

Notes
Article history
The contractual start date for this research was in April 2021. This article began editorial review in March 2023 and was accepted for publication in February 2024. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The Public Health Research editors and publisher have tried to ensure the accuracy of the authors’ article and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this article.
Permissions
Copyright statement
Copyright © 2024 Breheny et al. This work was produced by Breheny et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaptation in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
2024 Breheny et al.
Background and introduction
Health-related quality of life (HRQL) is described as emotional and physical functioning that contributes to overall quality of life1 and is an important factor in healthcare and policy decision-making. 2 Capability well-being measures broaden the scope and are complementary to HRQL when evaluating the cost-effectiveness of health and well-being interventions delivered outside of NHS settings (e.g. public health). Measures such as the EQ-5D,3,4 ICEpop CAPability measure for Adults (ICECAP-A) and Child Health Urtility 9 Dimension (CHU9D)5 were developed for use in evaluating the cost-effectiveness of health and well-being interventions for adults and children. Measures of socio-economic position including income and poverty level are important contributors to both HRQL and capability well-being. 6 The relationships between these variables are, however, complex, as access to healthcare can be socially patterned, while income can moderate availability of resources that enhance quality of life (e.g. the option to engage in recreational activities) or support an adequate standard of living (e.g. sufficient food). 6,7
The COVID-19 lockdowns had a negative impact on the UK population’s mental health and well-being,8–10 although ongoing implications are still unclear and may be unequally distributed with different facets (e.g. sadness, optimism) impacted in different ways. The ending of lockdowns was associated with an improvement in mental health for the majority of children; however, the negative effects persisted in low-income families9 and as such warrant further examination. The COVID-19 pandemic caused financial insecurity and hardship for many UK families11 and the UK ‘cost of living crisis’ is further compounding these issues. 12 These coinciding challenges may have had a detrimental impact on the population’s quality of life and well-being. For example, evidence has shown that in summer 2020 financial stress was associated with worse family well-being. 13,14 As such it is important to understand the links between these variables as the pandemic progressed. Despite its importance to policy-makers and in contrast to mental health, HRQL during the COVID-19 pandemic and period of recovery is relatively unexplored. A systematic review identified only six studies comparing pre and during COVID-19 lockdown HRQL15 in children, none of which were UK based. The majority (four of the six) of studies indicated a decline in HRQL. Similar findings are available for adults and also showed a decline, but again the data are limited. 16
Reported reductions in physical activity during COVID-19 lockdowns among both adults and children17–20 could be related to declines in HRQL and well-being. Evidence does suggest a positive relationship between physical activity and HRQL in adults21,22 and children,23 although the strength of this relationship in children is uncertain. Methodological factors such as use of a proxy rating of HRQL and measurement of physical activity contribute to this uncertainty. 23 Studies that explored this relationship during the pandemic were also limited by these issues. A study of Spanish and Brazilian children during the pandemic found that those meeting 24-hour movement guidelines had higher parent-proxy measured HRQL. 24 This is, however, in contrast to data from the UK Born in Bradford study, which reported that there was no observed relationship between self-reported physical activity and well-being among 7–13-year-old children. 25 Thus far, evidence exploring the relationship between HRQL and physical activity during the pandemic is limited to children and seems to be uncertain. There is a need to use child-reported measures of HRQL and expand the evidence base to associations in adults.
The COVID-19 pandemic has had demonstrable negative impacts on health and well-being and physical activity but the association between them is uncertain. Furthermore, current evidence is reliant on self-reported physical activity, which has particular limitations when assessing physical activity among children and young people. 25 As such, more information is needed on the effects of the pandemic on HRQL and its relationship with physical activity. The Active-6 project reported that UK children’s physical activity following COVID-19 lockdowns was lower than pre-pandemic levels in the short term, and sedentary activity was higher. 18 Screen viewing time was higher than before the lockdowns. 26 Qualitative interviews with Active-6 participants suggested that the lockdowns exacerbated fatigue and children felt emotionally overwhelmed. 27 HRQL, capability well-being and family financial strain were also collected in the study, so provide an opportunity to explore the relationship between physical activity and HRQL outcomes post COVID-19 lockdowns. This forms a unique and policy-relevant resource for intervention development and policy-making, particularly as there is currently no UK-based evidence which has examined financial hardship and its implications for the population’s health and well-being.
Aims and objectives
The aim of this paper is to assess the differences in parent and child HRQL and capability well-being during the short- and medium-term post-lockdown phases of the COVID-19 pandemic. The relationships between these outcomes, family financial strain and accelerometer-measured physical activity are also explored.
Methods
The data in this paper are part of the Active-6 study, which examined the impact of the COVID-19 pandemic on the physical activity and sedentary behaviour of 10–11-year-old children and their parents/carers. 18,26–31 We report child and parent/carer questionnaire and accelerometer data collected at two time points post COVID-19 lockdowns, to assess physical activity and related measures18 in the short- and medium-term post-lockdown phases of the pandemic.
Schools in the southwest of England were recruited from a sample of 50 that had previously participated in the B-Proact1v longitudinal study between 2017 and 2018. 32 All children aged 10–11 and one parent or carer per family were eligible to take part, including all children in families where there were two or more eligible children. Detailed information on recruitment is reported elsewhere. 17 Data were collected in two waves, with 23 schools participating in Wave 1 (May–December 2021) and 27 schools in Wave 2 (January–July 2022), including 22 participating in both waves, with 393 and 436 child–parent pairs recruited, respectively. Sample size calculations were conducted for the primary outcome of the Active-6 study only (difference in children’s weekday MVPA). 28
Data collection and measures
Parents/carers and children completed separate online questionnaires which included questions on financial strain, capability well-being and HRQL. Parents reported their gender, age group and ethnicity and their child’s gender and date of birth, as well as the highest educational qualification in the household [recoded as ‘Up to A level (exam at age 18) or equivalent’ and ‘University degree (or equivalent) and higher’]. Index of Multiple Deprivation (IMD33) rank was calculated from home postcode. IMD rank is a continuous measure generated by ranking all neighbourhoods in England according to their level of relative deprivation on 39 indices.
Physical activity
Physical activity data were collected using accelerometers. Adults and children wore a waist-worn ActiGraph wGT3X-BT accelerometer (Actigraph LLC, Florida, USA) during waking hours for seven consecutive days, and accelerometer data were processed using an open-source R script. 34,35 Data between midnight and 6 a.m. were excluded, and a valid day was defined as at least 500 minutes of data, excluding intervals of ≥ 60 minutes of zero counts, allowing up to 2 minutes of interruptions. 36 Mean weekday minutes of moderate-to-vigorous physical activity (MVPA) were derived for participants who provided at least two valid weekdays of data using Evenson et al. 37 thresholds for children and Troiano et al. 38 thresholds for adults.
Adult health-related quality of life: EQ-5D-5L and EQ-5D VAS
The EQ-5D-5L4,39 is a generic five-dimension preference-based measure assessing adults’ HRQL ‘today’. Questions address domains of usual activities, mobility, anxiety/depression, self-care and pain/discomfort with five response options, which were scored by applying population preference weights to create a utility score, using the van Hout et al. 40 algorithm (as only categorised parent ages were available). Scores are anchored at 0 (as bad as death) and 1 (best HRQL), with scores ˂ 0 reflecting health states valued as worse than death. The five items are supplemented by a visual analogue scale (EQ-5D VAS), where individuals rate their health on a scale from 0 to 100.
Adult capability well-being: ICECAP-A
The ICECAP-A is a five-item measure of capability well-being for the adult general population ‘at the moment’. 41,42 The five attributes assessed are attachment, stability, achievement, enjoyment and autonomy, and each question has four response options. The measure is scored by applying preference weights to produce a capability well-being index score,43 ranging between 0 and 1, with higher scores reflecting better capability well-being.
Child health-related quality of life: CHU9D
The CHU9D is a paediatric generic measure of health-related quality of life ‘today’,44,45 developed with UK children. It has nine items with five response options for each, covering areas deemed important to their lives (e.g. tiredness, school life, friendships). Preference weights are applied to generate a utility score5 between 0.33 and 1, with higher scores reflecting better HRQL.
Child capability well-being
Child capability well-being was measured using eight items that were based on the seven items in the UK CONTRAST study (Appendix 1). These were preliminary versions of items comprising a new measure of children’s capability well-being. 46 The changes made were small alterations to the wording and the addition of an extra question. Specifically, in Active-6 children reflected on their well-being compared to before the January 2021 lockdown, whereas the CONTRAST questions referred to the period before the March 2020 lockdown. The additional question focused on the ability to discover and learn. Each of the eight questions had five Likert response options, which were summed to produce a total score between 8 and 32, with individual items summarised by the mean.
Family Economic Strain Scale
The Family Economic Strain Scale (FESS) is a 13-item validated measure of financial difficulties experienced by families,47 which performs well in single-parent and two-parent families, and has good construct validity. 47 Parents reported the frequency of experiencing strain (e.g. putting off activities) on a five-point Likert scale, and a final item asked them to estimate their income in relation to other families. Items were summed to generate a total economic strain score, between 13 and 65, with higher scores reflecting greater strain.
