

Notes
Article history
The research reported in this issue of the journal was funded by the PHR programme as project number 13/90/16. The contractual start date was in April 2015. The final report began editorial review in December 2017 and was accepted for publication in April 2018. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The PHR editors and production house have tried to ensure the accuracy of the authors’ report and would like to thank the reviewers for their constructive comments on the final report document. However, they do not accept liability for damages or losses arising from material published in this report.
Declared competing interests of authors
Rona Campbell is a member of the National Institute for Health Research (NIHR) Public Health Research Funding Board and is a NIHR Senior Investigator. Russell Jago is a member of the NIHR Public Health Research Board. William Hollingworth is a member of the NIHR Health Technology Assessment Clinical Evaluation and Trials Board.
Permissions
Copyright statement
© Queen’s Printer and Controller of HMSO 2019. This work was produced by Sebire et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This issue may be freely reproduced for the purposes of private research and study and extracts (or indeed, the full report) may be included in professional journals provided that suitable acknowledgement is made and the reproduction is not associated with any form of advertising. Applications for commercial reproduction should be addressed to: NIHR Journals Library, National Institute for Health Research, Evaluation, Trials and Studies Coordinating Centre, Alpha House, University of Southampton Science Park, Southampton SO16 7NS, UK.
2019 Queen’s Printer and Controller of HMSO
Chapter 1 Introduction and background
Physical activity among girls
Physical activity (PA) in adulthood is associated with a reduced risk of heart disease, stroke, type 2 diabetes mellitus and all-cause mortality. 1 Being physically active in childhood has been associated with lower levels of cholesterol and blood lipids and favourable blood pressure and body composition. 2 Sedentary behaviour in children and adolescents has been associated with adiposity3 and insulin resistance,4 both markers of metabolic syndrome. 5 PA is also associated with adolescent mental health and well-being, including improved self-esteem,6 self-image,7 lower levels of stress8 and academic performance. 9 Despite the benefits, girls are less active than boys at all ages,10–12 the age-related decline in girls’ PA levels (7% per year) being greater and occurring at younger ages than for boys (5% per year). 13 A recent study reported that 68% of girls aged 15 years in the UK accumulated less than the recommended minimum of 60 minutes of moderate to vigorous physical activity (MVPA) per day. 14 As PA tracks moderately from adolescence into adulthood,15 increasing PA levels, especially among girls, is important.
Several psychosocial factors underpin girls’ PA including enjoyment, perceived competence, self-efficacy and physical self-perceptions. 16 Findings from qualitative studies suggest that changes to friendship groups, peer support, perceived competence, competing priorities, self-presentational concerns and ‘sporty’ gender stereotypes experienced during the transition from primary to secondary school may contribute to the observed decline in girls’ PA. 17–19 PA interventions aimed at young girls have produced small positive effects, the effect being larger for interventions that targeted girls only (vs. those that targeted girls and boys) and that used multifaceted designs and educational content. 20 The promotion of young people’s health in schools is a public health priority,21 it is easier to recruit through schools, and school-based interventions can have broad reach over time. However, a recent meta-analysis22 of school-based interventions, which used objective measures of PA in adolescents, found weak evidence for small effects (a standardised mean difference of 0.02 for total activity and 0.24 for MVPA). These interventions comprised traditional top-down strategies including activity breaks in class, health education/information provision, extra physical education (PE) lessons and pedometer-based self-monitoring.
The Physical Activity 4 Everyone multicomponent school-based intervention in Australia23 increased adolescents’ MVPA by 7 minutes [95% confidence interval (CI) 2.7 to 11.4 minutes; p = 0.002] at 2 years of follow-up compared with controls. However, the intervention was more effective in boys (10-minute increase) than in girls (4-minute increase), resource heavy (e.g. providing an expert health and PE teacher to each school 1 day per week) and expensive (£227 per student, £33 per minute of MVPA). 24 To achieve a population-level increase in girls’ activity, more cost-effective and scalable approaches are needed. The evidence suggests that, by focusing school-based interventions on top-down provision of education and short-term structured PA,25 the potential power of peers to influence girls’ activity has been underutilised. New creative ideas are needed that take advantage of the complexity of the system surrounding girls’ PA, such as their peer groups.
Peers and physical activity
A 2012 systematic review26 identified six ways in which peers can influence PA: peer social support, presence of peers during PA, peer norms (one study), friendship quality, peer affiliation to certain groups and peer victimisation (i.e. being the subject of aggressive behaviour). Consistent positive associations were found between peer support, the presence of peers, peer norms, friendship quality and adolescent PA levels. 26 Social network research supports this, showing that adolescents have friends with similar PA levels and behaviours to themselves and that adolescents may moderate their PA behaviour over time to be more like that of their friends’. 27 Both systematic reviews support the view that peer-led interventions are a possible avenue to increasing adolescent PA. There is a need to capitalise on existing peer processes in schools by promoting peer support and enhancing peer communication skills, specifically among girls. 26
Peer-led health interventions
Peer-led interventions have targeted several health behaviours in young people including asthma, smoking, alcohol consumption and drug use, water versus sugar-sweetened beverage consumption, PA and sedentary behaviour. 28–31 The majority were delivered in secondary schools and trained peer leaders to formally educate younger peers using information provision and skill development. 32 Eight interventions were effective in changing a behavioural outcome, with three changing psychological mediators and the effects of two being less clear. A recent high-quality cluster randomised controlled trial (RCT),33 conducted in English secondary schools, of an intervention in which Year 9 students mentored Year 7 students in formal one-to-one meetings for 6 weeks did not increase the PA of Year 7 students (measured by accelerometery). Studies of peer-led PA interventions are limited by a lack of high-quality trial interventions. They do not consistently utilise behaviour change theory and peer-led intervention mechanisms limited to older students supporting younger students, and using formal methods (e.g. leading educational classes), which are time limited and intensive.
An alternative approach is to train peer supporters (PSs) to informally diffuse health promotion messages among their trusted peers. This is based on the diffusion of innovations (DOI) theory34 that conceptualises how ideas, beliefs or behaviours are informally communicated through members of a social system. The DOI approach was adopted in ASSIST (A Stop Smoking In Schools Trial), which included a process,35 economic36 and outcome28 evaluation.
To informally diffuse messages about the importance of not smoking for 10 weeks, ASSIST aimed to reduce smoking rates in secondary school-aged students and trained 15% of Year 8 students, who were identified by their year group peers as influential. The cluster RCT28 involved 10,730 12- to 13-year-olds in 59 schools across England and Wales. The training content aimed at increasing knowledge of smoking and its effects, to improve participants’ communication, negotiating, decision-making, empathy and group work skills.
ASSIST was effective in achieving a sustained reduction in the uptake of smoking 2 years after baseline. Students who received the intervention were less likely than those in the control condition to be smokers immediately after the intervention [odds ratio (OR) 0.75, 95% CI 0.55 to 1.01] and at 1 year (OR 0.77, 95% CI 0.59 to 0.99) and 2 years of follow-up (OR 0.85, 95% CI 0.72 to 1.01). 28,34 The economic evaluation of ASSIST showed that the intervention could be delivered at a ‘modest’ cost {mean total cost £5662 [standard deviation (SD) £1226] or £32 per student}. PS recruitment targets were met37 and attrition was low, with 87% of children (i.e. 816 out of 942 children) who were invited to be a PS being trained and carrying out their role. Attendance at follow-up sessions was high (> 86%). 38 Trainers noted that the training could be improved if the delivery pair had different delivery styles, expertise and experience. 37 PSs focused on their friends within their year group and tried to influence people they thought they could persuade not to take up the habit (as opposed to those already smoking). 38 Teachers believed that Year 8 was a suitable time for an intervention such as ASSIST to take place, as there are no examinations and the project complemented broader teaching (encouraging responsibility and promoting transferable skills). 39 These findings indicate that peer-led DOI-informed interventions can be effective in changing adolescent health behaviours.
The Activity and Healthy Eating in ADolescence (AHEAD) study40 tested the feasibility of the ASSIST model for preventing obesity in adolescents. The project was piloted and refined in one school before a feasibility study was conducted in six schools. The results showed that, although it was feasible to implement AHEAD, PSs found it hard to learn about both PA and healthy eating in appropriate detail to confidently support their peers. The intervention was resource and labour intensive and was, subsequently, relatively expensive. The AHEAD study was well received by participants, but ultimately showed no evidence of promise. 40 Learning from both ASSIST and the AHEAD study has informed the refinement of the Peer-Led physical Activity iNtervention for Adolescent girls (PLAN-A) intervention.
Theoretical background of the Peer-Led physical Activity iNtervention for Adolescent girls
Interventions that target theoretical mechanisms of behaviour change are likely to be more effective than those that do not. 41 However, few peer-led PA interventions explictly incorporate principles of commonly used behaviour change theories. 30 The present study combines two complementary theories: DOI34 and self-determination theory (SDT). 42 As a cornerstone of the study, DOI provides a framework for harnessing the influential capacities of change agents (e.g. Year 8 girls identified as opinion leaders by their peers) who can informally diffuse messages about being active among their peers and, in turn, influence changes in beliefs/attitudes that can change behaviours.
Self-determination theory concerns the personal and social conditions needed to foster high-quality and sustainable motivation for behaviours. Within SDT it is hypothesised that autonomous motivation for PA (based on authentic choices, inherent satisfaction or personal value) is associated with positive behavioural, affective and cognitive outcomes, whereas controlled motivation (based on guilt or compliance with others’ demands) undermines these outcomes. 43 Autonomous motivation is supported by the degree to which the social environment satisfies (and individuals perceive the satisfaction of) three psychological needs: autonomy, competence and relatedness. SDT has been applied extensively to research aimed at understanding motivation for PA among children and adolescents19,44,45 and used to guide PA interventions,46 including a peer-led PA intervention for older adults. 47
Research has identified positive associations between autonomous motivation and PA among secondary school-aged children48 and children’s positive affect, challenge-seeking48 and quality of life. 49 Furthermore, autonomous motivation is positively associated with psychological need satisfaction (i.e. greater perceptions of autonomy, competence and relatedness). 45,50 SDT is well suited to a peer-to-peer intervention because peers can create a social climate that can either undermine or facilitate their peers’ interest in, and levels of, PA. 30 They can also create health and affiliation motives, perceptions of competence, connectedness and social support and realistic choices and options of how to be physically active. 17,19 Further details of how SDT was incorporated into PLAN-A are shown in Chapter 2.
Overview of the Peer-Led physical Activity iNtervention for Adolescent girls
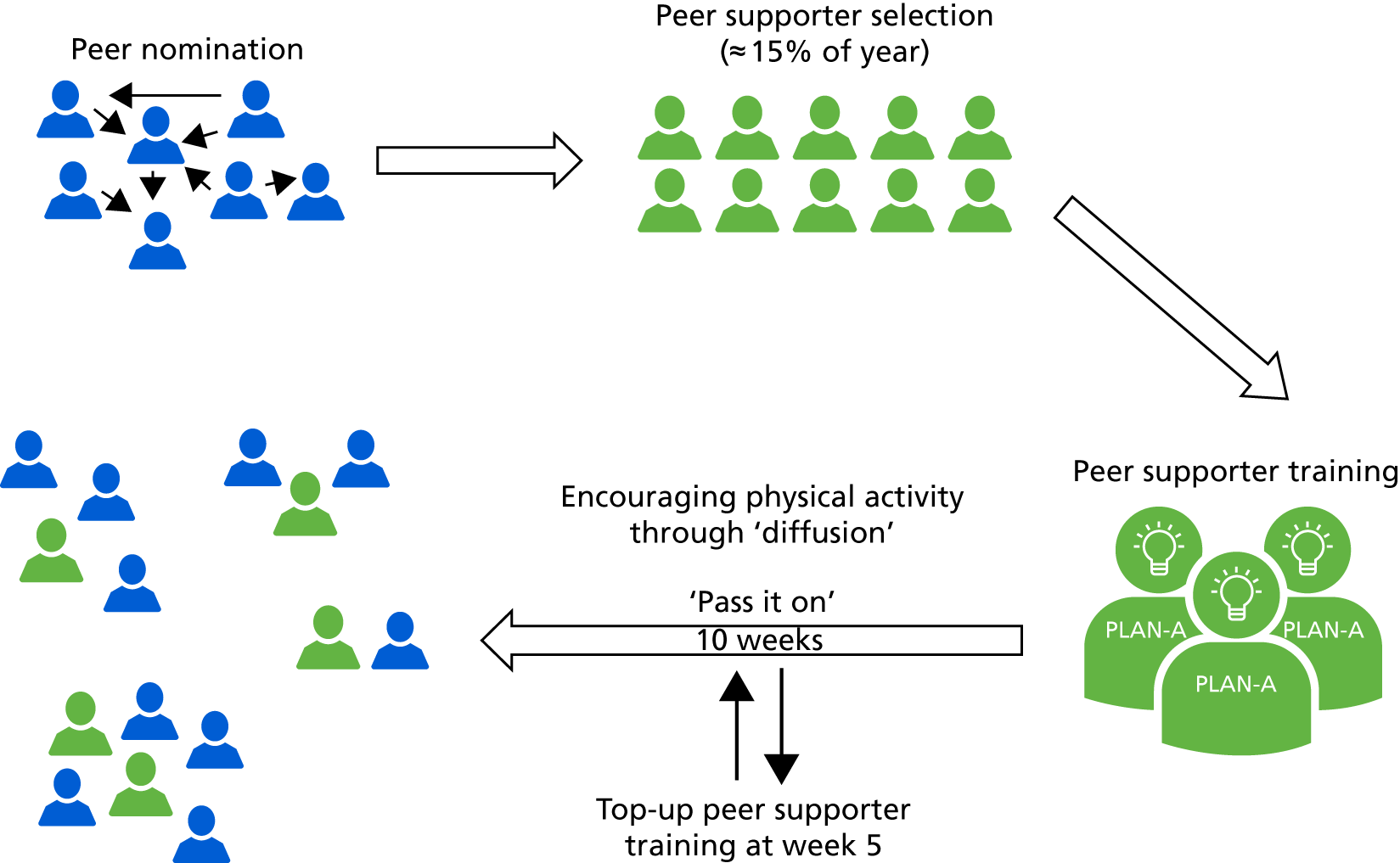
The ASSIST intervention model formed a template for PLAN-A (Figure 1). This was refined prior to piloting and feasibility testing. PSs were identified by Year 8 girls who nominated those they perceived to be influential in their school year. The highest scoring 18% were invited to be a PS, with the aim of ensuring that ≥ 15% became PSs. PSs attended a 2-day training course (plus a top-up day at week 5) to develop the skills, knowledge and confidence to promote PA among their peers. It should be noted that the ASSIST approach is to conduct four 1-hour in-school top-up training sessions with PS during the intervention period. However, feedback from stakeholders at the Centre for the Development and Evaluation of Complex Interventions for Public Health Improvement (DECIPHer)’s IMPACT (a not-for-profit company, with expertise in translation and impact of evidence-based public health and owners of ASSIST) and from teachers who had run ASSIST suggested that these sessions were poorly attended and lacked focus. As such, in PLAN-A these were replaced with a single day-long top-up day at week 5 of the intervention. External trainers, who had attended a 3-day training programme, delivered the PS training. The PS training was informed by phase 1 findings, was interactive and addressed issues central to girls’ PA. As previously discussed, the content was grounded in SDT. On completion of the training, PSs returned to school and informally promoted messages about increasing PA among their peers for 10 weeks. For details about the final intervention see Chapter 2, Description of the final intervention elements.
FIGURE 1.
The PLAN-A model.
Study aims and objectives
The study comprised two phases: phase 1, refinement and piloting and phase 2, a feasibility study.
Phase 1 objectives
-
Adapt and refine the ASSIST intervention to develop a PS training programme that focuses on promoting PA among Year 8 girls.
-
Develop an intervention logic model to refine in the feasibility trial.
Phase 2 objectives
-
Estimate the recruitment rate of PSs and non-PSs (NPSs), and monitor attendance at the PS training.
-
Qualitatively examine the acceptability of the intervention to students, trainers, schools and parents, and identify necessary refinements.
-
Report accelerometer and questionnaire data provision rates, examine data quality and explore the implications of missing accelerometer data in terms of how these data might be imputed in a definitive trial.
-
Estimate the potential effect of the intervention on daily accelerometer-derived MVPA and secondary PA-related and psychological variables immediately after the intervention (T1) and at 12 months after baseline (T2).
-
Estimate the school-related intraclass correlation (ICC) for daily MVPA.
-
Estimate the sample size for an adequately powered definitive trial evaluation.
-
Identify and test the feasibility of collecting the data needed to cost the intervention and conduct a cost-effectiveness analysis in a definitive trial.
-
Qualitatively examine parental views regarding allowing their child’s data to be used for data linkage with academic records kept by the National Pupil Database (NPD). Examine the completeness of data required to link participant data to educational attainment (via the NPD).
Progression criteria
The following criteria were established during protocol development and were used to inform on whether or not or how to proceed to a definitive trial:
-
Can we recruit trainers?
-
Is it feasible to implement the intervention in secondary schools?
-
Were the training and materials for the trainers and PSs acceptable?
-
Was the intervention acceptable to schools?
-
Were trial design and methods acceptable?
-
Does the intervention show evidence of promise to positively influence the proposed primary outcome (i.e. weekday MVPA)?
-
Indications of affordability and cost-effectiveness for local authorities.
-
Is there a positive view about data linkage from stakeholders involved (parents, schools, data custodians)? (See Chapter 3, Protocol amendments.)
Evidence of promise for weekday MVPA was a priori stated in the original trial protocol (version 1) as: ‘95% confidence intervals around the point estimate of the difference in means between trial arms on daily minutes in MVPA to include approximately 10-minute difference’.
Chapter 2 Phase 1: formative research and pilot study
Formative research
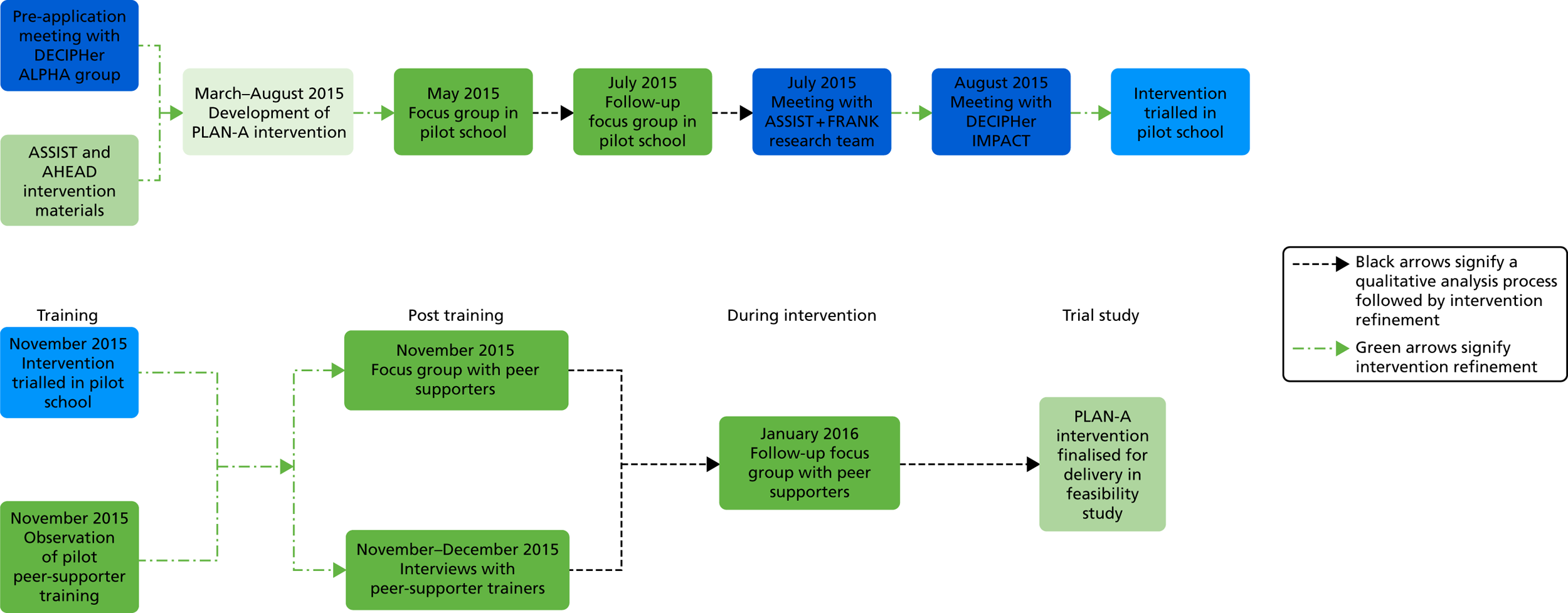
Formative research was conducted in 2015. The sequencing of phase 1 is shown in Figure 2; it comprised:
-
a focus group with the DECIPHer Advice Leading to Public Health Advancement (ALPHA) group (a research advisory group of young people) and an interview with a local secondary school teacher
-
a series of iterative focus groups with Year 8 girls in the pilot study school
-
sharing of practice and experience with the ASSIST+ FRANK51 team
-
a review of the proposed intervention by the chief operating officer of IMPACT.
FIGURE 2.
Sequence of phase 1 intervention refinement and piloting focus group with the DECIPHer ALPHA group.
The pilot study was granted ethics approval from the School for Policy Studies, University of Bristol (SPSREC14–15.A10) and was sponsored by the University of Bristol.
A semistructured focus group was conducted with six adolescent girls (aged 13–16 years) from the DECIPHer ALPHA public and patient involvement (PPI) group. A female PE teacher from a local secondary school was also interviewed. The focus group and interview were audio-recorded and the data were analysed using deductive thematic analysis using the question topics as a guide. 52 Table 1 shows the themes, summarised findings and the implications for the intervention design.
| Question topic | Findings | Implications for PLAN-A design |
|---|---|---|
| PS concept | Concept clear. Peers powerful in trends and PAa | Concept clear to Year 8 girlsa |
| Peer mentoring used in schoolsb | Schools open to peer mentoringa | |
| Supportive of 10-week intervention durationb | ||
| How to encourage PSs to participate | Sell the benefits (e.g. CV, certificates)a | Explore other benefits in phase 1 focus groupsa |
| Use videos from the pilot in recruitmenta | ||
| Refer to long-term benefitsa | Consider using videos of PSs from pilota | |
| Sign of kudos as nominated by peersb | ||
| PS training content and logistics | Off-site training and young adult female trainersa | Trainers and locationa |
| Consensus for girls only interventiona | ||
| Focus on health and not appearancea | Explore salient health messagesa | |
| Provide information on local PA opportunitiesa | ||
| Focus on PA primary–secondary transitionb | Identify local PA opportunitiesa | |
| Balance theory and practical learningb | ||
| PA terminology and how PA fits into the life of adolescents | Avoid complex terms, just talk normallya | Simplify termsa |
| Relate activity to Year 8 everyday lifea | Design activities to relate to Year 8 livesa | |
| Identify times for incidental PA (active travel)a | Peer education on incidental PAa | |
| Explore a day in the life of a Year 8 for PAa | ||
| Diffusing messages to peers | Peer supporting and compromise, not pressurea | Focus training on peers supporting, not ‘instructing’, and negotiation skillsa |
| Frame messages in Year 8 terms (e.g. ‘what are you doing tonight?’) to encourage PAa | ||
| Using social media | Support for Twitter (www.twitter.com; Twitter, Inc., San Francisco, CA, USA), Instagram (www.instagram.com; Facebook, Inc., Menlo Park, CA, USA) (‘active selfies’) and Facebook page (www.facebook.com; Facebook, Inc., Menlo Park, CA, USA). Better than textinga,b | Integrate social mediaa |
| Research team–peer and peer–peer idea-sharinga | Facilitate photo-sharinga |
Recruitment and description of the pilot study school
One pilot school was identified by Wiltshire Council to be above the median of the Pupil Premium (i.e. relatively more deprived) and which would give a robust early test of the intervention. Recruitment materials were sent to the head teacher, who then delegated responsibility to a school contact (assistant leader in learning in PE). A school study agreement form was completed. The school (N = 1086, students; n = 70, Year 8 girls) was located in a medium-sized town. The school was given £500 as a thank you for participating.
Iterative focus groups: round 1
Methods
Two semistructured focus groups (n = 16 participants, eight per group; duration 61–66 minutes) were conducted by two facilitators in May 2015 to explore girls’ views on PA barriers, PS recruitment, logistics and content of PS training and use of social media. Focus groups were audio-recorded, transcribed verbatim and analysed using thematic analysis52 to generate themes pertaining to intervention design and refinement. All participants provided informed consent and were given a £5 voucher in recognition of their time.
Results
Findings are presented under two themes (Recruitment materials and Intervention content) alongside mapping in which the girls’ views were included in the intervention design.
Recruitment materials
Both focus groups suggested that PLAN-A recruitment materials should highlight how their participation in the project would (1) help their peers; (2) improve their own (and PS) skills and knowledge; and (3) increase their potential to influence their peers and have their voice heard. These themes should be reflected on the PLAN-A website and a video would be a good method of communication for girls their age. Both focus groups recommended that recruitment materials provided an insight into the PA training activities. Certificates, endorsements in records of achievement and/or PLAN-A-branded clothing were not viewed as suitable incentives to participate.
Intervention content
Well-being and feeling good about oneself were seen as key facilitators. Time constraints, lack of confidence, competence and being seen by boys when exercising were barriers.
The characteristics of a good PS included confidence, good communication and leadership skills and an ability to encourage others. Girls wanted confirmation at the point of peer nomination that the peers whom they nominate do not need to be their friends. The characteristics that participants thought the trainers should have included patience, fun, having good knowledge about PA and being genuine in their relationship with the girls.
Both groups recommended that games should not be too childish and suggested focusing on topics such as making PA fun, how to fit PA into their day, how much PA to do and how to be a PS. Participants also suggested including role-play, reaction test games and parachute games.
Participants’ concerns about being a PS included peers not listening or disagreeing with what they said, not knowing what to say, being judged and teased.
These findings were used to refine the intervention content, including draft recruitment materials, PS training timetable and study logos, that were then further explored from the user’s perspective in the second round of focus groups.
Iterative focus groups: round 2
Methods
Participants were the same girls who had participated in round 1. A topic guide was developed to explore girls’ preferences for the study logo, feedback on recruitment materials, the PS training timetable, how best to communicate with PSs (e.g. using e-mails), how to make training fun and engaging, and dealing with potential bullying. Focus groups were between 40 and 42 minutes in duration, they were audio-recorded, transcribed verbatim and analysed thematically, as in round 1. Participants were each given a £5 voucher.
Results
The findings are similarly organised into Recruitment materials and Intervention content themes.
Recruitment materials
Suggested revisions to the recruitment materials included having less text and more pictures, emphasising the fun side and benefits of the training, giving further details of what the PS training would entail and reiterating that PSs did not have to be good at sport. Participants selected a favourite logo and guided the colour and the tag line ‘peer-power active girls’.
Intervention content
Incorporating yoga was a considered a good idea, but the word ‘yoga’ may be off-putting to some. Key points for creating a fun atmosphere included a non-serious environment, playing music at times and preventing individuals from dominating discussions.
Participants suggested bean bag games and further creative tasks, such as poster-making. Although participants from both groups thought the term ‘energiser’ was appropriate for activities to refresh the group, one group suggested the term ‘circle time’ was childish. Participants had concerns about PSs receiving support via e-mail, including being e-mailed by ‘strangers’.
Participants were asked about receiving e-mails to remind them of the PS role. Platforms such as Facebook were popular but pupils reported that its use was not permitted within school, thus preventing a school-based project from endorsing its use. The idea of contact via short messaging service (SMS) text was not raised by the students, but was supported when prompted. However, some participants raised concerns about sharing their personal mobile number with the research team and being contacted by ‘strangers’ (i.e. members of the PLAN-A team/trainers). Students also demonstrated inconsistent use of school e-mail, with some not using it and others checking it only in information technology lessons. A common theme for e-mail and social media contact was that participants did not want to be contacted too frequently (e.g. every few weeks was suggested as suitable).
Summary
Phase 1 resulted in the co-production of the draft PLAN-A, which was taken forward to pilot testing. The ASSIST intervention framework was successfully blended with the views and preferences of the user group. A description of how these findings were incorporated in to the final intervention is presented in Appendix 1.
Pilot study
Aims and objectives
The objective of the pilot study was to test the student recruitment approach and rehearse the peer nomination and PS selection processes, train the trainers and test the PS training (see Chapter 2, Description of the final intervention elements for details). In evaluating the delivery and receipt of the pilot intervention to identify refinements, the process evaluation methods were also piloted.
Methods
School and participant recruitment
Recruitment of the pilot school is presented in Recruitment and description of the pilot study school. A recruitment briefing was given to all Year 8 girls (N = 70; a new Year 8 cohort not involved in the formative work) to introduce PLAN-A and explain the role of the pilot school. Students were invited to ask questions and received parent and child information packs (distributed to absent girls by the school contact). Parents signed an opt-out form if they did not wish their child to participate. Parents of PSs provided written informed consent for their daughters to attend the training and PSs provided assent.
Peer supporter nomination, selection and recruitment
All consenting students completed a peer nomination questionnaire. The analysis of peer nomination questionnaires and the selection of PSs was carried out in accordance with the PLAN-A peer nomination standard operating procedure (SOP). This mirrored the ASSIST process: the 18% of students who received the most nominations were selected, with the aim of 15% of the year group being trained as PSs. Commensurate with ASSIST protocols, in which the cut-off point of 18% included multiple students, all of these students were invited to be a PS. Students who were selected to be a PS were invited to a meeting held within school that outlined what the nomination meant, the PS role and training. Students were provided with written information for themselves and their parents and were asked to provide written assent and parent consent to participate as a PS.
Trainer recruitment
A list of trainers was generated through local contacts and searches of sports development, youth work and health promotion organisations near to the pilot school. Two trainers were recruited to deliver the pilot PS training. In line with ASSIST28 and the AHEAD study,40 trainers were recruited to have between them a combination of subject (PA/health promotion) expertise and experience in teaching or leading groups of adolescents (e.g. theatre and/or youth work experience). Both trainers met informally with the principal investigator and project manager, who explained the study and informally assessed the trainers’ fit with the role.
Pilot train the trainers course
The two trainers received a 3-day training course, covering all aspects of the study (see Description of final intervention elements for a full description of the course). The training was provided by three study staff (MJE, KB and JM).
Pilot peer supporter training
The 2-day PS training was piloted in a venue close to the school site (see Description of final intervention elements). Following the training, PSs were asked to support their peers in school, as instructed in the training, for 5 weeks. This time was deemed sufficient for the girls to experience the PS role and to identify any challenges associated with it. Given the short time frame between the pilot study and the delivery of the intervention in the feasibility study, the top-up PS training was not included in the pilot.
Quantitative measures
Participant recruitment and retention
The number and percentage of participants who opted out of the study was recorded in addition to the number of girls attending peer nomination, the number of girls invited to be a PS and the percentage of girls who consented.
Peer supporter training attendance and adverse events
Trainers recorded the attendance of girls at each day of the PS training and reasons for absence. Trainers recorded adverse events and reported them to the research team.
Trainer questionnaire
Trainers completed an evaluation questionnaire following delivery of the PS training (see Appendix 2). The measures were adapted from a similar questionnaire used in the AHEAD study. 40 Achievement of PS training objectives was assessed through trainers’ perceptions that the training achieved key objectives of increasing PS knowledge, interpersonal skills, communication skills and confidence to be a PS using a four-point scale (0 = ‘not well at all’ to 3 = ‘very well’). Perception of the PS response to training was measured using four items (engagement, involvement, enjoyment and interest) and scored from 0 (‘not at all’) to 3 (‘very’). The training arrangements (e.g. suitability of training space) were rated on a five-point scale (0 = ‘poor’ to 4 = ‘excellent’).
Peer supporter questionnaire
Peer supporters completed an evaluation questionnaire at the end of the training (see Appendix 3) that assessed enjoyment, views on training content and logistics and perceived trainer autonomy support. Enjoyment of the training was rated using a five-point scale (1 = ‘not at all’ to 5 = ‘a lot’) and open text responses. Ten items assessed PSs’ views on the content and logistics of the training (e.g. ‘I understand my role as a PS’, ‘the length of the training was about right’) using a scale ranging from 0 (‘disagree a lot’) to 4 (‘agree a lot’). The Sport Climate Questionnaire53 measured PSs’ perceptions that trainers were autonomy supportive with five items (e.g. the PLAN-A trainers provided me with choices and options) anchored by responses ranging from 0 (‘disagree a lot’) to 4 (‘agree a lot’). The mean of the five items was derived to produce an autonomy support score for each training pair.
Observation of the pilot peer supporter training
A researcher who worked on the AHEAD study, and was familiar with the PS training approach, observed the PS training to assess fidelity. An observation form (see Appendix 4) was developed to record the timing of training components and to record whether or not individual activity objectives were met (0 = objective fulfilled ‘not at all’ to 3 = objective fulfilled ‘lots’). PS engagement was estimated from 0 (‘not at all’) to 3 (‘very’) for each activity. Notes documenting the extent to which trainers’ delivery style was need-supportive, elements that worked and those that did not were made.
Qualitative measures
Peer supporter focus groups
Focus groups with PSs (n = 10) were conducted at two time points: (1) the day after the second day of PS training (‘post training’) and (2) approximately 5 weeks after training (‘during intervention’). At both time points, PSs were divided into two groups of five. The post-training focus group guide focused on identifying improvements and participants’ experiences of the training and views on trainers. The during-intervention focus group guide examined the girls’ experiences of being a PS, feelings of preparedness, what actions they had taken, what had/had not worked and what their Year 8 peers thought of their role. Focus groups ranged from 25 to 30 minutes in duration.
Trainer interviews
Both trainers were interviewed separately (interview lengths were 63 and 52 minutes) by Kathryn Banfield. The trainer interview guide considered both the train the trainers workshop and the delivery of the PS training, including the content and logistics of training, what worked/what did not, potential changes and how to engage the PSs. Interviews and focus groups were recorded using an encrypted digital recorder (Olympus DS-3500; Olympus, KeyMed House, Southend-on-Sea, UK), then transcribed verbatim and anonymised.
Quantitative analysis
Quantitative data were analysed descriptively using means and SDs for each trainer or number and per cent of participants, as appropriate. Data from open-ended questions on the PS evaluation forms (e.g. ‘to make the training better you could . . .’) were reduced to qualitatively similar categories and a frequency count was derived.
Qualitative analysis
The framework method54 was used to produce a matrix for constant comparison to synthesise the data from the PSs and the trainers. This method facilitates the combination of inductive and deductive analysis. Data were analysed using the following steps:
-
Kathryn Banfield, Mark J Edwards and Joe Matthews read and re-read each transcript and listened to audio-recordings to become familiar with and write initial impressions of the data.
-
Initial codes for each informant group were created. For the purposes of deductive analysis, predefined codes were broad (Table 2). In addition, codes were inductively developed by the three researchers independently. To ensure consistency and agreement, each researcher independently coded the same transcript from each informant group.
-
The three researchers discussed the codes and agreed a refined set of codes that could be applied to the remaining transcript(s). An analytical framework was developed for PSs and trainers.
-
Each framework was applied to the remaining transcripts by the three researchers (KB, MJE and JM) using NVivo (version 10; QSR International, Warrington, UK). Each researcher applied the framework to a different set of transcripts (trainer, post-training and during-intervention focus groups) and this was cross-checked by another researcher to ensure consistency and agreement of coding. New codes that emerged were discussed and amendments were made to each framework.
-
Coded data were charted into a framework matrix in NVivo to summarise the data for PSs and trainers by category, including representative quotations.
-
Codes were interpreted and themes generated through frequent meetings to review the coding matrix. The three researchers (KB, MJE and JM) agreed on illustrative quotations.
The frameworks were triangulated between informant groups to assess convergence.
| Code | Informant group | Description |
|---|---|---|
| Recruitment/initial involvement | Trainer and PS | How the participant(s) became involved, thoughts on the recruitment process and reasons for involvement |
| Training the trainers | Trainer | Thoughts on the logistics of the training (venue, length and resources) and the content |
| PS training logistics | Trainer and PS | Views on the training venue, timings, length and catering for the training |
| PS training content | Trainer and PS | What was enjoyed and what was not, activities or elements of the training that worked and did not work. Any improvements to the content or adaptations made to activities |
| Delivering the PS training | Trainers | Experience of delivering the training to the girls, how prepared they felt and difficulties they had |
| Impact of the PS training | Trainer and PS | Evidence of how the training helped the girls become PSs or how it has developed their skills |
| Views on trainers | PSs | What the trainers were like and their delivery style |
| Impact on other girls in Year 8 | PSs | What PSs have done to encourage other girls to be active and whether or not they were successful |
| Support for PSs | PSs | Whether or not the PSs helped each other, whether or not they needed help and how the study can encourage them to peer support |
| Need support | Trainer and PS | Evidence of trainers providing autonomy support by providing positive feedback, offering choice, setting out clear expectations and being empathetic. It also includes evidence of genuine interest in the girls’ lives and nurturing individual interests |
Qualitative notes collected by the observer were used as a reference point for intervention refinements only. Formal analysis was not conducted. The qualitative and quantitative findings were blended to provide a rich mixed-methods evaluation.
Results
Participant recruitment, peer nomination, peer supporter selection and recruitment
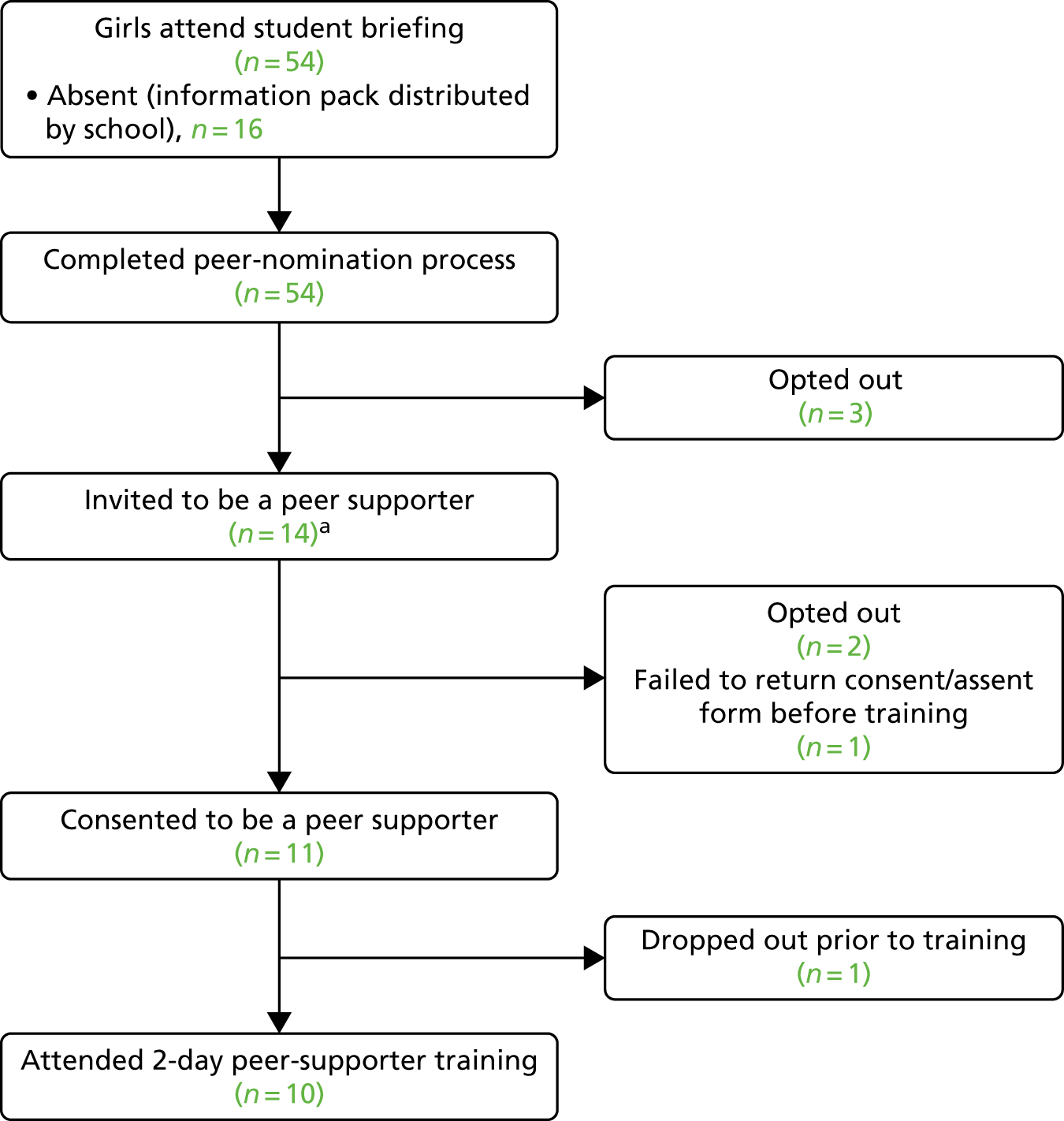
Participant recruitment flow is summarised in Figure 3. Of the 70 Year 8 girls, 54 (77%) attended the study briefing. Three (4%) study opt-out forms were returned. A total of 54 girls completed the peer nomination questionnaire, and the two researchers who led this process were satisfied that no amendments were required. The PS selection process was successful and 14 girls (20%) were invited to be a PS, all of whom attended the briefing meeting. The meeting was well received and 11 girls (16%) provided assent and parent consent to participate in the training.
FIGURE 3.
Flow diagram of PS recruitment in the pilot study. a, Number of Year 8 girls invited to PS meeting was > 18% as, in accordance with the ASSIST protocol, any student with an equal number of nominations as the final nominee was also invited to the training.
When PSs reflected on the peer nomination process they commented that the majority of PSs were from the same friendship group (many from the netball team) and believed that most of their friends were physically active:
. . . a lot of the people chosen are from the same friend group anyway, so there’s a lot of different people in the school who won’t have any friends that will have been voted for . . .
Post-training focus group 1
One participant suggested that rewording the peer nomination form to refer to ‘their closest friends’ could increase the diversity nominations across friendship groups:
I think maybe if you’d got everybody to write down, I don’t know, their five closest friends, then you could have a person from every friendship group.
Post-training focus group 1
Reasons PSs gave for wanting to be a PS included wanting ‘to help me help more people’ and personal skill development:
. . . you could benefit a lot of skills, not just for use in school but for when you get older for your jobs and stuff like that.
Post-training focus group 1
One participant took part because she thought the course would be focused on playing sports:
I thought it was to do with sports, to be honest.
Post-training focus group 2
During the PS meeting, participants suggested that they would prefer to wear PE kit, which the school contact agreed with. For the feasibility study, a decision was taken to recommend that the girls wear comfortable, casual clothing so as to (1) highlight that the training is not a sports event, (2) avoid the potential negative connotations of PE or PE kit for some PSs and (3) separate the PLAN-A training from school.
Recruitment of trainers
Two female trainers were recruited and, as planned, shared a mixture of expertise in delivering PA/sports coaching to young people, and in theatre and youth work settings.
Train the trainers
Overall, the training was delivered according to plan with little deviation from the schedule. Key feedback from the trainers was to provide more active, hands-on activities early in the training, before agreeing the group rules.
Intervention materials
All training and intervention materials, including the session plans and trainers’ guide, were seen as useful and clear. One trainer felt that the session plans presented too much information for use in the training (see Chapter 2, Peer supporter training, Logistics and resources).
Structure and venue
Trainers felt that there was insufficient training time for them to understand the content of the activities and allow them to ‘sink in’ (Trainer 1) and that the training was carried out too far ahead of the PS training delivery. Both trainers suggested lengthening the training to allow more time to practise each activity rather than just talk through them. The venue was considered satisfactory, but too small:
I think you could have done more learning by practise, by doing, because then you actually fully understand what the exercise is and how it works and what you’re trying to get from it.
Trainer 1
The training was well received, with clear information delivered with sufficient depth. Trainer 2 felt that there could have been more detail on the background of the project that they could disseminate to PSs:
If you went through it [background information] a little bit more, I think when we then said it to the girls I think it might have flowed a lot better rather than just saying, ‘OK, that’s that.’ It might have been nice to go in depth.
Trainer 2
Feelings of preparedness
Both trainers felt insufficiently prepared to deliver the PS training based on the train the trainers event alone. One trainer revisited the content in their own time, the other wanted to but did not have time:
There maybe needs to be another couple of hours added on, to maybe 2 top-up days, just to really go through it . . . I don’t think I was prepared enough in terms of knowing each activity off by heart.
Trainer 2
In response to this, the week before delivery of the PS training, a half-day meeting was held to allow trainers to prepare. The trainers found the extra meeting useful and the timing, structure and content of the 3-day train the trainers event was revised in light of these findings.
Peer supporter training
Attendance
Attendance was 91% (n = 10) at both training days; one girl did not attend because of a disagreement with another PS outside the PLAN-A training.
Logistics and resources
The PS training space and venue were rated ‘adequate’ by both trainers (Figure 4) and PSs (see Figure 7). This was largely because of its small size and lack of break-out space. This led to an environment in which it was difficult to concentrate. The observer also felt that the layout of the room (including a lack of tables) led to a very informal learning environment. Trainers and PSs rated the refreshments for the training highly (see Figures 4 and 7).
FIGURE 4.
Trainer ratings of PS training arrangements.
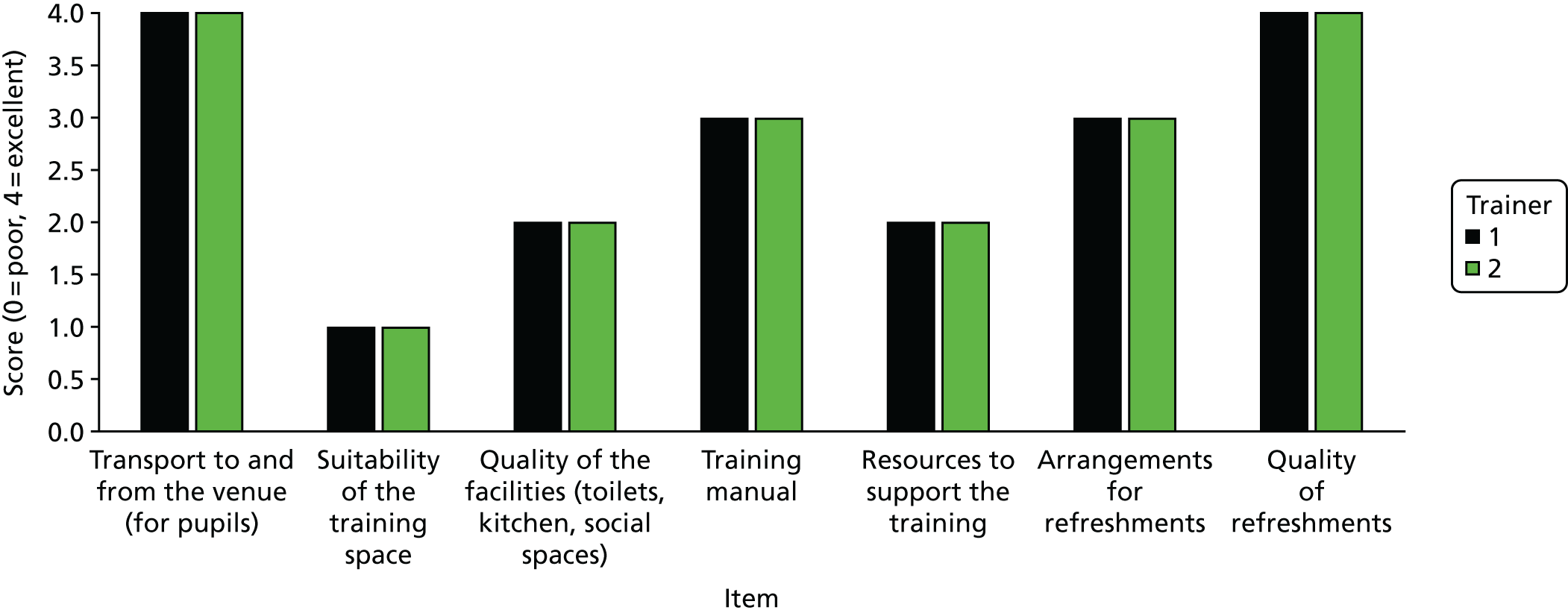
The training manual and resources were considered to be ‘very good’ and ‘good’, respectively, by the trainers (see Figure 4). Trainers agreed that the session plans were helpful and clear, but suggested condensing the quantity of information to make delivery easier:
There’s too much going on on the page . . . I don’t think you can take that in and use that as a thing to use in the classroom, for me.
