partly because that valued identity had changed as new domestic, work and even the mature drinker role had been adopted). Ultimately, it was seen to change one's character and desired behaviours:
I think it hampers your personality on all points, and that’s not always a good thing. I mean, you can say things you regret or those feelings that have been sitting on your mind or your boss, maybe you shouldn’t say something if you’re at a work night out, or a girl, that you’d maybe regret the next day, when you've left a text or a comment on a social network site or anything. And you’re like, this seemed like a good idea at the time. . . [laughter]
Tony, aged 28 years
My dad said to me at one point, he says, I always know when you’re back on the drink or drugs, you’re an obnoxious little shit.
Ross, aged 37 years
. . . she just says ‘I don’t like you when you drink, I don’t like your attitude and the way you are.’ She says I get quite aggressive.
Jim, aged 31 years
The most common seemingly powerful consequences of alcohol consumption for participants were in relation to aggression and physical violence. Many participants knew of others who had been in trouble with the police (including assault and murder), while others had personal experience:
Yeah. I’ve been arrested and put in the cells overnight and stuff like that. I’ve been in quite a few fights because of it, so.
Ben, aged 38 years
When I used to drink, if I drank whisky, it just made me drowsy. I’d get a heavy hangover and I’d probably start fighting with somebody.
Graeme, aged 43 years
Although there was widespread awareness of a range of negative consequences from alcohol consumption, it was interesting to note that explanations for changes in participants' drinking were rooted in past personal experience of these issues rather than knowledge of their more abstract existence and risk. The most important of these appeared to be the impact on the person's children, although multiple causes were often seen to combine.
The main reason for me is one, no more criminal record. Two, I’ve got two children that I haven’t seen for two years now. And obviously the money as well. And health. My brother’s only 40 and he drinks and he had a stroke last year, so that’s a bit worrying when you’ve got heart problems in the family as well, so I thought, I’ll stop as well, so.
Ben, aged 38 years
Other reported triggers to changing included the financial impact, e.g. falling behind in paying bills, and personal health events. Although most examples related to the individual's own personal experience of a substantive problem, a few individuals did indicate that it was the observed experience of a close friend or relative which had prompted their change in drinking. In earlier discussions regarding consequences of excessive drinking, participants frequently reported the consequences that they had observed in other people; however, observations only appeared to motivate actual reported change in the participant when it was someone close to them. This suggested that in some instances vicarious experience may prompt change, or at least intentions to change consumption patterns.
Discussion
Men reported a significant change in their drinking motives from when they were younger. This stemmed from a shift in the private purpose and social roles facilitated by alcohol use. Alcohol was now predominantly used as a form of reward, relaxation and release from life pressures. Patterns of consumption were also influenced by obligations to a range of competing social roles including parent, partner and employee that had not been extant when younger. Knowledge of the negative experiences of alcohol was detailed and widespread. However, reported changes in behaviour appeared rooted in concrete personal or vicarious experience of these issues rather than more abstract risk.
The importance of the ‘mature drinker’ role
Our data suggest that contemporary society may have a particular set of expectations and beliefs about the more ‘mature drinker’: someone who can tolerate greater amounts of alcohol without becoming drunk, has greater self-discipline, is more likely to be able to resist social pressures to drink, and drinks as a means of reward, relaxation and release. The existence of such a set of social expectancies is perhaps evident in the way society may interpret public drunkenness by a teenager or person in their early 20s differently compared with a man in his 40s. The existence of the ‘mature drinker’ role and the individual's desire to conform/live up to the identity it affords may prove useful in both behavioural interventions and those employing more social marketing approaches. 49,50
The development of competing social roles and identities as an explanation for changes in drinking behaviour with age
Our findings also show that reasons for alcohol consumption among older disadvantaged men differ from their younger counterparts. Therefore, brief interventions to tackle the problem must incorporate different approaches. The literature suggests the perceived benefits of alcohol (alcohol expectancies) for young people include mood enhancement and enjoyment, stress relief and escapism, easier socialising and social success, and conformity with peers. 51,52 Thus, three different types of drinkers have been identified: enhancement drinkers, social drinkers and coping drinkers. 53 Although similar benefits were stressed by the older men in this study, there was a clear shift in emphasis away from the use of alcohol as a means of achieving valued social identities, social confidence and group membership (‘freedom to’), towards a greater value attached to the use of alcohol as reward, relaxation and release (‘freedom from’). Such changes were clearly rooted in changes in social identities and roles acquired as men grew older. They became employees, partners and fathers – roles and responsibilities which had the potential to constrain alcohol consumption, or at least excessive drinking. The existence of these competing roles as a constraint may provide a means through which potential behavioural interventions may operate. The power of social roles to influence behaviour comes from the potential social sanctions applied when expectations and duties associated with those roles are not fulfilled (e.g. failing to be a good employee, partner or parent). 54 Consequently, the psychological concept of ‘subjective norm’ (an individual's perception of social normative pressures, or relevant others' beliefs that he or she should or should not perform such behaviour55) may be helpful in future behavioural interventions for this population.
Studies have shown that peer pressure is a significant factor in the level of alcohol consumption among young people. 56 Low levels of drinking refusal self-efficacy have been found to increase the acquisition and maintenance of binge drinking. 57 However, the adult version of the Drinking Motives Questionnaire (DMQ) has no scale to measure peer (conformity) motives, because it assumes the influence of peer pressure declines with age. 53 Although this, to a large extent, is true, our findings suggest the influence of peers and social networks on the older cohort may be more complex and subtle than first assumed. Although some men felt that their friends were more accepting of their decisions to slow their drinking down, other men still felt pressure from their peers to consume large amounts of alcohol. In the second context it was the behaviour – the consumption of alcohol – that signified membership of the group and gave the men a sense of belonging. The men's refusal self-efficacy therefore largely depended on whether the group was predominantly defined by its drinking behaviour or another organising factor. A brief intervention might therefore highlight that the men have a choice about the different social networks they are accessing, and that this choice will affect the amount of alcohol they consume and ultimately their health and well-being.
Alcohol and role incompatibilities: the potential of ‘developing discrepancy’
Drinking was a component of many rituals that were deeply satisfying to the older men in the study, and which reinforced the pleasure because of this association. Yet many of the benefits the men identified were not compatible with being very drunk. This presents an opportunity to highlight the inconsistency between an individual's drinking habits and the intended aims of drinking. Thus, brief interventions could highlight the mismatch between being drunk, and success in socialising, working, ‘doing good turns’ and feeling good about oneself. The utilisation of such discrepancies is at the centre of MI, suggesting that this approach may be effective, or at least a contributory approach, to behavioural strategies in this area. Indeed, the efficacy of MI in addressing drinking behaviours has demonstrated success in meta-analyses,58 and the feasibility of implementing it through brief intervention formats has been shown. 59
Concrete personal or vicarious experience as a trigger for behaviour change
Young people tend to believe that they will not come to harm, and that drinking will have few negative consequences. 51 Thus, they are unlikely to modify dangerous drinking habits because they do not perceive themselves as being susceptible to harm. On the contrary, such beliefs are associated with increased levels of consumption. 60 However, in marked contrast, the older men in our study believed they were susceptible to (or had actually experienced) the health and social consequences of excessive alcohol consumption. The most frequently cited negative consequences were the risk of injury or criminal record (through aggression and violence); serious illness (such as liver disease or stroke); family disruption and separation; and financial drain. Critically, a minority believed that any health damage was irreversible and therefore saw little point in reducing alcohol consumption.
However, although acknowledgement of the existence of these dangers was widespread, it appeared only to be those who had experienced them personally (or vicariously through a very close family member or friend) who reported them as a driver to behaviour change. This finding is unsurprising given both behavioural theory and empirical research elsewhere that suggests that beliefs that are less abstract and experientially more concrete are more likely to result in behaviour change. 61,62 Consequently, any intervention needs not only to present the true risks of alcohol, but wherever possible to ensure that this is expressed in non-abstract and more direct or even concrete/experiential terms. This may include anything from the use of graphics over abstract text, through to reminding people of key past negative personal experiences of alcohol and its impact on others. Although some participants were sceptical regarding the use of images in interventions, this centred primarily on the potential ambiguity of meanings within images compared with clear text. This is clearly important. Indeed, issues of what is now termed ‘visual literacy’ are well acknowledged and must be taken into consideration when designing any images. 63 Where such personal experiences do not exist then utilising those of close family, friends or even well-known and liked public figures may prompt similar results through vicarious experience. The potential of vicarious experience has been little studied but empirical evidence in other behavioural contexts suggests there may be potential for its use. 64 The potential of concrete personal experience as a motivator also raises questions regarding whether or not coinciding the timing of the delivery of the intervention to a point soon after any such experience may significantly improve its effectiveness. Certainly, concepts such as ‘triggers to action’65 and, more recently, the idea of the ‘teachable moment’66,67 would support this.
Conclusion
Interventions to reduce alcohol consumption among young to middle-aged men from disadvantaged backgrounds should acknowledge different motives for drinking and reducing consumption. The onset of wider competing social roles and reminding individuals of concrete personal negative experiences may be productive. Brief interventions need to reduce the frequency of heavy drinking among young to middle-aged disadvantaged men and increase their intentions to avoid becoming drunk. Our study suggests that this may be achieved through interventions which:
-
(a) highlight the discrepancy between being drunk and desired success in socialising; family, work and community relationships and roles; and feeling good about oneself
-
(b) show how behavioural change can heal the body, family and social relationships, and conserve (and enhance) financial resources
-
(c) are expressed through concrete experiential form, act as reminders of past personal negative experience of alcohol, or are timed to be delivered soon after such an experience
-
(d) promote success in achieving aspects of the ‘mature drinker’ role
-
(e) suggest men have a choice about the different social networks they can access, and that this choice will affect the amount of alcohol they consume.
Chapter 5 Developing the text messages
Introduction
The challenge in this study was to develop a brief intervention which could be delivered by text messages and images to a mobile telephone. A limitation of previous studies on text messages is the lack of a theoretical basis for the interventions. 23 This study adopted a systematic, transparent approach to message development. This began with reviews of the literature on empirical studies of brief alcohol interventions, text message interventions and behaviour change theories. The brief alcohol interventions identified the main design features required and identified some of the main design challenges to be solved. The text message studies identified many techniques for message design. A review of the literature on psychological models of behaviour change identified constructs which could form components of text messages for the intervention. A review of communication theory identified the best ways to render these components into text messages. A preliminary set of messages was prepared and tested in focus groups. The revised set of messages was then systematically checked against reviews of successful behaviour change techniques. This chapter describes these processes and the resulting set of theory-based text messages used in the intervention. The chapter also describes the design decisions for the control messages and the set of messages that were prepared.
Design features of published alcohol brief interventions
Brief interventions based on psychological theories have been developed to tackle alcohol-related problems. There is extensive evidence that brief interventions are effective. 7–10 Brief interventions are conventionally delivered face to face by a health-care professional such as a general practitioner (GP), nurse, psychiatrist, psychologist, alcohol worker or trained counsellor. The consultation can vary in length from 1 to 50 minutes, with patients receiving from one to seven sessions. Total duration of intervention may range from 10 to 175 minutes. The control groups generally receive much less contact, up to a maximum of 10 minutes.
The content of the intervention varies substantially across studies. 9 Early studies usually employed at least two techniques (raising awareness of the problem and giving advice about change) with the aim of increasing motivation to change. Other techniques, including emphasis on personal responsibility, provision of a menu of change options and enhancement of self-efficacy, were quickly added. 68 In addition, the intervention can be supported by an information leaflet, a self-help manual, a diary to record alcohol consumption, drinking goals and suggestions for alternatives to alcohol. A recent systematic review9 concluded that such interventions are derived from social cognition theories and can include the following elements: feedback on alcohol use, clarification of low-risk drinking, benefits of reducing consumption, harms of excessive consumption, motivational enhancement, coping strategies and a plan for reduced consumption. The systematic review confirms the finding from previous reviews that these interventions are effective, reducing total consumption by an average of 38 g of alcohol per week, 12.4% of baseline consumption.
Design features of published text message studies
Text messaging has been used to modify adverse health behaviours19,20 and to increase health-care uptake. 21,22 Delivering interventions through text messages to young to middle-aged men is attractive because ownership of mobile telephones is high in this group. Recent systematic reviews have shown that text messages can successfully change behaviour. 23,24,69 However, few of the primary papers described the behaviour change theories on which the intervention was based, although some studies mentioned the use of motivational messages. 23,24,69 Interactivity was an important feature of most interventions, commonly achieved by using text messages which requested responses.
Most of the primary text message studies which focused on improving the clinical care of patients provided feedback of test results, tailored advice, goal-specific prompts and direct contact with health-care professionals. 23,24,69 Studies trying to promote healthy behaviours provided advice, support and solutions for potential barriers to behaviour change. Many studies used supplementary material such as e-mails, websites, booklets and diaries. Interventions designed to change health behaviour relied mainly on the text messages, although a few provided access to other sources of support.
The number of texts and the frequency at which they were sent varied substantially between studies. One review paper23 commented that the frequency of sending texts depended on the target behaviour. Most studies had a predefined programme for message sending, although a few allowed participants to set their own frequency. The control groups generally received little attention with few, if any, text messages being sent.
Almost all studies tailored messages to the target individuals. Two studies which did not tailor messages experienced high attrition rates. 23 Tailoring could involve the use of first name or nickname, age-, gender- and culture-specific messages, current health status or behavioural preferences. A potential weakness of current studies is that most repeat some of the messages during the course of intervention delivery. Reinforcing the content of a message could be beneficial, but using the same words to do so could decrease the impact of the text. Furthermore, few studies use informal language. This is in marked contrast to the conventional texts which frequently dispense with the niceties of grammar and make regular use of abbreviations. 70 A formal style could result in less attention being paid to the messages.
Behaviour change theories
The theory of planned behaviour
The TPB has been widely used to predict intentions and behaviour. 12,71 It states that intention is the proximal determinant of behaviour and that the three main influencers of intention are attitudes, subjective norms and perceived behavioural control. 72 Attitudes are determined by beliefs about the desirable and undesired consequences of a behaviour, which lead to an overall evaluation of the behaviour. Subjective norms are the beliefs about the views of significant others (approval or disapproval). Perceived behaviour control was initially regarded as the extent to which internal factors, such as skills, and external factors influenced the individual's perceived control over the behaviour. More recently, perceived behavioural control has been subdivided into two factors:73 self-efficacy, that is, confidence in one's ability to perform the behaviour and the extent to which carrying out the behaviour is easy or difficult; and perceived control, perceptions of control over the behaviour and the extent to which the performance of the behaviour is within the individual's control. 74
Binge drinking has been extensively studied using the TPB,72,73,75 with implications for interventions to change behaviour. As attitude is a strong predictor of intention, focusing on the negative consequences of binge drinking has great promise. 75 Negative consequences are often described as negative alcohol expectancies and include hangover, vomiting, aggression and accidents. 76 These negative expectancies could be portrayed in text messages, encouraging participants towards preventive strategies. Subjective norms are another target to facilitate behaviour change. Although difficult to change at a population level, it would be possible to increase the salience of the views of significant others (parents, partners, close family) to encourage more moderate drinking. To ensure the significant other holds a more moderate view of drinking, the text message would need to direct the participant to those who would be pleased with a reduced consumption. Increasing drinking refusal self-efficacy is another promising approach. 77 Finally, the intervention could try to reinforce both self-efficacy and perceived behavioural control. Self-efficacy could be bolstered by acknowledging that change is difficult, while supporting continued effort for even modest improvements.
Motivational interviewing
Motivational interviewing was developed from clinical experience in the treatment of problem drinkers. 13 Recent meta-analyses have shown that it is an effective technique for treating problem behaviours. 36,58 It is a style of counselling that promotes behaviour change by helping individuals to decide for themselves that they wish to change. 13 Although it is directional, in that it seeks a specific behaviour change, MI avoids confrontation, or coercive approaches to behaviour change. 14 These are thought to make individuals defensive, increasing resistance to change. Instead MI empathises with individuals, recognising the legitimacy of their viewpoint while encouraging them to identify personal advantages of changing behaviour. Two further techniques are crucial to this approach. The first is to identify discrepancy between what the individual wants from a behaviour and the adverse outcomes which sometimes occur. For example, when drinking most people want to have fun and socialise, whereas if they become very drunk, arguments, violence or even physical collapse can prevent achieving the desired goals. MI encourages the individual to identify and describe this discrepancy for themselves, leading to a personal choice to change. That the individual, rather than the counsellor, identifies the need for change is seen as crucial to MI. 58
A second technique is to promote self-efficacy, an individual's belief in his or her ability to change behaviour. This can be done by encouraging individuals to make positive statements to reframe thinking about a behaviour. 78 Statements from the counsellor which affirm that behaviour change is difficult and that the individual should persevere under difficult circumstances can also promote self-efficacy. Another approach is to ask what would be the best outcome if behaviour were to change.
Motivational interviewing is traditionally delivered face to face,36 but it provides an attractive style for the design of the text messages. It suggests that approaches that emphasise autonomy, empathy and self-efficacy and avoid authority and adversarial content might be more effective and more acceptable. The emphasis on empathy would minimise any perception of the intrusiveness of the messages. This could occur with messages which were unsolicited and from an unknown source. The techniques of encouraging individuals to pursue discrepancies in their drinking behaviour, combined with improving self-efficacy also identify important content for the messages. Two other techniques of MI, avoid argument and roll with resistance, were deemed inappropriate for a text message intervention.
The approach of MI emphasises that advice giving should be avoided. This conflicts with the design of many brief interventions, particularly when delivered by health professionals, in which advice giving and an implicit appeal to professional authority are key ingredients of the behaviour change strategy. 9,68,79 Given the nature of the target group, healthy disadvantaged young men with few concerns about their drinking, avoidance of advice giving seemed the better choice. This view was supported by the focus group study, which showed the text messages offering tips to reduce drinking were unpopular.
The transtheoretical model
The TTM was developed in the 1970s as a synthesis of therapeutic approaches to behaviour change into a comprehensive model of change. 80 It has been used to explore change in drinking behaviour among individuals with alcohol problems. 81,82 It identifies a series of stages of readiness to change: from pre-contemplation (not thinking about cutting down), to contemplation, to preparation to change, to active behaviour change. 83 Motivation is seen as central to behaviour change84 at all stages of change. The model is driven by processes specific to each particular stage. These include: validating lack of readiness to change, encouraging re-evaluation of current behaviour, encouraging self-exploration not action, explaining and personalising risks, evaluating pros and cons of change, promoting new positive outcome expectations, helping identify and remove obstacles, helping patients identify social support and bolstering self-efficacy. 85
Reviews of behaviour change theories
Some recent reviews of theories of behaviour change have been concerned with giving guidance for the construction of interventions to change behaviour. One study identified, from a range of theories, a set of 12 theoretical constructs which explained behaviour. 86 A further study linked theoretical constructs to specific behaviour change techniques. 16 Another approach was to review the techniques commonly used in behaviour change studies, identifying those with theoretical support. 15 This led to a set of 26 defined techniques linked to specific theories. Finally, an evaluation of alcohol education leaflets identified 48 categories of message. 87 This was reduced to a set of 29 categories of message which target cognitive antecedents of drinking. Together these studies provided explicit descriptions of theory-based behaviour change techniques. These helped inspire the creation of text messages and provided a checklist against which the intervention messages could be compared to ensure that important techniques were not omitted. As expected,15 not all the techniques were appropriate for the target group or for delivery by text message. However, as the authors of the reviews suggested, identification of these techniques greatly aids the development of behaviour change interventions.
Communication theory
The design of the text messages was based on current communication theory. This draws attention to the series of steps from message receipt to behaviour change. To be effective a message must be attended to, comprehended, processed, accepted and acted on. 88 Communication theory identifies four features of a message which affect the likelihood of behaviour change: the source (i.e. credibility) of the message, its style and content, the nature of the recipient and the context (the circumstances in which the message is received). Each of these features affects the impact of the message on behaviour change. 89,90 The nature of the message comprises many facets, including its length, content (number of arguments), language and style (such as use of images). Important design features are the personal relevance of the message89 and whether the arguments are gain-framed (emphasising the benefits of moderate drinking) or loss-framed;91 gain-framed messages are much more persuasive in altering behaviour. Items can also be included to maintain interest (such as interesting and unexpected statements).
Conclusions from the literature review
The literature identified a series of key issues that had to be resolved:
-
What should be the style and tone of the messages?
-
Which harms of alcohol should be mentioned and how should these be displayed?
-
Which psychological models and behaviour change techniques are most appropriate for the target group and for delivery by mobile telephone?
-
Which components of the psychological models should be conveyed in the text messages?
-
In what sequence should the messages be sent?
-
How often should the messages be sent and at what times of day?
-
How could guidance to reduce consumption be given without patronising or preaching?
-
What should the balance be between serious and more whimsical messages?
-
Should the text messages be supplemented by other materials?
-
How many text messages should the control group receive?
Constructing a logical sequence of messages
The theories of communication and behaviour change, together with the reports of previous intervention studies, identify many key components for the intervention and important design features to take into account. However, they do not specify the sequence in which the components should be arranged to achieve maximum effect. Intuitively, a plausible sequence would be to review harms of current drinking, explore the benefits of moderated drinking then promote intentions to change behaviour. However, it would be preferable to have a theoretical justification of the sequence.
A second problem is that, although many drinkers are content with their current pattern of consumption, some wish to reduce their consumption. 11 This raises the question of whether or not different sets of messages should be sent to different types of drinkers. Brief interventions delivered face to face can establish how individuals view their alcohol consumption and whether or not they are thinking about reducing their consumption. A skilled counsellor can select the relevant components of the intervention and weave them into a coherent behaviour change strategy. This is more difficult with an automated text delivery system. It would be possible to screen each individual at baseline and, by clever programming, create a customised set of messages. However, this would increase the cost of the system if it was rolled out nationally as staff would be required to conduct screening interviews. As potential for national roll-out was a key requirement of the intervention, the need for simplicity meant that all participants would be given the same set of messages.
The TTM85 provided a convenient solution to the problem of presenting the messages in a logical order which is suitable for all drinkers. The texts were arranged in the sequence pre-contemplation (prompt re-evaluation of current behaviour), contemplation (focus on reasons for change), preparation (identify and overcome barriers to change) and action (promote self-efficacy, goal setting). One benefit of this model and the sequence of text messages is that it will be suitable for individuals irrespective of their stage of change at enrolment to the study. For example, those in the preparation stage will view the pre-contemplation messages as reinforcing their decision to do something about their drinking. Clearly this would not work if the messages were tedious or repetitive. A feature of this approach is that it encourages integration of behaviour change strategies from other theoretical models. Thus, the text messages make extensive use of the components of other theories of behaviour change.
Design decisions
Short Message Service (SMS) text messages can be no more than 160 characters in length. This meant that complex constructs from the psychological models had to be conveyed concisely. Mobile telephones can also send images through Multimedia Messaging Service (MMS) messages. At the time of the design of the intervention texts, not all mobile telephones could receive MMS images. However, given the speed of advance of mobile telephone technology it was concluded that, by the time the intervention was suitable for national roll-out, all telephones would support MMS messages.
Basis for the intervention
The intervention was to comprise a series of interactive text messages and images using communication theory,88,91,92 social cognition models,93 the TTM80 and the components of effective brief interventions for alcohol described by systematic reviews of interventions to tackle alcohol problems. 8–10 The text messages were all mapped to behaviour change models and techniques. A few examples will help clarify this mapping process:
-
Raising awareness of harms: ‘1 in 20 deaths a year in Scotland are caused by alcohol! Don't be the 1!’
-
Subjective norm: ‘Can U think of someone who'd be happy if U made a change! What would U hear them say?’
-
Drinking refusal self-efficacy: ‘Drinking too much can spoil a good night out & make U regret the things U did! Self-control = more fun!’
-
Outcome expectancy: ‘Some people change for the worse when they're incredibly drunk. Think of the benefits of taking it a wee bit easier.’
-
Goal setting: ‘Set yourself a goal & try to avoid alcohol on weekdays (Monday–Thursday). Give it a go!’
Credible source
The University of Dundee provided a credible source for the research project. The university logo was printed on all letters sent and appeared in the first text messages of the intervention. Thus, the introductory text used the university identity to welcome participants to the study. ‘Welcome, Dave! U are 1 of 60 men chosen by Dundee University for this important study on alcohol use’. This text had the additional benefits of making the men feel valued and building rapport.
Style and tone of the messages
The messages employed a simple, non-academic, friendly and non-confrontational language. Some messages contained quotes from the focus groups, suitably anonymised. The style of the messages changed across the intervention. The first text was a friendly welcome to the study using the participant's name, and the following texts were supportive, establishing rapport and making the men feel valued. However, the texts then became progressively more serious with the final messages emphasising the importance of behaviour change. The final text thanked the men for participating in the study.
The personal pronoun ‘you’ was used throughout, as it increases personal relevance and the processing of message arguments. 94 An early decision was to construct messages according to the conventions of texting, and to use the language of the target group. For example, the letter ‘u’ was used in place of ‘you’ and capitalised as ‘U’ to make it stand out. The abbreviated forms ‘it's’, ‘don't’, ‘I'll’ and ‘they're’ were used to create informality, but had the additional benefit of saving characters.
Unlike previous studies,23 no messages were repeated. Furthermore, the type and content of the messages was varied from day to day to maintain interest. Some messages were included because they might not be expected. For example, one text introduced a little-known side effect of heavy drinking, that it can cause ‘man boobs’ (male breasts).
Humour
Humour is thought to increase attention to messages, to increase their persuasiveness and to make them more memorable. 95,96 Humour was primarily used during the first 2 weeks of the study to engage the interest of the participants and build rapport with them. The jokes were designed to have sufficient appeal to be the kind you would want to show to your friends. Sharing texts would reinforce the impact of the message, increasing its salience and enlisting peer support for the study. As the target group was young to middle-aged men the humour had to be grounded in popular culture and included references to drunkenness and to sexual activity.
Tailoring of text messages
Tailoring is an essential feature of text messages. First name, or preferred name, was used for the first two and last two text messages of the intervention. Many messages reflected the drinking culture of the men which had been identified in focus groups, including drinking episodes with unfortunate consequences. The focus groups also provided examples of telling phrases which were used (anonymously) in the text messages. For example, one text used the expression of regret the day after a drinking session: ‘Many a weekend I've thought if I'd just went home at 8–9 p.m., I wouldn't be sitting here now feeling like a bag of shite’. When used, these quotes were attributed to individuals. To preserve anonymity individual names were replaced by the five most popular names given to babies born in Scotland in 1975; this was the mid-point of the years of birth of the study participants, 1966–85.
Gain-framing of messages
Conveying the adverse consequences of heavy drinking will help motivate participants to reduce their consumption. However, there is clear evidence that gain-framed messages are more effective than loss-framed ones. 91,97 To avoid loss-framing the messages about harms were frequently extended to conclude with the benefit of avoidance behaviour. For example, a text on the high death rate from alcohol was extended to wish the participant a long and healthy life. Similarly, the text on the high cost of alcohol was turned round to conclude with the amount that could be saved by cutting consumption.
Images
Images can enhance the coherence of the message (i.e. more clearly demonstrate how cause and effect are linked) by making behaviours and their consequences appear less abstract and more concrete. They can also help extend the narrative being developed, a particular benefit for short text messages. Images are often more memorable than verbal- or text-based messages. 98,99 In short, images can influence attitudes100,101 and intentions, thus increasing the likelihood of behaviour change.
Seventeen images, selected to be bright and colourful, were sent as MMS messages. They were designed to develop and extend the narrative and to make concrete the many harms of alcohol: impotence, vomiting, violence, crime, liver cirrhosis and death. For example, the way in which alcohol can make a peaceable individual aggressive was illustrated with a popular cartoon character, the Incredible Hulk™ (Marvel). The image of a jail was thought to be a powerful adjunct to a text conveying the risk of crime associated with heavy drinking. To ease the harshness of the message, a cartoon of the Monopoly™ (Hasbro) ‘Go to Jail’ character was used.
Paired messages
Five paired text messages, with the second message sent 3 minutes after the first, were used. This extends the time participants have to think about the content of the message. The device has several purposes: to enable more complex messages to be sent, to reinforce important concepts, and to extend the narrative of the previous message. For example, one text was used to seed an idea (a joke about the harms of alcohol) while the second encouraged reflection on the topic (i.e. can they think of any reasons for cutting down). This approach also introduces an element of novelty; when the participant opens a new message he cannot know whether a second will shortly follow.
Relapse
Two text messages to address relapse were built into the intervention. Relapse is common during behaviour change, particularly with behaviours like alcohol consumption. Individuals progress through the stages of change but often relapse to an earlier stage. 85 Thus, relapse was presented as a likely outcome: ‘If U aim to drink a little less on a night out but end up pissed, don't give up, it happens. Just try your best next time. Take care!’ The message provided encouragement on coping with unsuccessful attempts at cutting down.
Number, frequency and timing of message delivery
The question of when messages should be sent was resolved through an initial review of the target behaviour followed by testing of possible delivery schedules in the focus groups. Drinking patterns vary across the week, offering opportunities for different types of intervention. As many people drink more heavily at weekends, this creates two opportunities: early Friday evening before heavy drinking has started; and late morning or early afternoon on Sunday when drinkers experience regrets about the excesses of the previous nights. Between weekends there is a period of relative calm when mature reflection about the costs and benefits of drinking could be encouraged. The mid-week period is the time when a longer-term perspective can be taken on issues like money, relationships and health. Messages were designed to tap into these three opportunities: before drinking, after a heavy drinking episode and mid-week sobriety. Friday texts were sent at 1800 and Saturday texts at 1300–1400, in both cases before clients go out drinking. Sunday texts were generally later in the evening to give the participants a little more time to recover from a hangover. Mid-week texts, Monday to Thursday, were sent at selected times between 1200 and 2100. The aim was to avoid predictability.
A key question is the optimum number of messages to promote behaviour change: too few and the intervention will be ineffective, too many and messages will be unread with the risk that participants will withdraw from the study. The feasibility study opted for a moderate number of texts, 36, spread over a 28-day period. Thus, one message was sent each day but two introductory texts were sent on the first day and on five days pairs of linked messages were sent.
Interactivity
Conventional brief interventions involve a conversation between researcher and participant in which drinking motives, benefits and harms can be reviewed. Studies with automated delivery of text messages limit the opportunities for interaction. Questions can easily be incorporated into text messages and interactivity is a prominent feature of SMS-delivered interventions. 23 However, there is no opportunity to continue the dialogue, which restricts the use of questions to conversation-terminating events. An alternative approach is to take advantage of the finding that questions provoke more reflection on issues than statements or assertions. 102–104 Thus, questions were used to encourage participants to think about the key steps in the process to behaviour change: the potential benefits of drinking less, the people who would be pleased about moderated drinking (subjective norms) and self-efficacy about reducing drinking. A few questions were used primarily for humour to prevent messages being equated solely with serious issues.
Supplementary materials
Supplementary materials, such as websites and e-mail, could add to the effectiveness of an intervention. However, this potential gain is not without cost; it increases the demand placed on participants to access and use these materials. Making engagement with the intervention onerous was not attractive for this study. In studies of patients in clinical care, the additional burden of the supplementary materials might be welcomed because of perceived clinical need. This study recruited healthy individuals who were not seeking help for alcohol; they could potentially resent the invasion of their personal space. 23 Furthermore, using e-mail or websites to supplement the text messages would require daily access to an online computer, a facility which might not be available to all disadvantaged men. It was decided that the study should make as few demands on the participants as possible and thus supplementary materials were not used.
Control group messages
The aim of the control group messages was to promote engagement with the study and help retain individuals within the study. At the outset of the study participants were told that they were being recruited to a study on health and on alcohol. This would create an expectation of some level of involvement. The control package comprised 34 messages, delivered over 4 weeks. The messages addressed four topics – diet, physical activity, sexual health and mental health – with each topic lasting 1 week. The messages did not include any components of behaviour change theories, nor did they encourage behaviour change. It was, however, comparable to the intervention package in the duration and number of texts, the use of questions to elicit responses, the provision of health information and the frequent use of humour. Previous reviews have shown that in brief alcohol interventions the control group commonly receives little attention. 9,10
Improving the messages
Focus group comments on text messages
The design of the message content was assessed by members of the target population (11 disadvantaged men aged 21–55 years) in the focus groups. There was general support for both the acceptability and feasibility of a text messaging intervention. However, there was some scepticism and uncertainty as to its likely effect on substantive changes in drinking behaviours. Despite this there was broad agreement that a text would almost certainly always be read and that at the very least it would prompt a re-evaluation of drinking intentions.
