

Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 09/3005/09. The contractual start date was in April 2011. The final report began editorial review in November 2016 and was accepted for publication in June 2017. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
At the time of the study, Steven Cummins and Charlotte Clark were both members of the National Institute for Health Research (NIHR) Public Health Research Programme Funding Board. Steven Cummins was also funded by a NIHR Senior Research Fellowship.
Disclaimer
This report contains transcripts of interviews conducted in the course of the research and contains language that may offend some readers.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2018. This work was produced by Cummins et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2018 Queen’s Printer and Controller of HMSO
Chapter 1 Background
Health follows a social gradient, with those further up the socioeconomic scale experiencing better health. 1,2 In the UK, health inequalities have persisted over the past two decades, with the mortality gap between the most advantaged and disadvantaged groups standing at around 8 years. 3 Policies and interventions that tackle the wider socioeconomic and environmental determinants of poor health have been promoted by UK governments as important components of strategies to improve health and well-being, and to reduce health inequalities. 2,4 In recent years, large-scale programmes that tackle entrenched social and environmental deprivation through improvements in living conditions have become an increasing feature of the policy landscape. Such interventions have usually taken the form of large-scale urban regeneration and neighbourhood renewal programmes that have good potential to tackle health inequalities as they directly influence the wider social, economic and environmental determinants of physical and mental health. 5 Between 1980 and 2004 spending on such schemes in the UK was thought to have reached £11B. 6 In more recent years many of these schemes have been area based, and have thus involved the targeting of places that are considered to be in the greatest social and economic need. Such initiatives target areas of multiple deprivation and commonly comprise investment in schemes that might affect the key socioeconomic and environmental determinants of health, for example employment, housing, education, income and welfare. Much of this occurs through infrastructural improvements to the built environment such as new or upgraded transport links, the provision and upgrading of retail space, the creation of new green space, parks and public areas, and improvements in housing. General improvements in aesthetics and safety via neighbourhood redesign through lighting, furniture, public art, pedestrian zones and the amelioration of environmental stressors such as graffiti, litter and noise are also common components of regeneration programmes.
Despite continuing large-scale public investment, recent systematic reviews identify a dearth of evidence of the effectiveness of urban regeneration programmes in improving health and well-being, and alleviating health inequalities. 6–8 The evidence that does exist is weak with mixed findings. In the UK, studies investigating the health impacts of urban regeneration are rare and highly variable in terms of study quality and reported outcomes, and exist primarily in the grey literature. Although some studies with health indicators have reported improvements (e.g. mortality rates),9 previous research also suggests the possibility of negative effects. 10 Evaluations have tended to focus on socioeconomic outcomes (such as impacts on employment, education, income and housing quality) and have often neglected to assess effects on health outcomes. These evaluations of socioeconomic impacts have also been mixed, with the reporting of both positive and negative effects on socioeconomic factors, making it difficult to speculate as to the direction and nature of plausible indirect impacts on health. 10–12 Most studies are also focused on adults: evaluations of the impact of urban regeneration on young people and their families represent an important gap in the evidence, as adolescence may be a critical period for the emergence of health inequalities in later life.
Previous research therefore suggests that even though urban regeneration programmes have the potential to affect population health there is limited evidence to support this. Overall, the literature is clear: robust evaluations of the impact of urban regeneration programmes on the social determinants of health, and on health and behaviours, have rarely been undertaken and the evidence that does exist is of generally mixed quality. There has been little work on how impacts vary across population subgroups. Recently, there has been increasing demand from public health policy-makers, as well as practitioners, in urban planning for evidence that provides guidance to help ‘design-in’ health-promoting features of the urban environment, allowing them to maximise the health impact of new built infrastructure development. This might include design features that favour public and active modes of transport over the private motor car; increasing accessibility to resources that promote physical activity and well-being, such as green space, facilities for physical activity and more opportunities for leisure-time walking and cycling. The present study has therefore been designed to provide robust, longitudinal evidence on whether or not the large urban regeneration catalysed by the London 2012 Olympics has resulted in improvements in physical activity and psychological well-being.
The London 2012 Olympics as a catalyst for large-scale urban regeneration in east London
Hosting the London 2012 Olympic and Paralympic Games provided an opportunity to establish a quasi-experimental study of the effects of urban regeneration associated with the 2012 Olympics on physical activity and psychological well-being, as well as a wider range of health outcomes and behaviours. The components of the Olympic-related regeneration programme delivered in east London are common to the majority of urban regeneration programmes elsewhere (e.g. improvements in facilities, services, housing and built infrastructure). This presents an opportunity for wider learning around about the range and nature of positive and negative impacts on health and an exploration of the causal pathways between urban regeneration and health by linking specific individual components of regeneration to changes in specific outcomes and behaviours. Urban regeneration under investigation in this study is focused on east London, specifically the London boroughs of Hackney, Tower Hamlets, Newham, and Barking and Dagenham.
The east London boroughs included in this study comprise an ethnically diverse population of approximately 1.1 million people. This area is also relatively disadvantaged, with some of the most deprived neighbourhoods in the UK within its borders. The bid to host the London 2012 Games was centred on creating the first ‘Legacy Games’ and was predicated on leaving a lasting legacy for the residents of east London through improvements to infrastructure and housing, stimulating economic development and aiming to ‘inspire a generation’ to be more physically active. In the context of this study regeneration primarily consisted of the construction of services, infrastructure and facilities supporting the Olympic Park and Stratford City developments during late 2011 and 2012, plus the early legacy phases that were delivered from 2013. These developments covered an area of 7000 acres in the London Borough of Newham. The Legacy Masterplan13 outlines provision for a total of 2.9 million ft2 of retail and leisure space, 1.3 million ft2 of hotel space, a 6.6-million-ft2 commercial district, and 180,000 ft2 of new and refurbished community spaces. Regeneration components that are the focus of this study comprise ‘sustainable’ transport networks (rail and active travel corridors); new and refurbished civic spaces, parks and green areas; improvements in accessibility to services and facilities of communities on the fringe of the regeneration sites; and development of retail, business and community facilities. The main physical regeneration activities are summarised in Table 1.
| Date | Area | Main components |
|---|---|---|
| 2011–12 | Stratford City Development | Retail and leisure centre comprising 579,120 m2 of retail space (including Westfield Stratford City), 152,400 m2 of office and business space, new civic and public space |
| 2012–14 | Olympic Park | The Olympic Park consists of 2,460,000 m2 of regenerated land that consists of new green spaces and parkland, public space and play areas, world class sports venues (main stadium, aquatics centre, velodrome, BMX and mountain bike tracks, road cycle route) and associated facilities, and improved physical connectivity and accessibility to the Olympic Park from surrounding areas (foot and cycle paths, bridges, waterways, road and rail links). New housing associated with the former Athletes Village (East Village) |
| 2012–14 | Olympic Fringe | Area surrounding the Olympic Park will receive 900,000 m2 of improved green/civic space and improved connectivity to the main Olympic Park |
The London 2012 Olympic and Paralympic Games took place over a 6-week period from 27 July to 9 September 2012, with the park site closed for several years prior to these dates. After the completion of the Games, the Olympic Park entered legacy mode and was closed for refurbishment. It reopened to the public in phases between July 2013 and April 2014. A full timeline can be found here: https://web.archive.org/web/20161015003425/http://queenelizabetholympicpark.co.uk/our-story/transforming-east-london/timeline (accessed 13 September 2018).
Our study was therefore designed to answer a set of specific questions that linked elements of environment change related to urban regeneration in east London to changes in physical activity behaviour and psychological well-being to generate generalisable evidence on how the modification of urban environments might affect these health outcomes.
Primary research questions
The aim of this study, the Olympic Regeneration in East London (ORiEL) study, was to address the following primary research question:
-
What is the impact of urban regeneration on the social determinants of health (employment), health behaviours (physical activity) and health outcomes (mental health and well-being) of adolescents and their parents/carers?
We also aimed to answer the following secondary research questions:
-
How are any socioeconomic and health impacts distributed by age, sex and ethnicity?
-
What are the effects of specific components of the regeneration programme on physical activity and psychological well-being?
-
Are any socioeconomic and health impacts sustained over time?
It was not possible to investigate effects on a range of secondary outcomes (such as diet and obesity) within the time frame of the current grant. Further analyses of ORiEL data focusing on these areas are ongoing and we anticipate that findings will be published over the next 2 years.
This report
The report presented here is an original summary of a large body of ongoing research, some of which has been published, submitted or prepared for publication in peer-reviewed scientific journals. Given the space available, we have focused our report on the main findings of interest. As a consequence, the report is primarily focused on findings related to the adolescent cohort. Findings related to parents/carers are briefly described, but are limited in nature and scope, as we found few statistically significant associations with our primary outcomes of interest in cross-sectional, longitudinal and repeat cross-sectional analyses.
The work presented here is therefore a summary and further details on the study methods and the findings can be found in already published work. Further work will emerge from the data generated by the study. This work, when possible, is referenced in the text and is available from the London School of Hygiene and Tropical Medicine (LSHTM) Research Online website: http://researchonline.lshtm.ac.uk/ (accessed 13 September 2018).
Chapter 2 Methods
This chapter describes the research design and methods employed to evaluate the impact of Olympic-led urban regeneration on young people and their families. Here we describe the overall design of the study, respondent recruitment, fieldwork and data collection, the operationalisation of key variables and the general approach employed to analyse quantitative and qualitative data.
The content of this chapter updates previously published material contained in the protocol for the ORiEL study, published immediately before the London 2012 Olympic and Paralympic Games. For further details of the published study protocol, see Smith et al. 14
Research design
The ORiEL study is underpinned by a multilevel socioecological conceptual framework recognising that both individual and environmental risk factors are important for health. The implication is that action to improve health requires a focus not only on individual lifestyle and socioeconomic factors but also on the local environmental resources and opportunities available to those individuals. 15,16
Our main aim was to assess the impact of a multicomponent urban regeneration programme linked to the 2012 Olympic Games on the social determinants of health (employment), health behaviours (physical activity) and health outcomes (mental health and well-being) of adolescents and their parents or carers. The study was originally conceived as a natural quasi-experimental study of a school-based cohort of adolescents and their parents/carer, living within four east London boroughs (Hackney, Tower Hamlets, Newham and Barking and Dagenham), with a further in-depth qualitative study of a subsample of families enrolled in the cohort.
The overall study comprises two main elements:
-
A longitudinal controlled quasi-experimental quantitative study examining changes in health behaviour and health outcomes in a cohort of adolescent school pupils aged 11–12 at baseline, and their parents or primary carers (parent/carer). Residents in the intervention area (Newham) receiving urban regeneration were compared with those who live in comparison areas (Hackney, Tower Hamlets, and Barking and Dagenham) not receiving urban regeneration of this magnitude. Adolescent and parent/carer survey data were collected in three waves in intervention and comparison areas: wave 1 (baseline pre intervention, 2012), wave 2 (6 months post intervention, 2013) and wave 3 (18 months post intervention, 2014).
-
An in-depth longitudinal qualitative study of family experiences of, and attitudes towards regeneration in the intervention area and influences on socioeconomic status, health behaviours and health outcomes. The initial investigation comprised a subgroup of approximately 20 families at baseline that reflected the diversity of the survey sample. The qualitative study sample was drawn from wave 1 participants and was repeated at wave 2.
Study setting
The study took place in four London boroughs: Newham (intervention site), Barking and Dagenham, Tower Hamlets and Hackney (comparison sites). The boroughs have an estimated combined population of around 1.1 million residents17 and are significantly more disadvantaged than the London average. 18 For example, between 2011 and 2012 unemployment rates were 7.0% (compared with 5.1% in London),19 the incidence of violent crime was 22.0 offences per 1000 population per year (compared with 18.8 offences per 1000 population per year in London)20 and the proportion of the population with no educational qualifications was 22.0% (compared with 17.6% in London). 21 This setting was suitable for research of this type as area-based urban regeneration programmes that influence the socioeconomic and environmental determinants of health may be particularly beneficial for relatively disadvantaged communities with degraded infrastructure. 8
Methods: quantitative study
Sampling strategy
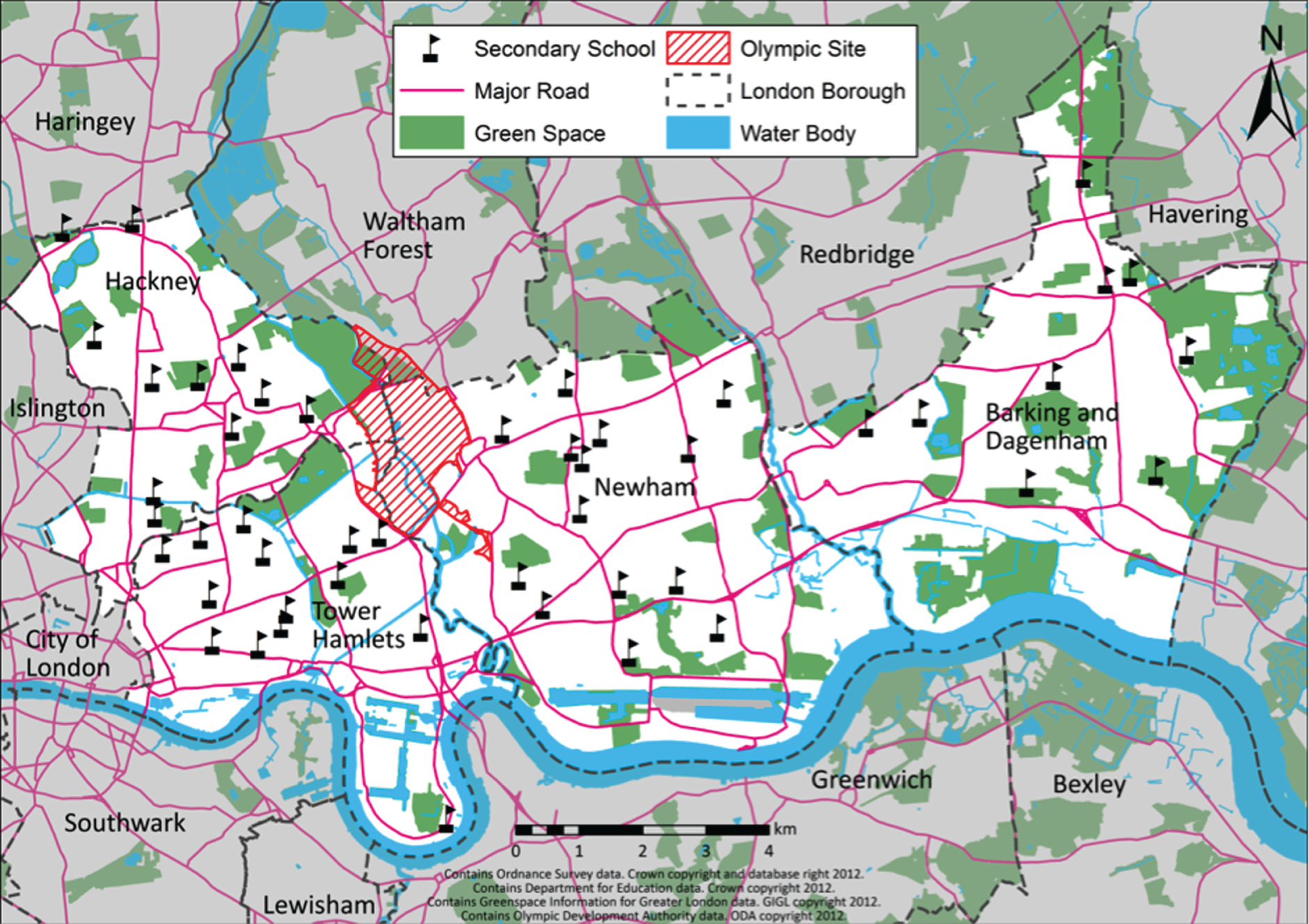
Participants at baseline were pupils aged 11–12 years (school year 7) who attended randomly selected state schools in the intervention and comparison boroughs, and their parents/carers. Schools were selected using simple randomisation within each borough, with refusals replaced by eligible schools from the same borough. Included adolescents were those with sufficient cognitive and language skills to complete a paper-based questionnaire, including those who required some assistance to do so. Special-needs schools, pupil referral units and independent schools were excluded. The total number of eligible schools in each borough was as follows: Newham, n = 14; Tower Hamlets, n = 14; Hackney, n = 11; and Barking and Dagenham, n = 9. The geographical location of these east London boroughs, and the schools’ position within them relative to the Olympic Park area, is shown on the map in Figure 1.
FIGURE 1.
Map showing the location of eligible schools adjacent to the Olympic Park in the London boroughs of Newham, Tower Hamlets, Hackney, and Barking and Dagenham. Map contains Ordnance Survey data, Crown copyright and database right 2012; Department for Education data, Crown copyright 2012; Greenspace Information for Greater London data, GIGL copyright 2012; and Olympic Development Authority data, ODA copyright 2012. Reproduced with permission from Smith et al. 14 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Study power
The study is powered to detect differences in our primary outcome measures of employment, mental well-being and physical activity. In the only high-quality controlled prospective study of neighbourhood change with related outcomes to those proposed here (the Moving to Opportunity study), the proportion of people employed increased by 13% among minority groups,22 and mental well-being scores, on a range of scales, improved by 8–33% for adults, and up to 25% for children. 23
On the basis of this, a plausible conservative minimum change in our primary outcomes (employment, mental well-being and physical activity) would be 8%. Given the finite number of schools available in the intervention area (n = 14) compared with comparison areas (n = 34), we assumed a 1 : 3 ratio for the number of participants in intervention and comparison arms, respectively.
A total sample size of 712 adolescents and 712 parents/carers at wave 3 was therefore, required to detect a difference of 8% with 80% power at a significance level of 5%. To take account of clustering by school, we assumed an intracluster correlation coefficient (ICC) of 0.02 (as our primary outcome is health related we expect a smaller ICC than that usually seen for measures such as educational attainment, which will be more highly school related). This results in a design effect of 2.48 with a total required sample size at second follow-up (wave 3) of 1766 adolescents (24 schools and 74 per school) and 1766 parents/carers. Our achieved adolescent sample size therefore has 80% power to detect the minimum difference of 8%, at the 5% significance level.
Recruitment
Adolescent survey
Participants were recruited through secondary schools in two ways: (1) school-based enrolment of adolescents aged 11–12 years in year 7, and (2) recruitment of parents/carers through the surveyed adolescents. Schools were incentivised by a single donation of £1000 paid after completion of the baseline survey.
Adolescent recruitment began by asking the borough-level administrators (local education authorities/learning trusts) to encourage schools to participate. This approach has been previously successful in recruiting primary schools, albeit outside London. 24 However, all four boroughs suggested that we contact schools directly. A letter of invitation was sent to school principals (and members of their senior leadership team), followed by a telephone call. This resulted in the recruitment of 10 schools. The remaining schools were recruited from an e-mail campaign targeting heads of year and subject leaders who might find the ORiEL project of academic interest to their students (e.g. physical education, geography, sociology). Overall, 42 of the 48 eligible schools were approached to recruit the final 25 schools needed. The most common reason for schools refusing was ‘research fatigue’. This suggests that personal preferences of organising staff were a cause of refusal rather than pupil characteristics. Further details can be found in Smith et al. 14
Respondents were recruited from six schools in each of the London boroughs of Newham, Hackney, and Barking and Dagenham and from seven schools in Tower Hamlets (Table 2). The cross-sectional baseline survey respondents comprised 3095 adolescents in year 7 of secondary school (aged 11–12 years) who completed a paper-based questionnaire during the 6 months (January to July 2012) prior to the start of the London 2012 Olympic and Paralympic Games. To maximise the sample, the whole school year was surveyed in seven schools that had relatively small year groups. The remaining 18 larger schools provided an allocation of mixed-ability adolescents selected on the basis of school timetabling. Adolescents were followed up at approximately 6 months (January to July 2013) and 18 months (January to July 2014) post intervention. Schools were surveyed as close to the same month of each year, when possible, in order to minimise seasonality effects. The cross-sectional sample was larger at follow-up than at baseline owing to a deliberate oversampling strategy. This was a logistical requirement given that the cohort members became dispersed over time to many different classes across the school timetables at first follow-up (year 8).
| School | Wave cross-section | Wave 1/2/3 cohort | ||
|---|---|---|---|---|
| 1 | 2 | 3 | ||
| Newham | ||||
| 1 | 163 | 155 | 152 | 108 |
| 2 | 126 | 158 | 151 | 93 |
| 3 | 136 | 145 | 147 | 98 |
| 4 | 209 | 229 | 228 | 145 |
| 5 | 112 | 103 | 91 | 81 |
| 6 | 147 | 145 | 155 | 103 |
| Mean | 149 | 156 | 154 | 105 |
| Total | 893 | 935 | 924 | 628 |
| Hackney | ||||
| 7 | 156 | 158 | 138 | 112 |
| 8 | 95 | 98 | 86 | 74 |
| 9 | 100 | 105 | 96 | 81 |
| 10 | 124 | 126 | 129 | 99 |
| 11 | 111 | 104 | 103 | 84 |
| 12 | 143 | 168 | 174 | 103 |
| Mean | 122 | 127 | 121 | 92 |
| Total | 729 | 759 | 726 | 553 |
| Tower Hamlets | ||||
| 13 | 105 | 115 | 105 | 85 |
| 14 | 95 | 95 | 89 | 73 |
| 15 | 104 | 103 | 101 | 77 |
| 16 | 116 | 130 | 146 | 85 |
| 17 | 121 | 120 | 105 | 85 |
| 18 | 127 | 120 | 113 | 90 |
| 19 | 135 | 136 | 118 | 89 |
| Mean | 115 | 117 | 111 | 83 |
| Total | 803 | 819 | 777 | 582 |
| Barking and Dagenham | ||||
| 20 | 130 | 133 | 87 | 77 |
| 21 | 105 | 111 | 86 | 73 |
| 22 | 100 | 110 | 108 | 87 |
| 23 | 113 | 112 | 115 | 99 |
| 24 | 112 | 105 | 101 | 80 |
| 25 | 103 | 129 | 117 | 75 |
| Mean | 111 | 117 | 102 | 82 |
| Total | 663 | 700 | 614 | 491 |
| Overall mean | 124 | 129 | 123 | 90 |
| Total | 3088 | 3213 | 3041 | 2254 |
The final sample featured single- and mixed-sex schools and drew on the largest and smallest schools in the four boroughs, which were affiliated to a range of religious denominations.
Table 3 compares the sociodemographic profile of the ORiEL sample at baseline with census data. The sociodemographic characteristics of the ORiEL baseline sample were broadly similar to the equivalent population observed by the 2011 census, with some exceptions. The ORiEL sample was slightly under-represented in terms of female respondents and Bangladeshi and white UK respondents; this ethnic difference contrasted with an ORiEL over-sample of white other and mixed white ethnic groups. The high proportion of white other groups included recent migrants from European Union states and will have contributed significantly to the higher than expected numbers of participants born overseas. Overall, the baseline response rate was 87% and the study sample (n = 3095 in school year 7) can be estimated at approximately 25% of the entire age group attending state schools in the catchment areas (n = 12,136 in school year 6).
| Variable | ORiEL study sample at 2012 baseline, n (%) | 2011 Census in ORiEL catchment area, n (%)a |
|---|---|---|
| Genderb | ||
| Male | 1756 (56.6) | 6205 (51.1) |
| Female | 1347 (44.4) | 5938 (48.9) |
| Ethnic groupc | ||
| White: UK | 598 (19.5) | 13,328 (24.0) |
| White: other | 399 (13.0) | 4454 (7.4) |
| White: mixed | 380 (12.4) | 4648 (7.7) |
| Asian: Indian | 108 (3.5) | 2846 (4.2) |
| Asian: Pakistani | 130 (4.2) | 2888 (4.1) |
| Asian: Bangladeshi | 508 (16.6) | 12,976 (22.4) |
| Asian: other | 27 (0.9) | 1943 (3.0) |
| Black: Caribbean | 147 (4.8) | 2772 (4.6) |
| Black: African | 364 (11.9) | 8666 (14.3) |
| Black: other | 242 (7.9) | 2511 (4.2) |
| Other | 163 (5.3) | 2392 (4.0) |
| Nativityc | ||
| Born overseas | 628 (20.7) | 26,697 (12.2) |
| Boroughb | ||
| Newham | 895 (28.8) | 3967 (32.7) |
| Tower Hamlets | 807 (26.0) | 2771 (22.8) |
| Barking and Dagenham | 670 (21.6) | 2559 (21.1) |
| Hackney | 733 (23.6) | 2839 (23.4) |
| Economic activityd | ||
| Both unemployed | 279 (10.4) | 23,536 (11.7) |
| One parent/carer employed | 941 (35.07) | 67,187 (33.4) |
| Both parents/carers employed | 1054 (39.28) | 61,638 (30.6) |
| Lone parent/carer employed | 235 (8.76) | 23,145 (11.5) |
| Lone parent/carer unemployed | 174 (6.49) | 25,917 (12.9) |
Parent/carer survey
The recruitment of parents/carers was carried out under contract with an external market research agency using face-to-face interviewer-administered questionnaires. Owing to data protection legislation, schools were unable to supply the home addresses of parents/carers of children enrolled in the study. We therefore asked adolescents to volunteer their home address during the completion of their questionnaires and this information was then passed on to the market research organisation for recruitment. Parents/carers received a letter of invitation to participate along with an incentive of an automatic entry into a prize draw in which five people would win £100. The overall response rate was 60%, a high response rate for east London, which has been historically difficult to enumerate. 25 However, the achieved sample size of the baseline cross-section was a considerably smaller than the adolescent sample because invitations to participate could be sent only to homes with a valid address provided by the adolescent during the survey session (Table 4). We were also obliged under the terms of the Market Research Society guidelines to ask all adult participants whether or not they would be willing to participate in the follow-up interview. Consequently, 37% of respondents opted out of the potential follow-up cohort at baseline. Because of the loss to follow-up, the study protocol was amended for follow-up data collection. The modified parent/carer survey adopted a repeat cross-sectional design, although a nested cohort was retained at each wave of data collection. This approach was agreed with the National Institute for Health Research (NIHR) as an appropriate compromise.
| Borough | Wave | ||
|---|---|---|---|
| 1 | 2 | 3 | |
| Newham | |||
| Total | 389 | 365 | 343 |
| Hackney | |||
| Total | 253 | 193 | 257 |
| Tower Hamlets | |||
| Total | 286 | 246 | 234 |
| Barking and Dagenham | |||
| Total | 317 | 219 | 161 |
| Total | 1245 | 1023 | 995 |
Data collection
Adolescent questionnaire
A paper-based questionnaire, based on validated tools and instruments listed below, was administered to assess individual and household sociodemographic characteristics, mental health and well-being, and physical activity of participating adolescents. Core questionnaire items are outlined below.
Socioeconomic circumstances
Household socioeconomic circumstances were measured using the Revised Family Affluence Scale (FAS II),26 whether or not adolescents were receiving means-tested free school meals and whether or not parents/carers were in employment. FAS II is a four-item questionnaire that has been validated in adolescents cross-nationally26 and is predictive of physical activity, self-reported health and mental well-being, and dietary outcomes. 27 However, we did not use the FAS II in our subsequent analyses owing to a very poor reliability of the scale (Cronbach’s alpha ≤ 0.4). Instead we used receipt of free school meals as our main measure of socioeconomic circumstance.
Mental health and social support
Well-being, mental health and social support were assessed using three self-completed scales. The first of these is the Warwick–Edinburgh Mental Well-Being Scale (WEMWBS), a scale for assessing positive mental health/subjective well-being. 28 It has 14 positively worded item scales with five response categories (ranging from ‘none of the time’ to ‘all of the time’) and covers most aspects of positive mental health (positive thoughts and feelings), including both hedonic and eudaimonic perspectives. The total score ranges from 14 (lowest level of well-being) to 70 (highest level of well-being) and is reported as a mean value. The scale has been validated in adolescents29 and cross-culturally within Pakistani and Chinese subgroups. 30
Second, the Moods and Feelings Questionnaire (MFQ)31 is a 32-item questionnaire for depressive symptoms based on the Diagnostic and Statistical Manual of Mental Disorders Third Edition (Revised)32 (DSM-III-R) criteria for depression. The 13-item short form Moods and Feelings Questionnaire (SMFQ), based on the discriminating ability between the depressed and non-depressed, was completed by each adolescent. Each item is rated on a three-point scale: ‘true’, ‘sometimes true’, and ‘not true’, with respect to the events of the past 2 weeks. Scores range between 0 (lowest risk of depressive symptoms) and 26 (highest risk) and the variable was dichotomised with a total score of eight or more indicating clinically relevant depressive symptoms. 31 This scale was used in the previous Research with East London Adolescents: Community Health Survey (RELACHS) study33–35 of east London adolescents.
Third, the Multidimensional Scale of Perceived Social Support (MSPSS) is a reliable and validated 12-item instrument designed to assess perceptions about support from family, friends and a significant other. 36 It is rated on a seven-point Likert scale ranging from ‘very strongly agree’ to ‘very strongly disagree’. The scale has a high construct and discriminant validity and high test–retest reliability (α = 0.92). 36 Summed scores for each domain and the overall total score were split into tertiles because of a skewed positive distribution.
Physical activity and sedentary behaviour
Physical activity and sedentary behaviour were assessed using the self-completed Youth Physical Activity Questionnaire (Y-PAQ). 37 This instrument was developed by the Medical Research Council (MRC) Epidemiology Unit in Cambridge. The validated questionnaire assesses accumulated time spent physically active and taking part in sedentary behaviours. 38 Estimates of total physical activity are comparable with previous population-based studies in a similar age group in Britain and other European countries. 39 A standard procedure was used to clean the Y-PAQ data and to account for extreme cases of overestimation of time and frequency of physical activity. The procedure sets outliers to a maximum value derived from validation studies and flags the value for the analyst.
Secondary outcomes and exposures
A range of sociodemographic, health-related and environmental variables were also collected. Participants were asked about their age, gender, home address and postcode, ethnicity (based on a question adapted from the 2011 Census for England and Wales),40 religion,41 cultural identity,42 country of birth, self-reported health,43 any long-term illnesses41,44 or mobility problems,44 smoking,45 drinking45 and dietary behaviours,46 parental interest in schooling,39,47 life events41,48 and education or employment expectations on reaching age. 41,47 The height and weight of participants were measured by the study team (Seca 899 scale, Seca 217 stadiometer, Seca Ltd, Birmingham, UK), with the exception of those individuals who declined to be measured or for whom an accurate reading was not possible, for example wheelchair users. These data were used to calculate body mass index (BMI) (taking age into account). Potential outliers for height and weight were noted during the measurement process and so confirm true cases of extreme values. Perceptions of the local cycling and walking environment were assessed using relevant items adapted from the Assessing Levels of Physical Activity and Fitness (ALPHA) environmental questionnaire. 48,49 Fifteen items were rated on a five-point scale (strongly agree to strongly disagree) with an additional item asking participants to rate in minutes how near they live to a range of neighbourhood resources. Finally, attitudes to the Olympic and Paralympic Games were investigated using an adapted version of the Department for Education’s questionnaire for evaluating schools’ engagement with the Games via the national Get Set initiative. 50 Questions examined excitement about the Games prior to the event and also frequency of use of the Olympic Park at follow-up. Adolescent questionnaires can be found in Appendices 1–3.
Parent/carer questionnaire
The content of the parent/carer questionnaire was similar to that of the adolescent questionnaire. The three primary outcomes (employment, mental health, and physical activity and behaviour) were identical but used instruments adapted for face-to-face adult interviews.
Primary outcome: employment
Parental/carer employment status was assessed using the standardised questions posed at the 2011 census for England and Wales. 40 Individual occupations were coded to SOC (Standard Occupational Classifications) 2010, which were further coded to the standard National Statistics Socioeconomic Classification System (NS-SEC). 51
Primary outcome: mental health
In addition to the WEMWBS assessment of positive well-being, parents/carers completed the Hospital Anxiety and Depression Scale (HADS). This is a validated 14-item questionnaire that detects depression and anxiety,52 with each item rated on a four-point scale with respect to the last week. Finally, experiences of job strain have been reported using a validated questionnaire assessing psychosocial job demands, decision latitude and social support at work. 53 Job characteristics are indicative of the quality of employment as well as being directly associated with mental health and cardiovascular outcomes. 54
Primary outcome: physical activity
Physical activities and behaviours were measured using the Recent Physical Activity Questionnaire (R-PAQ). The scale, developed by the MRC Epidemiology Unit at Cambridge University, describes the extent of physical activity around the house and travel to work patterns and determines recreational physical activity energy expenditure over the previous 4 weeks. This instrument has demonstrated validity for ranking individuals according to their time spent on vigorous-intensity activity and overall energy expenditure. 55
Secondary outcomes and exposures
Parent/carers’ sociodemographic factors included age, gender, relationship with the surveyed adolescent, ethnicity, religion, and their country of birth and that of their parents/carers. Socioeconomic indicators vary in their importance and meaning across the ethnic groups predominant in this east London sample. 56,57 Therefore, socioeconomic circumstances were captured using a battery of questions to assess the level of material deprivation, benefit receipts, financial difficulties and household living conditions. 58
A summary measure of physical and mental health was measured by the Short Form questionnaire-12 items (SF-12). 59 This is a shorter version of the Short Form-36 health questionnaire designed for use in clinical practice and research, health policy evaluations and general population surveys. 60 The SF-12 generated a mental component and physical component summary score and has been validated cross-culturally. 61 Adults additionally reported any specific physical or mental-health conditions from a list provided and described patterns of alcohol consumption, smoking and eating habits.
Neighbourhood perceptions were assessed by scales developed within the Multi-Ethnic Study of Atherosclerosis (MESA). 62 The six-item scale describes perceived aesthetic quality of the area, walkability of the environment, the availability of healthy foods, and levels of safety, violence and social cohesion within the neighbourhood.
Experiences and perceptions of discrimination were investigated by a seven-item questionnaire adapted from the Ethnic Minority Psychiatric Illness Rates in the Community (EMPIRIC) survey. 63,64
Respondents were asked a series of questions examining the extent of their participation and general attitudes towards the Olympic and Paralympic Games in 2012, adapted from wave 4 of the Understanding Society UK longitudinal study. 65 These questions distinguished between active participation, such as spectating, volunteering or being in paid employment at the Games, and passive engagement, namely watching events on television, listening on the radio or reading about them at home.
Fieldwork
Study protocols were drafted that detailed standard procedures in the preparation of fieldwork materials and duties and regulations during the in-school data collection. These quality management systems were implemented to ensure that all fieldworkers were trained to the same level and shared the same knowledge of the questionnaire. This helped to minimise the potential response bias introduced if fieldworkers provided differing levels of assistance or information to adolescents completing their questionnaire.
A pilot study was conducted on a subsample within a participating school to determine the appropriate length of the adolescent questionnaire, identify language or comprehension difficulties with the use of standard scales, and refine elements of the survey protocol focused on school and parental/carer consent, and adolescent assent. The questionnaire was designed so that the primary research outcomes were completed early in the schedule to ensure higher response rates, with secondary outcomes completed towards the end of the questionnaire, when there was a greater risk of non-response. For the main study at baseline, school-based data collection commenced in January 2012 and finished 3 weeks before the opening ceremony of the London 2012 Olympic and Paralympic Games, which were held on 27 July 2012.
Consent
One week prior to survey, the school provided each adolescent with an age-appropriate study information sheet and a study information sheet to take home to their parent/carer. The letter presented the opportunity for parents/carers to actively opt the adolescent out of the study at any time. Parental consent was therefore passively obtained if the opt-out form was not returned by the adolescent.
During the survey visit the questionnaire was explained orally prior to completion; all adolescents additionally provided active written assent prior to completing the survey, and all adolescents were reminded that they were free to withdraw at any time without consequence. Immediately following survey completion all students were provided with a copy of their assent form and a duplicate of the age-appropriate information sheet. They were invited to contact the ORiEL study team if they had further questions.
Written consent from the school Principal or authorised member of the school’s senior leadership team was obtained before fieldwork began in their school.
Response rates
Survey completion was defined as answering the final battery of questions. Any adolescent respondent who had a record of ‘non-compliance’ – either because the student was a random box ticker or it was obvious that the questionnaire was not being taken seriously – was removed from the database. This amounted to 18 individuals at wave 1, 15 individuals at wave 2 and 48 individuals at wave 3. Figures 2–4 show the percentage of respondents completing each item on the questionnaire at each wave, in which the x-axis represents the proportion of the questionnaire designated to each topic.
FIGURE 2.
The ORiEL baseline adolescent questionnaire: item completion by topic.
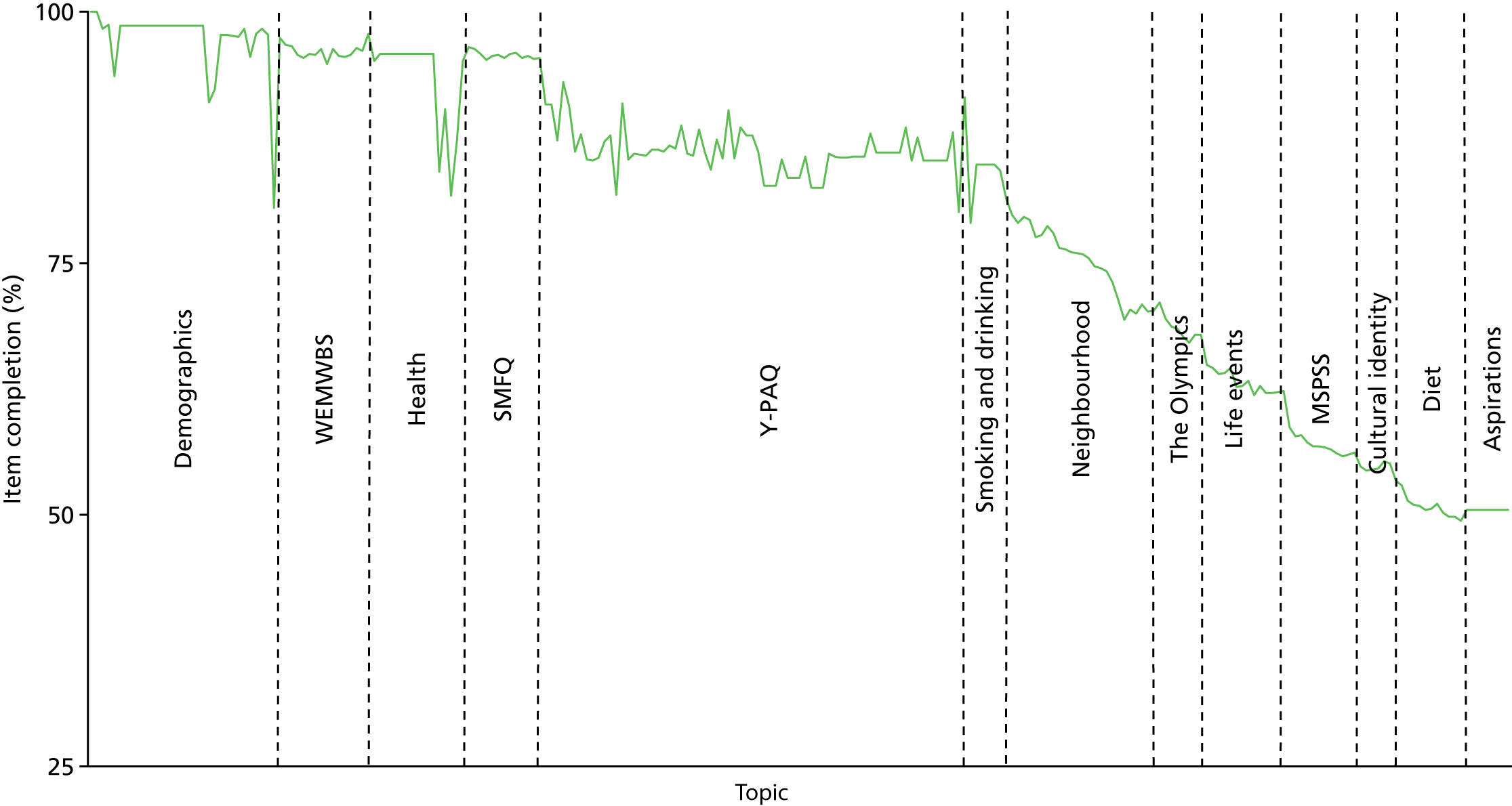
FIGURE 3.
The first ORiEL follow-up (wave 2) adolescent questionnaire: item completion by topic.
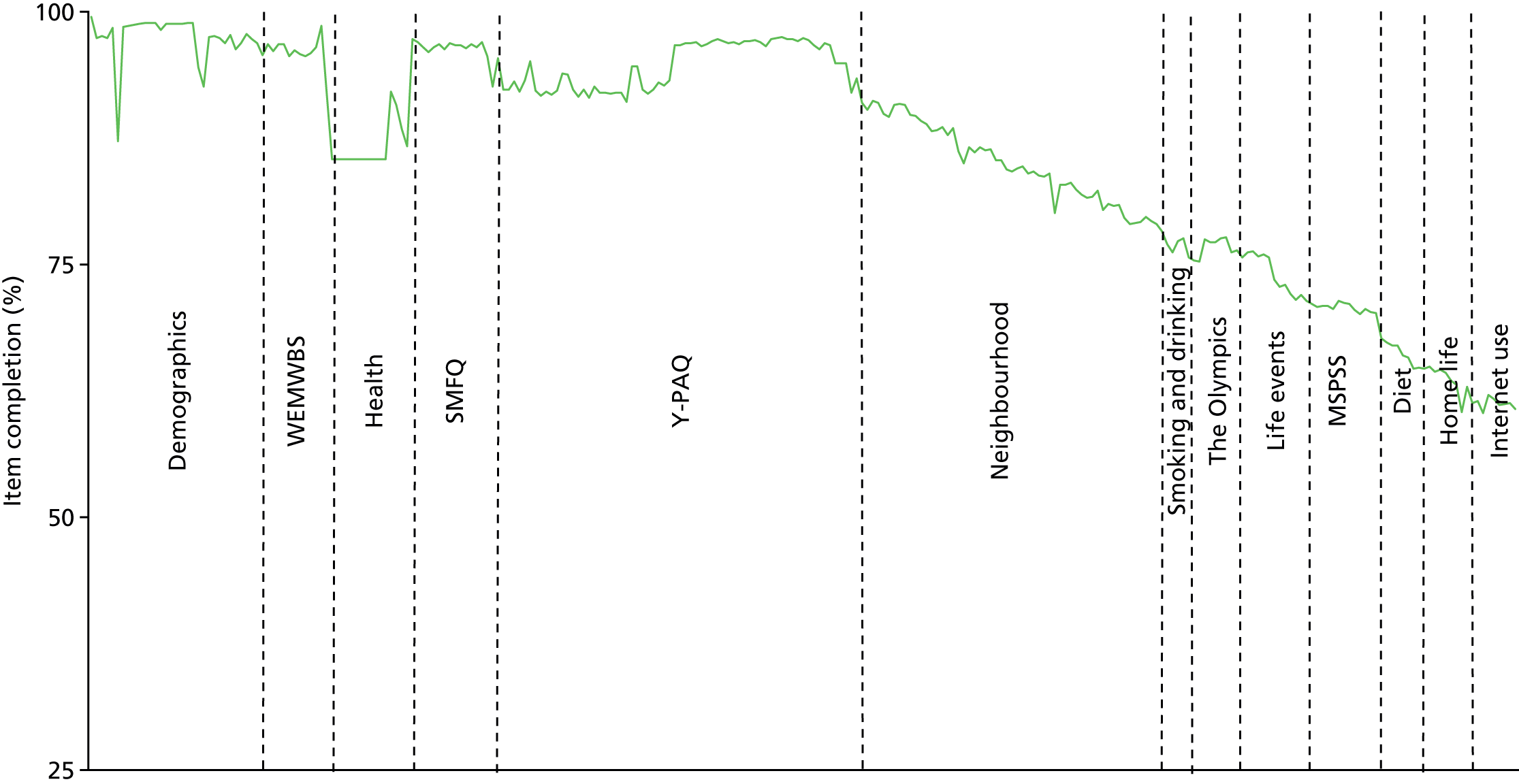
FIGURE 4.
The second ORiEL follow-up (wave 3) adolescent questionnaire: item completion by topic.
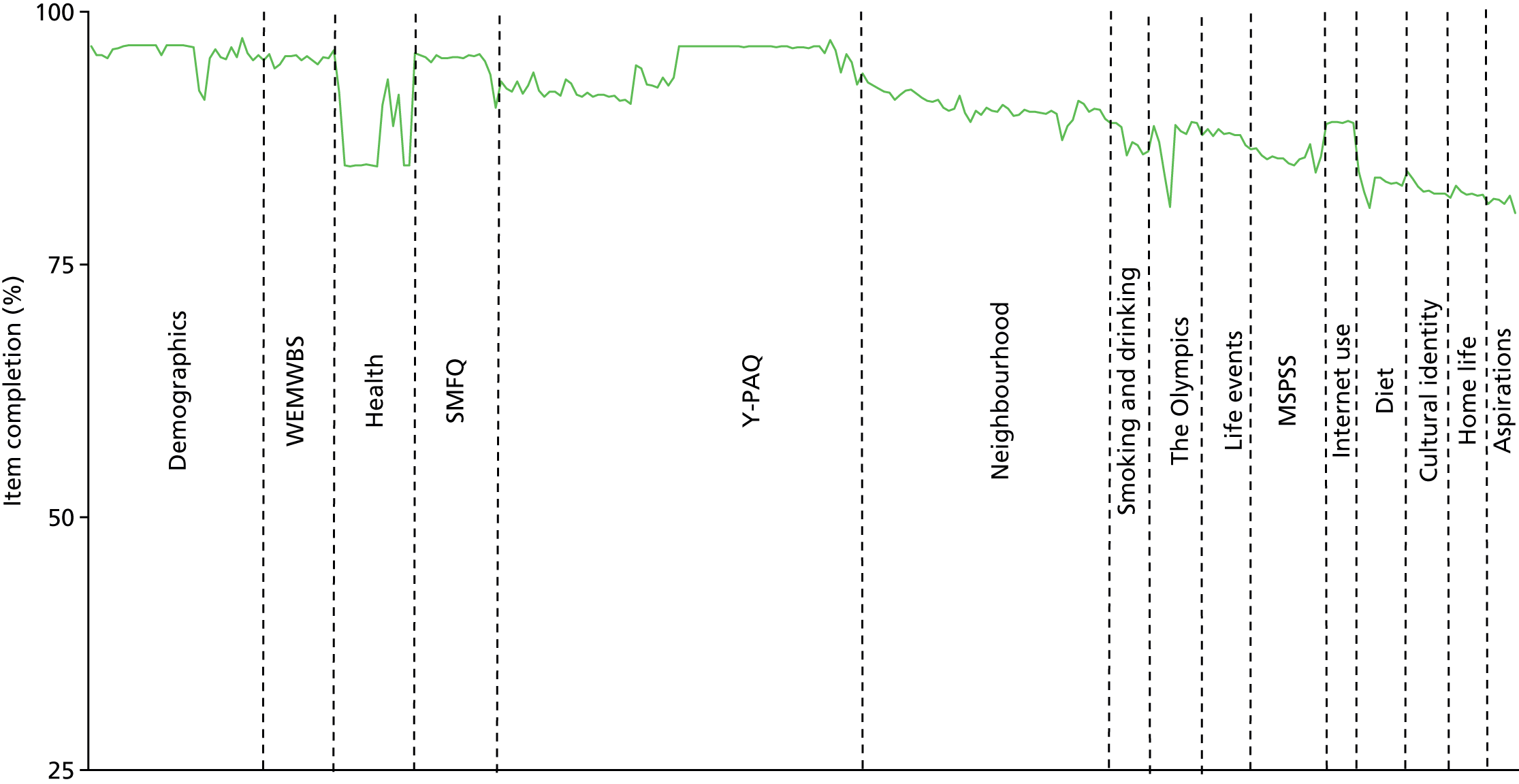
Full questionnaire completion at baseline was 50%, rising to 60% at first follow-up, increasing further still to 80% at second follow-up. Reasons for non-completion include unexpectedly short or interrupted questionnaire sessions; random sampling of streamed lower ability groups; higher levels of special educational needs; and lower than anticipated levels of literacy or English-language skills.
In order to invite parents/carers to participate in the study, we asked each adolescent participant for their home address. Overall, 88.8% of participants provided a valid home address at baseline. Addresses at first and second follow-up were derived by reconciling previous addresses with new details contained in the more recent follow-up questionnaires. This yielded addresses for 88.1% of participants at the first follow-up and for 86.7% at the second follow-up.
Parents/carers were also sent a letter of invitation describing the study’s aims and requesting participation in a doorstep interview. Those who did not wish to participate were asked to e-mail or ring the telephone number provided. If parents/carers did not opt out within 2 weeks of receiving the invitation, they were included in the doorstep interview schedule. Up to seven attempts to gain an interview were made before the participant was classified as a non-responder. Parents/carers were given the opportunity to refuse participation when first contacted by the market research fieldworkers and at any point during or after completion of the interview. Interviews were anonymised and parents/carers were linked to the relevant child.
Parent/carer interviews started in April 2012 and were completed by 27 July 2012. A market research agency administered the 35-minute face-to-face computer-assisted personal interview to consenting parents/carers and interviews were carried out at the parent/carer’s home address. To overcome any potential language problems, the parent/carer survey was translated into two of the most common non-English languages within the local community, namely Urdu and Bengali. Interviewers with particular language skills were allocated to specific participants, when required. All interviews were completed and had no missing data. The response rates were 60% at baseline, 51% at wave 2 and 57% at wave 3.
Data processing
Survey data entry was performed by an external agency with extensive experience in generating data files for longitudinal cohort studies. Variable names and coding structures were devised by the ORiEL research team and were implemented by the data entry contractor. Questionnaire data were double-punched and cleaned using range, consistency and logic checks. In a limited number of cases, the data were manually cleaned by ORiEL research staff when it was unclear to the third party what the correct coding should be.
Participants were allocated a unique identifier to allow us to track cohort members across waves while continuing to anonymise questionnaires. Adolescent and parent/carer names and addresses were stored separately from each other on encrypted USB drives. These were accessible by a single data custodian and were linked only temporarily by a unique identification number to produce lists of participants who were eligible for follow-up.
Environmental exposures and spatial data
Urban regeneration programmes related to the London 2012 Olympics were hypothesised to modify the built environment characteristics relevant to health either directly or indirectly. We therefore assessed whether or not environmental factors might be associated with health outcomes and behaviours at baseline and whether or not exposure to these environmental risks changed over the duration of our study.
All environmental and spatial data were obtained from a range of providers including local authority registers for food and alcohol, Transport for London, Ordnance Survey (OS) MasterMap, GiGL (Greenspace Information for Greater London) and Sport England. For further details, including information on the sourcing of all environmental data used within the study, see Appendix 4.
All data were cleaned and de-duplicated. A 10% random sample of environmental data for the food and alcohol establishments was selected and validated against Google StreetView.
We used ArcGIS, a geographical information system (GIS),66 to compute exposure to environmental risks. We identified five domains of environmental exposures that were relevant to the study:
-
the food environment
-
the alcohol environment
-
green space
-
sporting and recreation facilities
-
walkability.
In this report, owing to limitations of space, we focus our analyses on the main environmental exposures of interest that were hypothesised to be relevant to our primary outcomes and were most likely to change over the course of the study: green space and sporting and recreation facilities (see Chapter 4).
Environmental exposures: metric construction
In this study we use three distinct approaches to characterising environmental exposures: (1) proximity-based measures, (2) density-based measures and (3) ‘egocentric’ measures. A description of these is provided below.