Trainer 1
As a result, cue cards were developed that allowed the trainers to write their own notes about each activity to use in the PS training.
The girls found the PS booklets to be a helpful prompt of key information and good to show others what they did. They suggested that the booklet should be used more for reference by PSs rather than using it to write in during the training:
If you were to forget something, then you have a booklet to look back on. I feel maybe instead of copying it down you could have it written on the board and already written in the booklet.
Post-training focus group 2
The PSs felt that the PS diaries were a good idea; however, during the intervention the girls reported not using them because they forgot about them or did not want to record conversations:
I just don’t need it. I just can’t be bothered with it.
During-intervention focus group 2
Fidelity to the session plans
Given the time constraints, on day 1 two activities were not delivered: the ‘thought shower: why be active?’ (10 minutes in duration) and ‘post box’ (10 minutes in duration) activities. On day 2, the ‘relaxation activity’ (5 minutes in duration) was excluded.
The allocated time and observed delivery time for each activity are shown in Appendix 5. On day 1, three out of nine activities before lunch took more time than allocated to deliver (e.g. ‘what do we know already?’). Lunch was slightly longer than scheduled, which resulted in activities after lunch being excluded or shortened. On day 2, activities before and immediately after lunch were an average of 12 minutes longer than scheduled, again leading to activities in the afternoon being given less time. Qualitative findings supported the observations: trainers felt that there was too much content to deliver and a lack of time for discussion. As a result, both trainers suggested that the training should be extended and more time should be added for discussion:
It’s too much in 2 days . . . I think it would have been nice to spread it over 3 days if you keep the activities, have a bit longer for each of them.
Trainer 2
The observer recorded that trainers added in active games to energise girls when necessary. Despite intending to benefit the girls, these contributed to the drift from the schedule. In addition, the observer noted that trainers could have shortened some sessions that were longer than intended:
Too long was given for discussions amongst small groups/activities . . . The girls would then talk about ‘off task’ things . . . time could have been used better.
Observation note
The extent to which PS training objectives were met is reported in Table 3. For timetabled sessions that comprised more than one distinct activity, the mean objective fulfilment is reported. Seven activities (41.18%) across both days were not rated. The mean rating for activities was 3.00, suggesting that objectives were achieved. However, fulfilment of objectives was lower (1.00) for activities at the end of day 2.
| Day | |||
|---|---|---|---|
| 1 | 2 | ||
| Activity | Fulfilment, mean (SD) | Activity | Fulfilment, mean (SD) |
| Introduction | 3.00 (–) | Empowering girls’ confidence | 3.00 (0.00) |
| Getting to know each other | 3.00 (–) | Holding conversations | 3.00 (0.00) |
| Knowledge is power | 2.67 (0.58) | Communication skills | 3.00 (–) |
| Recognising your skills | 3.00 (–) | Gathering information | 3.00 (–) |
| A day in the life of a Year 8 | 3.00 (0.00) | Tricky issues | 1.00 (–) |
| Busting barriers | 3.00 (–) | Finishing up | 1.00 (–) |
| Day average | 2.89 (0.33) | Day average | 2.50 (0.93) |
| Average objective fulfilment | 2.71 (0.69) | ||
Both trainers felt they successfully enhanced PSs’ knowledge about PA, communication skills, interpersonal skills and understanding of their PS role (Figure 5). The objective to enhance PSs’ confidence to spread informal messages among their peers was not met well (1.5 ± 0.71); this supports PSs’ reported low confidence in this area (see Peer supporters’ experience of training).
FIGURE 5.
Trainer-rated achievement of pilot PS training objectives.
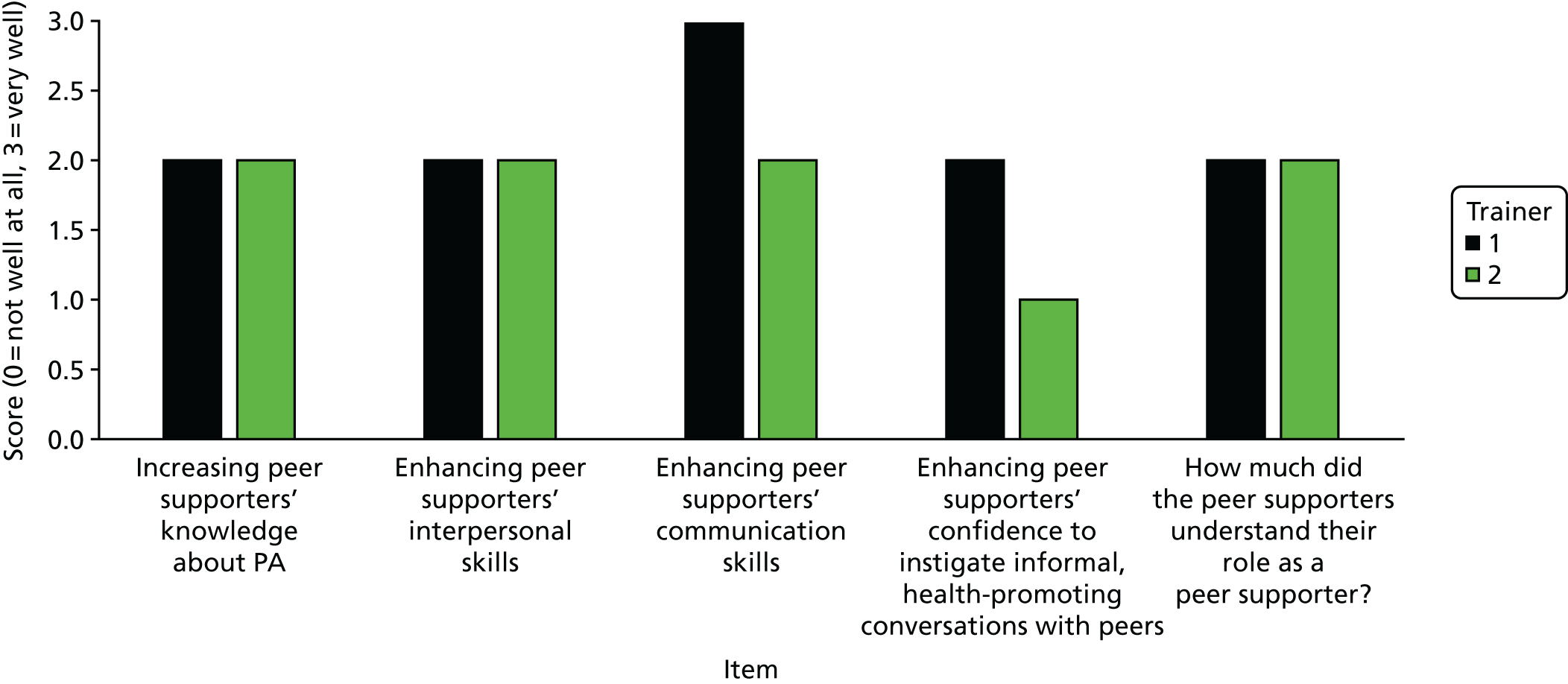
The qualitative data gave insight into why some objectives were not achieved fully, including losing focus because of activities over-running (and other activities being rushed), omitting key activities and trainers not being clear on general group rules:
When it came to the core message of it and becoming a PS, I think we did not do enough because we physically did not have enough time.
Trainer 2
Peer supporters’ experience of training
Peer supporters’ engagement with training was high on day 1 and slightly less so on day 2 (Table 4). A need to maintain engagement in the ‘communication skills’ and ‘finishing up’ activities was identified.
| Day | |||
|---|---|---|---|
| 1 | 2 | ||
| Activity section | Engagement, mean (SD) | Activity section | Engagement, mean (SD) |
| Introduction | 3.00 (–) | Empowering girls’ confidence | 3.00 (0.00) |
| Getting to know each other | 3.00 (–) | Holding conversations | 3.00 (0.00) |
| Knowledge is power | 3.00 (0.00) | Communication skills | 2.00 (0.00) |
| Recognising your skills | 3.00 (–) | Gathering information | 3.00 (–) |
| A day in the life of a Year 8 | 3.00 (0.00) | Tricky issues | 3.00 (–) |
| Busting barriers | 3.00 (–) | Finishing up | 2.00 (–) |
| Day average | 3.00 (0.00) | Day average | 2.67 (0.50) |
| Average engagement | 2.83 ± 0.38 | ||
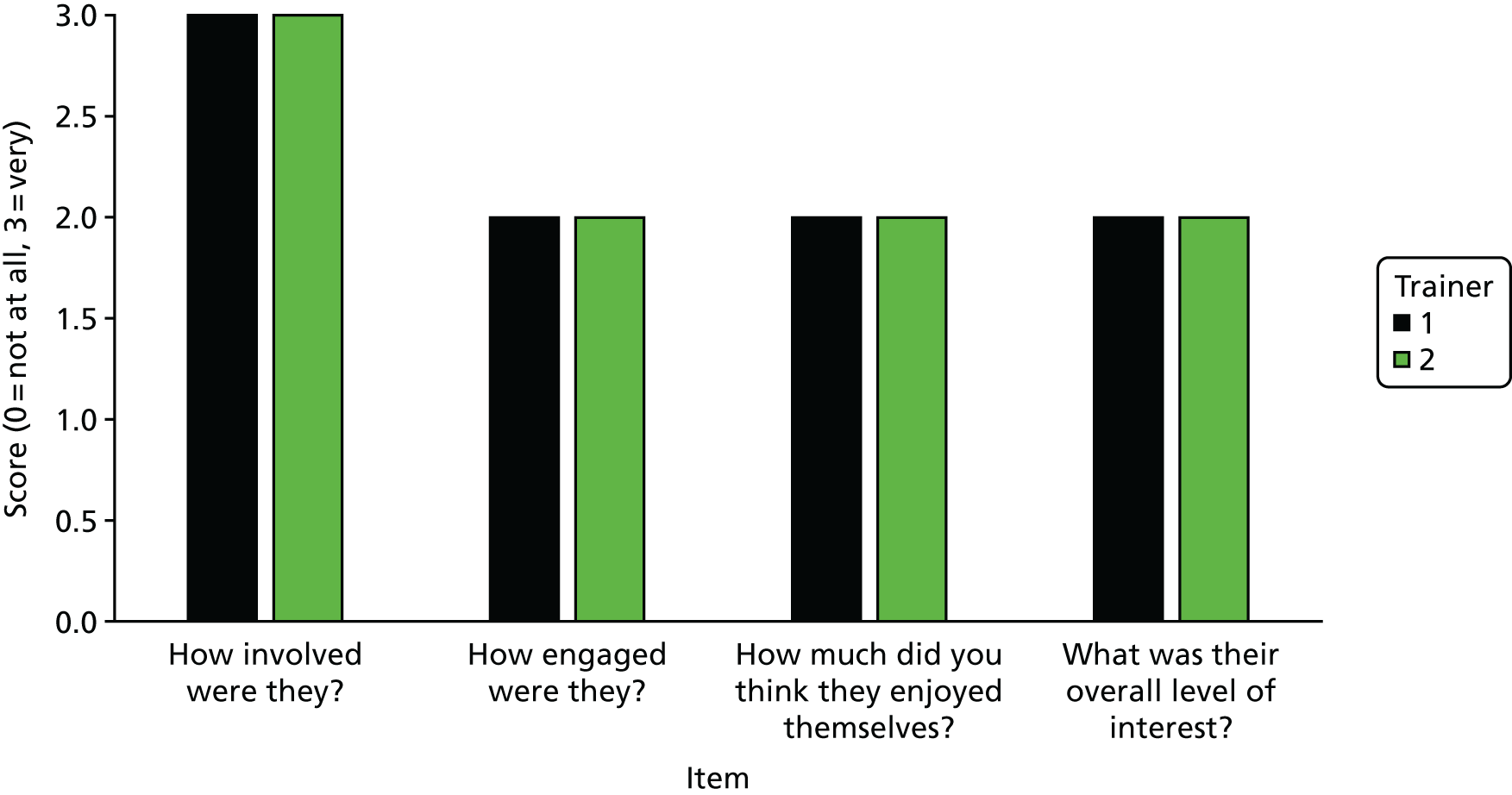
Figure 6 shows that the trainers felt the PSs were very involved throughout the training. They perceived the PSs to be somewhat engaged and interested. PSs wanted to discuss topics and ask questions throughout:
Every time we did something they wanted to talk about it. They were quite chatty and so they wanted to talk about things.
Trainer 1
That was quite good because you had to debate your point. That was quite good.
Post-training focus group 1
FIGURE 6.
Trainers’ ratings of PSs’ responses to the pilot training.
Girls were particularly engaged in activities that they could relate to and that involved being active:
It worked well because the video is so powerful. It was a ‘visual’ and some of them probably can relate to that . . . that’s why, because they can relate to those questions.
Trainer 2
However, although most activities were rated as highly engaging, there was evidence of some boredom, fatigue and distraction because of the ineffective timings of activities (i.e. rushing activities at the end of day 2), overuse of writing rather than more physical tasks and a disagreement between PSs on day 2:
Some silly[ness], some look bored [afternoon] day 2? Lethargic.
Observation notes
Some became distracted or I saw it in their face. OK, they might be looking but I could see they’re still not there.
Trainer 2
I just think there could have been more activities. . . . We probably learn more by doing stuff than writing because I think we get a bit bored writing.
Post-training focus group 1
Enjoyment over the 2-day training was moderate to high and was marginally higher on day 2 (3.80 ± 0.79) than on day 1 (3.30 ± 0.68). Open-ended responses revealed that all girls enjoyed the ‘listening train’ activity most and 60% felt they were good at role-play tasks. Activities that were more active and involved discussion and debate were also enjoyed, which supported trainers’ perceived drivers of engagement (see above):
I liked the big discussion we had about fitness between boys and girls and self-confidence. I liked that big debate.
Post-training focus group 2
Peer supporters believed that the training helped them understand their role; they enjoyed the games and learnt something new (Figure 7). Eighty per cent reported five different facts they learnt about PA in free text. The PSs felt prepared to support their friends by enhancing their knowledge, confidence and ability to empathise with others:
It does actually work, that you feel like you can go out and talk to people about it. It’s not just something that you do and then you forget about it.
Post-training focus group 1
Like, if one of your friends has an insecurity, you know how to understand them and how to talk to them about it.
Post-training focus group 1
FIGURE 7.
Peer supporter ratings of pilot training content.
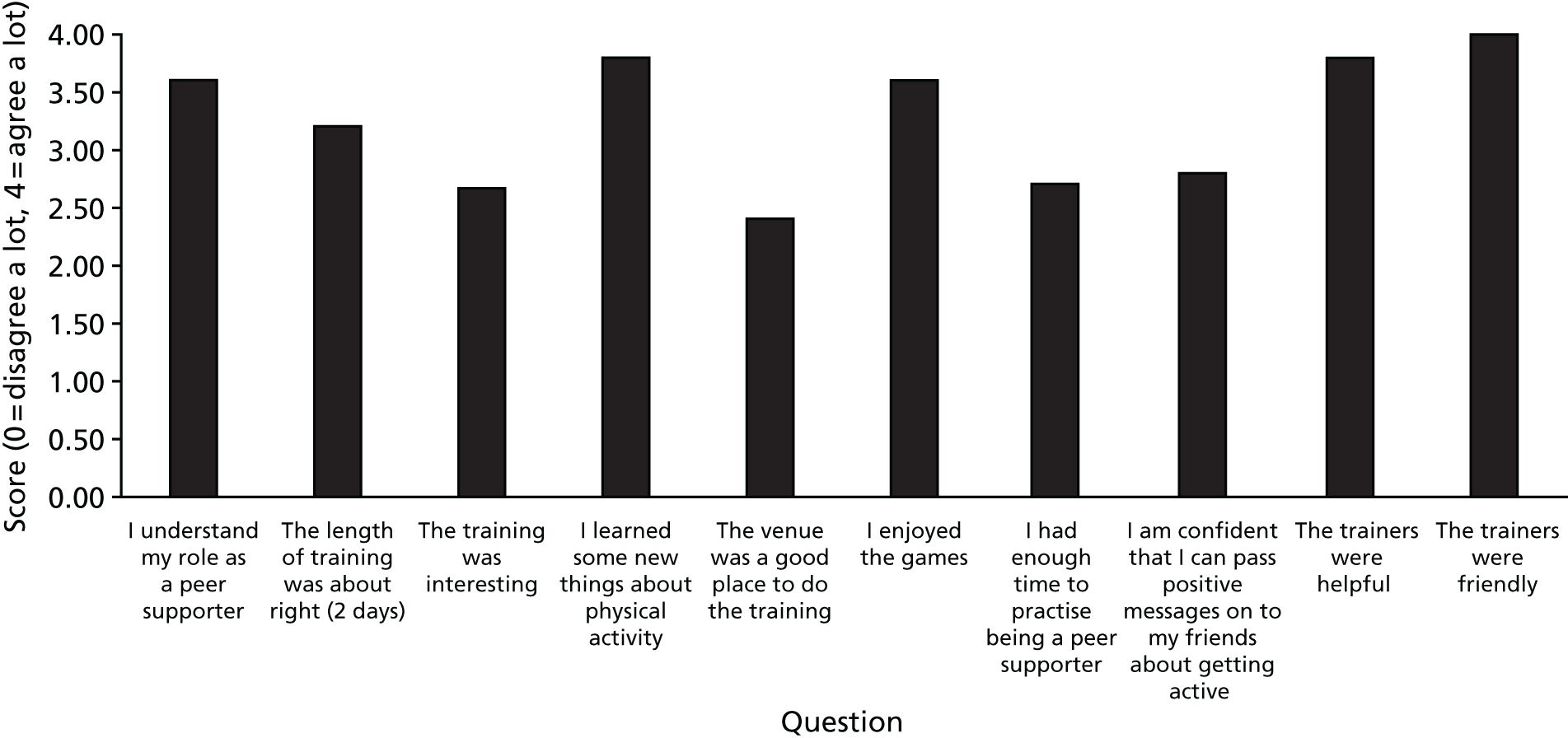
Trainers expressed concerns about the PSs’ ability to be realistic about how to peer support. This was also reflected in observation notes that questioned how empowered the girls were to make changes at school. Similarly, 60% of PSs suggested that more time could be devoted to practising being a PS, which would further enhance their confidence to be a PS (see Figure 7). Some PSs were unsure of how to use the facts they had learnt or how to start a conversation with their peers:
It feels like if we have all these facts – like, you can’t just casually slip a fact into, like, a conversation that you’re having with someone.
During-intervention focus group 2
Peer supporters thought that including more activities that focus on building confidence would improve the training:
Like with the confidence, we didn’t go a lot over how to be confident.
Yeah, because that’s like a major thing. If you’re going to help someone else you need to be confident in yourself as well.
Post-training focus group 1
Need-supportiveness of trainers and perceptions of need-support
On average, PSs reported relatively high levels of trainer autonomy support (3.42 ± 0.47; range 2.80–4.00) and thought that trainers were helpful (3.80 ± 0.42) and friendly (4.00 ± 0.00). Similarly, the observation documented that the trainers circulated among the girls, interacted with them and helped them with their tasks. The girls respected the trainers, commenting that they were different from teachers, made the training fun, were trusted, not boring and ‘understood us more than actual teachers’:
If you said something to them, you really felt you could trust them. They were just very friendly and stuff.
Post-training focus group 2
Autonomy support
Trainers provided autonomy by giving PSs choice within a structure of clear instructions and the opportunity to lead discussions and express their opinions:
They gave us lots of choices. They kind of said what to do but then they were giving you choices of how to do it, which was better than everybody saying, ‘you’ve got to do it like this’.
Post-training focus group 1
Trainers empathised with the PSs, and when the training required concentration or when engagement was low, they responded by incorporating elements that they felt the girls enjoyed:
In the lunchtimes, they were desperate to move. We were getting the tennis balls out and [Trainer 2] got some tunes on and was getting them dancing.
Trainer 1
Trainers frequently provided competence-based feedback, praising the girls’ efforts. Trainers circulated around the group asking questions and they provided help when needed. Both trainers reinforced the girls’ understanding of activities and provided them with the skills to become a PS, in particular ensuring that the girls were realistic about their role:
We talked a lot about being realistic. You’ve got to be realistic, so it’s not saying, ‘Right, let’s go for a 2-hour run.’ ‘Oh, but I don’t like running.’ Where do you go from there? ‘I want to watch TV.’ ‘Let’s go for a half-hour walk and then come and watch TV.’ So it’s that compromise . . .
Trainer 1
Trainers explicitly tried to help the PSs understand their role and spent time empowering the girls’ confidence to be a PS:
I think if they feel confident and empowered then they can go off and do anything. And I know that was quite a big part of the course, and I think we spent a lot of time doing that and I hope and think that went in.
Trainer 1
PSs, competence may have been undermined when the trainers rushed activities. Sometimes the PSs felt confused, and trainer 2 felt that some core messages were missed because of time constraints:
When it actually came to the core message of it and becoming a PS, I think we didn’t do enough of because we physically didn’t have enough time.
Trainer 2
Both trainers endeavoured to, and were successful in, forming trusting relations with the PSs within the short training window. Trainers valued the PSs’ opinions, empathised with them and were interested in them as individuals. The PSs described the trainers as ‘friends’ and felt that the trainers understood them:
They [the trainers] related well to the girls and their delivery style supported SDT. Connections between the girls and with trainers [are] clear.
Observation notes
They were trusting. If you said something to them, you really felt you could trust them. They were just very friendly and stuff.
Post-training focus group 2
I could see they’re still not there [engaged], and when they sat down is when I suggested different ideas as a group, because I know when I was that age I was a really, really shy girl so I wouldn’t want to say anything.
Trainer 2
Experience of being a peer supporter
What girls did to peer support
The PSs reported engaging in little peer-supporting activity. Efforts to peer support included suggesting active travel and leading by example:
We went to the gym last year just before the end of term, and, we kind of spoke to everyone about it, like a few of our friends. And then they invited a few of their friends to go.
During-intervention focus group 1
One of my friends, we were, coming back from town or something. She was like, ‘Oh, no, I’ll get my mum to pick us up.’ I was like, ‘Why can’t we walk, to get some exercise?’
During-intervention focus group 2
PSs felt that they encouraged their peers to walk more or go to the gym:
And [girl name] and [girl name] house are, like, an hour away from each other, and we walked, like, all the way.
During-intervention focus group 2
There were a number of instances of PSs talking to family or non-female Year 8 peers:
I had a conversation with this year seven, who was in my tutor [group].
During-intervention focus group 1
Challenges of being a peer supporter
The main challenges and reasons many girls did little peer supporting was that they lacked confidence in approaching peers and encouraging them to be active, particularly peers whom they did not know:
A bit awkward if I just went up to someone and told their friends. It would be a bit weird to just come up to her in person.
During-intervention focus group 1
Despite the PS training dedicating sessions to the when, where and how of starting conversations and overcoming challenges, a barrier to PS activity was knowing how and when to start a conversation. Participants suggested including more activities in the training to support this:
You might have told us, like, how to start the conversation or something. Because, in a conversation, we don’t really – it doesn’t really bring it up that much.
During-intervention focus group 2
Participants also reported that many of their friends are already active:
Most of the girls in our class are already really active, so it’s kind of not really.
During-intervention focus group 2
Perceived impact of the Peer-Led physical Activity iNtervention for Adolescent girls
The main impact that PSs perceived their role to have was improving their confidence and increasing their PA:
But it’s got me a lot more active, and it’s boosted my confidence a lot.
During-intervention focus group 1
The NPS Year 8 girls appeared to be aware of PLAN-A and were interested in it; however, PSs felt that it would be beneficial to have posters or to do a presentation to the rest of the year to raise awareness and help make their role easier:
I think more like getting all the girls together and talking about it, so, like, having like a presentation about what we’ve done because then all the girls will be in the room and nothing to be ashamed of.
During-intervention focus group 1
Ancillary accelerometer study
In addition to testing the intervention design, data collection methods were also tested with the pilot school. Year 8 girls from the pilot school were asked to wear either waist or wrist accelerometers, or both, for a short period; their thoughts about these different methods were qualitatively assessed to inform data collection for the feasibility trial (see Appendix 6).
Implications of phase 1 findings on the Peer-Led physical Activity iNtervention for Adolescent girls
The formative research carried out in phase 1 facilitated a user-centred refinement of the ASSIST intervention to form PLAN-A. The pilot study allowed the school, student and PS recruitment methods to be tested and refined. In addition, the peer nomination activity, train the trainers and PS training were delivered, rehearsed and critiqued. The key implications of the formative work and pilot study for the design of these intervention components are presented in Appendix 1.
Description of final intervention elements
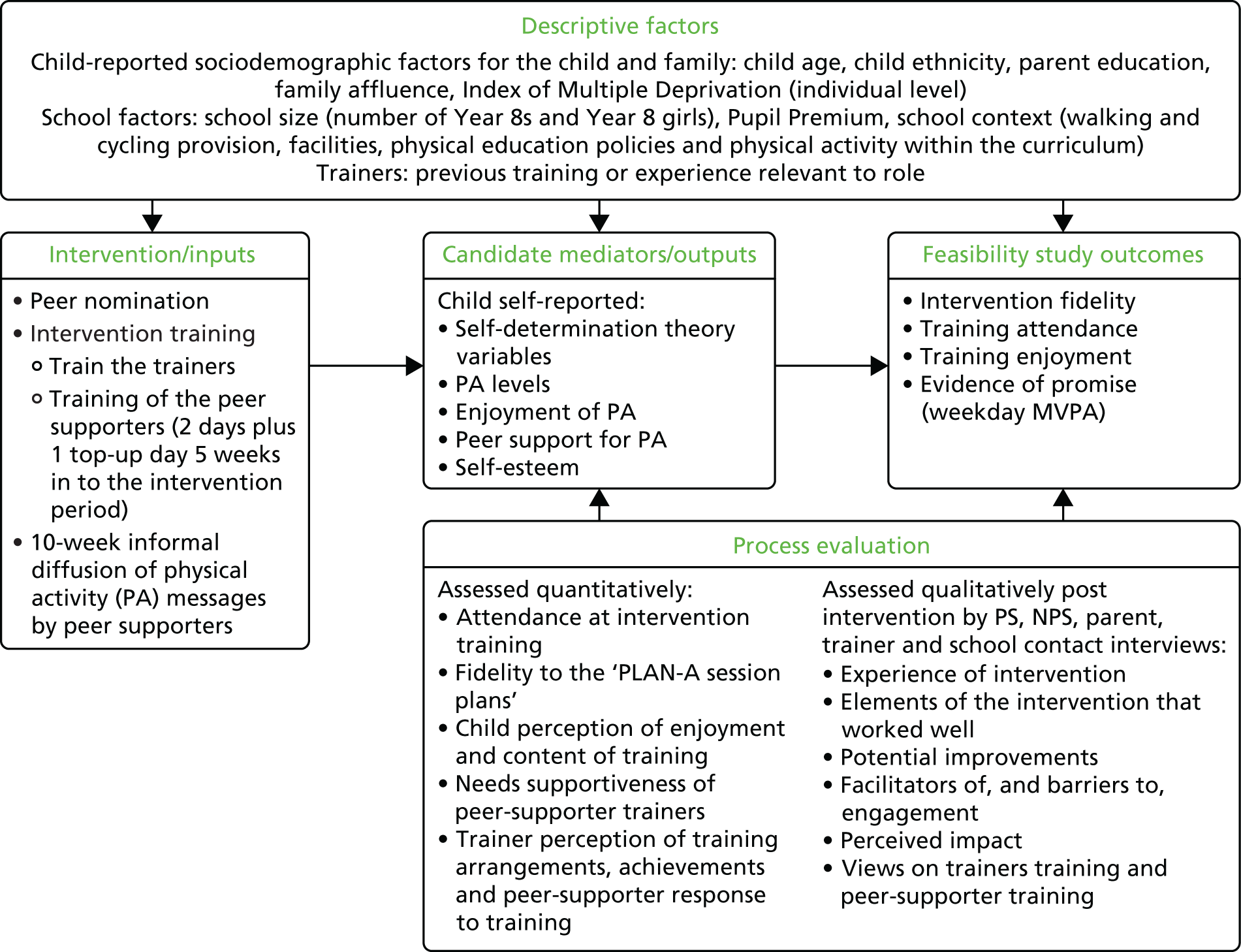
Figure 8 depicts the PLAN-A project logic model, including the process evaluation approaches taken to assess outputs and outcomes in addition to school context. The resources and elements of the intervention that were tested in phase 2 are presented in Table 5.
FIGURE 8.
The PLAN-A logic model.
| Intervention element | Description | Materials/resources needed |
|---|---|---|
| Peer nomination and selection | Peer nomination instructions read to all participating Year 8 girls, who then complete the peer nomination questionnaire | Peer nomination questionnaires and pens. Register, including list of girls who have opted out |
| Peer nomination analysis | Analyse the peer nomination questionnaires to determine which Year 8 girls will be invited to be a PS | Completed peer nomination forms, register and PLAN-A SOP for peer nomination analysis |
| PS meeting | Briefing for girls who have been nominated to be a PS. Explain the nomination and describe the PS role. Include time to answer questions | Student and parent information sheet, student assent form and parent consent form |
| Train the trainers 3-day workshop | 3-day training event, delivered by two PLAN-A staff, for the PS trainers. Training includes the theoretical underpinnings of PLAN-A, intervention content and time to practise delivery of the PS training activities. As delivery of the PS training is in pairs, the training provided opportunities for trainers to plan their delivery | Train the trainers Microsoft PowerPoint® (Microsoft Corporation, Redmond, WA, USA) presentation manager slides, 3-day training schedule and for each trainer a ‘trainers’ guide’ and ‘PLAN-A session plans’. A PLAN-A resources pack for each trainer pair that will be used to deliver the PS training (see below). In addition, an information leaflet detailing the logistics of each session |
|
||
| PLAN-A session plans (PS training): details on the objectives, resources, time required, how to set-up and deliver each activity across all 3 PS training days. Sections about how to use the manual and additional information (i.e. FAQs) | ||
| PS training (initial 2 days) | A 2-day training event for PSs that takes place within usual school hours. Preferably delivered at a venue off the school site, with catering and transport arranged by study staff. A staff member from the school will chaperone the PSs to the training and be available if any behaviour issues arise. Two trainers lead the PSs through PLAN-A material and prepare them for the role of a PS | PLAN-A resources pack used to deliver the training, including the PS booklet and diary (see below) |
|
||
| PS booklet and diary: a booklet including information about PLAN-A and the role of a PS, including tips, information and worksheets about activities from the training. A diary also forms part of this booklet, including useful links, tips and reminders about how to be a PS | ||
| PS training (top-up day) | A mid-intervention (approximately 5 weeks after the initial training) training day to refresh PSs on the aims and importance of their role and extend their knowledge of PA and being a PS. An opportunity to discuss any barriers to, or issues faced in, their role so far. Preferably use the same pair of trainers that delivered the initial 2-day training to maintain rapport | PLAN-A resources pack used to deliver the top-up training (see above) |
Self determination theory was used to inform the delivery and content of the PS training (Table 6). In terms of delivery, trainers were trained to facilitate the PS training in ways that support autonomy (e.g. empowerment to support peers and provide choice), competence (e.g. confidence in how to be an effective PS and support one’s peers’ competence to be active) and belonging (e.g. supportive network of PSs and being a trusted friend to one’s peers). The PS training was designed to encourage PSs to recognise and promote autonomous rather than controlled motivation for PA (focusing on health, challenge-seeking and social affiliation reasons rather than appearance and peer pressure), to support their peers’ needs for autonomy, competence and belonging and use autonomy-supportive language when diffusing PA messages (e.g. ‘I’m going to walk to school, will you come with me?’ versus ‘you need to do more activity so you do not get fat’).
| Training session/activity/tasks | Behaviour change technique56 | Behavioural mediators |
|---|---|---|
| PA content | ||
| PA knowledge: examining pre-existing knowledge, exploring PA myths, interactive tasks to find out what counts as PA, PA recommendations and levels of PA in adolescent girls |
|
Knowledge and competence |
| Fitting PA in: PSs analyse ‘A day in their life’, identify existing PA and sedentary time and places and means by which to add in PA. Working with others to support them to identify how to fit PA into daily life and practical activities to reduce sedentary time in a range of situations |
|
Autonomy, competence and relatedness |
| Busting barriers: identification and discussion of barriers adolescent girls face to being active. Problem-solving tasks to ‘bust’ the barriers |
|
Autonomy, competence and relatedness |
| Confidence and competence: watching a short video about girls’ PA stereotypes, discussing beliefs in groups and empowering through focusing on self-esteem and past success |
|
Autonomy, competence, relatedness and self-esteem |
| Goal-setting: learning how to set ‘SMART goals’ and planning two PS/activity goals |
|
Autonomy and competence |
| PS content | ||
| Identifying personal PS attributes: self-reflection on personal skills and interests which may make them a good PS |
|
Competence and self-esteem |
| Identifying PS skills: group work to develop a list and then pyramid of the most important PS skills |
|
Competence and autonomy |
| When, where, who: activity to identify the timing, situations and social circumstances in which to give peer support |
|
Competence and relatedness |
| Listening skills: interactive games to highlight key skills related to listening to peers about being active |
|
Competence and relatedness |
| Communication skills: written and practical role-play activities building awareness of communication skills and practising their use |
|
Competence and relatedness |
| PS role-play: reinforcement of key PA information/learning and combination with simple role-plays using sentence starters (e.g. ‘I was at this training the other day . . .’) |
|
Autonomy, competence and relatedness |
Template for intervention description and replication checklist
Table 7 summarises PLAN-A in accordance with the Template for Intervention Description and Replication (TIDieR) checklist. 57
| Item | Description |
|---|---|
| 1. Name | PLAN-A |
| 2. Why? | The primary aim of this study was to assess the feasibility of the PLAN-A peer-led intervention designed to increase the PA levels of adolescent girls. The aims of the feasibility study were to estimate recruitment, retention and attendance rates and examine the acceptability of the intervention to schools, trainers, PSs, NPSs and parents. The study also sought to test the feasibility of data collection and assess data provision rates, as well as examine the intervention’s effect on accelerometer-derived MVPA. An additional aim was to estimate school-related ICC for daily MVPA and sample size for a definitive trial |
| The MVPA levels of girls are lower than boys throughout childhood and adolescence, and they decline at a steeper rate. As girls become older, it is thought that this decline can be contributed to not only changes in their social context (friendship groups/peer support), but the perception of significant barriers to PA that begin to emerge. Research suggests that there is an urgent need for effective PA interventions for girls, and harnessing peer influence may be the answer | |
| Peers, through peer support, PA co-participation and creating positive peer norms for PA, can play a central role in adolescent girls’ PA. Social network research has also revealed that children within the same friendship group tend to have similar activity levels and may alter their activity levels to match their friends | |
| Utilising ‘peer power’ in an intervention alone may not be enough to see positive changes in PA behaviour. PLAN-A is based on the fundamental framework for using such influential change agents (PSs), DOI theory, as well as SDT, which aims to foster autonomous motivation for PA by satisfying autonomy, competence and social belonging among the girls. PLAN-A has the potential, therefore, to positively influence girls’ PA behaviour and motivation to be active | |
| 3. What? (Materials) | Training (train the trainers) was provided for the trainers hired to deliver the PS training. The training took place over the course of 3 consecutive days. Content covered the concept and principles behind PLAN-A, the theoretical underpinnings of the intervention, how to deliver the training to uphold these (particularly when in a challenging environment) and a rehearsal of all the activities that formed the PS training. Slides were used to support delivery |
| Each trainer was provided with a ‘trainers’ guide’ introducing PLAN-A (including its rationale and aims), detailing SDT principles, their role as a trainer, any practicalities or logistics, how to use the ‘session plans’ and a run through of the train the trainer training days | |
| The ‘PLAN-A session plans’ comprised a complete guide to all the activities to be delivered during the 2-day and top-up day PS training. The manual gave exact details of each activity, as well as resources needed, how to prepare and objectives for each activity | |
| Each PS received a PS booklet combined with a diary. Each trainer pair received a resource pack containing worksheets and materials to help deliver the training, as well as any technical equipment needed | |
| The booklet contained supporting materials and answers to various activities held within the training. The diary provided the PSs with an opportunity to record and reflect on the conversations they may have had with peers | |
| 4. What? (Procedures) | Recruitment letters were sent to secondary schools in the South Gloucestershire and Wiltshire council areas. Once schools expressed interest, a meeting was held between the PLAN-A project manager and the school contact for further discussion and to obtain a signed study agreement form. A student recruitment briefing was then held for all Year 8 girls in which they were told about PLAN-A and given information packs for themselves and their parents. Parents signed an opt-out form if they did not wish their daughter to take part |
| Peer nomination and data collection were held in all schools. Schools were then randomly assigned to intervention (n = 4) or control (n = 2) groups and were made aware of their allocation post-T0 data collection. This gave the schools and study team sufficient time to organise the PS training. Peer nomination analysis was completed for each intervention school | |
| A PS meeting was held with all the nominated PSs from each intervention school. This covered details about the role of a PS and the logistics and content of the PS training. PSs were given information packs for themselves and their parents. PSs had to return a signed parent consent and student assent form in order to attend the PS training | |
| All PSs received an initial 2-day PS training, delivered by two trainers. Half way through the intervention period they received a top-up day training session. The training gave the PSs the skills, knowledge and confidence to fulfil the role of a PS. Once training was complete, PSs returned to school and spread informal messages encouraging their peers to be active | |
| A process evaluation, using quantitative and qualitative methods, was conducted throughout the study to identify areas of success and required improvement. It also examined the acceptability of the intervention and its design, as well as assessing mechanisms of impact. PSs training attendance was recorded by trainers, and observations of each trainer pair on the 2-day and top-up day training were carried out to assess intervention fidelity, logistics and PS engagement. PSs and trainers completed a post-2-day and post-top-up day training evaluation form. PSs reported on enjoyment, knowledge gained, concerns about being a PS and perceived trainer autonomy support. Trainers reported on fulfilment of objectives, logistics and perceived student engagement. Semistructured interviews and focus groups were conducted with trainers, PSs, parents of PSs, school contacts and NPSs to gain feedback about the successes and any issues with the intervention. A school context audit was completed to assess level of PA provision, school policies to support PA and attitude towards PA | |
| 5. Who provided? | Female trainers with a background in delivering PA programmes, working with young people or in theatre were recruited to the study to deliver the PS training |
| A total of five trainers delivered the intervention; one trainer was unable to deliver any top-up day training and, therefore, another trainer took her place. All trainers completed a 3-day train the trainers programme approximately 1 week before delivery. Instructors were paid to attend the train the trainers programme and for each PS training they delivered | |
| 6. How? | PS training was provided to the top ≈ 18% of girls nominated to be a PS of each school (range in number of PSs at each school: 11–17) and delivered by two trainers. PSs then returned to school and informally diffused messages about PA to their friends |
| 7. Where? | PS training was delivered during the school day in the four intervention schools. Schools were located in South Gloucestershire and Wiltshire. The 2-day and top-up day sessions were delivered off the school site, usually in a town/local hall. PS training for one school was held within school grounds because the school was unable to release a staff member to attend the training |
| 8. When and how much? | Intervention schools received the initial 2-day PS training in February 2016 and received the top-up day midway through the intervention period in April 2016 (this was conducted in term time). The training days ran from ≈ 9:00 to 15.00 to reflect the usual school day. The intervention was 10 weeks; however, PSs were encouraged to peer support for as long as they felt necessary and, therefore, there was no defined period |
| 9. Tailoring | All trainers received the same training and resources for delivery and were encouraged to deliver the PS training in an autonomy-supportive style consistent with SDT. PSs from all schools received the same training, but delivered by different trainers, and sessions were observed for intervention fidelity |
| 10. Modifications | No modifications were made to the intervention |
| 11. How well? (Planned) | Observations assessed intervention fidelity, including the extent to which the trainers met activity objectives, delivered these in an autonomy-supportive style and any activities that were missed. PS, NPS and trainer focus groups and interviews evaluated the extent to which PSs had provided support and what impact this may have had |
| 12. How well? (Actual) | Across all 3 training days, fulfilment of activity objectives was rated as 2.66 ± 0.58 (mean ± SD), suggesting that the majority of objectives were achieved during the delivery of the activities. Observations witnessed that, for the majority of the training, trainers adhered to the principles of SDT by ensuring that PS opinions felt valued and by attempting to provide choice and making efforts to bond with the girls. Activities that were not delivered were those that were suggested in the manual to be missed if trainers needed to make time |
| Both PSs and trainers reported making efforts to support and encourage peers to be more active by providing knowledge, co-participating in PA and being subtle in their attempts. Some NPSs were sceptical about the amount of peer support they had received |
Summary of phase 1
Phase 1 of PLAN-A was designed to test all intervention elements, from recruitment through to intervention delivery. As a result, a number of intervention elements were changed or adapted to take into consideration the views of the Year 8 girls, PSs and trainers. The PS recruitment process was refined to focus on how PSs should take pride in being nominated and the benefits they would gain from being a PS. Training content and expectations were also made clear to the PSs on recruitment. Trainers were recruited based on characteristics described by Year 8 girls and the train the trainers activity was adapted so that there was enough time to practically run through all activities and for trainers to familiarise themselves with the content, based on trainer suggestions. It was ensured that the PS training content was active and practical, rather than involving too much writing and listening, as well as concentrating on boosting PSs’ confidence to talk to others by practising peer support and covering what to do if they come across any difficulties or issues when peer supporting. These changes led to the creation of the final intervention that was implemented in phase 2: the feasibility trial.
Chapter 3 Phase 2: feasibility study design and methods
Trial design
The study was a two-arm cluster randomised controlled feasibility study in secondary schools to compare PLAN-A against a usual-practice control. A mixed-methods process evaluation was conducted in addition to a health economics evaluation. The methods and results are reported in line with CONsolidated Standards Of Reporting Trials (CONSORT) guidelines for pilot and feasibility trials,58 the COnsolidated criteria for REporting Qualitative research (COREQ) checklist,59 the TIDieR framework57 and the Consolidated Health Economics Evaluation Reporting Standards (CHEERS) checklist. 60 The trial was registered with the International Standard Registered Clinical/soCial sTudy Number (as ISRCTN12543546) prior to data collection.
Protocol amendments
The original study protocol was submitted to the National Institute for Health Research (NIHR) on 26 April 2013 and was published on 15 January 2016. 55 A small number of revisions were made to the protocol following NIHR approval during the study and are summarised in Table 8.
| Date | Amendment to protocol |
|---|---|
| September 2015 | The number of parents of PSs to be interviewed was reduced from 24 to 10–12 |
| Participants are to be included in the analysis of evidence of promise if they provide at least 2 days of valid weekday accelerometer data | |
| January 2016 | The TSC chairperson requested to be made aware of any adverse events |
| April 2016 | If more than six schools volunteer to participate, schools will be randomly selected |
| Added semistructured interviews to be conducted with trainers | |
| Semistructured interviews to be conducted with trainers following the top-up training | |
| Substantial discussion with the Trial Management Group and data linkage experts suggested that a positive qualitative view on data linkage from parents, school management and education and health data custodians (including the NPDs) would be more appropriate than requesting stakeholders provide consent to a hypothetical scenario | |
| An exploratory accelerometer comparison study to be conducted during the pilot phase to investigate wrist-worn vs. waist-worn accelerometers |
Methods
Ethics and governance
The study was granted ethics approval from the School for Policy Studies, University of Bristol (SPSREC14–15.A27), and was sponsored by the University of Bristol. Parents were given study information and parental informed opt-out consent was obtained covering both the quantitative and qualitative data collections. Parents of PSs provided written informed consent and students gave written informed assent. All adults involved in the research (e.g. trainers) gave written informed consent. Adverse events during data collection or when the intervention was being delivered were recorded and reported to the chairperson of the Trial Steering Committee (TSC) and the chairperson of the Ethics Committee.
Local advisory group
A local advisory group (LAG) was formed to advise on the delivery of PLAN-A and provide support for issues regarding recruitment and training, as well as other school-based matters. The group was made up of teachers, PA experts and council staff. This improved the relevance and real-world application of the study. The group met three times over the course of the study and provided crucial information on the recruitment of PSs and trainers, bullying and behaviour management, the use of social media and how to effectively disseminate the study results to stakeholders.
Trial Steering Committee
A TSC was established to supervise the overall conduct of the trial on behalf of the funder. Members comprised individuals, independent of the investigators and funders, from other universities and government organisations. The committee met five times throughout the course of the trial, monitoring trial progress and offering advice on aspects of the trial from ethics to statistical issues. In addition, members provided guidance on the future of PLAN-A.
Sampling and participants
To be eligible for inclusion in the study schools had to:
-
be state-maintained mainstream secondary schools
-
be located in Wiltshire and South Gloucestershire
-
have girls in Year 8
-
be above the median of the local Pupil Premium (i.e. more deprived: Wiltshire = £115,000 and South Gloucestershire = £145,000 for 2014/15)61
-
not be currently implementing the ASSIST study intervention.
Eligible schools (N = 30: South Gloucestershire, n = 9, and Wiltshire, n = 21) were invited to participate in writing, followed by follow-up telephone calls and e-mails. In collaboration with Wiltshire Council, PLAN-A staff were advised to initially contact four schools that had previously proven difficult to engage in research and reach with health-based interventions. Consenting schools were selected on a first-come-first-served basis in line with the stratification by local authority (LA). A school contact teacher was designated to the study and a short, standardised briefing was delivered to all Year 8 girls in each school. This explained the study, participation, randomisation, data collection and PLAN-A. Students were able to ask questions and were provided with written student and parent information sheets and a parent opt-out consent form.