What it might do, it would certainly make you think. It would certainly, it might be one little trigger and it might stop you there rather than going that little bit more.
Simon, aged 27 years
This suggested that a text might nudge the individual in the direction of behaviour change.
A lot of people are weak-willed so obviously they cannot do it on their own so they need that support there to help them to take the first step.
Brian, aged 29 years
Although nudging might be acceptable, urging behaviour change would not.
I always felt that nobody could dictate to you . . . I mean I live my life the way I see fit and I wouldn’t tell anybody else what way they should live, that's just the way I am.
Harry, aged 50 years
Interactivity of texting (i.e. requesting a participant to text back) was seen as generally plausible.
Just texting back wouldn’t put you out in any way, you know?
Tony, aged 28 years
However, there were indications that some texts might be ignored if they appeared to be from commercial companies or if the timing was inappropriate. The issue of frequency and timing was therefore explored in more depth. All focus groups appeared to concur that 2–4 texts per week maximum was appropriate. Suggestions for timing highlighted the effect of drinking on the individual's ability to make judgements and therefore the potential importance of both pre-drinking prompts and early-evening reminders.
I’d need a text when I’m sober so that it’s more of a thought-provoking text to say, well you know what, maybe tonight, I’ll not go, I’ll do something else. Because I think once I’m in the pub and I’m a round in, it’ll take a hell of a lot more than text messages, if I’m in the mood, to tell me to go home.
Simon, aged 27 years
Once on a Friday, a Friday afternoon. Because on a Friday you know what I mean, a lot of people go out drinking. And then Monday mornings, to remind them because they did get drunk all over the weekend. And then they’ve got an incentive for the next week to try and keep them off it.
Ben, aged 38 years
Given participants' indication that the receipt of between two and four texts per week might be acceptable, the question of how to sustain engagement with the texts was explored. Central to a tactic of sustained engagement was the use of humour. However, humour was again perceived by participants to potentially lead to more indirect or ‘diluted’ messages, therefore resulting in reduced effectiveness. Thus, humour was used sparingly and was avoided in the texts promoting behaviour change.
Do you want people to focus on the joke or do you want people to focus on the message? If you send a cracking joke with that text then it might take the focus off the actual text in the first place. Whereas you’d think that was a brilliant joke and you’d forget where it came from.
Simon, aged 27 years
One focus group was held with three women from areas of high deprivation. This was to give a different (but relevant) perspective on men's reasons for drinking, awareness of harms and likelihood of responding to the intervention. Women who participated were partners of men who met the entry criteria.
The women confirmed that their partners were regular heavy drinkers who drank mainly at home.
Well he drinks every weekend, for the weekend.
Claire, aged 19 years
They suggested that their partners drank because of boredom or to relax, but also because it is part of the culture.
Probably because they have been brought up round alcohol.
Janine, aged 19 years
The women were shown the text messages and asked how they thought their partners would respond to them. However, all of the women were more likely to give a personal reaction to the messages, and discussed what effect the texts would have on their own drinking. For some of the messages they said that they did not know how a man would respond. However, for a message which suggested that participants might try to reduce their drinking, the women thought it could be counterproductive because men don't like to be told.
Yes because a guy was, like a guy that likes his drink and goes out with his mates and if they were to read that they’d be like oh right, go and get a drink.
Mairi, aged 38 years
However, they conceded that some of the messages were likely to make some men think about their drinking.
It can hit home with some but not all.
Claire, aged 19 years
The women also indicated that they would be supportive if their partners were taking part in the study. In response to being shown the text message ‘Let friends and family know you are trying to cut down, tell them about this study and they may give you their support’, they said:
I would give my man support.
Janine, aged 37 years
I like it.
Claire, aged 19 years
Incorporation of effective behaviour change techniques
The messages were continually mapped onto 26 behaviour change techniques described in a recent review by Abraham and Michie15 on theory-based techniques used in interventions. This helped to identify any gaps in the strategies used, enabling new messages to be developed to strengthen the intervention. The final intervention included 15 behaviour change techniques from the list of 26. For example, the technique of gaining social support for behaviour change was used in the text: ‘let friends & family know if you are trying to cut down. Tell them about this study & they may give U their support’. Some texts incorporated more than one technique. The text ‘drinking too much can spoil a good night out & make U regret the things U did! Self control = more fun!’ provided information on consequences, prompted self-monitoring of behaviour and provided motivation for change.
Discussion
This is the first study of behaviour change through text messages which has described the theoretical and empirical basis of the intervention. The intervention texts were developed following a review of several types of literature: brief interventions for alcohol; interventions delivered by text message; psychological models and techniques of behaviour change and communication theory. The study has employed the range of methods which were used in previous text message studies, but also introduced new techniques intended to increase the effectiveness of the intervention: paired messages, images, texting conventions and the language of the target group. The comprehensive review of potential behaviour change strategies, together with a specification of the design challenges and opportunities, enabled a coherent sequence of messages to be constructed. These messages were tested and improved through focus groups. At the forefront of the design process was the target behaviour – binge drinking – and the habits, attitudes, intentions and consequences of that behaviour. The result was an intervention tailored not just to the individual and his social group, but to the target behaviour, the delivery vehicle, and to a wide range of theoretical and empirical behaviour change strategies.
The text messages were organised following the TTM, in which texts followed the sequence pre-contemplation, contemplation, preparation and action. However, these texts were informed by components of communication theory, the TPB, MI and reviews of effective techniques of behaviour change. This was achieved in an iterative process in which messages were written then reviewed to identify opportunities for the inclusion of further behaviour change strategies. By careful use of language an array of behaviour change texts were compressed into 36 user-friendly SMS and MMS messages. This was a substantial achievement given the restrictions of an intervention delivered by text message and the limited number of texts. Not surprisingly this process took several months to complete.
The text messages also employed several devices to increase the potential effectiveness of the intervention. The timing of the texts was designed for the target behaviour, weekend binge drinking. Gain-framing and humour were used to make potentially threatening messages more palatable. Two techniques, interactivity and paired messages, increased the time for reflection on the content of the messages. Interactivity, requesting responses to selected messages, would have a similar effect. The use of these techniques is particularly valuable for messages conveying important components of the behaviour change strategy. Although the intervention was delivered automatically by computer, it was carefully tailored to the target group and the individual. It used personal names and used an appropriate style and tone for the texts.
The use of text messages offers several advantages for a study targeting disadvantaged men, a group known to be resistant to conventional health promotion. The intervention delivery was not face to face. This meant that the men did not need to attend a specific appointment. Instead the men could access the intervention when it was convenient to them. It also allowed the men to access previous messages and to share messages with friends. These benefits will result in increased exposure to the intervention. Possibly the greatest benefit of text messaging is that the intervention could be rolled out to large numbers of individuals at low cost. The cost-effectiveness of the intervention will be tested in the full trial which follows this feasibility study.
In summary, this study has designed an empirically and theoretically based intervention which has been tailored to the target group and customised to suit the delivery mechanism (text messages). The feasibility study will assess the acceptability and potential for behaviour of the intervention, as well as identifying ways to improve the intervention.
Chapter 6 Recruitment strategies
Introduction
Trials of brief interventions on alcohol have predominantly recruited participants through health-care settings, particularly primary care. 8,9,36 As this study was aimed at community-dwelling individuals, it seemed sensible to use the electronic patient records systems held by GPs. However, this method may not be sufficient to recruit the target group, men aged 25–44 years. These men are usually healthy and are seldom in contact with health services, so an alternative recruitment method is needed.
This chapter reviews the literature on techniques to increase participation in research studies to identify strategies to improve recruitment. It then describes a recruitment strategy used in parallel with recruitment through primary care, and reports on strengths and weaknesses of each method. In view of the anticipated difficulty of recruiting disadvantaged young to middle-aged men, RDS was used alongside recruitment through primary care. RDS provides a method for recruiting hard-to-reach groups. 37,38 The technique assumes that the target population is distributed through a number of socially networked groups and is thus suitable for a group behaviour such as drinking.
Techniques to promote recruitment
Several techniques have been shown to increase recruitment rates. As non-contact makes at least as large a contribution to failure to recruit as does refusal to participate,105,106 both non-contact and refusal were addressed. Systematic reviews show that repeated attempts at contact and monetary incentives increase recruitment to research studies. 45,107 Strategies which have been found to be effective in general population groups31,32,44,107–110 are shown in Box 2. Similar strategies have been identified for recruiting hard-to-reach and minority groups, although particular emphasis is given to culturally sensitive study materials, multiple recruitment strategies and incentives. 111–115
Financial or other appropriate incentives
Multiple attempts at contact
Personalised approaches
Assurances of confidentiality
Direct personal contact (by telephone or in person)
Letter in advance of contact attempt
Shorter questionnaire
Sponsorship by prestigious body such as a university
Methods
Participants
Men aged 25–44 years living in areas of high deprivation were recruited. Deprivation was measured using the SIMD,46 which is similar to the English Index of Multiple Deprivation. 116
Inclusion/exclusion criteria
Men were included in the study if they had two or more episodes of heavy drinking (≥ 8 units in a single session) in the preceding month. Men currently attending care at an alcohol problem service and men who would not be contactable by mobile telephone for any part of the intervention and follow-up period were excluded.
Recruitment methods
The invitation letter, participant information leaflet and consent form are presented in Appendix 2. The screening questionnaire is in Appendix 3.
Strategy 1: recruitment through primary care
Potential participants were identified from the practice lists of three GPs. These lists provide data on age, telephone numbers and postcode, which facilitate selection of men aged 25–44 years from areas of deprivation. Postcode was used to derive the SIMD score. 117 Potential participants randomly selected from the two most disadvantaged deciles were sent a letter by their GP inviting them to take part. The letter was personally addressed, mentioned the University of Dundee and stated that a financial reward would be given. The accompanying participant information leaflet carried the university's logo and stressed the confidentiality of the study. An opt-out strategy was used for recruitment. The names, addresses and telephone numbers of those who did not decline to take part were provided to the researchers by the GPs. Contact with these individuals was made by telephone approximately 2 weeks after the GP letter. The researcher described the study to these individuals, answered any questions and asked them if they wished to participate.
Up to six attempts were made to contact by telephone the men who did not opt out, at different times of the day and on different days of the week. Those who agreed to take part when contacted were asked to complete the screening questionnaire to determine eligibility. Ethical consent was then obtained from suitable individuals. On completion of the baseline questionnaire, participants were sent an initial £10 gift voucher to offset any charges incurred by receiving and responding to text messages. They were also sent a £5 gift voucher for each week of the study and a £10 voucher for completing the outcome assessment.
Strategy 2: respondent-driven sampling
Respondent-driven sampling begins with the identification of ‘seed’ individuals obtained from different locations. In this study, seeds were recruited from several venues in areas of high deprivation. The seed individuals identified suitable subjects from their social networks and recruited them to the study. A key element of the technique was the use of incentives to each seed person for taking part in the study and for each of the individuals they recruited. All participants recruited by this method also received the sequence of gift vouchers as described in recruitment strategy 1. In addition, the seed individuals received a £5 gift voucher for each person they recruited.
Potential seed individuals contacted directly were told about the nature of the study, the financial incentives and the sponsorship by the university. They were also given participant information leaflets as described for recruitment strategy 1. Individuals nominated by seeds were given the same information by telephone and were sent a copy of the participant information leaflet by post. This was followed up by another telephone call to explain the nature of the study and obtain informed consent as described below.
Initial screening and informed consent
Individuals identified by the recruitment strategies were screened by a telephone call from a researcher to establish current drinking levels. Those who reported binge drinking (≥ 8 units in a single session) at least twice in the previous 30 days were identified as potential participants. The details on the participant information leaflet were explained, such as their right to withdraw from the study at any time and the confidentiality of the data. Verbal consent was sought after potential participants confirmed that they had understood the contents of the information leaflet. Those who agreed to participate were sent a text message which asked them to reply to the message if they wanted to take part in the study. This meant that potential participants had to indicate their consent to participate by taking the positive action of responding to a text message. During the screening interview a consent form was completed by the research fellow. When the consent text was received, the date and time of obtaining consent was recorded and the form was signed by the research fellow. The consenting text was retained as proof of consent.
Results
Recruitment
Recruitment began on 17 March 2011 and was completed on 12 June 2011. A total of 67 men were recruited, exceeding the target of 60. The over-recruitment occurred because of the yield from the final GP. As the response rate could not be predicted, letters of invitation were sent to all 120 men randomly selected from the GP list at that practice. Recruitment could have been stopped when the intended target of 60 participants was achieved, but it seemed unwise, and possibly unethical, to write to men about a study then subsequently fail to invite them to participate.
Yield from recruitment through primary care
Identifying men living in areas of deprivation from practice databases proved straightforward. A random sample was taken of men on the practice lists who were in the appropriate age and deprivation categories. The sample taken allowed for anticipated loss due to failure to contact, ineligibility (do not binge drink frequently) and refusal. GPs screened these samples to exclude candidates because of concerns about health or family problems. The GPs noted that screening the lists of men was difficult because few of the men attended their doctor regularly. Almost all the men (89%) had telephone numbers, either landline or mobile, in their GP records and few (3%) were excluded by their GP (Table 4).
| GP number | Men identified | Men contacted | Men with no telephone number | Invalid postal address | Requested not to take part | Men to be telephoned |
|---|---|---|---|---|---|---|
| 1 | 75 | 75 | 0 | 3 | 5 | 67 |
| 2 | 120 | 106 | 10 | 2 | 2 | 92 |
| 3 | 120 | 115 | 24 | 4 | 3 | 84 |
As expected, some of the telephone numbers were invalid (Table 5); in fact, 25% of numbers tested were invalid. As up to six attempts were made to contact the men (covering daytime, evenings and weekends) it was expected that most men would answer the telephone. In the event, 18% of those with valid telephone numbers did not answer the telephone. Of those contacted, 31% refused to participate and a further 40% were found to be ineligible because they did not binge drink regularly. As a result, 29% of those contacted were recruited.
| GP number | Invalid telephone number | Wrong person answered | Never answered | Not interested | Not eligible | Recruited |
|---|---|---|---|---|---|---|
| 1 | 19 | 1 | 12 | 16 | 15 | 4 |
| 2 | 20 | 4 | 10 | 23 | 18 | 17 |
| 3 | 22 | 7 | 12 | 10 | 17 | 16 |
Lessons from recruitment through primary care
Recruitment through primary care is subject to losses from failure to contact (missing or incorrect telephone numbers) or refusal to take part. Ineligibility, because of low frequency of binge drinking, was a major reason for failure to recruit. Some men appeared concerned that the approach might be part of a scam to steal money. This was more marked when first-approach telephone calls came from an institutional 0845 telephone number. Use of a dedicated study mobile telephone number overcame this difficulty. As participants are randomised to treatment group, losses to recruitment will not affect internal validity of the study. Trials recruiting through this route should contact substantially more individuals than required to allow for these losses.
Yield from recruitment through respondent-driven sampling
In total, 30 men were recruited over a 5-week period. The sample of 30 men comprised 12 who did not nominate any friends and seven who nominated 11 friends in total. All of the nominated friends were recruited to the study. The venues through which men were recruited are shown in Table 6 (nominees have been allocated to the venue on the nominator). Multiple locations were used to ensure recruitment of individuals from different social networks. Recruitment took place during the day, in the evening and at the weekend.
| Locations for recruitment | Number recruited |
|---|---|
| Sports centres, outdoor and indoor football pitches, snooker halls | 5 |
| Community centres | 0 |
| Colleges of further education | 3 |
| Workplaces: hospital and university porters and cleaners | 8 |
| Shopping centres, cafes | 0 |
| Bars | 4 |
| Criminal justice service | 5 |
| Other informal contacts | 5 |
| Libraries | 0 |
Lessons from the respondent-driven sampling
Modes of recruitment
In total, 30 men were recruited from a variety of venues. More men were recruited from some venues than others, but interpreting this is problematic. At venues where groups of men were present it was not possible to count the number approached because they entered and left together. For example, teams of men at sports centres would be leaving at the same time. Thus, it was not possible to identify who had heard the initial request for attention, who had to leave quickly because of other engagements and who was not interested in the study.
Young and middle-aged men are willing to be stopped opportunistically at a wide range of settings. Approaching small groups was more productive than approaching single men, possibly because of the security of belonging to a group. In a group, the first response made, either in support of or against the study, often set the tone for the whole group. Timing is crucial for recruitment through sporting activities, as the men often wish to hurry away when the activity is finished.
Recruitment at some settings (e.g. snooker halls and slot machine venues) proved problematic. Staff at these venues wished to protect their clients from being disturbed. This was quickly established at the first contact and these venues were removed from the list. At other settings, such as community centres and sports clubs, many or all of the men were ineligible because they did not binge drink frequently.
Further education staff can greatly expedite the recruitment of men through their settings; they know and are known by the potential recruits, giving an opportunity for a personal touch in recruitment. Recruitment through work settings can be effective. However, in contrast to the community and further education settings, involvement of managerial staff in workplace settings could be counter-productive. Although the managers were keen to help identify men, recruitment was poor. It is possible that the men were concerned that information on their alcohol consumption would be passed to their employers. An alternative strategy, where the manager gave approval but the researcher did the recruitment, proved more successful.
Some bar staff were willing to nominate regular customers, although many other staff were reluctant to do so. Although there were few men in shopping centres, informal approaches were potentially useful, as the men appeared to have more time to chat. There were very few single men or groups of men in cafes.
Nomination of peers
Each of the recruited men was asked to nominate friends for possible inclusion in the study. Despite being offered financial reward for this (£5 for each friend nominated), only seven men did so. The rate of nomination was lower than in previous reports. 118,119 It is possible that the focus of the study on binge drinking inhibited men from nominating friends. Alternatively it could be that the nominators did not know enough about the study to feel confident in nominating a friend. Interestingly, one man who nominated two friends was never recruited to the study although he had said that he would take part.
Distribution by deprivation category
Deprivation was measured by the SIMD, in which decile 1 is high deprivation (Table 7). Although most of the men lived in areas of high deprivation, a few were from areas of low deprivation. Assessing the socioeconomic status of potential recruits during the recruitment proved problematic. It was decided it would have been impolite to ask the men directly whether or not they were from disadvantaged areas. In a full efficacy trial it would be possible to conduct a subgroup analysis which excluded the men from the least deprived areas. This could be accompanied by over-recruitment to ensure the intended sample size is achieved after the exclusions.
| Deprivation category (deciles) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| Number of men | 7 | 7 | 7 | 4 | 3 | 0 | 0 | 0 | 2 |
Additional venues for recruitment
Many people in the target group (binge drinking young and middle-aged socially disadvantaged men) are hidden because they do not participate in community activities. It proved difficult to recruit these men from community-based activities or sports centres, even though they are located in areas of high deprivation. Thus, instead of recruiting from organised activities, effort should be directed to venues in areas of high deprivation where these people must go, such as:
-
post offices
-
pharmacies
-
common areas in high-rise buildings
-
organisations/training centres where long-term unemployed people are required to attend.
Other lessons learned
Several observations were made during the conduct of the telephone calls. As these were unexpected findings, data recording procedures had not been put in place to record them. Thus, they could not be quantified.
-
Some men found the information given about the study did not fully explain what would be involved. Although further information was given during recruitment, it is possible that some men may not have asked for clarification, and instead refused to participate. Forming a rapport at the first telephone call and actively exploring concerns about participation can prevent this loss of participants.
-
People who drink a lot may be unwilling to disclose this to a stranger. They would thus be classed as not meeting the entry criteria. Establishing rapport, emphasising the confidential nature of the data and stressing the benefits of the research will minimise this problem.
Discussion
This study has shown it is possible to recruit sufficient disadvantaged men in early mid-life using recruitment through GPs or through RDS. Although this study focused on a difficult-to-recruit group it easily exceeded its recruitment target. Based on previous research,18 it is likely that the use of incentives contributed to the successful recruitment. The other recruitment techniques, particularly personalised approaches, credibility of the source and assurances of confidentiality, are likely to have played their part.
Both methods of recruitment proved successful. Recruitment through primary care is a well-tested strategy for trials of brief interventions for alcohol. In this study the intended sample size was easily attained, although only a subsample of men from the three GPs were approached. It also showed that failure to contact was a greater cause of non-inclusion than was refusal to participate. Recruitment through RDS was also successful in recruiting disadvantaged young men. This method has the potential to recruit large numbers of individuals, because of the many venues from which participants could be recruited. This method of recruitment requires a period of preliminary fieldwork to identify suitable venues and to negotiate approval to recruit through them.
This study was designed with a view to national roll-out. To keep costs low, a national study would require a low level of staff involvement in recruitment. Thus, the study developed and tested a non-contact method for recruiting and obtaining informed consent. This method proved successful. An additional benefit of the minimal-contact recruitment strategy is that the process of entry to the study does not become part of the behaviour change intervention. Thus, the intervention tested in this feasibility study and the proposed full trial will be the same as that used in any national roll-out.
Chapter 7 Randomisation and baseline characteristics
Introduction
Following the initial screening, informed consent and recruitment, participants were entered into the trial and randomised to the intervention or control group. Baseline data on all the recruited individuals were obtained by telephone interview. The aim was to describe the demographic characteristics and alcohol consumption for comparison with other studies. Data on the primary and secondary outcome measures were also collected, as were data on drinking intentions. This chapter reports on the results of the randomisation and the baseline interviews to assess whether or not study procedures worked satisfactorily and to determine the characteristics of the men recruited to the study.
Methods
Randomisation and blinding
After obtaining informed consent, participants were randomised to receive intervention or control messages by a three-way collaboration between the Schools of Medicine and Computing at the University of Dundee and the University of Glasgow Clinical Trials Unit. The processes were repeatedly tested in isolation then in combination. Handshaking between the Glasgow and Dundee computer systems required careful attention.
A web-based randomisation strategy was provided by the University of Glasgow Clinical Trials Unit. After consent had been obtained by the research fellow in the School of Medicine, Dundee, participants were allocated a unique study ID number. This, together with method of recruitment (GP or RDS), was entered into the randomisation website. Randomisation, allocation ratio 1 : 1, was stratified by recruitment strategy (GP or RDS) and was restricted using a block size of four.
The research fellow at the Medical School entered key participant information (ID, date of recruitment and participant's preferred name) into a website provided by the School of Computing at the University of Dundee. The Clinical Trials Unit sent the randomisation codes, with participant ID, directly to the School of Computing which then combined the randomisation code data with the participant information. The School of Computing managed the computerised delivery of the intervention. It was thus able to send a predetermined sequence of text messages (intervention or control) which were tailored to individual participants. The date of recruitment was used to start messages on the first Monday following recruitment. Thus, the School of Medicine research fellow who recruited participants and conducted baseline and follow-up interviews was not involved in the randomisation or the delivery of the intervention. Furthermore, the research team in the School of Medicine remained blind to treatment status until after the analysis of the primary and secondary outcomes.
Baseline interview
The baseline interview was conducted by telephone at a time suitable for the participants prior to the delivery of the first of the text messages. Interviews typically took 15–20 minutes, although occasionally longer. The interview largely comprised closed questions. A blank pro forma was completed during the interview and checked for completeness after the interview.
Baseline questionnaire (see Appendix 4)
Data were collected on age, address (to derive an area-based measure of deprivation), employment status and educational attainment. Questions on alcohol consumption were taken from the US Behavioral Risk Factor Surveillance System. 120 This enabled total consumption and frequency of binge drinking to be measured. Alcohol consumption was measured over the 30 days prior to interview to capture patterns of drinking which could vary from week to week. In addition, the frequency of drinking substantially in excess of the conventional binge drinking level (i.e. ≥ 16 units in a session) was recorded. The Fast Alcohol Screening Test (FAST)121 was used to determine hazardous drinking because it is short and thus suitable for telephone use. Questions on refusal skills were taken from the Drinking Refusal Self-efficacy Questionnaire. 122 The Readiness to Change Questionnaire123 was used to measure the stage of intention to reduce consumption. A separate question was also added on intentions to reduce drinking. Questions were also asked on knowledge of the harms of alcohol, the definition of binge drinking, the benefits of moderate drinking and whether or not current drinking was perceived to be harmful. The questions on harms were not restricted to health, but were left open so that any type of harm could be mentioned. The question on the benefits of moderated drinking was similarly unrestricted. The questionnaire was piloted and modifications were made to several questions.
Reported alcohol consumption (pints, bottles, etc.) was converted to units of alcohol. The free text answers to two questions (harms of drinking and benefits of moderated drinking) were listed and coded as short term (e.g. hangover, violence and accidents) and long term (e.g. cirrhosis, family break-up and addiction).
Statistical methods
Descriptive statistics were used to explore the characteristics of the intervention and control groups at baseline. Blinding was preserved until outcome data were collected and analysed. Until blinding was broken treatment groups were assigned arbitrary codes 1 and 2 by the School of Computing. The coding key was concealed until after the analyses. As part of the assessment of the two recruitment strategies a comparison was made of the participants recruited from primary care and through RDS. The chi-squared test was used for categorical data and the t-test for continuous data to test whether or not the men in the two recruitment strategies differed.
Results
The processes for entry into the trial, allocation of a unique ID number, and sequential addition of randomisation code and personal name worked well. A flow diagram giving the recruitment of participants to the trial, randomisation and follow-up is given in Figure 1. Data collection at baseline was successful. The questions were readily understood and a full data set was obtained on all participants. In particular, the set of questions to describe drinking patterns (total consumption, frequencies of binge drinking, heavy binge drinking and moderate drinking days) were answered without difficulty.
FIGURE 1.
Consolidated Standards of Reporting Trials (CONSORT) 2010 flow diagram.
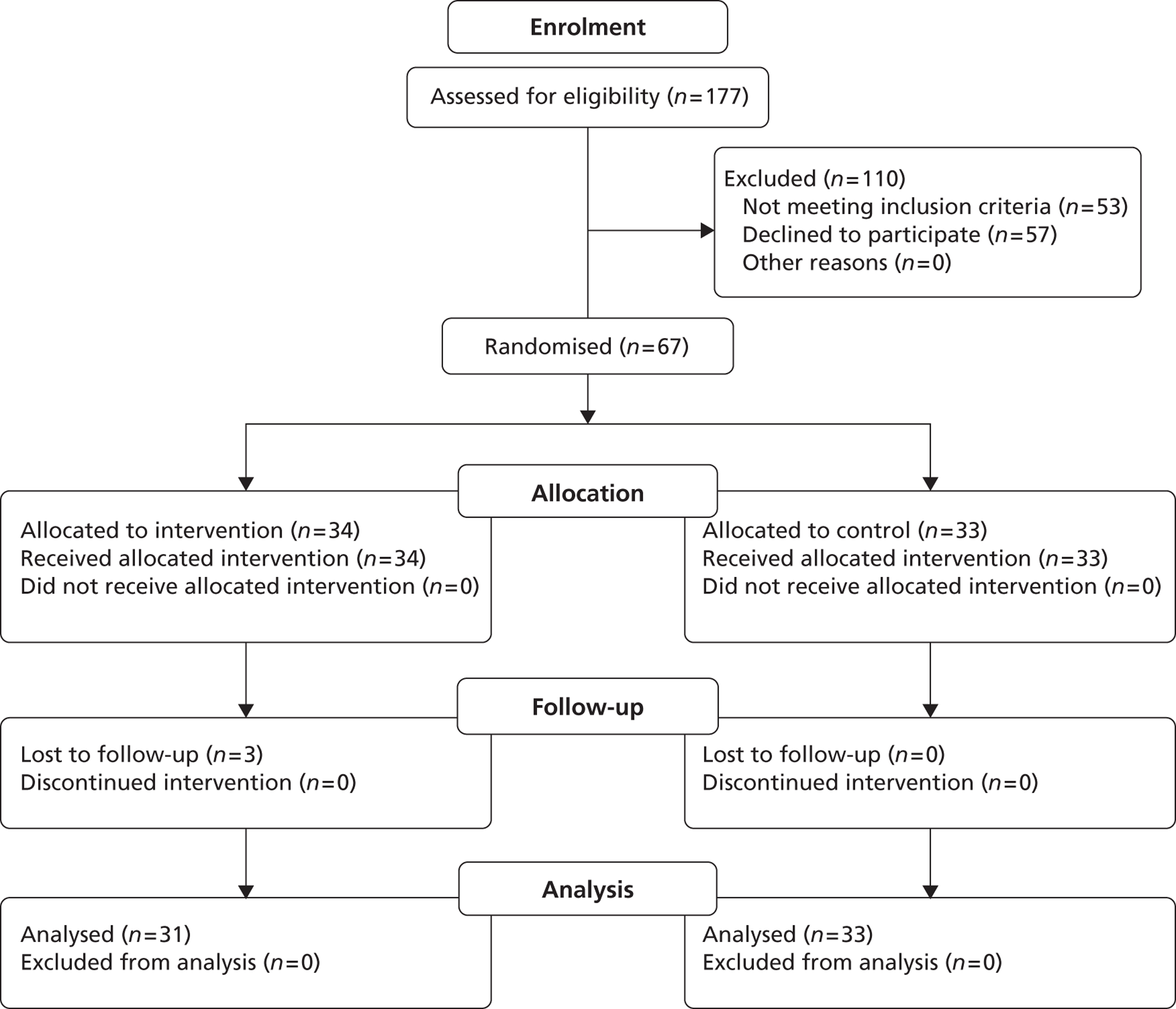
All participants were retained in the groups to which they were originally allocated. To ensure comparability between baseline and outcome data, baseline analyses (see Tables 8–16) only included men successfully followed up (only 3 of 67 men were lost to follow-up, see Chapter 10). The intervention and control groups were compared on demographic factors, alcohol consumption, awareness of harms and refusal self-efficacy. The participants were spread across the age range 25–44 years, almost four-fifths were in the lowest two deprivation deciles and over half only had school-level qualifications (Table 8). Twice as many participants were employed as unemployed and most lived with a partner. The intervention and control groups were similar on all demographic factors.