Proximity-based measures
Proximity to the nearest environmental resource is estimated according to the shortest path distance in metres on the road network. The road network is given by the OS survey MasterMap Integrated Transport Network. The resolution of the distance, in all but a small number of cases, is address-point to address-point. For an aggregate of environmental resource types, the minimum distance for those types represents the shortest distance to a member of that aggregate class. Metric creation used the Esri ArcGIS version 10.3 network (Esri, Redlands, CA, USA) analyst extension.
Proximity measures were created for food establishments, premises selling alcohol, green spaces (access points), and sports and recreation facilities.
Density-based measures
An adaptive kernel density estimation (aKDE) approach is used to compute density surfaces covering the study area for which comprehensive point location data have been collected. The aKDE is carried out in the R package (The R Foundation for Statistical Computing, Vienna, Austria) sparr (http://cran.r-project.org/web/packages/sparr/sparr.pdf); map outputs have a cell size of 25 m, and intensity values indicate the estimated relative density of a given environmental resource type per km2 for the area covered by a given cell.
We used aKDE, as opposed to the standard fixed-bandwidth kernel density estimation, owing to the highly clustered nature of observations within the various environmental resource data sets. A fixed bandwidth approach would probably produce unsatisfactory results, over-smoothing areas with high resource numbers and under-smoothing areas with low numbers, resulting in a density surface that inadequately captures variation in density. An adaptive approach better preserves the locally varying densities across the study area.
The aKDE method computes a density based upon a Gaussian (normal) kernel, and employs adaptive smoothing on the basis of a ‘pilot bandwidth’. Fitting a locally adaptive kernel is an optimisation problem; the use of a pilot bandwidth simply acts to help limit the size of the bandwidth to within realistic bounds. The pilot bandwidth is first calculated in sparr using leave-one-out least-squares cross-validation (LSCV). In practice, this method can be unreliable for computing fixed bandwidths and has a tendency towards conservative estimates that over-smooth spatial data. However, as pilot bandwidth inputs for aKDE, they are effective at narrowing the search space so that a density surface can be computed in a reasonable time.
Density-based measures better represent the local availability of environmental resources than do proximity-based measures, although the two are closely related. Density-based measures incorporate the combined effect of all nearby resources, whereas proximity-based measures generally restrict investigation to the nearest resource, or the nearest k resources.
A density value representing environmental resources of different types per km2 was calculated for each respondent, and for each environmental resource type. Density values were summed within environmental themes (e.g. food environment, alcohol environment) in order to provide a density for a chosen aggregate of resource types within that environment theme.
Metric creation used the ESRI’s ArcGIS version 10.3 spatial analyst extension, and R version 3.0.2 with sparr 0.3–4, and spatstat 1.36–0. 67
Density-based measures were created for food establishments, premises selling alcohol, and sports and recreation facilities. Density-based measures could not be created for green-space access as it is not possible to compute a kernel density value for polygon data.
Egocentric measures
An egocentric residential neighbourhood is created for each study respondent based on an 800-m road network buffer, using the same reference data as the proximity-based measure. This distance is widely used in epidemiological literature as representing the 10-minute walking distance of an average person, and is therefore said to represent the likely extent of the immediate residential neighbourhood. 68
Using respondent home address, we computed a set of bespoke neighbourhood buffers for each ORiEL respondent. We counted the occurrences of each environmental resource that fell within each buffer to measure how many resources an individual can reach for a given egocentric neighbourhood. When green space is concerned, we count the number of access points for distinct green spaces that are contained within each egocentric neighbourhood (e.g. parks), avoiding the repeated count of the same green space if an individual can access more than one entrance point.
Egocentric neighbourhoods also underlie the creation of the walkability index. All the components of walkability are captured subject to the 800-m network buffer. We used the egocentric neighbourhood as a ‘cookie cutter’ in order to compute the denominators for each walkability component as follows:
-
Residential density is computed as the count of domestic addresses as a ratio of the area of residential building footprints within each egocentric 800-m neighbourhood.
-
Intersection density is computed as the count of junctions connected to three or more edges (loosely, streets) as a ratio of the kilometres of road within each egocentric 800-m neighbourhood.
-
Land use mix is computed using the normalised Shannon entropy formula69 for each egocentric neighbourhood, which effectively measures the evenness with which the three categories are distributed within the 800-m buffer. Residential, office and commercial land uses are computed as proportions of combined land use based on the building footprint area of buildings belonging to each category. Assigning building footprints to office, commercial or residential usage is done using the National Land Use Database classification implemented in the OS MasterMap AddressLayer 2 data.
Metric creation used the ESRI’s ArcGIS version 10.3 network, including the network analyst extension.
Egocentric measures were created for food establishments, premises selling alcohol, green spaces (access points to green spaces), sports and recreation facilities, and walkability.
Further details of analyses can be found in the relevant results chapters.
General approach to analysis
Many different quantitative analyses are summarised in this report. Further details on specific analyses can be found in the relevant chapters or in previously published papers. These are signposted in the text. Our overall approach was to use regression modelling to estimate associations between our dependent and independent variables, adjusting for hypothesised confounders. We employed a range of approaches including linear, logistic and multilevel regression depending on the data structure and outcomes under investigation. Some models were stratified by a priori effect modifiers, a key example being gender for analyses with physical activity as the main outcome. Multiple imputation was used to impute missing data (see the methods sections in each specific results chapter for further details) for the adolescent data set. There were no missing data in the parent or carer data set.
Intervention and comparison groups
Participants residing within Newham at baseline and subsequent waves of the study were considered to have received a greater ‘dose’ of urban regeneration. Participants residing in Barking and Dagenham, Hackney and Tower Hamlets at baseline and subsequent waves of the study were considered not to have received urban regeneration (or not such a strong dose of regeneration) and, therefore, formed the comparison group.
At baseline, participants were asked to give consent to be followed up even if they moved during the lifetime of the study. Pupils who moved to attend a different school already participating in the ORiEL study were followed up at their new school when possible. When pupils moved outside the study schools, these were no longer followed up as the administration cost involved was considered too high given the relatively small numbers involved. Very few participants moved schools across the waves, so an intent-to-treat (ITT) approach was taken for the analyses, based on the following approach. All participants are analysed as if they had remained living in the same borough that they lived in at baseline for subsequent waves.
This therefore involved analysis of the change in well-being, mental health and physical activity before the Olympics, 6 months after the Olympics and 18 months after the Olympics for Newham, compared with Tower Hamlets, Barking and Dagenham, and Hackney, using all those who took part at baseline. Some individuals may have moved boroughs during the project, swapping from control to intervention school, from intervention to control school, from one control school to another, or from one intervention school to another. More simply, they may have dropped out or moved out of the area completely. The ITT approach does not take into account any movement between schools or drop out after baseline. ITT is the typical approach taken in randomised controlled trials, based on the argument that it preserves randomisation. Alongside ITT, other sensitivity analyses were conducted and compared.
Attrition and missing data
Participant non-response was present in individual questionnaire items and by wave, introducing attrition. Attrition was explored through missing data patterns and logistic regression, investigating predictors of missingness by wave. Missingness by wave was not found to be associated with any predictors and supported the assumption that attrition followed a missing completely at random (MCAR) mechanism. With a MCAR mechanism we were able to create a non-biased cohort of adolescents present at all three waves.
For each analysis, the missing data mechanism was explored for individual questionnaire items. We found no violations against the assumption that the missing data mechanism is missing at random (MAR). Data were imputed using multiple imputation to gain statistical power, and sensitivity analysis was explored to check if inferences were robust to the MAR assumption. The imputation methodology used in each analysis is described in more detail in each of the results chapters.
Weighting
Design weights have been derived to address over- or under-sampling of specific cases or for disproportionate stratification and sample clustering. These weights are used when we want the sample under investigation to be representative of the population. Design weights are used in analyses in which clustering is considered a nuisance to be controlled for. When clustering or area effects are a point of interest, then a hierarchical multilevel model has been used to estimate these effects. Non-response weights for the data sets are not necessary; rather, we have adjusted our models for a range of covariates known to predict non-response such as age, gender and ethnicity.
Methods: qualitative study
The qualitative component of the ORiEL study aimed to examine local perceptions and experiences of the Olympic event and associated regeneration. This primarily consisted of an in-depth longitudinal qualitative study of family experiences and perceptions of the London 2012 Games and associated regeneration in Newham, the main Olympic borough. This entailed two waves of qualitative data collection, with the first period of fieldwork commencing immediately after the Games (2012) and the second wave a year later (2013). Here we describe data collection and our overall approach to analysis.
Recruitment and sampling
The qualitative sample comprised both a family sample and an adolescent sample. At wave 1 a total of 66 participants took part (Table 5). At wave 2 this fell to 40.
| Participants | Characteristic | Number of participants |
|---|---|---|
| Adult core participants (20 in total) | Sex | |
| Male | 8 | |
| Female | 12 | |
| Age (years) | ||
| Range | 20–55 | |
| Median | 40.5 | |
| Ethnicity | ||
| White British | 5 | |
| White other | 3 | |
| Black African | 4 | |
| Black British | 1 | |
| Indian | 1 | |
| Pakistani | 1 | |
| Bangladeshi | 1 | |
| Asian British | 2 | |
| Asian other | 1 | |
| Mixed | 1 | |
|
Those also in attendance at family narrative interviews (1) young people (19 in total) |
Sex | |
| Male | 10 | |
| Female | 9 | |
| Age (years) | ||
| 12 | 10 | |
| 13 | 6 | |
| 15 | 2 | |
| 16 | 1 | |
| Ethnicity | ||
| White British | 4 | |
| Black African | 3 | |
| Black British | 1 | |
| Indian | 2 | |
| Pakistani | 1 | |
| Bangladeshi | 1 | |
| Asian British | 2 | |
| Asian other | 2 | |
| Mixed | 3 | |
| (2) adults (1 in total) | Sex | |
| Female | 1 | |
| Age (years) | ||
| 45 | 1 | |
| Ethnicity | ||
| Asian other | 1 | |
| Adolescent core participants (26 in total) | Sex | |
| Male | 12 | |
| Female | 14 | |
| Age (years) | ||
| 12 | 13 | |
| 13 | 7 | |
| 14 | 4 | |
| 15 | 2 | |
| Ethnicity | ||
| White British | 8 | |
| White other | 6 | |
| Black African | 3 | |
| Black British | 1 | |
| Indian | 2 | |
| Pakistani | 2 | |
| Asian British | 2 | |
| Mixed | 2 | |
Family sample
Participants were recruited via the parent/carer quantitative survey. We wrote to all survey participants who had indicated that they were willing to be contacted again with a view to participating in further research. These letters were followed up with a telephone call inviting them to participate in the qualitative study. In total, 130 people were contacted in this way, of whom 20 made themselves available for interview at wave 1. We asked that these core participants invite other members of their household to participate in interviews as they saw fit. In all, an additional 19 young people and one spouse also took part. At wave 2 this fell to 15 core participants and an additional 13 of their family members.
Adolescent sample
In total, 26 adolescent core participants (12 boys and 14 girls) were recruited from three participating schools at wave 1 (two in Newham and a pilot in a neighbouring borough). School contacts, who served as gatekeepers for qualitative recruitment, were each asked to select up to nine students from their year 8 and 9 cohorts to participate in a half-day video focus group workshop. At wave 2 the pilot school dropped out and a total of 12 adolescents participated in the focus group workshops.
Data collection
Data were collected in three phases, with the same data collection activities used at both waves:
-
family narrative interviews with the family sample
-
go-along interviews with a subset of the family sample
-
school video focus group workshops with the adolescent sample.
Family narrative interviews
A family narrative interview was conducted with each of the families. The typical format for this was an interview with a parent/carer (core participant recruited from the adult survey) and their children. However, adult participants often invited other family members to participate, and sometimes the other family members decided themselves to join in. Two of the adult participants wanted to be interviewed alone without any other family members present. At wave 1, participants were asked to provide a narrative account of their experience of the Games and whether or not they felt that it affected them personally. The interview then moved on to focus on what had changed in their local area and daily life, and how they perceived their neighbourhood. At wave 2, we asked the families to revisit their original narratives and update us on events between waves. These interviews provided insight into how the Games were experienced as a spectacle in their own right and how participants positioned the Games and regeneration in relation to their own lives, trajectories and local areas.
Go-along interviews
A go-along interview is a mixture of observation and interview concentrated around a particular site, journey or activity. 70 The researcher can accompany the participant(s) on a routine journey or activity to a specific place or request that the participant give them a ‘tour’ of part of their familial environment. In this way the interviews can provide direct experience of the natural habitats of informants, and access to their practices and perceptions as they unfold in real time and space. 71 The accounts and narratives made by all participants in the preceding family interviews (described above) were extended in the go-along interviews with the aim of understanding how participants experienced these sites and how they related them to their own lives and practices.
School video focus group workshops
Half-day workshops were organised with three participating schools. Focus groups were used because these interviews generate rich information within a social context in which interaction between participants can reveal cultural values and group norms that may not arise in individual interviews. 72 The first half of the sessions was a focus group interview on participants’ perceptions and experiences of the Games and of their local neighbourhoods, followed by small group work in which students were split into groups and given the task of interviewing each other about aspects of neighbourhood experience arising from the focus group discussion. Safety and crime was a popular choice of topic for participants. The sessions were video recorded so that they could be viewed by these participants at the next wave of data collection and serve as a prompt for reflection and discussion. At wave 2 we showed the participants clips from wave 1 and asked them to update us and reflect on their contributions to the previous wave.
Ethics and informed consent
All parent/carer core participants (family sample) were provided with a study information sheet, a consent form, and a verbal explanation of what would happen to their data and of their right to withdraw at any time. It was also explained to them that other members of the household could participate in the narrative family interviews and go-along interviews at their discretion. In the case of the video focus group workshops, contact teachers were given opt-out parental/carer consent forms and information sheets to send out to the parents/carers of those adolescents they selected to participate. At the outset of the workshop sessions, separate consent forms and information sheets were distributed to deal with both the interview data and the video footage. It was explained to participants that their data would be anonymised and that they could withdraw from the study at any time. We also provided contact details should the participants wish to ask further questions of the research team. Full ethics approval for the qualitative study was obtained from the Queen Mary Research Ethics Committee.
Data analysis
Transcripts were analysed verbatim and were used to facilitate a narrative analysis of the whole data set for each sample (family and adolescent). Narrative approaches are particularly useful for understanding lived experiences of health because they examine how social conditions are perceived and handled and, thereby, how they constrain the freedom of individuals to act in such ways that these conditions could be transformed or avoided. 73 By analysing the data in this way, the researchers can examine how individuals interpret biographical experiences, and broader social trends and events, such as the Olympic Games, and how they position themselves in relation to them. It is the interpretation expressed by the participant that is important, namely how they explain their circumstances and account for their behaviours and perceptions, and how they construct narratives in analytically persuasive ways. 73
NVivo 9 (QSR International UK, Daresbury, Cheshire, UK) software was used to facilitate a qualitative longitudinal analysis of the data set. The aim of the analysis was to investigate the lived experiences of the social determinants of health and how these may have changed in the year after the Olympic Games. In order to understand the causal processes by which social conditions (such as housing) shape health, it is necessary to examine both how social conditions are perceived and how they constrain the freedom of individuals to act in such ways that these conditions could be transformed or avoided. 73 Data from all elements of the qualitative work were combined for analysis. As a result, the qualitative data set was large and multimodal, comprising a total of 632 pages of transcribed interviews, 38 pages of field notes and 211 minutes of video-recording. The stages of the analysis were as follows:
-
thematic coding of the whole data set
-
identification of narrative episodes and the production of a list of core narratives for comparison across waves
-
identifying and describing the progression and sequencing of themes into narrative sense-making within these episodes
-
tracking the changes and continuities of the conceptual categories and substantive content of personal narratives between waves
-
examining the way in which individuals deploy wider cultural discourses within their personal narratives74 and draw upon shared meanings. 74
Feedback for participants
For both arms of the study newsletters were produced annually to inform participants and schools of the emerging findings of the study. In addition, we volunteered to undertake masterclasses on social research methods for schools with a sixth form and produced certificates for schools that recognised their participation in the study.
Ethics approval
Overall, the study operated to the highest ethics standards and the study gained approval from the Queen Mary University of London Ethics Committee (QMREC2011/40), the Association of Directors of Children’s Services (RGE110927) and the London Boroughs Research Governance Framework (CERGF113).
Chapter 3 Social patterning of health and well-being in the ORiEL study
In the previous chapter we described the general methodological approach to this study and the data collected. In this chapter, we describe the patterning of our key primary health and well-being outcomes, for both adolescents and their parents/carers, with the aim of exploring and describing social inequalities in health in these groups within our baseline data. To do this, and for reasons of space, we focused on two key sets of outcomes: (1) the social patterning of physical activity and mental health for adolescents, and (2) the social patterning of employment for parents and carers.
Individual sociodemographic factors and perceptions of the environment as determinants of inequalities in adolescent physical and psychological health
In this section we describe the social patterning of health and well-being in the baseline survey of adolescents in the study. We explore associations between demographic, socioeconomic and environmental factors and physical/sedentary activity, physical health and psychological well-being. Full results can be found in Smith et al. 75
Methods
Results from the cross-sectional baseline survey are presented here and come from 3105 adolescents in year 7 of secondary school (aged 11–12 years) who completed a paper-based questionnaire during the 6 months (January to July 2012) prior to the start of the London 2012 Olympic and Paralympic Games.
Outcome measures
As described in Chapter 2, validated instruments were deployed to assess a range of health outcomes. The main items of interest for this analysis were mental well-being, depression, physical activity and sedentary behaviour, self-rated health and long-term illness or disability. These were operationalised as described in the following sections.
Mental well-being
Mental well-being was assessed using the WEMWBS. 28 This is a positively worded 14-point scale with five response categories capturing eudaimonic and hedonic perspectives of positive mental health. The total score ranges from 14 (lowest well-being) to 70 (highest well-being) and is reported as a mean value within groups. It has been validated in adolescents29 and cross-culturally,30 and was introduced as a core module to the nationally representative Health Survey for England in 2010. 43
Depressive symptoms
Depressive symptoms were investigated using the SMFQ. 31 This is a validated 13-item short form of the 32-item MFQ scored on a three-point scale of ‘true’, ‘sometimes true’ or ‘not true’. Scores range between 0 and 26, with total score of 8 or more indicating depressive symptoms.
Physical activity and sedentary behaviour
This was estimated using the self-reported Y-PAQ. 39 This questionnaire assesses the accumulated time spent physically active or sedentary, respectively, over the previous 7 days outside school. The total time spent physically active in recreational games and sports outside school was derived. Conversely, the total time involved in sedentary activities, including screen time, was also estimated for outside school. Individuals reporting > 75 hours of total activity per week (outside school) were excluded from the analysis because of probable over-reporting of time.
Self-rated health
Participants were asked to rate their own health in general and responses were dichotomised to fair/poor/very poor as opposed to good/very good. 44
Long-term illness or disability
Long-term illness or disability was defined as a health problem that has troubled the participant over a period of time, or that is likely to affect the participant over a period of time. 45 Examples included asthma, anaemia, eczema, type 1 and 2 diabetes mellitus, epilepsy, hearing and eyesight problems, and chronic fatigue syndrome.
Individual demographic, social and environmental factors
The distribution of health outcomes described above was explored across a range of individual demographic and household socioeconomic indicators as well as by individual perceptions of the local environment. These were are described in the following sections.
Demographic indicators
These included borough of residence, gender, ethnicity and whether or not the respondent was born in the UK. Self-reported ethnicity used the wording and adapted categories of the England and Wales census 2011. 40 These sample-specific and age-appropriate categories were derived via extensive piloting to capture the characteristics of the highly ethnically diverse sample in east London. The analysis includes the seven largest groups in the study, namely white UK, white mixed (‘white UK and any other background’), Indian, Pakistani, Bangladeshi, black Caribbean and black African. All other ethnic minority groups collapsed to the other category for analysis by health outcome.
Socioeconomic indicators
Adolescents were asked whether or not their parents/carers ‘had a job’ to determine if both parents/carers were not in paid employment (unemployed), if one parent was not in paid employment (one employed), if both were in paid employment (both employed) or if they were cared for by a lone parent carer in paid employment (lone parent employed) or a lone parent carer who was not employed (lone parent unemployed). Household socioeconomic circumstances were quantified by the FAS. 26 This four-item scale has been validated in young people cross-nationally26 and is predictive of physical activity and self-reported general and mental health. Adolescents were additionally asked whether or not they were in receipt of means-tested free school meals.
Perceptions of the environment
Adolescents were asked for their perception of their local neighbourhood, defined as the area they could walk to within 15 minutes from their house, using selected domains from an adapted and age-appropriate ALPHA questionnaire. 49 Statements about perceptions of neighbourhood safety, aesthetics and walkability/cycleability were rated on a four-point scale (strongly agree to strongly disagree) with an additional domain asking how near in minutes participants lived to a range of businesses or services. Owing to a positively skewed distribution of the summed scores, all four domains were split into tertiles representing a relatively positive, mixed or negative perception of each environmental characteristic.
Statistical analysis
Analyses presented here were completed using Stata 13.1 (Stata Corp LP, College Station, TX, USA). There are four stages to the analysis. The first stage uses the total sample available for each outcome to estimate the unadjusted mean mental well-being total score, mean total time spent in physical/sedentary activity, and the proportion self-reporting fair/(very) poor general health, long-term illness and depressive symptoms for all participating adolescents across the range of demographic, socioeconomic and environmental indicators. An unpaired t-test (for mean outcomes) or logistic regression (for binary outcomes) was used to test for significant differences between subcategories of covariates. The second stage repeated this analysis using a complete-case sample for each outcome. In the third stage, the prevalence of each outcome was then fully adjusted for all demographic, socioeconomic and environmental factors using a complete-case mixed-effects linear regression and a logistical (logit) regression model to account for clustering at the school level. Likelihood ratio tests were used to assess whether or not the variance for each outcome was attributable to the clustering effect within schools. Finally, the relationship between all health outcomes was examined using mixed-effects logistic and linear regression to account for clustering, adjusted for gender, country of birth, ethnicity, borough, parental carer employment, family affluence and all neighbourhood characteristics.
Results
The sociodemographic characteristics of the ORiEL baseline sample were broadly similar to a cohort of similar ages observed at the most recent 2011 census with some exceptions (see Table 3 for a description). Overall, the response rate was 87% (n = 3105 in school year 7). The archived study sample can be estimated at approximately 25% of the entire age group attending state schools in the catchment areas (n = 12,136 in school year 6).
The following tables (see Tables 6 to 11) present observations based on the analytic complete-case sample. The total sample available for analysis is also shown in each table and demonstrates that differences in prevalence and trends across categories of covariates did not differ greatly between the total sample available for analysis and the complete-case sample used to fully account for demographic, socioeconomic and environmental factors.
Mental health and well-being
The complete case-analysis observed that females self-reported significantly lower mental well-being than their male counterparts, but there were no differences according to ethnic group or generation (Table 6). Well-being was lowest in adolescents in Newham and was significantly higher in those attending schools in Tower Hamlets and Barking and Dagenham. Overall, there was a mixed relationship between well-being and socioeconomic disadvantage; there was a gradient effect, with well-being increasing significantly with increasing family affluence, but no differences were apparent according to free school meal status. After full adjustment, adolescents with a lone parent not in paid employment had significantly higher levels of well-being than adolescents with two parents/carers not in paid employment. However, for all environmental factors there was a statistically significant gradient effect, with those perceiving the neighbourhood more positively being more likely to report higher mental well-being scores. These differences remained after full adjustment. Such patterns were broadly similar for the prevalence of depressive symptoms (Table 7). In unadjusted and adjusted models, females were more likely to be at risk of depressive symptoms, with no variation by socioeconomic background. However, after full adjustment only Indian adolescents were significantly less likely to report depressive symptoms than the white UK group. As observed for mental well-being, there was a significant association between negative perceptions of neighbourhood safety and aesthetics and a greater risk of depressive symptoms. This observation was also significant after full adjustment.
| Variables | Full sample, unadjusted mean, % (n)b | Analytic sample (N = 1689) | |
|---|---|---|---|
| Unadjusted mean, % (n) | Fully adjusted mean (95% CI)c | ||
| Demographic | |||
| Gender | |||
| Maled | 51.6 (1692) | 52.3 (898) | 52.3 (51.7 to 52.9) |
| Female | 50.5 (1293)*** | 50.8 (791)*** | 50.8*** (50.2 to 51.4) |
| Ethnic group | |||
| White: UKd | 51.0 (579) | 51.4 (352) | 51.3 (50.4 to 52.3) |
| White: mixed | 50.9 (362) | 51.3 (183) | 51.4 (50.1 to 52.6) |
| Asian: Indian | 51.6 (106) | 52.6 (71) | 52.5 (50.5 to 54.5) |
| Asian: Pakistani | 49.8 (125) | 49.9 (78) | 50.4 (48.5 to 52.4) |
| Asian: Bangladeshi | 50.9 (500) | 51.5 (335) | 51.3 (50.3 to 52.3) |
| Black: Caribbean | 52.6 (138) | 52.6 (65) | 52.7 (50.6 to 54.8) |
| Black: African | 52.0 (342) | 51.8 (172) | 51.7 (50.4 to 53.0) |
| Other | 51.1 (803) | 51.9 (433) | 52.0 (51.1 to 52.8) |
| Nativity | |||
| UK bornd | 51.1 (2344) | 51.6 (1376) | 51.6 (51.2 to 52.1) |
| Born overseas | 51.3 (595) | 51.6 (313) | 51.5 (50.5 to 52.5) |
| Borough | |||
| Newhamd | 50.3 (856) | 50.7 (421) | 50.8 (50.0 to 51.6) |
| Tower Hamlets | 51.7 (790)** | 51.9 (476)* | 51.9 (51.1 to 52.7) |
| Barking and Dagenham | 51.7 (641)** | 52.1 (414)* | 52.5* (51.6 to 53.3) |
| Hackney | 51.1 (698) | 51.5 (378) | 51.1 (50.2 to 52.0) |
| Socioeconomic | |||
| Parental economic activity | |||
| Both unemployedd | 50.7 (273) | 50.8 (185) | 51.0 (49.6 to 52.4) |
| One parent/carer employed | 51.1 (920) | 51.7 (580) | 51.9 (51.2 to 52.6) |
| Both parents/carers employed | 51.7 (1020) | 51.9 (665) | 51.5 (50.7 to 52.2) |
| Lone parent/carer employed | 50.4 (229) | 50.6 (144) | 50.7 (49.3 to 52.2) |
| Lone parent/carer unemployed | 52.0 (171) | 52.3 (100) | 53.2* (51.5 to 55.0) |
| Does not live with parents/carers | 47.6 (28) | 49.3 (15) | 49.5 (45.0 to 54.0) |
| Family affluencee | |||
| Lowd | 50.2 (302) | 50.1 (179) | 50.0 (48.8 to 51.3) |
| Moderate | 50.8 (1527) | 51.3 (906) | 51.3* (50.8 to 51.9) |
| High | 51.9 (1034)** | 52.5 (604)* | 52.5** (51.8 to 53.2) |
| Free school meals | |||
| No mealsd | 51.3 (1758) | 51.7 (1100) | 51.6 (51.0 to 52.1) |
| Receives free meals | 50.8 (1173) | 51.4 (589) | 51.6 (50.8 to 52.4) |
| Environmental | |||
| Neighbourhood safetyf | |||
| Safed | 52.8 (619) | 53.3 (456) | 52.4 (51.6 to 53.2) |
| Mixed | 51.7 (762)* | 51.8 (573)* | 51.7 (51.0 to 52.4) |
| Not safe | 50.0 (942)*** | 50.3 (660)*** | 50.9* (50.2 to 51.6) |
| Neighbourhood aestheticsf | |||
| Pleasantd | 53.8 (554) | 53.8 (439) | 53.6 (52.7 to 54.4) |
| Mixed | 51.7 (676)*** | 52.0 (508)*** | 51.9** (51.2 to 52.7) |
| Unpleasant | 49.8 (1050)*** | 50.0 (742)*** | 50.2** (49.5 to 50.8) |
| Neighbourhood walk/cycleabilityf | |||
| Easy to walk/cycled | 52.8 (478) | 53.1 (367) | 53.2 (52.3 to 54.1) |
| Mixed | 50.8 (616)*** | 51.0 (487)*** | 51.2** (50.5 to 52.0) |
| Not easy to walk/cycle | 51.3 (1067)*** | 51.3 (835)** | 51.1** (50.5 to 51.7) |
| Proximity to businesses and servicesf | |||
| Close byd | 52.8 (626) | 53.0 (480) | 52.7 (52.0 to 53.5) |
| Mixed | 51.6 (809)* | 51.9 (581)* | 52.0 (51.3 to 52.7) |
| Far away | 50.4 (890)*** | 50.2 (628)*** | 50.3** (49.7 to 51.0) |
| Likelihood ratio test vs. linear regression | p = 1.00 | ||
| Variables | Full sample, prevalence, % (n)a | Analytic sample (N = 1641) | |
|---|---|---|---|
| Prevalence, % (n) | Fully adjusted odds ratio (95% CI)b | ||
| Demographic | |||
| Gender | |||
| Malec | 18.4 (1584) | 16.2 (872) | 1.00 (–) |
| Female | 27.5 (1237)*** | 27.4 (769)*** | 2.06*** (1.60 to 2.65) |
| Ethnic group | |||
| White: UKc | 24.8 (552) | 25.2 (345) | 1.00 (–) |
| White: mixed | 24.2 (343) | 25 (180) | 1.04 (0.67 to 1.63) |
| Asian: Indian | 15.8 (101) | 11.8 (68)* | 0.41* (0.18 to 0.91) |
| Asian: Pakistani | 24.6 (122) | 23.7 (76) | 0.82 (0.44 to 1.53) |
| Asian: Bangladeshi | 18.5 (487)* | 17.5 (326)* | 0.66 (0.43 to 1.03) |
| Black: Caribbean | 20.7 (135) | 24.2 (66) | 1.07 (0.56 to 2.05) |
| Black: African | 21.1 (313) | 19.1 (162) | 0.79 (0.48 to 1.29) |
| Other | 23.8 (741) | 21.5 (418) | 0.88 (0.61 to 1.27) |
| Nativity | |||
| UK bornc | 22.3 (2222) | 21.7 (1337) | 1.00 (–) |
| Born overseas | 22.2 (554) | 20.4 (304) | 1.02 (0.73 to 1.45) |
| Borough | |||
| Newhamc | 24.5 (795) | 22.9 (406) | 1.00 (–) |
| Tower Hamlets | 19.3 (751)* | 19.3 (466) | 0.78 (0.54 to 1.14) |
| Barking and Dagenham | 24.4 (607) | 23 (400) | 0.91 (0.62 to 1.34) |
| Hackney | 21.6 (668) | 20.9 (369) | 0.80 (0.54 to 1.19) |
| Socioeconomic | |||
| Parental economic activity | |||
| Both unemployedc | 25.6 (262) | 23.1 (182) | 1.00 (–) |
| One parent/carer employed | 21.5 (871) | 21.8 (559) | 0.84 (0.53 to 1.33) |
| Both parents/carers employed | 21.2 (970) | 20.4 (652) | 0.72 (0.43 to 1.20) |
| Lone parent/carer employed | 25.3 (217) | 22.3 (139) | 0.71 (0.39 to 1.31) |
| Lone parent/carer unemployed | 20.9 (163) | 18.8 (96) | 0.52 (0.27 to 1.00) |
| Does not live with parent/carer | 29.6 (27) | 46.2 (13) | 2.23 (0.67 to 7.41) |
| Family affluenced | |||
| Lowc | 25.3 (273) | 25.5 (165) | 1.00 (–) |
| Moderate | 22.4 (1459) | 21.6 (885) | 0.83 (0.55 to 1.24) |
| High | 21.4 (967) | 20.1 (591) | 0.73 (0.47 to 1.13) |
| Free school meals | |||
| No mealsc | 21.6 (1667) | 21.3 (1074) | 1.00 (–) |
| Receives free meals | 23.3 (1106) | 21.7 (567) | 0.91 (0.66 to 1.25) |
| Environmental | |||
| Neighbourhood safetye | |||
| Safec | 16.1 (597) | 15.5 (446) | 1.00 (–) |
| Mixed | 19.7 (731) | 18.9 (556) | 1.06 (0.75 to 1.51) |
| Not safe | 29.3 (895)*** | 27.9 (639)*** | 1.53* (1.08 to 2.17) |
| Neighbourhood aestheticse | |||
| Pleasantc | 15.8 (537) | 13.8 (427) | 1.00 (–) |
| Mixed | 19.5 (647) | 19.3 (493)* | 1.41 (0.97 to 2.05) |
| Unpleasant | 28.2 (997)*** | 27.5 (721)*** | 2.09*** (1.46 to 2.99) |
| Neighbourhood walk/cycleabilitye | |||
| Easy to walk/cyclec | 21.4 (454) | 20.6 (350) | 1.00 (–) |
| Mixed | 23.8 (589) | 23 (470) | 1.12 (0.79 to 1.59) |
| Not easy to walk/cycle | 21.5 (1039) | 21 (821) | 1.09 (0.79 to 1.51) |
| Proximity to businesses and servicese | |||
| Close byc | 20.1 (602) | 20 (465) | 1.00 (–) |
| Mixed | 19.8 (774) | 19.7 (563) | 0.93 (0.67 to 1.28) |
| Far away | 25.7 (860)* | 24.1 (613) | 1.17 (0.86 to 1.60) |
| Likelihood ratio test vs. logistic regression | p = 0.31 | ||
Physical and sedentary activity
In unadjusted complete-case models, girls spent significantly fewer hours (12.6 hours) than boys (14.0 hours) participating in physical activity (Table 8). This was consistent with girls spending a significantly greater number of hours per week in sedentary activity (35.6 hours) than boys (33.2 hours) (Table 9). Indian adolescents reported significantly higher participation in physical activity than the white UK comparison group, but there were no other ethnic differences in either physical or sedentary behaviour. There was mixed evidence of a socioeconomic influence on activity. There was a significant increase in the hours spent physically active with increasing family affluence, but no differences in physical and sedentary activity were observed for other socioeconomic factors. In terms of neighbourhood effects on activity, adolescents who described their neighbourhoods as more amenable to walking and cycling were significantly more likely to be physically active and less likely to be sedentary than those who described the neighbourhood as more difficult to walk or cycle in. All differences remained significant in fully adjusted models. Variation in the number of hours spent sedentary was significant at school level.
| Variables | Full sample, unadjusted mean, % (n)a | Analytic sample (N = 1060) | |
|---|---|---|---|
| Unadjusted mean, % (n)b | Fully adjusted mean (95% CI)c | ||
| Demographic | |||
| Gender | |||
| Maled | 14.4 (1068) | 14 (550) | 14.0 (13.3 to 14.8) |
| Female | 12.8 (872)*** | 12.6 (510)* | 12.6* (11.8 to 13.4) |
| Ethnic group | |||
| White: UKd | 13.6 (378) | 13.4 (231) | 13.5 (12.2 to 14.7) |
| White: mixed | 15 (232) | 13.8 (111) | 13.8 (12.0 to 15.5) |
| Asian: Indian | 16.7 (71)* | 17.8 (49)* | 17.6* (15.0 to 20.3) |
| Asian: Pakistani | 12.8 (87) | 12.2 (48) | 12.2 (9.6 to 14.9) |
| Asian: Bangladeshi | 12.3 (355) | 12.3 (233) | 12.4 (11.1 to 13.8) |
| Black: Caribbean | 13 (89) | 14.4 (39) | 14.8 (11.9 to 17.8) |
| Black: African | 13.7 (212) | 13.1 (91) | 13.0 (11.1 to 15.0) |
| Other | 14 (498) | 13.4 (258) | 13.2 (12.0 to 14.4) |
| Nativity | |||
| UK bornd | 13.6 (1515) | 13.2 (878) | 13.2 (12.5 to 13.8) |
| Born overseas | 13.9 (386) | 13.9 (182) | 14.3 (12.8 to 15.7) |
| Borough | |||
| Newhamd | 13.8 (567) | 13.7 (266) | 13.5 (12.4 to 14.6) |
| Tower Hamlets | 13.5 (530) | 12.4 (315) | 12.6 (11.5 to 13.7) |
| Barking and Dagenham | 13.5 (410) | 13.7 (257) | 14.0 (12.8 to 15.1) |
| Hackney | 14 (433) | 13.9 (222) | 13.5 (12.2 to 14.8) |
| Socioeconomic | |||
| Parental economic activity | |||
| Both unemployedd | 13.4 (195) | 13.3 (131) | 14.1 (12.2 to 16.0) |
| One parent/carer employed | 13.8 (600) | 13.3 (361) | 13.7 (12.7 to 14.7) |
| Both parents/carers employed | 13.7 (643) | 13.2 (412) | 12.6 (11.6 to 13.7) |
| Lone parent/carer employed | 13.7 (137) | 13.9 (80) | 13.7 (11.7 to 15.8) |
| Lone parent/carer unemployed | 13.3 (119) | 13.5 (70) | 13.8 (11.4 to 16.1) |
| Does not live with parents/carers | 16.8 (16) | 14.9 (6) | 13.5 (6.0 to 21.0) |
| Family affluencee | |||
| Lowd | 11.6 (223) | 11.1 (132) | 10.9 (9.2 to 12.5) |
| Moderate | 13.4 (1001)* | 13.1 (572)* | 13.1* (12.4 to 13.9) |
| High | 15.1 (623)** | 14.6 (356)*** | 14.6** (13.6 to 15.6) |
| Free school meals | |||
| No mealsd | 13.7 (1164) | 13.2 (700) | 13.1 (12.4 to 13.9) |
| Receives free meals | 13.8 (739) | 13.6 (360) | 13.8 (12.6 to 14.9) |
| Environmental | |||
| Neighbourhood safetyf | |||
| Safed | 13.4 (393) | 13.3 (282) | 13.4 (12.2 to 14.5) |
| Mixed | 13.7 (491) | 13.5 (370) | 13.4 (12.5 to 14.4) |
| Not safe | 13.4 (587) | 13.2 (408) | 13.3 (12.3 to 14.2) |
| Neighbourhood aestheticsf | |||
| Pleasantd | 13.6 (343) | 13.5 (271) | 13.6 (12.5 to 14.8) |
| Mixed | 13.3 (437) | 13.2 (322) | 13.2 (12.1 to 14.2) |
| Unpleasant | 13.7 (671) | 13.4 (467) | 13.3 (12.4 to 14.2) |
| Neighbourhood walk-cycleabilityf | |||
| Easy to walk/cycled | 14.9 (277) | 15 (218) | 15.1 (13.9 to 16.3) |
| Mixed | 13.1 (397)* | 13.2 (310)* | 13.2* (12.2 to 14.3) |
| Not easy to walk/cycle | 13 (687)** | 12.7 (532)** | 12.7** (11.9 to 13.5) |
| Proximity to businesses and servicesf | |||
| Close byd | 14.4 (367) | 14.4 (286) | 14.4 (13.3 to 15.5) |
| Mixed | 12.6 (522)* | 12.6 (367)* | 12.6* (11.7 to 13.6) |
| Far away | 13.7 (567) | 13.3 (407) | 13.3 (12.4 to 14.2) |
| Likelihood ratio test vs. linear regression | p = 0.20 | ||
| Variables | Full sample, unadjusted mean, % (n)a | Analytic sample (N = 1060) | |
|---|---|---|---|
| Unadjusted mean, % (n)b | Fully adjusted mean (95% CI)c | ||
| Demographic | |||
| Gender | |||
| Maled | 29.7 (1068) | 33.2 (550) | 33.1 (31.9 to 34.3) |
| Female | 31.9 (872)** | 35.6 (510)** | 35.5** (34.2 to 36.8) |
| Ethnic group | |||
| White: UKd | 31.8 (378) | 34.1 (231) | 33.9 (32.0 to 35.8) |
| White: mixed | 29.3 (232) | 34.1 (111) | 34.1 (31.4 to 36.8) |
| Asian: Indian | 31.7 (71) | 34.8 (49) | 34.5 (30.5 to 38.5) |
| Asian: Pakistani | 29.6 (87) | 34.1 (48) | 34.1 (30.0 to 38.2) |
| Asian: Bangladeshi | 31.2 (355) | 33.4 (233) | 33.6 (31.5 to 35.6) |
| Black: Caribbean | 32.5 (89) | 36.1 (39) | 35.9 (31.4 to 40.4) |
| Black: African | 31 (212) | 37.4 (91) | 37.2 (34.3 to 40.2) |
| Other | 29.8 (498) | 34.1 (258) | 34.0 (32.2 to 35.8) |
| Nativity | |||
| UK bornd | 31.4 (1515) | 34.4 (878) | 34.5 (33.5 to 35.5) |
| Born overseas | 28.9 (386) | 34.2 (182) | 33.3 (31.1 to 35.5) |
| Borough | |||
| Newhamd | 29.7 (567) | 35 (266) | 35.2 (33.3 to 37.0) |
| Tower Hamlets | 31.7 (530)* | 34.1 (315) | 34.3 (32.6 to 36.1) |
| Barking and Dagenham | 30.3 (410) | 33.9 (257) | 33.5 (31.6 to 35.4) |
| Hackney | 31.3 (433) | 34.3 (222) | 34.0 (31.9 to 36.0) |
| Socioeconomic | |||
| Parental economic activity | |||
| Both unemployedd | 31.7 (195) | 34.8 (131) | 34.2 (31.3 to 37.2) |
| One parent/carer employed | 29.8 (600) | 33.3 (361) | 33.2 (31.6 to 34.7) |
| Both parents/carers employed | 31.6 (643) | 35 (412) | 35.2 (33.6 to 36.8) |
| Lone parent/carer employed | 33.3 (137) | 33.7 (80) | 33.9 (30.7 to 37.1) |
| Lone parent/carer unemployed | 32.9 (119) | 35.9 (70) | 35.0 (31.4 to 38.6) |
| Does not live with parents/carers | 26.4 (16) | 32.5 (6) | 32.2 (20.8 to 43.7) |
| Family affluencee | |||
| Lowd | 31.1 (223) | 33.9 (132) | 33.7 (31.2 to 36.2) |
| Moderate | 31.4 (1001) | 34.6 (572) | 34.5 (33.3 to 35.7) |
| High | 30.4 (623) | 34 (356) | 34.1 (32.5 to 35.6) |
| Free school meals | |||
| No mealsd | 31.3 (1164) | 34 (700) | 33.9 (32.7 to 35.1) |
| Receives free meals | 30 (739) | 35 (360) | 35.0 (33.2 to 36.8) |
| Environmental | |||
| Neighbourhood safetyf | |||
| Safed | 32.8 (393) | 33.5 (282) | 33.4 (31.7 to 35.2) |
| Mixed | 35 (491)* | 35.3 (370) | 35.3 (33.8 to 36.8) |
| Not safe | 33 (587) | 34 (408) | 33.9 (32.4 to 35.4) |
| Neighbourhood aestheticsf | |||
| Pleasantd | 34.1 (343) | 34.2 (271) | 34.2 (32.4 to 36.0) |
| Mixed | 33.3 (437) | 34.7 (322) | 34.7 (33.1 to 36.3) |
| Unpleasant | 33.3 (671) | 34.1 (467) | 34.0 (32.6 to 35.4) |
| Neighbourhood walk-cycleabilityf | |||
| Easy to walk/cycled | 31.8 (277) | 32.9 (218) | 32.8 (30.9 to 34.7) |
| Mixed | 34.4 (397)* | 35 (310) | 34.7 (33.1 to 36.4) |
| Not easy to walk/cycle | 34 (687)* | 34.6 (532) | 34.6 (33.3 to 35.8) |
| Proximity to businesses and servicesf | |||
| Close byd | 32.9 (367) | 33.7 (286) | 33.7 (32.0 to 35.4) |
| Mixed | 33.6 (522) | 34.3 (367) | 34.0 (32.6 to 35.5) |
| Far away | 33.7 (567) | 34.8 (407) | 34.9 (33.4 to 36.3) |
| Likelihood ratio test vs. linear regression | p ≤ 0.001 | ||
Self-rated general health
The proportion of respondents reporting fair/very poor health by a range of factors is shown in Table 10. Over one-quarter of girls (28.6%) reported fair/very poor health, but the prevalence was significantly lower for boys (20.6%). Bangladeshi and black African adolescents were significantly more likely to report poor health than white UK adolescents after full adjustment. There was weak evidence of a socioeconomic gradient in self-rated health. Although adolescents with both parents/carers in employment were significantly less likely to report poor health, as were those who did not have free school meals, these differences were no longer significant in fully adjusted models. However, there was a strong and consistent association between positive perceptions of the neighbourhood and better reported general health across all three neighbourhood domains. These associations were also observed in fully adjusted models.
| Variables | Full sample, prevalence, % (n)a | Analytical sample (N = 1687) | |
|---|---|---|---|
| Prevalence, % (n) | Fully adjusted odds ratio (95% CI)b | ||
| Demographic | |||
| Gender | |||
| Malec | 21.8 (1723) | 20.6 (899) | 1.00 (–) |
| Female | 26.8 (1315)** | 28.6 (788)*** | 1.67*** (1.32 to 2.12) |
| Ethnic group | |||
| White: UKc | 19 (590) | 20.2 (351) | 1.00 (–) |
| White: mixed | 25.5 (373)* | 25.4 (185) | 1.41 (0.90 to 2.20) |
| Asian: Indian | 21.3 (108) | 21.1 (71) | 1.18 (0.61 to 2.27) |
| Asian: Pakistani | 25.8 (128) | 26.3 (76) | 1.37 (0.75 to 2.51) |
| Asian: Bangladeshi | 30.5 (501)** | 29.9 (334)** | 1.65* (1.10 to 2.48) |
| Black: Caribbean | 22.2 (144) | 22.4 (67) | 1.29 (0.67 to 2.51) |
| Black: African | 24.5 (355)* | 27.4 (175)* | 1.81* (1.15 to 2.86) |
| Other | 23.2 (810)* | 22 (428) | 1.33 (0.91 to 1.93) |
| Nativity | |||
| UK bornc | 25 (2372) | 25.4 (1372) | 1.00 (–) |
| Born overseas | 19.5 (614)** | 19.7 (315)* | 0.64** (0.46 to 0.90) |
| Borough | |||
| Newhamc | 25.8 (875) | 28.8 (420) | 1.00 (–) |
| Tower Hamlets | 27.4 (793) | 27.9 (476) | 0.87 (0.62 to 1.21) |
| Barking and Dagenham | 21.5 (657)* | 21 (415)** | 0.64* (0.45 to 0.91) |
| Hackney | 20.2 (713)** | 18.4 (376)*** | 0.53** (0.36 to 0.77) |
| Socioeconomic | |||
| Parental economic activity | |||
| Both unemployedc | 28.8 (278) | 29 (186) | 1.00 (–) |
| One parent/carer employed | 25 (929) | 24.7 (575) | 0.81 (0.53 to 1.25) |
| Both parents/carers employed | 20.9 (1036)** | 21.5 (671)* | 0.82 (0.51 to 1.31) |
| Lone parent/carer employed | 21.6 (227) | 22.9 (140) | 0.85 (0.47 to 1.52) |
| Lone parent/carer unemployed | 28.1 (171) | 30 (100) | 1.06 (0.60 to 1.87) |
| Does not live with parent/carer | 41.4 (29) | 53.3 (15) | 3.80 (1.24 to 11.66) |
| Family affluenced | |||
| Lowc | 25.6 (308) | 26.3 (179) | 1.00 (–) |
| Moderate | 24.7 (1548) | 25.5 (909) | 1.05 (0.71 to 1.54) |
| High | 22.6 (1048) | 21.9 (599) | 0.99 (0.65 to 1.50) |
| Free school meals | |||
| No mealsc | 22.2 (1783) | 22.7 (1103) | 1.00 (–) |
| Receives free meals | 26.6 (1197)** | 27.4 (584)* | 1.01 (0.75 to 1.37) |
| Environmental | |||
| Neighbourhood safetye | |||
| Safec | 18.6 (625) | 18.7 (460) | 1.00 (–) |
| Mixed | 24.5 (758)** | 24.6 (568)* | 1.31 (0.95 to 1.80) |
| Not safe | 27.7 (949)*** | 27.9 (659)*** | 1.45* (1.04 to 2.01) |
| Neighbourhood aestheticse | |||
| Pleasantc | 20.1 (551) | 20.5 (435) | 1.00 (–) |
| Mixed | 20.9 (681) | 20.7 (513) | 1.01 (0.73 to 1.41) |
| Unpleasant | 28 (1056)*** | 29.1 (739)** | 1.45* (1.06 to 1.99) |
| Neighbourhood walk-cycleabilitye | |||
| Easy to walk/cyclec | 19.8 (475) | 20.1 (364) | 1.00 (–) |
| Mixed | 24.9 (618)* | 25.1 (486) | 1.32 (0.94 to 1.86) |
| Not easy to walk/cycle | 25.7 (1076)* | 25.7 (837)* | 1.51* (1.10 to 2.07) |
| Proximity to businesses and servicese | |||
| Close byc | 21 (629) | 20.2 (476) | 1.00 (–) |
| Mixed | 23 (816) | 23.4 (582) | 1.13 (0.83 to 1.53) |
| Far away | 27.9 (896)** | 28.3 (629)** | 1.51** (1.12 to 2.04) |
| Likelihood ratio test vs. logistic regression | p = 0.47 | ||
Long-term illness
Table 11 shows the prevalence estimates and factors associated with having a long-term illness. There were no gender differences in long-term illness. Prevalence varied widely among ethnic groups. Participants from the black Caribbean and white mixed groups were significantly more likely to report a long-term illness than their white UK counterparts in unadjusted models. After adjustment, participants from the ‘other’ ethnic group were also significantly more likely to report a long-term illness. Adolescents born overseas were significantly less likely to report having a long-term illness, but this finding was not significant following adjustment. There were no associations between any of the socioeconomic indicators and long-term illness. However, there was a graded increase in the odds of having a long-term illness as perceptions of neighbourhood safety and aesthetics worsened, although this finding was no longer significant for the case of aesthetics after adjusting for covariates. No association was observed for walk/cycleability or proximity to services in the local area.
| Variables | Full sample, prevalence, % (n)a | Analytical sample (N = 1689) | |
|---|---|---|---|
| Prevalence, % (n) | Fully adjusted mean (95% CI)b | ||
| Demographic | |||
| Gender | |||
| Malec | 42.1 (1694) | 40.9 (898) | 1.00 (–) |
| Female | 42.6 (1310) | 41 (791) | 1.02 (0.84 to 1.25) |
| Ethnic group | |||
| White: UKc | 42.8 (584) | 38.6 (352) | 1.00 (–) |
| White: mixed | 48.4 (364) | 50.5 (184)* | 1.75** (1.20 to 2.54) |
| Asian: Indian | 40.2 (107) | 36.6 (71) | 1.03 (0.59 to 1.79) |
| Asian: Pakistani | 48 (127) | 42.1 (76) | 1.18 (0.70 to 2.01) |
| Asian: Bangladeshi | 39.9 (499) | 38.3 (334) | 1.01 (0.72 to 1.44) |
| Black: Caribbean | 51.1 (139) | 52.2 (67)* | 1.87* (1.09 to 3.22) |
| Black: African | 31.5 (349)* | 32.8 (174) | 0.87 (0.58 to 1.31) |
| Other | 43 (805) | 42.7 (431) | 1.36* (1.00 to 1.86) |
| Nativity | |||
| UK bornc | 43.2 (2342) | 42.1 (1372) | 1.00 (–) |
| Born overseas | 38 (610)* | 36 (317)* | 0.77 (0.58 to 1.02) |
| Borough | |||
| Newhamc | 42.3 (863) | 41.3 (421) | 1.00 (–) |
| Tower Hamlets | 43.1 (789) | 41.7 (477) | 1.02 (0.76 to 1.37) |
| Barking and Dagenham | 41.9 (642) | 40.8 (414) | 0.98 (0.73 to 1.33) |
| Hackney | 42 (710) | 39.5 (377) | 0.81 (0.59 to 1.11) |
| Socioeconomic | |||
| Parental economic activity | |||
| Both unemployedc | 44.4 (277) | 39.8 (186) | 1.00 (–) |
| One parent/carer employed | 41.8 (922) | 40.1 (574) | 0.99 (0.67 to 1.45) |
| Both parents/carers employed | 41.3 (1024) | 41.3 (671) | 1.00 (0.65 to 1.53) |
| Lone parent/carer employed | 41.9 (229) | 40.6 (143) | 0.95 (0.58 to 1.58) |
| Lone parent/carer unemployed | 46.2 (171) | 46 (100) | 1.21 (0.72 to 2.01) |
| Does not live with parent/carer | 41.4 (29) | 40 (15) | 0.92 (0.0 to 2.81) |
| Family affluenced | |||
| Lowc | 39.3 (303) | 39.3 (178) | 1.00 (–) |
| Moderate | 43.2 (1534) | 42.2 (912) | 1.15 (0.82 to 1.61) |
| High | 41 (1034) | 39.4 (599) | 0.99 (0.69 to 1.42) |
| Free school meals | |||
| No mealsc | 41.5 (1755) | 41.1 (1101) | 1.00 (–) |
| Receives free meals | 43.2 (1188) | 40.6 (588) | 0.89 (0.68 to 1.16) |
| Environmental | |||
| Neighbourhood safetye | |||
| Safec | 38.2 (621) | 38 (460) | 1.00 (–) |
| Mixed | 39.2 (755) | 36.7 (570) | 0.94 (0.72 to 1.22) |
| Not safe | 47.3 (942)* | 46.6 (659)** | 1.35* (1.03 to 1.78) |
| Neighbourhood aestheticse | |||
| Pleasantc | 37.5 (550) | 36.6 (437) | 1.00 (–) |
| Mixed | 41.9 (677) | 40.5 (511) | 1.16 (0.89 to 1.53) |
| Unpleasant | 44.2 (1051)** | 43.7 (741)* | 1.17 (0.89 to 1.54) |
| Neighbourhood walk-cycleabilitye | |||
| Easy to walk/cycle | 43 (474) | 43.1 (364) | 1.00 (–) |
| Mixed | 40.1 (614) | 39.2 (485) | 0.81 (0.61 to 1.07) |
| Not easy to walk/cycle | 41.1 (1074) | 41 (840) | 0.95 (0.74 to 1.23) |
| Proximity to businesses and servicese | |||
| Close by | 41.9 (626) | 39.9 (481) | 1.00 (–) |
| Mixed | 41.6 (806) | 41.9 (580) | 1.09 (0.85 to 1.40) |
| Far away | 42.9 (892) | 40.8 (628) | 1.02 (0.79 to 1.31) |
| Likelihood ratio test vs. logistic regression | p = 0.39 | ||
The co-occurrence of selected health outcomes after full adjustment for all covariates is described in Table 12. Poor general health, having a long-term illness, lower levels of mental well-being and having depressive symptoms were all strongly associated with one another. However, there were no significant associations between the mean hours spent physically active or sedentary and all other health outcomes.
| Health outcome | Health outcome | ||||
|---|---|---|---|---|---|
| Has long-term illness, odds ratio (95% CI) | Has depressive symptoms, odds ratio (95% CI) | Mean WEMWBS score (95% CI)a | Mean hours of sedentary activity (95% CI)a | Mean hours of physical activity (95% CI)a | |
| Fair/poor general health | 1.51 (1.20 to 1.92)*** | 2.17 (1.65 to 2.84)*** | –3.78 (–4.74 to 2.81)*** | 1.85 (–0.18 to 3.88) | 0.25 (–1.09 to 1.58) |
| Has long-term illness | – | 1.59 (1.24 to 2.05)*** | –1.38 (–2.21 to –0.55)** | 0.10 (–1.66 to 1.85) | 0.16 (–0.99 to 1.31) |
| Has depressive symptoms | – | – | –7.87 (–8.83 to 6.91)*** | 2.38 (0.20 to 4.56) | –0.16 (–1.56 to 1.27) |
| Mean WEMWBS score | – | – | – | 0.03 (–0.01 to 0.06) | 0.05 (–0.01 to 0.10) |
| Mean hours sedentary activity | – | – | – | – | –0.21 (–0.30 to –0.12) |
Summary
Here we aimed to identify the sociodemographic and environmental determinants of a range of physical and mental health outcomes in an inner-city school-based population of adolescents aged 11–12 years. Evidence for socioeconomic inequalities in health at this age appeared to be mixed. Although physical activity increased with family affluence and general health was worse in those receiving free school meals, there was a mixed relationship with well-being and no relationship with depressive symptoms or long-term illness. However, the impact of the environment was much stronger and consistent across a range of neighbourhood metrics. Concurrent with previous findings across national contexts, adolescents who perceived their neighbourhoods positively had better mental health,76,77 reported better general health,78 were more likely to take part in physical exercise79,80 and were less likely to have a long-term illness. The association between neighbourhood perceptions and health has been repeatedly explained by the socioeconomic and demographic characteristics of the individuals. Here we controlled for a range of these confounding factors, which attenuated the associations, but overall they remained significant for all outcomes. In terms of demographics there were strong gender differences, with girls more likely to have poorer mental health, report poorer general health and lead more of a sedentary lifestyle than boys. Ethnic differences in reported general health in particular suggest that there are important differences between groups that must be fully understood when attempting to explain health inequalities in adolescents.