Interpretation of HRQL and well-being outcomes
We interpreted outcomes in reference to recent published norms. The most recently published EQ-5D-3L norms for the 35–44 age group (which is the most represented group in Active-6) are 0.94 (SD 0.17) (EQ-5D utility) and 81.1 (SD 19.0) (EQ-5D VAS)48 (Table 1). These values were obtained from a pooled dataset from five European countries (France, Germany, Italy, Spain and the UK). A recent UK-based study of 1071 members of the general population had a mean ICECAP-A score of 0.81 (SD 0.19). 16 Mean baseline CHU9D scores of 0.83 (SD 0.14)49 and 0.84 (SD 0.11)50 were obtained in two UK-based public health trials, so could be used as comparisons.
| Measure | Domain | Population | Range | UK norm, or comparable score | Direction of interpretation |
|---|---|---|---|---|---|
| EQ-5D-5L | Parent HRQL | Parent | −0.594 to 1 | 0.94 | Higher score indicated higher HRQL |
| EQ-5D VAS | Parent self-reported health | Parent | 0–100 | 81.1 | Higher score indicates higher self-rated health |
| ICECAP-A | Parent capability well-being | Parent | 0–1 | 0.81 | Higher score indicates more capability well-being |
| CHU9D | Child HRQL | Child | 0.33–1 | 0.83–0.84 | Higher score indicates higher HRQL |
| Child capability well-being | Child capability well-being | Child | 8–32 | N/A | Lower score indicates more capability well-being |
| FESS | Family financial strain | Family (parent completed) | 13–65 | N/A | Lower score indicates lower financial strain |
Analysis
Unless indicated, all analyses followed the study health economics analysis plan which was pre-agreed with the independent study steering committee before data analysis. 51 Missing data were examined and due to low missingness no imputation was conducted. Parent HRQL (EQ-5D-5L, EQ-5D VAS) and capability well-being (ICECAP-A), child HRQL (CHU9D) and capability well-being (capability questions) and financial strain (FESS) were summarised for Wave 1 and Wave 2 using descriptive statistics and histograms, with data presented by gender and wave-specific FESS score quartile. Missing questionnaire data were tabulated by wave. Consistent with standard practice within the field, linear regression was used for the HRQL and capability well-being outcome analyses. 52 Unadjusted and adjusted models were run, with the adjusted models forming our primary analyses. All statistical analyses were conducted in StataMP version 17 (StataCorp LP, College Station, TX, USA)53 and mixed-effect models were used to account for the study design, with repeated children and parents nested within schools, to answer the following questions:
1. Does HRQL and capability well-being differ between waves?
Linear mixed-effect models were used to model parent differences in HRQL (EQ-5D, EQ-5D VAS), capability well-being (ICECAP-A) and financial strain (FESS) between waves, with wave included as a categorical variable, and models adjusted for parent age, gender, IMD rank (treated as a continuous variable) and highest household education. Similarly, child differences in HRQL (CHU9D) between waves were modelled with linear mixed-effect models adjusted for child gender, IMD rank and highest household education.
2. Were differences in HRQL/capability well-being between waves mediated by MVPA?
The adjusted models in the previous section were extended to include parent mean weekday MVPA (child mean weekday MVPA for child models) as a covariate and compared to the unmediated models.
3. Is there a relationship between financial strain and HRQL/capability well-being?
Health-related quality of life and capability well-being measures were plotted against financial strain (FESS score), and linear mixed-effect models were used to model the association, with HRQL measures as outcomes, and FESS as an independent variable. Models were adjusted for the same covariates as in question 1. This was an exploratory post hoc analysis.
4. Does financial strain moderate differences in HRQL/capability well-being between waves?
The model from question 3 was extended to include a wave-FESS interaction term to estimate the potential moderating effect. The FESS variable was centred to aid interpretation as differences reflect the effect deviating from the average FESS score. This was an exploratory post hoc analysis.
Patient and participant involvement and equality, diversity and inclusion
Patient and public involvement (PPI) has been a core component of the Active-6 project. A range of stakeholders were engaged in designing the study, developing materials and planning dissemination. Our stakeholders included Year 6 children, teachers, parents and school staff. Parent representatives provided useful feedback on interim findings that enhanced our interpretation and highlighted additional analyses that would be informative for families and schools. Children from participating schools have also provided feedback on dissemination materials through PPI groups.
Despite efforts to recruit schools from deprived and affluent areas, the samples included in these analyses were not ethnically diverse, and lower socio-economic groups were under-represented. In addition, the adult sample is majority female. These factors can be partially attributed to difficulties conducting research in a pandemic and disruptions to work and family life. Equality, diversity and inclusion (EDI) was an important consideration in other components of the Active-6 project where it was feasible to intentionally sample underrepresented groups. These wider projects have contributed to the interpretation of our findings and considerations of policy implications.
Results
The majority of the parent/carers were female, White British and aged 40–44 years (Table 2). Around two-fifths lived in areas in the lowest deprivation quintile (Wave 1 45.3% and Wave 2 39.5%), and over half were educated to degree level or higher, indicating an affluent, educated sample. Questionnaire missing data were low and ranged from 6% (Wave 1 FESS) to 8% (Wave 2 EQ-5D-5L and EQ-5D VAS) (Appendix 1, Table 8). In both waves mean adult and child HRQL values were high, as would be expected in a non-clinical sample. Mean adult HRQL was lower than previously published norms, but capability well-being was higher than comparable pre-pandemic data. Mean child HRQL was higher than pre-pandemic comparable data. Adult and child HRQL measures were negatively skewed. A ceiling effect was observed for the EQ-5D-5L, with 41% scoring the maximum score at Wave 1 and 36% at Wave 2 (Table 3).
| Wave 1 (N = 393) N (%) |
Wave 2 (N = 436) N (%) |
||||
|---|---|---|---|---|---|
| Adults | |||||
| Gender | Male | 91 (23) | 97 (22) | ||
| Female | 297 (76) | 332 (76) | |||
| Missing | 5 (1) | 7 (2) | |||
| Age group | <30 | 3 (1) | 5 (1) | ||
| 30–34 | 35 (9) | 26 (6) | |||
| 35–39 | 80 (20) | 90 (21) | |||
| 40–44 | 136 (35) | 147 (34) | |||
| 45–49 | 94 (24) | 112 (26) | |||
| 50+ | 40 (10) | 49 (11) | |||
| Missing | 5 (1.3) | 7 (2) | |||
| Ethnicity | White British | 310 (79) | 323 (74) | ||
| Other | 53 (14) | 70 (16) | |||
| Prefer not to say | 5 (1) | 8 (2) | |||
| Missing | 25 (6) | 35 (8) | |||
| Highest household education | Up to A level | 131 (33) | 162 (37) | ||
| University degree or higher | 257 (65) | 267 (61) | |||
| Missing | 5 (1) | 7 (2) | |||
| IMD quintile | 1 most deprived | 31 (8) | 31 (7) | ||
| 2 | 37 (9) | 60 (14) | |||
| 3 | 48 (12) | 62 (14) | |||
| 4 | 95 (24) | 107 (25) | |||
| 5 least deprived | 178 (45) | 172 (40) | |||
| Missing | 4 (1) | 4 (1) | |||
| Children | |||||
| Gender | Male | 198 (50) | 212 (49) | ||
| Female | 193 (49) | 224 (51) | |||
| Other | 2 (1) | 0 (0) | |||
| Mean | SD | Mean | SD | ||
| Age, years | 10.9 | (0.4) | 11.1 | (0.3) | |
| Domain | Measure | Wave 1 | Wave 2 | ||
|---|---|---|---|---|---|
| Mean (SD) | N (%) scoring highest value | Mean (SD) | N (%) scoring highest value | ||
| Adult HRQL | EQ-5D-5L | 0.860 (0.166) | 147 (41) | 0.848 (0.171) | 146 (36) |
| Adult self-rated health | EQ-5D VAS | 76.7 (16.1) | 13 (4) | 76.1 (17.4) | 18 (5) |
| Adult capability well-being | ICECAP-A | 0.882 (0.114) | 53 (15) | 0.883 (0.124) | 65 (16) |
| Child HRQL | CHU9D | 0.884 (0.086) | 31 (8) | 0.885 (0.086) | 43 (11) |
| Child capability well-being | Sum of 8 items | 18.28 (5.63) | 18.11 (5.77) | ||
| Family financial strain | FESS | 26.3 (10.1) | 10 (3) | 27.5 (10.3) | 6 (2) |
Does HRQL and capability well-being differ between waves?
There were no notable differences in mean EQ-5D-5L, EQ-5D VAS, ICECAP-A or financial strain scores between Wave 1 and 2 (Table 3). Mean scores for children’s capability well-being items were skewed towards lower values, indicating that participants rated their capability well-being as better when reflecting on their current state compared to the previous lockdown (Table 3). There were no notable differences between boys and girls or between waves. The total score (sum of the Likert responses) was also comparable between waves.
Mixed-effect models showed no evidence of differences in adults’ or children’s HRQL and capability well-being between waves (Table 4), but family financial strain increased between waves by 1.14 points (adjusted 95% CI 0.15 to 2.12).
| Unadjusted model | Adjusted modela | ||||||
|---|---|---|---|---|---|---|---|
| Difference between waves | 95% confidence interval | p-value | Difference between waves | 95% confidence interval | p-value | ||
| Adult HRQL | EQ-5Da | −0.008 | −0.026 to 0.011 | 0.432 | −0.005 | −0.023 to 0.014 | 0.629 |
| Adult self-rated health | EQ-5D VASa | −0.56 | −2.63 to 1.52 | 0.598 | −0.18 | −2.24 to 1.88 | 0.864 |
| Adult capability well-being | ICECAP-Aa | 0.000 | −0.014 to 0.014 | 0.981 | 0.001 | −0.013 to 0.015 | 0.914 |
| Family financial strain | FESSa | 1.19 | 0.19: 2.19 | 0.019 | 1.14 | 0.15 to 2.12 | 0.024 |
| Child HRQL | CHU9Db | 0.005 | −0.005 to 0.015 | 0.323 | 0.006 | −0.004 to 0.016 | 0.234 |
Does MVPA have a mediating effect on HRQL and capability well-being?