Most men (84%) were classified as hazardous drinkers (FAST-positive) (Table 9). The common pattern of alcohol consumption was one of occasional heavy drinking episodes interspersed between periods of complete abstinence. The men all had regular binge drinking sessions, with one third having six or more binge drinking sessions per month. More than two-thirds of the men had binge drinking sessions at which they consumed ≥ 16 units of alcohol in a session (twice the conventional binge drinking level of 8 units of alcohol). However, more than three-quarters of participants had at least 21 alcohol-free days per month. Consequently, the average weekly consumption was relatively moderate at 22.4 units. This is close to the recommended maximum weekly consumption of 21 units.
| Factor | Control group (N = 33), n (%) | Intervention group (N = 31), n (%) | Total (N = 64), n (%) |
|---|---|---|---|
| Participants' age (years) | |||
| 25–29 | 13 (39) | 7 (23) | 20 (31) |
| 30–34 | 6 (18) | 5 (16) | 11 (17) |
| 35–39 | 9 (27) | 9 (29) | 18 (28) |
| 40–44 | 5 (15) | 10 (32) | 15 (23) |
| Marital status | |||
| Married/lives with a partner | 21 (64) | 16 (52) | 37 (58) |
| Single | 12 (36) | 15 (48) | 27 (42) |
| SIMD decile | |||
| 1 (most deprived) | 14 (42) | 13 (42) | 27 (42) |
| 2 | 11 (33) | 12 (39) | 23 (36) |
| 3 | 5 (15) | 1 (3) | 6 (9) |
| ≥ 4 | 3 (9) | 5 (16) | 8 (13) |
| Employment status | |||
| Employed | 25 (76) | 18 (58) | 43 (67) |
| Unemployed | 8 (24) | 13 (42) | 21 (33) |
| Highest educational attainment | |||
| University degree | 6 (18) | 4 (13) | 10 (16) |
| Vocational qualification/further training | 9 (27) | 11 (36) | 20 (31) |
| High school | 18 (55) | 16 (52) | 34 (53) |
| Factor | Control group (N = 33), n (%) | Intervention group (N = 31), n (%) | Total (N = 64), n (%) |
|---|---|---|---|
| Hazardous drinkers (positive FAST) | 28 (85) | 26 (84) | 54 (84) |
| Frequency of ≥ 8 units of alcohol in a single occasion in the last year | |||
| Less than monthly | 2 (6) | 5 (16) | 7 (11) |
| Monthly | 20 (61) | 13 (42) | 33 (52) |
| Weekly | 10 (30) | 10 (32) | 20 (31) |
| Daily or almost daily | 1 (3) | 3 (10) | 4 (6) |
| Total consumption in previous 30 days (units) | |||
| 16–50 | 9 (27) | 15 (48) | 24 (38) |
| 51–84 | 9 (27) | 6 (19) | 15 (23) |
| 85–120 | 8 (24) | 3 (10) | 11 (17) |
| > 120 | 7 (21) | 7 (23) | 14 (22) |
| Alcohol consumption | |||
| Mean consumption in past 30 days [units (SD)] | 89.5 (65.6) | 103.3 (137.2) | 96.2 (105.8) |
| Average weekly consumption [units (SD)] | 20.9 (15.3) | 24.0 (32.0) | 22.4 (24.7) |
| Number of binge drinking days in previous 30 days (≥ 8 units in one session) | |||
| 2 | 14 (42) | 13 (42) | 27 (42) |
| 3–5 | 6 (18) | 9 (29) | 15 (23) |
| > 5 | 13 (39) | 9 (29) | 22 (34) |
| Units usually consumed during a binge drinking session | |||
| 8–10 | 7 (21) | 6 (19) | 13 (20) |
| 11–14 | 8 (24) | 10 (32) | 18 (28) |
| 15–19 | 8 (24) | 9 (29) | 17 (27) |
| ≥ 20 | 10 (30) | 6 (19) | 16 (25) |
| Number of heavy binge drinking days in previous 30 days (≥ 16 units in one session) | |||
| 0 | 8 (24) | 11 (35) | 19 (30) |
| 1–2 | 13 (39) | 6 (19) | 19 (30) |
| 3–5 | 8 (24) | 6 (19) | 14 (22) |
| 6–10 | 4 (12) | 6 (19) | 10 (16) |
| > 10 | 0 | 2 (6) | 2 (3) |
| Number of moderate drinking days in previous 30 days (< 8 units in one session) | |||
| 0 | 11 (33) | 18 (58) | 29 (45) |
| 1–2 | 13 (39) | 7 (23) | 20 (31) |
| 3–5 | 5 (15) | 5 (16) | 10 (16) |
| > 5 | 4 (12) | 1 (3) | 5 (8) |
| Number of alcohol-free days in previous 30 days | |||
| < 10 | 2 (6) | 5 (16) | 7 (11) |
| 11–20 | 7 (21) | 2 (6) | 9 (14) |
| 21–24 | 7 (21) | 6 (19) | 13 (20) |
| 25–30 | 17 (52) | 18 (58) | 35 (55) |
Few men (5%) knew the conventional definition of binge drinking (8 units in a session) and most thought it was much higher (Table 10). Consistent with the episodic pattern of drinking, most men were unaware that this level of drinking is harmful. Although most men were drinking hazardously, only 25% believed that their drinking was harmful.
| Factor | Control group (N = 33), n (%) | Intervention group (N = 31), n (%) | Total (N = 64), n (%) |
|---|---|---|---|
| How many units of alcohol is binge drinking? | |||
| ≤ 8 | 2 (6) | 1 (3) | 3 (5) |
| 9–14 | 11 (33) | 10 (32) | 21 (33) |
| 15–20 | 13 (39) | 12 (39) | 25 (39) |
| > 20 | 6 (18) | 7 (23) | 13 (20) |
| Don't know | 1 (3) | 1 (3) | 2 (3) |
| Drinking 8 units of alcohol in a single session is harmful | |||
| Strongly agree | 6 (18) | 5 (16) | 11 (17) |
| Agree | 7 (21) | 8 (26) | 15 (23) |
| Don't know | 1 (3) | 4 (13) | 5 (8) |
| Disagree | 12 (36) | 6 (19) | 18 (28) |
| Strongly disagree | 7 (21) | 8 (26) | 15 (23) |
| My current level of drinking is harmful to my health | |||
| Strongly agree | 6 (18) | 4 (13) | 10 (16) |
| Agree | 3 (9) | 3 (10) | 6 (9) |
| Don't know | 7 (21) | 7 (23) | 14 (22) |
| Disagree | 6 (18) | 5 (16) | 11 (17) |
| Strongly disagree | 11 (33) | 12 (39) | 23 (36) |
| The benefits from my drinking outweigh the harms it causes | |||
| Strongly agree | 5 (15) | 8 (26) | 13 (20) |
| Agree | 4 (12) | 5 (16) | 9 (14) |
| Don't know | 6 (18) | 5 (16) | 11 (17) |
| Disagree | 9 (27) | 5 (16) | 14 (22) |
| Strongly disagree | 9 (27) | 8 (26) | 17 (27) |
Although most men reported a pattern of heavy binge drinking, almost 60% reported that their drinking never impacts on what they are normally expected to do (from the FAST questionnaire). Most men stated they had occasionally been unable to remember what happened during a drinking session, with 27% stating that this happens at least monthly.
Almost all (97%) of the men identified one or more harms of heavy drinking (Table 11), with most identifying two or three harms. The men identified similar numbers of short-term harms (such as hangovers or fights) and chronic harms (such as cirrhosis). Most men (91%) identified benefits of more moderate drinking. However, the men were very much more likely to identify short-term benefits than benefits which accrued in the longer term.
| Factor | Control group (N = 33), n (%) | Intervention group (N = 31), n (%) | Total (N = 64), n (%) |
|---|---|---|---|
| Harms of heavy drinking | |||
| Total number of harms of heavy drinking identified | |||
| 0–1 | 6 (18) | 9 (29) | 15 (23) |
| 2–3 | 21 (64) | 14 (45) | 35 (55) |
| ≥ 4 | 6 (18) | 8 (26) | 14 (22) |
| Number of short-term harms identified | |||
| 0–1 | 19 (58) | 21 (68) | 40 (63) |
| 2–3 | 12 (36) | 9 (29) | 21 (33) |
| ≥ 4 | 2 (6) | 1 (3) | 3 (5) |
| Number of chronic harms identified | |||
| 0–1 | 24 (73) | 20 (65) | 44 (69) |
| 2–3 | 9 (27) | 10 (32) | 19 (30) |
| ≥ 4 | 0 | 1 (3) | 1 (2) |
| Benefits of moderate drinking | |||
| Total number of benefits of moderate drinking identified | |||
| 0–1 | 9 (27) | 9 (29) | 18 (28) |
| 2–3 | 23 (70) | 18 (58) | 41 (64) |
| ≥ 4 | 1 (3) | 4 (13) | 5 (8) |
| Number of short-term benefits identified | |||
| 0–1 | 12 (36) | 11 (35) | 23 (36) |
| 2–3 | 20 (61) | 17 (55) | 37 (58) |
| ≥ 4 | 1 (3) | 3 (10) | 4 (6) |
| Number of long-term benefits identified | |||
| 0–1 | 33 (100) | 29 (94) | 62 (97) |
| 2–3 | 0 | 2 (6) | 2 (3) |
Despite awareness of the harms of heavy drinking and the benefits of moderate drinking, 42% had never considered reducing their alcohol consumption. The Readiness to Change Questionnaire123 showed that most men (61%) were in the pre-contemplation stage and few were taking action to cut down (Table 12).
| Factor | Control group (N = 33), n (%) | Intervention group (N = 31), n (%) | Total (N = 64), n (%) |
|---|---|---|---|
| Have you ever considered cutting down on your alcohol consumption? | |||
| No | 12 (36) | 15 (48) | 27 (42) |
| Yes, but not in the last 3 months | 12 (36) | 11 (35) | 23 (36) |
| Yes, in the last 3 months | 9 (27) | 5 (16) | 14 (22) |
| Do you have any plans to cut down on your drinking in the future? | |||
| Not at all | 14 (42) | 16 (52) | 30 (47) |
| I am thinking about it | 14 (42) | 12 (39) | 26 (41) |
| I have already made a plan | 5 (15) | 3 (10) | 8 (13) |
| Stage of readiness to change | |||
| Pre-contemplation | 18 (55) | 21 (68) | 39 (61) |
| Contemplation | 10 (30) | 6 (19) | 16 (25) |
| Action | 5 (15) | 4 (13) | 9 (14) |
Questions on refusing drinks were taken from the Drinking Refusal Self-efficacy Questionnaire. 122 Most men think they are able to refuse alcohol in many social situations (e.g. going out to eat, watching television) (Table 13). However, they find it much more difficult to refuse when offered a drink or when their friends are drinking.
| Factor | Control group (N = 33), n (%) | Intervention group (N = 31), n (%) | Total (N = 64), n (%) |
|---|---|---|---|
| I could resist alcohol when I go out to eat | |||
| Strongly agree | 28 (85) | 26 (84) | 54 (84) |
| Agree | 2 (6) | 2 (6) | 4 (6) |
| Don't know | 1 (3) | 2 (6) | 3 (5) |
| Disagree | 0 | 0 | 0 |
| Strongly disagree | 2 (6) | 1 (3) | 3 (5) |
| I could resist alcohol when I am watching television | |||
| Strongly agree | 25 (76) | 24 (77) | 49 (77) |
| Agree | 3 (9) | 2 (6) | 5 (8) |
| Don't know | 1 (3) | 2 (6) | 3 (5) |
| Disagree | 1 (3) | 0 | 1 (2) |
| Strongly disagree | 3 (9) | 3 (10) | 6 (9) |
| I could resist alcohol if someone offered me a drink | |||
| Strongly agree | 16 (48) | 12 (39) | 28 (44) |
| Agree | 9 (27) | 9 (29) | 18 (28) |
| Don't know | 1 (3) | 3 (10) | 4 (6) |
| Disagree | 3 (9) | 4 (13) | 7 (11) |
| Strongly disagree | 4 (12) | 3 (10) | 7 (11) |
| I could resist alcohol when my friends are drinking | |||
| Strongly agree | 7 (21) | 11 (35) | 18 (28) |
| Agree | 9 (27) | 7 (23) | 16 (25) |
| Don't know | 4 (12) | 2 (6) | 6 (9) |
| Disagree | 6 (18) | 6 (19) | 12 (19) |
| Strongly disagree | 7 (21) | 5 (16) | 12 (19) |
| I could resist alcohol when I am bored | |||
| Strongly agree | 24 (73) | 23 (74) | 47 (73) |
| Agree | 5 (15) | 3 (10) | 8 (13) |
| Don't know | 1 (3) | 1 (3) | 2 (3) |
| Disagree | 1 (3) | 2 (6) | 3 (5) |
| Strongly disagree | 2 (6) | 2 (6) | 4 (6) |
Comparison of subjects recruited by the two sampling strategies
The different methods used in the two sampling strategies could potentially recruit different types of individuals. This was explored by comparing the two groups by their demographic characteristics, patterns of alcohol consumption and intentions for future drinking.
The men recruited through RDS were more likely to be unemployed and less likely to be married (Table 14). In addition, they drank more than twice as much as the men recruited through GP and had many more binge drinking days: only 17% of the GP sample had six or more binge drinking days, whereas more than half (57%) of men from RDS had six or more binge drinking days (Table 15). The RDS men also had many more heavy binge drinking days (consuming ≥ 16 units in one session). Consequently, the RDS sample had fewer alcohol-free days.
| Factor | GP (N = 36), n (%) | RDS (N = 28), n (%) | Total (N = 64), n (%) | p-valuea |
|---|---|---|---|---|
| Marital status | ||||
| Married/lives with a partner | 27 (75) | 10 (36) | 37 (58) | 0.002 |
| Single | 9 (25) | 18 (64) | 27 (42) | |
| SIMD decile | ||||
| 1 (most deprived) | 20 (56) | 7 (25) | 27 (42) | < 0.0001 |
| 2 | 16 (44) | 7 (25) | 23 (36) | |
| 3 | 0 | 6 (21) | 6 (9) | |
| ≥ 4 | 0 | 8 (29) | 8 (13) | |
| Employment status | ||||
| Employed | 28 (78) | 15 (54) | 43 (67) | 0.041 |
| Unemployed | 8 (22) | 13 (46) | 21 (33) | |
| Highest educational attainment | ||||
| High school | 17 (47) | 17 (61) | 34 (53) | 0.064 |
| Vocational qualification/further training | 10 (28) | 10 (36) | 20 (31) | |
| University degree | 9 (25) | 1 (4) | 10 (16) | |
The higher frequency of binge and heavy binge drinking days had consequences. The men from RDS were much more likely to have episodes where they forgot what they had done during a binge drinking session (see Table 15). They were also much more likely to be thinking about making plans to cut down their drinking in the future (Table 16). The Readiness to Change Questionnaire confirmed this difference: three-quarters of the GP sample were in pre-contemplation, whereas 57% of the RDS sample were in contemplation or action.
| Factor | GP (N = 36), n (%) | RDS (N = 28), n (%) | Total (N = 64), n (%) | p-value |
|---|---|---|---|---|
| Mean consumption in past 30 days [units (SD)] | 65.51 (50.44) | 139.50 (139.16) | 96.20 (105.8) | 0.003a |
| Number of binge drinking days in previous 30 days (≥ 8 units in one session) | ||||
| 2–5 | 30 (83) | 12 (43) | 42 (66) | 0.002b |
| > 5 | 6 (17) | 16 (57) | 22 (34) | |
| Mean number of units usually consumed during a binge drinking session [units (SD)] | 15.49 (4.79) | 15.58 (5.80) | 15.53 (5.21) | 0.942a |
| Number of heavy binge drinking days in previous 30 days (≥ 16 units in one session) | ||||
| 0–5 | 34 (94) | 18 (64) | 52 (81) | 0.014b |
| ≥ 6 | 2 (6) | 10 (36) | 12 (19) | |
| Number of alcohol-free days in previous 30 days | ||||
| 0–20 | 6 (17) | 10 (36) | 16 (25) | 0.002b |
| 21–30 | 30 (83) | 18 (64) | 48 (75) | |
| How often during the last year have you been unable to remember what happened the night before because you had been drinking? | ||||
| Less than monthly | 34 (94) | 13 (46) | 47 (73) | 0.001b |
| More than once per month | 2 (6) | 15 (54) | 17 (27) | |
| Drinking 8 units of alcohol in a single session is harmful | ||||
| Strongly agree | 5 (14) | 6 (21) | 11 (17) | 0.231b |
| Agree | 6 (17) | 9 (32) | 15 (23) | |
| Don't know | 3 (8) | 2 (7) | 5 (8) | |
| Disagree | 14 (39) | 4 (14) | 18 (28) | |
| Strongly disagree | 8 (22) | 7 (25) | 15 (23) | |
| Factor | GP (N = 36), n (%) | RDS (N = 28), n (%) | Total (N = 64), n (%) | p-valuea |
|---|---|---|---|---|
| Do you have any plans to cut down on your drinking in the future? | ||||
| Not at all | 21 (58) | 9 (32) | 30 (47) | 0.015 |
| I am thinking about it | 9 (25) | 17 (61) | 26 (41) | |
| I have already made a plan | 6 (17) | 2 (7) | 8 (13) | |
| Stage of readiness to change | ||||
| Pre-contemplation | 27 (75) | 12 (43) | 39 (61) | 0.011 |
| Contemplation | 4 (11) | 12 (43) | 16 (25) | |
| Action | 5 (14) | 4 (14) | 9 (14) | |
Discussion
The study succeeded in randomising men using a procedure designed to ensure that the research team which collected and analysed the data were blind to intervention status. The baseline data confirmed that the participants were socially disadvantaged: educational attainment was low and the level of unemployment was high. Although it was thought that telephone collection of data might be challenging, complete data sets were obtained on all men recruited. This suggests that once the men have understood about the study and agreed to participate they will co-operate fully with the study procedures.
The study group is a high priority for intervention as most men were drinking at hazardous levels. However, few thought their current consumption is harmful, possibly because their total weekly consumption was modest. The perceived low level of harm may explain why most men did not intend to reduce their consumption. This is surprising as there was a high awareness of both the harms of alcohol and the benefits of moderate drinking. These baseline results are consistent with the focus groups' findings (see Chapter 4). They provide an opportunity for intervention, by drawing attention to the inconsistency between their knowledge and their intentions. MI, a technique included in the intervention text messages, uses such discrepancies to stimulate change thinking and to negotiate commitment to change. 124 The baseline results also indicate that, given the high levels of knowledge, there would be little advantage to further education on harms. Instead, techniques should be used to make the harms more concrete, immediate and personally relevant.
An important finding was that, once recruited, all men completed the conventional alcohol assessments in the baseline questionnaires. A concern about possible loss of interest during the telephone interview did not materialise. The study had to overcome one methodological problem for data collection. Much of the data collected at baseline and follow-up involved the use of Likert scales. These are simple to complete when presented as a visual scale, but present a challenge for telephone interviews. To overcome this, each question was asked in a phased way, first determining whether the participant agreed/disagreed with the main statement, then gauging the strength of this view. This method has been used previously not for its convenience for use by telephone, but because it is a better gauge of participants' preferences. 125
Most of the men have a pattern of drinking, with episodes of heavy binge drinking interspersed with many alcohol-free days. This type of drinking, often termed risky single occasion drinking (RSOD), has been widely documented in adolescents and young people. 126,127 The peak age for RSOD is 21–22 years, after which it falls substantially in frequency. 128 In studies of older adults this pattern of drinking was either not assessed or was found to be rare. 129 The finding in this study raises the question of whether or not ROSD persists throughout life among disadvantaged men.
Despite frequent RSOD, the overall weekly consumption of alcohol in this study was not high, only slightly exceeding the recommended level of weekly drinking. This is in contrast to previous research in adolescents showing that RSOD is commonly accompanied by a high level of total consumption. 128 The novel finding in this study is a consequence of the high frequency of alcohol-free days. The overall modest level of consumption was unexpected given that the entry criterion for the study was regular binge drinking. This pattern of drinking with frequent ROSD could explain why levels of alcohol-related morbidity and mortality are high among the disadvantaged130,131 although their overall consumption is lower than more affluent groups. 3 A key question to help understand the social inequalities in alcohol-related mortality is whether or not episodic heavy drinking in disadvantaged men is established in adolescence.
The average consumption of alcohol over a 30-day period in this study was 96.2 units, corresponding to 22.4 units per week, or 180 g of alcohol per week. This is much lower than the average of 306 g per week found in a recent systematic review of alcohol brief interventions. 9 The high level of consumption reported in that review probably occurred because most of the studies in the review set an entry criterion which specified a minimum alcohol consumption, typically > 21 units per week. The present study has also recruited individuals who were more socially disadvantaged. The recent systematic review9 found that, when reported, the majority of men in previous trials were in employment and had at least a college education. These differences from previous trials emphasise the need to determine whether or not alcohol brief interventions can be effective among disadvantaged young to middle-aged men.
Knowledge of the definition of binge drinking was very poor. Most men were willing to hazard a guess at the level of binge drinking, but they almost always overestimated it. This indicates that recent campaigns on binge drinking have failed to convey this information, at least to this section of the population. The result needs to be tested in other studies.
The analysis has shown that although the men could resist alcohol in some situations, they found it difficult to resist peer pressure. This is consistent with the existence of both private purpose and social roles for drinking, which were described in Chapter 4. This confirms that peer pressure should be one of the targets for an intervention to reduce the frequency of binge drinking.
The scale of the differences between individuals recruited through GP compared with those from RDS was unexpected. Those recruited by RDS were on average less well educated and more likely to be unemployed. RDS also recruited many more individuals at high risk of alcohol-related harm than did recruitment through GPs. Not only did they binge drink much more frequently, but this was often associated with instances of memory loss. To our knowledge a direct comparison of participants recruited by the two techniques has not previously been made.
This finding raises the question of why these harmful drinkers were not recruited through the GP sampling. It is possible that many disadvantaged men with high-risk drinking patterns are marginalised in society to such an extent that they are reluctant to respond to contact by letter or telephone. These men may constitute a hidden population which can be accessed only through community outreach recruitment strategies. 132,133 The finding that failure to contact was the main reason for non-recruitment through primary care (see Chapter 6) supports the concept of a hidden population. RDS employed personal approaches in settings familiar to the men which allowed the nature of the study to be explained. This could encourage participation. Studies which recruit participants through a single mechanism, particularly through health-care settings, may miss many high-risk drinkers. For the full trial it is recommended that more than one recruitment strategy be used.
In summary, the study procedures all worked well. The randomisation strategy was successful and complete baseline data were obtained on all men. Knowledge of the conventional definition of binge drinking was low. The participants had an unusual pattern of drinking, with occasional episodes of heavy binge drinking interspersed between periods of complete abstinence. Consequently, the men had moderate total alcohol consumption, lower than in previous trials of alcohol brief interventions. The pattern of drinking in this study may be particularly harmful to health and to society. The effectiveness of brief interventions needs to be tested in this group in a full trial. The study found that heavy binge drinking was common despite a high level of awareness of the harms of binge drinking. This discrepancy, using the techniques of MI, provides a lever for behaviour change.
Chapter 8 Retention strategy
Introduction
Retaining participants within a trial and successfully recording the outcome measures are key requirements for a high-quality clinical trial. Failure to retain individuals within a trial can threaten both internal and external validity of its findings. 134,135 Loss of more individuals from one study arm than the other could lead to biased estimates of treatment effect. Selective loss of specific groups of individuals can limit the generalisability of the findings. Recent studies have emphasised the importance of developing a strategy to ensure high retention in randomised trials. 136,137 Robinson et al. 135 argue that, given the cost of mounting, running and analysing a trial, it would be only prudent to put effort into ensuring retention of individuals.
A rule of thumb for retention rates in clinical trials has been proposed by several authors;136,138 a < 5% loss to follow-up is of little concern, whereas a > 20% loss casts serious doubts on the validity of the trial. Achieving high retention rates may be more challenging in interventions delivered in community settings than those in clinical settings. One review of community trials found loss to follow-up rates between 1% and 56% with a median rate of 24%. 134 If the 20% cut-off had been applied two-thirds of trials would be discarded. Trials of brief interventions for alcohol also experience high loss to follow-up. Reviews have found that the average attrition rates are usually well above the 20% threshold. 8,9,139 This chapter reviews the development of a strategy to maximise retention within the trial and reports on its impact.
Developing a retention strategy
Recent review papers have identified a variety of techniques to increase retention in follow-up studies. 135,140,141 Box 3 summarises the key findings. Rather than focusing on technical issues of achieving contact, the strategies emphasise cultural and person-sensitive approaches. They also emphasise that all stages of the study, from recruitment strategy to outcome assessment, should be designed to achieve a high recruitment.
Create project identity
Build and maintain rapport
-
establish good personal relationships
-
clear explanation of the nature of the study
-
assurance of confidentiality
-
culturally sensitive materials
-
make participation enjoyable and effortless, convenient and rewarding
-
keep in regular contact (telephone, mail, e-mail)
-
send reminders about follow-up interviews
Use financial or other relevant incentives
Establish tracking mechanisms
Create follow-up strategy
-
multiple attempts at follow-up
-
flexible scheduling of interview times
Application of recommended retention strategies
The retention strategy of this feasibility study applied the recommended strategies within three components of study design: the method of recruitment, the nature of the intervention and the outcome assessment (Box 4). Several of the techniques which were included in the recruitment strategy were also useful for retention. These included using the university logo to establish the credibility of the research team. Financial incentives were used to recruit and retain participants.
Several techniques to promote retention were incorporated into the intervention. The messages were tailored to the target group, using preferred first name, and using quotes from focus groups to capture appropriate language. Questions were asked in the text messages throughout intervention delivery to promote interaction. Possibly the most important feature was the design of the intervention, which was enjoyable as well as informative. The behaviour change strategies were presented using texts and images designed to appeal to the target group. Texts on the harms of alcohol were designed to be gain-framed rather than loss-framed. Regular contact was maintained, and personal names were used.
Use of university logo on all correspondence
Use of preferred name of correspondents
Clear explanation of study details with an emphasis on confidentiality of the findings
Financial incentives for participation
InterventionNon-contact intervention
Use of acceptable medium for intervention delivery (texts by mobile telephone)
Use of culturally sensitive language in text messages
Frequent use of humour
Requests for responses to text messages
Weekly incentive with accompanying letter
Outcome assessmentMaintain regular contact
Financial incentive for completing follow-up interview
Initial letter reminding participants about the study and the financial incentive
Text message to remind participants that follow-up was imminent
Multiple attempts at contact, varied by day of week and time of day
Impact of the strategies
The retention rate in the trial was 96% (64/67). Three men from the intervention group were lost to follow-up, of whom two were recruited by RDS. Two were aged between 25 and 29 years and were single, while the third was aged > 40 years and was married. Two of the men were in employment and both had vocational training after leaving school. The men lost to follow-up drank infrequently but they all drank in excess of 16 units in each drinking session. These men were in pre-contemplation on the Readiness to Change Questionnaire and two reported that they had no plans to cut down on their drinking.
The retention rate in this study is substantially higher than most studies of brief alcohol interventions9 and most studies of community-based interventions. 134 The result is more remarkable because it was achieved with disadvantaged men, a group recognised to be difficult to retain in research studies.
It was not possible to identify which component(s) of the recruitment strategy contributed to this success. However, there is clear evidence that many of the men valued the experience of taking part in the study. Following the final text message to the participants, which thanked the participants for taking part, some men spontaneously texted to thank the researcher. Their comments show how much they enjoyed participating, confirming the high level of engagement identified in the process evaluation:
No worries my pleasure.
Well really enjoyed some of the interesting facts so ur welcome Donald.
Thank for all the texts some were really funny good luck with your study thanks again look forward to chatting in a couple of months.
It was fun.speak soon bud.
Okay its been gud taking part in ur study!and i wul hear from you in 2 months then ok spk to then k from <<NAME>>!
Summary
Through the use of multiple evidence-based strategies embedded throughout the study, a retention rate of 96% was achieved with a difficult-to-reach group. Interventions delivered by mobile telephone which tackle adverse health behaviours typically have retention rates of 70–90%23,24,69 so the present study ranks among the highest. The finding was unexpected because disadvantaged individuals are more likely to be lost to follow-up. 142,143
The use of incentives may have played a part, as one trial which gave a lower incentive to the intervention group at follow-up had higher attrition in that group. 69 It seems likely that the features of the intervention, tailoring to the target group and the use of humour and interactivity led to a high level of retention. This suggests that future studies should ensure not only that their interventions are theoretically and empirically based, but also that they are sufficiently enjoyable and rewarding to promote engagement and retention in the study.
Chapter 9 Outcome assessment
Introduction
A key aim of the feasibility study was to determine whether or not the primary and secondary outcomes of the proposed full trial could be measured on all participants. These items were also measured at baseline, enabling changes in drinking patterns to be identified. This feasibility study was not powered to detect significant differences on these measures, but it can identify whether or not the observed changes are in the appropriate direction. Thus, this chapter describes the impact of the intervention on total consumption, patterns of drinking, intentions to reduce consumption, beliefs about harms and drinking self-efficacy.
Methods
Outcomes were measured by telephone interview at 3 months after the baseline assessment. A few days before an attempt was made at telephone contact, the individuals were sent a text reminding them of the study and of the £10 gift voucher awarded after completion of the outcome assessment. Multiple attempts were made at contact, using different times of day and days of the week. For men recruited by GP, further information was sought on one man who could not be contacted. This yielded a new telephone number for that man who was then successfully followed up. For men recruited by RDS, contact was made with seeds or nominees. No further men were followed up by this method, although it did identify that one man was unavailable because he was in prison.
All the questions in the baseline questionnaire were asked at the outcome assessment to enable changes on these measures to be assessed. The primary outcome measure for the proposed full trial was the change in frequency of heavy drinking (consumption of ≥ 8 units in a single session). This measure of consumption has been used for many years in national surveys of alcohol consumption. 11,144 Self-reported alcohol consumption is the primary outcome measure used in almost all randomised trials testing interventions to reduce alcohol consumption. 9 Secondary outcomes assessed the extent to which the intervention influenced perceptions of harms, benefits of moderated drinking and intentions for future drinking. In addition, questions were asked about receipt of the text messages, whether or not these messages were shared with others and whether or not involvement in the study had been worthwhile (see Appendix 5).
Statistical methods
The protocol stated that the study was not powered to detect the effects of the intervention and formal hypothesis testing was not appropriate. It specified that only descriptive analyses would be undertaken. The tabulations are presented primarily to demonstrate that the outcomes can be readily measured and the data for the full trial would be in the appropriate form for analysis.
Results
Changes in drinking
Alcohol consumption was measured over a 30-day period. Compared with baseline, men in the intervention group reduced their frequency of binge drinking (≥ 8 units in a session) slightly more than men in the control group (Table 17). A similar greater reduction in the frequency of heavy binge drinking (≥ 16 units in a session) was also seen in the intervention group compared with the control group. These changes were matched by a greater increase in the number of days of moderate drinking in the intervention group. The total amount of alcohol consumed by the intervention and control groups fell by similar amounts.
Intentions to reduce consumption and beliefs about harms
Slightly more men in the intervention group moved from not having a plan to cut down their drinking to having such a plan (Table 18). A similar result was seen in the Readiness to Change Questionnaire, in which more men in the intervention group moved to being in the action stage of changing their drinking.
| Factor | Baseline | Follow-up |
|---|---|---|
| Mean number of binge drinking days in previous 30 days (≥ 8 units in one session) | ||
| Control group | 5.42 | 5.36 |
| Intervention group | 6.32 | 5.77 |
| Mean number of units usually consumed during a binge drinking session | ||
| Control group | 16.29 | 12.85 |
| Intervention group | 14.72 | 13.80 |
| Mean number of heavy binge drinking days in previous 30 days (≥ 16 units in one session) | ||
| Control group | 2.64 | 2.52 |
| Intervention group | 3.68 | 2.77 |
| Mean alcohol consumption in past 30 days (units) | ||
| Control group | 89.54 | 82.92 |
| Intervention group | 103.28 | 96.32 |
| Mean number of moderate drinking days in previous 30 days (< 8 units in one session) | ||
| Control group | 2.30 | 2.48 |
| Intervention group | 1.35 | 2.06 |
| Mean number of alcohol-free days in previous 30 days | ||
| Control group | 22.27 | 22.15 |
| Intervention group | 22.32 | 22.16 |
| Factor | Control group (N = 33), n (%) | Intervention group (N = 31), n (%) | ||
|---|---|---|---|---|
| Baseline | Follow-up | Baseline | Follow-up | |
| Do you have any plans to cut down on your drinking in the future? | ||||
| Not at all | 14 (42) | 12 (36) | 16 (52) | 14 (45) |
| I am thinking about it | 14 (42) | 10 (30) | 12 (39) | 5 (16) |
| I have already made a plan | 5 (15) | 11 (33) | 3 (10) | 12 (39) |
| Stage of readiness to change | ||||
| Pre-contemplation | 18 (55) | 16 (48) | 21 (68) | 17 (55) |
| Contemplation | 10 (30) | 9 (27) | 6 (19) | 3 (10) |
| Action | 5 (15) | 8 (24) | 4 (13) | 11 (35) |
Knowledge about drinking and drinking refusal self-efficacy
There was a marked increase in knowledge of the definition of binge drinking level in both intervention and control groups (Table 19). This could have occurred because the baseline questionnaire explicitly stated that binge drinking was 8 units in a session (the question investigated whether or not the men thought that this level of drinking could be harmful). In contrast to knowledge, awareness that drinking 8 units of alcohol in a session was harmful remained unchanged. This suggests that the intervention did not address this issue adequately. There was a large fall in the number of men in the intervention group who thought the benefits of their drinking outweighed its harms. The control group increased slightly on this measure.