Trainers were recruited using snowball sampling and word of mouth, with the aim of reaching trainers with expertise in both PA promotion and youth work/drama. A recruitment advert was distributed to relevant organisations (e.g. Active Trowbridge, Nuffield Health, Travelling Light Theatre and Youth Action Wiltshire). Interested individuals contacted the study team and had an informal meeting to discuss the project and assess their fit with the recruitment criteria set out by Year 8 girls in the formative phase.
Sample size
As this was a feasibility study, a sample size calculation was not performed. We chose to recruit six schools to provide sufficient variety of schools and student numbers in which to test recruitment, retention and acceptability of the intervention, PLAN-A, and feasibility of the research to evaluate it. Participants were Year 8 girls and all girls in Year 8 were eligible to participate.
Randomisation
The unit of randomisation was school. After baseline data collection was complete, six schools were randomly allocated, stratified at an intervention-to-control ratio of 2 : 1 within the LA area (i.e. Wiltshire and South Gloucestershire). Two schools were allocated to the control arm and four schools were allocated to the PLAN-A arm by a member of the Bristol Randomised Trials Collaboration (BRTC), who was independent of the study and blind to the school identity. The lead and research associate statistician and all team members apart from the project manager, research assistants and fieldworkers were blind to allocation.
Intervention and control group provisions
The four intervention schools received PLAN-A, as described in Chapter 2, Description of final intervention elements. One PLAN-A school was not able to release a member of school staff to chaperone students to the off-site PS training and, as such, it was negotiated with the school that training would be held in the school. Peer nomination occurred in September 2015 and PS selection and recruitment took place in December 2015, with the initial 2-day PS training in February 2016 and the 1-day top-up training in April 2016. Control schools did not receive PLAN-A and continued with normal practice; all students completed identical measurements to the PLAN-A schools.
Measures
Accelerometer and questionnaire measures were collected at baseline [time 0 (T0): the beginning of Year 8, September–October 2015], immediately post intervention [time 1 (T1): the end of Year 8, May–June 2016] and follow-up [time 2 (T2): the beginning of Year 9, September–October 2016]. All questionnaire measures at each time point, apart from the EuroQol-5 Dimensions, child-friendly version (EQ-5D-Y) and KIDSCREEN,62 were completed using a Samsung Galaxy Tab 4 (Samsung Electronics Limited, Surrey, UK). Demographic information was collected at T0 only. Process evaluation measures were taken throughout the course of the project with key times being the training observations and evaluations in February and April 2016 and qualitative work in February, April and May 2016. Students received a retail voucher (£5 for T0 and £10 for each follow-up, i.e. T1 and T2) in recognition of the time given to each data collection. Participating schools (i.e. PLAN-A and control) received £500 and a summary of the findings in recognition of the time devoted to accommodating the study.
Participant demographic characteristics
Age
Participants’ age at baseline (T0) was calculated from self-reported date of birth.
Ethnicity
Ethnic background was self-reported by selecting 1 of 13 descriptions based on the 2011 UK Census [www.ethnicity-facts-figures.service.gov.uk/ethnicity-in-the-uk/ethnic-groups-and-data-collected (accessed 13 September 2018)].
Socioeconomic position
Participants’ socioeconomic position was estimated using multiple measures. First, participants self-reported their home postcode and this was used to calculate an Index of Multiple Deprivation (IMD) using the English Indices of Deprivation 201063 for each participant. Second, students reported the highest level of parent education [i.e. up to General Certificate of Secondary Education (GCSE) or similar; Advanced Levels (A Levels)/National Vocational Qualification (NVQ)/General National Vocational Qualification (GNVQ); or university/college degree] and their receipt of free school meals (i.e. yes, no, rather not say). Third, participants completed the four-item Family Affluence Scale that assesses family car ownership (no or yes one, yes two or more), whether or not the child has their own bedroom (no or yes), number of family holidays in the past year (not at all, once, twice, more than twice) and family computer ownership (none, one, two, more than two). 64,65
Recruitment and retention to trial and intervention
Recruitment of schools and Year 8 girls (opt-out consent rate) was recorded at T0 and retention was recorded at T1 and T2. Recruitment of PSs and trainers was recorded by the field team. Attendance of PSs at the briefing meeting and at each PS training day and the PS and the PS parent consent rate were also recorded by the field team.
Physical activity and sedentary time
A waist-worn ActiGraph accelerometer (model wGT3X-BT; ActiGraph LLC, FL, USA) was worn by each participant at each time point during waking hours and recorded data at 30 Hz for 7 days. Participants were asked to remove the accelerometer when showering/bathing, participating in water sports and sleeping at night. ActiGraph accelerometers provide reproducible and valid estimates of PA among adolescents. 66 Non-wear time was classified as periods of ≥ 60 minutes of zero counts and was removed from the data set. Provision of accelerometer data at each time point was a primary outcome of the feasibility study. To assess the secondary outcome of the potential effect of the intervention on girls’ MVPA, participants who provided at least 2 valid days, where a valid day was defined as recording at least 500 minutes of data between 05:00 and 23:59, were included in the analysis. Mean daily minutes of MVPA on weekdays and weekend day(s) was estimated using the Evenson cut-off point [≥ 2296 counts per minute (CPM)], as this threshold is the most accurate for adolescents. 67,68 Participants’ weekday and weekend minutes of sedentary time were estimated using a cut-off point of ≤ 100 CPM. 68
School travel mode
Two single-item questions were used to assess usual travel mode to and from school with four response options (i.e. walk, cycle/scoot, car, bus/train).
Screen viewing
Self-reported leisure time screen viewing was reported separately for a normal school (week)day and weekend day in the following categories: TV/DVD, computer/laptop, telephone/smartphone, console games and handheld console. Seven response options were used: none, < 1 hour, 1–2 hours, 2–3 hours, 3–4 hours, 4–5 hours and > 5 hours.
Psychosocial measures
Physical activity motivation
In line with SDT,42 participants completed a 19-item version of the behavioural regulations in exercise questionnaire [Behavioral Regulation in Exercise Questionnaire 2 (BREQ-2)]69 assessing (1) intrinsic motivation (four items, e.g. ‘I am physically active because it’s fun’), (2) identified motivation (four items, e.g. ‘I am physically active because it’s fun’), (3) introjected motivation (three items, e.g. ‘I feel guilty when I’m not physically active’), (4) external motivation (four items, e.g. ‘I am physically active because other people say I should be’) and (5) amotivation (four items, e.g. ‘I think being physically active is a waste of time’). Participants indicated their agreement with each statement using a five-point Likert scale ranging from 0 (not true for me) to 4 (very true for me). Composite autonomous (mean of intrinsic and identified) and controlled (mean of introjected and external) scores were calculated.
Physical activity psychological need satisfaction
Participants’ perceptions of autonomy (six items, e.g. ‘I feel I’m active because I want to be’), competence (six items, e.g. ‘I am pretty skilled at different physical activities’) and relatedness (five items, e.g. ‘I feel understood’) were assessed using a seven-point Likert scale ranging from 1 (not at all true) to 7 (very true). 48,70 Participants rated how ‘like them’ each statement was. Item means for each need variable were calculated.
Self-esteem
The nine-item Self-Description Questionnaire,71 which contained four positively worded (e.g. ‘most things I do, I do well’) and five negatively worded (e.g. ‘I do not have much to be proud of’) items, was used to assess self-esteem. Participants rated how true or false each description was for them using a six-point Likert scale ranging from 1 (false – not like me at all) to 6 (true – very much like me). A mean of the items was calculated.
Physical activity self-efficacy
Eight items were used to assess participants’ self-efficacy to be physically active in different situations (e.g. ‘I can be physically active most days after school’). 72 Participants indicated their endorsement of each statement using three responses (no, not sure and yes). A mean of the items was calculated.
Physical activity social support
Six items assessing social support from friends for PA were taken from a broader questionnaire measuring factors associated with PA in adolescents. 73 Participants read the stem ‘Thinking about your close friendship group how often do they do the following’ and rated each item (e.g. invite you to engage in PA with them) using a four-point Likert scale ranging from 0 (never) to 3 (always). Items covered social support in the form of encouragement, involvement, co-participation, talking about PA and giving positive comments. A mean score of the items was calculated.
At each time point, participants were asked two questions to assess their perceptions that others in their year (1) spoke to them about PA (‘has anyone in your year group talked with you recently about PA?’; response options: yes, no, not sure) and (2) whether or not they felt it helped them be more active [‘did talking to anyone in your year help you to be more active?’; response options: yes, no, not sure, NA (not applicable)].
Peer norms for physical activity
The six-item Social Support Scale74 was used to measure three factors of peer-based social support. Prevalence of friends’ PA was assessed with two items (e.g. ‘how many of your close friends would you say are physically active?’), scored using a four-point scale (0 = none to 3 = all). Perceived importance placed on PA by peers was measured using two items (e.g. ‘how important do you think it is to your close friends to be physically active?’), scored using a three-point scale (0 = not important at all to 2 = very important). Peer acceptance of the participant’s level of PA was assessed using two items (e.g. ‘my friends encourage me to be physically active’), scored using a 4-point scale (0 = disagree a lot to 3 = agree a lot). A mean score of the items was calculated for prevalence, importance and acceptance.
Health-related quality of life
The KIDSCREEN-10 Index,62 which is a unidimensional measure representing a global score for the factors included in the longer KIDSCREEN questionnaires, was completed. Participants responded to 10 items (e.g. ‘have you felt fit and well?’), reporting in the context of the last week, using options from ‘not at all’ to ‘extremely’. Scoring was undertaken in line with the questionnaire manual. 62
Data linkage
The original protocol included assessing the proportion of participants providing consent and the necessary data to allow the link to health and education data to be made. Discussion with the Trial Management Group, TSC and further research established that these original aims were not appropriate (see Table 8). It was decided that a qualitative examination of parents’ views on data linkage would be undertaken (see Chapter 3, Qualitative data collection); this received ethics approval. The proportions of participant demographic data (i.e. full name, date of birth and home postcode) required for data linkage was also examined (see Chapter 3, Data analysis, Statistical methods and analysis). School management were asked to complete a short questionnaire to assess whether or not schools would be willing to provide the unique pupil number for children taking part and address any concerns with data linkage.
Health economics methods
Aims
The aim of the economic evaluation was to assess the feasibility of collecting the data required to cost the intervention and to conduct a cost-effectiveness analysis in a definitive trial. The analysis also aimed to explore the affordability and potential cost-effectiveness of the intervention.
Resource use
We measured resources from a public sector perspective, assuming that, if adopted more widely, the intervention would be funded by local government or academy schools. Data were collected during the trial using expense claim and data collection forms completed by the research team, school contacts and students. Resource use was divided into three categories (1) development of the intervention, (2) preparation for delivering the intervention and (3) delivering the intervention.
-
Resources used in the development of the intervention: the intervention was developed by the research team and was based on other peer-led interventions. More information can be found in Chapter 1, Peer-led health interventions. Hours spent developing the intervention were retrospectively recorded by university staff and on expense claim forms completed by non-university staff. Time spent by the research team was multiplied by their hourly wage to estimate the cost of intervention development.
-
Resources used in preparation for delivering the intervention: train the trainers training was delivered by three members of the research team to five trainers over 3 days in individual and jointly delivered sessions (see Chapter 2, Description of final intervention elements). Non-staff resources, recorded on spreadsheets by the study administrator, included venue hire, printing and refreshment expenses. In addition, travel and parking costs were recorded on expense claim forms by trainers.
-
Resources used in delivering the intervention: delivery of the intervention included (1) pre-intervention preparation, (2) student briefing, (3) peer nomination, (4) PS meeting, (5) 2-day PS training and (6) 1-day top-up training session. Fieldworkers delivered the student briefing, peer nomination and PS meeting. Two trainers per school conducted the training and top-up sessions. Further information is presented in Chapter 2, Description of final intervention elements. Pre-intervention costs included administration for training days and sourcing of intervention resources. The student briefing, peer nomination and PS meeting were all conducted within the schools, with associated fieldworker time and travel costs recorded using expense claim forms for each school. Student and school contact time was also retrospectively recorded by school contacts and the research team using an observation form. Printing costs for materials used during the PS meeting were also recorded using the project budget database.
The 2-day and top-up day training were planned to take place outside the schools. This occurred in three schools. For one school, a school staff member was unable to accompany the PSs to offsite training and, therefore, the training took place within the school. Resources recorded included trainer time and travel, student and school contact time, printing, equipment and refreshments. For training that took place off site, venue costs and travel costs for PSs and school contacts were recorded by the study team using the project budget database.
Preference-based quality of life
Students’ quality of life was assessed using the EQ-5D-Y75 at baseline, immediately post intervention and 12 months following baseline. The EQ-5D-Y has five domains: ‘mobility’, ‘looking after myself’, ‘usual activities’, ‘pain or discomfort’ and ‘feeling worried, sad or unhappy’. Each domain has three response options from ‘no problems’/‘no pain’/‘not worried, sad or unhappy’ to ‘a lot of problems’/‘a lot of pain’/‘very worried, sad or unhappy’. EQ-5D-Y responses are combined with utility weights76 and time spent in each state to estimate quality-adjusted life-years (QALYs); 1 QALY is equivalent to a year spent in perfect health and 0 is equivalent to death. The inclusion of the EQ-5D-Y allowed the exploration of whether or not any increase in MVPA during the 12-month period would be reflected in improved self-reported health-related quality of life.
Process evaluation methods
A mixed-methods process evaluation was conducted to document and assess training attendance, receipt of training, intervention fidelity and the experiences of being a PS and to identify further intervention refinements. The process evaluation also sought to understand the context in which the intervention was delivered. The majority of the methods used are identical to those used and described in the pilot study (see Chapter 2, Pilot study). As such, reference will be made to these descriptions with additional methods described in Process evaluation quantitative analysis and Process evaluation qualitative analysis. Initially, however, the quantitative measures used and the different qualitative data collected will be described.
Quantitative measures used
Peer supporter training attendance, activities omitted and adverse events
Trainers recorded PS attendance and reasons for absence at the initial 2-day PLAN-A training and the top-up day using attendance registers. Trainers recorded any training activities that were omitted. Reasons for PSs withdrawing from their role were recorded. Trainers were asked to record adverse events at both the train the trainers and PS training.
Trainer evaluation of peer supporter training
Trainers evaluated the 2-day and top-up day training using a pro forma that assessed various PS training elements (i.e. resource, fulfilment of objectives, student engagement) (see Appendix 2 and Chapter 2, Pilot study).
Peer supporter questionnaire
At the end of the second day of the 2-day training and the top-up day training, all PSs rated their enjoyment, views on training content and logistics and trainer autonomy support using the questionnaire developed in the pilot study (see Appendix 3 and Chapter 2, Pilot study).
Observation of the peer supporter training
Each training pair was observed by the process evaluation research associate once when delivering each of day 1 and 2 and the top-up day. The observation form in Appendix 4 (see Chapter 2, Pilot study) was used with the addition of the top-up day activities.
School context
School context was assessed using multiple indicators.
School description
School size (number of students in whole school and in Year 8) and Pupil Premium data were provided by the school contact.
School physical activity provision
The presence [yes (1), no (0)] of walking and cycling provisions/infrastructure and the quantity and quality (poor, adequate, good) of sports/play facilities were assessed using items from a previously developed audit,77 with three items added (i.e. dance space, outdoor learning space and allotments) based on suggestions from members of the LAG (see Appendix 7). A member of the field team completed the audit during a school visit.
School physical activity policy
School contacts completed a questionnaire assessing the school’s policies on and budget for PE, attitudes towards encouraging PA (nine items) and the promotion of PA throughout the curriculum (five items)78 (see Appendix 7). Items that did not fit the UK context were removed and others were revised to capture written and unwritten policies. Based on LAG advice, three questions were added to assess the offer of cycle training and policies and facilities to encourage staff to be active.
School-level built environment
Information about the number of school playgrounds and their size, land use, road networks and cycle paths was established from a combination of satellite imagery and 1 : 10,000 maps79 within an 800-m radius around the school site. Playgrounds and fields were created as polygons in ArcGIS [version 10.4; ESRI (UK) Limited, Aylesbury, UK] and school shapefiles were imported into the open-source software R (The R Foundation for Statistical Computing, Vienna, Austria) to calculate the areas of each school’s fields and playgrounds. The following spatial data were also imported (1) road network and road nodes, from the Ordnance Survey’s MasterMap® Integrated Transport Network roads and road nodes,80 (2) footpaths and cycle paths, from the Ordnance Survey’s MasterMap Integrated Transport Network urban paths80 and (3) the Land Cover Map 2007. 81 Intersection density was calculated (number of intersections within the 800-m radius around schools/school area in km2). Land cover diversity was calculated using Shannon’s index of diversity from the Land Cover Map 2007 and road lengths, footpath lengths (excluding pavements) and cycle path lengths (excluding cycle lanes on roads) were also calculated.
Qualitative data collection
At the end of the 10-week intervention period (post-T1 data collection), focus groups and interviews were conducted with six stakeholders involved in PLAN-A (i.e. PSs, NPSs Year 8 girls, trainers, parents of PSs, school contacts and control school students). Focus groups and interviews were recorded using an encrypted digital recorder (Olympus DS-3500, Olympus Europa SE & Co., Hamburg, Germany), transcribed verbatim and transcripts were anonymised.
Peer supporter focus groups
One focus group per intervention school was held with PSs on school premises (n = 28; duration range 39–49 minutes). Seven participants per focus group were selected using a random number generator to select students from an alphabetically ordered list of names. These focus groups discussed recruitment to the project, training logistics and content, their views on the trainers and their perceptions of trainer support for autonomy, competence and relatedness, experiences of participating in the intervention, preparedness, actions and approaches taken to provide peer support (what worked and what was challenging) and perceived impact on themselves and their peers. The focus group in school 4 additionally discussed the dynamics of the PS training that was held in that school.
Non-peer supporter focus groups
One focus group was held with a NPS per intervention school (n = 24; duration range 21–49 minutes). Participants were purposively selected to include girls from across the range of baseline MVPA (random sampling within MVPA tertiles). Two girls from low-, medium- and high-baseline MVPA tertiles were selected and invited per school. These focus groups covered awareness of the project, including thoughts on who the PSs were (noting that the intervention model may mean some girls were not aware of this) and how they felt about not being a PS. The focus groups also discussed the perceived impact of the intervention on Year 8 girls (i.e. conversations they had, if any, how they were conducted, whether or not the information was well received and its impact).
Trainer interviews
Two interviews were conducted with each trainer, one (face-to-face interview) in the week after they had delivered their last 2-day training (n = 5; range 45–59 minutes) and one (telephone interview) after their last top-up day delivery (n = 4; range 32–50 minutes). The interview questions were similar to those used in the pilot and covered views on the train the trainers and PS training, (logistics, content, resources and improvements) and experiences of delivering the training in the school(s) setting.
School contact interviews
At the end of the 10-week intervention period, interviews were conducted with all school contacts (n = 6), either face to face or by telephone (duration range 14–43 minutes). The intervention school contact interview addressed their involvement in the project and logistics, including communication and support from the study team. If applicable, they were encouraged to articulate their thoughts on the PS training and perceived impact of the intervention on PSs and Year 8 students as a whole, as well as their thoughts on the sustainability of PLAN-A. The control school contact interviews guide covered involvement in the study, logistical issues and views on being randomised to the control group.
Parents of peer supporters’ interviews
Telephone interviews were conducted with three randomly selected parents of PSs in each intervention school (n = 12; duration range 20–34 minutes). The interviews explored parental involvement with the project and their daughter’s role as a PS, their thoughts (if any) on the PS training, the perceived impact on their daughter and her response to, and experience of, the PS role. Parental views on allowing their child’s data to be used for data linkage with academic records kept by the NPD [www.gov.uk/government/publications/national-pupil-database-user-guide-and-supporting-information (accessed 8 November 2018)] were qualitatively examined.
Control school participant focus groups
Focus groups were conducted with participants in both control schools (n = 12; 25 and 26 minutes’ duration). Two girls from each low-, medium- and high-baseline MVPA tertiles were selected and invited for each focus group. In these, the girls’ understanding of PLAN-A was explored, together with their thoughts on all elements of data collection and ideas on how to disseminate the project findings.
Field team reflective notes
Following T2 data collection, field staff made notes on their experience of working with the school, the school staff and participants. These notes were aligned with the results from the school context measures to create a rich description of context.
Data analysis
Statistical methods and analysis
Summary statistics are presented for the two arms at baseline (T0) according to demographics [age, ethnicity, socioeconomic status (IMD), family affluence] and for accelerometer measures including MVPA. Means and SDs are presented for continuous variables unless markedly skewed in which case the median and interquartile range are presented. Feasibility data, such as school and student recruitment and retention through the study, are presented as a CONSORT flow chart for schools allocated to the PLAN-A and control arms (see Figure 9). Recruitment of PSs, accelerometer and questionnaire data provision and provision of the data needed for data linkage (i.e. full name, date of birth and home postcode) are also summarised descriptively.
Summary statistics for the (definitive trial) primary and secondary outcomes are presented by intervention and control group according to the allocation of the student’s school (i.e. an intention-to-treat analysis). The adjusted differences in means between intervention and control groups were estimated using mixed-effects linear regression, with variance in the outcome at the school level accommodated by inclusion of school as a normal distribution random effect, and any remaining differences in the baseline assessment of the outcome measure, and LA (by which the randomisation was stratified) being accommodated for by its inclusion as a covariate. Each difference in means is presented with its 95% CI. A sensitivity analysis, with further adjustment for variables found to differ between intervention and control groups at baseline, was prespecified.
Further sensitivity analyses assessing the impact of ≥ 5% missing MVPA measures were prespecified. First, missing MVPA data have been imputed for T1 and T2 in turn using multiple imputation by chained equations,82 as implemented in Stata® statistical software (version 14.2; StataCorp LP, College Station, TX, USA). Fifty imputed data sets were generated for MVPA at each time point and the mixed-effects linear regression analysis described in the paragraph above was applied to these data. Imputation equations used the following variables in addition to those used in the regression analysis of MVPA: weekday and weekend screen time, mobile phone use, peer norms for PA, KIDSCREEN scores, autonomous motivation, PA self-efficacy, peer support help and family affluence. Second, MVPA measurements based on ≥ 1 valid days of accelerometer wear (rather than ≥ 2 valid days for the primary analysis) were used to estimate the adjusted difference between intervention and control groups in mean MVPA.
On the recommendation of the TSC, an exploratory post hoc analysis investigated whether or not the PSs derived any more or less benefit from the intervention than the other participants. A binary covariate identifying participants who were either nominated as PSs or not was added to the regression model used for the analysis of MVPA, and a p-value was calculated for the test of the null hypothesis of equal effect of the intervention on PSs and NPSs.
To inform the calculation of the sample size for a definitive trial, the school-level ICC coefficient for weekday MVPA was estimated in a variance component random-effects analysis. Acknowledging that this gives an imprecise estimate in a study of this size, the study data were compared with ICC estimates from other studies involving students of a similar age. 23,83,84 Estimates of the ICC from this study were calculated according to the analysis of variance (ANOVA) method using the Stata (version 14.2) loneway command; this estimates the proportion of total variation in the outcome variable measurements that is between (or explained by) the schools. Estimates of the standard deviation of MVPA, and the correlation between MVPA at baseline and follow-up, were obtained in the same way. The number of participating students per school was informed by this feasibility study (i.e. an average of 70 girls per school). These estimates were used to inform a sample size calculation for a definitive trial of PLAN-A. Sample sizes were calculated using Stata (version 14.2), for assumed true differences in mean MVPA between intervention and control groups (differences of 6, 8 and 10 minutes per weekday), and for 80% and 90% statistical power at the two-sided 5% significance level. The general approach is to calculate the sample size using the standard approach and ignoring clustering by school in the first instance and then to multiply that sample size by the design effect:
k being the number of participants at each school (cluster size) and ICC being the intraclass correlation coefficient.
Process evaluation quantitative analysis
Quantitative data analysis for the feasibility process evaluation was identical to the methods used in the pilot study (see Chapter 2, Pilot study).
School context
A ‘school PA suitability’ score was calculated as a sum of the scores from the cycling, walking and sports and play components, with the maximum score being 46. Facilities (e.g. marked pedestrian crossings) were scored as present (1) or not (0). The quantity of facilities was weighted relative to the mean number of each facility across all schools (0 = none, 1 = 1 to mean plus 1 SD, 2 = > mean plus 1 SD). 77 The modal quality of PA provision was reported by school. For school PA policies, a policy (maximum score = 10) and curriculum score (maximum score = 8) were calculated per school using the appropriate items. High scores represent a strong attitude towards PA provision, appropriate policies and strong evidence of PA being promoted throughout the curriculum.
Process evaluation qualitative analysis
Interviews and focus groups
The framework method54 and steps previously described in Chapter 2, Pilot study, were used to analyse interview and focus group data. For this study, this included all participant groups (i.e. PSs, NPSs, trainers, school contacts, parents of PSs and control school Year 8 girls). This approach facilitated the use of both inductive (i.e. allowing themes to emerge) and deductive (i.e. preplanned topics to be explored) coding. For deductive analysis, predefined codes for each group were broad (focusing on intervention delivery, experience and theoretical fidelity; see Appendix 8). In addition, codes were inductively developed by Kathryn Banfield, Mark J Edwards and Joe Matthews, who independently coded the same transcript from each participant group. Frameworks for each group were applied by the following researchers: school contact and trainer interviews (MJE), NPS and PS focus groups (KB) and parent interviews and control school focus groups (JM). To present a rich and detailed picture of the data collected for the feasibility study, the qualitative and quantitative results are presented alongside each other.
Observation analysis
To allow for a clear comparison between each trainer pair, observation data for all trainer pairs were reduced to two categories. These were the similarities and differences between trainer pair per activity for day 1, day 2 and the top-up day. For each activity, the similarities and differences were split into general comments and observations of theoretical fidelity.
Economic evaluation
Valuation of costs and outcomes
University staff time was costed using basic salary, national insurance and superannuation. External trainers were costed using the cost per hour they were paid during the trial (Table 9). The time spent by school contacts (PE teachers and student support staff) involved in PLAN-A was not valued because the time involved was relatively small and it was assumed to be part of normal teaching duties. No school hired supply teachers to cover for teacher time spent on PLAN-A-related meetings or training. All costs were valued in GBP (Great British pounds) for the year 2016. No discounting was required given that all costs and consequences were captured in year 1.
| Staff | Cost (£) per hour |
|---|---|
| Fieldworker | 19.62 |
| Research administrator | 19.62 |
| Research associate | 28.19 |
| Senior research associate | 31.81 |
| Senior lecturer | 45.60 |
| Trainer, as paid during the trial | 22.70 |
| Trainer, Hay band 6 or 7 | 15.64 |
Analysis of costs
The average cost of intervention delivery per school and per Year 8 girl was calculated. All Year 8 girls were included in the estimate of cost per Year 8 girl regardless of whether or not they consented to participate in the trial, as all can potentially benefit from the intervention.
Analysis of preference-based quality of life
Given the absence of a paediatric valuation for the EQ-5D-Y, the UK adult tariff76 was applied to derive utility values, and QALYs were estimated using the area under the curve approach. 85 Mean EQ-5D-Y utility values and QALYS were estimated along with the SD and 95% CIs. To compare intervention and control arms, the difference in means was estimated and for QALYS this was adjusted for baseline EQ-5D-Y, trial arm, LA and school-level clusters using multilevel mixed-effects linear regression. We estimated the additional cost per 10-minute increase of mean weekday MVPA at 12 months per Year 8 girl. This analysis was designed to explore the affordability and potential cost-effectiveness of the intervention rather than provide a definitive comparison.
Sensitivity and further analyses
In practice, it is possible that this intervention would be delivered by LA health improvement officers. For this reason, in a sensitivity analysis, fieldworkers and trainers who delivered the intervention were costed using Hay band 6 or 7 from the LA Hay band scale (provided by a LAG member from one of the project partner local councils). Further sensitivity analysis explored the impact of different assumptions on the cost of the ‘train the trainers’ event. In this analysis, we assumed that 10 PS trainers were trained by two trainers (health improvement officers) and the 3-day PS training was conducted at an external venue at a cost of £210 per day.
In further post hoc analyses Pearson’s correlation coefficients were estimated to explore the correlation between mean weekday minutes of MVPA and EQ-5D-Y score at baseline, post intervention and 12 months. Pearson’s correlation coefficients were also estimated to explore the correlation between change in mean weekday MVPA minutes and EQ-5D-Y score from baseline to 12-month follow-up. These correlations were estimated to explore whether or not EQ-5D-Y is likely to be a responsive outcome in a definitive trial in which the primary outcome is to increase MVPA.
Chapter 4 Feasibility study results
Recruitment
Figure 9 presents the CONSORT diagram and detail on recruitment and retention throughout the study.
FIGURE 9.
Trial profile for PLAN-A (CONSORT flow diagram). a, Returned at T2; b, took part in T2; and c, present at T2.
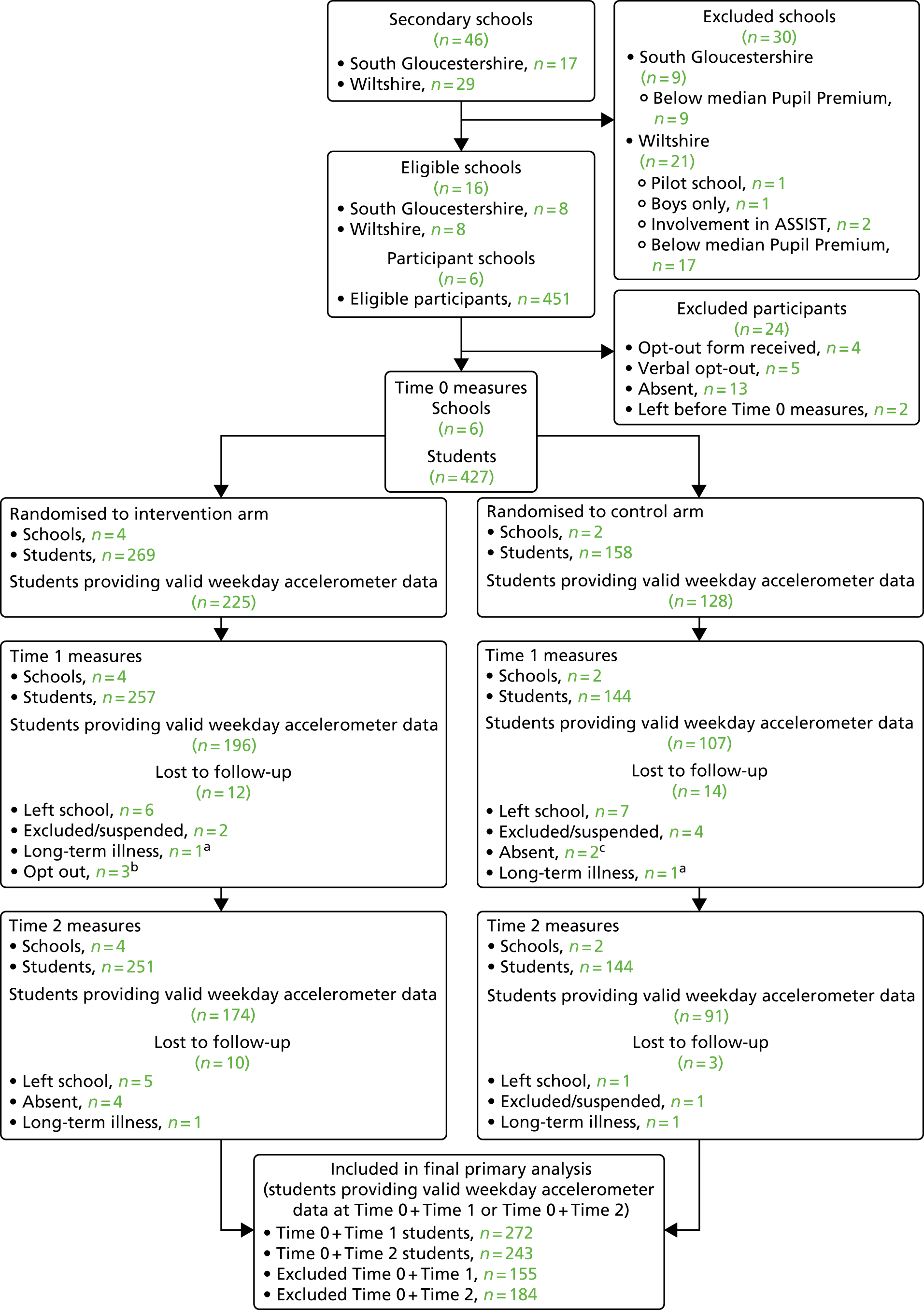
School recruitment
There were 46 secondary schools in the two study areas; 30 schools were ineligible (26 were below the median Pupil Premium). The 16 remaining schools (eight in each LA area) were invited to participate. Eight (50%) schools accepted (six feasibility schools, one pilot school, one reserve), one (6.25%) declined after expressing initial interest and seven (43.75%) failed to respond to the study invitation.
Participant (student) recruitment
The recruitment briefing was delivered to 451 Year 8 girls. Four girls (0.89%) returned opt-out forms and 20 girls (4.43%), despite not handing in an opt-out form, chose not to take part resulting in a 94.68% participation rate across the six schools (Table 10). A total of 427 girls from six secondary schools were recruited (PLAN-A arm, n = 269; control arm, n = 158).
| School ID | Number of Year 8 girls | |||||
|---|---|---|---|---|---|---|
| Total | Opted-out (%) | Did not participate (other reason) (%) | Consenting (%) | Invited to be PS (%a) | Consenting PSs (%a) | |
| 1b | 73 | 1 (1.37) | 0 (0.00) | 72 (98.63) | – | – |
| 2 | 58 | 0 (0.00) | 3 (5.17) | 55 (94.83) | 13 (22.41) | 13 (22.41) |
| 3 | 96 | 3 (3.13) | 5 (5.21) | 88 (91.67) | 18 (18.75) | 17 (17.70)c |
| 4 | 66 | 0 (0.00) | 2 (3.03) | 64 (96.97) | 12 (18.18) | 11 (16.67) |
| 5b | 89 | 0 (0.00) | 3 (3.37) | 86 (96.63) | – | – |
| 6 | 69 | 0 (0.00) | 7 (10.15) | 62 (89.86) | 14 (20.29) | 14 (20.29) |
| School average | 75.16 | 0.67 (0.75) | 3.33 (4.48) | 71.16 (94.68) | 14.25 (19.91) | 13.75 (18.29) |
| Intervention arm | 289 | 3 (1.04) | 17 (5.88) | 269 (93.07) | 57 (19.72) | 55 (19.03) |
| Control arm | 162 | 1 (0.62) | 3 (1.85) | 158 (97.53) | – | – |
| Total | 451 | 4 (0.89) | 20 (4.43) | 427 (94.68) | 57 (19.72) | 55 (19.03) |
Peer supporter recruitment
Peer nomination resulted in 57 girls being invited to be a PS; 56 attended the PS meeting and 55 (96.49%) consented to the role. One PS withdrew before the training citing reasons including low confidence and PA motivation, resulting in 54 PSs. The number of PSs per school ranged from 11 (16.67% Year 8 girls) to 17 (17.71% Year 8 girls) (see Table 10).
Trainer recruitment
Expressions of interest were received from 10 potential trainers with a range of experience in youth work, PA or both. Five female trainers were recruited: two had experience in drama and working with young people and three had experience in PA and working with young people (Table 11).
| Trainer ID | Characteristic | ||
|---|---|---|---|
| Age (years) | Education level | Employment, experience or training | |
| A | 41 | First degree/diploma/HNC/HND or equivalent | Co-artistic director of theatre company |
| B | 28 | Higher degree (e.g. MSc, PhD) or equivalent | Masters of Nutrition, Physical Activity and Public Health. Walking for health leader and promoter |
| C | 21 | A Levels/NVQs/GNVQs or equivalent | Community sports coach |
| D | 45 | First degree/diploma/HNC/HND or equivalent | Freelance personal training, tennis club coach and fitness advisor |
| E | 34 | First degree/diploma/HNC/HND or equivalent | Self-employed yoga teacher/holistic therapist/youth mentor. Senior youth worker and project co-ordinator community youth project |
Data provision
Accelerometer return and data provision rates are shown in Table 12. Return rates were high (> 85%) at each time point and only differed markedly between arms at T1, in which return was approximately 10% lower in the control than in the PLAN-A arm. The wear-time criteria was met by 82.63%, 71.13% and 62.21% of participants at T0, T1 and T2, respectively. A lower proportion of participants in the control arm, than in the PLAN-A arm, met the wear-time criteria at T1 (5%) and T2 (7%). A total of 64% of participants provided valid accelerometer data at both T0 and T1, and 57% participants provided valid data at T0 and T2.
| Accelerometer device status | Trial arm, n (%) | Total, n (%a) | |
|---|---|---|---|
| Control | PLAN-Aa | ||
| T0 | |||
| Accelerometer returned | 153 (96.84) | 258 (96.27) | 411 (96.48) |
| Validb | 128 (81.01) | 224 (83.58) | 352 (82.63) |
| Invalidc | 25 (15.82) | 34 (12.69) | 59 (13.85) |
| Missingd | 5 (3.16) | 10 (3.73) | 15 (3.52) |
| T1 | |||
| Accelerometer returned | 135 (85.44) | 255 (95.15) | 390 (91.55) |
| Valid | 107 (67.72) | 196 (73.13) | 303 (71.13) |
| Invalid | 27 (17.09) | 54 (20.15) | 81 (19.01) |
| Missing | 24 (15.19) | 18 (6.71) | 42 (9.86) |
| T2 | |||
| Accelerometer returned | 140 (88.61) | 241 (89.93) | 381 (89.44) |
| Valid | 91 (57.59) | 174 (64.93) | 265 (62.21) |
| Invalid | 44 (27.85) | 66 (24.63) | 110 (25.82) |
| Missing | 23 (14.56) | 28 (10.45) | 51 (11.97) |
| T0 and T1 | |||
| Valid | 95 (60.13) | 177 (66.04) | 272 (63.85) |
| T0 and T2 | |||
| Valid | 81 (51.27) | 162 (60.45) | 243 (57.04) |
Questionnaire data provision is shown in Table 13. Completion of the psychosocial questionnaire using the tablets exceeded 90% at each time point and was very similar between trial arms. Completion of the quality-of-life measures (i.e. KIDSCREEN-10 and EQ-5D-Y), which were administered on paper, was slightly lower but still high, with completion rates of > 87% at all time points.
| Questionnaire | Trial arm, n (%) | Total, n (%) | |
|---|---|---|---|
| Control | PLAN-A | ||
| T0 | |||
| Psychosocial questionnaire | 157 (99.37) | 269 (100.00) | 426 (99.77) |
| EQ-5D-Y | 153 (96.84) | 260 (96.65) | 413 (96.72) |
| KIDSCREEN-10 | |||
| Complete | 146 (92.41) | 252 (93.68) | 398 (93.21) |
| Partial | 9 (5.70) | 16 (5.95) | 25 (5.85) |
| Missing | 3 (1.90) | 1 (0.37) | 4 (0.94) |
| T1 | |||
| Psychosocial questionnaire | 144 (91.14) | 257 (95.54) | 401 (93.91) |
| EQ-5D-Y | 138 (87.34) | 257 (95.54) | 395 (92.51) |
| KIDSCREEN-10 | |||
| Complete | 137 (86.71) | 245 (91.08) | 382 (89.46) |
| Partial | 6 (3.80) | 12 (4.46) | 18 (4.22) |
| Missing | 15 (9.49) | 12 (4.46) | 27 (6.32) |
| T2 | |||
| Psychosocial questionnaire | 144 (91.14) | 251 (93.31) | 395 (92.51) |
| EQ-5D-Y | 156 (98.73) | 268 (99.63) | 424 (99.30) |
| KIDSCREEN-10 | |||
| Complete | 141 (89.24) | 238 (88.48) | 379 (88.76) |
| Partial | 3 (1.90) | 13 (4.83) | 16 (3.75) |
| Missing | 14 (8.86) | 18 (6.69) | 32 (7.49) |
Data linkage
The three variables needed to perform data linkage (i.e. full name, date of birth and home postcode) were collected for 88.76% (i.e. 379 out of 427) of students. This was solely limited by the provision of full postcode information, as full name and date of birth information were collected for all students. Three (50%) of the schools returned the completed data linkage questionnaire. Responses from one school indicated that it had concerns with the concept of data linkage that would need to be addressed before children and parents were involved, and that it would not provide the Unique Student Number identifier; however, no further details of these concerns were provided in the free-text fields. The other two schools indicated that they had no concerns and would provide the Unique Student Number identifier, assuming that parental consent was sought.
Baseline data
Baseline data are described in Table 14. Medians and lower and upper quartiles are presented for IMD and accelerometer variables, as these data were skewed. Overall, the trial arms were well balanced. IMD score (i.e. level of deprivation) was slightly higher in the intervention than in the control group, suggesting increased levels of deprivation in the PLAN-A arm, although both median scores were in the second quintile range (i.e. 8.5–13.8) of the least deprived households in England. Accelerometer-assessed MVPA was similar between study arms. Participants in the PLAN-A arm recorded more minutes of light PA and weekday sedentary time. Psychosocial variables were similar. KIDSCREEN-10 t-scores, indicating health-related quality of life, approximated European and UK norm values for girls aged 12–18 years (i.e. were within ± half a SD of the threshold of the reference group mean). 62
| Variable | Trial arm | |
|---|---|---|
| Control | PLAN-A | |
| Age (years), n; mean (SD) | 158; 13.53 (0.29) | 269; 13.50 (0.30) |
| Family affluence, n; mean (SD) | 157; 6.92 (1.70) | 269; 6.96 (1.59) |
| Receiving free school meals, n (%) | 22 (14.01) | 30 (11.15) |
| Ethnicity, n (%) | ||
| White British | 125 (79.62) | 232 (86.25) |
| White other | 9 (5.73) | 9 (3.35) |
| Mixed | 5 (3.19) | 7 (2.60) |
| Other | 18 (11.47) | 21 (7.81) |
| IMD score, n; median (IQR) | 134; 9.99 (7.09–16.50) | 245; 11.93 (6.69–18.60) |
| MVPA (minutes), n; median (IQR) | ||
| Weekday | 128; 56.38 (45.44–73.60) | 225; 52.50 (40.67–68.90) |
| Weekend | 69; 38.58 (21.50–62.00) | 155; 38.33 (23.83–59.58) |
| Overall | 128; 54.51 (42.98–71.42) | 225; 50.50 (40.33–63.83) |
| LPA (minutes), n; median (IQR) | ||
| Weekday | 127; 167.37 (144.67–191.0) | 225; 177.27 (150.58–202.92) |
| Weekend | 69; 174.92 (139.50–197.50) | 155; 173.50 (138.08–209.00) |
| Overall | 128; 92.37 (51.56–164.04) | 225; 145.93 (54.56–182.15) |
| Sedentary (minutes), n; median (IQR) | ||
| Weekday | 128; 467.07 (418.03–524.73) | 225; 505.63 (450.57–551.0) |
| Weekend | 69; 428.25 (367.25–520.17) | 154; 443.96 (393.17–513.58) |
| Overall | 128; 387.25 (59.36–487.71) | 225; 454.13 (75.70–519.81) |
| 60 minutes MVPA per, n (%) | ||
| Weekday | 54 (42.19) | 87 (38.67) |
| Weekend day | 20 (28.99) | 36 (23.23) |
| Travel mode to school, n (%) | ||
| Walk | 93 (59.24) | 149 (55.39) |
| Cycle | 17 (10.83) | 18 (6.69) |
| Car | 25 (15.92) | 58 (21.56) |
| Bus/train | 22 (14.01) | 44 (16.36) |
| Travel mode from school, n (%) | ||
| Walk | 92 (58.60) | 160 (59.48) |
| Cycle | 16 (10.19) | 19 (7.06) |
| Car | 25 (15.92) | 43 (16.99) |
| Bus/train | 24 (15.29) | 47 (17.47) |
| Self-esteem, n; mean (SD) | 157; 4.91 (0.88) | 269; 4.69 (0.96) |
| Motivation, n; mean (SD) | ||
| Autonomous | 157; 3.82 (0.87) | 269; 3.77 (0.81) |
| Controlled | 157; 2.50 (0.87) | 269; 2.45 (0.78) |
| Amotivation | 157; 1.51 (0.80) | 269; 1.44 (0.65) |
| Need satisfaction, n; mean (SD) | ||
| Autonomy | 157; 5.60 (1.21) | 269; 5.49 (1.18) |
| Competence | 157; 5.11 (1.40) | 269; 4.87 (1.52) |
| Relatedness | 157; 5.53 (1.58) | 269; 5.32 (1.51) |
| PA self-efficacy, n; mean (SD) | 157; 2.55 (0.37) | 269; 2.49 (0.39) |
| Peer PA norm, n; mean (SD) | ||
| Importance | 157; 2.40 (0.53) | 269; 2.34 (0.49) |
| Acceptance | 157; 2.38 (0.84) | 269; 2.46 (0.75) |
| Prevalence | 157; 2.82 (0.70) | 269; 2.77 (0.68) |
| PA social support from friends, n; mean (SD) | 157; 2.78 (0.71) | 269; 2.70 (0.72) |
| KIDSCREEN-10, n; mean (SD) | ||
| t-scorea | 146; 49.77 (9.64) | 252; 49.77 (9.61) |
| r-scoreb | 146; –0.10 (0.90) | 252; –0.18 (0.55) |
| EQ-5D-Y, n; mean (SD) | 153; 79.09 (16.91) | 260; 72.00 (18.74) |
Characteristics of peer supporters and non-peer supporters
The baseline characteristics of the PSs and the NPSs are presented in Table 15. For this analysis, students who were nominated as PSs in PLAN-A and control schools were included. PSs had higher family affluence, although similar IMD to NPSs, and a greater proportion of PSs than NPSs were of white ethnicity. PSs recorded approximately 12 minutes more MVPA on weekdays and weekends and less sedentary time (mainly because of weekday activity) than NPSs. A total of 59% of PSs versus 35% of NPSs met the PA guidelines, and more PSs than NPSs walked to and from school. PSs also reported higher self-esteem, PA-based autonomous motivation, need satisfaction, stronger social support and peer norms for activity.
| Variable | Students | |
|---|---|---|
| PSsa | NPSs | |
| Age (years), n; mean (SD) | 83; 13.59 (0.27) | 344; 13.50 (0.30) |
| Family affluence, n; mean (SD) | 83; 7.48 (1.48) | 343; 6.82 (1.64) |
| Receiving free school meals, n (%) | 5 (6.02) | 47 (13.70) |
| Ethnicity, n (%) | ||
| White British | 75 (90.36) | 282 (82.22) |
| White other, n (%) | 1 (1.20) | 17 (4.96) |
| Mixed, n (%) | 2 (2.41) | 10 (2.92) |
| Other, n (%) | 5 (6.03) | 34 (9.90) |
| IMD score, n; median (IQR) | 78; 10.99 (5.69–18.60) | 301; 11.05 (6.77–18.20) |
| MVPA (minutes), n; median (IQR) | ||
| Weekday | 71; 63.83 (51.43–77.88) | 282; 51.79 (40.67–67.92) |
| Weekend | 41; 49.83 (35.67–68.00) | 183; 37.17 (21.92–56.83) |
| Overall | 71; 60.36 (50.50–72.56) | 282; 49.79 (39.69–64.83) |
| LPA (minutes), n; median (IQR) | ||
| Weekday | 71; 171.77 (152.83–194.93) | 281; 173.11 (146.67–201.73) |
| Weekend | 42; 165.79 (135.50–208.50) | 182; 173.83 (142.08–204.67) |
| Overall | 71; 127.61 (59.92–178.03) | 282; 132.44 (51.58–177.33) |
| Sedentary (minutes), n; median (IQR) | ||
| Weekday | 71; 469.71 (422.67–524.37) | 282; 498.63 (437.27–546.47) |
| Weekend | 40; 428.71 (377.17–469.08) | 183; 437.83 (385.08–526.50) |
| Overall | 71; 418.03 (60.57–489.89) | 282; 448.90 (67.11–518.33) |
| 60 minutes of MVPA per, n (%) | ||
| Weekday | 42 (59.15) | 99 (35.11) |
| Weekend day | 13 (31.71) | 43 (23.5) |
| Travel mode to school, n (%) | ||
| Walk | 52 (62.65) | 190 (55.39) |
| Cycle | 5 (6.02) | 30 (8.75) |
| Car | 15 (18.07) | 68 (19.83) |
| Bus/train | 11 (13.25) | 55 (16.03) |
| Travel mode from school, n (%) | ||
| Walk | 53 (63.86) | 199 (58.02) |
| Cycle | 4 (4.82) | 31 (9.04) |
| Car | 11 (13.25) | 57 (16.62) |
| Bus/train | 15 (18.07) | 56 (16.33) |
| Self-esteem, n; mean (SD) | 83; 5.20 (0.69) | 343; 4.66 (0.95) |
| Motivation, n; mean (SD) | ||
| Autonomous | 83; 4.31 (0.55) | 343; 3.67 (0.84) |
| Controlled | 83; 2.52 (0.74) | 343; 2.46 (0.83) |
| Amotivation | 83; 1.23 (0.49) | 343; 1.52 (0.74) |
| Need satisfaction, n; mean (SD) | ||
| Autonomy | 83; 6.21 (0.76) | 343; 5.37 (1.22) |
| Competence | 83; 5.87 (1.05) | 343; 4.73 (1.48) |
| Relatedness | 83; 6.12 (0.98) | 343; 5.22 (1.60) |
| PA self-efficacy, n; mean (SD) | 83; 2.72 (0.24) | 343; 2.46 (0.39) |
| Peer PA norm, n; mean (SD) | ||
| Importance | 83; 2.55 (0.43) | 343; 2.32 (0.51) |
| Acceptance | 83; 2.66 (0.77) | 343; 2.38 (0.78) |
| Prevalence | 83; 3.04 (0.59) | 343; 2.73 (0.69) |
| PA social support from friends, n; mean (SD) | 83; 3.13 (0.63) | 343; 2.63 (0.70) |
| KIDSCREEN-10, n; mean (SD) | ||
| t-scoreb | 77; 50.32 (6.92) | 321; 49.64 (10.15) |
| r-scorec | 77; –0.14 (0.45) | 321; –0.16 (0.75) |
| EQ-5D-Y, n; mean (SD) | 82; 80.21 (14.19) | 331; 73.24 (19.05) |
Attendance at peer supporter training
Attendance rates at the PS training was very high across all training days, with 94% (i.e. 53 out of 55) of PSs attending all of the training. See Chapter 6, Peer supporter training: attendance at peer supporter training for complete attendance data.