There was no evidence that MVPA had any mediating effect on differences in HRQL and well-being, with similar wave estimates in both models for all outcomes tested (Table 5).
| Covariate | Unmediated model | Mediated modela | |||||
|---|---|---|---|---|---|---|---|
| Estimate | 95% confidence interval | p-value | Estimate | 95% confidence interval | p-value | ||
| Adult HRQL (EQ-5D) | Wave difference | −0.005 | −0.023 to 0.014 | 0.629 | −0.003 | −0.024 to 0.018 | 0.806 |
| MVPA | 0.001 | −0.000 to 0.001 | 0.347 | ||||
| Adult self-rated health (EQ-5D VAS) | Wave difference | −0.18 | −2.24 to 1.88 | 0.864 | −0.67 | −2.79 to 1.44 | 0.532 |
| MVPA | 0.04 | 0.00 to 0.08 | 0.064 | ||||
| Adult capability well-being (ICECAP-A) | Wave difference | 0.001 | −0.013 to 0.015 | 0.914 | −0.001 | −0.016 to 0.013 | 0.859 |
| MVPA | 0.001 | 0.000 to 0.001 | 0.024 | ||||
| Child HRQL (CHU9D) | Wave difference | 0.006 | −0.004 to 0.016 | 0.234 | 0.008 | −0.003 to 0.019 | 0.166 |
| MVPA | 0.001 | 0.000 to 0.000 | 0.679 | ||||
Is there a relationship between financial strain and HRQL and capability well-being?
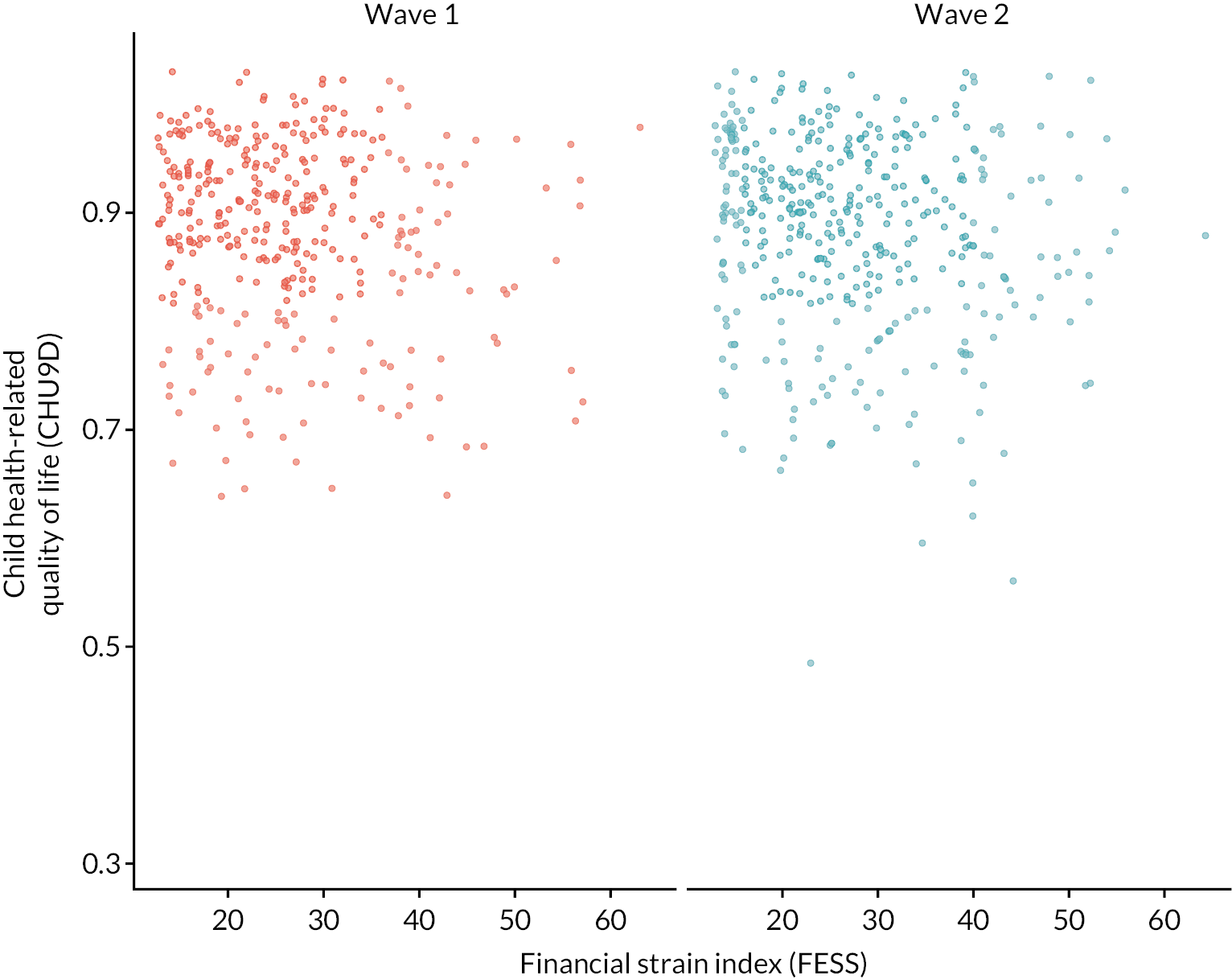
Adult HRQL and capability well-being measures were inversely associated with financial strain, with HRQL decreasing as financial strain increased (Figures 1–4; Appendix 1, Table 9). For children (CHU9D), the relationship was less clear, with a slight non-linear association (Appendix 1, Table 9; Figure 4). The linear relationship between financial strain and measures of HRQL/capability well-being was modelled explicitly via mixed models (Table 6). Coefficients reflect the change in outcome measure as a result of an increase of 10 points in FESS score (scale 13–65). All coefficients are negative, indicating that as financial strain increases, HRQL/capability well-being decreases in both adults and children. The association was smaller for children (CHU9D) than adults.
| Outcome | Unadjusted model | Adjusted model | |||||
|---|---|---|---|---|---|---|---|
| Difference in outcomea | 95% confidence interval | p-value | Difference in outcomea | 95% confidence interval | p-value | ||
| Adult HRQL | EQ-5D-5L | −0.05 | −0.07 to −0.04 | < 0.001 | −0.05 | −0.06 to −0.04 | < 0.001 |
| Adult self-rated health | EQ-5D-VAS | −5.95 | −7.05 to −4.84 | < 0.001 | −5.72 | −6.89 to −4.55 | < 0.001 |
| Adult capability well-being | ICECAP-A | −0.05 | −0.06 to −0.04 | < 0.001 | −0.05 | −0.06 to −0.05 | < 0.001 |
| Child HRQL | CHU9D | −0.01 | −0.02 to 0.00 | 0.001 | −0.01 | −0.01 to 0.00 | 0.010 |
FIGURE 1.
Scatter plot of parent/carer HRQL against financial strain. Note that points are jittered to avoid overplotting due to the underlying discrete nature of variables.
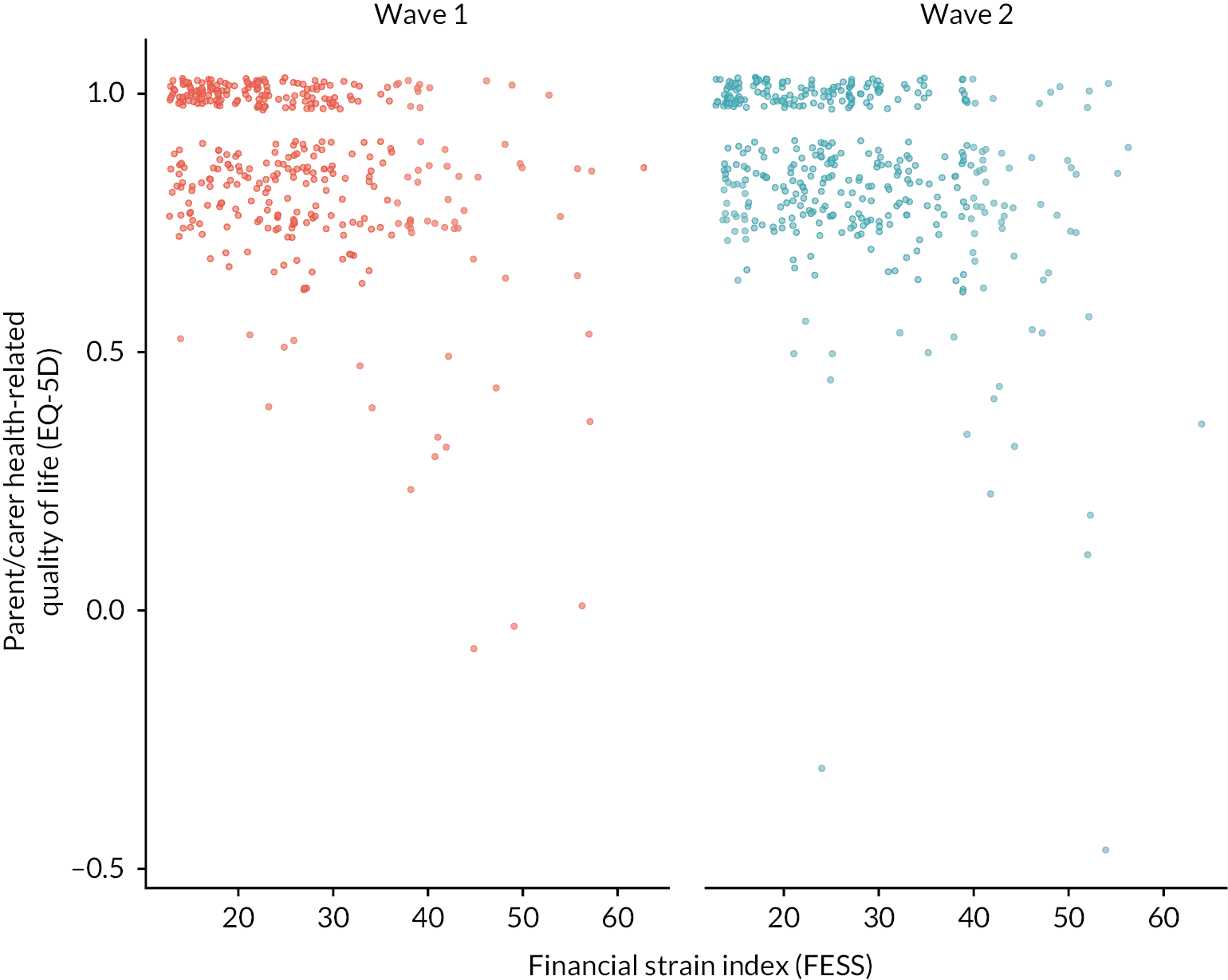
FIGURE 2.