Knowledge about the harms of heavy drinking and the benefits of moderate drinking were unchanged (Table 20). This most probably reflects the very high levels of knowledge at baseline. Drinking refusal self-efficacy also remained largely unchanged (Table 21).
| Factor | Agree at baseline, n (%) | Agree at follow-up, n (%) |
|---|---|---|
| 8 units of alcohol constitutes binge drinking | ||
| Control group | 2 (6) | 12 (36) |
| Intervention group | 1 (3) | 7 (23) |
| Drinking 8 units of alcohol in a single session is harmful | ||
| Control group | 13 (39) | 12 (36) |
| Intervention group | 13 (42) | 15 (48) |
| My current level of drinking is harmful to my health | ||
| Control group | 9 (27) | 14 (42) |
| Intervention group | 7 (23) | 6 (19) |
| The benefits from my drinking outweigh the harms it causes | ||
| Control group | 9 (27) | 10 (30) |
| Intervention group | 13 (42) | 7 (23) |
| Factor | Control group (N = 33), n (%) | Intervention group (N = 31), n (%) | ||
|---|---|---|---|---|
| Baseline | Follow-up | Baseline | Follow-up | |
| Harms of heavy drinking | ||||
| Total number of harms of heavy drinking identified | ||||
| 0–1 | 6 (18) | 7 (21) | 9 (29) | 7 (23) |
| 2–3 | 21 (64) | 19 (58) | 14 (45) | 15 (48) |
| ≥ 4 | 6 (18) | 7 (21) | 8 (26) | 9 (29) |
| Benefits of moderate drinking | ||||
| Total number of benefits of moderate drinking identified | ||||
| 0–1 | 9 (27) | 9 (27) | 9 (29) | 3 (10) |
| 2–3 | 23 (70) | 22 (67) | 18 (58) | 23 (74) |
| ≥ 4 | 1 (3) | 2 (6) | 4 (13) | 5 (16) |
| Factor | Agree at baseline, n (%) | Agree at follow-up, n (%) |
|---|---|---|
| I could resist alcohol when I go out to eat | ||
| Control group | 30 (91) | 29 (88) |
| Intervention group | 28 (90) | 30 (97) |
| I could resist alcohol when I am watching television | ||
| Control group | 28 (85) | 30 (91) |
| Intervention group | 26 (84) | 29 (94) |
| I could resist alcohol if someone offered me a drink | ||
| Control group | 25 (76) | 24 (73) |
| Intervention group | 21 (68) | 23 (74) |
| I could resist alcohol when my friends are drinking | ||
| Control group | 16 (48) | 21 (64) |
| Intervention group | 18 (58) | 18 (58) |
| I could resist alcohol when I am bored | ||
| Control group | 29 (88) | 29 (88) |
| Intervention group | 26 (84) | 28 (90) |
Potential for contamination
An unexpected finding was the extent to which study participants discussed the text messages with friends and family members. Almost all participants (95%) mentioned the study to at least one person and 42% discussed it with more than five people. It is possible that socially marginalised groups have close social networks that facilitate such sharing. This raises the possibility that, in an individually randomised trial, the control group could be contaminated by intervention group messages. This observation was made as part of the extensive process evaluation conducted within the study: in this case sharing was a measure of engagement.
Discussion
The study achieved a main aim of the feasibility study: to demonstrate that the outcomes measures could be successfully recorded. Although not powered to detect effectiveness, the results of the feasibility study are compatible with the intervention being effective. The men in the intervention group reported a larger reduction in the primary outcome of the full trial, the frequency of binge drinking. The reduction in the frequency of binge drinking days was accompanied by an increase in the frequency of moderate drinking days. There was a slightly greater increase in intention to reduce drinking in the intervention group. The Readiness to Change Questionnaire showed that more men in the intervention group were at the action stage at follow-up.
The pattern of drinking in this study, episodes of very heavy drinking interspersed among many alcohol-free days, raises the question of what should be the main aim of brief interventions: to reduce total consumption or to reduce the frequency of binge drinking? This feasibility study proposed that the frequency of binge drinking should be the primary outcome. Most trials of brief interventions have used total consumption as the primary outcome,9 with only a few assessing the impact of the intervention on binge drinking. Although reducing consumption is desirable, it is more important for disadvantaged young to middle-aged men to reduce the frequency of heavy binge drinking. Binge drinking is more likely to cause serious short-term harms, such as antisocial behaviour, accidents, violence and criminal behaviour. 1 Preventing these harms would bring immediate benefits to the men themselves as well as to the wider society. In contrast, reducing total consumption will reduce long-term health harms, but may have much less impact on these short-term societal harms. It is recommended that the frequency of binge drinking remain the primary outcome for the full trial.
A possible weakness of the intervention is that it did not place particular emphasis on closing the intention–behaviour gap. 145,146 One of the theoretical models underpinning the intervention, the TPB, has been criticised for addressing intention to change behaviour, but not taking the final step and promoting behaviour change. A more recent model, the health action process approach (HAPA),146 goes beyond intention to seek commitment to action and to the promotion of sustained change. Thus, for the full trial the intervention will be extended with new texts created to promote goal setting, to gain commitment to action, to overcome barriers to action and to promote maintenance of the reduced frequency of binge drinking. Goal planning may also enhance self-efficacy. 87 The results of the extensive process evaluation in this study (see Chapter 10) indicate that the increased number of texts would be welcomed.
Both intervention and control groups showed an increase in the level of awareness of the formal definition of binge drinking. This could have occurred because the baseline questionnaire included a question which explicitly stated that binge drinking was 8 units in a session. It has been suggested that administration of an alcohol screening questionnaire could be sufficient to influence alcohol consumption. 9 If so, the baseline questionnaire could have alerted the control group to the harms of heavy drinking. This is supported by the post-trial assessment (see Chapter 11); men in the control group mentioned that a memorable lesson from the study was that four pints constituted binge drinking. The effect of this would be to reduce the observed difference in frequency of binge drinking between intervention and control groups. This question should be omitted from the baseline questionnaire for the full trial.
The levels of knowledge of harms of drinking and benefits of moderated drinking remained unchanged from the very high levels at baseline. This is consistent with the finding from the focus groups (see Chapter 4) that the men were old enough to have direct experience of harm, either personally or to close family or friends. These results suggest that harms and benefits should not be used as secondary outcome measures. Furthermore, instead of raising the issue of harms, the intervention should focus on making the harms concrete and personally relevant. The lack of impact on drinking refusal skills suggests that the intervention for the full trial should also incorporate additional text messages on this topic.
The observation that study participants discussed the text messages with friends and family members was made as part of the extensive process evaluation conducted within the study. For the process evaluation, sharing was a measure of engagement with the intervention, a desirable attribute. However, for a full trial message sharing could be problematic. As RDS aims to recruit several individuals from close social networks, contamination of the control group could occur. All techniques which employ chain referral methods, such as snowball sampling, targeted sampling and RDS, are vulnerable to this problem.
Contamination, if it occurred, would be a serious issue. RDS has previously been used in surveys where the aim is to provide unbiased population estimates. 37,38 Contamination is less of a problem for surveys than it is for randomised trials. In recruitment of hard-to-reach groups for randomised controlled trials, there is clearly a tension between representativeness and potential for contamination. The use of chain referral methods, such as RDS, will increase representativeness at the price of contamination. Maintaining the internal validity of the trial is much more important than obtaining unbiased population estimates.
The potential for contamination of control group participants is widely recognised, although there is little empirical evidence that it occurs. 147 If true contamination occurred this would reduce the observed effect size of an intervention. Complex interventions (with multiple components) aimed at behaviour change are thought to be resistant to contamination. 148 To impact on the control group the contamination would have to transfer sufficient content of the intervention to change behaviour. 149 A recent study of reduction of high-risk sexual behaviour provided empirical evidence that, although there was communication between intervention and control group participants, this had no impact on study outcomes. 150 Contamination may thus be a theoretical possibility which seldom occurs in practice. Despite the possible reassurance, the potential for contamination is sufficiently serious that steps must be taken to avoid it.
The guidance for trials in which contamination could occur is to avoid the problem in the study design. 147 In this study contamination could occur in the RDS because there will be shared social networks. 148 To avoid this, an alternative recruitment strategy for hard-to-reach individuals should be used. Time–space sampling151,152 is a method that recruits from venues which the target group is known to frequent and involves sampling at selected times of day and days of the week. It does not use the technique (chain referral) which could lead to contamination. The approach requires initial fieldwork to identify appropriate venues and suitable times for recruitment. Adoption of time–space sampling, incorporating initial fieldwork, would provide a sampling strategy that recruits widely from the target population while avoiding the problem of contamination. In a full trial the use of multiple venues, with one or two participants recruited from each venue, should reduce the possibility of recruiting individuals from the same social network.
The propensity to share messages has an important beneficial consequence for roll-out of an effective intervention. Sharing messages will spread awareness of the intervention and could increase uptake. Furthermore, conversation about the shared messages could increase the effectiveness of the intervention by promoting reflection on the content of the messages. The sharing could help address misperceptions about peers' consumption and lead to the approval of significant others for a reduction in the frequency of binge drinking. These are important components of strategies for behaviour change. 86 The communication effect could be similar to viral marketing,153,154 in which word-of-mouth spread of a topic creates a groundswell of interest. Viral marketing is used by the industry to promote drinking, so it would seem appropriate to use the technique to reverse the process. It could be one mechanism of promoting culture change about the acceptability of binge drinking and its undesirable consequences.
In summary, the outcomes were successfully measured on all subjects who were followed up, including the primary and secondary outcomes for the proposed full trial. This feasibility study has also identified ways in which the intervention for the full trial should be modified to increase its effectiveness.
Chapter 10 Novel methods for process evaluation
Introduction
A critical component in the development and piloting of a new intervention is to determine what factors contribute to the overall success, or indeed failure, of the intervention. 40 Process evaluation in trials of behaviour change interventions investigates the extent to which an intervention is delivered as it was intended. 40,155,156 It is used to investigate whether or not the components of the intervention are delivered consistently and accurately to the target group. 155,157 Process evaluation may also be used to monitor engagement with the intervention and to determine what individual-level factors influence engagement. 158 Most importantly, careful process evaluation can help to identify: why an intervention was less successful than intended; what factors could have contributed to a successful intervention; and how further improvements could be made to the design or delivery of an intervention. 159,160
Three essential dimensions for assessing the extent to which an intervention has been delivered as intended are fidelity, dose and reach. 155 Fidelity measures the quality of delivery of the intervention, dose monitors how much of the intervention was delivered and how much was received by participants, and reach assesses the extent to which the intervention makes contact with or is received by the target group. Frameworks based on these dimensions have been created to evaluate studies and programmes, frequently with additional components including recruitment (of participants and agencies or personnel to deliver the intervention), context, barriers to implementation and maintenance (retention of participants). 161–164
Process evaluation often involves interviews, focus groups or observational studies, with both study participants and those delivering the intervention. 158 A challenge for non-contact interventions is to measure process without introducing personal contact into the study. This would change the nature of the intervention. There is a need to introduce new measures which do not interfere with the delivery of the intervention for non-contact interventions.
Research questions
-
To what extent were the text messages delivered as intended?
-
Were the messages opened, read and responded to by participants?
-
Did specific text messages successfully tap into key components of the behaviour change strategy?
-
Was the intervention acceptable to participants?
Methods
For this feasibility study, four methods of process evaluation were used. Fidelity of the delivery of the intervention was assessed from data captured by the computer system which monitored intervention delivery. It is possible to monitor receipt of text messages by individual telephone, which is equivalent to interviewing or observing those delivering an intervention. Engagement with the study was monitored by asking questions in text messages. The frequency of responses to these provided a measure of engagement with the intervention and assessed retention in the study. Content analysis of the responses given provided a method to ascertain the nature of engagement with components of the behaviour change intervention. This also identified parts of the intervention that were misunderstood or ambiguous. Finally, conventional process evaluation through interviews with participants at follow-up was undertaken to investigate the reported acceptability and impact of the study.
Research question 1: fidelity of the delivery of the intervention
The intervention comprised a combination of SMS messages (text messages) and MMS messages. The delivery was administered by a computer program at the Computing Department at the University of Dundee. SMS messages can be tracked to determine whether or not they were delivered to the telephone (it is not possible to track MMS messages). When SMS messages were not delivered to the telephone immediately, the computer program continued to try to send the message for 24 hours. If the message could not be delivered during this period, this was recorded as a delivery failure and the programme would then send the next message in the sequence.
Data captured on the delivery status of the SMS messages were recorded as: delivered (the telephone had reception and was switched on); undelivered (the telephone was switched off or it had no signal for 24 hours); or no status returned. The program did not record whether or not messages delivered to the telephones were opened. The proportion of SMS messages delivered to participants in the intervention and control groups was monitored as a measure of fidelity of the delivery of the intervention.
Research question 2: responses to text messages and characteristics of responders
Both the intervention and control packages included questions asked in text messages. The primary purpose of these questions was to promote engagement and to maximise retention of participants in the study. Responses to the text messages were received and collated by the Computing Department at the University of Dundee. The anonymised messages were screened daily by a member of the research team who was not involved in recruiting the participants or delivering the intervention. This ensured that any specific requests (e.g. to withdraw from the study, to find out where to get help for an alcohol problem, or a change in telephone number) could be dealt with.
On completion of the study, the collated data were analysed to gauge engagement and to examine the type of the men who responded by demographic characteristics and drinking history. The FAST121 and the Readiness to Change Questionnaire123 were used to measure hazardous drinking and attitudes to drinking behaviour. Intervention and control data were analysed separately. Study participants were categorised as high responders or low responders. High responders in the intervention group were men who replied to seven or more of the nine questions asked, whereas high responders in the control group were those who responded to at least three of the four questions asked.
Research question 3: content analysis of the responses received
Participants in the intervention group received a series of 36 SMS and MMS messages. These incorporated behaviour change techniques using social cognition models93 and MI124 which were organised by the stages of the TTM of behaviour change. 165 Nine of the 36 messages requested a response to a specific question. The questions were carefully crafted to reinforce specific components of the intervention.
Control group participants received 34 SMS and MMS messages on four health topics: healthy eating, physical activity, sexual health and mental health. One message each week asked a multiple-choice question on the topic of the week. The control package was designed to provide information on each topic and to be interesting and funny as a means of keeping the men engaged. The content of the messages did not incorporate any behaviour change techniques.
Responses to the messages confirmed that the participants had: opened and read the message; understood the question; reflected on the content/context of the question; and given an appropriate and considered response. Analysis of content of the messages from the intervention group participants permitted an assessment of engagement with the study and with the psychological constructs of the intervention. Responses to the questions gave an indication of engagement with behavioural antecedents to reduced drinking:
-
recognition of reasons for drinking
-
awareness of the harms of heavy drinking
-
perceived benefits of drinking less
-
subjective norms (perception of significant others' beliefs about their drinking)
-
control beliefs (beliefs about factors that facilitate drinking less or impede drinking less)
-
perceived behavioural control (perceived ease or difficulty in drinking less)
-
behavioural intentions.
In addition, responses to the questions were used to determine whether or not the messages were understood and how they may be modified and improved for the full trial.
Research question 4: acceptability and impact of the intervention
Following the outcome assessment questionnaire which was completed by telephone interview, participants were asked a further 10 questions about their experience in taking part in the study. The questionnaire comprised both closed and open questions on the acceptability of the study, whether or not they had encountered any problems with the delivery of the intervention, and also if they had gained anything from taking part. Open questions encouraged men to reflect on what they may have learned, whether or not the intervention encouraged them to think about their health, whether or not they felt the need to improve their own health and any changes they were thinking about making or had made. This was designed to give insight into ways in which the intervention and control packages and their delivery could be improved.
Results
Research question 1: fidelity of the delivery of the intervention
The intervention package included 19 SMS messages while the control package included 14 messages. The MMS messages (17 for the intervention group and 20 for the control group) could not be tracked. A total of 1108 SMS messages were sent to the 67 participants during the intervention period. Of these, 1053 messages (95%) were delivered to the participants' telephones. Of the remaining 55 messages, 45 were recorded as undelivered (the telephone was switched off or it had no signal for 24 hours); no delivery status was recorded for the remaining 10 messages. Only 11 men failed to receive all of the messages, eight from the intervention group and three control group participants. The number of failed messages among these 11 participants ranged from 1 to 13, with a median five messages missed.
Research question 2: responses to text messages and characteristics of responders
Intervention group
Thirty of the 34 study participants (88%) in the intervention group responded to the text messages that asked questions (Figure 2). More than half (18 men) replied to seven or more of the nine questions, with two replying to all nine questions and a further nine men answering eight questions. Of the four men who did not respond to any of the questions, two were also lost to follow-up.
FIGURE 2.
Intervention group: participants' text message responses to the nine questions.
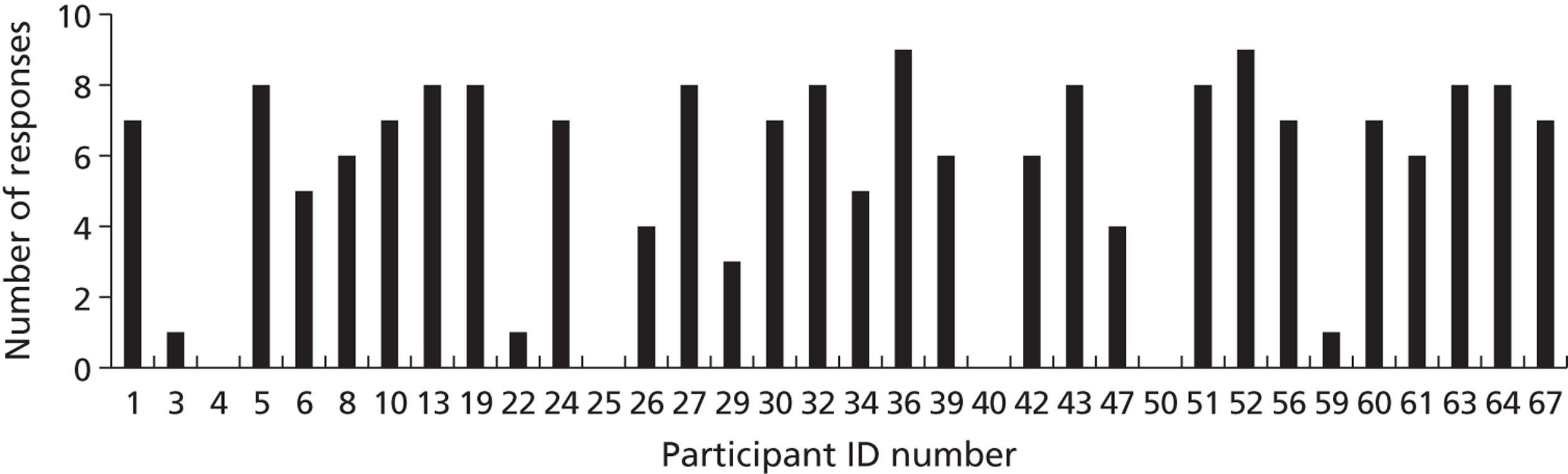
More than 82% of men in the intervention group responded to the first question (Figure 3). For the remaining eight questions, an average of 20 men responded. Overall, there was little evidence of attenuation during the intervention period. In addition to replying to the questions posed, many of the men commented on other text messages. Nineteen of the 27 messages which did not request a response received at least one reply (see Figure 3). Responses to these messages simply acknowledged that the message was delivered, expressed empathy with the message, or responded to the humour in the message.
FIGURE 3.
Intervention group: total number of responses to text messages.
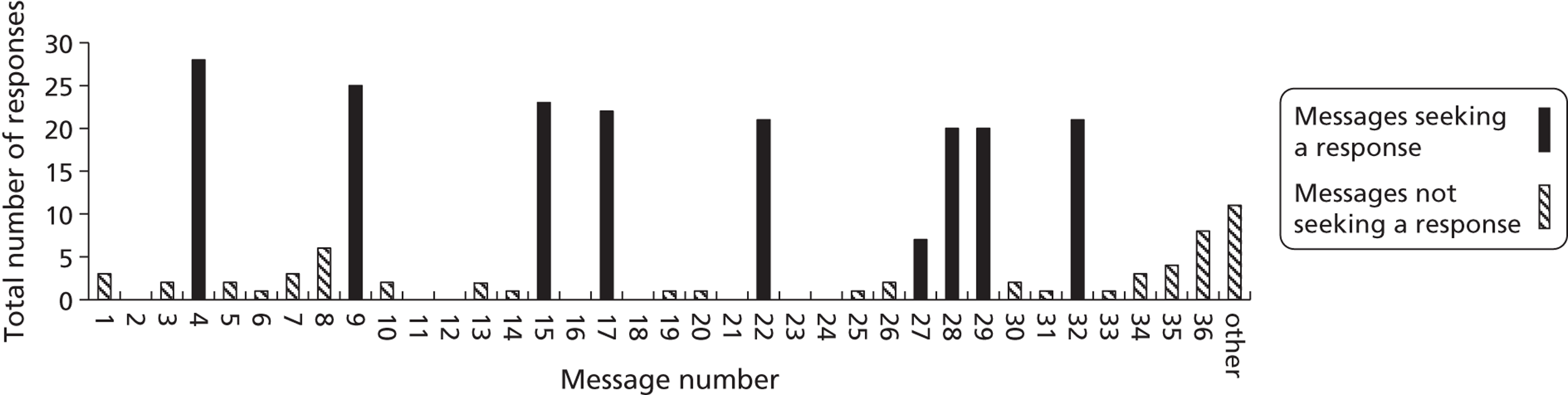
Characteristics of the men in the intervention group who responded
A comparison of high and low responders was made to explore the factors which influenced engagement with the study. High responders [those who responded to seven or more of the questions posed (n = 17)] were more likely to be married or living with a partner (71% of high responders vs 29% of low responders) and were more likely to be in employment (77% vs 36%). More of the high responders were recruited from GPs than through RDS (71% vs 43%). The high responders were more likely to report that they had fewer (two or less) heavy binge drinking days (≥ 16 units in one session) in the previous 30 days (65% vs 43%). However, more of the high responders were at the pre-contemplation stage on the Readiness to Change Questionnaire (77% vs 57%). 123 Factors that did not influence the frequency of responding included age, educational attainment, level of deprivation, frequency of binge drinking and FAST score. 121
Control group
Thirty-one of the 33 participants (94%) from the control group responded to the text message questions (Figure 4). One-third of the men answered all four questions and another third answered three of the four.
FIGURE 4.
Control group: participants' text message responses to the four questions.
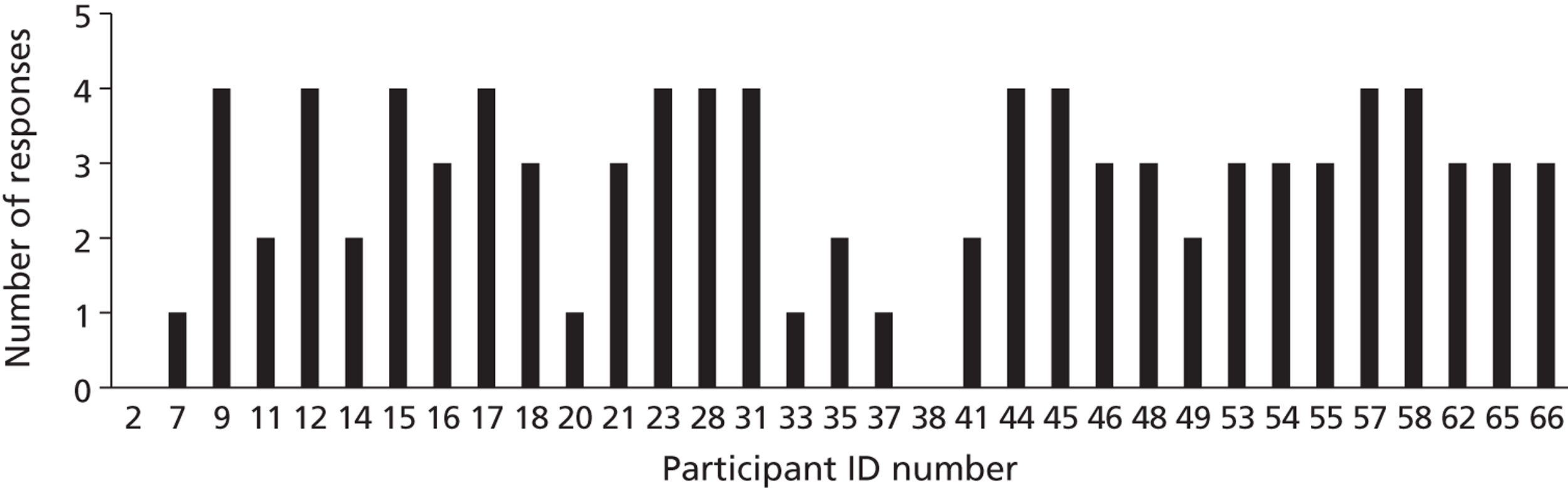
Fourteen of the text messages that did not seek a response elicited comments from participants (Figure 5). The majority of comments on these texts were in response to humorous messages. More men answered the questions during the second half of the study, and 100% of the control group remained in the study at follow-up.
FIGURE 5.
Control group: total number of responses to texts.
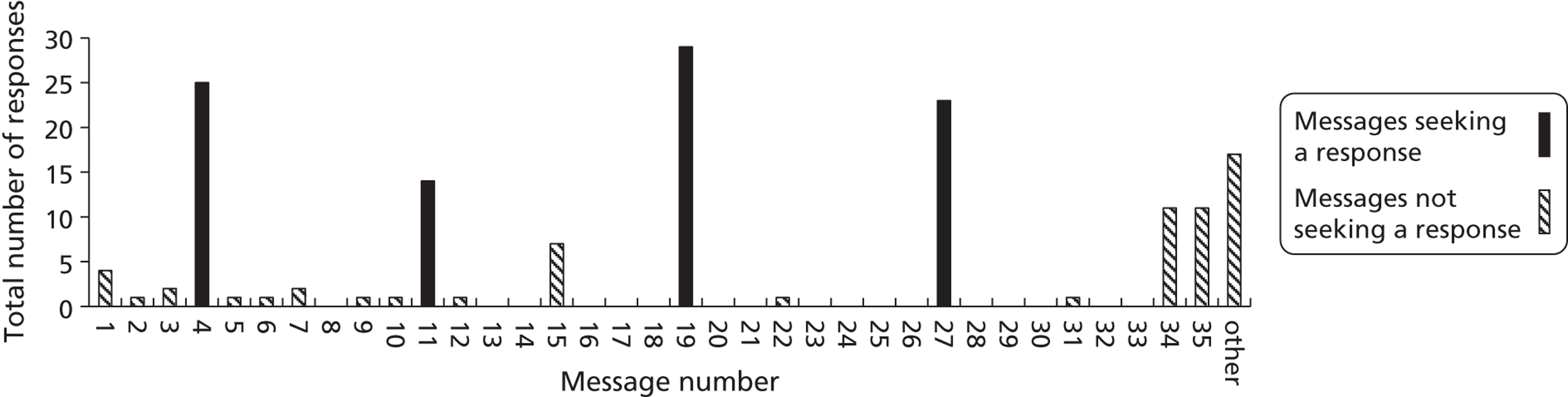
Characteristics of the men in the control group who responded
Comparing high and low responders (three or four responses vs two or fewer) showed that, like the intervention group, high responders were more likely to be married or living with a partner (73% vs 46%) and were more likely to be in employment (82% vs 63%). Fewer of the high responders (n = 22) were in the younger age group (27% vs 64%). More of the high responders were recruited from GPs (68% vs 27%). High responders were less likely to report binge drinking days (≥ 8 units in one session) on more than three occasions in the previous 30 days (50% vs 73%). More of the high responders were at the pre-contemplation stage on the Readiness to Change Questionnaire (64% vs 36%). Factors that did not influence the frequency of responding included educational attainment, level of deprivation, frequency of heavy binge drinking (≥ 16 units in one session) and FAST score.
Research question 3: content of the responses received
Intervention group
Engagement with the study was assessed through the nature of text messages received from participants. Responses to the questions monitored engagement with behavioural antecedents to reducing drinking.
Recognition of reasons for drinking
An early message (text number 4) was designed to identify the type of drinkers in the study, based on the DMQ,53 which categorises reasons for drinking as social, coping or enhancement. The message asked: ‘What's the main reason U drink? A It's a habit; B To feel better; C To have fun; D To cope; E To wash down your chips. Text me your answer’.
The majority of men (n = 23) indicated that they drink ‘to have fun’ and some gave more than one answer. Four men said that their drinking was ‘a habit’, while another five reported that they drink ‘to feel better’. Only one man said that he drank ‘to cope’. Two said none of the options applied, while one said he drank ‘to wash down his chips’. Two men proposed other reasons for drinking:
To unwind and help relax.
To have fun socialise and let my hair down. I work hard all week and when I get the chance I feel I deserve to enjoy my weekend.
Awareness of the harms of heavy drinking/perceived benefits of drinking less
Text number 9, ‘Can U think of any reasons why it may be a good idea for U to cut down a bit on your drinking? Text me your answer!’, was designed to encourage re-evaluation of current drinking behaviour. It was posed as a question so that the participant would not only voice an argument for change, but write it down in a text and return it to the researcher. Responses to the question fell into four categories.
Immediate benefits:
Not suffering with a hangover.
Feelin rough hangovers getin into silly situations getin into trouble all these things get u at some point with 2 much drinkin!
I wouldn't feel like crap in the morning, and my wallet would have more money in it!
I would want to cut down drinking to enjoy my night more and not forget parts of it. it would save on cash and avoid sore heads in the morning.
Health benefits:
Unhealthy and bad liver.
To stay healthier later in life.
For my health ageing of my skin.
Im putting on a lot of weight. And my health suffering as a result.
Family reasons:
To get fit and stay healthy for my family.
Live longer for my kids.
Financial benefits:
Money.
Save money no get hungover.
Text numbers 14 and 15 were delivered in quick succession, and were designed to encourage the participants to think about the pros and cons of changing their drinking patterns. The first simply asked ‘How much would U save every month if U drank half as much?’ The second, delivered 3 minutes later, said ‘Kerching! Kerching! Please count up your savings & text me the sum!’ Twenty-four of the 34 men answered the question. Their estimated savings ranged from £10 to £690 (two men said ≥ £600 and one said ‘400 quid easy’). Many of the responses indicated that the men had tried to do the calculation:
Hard 2 tell. But i would have at least saved 24 pound so far this week.
Im not sure but i think a good wee sum.
About between fifty and eighty pounds and thats a fact.
£200 a month or more easy. That would be on carry outs and the pub.
The next two text messages (text numbers 16 and 17) developed this theme by asking how saving money could enable them to buy items they wanted. This transforms potential benefits from the abstract to concrete. The first message stated ‘By saving up your cash U could treat yourself to something special!’ The second, delivered 3 minutes later, said ‘Try to picture what U would like to buy & text me back your answer!’ The men easily identified a range of ways to spend the saved money from simple treats to extravagant holidays. Responses demonstrated that the men had thought carefully:
Saving that money would help me take my girlfriend out for a meal now and then.
Definitely a car possibly a few more holidays – love buying designer clothes.
Xbox 360 with Kinect.
A 3d television that would be good or a nice holiday in the sun braw.
Trek 2.5 road bike – cost £1650.00 RR.
Holiday to Australia for 3 weeks.
One text message was a direct quote taken from a focus group: ‘Andy from Dundee says – “I cut back on my drinking because my father in law died of it” What would be a good reason for U to cut back? Text me back!’ It elicited deeply personal responses on the long-term benefits of reducing:
I really wanna stay out of trouble and not become the person I can be after a few too many.
I would b able to make the most of the next day rather than feeling shite.
Ive have tryed because i seen my dad nearly die.
Good reason for me cutting back was again, looking after my son. I can't allow drinking to interfere with my job either. My Grandad was an alcoholic, so I know the health risks associated with booze.
So i,m able to be here for my kids to grow up and have kids them self.
For my health so I can prolong my life and spend time with my family and money which could be better used on other things.
Subjective norms
Text number 22 asked ‘Can U think of someone who'd be happy if you made a change! What would U hear them say? Please text me your answer?’ This text message tried to get participants to identify people who would approve of their decision to reduce their alcohol consumption, to increase their self-efficacy about making a decision to change. This question elicited deeply personal responses. Parents, partners, family members and friends were identified as people who would be pleased to see a reduction in drinking. Some men gave detailed responses on what their family and friends would say:
Thats brilliant what u have done,maybe we can do something at the weekend.
yes my friends & family would say well done & good on you keep it up & stay focused & positive abou life because u only get 1 chance.
My partner. She would be happy for health reasons. That i would maybe lose weight.
Two of the men gave a light-hearted but nevertheless thoughtful response:
They would say what a peaceful night not having to deal with a drunken ass.
My dad. Its good ur no phoning me for a lift at 2am!
Only one man did not give a positive response to this question:
She drinks more than me so she will probably ask if I want a drink.
Control beliefs/perceived behavioural control
Text number 32, the final question in the intervention package, was a multiple-choice question which was intended to both motivate and challenge the participants. It was also designed to encourage the belief that change is possible. The message stated, ‘Many people find it easy to reduce their drinking. Do U think U could if U tried? A Yes; B No; C Maybe. Please text me your answer!’ This question was given an overwhelming positive response by the men who responded. Seventeen of the 21 who responded answered yes, with one man saying ‘A,,,, for sure’. Four men said ‘maybe’ and none said ‘no’.