Evidence of promise
Physical activity variables
Table 16 shows that at T1 (immediately after the 10-week intervention period, i.e. the end of Year 8) there was no evidence of a difference between PLAN-A and control groups for weekday MVPA or weekend day MVPA. There was some evidence that the girls in the PLAN-A arm were less sedentary than the control arm on weekdays at T1 (–31.8 minutes, 95% CI –57.44 to –6.18 minutes). In addition, there was some evidence that the control arm performed a higher volume of activity (i.e. CPM) at weekends, although the CI was wide (–124.24 CPM, 95% CI –213.48 CPM to –35.01 CPM).
| Variable | Trial arm, n; mean (SD) | PLAN-A vs. control, adjusted difference in means (95% CI)a | |
|---|---|---|---|
| Control | PLAN-A | ||
| T1 | |||
| MVPA (minutes) per | |||
| Weekdayb | 95; 61.19 (22.10) | 177; 60.72 (22.45) | 1.11 (–4.31 to 6.55) |
| Weekend day | 37; 45.07 (30.21) | 91; 41.80 (27.49) | –3.88 (–13.57 to 5.81) |
| CPM per | |||
| Weekday | 95; 503.18 (167.75) | 177; 501.35 (163.75) | 35.71 (–14.12 to 85.53) |
| Weekend | 37; 545.69 (363.10) | 91; 426.11 (212.75) | –124.24 (–213.4 to –35.01) |
| LPA (minutes) per | |||
| Weekday | 95; 163.00 (337.40) | 177; 170.26 (43.67) | 0.86 (–10.40 to 12.12) |
| Weekend | 29; 186.75 (48.74) | 77; 165.48 (51.71) | –20.3 (–40.67 to 0.04) |
| Sedentary (minutes) per | |||
| Weekday | 95; 522.37 (87.74) | 177; 509.87 (81.67) | –31.8 (–57.44 to –6.18) |
| Weekend | 37; 461.29 (112.19) | 91; 534.73 (188.56) | 67.43 (–51.34 to 186.20) |
| T2 | |||
| MVPA (minutes) per | |||
| Weekdayb | 81; 54.31 (19.56) | 162; 58.65 (22.21) | 6.09 (1.43 to 10.76) |
| Weekend day | 35; 37.95 (32.14) | 74; 46.57 (37.52) | 11.45 (–2.25 to 25.15) |
| CPM per | |||
| Weekday | 81; 463.10 (154.72) | 162; 483.26 (149.95) | –11.50 (–31.42 to 8.42) |
| Weekend | 35; 421.88 (307.58) | 74; 479.38 (311.92) | 83.94 (–37.05 to 204.93) |
| LPA (minutes) per | |||
| Weekday | 81; 151.89 (34.53) | 161; 155.63 (37.50) | 0.30 (–7.80 to 8.40) |
| Weekend | 27; 160.27 (46.95) | 63; 163.12 (46.99) | 0.96 (–18.89 to 20.82) |
| Sedentary (minutes) per | |||
| Weekday | 81; 511.65 (103.21) | 162; 510.78 (85.29) | –23.26 (–43.73 to –2.79) |
| Weekend | 35; 473.06 (93.74) | 74; 471.95 (97.20) | –5.25 (–41.19 to 30.69) |
At T2 there was evidence for a between-group difference in weekday MVPA in favour of the PLAN-A arm (6.09 minutes), with the 95% CI exceeding 10 minutes of MVPA per day (95% CI 1.43 to 10.76 minutes). The data suggested that the between-group difference was based on the PLAN-A arm girls maintaining their baseline level of MVPA, while the MVPA of the girls in the control group decreased over time. Similar to T1, there was some evidence that the girls in the PLAN-A arm were also less sedentary on weekdays at T2 (–23.26 minutes, 95% CI –43.73 to –2.79 minutes).
Sensitivity analysis
Data imputation
Table 17 shows the results of the adjusted regression analysis on the likely primary outcome at T1 and T2 in a future definitive trial based on the imputed data set. This sensitivity analysis explored whether or not there was comparable evidence of promise under the assumption of accelerometer data being ‘missing at random’ (i.e. < 2 valid days). The results were very similar to the complete-case analysis in both point estimate and 95% CIs (see Table 16).
| Data | Trial arm, n; mean (SD) | PLAN-A vs. control, adjusted difference in means (95% CI)a | |
|---|---|---|---|
| Control | PLAN-A | ||
| Imputed data | |||
| T1 | |||
| MVPA per weekday (minutes)b | 158; 61.72 (22.84) | 269; 60.66 (24.19) | 2.70 (–2.30 to 7.71) |
| T2 | |||
| MVPA per weekday (minutes)b | 158; 55.25 (20.34) | 269; 59.69 (23.19) | 6.89 (2.60 to 11.18) |
| Complete data for which ≥ 1 valid day of accelerometer data were provided | |||
| T1 | |||
| MVPA per weekday (minutes)b | 110; 62.45 (22.87) | 214; 62.17 (26.19) | 2.42 (–2.60 to 7.44) |
| T2 | |||
| MVPA per weekday (minutes)b | 102; 55.00 (20.86) | 193; 58.90 (22.84) | 6.29 (1.69 to 10.90) |
Complete data using ≥ 1 valid days of accelerometer data
A second sensitivity analysis (see Table 17) relaxed the criterion for participant inclusion based on their accelerometer data from ≥ 2 valid days to ≥ 1 valid days of data. Again, this analysis led to identical conclusions regarding the potential effect of the intervention on MVPA.
Intervention effects for peer supporters and non-peer supporters (exploratory)
Comparing the intervention effect between PSs and NPSs (Table 18), there is evidence that PSs benefit more from the intervention at T1 than NPSs, but there is no evidence of a difference between the two subgroups at T2.
| Subgroup | Trial arm, n; mean (SD) | Adjusted difference in means (95% CI)a | |
|---|---|---|---|
| Control | PLAN-A | ||
| T1 | |||
| Whole sample | 95; 61.19 (22.10) | 177; 60.72 (22.45) | 1.12 (–4.31 to 6.55) |
| PSs | 16; 57.49 (27.34) | 40; 65.97 (20.64) | 14.20 (3.16 to 25.25) |
| NPSs | 79; 61.94 (21.01) | 137; 59.19 (22.80) | –0.85 (–5.53 to 3.83) |
| Interaction between cohort and trial arm on weekday MVPA | p = 0.018 | ||
| T2 | |||
| Whole sample | 81; 54.31 (19.56) | 162; 58.65 (22.21) | 6.09 (1.43 to 10.76) |
| PSs | 12; 60.14 (15.15) | 40; 61.73 (22.47) | 2.06 (–9.35 to 13.48) |
| NPSs | 69; 53.30 (20.15) | 122; 57.65 (22.12) | 6.69 (1.63 to 11.76) |
| Interaction between cohort and trial arm on weekday MVPA | p = 0.78 | ||
Psychosocial variables
Internal consistency statistics (Cronbach’s α) are reported in Appendix 9. With the exception of the peer PA norm (acceptance) variable, which exhibited low internal consistency at all time points, all psychosocial composite variables had good internal consistency at all time points. Table 19 shows the adjusted multivariable regression results for psychosocial variables. There was little evidence of any differences between the PLAN-A and control arms on any of the variables at T1 or T2. There was no evidence of harm or detriment to these variables because of the intervention.
| Variable | Trial arm, n; mean (SD) | PLAN-A vs. control, adjusted difference in means (95% CI)a | |
|---|---|---|---|
| Control | PLAN-A | ||
| T1 | |||
| Self-esteem | 144; 4.73 (1.02) | 257; 4.54 (1.04) | –0.06 (–0.23 to 0.11) |
| Motivation | |||
| Autonomous | 144; 3.75 (0.82) | 257; 3.67 (0.83) | –0.02 (–0.16 to 0.12) |
| Controlled | 144; 2.34 (0.79) | 257; 2.37 (0.79) | 0.06 (–0.07 to 0.20) |
| Amotivation | 144; 1.51 (0.75) | 257; 1.49 (0.70) | 0.02 (–0.28 to 0.32) |
| Need satisfaction | |||
| Autonomy | 144; 5.52 (1.19) | 257; 5.50 (1.11) | 0.07 (–0.18 to 0.32) |
| Competence | 144; 5.01 (1.33) | 257; 4.81 (1.36) | –0.05 (–0.26 to 0.15) |
| Relatedness | 144; 5.28 (1.65) | 257; 5.17 (1.51) | –0.02 (–0.39 to 0.34) |
| PA self-efficacy | 144; 2.51 (0.38) | 257; 2.52 (0.39) | 0.05 (–0.05 to 0.15) |
| Peer PA norm | |||
| Importance | 144; 2.22 (0.50) | 257; 2.24 (0.52) | 0.04 (–0.06 to 0.14) |
| Acceptance | 144; 2.43 (0.73) | 257; 2.36 (0.76) | –0.10 (–0.30 to 0.11) |
| Prevalence | 144; 2.69 (0.66) | 257; 2.70 (0.66) | 0.02 (–0.19 to 0.22) |
| PA social support from friends | 144; 2.73 (0.58) | 257; 2.62 (0.64) | –0.06 (–0.17 to 0.05) |
| T2 | |||
| Self-esteem | 144; 4.67 (0.94) | 251; 4.62 (1.04) | 0.09 (–0.08 to 0.25) |
| Motivation | |||
| Autonomous | 144; 3.62 (0.90) | 251; 3.57 (0.89) | 0.02 (–0.13 to 0.17) |
| Controlled | 144; 2.39 (0.77) | 251; 2.30 (0.74) | –0.06 (–0.19 to 0.08) |
| Amotivation | 144; 1.54 (0.77) | 251; 1.57 (0.74) | 0.05 (–0.24 to 0.33) |
| Need satisfaction | |||
| Autonomy | 144; 5.49 (1.16) | 251; 5.39 (1.17) | –0.001 (–0.22 to 0.22) |
| Competence | 144; 4.90 (1.33) | 251; 4.85 (1.39) | 0.15 (–0.06 to 0.35) |
| Relatedness | 144; 5.25 (1.56) | 251; 5.20 (1.43) | 0.06 (–0.21 to 0.32) |
| PA self-efficacy | 144; 2.47 (0.37) | 251; 2.46 (0.42) | 0.04 (–0.03 to 0.10) |
| Peer PA norm | |||
| Importance | 144; 2.25 (0.49) | 251; 2.23 (0.52) | 0.003 (–0.10 to 0.10) |
| Acceptance | 144; 2.45 (0.72) | 251; 2.33 (0.72) | –0.12 (–0.33 to 0.09) |
| Prevalence | 144; 2.80 (0.71) | 251; 2.70 (0.68) | –0.08 (–0.27 to 0.12) |
| PA social support from friends | 144; 2.70 (0.72) | 251; 2.63 (0.66) | –0.01 (–0.17 to 0.14) |
Physical activity social support
Figure 10 shows that in the PLAN-A schools, immediately after the intervention period, there was an increase (9%) in the number of Year 8 girls believing that someone in their year group had spoken to them recently about PA, compared with a decrease (12%) at this time point in the control arm schools. At T2, scores in both schools had returned to approximately baseline values, albeit slightly higher relative to baseline in PLAN-A schools. Figure 11 shows that, at baseline, a similar proportion of girls in control and PLAN-A schools thought that talking to someone in their year had helped them to be more active (41–42%). However, at T1, although this level of belief was maintained in PLAN-A schools, in control arm schools there was a 5% decrease. At T2, 34.7% and 27.8% of girls agreed with this statement in PLAN-A and control arm schools, respectively.
FIGURE 10.
Responses (% yes, no, not sure) to peer support question 1 ‘has anyone in your year group talked with you recently about PA?’ at each time point.
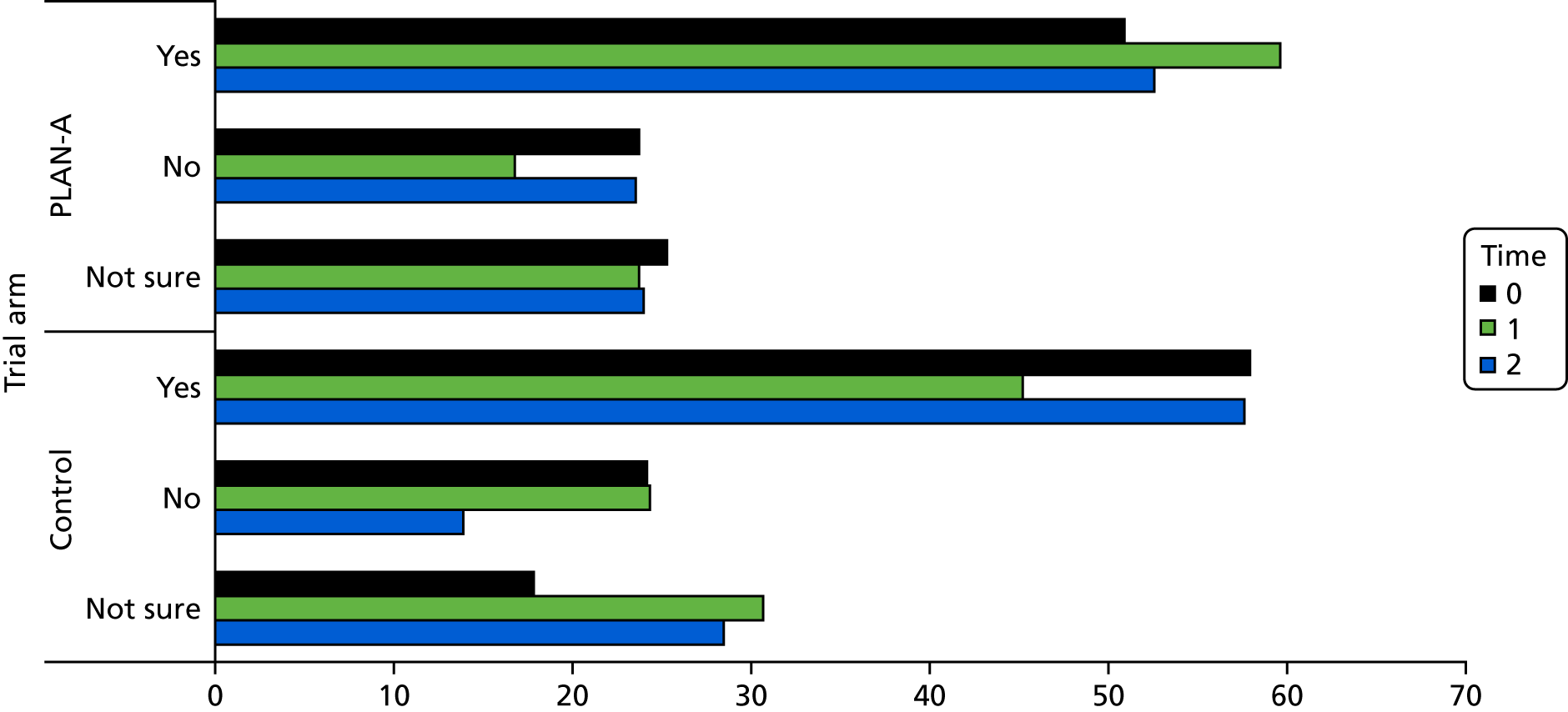
FIGURE 11.
Responses (% yes, no, not sure, NA) to peer support question 1 ’did talking to anyone in your year help you to be more active?’ at each time point. NA, not applicable.
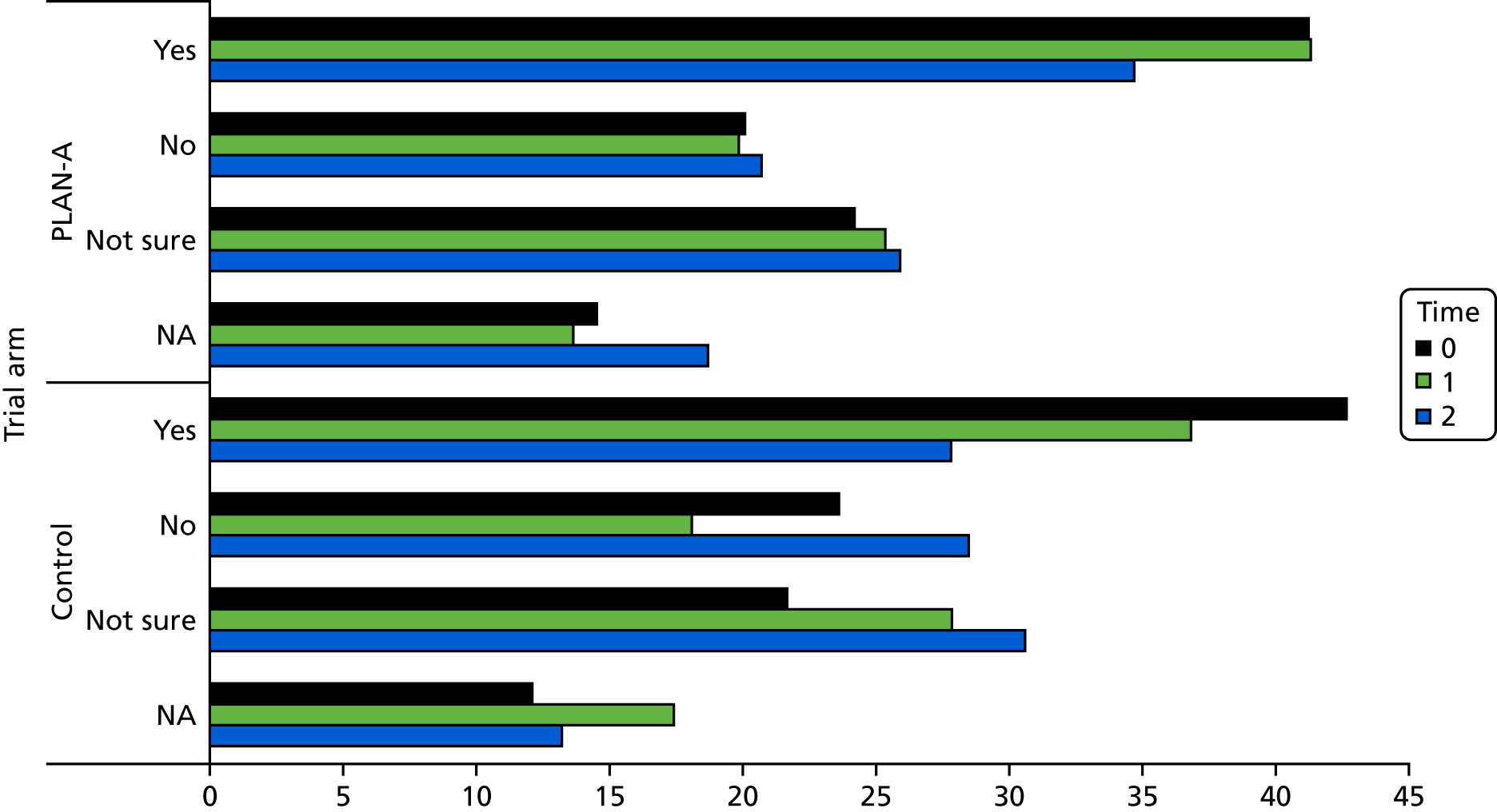
Sample size for a definitive trial
The ICC on the primary outcome for a definitive trial (i.e. weekday minutes of MVPA) from the PLAN-A arm at each time point is shown in Table 20 alongside ICC estimates of accelerometer-assessed MVPA from other studies involving adolescent girls. Based on these findings, sample size calculations for a definitive trial were based on an ICC of 0.01, but scenarios were also modelled in which the ICC was 0.02 and 0.03.
| Study | Sample characteristics | Physical activity variable | ICC (95% CI)a |
|---|---|---|---|
| PLAN-A (T0) | Year 8 girlsb (UK) | Weekday MVPA | < 0.00 (0.00 to 0.09) |
| PLAN-A (T1) | Year 8 girls (UK) | Weekday MVPA | 0.02 (0.00 to 0.06) |
| PLAN-A (T2) | Year 8 girls (UK) | Weekday MVPA | < 0.0001 (0.00 to 0.03) |
| Bristol Girls’ Dance Project83 | Year 7 girlsc (UK) | Weekday MVPA | 0.018 (< 0.001 to 0.087) |
| Trial for Activity in Adolescent Girls84 | 11- to 12-year-old girls (USA) | Weekday MVPA | 0.03 |
| Physical Activity 4 Everyone23 | 12- to 14-year-old boys and girls (Australia) | Total MVPA | 0.03 |
The results of the sample size calculations are shown in Table 21. To detect a 10-minute between-arm difference in weekday MVPA with 90% power, at the 5% significance level, and with a design effect of 1.7 (based on 70 students per school), 560 students are required (i.e. 280 per arm), inflated to 800 students in 12 schools to account for a 30% loss to follow-up. Keeping all other parameters the same and using a smaller between-arm difference in MVPA of 6 minutes (i.e. the point estimate from this feasibility study), 980 students are required (i.e. 490 per arm), inflated to 1400 students (700 per arm) in 20 schools to account for a 30% loss to follow-up.
| Between-arm difference in weekday MVPA (minutes) | Power (%) | Number of students | Number of schools | |
|---|---|---|---|---|
| Uninflated | Inflated | |||
| 10 | 90 | 560 | 800 | 12 |
| 10 | 80 | 420 | 600 | 10 |
| 8 | 90 | 700 | 1000 | 16 |
| 8 | 80 | 560 | 800 | 12 |
| 6 | 90 | 980 | 1400 | 20 |
| 6 | 80 | 840 | 1200 | 18 |
Should the ICC be 0.02 or 0.03, 800 girls in 12 schools or 1000 girls in 16 schools would be required, respectively, (after inflation for loss to follow-up) to detect a 10-minute between-arm difference in weekday MVPA with 90% power. As such, conducting a definitive trial involving 20 schools and 1400 girls would provide acceptable statistical power to detect a 6-minute difference in weekday MVPA or a 10-minute difference in MVPA should the ICC be larger than anticipated.
Adverse events
No adverse events or instances of bullying, among the girls of PLAN-A, were reported in any school.
Chapter 5 Health economics evaluation results
Intervention development
Total time spent in the initial development of PLAN-A was 185 hours, at a cost of £6533 (see Appendix 10).
Train the trainers
The total cost of ‘train the trainers’ was £3430 (Table 22), including the time and travel of trainers and of those delivering the training, training materials, venue hire and refreshments. The training was held at the University of Bristol Students’ Union for 2 days, at a cost of £120, and in a university building for the third day at no cost. The total cost of training the trainers, per trainer, was, on average, £686. In a sensitivity analysis, with 10 trainers, the cost was, on average, £502 per trainer trained.
| Staff costs | Time (hours) | Cost (£) | |
|---|---|---|---|
| Unit | Totala | ||
| Administration | |||
| Research administrator | 24 | 20 | 471 |
| Training delivery | |||
| Research associate | 15 | 28 | 423 |
| Fieldworker | 15 | 20 | 294 |
| Senior lecturer | 0.5 | 46 | 23 |
| Trainers | |||
| Trainer A | 15 | 23 | 341 |
| Trainer B | 15 | 23 | 341 |
| Trainer Cb | 12.5 | 23 | 284 |
| Trainer D | 15 | 23 | 341 |
| Trainer E | 15 | 23 | 341 |
| Total staff costs | – | – | 2857 |
| Non-staff costs | |||
| Category | |||
| Venue hire | – | – | 120 |
| Resource printing | – | – | 78 |
| Refreshments | – | – | 162 |
| Trainer car parking | – | – | 84 |
| Trainer travel | – | – | 129 |
| Total non-staff costs | 573 | ||
| Total train-the-trainer cost | 3430 | ||
| Average cost per trainer trained | 686 | ||
Delivery of the Peer-Led physical Activity iNtervention for Adolescent girls
The PLAN-A delivery costs are presented in Table 23 and the time spent by school contacts and Year 8 girls during intervention delivery is presented in Appendix 11. The average cost of peer nomination across the four PLAN-A schools was £111. Peer nomination required one fieldworker to visit each school and took 25 minutes for Year 8 girls to complete. School 4 had two peer nomination sessions: one with one half of the Year 8 girls and the second with the other half. The average cost per school of delivering the 2-day PS training was £1490 and £794 for the top-up day PS training. The total cost of delivering PLAN-A in each school varied from £2309 to £3235. Items that impacted the cost of delivering PS training included trainer time and travel costs, whether or not the students and school contact incurred travel costs and whether the training was delivered in or outside school. The total cost of the PLAN-A was, on average, £2685 per school and £37 per Year 8 girl. PSs who attended the student briefing, peer nomination, PS meeting and all 3 days of PS training spent, on average, 16 hours and 34 minutes taking part in PLAN-A. In a sensitivity analysis, costing fieldworkers and trainers at Hay band 6 or 7, the average cost was £2311 per school and £32 per Year 8 girl.
| Item | School, total cost (£); average cost (£) per Year 8 girla | All schools (n = 289b) | |||||
|---|---|---|---|---|---|---|---|
| 2 (n = 58b) | 3 (n = 96b) | 4c (n = 66b) | 6 (n = 69b) | Total cost (£) | Average cost (£) per schoola | Average cost (£) per Year 8 girla | |
| Pre-intervention preparation | 122.64; 2.11 | 122.64; 1.28 | 122.64; 1.86 | 122.64; 1.78 | 490.55 | 122.64 | 1.70 |
| Student briefing | 77.46; 1.34 | 79.26; 0.83 | 26.57; 0.40 | 40.41; 0.59 | 223.71 | 55.93 | 0.77 |
| Peer nomination | 115.43; 1.99 | 136.01; 1.42 | 98.51; 1.49 | 94.39; 1.37 | 444.35 | 111.09 | 1.54 |
| PS meeting | 122.10; 2.11 | 117.00; 1.22 | 65.94; 1.00 | 78.15; 1.13 | 383.20 | 95.80 | 1.33 |
| 2-day PS training | |||||||
| Trainer fees and travel | 908.94; 15.67 | 656.80; 6.84 | 764.68; 11.59 | 609.80; 8.84 | 2940.22 | 735.06 | 10.17 |
| Student and school contact travel | 250.00; 4.31 | 190.00; 1.98 | 0.00; 0.00 | 0.00; 0.00 | 440.00 | 110.00 | 1.52 |
| Venue hire | 200.00; 3.45 | 252.00; 2.63 | 0.00; 0.00 | 114.80; 1.66 | 566.80 | 141.70 | 1.96 |
| Refreshments | 200.84; 3.46 | 264.56; 2.76 | 219.50; 3.33 | 219.50; 3.18 | 904.40 | 226.10 | 3.13 |
| Resources and equipment | 315.48; 5.44 | 163.08; 1.70 | 315.47; 4.78 | 315.48; 4.57 | 1109.51 | 277.38 | 3.84 |
| 2-day PS training total | 1875.26; 32.33 | 1526.44; 15.90 | 1299.65; 19.69 | 1259.58; 18.25 | 5960.93 | 1490.23 | 20.63 |
| Top-up PS training | |||||||
| Trainer fees and travel | 383.08; 6.60 | 328.30; 3.42 | 368.15; 5.58 | 347.73; 5.04 | 1427.26 | 356.82 | 4.94 |
| Student and school contact travel | 150.00; 2.59 | 95.00; 0.99 | 0.00; 0.00 | 0.00; 0.00 | 245.00 | 61.25 | 0.85 |
| Venue hire | 100.00; 1.72 | 175.00; 1.82 | 0.00; 0.00 | 57.40; 0.83 | 332.40 | 83.10 | 1.15 |
| Refreshments | 115.72; 2.00 | 115.72; 1.21 | 153.85; 2.33 | 153.85; 2.23 | 539.14 | 134.79 | 1.87 |
| Resources and equipment | 157.74; 2.72 | 157.74; 1.64 | 157.74; 2.39 | 157.75; 2.29 | 630.97 | 157.74 | 2.18 |
| Top-up PS training total | 906.54; 15.63 | 871.76; 9.08 | 679.74; 10.30 | 716.73; 10.39 | 3174.77 | 793.69 | 10.99 |
| Post-intervention materials | 15.96; 0.28 | 15.96; 0.17 | 15.96; 0.24 | 15.96; 0.23 | 63.84 | 15.96 | 0.22 |
| Total intervention cost | 3235.40; 55.78 | 2869.08; 29.89 | 2309.01; 34.98 | 2327.86; 33.74 | 10,741.35 | 2685.34 | 37.17 |
Cost per increase in weekday moderate to vigorous physical activity
With the mean cost of PLAN-A at £37 per Year 8 girl and the adjusted difference in mean weekday MVPA minutes at 6.1 minutes, it was estimated that, on average, the cost per 10-minute increase in mean weekday MVPA at 12 months was £61.01 per Year 8 girl, and ranged from £38 to £162 between schools.
Quality of life
The number of missing EQ-5D-Y data were relatively low, but increased over time in both PLAN-A and control arms, and was slightly higher in the control arm (see Appendix 12). Complete data were available for the estimation of QALYs for 88% of i PLAN-A and 82% of control participants. Of those participants with missing EQ-5D-Y scores, 81% had all items in the EQ-5D-Y missing. Unadjusted EQ-5D-Y scores and estimated QALYs are presented in Table 24. Differences between arms were small and the CIs included zero. EQ-5D-Y scores in both arms decreased between baseline and post intervention, and increased between post intervention and 12 months’ follow-up. There was no evidence of an association between EQ-5D-Y scores and weekday MVPA (see Appendix 13).
| Variable | Trial arm, n; mean score (SD, 95% CI) | Difference in means (95% CI) | |
|---|---|---|---|
| PLAN-A | Control | ||
| EQ-5D-Y | |||
| Baseline | 264; 0.837 (0.202, 0.813 to 0.861) | 152; 0.844 (0.208, 0.811 to 0.878) | –0.007 (–0.048 to 0.033) |
| Post intervention | 254; 0.812 (0.227, 0.784 to 0.840) | 143; 0.836 (0.185, 0.805 to 0.866) | –0.024 (–0.067 to 0.020) |
| 12 months | 249; 0.831 (0.204, 0.806 to 0.857) | 141; 0.875 (0.176, 0.846 to 0.904) | –0.044 (–0.084 to –0.004) |
| QALYsa | 238; 0.830 (0.176, 0.808 to 0.852) | 130; 0.856 (0.142, 0.831 to 0.880) | –0.015 (–0.038 to 0.007) |
Summary
It is possible to record all the information required to estimate the cost of the PLAN-A per school and per Year 8 girl. It was also able to capture the quality-of-life data to estimate QALYs.
On average, PLAN-A cost £2685 per school to deliver, which equated to £37 per Year 8 girl. The cost per 10-minute increase in mean weekday MVPA was £61 per Year 8 girl at 12 months, but there was no evidence of an association between increased MVPA and higher self-reported health-related quality of life. The upfront development cost of PLAN-A was £6533 and the total cost of training the trainers was £3430 or £686 per trainer trained. Training more trainers at the same time could reduce this cost.
Chapter 6 Process evaluation results
Peer nomination
Outcome of peer nomination
The peer nomination process was largely successful. A small number of students copied others or felt pressure to nominate those that their friends had, but the majority of students nominated confident or active peers as they thought they would make legitimate PSs. Consistent across all schools and stakeholder groups was the perception that the girls selected to be a PS were ‘sporty’, ‘confident’, ‘outgoing’ and ‘self-motivated’, and this was the main reason for their nomination:
I think it’s because we’re all like quite sporty people.
School 2, PS focus group
If you have a non-active person telling you to be active, you wouldn’t listen to them as much would you? Because you think, well why should I, you’re not.
School 3, NPS focus group
Views on whether or not nomination had identified the influential PSs who were representative of the Year 8 girls varied between and within schools. For example, in schools 2 and 4, PSs thought that they represented different friendship groups, whereas NPSs thought that girls from the same ‘popular-type groups’ were selected. In school 2, trainers felt that the girls who were nominated could have been influential for the wrong reasons, describing them as ‘bullies’ (trainer B, top-up training day):
I think there was [sic] quite a few [girls] from lots of different ones [friendship groups].
School 2, PS focus group
There was evidence that some NPSs in school 3 viewed the PSs as potentially influential despite not being close friends:
I’m not close friends with them, but I can talk to them, but I don’t count them as friends.
School 3, NPS focus group
In one school, some PSs felt that their potential network of influence was reduced, as some of their friends were also PSs:
A lot of my friends went on the PLAN-A thing . . . like literally everybody that’s in our like group of friends went, and you kind of ran out of friends [to support].
School 6, PS focus group
Views on being nominated
There was consensus across participant groups that PSs were proud and happy to have been nominated and that they felt their nomination reflected their peers’ trust, support or confidence in their ability to be a PS. Parents suggested that their daughters were ‘shocked’, ‘proud’ and ‘really pleased’ to be nominated:
I felt quite privileged ‘cause like not everyone gets chosen, it’s nice that everyone like us gets chosen over everyone else really.
School 6, PS focus group
She was really pleased I think that people thought she could do it and like I said it just boosted her confidence.
School 2, parent
Consenting to be a peer supporter
Peer supporters were interested in becoming a PS because they liked the PLAN-A concept and wanted to help others be active:
I like the idea of helping others become more active . . . it’s the idea of helping my friends to do more stuff like inside or outside physically active [sic].
School 3, PS focus group
Peer supporters’ parents thought that the role aligned with their daughter’s characteristics, such as ‘wanting to help other people’ (school 4, parent), being ‘caring’ (school 2, parent) and having an interest in sports:
She’s just always looking for something sports wise and activity wise . . . not just for herself. So . . . I think that’s its appeal for her.
School 3, Parent
Non-peer supporters on not being nominated
Most NPSs did not mind or were relieved at not being a PS, providing some evidence that the nomination process was effective in identifying students who were sufficiently confident to influence the PA of their peers:
I didn’t want to do it because I didn’t want to have to meet new people. I don’t like talking to people who I don’t know and that made me feel really awkward about doing it.
School 4, NPS focus group
In contrast, a small number of NPSs were disappointed at not being nominated:
I like, didn’t want to do it, but when everyone else got chosen, I was a bit like, ‘well, does that mean that all of my other year group don’t think I’m good enough to do it?’.
School 4, NPS focus group
Trainer recruitment
Trainers’ personal interest in increasing adolescent girls’ PA was the main reason for their involvement:
I really am interested in PA with girls . . . I’m really passionate about that, so I thought it would be really good to have my passion, share that with these girls and motivate them to try and get other girls active . . . It was something that I’ve always wanted to do in terms of getting more females, especially, more involved in sport.
Trainer B
Train the trainers
Training was delivered over 3 days in a university studio space. All five trainers attended each of the 3 training days, except for one trainer who left 1 hour early on day 3. In general, the training was thought to be comprehensive and well delivered. The venues and duration of the training were adequate. Several trainers identified that the time lag between their training and delivering the PS top-up day training was too long. The trainers valued having time to practise delivering the activities:
There was nothing that you guys didn’t explain thoroughly . . . because we did every activity we were going to do, it gave us enough time to think about it and think how you would do it with 11, 15, 20 girls.
Trainer B
Trainer pairs were given time to work together to plan delivery, explore the resources or rehearse activities. On reflection, some trainers believed that they could have used this time more effectively by practising the delivery of activities:
. . . we used a lot of that time for writing notes, but in hindsight, it probably would have been useful to do some run throughs.
Trainer E
Trainers understood the explanation of SDT, found it interesting and motivating and agreed with the rationale for delivering the PS training consistent with SDT:
I think it was good to hear that [about SDT] for us to then kind of reinforce why we’re doing and why we want to motivate the girls and it just helps motivate us more to want to motivate the girls . . .
Trainer B
I think girls particularly need that encouragement and support and that motivational talk and confidence building, I think yeah they really can benefit from it.
Trainer A
The SDT principles aligned with the existing coaching/teaching practices of some trainers, but challenged the approach of one:
. . . my work’s been mainly [sports] coaching, so there’s not been a huge amount of group discussions about things. . . . And it’s more when I’m coaching, I’m more giving instructions.
Trainer D
The theoretical background ‘made sense’ and ‘was explained well’ (trainer B), but trainers suggested that this element should also be covered at the end of the training to revisit the theoretical concepts in light of the ‘context of what we are doing and the games we are playing with the girls and why we are playing those games’ (trainer B). Trainers A and B also wanted more guidance on how to deal with disruptive behaviour during the PS training while not undermining the theoretical principles of SDT:
It would have been nice to have somebody say to us ‘if they’re misbehaving 100% it’s okay for you to discipline’ and maybe give techniques and suggestions how to do that . . .
Trainer B
Trainers rated the trainers guide and resources to deliver the PS training as ‘very good’ or ‘excellent’ (see Appendix 14). The PS training manual was thorough, well presented and supported fidelity to the intervention (‘what to try’) and theory (‘remember to say’):
It [the trainers’ guide] was really thorough, really good . . . and then the manual I thought was really good, it was really well done, everything was laid out perfectly, I think everything you needed was in there . . . even like just little tips of what to try and remember to say, so it wasn’t like we left the training and didn’t have exactly what you guys had said.
Trainer B
All of the trainers felt prepared to deliver the PS training; however, the majority spoke about having to do additional preparatory work and two delivery pairs planned to meet up before the PS training. Some anticipated needing to recap on the top-up day content because of the gap between the train the trainers day and the delivery of the training to the PSs:
We’ve [trainers B and E] already talked about meeting up for like 1 hour for just a coffee beforehand and going over it again together.
Trainer B
I’ve now got time where I can go through it . . . then I can make sure that I know what I’m doing. I don’t know whether it would be useful to have like a little top-up day for us.
Trainer C
Peer supporter training
Attendance at peer supporter training
Attendance at all 3 days of the PS training was high, ranging between 90.91% and 100% (Table 25). In the majority of cases, absences were because of participant illness. In one case (school 2), a student had already been absent from school in the same week and her parents requested that she not attend. Attendance at training was not different in the school where training was delivered within the school setting (school 4) compared with the other schools where training was delivered off site.
| School ID (number of Year 8 girls) | Number of PSs | Attendance, n (%) | |||||
|---|---|---|---|---|---|---|---|
| Invited to training | Consenting to role | Day 1 | Day 2 | Days 1 and 2 | Top-up training day | All 3 days | |
| 2 (55) | 13 | 13 | 13 (100) | 13 (100) | 13 (100) | 12 (92.31)a | 12 (92.31) |
| 3 (88) | 17 | 17 | 17 (100) | 17 (100)b | 17 (100) | 17 (100) | 17 (100) |
| 4 (64) | 12 | 11 | 10 (90.91)c | 11 (100) | 10 (90.91) | 11 (100) | 10 (90.91) |
| 6 (69) | 14 | 14 | 13 (92.86)c | 13 (92.86)c | 13 (92.86) | 13 (92.86)d | 13 (92.86) |
Transport and refreshments
Trainers’ ratings of the PS training logistics are presented in Appendix 14; ratings were based on a 0 to 4 scale, with 0 = poor and 4 = excellent. School contacts and trainers felt that the transport provided to and from the training venue was well organised (mean 3.63, SD 1.06). The arrangements for refreshments were rated as ‘very good’ by trainers; however, the quality of the food varied between schools during the 2-day training (mean 2.00, SD 0.93), improving at the top-up day (3.75 ± 0.46). PSs and trainers suggested that there needed to be a wider selection of more ‘simple’ foods.
Venue
Training for three schools was delivered at four non-school off-site venues (three of these gave sole access to a large hall with a break-out space, tables, chairs and kitchen/toilet facilities; one venue was a small room among office space, with no break-out space and shared access to facilities with office workers). Trainers rated two of the venues as suitable and valued having sufficient space and facilities:
That [school 2 venue] was good, that was a perfect space, there was plenty of room for us and then having the kitchen separate and the bathrooms we had to ourselves, that worked really well, that was a really big space.
Trainer B, top-up
Trainers (see Appendix 14) and PSs (see Table 30) in schools 3 and 4 rated the training venues as adequate (0.50 ± 0.71 and 1.50 ± 0.71, respectively). The venue for school 3 was considered unsuitable because it was among a number of offices and there was no safe outdoor space. This venue was changed for the top-up day and received higher scores (see Appendix 14). Trainers thought that the venue size, layout and location was an important influence on the energy and engagement levels of the PSs:
If the girls are tired, if they’re just not feeling it, if the, if the [sic] venue’s not suitable, then I think that all brings them down.
Trainer C
Holding the peer supporter training within a school
In school 4, PS training was held on the school grounds. This provided trainers some more time to deliver each training day (because they did not have to travel to the training venue after registration at school). However, other students and PS commitments (e.g. music lessons) caused distractions. The trainers suggested that if a location that is separate from other students was available, then this would support delivery of the training within the school:
When you’re at school you have more time and I liked that . . . it was nice to have longer to do the reflection and relaxation thing, I almost prefer at the school, if there was a room where nobody was going to come into.
Trainer B
The school contact recognised that although PSs felt privileged ‘they would probably [have] felt more special if they were going out for the day’. PSs liked that the training was held within the school because it was familiar; however, PSs also recognised that they needed a bigger space and felt the usual school day structure (including the bell) was distracting:
that was better because you’re in the place where you knew.
and if you needed to go anywhere you knew where it was.
School 4, PS focus group
Length of training
The length of training was acceptable to PSs (see Table 30), school contacts and trainers, whereas some trainers thought that it was a long/intense day for the PSs and provided longer breaks. However, the PSs commented that the amount of activities ‘did not make the day feel really long’ (school 4, PS focus group). Although a greater number of shorter training days was suggested as an alternative, the structure of 2 consecutive days was acceptable and gave continuity to the training:
I think it’s the right approach 2 consecutive days, because you get that continuation. It’s whether they could have done 3 half-days with lunch, I don’t know?
Trainer D
Parents reported being aware of the training arrangements and were happy for their daughters to take the required 3 days out of usual lessons:
I think it was worthwhile, yes absolutely, to try and let’s say the recognition and the confidence building, the kind of soft skills that she got, absolutely I think 3 days is fine.
School 2, Parent
Timings of activities
The trainers were largely successful in delivering most activities close to time throughout days 1 and 2 (see Appendix 15). A minority of activities varied greatly from the allocated delivery time. For example, the ‘A day in my life: part 1’ activity on day 1 took an average of 18 (± 13.0) minutes longer to deliver than allocated and trainers took 15 (± 1.0) minutes less to deliver the ‘Introduction to “Like a girl”‘ activity. In general, the time allocated for the ‘post box’ was not used and lunch often over-ran.
The timings of activities on the top-up training were more varied than days 1 and 2 (see Appendix 15), with approximately half running close to the allocated time. Specific activities that were not delivered to time included ‘Our challenges’ (9 minutes longer) and ‘Self-esteem tree’ (15 minutes shorter).
Trainers and PSs indicated that the timing of activities was achievable and ‘did not all feel like one bit was rushed’ (school 4, PS focus group). The time of day, the venue and the engagement level of the PSs affected timing of delivery:
I think most of the lengths were fine, ‘cause a lot of them we did fill up the time allotted, some of the ones we didn’t were like the introduction at the beginning of the day, especially because they’re not talkative yet ‘cause they’re not comfortable with you yet an [sic] they’re not in the zone . . .
Trainer B
The importance of having access to outside space and PA opportunities during breaks in order to help keep focus was made clear:
I kind of felt like I was stuck inside and sometimes it was like sunny outside and I kind of just wanted to go outside rather than being inside the whole time.
School 6, PS focus group
. . . when they had the breaks and they had all the skipping ropes out. They were really happy just to do that.
School 6, school contact
Each trainer pair was observed once throughout the 2-day training and on the top-up day training. Observational findings show that throughout all of the training days, all trainer pairs skipped or adapted some activities. This flexible adaptation worked well in general; however, on a handful of occasions this had a detrimental effect resulting in PSs losing focus or sitting down and writing for longer periods of time:
. . . we added in another warm-up thing at the beginning. . . . Because I think they all really enjoyed that sense of playfulness and part of the thing of them being away from school.