Scatter plot of parent/carer EQ-5D VAS against financial strain. Note that points are jittered to avoid overplotting due to the underlying discrete nature of variables.
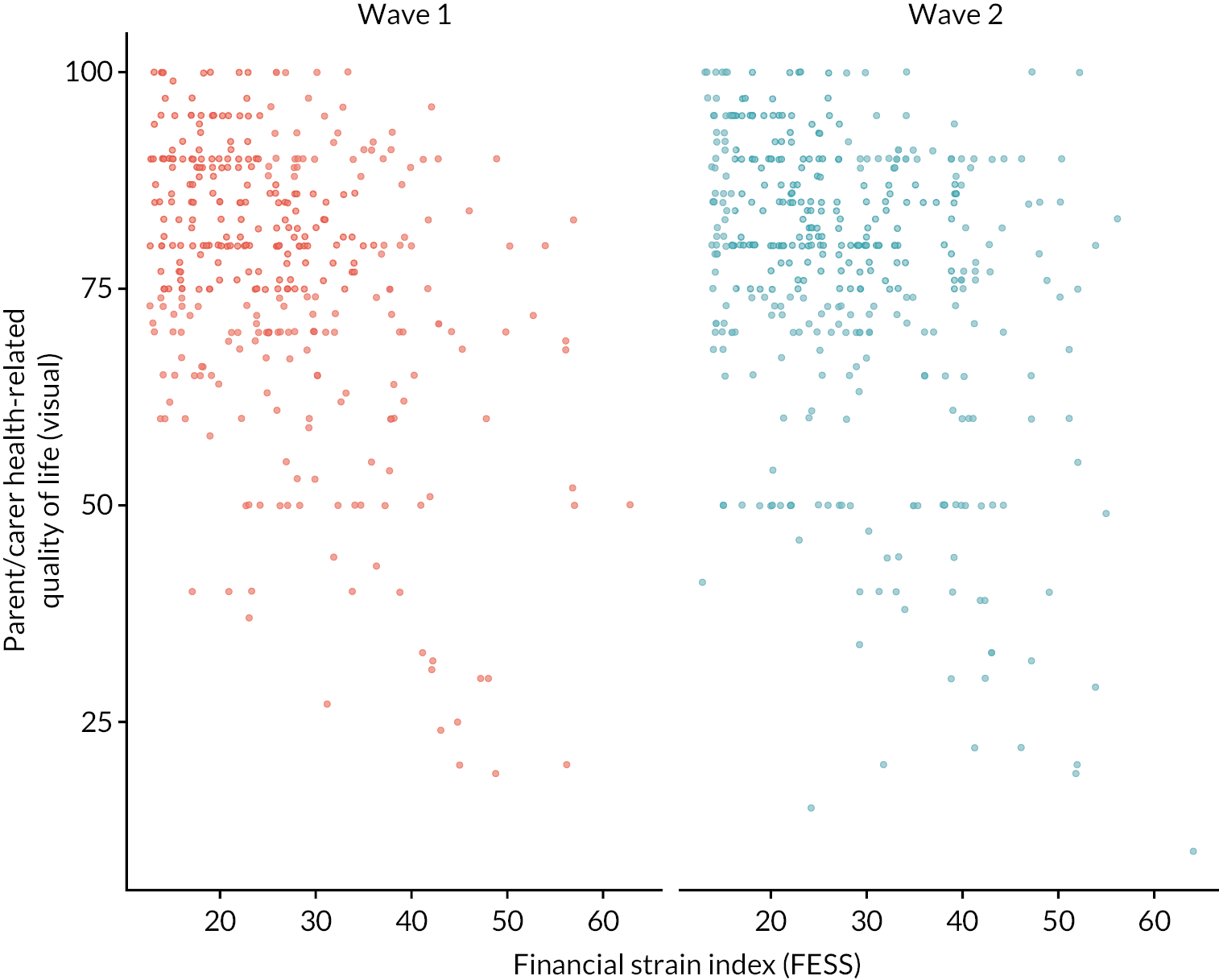
FIGURE 3.
Scatter plot of parent/carer capability well-being (ICECAP-A) against financial strain. Note that points are jittered to avoid overplotting due to the underlying discrete nature of variables.
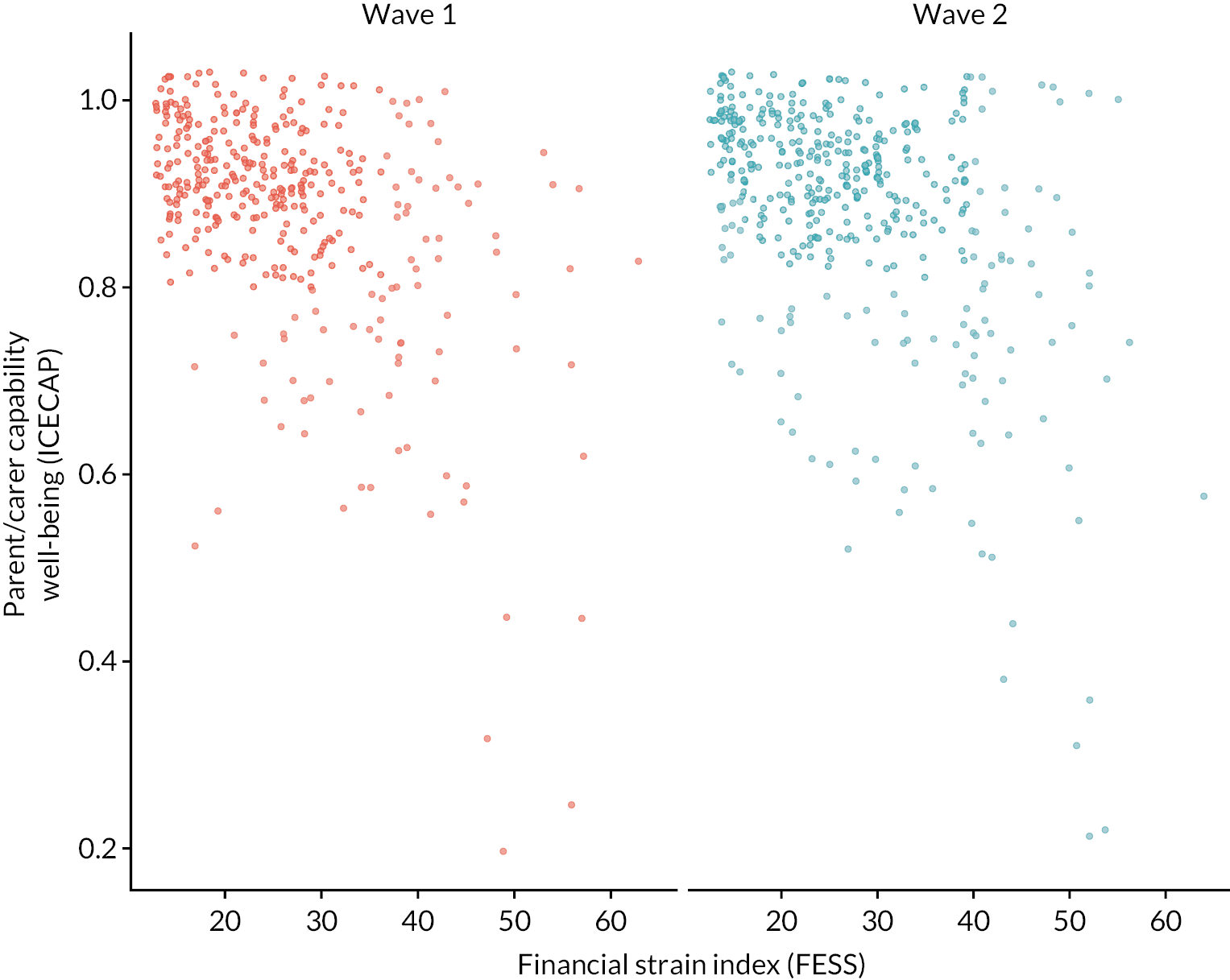
FIGURE 4.
Scatter plot of child HRQL (CHU9D) against parent-reported financial strain. Note that points are jittered to avoid overplotting due to the underlying discrete nature of variables.
Does financial strain moderate any differences in HRQL and capability well-being between waves?