Behavioural intentions
One of the last messages (text number 34) stated ‘Liver disease (cirrhosis) is the major cause of death in heavy drinkers. Drinking less will greatly reduce your risk of liver failure.’ One spontaneous response to this message was:
Im away 2 try and cut down or stop from monday.
Identifying ways to improve the intervention
Ambiguous question
One question was misinterpreted by approximately half of the men who responded, text number 28, ‘Can U think of any obstacles or barriers that stop U drinking a bit less each week? Text me your answer!’ Although the question asked for barriers to reducing alcohol consumption, some men listed factors which facilitated drinking less:
Work goin someplace in the car. Kids commitments.
Driving and work and playing football and definitely when I look after my daughter!
yes Driving.
Prices going up.
Yea money,, getting up early for work with hangover,, and prices in pubs,,,, wow.
Eight of the 12 men who appeared to interpret the question correctly felt there were no real barriers if the individual is committed to changing:
There is nothing to stop me drink less if that was what I wanted.
there isn't much that can stop me apart from me myself. anything else is just an excuse
I have no obstacles or barriers that stop me drinking a bit less each week, it's more of a lifestyle choice for me, and the fact I'm raising my son on my own.
Some men, however, were able to identify barriers:
I dont always know when iv had enough.
My friends asking me to meet them in the pub for a couple.
Boredom habit stress.
The question was effective in encouraging the men to identify barriers, so it should be retained in the full trial, but should be re-phrased to be more easily understood.
Unpopular question
One question proved unpopular, with only seven men answering it. Text number 27, ‘How much did U spend on alcohol this week – Please text me your answer!’, incorporated the image of a man with no money in his pockets and a banner saying ‘SKINT!’ This message was designed to make the participants think about the pros and cons of drinking, and to highlight the negative consequences. The amount spent ranged from zero to:
55 quid I reckon which isn't bad! I think;-)
Ive spent seventy six pounds this week ok mate
Those who responded gave appropriate answers, so it is unlikely that the question was misunderstood. The men had already answered questions that addressed how much money they could save if they drank less. Thus, the low response may suggest that participants felt the topic had already been covered. Most studies repeat messages given in an intervention as a means of reinforcing the intervention. 23 This message contained one of the few loss-framed questions, and indicates that this approach should be avoided in the full trial.
Control group
All of the questions posed to the control group had multiple-choice answers (e.g. what proportion of Scottish men are overweight or obese? Which is the most common sexually transmitted disease?) The correct answers were sent to the men 2 hours later. The majority of responses received were single letter (A–D), but some men wrote out the answers in full. Responses to the other text messages were typically a comment on a humorous text message.
Research question 4: follow-up questionnaire
The follow-up questionnaire was completed by telephone interview 3 months after recruitment to the study. Of the 67 men recruited, 64 (96%) completed the study. The three men lost to follow-up belonged to the intervention group. This section describes reported access to the text messages and reported acceptability and impact of the intervention. The results of the impact of the intervention on the primary and secondary outcome measures are given in Chapter 9.
Access to the intervention
Ten men reported that they had problems opening some of the messages (Table 22). However, all of the participants managed to resolve the problems. Four men, whose telephones could not receive images, were given new, low-cost mobile telephones. The remainder managed to open the images through the internet on a personal computer or contacted the service provider to find out how to open images on their telephones.
Acceptability and impact of the intervention
More than one third of the men reported that they would have liked more text messages. None would have wanted to receive fewer messages (see Table 22). Only one man reported that the timing of the messages could be inconvenient (while he was at work).
Willingness to share text messages with family and friends was used as a marker of acceptability of the intervention. The majority of the participants (95%), from the intervention and control groups, told other people about the study. More than 40% had discussed the study with more than five people and more than a quarter of participants had forwarded texts to friends and family members.
Almost all participants (94% from both groups) felt that taking part in the study was worthwhile, and when asked to give a score out of 10 for the study all said ≥ 6, with more than one third giving a score of 9 or 10 out of 10. The majority of men from both groups reported that they benefited from taking part in the study. More than 90% of participants from both groups said that they found the study informative (Table 23). The majority (86%) were encouraged to think about their health, and half of the men said that they wanted to make changes to improve their health. There was no statistically significant difference between the intervention and control groups in responses to any of the questions. Almost 80% of participants from both groups reported that the messages made them want to make changes to improve their health. In addition, just over half (58%) of the intervention group and 42% of the control group reported that the study helped them to reduce the amount they drank.
| Factor | Control (N = 33), n (%) | Intervention (N = 31), n (%) | Total (N = 64), n (%) | p-value |
|---|---|---|---|---|
| Did you manage to open all the text messages? | ||||
| Yes | 30 (91) | 24 (77) | 54 (84) | 0.137 |
| No | 3 (9) | 7 (23) | 10 (16) | |
| Did you receive any text messages at inconvenient times? | ||||
| Yes | 1 (3) | 0 | 1 (2) | 0.329 |
| No | 32 (97) | 31 (100) | 63 (98) | |
| Do you think the number of texts received was appropriate? | ||||
| Thought the number of texts was appropriate | 21 (64) | 21 (68) | 42 (66) | 0.730 |
| Wanted more | 12 (36) | 10 (32) | 22 (34) | |
| Wanted fewer | 0 | 0 | 0 | |
| Do you send the texts to anyone? | ||||
| Yes | 8 (24) | 9 (29) | 17 (27) | 0.665 |
| No | 25 (76) | 22 (71) | 47 (73) | |
| How many people did you mention the study to? | ||||
| None | 1 (3) | 2 (6) | 3 (5) | 0.657 |
| 1–5 | 18 (55) | 16 (52) | 34 (53) | |
| 6–10 | 8 (24) | 10 (32) | 18 (28) | |
| > 10 | 6 (18) | 3 (10) | 9 (14) | |
| Would you recommend the study to anyone? | ||||
| Yes | 33 (100) | 27 (87) | 60 (94) | 0.103 |
| No | 0 | 1 (3) | 1 (2) | |
| Maybe | 0 | 3 (10) | 3 (5) | |
| Do you think it was worthwhile taking part in the study? | ||||
| Yes | 31 (94) | 29 (94) | 60 (94) | 0.669 |
| No | 2 (6) | 2 (6) | 4 (6) | |
| What score would you give the study on a scale of 1–10? | ||||
| 6–7 | 4 (12) | 6 (19) | 10 (16) | 0.592 |
| 8 | 17 (52) | 14 (45) | 31 (48) | |
| 9 | 5 (15) | 3 (10) | 8 (13) | |
| 10 | 7 (21) | 8 (26) | 15 (23) | |
| Factor | Control (N = 33), n (%) | Intervention (N = 31), n (%) | Total (N = 64), n (%) | p-value |
|---|---|---|---|---|
| Did you learn anything from taking part in the study? | ||||
| Yes | 30 (91) | 29 (94) | 59 (92) | 0.530 |
| No | 3 (9) | 2 (6) | 5 (8) | |
| Did any of the messages encourage you to think about your health? | ||||
| Yes | 27 (82) | 28 (90) | 55 (86) | 0.270 |
| No | 6 (18) | 3 (10) | 9 (14) | |
| Did any of the messages make you want to change or improve your health? | ||||
| Yes | 26 (79) | 24 (77) | 50 (78) | 0.244 |
| No | 1 (3) | 4 (13) | 5 (8) | |
| Missing | 6 (18) | 3 (10) | 9 (14) | |
| Do you think taking part in this study helped to reduce the amount you drink? | ||||
| Yes | 14 (42) | 18 (58) | 32 (50) | 0.373 |
| No | 11 (33) | 9 (29) | 20 (31) | |
| Maybe | 8 (24) | 4 (13) | 12 (19) | |
Discussion
This feasibility study has shown that the client group (disadvantaged young and middle-aged men) are very willing to actively engage in a study with an interactive intervention. Through careful process evaluation the study has shown that participants had not only received, opened and read the messages, but thought deeply about the content and had taken the time to respond. Many of the men gave carefully considered personal responses to the questions set. The study has also shown that interest in the intervention was maintained for the duration of the study period. There was very little attenuation in the number of men responding to text messages, with > 60% replying to the final question.
Fidelity of delivery of the intervention is crucial. 155 An important advantage of interventions delivered by mobile telephone is that the fidelity of delivery can be accurately measured. The computer system which delivered the SMS messages recorded that almost all (95%) of the messages were successfully delivered to the telephones of the participants. The high number of responses to the intervention text messages implies that the men opened all of the messages, confirming that exposure to the intervention was comprehensive.
Bellg et al. 166 purport that measuring fidelity of delivery goes beyond ensuring that the content of the intervention is constant and that those delivering it are trained. Participants should understand the information given, particularly if literacy levels are low. This study monitored comprehension of the messages by assessing the nature of responses to the questions. The men clearly understood the language used. This was confirmed in interviews at the end of the study with one man reporting that ‘Anybody could have understood the messages even if you were dyslexic’.
A key finding is the value of content analysis of the responses to questions asked. This provides a further important dimension of fidelity that has not been previously reported. 23 There are several advantages of using this methodology. Critically, the process evaluation does not alter the delivery of the intervention. The study was designed to have a non-contact intervention. Obtaining process data through interview or focus groups would have altered the characteristics of the intervention. Another attraction of this method is that it is unobtrusive. The questions were embedded in a series of non-threatening text messages, which participants could choose to ignore, with no likelihood of being pressed for an answer. The result was that personal questions were asked in a way which elicited deeply personal and apparently honest answers.
Answering questions by text message allowed participants to give a considered response to the questions asked, a luxury not afforded during a face-to-face interview. This incorporates a technique used in MI, and is particularly apposite for the questions asked in this study. Participants were asked to reflect on aspects of their drinking behaviour (e.g. reasons for trying to reduce consumption), identify who would be pleased with changes made and identify potential financial benefits of reduced consumption. Reflecting on these questions, formulating and writing down the answers, reinforced the messages. While this was an integral part of the intervention, it also served as a valuable tool for process evaluation.
A notable feature of the responses to text questions is that there was a high level of engagement from the start of the study with little sign of attenuation during the course of the intervention. Another early indication that the men were willing to engage in a narrative was in responses to multiple-choice questions. Very few men gave the one-letter multiple-choice answer: instead they transcribed the whole answer (e.g. in response to the question on reasons for drinking a typical reply was ‘C – to have fun’). This raises the question of why men were so willing to respond to the text questions. It may be because text messages are viewed as part of a conversation to which responses are expected. 167 Certainly the high response indicates that men were comfortable with the study.
For this study, this dialogue was initiated by the process of obtaining consent by text message. Thus, a relationship was established, and the source was seen to be credible, an important factor in engagement. 168 This high success may have been achieved because one entry criterion for the study was that participants should have access to a mobile telephone for the duration of the study.
All process evaluation components were also measured in the control group. Control group participants were also fully engaged with the study, with 100% retention at follow-up. This has important implications for the full trial. The control group package must be interesting enough to keep participants engaged in order to avoid differential loss from the control group during the trial. The messages were designed to give health information only, but in a way that did not antagonise the participants. Further, to avoid bias, the control participants should be given a similar amount of attention and support as the intervention participants. 169,170 The text questions provide this attention.
Conclusion
The interactive nature of the intervention was successful in engaging participants, both in the intervention and control arms of the study. This feasibility study has identified a new and very useful tool for process evaluation in assessing complex interventions delivered electronically. Content analysis of responses to text messages not only confirms fidelity of the delivery of the intervention. It measures the extent of engagement with components of the behaviour change strategy, identifies ambiguity in messages and highlights gaps in the intervention and areas for improvement. Retention in the study, at 96%, confirmed that the overall design was acceptable to the target group.
Chapter 11 Post-trial assessment
Introduction
The final evaluation of the study involved telephone interviews with 20 of the men who had participated in the feasibility trial. This was designed to clarify which components of the recruitment process and intervention and control packages were acceptable to the men and whether or not the intervention package influenced drinking patterns. Participants were also asked to identify ways in which the study could be improved. This evaluation is recommended for trials of complex interventions. 160
Aims
To identify:
-
participants' motivation for taking part in the study
-
reasons for their engagement with the components of the intervention
-
areas where improvements to study design could be made.
Methods
Semi-structured interviews were conducted by telephone with 20 men. Participants were selected so that 10 men from the intervention group and 10 from the control group were included. Five men from each group had been recruited by RDS and five from GPs. Interviews were conducted after the follow-up questionnaire had been completed. The interviews were designed to explore the participants' reasons for taking part in the study and the acceptability of all stages of the recruitment process. The men were asked to identify ways in which the delivery of the intervention could be improved, whether or not aspects of the intervention had caused them to review their drinking patterns or consider moderating their drinking. Participants were also asked to reflect on and report factors which might limit their ability to drink less (see Appendix 6).
Men in the intervention group received 36 messages which used social cognition models, MI techniques and components of behaviour change strategies to encourage a reduction in binge drinking. The control group received 34 messages on four health topics: healthy diet, physical activity, sexual health and mental health. These messages did not incorporate any behaviour change techniques. However, the control messages were comparable to the intervention package in the duration and number of texts, the use of questions to elicit responses, the provision of health information and the frequent use of humour.
Results
Characteristics of participants
The Phase 3 participants were representative of the whole study population. Five men participated from each of the four age groupings from 25 to 44 years. Half of the men were married and 9 of the 20 men were in employment. Thirteen men had received no education after leaving school and half of them lived in the most socioeconomically disadvantaged areas of the city. Twelve men were in the pre-contemplation stage on the Readiness to Change Questionnaire,123 although 13 indicated at baseline that they had at least thought about cutting down on their drinking. Almost all (90%) of the men were drinking hazardously at baseline (i.e. had a positive FAST). 121
Factors influencing the decision to take part in the study
Curiosity and self-interest were most commonly given as the main reasons for taking part in the study (e.g. ‘Just to see what it was. I was curious’). Others were interested because the study was about alcohol. One man said that he thought the study would help to ‘try to take care of my alcohol problem’, one reported that he took part because he was in the process of trying to stop drinking, and another said he ‘was thinking about it anyway’. However, it appeared that alcohol as a topic had appeal even when the participant was not considering cutting down: ‘I thought it would be interesting topic. It [alcohol] was medium to a big part of my life’.
Several men took an altruistic approach. One man felt that it was ‘Important that people give their views and if it helps you [the researcher]’, whereas another said it would be ‘Good experience to help out’. Some men who were recruited through RDS appeared to want to please the person who had nominated them: ‘Mentioned by a friend and thought I would see what it was about’ or simply ‘My friend asked me’.
One man, recruited by RDS, appreciated being asked, although he clearly had apprehensions. He said that he wanted to take part ‘because nobody offered me these type of questions before’. He was encouraged because the study was conducted by telephone: ‘I didn't have to face the person’. He confessed he would be concerned about ‘a clash of personality’.
Six of the 20 men stated that they had doubts and concerns about taking part when asked directly. These were often general uncertainties: ‘Didn't know what was letting myself into, what was in store’, although these apprehensions were short-lived with one man saying they were ‘not borne out by the study’. Two men were concerned that they were being judged as alcoholics. One was ‘Afraid about what you were going be told. Would I get classed as an alcoholic?’, whereas another said ‘I was worried it was like the AA’. The participant information pack helped to alleviate worries: ‘Got the letter and read it and that helped a lot’. Four participants who were recruited by friends (RDS) thought that the decision to take part could have been easier if they were given more information by text message, e-mail or by a trustworthy person.
Nineteen of the 20 men said that at the end of the study they would be willing to nominate a friend to take part. The most common reason given was that the men felt a benefit from taking part and that the study raised awareness on health issues: ‘Good idea to improve the health of the community’. Although men in the control group did not receive any messages on alcohol, similar numbers from the intervention and control groups said that they would nominate friends to raise awareness on alcohol and help them with alcohol-related problems:
make them thinks about their drinking and what it's doing to them.
Cause I have got a few friends in same situation as me. And they could do with the help as well.
One man from each group (intervention and control) said they would nominate someone for entertainment value: ‘Such a good study, and you learn a lot from it! The text messages always fun to receive as well’. Credibility of the source of the messages was important. One man said he would nominate a friend ‘because you are from the university and he will know you are trying to help’. One man was dubious about whether or not his friends would take part if nominated, although he believed the study would benefit them: ‘a few friends that I think would benefit but they wouldn't take part’. Only one man said that he would nominate a friend for financial benefit.
Likes and dislikes
When asked specifically what they liked about the study, most participants commented on the appeal and acceptability of the overall approach. The comments indicated that both the method of delivery and the content of the messages were appropriate for the target group. One man summarised this succinctly: ‘Liked the style and the way it was delivered. Up to date, not letters. Felt direct’. Another commented that the study ‘Made you think about it in a non-serious way. More relaxed about it. If it was too serious, I would be less willing to think about’. Another man concurred saying that it ‘Didn't feel like it was pointing the finger’. The humour also appealed to the men: ‘I thought it was a good laugh. It cheered me up when I got it’.
Two men from the intervention group commented on the timing of the delivery of the text messages: ‘The randomness of the texts was good. They came in at times that stopped me from drinking. Seven out of 10 texts made me change my mind from drinking’.
Men from the control group also reported on the usefulness of the text messages, although they were given general health promotion messages only: ‘Couple of messages that opened your eyes to things that you didn't know before’ and ‘No pressure. Some of them were interesting. The questions were good, gave me something to do’.
The participants were hesitant in divulging details of anything they didn't like about the study. One participant said ‘The initial telephone call. I felt you were maybe trying to accuse me of being an alcoholic. Maybe trying to trip me up’. However, his apprehensions were fully resolved during the initial telephone call.
Opportunities for improvement
Participants were asked to consider how the intervention and control messages could be improved. The majority of men were satisfied, with some commenting that they enjoyed the texts. One man commented that ‘Anybody could have understood the messages even if you were dyslexic’. Only one man commented on the timing of the message delivery. He reported that he did not like receiving messages when he was out drinking. However, on reflection he decided ‘in long run [the intervention] has had a good effect, but at the time not good, but now think maybe it was good I got them’.
Most comments were suggestions on how to improve the images. The images were clearly important in reinforcing the text messages. One participant noted that the ‘ones with the pictures made me think more’, whereas another man said that the ‘ones with pictures – remembered better’ and suggested it maybe better to ‘put them all with pictures’. One man suggested introducing animation to the images and another wanted the ‘Cartoon pictures more life like. . . Real life’. He thought that he did not associate the images with himself if they were in cartoon format. One participant suggested the images could contain adult humour or be ‘a bit cheekier’.
Influences on drinking patterns
The majority of men from both groups reported that taking part in this part of the study made them think about changing their drinking. When asked if they could remember what made them want to change, the most common response was for family and health reasons:
My daughter is only 4½. Want to be with her as long as possible.
To save my health for my family.
One of the texts came through and I showed it to my daughter, and she said ‘you are going to have to do something about your drinking Dad’.
Men in the intervention group tended to give general answers about the effect of the intervention package and reasons for wanting to change:
The whole survey altogether.
Thinking about it, it was making me actively think about it. Text messages were making me think about it. It has been a good thing.
Reading the texts and make you think.
However, men in the control group who had not received the intervention text messages also reported that the study made them think about changing their drinking. They also recalled information given in the baseline questionnaire:
It was the binge drinking units in the questionnaire at the start.
Not to binge drink. Realising 4 pints is binge drinking.
Something I was doing anyway, but binge drinking of 4 made me think again.
Reading about facts. Did not think 4 pints is binge drinking.
Moving on from desire to change, the men were asked ‘Do you think you did change in any way?’
Several men from the intervention group reported that they had changed:
Drunk less, only one binge a month.
Yes, thought more about it and have cut back some weeks certainly.
Yes. Doing more stuff. When I went out drank juice, went to gym more, took my daughter out more.
A bit, but in the process of changing.
Yes, definitely, drink a lot less.
However, men in the control group also reported actual changes:
Took more interest in walking more. Don’t drink as much. Don’t down 3 to 4 pints each time.
Yes, bit more aware of drinking.
Yes – during my time of study had more alcohol in the fridge but was not going to the fridge. Was gradually drinking slower.
Yeah, more conscious of what I am drinking.
Two men, both from the control group, realised that they had not changed, but reported that this was due to family problems:
Not sure, as had a blow out as had problems with girlfriend.
No because a bad time with family, broke with missus.
Barriers to reducing drinking
Following discussions around the impact of the study, the men were asked to consider what the barriers would be to anyone who wanted to reduce their drinking. A few men from each group were unable to identify any barriers: ‘If they are going to do it they are going to do it’. One man thought it was about ‘Being able to control themselves, once you go past the limit its difficult to control yourself’. Overcoming addiction was highlighted by several men, some of whom felt lack of willpower was the barrier:
If you’re addicted, it’s about willpower.
Too hard, not got the will-power. It’s psychological.
Some men realised that drinking was a habit and the barrier is ‘Changing their habit, it's a bad habit. If you are in a rut, it is trying to find something to do. Fill in your time better’. Others identified peer pressure, unemployment, boredom and potential barriers. One man thought the main barriers were ‘Availability and price, supermarket cheap vodka, cheap beer’.
In an attempt to identify ways of improving and enhancing the impact of the intervention, participants were then asked if they could think of anything that would help people to cut down.
Two men felt it was entirely up to the individual and the answer was about self-control: ‘You have to make your mind up yourself’.
Six men felt that having support, both from family members and from a doctor would help. Others had thought of ways to reduce the amount consumed in sessions. One man identified two strategies: ‘Count up how many you would normally have and then reduce 1 or 2 pints a time, or keep the bank card at home’. Others proposed strategies to avoid drinking situations: ‘Getting out and doing more, and not sitting in the house. Going out for walks, to clear your head’. Another was aware that being employed was one of the best ways to reduce: ‘Something that doesn't stress people out. Having a job helps people cut down’.
One man proposed a complicated strategy to reduce gradually in order to avoid withdrawal problems: ‘Try to get them to drink half as much! Even ¾ as much, to stop them rattling. Then ½ for 4 days. Then ¼ lager for 2 weeks. Then few tins of lager. If they come straight down they can have a heart attack or die on their own puke’.
Some men reported that this study had helped them and had the potential to help other people:
The initial survey. I thought when I came off the telephone – I have a bit of a problem. The text made you think twice about drinking. Not all but some of them.
Show them the messages that might help them. It helped me and it helped my friend as well because I showed him the messages and pictures and he used to drink a lot, now he has calmed down. I saved the pictures and went round and showed him.
The final question asked of participants was whether or not the gift vouchers (£10 on completion of the baseline questionnaire, £20 during the intervention period and £10 each for the follow-up questionnaire and the in-depth interview) encouraged them to stay in the study. Two-thirds of the men said that it did. Some reported how they used them, for example ‘bought kids toys’ or ‘saved them up and bought some aftershave’. For some the vouchers were seen as a ‘a little reward, little bonus’. The remainder of the men said they were not influenced by the vouchers: ‘I enjoyed the texts. The vouchers was just a bonus’ and ‘Would have done it anyway’.
Discussion
The post-trial assessment with 20 participants provided insight into all aspects of the study. Some men were apprehensive when they were first approached and were unclear about the nature of the study, or whether or not they would be judged to be an alcoholic. These apprehensions were allayed, in some cases, by the participant information leaflet, and also by the first telephone conversation with the research fellow. An informal and friendly approach in the initial telephone contact was essential for facilitating recruitment. The main reason for taking part was curiosity about what would be involved and a general interest in the topic. Some men appreciated being asked to take part and thus felt valued. The men also demonstrated altruism in their decision to take part. Future recruitment should emphasise the importance of each individual's contribution to the study.
The attractive and informal style of the text messages was popular with the men as they did not come across as didactic or threatening. By the end of the study almost all the men said they had found the experience sufficiently worthwhile that they would recommend participation to their friends. This suggests that interventions should be designed to be enjoyable to promote engagement with the behaviour change strategies. Variety of content and timing of the messages was also important. As was expected,94,95 images were thought to be more memorable and to convey information and ideas more clearly than text. However, realistic pictures were thought likely to be more effective than the cartoon style that was used. The images will be modified for the full trial.
The modest financial incentives given at recruitment, at regular intervals during the intervention period and at the follow-up interview were important. The majority of men stated that these incentives encouraged them to stay in the study. Although many also said that they would have taken part without them, this may be a view of hindsight; having experienced the intervention, and enjoyed it, the men may have concluded that participation would have been worthwhile without the incentives. If so, it is likely that the incentives would have encouraged participation at recruitment and the early stages of intervention delivery. The literature shows that incentives are effective45,107 so it would seem wise to use them for the full trial.
The men confirmed that the intervention had made them think about changing their drinking habits. However, this was generally not just a simple wish to drink less. Instead it involved more engagement with close family and adopting new behaviours as an alternative to drinking. This suggests that text messages which ask the men about what activities they could do more of if they drank less could be added to the intervention. The comments that drinking was a habit support the idea of promoting new activities as a means of breaking the habit.
The finding that men in the control group felt that participation in the study increased their awareness of alcohol and willingness to reduce consumption has important implications. It is possible that the control messages, although intended to be neutral, elicited behaviour change. This could have been because the control messages were comparable to the intervention package in the duration and number of texts, the use of questions to elicit responses, the provision of health information and the frequent use of humour. The resulting engagement with the health messages could have led to a reappraisal of many aspects of life including drinking. The aim of the control messages was to promote retention in the study. As retention of the controls was 100% and the levels of satisfaction with the study were very high, a less active control package would still promote retention. Thus, for the full trial the number of control texts should be reduced, as should the amount of health information.
Several men in the control group reported that the baseline questionnaire prompted a reassessment of current drinking. It has been suggested that a screening questionnaire used to assess that participants meet the alcohol consumption entry criterion may be sufficient to prompt behaviour changes. 9 The baseline questionnaire stated the definition of binge drinking and asked questions on current alcohol consumption, the harms of alcohol, the benefits of moderated drinking, drinking refusal skills and readiness to change. These topics are also components of the behaviour change strategy for the intervention group. They were included in the baseline questionnaire to measure whether or not, at outcome, these components had been changed to a greater extent in the intervention group than the control. To prevent the baseline questionnaire from acting as an intervention, fewer questions should be asked in the full trial. The complete set of questions could still be asked at follow-up and, combined with the extensive process measures described in Chapter 10, should still identify which components of the intervention were associated with reduced binge drinking.
In summary, the post-trial assessment provided insight into the recruitment process, the reasons for high levels of engagement with the intervention and ways in which the study could be improved. In particular, it suggested ways to improve recruitment and identified new behaviour change opportunities which could be added to the intervention. It also identified modifications to be made to the baseline questionnaire and the control group messages to ensure that these did not prompt a re-evaluation of drinking intentions.
Chapter 12 Summary and conclusions
This study has successfully tested the feasibility of all aspects of a behaviour change intervention study which used text messages to deliver a brief alcohol intervention to disadvantaged men in early mid-life. Because the target group has been little studied and the design and delivery of the intervention posed interesting challenges, the study provided the opportunity to make a series of important theoretical and methodological advances. The use of extensive process measures shed light on all aspects of study design and conduct including the recruitment strategy and the design, delivery and impact of the intervention. The results of the study have been discussed fully in the main chapters of the report.
This chapter presents the main findings from each chapter, assesses the extent to which the aims of the feasibility study have been met, and concludes with modifications to be made to the proposed full trial. It should be noted that the term feasibility study is used here. In fact this study contains elements of both a feasibility study and a pilot study. The research could be described as feasibility because it assesses whether or not the full trial could be done (e.g. availability of participants, willingness to be randomised, follow-up rates). However, it also fits with the definition of pilot study: a version of the main study run in miniature. The term feasibility has been chosen because it captures the exploratory and developmental spirit of the study.
Main findings
Focus group analysis
-
Explanations for current drinking patterns and their change over time appear rooted in shifts in three interacting conceptual areas: private purpose (the individual's personal reasons for drinking), social roles (expectations, duties and sanctions on drinking) and concrete experience (of the adverse effects of excess drinking).
-
The set of social expectations stem from recognition of the person's wider social roles and responsibilities (employee, husband/partner, parent) and abilities (self-discipline/control, ability to tolerate alcohol, judge limits and resist social pressure).
-
Drinking motives had significantly changed from when the men were younger. This stemmed from a shift in the private purpose and social roles facilitated by alcohol use. It was accompanied by a shift from ‘freedom to’ enjoy the pleasures of alcohol to ‘freedom from’ life stresses through the use of alcohol.
-
Consumption was influenced by obligations to a range of competing social roles including parent, partner and employee that had not been extant when younger. In addition, recognitions of these changes produced what might be termed a ‘mature drinker’ role with associated expectations.
-
The mature drinker was viewed as someone who can tolerate greater amounts of alcohol without becoming drunk, has greater self-discipline, is more likely to be able to resist social pressures to drink, and drinks as a means of reward, relaxation and release from life pressures.
-
Knowledge of the negative experiences of alcohol was detailed and widespread. However, reported changes in behaviour appeared rooted in concrete personal or vicarious experience of these issues rather than more abstract risk.
-
Peers and social networks influenced drinking in this group in complex and subtle ways. Although some men felt that their friends were more accepting of their decisions to slow their drinking down, other men still felt pressure from their peers to consume large amounts of alcohol. In the second context, the consumption of alcohol signified membership of the group and gave the men a sense of belonging.
-
Drinking refusal self-efficacy largely depended on whether the group was predominantly defined by its drinking behaviour or another organising factor. A brief intervention might therefore highlight that the men have a choice about the different social networks they are accessing, and that this choice will affect the amount of alcohol they consume and ultimately their health and well-being.
-
There was often a marked discrepancy between an individual's drinking habits and the intended aims of drinking. Thus, brief interventions could highlight the mismatch between being drunk, and success in socialising, working, ‘doing good turns’ and feeling good about oneself.
Recruitment
-
10. The intended target of 60 men from disadvantaged areas was easily exceeded using two recruitment strategies: through GP lists and by RDS. The use of evidence-based techniques may have assisted the recruitment.
-
11. Obtaining ethical consent from individuals recruited through GP posed a challenge because there was no face-to-face contact. This was overcome by obtaining consent by a confirmatory text message.
-
12. Recruitment by RDS required prior fieldwork to establish suitable venues for recruitment. The study found that participants could be recruited if approached in familiar settings. For the full trial, venues such as post offices, training centres for the unemployed, pharmacies and communal areas in high-rise buildings could be used.
-
13. Flexible recruitment strategies involving multiple attempts at contact at different times of the day and days of the week are essential.
-
14. Some potential respondents were concerned that the initial approaches might be part of a scam to steal money. This was more marked when first approach telephone calls came from an institutional 0845 telephone number. Use of a dedicated study mobile telephone number overcame this difficulty.
Baseline characteristics
-
15. The men in this study were socially disadvantaged whereas those recruited to previous studies on alcohol brief interventions were mostly well educated and in employment.
-
16. Baseline interviews were successfully conducted by telephone. Data on alcohol consumption over a 30-day period, including total consumption and frequency of binge drinking, heavy binge drinking and alcohol-free days were obtained.
-
17. Binge drinking was common, with 57% of men consuming ≥ 8 units of alcohol in a session at least three times per week. In addition, 25% of men drank at least 20 units in a session.
-
18. Most men were drinking at a hazardous level (84% had a positive test score on the FAST screening questionnaire).
-
19. Randomisation was successful and the intervention and control groups were balanced at baseline.
-
20. Participants recruited by RDS were less well educated and more likely to be unemployed. These men may be marginalised in society to such an extent that they have become a hidden group.
-
21. Men recruited through RDS were much more likely to be drinking hazardously. These men also frequently suffered episodes of memory loss following drinking sessions. Recruiting solely through GP would miss high-risk drinkers.
-
22. Knowledge of the conventional definition of binge drinking was low, with most men guessing the level was much higher. There is an opportunity to incorporate education on binge drinking into the intervention.
-
23. RSOD was common, with episodes of heavy binge drinking interspersed with many alcohol-free days. This pattern of drinking has not been previously described in this age group. This type of drinking could explain why disadvantaged men are at such high risk of alcohol-related harms, even although the total alcohol consumed is not high.
-
24. Heavy binge drinking was common despite a high level of awareness of the harms of binge drinking. This discrepancy, using the techniques of MI, provides a lever for behaviour change.