Trainer E, top-up
The trainers were successful in giving clear instructions and facilitating the smooth running of each day, particularly on the top-up day during which the trainers gave a good recap about the project. Over-running on activities was usually because of the trainer’s attempts to consider and listen to all opinions in discussion tasks. In some instances, less important elements of activities were focused on leading to a reduction in PA engagement and later activities being rushed.
Materials and resources
The ‘session plans’ and resources used to deliver the training were both rated as very good (3.25 ± 0.46 and 3.87 ± 0.35, respectively; see Appendix 14):
I think it is really, really useful to have that [trainers’ guide] as a backup information definitely because especially for someone like me you know that is not my background and I don’t know a lot of the theory behind it . . .
Trainer A
There were mixed views on the ‘PS booklet’ and ‘diary’. Some PSs described them as a prompt to converse with peers and a source of information, whereas others used them only ‘once or twice’ (school 3, PS focus group). Observations noted that this resource was not effectively introduced by any of the trainers to any of the PSs:
I think it [PS booklet] helps you remember some more, because you had the book and it told you what to do and how to start what you were saying to someone.
School 4, PS focus group
Some parents reported seeing their daughter using the booklet or looking through it with her:
I went through all the book with her and she really was really taking the stuff on board.
School 4, Parent
Delivering in trainer pairs
On the whole, trainer pairs worked well together and benefited from the support and energy that delivering the training in pairs brought. Trainers suggested that they should deliver in pairs for both the 2-day and top-up day training to maintain the rapport formed with the PSs:
I think working as a pair is a really good thing. I think doing it on your own would be quite hard and intense and being able to share it and have someone to you know have that back-up and you know different energies and qualities.
Trainer A
I guess now looking back I don’t think it’s [having a different trainer for the top-up day] ideal because they don’t know me . . . it was nice to have the girls get to know you especially from the beginning . . . It’s like, then they come on that second day and they know they’re going to trust you already.
Trainer B
There were a small number of difficulties in pair delivery as a result of different levels of communication skills, student management and flexibility in delivery within pairs:
I think [trainer] was just trying to stick to the plan of the thing quite a lot.
Trainer ID concealed for anonymity
View on the content of the peer supporter training
Table 26 shows that the PSs enjoyed all 3 days of the training. Enjoyment increased from day 1 to day 2 (mean ± SD = 3.60 ± 0.77 and 4.24 ± 0.58, respectively). Enjoyment levels were similar on the top-up day to day 1. Trainers’ perception of PS enjoyment was similar to the PS ratings of enjoyment (Table 27).
| School ID | Training time point, mean (SD) | ||
|---|---|---|---|
| Day 1 | Day 2 | Top-up day | |
| 2 | 4.00 (0.82) | 4.54 (0.52) | 3.75 (0.62) |
| 3 | 3.06 (0.56) | 3.82 (0.39) | 3.47 (0.72) |
| 4 | 3.90 (0.74) | 4.36 (0.67) | 3.64 (0.51) |
| 6 | 3.38 (0.96) | 4.23 (0.73) | 3.54 (0.52) |
| Total | 3.60 (0.77) | 4.24 (0.58) | 3.58 (0.60) |
| Question | School ID | All schools, mean (SD) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2 | 3 | 4 | 6 | ||||||||||
| Mean (SD) | Trainer B | Trainer E | Mean (SD) | Trainer C | Trainer A | Mean (SD) | Trainer B | Trainer E | Mean (SD) | Trainer A | Trainer D | ||
| 2-day training | |||||||||||||
| How involved were they? | 2.00 (0.00) | 2.00 | 2.00 | 2.00 (0.00) | 2.00 | 2.00 | 3.00 (0.00) | 3.00 | 3.00 | 2.50 (0.71) | 3.00 | 2.00 | 2.38 (0.52) |
| How engaged were they? | 2.00 (0.00) | 2.00 | 2.00 | 2.50 (0.71) | 3.00 | 2.00 | 3.00 (0.00) | 3.00 | 3.00 | 2.50 (0.71) | 3.00 | 2.00 | 2.50 (0.54) |
| How much did you think they enjoyed themselves? | 2.00 (0.00) | 2.00 | 2.00 | 2.00 (0.00) | 2.00 | 2.00 | 3.00 (0.00) | 3.00 | 3.00 | 2.00 (0.00) | 2.00 | 2.00 | 2.25 (0.46) |
| What was their overall level of interest? | 2.00 (0.00) | 2.00 | 2.00 | 2.00 (0.00) | 2.00 | 2.00 | 3.00 (0.00) | 3.00 | 3.00 | 2.00 (0.00) | 2.00 | 2.00 | 2.25 (0.46) |
| Question | Mean (SD) | Trainer B | Trainer C | Mean (SD) | Trainer C | Trainer D | Mean (SD) | Trainer B | Trainer E | Mean (SD) | Trainer B | Trainer D | All schools, mean (SD) |
| Top-up day training | |||||||||||||
| How involved were they? | 1.50 (0.71) | 1.00 | 2.00 | 3.00 (0.00) | 3.00 | 3.00 | 2.50 (0.71) | 2.00 | 3.00 | 1.50 (0.71) | 1.00 | 2.00 | 2.13 (0.84) |
| How engaged were they? | 1.50 (0.71) | 2.00 | 1.00 | 3.00 (0.00) | 3.00 | 3.00 | 2.50 (0.71) | 2.00 | 3.00 | 1.50 (0.71) | 1.00 | 2.00 | 2.13 (0.84) |
| How much did you think they enjoyed themselves? | 1.50 (0.71) | 2.00 | 1.00 | 2.00 (0.00) | 2.00 | 2.00 | 2.50 (0.71) | 2.00 | 3.00 | 2.00 (0.00) | 2.00 | 2.00 | 2.00 (0.54) |
| What was their overall level of interest? | 2.00 (0.00) | 2.00 | 2.00 | 2.50 (0.71) | 3.00 | 2.00 | 2.50 (0.71) | 2.00 | 3.00 | 1.50 (0.71) | 1.00 | 2.00 | 2.13 (0.64) |
Qualitative evidence from all stakeholders suggested that PSs liked the novelty, participatory inclusiveness and autonomy of the training:
I think they enjoyed it. There was laughter, which is always a good sign.
Trainer C
I think it was about it being different; we hadn’t done anything like it before so it was just nice to try something new . . . It was a lot more we were involved, in classes we just get a teacher telling us things.
School 4, PS focus group
PSs found the training activities enjoyable and interesting (see Table 30). In particular, active games, competitions, working together and interactive activities (e.g. role-plays, discussions about videos) were enjoyable (see Appendix 17) and engaging because they differed from usual school-based learning:
I liked the alphabet game. It got us all together and it was like a competition and it made us think more as a group.
School 3, PS focus group
I think the things that are less like school are even better because they think then this is fun day, and then it’s less like they don’t even realising how much they’re learning at the moment, they’re just having fun.
Trainer B
. . . the discussions that come out of that ‘Like a Girl’ video exercise afterwards I think are brilliant in terms of what is going on in their groups . . .
Trainer A
They loved that video [Like a Girl] and they talked about that for ages.
School 2, school contact
Trainers and school contacts felt that the large majority of training activities were well conceived, flowed well, provided a clear message and were pitched at the right level. However, PSs from one school found some wording difficult to understand and struggled to give their opinion:
It probably meant something simple but it was a bigger word that no one really understood and that one didn’t have as many answers.
School 3, PS focus group
A lot of us struggled when we had to give our opinion on why picked stuff [sic] because you feel like you’re either going to be wrong [sic].
School 3, PS focus group
In contrast to the interactive tasks, PSs lost focus and struggled with behaviour when activities covered information that they already knew, and they did not enjoy activities that involved lots of writing, sitting and listening or repetition (see Appendix 17):
. . . the odd little bit that may have been a little bit wishy-washy in the sense that it is something that the kids were already aware of. And maybe that could have been why they lost concentration at times – or was less engaging.
School 2, school contact
It took ages and I think we remembered it more than they thought we would of [sic], so we didn’t really need to go through all of it again.
School 4, PS focus group
I think just sometimes sitting down for a bit longer than other times. . . . I think it is probably listening for a long time.
School 6, PS focus group
Many PSs believed that the 3-day training would be more active/sporty than it was:
I thought it was going to be more active. We talked a lot about being confident and stuff and I thought we were going to play some activities like, I don’t know, run round a field or something like that but we didn’t.
School 3, PS focus group
Although script writing and role-play was relatively unpopular at the 2-day training, it was the most enjoyed activity during the top-up day (see Appendix 17). This may reflect the PSs seeing the relevance of role-play at the top-up training, having had experienced being a PS for 5 weeks or their growing confidence:
I think some of the girls are kind of quite outgoing, confident, so the whole role-playing thing was great for them, they loved it. Whereas other girls, that’s their idea of hell and so for them that isn’t their thing so basically they’re a little bit out of their comfort zone.
School 3, school contact
Trainers reported that PSs also found it hard to understand the goal-setting task:
They found it [SMART (specific, measurable, achievable, realistic and timely) goals] quite hard to do it or they maybe misunderstood that it was in relation to . . . It’s more of a workplace, an adult thing . . . they did struggle a bit to get to grips with that one.
Trainer D
Most PSs would recommend the training to potential PSs, citing that it was fun and educational and motivated them to increase their PA:
You learn so much more and it really does change your mind about things.
School 2, PS focus group
I think it’s [sic] made me more confident.
School 3, PS focus group
The extent to which each training activity objective was achieved was assessed by the observer (see Appendix 18). For the majority of activities, objectives were achieved to at least some extent or lots on all training days and there was little variation between trainer pairs. When learning objectives were not achieved well [e.g. day 2 ‘communication skills’ (mean 1.75, SD 0.71)], the observations showed that delivery of the activity was suboptimal through either poor explanation, poor use of space or a lack of linking the activity to the role of a PS.
Peer supporter engagement with the training
On the whole, trainers and school contacts thought that the PSs had a positive attitude towards the training and their role as a PS. Trainers agreed that the PSs were excited and felt that they were ‘in a privileged position’ (trainer A) to attend the training:
I think the girls were really positive, they were positive about the whole event.
School 2, school contact
They seemed enthusiastic to be there. And they still seemed like something that was important to them.
Trainer E
In some cases, trainers thought PSs viewed the training as ‘a day out of school’ (trainer B, top-up), and in school 2 the trainers felt the PSs ‘were not really that fussed about it [being a PS]’ (trainer C, top-up). These findings are supported by the trainer survey findings (see Table 27).
Peer supporters engaged well in the activities on all 3 days. Engagement decreased throughout the afternoon of day 1, which corresponds with the lower enjoyment levels on day 1 (see Table 26). However, engagement was maintained throughout day 2 and the top-up day. Engagement levels did not differ between trainer pair/school and no particular activities elicited poor engagement. Notes from the observer’s and trainers’ evaluations support this; trainers rated the PSs as being engaged in the 2-day training (mean 2.50, SD 0.54) and top-up day (mean 2.13, SD 0.84) and were involved and interested in the activities:
You could tell they were really listening and not just pretending to listen, it was like they wanted to be there . . . when they were giving answers it was like they had the read the book! The way that they were genuinely understanding what we were talking about . . . what we were saying to them was getting through to them and they understood it.
Trainer B
However, the scores indicate some room for improvement and the qualitative evidence suggested that PSs were less engaged and/or lost concentration during longer and less varied or (inter)active tasks. At these times, the trainers found delivery difficult, particularly when PSs could not report any PS actions:
I would try and ask them . . . ‘Well, can you see yourself in a conversation?’ I wouldn’t get anything. Nobody would even shake their head yes or no. It was flat, nothing. . . . So then I felt like, ‘well now I’m putting things in their head and I’m assuming’ but they weren’t talking.
Trainer B
Peer supporter engagement was also influenced by the characteristics and behaviour of the group. School 6 in particular was challenging to engage and work with, with both trainers describing it as ‘like pulling teeth’ (trainer B). Behaviour problems in school 2 affected the level of engagement and interest. This is supported by the data in Table 27 that show lower interest and involvement for schools 2 and 6. In school 2, such behaviour made the trainers question how these PSs would carry out their role and how they would talk to others:
We were kind of thinking ‘oh my gosh, if they go and talk to their friends like this, it’s not going to be encouraging them, that’s really going to put them off’.
Trainer E
Interestingly, PSs recognised when their behaviour was poor and challenging for the trainers:
‘Cause we are still like kids, if we do something [wrong] and they like tell us off, but it won’t go into our heads straight away. If they tell us to stop talking then us being like kids we always try to finish the conversation . . .
School 2, PS focus group
Impact of training on peer supporters
Peer supporters felt that their confidence to promote PA among their peers increased as a result of completing the 2-day training (mean 3.33, SD 0.68) and top-up day (mean 3.38, SD 0.69) (see Table 30). Despite this, PSs commonly wanted further support to develop confidence to talk to people and start a conversation and with what to say (Table 28).
| Category | Frequency reported (n) | ||||
|---|---|---|---|---|---|
| School ID | Total | ||||
| 2 | 3 | 4 | 6 | ||
| Confidence to talk to people | 3 | 7 | 4 | 4 | 18 |
| How to start a conversation, knowing what to say and when | 2 | 3 | 1 | 4 | 10 |
| Being patient and tolerant | 5 | 1 | 0 | 0 | 6 |
| Being persuasive | 1 | 1 | 0 | 2 | 4 |
| Building other people’s confidence | 1 | 2 | 0 | 0 | 3 |
| Fun ideas of ways to get people active | 0 | 0 | 2 | 1 | 3 |
Trainers expressed some reservations (Table 29) about whether or not the training increased PS confidence to instigate conversations with their peers (mean 2.63, SD 0.74) and, in a minority of cases, questioned how realistic some of the PS-generated practice conversations were:
Sometimes when they were writing conversations I was thinking ‘is this really a conversation you know you would have?’.
Trainer A
| Objective | School ID | All schools, mean (SD) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2 | 3 | 4 | 6 | ||||||||||
| Mean (SD) | Trainer B | Trainer E | Mean (SD) | Trainer C | Trainer A | Mean (SD) | Trainer B | Trainer E | Mean (SD) | Trainer A | Trainer D | ||
| 2-day training | |||||||||||||
| Increase PSs’ PA knowledge | 2.50 (0.71) | 2.00 | 3.00 | 2.50 (0.71) | 2.00 | 3.00 | 2.50 (0.71) | 2.00 | 3.00 | 2.50 (0.71) | 2.00 | 3.00 | 2.50 (0.54) |
| Enhance PSs’ interpersonal skills | 1.50 (0.71) | 1.00 | 2.00 | 2.00 (0.00) | 2.00 | 2.00 | 2.50 (0.71) | 2.00 | 3.00 | 2.50 (0.71) | 2.00 | 3.00 | 2.13 (0.64) |
| Enhance PSs’ communication skills | 1.50 (0.71) | 1.00 | 2.00 | 2.00 (0.00) | 2.00 | 2.00 | 2.50 (0.71) | 2.00 | 3.00 | 2.50 (0.71) | 2.00 | 3.00 | 2.13 (0.64) |
| Enhance PSs’ confidence starting peer conversations | 1.50 (0.71) | 1.00 | 2.00 | 3.00 (0.00) | 3.00 | 3.00 | 3.00 (0.00) | 3.00 | 3.00 | 3.00 (0.00) | 3.00 | 3.00 | 2.63 (0.74) |
| PSs’ understanding of their role | 1.50 (0.71) | 1.00 | 2.00 | 2.50 (0.71) | 2.00 | 3.00 | 3.00 (0.00) | 3.00 | 3.00 | 2.50 (0.71) | 3.00 | 2.00 | 2.38 (0.52) |
The qualitative evidence supported the scores in Table 30 that show that the PSs understood their role. The girls demonstrated that their role was not to talk to students they did not know, that they knew when it was appropriate to offer support and that they understood that there are different forms of PA to suggest:
Knowing that a lot of things are exercise was really reassuring, you are doing exercise, it’s just not in some other ways [sic].
School 4, PS focus group
| Statement | School ID, mean (SD) | Total, mean (SD) | |||
|---|---|---|---|---|---|
| 2 | 3 | 4 | 6 | ||
| 2-day training | |||||
| I understand my role as a PS | 3.92 (0.29) | 3.76 (0.44) | 3.82 (0.41) | 3.91 (0.30) | 3.84 (0.37) |
| The length of training was about right | 3.67 (0.65) | 2.82 (0.81) | 3.27 (0.79) | 3.45 (0.69) | 3.25 (0.80) |
| The training was interesting | 3.50 (0.52) | 2.59 (0.87) | 3.36 (0.51) | 2.91 (0.83) | 3.04 (0.80) |
| I learned some new things about PA | 3.83 (0.39) | 3.24 (0.90) | 3.91 (0.30) | 3.64 (0.51) | 3.61 (0.67) |
| The venue was a good place to do the training | 3.17 (1.12) | 2.59 (0.87) | 2.18 (0.87) | 2.45 (1.13) | 2.51 (1.16) |
| I enjoyed the games | 3.42 (0.79) | 3.24 (0.83) | 3.55 (0.52) | 3.60 (0.52) | 3.42 (0.70) |
| I had enough time to practise being a PS | 3.42 (0.67) | 2.29 (1.26) | 3.09 (0.83) | 3.09 (0.94) | 3.10 (0.83) |
| I am confident that I can pass positive messages on to my friends about getting active | 3.75 (0.45) | 3.24 (0.83) | 3.36 (0.92) | 3.00 (0.63) | 3.33 (0.68) |
| The trainers were helpful | 3.83 (0.39) | 2.88 (0.86) | 3.55 (0.52) | 3.30 (0.68) | 3.52 (0.58) |
| The trainers were friendly | 3.83 (0.39) | 3.24 (0.56) | 4.00 (0.00) | 3.80 (0.63) | 3.80 (0.54) |
| Top-up day training | |||||
| I understand my role as a PS | 3.83 (0.39) | 3.94 (0.24) | 4.00 (0.00) | 3.85 (0.38) | 3.91 (0.30) |
| One top-up day was enough | 3.17 (0.84) | 3.18 (0.66) | 3.18 (0.64) | 3.08 (1.32) | 3.15 (0.86) |
| The training gave me new tips and help on being a PS | 3.42 (0.52) | 3.06 (0.90) | 2.73 (1.00) | 3.31 (0.75) | 3.13 (0.83) |
| I learned some new things about PA | 3.08 (1.08) | 2.82 (0.81) | 2.55 (1.37) | 3.00 (0.85) | 2.87 (1.01) |
| The training reminded me of important things about being active | 3.42 (1.00) | 3.18 (0.53) | 2.82 (1.17) | 3.38 (0.65) | 3.21 (0.84) |
| I enjoyed the games | 3.50 (0.80) | 3.41 (0.94) | 3.09 (0.94) | 3.23 (0.83) | 3.32 (0.87) |
| I had enough time to practise being a PS | 3.33 (0.89) | 3.00 (0.79) | 3.18 (1.08) | 3.00 (1.08) | 3.11 (0.93) |
| I am confident that I can pass positive messages on to my friends about getting active | 3.25 (0.87) | 3.29 (0.59) | 3.45 (0.69) | 3.54 (0.66) | 3.38 (0.69) |
| The trainers were helpful | 2.92 (1.08) | 3.12 (0.60) | 3.73 (0.47) | 3.31 (0.75) | 3.25 (0.78) |
| The trainers were friendly | 3.08 (0.90) | 3.18 (0.73) | 3.73 (0.47) | 3.69 (0.48) | 3.40 (0.72) |
Peer supporters reported gaining new knowledge about PA among girls, PA guidelines and benefits and the distinction between PA and sport (see Table 30; see Appendix 19). In addition, PSs reported building their communication skills and self-confidence. This corresponds with the trainer-rated achievement of objectives (see Table 29; Table 31), including enhancing PS knowledge of PA and their interpersonal and communication skills. Focus group evidence supported the quantitative findings and demonstrated how improvements in having the confidence to talk to others, problem-solving and PA knowledge worked together:
When you have the right information, [it] sort of gives you confidence and they [the trainers] said to go round obstacles that might occur.
School 4, PS focus group
| Objective | School ID | All schools, mean (SD) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2 | 3 | 4 | 6 | ||||||||||
| Mean (SD) | Trainer B | Trainer C | Mean (SD) | Trainer C | Trainer D | Mean (SD) | Trainer B | Trainer E | Mean (SD) | Trainer B | Trainer D | ||
| Top-up day training | |||||||||||||
| Increase PSs’ PA knowledge | 1.50 (0.71) | 1.00 | 2.00 | 2.50 (0.71) | 2.00 | 3.00 | – | – | 2.00 | 1.50 (0.71) | 1.00 | 2.00 | 1.86 (0.69) |
| Enhance PSs’ interpersonal skills | 1.00 (0.00) | 1.00 | 1.00 | 2.50 (0.71) | 2.00 | 3.00 | 1.50 (0.71) | 1.00 | 2.00 | 1.50 (0.71) | 1.00 | 2.00 | 1.63 (0.74) |
| Enhance PSs’ communication skills | 1.00 (0.00) | 1.00 | 1.00 | 2.00 (0.00) | 2.00 | 2.00 | 1.50 (0.71) | 1.00 | 2.00 | 2.00 (0.00) | 2.00 | 2.00 | 1.63 (0.52) |
| Enhance PSs’ confidence starting peer conversations | 1.00 (0.00) | 1.00 | 1.00 | 3.00 (0.00) | 3.00 | 3.00 | 2.50 (0.71) | 2.00 | 3.00 | 2.00 (0.00) | 2.00 | 2.00 | 2.13 (0.84) |
| PSs’ understanding of their role | 1.00 (0.00) | 1.00 | 1.00 | 2.50 (0.71) | 2.00 | 3.00 | 2.50 (0.71) | 2.00 | 3.00 | 1.50 (0.71) | 1.00 | 2.00 | 1.88 (0.84) |
Trainers’ perceptions of achieving the training objectives were generally lower on the top-up day than on the 2-day training. This may be because there is a ceiling effect following the high achievement rates at the 2-day training and it suggests that different objectives should be assessed after the top-up day. This finding may also be because of the poor achievement of objectives in school 2. The qualitative work indicated that this was a result of the behaviour of the children in school 2; trainers felt that the time they spent trying to manage this may have had an impact on what they managed to achieve throughout the training. This was not experienced in any other schools.
As a result of improving PS knowledge and their confidence to talk to people, the PSs felt prepared to support their friends, and their parents agreed:
Like slipping it into a conversation was pretty easy after we learnt how to do it [agreement]. Like before you’d be like ‘urrrr’ . . . But, yeah, learning it I think it actually helped.
School 4, PS focus group
However, some PSs were apprehensive to peer support because they were unsure of how to start and have a conversation promoting PA:
They didn’t tell you so much about going up to people and like how to start off the conversation.
School 6, PS focus group
Peer supporters reported an increased personal awareness of their activity levels and those of girls in England, which motivated them to increase their PA:
It like changed how like active you were, because like I wasn’t very active but then I’ve heard like only 8% of girls are active, so I started being more active.
School 6, PS focus group
Furthermore, in the schools where the year group was structured in two halves, PLAN-A helped integrate the two sides of the year and build friendships:
I think it’s also good that we interact with the other side of the year and sort of made friends with them as well.
School 4, PS focus group
The trainers, PSs and school contacts believed that the top-up day was an important and beneficial element of the training. Key content involved revisiting important PA information, supporting confidence and exploring how to communicate, providing a reminder of the PS objective/role and encouragement to continue peer supporting:
I think the top-up day kind of enforced [reinforced] the fact that you are actually trying to do something important.
Trainer C, top-up
Just to remind us . . . because after you have been to a top-up day we always think ‘we need to do this’ and then I’ll forget about it.
School 2, PS focus group
Self-determination theory outcomes, theoretical fidelity and participant perceptions
Need-supportiveness of trainers and peer supporters’ perceptions of need support
Peer supporters rated the trainer autonomy support as high during the 2-day training (mean 3.31, SD 0.63; possible range 0–4) and slightly lower at the top-up day (mean 2.92, SD 0.80). These scores are reflected in the qualitative findings; however, there was no clear explanation for the lower scores at the top-up day.
Autonomy support
Both the PSs and the trainers felt that during the training, the girls were given a variety of options and choices and felt that their input was valued. The PSs appreciated the way this was inclusive, which fostered rapport with the trainers:
They understood. They were saying it nicely, not telling us like do that, do this.
School 3, PS focus group
. . . they were supportive to everyone who was saying their reasons, they were supportive to everyone.
School 4, PS focus group
Peer supporters enjoyed being involved in the direction of the training; however, they felt more controlled in the PS role-play activity. This, in combination with the long training day, was seen to contribute to a lack of engagement in one school:
We had to act it [a role-play] out.
School 2, PS focus group
The trainers were really good. Sometimes maybe they could have spoken to or bonded with the girls a little bit differently to play to the girls’ strengths. Rather than ‘this is how we’re going to do it’. Just because it was a long day for the girls with it being full days . . .
School 2, school contact
Trainers provided regular positive feedback and supported learning by using role models in the group:
You know like saying ‘this is really good. Do you mind saying that out loud?’
Trainer B, top-up
Trainers ensured that the PSs felt comfortable sharing their views and answered their questions, which made the PSs feel understood and valued:
They [the trainers] understood what I was saying and they just didn’t keep skipping people out . . .
School 4, PS focus group
Competence support
Trainers took an informational approach to explaining the PS role, making it clear that PSs should feel comfortable with the peers they talk to and helping them develop realistic support/diffusion strategies. Most trainer pairs made sure that the PSs fully understood how to implement their new knowledge in a peer-supporting scenario:
I want to get through everything I can to them and to try and get them to understand their role as a PS.
Trainer C, top-up
Trainers were supportive when PSs reported undertaking little peer supporting:
We did kind of make a point of saying to them ‘it is OK if you haven’t had any conversations yet. You know, that’s completely fine. Nobody will be cross about that or annoyed. And if you haven’t it’s just good and helpful for us to know why you haven’t and you know to just be able to talk about it’.
Trainer E, top-up
At times, the trainers could have given more detailed answers to PSs’ questions, and there were occasions when trainers did not address important issues or correct PSs on key mistakes throughout the training. In addition, trainer pair B and E did not circulate among the group to support the girls as much as the other trainers. Some trainers focused too much on having conversations as a way to peer support and did not make it clear that there were other methods (e.g. co-participation). However, trainers recognised when PSs needed help and broke activities down into simpler steps and used teamwork activities to provide reassurance:
. . . because it was tricky with the second school, we used something [team-building activities] that we had seen the girls [from another school] doing and it worked really well.
Trainer E
The delivery in trainer pairs and good working relationships between trainers facilitated the provision of competence support by accommodating girls working at different paces:
I think [trainer E] and I worked well together, if I was then trying to help the group that was still going, she would go over and say ‘OK well why don’t you start thinking about this’ and I think that’s why it’s good that there’s two of you . . .
Trainer B
Trainers also used structure to support PS competence, demonstrating strong fidelity to the breadth of autonomy support concepts:
[Trainer E] and I had to actually go back to our rules for the day and say ‘remember we said this was a rule for today, you need to be listening to us as well’ . . .
Trainer B
Poor PS behaviour challenged the balance between structure and autonomy support in school 2. One trainer was concerned that the PSs may feel negative towards the project as a result and put in place strategies to resolve this challenge:
We were quite concerned that the amount of times we had to say to them ‘okay, it’s time to be quiet now’ . . . they were going to end up not liking us and the not liking us would impact on how positive they felt about the study, about being a PS. So we were really trying to combat that on the second day, to be really encouraging.
Trainer E
This was echoed by the PSs who, on occasion, felt that the trainers were ‘kind of strict and stuff and it got kind of annoying’ and they could ‘lighten up a bit’ (school 2, PS focus group) but who suggested that this was necessary when they were misbehaving. By the end of the 2-day training, the trainers felt confident that the PSs were capable of peer supporting:
We felt like they were all totally capable of it and they all got the idea.
Trainer E, top-up
Relatedness support
The PSs agreed that the trainers were both helpful (mean 3.25, SD 0.78) and friendly (mean 3.40, SD 0.72), for the 2-day and top-up day training (see Table 29). The qualitative results support this; school contacts and PSs agreed that the trainers delivered the training effectively, were very friendly, made the PSs feel valued and listened to, and had positive interpersonal interactions:
They were loud enough and like they interacted with us and they were funny.
School 3, PS focus group
The trainers were described positively as ‘not like teachers’ (school 6, school contact), approachable, understanding and supportive:
. . . you have that sense of when you go into a room with the teachers you know that you have to do the lesson but with the trainers they were more approachable, you were quite happy to have their interaction.
School 6, school contact
There was strong evidence from school contacts, trainers and PSs that the majority of trainers found it easy and were successful in forming a rapport with the PSs. The trainers felt a sense of trust from the girls and the girls felt understood by the trainers:
I thought the young girl [trainer], the girls really related to well.
School 3, school contact
I think it was quite easy for me to build rapport with them.
Trainer C, top-up
Trainers built relatedness with the PSs by talking/mutual sharing with the girls about life outside PLAN-A, including their PA. Central to this was listening to and valuing the girls’ opinions and inspiring the PSs through role modelling:
. . . they answered a lot of questions about themselves and how they’re active and [trainer C] was on about she does [sport] . . .
And she goes to the gym three times a week or whatever.
And [trainer A] goes running and it helped us feel more comfortable because they’re active.
And they were telling us a bit about themselves because we told them a bit about ourselves.
And like how they be active so that can influence us on how they’re active.
School 3, PS focus group
Other strategies used to support relatedness included circulating among PSs during activities to provide help, frequent verbal interactions, encouraging teamwork, working on tasks with the PSs, asking and answering lots of questions, listening to all PSs and giving clear explanations. This was supported by the training observations:
[We would] sometimes sit on the floor with them . . . so when we would then discuss it . . . I really think they liked that because we were all on the same level.
Trainer B
The trainers empathised with the PSs and understood the challenges and difficulties of being an adolescent girl. This helped them understand the challenges of being a PS:
I think we forget how much is going on in their lives and how much they’re doing on a daily basis and a weekly basis and the hunt for time is just so different for them.
Trainer B, top-up
In some instances, trainers used the relatedness they built within the group to encourage less confident PSs to engage in the training:
. . . we knew there was one we wanted to work with, a certain girl, ‘cause she brought her out of her shell, it was really nice, and she was way more talkative and they were talking about good things, it was nice to see that . . .
Trainer B
There was evidence that the intervention design and materials facilitated the development of relatedness between trainers and PSs:
I think it helped [that] on day 1, we did the personal profiles.
Trainer C
I guess it is nice because you’re taking them out of their usual situation and giving them something a bit different, so in that sense it’s quite easy to build a rapport, because you are doing something fun with them.
Trainer E
Forming a relationship with the PSs was helpful when trainers returned to deliver the top-up day training, which they found easier to deliver because they knew the PSs and the PSs liked seeing the same trainers again:
It was really nice that she was on all the training so she was on the 2 days and she was on the top-up day as well. I think that was really nice because they could relate back to what they had done before . . .
School 3, school contact
Challenges of delivering the peer supporter training in line with self-determination theory principles
Despite evidence for high fidelity to the SDT-based motivational climate, trainers also experienced barriers to need support, most commonly poor behaviour/disruption by PSs, low engagement and large groups. At school 2, in particular, student disruption often resulted in activities not being covered in necessary depth and the chaperone having to manage the disruption:
So I think that’s why it was hard with people who are super misbehaving because I felt like that was taking away from what PLAN-A actually is and what we’re supposed to be as PLAN-A trainers.
Trainer B, top-up
When the PSs were less proactively engaged, some trainers referred to identifying alternative, more controlling, strategies to activities to encourage PSs to engage:
. . . if somebody is really not having it and they’re really not like talking, if there’s then like another option [of the activity], that either forces them to talk . . .
Trainer B, top-up
Furthermore, one trainer found it difficult to support competence and build strong relationships with a large group of PSs:
. . . it’s just being mindful that if you’ve got that big a group then if you’ve got two trainers there they need to be able to support them . . .
Trainer D
It was also felt that the length of the training days had a negative effect on the relationships the trainers had established with the PSs. In contrast, 2 days was believed to be a rather short time in which to build a relationship:
I think to build positive relationships is really important for it to work and I think towards the end of both days that was a bit more of a struggle.
School 2, school contact
Peer supporter autonomy support
There was evidence to suggest that the PSs adopted need-supportive approaches to encourage their peers to be active, including listening to their friends to identify their preferences, considering what their peers enjoy and providing choice:
I just took on board what she said she wanted to do and I was giving her options.
School 3, PS focus group
Both PSs and NPSs indicated that PSs used autonomy-supportive language to motivate their peers by being encouraging, being empathic, minimising the importance of ability and not dictating what their friends should or should not do:
I’ve just tried to encourage people to do it like when they’re feeling down about it we’re like ‘you can do it – it’s fine, don’t worry. It doesn’t matter if you’re good or bad at it you can still do it’.
School 2, PS focus group
The person I spoke to said I could try and do some more physical activities outside of school or possibly try harder sometimes in PE because I’m not fond of PE.
School 2, NPS focus group
On the other hand, some NPSs believed that PSs could be ‘bossy’ (school 3, NPS focus group) or controlling (although it was clear that these views were reporting hypothetical situations and not actual interactions with PSs). However, trainers believed that PSs in one school seemed more confrontational, abrupt and less empathic towards less active girls than students in other schools. As such, being a PS may have challenged this communication style:
I think others [in school 2] knew their role as a PS but they’re not really portraying that as such in they’re being quite forceful and probably quite mean to the other girls . . .
Trainer C, top-up
Experience of being a peer supporter
Peer supporters suggested that their role was ‘quite cool’ (school 4, PS focus group) and that they ‘liked it’ (school 3, PS focus group). This view was reinforced by a parent who said that her daughter ‘loved it, yes she really enjoyed it’ (school 2, parent). Similarly, the school contact for school 4 agreed that PSs liked their PLAN-A experience:
I think the girls who are mentors [PSs] have had a really positive experience, they’ve really enjoyed the sessions, it’s been really good.
School 4, school contact
There was consensus that PSs felt proud and privileged to be a PS and recognised a sense of achievement in being able to help their friends:
I think there’s that kind of achievement in being able to speak to your friends in that way and being a PS.
School 4, PS focus group
Evidence of peer supporter diffusion
There was evidence from all stakeholders to suggest that the PSs made numerous attempts to peer support using different strategies:
I have overheard conversations because some of the mentors [PS] have been in my tutor group and even the girls saying to the boys ‘wow, you’re just always on the computer’.
School 2, school contact
What I quite often hear at the moment after that [PS training] is the girls will say to each other ‘for goodness sake woman up’.
School 2, school contact
A good few of them definitely had conversations.
Trainer B, top-up
Efforts to support peers included sharing knowledge with friends and offering to co-participate in clubs, sports, daily PA and active play. The PSs reported being empathetic to their friends and trying to encourage them to try new activities and persist with those in which they were already engaged:
There is a couple [of girls] [sic] actually, who I know got their friends joining [sic] a club doing a sport . . . and said that now a friend was doing a sports club or doing a different after-school club.
Trainer B, top-up
Whereas before they go [sic] to a youth club and I used to drop them off, now she’s walking. She gets her friends to call, they call for each other and they walk.
School 3, Parent
You know [NPS girl] because she is really good at athletics? She like . . .
Puts herself down a lot, doesn’t she?
Yeah, and then I have like let her join the athletics club with me. Because she is very good at high jumping.
So, you’ve tried to convince her to join the club with you? Have you succeeded yet?
Nearly there.
School 2, PS focus group
I do rounders, so me and [PS12] went up and spoke to her and said do you want to come and do rounders with us, you can come it’s all OK . . . she actually really enjoys it.
School 3, PS focus group
There was evidence that PSs carefully considered their diffusion attempts:
I tried to incorporate something that they liked. Erm, ‘cause some of my friends like to dance so it’s finding something that they like and encouraging them to do that more.
School 6, PS focus group
. . . at the top-up day we had a talk about when you’re in the car and talking about it and me and my friend were having a lift to go to someone’s house and we were talking about it and we ended up getting out the car early and then actually walking a bit because I was talking to her about all the benefits and we hadn’t done anything that day and we need to do stuff . . .
School 3, PS focus group
Generally, PSs felt that support given to close friends was more likely to be accepted and met with a positive attitude, and this was supported by NPSs who reported listening to PSs and accepting the support given if it was provided in an encouraging and polite way:
I feel [that] if I talk to my friend about it they won’t sort of be stubborn about it and when it’s coming from a friend or someone that they’re close with then they’re more sort of open about being active and what they would like to do, maybe rather than . . . So I feel that it’s sort of better coming from a friend.
School 4, PS focus group
If they say it [encouraging to be active] politely then yeah [they would try to be active], but if they get rude then probably not.
School 6, NPS focus group
The PSs in school 2 reported that it took time for some girls to accept support and that they persisted with their efforts. However, in school 6, NPSs were initially receptive ‘but they just sort of gave up after a while’ (school 6, PS focus group):
At first, yeah [NPS] was very negative about it, but over time she changed a lot – her mind . . . so we don’t want to give up on her because she does have potential, I think.
School 2, PS focus group
Trainers and PSs also reported that they had initially practised their role with family members as opposed to their peers; many found this easier:
She wasn’t actually talking to peers so she was trying to do it but she was doing it with her mum and her dad and her grandmother and her sister.
Trainer B, top-up
Despite the evidence of these PS activities, the trainers reported that many PSs seemed to have done little to peer support at the top-up training:
Some were like clearly covering up that they hadn’t done it and saying they had.
Trainer B, top-up
I just got the impression, particularly with the first school [school 6], that I’m not sure how much they were doing.
Trainer D, top-up
This was supported by many NPS:
No, no-one said anything to me.
School 4, NPS focus group
However, in line with their role, some PSs suggested that with effective peer support:
People might not know that you’re doing it.
School 2, PS focus group
They didn’t really know I was peer supporting because with some friends we did it quite subtly.
School 2, PS focus group
. . . you have just got to like every now and then just say something like ‘do you want to walk to school with me?’ or something or ‘why don’t you do PE today? Like have a go at it’.
School 2, PS focus group
Challenges to being a peer supporter
Peer supporters experienced a variety of challenges to communicating messages to their peers and commonly worked with other PSs in their school to ‘give each other advice’ (school 2, PS focus group) and discuss challenges. Some thought that support could be misconstrued as critique:
It’s annoying when you’re trying to speak to someone and they’re saying that you’re really fat and I’m like ‘no, we’re just talking to you about it’.
School 2, PS focus group
. . . when we were talking to people I did panic in my brain because if I say something wrong it’s going to sound rude and I’d hate it if someone said it to me . . . then I realised that if I just break it down and say it in a way that I’d want to be told then . . .
School 3, PS focus group
Others (from school 6) felt that their influence was limited as many of their friends were PSs:
A lot of my friends went on the PLAN-A thing, so it’s kind of difficult to know. Like literally everybody that’s in our like group of friends went and you kind of ran out of friends.
School 6, PS focus group
Some PSs faced challenges in being persuasive, although the majority of these views were given by the adult participant; views from PSs reflected anxiety of hypothetical situations where their advice was challenged:
I think she understood, but I just think she found it difficult to actually make other people listen.
School 4, Parent
Mm, they [NPS] may say, ‘I’m not going to do this; why should I? Like do you carry on encouraging them or do you agree with them or if I said to someone ‘no’, it sounded like I was a bit sort of nervous about talking to them . . . they would then sort of know that they wouldn’t feel as comfortable talking to me about anything.
School 4, PS focus group
Most PSs felt that their attempts to provide support were accepted by their peers and only on a few occasions was this not welcomed or ignored. NPSs gave a variety of reasons why they ignored or did not receive peer support, including finding it annoying and that PSs may have felt embarrassed. Although not referring to receiving peer support directly, one NPS referred to the need for PSs to not be pressurising:
There’s kind of this pressure when people are like, ‘oh, come on, do more sports!’, you know, ‘it’ll get you more fit.’[sic] . . . we get that enough from teachers telling us to be more physically active. I don’t want to hear that from people who I’m close to.
School 4, NPS focus group
The perceived effect of the Peer-Led physical Activity iNtervention for Adolescent girls
The perceived effect of the Peer-Led physical Activity iNtervention for Adolescent girls on Year 8 girls (non-peer supporters)
The various stakeholders believed that PLAN-A had potential positive effects including increased participation in PA (e.g. extracurricular activities, daily PA or planned exercise), improved intrayear relations and knowledge of the importance of PA. One student reflected that a PS had helped her ‘realise that some sports are actually more fun than others’ (school 6, NPS focus group). In one school, students who were not nominated to be PSs appeared to take on the role of a PS by talking to others, this was perceived to be because these students did not want to ‘miss out’ and wanted to ‘be seen in the same way that PSs are’ (school 2, school contact):
It is good and it helps confidence and it makes people feel like people do trust them [PS], people do look up to them [PS] and people do actually think I would want them [PS] to do stuff with her; I want to be active with her [a PS].
School 3, PS focus group
They’ve grown in confidence again, I’m not sure whether I could say wholeheartedly that’s because of PLAN-A . . . Because it’s, they’ve matured because they feel more settled in the tutor group. But they are very happy to be themselves and not be a follower.
School 2, school contact
Some of them, like in my group a lot of them did actually start going to the gym now but I don’t know if it was ‘you’re allowed to go to the gym now let’s go for it’ or if it was ‘we should do this because of PLAN-A’.
School 2, NPS focus group
Non-peer supporters demonstrated some understanding of PLAN-A, but could not explain it fully. In their view, any impact that PLAN-A had on other girls within Year 8 was minimal and, if any, was short-lived. Reasons given for this were a lack of interfriendship group communication, ignoring advice or not being spoken to by a PS:
I’m that kind of person that will take it on for a day and then forget about it the next day . . .
School 2, NPS focus group
I don’t think that people should like encourage us because if we wanted to do it then we would do it but like them telling us, isn’t going to really change our opinion of if we want to do it or not.
School 3, NPS focus group
The impact of the Peer-Led physical Activity iNtervention for Adolescent girls on peer supporters
The perceived impact of the PS training on PS knowledge, motivation and PA is reported in Chapter 6, Peer supporter training, Impact of training on peer supporters. The most commonly reported effect of PLAN-A and actually being a PS was its positive effect on PSs’ self-confidence and self-perceptions. In addition to the pride and privilege associated with being nominated by one’s peers (see Chapter 6, Peer nomination), parents felt their daughters had ‘definitely become more confident’ (school 4, parent) and used terms such as ‘feel valued’, ‘empowered’ and ‘more assertive’:
I think it’s done their confidence a world of good and, like I say, they’ve taken quite a lot of pride in what they’re doing because they’ve been chosen to do it.
School 2, school contact
Although the NPSs identified an increased sense of confidence in the PSs, in school 3 they interpreted this negatively, describing PSs as ‘a bit more boastful’, with one girl suggesting that ‘it’s not good for the rest of us, because they are cocky’. Girls in school 4 suggested that the PSs were ‘confident anyway’ and that ‘they get a bit big headed, just ‘cause they did get chosen’.
There was also a perception that PSs were more empathetic in general with their peer group:
It’s just the everyday getting along. The supporting in a classroom and not if somebody gets something wrong – not laughing. You know, they are much more aware of people’s feelings themselves.
School 2, school contact
There was a clear understanding that being active was more than just participation in ‘sport’. Some girls claimed that their participation in PLAN-A had changed the way in which they think, and for many it led to an increase in their own PA levels:
It’s definitely helped me be a better person. It’s realised [sic] that I am active, I don’t have to just have to do loads of sports, I can just walk around the house, go up and down the stairs and I end up doing a lot of active things. It has helped me become a better person in how I talk to people as well, like making me think before I say to some people like I know that before I probably, if we didn’t have the PLAN-A thing, I probably would have just gone to someone, ‘oh you need to be active, come on a run’ and I think that would have then ended up not working.
School 3, PS focus group
I think it’s all the facts and it does make you realise how important it actually is having exercise.
I want to prove people wrong who say that girls aren’t as active as boys. Want to prove them wrong and say we are.
Like boys will still say, ‘ah, you run like a girl’ or something that’s like . . . you just want to prove them wrong. ‘Shut up’.
School 2, PS focus group
School context
School policy and attitude towards physical activity
The control (mean 6.00, SD 1.41) and PLAN-A (mean 5.75, SD 1.71) schools scored similarly with regard to policies to encourage PA and PE (Table 32). One control school reported its annual PE budget and this was approximately £700 higher, on average, than PLAN-A schools. School 3 scored lowest (4.00) overall on policy and attitudes, reflecting few written PA policies and provisions, such as cycle training. School 4 was the highest scoring, reflecting a broad range of support for both staff and student PA and PE. All schools reported facilities to support staff PA (e.g. showers/changing); however, no schools required staff to receive training on PA promotion. The qualitative interviews revealed that schools 2 and 5 were involved in a variety of schemes and programmes (This Girl Can, Healthy Schools) to encourage student PA.
| Policy | School ID | Trial arm, n (%) | ||||||
|---|---|---|---|---|---|---|---|---|
| 1a,b | 2a | 3c | 4a | 5b,c | 6c | Control (N = 2 schools) | PLAN-A (N = 4 schools) | |
| Number of pupils in whole school/number of pupils in Year 8 | 929/159 | 867/143 | 1281/222 | 1347/156 | 1939/178 | 996/141 | – | – |
| Written policy that PE programme follows specific standards or guidelines | ✓ | ✓ | ✓ | ✓ | ✓ | Do not know | 2 (100) | 3 (75) |
| Written policy that requires a specific number of minutes or days of PE per week or that students have PE | ✗ | ✗ | ✗ | ✓ | ✓ | ✓ | 1 (50) | 2 (50) |
| If ‘no’, is there a ‘policy’ that is not formally recorded or written? | ✗ | ✗ | ✗ | – | – | – | – | – |
| Written policy that encourages students to walk or bike to school (e.g. Bike It) | ✓ | ✓ | ✗ | ✓ | Do not know | ✗ | 1 (50) | 2 (50) |
| Offer cycle training (e.g. Bikeability) | ✗ | ✗ | Do not know | ✓ | ✓ | ✓ | 1 (50) | 2 (50) |
| Written policy that requires all school personnel to receive professional development on PA promotion? | ✗ | ✗ | Do not know | ✗ | ✗ | ✗ | 0 (0) | 0 (0) |
| Does your school (have a written policy that) encourage(s) staff to be active (e.g. cycle schemes)? | ✗ | ✓ | ✗ | Do not know | ✓ | ✗ | 1 (50) | 1 (25) |
| Provide facilities which support the staff to be active (e.g. showers, cycle parking) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 2 (100) | 4 (100) |
| Have a budget allocation for PE equipment and supplies | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | 2 (100) | 4 (100) |
| If ‘yes’, on average how much does the school spend on PE equipment per year? (£) | Do not know | 1000 | 2000 | 4000 | 3000 | – | 3000 | 2333 |
| Involvement of PE teacher in PE budget decisions | Somewhat | – | Somewhat | Great deal | Somewhat | Great deal | Somewhat | Great deal |
| Scored | 5 | 5 | 4 | 8 | 7 | 6 | 6.00 ± 1.41 | 5.75 ± 1.71 |
Physical activity within the curriculum was scored similarly in both PLAN-A and control schools (Table 33); however, both scores are relatively low, providing limited evidence for the promotion of PA across the curriculum, outside PE. Half of schools used PA in other subjects aside from PE, primarily in personal, social, health, economic (PSHE) education. Two PLAN-A schools encouraged staff members to promote PA to students. Mostly, the delivery of PE is not often compromised for other needs. However, in four out of the six schools, children are sometimes withheld from PE for other academic subjects, which is supported by the interview findings:
I think the schools at the moment are under so much pressure to get like the academic side, sometimes they forget the other [PA] side.