Labour market status and psychological health and well-being in parents/carers
In this section we describe the social patterning of employment, unemployment and psychological health and well-being in parents/carers in each wave of the study. We then explore associations between labour market status and psychological health and well-being. In order to do this, we answer the following research questions:
-
What is the prevalence of employment, unemployment and economic activity among primary respondents, and how does this change over time?
-
What proportion of primary respondents reside in a workless household, that is, a household in which no resident adult is employed? How does this change over time?
-
Is individual-level labour market status associated with psychological distress or psychological well-being, independently of demographic characteristics?
-
Is household-level worklessness associated with psychological distress or psychological well-being, independently of demographic characteristics?
Methods
Three cross-sectional analytical samples were derived to allow complete-case analysis of each wave. Two exposure variables were derived: (1) individual-level employment status (employed, economically inactive, unemployed); and (2) household worklessness status (primary respondent residing in a household where no resident adult reports employment, primary respondent residing in a household where at least one resident adult reports employment). Two mental health outcomes were utilised: (1) psychological distress (anxiety or depression risk) as measured by the HADS; and (2) psychological well-being as measured by the WEMWBS. These two outcomes were both dichotomised to create binary outcomes indicating caseness.
Descriptive analyses of the two exposure variables was undertaken for each wave. In order to investigate the relationships between individual and household labour market disadvantage and the two complementary mental health outcomes, four pairs of nested multivariate logistic regression models were fitted using baseline cross-sectional data. Age, sex and ethnic group were adjusted for in each case.
Results
The most prevalent individual-level labour market status was employment, accounting for 42% of primary respondents at wave 1, 43% at wave 2 and rising to 51% at wave 3. Table 13 shows the distribution of labour market status at each wave for repeated cross-sections of primary respondents. Approximately one-third of individuals were economically inactive because of homemaking and care-giving responsibilities. Labour market non-participation owing to long-term sickness accounted for 3% of respondents at waves 1 and 2, rising to 5% at wave 3. In total, 15% of individuals reported being unemployed (either actively searching for work or not) at wave 1. This decreased substantially to 9% at wave 2 and 7% at wave 3.
| Respondent labour market status | Frequency (%) | ||
|---|---|---|---|
| Wave 1 | Wave 2 | Wave 3 | |
| In work | 538 (42.4) | 448 (43.58) | 523 (50.53) |
| Retired | 20 (1.58) | 17 (1.65) | 14 (1.35) |
| Student | 41 (3.23) | 19 (1.85) | 35 (3.38) |
| Homemaker | 388 (30.58) | 368 (35.8) | 328 (31.69) |
| Long-term sickness | 37 (2.92) | 35 (3.4) | 51 (4.93) |
| Unemployed | 195 (15.37) | 89 (8.66) | 72 (6.96) |
| Refused/other | 50 (3.94) | 52 (5.06) | 12 (1.16) |
| Total | 1269 (100) | 1028 (100) | 1035 (100) |
Table 14 describes the distribution of primary respondents residing in a workless household, that is, an address at which no resident adult reported being employed. Across all three waves the majority of households included at least one working adult: 67% at wave 1, 70% at wave 2 and 69% at wave 3.
| Household work status | Frequency (%) | ||
|---|---|---|---|
| Wave 1 | Wave 2 | Wave 3 | |
| Working household | 820 (67.10) | 569 (69.65) | 654 (68.99) |
| Workless household | 402 (32.90) | 248 (30.35) | 294 (31.01) |
| Total | 1222 (100) | 817 (100) | 948 (100) |
Regarding the relationship between labour market status and mental health, results from the baseline data corroborate findings from a large and consistent body of previous research. Individual- and household-level labour market disadvantage is significantly associated with greater odds of psychological distress, and with lower odds of psychological well-being. Table 15 shows that, irrespective of gender, age and ethnicity, unemployed individuals were 70% more likely to be at risk of anxiety or depression than employed individuals [adjusted odds ratio (aOR) 1.71, 95% confidence interval (CI) 1.18 to 2.47]. Likewise, economically inactive respondents (primarily homemakers) were 60% more likely to be at risk of minor psychiatric morbidity (aOR 1.59, 95% CI 1.17 to 2.16) than their working counterparts.
| Outcome: HADS caseness (n = 1050) | Model | |||||
|---|---|---|---|---|---|---|
| 1 | 2 | |||||
| OR | p-value | 95% CI | OR | p-value | 95% CI | |
| Respondent employed | 1 | 1 | ||||
| Respondent inactive | 1.77 | < 0.001 | 1.34 to 2.34 | 1.59 | 0.003 | 1.17 to 2.16 |
| Respondent unemployed | 1.70 | 0.004 | 1.18 to 2.44 | 1.71 | 0.005 | 1.18 to 2.47 |
| Age | 1.02 | 0.017 | 1.00 to 1.04 | |||
| Gender | ||||||
| Male | 1.00 | |||||
| Female | 1.52 | 0.015 | 1.08 to 2.12 | |||
| Ethnicity | ||||||
| White: UK | 1.00 | |||||
| White: mixed | 1.54 | 0.324 | 0.65 to 3.61 | |||
| Asian: Indian | 1.24 | 0.492 | 0.67 to 2.32 | |||
| Asian: Pakistani | 1.00 | 0.996 | 0.53 to 1.89 | |||
| Asian: Bangladeshi | 1.10 | 0.627 | 0.75 to 1.62 | |||
| Black: Caribbean | 1.23 | 0.501 | 0.67 to 2.27 | |||
| Black: African | 0.63 | 0.036 | 0.41 to 0.97 | |||
| Other ethnicity | 1.05 | 0.795 | 0.72 to 1.54 | |||
The results presented in Table 16 suggest that household-level labour market attachment also predicts the psychological distress status of individuals. Respondents from workless households were 2.5 times more likely to be at risk of anxiety or depression than those residing in a household where at least one adult works, after adjustment for demographic characteristics (aOR 2.49, 95% CI 1.90 to 3.27). Across both individual- and household-level labour market status models, being female was associated with greater odds of psychological distress and emerged as a statistically significant covariate. Although the majority of ethnic groups were not significantly different from the white British reference category with regard to their HADS caseness, and the ethnicity variable was not a statistically significant covariate overall, those of black African origin were significantly less likely to be at risk of anxiety and depression when accounting for age, gender and labour market status.
| Outcome: HADS caseness (n = 1054) | Model | |||||
|---|---|---|---|---|---|---|
| 1 | 2 | |||||
| OR | p-value | 95% CI | OR | p-value | 95% CI | |
| Household not workless | 1 | 1 | ||||
| Household workless | 2.45 | < 0.001 | 1.88 to 3.20 | 2.49 | < 0.001 | 1.90 to 3.27 |
| Age | 1.02 | 2.51 | 0.01 to 1.00 | |||
| Male | 1 | 1 | ||||
| Female | 1.56 | 0.007 | 1.13 to 2.16 | |||
| White: UK | 1 | 1 | ||||
| White: mixed | 1.42 | 0.433 | 0.59 to 3.39 | |||
| Asian: Indian | 1.47 | 0.227 | 0.79 to 2.76 | |||
| Asian: Pakistani | 1.14 | 0.683 | 0.61 to 2.14 | |||
| Asian: Bangladeshi | 1.22 | 0.305 | 0.83 to 1.80 | |||
| Black: Caribbean | 1.20 | 0.549 | 0.66 to 2.20 | |||
| Black: African | 0.60 | 0.023 | 0.39 to 0.93 | |||
| Other ethnicity | 1.11 | 0.581 | 0.76 to 1.64 | |||
Tables 17 and 18 suggest that individual- and household-level worklessness are associated with reduced odds of psychological well-being: a concept related to but distinct from the dimensions of negative affect measured by HADS. Controlling for age, sex and ethnicity, respondents who were unemployed or economically inactive were twice as likely as their employed counterparts to fall below the UK population average for psychological well-being, as measured by WEMWBS.
| Outcome: WEMWBS caseness (n = 1050) | Model | |||||
|---|---|---|---|---|---|---|
| 1 | 2 | |||||
| OR | p-value | 95% CI | OR | p-value | 95% CI | |
| Respondent employed | 1 | 1 | ||||
| Respondent inactive | 2.10 | < 0.001 | 1.45 to 3.06 | 2.04 | 0.001 | 1.36 to 3.06 |
| Respondent unemployed | 1.93 | 0.007 | 1.20 to 3.10 | 2.09 | 0.003 | 1.28 to 3.40 |
| Age | 1.03 | 0.001 | 1.01 to 1.06 | |||
| Male | 1 | |||||
| Female | 1.30 | 0.247 | 0.83 to 2.03 | |||
| White: UK | 1 | |||||
| White: mixed | 0.91 | 0.872 | 0.29 to 2.83 | |||
| Asian: Indian | 0.56 | 0.215 | 0.22 to 1.40 | |||
| Asian: Pakistani | 0.71 | 0.417 | 0.31 to 1.63 | |||
| Asian: Bangladeshi | 0.80 | 0.356 | 0.49 to 1.29 | |||
| Black: Caribbean | 0.84 | 0.662 | 0.38 to 1.86 | |||
| Black: African | 0.40 | 0.003 | 0.22 to 0.73 | |||
| Other ethnicity | 0.97 | 0.907 | 0.61 to 1.56 | |||
| Outcome: WEMWBS caseness (n = 1050) | Model | |||||
|---|---|---|---|---|---|---|
| 1 | 2 | |||||
| OR | p-value | 95% CI | OR | p-value | 95% CI | |
| Household not workless | 1 | 1 | ||||
| Household workless | 2.64 | < 0.001 | 1.90 to 3.67 | 2.68 | < 0.001 | 1.91 to 3.76 |
| Age | 1.04 | 0.001 | 1.02 to 1.06 | |||
| Male | 1 | |||||
| Female | 1.35 | 0.165 | 0.88 to 2.06 | |||
| White: UK | 1 | |||||
| White: mixed | 0.84 | 0.761 | 0.27 to 2.63 | |||
| Asian: Indian | 0.70 | 0.453 | 0.28 to 1.77 | |||
| Asian: Pakistani | 0.79 | 0.575 | 0.34 to 1.82 | |||
| Asian: Bangladeshi | 1.02 | 0.921 | 0.63 to 1.66 | |||
| Black: Caribbean | 1.06 | 0.871 | 0.51 to 2.20 | |||
| Black: African | 0.39 | 0.003 | 0.21 to 0.73 | |||
| Other ethnicity | 1.09 | 0.709 | 0.68 to 1.76 | |||
Table 18 shows that residing in a workless household increases the odds of scoring below the UK population average for psychological well-being by a factor of 2.7, after adjustment for demographic characteristics (aOR 2.68, 95% CI 1.91 to 3.76). When the outcome under consideration was changed to psychological well-being as opposed to psychological distress, gender no longer emerged as a significant covariate. However, consistent with the HADS models, those with black African ethnicity were significantly less likely to score below the UK population well-being average than their white British counterparts.
Summary of findings
Employment was the most prevalent labour market status for primary respondents at all three waves. The proportion of primary respondents in work increased from 42% at wave 1 to 51% at wave 3. This could be driven by a range of underlying factors and it should be noted that, as these are repeated cross-sections, the proportion of primary respondents in work does not necessarily indicate transitions from unemployment to employment within individuals, but could be more reflective of the changing composition of the sample. One might expect, however, that making the transition from full-time homemaking to employment is a common experience for parents/carers of early secondary-school-age children. It is also possible that changing secular trends, such as an increase in vacancy rates in the local economy, could have addressed an unmet need for employment over this period. The relatively static proportion of household worklessness over the same period, however, does not support the latter interpretation. Further research is required to unpack these mechanisms. Around one-third of primary respondents resided in households with no working adult. As hypothesised, and in support of previous research, individual- and household-level worklessness were both significant predictors of psychological distress and poor psychological well-being, despite adjustment for demographic factors.
Chapter 4 Impacts on adolescent and parent physical activity and the physical activity environment
In this chapter we prospectively investigate changes in adolescent physical activity and sedentary behaviour, as measured by screen time, before and after the London 2012 Olympic and Paralympic Games and explore the social patterning of environmental change related to the ‘legacy’ phase of the Olympic Park. It was hypothesised that the goal of increasing adolescent physical activity through the London 2012 Olympic Games might be achieved through two main mechanisms: first, in the short term, through a ‘demonstration’ effect, by which young people would be inspired to participate in sport through having the Games on their ‘doorstep’; second, in the longer term, through the ‘legacy’ effect of the regeneration of urban infrastructure locally and the development of environmental resources supportive of physical activity, such as increased access to high-quality sporting facilities, improved green and public open space, and increased opportunities for walking and cycling primarily centred on the redevelopment of the Queen Elizabeth Olympic Park.
Impacts on adolescent physical activity
We explored the impacts on adolescent physical activity in two complementary ways. First, we assessed impacts at 6 months (demonstration effects) and 18 months (legacy effects) after the Games on an ITT basis by comparing adolescents living in the primary host borough (Newham), which was the primary focus of Olympic activity, with adolescents living in three comparison boroughs (Tower Hamlets, Hackney, and Barking and Dagenham). Second, we assessed whether or not longitudinal changes in physical activity and screen time were moderated by level of ‘engagement’ with the Games at 6 months, and by use of the Olympic Park at 18 months in the entire cohort.
Methods
Study design and participants
This longitudinal quasi-experimental study followed a cohort of adolescents recruited from schools in the London boroughs of Barking and Dagenham, Hackney, Newham and Tower Hamlets over a 3-year period (see Chapter 2). The participants, in year 7 at baseline (age 11–12 years, January–June 2012), were first followed up in year 8 (wave 2, age 12–13 years, January–June 2013), 6–11 months after the London 2012 Games and again in year 9 (wave 3, age 13–14 years, January–June 2014), 18–23 months after the London 2012 Games. Timing of follow-up for each school was matched by month to reduce seasonality effects. The baseline survey sample comprised 3106 respondents. After excluding respondents who moved schools between waves (n = 8), the final longitudinal cohort for this analysis comprised 2254 adolescents who participated in all three waves, representing an overall retention rate of 73%.
Intervention and control areas
The London Borough of Newham, where the London 2012 Olympic Games were mainly hosted and where the majority of focused regeneration occurred, acted as the intervention area. In the context of this analysis, Olympic-led regeneration in Newham consisted primarily of the construction of infrastructure and facilities supporting the Olympic Park prior to the Games, and subsequent legacy redevelopment of the Queen Elizabeth Olympic Park, which reopened to the public in phases from July 2013 www.queenelizabetholympicpark.co.uk (accessed May 2018). Regeneration components plausibly affecting the outcomes reported here, and outlined in the Legacy Masterplan,13 include the development of ‘sustainable’ transport networks (rail and walking/cycling corridors) to promote active travel; the provision of new and refurbished recreation and leisure facilities to promote formal physical activity; and new and refurbished civic space, parks and green areas to promote leisure-time and routine physical activity.
Data and variables
Physical activity and screen time was assessed using the Y-PAQ. 39 The Y-PAQ is a validated self-reported tool that captures the frequency and duration of a range of physical and sedentary activities over the past 7 days. In addition, it records frequency and duration of screen-based activities, such as TV viewing, internet use and gaming. Respondents who reported > 75 hours of total activity per week were excluded from analysis. Total hours spent physically active or undertaking screen-based activities were calculated for each respondent. Time spent physically active per week was highly positively skewed, with the majority of adolescents reporting few hours of activity, whereas screen time per day was negatively skewed. Time spent physically active was therefore categorised to either ‘active’ or ‘inactive’ based on whether or not the adolescents met the current UK Department of Health and Social Sciences recommendation of 60 minutes of physical activity per day. 81 Screen time was used as a marker of sedentariness and was dichotomised into ‘sedentary’ or ‘not sedentary’ at the internationally recognised cut-off of no more than 2 hours per day. 82
Engagement with the London 2012 Olympic and Paralympic Games
Engagement with the London 2012 Games was assessed using a question from the national evaluation of the London 2012 education programme (Get Set) (ref 5). Respondents were asked ‘How excited do you feel about the 2012 Olympic Games being held in London?’, with responses ranked on a 1 to 10 scale, where 10 was the most excited. Data were categorised into low (1–4), moderate (5–7) and high (8–10) levels of engagement.
Use of the Olympic Park
Use of the Olympic Park was assessed using the question ‘How often do you visit the Olympic Park?’. Responses were every day, once a week, 2–3 times per month, once a month, less than once a month, and never visited. Data were categorised into never visited, less than once a month, and more than once a month in order to adequately power statistical analyses.
Covariates
A range of factors hypothesised to act as confounders between exposure to the games and its legacy were identified: age (in months), gender, ethnicity (white UK, white mixed, Asian Indian, Asian Pakistani, Asian Bangladeshi, black Caribbean, black African, other), means-tested free school meals (yes/no), home language (English/other), household composition (both parents/carers, single parent/carer or neither parent/carer at home), self-rated health (five-point categorical scale collapsed to very good/good versus fair/poor/very poor), long-term limiting illness (yes/no; defined as a health problem that has troubled them over a period of time, or is likely to affect them over a period of time), BMI (z-scored), days between surveys and days from opening ceremony.
Statistical analysis
Survey weights were applied to all analyses by the use of the .svy commands in Stata 14 SE (StataCorp LP, College Station, TX, USA). Weighting was deployed to account for differing probabilities of being selected in each school. Descriptive analysis of baseline data explores the extent to which physical and sedentary activity and screen time, as well as pre engagement with the Olympic Games, covaries across the range of selected social, economic and demographic characteristics. Data were imputed under a MAR assumption83 with a joint multivariate normal modelling approach through the Bayesian estimation method Markov chain Monte Carlo (MCMC). A burn-in of 20,000 iterations was used to stabilise the Markov chains and a further 25,000 iterations were run, creating 50 imputed data sets at every 500th iteration. We tested whether or not there were longitudinal changes in the proportion of individuals reporting > 60 minutes of physical activity per day and < 2 hours of screen time per day before and after the Games by (1) intervention versus control areas (at 6 and 18 months), (2) levels of pre-engagement (at 6 months) and (3) use of the Olympic Park (at 18 months). When appropriate, we present gender-stratified results.
Logistic regression models derived the fully adjusted odds of reporting > 60 minutes per day of physical activity post Games in the lesser engaged groups compared with the highly engaged group (reference category), after accounting for activity pre Games. This was repeated for screen time.
Results
Descriptive data on the analytic sample by survey wave are presented in Table 19. The majority of participants were male (56.7%), with 27.9% drawn from schools in Newham (the main geographical focus of regeneration). The sample was ethnically diverse, with the largest groups being white UK (16.9%), Asian Bangladeshi (15.0%) and white other (14.5%); 36.9% qualified for means-tested free school meals. Over one-fifth (20.2%) of the sample reported undertaking less than the recommended 60 minutes of physical activity a day at baseline, and this increased at each subsequent wave (wave 2 = 24.3%; wave 3 = 30.2%). The proportion of participants reporting 2 or more hours of screen time a day, a marker of sedentariness, increased from 68% at baseline to 75.6% at final follow-up. At wave 3, 18–23 months after the Games had finished, 55.1% of the sample had reported never visiting the Olympic Park.
| Variables | Wave | |||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | ||||
| n (%) | % Missing | n | % Missing | n | % Missing | |
| Gender | ||||||
| Male | 1271 (56.3) | – | – | – | – | – |
| Female | 983 (43.7) | 0.00 | – | – | – | – |
| Ethnicity | ||||||
| White: UK | 380 | – | – | – | – | – |
| White: mixed | 190 | – | – | – | – | – |
| Asian: Indian | 85 | – | – | – | – | – |
| Asian: Pakistani | 86 | – | – | – | – | – |
| Asian: Bangladeshi | 337 | – | – | – | – | – |
| Black: Caribbean | 111 | – | – | – | – | – |
| Black: African | 249 | – | – | – | – | – |
| Other | 816 | 0.00 | – | – | – | – |
| Free school meals | ||||||
| No | 1376 | – | 1404 | 1503 | – | |
| Yes | 832 | 2.00 | 810 | 1.77 | 716 | 1.55 |
| General health | ||||||
| Good/very good | 1696 | – | 1676 | – | 1655 | – |
| Fair/poor | 522 | 1.60 | 557 | 0.93 | 577 | 0.98 |
| Limiting illness | ||||||
| No | 1310 | – | 1119 | – | 1163 | – |
| Yes | 867 | 3.42 | 803 | 14.73 | 767 | 14.37 |
| BMI z-score | 2061 | 8.56 | 2069 | 8.21 | 2099 | 6.88 |
| Language at home | ||||||
| English | 1418 | – | – | – | – | – |
| Other | 820 | 0.71 | – | – | – | – |
| Household composition | ||||||
| Both parents/carers | 1503 | 1544 | 1510 | – | ||
| Single parent/neither parent/carer | 718 | 1.46 | 690 | 0.89 | 728 | 0.71 |
| Borough | ||||||
| Newham | 628 | – | – | – | – | – |
| Tower Hamlets | 582 | – | – | – | – | – |
| Barking and Dagenham | 491 | – | – | – | – | – |
| Hackney | 553 | 0.00 | – | – | – | – |
| Physical activity | ||||||
| < 1 hours a day | 456 | – | 548 | – | 680 | – |
| ≥ 1 hours a day | 1734 | 2.84 | 1689 | 0.75 | 1562 | 0.53 |
| Screen time | ||||||
| < 2 hours a day | 542 | – | 531 | – | 515 | – |
| ≥ 2 hours a day | 1533 | 7.94 | 1666 | 2.53 | 1703 | 1.60 |
| Pre-Games excitement | ||||||
| Low | 307 | – | – | – | – | – |
| Moderate | 610 | – | – | – | – | – |
| High | 698 | 28.35 | – | – | – | – |
| How often do you visit the Olympic Park? | ||||||
| Never visited | – | – | – | – | 1243 | – |
| Less than once a month | – | – | – | – | 572 | – |
| More than once a month | – | – | – | – | 214 | 9.98 |
Demonstration effects at 6 months
Table 20 shows changes in meeting the daily recommended amount of physical activity between baseline (wave 1) and the 6-month follow-up (wave 2). In fully adjusted models, compared with those who remained active, adolescents who became inactive were less likely to come from the intervention borough (Newham) than from the comparison boroughs [relative risk (RR) = 0.69, 95% CI 0.51 to 0.93], indicating that a transition to inactivity was less likely in Newham than in the comparison boroughs. For those who remained inactive or became active, no statistically significant differences between control and intervention boroughs were observed. For screen time, no differences in transitions were observed between intervention and comparison boroughs. No interactions were observed for gender and free school meal status for either outcome.
| Borough | Physical activity, RR (95% CI) | Screen time, RR (95% CI) | |||||
|---|---|---|---|---|---|---|---|
| Remained inactive | Became active | Became inactive | Increased screen time | Continued high-level screen time | Decreased screen time | ||
| Wave 1 to wave 2 | |||||||
| Adjusted for age | |||||||
| Control groupa | |||||||
| Intervention | 0.79 (0.55 to 1.12) | 1.09 (0.80 to 1.48) | 0.69* (0.51 to 0.93) | 1.19 (0.80 to 1.78) | 1.33 (0.95 to 1.87) | 1.08 (0.71 to 1.63) | |
| Fully adjustedb | |||||||
| Control groupa | |||||||
| Intervention | 0.86 (0.60 to 1.23) | 1.05 (0.77 to 1.44) | 0.69* (0.51 to 0.94) | 1.08 (0.71 to 1.63) | 1.21 (0.85 to 1.72) | 0.97 (0.64 to 1.48) | |
| Wave 1 to wave 3 | |||||||
| Adjusted for age | |||||||
| Control groupa | |||||||
| Intervention | 0.79 (0.56 to 1.11) | 1.20 (0.88 to 1.66) | 0.90 (0.69 to 1.16) | 1.37 (0.91 to 2.08) | 1.45* (1.00 to 2.09) | 1.36 (0.89 to 2.10) | |
| Fully adjustedb | |||||||
| Control groupa | |||||||
| Intervention | 0.83 (0.58 to 1.17) | 1.22 (0.88 to 1.69) | 0.93 (0.71 to 1.22) | 1.27 (0.83 to 1.96) | 1.33 (0.90 to 1.95) | 1.25 (0.80 to 1.95) | |
Table 21 reports changes in physical activity across the whole cohort by levels of engagement with the Olympic Games between baseline (wave 1) and the 6-month follow-up (wave 2). Those with low levels of engagement were more likely to remain inactive (RR 1.79, 95% CI 1.20 to 2.66), more likely to become inactive (RR 1.52, 95% CI 1.05 to 2.19) and more likely to become active (RR 1.95, 95% CI 1.31 to 2.91) than those who were active at both waves after adjustment for hypothesised confounders. In the fully adjusted gender-stratified models, low levels of engagement in males was associated with a higher likelihood of becoming active (RR 2.19, 95% CI 1.24 to 3.87) and becoming inactive (RR 1.77, 95% CI 1.07 to 2.94). For females, low levels of engagement were associated with remaining inactive (RR 1.77, 95% CI 1.02 to 3.06). For screen time, those with low levels of engagement with the Games were more likely to become sedentary (RR 1.70, 95% CI 1.00 to 2.87) than those who were not sedentary at both baseline and the 6-month follow-up (Table 22). No other significant effects were observed.
| Engagement | Physical activity, RR (95% CI) | |||||
|---|---|---|---|---|---|---|
| Remained inactive | Became active | Became inactive | Remained inactive | Became active | Became inactive | |
| Adjusted for age | ||||||
| Pre-Games excitement | ||||||
| Higha | ||||||
| Moderate | 1.25 (0.88 to 1.78) | 1.40* (1.00 to 1.95) | 1.54** (1.15 to 2.04) | |||
| Low | 1.92*** (1.29 to 2.86) | 2.00*** (1.36 to 2.93) | 1.54* (1.08 to 2.20) | |||
| Fully adjustedb | ||||||
| Pre-Games excitement | ||||||
| Higha | ||||||
| Moderate | 1.19 (0.83 to 1.71) | 1.38 (0.98 to 1.94) | 1.49** (1.11 to 1.99) | |||
| Low | 1.79** (1.20 to 2.66) | 1.95*** (1.31 to 2.91) | 1.52* (1.05 to 2.19) | |||
| Fully adjusted,b stratified by gender | Male | Female | ||||
| Pre-Games excitement | ||||||
| Higha | ||||||
| Moderate | 1.76* (1.04 to 2.98) | 1.56 (0.95 to 2.57) | 1.80** (1.19 to 2.71) | 0.85 (0.51 to 1.40) | 1.19 (0.74 to 1.90) | 1.30 (0.85 to 1.97) |
| Low | 1.66 (0.89 to 3.13) | 2.19** (1.24 to 3.87) | 1.77* (1.07 to 2.94) | 1.77* (1.02 to 3.06) | 1.74 (0.98 to 3.08) | 1.27 (0.74 to 2.17) |
| Fully adjusted,b stratified by free school meals | No free school meal (n = 1405 to 1406) | Free school meal (n = 848 to 849) | ||||
| Pre-Games excitement | ||||||
| Higha | ||||||
| Moderate | 1.12 (0.70 to 1.79) | 1.39 (0.90 to 2.13) | 1.65** (1.14 to 2.37) | 1.39 (0.76 to 2.54) | 1.40 (0.80 to 2.45) | 1.27 (0.77 to 2.10) |
| Low | 1.38 (0.81 to 2.35) | 2.03** (1.23 to 3.34) | 1.39 (0.85 to 2.25) | 2.92*** (1.54 to 5.53) | 1.81 (0.92 to 3.55) | 1.75 (0.98 to 3.12) |
| Engagement | Screen time, RR (95% CI) | |||||
|---|---|---|---|---|---|---|
| Increased | Remained high-level | Decreased | Increased | Remained high-level | Decreased | |
| Adjusted for age | ||||||
| Pre-Games excitement | ||||||
| Higha | ||||||
| Moderate | 1.00 (0.67 to 1.48) | 0.89 (0.64 to 1.23) | 1.11 (0.75 to 1.64) | |||
| Low | 1.67 (1.00 to 2.78) | 1.47 (0.94 to 2.30) | 0.99 (0.56 to 1.75) | |||
| Fully adjustedb | ||||||
| Pre-Games excitement | ||||||
| Higha | ||||||
| Moderate | 1.03 (0.69 to 1.54) | 0.94 (0.67 to 1.31) | 1.13 (0.75 to 1.68) | |||
| Low | 1.70* (1.00 to 2.87) | 1.50 (0.95 to 2.38) | 0.95 (0.53 to 1.70) | |||
| Fully adjusted,b stratified by free school meals | No free school meal (n = 1405 to 1406) | Free school meal (n = 848 to 849) | ||||
| Pre-Games excitement | ||||||
| Higha | ||||||
| Moderate | 1.38 (0.84 to 2.26) | 1.33 (0.88 to 2.03) | 1.46 (0.88 to 2.41) | 0.60 (0.28 to 1.28) | 0.45* (0.24 to 0.84) | 0.64 (0.31 to 1.31) |
| Low | 1.45 (0.74 to 2.85) | 1.72 (0.96 to 3.07) | 1.03 (0.49 to 2.16) | 1.87 (0.74 to 4.73) | 1.07 (0.47 to 2.42) | 0.75 (0.28 to 1.99) |
Legacy effects at 18 months
Table 20 shows changes in meeting physical activity recommendations between baseline (wave 1) and the 18-month follow-up (wave 3). In the fully adjusted models there were no statistically significant differences between intervention and comparison boroughs for all physical activity and screen time transitions.
In order to assess the effect of the infrastructural legacy of the Olympic Park we also explored whether or not visiting the Olympic Park at 18 months was associated with transitions in physical activity and screen time. Table 23 shows that there was a graded effect of visiting the Olympic Park (less than once a month to more than once a month) for those who remained inactive and those who became active. Those who visited the Olympic Park more than once a month were the least likely to remain inactive (RR 0.11, 95% CI 0.02 to 0.48) and the least likely to become inactive (RR 0.38, 95% CI 0.24 to 0.60) of those who were active at both baseline and at the 18-month follow-up. However, study respondents were also less likely to become active if they visited the Olympic Park more than once a month (RR 0.52, 95% CI 0.30 to 0.90) than the always active group. In gender-stratified models, males who visited the park more than once a month were less likely to remain inactive (RR 0.11, 95% CI 0.02 to 0.48) and less likely to become inactive (RR 0.42, 95% CI 0.23 to 0.76). For females, associations were observed for all three physical activity transitions, with respondents less likely to remain inactive (RR 0.31, 95% CI 0.13 to 0.74), less likely to become inactive (RR 0.36, 95% CI 0.18 to 0.73) and less likely to become active (RR 0.24, 95% CI 0.08 to 0.74) than the always active group.
| Frequency of visit | Physical activity, RR (95% CI) | |||||
|---|---|---|---|---|---|---|
| Remained inactive | Became active | Became inactive | Remained inactive | Became active | Became inactive | |
| Adjusted for age | ||||||
| How often do you visit the Olympic Park? | ||||||
| Never visiteda | ||||||
| Less than once a month | 0.65* (0.46 to 0.91) | 0.82 (0.59 to 1.15) | 0.66** (0.50 to 0.85) | |||
| More than once a month | 0.20*** (0.10 to 0.44) | 0.49** (0.28 to 0.84) | 0.36*** 0(.23 to 0.57) | |||
| Fully adjustedb | ||||||
| How often do you visit the Olympic Park? | ||||||
| Never visiteda | ||||||
| Less than once a month | 0.68* (0.47 to 0.96) | 0.91 (0.65 to 1.28) | 0.67** (0.52 to 0.88) | |||
| More than once a month | 0.22*** (0.11 to 0.47) | 0.52* (0.30 to 0.90) | 0.38*** (0.24 to 0.60) | |||
| Fully adjusted,b stratified by gender | Male | Female | ||||
| How often do you visit the Olympic Park? | ||||||
| Never visiteda | ||||||
| Less than once a month | 0.80 (0.49 to 1.32) | 0.85 (0.53 to 1.37) | 0.71 (0.50 to 1.03) | 0.56* (0.34 to 0.93) | 1.02 (0.62 to 1.68) | 0.65* (0.43 to 0.98) |
| More than once a month | 0.11** (0.02 to 0.48) | 0.75 (0.39 to 1.44) | 0.42** (0.23 to 0.76) | 0.31** (0.13 to 0.74) | 0.24* (0.08 to 0.74) | 0.36** (0.18 to 0.73) |
| Fully adjusted,b stratified by free school meals | No free school meal (n = 1405 to 1406) | Free school meal (n = 848 to 849) | ||||
| How often do you visit the Olympic Park? | ||||||
| Never visiteda | ||||||
| Less than once a month | 0.69 (0.45 to 1.07) | 0.93 (0.61 to 1.43) | 0.72* (0.52 to 1.00) | 0.69 (0.37 to 1.29) | 0.90 (0.51 to 1.61) | 0.57* (0.35 to 0.93) |
| More than once a month | 0.25** (0.10 to 0.58) | 0.27** (0.11 to 0.66) | 0.34*** (0.18 to 0.63) | 0.15* (0.03 to 0.68) | 0.84 (0.38 to 1.83) | 0.43* (0.22 to 0.85) |
For sedentary behaviour, Table 24 shows that females who visited the Olympic Park less than once per month were less likely to become less sedentary (RR 0.39, 95% CI 0.21 to 0.73). No other significant associations for sedentary behaviour were observed.
| Frequency of visit | Screen time, RR (95% CI) | |||||
|---|---|---|---|---|---|---|
| Increased | Remained high-level | Decreased | Increased | Remained high-level | Decreased | |
| Adjusted for age | ||||||
| How often do you visit the Olympic Park? | ||||||
| Never visiteda | ||||||
| Less than once a month | 0.87 (0.58 to 1.32) | 0.84 (0.58 to 1.20) | 0.64* (0.41 to 0.98) | |||
| More than once a month | 1.03 (0.54 to 1.98) | 1.07 (0.61 to 1.89) | 1.31 (0.69 to 2.48) | |||
| Fully adjustedb | ||||||
| How often do you visit the Olympic Park? | ||||||
| Never visiteda | ||||||
| Less than once a month | 0.92 (0.61 to 1.40) | 0.86 (0.60 to 1.24) | 0.67 (0.43 to 1.04) | |||
| More than once a month | 0.99 (0.50 to 1.93) | 1.00 (0.55 to 1.81) | 1.28 (0.66 to 2.46) | |||
| Fully adjusted,b stratified by gender | Male | Female | ||||
| How often do you visit the Olympic Park? | ||||||
| Never visiteda | ||||||
| Less than once a month | 1.40 (0.73 to 2.68) | 1.11 (0.62 to 2.00) | 1.19 (0.61 to 2.34) | 0.65 (0.37 to 1.13) | 0.78 (0.48 to 1.26) | 0.39** (0.21 to 0.73) |
| More than once a month | 0.77 (0.32 to 1.89) | 0.80 (0.37 to 1.76) | 0.87 (0.35 to 2.15) | 1.25 (0.46 to 3.37) | 1.18 (0.48 to 2.92) | 1.74 (0.67 to 4.54) |
Summary
This section investigated both demonstration (at 6 months) and legacy (at 18 months) effects of the London 2012 Olympic Games on adolescent physical activity and screen time. For demonstration effects, 6 months after the games had finished, living in Newham (the intervention borough) was associated with a lower likelihood of becoming inactive than living in surrounding comparison boroughs. However, the London 2012 Games was not associated with adolescent residents becoming more active. When stratifying by ‘engagement’ with the Games, contradictory results were observed. For males, low levels of engagement were associated with an increased risk of becoming inactive, and with becoming more active. However, in females, low levels of engagement were associated with remaining inactive.
For legacy effects, as measured at 18 months, there were no differences in physical activity and screen-time transitions between intervention and comparison boroughs for all physical activity and screen-time transitions. At 18 months, 44.9% of the sample reported never having visited the Olympic Park. However, of those who did visit, male adolescents who visited the park more than once a month were less likely to become inactive and to remain inactive. The pattern for females was similar, with females less likely to remain inactive, less likely to become inactive but also less likely to become active if they visited the Olympic Park more than once a month.
Overall, there was no consistent evidence for a demonstration effect of the London 2012 Games on physical activity. In terms of legacy effects, there was some evidence that use of the Olympic Park was associated with a lower risk of becoming or remaining inactive; however, this was not matched by any observed transition from being inactive to active. Therefore, there may have been some minor arrest of secular declines in adolescent physical activity at wave 3 for park users, but there was no concomitant increase in the proportion of adolescents meeting physical activity recommendations as a result of use of the Olympic Park.
Changes in parental/carer physical activity
In this section, for completeness, we briefly describe changes in physical activity within the longitudinal parent/carer data. We cover this only briefly as we have limited data available owing to the changes in the design of the parent/carer survey, high levels of missingness and inconsistency in findings. Further analyses of the cross-sectional data to try to make further sense of these are ongoing. Table 25 shows the percentage of parents/carers meeting the recommended number of minutes of exercise (≥ 150 minutes) per week over the three waves of the study by intervention versus comparison areas. There are inconsistent patterns over waves, but this is limited by low sample size. Table 26 shows the same data as the odds of meeting physical activity recommendations in the intervention area versus the comparison area over each wave. Residents of the intervention borough (Newham) have greater odds of meeting physical activity recommendations in waves 1 and 2, but have reduced odds at wave 3. We are unable to draw any firm conclusions from these data at present.
| Recommended level of physical activity | Wave, n (%) | |||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | ||||
| Control | Intervention | Control | Intervention | Control | Intervention | |
| Not meeting recommendation | 26 (18.4) | 55 (20.1) | 16 (16.3) | 15 (25.4) | 22 (18.5) | 7 (17.1) |
| Meeting recommendation | 115 (81.6) | 219 (79.9) | 82 (83.7) | 44 (74.6) | 97 (81.5) | 34 (82.9) |
| Group | Wave, OR (95% CI) | ||
|---|---|---|---|
| 1 | 2 | 3 | |
| Control | |||
| Newham | 1.11 (0.66 to 1.87) | 1.75 (0.79 to 3.86) | 0.91 (0.36 to 2.31) |
Impacts on the adolescent physical activity environment
In this section we focus on assessing the social patterning of Olympic-related improvements to the physical activity environment. The most tangible physical legacy for post-Olympic east London was the opening of the Queen Elizabeth Olympic Park, which consists of new high-quality parkland and three world-class sporting facilities: the Aquatics Centre, the Copper Box Sports Centre and the Lee Valley VeloPark. Other aspects of physical legacy upon which the Olympic bid was based were either already in place, such as the transport connections through Stratford, or will be developed in the future, such as new residential development. Figure 5 depicts the pre-development Olympic Park site alongside the proposed post-Olympic development. Based on current plans, the area will undergo transformation from mostly light-industrial use with significant railway lands, to a mixed-use area with significant residential, commercial/retail, green and sporting infrastructure that is better connected to the surrounding neighbourhoods of east London.
FIGURE 5.
Map of the Olympic Park site prior to development (2007) and the proposed Olympic Park in legacy mode (2012). Maps contain data from Ordnance Survey MasterMap Data, Crown Copyright 2007; Ordnance Survey MasterMap Data, Crown Copyright 2012; and Legacy Redevelopment Data, Copyright 2012 Olympic Park Legacy Company.
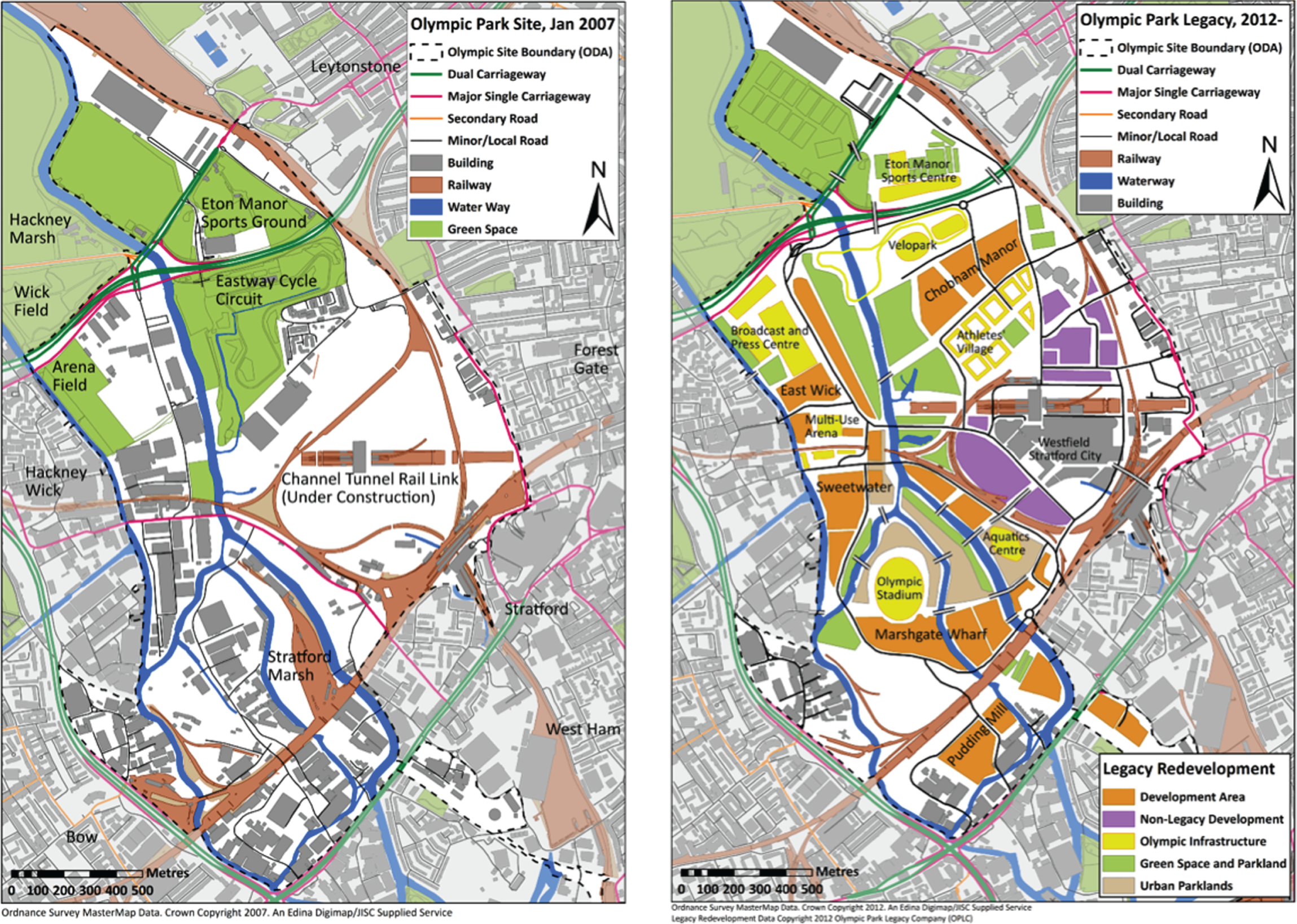
The Olympic site was removed from public usage shortly after the Games were awarded in order to facilitate development. From 2008 the entire area was closed to the public, with no access through the site, and was reopened for the London 2012 Olympic and Paralympic Games. After the Games finished, the park was closed and moved into legacy phase, during which it was converted for public use. The Olympic Park was partially reopened to the public on 27 July 2013 on the first anniversary of the Games, when parts of the south and north park and Copper Box Sports Centre were opened. Subsequently the VeloPark and Aquatics Centre and remaining areas of the south park were opened in phases up to April 2014. Adolescents in the ORiEL study were 6 years old when the Olympic Park area was first closed for redevelopment. The redeveloped Olympic Park therefore represents an opportunity to access an entirely new part of east London for these young people.
In this section we focus on the two most visible physical legacies of the Games that may relate directly to physical activity behaviours: the provision of new green space and new public sports facilities. We assess whether or not the provision of new high-quality green space and sporting facilities has made environments supportive of physical activity more accessible and for whom.
We therefore answer the following research questions:
-
Has accessibility to environments supportive of physical activity changed in response to Olympic-led regeneration?
-
Is this change patterned by socioeconomic position?
Methods
Environmental change metrics were computed that characterised the change in individuals’ potential to access green space and sports facilities between wave 1 (baseline) and wave 3 of the adolescent school-based survey. We then considered how exposure to environmental change varied on the basis of key socioeconomic variables. The analytical sample comprised adolescents who were present at wave 1 (baseline) and wave 3, did not move school during that time, were not observed by study invigilators as ‘cheating or chatting’ and from whom environmental data were also observed at both waves. This leaves a cohort of 1853 respondents.
Measuring change in physical activity environments
As detailed in Chapter 2, we computed a range of environmental metrics measured at each wave from which to create measures of individual environmental change. Here we focus on access to sporting facilities and green space.
Access to sporting facilities
Redevelopment of the Olympic Park introduced several new opportunities to access sporting facilities and, therefore, we wanted to capture this change in provision. Density measures are particularly well suited to do this; however, the actual density value is difficult to interpret as differences are small, and the meaning of any change is hard to grasp. As a result, rather than using the absolute change in density we assessed relative change as a percentage difference from the measure at wave 1 (baseline) to wave 3. For each individual, for each sports facility category, we calculated the change in density at the point at which new Olympic sports facilities became available as an increase or decrease from the density of provision available to that individual at baseline. In this analysis we focus on all public sports facilities, which represent the wider sporting legacy of the games. Although we cannot fully distinguish Olympic-related provision from other changes across the study site, it is evident that the new venues within the Olympic Park were responsible for the majority of change in the density of public sports facilities. Figure 6 classifies the ORiEL study area based on the percentage change in density between wave 1 (baseline) and wave 3, demonstrating that the largest positive changes in access are centred around the Olympic Park area, extending westward. Much of Barking and Dagenham experienced some amount of negative change.
FIGURE 6.
Change in density of sports facilities in the ORiEL study boroughs.