Intervention design
-
25. The content of the intervention text messages was derived from seven types of literature: alcohol brief interventions, text message interventions, two psychological models (the TPB and the TTM), MI, communication theory and reviews of specific behaviour change techniques.
-
26. The literature reviews identified several issues to be resolved including style and tone of the texts, the specific behaviour change strategies to be included, and the sequence and frequency of the messages.
-
27. A combination of SMS texts and MMS messages with images were used to deliver the intervention. The images provided colour and variety and were used to complement the text messages.
-
28. Despite the restriction of SMS texts to a maximum of 160 characters, the components of behaviour change strategies were successfully presented in the messages.
-
29. The user group representatives provided insight into drinking motives and behaviour which identified opportunities for behaviour change. They also helped ensure that the interventions were acceptable and the outcomes were relevant and measurable.
-
30. Messages were tailored to the target group and the individual by embedding them in the language and the drinking culture of disadvantaged young men. The messages used popular texting terms and abbreviations. The participant's first or preferred name was used, particularly in the early text messages.
-
31. The text messages emphasised the credibility of the source (University of Dundee), used the informal style and abbreviations of everyday text messages and made frequent use of humour.
-
32. A variety of techniques were employed to increase message effectiveness: tailoring of messages; use of gain-framed texts; pairing of messages; inclusion of questions to promote interactivity.
-
33. Images were designed to develop and extend the narrative and to make concrete the harms of alcohol.
-
34. The messages were constructed to take advantage of the conventional pattern of heavy weekend drinking. Messages were designed to tap into three windows of opportunity: before weekend drinking, after a heavy drinking episode and mid-week sobriety.
-
35. The initial set of messages were tested in focus groups and improvements made. They were then mapped against reviews of behaviour change techniques to ensure that relevant techniques were not overlooked.
-
36. The control group received a similar number of texts, but these were intended to have no influence on drinking behaviour. The control texts addressed four health behaviours: diet, physical activity, sexual health and mental health.
Intervention delivery
-
37. Delivery of the messages was computerised, and followed the same schedule for all men. Messages began on the Monday morning following recruitment and continued for 28 days. This enabled messages to be tailored to day of the week.
-
38. The computerised system could identify receipt of SMS text messages and could collect responses from the participants. This enabled messages to be terminated for individuals who wished to withdraw from the study. In the event no-one asked to leave.
-
39. The use of a computerised system for the automated delivery of the text messages means that large numbers of men could be targeted at low cost.
Retention
-
40. Through the use of multiple evidence-based strategies embedded throughout the study, a retention rate of 96% was achieved with a difficult-to-retain group.
-
41. Over 90% of men thought that participation in the study was informative and worthwhile. The text messages were very popular and many men would have liked more text messages.
-
42. Three features of the messages – anticipation of the content of the next message, the varied time of sending of the messages and the frequent use of humour – may have contributed to the popularity of the study.
Process evaluation of the delivery and impact of the intervention
-
43. Novel methods of process evaluation were employed in this study. These shed light on the fidelity of delivery of the intervention and on the impact of the components of the intervention. The novel methods complement and strengthen conventional process measures.
-
44. The fidelity of delivery of the text messages can be successfully measured through the computer system which managed the sending of the messages. Overall, 95% of SMS text messages were delivered to the participants' telephones.
-
45. The computer system also captured responses to text messages. Responses to text messages were common, particularly for texts which asked questions. However, many participants responded to other texts.
-
46. Eighty-eight per cent of men in the intervention group responded to one or more text questions. Over half of the men replied to at least seven of the nine texts which asked questions. Frequency of responding did not vary by age, social deprivation or level of hazardous drinking, suggesting this approach is suitable for different types of drinkers.
-
47. There was no evidence that the frequency of responding decreased over the duration of the intervention, suggesting that, once enlisted, engagement is maintained.
-
48. The questions gave the men the opportunity to think about the components of the behaviour change strategy. The questions thus form an important element of the behaviour change strategy.
-
49. Analysis of the content of the responses showed that the men gave considered and personal responses to the questions, indicating a high level of engagement with the texts.
-
50. Analysis of specific questions identified which of the components of the causal chain to behaviour change was achieving the intended response. The effective components included: subjective norms, control beliefs, perceived behavioural control and behavioural intentions.
-
51. The process evaluation provides strong evidence that the proposed full trial will be a technical success.
-
52. Men in the control group also showed a high readiness to respond to text questions. These questions concerned other health behaviours: sexual health, mental health, physical activity and diet. This indicates that the text message questions can be successfully used in studies targeting other health behaviours.
-
53. Given the highly informative nature of the text question responses, they should be a feature of feasibility studies of interventions delivered electronically.
-
54. This type of process measure is unobtrusive and gives real-time feedback on the components of the intervention.
-
55. As text message questions have the potential to increase the effectiveness of the intervention, they should be used for each of the key components of the behaviour change strategy.
-
56. Two text messages were found to be inadequate; one was ambiguous and the other (a loss-framed message) received a poor response. These messages will be changed for the full trial.
-
57. Almost all (95%) of the men told someone else about the study and 40% discussed it with more than five people. This could increase the impact of the intervention on social norms (gaining support from family and friends). It could also facilitate national roll-out of the intervention, promoting uptake in the general population. Through this mechanism the intervention could act to promote culture change by encouraging discussion of the benefits of more moderate drinking.
-
58. The extent to which study participants discussed the text messages with friends and family members has an unexpected consequence for RDS. As this technique aims to recruit several individuals from close social networks, contamination of the control group could occur. Abandoning the community outreach recruitment strategy would seem unwise, since recruiting only through GP would exclude many high-risk drinkers. The solution is to use an alternative strategy, time–space sampling. This technique recruits individuals from multiple venues, but avoids recruiting groups of individuals from the same social network.
Outcome assessment
-
59. The primary and secondary outcomes proposed for the full trial were successfully measured on all subjects who were followed up.
-
60. More men in the intervention group reduced their frequency of binge drinking, and heavy binge drinking, than in the control group. There was also a greater increase in the number of moderate drinking days in the intervention group.
-
61. More men in the intervention group increased intention to reduce their alcohol consumption, as measured by the Readiness to Change Questionnaire and a question specifically about intentions. These changes were accompanied by a fall in the number of men who thought the benefits of their drinking outweighed its harms.
-
62. The success of the intervention most likely reflects four key design features.
-
The use of a delivery medium, the mobile telephone, which is an attractive, valued means of communication by the target group. It gave the men control over when they read the messages and gave them time to reflect on them and respond to them if they chose (most men did respond).
-
The consistent use of a friendly supportive style in which behaviour change strategies were interspersed with novelty and humour. The messages were of sufficient popularity to be shared widely with friends and family.
-
The use of questions to encourage extended engagement with the behaviour change strategies. These questions elicited carefully thought-out, highly personal responses.
-
The phrasing of text messages in the language of the target group, based on the focus groups conducted prior to and during intervention development.
-
-
63. There was a high awareness of both the harms of alcohol and the benefits of moderate drinking in both intervention and control groups. This indicates that these items should not, as was proposed in the protocol, be used as secondary outcome measures.
-
64. The feasibility study identified that drinking refusal self-efficacy was not influenced by the intervention. For the full trial the intervention will be improved by giving increased emphasis on self-efficacy.
Post-trial assessment
-
65. The main reasons for taking part in the study were curiosity about the study, interest in the topic of alcohol and feeling valued.
-
66. In the recruitment process, more emphasis could be placed on the importance of each individual to the research study. The potential to help others could also be stressed.
-
67. Some men expressed initial concerns about participation, particularly being classed as an alcoholic and uncertainty about what the study would involve.
-
68. The majority of men thought that the financial incentives promoted retention within the study.
-
69. By the end of the study almost all the men said they had found the experience sufficiently worthwhile that they would recommend participation to their friends.
-
70. The friendly style and the varied content, particularly the use of humour, were highly valued by the participants.
-
71. Text messages with images were thought to have had more impact than text messages alone. Making images more realistic could increase their relevance to the participants.
-
72. Men in the intervention group thought that the study increased intention to change drinking, through concerns about personal health and their families.
-
73. Some men in the control group reported being very surprised by the statement in the baseline questionnaire that consumption of four pints constituted binge drinking. They may also have been influenced by baseline questions on the harms of alcohol and the benefits of moderated drinking. These questions should be omitted for the full trial.
-
74. The control messages may also have influenced drinking intentions. This could be because the control messages were comparable to the intervention package in the duration and number of texts, the use of questions to elicit responses, the provision of health information and the frequent use of humour. Thus, for the full trial the number of control texts should be reduced, as should the amount of health information. This would make the control group messages more comparable to those used in conventional alcohol brief interventions.
Implications for other research studies
-
75. Questions embedded in text messages provide a simple method of process evaluation for trials of behaviour change interventions delivered by electronic media. The questions should tap into key components of the behaviour change strategy, to assess the extent of engagement with each component. Rather than being intrusive, this method of process evaluation may promote engagement with the intervention and thus increase its effectiveness.
-
76. Follow-up rates are likely to be higher if the intervention is inherently enjoyable. Behaviour change interventions should address the enjoyability of their intervention. The challenge is to make sure the intervention is not boring or ‘preachy’.
-
77. The intervention and delivery method could easily be rolled out for use with other social groups and other adverse health behaviours. The responses to the control group text messages showed a high willingness to engage in improving mental health, sexual health, physical activity and diet.
Does the feasibility study indicate that a full trial should be conducted?
The feasibility study sought to answer three questions to determine whether or not a full trial of the intervention should be conducted.
-
What are the best ways to recruit and retain disadvantaged men in a study aimed at reducing the frequency of heavy drinking?
-
What is the type of content and timing of the delivery of a series of text messages and images that is most likely to engage young to middle-aged men?
-
Is the intervention likely to be an acceptable way to influence the frequency of heavy drinking?
Recruitment and retention
Recruitment was successful. It is recommended that GP recruitment together with a community outreach strategy be used in the full trial. RDS, by recruiting several individuals from close social networks, could lead to contamination of the control group. An alternative strategy, time–space sampling, could be used. Retention, at 96%, was very high and the existing strategies to promote retention should be maintained in the full trial.
Content and timing of messages
The messages were derived from an extensive review of several relevant fields of research. Components of behaviour change theories and techniques were successfully conveyed in short text messages and images. The content and timing of the messages was carefully planned to fit with the pattern of drinking of the target group. The high level of engagement with the messages indicates that the content was warmly received. The spontaneous ‘thank-you’ text messages at the end of the study support this conclusion. The post-trial evaluation showed that the frequency and timing of the messages was not only acceptable but also popular.
Influence on heavy drinking
The study was not powered to detect changes in drinking. However, the frequency of binge drinking reduced slightly more in the intervention group. In addition, there was a greater improvement in intentions to reduce drinking in the intervention group. These findings, together with the high level of engagement with the intervention, are compatible with the intervention being effective.
Summary
In summary, this study has successfully tested the feasibility of all aspects of a behaviour change intervention study which used text messages to deliver a brief alcohol intervention to disadvantaged men in early mid-life. The use of extensive process measures has shed light on many aspects of study design and conduct including the recruitment strategy and the design, delivery and impact of the intervention. This study design has demonstrated the potential to recruit, engage and modify drinking behaviour among disadvantaged young to middle-aged men. We recommend that a full trial of the intervention be carried out to assess the effectiveness of the intervention. We further recommend that a cost-effectiveness study be incorporated into the trial to determine whether or not the approach is truly a low-cost method of reaching large numbers of disadvantaged men.
Modifications to the full randomised controlled trial
This feasibility study has identified several ways in which the design of the full trial could be improved. These cover the recruitment strategy, intervention, process measures and outcome measures. These revisions will improve the conduct of the stages of the trial and increase the effectiveness of the intervention. This section only mentions issues which arose from the feasibility study it does not attempt to provide a protocol for the full trial.
Recruitment strategies
-
The evidence-based recruitment techniques should be retained for the full trial.
-
In the recruitment process, more emphasis could be placed on the importance of each individual to the research study. The potential to help others could also be stressed.
-
Given the differences in the types of drinkers recruited by the GP and community outreach strategies, it is recommended that both GP and community outreach recruitment strategies be used. With each method recruiting 50% of the intended sample, coverage of all types of drinkers will be achieved.
-
As RDS could give rise to contamination of the control group, an alternative outreach strategy, time–space sampling, should be employed. This recruits from areas which the target group is known to frequent and stresses the need for flexibility of setting, time of day and day of the week for recruitment. It requires initial fieldwork to identify a wide range of venues and suitable times for recruitment.
Randomisation
-
5. As the randomisation method used in the feasibility study was successful and maintained blindness of the research team which collected and analysed baseline and outcome data, it should be used again.
-
6. Randomisation should be stratified by recruitment method because of the difference in the types of men recruited by the two recruitment strategies. This will enable the analysis to determine whether or not the impact of the intervention differs between the two types of men.
Baseline questionnaire
-
7. The question which gives information on the definition of binge drinking should be deleted as it could lead to contamination of the control group. This question will still be asked at follow-up.
-
8. Fewer questions should be asked about the harms of alcohol, the benefits of moderated drinking and intentions about future drinking to ensure that the baseline questionnaire does not act as part of the intervention. This will be important for national roll-out, which would not involve the administration of a baseline questionnaire.
The intervention
-
9. The use of the novel method of process evaluation identified a text message which was misunderstood and another which elicited a poor response. These will be modified.
-
10. Information on the conventional level of binge drinking (≥ 8 units in a session) should be added to the intervention. The post-trial evaluation showed that the men were surprised to learn that as little as four pints constituted binge drinking.
-
11. The analysis of the follow-up data revealed that there was insufficient improvement in self-efficacy to refuse a drink. Additional texts should be created to address this.
-
12. Negative experience of alcohol should be presented in a more concrete manner to increase impact.
-
13. More attention should be given to the discrepancy between drinking aims (relaxing, having fun and socialising) and the consequences of heavy drinking.
-
14. The intervention should be extended to incorporate the HAPA, which seeks commitment to action and also promotes maintenance. Thus, new texts will be created to promote goal setting, to gain commitment to action, to overcome barriers to action and to promote maintenance of the reduced frequency of binge drinking.
-
15. The planned modifications will increase the length of the intervention. Feedback from the participants indicated that additional text messages would be welcomed. Because of the affection that the intervention generated in many participants, it would seem sensible to taper the last few messages over several weeks.
-
16. The control messages should be fewer in number and give less information about health. This will ensure that the control messages do not prompt a re-evaluation of drinking behaviour. This would make the control group messages more comparable to those used in conventional alcohol brief interventions.
Outcome assessment
-
17. The primary outcome should remain the frequency of binge drinking. It is the most appropriate measure for men whose drinking pattern is episodes of very heavy drinking interspersed between periods of abstinence.
-
18. The secondary outcome measures should be changed. Awareness of harms of drinking and benefits of moderated drinking should be omitted as levels of knowledge are high in the target group. Total consumption should be added as a secondary outcome. Goal setting and action planning could also be secondary outcome measures.
Process measures
-
19. Additional process measure questions will need to be added to the intervention to check that the proposed new texts on goal setting and action have the desired impact.
-
20. New process measures on self-efficacy should also be added.
The proposed revisions to the study protocol clearly demonstrate the value of conducting a feasibility study prior to a full trial. Although the broad structure of the study is unchanged, important changes will be made to all phases of the trial. These will improve internal and external validity and, crucially, increase the effectiveness of the intervention.
Acknowledgements
We are grateful to the men who participated willingly in the study. We would like to thank the three GPs for helping recruit participants. Recruitment through GPs was co-ordinated through the Scottish Primary Care Research Network, and we are grateful to Marie Pitkethley and Kim Stringer for the efforts they made to make this a success. Recruitment by RDS would not have been possible without the active support of many community groups that helped to nominate potential participants: Claverhouse Training, Angus College, the Dundee Criminal Justice team, Dundee Saturday Football League, staff of community centres and a community nurse.
Contribution of authors
Professor Iain Crombie (Professor of Public Health) was the chief investigator for the study. He conceived and designed the study, supervised its conduct and led the writing of the report.
Dr Donald Falconer (Research Fellow) designed the intervention and control text messages, identified suitable images, recruited the participants, collected the data and contributed to the writing of the report.
Dr Linda Irvine (Lecturer in Public Health) contributed to the study design, was project manager for the study, led the data analysis and contributed to the writing of the report.
Professor Brian Williams (Director of the Nursing, Midwifery and Allied Health Professions Research Unit) contributed to the study design and conduct, led the focus group analysis and contributed to the writing of the report.
Professor Ian Ricketts (Professor of Assistive Systems and Healthcare Computing) was responsible for the computerised system which sent the messages and contributed to the study design and conduct.
Professor Gerry Humphris (Professor of Health Psychology) contributed to the study design and conduct and contributed to the writing of the report.
Professor John Norrie [Professor of Clinical Trials and Biostatistics, Director, Centre for Healthcare Randomised Trials (CHaRT)] was responsible for the web-based randomisation system, contributed to the study design and contributed to the writing of the report.
Dr Peter Rice (Consultant Psychiatrist) contributed to the study design.
Dr Peter Slane (General Practitioner) contributed to the study design and advised on the recruitment strategy.
Contribution of the research team
Ms Claire Jones (Research Assistant) created, ran and monitored the message delivery system, the system for recording receipt of SMS texts and the mechanism for storing text message responses from participants.
Mr Philip Vaughan (Lecturer) created the images used with the text messages.
Dr Joanne Coyle (Senior Research Fellow) ran the focus groups and helped analyse the transcripts.
Terri (User Group Representative) attended steering group meetings and contributed to the study design.
Bryan (User Group Representative) attended steering group meetings and contributed to the study design.
Disclaimers
This report contains transcripts of focus groups and interviews conducted in the course of the research. Quotes from the transcripts contain language that may offend some readers.
References
- Alcohol misuse: tackling the UK epidemic. London: BMA; 2008.
- The societal cost of alcohol misuse in Scotland for 2007. Edinburgh: Scottish Government; 2010.
- Statistics on alcohol: England, 2011. London: The Health and Social Care Information Centre; 2011.
- Alcohol-use disorders: preventing the development of hazardous and harmful drinking. NICE public health guidance 24. London: NICE; 2010.
- Mackenbach JP, Stirbu I, Roskam A-JR, Schaap MM, Menvielle G, Leinsalu M, et al. Socioeconomic inequalities in health in 22 European countries. N Engl J Med 2008;358:2468-81. http://dx.doi.org/10.1056/NEJMsa0707519.
- Overview of Scotland’s health and NHS performance in 2006/07. Edinburgh: Audit Scotland; 2007.
- Raistrick D, Heather N, Godfrey C. Review of the effectiveness of treatment for alcohol problems. London: The National Treatment Agency for Substance Misuse; 2006.
- Bertholet N, Daeppen JB, Wietlisbach V, Fleming M, Burnand B. Reduction of alcohol consumption by brief alcohol intervention in primary care: systematic review and meta-analysis. Arch Intern Med 2005;165:986-95. http://dx.doi.org/10.1001/archinte.165.9.986.
- Kaner EF, Dickinson HO, Beyer F, Campbell F, Schlesinger C, Heather N, et al. Effectiveness of brief alcohol interventions in primary care populations. Cochrane Database Syst Rev 2007;2.
- Moyer A, Finney J, Swearingen C, Vergun P. Brief interventions for alcohol problems: a meta-analytic review of controlled investigations in treatment-seeking and non-treatment-seeking populations. Addiction 2002;97:279-92. http://dx.doi.org/10.1046/j.1360-0443.2002.00018.x.
- Bromley C, Given L, Ormston R. The Scottish Health Survey 2009. Edinburgh: Scottish Government; 2010.
- Conner M, Sparks P, Conner M, Norman P. Predicting health behaviour. Buckingham: Open University Press; 2005.
- Rollnick S, Miller WR. What is Motivational Interviewing?. Behav Cognit Psychother 1995;23:325-34. http://dx.doi.org/10.1017/S135246580001643X.
- Rubak S, Sandboek A, Lauritzen T, Christensen B. Motivational interviewing: a systematic review and meta-analysis. Br J Gen Pract 2005;55:305-12.
- Abraham C, Michie S. A taxonomy of behavior change techniques used in interventions. Health Psychol 2008;27:379-87. http://dx.doi.org/10.1037/0278-6133.27.3.379.
- Michie S, Johnston M, Francis J, Hardeman W, Eccles M. From theory to intervention: mapping theoretically derived behavioural determinants to behaviour change techniques. Appl Psychol 2008;57:660-80. http://dx.doi.org/10.1111/j.1464-0597.2008.00341.x.
- Glasgow RE, McKay HG, Piette JD, Reynolds KD. The RE-AIM framework for evaluating interventions: what can it tell us about approaches to chronic illness management?. Patient Educ Coun 2001;44:119-27. http://dx.doi.org/10.1016/S0738-3991(00)00186-5.
- Drummond C, Oyefeso A, Phillips T, Cheeta S, Deluca P, Perryman K, et al. Alcohol Needs Assessment Research Project (ANARP). The 2004 national alcohol needs assessment for England. London: Department of Health; 2005.
- Vidrine DJ, Arduino RC, Lazev AB, Gritz ER. A randomized trial of a proactive cellular telephone intervention for smokers living with HIV/AIDS. AIDS 2006;20:253-60. http://dx.doi.org/10.1097/01.aids.0000198094.23691.58.
- Rodgers A, Corbett T, Bramley D, Riddell T, Wills M, Lin RB, et al. Do u smoke after txt? Results of a randomised trial of smoking cessation using mobile telephone text messaging. Tob Control 2005;14:255-61. http://dx.doi.org/10.1136/tc.2005.011577.
- Geraghty M, Glynn F, Amin M, Kinsella J. Patient mobile telephone ‘text’ reminder: a novel way to reduce non-attendance at the ENT out-patient clinic. J Laryngol Otol 2008;122:296-8. http://dx.doi.org/10.1017/S0022215107007906.
- Franklin VL, Greene A, Waller A, Greene SA, Pagliari C. Patients’ engagement with ‘Sweet Talk’ – a text messaging support system for young people with diabetes. J Med Internet Res 2008;10. http://dx.doi.org/10.2196/jmir.962.
- Fjeldsoe BS, Marshall AL, Miller YD. Behavior change interventions delivered by mobile telephone short-message service. Am J Prev Med 2009;36:165-73. http://dx.doi.org/10.1016/j.amepre.2008.09.040.
- Cole-Lewis H, Kershaw T. Text messaging as a tool for behavior change in disease prevention and management. Epidemiol Rev 2010;32:56-69. http://dx.doi.org/10.1093/epirev/mxq004.
- Blaxter M. Evidence for the effect on inequalities in health of interventions designed to change behaviour. Bristol: Department of Social Medicine, University of Bristol; 2007.
- Michie S, Jochelson K, Markham WA, Bridle C. Low-income groups and behaviour change interventions: a review of intervention content, effectiveness and theoretical frameworks. J Epidemiol Community Health 2009;63:610-22. http://dx.doi.org/10.1136/jech.2008.078725.
- Galea S, Tracy M. Participation rates in epidemiologic studies. Ann Epidemiol 2007;17:643-53. http://dx.doi.org/10.1016/j.annepidem.2007.03.013.
- Keeter S, Kennedy C, Dimock M, Best J, Craighill P. Gauging the impact of growing nonresponse on estimates from a national RDD telephone survey. Public Opinion Quarterly 2006;70:759-79. http://dx.doi.org/10.1093/poq/nfl035.
- van der Wouden JC, Blankenstein AH, Huibers MJH, van der Windt DAWM, Stalman WAB, Verhagen AP. Survey among 78 studies showed that Lasagna’s law holds in Dutch primary care research. J Clin Epidemiol 2007;60:819-24. http://dx.doi.org/10.1016/j.jclinepi.2006.11.010.
- Bower P, Wilson S, Mathers N. Short report: how often do UK primary care trials face recruitment delays?. J Fam Prac 2007;24:601-3. http://dx.doi.org/10.1093/fampra/cmm051.
- Treweek S, Mitchell E, Pitkethly M, Cook J, Kjeldstrøm M, Johansen M, et al. Strategies to improve recruitment to randomised controlled trials. Cochrane Database Syst Rev 2010;4.
- Watson JM, Torgerson DJ. Increasing recruitment to randomised trials: a review of randomised controlled trials. BMC Med Res Methodol 2006;6. http://dx.doi.org/10.1186/1471-2288-6-34.
- Lorant V, Demarest S, Miermans PJ, Van Oyen H. Survey error in measuring socio-economic risk factors of health status: a comparison of a survey and a census. Int J Epidemiol 2007;36:1292-9. http://dx.doi.org/10.1093/ije/dym191.
- Goodman A, Gatward R. Who are we missing? Area deprivation and survey participation. Eur J Epidemiol 2008;23:379-87. http://dx.doi.org/10.1007/s10654-008-9248-0.
- Turrell G, Patterson C, Oldenburg B, Gould T, Roy MA. The socio-economic patterning of survey participation and non-response error in a multilevel study of food purchasing behaviour: area- and individual-level characteristics. Public Health Nutri 2003;6:181-9. http://dx.doi.org/10.1079/PHN2002415.
- Vasilaki EI, Hosier SG, Cox WM. The efficacy of motivational interviewing as a brief intervention for excessive drinking: a meta-analytic review. Alcohol Alcohol 2006;41:328-35. http://dx.doi.org/10.1093/alcalc/agl016.
- Abdul-Quader AS, Heckathorn DD, Sabin K, Saidel T. Implementation and analysis of respondent driven sampling: lessons learned from the field. J Urban Health 2006;83:i1-5. http://dx.doi.org/10.1007/s11524-006-9108-8.
- Heckathorn DD. Respondent-driven sampling: a new approach to the study of hidden populations. Social Problems 1997;44:174-99. http://dx.doi.org/10.2307/3096941.
- Johnston LG, Malekinejad M, Kendall C, Iuppa IM, Rutherford GW. Implementation challenges to using respondent-driven sampling methodology for HIV biological and behavioral surveillance: field experiences in international settings. AIDS Behav 2008;12:S131-41. http://dx.doi.org/10.1007/s10461-008-9413-1.
- Craig P, Dieppe P, Macintyre S, Mitchie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: new guidance. London: Medical Research Council; 2008.
- Pope C, Mays N. Reaching the parts other methods cannot reach: an introduction to qualitative methods in health and health services research. BMJ 1995;311:42-5. http://dx.doi.org/10.1136/bmj.311.6996.42.
- Murphy E, Dingwall R, Greatbatch D, Parker S, Watson P. Qualitative research methods in health technology assesment: a review of the literature. Health Technol Assess 1998;2.
- Mays N, Pope C. Qualitative research: rigour and qualitative research. BMJ 1995;311:109-12. http://dx.doi.org/10.1136/bmj.311.6997.109.
- Edwards P, Cooper R, Roberts I, Frost C. Meta-analysis of randomised trials of monetary incentives and response to mailed questionnaires. J Epidemiol Community Health 2005;59:987-99. http://dx.doi.org/10.1136/jech.2005.034397.
- Smith W, Chey T, Jalaludin B, Salkeld G, Capon T. Increasing response rates in telephone surveys: a randomized trial. J Public Health Med 1995;17:33-8.
- Scottish indices of deprivation. Oxford: University of Oxford; 2003.
- Barbour R, Kitzinger J. Developing focus group research. London: Sage; 1998.
- Ritchie J, Spencer L, Bryman A, Burgess RG. Analyzing qualitative data. New York, NY: Routledge; 1994.
- Stead M, Gordon R, Angus K, McDermott L. A systematic review of social marketing effectiveness. Health Education 2007;107:126-91. http://dx.doi.org/10.1108/09654280710731548.
- Gordon R, McDermott L, Stead M, Angus K. The effectiveness of social marketing interventions for health improvement: what’s the evidence?. Public Health 2006;120:1133-9. http://dx.doi.org/10.1016/j.puhe.2006.10.008.
- Engineer R, Phillips A, Thompson J, Nicholls J. Home Office Research Study 262. Drunk and disorderly: a qualitative study of binge drinking among 18- to 24-year-olds. London: Home Office Research, Development and Statistics Directorate; 2003.
- Larimer ME, Cronce JM. Identification, prevention, and treatment revisited: individual-focused college drinking. Addict Behav 2007;32:2439-68. http://dx.doi.org/10.1016/j.addbeh.2007.05.006.
- Cooper ML, Russell M, Skinner JB, Windle M. Development and validation of a three-dimensional measure of drinking motives. Psychol Assess 1992;4:123-32. http://dx.doi.org/10.1037/1040-3590.4.2.123.
- Smith E. Social psychology. New York, NY: Psychology Press; 2007.
- Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Processes 1991;50:179-221. http://dx.doi.org/10.1016/0749-5978(91)90020-T.
- Ali MM, Dwyer DS. Social network effects in alcohol consumption among adolescents. Addictive Behaviors 2011;35:337-42. http://dx.doi.org/10.1016/j.addbeh.2009.12.002.
- Oei TP, Morawska A. A cognitive model of binge drinking: the influence of alcohol expectancies and drinking refusal self-efficacy. Addict Behav 2004;29:159-79. http://dx.doi.org/10.1016/S0306-4603(03)00076-5.
- Burke BL, Arkowitz H, Menchola M. The efficacy of motivational interviewing: a meta-analysis of controlled clinical trials. J Consult Clin Psychol 2003;71:843-61. http://dx.doi.org/10.1037/0022-006X.71.5.843.
- Dunn C, Deroo L, Rivara FP. The use of brief interventions adapted from motivational interviewing across behavioral domains: a systematic review. Addiction 2001;96:1725-42. http://dx.doi.org/10.1046/j.1360-0443.2001.961217253.x.
- Dijkstra A, Sweeney L, Gebhardt W. Social cognitive determinants of drinking in young adults: beyond the alcohol expectancies paradigm. Addict Behav 2001;26:621-773. http://dx.doi.org/10.1016/S0306-4603(00)00153-2.
- Leventhal H, Diefenbach M, Leventhal E. Illness cognition: using common sense to understand treatment adherence and affect cognition interactions. Cognit Ther Res 1992;16:143-63. http://dx.doi.org/10.1007/BF01173486.
- Langer M, Ringler M, Reinold E. Psychological effects of ultrasound examinations: changes of body perception and child image in pregnancy. Psychosom Obstet Gynecol 1988;8:199-208. http://dx.doi.org/10.3109/01674828809016788.
- Avgerinou M, Ericson J. A review of the concept of visual literacy. Br J Educ Tech 1997;28:280-91. http://dx.doi.org/10.1111/1467-8535.00035.
- Hoddinott P, Kroll T, Raja A, Lee AJ. Seeing other women breastfeed: how vicarious experience relates to breastfeeding intention and behaviour. Matern Child Nutr 2010;6:134-46.
- Harrison JA, Mullen PD, Green LW. A meta-analysis of studies of the Health Belief Model with adults. Health Educ Res 1992;7:107-16. http://dx.doi.org/10.1093/her/7.1.107.
- McBride CM, Puleo E, Pollak KI, Clipp EC, Woolford S, Emmons KM. Understanding the role of cancer worry in creating a ‘teachable moment’ for multiple risk factor reduction. Soc Sci Med 2008;66:790-80. http://dx.doi.org/10.1016/j.socscimed.2007.10.014.
- McBride CM, Emmons KM, Lipkus IM. Understanding the potential of teachable moments: the case of smoking cessation. Health Educ Res 2003;18:156-70. http://dx.doi.org/10.1093/her/18.2.156.
- Bien TH, Miller WR, Tonigan JS. Brief interventions for alcohol problems: a review. Addiction 1993;88:315-36. http://dx.doi.org/10.1111/j.1360-0443.1993.tb00820.x.
- Whittaker R, Borland R, Bullen C, Lin RB, McRobbie H, Rodgers A. Mobile phone-based interventions for smoking cessation. Cochrane Database Syst Rev 2009;4.
- Varnhagen CK, McFall GP, Pugh N, Routledge L, Sumida-MacDonald H, Kwong TE. lol: new language and spelling in instant messaging. Read Writ 2010;23:719-33. http://dx.doi.org/10.1007/s11145-009-9181-y.
- Darker CD, French DP, Eves FF, Sniehotta FF. An intervention to promote walking amongst the general population based on an ‘extended’ theory of planned behaviour: a waiting list randomised controlled trial. Psychol Health 2010;25:71-88. http://dx.doi.org/10.1080/08870440902893716.