School 6, school contact
| PA in the wider curriculum | School ID [subjects] | Trial arm, n (%) [subjects] | ||||||
|---|---|---|---|---|---|---|---|---|
| 1a,b | 2a | 3c | 4a | 5c,d | 6c | Control (N = 2) | PLAN-A (N = 4) | |
| Number of pupils in school/number of pupils in Year 8 | 929/159 | 867/143 | 1281/222 | 1347/156 | 1939/178 | 996/141 | – | – |
| PA used in other non-PE KS3 subjects? (subjects) | ✓ (PSHE) | ✗ | ✓ (science, geography, PSHE and outdoor education) | ✗ | ✗ | ✓ (PSHE) | 1 (50) (PSHE) | 2 (50%) (PSHE, science, geography and outdoor education) |
| Do class teachers provide regular PA breaks in the school day beyond PE and break? (Energisers) | ✗ | ✗ | ✓ (individual teachers) | ✗ | Do not know | ✗ | 0 (0) | 1 (25) |
| Does the school encourage class teachers to promote PA to students? | ✗ | ✗ | Do not know | ✓ | ✗ | ✓ | 0 (0) | 2 (50) |
| How often do teachers withhold students from PE to fulfil other academic requirements? | Rarely | Rarely | Sometimes | Sometimes | Sometimes | Sometimes | Rarely/sometimes | Sometimes |
| How often is the delivery of PE compromised because of competing demands for PE space (e.g. for examinations or assemblies)? | Rarely | Rarely | Sometimes | Sometimes | Sometimes | Rarely | Rarely/sometimes | Rarely/sometimes |
| Other comments about how PA is thought of or prioritised in your school? | Taking part in a future trial to improve mental health using tutor time |
Staff support PE allowing students to attend fixtures in the school day Staff see the benefits of PA, but it is often not prioritised |
– |
Academic grades come first Core PE time facilities can be taken |
– | – | One school involved in a mental health trial | PA and PE is important, but other areas usually take priority |
| Scorec | 5 | 4 | 4 | 3 | 2 | 5 | Mean 3.50 (SD 2.12) | Mean 4.00 (SD 0.82) |
School physical activity provision
The audit of school-level PA provision (i.e. quality of cycling, walking and sports/play provisions) ranged from 13 to 25 out of 46 (Table 34), with higher scores indicating greater provision. The two lowest total scores (13 and 16) were from the PLAN-A schools; this is supported by the number of active after-school clubs offered in the same schools (20% and 37.5% of all clubs offered are physically active, respectively). School 4 scored highest (25 out of 46), commensurate with its high score for policies on PE and attitude towards PA. Although parents and students from this school thought that the sports facilities were excellent, space and equipment were not always accessible:
I heard that [the school has their own ‘sports facility’] the other day. I thought that was brilliant.
School 4, parent
| PA provision | School ID | Trial arm, mean (SD) | ||||||
|---|---|---|---|---|---|---|---|---|
| 1a,b | 2a | 3c | 4a | 5b,c | 6c | Control (N = 2) | PLAN-A (N = 4) | |
| Number of pupils in school/number of pupils in Year 8 | 929/159 | 867/143 | 1281/222 | 1347/156 | 1939/178 | 996/141 | – | – |
| Cycling provision (scale of 0–9) | 5 | 3 | 4 | 7 | 6 | 6 | 5.5 (0.71) | 5 (1.83) |
| Walking provision (scale of 0–5) | 4 | 1 | 2 | 5 | 4 | 4 | 4 (0.00) | 3 (1.83) |
| Sports and play facility provision (scale of 0–32) | 11 | 9 | 10 | 13 | 9 | 10 | 10 (1.41) | 10.5 (1.73) |
| Modal quality of facility provision | Good | Adequate | Good | Good | Good | Good | Good | Good |
| Total school PA provision (scale of 0–46) | 20 | 13 | 16 | 25 | 19 | 20 | 19.5 (0.71) | 18.5 (5.20) |
One school contact recognised the need for appropriate equipment and space to encourage girls to be active, but the school may not have the capacity to do this:
[At the training] when they had the breaks and they had all the skipping ropes out and they were really happy just to do that. There was no boys around so they were not inhibited and I would love them to be able to do that somewhere but I’m not sure we’ve got the facility to do it but . . . they’re too embarrassed to do these activities so they don’t.
School 6, school contact
Five schools provided after-school activity club data. Out of the clubs provided for, and available to, Year 8s, approximately 50% were categorised as active in three schools; 37.50% of active clubs in school 4 were for girls only.
Physical activity facilities were rated as good at five out of six schools and adequate in school 2 (see Table 34). Of the three schools that had a written policy to encourage active travel (see Table 32), school 2 had relatively low scores for cycling and walking provision. When referring to PA in school, students commonly referred to formal sports or PE opportunities rather than broader opportunities such as cycling or walking:
And there’s clubs as well [sic].
Yeah, there are quite a few clubs [netball, rounders, badminton . . .
There’s a girls’ fitness club as well.
School 3, NPS focus group
School-level built environment
Table 35 provides a description of school grounds and the area within an 800-m buffer around each school. School field areas at PLAN-A schools were approximately 9000 m2 larger than school field areas at control schools. The area of school playground and field do not appear to align with the data on level of sports and play precision within each school. The length (9952.67 m vs. 6381.04 m) and density (3.56 km/km2 vs. 2.39 km/km2) of footpaths within the buffer was greater in control schools than in the PLAN-A schools. The data align with the scores in Table 34 in which school 2 scored lowest on walking provision; Table 35 shows that there are no footpaths within its buffer area. The majority of schools have no cycle paths within their buffer area; however, it is important to note that data are not available for cycle lanes that are part of roads or pavements, which are more common in England than separate cycle lanes. Therefore, these data do not agree with the cycling provision data in Table 34. The size of grassland areas is greater at control schools than at PLAN-A schools, and urban and suburban areas are larger at PLAN-A schools than at control schools.
| School-built environment | School ID | Trial arm | ||||||
|---|---|---|---|---|---|---|---|---|
| 1a,b | 2a | 3c | 4a | 5b,c | 6c | Control (N = 2) | PLAN-A (N = 4) | |
| Number of pupils in whole school/number of pupils in Year 8 | 929/159 | 867/143 | 1281/222 | 1347/156 | 1939/178 | 996/141 | – | – |
| Area of the 800-m buffer around the school (m2) | 2,789,475.72 | 2,445,852.68 | 2,972,084.43 | 2,593,431.59 | 2,802,378.75 | 2,624,256.54 | 2,795,927.23 | 2,658,906.31 |
| Area of school playground (m2) | 6560.29 | 3580.92 | 13,490.27 | 8453.11 | 9092.42 | 3394.57 | 7826.35 | 7229.72 |
| Area of school field (m2) | 74,341.49 | 83,306.06 | 40,670.06 | 28,518.99 | 3947.68 | 41,639.40 | 39,144.59 | 48,533.63 |
| Number of road intersections within buffer | 508 | 253 | 320 | 798 | 469 | 471 | 488.50 | 460.50 |
| Intersection density (intersections/km2) | 182.11 | 103.44 | 107.67 | 307.70 | 167.36 | 179.48 | 174.74 | 174.57 |
| Length of road (excluding motorways) within buffer (m) | 43,361.45 | 21,883.17 | 23,037.77 | 53,634.39 | 34,438.39 | 30,886.24 | 38,899.92 | 32,360.39 |
| Length of footpath within buffer (m) | 9920.16 | 0 | 5184.89 | 10,300.80 | 9985.17 | 10,038.48 | 9952.67 | 6381.04 |
| Footpath density within buffer (km/km2) | 3.56 | 0 | 1.74 | 3.97 | 3.56 | 3.83 | 3.56 | 2.39 |
| Length of cycle path with buffer (m) | 0 | 0 | 0 | 0 | 1246.31 | 0 | 623.16 | 0.00 |
| Cycle path density within buffer (km/km2) | 0 | 0 | 0 | 0 | 0.44 | 0 | 0.22 | 0.00 |
| Area of woodland within the buffer (m2) | 19,152.53 | 30,199.76 | 8009.64 | 49,073.70 | 49,293.20 | 62,874.84 | 37,539.49 | 34,222.86 |
| Area of grassland within the buffer (m2) | 348,841.55 | 887,984.88 | 1,618,850.32 | 109,068.82 | 664,242.51 | 491,693.29 | 776,899.32 | 506,542.03 |
| Area of urban land within buffer (m2) | 102,134.99 | 0.00 | 43,695.42 | 26,116.45 | 47,706.60 | 42,289.06 | 28,025.23 | 74,920.79 |
| Area of suburban land within buffer (m2) | 1,973,597.03 | 913,785.59 | 688,209.43 | 2,290,203.81 | 1,453,322.49 | 1,343,693.99 | 1,308,973.20 | 1,713,459.76 |
Year group structure
All schools taking part in PLAN-A had a tutor system by which the year group was split in half. As such, girls in different halves of the year often were in different classes and did not interact. This influenced friendship groups, with girls often more likely to be friends with others in their half of the year:
Because we don’t see each other much, we’re never in any of the same lessons . . .
School 4, PS focus group
It also influenced peer nomination in some cases:
I’m on one side of the year so I chose the people who were on my side of the year that I knew were good at it but obviously I wouldn’t know the people on the other side of the year so I didn’t put [nominate] any of them.
School 3, NPS focus group
Awareness of and school-based support for the project
Awareness of PLAN-A was generally restricted to either the Year 8 students or the PE staff. In some schools, by focusing on PA promotion, PLAN-A was only considered important in the PE department. Among intervention schools, the level of priority depended on whether or not it fitted with the schools’ objectives and if it had the potential to be successful:
I don’t know about the school priorities, within the PE department it fits in very well with trying to promote PA . . .
School 4, school contact
The degree of support given by both school contacts and school leadership to the project was governed by contextual factors, such as changes in school senior management, work patterns of school contacts and teacher workload (data collection, accommodating the PS training and encouraging the PSs). In general, however, school contacts were helpful and facilitation of the study within schools was simple. In the school in which PS training was delivered in-school rather than off-site, there was a change in head teacher between initial school enrolment and intervention delivery:
The original head was really supportive towards it and I suppose the others have been – it’s not their thing – so it wasn’t a priority as such whereas [former head teacher] was very much keen to get involved.
School 4, school contact
School context summary
There were minimal variations between schools, as seen throughout the process evaluation. The majority of those that did exist (i.e. the behaviour issues in school 2 and poor PS engagement in school 6) could not be clearly linked to any school context factors. However, the year group structure can explain the barriers that some PSs experienced while trying to carry out their role as a PS. The split year group in most schools made it difficult for PSs to support girls outside the PS group and approach those in the other half of the year. Aside from this, evidence suggests that PLAN-A appears to be robust to a variety of contexts.
Data linkage
The parent interview data were grouped into two related themes covering parents’ understanding and support for data linkage and their concerns.
Parent understanding of and support for data linkage
The majority of parents understood the description of data linkage given; only a minority wanted additional information. All parents stated that they would be likely to consent to their daughter’s health and education data being used for data linkage, with some wanting to discuss it with their partner and/or seeking their daughter’s consent:
Yes [I would consent] if she wanted to do it.
School 4, parent
Parents supported data linkage as a contemporary and valuable scientific resource: ‘in this day and age it is something that needs to be done’ (school 4, parent), and commonly described their expectation that the process was secure and undertaken with appropriate governance so that data were ‘safe’ and ‘used positively’.
Most parents suggested that they would consent to data linkage studies until their daughter completed secondary or further education. Some parents would provide consent indefinitely, whereas others wanted to be able to review their consent in the future:
In principle, I would probably say until the end of school but it would be nice to be given the option on a yearly basis or whatever to change your mind, not that I probably would . . .
School 2, parent
Some parents suggested that the consent for data linkage should pass to their daughter either upon leaving school or at the age of 16 or 18 years:
I kind of think that then she’d be of an age, 18 [years], that, you know if you wanted to carry on it would be in her hands then. She’d be adult enough to say, ‘do you know what, now remove me’.
School 3, parent
Parents’ concerns
The majority of parents raised a range of concerns regarding anonymity, data security, potential negative effects of data linkage and who would have access to the data:
You know, where does that information go? Would it have her name, date of birth, etc.? So yes, I would want to know a lot more about it before I could be comfortable.
School 4, parent
I mean, because obviously of her age . . . it’s all secure isn’t it?
School 3, parent
I wouldn’t want to agree to something when she’s 12 years old that when she’s 30 years old might have a detrimental effect on her.
School 4, parent
Chapter 7 Discussion
This chapter summarises the main findings, with reference to how evidence can be provided to inform the definitive trial progression criteria. Findings are organised into two sections: (1) Intervention feasibility, acceptability and evidence of promise and (2) Research feasibility and acceptability. The findings are discussed in line with previous literature, and implications for research and practice are suggested. The definitive trial progression criteria and the evidence for them are summarised in Table 36.
| Progression criteria | Evidence | Criterion met? |
|---|---|---|
| Can we recruit PS trainers? | Five trainers recruited and trained (to include one reserve) | Yes |
| Is it feasible to implement the intervention in secondary schools? | A total of 55 PSs were recruited and trained, meeting the target in each school (range 18–22%). Focus groups with PSs/NPS support feasibility | Yes |
| Were the training and materials for the trainers and PSs acceptable? | Interviews/focus groups with trainers, parents and PSs support acceptability. High (96.8%) attendance at PS training. Training was enjoyed (score 3.8/5). Minimal content tweaks identified to improve some elements | Yes |
| Was the intervention acceptable to schools? | Interviews with school contacts support acceptability and positive views about the intervention and its potential effect | Yes |
| Were the trial design and methods acceptable? | Target of six schools recruited and retained. A total of 427 (94.7%) Year 8 girls participated. Questionnaire data provision > 92% at all time points. Accelerometer return rates were high (> 86%) and exceeded the progression criteria (70%). Provision of 2 valid days of accelerometer data exceeded 70% at T0 and T1, and was 62% at T2 | Yes |
| Does the intervention show evidence of promise to positively influence the proposed primary outcome (i.e. weekday MVPA)? | No evidence of between-intervention difference at T1 (end of Year 8). At T2 (start of Year 9), between-intervention difference = 6.1 minutes (95% CI 1.4 to 10.8 minutes) favouring the PLAN-A arm after adjustment. In addition, PLAN-A did less sedentary time per day at T1 (–32 minutes, 95% CI –57.4 to –6.2 minutes) and T2 (–23 minutes, 95% CI –43.7 to –2.8 minutes) than the control group after adjustment | Yes |
| Indications of affordability and cost-effectiveness for LAs | The mean cost of intervention delivery was £2685 per school (range £2309–3235), equating to £37 per Year 8 girl (range £30–56) and £61 (range £38–162) per 10-minute increase in mean weekday MVPA | Yes |
| Is there a positive view about data linkage from stakeholders involved (parents, schools, data custodians)? | There was a positive qualitative view on data linkage from parents, schools and data custodians. A total of 88.76% of participants had complete data needed to perform linkage to education records | Yes |
Intervention feasibility, acceptability and evidence of promise
Intervention refinement and piloting
The PLAN-A was based on the successful ASSIST28 intervention model, reworked to focus on influential Year 8 girls supporting their close friends’ PA. In line with recommendations for early intervention development and adaptation86,87 and a core focus of the NIHR through NIHR INVOLVE, phase 1 of the study involved extensive and iterative formative PPI. This included consultation with the DECIPHer ALPHA young persons’ advisory group followed by rounds of focus groups with Year 8 girls (using a ‘design–listen–refine’ cycle). The focus groups identified relevant barriers to PA, which the girls wanted help to overcome, how best to frame PS recruitment, PS training content, characteristics of PS trainers, design of the study logo and using social media in the intervention. The result was a co-designed intervention that, although remaining faithful to the ASSIST intervention model and structure, was adapted to include content focused on PA-based issues that were relevant for Year 8 girls, used appropriate terminology and equipped girls with the skills and confidence to support their peers.
The intervention was piloted in one school to identify key problems before the feasibility trial. The evaluation of the pilot identified a number of issues, including where insufficient or surplus time had been allocated to various PS training activities, the need to include more active tasks and more activities focused on the ‘how to’ of peer support and a clearer idea of the physical space requirements for PS training (i.e. all need a break-out space if possible). The pilot intervention test also provided an initial deployment of the peer nomination and selection process, as well as the majority of process evaluation methods (observations, interviews, focus groups) that were then used in the feasibility trial. In summary, the refinement and piloting stage of the current study was central to the development of an intervention with a higher likelihood of acceptance, which was further tested in the feasibility trial.
Peer nomination and peer supporter selection
Phase 2 comprised a feasibility trial of PLAN-A in six secondary schools, all above the median local Pupil Premium (i.e. schools serving more deprived communities). The peer nomination process was implemented as planned. The idea of being a PS was popular with the students: 97% (n = 55) of those invited gave consent to attend the PS training. This represented 18–22% of the Year 8 cohort of girls in each school. This proportion of PSs within each year group is stipulated in DOI theory34 and the ASSIST intervention28 as necessary for there to be sufficient opinion leaders within a social group to make peer support effective. Commensurate with findings from ASSIST,38 PSs valued and felt pride in being nominated and in their role. Some parents believed that the nomination alone had enhanced their daughter’s confidence. PSs were motivated largely by altruism in the form of helping others to be active.
The peer nomination process adopted in ASSIST28 and PLAN-A sets it apart from most PA interventions that involve a peer support component. It is common for peer mentoring to be hierarchical, in that older students (e.g. Year 10) are assigned an individual or group of younger students (e.g. Year 7) to mentor on a more formal basis. 33,88–90 The most robust study of this peer mentoring model,33 a cluster RCT in 1495 young people in 60 schools in the north of England, showed no effect of the intervention on accelerometer-assessed PA. In contrast, the peer nomination process adopted in PLAN-A allows the intervention to capitalise on the potential influence of close-knit peer groups. As PLAN-A is led by key influencers from within peer groups, it is reasoned that they are sufficiently similar (i.e. in age, interests, life and educational stage and context and priorities) to both understand and influence their close friends. There is also evidence to support the influence of peers’ PA modelling, co-participation and encouragement on the PA levels of adolescent girls,91 and that peer support can partly buffer the effect of low self-efficacy on PA levels among girls. 92 On average, the students selected to be a PS did approximately 12 minutes more MVPA on weekdays and weekends and were less sedentary on weekdays than NPS at baseline. They also had a more favourable profile on some psychosocial attitudes towards being active. These findings agree with qualitative reports in some focus groups that more active girls had been nominated and that some PSs experienced difficulty in supporting others to be active as their friends were also trained as PSs. However, equally, there was the view from focus groups that PSs represented a variety of friendship groups and that PSs would have more legitimacy if they were active versus less active. Several ways of controlling peer nomination to recruit PSs, who are as active as the NPSs and well distributed through all friendship groups, and its advantages and disadvantages, are shown in Table 37.
| Peer nomination method | Advantages | Disadvantages |
|---|---|---|
| Open peer nomination (as used in feasibility study) | Entirely student led | Potential for limited coverage of PSs in all friendship groups |
| Reflects current social structures | Potential for friends to be selected and have limited influence beyond other PSs | |
| Students can nominate any other student, allowing nomination of influential peers based on one’s own view | Potentially disappointing for those not selected | |
| Empowering and motivating for PS | ||
| Open peer nomination plus teacher screening to select across friendship groups | Potential to get a PS in a range of friendship groups | Teacher views may not represent friendship groups |
| Knowledge of friendship groups likely to vary among different teachers | ||
| Added teacher burden | ||
| Potentially disempowering to participants (i.e. not trusted to identify PS) | ||
| Nomination constrained to different teacher-identified friendship groups | Potential to get a PS in a range of friendship groups | Teacher views may not represent friendship groups |
| ‘Influential’ peers may not always be within overt friendship groups | ||
| There may not be naturally influential girls in each peer group, limiting their influence | ||
| Social network analysis (i.e. measure friendship ties and select ‘well-connected’ girls across a year group). Could stratify by PA level if pre-assessed | Time, cost and resource intensive, higher participant burden (additional data collection needed) | Number of ties to other peers may not equal influence |
| ‘Objective ties’ may not represent the most ‘influential’ (i.e. leaders, trust etc); ties may be more superficial | Not peer led, potentially disempowering and removes motivational sense of pride in being highly thought of by one’s peers |
An unexpected influence on peer nomination was that the school year groups were structured as two relatively separate halves. The process evaluation revealed the existence of these structures in all schools and a tendency for students to nominate girls in their half of the year. This resulted in perceptions of unequal recruitment of PSs from each half or for PSs to feel that their influence was limited by having limited opportunities within school to interact with girls from the other half of the year. Future implementations of interventions using the peer nomination approach should determine how school year groups are split or structured and consider running peer nomination in ways that take account of the structure.
The process evaluation provided scant evidence that peer nomination had detrimental effects on the girls not selected to be a PS. No adverse events related to bullying were reported through either the adverse events reporting protocol or the school contact interviews. There was a small amount of disappointment voiced from some NPS girls in not being nominated, but this was not a commonly reported experience and there was no qualitative evidence that NPS girls’ PA was discouraged as a result of not being selected. Notwithstanding this, in a larger trial, with a greater number and diversity of participants, it is possible that some negative effects of not being selected may be seen. Therefore, it would be prudent to review the script with which the peer nomination process is delivered to ensure that terms such as ‘popular’ are not used (as was the case in this study).
Trainer recruitment and train the trainers
Five women were recruited and attended the train the trainers 3-day workshop. Trainers had a variety of backgrounds (e.g. youth work, theatre, yoga instruction, health promotion, coaching) and were paired as intended (balancing experience in PA promotion and working with young people). In this study, trainers were recruited using adverts and group contacts. Some trainers were self-employed, while others were employed by the LA (health promotion) or town council sports development teams. This profile is similar to the trainers recruited in ASSIST including youth workers, smoking cessation staff, teachers and NHS health improvement leaders. 93 Looking toward a larger trial and/or future wider dissemination, it will be important to identify a sustainable source of trainers while ensuring that the personal characteristics that were viewed as successful in this study (see below) are maintained.
The train the trainers course was effective and trainers found the materials and resources helpful. Trainers reported wanting a recap on theoretical principles and further advice on managing disruptive behaviour. Trainers also needed to use time (unpaid) outside the training to prepare for the delivery. Although it would be expensive to pay for all preparation time, future interventions could build in some personal preparation time. Alternatively, if trainers were identified through employers such as LAs, PLAN-A delivery would form part of their contracted tasks and some preparation time may be incorporated.
Trainers largely delivered the PS training with high fidelity to the training manual and in a manner that was consistent with SDT,46 supporting the PSs autonomy, competence and relatedness as planned. Challenges to this included disruptive behaviour, low PS engagement and long training activities. Previous school-based PA interventions based on SDT have identified similar challenges (i.e. delivering in an autonomy-supportive manner when facing disruptive behaviour). 94,95 Although the train the trainers’ workshops attempted to learn from these studies and provide advice on the use of structure and agreed ground rules, trainers requested greater practical guidance.
Focus groups with PSs reinforced the importance of the trainers’ ability to quickly build a strong and genuine rapport between themselves and the PSs, which was the foundation of much of the enjoyment and engagement in the PS training. PSs highly valued the autonomy-supportive approach of the trainers (with clear qualitative reports by PSs of trainer support for competence, autonomy and relatedness), identifying that their interpersonal style was different (i.e. more autonomy supportive) than their usual teachers. Many examples of autonomy support and enjoyment centred on when trainers delivered the training with flexible adaptation of the intervention materials and trainers being attuned to the PSs (e.g. recognising when it was appropriate to move on or spend more time on a task, and including their own experiences and skills, such as yoga in warm-up activities). As such, trainer innovations96 were in accordance with, and facilitated, the SDT underpinning of the intervention. Previous studies have identified drift (when adaptations are not in line with the spirit or theoretical underpinning of the intervention)94,95 in intervention delivery; however, this was not commonly seen in the delivery of PLAN-A. Consistent with previous research in which PA/educational intervention deliverers have been trained to deliver sessions based on SDT,94,97,98 this study suggests that trainers welcome the approach, and that it is possible to train deliverers to adopt this method and for them to deliver it in practice. Refinements to the train the trainers elements are shown in Appendix 20.
Peer supporter training and peer supporter experiences
Peer supporter training was held at non-school off-site venues for students from three out of the four schools. One school was unable to release a member of staff to chaperone the students at the training because of financial and staffing constraints. In this school, the PS training was conducted on the school site. Insight from the LAG suggested that this finding reflects the current challenging financial climate for schools. Delivery of the training in school had advantages (e.g. more time to conduct training) and disadvantages (e.g. small training space, disruption by other students using nearby rooms and a less marked sense of privilege among the PSs who were not taken off-site). Although off-site delivery is preferable, on-site PS training is feasible if carefully managed and could represent a pragmatic balance between intervention fidelity and acceptability to schools in the current challenging financial climate.
A key amendment to the ASSIST intervention approach was that, in addition to the initial 2 consecutive days of PS training, PLAN-A included a 1-day top-up training session (5 weeks after the initial 2 days) rather than four 1-hour in-school sessions (as implemented in ASSIST and the AHEAD study). Findings from the AHEAD study suggested that trainers found it more difficult to motivate PSs and deliver the in-school training. 40 In addition, feedback from the LAG (including representatives who had commissioned and delivered ASSIST) suggested that the four in-school visits yielded relatively poor engagement compared with the 2-day training. In PLAN-A, the top-up day built on the strong rapport between the PSs and the trainers and was valued as a good time to refresh key learning objectives, solve problems and re-energise the PSs. Trainers voiced some concerns about the length of the training days and suggested the option of adding another top-up day. However, it is felt that PS engagement could be improved through small changes to the training day content and structure that would be more financially viable than adding a further training day (this would cost approximately £1000 per school).
The PS training was successful with very high attendance (90–100%). PSs had fun, were engaged with most tasks and liked the trainers. Training helped the PSs prepare for their role; however, they would have liked some tasks to be more active (a finding replicated in the AHEAD study40) and greater help on how to start conversations about PA. Attending the training and being a PS had a number of perceived positive impacts on the girls: it increased their confidence to talk to others, improved their social connections, as well as increasing their drive to help their peers and maintain their activity levels. Similar to a recent process evaluation of the implementation of ASSIST in Scotland,93 PSs, NPSs and trainers raised questions about the level of diffusion of messages from PS to their friends. However, PSs reported employing numerous strategies to support their peers including sharing knowledge, giving encouragement and co-participation in sport and daily activity (e.g. active travel). Central to PS-reported efforts to peer support was their ability to empathise with their friends and be subtle in their support. This is suggestive of good theoretical fidelity, in that the PSs were faithful to the SDT-based foundations of the intervention (i.e. supporting and developing each other’s autonomy to be active in ways that suit them, rather than pressuring their peers, which was found to be an expectation that some students had pre training). Challenges to peer support included anticipating hostility, worries of offending others and difficulties in approaching peers; however, PSs reported that the anticipation of these factors was often worse than the reality and they were able to use an empathic and subtle approach to peer support to good effect.
The results of the feasibility study identified a number of refinements that could be made to the intervention if it was taken forward in a definitive trial; these are summarised below in Table 38 and further details are in Appendix 20. Refinements focus on the physical training space, manipulating the training structure and content to optimise engagement, simplifying some activities and terminology and adding more active training content, including practical guidance on the ‘how to’ of peer supporting. All of these changes are simple, would not change the core intervention design and are possible within current intervention cost estimates.
| Intervention element | Refinement |
|---|---|
| Train the trainers | Cover principles of SDT more than once in the training |
| PS training | Consider the trainer-to-PS ratio |
| Offer outdoor space for breaks and more equipment | |
| Move more writing-based tasks to the morning and add in active games to break learning up | |
| Emphasise using the PS booklet and diary | |
| Allow space in PS booklet for blank notes pages and diagrams with speech bubbles | |
| Make the group sizes for each activity clearer to trainers | |
| Add more practical/active- or interactive-learning activities | |
| Provide more information on how to overcome challenges faced as a PS | |
| Give more specific examples about who PSs should support and how to do so | |
| Add in or adapt activities to involve more teamwork | |
| Consider suggesting alternative methods to meet task learning objectives under certain conditions (e.g. low student engagement) | |
| Simplify the terminology in some activities (e.g. sedentary) |
Evidence of promise to affect girls’ physical activity
The quantitative analysis for evidence of promise showed no evidence for a difference in minutes of weekday MVPA between control and PLAN-A arms at T1 (end of Year 8), but there was a 6.1-minute difference (95% CI 1.43 to 10.76 minutes) in weekday MVPA favouring the PLAN-A arm at T2 (i.e. beginning of Year 9). The CI exceeded 10 minutes, which is a level of daily MVPA considered to have important implications for health. 99 The between-intervention difference reflected a prevention of the decline in MVPA (seen in the control group) between the beginning of Years 8 and 9. The study also found that PLAN-A held promise to reduce the time that girls spend sedentary (i.e. sitting, lying down) as measured by accelerometer. At T1, girls in PLAN-A schools did 32 minutes less sedentary time per weekday (95% CI –57.44 to –6.18 minutes) than girls in control schools. This finding was largely replicated at T2, with girls in PLAN-A schools doing 23 minutes less sedentary time per weekday (95% CI –43.73 to –2.79 minutes). The findings were consistent when missing data were imputed and when the accelerometer validity criterion was reduced to 1 valid weekday. The results of the exploratory interaction analysis must be treated with caution, but suggested that PLAN-A might be more effective on PSs than NPSs at T1. However, there was no evidence for this at T2; when combined with the finding of evidence of promise at T2, this could indicate that the PSs had managed to diffuse the PA messages more successfully to their peers by this time point. In contrast to this, at T2, PLAN-A arm participants reported having been spoken to by a friend about PA less frequently than at T1. However, in process evaluation focus groups, the PSs believed that some of their peer support was subtle rather than overt; this is in line with the informal nature of PLAN-A and may suggest that PSs became more effective at peer support by T2 and explain these divergent findings.
Given the lack of interventions with evidence of effectiveness to increase (or maintain) adolescent girls’ PA, this finding is promising. Reviews of PA interventions for girls have shown very small positive effects,100 with an average effect of approximately 4 minutes of MVPA per day. 101 There was no effect on the accelerometer-assessed weekday MVPA of Year 7 girls in a robust RCT of an after-school dance intervention versus control. 83 A recent RCT of a multicomponent school-based intervention (Girls in Sport) in Australia,102 involving 1518 girls, aged 13 years at baseline, reported no effect on accelerometer-assessed MVPA. Among interventions that have shown effectiveness, the RCT of Physical Activity 4 Everyone, a multicomponent school-based intervention in Australia, showed that the effect in girls (4.0 minutes MVPA per day, 95% CI 0.01 to 8.0 minutes) was less than half that of the effect in boys (10.4 minutes MVPA per day, 95% CI 2.1 to 18.0 minutes). 23 Finally, there was no evidence of promise that the AHEAD intervention affected the MVPA of the boys and girls included. 40 Should the evidence of effectiveness of PLAN-A be replicated or increased (e.g. to 10 minutes MVPA per day) in a definitive trial, the intervention would be one of the most effective to date. In comparison to multicomponent school-based intervention approaches, such as Physical Activity 4 Everyone, PLAN-A is relatively simple, focused and a low burden for schools. As such, in addition to its potential effect on PA, PLAN-A also has the potential to be widely implemented in schools.
Reflections on the logic model
The logic model for the intervention was largely supported and it serves as a foundation for a definitive trial. Qualitative support was demonstrated for the proposed mediators of PLAN-A (i.e. SDT variables); however, this was largely based on the experiences of PSs, rather than NPSs, and there was no quantitative evidence that these variables changed as a result of the intervention. This may reflect a true lack of change, be as a result of the low power to detect changes or be as a result of measures with low sensitivity to change. To better understand mediation of the intervention effect, in a future trial there is a need to more fully explore what PSs did to support their peers and girls’ perceptions of this, in addition to more general PA social support, as these are likely key mediators (in addition to more abstract concepts, such as need satisfaction or motivation quality). Measuring these psychosocial factors with appropriate depth and precision is challenging, especially within the context of interventions, such as PLAN-A, which rely (at least partially) on subtle diffusion/support. The qualitative data in this study suggested that such support may not be in the conscious awareness of those receiving it, which further complicates its measurement. There is likely to be no single, simple solution (or questionnaire) to resolve this issue. Rather, further in-depth mixed-methods approaches involving both PSs and NPSs, in addition to more frequent monitoring (including the potential use of online resources to record peer support) of PS actions are needed.
Health economics: indications of affordability and potential cost-effectiveness
This study has established that it is feasible to both collect and cost resource-use data to estimate the cost-effectiveness of delivering PLAN-A. The study was able to collect all the costs associated with train the trainers (including estimates of how the cost would alter if more PSs were trained in a different location) and the information required to estimate the cost of the intervention per school and per Year 8 girl, including PS and Year 8 girl time attending PLAN-A meetings and training. As such, the study developed a robust and effective methodology for capturing cost data that could be applied in a definitive trial.
When compared with other studies, PLAN-A has the potential to be good value. PLAN-A cost an average of £2685 per school and £37 per Year 8 girl. Based on the identified 6.1-minute difference in weekday minutes of MVPA between trial arms, on average the cost per 10-minute increase in mean weekday MVPA at 12 months was £61.01 per Year 8 girl. For comparison, in the cost-effectiveness analysis conducted alongside the Physical Activity 4 Everyone in Australia,23 a societal perspective was taken and resource use measured included personnel costs, materials and printing. Opportunity costs for personnel time were estimated only for activities that took place outside usual PE and sport time. Participants in the PLAN-A arm were more active at 24 months (adjusted difference in mean daily MVPA 7.0 minutes, 95% CI 2.7 to 11.4 minutes). The intervention cost over 24 months was £240 per student and this equated to £34 (95% CI £21 to £90) per additional minute (or £340 per 10 minutes) of MVPA (conversion rate used, AUD$1 = £0.609317; date of exchange, 8 August 2017). In the UK, the Bristol Girls’ Dance Project83 provided after-school dance sessions for adolescent girls and effectiveness and cost-effectiveness were estimated. The intervention cost per girl was £73 (95% CI £71 to £75); however, there was no evidence that girls in the intervention arm were more active than girls in the control arm.
The PLAN-A was based on the ASSIST smoking preventing intervention model,28 which involved peer nomination, PS training and informal diffusion. A public-sector costing perspective was taken, similar to that used in the present study. The total cost of the ASSIST intervention per school was £5662 [including costs for a teacher chaperone for PS training (£633/school)]. The ASSIST intervention was estimated to cost £32 (95% CI £30 to £34) per student and, at 2 years post baseline, the incremental cost per student not smoking was £1500 (95% CI £669 to £9947). The AHEAD intervention,40 which used the PS model to target change in healthy eating and PA in secondary schools, cost £11,289 per school and was considered too expensive to replicate on a larger scale.
There was no evidence that the intervention could affect quality of life, as measured using the EQ-5D-Y. A limitation of the EQ-5D-Y is its focus on health outcomes; however, PLAN-A is a public health intervention that has the potential to impact quality of life more broadly. Given the focus of the EQ-5D-Y and given that we did not expect to see significant changes in the health of a largely healthy group, the limited variation in EQ-5D-Y scores and lack of association between EQ-5D-Y and MVPA was unsurprising.
Research feasibility and acceptability
This study has demonstrated the feasibility of the research methods required to conduct a robust mixed-methods evaluation of PLAN-A in a definitive trial. School recruitment targets were met, despite recruiting from a restricted pool of schools, having excluded schools below the local Pupil Premium median and those already implementing ASSIST in Year 8. No schools withdrew from the study; however, a change of senior leadership in one school between recruitment (pre-summer holiday break) and subsequent contact in the autumn term resulted in less senior support for the school’s involvement in the study and a reluctance to release a member of staff to chaperone PSs to the training. The school context information indicated that in one school, the Ofsted rating changed considerably between recruitment and the time of organising the intervention period. This school continued to participate in all study elements; however, as discussed in Chapter 6, Peer supporter training, Training logistics, PS training was held on the school site. Participant opt-out rates were very low (0.89%) and the opt-out consent procedure was effective, as it fitted both the nature of the research (i.e. whole school year measurement) and intervention (i.e. low risk, diffusion). Participant drop out was low, with the majority of participants taking part in all measurement points (94% at T1 and 93% at T2) and those participants who were lost to follow-up were lost because of leaving school, exclusion from school, illness or absence on the measurement day.
Provision of quantitative survey data was very high (> 90% at each time point), which supports the use of tablet-based questionnaires. Accelerometer return rates were also high (> 85% at each time point), thus the progression criteria of a 70% accelerometer return rate was met. Despite this, compliance with wear-time criteria was variable, with 83%, 71% and 62% of students providing a minimum of 2 valid days of accelerometer data at T0, T1 and T2, respectively. These levels of data provision are slightly higher than those reported in the AHEAD study,40 a previous school-based intervention using the ASSIST PS method that targeted healthy eating and PA and in which 79% and 60% of students provided at least 3 days of valid data at baseline and at the 4- to 5-month follow-up, respectively. The baseline provision rate is also similar to that reported in a school-based cluster RCT in Australia (84% providing at least 3 days of data),23 which used the waist-worn accelerometer used in the present study. Other secondary school-based trials have reported lower data provision levels and rates of inclusion of participants in primary outcome analysis. For example, in the GoActive feasibility trial,89 55% of students provided 1 valid day of data at baseline and follow-up, and in the MOVE cluster RCT33 the provision of valid accelerometer data ranged from 42% to 57% in the intervention groups.
The whole-year-group approach to data collection in PLAN-A is ambitious and different from other studies in which a subsample of students participate in accelerometer measurement103 or the intervention and measurement focuses on a self-selected group. 83 From this perspective, the accelerometer return rates are excellent and the provision of valid data at baseline and T1 was high. Although provision of valid accelerometer data at T2 is comparatively lower, the level of missing accelerometer data (i.e. not wearing the monitor at all on measurement days) was low at each time point. This indicates that the girls were willing to wear the accelerometers, but that strategies are needed to ensure that they are worn for sufficient time on enough days in a future definitive trial. Such strategies include incentivising sufficient wear time rather than monitor return, amending the study design to reduce participant fatigue (i.e. accelerometery at baseline and at the beginning of Year 9 in the first instance) or using alternative accelerometers (e.g. wrist-worn units) that may result in greater compliance. The ancillary accelerometer study that was conducted suggested that wear time from the wrist-worn GENEActiv (Activinsights Ltd, Kimbolton, UK) accelerometer was high (4–5 valid days, 100% return rate).
With regard to collecting the data necessary to link study data to academic outcomes data using the NPD, we collected the necessary quantitative data (i.e. full name, postcode and date of birth) for the majority of participants. Parents were generally supportive of data linkage and had some concerns about data security, which is a common issue in data linkage research. 104 Parents were supportive of providing parental consent until their daughter left school, after which the girls were expected to take control of consent. Study findings identified that it is important to explain to parents the issues of anonymity and data security alongside the length of time for which consent will last, and that it would be necessary therefore to have additional consent procedures if data linkage is to be extended beyond school-leaving age (at either 16 or 18 years of age). Only 50% of schools responded to the data linkage questionnaire, with one school recording unspecified concerns and two not having concerns assuming parental consent. Although the findings should be interpreted with caution, it is likely that data linkage would require negotiation and careful discussion with each school, but would ultimately hinge on parental consent. Based on the findings, it may be challenging to initiate these conversations in some schools.
Process evaluation is a key component of complex intervention research105 and in this study we conducted a mixed-methods process evaluation of PLAN-A, explored the feasibility of these methods and used the resultant data to understand intervention implementation and mechanisms of impact and to identify weaknesses and potential improvements. Participation in the process evaluation research elements was very high and we recruited the target number of PSs, NPSs, parents of PSs and school contacts and involved the trainers in multiple interviews and surveys. The level of depth of the semistructured focus groups and interviews was excellent and they provided a rich resource. The study also developed and piloted an observation tool to examine PS training fidelity and piloted adapted measures of school PA environment and policy, which were deployed without problems. The assessment of intervention fidelity by the PS (i.e. what they did to peer support and how they did it) is challenging because of the subtle support given within close peer groups, which is not directly observable. Following the ASSIST approach, in this study diaries were provided for PSs to record conversations they had with peers (as an intervention resource, rather than data collection tool); however, the PS trainers reported that these had been infrequently used when they viewed them at the top-up training. More frequent data collection (e.g. text- or e-mail-prompted provision of information) is an alternative option, but the more regular contact from the project team could become part of the intervention and may not be sustainable in a scaled-up trial because of additional cost and administration needs. In a definitive trial, fidelity could be assessed by the addition of a specific questionnaire for PSs at weeks 5 (top-up training) and 10 (end of formal intervention period) to collect information on the types, frequency and specific examples of support given.
In summary, although improvements are needed in the assessment of peer support fidelity, it is feasible to conduct an in-depth process evaluation, and we have developed a wealth of research resources that could be used within the evaluation of a definitive trial.
Together, the results suggest that a definitive trial to compare the effectiveness and cost-effectiveness of PLAN-A on Year 8 girls’ weekday MVPA intervention with usual practice control is warranted. Based on the sample size calculations above, we propose conducting a two-arm cluster RCT involving 20 schools: 10 intervention schools and 10 control schools, with embedded process and economic evaluations.
Strengths and limitations
A main strength of this study was its use of robust methodology appropriate to examine the feasibility of the PLAN-A intervention and the research required to evaluate the intervention in a future cluster RCT. This methodology has resulted in the collection of a broad range of evidence for feasibility that has been mapped on to a clearly articulated set of definitive trial progression criteria. The study protocol was submitted prior to the collection of baseline data and the reporting in this document has been (and in forthcoming peer-reviewed papers will be) commensurate with the CONSORT guidelines for pilot and feasibility trials,58 the COREQ checklist59 and the TIDieR framework,57 resulting in transparency from study conception to dissemination, which was monitored by an independent TSC. A further strength is that the formative phase of the present research included a strong PPI element to ensure that the intervention content was co-designed. This led to the development of an intervention, tested in phase 2, that was relevant, appropriate and acceptable to the Year 8 girls and the avoidance of easily identifiable pitfalls in the feasibility study. The use of a LAG also ensured that the project took account of, and learnt from, stakeholders working in schools and public health. The detailed mixed-methods process evaluation was conducted in line with Medical Research Council (MRC)’s recommendations,105 including gathering views from multiple stakeholders, using quantitative and qualitative methods and capturing the intervention context. The use of purposive sampling for the NPS interviews also avoided limitations associated with self-selecting samples. The collection of PA data using accelerometers also overcomes self-report limitations of PA questionnaires.
A limitation of the study was that we did not include parents of NPS students whose views on the intervention may be different from those of the parents of PS students, although the knowledge of the intervention in this group is likely to be very low. Furthermore, although the involvement of six schools was sufficient to establish feasibility, generalisability of the findings to other schools is limited. In particular, the findings from the two control schools may not represent the likely response from other schools allocated to the control arm in a definitive trial and, ideally, there would have been an equal balance in the number of schools between arms. We also did not measure school year group structure before peer nomination which, as the year groups were often split in half, had a bearing on both peer nomination and the potential for peers to support girls across the year group. Although the qualitative results supported the logic model and its theoretical underpinning, the study did not see any consistent or meaningful evidence of change in the proposed psychosocial mediators. These contrasting findings may reflect a lack of change in these variables or that the quantitative measures are not sufficiently sensitive to change. Further work is needed to develop tools that are sensitive to changes that may occur. In terms of the health economic evaluation, the study did not capture, and thus quantify, the opportunity cost of Year 8 girls’ time spent discussing the intervention with one another; however, in practice, this would be difficult to measure with enough accuracy for the outcome to be helpful. A limitation in the study estimates is that the cost of equipment was divided by the number of training days; however, these items can be re-used and, therefore, equipment costs are likely to be an overestimate. This feasibility study was not designed to have sufficient statistical power to provide a precise estimate of cost-effectiveness. Finally, this study was not able to resolve whether or how best to include social media in the intervention. Social media is pervasive in young people’s lives and central to how they communicate with their peers. Estimates suggest that 26% of 8- to 11-year-olds and 74% of 12- to 15-year-olds have a social media profile [e.g. platforms such as Facebook (Facebook, Inc., Menlo Park, CA, USA), Snapchat (Snap Inc., Venice, CA, USA), Pinterest (Pinterest, Inc., San Francisco, CA, USA), Instagram (Facebook, Inc., Menlo Park, CA, USA) and Twitter (Twitter, Inc., San Francisco, CA, USA)]. 106 However, the minimum age to register a profile on most of these platforms is 13 years [18 years for YouTube (YouTube, LLC, San Bruno, CA, USA), 13 years with parent permission]. As Year 8 girls are aged 12–13 years, it would be inappropriate to actively promote the use of social media and/or add social media intervention components (e.g. Facebook groups for PSs) from the beginning of Year 8. Furthermore, it would also be inappropriate for a school-based intervention to encourage the use of social media (mainly accessed using mobile phones), which could contradict the school’s mobile phone and social media policies (which are likely to be varied). Further developmental work is needed to understand better how best to acknowledge and/or integrate highly influential social media platforms in to interventions like PLAN-A, which involve young people’s social networks.
Implications for research and policy
This study adds to other studies28,51 that support the design of health behaviour interventions for young people to target their core social networks and the potential positive power of peer influence. As the ASSIST approach to peer-diffusion and our application of it to target PA differs from other peer-led PA interventions, this presents an interesting avenue for future interventions involving peers.
The evidence gathered supports the conduct of further research, specifically a definitive trial of the effectiveness and cost-effectiveness of PLAN-A. The results of the feasibility study can guide key considerations in the design of a definitive trial including (1) reducing the burden of accelerometer data collection and the potential removal of the immediate post-intervention measure (leaving baseline and 1 year follow-up) to optimise compliance, (2) ensuring peer nomination accounts for year group structure, (3) improved monitoring of peer support actions and (4) refined PS training activities.
For schools and policymakers, PLAN-A is a promising intervention approach because, when compared with other multicomponent or peer interventions, this intervention appears to be low cost and low burden for schools. If the PLAN-A intervention is found to be effective in a definitive trial, it will be important to identify a logistically and financially sustainable dissemination package (which considers who the trainers are and how the intervention provision is organised) that is acceptable to commissioners and service providers. When deciding whether or not to participate in the PLAN-A intervention, schools should consider the time a school contact will need to commit to PLAN-A, both for organising PLAN-A-related meetings and time spent at the training days. In this study, it was found that, in general, schools did not hire supply teachers; however, if the schools were required to, this would incur a cost for the school.