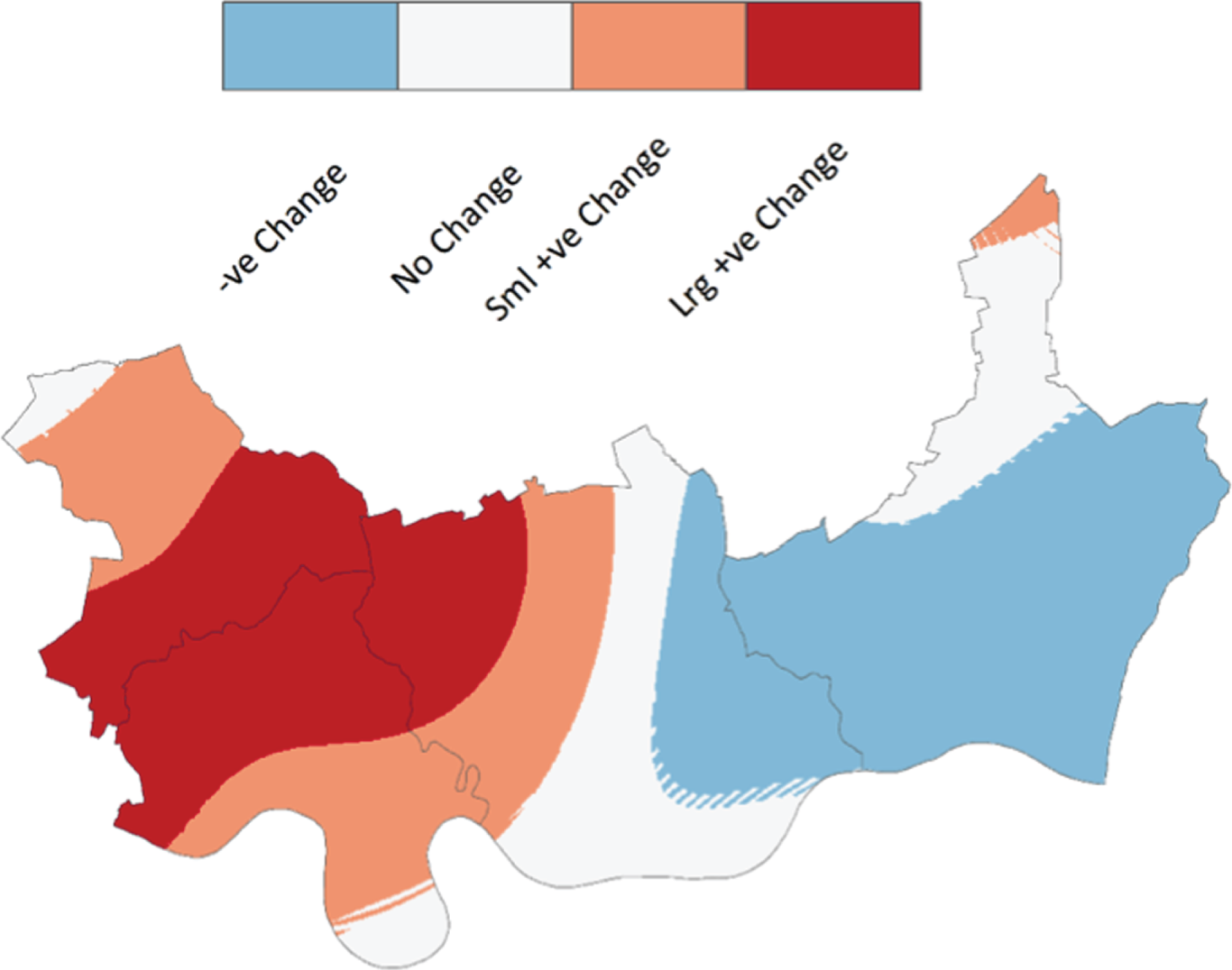
Access to green space
Characterising individual change in access to green space was challenging, given that most change in green space is concentrated within the Olympic Park itself (see Figure 5) and not distributed across east London. In addition, it became clear that green space is relatively abundant within east London. This means that, for respondents, the new green-space provision catalysed by the development of the Olympic Park is unlikely to be the nearest green space for any participant. This suggests that simple ‘nearest neighbour’ accessibility metrics that are the standard approach in the field would not adequately capture environmental change. This suggests that we need to treat the Olympic Park as an addition to existing green infrastructure rather than exclusively as a new, closer destination for local people. As with the sports facilities metric, a density measure would be well suited here; however, we cannot calculate one for polygonal data, which are what the available green-space data are based upon. Therefore, for each individual we computed a measure of the average (mean) distance to their nearest three ‘metropolitan parks’ at wave 1 (baseline) and wave 3. We used changes in that average to quantify exposure to the new Olympic Park green space. This change is then expressed as the relative percentage change (as we used for the sports facilities metric). The ‘metropolitan parks’ categorisation used as the basis for this metric is an official park category (used in the London Plan)84 that denotes large size, high quality and high amenity.
Figure 7 demonstrates the percentage change in access to green space interpolated over the ORiEL study area and represented using four change categories. A similar kind of spatial pattern as in Figure 6 is evident, with few negative changes. The negative changes that do exist appear to be the result of changes to the road network structure, leading to some individuals travelling slightly further at wave 3 to get to the same metropolitan parks and hence forming a small negative change category.
FIGURE 7.
Change in access to green space in the ORiEL study boroughs.
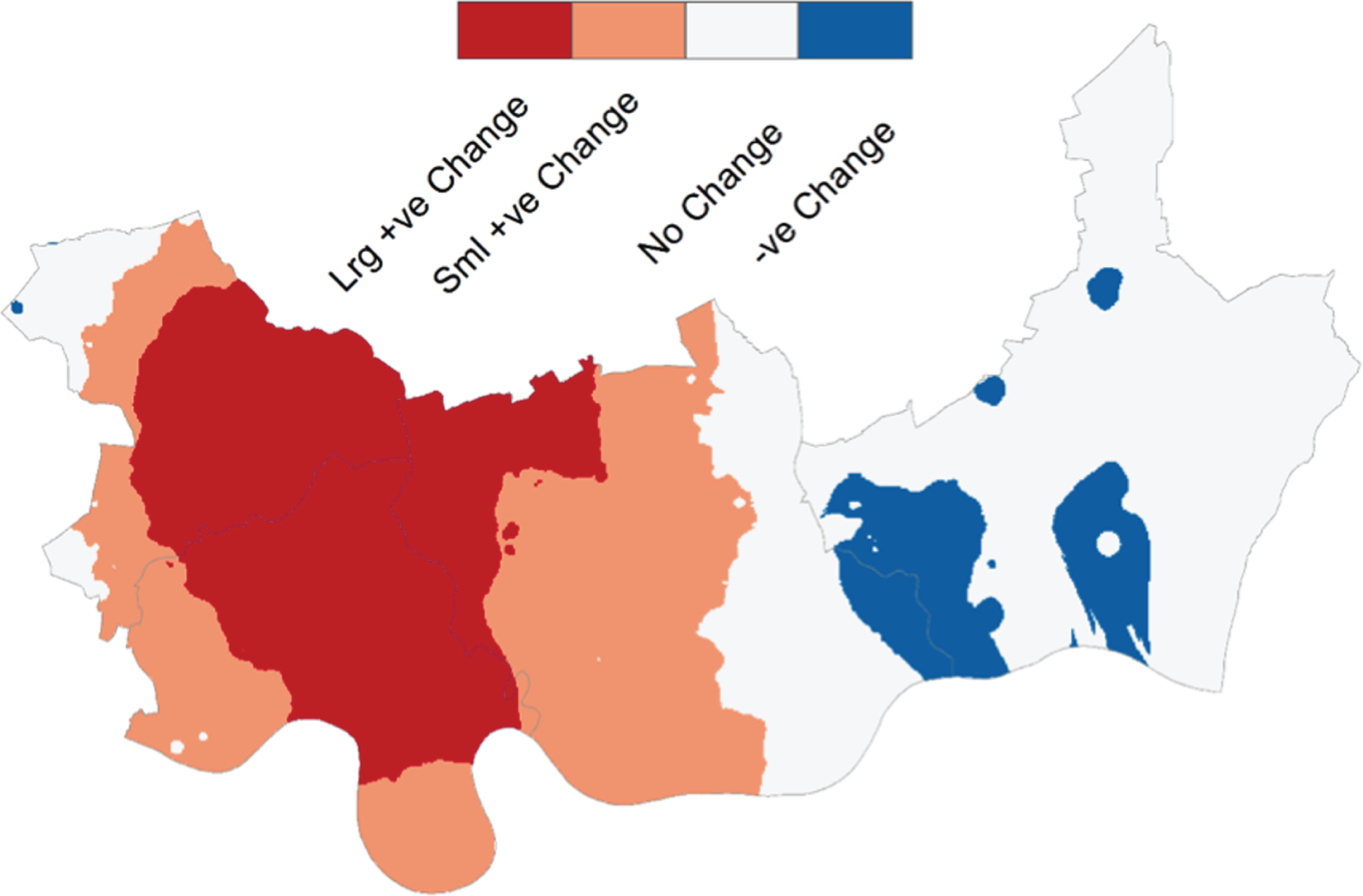
Environmental change: use of a four-category change variable
The raw distributions of percentage environmental change for sports facilities and green space did not fit any known distribution, and the data could not be transformed for normality. Distributions are strongly multimodal, with the largest peaks clustered around zero and smaller peaks for a range of positive change values. This distribution is likely to be as a result of the spatially clustered nature of the sample around schools. In order to meaningfully use these data, we took a pragmatic approach. First, we acknowledged that change values were meaningful: values clustered around zero indicated no or little change between the two time points; negative change values for densities (of sport facilities) and positive change values for distances (to green space) indicated a worsening environment for a given individual; and positive change values for densities (or sport facilities) or negative change values for distances (to green space) indicated an improving environment. On this basis we first created four categories to accurately represent any meaningful change that occurred. These are presented in Tables 27 and 28. Negative change categories were generally small, and tended towards small changes; however, the positive change categories tended to include larger numbers of people and a larger spread of data values. The positive change group was multimodal so we split those who experienced positive change in two and created similarly sized groups.
| Category | Change (%) | Non-movers, n (%) |
|---|---|---|
| No change | –3.0 ≥ χ ≤ 3.0 | 337 (18.2) |
| Negative change | χ < –3.0 | 371 (20.0) |
| Small positive change | 3.0 ≥ χ < 18.0 | 587 (31.7) |
| Large positive change | χ > 18.0 | 558 (30.1) |
| Total | 1853 (100.0) | |
| Category | Change (%) | Non-movers, n (%) |
|---|---|---|
| No change | –0.5 ≥ χ ≤ 0.5 | 584 (31.5) |
| Negative change | χ > 0.5 | 62 (3.3) |
| Small positive change | –15.0 ≥ χ < –0.5 | 598 (32.3) |
| Large positive change | χ < –15.0 | 609 (32.9) |
| Total | 1853 (100.0) | |
Analytical strategy
We used descriptive statistics, simple hypothesis testing and multinomial and logistic regression to undertake a complete-case analysis of the data. We computed robust standard errors in regression modelling to account for the clustered nature of the sample. We also stratified our regression analyses by sex when appropriate.
We investigated whether or not change in access to sports facilities or green space was patterned by key socioeconomic variables. These variables were sex (male/female); ethnicity (eight categories, see Chapter 2); free school meals (yes/no); family affluence scale categories (low/moderate/high); time in the UK (all my life/> 10 years/6–10 years/< 5 years); English as main language spoken at home (yes/no); household composition (lives with mother and father/mother or father/neither); and 2015 neighbourhood Income Deprivation Affecting Children (IDACI) quintile for London. 85
Results
Table 29 summarises the results of initial bivariate analyses. We found no evidence of an association between our environmental change measures and gender, English as main language or household composition. We found evidence of an association between environmental change in both green space and sports facilities and ethnicity, free school meals, family affluence, time in the UK and IDACI 2015 for London.
| Variable | n (missing; missing %) | Green space χ2 (p) | Sports facilities χ2 (p) |
|---|---|---|---|
| Gender | 1853 (0; 0) | 5.65 (0.130) | 1.6812 (0.641) |
| Ethnicity | 1853 (0; 0) | 131.24 (< 0.000) | 108.68 (< 0.000) |
| Free school meals | 1819 (34; 1.8) | 24.79 (< 0.000) | 25.48 (< 0.000) |
| Family affluence | 1787 (66; 3.6) | 14.75 (0.022) | 19.94 (0.003) |
| Time in the UK | 1834 (19; 1.0) | 25.92 (0.002) | 34.15 (< 0.000) |
| English main language | 1845 (8; 0.4) | 14.03 (0.003) | 1.93 (0.587) |
| Household composition | 1831 (22; 1.2) | 4.53 (0.604) | 4.37 (0.626) |
| IDACI London | 1853 (0; 0) | 274.76 (< 0.000) | 269.87 (< 0.000) |
Tables 30 and 31 report, for multivariate models, the relative RRs (RRRs) of any environmental change compared with no environmental change (the reference category) by key socioeconomic factors. Table 30 reports RRRs for percentage change in the access to green-space measure (mean distance to nearest three metropolitan parks). In unadjusted analyses the Asian Bangladeshi group experienced a greater improvement in access to green space in both positive change categories than the reference group. The black Caribbean group also experienced a small positive improvement in access. Recipients of free school meals and those of moderate family affluence were also more likely to experience improvements in green-space accessibility. Residents of more disadvantaged neighbourhoods were also more likely to have improved access to green space than residents of the most advantaged neighbourhoods.
| Variable | Change in access to green space | |||||
|---|---|---|---|---|---|---|
| Negative vs. no change | Small positive vs. no change | Large positive vs. no change | ||||
| RRR | SE | RRR | SE | RRR | SE | |
| Gender | ||||||
| Male | 1.00 | – | 1.00 | – | 1.00 | – |
| Female | 1.02 | 0.164 | 0.852 | 0.183 | 0.766 | 0.200 |
| Ethnicity | ||||||
| White: UKa | 1.00 | – | 1.00 | – | 1.00 | – |
| White: mixed | 0.59 | 0.349 | 1.42 | 0.480 | 1.46 | 0.394 |
| Asian: Indian | 1.40 | 1.146 | 2.36 | 1.883 | 1.22 | 0.897 |
| Asian: Pakistani | 1.14 | 0.640 | 2.42 | 1.646 | 0.41 | 0.271 |
| Asian: Bangladeshi | 0.79 | 0.466 | 4.47* | 2.702 | 6.33*** | 3.439 |
| Black: Caribbean | 0.51 | 0.661 | 2.34* | 1.020 | 2.53 | 1.266 |
| Black: African | 1.74 | 1.038 | 1.67 | 0.648 | 1.74 | 0.610 |
| Other | 1.16 | 0.329 | 1.57 | 0.531 | 1.38 | 0.458 |
| Free school meals | ||||||
| No | 1.00 | – | 1.00 | – | 1.00 | – |
| Yes | 1.44 | 0.289 | 1.60** | 0.292 | 1.80** | 0.392 |
| Family affluence | ||||||
| Higha | 1.00 | – | 1.00 | – | 1.00 | – |
| Moderate | 1.50 | 0.533 | 1.32* | 0.158 | 1.44* | 0.219 |
| Low | 0.98 | 0.478 | 1.20 | 0.310 | 1.77 | 0.534 |
| Time in the UK | ||||||
| All my lifea | 1.00 | – | 1.00 | – | 1.00 | – |
| > 10 years | 2.03** | 0.491 | 1.17 | 0.244 | 1.22 | 0.343 |
| 6–10 years | 0.45 | 0.206 | 0.74 | 0.150 | 0.53* | 0.138 |
| < 6 years | 0.46 | 0.416 | 0.82 | 0.261 | 0.43** | 0.129 |
| IDACI quintile (London) | ||||||
| 1 – most depriveda | 1.00 | – | 1.00 | – | 1.00 | – |
| 2 | 0.85 | 0.276 | 0.76 | 0.213 | 0.26*** | 0.066 |
| 3 | 0.24 | 0.105 | 1.00 | 0.416 | 0.15*** | 0.066 |
| 4 | 0.00*** | 0.000 | 0.44 | 0.200 | 0.04*** | 0.022 |
| 5 – least deprived | 0.00*** | 0.000 | 1.52 | 1.783 | 0.00*** | 0.000 |
| Variable | Change in density of sports facilities | |||||
|---|---|---|---|---|---|---|
| Negative vs. no change | Small positive vs. no change | Large positive vs. no change | ||||
| RRR | SE | RRR | SE | RRR | SE | |
| Gender | ||||||
| Male | 1.00 | – | 1.00 | – | 1.00 | – |
| Female | 1.10 | 0.234 | 0.93 | 0.179 | 0.98 | 0.302 |
| Ethnicity | ||||||
| White: UKa | 1.00 | – | 1.00 | – | 1.00 | – |
| White: mixed | 0.96 | 0.289 | 1.07 | 0.464 | 1.40 | 0.447 |
| Asian: Indian | 0.87 | 0.506 | 1.64 | 1.115 | 0.56 | 0.309 |
| Asian: Pakistani | 1.64 | 0.985 | 2.29 | 1.645 | 0.28* | 0.177 |
| Asian: Bangladeshi | 0.66 | 0.337 | 2.45 | 1.492 | 3.53* | 2.057 |
| Black: Caribbean | 0.93 | 0.401 | 1.97 | 1.196 | 1.65 | 0.738 |
| Black: African | 1.47 | 0.689 | 1.77 | 0.852 | 1.73 | 0.573 |
| Other | 1.01 | 0.343 | 1.26 | 0.583 | 1.39 | 0.413 |
| Free school meals | ||||||
| No | 1.00 | – | 1.00 | – | 1.00 | – |
| Yes | 0.80 | 0.137 | 1.40 | 0.305 | 1.54* | 0.287 |
| Family affluence | ||||||
| Higha | 1.00 | – | 1.00 | – | 1.00 | – |
| Moderate | 1.03 | 0.190 | 0.93 | 0.169 | 1.56* | 0.287 |
| Low | 0.91 | 0.234 | 1.08 | 0.323 | 1.65 | 0.424 |
| Time in the UK | ||||||
| All my lifea | 1.00 | – | 1.00 | – | 1.00 | – |
| > 10 years | 0.93 | 0.295 | 0.77 | 0.240 | 0.99 | 0.286 |
| 6–10 years | 1.36 | 0.305 | 0.78 | 0.182 | 0.68 | 0.149 |
| < 6 years | 0.73 | 0.245 | 0.39*** | 0.088 | 0.36*** | 0.102 |
| IDACI quintile (London) | ||||||
| 1 – most depriveda | 1.00 | – | 1.00 | – | 1.00 | – |
| 2 | 0.99 | 0.324 | 0.44 | 0.171 | 0.25*** | 0.080 |
| 3 | 0.66 | 0.333 | 0.54 | 0.283 | 0.08*** | 0.043 |
| 4 | 2.24 | 1.421 | 1.74 | 0.894 | 0.19*** | 0.098 |
| 5 – least deprived | 0.85 | 1.156 | 4.39 | 6.148 | 0.26 | 0.403 |
Table 31 reports unadjusted RRRs for percentage change in the density of sports facilities for ORiEL baseline respondents. Similarly to the results presented for green space, the Asian Bangladeshi group experienced improvements in access to sport facilities, highlighting how geographically concentrated this group is in the area of highest change. Recipients of free school meals and those of moderate family affluence were also more likely to experience a large positive change in access to sports facilities.
Socioeconomic variables that were significantly associated with environmental changes in bivariate analysis were included within a final multivariate model. Tables 32 and 33 show that, although some attenuation occurred, the sociodemographic variables associated with change in access to green space and sports facilities remain the same. The Asian Bangladeshi group, the black African group and those receiving free school meals benefited from improvements in access to green space. The Asian Bangladeshi group, the black African group and the Asian Pakistani group benefited from improvements in access to sports facilities.
| Variable | Change in acess to green space | |||||
|---|---|---|---|---|---|---|
| Negative vs. no change | Small positive vs. no change | Large positive vs. no change | ||||
| RRR | SE | RRR | SE | RRR | SE | |
| Free school meals | 1.37 | 0.307 | 1.53* | 0.277 | 1.63* | 0.356 |
| Recent migrant | 0.35 | 0.193 | 0.73 | 0.143 | 0.49*** | 0.097 |
| White: UKa | 1.00 | – | 1.00 | – | 1.00 | – |
| White: mixed | 0.58 | 0.349 | 1.31 | 0.435 | 1.37 | 0.376 |
| Asian: Indian | 1.59 | 1.327 | 2.48 | 2.046 | 1.40 | 1.030 |
| Asian: Pakistani | 1.25 | 0.723 | 2.44 | 1.666 | 0.44 | 0.288 |
| Asian: Bangladeshi | 0.80 | 0.468 | 4.27* | 2.560 | 5.99** | 3.203 |
| Black: Caribbean | 0.60 | 0.773 | 2.56* | 1.182 | 2.72 | 1.418 |
| Black: African | 2.33 | 1.394 | 1.84 | 0.756 | 2.12* | 0.733 |
| Other | 1.35 | 0.351 | 1.60 | 0.593 | 1.55 | 0.523 |
| Variable | Change in density of sports facilities | |||||
|---|---|---|---|---|---|---|
| Negative vs. no change | Small positive vs. no change | Large positive vs. no change | ||||
| RRR | SE | RRR | SE | RRR | SE | |
| Free school meals | 0.78 | 0.134 | 1.30 | 0.274 | 1.35 | 0.241 |
| Recent migrant | 0.90 | 0.212 | 0.49*** | 0.093 | 0.48*** | 0.099 |
| White: UKa | 1.00 | – | 1.00 | – | 1.00 | – |
| White: mixed | 0.99 | 0.314 | 1.01 | 0.418 | 1.38 | 0.434 |
| Asian: Indian | 0.85 | 0.501 | 1.78 | 1.191 | 0.63 | 0.342 |
| Asian: Pakistani | 1.61 | 0.998 | 2.40 | 1.708 | 0.22* | 0.148 |
| Asian: Bangladeshi | 0.67 | 0.346 | 2.40 | 1.455 | 3.44* | 1.987 |
| Black: Caribbean | 1.02 | 0.403 | 2.27 | 1.331 | 1.88 | 0.826 |
| Black: African | 1.50 | 0.700 | 2.21 | 1.003 | 2.12* | 0.700 |
| Other | 1.08 | 0.409 | 1.52 | 0.699 | 1.63 | 0.490 |
Summary
Environmental change relevant to physical activity, as a result of the development of new Olympic infrastructure, is concentrated spatially. Therefore, the main beneficiaries of this investment will be groups that also cluster spatially in the neighbourhoods surrounding the Olympic Park. The analyses presented here suggest that these groups include Asian Bangladeshi groups and black Caribbean groups, who experience improvements in access to environmental improvements compared with the white British group. We also observe that, in terms of access to green space, adolescents who receive free school meals (a marker of material disadvantage) see greater improvements than those who do not qualify. This suggests that, for some markers of social position, investment in environmental infrastructure that is supportive of physical activity benefits some minority ethnic and disadvantaged adolescents proportionally more. This is in line with the underlying rationale for investing in an Olympic legacy of east London, although some disadvantaged groups benefit more than others.
Chapter 5 Evaluating impacts on adolescent and parent psychological well-being
In the preceding chapters we outlined our methodological approach for evaluating the impact of the London 2012 Olympic and Paralympic Games, described the baseline characteristic of our adolescent and parent samples and outlined the impacts of London 2012 and its infrastructural legacy on physical activity and sedentary behaviour. In this chapter, we report our evaluation of the impacts on psychological health and well-being.
The aim in this chapter was to explore the following primary research question:
-
What is the impact of urban regeneration on the mental health and well-being of adolescents and their parents/carers?
We take two approaches based on the sample population under consideration. First, we explore the impacts on adolescents using the longitudinal data from all three waves of the adolescent sample. Second, we track changes in parents/carers using repeated cross-sectional parental survey. The findings reported here are preliminary; a range of further data analyses are currently being undertaken and will be submitted for publication over the next 12–18 months.
Impacts on adolescent psychological health and well-being
In this section we systematically explore impacts on our primary adolescent psychological health and well-being measures on an outcome-by-outcome basis. Based on a per-protocol analysis, we utilise a longitudinal approach and compare differences in the impact of the Games on our outcomes by intervention and comparison boroughs over time.
Methods
Primary outcomes
Adolescent well-being
Subjective well-being was assessed by the WEMWBS, a 14-item (five response category) self-report measure of subjective positive well-being, at waves 1, 2 and 3. 30 Continuous scores were used for analyses examining changes in well-being over time. Pre–post absolute change in the WEMWBS scores between waves 1 and 2 and between waves 1 and 3 was calculated by subtracting the wave 1 score from the wave 2 or wave 3 score for each individual, respectively.
Adolescent depressive symptoms
Negative affect was assessed by depressive symptoms using the self-report SMFQ, a 13-item (three-response category) self-report measure. 31 A score of ≥ 8 indicates significant depressive symptoms. In RELACHS we allowed one item to be imputed if missing;35 if more than one item was missing we set the whole scale as missing. We followed the same scoring rules in ORiEL.
Sociodemographic and neighbourhood covariates
The following covariates, available at each wave, were identified a priori from existing literature: age in cohort (months); gender; ethnicity (assessed using an 11-category variable based on the 2011 UK census); years in UK; number of parents/carers the participant lived with; parental income; bullied at school in the past 12 months; receiving free school meals; long-term illness; number of life events; whether or not moved neighbourhood since last wave; and the number of days since the opening ceremony of the Olympics that the participant completed the questionnaire. Social support from family and friends were assessed using the MSPSS,36 with scores divided into tertiles representing low-, medium- and high-level support. See Table 34 for further details of these measures.
Dealing with missing data and multiple imputation strategy
Weights were derived to take account of unequal probabilities of school and pupil selection. Prevalence and missing data rates for the outcomes and covariates were examined: missing values ranged from 0.0% to 45.2%. We found no evidence against the assumption that data were MAR. 83 We imputed the data using multilevel multiple imputation in the REALCOM software (Realcom Applications, Coleorton, Leicestershire, UK), which uses a joint multivariate normal modelling approach through the MCMC method. We imputed with two levels (first = wave and second = adolescent) with all of the outcomes and covariates as fixed effects. Interaction terms between gender and the intervention, and between free school meals and the intervention, were also included. The imputation model was chosen to be congenial86 with the most saturated model of interest; auxiliary variables were included to strengthen the MAR assumption. We used a ‘burn-in’ period of 25,000 iterations, followed by 50,000 iterations producing a data set every 1000th iteration, resulting in 50 imputed data sets. The MCMC chains were examined to check for convergence.
Statistical analyses
Analyses were carried out using Stata version 14 (StataCorp LP, College Station, TX, USA). Standard descriptive statistics are reported. For categorical outcomes, the prevalence and 95% CI were calculated; for continuous outcomes, the mean/median, standard deviation and range were calculated. Crude and adjusted multilevel linear and logistic regression models were run to assess the impact of urban regeneration (intervention vs. comparison) on short-term (wave 1 to wave 2) and longer term (wave 1 to wave 3) change in adolescent well-being and depressive symptoms. The models were adjusted for baseline demographic factors; household factors; family and friend social support; and psychological factors (see Table 34 for variable details). An additional adjustment for baseline WEMWBS was made to the adjusted model for well-being to test the sensitivity of the findings for baseline well-being. Interactions between the intervention and gender, and between the intervention and free schools meals, were tested: models were stratified when the interactions had a p-value of ≤ 0.05. Robustness of inference to the MAR assumption applied within the imputation of missing observations was explored through sensitivity analysis. Two methods were used: the first replaced missing observations with unrealistic extreme settings; if inferences were not robust, the second method was used, which applied more realistic settings through tipping point sensitivity analysis. The sensitivity analysis suggested that inferences were robust to realistic departures from the MAR assumption.
Results
Descriptive analysis of adolescent mental health and well-being (waves 1, 2 and 3)
The following sections present data from 2254 adolescents who participated at all three waves (73% of the wave 1 sample). Table 34 shows the prevalence for the outcomes and covariates at each wave. In total, 27.9% of the participants were from schools in the intervention borough of Newham and 72.1% were from schools in the comparison boroughs (Barking and Dagenham, Hackney, and Tower Hamlets). Participants were ethnically diverse: the largest groups described themselves as white UK (16.9%), Asian Bangladeshi (15.0%) and white other (14.5%).
| Variable | Wave | |||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | ||||
| n (%) | Missing (%) | n (%) | Missing (%) | n (%) | Missing (%) | |
| Intervention | ||||||
| Intervention | 2254 | 0.00 | ||||
| No | 1626 (72.14) | |||||
| Yes | 628 (27.86) | |||||
| Outcome | ||||||
| SMFQ | 2068 | 8.25 | 2116 | 6.12 | 2155 | 4.39 |
| Not depressed | 1618 (78.24) | 1676 (79.21) | 1633 (75.78) | |||
| Depressed (≥ 8) | 450 (21.76) | 440 (20.79) | 522 (24.22) | |||
| Cronbach’s α | 0.873 | 0.897 | 0.914 | |||
| WEMWBS | 1943 | 13.8 | 2016 | 10.56 | 2085 | 7.5 |
| Mean (SD) | 51.25 (9.01) | 51.62 (9.68) | 51.24 (10.12) | |||
| Cronbach’s α | 0.838 | 0.882 | 0.902 | |||
| Baseline demographic | ||||||
| Gender | 2254 | 0.00 | ||||
| Male | 1271 (56.39) | |||||
| Female | 983 (43.61) | |||||
| Ethnicity | 2254 | 0.00 | ||||
| White: UK | 380 (16.86) | |||||
| White: other | 326 (14.46) | |||||
| White: mixed | 190 (8.43) | |||||
| Asian: Indian | 85 (3.77) | |||||
| Asian: Pakistani | 86 (3.82) | |||||
| Asian: Bangladeshi | 337 (14.95) | |||||
| Asian: other | 72 (3.19) | |||||
| Black: Caribbean | 111 (4.92) | |||||
| Black: African | 249 (11.05) | |||||
| Black: other | 263 (11.67) | |||||
| Other | 155 (6.88) | |||||
| Time in the UK | 2221 | 1.46 | ||||
| All my life | 1629 (73.35) | |||||
| > 10 years | 174 (7.83) | |||||
| < 6–10 years | 190 (8.55) | |||||
| Less than 6 years | 228 (10.27) | |||||
| Long-term illness | 2153 | 4.48 | ||||
| No | 1898 (88.16) | |||||
| Yes | 255 (11.84) | |||||
| Household | ||||||
| Parental income | 1984 | 11.98 | 2104 | 6.65 | 2090 | 7.28 |
| Two | 796 (40.12) | 813 (38.64) | 832 (39.81) | |||
| One | 832 (41.94) | 883 (41.97) | 891 (42.63) | |||
| None | 356 (17.94) | 408 (19.39) | 367 (17.56) | |||
| Household composition | 2221 | 1.46 | 2234 | 0.89 | 2238 | 0.71 |
| Lives with both parents/carers | 1503 (67.67) | 1544 (69.11) | 1510 (67.47) | |||
| Lives with one parent/carer | 673 (30.30) | 643 (28.78) | 688 (30.74) | |||
| Lives with no parent/carer | 45 (2.03) | 47 (2.10) | 40 (1.79) | |||
| Moved neighbourhood since previous wave | 1914 | 15.08 | 2137 | 5.19 | 2167 | 3.86 |
| No | 1746 (91.22) | 1977 (92.51) | 2022 (93.31) | |||
| Yes | 168 (8.78) | 160 (7.49) | 145 (6.69) | |||
| Free school meals | 2208 | 2.04 | 2214 | 1.77 | 2219 | 1.55 |
| No | 1376 (62.3) | 1404 (63.4) | 1503 (67.7) | |||
| Yes | 832 (37.7) | 810 (36.6) | 716 (32.3) | |||
| Social support | ||||||
| MSPSS family | 1236 | 45.16 | 1663 | 26.22 | 1962 | 12.95 |
| Low tertile | 378 (30.58) | 530 (31.87) | 642 (32.72) | |||
| Medium tertile | 392 (31.72) | 475 (28.56) | 586 (29.87) | |||
| High tertile | 466 (37.70) | 658 (39.57) | 734 (37.41) | |||
| Cronbach’s α | 0.872 | 0.897 | 0.907 | |||
| MSPSS friend | 1239 | 45.03 | 1656 | 26.53 | 1958 | 13.13 |
| Low tertile | 349 (28.17) | 495 (29.89) | 649 (33.15) | |||
| Medium tertile | 470 (37.93) | 592 (35.75) | 634 (32.38) | |||
| High tertile | 420 (33.90) | 569 (34.36) | 675 (34.47) | |||
| Cronbach’s α | 0.901 | 0.925 | 0.942 | |||
| Psychological | ||||||
| Ever bullied | 1463 | 35.09 | ||||
| No | 948 (64.80) | |||||
| Yes | 515 (35.20) | |||||
| Negative life events | 1663 | 26.22 | 1910 | 15.26 | 2001 | 11.22 |
| 0 | 865 (52.01) | 691 (36.18) | 481 (24.04) | |||
| 1 | 373 (22.43) | 469 (24.55) | 499 (24.94) | |||
| 2 | 235 (14.13) | 334 (17.49) | 372 (18.59) | |||
| 3+ | 190 (11.43) | 416 (21.78) | 649 (32.43) | |||
Over one-fifth of the sample reported depressive symptoms at each wave (wave 1, 21.7%; wave 2, 20.8%; wave 3, 24.2%). The mean well-being score was 51 at each wave. Baseline depressive symptoms were higher in the intervention group than in the comparison group (27% vs. 20%: unadjusted OR 1.49; p = 0.024) and baseline well-being scores were lower in the intervention group than in the comparison group [50.7 standard error (SE) (0.6) vs. 53.0 SE (0.2); p = 0.001]. These findings indicate that adolescents attending schools in the London Borough of Newham had higher rates of depressive symptoms and lower levels of well-being at the start of the study than adolescents attending schools in the boroughs of Barking and Dagenham, Hackney and Tower Hamlets.
Table 35 shows the change in SMFQ scores between wave 1 and wave 2. In total, 66.69% of the sample remained not depressed, with 11.36% becoming depressed, 10.24% remaining depressed and 11.71% being no longer depressed. Table 35 also shows the change in SMFQ scores between wave 1 and wave 3. In total, 64.50% of the sample remained not depressed, with 13.56% becoming depressed, 11.12% remaining depressed and 10.82% being no longer depressed.
| Variable | Change between the waves, % (95% CI) | |
|---|---|---|
| Wave 1 to wave 2 | Wave 1 to wave 3 | |
| Not depressed | 66.69 (62.85 to 70.54) | 64.50 (60.70 to 68.30) |
| Intervention | ||
| Comparison group | 69.14 (65.55 to 72.73) | 66.78 (63.59 to 69.97) |
| Newham | 60.36 (53.42 to 67.30) | 58.59 (50.58 to 66.60) |
| Gender | ||
| Male | 73.25 (69.80 to 76.69) | 72.46 (69.28 to 75.63) |
| Female | 58.43 (52.92 to 63.93) | 54.46 (48.76 to 60.15) |
| Free school meals | ||
| No | 66.07 (61.94 to 70.19) | 63.90 (59.87 to 67.93) |
| Yes | 67.76 (62.82 to 72.70) | 65.51 (60.72 to 70.29) |
| Became depressed | 11.36 (9.66 to 13.07) | 13.56 (12.02 to 15.10) |
| Intervention | ||
| Comparison group | 10.91 (9.45 to 12.37) | 13.27 (11.73 to 14.82) |
| Newham | 12.53 (7.85 to 17.21) | 14.30 (10.58 to 18.02) |
| Gender | ||
| Male | 8.34 (6.76 to 9.92) | 9.13 (7.87 to 10.39) |
| Female | 15.17 (12.39 to 17.96) | 19.15 (15.71 to 22.58) |
| Free school meals | ||
| No | 12.17 (10.10 to 14.25) | 14.34 (12.41 to 16.27) |
| Yes | 9.98 (7.75 to 12.22) | 12.24 (9.86 to 14.61) |
| No longer depressed | 11.71 (9.92 to 13.49) | 10.82 (9.21 to 12.44) |
| Intervention | ||
| Comparison group | 10.93 (8.96 to 12.89) | 9.88 (8.56 to 11.21) |
| Newham | 13.73 (10.70 to 16.76) | 13.25 (9.30 to 17.2) |
| Gender | ||
| Male | 11.76 (9.61 to 13.91) | 12.41 (10.42 to 14.39) |
| Female | 11.64 (9.40 to 13.88) | 8.82 (6.40 to 11.24) |
| Free school meals | ||
| No | 11.70 (9.58 to 13.81) | 10.06 (8.44 to 11.67) |
| Yes | 11.72 (8.88 to 14.56) | 12.12 (9.46 to 14.78) |
| Remained depressed | 10.24 (8.23 to 12.25) | 11.12 (8.60 to 13.65) |
| Intervention | ||
| Comparison group | 9.02 (7.41 to 10.63) | 10.07 (8.04 to 12.10) |
| Newham | 13.38 (8.98 to 17.79) | 13.86 (7.54 to 20.18) |
| Gender | ||
| Male | 6.65 (4.47 to 8.84) | 6.01 (3.65 to 8.36) |
| Female | 14.76 (11.22 to 18.29) | 17.58 (13.98 to 21.17) |
| Free school meals | ||
| No | 10.06 (7.49 to 12.64) | 11.70 (8.70 to 14.71) |
| Yes | 10.54 (8.12 to 12.95) | 10.13 (7.60 to 12.67) |
Table 36 shows the change in well-being scores between wave 1 and wave 2, and between wave 1 and wave 3. In the total sample, changes in well-being scores were small in magnitude, with a positive change of 0.43 (95% CI –0.31 to 1.16) between wave 1 and wave 2, and a positive change of 0.09 (95% CI –0.74 to 0.92) between wave 1 and wave 3. Change scores for well-being were negative for females and positive for males at both time-points. Slightly larger positive change scores were observed for the intervention site (Newham) than the comparison group at wave 1 to wave 2. Positive change scores were observed for the intervention site (Newham) from wave 1 to wave 3, while a small negative change was observed for the comparison group. There was little difference in change scores in well-being by free school meal status at wave 1 and wave 2; participants receiving free school meals showed a small negative change in levels of well-being between wave 1 and wave 3, whereas participants not receiving free school meals showed a small positive change in levels of well-being between waves 1 and 3.
| Variable | Change between the waves, % (95% CI) | |
|---|---|---|
| Wave 1 to wave 2 | Wave 1 to wave 3 | |
| Mean well-being change | 0.43 (–0.31 to 1.16) | 0.09 (–0.74 to 0.92) |
| Intervention | ||
| Comparison group | 0.27 (–0.54 to 1.08) | –0.25 (–1.15 to 0.64) |
| Newham | 0.84 (–0.75 to 2.43) | 0.98 (–0.78 to 2.74) |
| Gender | ||
| Male | 0.98 (0.08 to 1.89) | 1.43 (0.56 to 2.30) |
| Female | –0.27 (–0.11 to 0.56) | –1.60 (–2.65 to 0.54) |
| Free school meals | ||
| Yes | 0.34 (–0.63 to 1.31) | –0.32 (–1.21 to 0.57) |
| No | 0.57 (–0.28 to 1.41) | 0.78 (–0.50 to 2.06) |
Impact of urban regeneration on change in adolescent mental health
Change in depressive symptoms from wave 1 to wave 2
Table 37 shows the changes in SMFQ outcome between wave 1 and wave 2. In the fully adjusted models, adolescents who were ‘no longer depressed’ (RRR 1.53, 95% CI 1.07 to 2.20) or who ‘remained depressed’ (RRR 1.78, 95% CI 1.12 to 2.83) were more likely to be from the intervention borough than from the comparison boroughs, compared with those who were not depressed. ‘Remaining depressed’ was also associated with female gender (RRR 2.94, 95% CI 1.92 to 4.51), low family support (RRR 2.36, 95% CI 1.58 to 3.52), being bullied (RRR 2.53, 95% CI 1.69 to 3.78), long-term illness (RRR 1.98, 95% CI 1.26 to 3.09) and experiencing one, two, or three or more life events (RRR 1.88, 95% CI 1.22 to 2.91; RRR 2.24, 95% CI 1.56 to 3.21; RRR 2.91, 95% CI 1.64 to 3.09) and was more likely for Asian Bangladeshi adolescents (RRR 1.76, 95% CI 1.04 to 2.95). Becoming ‘no longer depressed’ was associated with low family support (RRR 1.70, 95% CI 1.21 to 2.37), being bullied (RRR 1.84, 95% CI 1.34 to 2.53), and experiencing two or three or more life events (RRR 2.03, 95% CI 1.37 to 2.99; RRR 2.12, 95% CI 1.26 to 3.58), and was less likely for Asian Indian adolescents (RRR 0.17, 95% CI 0.03 to 0.99). ‘Becoming depressed’ was more likely for females (RRR 2.34, 95% CI 1.71 to 3.21) and those experiencing three or more life events (RRR 1.69, 95% CI 1.05 to 2.71). No interactions between the intervention and gender or entitlement to free school meals were observed for depressive symptoms (p > 0.05).
| Variable | Change in depressive symptoms, RRR (95% CI) | |||||
|---|---|---|---|---|---|---|
| Became depressed | No longer depressed | Remained depressed | ||||
| Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted | |
| Intervention | 1.32 (0.81 to 2.12) | 1.44 (0.95 to 2.17) | 1.44* (1.03 to 2.02) | 1.53* (1.07 to 2.20) | 1.70* (1.04 to 2.77) | 1.78* (1.12 to 2.83) |
| Femalea | 2.34*** (1.71 to 3.21) | 1.21 (0.91 to 1.61) | 2.94*** (1.92 to 4.51) | |||
| Age (months) | 1.02 (0.97 to 1.06) | 0.98 (0.94 to 1.02) | 1.00 (0.95 to 1.05) | |||
| Ethnicityb | ||||||
| White: other | 0.84 (0.42 to 1.67) | 0.61 (0.33 to 1.12) | 0.91 (0.57 to 1.45) | |||
| White: mixed | 1.04 (0.56 to 1.93) | 1.02 (0.57 to 1.81) | 0.68 (0.39 to 1.17) | |||
| Asian: Indian | 0.44 (0.16 to 1.17) | 0.17* (0.03 to 0.99) | 0.60 (0.29 to 1.25) | |||
| Asian: Pakistani | 0.84 (0.46 to 1.55) | 0.87 (0.34 to 2.25) | 1.76* (1.04 to 2.95) | |||
| Asian: Bangladeshi | 0.79 (0.42 to 1.49) | 0.86 (0.53 to 1.39) | 0.78 (0.42 to 1.46) | |||
| Asian: other | 0.97 (0.41 to 2.30) | 1.11 (0.38 to 3.27) | 0.46 (0.16 to 1.34) | |||
| Black: Caribbean | 1.10 (0.45 to 2.70) | 1.04 (0.59 to 1.84) | 0.79 (0.29 to 2.17) | |||
| Black: African | 0.64 (0.33 to 1.23) | 0.96 (0.54 to 1.72) | 0.94 (0.49 to 1.79) | |||
| Black: other | 0.64 (0.36 to 1.11) | 1.17 (0.67 to 2.02) | 0.74 (0.34 to 1.59) | |||
| Other | 0.98 (0.56 to 1.73) | 0.89 (0.36 to 2.21) | 1.04 (0.56 to 1.92) | |||
| Lived in the UKc | ||||||
| ≥ 10 years | 1.16 (0.58 to 2.32) | 1.23 (0.69 to 2.20) | 1.07 (0.57 to 2.01) | |||
| 6–10 years | 1.02 (0.53 to 1.95) | 0.82 (0.49 to 1.38) | 1.29 (0.58 to 2.87) | |||
| < 6 years | 1.37 (0.89 to 2.13) | 1.17 (0.70 to 1.98) | 1.27 (0.62 to 2.58) | |||
| Days since the Olympicsd | 1.00 (1.00 to 1.01) | 1.00 (1.00 to 1.00) | 1.00 (1.00 to 1.01) | |||
| Parental incomee | ||||||
| 1 | 0.86 (0.57 to 1.30) | 0.96 (0.69 to 1.34) | 1.15 (0.76 to 1.75) | |||
| None | 0.66 (0.34 to 1.27) | 0.91 (0.62 to 1.33) | 0.88 (0.49 to 1.60) | |||
| Parents/carers living withf | ||||||
| 1 | 0.97 (0.68 to 1.38) | 0.84 (0.60 to 1.18) | 0.86 (0.54 to 1.39) | |||
| 0 | 1.16 (0.38 to 3.54) | 0.78 (0.19 to 3.11) | 1.62 (0.66 to 3.96) | |||
| Moved neighbourhoodg | 1.39 (0.93 to 2.09) | 1.23 (0.71 to 2.14) | 1.34 (0.64 to 2.79) | |||
| Free school meals | 0.91 (0.66 to 1.26) | 0.92 (0.64 to 1.33) | 1.05 (0.75 to 1.48) | |||
| MSPSS family (tertiles)h | ||||||
| Low tertile | 1.35 (0.93 to 1.97) | 1.70** (1.21 to 2.37) | 2.36*** (1.58 to 3.52) | |||
| Medium tertile | 1.27 (0.87 to 1.84) | 1.01 (0.73 to 1.39) | 1.38 (0.89 to 2.14) | |||
| MSPSS friend (tertiles)i | ||||||
| Low tertile | 0.87 (0.54 to 1.40) | 1.02 (0.72 to 1.44) | 1.02 (0.59 to 1.77) | |||
| Medium tertile | 0.93 (0.63 to 1.36) | 0.99 (0.67 to 1.47) | 0.80 (0.51 to 1.26) | |||
| Bullied | 1.19 (0.86 to 1.64) | 1.84*** (1.34 to 2.53) | 2.53*** (1.69 to 3.78) | |||
| Negative life eventsj | ||||||
| 1 | 1.38 (0.88 to 2.16) | 1.22 (0.87 to 1.73) | 1.88** (1.22 to 2.91) | |||
| 2 | 1.56 (0.89 to 2.72) | 2.03*** (1.37 to 2.99) | 2.24*** (1.56 to 3.21) | |||
| 3+ | 1.69* (1.05 to 2.71) | 2.12** (1.26 to 3.58) | 2.91*** (1.64 to 5.19) | |||
| Long-term illness | 1.53 (0.91 to 2.58) | 1.49 (0.97 to 2.29) | 1.98** (1.26 to 3.09) | |||
Change in depressive symptoms between wave 1 and wave 3
Table 38 shows the changes in SMFQ outcome between wave 1 and wave 3. In the fully adjusted models, compared with adolescents who were not depressed, adolescents who ‘remained depressed’ (RRR 1.93, 95% CI 1.01 to 3.70) were more likely to be from the intervention borough than from the comparison boroughs. ‘Remaining depressed’ was also associated with female gender (RRR 3.98, 95% CI 2.70 to 5.86), low family support (RRR 2.11, 95% CI 1.34 to 3.32), being bullied (RRR 2.55, 95% CI 1.79 to 3.64), experiencing one, two, or three or more life events (RRR 1.78, 95% CI 1.17 to 2.70; RRR 2.42, 95% CI 1.53 to 3.83; RRR 2.82, 95% CI 1.61 to 4.94) and long-term illness (RRR 1.62, 95% CI 1.07 to 2.44), but was less likely for Asian Indian adolescents (RRR 0.39, 95% CI 0.18 to 0.82). The intervention was not associated with ‘becoming depressed’ or becoming ‘no longer depressed’. Becoming ‘no longer depressed’ was associated with living in the UK for less than 6 years (RRR 2.05, 95% CI 1.08 to 3.89), low family support (RRR 1.73, 95% CI 1.23 to 2.42), being bullied (RRR 1.70, 95% CI 1.22 to 2.37), long-term illness (RRR 1.46, 95% CI 1.01 to 2.11) and experiencing two or three or more life events (RRR 1.89, 95% CI 1.26 to 2.83; RRR 2.30, 95% CI 1.28 to 4.14). ’Becoming depressed’ was more likely for females (RRR 2.89, 95% CI 2.06 to 4.06), living in the UK for less than 6 years (RRR 1.75, 95% CI 1.17 to 2.62) and having one or three or more life events (RRR 1.50, 95% CI 1.05 to 2.14; RRR 1.79, 95% CI 1.16 to 2.77), but was less likely for Asian Indian adolescents (RRR 0.42, 95% CI 0.18 to 0.96). No interactions between the intervention and gender or between the intervention and entitlement to free school meals were observed for depressive symptoms (p > 0.05).
| Factor | Change in depressive symptoms, RRR (95% CI) | |||||
|---|---|---|---|---|---|---|
| Became depressed | No longer depressed | Remained depressed | ||||
| Unadjusted | Adjusted | Unadjusted | Adjusted | Unadjusted | Adjusted | |
| Intervention | 1.23 (0.82 to 1.83) | 1.30 (0.97 to 1.76) | 1.53* (1.07 to 2.17) | 1.39 (0.88 to 2.18) | 1.57 (0.83 to 2.95) | 1.93* (1.01 to 3.70) |
| Femalea | 2.89*** (2.06 to 4.06) | 0.93 (0.62 to 1.39) | 3.98*** (2.70 to 5.86) | |||
| Age (months) | 1.03 (0.99 to 1.06) | 0.98 (0.94 to 1.02) | 1.00 (0.95 to 1.04) | |||
| Ethnicityb | ||||||
| White: other | 1.10 (0.59 to 2.04) | 0.71 (0.39 to 1.29) | 0.93 (0.54 to 1.60) | |||
| White mixed | 1.31 (0.82 to 2.12) | 1.10 (0.68 to 1.79) | 0.75 (0.46 to 1.21) | |||
| Asian: Indian | 0.42* (0.18 to 0.96) | 0.33 (0.08 to 1.30) | 0.39* (0.18 to 0.82) | |||
| Asian: Pakistani | 1.23 (0.69 to 2.22) | 1.80 (0.92 to 3.51) | 0.93 (0.38 to 2.28) | |||
| Asian: Bangladeshi | 1.47 (0.90 to 2.39) | 1.00 (0.64 to 1.58) | 0.85 (0.46 to 1.60) | |||
| Asian: other | 0.98 (0.47 to 2.05) | 1.23 (0.41 to 3.71) | 0.47 (0.15 to 1.50) | |||
| Black: Caribbean | 0.86 (0.25 to 3.00) | 0.96 (0.43 to 2.12) | 0.82 (0.32 to 2.15) | |||
| Black: African | 1.04 (0.66 to 1.63) | 1.38 (0.78 to 2.43) | 0.74 (0.35 to 1.55) | |||
| Black: other | 0.72 (0.38 to 1.34) | 1.27 (0.75 to 2.15) | 0.75 (0.33 to 1.75) | |||
| Other | 1.48 (0.83 to 2.61) | 1.02 (0.40 to 2.60) | 1.07 (0.57 to 2.00) | |||
| Lived in the UKc | ||||||
| ≥ 10 years | 1.11 (0.71 to 1.74) | 1.37 (0.68 to 2.78) | 0.93 (0.53 to 1.64) | |||
| 6–10 years | 1.10 (0.65 to 1.85) | 1.14 (0.65 to 2.01) | 0.96 (0.45 to 2.04) | |||
| < 6 years | 1.75** (1.17 to 2.62) | 2.05* (1.08 to 3.89) | 0.70 (0.37 to 1.33) | |||
| Days since the Olympicsd | 1.00** (1.00 to 1.01) | 1.00 (1.00 to 1.00) | 1.00 (1.00 to 1.01) | |||
| Parental incomee | ||||||
| 1 | 0.76 (0.54 to 1.07) | 0.83 (0.63 to 1.10) | 1.26 (0.74 to 2.13) | |||
| None | 0.69 (0.40 to 1.19) | 0.79 (0.48 to 1.29) | 1.01 (0.59 to 1.74) | |||
| Parents/carers living withf | ||||||
| 1 | 1.01 (0.75 to 1.37) | 0.84 (0.56 to 1.28) | 0.88 (0.59 to 1.33) | |||
| 0 | 1.66 (0.61 to 4.48) | 0.58 (0.14 to 2.36) | 2.05 (0.88 to 4.77) | |||
| Moved neighbourhoodg | 1.46 (0.92 to 2.32) | 1.33 (0.87 to 2.03) | 1.27 (0.68 to 2.38) | |||
| Free school meals | 0.96 (0.69 to 1.33) | 1.18 (0.81 to 1.72) | 0.77 (0.59 to 1.01) | |||
| MSPSS family (tertiles)h | ||||||
| Low tertile | 1.23 (0.76 to 1.99) | 1.73** (1.23 to 2.42) | 2.11** (1.34 to 3.32) | |||
| Medium tertile | 1.30 (0.87 to 1.94) | 1.18 (0.77 to 1.80) | 1.15 (0.73 to 1.81) | |||
| MSPSS friend (tertiles)i | ||||||
| Low tertile | 1.14 (0.78 to 1.65) | 1.03 (0.72 to 1.47) | 1.14 (0.67 to 1.94) | |||
| Medium tertile | 1.13 (0.77 to 1.65) | 1.00 (0.66 to 1.53) | 0.88 (0.57 to 1.33) | |||
| Bullied | 1.12 (0.80 to 1.58) | 1.70** (1.22 to 2.37) | 2.55*** (1.79 to 3.64) | |||
| Negative life eventsj | ||||||
| 1 | 1.50* (1.05 to 2.14) | 1.31 (0.81 to 2.13) | 1.78** (1.17 to 2.70) | |||
| 2 | 1.49 (0.85 to 2.63) | 1.89** (1.26 to 2.83) | 2.42*** (1.53 to 3.83) | |||
| 3+ | 1.79* (1.16 to 2.77) | 2.30** (1.28 to 4.14) | 2.82*** (1.61 to 4.94) | |||
| Long-term illness | 0.86 (0.51 to 1.46) | 1.46* (1.01 to 2.11) | 1.62* (1.07 to 2.44) | |||
Change in psychological well-being between wave 1 and wave 2
There was only a small change in well-being scores between the waves (wave 1 to wave 2, µ = –0.02, SE 0.03). Table 39 shows that there intervention had no effect on change in well-being between wave 1 and wave 2. A negative change in well-being between wave 1 and wave 2 was predicted by baseline well-being (β = –0.72, 95% CI –0.78 to –0.66), being female (β = –2.04, 95% CI –3.12 to –0.97), having low or medium family support (β = –1.68, 95% CI –2.79 to –0.58; β = –1.42, 95% CI –2.64 to –0.21) and being bullied (β = –1.15, 95% CI –1.99 to –0.31). A positive change in well-being between wave 1 and wave 2 was predicted by being of Asian Indian (β = 2.61, 95% CI 0.14 to 5.07) or ‘other’ ethnicity (β = 1.31, 95% CI 0.11 to 2.50). In terms of well-being, no interactions were observed between the intervention and gender or between the intervention and entitlement to free school meals (p > 0.05).