To test whether financial strain had a moderating effect on the association between wave and HRQL/capability well-being we included a wave-FESS interaction term, for an increase of 10 points on the FESS scale (Table 7). All interaction estimates were small and did not indicate that financial strain moderated the effect of wave.
| Wave 1 | Wave 2 | |||||
|---|---|---|---|---|---|---|
| Estimatea | 95% confidence interval | Estimatea | 95% confidence interval | p-valueb | ||
| Adult HRQL | EQ-5D-5L | −0.051 | −0.067 to −0.035 | −0.049 | −0.0664 to −0.035 | 0.852 |
| Adult self-rated health | EQ-5D VAS | −5.931 | −7.21 to −4.341 | −5.474 | −6.943 to −4.006 | 0.650 |
| Adult capability well-being | ICECAP-A | −0.052 | −0.063 to −0.041 | −0.056 | −0.066 to −0.046 | 0.503 |
| Child HRQL | CHU9D | −0.008 | −0.016 to 0.001 | −0.011 | −0.019 to −0.003 | 0.529 |
All models allow for clustering at school and individual level and are adjusted for IMD and highest household education. Parent models additionally adjust for parent gender and age group, and child models additionally adjust for child gender.
Discussion
The Active-6 project collected detailed data on HRQL, capability well-being, and financial strain in the period after the COVID-19 lockdowns were lifted in addition to accelerometer-measured MVPA. The data presented in this study make an important contribution to the field as to the best of our knowledge there is no comparable study that has used the CHU9D to measure children’s HRQL in the short to medium term after lockdown.
There were no differences in HRQL and capability well-being in either adults or children when comparing the short and medium post-lockdown phases of the pandemic. The Australian DETECT study54 collected adolescent (aged 12–18) CHU9D data from May 2020, finding higher levels of distress compared to data collected six years before. It is important to note, however, that the DETECT team did not score the CHU9D using recommended scoring algorithms, which limits comparability to our study and the wider field. Active-6 children’s HRQL and parent capability well-being were better than observed in studies of similar populations observed before the COVID-19 pandemic (CHU9D 0.83–0.84,49,50 ICECAP-A 0.8116). Related qualitative studies suggested some Active-6 child participants experienced increased mental health challenges, such as emotional overwhelm, and physical fatigue in the short-term post-lockdown phase. 27 Sadness and tiredness are facets of HRQL measured by the CHU9D, yet the scores we observed did not support the qualitative data. Interview and focus-group participants may not be representative of the Active-6 sample, however, or the CHU9D may not be sensitive to COVID-19 lockdown-related changes. In contrast to child HRQL, adult HRQL was below the 2014 estimates of population norms (estimate 0.9448) in both waves. While we are unable to explore causation using the Active-6 dataset due to lack of pre-COVID-19 data, many aspects of the experience of the COVID-19 pandemic and related lockdowns could have contributed to poorer adult HRQL. For example, social isolation could have exacerbated mental health difficulties and COVID-19 infection could have disrupted families’ usual activities.
It might be expected that lockdowns would impact capability well-being more than HRQL due to the measures’ focus on broader outcomes; however, we saw no difference in adult or child capability well-being between the two waves. It may be that any changes in HRQL or capability well-being during lockdowns were alleviated by the lifting of restrictions or that changes persisted post-lockdown, thus any differences were not evident at Wave 1 data collection. Alternatively, the measures used could be insensitive to impacts of lockdowns, or lockdowns may have had no effect on HRQL or capability well-being at all. For children’s capability well-being, the Active-6 findings are markedly different to those found in the CONTRAST study. 55 In CONTRAST, the majority of domains indicated no change or worsening since pre-COVID-19 where only ‘feeling safe and at ease’, ‘being able to seek support’ and questions regarding relationships reported no change or a positive impact. In Active-6 data, most responses indicated that children’s capability well-being had improved since the lockdown. These differences may be due to the CONTRAST study’s older sample (aged 11–15), the data collection during different phases of the pandemic or other demographic characteristics. Despite piloting, children aged 10–11 may have struggled to understand and answer the questions in Active-6. The CONTRAST study’s recruitment using social media could also contribute to these differences.
Families experiencing the most financial strain had worse HRQL and capability well-being, with scores well below population norms. Children from families experiencing most financial strain also appeared to have lower HRQL. This observed relationship between greater financial strain and lower HRQL/capability well-being is an important finding for future research and policy. Adult HRQL and capability well-being scores for families reporting the highest level of financial strain were below population norms and the comparable population scores. Similar relationships have been observed in the USA and Canada, where financial insecurity or material hardship (e.g. inability to afford food or rent) were associated with poorer family well-being at repeated time points during the pandemic,14 and increased financial stress was associated with increased socioemotional and behavioural difficulties in children. 56 Our finding that financial strain appeared to increase slightly between Wave 1 and Wave 2 could reflect early effects of the ‘cost of living crisis’12 on health and well-being. Equally, the economic impacts of COVID-19 may have accumulated over time, with families initially able to absorb changes in income due to reduced opportunities to spend disposable income on holidays or leisure activities, for example. Qualitative findings from the Active-6 study indicate that children’s extra-curricular physical activity behaviour has changed, with participation in more affordable school-based active clubs increasing. 31 This may reflect how families have had to adapt to the new economic context.
Family financial strain showed indications of worsening between data collection waves, but differences are difficult to interpret. There is limited use of the FESS in the UK, so the interpretation of absolute values and the impact of those changes in the context of this study is challenging. Mean scores obtained in the FESS validation study47 (conducted in 1997 in the USA) were 43.30 for single mothers and ranged from 29 to 30 for single and married fathers and married mothers. Mean scores in Active-6 were 26.3 (Wave 1) and 27.5 (Wave 2), suggesting marginally less financial strain, although our data were collected 25 years later and in a different context. Nevertheless, our study provides a unique insight into the financial challenges facing the UK population during the pandemic and as the ‘cost of living crisis’ begins to deepen, and therefore will provide a useful resource for future studies. Perceived financial strain could be an important measure to collect in future research. IMD (derived from home postcode) is typically used as an indicator of deprivation; however, financial shocks such as loss of income are unlikely to affect a family’s residential address immediately, if at all. Identifying individuals or families unable to afford resources crucial for living healthy and fulfilling lives may be advantageous for quickly highlighting more targeted opportunities for public health interventions.
Physical activity had no mediating effect on differences in adult and child HRQL/capability well-being between waves. Existing evidence exploring associations between children’s physical activity and HRQL/well-being during the pandemic is mixed,24,25 although no mediation analysis examining phases of the pandemic has been conducted. Our finding that those experiencing most financial strain had poorest HRQL could have implications for the provision of interventions aiming to improve population well-being through physical activity. To avoid exacerbating inequalities, affordability of new interventions and the financial situation of the target population should be important physical activity policy-making considerations.
Strengths, limitations and future research
The Active-6 project collected data on the financial pressures experienced by England-based families, with linked data on HRQL and capability well-being in adults and children. Device-determined physical activity enabled exploration of the association of HRQL and capability well-being with activity levels. To the best of our knowledge, no other studies provide such insights into the ongoing impacts of the COVID-19 pandemic. There were also minimal missing data. The study is limited by the lack of pre-COVID-19 health economics data. We attempted to mitigate this by comparing values to population norms or pre-pandemic estimates. Ceiling effects observed reflect the non-clinical context of this study and are a recognised challenge in population-based studies. 57 Despite efforts to recruit participants from low socio-economic groups, participation was limited. There were also more female than male parents and most participants were White British. This limited our ability to explore possible inequalities across socio-economic groups, ethnicities and genders. Adult HRQL was lower post-lockdowns compared to pre-COVID-19 norms. Future research should monitor this to ascertain whether this is a continuing trend. Whether the association between HRQL and financial strain persisted as the ‘cost of living crisis’ continued should also be explored further. Qualitative research that examined this association would have provided valuable context to our findings and guided the design of future research addressing the longer-term effects.
Conclusions
Active-6 is the first study to explore the relationships between perceived financial hardship, HRQL capability well-being, and physical activity during the COVID-19 pandemic. We used validated outcome measures recommended for use in UK policy-making. While HRQL and capability well-being showed no differences as the pandemic progressed, families experiencing financial hardship had notably worse HRQL and capability well-being in both waves. This was most pronounced in children of parents reporting most financial difficulties. Using robust methods to collect accelerometer data, we did not observe a mediating effect of physical activity on HRQL.
Additional information
Contributions of authors
Katie Breheny (https://orcid.org/0000-0001-6886-4049) (Research Fellow, Health Economics) conducted the analysis of all models and led the writing of the manuscript.
Ruth Salway (https://orcid.org/0000-0002-3242-3951) (Research Fellow, Statistics) advised on statistical analysis and interpretation and edited the paper for intellectual content.
Danielle House (https://orcid.org/0000-0001-6171-9922) (Senior Research Associate, Study Manager) oversaw data collection in Wave 2, managed the project and edited the paper for intellectual content.
Robert Walker (https://orcid.org/0000-0001-9901-5285) (Senior Research Associate, Qualitative Lead) supported the development of the paper and edited the paper for intellectual content.
Lydia Emm-Collison (https://orcid.org/0000-0002-5493-3223) (Steering Group Member) supported the development of the paper and edited the paper for intellectual content.
Kate Sansum (https://orcid.org/0000-0003-3392-6750) (Fieldworker) conducted Wave 2 data collection, supported the development of the paper and edited the paper for intellectual content.
Joanna G Williams (https://orcid.org/0000-0002-4737-1760) (Steering Group Member) supported the development of the paper and edited the paper for intellectual content.
Frank de Vocht (https://orcid.org/0000-0003-3631-627) (Steering Group Member) supported the development of the paper and edited the paper for intellectual content.