Conclusion
The PLAN-A intervention was acceptable to students, teachers, parents and trainers. It was feasible to conduct a cluster RCT, including process and economic evaluations to study the intervention. The quantitative and qualitative data demonstrated that the PLAN-A intervention has promise to positively affect girls’ PA levels. Together, these findings meet the criteria for progression to a definitive trial of the PLAN-A intervention.
Acknowledgements
The study was carried out with the support of DECIPHer, a UK Clinical Research Collaboration (UKCRC) Public Health Research Centre of Excellence. Joint funding (MR/KO232331/1) from the British Heart Foundation, Cancer Research UK, the Economic and Social Research Council, MRC, the Welsh Government and the Wellcome Trust, under the auspices of the UKCRC, is gratefully acknowledged. This study was designed and delivered in collaboration with the BRTC, a UKCRC-registered clinical trials unit (CTU) in receipt of NIHR CTU support funding. The intervention costs were provided by the respective LAs in which the study schools were located; these LAs were South Gloucestershire Council and Wiltshire Council. Russell Jago is partly funded by the NIHR Collaboration for Leadership in Applied Health Research and Care West (CLAHRC West) at University Hospitals Bristol NHS Foundation Trust. None of the funders had involvement in the TSC, data collection analysis or interpretation or the writing of study results.
We would like to thank members of the LAG, including Nick Bolton, Healthy Schools and Personal, Social, Health and Economic Education (PSHE) support; Wiltshire Council; Sarah Heathcote, Head of Public Health, Wiltshire Council; Sarah Godsell, Partnership Officer, South Gloucestershire Council; Sally Good, Chief Executive Officer of DECIPHer Impact; Nancy Strickland, PE teacher, Wiltshire Council; Phoebe Kalungi, Public Health Specialist, Wiltshire Council; Katie Davies, Public Health Specialist, Wiltshire Council; and Ruth Sampson, Health Improvement Specialist, Sirona Care and Health.
We would like to extend our gratitude to the members of the TSC: Dr Katrina Wyatt (chairperson), University of Exeter; Dr Paul Ewings, Taunton and Somerset NHS Trust; Trish Gorely, University of Stirling; and Professor Russell Jago, University of Bristol for the continued support and advice throughout the course of the study. In addition, we would also like to thank Dr Mark Edwards (Trial Manager), Miss Lisa Campbell (study administrator) and Joe Matthews (fieldworker) for the successful conduct and execution of the study; Dr Duncan Proctor for conducting the geographical mapping analysis; Sarah Bell for her contributions to the development of the intervention; and Dr Chris Metcalfe for support with the statistical analysis and reporting.
A special thank you must go to the trainers, school staff, child participants and parents for their involvement in the study.
Contributions of authors
Simon J Sebire (Senior Lecturer in Physical Activity and Public Health) was the principal investigator and obtained the funds for the study. He co-wrote the first version of the final report, co-led the development of the study methods and design and analysed the qualitative process evaluation data.
Kathryn Banfield (Research Associate) led on the process evaluation, co-wrote the first version of the final report, developed the process evaluation and was responsible for collecting process evaluation data, drafted the methods and results chapters for the process evaluation and analysed the qualitative process evaluation data.
Rona Campbell (Professor of Public Health Research) was a co-applicant and co-led the development of the study methods and design.
Mark J Edwards (Senior Research Associate) was trial manager, co-wrote the first version of the final report and analysed the qualitative process evaluation data.
Ruth Kipping (Senior Research Fellow in Epidemiology and Public Health) was a co-applicant.
Bryar Kadir (Research Associate in Medical Statistics) was responsible for leading the statistical analysis and provided the main link to the BRTC, a UKCRC-registered CTU.
Kirsty Garfield (Research Associate in Health Economics) designed and conducted the economic analysis for the study and drafted the corresponding sections for the report.
Joe Matthews (Fieldworker) led on data collection in schools and data processing, cleaned and managed accelerometer data and analysed the qualitative process evaluation data.
Peter S Blair (Reader in Medical Statistics) was a co-applicant and co-led the development of the study methods and design. He was responsible for leading the statistical analysis and provided the main link to the BRTC, a UKCRC-registered CTU.
Ronan A Lyons (Clinical Professor of Public Health) was a co-applicant and co-led the development of the study methods and design.
William Hollingworth (Professor of Health Economics) was a co-applicant and co-led the development of the study methods and design. He designed and conducted the economic analysis for the study and drafted the corresponding sections for the report.
Russell Jago (Professor of Paediatric Physical Activity and Public Health) was a co-applicant.
All authors reviewed various sections of the report and made critical revisions to relevant sections. All authors approved the final submission.
Publications
Sebire S, Edwards M, Campbell R, Jago R, Kipping R, Banfield K, et al. Protocol for a feasibility cluster randomised controlled trial of a peer-led school-based intervention to increase the physical activity of adolescent girls (PLAN-A). Pilot Feasibility Stud 2016;2:2.
Sebire S, Edwards M, Campbell R, Jago R, Kipping R, Banfield K, et al. Update to a protocol for a feasibility cluster randomised controlled trial of a peer-led school-based intervention to increase the physical activity of adolescent girls (PLAN-A). Pilot Feasibility Stud 2016;2:68.
Sebire SJ, Jago R, Banfield K, Edwards MJ, Campbell R, Kipping R, et al. Results of a feasibility cluster randomised controlled trial of a peer-led school-based intervention to increase the physical activity of adolescent girls (PLAN-A). Int J Behav Nutr Phys Act 2018;15:50.
Sebire S, Banfield K, Jago R, Edwards M, Campbell R, Kipping R, et al. A process evaluation of the PLAN-A intervention (PEER-Led physical Activity iNtervention for Adolescent girls). BMC Public Health 2019;19:1203.
Data-sharing statement
All data requests should be submitted to the corresponding author for consideration. Access to available anonymised data may be granted following review.
Disclaimers
This report presents independent research funded by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care. If there are verbatim quotations included in this publication the views and opinions expressed by the interviewees are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, NETSCC, the PHR programme or the Department of Health and Social Care.
References
- Chief Medical Officers . Start Active, Stay Active: A Report on Physical Activity from the Four Home Countries 2011.
- Janssen I, Leblanc AG. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int J Behav Nutr Phys Act 2010;7. https://doi.org/10.1186/1479-5868-7-40.
- Steele RM, van Sluijs EM, Cassidy A, Griffin SJ, Ekelund U. Targeting sedentary time or moderate- and vigorous-intensity activity: independent relations with adiposity in a population-based sample of 10-y-old British children. Am J Clin Nutr 2009;90:1185-92. https://doi.org/10.3945/ajcn.2009.28153.
- Sardinha LB, Andersen LB, Anderssen SA, Quitério AL, Ornelas R, Froberg K, et al. Objectively measured time spent sedentary is associated with insulin resistance independent of overall and central body fat in 9- to 10-year-old Portuguese children. Diabetes Care 2008;31:569-75. https://doi.org/10.2337/dc07-1286.
- Ardern CI, Janssen I. Metabolic syndrome and its association with morbidity and mortality. Appl Physiol Nutr Metab 2007;32:33-45. https://doi.org/10.1139/h06-099.
- Biddle SJ, Asare M. Physical activity and mental health in children and adolescents: a review of reviews. Br J Sports Med 2011;45:886-95. https://doi.org/10.1136/bjsports-2011-090185.
- Kirkcaldy BD, Shephard RJ, Siefen RG. The relationship between physical activity and self-image and problem behaviour among adolescents. Soc Psychiatry Psychiatr Epidemiol 2002;37:544-50. https://doi.org/10.1007/s00127-002-0554-7.
- Norris R, Carroll D, Cochrane R. The effects of physical activity and exercise training on psychological stress and well-being in an adolescent population. J Psychosom Res 1992;36:55-6. https://doi.org/10.1016/0022-3999(92)90114-H.
- Dwyer T, Sallis JF, Blizzard L, Lazarus R, Dean K. Relation of academic performance to physical activity and fitness in children. Pediatric Exercise Science 2001;13:225-37. https://doi.org/10.1123/pes.13.3.225.
- Nader PR, Bradley RH, Houts RM, McRitchie SL, O’Brien M. Moderate-to-vigorous physical activity from ages 9 to 15 years. JAMA 2008;300:295-30. https://doi.org/10.1001/jama.300.3.295.
- Bauman AE, Reis RS, Sallis JF, Wells JC, Loos RJ, Martin BW. Lancet Physical Activity Series Working Group . Correlates of physical activity: why are some people physically active and others not?. Lancet 2012;380:258-71. https://doi.org/10.1016/S0140-6736(12)60735-1.
- Inchley JC, Currie DB, Todd JM, Akhtar PC, Currie CE. Persistent socio-demographic differences in physical activity among Scottish schoolchildren 1990-2002. Eur J Public Health 2005;15:386-8. https://doi.org/10.1093/eurpub/cki084.
- Dumith SC, Gigante DP, Domingues MR, Kohl HW. Physical activity change during adolescence: a systematic review and a pooled analysis. Int J Epidemiol 2011;40:685-98. https://doi.org/10.1093/ije/dyq272.
- Collings PJ, Wijndaele K, Corder K, Westgate K, Ridgway CL, Dunn V, et al. Levels and patterns of objectively-measured physical activity volume and intensity distribution in UK adolescents: the ROOTS study. Int J Behav Nutr Phys Act 2014;11. https://doi.org/10.1186/1479-5868-11-23.
- Twisk JW, Kemper HC, van Mechelen W. Tracking of activity and fitness and the relationship with cardiovascular disease risk factors. Med Sci Sports Exerc 2000;32:1455-61. https://doi.org/10.1097/00005768-200008000-00014.
- Biddle SJH, Whitehead SH, O’Donovan TM, Neville ME. Correlates of participation in physical activity for adolescent girls: a systematic review of recent literature. J Phys Act Health 2005;2:421-32. https://doi.org/10.1123/jpah.2.4.423.
- Slater A, Tiggemann M. ‘Uncool to do sport’: A focus group study of adolescent girls’ reasons for withdrawing from physical activity. Psychol Sport Exerc 2010;11:619-26. https://doi.org/10.1016/j.psychsport.2010.07.006.
- Knowles AM, Niven AG, Fawkner SG. Adopting a narrative approach to understanding physical activity behaviour in adolescent girls. Qual Res Sport, Exerc &Amp; Health 2013;6:62-76. https://doi.org/10.1080/2159676X.2013.766816.
- Gillison F, Sebire S, Standage M. What motivates girls to take up exercise during adolescence? Learning from those who succeed. Br J Health Psychol 2012;17:536-50. https://doi.org/10.1111/j.2044-8287.2011.02053.x.
- Biddle SJ, Braithwaite R, Pearson N. The effectiveness of interventions to increase physical activity among young girls: a meta-analysis. Prev Med 2014;62:119-31. https://doi.org/10.1016/j.ypmed.2014.02.009.
- HM Government . Childhood Obesity: A Plan for Action 2016.
- Borde R, Smith JJ, Sutherland R, Nathan N, Lubans DR. Methodological considerations and impact of school-based interventions on objectively measured physical activity in adolescents: a systematic review and meta-analysis. Obes Rev 2017;18:476-90. https://doi.org/10.1111/obr.12517.
- Sutherland RL, Campbell EM, Lubans DR, Morgan PJ, Nathan NK, Wolfenden L, et al. The Physical Activity 4 Everyone Cluster Randomized Trial: 2-year outcomes of a school physical activity intervention among adolescents. Am J Prev Med 2016;51:195-20. https://doi.org/10.1016/j.amepre.2016.02.020.
- Sutherland R, Reeves P, Campbell E, Lubans DR, Morgan PJ, Nathan N, et al. Cost effectiveness of a multi-component school-based physical activity intervention targeting adolescents: the ‘Physical Activity 4 Everyone’ cluster randomized trial. Int J Behav Nutr Phys Act 2016;13. https://doi.org/10.1186/s12966-016-0418-2.
- Dobbins M, De Corby K, Robeson P, Husson H, Tirilis D. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6–18. Cochrane Database Syst Rev 2009;1. https://doi.org/10.1002/14651858.CD007651.
- Fitzgerald A, Fitzgerald N, Aherne C. Do peers matter? A review of peer and/or friends’ influence on physical activity among American adolescents. J Adolesc 2012;35:941-58. https://doi.org/10.1016/j.adolescence.2012.01.002.
- Macdonald-Wallis K, Jago R, Sterne JA. Social network analysis of childhood and youth physical activity: a systematic review. Am J Prev Med 2012;43:636-42. https://doi.org/10.1016/j.amepre.2012.08.021.
- Campbell R, Starkey F, Holliday J, Audrey S, Bloor M, Parry-Langdon N, et al. An informal school-based peer-led intervention for smoking prevention in adolescence (ASSIST): a cluster randomised trial. Lancet 2008;371:1595-602. https://doi.org/10.1016/S0140-6736(08)60692-3.
- Mellanby AR, Rees JB, Tripp JH. Peer-led and adult-led school health education: a critical review of available comparative research. Health Educ Res 2000;15:533-45. https://doi.org/10.1093/her/15.5.533.
- Martin Ginis KA, Nigg CR, Smith AL. Peer-delivered physical activity interventions: an overlooked opportunity for physical activity promotion. Transl Behav Med 2013;3:434-43. https://doi.org/10.1007/s13142-013-0215-2.
- Smit CR, de Leeuw RNH, Bevelander KE, Burk WJ, Buijzen M. A social network-based intervention stimulating peer influence on children’s self-reported water consumption: a randomized control trial. Appetite 2016;103:294-301. https://doi.org/10.1016/j.appet.2016.04.011.
- Harden A, Oakley A, Oliver S. Peer-delivered health promotion for young people: a systematic review of different study designs. Health Educ J 2001;60:339-53. https://doi.org/10.1177/001789690106000406.
- Tymms PB, Curtis SE, Routen AC, Thomson KH, Bolden DS, Bock S, et al. Clustered randomised controlled trial of two education interventions designed to increase physical activity and well-being of secondary school students: the MOVE Project. BMJ Open 2016;6. https://doi.org/10.1136/bmjopen-2015-009318.
- Rogers EM. Diffusion of Innovations. New York, NY: The Free Press; 1983.
- Audrey S, Holliday J, Parry-Langdon N, Campbell R. Meeting the challenges of implementing process evaluation within randomized controlled trials: the example of ASSIST (A Stop Smoking in Schools Trial). Health Educ Res 2006;21:366-77. https://doi.org/10.1093/her/cyl029.
- Hollingworth W, Cohen D, Hawkins J, Hughes RA, Moore LA, Holliday JC, et al. Reducing smoking in adolescents: cost-effectiveness results from the cluster randomized ASSIST (A Stop Smoking In Schools Trial). Nicotine Tob Res 2012;14:161-8. https://doi.org/10.1093/ntr/ntr155.
- Holliday J, Audrey S, Moore L, Parry-Langdon N, Campbell R. High fidelity? How should we consider variations in the delivery of school-based health promotion interventions?. Health Educ J 2009;68:44-62. https://doi.org/10.1177/0017896908100448.
- Audrey S, Holliday J, Campbell R. It’s good to talk: adolescent perspectives of an informal, peer-led intervention to reduce smoking. Soc Sci Med 2006;63:320-34. https://doi.org/10.1016/j.socscimed.2005.12.010.
- Audrey S, Holliday J, Campbell R. Commitment and compatibility: teachers’ perspectives on the implementation of an effective school-based, peer-led smoking intervention. Health Educ J 2008;67:74-90. https://doi.org/10.1177/0017896908089387.
- Bell SL, Audrey S, Cooper AR, Noble S, Campbell R. Lessons from a peer-led obesity prevention programme in English schools. Health Promot Int 2017;32:250-9. https://doi.org/10.1093/heapro/dau008.
- Michie S. Designing and implementing behaviour change interventions to improve population health. J Health Serv Res Policy 2008;13:64-9. https://doi.org/10.1258/jhsrp.2008.008014.
- Deci EL, Ryan RM. The ‘what’ and ‘why’ of goal pursuits: human needs and the self-determination of behavior. Psychol Inq 2000;11:227-68. https://doi.org/10.1207/S15327965PLI1104_01.
- Standage M, Ryan RM, Roberts GC, Treasure DC. Advances in Motivation in Sport and Exercise. Champaign, IL: Human Kinetics; 2012.
- Teixeira PJ, Carraça EV, Markland D, Silva MN, Ryan RM. Exercise, physical activity, and self-determination theory: a systematic review. Int J Behav Nutr Phys Act 2012;9. https://doi.org/10.1186/1479-5868-9-78.
- Sebire SJ, Jago R, Fox KR, Edwards MJ, Thompson JL. Testing a self-determination theory model of children’s physical activity motivation: a cross-sectional study. Int J Behav Nutr Phys Act 2013;10. https://doi.org/10.1186/1479-5868-10-111.
- Fortier MS, Duda JL, Guerin E, Teixeira PJ. Promoting physical activity: development and testing of self-determination theory-based interventions. Int J Behav Nutr Phys Act 2012;9. https://doi.org/10.1186/1479-5868-9-20.
- Buman MP, Giacobbi PR, Dzierzewski JM, Aiken Morgan A, McCrae CS, Roberts BL, et al. Peer volunteers improve long-term maintenance of physical activity with older adults: a randomized controlled trial. J Phys Act Health 2011;8:257-66. https://doi.org/10.1123/jpah.8.s2.s257.
- Standage M, Duda JL, Ntoumanis N. A test of self-determination theory in school physical education. Br J Educ Psychol 2005;75:411-33. https://doi.org/10.1348/000709904X22359.
- Gillison FB, Standage M, Skevington SM. Relationships among adolescents’ weight perceptions, exercise goals, exercise motivation, quality of life and leisure-time exercise behaviour: a self-determination theory approach. Health Educ Res 2006;21:836-47. https://doi.org/10.1093/her/cyl139.
- Sebire SJ, Standage M, Vansteenkiste M. Examining intrinsic versus extrinsic exercise goals: cognitive, affective, and behavioral outcomes. J Sport Exerc Psychol 2009;31:189-210. https://doi.org/10.1123/jsep.31.2.189.
- White J, Hawkins J, Madden K, Grant A, Er V, Angel L, et al. Adapting the ASSIST model of informal peer-led intervention delivery to the Talk to FRANK drug prevention programme in UK secondary schools (ASSIST + FRANK): intervention development, refinement and a pilot cluster randomised controlled trial. Public Health Res 2017;5. https://doi.org/10.3310/phr05070.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol 2006;3:77-101. https://doi.org/10.1191/1478088706qp063oa.
- Amorose AJ, Anderson-Butcher D. Autonomy-supportive coaching and self-determined motivation in high school and college athletes: a test of self-determination theory. Psychol Sport Exerc 2007;8:654-70. https://doi.org/10.1016/j.psychsport.2006.11.003.
- Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol 2013;13. https://doi.org/10.1186/1471-2288-13-117.
- Sebire SJ, Edwards MJ, Campbell R, Jago R, Kipping R, Banfield K, et al. Protocol for a feasibility cluster randomised controlled trial of a peer-led school-based intervention to increase the physical activity of adolescent girls (PLAN-A). Pilot Feasibility Stud 2016;2. https://doi.org/10.1186/s40814-015-0045-8.
- Michie S, Ashford S, Sniehotta FF, Dombrowski SU, Bishop A, French DP. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: the CALO-RE taxonomy. Psychol Health 2011;26:1479-98. https://doi.org/10.1080/08870446.2010.540664.
- Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014;348. https://doi.org/10.1136/bmj.g1687.
- Eldridge SM, Chan CL, Campbell MJ, Bond CM, Hopewell S, Thabane L, et al. PAFS consensus group . CONSORT 2010 statement: extension to randomised pilot and feasibility trials. Pilot Feasibility Stud 2016;2. https://doi.org/10.1186/s40814-016-0105-8.
- Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care 2007;19:349-57. https://doi.org/10.1093/intqhc/mzm042.
- Husereau D, Drummond M, Petrou S, Carswell C, Moher D, Greenberg D, et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS) – explanation and elaboration: a report of the ISPOR Health Economic Evaluation Publication Guidelines Good Reporting Practices Task Force. Value Health 2013;16:231-50. https://doi.org/10.1016/j.jval.2013.02.002.
- Education Funding Agency . Pupil Premium: Funding Allocations 2015 to 2016 2015.
- Europe TKG . The KIDSCREEN Questionnaires: Quality of Life Questions for Children and Adolescents 2006.
- Ministry of Housing, Communities and Local Government . English Indices of Deprivation 2010 2011.
- Boyce W, Torsheim T, Currie C, Zambon A. The Family Affluence Scale as a measure of national wealth: validation of an adolescent self-report measure. Soc Indic Res 2006;78:473-87. https://doi.org/10.1007/s11205-005-1607-6.
- Currie C, Molcho M, Boyce W, Holstein B, Torsheim T, Richter M. Researching health inequalities in adolescents: the development of the Health Behaviour in School-Aged Children (HBSC) Family Affluence Scale. Soc Sci Med 2008;66:1429-36. https://doi.org/10.1016/j.socscimed.2007.11.024.
- De Vries SI, Van Hirtum HW, Bakker I, Hopman-Rock M, Hirasing RA, Van Mechelen W. Validity and reproducibility of motion sensors in youth: a systematic update. Med Sci Sports Exerc 2009;41:818-27. https://doi.org/10.1249/MSS.0b013e31818e5819.
- Trost SG, Loprinzi PD, Moore R, Pfeiffer KA. Comparison of accelerometer cut points for predicting activity intensity in youth. Med Sci Sports Exerc 2011;43:1360-8. https://doi.org/10.1249/MSS.0b013e318206476e.
- Evenson KR, Catellier DJ, Gill K, Ondrak KS, McMurray RG. Calibration of two objective measures of physical activity for children. J Sports Sci 2008;26:1557-65. https://doi.org/10.1080/02640410802334196.
- Markland D, Tobin V. A modification to the Behavioural Regulation in Exercise Questionnaire to include an assessment of amotivation. JSEP 2004;26:191-96. https://doi.org/10.1123/jsep.26.2.191.
- McAuley E, Duncan T, Tammen VV. Psychometric properties of the Intrinsic Motivation Inventory in a competitive sport setting: a confirmatory factor analysis. Res Q Exerc Sport 1989;60:48-5. https://doi.org/10.1080/02701367.1989.10607413.
- Marsh HW. Self Description Questionnaire (SDQ) III: A Theoretical and Empirical Basis for the Measurement of Multiple Dimensions of Late Adolescent Self-Concept: A Test Manual and a Research Monograph. Sydney, NSW: University of Western Sydney, Faculty of Education; 1992.
- Bartholomew JB, Loukas A, Jowers EM, Allua S. Validation of the physical activity self-efficacy scale: testing measurement invariance between Hispanic and Caucasian children. JPAH 2006;3:70-8. https://doi.org/10.1123/jpah.3.1.70.
- de Farias Junior JC, da Silva Lopes A, Siqueira Reis R, do Nascimento JV, Borgatto AF, Hallal PC. Development and validation of a questionnaire measuring factors associated with physical activity in adolescents. Braz J Mother Infant Health 2011;11:301-12. https://doi.org/10.1590/S1519-38292011000300011.
- Ling J, Robbins LB, Resnicow K, Bakhoya M. Social support and peer norms scales for physical activity in adolescents. Am J Health Behav 2014;38:881-9. https://doi.org/10.5993/AJHB.38.6.10.
- Wille N, Badia X, Bonsel G, Burström K, Cavrini G, Devlin N, et al. Development of the EQ-5D-Y: a child-friendly version of the EQ-5D. Qual Life Res 2010;19:875-86. https://doi.org/10.1007/s11136-010-9648-y.
- Dolan P, Gudex C, Kind P, Williams A. A Social Tariff for EuroQol: Results from a UK General Population Survey. York: Centre for Health Economics, University of York; 1995.
- Jones NR, Jones A, van Sluijs EM, Panter J, Harrison F, Griffin SJ. School environments and physical activity: the development and testing of an audit tool. Health Place 2010;16:776-83. https://doi.org/10.1016/j.healthplace.2010.04.002.
- Lounsbery MA, McKenzie TL, Morrow JR, Holt KA, Budnar RG. School physical activity policy assessment. J Phys Act Health 2013;10:496-503. https://doi.org/10.1123/jpah.10.4.496.
- (GB) OS . OS VectorMap® Local [TIFF Geospatial Data] 2017. www.ordnancesurvey.co.uk/business-and-government/products/vectormap-local.html (accessed 10 January 2019).
- (GB) OS . MasterMap® Integrated Transport Network Layer [GML2 Geospatial data]: Tiles: GB 2016. www.ordnancesurvey.co.uk/business-and-government/help-and-support/products/itn-layer.html (accessed 10 January 2019).
- CEH . Land Cover Map 2007 2008. www.ceh.ac.uk/services/land-cover-map-2007 (accessed 10 January 2019).
- White IR, Royston P, Wood AM. Multiple imputation using chained equations: issues and guidance for practice. Stat Med 2011;30:377-99. https://doi.org/10.1002/sim.4067.
- Jago R, Edwards MJ, Sebire SJ, Tomkinson K, Bird EL, Banfield K, et al. Effect and cost of an after-school dance programme on the physical activity of 11–12 year old girls: the Bristol Girls Dance Project, a school-based cluster randomised controlled trial. Int J Behav Nutr Phys Act 2015;12. https://doi.org/10.1186/s12966-015-0289-y.
- Murray DM, Stevens J, Hannan PJ, Catellier DJ, Schmitz KH, Dowda M, et al. School-level intraclass correlation for physical activity in sixth grade girls. Med Sci Sports Exerc 2006;38:926-36. https://doi.org/10.1249/01.mss.0000218188.57274.91.
- Manca A, Hawkins N, Sculpher MJ. Estimating mean QALYs in trial-based cost-effectiveness analysis: the importance of controlling for baseline utility. Health Econ 2005;14:487-96. https://doi.org/10.1002/hec.944.
- Staley K. ‘Is it worth doing?’ Measuring the impact of patient and public involvement in research. Res Involv Engagem 2015;1. https://doi.org/10.1186/s40900-015-0008-5.
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. Int J Nurs Stud 2013;50:587-92. https://doi.org/10.1016/j.ijnurstu.2012.09.010.
- Smith LH. Piloting the use of teen mentors to promote a healthy diet and physical activity among children in Appalachia. J Spec Pediatr Nurs 2011;16:16-2. https://doi.org/10.1111/j.1744-6155.2010.00264.x.
- Corder K, Brown HE, Schiff A, van Sluijs EM. Feasibility study and pilot cluster-randomised controlled trial of the GoActive intervention aiming to promote physical activity among adolescents: outcomes and lessons learnt. BMJ Open 2016;6. https://doi.org/10.1136/bmjopen-2016-012335.
- Santos RG, Durksen A, Rabbanni R, Chanoine JP, Lamboo Miln A, Mayer T, et al. Effectiveness of peer-based healthy living lesson plans on anthropometric measures and physical activity in elementary school students: a cluster randomized trial. JAMA Pediatr 2014;168:330-7. https://doi.org/10.1001/jamapediatrics.2013.3688.
- Verloigne M, Cardon G, De Craemer M, D’Haese S, De Bourdeaudhuij I. Mediating effects of self-efficacy, benefits and barriers on the association between peer and parental factors and physical activity among adolescent girls with a lower educational level. PLOS ONE 2016;11. https://doi.org/10.1371/journal.pone.0157216.
- Hamilton K, Warner LM, Schwarzer R. The role of self-efficacy and friend support on adolescent vigorous physical activity. Health Educ Behav 2017;44:175-81. https://doi.org/10.1177/1090198116648266.
- Dobbie F, Purves R, McKell J, Dougall N, White J, Campbell R, et al. A Process Evaluation of the Implementation of Assist in Scotland: Final Report 2017.
- Sebire SJ, Edwards MJ, Fox KR, Davies B, Banfield K, Wood L, et al. Delivery and receipt of a self-determination-theory-based extracurricular physical activity intervention: exploring theoretical fidelity in action 3:30. J Sport Exerc Psychol 2016;38:381-95. https://doi.org/10.1123/jsep.2015-0217.
- Sebire SJ, Kesten JM, Edwards MJ, May T, Banfield K, Tomkinson K, et al. Using self-determination theory to promote adolescent girls’ physical activity: Exploring the theoretical fidelity of the Bristol Girls Dance Project. Psychol Sport Exerc 2016;24:100-10. https://doi.org/10.1016/j.psychsport.2016.01.009.
- Bumbarger B, Perkins D. After randomised trials: issues related to dissemination of evidence-based interventions. J Child Serv 2008;3:55-64. https://doi.org/10.1108/17466660200800012.
- Sebire SJ, Edwards MJ, Kesten JM, May T, Banfield KJ, Bird EL, et al. Process evaluation of the Bristol Girls Dance Project. BMC Public Health 2016;16. https://doi.org/10.1186/s12889-016-3010-4.
- Aelterman N, Vansteenkiste M, Van Keer H, De Meyer J, Van den Berghe L, Haerens L. Development and evaluation of a training on need-supportive teaching in physical education: qualitative and quantitative findings. Teach Teach Educ 2013;29:64-75. https://doi.org/10.1016/j.tate.2012.09.001.
- Ekelund U, Luan J, Sherar LB, Esliger DW, Griew P, Cooper A. International Children’s Accelerometry Database (ICAD) Collaborators . Moderate to vigorous physical activity and sedentary time and cardiometabolic risk factors in children and adolescents. JAMA 2012;307:704-12. https://doi.org/10.1001/jama.2012.156.
- Owen MB, Curry WB, Kerner C, Newson L, Fairclough SJ. The effectiveness of school-based physical activity interventions for adolescent girls: a systematic review and meta-analysis. Prev Med 2017;105:237-49. https://doi.org/10.1016/j.ypmed.2017.09.018.
- Metcalf B, Henley W, Wilkin T. Effectiveness of intervention on physical activity of children: systematic review and meta-analysis of controlled trials with objectively measured outcomes (EarlyBird 54). BMJ 2012;345. https://doi.org/10.1136/bmj.e5888.
- Okely AD, Lubans DR, Morgan PJ, Cotton W, Peralta L, Miller J, et al. Promoting physical activity among adolescent girls: the Girls in Sport group randomized trial. Int J Behav Nutr Phys Act 2017;14. https://doi.org/10.1186/s12966-017-0535-6.
- Edwardson CL, Harrington DM, Yates T, Bodicoat DH, Khunti K, Gorely T, et al. A cluster randomised controlled trial to investigate the effectiveness and cost effectiveness of the ‘Girls Active’ intervention: a study protocol. BMC Public Health 2015;15. https://doi.org/10.1186/s12889-015-1886-z.
- Jones KH, Laurie G, Stevens L, Dobbs C, Ford DV, Lea N. The other side of the coin: harm due to the non-use of health-related data. Int J Med Inform 2017;97:43-51. https://doi.org/10.1016/j.ijmedinf.2016.09.010.
- Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015;350. https://doi.org/10.1136/bmj.h1258.
- Ofcom . Children and Parents: Media Use and Attitudes Report 2016 2017. www.ofcom.org.uk/research-and-data/media-literacy-research/childrens/children-parents-2017 (accessed 8 November 2018).
- Chandler JL, Brazendale K, Beets MW, Mealing BA. Classification of physical activity intensities using a wrist-worn accelerometer in 8–12-year-old children. Pediatr Obesity 2016;11:120-7.
Appendix 1 Key findings from formative work and their implications on phase 2
| Source | Key findings | Intervention refinement |
|---|---|---|
| Recruitment materials/peer nomination | ||
| Iterative focus group: round 1 and 2; DIFG; and observations |
|
|
| Characteristics of PSs and trainers | ||
| Iterative focus group: round 1 |
|
|
| Train the trainers | ||
| Trainer 1 and 2; and observations |
|
|
| Expectations of PS training | ||
| Iterative focus groups: round 1; PTFG; and observations |
|
|
| Concerns about being a PS | ||
| Iterative focus groups: round 1 |
|
|
| PS training content | ||
| Iterative focus groups: round 1 and 2; trainer 1 and 2; PTFG; DIFG; and observations |
|
|
| Individual activity changes | ||
| PTFG; trainer 1 and 2; and observations |
|
|
| Intervention materials | ||
| Iterative focus groups: round 1 and 2; trainer 1 and 2 |
|
|
| PS training logistics | ||
| PTFG; trainer 1 and 2; and observations |
|
|
Appendix 2 Trainer peer supporter training evaluation form
Appendix 3 Peer supporter training evaluation form
Appendix 4 Peer supporter training observation form
Appendix 5 Observed versus allocated time for pilot training activities on days 1 and 2
FIGURE 12.
Observed vs. allocated time for pilot training activities on day 1.
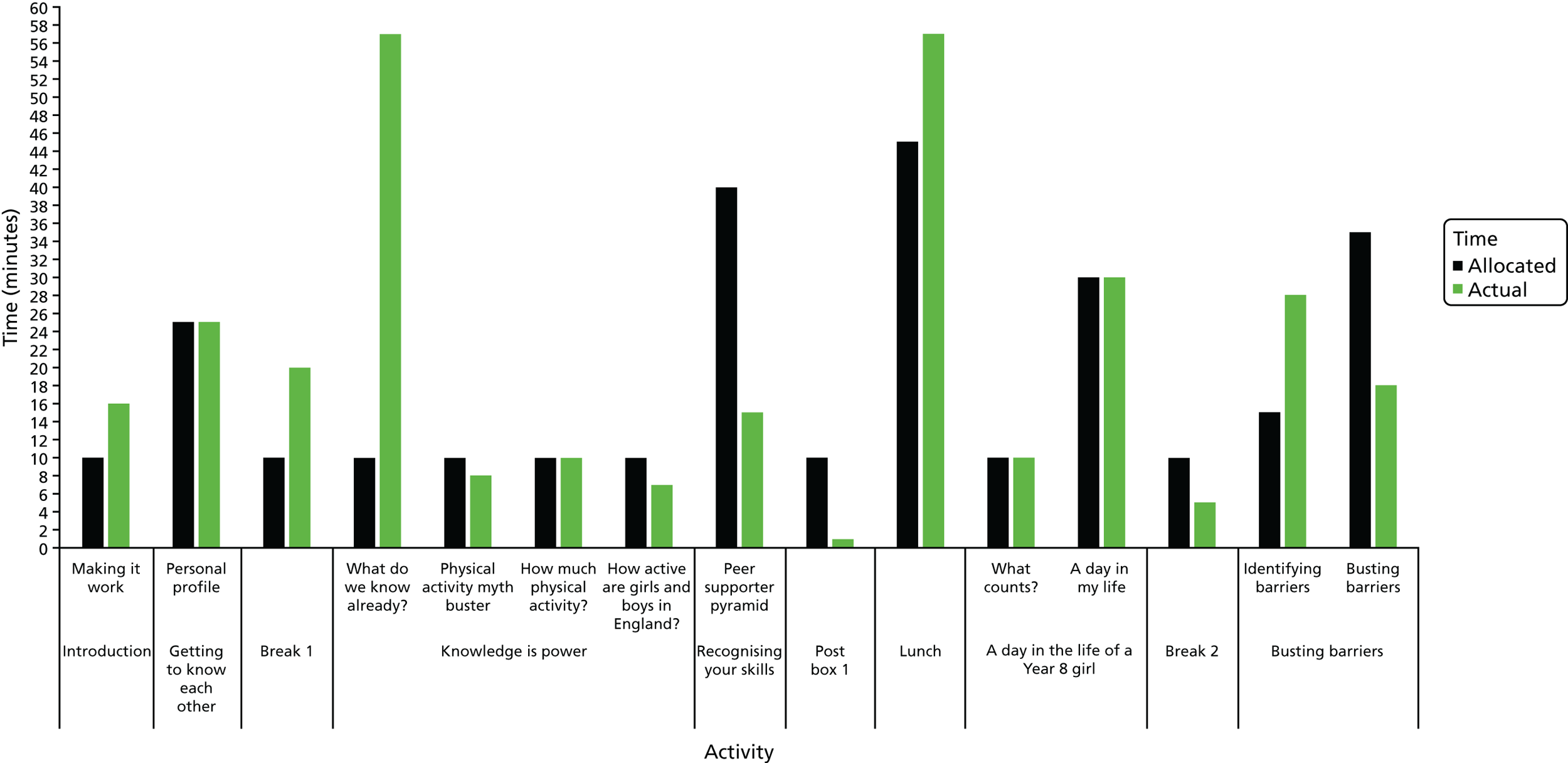
FIGURE 13.
Observed vs. allocated time for pilot training activities on day 2.
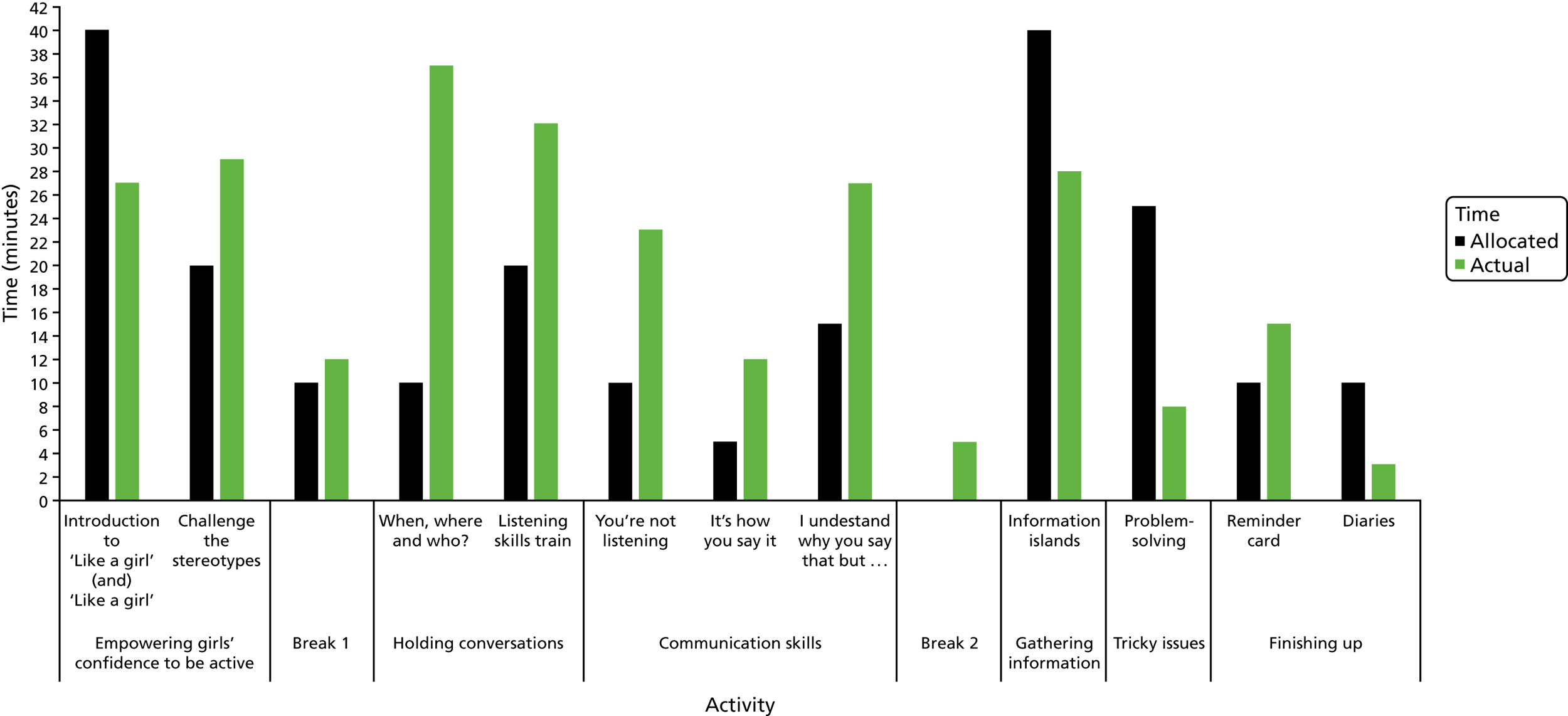
Appendix 6 Ancillary accelerometer study
Study context
This substudy was developed in response to the research team’s experience at baseline data collection and subsequent discussions with, and recommendations of, the TSC (in December 2015).
It was originally proposed that participants in two schools would wear both a wrist- and waist-worn ActiGraph accelerometers to explore the differences in wear-time compliance, as well as the agreement between the data derived from the two devices. Anecdotal reports from participants during T0 data collection suggested that wearing the two accelerometers would be burdensome and could reduce accelerometer return at T1, which is a key progression criterion. The TSC also highlighted that the plan would not sufficiently address the aims (i.e. there are specific existing studies comparing compliance with wrist- vs. waist-worn accelerometers).
The TSC proposed an alternative qualitative design that would explore the acceptability of different accelerometers among Year 8 girls, with the intention that the findings could inform the adoption or removal of the wrist- and waist-worn monitoring protocol at T1. The proposed design was approved by the NIHR (on 5 February 2016).
Objectives
To qualitatively examine girls’ views on wearing waist and wrist accelerometers, and both devices concurrently, as this was proposed in the NIHR protocol; and to present data showing wear time for descriptive purposes. The three groups tested were:
-
a waist-worn ActiGraph WGT3X-BT accelerometer
-
a wrist-worn GENEActiv accelerometer
-
a wrist- and hip-worn ActiGraph WGT3X-BT, worn at the same time.
School and participant recruitment
The PLAN-A pilot school hosted the study. Seventy Year 8 girls from the pilot school were invited to participate. Written parental consent and assent from the young women were required for participation. The study took place in March/April 2016.
Methods/design
Consenting participants (n = 21, 30% of those eligible) were randomly allocated, in equal numbers, to wear either (1) one waist-worn ActiGraph WGT3X-BT, (2) one wrist-worn GENEActiv or (3) a waist- and wrist-worn ActiGraph WGT3X-BT. Participants were asked to wear their allocated accelerometer(s) for 7 days, following the feasibility study protocol.
Three semistructured focus groups were conducted for participants in each group (n = 21) and ranged from 12 to 26 minutes in duration (mean duration 17.42 minutes). Questions focused on participants’ experiences of wearing each accelerometer and wearing two accelerometers concurrently. Interviews were digitally recorded, transcribed verbatim and anonymised.
The ancillary accelerometer study was approved by the School for Policy Studies Ethics Committee at the University of Bristol as an amendment to the main feasibility study approval.
Analysis
Qualitative data
Directed thematic analysis was undertaken examining the following a priori issues: (1) views on the device prior to wearing them, (2) peer and family perception of the device, (3) participants’ experience of wearing the device and (4) which device participants would prefer to wear. The initial analysis was undertaken by an experienced qualitative researcher (ME), and was triangulated and refined by a second researcher (JM). Key quotations that represented the breadth of participants’ experiences were selected and checked by both analysts.
Quantitative data
ActiGraph data were downloaded via ActiLife 1.7 (ActiGraph, LLC, Pensacola, FL, USA) and analysed using Kinesoft (Kinesoft, SK, Canada). The GENEActiv data were downloaded using GENEActiv software. Given the difference in device placement, multiple analysis protocols were followed. ActiGraph waist data were analysed in line with the PLAN-A intervention protocol. Wrist-worn ActiGraph data were analysed in accordance with recommendations of Chandler et al. 107 (Axis 1). GENEActiv data were analysed using a Microsoft Excel® (Microsoft Corporation, Redmond, WA, USA), macro analysis spreadsheet, supplied by GENEActiv. GENEActiv Open Platforms [https://open.geneactiv.org/geneactiv_macros.html (accessed 27 November 2018)] was used to interpret data.
Results
Qualitative results
Views towards the device before having experienced wearing them
The group of girls assigned to the GENEActiv watches was the most positive about their device allocation, and the appraisal became more pronounced when compared with the ActiGraph devices:
It looks more stylish [than an ActiGraph].
Ours [GENEActiv] was quite flat and theirs [ActiGraph] is quite chunky.
Participants who were assigned both the ActiGraph waist and the ActiGraph wrist devices were less happy with their allocation:
When I had both and I found out what they looked like, I would have preferred just to have the waist one because, I’m not going to lie, they’re not too attractive, it’s a big thing poking out of your wrist. The black ones were better [GENEActiv] because you could disguise it to look like a watch.
Some participants saw the waist-only ActiGraph as being ‘easy to hide’, whereas others saw it as ‘a big lumpy thing’. Girls liked that ‘it was not beeping or flashing constantly’, but felt that a more inconspicuous colour would be better:
If it was black it wouldn’t be too bad, it’s bright red, if I see someone walk out with that I think, ‘why have they got a red thing sticking out of them’.
Social and familial perceptions of the devices
Girls assigned to the waist- and wrist-worn ActiGraph group were more concerned about other people’s perceptions of their devices than the other two groups. There were few comments from other people about the waist-worn ActiGraph as their peers ‘did not really notice’.
Views towards the GENEActiv devices comprised general approval mixed with scepticism. Peers were seen to ‘quite like it’, but although some family members ‘thought it was a normal watch’ others thought it was a tracking tag. The GENEActiv device was approved of ‘because of what it does and [because] it looks really nice’.
The wrist-worn ActiGraph received the most apprehension from family and friends. The devices were frequently commented on and the girls received increased attention from people asking them to explain what was on their wrist and for what purpose:
The watch one [wrist-worn ActiGraph] was a bit of a problem, because everyone was coming up to us asking us loads of questions. My dad thought I was on tag. It was just like it was really ugly.
People nowadays are really judgemental about things, so it would be better if I just held it [wrist-worn ActiGraph]. But the hip one was fine, because you could just wear it under your clothes. I would prefer just to have the belt, so I don’t have to worry about hiding the watch.
Experience of wearing the accelerometers
Girls reported few issues with wearing the waist-worn ActiGraph. One respondent reported that she ‘did not really mind it’, with others suggesting that ‘it was not itchy’ and it ‘was all right with sports.’ Negative comments related to wearing it comfortably with a variety of clothing.
Experiences of wearing the GENEActiv devices were positive. The only negative comments were related to the size, in that the girls found ‘it was quite big for us’:
It just feels like you have a watch on.
The majority of girls found the wrist-worn ActiGraph difficult to wear because of the size of the device in comparison to their wrist size:
I don’t think hardly [any] people like the watch [wrist-worn ActiGraph] because when we were going out on Saturday, we didn’t want to wear it because it’s like big and chunky.
Which device would girls like to wear if participating in the study again?
The wrist-worn ActiGraph was the least desirable single device option; however, wearing both a waist- and wrist-worn ActiGraph was viewed more unfavourably. Girls who wore the GENEActiv device unanimously preferred to wear it again in a future project. The majority of views related to physical (dis)comfort and appearance and, as such, wearing a wrist-worn ActiGraph was the least desirable mode. ActiGraph devices were not seen as visually desirable; however, wearing an ActiGraph on the waist was favoured over the wrist as it is easier to hide:
You can hide the hip one.
Quantitative results
The primary objective of this study was to gather participants’ experiences of wearing the different accelerometers. Although the accelerometers recorded data and the data were downloaded and analysed, the analysis is descriptive (as the study was not powered, nor was it intended, to use these data to identify representative differences in compliance and/or wear time).