| Change in well-being, coef (95% CI) | ||||||
|---|---|---|---|---|---|---|
| Wave 1 to wave 2 | Wave 1 to wave 3 | |||||
| Unadjusted | Adjusted | Adjusted + baseline WEMWBS | Unadjusted | Adjusted | Adjusted + baseline WEMWBS | |
| Intervention | 0.58 (–1.21 to 2.36) | 0.18 (–1.45 to 1.80) | –0.50 (–1.86 to 0.85) | 1.23 (–0.74 to 3.20) | 0.52 (–0.95 to 1.99) | –0.07 (–1.59 to 1.44) |
| WEMWBS baseline | n/a | –0.72*** (–0.78 to –0.66) | n/a | –0.71*** (–0.77 to –0.64) | ||
| Femalea | –1.15** (–1.94 to –0.35) | –2.04*** (–3.12 to –0.97) | –2.81*** (–3.73 to –1.89) | –3.65*** (–4.72 to –2.58) | ||
| Age (months) | 0.02 (–0.12 to 0.17) | 0.04 (–0.08 to 0.16) | –0.10 (–0.25 to 0.05) | –0.06 (–0.18 to 0.05) | ||
| Ethnicityb | ||||||
| White: other | 0.64 (–1.02 to 2.30) | 1.15 (–0.61 to 2.91) | 0.31 (–1.28 to 1.91) | 0.73 (–0.80 to 2.26) | ||
| White mixed | 1.06 (–1.04 to 3.15) | 1.06 (–0.65 to 2.77) | 1.14 (–1.71 to 3.98) | 1.11 (–1.17 to 3.38) | ||
| Asian: Indian | 1.49 (–1.22 to 4.20) | 2.61* (0.14 to 5.07) | 3.28** (1.27 to 5.29) | 4.23*** (2.60 to 5.87) | ||
| Asian: Pakistani | –0.17 (–1.77 to 1.43) | –0.61 (–2.03 to 0.82) | 0.82 (–1.02 to 2.65) | 0.29 (–1.57 to 2.15) | ||
| Asian: Bangladeshi | –0.07 (–1.74 to 1.61) | –0.18 (–1.86 to 1.50) | 1.02 (–1.11 to 3.15) | 0.92 (–1.04 to 2.88) | ||
| Asian: other | 1.90 (–1.21 to 5.00) | 0.67 (–1.65 to 2.99) | 0.97 (–2.69 to 4.64) | –0.19 (–3.09 to 2.71) | ||
| Black: Caribbean | –0.77 (–4.22 to 2.68) | 0.53 (–2.52 to 3.58) | –2.46 (–5.59 to 0.67) | –1.20 (–4.42 to 2.01) | ||
| Black: African | 1.65 (–0.55 to 3.85) | 1.94 (–0.12 to 4.00) | 2.09* (0.31 to 3.87) | 2.29** (0.71 to 3.88) | ||
| Black: other | 1.22 (–0.93 to 3.36) | 1.61 (–0.31 to 3.52) | 1.62 (–0.09 to 3.33) | 1.98* (0.41 to 3.54) | ||
| Other | 1.20 (–0.07 to 2.48) | 1.31* (0.11 to 2.50) | 0.20 (–1.44 to 1.85) | 0.25 (–1.13 to 1.63) | ||
| Lived in the UKc | ||||||
| ≥ 10 years | 1.50 (–0.06 to 3.06) | 0.81 (–0.93 to 2.54) | 2.21** (0.61 to 3.82) | 1.56 (–0.47 to 3.58) | ||
| 6–10 years | 0.28 (–2.01 to 2.57) | 0.75 (–1.18 to 2.68) | –0.22 (–1.63 to 1.18) | 0.16 (–1.12 to 1.43) | ||
| < 6 years | 0.76 (–1.30 to 2.82) | 0.23 (–1.34 to 1.79) | 1.19 (–0.71 to 3.09) | 0.67 (–0.67 to 2.01) | ||
| Days since the Olympicsd | –0.01 (–0.03 to 0.01) | –0.01 (–0.02 to 0.01) | –0.01 (–0.02 to 0.00) | 0.00 (–0.02 to 0.01) | ||
| Parental incomee | ||||||
| 1 | 0.52 (–0.45 to 1.49) | 0.24 (–0.44 to 0.93) | 0.17 (–1.11 to 1.44) | –0.09 (–1.08 to 0.90) | ||
| None | –1.07 (–3.05 to 0.91) | –0.73 (–2.25 to 0.80) | –0.45 (–2.59 to 1.68) | –0.02 (–1.57 to 1.52) | ||
| Parents/carers living withf | ||||||
| 1 | –0.98 (–2.04 to 0.07) | –0.81 (–1.80 to 0.17) | –0.65 (–1.80 to 0.50) | –0.47 (–1.41 to 0.48) | ||
| 0 | 2.37 (–1.76 to 6.51) | 0.80 (–1.78 to 3.38) | –0.89 (–5.81 to 4.03) | –2.43 (–5.50 to 0.63) | ||
| Moved neighbourhoodg | –0.33 (–2.35 to 1.69) | –0.69 (–2.20 to 0.83) | –0.62 (–2.41 to 1.17) | –0.92 (–2.59 to 0.76) | ||
| Free school meals | 0.55 (–0.73 to 1.84) | 0.22 (–0.79 to 1.24) | 0.98 (–0.38 to 2.34) | 0.66 (–0.54 to 1.86) | ||
| MSPSS family (tertiles)h | ||||||
| Low tertile | 1.15 (–0.15 to 2.45) | –1.68** (–2.79 to –0.58) | 1.44* (0.28 to 2.60) | –1.33** (–2.22 to –0.45) | ||
| Medium tertile | 0.07 (–1.47 to 1.62) | –1.42* (–2.64 to –0.21) | 0.43 (–0.90 to 1.75) | –1.04 (–2.12 to 0.03) | ||
| MSPSS friend (tertiles)i | ||||||
| Low tertile | 1.42* (0.20 to 2.65) | 0.09 (–0.89 to 1.07) | 1.20 (0.00 to 2.40) | –0.14 (–1.29 to 1.01) | ||
| Medium tertile | 0.79 (–0.58 to 2.16) | 0.51 (–0.66 to 1.68) | –0.25 (–1.61 to 1.12) | –0.54 (–1.82 to 0.74) | ||
| Bullied | –0.64 (–1.54 to 0.25) | –1.15** (–1.99 to –0.31) | –0.66 (–1.65 to 0.33) | –1.15* (–2.03 to –0.27) | ||
| Negative life eventsj | ||||||
| 1 | –0.24 (–1.41 to 0.93) | –0.39 (–1.38 to 0.61) | –0.29 (–1.48 to 0.91) | –0.43 (–1.43 to 0.57) | ||
| 2 | 1.14 (–0.43 to 2.71) | 0.37 (–0.96 to 1.70) | –0.29 (–1.61 to 1.04) | –1.09 (–2.36 to 0.18) | ||
| 3+ | 0.76 (–0.53 to 2.06) | –0.62 (–1.93 to 0.68) | 1.02 (–0.08 to 2.12) | –0.40 (–1.55 to 0.75) | ||
| Long-term illness | 0.39 (–1.66 to 2.43) | –0.98 (–2.44 to 0.48) | 0.97 (–1.13 to 3.06) | –0.38 (–1.88 to 1.12) | ||
Change in levels of well-being between wave 1 and wave 3
There was only a small change in well-being scores between the waves (wave 1 and wave 3, µ = –0.04, SE 0.04). Table 39 shows that there the intervention had no effect on change in well-being between wave 1 and wave 3. A negative change in well-being between wave 1 and wave 3 was predicted by baseline well-being (β = –0.71, 95% CI –0.77 to –0.64), being female (β = –3.65, 95% CI –4.72 to –2.58), having low family support (β = –1.33, 95% CI –2.22 to –0.45) and being bullied (β = –1.15, 95% CI –2.03 to –0.27). A positive change in well-being between wave 1 and wave 3 was predicted by being of Asian Indian (β = 4.23, 95% CI 2.60 to 5.87), black African (β = 2.29, 95% CI 0.71 to 3.88) or black other ethnicity (β = 1.98, 95% CI 0.41 to 3.54). In terms of well-being, no interactions were observed between the intervention and gender or between the intervention and free school meals (p > 0.05).
Summary
The adolescent study suggests that the urban regeneration associated with the London 2012 Olympic Games had little positive effect on mental health in terms of depressive symptoms or levels of well-being. Although urban regeneration was associated with becoming ‘no longer depressed’ in the shorter term (6-months post regeneration), this was the only positive impact observed. This positive effect was not sustained at 18 months post regeneration. Urban regeneration may actually have maintained depressive symptoms. Our hypotheses that adolescents living in areas that are receiving urban regeneration would have greater positive change in well-being and better mental health post regeneration than adolescents receiving less or no urban regeneration were refuted.
Impacts on parental psychological health and well-being
In this section we explore parental psychological health and well-being measures on an outcome-by-outcome basis. We analyse three waves of cross-sectional data to describe changes in the strength and magnitude of association with our outcomes over time. Future analyses will extend the current descriptive approach.
Methods
Primary outcomes
Parental well-being
Parents/carers also completed the WEMWBS (see Adolescent well-being). For these analyses, low levels of well-being were defined as a score less than one standard deviation (SD) below the mean and high levels of well-being were defined as a score of more than one SD above the mean. 87 Those scoring within one SD of the mean were defined as having average levels of well-being.
Parental anxiety and depressive symptoms
Parents/carers completed the HADS. The scale can be split into two subscales (anxiety and depression), with scores ranging from 0 to 21. These subscales can be dichotomised using the cut off of scores that are ≥ 8 to represent anxiety or depression. 88 For these analyses we have used the dichotomised scales.
Sociodemographic, neighbourhood and discrimination covariates
A range of sociodemographic, neighbourhood and discrimination factors that might influence mental health were identified a priori from the literature. We investigated whether or not these factors were associated with parental/carer well-being, anxiety symptoms and depressive symptoms.
The following demographic factors were included: age (years); gender; ethnicity (assessed using an 11-category variable based on the 2011 UK Census); highest educational qualification; current employment status; highest NS-SEC in the household; marital status; home ownership; receipt of any benefit(s); born in the UK; and long-term illness.
The following accommodation and neighbourhood factors were included: access to a garden; satisfaction with accommodation; frequency of visits to green spaces; self-reports of damp, vibrations, dust and mould in the house; and the following scales from the MESA measure – neighbourhood aesthetics, neighbourhood safety, neighbourhood social cohesion and neighbourhood violence. 62
The following discrimination measures were included:64 insulted because of ethnicity in the past 12 months; ever refused a job as a result of discrimination; and ever treated unfairly at work because of ethnicity. See Table 40 for further details of these measures.
Missingness and multiple imputation models
Prevalence and missing data rates for the outcomes and covariates were examined: missing values ranged from 0.0% to 36.5%. We found no evidence against the assumption that data were MAR. 83 We imputed the data separately for each wave using multiple imputation by chained equations using the Stata ice package. We used 50 cycles of the imputation algorithm producing 25 data sets for wave 1, 35 for wave 2 and 40 for wave 3. The number of data sets produced for each wave was chosen to be greater than the variable with the largest percentage of missing data. The imputation model was chosen to be congenial86 with the most saturated model of interest.
Analysis
Cross-sectional univariate and multivariate logistic regression models were run to assess the impact of regeneration on rates of parental/carer mental health. The models were run in several stages to assess the effect of the intervention on parental mental health:
-
Model 1 – univariate regression analyses examined the initial associations between the intervention, sociodemographic, neighbourhood and discrimination factors with each outcome.
-
Model 2 – multivariate regression analyses simultaneously adjusted for all factors that were significantly associated (p ≤ 0.05) with the outcome in model 1, with the exception of the multiple poverty score.
-
Model 3 – model 2, with additional adjustment for the multiple poverty score.
Interactions between intervention and gender were examined in model 2. If the interaction was significant (p ≤ 0.05), models 1 and 2 were re-run stratified by gender.
Three sets of cross-sectional models were run examining each outcome separately at wave 1, wave 2 and wave 3.
Results
Descriptive analysis of parent mental health and well-being (waves 1, 2 and 3)
In total, 1233 parents/carers completed the survey at wave 1, 1023 at wave 2 and 995 at wave 3. Table 40 shows the prevalence of the outcomes and covariates at each wave. At each wave, approximately one-third of the sample was from the intervention borough of Newham. In total, 74% of the sample at each wave was female. The sample was drawn from a range of ethnic groups at each wave. At waves 1 and 2, 42% of the participants were in employment, compared with 49% at wave 3. Over half the sample at each wave reported receiving benefits.
| Variable | Wave | |||||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | ||||
| n (%) | Missing (%) | n (%) | Missing (%) | n (%) | Missing (%) | |
| Intervention | ||||||
| Intervention | 1233 | 0.00 | 1023 | 0.00 | 995 | 0.00 |
| Comparison group | 845 (68.53) | 658 (64.32) | 652 (65.53) | |||
| Newham | 388 (31.47) | 365 (35.68) | 343 (34.47) | |||
| Outcome | ||||||
| HADS anxiety | 1233 | 0.00 | 1019 | 0.39 | 995 | 0.00 |
| No anxiety | 786 (63.75) | 786 (77.13) | 676 (67.94) | |||
| Anxiety (≥ 8) | 447 (36.25) | 233 (22.87) | 319 (32.06) | |||
| Cronbach’s α | 0.67 | 0.68 | 0.66 | |||
| HADS depression | 1233 | 0.00 | 1019 | 0.39 | 995 | 0.00 |
| Not depressed | 959 (77.78) | 846 (83.02) | 778 (78.19) | |||
| Depressed (≥ 8) | 274 (22.22) | 173 (16.98) | 217 (21.81) | |||
| Cronbach’s α | 0.49 | 0.53 | 0.44 | |||
| WEMWBS | 1233 | 0.00 | 1019 | 0.39 | 995 | 0.00 |
| Below 1 SD from mean | 199 (16.14) | 166 (16.29) | 132 (13.27) | |||
| Within 1 SD of mean | 807 (65.45) | 671 (65.85) | 728 (73.17) | |||
| Above 1 SD from mean | 227 (18.41) | 182 (17.86) | 135 (13.57) | |||
| Cronbach’s α | 0.92 | 0.94 | 0.91 | |||
| Demographic | ||||||
| Age | 1058 | 14.19 | 703 | 31.28 | 632 | 36.48 |
| Mean age in years (SD) | 40.17 (8.10) | 41.69 (7.98) | 42.12 (7.96) | |||
| Gender | 1233 | 0.00 | 1021 | 0.20 | 995 | 0.00 |
| Male | 332 (26.93) | 264 (25.86) | 257 (25.83) | |||
| Female | 901 (74.07) | 757 (74.14) | 738 (74.17) | |||
| Ethnicity | 1226 | 0.57 | 990 | 3.23 | 871 | 12.46 |
| White | 285 (23.25) | 216 (21.82) | 199 (22.85) | |||
| Asian: Indian | 55 (4.49) | 47 (4.75) | 43 (4.94) | |||
| Asian: Pakistani | 64 (5.22) | 55 (5.56) | 47 (5.40) | |||
| Asian: Bangladeshi | 269 (21.94) | 247 (24.95) | 197 (22.62) | |||
| Black: Caribbean | 70 (5.71) | 46 (4.65) | 49 (5.63) | |||
| Black: African | 211 (17.21) | 179 (18.08) | 140 (16.07) | |||
| Other | 272 (22.19) | 200 (20.20) | 196 (22.50) | |||
| Top education | 1233 | 0.00 | 1003 | 1.96 | 982 | 1.31 |
| NVQ 1/2 | 329 (26.68) | 229 (22.83) | 196 (19.96) | |||
| NVQ 3 | 106 (8.60) | 79 (7.88) | 98 (9.98) | |||
| NVQ 4/5 | 232 (18.82) | 166 (16.55) | 174 (17.72) | |||
| Other | 287 (23.28) | 243 (24.23) | 230 (23.42) | |||
| None | 279 (22.63) | 286 (28.51) | 284 (28.92) | |||
| Employment | 1233 | 0.00 | 1019 | 0.39 | 995 | 0.00 |
| Yes | 518 (42.01) | 427 (41.90) | 486 (48.84) | |||
| No | 715 (57.99) | 592 (58.10) | 509 (51.16) | |||
| Household NS-SEC | 1219 | 1.15 | 850 | 16.91 | 700 | 29.65 |
| Not applicable | 426 (34.95) | 372 (43.76) | 403 (57.57) | |||
| Higher managerial | 232 (19.03) | 128 (15.06) | 69 (9.86) | |||
| Intermediate | 97 (7.96) | 67 (7.88) | 47 (6.71) | |||
| Semiroutine, etc. | 464 (38.06) | 283 (33.29) | 181 (25.86) | |||
| Marital status | 1233 | 0.00 | 1023 | 0.00 | 995 | 0.00 |
| Never married/no civil partnership | 272 (22.06) | 195 (19.06) | 170 (17.09) | |||
| Married/civil partnership | 794 (64.40) | 671 (65.59) | 666 (66.93) | |||
| Divorced, separated, widowed | 167 (13.54) | 157 (15.35) | 159 (15.98) | |||
| Home ownership | 1233 | 0.00 | 1007 | 1.56 | 992 | 0.30 |
| Owned/mortgaged | 288 (23.36) | 252 (25.02) | 226 (22.78) | |||
| Social rent | 660 (53.53) | 611 (60.68) | 578 (58.27) | |||
| Private rent | 251 (20.36) | 134 (13.31) | 173 (17.44) | |||
| Other | 34 (2.76) | 10 (0.99) | 15 (1.51) | |||
| Benefitsa | 1233 | 0.00 | 860 | 15.93 | 923 | 7.24 |
| Yes | 673 (54.58) | 521 (60.58) | 579 (62.73) | |||
| No | 560 (45.42) | 339 (39.42) | 344 (37.27) | |||
| Born in the UK | 1233 | 0.00 | 1023 | 0.00 | 995 | 0.00 |
| Yes | 431 (34.96) | 199 (19.45) | 173 (17.39) | |||
| No | 802 (65.04) | 824 (80.55) | 822 (82.61) | |||
| Multiple poverty score26 | 1233 | 0.00 | 858 | 16.13 | 923 | 7.24 |
| 0 | 172 (13.95) | 125 (14.57) | 124 (13.43) | |||
| 1 | 287 (23.28) | 219 (25.52) | 168 (18.20) | |||
| 2 | 359 (29.12) | 276 (32.17) | 271 (29.36) | |||
| 3 | 313 (25.39) | 196 (22.84) | 271 (29.36) | |||
| 4 | 102 (8.27) | 42 (4.90) | 89 (9.64) | |||
| Long-term illness | 1199 | 2.76 | 1023 | 0.00 | 995 | 0.00 |
| Yes | 448 (37.36) | 364 (35.58) | 363 (36.48) | |||
| No | 751 (62.64) | 659 (64.42) | 632 (63.52) | |||
| Accommodation and neighbourhood | ||||||
| Access to garden | 1233 | 0.0 | 1016 | 0.68 | 828 | 16.78 |
| Yes | 815 (66.10) | 677 (66.63) | 548 (66.18) | |||
| No | 418 (33.90) | 339 (33.37) | 280 (33.82) | |||
| Accommodation satisfaction | 1233 | 0.00 | 1021 | 0.20 | 995 | 0.00 |
| Very/fairly/neither satisfied nor dissatisfied | 1031 (83.62) | 853 (83.55) | 830 (83.42) | |||
| Slightly/very dissatisfied | 202 (16.38) | 168 (16.45) | 165 (16.58) | |||
| How often do you visit green spaces? | 1233 | 0.00 | 1021 | 0.20 | 995 | 0.00 |
| Weekly | 540 (43.80) | 408 (39.96) | 524 (52.66) | |||
| Once a fortnight or month | 343 (27.82) | 270 (26.44) | 216 (21.71) | |||
| Several times a year/never | 350 (28.39) | 343 (33.59) | 255 (25.63) | |||
| Neighbourhood aesthetics | 1214 | 1.54 | 1005 | 1.76 | 972 | 2.31 |
| Mean (SD) | 2.66 (0.81) | 2.71 (0.76) | 2.72 (0.73) | |||
| Cronbach’s α | 0.71 | 0.73 | 0.72 | |||
| Neighbourhood safety | 1208 | 2.03 | 1011 | 1.17 | 979 | 1.61 |
| Mean (SD) | 2.78 (1.09) | 2.74 (0.98) | 2.61 (0.90) | |||
| Cronbach’s α | 0.80 | 0.81 | 0.80 | |||
| Neighbourhood social cohesion | 1155 | 6.33 | 903 | 11.73 | 923 | 7.24 |
| Mean (SD) | 2.34 (0.96) | 2.36 (0.81) | 2.35 (0.76) | |||
| Cronbach’s α | 0.89 | 0.87 | 0.85 | |||
| Neighbourhood violence | 1009 | 18.2 | 784 | 23.36 | 854 | 14.17 |
| Mean (SD) | 3.39 (0.80) | 3.49 (0.73) | 3.42 (0.69) | |||
| Cronbach’s α | 0.84 | 0.83 | 0.80 | |||
| Damp in house | 1233 | 0.00 | 1016 | 0.68 | 995 | 0.00 |
| Yes | 268 (21.74) | 272 (26.77) | 311 (31.26) | |||
| No | 965 (78.26) | 744 (73.23) | 684 (68.74) | |||
| Vibrations in house | 1233 | 0.00 | 1016 | 0.68 | 995 | 0.00 |
| Yes | 42 (3.41) | 23 (2.26) | 38 (3.82) | |||
| No | 1191 (96.59) | 993 (97.74) | 957 (96.18) | |||
| Dust in house | 1233 | 0.00 | 1016 | 0.68 | 995 | 0.00 |
| Yes | 85 (6.89) | 53 (5.22) | 112 (11.26) | |||
| No | 1148 (93.11) | 963 (94.78) | 883 (88.74) | |||
| Mould in house | 1233 | 0.00 | 1016 | 0.68 | 995 | 0.00 |
| Yes | 194 (15.73) | 183 (18.01) | 206 (20.70) | |||
| No | 1039 (84.27) | 833 (81.99) | 789 (79.30) | |||
| Discrimination | ||||||
| Insulted because of to ethnicity | 1233 | 0.00 | ||||
| Yes | 63 (5.11) | |||||
| No | 1170 (94.89) | |||||
| Refused job as a result of discrimination | 1233 | 0.00 | ||||
| Yes | 42 (3.41) | |||||
| No | 1191 (96.59) | |||||
| Treated unfairly at work because of ethnicity | 1233 | 0.00 | ||||
| Yes | 32 (2.60) | |||||
| No | 662 (53.69) | |||||
| Not applicable | 539 (43.71) | |||||
Rates of anxiety symptoms varied across the waves. One-third of the sample reported anxiety at wave 1 (36.25%) and wave 3 (32.06%), with only one-fifth reporting anxiety at wave 2 (22.87%). One-fifth of the sample reported depression at wave 1 (22.22%) and wave 3 (21.81%), with one-sixth reporting depression at wave 2 (16.98%). The prevalence of low levels of well-being was similar at waves 1 and 2 (16.14% and 16.29%, respectively) but were slightly lower at wave 3 (13.27%). High levels of well-being were seen to be similar at wave 1 and wave 2 (18.41% and 17.86%, respectively), but were slightly lower at wave 3 (13.57%).
Associations between the intervention and parental well-being
Table 41 shows the association of living in the intervention borough of Newham with well-being at each wave. At wave 1, participants living in Newham were more likely to report higher levels of well-being than participants living in the comparison area (RRR 2.31, 95% CI 1.70 to 3.13). However, at wave 3 participants living in Newham were less likely to report higher levels of well-being than participants living in the comparison area (RRR 0.51, 95% CI 0.33 to 0.79). Levels of low well-being did not differ between the intervention and the comparison areas at any wave.
| Wave | Borough | WEMWBS, RRR (95% CI) | |
|---|---|---|---|
| Below 1 SD from mean | Above 1 SD from mean | ||
| Wave 1 intervention | Newham | 1.14 (0.81 to 1.6) | 2.31*** (1.70 to 3.13) |
| Wave 2 intervention | Newham | 0.83 (0.58 to 1.2) | 0.94 (0.67 to 1.32) |
| Wave 3 intervention | Newham | 0.86 (0.58 to 1.27) | 0.51** (0.33 to 0.79) |
Well-being at wave 1
Associations between sociodemographic and neighbourhood factors with well-being at wave 1 are reported in Table 42. In univariate analyses low levels of well-being was associated with increasing age, having no formal educational qualifications, unemployment, being either single (never married), widowed, divorced or separated, living in social rented accommodation and being on benefits. Long-term illness and an increasing score on the multiple poverty score were also associated with lower levels of well-being (Table 42). Black African ethnicity was associated with reduced risk of low levels of well-being.
| Variable | WEMWBS RRR (95% CI) | |
|---|---|---|
| Below 1 SD from mean | Above 1 SD from mean | |
| Age | 1.04*** (1.02 to 1.06) | 1.01 (0.99 to 1.03) |
| Gendera | ||
| Female | 1.09 (0.76 to 1.57) | 0.69* 0.5 to 0.95 |
| Ethnicityb | ||
| Asian: Indian | 0.59 (0.22 to 1.60) | 2.87** (1.49 to 5.53) |
| Asian: Pakistani | 0.91 (0.44 to 1.89) | 0.88 (0.40 to 1.94) |
| Asian: Bangladeshi | 0.82 (0.52 to 1.29) | 0.96 (0.60 to 1.53) |
| Black: Caribbean | 0.96 (0.48 to 1.95) | 1.36 (0.69 to 2.70) |
| Black: African | 0.47** (0.26 to 0.83) | 1.71* (1.09 to 2.69) |
| Other | 1.13 (0.73 to 1.73) | 1.10 (0.69 to 1.75) |
| Top educationc | ||
| NVQ 3 | 0.91 (0.46 to 1.79) | 0.80 (0.44 to 1.44) |
| NVQ 4/5 | 0.91 (0.53 to 1.56) | 1.49 (0.99 to 2.24) |
| Other | 1.21 (0.76 to 1.94) | 1.03 (0.69 to 1.56) |
| None | 2.36*** (1.54 to 3.61) | 0.64 (0.40 to 1.03) |
| Employmentd | ||
| No | 1.83*** (1.31 to 2.57) | 0.76 (0.57 to 1.02) |
| Household NS-SECe | ||
| Intermediate | 0.81 (0.35 to 1.84) | 0.35** (0.17 to 0.72) |
| Semiroutine, etc. | 1.61 (0.96 to 2.70) | 0.69 (0.47 to 1.02) |
| Marital statusf | ||
| Never married/CP | 1.53* (1.05 to 2.22) | 1.04 (0.72 to 1.48) |
| Separated, divorced, widowed | 1.80** (1.18 to 2.73) | 0.52* (0.30 to 0.89) |
| Home ownershipg | ||
| Social rent | 1.69* (1.11 to 2.56) | 0.79 (0.55 to 1.12) |
| Private rent | 1.14 (0.68 to 1.92) | 0.90 (0.59 to 1.39) |
| Other | 1.03 (0.33 to 3.17) | 1.13 (0.48 to 2.66) |
| Benefitsh,i | ||
| Yes | 1.49* (1.08 to 2.05) | 0.87 (0.65 to 1.17) |
| Born in the UKd | ||
| No | 0.82 (0.59 to 1.12) | 1.07 (0.78 to 1.46) |
| Multiple poverty scorej | ||
| 1 | 2.15* (1.05 to 4.39) | 1.27 (0.79 to 2.04) |
| 2 | 2.84** (1.43 to 5.61) | 1.23 (0.78 to 1.95) |
| 3 | 4.06*** (2.07 to 7.98) | 0.91 (0.56 to 1.50) |
| 4 | 4.75*** (2.23 to 10.14) | 0.33* (0.13 to 0.82) |
| Long-term illnessh | ||
| Yes | 2.65*** (1.92 to 3.66) | 0.61** (0.43 to 0.85) |
| Access to gardend | ||
| No | 1.07 (0.78 to 1.49) | 1.02 (0.74 to 1.39) |
| Accommodation satisfactionk | ||
| Slightly/very dissatisfied | 1.58* (1.09 to 2.30) | 0.58* (0.36 to 0.92) |
| How often do you visit green spaces?l | ||
| Once a fortnight or month | 0.79 (0.54 to 1.17) | 0.62* (0.43 to 0.91) |
| Several times a year/never | 1.05 (0.73 to 1.52) | 0.88 (0.62 to 1.25) |
| Neighbourhood aesthetics | ||
| Higher score = worse | 1.42*** (1.17 to 1.72) | 0.69*** (0.57 to 0.84) |
| Neighbourhood safety | ||
| Higher score = worse | 1.24** (1.07 to 1.44) | 0.62*** (0.53 to 0.72) |
| Neighbourhood social cohesion | ||
| Higher score = worse | 1.31*** (1.12 to 1.54) | 0.61*** (0.51 to 0.73) |
| Neighbourhood violence | ||
| Lower score = worse | 0.64*** (0.53 to 0.77) | 1.23 (0.99 to 1.54) |
| Insulted because of ethnicityh | ||
| Yes | 0.96 (0.47 to 1.96) | 0.93 (0.47 to 1.83) |
| Refused job because of discriminationh | ||
| Yes | 1.17 (0.52 to 2.60) | 0.76 (0.31 to 1.85) |
| Treated unfairly at work owing to ethnicityh | ||
| Yes | 1.45 (0.53 to 3.99) | 1.47 (0.63 to 3.44) |
| Damp in househ | ||
| Yes | 1.56* (1.10 to 2.20) | 0.61* (0.41 to 0.92) |
| Vibrations in househ | ||
| Yes | 1.32 (0.61 to 2.84) | 0.63 (0.24 to 1.64) |
| Dust in househ | ||
| Yes | 2.09** (1.26 to 3.46) | 0.53 (0.25 to 1.13) |
| Mould in househ | ||
| Yes | 1.59* (1.08 to 2.35) | 0.79 (0.51 to 1.23) |
Low levels of well-being were also related to poor neighbourhood conditions, unsafe neighbourhoods, low levels of neighbourhood social cohesion, violence in the neighbourhood and being slightly or very dissatisfied with accommodation at wave 1 (see Table 42). In terms of housing conditions, damp, dust and mould were associated with lower levels of well-being.
High levels of well-being at wave 1 were associated with being male and being of Indian or black African ethnicity (see Table 42). In households with intermediate or semi-routine NS-SEC occupations, higher levels of well-being were less likely than average well-being to be associated with being widowed, divorced and separated and having a long-term illness. Poor neighbourhood conditions, unsafe neighbourhoods, low levels of neighbourhood social cohesion and being slightly or very dissatisfied with accommodation at wave 1 was associated with a reduced risk of high levels of well-being. Visiting green space once a fortnight or once a month compared with visiting weekly was associated with a lower likelihood of high levels of well-being relative to the average well-being. Having damp in the house was also associated with a lower likelihood of high levels of well-being.
Table 43 shows the multivariate associations between sociodemographic and neighbourhood factors with parental carer well-being at wave 1. Low levels of well-being were associated with age, having no formal educational qualifications, a multiple poverty score of 3 or greater and having a long-term illness in analyses mutually adjusted for age, gender, ethnicity, no formal educational qualifications, employment, household NS-SEC, marital status, home ownership, receipt of benefits and long-term illness (see Table 43). Adjustment for the multiple poverty score made very little change to the associations. In adjusted analyses, only neighbourhood violence was associated with increased risk of low levels of well-being, which was not influenced by further adjustment for multiple poverty score at wave 1.
| Variable | WEMWBS, RRR (95% CI) | |||
|---|---|---|---|---|
| Below 1 SD from mean | Above 1 SD from mean | Below 1 SD from mean | Above 1 SD from mean | |
| Intervention | ||||
| Newham | 1.41 (0.95 to 2.08) | 2.07*** (1.47 to 2.9) | 1.23 (0.82 to 1.84) | 2.23*** (1.55 to 3.2) |
| Age | 1.03* (1 to 1.05) | 1 (0.98 to 1.03) | 1.03* (1 to 1.05) | 1 (0.98 to 1.03) |
| Gendera | ||||
| Female | 1 (0.65 to 1.55) | 0.83 (0.57 to 1.21) | 0.95 (0.61 to 1.48) | 0.87 (0.6 to 1.27) |
| Ethnicityb | ||||
| Asian: Indian | 0.74 (0.25 to 2.19) | 2.7** (1.26 to 5.75) | 0.72 (0.24 to 2.14) | 2.65* (1.24 to 5.68) |
| Asian: Pakistani | 1.54 (0.66 to 3.61) | 0.65 (0.27 to 1.54) | 1.39 (0.59 to 3.31) | 0.66 (0.28 to 1.59) |
| Asian: Bangladeshi | 0.87 (0.5 to 1.53) | 0.9 (0.52 to 1.58) | 0.77 (0.44 to 1.37) | 0.96 (0.54 to 1.69) |
| Black: Caribbean | 1.28 (0.58 to 2.81) | 1.33 (0.63 to 2.8) | 1.2 (0.55 to 2.65) | 1.39 (0.66 to 2.95) |
| Black: African | 0.62 (0.32 to 1.18) | 1.34 (0.8 to 2.27) | 0.56 (0.29 to 1.07) | 1.42 (0.83 to 2.41) |
| Other | 1.31 (0.77 to 2.22) | 0.98 (0.57 to 1.7) | 1.23 (0.72 to 2.1) | 1.03 (0.59 to 1.8) |
| Top educationc | ||||
| NVQ 3 | 0.93 (0.45 to 1.92) | 0.74 (0.39 to 1.41) | 0.95 (0.46 to 1.98) | 0.71 (0.37 to 1.35) |
| NVQ 4/5 | 1.38 (0.73 to 2.63) | 1.16 (0.7 to 1.91) | 1.49 (0.78 to 2.85) | 1.11 (0.67 to 1.84) |
| Other | 1.51 (0.87 to 2.64) | 0.88 (0.54 to 1.43) | 1.54 (0.88 to 2.7) | 0.85 (0.52 to 1.39) |
| None | 2.87*** (1.73 to 4.77) | 0.62 (0.36 to 1.05) | 2.95*** (1.76 to 4.93) | 0.6 (0.35 to 1.03) |
| Employmentd | ||||
| No | 1.13 (0.69 to 1.83) | 0.64 (0.41 to 1.01) | 1.15 (0.7 to 1.86) | 0.63 (0.4 to 1) |
| Household NS-SECe | ||||
| Intermediate | 0.91 (0.37 to 2.21) | 0.44* (0.2 to 0.96) | 0.81 (0.33 to 1.97) | 0.45* (0.21 to 0.98) |
| Semiroutine, etc. | 1.54 (0.83 to 2.86) | 0.96 (0.59 to 1.57) | 1.34 (0.72 to 2.52) | 1.01 (0.61 to 1.67) |
| Marital statusf | ||||
| Never married/CP | 1.28 (0.80 to 2.04) | 1.03 (0.66 to 1.6) | 1.19 (0.74 to 1.92) | 1.08 (0.69 to 1.69) |
| Separated, divorced, widowed | 1.45 (0.88 to 2.39) | 0.54* (0.3 to 0.98) | 1.38 (0.84 to 2.29) | 0.55* (0.3 to 1) |
| Home ownershipg | ||||
| Social rent | 0.98 (0.59 to 1.63) | 1.11 (0.71 to 1.71) | 0.82 (0.48 to 1.39) | 1.19 (0.76 to 1.88) |
| Private rent | 0.89 (0.48 to 1.65) | 0.92 (0.56 to 1.53) | 0.75 (0.4 to 1.4) | 0.97 (0.58 to 1.62) |
| Other | 0.7 (0.21 to 2.37) | 1.29 (0.52 to 3.25) | 0.63 (0.18 to 2.17) | 1.38 (0.55 to 3.5) |
| Long-term illnessh | ||||
| Yes | 1.92*** (1.32 to 2.79) | 0.68* (0.46 to 0.99) | 1.76** (1.2 to 2.58) | 0.74 (0.5 to 1.09) |
| Accommodation satisfactioni | ||||
| Slightly/very dissatisfied | 1.01 (0.63 to 1.62) | 0.89 (0.53 to 1.52) | 1.01 (0.63 to 1.63) | 0.9 (0.53 to 1.53) |
| How often do you visit green spaces?j | ||||
| Once a fortnight or month | 0.94 (0.61 to 1.43) | 0.7 (0.47 to 1.05) | 0.96 (0.63 to 1.47) | 0.72 (0.48 to 1.08) |
| Several times a year/never | 1.06 (0.71 to 1.6) | 1.04 (0.71 to 1.52) | 1.12 (0.74 to 1.7) | 1.01 (0.68 to 1.48) |
| Neighbourhood aesthetics | ||||
| Higher score = worse | 1.17 (0.92 to 1.49) | 0.98 (0.78 to 1.24) | 1.15 (0.9 to 1.47) | 0.98 (0.77 to 1.24) |
| Neighbourhood safety | ||||
| Higher score = worse | 0.97 (0.79 to 1.18) | 0.7*** (0.57 to 0.85) | 0.95 (0.78 to 1.16) | 0.7*** (0.58 to 0.86) |
| Neighbourhood social cohesion | ||||
| Higher score = worse | 1.14 (0.92 to 1.41) | 0.81 (0.63 to 1.02) | 1.15 (0.93 to 1.43) | 0.79 (0.62 to 1.01) |
| Neighbourhood violence | ||||
| Lower score = worse | 0.64*** (0.49 to 0.83) | 0.98 (0.76 to 1.27) | 0.64*** (0.49 to 0.83) | 0.96 (0.75 to 1.25) |
| Damp in househ | ||||
| Yes | 1.23 (0.78 to 1.94) | 0.81 (0.5 to 1.31) | 1.18 (0.75 to 1.87) | 0.84 (0.52 to 1.37) |
| Dust in househ | ||||
| Yes | 1.58 (0.87 to 2.88) | 0.64 (0.28 to 1.46) | 1.54 (0.85 to 2.81) | 0.71 (0.31 to 1.63) |
| Mould in househ | ||||
| Yes | 1.08 (0.65 to 1.8) | 1.06 (0.62 to 1.82) | 1.04 (0.62 to 1.74) | 1.06 (0.62 to 1.82) |
| Multiple poverty scorek | ||||
| 1 | 1.95 (0.91 to 4.19) | 1.18 (0.7 to 2.01) | ||
| 2 | 2.1 (0.98 to 4.51) | 1.04 (0.59 to 1.81) | ||
| 3 | 2.67* (1.21 to 5.92) | 0.73 (0.39 to 1.38) | ||
| 4 | 3.11* (1.28 to 7.54) | 0.33* (0.12 to 0.91) | ||
High levels of well-being were associated with living in the intervention area and being of Asian Indian ethnicity, whereas decreased likelihood of high levels of well-being were associated with unemployment, being widowed, divorced or separated, being in an intermediate NS-SEC group and having a long-term illness (see Table 43). Further adjustment for multiple poverty scores made very little difference to the magnitude of the risk of these factors for high levels of well-being (see Table 43). Being in an unsafe neighbourhood was associated with decreased odds of high levels of well-being at wave 1 (see Table 43).
Well-being at wave 2
Associations between sociodemographic and neighbourhood factors and well-being at wave 2 are reported in Table 44. At wave 2, low levels of well-being were associated with having never married, being widowed, divorced or separated, living in households with intermediate or semiroutine NS-SEC occupations, and having a long-term illness. Having a multiple poverty score of 2 or 3, but not 4, was also associated with lower levels of well-being. There was a lower risk of low levels of well-being among those of Asian Bangladeshi and black African ethnicity, and among those participants not born in the UK. At wave 2, poor neighbourhood conditions, unsafe neighbourhoods, low levels of social cohesion and high levels of violence were associated with lower levels of well-being. Being slightly or very dissatisfied with accommodation was associated with low levels of well-being, as were vibrations and dust in the house.
| Variable | WEMWBS, RRR (95% CI) | |
|---|---|---|
| Below 1 SD from mean | Above 1 SD from mean | |
| Age | 1.02 (0.99 to 1.04) | 0.98 (0.96 to 1.01) |
| Gendera | ||
| Female | 0.96 (0.65 to 1.42) | 0.84 (0.58 to 1.20) |
| Ethnicityb | ||
| Asian: Indian | 0.45 (0.17 to 1.24) | 1.16 (0.50 to 2.65) |
| Asian: Pakistani | 0.54 (0.22 to 1.3) | 1.11 (0.50 to 2.48) |
| Asian: Bangladeshi | 0.54* (0.33 to 0.88) | 0.78 (0.46 to 1.33) |
| Black: Caribbean | 1.10 (0.51 to 2.38) | 1.19 (0.50 to 2.84) |
| Black: African | 0.47* (0.26 to 0.84) | 1.93* (1.16 to 3.19) |
| Other | 0.84 (0.51 to 1.38) | 1.29 (0.76 to 2.18) |
| Top educationc | ||
| NVQ 3 | 0.89 (0.43 to 1.82) | 1.66 (0.87 to 3.15) |
| NVQ 4/5 | 0.67 (0.38 to 1.19) | 1.41 (0.83 to 2.38) |
| Other | 0.64 (0.38 to 1.06) | 0.98 (0.59 to 1.62) |
| None | 1.09 (0.69 to 1.71) | 1.17 (0.72 to 1.89) |
| Employmentd | ||
| No | 1.07 (0.76 to 1.52) | 0.63** (0.45 to 0.87) |
| Household NS-SECe | ||
| Intermediate | 2.47* (1.02 to 5.99) | 0.89 (0.43 to 1.86) |
| Semiroutine, etc. | 1.79 (0.91 to 3.53) | 0.98 (0.61 to 1.59) |
| Marital statusf | ||
| Never married/CP | 1.60* (1.04 to 2.46) | 1.12 (0.74 to 1.70) |
| Separated, divorced, widowed | 1.97** (1.27 to 3.06) | 0.76 (0.45 to 1.27) |
| Home ownershipg | ||
| Social rent | 1.53 (1.00 to 2.36) | 1.08 (0.74 to 1.58) |
| Private rent | 1.03 (0.55 to 1.91) | 0.59 (0.32 to 1.09) |
| Other | –h | –h |
| Benefitsi,j | ||
| Yes | 1.31 (0.90 to 1.90) | 0.77 (0.54 to 1.09) |
| Born in the UKd | ||
| No | 0.66* (0.44 to 0.99) | 0.83 (0.55 to 1.24) |
| Multiple poverty scorek | ||
| 1 | 1.49 (0.66 to 3.35) | 0.75 (0.45 to 1.24) |
| 2 | 2.36* (1.12 to 4.95) | 0.61 (0.37 to 1.02) |
| 3 | 3.39** (1.60 to 7.20) | 0.54* (0.31 to 0.95) |
| 4 | 2.39 (0.87 to 6.54) | 0.26* (0.08 to 0.91) |
| Long-term illnessi | ||
| Yes | 2.17*** (1.54 to 3.07) | 0.67* (0.46 to 0.97) |
| Access to gardend | ||
| No | 1.16 (0.81 to 1.66) | 1.04 (0.74 to 1.48) |
| Accommodation satisfactionl | ||
| Slightly/very dissatisfied | 2.22*** (1.49 to 3.31) | 0.70 (0.42 to 1.16) |
| How often do you visit green spaces?m | ||
| Once a fortnight or month | 0.85 (0.54 to 1.34) | 1.06 (0.71 to 1.59) |
| Several times a year/never | 1.34 (0.91 to 1.98) | 1.03 (0.70 to 1.52) |
| Neighbourhood aesthetics | ||
| Higher score = worse | 1.40** (1.12 to 1.75) | 0.64*** (0.51 to 0.81) |
| Neighbourhood safety | ||
| Higher score = worse | 1.51*** (1.27 to 1.79) | 0.78** (0.65 to 0.93) |
| Neighbourhood social cohesion | ||
| Higher score = worse | 1.93*** (1.57 to 2.37) | 0.67** (0.52 to 0.87) |
| Neighbourhood violence | ||
| Lower score = worse | 0.62*** (0.50 to 0.78) | 1.50** (1.12 to 2.02) |
| Damp in housei | ||
| Yes | 1.26 (0.87 to 1.83) | 0.96 (0.66 to 1.40) |
| Vibrations in housei | ||
| Yes | 3.32* (1.29 to 8.54) | 1.89 (0.64 to 5.64) |
| Dust in housei | ||
| Yes | 2.44** (1.31 to 4.54) | 0.73 (0.30 to 1.79) |
| Mould in housei | ||
| Yes | 1.44 (0.95 to 2.19) | 1.20 (0.79 to 1.83) |
There was an increased likelihood of high levels of well-being in participants of black African ethnicity. There was a lower likelihood of high levels of well-being among those who were unemployed, who had a long-term illness or who had a multiple poverty score of 3 or greater (see Table 44). Poor neighbourhood conditions, unsafe neighbourhoods, neighbourhood violence and low levels of social cohesion were associated with lower likelihoods of high levels of well-being (see Table 44).
Table 45 shows the multivariate associations between sociodemographic and neighbourhood factors with well-being at wave 2. At wave 2 only long-term illness was associated with increased odds of low levels of well-being (see Table 45). At wave 2, low levels of neighbourhood social cohesion was associated with increased odds of low levels of well-being, unchanged by further adjustment for multiple poverty score (see Table 45). Dissatisfaction with accommodation was associated with increased risk of low levels of well-being, but this finding became non-significant after adjustment for multiple poverty score at wave 2 (see Table 45).
| Variable | WEMWBS, RRR (95% CI) | |||
|---|---|---|---|---|
| Below 1 SD from mean | Above 1 SD from mean | Below 1 SD from mean | Above 1 SD from mean | |
| Ethnicitya | ||||
| Asian: Indian | 0.54 (0.18 to 1.58) | 1.31 (0.53 to 3.23) | 0.52 (0.17 to 1.54) | 1.31 (0.53 to 3.26) |
| Asian: Pakistani | 0.72 (0.28 to 1.88) | 1.32 (0.55 to 3.14) | 0.74 (0.28 to 1.96) | 1.27 (0.53 to 3.07) |
| Asian: Bangladeshi | 0.74 (0.39 to 1.37) | 0.98 (0.51 to 1.88) | 0.69 (0.37 to 1.31) | 1.04 (0.54 to 2.01) |
| Black: Caribbean | 1.07 (0.46 to 2.51) | 1.24 (0.49 to 3.15) | 1.08 (0.46 to 2.54) | 1.32 (0.51 to 3.40) |
| Black: African | 0.56 (0.28 to 1.13) | 2.23** (1.21 to 4.09) | 0.53 (0.26 to 1.07) | 2.34** (1.27 to 4.34) |
| Other | 1.06 (0.59 to 1.91) | 1.49 (0.81 to 2.75) | 1.07 (0.59 to 1.95) | 1.47 (0.79 to 2.73) |
| Employmentb | ||||
| No | 0.78 (0.44 to 1.38) | 0.79 (0.48 to 1.29) | 0.73 (0.41 to 1.30) | 0.81 (0.49 to 1.35) |
| Household NS-SECc | ||||
| Intermediate | 2.47 (0.94 to 6.48) | 0.89 (0.41 to 1.93) | 2.10 (0.76 to 5.82) | 1.02 (0.46 to 2.28) |
| Semiroutine, etc. | 1.90 (0.90 to 4.01) | 1.15 (0.67 to 1.99) | 1.59 (0.71 to 3.56) | 1.38 (0.76 to 2.51) |
| Marital statusd | ||||
| Never married/CP | 0.92 (0.55 to 1.54) | 1.23 (0.76 to 1.99) | 0.82 (0.48 to 1.40) | 1.37 (0.83 to 2.24) |
| Separated, divorced, widowed | 1.52 (0.92 to 2.51) | 0.71 (0.41 to 1.24) | 1.37 (0.82 to 2.31) | 0.82 (0.46 to 1.45) |
| Born in the UKb | ||||
| No | 0.67 (0.41 to 1.11) | 0.66 (0.40 to 1.08) | 0.66 (0.40 to 1.10) | 0.68 (0.41 to 1.13) |
| Long-term illnesse | ||||
| Yes | 2.05*** (1.42 to 2.98) | 0.72 (0.49 to 1.05) | 2.01*** (1.38 to 2.93) | 0.73 (0.50 to 1.08) |
| Accommodation satisfactionf | ||||
| Slightly/very dissatisfied | 1.62* (1.01 to 2.58) | 0.88 (0.50 to 1.54) | 1.53 (0.95 to 2.45) | 0.91 (0.51 to 1.61) |
| Neighbourhood aesthetics | ||||
| Higher score = worse | 0.90 (0.68 to 1.19) | 0.75* (0.57 to 0.98) | 0.90 (0.68 to 1.19) | 0.75* (0.57 to 0.99) |
| Neighbourhood safety | ||||
| Higher score = worse | 1.15 (0.91 to 1.46) | 0.96 (0.77 to 1.20) | 1.13 (0.89 to 1.44) | 0.97 (0.78 to 1.22) |
| Neighbourhood social cohesion | ||||
| Higher score = worse | 1.63*** (1.23 to 2.16) | 0.79 (0.57 to 1.11) | 1.64*** (1.23 to 2.19) | 0.79 (0.56 to 1.11) |
| Neighbourhood violence | ||||
| Lower score = worse | 0.98 (0.71 to 1.35) | 1.16 (0.81 to 1.66) | 0.96 (0.69 to 1.31) | 1.15 (0.80 to 1.66) |
| Vibrations in housee | ||||
| Yes | 1.68 (0.51 to 5.61) | 2.82 0.78 to 10.17 | 1.87 (0.56 to 6.27) | 3.04 (0.82 to 11.33) |
| Dust in housee | ||||
| Yes | 1.56 (0.71 to 3.41) | 0.69 (0.24 to 2.00) | 1.39 (0.63 to 3.06) | 0.73 (0.25 to 2.18) |
| Multiple poverty scoreg | ||||
| 1 | 1.20 (0.49 to 2.91) | 0.74 (0.42 to 1.31) | ||
| 2 | 1.88 (0.80 to 4.43) | 0.62 (0.34 to 1.14) | ||
| 3 | 2.38 (0.98 to 5.78) | 0.56 (0.29 to 1.11) | ||
| 4 | 1.19 (0.36 to 3.97) | 0.29 (0.08 to 1.11) | ||
At wave 2 being of black African ethnicity was associated with increased odds of high levels of well-being. Further adjustment for multiple poverty score slightly increased the odds of people of black African ethnicity having higher levels of well-being (see Table 45).