Russell Jago (https://orcid.org/0000-0002-3394-0176) (Principal Investigator, Active-6) led the project, oversaw all aspects of study design and interpretation, supported the development of the paper and edited the paper for intellectual content.
William Hollingworth (https://orcid.org/0000-0002-0840-6254) (Steering Group Member, Health Economics) oversaw all aspects of the economic design and analysis and edited the paper for intellectual content.
Disclosure of interests
Full disclosure of interests: Completed ICMJE forms for all authors, including all related interests, are available in the toolkit on the NIHR Journals Library report publication page at https://doi.org/10.3310/LYJG6305.
Primary conflicts of interest: Russell Jago, Katie Breheny, Frank de Vocht and William Hollingworth are partly funded by the National Institute for Health and Care Research Applied Research Collaboration West (NIHR ARC West). Russell Jago is partly funded by the National Institute for Health and Care Research Bristol Biomedical Research Centre, and was a member of the PHR Prioritisation Group 11 October 2019–12 October 2021, and a member of the PHR – Research Funding Board 1 June 2014–12 October 2021. Frank de Vocht has been on the NIHR Public Health Research Funding Board since 8 October 2019. William Hollingworth was a member of the HTA Clinical Evaluation and Trials Committee 1 July 2016–31 March 2021. Katie Breheny is a member of the ICECAP questionnaires Management Group.
Data-sharing statement
All data requests should be submitted to the corresponding author for consideration. Access to anonymised data may be granted following review.
Ethics statement
Ethical approval was gained from the School of Policy Studies Ethics Committee at the University of Bristol, UK (Ref SPSREC/20-21/150) on 9 March 2021. The project was listed on the Research Registry [Assessing the Impact of COVID-19 on the Physical Activity of Year 6 Children and Their Parents: Identifying Scalable Actions to Mitigate Adverse Impacts and Provide Rapid Evidence to Policy Makers. 2021. URL: www.researchregistry.com/browse-the-registry#home/registrationdetails/604b4760d539c90020642be6/ (accessed 27 January 2023)]. 58
Information governance statement
The University of Bristol is committed to handling all personal information in line with the UK Data Protection Act (2018) and the General Data Protection Regulation (EU GDPR) 2016/679. Under the Data Protection legislation, the University of Bristol is the Data Controller, and you can find out more about how we handle personal data, including how to exercise your individual rights and the contact details for our Data Protection Officer here (www.bristol.ac.uk/secretary/data-protection/).
Study registration
The study is registered on the Research Registry (project 6646).
Funding
This article presents independent research funded by the National Institute for Health and Care Research (NIHR) Public Health Research programme as award number NIHR131847.
Department of Health and Social Care disclaimer
This publication presents independent research commissioned by the National Institute for Health and Care Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, MRC, NIHR Coordinating Centre, the PHR programme or the Department of Health and Social Care.
This article reports on one component of the research award ‘Assessing the impact of COVID-19 on the physical activity of Year 6 children and their parents: Identifying scalable actions to mitigate adverse impacts & provide rapid evidence to policy makers (ACTIVE-6)’. Other articles published as part of this thread are:
Salway R, Foster C, de Vocht F, Tibbitts B, Emm-Collison L, House D, et al. Accelerometer-measured physical activity and sedentary time among children and their parents in the UK before and after COVID-19 lockdowns: a natural experiment. Int J Behav Nutr Phys Act 2022;19:51. https://doi.org/10.1186/s12966-022-01290-4
Walker R, House D, Emm-Collison L, Salway R, Tibbitts B, Sansum K, et al. A multi-perspective qualitative exploration of the reasons for changes in the physical activity among 10–11-year-old children following the easing of the COVID-19 lockdown in the UK in 2021. Int J Behav Nutr Phys Act 2022;19:114. https://doi.org/10.1186/s12966-022-01356-3
Jago R, Salway R, House D, Walker R, Emm-Collison L, Sansum K, et al. Short and medium-term effects of the COVID-19 lockdowns on child and parent accelerometer-measured physical activity and sedentary: a natural experiment. Int J Behav Nutr Phys Act 2023;20:42. https://doi.org/10.1186/s12966-023-01441-1
Salway R, Walker R, Sansum K, House D, Emm-Collison L, Reid T, et al. Screen-viewing behaviours of children before and after the 2020–21 COVID-19 lockdowns in the UK: a mixed methods study. BMC Public Health 2023;23:116. https://doi.org/10.1186/s12889-023-14976-6
Walker R, House D, Salway R, Emm-Collison L, Hollander L, Sansum K, et al. The new normal for children’s physical activity and screen viewing: a multi-perspective qualitative analysis of behaviours a year after the COVID-19 lockdowns in the UK. BMC Public Health 2023;23:1432. https://doi.org/10.1186/s12889-023-16021-y
Emm-Collison L, Walker R, Salway R, House D, Sansum K, Breheny K, et al. Exploring parents’ physical activity motivation during the COVID-19 pandemic: a mixed methods study from a self-determination theory perspective. Public Health Res 2024;27 March:1–35 [published online ahead of print] https://doi.org/10.3310/KPKW8220
Salway R, de Vocht F, Emm-Collison L, Sansum L, House D, Walker R, et al. Comparison of children’s physical activity profiles before and after COVID-19 lockdowns: a latent profile analysis. PLOS ONE 2023;18(11):e0289344. https://doi.org/10.1371/journal.pone.0289344
Walker R, Salway R House D, Emm-Collison L, Breheny K, Sansum K, et al. The status of active after-school clubs among primary school children in England (UK) after the COVD-19 lockdowns: implications for policy and practice. Int J Behav Nutr Phys Act 2023;20:120. https://doi.org/10.1186/s12966-023-01499-x
House D, Walker R, Salway R, Emm-Collison L, Breheny K, Sansum K, et al. The impact of the COVID-19 pandemic on the physical activity environment in English primary schools: a multi-perspective qualitative analysis. Public Health Res 2024;7 Feb:1–37 [published online ahead of print] https://doi.org/10.3310/KLML4701
Salway R, House D, Walker R, Emm-Collison L, Breheny K, Sansum K, et al. Between-school differences (school variation) in children’s MVPA before and after COVID-19 lockdowns: a multilevel model analysis. Public Health Res (in press).
Jago R, House D, Salway R, Walker R, Emm-Collison L, Sansum K, Breheny K, Churchward S, Williams J, Hollingworth W, and de Vocht F. Assessing the impact of COVID-19 on the physical activity of 10- to 11-year-old children and their parents: Active-6 a mixed-methods study. Public Health Res (in press).
For more information about this research please view the award page https://fundingawards.nihr.ac.uk/award/NIHR131847
About this article
The contractual start date for this research was in April 2021. This article began editorial review in March 2023 and was accepted for publication in February 2024. The authors have been wholly responsible for all data collection, analysis and interpretation, and for writing up their work. The Public Health Research editors and publisher have tried to ensure the accuracy of the authors’ article and would like to thank the reviewers for their constructive comments on the draft document. However, they do not accept liability for damages or losses arising from material published in this article.
This article was published based on current knowledge at the time and date of publication. NIHR is committed to being inclusive and will continually monitor best practice and guidance in relation to terminology and language to ensure that we remain relevant to our stakeholders.
Copyright
Copyright © 2024 Breheny et al. This work was produced by Breheny et al. under the terms of a commissioning contract issued by the Secretary of State for Health and Social Care. This is an Open Access publication distributed under the terms of the Creative Commons Attribution CC BY 4.0 licence, which permits unrestricted use, distribution, reproduction and adaption in any medium and for any purpose provided that it is properly attributed. See: https://creativecommons.org/licenses/by/4.0/. For attribution the title, original author(s), the publication source – NIHR Journals Library, and the DOI of the publication must be cited.
List of abbreviations
- CHU9D
- Child Health Utility 9 Dimension
- EDI
- equality, diversity and inclusion
- FESS
- Family Economic Strain Scale
- HRQL
- health-related quality of life
- IMD
- Index of Multiple Deprivation
- MVPA
- moderate to vigorous physical activity
- PPI
- patient and public involvement
- SD
- standard deviation
References
- Torrance GW. Utility approach to measuring health-related quality of life. J Chron Dis 1987;40:593-60. https://doi.org/10.1016/0021-9681(87)90019-1.
- NICE . NICE Health Technology Evaluations: The Manual 2022.
- Brooks R. EuroQol: the current state of play. Health Pol 1996;37:53-72. https://doi.org/10.1016/0168-8510(96)00822-6.
- Herdman M, Gudex C, Lloyd A, Janssen MF, Kind P, Parkin D, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res: Int J Qual Life Aspect Treat Care Rehab 2011;20:1727-36. https://doi.org/10.1007/s11136-011-9903-x.
- Stevens K. Valuation of the Child Health Utility 9D Index. PharmacoEcon 2012;30:729-47. https://doi.org/10.2165/11599120-000000000-00000.
- Baldwin S, Godfrey C, Propper C. Quality of Life: Perspectives and Policies. London: Routledge; 1994.
- Fenge L-A, Hean S, Worswick L, Wilkinson C, Fearnley S, Ersser S. The impact of the economic recession on well-being and quality of life of older people. Health Soc Care Commun 2012;20:617-24. https://doi.org/10.1111/j.1365-2524.2012.01077.x.
- Creswell C, Shum A, Pearcey S, Skripkauskaite S, Patalay P, Waite P. Young people’s mental health during the COVID-19 pandemic. Lancet Child Adolesc Health 2021;5:535-7. https://doi.org/10.1016/S2352-4642(21)00177-2.