Table 39 shows wear protocol compliance. Wear time exceeded the thresholds used in the PLAN-A feasibility study (i.e. 2 valid weekdays) for all devices, although there is greater wear time in the GENEActiv group.
| Device | Return, n (%) | Number of valid days, mean (range) | Mean wear time (hours/valid day) | ||||
|---|---|---|---|---|---|---|---|
| Total | Weekdays | Weekend days | Total | Weekdays | Weekend days | ||
| Wrist- and waist-worn ActiGraph | |||||||
| ActiGraph, wrist worna | 7 (100) | 5.57b (4–7) | 4.14b (4–5) | 1.43b (0–2) | 12.30 | 12.04 | 13.56 |
| ActiGraph, waist worna | 7 (100) | 5.57b (4–7) | 4.00b (3–5) | 1.57b (0–2) | 11.73 | 11.81 | 11.58 |
| Waist-worn ActiGraph | |||||||
| ActiGraph, waist worn | 7 (100) | 4.00b (2–5) | 2.86b (2–4) | 1.14b (0–2) | 11.78 | 11.85 | 11.40 |
| GENEActiv | |||||||
| GENEActiv | 7 (100) | 4.71c (4–5) | 3.00c (–) | 1.86c (1–2) | 19.74d | 20.32d | 18.76d |
Conclusions
Qualitatively, the GENEActiv device was viewed most favourably, as it was initially seen to be ‘cool’, like wearing a watch. The waist-worn ActiGraph device was acceptable, but caused some discomfort and several girls did not like its appearance. The group wearing both waist- and wrist-worn ActiGraph devices had the most reservations and were the least satisfied with their experience. This group voiced concerns in relation to appearance, family and friends asking questions, fit and discomfort. The findings suggest that asking girls in two schools to wear both a waist- and wrist-worn ActiGraph would be detrimental to the feasibility study. Participants would be frustrated with wearing wrist- and waist-worn devices concurrently and issues related to appearance, unwanted attention from others, discomfort and inconvenience may compromise data provision on which a primary progression criterion is based.
The findings also provide useful information that can help guide the decision of which activity monitor could be used in a definitive trial. Participants would be most accepting of either the waist-worn ActiGraph (as currently used) or the wrist-worn GENEActiv device.
Appendix 7 School context questionnaire
Appendix 8 Deductive codes for the feasibility qualitative analysis
| Code | Description |
|---|---|
| PSs | |
| Recruitment | Why the girls wanted to be involved and become a PS |
| Peer nomination | What they thought of the peer nomination process, which people got nominated and how it could be changed |
| PS training | Thoughts on where the training was held, how long the training was, the catering and the amount of training |
| Experience of PS training | Thoughts on the content and type of activities, what was enjoyed and what was disliked |
| Impact of the PS training | What the PSs learnt during the training, how it has changed them (views about being active), effects on friendship groups and how it has prepared them to be a PS |
| Views on PS trainers | Were the trainers liked and why? Comments on teaching style and improvements they could have made |
| Experience of being a PS | How they have found being a PS (have they enjoyed it), what have they liked/disliked, what have they done to peer support, who have they talked to? Was it easy/hard? What has been challenging? |
| Impact of PSs on others | Any perceived impact the PS think they may have had on other girls in their year or outside school |
| Suggestions for the future | Anything the PSs suggest changing or adding with regard to the PS training, peer nomination or intervention |
| NPSs | |
| Views towards PA | General attitudes towards PA, did the girls talk about PLAN-A before they were prompted? |
| About the PSs | Did the girls know who they were? If so how? Were the PSs the right people to peer support? |
| Impact of PSs on others | What the PSs talked about or did to peer support, did it help change their level of activity or attitudes towards being active? Did it have any effect on friendship groups? |
| Feelings of not being a PS | How the girls felt about not being picked to be a PS and whether or not they felt the need to take on the role of a PS and help their friends |
| Impact of PLAN-A on PSs | Whether or not the NPSs felt that the PSs had changed as a result of being a PS; for example, a change in levels of confidence |
| Needs supportiveness | Anything that suggests the PSs were autonomy-supportive in encouraging the girls to be more active. Perceptions of their own feelings of autonomy and any reference to motivation or reasons why they are or are not active (as a result of influence from a PS) |
| Trainers | |
| Post-2-day training | |
| Recruitment/initial involvement | How the trainer became involved, thoughts on the recruitment process and why they became involved |
| Training the trainers | Thoughts on the logistics of the training (venue, length and resources) and the content |
| Post-2-day and top-up day | |
| PS training logistics | Views on the training venue, timings, length and catering for the training |
| Training content | What was enjoyed and what was not, activities or elements of the training that worked and didn’t work. Any improvements to the content or adaptations made to activities |
| Delivering the PS training | Experience of delivering the training to the girls, how prepared they felt and difficulties they had. How they felt delivering to a different group of girls during the top-up day training (if applicable) |
| Impact of the training | Evidence of how the training helped the girls become PSs or how it has developed their skills |
| Working with the other trainer | How they felt the trainer dynamics worked and how it affected delivery. How they felt if they had to work with a different trainer during the top-up day |
| School contacts | |
| Intervention and control | |
| Recruitment/initial involvement | How the contact became involved, thoughts on the recruitment process and why they became involved |
| Project understanding | Thoughts on the logistics of the training (venue, length and resources) and the content |
| Role in facilitating the project | How the contacts perceived what their role was in the project, how they found carrying out this role, their level of involvement in the project |
| Communication and organisation of the study team | How the contacts felt about the quality and level of communication to both them and the participants. Any comments regarding the organisation of the project within school |
| Intervention | |
| PS training | Thoughts on the content and logistics of the PS training |
| Impact of PLAN-A | Any impact it has had on the PSs, NPSs and on the school |
| Problems | Issues regarding bullying as a result of the PLAN-A intervention |
| Sustainability | Thoughts on whether or not the PLAN-A intervention could continue in school |
| School context | Anything regarding school priority for PA, staff awareness of the PLAN-A intervention, level of involvement of school contact or school ethos that could explain the reasoning behind results |
| Perceived trainer autonomy support | Comments regarding needs supportive motivation and teaching styles or controlling teaching styles |
| Control | |
| Impact of PLAN-A | Any impact Year 8 girls or the school have had as a result of being a control school, any potential impact a project like this could have and any exposure to the school about the PLAN-A intervention |
| Parent | |
| Views on PA among girls | Opinions on the importance of girls being active |
| Level of involvement in PLAN-A | How much do the parents know about the PLAN-A intervention, what do they think their daughter’s role as a PS involves and have they provided any support? |
| PS/parent communication | Has their daughter talked about the training or what she does to peer support? |
| Impact of being a PS | Thoughts on how their daughter has found being a PS, what impact has it had on their daughter’s social skills, PA levels and self-esteem or confidence? |
| What their daughter has done to peer support | Any evidence that their daughter has encouraged their friends to be active, what have they done and who with? |
| Problems/issues | Any issues regarding bullying or challenges carrying out the role of a PS? |
| PS training | Perceptions of whether or not it prepared their daughter to fulfil her role and thoughts on the logistics of the training (how they felt about their daughter taking 3 days out of school to take part) |
| Data linkage | Understanding of data linkage and whether or not they would consent to their daughter taking part |
Appendix 9 Internal consistency scores for psychosocial variables at each time point
| Variable | Time point | ||
|---|---|---|---|
| T0 | T1 | T2 | |
| Self-esteem | 0.87 | 0.90 | 0.90 |
| Motivation | |||
| Autonomous | 0.73 | 0.76 | 0.80 |
| Controlled | 0.87 | 0.88 | 0.90 |
| Amotivation | 0.75 | 0.79 | 0.76 |
| Need satisfaction | |||
| Autonomy | 0.77 | 0.78 | 0.81 |
| Competence | 0.91 | 0.90 | 0.90 |
| Relatedness | 0.92 | 0.93 | 0.94 |
| PA self-efficacy | 0.72 | 0.74 | 0.75 |
| Peer PA norm | |||
| Importance | 0.71 | 0.75 | 0.80 |
| Acceptance | 0.51 | 0.49 | 0.41 |
| Prevalence | 0.71 | 0.67 | 0.70 |
| PA social support from friends | 0.88 | 0.85 | 0.88 |
Appendix 10 Costs of intervention development
| Staff role | Units (hours) | Cost (£) | |
|---|---|---|---|
| Unit | Totala | ||
| Senior lecturer | 86 | 46 | 3921 |
| Research associate | 74.5 | 28 | 2100 |
| Research administrator | 16 | 20 | 314 |
| Fieldworker | 6 | 20 | 118 |
| Senior research associate | 2.5 | 32 | 80 |
| Total cost of intervention development | 6533 | ||
Appendix 11 School contact, Year 8 girls and peer supporter time
| Time | School ID, number of people; time (hours) | |||
|---|---|---|---|---|
| 2 (N = 58a) | 3 (N = 96a) | 4 (N = 66a) | 6 (N = 69a) | |
| School contact time | ||||
| Student briefing | 1; 1.0 | 1; 0.5 | 1; 1.0 | 1; 0.5 |
| Peer nomination | 1; 0.4 | 2; 0.7 | 1; 1.3 | 2; 0.7 |
| PS meeting | 1; 0.3 | 1; 0.3 | 1; 0.3 | 1; 0.3 |
| 2-day PS training | 1; 12.0 | 1; 11.8 | 1; 1.5 | 1; 12.1 |
| Top-up PS training | 1; 5.9 | 1; 5.9 | 0; 0.0 | 1; 6.0 |
| Year 8 girls’ time | ||||
| Student briefing | 58; 0.3 | 96; 0.3 | 66; 0.3 | 69; 0.3 |
| Peer nomination | 55; 0.4 | 88; 0.4 | 64; 0.4 | 62; 0.4 |
| PS time | ||||
| PS meeting | 12; 0.3 | 18; 0.3 | 12; 0.3 | 14; 0.3 |
| 2-day PS training, day 1 | 13; 5.1 | 17; 4.9 | 10; 5.7 | 13; 4.7 |
| 2-day PS training, day 2 | 13; 5.4 | 16; 5.3 | 11; 6.0 | 13; 4.9 |
| Top-up PS training | 12; 5.2 | 17; 5.2 | 11; 5.7 | 13; 5.0 |
Appendix 12 EuroQol-5 Dimensions, child-friendly version and quality-adjusted life-year data missingness, by trial arm
| Data | Trial arm, number missing (%) | |
|---|---|---|
| PLAN-A (N = 269) | Control (N = 158) | |
| EQ-5D-Y | ||
| Baseline | 5 (2) | 6 (4) |
| Post intervention | 15 (6) | 15 (9) |
| 12 months | 20 (7) | 17 (11) |
| QALYs | 31 (12) | 28 (18) |
Appendix 13 Correlation between mean weekday moderate to vigorous physical activity minutes and EuroQol-5 Dimensions, child-friendly version scores
| Correlation | Pearson’s correlation coefficient (p-value) |
|---|---|
| Baseline (T0) MVPA vs. EQ-5D-Y | 0.086 (0.112) |
| Post-intervention (T1) MVPA vs. EQ-5D-Y | 0.054 (0.354) |
| 12-month (T2) MVPA vs. EQ-5D-Y | –0.053 (0.391) |
| MVPA vs. EQ-5D-Y change between baseline and 12 months | 0.020 (0.767) |
FIGURE 14.
Correlation between change in EQ-5D-Y score and change in mean minutes of MVPA from baseline to 12 months.
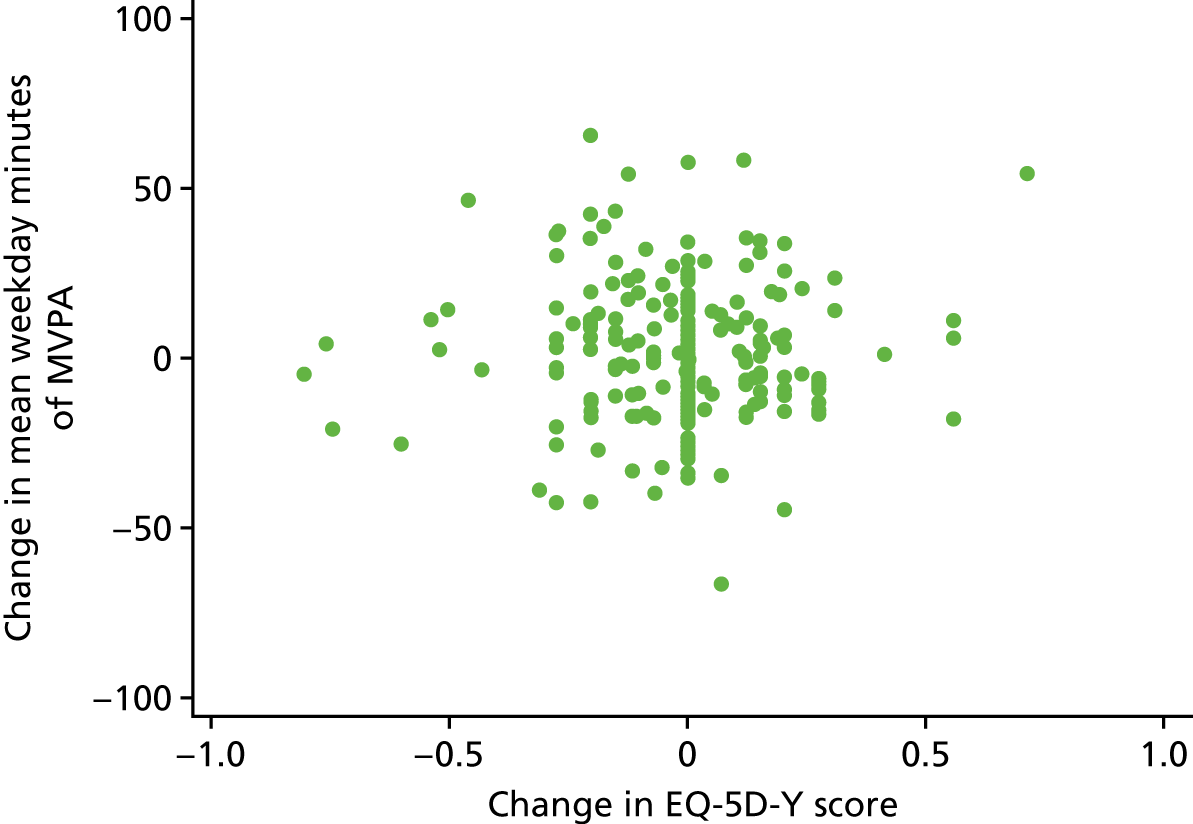
Appendix 14 Trainers’ evaluation of the training arrangements
| Training | School ID | All schools, mean (SD) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2 | 3 | 4 | 6 | ||||||||||
| Mean (SD) | Trainer | Mean (SD) | Trainer | Mean (SD) | Trainer | Mean (SD) | Trainer | ||||||
| 2-day training | |||||||||||||
| Training feature | B | E | C | A | B | E | A | D | |||||
| Transport to and from the venue (for students) | 3.50 (0.71) | 3.00 | 4.00 | 3.00 (0.00) | 3.00 | 3.00 | – | NA | NA | 3.00 (1.41) | 2.00 | 4.00 | 3.63 (1.06) |
| Suitability of the training space | 4.00 (0.00) | 4.00 | 4.00 | 0.50 (0.71) | 1.00 | 0.00 | 1.50 (0.71) | 2.00 | 1.00 | 3.50 (0.71) | 3.00 | 4.00 | 2.38 (1.60) |
| Quality of the facilities (toilets, kitchen, social spaces) | 3.00 (0.00) | 3.00 | 3.00 | 1.00 (0.00) | 1.00 | 1.00 | 2.00 (0.00) | 2.00 | 2.00 | 2.50 (0.71) | 3.00 | 2.00 | 2.13 (0.84) |
| Location (distance from school) | 3.00 (0.00) | 3.00 | 3.00 | 2.00 (0.00) | 2.00 | 2.00 | – | NA | NA | – | 2.00 | – | 3.38 (1.41) |
| Training manual | 3.50 (0.71) | 4.00 | 3.00 | 3.00 (0.00) | 3.00 | 3.00 | 3.00 (0.00) | 3.00 | 3.00 | 3.50 (0.71) | 3.00 | 4.00 | 3.25 (0.46) |
| Resources to support the training | 4.00 (0.00) | 4.00 | 4.00 | 3.50 (0.71) | 3.00 | 4.00 | 4.00 (0.00) | 4.00 | 4.00 | 4.00 (0.00) | 4.00 | 4.00 | 3.87 (0.35) |
| Arrangements for refreshments | 2.50 (2.12) | 1.00 | 4.00 | 2.50 (0.71) | 3.00 | 2.00 | 3.50 (0.71) | 3.00 | 4.00 | 3.50 (0.71) | 3.00 | 4.00 | 3.00 (1.07) |
| Quality of refreshments | 1.00 (0.00) | 1.00 | 1.00 | 2.50 (0.71) | 3.00 | 2.00 | 3.00 (0.00) | 3.00 | 3.00 | 1.50 (0.71) | 1.00 | 2.00 | 2.00 (0.93) |
| Top-up day training | |||||||||||||
| Training feature | B | C | C | D | B | E | B | D | |||||
| Transport to and from the venue (for students) | 3.50 (0.71) | 4.00 | 3.00 | 3.00 (1.41) | 4.00 | 2.00 | – | NA | NA | 3.00 (0.00) | 3.00 | 3.00 | 3.63 (1.06) |
| Suitability of the training space | 4.00 (0.00) | 4.00 | 4.00 | 4.00 (0.00) | 4.00 | 4.00 | 1.00 (0.00) | 1.00 | 1.00 | 3.50 (0.71) | 4.00 | 3.00 | 3.13 (1.36) |
| Quality of the facilities (toilets, kitchen, social spaces) | 3.50 (0.71) | 4.00 | 3.00 | 4.00 (0.00) | 4.00 | 4.00 | 1.50 (0.71) | 2.00 | 1.00 | 3.00 (1.41) | 4.00 | 2.00 | 3.00 (1.20) |
| Location (distance from school) | 3.00 (1.41) | 4.00 | 2.00 | 4.00 (1.41) | 3.00 | – | – | 4.00 | – | 3.50 (0.71) | 4.00 | 3.00 | 3.75 (1.04) |
| Training manual | 3.50 (0.71) | 4.00 | 3.00 | 3.00 (0.00) | 3.00 | 3.00 | 3.50 (0.71) | 4.00 | 3.00 | 3.50 (0.71) | 4.00 | 3.00 | 3.38 (0.52) |
| Resources to support the training | 3.50 (0.71) | 4.00 | 3.00 | 3.00 (0.00) | 3.00 | 3.00 | 4.00 (0.00) | 4.00 | 4.00 | 3.50 (0.71) | 4.00 | 3.00 | 3.50 (0.54) |
| Arrangements for refreshments | 3.50 (0.71) | 4.00 | 3.00 | 3.50 (0.71) | 4.00 | 3.00 | 3.00 (1.41) | 2.00 | 4.00 | 3.00 (0.00) | 3.00 | 3.00 | 3.25 (0.71) |
| Quality of refreshments | 3.50 (0.71) | 4.00 | 3.00 | 3.50 (0.71) | 3.00 | 4.00 | 4.00 (0.00) | 4.00 | 4.00 | 4.00 (0.00) | 4.00 | 4.00 | 3.75 (0.46) |
Appendix 15 Observed versus allocated time for training activities on day 1, 2 and top-up day
FIGURE 15.
Observed vs. allocated time for training activities on day 1.
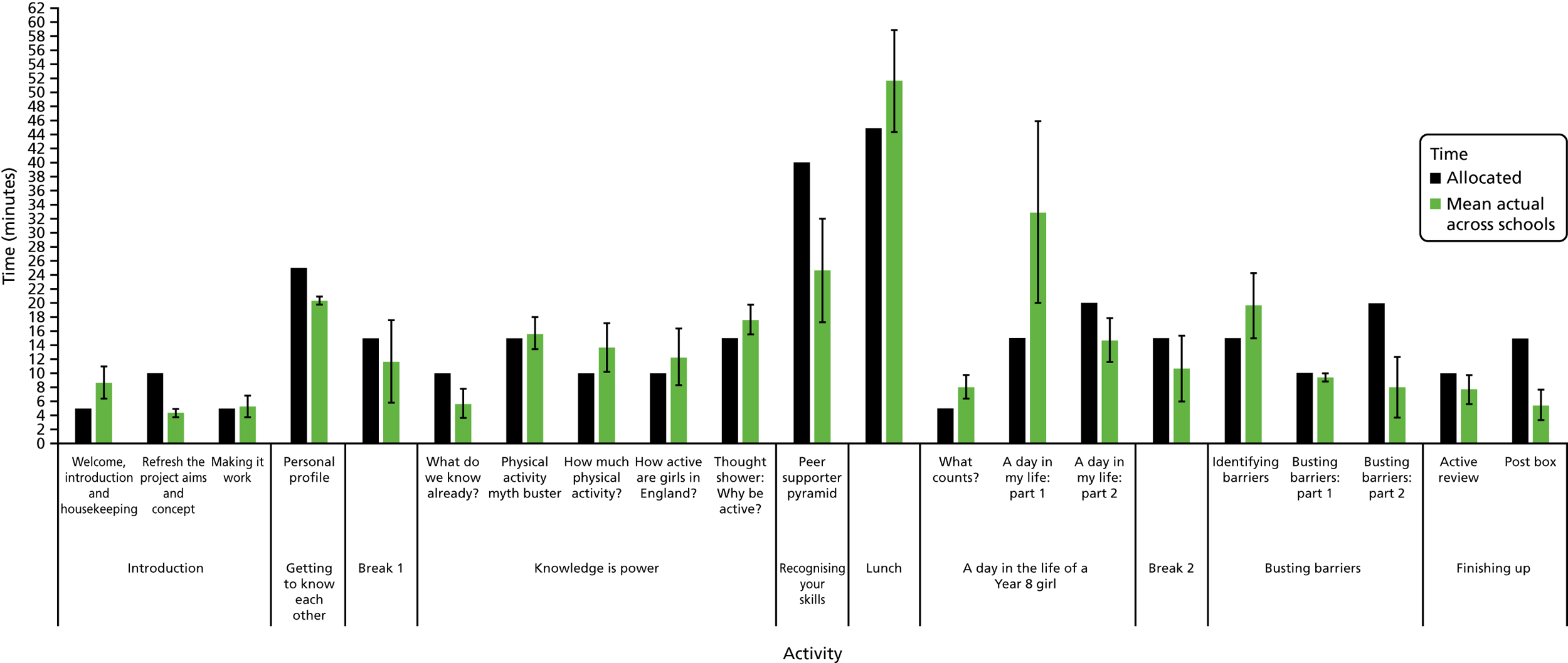
FIGURE 16.
Observed vs. allocated time for training activities on day 2.
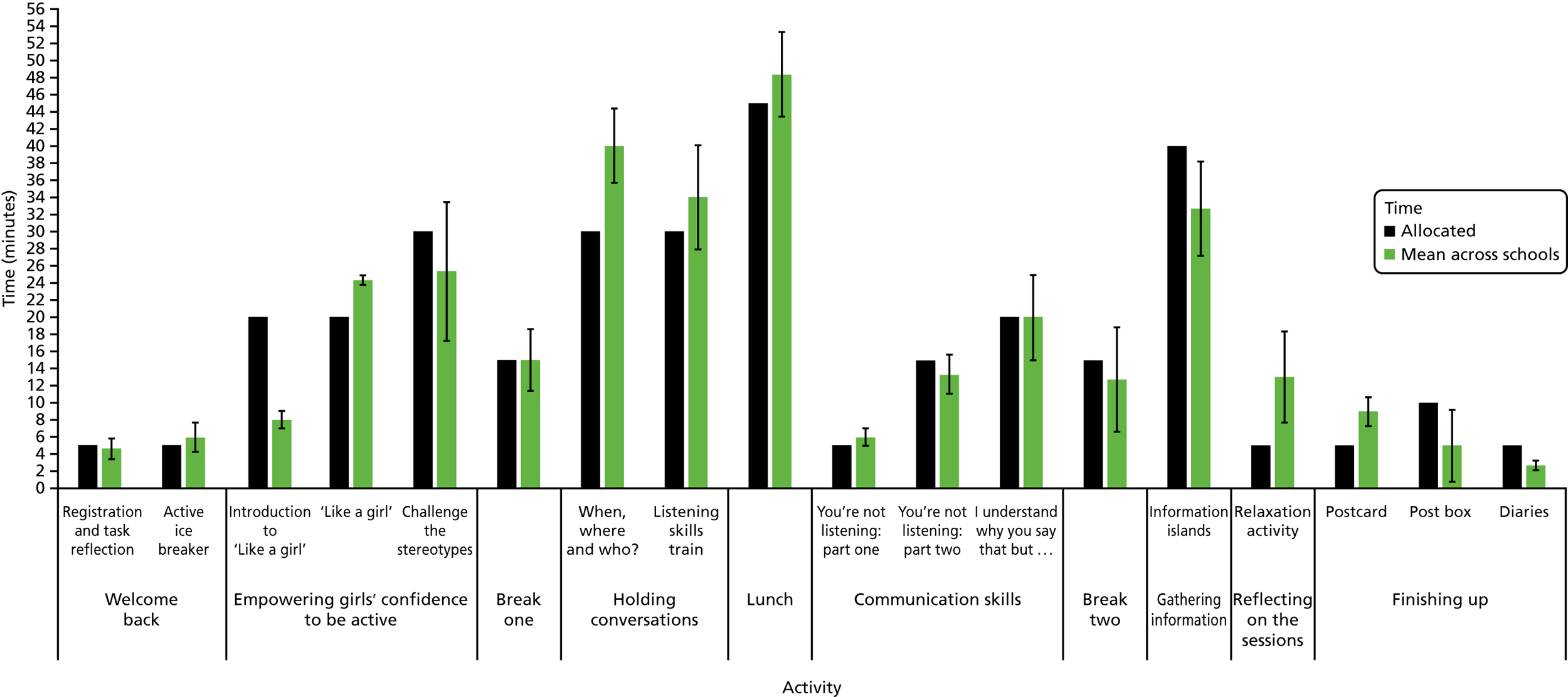
FIGURE 17.
Observed vs. allocated time for training activities on the top-up day.
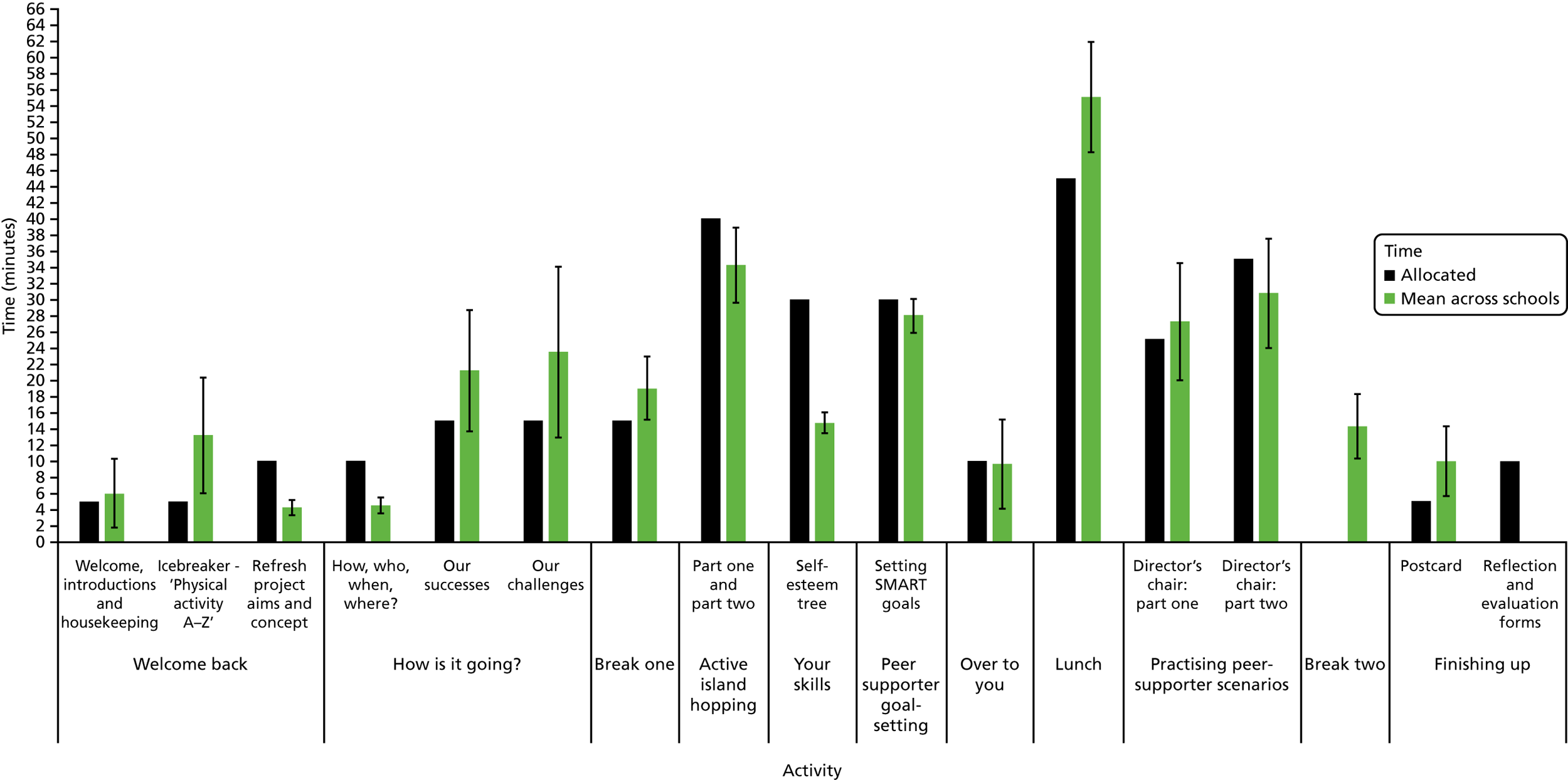
Appendix 16 Observed peer supporter engagement per activity section for each trainer pair
| Activity section (engagement) | Trainer pair (school) | Average rating per activity section, mean (SD)a | |||||||
|---|---|---|---|---|---|---|---|---|---|
| B and E (2) | A and C (3) | B and E (4) | A and D (6) | ||||||
| Day 1 | |||||||||
| Introduction | b | 2.33 | 2.33 | 2.67 | 2.44 (0.73) | ||||
| Getting to know each other | b | 3.00 | 3.00 | 3.00 | 3.00 (0.00) | ||||
| Knowledge is power | b | 2.80 | 2.80 | 3.00 | 2.87 (0.35) | ||||
| Recognising your skills | b | 3.00 | 3.00 | 3.00 | 3.00 (0.00) | ||||
| A day in the life of a Year 8 girl | b | 2.67 | 2.67 | 2.67 | 2.67 (0.50) | ||||
| Busting barriers | b | 2.33 | 1.67 | 2.33 | 2.11 (0.60) | ||||
| Finishing up | b | 2.00 | 2.00 | 1.50 | 1.80 (0.84) | ||||
| Average, mean (SD) | – | – | 2.56 | 0.62 | 2.47 | 0.72 | 2.61 | 0.61 | 2.55 (0.64) |
| Day 2 | |||||||||
| Welcome back | b | 2.00 | 2.50 | 2.00 | 2.17 (0.98) | ||||
| Empowering girls’ confidence | b | 3.00 | 2.67 | 2.67 | 2.78 (0.44) | ||||
| Holding conversations | b | 2.50 | 3.00 | 3.00 | 2.83 (0.41) | ||||
| Communication skills | b | 2.50 | 2.33 | 2.33 | 2.38 (0.74) | ||||
| Gathering information | b | 3.00 | 3.00 | 3.00 | 3.00 (0.00) | ||||
| Tricky issues | b | 0.00c | 3.00 | 0.00c | 3.00 (0.00) | ||||
| Reflecting on the sessions | b | 3.00 | 2.00 | 2.00 | 2.33 (0.58) | ||||
| Finishing up | b | 3.00 | 2.50 | 2.33 | 2.63 (0.74) | ||||
| Average, mean (SD) | – | – | 2.71 | 0.61 | 2.60 | 0.51 | 2.47 | 0.83 | 2.59 (0.66) |
| B and C (2) | C and D (3) | B and E (4) | B and D (6) | Average rating per activity section, mean (SD) | |||||
| Top-up day | |||||||||
| Welcome back | 2.67 | 2.33 | 2.67 | 2.67 | 2.58 (0.51) | ||||
| How is it going? | 2.67 | 2.67 | 2.33 | 2.67 | 2.58 (0.51) | ||||
| Active island hopping | 1.00 | 3.00 | 3.00 | 3.00 | 2.50 (1.00) | ||||
| Your skills | 3.00 | 3.00 | 3.00 | 3.00 | 3.00 (0.00) | ||||
| PS goal-setting | 3.00 | 3.00 | 2.00 | 2.00 | 2.50 (0.58) | ||||
| Over to you | 0.00c | 2.00 | 3.00 | 1.00 | 2.00 (1.00) | ||||
| Practising PS scenarios | 2.00 | 3.00 | 3.00 | 3.00 | 2.86 (0.38) | ||||
| Finishing up | 2.50 | 3.00 | 3.00 | 3.00 | 2.83 (0.41) | ||||
| Average, mean (SD) | 2.50 | 0.67 | 2.71 | 0.47 | 2.69 | 0.48 | 2.62 | 0.65 | 2.63 (0.56) |
Appendix 17 Peer supporter reported most and least enjoyable training elements
| Training elements | School ID, frequency reported (n) | Total frequency reported (N) | |||
|---|---|---|---|---|---|
| 2 | 3 | 4 | 6 | ||
| Most enjoyable training elements | |||||
| 2-day training | |||||
| Listening train game | 7 | 5 | 7 | 9 | 28 |
| Energiser (ball game) | – | 9 | 1 | – | 10 |
| Busting barriers | 1 | – | – | 5 | 6 |
| Script writing and role-play | – | 1 | 3 | – | 4 |
| Teamwork | 2 | 1 | – | – | 3 |
| Top-up day training | |||||
| Script writing and role-play | 4 | 11 | 10 | 12 | 37 |
| The ball game | 1 | 7 | 2 | – | 10 |
| The hula hoop game | 7 | – | – | – | 7 |
| Active island hopping | – | – | – | 2 | 2 |
| Self-esteem tree | – | 2 | – | – | 2 |
| Least enjoyable training elements | |||||
| 2-day training | |||||
| Lots of writing | 2 | 2 | – | 4 | 8 |
| Not much PA | – | 6 | 1 | 1 | 8 |
| Waiting around (standing or sitting) | 1 | 3 | 2 | 1 | 7 |
| Stopping to talk or listen a lot | 2 | – | 1 | 2 | 5 |
| Nothing | 4 | – | 1 | – | 5 |
| Top-up day training | |||||
| Active island hopping | – | 5 | 4 | 2 | 11 |
| Lots of writing | 2 | 2 | 1 | 4 | 9 |
| Sitting down a lot | – | 3 | 2 | 1 | 6 |
| Role-play/acting | 2 | 1 | – | 2 | 5 |
| Nothing | 1 | 2 | – | – | 3 |
Appendix 18 Observed fulfilment of manualised activity objectives per trainer pair
| Activity section (objective) | Trainer pair (school) | Average rating per activity section, mean (SD)a | |||
|---|---|---|---|---|---|
| B and E (2) | A and C (3) | B and E (4) | A and D (6) | ||
| Day 1 | |||||
| Introduction | b | 3.00 | 3.00 | 2.67 | 2.89 (0.33) |
| Getting to know each other | b | 3.00 | 3.00 | 1.00 | 2.33 (1.15) |
| Knowledge is power | b | 3.00 | 2.60 | 2.80 | 2.80 (0.41) |
| Recognising your skills | b | 3.00 | 3.00 | 3.00 | 3.00 (0.00) |
| A day in the life of a Year 8 girl | b | 2.33 | 3.00 | 3.00 | 2.78 (0.44) |
| Busting barriers | b | 2.33 | 2.33 | 2.00 | 2.22 (0.83) |
| Finishing up | b | 2.50 | 2.00 | 2.50 | 2.40 (0.55) |
| Average rating per trainer pair day 1, mean (SD) | – | 2.72 (0.57) | 2.71 (0.59) | 2.56 (0.62) | 2.66 (0.59) |
| Day 2 | |||||
| Welcome back | b | 2.00 | 3.00 | 2.00 | 2.33 (1.03) |
| Empowering girls’ confidence | b | 3.00 | 3.00 | 2.50 | 2.83 (0.41) |
| Holding conversations | b | 3.00 | 3.00 | 2.50 | 2.83 (0.41) |
| Communication skills | b | 2.50 | 2.00 | 1.00 | 1.75 (0.71) |
| Gathering information | b | 2.00 | 3.00 | 3.00 | 2.67 (0.58) |
| Tricky issues | b | 0.00c | 3.00 | 0.00c | 3.00 (0.00) |
| Reflecting on the sessions | b | 3.00 | 2.00 | 3.00 | 2.67 (0.58) |
| Finishing up | b | 3.00 | 2.50 | 2.67 | 2.75 (0.46) |
| Average rating per trainer pair day 2, mean (SD) | – | 2.69 (0.63) | 2.64 (0.50) | 2.21 (0.89) | 2.51 (0.71) |
| B and C (2) | C and D (3) | B and E (4) | B and D (6) | Average rating per activity section, mean (SD)a | |
| Top-up day | |||||
| Welcome back | 3.00 | 2.50 | 3.00 | 3.00 | 2.88 (0.35) |
| How is it going? | 2.67 | 2.67 | 2.67 | 2.67 | 2.67 (0.49) |
| Active island hopping | 2.00 | 3.00 | 3.00 | 3.00 | 3.00 (0.50) |
| Your skills | 3.00 | 3.00 | 3.00 | 3.00 | 3.00 (0.00) |
| PS goal-setting | 3.00 | 3.00 | 3.00 | 3.00 | 3.00 (0.00) |
| Over to you | 0.00c | 3.00 | 3.00 | 2.00 | 2.67 (0.58) |
| Practising PS scenarios | 2.00 | 3.00 | 3.00 | 3.00 | 2.86 (0.38) |
| Finishing up | 3.00 | 2.00 | 3.00 | 3.00 | 2.60 (0.55) |
| Average rating per trainer pair top-up day, mean (SD) | 2.70 (0.48) | 2.69 (0.48) | 2.92 (0.29) | 2.83 (0.39) | 2.79 (0.41) |
Appendix 19 Peer supporters’ open response reports of what they learnt during the training
| Notion | School ID, frequency reported (n) | Total frequency reported (N) | |||
|---|---|---|---|---|---|
| 2 | 3 | 4 | 6 | ||
| 2-day training | |||||
| You need to do 1 hour of moderate-intensity PA per day (which can be broken down) | 11 | 25 | 7 | 10 | 53 |
| Only 8% of girls their age are active for 1 hour a day | 8 | 2 | 8 | 9 | 27 |
| Exercise improves grades | 9 | 9 | 3 | 3 | 24 |
| Different ways of being active (not always sport) | 6 | 5 | 5 | 8 | 24 |
| PA helps your skin | 2 | 16 | 1 | – | 19 |
| 20–25% primary school children are active for 1 hour a day | – | – | 5 | 5 | 10 |
| PA prevents illness and heart disease | 1 | 5 | 1 | 2 | 9 |
| ‘Like a girl’ is a good thing | 3 | – | 1 | 4 | 8 |
| Be proud of yourself | 2 | – | 3 | – | 5 |
| Do not let barriers or excuses get in the way of being active | 2 | – | 1 | 2 | 5 |
| How to talk to people | 1 | 2 | 2 | – | 5 |
| Top-up day training | |||||
| PA helps your skin | 1 | 17 | – | 2 | 20 |
| PA improves grades | 4 | 6 | 2 | 4 | 16 |
| You need to do 1 hour of moderate-intensity PA per day (which can be broken down) | 3 | 6 | 1 | 3 | 15 |
| Activity is not always sport, going to the gym or a club | 3 | – | 7 | 4 | 14 |
| Be kind, encouraging, trustworthy and positive | 1 | 3 | – | 5 | 9 |
| PA is important for your health | 6 | 2 | 1 | – | 9 |
| PA helps weight loss | – | 3 | 3 | 3 | 9 |
| PA helps you sleep | – | 3 | – | 5 | 8 |
| How to use SMART to plan what to say and do | 4 | – | – | 4 | 8 |
| How to influence and support people to be active | – | 3 | 1 | 3 | 7 |
| PA clears your mind, helps you concentrate and makes you more alert | – | 1 | 5 | 1 | 7 |
| Exercise makes you happy and improves your mood | 3 | 2 | 2 | – | 7 |
Appendix 20 Suggested intervention refinements
| Source | Suggested Improvement | Reason for suggested improvement | Action required |
|---|---|---|---|
| Train the trainers | |||
| Trainer | Cover principles of SDT more than once in the training | Trainers felt they needed reminding about SDT and how to use it with the PSs after the training. They would have more questions about it in light of going through the activities | Create time during training day 3 to reinforce SDT |
| PS training | |||
| Training logistics | |||
| Trainer 5 | Consider the trainer-to-PS ratio | Too high a PS-to-trainer ratio may have a negative effect on deliverya | To establish an ideal PS-to-trainer ratio and consider multiple groups in larger schools |
| Focus group, trainer, training observation | Offer outdoor space for breaks and more equipment | Staying in the same space all day challenged PS engagement and focus. PSs enjoyed using the hoops and skipping ropes in the breaks | Ensure training venues have suitable outdoor space for the PSs to use during break and provide a wider variety of equipment |
| Training structure | |||
| Trainer | Change the structure of the day | Activities requiring more concentration worked better in the morning. More active tasks were good at re-engaging the PSs, which was needed in the afternoon | Move more writing-based tasks to the morning and add in active games to break it up |
| Focus group, school contact, trainer | Spread the training out/make shorter or have another top-up day | The training days were quite long, by spreading the days out it would help their focus, engagement and enjoyment. An additional top-up day would act as a ‘boost’ to continue peer supporting | Spread the initial 2-day training over 3 shorter days with a school day in between. Have 2 top-up days spread evenly throughout the intervention |
| Materials and resources | |||
| Trainer, training observation | Need more emphasis on using the PS booklet and diary | The booklet was not introduced by any of the trainers or used effectively throughout the training, this could have helped the PSs | Include a section at the beginning of the manual to make time to introduce the booklet and make it clear when to use it throughout the training |
| Focus group | Space for own notes and how to start conversations in the PS booklet | PSs wanted space to be able to write their own notes to help them remember more effectively. They also wanted a simple way to help them have conversations (pictures) | Allow space in booklet for blank note pages and diagrams with speech bubbles |
| Trainer 2 | Make the group sizes for each activity clearer | This trainer did not want the PSs losing focus while she struggled to find what groups to divide them into | Add group size to the top of the description of each activity in the ‘session plan’ book |
| Training content | |||
| Focus group, trainer, training observation | Add more practical/active- or interactive-learning activities | PS focus was challenged when activities were mainly writing/sitting down. Games and fun competition would increase enjoyment/engagement | Incorporate competition elements into the activities involving lots of writing. Intersperse active games throughout the training days |
| Trainer 4 | Provide more information on how to overcome challenges faced as a PS | Trainer felt that the small amount of training covering solutions to problems was not sufficient for the girls to remember how to deal with such situations | Refine certain activities (i.e. busting barriers) to focus more on solving problems |
| School contact, trainer | Give more specific examples about who PSs should support and how to do so | This was covered, however more specific examples of what to do to get peers more active in realistic ways | Adapt or add an activity that focuses on ‘brain-storming’ ideas about how to give realistic peer support with opportunity to practise |
| Focus group, trainer | Add in or adapt activities to involve more teamwork | Needed to help make the PSs feel comfortable with each other and team games introduce a sense of playfulness which the girls enjoy | Add further team-building tasks at the start of training days and during breaks |
| Focus group, trainer | Alternative instructions for certain tasks or additional (optional) activities | On some occasions activities did not work if girls were not talkative or could not give peer-support examples. Alternative methods to meet the learning objectives are needed | Identify activities where this could be a problem and add alternative steps or activities |
| Trainer 5 | Ensure each PS is given a role in every activity | In a few activities some PSs could disengage and let others do the task | Make it clear what each PS should be doing in every activity |
| Focus group, trainer, training observation | Change the terminology in some activities | Some of the terminology in a selection of activities made it difficult for the PSs to understand what to do (i.e. relevant, irrelevant and sedentary) | Simplify terminology |
| Individual activity changes | |||
| Trainer 1 | ‘Introduction’ | Energise the PSs and facilitate early positive rapport with each other | Add in a team-building game in the introduction |
| Trainer 3 | ‘Knowledge is power’ | Having PSs guess the answers in this section took a long time and it was repetitive, PSs got bored | Incorporate a more active approach to answering questions |
| Trainer | ‘The self-esteem tree’ | PSs wrote the same characteristic for each person if they did not know them. It presented an opportunity for the PSs to be negative about each other | Encourage girls to think of different things to write or change activity so other PSs do not see what is already written |
| Trainer, training observation | ‘SMART goal-setting’ | PSs struggled to grasp the concept of what a SMART goal was and how to make a realistic goal from this | Remove the ‘SMART’ element from the goal-setting |
| Trainer 4 | ‘Director’s chair’ | Some PSs did not understand when or how they should be directing | Simplify this task: add a hand-out/slide with examples of how to direct a scene |
List of abbreviations
- A level
- Advanced level
- AHEAD
- Activity and Healthy Eating in ADolescence
- ALPHA
- Advice Leading to Public Health Advancement
- ASSIST
- A Stop Smoking In Schools Trial
- BRCT
- Bristol Randomised Trials Collaboration
- CI
- confidence interval
- CONSORT
- CONsolidated Standards Of Reporting Trials
- COREQ
- COnsolidated criteria for REporting Qualitative research
- CPM
- counts per minute
- CTU
- clinical trials unit
- DECIPHer
- Centre for the Development and Evaluation of Complex Interventions for Public Health Improvement
- DOI
- diffusion of innovations
- EQ-5D-Y
- EuroQol-5 Dimensions, child-friendly version
- GNVQ
- General National Vocational Qualification
- ICC
- intraclass correlation
- IMD
- Index of Multiple Deprivation
- LA
- local authority
- LAG
- local advisory group
- MRC
- Medical Research Council
- MVPA
- moderate to vigorous physical activity
- NIHR
- National Institute for Health Research
- NPD
- National Pupil Database
- NPS
- non-peer supporter
- NVQ
- National Vocational Qualification
- OR
- odds ratio
- PA
- physical activity
- PE
- physical education
- PLAN-A
- Peer-Led physical Activity iNtervention for Adolescent girls
- PPI
- public and patient involvement
- PS
- peer supporter
- PSHE
- personal, social, health, economic
- QALY
- quality-adjusted life-year
- RCT
- randomised controlled trial
- SD
- standard deviation
- SDT
- self-determination theory
- SOP
- standard operating procedure
- T0
- baseline
- T1
- follow-up 1
- T2
- follow-up 2
- TIDieR
- Template for Intervention Description and Replication
- TSC
- Trial Steering Committee
- UKCRC
- UK Clinical Research Collaboration