Well-being at wave 3
Univariate associations between sociodemographic and neighbourhood factors with well-being at wave 3 are reported in Table 46. At wave 3, low levels of well-being were associated with increasing age, unemployment, having a long-term illness and a multiple poverty score of 1 or greater (see Table 46). Being of Bangladeshi, black African or ‘other’ ethnicity was related to a lower risk of low levels of well-being. At wave 3, visiting green spaces once a fortnight, once a month or only several times a year was associated with low levels of well-being. Poor neighbourhood conditions, unsafe neighbourhoods, low levels of social cohesion and high levels of violence were associated with low levels of well-being. Similarly, being slightly or very dissatisfied with accommodation and damp, dust and mould in the house were associated with low levels of well-being.
| Variable | WEMWBS, RRR (95% CI) | |
|---|---|---|
| Below 1 SD from mean | Above 1 SD from mean | |
| Age | 1.04* (1.01 to 1.06) | 1.01 (0.98 to 1.03) |
| Gendera | ||
| Female | 1.13 (0.73 to 1.75) | 0.89 (0.59 to 1.34) |
| Ethnicityb | ||
| Asian: Indian | 1.03 (0.42 to 2.58) | 1.79 (0.75 to 4.29) |
| Asian: Pakistani | 1.67 (0.75 to 3.70) | 1.90 (0.79 to 4.55) |
| Asian: Bangladeshi | 0.54* (0.30 to 0.98) | 1.13 (0.63 to 2.03) |
| Black: Caribbean | 0.90 (0.40 to 2.05) | 0.47 (0.14 to 1.61) |
| Black: African | 0.46* (0.22 to 0.94) | 1.77 (0.98 to 3.19) |
| Other | 0.56* (0.32 to 0.99) | 0.73 (0.39 to 1.36) |
| Top educationc | ||
| NVQ 3 | 0.82 (0.39 to 1.70) | 1.13 (0.56 to 2.27) |
| NVQ 4/5 | 0.84 (0.45 to 1.56) | 1.67 (0.96 to 2.91) |
| Other | 0.52* (0.28 to 0.95) | 0.62 (0.34 to 1.14) |
| None | 1.21 (0.73 to 2.01) | 0.85 (0.49 to 1.49) |
| Employmentd | ||
| No | 2.29*** (1.54 to 3.41) | 0.62* (0.43 to 0.91) |
| Household NS-SECe | ||
| Intermediate | 1.28 (0.46 to 3.54) | 0.48 (0.19 to 1.17) |
| Semiroutine, etc. | 0.80 (0.34 to 1.86) | 0.51 (0.26 to 1.00) |
| Marital statusf | ||
| Never married/CP | 1.31 (0.81 to 2.13) | 0.77 (0.45 to 1.31) |
| Separated, divorced, widowed | 1.57 (0.98 to 2.54) | 0.86 (0.50 to 1.46) |
| Home ownershipg | ||
| Social rent | 1.21 (0.75 to 1.96) | 0.45*** (0.30 to 0.68) |
| Private rent | 0.75 (0.39 to 1.45) | 0.51* (0.29 to 0.89) |
| Other | 1.09 (0.23 to 5.21) | 0.56 (0.12 to 2.63) |
| Benefitsh,i | ||
| Yes | 1.46 (0.95 to 2.24) | 0.48*** (0.33 to 0.70) |
| Born in the UKd | ||
| No | 0.83 (0.52 to 1.33) | 0.94 (0.58 to 1.52) |
| Multiple poverty scorej | ||
| 1 | 3.03 (0.97 to 9.44) | 0.60 (0.34 to 1.07) |
| 2 | 4.51** (1.56 to 13.02) | 0.44** (0.25 to 0.76) |
| 3 | 6.03*** (2.11 to 17.21) | 0.41** (0.23 to 0.72) |
| 4 | 4.31* (1.33 to 13.94) | 0.53 (0.25 to 1.11) |
| Long-term illnessh | ||
| Yes | 2.64*** (1.81 to 3.86) | 0.82 (0.55 to 1.22) |
| Access to gardend | ||
| No | 0.94 (0.62 to 1.42) | 0.63* (0.40 to 0.98) |
| Accommodation satisfactionk | ||
| Slightly/very dissatisfied | 1.67* (1.07 to 2.61) | 0.70 (0.40 to 1.23) |
| How often do you visit green spaces?l | ||
| Once a fortnight or month | 2.01** (1.24 to 3.28) | 1.35 (0.86 to 2.14) |
| Several times a year/never | 2.98*** (1.93 to 4.60) | 1.30 (0.83 to 2.03) |
| Neighbourhood aesthetics | ||
| Higher score = worse | 1.56*** (1.21 to 2.00) | 0.79 (0.60 to 1.03) |
| Neighbourhood safety | ||
| Higher score = worse | 1.57*** (1.29 to 1.92) | 0.89 (0.72 to 1.10) |
| Neighbourhood social cohesion | ||
| Higher score = worse | 2.04*** (1.61 to 2.58) | 1.04 (0.80 to 1.34) |
| Neighbourhood violence | ||
| Lower score = worse | 0.75* (0.57 to 0.97) | 0.98 (0.74 to 1.30) |
| Damp in househ | ||
| Yes | 1.55* (1.06 to 2.27) | 0.90 (0.60 to 1.36) |
| Vibrations in househ | ||
| Yes | 1.81 (0.80 to 4.11) | 1.08 (0.41 to 2.88) |
| Dust in househ | ||
| Yes | 1.93** (1.17 to 3.20) | 0.93 (0.50 to 1.72) |
| Mould in househ | ||
| Yes | 1.61* (1.05 to 2.45) | 1.03 (0.65 to 1.63) |
Unemployment, social renting, being on benefits and a multiple poverty score of 2 or 3 were associated with a lower likelihood of high levels of well-being at wave 3 (see Table 46). Having no access to a garden was associated with a lower likelihood of high levels of well-being at wave 3.
Table 47 shows the multivariate associations between sociodemographic and neighbourhood factors and well-being at wave 3. At wave 3 increasing age, being of Asian Pakistani ethnicity and being unemployed were associated with an increased risk of low levels of well-being. Having ‘other’ educational qualifications was associated with a reduced risk of low levels of well-being (see Table 47). After adjustment for multiple poverty score, associations with Asian Pakistani ethnicity became non-significant. Multiple poverty score was strongly associated with increased odds of low levels of well-being. At wave 3, visiting green spaces only several times a year or less often was associated with an increased risk of low levels of well-being, even after adjusting for multiple poverty score (see Table 47). Low social cohesion was also associated with an increased risk of low levels of well-being at wave 3, this was maintained after adjustment for multiple poverty score (see Table 47).
| Variable | WEMWBS, RRR (95% CI) | |||
|---|---|---|---|---|
| Below 1 SD from mean | Above 1 SD from mean | Below 1 SD from mean | Above 1 SD from mean | |
| Intervention | ||||
| Newham | 0.79 (0.49 to 1.26) | 0.46*** (0.28 to 0.74) | 0.72 (0.45 to 1.16) | 0.46** (0.28 to 0.75) |
| Age | 1.04** (1.01 to 1.08) | 1.00 (0.97 to 1.03) | 1.05** (1.01 to 1.08) | 1.00 (0.97 to 1.03) |
| Ethnicitya | ||||
| Asian: Indian | 1.62 (0.58 to 4.53) | 2.16 (0.84 to 5.54) | 1.78 (0.61 to 5.15) | 2.04 (0.78 to 5.34) |
| Asian: Pakistani | 2.86* (1.12 to 7.32) | 3.09* (1.19 to 8.01) | 2.39 (0.92 to 6.20) | 3.54* (1.34 to 9.39) |
| Asian: Bangladeshi | 0.62 (0.31 to 1.25) | 2.01* (1.01 to 3.99) | 0.58 (0.28 to 1.19) | 2.08* (1.04 to 4.16) |
| Black: Caribbean | 0.76 (0.30 to 1.93) | 0.52 (0.15 to 1.86) | 0.65 (0.25 to 1.69) | 0.56 (0.16 to 2.01) |
| Black: African | 0.52 (0.23 to 1.18) | 2.50** (1.28 to 4.88) | 0.46 (0.20 to 1.07) | 2.61** (1.33 to 5.14) |
| Other | 0.83 (0.43 to 1.62) | 1.10 (0.55 to 2.21) | 0.85 (0.43 to 1.67) | 1.11 (0.55 to 2.23) |
| Top educationb | ||||
| NVQ 3 | 0.78 (0.35 to 1.77) | 0.97 (0.46 to 2.02) | 0.86 (0.37 to 1.99) | 0.94 (0.45 to 1.96) |
| NVQ 4/5 | 0.96 (0.48 to 1.93) | 1.26 (0.68 to 2.33) | 1.20 (0.59 to 2.46) | 1.13 (0.59 to 2.14) |
| Other | 0.50 (0.25 to 1.00) | 0.54 (0.28 to 1.05) | 0.52 (0.26 to 1.06) | 0.53 (0.27 to 1.03) |
| None | 1.06 (0.60 to 1.87) | 0.83 (0.46 to 1.50) | 1.03 (0.58 to 1.83) | 0.84 (0.46 to 1.52) |
| Employmentc | ||||
| No | 2.37*** (1.51 to 3.72) | 0.71 (0.46 to 1.10) | 2.31*** (1.46 to 3.67) | 0.72 (0.47 to 1.12) |
| Home ownershipd | ||||
| Social rent | 1.31 (0.72 to 2.37) | 0.57* (0.34 to 0.96) | 0.86 (0.46 to 1.60) | 0.64 (0.37 to 1.12) |
| Private rent | 1.01 (0.47 to 2.16) | 0.79 (0.42 to 1.50) | 0.74 (0.34 to 1.63) | 0.89 (0.46 to 1.74) |
| Other | 1.21 (0.22 to 6.65) | 0.65 (0.13 to 3.22) | 0.88 (0.15 to 5.23) | 0.70 (0.14 to 3.49) |
| Access to gardenc | ||||
| No | 0.77 (0.46 to 1.30) | 0.64 (0.37 to 1.09) | 0.76 (0.45 to 1.28) | 0.65 (0.38 to 1.12) |
| Accommodation satisfactione | ||||
| Slightly/very dissatisfied | 1.03 (0.59 to 1.80) | 0.80 (0.42 to 1.53) | 1.01 (0.57 to 1.78) | 0.82 (0.43 to 1.57) |
| How often do you visit green spaces?f | ||||
| Once a fortnight or month | 1.98* (1.16 to 3.36) | 1.25 (0.76 to 2.05) | 1.91* (1.12 to 3.28) | 1.25 (0.76 to 2.06) |
| Several times a year/never | 2.56*** (1.57 to 4.16) | 1.26 (0.78 to 2.05) | 2.57*** (1.57 to 4.22) | 1.26 (0.77 to 2.06) |
| Neighbourhood aesthetics | ||||
| Higher score = worse | 0.96 (0.68 to 1.35) | 0.80 (0.58 to 1.12) | 0.97 (0.68 to 1.37) | 0.81 (0.58 to 1.12) |
| Neighbourhood safety | ||||
| Higher score = worse | 1.28 (0.94 to 1.74) | 0.87 (0.65 to 1.16) | 1.27 (0.92 to 1.73) | 0.86 (0.64 to 1.16) |
| Neighbourhood social Cohesion | ||||
| Higher score = worse | 1.77*** (1.27 to 2.46) | 1.25 (0.90 to 1.74) | 1.79*** (1.27 to 2.51) | 1.26 (0.90 to 1.76) |
| Neighbourhood violence | ||||
| Lower score = worse | 1.23 (0.83 to 1.84) | 0.84 (0.59 to 1.21) | 1.25 (0.83 to 1.87) | 0.83 (0.58 to 1.20) |
| Damp in houseg | ||||
| Yes | 1.25 (0.73 to 2.13) | 0.96 (0.57 to 1.61) | 1.20 (0.70 to 2.04) | 0.97 (0.58 to 1.63) |
| Dust in houseg | ||||
| Yes | 1.22 (0.66 to 2.27) | 0.81 (0.40 to 1.65) | 1.17 (0.62 to 2.19) | 0.81 (0.40 to 1.66) |
| Mould in houseg | ||||
| Yes | 0.97 (0.53 to 1.79) | 1.48 (0.81 to 2.71) | 1.01 (0.55 to 1.85) | 1.49 (0.81 to 2.75) |
| Multiple poverty scoreh | ||||
| 1 | 3.25 (0.96 to 10.97) | 0.73 (0.38 to 1.40) | ||
| 2 | 6.07** (1.88 to 19.62) | 0.67 (0.34 to 1.31) | ||
| 3 | 6.31** (1.94 to 20.51) | 0.59 (0.29 to 1.20) | ||
| 4 | 4.74* (1.24 to 18.19) | 0.73 (0.30 to 1.77) | ||
Being of black African ethnicity or of Asian Pakistani ethnicity was associated with an increased risk of high levels of well-being, whereas living in the intervention area, being on benefits and social renting was associated with a reduced risk of high levels of well-being (see Table 46 ). After adjustment for multiple poverty score, the association of the intervention area and of being of black African ethnicity with high levels of well-being was maintained; being of Asian Pakistani ethnicity also showed a positive association (see Table 47).
Living in the intervention area and anxiety at waves 1, 2 and 3
Table 48 shows the association of living in the intervention borough of Newham with anxiety at each wave. At wave 1, participants living in Newham were less likely to report anxiety than participants living in the comparison area (RRR 0.77, 95% CI 0.60 to 1.00). However, at wave 3 participants living in Newham were more likely to report anxiety than participants living in the comparison area (RRR 1.68, 95% CI 1.28 to 2.22). No differences were observed at wave 2.
| Wave | Borough | HADS anxiety, OR (95% CI) |
|---|---|---|
| Wave 1 intervention | Newham | 0.77* (0.60 to 1.00) |
| Wave 2 intervention | Newham | 0.88 (0.65 to 1.20) |
| Wave 3 intervention | Newham | 1.68*** (1.28 to 2.22) |
Anxiety at wave 1
Table 49 shows the univariate associations of the sociodemographic and neighbourhood characteristics with anxiety at wave 1. Being female, being unemployed, never having been married, being widowed, divorced or separated, being on benefits, social renting, having a long-term illness and having a multiple poverty score of 2 or greater were associated with increased likelihood of above threshold anxiety symptoms (see Table 49). Being of black African ethnicity was associated with reduced odds of anxiety symptoms. At wave 1, poor neighbourhood conditions, unsafe neighbourhoods, low levels of social cohesion and high levels of violence were associated with increased odds of anxiety symptoms (see Table 49). Being slightly or very dissatisfied with accommodation, and having damp, vibrations or mould in the house were also associated with anxiety symptoms. Being insulted because of ethnicity was also associated with increased odds of anxiety symptoms.
| Variable | HADS anxiety, OR (95% CI) |
|---|---|
| Age | 1.01 (1.00 to 1.03) |
| Gendera | |
| Female | 1.70*** (1.29 to 2.23) |
| Ethnicityb | |
| Asian: Indian | 0.88 (0.48 to 1.60) |
| Asian: Pakistani | 0.75 (0.42 to 1.32) |
| Asian: Bangladeshi | 0.83 (0.58 to 1.17) |
| Black: Caribbean | 0.70 (0.40 to 1.23) |
| Black: African | 0.63* (0.43 to 0.92) |
| Other | 1.11 (0.79 to 1.56) |
| Top educationc | |
| NVQ 3 | 1.05 (0.66 to 1.67) |
| NVQ 4/5 | 0.88 (0.62 to 1.27) |
| Other | 1.31 (0.95 to 1.82) |
| None | 1.32 (0.95 to 1.83) |
| Employmentd | |
| No | 1.74*** (1.37 to 2.22) |
| Household NS-SECe | |
| Intermediate | 0.94 (0.56 to 1.59) |
| Semiroutine, etc. | 1.12 (0.80 to 1.58) |
| Marital statusf | |
| Never married/CP | 1.39* (1.05 to 1.85) |
| Separated, divorced, widowed | 2.14*** (1.53 to 3.00) |
| Home ownershipg | |
| Social rent | 1.38* (1.03 to 1.86) |
| Private rent | 1.07 (0.75 to 1.54) |
| Other | 1.02 (0.48 to 2.18) |
| Benefitsh,i | |
| Yes | 1.47*** (1.16 to 1.86) |
| Born in the UKd | |
| No | 0.92 (0.72 to 1.17) |
| Multiple poverty scorej | |
| 1 | 1.15 (0.75 to 1.76) |
| 2 | 1.60* (1.07 to 2.40) |
| 3 | 2.03*** (1.35 to 3.05) |
| 4 | 3.72*** (2.21 to 6.25) |
| Long-term illnessh | |
| Yes | 2.64*** (2.07 to 3.37) |
| Access to gardend | |
| No | 1.14 (0.89 to 1.46) |
| Accommodation satisfactionk | |
| Slightly/very dissatisfied | 1.55** (1.15 to 2.11) |
| How often do you visit green spaces?l | |
| Once a fortnight or month | 0.79 (0.59 to 1.05) |
| Several times a year/never | 0.95 (0.72 to 1.25) |
| Neighbourhood aesthetics | |
| Higher score = worse | 1.60*** (1.38 to 1.86) |
| Neighbourhood safety | |
| Higher score = worse | 1.26*** (1.13 to 1.41) |
| Neighbourhood social cohesion | |
| Higher score = worse | 1.40*** (1.23 to 1.59) |
| Neighbourhood violence | |
| Lower score = worse | 0.58*** (0.50 to 0.69) |
| Insulted because of ethnicityh | |
| Yes | 2.01** (1.21 to 3.34) |
| Refused job as a result of discriminationh | |
| Yes | 1.80 (0.97 to 3.33) |
| Treated unfairly at work because of ethnicityh | |
| Yes | 1.16 (0.55 to 2.45) |
| Damp in househ | |
| Yes | 1.43* (1.09 to 1.89) |
| Vibrations in househ | |
| Yes | 2.19* (1.18 to 4.07) |
| Dust in househ | |
| Yes | 1.46 (0.94 to 2.28) |
| Mould in househ | |
| Yes | 1.50* (1.10 to 2.04) |
In multivariate analysis at wave 1, being female, being of ‘other’ ethnicity, being unemployed, being widowed, divorced or separated, having a multiple poverty score of 4 and having a long-term illness were associated with an increased risk of anxiety symptoms adjusting for gender, ethnicity, employment, marital status, eligibility for benefits and long-term illness (Table 50). Further adjustment for multiple poverty score reduced the odds of increased anxiety symptoms associated with long-term illness. Poor neighbourhood conditions and high levels of violence in the neighbourhood were associated with increased risk of anxiety symptoms at wave 1 in adjusted analyses, including adjusting for multiple poverty score (see Table 50). Being insulted because of ethnicity was also associated with increased odds of anxiety symptoms, which was maintained after further adjustment for multiple poverty score (see Table 50).
| Variable | HADS anxiety, OR (95% CI) | |
|---|---|---|
| Unadjusted | Adjusted | |
| Intervention | ||
| Newham | 0.92 (0.69 to 1.22) | 0.81 (0.60 to 1.10) |
| Gendera | ||
| Female | 1.44* (1.06 to 1.96) | 1.39* (1.02 to 1.89) |
| Ethnicityb | ||
| Asian: Indian | 1.40 (0.72 to 2.72) | 1.41 (0.72 to 2.75) |
| Asian: Pakistani | 1.18 (0.62 to 2.24) | 1.11 (0.58 to 2.12) |
| Asian: Bangladeshi | 1.21 (0.80 to 1.83) | 1.10 (0.72 to 1.67) |
| Black: Caribbean | 0.92 (0.51 to 1.68) | 0.88 (0.48 to 1.61) |
| Black: African | 0.93 (0.60 to 1.43) | 0.88 (0.57 to 1.37) |
| Other | 1.71** (1.15 to 2.54) | 1.60* (1.07 to 2.40) |
| Employmentc | ||
| No | 1.65*** (1.25 to 2.18) | 1.62*** (1.23 to 2.15) |
| Marital statusd | ||
| Never married/CP | 1.11 (0.79 to 1.56) | 1.03 (0.73 to 1.45) |
| Separated, divorced, widowed | 1.74** (1.19 to 2.55) | 1.65* (1.12 to 2.43) |
| Home ownershipe | ||
| Social rent | 0.85 (0.60 to 1.20) | 0.73 (0.51 to 1.05) |
| Private rent | 0.93 (0.62 to 1.40) | 0.81 (0.53 to 1.23) |
| Other | 0.78 (0.34 to 1.80) | 0.73 (0.31 to 1.68) |
| Long-term illnessf | ||
| Yes | 2.29*** (1.75 to 3.00) | 2.10*** (1.59 to 2.76) |
| Accommodation satisfactiong | ||
| Slightly/very dissatisfied | 1.07 (0.74 to 1.55) | 1.05 (0.73 to 1.53) |
| Neighbourhood aesthetics | ||
| Higher score = worse | 1.33** (1.11 to 1.60) | 1.32** (1.09 to 1.59) |
| Neighbourhood safety | ||
| Higher score = worse | 0.92 (0.79 to 1.07) | 0.91 (0.78 to 1.06) |
| Neighbourhood social cohesion | ||
| Higher score = worse | 1.14 (0.96 to 1.35) | 1.15 (0.97 to 1.37) |
| Neighbourhood violence | ||
| Lower score = worse | 0.63*** (0.52 to 0.77) | 0.63*** (0.52 to 0.77) |
| Insulted because of ethnicityf | ||
| Yes | 1.92* (1.09 to 3.40) | 1.86* (1.05 to 3.31) |
| Damp in housef | ||
| Yes | 1.08 (0.76 to 1.54) | 1.04 (0.73 to 1.49) |
| Vibrations in housef | ||
| Yes | 1.51 (0.75 to 3.04) | 1.36 (0.67 to 2.75) |
| Mould in housef | ||
| Yes | 1.01 (0.68 to 1.49) | 0.99 (0.67 to 1.47) |
| Multiple poverty scoreh | ||
| 1 | 1.09 (0.68 to 1.74) | |
| 2 | 1.43 (0.89 to 2.28) | |
| 3 | 1.65* (1.00 to 2.72) | |
| 4 | 2.57** (1.39 to 4.75) | |
Anxiety at wave 2
Table 51 shows the univariate associations of the sociodemographic and neighbourhood characteristics with anxiety at wave 2. At wave 2, increasing age, being unemployed, being never married or being widowed, divorced or separated, being on benefits, having a long-term illness and a multiple poverty score of 1 or greater were associated with increased odds of anxiety symptoms (see Table 51). Having an educational level of National Vocational Qualification (NVQ) 4/5 was associated with reduced odds of anxiety symptoms. At wave 2, poor neighbourhood conditions, unsafe neighbourhoods, low levels of social cohesion and high levels of violence were associated with increased odds of anxiety symptoms (see Table 51). Being slightly or very dissatisfied with accommodation and having damp, vibrations or dust in the house were also associated with anxiety symptoms.
| Variable | HADS anxiety, OR (95% CI) |
|---|---|
| Age | 1.02* (1.00 to 1.04) |
| Gendera | |
| Female | 1.41 (0.99 to 2.00) |
| Ethnicityb | |
| Asian: Indian | 0.82 (0.39 to 1.72) |
| Asian: Pakistani | 1.20 (0.63 to 2.28) |
| Asian: Bangladeshi | 0.75 (0.49 to 1.15) |
| Black: Caribbean | 0.97 (0.47 to 1.99) |
| Black: African | 0.68 (0.42 to 1.09) |
| Other | 0.64 (0.40 to 1.02) |
| Top educationc | |
| NVQ 3 | 0.94 (0.53 to 1.66) |
| NVQ 4/5 | 0.46** (0.27 to 0.76) |
| Other | 0.74 (0.49 to 1.13) |
| None | 0.74 (0.50 to 1.10) |
| Employmentd | |
| No | 1.38* (1.02 to 1.86) |
| Household NS-SECe | |
| Intermediate | 1.55 (0.70 to 3.44) |
| Semiroutine, etc. | 1.73 (0.98 to 3.04) |
| Marital statusf | |
| Never married/CP | 1.56* (1.07 to 2.27) |
| Other | 2.61*** (1.79 to 3.82) |
| Home ownershipg | |
| Social rent | 1.43 (0.99 to 2.07) |
| Private rent | 1.63 (0.99 to 2.68) |
| Other | 0.48 (0.06 to 3.88) |
| Benefitsh,i | |
| Yes | 1.45* (1.04 to 2.01) |
| Born in the UKd | |
| No | 0.95 (0.66 to 1.37) |
| Multiple poverty scorej | |
| 1 | 2.19* (1.09 to 4.41) |
| 2 | 2.76** (1.41 to 5.43) |
| 3 | 4.86*** (2.47 to 9.57) |
| 4 | 8.3*** (3.45 to 19.98) |
| Long-term illnessh | |
| Yes | 2.41*** (1.79 to 3.25) |
| Access to gardend | |
| No | 1.14 (0.83 to 1.54) |
| Accommodation satisfactionk | |
| Slightly/very dissatisfied | 1.72** (1.19 to 2.47) |
| How often do you visit green spaces?l | |
| Once a fortnight or month | 0.94 (0.65 to 1.36) |
| Several times a year/never | 0.97 (0.69 to 1.37) |
| Neighbourhood aesthetics | |
| Higher score = worse | 1.32** (1.09 to 1.60) |
| Neighbourhood safety | |
| Higher score = worse | 1.45*** (1.24 to 1.68) |
| Neighbourhood social cohesion | |
| Higher score = worse | 1.65*** (1.38 to 1.98) |
| Neighbourhood violence | |
| Lower score = worse | 0.54*** (0.44 to 0.66) |
| Damp in househ | |
| Yes | 1.52** (1.11 to 2.09) |
| Vibrations in househ | |
| Yes | 2.59* (1.12 to 5.98) |
| Dust in househ | |
| Yes | 2.13** (1.20 to 3.79) |
| Mould in househ | |
| Yes | 1.33 (0.93 to 1.92) |
Table 52 shows the multivariate analyses for anxiety at wave 2. At wave 2, being widowed, divorced or separated or having a long-term illness was associated with increased odds of anxiety symptoms. These odds were slightly reduced after adjustment for multiple poverty score, which was strongly associated with increased odds of anxiety symptoms (see Table 52). Having education qualifications at NVQ 4/5 level was associated with decreased odds of anxiety symptoms but this became non-significant after adjustment for multiple poverty score. At wave 2, high levels of violence in the neighbourhood and low levels of social cohesion were associated with increased odds of anxiety symptoms and this remained after adjustment for multiple poverty score (see Table 52).
| Variable | HADS anxiety, OR (95% CI) | |
|---|---|---|
| Unadjusted | Adjusted | |
| Age | 1.02 (1.00 to 1.04) | 1.02* (1.00 to 1.05) |
| Top educationa | ||
| NVQ 3 | 1.10 (0.60 to 2.04) | 1.21 (0.65 to 2.28) |
| NVQ 4/5 | 0.45** (0.25 to 0.79) | 0.58 (0.32 to 1.05) |
| Other | 0.84 (0.53 to 1.34) | 0.88 (0.55 to 1.41) |
| None | 0.86 (0.55 to 1.34) | 0.90 (0.57 to 1.42) |
| Employmentb | ||
| No | 1.14 (0.81 to 1.60) | 1.02 (0.72 to 1.46) |
| Marital statusc | ||
| Never married/CP | 1.19 (0.78 to 1.81) | 1.04 (0.68 to 1.61) |
| Separated, divorced, widowed | 2.06*** (1.37 to 3.09) | 1.65* (1.07 to 2.53) |
| Long-term illnessd | ||
| Yes | 2.02*** (1.46 to 2.80) | 1.96*** (1.41 to 2.72) |
| Accommodation satisfactione | ||
| Slightly/very dissatisfied | 1.10 (0.72 to 1.70) | 1.04 (0.67 to 1.61) |
| Neighbourhood aesthetics | ||
| Higher score = worse | 0.90 (0.70 to 1.14) | 0.91 (0.71 to 1.16) |
| Neighbourhood safety | ||
| Higher score = worse | 1.09 (0.89 to 1.34) | 1.07 (0.87 to 1.32) |
| Neighbourhood social cohesion | ||
| Higher score = worse | 1.32* (1.03 to 1.69) | 1.29* (1.00 to 1.66) |
| Neighbourhood violence | ||
| Lower score = worse | 0.67** (0.51 to 0.88) | 0.65** (0.49 to 0.85) |
| Damp in housed | ||
| Yes | 1.21 (0.84 to 1.74) | 1.11 (0.76 to 1.60) |
| Vibrations in housed | ||
| Yes | 1.78 (0.63 to 5.02) | 1.81 (0.64 to 5.14) |
| Dust in housed | ||
| Yes | 1.26 (0.61 to 2.61) | 1.09 (0.52 to 2.28) |
| Multiple poverty scoref | ||
| 1 | 2.02 (0.96 to 4.24) | |
| 2 | 2.35* (1.12 to 4.95) | |
| 3 | 3.6*** (1.68 to 7.70) | |
| 4 | 4.67** (1.73 to 12.57) | |
Anxiety at wave 3
At wave 3 being female, being unemployed, working in a semiroutine occupation, being never married, being widowed, divorced or separated, living in social rented accommodation or ‘other’ accommodation, being on benefits, having a multiple poverty score of 2 or greater and having a long-term illness were associated with increased odds of anxiety symptoms (Table 53). However, being educated to NVQ 4/5 level or having ‘other’ educational qualifications was associated with lower odds of anxiety symptoms (see Table 53). At wave 3, poor neighbourhood conditions, unsafe neighbourhoods, low levels of social cohesion and high levels of violence were associated with increased odds of anxiety symptoms (see Table 53). Being slightly or very dissatisfied with accommodation, visiting green spaces once a fortnight or less often and having damp, vibrations, dust or mould in the house were also associated with increased odds of anxiety symptoms.
| Variable | HADS anxiety, OR (95% CI) |
|---|---|
| Age | 1.01 (0.99 to 1.03) |
| Gendera | |
| Female | 1.43* (1.04 to 1.97) |
| Ethnicityb | |
| Asian: Indian | 0.95 (0.48 to 1.88) |
| Asian: Pakistani | 1.31 (0.69 to 2.50) |
| Asian: Bangladeshi | 0.68 (0.44 to 1.03) |
| Black: Caribbean | 1.05 (0.55 to 1.98) |
| Black: African | 0.81 (0.51 to 1.28) |
| Other | 0.84 (0.55 to 1.28) |
| Top educationc | |
| NVQ 3 | 0.94 (0.57 to 1.57) |
| NVQ 4/5 | 0.59* (0.38 to 0.93) |
| Other | 0.59* (0.39 to 0.89) |
| None | 1.08 (0.74 to 1.58) |
| Employmentd | |
| No | 1.47** (1.13 to 1.93) |
| Household NS-SECe | |
| Intermediate | 1.91 (0.83 to 4.42) |
| Semiroutine, etc. | 2.17* (1.18 to 4.01) |
| Marital statusf | |
| Never married/CP | 1.57* (1.10 to 2.24) |
| Separated, divorced, widowed | 2.04*** (1.43 to 2.92) |
| Home ownershipg | |
| Social rent | 1.78*** (1.25 to 2.53) |
| Private rent | 1.52 (0.98 to 2.37) |
| Other | 3.72* (1.29 to 10.74) |
| Benefitsh,i | |
| Yes | 1.59** (1.19 to 2.13) |
| Born in the UKd | |
| No | 0.87 (0.61 to 1.22) |
| Multiple poverty scorej | |
| 1 | 1.73 (0.97 to 3.07) |
| 2 | 2.19** (1.28 to 3.73) |
| 3 | 2.84*** (1.68 to 4.82) |
| 4 | 5.82*** (3.12 to 10.86) |
| Long-term illnessh | |
| Yes | 3.28*** (2.49 to 4.34) |
| Access to gardend | |
| No | 1.07 (0.80 to 1.45) |
| Accommodation satisfactionk | |
| Slightly/very dissatisfied | 2.00*** (1.42 to 2.81) |
| How often do you visit green spaces?l | |
| Once a fortnight or month | 1.10 (0.78 to 1.56) |
| Several times a year/never | 1.85*** (1.36 to 2.54) |
| Neighbourhood aesthetics | |
| Higher score = worse | 1.57*** (1.30 to 1.89) |
| Neighbourhood safety | |
| Higher score = worse | 1.41*** (1.22 to 1.64) |
| Neighbourhood social cohesion | |
| Higher score = worse | 1.55*** (1.29 to 1.86) |
| Neighbourhood violence | |
| Lower score = worse | 0.60*** (0.49 to 0.74) |
| Damp in househ | |
| Yes | 1.63*** (1.23 to 2.16) |
| Vibrations in househ | |
| Yes | 2.45** (1.27 to 4.69) |
| Dust in househ | |
| Yes | 2.17*** (1.46 to 3.23) |
| Mould in househ | |
| Yes | 1.76*** (1.28 to 2.41) |
Table 54 shows the multivariate analyses for parental anxiety at wave 3. At wave 3, living in the intervention area, being in a semiroutine occupation, being widowed, divorced or separated and having a long-term illness were associated with increased odds of anxiety symptoms. These odds were minimally reduced after further adjustment for multiple poverty score (see Table 54). Scoring 4 on the multiple poverty score was also associated with increased odds of anxiety symptoms. At wave 3, visiting green spaces only several times a year or never was associated with increased odds of anxiety symptoms, which was maintained after adjusting for multiple poverty score (see Table 54). High levels of neighbourhood violence were also associated with increased odds of anxiety symptoms at wave 3 and this was maintained after adjustment for multiple poverty score (see Table 54).
| Variable | HADS anxiety, OR (95% CI) | |
|---|---|---|
| Unadjusted | Adjusted | |
| Intervention | ||
| Newham | 1.97*** (1.42 to 2.74) | 1.97*** (1.41 to 2.74) |
| Gendera | ||
| Female | 1.23 (0.85 to 1.80) | 1.21 (0.82 to 1.77) |
| Top educationb | ||
| NVQ 3 | 1.01 (0.57 to 1.77) | 1.11 (0.62 to 1.96) |
| NVQ 4/5 | 0.82 (0.46 to 1.44) | 0.88 (0.50 to 1.57) |
| Other | 0.55* (0.34 to 0.90) | 0.57* (0.35 to 0.92) |
| None | 0.97 (0.63 to 1.49) | 0.95 (0.62 to 1.47) |
| Employmentc | ||
| No | 1.27 (0.65 to 2.51) | 1.40 (0.71 to 2.79) |
| Household NS-SECd | ||
| Intermediate | 1.70 (0.65 to 4.46) | 1.57 (0.59 to 4.21) |
| Semiroutine, etc. | 2.55* (1.14 to 5.72) | 2.47* (1.10 to 5.56) |
| Marital statuse | ||
| Never married/CP | 1.10 (0.72 to 1.68) | 1.06 (0.69 to 1.63) |
| Separated, divorced, widowed | 1.92** (1.26 to 2.91) | 1.86** (1.21 to 2.84) |
| Home ownershipf | ||
| Social rent | 1.20 (0.78 to 1.82) | 1.06 (0.68 to 1.66) |
| Private rent | 1.33 (0.79 to 2.24) | 1.17 (0.68 to 2.00) |
| Other | 3.12 (0.92 to 10.63) | 3.17 (0.92 to 10.93) |
| Long-term illnessg | ||
| Yes | 3.19*** (2.35 to 4.33) | 3.09*** (2.26 to 4.22) |
| Accommodation satisfactionh | ||
| Slightly/very dissatisfied | 1.29 (0.85 to 1.95) | 1.27 (0.83 to 1.93) |
| How often do you visit green spaces?i | ||
| Once a fortnight or month | 1.03 (0.70 to 1.53) | 1.01 (0.68 to 1.50) |
| Several times a year/never | 1.58* (1.10 to 2.27) | 1.61* (1.12 to 2.31) |
| Neighbourhood aesthetics | ||
| Higher score = worse | 1.02 (0.80 to 1.32) | 1.00 (0.78 to 1.29) |
| Neighbourhood safety | ||
| Higher score = worse | 1.03 (0.83 to 1.29) | 1.07 (0.85 to 1.34) |
| Neighbourhood social cohesion | ||
| Higher score = worse | 1.22 (0.95 to 1.56) | 1.19 (0.92 to 1.53) |
| Neighbourhood violence | ||
| Lower score = worse | 0.72* (0.54 to 0.97) | 0.75 (0.55 to 1.01) |
| Damp in houseg | ||
| Yes | 1.03 (0.70 to 1.53) | 1.03 (0.70 to 1.53) |
| Vibrations in houseg | ||
| Yes | 1.56 (0.72 to 3.41) | 1.51 (0.68 to 3.36) |
| Dust in houseg | ||
| Yes | 1.43 (0.86 to 2.39) | 1.36 (0.81 to 2.29) |
| Mould in houseg | ||
| Yes | 1.01 (0.65 to 1.59) | 1.03 (0.66 to 1.63) |
| Multiple poverty scorej | ||
| 1 | 1.19 (0.62 to 2.31) | |
| 2 | 1.31 (0.69 to 2.49) | |
| 3 | 1.35 (0.70 to 2.59) | |
| 4 | 2.89** (1.35 to 6.20) | |
Living in the intervention area and depressive symptoms at waves 1, 2 and 3
Table 55 shows the association of living in the intervention borough of Newham rather than in the comparison areas with depressive symptoms at each wave. At wave 3, participants living in Newham were more likely to report depressive symptoms than participants living in the comparison area (RRR 1.55, 95% CI 1.14 to 2.10). No differences were observed at wave 1 or wave 2.
| Wave | Borough | HADS depression, OR (95% CI) |
|---|---|---|
| Wave 1 intervention | Newham | 0.91 (0.68 to 1.22) |
| Wave 2 intervention | Newham | 1.13 (0.81 to 1.59) |
| Wave 3 intervention | Newham | 1.55** (1.14 to 2.10) |
Depressive symptoms at wave 1
Table 56 shows the univariate associations of sociodemographic and neighbourhood characteristics on parental depressive symptoms at wave 1. At wave 1, being older, being of Bangladeshi or ‘other’ ethnicity, having no formal educational qualifications, being unemployed, being widowed, divorced or separated, living in social rented accommodation, receiving benefits, having a long-term illness and having a multiple poverty score of 1 or greater were associated with increased odds of depressive symptoms (see Table 56). Poor neighbourhood conditions and being in an unsafe neighbourhood with low levels of social cohesion and high levels of violence were associated with increased odds of depressive symptoms at wave 1 (see Table 56). Being slightly or very dissatisfied with accommodation, or having damp, dust or mould in the house were also associated with increased odds of depressive symptoms. In addition, being treated unfairly at work because of ethnicity was associated with increased odds of depressive symptoms. This was similar to the results for anxiety at wave 1.
| Variable | HADS depression, OR (95% CI) |
|---|---|
| Age | 1.04*** (1.03 to 1.06) |
| Gendera | |
| Female | 0.86 (0.64 to 1.16) |
| Ethnicityb | |
| Asian: Indian | 0.57 (0.23 to 1.40) |
| Asian: Pakistani | 1.70 (0.90 to 3.19) |
| Asian: Bangladeshi | 1.91** (1.28 to 2.85) |
| Black: Caribbean | 1.46 (0.78 to 2.72) |
| Black: African | 0.85 (0.52 to 1.37) |
| Other | 1.59* (1.06 to 2.39) |
| Top educationc | |
| NVQ 3 | 0.89 (0.51 to 1.55) |
| NVQ 4/5 | 0.64 (0.40 to 1.00) |
| Other | 1.12 (0.77 to 1.65) |
| None | 1.77** (1.22 to 2.55) |
| Employmentd | |
| No | 2.44*** (1.81 to 3.28) |
| Household NS-SECe | |
| Intermediate | 1.19 (0.62 to 2.29) |
| Semiroutine, etc. | 1.46 (0.95 to 2.27) |
| Marital statusf | |
| Never married/CP | 1.13 (0.81 to 1.57) |
| Separated, divorced, widowed | 1.72** (1.18 to 2.49) |
| Home ownershipg | |
| Social rent | 1.79*** (1.26 to 2.53) |
| Private rent | 0.82 (0.52 to 1.31) |
| Other | 1.23 (0.51 to 2.99) |
| Benefitsh,i | |
| Yes | 1.70*** (1.29 to 2.25) |
| Born in the UKd | |
| No | 1.23 (0.92 to 1.64) |
| Multiple poverty scorej | |
| 1 | 2.01* (1.10 to 3.66) |
| 2 | 2.53** (1.43 to 4.50) |
| 3 | 3.93*** (2.23 to 6.96) |
| 4 | 7.7*** (4.03 to 14.69) |
| Long-term illnessh | |
| Yes | 3.89*** (2.91 to 5.19) |
| Access to gardend | |
| No | 1.21 (0.91 to 1.60) |
| Accommodation satisfactionk | |
| Slightly/very dissatisfied | 2.15*** (1.55 to 2.98) |
| How often do you visit green spaces?l | |
| Once a fortnight or month | 0.85 (0.61 to 1.19) |
| Several times a year/never | 1.04 (0.75 to 1.43) |
| Neighbourhood aesthetics | |
| Higher score = worse | 1.36*** (1.15 to 1.60) |
| Neighbourhood safety | |
| Higher score = worse | 1.29*** (1.14 to 1.46) |
| Neighbourhood social cohesion | |
| Higher score = worse | 1.27*** (1.10 to 1.46) |
| Neighbourhood violence | |
| Lower score = worse | 0.66*** (0.56 to 0.79) |
| Insulted because of ethnicityh | |
| Yes | 1.00 (0.54 to 1.84) |
| Refused job as a result of discriminationh | |
| Yes | 1.10 (0.53 to 2.26) |
| Treated unfairly at work because of ethnicityh | |
| Yes | 2.26* (1.04 to 4.90) |
| Damp in househ | |
| Yes | 1.65*** (1.22 to 2.24) |
| Vibrations in househ | |
| Yes | 1.42 (0.72 to 2.81) |
| Dust in househ | |
| Yes | 2.14*** (1.34 to 3.40) |
| Mould in househ | |
| Yes | 1.89*** (1.35 to 2.64) |
Table 57 shows the multivariate associations for depressive symptoms at wave 1. At wave 1, increasing age, being of Pakistani, Bangladeshi or ‘other’ ethnicity, having no formal educational qualifications, being unemployed, being widowed, divorced or separated and having a long-term illness were associated with increased odds of depressive symptoms adjusting for age, ethnicity, education, employment, marital status, home ownership, receipt of benefits and long-term illness (see Table 57). These odds changed very little after further adjustment for multiple poverty score, which was itself strongly associated with depressive symptoms, except for the odds associated with Pakistani and Bangladeshi ethnicity and long-term illness, which were slightly reduced. At wave 1, high levels of neighbourhood violence were associated with increased odds of depressive symptoms in adjusted analyses, including after adjustment for multiple poverty score (see Table 57).
| Variable | HADS depression, OR (95% CI) | |
|---|---|---|
| Unadjusted | Adjusted | |
| Age | 1.04*** (1.01 to 1.06) | 1.04*** (1.02 to 1.06) |
| Ethnicitya | ||
| Asian: Indian | 0.92 (0.34 to 2.47) | 0.92 (0.34 to 2.49) |
| Asian: Pakistani | 3.73*** (1.76 to 7.89) | 3.36** (1.57 to 7.21) |
| Asian: Bangladeshi | 2.59*** (1.56 to 4.31) | 2.27** (1.35 to 3.82) |
| Black: Caribbean | 2.01 (0.99 to 4.08) | 1.95 (0.95 to 3.98) |
| Black: African | 1.43 (0.81 to 2.50) | 1.29 (0.73 to 2.28) |
| Other | 2.66*** (1.60 to 4.43) | 2.44*** (1.45 to 4.09) |
| Top educationb | ||
| NVQ 3 | 0.86 (0.47 to 1.59) | 0.92 (0.49 to 1.72) |
| NVQ 4/5 | 0.90 (0.53 to 1.54) | 1.05 (0.61 to 1.81) |
| Other | 0.98 (0.62 to 1.56) | 1.06 (0.66 to 1.70) |
| None | 1.58* (1.02 to 2.44) | 1.69* (1.08 to 2.63) |
| Employmentc | ||
| No | 1.89*** (1.35 to 2.66) | 1.87*** (1.33 to 2.64) |
| Marital statusd | ||
| Never married/CP | 1.28 (0.84 to 1.95) | 1.15 (0.75 to 1.75) |
| Separated, divorced, widowed | 1.62* (1.05 to 2.52) | 1.54 (0.99 to 2.41) |
| Home ownershipe | ||
| Social rent | 1.06 (0.69 to 1.65) | 0.87 (0.55 to 1.37) |
| Private rent | 0.74 (0.42 to 1.28) | 0.57 (0.32 to 1.01) |
| Other | 1.10 (0.40 to 2.99) | 0.99 (0.36 to 2.74) |
| Long-term illnessf | ||
| Yes | 2.80*** (2.01 to 3.91) | 2.50*** (1.78 to 3.52) |
| Accommodation satisfactiong | ||
| Slightly/very dissatisfied | 1.38 (0.91 to 2.10) | 1.40 (0.92 to 2.13) |
| Neighbourhood aesthetics | ||
| Higher score = worse | 1.04 (0.83 to 1.30) | 1.02 (0.82 to 1.28) |
| Neighbourhood safety | ||
| Higher score = worse | 1.09 (0.91 to 1.30) | 1.07 (0.9 to 1.28) |
| Neighbourhood social cohesion | ||
| Higher score = worse | 1.05 (0.86 to 1.28) | 1.06 (0.87 to 1.30) |
| Neighbourhood violence | ||
| Lower score = worse | 0.67*** (0.53 to 0.84) | 0.67*** (0.53 to 0.84) |
| Damp in housef | ||
| Yes | 1.15 (0.76 to 1.73) | 1.12 (0.74 to 1.70) |
| Dust in housef | ||
| Yes | 1.37 (0.78 to 2.40) | 1.29 (0.73 to 2.26) |
| Mould in housef | ||
| Yes | 1.25 (0.79 to 1.96) | 1.20 (0.76 to 1.90) |
| Multiple poverty scoreh | ||
| 1 | 1.76 (0.91 to 3.39) | |
| 2 | 1.81 (0.95 to 3.47) | |
| 3 | 2.39** (1.23 to 4.65) | |
| 4 | 4.55*** (2.15 to 9.64) | |
Depressive symptoms at wave 2
Table 58 shows the univariate associations of sociodemographic and neighbourhood characteristics on parental/carer depressive symptoms at wave 2. At wave 2, increasing age, unemployment, intermediate or semiroutine occupation, being widowed, divorced or separated, living in social, rented or privately rented accommodation, being in receipt of benefits, having a long-term illness and a multiple poverty score of 1 or greater were associated with increased odds of depressive symptoms (see Table 58). Having educational qualifications of NVQ 4/5 level was associated with reduced odds of depressive symptoms at wave 2 (see Table 58). At wave 2, being in an unsafe neighbourhood with low levels of social cohesion and high levels of violence was associated with increased odds of depressive symptoms (see Table 58). Being slightly or very dissatisfied with accommodation was also associated with increased odds of depressive symptoms.
| Variable | HADS depression, OR (95% CI) |
|---|---|
| Age | 1.05*** (1.03 to 1.07) |
| Gendera | |
| Female | 0.96 (0.66 to 1.38) |
| Ethnicityb | |
| Asian: Indian | 0.79 (0.33 to 1.89) |
| Asian: Pakistani | 1.08 (0.52 to 2.28) |
| Asian: Bangladeshi | 0.80 (0.49 to 1.29) |
| Black: Caribbean | 1.44 (0.68 to 3.08) |
| Black: African | 0.62 (0.35 to 1.08) |
| Other | 1.03 (0.63 to 1.69) |
| Top educationc | |
| NVQ 3 | 0.64 (0.30 to 1.34) |
| NVQ 4/5 | 0.32*** (0.16 to 0.63) |
| Other | 0.89 (0.56 to 1.44) |
| None | 1.32 (0.85 to 2.03) |
| Employmentd | |
| No | 2.43*** (1.68 to 3.50) |
| Household NS-SECe | |
| Intermediate | 3.87* (1.34 to 11.21) |
| Semiroutine, etc. | 4.11** (1.71 to 9.85) |
| Marital statusf | |
| Never married/CP | 1.30 (0.86 to 1.98) |
| Separated, divorced, widowed | 1.55* (1.01 to 2.40) |
| Home ownershipg | |
| Social rent | 1.60* (1.04 to 2.48) |
| Private rent | 2.09** (1.20 to 3.65) |
| Other | 0.78 (0.10 to 6.32) |
| Benefitsh,i | |
| Yes | 1.63* (1.12 to 2.37) |
| Born in the UKd | |
| No | 0.87 (0.58 to 1.30) |
| Multiple poverty scorej | |
| 1 | 2.71* (1.03 to 7.12) |
| 2 | 4.20** (1.69 to 10.48) |
| 3 | 6.78*** (2.78 to 16.5) |
| 4 | 7.50*** (2.46 to 22.87) |
| Long-term illnessh | |
| Yes | 2.27*** (1.63 to 3.16) |
| Access to gardend | |
| No | 1.21 (0.86 to 1.70) |
| Accommodation satisfactionk | |
| Slightly/very dissatisfied | 1.83** (1.23 to 2.72) |
| How often do you visit green spaces?l | |
| Once a fortnight or month | 1.12 (0.74 to 1.70) |
| Several times a year/never | 1.33 (0.91 to 1.95) |
| Neighbourhood aesthetics | |
| Higher score = worse | 1.22 (0.98 to 1.51) |
| Neighbourhood safety | |
| Higher score = worse | 1.34*** (1.14 to 1.58) |
| Neighbourhood social cohesion | |
| Higher score = worse | 1.40*** (1.15 to 1.70) |
| Neighbourhood violence | |
| Lower score = worse | 0.68** (0.53 to 0.86) |
| Damp in househ | |
| Yes | 1.31 (0.91 to 1.87) |
| Vibrations in househ | |
| Yes | 1.73 (0.67 to 4.44) |
| Dust in househ | |
| Yes | 1.63 (0.85 to 3.12) |
| Mould in househ | |
| Yes | 1.48 (0.99 to 2.20) |
Table 59 shows the multivariate associations for parental depressive symptoms at wave 2. At wave 2, increasing age, having an intermediate or semiroutine household occupation and long-term illness were associated with increased odds of depressive symptoms (see Table 59). After further adjustment for multiple poverty score, only age and long-term illness still led to significantly increased ORs (see Table 59). Having a multiple poverty score of 2 or more was associated with increased odds of depressive symptoms.