- Burgess L, Skripkauskaite S, Waite P, Creswell C. Children’s Mental Health Symptoms Two Years After the Start of the Pandemic: March 2020 to March 2022 (Report 12) – Co-SPACE Study. 2022.
- Moore G, Anthony R, Angel L, Hawkins J, Morgan K, Copeland L, et al. Mental health and life satisfaction among 10–11-year-olds in Wales, before and one year after onset of the COVID-19 pandemic. BMC Publ Health 2022;22. https://doi.org/10.1186/s12889-022-12752-6.
- Powell A, Francis-Devine B, Clark H. Coronavirus: Impact on the Labour Market. London: Commons Library; 2022.
- Institute for Government . Cost of Living Crisis 2022. www.instituteforgovernment.org.uk/explainer/cost-living-crisis (accessed 11 January 2023).
- Stevenson C, Wakefield JRH, Bowe M, Kellezi B, Jones B, McNamara N. Weathering the economic storm together: family identification predicts future well-being during COVID-19 via enhanced financial resilience. J Fam Psychol 2022;36:337-45.
- Gonzalez MR, Brown SA, Pelham Iii WE, Bodison SC, McCabe C, Baker FC, et al. Family well-being during the COVID-19 pandemic: the risks of financial insecurity and coping. J Res Adolesc 2022;33:43-58. https://doi.org/10.1111/jora.12776.
- Nobari H, Fashi M, Eskandari A, Villafaina S, Murillo-Garcia A, Pérez-Gómez J. Effect of COVID-19 on health-related quality of life in adolescents and children: a systematic review. Int J Environ Res Public Health 2021;18. https://doi.org/10.3390/ijerph18094563.
- Mitchell PM, Morton RL, Hiligsmann M, Husbands S, Coast J. Estimating loss in capability wellbeing in the first year of the COVID-19 pandemic: a cross-sectional study of the general adult population in the UK, Australia and the Netherlands. Eur J Health Econ 2022;24:609-19. https://doi.org/10.1007/s10198-022-01498-y.
- Jago R, Salway R, House D, Walker R, Emm-Collison L, Sansum K, et al. Short and medium-term effects of the COVID-19 lockdowns on child and parent accelerometer-measured physical activity and sedentary time: a natural experiment. Int J Behav Nutr Phys Activ 2023;20. https://doi.org/10.1186/s12966-023-01441-1.
- Salway R, Foster C, de Vocht F, Tibbitts B, Emm-Collison L, House D, et al. Accelerometer-measured physical activity and sedentary time among children and their parents in the UK before and after COVID-19 lockdowns: a natural experiment. Int J Behav Nutr Phys Activ 2022;19. https://doi.org/10.1186/s12966-022-01290-4.
- Wunsch K, Kienberger K, Niessner C. Changes in physical activity patterns due to the COVID-19 pandemic: a systematic review and meta-analysis. Int J Environ Res Public Health 2022;19. https://doi.org/10.3390/ijerph19042250.
- Park AH, Zhong S, Yang H, Jeong J, Lee C. Impact of COVID-19 on physical activity: a rapid review. J Glob Health 2022;12. https://doi.org/10.7189/jogh.12.05003.
- Bize R, Johnson JA, Plotnikoff RC. Physical activity level and health-related quality of life in the general adult population: a systematic review. Prev Med 2007;45:401-15. https://doi.org/10.1016/j.ypmed.2007.07.017.
- Feeny D, Garner R, Bernier J, Thompson A, McFarland BH, Huguet N, et al. Physical activity matters: associations among body mass index, physical activity, and health-related quality of life trajectories over 10 years. J Phys Act Health 2014;11:1265-75. https://doi.org/10.1123/jpah.2012-0268.
- Marker AM, Steele RG, Noser AE. Physical activity and health-related quality of life in children and adolescents: a systematic review and meta-analysis. Health Psychol 2018;37:893-90. https://doi.org/10.1037/hea0000653.
- López-Gil JF, Tremblay MS, Tapia-Serrano MA, Tárraga-López PJ, Brazo-Sayavera J. Meeting 24 h movement guidelines and health-related quality of life in youths during the COVID-19 lockdown. Appl Sci 2022;12. https://doi.org/10.3390/app12168056.
- Pybus K, Kelly B, Hou B, Ajebon M, McIvor C, Bingham D, et al. Changes in children’s wellbeing in Bradford during COVID-19: the Born in Bradford COVID-19 longitudinal research study [version 2]. Wellc Open Res 2022;7. https://doi.org/10.12688/wellcomeopenres.17642.2.
- Salway R, Walker R, Sansum K, House D, Emm-Collison L, Reid T, et al. Screen-viewing behaviours of children before and after the 2020–21 COVID-19 lockdowns in the UK: a mixed methods study. BMC Public Health 2023;23. https://doi.org/10.1186/s12889-023-14976-6.
- Walker R, House D, Emm-Collison L, Salway R, Tibbitts B, Sansum K, et al. A multi-perspective qualitative exploration of the reasons for changes in the physical activity among 10–11-year-old children following the easing of the COVID-19 lockdown in the UK in 2021. Int J Behav Nutr Phys Activ 2022;19. https://doi.org/10.1186/s12966-022-01356-3.
- Jago R. Assessing the impact of COVID-19 on the physical activity of Year 6 children and their parents: identifying scalable actions to mitigate adverse impact & provide rapid evidence to olicy Makers (ACTIVE-6) 2021. https://fundingawards.nihr.ac.uk/award/NIHR131847 (accessed 27 January 2023).
- Salway R, de Vocht F, Emm-Collison L, Sansum K, House D, Walker R, et al. Comparison of children’s physical activity profiles before and after COVID-19 lockdowns: a latent profile analysis. PLOS ONE 2023;18. https://doi.org/10.1371/journal.pone.0289344.
- Walker R, House D, Salway R, Emm-Collison L, Hollander LE, Sansum K, et al. The new normal for children’s physical activity and screen viewing: a multi-perspective qualitative analysis of behaviours a year after the COVID-19 lockdowns in the UK. BMC Publ Health 2023;23. https://doi.org/10.1186/s12889-023-16021-y.
- Walker R, Salway R, House D, Emm-Collison L, Breheny K, Sansum K, et al. The status of active after-school clubs among primary school children in England (UK) after the COVD-19 lockdowns: implications for policy and practice. Int J Behav Nutr Phys Activ 2023;20. https://doi.org/10.1186/s12966-023-01499-x.
- Jago R, Salway R, Emm-Collison L, Sebire SJ, Thompson JL, Lawlor DA. Association of BMI category with change in children’s physical activity between ages 6 and 11 years: a longitudinal study. Int J Obes (Lond) 2020;44:104-13. https://doi.org/10.1038/s41366-019-0459-0.
- National Statistics . English Indices of Deprivation 2019.
- R Core Team . R: A Language and Environment for Statistical Computing 2020.
- Salway R. Accelerometer Processing Code. 2022.
- Cooper AR, Goodman A, Page AS, Sherar LB, Esliger DW, van Sluijs EMF, et al. Objectively measured physical activity and sedentary time in youth: the International children’s accelerometry database (ICAD). Int J Behav Nutr Phys Activ 2015;12. https://doi.org/10.1186/s12966-015-0274-5.
- Evenson KR, Catellier DJ, Gill K, Ondrak KS, McMurray RG. Calibration of two objective measures of physical activity for children. J Sports Sci 2008;26:1557-65. https://doi.org/10.1080/02640410802334196.
- Troiano RP, Berrigan D, Dodd KW, Mâsse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc 2008;40:181-8. https://doi.org/10.1249/mss.0b013e31815a51b3.
- Feng YS, Kohlmann T, Janssen MF, Buchholz I. Psychometric properties of the EQ-5D-5L: a systematic review of the literature. Qual Life Res 2021;30:647-73. https://doi.org/10.1007/s11136-020-02688-y.
- van Hout B, Janssen MF, Feng Y-S, Kohlmann T, Busschbach J, Golicki D, et al. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health: J Int Soc Pharmacoecon Outc Res 2012;15:708-15. https://doi.org/10.1016/j.jval.2012.02.008.
- Al-Janabi H, Flynn T N, Coast J. Development of a self-report measure of capability wellbeing for adults: the ICECAP-A. Qual Life Res 2012;21:167-76. https://doi.org/10.1007/s11136-011-9927-2.
- Afentou N, Kinghorn P. A systematic review of the feasibility and psychometric properties of the ICEpop CAPability measure for adults and its use so far in economic evaluation. Value Health 2020;23:515-26. https://doi.org/10.1016/j.jval.2019.12.010.
- Flynn TN, Huynh E, Peters TJ, Al-Janabi H, Clemens S, Moody A, et al. Scoring the Icecap-a capability instrument: estimation of a UK general population tariff. Health Econ 2015;24:258-69. https://doi.org/10.1002/hec.3014.
- Stevens K. Developing a descriptive system for a new preference-based measure of health-related quality of life for children. Qual Life Res: Int J Qual Life Aspect Treat Care Rehab 2009;18:1105-13. https://doi.org/10.1007/s11136-009-9524-9.
- Rowen D, Keetharuth AD, Poku E, Wong R, Pennington B, Wailoo A. A review of the psychometric performance of selected child and adolescent preference-based measures used to produce utilities for child and adolescent health. Value Health: J Int Soc Pharmacoecon Outc Res 2021;24:443-60. https://doi.org/10.1016/j.jval.2020.09.012.
- Husbands S, Mitchell P, Floredin I, Peters T, Kinghorn P, Byford S, et al. The children and young people quality of life study: a protocol for the qualitative development of attributes for capability wellbeing measures for use in health economic evaluation with children and young people. Wellc Open Res 2022;7. https://doi.org/10.12688/wellcomeopenres.17801.1.