- Murgraff V, McDermott MR, Walsh J. Exploring attitude and belief correlates of adhering to the new guidelines for low-risk single-occasion drinking: an application of the theory of planned behaviour. Alcohol Alcohol 2001;36:135-40. http://dx.doi.org/10.1093/alcalc/36.2.135.
- Norman P, Armitage CJ, Quigley C. The theory of planned behavior and binge drinking: assessing the impact of binge drinker prototypes. Addict Behav 2007;32:1753-68. http://dx.doi.org/10.1016/j.addbeh.2006.12.009.
- Tavousi M, Hidarnia AR, Montazeri A, Hajizadeh E, Taremain F, Ghofranipour F. Are perceived behavioral control and self-efficacy distinct constructs?. Eur J Sci Res 2009;30:146-52.
- Norman P, Conner M. The theory of planned behaviour and binge drinking: assessing the moderating role of past behaviour within the theory of planned behaviour. Br J Health Psychol 2006;11:55-70. http://dx.doi.org/10.1348/135910705X43741.
- Leigh BC, Stacy AW. Alcohol outcome expectancies: scale construction and predictive utility in higher order confirmatory models. Psychol Assess 1993;5:216-29. http://dx.doi.org/10.1037/1040-3590.5.2.216.
- Young RM, Connor JP, Ricciardelli LA, Saunders JB. The role of alcohol expectancy and drinking refusal self-efficacy beliefs in university student drinking. Alcohol Alcohol 2006;41:70-5. http://dx.doi.org/10.1093/alcalc/agh237.
- Bundy C. Changing behaviour: using motivational interviewing techniques. J Roy Soc Med 2004;97:43-7.
- Emmen MJ, Schippers GM, Bleijenberg G, Wollersheim H. Effectiveness of opportunistic brief interventions for problem drinking in a general hospital setting: systematic review. BMJ 2004;328:318-20B. http://dx.doi.org/10.1136/bmj.37956.562130.EE.
- Prochaska JO, DiClemente CC. Trans-theoretical therapy – toward a more integrative model of change. Psychother Theor Res Pract 1982;19:276-88. http://dx.doi.org/10.1037/h0088437.
- Heather N, Hoenekopp J, Smailes D, Team UR. Progressive stage transition does mean getting better: a further test of the transtheoretical model in recovery from alcohol problems. Addiction 2009;104:949-58. http://dx.doi.org/10.1111/j.1360-0443.2009.02578.x.
- Bertholet N, Horton NJ, Saitz R. Improvements in readiness to change and drinking in primary care patients with unhealthy alcohol use: a prospective study. BMC Public Health 2009;9. http://dx.doi.org/10.1186/1471-2458-9-101.
- Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking – toward an integrative model of change. J Consult Clin Psychol 1983;51:390-5. http://dx.doi.org/10.1037/0022-006X.51.3.390.
- DiClemente CC, Schlundt D, Gemmell L. Readiness and stages of change in addiction treatment. Am J Addict 2004;13:103-19. http://dx.doi.org/10.1080/10550490490435777.
- Prochaska JO, DiClemente CC, Norcross JC. In search of how people change. Applications to addictive behaviors. Am Psychol 1992;47:1102-14. http://dx.doi.org/10.1037/0003-066X.47.9.1102.
- Michie S, Johnston M, Abraham C, Lawton R, Parker D, Walker A, et al. Making psychological theory useful for implementing evidence based practice: a consensus approach. Qual Saf Health Care 2005;14:26-33. http://dx.doi.org/10.1136/qshc.2004.011155.
- Abraham C, Southby L, Quandte S, Krahe B, van der Sluijs W. What’s in a leaflet? Identifying research-based persuasive messages in European alcohol-education leaflets. Psychol Health 2007;22:31-60. http://dx.doi.org/10.1080/14768320600774405.
- Fishbein M, Cappella JN. The role of theory in developing effective health communications. J Commun 2006;56:S1-17. http://dx.doi.org/10.1111/j.1460-2466.2006.00280.x.
- Briñol P, Petty RE. Fundamental processes leading to attitude change: implications for cancer prevention communications. J Commun 2006;56:S81-104. http://dx.doi.org/10.1111/j.1460-2466.2006.00284.x.
- Whittaker R, Maddison R, McRobbie H, Bullen C, Denny S, Dorey E, et al. A multimedia mobile phone-based youth smoking cessation intervention: findings from content development and piloting studies. J Med Internet Res 2008;10. http://dx.doi.org/10.2196/jmir.1007.
- Rothman AJ, Bartels RD, Wlaschin J, Salovey P. The strategic use of gain- and loss-framed messages to promote healthy behavior: how theory can inform practice. J Commun 2006;56:S202-20. http://dx.doi.org/10.1111/j.1460-2466.2006.00290.x.
- Viswanath K, Emmons KM. Message effects and social determinants of health: its application to cancer disparities. J Commun 2006;56:238-64. http://dx.doi.org/10.1111/j.1460-2466.2006.00292.x.
- Conner M, Norman P. Predicting health behaviour. Buckingham: Open University Press; 2005.
- Burnkrant RE, Unnava HR. Self-referencing – a strategy for increasing processing of message content. Pers Soc Psychol Bull 1989;15:628-38. http://dx.doi.org/10.1177/0146167289154015.
- Galloway G. Humor and ad liking: evidence that sensation seeking moderates the effects of incongruity-resolution humor. Psychol Market 2009;26:779-92. http://dx.doi.org/10.1002/mar.20299.
- Gold J, Lim MSC, Hellard ME, Hocking JS, Keogh L. What’s in a message? Delivering sexual health promotion to young people in Australia via text messaging. BMC Public Health 2010;10. http://dx.doi.org/10.1186/1471-2458-10-792.
- Latimer AE, Brawley LR, Bassett RL. A systematic review of three approaches for constructing physical activity messages: What messages work and what improvements are needed?. Int J Behav Nutr Phys Activ 2010;7. http://dx.doi.org/10.1186/1479-5868-7-36.
- Paivio A, Walsh M, Bons T. Concreteness effects on memory: when and why?. J Exp Psychol Learn Mem Cognit 1994;20:1196-204. http://dx.doi.org/10.1037/0278-7393.20.5.1196.
- Gardner MP, Houston MJ. The effects of verbal and visual components of retail communications. J Retailing 1986;62:64-78.
- Babin LA, Burns AC. Effects of print ad pictures and copy containing instructions to imagine on mental imagery that mediates attitudes. J Advert 1997;26:33-44.
- Burns AC, Biswas A, Babin LA. The operation of visual imagery as a mediator of advertising effects. J Advert 1993;22:71-85.
- Howard DJ. Rhetorical question effects on message processing and persuasion – the role of information-availability and the elicitation of judgment. J Exp Soc Psychol 1990;26:217-39. http://dx.doi.org/10.1016/0022-1031(90)90036-L.
- Petty RE, Cacioppo JT, Heesacker M. Effects of rhetorical questions on persuasion – a cognitive response analysis. J Pers Soc Psychol 1981;40:432-40. http://dx.doi.org/10.1037/0022-3514.40.3.432.
- Swasy JL, Munch JM. Examining the target of receiver elaborations – rhetorical question effects on source processing and persuasion. J Consum Res 1985;11:877-86. http://dx.doi.org/10.1086/209023.
- Parry O, Bancroft A, Gnich W, Amos A. Nobody home? Issues of respondent recruitment in areas of deprivation. Crit Publ Health 2001;11:305-17. http://dx.doi.org/10.1080/09581590110094585.
- Lynn P, Clarke P. Separating refusal bias and non-contact bias: evidence from UK national surveys. The Statistician 2002;51:319-33. http://dx.doi.org/10.1111/1467-9884.00321.
- Edwards PJ, Roberts I, Clarke MJ, DiGuiseppi C, Wentz R, Kwan I, et al. Methods to increase response to postal and electronic questionnaires. Cochrane Database Syst Rev 2009;3.
- Nakash RA, Hutton JL, Jørstad-Stein EC, Gates S, Lamb SE. Maximising response to postal questionnaires – a systematic review of randomised trials in health research. BMC Med Res Methodol 2006;6. http://dx.doi.org/10.1186/1471-2288-6-5.
- McDonald PW. Population-based recruitment for quit-smoking programs: an analytic review of communication variables. Prev Med 1999;28:545-57. http://dx.doi.org/10.1006/pmed.1998.0479.
- Harrison RA, Cock D. Increasing response to a postal survey of sedentary patients – a randomised controlled trial. BMC Health Serv Res 2004;4. http://dx.doi.org/10.1186/1472-6963-4-31.
- Gilliss CL, Lee KA, Gutierrez Y, Taylor D, Beyene Y, Neuhaus J, et al. Recruitment and retention of healthy minority women into community-based longitudinal research. J Wom Health Gend Base Med 2001;10:77-85. http://dx.doi.org/10.1089/152460901750067142.
- Yancey AK, Ortega AN, Kumanyika SK. Effective recruitment and retention of minority research participants. Annu Rev Publ Health 2006;27:1-28. http://dx.doi.org/10.1146/annurev.publhealth.27.021405.102113.
- Southern DA, Lewis S, Maxwell CJ, Dunn JR, Noseworthy TW, Corbett G, et al. Sampling ‘hard-to-reach’ populations in health research: yield from a study targeting Americans living in Canada. BMC Med Res Methodol 2008;8. http://dx.doi.org/10.1186/1471-2288-8-57.
- Schoenfeld ER, Greene JM, Wu SY, O’Leary E, Forte F, Leske MC. Recruiting participants for community-based research: the Diabetic Retinopathy Awareness Program. Ann Epidemiol 2000;10:432-40. http://dx.doi.org/10.1016/S1047-2797(00)00067-3.
- Harkins C, Shaw R, Gillies M, Sloan H, MacIntyre K, Scoular A, et al. Overcoming barriers to engaging socio-economically disadvantaged populations in CHD primary prevention: a qualitative study. BMC Public Health 2010;10. http://dx.doi.org/10.1186/1471-2458-10-391.
- The English indices of deprivation 2010. London: Neighbourhoods Statistical Release; 2011.
- Scottish Index of Multiple Deprivation 2004. Edinburgh: Technical Report Scottish Executive; 2004.
- Reisner SL, Mimiaga MJ, Johnson CV, Bland S, Case P, Safren SA, et al. What makes a respondent-driven sampling ‘seed’ productive? Example of finding at-risk Massachusetts men who have sex with men. J Urban Health 2010;87:467-79. http://dx.doi.org/10.1007/s11524-010-9439-3.
- Malekinejad M, Johnston LG, Kendall C, Kerr LRFS, Rifkin MR, Rutherford GW. Using respondent-driven sampling methodology for HIV biological and behavioral surveillance in international settings: a systematic review. Aids Behav 2008;12:S105-30. http://dx.doi.org/10.1007/s10461-008-9421-1.
- Stahre M, Naimi T, Brewer R, Holt J. Measuring average alcohol consumption: the impact of including binge drinks in quantity-frequency calculations. Addiction 2006;101:1711-18. http://dx.doi.org/10.1111/j.1360-0443.2006.01615.x.
- Manual for the Fast Alcohol Screening Test (FAST). London: Health Development Agency; 2002.
- Oei TP, Young RS, Allen JP, Wilson VB. Assessing alcohol problems. A guide for clinicians and researchers. Bethesda, MD: National Institute on Alcohol Abuse and Alcoholism; 2003.
- Heather N, Hoenekopp J. A revised edition of the Readiness to Change Questionnaire Treatment Version. Addict Res Theory 2008;16:421-33.
- Rollnick S, Miller WR, Butler CC. Motivational interviewing in health care. Helping patients change behavior. New York, NY: The Guilford Press; 2008.
- Albaum G. The Likert scale revisited: an alternate version. J Market Res Soc 1997;39:331-48.
- Murgraff V, Parrott A, Bennett P. Risky single-occasion drinking amongst young people – definition, correlates, policy, and intervention: a broad overview of research findings. Alcohol Alcohol 1999;34:3-14. http://dx.doi.org/10.1093/alcalc/34.1.3.
- Gmel G, Gaume J, Faouzi M, Kulling J-P, Daeppen J-B. Who drinks most of the total alcohol in young men – risky single occasion drinking as normative behaviour. Alcohol Alcohol 2008;43:692-7. http://dx.doi.org/10.1093/alcalc/agn070.
- Gmel G, Kuntsche E, Rehm J. Risky single-occasion drinking: bingeing is not bingeing. Addiction 2010;106:1037-45. http://dx.doi.org/10.1111/j.1360-0443.2010.03167.x.
- Roerecke M, Greenfield TK, Kerr WC, Bondy S, Cohen J, Rehm J. Heavy drinking occasions in relation to ischaemic heart disease mortality – an 11–22 year follow-up of the 1984 and 1995 US National Alcohol Surveys. Int J Epidemiol 2011;40:1401-10. http://dx.doi.org/10.1093/ije/dyr129.
- Erskine S, Maheswaran R, Pearson T, Gleeson D. Socioeconomic deprivation, urban–rural location and alcohol-related mortality in England and Wales. BMC Public Health 2010;10. http://dx.doi.org/10.1186/1471-2458-10-99.
- Romeri E, Baker A, Griffiths C. Alcohol-related deaths by occupation, England and Wales, 2001–05. Health Stat Q 2007;35:6-12.
- Muhib FB, Lin LS, Stueve A, Miller RL, Ford WL, Johnson WD, et al. A venue-based method for sampling hard-to-reach populations. Publ Health Rep 2001;116:216-22. http://dx.doi.org/10.1093/phr/116.S1.216.
- Heckathorn DD, Semaan S, Broadhead R, Hughes J. Extensions of respondent-driven sampling: a new approach to the study of injection drug users aged 18–25. AIDS Behav 2002;6:55-67. http://dx.doi.org/10.1023/A:1014528612685.
- Davis LL, Broome ME, Cox RP. Maximizing retention in community-based clinical trials. J Nurs Scholarsh 2002;34:47-53. http://dx.doi.org/10.1111/j.1547-5069.2002.00047.x.
- Robinson KA, Dennison CR, Wayman DM, Pronovost PJ, Needham DM. Systematic review identifies number of strategies important for retaining study participants. J Clin Epidemiol 2007;60:757-65. http://dx.doi.org/10.1016/j.jclinepi.2006.11.023.
- Schulz KF, Grimes DA. Sample size slippages in randomised trials: exclusions and the lost and wayward. Lancet 2002;359:781-5. http://dx.doi.org/10.1016/S0140-6736(02)07882-0.
- Goldberg JH, Kiernan M. Innovative techniques to address retention in a behavioral weight-loss trial. Health Educ Res 2005;20:439-47. http://dx.doi.org/10.1093/her/cyg139.
- Fewtrell MS, Kennedy K, Singhal A, Martin RM, Ness A, Hadders-Algra M, et al. How much loss to follow-up is acceptable in long-term randomised trials and prospective studies?. Arch Dis Child 2008;93:458-61. http://dx.doi.org/10.1136/adc.2007.127316.
- Edwards AGK, Rollnick S. Outcome studies of brief alcohol intervention in general practice: the problem of lost subjects. Addiction 1997;92:1699-704. http://dx.doi.org/10.1111/j.1360-0443.1997.tb02890.x.
- McKenzie M, Tulsky JP, Long HL, Chesney M, Moss A. Tracking and follow-up of marginalized populations: A review. J Health Care Poor Underserved 1999;10:409-29. http://dx.doi.org/10.1353/hpu.2010.0697.
- Fowler HS, Aubry T. Conducting evaluation research with hard-to-follow populations: adopting a participant-centred approach to maximize participant retention. Can J Program Eval 2004;19:89-108.
- Chang M-W, Brown R, Nitzke S. Participant recruitment and retention in a pilot program to prevent weight gain in low-income overweight and obese mothers. BMC Public Health 2009;9. http://dx.doi.org/10.1186/1471-2458-9-424.
- El-Khorazaty MN, Johnson AA, Kiely M, El-Mohandes AA, Subramanian S, Laryea HA, et al. Recruitment and retention of low-income minority women in a behavioral intervention to reduce smoking, depression, and intimate partner violence during pregnancy. BMC Public Health 2007;7. http://dx.doi.org/10.1186/1471-2458-7-233.
- Health survey for England. London: The NHS Centre for Health and Social Care; 2008.
- Sniehotta FF. Towards a theory of intentional behaviour change: plans, planning, and self-regulation. Br J Health Psychol 2009;14:261-73. http://dx.doi.org/10.1348/135910708X389042.
- Schwarzer R. Modeling health behaviour change: How to predict and modify the adoption and maintenance of health behaviours. Appl Psychol 2008;57:1-29. http://dx.doi.org/10.1111/j.1464-0597.2007.00325.x.
- Keogh-Brown MR, Bachmann MO, Shepstone L, Hewitt C, Howe A, Ramsay CR, et al. Contamination in trials of educational interventions. Health Technol Assess 2007;11.
- Howe A, Keogh-Brown M, Miles S, Bachmann M. Expert consensus on contamination in educational trials elicited by a Delphi exercise. Medical Education 2007;41:196-204. http://dx.doi.org/10.1111/j.1365-2929.2006.02674.x.
- Torgerson DJ. Contamination in trials: is cluster randomisation the answer?. BMJ 2001;322:355-7. http://dx.doi.org/10.1136/bmj.322.7282.355.
- Lang DL, DiClemente RJ, Hardin JW, Crosby RA, Salazar LF, Hertzberg VS. Threats of cross-contamination on effects of a sexual risk reduction intervention: fact or fiction. Prev Sci 2009;10:270-5. http://dx.doi.org/10.1007/s11121-009-0127-z.
- Semaan S. Time-space sampling and respondent-driven sampling with hard-to-reach populations. Methodol Innov Online 2010;5:60-75.
- Agadjanian V, Zotova N. Sampling and surveying hard-to-reach populations for demographic research: A study of female labor migrants in Moscow, Russia. Demogr Res 2012;26:131-50. http://dx.doi.org/10.4054/DemRes.2012.26.5.
- De Bruyn A, Lilien GL. A multi-stage model of word-of-mouth influence through viral marketing. Int J Res Market 2008;25:151-63. http://dx.doi.org/10.1016/j.ijresmar.2008.03.004.
- Welker CB. The paradigm of viral communication. Inform Serv Use 2002;2:3-8.
- Steckler A, Linnan L. Process evaluation for public health interventions and research. San Francisco, CA: Jossey Bass; 2002.
- Toroyan T, Oakley A, Laing G, Roberts I, Mugford M, Turner J. The impact of day care on socially disadvantaged families: an example of the use of process evaluation within a randomized controlled trial. Child Care Health Dev 2004;30:691-8. http://dx.doi.org/10.1111/j.1365-2214.2004.00481.x.
- Schneider M, Hall WJ, Hernandez AE, Hindes K, Montez G, Pham T, et al. Rationale, design and methods for process evaluation in the HEALTHY study. Int J Obes 2009;33:S60-7. http://dx.doi.org/10.1038/ijo.2009.118.
- Oakley A, Strange V, Bonell C, Allen E, Stephenson J, Team RS. Health services research – process evaluation in randomised controlled trials of complex interventions. BMJ 2006;332:413-16. http://dx.doi.org/10.1136/bmj.332.7538.413.
- Graff FS, Morgan TJ, Epstein EE, McCrady BS, Cook SM, Jensen NK, et al. Engagement and retention in outpatient alcoholism treatment for women. Am J Addict 2009;18:277-88. http://dx.doi.org/10.1080/10550490902925540.
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ 2008;337.
- Linnan L, Steckler A, Steckler A, Linnan L. Process evaluation for public health interventions and research. San Francisco, CA: Jossey Bass; 2002.
- Glasgow R, Vogt T, Boles S. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Publ Health 1999;89:1322-7. http://dx.doi.org/10.2105/AJPH.89.9.1322.
- Saunders RP, Evans MH, Joshi P. Developing a process-evaluation plan for assessing health promotion program implementation: a how-to guide. Health Promot Pract 2005;6:134-47. http://dx.doi.org/10.1177/1524839904273387.
- Baranowski T, Stables G. Process evaluations of the 5-a-Day projects. Health Educ Behav 2000;27:157-66. http://dx.doi.org/10.1177/109019810002700202.
- Prochaska JO, Redding CA, Evers K, Glanz K, Rimer BK, Viswanath K. Health behavior and health education: theory, research, and practice. San Francisco, CA: John Wiley & Sons; 2008.
- Bellg AJ, Borrelli B, Resnick B, Hecht J, Minicucci DS, Ory M, et al. Enhancing treatment fidelity in health behavior change studies: Best practices and recommendations from the NIH behavior change consortium. Health Psychol 2004;23:443-51. http://dx.doi.org/10.1037/0278-6133.23.5.443.
- Spagnolli A, Gamberini L. Interacting via SMS: practices of social closeness and reciprocation. Br J Soc Psychol 2007;46:343-64. http://dx.doi.org/10.1348/014466606X120482.
- Tsang MM, Ho SC, Liang TP. Consumer attitudes toward mobile advertising: an empirical study. Int J Electron Commerce 2004;8:65-78.
- Safer DL, Hugo EM. Designing a control for a behavioral group therapy. Behav Ther 2006;37:120-30. http://dx.doi.org/10.1016/j.beth.2005.06.001.
- Lohr JM, DeMaio C, McGlynn FD. Specific and nonspecific treatment factors in the experimental analysis of behavioral treatment efficacy. Behav Modif 2003;27:322-68. http://dx.doi.org/10.1177/0145445503027003005.
Appendix 1 Study protocol
1. Project title
Reducing alcohol-related harm in disadvantaged men: development and feasibility assessment of a brief intervention delivered by mobile telephone.
2. Background
2.1 Existing research
Alcohol-related morbidity and mortality represent a major public health challenge. The cost of alcohol to society has been estimated at more than £55 billion per year in England1 and more than £2 billion per year in Scotland. 2 These costs occur through lost productivity, increased health-care and other public sector costs and through social disruption. Alcohol-related harms are not evenly distributed in the population. People who are socially disadvantaged are at a substantially higher risk of developing alcohol-related diseases. 3,4 Levels of binge drinking are highest among young and disadvantaged men. 5 There is a pressing need to change the culture of drinking among this group in order to prevent alcohol-related problems in later life.
2.2 Risks and benefits
The proposed intervention involves a novel method of delivery of a brief intervention to reduce hazardous drinking. Brief interventions to reduce harmful drinking have been widely used in health-care settings and no reports of risk have been made. 6 The potential benefits to the participants are the health and social benefits which accrue from adopting more moderate drinking habits. Society will benefit from reduced social disruption resulting from drunkenness, reduced healthcare costs and from reduced sickness absence from the health effects of excess consumption.
2.3 Rationale
The group who drink most alcohol and binge drink most frequently are young to middle-aged disadvantaged men. 5 Men aged 25–44 years are seldom in contact with health services and few are in full-time education. They will therefore not be reached by current initiatives to tackle excessive drinking. Targeting this group would lead to reductions in heavy drinking before chronic health harms develop. This group may be receptive to brief interventions: 27% of young men reported feeling the need to cut down on their drinking. 5
Brief interventions based on psychological theories have been developed to tackle alcohol-related problems. There is extensive evidence that brief interventions are effective. 6–9 Thus there is a need to develop alternative methods of delivering brief interventions to disadvantaged men aged 25–44 years. Given the extent of the current problem, the delivery methods need to be able to contact large numbers of individuals at low cost.
Text messaging has been used to modify adverse health behaviours10,11 and to increase healthcare uptake. 12,13 This approach is well suited to young to middle-aged men because their ownership of mobile telephones is high. This method has been successfully used as a smoking cessation tool in New Zealand11 and the intervention is being implemented nationally in a government funded programme. 14 Text messaging is also one component of the NHS stop smoking programme in England. 15
The text messages can be supported and reinforced by visual images. There is evidence that psychological theory can be embedded in visual media (e.g. posters, pictures in leaflets, films or animations) and alongside verbal and/or textual explanation, can improve patient understanding and self-care behaviours. 16 The use of images can enhance the coherence of the message (i.e. more clearly demonstrate how cause and effect are linked) by making the symptoms and their consequences appear less abstract and more concrete. Increasing coherence17 and concreteness18 in relation to illness and risk perceptions have been shown to influence attitudes19,20 and intentions and increase the likelihood of behaviour change. Visual media is acceptable to patients and, due to its less abstract and more concrete nature, may be more memorable than verbal or text based messages. 21,22 Images may therefore be an effective and acceptable adjunct to text messaging to increasing coherence and concreteness about alcohol-related harm and the benefits of moderate drinking.
The important question is whether text messaging could be helpful in tackling harmful drinking. Alcohol presents different challenges to the stop smoking campaign. Alcohol consumption is widely viewed as acceptable and in moderate amounts may be good for health. Further changing adverse health behaviours among disadvantaged groups is challenging because the uptake of health promotion interventions is much lower than in more advantaged groups. 23 Thus we need to determine whether a brief intervention delivered by mobile telephone will help moderate heavy drinking among young to middle-aged disadvantaged men.
3. Research objectives
The objective of the planned research is to develop and test the feasibility of a novel intervention to reduce the frequency of heavy drinking among young to middle-aged disadvantaged men. The intervention has been developed from brief interventions which have been successful when delivered by face-to-face interviews, but will use mobile telephone technology to deliver a series of text and images. If the development and pilot evaluation are successful, the intervention will be tested in a full-scale randomised controlled trial in a further study for which new funding will be sought.
Research questions of the full-scale trial of the novel intervention
Can a brief intervention delivered by mobile telephone:
-
Reduce the frequency of heavy drinking by disadvantaged men
-
Increase awareness of the harms of excessive drinking
-
Increase intentions to avoid becoming drunk
-
Increase self-efficacy for refusing drinks
The need for the feasibility study
The intervention to be used in the proposed trial has several components and thus is a complex intervention. The MRC framework for complex interventions recommends that the feasibility of all aspects of the trial be piloted and that the causal mechanism by which the intervention will work should be tested in advance of a formal trial. 24 The methods of recruitment to the trial and the retention of participants within it need to be piloted. The disadvantaged are recognised to be a difficult group to recruit so the proposed recruitment strategy needs to be tested. The potential for the intervention to influence beliefs and attitudes also needs to be assessed. Previous research has evaluated interventions delivered by face-to-face interview, often conducted by a health professional within a health-care setting. The acceptability of the use of mobile telephones to deliver the intervention and the potential of the intervention to influence drinking behaviour need to be assessed. We therefore propose to conduct a preliminary study to develop the recruitment strategies, to finalise the design of the intervention, to assess retention in the study and to investigate the likelihood of the intervention being effective.
Aims of the feasibility study
To investigate the feasibility and likelihood of success of a complex intervention to reduce the frequency of heavy drinking among young to middle-aged disadvantaged men.
Research questions of the feasibility study
-
What are the best ways to recruit and retain disadvantaged men in a study aimed at reducing the frequency of heavy drinking?
-
What is the type of content and timing of the delivery of a series of text messages and images that is most likely to engage young to middle-aged men?
-
Is the intervention likely to be an acceptable way to influence the frequency of heavy drinking?
4. Research design
Overview
The study will be conducted in three phases. Phase 1 will comprise six focus groups to develop the recruitment strategy, to optimise the design of the text messages and images and to determine the most acceptable sequence for their delivery. Phase 2 will involve the recruitment of 60 participants who will be randomised to receive either the alcohol intervention or a general health promotion intervention. The interventions will be delivered to mobile telephones using a programmed computer system. Participants will be followed-up for 3 months to assess recruitment and retention, willingness to respond to text messages and to complete the final assessment of drinking behaviour. Phase 3 will involve in-depth interviews with 20 participants to assess the acceptability of the intervention, the impact it had on their willingness to moderate their drinking and factors which might limit their ability to drink less.
For clarity of presentation Phase 1 will be described here because it is short and does not fit readily with the types of information elicited in Sections 5–10.
Phase 1 Focus groups
Focus group participants will be purposively recruited from several venues in areas of high deprivation: Sunday amateur football clubs, public houses and betting shops. Five of the six focus groups will be held with men aged 25–44 years. Potential participants will be men who have consumed eight or more units of alcohol during a single session on at least two occasions during the previous four weeks. The sixth focus group will be with women. A women only focus group is included because this will give a different perspective on men's reasons for drinking, refusal skills, awareness of harms and likelihood of responding to the intervention. Women who participate will be partners of men who meet the entry criteria.
The Focus groups will review the methods to be employed in Phase 2. Specifically it will investigate:
-
strategies to recruit and retain disadvantaged men in a study on drinking
-
the appropriateness of the theoretical approach underpinning the intervention
-
the acceptability of the components of the intervention
-
the acceptability of the recruitment process (credibility of source, invitation letter, initial screening telephone call).
The discussion on the design of text messages will explore:
-
the types of questions that are acceptable; the language used to describe drinking and its consequences; beliefs and attitudes about the benefits and potential harms of alcohol; and attitudes to receiving messages on drinking (credibility, perceived relevance, likelihood of influencing drinking behaviour)
-
the design of the images that will induce interest and stimulate a review of drinking habits
-
total number of texts to be sent, frequency of sending texts, maximum length of texts
All interviews and focus group discussions will be digitally recorded and fully transcribed. Transcripts will be analysed using framework analysis. 25 Analysis will be facilitated by the use of text management software (NVivo) and carried out by a research fellow with formal training in qualitative research and practical experience of analysis. Two researchers will be involved in the analysis to ensure reliability of interpretation and coding.
4. Research design continued – Phases 2 and 3
The trial of feasibility and likely impact of the intervention will be assessed by carrying out all of the stages of a pragmatic randomised controlled trial.
Randomisation
The randomisation will be carried out by the Glasgow Clinical Trials Unit under the leadership of Professor J Norrie. After identifying and obtaining consent from an eligible participant the Research Assistant will contact the randomisation system at the Robertson Centre for Biostatistics, Glasgow Clinical Trials Unit. This randomisation system will be an Interactive Voice Response telephone system or accessed over the web. The randomisation system will then, after successfully randomising the participant, remotely contact the Dundee SMS text messaging server and the sequence of calls appropriate for that participant's randomised allocation will be set up.
Intervention delivery
The interventions will be delivered by an automated computer system, which will be programmed to send out text messages and images to mobile telephones in a predetermined sequence. The computer system will be devised and operated by the staff at the School of Computing at Dundee University under the direction of Professor I Ricketts.
The exchange of text messages with the clients will be via a secure server based within the School of Computing at the University of Dundee. Messages delivered to the client will appear to originate from the project's mobile telephone but the message content and client address will be assembled on the secure server and routed via the JISC funded JANET network to a UK based Mobile Network Service Provider and thereby to the clients. All replies from the clients will follow the reverse path. The Mobile Service Provider offers support for a variety of connections including email, web browser and individually tailored www solutions. In this feasibility study the team will provide the simplest solution compatible with providing an effective communication between the client and the project team. The secure server and associated software tools will be provided at no cost to the project.
Blinding
The researcher who collects both baseline and outcome data will not be involved in the randomization process or the delivery of the active and control interventions. Thus the researcher will be blinded to treatment group.
Stopping rule/Discontinuation criteria
The intervention is only delivered over a three month period. Extensive previous research on brief interventions to tackle harmful drinking have found no evidence of harm. The issue of discontinuation is not applicable to this study. However we will monitor any emerging safety issues such as reported increases in drinking or depression, which might be caused by the drinkers being confronted by these health messages about alcohol.
5. Study population
Study group
Men aged 25–44 years living in areas of high deprivation will be recruited. Deprivation is measured using the Scottish Index of Multiple Deprivation,26 which is similar to the English Index of Multiple Deprivation. Men will be recruited from the 25% of electoral wards with the highest deprivation scores. Individual level socio-economic position will be measured on all men recruited to the study. It will be measured using education, nature of housing and occupation (NS-SEC) following the recommendations of Galobardes et al. 27,28
Inclusion/exclusion criteria
Men will be included in the study if they have had two or more episodes of heavy drinking (≥ 8 units in a single session) in the preceding month. Exclusion criteria are: men who are currently attending care at an Alcohol Problem Service; and men who will not be contactable by mobile telephone for any part of the intervention period.
Recruitment strategy
Two recruitment strategies will be tested.
Strategy 1: Potential participants will be identified from GP practice lists which contain data on age, gender and postcode. Postcode will be used to derive the Index of Multiple Deprivation (SIMD) score. 29 Potential participants will receive a letter from their GP inviting them to take part. The telephone numbers of those willing to take part will be obtained using the techniques employed in a previous study by this group. 30 In that study telephone numbers were obtained for 99% of disadvantaged mothers of young children. Telephone numbers were obtained from a combination of GP records, extensive web searches of publicly available databases and further contacts with GP staff. Of those contacted by telephone 77% were recruited to the study.