| Variable | HADS depression, OR (95% CI) | |
|---|---|---|
| Unadjusted | Adjusted | |
| Age | 1.05*** (1.03 to 1.08) | 1.05*** (1.03 to 1.08) |
| Top educationa | ||
| NVQ 3 | 0.75 (0.34 to 1.65) | 0.81 (0.36 to 1.83) |
| NVQ 4/5 | 0.44* (0.21 to 0.96) | 0.50 (0.23 to 1.10) |
| Other | 0.92 (0.54 to 1.57) | 0.96 (0.55 to 1.66) |
| None | 1.23 (0.74 to 2.03) | 1.34 (0.80 to 2.23) |
| Employmentb | ||
| No | 1.33 (0.77 to 2.31) | 1.24 (0.71 to 2.17) |
| Household NS-SECc | ||
| Intermediate | 3.81* (1.23 to 11.76) | 3.14 (0.98 to 10.08) |
| Semiroutine, etc. | 2.99* (1.12 to 7.97) | 2.49 (0.91 to 6.82) |
| Marital statusd | ||
| Never married/CP | 1.13 (0.70 to 1.82) | 1.02 (0.62 to 1.65) |
| Separated, divorced, widowed | 1.00 (0.61 to 1.64) | 0.83 (0.50 to 1.40) |
| Home ownershipe | ||
| Social rent | 1.11 (0.67 to 1.83) | 0.81 (0.47 to 1.39) |
| Private rent | 1.88 (0.99 to 3.56) | 1.37 (0.70 to 2.68) |
| Other | 0.86 (0.09 to 7.99) | 0.79 (0.08 to 7.48) |
| Long-term illnessf | ||
| Yes | 1.83*** (1.27 to 2.65) | 1.76** (1.21 to 2.55) |
| Accommodation satisfactiong | ||
| Slightly/very dissatisfied | 1.34 (0.85 to 2.12) | 1.27 (0.80 to 2.02) |
| Neighbourhood safety | ||
| Higher score = worse | 1.11 (0.88 to 1.41) | 1.09 (0.86 to 1.38) |
| Neighbourhood social cohesion | ||
| Higher score = worse | 1.12 (0.85 to 1.47) | 1.14 (0.86 to 1.51) |
| Neighbourhood violence | ||
| Lower score = worse | 0.75 (0.53 to 1.05) | 0.75 (0.53 to 1.06) |
| Multiple poverty scoreh | ||
| 1 | 2.02 (0.70 to 5.82) | |
| 2 | 2.85* (1.01 to 8.05) | |
| 3 | 4.13** (1.46 to 11.68) | |
| 4 | 4.14* (1.14 to 15.00) | |
Depressive symptoms at wave 3
Table 60 shows the univariate associations of sociodemographic and neighbourhood characteristics on parental depressive symptoms at wave 3. At wave 3, increasing age, having no formal educational qualifications, being unemployed, being in a semiroutine occupation, living in social, rented or privately rented accommodation, being in receipt of benefits, having a long-term illness and having a multiple poverty score of 1 or greater were associated with an increased risk of depressive symptoms (see Table 60). At wave 3, visiting green spaces only several times a year or never was associated with increased odds of depressive symptoms. Poor neighbourhood conditions, unsafe neighbourhoods and low levels of social cohesion and high levels of violence were associated with an increased risk of depressive symptoms (see Table 60). Being slightly or very dissatisfied with housing was associated with increased odds of depressive symptoms, as was having damp or dust in the house (see Table 60).
| Variable | HADS depression, OR (95% CI) |
|---|---|
| Age | 1.03* (1.01 to 1.05) |
| Gendera | |
| Female | 1.03 (0.73 to 1.46) |
| Ethnicityb | |
| Asian: Indian | 0.97 (0.45 to 2.09) |
| Asian: Pakistani | 1.56 (0.79 to 3.07) |
| Asian: Bangladeshi | 0.73 (0.45 to 1.19) |
| Black: Caribbean | 0.69 (0.32 to 1.50) |
| Black: African | 0.82 (0.49 to 1.38) |
| Other | 0.87 (0.55 to 1.38) |
| Top educationc | |
| NVQ 3 | 1.12 (0.62 to 2.02) |
| NVQ 4/5 | 0.73 (0.42 to 1.24) |
| Other | 0.70 (0.43 to 1.16) |
| None | 1.88** (1.22 to 2.88) |
| Employmentd | |
| No | 1.82*** (1.34 to 2.48) |
| Household NS-SECe | |
| Intermediate | 2.54 (0.85 to 7.60) |
| Semiroutine, etc. | 2.69* (1.18 to 6.15) |
| Marital statusf | |
| Never married/CP | 0.90 (0.59 to 1.37) |
| Separated, divorced, widowed | 1.38 (0.93 to 2.05) |
| Home ownershipg | |
| Social rent | 2.04*** (1.34 to 3.12) |
| Private rent | 2.02** (1.21 to 3.37) |
| Other | 1.57 (0.42 to 5.90) |
| Benefitsh,i | |
| Yes | 1.54* (1.10 to 2.15) |
| Born in the UKd | |
| No | 0.99 (0.67 to 1.47) |
| Multiple poverty scorej | |
| 1 | 3.05** (1.39 to 6.69) |
| 2 | 4.23*** (2.02 to 8.85) |
| 3 | 4.51*** (2.15 to 9.44) |
| 4 | 5.41*** (2.38 to 12.28) |
| Long-term illnessh | |
| Yes | 2.53*** (1.86 to 3.44) |
| Access to gardend | |
| No | 1.03 (0.74 to 1.44) |
| Accommodation satisfactionk | |
| Slightly/very dissatisfied | 1.79** (1.23 to 2.59) |
| How often do you visit green spaces?l | |
| Once a fortnight or month | 1.03 (0.70 to 1.53) |
| Several times a year/never | 1.50* (1.06 to 2.13) |
| Neighbourhood aesthetics | |
| Higher score = worse | 1.32** (1.07 to 1.62) |
| Neighbourhood safety | |
| Higher score = worse | 1.20* (1.02 to 1.42) |
| Neighbourhood social cohesion | |
| Higher score = worse | 1.41*** (1.16 to 1.71) |
| Neighbourhood violence | |
| Lower score = worse | 0.76* (0.61 to 0.95) |
| Damp in househ | |
| Yes | 1.49* (1.09 to 2.05) |
| Vibrations in househ | |
| Yes | 1.12 (0.52 to 2.40) |
| Dust in househ | |
| Yes | 2.02*** (1.32 to 3.09) |
| Mould in househ | |
| Yes | 1.32 (0.92 to 1.89) |
Table 61 shows the multivariate associations for depressive symptoms at wave 3. At wave 3, living in the intervention area, increasing age, unemployment, having no formal educational qualifications, having a semiroutine household occupation, living in privately rented accommodation and having a long-term illness were associated with increased odds of depressive symptoms (see Table 61). Further adjustment for multiple poverty score had a minimal effect on the ORs for these risk factors (see Table 61). Having a multiple poverty score of 2 or more was associated with increased risk of depressive symptoms.
| Variable | HADS depression, OR (95% CI) | |
|---|---|---|
| Unadjusted | Adjusted | |
| Intervention | ||
| Newham | 1.70** (1.19 to 2.42) | 1.63** (1.14 to 2.32) |
| Age | 1.03* (1.00 to 1.06) | 1.04* (1.01 to 1.06) |
| Top educationa | ||
| NVQ 3 | 1.29 (0.69 to 2.42) | 1.41 (0.75 to 2.66) |
| NVQ 4/5 | 0.97 (0.52 to 1.83) | 1.09 (0.58 to 2.08) |
| Other | 0.59 (0.34 to 1.02) | 0.59 (0.34 to 1.03) |
| None | 1.59 (0.99 to 2.54) | 1.56 (0.98 to 2.50) |
| Employmentb | ||
| No | 1.97 (0.96 to 4.02) | 2.06 (0.99 to 4.28) |
| Household NS-SECc | ||
| Intermediate | 2.07 (0.67 to 6.42) | 1.95 (0.61 to 6.22) |
| Semiroutine, etc. | 2.52* (1.01 to 6.31) | 2.44 (0.96 to 6.20) |
| Home ownershipd | ||
| Social rent | 1.61 (0.99 to 2.61) | 1.31 (0.79 to 2.18) |
| Private rent | 2.08* (1.16 to 3.73) | 1.79 (0.98 to 3.26) |
| Other | 0.99 (0.22 to 4.50) | 0.91 (0.20 to 4.23) |
| Long-term illnesse | ||
| Yes | 2.29*** (1.62 to 3.22) | 2.23*** (1.57 to 3.16) |
| Accommodation satisfactionf | ||
| Slightly/very dissatisfied | 1.16 (0.75 to 1.82) | 1.12 (0.71 to 1.75) |
| How often do you visit green spaces?g | ||
| Once a fortnight or month | 1.00 (0.65 to 1.53) | 1.00 (0.65 to 1.53) |
| Several times a year/never | 1.18 (0.79 to 1.74) | 1.18 (0.80 to 1.75) |
| Neighbourhood aesthetics | ||
| Higher score = worse | 0.96 (0.74 to 1.26) | 0.95 (0.73 to 1.25) |
| Neighbourhood safety | ||
| Higher score = worse | 0.98 (0.77 to 1.25) | 0.99 (0.78 to 1.27) |
| Neighbourhood social cohesion | ||
| Higher score = worse | 1.21 (0.92 to 1.57) | 1.20 (0.92 to 1.57) |
| Neighbourhood violence | ||
| Lower score = worse | 0.84 (0.63 to 1.14) | 0.86 (0.64 to 1.17) |
| Damp in housee | ||
| Yes | 1.00 (0.68 to 1.47) | 1.00 (0.68 to 1.46) |
| Dust in housee | ||
| Yes | 1.68* (1.02 to 2.78) | 1.66* (1.00 to 2.76) |
| Multiple poverty scoreh | ||
| 1 | 2.24 (0.95 to 5.30) | |
| 2 | 2.81* (1.23 to 6.40) | |
| 3 | 2.32* (1.01 to 5.34) | |
| 4 | 2.79* (1.08 to 7.21) | |
Summary
At wave 1, there were higher levels of well-being in the urban regeneration area, but this was no longer the case by wave 3. Low levels of well-being did not differ between the urban regeneration area and the other areas across the three waves. At follow-up, in wave 3, there were higher levels of anxiety and depressive symptoms in the urban regeneration area than in the comparison areas. In general, there was a fairly consistent pattern of associations of indicators of social disadvantage, marital breakdown, long-term illness and poor neighbourhood conditions with low levels of well-being and higher scores on anxiety and depressive symptoms.
Chapter 6 Understanding the lived experience of Olympic-led regeneration in Newham
In this chapter we complement the quantitative analyses present in the preceding chapters with qualitative work that attempts to situate Olympic-related regeneration and change in the context of those residents who experienced it. Regeneration is both a process and an outcome, it can have physical, economic and social dimensions. 89 Urban regeneration is often framed as a means of addressing inequalities and exclusion by improving the built environment and local economy, and thereby providing enhanced employment, social, health, educational and recreational opportunities. 89
This qualitative study aimed to examine the lived experiences of regeneration for local families and young people. In doing so, it addresses a number of gaps in the literature on urban renewal in deprived areas. Specifically, with regard to young people, the impact of poverty on adolescents was, until recently, mostly overlooked. Few empirical studies on adolescents ground youth outcomes in inter-related social contexts, despite the growing consensus that a more complete understanding of how young people achieve social competency requires taking into account the multiple and inter-related contexts that young people inhabit and the factors that shape them. In addition to this, there remains little qualitative research addressing local perceptions of regeneration interventions.
Sporting mega-event-led regeneration has emerged as a discrete approach to urban renewal. 90 As with regeneration literature in general, there remains a lack of research addressing the lived experiences of sporting mega-events themselves and of associated regeneration. Experiences of place, and the meanings attached to them, may be a component of the complex ways in which material and social conditions interact to produce health inequality. 91 Investigating the impact of urban renewal on residents requires an understanding of how people use and perceive regenerated areas and facilities. In order to do this, we undertook a study that attempted to answer the following primary research question:
-
What is the ‘reach’ and experience of the London 2012 regeneration programme for Newham residents and how is it understood in relation to their family circumstances, health and well-being?
We conducted a longitudinal qualitative study of family experiences and perceptions of the London 2012 Olympic and Paralympic Games and the associated regeneration. We employed a range of methods over three phases of data collection:
-
family narrative interviews with a sample of families
-
go-along interviews with a subset of the family sample
-
school video focus groups with a sample of adolescents.
A full description of the methods and analytical approach used can be found in Chapter 2. We report the main findings below. All quotations used below are paraphrased from Thompson et al. 92,93
Main findings
Our analyses explored the residents’ narratives of change, or lack of change, in the Olympic period. Three particular themes were prominent in these narratives:
-
a legacy perceived as temporary, symbolic, largely positive but also somewhat superficial
-
a dominant narrative of social housing need as a pressing concern for local residents that was not addressed by Olympic regeneration
-
unexpected findings around local acceptance of securitisation and the absence of a ‘sporting legacy’.
Pre Olympics, and to a large extent post Olympics, Newham was described as a run-down and socially fragmented area very much in need of improvement and renewal. Respondent accounts depicted living in Newham as an experience of diverse and rapidly shifting populations, urban decay, and constant changes to the landscape and local services. The area was consistently described as being overcrowded and often chaotic. Several talked of housing blocks and amenities ‘going up’ or ‘coming down’. This was experienced by some as welcoming and dynamic but by others as insecure and threatening. Public services in the area, in particular ‘the council’, were depicted as inefficient, unfair and underfunded. Participants described being ‘disconnected’ from the services provided, as if these were at odds with their personal goals and needs. As a result, participants who mentioned them had limited faith in them. They described how ‘the people in charge don’t know what to do’ and so (allegedly) addressed big problems like the housing shortage or unemployment with a series of ‘stop gaps’ that were generally considered to be temporary and inadequate. In these narratives, participants consistently positioned themselves in opposition to those within the ‘system’ and adopted a binary taxonomy of ‘us’ and ‘them’. The area in general was described as being, aesthetically, in a state of decay. Litter, vandalism and dilapidated facilities in particular were seen as major problems in Newham and served to demoralise residents. Overall, when describing Newham before the Games, participants described a desperate need for improvements to both the physical and social environment.
Temporary and symbolic change as the dominant Olympic legacy
Overall, the changes and regeneration activities in Newham were described by participants as largely temporary in nature and focused on improving ‘the look’ of the area and putting on a series of celebratory community events. Despite the transient way in which these changes were described, residents were relatively positive about them and described how they had improved their lives, even if only in the short term. By contrast, more substantive and pressing local needs, most especially housing, were felt to be largely ignored by regeneration efforts.
Aesthetic improvements: ‘tidying up’ Newham
Improving ‘the look’ of the area by measures such as resurfacing roads, repainting and replacing street lighting meant that residents perceived and experienced their neighbourhood more positively. Relatively minor changes to the local physical environment sometimes had a significant impact on participants’ sense of well-being. They described how the Games had put Newham in the limelight and prompted a programme of ‘tidying up’ that improved the area and its image and enabled residents to feel proud rather than ashamed of where they lived. For example, David, a stay-at home father of two who lived very close to the Olympic Park, described how the changes were more than cosmetic:
It’s changed it 100%, you know, especially where the actual Olympics was based used to be like waste ground and train tracks and all that crap and what they’ve done to it is just amazing, you know, I’ve been over there a few times and it is just amazing, the whole area, just for that down there, it seems to have made people feel better about living in this area now, rather than stuck in the East End of London, you know, it’s more yeah well I’m living here now and it’s, I can come in, got more people coming in, more events, more upgrade in housing, no more it’s the slums of east London, more the London East, as I’ve heard people call it now instead of east London.
Despite a widespread sense of well-being and pride associated with the physical regeneration of the locality, there was also a strong sense that these improvements were temporary in nature, being for the benefit of the Games, and concentrated mostly in Stratford rather than occurring at the wider borough level as a whole.
The Stratford City Westfield shopping centre development was described as the most tangible and symbolic site of Olympic area improvement, providing a sense of aspiration and novelty. Although generally positive about this development and the income it might bring to the area, participants also perceived a rejection of the unadorned locality by the Olympic brand and a perceived need to make the area more presentable and ‘showcase’ it for visitors and investors. The Westfield development was even depicted as physically ‘blocking off’ the less salubrious parts of the borough. Participants pointed out that only some parts of the borough have been smartened up, and only temporarily so, giving a sense of artificial façade with the borough’s dirt and deprivation continuing, largely hidden from view. The westfield shopping centre was, for many participants, the most tangible and lasting aspect of the Olympic legacy.
Celebratory events: bringing residents together
Living in the host borough during the Olympic period provided a sense of community and belonging that was new to many residents. The numerous activities and events, along with the Games themselves, provided a respite from the frustration and lack of unity that they felt had previously characterised day-to-day life in Newham. Undoubtedly, the profile of Newham was raised and its reputation improved as a result of the Games. However, participants did not perceive the renewed sense of community pride to be permanent or necessarily to have any material benefits. The anticipated legacy seemed to be a symbolic rather than a material one. Other than possible revenue and employment from the Westfield shopping centre they did not envisage a legacy of direct benefits and more permanent community-level improvements. For example, the temporary Olympic site jobs, although exciting and unique, were also largely interpreted as further evidence of the transient nature of the event and its legacy, as yet more temporary measures or ‘stop gaps’ that failed to offer permanent solutions to problems in the area. Tasha, an unemployed 20-year-old, put it like this:
In terms of jobs I don’t think there are many jobs available right now around here, like so many people unemployed, jobs haven’t really increased, it was only during the Olympic times that people were like, oh yeah, we’ve got a job in the Olympics but our heads were thinking, OK, how long is that going to last, it’s until the Olympics are over, after that, I don’t know what the Olympic Park is used for now, I don’t think it’s used for anything.
Tasha was positive about the hosting of the Games overall and saw it as an event that brought attention and celebration and ‘got people talking’. However, when asked to comment in more detail about the possible impact on wider aspects of life in Newham, such as employment, she was doubtful as to how any material legacy or benefits might manifest themselves. ‘Spectacle’ alone was not viewed as sufficient to adequately address the many problems faced by Newham or to tangibly improve the lives of residents.
In many cases it was aesthetic improvements and community events that enabled residents to experience a more socially inclusive Newham. Social networks predict mental health. 94 Lawrence,94 in his study of neighbourhood satisfaction and self-rated mental health, found that the perceived environmental characteristics influencing this relationship included diversity, street connectivity, aesthetics and traffic loads. His suggested explanation for the mechanisms of this association is that perception of greenery encourages residents to enjoy the outdoors, where they are likely to meet their neighbours.
Enduring local needs not addressed by urban renewal: ‘the housing’
By far the most pressing local issue described by participants was a lack of affordable and social housing. Newham has one of the most acute housing shortages in London, with 32,000 of its residents on the social housing waiting list,95 and overcrowding is a well-documented problem. Private renting accounts for more than one-third of all households in the borough and is rising steadily owing to buy-to-let landlords increasingly setting themselves up as social landlords by renting to housing-benefit-supported tenants within the private rental sector. Participants of the qualitative study reported that Olympic regeneration, even the new social housing in the former Athletes’ Village site, did not adequately address this issue.
One of the defining characteristics of Newham, according to the residents interviewed, is its housing problems. All of the adult participants, and many of the adolescents, identified housing as an ‘issue’ for Newham, and often for themselves personally. There were a diverse range of narratives about various aspects of ‘the housing’. For those in the social housing system the most desired outcome was to obtain an affordable, permanent home of acceptable quality and size, without having to move out of the area. Pursuing this aim in the long term requires a strategy of ‘waiting it out’, which is characterised by the need to endure the temporary and insecure housing almost indefinitely while waiting to ‘get to the top of the (housing) list’. ‘Waiting it out’ is a strategy of patience, of keeping in contact with the relevant services and agencies, and persevering, but also one in which the locus of control is external. There is a degree of resignation to agency and decision-making being out of reach for an indefinite period of time in the hope of being ‘permanent’. In order to ‘stay on the list’ it is also often necessary to go into ‘temporary’ accommodation – most typically bed and breakfast hotels – for extended periods. Experiences of ‘temporary’ accommodation are far from positive. Accounts of these episodes were characterised by multiple moves, reported difficulties with landlords and other residents, and descriptions of poor-quality accommodation. Beth, a 41-year-old mother of three, and her 16-year-old son, Kam, gave a complex account of their family’s time in various bed and breakfast hotels before getting a permanent flat:
Eight months in bed and breakfast . . . Um, originally when we lived in East Ham he was just born, he was born in the July and we got evicted in the October actually on his birthday . . . They said to us ‘go down with the papers, you know, the eviction papers on the day of the eviction and they will give us temporary accommodation’. Which I was led to believe that they would give us accommodation, i.e. a house or a flat or something but we ended up in a bed and breakfast, which I turned down initially because that’s not what they led us to believe, Newham Council. And I was a bit upset so we went to stay with a friend for a while in Stratford . . . And we stayed there . . . Hmm, then you know like we felt that we’d overstayed our welcome in my friend’s house so I decided to go back to the Council and then they sent us to, Pragel Street sent us to Southend.
Oh yeah, that’s the one where we had to go underground, it was filled with illegal staff.
Yeah. It was like a building site so we came back with their stuff, um, his dad, we had to take like a personnel cruiser, a people cruiser . . . And there was five of us then, there was him, the two older boys, myself and my husband. It cost us £110 round trip to come back to London and the Council actually owes us that £110 ‘cause they said to me that they would reimburse the £110 for the taxi because we paid for our own taxi and we never saw a penny of that back . . . We had a nice contained little room, didn’t we?
Narratives of ‘waiting it out’ were full of long explanations of the factors that obscured this aim. Accounts are characterised by tensions between the permanent and the temporary, with a degree of resignation and even hopelessness. Such experiences and pressures had implications for health and well-being, and participants were very much aware of these.
Participants explained that ‘housing’ issues had an impact on their health in terms of both the poor-quality conditions (such as damp and structural defects) and the stress caused by the housing crisis. For example, Jalika, a 43-year-old mother of three, explained that overcrowding had caused significant problems for both her family and her health. By wave 2, Jalika’s husband had moved out of the family home. Jalika had also experienced a number of health scares, as she explains in the extract below:
And so I’m sharing the bedroom with Darren [son] who’s 4 years old and we were sharing the bed and it’s only on Sunday that I managed to find a bed at IKEA so I moved him in his bed now, but he’s still in the same room as me . . . and this, since we met last time it has caused a lot of trouble in the family. Yeah, because two teenagers, one child, no space for them to do their homework, to have peace and quiet with Darren around, it’s been, I would say 2013 has been hell for us [laughs]. I’m really, really struggling familywise, I’ve got a lot of problem[s] with my family at the moment so it would be nice if the school could take the responsibilities . . . [.] I was at the hospital yesterday even for a check-up, for the result, because of all the stress I went through this year I started to have some pains here and the breast pain on that side, so I went to see, I went to Newham, I went to see my GP, who referred me to the breast clinic sorry at Newham and I feel so scared because when the doctor touched it he quite felt a lump, and then he sent me straight to do some [laughs], and luckily it was, yesterday when I went for my result everything is fine. Ah, I didn’t know about it, but now I know [laughs]. I know what stress can cause now [laughs].
Jalika draws a direct causal relationship between her housing status and her health and family life. Once again, the ongoing pressure of inadequate housing is described as having a cumulative and corrosive impact. As can be seen in the quotation above, health is spoken about in very specific ways in relation to housing. In addition to housing problems causing and exacerbating health problems, illness and incapacity are, to an extent, commodified as resources in the course of interactions with ‘the housing’. When Jalika explains the extent and impact of her overcrowding problem she references her middle son’s health needs as a further rationale:
. . . for example my son needs his own bedroom, the one with a disability, why hasn’t he got that? It’s been 7 years, nearly 7 years we have been bidding for him to have his own room, it’s too much. And there’s no other way for me, even if I work they can’t put me on the, I can’t have a mortgage so I will have to bid on the council’s property, so it’s the same thing for me. So it has really been a struggle [laughs].
A recognised medical condition or complaint had the potential to confer additional ‘need’ and, thus, could be used as a pathway into social housing by either ‘getting on’ or ‘moving up’ the (housing) waiting list. Narratives of incapacity, need and housing included descriptions of a range of conditions including musculoskeletal disorders, mental health problems, arthritis and epilepsy, and participants told these stories about themselves and others.
Olympic change and regeneration altered the way in which residents perceived their local area. Preparations for the Games changed the landscape of Newham, with demolitions and new developments. The dominant housing narratives around Olympic regeneration were those concerning the East Village. Certainly, this development had considerable symbolic value for change and renewal in the area. Narratives of the East Village housing were relatively sparse at wave 1. By wave 2, these narratives had expanded to become more critical and speculative, and were incorporated into broader narratives about ‘the housing’. In this sense, narratives of Olympic housing are both interwoven with established housing narratives and, in some ways, stand apart from them. The selectivity of the social housing allocation process indicated, for some participants, that the regeneration of the area was motivated more towards gentrification than renewal. David and Sarah, parents of three young children by wave 2, articulated in this exchange from a family interview:
What places are these?
Olympic Park, Olympic Village . . . Yeah, and apparently Newham got 300 homes that they gave them.
Yeah, it’s all, it’s pretty much all gone to the Housing Association who at the moment are charging £176 but are making it really clear that that’s going to shoot up in the next couple of years.
Yeah, as soon as the old tenancy is up with, they’ve got to offer Council tenancy, a certain amount of tenancy length, once that’s up, they can charge pretty much whatever they want . . . yeah. No, that’s what a lot of people, they hear it and it says social but then, um, after a certain amount of time your tenancy is up they want you to go onto private.
David and Sarah assert that the provision of social housing in the East Village is a temporary, transitionary step, rather than a permanent solution.
Unexpected changes
Local narratives of Olympic change and, in the case of housing, lack of change, also generated some results that ran counter to wider narratives around the Olympics. Most notably, the broadly positive acceptance of increased security and surveillance in the run-up to the Games and the absence in the data of detailed health and sporting narratives.
Olympic securitisation
Securitisation, as a process, refers to the intensification of security measures, such as policing and surveillance, in response to a perceived threat. The Olympic securitisation of east London, in response to perceived internal and external threats that hosting the Games entailed, has received much scrutiny and been interpreted, by some analysts, as contributing to the militarisation and repression of urban spaces and populations. 96 Trepidation and concern over the anticipated ‘security legacy’ of the London Games centred on the assumption that expansion of security powers, measures and technologies by the state for the duration of the Games would become permanent. Measures such as the London Olympic and Paralympic Games Act (2006),97 which, among over things, gave the police and private security contractors extra powers to clamp down on ‘disruptive’ protests, and section 44 of the Terrorism Act (2000),98 which allowed the police to stop and search without suspicion, excited criticism and concern on these grounds. Fussey et al. 99 described this as control ‘creep’ and speculated that what remains of the security infrastructure after the Games is likely to have a significant impact upon everyday life for residents of east London.
However, for participants of our study, securitisation was described by participants in very positive terms. Securitisation of Olympic venues and of Newham more generally appeared to be welcomed. In particular, increased use of closed-circuit television (CCTV) surveillance and greater police presence were popular. Participants expressed little concern over these intensified security measures and positioned themselves as the ‘protected’, in contrast to the dangerous and undesirable ‘others’ who were the intended objects of securitisation and who made such strategies necessary. Newham was described by some as a markedly different place to live during the Games. Although certain areas, such as Westfield and Stratford town centre, had lots of visitors (which brought its own potential threats), residential life in Newham was quieter, calmer, less congested and with less traffic. However, the increased security and safety lasted only as long as the event, as Julie and Nisha, both residents of Stratford, explain:
The thing is, the thing is, when the Olympics was on to get in any of the parks, there was security at the gates, yeah, I think it should be like that all the time.
I think that’s the only problem, and that . . . it was so safe round here, the Olympics was such a big thing and they paid so much for security but then it’s like they’re protecting us so much with the Olympics, why aren’t they protecting us that much when it’s not the Olympics?
What was also notable were narratives that were absent from the data, given wider prevailing narratives in the media. There was very little anxiety about being watched or concern about what the footage might be used for. Rather, it was a case of if you had not done anything wrong then you would not have anything to fear from being watched. And as the protected, rather than the subjects of surveillance, CCTV did not present a problem, as demonstrated here in an extract from Minal and Vidip, a sister and brother aged 15 and 12 years:
And how do you feel about being watched with CCTV? Does that make you feel strange at all or you don’t mind?
No, I don’t mind it cos we don’t really do it like.
Cos we don’t do . . .
. . . something bad, so . . . it’s like quite a benefit for us . . .
As can be seen, the participants did not position themselves as the subjects of surveillance and security measures. Rather, they described themselves as the protected.
The absence of sporting and health narratives
At interview, eliciting narratives specifically about health was very challenging. The concept of actively maintaining health, rather than just treating illness, did not appear to be a topic about which participants had a great deal to say. Healthfulness was certainly less of a priority than more immediate concerns such as employment, safety and, of course, housing (although these are determinants of health, they were not presented as being so by respondents). Such absences in the data are, perhaps, unsurprising given that the research was carried out in a relatively deprived area and health considerations and behaviours can often be subsumed by more pressing problems in low socioeconomic status settings. 100 When health and well-being were discussed it was nearly always in relation to other areas of daily life and, overwhelmingly, in relation to housing and housing problems.
None of the participants responded positively when asked if they thought that Newham was a ‘healthy’ place. They described it as a very unhealthy place in terms of the ready availability of junk food and takeaways, particularly chicken shops that were often described as ‘temptations’. Queens Market (Green Street) was the exception to this and was talked about as a place for fruit and vegetables and ‘food from home’. Despite uniform descriptions of Newham as an unhealthy place in terms of food, the participants maintained that it was (or could be) quite easy to live a healthy lifestyle there. Participants talked about ‘being healthy’ in terms of making the right choices at the individual level, as the two quotations below demonstrate:
I think it’s just the people that, you can obviously choose, you can stop yourself from eating stuff like that and you can buy, I don’t know, something else from there like, yeah.
This is the people, because I know we’ve got all the shops out there. But it’s up to you if you actually want to go and eat those foods. There’s a gym just across the A13, so it’s not far. So, it’s up to them really. But I think it’s quite easy, because maybe you have more power to hold yourself back from doing whatever.
Being healthy was predominantly framed in terms of food and consumption, specifically of buying the right foods, rather than in terms of exercise. Comments about exercise and being active were less uniform. Adult participants commented that there were a variety of places to exercise (including three leisure centres), although few participants reported using them on the grounds of expense, time constraints and not ‘feeling safe’.
In terms of a health and/or sporting legacy there was a general perception that the Games had probably encouraged residents to exercise more or to try new activities, although only one participant actually reported doing more exercise. Adult participants talked about how schools had probably become more sporting and healthier, although adolescent participants themselves reported that they had not taken up any new activities in the long term (although some had tried new sports). Adults often commented that they felt ‘inspired’ by the Games but doubted that they would actually do any more sport and exercise as a result. Farrid, a father of two, explained that he doubted Newham residents had become more active as a result of the Games:
Once the Games are over and all that and they’ve said, oh yeah a lot of people will be, you know, sporty, nothing’s happened, no-one going to the park and jogging [both laugh] or another Mo Farah running around, I seen no difference to be honest with you, nothing.
So you don’t think necessarily it’s inspired people to do sport?
No no no, OK? Might be by 5% if that of the whole population, and probably even less than that to be honest with you, OK, but not, no, nothing fundamental, you know, there’s not gonna be a, you know, we’re not gonna win 50 gold medals next time, simple as that, alright OK?
Summary
Residents generally welcomed the unexpected chance to live in a cleaner, safer and more unified environment. The qualitative findings therefore suggest that the Olympics served to reduce and temporarily alleviate certain stressors in the social and physical environment and thereby had potentially positive impacts on health and well-being. Olympic preparations provided a small window of respite from some of the stresses and pressures of daily life in a relatively deprived area, an area that residents felt to be run-down, fragmented and unsafe. It offered opportunities for residents to use the built environment and mix with other residents that were not normally possible. Overall, it served to lessen participants’ sense of social exclusion and seemed to generate a sense of inclusion and respite, even if this was only temporary. However, it did not address the most dominant and emphatically articulated local need: housing.
Chapter 7 Discussion
Public expenditure on sporting mega-events, such as the London 2012 Olympic and Paralympic Games, is often justified by the hypothesised positive social, economic and health legacy benefits for local communities. Enhancing health and well-being through the vehicle of large-scale urban regeneration was one of the primary legacy benefits identified for the London 2012 Olympic Games, and upon which the original bid to host the Games was developed and won. However, evaluations of the health impacts of urban regeneration programmes find mixed evidence for a positive impact at the household, dwelling, neighbourhood or community-level directly on health or indirectly on the social determinants of health. We used the advent of the London 2012 Olympic Games to conduct an evaluation of the health and social impact of the Games. We employed quantitative and qualitative approaches to investigate the impacts of the Games on physical activity and psychological health and well-being, and to explore the social experiences of those living in the main host borough as it underwent Olympic-driven change.
In this chapter we discuss the main findings of the study to date and their implications for future research, under four headings: (1) describing inequalities in adolescent health and well-being in east London; (2) impacts on physical activity in adolescents and their parents/carers; (3) impacts on psychological health and well-being in adolescents and their parents/carers; and (4) understanding families’ lived experience of regeneration associated with the Games. We then give a brief account of our engagement with stakeholders and summarise the strengths and limitations of the study. The discussion presented here, as highlighted in Chapter 1, is necessarily a summary of selected findings from a large and complex study, and focuses on our primary outcomes from the adolescent cohort, which is where the main findings of interest were observed. Further detailed discussion of the material presented here can be found in the relevant peer-reviewed publications (see Publications). Further analysis of the large amount of quantitative data generated by the project is currently ongoing, and will generate further manuscripts for submission to peer-reviewed journals in due course.
Describing inequalities in adolescent health and well-being in east London
Socioeconomic inequalities in adolescent health
In our study we observed a limited socioeconomic gradient in adolescent health. This may reflect the equalisation hypothesis, albeit starting at an earlier age. The equalisation hypothesis suggests that adolescence may be a period of relative health equality compared with the marked health inequalities observed in early childhood and adulthood. 101,102 The hypothesis postulates that the health gap narrows between socioeconomic groups in early adolescence and has been observed for all-cause mortality, mental health, a range of health conditions and general health. 103–106 This phenomenon is attributed to school and peer influences outweighing home and family effects on health on entry to adolescence. However, this contrasts with a study based on nationally representative data purporting that equalisation occurs much later than previously proposed. 107 One explanation for this difference is the influence of the urban environment on young people. It is possible that peer influences are more pervasive and family influences weaker when growing up in an urban environment such as east London. The earlier age of equalisation observed in our study could be a consequence of adolescence occurring at an earlier age,108 accelerated by secular technological change and a high-density urban environment that may promote the onset of ‘adolescence’ at an earlier age.
Prevalence of adolescent health behaviours and outcomes
The overall prevalence of health behaviours and outcomes reported here are broadly comparable to similar studies of adolescents conducted in similar settings. 109 Similarly aged cohorts based in south-east London110 and east London35 have also noted that socioeconomic factors do not correlate with mental health, with the exception of a limited number of ethnic minority groups. This lack of socioeconomic difference may be explained by the relative social homogeneity of our study sample. In terms of self-rated general health, this outcome was associated with family wealth, albeit weakly. This is consistent with a comparison of material wealth and general health across 22 European countries describing similar, but declining, health inequality at this age. 111 Our study builds upon some earlier investigations describing a high prevalence of long-term illness in Afro-Caribbean young adults. 112 Our study suggests that such rates are likely to be driven by the black Caribbean group rather than by the black African group. However, there is a comparative lack of literature exploring the influence of the neighbourhood environment on mediating adolescent health outcomes. 101 The findings presented here suggest this as a useful focus for further analysis of this and other community-based studies. Future studies may examine the extent to which differences in the physical environment (e.g. green or blue spaces, housing) or the social environment (e.g. crime, social cohesion) may explain differences in health with a view to providing evidence for policies aimed at reducing health inequalities via area-based interventions.
Relationship between physical activity and mental health
Although previous research suggests that there is a positive association between physical activity, mental health113,114 and general physical health,114,115 no association was observed in this study. Although interventions aimed at increasing physical activity may well act as a means of reducing obesity and its comorbidities, within the social and environmental context experienced by this cohort of adolescents, physical activity appears unlikely to influence other health outcomes.
Impacts on physical activity and sedentary behaviour in adolescents and their parents/carers
Using a quasi-experimental design, and against a backdrop of a general secular decline in physical activity in adolescents, we found no evidence for demonstration effects at 6 months or legacy effects at 18 months for either males or females in the intervention borough compared with the control boroughs. However, at 18 months, at the time when hypothesised legacy effects would begin, we observed that male and female adolescents were less likely to become inactive or remain inactive if they visited the Olympic Park more than once a month. There was also no significant increase in the proportion of adolescents reaching minimum recommended physical activity levels. In addition, we found that those groups who primarily benefited from increased access to environmental resources supportive of physical activity as a result of redevelopment of the Olympic Park were from minority ethnic groups and were relatively disadvantaged (when using free school meals as an indicator).
Previous systematic reviews of the impacts of sporting mega-events on physical activity116,117 suggested that limited evidence exists for the effectiveness of such events in stimulating physical activity, and that this evidence was insufficient to either support or refute the presence of legacy impacts on health or socioeconomic outcomes. Mahtani et al. ’s117 review of reviews of the impact of Olympic and Paralympic Games suggested only that there was a dearth of studies and that high-quality evidence was urgently needed to measure the true impacts of these events. These reviews suggested that evidence for increases in sporting participation or an increase in physical activity were weak or inconclusive, with no evidence of changes in recreational behaviour. The exception to this was some evidence for an increase in sports participation after the Barcelona Olympic Games in 1992,116,118 although this was graded as low-quality evidence. More recent primary evidence has been produced by an ongoing evaluation of the 2014 Commonwealth Games in Glasgow. Initial findings from this small longitudinal study of adults (n = 414) has suggested that even though the Commonwealth Games were viewed positively, there were lower levels of sports participation and physical activity reported 4 months after the completion of the Commonwealth Games;119 however, this might be related to the effects of seasonality on physical activity participation.
Thus, the findings reported in our study tend to confirm those of previous research, namely that there is no evidence to support increases in adolescent physical activity through either short-term demonstration or medium-term legacy causal pathways after sporting mega-events. The most plausible causal mechanism by which any medium- to long-term increases in routine adolescent physical activity and reductions in sedentary behaviour was hypothesised to have occurred would be through the direct use of the redeveloped Olympic Park for leisure and recreation. Our findings provide some evidence that visiting the Olympic Park may play some role in reducing the risk of not meeting the recommended levels of physical activity. However, our adolescent respondents report that up to 23 months after the Games had finished only 55.1% of the sample had actually visited the Olympic Park, suggesting that further activities to encourage the routine use of the Olympic Park by local residents may be one possible way of optimising any physical activity legacy of the Games.
Observed effects on sedentary behaviour were inconsistent; at 6 months and at 18 months we found that no differences in sedentary behaviour (as measured by screen time) transitions were observed between the intervention and comparison boroughs. However, at 6 months we did observe that respondents with low levels of engagement with the Olympic Games were more likely to become sedentary after the Games. It is probable that the lack of observed effects is because of the secular increase in screen time during adolescence, and that this outweighs any direct effect of the Games and any indirect effect of the provision of new physical activity infrastructure.
No effects on physical activity or sedentary behaviour were observed for parents/carers. This is probably as a result of the point in the life course of the parents.
Changes to the physical activity environment
This study demonstrated that improvements to the physical activity environment were concentrated spatially. Given the spatially targeted nature of Olympic-related urban regeneration it is no surprise that environmental changes were highly localised and close to the Olympic Park. This ensured that the prime beneficiaries were those who were also geographically concentrated close to the Olympic Park, primarily the Asian Bangladeshi group and the black Caribbean group. We found no evidence that Olympic-related regeneration catalysed other physical activity environment improvements elsewhere in our study boroughs, or that investment in new sports facilities or green space focused on the Olympic Park resulted in the closure of services or amenities located elsewhere. This suggests that improvements to local environments may have been successfully targeted at those population groups who are relatively disadvantaged in the study sample.
Impacts on psychological health and well-being in adolescents and their parents/carers
Urban regeneration and adolescent depressive symptoms
This study found higher levels of depressive symptoms, in terms of ‘remaining depressed’, for adolescents living in Newham, the borough receiving urban regeneration, than in adolescents living in the three comparison boroughs. These findings replicate those of some previous studies of adult populations. 120 Urban regeneration has been found to be associated with increased feelings of social isolation,121 reduced social capital,121 increased exposure to stress122 and relative deprivation, all of which could influence mental health. Urban regeneration may not address residents’ concerns123,124 and may not influence psychosocial, lifestyle, safety or economic determinants of mental health. 125
However, the intervention borough of Newham had higher rates of depressive symptoms at all waves than the comparison boroughs, which may be explained by other unmeasured differences between the boroughs, such as social, economic and environmental determinants of mental health. 125 A previous cohort study of adolescent depressive symptoms in Newham, Tower Hamlets and Hackney between 2001 and 2005, the RELACHS study, found the highest rates of depressive symptoms in Hackney and the lowest rates in Newham,42 suggesting that borough differences in rates of mental health are changeable over relatively short time periods.
The intervention showed similar associations with ‘remaining depressed’ at the 6- and 18-month follow-up, with risk doubling. These effect sizes were similar in magnitude to those observed in our models for established psychosocial predictors of depressive symptoms such as gender, low family social support and being bullied. Known triggers for the onset of depression, such as exposure to negative life events and bullying, did not relate to onset of depressive symptoms (‘becoming depressed’) in our sample, although recent rather than lifetime exposure may be relevant for incidence of depression. Few ethnic differences in depressive symptoms were observed in the study.
Urban regeneration and adolescent well-being
There were no differences in change in well-being between the intervention and comparison boroughs. Little is known about predictors of adolescent well-being. In this study few factors predicted positive or negative change in well-being, which may be because little change in well-being was found over the three waves. Negative change was associated with baseline well-being and there was some suggestion that positive change was more likely for Asian Indian and black adolescents than for white UK adolescents. However, these ethnic differences have not been reported in other studies.
A systematic review of interventions using the WEMWBS found large variability in change scores for different interventions. 126 However, to date few studies have examined the impact of neighbourhood interventions on change in mean WEMWBS scores. Our study suggests that the WEMWBS may not be sensitive to change for evaluating neighbourhood population health interventions. In our adolescent population, well-being was a more stable trait than a changing state.
This large-scale quasi-experimental longitudinal study therefore provides limited evidence that the urban regeneration associated with the London 2012 Games had a positive effect on adolescent mental health in terms of depressive symptoms or well-being. Although urban regeneration was associated with becoming ‘no longer depressed’ in the shorter term, this was the only positive impact observed. In fact, urban regeneration may have maintained depressive symptoms for adolescents but this might be explained by differences between boroughs in the social and economic determinants of mental health.
Urban regeneration and other associations with parental/carer well-being
Parental/carer well-being does not seem to have been influenced by the urban regeneration in Newham, with the exception that the high levels of well-being observed at baseline in the regeneration area were no longer present at follow-up in wave 3. This is in keeping with generally poorer mental health at wave 3 in terms of anxiety and depressive symptoms in the regeneration area. The lack of change in low levels of well-being, as mentioned above for the adolescent cohort, may be because WEMWBS does not function well for measuring change in community samples. 127 There were fairly consistent associations across the waves between low levels of well-being and multiple poverty score, unemployment, poorer neighbourhood conditions, safety, social cohesion, violence and long-term illness. There are relatively few studies of adult well-being in community samples except, for instance, Weich et al. 128 who found associations between low levels of well-being and unemployment. In general, the associations mirror those found with depressive and anxiety symptoms. In contrast, there were relatively fewer positive associations with high levels of well-being, many of the same variables associated with low socioeconomic status reduced the odds of high levels of well-being. Consistently across the waves, being of black African ethnicity was associated with higher levels of well-being, but ethnic differences varied across waves and by adjustment for social disadvantage.
Urban regeneration and other associations with parental/carer depression
There were no differences in depressive symptoms between the urban regeneration areas and the other areas at waves 1 and 2, but by wave 3 there were significantly greater odds of depressive symptoms in the urban regeneration area. This is in keeping with the adolescent results and lends support to previous findings of the lack of effect or negative effect of regeneration on health,6 possibly because regeneration is associated with increased exposure to stress, social isolation and community disturbance. 121,122 Regeneration that does not take into account the preferences of the community is also less likely to improve mental health. 124
Depressive symptoms were associated with age but not gender in this sample. Depressive symptoms were associated with unemployment, social renting, being on benefits, multiple poverty score and long-term illness across the waves. These associations indicate some consistency across various measures of poverty and social disadvantage. The association of depressive symptoms with indicators of low socioeconomic status is consistent with other studies of deprived inner city areas such as south London129 as well as UK national surveys. 130 In our study depressive symptoms were also associated with dissatisfaction with housing, unsafe neighbourhoods, low levels of social cohesion and perceptions of high levels of neighbourhood violence. In multivariate analyses, adjustment for multiple poverty score may remove some of the effects of environmental factors that may be on the pathway from social disadvantage to mental ill-health. The association of perceived environmental factors and mental health should be interpreted with caution in cross-sectional analyses. Fagg et al. 101 in a study of east London adolescents found that those with poor mental health were more likely to perceive their area as disadvantaged in terms of amenities and were also more likely to feel alienated from their neighbourhood.
Urban regeneration and other associations with parental/carer anxiety
There were no differences in anxiety symptoms between the urban regeneration areas and the comparison areas at waves 1 and 2, but by wave 3 there were significantly greater odds of anxiety symptoms in the urban regeneration area. This is similar to the pattern of results found with depressive symptoms and may represent a response to the disruptive effects of regeneration in terms of stress, increased social isolation and possibly the perception that after the Olympics were over there were few positive legacies for those living in east London. A similar pattern of associations with social disadvantage was shown for anxiety symptoms. Anxiety symptoms across the waves were associated with unemployment, being never married, being widowed, divorced or separated, being on benefits, multiple poverty score, long-term illness, poor neighbourhood conditions, safety, social cohesion and violence. Damp and vibrations in the house were also associated with anxiety symptoms. Anxiety symptoms were associated with age on only one occasion but were more associated with gender.
Overall, there was no evidence that adult mental health differed across the first two waves of the study, but by wave 3 the odds of a higher level of well-being were lower and there were greater odds of greater anxiety and depressive symptoms in the regeneration area of Newham. It is plausible that the poorer mental health in Newham might be a consequence of the disruption related to regeneration, but it is difficult to disentangle this effect from the effects of social inequalities, long-term illness and generally poor neighbourhood environments. It may be that in order to see improvements in mental health there is a need for more targeted interventions with a focus on improving housing. 131 This does not rule out later positive effects from improved infrastructure in the regeneration area.
Understanding families’ lived experience of regeneration associated with the Games
A temporary and symbolic legacy
Attempts by Olympic and Paralympic host cities to improve the aesthetic conditions of deprived areas as part of larger mega-event-led regeneration reflect the contradictory intents of the host city to at once provide a welcoming area for visitors and revitalise areas for residents. Boyle and Haggerty132 suggest that aesthetic improvements during the 2010 Vancouver Winter Olympics were actions of urban governance intended to ‘regulate disorder’. Concerns in Vancouver rested on how visitors would perceive the city; it was important to the ‘brand’ that enduring memories were not of a deteriorating environment. 133 Newham residents articulate this in London in what they perceive as an attempt to hide away the ‘dirtiness’, in favour of the new facilities of the Westfield shopping centre and the Olympic Park. Westfield in particular was highlighted as being particularly important in the everyday lives of residents, perhaps more so than the Olympic Park itself. This perspective is well articulated by Watt,134 whose view of Newham as a laboratory for urban policy allows an understanding of how lower-income east Londoners encountered processes of change, particularly in terms of ‘gentrification’ and displacement. 135
At the same time, some Newham residents saw aesthetic improvements in more positive terms, in line with the aspirational context for regeneration. The redevelopment promised to bring money into the area and offered the possibility of a longer term legacy. The aesthetic improvement of neighbourhoods plays an important and positive functional role in public health and the ‘hope’ articulated by Newham residents, and the possibility of increased civic pride, factor into well-being. There is a large body of work demonstrating independent associations between the quality of the environment and health improvement. 136 However, less well known are the causal mechanisms that relate changes in the environment with changes in health and well-being. Leslie and Cerin137 put forward the view that neighbourhood satisfaction may mediate the association between perceived environmental characteristics and measures of mental health in adults. Furthermore, they assert that visible evidence of physical disorder in the form of graffiti, litter and vandalism may trigger negative emotions. Their study of the association between perceived environmental characteristics, neighbourhood satisfaction and self-rated mental health found that safety and walkability, social networks and traffic and noise were significant correlates of residents’ mental health. The authors suggest that this is indicative of neighbourhood aesthetics being a particularly important factor impacting on mental health and that having a more pleasant and appealing environment could benefit feelings of health.
Newham residents reported a strong sense of ‘spectacle’ during the Games, and many admitted to getting ‘caught up’ in the excitement, even if initially cynical or unengaged. Accounts of experiencing a sense of community belonging and pride during the Olympic period are perhaps unsurprising in light of the ‘festival’ effect of the Olympics. 118 Research on both the Calgary and Vancouver Winter Olympics showed that although concerns over cost and inconvenience were present before these events, by the post Game period there was a firm belief that the event was positive and showed the host city in a positive light. In many cases it was because of aesthetic improvements and organised community events around the Games that residents were able to experience a more socially inclusive Newham.
The spectacle of the Games and the ‘festival’ that surrounded it undoubtedly added to the sense of occasion and community belonging that participants spoke about. However, spectacle alone is inadequate to address the problems faced by Newham residents. The withdrawal of these short-lived opportunities was acutely felt, and served only to enforce the ongoing experience of exclusion and deprivation.
Housing: an unmet need
Participants spoke about ‘the housing’ as a system, comprising physical, social and administrative qualities that had a direct bearing on their health. This has to be understood as more than the cumulative effect of factors such as housing tenure, badly maintained properties and structural defects. Interactions with this housing system were experienced as difficult, unfair and demoralising. In this sense, narratives of ‘the housing’ are multidimensional and interwoven with stories about stress, agency, hope and frustration, all of which have bearing on health and well-being.
The East Village development (formally the Athletes Village) was much publicised and presented as one of the key elements of a housing legacy. However, as is demonstrably apparent in the discrepancy between the numbers of residents on the list for public housing and the quantity of affordable units planned, it was never designed to ‘solve’ this problem in its entirety. The conversion of the athletes’ accommodation into a housing development has become a common aspect of post Games regeneration for Olympic host cities. Arguably, such developments represent more of a symbolic legacy than a material one. 135
In some ways, accounts of Olympic housing are implicated in broader housing narratives of ‘waiting it out’. And yet, there are some marked differences in the way it is framed and the way it is experienced. Bernstock135 draws attention to the worrying return of allocating housing based on categories of being ‘deserving’ or ‘undeserving’ (proxied, in this case, on employment status) rather than need. An Olympic housing legacy for Newham was always going to be a somewhat contentious issue given that preparations for hosting the Games began with the high-profile demolition of social housing estates to make way for new developments. Tactics such as the issuing of compulsory purchase orders and the relocation of members of the Traveller community drew further public and press attention to housing issues in Newham. In post Olympic Newham, the East Village development has become synonymous with the 2012 housing legacy in its entirety. These factors, in combination with the huge investment in private housing developments in the area, have widely been interpreted as a dilution of initial legacy commitments of improving the quality of life for Newham residents. 135 According to the participants of this study housing is one of the most pressing needs for the local population and this need was not adequately addressed by the Olympic-led regeneration efforts.