- Hilton JM, Devall EL. The Family Economic Strain Scale: development and evaluation of the instrument with single- and two-parent families. J Family Econ Issues 1997;18:247-71. https://doi.org/10.1023/A:1024974829218.
- Janssen MF, Pickard AS, Shaw JW. General population normative data for the EQ-5D-3L in the five largest European economies. Eur J Health Econ: HEPAC: Health Econ Prev Care 2021;22:1467-75. https://doi.org/10.1007/s10198-021-01326-9.
- Adab P, Pallan MJ, Lancashire ER, Hemming K, Frew E, Barrett T, et al. Effectiveness of a childhood obesity prevention programme delivered through schools, targeting 6 and 7 year olds: cluster randomised controlled trial (WAVES study). BMJ 2018;360. https://doi.org/10.1136/bmj.k211.
- Connolly P, Miller S, Kee F, Sloan S, Gildea A, McIntosh E, et al. A cluster randomised controlled trial and evaluation and cost-effectiveness analysis of the Roots of Empathy schools-based programme for improving social and emotional well-being outcomes among 8- to 9-year-olds in Northern Ireland. Publ Health Res 2018;6:1-108. https://doi.org/10.3310/phr06040.
- Breheny K, Hollingworth W, Tibbitts B. The ACTIVE-6 Project: Detailed Health Economics Analysis Plan. Bristol: University of Bristol; 2021.
- Devlin N, Parkin D, Janssen B. Methods for Analysing and Reporting EQ-5D Data. Cham: Springer International; 2020.
- StataCorp . Stata Statistical Software: Release 17 2021.
- Thomas HM, Runions KC, Lester L, Lombardi K, Epstein M, Mandzufas J, et al. Western Australian adolescent emotional wellbeing during the COVID-19 pandemic in 2020. Child Adolesc Psychiat Ment Health 2022;16. https://doi.org/10.1186/s13034-021-00433-y.
- Pallan M, Adab P, Clarke J, Duff R, Frew E, Lancashire E, et al. Impacts of the First COVID-19 Lockdown on Learning, Health Behaviours and Mental Wellbeing in Young People Aged 11–15 Years. Birmingham: University of Birmingham Institute of Applied Health Research; 2021.
- McGill MG, Purkey E, Davison CM, Watson A, Bayoumi I. Financial stress during COVID-19: implications for parenting behaviour and child well-being. BMJ Paediatr Open 2022;6. https://doi.org/10.1136/bmjpo-2022-001569.
- Brazier J, Peasgood T, Mukuria C, Marten O, Kreimeier S, Luo N, et al. The EQ-HWB: overview of the development of a measure of health and wellbeing and key results. Value Health: J Int Soc Pharmacoecon Outc Res 2022;25:482-91. https://doi.org/10.1016/j.jval.2022.01.009.
- Research Registry . Assessing the Impact of COVID-19 on the Physical Activity of Year 6 Children and Their Parents: Identifying Scalable Actions to Mitigate Adverse Impacts and Provide Rapid Evidence to Policy Makers 2021. www.researchregistry.com/browse-the-registry#home/registrationdetails/604b4760d539c90020642be6/ (accessed 27 January 2023).
Appendix 1 Child capability well-being questions
The questions below are about how things have changed since the UK went into lockdown in January 2021.
We are interested in whether you think that you have been able to have more or less of these things since the January 2021 lockdown restrictions began. For each question below, please select which statement best describes how you feel at the moment.
1. Feeling safe and at ease
| I feel much more safe and at ease than I did before the start of the lockdown restrictions |
| I feel more safe and at ease than I did before the start of the lockdown restrictions |
| I feel as safe and at ease as I did before the start of the lockdown restrictions |
| I feel less safe and at ease than I did before the start of the lockdown restrictions |
| I feel much less safe and at ease than I did before the start of the lockdown restrictions |
2. Talking and support from people who care about me
| I am now able to talk to and seek support from the people who are there for me, much more than I could before the start of the lockdown restrictions |
| I am now able to talk to and seek support from the people who are there for me, more than I could before the start of the lockdown restrictions |
| I am now able to talk to and seek support from the people who are there for me, as much as I could before the start of the lockdown restrictions |
| I am now able to talk to and seek support from the people who are there for me, less than I could before the start of the lockdown restrictions |
| I am now able to talk to and seek support from the people who are there for me, much less than I could before the start of the lockdown restrictions |
3. Having fun
| I am now able to do a lot more of the things that I enjoy than I could before the start of the lockdown restrictions |
| I am now able to do more of the things that I enjoy than I could before the start of the lockdown restrictions |
| I am now able to do as many of the things that I enjoy as I could before the start of the lockdown restrictions |
| I am now able to do fewer of the things that I enjoy than I could before the start of the lockdown restrictions |
| I am now able to do a lot fewer of the things that I enjoy than I could before the start of the lockdown restrictions |
4. Being able to achieve things that are important to me (these might be things like schoolwork, hobbies and interests, sports)
| I am now able to achieve much more of what is important to me than I could before the start of the lockdown restrictions |
| I am now able to achieve more of what is important to me than I could before the start of the lockdown restrictions |
| I am now able to achieve as much of what is important to me as I could before the start of the lockdown restrictions |
| I am now able to achieve less of what is important to me than I could before the start of the lockdown restrictions |
| I am now able to achieve much less of what is important to me than I could before the start of the lockdown restrictions |
5. Relationships
5a. Relationships with people I live with
| My ability to feel close to the people I live with is much better than before the start of the lockdown restrictions |
| My ability to feel close to the people I live with is better than before the start of the lockdown restrictions |
| My ability to feel close to the people I live with is the same as before the start of the lockdown restrictions |
| My ability to feel close to the people I live with is worse than before the start of the lockdown restrictions |
| My ability to feel close to the people I live with is much worse than before the start of the lockdown restrictions |
5b. Relationships with family who I don’t live with
| My ability to feel close to family who I don’t live with is much better than before the start of the lockdown restrictions |
| My ability to feel close to family who I don’t live with is better than before the start of the lockdown restrictions |
| My ability to feel close to family who I don’t live with is the same as before the start of the lockdown restrictions |
| My ability to feel close to family who I don’t live with, is worse than before the start of the lockdown restrictions |
| My ability to feel close to family who I don’t live with is much worse than before the start of the lockdown restrictions |
5c. Relationships with friends
| My ability to feel close to friends is much better than before the start of the lockdown restrictions |
| My ability to feel close to friends is better than before the start of the lockdown restrictions |
| My ability to feel close to friends is the same as before the start of the lockdown restrictions |
| My ability to feel close to friends is worse than before the start of the lockdown restrictions |
| My ability to feel close to friends is much worse than before the start of the lockdown restrictions |
6. Being able to discover and learn
| I am able to discover and learn much more than I was before the start of lockdown restrictions |
| I am able to discover and learn more than I was before the start of lockdown restrictions |
| I am able to discover and learn as much as I was before the start of lockdown restrictions |
| I am able to discover and learn less than I was before the start of lockdown restrictions |
| I am able to discover and learn much less than I was before the start of lockdown restrictions |
| Domain | Measure | Wave 1, N = 393, N missing (%) | Wave 2, N = 436, N missing (%) |
|---|---|---|---|
| Adult HRQL | EQ-5D-5L | 31 (8) | 34 (8) |
| Adult self-rated health | EQ-5D VAS | 31 (8) | 33 (8) |
| Adult capability well-being | ICECAP-A | 29 (7) | 31 (7) |
| Children’s HRQL | CHU9D | 30 (8) | 31 (7) |
| Parent-reported financial strain | FESS | 33 (8) | 34 (8) |
| Measure | FESS quartile | Wave 1 | Wave 2 | |||
|---|---|---|---|---|---|---|
| Mean (SD) | N | Mean (SD) | N | |||
| Adult HRQL | EQ-5D-5L utility | 1 (lowest strain) | 0.920 (0.106) | 97 | 0.905 (0.106) | 114 |
| 2 | 0.877 (0.128) | 89 | 0.847 (0.177) | 92 | ||
| 3 | 0.870 (0.123) | 90 | 0.865 (0.117) | 95 | ||
| 4 (highest strain) | 0.759 (0.242) | 83 | 0.762 (0.233) | 97 | ||
| Adult self-rated health | EQ-5D-5L VAS | 1 (lowest strain) | 82.23 (11.43) | 97 | 82.52 (12.98) | 114 |
| 2 | 79.35 (13.61) | 89 | 78.83 (14.51) | 92 | ||
| 3 | 77.06 (13.47) | 90 | 75.61 (15.48) | 97 | ||
| 4 (highest strain) | 67.47 (20.81) | 83 | 66.82 (21.33) | 97 | ||
| Adult capability well-being | ICECAP-A | 1 (lowest strain) | 0.927 (0.067) | 97 | 0.934 (0.071) | 115 |
| 2 | 0.911 (0.073) | 89 | 0.903 (0.084) | 92 | ||
| 3 | 0.880 (0.088) | 90 | 0.885 (0.102) | 98 | ||
| 4 (highest strain) | 0.799 (0.166) | 84 | 0.800 (0.176) | 97 | ||
| Children’s HRQL | CHU9D | 1 (lowest strain) | 0.896 (0.075) | 95 | 0.905 (0.078) | 115 |
| 2 | 0.885 (0.082) | 89 | 0.881 (0.091) | 92 | ||
| 3 | 0.891 (0.079) | 90 | 0.880 (0.079) | 96 | ||
| 4 (highest strain) | 0.865 (0.087) | 84 | 0.868 (0.095) | 97 | ||