Systematic reviews show that repeated attempts at contact and monetary incentives increase recruitment to research studies. 31,32 Up to four attempts at contact by telephone will be made. Men who agree to take part will be offered an initial £10 gift voucher to offset any charges incurred by receiving and responding to text messages. They will also be sent a £5 gift voucher for each week of the study that they respond to text messages, and a £10 voucher for completing the outcome assessment.
Strategy 2: Respondent-driven sampling is a recently developed technique for surveying hard to reach groups, particularly those who engage in stigmatized or illegal behaviours. 33,34 It was designed to overcome the limitations of other techniques such as snowball sampling and key informant sampling. The technique assumes that the target population are distributed through a number of socially networked groups and is thus suitable for a group behaviour such as drinking. It has been extensively and successfully used with injecting drug users and groups at high risk of HIV infection. 35 The sampling strategy begins with the identification of a small number of ‘seed’ individuals obtained from different locations. In this study seeds will be recruited from several venues in areas of high deprivation: Sunday amateur football clubs, public houses and betting shops. The seed individuals identify suitable subjects from their social networks and recruit them to the study. To prevent over recruitment by individuals with large social networks each seed individual can only recruit a maximum of five individuals.
A key element of the technique is the use of incentives to each seed person for taking part in the study and for each of the individuals they recruit. Thus the seed individuals will receive a £5 gift voucher for each person they recruit. All participants recruited by this method will also receive the sequence of gift vouchers as described for Recruitment Strategy 1 (for joining and responding actively to the text messages).
Initial screening and Baseline assessment
Potential participants will be screened by a telephone call from a researcher to establish current drinking levels. Those who report binge drinking (≥ 8 units in a single session) at least twice in the previous four weeks will be recruited. They will also complete a short structured questionnaire that will include the validated CAGE questionnaire for alcohol dependence. 36
6. Planned intervention
Experimental intervention
A brief intervention to reduce harmful drinking will be delivered by text messages to a mobile telephone. A series of interactive text messages and images will be designed using messaging theory,37–39 social cognition models40 and systematic reviews of interventions to tackle alcohol problems. 6,8,9 The intervention has four components:
i Positive alcohol expectancies: the perceived benefits of heavy drinking
The literature suggests the perceived benefits of alcohol for young people are mood enhancement and enjoyment, stress relief and escapism, easier socialising and social success, and conformity with peers. 41 Many of these are not compatible with being very drunk. This presents the opportunity to explore the inconsistency between an individual's drinking habits and the intended aims of drinking. Thus text messages will discuss the mismatch between being drunk and having fun.
ii Subjective norms: misperceptions about peers' levels of alcohol consumption
Beliefs about how much peers drink have been found to be powerful predictors of drinking behaviour. 42 Many people overestimate what their peers drink and drink more in consequence. Systematic reviews have shown that personalised normative feedback is effective in reducing alcohol consumption and alcohol-related problems. 43,44 Thus text messages will state that many people overestimate what their peers drink and will reinforce this with data on current consumption by men of their age.
iii Perceptions of harms
Younger people who binge drink tend to view themselves as party drinkers or occasional drinkers and may be unaware of the long term harms of their drinking. 45 A belief that drinking will have few negative consequences is associated increased levels of consumption. 46 Young people tend to think that they will not come to harm, unless they have previously suffered harm. 41 The text messages will briefly present the true risks of alcohol.
iv Refusal self-efficacy
Low levels of drinking refusal self-efficacy have been shown to predict the acquisition and maintenance of binge drinking. 45 Thus texts will present techniques for refusing drinks and for leaving drinking situations early.
Message development
The design of the text messages will be based on current communication theory. This identifies the series of steps in the causal chain from message receipt to behaviour change. To be effective a message must be: attended to, comprehended, processed, accepted and acted on. 38 Communication theory identifies four features of a message which affect the likelihood of behaviour change: the source (i.e. credibility) of the message, its style and content, the nature of the recipient and the context (the circumstances in which the message is received). Each of these features affects the impact of the message on behaviour change. 14,47 The nature of the message comprises many facets including its length, content (number of arguments), language and style (such as use of images). Other design features are the personal relevance of the message,47 whether the arguments are gain-framed (emphasising the benefits of moderate drinking) or loss-framed37 and items included to maintain interest (such as interesting and unexpected statements). The design of the message content will be assessed by the user group (disadvantaged men aged 25–44) at the focus group stage.
Image development
The images will be developed by a collaborative team involving a sociologist, a psychologist, a computer scientist and design specialists from the Dundee 3D Visualisation Group. Team members (led by Dr Williams) have successfully created images linking obesity and risk of arteriosclerosis. The design process will embed psychological theory of behaviour change in the development of images. The images will increase participants' awareness of their susceptibility to alcohol-related harm and increase their confidence and skill in moderating alcohol consumption. The design follows a four stage sequential process in which professionals work with the user group (disadvantaged men aged 25–44) to review:
-
The theoretical basis: the creation of conceptual content
-
The structure: creating a visual narrative
-
The ‘look’: visual rendering of narrative and concepts
-
The interpretation and impact.
Delivery of the intervention
A series of 28 interactive text messages and images will be sent over a four week period. The frequency and timing of the messages will be determined following the focus group discussions. Each of the four components of the intervention will be addressed in several messages. Some of these messages will also ask a question which, when answered, will generate an appropriate automated response. A few messages of general interest, designed to promote retention in the trial, will also be sent.
Comparator intervention
The comparator group will receive the same number of text messages and images. These will cover the general health promotion messages from current government public health policy. 48 These include diet, physical activity, smoking and mental wellbeing. The text messages and images will be designed to maintain interest in study to ensure that the control group complete the outcome assessment.
7. Outcome measures
Outcomes will be measured by telephone interview at three months after the baseline assessment. The primary outcome measure will be the change in frequency of heavy drinking (consumption of ≥ 8 units in a single session). This measure of consumption has been used for many years in national surveys of alcohol consumption. 5,49 Self-reported alcohol consumption is the primary outcome measure used in almost all randomised trials testing interventions to reduce alcohol consumption. 6 Secondary outcomes will assess the extent to which the intervention has influenced perceptions of harms, benefits of moderated drinking, intentions for future drinking. The feasibility study will develop and test a short structured questionnaire which can be used in a telephone interview to measure these factors. The questionnaire will be completed at baseline and at outcome assessment to enable changes on these measures to be assessed.
Phase 3 Post trial evaluation
A more detailed assessment of the impact of the intervention will be made in a sub-sample of 20 randomly selected participants (10 intervention and 10 control). Face to face interviews will elicit their views on all aspects of Phase 2. It will explore their reasons for participating in the study and the stages of the recruitment process. It will also examine the ways that the delivery of the intervention could be improved, the aspects of the intervention that caused them to review their drinking patterns and consider moderating their drinking. It will also explore the factors which might limit their ability to drink less with the aim of identifying ways in which the intervention could be improved. The interviews will be recorded and transcribed. The transcripts will be analysed thematically to identify additional improvements that could be made to the recruitment process and the intervention.
8. Assessment and follow-up
8.1 For Phase 2 a short structured questionnaire will be administered by telephone at baseline and at three months. For Phase 3 an in-depth interview will be carried out within two weeks of completion of the Phase 2 interview.
8.2 Assessment of harms
This study involves a novel method of delivery of a widely used brief intervention to reduce harmful drinking. The method of delivery has been used for other types of health behaviour and no harms have been identified. However we will monitor any emerging safety issues such as reported increases in drinking or depression, which might be caused by the drinkers being confronted by these health messages about alcohol. In addition participants who report problems related to their drinking, either at the baseline assessment or follow-up will be advised to contact their GP.
9. Proposed sample size
The Phase 2 feasibility assessment will involve randomising 60 men to intervention or control. This will be sufficient to test the feasibility of all aspects of the study and to assess the components of the intervention package. Two recruitment strategies will be tested to obtain the 60 participants: recruitment from three multi-partner general practices; and a respondent-driven sampling. The Phase 3 post trial evaluation will involve a random sample of 20 men (10 intervention, 10 control).
10. Statistical analysis
As this is a feasibility study, formal hypothesis testing is not appropriate. Instead the analysis will assess the participants' experience of all aspects of the study. It will determine the appropriateness of the recruitment strategy and the design and delivery of the intervention. Descriptive statistics will be used to explore recruitment and retention rates. The analysis will also determine whether the outcome measures can be readily measured and whether they will enable the significance of changes in the outcome measures in the full trial to be analysed using paired t-tests, McNemar's test and the Wilcoxon test.
11. Ethical arrangements
The study will comply with the ESRC Research Ethics Framework. 50 Permission to conduct the study will be sought from the Tayside Committee on Medial Research Ethics. As this study involves a widely used brief intervention it raises few ethical issues. It is possible that the telephone interview will identify individuals with serious alcohol-related problems. These men will be asked to seek help from their own GPs. In addition, the researcher will ask permission to contact the GP about their alcohol problem, to increase the chance that they will receive the help they need.
Study participants will be informed that they can withdraw from the study at any time. If participants withdraw during the intervention period they will not receive further text messages. The study does not use any existing database.
12. Research governance
The University of Dundee will act as sponsor for the project. The governance of both the feasibility study and the subsequent full trial will be overseen by the Glasgow Clinical Trials Unit (GCTU), a fully registered NIHR CRN trials unit. As such, GCTU designs, conducts, analyses, reports and archives all its clinical studies to exacting regulatory, legal, ethical and scientific requirements, including Good Clinical Practice. As this is a study which is designed to develop and test the feasibility of a novel method of delivering a widely used brief intervention it is not necessary to have a Steering Committee and a DMEC at this stage. For the full trial which will follow this study, both a Steering Committee and a DMEC will be established.
13. Project timetable and milestones
Ethical permission will be sought and obtained before the start date of the project. Research staff will also be appointed before the study begins. The start date will be the 1st March 2010.
1st March 2010 – 11th April 2010: prepare for focus groups
-
Develop a schedule to be used for the focus groups
-
Identify and recruit organisations which have members suitable for the focus group
-
Establish acceptable recruitment procedures
-
Develop computer software to administer the sending of the text messages
12th April 2010 – 31st August 2010: conduct focus groups, design intervention
-
Recruit potential participants
-
Conduct the first three focus groups
-
Transcribe focus group discussions and begin analysis so that new topics or themes for discussion can be identified
-
Begin to develop the intervention and control packages in conjunction with the text message design team and the image design team
1st September 2010 – 30th November 2010: conduct and analyse focus groups, design intervention
-
Conduct the remaining three focus groups
-
Continue framework analysis of the focus group data
-
Further develop the messages and images and assess their acceptability in focus groups
-
Design baseline and follow up questionnaires
1st December 2010 – 15th January 2011: finalise design and pilot recruitment methods
-
Work with psychologist, sociologist, the image design group and the Department of Computing to finalise the text messages and images to be used in the intervention
-
Develop and pilot the screening interview and methods for gaining informed consent
-
Pilot the intervention
17th January 2011 – 13th February 2011: Test the feasibility of the two recruitment strategies
-
Recruitment Strategy 1
-
Recruit three GP practices who will provide participants for the feasibility study
-
Assist practices in identifying patients suitable for recruitment and in the preparation of letters of invitation
-
Search for mobile telephone numbers of potential participants
-
-
Recruitment Strategy 2
-
Test procedures for identifying seed individuals
-
Determine whether social networks are sufficiently large
-
14th February 2011 – 30th April 2011: Screen and recruit participants
-
Screen up to 180 potential participants to identify those eligible for randomisation
-
Recruit and randomise 60 subjects (6 per week)
-
Conduct baseline assessment
21st February 2011 – 31st August 2011: deliver intervention and follow up interviews
-
Deliver intervention over the 28 day period following randomisation
-
Conduct outcome assessment at 3 months
-
Recruit post-trial sub sample and conduct in depth interviews
1st September 2011 – 30th November 2011: analysis and report writing
Complete analysis
-
Complete final report for funding body
-
Prepare papers for publication
14. Expertise
All co-applicants contributed to the study design and to the writing of the protocol. Professor Crombie is an epidemiologist. He conceived the project and will supervise its conduct, help develop the intervention and participate in the analysis. Professor Norrie is a statistician and an experienced triallist. He will be responsible for randomisation of participants and governance arrangements for the trial. Professor Ricketts is a computer scientist. He will be responsible for the delivery of the text messages and images and for monitoring participant responses to these messages. Dr Williams is a medical sociologist. He will guide the conduct and analysis of the focus group data and will help to develop the intervention, particularly the design of the images. Professor Humphris is a health psychologist. He identified the relevant psychological models, and will help develop the intervention and participate in the analysis. Dr Rice is a consultant psychiatrist and head of the Tayside Alcohol Services. He has extensive experience in tackling alcohol-related problems, particularly in helping clients to reduce alcohol consumption. Dr Irvine is an experienced researcher. She will supervise the research assistant on a day-to-day basis and will assist with: conducting the focus groups; analysis of focus group data, developing the intervention, recruitment procedures; and analysis of the data. Dr Slane is a general practitioner. He advised on recruitment strategies for hard to reach groups and the use of brief interventions for alcohol. All co-applicants will contribute to the writing of the final report.
15. Members of the Public
Involving members of the public in the design of the intervention and in the delivery of the intervention is an essential part of this project. We will recruit two members of the user group community prior to the start of the study. They will initially be involved in the design of recruitment processes and the information leaflets and letters of invitation. This will ensure that the language used is appropriate and acceptable. The men will also have a role in planning the schedules to be used to guide focus group sessions. On completion of Phase 1, the men will join the design teams to ensure that the interventions are acceptable and the outcomes are relevant and measurable. The men will be invited to attend all project meetings, and will be strongly encouraged to attend the early study design meetings. The user group representatives will be identified through local community groups (e.g. football leagues, public houses and betting shops). Community group leaders will be approached and asked to nominate individuals who may be willing to take part in the study.
16. Justification of the costs
An experienced full time research assistant (grade 7 spine point 31) is required for 21 months to conduct the focus groups, analyse focus group data, help develop the intervention, recruit all trial participants, conduct baseline and follow-up interviews and analyse the outcome assessments.
Costs for conducting four focus groups and the 20 in-depth interviews include room hire at local community centres, travel expenses for the research assistant and participants, and gift vouchers to thank them for taking part in the study. Secretarial support (grade 2, spine point 2) for the transcription of focus group discussions will be required for two months at 50% whole time equivalent. A qualitative researcher (grade 8 spine point 40) will also be required for eight months at 25% whole time equivalent to assist with the analysis of the focus group data.
Image development by the Dundee 3D Visualisation Group at Dundee University will involve a design consultant (grade 8 spine point 40) who will be required for four months at 50% whole time equivalent.
Two user group representatives will be involved throughout the project. They will be invited to participate in project meeting and sessions to design the text messages and images used for the intervention. They will be reimbursed at £20 per session for their time plus £10 for travelling expenses.
Governance of the project and administration of the randomisation of participants will be overseen by the Glasgow Clinical Trials Unit. Randomisation will cost £1,500 and long term data archiving will cost a further £1,200.
A computer programmer (grade 7, spine point 32) will be required for two months to develop the computer system to administer the sending and receiving of text messages. A dedicated mobile telephone number will be required for the duration of the study (£35.50/month for 21 months). Sending a daily multimedia message (MMS) to each of 60 clients and receiving their text message (SMS) replies for the period of the evaluation will cost £1,700.
Participants in the feasibility trial need to be reimbursed for the use of their mobile telephones, as the study cannot be administered cost free to participants. There is also strong evidence that financial incentives promote recruitment and retention to research studies. Participants will be given a £10 gift voucher for agreeing to take part in the study, and will subsequently be given £5 per week if they respond by text message to the intervention. Finally they will be given a £10 voucher for completing the follow up interview. Thus, the 60 participants randomised will each receive £40 for completing the study.
Part of this study is to test respondent-driven sampling, where participants nominate others suitable for recruitment to the study. A fee of £5 is paid for every participant recruited. This method of recruitment has been shown to be successful in hard to reach groups.
A computer and printer will be required for the administration of the study, the development of text messages for the intervention, and the analysis of data. Landline calls to recruit participants, obtain consent and conduct baseline and follow up interviews will also be required. A modest sum will be required for stationery and printing costs for letters of invitation, information leaflets, data transcripts and reports. Although most of the scientific papers required will be available online it is estimated that ten will be obtained through interlibrary loan. Provision has been made for one person to attend one international public health conference. Finally, £1,700 will be required for advertising and recruitment costs.
References
- Lister G, Fordham R, Mugford M, Olukoga A, Wilson E, McVey D. 2007.
- Costs of Alcohol Use and Misuse in Scotland. The Scottish Government; 2008.
- Mackenbach JP, Stirbu I, Roskam A-JR, Schaap MM, Menvielle G, Leinsalu M, et al. Socioeconomic Inequalities in Health in 22 European Countries. The New England Journal of Medicine 2008;358:2468-81.
- Overview of Scotland’s health and NHS performance in 2006/07. Edinburgh; 2007.
- Bromley C, Sproston K, Sheldon N. The Scottish Health Survey – 2003. Edinburgh: Scottish Executive; 2005.
- Kaner EF, Beyer F, Dickinson HO, Pienaar E, Campbell F, Schlesinger C, et al. Effectiveness of brief alcohol interventions in primary care populations. Cochrane Database of Systematic Reviews 2007. URL: 10.1002/14651858.CD004148.pub3.
- Raistrick D, Heather N, Godfrey C. Review of the effectiveness of treatment for alcohol problems. London: The National Treatment Agency for Substance Misuse; 2006.
- Bertholet N, Daeppen JB, Wietlisbach V, Fleming M, Burnand B. Reduction of alcohol consumption by brief alcohol intervention in primary care: systematic review and meta-analysis. Arch Intern Med 2005;165:986-95.
- Moyer A, Finney J, Swearingen C, Vergun P. Brief interventions for alcohol problems: a meta-analytic review of controlled investigations in treatment-seeking and non-treatment-seeking populations. Addiction 2002;97:279-92.
- Vidrine DJ, Arduino RC, Lazev AB, Gritz ER. A randomized trial of a proactive cellular telephone intervention for smokers living with HIV/AIDS. AIDS 2006;20:253-60.
- Rodgers A, Corbett T, Bramley D, Riddell T, Wills M, Lin RB, et al. Do u smoke after txt? Results of a randomised trial of smoking cessation using mobile phone text messaging. Tob Control 2005;14:255-61.
- Geraghty M, Glynn F, Amin M, Kinsella J. Patient mobile telephone ‘text’ reminder: a novel way to reduce non-attendance at the ENT out-patient clinic. J Laryngol Otol 2008;122:296-8.
- Franklin VL, Greene A, Waller A, Greene SA, Pagliari C. Patients’ Engagement With ‘Sweet Talk’ – a Text Messaging Support System for Young People With Diabetes 2008;10.
- Whittaker R, Maddison R, McRobbie H, Bullen C, Denny S, Dorey E, et al. A multimedia mobile phone-based youth smoking cessation intervention: findings from content development and piloting studies. J Med Internet Res 2008;10.
- NHS Choices . Smokefree n.d. URL: http://smokefree.nhs.uk/what-suits-me/support-at-home/.
- Krouse HJ. Video modelling to educate patients. Journal of Advanced Nursing 2001;33:748-57.
- Hall S, Weinman J, Marteau TM. The motivating impact of informing women smokers of a link between smoking and cervical cancer: the role of coherence. Health Psychology 2004;23:419-24.
- Shahab L, Hall S, Marteau T. Showing smokers with vascular disease images of their arteries to motivate cessation: a pilot study. British Journal of Health Psychology 2007;12:275-83.
- Babin LA, Burns AC. Effects of print ad pictures and copy containing instructions to imagine on mental imagery that mediates attitudes. Journal of Advertising 1997;26:33-44.
- Burns AC, Biswas A, Babin LA. The operation of visual imagery as a mediator of advertising effects. Journal of Advertising 1993;22:71-85.
- Paivio A, Walsh M, Bons T. Concreteness effects on memory: when and why?. Journal of Experimental Psychology: Learning, Memory and Cognition 1994;20:1196-204.
- Gardner MP, Houston MJ. The effects of verbal and visual components of retail communications. Journal of Retailing 1986;62:64-78.
- Goddard M, Smith P. Equity of access to health care services: theory and evidence from the UK. Soc Sci Med 2001;53:1149-62.
- Craig P, Dieppe P, Macintyre S, Mitchie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: new guidance. Medical Research Council; 2008.
- Ritchie J, Spencer L, Bryman A, Burgess RG. Analysing qualitative data. London: Routledge; 1994.
- Scottish Indices of Deprivation. University of Oxford; 2003.
- Galobardes B, Shaw M, Lawlor DA, Lynch JW, Davey Smith G. Indicators of socioeconomic position (part 1). J Epidemiol Community Health 2006;60:7-12.
- Galobardes B, Shaw M, Lawlor DA, Lynch JW, Davey Smith G. Indicators of socioeconomic position (part 2). J Epidemiol Community Health 2006;60:95-101.
- Office of the Chief Statistician . Scottish Index of Multiple Deprivation 2004 Technical Report 2004. URL: http://www.scotland.gov.uk/Resource/Doc/26350/0025281.pdf.
- Crombie IK, Kiezebrink K, Irvine L, Wrieden WL, Swanson V, Power K, et al. What maternal factors influence the diet of 2-year-old children living in deprived areas? A cross-sectional survey. Public Health Nutrition 2008. URL: 10.1017/S1368980008003819.
- Edwards PJ, Roberts IG, Clarke MJ, DiGuiseppi C, Wentz R, Kwan I, et al. Methods to increase response rates to postal questionnaires. Cochrane Database of Systematic Reviews 2007. URL: 10.1002/14651858.MR000008.pub3.
- Smith W, Chey T, Jalaludin B, Salkeld G, Capon T. Increasing response rates in telephone surveys: a randomized trial. J Public Health Med 1995;17:33-8.
- Abdul-Quader AS, Heckathorn DD, Sabin K, Saidel T. Implementation and analysis of respondent driven sampling: lessons learned from the field. J Urban Health 2006;83:i1-5.
- Heckathorn DD. Respondent-driven sampling: a new approach to the study of hidden populations. Social Problems 1997;44:174-99.
- Johnston LG, Malekinejad M, Kendall C, Iuppa IM, Rutherford GW. Implementation Challenges to Using Respondent-Driven Sampling Methodology for HIV Biological and Behavioral Surveillance: Field Experiences in International Settings. AIDS Behav 2008;12:S131-S141.
- Ewing JA. Detecting alcoholism. The CAGE questionnaire. JAMA 1984;252:1905-7.
- Rothman AJ, Bartels RD, Wlaschin JS, P. The strategic use of gain- and loss-framed messages to promote healthy behavior: how theory can inform practice. Journal of Communication 2006;56:S202-S220.
- Fishbein M, Cappella JN. The Role of Theory in Developing Effective Health Communications. Journal of Communication 2006;56:S1-S17.
- Viswanath K, Emmons KM. Message Effects and Social Determinants of Health: Its Application to Cancer Disparities. Journal of Communication 2006;56:S238-S264.
- Conner M, Norman P. Predicting Health Behaviour. Open University Press; 2005.
- Engineer R, Phillips A, Thompson J, Nicholls J. Home Office Research Study 262. Drunk and disorderly: a qualitative study of binge drinking among 18- to 24-year-olds. London: Home Office Research, Development and Statistics Directorate; 2003.
- Wild TC. Personal drinking and sociocultural drinking norms: a representative population study. J Stud Alcohol 2002;63:469-75.
- Carey KB, Scott-Sheldon LA, Carey MP, DeMartini KS. Individual-level interventions to reduce college student drinking: a meta-analytic review. Addict Behav 2007;32:2469-94.
- Larimer ME, Cronce JM. Identification, prevention, and treatment revisited: individual-focused college drinking. Addict Behav 2007;32:2439-68.
- Oei TP, Morawska A. A cognitive model of binge drinking: the influence of alcohol expectancies and drinking refusal self-efficacy. Addict Behav 2004;29:159-79.
- Dijkstra A, Sweeney L, Gebhardt W. Social cognitive determinants of drinking in young adults: Beyond the alcohol expectancies paradigm. Addict Behav 2001;26:621-773.
- Briñol P, Petty RE. Fundamental Processes Leading to Attitude Change: Implications for Cancer Prevention Communications. Journal of Communication 2006;56:S81-S104.
- Choosing Health: Making healthy choices easier. London: UK Parliament; 2004.
- Health Survey for England. London; 2008.
- Economic and Social Research Council (ESRC) . Research Ethics Framework (REF) 2005. URL: http://www.esrcsocietytoday.ac.uk/ESRCInfoCentre/Images/ESRC_Re_Ethics_Frame_tcm6-11291.pdf.
Appendix 2 Letter of invitation, participant information leaflet and consent form
Letter of invitation from GP (on GP-headed notepaper)
Ref: GP/PID
Dear Mr
A study on health and alcohol
We would like your help with a research study. A group from the University of Dundee are doing a research study about health and alcohol consumption among young to middle-aged men. They are doing this because some people in this age group drink in ways that is harmful to their health. The researchers want to talk to men to try to identify ways to encourage people to reduce the frequency of drinking at harmful levels. The enclosed leaflet tells you more about the study.
If you decide to take part in the study a researcher will get in touch with you by telephone. You will be asked some questions and will receive some text messages over a period of four weeks. Three months after the first telephone interview, the researcher will get in touch again to ask some more questions. The amount of time this would take is small. You will receive gift vouchers to thank you for taking part in the study and will be reimbursed for any costs incurred.
Please read the enclosed information leaflet carefully. If you do not wish to take part, please return the enclosed card. However, if you are interested in taking part, or if you would like to find out more about the study, you do not have to do anything at this stage. If you do not return the card we will give your name to the researcher working on the study. He will contact you within the next four weeks to discuss the study. For further information you can speak to [contact details given].
Thank you for your help
Yours sincerely
08/10/2009, Version 1

Department of Public Health
Division of Clinical & Population Sciences & Education
Head of Department Professor I K Crombie
A study on health and alcohol
Participant information leaflet
We invite you to take part in a research study. Before you decide, we would like you to understand why the research is being done and what it would involve for you. We are therefore providing you with the following information. Please take time to read it carefully and discuss it with others if you wish. When you have read the information provided, one of our team will go through it with you and answer any questions you have. This will take about 10 minutes. Be sure to ask us if there is anything that is not clear or if you would like more information. Take time to decide whether or not you wish to take part. Thank you for taking the time to read this.
Purpose of the study
This is a study about health and alcohol consumption among young to middle-aged men. Some men in this age group drink too much and we want to find ways to encourage them to reduce the frequency of drinking at harmful levels. We therefore want to look at alcohol consumption among a group of men, find out about their reasons for drinking, their intentions about drinking in the future and how these change over time.
Men will be invited to take part if they have had at least two days in the past month where they have consumed more than eight units of alcohol in one session. (A unit of alcohol is half a pint of normal strength beer, one measure of spirits or one small glass of wine).
What we would like you to do
After you have read this leaflet and have had a few days to think about it, a researcher will call you back to see if you wish to take part. If you give consent you will be asked some questions about yourself and how much you drink to see if you are eligible for the study. If you are eligible, we will send you a series of text messages with images over the next four weeks. The men taking part in the study will be put into two groups who will receive different text messages. Three months after the telephone interview, the researcher will get in touch by telephone again to ask some more questions.
At the end of the three month period we would like to conduct longer interviews with a few of the men who have taken part. We will choose some names at random (20 of the 60 men involved in the study). If you are selected, the researcher will contact you by telephone or text message to arrange a suitable time and place for the interview.
Why have I been chosen?
Men living in areas of Dundee, selected by postcode area, are being invited to take part. Your GP has randomly selected men in this age group to be contacted to ask if they would be willing to take part. To take part you must be available to be contacted by mobile telephone over a three month period.
Do I have to take part?
It is up to you to decide whether or not to take part. We will explain the study and go through the information leaflet. If you do decide to take part you will be asked to give consent. To do this you will be asked to reply to a text message from us to confirm that you are willing to take part. Participation in this study is entirely voluntary and you are free to refuse to take part or to withdraw from the study at any time without having to give a reason and without this affecting your future medical care or your relationship with medical staff looking after you.
Expenses and payment
You will be given gift vouchers as a thank you for taking part in the study and to reimburse you for the cost of any text messages you send to us. You will be sent a £10 gift voucher after you have completed the first telephone interview. You will then receive a £5 gift voucher each week for four weeks if you respond to the text messages you have received. You will also receive another £10 voucher when you complete the second telephone interview. Finally, those who take part in the detailed interview at the end of the three month period will receive a further £10 gift voucher.
What are the possible benefits of taking part?
Throughout the study we will give you information on health issues. You may find these useful in helping you to make healthier choices.
Confidentiality
Any information collected during the course of the study will be maintained on a confidential basis and access will be restricted to people conducting the study. Your name will not be disclosed, nor will details of your answers be given to anyone. With your permission, the telephone interviews with the researcher will be recorded and typed up as a written document or transcript. The transcripts will then be examined to ensure that all of the important information has been captured. The transcripts will not contain your name or any information about you that would allow you to be identified. The only people who will have access to the transcripts are the researchers. Some of your comments may be included in a report on the study, but these will be completely anonymous.
What will happen to the results of the research study?
The overall findings of the study may be published in a scientific journal, but these will not mention you in any way. If you would like to receive information about the results of the study, please let us know, and we will forward a summary of the findings to you at the end of the study.
Who has designed and reviewed the study?
The study has been designed by a group of researchers from The Universities of Dundee, Glasgow and St Andrews and NHS Tayside. Funding has been provided by the National Institute for Health Research. The Tayside Committee on Medical Research Ethics A, which has responsibility for scrutinising all proposals for medical research on humans in Tayside, has examined the proposal and has raised no objections from the point of view of medical ethics. It is a requirement that your records in this research be made available for scrutiny by monitors from the University of Dundee and NHS Tayside, whose role it is to check that research is properly conducted and the interests of those taking part are adequately protected.
Concerns or complaints about the research
If you have a concern about any aspect of this study, you should ask to speak to [contact details given] who will do her best to answer your questions. If you remain unhappy and wish to complain formally, you can do this by contacting [contact details given] who is the project leader.
Thank you for taking the time to read this information sheet and considering taking part.
To obtain further information
If you have any questions about this research, please contact [contact details given] who will be happy to discuss the study or answer any questions you may have.
Appendix 3 Screening questionnaire
Appendix 4 Baseline questionnaire
References
- Manual for the Fast Alcohol Screening Test (FAST). London: Health Development Agency; 2002.
- Oei TP, Hasking PA, Young RM. Drinking refusal self-efficacy questionnaire-revised (DRSEQ-R): a new factor structure with confirmatory factor analysis. Drug Alcohol Depend 2005;78:297-30.
- Heather N, Hoenekopp J. A revised edition of the Readiness to Change Questionnaire Treatment Version. Addiction Res Theor 2008;16:421-33.
Appendix 5 Follow-up questionnaire
References
- Oei TP, Hasking PA, Young RM. Drinking refusal self-efficacy questionnaire-revised (DRSEQ-R): a new factor structure with confirmatory factor analysis. Drug Alcohol Depend 2005;78:297-30.
- Heather N, Hoenekopp J. A revised edition of the Readiness to Change Questionnaire Treatment Version. Addiction Res Theor 2008;16:421-33.
Appendix 6 Post-trial assessment
List of abbreviations
- DMQ
- Drinking Motives Questionnaire
- FAST
- Fast Alcohol Screening Test
- GP
- general practice/general practitioner
- HAPA
- health action process approach
- MI
- motivational interviewing
- MMS
- Multimedia Messaging Service
- RDS
- respondent-driven sampling
- RSOD
- risky single occasion drinking
- SIMD
- Scottish Index of Multiple Deprivation
- SMS
- Short Message Service
- TPB
- theory of planned behaviour
- TTM
- transtheoretical model
All abbreviations that have been used in this report are listed here unless the abbreviation is well known (e.g. NHS), or it has been used only once, or it is a non-standard abbreviation used only in figures/tables/appendices, in which case the abbreviation is defined in the figure legend or in the notes at the end of the table.