Security and securitisation as ‘respite’
Our study suggests that the experience and perception of increased security reported by residents were largely positive. These findings are at odds with the critiques of Olympic or mega-event securitisation as militaristic and potentially marginalising. 138,139 That is not to attempt to discredit these critiques or dismiss the questions about social justice, civil liberties and state power that they raise. Rather, the disparity highlights both a difference in values and the fact that experiences of security and securitisation may need to be understood contextually.
Critiques of mega-event securitisation tend to be contextualised in relation to the rise of ‘military urbanism’,96 the identification of urban areas as particularly problematic and the late neo-liberal programme of fortifying and modifying urban spaces in order to surveille and control populations. These critiques draw largely on ideas that argue that a focus on ‘security’ is being used to facilitate the erosion of truly ‘private’ spaces and the individual rights and liberties that are afforded within them, meaning that rights abuses can be committed in the name of security.
Goldstein140 observes that the security–rights conflict is a distinctly neo-liberal phenomenon, especially in the context of insecure and even violent daily life for marginalised urban communities within unequal societies. He advocates for an understanding of securitisation as a process of constructing a collective understanding of something as a particular kind of danger and a threat to society and security, making securitisation a physical and a social process. Successful securitisation therefore depends on a willingness to accept the legitimacy of the perceived security threat and framing of the object(s) of securitisation as dangerous. In other words, security is not just deployed by the state in a top-down process. It is taken up by citizens and community groups as well. Individuals accept, take up and enact securitisation, justify its deployment and engage in the valuing of ‘security’ as a necessary priority over ‘rights’. For Goldstein, this approach is vital to establishing a critical anthropology of security, a perspective on security as made and understood by actors and groups outside the state and its official institutions of security as a lived social experience. 140 Such an analysis may go some way to explaining the lack of concern for issues such as privacy and democracy in the narratives of participants, the high value they placed on safety and security, and the ways in which they used the potential threat of ‘others’ to explain and legitimise securitisation. Participants were active agents in the social construction of securitisation rather than passive recipients.
Trepidation over the anticipated ‘security legacy’ of the London Games centred on the fear that the markedly visible expansion of security by the state for the duration of the Games would become permanent and oppressive. Measures such as the London Olympic and Paralympic Games Act (2006),97 which, among over things, gave the police and private security contractors extra powers to clamp down on ‘disruptive’ protests excited criticism on these grounds. Findings from both London and Vancouver showed that, for low-income young people, the reordering of Olympic cities resulted in exclusion from former recreational spaces, increased surveillance and detrimental effects on social participation. 138
In our study, respondents accepted the legitimacy of the perceived security threat and actively welcomed intensified security. Rather than be concerned that securitisation would become entrenched and linger on after the Games, they actually hoped that securitisation activity would remain in place and were disappointed when security lessened after the events. Instead of being a tool of restriction, participants explained that it allowed them to go out more, to go to places that they would not normally venture into and to stay out after dark (which would not normally be considered safe). Narratives of experience in securitised spaces, far from being negative, were very positive and were centred around ‘respite’ from the security and safety concerns routinely experienced as part of everyday life in Newham. Experiences of Olympic securitisation therefore fitted into this wider expressed desire for increased safety and security in the locality, and enduring concerns over crime and personal safety. Participants described life in Newham as being characterised by feeling insecure, unsafe and having a fear of crime. In this context, desiring increased securitisation and protection seems a logical response to the respondents’ own experiences.
Engagement with stakeholders
We engaged with a variety of stakeholders at key stages of the research process. During the development of the proposal for this study we convened a half-day workshop with representatives from the Olympic host boroughs for the Olympics, planning, economic development and public health, school teachers, the director of public health at the Greater London Authority and other community stakeholders. The purpose of this meeting was to outline our ideas for evaluation and to gain insight and feedback into the plausible changes that were expected as a result of the Olympics within the host boroughs, their expected impacts on health (and the determinants of health) and any other probable impacts that were perceived to be important to the local community, both positive and negative. Insights from this meeting were used to modify our primary outcomes of interest (we collected data on adult employment status in order to capture economic impacts) and to suggest a school-based study rather than a community study for reasons of recruitment and retention.
During the start-up phase of the project (September 2011) we hosted a half-day seminar for community groups, outlining the fieldwork we were about to undertake and inviting feedback into recruitment methods, particularly for the qualitative fieldwork. Unfortunately, this was relatively poorly attended, with particular representation from housing and environmental groups rather than those with an interest in health improvement.
Throughout the project, particularly during the 3-year fieldwork phase, we maintained a strong dialogue with the 25 schools enrolled into the study. We engaged with the schools by offering to conduct masterclasses in social research methods and geography (year 12–13 students), attending parent’s events and producing regular newsletters for classroom use about project findings.
Final dissemination has yet to happen as final main analyses have only just been finished for the completion of this report; however, we are in contact with a range of interested parties and local authorities (local councillors and directors of public health) about hosting an event focused on ‘healthy urban communities’ in which we will be able to disseminate the main findings of the study.
Challenges, strengths and limitations of the study
Challenges of the study
We experienced a number of challenges relating to the design and conduct of the study. These were recruiting and retaining parents/carers in the study; practical management of school-based fieldwork; and collecting and using environmental data. First, the parental element of the study was originally designed as a prospective controlled quasi-experimental study with face-to-face data collection at baseline and second follow-up, and a postal survey at first follow-up. However, there were challenges related to the recruitment of parents/carers at baseline that were unforeseen at the time of application and which required us to seek permission to modify the design of this element of the project. Lower than expected recruitment of parents/carers occurred for two main reasons:
-
Denial of ethics approval to obtain parental/carers home address from the school of each adolescent respondent. This required the primary collection of home address from each child enrolled in our study. Baseline child-reported address was of varied quality as children either did not know their full home address, provided an inaccurate or incomplete home address, or refused to supply a home address.
-
Parental response rate was somewhat lower than expected (63% vs. 75% response rate).
As a result, the number of eligible home addresses used to contact and enrol parents/carers was lower than anticipated, resulting in a lower than expected recruitment at baseline (and thus a reduction in expected numbers at follow-up). The solution was to modify the design in order to maximise statistical power and boost parental enrolment. We therefore modified the design of the parental survey from a prospective design to one that employs a repeat cross-sectional study with a nested prospective cohort. This enabled us to:
-
boost the number of parents/carers enrolled in the repeat cross-sectional part of study by recollecting child-provided addresses at first and second follow-up. This allowed us to clean any inaccurate addresses provided at wave 1 in order to arrange a first interview during wave 2 fieldwork, allowing us to visit those parents/carers who did not respond at wave 1;
-
ensure minimal loss to statistical power in repeat cross-sectional analyses by aiming to maintain an n at each wave similar to that at baseline;
-
retain a prospective element, although inevitably with a loss of statistical power.
Second, the practical management of the school-based fieldwork was far more onerous that originally envisaged. Enrolment of schools took 8 months, scheduling of school visits was also challenging owing to school-link-staff turnover and the time pressure on teaching staff. We were also required to visit each school on more than one occasion at each of the three waves of data collection owing to scheduling of classes for data collection and to ‘mop-up’ students who were absent on the day of the initial and subsequent study visits. At each wave, between 50 and 60 separate school visits by a minimum of four to six study staff were required over a 5- to 7-month period each year, for 3 years. This, combined with data entry, cleaning and coding, meant that fieldwork and initial data processing took 4 years, rather than the 3 years originally planned for it. This had knock-on effects on the amount of data analysis that was able to be conducted within the lifetime of the project. However, the dedication of the fieldwork team and the intensive nature of data collection yielded very high overall response rates [wave 1, 86.4% (n = 3088); wave 2, 83.9% (n = 3213); wave 3, 75.8% (n = 3014)], with an overall retention rate of 73% from baseline (n = 2254).
Third, the collection and use of environmental data was very challenging owing to the fragmented and uneven nature of local authority data, differences in the temporality of spatial data and the large amount of data cleaning, validation and processing that was required. Although these data are now of very high quality, their analysis was inevitably slower than expected and papers emerging from this work are only likely to be submitted in 2017 after the completion of this report.
Strengths of the study
The key strengths of the study were the extremely high-quality adolescent cohort, which had a very high retention rate of 73%, consistent with best practice in other school-based cohorts,141 overcoming a limitation of many previous studies in this field. 33 The adolescent cohort also had a large and representative sample, which is indicative of the ethnic super-diversity in east London. This was one of the first studies to examine the longitudinal effects of urban regeneration on physical activity and mental health of an adolescent population. Few participants relocated during the study, attrition was very low and multiple imputation was employed to deal with missing data. The adolescent cohort also provides a very high-quality observational data set of both individual and environmental longitudinal data that provides a rich base upon which to conduct further analyses.
We also collected qualitative data, which was essential in further exploring previously unanticipated findings around family perceptions of the Olympic-response to security and safety. By conducting longitudinal qualitative work we were able to elucidate how perceptions of the Olympic Games and its legacy changed over time, and this has provided valuable insights into the concerns of the local community in the context of embedded and long-term community disadvantage.
Limitations of the study
In the adolescent cohort, exposure to regeneration was determined by school location, which may have resulted in exposure misclassification in relation to regeneration for some participants. It is extremely difficult to characterise the exact dose of regeneration that each adolescent received, or to determine exactly when regeneration begins and ends; a small degree of regeneration may have started prior to baseline and continued beyond our 18-month follow-up. There may also be contamination between the intervention and comparison boroughs owing to geographic proximity. The regeneration was highly localised, resulting in most of Newham remaining unchanged. Positive effects of urban regeneration on physical activity and mental health may therefore be demonstrated over a longer time period than that of our follow-up period.
The parent carer sample for the study was selected on the basis of adolescents within schools. Thus, the parent or carer sample was secondary in this selection process and might comprise any available adult within the adolescent pupil’s household, although preference was given to a parent or carer. The sample of adults who were parents or carers of the adolescents in the study is not representative of the population of adults in east London. It was also difficult to recruit the same adults across the three waves of data collection (see Challenges of the study above). Thus, planned longitudinal analysis in change of mental health across the study in parallel to what was achieved with the adolescent sample was not possible. However, given the challenges of recruitment to surveys in east London, the sample achieved at each of the three waves was substantial compared with previous surveys and did allow for comparison of repeated cross-sectional analyses by wave. The findings for all three outcomes were more consistent at waves 1 and 3 than at wave 2. This may be related to a different type of sample being selected at wave 2. Given these changes in design the conclusions that can be drawn from these data are potentially limited.
In terms of the qualitative work, data were limited in two ways. First, the qualitative sample was entirely Newham based, so we could not make any comparisons with other areas. Second, the two waves of data collection were only 12 months apart and were both post Games. An additional wave of pre-Games data collection would have added further depth to the narrative analysis.
Finally, the study coincided with the start of large (and continuing) cuts in public spending for locally delivered services. This inevitably had an impact on the primary outcomes investigated in this study. For example, schools reported that funding for the School Sports Partnership were cut by up to 90% during and after the Games. This directly impacted on schools’ ability to deliver physical activity programming and cut initiatives to enhance sports participation.
The limitations described above do impact the ability of the study to identify positive effects of regeneration on the health outcomes studied here; however, the consistent lack of a narrative generated around health improvement from both the quantitative and qualitative elements of the study suggest that mega-event-related regeneration is unlikely to have major impacts on health in the short term.
Implications for future research
This study provided the highest quality data to date on the short- and medium-term social and health impacts of sporting mega-events. In addition to investigating short-term demonstration effects, we used event-related urban regeneration as a vehicle to examine the impacts of medium-term physical legacy. Future research should seek to replicate the findings reported here, with larger and more representative adult longitudinal data. In addition, a key issue in improving future research and practice would be to routinely collect objective physical activity data through accelerometers, something that we were unable to do because of cost considerations. We were also unable to explore equity effects as much as we had anticipated as the sample was relatively homogeneously deprived. This was mainly because of the relatively disadvantaged nature of the east London population. Further evaluative research should therefore ensure that the underlying sample is more socioeconomically diverse, although this may be challenging as large-scale sporting events with a legacy element typically target relatively disadvantaged communities. If it is possible to increase socioeconomic diversity this would form a useful basis from which to investigate impacts by differential social group. This could potentially be a future research priority.
A key issue not discussed above is whether or not Olympic-led regeneration is equivalent to mainstream urban renewal programmes. It is difficult to draw any conclusions about this from the current study. It is true that investment in, and changes to, the built urban form identified in this study are common to many other urban change programmes (such as improvements in green space, improvement in facilities and investment in new transport infrastructure) and, therefore, can be seen as equivalent. However, it would be fair to say that it is difficult here to unpick whether or not these changes might have acted synergistically with the ‘spectacle’ of the Games. Given the relative lack of impact identified in this study, we would speculate that the Games provided little extra in terms of health impact in the medium term. As a result, it would be useful if future research could further investigate the extent to which community acceptability of regeneration planning and community involvement in the actual design of the post Olympic built landscape might have resulted in a more tangible impact on the health and well-being of local residents. Given the long lead-in time related to community consultation in this context, this was unfortunately outside the remit of this study. We recommend that future studies incorporate a strand of work dedicated to this area.
Finally, natural experiments such as this require flexibility from both funders and researchers. In this study, the final form and nature of the Olympic Park was not known at the time of application, thus we had to be sensitive to the final composition of the legacy elements of the Olympic Park in our analyses and had to redesign elements of the study in order to boost recruitment of parent carer participants.
Conclusion
Studies that evaluate the health impacts of sporting mega-events are rare, with inconsistent findings. However, this large-scale quasi-experimental study provides limited evidence that the London 2012 Olympic and Paralympic Games had any positive effect on adolescent or parental/carer physical activity, mental health or well-being. Limited evidence was found for any changes in the social determinants of health (in this case operationalised as changes in labour market status). The qualitative study found that residents generally welcomed the unexpected chance to live in a cleaner, safer and more unified environment. The findings suggest that the Olympics served to generate only temporary respite by alleviating certain social and physical environment stressors and lessen participants’ sense of social exclusion. Given the level of public expenditure on such events, further evaluations of the demonstration and legacy health effects are required in order to improve generalisability and strengthen causal inference in an area of research that still relies on a very limited evidence base.
Acknowledgements
Contributions of others
We would like to thank Mark Petticrew, Adrian Renton and Derek Moore, all of whom contributed to the design of the study and are involved in publications arising from the study, but did not comment on the final report. Special thanks to Ellen Flint for undertaking analyses of the employment data and drafting material for inclusion here.
The authors would also like to thank the study participants, who gave their time, patience and permission to be involved in the study over multiple years; and the schools and school teachers involved in the project from its inception. We also wish to thank the time and dedication of fieldwork staff including: Lianne Austin, Rebecca Evans, Shaneka Foster, Jannat Hossain, Danielle House, Vanathi Tharmaratnam and Bukola Thompson.
Contributions of authors
Steven Cummins (Professor of Population Health) led the design and execution of the study, oversaw study analyses and publications, and led the preparation of the final report.
Charlotte Clark (Reader in Environmental and Mental Health Epidemiology) led the design and execution of the study, oversaw study analyses and publications, and contributed chapters to the final report.
Daniel Lewis (Research Fellow in Spatial Analysis) was the lead researcher for environmental data collection and analysis, conducted analysis, contributed to publications and led the spatial analyses produced for this report.
Neil Smith (Research Fellow in Epidemiology and Survey Manager) led and managed the fieldwork for the study, contributed to study design, undertook initial analyses of survey data, led early publications and commented on the final report.
Claire Thompson (Research Fellow in Qualitative Research) was the lead researcher for the qualitative longitudinal data collection and analysis, led the writing of qualitative publications and wrote the qualitative chapter in this report.
Melanie Smuk (Research Fellow in Medical Statistics) developed and implemented the multiple imputation strategy, conducted statistical analyses and contributed to chapters in the final report.
Stephen Stansfeld (Professor of Psychiatry) led the design and execution of the study, oversaw study analyses and publications, and contributed to chapters in the final report.
Stephanie Taylor (Professor of Primary Care) contributed to the design and execution of the study, contributed to study analyses and commented on the final report.
Amanda Fahy (Field Researcher) co-ordinated and undertook fieldwork, undertook data cleaning and preliminary analysis, and contributed to drafting the methods chapter.
Trish Greenhalgh (Professor of Primary Care) contributed to the design and execution of the qualitative element of the study, oversaw qualitative analyses and contributed to qualitative publications, and commented on the final report.
Sandra Eldridge (Professor of Biostatistics) contributed to the design and execution of the study, conducted power calculations and contributed to quantitative data analyses, and commented on the final report.
Publications
Smith N, Clark C, Fahy A, Tharmaratnam V, Lewis D, Thompson C, et al. The Olympic Regeneration in East London (ORiEL) study: protocol for prospective controlled quasi-experiment to evaluate the impact of urban regeneration on young people and their families. BMJ Open 2012;2:e001840.
Selvanayagam M, Thompson C, Taylor S, Cummins S, Bourke L. How might the London 2012 Olympics influence health and health inequalities? Local newspaper analysis of pre games pathways and impacts. BMJ Open 2012;2:e001791.
Thompson C, Lewis D, Greenhalgh T, Taylor SCJ, Cummins S. A health and social legacy for east London: narratives of ‘problem’ and ‘solution’ around London 2012. Sociol Res Online 2013;18:1.
Smith NR, Lewis D, Fahy A, Eldridge S, Taylor S, Moore D, et al. Individual sociodemographic factors and perceptions of the environment as determinants of inequalities in adolescent physical and psychological health: the Olympic Regeneration in East London (ORiEL) study. BMC Public Health 2015;15:150.
Smith NR, Clark C, Smuk M, Cummins S, Stansfeld S. The influence of social support on ethnic differences in well-being and depression in east London adolescents: findings from the prospective Olympic Regeneration in East London (ORiEL) study. Soc Psychiatry Psychiatr Epidemiol 2015;50:1701–11.
Thompson C, Lewis D, Greenhalgh T, Smith NR, Fahy A, Cummins S. ‘Everyone was looking at you smiling’: east London residents’ experiences of the 2012 Olympics and its legacy on the social determinants of health. Health Place 2015;36:18–24.
Fahy A, Stansfeld SA, Smith NR, Smuk M, Cummins S, Clark C. Longitudinal associations between cyberbullying involvement and adolescent mental health. J Adolesc Health 2016;59:502–9.
Clary C, Lewis D, Smith NR, Flint E, Kestens Y, Cummins S. The local food environment and fruit and vegetable intake: a geographically weighted regression approach in the ORiEL study. Am J Epidemiol 2016;184:837–46.
Thompson C, Lewis D, Smith NR, Petticrew M, Fahy A, Greenhalgh T, et al. ‘I don’t know how I’m still standing’: a Bakhtinian analysis of housing narratives in post-Olympic east London. Soc Sci Med 2017;177:27–34.
Clark C, Smuk M, Cummins S, Eldridge S, Fahy A, Lewis D, et al. An Olympic Legacy? Does urban regeneration associated with the London 2012 Olympic Games impact on adolescent mental health? Am J Epidemiol 2018;187:474–83.
Thompson C, Lewis D, Taylor S. The use of video recording in longitudinal focus group research. In Barbour R, Morgan D, editors. A New Era of Focus Groups: Challenge Innovation Practice. London: Palgrave; 2017. pp. 207–25.
Shareck M, Lewis DJL, Smith NR, Clary C, Cummins S. Associations between home and school neighbourhood food environments and adolescents’ fast-food and sugar-sweetened beverage intakes: findings from the Olympic Regeneration in East London (ORiEL) Study. Public Health Nutr 2018;21:2842–51.
Thompson C, Lewis D, Ponsford R, Cummins S. Fast-food, everyday life and health: a qualitative study of ‘chicken shops’ in east London. Appetite 2018;128:7–13.
Data-sharing statement
All data requests should be submitted to the corresponding author for consideration. Access to available anonymised data may be granted following review.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care.
References
- Wilkinson R, Pickett K. The Spirit Level. Why More Equal Societies Almost Always Do Better. London: Penguin; 2010.
- Marmot M. Fair Society, Healthy Lives. Strategic Review of Health Inequalities in England Post-2010. London: The Marmot Review; 2010.
- Health Inequalities (3rd Report). London: The Stationery Office; 2009.
- Wanless D. Securing Good Health for the Whole Population. London: HM Treasury/Department of Health and Social Sciences; 2004.
- Thomson H. A dose of realism for healthy urban policy: lessons from area-based initiatives in the UK. J Epidemiol Community Health 2008;62:932-6. https://doi.org/10.1136/jech.2007.068775.
- Thomson H, Atkinson R, Petticrew M, Kearns A. Do urban regeneration programmes improve public health and reduce health inequalities? A synthesis of the evidence from UK policy and practice 1980 to 2004. J Epidemiol Community Health 2006;60:108-15. https://doi.org/10.1136/jech.2005.038885.
- Elliott E, Landes R, Popay J. Regeneration and Health: A Selected Review of Research. Leeds: Nuffield Institute of Health, University of Leeds; 2001.
- Curtis S, Cave B, Coutts A. Is urban regeneration good for health? Perceptions and theories of the health impacts of urban change. Environ Plann C Gov Policy 2002;20:517-34. https://doi.org/10.1068/c02r.
- Brennan A, Rhodes J, Tyler P. Evaluation of the Single Regeneration Budget Challenge Fund: Second Final Evaluation of two SRB Short Duration Case Studies. Cambridge: University of Cambridge; 1999.
- Rhodes J, Tyler P, Brennan A. Lessons and Evaluation Evidence from Ten Single Regeneration Budget Case Studies: Mid-Term Report. London: Department for Transport, Local Government and the Regions; 2002.
- Baldock RO. Ten years of the urban programme 1981–91: the impact and implications of its assistance to small businesses. Urban Studies 1998;35:2063-83. https://doi.org/10.1080/0042098984006.
- Thomson H, Petticrew M, Morrison D. Health effects of housing improvement: systematic review of intervention studies. BMJ 2001;323:187-90. https://doi.org/10.1136/bmj.323.7306.187.
- Opportunities for 2012: Legacy Update. London: London Development Agency; 2009.
- Smith NR, Clark C, Fahy AE, Tharmaratnam V, Lewis DJ, Thompson C, et al. The Olympic Regeneration in East London (ORiEL) study: protocol for a prospective controlled quasi-experiment to evaluate the impact of urban regeneration on young people and their families. BMJ Open 2012;2.
- Diez Roux AV, Mair C. Neighborhoods and health. Ann N Y Acad Sci 2010;1186:125-45. https://doi.org/10.1111/j.1749–6632.2009.05333.x.
- Macintyre S, Ellaway A, Cummins S. Place effects on health: how can we conceptualise, operationalise and measure them?. Soc Sci Med 2002;55:125-39. https://doi.org/10.1016/S0277-9536(01)00214-3.
- Office for National Statistics . 2011 Census: KS101UK Usual Resident Population, Local Authorities in the United Kingdom 2015. www.ons.gov.uk/ons/rel/census/2011-census/key-statistics-and-quick-statistics-for-local-authorities-in-the-united-kingdom---part-1/rft-ks101uk.xls (accessed 21 September 2015).
- McLennan D, Barnes H, Noble M, Davies J, Garratt E, Dibben C. The English Indices of Deprivation 2010. London: Department for Communities and Local Government; 2011.
- Office for National Statistics . 2011 Census: KS601UK Economic Activity, Local Authorities in the United Kingdom 2015. www.ons.gov.uk/ons/rel/census/2011-census/key-statistics-and-quick-statistics-for-local-authorities-in-the-united-kingdom---part-2/rft-ks601uk.xls (accessed 21 September 2015).
- Metropolitan Police Service . Crime Mapping: Data Tables: Year End Figures (fixed) 2012. http://maps.met.police.uk/datatables/borough_2011–12.xls (accessed 21 September 2015).
- Office for National Statistics . 2011 Census: KS501UK Qualifications and Students, Local Authorities in the United Kingdom 2015. www.ons.gov.uk/ons/rel/census/2011-census/key-statistics-and-quick-statistics-for-local-authorities-in-the-united-kingdom---part-2/rft-ks501uk.xls (accessed 21 September 2015).
- Fauth RC, Leventhal T, Brooks-Gunn J. Short-term effects of moving from public housing in poor to middle-class neighborhoods on low-income, minority adults’ outcomes. Soc Sci Med 2004;59:2271-84. https://doi.org/10.1016/j.socscimed.2004.03.020.
- Leventhal T, Brooks-Gunn J. Moving to opportunity: an experimental study of neighborhood effects on mental health. Am J Public Health 2003;93:1576-82. https://doi.org/10.2105/AJPH.93.9.1576.
- Lawlor DA, Jago R, Noble SM, Chittleborough CR, Campbell R, Mytton J, et al. The Active for Life Year 5 (AFLY5) school based cluster randomised controlled trial: study protocol for a randomized controlled trial. Trials 2011;12. https://doi.org/10.1186/1745-6215-12-181.
- Office for National Statistics . Office for National Statistics: 2011 Census Response Rates 2011. https://web.archive.org/web/20180407053517/http://webarchive.nationalarchives.gov.uk/20160105160709/http://www.ons.gov.uk/ons/guide-method/census/2011/the-2011-census/2011-census-questionnaire-content/2011-census-questions---england.pdf (accessed 25 July 2018).
- Boyce W, Torsheim T, Currie C, Zambon A. The family affluence scale as a measure of national wealth: validation of an adolescent self-report measure. Soc Indic Res 2006;78:473-87. https://doi.org/10.1007/s11205-005-1607-6.
- Currie C, Molcho M, Boyce W, Holstein B, Torsheim T, Richter M. Researching health inequalities in adolescents: the development of the Health Behaviour in School-Aged Children (HBSC) family affluence scale. Soc Sci Med 2008;66:1429-36. https://doi.org/10.1016/j.socscimed.2007.11.024.
- Tennant R, Hiller L, Fishwick R, Platt S, Joseph S, Weich S, et al. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): development and UK validation. Health Qual Life Outcomes 2007;5. https://doi.org/10.1186/1477-7525-5-63.
- Clarke A, Friede T, Putz R, Ashdown J, Martin S, Blake A, et al. Warwick-Edinburgh Mental Well-being Scale (WEMWBS): validated for teenage school students in England and Scotland. A mixed methods assessment. BMC Public Health 2011;11. https://doi.org/10.1186/1471-2458-11-487.
- Stewart-Brown SL, Platt S, Tennant A, Maheswaran H, Parkinson J, Weich S, et al. The Warwick-Edinburgh Mental Well-being Scale (WEMWBS): a valid and reliable tool for measuring mental well-being in diverse populations and projects. J Epidemiol Community Health 2011;65:A38-9. https://doi.org/10.1136/jech.2011.143586.86.
- Angold A, Costello EJ, Messer SC, Pickles A, Winder F, Silver D. Development of a short questionnaire for use in epidemiological studies of depression in children and adolescents. Int J Methods Psychiatr Res 1995;5:237-49.
- Diagnostic and Statistical Manual of Mental Disorders (3rd ed. Revised). Washington, DC: American Psychiatric Association; 1987.
- Clark C, Haines MM, Head J, Klineberg E, Arephin M, Viner R, et al. Psychological symptoms and physical health and health behaviours in adolescents: a prospective 2-year study in east London. Addiction 2007;102:126-35. https://doi.org/10.1111/j.1360-0443.2006.01621.x.
- Klineberg E, Clark C, Bhui KS, Haines MM, Viner RM, Head J, et al. Social support, ethnicity and mental health in adolescents. Soc Psychiatry Psychiatr Epidemiol 2006;41:755-60. https://doi.org/10.1007/s00127-006-0093-8.
- Stansfeld SA, Haines MM, Head JA, Bhui K, Viner R, Taylor SJC, et al. Ethnicity, social deprivation and psychological distress in adolescents: school-based epidemiological study in east London. Br J Psychiatry 2004;185:233-8. https://doi.org/10.1192/bjp.185.3.233.
- Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Pers Assess 1988;52:30-41. https://doi.org/10.1207/s15327752jpa5201_2.
- MRC Epidemiology Unit, University of Cambridge . Youth Physical Activity Questionnaire (YPAQ) n.d. www.mrc-epid.cam.ac.uk/wp-content/uploads/2014/08/YPAQ.pdf (accessed 13 September 2018).
- van Sluijs E, Skidmore P, Mwanza K, Jones A, Callaghan A, Ekelund U, et al. Physical activity and dietary behaviour in a population-based sample of British 10-year old children: the SPEEDY study (Sport, Physical activity and Eating behaviour: Environmental Determinants in Young people). BMC Public Health 2008;8. https://doi.org/10.1186/1471-2458-8-388.
- Corder K, van Sluijs EM, Wright A, Whincup P, Wareham NJ, Ekelund U. Is it possible to assess free-living physical activity and energy expenditure in young people by self-report?. Am J Clin Nutr 2009;89:862-70. https://doi.org/10.3945/ajcn.2008.26739.
- Office for National Statistics . Office for National Statistics: 2011 Census Questionnaire Content for England 2011. www.ons.gov.uk/ons/guide-method/census/2011/the-2011-census/2011-census-questionnaire-content/2011-census-questions---england.pdf.
- Health of Young People in East London. London: Institute of Community Health Sciences, Queen Mary University of London; 2003.
- Bhui K, Lawrence A, Klineberg E, Woodley-Jones D, Taylor S, Stansfeld S, et al. Acculturation and health status among African-Caribbean, Bangladeshi and white British adolescents – validation and findings from the RELACHS study. Soc Psychiatry Psychiatr Epidemiol 2005;40:259-66. https://doi.org/10.1007/s00127-005-0890-5.
- Craig R, Mindell J. Health Survey for England 2010. London: The Information Centre; 2011.
- Office for National Statistics . Life Opportunities Survey: Questionnaire V4.1 2009.
- The Health Survey for England . Household Questionnaire. UK Data Archive Study Number 726 2011.
- Wardle J, Sutton S, Jarvis M. HABITS – The Health and Behaviours in Teenagers Study. London: University College London; 1998.
- Haselden L, Angle H, Hickman M. Young People and Health: Health Behaviour in School-Aged Children. London: Health Education Authority; 1999.
- Spittaels H, Foster C, Oppert JM, Rutter H, Oja P, Sjostrom M, et al. Assessment of environmental correlates of physical activity: development of a European questionnaire. Int J Behav Nutr Phys Act 2009;6. https://doi.org/10.1186/1479-5868-6-39.
- Spittaels H, Verloigne M, Gidlow C, Gloanec J, Titze S, Foster C, et al. Measuring physical activity-related environmental factors: reliability and predictive validity of the European environmental questionnaire ALPHA. Int J Behav Nutr Phys Act 2010;7. https://doi.org/10.1186/1479-5868-7-48.
- Bunt K, Llewellyn-Thomas S, Campbell-Hall V, Johns E. Schools’ and Colleges’ Engagement with the 2012 Olympic and Paralympic Games: PE and Sport. Department of Health and Social Sciences; 2011.
- Rose D, Pevalin DJ. The National Statistics Socioeconomic Classification (NS-SEC Rebased on the SOC2010). Basingstoke: Palgrave Macmillan; 2011.
- Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand 1983;67:361-70. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x.
- Karasek RA. Job demands, job decision latitude, and mental strain: implications for job redesign. Adm Sci Q 1979;24:285-308. https://doi.org/10.2307/2392498.
- Bosma H, Marmot MG, Hemingway H, Nicholson AC, Brunner E, Stansfeld SA. Low job control and risk of coronary heart disease in Whitehall II (prospective cohort) study. BMJ 1997;314:558-65. https://doi.org/10.1136/bmj.314.7080.558.
- Besson H, Brage S, Jakes RW, Ekelund U, Wareham NJ. Estimating physical activity energy expenditure, sedentary time, and physical activity intensity by self-report in adults. Am J Clin Nutr 2010;91:106-14. https://doi.org/10.3945/ajcn.2009.28432.
- Davey Smith G. Learning to live with complexity: ethnicity, socioeconomic position, and health in Britain and the United States. Am J Public Health 2000;90:1694-8. https://doi.org/10.2105/AJPH.90.11.1694.
- Nazroo JY. The Health of Britain’s Ethnic Minorities: Findings from a National Survey. London: Policy Studies Institute; 1997.
- Centre for Longitudinal Studies . Millennium Cohort Study: Data Dictionary 2015. www.cls.ioe.ac.uk/datadictionary/page.asp?section=000100010003000400020001&sectionTitle=A%2E+Main+Interview (accessed 22 September 2015).
- Ware J, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care 1996;34:220-33. https://doi.org/10.1097/00005650-199603000-00003.
- Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Med Care 1992;30:473-83. https://doi.org/10.1097/00005650-199206000-00002.
- Gandek B, Ware JE, Aaronson NK, Apolone G, Bjorner JB, Brazier JE, et al. Cross-validation of item selection and scoring for the SF-12 health survey in nine countries: results from the IQOLA project. J Clin Epidemiol 1998;51:1171-8. https://doi.org/10.1016/S0895-4356(98)00109-7.
- Mujahid MS, Diez Roux AV, Morenoff JD, Raghunathan T. Assessing the measurement properties of neighborhood scales: from psychometrics to ecometrics. Am J Epidemiol 2007;165:858-67. https://doi.org/10.1093/aje/kwm040.
- Bhui K, Stansfeld S, McKenzie K, Karlsen S, Nazroo J, Weich S. Racial/ethnic discrimination and common mental disorders among workers: findings from the EMPIRIC Study of Ethnic Minority Groups in the United Kingdom. Am J Public Health 2005;95:496-501. https://doi.org/10.2105/AJPH.2003.033274.
- Sproston K, Nazroo JY. Ethnic Minority Psychiatric Illness Rates in the Community (EMPIRIC): Quantitative Report. London: Department of Health and Social Sciences; 2002.
- Understanding Society: Wave 4, 2012–2013[computer file]. Colchester; 2014.
- Longley P. Geographic Information Systems & Science. Hoboken, NJ: John Wiley & Sons; 2011.
- Baddeley A, Turner R. spatstat: an R package for analyzing spatial point patterns. J Stat Softw 2005;12:1-42. https://doi.org/10.18637/jss.v012.i06.
- Planning for Walking. London: Chartered Institution of Highways and Transportation; 2015.
- Shannon CE. A Mathematical Theory of Communication. Bell System Technical Journal 1948;27:379-423. https://doi.org/10.1002/j.1538-7305.1948.tb01338.x.
- Carpiano RM. Come take a walk with me: the ‘go-along’ interview as a novel method for studying the implications of place for health and well-being. Health Place 2009;15:263-72. https://doi.org/10.1016/j.healthplace.2008.05.003.
- Kusenbach M. Street phenomenology: the go-along as ethnographic research tool. Ethnography 2003;4:455-85. https://doi.org/10.1177/146613810343007.
- Robinson N. The use of focus group methodology – with selected examples from sexual health research. J Adv Nurs 1999;29:905-13. https://doi.org/10.1046/j.1365-2648.1999.00966.x.
- Williams GH. Knowledgeable narratives. Anthropol Med 2000;7:135-40. https://doi.org/10.1080/136484700109395.
- Squire C, Squire C, Andrews M, Tamboukou M. Doing Narrative Research. London: Sage; 2008.
- Smith NR, Lewis DJ, Fahy A, Eldridge S, Taylor SCJ, Moore DG, et al. Individual sociodemographic factors and perceptions of the environment as determinants of inequalities in adolescent physical and psychological health: the Olympic Regeneration in East London (ORiEL) study. BMC Public Health 2015;15. https://doi.org/10.1186/s12889-015-1459-1.
- Aneshensel CS, Sucoff CA. The neighborhood context of adolescent mental health. J Health Soc Behav 1996;37:293-310. https://doi.org/10.2307/2137258.
- Ivert A-K, Levander M. Adolescents’ perceptions of neighbourhood social characteristics – is there a correlation with mental health?. Child Ind Res 2014;7:177-92. https://doi.org/10.1007/s12187-013-9210-x.
- Franzini L, Caughy M, Spears W, Fernandez Esquer ME. Neighborhood economic conditions, social processes, and self-rated health in low-income neighborhoods in Texas: a multilevel latent variables model. Soc Sci Med 2005;61:1135-50. https://doi.org/10.1016/j.socscimed.2005.02.010.
- Mota J, Almeida M, Santos P, Ribeiro JC. Perceived neighborhood environments and physical activity in adolescents. Prev Med 2005;41:834-36. https://doi.org/10.1016/j.ypmed.2005.07.012.
- Timperio A, Crawford D, Telford A, Salmon J. Perceptions about the local neighborhood and walking and cycling among children. Prev Med 2004;38:39-47. https://doi.org/10.1016/j.ypmed.2003.09.026.
- UK Physical Activity Guidelines. London: Department of Health and Social Sciences; 2011.
- Tremblay MS, Leblanc AG, Janssen I, Kho ME, Hicks A, Muruments K, et al. Canadian sedentary behaviour guidelines for children and youth. Appl Physiol Nutr Metab 2011;36:59-64. https://doi.org/10.1139/H11-012.
- Rubin DB. Multiple Imputation for Nonresponse in Surveys. New York, NY: John Wiley & Sons; 1987.
- The London Plan. The Spatial Development Strategy for London Consolidated with Alterations Since 2011. London: Greater London Authority; 2016.
- Index of Deprivation Affecting Children (2015). London: Department for Communities and Local Government; 2015.
- Meng XL. Multiple-imputation inferences with uncongenial sources of input (with discussion). Stat Sci 1994;9:538-73. https://doi.org/10.1214/ss/1177010269.
- Stranges S, Chandimali Samaraweera P, Taggart F, Kandala N, Stewart-Brown S. Major health-related behaviours and mental well-being in the general population: the Health Survey for England. BMJ Open 2014;4. https://doi.org/10.1136/bmjopen-2014-005878.
- Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res 2002;52:69-77. https://doi.org/10.1016/S0022-3999(01)00296-3.
- Meegan R, Mitchell A. ‘It’s not community round here, it’s neighbourhood’: neighbourhood change and cohesion in urban regeneration. Urban Studies 2001;38:2167-94. https://doi.org/10.1080/00420980120087117.
- Misener L, Mason DS. Creating community networks: can sporting events offer meaningful sources of social capital?. Managing Leisure 2006;11:39-56. https://doi.org/10.1080/13606710500445676.
- Wakefield S, McMullan C. Healing in places of decline: (re)imagining everyday landscapes in Hamilton, Ontario. Health Place 2005;11:299-312. https://doi.org/10.1016/j.healthplace.2004.05.001.
- Thompson C, Lewis DJ, Greenhalgh T, Smith NR, Fahy AE, Cummins S. ‘Everyone was looking at you smiling’: east London residents’ experiences of the 2012 Olympics and its legacy on the social determinants of health. Health Place 2015;36:18-24. https://doi.org/10.1016/j.healthplace.2015.08.008.
- Thompson C, Lewis DJ, Greenhalgh T, Smith NR, Fahy A, Cummins S. ‘I don’t know how I’m still standing’ a Bakhtinian analysis of social housing and health narratives in east London. Soc Sci Med 2017;177:27-34. https://doi.org/10.1016/j.socscimed.2017.01.054.
- Lawrence RJ. Housing and health: from interdisciplinary principles to transdisciplinary research and practice. Futures 2004;36:487-502. https://doi.org/10.1016/j.futures.2003.10.001.
- Council’s Move Highlights Severity of Problem in Newham. London: Caritas Anchor House; 2012.
- Giulianotti R, Klauser F. Security governance and sport mega-events: toward an interdisciplinary research agenda. J Sport Soc Issues 2010;34:49-61. https://doi.org/10.1177/0193723509354042.
- London Olympic and Paralympic Games Act. London: The Stationery Office; 2006.
- Terrorism Act. London: The Stationery Office; 2000.
- Fussey P, Coaffee J, Armstrong G, Hobbs D. Securing and Sustaining the Olympic City: Reconfiguring London for 2012 and Beyond. London: Ashgate; 2011.
- Wills W, Backett-Milburn K, Roberts M, Lawton L. The framing of social class distinctions through family food and eating practices. Sociol Rev 2011;59:725-40. https://doi.org/10.1111/j.1467-954X.2011.02035.x.
- Fagg J, Curtis S, Stansfeld S, Congdon P. Psychological distress among adolescents, and its relationship to individual, family and area characteristics in east London. Soc Sci Med 2006;63:636-48. https://doi.org/10.1016/j.socscimed.2006.02.012.
- West P. Health inequalities in the early years: is there equalisation in youth?. Soc Sci Med 1997;44:833-58. https://doi.org/10.1016/S0277-9536(96)00188-8.
- Blane D, Bartley M, Smith GD, Filakti H, Bethune A, Harding S. Social patterning of medical mortality in youth and early adulthood. Soc Sci Med 1994;39:361-6. https://doi.org/10.1016/0277-9536(94)90132-5.
- Dibben C, Popham F. Are health inequalities evident at all ages? An ecological study of English mortality records. Eur J Public Health 2013;23:39-45. https://doi.org/10.1093/eurpub/cks019.
- Spencer NJ. Social equalization in youth: evidence from a cross-sectional British survey. Eur J Public Health 2006;16:368-75. https://doi.org/10.1093/eurpub/cki222.
- Wickrama K, Noh S, Elder GH. An investigation of family SES-based inequalities in depressive symptoms from early adolescence to emerging adulthood. Adv Life Course Res 2009;14:147-61. https://doi.org/10.1016/j.alcr.2010.04.001.
- Vallejo-Torres L, Hale D, Morris S, Viner RM. Income-related inequality in health and health-related behaviour: exploring the equalisation hypothesis. J Epidemiol Community Health 2014;68:615-21. https://doi.org/10.1136/jech-2013-203306.
- Sawyer SM, Azzopardi PS, Wickremarathne D, Patton GC. The age of adolescence. Lancet Child Adolesc Health 2018;2:223-8. https://doi.org/10.1016/S2352-4642(18)30022-1.
- Harding S, Whitrow M, Maynard MJ, Teyhan A. Cohort profile: the DASH (Determinants of Adolescent Social well-being and Health) study, an ethnically diverse cohort. Int J Epidemiol 2007;36:512-17. https://doi.org/10.1093/ije/dym094.
- Maynard MJ, Harding S, Minnis H. Psychological well-being in black Caribbean, black African, and white adolescents in the UK Medical Research Council DASH study. Soc Psychiatry Psychiatr Epidemiol 2007;42:759-69. https://doi.org/10.1007/s00127-007-0227-7.
- Torsheim T, Currie C, Boyce W, Kalnins I, Overpeck M, Haugland S. Material deprivation and self-rated health: a multilevel study of adolescents from 22 European and North American countries. Soc Sci Med 2004;59:1-12. https://doi.org/10.1016/j.socscimed.2003.09.032.
- Saxena S, Eliahoo J, Majeed A. Socioeconomic and ethnic group differences in self reported health status and use of health services by children and young people in England: cross sectional study. BMJ 2002;325:520-3. https://doi.org/10.1136/bmj.325.7363.520.
- Biddle SJ, Asare M. Physical activity and mental health in children and adolescents: a review of reviews. Br J Sports Med 2011;45:886-95. https://doi.org/10.1136/bjsports-2011-090185.
- Penedo FJ, Dahn JR. Exercise and well-being: a review of mental and physical health benefits associated with physical activity. Curr Opin Psychiatry 2005;18:189-93. https://doi.org/10.1097/00001504-200503000-00013.
- Galán I, Boix R, Medrano MJ, Ramos P, Rivera F, Pastor-Barriuso R, et al. Physical activity and self-reported health status among adolescents: a cross-sectional population-based study. BMJ Open 2013;3. https://doi.org/10.1136/bmjopen-2013-002644.
- McCartney G, Thomas S, Thomson H, Scott J, Hamilton V, Hanlon P, et al. The health and socioeconomic impacts of major multi-sport events: systematic review 1978 to 2008. BMJ 2010;340. https://doi.org/10.1136/bmj.c2369.
- Mahtani KR, Protheroe J, Slight SP, Demarzo MM, Blakeman T, Barton CA, et al. Can the London 2012 Olympics ‘inspire a generation’ to do more physical or sporting activities? An overview of systematic reviews. BMJ Open 2013;3. https://doi.org/10.1136/bmjopen-2012-002058.
- Weed M, Coren E, Fiore J, Mansfield L, Wellard I, Chatziefstathiou D. A Systematic Review of the Evidence Base for Developing a Physical Activity and Health Legacy from the London 2012 Olympic and Paralympic Games. London: Department of Health and Social Sciences; 2009.
- Cleland C, Stewart S, Clark J, Kearns S, Ellaway A. GoWell East: Studying Change in Glasgow’s East End. Headline Indicators Report for Wave 2 (2015) in Comparison With Wave 1 (2012) n.d. www.gowellonline.com/publications/384_gowell_east_headline_indicators_comparison_report (accessed 25 July 2018).
- Clark C, Myron R, Stansfeld S, Candy B. A systematic review of the evidence on the effect of the built and physical environment on mental health. J Public Ment Health 2007;6:14-27. https://doi.org/10.1108/17465729200700011.
- Rogers A, Huxley P, Evans S, Gately C. More than jobs and houses: mental health, quality of life and the perceptions of locality in an area undergoing urban regeneration. Soc Psychiatry Psychiatr Epidemiol 2008;43:364-72. https://doi.org/10.1007/s00127-008-0316-2.
- Thomas RW, Evans S, Gately C, Stordy J, Huxley P, Rogers A, et al. State-event relations among indicators of susceptibility to mental distress in Wythenshawe in the UK. Soc Sci Med 2002;55:921-35. https://doi.org/10.1016/S0277-9536(01)00226-X.
- Clark J, Kearns A, Cleland C. Spatial scale, time and process in mega-events: the complexity of host community perspectives on neighbourhood change. Cities Environ 2016;53:87-9. https://doi.org/10.1016/j.cities.2016.01.012.
- Huxley P, Evans S, Leese M, Gatley C, Rogers A, Thomas R, et al. Urban regeneration and mental health. Soc Psychiatry Psychiatr Epidemiol 2004;39:208-85. https://doi.org/10.1007/s00127-004-0739-3.
- Kearns A, Mason P. Regeneration, relocation and health behaviours in deprived communities. Health Place 2015;32:43-58. https://doi.org/10.1016/j.healthplace.2014.12.012.
- Maheswaran H, Weich S, Powell J, Stewart-Brown S. Evaluating the responsiveness of the Warwick Edinburgh Mental Well-Being Scale (WEMWBS): group and individual level analysis. Health Qual Life Outcomes 2012;10. https://doi.org/10.1186/1477-7525-10-156.
- Phillips G, Bottomley C, Schmidt E, Tobi P, Lais S, Yu G, et al. Well London phase-1: results among adults of a cluster-randomised trial of a community engagement approach to improving health behaviours and mental well-being in deprived inner-city neighbourhoods. J Epidemiol Community Health 2014;68:606-14. https://doi.org/10.1136/jech-2013-202505.
- Weich S, Brugha T, McManus S, Bebbington P, Jenkins R, Cooper C, et al. Mental well-being and mental illness: findings from the Adult Psychiatric Morbidity Survey for England 2007. Br J Psychiatry 2011;199:23-8. https://doi.org/10.1192/bjp.bp.111.091496.
- Hatch S, Frissa S, Verdecchia M, Stewart R, Fear NT, Reichenberg A, et al. Identifying sociodemographic and socioeconomic determinants of health inequalities in a diverse London community: the South East London Community Health (SELCoH) study. BMC Public Health 2011;11. https://doi.org/10.1186/1471-2458-11-861.
- McManus S, Meltzer H, Brugha T, Bebbington P, Jenkins R. Adult Psychiatric Morbidity in England, 2007: Results of a Household Survey. Leeds: NHS Digital; 2009.
- Egan M, Lawson L, Kearns A, Conway E, Neary J. Neighbourhood demolition, relocation and health. A qualitative longitudinal study of housing-led urban regeneration in Glasgow, UK. Health Place 2015;33:101-8. https://doi.org/10.1016/j.healthplace.2015.02.006.
- Boyle P, Haggerty KD. Civil cities and urban governance: regulating disorder in Vancouver. Urban Studies 2011;48:3185-201. https://doi.org/10.1177/0042098011422391.
- Pevalin DJ. Socioeconomic inequalities in health and service utilization in the London borough of Newham. Public Health 2007;121:596-602. https://doi.org/10.1016/j.puhe.2006.12.015.
- Watt P. ‘It’s not for us’: regeneration, the 2012 Olympics and the gentrification of east London. City 2013;17:99-118. https://doi.org/10.1080/13604813.2012.754190.
- Bernstock P. Olympic Housing: a Review of London 2012’s Legacy. Farnham: Ashgate; 2013.
- Burns T. Update on East Village, E20 – A Legacy Neighbourhood for London. Regional Focus. East Thames Group. London: The Housing Forum; 2014.
- Leslie E, Cerin E. Are perceptions of the local environment related to neighbourhood satisfaction and mental health in adults?. Prev Med 2008;47:273-8. https://doi.org/10.1016/j.ypmed.2008.01.014.
- Kennelly J, Watt P. Sanitizing public space in Olympic host cities: the spatial experiences of marginalized youth in 2010 Vancouver and 2012 London. Sociology 2011;45:765-81. https://doi.org/10.1177/0038038511413425.
- Fussey P, Coaffee J, Haggerty K, Bennett C. Security Games: Surveillance and Control at Megaevents. London: Routledge; 2011.
- Goldstein DM. Towards a critical anthropology of security. Curr Anthropol 2010;51:487-51. https://doi.org/10.1086/655393.
- Booker CL, Harding S, Benzeval M. A systematic review of the effect of retention methods in population-based cohort studies. BMC Pub Health 2011;11. https://doi.org/10.1186/1471-2458-11-249.
Appendix 1 Wave 1 survey: baseline (2012)
Appendix 2 Wave 2 survey: 6-month follow-up (2013)
Appendix 3 Wave 3 survey: 18-month follow-up (2014)
List of abbreviations
- aKDE
- adaptive kernel density estimation
- ALPHA
- Assessing Levels of Physical Activity and Fitness
- aOR
- adjusted odds ratio
- BMI
- body mass index
- CCTV
- closed-circuit television
- CI
- confidence interval
- EMPIRIC
- Ethnic Minority Psychiatric Illness Rates in the Community survey
- FAS II
- Revised Family Affluence Scale
- GIS
- geographical information system
- HADS
- Hospital Anxiety and Depression Scale
- ICC
- intracluster correlation coefficient
- IDACI
- Income Deprivation Affecting Children index
- ITT
- intent to treat
- LSCV
- least-squares cross-validation
- MAR
- missing at random
- MCAR
- missing completely at random
- MCMC
- Markov chain Monte Carlo
- MESA
- Multi-Ethnic Study of Atherosclerosis
- MFQ
- Moods and Feelings Questionnaire
- MRC
- Medical Research Council
- MSPSS
- Multi-dimensional Scale of Perceived Social Support
- NIHR
- National Institute for Health Research
- NS-SEC
- National Statistics Socioeconomic Classification System
- NVQ
- National Vocational Qualifications
- OR
- odds ratio
- ORiEL
- Olympic Regeneration in East London
- OS
- Ordnance Survey
- RELACHS
- Research with East London Adolescents: Community Health Survey
- R-PAQ
- Recent Physical Activity Questionnaire
- RR
- risk ratio
- RRR
- relative risk ratio
- SD
- standard deviation
- SDQ
- strengths and difficulties
- SE
- standard error
- SF-12
- Short Form questionnaire-12 items
- SMFQ
- Moods and Feelings Questionnaire short form
- WEMWBS
- Warwick–Edinburgh Mental Well-Being Scale
- Y-PAQ
- Youth Physical Activity Questionnaire